CADTH Health Technology Review
Anesthesia Care Provided by Nurses
Rapid Review
Authors: Srabani Banerjee, Nicole Askin
Abbreviations
ASA
American Society of Anesthesiologists
CI
confidence interval
CRNA
certified registered nurse anesthetist
ICER
incremental cost-effectiveness ratio
MSF-OCB
Médecins Sans Frontières-Operational Centre Brussels
NPA
non-physician anesthetist
OR
odds ratio
PA
physician anesthesiologist
QALY
quality-adjusted life-year
SR
systematic review
Key Messages
One systematic review, 4 primary studies (observational studies: 3 retrospective and 1 prospective), and 1 economic evaluation were identified.
A definitive conclusion is not possible regarding the clinical effectiveness of anesthesia provided by non-physician anesthetists compared with physician anesthetists, considering the evidence was from studies of low quality that were associated with considerable risk of bias, and there were inconsistencies in the findings.
The incremental cost-effectiveness ratio (ICER) for physician anesthesiologists compared with nurse anesthetists was US$77,400 per quality-adjusted life-year (QALY) gained. The 1-way sensitivity analyses showed that with an increase in the cost of nurse anesthetist professional services or an increase in the number of unexpected hospital days, the ICER values would fall below US$50,000 per QALY gained.
Context and Policy Issues
Anesthesia is a treatment with drugs (known as anesthetics) that is used for surgical and other interventional procedures, to produce analgesia (pain control), or lack of awareness of pain.1 Perioperative anesthetic care involves the maintenance of physiologic homeostasis (e.g., hemodynamic stability, oxygenation, ventilation, and temperature).1 Depending on the type of pain relief required, anesthesia may be administered by injection, inhalation, topical application, or skin patch.2 Generally, an anesthesiologist, and an anesthesia care team, including a Certified Registered Nurse Anesthetist (CRNA) or an Anesthesia Assistant, manage perioperative care.1 Risk factors for anesthesia complications include advanced age, diabetes, kidney disease, heart disease, high blood pressure, lung disease (such as asthma or chronic obstructive pulmonary disease), sleep apnea, neurologic disorders, and smoking.3 Aging population, increasing demand for surgery, and rising health care costs are some of the challenges that impact the provision of anesthesia services.4 To address some of these challenges, various anesthesia delivery models are being explored. Anesthetics may be administered by a physician anesthetist working alone or as part of a team or by non-physician anesthetists (NPAs) who may be working alone or as part of an anesthetic team.4 In some European countries, there is a move toward NPAs being able to induce general anesthesia for American Society of Anesthesiologists (ASA) categories ASA1 and ASA2, under the indirect supervision of a physician anesthetist.4 There is still much debate among anesthesia professionals and policy-makers, regarding the types of anesthesia delivery models that are appropriate and should be used.5
The purpose of this review is to summarize the evidence regarding clinical effectiveness and cost-effectiveness of anesthesia care provided by nurses versus anesthesia care provided by physicians.
Research Questions
What is the clinical effectiveness of anesthesia care provided by nurses versus anesthesia care provided by physicians?
What is the cost-effectiveness of anesthesia care provided by nurses versus anesthesia care provided by physicians?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, CINAHL, the Cochrane Library, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was nurse anesthetists. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses or network meta-analyses, any type of clinical trials or observational studies, or economic studies. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2011 and June 29, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients (any age) requiring anesthesia care for peri-operative, obstetrical, or diagnostic procedures. Patients (any age) receiving anesthesia care for chronic pain at a pain management clinic. |
Intervention | Anesthesia care provided independently by nurses or under the supervision or direction of a physician (e.g., physician orders the anesthetic, nurse administers the anesthesia care). Anesthesia care can include administration of the anesthesia for pain management, obstetrical procedures, diagnostic procedures, and surgical procedures as well as follow-up care in the preoperative/preprocedural, intraoperative/intraprocedural, and post-operative/postprocedural stages. |
Comparator | Anesthesia care administered by a physician/anesthesiologist |
Outcomes | Q1: Clinical effectiveness: (e.g., intraoperative emergency management, length of stay, mortality) Adverse events (e.g., hospital re-admission) Q2: Cost-effectiveness: (e.g., cost per QALY, ICERs, etc.) |
Study designs | HTAs, SRs, RCTs, NRSs, and economic evaluations |
HTA = health technology assessment; ICER = incremental cost-effectiveness ratio; NRS = non-randomized study; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, if they were duplicate publications, or if they were published before 2011. Studies that amalgamated non-physician groups into a comparative group (e.g., pharmacists and nurses) and studies that specified anesthesiology assistants only, were excluded. Studies in which it was unclear if the intervention or comparator satisfied the description in Table 1 were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)6 for systematic reviews (SRs), the Downs and Black checklist7 for non-randomized studies, and the Drummond checklist8 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
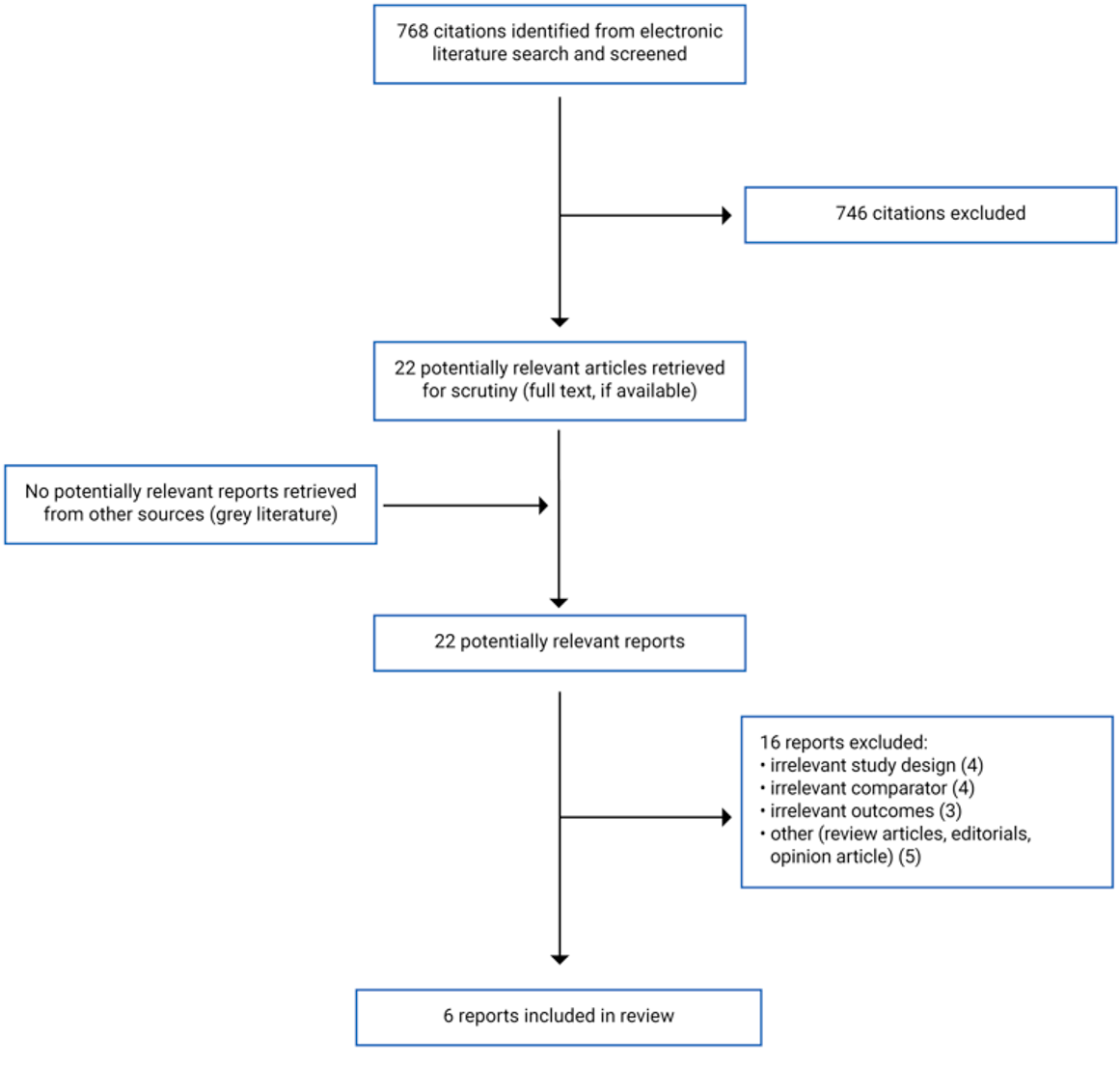
A total of 768 citations were identified in the literature search. Following screening of titles and abstracts, 746 citations were excluded and 22 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 22 potentially relevant articles, 16 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 1 SR,4 4 non-randomized studies,9-12 and 1 economic evaluation.13 Appendix 1 presents the PRISMA14 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One SR,4 4 non-randomized studies,9-12 and 1 economic evaluation13 were identified. The included SR had broader inclusion criteria than the present report. Specifically, it included studies on NPAs working independently versus physician anesthetists (PAs) working independently, and in addition other comparisons that were not relevant for the current report (such as NPAs working independently versus NPAs working in a team; and undirected NPAs versus directed NPAs). The SR included 6 studies of which 4 studies were relevant for this report. Only the characteristics and results of the subset of relevant studies will be described in this report.
The characteristics of the included publications (1 SR,4 4 non-randomized studies,9-12 and 1 economic evaluation13) are described below, and details are presented in Appendix 2.
Study Design
Systematic Review
The SR4 was published in 2014 and included 4 relevant studies published between 2003 and 2010. All the studies were retrospective cohort studies using routinely collected hospital or administrative data. The results were described narratively.
Primary studies
The 4 included primary studies9-12 were non-randomized studies and were published between 2012 and 2020. Of these, 3 studies9-11 were retrospective studies involving analyses of data from databases, and 1 study12 was a prospective study involving multiple centres. Settings for these studies varied. The study by Kudsk-Iversen et al.11 was in the context of active conflict or assessment of health care gaps, and the settings were hospital facilities ranging from basic health centers to tertiary referral centers. The study by Negrusa et al.9 considered both inpatient and outpatient settings. The study by Memtsoudis10 considered freestanding ambulatory surgery facilities and hospital-based settings. The study by Gellerfors et al.12 considered emergency service systems that included rapid response car- and helicopter-based pre-hospital critical care settings.
Economic evaluation
The economic evaluation13 was a cost-effectiveness study, reported on incremental cost per QALY, and was published in 2016. The time horizon was 1 year. The perspective was not stated. Clinical data were obtained from the literature and cost data were obtained from the US Department of Labor, Bureau of Labor Statistics, Consumer price index, and the literature. It was assumed that there were no differences between the intervention and comparator groups in complication rates (excluding unexpected disposition). Sensitivity analyses were conducted by varying post-discharge costs and utility values; and professional service costs.
Country of Origin
Systematic review
The first author of the SR4 was from the UK, and the 4 relevant included studies in this SR were from the US.
Primary studies
The first author of the included primary studies were from the UK,11 the US,9,10 and Sweden.12 Two studies9,10 were conducted in the US. The study by Kudsk-Iversen et al.11 was on humanitarian surgical projects run by the Médecins Sans Frontières-Operational Centre Brussels (MSF-OCB). The study by Gellerfors et al.12 was conducted in the Nordic countries.
Economic evaluation
The first author of the economic evaluation13 was from the US and the study was conducted in the US.
Patient Population
Systematic review
The SR4 involved patients undergoing various surgical procedures. The sample size (expressed as the number of patients, hospitalizations, or surgical procedures) in the 4 relevant studies ranged between 134,806 and 481,440. Of the 4 included studies, for 2 studies the patient age was more than 65 years, for 1 study all ages were considered, and for 1 study age was not reported.
Primary studies
Two studies,9,11 were on patients undergoing various surgical procedures, 1 study10 was on patients undergoing knee or shoulder surgery, and 1 study12 was on pre-hospital patients needing emergency tracheal intubation. In the study by Kudsk-Iversen et al.11 the median ages ranged between 23 and 27 years. In the study by Negrusa et al.9 the mean age was 52 years. In the study by Memtsoudis et al.,10 the majority of patients were in the age range 15 to 64 years. In the study by Gellerfors et al.12 the median age was 62 years.
Economic evaluation
The economic evaluation13 involved patients undergoing ambulatory knee and shoulder surgery.
Interventions and Comparators
Systematic review
The SR4 compared NPAs working independently with PAs working independently. The relevant studies in this SR were conducted in the US where NPAs represented CRNAs.
Primary studies
Various comparisons were investigated in the primary studies. In the study by Kudsk-Iversen et al.11 anesthesiologist-led anesthesia care and nurse anesthetist-led anesthesia care were compared. In the study by Gellerfors et al.12 critical care by physician anesthetist-led teams and that by nurse anesthetist-led teams were compared. In the study by Negrusa et al.9 anesthesia care by anesthesiologists was compared with various delivery models (CRNA only and CRNA plus various levels of supervision). In the study by Memtsoudis et al.10 anesthesiologists only and CRNAs only were compared.
Economic evaluation
The economic evaluation13 compared services provided by physician anesthesiologists with those provided by nurse anesthetists.
Outcomes
Systematic review
The SR4 reported on complications and mortality, and the time periods investigated were between 1993 and 2005. Follow-up durations were not reported.
Primary studies
Outcomes reported in the primary studies included mortality,11 complications,9 unexpected disposition,10 and intubation success rates.12 Unexpected disposition was described by the authors10 as disposition other than discharge to the patient’s primary residence, such as disposition to observation status, discharge to a postsurgical or recovery care facility, or admission as an inpatient at the hospital. The time periods investigated were between 1994 and 2017. Follow-up durations were not reported.
Economic evaluation
The economic evaluation13 reported the incremental cost (2014 US$) per QALY gained (i.e., ICER).
Summary of Critical Appraisal
An overview of the critical appraisal of the included SR, primary studies, and economic evaluation is summarized below. Additional details regarding the strengths and limitations of the included SR, primary studies, and economic evaluation are provided in Appendix 3.
Systematic Review
In the SR,4 the objective was stated, the literature search included multiple databases, study selection was described, lists of included and excluded studies were presented, and article selection and data extraction were done independently by 2 or 3 reviewers. Quality assessment was conducted, and the authors reported that the risk of bias was considerable. Hence the validity of the findings is unclear. The authors declared their conflicts of interest and potential for bias seemed unlikely. The results were described narratively; the authors reported the results were too disparate to present together in a forest plot. The authors reported that publication bias could not be assessed as the number of included studies was low. Hence potential for publication bias cannot be ruled out.
Primary Studies
In all the 4 included primary studies,9-12 the objective was stated; and the characteristics of the patients, interventions and outcomes were described but the descriptions of patients and interventions were limited. All 4 studies were non-randomized studies, with 3 being retrospective studies,9-11 using database data, and 1 study12 being prospective. These studies have inherent biases such as selection bias, and reporting bias, hence could impact the validity of the findings. In all 4 studies the conflicts of interest were reported by the authors; in 2 of the studies,10,11 potential for bias seemed unlikely, and for 2 studies9,12 potential for bias could not be ruled out.
Economic Evaluation
In the economic evaluation13 the objective, the strategies compared, the time horizon (1 year), and the sources of clinical data and costs were stated. An incremental analysis was conducted and ICER values were presented. Sensitivity analyses, by varying different parameters were conducted to determine the impact of the parameters on ICER values. Conclusions were consistent with the findings. The model used in the economic evaluation was not described. The perspective was not stated, hence the specific situation for which the findings would be applicable was unclear. The analysis was based on the assumption that all complication rates (except unexpected disposition) were identical between the 2 strategies. As no justification for this assumption was provided by the authors, the validity of this assumption was unclear. The conflicts of interest of the authors were not presented, hence the potential for bias cannot be ruled out.
Summary of Findings
Main findings from the included publications are presented below. Additional details of the main findings and the authors’ conclusions are presented in Appendix 4.
Clinical Effectiveness of Anesthesia Care Provided by Nurses
Mortality
Mortality was reported in 1 SR4 and 1 primary study.11
In the systematic review,4 all the 4 relevant included studies reported on mortality. In 2 studies, there was no difference in risk of death in women undergoing Caesarean section with anesthetics given by different providers (NPAs working independently compared with PAs working independently). In 1 study, there was no difference in risk of death in patients undergoing surgery between the 2 different types of providers. In 1 study, the risk of death in patients undergoing surgery was lower when the anesthetics were given by NPAs compared with PAs, both working independently.
In 1 study11 involving patients undergoing various types of surgery, the mortality was numerically lower with nurse anesthetist-led procedures compared with physician anesthesiologist-led procedures, but the statistical significance was not reported.
Complications
Complications were reported in 1 SR,4 and 1 primary study.9
In the systematic review,4 3 included studies reported on complications. In 2 studies, there was no difference in risk of anesthesia-related complications in women undergoing Caesarean section with anesthetics given by NPAs compared with that by PAs, both working independently. In the third study, there was some indication that the risk of anesthesia-related complications in patients undergoing surgery was lower when the anesthetics were given by NPAs compared with PAs, both working independently; however, not all of the relevant findings were statistically significant.
In 1 study9 involving patients undergoing various types of surgeries, there were no statistically significant between-group differences for each of the 4 groups involving CRNAs (CRNAs alone or CRNAs plus various levels of anesthesiologist involvement) compared with anesthesiologists alone (95% CI for odds ratio [OR] included 1).
Unexpected disposition
One study10 reported on unexpected disposition.
In the study by Memtsoudis et al.10 involving patients undergoing knee and shoulder surgery, there was a statistically significantly greater risk of unexpected disposition with CRNAs compared with anesthesiologists (95% CI of OR did not include 1). There was no statistically significant difference in risk of unexpected disposition with CRNAs plus anesthesiologists compared with anesthesiologists alone (95% CI of OR included 1).
Tracheal intubation
One study12 reported on the rate of success with tracheal intubation in patients with various conditions and requiring intubation. The success rate was statistically significantly lower with nurse anesthetist-led groups compared with physician anesthetist-led groups (P = 0.03), in pre-hospital advanced airway management.
Cost-Effectiveness of Anesthesia Care Provided by Nurses
The incremental cost per QALY for physician anesthesiologists compared with nurse anesthetists was $77,400 per QALY gained. The 1-way sensitivity analyses showed that by increasing the cost of nurse anesthetist professional services by 5% and 20%, the ICER values were respectively US$54,000 per QALY gained and US$7,200 per QALY gained. It also showed, that if the length of stay due to unexpected hospitalization increased from 2.5 days (for base-case) to 5 days or 10 days, the ICER values were respectively US$17,400 per QALY gained and US$15,900 per QALY gained. The 2-way sensitivity analysis showed that in general, lower assumed excess risk associated with nurse anesthetist administration and lower assumed cost per hospitalization yielded higher incremental cost per QALY estimates.
Limitations
All the primary studies as well as the studies included in the SR were non-randomized studies (observational studies, with the majority being retrospective studies) which have inherent biases such as selection bias, and reporting bias. There is potential for selection and reporting bias due to the number of possible codes for diagnoses and interventions that can be used in databases. hence the validity of the findings is unclear. Comparability of the patients in the different interventions groups is unclear and this could impact the findings. For example, it is possible that the sicker patients may be treated by the PA rather than the NPA. Also, it was unclear if patients undergoing more serious surgical procedures were treated by the PA rather than the NPA. The types of anesthesia used were not specified in the studies, hence it is possible that outcomes obtained in the intervention and comparator groups were due to the differences in the anesthesia type used, rather than the differences in the anesthesia care providers. In the light of these possibilities, the validity of the findings is unclear.
None of the clinical studies were conducted in Canada, hence the generalizability of the findings to the Canadian context is unclear. Also, the economic evaluation pertains to the US context, hence the generalizability of the economic findings to the Canadian context is unclear.
Conclusions and Implications for Decision- or Policy-Making
One SR, 4 primary studies (observational studies: 3 retrospective and 1 prospective), and 1 economic evaluation were identified. Outcomes reported included, mortality, complications, and unexpected dispositions for patients undergoing surgery; and intubation success in patients, in car- and helicopter-based pre-hospital critical care settings.
For patients undergoing surgical procedures, there was no difference in mortality (2 studies in the SR,4) or the mortality was lower (1 study in the SR4 and 1 primary study11) in the NPA group compared with the PA group. There was no difference in complications (3 studies in the SR4 and 1 primary study9) in the NPA group compared with the PA group, however in the majority of cases the statistical significance was not reported. There was statistically significantly greater risk of unexpected disposition with anesthesia by CRNAs compared with that by anesthesiologists (1 study10). There was a statistically significantly lower success rate with tracheal intubation by nurse anesthetists compared with PAs (1 study12).
A definite conclusion is not possible regarding whether 1 type of anesthesia care is better or not different than another, considering the studies were of low quality and were associated with considerable risk of bias, the complexity of perioperative care, and confounding factors.
The ICER for physician anesthesiologists compared with nurse anesthetists was US$77,400 per QALY gained. The 1-way sensitivity analyses showed that with increase in the cost of nurse anesthetist professional services or increase in the number of unexpected hospital days, the ICER values would fall below US$50,000 per QALY gained. The validity of the findings is unclear, as the economic evaluation was based on clinical data from a few selected studies, whose qualities were not reported.
Further research is needed to definitively determine the clinical effectiveness and cost-effectiveness of anesthesia provided by nurse-led care compared with that provided by anesthesiologists. Randomized controlled studies are unlikely to be conducted due to ethical reasons and logistical difficulties with respect to allocation concealment and blinding. Well-defined prospective studies, with a mechanism in place to ensure accuracy in database coding and consistency in recording of data with respect to patients and the anesthesia care provided, are needed to understand the clinical effectiveness of anesthesia care by the different providers. Also, well conducted economic evaluations taking into consideration important factors (such as different perspectives, and different compositions of the anesthesia care team) are needed to better understand the cost-effectiveness of anesthesia care provided by different providers.
References
1.Falk SA, Fleisher LA. Overview of anesthesia. In: Jones SB, ed. UpToDate. Waltham (MA): UpToDate; 2020: http://www.uptodate.com. Accessed 2021 Jun 30.
2.National Institute of General Medical Sciences, NIH. Anesthesia. 2020; https://www.nigms.nih.gov/education/fact-sheets/Pages/anesthesia.aspx. Accessed 2021 Jul 24.
3.Cleveland Clinic. Anesthesia. https://my.clevelandclinic.org/health/treatments/15286-anesthesia. Accessed 2021 Jul 24.
4.Lewis SR, Nicholson A, Smith AF, Alderson P. Physician anaesthetists versus non-physician providers of anaesthesia for surgical patients. Cochrane Database Syst Rev. 2014(7):CD010357. PubMed
5.Hoyem RL, Quraishi JA, Jordan L, Wiltse Nicely KL. Advocacy, research, and anesthesia practice models: key studies of safety and cost-effectiveness. Policy, Politics, & Nursing Practice. 2019;20(4):193-204. PubMed
6.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
7.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
8.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 Jul 24.
9.Negrusa B, Hogan PF, Warner JT, Schroeder CH, Pang B. Scope of practice laws and anesthesia complications: No measurable impact of certified registered nurse anesthetist expanded scope of practice on anesthesia-related complications. Med Care. 2016;54(10):913-920. PubMed
10.Memtsoudis SG, Ma Y, Swamidoss CP, Edwards AM, Mazumdar M, Liguori GA. Factors influencing unexpected disposition after orthopedic ambulatory surgery. J Clin Anesth. 2012;24(2):89-95. PubMed
11.Kudsk-Iversen S, Trelles M, Ngowa Bakebaanitsa E, et al. Anaesthesia care providers employed in humanitarian settings by Medecins Sans Frontieres: a retrospective observational study of 173 084 surgical cases over 10 years. BMJ Open. 2020;10(3):e034891. PubMed
12.Gellerfors M, Fevang E, Backman A, et al. Pre-hospital advanced airway management by anaesthetist and nurse anaesthetist critical care teams: a prospective observational study of 2028 pre-hospital tracheal intubations. Br J Anaesth. 2018;120(5):1103-1109. PubMed
13.Ohsfeldt RL, Miller TR, Schneider JE, Scheibling CM. Cost impact of unexpected disposition after orthopedic ambulatory surgery associated with category of anesthesia provider. J Clin Anesth. 2016;35:157-162. PubMed
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Lewis et al. 2014,4 UK. Funding: National Institute for Health Research Cochrane Collaboration Programme Grant | SR, findings described narratively. It included a total of 6 non-randomized studies of which 4 studies were relevant (Study 1, Study 2, Study 3, and Study 4) conducted in the US, and published between 2003 and 2010. All the studies were retrospective cohort studies using routinely collected hospital or administrative data. Inclusion criteria: RCTs and non-randomized studies; patients of any age undergoing surgery; and anesthesia provided by PAs or NPAs. Exclusion criteria: not explicitly stated. Aim: to assess the safety and effectiveness of different anesthetic providers for patients undergoing surgery | Two studies (Studies 2 and 4) were on obstetric patients; and 2 studies (Studies 1 and 3) were on patients undergoing various surgical procedures. Population size: 481,440 hospitalizations (Study 1); 271,350 Caesarean sections (Study2); 404,194 patients (Study 3); and 134,806 patients undergoing Caesarean section (Study 4) Age: Study 1 and 3 used US Medicare data, hence the population studied was over 65 years. In Study 2, 12% < 20 years, 74% 20 to 34 years, and 14% ≥ 35 years. In Study 4, NR. % Female: NR ASA level: NR | Anesthesia providers PAs and NPAs compared. (Definitions: PAs are personnel who are medically qualified and NPAs are personnel who provide anesthesia without a medical qualification) | Outcomes: Mortality, and complications Time period investigated: 1999 to 2005 (Study 1); 1999 to 2001 (Study 2); 1995 to 1997 (Study 3); and 1993 to 2004 (Study 4) Length of follow-up: NR |
ASA = American Association of Anesthesiologists; NPA = non-physician anesthetist; NR = not reported; PA = physician anesthetist, RCT = randomized controlled trial; SR = systematic review, Study 1 = Dulisse 2010; Study 2 = Needleman 2009; Study 3 = Pine 2003; Study 4 = Simonson 2007.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Kudsk-Iversen et al. 2020. UK11 Funding: Of the 10 authors, 1 author received funding from NIHR and 1 author received a Wellcome Trust Senior Fellowship for an unrelated research project. | Analysis of routine case-level data linked with routine program-level data from surgical projects run by MSF-OCB. Setting: Humanitarian settings. Hospital facilities ranging from basic health centers to tertiary referral centers; 52 sites in 23 countries. Context: active conflict or assessment of stable health care provision gaps. Aim: to assess the different categories of anesthesia providers and the nature and volume of their workload in humanitarian surgical projects. | Patients undergoing surgery (minor surgery; obstetric and gynecological, visceral, and orthopedic surgery). Conflict context. N = 33,763 in PA, and 3,798 in NUA. Age (years) (median [IQR]): 23 (15 to 33) in PA, and 25 (16 to 34) in NUA. % Female: 37% in PA, and 50% in NUA ASA level (IQR):1 (1 to 2) in PA, and 1 (1 to 2) in NUA Health care gap context. N = 78,126 in PA, and 28,559 in NUA Age (years) (median [IQR]): 28 (19 to 37) in PA, and 26 (20 to 34) in NUA % Female: 50% in PA, and 79% in NUA ASA level (IQR): 1 (1 to 2) in PA, and1 (1 to 2) in NUA | Anesthesiologist-led (PA) anesthesia care compared with nurse anesthetist-led (NUA) anesthesia care. | Outcomes: Mortality Time period investigated: 2008 to 2017 Length of follow-up: NR |
Gellerfos et al. 2018.12 Sweden. Funding received from Swedish Medical Association, ALF-Grant Stockholm Country Council, and the Laerdahl Foundation. | Prospective observational study. Setting: multi-centre; national emergency services systems that included rapid response car- and helicopter-based pre-hospital critical care. Aim: to assess success and complication rates of pre-hospital tracheal intubation performed by physician anesthetist-led or nurse anesthetist-led pre-hospital critical care teams | Patient categories included: trauma, cardiac arrest, cardiac disease, stroke, hemorrhage, seizures, asthma, COPD, ENT disease, intoxication, and other. N = 2026. Age (years) (median [IQR]): 62 (45 to 74). % Female: 33.1% ASA value (median): 2 | Anesthesia by physician anesthetist-led teams compared with nurse anesthetist-led teams. | Outcomes: pre-hospital tracheal intubation success rate Time period investigated: May 2015 to November 2016. Length of follow-up: NR |
Negrusa et al. 2016.9 US. Funding: unclear. It was reported that this work was supported by the AANA and the AANA foundation. | Retrospective study. Logistic regression analysis using data from the Optum Research Database, a database of deidentified health care claims of individuals insured by United Health care, a major US health insurer, and other claims processed by Optum. Setting: inpatient and outpatient (6% of procedures were conducted in rural areas). Aim: to assess if there are differences in anesthesia complications across different delivery models and other factors. | Patients of all ages undergoing various types of surgeries (gynecological, orthopedic, urology, head and neck, cardiac, vascular, and other). N = 5,740,470 anesthesia-specific procedures were recorded in the database. Age (mean): 52 years. % Female: 60%. ASA level: NR | Various anesthetic delivery models were compared using the model with anesthesiologist only as the reference. Delivery models: CRNA only; Medical direction 1:1; Medical direction 1:2-4; and; Supervision 1: > 4. The notations 1:1, 1:2-4, and 1: > 4 refer to the anesthesiologist to CRNA ratio. | Outcomes: anesthesia-related complications. Time period investigated: 2011 to 2012. Length of follow-up: NR |
Memtsoudis et al. 2012.10 US. Funding: Funded by the Department of Anesthesiology, Hospital for Special Surgery, the Center for Education and Research in Therapeutics, and the Clinical Translational Science Center. | Retrospective study. Logistic regression analysis using data (collected for NSAS) from CDC. Setting: freestanding ambulatory surgery facilities and hospital-based settings. Aim: to assess if there are differences in unexpected disposition with different anesthesia providers and other factors. | Patients undergoing ambulatory knee and shoulder surgery. N = 6,942 (entries from NSAS database); the weighted N representing the national sample equivalent is 2,405,022. Age: all ages with majority being in the range 15 and 64 years. Majority of patients were male. ASA level: NR | Anesthesia by anesthesiologists compared with CRNAs. | Outcomes: unexpected disposition status after ambulatory knee and shoulder surgery. (Unexpected disposition status referred to disposition other than discharge to the patient’s primary residence, such as discharge to observation status, discharge to a postsurgical/recovery care facility, hospital admission as an inpatient) Time period investigated: 1994 to1996, and 2006. Length of follow-up: NR |
AANA = American Association of Nurse Anesthetists; ASA = American Association of Anesthesiologists; ENT = ear-nose-throat-; CDC = Centers for Disease Control; COPD = chronic obstructive pulmonary disease; CRNA = certified registered nurse anesthetist; IQR = interquartile range; MSF-OCB = Médecins Sans Frontières-Operational Centre Brussels; NUA = nurse anesthesiologist-led; NSAS = National Survey of Ambulatory Surgery; NR = not reported; PA = physician anesthesiologist-led.
For ASA values, higher values indicate worse health.
Table 4: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
Ohsfeldt et al. 2016,13 US. Study funded by ASA. | Cost-effectiveness analysis. Time horizon: 1 year Perspective: NR | Patients undergoing orthopedic ambulatory surgery | Anesthesia by physician anesthesiologists vs. nurse anesthesiologists | ICER (incremental cost per QALY) reported. 1-way and 2-way sensitivity analyses conducted. | Clinical data and utility values were obtained mostly from the literature. Risk of death for all groups was taken as 1 based on author’s assumption. Cost data (2014$) were obtained from the US Department of Labor, Bureau of Labor Statistics, Consumer price index and the literature. | Assumptions for the base-case model: No difference between the intervention and comparator groups of patients in rates for other serious complications (i.e., excluding unexpected disposition). Anesthesia supply costs were same for all types of anesthesia providers. |
ASA = American Society of Anesthesiologist; ICER = incremental cos-effectiveness ratio; NR = not reported; QALY = quality-adjusted life-year.
Appendix 3: Critical Appraisal of Included Publications
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 26
Strengths | Limitations |
Lewis et al. 2014,4 UK. | |
The objective was clearly stated Multiple databases (Medline, Embase, and CINAHL, [from 1985 to February 2014]; CENTRAL [Cochrane Library 2014, Issue 2]) were searched. Also, trial registries and grey literature were searched Study selection was described, and a flow chart was presented A list of included studies was provided A list of excluded studies was provided. Article selection was done by 2 reviewers Data extraction was done by 3 reviewers using a paper-based data extraction form. Quality assessment was conducted using the specific NRS risk of bias tool presented at the UK Contributor’s Meeting 2012. The authors reported that there was considerable risk of bias due to confounding and selection bias. Characteristics of the included studies were presented The authors reported that the results from the included studies were too disparate to display together in a forest plot so results were described narratively. Conflicts of interest of the authors were declared, and potential for bias seemed unlikely. | Publication bias could not be assessed as the number of included studies was low, hence potential for publication bias cannot be ruled out. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black checklist7
Strengths | Limitations |
Kudsk-Iversen et al. 2020, 11 UK | |
The objective was clearly stated. Patient characteristics, intervention and outcomes were described. Conflicts of interest were declared. Of the 10 authors, 7 authors were employed by MSF-OCB. Data used for the analysis were from surgical projects run by MSF-OCB. Therefore, it is possible that as the authors could control the data collection, all relevant data were collected. | The inclusion and exclusion criteria were not explicitly stated. Although patient characteristics and interventions were described, details were limited. It is unclear if power calculations were done to determine the appropriate sample size. It is a non-randomized study - retrospective observational study – with inherent biases. Confidence intervals or P values were not presented. It was mentioned in the conflicts of interest section that of the 10 authors, 7 authors were employed by MSF-OCB. Data used for the analysis were from surgical projects run by MSF-OCB. Therefore, there may be some selectivity in the type of data collected which may bias findings. |
Gellerfos et al. 2018,12 Sweden | |
The objective was clearly stated. Patient characteristics, intervention and outcomes were described, but details of patient characteristics and interventions were limited. P values were reported. It was reported that the authors had no personal financial gains from the study. | The inclusion and exclusion criteria were not explicitly stated. It is unclear if power calculations were done to determine the appropriate sample size. It is a non-randomized study – prospective observational study – with inherent biases. |
Negrusa et al. 2016,9 US | |
The objective was clearly stated. Patient characteristics, intervention and outcomes were described but details of patient characteristics and interventions were limited. Power calculations were conducted, and the appropriate sample size was used. Confidence intervals and P values were presented. The authors reported that there were no conflicts of interest. (Of note, the authors were employees of The Lewin Group. The Lewin Group is a wholly owned subsidiary of Optum Public Sector Solutions Inc., which in turn is a wholly owned subsidiary of OptumInsight, a UnitedHealth Group.) | The inclusion and exclusion criteria were not explicitly stated. It is a non-randomized study – retrospective study – with inherent biases. Since logistic regression analysis of data from a commercial private insurance database was conducted, there could be some bias in the data selected. Further, as the data were from a private insurance database, the generalizability of the findings to a wider population is likely to be limited. |
Memtsoudis et al. 2012.10 US | |
The objective was clearly stated Patient characteristics, intervention and outcomes were described but details of patient characteristics and interventions were limited. Confidence intervals and P values were presented. The authors reported that there were no conflicts of interest. | The inclusion and exclusion criteria were not explicitly stated. It is unclear if power calculations were conducted and if the appropriate sample size was used. It is a non-randomized study – retrospective study – with inherent biases. Since logistic regression analysis of data from a national database was conducted, there could be some bias in the data selected. |
MSF-OCB = Médecins Sans Frontières-Operational Centre Brussels.
Table 7: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist8
Strengths | Limitations |
Ohsfeldt et al. 2016,13 US | |
Objectives were stated. The strategies compared were stated (physician anesthesiologist alone and nurse anesthetist alone). Time horizon (1 year) was stated. Sources for the clinical and cost data were stated. Incremental analyses were conducted. Sensitivity analyses (1-way and 2-way) were conducted. Conclusions were consistent with findings. | Perspective was not stated. The model used for the economic evaluation was not presented. Conflicts of interest of the authors were not presented. |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 8: Summary of Findings Included Systematic Review
Main study findings | Authors’ conclusion |
Lewis et al. 2014,4 UK | |
Findings are based on non-randomized studies. Mortality There was no difference in risk of death in women undergoing Caesarean section with anesthetic given by NPA working independently compared with anesthetic given by PA working independently (2 studies: Needleman 2009, and Simonson 2007). There was no significant difference in mortality in individuals undergoing surgery with anesthetics provided by NPAs working independently compared with anesthetics provided by PAs working independently, in both adjusted and unadjusted analyses (1 study: Pine 2003). In 1 study, results were based on anesthesia provided to individuals undergoing surgery by PAs working independently in the non-opt-out states, as the reference group. The risk of mortality was lower in individuals undergoing surgery with anesthetics given by NPAs working independently (in both opt-out and non-opt-out states) compared with anesthetics given by PAs working independently (1 study: Dulisse 2010). This study did not adjust for hospital characteristics.
*Significant difference reported by study authors P = 0.05. | “No definitive statement can be made about the possible superiority of one type of anaesthesia care over another. The complexity of perioperative care, the low intrinsic rate of complications relating directly to anaesthesia, and the potential confounding effects within the studies reviewed, all of which were non-randomized, make it impossible to provide a definitive answer to the review question.” (p. 2)4 |
Complications There was no difference in risk of anesthesia-related complications in women undergoing Caesarean section with anesthetics given by NPAs working independently compared with anesthetics given by PAs working independently (2 studies: Needleman 2009, and Simonson 2007). In 1 study (Dulisse 2010), results were based on anesthesia provided to individuals undergoing surgery by PAs working independently in the non-opt-out states, as the reference group. There was some indication that the risk of anesthesia-related complications in individuals undergoing surgery with anesthetics given by NPAs working independently was lower compared with anesthetics given by PAs working independently, however, not all the relevant findings were statistically significant.
*Significant difference reported by study authors P = 0.05. (Note: Opt-out states refer to US states that had opted out of the federal insurance requirements for reimbursement that PAs supervise or direct NPAs.) | |
NPA = non-physician anesthetist;. OR = odds ratio; PA physician anesthetist; SR = systematic review.
Table 9: Summary of Findings of Included Primary Clinical Studies
Main study findings | Authors’ conclusion |
Kudsk-Iversen et al. 2020,11 UK | |
Findings from an observational study involving analysis of data from MSF-OCB. Context: conflict Mortality: 0.3% in PA, and 0.2% in NUA Context: health care gap Mortality: 0.3% in PA, and 0.1% in NUA | “Our findings contribute to existing knowledge of the nature of anesthetic provision in humanitarian settings, while demonstrating the value of high-quality, routine data collection at scale in this sector. Further evaluation of perioperative outcomes associated with different models of humanitarian anesthetic provision is required.” (p. 1 of 9)11 |
Gellerfors et al. 2018,12 Sweden | |
Findings from a prospective observational study of pre-hospital advanced airway management. Tracheal intubation success rate The tracheal intubation success rates were 97.6% for the nurse anesthetist-led group, and 99% for the physician anesthetist-led group, P = 0.03. | “When performed by experienced physician anaesthetists and nurse anaesthetists, pre-hospital tracheal intubation was completed rapidly with high success rates and a low incidence of complications.” (p. 1103)12 |
Negrusa et al. 2016,9 US | |
Likelihood of anesthesia-related complications (expressed as ORs) This was determined by logistic regression using data from a commercial database of privately insured persons. The delivery model with anesthesiologist only was considered the reference category for the 4 delivery models presented below. An OR estimate greater (less) than 1 and statistically significant, indicates that the deliver model increases (decreases) the odds of a complication. Inpatient procedures CRNA only, OR (95% CI), 1.149 (0.954 to 1.385), P = 0.142. MD 1:1, OR (95% CI), 1.042 (0.826 to 1.313), P = 0.730. MD 1:2-4, OR (95% CI), 1.160 (0.951 to 1.415), P = 0.144. Supervision 1: > 4, OR (95% CI), 1.080 (0.537 to 2.173), P = 0.830. | “The primary finding of this study is that there is no statistically significant difference in the risk of anesthesia complications based on the degree of restrictions placed on CRNAs by state SOP laws. Nor is there evidence that the risk of complications varies by delivery model.” (p.919)9 |
Outpatient procedures CRNA only, OR (95% CI), 1.009 (0.740 to 1.377), P = 0.954. MD 1:1, OR (95% CI), 1.22 (0.814 to 1.545), P = 0.482. MD 1:2-4, OR (95% CI), 1.320 (0.970 to 1.797), P = 0.077. Supervision 1: > 4, OR (95% CI), 1.363 (0.572 to 3.249), P = 0.485. (The notations 1:1, 1:2-4, and 1: > 4 refer to the anesthesiologist to CRNA ratio.) The findings for the delivery system with CRNA only indicate that the hypothesis that the risk of anesthesia-related complications is the same whether the anesthesia is delivered by a CRNA acting alone or by an anesthesiologist acting alone cannot be rejected. | |
Memtsoudis et al. 2012,10 US | |
Risk of unexpected disposition This was determined by logistic regression using data from NSAS. Anesthesia provided by anesthesiologists was considered as the reference. Knee and shoulder surgery CRNA, OR (95% CI), 1.80 (1.09 to 2.99), P = 0.0229 | “We found an increased risk of adverse disposition in cases where the anesthesia provider was a non-anesthesiology professional.” (p. 2 of 11)10 |
ACT = anesthesia care team; CI = confidence interval; CRNA = certified registered nurse anesthetist; MD = medical direction; MSF-OCB = Médecins Sans Frontières-Operational Centre Brussels; NR = not reported; NSAS = National Survey of Ambulatory Surgery; NUA = nurse anesthesiologist-led; PA = physician anesthesiologist-led; OR = odd’s ratio; PACU = post-anesthetic care unit; RR = relative risk; SO = solo anesthesiologist.
Table 10: Summary of Findings of Included Economic Evaluation
Main study findings | Authors’ conclusion |
Ohsfeldt et al. 2016,13 US. | |
Cost-effectiveness (cost in 2014 US$) Base case Expected costs over 1-year period per ambulatory procedure were $807 for a physician anesthesiologist, and $776 for a nurse anesthetist. Unexpected admissions were 4.57% for a physician anesthesiologist, and 6.90% for a nurse anesthetist. QALYs were 0.9965 for a physician anesthesiologist, and 0.9961 for a nurse anesthetist. The incremental cost per unexpected admission for a physician anesthesiologist compared with a nurse anesthetist was $1325 per unexpected admission. The incremental cost per QALY for a physician anesthesiologist compared with a nurse anesthetist was $77,400 per QALY gained. Sensitivity analyses Results for the 1-way sensitivity analyses with different scenarios are presented below. (For the base case the LOS for unexpected hospitalizations was 2.5 days.) Incremental cost ($) per unexpected admission were 1,225 considering post-discharge costs and disutility (5 days). 1,125 considering post-discharge costs and disutility (10 days). 924 considering base-case NUA professional services cost + 5%. 524 considering base-case NUA professional services cost + 10%. 123 considering base-case NUA professional services cost + 15%. Cost saving considering base-case NUA professional + 20%. Incremental cost ($) per QALY (i.e., ICER) 15,900 considering post-discharge costs and disutility (5 days). 6,600 considering post-discharge costs and disutility (10 days). | “Provision of anesthesia for ambulatory knee and shoulder procedures by physician anesthesiologists results in better health outcomes, at a reasonable additional cost, compared with procedures with NA-administered anesthesia, at least when using updated cost-effectiveness willingness-to-pay benchmarks.” (p. 157)13 |
54,000 considering base-case NUA professional services cost + 5%. 30,600 considering base-case NUA professional services cost + 10%. 7,200 considering base-case NUA professional services cost + 15%. Cost saving considering base-case NUA professional + 20%. The 2-way sensitivity analysis showed that in general, lower assumed excess risk associated with nurse anesthetist administration and lower assumed cost per hospitalization yielded higher incremental cost per QALY estimates. | |
ICER = incremental cost-effectiveness ratio; LOS = length of stay; NA = nurse anesthetist; NUA = nurse anesthetist; QALY = quality-adjusted life-year; RR = relative risk; WTP = willingness-to-pay.
Appendix 5: References of Potential Interest
Studies with alternative comparators
1.Yin L, Shui X, Zuo J, Yang Q, Jiang X, Liao L. No harm found when the scope of practice of nurse anesthetists is expanded to the whole process of anesthetic care and under indirect supervision of anesthesiologists: a time series study. Int J Nurs Stud. 2021;117:103881. PubMed
2.Dony P, Seidel L, Pirson M, Forget P. Anaesthesia care team improves outcomes in surgical patients compared with solo anaesthesiologist: an observational study. Eur J Anaesthesiol. 2019;36(1):64-69. PubMed
3.Charles LA, Korejwa E, Kent DC, Raniero D. Specially trained registered nurses can safely manage epidural analgesia infusion in laboring patients. J Perianesth Nurs. 2015;30(3):209-214. PubMed
4.Guimaraes ES, Campbell EJ, Richter JM. The safety of nurse-administered procedural sedation compared to anesthesia care in a historical cohort of advanced endoscopy patients. Anesth Analg. 2014;119(2):349-356. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca