CADTH Health Technology Review
Medications Containing Low-Dose Codeine for the Treatment of Pain and Coughs
Rapid Review
Authors: Calvin Young, Hannah Loshak
Abbreviations
AMSTAR 2
A MeaSurement Tool to Assess systematic Reviews 2
RCT
randomized controlled trial
Key Messages
Codeine and codeine-containing medicines are used to treat people experiencing pain or cough symptoms. Whereas most products containing codeine require a prescription in Canada, some jurisdictions permit over-the-counter sales of products containing low doses of codeine mixed with other non-narcotic medicinal ingredients.
Three overviews of reviews and 13 systematic reviews of variable methodological quality failed to identify studies on the effectiveness of low-dose codeine (i.e., 8 mg of codeine per tablet or 20 mg of codeine per 30 mL in liquid products) for the treatment of pain or coughs.
There is a lack of evidence on the clinical effectiveness of oral analgesics and oral antitussives containing low doses of codeine.
Context and Policy Issues
Codeine is an alkaloid opiate compound derived from the opium poppy plant and has been used to treat pain and cough symptoms for centuries.1,2 Codeine exerts its analgesic effect after it is metabolized to morphine in the liver by the enzyme cytochrome P-450 2D6.3 Morphine primarily acts as an agonist of the mu (μ) and kappa (κ) opioid receptors, and activation of these receptors inhibits the transmission of nociceptive signals.4,5 As an antitussive medication (cough suppressant), codeine likely suppresses cough by acting on brainstem opioid receptors and on receptors on sensory nerve endings in the airways.6-8 While codeine is often considered to be less potent than other opioids, some of the adverse effects associated with its short- and long-term use include constipation, nausea, vomiting, respiratory depression, cognitive impairment; and a risk for substance addiction, misuse, and abuse.9,10 Individual variability with codeine metabolism due to genetic polymorphism affecting cytochrome P-450 2D6 impacts the risk for experiencing these adverse effects (e.g., those who are rapid metabolizers may be at an increased risk, as they will be exposed to higher levels of morphine).2,11
Opioids, including codeine and other morphine derivatives, are regulated as Schedule I drugs by Health Canada's Controlled Drugs and Substances Act.12,13 While medications containing codeine generally require a prescription for their use, many Canadian jurisdictions permit the sale of over-the-counter products containing codeine mixed with other non-narcotic medicinal ingredients (e.g., acetaminophen, acetylsalicylic acid) provided the dose of codeine in these products does not exceed 8 mg per tablet or 20 mg per 30 mL of liquid medication.12 Other jurisdictions in Canada and internationally ― including Manitoba, Australia, Hong Kong, Japan, New Zealand, the United Arab Emirates, and the US14-17 ― have reclassified codeine-containing products as prescription-only medicines because of concerns related to patient safety and the contributions these products make toward the ongoing opioid crisis.14 Regardless of their over-the-counter availability, the use of codeine-containing products is generally not recommended in children because of these concerns.11,18,19
CADTH previously reviewed the effectiveness of codeine with no dose restrictions for a number of indications, such as acute dental pain20 and acute extremity pain;21 acute pain in children;22 pain related to osteoarthritis of the knee and hip and23 Caesarean section;24 and pain as a result of orthopedic surgery,25 urological surgery, and general surgery.26 While various levels of evidence were identified for each of these indications, there is uncertainty in the effectiveness of medications containing small quantities of codeine for the treatment of pain or cough. Therefore, the objective of this report is to summarize the evidence regarding the clinical effectiveness of oral analgesic and oral antitussive medications containing up to 8 mg of codeine per tablet or 20 mg of codeine per 30 mL of liquid for the treatment of individuals with pain or cough symptoms.
Research Questions
What is the clinical effectiveness of medications containing low-dose codeine for the treatment of pain?
What is the clinical effectiveness of medications containing low-dose codeine for the treatment of cough?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE via Ovid, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were codeine and cough or pain. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016 and June 21, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Individuals of any age with pain or cough symptoms |
Intervention | Q1: Oral analgesic medications containing ≤ 8 mg codeine per tablet or ≤ 20 mg of codeine per 30 mL in liquid products alone or in combination with additional non-narcotic medicinal ingredients Q2: Oral antitussive medications containing ≤ 8 mg codeine per tablet or ≤ 20 mg of codeine per 30 mL in liquid products alone or in combination with additional non-narcotic medicinal ingredients |
Comparator | Q1: Placebo, oral analgesic medications, including alternative codeine-containing products (i.e., those containing > 8 mg but ≤ 30 mg codeine per tablet or > 20 mg of codeine per 30 mL in liquid products alone or in combination with additional non-narcotic medicinal ingredients) Q2: Placebo, oral antitussive medications, including alternative codeine-containing products (i.e., those containing > 8 mg but ≤ 30 mg codeine per tablet or > 20 mg of codeine per 30 mL in liquid products alone or in combination with additional non-narcotic medicinal ingredients) |
Outcomes | Clinical benefits (e.g., pain levels, need for additional pain medication, function, cough symptoms, cough frequency or severity, quality of life) and harms (e.g., adverse events [e.g., drowsiness, irritated stomach, nausea, opioid dependence, constipation, headache, dizziness], overdose, misuse, withdrawals) |
Study designs | HTAs, SRs, RCTs, and non-randomized studies |
HTAs= health technology assessments; RCTs = randomized controlled trials; SRs= systematic reviews.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2016. Studies that did not adequately describe the dose of codeine in analgesic or antitussive medications that participants received were also excluded.
Critical Appraisal of Individual Studies
The included systematic reviews (including overviews of reviews) were critically appraised by 1 reviewer using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)27 as a guide. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
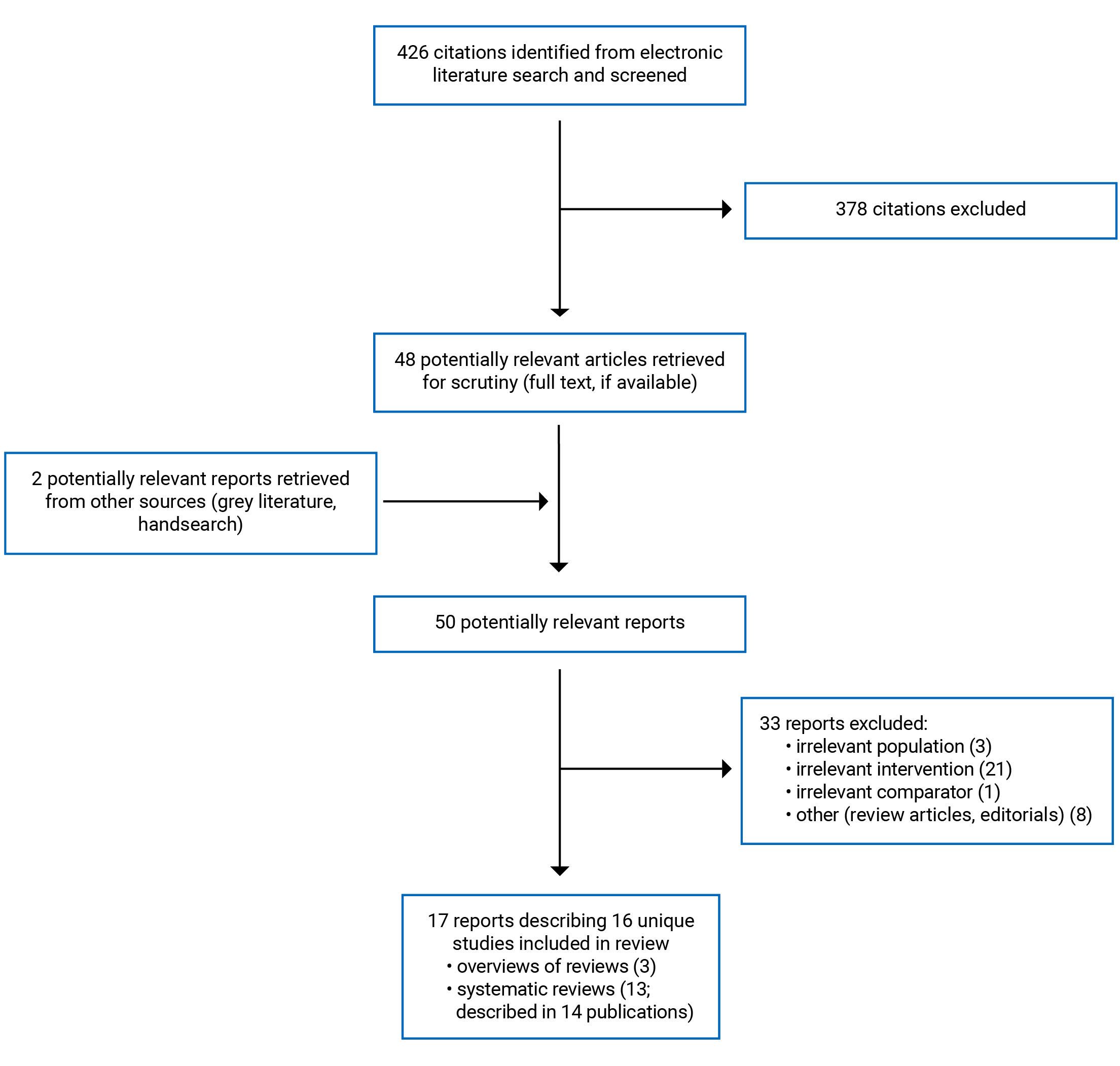
A total of 426 citations were identified in the literature search. Following the screening of titles and abstracts, 378 citations were excluded and 48 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 50 potentially relevant articles, 33 publications were excluded for various reasons and 17 publications met the inclusion criteria and were included in this report. These comprised 3 overviews of reviews28-30 (i.e., systematic reviews of systematic reviews) and 13 systematic reviews31-44 (5 with meta-analysis31-33,37,42,44 and1 with network-meta analysis),38 1 of which was reported in 2 publications.32,33 Appendix 1 presents the PRISMA45 flow chart of the study selection. Additional references of potential interest are provided in Appendix 4.
Summary of Study Characteristics
Three overviews of reviews28-30 and 13 systematic reviews31-44 (5 with meta-analysis31-33,37,42,44 and 1 with network-meta analysis)38 were identified for inclusion in this review. Of these, 3 overviews of reviews28-30 and 10 systematic reviews31-41 were specific to pain, 2 systematic reviews42,43 were specific to cough, and 1 systematic review44 examined both pain and cough. Detailed study characteristics are available in Appendix 2, Table 2. Recognizing that gender is a spectrum, when the terms “mother” or “women” were used in the included studies, we retained these terms in our reporting on these studies.
All included overviews of reviews28-30 and systematic reviews31-44 had objectives and inclusion criteria that were broader than the current report (i.e., wider in scope), mostly relating to the eligible interventions and comparators. Of the overviews of reviews and systematic reviews that were specific to pain conditions, the included studies covered any opioid for the treatment of adults with non-cancer pain,28 adults with cancer-related pain,29 children with chronic non-cancer pain,39 and children with cancer-related pain;40 pharmacological and non-pharmacological interventions for the treatment of adults with chronic tension-type headache and30 any analgesic medications for adults undergoing surgical dental implant placement;31 pharmacologic and non-pharmacologic interventions to prevent or treat episodes of primary headaches in women who were pregnant, attempting to become pregnant, postpartum, or breastfeeding;32,33 any oral medications used for pain control in adults who underwent endodontic treatments,34 any pain control preparation for people who underwent otologic surgery,35 low-dose codeine products (defined by the authors as ≤ 30 mg) in adults36 or people of all ages,37 systemic pharmaceutical for adults with chronic cancer pain,38 and oral paracetamol with or without codeine or dihydrocodeine for the treatment of adults with chronic neuropathic pain conditions.41 As for the 2 systematic reviews42,43 that were specific to cough conditions, 1 systematic review42 included studies of any drug or non-drug treatments for people (16 years of age and older) with subacute cough, while 1 systematic review43 included studies of codeine or codeine derivatives for the treatment of children with chronic cough. The final included systematic review44 summarized evidence for both pain and cough conditions, and included studies of codeine-based antitussive agents at doses that could be achieved using over-the-counter medications in Australia.
Two overviews of reviews included Cochrane systematic reviews that were published up to May 201729 and March 2017.28 The overview of reviews by Ghadiri-Sani and Silver30 included systematic reviews and randomized controlled trials (RCTs) published up to December 2013. Twelve systematic reviews31,34-44 only included RCTs. These systematic reviews included RCTs that were published up to November 2020,31 January 2019,36 August 2018,37,38 June 2018,35 December 2017,34 February 2017,40,42 September 2016,39 July 2016,41 June 2016,43 and December 2015.44 One systematic review32,33 included studies of any design (e.g., RCTs, non-randomized comparative studies, single-group studies, and N-of-1 trials) that were published up to June 2020.
Despite being eligible for inclusion, none of the overviews of reviews28-30 or systematic reviews31-44 identified studies that evaluated the clinical effectiveness of the intervention of interest for this report ― namely oral analgesic or antitussive medications containing 8 mg or less of codeine per tablet for the management of pain or cough symptoms in individuals of any age or 20 mg or less of codeine per 30 mL in liquid products alone or in combination with additional non-narcotic medicinal ingredients. While the overviews of reviews28-30 and systematic reviews31-44 often included many studies addressing their objectives and research questions, these studies examined products containing higher doses of codeine than what is relevant to the current report.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3, Table 3.
Overviews of Reviews and Systematic Reviews
The 3 overviews of reviews28-30 and 13 systematic reviews31-44 (5 with meta-analysis31-33,37,42,44 and 1 with network-meta analysis)38 were considered to be of variable methodological quality based on the assessments using AMSTAR 2.27 All included overviews28-30 and systematic reviews31-44 had clearly defined objectives and study eligibility criteria (that included components of population, intervention, comparator, and outcomes), provided the dates when literature searches were conducted, and described literature search restrictions (e.g., restrictions on publication date or language). Two overviews of reviews28,29 and the 13 systematic reviews31-44 also provided key search terms. These methodological strengths increase the reproducibility of the literature searches. In addition, literature searches were conducted in multiple databases in 1 overview30 and 12 systematic reviews,31-35,37-44 increasing the number of citations to be considered for inclusion in the review. The methods for article selection, data extraction, and quality assessment were well-documented and were conducted in duplicate or triplicate (with the exception of article selection and data extraction in the overview by Ghadiri-Sani and Silver;30 quality assessment in the review by Saldanha et al.;32,33 article selection and quality assessment in the review by Celic et al.;36 and study selection, data extraction, and quality assessment in the review by Campbell et al.;35 where it was unclear if these were conducted by a single author or in duplicate), decreasing the likelihood for inconsistency in these processes. All overviews of reviews28-30 and systematic reviews31-38,42,44 that identified studies that met their eligibility criteria described the included studies in adequate detail and assessed the methodological quality of included studies using satisfactory techniques.
As for methodological limitations, it was unclear whether the review methods were established before conducting the review in 1 overview of reviews30 and 6 systematic reviews,35-38,42,44 as there was no mention of a published protocol, increasing the risk for reporting bias. One overview of reviews30 and 7 systematic reviews34-38,42,44 did not include a list of studies excluded after full-text review, decreasing transparency in the review process. None of the authors of the included overviews28-30 and systematic reviews31-44 provided justification for their selection of eligible study designs (1231,34-44 of the 1331-44 systematic reviews only included RCTs). The authors of 2 overviews28,30 did not assess or describe the quality of the evidence summarized within the systematic reviews included in their overviews. Additionally, the included reviews did not incorporate searches for grey literature, increasing the risk that relevant studies produced outside of traditional publishing and distribution channels were not captured. Finally, the authors of 1 systematic review44 did not disclose their potential conflicts of interest, 1 systematic review36 was funded by industry, and it was unclear if financial support was received for the overview of reviews by Ghadiri-Sani and Silver30 and the systematic review by Khouly et al.31
Additional critical appraisal considerations outlined in the AMSTAR 2,27 such as the appropriateness of methods used in evidence syntheses, were not assessed, as there were no primary studies relevant to the current report identified in the included reviews and thus does not impact the interpretation of the evidence made in this report.
Summary of Findings
Clinical Effectiveness of Medications Containing Low-Dose Codeine for the Treatment of Pain
No relevant evidence regarding the clinical benefits or harms of medications containing low-dose codeine (i.e., 8 mg of codeine or less per tablet or 20 mg of codeine or less per 30 mL in liquid products) alone or in combination with additional non-narcotic medicinal ingredients for the treatment of pain was identified; therefore, no summary can be provided.
Clinical Effectiveness of Medications Containing Low-Dose Codeine for the Treatment of Cough
No relevant evidence regarding the clinical benefits or harms of medications containing low-dose codeine (i.e., 8 mg of codeine or less per tablet or 20 mg of codeine or less per 30 mL in liquid products) alone or in combination with additional non-narcotic medicinal ingredients for the treatment of cough was identified; therefore, no summary can be provided.
Limitations
Based on the findings of this report, there appears to be a lack of relevant published evidence regarding the clinical benefits or harms of medications containing low-dose codeine (i.e., 8 mg of codeine or less per tablet or 20 mg of codeine or less per 30 mL in liquid products) for the treatment of people, of any age, with pain or cough symptoms. It should be noted that, while these doses of codeine reflect the maximum dose permitted in over-the-counter products in Canada, these thresholds likely vary by jurisdiction and there may be published literature examining the clinical effectiveness of codeine-containing medications available as over-the-counter products in other countries (i.e., products with higher doses of codeine than those permitted in over-the-counter products in Canada).
Conclusions and Implications for Decision- or Policy-Making
Three overviews of reviews28-30 and 13 systematic reviews31-44 were included in this review. However, these publications28-44 failed to identify any studies that examined codeine products at doses relevant to this review. The data summarized in these overviews of reviews28-30 and systematic reviews31-44 were from studies that examined products containing higher doses of codeine. Therefore, no conclusions regarding the clinical effectiveness of analgesics or antitussives containing up to 8 mg of codeine per tablet or up to 20 mg of codeine per 30 mL in liquid products can be provided.
Future research examining the clinical effectiveness of these low-dose codeine-containing products for the treatment of pain and cough symptoms is warranted to provide decision-makers with an increased understanding of the potential role of these medicines.
References
1.Rosenblum A, Marsch LA, Joseph H, Portenoy RK. Opioids and the treatment of chronic pain: controversies, current status, and future directions. Exp Clin Psychopharmacol. 2008;16(5):405-416. PubMed
2.On PC. Updates in treatment of adults with chronic cough. Am J Manag Care. 2020;26(11 Suppl):S239-s245. PubMed
3.Smith HS. Opioid metabolism. Mayo Clin Proc. 2009;84(7):613-624. PubMed
4.Pacifici GM. Metabolism and pharmacokinetics of morphine in neonates: a review. Clinics (Sao Paulo). 2016;71(8):474-480. PubMed
5.Al-Hasani R, Bruchas MR. Molecular mechanisms of opioid receptor-dependent signaling and behavior. Anesthesiology. 2011;115(6):1363-1381. PubMed
6.Bolser DC. Central mechanisms II: pharmacology of brainstem pathways. Handb Exp Pharmacol. 2009(187):203-217. PubMed
7.Bolser DC, Davenport PW. Codeine and cough: an ineffective gold standard. Curr Opin Allergy Clin Immunol. 2007;7(1):32-36. PubMed
8.Belvisi MG, Geppetti P. Cough • 7: Current and future drugs for the treatment of chronic cough. Thorax. 2004;59(5):438-440. PubMed
9.Peechakara BV, Gupta M. Codeine. Treasure Island (FL): StatPearls Publishing; 2021: https://www.ncbi.nlm.nih.gov/books/NBK526029/. Accessed 2021 Jul 16.
10.Tay EMY, Roberts DM. A spotlight on the role, use, and availability of codeine and the implications faced. Expert Rev Clin Pharmacol. 2018;11(11):1057-1059. PubMed
11.Constant I, Ayari Khalfallah S, Brunaud A, et al. How to replace codeine after tonsillectomy in children under 12 years of age? Guidelines of the French Oto-Rhino-Laryngology--Head and Neck Surgery Society (SFORL). Eur Ann Otorhinolaryngol Head Neck Dis. 2014;131(4):233-238. PubMed
12.Health Canada. Canada Gazette, Part I, volume 151, number 36: government notices. 2017; http://www.gazette.gc.ca/rp-pr/p1/2017/2017-09-09/html/notice-avis-eng.html#ne3. Accessed 2021 Jul 19.
13.Richard G, Ojala V, Ojala A, Bowles SK, Banh HL. Monitoring programs for drugs with potential for abuse or misuse in Canada. Can Pharm J (Ott). 2012;145(4):168-171. PubMed
14.MacKinnon JIJ. Tighter regulations needed for over-the-counter codeine in Canada. Can Pharm J (Ott). 2016;149(6):322-324. PubMed
15.Government of Western Australia Department of Health. Codeine. 2018; https://ww2.health.wa.gov.au/Articles/A_E/Codeine. Accessed 2021 Jul 19.
16.bpacNZ. Codeine: all formulations prescription only. 2020; https://bpac.org.nz/2020/codeine.aspx. Accessed 2021 Jul 19.
17.Australian Government Department of Health. Update on the proposal for the rescheduling of codeine products. 2016; https://www.tga.gov.au/media-release/update-proposal-rescheduling-codeine-products. Accessed 2021 Jul 19.
18.Health Canada. Non-prescription pain relief products containing codeine are not recommended for use in people under 18 years of age. 2020; https://healthycanadians.gc.ca/recall-alert-rappel-avis/hc-sc/2020/73635a-eng.php. Accessed 2021 Jul 21.
19.Jin J. Risks of codeine and tramadol in children. JAMA. 2017;318(15):1514-1514. PubMed
20.Codeine for acute dental pain and acute pain related to dental procedures. (CADTH Health technology review). Ottawa (ON): CADTH; 2021: https://cadth.ca/sites/default/files/pdf/htis/2021/RC1325-Codeine-Dental-Pain%20Final.pdf. Accessed 2021 Jul 21.
21.Codeine for acute extremity pain. (CADTH Health technology review). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/pdf/htis/2021/RC1324%20Codeine%20for%20Acute%20Extremity%20Pain%20Final.pdf. Accessed 2021 Jul 21.
22.Codeine for pediatric patients with acute pain: a review of clinical effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1200%20Codeine%20for%20Pediatric%20Patients%20Final.pdf. Accessed 2021 Jul 21.
23.Codeine for pain related to osteoarthritis of the knee and hip: a review of clinical effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/pdf/htis/2020/RC1323%20Codeine%20for%20Osteoarthritis%20Pain%20Final.pdf. Accessed 2021 Jul 21.
24.Codeine for pain related to Caesarean section. (CADTH Health technology review). Ottawa (ON): CADTH; 2021: https://cadth.ca/sites/default/files/pdf/htis/2021/RC1326%20Codeine%20for%20C-section%20Pain%20Final.pdf. Accessed 2021 Jul 21.
25.Codeine for acute pain in patients undergoing orthopedic surgery: a review of clinical effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1199%20Codeine%20for%20Orthopaedic%20Pts%20Final.pdf. Accessed 2021 Jul 21.
26.Codeine for acute pain for urological or general surgery patients: a review of clinical effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1201%20Codeine%20for%20Urological%20Pts%20Final.pdf. Accessed 2021 Jul 21.
27.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
28.Els C, Jackson TD, Kunyk D, et al. Adverse events associated with medium- and long-term use of opioids for chronic non-cancer pain: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2017;10:CD012509. PubMed
29.Wiffen PJ, Wee B, Derry S, Bell RF, Moore RA. Opioids for cancer pain - an overview of Cochrane reviews. Cochrane Database Syst Rev. 2017;7:CD012592. PubMed
30.Ghadiri-Sani M, Silver N. Headache (chronic tension-type). Clin Evid. 2016;05:05.
31.Khouly I, Braun RS, Ordway M, et al. Post-operative pain management in dental implant surgery: a systematic review and meta-analysis of randomized clinical trials. Clin Oral Investig. 2021;25(5):2511-2536. PubMed
32.Saldanha IJ, Cao W, Bhuma MR, et al. Management of primary headaches during pregnancy, postpartum, and breastfeeding: a systematic review. Headache. 2021;61(1):11-43. PubMed
33.Saldanha IJ, Roth JL, Chen KK, et al. Management of primary headaches in pregnancy. Rockville (MD): Agency for Healthcare Research and Quality; 2020: https://effectivehealthcare.ahrq.gov/products/headaches-pregnancy/research. Accessed 2021 Jul 21.
34.Santini M, Da Rosa RA, Ferreira MB, et al. Medications used for prevention and treatment of postoperative endodontic pain: a systematic review. Eur Endod J. 2021;6(1):15-24. PubMed
35.Campbell HT, Yuhan BT, Smith B, et al. Perioperative analgesia for patients undergoing otologic surgery: an evidence-based review. Laryngoscope. 2020;130(1):190-199. PubMed
36.Celic I, Bach-Rojecky L, Mercep I, Soldo A, Petrak AK, Bucan A. Resolving issues about efficacy and safety of low-dose codeine in combination analgesic drugs: a systematic review. Pain Ther. 2020;9(1):171-194. PubMed
37.Abdel Shaheed C, Maher CG, McLachlan AJ. Efficacy and safety of low-dose codeine-containing combination analgesics for pain: systematic review and meta-analysis. Clin J Pain. 2019;35(10):836-843. PubMed
38.Huang R, Jiang L, Cao Y, et al. Comparative efficacy of therapeutics for chronic cancer pain: a Bayesian network meta-analysis. J Clin Oncol. 2019;37(20):1742-1752. PubMed
39.Cooper TE, Fisher E, Gray AL, et al. Opioids for chronic non-cancer pain in children and adolescents. Cochrane Database Syst Rev. 2017;7:CD012538. PubMed
40.Wiffen PJ, Cooper TE, Anderson AK, et al. Opioids for cancer-related pain in children and adolescents. Cochrane Database Syst Rev. 2017;7:CD012564. PubMed
41.Wiffen PJ, Knaggs R, Derry S, Cole P, Phillips T, Moore RA. Paracetamol (acetaminophen) with or without codeine or dihydrocodeine for neuropathic pain in adults. Cochrane Database Syst Rev. 2016;12:CD012227. PubMed
42.Speich B, Thomer A, Aghlmandi S, Ewald H, Zeller A, Hemkens LG. Treatments for subacute cough in primary care: systematic review and meta-analyses of randomised clinical trials. Br J Gen Pract. 2018;68(675):e694-e702. PubMed
43.Gardiner SJ, Chang AB, Marchant JM, Petsky HL. Codeine versus placebo for chronic cough in children. Cochrane Database Syst Rev. 2016;7:CD011914. PubMed
44.Abdel Shaheed C, Maher CG, McLachlan A. Investigating the efficacy and safety of over-the-counter codeine containing combination analgesics for pain and codeine based antitussives. Sydney (AU): Therapeutic Goods Administration; 2016: https://www.tga.gov.au/sites/default/files/review-efficacy-and-safety-over-counter-codeine-combination-medicines.pdf. Accessed 2021 Jul 8.
45.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Overviews of Reviews and Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Pain | ||||
Overviews of reviews | ||||
Els et al. (2017)28 Canada Funding source: Workers' Compensation Board of Alberta, Canada. | Study design: Overview of Cochrane systematic reviews. Number of included studies: A total of 16 systematic reviews were included in the overview. Of these, 14 were included in the quantitative synthesis. None of the data summarized from the included systematic reviews were relevant to the current report. | Studies of adults with chronic non-cancer pain due to any condition were included. | Interventions: Any opioid agent (any dose, frequency, or route of administration) used on a medium-term (2 weeks to 2 months) or long-term basis (2 months or longer). Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo, non-opioid pharmacological interventions, or non-pharmacological interventions. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes: Adverse events (e.g., number of participants with any adverse event, number of deaths, proportion of patients who experienced addiction, cognitive dysfunction, constipation, depressive symptoms, endocrine dysfunction, infection, respiratory depression, sexual dysfunction, anorexia, diarrhea, dizziness, drowsiness Follow-up: Varied by individual study. |
Wiffen et al. (2017a)29 UK Funding source: The National Institute for Health Research. | Study design: Overview of Cochrane systematic reviews of RCTs. Number of included studies: 9 systematic reviews were included in the overview. None of the data summarized from the included systematic reviews were relevant to the current report. | Systematic reviews of adults with pain associated with active cancer (i.e., pain due to cancer or its treatment) were included. | Interventions: Opioid drugs. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo or active comparators (e.g., alternative opioid drugs). Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: Varied by individual study. |
Ghadiri-Sani and Silver (2016)30 UK Funding source: NR. | Study design: Overview of systematic reviews and RCTs. For RCTs to be eligible they needed to be at least single-blinded and include at least 20 individuals (10 per treatment arm). Number of included studies: This review updated previously published work and identified an additional 3 systematic reviews and 1 RCT for inclusion. None of the data summarized from the included systematic reviews or RCTs were relevant to the current report. | Studies of adults (> 16 years of age) with chronic tension-type headache (i.e., headaches on 15 or more days a month for at least 3 months, pain that is bilateral, pressing, or tightening in quality and non-pulsating, of mild or moderate intensity which does not worsen with routine physical, and without moderate or severe nausea or vomiting). | Interventions: Pharmacological and non-pharmacological (e.g., acupuncture and cognitive behavioural therapy) interventions. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo, no treatment, alternative pharmacological or non-pharmacological interventions. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: Varied by individual study. |
Systematic reviews | ||||
Khouly et al. (2021)31 US Funding source: NR. | Study design: Systematic review and meta-analysis of RCTs. For RCTs to be eligible they needed to include at least 10 people per treatment group. Number of included studies: In total, 9 RCTs were included in the systematic review. None of the included RCTs were relevant to the current report. | Studies of overall healthy human adult patients (≥ 18 years) undergoing surgical dental implant placement were included. | Interventions: Any analgesic medications. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo, no treatment, or alternative analgesic medications. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: A minimum follow-up duration of 12 hours was required for inclusion; however, the total follow-up duration varied by individual study. |
Saldanha et al. (2021)32 and Saldanha et al. (2020)33 US Funding source: The Agency for Health care Research and Quality. | Study design: Systematic review and meta-analysis of primary studies of any design (e.g., RCTs, non-randomized comparative studies, single-group studies, and N-of-1 trials). Number of included studies: In total, 16 studies (reported in 26 articles) were included in the review. None of the included studies were relevant to the current report. | Studies of women who were pregnant, attempting to become pregnant, postpartum (i.e., up to 12 months post-delivery), or breastfeeding (for any length of time) with a history of primary headache or with acute episodes of primary headache were eligible for inclusion. | Interventions: Pharmacologic and non-pharmacologic interventions to prevent or treat episodes of primary headaches (migraine, tension headache, cluster headache, and other trigeminal autonomic cephalgias). Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: No treatment, placebo, or alternative pharmacologic and non-pharmacologic interventions. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: Varied by individual study. |
Santini et al. (2021)34 Brazil Funding source: No funding was received for this work. | Study design: Systematic review of RCTs. Number of included studies: 10 RCTs were included in the review. None of the included studies were relevant to the current report. | Studies of adults who underwent endodontic treatments for any type of pulpal or periapical diagnosis were included. | Interventions: Any oral medications used for pain control following endodontic intervention. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo or alternative oral medications used for pain control. | Outcomes:
Follow-up: Varied by individual study. |
Campbell et al. (2020)35 US Funding source: No funding was received for this work. | Study design: Systematic review of RCTs. Number of included studies: In total, 23 RCTs were included in the systematic review. None of the included RCTs were relevant to the current report. | Studies of people who underwent otologic surgery (e.g., myringotomy, ossiculoplasty, tympanostomy, stapedectomy, tympanoplasty, cochlear implant, acoustic neuroma, ear surgery, neurotology) were included. | Intervention: Any pain control preparation. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Any comparator. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: Varied by individual study. |
Celic et al. (2020)36 Croatia Funding source: A project by the Croatian Chamber of Pharmacists funded by PLIVA Hrvatska and Alkaloid AD Skopje. | Study design: Systematic review of RCTs. The review included an analysis of efficacy and of safety. Number of included studies: 16 RCTs were included in the efficacy review and 20 RCTs were included in the safety review. None of the included RCTs were relevant to the current report. | Studies of adults with acute pain due to any reason were included. | Interventions: For the efficacy review, low-dose (≤ 30 mg) codeine alone or in combination with other non-opioid analgesic drugs. For the safety evaluation, any medicines containing codeine either alone or in combinations, regardless of the dose. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo or alternative analgesics. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: Varied by individual study. |
Abdel Shaheed et al. (2019)37 Australia Funding source: The Therapeutic Goods Administration. | Study design: Systematic review and meta-analysis of RCTs. Number of included studies: 10 RCTs were included in the systematic review and meta-analysis. None of the included studies were relevant to the current report. | Studies of people with any pain condition were eligible for inclusion. | Interventions: Low-dose (≤ 30 mg) codeine in combination with an NSAID (e.g., ibuprofen or Aspirin) or paracetamol. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo. | Outcomes:
Follow-up: Varied by individual study. Outcomes were grouped into 3 lengths of follow-up: immediate (3 hours after treatment initiation), short-term (4 to 6 hours after treatment initiation), and intermediate term (≥ 7 hours after treatment initiation). |
Huang et al. (2019)38 China Funding source: National Natural Science Foundation of China grants, a Key Program of Natural Science Research of Higher Education of Anhui Province grant, a Key Program for Excellent Young Talents in College and University of Anhui Province grant, and a Special Foundation for Science and Technology Development of Anhui Province grant. | Study design: Systematic review and network meta-analysis of RCTs. Number of included studies: A total of 81 RCTs were included. None of the included RCTs were relevant to the current report. | Studies of adults (≥ 18 years of age) with chronic cancer-related pain were eligible for inclusion. Excluded: Studies of patients experiencing episodes of acute pain (i.e., breakthrough pain) that are superimposed on their background chronic pain. | Interventions: Systemic pharmaceutical interventions (alone or in combination) for chronic cancer pain. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo or alternative active treatments. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: Varied by individual study. |
Cooper et al. (2017)39 Australia Funding source: The National Institute for Health Research. | Study design: Systematic review of RCTs. Number of included studies: No eligible studies were identified or included in the review. | Studies of children and adolescents (≤ 17 years of age) with chronic non-cancer pain in any setting. | Interventions: Opioids of any dose and any route. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo or any active treatment. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: NA. |
Wiffen et al. (2017b)40 UK Funding source: The National Institute for Health Research. | Study design: Systematic review of RCTs. Number of included studies: No eligible studies were identified or included in the review. | Studies of children and adolescents (≤ 17 years of age) with cancer-related pain in any setting. | Interventions: Opioids of any dose and any route. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo or any active treatment. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: NA. |
Wiffen et al. (2016)41 UK Funding source: The National Institute for Health Research. | Study design: Systematic review of RCTs. For RCTs to be eligible they needed to be at least 2 weeks in duration. Number of included studies: No eligible studies were identified or included in the review. | Studies of adults (≥ 18 years of age) with 1 or more chronic neuropathic pain conditions (e.g., cancer-related neuropathy, central neuropathic pain, HIV neuropathy, painful diabetic neuropathy, phantom limb pain, spinal cord injury) were included. | Interventions: Oral paracetamol with or without codeine ordihydrocodeine at any dose. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo or any active comparator. Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: NA. |
Cough | ||||
Systematic reviews | ||||
Speich et al. (2018)42 Switzerland Funding source: The Research Foundation of the University of Basel. | Study design: Systematic review and meta-analysis of RCTs. Number of included studies: A total of 6 RCTs were included. None of the included RCTs were relevant to the current report. | Studies of people (≥ 16 years of age) with subacute cough (i.e., cough lasting between 3 to 8 weeks) and without known chronic respiratory diseases or other related diagnoses with overlapping symptoms were included. Additionally, studies of people with slightly shorter or longer cough duration (i.e., between 2 weeks and 10 weeks) or with a less specific definition of subacute cough (e.g., no maximum duration of cough was reported) were evaluated given the arbitrary definition of subacute cough. | Intervention: Any drug or non-drug treatments, including traditional Western cough remedies or medicines, herbal or other natural products, and preparations with minimal processing from the Europe or North America. Chinese or Asian herbal medicines were not considered eligible. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Any comparator (e.g., placebo, alternative drug or non-drug treatments, no treatment, usual care). Only studies that used placebo or oral analgesic medications as comparators were considered relevant to the current report. | Outcomes:
Follow-up: Varied by individual study. |
Gardiner et al. (2016)43 Australia Funding source: The National Institute for Health Research, the National Health and Medical Research Council, the Lung Foundation of Australia, and the Queensland University of Technology. | Study design: Systematic review of RCTs. Number of included studies: No eligible studies were identified or included in the review. | Studies of children (< 18 years of age) with chronic cough (i.e., cough with duration ≥ 4 weeks at the time of intervention) were included. Excluded: Studies of people with acute cough. | Interventions: Codeine or codeine derivatives, alone or in combination with other active ingredients. Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo. | Outcomes:
Follow-up: NA. |
Mixed (i.e., pain and cough) | ||||
Systematic reviews | ||||
Abdel Shaheed et al. (2016)44 Australia Funding source: The Therapeutic Goods Administration. | Study design: Systematic review and meta-analysis of RCTs. Number of included studies: 14 RCTs were included in the review (10 RCTs on pain and 4 RCTs on cough). None of the included RCTs were relevant to the current report. | Studies of people with pain or cough conditions were eligible for inclusion. | Interventions: Codeine combination analgesics and codeine-based antitussive agents at doses that could be achieved using over-the-counter medications in Australia (as of the time that the report was produced). Only studies that examined products containing low-dose codeine (as defined in our selection criteria) were considered relevant to the current report. Comparators: Placebo or alternative doses of the same drug or combination product. | Outcomes:
Follow-up: Varied by individual study. Outcomes were grouped into 3 lengths of follow-up: immediate (3 hours after treatment initiation), short-term (4 to 6 hours after treatment initiation), and intermediate term (≥ 7 hours after treatment initiation). |
N = number of participants; NA = not applicable; NR = not reported; NSAID = nonsteroidal anti-inflammatory drug; RCT = randomized controlled trial.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Overviews of Reviews and Systematic Reviews, Using AMSTAR 227
Strengths | Limitations |
Overviews of reviews | |
Els et al. (2017)28 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review Key search terms, dates of search (up to March 2017), and search restrictions were provided (e.g., no language restrictions were applied) A flow chart of study selection was provided Study selection, data extraction, and quality assessment were conducted by at least 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) The review authors described the included studies in adequate detail The methodological quality of included systematic reviews was assessed using satisfactory techniques (i.e., AMSTAR) Review authors disclosed their potential conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | The authors did not provide justification for their selection of eligible study designs (i.e., Cochrane systematic reviews) The electronic literature searches were limited to 1 database (i.e., the Cochrane Database of Systematic Reviews) A grey literature search was not completed The quality of included studies and of the evidence within the included systematic reviews was not assessed |
Wiffen et al. (2017a)29 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review Key search terms, dates of search (up to May 2017), and search restrictions were provided (e.g., no language restrictions were applied) Study selection, data extraction, and quality assessment were conducted by at least 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) The review authors described the included studies in adequate detail The methodological quality of included systematic reviews was assessed using satisfactory techniques (i.e., AMSTAR) The quality of the evidence within the included systematic reviews was discussed Review authors disclosed their potential conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | The authors did not provide justification for their selection of eligible study designs (i.e., Cochrane systematic reviews of RCTs) The electronic literature searches were limited to 1 database (i.e., the Cochrane Database of Systematic Reviews) A grey literature search was not completed A flow chart of study selection was not provided |
Ghadiri-Sani and Silver (2016)30 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes Multiple databases were searched (i.e., MEDLINE, Embase, the Cochrane Database of Systematic Reviews, DARE, and the Health Technology Assessment database) Dates of search (up to December 2013) and search restrictions were provided (e.g., only studies published in English were eligible) The review authors described the included studies in adequate detail Review authors disclosed their potential conflicts of interest related to this review | It was unclear whether the review methods were established before conducting the review (no mention of a protocol); however, the inclusion and exclusion criteria were agreed to a priori The authors did not provide justification for their selection of eligible study designs (i.e., systematic reviews and RCTs) A grey literature search was not completed Key search terms were not provided A flow chart of study selection was not provided A list of studies excluded after full-text review was not provided It was unclear if article selection and data extraction were conducted in duplicate The quality of included studies and of the evidence within the included systematic reviews was not assessed Sources of funding were not reported |
Systematic reviews | |
Khouly et al. (2021)31 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review (PROSPERO registration number CRD42018099324) Multiple databases were searched (i.e., PubMed, CINAHL, Embase, and DOSS). Additionally, reference lists of the identified studies and relevant were checked for additional potentially relevant records Key search terms, dates of search (up to November 2020), and search restrictions were provided (e.g., no language restrictions were applied) A flow chart of study selection was provided A list of studies excluded after full-text review, along with reasons for exclusion, was provided Study selection, data extraction, and quality assessment were conducted by at least 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using satisfactory techniques (i.e., the Cochrane Risk of Bias tool) Review authors stated that they had no conflicts of interest related to this review | The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed Sources of funding were not reported |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review (PROSPERO registration number CRD42020158310) Multiple databases were searched (i.e., MEDLINE, Embase, CENTRAL, and CINAHL). Additionally, clinical trial registries and reference lists of clinical practice guidelines and systematic reviews were checked for additional potentially relevant records Key search terms, dates of search (up to June 2020), and search restrictions were provided (e.g., no language restrictions were applied) A flow chart of study selection was provided A list of studies excluded after full-text review, along with reasons for exclusion, was provided Study selection was conducted by independent reviewers in duplicate (disagreements were resolved through discussion and consensus) Data extraction was performed by 1 reviewer and verified independently by a second reviewer The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using satisfactory techniques (i.e., the Cochrane Risk of Bias tool, the Risk of Bias in Nonrandomized Studies tool, or the National Heart, Lung, and Blood Institute Quality Assessment tool, depending on study design) Review authors stated that they had no conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | The authors did not provide justification for their selection of eligible study designs (i.e., RCTs, non-randomized comparative studies, single-group studies, and N-of-1 trials) A grey literature search was not completed It was unclear if quality assessment was conducted in duplicate |
Santini et al. (2021)34 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review (PROSPERO registration number CRD42020202071) Multiple databases were searched (i.e., MEDLINE, the clinical trials register of the Cochrane Library, LILACS, and SciELO). Additionally, reference lists of retrieved studies were checked for additional potentially relevant records Key search terms, dates of search (up to December 2017), and search restrictions were provided (e.g., only studies published in English were eligible) A flow chart of study selection was provided Study selection, data extraction, and quality assessment were conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using a satisfactory technique (i.e., the 5-point Jaded scale) Review authors stated that they had no conflicts of interest and received no financial support related to this review | The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed A list of studies excluded after full-text review was not provided (although the reasons for exclusion were) |
Campbell et al. (2020)35 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes Multiple databases were searched (i.e., PubMed/MEDLINE, Embase, and Cochrane Library) Key search terms, dates of search (up to June 2018), and search restrictions were provided (e.g., only studies published in English were eligible) A flow chart of study selection was provided The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using a satisfactory technique (i.e., the Cochrane Risk of Bias tool) Review authors stated that they had no conflicts of interest and received no financial support related to this review | It was unclear whether the review methods were established before conducting the review (no mention of a protocol) The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed A list of studies excluded after full-text review was not provided (although the reasons for exclusion were) It was unclear whether study selection, data extraction, and quality assessment were conducted in duplicate |
Celic et al. (2020)36 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes Key search terms, dates of search (up to January 2019), and search restrictions were provided (e.g., only studies published in English were eligible) A flow chart of study selection was provided Data extraction was conducted by 2 independent reviewers (a third reviewer checked for accuracy) The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using a satisfactory technique (i.e., the 11-item PEDro scale) Review authors disclosed their potential conflicts of interest related to this review | It was unclear whether the review methods were established before conducting the review (no mention of a protocol) The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) The electronic literature searches were limited to 1 database (i.e., MEDLINE) A grey literature search was not completed A list of studies excluded after full-text review was not provided (although the reasons for exclusion were) It was unclear whether study selection and quality assessment were conducted in duplicate This work was funded by industry |
Abdel Shaheed et al. (2019)37 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes Multiple databases were searched (i.e., MEDLINE, Embase, Cochrane Database of Systematic Reviews, CENTRAL, CINAHL, and PsycINFO). Additionally, reference lists of included RCTs and related systematic reviews were checked for additional potentially relevant records Key search terms, dates of search (August 2018), and search restrictions were provided (e.g., only studies published in English were eligible) A flow chart of study selection was provided Study selection, data extraction, and quality assessment were conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus) The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using a satisfactory technique (i.e., the 11-item PEDro scale) Review authors stated that they had no conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | It was unclear whether the review methods were established before conducting the review (no mention of a protocol) The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed A list of studies excluded after full-text review was not provided (although the reasons for exclusion were) |
Huang et al. (2019)38 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes Multiple databases were searched (i.e., MEDLINE, Embase, and CENTRAL). Additionally, reference lists of studies were checked for additional potentially relevant records Key search terms, dates of search (up to August 2018), and search restrictions were provided (e.g., studies published between 1970 and August 2018 were eligible, no language restrictions were applied) A flow chart of study selection was provided Study selection, data extraction, and quality assessment were conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus) The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using a satisfactory technique (i.e., modified version of the Cochrane Collaboration’s Risk-of-Bias Tool) Review authors stated that they had no conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | It was unclear whether the review methods were established before conducting the review (no mention of a protocol) The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed A list of studies excluded after full-text review was not provided (although the reasons for exclusion were) |
Speich et al. (2018)42 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes Multiple databases were searched (i.e., MEDLINE and CENTRAL). Additionally, reference lists of included trials, pertinent systematic reviews, and selected current clinical guidelines were checked for additional potentially relevant records Key search terms, dates of search (February 10th, 2017), and search restrictions were provided (e.g., studies published in English, German, Italian, Spanish, or French were eligible) A flow chart of study selection was provided Study selection, data extraction, and quality assessment were conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using a satisfactory technique (i.e., following Cochrane standards) Review authors stated that they had no conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | It was unclear whether the review methods were established before conducting the review (no mention of a protocol) The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed A list of studies excluded after full-text review was not provided (although the reasons for exclusion were) |
Cooper et al. (2017)39 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review Multiple databases were searched (i.e., MEDLINE, Embase, and CENTRAL). Additionally, online clinical trial registries and reference lists of retrieved studies and reviews were checked for additional potentially relevant records Key search terms, dates of search (up to September 2016), and search restrictions were provided (e.g., no language restrictions were applied) A flow chart of study selection was provided A list of studies excluded after full-text review, along with reasons for exclusion, was provided Study selection was conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) Data extraction and quality assessment were planned to be conducted in duplicate; however, there were no included studies, so these processes were not conducted The risk of bias of included primary studies was planned to be assessed using a satisfactory technique (i.e., using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions) Review authors disclosed their potential conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed |
Wiffen et al. (2017b)40 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review Multiple databases were searched (i.e., MEDLINE, Embase, and CENTRAL). Additionally, online clinical trial registries and reference lists of retrieved studies and reviews were checked for additional potentially relevant records Key search terms, dates of search (up to February 2017), and search restrictions were provided (e.g., no language restrictions were applied) A flow chart of study selection was provided A list of studies excluded after full-text review, along with reasons for exclusion, was provided Study selection was conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) Data extraction and quality assessment were planned to be conducted in duplicate; however, there were no included studies, so these processes were not conducted The risk of bias of included primary studies was planned to be assessed using a satisfactory technique (i.e., using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions) Review authors disclosed their potential conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed |
Abdel Shaheed et al. (2016)44 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes Multiple databases were searched (i.e., MEDLINE, Embase, Cochrane Database of Systematic Reviews, CENTRAL, CINAHL and PsycINFO). Additionally, reference lists of included RCTS and related systematic reviews were checked for additional potentially relevant records Key search terms, dates of search (up to December 2015), and search restrictions were provided (e.g., only studies published in English were eligible) A flow chart of study selection was provided Study selection, data extraction, and quality assessment were conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) The review authors described the included studies in adequate detail The risk of bias of included primary studies was assessed using a satisfactory technique (i.e., the 11-item PEDro scale) Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | It was unclear whether the review methods were established before conducting the review (no mention of a protocol) The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed A list of studies excluded after full-text review was not provided (although the reasons for exclusion were) The authors did not disclose any potential conflicts of interest |
Gardiner et al. (2016)43 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review Multiple databases were searched (i.e., Cochrane Airways Group Register of Trials, CENTRAL, MEDLINE, and Embase). Additionally, online clinical trial registries and reference lists of retrieved studies were checked for additional potentially relevant records Key search terms, dates of search (up to June 2016), and search restrictions were provided (e.g., no language restrictions were applied) A flow chart of study selection was provided A list of studies excluded after full-text review, along with reasons for exclusion, was provided Study selection was conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus, involving a third reviewer if necessary) Data extraction and quality assessment were planned to be conducted in duplicate; however, there were no included studies, so these processes were not conducted The risk of bias of included primary studies was planned to be assessed using a satisfactory technique (i.e., using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions) Review authors disclosed their potential conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed |
Wiffen et al. (2016)41 | |
The objectives and inclusion criteria were clearly stated and included components of population, intervention, comparator, and outcomes The review methods were established prior to conducting the review Multiple databases were searched (i.e., CENTRAL, MEDLINE, Embase, and the Oxford Pain Relief Database). Additionally, online clinical trial registries and reference lists of retrieved studies and review articles were checked for additional potentially relevant records Key search terms, dates of search (up to July 2016), and search restrictions were provided (e.g., no language restrictions were applied) A flow chart of study selection was provided A list of studies excluded after full-text review, along with reasons for exclusion, was provided Study selection was conducted by 2 independent reviewers (disagreements were resolved through discussion and consensus) Data extraction and quality assessment were planned to be conducted in duplicate; however, there were no included studies, so these processes were not conducted The risk of bias of included primary studies was planned to be assessed using a satisfactory technique (i.e., using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions) Review authors disclosed their potential conflicts of interest related to this review Sources of funding were disclosed and were unlikely to have had an effect on the findings of the review | The authors did not provide justification for their selection of eligible study designs (i.e., RCTs) A grey literature search was not completed |
AMSTAR = A MeaSurement Tool to Assess systematic Reviews; CENTRAL = Cochrane Central Register of Controlled Trials; CINAHL = Cumulative Index to Nursing and Allied Health Literature; DARE = Database of Abstracts of Reviews of Effects; DOSS = Dentistry & Oral Sciences Source; LILACS = Latin American and Caribbean Health Sciences Literature; MEDLINE = Medical Literature Analysis and Retrieval System Online; PEDro = Physiotherapy Evidence Database; RCT = randomized controlled trial; SciELO = Scientific Electronic Library Online.
Appendix 4: References of Potential Interest
Previous CADTH Reports
1.Codeine for acute pain: a synopsis of the evidence. Ottawa (ON): CADTH; 2021: https://cadth.ca/codeine-acute-pain-synopsis-evidence. Accessed 2021 Jul 27.
2.Policies to prevent harms from the co-prescribing of opioids and central nervous system depressant drugs (CADTH Environmental scan no. 72). Ottawa (ON): CADTH; 2020: https://cadth.ca/policies-prevent-harms-co-prescribing-opioids-and-central-nervous-system-depressant-drugs. Accessed 2021 Jul 27. Qualitative Studies.
3.Mishriky J, Stupans I, Chan V. Pharmacists' views on the upscheduling of codeine-containing analgesics to 'prescription only' medicines in Australia. Int J Clin Pharm. 2019;41(2):538-545. Study Protocols. PubMed
4.McCoy J, Nielsen S, Bruno R. Impact of removing nonprescription codeine in Australia: protocol for a prospective cohort study. JMIR Res Protoc. 2020;9(3):e15540. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca