CADTH Health Technology Review
Antipsychotic Drugs or Benzodiazepines for Rapid Tranquilization in Mental Health Facilities or Emergency Department Settings
Rapid Review
Authors: Gabrielle Brankston, Lory Picheca
Abbreviations
ABS
Agitated Behavior Scale
ACES
Agitation-Calmness Evaluation Scale
AE
adverse event
AIMS
Abnormal Involuntary Movement Scale
AMSS
Altered Mental Status Scale
IM
intramuscular
PANSS-EC
Positive and Negative Syndrome Scale Excited
RCT
randomized controlled trial
SR
systematic review
Key Messages
Evidence from 5 systematic reviews, 3 randomized controlled trials, and 4 observational studies provide inconsistent evidence regarding the comparative efficacy and safety of antipsychotic drugs and benzodiazepines for adults with acute aggression or agitation requiring rapid tranquilization in emergency department or mental health inpatient settings.
Overall, the evidence came from low- to moderate-quality studies. Some studies suggested different antipsychotic drugs and benzodiazepines, alone or in combination, have similar efficacy, whereas others favoured one treatment over another.
No studies differentiated between adults aged 18 to 64 years and those older than 65 years. Most studies included mixed ages or excluded patients older than 75 years.
No studies differentiated between aggression or agitation associated with psychiatric illness and other etiologies such as alcohol intoxication.
One guideline suggests initial treatment with intramuscular lorazepam, promethazine, or 1 of aripiprazole, droperidol, or olanzapine. If the desired outcome is not achieved with monotherapy, the guideline recommends an intramuscular combination of either promethazine plus haloperidol or lorazepam plus haloperidol.
Context and Policy Issues
Agitation can be defined as excessive verbal or motor activity that may lead to aggression or violence, while aggression entails an attempt to harm, hurt, or injure another person (emotional or physical), or damage property regardless of whether harm is sustained.1 Violence and aggression are common occurrences in health care settings and occur most frequently in inpatient psychiatric units and hospital emergency departments.2 To ensure the safety of both the patient and staff, clinical practice guidelines suggest that health care providers initially attempt verbal de-escalation for agitated or aggressive patients.1 Should verbal de-escalation be ineffective, alternative management approaches may be employed. One such modality, rapid tranquilization, refers to the use of medication to achieve a reduction in agitation or aggression. The goal of rapid tranquilization is to achieve calmness without sedation, thereby reducing the risk of harm to self and/or others while maintaining the ability of the patient to communicate.3 Health care providers typically use benzodiazepines and antipsychotic drugs, either alone or in combination, in the management of acutely agitated or aggressive patients.4-6
A Rapid Response report published by CADTH in 2015 found 3 randomized controlled trials (RCTs), 4 systematic reviews (SRs), and 1 clinical practice guideline relevant to the use of antipsychotic drugs and benzodiazepines for rapid tranquilization in acutely agitated or aggressive patients.7 This body of literature provided inconsistent evidence regarding the comparative efficacy and safety of antipsychotic drugs and benzodiazepines, with the exception of the evidence that intramuscular (IM) haloperidol is less effective and more harmful than other therapies.7 The 2015 report included a guideline suggesting the use of IM lorazepam or a combination of IM haloperidol and promethazine as rapid tranquilization for adults in emergency department or inpatient settings.7
Due to the inconsistent and inconclusive evidence from the previous report, the optimal approach for rapid tranquilization is not well-defined. Thus, the purpose of this Rapid Response report is to assess the extent to which there have been advances in the evidence informing the clinical efficacy of IM antipsychotic drugs and benzodiazepines for rapid tranquilization of adult inpatients of mental health facilities and emergency departments.
Research Questions
What is the clinical effectiveness of using intramuscular antipsychotic drugs and/or intramuscular benzodiazepines as rapid tranquilization for inpatients in mental health facilities or emergency departments?
What are the evidence-based guidelines for using intramuscular antipsychotic drugs and/or intramuscular benzodiazepines as rapid tranquilization for inpatients in mental health facilities or emergency departments?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, PsycINFO, the Cochrane Library, the University of York Centre for Reviews and Dissemination (CRD) databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were rapid tranquilization and psychosis. No filters were applied to limit the retrieval by study type. Comments, newspaper articles, editorials, conference abstracts, and letters were excluded. When possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and June 17, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. At the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Adult inpatients exhibiting severe or acute agitation, aggressive behaviour, or psychosis-induced aggression within a mental health facility or emergency department setting; adult inpatients with confirmed or suspected substance induced psychosis/agitation during intoxication (e.g., alcohol, stimulants [cocaine/crystal methamphetamine], cannabis) within a mental health facility or emergency department setting. Subgroups of interest:
|
Intervention | Rapid tranquilization achieved using any of the following (in any combination):
|
Comparator | Q1: Other antipsychotic drugs and/or other benzodiazepines Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., time to tranquilization, sedation, calm; level of agitation, aggression, calm); safety (e.g., side effects or adverse events [injury or mortality]) Q2: Recommendations regarding the use of antipsychotic medication or benzodiazepines for rapid tranquilization of aggressive or agitated patients |
Study designs | Health technology assessments, systematic reviews (with or without meta-analyses), randomized controlled trials, non-randomized studies, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Systematic reviews in which all relevant studies were included in another more recent or more comprehensive SR were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Clinical practice guidelines with unclear methodology were also excluded.
Randomized controlled trials were excluded if they did not meet the selection criteria in Table 1, were duplicate publications, or were captured in a selected SR. Additional ineligibility criteria excluded studies that focused on management of patients with delirium or excited delirium or those that were conducted in settings other than inpatient mental health or emergency department settings.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for SRs, the Questionnaire to Assess the Relevance and Credibility of a Network Meta-Analysis9 for network meta-analyses, the Downs and Black checklist10 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument11 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
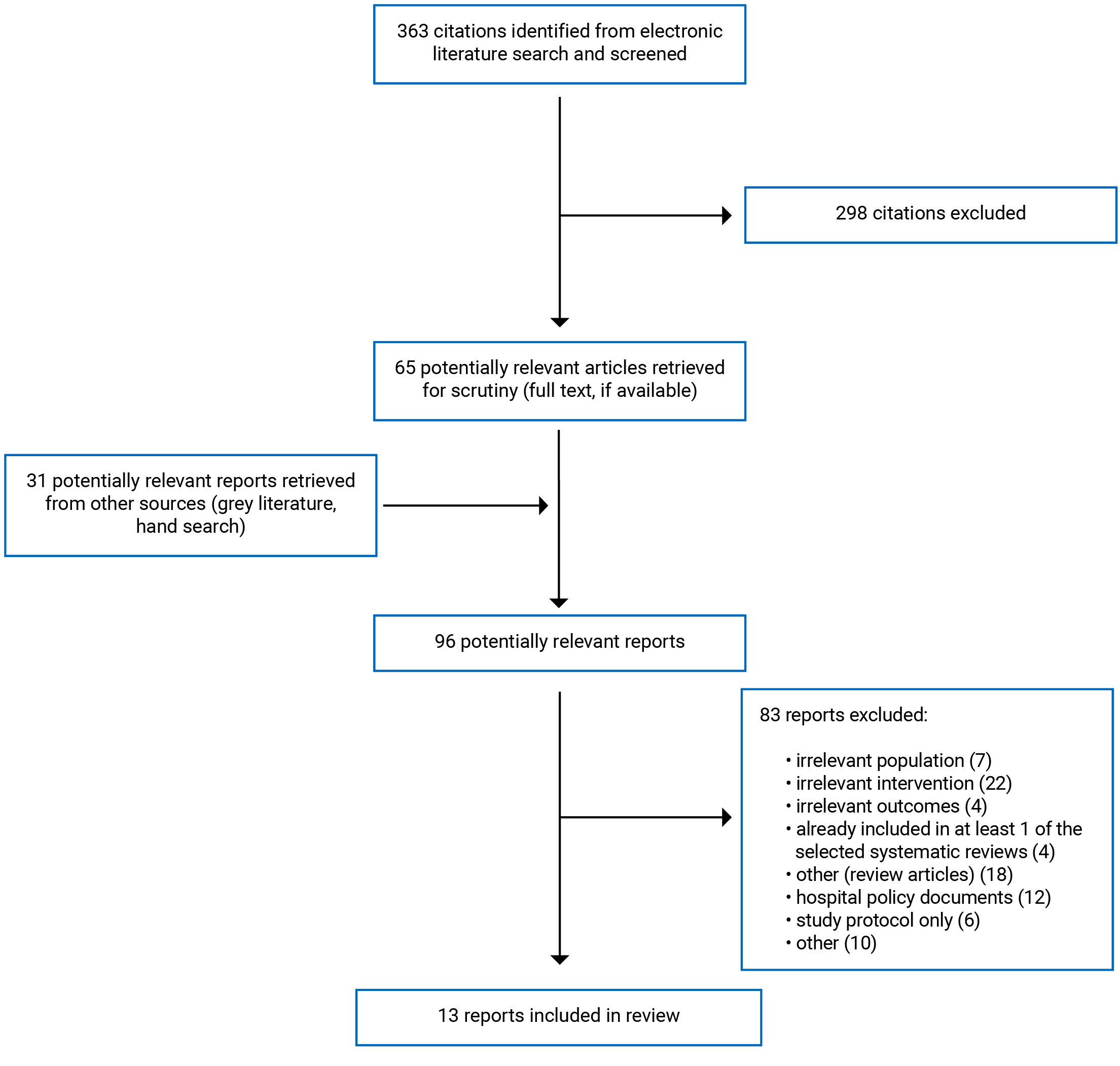
A total of 363 citations were identified in the literature search. Following screening of titles and abstracts, 298 citations were excluded and 65 potentially relevant reports from the electronic search were retrieved for full-text review. A total of 31 potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 83 publications were excluded for various reasons, and 13 publications met the inclusion criteria and were included in this report. These comprised 5 SRs, 3 RCTs, 4 non-randomized studies, and 1 evidence-based guideline. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)12 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6. Two references are descriptions of clinical practice guidelines that were published before the 2016 time frame. The remaining references are studies or SRs that do not appear to focus solely on IM antipsychotic drugs or IM benzodiazepines, but may provide information about the efficacy or safety of other drugs or other routes of administration for rapid tranquilization in the population of interest.
Summary of Study Characteristics
Details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Thirteen relevant reports were identified: 5 SRs,13-17 3 RCTs,18-20 4 observational studies,21-24 and 1 clinical practice guideline.1
Two of the 5 SRs had broader inclusion criteria than the present review.13,15 Specifically, both SRs included studies examining oral and/or IV routes of administration of benzodiazepines and antipsychotic medications in addition to IM administration.13,15 Only the characteristics and results of the subset of relevant studies (i.e., IM administration) are described in this report.
All SRs exclusively included RCTs (3 to 14 trials per review). One SR pooled data17 and 1 SR conducted a network meta-analysis16 for at least 1 outcome of interest. Three SRs provided a narrative evidence synthesis only.13-15 The publication year of the included studies within the SRs ranged from 1989 to 2017. The total number of patients enrolled in the eligible studies ranged from 15 to 448. There was overlap of 12 RCTs between 2 or more SRs (Appendix 5).
All 3 RCTs directly compared 2 or more therapies.18-20 Two RCTs involved a single study centre19,20 and 1 involved multiple centres within Hong Kong.18 All 4 observational studies compared 2 or more therapies.21-24 Three were prospective comparative studies,21,23,24 while 1 was a retrospective chart review.22
One evidence-based clinical practice guideline,1 published jointly by the British Association for Psychopharmacology (BAP) and the National Association of Psychiatric Intensive Care Units (NAPICU) in 2018, provided recommendations based on expert consensus for clinical practice in emergency and inpatient psychiatric settings to guide treatment by health care professionals with various options outlined according to their route of administration and category of evidence. Part of the recommendations included use of rapid tranquilization. It included evidence from SRs, RCTs, and observational studies. The quality of the evidence informing the recommendations was graded according to categories of evidence ranging from Ia (meta-analysis) to IV (expert opinion) as well as strength of recommendation ranging from A (based on category I evidence) to D (based on category IV evidence). A designation of S indicated standard practice based on expert opinion.
Country of Origin
The lead author of 1 SR each was from Australia,13 the US,14 and Denmark.15 Lead authors of 2 SRs were from Italy.16,17 Among the RCTs, 1 each was from China,18 Lebanon,19 and the US.20 Three observational studies were from the US21-23 and 1 was from Mexico.24 The joint BAP/NAPICU guidelines are from the UK.1
Patient Population
Four SRs focused on managing patients who exhibited agitated or aggressive behaviour due to an underlying mental illness.13,15-17 Most of the included trials enrolled patients with schizophrenia. One SR focused on managing patients with aggression and/or agitation for any reason in an emergency department setting.14 Three SRs included adult patients 18 years and older with no upper limit,13,14,16 while the other 2 SRs included adult patients 18 to 65 years15 and 18 to 69 years.17 No SR reported results stratified by age. Two SRs were focused on emergency department settings,14,17 2 SRs focused on mental health inpatients,15,16 and 1 SR included a mixture of the 2 settings.13
The 3 RCTs enrolled somewhat different patient populations. Age of patients enrolled ranged from 18 to 75 years,18 18 to 65 years,19 or 18 years and older with no upper limit.20 Two trials took place in the emergency department18,20 and 1 in a psychiatric hospital.19 Etiology of aggression and/or agitation was mainly psychiatric illness in 2 trials18,19 and mixed but mainly alcohol intoxication in 1 trial.20
All 4 of the observational studies took place in an emergency department setting.21-24 Etiology of aggression and/or agitation was schizophrenia in 1 study,24 while the 3 other studies focused on aggression and/or agitation mainly due to alcohol intoxication, with 10% to 17% due to psychiatric illness.21-23 All observational studies enrolled adult patients with no specified upper age limit.21-24
The BAP/NAPICU guidelines targeted health care professionals working in emergency psychiatric care or acute psychiatric inpatient care, general acute hospital, and forensic psychiatry involved in the management of adult patients with acute aggression or agitation requiring de-escalation.1
Interventions and Comparators
The SRs evaluated a variety of interventions including IM monotherapy and combination therapy in a variety of dosages. Paris et al. (2021) compared second-generation antipsychotic medications administered in short-acting formulations, including aripiprazole, olanzapine, and ziprasidone, with the first-generation antipsychotic medication haloperidol.16 One Cochrane review compared aripiprozole with haloperidol and olanzapine.17 Another review evaluated IM monotherapy with antipsychotic medications olanzapine, haloperidol, and droperidol compared with IM antipsychotic medication ziprasidone, combinations of IM antipsychotic and adjunct medication (e.g., haloperidol plus promethazine, haloperidol plus lorazepam, droperidol plus midazolam, haloperidol plus midazolam), and other medications (e.g., haloperidol, lorazepam, midazolam).14 Two SRs evaluated a number of medications including IM monotherapy with lorazepam 2 mg to 4 mg, olanzapine 10 mg, ziprasidone 10 mg to 20 mg, midazolam 5 mg to 15 mg, or droperidol 5 mg to 10 mg, as well as combinations of haloperidol 2.5 mg to 15 mg plus promethazine 20 mg to 50 mg, lorazepam 2 mg to 4 mg plus haloperidol 5 mg, haloperidol 2.5 mg plus midazolam 7.5 mg, and droperidol 5 mg plus midazolam 5 mg.13,15 Other medications considered were haloperidol 5 mg,15 flunitrazepam 1 mg, and promethazine 25 mg or 50 mg.13
The 3 RCTs evaluated different medications. Martel et al. (2021) compared each of droperidol (5 mg), lorazepam (2 mg), and 2 doses of ziprasidone (10 mg and 20 mg).20 Dib et al. (2021) evaluated triple therapy with haloperidol 5 mg plus promethazine 25 mg and chlorpromazine 100 mg versus dual therapy haloperidol 5 mg plus promethazine 25 mg.19 Chan et al. (2021) compared olanzapine with haloperidol and with midazolam.18
The observational studies evaluated olanzapine,21-24 droperidol,21,22 midazolam,23 and ziprasidone,23 while 3 of these studies also included haloperidol.22-24
The BAP/NAPICU guidelines considered IM monotherapy (e.g., lorazepam, midazolam) as well as IM benzodiazepines in combination with other medications (e.g., haloperidol, promethazine).1
Outcomes
The 5 SRs, 3 RCTs, and 4 observational studies evaluated treatment effects for a number of outcomes. Efficacy outcomes of interest included improvement in agitation and aggression, time to adequate sedation, need for additional (rescue) medications to treat agitation, proportion sedated in set time period, and adverse events (AEs). Common instruments to measure efficacy included the Agitated Behavior Scale (ABS), the Agitation-Calmness Evaluation Scale (ACES), the Positive and Negative Syndrome Scale (PANSS), as well as the PANSS-Excited Component (PANSS-EC). Investigators reported scores on these measures in a number of ways, including change from baseline to a certain time point, time to achieve a set reduction in score (e.g., 40% reduction in PANSS-EC score), or time to achieve a set score (e.g., 0 or less on agitation/aggression score). One RCT did not specify the tools used to determine efficacy.19 Three SRs13,14,17 and 3 individual studies reported on safety outcomes of interest, including rates of AEs and extrapyramidal symptoms.18,20-23 The Abnormal Involuntary Movement Scale (AIMS) was used to assess the presence of extrapyramidal symptoms in 1 study.24 Relevant efficacy and safety outcomes that the BAP/NAPICU guidelines considered in formulating recommendations were achievement of sedation, time to sedation, and AEs.1 Common instruments to measure efficacy included, as above, PANSS-EC and ACES.
Summary of Critical Appraisal
Systematic Reviews
One of the 5 SRs was a Cochrane review and therefore adhered to rigorous methodology and high reporting standards, including assessment of risk of bias among individual studies, exploration of heterogeneity (clinical, methodological, and statistical) between studies, robust statistical analyses, and evaluation of quality of the body of evidence using Grading of Recommendations Assessment, Development and Evaluation (GRADE).17 In addition, the search of relevant literature was completed relatively recently, in 2017.17 Strengths of the remaining 4 SRs were the inclusion of a comprehensive search strategy,13-16 3 SRs assessed the risk of bias of included studies,13,14,16 and the authors of 3 SRs registered their protocol with PROSPERO.13,14,16 One SR used a network meta-analysis approach and the authors followed PRISMA guidelines extended for network meta-analysis, selected studies and extracted data in duplicate by 2 reviewers, used random-effects models to pool data in meta-analyses, and provided a thorough description of the characteristics and results of included studies.16
A key limitation, however, was moderate to high risk of bias of the included studies in 2 of the SRs14,17 and 1 SR did not report any assessment of risk of bias of individual studies,15 thereby limiting our ability to evaluate the internal validity of the studies and judge the quality of the evidence. Threats to external validity included the study population representing only a subset of the source population of patients who would present with aggression or agitation. For example, 4 SRs included only patients with aggression or agitation secondary to underlying psychiatric illness,13,15-17 which excludes those with aggression and/or agitation associated with substance intoxication or another reason.
Randomized Controlled Trials
Authors of 2 RCTs reported registering their studies on ClinicalTrials.gov.18,19 Although described as a randomized trial, the study by Martel et al. (2021) did not mention the manner in which the randomization was generated nor the procedure for blinding investigators or patients to treatment allocation.20 Further, 1 RCT did not describe the method they used to conceal the randomization sequence, which raises the possibility of selection bias.20 The extent to which investigators across all trials blinded participants and study personnel also varied. Chan et al. (2021) reported blinding patients, health care providers, and study investigators,18 but Dib and colleagues reported not blinding outcome assessors in their study.19 Two trials used appropriate techniques to conduct statistical analyses18,20; however, the authors of the third trial did not describe their analysis in sufficient detail to assess.19
There is some uncertainty with respect to external validity in 2 trials. Due to staffing availability, Dib and colleagues excluded eligible patients presenting during late-night hours, which potentially contributed to selection bias.19 Chan et al. (2021) reported that external validity may have been threatened by several patients who were randomized and treated but subsequently did not provide consent to use their data in the analysis.18
Two trials used validated instruments to assess agitation and provided a priori criteria for determination of efficacy or outcomes: Altered Mental Status Scale (AMSS) and Behavioural Activity Rating Scale (BARS). However, Dib et al. (2021) provided no description of validated instruments or criteria for outcome measures.19
Observational Studies
Three prospective studies21,23,24 and 1 retrospective chart review22 are included. The 3 prospective studies reported using validated scales to assess outcomes,21,23,24 while 1 reported that the primary outcome (need for rescue sedation) is subject to the discretion of the treating clinician (i.e., not an objective measure).22
The potential for selection bias was considerable in several studies. For example, Cole et al. (2021) reported that patients who were not selected were younger, had lower ethanol concentrations, and were less agitated on arrival than those included in the study.21 Real Juarez et al. (2016) reported differences in the baseline level of agitation between treatment groups.24 In a retrospective chart review, Klein and colleagues identified that electronic medical record search criteria may not have captured all cases of aggression and/or agitation treated with an antipsychotic drug.22 Further, authors of 1 study reported that characteristics of screening misses and protocol violations were not reported; therefore, it was impossible to determine whether selected patients were representative of the source population.23
Two studies were conducted during a time period in which there was a shortage of 1 of the study medications21,22; therefore, patients in each group were not selected during the same time period. Similarly, in lieu of randomization, 1 study changed the medication provided every 3 weeks, so patients were not selected during the same time period.23 In 2 studies, treatment allocation was based on physician choice for all patients24 or in instances when the attending physician disagreed with the study treatment allocation.23
Guidelines
The objectives, research questions, and target users of the BAP/NAPICU guidelines were well-defined; however, although the methods used in the development of guidelines were evidence-based, they lacked reporting detail.1 For example, “experts” were involved in the review of literature and guideline development but the experts were neither defined nor identified in the report.1 Further, there was no description of the method of selection for relevant literature and no search terms were identified.1 Finally, the authors reported the guidelines were finalized using expert consensus after review of the literature; however, there was no description of the method used to achieve consensus.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions. There was some overlap in the primary studies that were included in the SRs. Data from narrative reviews are presented only once. A citation matrix illustrating the degree of overlap is presented in Appendix 5.
Clinical Effectiveness
Research question 1: What is the clinical effectiveness of using intramuscular antipsychotic drugs and/or intramuscular benzodiazepines as rapid tranquilization for inpatients in mental health facilities or emergency departments?
Antipsychotic Drugs Versus Other Antipsychotic Drugs
Improvement in Aggression or Agitation Scale
Direct comparisons of antipsychotic drugs in 1 SR showed the second-generation antipsychotic drug olanzapine was more effective at reducing agitation than the first-generation antipsychotic drug haloperidol plus adjunctive medication.14 Another SR found the second-generation antipsychotic drug olanzapine more effective than aripiprazole in improvement in agitation at 2 hours.17 In contrast, 1 prospective observational study found no difference in the effectiveness of 2 doses of haloperidol and olanzapine for rapid tranquilization of patients with agitation.24
Time to Adequate Sedation
One prospective observational study compared first- and second-generation antipsychotic drugs in terms of time to sedation and found no difference between droperidol and olanzapine.21
Proportion or Number Adequately Sedated
Indirect pairwise comparisons from a network meta-analysis found that the number of patients responding at 24 hours was not different among olanzapine, haloperidol, and aripiprazole; however, in terms of the number of responders at 2 hours, olanzapine was superior to aripiprazole.16 Available direct pairwise comparisons showed similar results.16
One low-quality RCT found a significant difference in the proportion who were adequately sedated at 40 minutes, but at no other time point with the addition of chlorpromazine to the combination of haloperidol plus promethazine.19
The proportion of patients adequately sedated by 15 minutes was found to be similar for the first-generation antipsychotic drug droperidol and the second-generation antipsychotic drug olanzapine.21
Need for Rescue or Additional Medication
One observational study found patients receiving the first-generation antipsychotic drug haloperidol were more likely to require rescue sedation compared with droperidol and olanzapine, supporting that olanzapine and droperidol may be more effective than haloperidol for achieving adequate sedation in agitated patients.22 However 1 SR and 1 RCT found patients receiving second-generation antipsychotic drugs (aripiprazole, olanzapine) were more likely to require repeat medication for tranquilization than those receiving first-generation antipsychotic drugs (haloperidol, droperidol).17,21
Antipsychotic Drugs Versus Benzodiazepines
Improvement in Aggression or Agitation Scale
In 1 narrative SR, a study at moderate risk of bias found ziprasidone had the least reduction in agitation at 15 minutes versus both midazolam and droperidol but was superior to midazolam at 45 minutes, and had the greatest reduction in agitation compared with the other medications at 60 minutes.14 A second narrative SR found lorazepam to be of similar efficacy to haloperidol but inferior to olanzapine.15 Midazolam was found to be superior to haloperidol.15 In combination therapy, haloperidol plus lorazepam was found to be more effective than lorazepam alone (3 studies), olanzapine alone (1 study), and haloperidol alone (2 studies).15 The combination of haloperidol plus midazolam was found to be more effective than haloperidol plus promethazine, ziprasidone, and olanzapine.15 A third narrative SR found the combination of haloperidol plus promethazine to be more effective than haloperidol alone within 20 minutes.13 No significant differences were found for a number of comparisons. For example, similar effects were found for flunitrazepam and haloperidol as well as haloperidol plus promethazine and lorazepam or olanzapine.13 Improvement in agitation and/or aggression was not found to be different between olanzapine, ziprasidone, haloperidol alone, or haloperidol plus midazolam.13
Time to Adequate Sedation
As part of a narrative SR, Kousgaard and colleagues found time to sedation to be shorter for midazolam compared with haloperidol (alone or in combination with promethazine) but was similar to lorazepam.15 A separate narrative SR found midazolam to have a significantly shorter time to onset of sedation than lorazepam, haloperidol, or ziprasidone but longer time to onset than droperidol.13 Droperidol was found to be faster acting than ziprasidone.13 The combination of haloperidol plus promethazine acted more quickly than lorazepam.13
An RCT found patients receiving midazolam to achieve sedation more quickly than patients receiving olanzapine or haloperidol.18 Similarly, an observational study found midazolam to provide faster sedation time compared with ziprasidone or haloperidol but similar time to sedation compared with olanzapine.23
Proportion or Number Adequately Sedated
One study within an SR reported the combination of haloperidol plus promethazine was superior to lorazepam in terms of the proportion sedated.15 One good-quality RCT found the proportion adequately sedated at 15 minutes was greatest for droperidol (64% of patients sedated) compared to 25%, 35%, and 29% for ziprasidone (10 mg), ziprasidone (20 mg), and lorazepam, respectively.20 One good-quality RCT found a greater proportion of patients were sedated with midazolam compared with olanzapine and haloperidol; however, no significant differences were observed for haloperidol compared with olanzapine.18
Need for Rescue or Additional Medication
In a prospective observational study, Klein and colleagues found that 40% of patients receiving the benzodiazepine midazolam required additional medication for sedation compared with 20% receiving haloperidol 10 mg, 33% receiving haloperidol 5 mg, 21% receiving olanzapine, and 24% receiving ziprasidone.23 In contrast, 1 narrative SR found, in 1 study, more patients given midazolam required rescue medication to achieve adequate sedation compared with droperidol or ziprasidone.13 However, 1 good-quality RCT found no significant differences between midazolam, olanzapine, and haloperidol in the requirement for rescue sedation.18 More people treated with olanzapine needed additional sedation within 4 hours to maintain tranquilization compared with the combination of haloperidol plus promethazine.13
Adverse Events
One SR found no significant differences in the incidence of AEs between second-generation and first-generation antipsychotic drugs.14 However, Ostinelli and colleagues found fewer extrapyramidal symptoms and fewer reports of insomnia during 24 hours in patients administered aripiprazole compared with haloperidol.17 Fewer patients receiving aripiprazole reported somnolence over a 24-hour period compared with olanzapine.17 One SR found haloperidol plus midazolam to have the highest proportion of patients with AEs.13 In addition, 1 RCT found respiratory AEs occurred in 4% of patients with droperidol and 7% of olanzapine, while extrapyramidal AEs were more common with droperidol compared with olanzapine.21 In 1 RCT, Chan et al. (2021) found no differences between midazolam, olanzapine, and haloperidol in adverse effects including oxygen desaturation, dry mouth, dystonia, cardiac arrest, and QT prolongation.18
Respiratory depression was reported in significantly fewer patients receiving droperidol in an RCT compared with ziprasidone and lorazepam; however, QTc durations were similar in all groups.20 Similarly, an SR found respiratory distress was experienced by significantly more midazolam patients than the patients given droperidol or ziprasidone.13
Evidence-Based Guidelines
Research question 2: What are the evidence-based guidelines for using intramuscular antipsychotic drugs and/or intramuscular benzodiazepines as rapid tranquilization for inpatients in mental health facilities or emergency departments?
Joint BAP/NAPICU Guideline
Based on standard of care (S recommendation), the guidelines recommend that IM monotherapy should be considered before IM combinations for rapid tranquilization.1
Rapid Tranquilization Intramuscular Monotherapy
For rapid tranquilization IM monotherapy, the BAP/NAPICU guideline1 recommends lorazepam (quality of evidence Ib; A) OR promethazine (quality of evidence extrapolated Ia; D) OR 1 of aripiprazole (quality of evidence Ia; A), droperidol (quality of evidence Ib; A), or olanzapine (quality of evidence Ib; A). Midazolam is not recommended due to the risk of respiratory depression (quality of evidence Ia; A). Haloperidol is not recommended as monotherapy even though there is evidence of its effectiveness because measures need to be in place to offset adverse effects (quality of evidence Ia; A). Based on standard of care (S recommendation), clonazepam and diazepam are not recommended due to a lack of supporting evidence for use in rapid tranquilization.
Rapid Tranquilization Intramuscular Combinations
For rapid tranquilization IM combinations, the BAP/NAPICU guideline1 recommends promethazine plus haloperidol (quality of evidence Ia; A) OR lorazepam plus haloperidol (quality of evidence Ia; A). Based on standard of care, flumazenil must be immediately available when using parenteral benzodiazepines due the risk of respiratory depression. There is little evidence of efficacy for the combination of lorazepam plus promethazine.
Limitations
There were several important limitations among SRs and individual studies of antipsychotic drugs or benzodiazepines as rapid tranquilization in inpatients of mental facilities and emergency departments. Thus, there is some uncertainty in terms of the validity of the results. Three of the included SRs were narrative reviews only and included several medications and dosages which made synthesis of the evidence challenging. Further, the shortcomings of the primary studies limited the utility of the SRs, primarily due to poor quality of reporting and design of the individual trials, and the quality of the underlying evidence that led to conclusions was very poor to moderate. Limitations among the 3 RCTs and observational studies were the variability in methodology, including the allocation process and the extent to which participants and study personnel were fully blinded to treatment allocation. Furthermore, the population characteristics in the individual studies were quite varied in the etiology of agitation and/or aggression, making it challenging to make comparisons or draw generalizable conclusions. Investigators used a range of instruments to measure efficacy outcomes, which limits the utility of results and precludes comparisons across trials. The BAP/NAPICU guidelines did not provide a thorough account of the details of the literature review to inform their recommendations. Another limitation of the guidelines was the unclear decision-making and consensus process between the evidence and final recommendations. No evidence was found for the efficacy of antipsychotic drugs or benzodiazepines in the elderly population, nor did researchers stratify by age group when adults of all ages were included. Similarly, there was a lack of stratification by prior antipsychotic drug use. Four studies reported whether patients had received antipsychotic medication before rapid tranquilization; however, no study stratified or discussed outcomes in this context.
Conclusions and Implications for Decision- or Policy-Making
The management of patients exhibiting agitated, threatening, or destructive behaviour in mental health facilities and emergency departments remains challenging. Although there is evidence that antipsychotic drugs and benzodiazepines are effective in rapid tranquilization of acutely agitated and/or aggressive patients, the literature base lacks consistency in terms of specific comparisons, making it challenging to draw conclusions about which medications or combination of medications result in superior outcomes. Five SRs, 3 RCTs, 4 observational studies, and 1 guideline document were included in this report. The evidence is somewhat inconsistent in terms of the comparative efficacy and safety of medications. Some studies suggested the given comparisons or combinations were similar, whereas others favoured one treatment over another.
A 2015 CADTH Rapid Response report on this topic7 also found inconsistent evidence regarding the comparative efficacy and safety of antipsychotic drugs and benzodiazepines. However, the authors noted there was consistent evidence that IM haloperidol is less effective and more harmful than other therapies. The results from the current review are more heterogeneous. Although 1 SR and 3 individual studies reported haloperidol alone or in combination with other medications to be inferior to other first-generation antipsychotic drugs, second-generation antipsychotic drugs, or benzodiazepines,14,18,22,23 2 SRs reported superiority over second-generation antipsychotic drugs.15,17 Others reported mixed results13 or no difference in efficacy.24 The 2015 report included a guideline that suggested the use of IM lorazepam or a combination of IM haloperidol and promethazine as rapid tranquilization for adults in inpatient psychiatric or emergency department settings.7
In the current review, we found 1 guideline that recommends IM monotherapy should be considered before IM combinations. Similar to the most recent CADTH Rapid Response report, the current review includes a guideline recommending IM monotherapy with lorazepam, promethazine, or 1 of aripiprazole, droperidol, or olanzapine. For IM combinations, the guideline recommends promethazine plus haloperidol or lorazepam plus haloperidol.1
There is a need to conduct high-quality research studies that provide more definitive evidence of the efficacy and safety of the different treatments for rapid tranquilization. Future research should evaluate the use of antipsychotic drugs and benzodiazepines among more specific populations, such as patients older than 65 years. Investigators should attempt to differentiate dosages in terms of patients presenting who have had prior exposure to antipsychotic drugs, whether in the pre-hospital setting or as a routine medication taken for psychiatric illness. Further, outcomes stratified by etiology of aggression and/or agitation would allow for a more customized approach to treatment.
References
1.Patel MX, Sethi FN, Barnes TR, et al. Joint BAP NAPICU evidence-based consensus guidelines for the clinical management of acute disturbance: de-escalation and rapid tranquillisation. J Psychopharmacol. 2018;32(6):601-640. PubMed
2.Cookson J. Rapid tranquillisation: the science and advice. BJPsych Advances. 2018;24(5):346-358.
3.National Collaborating Centre for Mental Health. Violence and aggression: short-term management in mental health, health and community settings. NICE guideline N10. Updated edition. Leicester (UK): British Psychological Society; 2015: https://www.nice.org.uk/guidance/ng10/evidence/full-guideline-70830253. Accessed 2021 Jul 12.
4.Hatta K, Katayama S, Morikawa F, et al. A prospective naturalistic multicenter study on choice of parenteral medication in psychiatric emergency settings in Japan. Neuropsychopharmacol. 2018;38(3):117-123. PubMed
5.Paton C, Adams CE, Dye S, Fagan E, Okocha C, Barnes TR. The pharmacological management of acute behavioural disturbance: data from a clinical audit conducted in UK mental health services. J Psychopharmacol. 2019;33(4):472-481. PubMed
6.Yap CYL, Taylor DM, Kong DCM, et al. Management of behavioural emergencies: a prospective observational study in Australian emergency departments. J Pharm Pract Res. 2019;49(4):341-348.
7.Use of antipsychotics and/or benzodiazepines as rapid tranquilization in in-patients of mental facilities and emergency departments: a review of the clinical effectiveness and guidelines. Rapid response report: summary with critical appraisal. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/pdf/htis/oct-2015/RC0718%20Antipsychotics%20for%20rapid%20tranq%20Final.pdf. Accessed 2021 Jul 16.
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. Appendix A: questionnaire to assess the relevance and credibility of a network meta-analysis. PubMed
10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
11.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Jul 19.
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Muir-Cochrane E, Grimmer K, Gerace A, Bastiampillai T, Oster C. Safety and effectiveness of olanzapine and droperidol for chemical restraint for non-consenting adults: a systematic review and meta-analysis. Australas Emerg Care. 2021;24(2):96-111. PubMed
14.Schneider A, Mullinax S, Hall N, Acheson A, Oliveto AH, Wilson MP. Intramuscular medication for treatment of agitation in the emergency department: a systematic review of controlled trials. Am J Emerg Med. 2020;09:09.
15.Kousgaard SJ, Licht RW, Nielsen RE. Effects of intramuscular midazolam and lorazepam on acute agitation in non-elderly subjects - a systematic review. Pharmacopsychiatry. 2017;50(4):129-135. PubMed
16.Paris G, Bighelli I, Deste G, et al. Short-acting intramuscular second-generation antipsychotic drugs for acutely agitated patients with schizophrenia spectrum disorders. A systematic review and network meta-analysis. Schizophr Res. 2021;229:3-11. PubMed
17.Ostinelli EG, Jajawi S, Spyridi S, Sayal K, Jayaram MB. Aripiprazole (intramuscular) for psychosis-induced aggression or agitation (rapid tranquillisation). Cochrane Database Syst Rev. 2018;1(1):CD008074. PubMed
18.Chan EW, Lao KSJ, Lam L, et al. Intramuscular midazolam, olanzapine, or haloperidol for the management of acute agitation: a multi-centre, double-blind, randomised clinical trial. EClinicalMedicine. 2021;32:100751. PubMed
19.Dib JE, Yaacoub HE, Ikdais WH, et al. Rapid tranquillisation in a psychiatric emergency hospital in Lebanon: TREC-Lebanon - a pragmatic randomised controlled trial of intramuscular haloperidol and promethazine v. intramuscular haloperidol, promethazine and chlorpromazine. Psychol Med. 2021:1-9. PubMed
20.Martel ML, Driver BE, Miner JR, Biros MH, Cole JB. Randomized double-blind trial of intramuscular droperidol, ziprasidone, and lorazepam for acute undifferentiated agitation in the emergency department. Acad Emerg Med. 2021;28(4):421-434. PubMed
21.Cole JB, Stang JL, DeVries PA, Martel ML, Miner JR, Driver BE. A prospective study of intramuscular droperidol or olanzapine for acute agitation in the emergency department: a natural experiment owing to drug shortages. Ann Emerg Med. 2021:Apr 9. Online ahead of print.
22.Klein LR, Driver BE, Horton G, Scharber S, Martel ML, Cole JB. Rescue sedation when treating acute agitation in the emergency department with intramuscular antipsychotics. J Emerg Med. 2019;56(5):484-490. PubMed
23.Klein LR, Driver BE, Miner JR, et al. Intramuscular midazolam, olanzapine, ziprasidone, or haloperidol for treating acute agitation in the emergency department. Ann Emerg Med. 2018;72(4):374-385. PubMed
24.Real Juarez D, Diaz-Castro L, Cabello-Rangel H. A naturalistic comparison study of effectiveness of intramuscular olanzapine and intramuscular haloperidol in acute agitated patients with schizophrenia. Neuropsychiatry. 2016;6(5):229-235.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Muir-Cochrane et al. (2021)13 Australia Funding source: No funding received | 23 RCTs total 12 RCTs relevant to present review Total number of patients per trial: 20-316 | Adults (18 + years) with uncontrolled aggression, anxiety, or violence, who are likely to cause harm to themselves or others, because of mental health disorders (with/without substance abuse). Setting: Inpatients or emergency department (12 studies) No indication of prior antipsychotic medication | Lorazepam (3 studies) Lorazepam + Haloperidol (6 studies) Haloperidol + Promethazine (6 studies) Haloperidol + Midazolam (2 studies) Olanzapine (2 studies) Droperidol (3 studies) Droperidol + Midazolam (1 study) Ziprasidone (3 studies) Midazolam (4 studies) Flunitrazepam (1 study) Promethazine (1 study) *dosages varied | Outcomes: Improvement in aggression/agitation scales (9 studies) Sedation scale (1 study) Time to calm/sedation (5 studies) Use of additional sedation (5 studies) Length of stay (2 studies) Proportion sedated in set time period (4 studies) Further violent episodes (3 studies) Adverse events (12 studies) Follow-up: Up to 12 hours |
Paris et al. (2021)16 Italy Funding source: Consorzio Bacino Imbrifero Montano Dell'Oglio, Italy | 10 RCTs Total number of patients per trial: 49-448 | Adults (18 + years) diagnosed with schizophrenia, schizophreniform or schizoaffective disorder who presented acute agitation Setting: NR No indication of prior antipsychotic medication | Second-generation antipsychotics administered in IM short-acting formulations Aripiprazole (2 studies) Olanzapine (6 studies) Ziprasidone (2 studies) First-generation antipsychotic Haloperidol (5 studies) | Outcomes: Number of patients having responded to treatment at 2 hour Number of responders at 24 hour Responders: ≥ 40% reduction in PEC score (8 studies) ≥ 2 point reduction in BARS score (2 studies) Follow-up: 24 hours |
Schneider et al. (2020)14 US Funding source: NA | 8 RCTs (but 3 were excluded from analysis due to high risk of bias) Total number of patients per trial: 91-150 | Adults (18 + years) who were acutely agitated for any reason Setting: Emergency Department (Regular – 6 studies; or psychiatric – 2 studies) No indication of prior antipsychotic medication | Intervention: IM Antipsychotic medications (Olanzapine, Haloperidol, Droperidol) Comparators: IM Antipsychotic medications (Ziprasidone) IM Antipsychotic + adjunct medication (Haloperidol + promethazine, Haloperidol + Lorazepam, Droperidol + midazolam, Haloperidol + midazolam) Other medications (Haloperidol, Lorazepam, Midazolam) | Outcomes: Reduction in agitation rating scale (OASS [1], ABS [1], AMSS [2], ACES [1] Adverse effects Follow-up: up to 24 hours |
Ostinelli et al. (2018)17 Italy Funding source: Università degli Studi di Milano; Rotherham, Doncaster and South Humber NHS Foundation Trust; Cyprus University of Technology; UK LLP; Cygnet Hospital Derby, UK; Melbourne Neuropsychiatry Centre | 3 RCTs Total number of patients per trial: 80-448 per trial | Adults (18-69 years) presenting with psychosis-induced aggression and/or agitation Schizophrenia (74.4%), schizoaffective disorder (24.9%), schizophreniform disorder (0.7%) Setting: Emergency department No indication of prior antipsychotic medication | IM Aripiprozole 9.75mg IM Haloperidol 6.5-7.5mg IM Olanzapine 10mg | Outcomes: Primary: Tranquil or asleep by 30 minutes Need for repeated rapid tranquilization Secondary: Tranquil/asleep > 30 minutes Time to tranquilization and/or sleep Change in aggression/agitation Duration of hospital stay Adverse events Follow-up: 30 minutes - 24 hours |
Kousgaard et al. (2017)15 Denmark Funding source: Affiliated research institution | 16 RCTs 14 RCTs relevant to this review Total number of patients per trial: 15-301 | Adults (18-65 years) with aggression and/or agitation because of mental health disorders Setting: Psychiatric setting No indication of prior antipsychotic medication | IM Lorazepam 2-4 mg IM Haloperidol 5 mg IM Midazolam 5-15 mg IM Olanzapine 10 mg IM Droperidol 5-10 mg IM Ziprasidone 10-20 mg IM Haloperidol 2.5-15 mg + IM Promethazine 20-50 mg IM Lorazepam 2-4 mg + IM Haloperidol 5 mg IM Haloperidol 2.5 mg + IM Midazolam 7.5 mg IM Droperidol 5 mg + IM Midazolam 5 mg | Improvement in Aggression or Agitation Scale Duration of violence/aggression Time to sedation Proportion sedated Follow-up: up to 24 hours |
IM = intramuscular; PEC = Positive and Negative Syndrome Scale – Excited Component; BARS = Behaviour Activity Rating Scale; OASS = Overt Agitation Severity Score, ABS = Agitated Behavior Scale; AMSS = Altered Mental Status Scale; ACES = Agitation and Calmness Evaluation Scale.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Randomized controlled trials | ||||
Chan et al. (2021)18 China Funding source: Research Grants Council (Early Career Scheme), Hong Kong | RCT Multi-centre within Hong Kong | Inclusion criteria were: patients aged 18-75 years; and requiring parenteral drug sedation for acute agitation at the treating physician’s discretion. Patients who had received oral or parenteral sedative drug(s) within 12 hour, either as usual medications or pre-hospital acute agitation management, were eligible Setting: Emergency department IM Midazolam (n = 56); median age 44 years; 61% male; 2% received prior sedation; etiology of agitation – alcohol intoxication (28%), substance abuse (31%), psychological illness (87%), non-compliance to usual medication (47%), suicidal ideation (34%) IM Olanzapine (n = 54); median age 40 years; 70% male; 2% received prior sedation; etiology of agitation – alcohol intoxication (23%), substance abuse (27%), psychological illness (83%), non-compliance to usual medication (43%), suicidal ideation (33%) IM Haloperidol (n = 57); median age 42 years; 42% male; 2% received prior sedation; etiology of agitation – alcohol intoxication (25%), substance abuse (37%), psychological illness (84%), non-compliance to usual medication (35%), suicidal ideation (35%) | IM Olanzapine 5 mg IM Haloperidol 5 mg IM Midazolam 5 mg | Time to achieve adequate sedation Proportion of patients adequately sedated at 10, 20, 30, 45, and 60 minute Proportion of patients requiring a second dose of study drug and/or alternative drug(s) to achieve initial adequate sedation Proportion of patients with corrected QT interval (QTc) prolongation on the ECG Adverse events reported after study drug administration Proportion of patients with a sedation score of 0 (observed asleep) after study drug administration Emergency department LOS Follow-up: 60 minutes – 5 + hours (for LOS) |
Dib et al. (2021)19 Lebanon Funding source: NR | RCT Single-centre | Inclusion criteria: Adult (18- 65 years) patients of psychiatric hospital, requiring acute intramuscular sedation because of aggression, agitation, or violence IM HPC (n = 51), median age 36 years, 46% male, 85% already taking antipsychotic medication; etiology of agitation – psychosis (58%), substance abuse (6%), intellectual disability (6%), psychological (2%), unknown (26%) IM HP (n = 43), median age 35 years, 44% male, 85% already on antipsychotic medication; etiology of agitation – psychosis (56%), substance abuse (10%) intellectual disability (2%), psychological (0%), unknown (21%) | Haloperidol 5mg + Promethazine 25mg + Chlorpromazine 100mg (HPC) Haloperidol 5mg + Promethazine 25 mg (HP) | Primary: calm or tranquil at 20, 40, 60 and 120 minutes Secondary: asleep, restrained/straitjacket applied, left the ward (at 20, 40, 60 and 120 minute), recurrence of index aggression, new aggressive event beyond the 120-minute time interval, medications used, serious adverse event Follow-up: 2 weeks |
Martel et al. (2021)20 US Funding source: NR | RCT Single-centre | Inclusion criteria: Adults aged ≥ 18 years requiring parenteral sedation for acute agitation Setting: Emergency department No indication of prior antipsychotic medication IM Droperidol (n = 25); median age 39 years; 84% male; etiology of agitation – alcohol intoxication (76%), drug intoxication (4%), head injury (12%), primary psychiatric etiology (12%) IM Ziprasidone (10 mg) (n = 28); median age 40 years; 68% male; etiology of agitation – alcohol intoxication (68%), drug intoxication (7%), head injury (11%), primary psychiatric etiology (18%) IM Ziprasidone (20 mg) (n = 31); median age 41 years; 77% male; etiology of agitation – alcohol intoxication (81%), drug intoxication (13%), head injury (16%), primary psychiatric etiology (13%) IM Lorazepam (n = 31); median age 39 years; 74% male; etiology of agitation – alcohol intoxication (81%), drug intoxication (10%), head injury (27%), primary psychiatric etiology (17%) | IM Droperidol 5 mg IM Ziprasidone 10 mg IM Ziprasidone 20 mg IM Lorazepam 2 mg | Proportion adequately sedated at 15 minutes Need for additional sedating medication ED length of stay Respiratory depression Follow-up: < 24 hours |
Observational studies | ||||
Cole et al. (2021)21 US Funding source: NR | Prospective observational study | Inclusion criteria: Patients with acute agitation Setting: Emergency department intoxication unit IM Droperidol (n = 538); median age 40 years; 70% male; < 5% received pre-hospital medication for agitation; etiology of agitation – alcohol intoxication (86%), drug intoxication (15%), psychiatric illness (12%), medical etiology (2%) IM Olanzapine (n = 719); median age 43 years; 75% male; < 5% received pre-hospital medication for agitation; etiology of agitation – alcohol intoxication (87%), drug intoxication (13%), psychiatric illness (13%), medical etiology (1%) | IM Droperidol 5 mg IM Olanzapine 10 mg | Time to adequate sedation Need for additional (rescue) medications to treat agitation Total time in the ED Adverse events Follow-up: NR |
Klein et al. (2019)22 US Funding Source: NR | Retrospective observational study | Adults (18 years of age and older) patients receiving a parenteral antipsychotic for sedation with a chief complaint of “Altered Mental Status” Setting: Emergency department No indication of prior antipsychotic medication IM Droperidol (n = 4,947); median age 40 years; 74% male; etiology of agitation – alcohol intoxication (92%), drug intoxication (8%), psychiatric (11%), medical (0.2%) IM Olanzapine (n = 8,825); median age 35 years; 75% male; etiology of agitation – alcohol intoxication (93%), drug intoxication (7%), psychiatric (10%), medical (0.3%) IM Haloperidol (n = 2,146); median age 38 years; 77% male; etiology of agitation – alcohol intoxication (92%), drug intoxication (7%), psychiatric (10%), medical (0.6%) | IM Droperidol IM Olanzapine IM Haloperidol *dosages not reported | Rescue sedation administered within 1 hour of initial sedative. Rescue sedation at any time during the encounter Serious adverse events or extrapyramidal side effects Follow-up: NR |
Klein et al. (2018)23 US Funding source: NR | Prospective observational study | Patients were eligible for inclusion in the study if they received medication to treat acute agitation in the ED during the 15-week protocol. IM Midazolam (n = 127); median age 40 years; 76% male; 1% received prior antipsychotic; etiology of agitation – alcohol intoxication (82%), drug intoxication (17%), psychiatric illness (17%), medical (1%) IM Olanzapine (n = 163); median age 45 years; 69% male; 3% received prior antipsychotic; etiology of agitation – alcohol intoxication (90%), drug intoxication (11%), psychiatric illness (12%), medical (1%) IM Ziprasidone (n = 145); median age 40 years; 75% male; 2% received prior antipsychotic; etiology of agitation – alcohol intoxication (90%), drug intoxication (10%), psychiatric illness (10%), medical (1%) IM Haloperidol 5mg (n = 151); median age 40 years; 67% male; 1% received prior antipsychotic; etiology of agitation – alcohol intoxication (90%), drug intoxication (17%), psychiatric illness (9%), medical (1%) IM Haloperidol 10mg (n = 151); median age 38 years; 71% male; 1% received prior antipsychotic; etiology of agitation – alcohol intoxication (85%), drug intoxication (15%), psychiatric illness (9%), medical (1%) | IM Midazolam 5mg IM Olanzapine 10mg IM Ziprasidone 20mg IM Haloperidol 5mg IM Haloperidol 10mg | Proportion of patients adequately sedated (defined as AMSS score < 1). Median difference in AMSS score from baseline at 15 minutes Rescue medications administered (before and after adequate sedation achieved), Time to adequate sedation Adverse events. Follow-up: 120 minutes |
Real Juarez et al. (2016)24 Mexico Funding source: NR | Prospective observational study | Adult patients with previous diagnosis of schizophrenia, had total scores of 14 or higher on the PANSS-EC with a score of 4 or higher on at least 1 item, and the treating psychiatrist concluded that the patient needed to be treated with an IM injection, of olanzapine or of haloperidol, which are the 2 most used and available antipsychotics in hospital emergency services No indication of prior antipsychotic medication IM Haloperidol 5 mg (n = 11), mean age 38 years, 55% male IM Haloperidol 10mg (n = 32), mean age 34 years, 44% male IM Olanzapine 10mg (n = 15), mean age 34 years, 60% male | IM Olanzapine 10mg IM Haloperidol 5mg IM Haloperidol 10mg | PANSS-EC at 0, 30, 60, 90, and 120 minutes Abnormal Involuntary Movements Scale (AIMS) were taken to assess the presence of extrapyramidal symptoms (adverse effects) Follow-up: 120 minutes |
AMSS = Altered Mental Status Scale; ECG = electrocardiogram; ED = emergency department; IM = intramuscular; LOS = length of stay; NR = not reported; PANSS-EC = Positive and Negative Syndrome Scale Excited.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommend-ations development and evaluation | Guideline validation |
Patel et al. (2018)1 | ||||||
Intended users: Health care professionals working in emergency psychiatric care or acute psychiatric inpatient care, general acute hospital and forensic psychiatry Target population: Adults; excludes children and young people, those with a learning disability or traumatic brain injury, or older adults with or without dementia. | IM monotherapy (IM Lorazepam, IM Midazolam) IM benzodiazepines in combination with other medications (haloperidol, promethazine) | “Primary outcome measures are multiple, diverse and measured at different pre-set time points. Further, they commonly include achieving sedation or the state of falling asleep or time to desirable state. The proportions of participants who become calm are not consistently reported.” | Systematic reviews, RCTs and observational studies were identified from PubMed, MEDLINE, and Embase and from the Cochrane Database. Published NICE guidelines on RT were also considered Evidence selection: NR Evidence synthesis: discussion among expert panel | Categories of evidence: Ia: Evidence from meta-analysis of RCTs Ib: Evidence from at least 1 RCT IIa: Evidence from at least 1 controlled study without randomization IIb: Evidence from at least 1 other type of quasi-experimental study III: Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies and case-control studies IV: Evidence from expert committee reports or opinions and/or clinical experience of respected authorities Strength of recommendation: A: Based on category I evidence, at least 1 large, good-quality, RCT or replicated, smaller, RCTs B: Based on category II evidence, at least 1 large, good-quality, RCT or replicated, smaller, RCTs, or extrapolated a recommendation from category I evidence C: Based on category III evidence or extrapolated recommendation from category I or II evidence D: Based on category IV evidence or extrapolated a recommendation from category I, II or III evidence S: Standard of practice | Consensus Literature review and discussion | Internal review by experts |
IM = intramuscular; NR = not reported; RCT = randomized controlled trial; RT = rapid tranquilization.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 28 and the ISPOR Questionnaire9
Strengths | Limitations |
Muir-Cochrane et al. (2021)13 | |
Protocol was registered with PROSPERO in 2017 Used comprehensive search strategy Assessed risk of bias of included studies | Data extraction was completed by only 1 reviewer Reporting of outcomes was disorganized Study conclusions were based on a meta-analysis of only 2 RCTs (out of 23 total RCTs) Multiple settings, dosages, and routes of administration were included Narrative review |
Paris et al. (2021)16 | |
Protocol was registered with PROSPERO Authors followed PRISMA guidelines extended for network meta-analysis Search was recent; conducted in March 2020 Included RCTs all had low to moderate risk of bias Included sensitivity analysis excluding studies that used pseudoplacebo or ineffective dose as comparator Provided analyses of both direct and indirect comparisons between treatments Authors used random-effects models to pool data in meta-analyses Characteristics and results of individual studies were well-described Study selection and data extraction completed in duplicate by 2 reviewers | Included only patients with schizophrenia, schizophreniform, or schizoaffective disorder with acute agitation Did not report on adverse events Potential conflict of interest for the supervising author |
Schneider et al. (2020)14 | |
Protocol was registered with PROSPERO Search was recent; conducted in February 2020 Comprehensive search strategy | No description of data extraction process Included studies were not well-described in terms of population characteristics Evidence was limited, heterogeneous, and at moderate to high risk of bias |
Ostinelli et al. (2018)17 | |
Cochrane review adheres to the reporting standards of the Cochrane Collaboration Studies were screened in duplicate. Authors assessed risk of bias of included studies. Authors considered clinical, methodological, and statistical heterogeneity between studies. Authors conducted subgroup analyses to explain heterogeneity. Authors evaluated quality of body of evidence using the GRADE approach. | Search is not recent; conducted in 2014 and 2017 For the 2017 search, only 1 author inspected citations, identified relevant abstracts, and extracted data Only 10% of data extraction was performed in duplicate Authors used fixed-effects models to pool data, which assumes no heterogeneity between studies |
Kousgaard et al. (2017)15 | |
Comprehensive search strategy Specific inclusion/exclusion criteria Characteristics of included studies were well-described | Assessment of risk of bias of individual studies not reported Data extraction process was not well-described Narrative review only and did not differentiate between outcomes in determining superiority of 1 medication over another |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; GRADE = Grades of Recommendation, Assessment, Development and Evaluation; ISPOR = International Society for Pharmacoeconomics and Outcomes Research.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist10
Strengths | Limitations |
Chan et al. (2021)18 | |
Randomization – method was suitable (computer generated) Double Blinded – study personnel were not involved in administering medication Sample size calculation included Loss to follow-up was minimal | Discontinued study before completion due to civil unrest therefore did not obtain the projected sample size External validity may be threatened by 36 patients who were randomized and treated but subsequently did not provide consent to use their data in the analysis Did not describe the source population in terms of etiology of agitation and there is therefore some uncertainty with respect to external validity |
Dib et al. (2021)19 | |
Part of the TREC-Lebanon Trials Randomization method was sound (computer generated) Treatment allocation was concealed until the patient entered the study | Unconventional blinding system – medical resident was blinded to treatment allocation until complete, then unblinded to collect outcome data Eligible patients presenting during late-night hours were not included because no study staff were available at that time (n = 134) Statistical analysis not well-described No sample size calculation No description of criteria for outcomes (e.g., agitation scale) Stated their acceptable p-value but did not report any p-values in the results Stated their analysis included number needed to treat but did not report in the results |
Martel et al. (2021)20 | |
Randomized Double blinded Used validated instruments to assess agitation and determine efficacy/outcomes – Altered Mental Status Scale (AMSS) and Behavioural Activity Rating Scale (BARS) Sample size calculation provided | Method of randomization was not reported Method of blinding/treatment concealment was not reported Reason for ineligibility was not provided for patients who were deemed ineligible for the study |
Cole et al. (2021)21 | |
Used validated instruments to assess agitation and determine efficacy/outcomes – Altered Mental Status Scale (AMSS) Sample size calculation provided | Not randomized Some patients were selected during a time period in which there was a shortage of 1 of the medications therefore patients in each treatment group were not selected during the same time period Patients who were not selected were younger, had lower ethanol concentrations, and were less agitated on arrival |
Klein et al. (2019)22 | |
Data abstractors and research personnel were blinded to treatment status | Retrospective chart review EMR search criteria may not have captured all cases of aggression/agitation treated with an antipsychotic Primary outcome (need for rescue sedation) is subject to the discretion of the treating clinician (i.e., not an objective measure) A drug shortage in 2013 limited access to Droperidol It is possible that some patients were given other medications concomitantly that were not reported in the results |
Klein et al. (2018)23 | |
Prospective study Used validated instrument to assess agitation and determine efficacy/outcomes – Altered Mental Status Scale (AMSS) Provided sample size calculation | Medication given changed every 3 weeks, so patients were not selected for each treatment during same time period Attending physician could break protocol if they determined that a different medication was indicated according to the clinical scenario Characteristics of screening misses and protocol violations were not reported |
Real Juarez et al. (2016)24 | |
Prospective study Used validated instruments to assess agitation and to determine efficacy/outcomes – PANSS-EC; AIMS | Treatment allocation based on physician choice Included only patients with schizophrenia-related agitation Not randomized No report of blinding research personnel of treatment allocation Differences in baseline level of agitation between treatment groups Conducted post hoc subgroup analyses |
AIMS = Abnormal Involuntary Movement Scale; PANSS-EC = Positive and Negative Syndrome Scale Excited Component.
Table 7: Strengths and Limitations of Guideline Using AGREE II11
Item | Patel et al. (2018)1 |
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Unclear; excluded children, young people, those with learning disability or traumatic brain injury, or elderly people with or without dementia. Guideline method gave no specific age group or inclusion criteria |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Unclear; ‘experts’ were involved in review of literature and guideline development but were not defined in the report |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | No |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Unclear; reported searching several databases but no search terms were identified |
8. The criteria for selecting the evidence are clearly described. | No; there was no description of the methods for selecting the evidence to review |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Unclear; it was reported that ‘experts’ met and discussed the literature base however, there was no specific description of how exactly the recommendations were formulated or how consensus was achieved |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | Yes |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear; the British Association for Psychopharmacology (BAP) and the National Association of Psychiatric Intensive Care and Low Secure Units (NAPICU) were reported as providing the funds for the expert group meetings however, there was no statement indicating that these organizations did not influence the content of the guideline |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Summary of Findings Included Systematic Reviews and Network Meta-Analyses
Muir-Cochrane et al. (2021)13
Main Study Findings
Efficacy of reducing agitation/aggression:
Lorazepam + haloperidol was significantly better than lorazepam alone in acutely agitated patients (1 study)
Midazolam was not different than lorazepam or haloperidol (1 study)
Midazolam successfully sedated more patients at 20 minutes than haloperidol + lorazepam (1 study)
Haloperidol + promethazine is not different than lorazepam (1 study)
Olanzapine is not different than ziprasidone, haloperidol alone, haloperidol + promethazine, haloperidol + midazolam within 12 hours (1 study)
Midazolam and droperidol were more effective than ziprasidone (1 study)
Statistically significant at P < 0.05
Haloperidol + promethazine was more effective than haloperidol alone within 20 minutes (1 study)
Haloperidol + midazolam, and olanzapine, were more effective than haloperidol + promethazine, or ziprasidone, in reducing agitation without incurring AEs for people with acute psychomotor agitation (1 study)
Haloperidol + promethazine, and olanzapine were both effective in producing tranquilization within 15 minutes, and neither incurred notable AEs (1 study)
Flunitrazepam (1 mg) and haloperidol (5 mg) had similar effects on reducing aggression within 90 minutes of administration (1 study)
Time to sedation:
Midazolam has a significantly shorter time to onset of sedation and a more rapid time to arousal than lorazepam or haloperidol.
Haloperidol + promethazine acted more quickly than lorazepam (1 study)
Midazolam and droperidol were faster acting and more effective than ziprasidone (1 study)
Droperidol faster acting than midazolam. There was no additional benefit in using the combination administration of droperidol + midazolam (1 study)
Requiring additional sedation:
Fewer patients given droperidol or ziprasidone required rescue medication to achieve adequate sedation, compared with midazolam (1 study)
More people treated with olanzapine versus haloperidol + promethazine needed additional sedation within 4 hours to maintain tranquilization (1 study)
Adverse events:
Haloperidol + midazolam had the poorest results versus olanzapine in terms of unalleviated aggression, and the highest percentage of people with AEs (1 study)
Respiratory distress was experienced by significantly more midazolam patients than the patients given droperidol or ziprasidone (1 study)
Authors’ Conclusion
“This study provides clear guidance than 5 mg olanzapine delivered intramuscularly is both safe and effective in quickly producing calm in potentially distressing situations, and that it is as effective, and safer, than higher doses.” (p. 109)13
Paris et al. (2021)16
Main Study Findings
Efficacy:
Primary outcome: Responders at 2 hours:
Ziprasidone versus olanzapine: risk ratio (RR) = 1.26; 95% confidence interval (CI), 0.76 to 2.09
Ziprasidone versus aripiprazole: RR = 1.55; 95% CI, 0.94 to 2.56
Ziprasidone versus haloperidol: RR = 1.42; 95% CI, 0.86 to 2.34
Olanzapine versus aripiprazole: RR = 1.24; 95% CI, 1.05 to 1.45)
Statistically significant at P < 0.05
Olanzapine versus haloperidol: RR = 1.13; 95% CI, 0.99 to 1.28
Haloperidol versus aripiprazole: RR = 1.10; 95% CI, 0.95 to 1.27
Secondary outcome: Responders at 24 hours:
Olanzapine versus haloperidol: RR = 0.99; 95% CI, 0.83 to 1.19
Olanzapine versus aripiprazole: RR = 1.06; 95% CI, 0.91 to 1.22
Haloperidol versus aripiprazole: RR = 1.06; 95% CI, 0.85 to 1.34
Authors’ Conclusion
“The main results were: compared to placebo, a significantly higher proportion of participants in the aripiprazole, haloperidol, olanzapine and ziprasidone groups showed a clinically significant reduction in the PEC agitation score at 2 h and at 24 h, except ziprasidone for which no results at 24 h were available. All in all, 409/700 (58.42%) participants receiving second-generation antipsychotics responded at 2 h, in comparison with 97/326 (29.75%) receiving placebo. There were no significant differences between drugs, except that olanzapine outperformed aripiprazole.” (p. 8)16
“When compared with haloperidol, neither aripiprazole nor olanzapine nor ziprasidone showed a statistically significant difference in agitation at 2 h. This finding does not support the hypothesis of a possible superiority of some “atypical” compared to “typical” antipsychotics (Leucht et al., 2009a).” (p. 8)16
“In the “head-to-head” comparisons between aripiprazole, olanzapine and ziprasidone the only statistically significant difference emerged between olanzapine and aripiprazole, where the former was more effective in reducing agitation at 2 hour.” (p. 8)16
“this meta-analysis confirmed the efficacy of IM short-acting second-generation antipsychotics in reducing agitation in patients with schizophrenia compared to placebo, while there was no superiority compared to haloperidol. Olanzapine was somewhat more efficacious than aripiprazole for this purpose.” (p. 10)16
Schneider et al. (2020)14
Main Study Findings
Qualitative assessment of efficacy:
Olanzapine was more effective at reducing agitation than haloperidol plus either adjunctive medication, and the number of adverse events was similar between medications (2 studies). Ziprasidone had the least reduction in agitation at 15 minutes versus both midazolam and droperidol but was superior to midazolam at 45 minutes and had the greatest reduction in agitation compared to the other medications at 60 minutes or longer (1 study).
Adverse effects:
Extrapyramidal symptoms (dystonia, akathisia, parkinsonism, tardive dyskinesia)
Haloperidol + midazolam: 10% to 44%
Haloperidol + promethazine: 16.7% to 74.1%
Haloperidol alone: 16.7% to 20%
Lorazepam: 3%
Haloperidol + lorazepam: 6%
Olanzapine: 56%
Ziprasidone: 8.7% to 52.2%
Midazolam alone: 2.1%
Droperidol alone: 2%
Excessive sedation
Haloperidol + midazolam: 40%
Haloperidol + promethazine: 3%
Haloperidol: 10%
Olanzapine: 3.3%
Ziprasidone: 10%
QT prolongation
Droperidol: 6.5%
Midazolam: 6.9%
Droperidol + midazolam: 13.8%
Hypotension
Haloperidol + midazolam: 16.7%
Haloperidol + promethazine: 10%
Olanzapine: 3.3%
Ziprasidone: 20%
Midazolam: 3.4%
Droperidol + midazolam: 3.4%
Authors’ Conclusion
“Agitation is a common presenting symptom in the ED setting. Unfortunately, the existing evidence is limited, heterogeneous, and at moderate or high risk of bias. Based only off studies at a moderate risk of bias, SGAs likely reduce agitation as effectively as FGAs plus an adjunctive medication with a similar or lower risk of side effects in patients who are not alcohol-intoxicated. Given the immense clinical importance and interest, the field of emergency medicine would benefit from further study in this domain, but existing FDA regulations have largely stopped prospective randomized trials of agitated participants. Further high-quality, randomized, prospective studies are needed.” (p. 6)14
Ostinelli et al. (2018)17
Main Study Findings
Efficacy:
Aripiprazole versus haloperidol
Repeated need for tranquilization: RR = 1.28; 95% CI, 1.00 to 1.63 (2 RCTs)
Statistically significant at P < 0.05
PANSS-EC reduction (of ≥ 40% from baseline): RR = 0.94; 95% CI, 0.80 to 1.11 (2 RCTs)
Change score ABS at approximately 2 hours: mean difference (MD) = 0.55; 95% CI, −1.00 to 2.10 (2 RCTs)
Change score ACES at approximately 2 hours MD = 0.12; 95% CI, −0.30 to 0.55 (2 RCTs)
Change score PANSS-EC (total sample) at approximately 2 hours: MD = 0.48; 95% CI, −1.16 to 2.12 (1 RCT)
Change score PANSS-EC (schizophrenia subgroup) at approximately 2 hours: MD = 0.07; 95% CI, −0.99 to 1.13 (2 RCTs)
Change score ACES (non-sedated patients) at approximately 2 hours: MD = 0.12; 95% CI, −0.82 to 1.06 (2 RCTs)
AEs at approximately 2 hours: MD = 0.26; 95% CI, −0.68 to 1.19 (2 RCTs)
Number not responding to first injection: RR = 1.18; 95% CI, 0.78 to 1.79 (1 RCT)
Number requiring benzodiazepine within 24 hours: RR = 0.79; 95% CI, 0.46 to 1.35 (2 RCTs)
Clinical Global Impressions Improvement end point score (total sample): MD = 0.02; 95% CI, −0.19 to 0.23 (2 RCTs)
Clinical Global Impressions Improvement end point score (schizophrenia subgroup): MD = 0.02; 95% CI, −0.44 to 0.48 (1 RCT)
Clinical Global Impressions Severity change score: MD = −0.07; 95% CI, −0.36 to 0.22 (2 RCTs)
PANSS-derived BPRS change score at 2 hours: MD = 2.03; 95% CI, −1.70 to 5.76 (1 RCT)
PANSS-derived BPRS change score positive subscale at 2 hours: MD = 0.23; 95% CI, −0.82 to 1.28 (1 RCT)
Aripiprazole versus olanzapine
Improvement in agitation at 2 hours: RR = 0.77; 95% CI, 0.60 to 0.99 (1 RCT)
Statistically significant at P < 0.05
ACES change scores at 2 hours: MD = 0.58; 95% CI, 0.10 to 1.06 (1 RCT)
PANSS-EC change scores at 2 hours: MD = 3.30; 95% CI, 1.25 to 5.35 (1 RCT)
Statistically significant at P < 0.05
Clinical Global Impressions Severity change scores: MD = 0.58; 95% CI, 0.01 to 1.15 (1 RCT)
Adverse effects:
Aripiprazole versus haloperidol
1 or more drug-related adverse effects during 24 hours: RR = 0.91; 95% CI, 0.61 to 1.35 (1 RCT)
Onset or worsening of adverse effects after the second injection: RR = 0.74; 95% CI, 0.57 to 0.96 (1 RCT)
Statistically significant at P < 0.05
Serious adverse effects: RR = 1.73; 95% CI, 0.54 to 5.52 (2 RCTs)
Insomnia during 24 hours (1 RCT, n = 358, RR = 0.48; 95% CI, 0.23 to 0.97)
Statistically significant at P < 0.05
“Over”-sedated: RR = 0.60; 95% CI, 0.34 to 1.07 (1 RCT)
Somnolence: RR = 0.81; 95% CI, 0.41 to 1.58 (2 RCTs)
Dizziness: RR = 1.41; 95% CI, 0.66 to 3.01 (2 RCTs)
Tachycardia: RR = 4.07; 95% CI, 0.47 to 35.31 (1 RCT)
Sinus tachycardia: RR = 0.15; 95% CI, 0.01 to 2.75 (1 RCT)
Extrapyramidal symptoms: RR = 0.29; 95% CI, 0.12 to 0.70 (2 RCTs)
Statistically significant at P < 0.05
Akathisia: RR = 0.51; 95% CI, 0.13 to 1.94 (1 RCT)
Dystonia: RR = 0.25; 95% CI, 0.03 to 2.21 (1 RCT)
Nausea within 24 hours (2 RCTs, n = 471, RR = 5.52; 95% CI, 1.63 to 18.70).
Pain at injection site within 24 hours: RR = 3.12; 95% CI, 0.75 to 12.91 (2 RCTs)
Agitation within 24 hours: RR = 1.04; 95% CI, 0.42 to 2.58 (2 RCTs)
Headache within 24 hours: RR = 1.16; 95% CI, 0.62 to 2.18 (2 RCTs)
Vomiting within 24 hours: RR = 2.04; 95% CI, 0.19 to 21.82 (1 RCT)
Aripiprazole versus olanzapine
At least 1 adverse effect: RR = 0.75; 95% CI, 0.45 to 1.24 (1 RCT)
Somnolence during 24 hours: RR = 0.25; 95% CI, 0.08 to 0.82 (1 RCT)
Statistically significant at P < 0.05
Rigidity within 24 hours: RR = 1.33; 95% CI, 0.32 to 5.58 (1 RCT)
Tremor within 24 hours: RR = 1.50; 95% CI, 0.26 to 8.50 (1 RCT)
Akathisia at 2 hours: MD = −0.05; 95% CI, −0.26 to 0.16 (1 RCT)
Akathisia at 24 hours: MD = −0.03; 95% CI, −0.29 to 0.23 (1 RCT)
Headache: RR = 2.00; 95% CI, 0.19 to 21.18 (1 RCT)
Nausea: RR = 3.00; 95% CI, 0.13 to 71.51 (1 RCT)
Pain at injection site: RR = 2.67; 95% CI, 0.76 to 9.33 (1 RCT)
Authors’ Conclusion
“The available evidence is of poor quality but there is some evidence aripiprazole is effective compared to placebo and haloperidol, but not when compared to olanzapine. However, considering that evidence comes from only three studies, caution is required in generalizing these results to real-world practice. This review firmly highlights the need for more high-quality trials on intramuscular aripiprazole in the management of people with acute aggression or agitation.” (p. 2)17
“In this review, the superiority of aripiprazole in comparison to placebo but not haloperidol is reported. Concerning the last comparison, people allocated to aripiprazole required more injections, a potentially complex issue to manage in an acute real world setting; whilst experiencing nausea was more common to participants in the aripiprazole group, haloperidol tended to cause more extrapyramidal symptoms side effects. Olanzapine was found to be more effective than aripiprazole, and tended to cause more somnolence side effects. Evidence is limited by the small number of trials available. Further good-quality research is needed to confirm these results and to provide missing but clinically relevant outcomes, as well as to compare aripiprazole with other atypical antipsychotics.” (p. 34)17
Kousgaard et al. (2017)15
Main Study Findings
Improvement in Aggression or Agitation Scale:
Lorazepam 2 mg similar to haloperidol 5 mg (2 studies)
Lorazepam 2 mg inferior to olanzapine 10 mg (1 study)
Haloperidol 5 mg + lorazepam 2 mg superior to olanzapine 10 mg (1 study)
Haloperidol 5 mg + lorazepam 4 mg superior to haloperidol 5 mg > lorazepam 4 mg (1 study)
Haloperidol 5 mg + lorazepam 2 mg superior to haloperidol 5 mg > lorazepam 2 mg (1 study)
Lorazepam 2 mg inferior to haloperidol 5 mg + lorazepam 2 mg (1 study)
Midazolam 5 mg superior to haloperidol 5 mg (1 study)
Midazolam 5 mg superior to droperidol 5 mg superior to ziprasidone 20 mg (1 study)
Haloperidol 2.5 mg + midazolam 7.5 mg superior to haloperidol 2.5 mg + promethazine 25 mg superior to ziprasidone 10 mg superior to olanzapine 10 mg (1 study)
Duration of violence/aggression
Droperidol 5 mg + midazolam 5 mg similar to midazolam 10 mg similar to droperidol 10 mg (1 study)
Time to sedation
Midazolam 7.5 mg to 15 mg superior to haloperidol 5 mg to 10 mg + promethazine 35 mg to 50 mg (1 study)
Lorazepam 2 mg similar to midazolam 5 mg superior to haloperidol 5 mg (1 study)
Midazolam versus haloperidol statistically significant at P < 0.05
Proportion sedated
Lorazepam 4 mg inferior to haloperidol 10 mg + promethazine 20 mg to 50 mg (1 study)
Authors’ Conclusion
“In summary, based on our review, it is unclear whether lorazepam IM or midazolam IM is as efficacious as an antipsychotic IM. It is a bit more certain that the combination of 1 of these benzodiazepines IM and a low dose typical antipsychotic IM is more efficacious than the benzodiazepine and the antipsychotic given as monotherapy. However, there is no doubt that the benzodiazepines are less likely to be associated with treatment emergent side effects, as compared to antipsychotic drugs. Translating this into clinical practice, a benzodiazepine IM should be chosen ahead of an antipsychotic IM, at least ahead of a typical antipsychotic. Addition of benzodiazepine treatment in patients already treated with antipsychotic drugs, who experience acute agitation, is also supported by the results in the current review.” (p. 134)15
Summary of Findings of Included Primary Clinical Studies
Chan et al. (2021)18
Main Study Findings
Median time to sedation:
Midazolam: 8.5 minutes (95% CI, 8.5 to 59.5),
Olanzapine: 11.5 minutes (95% CI, 7.5 to 67.0)
Haloperidol: 23.0 minutes (95% CI, 6.0 to 53.5)
Proportion adequately sedated 10 minutes after the initial dose:
Midazolam: 52%
Olanzapine: 34%
Haloperidol: 21%
Proportion adequately sedated 20 minutes after the initial dose:
Midazolam: 79%
Olanzapine: 60%
Haloperidol: 41%
Proportion adequately sedated 30 minutes after the initial dose:
Midazolam: 91%
Olanzapine: 74%
Haloperidol: 63%
Proportion adequately sedated 45 minutes after the initial dose:
Midazolam: 91%
Olanzapine: 81%
Haloperidol: 82%
Proportion adequately sedated 60 minutes after the initial dose:
Midazolam: 98%
Olanzapine: 87%
Haloperidol: 97%
The proportion of patients sedated by time Kaplan-Meier curves:
Significant differences were detected in the Kaplan-Meier curves for midazolam compared with olanzapine (P = 0.03) and haloperidol (P = 0.002); however, this was not observed for haloperidol compared with olanzapine (P = 0.78).
Administered second dose of study medication
Midazolam: 23%
Olanzapine: 28%
Haloperidol: 32%
(P = 0.61)
Administered alternative sedatives
Midazolam: 16%
Olanzapine: 11%
Haloperidol: 12%
(P = 0.72)
Length of stay
Midazolam: 4.52 hours (95% CI, 2.63 to 8.69)
Olanzapine: 4.01 hours (95% CI, 2.31 to 6.42)
Haloperidol: 4.02 hours (95% CI, 2.32 to 6.87)
(P = 0.73)
Adverse effects (oxygen desaturation, dry mouth, dystonia, cardiac arrest):
Midazolam: 4%
Olanzapine: 6%
Haloperidol: 5%
(P = 0.91)
QT prolongation
Midazolam: 23%
Olanzapine: 17%
Haloperidol: 23%
(P = 0.59)
Fell asleep after treatment
Midazolam: 50%
Olanzapine: 19%
Haloperidol: 30%
(P < 0.01)
Authors’ Conclusion
“Our study indicates that intramuscular midazolam was more effective at 5-10 mg doses compared with olanzapine or haloperidol for acute agitation in ED settings, regardless of aetiology. Intramuscular midazolam’s faster sedation time may deem it preferable as an initial sedation agent. Intramuscular midazolam, olanzapine, and haloperidol effectively sedated ED patients with acute agitation within 60 min. Although adverse event rates did not differ significantly, the potential risk of extrapyramidal side effects for haloperidol should be noted.
Given the potential risk of adverse events, intramuscular midazolam or olanzapine should be considered over haloperidol for undifferentiated acute agitation in EDs. As this study includes only 3 of the most commonly prescribed sedatives in a local setting, further investigation to compare other sedatives is warranted.” (p. 7)18
Dib et al. (2021)19
Main Study Findings
Haloperidol 5 mg + promethazine 25 mg (HP) versus haloperidol 5 mg + promethazine 25 mg + chlorpromazine 100 mg (HPC)
Number of patients calm
20 minutes: RR = 0.84 (95% CI, 0.47 to 1.50)
40 minutes: RR = 0.66 (95% CI, 0.49 to 0.90)
60 minutes: RR = 0.84 (95% CI, 0.69 to 1.03)
120 minutes: RR = 0.81 (95% CI, 0.66 to 0.98) — reported in the study text as “the difference was gone”
Authors’ Conclusion
“TREC-Lebanon suggests that addition of chlorpromazine adds little to the potent, safe and well-researched combination of HP.” (p. 6)19
Martel et al. (2021)20
Main Study Findings
Proportion adequately sedated at 15 minutes:
Droperidol was most effective with 64% of patients sedated, compared to 25%, 35%, and 29% for ziprasidone (10 mg), ziprasidone (20 mg), and lorazepam, respectively
Difference in proportion adequately sedated at 15 minutes:
Droperidol versus lorazepam: 33 (95% CI, 8 to 58)
Droperidol versus 10 mg of ziprasidone: 39 (95% CI, 14 to 64)
Droperidol versus 20 mg of ziprasidone: 29 (95% CI, 3 to 54)
10 mg of ziprasidone versus lorazepam: −6 (95% CI, −29 to 17)
10 mg of ziprasidone versus 20 mg of ziprasidone: −10 (95% CI, −34 to 13)
20 mg of ziprasidone versus lorazepam: 4 (95% CI, −19 to 28)
Difference in reduction in median AMSS from baseline to 15 minutes:
Droperidol versus lorazepam: 2 (95% CI, 0 to 3)
Droperidol versus ziprasidone (10 mg): 1 (95% CI, 0 to 2)
Droperidol versus ziprasidone (20 mg): 1 (95% CI, 0 to 2)
Ziprasidone (10 mg) versus lorazepam: 1 (95% CI, −1 to 1)
Ziprasidone (10 mg) versus ziprasidone (20 mg): 0 (95% CI, −1 to 1)
20 mg of ziprasidone versus lorazepam: 0 (95% CI, −1 to 0)
Adverse events:
Respiratory depression
Droperidol: 12%
Ziprasidone (10 mg): 36%
Ziprasidone (20 mg): 39%
Lorazepam: 48%
(P = 0.04)
One patient who received ziprasidone (20 mg) had persistent agitation. One patient receiving droperidol experienced atrial flutter. Two patients experienced dystonia, 1 who received droperidol and 1 who received ziprasidone (20 mg).
QTc durations were similar in all groups (P = 0.52).
Authors’ Conclusion
“Droperidol was more effective for sedation and was associated with fewer episodes of respiratory depression than lorazepam or either dose of ziprasidone.” (p. 432)20
Cole et al. (2021)21
Main Study Findings
Time to adequate sedation, median (IQR)
Droperidol: 16 minutes (10 to 30)
Olanzapine: 17.5 minutes (10 to 31)
Time to sedation, Cox proportional hazard model
Droperidol versus olanzapine 1.12 (95% CI, 1.00 to 1.25)
Proportion of patients adequately sedated before 15 minutes
Droperidol: 38%
Olanzapine: 42%
Absolute difference: –4% (95% CI, –9% to 2%)
Nadir AMSS scores
Droperidol (median AMSS score –2)
Olanzapine (median AMSS score –3)
Change in median AMSS score from baseline to 15 minutes, median (IQR) droperidol 2 (1 to 3) olanzapine 2 (1 to 3)
Proportion requiring additional medication for agitation
Droperidol: 17%
Olanzapine: 24%
Absolute difference: –8% (95% CI, –12% to –3%)
Time until first rescue medication given, median (IQR), min Droperidol 36 (20 to 60) olanzapine 37 (22 to 64)
Total time in the emergency department, median (IQR)
Olanzapine: 444 minutes (349 to 543)
Droperidol: 500 minutes (391 to 631)
Median difference: −59 minutes (95% CI, –78 to –40 minutes).
Adverse events
Respiratory AE occurred in 4% of patients with droperidol and 7% of olanzapine
Extrapyramidal AEs were more common with droperidol (n = 6; 1%) than olanzapine (n = 1).
Authors’ Conclusion
Despite a number of limitations that may affect external validity of the results such as the study design and the fact that patients largely had agitation secondary to alcohol intoxication, the data suggest both olanzapine and droperidol are effective medications for acute agitation in the emergency department. The advantages of droperidol include fewer total injections, which could improve safety for both patients and caregivers, and a shorter length of stay. These advantages are countered by an increased risk of extrapyramidal adverse effects with droperidol.
Klein et al. (2019)22
Main Study Findings
Rescue sedation required at 1 hour: n (%; 95% CI):
Droperidol: 547 (11%; 10% to 12%)
Olanzapine: 988 (11%; 10% to 12%)
Haloperidol: 390 (18%; 17% to 20%)
Rescue sedation: during entire ED encounter n (%; 95% CI):
Droperidol: 832 (17%; 16% to 18%)
Olanzapine: 1,665 (19%; 18% to 20%)
Haloperidol: 390 (26%; 24% to 28%)
Difference in proportion of patients receiving rescue sedation (95% CI):
Droperidol versus olanzapine: 0% (−1 to 1%)
Droperidol versus haloperidol: −7% (−9 to −5%)
Olanzapine versus haloperidol: −7% (−9 to −5%)
Authors’ Conclusion
“At 1 h, droperidol and olanzapine resulted in the lowest rates of rescue medication administration (11% for each) compared with haloperidol (18%). Adverse events were relatively uncommon. Our findings support that olanzapine and droperidol may be more effective than haloperidol for achieving adequate sedation in agitated patients.” (p. 488)22
Klein et al. (2018)23
Main Study Findings
Time to adequate sedation, median (IQR), min:
Midazolam: 12 (19 to 22)
Olanzapine: 14 (10 to 28)
Ziprasidone: 17 (13 to 30)
Haloperidol 5 mg: 20 (15 to 32)
Haloperidol 10 mg: 19 (13 to 31)
Rescue medications entire encounter, n (%)
Midazolam: 52 (40)
Olanzapine 34 (21)
Ziprasidone: 35 (24)
Haloperidol 5 mg: 50 (33)
Haloperidol 10 mg: 30 (20)
Time in emergency department, median (IQR), min
Midazolam: 423 (364 to 554)
Olanzapine: 429 (351 to 598)
Ziprasidone: 454 (374 to 581)
Haloperidol 5 mg: 405 (299 to 504)
Haloperidol 10 mg: 443 (335 to 554)
Difference in proportion adequately sedated, % (95% CI)
Midazolam versus olanzapine: 9 (–1 to 20)
Midazolam versus ziprasidone: 18 (6 to 29)
Midazolam versus haloperidol 5 mg: 30 (19 to 41)
Midazolam versus haloperidol 10 mg: 28 (17 to 39)
Olanzapine versus ziprasidone: 8 (–3 to 19)
Olanzapine versus haloperidol 5 mg: 20 (10 to 31)
Olanzapine versus haloperidol 10 mg: 18 (7 to 29)
Ziprasidone versus haloperidol 5 mg: 12 (1 to 23)
Ziprasidone versus haloperidol 10 mg: 10 (0 to 21)
Haloperidol 10 mg versus haloperidol 5 mg: 2 (–9 to 13)
Change in median AMSS from baseline to 15 minutes (95% CI):
Midazolam versus olanzapine: –1 (–1 to 0)
Midazolam versus ziprasidone: –1 (–0.5 to 0.5)
Midazolam versus haloperidol 5 mg: –2 (–2.5 to –1.5)
Midazolam versus haloperidol 10 mg: –2 (–2.5 to –1.5)
Olanzapine versus ziprasidone: 0 (–0.5 to 0.5)
Olanzapine versus haloperidol 5 mg: –1 (–1.5 to –1)
Olanzapine versus haloperidol 10 mg: –1 (–1.5 to –0.5)
Ziprasidone versus haloperidol 5 mg: –1 (–1.5 to –0.5)
Ziprasidone versus haloperidol 10 mg: –1 (–1.5 to –0.5)
Haloperidol 10 mg versus haloperidol 5 mg: 0 (–0.5 to 0.5)
Authors’ Conclusion
“…treatment of acute agitation with intramuscular midazolam resulted in a greater proportion of patients adequately sedated at 15 minutes and greater median reduction in Altered Mental Status Scale scores at 15 minutes compared with haloperidol, ziprasidone, and olanzapine, although the comparison with olanzapine was not significant. Olanzapine resulted in more effective sedation than haloperidol. Similar adverse event profiles were observed for each treatment.” (p. 384)23
Real Juarez et al. (2016)24
Main Study Findings
Overall (mean ± SD)
PANSS-EC basal
IM Haloperidol 5 mg: 27.3 (5.35)
IM Haloperidol 10 mg: 31.8 (3.15)
IM Olanzapine: 29.2 (2.9)
PANSS-EC 30 minutes
IM Haloperidol 5 mg: 23.8 (8.42)
IM Haloperidol 10 mg: 24.72 (4.06)
IM Olanzapine: 21.6 (5.49)
PANSS-EC 60 minutes
IM Haloperidol 5 mg: 18.0 (7.81)
IM Haloperidol 10 mg: 17.5 (3.45)
IM Olanzapine: 17.4 (5.36)
PANSS-EC 90 minutes
IM Haloperidol 5 mg: 14.27 (5.68)
IM Haloperidol 10 mg: 14.25 (2.09)
IM Olanzapine: 14.27 (4.11)
PANSS-EC 120 minutes
IM Haloperidol 5 mg: 12.73 (5.27)
IM Haloperidol 10 mg: 12.78 (2.06)
IM Olanzapine: 12.80 (3.45)
Moderate agitation (mean)
PANSS-EC basal
IM Haloperidol 5 mg: 22
IM Haloperidol 10 mg: 28
IM Olanzapine: 27
PANSS-EC 30 minutes
IM Haloperidol 5 mg: 16
IM Haloperidol 10 mg: 21
IM Olanzapine: 21
PANSS-EC 60 minutes
IM Haloperidol 5 mg: 13
IM Haloperidol 10 mg: 14
IM Olanzapine: 14.5
PANSS-EC 90 minutes
IM Haloperidol 5 mg: 10
IM Haloperidol 10 mg: 12
IM Olanzapine: 12.5
PANSS-EC 120 minutes
IM Haloperidol 5 mg: 9
IM Haloperidol 10 mg: 11
IM Olanzapine: 12
Severe Agitation (mean)
PANSS-EC basal
IM Haloperidol 5 mg: 32
IM Haloperidol 10 mg: 34
IM Olanzapine: 31
PANSS-EC 30 minutes
IM Haloperidol 5 mg: 26
IM Haloperidol 10 mg: 27
IM Olanzapine: 24.5
PANSS-EC 60 minutes
IM Haloperidol 5 mg: 18
IM Haloperidol 10 mg: 19
IM Olanzapine: 21
PANSS-EC 90 minutes
IM Haloperidol 5 mg: 12
IM Haloperidol 10 mg: 15
IM Olanzapine: 16.5
PANSS-EC 120 minutes
IM Haloperidol 5 mg: 11
IM Haloperidol 10 mg: 13
IM Olanzapine: 13.5
Authors’ Conclusion
The authors concluded that there is no difference in the effectiveness of these antipsychotic drugs for rapid tranquilization of patients with agitation.
Summary of Recommendations in Included Guideline
Patel et al. (2018)1
Recommendations
The treatment algorithm provided in the guideline includes both fundamental principles and interventions (pre-rapid tranquilization, rapid tranquilization, and considerations for nonresponse). The interventions are organized in a linear stepwise manner considering that there is an increased likelihood of requiring a later-stage interventional category, if earlier and generally less restrictive interventions have been tried and not had the desired outcome, the clinical state is worsening, the risks are increasing, or patient engagement is challenging.
For rapid tranquilization intramuscular monotherapy, the guideline recommends:
IM lorazepam OR
IM promethazine OR
One of IM aripiprazole, IM droperidol, IM olanzapine
For rapid tranquilization intramuscular combinations, the guideline recommends:
IM promethazine + IM haloperidol OR
IM lorazepam + IM haloperidol
Quality of Evidence and Strength of Recommendations
Category of evidence:
Ia: Evidence from meta-analysis of RCTs
Ib: Evidence from at least 1 RCT
IIa: Evidence from at least 1 controlled study without randomization
IIb: Evidence from at least 1 other type of quasi-experimental study
III: Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies and case-control studies
IV: Evidence from expert committee reports or opinions and/or clinical experience of respected authorities
Strength of recommendation:
A: Based on category I evidence
B: Based on category II evidence, or extrapolated a recommendation from category I evidence
C: Based on category III evidence or extrapolated recommendation from category I or II evidence
D: Based on category IV evidence or extrapolated recommendation from category I, II, or III evidence
S: Standard of practice
IM monotherapy:
IM lorazepam is effective (Ib; A).
Parenteral benzodiazepines have safety concerns due the risk of respiratory depression. Thus, wherever they are used, flumazenil must be immediately available (S).
IM promethazine may be effective (extrapolated Ia; D)
IM aripiprazole is effective (Ia; A).
IM droperidol is effective and a baseline electrocardiogram (ECG) is advised before use due to the risk of QTc prolongation (Ib; A).
IM olanzapine is effective, but it should only be administered by itself and not concurrently with IM benzodiazepines due to risk of hypotension; thus, there should be an interval of at least 1 hour between the 2 (Ia; A).
IM clonazepam is not recommended due to a relative lack of supporting evidence for use in rapid tranquilization (S).
IM diazepam is not recommended due to lack of evidence for use in rapid tranquilization (S).
IM midazolam is not recommended due to the risk of respiratory depression (Ia; A).
IM haloperidol is not recommended as monotherapy even though it has evidence of effectiveness, and a baseline ECG is advised, as measures need to be in place to offset its adverse effects and especially for the risk of acute dystonia (Ia; A).
IM levomepromazine is not recommended, even though it has some evidence of effectiveness, as there is potential evidence for a risk of cardiovascular adverse effects, especially hypotension (III; C).
Rapid tranquilization IM monotherapy should be considered before rapid tranquilization IM combinations (S).
IM combinations:
IM promethazine plus IM haloperidol is effective and a baseline ECG is advised before haloperidol use due to the risk of QTc prolongation (Ia; A).
IM lorazepam plus IM haloperidol is effective and a baseline ECG is advised before haloperidol use due to the risk of QTc prolongation (Ia; A).
Parenteral benzodiazepines have safety concerns due the risk of respiratory depression. Thus, wherever they are used, flumazenil must be immediately available (S).
IM lorazepam plus IM promethazine is not recommended due to lack of evidence for efficacy for this combination (S).
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 8: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Muir-Cochrane et al. (2021)13 | Paris et al. (2021)16 | Schneider et al. (2020)14 | Ostinelli et al. (2018)17 | Kousgaard et al. (2017)15 |
Alexander J, et al. Br J Psychiatry 2004;185:63–69 | Yes | No | No | No | Yes |
Andrezina R, et al. Psychopharmacology 2006;188(3):281–92 | No | Yes | No | Yes | No |
Baldacara L, et al. Braz J Psychiatry. 2011;33:30–9 | Yes | No | Yes | No | No |
Battaglia J, et al. Am J Emerg Med. 1997;15:335–40. | No | No | Yes | No | Yes |
Bieniek SA, et al. Pharmacotherapy 1998;18:57–62 | Yes | No | No | No | Yes |
Breier A et al. Arch. Gen. Psychiatry 2002;59 (5), 441–448. | No | Yes | No | No | No |
Bristol-Myers Squibb. http://www.clinicalstudyresults.org/ 2005 | No | No | No | Yes | No |
Chan HY et al. J Clin Psychopharmacol. 2014 Jun;34(3):355-8 | No | Yes | No | No | No |
Daniel DG, et al. Psychopharmacology 2001;155 (2), 128–134 | No | Yes | No | No | No |
Dorevitch A, et al. Am J Psychiatry 1999;156:142-4 | Yes | No | No | No | No |
Foster S, et al. Int Clin Psychopharmacol 1997; 12: 175–179 | No | No | No | No | Yes |
Garza-Trevino ES, et al. Am J Psychiatry 1989; 146: 1598–1601 | No | No | No | No | Yes |
Huang CLC, et al. J Formos Med Assoc 2015; 114: 438–445 | No | No | No | No | Yes |
Huf G, et al. BMJ 2003; 27:708–713 | Yes | No | No | No | Yes |
Huf G, et al. BMJ 2007;335:869 | Yes | No | No | No | No |
Isbister GK, et al. Ann Emerg Med. 2010;56:392–401 | No | No | Yes | No | Yes |
Isbister GK, et al. Ann Emerg Med. 2017;69(3):337-9 | Yes | No | No | No | No |
Katagiri H, et al. BMC psychiatry 2013;13 (1), 230 | No | Yes | No | No | No |
Kittipeerachon M, et al. Schizophrenia Research 2016;176(2-3):231–8 | No | Yes | No | Yes | No |
Lesem MD, et al. The Journal of clinical psychiatry 2001;62 (1), 12–18. | No | Yes | No | No | No |
Mantovani C, et al. J Clin Psychopharmacol. 2013;33:306–12. | Yes | No | Yes | No | Yes |
Martel M, et al. Acad Emerg Med. 2005;12:1167–72. | Yes | No | Yes | No | Yes |
Meehan K, et al. J Clin Psychopharmacol 2001;21:389–397 | No | No | No | No | Yes |
Nobay F, et al. Acad Emerg Med 2004; 11: 744–749 | Yes | No | No | No | Yes |
Ono 2009a | No | Yes | No | No | No |
Raveendran NS, et al. BMJ (Clinical research Ed.) 2007;335 (7625), 865 | Yes | No | Yes | No | No |
Salzman C, et al. J Clin Psychiatry 1991; 52: 177–180 | No | No | No | No | Yes |
Tran-Johnson TK, et al. 2007 J Clin Psychiatry 68: 111–119. | No | Yes | No | No | No |
Veser FH, et al. J Psychiatr Pract 2006; 12: 103–108 | No | No | No | No | Yes |
Wright, P, et al. AJP 2001;158 (7), 1149–1151 | No | Yes | No | No | No |
Wyant M, et al. Psychopharmacol Bull 1990;26:126–129 | No | No | No | No | Yes |
aFull citation not provided in review (Paris et al. [2021]).
Appendix 6: References of Potential Interest
Previous CADTH Reports
1.Use of antipsychotics and/or benzodiazepines as rapid tranquilization in in-patients of mental facilities and emergency departments: a review of the clinical effectiveness and guidelines. Rapid response report: summary with critical appraisal. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/pdf/htis/oct-2015/RC0718%20Antipsychotics%20for%20rapid%20tranq%20Final.pdf. Accessed 2021 Jul 16
Review Articles
2.Ostinelli EG, Brooke-Powney MJ, Li X, Adams CE. Haloperidol for psychosis-induced aggression or agitation (rapid tranquillisation). Cochrane Database Syst Rev. 2017 07 31;7(7):CD009377.
Additional References
3.National Collaborating Centre for Mental Health. Violence and aggression: short-term management in mental health, health and community settings. NICE guideline N10. Updated edition. Leicester (UK): British Psychological Society; 2015: https://www.nice.org.uk/guidance/ng10/evidence/full-guideline-70830253. Accessed 2021 Jul 12
4.Roppolo LP, Morris DW, Khan F, et al. Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation). J Am Coll Emerg Physicians Open. 2020 Oct;1(5):898-907. PubMed
5.Vieta E, Garriga M, Cardete L, et al. Protocol for the management of psychiatric patients with psychomotor agitation. BMC Psychiatry. 2017 Sep 8;17(1):328. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca