CADTH Health Technology Review
Chlorhexidine Gluconate for Skin Preparation During Catheter Insertion and Surgical Procedures
Rapid Review
Authors: Kylie Tingley, Mê-Linh Lê
Abbreviations
CHG
chlorhexidine gluconate
HAI
health care–associated infection
ICU
intensive care unit
MDRO
multi-drug–resistant organism
MRSA
methicillin-resistant Staphylococcus aureus
SR
systematic review
RCT
randomized controlled trial
VRE
vancomycin-resistant enterococci
Key Messages
There is a lack of evidence on the clinical effectiveness of chlorhexidine gluconate wipes for patients being prepped for urinary catheter insertion in acute or community care. More research in this area is needed.
In critical care settings, bathing with chlorhexidine gluconate wipes results in either a reduction or no difference in the risk of infection compared to bathing with soap and water.
The results from 1 study demonstrated that using chlorhexidine gluconate‒impregnated cloths the night before and morning of admission pre-surgery reduced infections at the site of the prosthetic in patients undergoing total joint arthroplasty when compared to standard soap and water bathing.
When reported, adverse events associated with chlorhexidine gluconate wipes included mild skin irritation.
Context and Policy Issues
Health care–associated infections (HAIs), many of which are preventable, represent a large proportion of adverse events experienced by those receiving care in the Canadian health care system. It is estimated that the prevalence of patients in Canada with at least 1 HAI was 7.9% in 2017 and that device-associated infections accounted for 35.6% of all HAIs.1 It is also estimated that 9% of HAIs observed in Canadian hospitals were caused by an antimicrobial-resistant organism such as, for example, methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE).1 The management of HAIs in Canada incurs substantial costs to the health care system, contributes to lengthier hospital stays, and places an added burden on an already strained system.2 For example, the Canadian Institute for Health Information estimated that HAIs were associated with a cost of $281 million dollars in 2014–2015.3 Infection prevention measures, such as skin cleaning before a procedure or at regular intervals for venous access sites, have been implemented as a strategy to reduce the prevalence HAIs.
Chlorhexidine gluconate (CHG) is an antiseptic that can be used for skin cleaning and has been shown to be effective against a wide range of organisms, including some antimicrobial-resistant organisms.4 CHG is manufactured in several different formulations and concentrations, such as hand scrubs, concentrated solutions that can be diluted with water or alcohol, and CHG-impregnated wipes or sponges.5 While disposable CHG wipes may be convenient, offer good contact with the skin, and uniformity in skin coverage, there are remaining questions regarding their clinical effectiveness compared to other CHG products and skin cleaning techniques.
The objective of this report is to summarize the evidence regarding the clinical effectiveness of CHG wipes for infection prevention in patients being prepped for urinary catheter insertion and in patients who are preoperative and/or in critical care settings.
Research Questions
What is the clinical effectiveness of chlorhexidine gluconate wipes for infection prevention in patients being prepped for a urinary catheter insertion?
What is the clinical effectiveness of chlorhexidine gluconate wipes for infection prevention in patients who are preoperative and/or admitted to the critical care setting?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy consisted of both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were chlorhexidine and wipes/skin preparation, and urinary catheters or surgical intensive care unit or critical care settings. Search filters were applied to limit to health technology assessments, systematic reviews (SRs), meta-analyses, network meta-analyses, all types of clinical trials, and observational studies. The initial search was limited to English-language documents published between January 1, 2016 and June 22, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Q1: Patients in the acute care or community (e.g., LTC or home) setting being prepped for a urinary catheter insertion Q2: Preoperative patients and/or patients in the critical care setting |
Intervention | Q1: CHG wipes or prep sticks (e.g., 0.1% to 0.5% CHG formulation) Q2: CHG wipes (e.g., 2% CHG) or CHG sponge (e.g., 4% CHG) |
Comparator | Q1: PVP wipes, saline cleansing/wipes Q2: Soap and water (e.g., using soap cleanser) |
Outcomes | Q1: Clinical effectiveness: infection rate (i.e., catheter-associated urinary tract infections, hospital-acquired urinary tract infections); adverse events (e.g., skin irritation, chlorhexidine resistance) Q2: Clinical effectiveness: infection rate (i.e., surgical site infections, level of antibiotic-resistant organisms (e.g., MRSA) or drug-resistant microbes; adverse events (e.g., skin irritation, chlorhexidine resistance) |
Study designs | HTA, systematic reviews, randomized controlled trials, non-randomized studies |
CHG = chlorhexidine gluconate; HTA = health technology assessment; LTC = long-term care; MRSA = methicillin-resistant Staphylococcus aureus; PVP = polyvinylpyrrolidone.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)6 for SRs and the Downs and Black checklist7 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
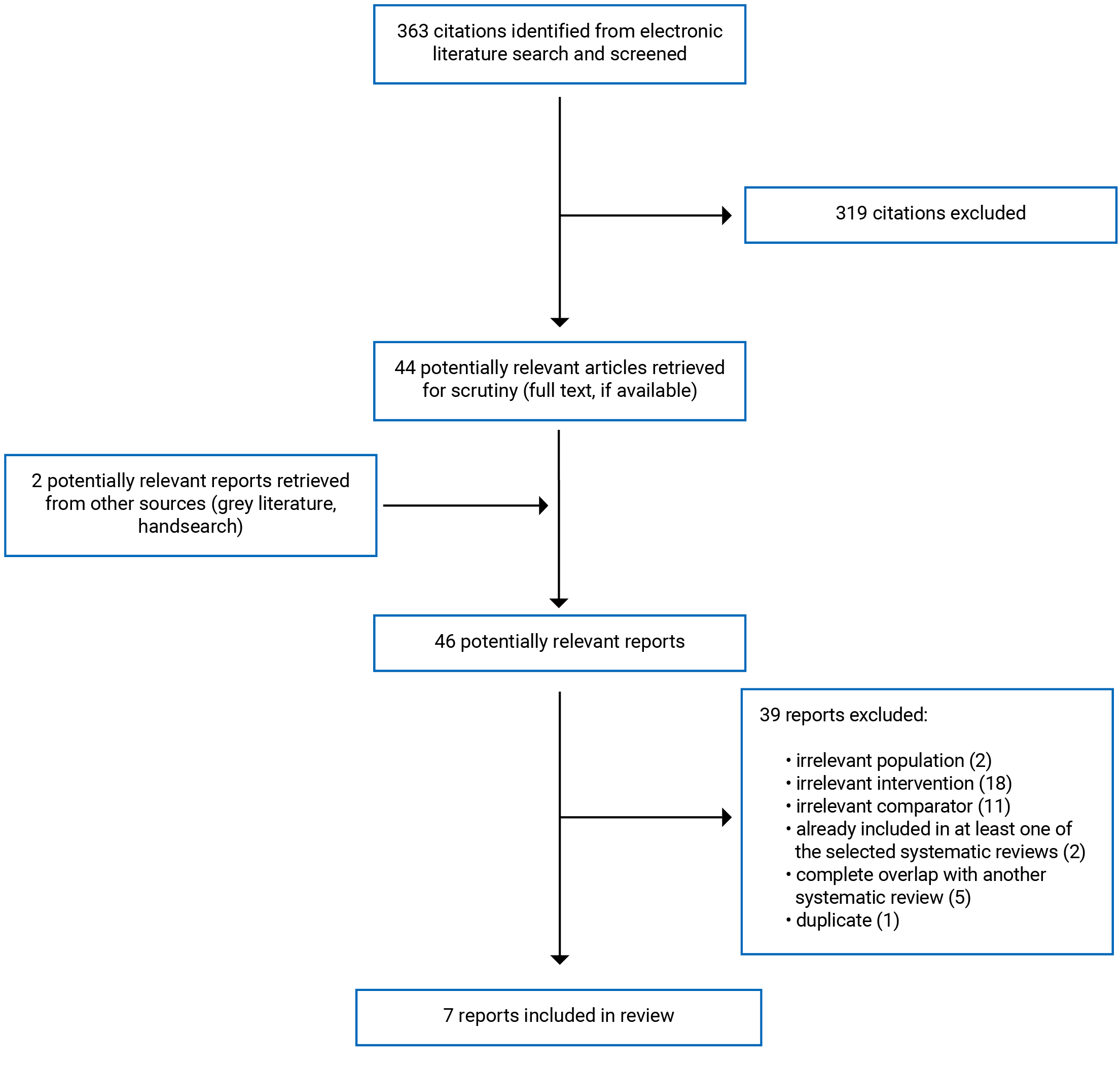
A total of 363 citations were identified in the literature search. Following the screening of titles and abstracts, 319 citations were excluded and 44 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 39 publications were excluded for various reasons and 7 publications met the inclusion criteria and were included in this report. These comprised 2 SRs,8,9 1 randomized controlled trial (RCT),10 and 4 non-randomized studies.11-14 Appendix 1 presents the PRISMA15 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Two SRs,8,9 1 RCT,10 and 4 non-randomized studies11-14 were identified and included in this report. Additional details regarding the characteristics of included publications are provided in Appendix 2.
The 2 included SRs8,9 had broader inclusion criteria than the current review. Specifically, both SRs8,9 included studies examining the effects of CHG bathing (not specific to CHG wipes) on the incidence of hospital-acquired infections compared to usual care or non-CHG bathing. In addition, the SR conducted by Musuuza et al. (2019)9 included any adult health care setting, whereas the SR conducted by Huang et al. (2016)8 focused specifically on adult intensive care unit (ICU) settings. Only the characteristics and results of the subset of relevant studies will be described in this report.
Study Design
One SR included RCTs, cluster randomized trials, and non-randomized studies published from inception to January 4, 2019.9 The second SR also included RCTs and non-randomized studies (interrupted time series studies and before-and-after studies), and included studies from inception to December 31, 2014.8 Of the 26 studies (8 RCTs and 18 non-randomized studies) included in the SR by Musuuza et al.,9 only primary studies that compared bathing with CHG wipes versus soap and water in ICU settings were relevant to this report (i.e., 2 RCTs and 7 non-randomized studies). Of the 15 studies included in the SR by Huang et al.,8 only primary studies that compared bathing with CHG wipes versus soap and water in ICU settings were relevant to this report (i.e., 1 RCT and 6 non-randomized studies). The overlap of primary studies relevant to the current review and included in both SRs is provided in Appendix 5.
One single-centre RCT published in 2016 by Kapadia et al.10 was included.
The remaining 4 studies were non-randomized designs. The study by Tien et al. was a prospective, cluster, quasi-experimental controlled before-and-after study.14 The study by Kengen et al. was a retrospective, single-centre, sequential period, interrupted time series design in which the outcomes were measured monthly over an 11-month control period and then again during an 11-month intervention period.12 Garrido-Benedicto et al. (2017) and Ruiz et al. (2017) both conducted prospective, single-centre before-and-after studies.11,13
Country of Origin
One of the included SRs was conducted by a research group in the US9 and the other was conducted by a research group in China.8 Among the primary clinical studies included, 2 were conducted in Spain11,13 and the remaining 3 were conducted in Taiwan,14 Australia,12 and the US.10
Patient Population
One SR had broader inclusion criteria than the inclusion criteria for this review. The SR by Musuuza et al. (2019) included studies on hospitalized adults from the ICU, general hospital units, and long-term acute care setting, which were eligible for inclusion.9
Kapadia et al. recruited adult patients from a single centre undergoing a joint arthroplasty, specifically a total knee or hip arthroplasty.10
As previously mentioned, Kapadia et al. recruited patients pre-surgery;10 the remaining 6 studies focused on adult patients admitted to critical care settings. The study settings for these publications included medical and/or surgical ICUs,8,9,11-13 general ICUs,14 coronary care units,9,14 cardiac ICUs,9,14 stroke units,14 emergency care units,14 trauma ICUs,8,9 and bone marrow transplant units.9
Interventions and Comparators
The SRs conducted by Musuuza et al. (2019)9 and Huang et al. (2016)8 had broader inclusion criteria for interventions and comparators than the current report. Musuuza et al.9 included studies with any CHG bathing intervention (e.g., CHG wipes, diluted CHG solution) compared with non-CHG bathing (not otherwise described). All 9 primary studies identified in the SR by Musuuza et al. (2019)9 that met eligibility criteria for this report compared 2% CHG-impregnated wipe bathing with soap and water bathing. Huang et al. (2016)8 also included studies comparing daily CHG bathing, regardless of formulation, compared with daily soap and water or routine care bathing. All 7 primary studies identified in the SR by Huang et al. (2016)8 that met eligibility criteria for this report compared daily 2% CHG-impregnated wipes with daily soap and water bathing.
Four of the included primary studies evaluated bathing with 2% CHG-impregnated washcloths.10,12-14 All 2% CHG wipes were commercially prepared by either Clinell Chlorhexidine Wash Cloths, Clinell (GAMA Healthcare) London, UK;13 Teleflex Medical Australia, Sydney, New South Wales;12 TBF Biotech, Taipei, Taiwan;14 or Sage Products LLC, Illinois, US.10 The study by Garrido-Benedicto et al. evaluated 4% CHG-impregnated sponge (Dispomedic sponge C, CV Médica, Tarragona, Spain).11 CHG bathing of patients in the ICU was performed daily as the intervention (or every second day) in 4 primary studies.11-14 Kapadia et al. instructed study participants to use 6 2% CHG-impregnated cloths the night and morning before their surgery.10 In all 5 of the included primary studies, soap and water was the comparator.10-14
Outcomes
Kapadia et al.10 evaluated the incidence of deep periprosthetic infection as their primary outcome.10 The remaining 6 studies included in this review evaluated a range of outcomes related to the clinical effectiveness of CHG bathing, including the incidence or prevalence rates of hospital-acquired bloodstream infections;9 catheter-related bloodstream infections8 and catheter-associated urinary tract infections;8 ventilator-associated pneumonia;8 the acquisition of MRSA, VRE, or other multi-drug–resistant organism (MDRO);8,11-14 health care facility–onset Clostridium difficile infection cases between 48 hours after ICU admission through to 48 hours after ICU discharge;12 and blood culture contamination.11 Five studies reported on adverse events.8,10,11,13,14
Summary of Critical Appraisal
Systematic Reviews
Strengths of both SRs8,9 were related to publication or registration of methods a priori, the comprehensive literature search, the use of appropriate risk of bias assessments, their adequate explanations for any heterogeneity observed, and discussion of publication bias. Defining the protocol for an SR a priori coupled with comprehensive reporting reduces the risk of bias, particularly reporting bias, and increases the transparency and reproducibility of the review. Comprehensive literature searching reduces the risk of missing potentially relevant studies and in turn, provides a more complete picture of the literature at the time. In addition, conducting adequate risk of bias assessments and assessing possible explanations for observed heterogeneity strengthens the validity of the results.
Regarding limitations, in both SRs, details were missing as to which studies were excluded from the review and the authors did not report on the funding sources for the included studies. Without details for excluded studies, no conclusions can be drawn about their potential impact. It is important to report the funding sources for included studies so that the potential for industry bias of the primary studies can be adequately considered. Given that the majority of primary studies included in each SR were non-randomized, it may limit the certainty of the findings from the review; however, authors of both SRs did report that most of the included non-randomized studies were of high quality according to their risk of bias assessments. In addition, some aspects of the SR conducted by Huang et al.8 were not clear; for example, the authors did not report whether study selection was done in duplicate or not, which could have led to errors in study selection. There were also some inconsistencies noted in the reporting of primary study characteristics in the SR conducted by Huang et al.,8 contributing to uncertainty about reporting in the remainder of the article. Huang et al.8 also did not report on the funding source of the review or the potential conflicts of interest of the authors, which increases the risk of industry bias.
Randomized Controlled Trial
One RCT10 was included in this report. The reporting of this study’s objective, inclusion and exclusion criteria, intervention, comparator, and main outcome were all well-described, which is a strength when it comes to transparency and reproducibility of results. Study participants were randomized using a computer-generated algorithm; thus, balancing potential unmeasured confounding factors and reducing the risk of selection bias. Authors report in the discussion that the study was double-blinded; however, there were no details provided in the methods section about the blinding procedures. Another limitation of this study is the lack of description for participants who were randomized but did not complete the study. Kapadia and colleagues10 reported that 35 participants (11.4%) in the intervention group and 8 (2.9%) in the control group did not complete the study. This unequal dropout between study arms increases the risk of attrition bias and potentially creates imbalances among participant characteristics, and it is unclear what contributed to the higher dropout rate in the intervention group. Kapadia et al.10 also used a per-protocol analysis rather than an intention-to-treat analysis, which may have affected the study findings. An intention-to-treat analysis more accurately reflects real-world clinical practice, where dropout and noncompliance would happen, and keeps the statistical power unchanged. Another potential limitation is possible compliance issues among the intervention group as acknowledged by the study authors in their discussion; however, no data were provided to assess study participant compliance with the assigned intervention.
Non-Randomized Studies
There were 4 non-randomized studies included in this review; 3 before-and-after studies,11,13,14 and 1 interrupted times series study.12 These 4 studies provided good descriptions of their objectives, inclusion and exclusion criteria, intervention, comparators, and main outcomes. Comprehensive reporting is a strength, as it improves the transparency and reproducibility of results. In addition, the statistical analyses that were conducted for the main outcome in each of the 4 studies were appropriate, which increases the internal validity of the study.
There were several limitations associated the 4 non-randomized studies and the results from these studies should be interpreted with caution. Without randomization, there is a risk that the association between an intervention and an outcome is due to unmeasured confounding factors (e.g., variation in staff practices and compliance or patient characteristics during the study periods), which threatens the internal validity of the study. Before-and-after studies are also subject to history bias because data are collected from 2 different time periods. As well, before-and-after studies are at risk of the Hawthorne effect, whereby behaviour changes when subjects know they are being observed. For example, it is unknown whether the vigilance of the ICU care staff regarding bathing techniques used on patients differed after the implementation of the CHG intervention compared to the pre-intervention period. Interrupted time series design, such as that used by Kengen et al.,12 are also subject to problems with confounders that vary over time, as their design is similar to that of a before-and-after study, but the data collection and analyses may be more robust.
All 4 studies were conducted in settings that would be representative of usual care for those in an ICU; however, 2 studies limited their study populations to those who had been in the ICU for more than 48 hours11 or more than 24 hours.12 While this is likely reflective of the focus on newly acquired HAIs, this may exclude some patients who may still require bathing and who may represent a clinically different group of patients. In addition, Tien et al.14 assigned 4 ICUs with a higher baseline VRE-HAIs incidence to provide 2% CHG bathing on a daily (or every 2 days) basis to all patients in the CHG group, while 4 ICUs with a lower baseline VRE-HAIs incidence were assigned to provide standard care (without 2% CHG bathing) to all patients in the standard care group. This could have led to an overestimate of the intervention effect, as the baseline rate of VRE-HAI was different between the 2 groups.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of CHG Wipes for Infection Prevention in Patients Being Prepped for a Urinary Catheter Insertion
No relevant evidence regarding CHG wipes for infection prevention in patients being prepped for a urinary catheter insertion was identified; therefore, no summary can be provided.
Clinical Effectiveness of CHG Wipes for Infection Prevention in Patients Pre-Surgery or Admitted to the Critical Care Setting
Two SRs,8,9 1 RCT,10 and 4 non-randomized studies11-14 were identified and included in this report. The studies included in this review reported results pertaining to rates of surgical site infections,10 health care–associated infections8,9,11-14, blood culture contamination,11 and adverse events.8,10,11,13,14 There was some overlap in the primary studies that were included in the SRs (see Appendix 5); however, as the results of the SRs are presented narratively, the data are only presented once by primary study.
Surgical Site Infections
One primary study was identified with respect to using CHG wipes for infection prevention pre-surgery.10 The results from this RCT demonstrated that using 2% CHG-impregnated cloths the night before and morning of admission significantly reduced the likelihood of deep periprosthetic infections in patients undergoing total joint arthroplasty (hip and knee) when compared to standard soap and water bathing. This result was associated with a wide confidence interval, which suggests some uncertainty in the finding.
Health Care–Associated Bloodstream Infections
Nine primary studies included in the SR by Musuuza et al. (2019)9 that were eligible for this review reported on health care–associated bloodstream infections and there was complete overlap among the eligible primary studies from the Huang et al. (2016)8 SR addressing this outcome; thus, the results from the relevant studies are only reported once. A citation matrix illustrating the degree of overlap is presented in Appendix 5. Of these 9 primary studies, 5 reported an incidence rate ratio that suggested a statistically significant reduction in health care–associated bloodstream infections when comparing bathing with CHG-impregnated wipes versus soap and water bathing, and 4 studies suggested no difference between groups. Together, these data suggest that 2% CHG bathing either reduces or has no difference in the risk of hospital-associated bloodstream infections compared with soap and water bathing.
Catheter-Associated Urinary Tract Infections
Four studies included in the SR by Huang et al. (2016)8 that were eligible for this review reported on catheter-associated urinary tract infections. Of these 4 studies, 1 study reported a risk ratio that suggested a statistically significant reduction in catheter-associated urinary tract infections when comparing bathing with CHG-impregnated wipes versus soap and water bathing, and 3 studies reported no difference between groups. Together, these data suggest that 2% CHG bathing either reduces the risk of catheter-associated urinary tract infections or has no effect compared with soap and water bathing.
Ventilator-Associated Pneumonia
Three studies included in the SR by Huang et al. (2016)8 that were eligible for this review reported on ventilator-associated pneumonia. All 3 studies reported no difference in ventilator-associated pneumonia when comparing bathing with CHG-impregnated wipes versus soap and water bathing.
Acquisition of MRSA, VRE, or Another MDRO
Two studies included in the SR by Huang et al. (2016)8 that were eligible for this review reported on the acquisition of MRSA. Both studies reported no difference in the acquisition of MRSA when comparing bathing with CHG-impregnated wipes versus soap and water bathing.
Among the primary studies included in this report, Tien et al.14 showed that daily bathing with 2% CHG wipes was associated with a lower risk of VRE-HAI after adjusting for the effects of VRE carriage at ICU entry and the length of hospital stay. Conversely, Kengen et al.12 demonstrated no difference in the incidence rates of newly acquired MRSA among ICU patients. Similarly, Ruiz et al.13 reported no reductions in the overall incidence of nosocomial infections or those infections caused by MDROs (i.e., MRSA, VRE, multi-drug–resistant gram-negative organisms, Clostridium difficile) when comparing CHG bathing to soap and water bathing.
Blood Culture Contamination
Two non-randomized studies reported on the incidence of blood culture contamination. Garrido-Benedicto et al.11 reported that the use of 4% CHG-impregnated sponges significantly reduced the incidence of positive blood cultures compared to soap and water bathing. However, Kengen et al.12 reported no difference in the risk of in the blood culture contamination when 2% CHG wipe bathing was compared to soap and water bathing, and their interrupted time series analysis showed no change in the month-to-month trend in the number of positive blood cultures.
Adverse Events
One SR8,9 and 4 primary studies reported on adverse skin reactions.10,11,13,14 Kapadia et al. reported that red wheals occurred in 1 of 275 patients in the CHG intervention group but was resolved with 2 days. Huang et al.8 reported that 1 primary study included in their SR noted that 3 study participants were excluded from the CHG arm of the study because of a rash; however, it was later determined that the rash was not due to CHG bathing. No further details were reported. The remaining 3 studies reported no adverse skin reactions. No other adverse events were reported.
Limitations
The primary limitation of this review is the lack of evidence regarding the clinical effectiveness of CHG wipes for infection prevention among patients being prepped for urinary catheter insertion, as well as for preoperative patients. A single study was identified regarding CHG wipes for infection prevention in patients who were preoperative. Additionally, while the non-randomized studies included in the SRs were assessed by the authors to have a low risk of bias, there were no other high-quality primary studies identified in this report regarding the clinical effectiveness of CHG wipes for infection prevention among patients in critical care settings.
Most of the studies took place at a single site and none of the studies were conducted in Canada. Thus, the generalizability to the Canadian context is unclear.
Conclusions and Implications for Decision- or Policy-Making
This review comprised 2 SRs,8,9 1 RCT,10 and 4 non-randomized studies11-14 evaluating the clinical effectiveness of CHG wipes for infection prevention among patients pre-surgery or in critical care settings. No literature was identified with respect to the clinical effectiveness of CHG wipes for infection prevention among patients being prepped for a urinary catheter insertion.
Based on the evidence summarized, there appears to be a modest association between CHG wipes and reduction in surgical site infections10 when compared to cleansing with soap and water; however, this finding is based on 1 RCT and there is some uncertainty in the finding. The results were mixed for the association of CHG wipes with reduction in health care–associated blood stream infections;8,9,12,14 catheter-associated urinary tract infections;8 acquisition of MRSA, VRE, or another MDRO;12-14 and blood culture contamination11,12 compared to soap and water. In some studies, there was a statistically significant reduction of health care–associated bloodstream infections;9 catheter-related urinary tract infections;8 the acquisition of MRSA, VRE, or another MDRO;8,14 and blood culture contamination11 when CHG wipes were used in critical care settings compared to soap and water. In other studies, however, no differences were observed between intervention groups.8,9,12,13 No difference was observed between bathing with CHG wipes compared to soap and water for the incidence of ventilator-associated pneumonia among patients in the ICU. Thus, we can conclude that, compared to bathing with soap and water, bathing with CHG-impregnated wipes in critical care settings results in either a reduction or no difference in the risk of infection but does not increase the risk of infection. For adverse events, 2 studies8,10 reported mild adverse skin reactions during the CHG bathing period, while 3 other studies11,13,14 reported no adverse events. Bathing with CHG-impregnated wipes appears to be safe.
The limitations of the included literature (e.g., unequal dropout in the RCT, potential for unmeasured confounding in non-randomized studies) should be considered when interpreting the findings of this report. More robust research using well-designed, high-quality studies is required to support the clinical effectiveness and subsequent decision-making regarding the use of CHG-impregnated wipes versus soap and water for infection prevention in pre-surgical and critical care settings.
A previous CADTH report from 2016 that reviewed the clinical and cost-effectiveness evidence regarding CHG wipes for infection prevention in adult patients in acute or critical care settings also identified conflicting evidence regarding the clinical effectiveness of CHG wipes in critical care settings based on the review of 5 publications.16
References
1.Mitchell R, Taylor G, Rudnick W, et al. Trends in health care–associated infections in acute care hospitals in Canada: an analysis of repeated point-prevalence surveys. CMAJ. 2019;191(36):E981-E988. PubMed
2.Tessier L, Guilcher SJT, Bai YQ, Ng R, Wodchis WP. The impact of hospital harm on length of stay, costs of care and length of person-centred episodes of care: a retrospective cohort study. CMAJ. 2019;191(32):E879-E885. PubMed
3.Measuring patient harm in Canadian hospitals. Ottawa (ON): Canadian Institute for Health Information; 2016: https://secure.cihi.ca/free_products/cihi_cpsi_hospital_harm_en.pdf. Accessed 2021 Jul 18.
4.Lim KS, Kam PC. Chlorhexidine--pharmacology and clinical applications. Anaesth Intensive Care. 2008;36(4):502-512. PubMed
5.Chlorhexidine gluconate (topical): drug information. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: https://www.uptodate.com. Accessed 2021 Jun 23.
6.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
7.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
8.Huang HP, Chen B, Wang HY, He M. The efficacy of daily chlorhexidine bathing for preventing healthcare-associated infections in adult intensive care units. Korean J Intern Med. 2016;31(6):1159-1170. PubMed
9.Musuuza JS, Guru PK, O'Horo JC, et al. The impact of chlorhexidine bathing on hospital-acquired bloodstream infections: a systematic review and meta-analysis. BMC Infect Dis. 2019;19(1):416. PubMed
10.Kapadia BH, Elmallah RK, Mont MA. A randomized, clinical trial of preadmission chlorhexidine skin preparation for lower extremity total joint arthroplasty. J Arthroplasty. 2016;31(12):2856-2861. PubMed
11.Garrido-Benedicto P, Cueto-Quintana P, Farre-Termens E, Marine-Cabre M, Riba-Reig J, Molina-Chueca R. Effect of daily cleaning with chlorhexidine on the incidence of contamination of blood cultures in the critical patient. Enferm Intensiva. 2017;28(3):97-104. PubMed
12.Kengen R, Thoonen E, Daveson K, et al. Chlorhexidine washing in intensive care does not reduce bloodstream infections, blood culture contamination and drug-resistant microorganism acquisition: an interrupted time series analysis. Crit Care Resusc. 2018;20(3):231-240. PubMed
13.Ruiz J, Ramirez P, Villarreal E, et al. Daily bathing strategies and cross-transmission of multidrug-resistant organisms: Impact of chlorhexidine-impregnated wipes in a multidrug-resistant gram-negative bacteria endemic intensive care unit. Am J Infect Control. 2017;45(10):1069-1073. PubMed
14.Tien KL, Wang JT, Sheng WH, et al. Chlorhexidine bathing to prevent healthcare-associated vancomycin-resistant Enterococcus infections: A cluster quasi-experimental controlled study at intensive care units. J Formos Med Assoc. 2021;120(3):1014-1021. PubMed
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
16.Chlorhexidine gluconate wipes for infection prevention in acute and critical care: a review of clinical effectiveness and cost-effectiveness. Rapid response report: summary with critical appraisal. Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/pdf/htis/apr-2016/RC0769%20Chlorhexidine%20Wipes%20Final.pdf. Accessed 2021 Jul 19.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews and Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Relevant clinical outcomes, length of follow-up |
Musuuza et al. (2019)9 US Funding source: Agency for Healthcare Research and Quality [R18HS024039] and the United States Veterans Affairs National Center for Patient Safety Center of Inquiry | All included studies:
Relevant included studies:
| Eligible populations:
Relevant population:
| Eligible interventions:
Relevant intervention:
Eligible comparators:
Relevant comparator:
|
Follow-up: NR |
Huang et al. (2016)8 China Funding source: NR | All included studies:
Relevant included studies:
|
| Eligible intervention:
Relevant intervention:
Eligible comparators:
Relevant comparator:
|
Follow-up: NR |
CHG = chlorhexidine gluconate; ICU = intensive care unit; MRSA = Methicillin-resistant Staphylococcus aureus; NR = not reported; RCT = randomized controlled trial; VRE = vancomycin-resistant Enterococcus.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Randomized Controlled Trials | ||||
Kapadia et al. (2016)10 US Funding source: Sage Products, LLC | Study design: single-centre, prospective, randomized controlled trial Setting: tertiary care centre Objective: to compare chlorhexidine cloths to standard-of-care antiseptic bathing in patients before total join arthroplasty to evaluate any differences in periprosthetic infection risk | Adult patients undergoing a joint arthroplasty, specifically a total knee arthroplasty or total hip arthroplasty Number of patients: N = 539 Mean (SD) age and % female:
| Intervention: 2 packets containing 6 2% CHG-impregnated cloths (Sage Products LLC), along with instructions for use the night before and morning of surgery N = 272 Comparator: bathing instructions with antibacterial soap and water the night before surgical admission N = 267 | Outcomes:
Follow-up:
|
Non-Randomized Studies | ||||
Tien et al. (2021)14 Taiwan Funding source: PBF Biotech (Taipei, Taiwan) provided CHG wipes, otherwise, no funding source reported | Study design: Cluster quasi-experimental controlled before-and-after study Setting: 8 medical ICU of the National Taiwan University Hospital (80 beds in total) Objective: to assess the effect of CHG bathing to prevent VRE-HAIs at ICUs | Adult patients in ICU Number of patients: N = 4,800 in total Median age (IQR) and % female: Intervention:
Standard of care:
68 (58-79) and 36.7% Intervention period: 68 (57-79) and 36.3% | Intervention: whole body bathing with 2% CHG-impregnated paper towel (PBF Biotech, Taipei, Taiwan) daily or every 2 days N = 1,501 Comparator: daily wiping bath using commercial cleansing lotion not containing CHG N = 3,299 | Outcomes:
Follow-up:
|
Kengen et al. (2018)12 Australia Funding source: NR | Study design: single-centre, retrospective, open-label, sequential period, interrupted time series design Setting: ICU of the Canberra Hospital (31 bed mixed medical and surgical ICU) Objective: to investigate the effect of implementation of a policy of daily chlorhexidine washing on rates of bloodstream infections, blood culture contamination, newly acquired MDRO isolates and Clostridium difficile infections | Adult ICU patients, excluded if ICU stay was < 24 hours or had an allergy to chlorhexidine Number of patients: N = 6,334 in total Mean age (SD) and % female:
| Intervention: daily chlorhexidine washes (2% chlorhexidine-impregnated washcloths (Teleflex Medical Australia, Sydney, NSW) were to be used according to the supplier’s instructions)
Comparator: daily washes with water and soap
| Outcomes:
Follow-up:
|
Garrido-Benedicto et al. (2017)11 Spain Funding source: NR | Study design: single-centre, prospective, quasi-experimental, non-randomized, single blind, pre-post-design Setting: medical-surgical intensive care unit in the Hospital Universitari Sant Joan de Reus (12-bed) Objective: to evaluate the efficacy of daily cleaning with 4% chlorhexidine-impregnated sponges in decreasing contamination of blood cultures in critically-ill patients | Adult ICU patients admitted for > 48 hours; patients with > 20% skin disruption, who were pregnant, or had an allergy to chlorhexidine were excluded Number of patients: N = 237 Median age (IQR) and % female:
| Intervention: body sponges impregnated with 4% chlorhexidine digluconate (Dis- pomedic sponge C, CV Médica, Tarragona, Spain),
Comparator: warm water and CR-32 antiseptic-free dermatological soap (José Collado S.A., Barcelona, Spain)
| Outcomes:
Follow-up:
|
Ruiz et al. (2017)13 Spain Funding source: NR | Study design: single-centre, prospective, non-randomized, before-and-after study Setting: nonsurgical ICU (24 bed) at a university hospital (Hospital La Fe) Objective: to assess the impact on the nosocomial colonization and infection caused by MDRO by introducing CHG-impregnated wipes into the daily bathing of patients admitted to an ICU | Adult ICU patients Number of patients: N = 3,235 Mean age (SD) and % female:
| Intervention: CHG wipes (Clinell Wash Cloths; Clinell; Health care, London, UK), impregnated with 2% CHG plus softening agents were introduced for the daily bathing of patients on mechanical ventilation, and for those patients colonized by MDROs
Comparator: traditional wash with soap and water for the daily bathing of ICU patients on mechanical ventilation, and for those patients colonized by MDROs
| Outcomes:
Follow-up:
|
CHG = chlorhexidine gluconate; HAI = hospital-acquired infection; ICU = intensive care unit; IQR = interquartile range; MDRO = multi-drug‒resistant organisms; MRSA = Methicillin-resistant Staphylococcus aureus; NR = not reported; SD = standard deviation; VRE = vancomycin-resistant Enterococcus.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 26
Strengths | Limitations |
Musuuza et al. (2019)9 | |
Review was conducted according to PRISMA and MOOSE guidelines and was registered with PROSPERO (CRD42015032523) Inclusion criteria included PICO components Review methods were established a priori A comprehensive search strategy was used (searched at least 2 databases, provided keywords and/or search strategy, searched the reference lists/bibliographies of included studies) Study selection was done in triplicate and data extraction was done in duplicate Included studies were described in adequate detail regarding PICO and study design Authors used Cochrane Collaboration Tool to assess the risk of bias of the individual studies included in the review Authors discussed the risk of bias assessment results of individual studies when discussing their results (i.e., conducted subgroup analyses based on RCT or CRT vs. non-randomized studies, bundled vs. non-bundled interventions, CHG wipes vs. CHG solution, and ICU vs. non-ICU settings) Authors provided adequate explanation for heterogeneity observed in the results of the primary studies through statistical analysis Authors conducted and discussed graphical and statistical test for publication bias Authors reported funding sources and potential conflicts of interest for conducting the review | Selection of study designs included in the review was not clearly explained Authors did not report if trial registries or grey literature was searched. Authors did not provide a list of excluded studies with reasons for exclusion Authors did not report on the sources of funding or conflicts of interest for the included studies |
Huang et al. (2016)8 | |
Review was conducted according to PRISMA guidelines and was registered with PROSPERO (CRD42014014973) Inclusion criteria included PICO components Review methods were established a priori A comprehensive search strategy was used (searched at least 2 databases, provided keywords and/or search strategy, searched the reference lists/bibliographies of included studies) Data were extracted from included studies in duplicate Included studies were described in adequate detail regarding PICO and study design Authors used Cochrane Risk of Bias tool to assess the risk of bias for RCTs and the Newcastle-Ottawa Quality Assessment Scale to assess the quality of non-randomized studies included in the review Authors discussed the RoB assessment results of individual studies when discussing their results Authors provided adequate explanation for heterogeneity observed in the results of the primary studies through statistical analysis | Selection of study designs included in the review was not clearly explained Authors did not report if trial registries or grey literature was searched Authors did not report whether study selection was done in duplicate Authors did not provide a list of excluded studies with reasons for exclusion Authors did not report on the sources of funding or conflicts of interest for the included studies Authors did not adequately investigate the impact of publication bias on the results of the SR Authors did not report the funding source or potential conflicts of interest for the authors conducting the review Discrepancies were noted in the reporting of study characteristics for studies that overlapped with Musuuza et al. (2019),9 which leads to uncertainty about other aspects of reporting for this study |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; MOOSE = Meta-analyses Of Observational Studies in Epidemiology; PICO = population, intervention, comparator, outcome; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-analyses; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist7
Strengths | Limitations |
Randomized controlled trial | |
Kapadia et al. (2016)10 | |
Study objective was clearly described Outcomes to be measured were clearly described, and were valid and reliable Inclusion/exclusion criteria and participant characteristics were clearly described Intervention and comparator were clearly described Randomization procedures were clearly reported Sample size calculation was reported Data analyses were planned a priori Main findings were clearly described Estimates of random variability for the main outcomes were clearly described All important adverse events were reported Actual probability values were reported for the main outcomes Statistical tests used to assess the main outcomes were appropriate with sufficient statistical power to detect a difference | Characteristics of participants who were randomized but did not complete the study were not described and the numbers of non-participants differed between study groups (N = 35 in intervention group, N = 8 in control group) Study was conducted in US at a single tertiary care centre; thus, findings may not be generalizable to Canada or to other centres Study authors acknowledged in their discussion that some study participants may not have reliably followed directions for the intervention they were assigned; however, no data were reported to support this Per-protocol analysis was conducted instead of intention-to-treat; thus, increasing the risk of imbalanced patient characteristics between study arms Authors reported that the study was double-blinded in the Discussion, but no details provided in the Methods |
Non-randomized studies | |
Tien et al. (2021)14 | |
Study objective was clearly described Outcomes to be measured were clearly described, and were valid and reliable Inclusion/exclusion criteria and participant characteristics were clearly described Intervention and comparator were clearly described Data analyses were planned a priori Main findings were clearly described Statistical tests used to assess the main outcomes were appropriate All-important adverse events were reported | Non-randomized, the 4 ICUs with a higher baseline VRE-HAIs incidence were assigned to provide 2% CHG bathing on a daily (or every 2 days) basis to all patients (CHG group), while the 4 ICUs with a lower baseline VRE-HAIs incidence were assigned to provide standard care (without 2% CHG bathing) to all patients (standard care group) Study was conducted in Taiwan in a single hospital across 8 ICUs; thus, findings may not be generalizable to Canada or to other centres Authors did not discuss statistical power |
Kengen et al. (2018)12 | |
Study objective was clearly described Outcomes to be measured were clearly described, and were valid and reliable Inclusion and exclusion criteria and participant characteristics were clearly described Intervention and comparator were clearly described Data analyses were planned a priori Main findings were clearly described Actual probability values were reported for the main outcomes Estimates of random variability for the main outcomes were clearly described | Retrospective, non-randomized Study was conducted in Australia in a single hospital ICU; thus, findings may not be generalizable to Canada or to other centres Potentially insufficient statistical power to detect changes in infection and colonization rates No measure of nursing staff compliance in administration of study intervention Potential for unmeasured confounding |
Garrido-Benedicto et al. (2017)11 | |
Study objective was clearly described Outcomes to be measured were clearly described, and were valid and reliable Inclusion and exclusion criteria and participant characteristics were clearly described Intervention and comparator were clearly described Data analyses were planned a priori Main findings were clearly described Estimates of random variability for the main outcomes were clearly described Statistical tests used to assess the main outcomes were appropriate with sufficient statistical power to detect a difference All-important adverse events were reported | Non-randomized Actual probability values were not reported for the main outcomes Study was conducted in Spain in a single hospital ICU; thus, findings may not be generalizable to Canada or to other centres |
Ruiz et al. (2017)13 | |
Study objective was clearly described Outcomes to be measured were clearly described Inclusion/exclusion criteria and participant characteristics were clearly described Intervention and comparator were clearly described Data analyses were planned a priori Main findings were clearly described Statistical tests used to assess the main outcomes were appropriate All-important adverse events were reported | Non-randomized Study was conducted in Spain in a single hospital ICU; thus, findings may not be generalizable to Canada or to other centres Only patients who required mechanical ventilation or were colonized with multi-drug‒resistant organism(s) were subject to the intervention of CHG bathing while in ICU, rather than entire ICU population as a means to control spread of MDROs Actual probability values were not reported for the main outcomes Authors did not discuss statistical power |
CHG = chlorhexidine gluconate; ICU = intensive care unit; MDRO = multi-drug‒resistant organisms.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Summary of Findings Included Systematic Reviews and Meta-Analyses
Musuuza et al. (2019)9
Main Study Findings
SR and meta-analysis of RCTs, cluster randomized trials and quasi-experimental studies to examine the effect of CHG bathing on prevention of HABSIs and assessed fidelity to implementation of this behavioural intervention in adult health care settings.
Relevant primary studies: The SR included 26 studies (8 RCTs and 18 non-randomized studies) that measured the clinical effectiveness of CHG bathing on prevention of hospital-acquired bloodstream infection (HABSIs); however, only primary studies that compared bathing with CHG wipes versus soap and water in critical care settings were relevant to this report (2 RCTs and 7 non-randomized studies). Although the SR included meta-analyses, there was no meta-analysis specific to the primary studies relevant to the current report. Therefore, relevant results were summarized individually by primary study.
Summary of relevant findings from the systematic review:
Health care associated bloodstream infections
Bleasdale et al. (2007)
CHG wipes versus soap and water: incidence rate ratio (IRR) = 0.39 (95% confidence interval [CI], 0.18 to 0.86)
Boonyasiri et al. (2016)
CHG wipes versus soap and water: IRR = 1.27 (95% CI, 0.23 to 6.86)
Cassir et al. (2015)
CHG wipes versus soap and water: IRR = 0.50 (95% CI, 0.25 to 0.97)
Dixon and Carver (2010)
CHG wipes versus soap and water: IRR = 0.28 (95% CI, 0.12 to 0.64)
Duszyńska et al. (2017)
CHG wipes versus soap and water: IRR = 0.32 (95% CI, 0.14 to 0.71)
Holder and Zellinger (2009)
CHG wipes versus soap and water: IRR = 1.00 (95% CI, 0.22 to 4.47)
Kassakian et al. (2011)
CHG wipes versus soap and water: IRR = 0.96 (95% CI, 0.31 to 2.98)
Popovich et al. (2009)
CHG wipes versus soap and water: IRR = 0.13 (95% CI, 0.03 to 0.54)
Popovich et al. (2010)
CHG wipes versus soap and water: IRR = 1.14 (95% CI, 0.59 to 2.18)
Author’s Conclusion
“We found that CHG bathing of patients is associated with a consistent, clinically important, and statistically significant reduction in the risk of HABSIs. This effect was consistent across study settings, study designs, whether the intervention was bundled or not, and whether a no-rinse approach (i.e., CHG-impregnated wipes) or CHG solution requiring rinsing was used.” (p.6)
Huang et al. (2016)8
Main Study Findings
SR and meta-analysis of RCTs, cluster randomized trials and quasi-experimental studies to determine whether daily CHG bathing significantly decreases the rates of HAIs in adult ICUs.
Relevant primary studies: The SR included 15 studies (3 RCTs and 12 non-randomized studies) that measured the clinical effectiveness of CHG bathing on prevention of HAIs; however, only primary studies that compared bathing with CHG wipes versus soap and water in critical care settings were relevant to this report (1 RCTs and 6 non-randomized studies). Although the SR included meta-analyses, there was no meta-analysis specific to the primary studies relevant to the current report. Therefore, relevant results were summarized individually by primary study. Results that overlap with those reported by Musuuza and colleagues9 are not repeated here (see Appendix 5 for overlap).
Summary of relevant findings from the systematic review:
Catheter-associated urinary tract infections
Bleasdale et al. (2007)
CHG wipes versus soap and water: RR = 0.73 (95% CI, 0.36 to 1.51)
Cassir et al. (2015)
CHG wipes versus soap and water: RR = 0.27 (95% CI, 0.09 to 0.80)
Popovich et al. (2009)
CHG wipes versus soap and water: RR = 0.78 (95% CI, 0.39 to 1.57)
Popovich et al. (2010)
CHG wipes versus soap and water: RR = 1.34 (95% CI, 0.71 to 2.50)
Ventilator-associated pneumonia
Bleasdale et al. (2007)
CHG wipes versus soap and water: RR = 0.98 (95% CI, 0.49 to 1.93)
Popovich et al. (2009)
CHG wipes versus soap and water: RR = 0.92 (95% CI, 0.40 to 2.10)
Popovich et al. (2010)
CHG wipes versus soap and water: RR = 0.64 (95% CI, 0.39 to 1.04)
Acquisition of MRSA
Popovich et al. (2009)
CHG wipes versus soap and water: RR = 0.87 (95% CI, 0.35 to 2.17)
Popovich et al. (2010)
CHG wipes versus soap and water: RR = 1.52 (95% CI, 0.47 to 4.99)
Acquisition of VRE
Popovich et al. (2009)
CHG wipes versus soap and water: RR = 0.60 (95% CI, 0.15 to 2.40)
Popovich et al. (2010)
CHG wipes versus soap and water: RR = 2.12 (95% CI, 0.51 to 8.85)
Vernon et al. (2006)
CHG wipes versus soap and water: RR = 0.35 (95% CI, 0.21 to 0.58)
Adverse events
Bleasdale et al. (2006)
“…three subjects were excluded from the CHG arm after developing rashes; however, it was ultimately determined not to be due to CHG” (p.1166)
Author’s Conclusion
“This further meta-analysis demonstrated that daily CHG bathing had an overwhelming effect on decreasing the rates of the composite primary outcomes, including CRBSI, CAUTI, VAP, and acquisition of MRSA and VRE.” (p.1166)
Summary of Findings of Included Primary Clinical Studies
Randomized Controlled Trial — Main Study Findings
Kapadia et al. (2016)10
Periprosthetic infections, n (%)
9 (1.6%) periprosthetic infections in the entire population of 554 arthroplasties
Deep periprosthetic infections, n (%)
CHG cohort (N = 275): 1 (0.4%);
Standard-of-care cohort (N = 279): 8 (2.9%)
(P = 0.038)
Standard of care versus CHG cohort: odds ratio (OR) = 8.15 (95% confidence interval [CI] = 1.01 to 65.6; P = 0.049)
Superficial periprosthetic infections, n (%)
CHG cohort (N = 275): 1 (0.4%)
Standard-of-care cohort (N = 279): 5 (2.5%)
Adverse events
“Red wheals occurred in one treated patient, which resolved within 2 days with local wound care” (p.2859)
Author’s Conclusion
“In this study, chlorhexidine gluconate-impregnated cloths the night before and morning of admission significantly decreased periprosthetic infections in TJA [total joint arthroplasty] patients when compared to standard antiseptic bathing overall (OR 8.15).” (p.2859)
Non-Randomized Studies — Main Study Findings
Tien et al. (2021)14
CHG bathing
independently associated with a 70% lower risk of VRE-HAIs (adjusted OR = 0.3, 95% CI,0.2 to 0.7, P = 0.006), after adjusting for effects of VRE carriage at entry to ICUs and the length of hospital stay
all types of VRE-HAIs decreased during the intervention period, including bloodstream, urinary tract, surgical site, and cardiovascular infections
VRE carriage at entry to ICUs was a major risk factor for VRE-HAIs (adjusted OR = 4.5, 95% CI, 2.4 to 8.3, P < 0.0001)
Standard of care
No effect on the risk of VRE-HAIs (adjusted OR = 1.8, 95% CI, 0.7 to 4.7, P = 0.259)
VRE carriage at entry to ICUs was a major risk factor for VRE-HAIs (adjusted OR = 7.9, 95% CI, 3.0 to 21.1, P < 0.0001)
Adverse effects
No rash or allergy occurred. No adverse events other than skin dryness was reported
Author’s Conclusion
“This is the first study to examine the effect of daily 2% CHG bathing on VRE-HAIs incidence at ICUs, in the context of active VRE surveillance. Our results show that 2% CHG bathing was independently associated with a 70% lower risk of VRE-HAIs. In contrast, standard care during the same period had no effect on the incidence of VRE-HAIs. This provides a strong evidence that the observed decrease in VRE-HAIs in the CHG group is the effect of 2% CHG bathing, rather than the effect of advances in standard care during the same period.” (p.1017)
“In conclusion, CHG bathing is a simple, safe, and highly effective approach to prevent VRE-HAIs at ICUs, in the context of active VRE surveillance with contact isolation. Further investigations on using CHG bathing to prevent VRE-HAIs in non-ICUs settings are warranted.” (p.1020)
Kengen et al. (2018)12
Main Study Findings
Blood culture contamination in ICU
Total positive blood cultures, soap and water group versus CHG washing group:
unadjusted risk ratio [RR] = 0.85 (95% CI, 0.68 to 1.07, P = 0.17)
adjusteda RR = 0.80 (95% CI 0.61 to 1.03, P = 0.09)
Total clinically significant blood cultures, soap and water group versus CHG washing group
unadjusted RR = 0.84 (95% CI 0.58 to 1.22, P = 0.37)
adjusteda RR = 0.76 (95% CI 0.51 to 1.13, P = 0.17)
Gram to negative cultures, soap and water group versus CHG washing group
unadjusted RR = 0.75 (95% CI 0.38 to 1.49, P = 0.41)
adjusteda RR = 0.43 (95% CI 0.18 to 1.00, P = 0.05)
Gram to positive cultures, soap and water group versus CHG washing group
unadjusted RR = 0.91 (95% CI 0.72 to 1.16, P = 0.46)
adjusteda RR = 0.85 (95% CI 0.67 to 1.09, P = 0.21)
Yeast cultures, soap and water group versus CHG washing group
unadjusted RR = 0.89 (95% CI 0.32 to 2.49, P = 0.82)
adjusteda RR = 0.62 (95% CI 0.20 to 1.94, P = 0.41)
Interrupted time series [ITS] analysis
No statistically significant change in month-to-month number of positive blood cultures during the pre-intervention period (P = 0.72) or during the intervention period (P = 0.29)
New acquisition of multi-drug–resistant organisms (MDROs) in the ICU
Total MDRO acquisitions, soap and water group versus CHG washing group:
unadjusted RR = 1.27 (95% CI 0.83 to 1.93, P = 0.27)
adjusteda RR = 0.99 (95% CI 0.62 to 1.24, P = 0.97)
MRSA acquisitions, soap and water group versus CHG washing group:
unadjusted RR = 0.83 (95% CI 0.32 to 2.14, P = 0.70)
adjusteda RR = 1.23 (95% CI 0.42 to 1.30, P = 0.89)
VRE acquisitions, soap and water group versus CHG washing group:
unadjusted RR = 1.85 (95% CI 0.54 to 1.66, P = 0.86)
adjusteda RR = 0.74 (95% CI 0.42 to 1.30, P = 0.29)
Multi-drug–resistant gram-negative (MRGN) acquisitions, soap and water group versus CHG washing group:
unadjusted RR = 1.29 (95% CI 0.55 to 3.02, P = 0.56)
adjusteda RR = 2.29 (95% CI 0.81 to 6.49, P = 0.12)
New Clostridium difficile cases, soap and water group versus CHG washing group
incidence rate (IR) 0.79 vs 2.01 cases per 1,000 patient days, P = 0.16
ITS analysis
No significant changes in the month-to-month trend of MRSA, VRE or MRSA + VRE + MRGN positive cultures (slope change; P = 0.47; P = 0.13; P = 0.10, respectively)
a Adjusted for: patient age, sex, Acute Physiology and Chronic Health Evaluation (APACHE) III score, mechanical ventilation, intensive care unit and hospital length of stay, comorbid conditions, admission source, and the monthly prevalence of hospital-wide positive cultures.
Author’s Conclusion
“In this single-centre, retrospective, open-label, sequential period, ITS analysis, implementation of a unit-level policy of once daily washing with chlorhexidine, compared with water and soap, was not associated with a reduction in the number of clinically significant blood cultures, blood culture contamination, or ICU-associated new acquisition of MDRO.” (p.236)
Garrido-Benedicto et al. (2017)11
Main Study Findings
Blood culture contamination, n (%)
CHG intervention group (N = 111 blood cultures taken): 7 (6.3%)
Control group (N = 148 blood cultures taken): 23 (15.6%)
(P < 0.05)
Control group versus CHG intervention group: OR = 2.73 (95% CI, 1.13 to 6.63 P < 0.05)
Adverse events:
No skin alterations were detected during the study period
No differences in SCORing Atopic Dermatitis [SCORAD] scores between groups
Author’s Conclusion
“The use of 4% chlorhexidine soap in the daily washing of critical patients reduces the incidence of blood culture contamination, and its effect lasts over time. A low rate of blood culture contamination is a quality of care marker. It gives rise to cost savings due to the use of diagnostic tests and unnecessary treatments, as well as aiding the clinical management of patients.” (p.103)
Ruiz et al. (2017)13
Main Study Findings
Colonization by MDROs
Pre-intervention period:
no statistically significant trends were observed in the incidence of colonization by MDROs during ICU stay (Beta = − 0.04; r2 = 0.085; P = 0.227)
Intervention period:
statistically significant reduction was observed in the incidence of patients colonized by MDROs over the months (Beta = –0.209; r2 = 0.549; P = 0.027).
Pre-intervention period versus intervention period:
statistically significant difference was found between pre-intervention and intervention colonization slopes (P < 0.01).
statistically significant differences were found in the total (22.0% versus 18.4%; P = 0.01) and gram-negative (19.9% vs 16.8%; P = 0.02) number of patients colonized between the pre- and post-intervention periods, and the colonization pressure caused by MDROs (29.6% versus 15.8%; P < 0.01), respectively
Infections caused by MDROs
no reduction in the overall incidence of nosocomial infections regarding the equivalent period before the intervention (pre-intervention: 11.45 versus post-intervention: 9.97 per 1,000 patients day; P = 0.934), or in those caused by MDROs (pre-intervention: 4.84 versus post-intervention: 5.05 per 1,000 patients day; P = 0.956)
Adverse events
none of the participants had a moderate/severe skin reaction
Author’s Conclusion
“Our study demonstrates the association between daily bathing of the critical patient with CHG-impregnated wipes and the reduction of MDRO colonization, even in an endemic situation caused by multidrug-resistant gram-negative bacteria.” (p.1071)
“In conclusion, the use of CHG-impregnated wipes is an effective tool in the reduction of cross-transmission by MDROs, and therefore on the colonization rate by MDROs, even in an endemic situation because of multidrug-resistant gram-negative bacteria. It is possible that the inefficiency of standard measures for the control of MDRO transmission could be because of high inoculum (colonization pressure of 29.6%), and that the use of CHG could have helped control the situation by means of the reduction of this inoculum.” (p.1073)
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 6: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Huang (2016)8 | Musuuza (2019)9 |
Bleasdale et al. Arch Intern Med. 2007;167(19):2073–9. | Yes | Yes |
Boonyasiri et al. Infect Control Hosp Epidemiol. 2016;37(3):245–53. | No | Yes |
Cassir et al. Eur J Clin Microbiol Infect Dis. 2015;34(5):999–1004. | Yes | Yes |
Dixon and Carver. Am J Infect Control. 2010;38(10):817–21. | Yes | Yes |
Duszyńska et al. Anaesthesiol Intensive Ther. 2017;49(1):28–33. | No | Yes |
Holder and Zellinger. J Clin Outcomes Manag. 2009;16(11):509–13. | Yes | Yes |
Kassakian et al. Infect Control Hosp Epidemiol. 2011;32(3):238–43. | No | Yes |
Popovich et al. Infect Control Hosp Epidemiol. 2009;30(10):959–63. | Yes | Yes |
Popovich et al. Intensive Care Med. 2010;36(5):854–8. | Yes | Yes |
Vernon et al. Arch Intern Med 2006;166:306-312. | Yes | No |
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
CADTH. 2020. Antisepsis for Urinary Catheter Insertion: A Review of Clinical Effectiveness and Guidelines. https://www.cadth.ca/antisepsis-urinary-catheter-insertion-review-clinical-effectiveness-and-guidelines
CADTH 2019. Chlorhexidine Gluconate for Skin Preparation during Minor Procedures: Clinical Effectiveness and Guidelines https://www.cadth.ca/chlorhexidine-gluconate-skin-preparation-during-minor-procedures-clinical-effectiveness-and
CADTH 2016. Chlorhexidine Gluconate Wipes for Infection Prevention in Acute and Critical Care: A Review of Clinical Effectiveness and Cost-Effectiveness https://www.cadth.ca/chlorhexidine-gluconate-wipes-infection-prevention-acute-and-critical-care-review-clinical
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca