CADTH Health Technology Review
Palonosetron for Patients Undergoing High or Moderate Emetogenic Chemotherapy
Rapid Review
Authors: Khai Tran, Hannah Loshak
Abbreviations
AC
anthracycline and cyclophosphamide
AE
adverse event
ASCO
American Society of Clinical Oncology
CC
complete control
CCO
Cancer Care Ontario
CI
confidence interval
CINV
chemotherapy-induced nausea and vomiting
CP
complete protection
CR
complete response
DEX
dexamethasone
ESMO
European Society of Medical Oncology
FLIE
Functional Living Index-Emesis
HEC
highly emetogenic chemotherapy
5-HT3
5-hydroxytryptamine-3
ICER
incremental cost-effectiveness ratio
IR
incomplete response
ITT
intention-to-treat
IV
intravenous
JPY
Japanese yen
MASCC
Multinational Association of Supportive Care in Cancer
MAT
MASCC Antiemesis Tool
MEC
moderate emetogenic chemotherapy
NCCN
National Comprehensive Cancer Network
NEPA
netupitant-palonosetron
NK1
neurokinin-1
NMB
net monetary benefit
POGO
Pediatric Oncology Group of Ontario
QALD
quality-adjusted life-day
QALY
quality-adjusted life-year
QoL
quality of life
RA
receptor antagonist
RCT
randomized controlled trial
SR
systematic review
TC
total control
WTP
willingness-to-pay
Key Messages
This report identified high to moderate quality evidence from clinical studies and economic evaluations, as well as high-quality guidelines regarding the use of palonosetron in the prevention of chemotherapy-induced nausea and vomiting in adult and pediatric patients receiving different emetogenic chemotherapies. Interpretations of the findings should be taken with caution because of the presence of some identified limitations in both clinical and economic evidence.
In adult patients receiving high emetogenic chemotherapy, a fixed antiemetic combination of netupitant and palonosetron (NEPA) plus dexamethasone demonstrated noninferiority relative to a triple regimen of granisetron-aprepitant-dexamethasone. Similarly, palonosetron had similar efficacy compared to granisetron with the co-administration of neurokinin 1 receptor antagonist (e.g., aprepitant or fosaprepitant) and dexamethasone. However, in the absence of aprepitant, a 2-drug combination of palonosetron-dexamethasone appeared to be significantly more effective than granisetron-dexamethasone for the prevention of both acute and delayed emesis.
In adult patients receiving moderate emetogenic chemotherapy, palonosetron plus dexamethasone was found to be noninferior compared with ondansetron plus dexamethasone. Similar efficacy was also observed between palonosetron plus dexamethasone and transdermal granisetron plus dexamethasone.
In a mixed population of adult patients receiving high or moderate emetogenic chemotherapy, a palonosetron regimen appeared to have greater efficacy than ondansetron for delayed emesis. The efficacy of triple regimen of palonosetron-aprepitant-dexamethasone and granisetron-aprepitant-dexamethasone was comparable at all phases.
In pediatric patients receiving high emetogenic chemotherapy, palonosetron plus dexamethasone had similar efficacy compared with ondansetron plus dexamethasone in the acute phase, but was more effective in delayed and overall phases of chemotherapy-induced nausea and vomiting.
In a mixed population of pediatric patients receiving high or moderate emetogenic chemotherapy, palonosetron plus dexamethasone was noninferior to ondansetron plus dexamethasone.
There were no significant differences between palonosetron and ondansetron or between palonosetron and granisetron treatment regimens in adverse events or quality of life.
A cost-utility analysis revealed that NEPA plus dexamethasone was dominant (i.e., cost less, more effective) relative to granisetron-aprepitant-dexamethasone and ondansetron-aprepitant or fosaprepitant-dexamethasone in adult patients receiving high emetogenic chemotherapy. In contrast, double or triple regimens of palonosetron was not cost-effective compared to granisetron regimens, mainly due to large difference in price and small quality-adjusted life-years gained. These economic evaluations may not be applicable to the Canadian context.
The identified high-quality guidelines have recommendations on the use of specific antiemetic regimens for adult and pediatric patients receiving high emetogenic chemotherapy or moderate emetogenic chemotherapy and suggest that palonosetron may be offered as an alternative to other 5-hydroxytryptamine-3 receptor antagonists and that 1 5-hydroxytryptamine-3 receptor antagonist is not preferred over another based on the available evidence.
Context and Policy Issues
Chemotherapy-induced nausea and vomiting (CINV) is 1 of the most debilitating side effects of cancer therapy, affecting up to 80% of chemotherapy patients.1 Chemotherapy drugs are classified according to the associated risk of causing CINV: minimal (less than 10%), low (10% to 30%), moderate (30% to 90%), and high (greater than 90%).2 High emetogenic chemotherapy (HEC) drugs include a high dose of cisplatin, a high dose of cyclophosphamide (1,500 mg/m2 or more), and a combination of anthracycline and cyclophosphamide (AC).2 Moderate emetogenic chemotherapy (MEC) regimens are more variable including carboplatin, oxaliplatin, doxorubicin, and cyclophosphamide.2
CINV symptoms can manifest at various time points after chemotherapy. There are 3 distinct types of CINV:
Acute CINV occurs within 24 hours after administration of chemotherapy, with acute vomiting and nausea, and is primarily mediated by the 5-hydroxytryptamine-3 (5-HT3) receptor antagonist.
Delayed CINV occurs from 24 hours to 5 days after chemotherapy and is predominantly mediated by the neurokinin 1 (NK1) receptor antagonists.
Anticipatory CINV occurs before chemotherapy treatment as a conditioned response because of the development of significant CINV from the previous chemotherapy cycles, mediated by both physiologic and psychological mechanisms.2,3
The management of CINV has been facilitated from the development of various antiemetic agents with different mechanisms of action. Three most commonly used medications for antiemetic prophylaxis are 5-HT3 receptor antagonists (5-HT3 RA), NK1 RA, and corticosteroids, usually dexamethasone (DEX).3,4 Other antiemetic agent such as olanzapine, an atypical antipsychotic, has been used for acute and delayed CINV.3,4 These antiemetic agents are used in specific combinations depending on the emetogenicity of the chemotherapy regimen given to different population (i.e., adults or children).3,4 Currently available 5-HT3 RAs for CIVN include ondansetron, granisetron, dolasetron, and palonosetron.3,4 The NK1 RA include aprepitant, fosaprepitant, and rolapitant.3,4
On March 14, 2012, Health Canada issued a Notice of Compliance for the IV and oral formulation of palonosetron. IV palonosetron is indicated in adults for “the prevention of acute and delayed nausea and vomiting associated with MEC and the prevention of acute nausea and vomiting associated with HEC, including high dose cisplatin. Oral palonosetron is indicated in adults for the prevention of acute nausea and vomiting associated with MEC”.5 Palonosetron is a long-lasting, second-generation agent, with higher affinity and binding capacity to 5-HT3 receptor, and thus has a longer half-life of 40 hours compared to first-generation 5-HT3 RAs, ondansetron, granisetron, dolasetron, and with a half-life of 3 to 9 hours.6 Due to its long half-life, palonosetron has been suggested to produce best treatment responses in both acute and delayed CINV of varying emetogenicity.6 On September 28, 2017, Health Canada issued a Notice of Compliance for netupitant/palonosetron (NEPA) — a combination of a highly selective NK1 RA netupitant (300 mg) and palonosetron (0.5 mg) — in combination with DEX, for once-per-cycle treatment in adult patients for the “prevention of acute and delayed nausea and vomiting associated with HEC and prevention of acute nausea and vomiting associated with MEC therapy that is uncontrolled by a 5-HT3 RA.”7,8
Over the past decades, the development of new antiemetic drugs has progressed and shown promising results in the prevention of CINV. Particularly, the appearance of second-generation of 5-HT3 receptor palonosetron and its combination with netupitant in NEPA has urged a literature review on the clinical effectiveness and cost-effectiveness of these drugs relative to other 5-HT3 RAs. Both dosage forms of palonosetron (IV and oral) were reviewed by the CADTH Common Drug Review in 2012.9-12 The combination product palonosetron-netupitant (Akynzeo) was reviewed in 2017.13-15 Since then, new evidence and guidelines have emerged on the use of palonosetron as monotherapy or in combination with netupitant to treat adults and children with CINV. The aim of this report is to review the clinical effectiveness and cost-effectiveness of palonosetron for the prevention of CINV in patients receiving HEC or MEC. The report also summarizes the evidence-based guidelines regarding the use of palonosetron for the prevention CINV in patients receiving HEC or MEC.
Research Questions
What is the clinical effectiveness of palonosetron for the prevention of CINV in patients receiving HEC or MEC?
What is the cost-effectiveness of palonosetron for the prevention of CINV in patients receiving HEC or MEC?
What are the evidence-based guidelines regarding the use of palonosetron for the prevention CINV in patients receiving HEC or MEC?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and Embase via OVID, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was palonosetron. No filters were applied to limit the retrieval by study type. Conference reviews and conference abstracts were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016 and May 28, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients with cancer undergoing HEC or MEC |
Intervention | Palonosetron (injectable or oral capsule) as monotherapy or co-administered with NK1 RA or dexamethasone |
Comparator | Ondansetron or granisetron as monotherapy or co-administered with NK1 RA or dexamethasone |
Outcomes | Q1: Clinical effectiveness (e.g., nausea, vomiting, patient satisfaction, noninferiority, superiority, complete response) Q2: Cost-effectiveness (e.g., ICERs, QALYs) Q3: Recommendations regarding best practices for the prevention of nausea and vomiting secondary to chemotherapy using palonosetron |
Study Designs | HTA, SR, RCT, economic evaluations and evidence-based guidelines |
HEC = high emetogenic chemotherapy; HTA = health technology assessment; ICER = incremental cost-effectiveness ratio; MEC = moderate emetogenic chemotherapy; NK1 RA = neurokinin 1 receptor antagonist; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Older guidelines that had been updated and guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)16 for systematic reviews, the Downs and Black checklist17 for randomized studies, the Drummond checklist18 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument19 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
A total of 403 citations were identified in the literature search. Following the screening of titles and abstracts, 350 citations were excluded and 53 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 28 publications were excluded for various reasons and 27 publications of 23 unique studies met the inclusion criteria and were included in this report. These comprised 1 systematic review (SR), 12 randomized controlled trials, RCTs, 5 economic evaluations, and 5 evidence-based guidelines. Appendix 1 presents the PRISMA flow chart20 of the study selection.
Summary of Study Characteristics
The detailed characteristics of the included SR21 (Table 2), primary clinical studies (RCTs)22-35 (Table 3), economic studies36-40 (Table 4), and guidelines41-47 (Table 5) are provided in Appendix 2.
Study Design
The SR21 included 26 studies comparing ondansetron with other 5-HT3 RA treatments, of which 6 RCTs compared ondansetron with palonosetron. The RCTs included in the SR were published between 2003 to 2013.
The additional 12 included RCTs published in 14 reports comprised 7 open-label22,23,25-27,31,34 and 5 double-blind24,28-30,32,33,35 trials. Ten RCTs were parallel22-25,27-30,32-35 and 2 were cross-over26,31 in design. Sample size calculation was performed and reported in 9 RCTs.23-25,27,29,31,32,34,35 The efficacy results were analyzed using intention-to-treat approach in 2 RCTs28,31 and per-protocol analysis or not was reported in the other 10 studies.22-27,29,30,32-35
Of the 5 included economic studies, 4 were cost-utility analysis36,37,39,40 and 1 was a cost-effectiveness analysis.38
The cost-utility analysis by Botteman et al. (2020)36 was conducted using the efficacy data from a phase III noninferior RCT by Zhang et al. (2018)29 to determine the cost-effectiveness of NEPA relative to the granisetron-aprepitant regimen for HEC. The analyses were performed from the US health care perspective, with a time horizon of 5 days. The utilities values of 0.90, 0.70, and 0.24 were assigned for the outcomes of complete protection (CP), complete response (CR), and incomplete response (IR), respectively. The costs of antiemetic prophylaxis, rescue medications, and medical costs of CINV-related events were assigned into the analysis based on usage observed in the trial. Costs were adjusted at 2018 US dollars.
The cost-utility analysis by Kashiwa and Matsushita (2019)37 was conducted using the efficacy data of a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35 to assess the cost-effectiveness of a triple regimen of palonosetron relative to granisetron for cisplatin-containing HEC. The analyses were performed from the Japanese health care payer perspective, with a time horizon of 5 days. The utilities values of 0.90, 0.70, and 0.20 were assigned for the outcomes of CP, CR, and IR, respectively. Costs considered in the analyses included direct medical costs associated with CINV prevention and medical fees incurred by CINV. Costs were adjusted at 2018 US dollars (US$1 = 112.17 Japanese yen [JPY]).
The cost-effectiveness analysis by Shimizu et al. (2018)38 was also conducted using the efficacy data of a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35 to assess the cost-effectiveness of a triple regimen of palonosetron relative to granisetron for cisplatin-containing HEC. The analyses were performed from the Japanese health care payer perspective, with a time horizon of 5 days. The costs of drugs and total medical costs were considered in the analysis. Costs were adjusted at 2018 US dollars (US$1 = 110.57 JPY).
The cost-utility analysis by Du et al. (2017)39 was conducted using the efficacy data of 2 pivotal phase III RCTs to compare the cost-effectiveness among 3 5-HT3 RAs (i.e., palonosetron, ondansetron, and granisetron) in the presence of DEX for HEC. The analyses were performed from the Chinese health care perspective, with a time horizon of 5 days. The utilities values of 9.02, 7.74, and 2.28 were assigned for the outcomes of CR, nausea but not receive medication, and failure, respectively. Only direct medical costs (i.e., antiemetic drugs and rescue drugs) were considered in the analyses. Costs were adjusted at 2014 US dollars.
The cost-utility analysis by Restelli et al. (2017)40 was conducted using the efficacy data of 3 RCTs48-50 to determine the cost-effectiveness of NEPA-DEX relative to other comparators for HEC or MEC. The analyses were performed from the Italian National Health Service perspective, with a time horizon of 5 days. The utilities values of 0.77, 0.60, and 0.26 were assigned for the outcomes of CP, CR, and IR, respectively. Direct medical costs, costs management of adverse events (AEs), and costs for the management of CINV episodes were considered in the analysis. Costs were adjusted at year 2016, in Euros.
All 5 included guidelines were updated versions of the previous American Society of Clinical Oncology (ASCO) guideline,41 National Comprehensive Cancer Network (NCCN) guideline,42 Cancer Care Ontario (CCO) guideline,43 Pediatric Oncology Group of Ontario (POGO) guideline,44 and Multinational Association of Supportive Care in Cancer/ European Society of Medical Oncology (MASCC/ESMO) guideline.45-47 All guidelines were developed to provide recommendations on the use of antiemetics for the prevention of CINV. A systematic literature review search was conducted for all included guidelines. The quality of evidence and the strength of recommendations were assessed and reported in 4 guidelines: ASCO,41 NCCN,42 POGO,44 and MASCC/ESMO.45-47 In the CCO guideline,43 the quality of evidence was assessed, but the level of evidence and the strength of recommendations were not provided for each recommendation. Recommendations in all guidelines were developed by expert panels and the guidelines were reviewed by external reviewers and published either on their websites or in peer-reviewed journals.
Country of Origin
The SR21 was conducted by authors from Brazil and was published in 2016.
The RCTs were conducted by authors in Egypt,22 the Netherlands,23 Japan,24,26,31,35 India,25,27 China,28-30 Korea,34 the US and multiple countries in Latin America, Western and Eastern Europe, and Russia.32,33 Two RCTs were published in 2021,22,23 1 in 2020,24 2 in 2019,25,26 3 in 2018,27-29 and 4 in 2016.31,32,34,35 Four RCTs were designed to test the noninferiority of palonosetron compared to ondansetron23,27,32 or to granisetron.29 The noninferiority margin was set at –10%,29 –15%27,32 or –20%.23 Noninferiority was demonstrated if the lower limit of the confidence interval (CI) for the difference between palonosetron and its comparator (ondansetron or granisetron) in the incidence of primary outcome was greater than the noninferiority margin.
The economic studies were conducted by authors from US,36 Japan,37,38 China,39 and Italy.40 The studies were published in 2020,36 2019,37 2018,38 and 2017.39,40
The guidelines were conducted by authors from US,41,42 Canada,43,44 and multiple countries including Canada, the US, and European countries.45-47
Patient Population
Patients in the RCTs included in the SR21 were adults with various cancer types (e.g., breast, lung, bladder, colon, rectum, gastric, lymphoma, leukemia, other) who were scheduled to receive HEC (3 RCTs) or MEC (3 RCTs). The mean age ranged between 52 years and 56 years, and the percent of females ranged between 36% and 100% (breast cancer).
Eight RCTs22-24,26,29-31,34,35 involved adult cancer patients with mean ages ranging from 49 to 68 years, and the proportion of females varied from 20% to 100% (breast cancer). Five RCTs included patients naive to chemotherapy who were scheduled to receive HEC,22,24,29-31,35 1 RCT included patients naive to chemotherapy who were scheduled to receive MEC,23 1 RCT included patients naive to chemotherapy who were scheduled to receive HEC or MEC,26 and 1 RCT included patients with or without previous chemotherapy who were scheduled to receive MEC.34 The types of cancer were mainly lung,22,26,29,30,35 breast,22,24 colon and rectum,23 and stomach.31 One RCT did not report cancer type.34
There were 4 RCTs25,27,28,32,33 involving pediatric patients with mean age ranging from 5 to 8 years and the proportion of females ranged between 28% to 52%. Two RCTs included patients naive to chemotherapy who were scheduled to receive HEC or MEC,25,27 1 RCT included patients with or without previous chemotherapy who were scheduled to receive HEC or MEC,32,33 and 1 RCT included patients with or without previous chemotherapy who were scheduled to receive HEC.28 The types of cancer included both hematological cancer and solid tumour.
Patients in all economic studies were adults with cancer, naive to chemotherapy, who were scheduled to receive HEC;36-39 or adult cancer patients naive to chemotherapy who were scheduled to receive HEC or MEC.40
All included guidelines41-47 were developed for health care providers involved in the treatment and care for cancer patients including oncologists, pharmacists, and nurses. The target population of the ASCO guideline41 and the MASCC/ESMO guidelines45-47 are adult patients receiving HEC or MEC, and pediatric patients receiving HEC or MEC. The target population of the NCCN guideline42 are adult patients receiving HEC or MEC parenteral anticancer drugs and adult patients receiving HEC or MEC oral anticancer drugs. The target population of the CCO guideline43 are adult patients receiving HEC or MEC, a single day of IV chemotherapy or a multiple day of IV chemotherapy. The target population of the POGO guideline44 is pediatric patients receiving HEC or MEC.
Interventions and Comparators
The SR21 included 6 RCTs that compared ondansetron with palonosetron. Ondansetron doses varied from 32 mg administered orally, or from 8 mg to 32 mg administered intravenously. The palonosetron dose was 0.25 mg administered either orally or IV. Meta-analysis was performed and subgroup analysis was conducted.
Among RCTs involving adult patients, 2 RCTs compared a dual regimen of palonosetron-DEX versus granisetron-DEX,22,34 1 RCT compared palonosetron-DEX versus ondansetron-DEX versus ondansetron-DEX-metoclopramide,23 3 RCTs compared a regimen of palonosetron-aprepitant or fosaprepitant-DEX versus granisetron-aprepitant or fosaprepitant-DEX,24,26,35 1 RCT compared NEPA oral (netupitant 300 mg and palonosetron 0.5 mg)-DEX versus granisetron-aprepitant-DEX,29 and 1 RCT compared palonosetron-DEX versus granisetron-aprepitant-DEX,31
Among RCTs involving pediatric patients, 3 RCTs compared dual regimens of palonosetron-DEX versus ondansetron-DEX,25,28,32 and 1 RCT compared a dual regimen of palonosetron-DEX versus ondansetron-DEX for MEC and a triple regimen of palonosetron-fosaprepitant-DEX versus of ondansetron-fosaprepitant-DEX for HEC.27
The cost-utility analysis by Botteman et al. (2020)36 assessed the cost-effectiveness of NEPA-DEX relative to granisetron-aprepitant-DEX in patients following HEC.
The cost-utility analysis by Kashiwa and Matsushita (2019)37 and the cost-effectiveness analysis by Shimizu et al. (2018)38 determined the cost-effectiveness of a triple regimen of palonosetron-aprepitant-DEX versus granisetron-aprepitant-DEX in patients following HEC.
The cost-utility analysis by Du et al. (2017)39 estimated which of the 3 treatment strategies consisting of palonosetron-DEX, ondansetron-DEX, and granisetron-DEX was the most cost-effective option in patients following HEC.
The cost-utility analysis by Restelli et al. (2017)40 estimated the cost-effectiveness of NEPA-DEX compared with other regimens such as palonosetron-aprepitant-DEX, palonosetron-fosaprepitant-DEX, ondansetron-aprepitant/DEX, and ondansetron-fosaprepitant-DEX in patients following HEC or MEC.
All included guidelines41-47 considered the efficacy and safety of antiemetic drugs including 5-HT3 RA and NK-1 RA used concomitantly with DEX, which were formulated in different regimens for HEC or MEC.
Outcomes
The efficacy outcomes examined in the SR21 were acute nausea, acute vomiting, delayed nausea, and delayed vomiting. The AEs that were assessed included headache, constipation, diarrhea, and dizziness. The acute phase was defined as 0 to 24 hours after chemotherapy and the delayed phase was from more than 24 hours to 120 hours. Follow-up periods were not reported.
The clinical outcomes considered in the RCTs included CR, total control (TC), complete control (CC), CP, nausea, vomiting, and no use of rescue antiemetic medication. CR was defined as no vomiting and no use of antiemetic medication. CP was defined as no nausea and no vomiting. TC was defined as no vomiting, no use of antiemetic medication and no nausea. CC was defined as no vomiting, no use of antiemetic medication and no more than mild nausea. These outcomes were assessed for acute (within 24 hours), delayed (24 to 120 hours), and overall (0 to 120 hours) period after completion of chemotherapy. Other outcomes considered in the RCTs were the MASCC Antiemetic Tool (MAT) questionnaire, quality of life (QoL) assessed using the Functional Living Index-Emesis (FLIE), and AEs. The MAT questionnaire was a validated tool and an 8-item scale for the assessment of acute and delayed CINV that is completed once per cycle of chemotherapy. The FLIE questionnaire consists of 9 nausea-specific items and 9 vomiting-specific items. Responses were marked on 100 mm visual analogue scale (VAS), with anchors of 1 and 7. A total FLIE score of higher than 108 was considered as “no or minimal impact on daily life.” All RCTs, except one (follow-up of 3 days),34 had a follow-up period of 5 days (120 hours).
The primary outcomes in the cost-utility analysis by Botteman et al. (2020)36 were net monetary benefit (NMB) and the probability that NEPA/DEX is cost-effective versus granisetron-aprepitant-DEX. NMB was calculated with the formula: NMB = quality-adjusted life-day (QALD) difference / 365.25 x $25,000 – cost difference. The willingness-to-pay (WTP) per quality-adjusted life-year (QALY) gained threshold was set at $25,000. A positive NMB suggests that NEPA is cost-effective at the $25,000 per QALY threshold. The higher the NMB, the more cost-effective NEPA is. A sensitivity analysis was conducted using a 1-way and probabilistic sensitivity analysis approach to confirm the robustness of the base-case results.
In the cost-utility analysis by Kashiwa and Matsushita (2019),37 cost-effectiveness was calculated from the costs incurred in antiemetic therapy and QALYs for 5 days. The incremental cost-effectiveness ratio (ICER) of the base case was calculated by dividing the incremental cost between regimens divided by incremental QALYs between regimens. The WTP threshold was 5,000,000 JPY per QALY (US$44,575 per QALY). One-way and probabilistic sensitivity analyses were conducted to assess the uncertainty and robustness of the model.
In the cost-effectiveness analysis by Shimizu et al. (2018),38 the cost-effectiveness ratio was calculated by dividing the mean cost of antiemetic used in each group by the number of CR. The ICER was calculated as the difference in mean cost between groups divided by the difference in CR rates between groups. One-way sensitivity analysis of branded and generic drugs as rescue medication was carried out to calculate the ICER range.
In the cost-utility analysis by Du et al. (2017),39 the ICER was estimated for palonosetron or ondansetron compared with granisetron. The WTP threshold was set at US$22,515. One-way and probabilistic sensitivity analyses were conducted to reflect the uncertainty and robustness of the model.
In the cost-utility analysis by Restelli et al. (2017),40 the ICER of NEPA-DEX was compared with palonosetron-aprepitant-DEX, palonosetron-fosaprepitant-DEX, ondansetron-aprepitant-DEX, and ondansetron-fosaprepitant-DEX. A 1-way sensitivity analysis was conducted to test the robustness of the results.
All included guidelines41-47 considered evidence-based on efficacy and safety outcomes of antiemetic drugs for the prevention of CINV, for the development of the recommendations.
Summary of Critical Appraisal
The detailed quality assessments of the included SR21 (Table 6), RCTs22-35 (Table 7 and Table 8), economic studies36-40 (Table 9), and guidelines41-47 (Table 10) are presented in Appendix 3.
The SR21 was explicit in its objective and inclusion criteria for the review and selection of study design for inclusion, and included a comprehensive literature search strategy. Study selection was performed in duplicate, but it was unclear if data extraction was performed in duplicate. The SR did not report whether a protocol had been published before the conducting of the review. The SR also did not report the sources of funding of the studies included in their review, nor did they provide a list of excluded studies. The characteristics of the included studies were described in adequate detail. A modified Jadad scale and the Cochrane risk of bias (RoB) tool were used to assess the quality and RoB of the included studies. Meta-analysis was performed to combine the results and a subgroup analysis was conducted to assess the potential impact of RoB on the results. Statistical heterogeneity was observed and discussed. Publication bias was not investigated due to the small number of studies. Conflicts of interest were declared. Overall, the SR was of acceptable methodological quality.
All included RCTs22-35 were explicit in reporting (i.e., clearly described the objective of the study, the main outcomes, the characteristics of the participants, the interventions, differences in baseline characteristics between groups, and the main findings of the study). All RCTs22-35 provided estimates of the random variability (e.g., standard deviation or 95% CI) in the data of the main outcomes and actual P values for main outcomes. Of the included RCTs, 222,26 did not report AEs related to treatment drugs. As 4 RCTs22,26,27,31 were conducted with relatively small sample sizes (range from 70 to 116), it was not applicable to determine if the participants were representative of the entire population from which they were recruited. However, the treatment settings in all included RCTs were representative of the treatment received by most of the patients. Seven RCTs22,23,25-27,31,34 were open-label and 5 RCTs24,28-30,32,33,35 were double-blind, of which 229,30,32,33 were double-blind/double-dummy. The intervention and comparator groups in all included RCTs had the same follow-up. Appropriate statistical tests were used to assess the main outcomes, which were accurately measured. Patients in all intervention groups were recruited from the same population and over the same time period. Allocation concealment was only reported in 1 RCT.32,33 Analysis for efficacy and safety outcomes was performed using intention-to-treat (ITT) analysis in 2 RCTs.28,31 Sample size was determined in 9 RCTs23-25,27,29-35 and not reported in the other 3.22,26,28 Overall, the methodological quality of the included RCTs was moderate to high.
All included economic studies36-40 clearly stated the objectives, the economic importance of the research questions, the rationale for choosing the alternative comparators, the viewpoint of the analysis, and the type of economic evaluation that was conducted. Three studies37,39,40 justified the choice of form of economic evaluation in relation to the questions addressed. For data collection, all economic studies clearly stated the sources of effectiveness estimates, with details of the design and findings of those studies, the primary outcome measures for the economic evaluation, the methods to value benefits, the methods for the estimation of quantities and unit costs, currency and price data, and details of the model used (except for 2 studies,36,38 which did not have a model). For the analysis and interpretation of results, all economic studies clearly stated the time horizon of costs and benefits, details of statistical tests and CIs, and the approach to sensitivity analysis. All studies provided justification for the choice of variables for sensitivity analysis and the ranges over which the variables were varied. All studies reported incremental analysis and presented major outcomes in a disaggregated, as well as aggregated, form. The conclusions in all the studies were based on the data reported and were accompanied by the appropriate caveats. Overall, the included economic studies were of moderate to high methodological quality in study design, data collection, and analysis and interpretation of results.
All included guidelines41-47 were explicit in their scope and purpose (i.e., objectives, health questions, and populations), and had clear presentation (i.e., specific, and unambiguous recommendations, different options for management of the condition or health issue, and easy to find key recommendations). Regarding stakeholder involvement, all guidelines clearly defined target users and the development groups; however, it was unclear if the views and preferences of the patients were sought. For rigour of development, all guidelines reported details of systematic searches for evidence, criteria for selecting evidence, explicit link between recommendations and the supporting evidence, and methods of formulating the recommendations. All guidelines considered health benefits, side effects, and risks in formulating the recommendations; were peer-reviewed before publication; and provided a procedure for updating. All guidelines, except the CCO guideline,43 assessed and reported the strength of its recommendations. For applicability, the guidelines were explicit in facilitators and barriers to application, advice and/or tools on how the recommendations can be put into practice, resource implications, and monitoring and or auditing criteria. For editorial independence, all guidelines reported that the funding bodies had no influence on the content of the guidelines. The competing interests of the guideline development group members were reported. Overall, all included guidelines were of high methodological quality.
Summary of Findings
The main findings and authors’ conclusions of the SR21 (Table 11), RCTs22-35 (Table 12), economic studies36-40 (Table 13), and guidelines41-47 (Table 14) are presented in Appendix 4.
Clinical Effectiveness of Palonosetron for the Prevention of CINV in Patients Receiving HEC or MEC
The clinical efficacy and safety of palonosetron for the prevention of prevention CINV in adult and pediatric patients receiving HEC or MEC were reviewed and reported separately. One SR21 and 8 RCTs22-24,26,29-31,34,35 involved adult cancer patients, while 4 RCTs25,27,28,32,33 involved pediatric cancer patients.
Adult Patients Receiving HEC
Five RCTs22,24,29-31,35 included patients naive to chemotherapy who were scheduled to receive HEC.
Clinical Efficacy
The RCT by Mahrous et al. (2021)22 compared the efficacy of palonosetron-DEX with granisetron-DEX in patients receiving at least 4 cycles of HEC (cisplatin-based). The study found that palonosetron combined with DEX was significantly more effective than granisetron-DEX in the prevention of both acute (11.8% versus 89.1%; P < 0.0001) and delayed (47.06% versus 92.2%; P < 0.0001) nausea, as well as both acute (7.8% versus 43.8%; P < 0.0001) and delayed (23.5% versus 82.8%; P < 0.0001) vomiting.
The RCT by Matsumoto et al. (2020)24 compared the efficacy of the 3-drug combination of palonosetron-fosaprepitant-DEX with granisetron-fosaprepitant-DEX in patients receiving HEC (AC-based regimen). The study found no significant difference between palonosetron and granisetron regimens for the primary outcome, which was CR during the delayed phase (62.3% versus 60.4%; P = 0.8). There were also no significant differences for secondary outcomes such as acute CR, overall CR, acute vomiting, delayed vomiting, overall vomiting, acute nausea, and overall nausea. However, patients receiving the palonosetron regimen had a significantly lower incidence of nausea at the delayed phase compared to those receiving granisetron regimen (60% versus 72%; P = 0.029).
The RCT by Zhang et al. (2018)29 compared the efficacy of NEPA (a fixed antiemetic combination of netupitant and palonosetron)-DEX with granisetron-aprepitant-DEX in patients receiving cisplatin-based HEC. A subsequent publication30 of the same study examined the efficacy and safety of the regimens in a subset of a Chinese population, which was 80% of the overall population. The study found no significant difference between regimens for the primary outcome, which was CR during the overall phase (73.8% versus 72.4%; risk difference [RD] = 1.5%; 95% CI, –4.5% to 7.5%). The authors concluded that NEPA demonstrated noninferiority compared to a granisetron-aprepitant regimen, with a noninferiority margin set at –10%. Daily rates of patients with CINV over 5 days in the NEPA group declined from 16% to 8%, while those in the granisetron-aprepitant group remained between 13% and 15%. On day 5, 8.0% of patients in the NEPA group compared with 13.9% of patients in the granisetron group had CINV, P = 0.0063. For secondary outcomes, the study found no significant differences between regimens for no vomiting (acute, delayed, overall), no significant nausea (acute, delayed, overall), no nausea (acute, delayed, overall), and no use of rescue medication during the acute phase. However, a significantly higher proportion of patients in the NEPA group did not need to use rescue medication during the delayed phase (97.6% versus 94.7%; RD = 2.9%; 95% CI, 0.2% to 5.5%; P < 0.05) or during the overall phase (96.6% versus 93.5%; RD = 3.1%; 95% CI, 0.2 to 6.1; P < 0.05) compared to the granisetron-aprepitant group. For QoL, FLIE scores reflecting “no impact on daily life” showed no significant differences between groups for nausea, vomiting, or overall combined in the acute and delayed phases, except NEPA was significantly better with the nausea domain for the delayed phase (71.1% versus 65.1%; RD = 6.5%; 95% CI, 0.2% to 12.8%). The subgroup analysis of a subset of a Chinese population found similar results as those in the overall population.30
The RCT by Ishido et al. (2016)31 compared the efficacy of palonosetron-DEX versus granisetron-aprepitant-DEX in patients receiving cisplatin-based HEC. The results of the study showed no significant difference between groups for the primary outcome, which was CR during the overall phase (58.5% versus 67.4%; P = 0.399). For secondary outcomes, there were also no significant differences between groups for CR (acute, delayed), no vomiting (acute, delayed, overall), no nausea (acute, delayed, overall), no use of rescue medication (acute, delayed, overall), TC (acute, delayed, overall), and FLIE scores.
The RCT by Suzuki et al. (2016)35 compared the efficacy of a triple regimen of palonosetron-aprepitant-DEX with granisetron-aprepitant-DEX in patients receiving cisplatin-based HEC. The study found no significant difference between treatment groups in the primary outcome, which was CR during the overall phase (65.7% versus 51.9%; P = 0.0539). For secondary outcomes, there were also no significant differences between groups for CR, CC, and TC during the acute phase. Patients in the palonosetron regimen had significantly higher rates in CR at the delayed phase (67.2% versus 59.1%; P = 0.0142), CC during the delayed phase (65.2% versus 55.9%; P = 0.0053), CC during the overall phase (63.8% versus 55.9%; P = 0.0234), TC during the delayed phase (48.6% versus 41.4%; P = 0.0369), and TC during the overall phase (47.6% versus 40.7%; P = 0.0369). The palonosetron group had a longer time to treatment failure when compared with the granisetron group (hazard ratio = 0.81; 95% CI, 0.65 to 1.01; P = 0.063), although not statistically significantly different.
Safety
The RCT by Matsumoto et al. (2020)24 found that most of the AEs were of grade 1 and 2 based on the Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. The study reported no differences between palonosetron-fosaprepitant-DEX and granisetron-fosaprepitant-DEX groups for constipation (34% versus 27.5%), headache (13.2% versus 12%), infusion site reaction (20.3% versus 23.3%), and febrile neutropenia (5.4% versus 4.2%). Statistical comparisons were not conducted.
The RCT by Zhang et al. (2018)29 reported a comparable safety profile in overall AEs between treatment groups (NEPA 58.1% versus granisetron-aprepitant 57.5%) including constipation (8.0% versus 6.3%) and hiccups (2.7% versus 1.4%). Most AEs were of mild to moderate intensity. The study reported that there was more severe AEs in the granisetron-aprepitant group (10.8%) compared to the NEPA group (8.7%). Statistical comparisons were not conducted.
The RCT by Ishido et al. (2016)31 reported no significant difference between groups for any grade AEs, except constipation was significantly higher in the palonosetron group (17.1%) compared to the ondansetron group (2.3%); P = 0.028. There was no significant difference between groups for grade 3 or higher AEs.
The RCTs by Mahrous et al. (2021)22 and by Suzuki et al. (2016)35 did not report safety outcomes.
Adult Patients Receiving Moderate Emetogenic Chemotherapy
Two RCTs23,34 included patients who were scheduled to receive MEC. One RCT23 included patients naive to chemotherapy, while the other34 included patients with or without previous chemotherapy experience.
Clinical Efficacy
The RCT by van der Vorst et al. (2021)23 was conducted to demonstrate the noninferiority of 2 treatment regimens; i.e., palonosetron-DEX and ondansetron-DEX-metoclopramide relative to ondansetron-DEX. The results of the study showed no significant difference in primary outcome, which was TC at the delayed phase between palonosetron-DEX and ondansetron-DEX (55.6% versus 50.0%; 95% CI of difference, –12.0% to 23.2%), or between ondansetron-DEX-metoclopramide and ondansetron-DEX (56.1% versus 50.0%; 95% CI of difference, –11.3% to 23.5%). The authors concluded that both palonosetron-DEX and ondansetron-DEX-metoclopramide met the criteria for noninferiority relative to ondansetron/DEX, as the lower limit of the 95% CI of the differences between arms was greater than the noninferiority margin of –20%. There were no significant differences between the palonosetron-DEX and ondansetron-DEX groups for secondary outcomes such as TC at the acute phase and at the overall phase. Also, no significant differences were observed between the palonosetron-DEX and ondansetron-DEX groups for no vomiting, no significant nausea, no nausea, no use of rescue medication, CR, and CP at the acute, delayed, or overall phase. There were also no significant differences between palonosetron-DEX and ondansetron-DEX for QoL, as determined by FLIE scores.
The RCT by Seol et al. (2016)34 compared palonosetron-DEX with transdermal granisetron-DEX. The study found no significant different between treatment groups for the primary outcome, which was CR during the acute phase (79.8% versus 75.2%). The difference between granisetron and palonosetron groups was –4.6%; 95% CI, –13.6 to 4.4. There were also no significant differences between groups in secondary outcomes such as CR during the overall phase, CC (acute, overall), TC (acute, overall), and QoL, assessed by FLIE scores.
Safety
The RCT by van der Vorst et al. (2021)23 did not report palonosetron or ondansetron treatment-related AEs.
The RCT by Seol et al. (2016)34 reported no significant differences between palonosetron-DEX and transdermal granisetron-DEX groups in AEs including constipation, diarrhea, insomnia and rash.
Adult Patients Receiving Highly Emetogenic Chemotherapy or Moderate Emetogenic Chemotherapy
For adult patients receiving HEC or MEC, 1 SR21 and 1 RCT26 were included in this review. The SR21 included 6 RCTs published between 2003 and 2013 comparing ondansetron with palonosetron: 3 RCTs involving HEC and 3 involving MEC. The RoB of the RCTs were assessed by the authors as low (2 RCTs), unclear (2 RCTs), and high (2 RCTs).
Clinical Efficacy
In the comparison of ondansetron with palonosetron in the SR,21 meta-analysis results showed no significant difference in acute nausea (relative risk [RR] = 1.14; 95% CI, 0.78 to 1.66). However, palonosetron showed greater efficacy than ondansetron for delayed nausea (RR = 1.25; 95% CI, 1.01 to 1.56), acute vomiting (RR = 1.28; 95% CI, 1.02 to 1.59), and delayed vomiting (RR = 1.31; 95% CI, 1.01 to 1.69). Subgroup analysis revealed that palonosetron exhibited significantly greater efficacy for acute vomiting compared with ondansetron in the MEC subgroup (RR = 1.57; 95% CI, 1.15 to 2.15) but not in the HEC subgroup. In both HEC and MEC subgroups, the analyses showed no statistically significant differences in acute nausea between drugs.
The RCT by Tsubata et al. (2019)26 compared the 3-drug combination of palonosetron-aprepitant-DEX with granisetron-aprepitant-DEX in a mixed population receiving HEC or MEC. The study found no significant differences between groups in the primary outcome (i.e., MAT scores at delayed phase),or secondary outcomes (i.e., MAT scores at acute phase; FLIE scores for vomiting; FLIE scores for nausea; CR for acute, delayed, and overall phase; and overall TC). Subgroup analysis of each treatment group stratified by HEC or MEC showed no statistically significant differences.
Safety
The SR21 assessed AEs such as headache, constipation, diarrhea, and dizziness, and found no statistically significant difference between ondansetron and palonosetron.
The RCT by Tsubata et al. (2019)26 did not report safety outcomes.
Pediatric Patients Receiving Highly Emetogenic Chemotherapy
One RCT28 included patients with or without previous chemotherapy who were scheduled to receive HEC.
Clinical Efficacy
The RCT by Tan et al. (2018)28 compared the efficacy of 2 doses of palonosetron (5 mcg/kg and 10 mcg/kg)-DEX versus ondansetron-DEX. The results of the study showed no significant difference between treatment groups in CR rates for the acute phase (palonosetron 5 mcg/kg 69.1%, palonosetron 10 mcg/kg 69.7%, ondansetron 64.6%). However, patients in the palonosetron 10 mcg/kg group had significantly higher CR rate at the delayed phase (53.5% versus 32.8%; P < 0.017) and at the overall phase (42.7% versus 21.7%; P < 0.017) compared with the ondansetron group. Similarly, significant differences between palonosetron 10 mcg/kg group and the ondansetron group were observed for vomiting and nausea at the delayed and overall phases but not at the acute phase. There were no significant differences between the palonosetron 5 mcg/kg group and the ondansetron group for all outcomes assessed.
Safety
The RCT by Tan et al. (2018)28 reported no significant difference between treatment groups in AEs (palonosetron 5 mcg/kg 12.7%, palonosetron 10 mcg/kg 11.9%, ondansetron 13.2%). Most AEs were grade 1 and 2.
Pediatric Patients Receiving Highly Emetogenic Chemotherapy or Moderate Emetogenic Chemotherapy
Two RCTs25,27 included patients naive to chemotherapy who were scheduled to receive HEC or MEC and 1 RCT32,33 included patients with or without previous chemotherapy experience who were scheduled to receive HEC or MEC.
Clinical Efficacy
The RCT by Chaudhary et al. (2019)25 compared palonosetron-DEX with ondansetron-DEX. The study found no significant differences between treatment groups in CR and CP during all phases (acute, delayed, overall). There was also no significant difference between the treatment groups’ proportion of patients using rescue antiemetic medication.
The RCT by Jain et al. (2018)27 assessed the noninferiority of palonosetron-DEX versus ondansetron-DEX. The study found no significant difference between treatment groups in primary outcomes, which was CR at acute phase (83.3% versus 72.2%). The difference between groups was 11.1%; 97.5% CI, –6.95 to 28.39. The authors concluded that palonosetron was noninferior to ondansetron, as the lower limit of 97.5% CI of the difference was greater than the noninferiority margin of –15%.
The RCT by Kovacs et al. (2016)32,33 assessed the noninferiority of palonosetron-DEX versus ondansetron-DEX. Two doses of palonosetron (10 mcg/kg and 20 mcg/kg) were investigated. The study found no significant difference in primary outcome, which was CR during the acute phase between palonosetron 10 mcg/kg and ondansetron (54% versus 59%) and between palonosetron 20 mcg/kg and ondansetron (59% versus 59%). The difference between palonosetron 10 mcg/kg and ondansetron was –4.41%; 97.5% CI, –16.4 to 7.6. The authors concluded that noninferiority was not shown for palonosetron 10 mcg/kg, as the noninferiority margin was set at –15%. However, the difference between palonosetron 20 mcg/kg and ondansetron was 0.36% (97.5% CI, –11.7 to 12.4, and therefore noninferiority was shown for this dose. There were also no significant differences between the palonosetron 20 mcg/kg and ondansetron treatment groups for CR during the delayed phase (39% versus 28%) and during the overall phase (33% versus 24%). Compared with ondansetron, palonosetron 20 mcg/kg showed significant efficacy regarding several other secondary outcomes including vomiting during the acute phase (84% versus 73%; difference = 10.03%; 95%CI, 1.2 to 18.1), vomiting during the delayed phase (74% versus 58%; difference = 15.84%; 95%CI, 5.7 to 26.0), vomiting during the overall phase (69% versus 51%; difference = 17.46%; 95%CI, 7.0 to 27.9), no emetic episodes during the acute phase (80% versus 69%; difference = 11.25%; 95%CI, 2.0 to 20.5), no emetic episodes during the delayed phase (68% versus 53%; difference = 15.38%; 95%CI, 5.1 to 25.7), no emetic episodes during the overall phase (64% versus 46%; difference = 17.56%; 95%CI, 7.0 to 28.1), no delayed nausea (66% versus 51%; difference = 14.79%; 95%CI, 1.5 to 28.1), and no nausea during the overall phase (58% versus 43%; difference = 15.00%; 95%CI, 1.4 to 28.6). Outcomes showed no significant differences between 3 treatment groups for no use of antiemetic rescue medication during acute, delayed, and overall phases, and for nausea during the acute phase.
Safety
The RCT by Chaudhary et al. (2019)25 reported that both drugs were well-tolerated and found no difference between the palonosetron-DEX and ondansetron-DEX groups in AEs (22% versus 20%). Common AEs included abdominal pain, constipation, diarrhea, headache, and dizziness.
The RCT by Jain et al. (2018)27 reported the incidence of headache (palonosetron, 1 patient, versus ondansetron, 2 patients) and constipation (1 patient in each group). No serious AEs were observed in either groups.
The RCT by Kovacs et al. (2016)32,33 reported comparable drug-related, treatment-emergent AEs among 3 treatment groups (palonosetron 10 mcg/kg 4%, palonosetron 20 mcg/kg 4%, ondansetron 4%). Incidence of headache among treatment groups were 2%, less than 1%, and 1%, respectively. Incidence of dizziness among treatment groups was less than 1%, less than 1%, and 0, respectively.
Cost-Effectiveness of Palonosetron for the Prevention of CINV in Patients Receiving HEC or MEC
All 5 included economic studies36-40 involved adult patients.
Adult Patients Receiving Highly Emetogenic Chemotherapy
Two studies36-38 assessed the cost-effectiveness of palonosetron in patients naive to chemotherapy and 1 study39 included patients naive or non-naive to chemotherapy.
The cost-utility analysis by Botteman et al. (2020)36 assessed the cost-effectiveness of NEPA-DEX versus granisetron-aprepitant-DEX. Compared with the granisetron regimen, NEPA resulted in a non-significant gain of 0.09 QALD (95% CI, –0.06 to 0.25). In terms of costs, NEPA resulted in significant total per-patient cost reduction ($309; 95% CI, 4 to 624), mean decrease in medical costs of CINV-related events ($409; 95% CI, 215 to 612), reduction in study drug costs ($45; $531 versus $577), and reduction in rescue medication costs ($3 [95% CI, 1 to 5] versus $8 [95% CI, 2 to 17]). Joint bootstrap and probabilistic sensitivity analysis simulations revealed that NEPA resulted in lower costs and higher QALD; hence, it was considered as dominant in 86.5% of cases (located in bottom-right quadrant). With a WTP threshold of $25,000 per QALY gained, the probability of NEPA being cost-effective was 97.8% of cases. The NMB was found to be $315. Sensitivity and subgroup revealed that NEPA was cost-effective with all parameters investigated. NEPA was particularly highly cost-effective, with severe nausea defined as an 8.5-hour vomiting and/or retching threshold.
The cost-utility analysis by Kashiwa and Matsushita (2019)37 assessed the cost-effectiveness of a triple regimen of palonosetron-aprepitant-DEX versus granisetron-aprepitant-DEX based on the TRIPLE study by Suzuki et al. (2016).35 Compared with the granisetron regimen, the palonosetron regimen resulted in a 0.0006452 QALY gained. Regarding costs for palonosetron and granisetron regimens, the antiemetic drug costs were 27,406 JPY (US$244.33) and 13,707 JPY (US$122.20), rescue medication costs were 432 JPY (US$3.85) and 5,953 JPY (US$53.10), respectively. The medical costs were 1,580 JPY (US$14.09) for blood testing, 590 JPY (US$5.25) for pharmacy costs, and 1,374 JPY (US$12,25) for supplementary nutrition infusion. The incremental cost was 10,455 JPY (US$93.21), due to the higher total cost of the palonosetron regimen compared to the granisetron regimen (30,348 JPY [US$270.55] versus 19,893 JPY [US$177.35]). The ICER was estimated to be 16,204,591 JPY per QALY (US$144,465 per QALY), which was much higher than the WTP threshold of 5,000,000 JPY (US$44,575). At this WTP threshold, the probability of the palonosetron regimen being cost-effective was 3.64% of cases. Probabilistic sensitivity analysis revealed that the palonosetron regimen was more expensive but more effective (located in top-right quadrant). The authors concluded that the palonosetron regimen was not cost-effective for HEC in Japan. The authors suggested that with a 50% reduction in drug price for palonosetron, the ICER decreased to approximately 4,600,000 JPY per QALY (US$41,000 USD per QALY), and the acceptable price of palonosetron was estimated to be 7,743 JPY (US$69.03).
The cost-effectiveness analysis by Shimizu et al. (2018)38 assessed the cost-effectiveness of a triple regimen of palonosetron-aprepitant-DEX versus granisetron-aprepitant-DEX, also based on the TRIPLE study by Suzuki et al. (2016),35 as in the cost-utility analysis by Kashiwa and Matsushita (2019).37 The CR rates during the overall phase were 65.7% and 59.1% for the palonosetron regimen and granisetron regimen, respectively. The palonosetron regimen costed more than the granisetron regimen (27,863.8 JPY versus 15,342.8 JPY; cost difference 12,521 JPY). The costs of rescue medication were 59,292.7 JPY and 73,883.8 JPY for the palonosetron regimen and the granisetron regimen, respectively. The cost-effectiveness ratios for the palonosetron regimen and the granisetron regimen were 42,628.6 JPY per CR and 26,263.4 JPY per CR, respectively. The ICER was 189,171.6 JPY per CR,with a range between 189,044.8 to 189,215.5 JPY per CR. The authors found that the difference in price between palonosetron and granisetron was large and that was the main factor affecting the ICER.
The cost-utility analysis by Du et al. (2017)39 estimated which of the 3 antiemetic regimens (i.e., palonosetron-DEX, ondansetron-DEX, and granisetron-DEX) was the most cost-effective option. In terms of utilities, ondansetron resulted in a QALY loss of –0.00003 and palonosetron resulted in a QALY gained of 0.00056 compared with granisetron. The difference in drug cost between ondansetron and granisetron was US$25.95, and between palonosetron and granisetron it was US$93.64. Compared to granisetron, the ICER was US$–953,456.58 per QALY for ondansetron (more cost, less effective) and US$167,914.74 per QALY for palonosetron (more cost, more effective), which was higher than the WTP threshold of US$22,515 per QALY and was therefore not cost-effective. One-way sensitivity analysis revealed that the cost of palonosetron 0.25 mg was the most important parameter among the parameters evaluated. The authors suggested that the price of palonosetron per 0.25 mg must be decreased to US$23.41, a reduction of at least 69.7%, to be cost-effective.
Adult Patients Receiving Highly Emetogenic Chemotherapy or Moderate Emetogenic Chemotherapy
The cost-utility analysis by Restelli et al. (2017)40 estimated the cost-effectiveness of NEPA-DEX compared with other regimens such as palonosetron-aprepitant-DEX, palonosetron-fosaprepitant-DEX, ondansetron-aprepitant-DEX, and ondansetron-fosaprepitant-DEX. NEPA had higher utility value and costed less compared to all comparators. Cost-utility analysis revealed that NEPA was dominant compared with palonosetron-aprepitant-DEX (for HEC and MEC), palonosetron-fosaprepitant-DEX (for HEC and MEC), ondansetron-aprepitant-DEX (for HEC), and ondansetron-fosaprepitant-DEX (for HEC).
Guidelines
Two guidelines41,45-47 had recommendations for both adult and pediatric patients; 2 guidelines42,43 had recommendations for adult patients, only; and 1 guideline44 had recommendations for pediatric patients, only.
Adult Patients Receiving Highly Emetogenic Chemotherapy
The ASCO guideline (2020)41 recommends a 4-drug combination of an NK1 RA, a 5-HT3 RA (granisetron, ondansetron, palonosetron, dolasetron, tropisetron, or ramosetron), DEX, and olanzapine for adults receiving cisplatin, other high emetic–risk single agents, or a combination of AC. DEX and olanzapine should be continued on days 2 to 4 (level of evidence: high; strength of recommendation: strong).
The NCCN guideline (2020)42 recommends 1 of the 3 treatment options (A, B, C). With option A (preferred), the guideline recommends a 4-drug combination of olanzapine, NK1 RA (with 1 of: aprepitant, fosaprepitant, netupitant, fosnetupitant, or rolapitant), 5-HT3 RA (with 1 of: dolasetron, granisetron, ondansetron or palonosetron), and DEX for day 1. For days 2 to 4, the guideline recommends the use of olanzapine, aprepitant, and DEX. With treatment option B, the guideline recommends a 3-drug combination of olanzapine, palonosetron, and DEX for day 1. For days 2 to 4, the guideline recommends the use of olanzapine. With option C, the guideline recommends 3-drug combination of NK1 RA (with 1 of: aprepitant, fosaprepitant, netupitant, fosnetupitant, or rolapitant), 5-HT3 RA (with 1 of: dolasetron. granisetron, ondansetron, or palonosetron), and DEX for day 1. For days 2 to 4, the guideline recommends the use of aprepitant and DEX. All recommendations are category 2A (based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate).
The CCO guideline (2019)43 recommends a 4-drug combination of an NK1 RA (with 1 of: aprepitant, fosaprepitant, or NEPA), a 5-HT3 RA (with 1 of: granisetron, ondansetron, or palonosetron), dexamethasone, and olanzapine for day 1. On subsequent days, aprepitant is recommended for days 2 and 3 if the drug is started on day 1, DEX for days 2 to 4, and olanzapine for day 2 to 4. The level of evidence and the strength of recommendation are not provided.
The MASCC/ESMO guideline (2016)45-47 recommends a 3-drug combination of an NK1 RA (aprepitant, fosaprepitant, netupitant, or rolapitant), a 5-HT3 RA (granisetron, ondansetron, dolasetron, tropisetron, or palonosetron), and DEX given before chemotherapy for the prevention of non-AC HEC (MASCC level of confidence: high; MASCC level of consensus: high; ESMO level of confidence: I; Grade of recommendation: A). On days 2 to 4, the guideline suggests the use of DEX to prevent delayed nausea and vomiting (MASCC level of confidence: high; MASCC level or consensus: moderate; ESMO level of confidence: I; Grade of recommendation: B). In women with breast cancer receiving AC-based chemotherapy, the guideline recommends a 3-drug combination of an NK1 RA, a 5-HT3 RA, and DEX given before chemotherapy (MASCC level of confidence: high; MASCC level of consensus: high; ESMO level of confidence: I; Grade of recommendation: A). On days 2 and 3, the guideline suggests the use of aprepitant or DEX in women with breast cancer. Subsequent aprepitant should not be used if fosaprepitant, netupitant, or rolapitant has been used on day 1 (MASCC level of confidence: moderate; MASCC level of consensus: moderate; ESMO level of confidence: II; Grade of recommendation: B).
Adult Patients Receiving Moderate Emetogenic Chemotherapy
The ASCO guideline (2020)41 recommends a 3-drug combination of an NK1 RA, a 5-HT3 RA (granisetron, ondansetron, palonosetron, dolasetron, tropisetron, or ramosetron) and DEX (day 1) for patients treated with carboplatin area under the curve (AUC) ≥ 4 mg/min or other MEC (level of evidence: high; strength of recommendation: strong). For patients receiving cyclophosphamide, doxorubicin, oxaliplatin, or other MEC known to cause delayed nausea and vomiting, the guideline recommends continuing DEX on days to 2 to 3 (level of evidence: low; strength of recommendation: moderate).
The NCCN guideline (2020)42 recommends 1 of the 3 treatment options (D, E, F). With option D, the guideline recommends a 2-drug combination of 5-HT3 RA (with 1 of: dolasetron. granisetron, ondansetron, palonosetron) and dexamethasone for day 1. For days 2 and 3, the guideline recommends the use of DEX or a 5-HT3 RA monotherapy (granisetron, ondansetron, or dolasetron). With option E, the guideline recommends a 3-drug combination of olanzapine, palonosetron, and DEX for day 1. For days 2 and 3, the guideline recommends the use of olanzapine. With option F, the guideline recommends 3-drug combination of NK1 RA (with 1 of: aprepitant, fosaprepitant, netupitant, fosnetupitant, or rolapitant), 5-HT3 RA (with 1 of: dolasetron. granisetron, ondansetron, or palonosetron), and DEX for day 1. For days 2 and 3, the guideline recommends the use of aprepitant with or without DEX. All recommendations are category 2A (based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate).
The CCO guideline (2019)43 recommends a 2-drug combination of a 5-HT3 RA (with 1 of: granisetron, ondansetron, or palonosetron), and DEX for day 1. For subsequent days, no 5-HT3 RA or dexamethasone is recommended after day of chemotherapy. The level of evidence and the strength of recommendation are not provided.
The MASCC/ESMO guideline (2016)45-47 recommends a 2-drug combination of a 5-HT3 RA (granisetron, ondansetron, dolasetron, tropisetron or palonosetron) and DEX for the prevention of acute emesis in MEC (MASCC level of confidence: moderate; MASCC level of consensus: moderate; ESMO level of confidence: II; Grade of recommendation: B). The guideline suggests that DEX should be considered for days 2 and 3 in patients receiving MEC with a known potential for delayed emesis (MASCC level of confidence: low; MASCC level of consensus: moderate; ESMO level of confidence: III; Grade of recommendation: C). For all other patients receiving MEC, the guideline does not recommend routine prophylaxis for delayed emesis (MASCC level of confidence: no confidence possible; MASCC level of consensus: high; ESMO level of confidence: IV; Grade of recommendation: D).
Pediatric Patients Receiving Highly Emetogenic Chemotherapy
The ASCO guideline (2020)41 recommends a 3-drug combination of a 5-HT3 receptor antagonist (granisetron, ondansetron, palonosetron, dolasetron, tropisetron, or ramosetron), DEX, and aprepitant or fosaprepitant (level of evidence: intermediate; strength of recommendation: strong). For patients who are unable to receive aprepitant or fosaprepitant, the guideline recommends a 2-drug combination of a 5-HT3 receptor antagonist and DEX (level of evidence: intermediate; strength of recommendation: strong). For patients who are unable to receive DEX, the guideline recommends a 2-drug combination of palonosetron and aprepitant or fosaprepitant (level of evidence: intermediate; strength of recommendation: strong).
The POGO guideline (2017)44 recommends that children aged 6 months and older receive a 3-drug combination of a 5-HT3 RA (with 1 of: granisetron, ondansetron, or palonosetron), aprepitant, and DEX (level of evidence: moderate; strength of recommendation: strong). For children younger than 6 months, the guideline recommends a 2-drug combination of a 5-HT3 RA (with 1 of: granisetron, ondansetron, palonosetron) and DEX (level of evidence: moderate; strength of recommendation: strong). For children aged 6 months and older receiving HEC, which is known or suspect to interact with aprepitant, the guideline recommends a 2-drug combination of a 5-HT3 RA (with 1 of: granisetron, ondansetron, or palonosetron) and DEX (level of evidence: moderate; strength of recommendation: strong). For children aged 6 months and older who cannot receive DEX, the guideline recommends a 2-drug combination of palonosetron and DEX (level of evidence: moderate; strength of recommendation: strong). For children younger than 6 months who cannot receive DEX, the guideline suggests the use of palonosetron alone (level of evidence: moderate; strength of recommendation: weak). For all children receiving HEC, which is known or suspect to interact with aprepitant and who cannot receive DEX, the guideline suggests the use of palonosetron alone (level of evidence: moderate; strength of recommendation: weak).
The MASCC/ESMO guideline (2016)45-47 recommends a 3-drug combination of a 5-HT3 RA (granisetron, ondansetron, tropisetron, or palonosetron), aprepitant, and DEX (MASCC level of confidence: high; MASCC level of consensus: high; ESMO level of confidence: II; Grade of recommendation: B). For children who cannot receive DEX, the guideline recommends a 2-drug combination of a 5-HT3 RA and aprepitant (MASCC level of confidence: moderate; MASCC level of consensus: high; ESMO level of confidence: II; Grade of recommendation: B). When aprepitant is not feasible or desirable, the guideline recommends a 2-drug combination of a 5-HT3 RA, and DEX (MASCC level of confidence: moderate; MASCC level of consensus: high; ESMO level of confidence: II; Grade of recommendation: B).
Pediatric Patients Receiving Moderate Emetogenic Chemotherapy
The ASCO guideline (2020)41 recommends a 2-drug combination of a 5-HT3 RA (granisetron, ondansetron, palonosetron, dolasetron, tropisetron, or ramosetron) and DEX (level of evidence: intermediate; strength of recommendation: strong). For children who are unable to receive DEX, the guideline recommends a 2-drug combination of a 5-HT3 receptor antagonist and aprepitant or fosaprepitant (level of evidence: intermediate; strength of recommendation: strong).
The POGO guideline (2017)44 recommends that children receive a 2-drug combination of 5-HT3 RA (with 1 of: granisetron, ondansetron, or palonosetron) and DEX (level of evidence: moderate; strength of recommendation: strong). For children aged 6 months and older who cannot receive DEX, the guideline suggests a 2-drug combination of 5-HT3 RA (choose 1: granisetron, ondansetron, or palonosetron) and aprepitant (level of evidence: moderate; strength of recommendation: weak). For children younger than 6 months who cannot receive DEX, the guideline suggests the use of palonosetron alone (level of evidence: moderate; strength of recommendation: weak). For all children receiving MEC, which is known or suspect to interact with aprepitant, and who cannot receive DEX, the guideline suggests the use of palonosetron alone (level of evidence: moderate; strength of recommendation: weak).
The MASCC/ESMO guideline (2016)45-47 recommends a 2-drug combination of a 5-HT3 RA and DEX (MASCC level of confidence: moderate; MASCC level of consensus: high; ESMO level of confidence: II; Grade of recommendation: B). For children who cannot receive DEX, the guideline recommends a 2-drug combination of a 5-HT3 RA and aprepitant (MASCC level of confidence: moderate; MASCC level or consensus: high; ESMO level of confidence: II; Grade of recommendation: B).
Limitations
Although there has been a large body of clinical evidence within the past 5 years regarding the clinical effectiveness of palonosetron versus ondansetron and granisetron in the prevention of CIVN, the included SR and RCTs had several limitations. The SR21 was published in 2016 and its included studies for the comparison of palonosetron versus ondansetron were published between 2003 and 2013; hence, the evidence was quite outdated relative to the included RCTs. Studies included in the SR were heterogeneous in their treatment regimens of the interventions, sample size, type of cancer, type of chemotherapy, and concomitant used of corticosteroids. One of the limitations of the included RCTs was that treatment regimens including the dosage of the intervention drugs (i.e., palonosetron, ondansetron, and granisetron), schedule and mode of administration, and the use of concomitant medications such as NK1 RA and DEX, varied among studies even within the same type of chemotherapy and therefore would generate different results. Another limitation was that the primary outcome varied among studies and it was unclear how it was selected. It was also unclear how the noninferiority margin was determined in the noninferiority studies. Seven RCTs22,23,25-27,31,34 had open-label designs, which may allow the analysis to be vulnerable to detection bias. As 4 RCTs22,26,27,31 were conducted with relatively small sample sizes, the non-significant differences in certain outcomes between groups may be due to the lack of power. Patients’ comorbidities, concomitant addition medications or current home medications, could interfere with the medication used and were not assessed in the included studies. Also, subgroup analysis by patient risk factors of emesis such as age, sex, history of morning sickness, anxiety, and expectations of nausea and vomiting was not performed.
One of the limitations in the included economic evaluations36-40 was that the costs and benefits for treatment were limited to short time periods (i.e., 120 hours). All studies just focused on the effect of antiemetics within 120 hours in the first cycle of chemotherapy; therefore, the economic evaluations could not track the additional use of chemotherapy and additional use of antiemetics to prevent CINV. In the studies conducting cost-utility analysis, the utility values were based on data measured in other countries, which have different health care systems. The cost-utility analysis was based on a clinical efficacy trial so that the results may have high internal validity; however, the degree of external validity may be limited when extrapolating the results to different populations. Incidence and duration of treatment-related AEs were obtained from well-controlled trials that may not reflect real-word data. The cost-utility analysis did not include utility values associated with AEs of antiemetics; therefore, the costs associated with antiemetic prophylaxis may be underestimated. The included economic studies were conducted in countries other than Canada; therefore, the results have limited generalizability to the Canadian context (i.e., the Canadian health care system).
There were no significant methodological limitations of all included guidelines, except that the strength of recommendations in the CCO guideline43 was not graded.
Conclusions and Implications for Decision- or Policy-Making
This report identified 1 SR,21 12 RCTs22-35 and 5 economic studies36-40 assessing the clinical effectiveness and cost-effectiveness of palonosetron in comparison with other 5-HT3 RA, particularly ondansetron and granisetron, for the prevention of CINV in patients (adults and children) receiving HEC or MEC. This report also included 5 evidence-based guidelines41-47 providing recommendations on antiemetic regimens including palonosetron for the prevention of CINV in adult and pediatric patients receiving HEC or MEC.
In adult patients receiving HEC, NEPA — a fixed antiemetic combination of netupitant and palonosetron — co-administered with DEX demonstrated noninferiority relative to a triple regimen of granisetron-aprepitant-DEX. Similarly, the efficacy of a triple regimen of palonosetron-aprepitant-DEX or palonosetron-fosaprepitant-DEX was comparable with a triple regimen of granisetron-aprepitant-DEX or granisetron-fosaprepitant-DEX, respectively. In the absence of NK1 RA aprepitant in the palonosetron regimen, the efficacy between palonosetron-DEX and granisetron-aprepitant-DEX also did not differ. However, when aprepitant was removed from both treatment groups, a 2-drug combination of palonosetron-DEX appeared to be significantly more effective than granisetron-DEX for the prevention of both acute and delayed emesis.
In adult patients receiving MEC, a 2-drug combination of palonosetron-DEX was found to be noninferior compared with ondansetron-DEX in terms of delayed TC. Similar efficacy was also observed between palonosetron-DEX and transdermal granisetron-DEX for the prevention of CINV.
In mixed population of adult patients receiving HEC or MEC, meta-analysis results showed no significant difference in efficacy between the palonosetron and ondansetron regimens for acute nausea. Palonosetron, however, appeared to have greater efficacy than ondansetron for delayed nausea and acute and delayed vomiting. There was no significant difference in efficacy between a triple regimen of palonosetron-aprepitant-DEX and granisetron-aprepitant-DEX at all phases investigated.
In pediatric patients receiving HEC, dual therapy of palonosetron-DEX had similar efficacy compared with ondansetron-DEX in controlling acute CINV; however, palonosetron-DEX was more effective in controlling CINV at delayed and overall phases.
In a mixed population of pediatric patients receiving HEC or MEC, evidence showed that palonosetron-DEX was noninferior to ondansetron-DEX for the prevention of CINC.
The assessment of the safety profile and QoL showed no significant differences in AEs and “no or minimal impact on daily life” between the palonosetron and ondansetron or between the palonosetron and granisetron treatment regimens.
In adult patients receiving HEC, a cost-utility analysis revealed that NEPA-DEX was dominant (i.e., cost less, more effective) relative to granisetron-aprepitant-DEX. Cost-utility analysis also revealed that NEPA-DEX was dominant compared with ondansetron-aprepitant-DEX or ondansetron-fosaprepitant-DEX for the prevention of CINV in patients receiving HEC. In contrast, a triple regimen of palonosetron-aprepitant-DEX was not cost-effective compared to granisetron-aprepitant-DEX, as the palonosetron regimen was had a small QALY gain but was more expensive. Similarly, palonosetron-DEX was also not cost-effective compared with granisetron-DEX, mainly due to a large difference in price and a small QALY gained.
Three recent guidelines (ASCO,41 NCCN,42 and CCO43) recommend a 4-drug combination of olanzapine, NK1 RA, 5-HT3 RA, and DEX on day 1 for adult patients receiving HEC. The NCCN guideline42 recommends other treatment options such as a 3-drug combination of olanzapine, palonosetron, and DEX, or a 3-drug combination of NK1 RA, 5-HT3 RA, and DEX on day 1. Likewise, an older guideline MASCC/ESMO45-47 recommends a 3-drug combination of NK1 RA, 5-HT3 RA, and DEX given before chemotherapy to prevent CINV for adult patients receiving HEC.
The ASCO guideline41 recommends a 3-drug combination of NK1 RA, 5-HT3 RA, and DEX on day 1, while the other 3 guidelines (NCCN,42 CCO,43 and MASCC/ESMO45-47) had recommendations of a 2-drug combination of 5-HT3 RA and DEX on day 1 for adult patients receiving MEC. The NCCN guideline42 also recommends other treatment options such as a 3-drug combination of olanzapine, palonosetron, and DEX or a 3-drug combination of NK1 RA, 5-HT3 RA, and DEX for adult patients receiving MEC.
For pediatric patients receiving HEC, the ASCO,41 POGO,44 and MASCC/ESMO45-47 guidelines recommend a 3-drug combination of 5-HT3 RA, DEX, and aprepitant or fosaprepitant. For children who are unable to receive aprepitant or fosaprepitant, the guidelines recommend a 2-drug combination of 5-HT3 RA and DEX. For patients who are unable to receive DEX, the guidelines recommend a 2-drug combination of palonosetron, and aprepitant or fosaprepitant. The POGO guideline44 suggests the use of palonosetron alone for children receiving HEC (which is known or suspect to interact with aprepitant) who cannot receive DEX.
For pediatric patients receiving MEC, the ASCO,41 the POGO44 and MASCC/ESMO45-47 guidelines recommend a 2-drug combination of 5-HT3 RA and DEX. For children who are unable to receive DEX, the guidelines recommend a 2-drug combination of palonosetron, and aprepitant or fosaprepitant. For children receiving MEC (which is known or suspect to interact with aprepitant) who cannot receive DEX, the POGO guideline44 suggests the use of palonosetron alone.
This report summarizes evidence from a limited literature review between January 1, 2016 and May 28, 2021 on the efficacy and cost-effectiveness of palonosetron for the prevention of CINV in patients receiving HEC or MEC. This report also summarizes recommendations from recent guidelines on the use of antiemetic regimens for the prevention of CINV in patients receiving HEC or MEC. There were no economic evaluations of palonosetron conducted from the perspective of the Canadian health care system. Interpretations of the findings should be taken with caution due to the presence of identified limitations including heterogeneity in terms of treatment regimens, sample size, type of cancer, type of chemotherapy, and use of concomitant medications. There is a strong need to conduct economic evaluations of palonosetron based on the Canadian health care perspective and, ideally, the efficacy data from high-quality research involving the Canadian population.
While both dosage forms of palonosetron (IV and oral), as well as the combination product palonosetron-netupitant (Akynzeo) were reviewed by the CADTH Common Drug Review in 2012 and 2017, respectively, new evidence and guidelines have since emerged on the use of palonosetron as monotherapy or in combination with netupitant to treat adults and children with CINV. This report should not be interpreted as a reimbursement recommendation.
References
1.Canadian Cancer Survivor Network. Chemo-induced nausea and vomiting (CINV). https://survivornet.ca/learn/health-concerns-for-cancer-patients/chemo-induced-nausea-and-vomiting-cinv/, 2021 Jun 17.
2.Gupta K, Walton R, Kataria SP. Chemotherapy-Induced Nausea and Vomiting: Pathogenesis, Recommendations, and New Trends. Cancer Treat Res Commun. 2021;26(no pagination). PubMed
3.Hesketh PJ. Prevention and treatment of chemotherapy-induced nausea and vomiting in adults. In: Post T, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Jun 17.
4.Longstreth GF, Hesketh PJ. Characteristics of antiemetic drugs. In: Post T, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Jun 17.
5.Health Canada. Summary Basis of Decision - Aloxi®. 2020; https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailOne.php?lang=en&linkID=SBD00004, 2021 Jun 23.
6.Rao KV, Faso A. Chemotherapy-induced nausea and vomiting: optimizing prevention and management. Am Health Drug Benefits. 2012;5(4):232-240. PubMed
7.Health Canada. Summary Basis of Decision - Akynzeo. 2020; https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?lang=en&linkID=SBD00375, 2021 Jun 23.
8.Lorusso V, Russo A, Giotta F, Codega P. Management of Chemotherapy-Induced Nausea and Vomiting (CINV): A Short Review on the Role of Netupitant-Palonosetron (NEPA). Core Evid. 2020;15:21-29. PubMed
9.CADTH. Palonosetron hydrochloride - Aloxi (capsule). 2013; https://cadth.ca/palonosetron-hydrochloride-0. Accessed 2021 Jun 28.
10.CADTH. Palonosetron hydrochloride - Aloxi (injection). 2013; https://cadth.ca/palonosetron-hydrochloride. Accessed 2021 Jun 28.
11.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: palonosetron injection (Aloxi IV - Eisai Limited). Ottawa (ON): CADTH; 2013 May 15: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_Aloxi%20IV_may-17-13.pdf. Accessed 2021 Jun 28.
12.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: palonosetron capsule (Aloxi - Eisai Limited). 2012 Apr 24; https://www.cadth.ca/media/cdr/complete/cdr_complete_Aloxi%20PO_April-25-13.pdf. Accessed 2021 Jun 28.
13.CADTH. netupitant / palonosetron - Akynzeo. 2018; https://cadth.ca/netupitant-palonosetron, 2021 Jun 28.
14.Pharmacoeconomic Review Report: netupitant/palonosetron 300 mg/0.5 mg (Akynzeo - Purdue Pharma). Ottawa (ON): CADTH; 2018: www.ncbi.nlm.nih.gov/books/NBK533431/ Accessed 2021 Jun 28.
15.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: netupitant/palonosetron (Akynzeo — Purdue Pharma). 2018 Jun 18; https://cadth.ca/sites/default/files/cdr/complete/SR0548_cdr_complete_Akynzeo_June_22_18.pdf. Accessed 2021 Jun 28.
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
18.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 May 28.
19.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 May 28.
20.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
21.Simino GP, Marra LP, Andrade EI, et al. Efficacy, safety and effectiveness of ondansetron compared to other serotonin-3 receptor antagonists (5-HT3RAs) used to control chemotherapy-induced nausea and vomiting: systematic review and meta-analysis. Expert Rev Clin Pharmacol. 2016;9(9):1183-1194. PubMed
22.Mahrous MA, El-Azab GA, Tawfik HA. Evaluation of clinical outcomes and efficacy of palonosetron and granisetron in combination with dexamethasone in Egyptian patients receiving highly emetogenic chemotherapy. Cancer Chemother Pharmacol. 2021;88(1):121-129. PubMed
23.van der Vorst M, Toffoli EC, Beusink M, et al. Metoclopramide, Dexamethasone, or Palonosetron for Prevention of Delayed Chemotherapy-Induced Nausea and Vomiting After Moderately Emetogenic Chemotherapy (MEDEA): A Randomized, Phase III, Noninferiority Trial. Oncologist. 2021;26(1):e173-e181. PubMed
24.Matsumoto K, Takahashi M, Sato K, et al. A double-blind, randomized, multicenter phase 3 study of palonosetron vs granisetron combined with dexamethasone and fosaprepitant to prevent chemotherapy-induced nausea and vomiting in patients with breast cancer receiving anthracycline and cyclophosphamide. Cancer Medicine. 2020;9(10):3319-3327. PubMed
25.Chaudhary NK, John RR, Boddu D, Mahasampath G, Nesadeepam N, Mathew LG. Palonosetron is a Better Choice Compared With Ondansetron for the Prevention of Chemotherapy-induced Nausea and Vomiting (CINV) in a Resource-limited Pediatric Oncology Center: Results From a Randomized Control Trial. J Pediatr Hematol Oncol. 2019;41(4):294-297. PubMed
26.Tsubata Y, Nakao M, Amano Y, et al. Translational and Randomized Study of 5-HT3 Receptor Antagonists for Evaluation of Chemotherapy-induced Nausea and Vomiting Related Biomarkers. J Med Invest. 2019;66(3.4):269-274.
27.Jain S, Kapoor G, Koneru S, Vishwakarma G. A randomized, open-label non-inferiority study to compare palonosetron and ondansetron for prevention of acute chemotherapy-induced vomiting in children with cancer receiving moderate or high emetogenic chemotherapy. Support Care Cancer. 2018;26(9):3091-3097. PubMed
28.Tan J, Wang S, Liang X, et al. Palonosetron is nonsuperior to ondansetron in acute phase but provides superior antiemetic control in delayed phase for pediatric patients administered highly emetogenic chemotherapy. Pediatr Blood Cancer. 2018;65(2). PubMed
29.Zhang L, Lu S, Feng J, et al. A randomized phase III study evaluating the efficacy of single-dose NEPA, a fixed antiemetic combination of netupitant and palonosetron, versus an aprepitant regimen for prevention of chemotherapy-induced nausea and vomiting (CINV) in patients receiving highly emetogenic chemotherapy (HEC). Ann Oncol. 2018;29(2):452-458. PubMed
30.Chang J, Chen G, Wang D, et al. Efficacy of NEPA, a fixed antiemetic combination of netupitant and palonosetron, vs a 3-day aprepitant regimen for prevention of chemotherapy-induced nausea and vomiting (CINV) in Chinese patients receiving highly emetogenic chemotherapy (HEC) in a randomized Phase 3 study. Cancer Medicine. 2020;9(14):5134-5142. PubMed
31.Ishido K, Higuchi K, Azuma M, et al. Aprepitant, granisetron, and dexamethasone versus palonosetron and dexamethasone for prophylaxis of cisplatin-induced nausea and vomiting in patients with upper gastrointestinal cancer: a randomized crossover phase II trial (KDOG 1002). Anticancer Drugs. 2016;27(9):884-890. PubMed
32.Kovacs G, Wachtel AE, Basharova EV, Spinelli T, Nicolas P, Kabickova E. Palonosetron versus ondansetron for prevention of chemotherapy-induced nausea and vomiting in paediatric patients with cancer receiving moderately or highly emetogenic chemotherapy: a randomised, phase 3, double-blind, double-dummy, non-inferiority study. Lancet Oncol. 2016;17(3):332-344. PubMed
33.Kovacs G, Wachtel A, Basharova E, Spinelli T, Nicolas P, Kabickova E. Palonosetron compared with ondansetron in pediatric cancer patients: multicycle analysis of a randomized Phase III study. Fut Oncol. 2017;13(19):1685-1698. PubMed
34.Seol YM, Kim HJ, Choi YJ, et al. Transdermal granisetron versus palonosetron for prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy: a multicenter, randomized, open-label, cross-over, active-controlled, and phase IV study. Support Care Cancer. 2016;24(2):945-952. PubMed
35.Suzuki K, Yamanaka T, Hashimoto H, et al. Randomized, double-blind, phase III trial of palonosetron versus granisetron in the triplet regimen for preventing chemotherapy-induced nausea and vomiting after highly emetogenic chemotherapy: TRIPLE study. Ann Oncol. 2016;27(8):1601-1606. PubMed
36.Botteman M, Nickel K, Corman S, Turini M, Binder G. Cost-effectiveness of a fixed combination of netupitant and palonosetron (NEPA) relative to aprepitant plus granisetron (APR + GRAN) for prophylaxis of chemotherapy-induced nausea and vomiting (CINV): a trial-based analysis. Support Care Cancer. 2020;28(2):857-866. PubMed
37.Kashiwa M, Matsushita R. Cost-utility analysis of palonosetron in the antiemetic regimen for cisplatin-containing highly emetogenic chemotherapy in Japan. BMC Health Serv Res. 2019;19(1):438. PubMed
38.Shimizu H, Suzuki K, Uchikura T, et al. Economic analysis of palonosetron versus granisetron in the standard triplet regimen for preventing chemotherapy-induced nausea and vomiting in patients receiving highly emetogenic chemotherapy in Japan (TRIPLE phase III trial). J Pharm Health Care Sci. 2018;4:31. PubMed
39.Du Q, Zhai Q, Zhu B, Xu XL, Yu B. Economic evaluation of 5-HT3 receptor antagonists in combination with dexamethasone for the prevention of 'overall' nausea and vomiting following highly emetogenic chemotherapy in Chinese adult patients. J Oncol Pharm Pract. 2017;23(6):403-412. PubMed
40.Restelli U, Saibene G, Nardulli P, et al. Cost-utility and budget impact analyses of the use of NEPA for chemotherapy-induced nausea and vomiting prophylaxis in Italy. BMJ Open. 2017;7(7):e015645. PubMed
41.Hesketh PJ, Kris MG, Basch E, et al. Antiemetics: ASCO Guideline Update. J Clin Oncol. 2020;38(24):2782-2797. PubMed
42.Clinical Practice Guidelines in Oncology, Antiemesis V1.2021. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2020: www.nccn.org. Accessed 2021 Jun 5.
43.2019 Antiemetic Recommendations for Chemotherapy-Induced Nausea and Vomiting: A Clinical Practice Guideline. Toronto (ON): Cancer Care Ontario; 2019: https://www.cancercareontario.ca/en/AntiemeticGuideline. Accessed 2021 Jun 5.
44.Patel P, Robinson PD, Thackray J, et al. Guideline for the prevention of acute chemotherapy-induced nausea and vomiting in pediatric cancer patients: A focused update. Pediatr Blood Cancer. 2017;64(10). PubMed
45.Roila F, Molassiotis A, Herrstedt J, et al. 2016 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting and of nausea and vomiting in advanced cancer patients. Ann Oncol. 2016;27(Supplement 5):v119-v133. PubMed
46.Herrstedt J, Roila F, Warr D, et al. 2016 Updated MASCC/ESMO Consensus Recommendations: Prevention of Nausea and Vomiting Following High Emetic Risk Chemotherapy. Support Care Cancer. 2017;25(1):277-288. PubMed
47.Dupuis LL, Sung L, Molassiotis A, Orsey AD, Tissing W, van de Wetering M. 2016 updated MASCC/ESMO consensus recommendations: Prevention of acute chemotherapy-induced nausea and vomiting in children. Support Care Cancer. 2017;25(1):323-331. PubMed
48.Hesketh PJ, Rossi G, Rizzi G, et al. Efficacy and safety of NEPA, an oral combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy: a randomized dose-ranging pivotal study. Ann Oncol. 2014;25(7):1340-1346. PubMed
49.Aapro M, Rugo H, Rossi G, et al. A randomized phase III study evaluating the efficacy and safety of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy. Ann Oncol. 2014;25(7):1328-1333. PubMed
50.Gralla RJ, Bosnjak SM, Hontsa A, et al. A phase III study evaluating the safety and efficacy of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting over repeated cycles of chemotherapy. Ann Oncol. 2014;25(7):1333-1339. PubMed
51.ASCO Guidelines - Assessment of Study Quality, Strength of Evidence, and Strength of Recommendations. Alexandria (VA): American Society of Clinical Oncology; 2018: https://www.asco.org/sites/new-www.asco.org/files/content-files/practice-and-guidelines/documents/2018-Ratings-Evidence-Recommendations.pdf. Accessed 2021 Jun 21.
52.National Comprehensive Cancer Network. Development and update of guidelines. 2021; https://www.nccn.org/guidelines/guidelines-process/development-and-update-of-guidelines, 2021 Jun 21.
53.ESMO Standard Operating Procedures (SOPs) for Clinical Practice Guidelines (CPGs) and ESMO Magnitude of Clinical Benefit (ESMO-MCBS) scores. Lugano (CH): European Society for Medical Oncology: https://www.esmo.org/content/download/77789/1426712/file/ESMO-Clinical-Practice-Guidelines-Standard-Operating-Procedures.pdf. Accessed 2021 Jun 21.
54.Saito M, Aogi K, Sekine I, et al. Palonosetron plus dexamethasone versus granisetron plus dexamethasone for prevention of nausea and vomiting during chemotherapy: a double-blind, double-dummy, randomised, comparative phase III trial. Lancet Oncol. 2009;10(2):115-124. PubMed
55.Aapro MS, Grunberg SM, Manikhas GM, et al. A phase III, double-blind, randomized trial of palonosetron compared with ondansetron in preventing chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy. Ann Oncol. 2006;17(9):1441-1449. PubMed
56.Aapro M, Bernareggi A. Comparison of pharmacokinetic (PK) profiles of netupitant (NETU) and palonosetron (PALO) in Chinese and Caucasian healthy volunteers (HV). Ann Oncol. 2017;28(Supplement 10).
Appendix 1: Selection of Included Studies
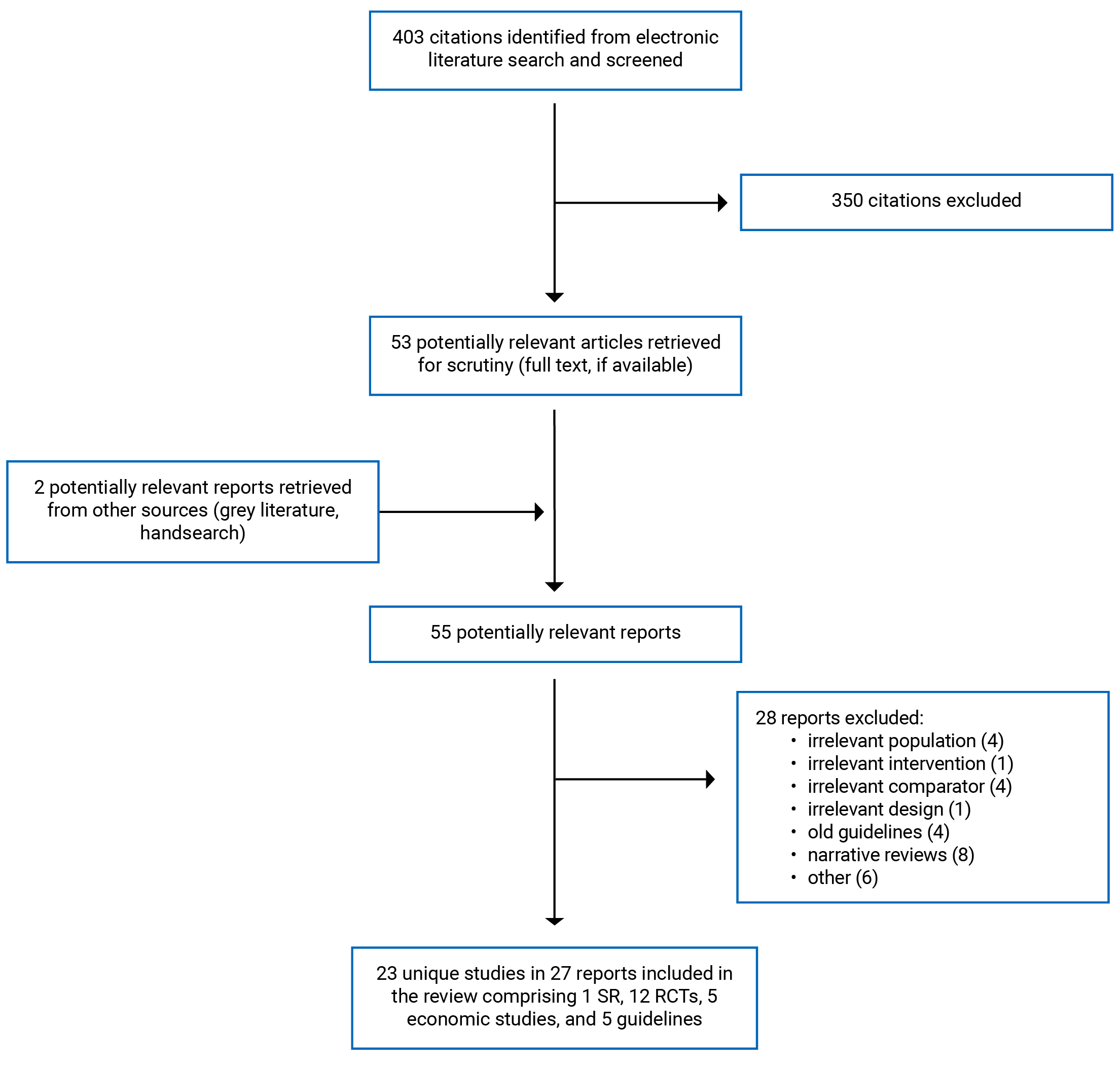
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Objectives, study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Simino et al. (2016)21 Brazil Funding: National Council for Scientific and Technological Development, Brazil | Objective: To assess the efficacy and safety of ondansetron in cancer patients undergoing chemotherapy with other 5-HT3 RA, such as granisetron, dolasetron, tropisetron and palonosetron Total: 26 studies (23 RCTs, 3 cohort studies); 6 RCTs comparing ondansetron with palonosetron Quality assessment tools: Jadad scale for RCTs; Newcastle-Ottawa scale for cohort studies | Adult cancer patients Mean age range: 52 to 56 years % female: 36 to 100 Cancer type: Breast, lung, bladder, colon, rectum, gastric, lymphoma, leukemia, other Type of chemotherapy: 3 RCTs with HEC; 3 RCTs with MEC | Ondansetron (32 mg orally, 8 mg IV to 32 mg IV) Palonosetron (0.25 mg orally, 0.25 mg IV) Concomitant medications such as NK1 RA or DEX were not reported | Outcomes:
|
AEs = adverse event; 5-HT3 RA = 5-hydroxytryptamine-3 receptor antagonist; NK1 RA = neurokinin-1 receptor antagonist; NR = not reported; RCT = randomized controlled trial.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Mahrous et al. (2021)22 Egypt Funding: The authors declared no funding received for this work | Open-label RCT, parallel, 2 arms, 1:1 ratio Sample size calculation: Unclear ITT analysis: Unclear | Adult cancer patients naïve to chemotherapy who were scheduled to receive 4 cycles of HEC (cisplatin-based) (N = 115) Mean age: 48.7 years % female: 59.5 Cancer type: Mainly breast and lung Chemotherapy: HEC (cisplatin-based) | Palonosetron IV 0.25 mg and DEX IV 16 mg (N = 51) Granisetron IV 1 mg and DEX IV 16 mg (N = 64) | Primary outcome:
Secondary outcome:
|
van der Vorst et al. (2021)23 The Netherlands Funding: NR | Phase III RCT, open-label, multicenter (6 sites), parallel, 3 arms, 1:1:1 ratio, noninferiority trial. Sample size calculation: Yes ITT analysis: No | Adult cancer patients naïve to chemotherapy who were scheduled for MEC (N = 230) Median age (range): 65.0 (40 to 84) years % female: 44.3 Cancer type: mainly colorectal (85.7%), ovarian (6.9%), lung (3.2%), gastric (2.1%), pancreatic (1.6%), other (0.5%) Chemotherapy (MEC):
| Arm 1 (N = 75; 12 did not complete study): Palonosetron 0.25 mg IV and DEX 8 mg IV on day 1 with no additional doses of antiemetics. Arm 2 (N = 77; 17 did not complete study): Ondansetron 8 mg IV on day 1 with DEX 4 mg orally twice daily on days 2 to 3 Arm 3 (N = 79; 13 did not complete study): Ondansetron 8 mg IV and DEX 8 mg on day 1 with metoclopramide 10 mg p.o. 3 times daily on days 2 to 3. | Primary outcome:
Secondary outcomes:
Follow-up: 5 days (120 hours) after chemotherapy |
Matsumoto et al. (2020)24 Japan Funding: NR | Phase III RCT, multicenter, double-blind, active-controlled, parallel, 2 arms, 1:1 ratio Sample size calculation: Yes ITT analysis: No | Breast cancer patients naïve to chemotherapy who were scheduled on AC-based regimen (N = 338) Median age (range): 54 (27 to 82) years % female: 100 Chemotherapy (HEC): AC-based | Palonosetron IV 0.75 mg on day1, DEX (12 mg at day 1, 8 mg at day 2 to 3), and fosaprepitant 150 mg on day 1 (N = 170) Granisetron IV 1 mg on day 1, DEX (12 mg at day 1, 8 mg at day 2 to 3), and fosaprepitant 150 mg on day 1 (N = 168) | Primary outcome:
Secondary outcomes:
Follow-up: 5 days (120 hours) |
Chaudhary et al. (2019)25 India Funding: Intramural research grant from Christian Medical College Vellore | RCT, single-centre, nonblinded, parallel, 2 arms, 1:1 ratio Sample size calculation: Yes ITT analysis: No | Children 3 to 17 years with cancer naïve to chemotherapy who were scheduled to receive HEC or MEC (N = 200). Mean age (range): 8.0 (3 to 16) years % female: 35.5 Cancer type:
Chemotherapy:
| Palonosetron IV (5 mcg/kg, max. 0.25 mg) single dose (N = 100). Ondansetron 0.15 mg/kg/dose IV on day 1, and orally on day 2 to 3 (N = 100). Both groups received DEX 5 mg/m2/dose IV (max. 8 mg) 12 hourly. | Outcomes:
The outcomes were assessed for acute (within 24 hours), delayed (24 to 120 hours), and overall (0 to 120 hours) period after completion of chemotherapy. Follow-up: 5 days (120 hours) after chemotherapy |
Tsubata et al. (2019)26 Japan Funding: NR | Open-label phase III RCT, single-centre, parallel, 2 arms, 1:1 ratio Sample size calculation: No ITT analysis: No | Adult cancer patients naïve to chemotherapy who were scheduled for HEC or MEC (N = 70) Median age: 68 years % female: 37% Cancer type:
Chemotherapy: HEC or MEC | HEC:
MEC:
| Primary outcome:
Secondary outcomes:
Follow-up: 5 days (120 hours) after chemotherapy |
Jain et al. (2018)27 India Funding: NR | Open-label RCT, parallel, 2 arms, 1:1 ratio Sample size calculation: Yes ITT analysis: No | Children from 2 to 18 years of age with cancer and naïve to chemotherapy, receiving HEC or MEC (N = 116) Mean age: 9.6 years % female: 27.8% Cancer type:
Chemotherapy: HEC or MEC | Palonosetron (N = 58) Ondansetron (N = 58) MEC:
HEC:
| Primary outcome:
Secondary outcome: • AEs Follow-up: 5 days (120 hours) after chemotherapy |
Tan et al. (2018)28 China Funding: NR | Phase III RCT, single-centre, double-blind, parallel, 3 arms, 1:1:1 ratio Sample size calculation: Unclear ITT analysis: Yes | Children from newborn (full term) to < 18 years with or without previous chemotherapy who were scheduled for HEC (N = 565). Mean age: 5.05 years % female: 51.9 Cancer type:
Chemotherapy: Cisplatin/cyclophosphamide (HEC) | Palonosetron IV (5 mcg/kg, max. 0.25 mg) on day 1 (N = 185) Palonosetron IV (10 mcg/kg, max. 0.5 mg) on day 1 (N = 186) Ondansetron 0.15 mg/kg/dose IV 30 minutes before chemotherapy, and every 8 hours thereafter on all chemotherapy days, max. 32 mg/day (N = 194) All 3 groups received DEX 5 mg/m2/dose IV 30 minutes before chemotherapy and 12 hours thereafter. | Outcomes:
The outcomes were assessed for acute (within 24 hours), delayed (24 to 120 hours), and overall (0 to 120 hours) period after completion of chemotherapy. Follow-up: 5 days (120 hours) after chemotherapy |
Zhang et al. (2018)29 and Chang et al. (2020)30 China, Taiwan, Thailand, Korea Funding: Helsinn Health care, SA, Lugano, Switzerland | Phase III RCT, multicenter, double-blind/double-dummy, single cycle, multi-country (30 sites in China, 5 in Taiwan, 3 in Thailand, and 8 in Korea), 2 arms, 1:1 ratio. Chang study looked at a subset of Chinese patients from the previous pivotal study by Zhang et al. (2018). Sample size calculation: Yes ITT analysis: No | Adult cancer patients naïve to chemotherapy and scheduled to receive first course of cisplatin-based (≥ 50 mg/m2) chemotherapy (N = 829; Chinese subset N = 667). Mean age: 54.6 years % female: 29.0% Cancer type: Mainly lung (58.3%) Chemotherapy (HEC):
Cisplatin ≥ 70 mg/m2 (59.1%) | NEPA oral (300 mg netupitant and 0.5 mg palonosetron) and oral DEX 12 mg on day 1; DEX 8 mg on day 2 to 4 (N = 413; Chinese subset N = 339). Granisetron IV 3 mg, oral aprepitant 125 mg, and oral DEX 12 mg on day 1; aprepitant 80 mg on day 2 to 3; DEX 8 mg on day 2 to 4 (N = 416; Chinese subset N = 328). | Primary outcome:
Secondary outcomes:
The outcomes were assessed at acute (0 to 24 hours), delayed (25 to 120 hours) and overall (0 to 120 hours) Follow-up: 5 days (120 hours) after chemotherapy |
Ishido et al. (2016)31 Japan Funding: NR | Phase II RCT, open-label, crossover, 2 arms, 1:1 ratio Sample size calculation: Yes ITT analysis: Yes | Adult cancer patients naïve to chemotherapy who were scheduled to receive 2 or more cycles of chemotherapy including cisplatin at a dose of ≥ 60 mg/m2 (N = 85) Median age (range): 65 (30 to 77) % female: 20.2% Cancer type:
Chemotherapy: Cisplatin-based (HEC) | Palonosetron IV 0.75 mg and 13.3 mg DEX on day 1; oral DEX 8 mg on day 2 to 4 (N = 42) Granisetron IV 3 mg, oral aprepitant 125 mg, and DEX IV 6.6 mg on day 1; oral aprepitant 80 mg and oral DEX 8 mg on day 2 to 4 (N = 43) During the second cycle, the study treatments were crossover | Primary outcome:
Secondary outcome:
The outcomes, except patients’ preference, were assessed within 120 hours during first treatment cycle. Follow-up: 5 days (120 hours) after chemotherapy |
Kovacs et al. (2016)32 and Kovacs et al. (2017)33 Multinational (US, Latin America, western and eastern Europe, and Russia) Funding: Helsinn Health care, SA (Lugano, Switzerland) | Phase III RCT, double-blind, double-dummy, multicenter (71 sites), parallel, 3 arms, 1:1:1 ratio, noninferiority study Sample size calculation: Yes ITT analysis: No | Children from newborn (full term) to < 17 years with or without previous chemotherapy who were scheduled for HEC or MEC (N = 502) Mean age: 8.2 years % female: 47% Cancer type:
Chemotherapy: HEC, MEC | Palonosetron IV 10 mcg/kg, max. 0.75 mg (N = 169) Palonosetron IV 20 mcg/kg, max. 1.50 mg (N = 169) Ondansetron IV 3 × 150 mcg/kg, max. 32 mg (N = 164) All patients received concomitant DEX (Dose NR) | Primary outcome:
Secondary outcomes:
The outcomes were assessed for acute (within 24 hours), delayed (24 to 120 hours), and overall (0 to 120 hours) Follow-up: 5 days (120 hours) after chemotherapy |
Seol et al. (2016)34 Korea Funding: NR | Phase 4 RCT, open-label, crossover, multicenter, active-controlled study Sample size calculation: Yes ITT analysis: No | Adult cancer patients (> 20 years) with or without previous chemotherapy who were scheduled to receive a MEC in 2 consecutive chemotherapy cycles (N = 196) Mean age: 59.6 years % female: 37.9 Cancer type: NR Chemotherapy: MEC | Palonosetron IV 0.25 mg administered at 30 minutes before chemotherapy on day 1 (N = 100 in the first period; N = 87 in the second period) Granisetron transdermal (N = 96 in the first period; N = 95 in the second period) All patients received concomitant DEX IV 10 mg on day 1 Washout period: NR | Primary outcome:
Secondary outcomes:
Follow-up: 3 days (72 hours) per period |
Suzuki et al. (2016)35 Japan Funding: Pharma Valley Center, the Shizuoka Organization of Creation Industries which is a public foundation operated by Shizuoka Prefecture in Japan | Phase III RCT, double-blind, multicenter, parallel, 2 arms, 1:1 ratio Sample size calculation: Yes ITT analysis: No | Adult cancer patients naïve to chemotherapy who were scheduled for cisplatin-based HEC (N = 842) Median age (range): 64 (25 to 83) % female: 25.5 Cancer type: Non-small-cell lung: 47.7%
Chemotherapy: HEC (cisplatin at ≥ 50 mg/m2 – based regimen) | Palonosetron IV 0.75 mg on day 1 (N = 421) Granisetron IV 1 mg on day 1 (N = 421) Patients in both arms received oral aprepitant (125 mg on day 1 and 80 mg/day on day 2 to 3), and DEX IV (9.9 mg on day 1, and 6.6 mg on day 2 to 4) | Primary outcome:
Secondary outcomes:
Follow-up: 5 days (120 hours) after chemotherapy |
AC = anthracycline and cyclophosphamide; CC = complete control; CP = complete protection; CR = complete response; DEX = dexamethasone; FLIE = Functional Living Index-Emesis; HEC = high emetogenic chemotherapy; ITT = intention-to-treat; IV = IV; max. = maximum; MASCC = Multinational Association of Supportive Care in Cancer; MAT = MASCC Antiemetic Tool; MEC = moderate emetogenic chemotherapy; NA = not applicable; NEPA = netupitant/palonosetron; NR = not reported; QoL = quality of life; NR = not reported; RCT = randomized controlled trial; TC = total control; VAS = visual analogue scale.
Table 4: Characteristics of Included Economic Evaluations
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
Botteman et al. (2020)36 US Funding: Helsinn Therapeutics US, Inc. | Cost-utility analysis Time horizon: 5 days Perspective: US health care | Adult cancer patients naïve to chemotherapy and scheduled to receive first course of cisplatin-based (≥ 50 mg/m2) chemotherapy (N = 828) as per a phase III noninferior RCT by Zhang et al. (2018)29 Mean age: 54.6 years % female: 29.0% Cancer type: Mainly lung (58.3%) Chemotherapy (HEC):
| NEPA oral (300 mg netupitant and 0.5 mg palonosetron) and oral DEX 12 mg on day 1; DEX 8 mg on day 2 to 4 (N = 412). Granisetron IV 3 mg, oral aprepitant 125 mg, and oral DEX 12 mg on day 1; aprepitant 80 mg on day 2 to 3; DEX 8 mg on day 2 to 4 (N = 416). | Primary outcome measures:
WTP per QALY gained threshold: $25,000 or lower ($100,000 in sensitivity analysis) NMB = QALD difference / 365.25 x $25,000 – cost difference. The higher NMB the more cost-effective NEPA is. 1-way sensitivity analysis Probabilistic multivariate sensitivity analysis | Clinical: From a phase III noninferior RCT by Zhang et al. (2018)29 Cost: Antiemetic prophylaxis, rescue medications, medical costs of CINV-related events. Costs were adjusted at 2018 USD Utilities: 0.90, 0.70, and 0.24 were assigned for the outcomes of CP, CR, and IR, respectively. QALDs were calculated by summing the patient’s quality-adjusted time over the 5-day trial; the maximum possible QALDs (i.e., having no CINV) for the period was 4.5 (i.e., 0.90 × 5 days) | Patients with worst nausea VAS scores were most likely to receive medical treatment for CINV. Any patient with VAS greater than 80 mm was assigned a $9,920 CINV cost. Any patient with a vomiting and/or retching duration more than 8.5 hours was assigned the 9,920 CINV cost. |
Kashiwa et al. (2019)37 Japan Funding: NA as reported by the authors | Cost-utility analysis Time horizon: 5 days Perspective: Health care payer perspective in Japan | Adult cancer patients naïve to chemotherapy who were scheduled for cisplatin-based HEC (N = 842) as per a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35 Median age (range): 64 (25 to 83) % female: 25.5 Cancer type: Non-small-cell lung: 47.7%
Chemotherapy: HEC (cisplatin at ≥ 50 mg/m2 – based regimen) | Palonosetron IV 0.75 mg on day 1 (N = 421) Granisetron IV 1 mg on day 1 (N = 421) Patients in both arms received oral aprepitant (125 mg on day 1 and 80 mg/day on day 2 to 3), and DEX IV (9.9 mg on day 1, and 6.6 mg on day 2 to 4) | A decision tree model consisted of the acute phase and the delayed phase. Cost-effectiveness was calculated from the costs incurred in antiemetic therapy and QALYs for 5 days. ICER was calculated for the base case. WTP threshold was 5,000,000 JPY/QALY (44,575 USD/QALY) Sensitivity analysis: 1-way and probabilistic sensitivity analysis | Clinical: From a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35 Cost: Direct medical costs associated with CINV prevention and medical fees incurred by CINV. Costs were adjusted at 2018 USD (1USD = 112.17 JPY) Utilities: 0.90, 0.70, and 0.20 were assigned for the outcomes of CP, CR, and IR, respectively. | The cost associated with the administration of chemotherapy other than the antiemetic therapy would be the same in both groups, and this cost was not included in the calculation. As there was no difference in overall AEs incidence between groups, costs relating to AEs were not included. |
Shimizu et al. (2018)38 Japan Funding: The authors declared no specific funding | Cost-effectiveness analysis Time horizon: 5 days Perspective: Health care payer perspective in Japan | Adult cancer patients naïve to chemotherapy who were scheduled for cisplatin-based HEC (N = 842) as per a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35 | Palonosetron IV 0.75 mg on day 1 (N = 421) Granisetron IV 1 mg on day 1 (N = 421) Patients in both arms received oral aprepitant (125 mg on day 1 and 80 mg/day on day 2 to 3), and DEX IV (9.9 mg on day 1, and 6.6 mg on day 2 to 4) | Cost-effectiveness ratio was calculated by dividing the mean cost of antiemetic used in each group by the number of CRs. ICER was calculated as difference in mean cost between groups divided by the difference in CR rates between groups. Sensitivity analysis: 1-way | Clinical: From a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35 Cost: Cost of drugs, and total medical cost adjusted at 2018 USD (1USD = 110.57 JPY) Utility: NA | Cost of chemotherapy and cost of treatment of AEs were not included. |
Du et al. (2017)39 China Funding: National Natural Science Foundation of China, and Science and Technology Commission of Shanghai Municipality | Cost-utility analysis Time horizon: 5 days Perspective: Chinese health care system | Adult cancer patients naïve and non-naive to chemotherapy from 2 pivotal phase III RCTs comparing palonosetron, ondansetron and granisetron, who were scheduled for HEC. Age: ≥ 18 years Other characteristics: NR | Palonosetron (0.25 or 0.75 mg) + DEX (12 mg IV on day 1 and 8 mg orally on day 2 and 3) Ondansetron (32 mg) + DEX Granisetron (3 mg) + DEX | A decision tree Markov model was used to evaluate the 3 treatment strategies. Cost per gained in perfect health Cost per QALY Cost per QALD ICER Sensitivity analysis: 1-way and probabilistic sensitivity analysis WTP threshold: USD 22,515 | Clinical: From 2 pivotal phase III RCTs comparing palonosetron, ondansetron and granisetron Cost: Only direct medical costs (antiemetic drugs and rescue drugs) adjusted at 2014 USD Utilities: 9.02, 6.74, and 2.28 for CR, NNR and failure, respectively | Assumed that 2/3 and 3/4 of patients, who failed prophylactic palonosetron and ondansetron/ granisetron, respectively, received rescue treatment. |
Restelli et al. (2017)40 Italy Funding: Italfarmaca SA | Cost-utility analysis Time horizon: 5 days Perspective: Italian National Health Service | Adult cancer patients who were scheduled to receive HEC or MEC based on 3 RCTs, 1 determined the netupitant dose in combination with palosetron,48 1 compared NEPA and palonosetron alone,49 and 1 compared NEPA vs. aprepitant plus palonodetron.50 | NEPA (fixed combination of netupitant/ palonosetron and DEX on day 1) Aprepitant + palonosetron (Apr 125 mg, palo 0.5 mg and DEX on day 1; Apr 80 mg on day 2 to 3) Fosaprepitant + palonosetron + DEX Aprepitant + ondansetron + DEX Fosaprepitant + ondansetron + DEX | ICUR of NEPA vs. other comparators was performed using a Markov model. The model considered a single cycle of chemotherapy. Patients transited through 3 mutually exclusive health states: CP, CR, and IR. Sensitivity analysis: 1-way | Cost: Direct medical costs, costs for management of AEs, and costs for management of CINV episodes. Costs were adjusted at year 2016 Utilities: 0.77, 0.60, and 0.26 for CP, CR, and IR, respectively. QADY was used due to short-term horizon. | Due to the clinical noninferiority of fosaprepitant and aprepitant and to a lack of data referred to therapies of fosaprepitant, the same odds ratio of aprepitant-based therapies were used. |
CINV = chemotherapy-induced nausea and vomiting; CP = complete protection; CR = complete response; DEX = dexamethasone; HEC = high emetogenic chemotherapy; ICER = incremental cost-effectiveness ratio; ICUR = incremental cost-utility ratio; IR = incomplete response; JPY = Japanese yen; MEC = moderate emetogenic chemotherapy; NA = not applicable; NEPA = netupitant/palonosetron; NMB = net monetary benefit; NNR = nausea but no rescue medication; QALD = quality-adjusted life-day; QALY = quality-adjusted life-year; RCT = randomized controlled trial; USD = US dollar; VAS = visual analogue scale; WTP = willingness-to-pay.
Table 5: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
ASCO Guideline Update, Hesketh et al. (2020)41 | ||||||
Intended users: Oncologists and other health care practitioners Target population: Adult and pediatric cancer patients, and their caregivers | New anticancer agents, antiemetics, and antiemetic regimens | Efficacy and safety outcomes of antiemetic regimens | Evidence is obtained through systematic search of the literature from PubMed and Cochrane Library databases. | The strength of recommendation and the level of evidencea were provided for each recommendation.b | Expert panel provided critical review and finalized the guideline recommendations. | The guidelines were circulated for external review. The guidelines were reviewed and approved by the Expert Panel and the ASCO Clinical Practice Guideline Committee before publication. |
NCCN Guideline Update (2020)42 | ||||||
Intended users: All individuals who impact decision-making in cancer care including physicians, nurses, pharmacists, payers, and many others. Target population: Adult patients receiving chemotherapy or radiotherapy for cancer treatment, and their caregivers | Antiemetics for prevention of chemotherapy-induced or radiotherapy-induced nausea and/or vomiting | Efficacy and safety outcomes of antiemetic agents | The NCCN guidelines are reviewed and updated at least annually. Electronic search was performed through PubMed database. Evidence was reviewed, discussed by the NCCN panel, and incorporated in the updated version of the guidelines. | The level of evidence depends on the quality of data, quantity of data and consistency of data. NCCN categories for recommendationsc | The NCCN Guidelines Development Group comprised the NCCN Guidelines Steering Committee, Panels specific to each of the Guidelines, and the NCCN Headquarters Team. Panel members reviewed literature evidence, discussed the evidence, and provided comments and responses, which were gathered to serve as basis for possible revisions or changes to the recommendations | Reviewed and approved by NCCN framework committee. Reviewed and revised from international feedback |
CCO Guideline Update (2019)43 | ||||||
Intended users: Medical oncologists, pharmacists, and nurses Target population: Adult patients receiving chemotherapy for cancer treatment | Antiemetics for prevention of chemotherapy-induced nausea and vomiting | Efficacy and safety outcomes of antiemetic agents | Systematic search of literature review was conducted. | The quality of evidence was assessed, but the level of evidence and the strength of recommendations were not provided for each recommendation. | The CCO Working Group met via teleconference and corresponded through email review and assess the quality of evidence, contributed to the development of the recommendations. | The guideline was circulated for expert review. |
POGO Guideline Update (2017)44 | ||||||
Intended users: Physicians, pharmacists, nurse practitioners, physician assistants, and nurses. Target population: Children receiving HEC or MEC for cancer treatment, and their caregivers. | Antiemetics for prevention of chemotherapy-induced nausea and vomiting | Efficacy and safety outcomes of antiemetic agents | Systematic search of literature review was conducted. | The quality of evidence and strength of recommendations were assessed using GRADE system. | Panel members reviewed the evidence, discussed, and contributed to the update of the recommendations. | The guideline was reviewed by experts and published in peer-reviewed journal. |
Intended users: Health care providers including physicians, nurses, pharmacists, psychologists, and those involving in the treatment and care for cancer patients Target population: Adults and children (1 month to < 18 years) receiving chemotherapy for cancer treatment, and their caregivers | Antiemetics for prevention of chemotherapy-induced nausea and vomiting | Efficacy and safety outcomes of antiemetic agents | Evidence is obtained through systematic search of main databases. | MASCC level of confidenced and MASCC level of consensuse ESMO level of evidencef and ESMO grade of recommendationg | Recommendations were developed through panel discussions after review of the evidence. The recommendations were revised, and differences in interpretations were resolved by consensus | Published in peer-reviewed journal |
ASCO = American Society of Clinical Oncology; CCO = Cancer Care Ontario; ESMO = European Society of Medical Oncology; GRADE = Grades of Recommendation Assessment, Development and Evaluation; HEC = high emetogenic chemotherapy; MASCC = Multinational Association of Supportive Care in Cancer; MEC = moderate emetogenic chemotherapy; NCCN = National Comprehensive Cancer Network; POGO = Pediatric Oncology Group of Ontario.
a“ASCO level of evidence:
High: High confidence that the available evidence reflects the true magnitude and direction of the net effect (e.g., balance of benefits vs. harms) and further research is very unlikely to change either the magnitude or direction of this net effect.
Intermediate: Intermediate confidence that the available evidence reflects the true magnitude and direction of the net effect. Further research is unlikely to alter the direction of the net effect, however it might alter the magnitude of the net effect.
Low: Low confidence that the available evidence reflects the true magnitude and direction of the net effect. Further research may change the magnitude and/or direction of this net effect.
Insufficient: Evidence is insufficient to discern the true magnitude and direction of the net effect. Further research may better inform the topic. Reliance on consensus opinion of experts may be reasonable to provide guidance on the topic until better evidence is available.
b“ASCO strength of recommendation:
Strong: There is high confidence that the recommendation reflects best practice. This is based on: a) strong evidence for a true net effect (e.g., benefits exceed harms); b) consistent results, with no or minor exceptions; c) minor or no concerns about study quality; and/or d) the extent of panelists’ agreement. Other compelling considerations (discussed in the guideline’s literature review and analyses) may also warrant a strong recommendation.
Moderate: There is moderate confidence that the recommendation reflects best practice. This is based on: a) good evidence for a true net effect (e.g., benefits exceed harms); b) consistent results, with minor and/or few exceptions; c) minor and/or few concerns about study quality; and/or d) the extent of panelists’ agreement. Other compelling considerations (discussed in the guideline’s literature review and analyses) may also w arrant a moderate recommendation.
Weak: There is some confidence that the recommendation offers the best current guidance for practice. This is based on: a) limited evidence for a true net effect (e.g., benefits exceed harms); b) consistent results, but with important exceptions; c) concerns about study quality; and/or d) the extent of panelists’ agreement. Other considerations (discussed in the guideline’s literature review and analyses) may also w arrant a weak recommendation.”51 (p.6)
c “Definitions for NCCN categories:
Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate
Category 2A: Based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate
Category 2B: Based upon lower-level evidence, there is NCCN consensus that the intervention is appropriate
Category 3: Based upon any level of evidence, there is major NCCN disagreement that the intervention is appropriate”52
d“MASCC level of scientific confidence:
High: repeated, randomized trials that were appropriately sized and well conducted
Moderate: at least on randomized trial, supported by well-conducted phase II trials, or possibly several well-conducted phase II studies
Low: formal clinical trials of a level less than that expressed above
Very low: clinical impression only
No confidence possible
e“MASCC level of consensus: high, moderate, or low”45 (p. v119)
fESMO level of evidence:
I: Evidence from at least one large randomized, controlled trial of good methodological quality (low potential of bias) or meta-analyses of well-conducted randomized trials without heterogeneity
II: Small randomized trials or large randomized trials with suspicion of bias (low methodological quality) or meta-analyses of such trials with demonstrated heterogeneity
III: Prospective cohort studies
IV: Retrospective cohort studies or case-control studies
V: Studies without control group, case reports, expert opinions
g“ESMO grade of recommendation:
A: Strong evidence for efficacy with a substantial clinical benefit, strongly recommended
B: Strong or moderate evidence for efficacy but with a limited clinical benefit, generally recommended
C: Insufficient evidence for efficacy or benefit does not outweigh the risk or the disadvantages (adverse events, costs, etc.), optional
D: Moderate evidence against efficacy or for adverse outcome, generally not recommended
E: Strong evidence against efficacy or for adverse outcome, never recommended”53 (p. 12)
Appendix 3: Critical Appraisal of Included Publications
Table 6: Strengths and Limitations of Systematic Review Using AMSTAR 216
Item | Simino et al. (2016)21 |
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes |
2. Did the report of the review contain an explicit statement that the review methods were established before the conduct of the review and did the report justify any significant deviations from the protocol? | No |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes – RCTs and observational studies |
4. Did the review authors use a comprehensive literature search strategy? | Yes |
5. Did the review authors perform study selection in duplicate? | Yes |
6. Did the review authors perform data extraction in duplicate? | NR |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | No |
8. Did the review authors describe the included studies in adequate detail? | Yes |
9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | Yes – Modified Jadad scale and Cochrane RoB tool |
10. Did the review authors report on the sources of funding for the studies included in the review? | No |
11. If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? | Yes |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Yes |
13. Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review? | Yes |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Yes |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | NA |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; NA = not applicable; NR = not reported; PICO = Population, Intervention, Comparator, Outcomes; RCT = randomized controlled trial; RoB = risk of bias.
Table 7: Strengths and Limitations of Clinical Studies Using the Downs and Black checklist17
Item | Mahrous et al. (2021)22 | Vorst et al. (2021)23 | Matsumoto et al. (2020)24 | Chaudhary et al. (2019)25 | Tsubata et al. (2019)26 | Jain et al. (2018)27 |
Reporting | ||||||
1. Is the hypothesis/aim/objective of the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
2. Are the main outcomes to be measured clearly described in the Introduction or Methods section? | Yes | Yes | Yes | Yes | Yes | Yes |
3. Are the characteristics of the patients included in the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
4. Are the interventions of interest clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
5. Are the distributions of principal confounders in each group of subjects to be compared clearly described? | NA - RCT | NA - RCT | NA - RCT | NA - RCT | NA - RCT | NA - RCT |
6. Are the main findings of the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
7. Does the study provide estimates of the random variability in the data for the main outcomes? | Yes – SD provided | Yes – 95% CI provided | Yes – 95% CI provided | No | Yes – SD provided | Yes – 95% CI provided |
8. Have all important adverse events that may be a consequence of the intervention being reported? | No – AEs was not reported, although it was stated in the methods as secondary outcome | Yes | Yes | Yes | No | Yes |
9. Have the characteristics of patients lost to follow-up been described? | NR – Flow diagram not provided | No | No | NR – Flow diagram not provided | NR – Flow diagram not provided | NA – No lost to follow-up |
10. Have actual P values been reported (e.g., 0.035 rather than < 0.05) for the main outcomes except where the P value is less than 0.001? | Yes | Yes | Yes | Yes | Yes | Yes |
External validity | ||||||
11. Were the subjects asked to participate in the study representative of the entire population from which they were recruited? | Unclear – small sample size | Probably yes | Probably yes | Probably yes | Unclear – small sample size | Unclear – small sample size |
12. Were the subjects who were prepared to participate representative of the entire population from which they were recruited? | Unclear – small sample size | Probably yes | Probably yes | Probably yes | Unclear – small sample size | Unclear – small sample size |
13. Were the staff, places, and facilities where the patients were treated, representative of the treatment the majority of the patients receive? | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity – bias | ||||||
14. Was an attempt made to blind study subjects to the intervention they have received? | No – Open-label | No – Open-label | Yes – double-blind | No – Open-label | No – Open-label | No – Open-label |
15. Was an attempt made to blind those measuring the main outcomes of the intervention? | No – Open-label | No – Open-label | Yes – double-blind | No – Open-label | No – Open-label | No – Open-label |
16. If any of the results of the study were based on “data dredging”, was this made clear? | NA | NA | NA | NA | NA | NA |
17. In trials and cohort studies, so the analyses adjust for different lengths of follow-up of patients, or in case-control studies, is the time period between the intervention and outcome the same for cases and controls? | NA | NA | NA | NA | NA | NA |
18. Were the statistical tests used to assess the main outcomes appropriate? | Yes | Yes | Yes | Yes | Yes | Yes |
19. Was compliance with the intervention/s reliable? | Yes | Yes | Yes | Yes | Yes | Yes |
20. Were the main outcome measures used accurate (valid and reliable)? | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity – confounding (selection bias) | ||||||
21. Were the patients in different intervention groups (trials and cohort studies) or were the cases and controls (case-control studies) recruited from the same population? | Yes | Yes | Yes | Yes | Yes | Yes |
22. Were study subjects in different intervention groups (trial and cohort studies) or were the cases and controls (case-controls studies) recruited over the same period of time? | Yes | Yes | Yes | Yes | Yes | Yes |
23. Were study subjects randomized to intervention groups? | Yes | Yes | Yes | Yes | Yes | Yes |
24. Was the randomized intervention assignment concealed from both patients and health care staff until recruitment was complete and irrevocable? | NR | NR | NR | NR | NR | NR |
25. Was the adequate adjustment for confounding in the analyses from which the main findings were drawn? | NA - RCT | NA - RCT | NA - RCT | NA - RCT | NA - RCT | NA - RCT |
26. Were losses of patients to follow-up taken into account? | NR | No – PP analysis | No – PP analysis | NR | NR | NA – No lost to follow-up |
27. Did the study have sufficient power to detect a clinically important effect where the P value for a difference being due to chance is less than 5%? | NR | Yes | Yes | Yes | NR | Yes |
AEs = adverse event; CI = confidence interval; ITT = intention-to-treat; NA = not applicable; NR = not reported; PP = per protocol; RCT = randomized controlled trial.
Table 8: Strengths and Limitations of Clinical Studies Using the Downs and Black checklist17 (continued)
Item | Tan et al. (2018)28 | Ishido et al. (2016)31 | Seol et al. (2016)34 | Suzuki et al. (2016)35 | ||
Reporting | ||||||
1. Is the hypothesis/aim/objective of the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
2. Are the main outcomes to be measured clearly described in the Introduction or Methods section? | Yes | Yes | Yes | Yes | Yes | Yes |
3. Are the characteristics of the patients included in the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
4. Are the interventions of interest clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
5. Are the distributions of principal confounders in each group of subjects to be compared clearly described? | NA - RCT | NA - RCT | NA - RCT | NA - RCT | NA - RCT | NA - RCT |
6. Are the main findings of the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
7. Does the study provide estimates of the random variability in the data for the main outcomes? | Yes – 95% CI provided | Yes – 95% CI provided | No | Yes – 95% CI provided | Yes – 95% CI provided | Yes – 95% CI provided |
8. Have all important adverse events that may be a consequence of the intervention being reported? | Yes | Yes | Yes | Yes | Yes | Yes |
9. Have the characteristics of patients lost to follow-up been described? | No | No | No | No | No | No |
10. Have actual P values been reported (e.g., 0.035 rather than < 0.05) for the main outcomes except where the P value is less than 0.001? | Yes | Yes | Yes | Yes | Yes | Yes |
External validity | ||||||
11. Were the subjects asked to participate in the study representative of the entire population from which they were recruited? | Probably yes | Probably yes | Unclear – small sample size | Probably yes | Probably yes | Probably yes |
12. Were the subjects who were prepared to participate representative of the entire population from which they were recruited? | Probably yes | Probably yes | Unclear – small sample size | Probably yes | Probably yes | Probably yes |
13. Were the staff, places, and facilities where the patients were treated, representative of the treatment the majority of the patients receive? | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity – bias | ||||||
14. Was an attempt made to blind study subjects to the intervention they have received? | Yes – Double-blind | Yes – Double-blind/double-dummy | No – Open-label | Yes – Double-blind/double-dummy | No – Open-label | Yes – Double-blind |
15. Was an attempt made to blind those measuring the main outcomes of the intervention? | Yes – Double-blind | Yes – Double-blind/double-dummy | No – Open-label | Yes – Double-blind/double-dummy | No – Open-label | Yes – Double-blind |
16. If any of the results of the study were based on “data dredging”, was this made clear? | NA | NA | NA | NA | NA | NA |
17. In trials and cohort studies, so the analyses adjust for different lengths of follow-up of patients, or in case-control studies, is the time period between the intervention and outcome the same for cases and controls? | NA | NA | NA | NA | NA | NA |
18. Were the statistical tests used to assess the main outcomes appropriate? | Yes | Yes | Yes | Yes | Yes | Yes |
19. Was compliance with the intervention/s reliable? | Yes | Yes | Yes | Yes | Yes | Yes |
20. Were the main outcome measures used accurate (valid and reliable)? | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity – confounding (selection bias) | ||||||
21. Were the patients in different intervention groups (trials and cohort studies) or were the cases and controls (case-control studies) recruited from the same population? | Yes | Yes | Yes | Yes | Yes | Yes |
22. Were study subjects in different intervention groups (trial and cohort studies) or were the cases and controls (case-controls studies) recruited over the same period of time? | Yes | Yes | Yes | Yes | Yes | Yes |
23. Were study subjects randomized to intervention groups? | Yes | Yes | Yes | Yes | Yes | Yes |
24. Was the randomized intervention assignment concealed from both patients and health care staff until recruitment was complete and irrevocable? | NR | NR | NR | Yes | NR | NR |
25. Was the adequate adjustment for confounding in the analyses from which the main findings were drawn? | NA – RCT | NA – RCT | NA – RCT | NA – RCT | NA – RCT | NA – RCT |
26. Were losses of patients to follow-up taken into account? | Yes – ITT analysis | Yes – ITT analysis | Yes – ITT analysis of first cycle | Yes – ITT analysis | No – PP analysis | No – PP analysis |
27. Did the study have sufficient power to detect a clinically important effect where the P value for a difference being due to chance is less than 5%? | NR | Yes | Yes | Yes | Yes | Yes |
AEs = adverse event; CI = confidence interval; ITT = intention-to-treat; NA = not applicable; NR = not reported; PP = per protocol; RCT = randomized controlled trial.
Table 9: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist18
Item | Botteman et al. (2020)36 | Kashiwa and Matsushita (2019)37 | Shimizu et al. (2018)38 | Du et al. (2017)39 | Restelli et al. (2017)40 |
Study design | |||||
1. The research question is stated. | Yes – Assess the cost-utility of NEPA vs. granisetron/ aprepitant regiment | Yes – Assess the cost-utility of triple regimen of palonosetron vs. triple regimen of granisetron | Yes – Assess the cost-effectiveness of triple regimen of palonosetron vs. triple regimen of granisetron | Yes – Assess the cost-utility of palonosetron vs. ondansetron vs. granisetron | Yes – Assess the cost-utility analysis of NEPA vs. other 4 3-drug combination regimens |
2. The economic importance of the research question is stated. | Yes – Less is known about the relative cost-effectiveness of NEPA in the US. | Yes – Although palonosetron was shown to be superior to granisetron, the economic evaluations have not been done. | Yes – No previous study directly compared the cost-effectiveness of palonosetron and granisetron. | Yes – Economic evaluations of these 3 drugs in the real-world setting of Chinese patients has not been determined. | Yes – Efficiency of resources allocation and sustainability of the use of NEPA |
3. The viewpoint(s) of the analysis are clearly stated and justified. | Yes – From the US health care perspective | Yes – From the health care perspective in Japan | Yes – From the health care perspective in Japan | Yes – From the Chinese health care perspective | Yes – Italian National Health Service perspective |
4. The rationale for choosing alternative programmes or interventions compared is stated. | Yes – Most guidelines recommend a 3-drug combination including NK1 RA, a 5-HT3 RA and dexamethasone | Yes – Used the results of an RCT | Yes – No previous study directly compared the cost-effectiveness of palonosetron and granisetron. | Yes – those are 3 main 5-HT3 RAs | Yes – New drugs of NK1 RA (aprepitant, fosaprepitant) in combination with palonosetron and ondansetron |
5. The alternatives being compared are clearly described. | Yes | Yes | Yes | Yes | Yes |
6. The form of economic evaluation used is stated. | Yes – Cost-utility analysis | Yes – Cost-utility analysis | Yes – Cost-effectiveness analysis | Yes – Cost-utility analysis | Yes – Cost-utility analysis |
7. The choice of form of economic evaluation is justified in relation to the questions addressed. | NR | Yes – Want to incorporate quality of life into the analysis. | NR | Yes – Want to incorporate quality of life into the analysis. | Yes – Want to incorporate quality of life into the analysis. |
Data collection | |||||
8. The source(s) of effectiveness estimates used are stated. | Yes – Based on a phase III noninferior RCT by Zhang et al. (2018)29 | Yes – Based on a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35 | Yes – Based on a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35 | Yes – Based on 2 pivotal phase III RCTs comparing palonosetron, ondansetron and granisetron | Yes – Based on 3 RCTs |
9. Details of the design and results of effectiveness study are given (if based on a single study). | Yes | Yes | Yes | Yes | Yes |
10. Details of the methods of synthesis or meta-analysis of estimates are given (if based on a synthesis of a number of effectiveness studies). | NA | NA | NA | No | No |
11. The primary outcome measure(s) for the economic evaluation are clearly stated. | Yes – Net monetary benefit and probability that NEPA is cost-effective relative to granisetron/ aprepitant regimen | Yes – ICER | Yes – ICER | Yes – ICER | Yes – ICER |
12. Methods to value benefits are stated. | Yes | Yes | Yes | Yes | Yes |
13. Details of the subjects from whom valuations were obtained were given. | Yes – Table of patient characteristics was provided | Yes – Described and referred to the clinical study | Yes – Table of patient characteristics was provided | Yes – Described and referred to the study | No – Referred to the clinical studies |
14. Productivity changes (if included) are reported separately. | NA – Only 5-day follow-up | NA – Only 5-day follow-up | NA – Only 5-day follow-up | NA – Only 5-day follow-up | NA – Only 5-day follow-up |
15. The relevance of productivity changes to the study question is discussed. | NA – Only 5-day follow-up | NA – Only 5-day follow-up | NA – Only 5-day follow-up | NA – Only 5-day follow-up | NA – Only 5-day follow-up |
16. Quantities of resource use are reported separately from their unit costs. | Yes | Yes | Yes | Yes | Yes |
17. Methods for the estimation of quantities and unit costs are described. | Yes | Yes | Yes | Yes | Yes |
18. Currency and price data are recorded. | Yes | Yes | Yes | Yes | Yes |
19. Details of currency of price adjustments for inflation or currency conversion are given. | Yes – 2018 USD | Yes – 2018 USD | Yes – 2018 USD | Yes – 2014 USD | Yes – 2016 € |
20. Details of any model used are given. | No model used | Yes – Decision tree | No model used | Yes – Decision tree | Yes – Markov model |
21. The choice of model used and the key parameters on which it is based are justified. | No model used | Yes | No model used | Yes | Yes |
Analysis and interpretation of results | |||||
22. Time horizon of costs and benefits is stated. | Yes – 5 days | Yes – 5 days | Yes – 5 days | Yes – 5 days | Yes – 5 days |
23. The discount rate(s) is stated. | NA | NA | NA | NA | NA |
24. The choice of discount rate(s) is justified. | NA | NA | NA | NA | NA |
25. An explanation is given if costs and benefits are not discounted. | NA | NA | NA | NA | NA |
26. Details of statistical tests and confidence intervals are given for stochastic data. | Yes | Yes | Yes | Yes | Yes |
27. The approach to sensitivity analysis is given. | Yes – 1-way and probabilistic sensitivity analysis | Yes - 1-way and probabilistic sensitivity analysis | Yes - 1-way sensitivity analysis | Yes - 1-way and probabilistic sensitivity analysis | Yes - 1-way sensitivity analysis |
28. The choice of variables for sensitivity analysis is justified. | Yes | Yes | Yes | Yes | Yes |
29. The ranges over which the variables are varied are justified. | Yes | Yes | Yes | Yes | Yes |
30. Relevant alternatives are compared. | No | No | No | No | No |
31. Incremental analysis is reported. | Yes | Yes | Yes | Yes | Yes |
32. Major outcomes are presented in a disaggregated as well as aggregated form. | Yes | Yes | Yes | Yes | Yes |
33. The answer to the study question is given. | Yes | Yes | Yes | Yes | Yes |
34. Conclusions follow from the data reported. | Yes | Yes | Yes | Yes | Yes |
35. Conclusions are accompanied by the appropriate caveats. | Yes | Yes | Yes | Yes | Yes |
5-HT3 RA = 5-hydroxytryptamine-3 receptor antagonist; ICER = incremental cost-effectiveness ratio; NA = not applicable; NK1 RA = neurokinin-1 receptor antagonist; NEPA = netupitant/palonosetron; NR = not reported; RCT = randomized controlled trial; WTP = willingness-to-pay.
Table 10: Strengths and Limitations of Guidelines Using AGREE II19
Item | ASCO, Hesketh et al. (2020)41 | NCCN (2020)42 | CCO (2019)43 | POGO (2017)44 | |
Domain 1: Scope and Purpose | |||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | |||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear | Unclear | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes | Yes |
Domain 3: Rigour of Development | |||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Unclear | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes | Yes | Yes | Yes |
Domain 4: Clarity of Presentation | |||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | |||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Yes | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | Yes | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes | Yes | Yes | Yes | Yes |
Domain 6: Editorial Independence | |||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes | Yes |
ASCO = American Society of Clinical Oncology; CCO = Cancer Care Ontario; ESMO = European Society of Medical Oncology; GRADE = Grades of Recommendation Assessment, Development and Evaluation; HEC = high emetogenic chemotherapy; MASCC = Multinational Association of Supportive Care in Cancer; MEC = moderate emetogenic chemotherapy; NCCN = National Comprehensive Cancer Network; POGO = Pediatric Oncology Group of Ontario.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings Included Systematic Review
Simino et al. (2016)21
Main study findings
Ondansetron versus Palonosetron
6 RCTs (2 low RoB, 2 unclear RoB, and 2 high RoB); N = 1,072
3 RCTs involving HEC and 3 RCTs involving MEC
Published from 2003 to 2013
Efficacy
Acute nausea (4 RCTs; N = 254)
Relative risk [RR] (95% CI) = 1.14 (0.78 to 1.66); P = 0.50; I2 = 0%
Delayed nausea (4 RCTs; N = 254)
RR (95% CI) = 1.25 (1.01 to 1.56); P = 0.04; I2 = 0%
Acute vomiting (6 RCTs; N = 1,072)
RR (95% CI) = 1.28 (1.02 to 1.59); P = 0.03; I2 = 13%
Delayed vomiting (6 RCTs; N = 1,072)
RR (95% CI) = 1.31 (1.01 to 1.69); P = 0.04; I2 = 72%
Efficacy (subgroup analysis)
Acute nausea
HEC: No statistically significant difference between drugs
MEC: No statistically significant difference between drugs
Acute vomiting
HEC: No statistically significant difference between drugs
MEC: RR (95% CI) = 1.57 (1.15 to 2.15); P = 0.004; I2 = 0%
Safety
Headache (4 RCTs; N = 1,002)
RR (95% CI) = 1.31 (0.83 to 2.08); P = 0.25; I2 = 0%
Constipation (4 RCTs; N = 859)
RR (95% CI) = 0.88 (0.47 to 1.65); P = 0.70; I2 = 0%
Diarrhea (3 RCTs; N = 628)
RR (95% CI) = 1.68 (0.41 to 6.95); P = 0.47; I2 = NA
Dizziness (2 RCTs; N = 463)
RR (95% CI) = 4.89 (0.85 to 28.32); P = 0.08; I2 = 0%
Authors’ conclusion
“Palonosetron exhibited greater efficacy than ondansetron for delayed nausea and acute and delayed vomiting.”21 (p. 1183)
Summary of Findings of Included Primary Clinical Studies
Mahrous et al. (2021)22
Main study findings
Palonosetron + DEX (N = 51) versus Granisetron + DEX (N = 64) in adult patients naive to chemotherapy who were scheduled to receive HEC
Efficacy
Acute nausea: 11.8% versus 89.1%; P < 0.0001
Delayed nausea: 47.06% versus 92.2%; P < 0.0001
Acute vomiting: 7.8% versus 43.8%; P < 0.0001
Delayed vomiting: 23.5% versus 82.8%; P < 0.0001
Use of rescue medication: 45.1% versus 96.9%
AEs: NR
Authors’ conclusion
“Palonosetron, combined with dexamethasone, is more effective than granisetron and dexamethasone combination against both acute and delayed emesis induced by highly emetogenic chemotherapy (HEC) cisplatin-based protocols and the combination of cyclophosphamide and anthracyclines (AC).”22 (p. 121)
van de Vorst et al. (2021)23
Main study findings
Palonosetron + DEX (Arm 1, N = 63) versus Ondansetron + DEX (Arm 2, N = 60) versus Ondansetron + DEX + Metoclopramide (Arm 3, N = 66) in adult patients naïve to chemotherapy who were scheduled to receive MEC
Efficacy
Primary outcome
Delayed TC (no emetic episodes, no use of rescue medication, no nausea)
Arm 1: 55.6% (95% CI, 42.5 to 68.1)
Arm 2: 50.0% (95% CI, 36.8 to 63.2)
Arm 3: 56.1% (95% CI, 43.3 to 68.3)
95% CI of difference between Arm 3 and Arm 2: −11.3% to 23.5%
95% CI of difference between Arm 1 and Arm 2: −12.0% to 23.2%
Both Arm 1 and Arm 3 met the criteria for noninferiority to Arm 2 (i.e., the lower limit of the 95% CI of the differences between arms was greater than the noninferiority margin of - 20%)
Secondary outcomes
Acute TC
Arm 1: 79.4% (95% CI, 67.3 to 88.5)
Arm 2: 85.0% (95% CI, 73.4 to 92.9)
Arm 3: 90.9% (95% CI, 81.3 to 96.6)
95% CI of difference between Arm 3 and Arm 2: −5.6% to 17.0%
95% CI of difference between Arm 1 and Arm 2: −19.2% to 7.6%
Overall TC
Arm 1: 51.5% (95% CI, 38.9 to 64.0)
Arm 2: 46.7% (95% CI, 33.7 to 60.0)
Arm 3: 54.0% (95% CI, 40.9 to 66.6)
95% CI of difference between Arm 3 and Arm 2: −10.3% to 24.9%
95% CI of difference between Arm 1 and Arm 2: −12.7% to 22.3%
No vomiting, Arm 1 – Arm 2 risk difference (95% CI)
Acute: −6.1% (−15.6 to 3.4)
Delayed: −10.5% (−23.6 to 2.6)
Overall: - 8.7% (−23.0 to 5.6)
No significant nausea, Arm 1 – Arm 2 risk difference (95% CI)
Acute: - 4.3% (−15.8 to 7.2)
Delayed: - 6.6% (−22.8 to 9.6)
Overall: - 6.5% (−23.1 to 10.1)
No nausea, Arm 1 – Arm 2 risk difference (95% CI)
Acute: 6.5% (−11.2 to 24.2)
Delayed: 2.5% (−15.1 to 20.1)
Overall: 1.0% (−16.6 to 18.6)
No rescue use, Arm 1 – Arm 2 risk difference (95% CI)
Acute: −2.8% (−20.8 to 14.9)
Delayed: 9.7% (−6.7 to 26.1)
Overall: 11.4% (−5.3 to 28.1)
CR (no emetic episodes, no use of rescue medication), Arm 1 – Arm 2 risk difference (95% CI)
Acute: −9.2% (−21.1 to 2.7)
Delayed: 11.7% (−5.4 to 28.8)
Overall: 11.8% (−5.6 to 29.2)
CP (no emetic episodes, no use of rescue medication, no significant nausea), Arm 1 – Arm 2 risk difference (95% CI)
Acute: −5.6% (−17.9 to 6.7)
Delayed: 5.6% (−12.0 to 23.2)
Overall: 7.3% (−10.3 to 24.9)
QoL (determined by FLIE scores; a total of FLIE score of > 108 was considered as “no or minimal impact on daily life”)
On day 2 – FLIE scores, mean ± SD:
Arm 1: 114 ± 21.7
Arm 2: 118 ± 17.5
Arm 3: 117 ± 22.4
On day 2 – Proportion of patients with “no or minimal impact on daily life”
Arm 1: 78.7%; P = 0.50 compared to Arm 2
Arm 2: 86.0%
Arm 3: 87.5%; P = 0.80 compared to Arm 2
On day 6 – FLIE scores, mean ± SD:
Arm 1: 114 ± 21.2
Arm 2: 114 ± 16.1
Arm 3: 114 ± 21.5
On day 6 – Proportion of patients with “no or minimal impact on daily life”
Arm 1: 80%; P = 0.21 compared to Arm 2
Arm 2: 70.9%
Arm 3: 78.1%; P = 0.37 compared to Arm 2
Safety (moderate to severe DEX-associated side effects; DSQ score 3 or 4)
Indigestion/reflux: 7.9% versus 1.7% versus 1.7%; NS
Insomnia: 4.8% versus 5.0% versus 4.5%; NS
Increased appetite: 14.4% versus 12.1% versus 16.7%; NS
Hiccups: 0.0% versus 3.3% versus 0.0%; NS
Agitation: 1.6% versus 3.3% versus 0.0%; NS
Depression: 3.2% versus 5.0% versus 1.5%; NS
Rash/acne: 4.8% versus 6.7% versus 10.6%; NS
Thrush/oral yeast infection: 9.5% versus 3.3% versus 3.0%; NS
Authors’ conclusion
The authors concluded that ondansetron + DEX + metoclopramide demonstrated noninferiority to ondansetron + DEX for delayed TC. Palonosetron + DEX also demonstrated noninferiority to ondansetron + DEX. There were no statistically significant differences for all secondary end points between treatment arms.
Matsumoto et al. (2020)24
Main study findings
Palonosetron + fosaprepitant + DEX versus Granisetron + fosaprepitant + DEX in breast cancer patients naïve to chemotherapy who were scheduled to receive HEC (AC-based regimen)
Efficacy
Primary outcome
CR during the delayed phase: 62.3% versus 60.4%; P = 0.8
Secondary outcomes
CR during the acute phase: 75.9% versus 73.2%; NS
CR during the overall phase: 54.9% versus 54.9%; NS
No vomiting
Acute: 95.7% versus 93.9%; NS
Delayed: 89.5% versus 82.3%; NS
Overall: 85.8% versus 79.9%; NS
No nausea
Acute: 51.2% versus 45.1%; NS
Delayed: 40.1% versus 28.0%; P = 0.029
Overall: 32.7% versus 24.4%; NS
Patient-reported outcomes: The frequency of nausea was significantly lower after administration of palonosetron regimen compared to granisetron regiment (P = 0.014).
Safety
Most of the AEs were of grade 1 and 2
Constipation: 34% versus 27.5%
Headache: 13.2% versus 12%
Infusion site reaction: 20.3% versus 23.3%
Febrile neutropenia: 5.4% versus 4.2%
Authors’ conclusion
“Palonosetron exerts efficacy against delayed CINV which is not better than that of the combination with granisetron for patients with breast cancer receiving 3 days dexamethasone and fosaprepitant after AC-based regimen, even though palonosetron reduced significantly delayed nausea. Both palonosetron and granisetron combined with steroids and NK-1 Ras are good options for CIVN prevention in patients with breast cancer receiving AC-based regimen. These patients are still at high risk of nausea, especially during the delayed phase. Administration of fosaprepitant in the peripheral vein with AC-based regimen should be avoided because it leads to higher risk of infusion site reaction.”24 (p. 3325)
Chaudhary et al. (2019)25
Main study findings
Palonosetron + DEX versus Ondansetron + DEX in children naïve to chemotherapy who were scheduled to receive HEC or MEC
Efficacy
CR
Acute: 88% versus 84%; P = 0.42
Delayed: 88% versus 79%: P = 0.09
Overall: 81% versus 72%; P = 0.21
CP
Acute: 84% versus 79%; P = 0.44
Delayed: 81% versus 67%; P = 0.06
Overall: 73% versus 60%; P = 0.10
Use of rescue antiemetics: 5% versus 4%
Safety
AEs: 22% versus 20%
Both drugs were well tolerated
Abdominal pain, constipation, diarrhea, headache, dizziness
Authors’ conclusion
“Palonosetron (5 µg/kg) seemed to be as efficacious and safe as ondansetron for the prevention of CINV. It is, however, a better choice in terms of cost and utilization of manpower for centers in resource-limited countries.”25 (p. 297)
Tsubata et al. (2019)26
Main study findings
Palonosetron + DEX versus Granisetron + DEX in adult patients naïve to chemotherapy who were scheduled to receive MEC or HEC (addition of aprepitant in both groups)
Efficacy
Primary outcome
MAT scores at delayed phase: 2.7 versus 3.5; P = 0.55
Secondary outcomes:
MAT scores at acute phase: No statistically significant different between groups (P = 0.61)
FLIE scores for vomiting domain: No statistically significant different between groups (P = 0.82)
FLIE scores for nausea domain: No statistically significant different between groups (P = 0.49)
CR
Acute: 80.0% versus 82.9%; NS
Delayed: 51.4% versus 48.6%; NS
Overall: 51.4% versus 48.6%; NS
TC
Overall: 31.7 versus 40.0; NS
Subgroup analysis of each treatment group stratified by HEC or MEC showed no statistically significant differences.
Authors’ conclusion
“For the primary endpoint, the score of the late phase on MAT questionnaire was not statistically different between PAL and GRA treatment groups.”26 (p. 269)
Jain et al. (2018)27
Main study findings
Palonosetron + DEX versus Ondansetron + DEX in children naïve to chemotherapy who were scheduled to receive MEC or HEC (addition of fosaprepitant in both groups)
Efficacy
Primary outcome
CR at acute phase: 83.3% versus 72.2%
Difference between groups (97.5% CI) = 11.1% (−6.95 to 28.39)
The lower limit of 97.5% CI of the difference was greater than −15% (noninferiority margin)
Safety
Headache: palonosetron (1 patient) versus ondansetron (2 patients)
Constipation: palonosetron (1 patient) versus ondansetron (1 patient)
No serious AEs
Authors’ conclusion
“We conclude that a single dose of palonosetron is safe and noninferior to ondansetron for prevention of acute CINV in children and is also cost-effective. For patients where dexamethasone cannot be used in the prophylactic regimen, alternative strategies need to be explored.”27 (p. 3096)
Tan et al. (2018)
Main study findings
Palonosetron (5 mcg/kg) + DEX versus Palonosetron (10 mcg/kg) + DEX versus Ondansetron + DEX in children with or without previous chemotherapy who were scheduled to receive HEC
Efficacy
CR
Acute: 69.1% versus 69.7% versus 64.6%
Delayed: 39.8% versus 53.5% versus 32.8%; P < 0.017 compared between palonosetron (10 mcg/kg) and ondansetron
Overall: 36.5% versus 42.7% versus 21.7%; P < 0.017 compared between palonosetron (10 mcg/kg) and ondansetron
No vomiting
Acute: 78.5% versus 81.1% versus 78.3%
Delayed: 58% versus 63.8% versus 46.6%; P < 0.017 compared between palonosetron (10 mcg/kg) and ondansetron
Overall: 51.9% versus 56.8% versus 40.2%; P < 0.017 compared between palonosetron (10 mcg/kg) and ondansetron
No nausea
Acute: 66.3% versus 67.6% versus 62.4%
Delayed: 49.7% versus 56.8% versus 36.0%; P < 0.017 compared between palonosetron (10 mcg/kg) and ondansetron
Overall: 42.0% versus 41.1% versus 22.2%; P < 0.017 compared between palonosetron (10 mcg/kg) and ondansetron
Safety
AEs: 12.7% versus 11.9% versus 13.2%; NS
Most AEs were grade 1 to 2
Authors’ conclusion
“In conclusion, this study showed that combination of palonosetron and dexamethasone is effective in controlling acute and delayed CINV, especially the latter. Palonosetron is nonsuperiority to ondansetron for acute CINV control and provides superior CINV control during the delayed phase. There was no significant difference in adverse effects between the palonosetron and ondansetron group.”27 (p. 6)
Zhang et al. (2018)29 and Chang et al. (2020)30
Main study findings
NEPA (netupitant and palonosetron) + DEX (N = 413) versus Granisetron + aprepitant + DEX (N = 416) in adult patients naive to chemotherapy who were scheduled to receive HEC
Efficacy (overall population)
Primary outcome
Overall CR: 73.8% versus 72.4% (95% CI, −4.5% to 7.5%)
RD (95% CI) = 1.5% (−4.5% to 7.5%)
NEPA demonstrated noninferiority compared to granisetron/aprepitant, as noninferiority margin set at −10%.
Daily rates of patients with CINV over 5 days:
NEPA: declined from 16% to 8%
Granisetron/aprepitant: remained between 13 and 15%
On day 5: 8.0% NEPA versus 13.9% granisetron/aprepitant; 95% CI, 1.7% to 10.2%; P = 0.0063
Secondary outcomes
No emesis – Rates; RD (95% CI)
Acute: 85.2% versus 87.5%; −2.2% (−6.9 to 2.4)
Delayed: 79.4% versus 76.2%; 3.3% (−2.4 to 8.9)
Overall: 75.0% versus 74.0%; 1.1% (−4.8 to 6.9)
No significant nausea – Rates; RD (95% CI)
Acute: 89.8% versus 87.3%; 2.6% (−1.7 to 6.9)
Delayed: 78.2% versus 72.8%; 5.4% (−0.4 to 11.2)
Overall: 75.7% versus 70.4%; 5.4% (−0.6 to 11.4)
No nausea – Rates; RD (95% CI)
Acute: 68.9% versus 67.8%; 1.2% (−5.1 to 7.5)
Delayed: 53.2% versus 54.3%; −1.1% (−7.9 to 5.7)
Overall: 49.3% versus 51.4%; −2.1% (−8.9 to 4.7)
No use of rescue medication – Rates; RD (95% CI)
Acute: 98.8% versus 98.3%; 0.5% (−1.2 to 2.1)
Delayed: 97.6% versus 94.7%; 2.9% (0.2% to 5.5%); P < 0.05
Overall: 96.6% versus 93.5%; 3.1% (0.2 to 6.1); P < 0.05
Proportion of patients with NIDL (based on FLIE)
No significant differences between groups for nausea, vomiting or overall combined in the acute and delayed phases, except NEPA was significantly better with nausea domain for the delayed phase (71.1% versus 65.1%; RD [95% CI] = 6.5% [0.2% to 12.8%])
Safety (Overall population)
AEs: 58.1% versus 57.5%
Constipation: 8.0% versus 6.3%
Hiccups: 2.7% versus 1.4%
Severe AEs: 8.7% versus 10.8%
Efficacy and Safety (Subset of Chinese population; 80% of the overall population)
Same results as those in the overall population.
Authors’ conclusion
“In conclusion, our study indicated that as a combination antiemetic targeting two antiemetic pathways with a single dose administered only once per cycle, NEPA offers a convenient and simplified prophylactic antiemetic that is at least as effective as a 3-day aprepitant regimen with granisetron.”29 (p. 457)
“In conclusion, this study exploring the efficacy or oral NEPA, a convenient and simplified combination antiemetic, in Chinese patients revealed that single-dose NEPA more effectively prevents CINV than a 3-day aprepitant/granisetron regimen during the latter days (3-5) post-chemotherapy.”30 (p. 5141)
Ishido et al. (2016)31
Main study findings
Palonosetron + DEX versus Granisetron + aprepitant + DEX in adult cancer patients naïve to chemotherapy who were scheduled to receive HEC
Efficacy
Primary outcome
Overall CR: 58.5% versus 67.4%; P = 0.399
Secondary outcomes
CR
Acute: 95.1% versus 95.3%; P = 0.961
Delayed: 58.5% versus 67.4%; P = 0.399
No vomiting
Acute: 97.6% versus 97.7%; P = 0.973
Delayed: 58.5% versus 81.4%; P = 0.025
Overall: 58.5% versus 81.4%; P = 0.025
No nausea
Acute: 95.1% versus 88.4%; P = 0.277
Delayed: 39.0% versus 39.5%; P = 0.962
Overall: 39.0% versus 39.5%; P = 0.962
No rescue medication
Acute: 97.6% versus 95.3%; P = 0.591
Delayed: 75.6% versus 67.4%; P = 0.409
Overall: 75.6% versus 67.4%; P = 0.409
TC
Acute: 90.2% versus 83.7%; P = 0.380
Delayed: 36.6% versus 39.5%; P = 0.781
Overall: 36.6% versus 39.5%; P = 0.781
Patients’ preference for treatment after second cycle (N = 35 in Palonosetron group and N = 26 in Granisetron group)
19.7% preferred palonosetron, 41.0% preferred granisetron, and 39.3% indicated no preference.
QoL (based on FLIE), % with NIDL
FLIE total score: 46.3% versus 48.8%; P = 0.819
Nausea domain total score: 39.0% versus 41.9%; P = 0.791
Vomiting domain total score: 53.7% versus 79.1%; P = 0.014
Safety
AEs
No significant difference between groups for any grade AEs, except constipation was significantly higher in the palonosetron group (17.1%) compared to ondansetron group (2.3%); P = 0.028.
No significant difference between groups for ≥ Grade 3 AEs.
Oral intake
The difference in oral intake rate between groups decreased with time. There was a trend toward decreased rates of oral intake in both groups.
Authors’ conclusion
Although the primary end point of complete response was not achieved, aprepitant/granisetron/dexamethasone combination therapy seems to be more effective than palonosetron/dexamethasone therapy for the prevention of HEC-induced vomiting.”31 (p. 890)
Main study findings
Palonosetron (10 mcg/kg) + DEX versus Palonosetron (20 mcg/kg) + DEX versus Ondansetron + DEX in children with or without previous chemotherapy who were scheduled to receive HEC or MEC
Efficacy
Primary outcome
Acute CR
54% versus 59% versus 59%
Difference between palonosetron (10 mcg/kg) and ondansetron = −4.41% (97.5% CI, −16.4 to 7.6). Noninferiority was not shown for this dose (noninferiority margin was set at −15%).
Difference between palonosetron (20 mcg/kg) and ondansetron = 0.36% (97.5% CI, −11.7 to 12.4). Noninferiority was shown for this dose.
Secondary outcomes
Delayed CR
29% versus 39% versus 28%
Difference between palonosetron (10 mcg/kg) and ondansetron = 0.42% (97.5% CI, −9.4 to 10.3)
Difference between palonosetron (20 mcg/kg) and ondansetron = 10.17% (97.5% CI, −0.1 to 20.4)
Overall CR
23% versus 33% versus 24%
Difference between palonosetron (10 mcg/kg) and ondansetron = −0.60% (97.5% CI, −10.0 to 8.8)
Difference between palonosetron (20 mcg/kg) and ondansetron = 8.25% (97.5% CI, −1.6 to 18.1)
No vomiting
Acute: 80% versus 84% versus 73%. Difference between palonosetron (10 mcg/kg) and ondansetron were not statistically significant, but palonosetron (20 mcg/kg) was significantly higher versus ondansetron (difference = 10.03%; 95%CI, 1.2 to 18.1)
Delayed: 68% versus 74% versus 58%. Difference between palonosetron (10 mcg/kg) and ondansetron were not statistically significant, but palonosetron (20 mcg/kg) was significantly higher versus ondansetron (difference = 15.84%; 95%CI, 5.7 to 26.0)
Overall: 59% versus 69% versus 51%. Difference between palonosetron (10 mcg/kg) and ondansetron were not statistically significant, but palonosetron (20 mcg/kg) was significantly higher versus ondansetron (difference = 17.46%; 95%CI, 7.0 to 27.9)
No emetic episodes
Acute: 73% versus 80% versus 69%. Difference between palonosetron (10 mcg/kg) and ondansetron were not statistically significant, but palonosetron (20 mcg/kg) was significantly higher versus ondansetron (difference = 11.25%; 95%CI, 2.0 to 20.5)
Delayed: 61% versus 68% versus 53%. Difference between palonosetron (10 mcg/kg) and ondansetron were not statistically significant, but palonosetron (20 mcg/kg) was significantly higher versus ondansetron (difference = 15.38%; 95%CI, 5.1 to 25.7)
Overall: 52% versus 64% versus 46%. Difference between palonosetron (10 mcg/kg) and ondansetron were not statistically significant, but palonosetron (20 mcg/kg) was significantly higher versus ondansetron (difference = 17.56%; 95%CI, 7.0 to 28.1)
No antiemetic rescue medication:
Acute: 69% versus 75% versus 76%. Both palonosetron groups were not statistically significant difference compared with ondansetron.
Delayed: 39% versus 45% versus 35%. Both palonosetron groups were not statistically significant difference compared with ondansetron.
Overall: 69% versus 75% versus 76%. Both palonosetron groups were not statistically significant difference compared with ondansetron.
Delayed: 36% versus 42% versus 33%. Both palonosetron groups were not statistically significant difference compared with ondansetron.
No nausea for children age ≥ 6 years
Acute: 65% versus 72% versus 67%. Both palonosetron groups were not statistically significant difference compared with ondansetron.
Delayed: 57% versus 66% versus 51%. Difference between palonosetron (10 mcg/kg) and ondansetron were not statistically significant, but palonosetron (20 mcg/kg) was significantly higher versus ondansetron (difference = 14.79%; 95%CI, 1.5 to 28.1)
Overall: 47% versus 58% versus 43%. Difference between palonosetron (10 mcg/kg) and ondansetron were not statistically significant, but palonosetron (20 mcg/kg) was significantly higher versus ondansetron (difference = 15.00%; 95%CI, 1.4 to 28.6)
Safety
AEs
At least 1 drug-related treatment-emergent AEs: 4% versus 4% versus 4%
Headache: 2% versus < 1% versus 1%
Dizziness: < 1% versus < 1% versus 0
Efficacy and Safety across multiple cycles of chemotherapy
“In all on-study chemotherapy cycles, complete response rates were higher in patients in the 20 µg/kg palonosetron group than the ondansetron group. Treatment-emergent adverse events were comparable between the palonosetron 20 µg/kg and ondansetron group.”33 (p. 1685)
Authors’ conclusion
“Noninferiority was shown for 20 µg/kg palonosetron during the acute phase of the first on-study chemotherapy cycle. 20 µg/kg palonosetron is now indicated in the European Medicines Agency and the US Food and Drug Administration for the prevention of chemotherapy-induced nausea and vomiting in pediatric patients aged 1 month to younger than 17 years.”32 (p. 332)
“Over four cycles of HEC/MEC, 20 µg/kg palonosetron was an efficacious and safe treatment for the prevention of chemotherapy-induced nausea and vomiting in pediatric cancer patients.”33 (p. 1685)
Seol et al. (2016)34
Main study findings
Palonosetron + DEX versus Granisetron (transdermal) + DEX in adult cancer patients with or without previous chemotherapy who were scheduled to receive a MEC in 2 consecutive chemotherapy cycles
Efficacy
Primary outcome:
CR during acute phase: 79.8% versus 75.2%
Difference between granisetron and palonosetron groups (95% CI) = −4.6% (−13.6 to 4.4)
Secondary outcomes:
CR during overall phase: No significant difference between groups
CC (acute, overall): No significant differences between groups
TC (acute, overall): No significant differences between groups
QoL (FLIE scores): No significant differences between groups during overall phase
Safety
AEs
Constipation: 5.0% versus 2.7%; NS
Diarrhea: 0.6% versus 1.1%; NS
Insomnia: 1.1% versus 2.1%; NS
Rash: 0 versus 0.5%; NS
Authors’ conclusion
“This study demonstrated granisetron transdermal delivery system (GTDS) is noninferior to palonosetron for relieving CINV in patients receiving MEC and patient’s satisfaction with GTDS being higher than with palonosetron. On the basis of the results of trial, GTDS could be a good therapeutic option for patients receiving MEC.”34 (p. 951)
Suzuki et al. (2016)35
Main study findings
Palonosetron + DEX + aprepitant versus Granisetron + DEX + aprepitant in adult cancer patients naïve to chemotherapy who were scheduled for HEC
Efficacy
Primary outcome
Overall CR: 65.7% versus 59.1%; P = 0.0539
Secondary outcomes
CR at acute phase: 91.8% versus 91.8%; P = 1.0000
CR at delayed phase: 67.2% versus 59.1%; P = 0.0142
CC
Acute: 90.1 versus 90.1%; P = 1.0000
Delayed: 65.2% versus 55.9%; P = 0.0053
Overall: 63.8% versus 55.9%; P = 0.0234
TC
Acute: 80.7% versus 80.6%; P = 1.0000
Delayed: 48.6% versus 41.4%; P = 0.0369
Overall: 47.6% versus 40.7%; P = 0.0369
Time to treatment failure
The palonosetron group had a longer time to treatment failure when compared with granisetron group
Hazard ratio (95% CI) = 0.81 (0.65 to 1.01); P = 0.063
Authors’ conclusion
“In conclusion, the present study did not show the superiority of palonosetron when compared with granisetron in the primary end point and should be concluded as a negative result. We, however, observed that palonosetron achieved the save efficacy as granisetron at the acute period as well as significantly higher CR, CC, and TC rates than granisetron at the delayed period, suggesting the need to discuss the clinical implications of these results in choosing 5-HT3 RA for controlling HEC-related CINV.”35 (p. 1605)
Summary of Findings of Included Economic Evaluations
Botteman et al. (2020)36
Main study findings
Cost-utility analysis of NEPA (netupitant/palonosetron) + DEX versus Granisetron + aprepitant + DEX in adult cancer patients naïve to chemotherapy and scheduled to receive HEC
Clinical efficacy – Based on a phase III noninferiority RCT by Zhang et al. (2018)29
Utility gained – Compared with granisetron regimen, NEPA resulted in a non-significant gained of 0.09 QALDs (95% CI, −0.06 to 0.25)
Costs (NEPA versus Granisetron regimen)
Total per-patient cost reduction: $309 (95% CI, 4 to 624)
Mean decrease in medical costs of CINV-related events: $409 (95% CI 215 to 612)
Reduction in study drug costs: $45 ($531 versus $577)
Reduction in rescue medication costs: $3 (95% CI 1 to 5) versus $8 (95% CI, 2 to 17)
Cost-utility analysis
Joint bootstrap and PSA simulations revealed that NEPA resulted in lower costs and higher QALDs, hence considered as dominant, in 86.5% of cases (located in bottom-right quadrant)
With WTP threshold of $25,000 per QALY gained, the probability of NEPA being cost-effective was 97.8% of cases.
NMB was $315
Sensitivity and subgroup analyses
NEPA was found to be cost-effective with all parameters investigated. NEPA was particularly highly cost-effective with severe nausea defined as 8.5-hour vomiting and/or retching threshold.
Authors’ conclusion
“Using patient-level outcomes data from a large comparative phase 3 trial as well as conservative cost and utilities assumptions, this analysis suggests that NEPA improves CINV outcomes at lower cost and is cost-effective relative to aprepitant-based regimens in CINV prevention for US patients receiving HEC. The cost reduction is principally due to a decrease in the occurrence of severe nausea with its associated medical cost and, to a lesser extent, a lower drug cost. This result is aligned with cost-effectiveness models assessing NEPA against comparator antiemetic prophylaxis, and supports the use of NEPA within oncology practices seeking to improve adherence to prophylaxis and optimize patient outcomes and cost-effectiveness.”36 (p. 864)
Kashiwa and Matsushita (2019)37
Main study findings
Cost-utility analysis of palonosetron + aprepitant + DEX versus granisetron + aprepitant + DEX in adult cancer patients naive to chemotherapy and scheduled to receive HEC
Clinical efficacy – Based on a phase III RCT (TRIPLE study) by Suzuki et a. (2016)35
Utility gained – Compared with granisetron regimen, palonosetron regimen resulted in a 0.0006452 QALY gained.
Costs
Antiemetic drugs: Palonosetron regimen 27,406 JPY (244.33 USD) versus granisetron regimen 13,707 JPY (122.20 USD).
Medical costs: 1,580 JPY (14.09 USD) for blood testing, 590 JPY (5.25 USD) for pharmacy costs, and 1,374 JPY (12,25 USD) for supplementary nutrition infusion.
Rescue medication costs: 432 JPY (3.85 USD) with palonosetron regimen and 5,953 JPY (53.1 USD) with granisetron regimen.
Cost-utility analysis
The incremental cost was 10,455 JPY (93.21 USD), due to higher total cost of palonosetron regimen compared to granisetron regimen (30,348 JPY [270.55 USD] versus 19,893 JPY [177.35 USD]).
The ICER was 16,204,591 JPY/QALY (144,465 USD/QALY).
Sensitivity analysis
One-way sensitivity analysis: CR rate in the delayed phase had largest effect on the increase in the ICER.
PSA revealed that palonosetron regimen resulted in more expensive and more effective (located in top-right quadrant).
With a WTP threshold of 5,000,000 JPY (44,575 USD) per QALY gained, the probability of palonosetron regimen being cost-effective was 3.64% of cases. Hence palonosetron regimen was not cost-effective for HEC in Japan.
With a 50% reduction in drug price for palonosetron, the ICER decreased to approximately 4,600,000 JPY/QALY (41,000 USD/QALY).
The acceptable price of palonosetron was estimated to be 7,743 JPY (69.03 USD), a 51.7% of the current price of 14,472 JPY.
Authors’ conclusion
“The use of PALO instead of GRA for the prevention of CINV in patients receiving HEC through the Japanese health insurance system is not cost-effective at this time. The cost of drugs, with the arrival of inexpensive generic drugs, will make a major contribution to its cost-effectiveness.”37 (p. 9)
Shimizu et al. (2018)38
Main study findings
Cost-effectiveness analysis of palonosetron + aprepitant + DEX versus granisetron + aprepitant + DEX in adult cancer patients naive to chemotherapy and scheduled to receive HEC
Clinical efficacy – Based on a phase III RCT (TRIPLE study) by Suzuki et al. (2016)35
Costs
Drug costs: Palonosetron regimen 27,863.8 JPY versus granisetron regimen 15,342.8 JPY; cost difference 12,521 JPY.
Rescue medication costs: Palonosetron regimen 59,292.7 JPY versus granisetron regimen 73,883.8 JPY
Cost-effectiveness ratio (CER)
The CERs for palonosetron regimen and granisetron regimen were 42,628.6 JPY/CR and 26,263.4 JPY/CR, respectively.
The ICER was 189,171.6 JPY/CR.
The range of ICER was 189,044.8 to 189,215.5 JPY/CR.
Authors’ conclusion
“We determined the CER and ICER, which served as indices of the cost-effectiveness of standard triplet antiemetic therapy for preventing CINV in patients receiving cisplatin-based HEC regimens in Japan. Also, we found that PALO 0.75 mg was more expensive than GRA 1 mg in the patients who received the cisplatin-based HEC regimen.”38 (p. 8)
Du et al. (2017)39
Main study findings
Cost-utility analysis of palonosetron + DEX versus ondansetron + DEX versus granisetron + DEX in adult cancer patients naive and non-naive to chemotherapy who were scheduled to receive HEC
Clinical efficacy – Based on 2 pivotal phase III RCTs comparing palonosetron, ondansetron and granisetron.54,55
Utilities – Compared to granisetron, ondansetron resulted in a QALY loss of −0.00003, and palonosetron resulted in a QALY gained of 0.00056.
Costs
Compared to granisetron, difference in drug cost was 25.95 USD for ondansetron and 93.64 USD for palonosetron.
Cost-utility analysis
Compared to granisetron, ICER was −953,456.58 USD/QALY for ondansetron (more cost, less effective) and 167,914.74 USD/QALY for palonosetron (more cost, more effective), which was higher than the WTP threshold of 22,515 USD/QALY and was therefore not cost-effective.
Sensitivity analysis
Among the parameters evaluated, the cost of palonosetron 0.25 mg was the most important parameter.
To be cost-effective, the price of palonosetron per 0.25 mg has to be decreased to 23.41 USD, a reduction of at least 69.7%.
PSA revealed that at the WTP threshold of 22,515 USD/QALY, granisetron strategy was cost-effective in 99.1% of the simulation.
Authors’ conclusion
“Our analysis suggests that, compared with palonosetron and ondansetron, 3 mg granisetron may be a cos0effective treatment option in the current Chinese healthcare setting”39 (p. 403)
“Moreover, palonosetron is not cost-effective in preventing ‘overall’ nausea and vomiting following highly emetogenic chemotherapy in Chinese patients.”39 (p. 403)
Restelli et al. (2017)56
Main study findings
Cost-utility analysis of 5 regimens (NEPA [NEPA] versus aprepitant + palonosetron [APR + PALO] versus fosaprepitant + palonosetron [fAPR + PALO] versus aprepitant + ondansetron [APR + ONDA] versus fosaprepitant + ondansetron [fAPR + ONDA]) in adult cancer patients who were scheduled to receive HEC or MEC
Clinical efficacy – Based on 3 RCTs48-50
For patients receiving HEC
Costs
NEPA €102.4 versus APR + PALO €132.5; difference -€30.2
NEPA €100.4 versus APR + ONDA €148.8; difference -€48.4
NEPA €102.4 versus fAPR + PALO €155.3; difference -€52.9
NEPA €100.4 versus fAPR + ONDA €171.7; difference -€71.4
Utilities (QALD)
NEPA 2.945 versus APR + PALO 2.684; difference + 0.261
NEPA 3.097 versus APR + ONDA 3.020; difference + 0.077
NEPA 2.945 versus fAPR + PALO 2.684; difference + 0.261
NEPA 3.097 versus fAPR + ONDA 3.020; difference + 0.077
Cost-utility analysis
NEPA is dominant compared to APR + PALO
NEPA is dominant compared to APR + ONDA
NEPA is dominant compared to fAPR + PALO
NEPA is dominant compared to fAPR + ONDA
For patients receiving MEC
Costs
NEPA €97.9 versus APR + PALO €125.1; difference -€27.2
NEPA €97.9 versus APR + PALO €145.9; difference -€48.0
Utilities (QALD)
NEPA 3.044 versus APR + PALO 2.992; difference + 0.052
NEPA 3.044 versus APR + PALO 2.992; difference + 0.052
Cost-utility analysis
NEPA is dominant compared to APR + PALO
NEPA is dominant compared to fAPR + PALO
Authors’ conclusion
“In conclusion, being aware of the limitations of the model and the lack of a probabilistic sensitivity analysis, the use of NEPA for the prophylaxis of CINV within the Italian context would lead to an efficient allocation of resources both for the treatment of patients receiving HEC (being dominant compared with APR + PALO, fAPR + PALO, APR + ONDA, fAPR + ONDA) and MEC (being dominant compared with APR + PALO, fAPR + PALO).”40 (p. 8)
Table 11: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
ASCO Guideline Update, Hesketh et al. (2020)41 | |
Adult patients receiving HEC “Adults treated with cisplatin and other high-emetic risk single agents should be offered a 4-drug combination of an NK1 receptor antagonist, a serotonin (5HT3) receptor antagonist*, dexamethasone, and olanzapine (day 1). Dexamethasone and olanzapine should be continued on days 2 to 4.”41 (p. 2783) | Level of evidence: High Strength of recommendation: Strong |
“Adults treated with anthracycline combined with cyclophosphamide should be offered a 4-drug combination of an NK1 receptor antagonist, a 5HT3 receptor antagonist, dexamethasone, and olanzapine (day 1). Dexamethasone and olanzapine should be continued on days 2 to 4.”41 (p. 2783) | Level of evidence: High Strength of recommendation: Strong |
Adult patients receiving MEC “Adults treated with carboplatin area under the curve (AUC) ≥ 4 mg/min should be offered a 3-drug combination of an NK1 receptor antagonist, a 5HT3 receptor antagonist and dexamethasone (day 1).”41 (p. 2783) | Level of evidence: High Strength of recommendation: Strong |
“Adults treated with moderate-emetic-risk antineoplastic agents (excluding carboplatin AUC ≥ 4 mg/min) should be offered a 2-drug combination of a 5HT3 receptor antagonist and dexamethasone (day 1)”41 (p. 2783). | Level of evidence: High Strength of recommendation: Strong |
“Adults treated with cyclophosphamide, doxorubicin, oxaliplatin, and other moderate-emetic-risk antineoplastic agents known to cause delayed nausea and vomiting may be offered dexamethasone on days to 2 to 3.”41 (p. 2783) | Level of evidence: Low Strength of recommendation: Moderate |
Pediatric patients receiving HEC “(Updated) Pediatric patients treated with high-emetic-risk antineoplastic agents should be offered a 3-drug combination of a 5HT3 receptor antagonist, dexamethasone, and aprepitant or fosaprepitant.”41 (p. 2785) | Level of evidence: Intermediate Strength of recommendation: Strong |
“(Updated) Pediatric patients treated with high-emetic-risk antineoplastic agents who are unable to receive aprepitant or fosaprepitant should be offered a 2-drug combination of a 5HT3 receptor antagonist and dexamethasone.”41 (p. 2785) | Level of evidence: Intermediate Strength of recommendation: Strong |
“(Updated) Pediatric patients treated with high-emetic-risk antineoplastic agents who are unable to receive dexamethasone should be offered a 2-drug combination of palonosetron and aprepitant or fosaprepitant.”41 (p. 2785) | Level of evidence: Intermediate Strength of recommendation: Strong |
Pediatric patients receiving MEC “Pediatric patients treated with moderate-emetic-risk antineoplastic agents should be offered a 2-drug combination of a 5HT3 receptor antagonist and dexamethasone.”41 (p. 2785) | Level of evidence: Intermediate Strength of recommendation: Strong |
“Pediatric patients treated with moderate-emetic-risk antineoplastic agents who are unable to receive dexamethasone should be offered a 2-drug combination of a 5HT3 receptor antagonist and aprepitant or fosaprepitant.”41 (p. 2785) | Level of evidence: Intermediate Strength of recommendation: Strong |
*5HT3 receptor antagonist: Granisetron, ondansetron, palonosetron, dolasetron, tropisetron, and ramosetron | |
NCCN Guideline Update (2020)42 | |
Adult patients receiving HEC parenteral anticancer agents Day 1: Choose 1 of the following 3 treatment options and start before anticancer therapy
Days 2, 3, 4:
| All recommendations are category 2A (Based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate) |
Adult patients receiving MEC parenteral anticancer agents Day 1: Choose 1 of the following 3 treatment options:
Days 2, 3:
| |
Adult patients receiving HEC or MEC oral anticancer agents
| |
CCO Guideline Update (2019)43 | |
Adult patients receiving HEC, a single day IV chemotherapy
Adult patients receiving MEC, a single day IV chemotherapy
Adult patients receiving HEC, multiple day IV chemotherapy
Adult patients receiving MEC, multiple day IV chemotherapy
| None |
POGO Guideline Update (2017)44 | |
Children receiving HEC “We recommend that children ≥ 6 months old receiving HEC which is not known or suspected to interact with aprepitant receive granisetron or ondansetron or palonosetron + dexamethasone + aprepitant.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Strong |
“We recommend that children < 6 months old receiving HEC receive granisetron or ondansetron or palonosetron + dexamethasone.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Strong |
“We recommend that children ≥ 6 months old receiving HEC which is known or suspected to interact with aprepitant receive granisetron or ondansetron or palonosetron + dexamethasone.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Strong |
“We recommend that children ≥ 6 months old receiving HEC which is not known or suspected to interact with aprepitant, and who cannot receive dexamethasone for CINV prophylaxis receive palonosetron + aprepitant.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Strong |
“We suggest that children < 6 months old receiving HEC and who cannot receive dexamethasone for CINV prophylaxis receive palonosetron.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Weak |
“We suggest that children receiving HEC, which is known or suspect to interact with aprepitant, and who cannot receive dexamethasone receive palonosetron.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Weak |
Children receiving MEC “We recommend that children receiving MEC receive granisetron or ondansetron or palonosetron + dexamethasone.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Strong |
“We suggest that children ≥ 6 months receiving MEC who cannot receive dexamethasone for CINV prophylaxis receive granisetron or ondansetron or palonosetron + aprepitant.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Weak |
“We suggest that children < 6 months receiving MEC who cannot receive dexamethasone for CINV prophylaxis receive palonosetron.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Weak |
“We suggest that children receiving MEC, which is known or suspected to interact with aprepitant, and who cannot receive dexamethasone receive palonosetron.”44 (p. 3) | Level of evidence: Moderate Strength of recommendation: Weak |
Recommended dose of palonosetron for children |
|
Adult patients receiving HEC “For the prevention of non-AC highly emetogenic chemotherapy, a three-drug regimen including single doses of a 5-HT3 RA (granisetron, ondansetron, dolasetron, tropisetron or palonosetron), dexamethasone and an NK1 RA (aprepitant, fosaprepitant, netupitant or rolapitant), given before chemotherapy is recommended.”45 (p. v122) | MASCC Level of confidence: High Level of consensus: High ESMO Level of evidence: I Grade of recommendation: A |
“In patients receiving non-AC highly emetogenic chemotherapy treated with a combination of an NK1 RA, 5-HT3 RA and dexamethasone to prevent acute nausea and vomiting, dexamethasone on days 2-4 is suggested to prevent delayed nausea and vomiting.”45 (p. v122) | MASCC Level of confidence: High Level of consensus: Moderate ESMO Level of evidence: I Grade of recommendation: B |
“In women with breast cancer treated with a combination of a 5-HT3 RA, dexamethasone and an NK1 RA (aprepitant, fosaprepitant, netupitant or rolapitant), given before chemotherapy is recommended.”45 (p. v123) | MASCC Level of confidence: High Level of consensus: High ESMO Level of evidence: I Grade of recommendation: A |
“In women with breast cancer treated with a combination of a 5-HT3 RA, dexamethasone and an NK1 RA to prevent acute nausea and vomiting, aprepitant or dexamethasone should be used on days 2 and 3 but not if fosaprepitant, netupitant or rolapitant has been used on day 1.”45 (p. v123) | MASCC Level of confidence: Moderate Level of consensus: Moderate ESMO Level of evidence: II Grade of recommendation: B |
“Olanzapine may be considered with a 5-HT3 RA plus dexamethasone, particularly when nausea is an issue, but using a 10 mg dose, patient sedation may be a concern.”45 (p. v124) | MASCC Level of confidence: Low Level of consensus: Low ESMO Level of evidence: II Grade of recommendation: B |
Adult patients receiving MEC “For the prevention of acute emesis in MEC-treated patients, a 5-HT3 RA plus dexamethasone is recommended.”45 (p. v125) | MASCC Level of confidence: Moderate Level of consensus: Moderate ESMO Level of evidence: II Grade of recommendation: B |
“In patients receiving MEC with a known potential for delayed emesis, the use of dexamethasone for days 2-3 can be considered.”45 (p. v125) | MASCC Level of confidence: Low Level of consensus: Moderate ESMO Level of evidence: III Grade of recommendation: C |
“No routine prophylaxis for delayed emesis can be recommended for all other patients receiving MEC.”45 (p. v125) | MASCC Level of confidence: No confidence possible Level of consensus: High ESMO Level of evidence: IV Grade of recommendation: D |
Children receiving HEC “In children receiving chemotherapy of high emetic risk, an antiemetic prophylaxis with a 5-HT3 RA (granisetron, ondansetron, tropisetron or palonosetron) plus dexamethasone plus aprepitant is recommended.”45 (p. v130) | MASCC Level of confidence: High Level of consensus: High ESMO Level of evidence: II Grade of recommendation: B |
“Children who cannot receive dexamethasone should receive a 5-HT3 RA plus aprepitant.”45 (p. v130) | MASCC Level of confidence: Moderate Level of consensus: High ESMO Level of evidence: II Grade of recommendation: B |
“When aprepitant administration is not feasible or desirable, the guideline recommends a 5-HT3 RA plus dexamethasone be given to children receiving highly emetogenic chemotherapy.”45 (p. v130) | MASCC Level of confidence: Moderate Level of consensus: High ESMO Level of evidence: II Grade of recommendation: B |
Children receiving MEC “Children receiving MEC should receive antiemetic prophylaxis with a 5-HT3 RA plus dexamethasone.”45 (p. v130) | MASCC Level of confidence: Moderate Level of consensus: High ESMO Level of evidence: II Grade of recommendation: B |
“Children who cannot receive dexamethasone should receive a 5-HT3 RA and aprepitant.”45 (p. v130) | MASCC Level of confidence: Moderate Level of consensus: High ESMO Level of evidence: II Grade of recommendation: B |
AC = anthracycline/cyclophosphamide; ASCO = American Society of Clinical Oncology; CCO = Cancer Care Ontario; ESMO = European Society of Medical Oncology; GRADE = Grades of Recommendation Assessment, Development and Evaluation; 5-HT3 RA = 5-hydroxytryptamine-3 receptor antagonist; HEC = high emetogenic chemotherapy; IV = IV; MASCC = Multinational Association of Supportive Care in Cancer; MEC = moderate emetogenic chemotherapy; NCCN = National Comprehensive Cancer Network; NEPA = netupitant/palonosetron; NK 1 RA = neurokinin 1 receptor antagonist; PO = by mouth; POGO = Pediatric Oncology Group of Ontario.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca