CADTH Health Technology Review
Vitamin D Supplementation for the Prevention of Falls and Fractures in Residents of Long-Term Care Facilities: A 2021 Update
Rapid Review
Authors: Srabani Banerjee, Holly Gunn, Carolyn Spry
Abbreviations
Ca
calcium
LTC
long-term care
RCT
randomized controlled trial
SR
systematic review
Key Messages
The relevant publications identified comprised 1 overview of systematic reviews and 2 systematic reviews.
There is a suggestion that for seniors living in long-term care facilities, compared to control, vitamin D supplementation, with or without calcium, may reduce the rate of falls and fractures; however, the reductions were not always statistically significant.
There were no statistically significant differences in the number of seniors who fell with vitamin D supplementation, with or without calcium, compared with control groups.
Findings need to be interpreted with caution, considering the limitations such as primary studies of variable quality (critically low to moderate) and lack of clarity with respect to the type of long-term care setting.
No cost-effectiveness studies regarding vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in long-term care facilities were identified.
No evidence-based guidelines regarding vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in long-term care facilities were identified.
Context and Policy Issues
Among seniors (i.e., the elderly population older than 65 years of age), falls and the associated complications are a serious problem.1 It impacts the individual, their family, and society. Falls may result in pain, fracture, functional impairment, disability, and death. During 2015‒2016, it was estimated that 11.9% of adults older than 40 years of age were living with diagnosed osteoporosis.2 Characteristics of osteoporosis include reduction in bone mass and fragmentation of the bone structure.3 The prevalence of osteoporosis increases with age. Seniors generally have osteoporosis, which makes them prone to the risk of fractures resulting from falls.3,4 Among the seniors in Canada, it has been estimated that the annual rate of falls will be 30% for those living in the community and 50% for those living in long-term care (LTC) facilities.1 Hence, preventive measures to maintain bone health and reduce falls are important.
Vitamin D plays an important role for maintenance of musculoskeletal health.3 Low vitamin D has been associated with bone loss and muscle weakness.3 Sunlight helps in vitamin D production. It has been reported that endogenous vitamin D production in persons aged older than 65 years is 25% of that in persons in the age range of 20 to 30 years, when exposed to the same amount of sunlight.4 In seniors, supplementation may be necessary to increase levels of vitamin D. There appears to be uncertainty with respect to the effectiveness of vitamin D supplementation in reducing falls and fractures in seniors living in LTC facilities.3,5
A previous 2019 CADTH report assessed the use of vitamin D supplementation for the prevention of falls and fractures in residents of LTC facilities.6 According to this report, moderate-quality evidence suggested that, for older adults, vitamin D supplementation may reduce the rate of falls but not the number of individuals who fall. Additionally, according to the report, vitamin D supplementation appeared to be less costly and more effective than no treatment; and the identified guidelines recommended standard dose (at least 1,000 IU daily) vitamin D supplementation and cautioned that high dose (more than 4,000 IU daily) resulted in higher fall rates than standard dose. This current report is an update and will review the evidence available since the publication of the 2019 CADTH report.6 It will summarize the evidence regarding the clinical effectiveness and cost-effectiveness of vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in LTCs; and also summarize the evidence-based guidelines regarding vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in LTC facilities.
Research Questions
What is the clinical effectiveness of vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in long-term care facilities?
What is the cost-effectiveness of vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in long-term care facilities?
What are the evidence-based guidelines regarding vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in long-term care facilities?
Methods
Literature Search Methods
The literature search strategy used in this report is an update of 1 developed for a previous CADTH report.6 For the current report, a limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, Canadian and major international health technology agencies, as well as a focused internet search. No filters were applied to limit the retrieval by study type. The initial search was limited to English-language documents published between January 1, 2014 and March 29, 2019. For the current report, database searches were rerun on June 8, 2021 to capture any articles published since the initial search date. The search of major health technology agencies was also updated to include documents published since March 29, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Studies reporting on residential dwelling were included if they were distinguished from community dwelling. Also, studies reporting on health-care dwelling or institutions were included if further descriptions were not presented to indicate these settings were not LTC facilities. Studies where the average age of the population was reported as 65 years or older were included.
Criteria | Description |
Population | Seniors (i.e., aged 65 years and older) residing in LTC facilities |
Intervention | Vitamin D supplementation in any formulation and dose, with or without calcium supplementation |
Comparator | Q1 and Q2: No vitamin D supplementation; different dosing of vitamin D Q3: Not applicable |
Outcomes | Q1: Effectiveness (e.g., falls reduction, fracture reduction); safety (e.g., adverse events or adverse health outcomes related to supplementation) Q2: Cost-effectiveness for preventing falls and fractures Q3: Recommendations regarding the prevention of falls and fractures (e.g., optimal use of vitamin D supplementation, optimal vitamin D supplementation, optimal dosing, who should and should not be supplemented) |
Study designs | HTAs, SRs, RCTs, economic evaluations, and evidence-based guidelines |
HTA = health technology assessment; LTC = long-term care; Q = question; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2019. Studies on individuals living in the community or on hospitalized patients were excluded. Studies on a combination of settings that did not present results separately for individuals living in LTC or similar facilities were excluded. Studies assessing the dietary intake of vitamin D were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using, as guidance, the A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)7 tool for systematic reviews. Summary scores were not calculated for the included publications; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
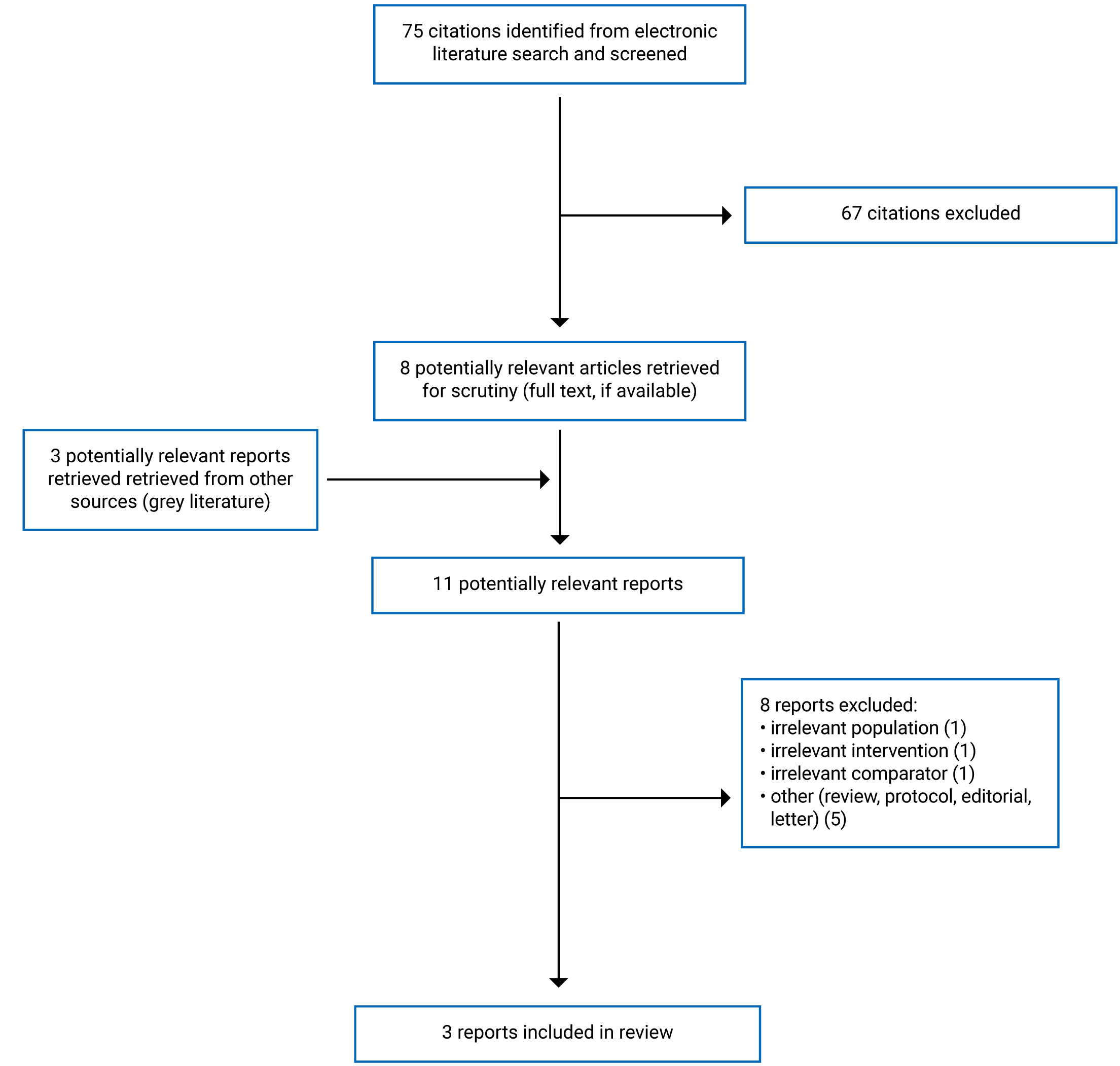
A total of 75 citations were identified in the literature search. Following the screening of titles and abstracts, 67 citations were excluded and 8 potentially relevant reports from the electronic search were retrieved for full-text review. Three potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 11 potentially relevant articles, 8 publications were excluded for various reasons and 3 publications met the inclusion criteria and were included in this report. These comprised 1 overview of systematic reviews (SRs)5 and 2 SRs.3,8 No economic evaluations or evidence-based guidelines were identified. Appendix 1 presents the PRISMA9 flow chart of the study selection.
Summary of Study Characteristics
One relevant overview of SRs5 and 2 relevant SRs3,8 were identified. The overview of SRs5 will henceforth be referred to simply as an overview. The overview and 2 SRs had broader inclusion criteria than the present review. Specifically, all 3 publications3,5,8 included studies involving individuals living in LTC facilities (i.e., residential dwellings, health-care dwellings, or institutions) in addition to those living in the community. Of note, as residential dwellings were distinguished from community dwellings, and no further details were provided, we considered residential dwellings as LTC facilities. Only the characteristics and results of the subset of relevant studies will be described in this report. The characteristics of the studies are described herein and details are presented in Appendix 2.
There was some overlap in the relevant studies included in the SR; it should therefore be noted that the findings from the SRs are not exclusive, as some primary studies were included in both SRs. A table depicting the degree of overlap in relevant primary studies is presented in Appendix 5.
Study Design
The overview by Chakhtoura et al.5 was published in 2020, the literature search period was up to August 2017, and alerts were set up for 2018. It included 6 relevant SRs published between 2012 and 2018, and narratively summarized the included SRs. The SR by Thanapluetiwong et al.8 was published in 2020 and the literature search period was up to January 2019. It included 14 relevant randomized controlled trials (RCTs) published between 1992 and 2017. The SR by Yao et al.3 was published in 2019 and the literature search period was up to December 31, 2018. It included 4 relevant RCTs published between 1992 and 2006. Both SRs included meta-analyses.
Country of Origin
The first author of the overview5 was from Lebanon; the first author of each SR was from Thailand8 and the UK, respectively.3 The countries for the primary studies included in the SRs that were included in the overview5 were not reported. The included RCTs in the 2 SRs3,8 were from Australia, Europe, and North America, with the majority being from Europe.
Patient Population
The overview and SRs included elderly individuals living in settings described as institutions3,5 and residential dwellings or health-care dwellings.8 In the overview by Chakhtoura et al.5 with 6 relevant SRs, the number of patients ranged from 2,013 to 6,186 (5 SRs) and was not reported for 1 SR, the age was older than 60 years, both sexes were included, and the proportions of females and males were not reported. In the SR by Thanapluetiwong et al.8 for the 14 relevant RCTs, the total number of individuals was 6,854 (range: 122 to 3,270), the ages of the individuals were 80 years and older (8 RCTs) and younger than 80 years (6 RCTs), and comprised 100% females (6 RCTs) or both sexes with proportions not specified (8 RCTs). In the SR by Yao et al.3 for the 4 relevant RCTs the total number of individuals was 8,714 (range 583 to 3,717), the mean ages of the individuals were between 84 years and 85 years, and the percentage of females ranged from 75% to 100% females.
Interventions and Comparators
In the overview by Chakhtoura et al.,5 the interventions and comparators included vitamin D versus control or placebo and vitamin D plus calcium (Ca) versus control or placebo; the authors seemed to use the terms placebo and control interchangeably. In the SR by Thanapluetiwong et al.,8 the intervention and comparators included vitamin D with or without Ca versus control and the type of control was not specified. In the SR by Yao et al.,3 the interventions and comparators included vitamin D with or without Ca versus control (i.e., placebo or no treatment).
The doses of vitamin D ranged from 100 IU/day to 2,285 IU/day. The doses of Ca ranged from 360 mg to 2,000 mg.
Outcomes
Outcomes included falls,5,8 hip fractures,3,5 and any fractures.3,5,8 For the included primary studies in the overview and SRs, the trial durations were from 1 month to 84 months,5 12 months or less or more than 12 months,8 and from 10 months to 24 months.3
Summary of Critical Appraisal
An overview of the critical appraisal of the included SRs is summarized herein. Additional details regarding the strengths and limitations of included SRs are provided in Appendix 3.
In the overview5 and the 2 SRs,3,8 the objective was clearly presented, the inclusion criteria were stated, multiple databases were searched, a list of included studies was presented, and author conflicts of interest were declared and were unlikely to result in bias. The list of excluded studies was presented in 1 SR3 but not in the other SR8 or overview.5 For both the SRs,3,8 the methods for the conducting of the SR were established a priori (i.e., the protocols were registered with PROSPERO the International Prospective Register of Systematic Reviews). For the overview,5 it was unclear if the methods had been established a priori; hence, the potential for bias cannot be ruled out. The flow chart for the article selection was presented in the 2 SRs3,8 but not in the overview.5 Article selection was done in duplicate in 2 publications3,8 but was unclear in 1 publication5; therefore, the potential for error in the latter SR cannot be ruled out. In all 3 publications,3,5,8 the characteristics of the included studies were described; however, details about the settings were lacking and were generally described as “institutions,” “residential dwelling,” or “health-care dwelling.” Hence, it was difficult to ascertain if all the included settings were specifically LTC facilities or if other types of settings were also included in those categories; in which case, the findings would not be solely for LTC facilities. In the 2 SRs,3,8 meta-analyses were appropriately conducted. In all 3 publications, the qualities of the included studies were assessed and were reported by review authors to be variable, ranging from critically low to moderate and this may therefore impact the validity of the findings. In 2 SRs,3,8 the publication bias was assessed and there was suggestion of publication bias. In the overview,5 the publication bias does not appear to have been assessed; therefore, it is unclear if there is a potential for bias.
Summary of Findings
Main findings from the included overview5 and SRs3,8 are presented herein. Additional details of the main findings of the overview and SR authors’ conclusions are presented in Appendix 4.
Clinical Effectiveness of Vitamin D Supplementation
The outcomes reported in the identified relevant publications were risk of falls,5,8 number of fallers,5 and fractures;3,5,8 the reported quality of evidence was variable. In the overview,5 the quality of evidence was reported by the authors to be critically low to moderate. In the SR by Yao et al.,3 the authors considered the overall risk of bias to be high. In the SR by Thanapluetiwong et al.,8 the authors reported the quality of the studies to be generally fair.
Falls
In the overview by Chakhtoura et al.5 for seniors living in institutions, there was a statistically significant reduction in the rate of falls with vitamin D supplementation with and without Ca compared to controls in 2 SRs included in the overview, and the between-group differences were not statistically significant in 2 SRs included in the overview. There were no statistically significant between-group differences with respect to the number of fallers with vitamin D supplementation with or without Ca compared to controls (placebo, Ca, or sometimes reported simply as control) based on findings from 3 SRs included in the overview.5
In the SR by Thanapluetiwong et al.8 for seniors living in health care dwellings, there was a statistically significant reduction in the rate of falls with vitamin D compared to control; whereas for those living in residential dwellings, there was no statistically significant between-group difference in the rate of falls.
Fractures
The overview5 reported on seniors living in institutions. The authors found there was a statistically significant between-group difference in the risk of hip fracture with vitamin D plus Ca compared to control or placebo, favouring vitamin D plus Ca (2 SRs). With respect to the risk of any fracture, 1 SR reported a statistically significant decrease in the risk of any fracture with vitamin D plus Ca compared to control or placebo and 1 SR reported no statistically significant difference with vitamin D compared to control.
The SR by Yao et al.3 also reported on seniors living in institutions. They found that the risk of hip fracture and the risk of any fracture were statistically significantly reduced with vitamin D plus Ca compared to control; however, for vitamin D compared to control, there were no statistically significant between-group differences in the risk of hip fracture or any fracture.
The SR by Thanapluetiwong et al.8 reported on seniors living in residential dwellings and health-care dwellings. They found that for both settings, the risk of fracture was statistically significantly reduced with vitamin D compared to control.
Cost-Effectiveness of Vitamin D Supplementation
No cost-effectiveness studies regarding vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in LTC facilities were identified.
Guidelines for Vitamin D Supplementation
No evidence-based guidelines regarding vitamin D supplementation for the prevention of falls and fractures in elderly patients residing in LTC facilities were identified.
Limitations
Studies involving residential dwellings, health-care dwellings, or institutionalized living have been included in this report. However, as details of these living facilities were not presented, it was difficult to ascertain if they were specifically LTC facilities for seniors; hence, it is possible that other types of facilities besides LTC facilities for seniors may also have been included in these categories (such as a possibility of hospitals being included as health-care dwellings and prisons being included in institutionalized living). In these other types of facilities, the dose and administration of vitamin D and the characteristics of the populations may be different from that in LTC facilities. The findings may therefore not exclusively reflect outcomes in seniors living in LTC facilities. Considering there was wide variation in the vitamin D doses examined in the primary studies and that no recent evidence-based guidelines on vitamin D supplementation were identified, it is difficult to comment on the implementation of vitamin D supplementation. There was some overlap in the primary studies included in the 2 SRs3,8 (i.e., a couple of studies were included in the meta-analyses of both these SRs); hence, findings were not exclusive. Additionally, for the SRs included in the overview,5 it was unclear which primary studies were included. Therefore, it is possible that some of the primary studies that were included in the 2 SRs3,8 may have also been included in the overview, in which case the findings of the overview would not be exclusive. As none of the publications reported on adverse events, the status of adverse events with interventions using vitamin D supplementation is unclear.
The generalizability of the findings to the Canadian context is unclear, as none of the studies (for which countries where the study was conducted were available) was conducted in Canada. However, since many of the primary studies were conducted in Europe, the LTC facilities may not be very different and so less likely to be an issue.
The included primary studies in the identified reviews were reported to be of variable quality (critically low to fair or moderate) by review authors, which could impact the validity of the findings.
Conclusions and Implications for Decision- or Policy-Making
One overview5 and 2 SRs3,8 were identified that reported on the clinical effectiveness of vitamin D supplementation with or without Ca compared to control, placebo, or no treatment for the prevention of falls and fractures in seniors residing in LTC facilities (institutions, residential dwellings, and health-care dwellings).
For vitamin D with or without Ca in comparison to control, results for the rate of falls in seniors in LTC settings were mixed; some reviews reported a statistically significant reduction in the rate of falls for seniors in institutional living (findings from 2 SRs included in 1 overview)5 or health care dwellings (1 SR),8 while others reported that the between-group differences were not statistically significant for seniors in institutional living (2 SRs included in 1 overview)5 or residential dwellings (1 SR).8 There were no statistically significant differences in the number of fallers with vitamin D supplementation (with or without Ca) compared to control (1 overview).5
For vitamin D plus Ca compared with control or placebo, there was a statistically significant reduction in the rate of hip fractures (1 overview and 1 SR).3,5 However, for vitamin D alone compared with control or placebo, there was no statistically significant between-group difference in the rate of hip fracture (1 SR).3 For vitamin D compared with control or placebo, results for the rate of any fracture in seniors in LTC settings were mixed; there was a statistically significant reduction in the rate of any fracture for residential dwelling or health care dwelling living (1 SR)8 and no statistically significant between-group difference for institutional living (1 overview and 1 SR).3,5
The findings from this current report were generally similar to the findings reported in the previous 2019 CADTH report,6 with some exceptions. In this current report, the findings regarding the reduction in the rate of falls with vitamin D supplementation compared to control were mixed, being statistically significant or not statistically significant based on 1 overview5 and 1 SR,8 whereas in the 2019 CADTH report,6 the rate of falls was statistically significantly reduced with vitamin D supplementation compared to control based on 1 SR. This difference in findings across CADTH reports is likely because of the included overview,5 for which multiple databases had been searched and in which the search period was different (2012 to 2018), and because the search included several SRs.
To better understand the role of vitamin D supplementation in reducing falls and fractures in seniors, further research is needed to determine definitively the subsets of seniors (such as living in specific LTC settings, age groups, ethnicity, and comorbidities) that are likely to benefit the most and which vitamin D doses are likely to be beneficial.
References
1.Cameron EJ, Bowles SK, Marshall EG, Andrew MK. Falls and long-term care: a report from the care by design observational cohort study. BMC Fam Pract. 2018;19(1):73. PubMed
2.Osteoporosis and related fractures in Canada: report from the Canadian Chronic Disease Surveillance System. Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/osteoporosis-related-fractures-2020/osteoporosis-related-fractures-2020.pdf?bcs-agent-scanner=d75da743-ac16-844e-8d7e-f80680a4f841. Accessed 2021 Jun 8.
3.Yao P, Bennett D, Mafham M, et al. Vitamin D and calcium for the prevention of fracture: a systematic review and meta-analysis. JAMA Network Open. 2019;2(12):e1917789-e1917789. PubMed
4.Hill TR, Aspray TJ. The role of vitamin D in maintaining bone health in older people. Ther Adv Musculoskelet Dis. 2017;9(4):89-95. PubMed
5.Chakhtoura M, Chamoun N, Rahme M, Fuleihan GE. Impact of vitamin D supplementation on falls and fractures-a critical appraisal of the quality of the evidence and an overview of the available guidelines. Bone. 2020;131:115112. PubMed
6.Tran K, Butcher R. Vitamin D supplementation for the prevention of falls and fractures in residents of long-term care facilities: a review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Apr: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1105%20Vit%20D%20in%20LTC%20Final.pdf. Accessed 2021 Jun 9.
7.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
8.Thanapluetiwong S, Chewcharat A, Takkavatakarn K, Praditpornsilpa K, Eiam-Ong S, Susantitaphong P. Vitamin D supplement on prevention of fall and fracture: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2020;99(34):e21506. PubMed
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Chakhtoura et al. (2020),5 Lebanon. Funding: partly supported by Fogarty International Center and Office of Dietary Supplements of the National Institute of Health. | Overview of SRs Total = 13 SRs. Relevant studies for this report = 6 SRs (published between 2012 and 2018; countries for the first authors of each SR were not reported). Inclusion criteria: SRs, MAs, RCTs and guidelines;a intervention: vitamin D supplementation; outcomes: fall and fracture; English articles published between 2012 and 2018. Exclusion criteria: SRs on patients with chronic diseases. Aim: to assess the beneficial effect of vitamin D supplementation on falls and fractures | Individuals living in long-term care facilities (institutions). Number of RCTs (in the 6 included SRs) ranged from 2 to 6, and the number of individuals ranged from 2,013 to 6,186 for 5 SRs and was not reported for 1 SR. Age: more than 60 years Both sexes. % Female: NR | Interventions and comparators: vit-D, vit-D2, or vit-D3 vs. control or placebo; vit-D3 + Ca vs. Ca; or vit-D + Ca vs. control or placebo. Doses of vit-D, vit-D2 or vit-D3 ranged from 100 IU/day to 2,285 IU/day. Doses of Ca ranged from 360 mg to 2000 mg. | Outcomes: fall and fracture (hip and any) Trial duration range: 1 month to 84 months |
Thanapleutiwong et al. (2020),8 Thailand. Funding: supported by the Research Unit for Metabolic Bone Disease in CKD patients, Faculty of Medicine, Chulalongkom University, Bangkok, Thailand. | SR with meta-analyses. Total studies = 47 RCTs. Relevant RCTs = 14 (7 on residential dwelling group, and 7 on health care dwelling group; 11 from Europe, 2 from Australia, and 1 from North America) published between 1992 and 2017. Setting types = 3 Relevant settings = 2 (residential and health care dwellings) Inclusion criteria: RCTs; no restrictions on sample size, study duration or language Exclusion criteria: not specified Aim: to assess the effect of vitamin D supplementation on fall and fracture for patients living in different settings. | Residential dwelling group (7 RCTs). Patient number = 5,487 (range: 122 to 3270). Age: ≥ 80 years (4 RCTs), < 80 years (3 RCTs). Sex: all females (4 RCTs), both females and males (3 RCTs). Health care dwelling group (7 RCTs). Patient number = 1,358 (range: 150 to 492). Age: ≥ 80 years (4 RCTs), < 80 years (3 RCTs). Sex: all females (2 RCTs), both females and males (5 RCTs). | Residential dwelling group (7 RCTs). Intervention: Vitamin D dose (IU), D3 (400, 800, or 1000) daily; or D2 (200, 400, 600, or 800) daily. With Ca (4 RCTs), without Ca (3 RCTs). Control: not described Health care dwelling group (7 RCTs). Intervention: Vitamin D dose (IU), D3 (400 or 800 daily; 800 mixed frequency; or 900,000 non-daily D2 (300,000 mixed frequency). With calcium (6 RCTs), without calcium (1 RCT). Control: not described D3 = cholecalciferol, D2 = ergocalciferol. | Outcomes: Fall, and fracture Primary study duration: For residential dwelling group, > 12 months (4 RCTs), ≤ 12 months (3 RCTs) For health care dwelling group, > 12 months (1 RCT) ≤ 12 months (6 RCTs) |
Yao et al. (2019),3 UK. Funding: Dr. Yao was supported by a Sino-British Fellowship Trust scholarship. | SR with meta-analyses. Total studies = 28 (RCT and observational). Relevant studies = 4 RCTs (setting: living in institution) published between 1992 and 2006. Countries where the RCTs were conducted were not reported. Setting types = 2. Relevant setting = 1 (institution) Inclusion criteria: RCTs (on vit-D, including at least 500 participants and reporting at least 10 fracture events) and observational studies (on vit-D and reporting at least 200 fracture events), English-language articles. Exclusion criteria: not explicitly stated. Aim: to assess the effect of vit-D on the risk of fracture | Individuals living in institutions. Patient number = 8,714 (range: 583 to 3717) Mean age (years) (range): 84 to 85. % Female (range): 75% to 100% | Intervention (vit-D with or without Ca) vs control (placebo or no treatment): 1100 IU/d vit-D vs. placebo (1 RCT); 400 IU/d vit-D vs. no treatment (1 RCT); 800 IU/d vit-D + 1200 Ca mg/d vs. placebo (2 RCTs) | Outcomes: fracture (hip or any) Duration: 10 months to 2 years |
Ca = calcium; RCT = randomized controlled trial; SR = systematic review; vit-D = vitamin D, vit-D2 = vitamin D2; vit-D3 = vitamin D3.
aOf note, none of the included guidelines in the overview were relevant for the current report and hence are not discussed here.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Systematic Reviews AMSTAR 27
Strengths | Limitations |
Chakhtoura et al., 2020,5 Lebanon. | |
The objective was clearly stated Multiple databases (MEDLINE, PubMed, and Embase), were searched from inception to August 2017. Pre-set alerts were used to identify SRs published in 2018. A list of included studies was provided Quality assessments of the included SRs were done by 2 reviewers using AMSTAR. Quality ranged from critically low to moderate. Characteristics of the SRs were described It was mentioned that the authors had no conflicts of interest. | Details of study selection were lacking, and a flow chart of study selection was not presented. A list of excluded studies was not provided Unclear if article selection was done by 2 reviewers Unclear if data extraction was done by 2 reviewers Unclear if publication bias was examined Details of the settings were not presented Unclear if overlap in the primary studies between the included SRs were assessed. Hence unclear if the findings from the individual systematic reviews were exclusive. |
Thanapleutiwong et al., 2020,8 Thailand. | |
The objective was clearly stated Multiple databases were searched, MEDLINE from 1990 to January 2019, and also Embase and Cochrane Central Register of Controlled Trials. Study selection was described, and a flow chart was presented A list of included studies was provided Article selection was done by 2 reviewers Quality assessment was conducted using the Jadad scale. Study quality was variable (majority being fair and a few being good) Characteristics of the study were described Meta-analysis was appropriately conducted. Publication bias was assessed using the Funnel plot and Egger’s test and the author’s reported there was potential for publication bias. The authors declared that there were no conflicts of interest. | A list of excluded studies was not provided It was unclear if data extraction was done in duplicate Details of the settings were not presented |
Yao et al., 2019,3 UK. | |
The objective was clearly stated Multiple databases (PubMed, Embase, Cochrane Central register of Controlled Trials, and ClinicalTrials.gov) were searched up to 31 December 2018. Study selection was described, and a flow chart was presented A list of included studies was provided. A list of excluded studies was provided. Data extraction was done independently by 2 reviewers. Quality assessment was conducted using the Cochrane risk of bias tool; overall risk of bias was high. Characteristics of the included studies were presented. Meta-analysis was appropriately conducted. Publication bias was assessed using the Funnel plot; asymmetry suggested possibility of publication bias. Conflicts of interest were declared, and it was reported that 1 author received a grant from the UK Medical Research Council. This is less likely to introduce bias. | Unclear if article selection was done in duplicate Details of the settings were not presented |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; SR = systematic review
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Summary of Findings Included Systematic Reviews
Main study findings
Chakhtoura et al., 2020,5 Lebanon
Overview of Systematic Reviews (SR)s
Results presented here pertain to seniors living in institutions.
Outcome: Falls
SR by Bolland et al., 2014; (quality = critically low).
No statistically significant between groups difference in the number of fallers for vitamin D (vit-D) compared with control, or vit-D + calcium (Ca) compared with control; (6 trials, N = 2,013).
SR by Cameron et al., 2018; (quality = moderate).
Risk reduction in falls with vit-D compared to control: 28%; statistically significant, P = NR; (4 trials, N = 4,580); with vit-D versus placebo, risk ratio (RR) (95% confidence interval [CI]) = 0.72 (0.55; 0.95), I2 = 62%.
No statistically significant between groups difference in the number of fallers for vit-D compared with control; (4 trials, N = 4,580); with vit-D versus placebo, RR (95% CI) = 0.92 (0.76 to 1.12), I2 = 42%.
SR by Cameron et al., 2012; (quality = low.)
Risk reduction in falls with vit-D3 + Ca compared to Ca: 29%; statistically significant, P = NR, and not statistically significant between groups difference in risk reduction in falls with vit-D2 compared to placebo; (4 trials, N = 4,580).
For vit-D3 + Ca versus Ca, for falls, RR (95% CI) = 0.71 (0.56 to 0.90), I2 = 0%, (2 studies).
For vit-D2 versus usual care or placebo, for falls, RR (95% CI) = 0.55 (0.19 to 1.64), I2 = 80%, (2 studies).
No statistically significant between groups difference in the number of fallers with vit-D3 + Ca compared to Ca, or vit-D2 + Ca compared to placebo; (6 trials, N = 6,186);
For vit-D3 + Ca versus Ca, for number of fallers, RR (95% CI) = 0.85 (0.69 to 1.05), I2 = 0%, (2 studies).
For vit-D2 versus usual care or placebo, for number of fallers, RR (95% CI) = 0.80 (0.38 to 1.71), I2 = 58%, (2 studies).
SR by Guo et al., 2014; (quality = critically low).
No statistically significant between groups difference in the rate of falls for vit-D compared with control, or vit-D + Ca compared with control; (6 trials, N = 4,934).
For vit-D versus control, for rate of falls, odds ratio (OR) (95% CI) = 0.98 (0.79 to 1.22), I2 = NA (4 trials).
For vit-D + Ca versus control, for rate of falls, OR 0.71 (0.45 to 1.12), I2 = NA (2 trials).
Outcome: fracture
SR by Avenell et al., 2014; (quality = moderate).
Risk reduction in hip fractures with vit-D + Ca compared to control or placebo: 25%; statistically significant, P = NR; (2 trials, N = 3,853).
Risk reduction in any fractures with vit-D + Ca compared to control or placebo: 13%; statistically significant, P = NR; (2 trials, N = 3,853).
For vit-D + Ca versus placebo, for vertebral fracture, RR (95% CI) = 0.89 (0.74 to 1.09), I2 = 0% (4 trials).
SR by Cameron et al., 2018; (quality = moderate).
No statistically significant between groups difference in the risk of any fractures for vit-D compared with control; (3 trials, N = 4,464).
SR by Weaver et al., 2016; (quality = critically low).
Risk reduction in hip fractures with vit-D + Ca compared to placebo: 29%; statistically significant, P = NR; (numbers of trials and individuals not reported [NR]).
Author’s conclusion
“While the effect on falls is inconsistent, CaD reduces the risk of fracture (hip and any fracture), as shown in meta-analyses pooling data of studies combining institutionalized and community individuals. The evidence is however limited by major shortcomings and heterogeneity. (p. 1 of 12)”5
(Note: this overview had broader inclusion criteria than the current report)
Thanapleutiwong et al., 2020,8 Thailand
Main study findings
Results (from meta-analyses) presented here pertain to residential dwelling and health-care dwelling
Outcome: Falls (vit-D compared to control)
For residential dwelling, RR (95% CI) = 0.957 (0.884 to 1.037); (10 study arms, 5562 individuals); statistically not significant; heterogeneity, I2 = 14%.
For health-care dwelling, RR (95% CI) = 0.717 (0.558 to 0.921); (8 study arms, 1600 individuals), statistically significant; heterogeneity I2 = 56%.
Outcome: Fracture (vit-D compared to control)
For residential dwelling, RR (95% CI) = 0.782 (0.665 to 0.919); (3 study arms, 4478 individuals), statistically significant; heterogeneity, I2 = 0%.
For health-care dwelling dwelling, RR (95% CI) = 0.517 (0.286 to 0.935); (6 study arms, 1293 individuals), statistically significant; heterogeneity, I2 = 0%.
Author’s conclusion
“The use of vitamin D supplement, especially vitamin D3 could reduce incidence of fall. Only vitamin D with calcium supplement showed benefit in fracture reduction. (p. 1 of 12)”8
(Note: this overview had broader inclusion criteria than the current report and included community dwelling besides residential dwelling, and health-care dwelling.)
Yao et al., 2019,3 UK
Main study findings
Results (from meta-analyses) presented here pertain to seniors living in institutions.
Outcome: fracture (vit-D or vit-D + Ca compared to control (placebo or no treatment)
Risk of hip fracture with vit-D compared to control, RR (95% CI) = 1.09 (0.88 to 1.35), (3 RCTs, 6301 individuals); between-group difference not statistically significant.
Risk of any fracture with vit-D compared to control, RR (95% CI) = 0.99 (0.85 to 1.17), (3 RCTs, 6301 individuals); between-group difference not statistically significant.
Risk of hip fracture with vit-D + Ca compared to control, RR (95% CI) = 0.69 (0.53 to 0.90), (2 RCTs, 3853 individuals); between-group difference statistically significant, favouring vit-D + Ca.
Risk of any fracture with vit-D + Ca compared to, RR (95% CI) = 0.76 (0.62 to 0.92), (2 RCTs, 3853 individuals) between-group difference statistically significant, favouring vit-D + Ca.
Author’s conclusion
“In this systematic review and meta-analysis, neither intermittent nor daily dosing with standard doses of vitamin D alone was associated with reduced risk of fracture, but daily supplementation with both vitamin D and calcium was a more promising strategy. (p. 2 of 14)”3
(Note: this overview had broader inclusion criteria than the current report and included institutionalized as well as non-institutionalized individuals.)
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 4: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Thanapluetiwong et al. 2020,8 Thailand | Yao et al. 2019,3 UK |
Berggren et al., Osteoporos Int 2008;19:801–9. | Yes | NA |
Bischoff et al., J Bone Miner Res 2003;18:343–51. | Yes | NA |
Bischoff-Ferrari et al., Osteoporos Int 2006;17:656–63. | Yes | NA |
Broe et al., J Am Geriatr Soc 2007;55:234–9. | Yes | NA |
Burleigh et al., Age Aging 2007;36:507–13. | Yes | NA |
Chapuy et al., Osteoporos Int 2002;13:257–64. | Yes | Yes |
Chapuy et al., NEngl J Med 1992;327:1637–42. | Yes | Yes |
Flicker et al., J Am Geriatr Soc 2005;53:1881–8. | Yes | NA |
Graafmans et al., Am J Epidemiol; 1996;143:1129–36. | Yes | NA |
Harwood et al., Age Aging 2004;33:45–51. | Yes | NA |
Latham et al., J Am Geriatr Soc 2003;51:291–9. | Yes | NA |
Law et al., Age Aging. 2006;35(5):482-486. | NA | Yes |
Meyer et al., J Bone Miner Res. 2002;17(4):709-715. | NA | Yes |
Neelemaat et al., J Am Geriatr Soc 2012;60:691–9. | Yes | NA |
Schwetz et al., Osteoporos Int 2017;28:3347–54. | Yes | NA |
Uusi-Rasi et al., JAMA Intern Med 2015;175:703–11. | Yes | NA |
NA = not applicable.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca