CADTH Health Technology Review
Vitamin D Supplementation for the Prevention and/or Treatment of Cardiovascular Disease, Cancer, and Other Conditions in Residents of Long-Term Care Facilities
Rapid Review
Authors: Keeley Farrell, Jennifer Horton
Abbreviations
AHRQ
Agency for Healthcare Research and Quality
CI
confidence interval
CVD
cardiovascular disease
GDS
Geriatric Depression Scale (short form, 15 questions)
OR
odds ratio
RCT
randomized controlled trial
WAIS-RC
Wechsler Adult Intelligence Scale-Revised
Key Messages
The results of 1 systematic review suggest that supplementation with vitamin D may provide some benefit for cancer-related mortality in older adults. It is unclear whether there is a benefit of vitamin D supplementation for all-cause mortality; however, no benefit was found for cardiovascular disease mortality, cardiovascular disease events, or cancer incidence.
There is limited and mixed evidence on the effectiveness of vitamin D supplementation for dementia and mild cognitive impairment in older adults.
The results of 1 systematic review suggest that vitamin D supplementation may provide protection against acute respiratory infections in the overall population; however, this result was not significant in the subgroup of patients older than 65 years.
No evidence-based guidelines were identified regarding vitamin D supplementation for the prevention and/or treatment of cardiovascular disease, cancer, and other conditions in elderly patients residing in long-term care facilities.
Context and Policy Issues
Low levels of vitamin D are common in older adults and associated with a variety of negative health outcomes.1 Studies have found associations between low levels of vitamin D and mortality — all-cause and cardiovascular disease (CVD) —2,3 and type 2 diabetes,1 dementia,4 cancer,5 heart failure,6 and respiratory tract infections.7 Since low levels of vitamin D are reversible, vitamin D supplementation may have a potential role in the prevention and/or treatment of conditions associated with low levels of vitamin D.
The main function of vitamin D is to enhance the intestinal absorption of calcium and phosphorous.7 Vitamin D can be obtained from dietary sources and is also produced by the skin after exposure to UV light.8 Vitamin D deficiency can result from reduced sunlight exposure or a limited dietary intake of vitamin D. Aging reduces the skin’s ability to produce vitamin D.9 When exposed to the same amount of sunlight, the capacity of the skin to produce vitamin D in adults aged 65 years has been estimated to be about 25% of that as compared to adults aged 20 to 30 years.10 This may be a contributing factor to the low levels of vitamin D that are commonly seen in older adults.
In Canada, more than 90% of long-term care residents were found to consume amounts of vitamins D, E, K, magnesium, and potassium below the estimated average requirement/adequate intake.11 Vitamin D supplements were shown to resolve inadequate intakes for 50% to 70% of participants.11 Vitamin D has an established role in bone health8 and vitamin D supplementation is recommended to prevent fractures in long-term care residents.12 However, the role of vitamin D supplementation in the prevention and/or treatment of other conditions in long-term care residents remains unclear. A summary of the available literature could help decision-makers to determine the appropriate use of vitamin D supplementation in long-term care facilities.
This report is part of a series of 3 CADTH reports on the use of vitamin D supplementation in residents of long-term care facilities. One of the reports aimed to summarize the effectiveness and guidelines of vitamin D supplementation for the prevention and/or treatment of COVID-19 in long-term care residents.13 The other report is an update to a 2019 CADTH report on the clinical effectiveness, cost-effectiveness, and evidence-based guidelines on the use of vitamin D supplementation for the prevention of falls and fractures in long-term care residents.14 The aim of the current report is to summarize the evidence regarding the clinical effectiveness and evidence-based guidelines of vitamin D supplementation for the prevention and/or treatment of CVD, cancer, and other conditions in elderly patients residing in long-term care facilities.
Research Questions
What is the clinical effectiveness of vitamin D supplementation for the prevention and/or treatment of cardiovascular disease, cancer, and other conditions in elderly patients residing in long-term care facilities?
What are the evidence-based guidelines regarding vitamin D supplementation for the prevention and/or treatment of cardiovascular disease, cancer, and other conditions in elderly patients residing in long-term care facilities?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were vitamin D and long-term care. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016 and June 8, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients (i.e., aged 65 years and older) residing in long-term care facilities |
Intervention | Vitamin D supplementation in any formulation and dose, with or without calcium supplementation |
Comparator | Q1: No vitamin D supplementation, different dosing of vitamin D, placebo Q2: Not applicable |
Outcomes | Q1: Effectiveness and safety for the prevention and/or treatment of cardiovascular disease, cancer, and other conditions Q2: Recommendations regarding the prevention and/or treatment of cardiovascular disease, cancer, and other conditions (e.g., optimal use of vitamin D supplementation, optimal vitamin D supplementation, optimal dosing, who should and should not be supplemented) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2016. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Studies where the average population age was younger than 65 years were excluded. Studies assessing the dietary intake of vitamin D from food sources (e.g., oily fish, red meat, liver)15 were excluded. Studies that only included outcomes pertaining to falls and fracture prevention, and coronavirus disease (COVID-19), were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)16 for systematic reviews and the Downs and Black checklist17 for randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
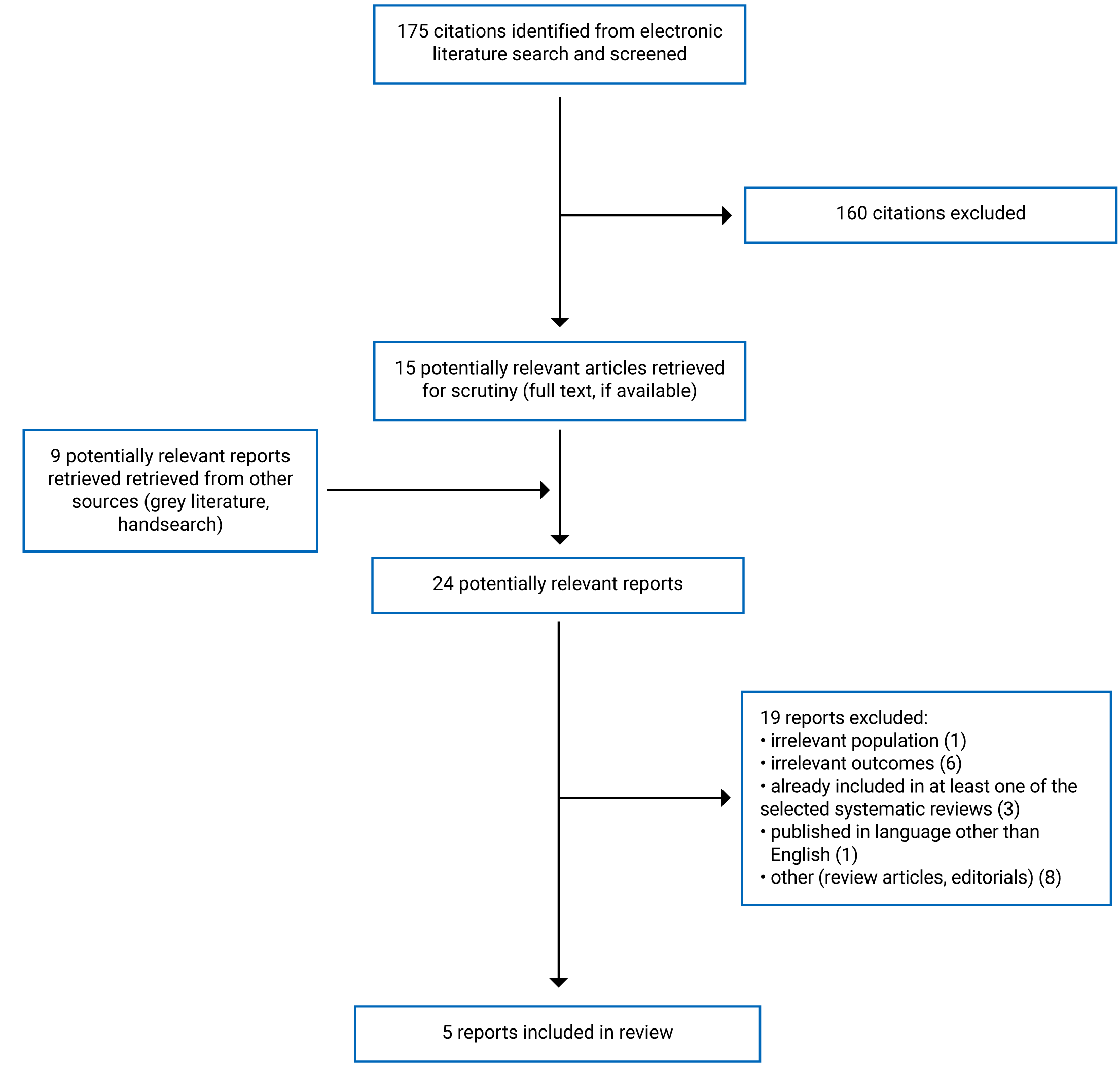
A total of 175 citations were identified in the literature search. Following screening of titles and abstracts, 160 citations were excluded and 15 potentially relevant reports from the electronic search were retrieved for full-text review. Nine potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 19 publications were excluded for various reasons and 5 publications met the inclusion criteria for question 1 and were included in this report. These comprised 3 systematic reviews and 2 randomized controlled trials (RCTs). Appendix 1 presents the PRISMA18 flow chart of the study selection. Additional references of potential interest are provided in Appendix 6.
No evidence-based guidelines regarding vitamin D supplementation for the prevention and/or treatment of CVD, cancer, and other conditions in elderly patients residing in long-term care facilities were identified.
Summary of Study Characteristics
All 319-21 included systematic reviews had broader inclusion criteria than the current review. Specifically, 2 of the systematic reviews19,21 included studies in adults of any age and 1 of the systematic reviews20 included studies in children and adults of any age. Additionally, 1 of the systematic reviews19 included studies of supplementation with any multivitamin/mineral (defined as 3 or more vitamins, minerals, or combinations of both), single nutrient, or functionally related nutrient pair; and 1 systematic review21 included studies of any intervention to prevent, delay, or slow age-related cognitive decline, mild cognitive impairment, and clinical Alzheimer-type dementia. Only the characteristics and results of the subset of relevant studies will be described in this report.
Two RCTs were identified that evaluated the clinical effectiveness of supplementation with vitamin D in older adults. The study by Yang et al. (2020)22 assessed cognitive function in older adults with mild cognitive impairment. The study by Alavi et al. (2019)23 assessed depression in older adults.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Of the 3 systematic reviews19-21 included in this report, 219,20 conducted meta-analyses.
The search time frame in the Agency for Healthcare Research and Quality (AHRQ) (2021)19 review was between January 2013 and August 28, 2020. Studies included in a previous US Preventive Services Task Force review on the same topic were also eligible. Seventy-eight trials met the inclusion criteria and 38 were relevant to the present review (35 RCTs and 3 cohort studies). Thirty RCTs were included in the meta-analysis. The 3 cohort studies, as well as RCTs that only reported harms outcomes, were not included in the meta-analysis. One included RCT overlaps with the Martineau et al. (2019)20 review. However, the 2 systematic reviews assessed different outcomes. A table depicting the overlap between primary studies in the included systematic reviews is provided in Appendix 5. Only primary studies that provide direct evidence relevant to this review were included in the overlap table.
The search time frame in Martineau et al. (2019)20 was anything published up to and including December 31, 2015. Twenty-seven RCTs met the inclusion criteria. Of these studies, 25 included acute respiratory infections outcomes and 11 were relevant to the present review. Individual patient data were obtained for all 25 studies and combined in the meta-analysis.
The search time frame in the AHRQ (2017)21 review was between January 2009 and September 2016. There were 263 trials that met the inclusion criteria, 1 of which is an RCT that is relevant to the present review. The results of this RCT were described narratively in the AHRQ (2017)21 review.
Two primary studies22,23 that evaluated the clinical effectiveness of supplementation with vitamin D in older adults were identified, both of which were RCTs.
Country of Origin
Two of the included systematic reviews were authored by researchers in the US19,21 and 1 was from the UK.20
The RCTs were conducted in China22 and Iran.23
Patient Population
AHRQ (2021)19 included community-dwelling adults without chronic disease. The subgroup relevant to the present review included 390,565 participants. The weighted average age was 66 years and 75% of participants were female.
Martineau et al. (2019)20 included participants of any age; however, the subgroup relevant to the present review included 1,232 adults older than 65 years. Summary characteristics for the subgroup of interest were not provided.
The relevant RCT in AHRQ (2017)21 included 4,143 women with normal cognition and with a mean age of 71 years.
Yang et al. (2020)22 included 183 participants aged 65 years or older with mild cognitive impairment who were not living in a nursing home. The mean age of participants was 67.22 years in the vitamin D group and 66.59 years in the placebo group. Participants were 46% and 43% male in the vitamin D and placebo groups, respectively.
Alavi et al. (2019)23 included 78 participants older than 60 years of age, with moderate to severe depression (defined as a score higher than 5 on the Geriatric Depression Scale). The mean age of participants was 68.7 years in the vitamin D group and 67 years in the placebo group. Participants were 49% and 51% female in the vitamin D and placebo groups, respectively.
Interventions and Comparators
AHRQ (2021)19 included studies with doses of vitamin D ranging from 20 to 5,000 IU per day that were administered from 1 month to 7 years. Some of the studies also included calcium, with doses ranging from 93 to 2,000 mg per day. Comparators included placebo, no intervention, and usual diet.
All studies included in the Martineau et al. (2019)20 meta-analysis administered vitamin D3 at a range of doses dispensed either daily, weekly, monthly, or every 3 months, for a duration from 7 weeks to 1.5 years. Comparators included placebo or supplementation with vitamin D at a different dose than the intervention.
In the relevant RCT included in the AHRQ (2017) review,21 the intervention group received supplementation with 400 IU vitamin D and 1,000 mg calcium daily for 8 years and the control group received placebo.
The interventions for both RCTs were vitamin D3 and the comparators were matched placebo.22,23 The intervention groups received 800 IU vitamin D3 daily for 12 months and 50,000 units of vitamin D3 weekly for 8 weeks in the Yang et al. (2020)22 and Alavi et al. (2019)23 trials, respectively.
Outcomes
AHRQ (2021)19 assessed cancer outcomes (cancer incidence, cancer-related mortality), cardiovascular outcomes (CVD incidence, CVD events, CVD-related mortality), all-cause mortality, and adverse events. Cancer incidence included any cancer or site-specific cancer. CVD incidence included coronary heart, peripheral artery, and cerebrovascular disease. CVD events included myocardial infarction and ischemic and hemorrhagic stroke.
Incidence of acute respiratory infection was assessed for the relevant subgroup in Martineau et al. (2019).20 Acute respiratory infections included upper and lower respiratory tract infections, as well as acute respiratory infections of unclassified location.
In the relevant RCT included in AHRQ (2017),21 incident probable dementia or mild cognitive impairment (reported as 1 pooled outcome) and cognitive performance were measured. Cognitive performance was measured using a variety of cognitive tests including the Mini-Mental State Examination, Digit Span Forward and Backward, California Verbal Learning Test, and the Benton Visual Retention Test.
Yang et al. (2020)22 assessed cognitive function using the Wechsler Adult Intelligence Scale-Revised (WAIS-RC) and full-scale intelligence quotient tests, which were administered by trained psychologists. The WAIS-RC contains 11 subtests including information, digit span, vocabulary, arithmetic, comprehension, similarity, picture completion, block design, object assembly, digit symbol, and picture arrangement. In both the WAIS-RC and the full-scale intelligence quotient tests, higher scores indicate better cognitive function.
Alavi et al. (2019)23 assessed depression using the short form Geriatric Depression Scale-15 (GDS-15). GDS-15 contains 15 dichotomous items and scores can range from 0 to 15. A score higher than 5 indicates mild to moderate depression and a score higher than 10 indicates severe depression. The study also assessed adverse events.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
All the included reviews had a clear research objective.19-21 The review methods for Martineau et al. (2019)20 were established a priori and the protocol was registered. For the other 2 reviews, it was unclear which components of the research methods were established a priori.19,21 This could introduce bias if methods were adjusted after the systematic review had begun. All of the included reviews had a comprehensive literature search strategy and described the methods in detail.19-21 Study selection was performed by at least 2 investigators in all the reviews. Performing study selection in duplicate helps to decrease the risk of bias in study selection. In both AHRQ (2021)19 and AHRQ (2017),21 data extraction was not performed in duplicate. However, a second reviewer checked data for accuracy. In all the reviews, the risk of bias was assessed independently by 2 reviewers using appropriate techniques.19-21 Both AHRQ (2021)19 and AHRQ (2017)21 provided a list of excluded studies and justifications; however, Martineau et al. (2019)20 did not. An unjustified exclusion of studies could bias the results of the review. Both systematic reviews that performed meta-analysis19,20 used appropriate methods. AHRQ (2021)19 used appropriate methods for the pooling of results, excluded studies at high risk of bias from the review, and assessed heterogeneity. Martineau et al. (2019)20 combined individual participant data from the included studies, performed a sensitivity analysis that excluded studies assessed to have an unclear risk of bias, and performed pre-specified subgroup analyses to explore heterogeneity and effect modification. Of the 2 systematic reviews that performed meta-analysis,19,20 only Martineau et al. (2019)20 discussed their investigation of publication bias. In AHRQ (2021),19 there is a risk of false-positive findings because of chance as a result of multiple analyses performed for each outcome. The sources of funding for all of the systematic reviews were reported; however, the sources of funding for the individual studies included in the reviews were not.19-21
Randomized Controlled Trials
In both studies,22,23 the objectives, outcomes, patient characteristics, interventions, and main findings were clearly described. However, adverse events were not reported in Yang et al. (2020).22 There were only a small number of participants lost to follow-up in both studies. Participants in Yang et al. (2020)22 were selected via multi-stage cluster random sampling. The recruitment method for participants in Alavi et al. (2019)23 was not described and therefore it is unclear whether the study sample is representative of the source population. In both studies, patients and researchers were blind to treatment allocation until the analyses were complete. Treatment compliance was assessed using medication counts in both studies,22,23 as well as self-reporting in Yang et al. (2020).22 The main outcome measures in both studies were valid and reliable. Participants were allocated to treatment groups based on a computer-generated randomization sequence in Yang et al. (2020)22 and computer-generated random numbers in Alavi et al. (2019).23 A power calculation was conducted a priori to determine the sample size in Alavi et al. (2019).23 However, it is unclear if this was done in Yang et al. (2020).22 There appears to be some imbalances in baseline characteristics between treatment groups in both studies.22,23 This could threaten the internal validity of the studies if the populations are systematically different between the treatment groups. In Yang et al. (2020),22 potential confounders were not discussed or adjusted for in the analyses. In Alavi et al. (2019),23 there was no description of the distribution of some confounders mentioned by the authors (i.e., severity of depression, depression treatment, sun exposure) between the treatment groups. There may be a risk of bias in the results of both studies because of the lack of adequate adjustment for confounding. In Yang et al. (2020),22 all analyses were conducted for the intention-to-treat population. However, in Alavi et al. (2019),23 the 2 participants lost to follow-up were not analyzed. As there was only 1 participant lost to follow-up in each group in Alavi et al. (2019),23 this may not have biased the results of the study.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Vitamin D Supplementation
As mentioned in the Study Design section of this report, there was 1 RCT that overlapped between the AHRQ (2021)19 and Martineau et al. (2019)20 systematic reviews. Although this study was included in both reviews, the outcomes reported did not overlap. A citation matrix depicting the overlap between the included systematic reviews is provided in Appendix 5. Only primary studies that provide direct evidence relevant to this review were included in the overlap table.
Cancer, Cardiovascular Disease, and Mortality
In AHRQ (2021),19 results from the meta-analysis showed that supplementation with vitamin D was associated with significantly lower odds of cancer-related mortality (odds ratio [OR] = 0.89; 95% confidence interval [CI], 0.80 to 0.99). Supplementation with vitamin D was also associated with lower odds of all-cause mortality. However, this result was not statistically significant (OR = 0.95; 95% CI, 0.89 to 1.00). No benefit of vitamin D supplementation was found for CVD mortality, CVD events, or cancer incidence.
Acute Respiratory Infection
In Martineau et al. (2019),20 results from the individual participant data meta-analysis showed that supplementation with vitamin D was associated with lower odds of acute respiratory infection in the subgroup of participants aged older than 65 years. However, this result was not statistically significant (adjusted OR = 0.86; 95% CI, 0.67 to 1.09; P = 0.21). In the overall group of participants of any age, vitamin D supplementation was associated with significantly lower odds of acute respiratory infection (adjusted OR = 0.88; 95% CI, 0.81 to 0.96; P = 0.003). The subgroup analysis did not find evidence that age was acting as an effect modifier for the relationship between vitamin D supplementation and acute respiratory infection (P value for interaction = 0.61).
Dementia and Mild Cognitive Impairment
The relevant RCT included in AHRQ (2017)21 did not find an association between vitamin D supplementation and the incidence of probable dementia or mild cognitive impairment. The study also found no benefit for vitamin D supplementation on cognitive performance based on several cognitive tests (i.e., the Mini-Mental State Examination, Digit Span Forward and Backward, California Verbal Learning Test, Benton Visual Retention Test).
Yang et al. (2020)22 found a significant increase in the full-scale intelligence quotient score over 12 months for the vitamin D group compared to the control group. The study also found significant improvements in some, but not all, the cognitive domain tests of the WAIS-RC in the vitamin D group compared to the control group.
Depression
Alavi et al. (2019)23 found that GDS-15 scores decreased from 9.25 to 7.48 in the vitamin D group (P = 0.0001), whereas there was a non-significant increase in the placebo group. The multiple regression analysis showed that the intervention group and score of depression before the study could explain 81.8% of the variance in the depression score after the intervention.
Adverse Events
Only 1 of the included systematic reviews and 1 RCT reported adverse events.
Several of the RCTs included in AHRQ (2021)19 reported no differences in the participants experiencing any adverse event, serious adverse event, or withdrawal due to adverse event between the intervention groups. The review found some evidence of an increased risk of kidney stones with the long-term use of vitamin D supplementation; however, results were mixed. The largest RCT included in the review found that 2.5% of participants taking vitamin D developed a kidney stone after 7 years compared with 2.1% in the placebo group (hazard ratio = 1.17; 95% CI, 1.02 to 1.34). One of the included cohort studies also found a statistically significant increased risk of kidney stones with the use of 1,000 IU/day or more of vitamin D after 20 years (hazard ratio = 1.38; 95% CI, 1.03 to 1.85). Other included studies did not find a significant association between kidney stones and vitamin D.
Alavi et al. (2019)23 reported no adverse events during the trial.
Evidence-Based Guidelines
No evidence-based guidelines were identified; therefore, a summary cannot be provided.
Limitations
No evidence-based guidelines regarding vitamin D supplementation for the prevention and/or treatment of CVD, cancer, and other conditions in elderly patients residing in long-term care facilities were identified. There was also limited evidence identified on the effectiveness of vitamin D supplementation in patients with dementia, mild cognitive impairment, and depression. Only 1 systematic review19 and 1 RCT23 reported on adverse events related to vitamin D supplementation.
The RCTs that looked at outcomes related to mild cognitive impairment and depression did not discuss minimal clinically important differences for the scales and cognitive tests used (i.e., WAIS-RC, full-scale intelligence quotient, GDS-15).22,23 It is unclear if the magnitude of benefits reported for vitamin D supplementation in these studies are clinically meaningful.
Martineau et al. (2019)20 conducted their individual participant data meta-analysis in patients of all ages and only included patients older than the age of 65 as a subgroup analysis for the primary outcome.
AHRQ (2021)19 included 1 relevant study from Canada. However, the other systematic reviews did not include any relevant Canadian studies.20,21 Both included RCTs were also conducted outside of Canada.22,23 Therefore, it is unclear whether the results summarized in this report are generalizable to Canadian patients.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 3 systematic reviews19-21 and 2 RCTs22,23 on the clinical effectiveness of supplementation with vitamin D. No evidence-based guidelines were identified.
The findings of the included systematic reviews and RCTs suggest that supplementation with vitamin D may provide some benefit to older adults for specific clinical outcomes. The results of 1 systematic review suggest that supplementation with vitamin D may provide some benefit for cancer-related mortality in older adults.19 Martineau et al. (2019)20 found that supplementation with vitamin D was associated with lower odds of acute respiratory infection; however, this result was not significant in the subgroup of patients older than the age of 65. Results for the effectiveness of vitamin D supplementation for dementia and mild cognitive impairment were mixed. The relevant RCT included in AHRQ (2017)21 did not find a benefit of vitamin D supplementation for the incidence of probable dementia or mild cognitive impairment, or any benefit of performance on cognitive tests in women with normal cognition. In contrast, the RCT by Yang et al. (2020)22 found significant improvements in several cognitive tests in older adults with mild cognitive impairment; however, it is uncertain whether these improvements are clinically meaningful. Similarly, it is uncertain whether the improvements in depression found in Alavi et al. (2019)23 are clinically meaningful.
Adverse events were assessed in 1 systematic review and 1 RCT. Several RCTs included in AHRQ (2021)19 reported no differences in adverse events between intervention groups. The review found some evidence of an increased risk of kidney stones associated with vitamin D supplementation; however, results were mixed. Alavi et al. (2019)23 reported no adverse events during the trial.
A 2019 CADTH report aimed to summarize the evidence on the clinical effectiveness, cost-effectiveness, and evidence-based guidelines on the use of vitamin D supplementation for the prevention of falls and fractures in residents of long-term care facilities.24 The report concluded that vitamin D supplementation may reduce the rate of falls (i.e., number of falls) but not the risk of falling (i.e., number of individuals who fall) in residents of long-term care facilities.
Gaps in the evidence, as well as methodological limitations of the included studies, make it difficult to draw conclusions on the clinical effectiveness of vitamin D supplementation in older adults residing in long-term care facilities. Specifically, additional high-quality studies on the effectiveness of vitamin D supplementation in patients with dementia, mild cognitive impairment, and depression would reduce uncertainty. Future studies on the effectiveness of vitamin D supplementation for reducing acute respiratory infections specific to older adults residing in long-term care facilities would also reduce uncertainty.
References
1.Lucato P, Solmi M, Maggi S, et al. Low vitamin D levels increase the risk of type 2 diabetes in older adults: A systematic review and meta-analysis. Maturitas. 2017;100:8-15. PubMed
2.Yang J, Ou-Yang J, Huang J. Low serum vitamin D levels increase the mortality of cardiovascular disease in older adults: A dose–response meta-analysis of prospective studies. Medicine. 2019;98(34):e16733. PubMed
3.Pérez-López FR, Chedraui P, Fernández-Alonso AM. Vitamin D and aging: beyond calcium and bone metabolism. Maturitas. 2011;69(1):27-36. PubMed
4.Arnljots R, Thorn J, Elm M, Moore M, Sundvall PD. Vitamin D deficiency was common among nursing home residents and associated with dementia: a cross sectional study of 545 Swedish nursing home residents. BMC geriatr. 2017;17(1):229. PubMed
5.Garland CF, Garland FC, Gorham ED, et al. The role of vitamin D in cancer prevention. Am J Public Health. 2006;96(2):252-261. PubMed
6.Porto CM, Silva VDL, da Luz JSB, Filho BM, da Silveira VM. Association between vitamin D deficiency and heart failure risk in the elderly. ESC Heart Fail. 2018;5(1):63-74. PubMed
7.Kuwabara A, Tsugawa N, Ao M, Ohta J, Tanaka K. Vitamin D deficiency as the risk of respiratory tract infections in the institutionalized elderly: A prospective 1-year cohort study. Clin Nutr ESPEN. 2020;40:309-313. PubMed
8.Bouillon R, Marcocci C, Carmeliet G, et al. Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocr Rev. 2019;40(4):1109-1151. PubMed
9.MacLaughlin J, Holick MF. Aging decreases the capacity of human skin to produce vitamin D3. J Clin Invest. 1985;76(4):1536-1538. PubMed
10.Hill TR, Aspray TJ. The role of vitamin D in maintaining bone health in older people. Ther. 2017;9(4):89-95. PubMed
11.Keller HH, Lengyel C, Carrier N, et al. Prevalence of inadequate micronutrient intakes of Canadian long-term care residents. Br J Nutr. 2018;119(9):1047-1056. PubMed
12.Papaioannou A, Santesso N, Morin SN, et al. Recommendations for preventing fracture in long-term care. Can Med Assoc J. 2015;187(15):1135. PubMed
13.Vitamin D Supplementation for the Prevention or Treatment of COVID-19 in Residents of Long-Term Care Facilities. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/vitamin-d-supplementation-prevention-or-treatment-covid-19-residents-long-term-care-facilities. Accessed 7 Jul 2021.
14.Vitamin D Supplementation for the Prevention of Falls and Fractures in Residents of Long-Term Care Facilities: A 2021 Update. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/vitamin-d-supplementation-prevention-falls-and-fractures-residents-long-term-care-facilities-2021 Accessed 8 Jul 2021.
15.Vitamin D. Health A to Z 2020; https://www.nhs.uk/conditions/vitamins-and-minerals/vitamin-d/ Accessed 13 Jul 2021.
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
19.Kaiser Permanente Evidence-based Practice Center, O’Connor EA, Evans CV, et al. Vitamin and Mineral Supplements for the Primary Prevention of Cardiovascular Disease and Cancer: A Systematic Evidence Review for the U.S. Preventive Services Task Force. Evidence Synthesis Number 209. Rockville (MD): Agency for Healthcare Research and Quality; 2021: https://www.uspreventiveservicestaskforce.org/home/getfilebytoken/ejxWP-aWZCjDoae4YnSGZ3 Accessed 23 Jun 2021.
20.Martineau AR, Jolliffe DA, Greenberg L, et al. Vitamin D supplementation to prevent acute respiratory infections: individual participant data meta-analysis. Health Technol Assess. 2019;23:1. PubMed
21.Minnesota Evidence-Based Practice Center, Kane RL, Butler M, et al. Interventions To Prevent Age-Related Cognitive Decline, Mild Cognitive Impairment, and Clinical Alzheimer’s-Type Dementia Comparative Effectiveness Review Number 188. Rockville (MD): Agency for Healthcare Research and Quality; 2017: https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/cognitive-decline_research-2017.pdf. Accessed 23 Jun 2021.
22.Yang T, Wang H, Xiong Y, et al. Vitamin D Supplementation Improves Cognitive Function Through Reducing Oxidative Stress Regulated by Telomere Length in Older Adults with Mild Cognitive Impairment: A 12-Month Randomized Controlled Trial. J Alzheimers Dis. 2020;78(4):1509-1518. PubMed
23.Alavi NM, Khademalhoseini S, Vakili Z, Assarian F. Effect of vitamin D supplementation on depression in elderly patients: A randomized clinical trial. Clin Nutr. 2019;38(5):2065-2070. PubMed
24.Vitamin D Supplementation for the Prevention of Falls and Fractures in Residents of Long-Term Care Facilities: A Review of Clinical Effectiveness, CostEffectiveness, and Guidelines. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1105%20Vit%20D%20in%20LTC%20Final.pdf Accessed 6 Jul 2021.
Appendix 1: Selection of Included Studies
Note that Appendix 1 through 5 have been formatted for accessibility but have not been copy-edited.
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews and Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
AHRQ (2021)19 US AHRQ | 78 trials in total; 35 RCTs and 3 cohort studies relevant to the present review | Inclusion criteria: community-dwelling adults aged ≥ 18 years without chronic disease Relevant population: weighted average age of 66 years, 75% female, weighted average BMI of 28.5 kg/m2, median for baseline 25(OH)D serum level was 63 nmol/L | Eligible interventions: Supplementation with multivitamins/minerals, single nutrients, or functionally related pairs Relevant intervention: Supplementation with vitamin D (with or without calcium) Comparators: placebo, no intervention, usual diet | Outcomes: Cancer incidence, CVD incidence, CVD events (myocardial infarction and ischemic and hemorrhagic stroke), heart failure, mortality (all-cause, CVD-related, or cancer-related) Serious adverse events, withdrawals due to adverse events, nonserious adverse events reported by at least 5% of study sample Follow-up: 1 month to 26 years |
Martineau et al. (2019)20 UK National Institute for Health Research | 27 RCTs total; 11 RCTs relevant to the present review | Inclusion criteria: Participants of any age Relevant population: Adults aged > 65 years | Intervention: Supplementation with vitamin D3 or vitamin D2 Comparators: placebo, supplementation with vitamin D at a different dose than intervention | Outcomes: incidence of ARI, incidence of upper respiratory tract infection and lower respiratory tract infection, incidence of hospital admission for ARI, use of antimicrobials for treatment of ARI, work/school absence as a result of ARI, incidence of severe asthma exacerbation, incidence of severe COPD exacerbation, serious adverse events, adverse reactions to vitamin D, mortality Follow-up: 7 weeks to 1.5 years |
AHRQ (2017)21 US AHRQ | 263 studies total; 1 RCT relevant to the present review | Inclusion criteria: Adults with normal cognition and/or mild cognitive impairment Relevant population: Women with normal cognition, mean age of 71 years | Eligible interventions: interventions to prevent, delay, or slow age-related cognitive decline, mild cognitive impairment, and clinical Alzheimer-type dementia Relevant intervention: Supplementation with 400 IU vitamin D and 1000 mg calcium (optional use of additional 600 mg vitamin D and 1000 mg calcium) Comparators: placebo, usual care, waitlist, information or attention control, active control Relevant comparator: placebo | Outcomes: cognitive performance measured with validated instruments, biomarker measures associated with clinical Alzheimer-type dementia, and incident mild cognitive impairment or clinical Alzheimer-type dementia Follow-up: 7.8 years (mean) |
25(OH)D = 25-hydroxyvitamin D; AHRQ = Agency for Healthcare Research and Quality; ARI = acute respiratory infection; BMI = body mass index; COPD = chronic obstructive pulmonary disease; CVD = cardiovascular disease; RCT = randomized controlled trial.
Table 3: Characteristics of Included Randomized Controlled Trials
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Yang et al. (2020)22 China National Natural Sciences Foundation of China, CNS-ZD Tizhi and Health Fund | RCT | Inclusion criteria: Participants aged ≥ 65 years with no terminal illness or mental disorders and not living in a nursing home who were assessed to have mild cognitive impairment Baseline characteristics: Vitamin D group: mean age of 67.22 years, 46.24% male, mean BMI of 24.68 kg/m2, mean 25(OH)D3 of 19.07 ng/mL, MMSE 22.76, history of hypertension in 46.24%, diabetes in 18.28%, and cardiopathy in 5.38% Placebo group: mean age of 66.59 years, 43.33% male, mean BMI of 25.66 kg/m2, mean 25(OH)D3 of 19.78 ng/mL, MMSE 22.40, history of hypertension in 26.67%, diabetes in 11.11%, and cardiopathy in 6.67% | Intervention: 2 oral tablets containing 800 IU vitamin D3 (400 IU/tablet) daily Comparator: placebo daily | Outcomes: cognitive function assessed via WAIS-RC and FSIQ, blood biomarkers Follow-up: 12 months |
Alavi et al. (2019)23 Iran Kashan University of Medical Sciences | RCT | Inclusion criteria: Patients aged > 60 years who were under treatment for depression, no history of mental illness other than depression, no history of physical disability, and GDS score above 5 that represents moderate to severe depression Baseline characteristics: Vitamin D group: mean age of 68.7 years, 48.7% female, mean baseline 25(OH)D3 concentration of 22.57 ng/mL, 51.3% had hypertension, 38.5% had diabetes, 52.3% had a history of depression Placebo: mean age of 67 years, 51.3% female, mean baseline 25(OH)D3 concentration of 21.2 ng/mL, 66.7% had hypertension, 56.4% had diabetes, 32.9% had a history of depression | Intervention: 50,000 units of vitamin D3 pearl weekly for 8 weeks at mealtime Comparator: placebo weekly | Outcomes: GDS-15 questionnaire, 25(OH)D3 Follow-up: 8 weeks |
25(OH)D3 = 25-hydroxyvitamin D3; BMI = body mass index; FSIQ = full-scale intelligence quotient; GDS = geriatric depression scale; MMSE = mini-mental state examination; RCT = randomized controlled trial; WAIS-RC = Wechsler Adult Intelligence Scale-Revised.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 216
Strengths | Limitations |
AHRQ (2021)19 | |
Clear objective Comprehensive literature search strategy and detailed methods described Study selection performed in duplicate List of excluded studies and justifications provided Two investigators independently assessed the studies’ risk of bias based on an adaptation of the US Preventive Service Task Force methods Appropriate methods for meta-analysis were described Studies rated as ‘poor’ quality were excluded from the review Non-randomized studies were not included in meta-analysis Source of funding reported | Unclear which components of the research methods were established a priori Data were not extracted in duplicate however, a second reviewer checked data for accuracy Comparator groups for included studies were not described in detail Sources of funding for individual studies included in the review were not reported Investigation of publication bias was not described Risk of false-positive findings due to chance as a result of multiple analyses |
Martineau et al. (2019)20 | |
Clear objective Comprehensive literature search strategy and detailed methods described Review methods established a priori; protocol registered with PROSPERO Three investigators determined which trials met eligibility criteria Characteristics of included studies were described in detail Two investigators independently assessed studies using the Cochrane Collaboration risk of bias tool Individual patient data from the included studies was combined in meta-analysis and heterogeneity was assessed Authors performed a sensitivity analysis removing studies assessed as being at unclear risk of bias Pre-specified subgroup analyses were performed to explore causes of heterogeneity and identify effect modifiers Publication bias was investigated and discussed Source of funding reported | List of excluded studies not provided Sources of funding for individual studies included in the review were not reported |
AHRQ (2017)21 | |
Clear objective Comprehensive literature search strategy and detailed methods described Study selection performed in duplicate List of excluded studies and justifications provided Characteristics of included studies were described in detail Two investigators independently assess risk of bias using an instrument based on Agency for Health care research and Quality guidance Source of funding reported | Unclear which components of the research methods were established a priori Data were not extracted in duplicate however, a second reviewer checked data for accuracy Sources of funding for individual studies included in the review were not provided |
AHRQ = Agency for Healthcare Research and Quality; AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist17
Strengths | Limitations |
Yang et al. (2020)22 | |
Objective, outcomes, patient characteristics, interventions, and main findings were clearly described There were a small number of participants lost to follow-up in each group Participants were selected via multi-stage cluster random sampling Participants in different intervention groups were recruited over the same period of time Participants, researchers and medical staff were blind to treatment allocation until the statistical analyses were complete Treatment compliance was assessed based on self-report as well as medication counts The main outcome measures were valid and reliable Participants were allocated to treatment groups based on a computer-generated randomization sequence All analyses were conducted for the intention-to-treat population | Adverse events are not reported Potential confounders are not discussed or adjusted for in the analyses There appear to be some imbalances in baseline characteristics between treatment groups It is unclear whether a power calculation was conducted a priori to determine sample size The results of the study may not be generalizable to Canadian patients residing in long-term care |
Alavi et al. (2019)23 | |
Objective, outcomes, patient characteristics, interventions, main findings, and confounders were clearly described There was only 1 patient lost to follow-up in each group Patients and researchers were blind to treatment allocation until the main analyses were completed Statistical tests used to assess main outcomes were appropriate Treatment compliance was assessed using medication counts The main outcome measures were valid and reliable Random assignment was conducted using computer-generated random numbers A power calculation was conducted a priori to determine sample size | Recruitment method for study participants was not described There appear to be some imbalances in baseline characteristics between treatment groups The 2 patients lost to follow-up were not analyzed The distribution of some confounders in the different treatment groups was not described The statistical analysis did not adjust for multiplicity The results of the study may not be generalizable to Canadian patients residing in long-term care |
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 6: Summary of Findings Included Systematic Reviews and Meta-Analyses
Main study findings | Authors’ conclusion |
AHRQ (2021)19 | |
Results from meta-analysis of 30 RCTs: end point (number of studies), OR (95% CI)
Note: A value < 1 favours vitamin D *Data were insufficient for meta-analysis so findings from the largest and most comprehensive study are presented Adverse events: “Several RCTs reported no differences in the percent of participants experiencing any adverse event any serious adverse events or withdrawal due to adverse events (p. 29)”19 “While most trials reporting kidney stones had very few events, the largest trial indicated a small increased risk. In the WHI, 2.5% of participants taking 400 IU vitamin D and 1000 mg calcium daily developed a kidney stone after 7 years, compared with 2.1% in the placebo group (HR, 1.17 [95% CI, 1.02 to 1.34). The VITamin D and OmegA-3 trial (VITAL) found a similar effect size, although it was not statistically significant (HR, 1.12 [95% CI, 0.99 to 1.28]); 3.7% in those taking 2000 IU/day vitamin D vs. 3.3% in the placebo group after 5.3 years developed a kidney stone. (p. 29).”19 “In addition, 2 of the cohort studies found an increased risk of kidney stones with use of 1000 IU/day or more of vitamin D after 20 to 26 years, compared with no vitamin D use, but only 1 of these findings was statistically significant. There was no suggestion of increased risk with lower doses in either of these studies. The third cohort study, NHS-I, found no association between any dose of vitamin D and kidney stones (p. 29-30).”19 | “Vitamin and mineral supplementation provides little to no benefit in preventing cancer, CVD, and death, with the exception of a benefit for cancer-related mortality and a possible small benefit for all-cause mortality with vitamin D use (p. 57).”19 |
Martineau et al. (2019)20 | |
Results from individual participant data meta-analysis, proportion of patients experiencing at least 1 ARI:
Note: A value < 1 favours vitamin D *Adjusted for age, sex and study duration | “In the study population as a whole, vitamin D supplementation reduced the risk of experiencing at least one ARI (p. 31).”20 |
AHRQ (2017)21 | |
Results from 1 RCT relevant to this report:
| No benefit on cognitive performance or incident mild cognitive impairment or clinical Alzheimer-type dementia for vitamin D with calcium in women was shown based on low-strength evidence. |
AHRQ = Agency for Healthcare Research and Quality; ARI = acute respiratory infection; CI = confidence interval; CVD = cardiovascular disease; HR = hazard ratio; NHS-I = Nurses’ Health Study; OR = odds ratio; RCT = randomized controlled trial; SE = standard error; WHI = Women’s health Initiative study.
Table 7: Summary of Findings of Included Randomized Controlled Trials
Main study findings | Authors’ conclusion |
Yang et al. (2020)22 | |
FSIQ: Repeated-measures ANOVA results:
Mixed-model repeated-measures ANOVA results:
Cognitive domain tests of WAIS-RC:
Note: in all tests higher scores indicate better cognitive function | “In conclusion, this randomized placebo-controlled trial found that daily oral vitamin D supplementation (800 IU/day) for 12 months may significantly improve cognitive function through reducing oxidative stress regulated by increased telomere length in Chinese older adults with MCI. The results provide a possible direction for preventing cognitive decline in order adults. Larger scale and longer duration trials for vitamin D are needed in the future (p. 1517).”22 |
Alavi et al. (2019)23 | |
GDS-15 scores:
GDS-15 scores difference:
Patients diagnosed with severe* depression:
Multiple regression analysis:
*GDS-15 score 5 to 10 = mild to moderate depression, > 10 = severe depression Adverse events:
| “In conclusion vitamin D supplementation significantly decreased GDS score in older adults. According to our findings the older adults who are under treatment of depression could clinically benefit from vitamin D prescription. Although, there is a need for more well designed randomized clinical trials in this field (p. 2069).”23 |
CI = confidence interval; FSIQ = full-scale intelligence quotient; GDS = geriatric depression scale; MCI = mild cognitive impairment; NR = not reported; SD = standard deviation; WAIS-RC = Wechsler Adult Intelligence Scale-Revised.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Table 8: Overlap in Relevant Primary Studies between Included Systematic Reviews
Primary study citation | AHRQ (2021)19 | Martineau et al. (2019)20 |
Aloia JF, et al. Arch Intern Med. 2005,165(14):1618-23. | Yes | No |
Aloia J, et al. J Bone Miner Res. 2018;33(11):1916-22. | Yes | No |
Avenell A, et al. J Clin Endocrinol Metab. 2012;97(2):614-22. | Yes | No |
Baeksgaard L, et al. Osteoporos Int. 1998;8(3):255-60. | Yes | No |
Baron JA, et al. N Engl J Med. 2015;373(16):1519-30. | Yes | No |
Bischoff-Ferrari HA, et al. JAMA. 2020;324(18):1855-68. | Yes | No |
Brisson J, et al. Cancer Epidemiol Biomarkers Prev. 2017;26(8):1233-41. | Yes | No |
Cooper L, et al. Am J Clin Nutr. 2003;77(5):1324-9. | Yes | No |
Dawson-Hughes B, et al. Ann Intern Med. 1991;115(7):505-12. | Yes | No |
Dawson-Hughes B, et al. N Engl J Med. 1997;337(10):670-6. | Yes | No |
Dean AJ, et al. PLoS ONE. 2011;6(11):e25966 | Yes | No |
Dukas L, et al. J Am Geriatr Soc. 2004;52(2):230-6. | Yes | No |
Fedirko V, et al. Cancer Prev Res (Phila). 2009;2(3):213-23. | Yes | No |
Gallagher JC, et al. J Clin Endocrinol Metab. 2001;86(8):3618-28. | Yes | No |
Glendenning P, et al. J Bone Miner Res. 2012;27(1):170-6. | Yes | No |
Grady D, et al. J Clin Endocrinol Metab. 1991;73(5):1111-7. | Yes | No |
Kenny AM, et al. J Am Geriatr Soc. 2003;51(12):1762-7. | Yes | No |
Komulainen M, et al. J Clin Endocrinol Metab. 1999;84(2):546-52. | Yes | No |
Lappe JM, et al. Am J Clin Nutr. 2007;85(6):1586-91. | Yes | No |
Lappe J, et al. JAMA. 2017;317(12):1234-43. | Yes | No |
Lips P, et al. Ann Intern Med. 1996;124(4):400-6. | Yes | No |
Pittas AG, et al. N Engl J Med. 2019. PMID:31173679. | Yes | No |
Manson JE, et al. N Engl J Med. 2018. PMID:30415629. | Yes | No |
Murdoch DR, et al. JAMA. 2012;308(13):1333-9. | Yes | Yes |
Rake C, et al. Health Technol Assess. 2020;24(10):1-53. | Yes | No |
Salovaara K, et al. J Bone Miner Res. 2010;25(7):1487-95. | Yes | No |
Sanders KM, et al. JAMA. 2010;303(18):1815-22. | Yes | No |
Scragg R, et al. JAMA Cardiol. 2017;2(6):608-16. | Yes | No |
Toss G and Magnusson P. Eur J Nutr. 2012;51(8):939-45. | Yes | No |
Trivedi DP, et al. BMJ. 2003;326(7387):469. | Yes | No |
Uusi-Rasi K, et al. JAMA Intern Med. 2015;175(5):703-11. | Yes | No |
Wactawski-Wende J, et al. N Engl J Med. 2006;354(7):684-96. | Yes | No |
Witham MD, et al. Hypertension. 2014;63(4):706-12. | Yes | No |
Wood AD, et al. J Clin Endocrinol Metab. 2012;97(10):3557-68. | Yes | No |
Zittermann A, et al. Am J Clin Nutr. 2009;89(5):1321-7. | Yes | No |
Ferraro PM, et al. J Urol. 2017;197(2):405-10. | Yes | No |
Feskanich D, et al. JAMA. 2002;287(1):47-54. | Yes | No |
Taylor EN, et al. J Am Soc Nephrol. 2004;15(12):3225-32. | Yes | No |
Li-Ng M, et al. Epidemiol Infect. 2009;137(10):1396-404. | No | Yes |
Lehouck A, et al. Ann Intern Med. 2012;156:105-14. | No | Yes |
Bergman P, et al. BMJ Open. 2012;2:e001663. | No | Yes |
Rees JR, et al. Clin Infect Dis. 2013;57(10):1384-92. | No | Yes |
Tran B, et al. Am J Clin Nutr. 2014;99(1):156-61. | No | Yes |
Martineau AR, et al. Lancet Respir Med. 2015;3(2):120-30. | No | Yes |
Martineau AR, et al. Thorax. 2015;70:451-7. | No | Yes |
Martineau AR, et al. Thorax. 2015;70:953-60. | No | Yes |
Castro M, et al. JAMA. 2014;311(20):2083-91. | No | Yes |
Denlinger LC, et al. Am J Respir Crit Care Med. 2016;193(6):634-41. | No | Yes |
Ginde AA, et al. J Am Geriatr Soc. 2017;65(3):496-503. | No | Yes |
AHRQ = Agency for Healthcare Research and Quality.
Note: Yes indicates the primary study was included within the systematic review; No indicates the primary study was not included within the systematic review.
Appendix 6: References of Potential Interest
Previous CADTH Reports
1.Vitamin D Supplementation for the Prevention of Tuberculosis Infection: Clinical Effectiveness and Guidelines. Ottawa (ON): CADTH; 2020 Mar. https://www.cadth.ca/vitamin-d-supplementation-prevention-tuberculosis-infection-clinical-effectiveness-and-guidelines Accessed 7 Jul 2021.
2.Calcium and Vitamin D Supplementation for Adults: Safety and Guidelines. Ottawa (ON): CADTH; 2018 Jun. https://www.cadth.ca/calcium-and-vitamin-d-supplementation-adults-safety-and-guidelines Accessed 8 Jul 2021.
3.Vitamin D for the Treatment or Prevention of Multiple Sclerosis: A Review of the Clinical Effectiveness. Ottawa (ON): CADTH; 2016 Mar. https://www.cadth.ca/vitamin-d-treatment-or-prevention-multiple-sclerosis-review-clinical-effectiveness Accessed 7 Jul 2021.
Review Articles
4.Ebeling PR, Adler RA, Jones G, et al. Management of endocrine disease: Therapeutics of Vitamin D. Eur J Endocrinol. 2018;179(5):R239-R259. PubMed
Additional References
5.Arnedo-Pena A, Juan-Cerdan JV, Romeu-Garcia M, et al. Vitamin D status and latent tuberculosis infection: conversion in nursing homes, Spain. Int J Tuberc Lung Dis. 2020;24(3):278-286. PubMed
6.Azzam E, Elsabbagh N, Elgayar N, Younan D. Relation between vitamin D and geriatric syndrome. Clin Nutr ESPEN. 2020;35:123-127. PubMed
7.Arnljots R, Snaebjornsson Arnljots E, Thorn J, et al. Bacteriuria and vitamin D deficiency: a cross sectional study of 385 nursing home residents. BMC Geriatr. 2019;19(1):381. PubMed
8.Carlsson M, Wanby P, Brudin L, et al. Older Swedish Adults with High Self-Perceived Health Show Optimal 25-Hydroxyvitamin D Levels Whereas Vitamin D Status Is Low in Patients with High Disease Burden. Nutrients. 2016;8(11):11. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca