CADTH Health Technology Review
Conventional Disease-Modifying Antirheumatic Drugs for the Treatment of Rheumatoid Arthritis
Rapid Review
Authors: Shannon Hill, Nina Frey
Abbreviations
ACR
American College of Rheumatology
AGREE
Appraisal of Guidelines for Research & Evaluation
APLAR
Asia Pacific League of Associations for Rheumatology
CRA
Canadian Rheumatology Association
csDMARD
conventional synthetic disease-modifying antirheumatic drug
DMARD
disease-modifying antirheumatic drug
EULAR
European League Against Rheumatism
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HCQ
hydroxychloroquine
JAK
Janus kinase
LEF
leflunomide
MTX
methotrexate
NICE
National Institute for Health and Care Excellence
RA
rheumatoid arthritis
SIGN
Scottish Intercollegiate Guidelines Network
SR
systematic review
SSZ
sulfasalazine
tsDMARD
targeted synthetic disease-modifying antirheumatic drug
Key Messages
Nine evidence-based guidelines were identified that recommend the use of conventional synthetic disease-modifying antirheumatic drugs as a first-line therapy for patients with rheumatoid arthritis prior to using biologic disease-modifying antirheumatic drugs or Janus kinase inhibitors.
Methotrexate monotherapy was the most commonly recommended conventional synthetic disease-modifying antirheumatic drug recommended as first-line therapy by the included guidelines.
Eight of the included guidelines recommend combination therapy using multiple conventional synthetic disease-modifying antirheumatic drugs if monotherapy is ineffective and 4 included guidelines recommend the use of glucocorticoids in combination with conventional synthetic disease-modifying antirheumatic drugs.
Context and Policy Issues
Rheumatoid arthritis (RA) is a chronic, systemic, autoimmune disease that can affect the entire body.1,2 RA is characterized by inflammation in the lining of the joints and other tissue, causing swelling, pain, and stiffness, which can lead to permanent joint damage.1 RA is a debilitating chronic disease and people with RA are often at a higher risk of mortality because of associated comorbidities such as cardiovascular disease.3,4 In Canada, approximately 374,000 people aged 16 or older are currently living with diagnosed RA and approximately 1% of the global population is affected by RA.1 The prevalence and incidence of diagnosed RA generally increases with age and females in Canada are more likely to experience diagnosed RA compared to males.1
There is no cure for RA; however, early diagnosis and treatment can play a large role in reducing symptoms, preventing lasting joint damage, and reducing the risk of developing comorbidities.1,2 Early treatment for RA (e.g., as soon as a patient is diagnosed) can mean that disease remission is more likely.2 A “treat-to-target” strategy is often used in RA management, where the target for patient treatment is remission or low disease activity when remission is not possible.5
Disease-modifying antirheumatic drugs (DMARDs) are commonly used course in the treatment for RA because they slow disease progression and provide symptom relief.4 RA treatment regimens can consist of conventional synthetic DMARDs (csDMARDs), biologic DMARDs, or targeted synthetic DMARDs (tsDMARDs). Common csDMARDs include methotrexate (MTX), leflunomide (LEF), sulfasalazine (SSZ), and antimalarials such as hydroxychloroquine (HCQ).4 Biologic DMARDs usually include either tumour necrosis factor inhibitors or non-tumour necrosis factor inhibitors. Janus kinase (JAK) inhibitors are a commonly used tsDMARD in advanced RA treatment.5 csDMARDs were the first DMARD agents approved for RA treatment, are the most commonly prescribed treatment for RA, and are typically the least expensive.4 csDMARD monotherapy is typically the first course of treatment for newly diagnosed individuals. However, if disease progression continues, then additional csDMARDs may be added as a “step-up” approach, followed by adding or switching to biologic DMARDs or JAK inhibitors if disease progression does not slow down.4,5 Glucocorticoids are also commonly used on a short-term basis in the treatment of RA. Glucocorticoids, which have anti-inflammatory and immunosuppressive effects, may also be used as an adjunct therapy when a patient is starting a new DMARD treatment or changing from one DMARD to another.6 DMARD therapy for the treatment and management of RA has shown to be effective in providing symptom relief and slowing disease progression; however, there are a variety of treatment approaches that may be used to manage RA disease progression and evidence-based guidance is helpful in determining the best course of action for patients with RA.
The purpose of this report is to review the evidence-based guidelines regarding the use of csDMARD therapy prior to the use of biologic DMARDs or JAK inhibitors. Evidence-based guidelines containing recommendations related to the use of csDMARDs, combination approaches for csDMARD therapy, csDMARD trial periods, and combining glucocorticoids with csDMARD therapy will be sought for this report and any relevant recommendations will be summarized.
Research Question
What are the evidence-based guidelines regarding the use of conventional disease-modifying antirheumatic drugs prior to the use of biologic disease-modifying antirheumatic drugs or Janus kinase inhibitors for the treatment of rheumatoid arthritis?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and rheumatoid arthritis. A search filter was applied to limit retrieval to clinical practice guidelines. The search was also limited to documents published between January 01, 2011 and April 05, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Adults with moderate to severe rheumatoid arthritis that have yet to be treated with biologic DMARDs or JAK inhibitors |
Intervention | csDMARDs including but not limited to MTX, LEF, SSZ, HCQ, AZA, tacrolimus, cyclosporine, gold, and doxycycline |
Comparator | Not applicable |
Outcomes | Recommendations for the best practices regarding the use of csDMARDs prior to biologic DMARDs or JAK inhibitors including which csDMARDs to use, combination approaches for csDMARDs use (single, dual, triple therapy, O’Dell protocol), length of csDMARD trial period prior to using biologic DMARDs or JAK inhibitors, and recommendations for glucocorticoids in combination with csDMARDs |
Study designs | Evidence-based guidelines |
AZA = azathioprine; csDMARD = conventional synthetic disease-modifying antirheumatic drug; DMARD = disease-modifying antirheumatic drug; HCQ = hydroxychloroquine; JAK = Janus kinase; LEF = leflunomide; MTX = methotrexate; SSZ = sulfasalazine.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published prior to 2011. Guidelines with unclear methodology were also excluded and only the most recent version of each guideline was eligible for inclusion in this report.
Critical Appraisal of Individual Studies
The included publications were critically appraised by one reviewer using the Appraisal of Guidelines for Research & Evaluation (AGREE) II instrument for guidelines as a guide.7 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
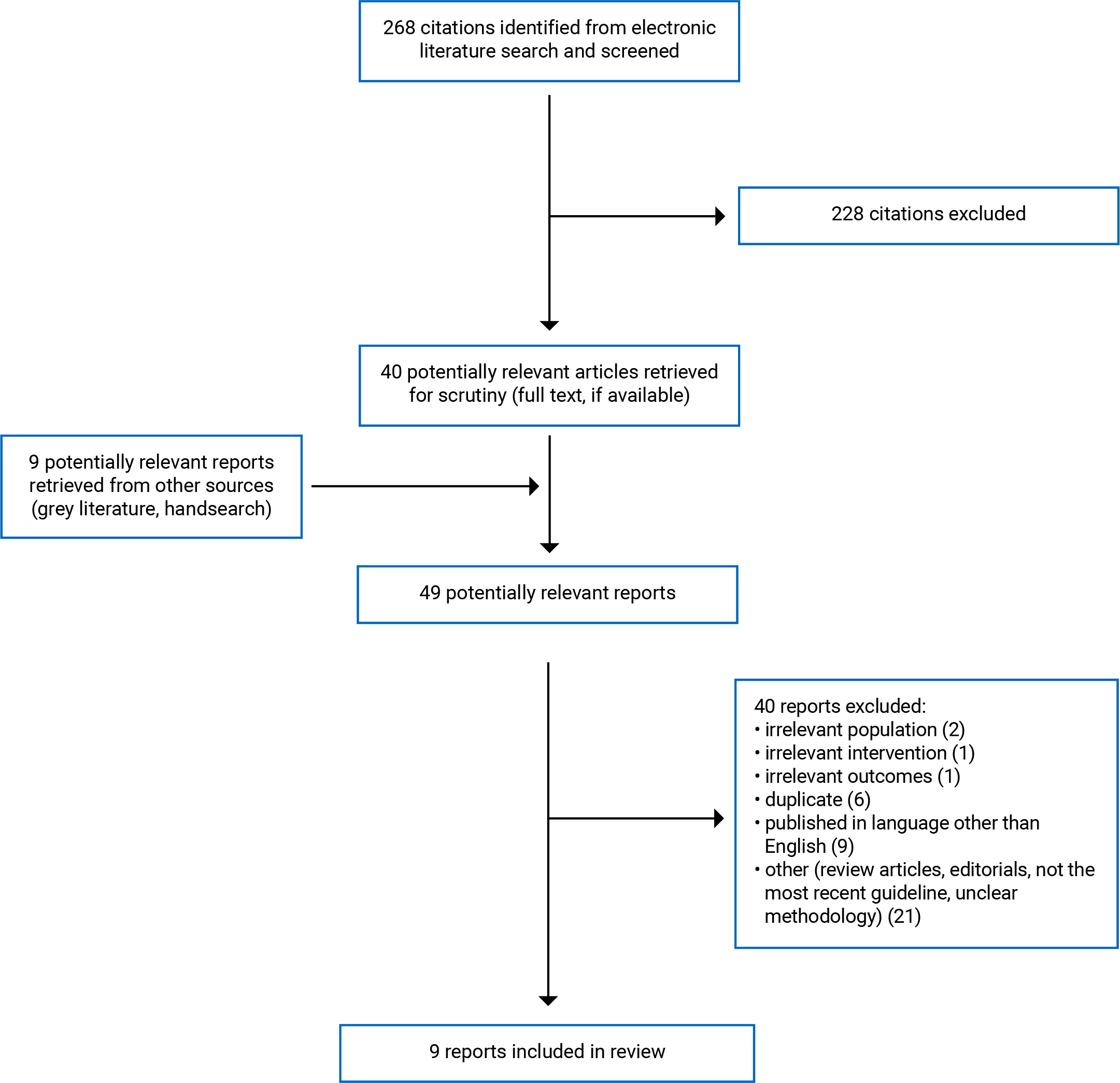
A total of 268 citations were identified in the literature search. Following the screening of titles and abstracts, 228 citations were excluded and 40 potentially relevant reports from the electronic search were retrieved for full-text review. Nine potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 40 publications were excluded for various reasons and 9 publications met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA8 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Nine relevant evidence-based guidelines9-17 were identified. The characteristics of the included evidence-based guidelines are subsequently summarized. Many of the identified evidence-based guidelines include information related to the general management and treatment of RA; however, only information related to recommendation for the use of csDMARD therapy prior to biologic DMARDs or JAK inhibitors will be presented in this report. Additional details regarding the characteristics of included guidelines are provided in Appendix 2.
Study Design
The 9 relevant guidelines were developed by the European League Against Rheumatism (EULAR),9 the Asian Pacific League of Associations for Rheumatology (APLAR),10 the French Society for Rheumatology,11 the Brazilian Society of Rheumatology,12 the NICE–National Institute of Health and Care Excellence,13 the American College of Rheumatology (ACR),14 the ICARUS Project by Todoerti et al.,15 the Canadian Rheumatology Association (CRA),16 and the Scottish Intercollegiate Guidelines Network (SIGN).17
Each evidence-based guideline9-17 was informed by a systematic review (SR) of evidence regarding the management and treatment of patients with RA. The quality of the evidence informing the recommendations and the strength of the recommendations were appraised using a variety of methods. Three guidelines9,11,15 determined the level of evidence and strength of recommendations using the Oxford Centre for Evidence-Based Medicine tool.18 For the tool, the level of evidence ranges from 1 (high-quality evidence including SRs of randomized controlled trials) to 5 (very low-quality evidence including expert opinion).18 Based on the quality of evidence used to inform the recommendations, each recommendation is graded between A (recommendation is based on consistently high-quality evidence) to D (recommendation is based on consistently low-quality evidence).18 The Grading of Recommendations Assessment, Development and Evaluation (GRADE)19 approach was used to evaluate the quality of evidence used to inform the recommendations for 4 guidelines.10,12-14 However, strengths of recommendations were only reported in the ACR guideline.14 According to GRADE, evidence quality can be rated as “high,” “moderate,” “low,” or “very low.” The guideline by the CRA16 sought previous evidence-based guidelines within the SR process and appraised the quality of existing guidelines using the AGREE model.7 A custom grading system was used to give the evidence informing the recommendation a designation between 1 (high-quality evidence) and 4 (very low-quality evidence) and the strength of recommendation a designation between “A” (strong recommendation) and “D” (consensus recommendation). This customized grading system was informed by the original levels of evidence and strengths of recommendations from each included guideline identified from the SR. One guideline by SIGN17 used an internal methodology to grade the quality of evidence used to inform recommendations. This grading system designated recommendations between “A” (recommendation based on high-quality evidence) and “D” (recommendation based on very low-quality evidence).
Six guidelines9,10,12,14-16 were developed using a voting process to determine the agreement of the drafted recommendations and 3 guidelines were developed through consensus.11,13,17
Country of Origin
Five guidelines were intended for broad use in Europe9 or for use in specific European nations including France,11 Italy,15 Scotland,17 and the UK, in general.13 The guideline from APLAR was intended for use in the Asian-Pacific region.10 The guideline from the Brazilian Society of Rheumatology was intended for use in Brazil.12 Two guidelines were intended for use in North America, specifically in Canada16 and the US.14
Patient Population
The intended users for each of the guidelines were rheumatologists or other health care professionals providing care for patients with RA.9-17 The target population for each of the guidelines was adult patients with RA.9-17
Relevant Interventions
The evidence-based guidelines considered a broad range of recommendations for the treatment of patients with RA. The interventions that were relevant to this report were csDMARDs as a first-line therapy for the treatment of patients with RA.9-17 The guideline by Todoerti et al.15 focused primarily on the use of MTX for the treatment of rheumatic diseases, with a focus on patients with RA.
Outcomes
The included guidelines considered relevant patient-related outcomes like treatment efficacy,9,12,16,17 patient safety,9,12,15-17 quality of life,11,13 disease activity and patient functionality,10,11,13,14,16 and cost of csDMARDs.14
Summary of Critical Appraisal
An overview of the critical appraisal using the AGREE II7 instrument follows. Additional details regarding the strengths and limitations of the included guidelines are provided in Appendix 3.
In each included guideline, the scope and purpose were described, including the overall objective of the guideline and population of interest. Five of the included guidelines12-14,16,17 clearly described the health questions covered by the guideline. Six of the guidelines9,11,13,14,16,17 provided a description of the guideline development groups, which included relevant professionals in the field of rheumatology and members of the target population. Each guideline used a systematic method to search for, collect, and appraise the quality of evidence; however, 4 guidelines10-12,15 provided limited or no information regarding the inclusion criteria. Seven guidelines10,12-16 provided an explicit link between the recommendations and supporting evidence. Five guidelines9,10,13,14,17 provided a clear indication that the guidelines and recommendations were externally reviewed prior to publication. Each guideline presented recommendations clearly, with the key recommendations easily identified, and gave different options for RA management. One guideline13 described barriers and facilitators for recommendations application, provided advice for putting recommendations into practice, addressed potential resource implications of recommendations, and presented monitoring and auditing criteria within the guideline. Four guidelines10,12,13,17 provided clear indication that any views from the funding bodies did not influence the content of the guideline; for the remaining 5 guidelines,9,11,14-16 it was unclear whether the recommendations were influenced by funders. Five guidelines9,11-14 provided information related to competing interests among the guideline development groups, while 3 guidelines did not provide information10,15,16 and 1 provided unclear information.17 Three of the 5 guidelines that provided information with competing interests did not report how these were addressed;9,11,12 however, 2 guidelines providing details regarding the actions taken to address competing interests were provided.13,14
Summary of Findings
The main recommendations are subsequently summarized. Appendix 4 presents the detailed recommendations and supporting evidence.
Guidelines
Each guideline provided recommendations regarding the use of csDMARDs as first-line therapy for patients with RA prior to the use of biologic DMARDs, JAK inhibitors, or other tsDMARDs.9-17 Furthermore, the guidelines provided recommendations regarding which csDMARDs should be considered at certain stages of a patient’s RA progression, the use of combination therapy as a treatment option, and the use of glucocorticoids in combination with regular DMARD treatment. None of the included guidelines provided recommendations regarding the length of the time csDMARDs should be used prior to switching to or adding biologic DMARDs or JAK inhibitors.
Recommendations Regarding csDMARDs as First-Line Therapy
Each of the 9 included guidelines9-17 recommend csDMARDs as the first-line treatment for patients diagnosed with RA (strong recommendation for 5 guidelines,9,11,15-17 conditional recommendation for 1 guideline,14 and strength or recommendation not reported for 3 guidelines).10,12,13 Seven of the included guidelines9-12,14-16 recommend that MTX monotherapy should be the csDMARD of choice to begin treatment for patients with RA. The guideline from ACR specifies csDMARD monotherapy should be used over double or triple therapy and that MTX should be used as a first-line treatment for patients with a moderate to high severity of RA.14 Additionally, the ACR guideline recommends MTX monotherapy, as evidence favours MTX monotherapy because of clinical benefits, lower risk, and cost.14 These recommendations were based on evidence that was assessed to be moderate- to high-quality. The guideline from NICE13 recommends that MTX, LEF, or SSZ monotherapies be offered as first-line treatment or within the first 3 months of persistent symptoms for RA (quality of evidence and strength of recommendation not reported). Lastly, the SIGN guideline recommends MTX and SSZ be considered as first-line therapy because of evidence of favourable efficacy and toxicity profiles (moderate- to high-quality evidence; strong recommendation).17
Recommendations Regarding Treatment Approach for csDMARDs
Five included guidelines9-13 provide recommendations regarding alternative csDMARD treatment options for when MTX is not well-tolerated or not reaching targeted treatment results. These 5 guidelines recommended that LEF, SSZ, or HCQ be used as alternative options for csDMARD monotherapy.9-13 Additionally, APLAR recommends that iguratimod, bucillamine, cyclosporine, intramuscular gold, or tacrolimus can be considered as alternatives to MTX depending on availability.10 Where reported, these recommendations were based on high-,9,11 moderate-,10 and low-quality evidence,9 and the strength of the recommendations ranged from strong to weak.9,11 The guideline by NICE did not report the quality of evidence or strength of recommendation13 and the guideline by APLAR and the Brazilian Society of Rheumatology did not report the strength of recommendation.10,12
Six of the included guidelines provide recommendations regarding the use of a combination approach for csDMARD treatment in patients for whom RA monotherapy is inadequate or not well-tolerated,11-13,15-17 and 3 guidelines provided recommendations for the use of a combination approach when disease activity is moderate to high.10,14,16 Six included guidelines recommend the use of combination therapy with csDMARDs when MTX monotherapy produces an inadequate response or is not well-tolerated.11-13,15-17 The Brazilian Society of Rheumatology and NICE recommend that LEF, SSZ, or HCQ be used in combination with MTX when monotherapy has failed (high level of agreement for the Brazilian Society of Rheumatology; quality of evidence and strength or recommendation not reported for NICE).12,13 The CRA recommends that MTX and LEF should be used with caution because of an association with high toxicity (high level of evidence; strong recommendation).16 Two recommendations by the French Society for Rheumatology and Todoerti et al. specify that combination therapy with both csDMARDs and biologic DMARDs should be considered (high level of evidence; moderate to strong recommendation).11,15 The APLAR, ACR, and CRA guidelines recommend combination therapy with csDMARDs when disease activity is moderate to high.10,14,16 APLAR recommends that combination csDMARD therapy be considered for patients with high disease activity, but that patients be monitored closely for therapy-related toxicities (low quality of evidence; low strength of recommendation).10 The ACR recommendation specifies that when disease activity remains moderate to high when using csDMARD monotherapy, combination therapy with csDMARDs or adding biological DMARDs should be considered over csDMARD monotherapy (low to moderate quality of evidence; strong recommendation).14
Recommendations Regarding Combination Therapy With Glucocorticoids
Four included guidelines9,11,13,16 provide recommendations regarding the use of glucocorticoids in combination with csDMARD for the treatment of RA. EULAR and French Society for Rheumatology strongly recommend that short-term glucocorticoids be considered when changing csDMARD treatment but tapered as rapidly as clinically feasible (high-quality evidence).9,11 Similarly, the NICE guidelines recommend that short-term glucocorticoids be considered when starting a new csDMARD treatment regime (quality of evidence and strength of recommendation not reported).13 The CRA guideline recommends that glucocorticoids be added to csDMARD treatment as part of an initial treatment strategy or bridging therapy (high quality of evidence; strong recommendation), and that they be tapered as rapidly as clinically feasible (very low quality of evidence; consensus-based recommendation).16 Lastly, the SIGN guideline17 recommends the use of low-dose oral corticosteroids in combination with csDMARDs (high-quality evidence; strong recommendation).
Limitations
No recommendations related to the trial period for csDMARDs prior to switching or adding biologic DMARDs or JAK inhibitors were identified; therefore, no summary can be provided. One included guideline that was published in 2012 was intended for use in Canada.16 Given differences in available treatments and the organization of care around the world, the applicability of the other guidelines to the Canadian context is unclear. There is a large variety of available csDMARDs that can be used to treat RA, but many of the recommendations in this report only focus on common csDMARDs such as MTX, LEF, SSZ, and HCQ. Only one guideline by APLAR10 provided a limited recommendation specifying the use of other available csDMARDs including cyclosporine, intramuscular gold, or tacrolimus.
Conclusions and Implications for Decision- or Policy-Making
This review comprised 9 evidence-based guidelines9-17 that provide recommendations regarding the use of csDMARD therapy, prior to using biologic DMARDs or JAK inhibitors, in patients with RA. These guidelines were developed by rheumatology associations in different countries and regions in Europe, North America, the Asian-Pacific region, and Brazil. Similar recommendations were found across each included guideline, including using csDMARD therapy as first-line treatment for patients starting treatment for RA,9-17 providing alternative recommendations for which csDMARDs to use as first-line treatment,9-13 using combination therapy when monotherapy is not effective,10-17 and adding glucocorticoids to treatment when switching or bridging between therapies.9,11,13,16 Furthermore, these recommendations have remained consistent over the past decade despite new evidence being used to inform more recent recommendations.
Overall, the guidelines included in this report generally support the use of csDMARDs as first-line therapy prior to switching to or adding biologic DMARDs or JAK inhibitors, are in favour of combination therapy with other csDMARDs when monotherapy is ineffective or not well-tolerated, and recommend glucocorticoid use for switching or bridging between csDMARD treatment.
References
1.Rheumatoid arthritis in Canada. Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/rheumatoid-arthritis.html. Accessed 2021 Apr 21.
2.RheumInfo. Rheumatoid arthritis. 2021; https://rheuminfo.com/diseases/rheumatoid-arthritis/. Accessed 2021 Apr 27.
3.Widdifield B, Bernatsky S, Bombardier C, al. e. Rheumatoid arthritis surveillance in Ontario: Monitoring the burden, quality of care and patient outcomes through linkage of administrative data. Healthcare Quarterly. 2015;18(3):7-10. PubMed
4.Padjen I, Crnogaj MR, Anic B. Conventional disease-modifying agents in rheumatoid arthritis - a review of their current use and role in treatment algorithms. Reumatologia. 2020;58(6):390-400. PubMed
5.Aletaha D, Smolen J. Diagnosis and management of rheumatoid arthritis: A review. JAMA. 2018;320(13):1360-1372. https://jamanetwork.com/journals/jama/article-abstract/2705192. Accessed 2021 Apr 27. PubMed
6.Akirov A. Considerations for the use of glucocorticoids in rheumatoid arthritis. Rheumatology Advisor. 2021. https://www.rheumatologyadvisor.com/home/rheumatoid-arthritis-advisor/potential-toxicity-associated-with-glucocorticoids-requires-care-and-vigilance/#:~:text=Glucocorticoids%20are%20used%20in%20patients,occurring%20as%20early%20as%20possible. Accessed 2021 Apr 27.
7.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Apr 27.
8.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
9.Smolen JS, Landewe RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685-699. PubMed
10.Lau CS, Chia F, Dans L, et al. 2018 update of the APLAR recommendations for treatment of rheumatoid arthritis. Int J Rheum Dis. 2019;22(3):357-375. PubMed
11.Daien C, Hua C, Gaujoux-Viala C, et al. Update of French society for rheumatology recommendations for managing rheumatoid arthritis. Joint Bone Spine. 2019;86(2):135-150. PubMed
12.Mota L, Kakehasi AM, Gomides APM, et al. 2017 recommendations of the Brazilian Society of Rheumatology for the pharmacological treatment of rheumatoid arthritis. Advances in Rheumatology. 2018;58(1):2. PubMed
13.National Institute for Health and Care Excellence. Rheumatoid athritis in adults: Management (NICE guideline ng100). 2018; https://www.nice.org.uk/guidance/ng100/resources/rheumatoid-arthritis-in-adults-management-pdf-66141531233989. Accessed 2021 Apr 25.
14.Singh JA, Saag KG, Bridges SL, Jr., et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care Res (Hoboken). 2016;68(1):1-25. PubMed
15.Todoerti M, Maglione W, Bernero E, et al. Systematic review of 2008-2012 literature and update of recommendations for the use of methotrexate in rheumatic diseases, with a focus on rheumatoid arthritis. Reumatismo. 2013;65(5):207-218. PubMed
16.Bykerk VP, Akhavan P, Hazlewood GS, et al. Canadian Rheumatology Association recommendations for pharmacological management of rheumatoid arthritis with traditional and biologic disease-modifying antirheumatic drugs. J Rheumatol. 2012;39(8):1559-1582. PubMed
17.Management of early rheumatoid arthritis: A national clinical guideline (SIGN publication no. 123). Edinburgh (GB): Scottish Intercollegiate Guideline Network (SIGN); 2011: https://www.sign.ac.uk/media/1061/sign123.pdf. Accessed 2021 Apr 25.
18.Oxford Centre for Evidence-Based Medicine: Levels of evidence. Oxford (GB): Centre for Evidence-Based Medicine; 2009: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009. Accessed 2021 Apr 25.
19.GRADE approach. London (GB): Cochrane Collaboration; 2021: https://training.cochrane.org/grade-approach. Accessed 2021 Apr 27.
20.Smolen JS, Landewe R, Bijlsma J, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. 2017;76(6):960-977. PubMed
21.Cochrane Handbook for Systematic Review of Interventions. London (GB): Cochrane Collaboration,; 2021: https://training.cochrane.org/handbook/current. Accessed 2021 Apr 27.
22.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
23.National Institute for Health and Care Excellence. Rheumatoid athritis in adults: Methods (NICE guideline ng100). 2018; https://www.nice.org.uk/guidance/ng100/documents/supporting-documentation-4. Accessed 2021 Apr 25.
24.A guidelines developer's handbook. Edinburgh (GB): Scottish Intercollegiate Guidelines Network (SIGN); 2019: https://www.sign.ac.uk/media/1050/sign50_2019.pdf. Accessed 2021 Apr 25.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
EULAR (2020)9 | ||||||
Intended users: Rheumatologists, RA patients, health professionals Target population: Patients with RA | Pharmacological therapy using DMARDs (monotherapy or combination therapy for csDMARDs [MTX, LEF, and SSZ], biologic DMARDs, and tsDMARDs) and glucocorticoids for RA |
| An SR was undertaken from the date of the last guideline publication (2016).20 Publication databases were searched for RCTs related to efficacy and safety. Data from the SR and suggestions from the steering committee were presented to a task force for discussion, suggestions for recommendation updates, and voting. | Risk of bias assessments were completed and quality of evidence was assessed using the Oxford Centre for Evidence-Based Medicine tool.18 A “level” designation for the quality of evidence was assigned between 1 (high-quality; SRs of RCTs) and 5 (very low-quality; expert opinion). Based on the quality of evidence, the recommendation was given a “grade” between A (consistently high-quality evidence) and D (consistently low-quality evidence). | Recommendations and overarching principles from the 2016 version were used to guide this guideline. A modified voting process was used by a task force to amend, change, and delete guiding principles and recommendations, and develop new recommendations based on any new evidence. | All task force members provided comments on the guideline manuscript. The guideline manuscript was submitted to the EULAR executive committee for review and approval. The final version of the guideline manuscript was submitted for peer review. |
APLAR (2019)10 | ||||||
Intended users: Clinicians providing management for RA patients Target population: Patients with RA | Targeted therapies (focusing on DMARD use including MTX, LEF, and SSZ) for the management of RA | Disease activity | A working group conducted an SR, with 10 research questions on the use of targeted therapy. Database searches for RCTs, observational studies, and meta-analyses were conducted. | GRADE19 was used to evaluate the quality of the evidence and SoR. One overall grade was assigned to each recommendation. The quality of evidence was rated as: high (very confident that the true effect lies close to that of the estimate of the effect); moderate (moderately confident in the effect estimate); low (confidence in the effect estimate is limited); very low (very little confidence in the effect estimate). Recommendations that lacked sufficient evidence were informed by expert advice and remained ungraded. | The working group drafted and refined recommendations based on the evidence and a final draft of recommendations was reviewed by an APLAR voting group. A modified Delphi technique was used to rate the agreement for each recommendation using a 5-point Likert scale and agreement by 75% of voting members was used as the threshold for acceptance of the recommendation. | Draft recommendations were externally reviewed by 2 independent reviewers and presented during the 2018 APLAR Congress and regional rheumatology conferences. Feedback was used to finalize the recommendations. |
French Society for Rheumatology (2019)11 | ||||||
Intended users: Rheumatologists and other primary health care providers Target population: Patients with RA | Diagnosis, treatment (including csDMARDs [MTX, LEF, SSZ] biologic DMARDs, tsDMARDs, and glucocorticoids), follow-up, management of remission, and management of comorbidities |
| An SR with 11 research questions was conducted by 2 task force members. Searches of MEDLINE (via PubMed) and abstracts published at meetings held by EULAR and ACR were conducted. | Quality of evidence for each recommendation was determined using the Oxford Centre for Evidence-Based Medicine tool.18 (Please refer to characteristics of the EULAR 2020 guideline9 for quality appraisal information.) | The task force drafted and finalized recommendations via email rounds. A panel of 40 experts reviewed and scored each recommendation from 0 (complete disagreement) to 10 (complete agreement). | NR |
Brazilian Society of Rheumatology (2018)12 | ||||||
Intended users: Rheumatologists Target population: Adults with RA | Use of csDMARDs for RA (including MTX, LEF, SSZ, and HCQ) |
| An SR with 10 research questions was conducted by 2 independent researchers. Database searches of MEDLINE, Embase, and Scopus were conducted and RCTs and SRs of RCTs were primarily sought. | The risk of bias for clinical trials was assessed using Cochrane Collaboration tools,21 and SRs were assessed using the AMSTAR tool.22 The quality of evidence was evaluated using the GRADE tool.19 (Please refer to characteristics of the APLAR 2019 guideline10 for quality appraisal information.) | A modified voting strategy was used to determine recommendations. When 70% of participants agreed with the statement, members then voted to assess the level of agreement using a numerical scale from 0 (completely disagree) to 10 (completely agree). | NR |
NICE (2018)13 | ||||||
Intended users: Health professionals; commissioners and providers; and people with RA, their families, and their care providers Target population: Patients with RA | Diagnosis and management of RA (including csDMARDs [MTX, LEF, SSZ, and HCQ] and glucocorticoids) |
| An SR based on previously developed review questions was undertaken to identify clinical and health economic-related evidence. Database searches were conducted and evidence was synthesized according to the NICE protocol.23 | The quality of evidence and SoR were assessed using GRADE.19 An overall quality grade was applied to each evidence outcomes using “high,” “moderate,” “low,” and “very low” designations. | The committee was presented with a summary of evidence. Recommendations were drafted and the “strength” of each recommendation based on the GRADE assessment was considered by the committee. The committee then agreed on the wording of the recommendations. | The guideline was subjected to a 6-week public consultation and feedback period as part of a quality assurance and peer-review process. |
ACR (2016)14 | ||||||
Intended users: Clinicians and patients with RA Target population: Patients with RA |
|
| An SR was undertaken. Database searches were conducted and SRs, RCTs, and observational studies were sought. | Evidence was evaluated based on GRADE19 criteria. Quality assessment included risk of bias, publication bias, inconsistency of results, indirectness of evidence, and imprecision. Quality of evidence was reported according to the GRADE designations of “high,” “moderate,” “low,” and “very low.” (Please refer to APLAR 201910 for quality appraisal information.) Recommendations received GRADE designations of “strong” (the panel was convinced that the benefits outweigh the harms) or “conditional” (uncertainty of harms and benefits due to low-quality evidence). | Evidence was delivered to a voting panel that voted on the direction and strength of the recommendations and used a modified voting strategy to determine the final decisions for each recommendation. | The final manuscript was reviewed by the ACR Guideline Subcommittee, ACR Quality of Care Committee, and the ACR Board of Directors, in addition to journal peer review. |
Todoerti et al. (2013)15 | ||||||
Intended users: Rheumatologists and clinicians supporting patients with rheumatic disease Target population: Patients with rheumatic disease, with a focus on RA | MTX for patients with rheumatic diseases, with a focus on RA | Safety | An SR was conducted. Database searches of PubMed and Embase were conducted to identify literature published between 2008 and 2012 to update the 2010 recommendations of the Italian consensus. | The quality of evidence was appraised by 2 Fellows according to the Oxford Centre for Evidence-Based Medicine tool.18 (Please refer to characteristics of the EULAR 2020 guideline9 for quality appraisal information.) | The evidence was presented to the panel of 36 Italian rheumatologists. Two meetings were held to discuss the evidence, formulate recommendations, and finalize the recommendations using a Delphi-like procedure. | NR |
CRA (2012)16 | ||||||
Intended users: Rheumatologists and primary prescribers of RA medication who are treating patients with RA Target population: Adult patients with RA | Pharmacological treatment for RA with traditional (conventional) DMARDs (including MTX and LEF), biologic DMARDs, and glucocorticoids |
| An SR was undertaken to identify clinical practice guidelines and consensus statements, with recommendations for DMARD use in RA. Database searches were conducted with additional grey literature and bibliography handsearches. | Quality of the guidelines was assessed using the AGREE instrument.7 LoE and SoR were adapted and graded using a custom system. New LoE and SoR designations were given to each recommendation based on the LoE and SoR from the guidelines. LoE: I — MAs, SRs of RCTs, or individual RCTs II — MAs, SRs of observational studies, or individual observational studies III — non-analytic studies (e.g., case reports) IV — expert opinion NR —recommendations not linked to evidence SoR: A — strong (direct level I evidence) B — moderate (direct level II evidence or extrapolated level I evidence) C — weak (direct level III evidence or extrapolated level II evidence) D — consensus (expert opinion based on very limited evidence) | Evidence and existing recommendations were presented to the working group and, if the recommendation was agreed upon, a Canadian recommendation was developed by adapting and rewording the presented recommendation. Canadian recommendations were voted on using a modified Delphi consensus technique, which included each participant using a voting scheme from 1 (strongly disagree) to 10 (strongly agree). Disagreements between votes were resolved by discussion and multiple rounds of voting until agreement. | Draft recommendations were reviewed by members of the CRA and feedback was used to finalize recommendations. A final review was completed by the CRA executive and received the official CRA endorsement. |
SIGN (2011)17 | ||||||
Intended users: Rheumatologists, general practitioners, rheumatology nurse specialists, physiotherapists, occupational therapists, dieticians, podiatrists, and pharmacists Target population: Patients with RA | Pharmacological treatment (including csDMARDs [MTX and SSZ] and low-dose corticosteroids) and multidisciplinary team involvement for patients with RA |
| The evidence was collected according to SIGN methodology.24 An SR was conducted. Database searches were conducted to identify evidence related to key guiding questions. | The quality of evidence was assessed and critically appraised using a variety of tools depending on the study design. Grades of recommendations were assigned as: A — at least one MA, SR, or RCT rated as 1++ and directly applicable to the target population, or a body of evidence consisting principally of studies rated as 1+ directly applicable to the target population and demonstrating an overall consistency of results B — a body of evidence including studies rated as 2++ directly applicable to the target population and demonstrating an overall consistency of results, or extrapolated evidence from studies rated as 1++ or 1+ C — a body of evidence including studies rated as 2+ directly applicable to the target population and demonstrating an overall consistency of results, or extrapolated evidence from studies rated as 2++ D — evidence level 3 or 4, or extrapolated evidence from studies rated as 2+ | Recommendation development was based on the evidence from the SR. Recommendations were formed through an informal consensus process. Advice from the editorial group or SIGN senior management team was used to settle any disagreement. | A draft of the guidelines was made available for public commentary on the SIGN website for 1 month. The draft guideline was also reviewed by an independent expert committee. A final quality check was completed by an editorial group from the SIGN Council. |
ACR = American College of Rheumatology; AGREE = Appraisal of Guidelines for Research & Evaluation; AMSTAR = A MeaSurement Tool to Assess systematic Reviews; APLAR = Asia Pacific League of Associations for Rheumatology; CRA = Canadian Rheumatology Association; csDMARD = conventional synthetic disease-modifying antirheumatic drug; DMARD = disease-modifying antirheumatic drug; EULAR = European League Against Rheumatism; GRADE = Grading of Recommendations Assessment, Development and Evaluation; HCQ = hydroxychloroquine; LEF = leflunomide; LoE = level of evidence; MA = meta-analysis; MTX = methotrexate; NICE = National Institute for Health and Care Excellence; NR = not reported; QoL = quality of life; RA = rheumatoid arthritis; RCT = randomized controlled trial; SIGN = Scottish Intercollegiate Guidelines Network; SoR = strength of recommendation; SR = systematic review; SSZ = sulfasalazine; tsDMARD = targeted synthetic disease-modifying antirheumatic drug.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Guidelines Using AGREE
Item | EULAR (2020)9 | APLAR (2019)10 | French Society for Rheumatology (2019)11 | Brazilian Society of Rheumatology (2018)12 | NICE (2018)13 | ACR (2016)14 | Todoerti et al. (2013)15 | CRA (2012)16 | SIGN (2011)17 |
Domain 1: Scope and Purpose | |||||||||
1. The overall objective(s) of the guideline is (are) specifically described. | Partially; details lacking | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | No | No | No | Yes | Yes | Yes | No | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | |||||||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Unclear; working group participants were mentioned but not described | Yes | Unclear; Rheumatoid Arthritis Committee was not outlined | Yes | Yes | Unclear; development group lacking detail | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | No | Yes | No | Yes | Yes | No | Yes | Yes |
6. The target users of the guideline are clearly defined. | Partially; details lacking | No | Yes | Partially; details lacking | Yes | Yes | No | Yes | Yes |
Domain 3: Rigour of Development | |||||||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Partially; details lacking | Yes | Yes | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Partially; details lacking | No | Partially; details lacking | Yes | Yes | No | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | No | No | No | Yes | Yes | No | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes | Yes | Yes | Partially; lacking details | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Unclear | Unclear | No | No | Yes | Yes | No | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Unclear; details lacking | Yes | Unclear; details lacking | Yes | Yes | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | Yes | Yes | No | No | Yes | Yes | No | Unclear; external review was not mentioned in the review phase | Yes |
14. A procedure for updating the guideline is provided. | No | No | No | No | Yes | Unclear; periodic updates were discussed but no specific procedure was described | No | Yes | Yes |
Domain 4: Clarity of Presentation | |||||||||
15. The recommendations are specific and unambiguous. | Partially; some details lacking | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | |||||||||
18. The guideline describes facilitators and barriers to its application. | No | Partially; details lacking | No | Yes | Yes | Yes | No | Yes | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No | No | Partially; details lacking | Yes | Yes | No | Partially; details lacking | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | Yes | No | No | Yes | Yes | No | No | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No | Partially; details lacking | No | Yes | No | No | No | Yes |
Domain 6: Editorial Independence | |||||||||
22. The views of the funding body have not influenced the content of the guideline. | Unclear; funding was provided by EULAR and numerous conflict of interest statements were provided | Yes | Unclear; no funding information was provided | Yes | Yes | Unclear; no funding information was provided | Unclear; no funding statement was provided | Unclear; funding information was provided but no statement related to influence was made | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Partially; but lacking details of how conflicts of interest were addressed | No | Partially; but lacking details of how conflicts of interest were addressed | Partially; but lacking details of how conflicts of interest were addressed | Yes | Yes | No | No | Unclear; information related to guideline develop-ment group members was provided but no conflicts of information were presented |
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence, strength of recommendations, GRADE, or level of agreement |
EULAR (2020)9 | |
Recommendation “Methotrexate (MTX) should be part of the first treatment strategy (p. 690).”9 Evidence informing this recommendation was not provided. | LoE: 1a (SR of RCTs) SoR: A (consistent level 1 studies)a |
Recommendation “In patients with contraindication to MTX (or early intolerance), leflunomide or sulfasalazine should be considered as part of the (first) treatment strategy (p. 690).”9 Evidence informing this recommendation was not provided. | LoE: 1a (SR of RCTs) SoR: A (consistent level 1 studies) |
Recommendation “Short-term GC should be considered when initiating or changing csDMARDs, in different dose regimens and routes of administration, but should be tapered as rapidly as clinically feasible (p. 692).”9 Three clinical trials suggested that MTX + GC showed similar effectiveness when compared to MTX + biologic DMARDs. | LoE: 1a (SR of RCTs) SoR: A (consistent level 1 studies) |
Recommendation “If the treatment target is not achieved with the first csDMARDs strategy, in the absence of poor prognostic factors, other csDMARDs should be considered (p. 692).”9 Evidence informing this recommendation was not provided. | LoE: 5 (expert opinion without explicit critical appraisal) SoR: D (level 5 evidenceb or troublingly inconsistent or inconclusive studies of any level) |
APLAR (2019)12 | |
Recommendation “Starting treatment with csDMARD monotherapy, preferably MTX, is recommended as soon as the diagnosis of RA is made (p. 359).”12 Evidence for the use csDMARDs, particularly MTX, as first-line therapy for patients diagnosed with RA was presented in previous 2016 EULAR20 and 2015 ACR14 treatment guidelines. The efficacy of using MTX monotherapy as first-line treatment for patients with RA was outlined in a 2014 SR and moderate-quality evidence from individual studies. The previous recommendation found in the 2015 version of this guideline presented 2 strong recommendations on csDMARDs as first-line RA treatment and that MTX is the preferred csDMARD. Based on current and past moderate-quality evidence, the previous 2 statements were integrated into 1 recommendation. | Quality of Evidence: Moderate (moderately confident in the effect estimate) SoR: NR |
Recommendation “Patients who cannot tolerate MTX may receive other csDMARDs such as LEF or SSZ as first-line treatment. HCQ, iguratimod, bucillamine, cyclosporine, intramuscular gold or tacrolimus may also be considered depending on availability (p. 361).”12 This recommendation is consistent with the previous recommendation in the 2015 version and is consistent with the 2016 EULAR20 treatment guideline. Three SRs and one RCT provided evidence for the efficacy of LEF compared to MTX. One SR and 2 RCTs support SSZ as an alternative to MTX. There were limited data on the efficacy of the other mentioned csDMARDs. | Quality of Evidence: Moderate (moderately confident in the effect estimate) SoR: NR |
Recommendation “In patients with high disease activity, combination csDMARD therapy should be considered, with close monitoring of therapy-related toxicities (p. 361).”12 This recommendation was based on RCTs in which patients with active RA were provided combination therapy. Four RCTs showed that triple therapy was more efficacious than monotherapy but was accompanied with higher hepatotoxicity. An additional 7 RCTs that looked at double or triple therapy versus monotherapy had similar findings. A previous Cochrane review from 2002 also showed higher efficacy in combination therapy compared to monotherapy. | Quality of Evidence: Low (confidence in the effect estimate is limited) SoR: NR |
French Society for Rheumatology (2019)11 | |
Recommendation “Methotrexate is the first-line DMARD in patients with active RA, starting at a dosage of at least 10 mg/week then reaching the optimal dosage within no more than 4–8 weeks (p. 141).”11 Evidence informing this recommendation was not provided. | LoE: 1a (SR of RCTs) SoR: A (consistent level 1 studies) |
Recommendation “In DMARD-naive patients who have contraindications or early intolerance to methotrexate, leflunomide and sulfasalazine are good alternatives (p. 141).”11 Evidence informing this recommendation was not provided. | LoE: 1a (SR of RCTs) SoR: A (consistent level 1 studies) |
Recommendation “While awaiting the effects of csDMARD therapy, oral or parenteral glucocorticoid therapy can be considered, in a low cumulative dosage, if possible for no longer than 6 months. The glucocorticoid dose should be tapered to nothing as promptly as possible (p. 141).”11 Evidence informing this recommendation was not provided. | LoE: 1a (SR of RCTs) SoR: B (consistent level 2c or 3 studies,d or extrapolations from level 1 studies) |
Recommendation “In patients with an inadequate response or intolerance to methotrexate, the treatment must be optimized. In patients with adverse prognostic factors, add-on bDMARD or tsDMARD therapy can be considered, using a TNFα antagonist, abatacept, an IL-6 pathway antagonist, a JAK inhibitor, or, under specific circumstances, rituximab. In patients without adverse prognostic factors, a switch to another csDMARD (leflunomide, sulfasalazine) or the combination of several csDMARDs can be considered; if this strategy fails or is contraindicated, targeted therapy (with a bDMARD or tsDMARD) should be considered (p.141).”11 Evidence informing this recommendation was not provided. | LoE: 1b (individual RCT) SoR: A (consistent level 1 studies) |
Brazilian Society of Rheumatology (2018)12 | |
Recommendation “The first line of treatment should be a csDMARD started as soon as the diagnosis of RA is established (p. 4).”12 Evidence for this recommendation was described as low to moderate. | LoA: 9.93 (mean score out of 10) Quality of evidence was described as low to moderate Strength of Recommendation: NR |
Recommendation “Methotrexate is the first-choice csDMARD (p. 6).”12 Moderate-quality evidence suggested that there was no significant difference in the efficacy of csDMARDs for most relevant outcomes including the number of painful and swollen joints, disease activity, pain, and functional capacity. High evidence suggested there were more adverse events with LEF compared to MTX; however, low to very low evidence suggested that MTX had the highest risk of hepatic pulmonary adverse events. | LoA: 10 Quality of evidence was described as very low to high Strength of Recommendation: NR |
Recommendation “Combination of two or more csDMARDs, including MTX, may be used as the first line of treatment (p. 6).”12 High to moderate evidence suggested that triple therapy with MTX + SSZ + HCQ and MTX + LEF compared with MTX monotherapy showed an improved response. Moderate to low evidence suggests that there was no clinically significant difference in MTX alone or in combination in other disease activities, radiographic progression, and therapeutic safety. | LoA: 9.62 Quality of evidence was described as low to high Strength of Recommendation: NR |
Recommendation “After failure of first-line therapy with MTX, therapeutic strategies include combining MTX with another csDMARD (leflunomide), with two csDMARDs (hydroxychloroquine and sulfasalazine), or switching MTX for another csDMARD (leflunomide or sulfasalazine) alone (p. 6).”12 Moderate to low evidence suggested combination therapies with MTX may provide a better response, with no significant difference in radiographic progression or adverse events from discontinuation. | LoA: 9.12 Quality of evidence was described as low to moderate Strength of Recommendation: NR |
NICE (2018)13 | |
Recommendation “For adults with newly diagnosed active RA:
“Consider short-term bridging treatment with glucocorticoids (oral, intramuscular or intra-articular) when starting new cDMARD (p. 9).”13 Overall evidence suggested that starting treatment with more than 1 csDMARD was no more effective than starting with a monotherapy csDMARD approach. Additionally, evidence from RCTs in DMARD-naive patients showed no difference in the effectiveness of MTX, LEF, and SSZ as monotherapies. The committee agreed that any of these csDMARDs may be used as first-line therapies. | Quality of evidence and strength of recommendations were NR |
Recommendation “Offer additional cDMARDs (oral methotrexate, leflunomide, sulfasalazine or hydroxychloroquine) in combination in a step-up strategy when the treatment target (remission or low disease activity) has not been achieved despite dose escalation (p. 9).”13 Evidence from RCTs was limited regarding the use of glucocorticoids for symptom relief in patients starting new DMARD therapy and no evidence was found regarding the effectiveness of glucocorticoids in terms of disease activity, QoL, or function. The committee agreed that the use of glucocorticoids may be considered on a case-by-case basis. | Quality of evidence and strength of recommendations were NR |
ACR (2016)14e | |
Recommendations for patients with symptomatic early RA: Recommendation “If the disease activity is moderate or high, in patients who have never taken DMARD:
Overall, 7 RCTs informed this recommendation. The strength for this recommendation is conditional because of low-quality evidence. Additionally, the evidence for this recommendation was shown to be imprecise. It was suggested that there was little difference in the benefit of double therapy over monotherapy and triple therapy may be desired by some patients. | SoR: Conditional (uncertainty of harms and benefits because of low-quality evidence) LoE: Moderate (further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate) LoE: High (further research is very unlikely to change our confidence in the estimate of effect) |
Recommendation “If disease activity remains moderate or high despite DMARD monotherapy (with or without glucocorticoids), use combination DMARDs or a TNFi or a non-TNF biologic (all choices with or without MTX, in no particular order of preference), rather than continuing DMARD monotherapy alone (p. 8).”14 One RCT provided low-quality evidence that suggested that when DMARD monotherapy was failing, adding treatment options is supported and recommending no additional treatment is not an option. | SoR: Strong (the benefits outweigh the harms) LoE: Low (further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate) |
Recommendations for patients with established RA Recommendation “If disease activity is moderate or high, in patients who have never taken DMARD:
Overall, 8 RCTs informed this recommendation. This recommendation is conditional because, despite positive evidence for tofacitinib, conflicting evidence suggested that benefit, risk, and cost favoured MTX monotherapy. The evidence for DMARD monotherapy over combination DMARD therapy was of low quality because evidence supporting the benefit of double therapy over monotherapy was indirect and imprecise. | SoR: Conditional (uncertainty of harms and benefits because of low-quality evidence) LoE: High (further research is very unlikely to change our confidence in the estimate of effect) LoE: High (further research is very unlikely to change our confidence in the estimate of effect) |
Recommendation “If disease activity remains moderate or high despite DMARD monotherapy, use combination traditional DMARDs or add a TNFi or a non-TNF biologic or tofacitinib (all choices with or without MTX, in no particular order of preference), rather than continuing DMARD monotherapy alone (p. 11).”14 Overall, 14 RCTs informed this recommendation. This recommendation is strong because clinical experience supported adding treatment options when DMARD monotherapy is failing. Additionally, voting supported biologic DMARD therapy used in combination with MTX because of evidence of efficacy compared to biologic DMARD monotherapy. | SoR: Strong (the benefits outweigh the harms) LoE: Moderate to very low (further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate; we are very uncertain about the estimate) |
Todoerti et al. (2013)15 | |
Recommendation “MTX must be considered the DMARD of first choice in RA patients both alone and in combination (with low dosage glucocorticoid and/or other DMARDs) (p. 209).”15 One meta-analysis and one RCT suggested that MTX-based treatment with the addition of a low-dose steroid (such as a glucocorticoid) improved outcomes related to radiographic progression and lower disease activity. | LoE: 2b (individual cohort study) SoR: B (consistent level 2 or 3 studies, or extrapolations from level 1 studies) |
Recommendation “In patients that are non-responders to MTX at the maximum tolerated dosage, combination therapy can be started with DMARD or a biological agent (p. 209).”15 One Cochrane review suggested that combining MTX with other DMARDs compared to MTX alone had no significant advantage in DMARD-naive or non-respondent patients, except for the combination of MTX + HCQ + SSZ (known as the O’Dell protocol). Additional evidence compared the efficacy of triple therapy to adding a biologic DMARD to therapy and suggested that the addition of the biologic DMARD improved clinical and radiographical outcomes. | LoE: 1b (individual RCT) SoR: B (consistent level 2 or 3 studies, or extrapolations from level 1 studies) |
CRA (2012)16 | |
Recommendation “Glucocorticoids (GC; oral, intramuscular, or intraarticular) can be added to DMARD therapy as part of the initial treatment strategy of patients with RA (I), and may be an option for managing flares, as bridge therapy while waiting for DMARD to take effect, or for symptom control if no other options exist (IV). GC should be used in the lowest possible dose and tapered as rapidly as clinically feasible (IV) (p. 1569).”16 One SR of RCTs that informed the EULAR 2010 guidelines suggested that short-term treatment with GC was beneficial for symptom control and inhibiting radiographic progression when added to DMARD monotherapy of combination therapy. Other evidence informing the NICE 2009 guidelines showed there was a discordance between strong evidence for the use of GC and the paucity of other research studies. Additional evidence from the EULAR 2007 guidelines suggested there was a risk of adverse events depending on the dosage of GC used. | LoE: I (meta-analyses, SRs of RCTs, or individual RCTs), IV (expert opinion) SoR: A (strong recommendation)/D (consensus recommendation) |
Recommendation “Methotrexate is the preferred DMARD with respect to efficacy and safety and should be the first DMARD used in patients with RA unless contraindicated (p.1569).”16 RCT and observational evidence from the EULAR 2010 guidelines suggested that MTX was effectives in DMARD-naive patients with early moderate to severe RA. Additionally, no other csDMARD or biologic DMARD monotherapies were shown to have better clinical efficacy compared to MTX. One SR supported the beneficial safety of long-term MTX. | LoE: I (meta-analyses, SRs of RCTs, or individual RCTs) SoR: A (strong recommendation) |
Recommendation “Initial combination therapy with traditional DMARD should be considered, particularly in patients with poor prognostic features, moderate-high disease activity, and in patients with recent-onset disease. Combination therapy should also be considered in patients who have an inadequate response to monotherapy (p. 1571).”16 RCT evidence informing the ACR 2008 guidelines suggested there was efficacy in DMARD combinations in different clinical situations. An SR of RCTs and observational studies informing the NICE 2009 guidelines suggested that several combinations (including GC) was superior to DMARD monotherapy. An SR of RCTs informing the EULAR 2010 guidelines found low-quality evidence in trials comparing combination therapy to monotherapy. | LoE: I (meta-analyses, SRs of RCTs, or individual RCTs) SoR: B (moderate recommendation) |
Recommendation “When treating with combination therapy, methotrexate (MTX) should be used as the anchor drug unless contraindicated. Combinations not including MTX can be considered on a case-by-case basis (p. 1571).”16 Evidence informing the NICE 2009 guideline and ACR 2008 guideline provided details for combination therapy in RA. At least 1 RCT showed increased efficacy for a number of combination therapies over monotherapy. | LoE: I (meta-analyses, SRs of RCTs, or individual RCTs) SoR: A (strong recommendation) |
Recommendation “Combination therapy with leflunomide (LEF) and methotrexate (MTX) should be used with caution as it is associated with higher toxicity (GI and liver) (I) and has no added benefit relative to other DMARD combinations (IV) (p. 1572).”16 Evidence from 1 RCT suggested combination therapy with MTX + LEF had better efficacy compared to MTX + placebo in patients with high disease activity. It should be noted that LEF was associated with the risk of severe liver injury. Additionally, several Canadian provincial formularies require patients to fail LEF or MTX + LEF prior to accessing biologic DMARD therapy. | LoE: I (meta-analyses, SRs of RCTs, or individual RCTs), IV (expert opinion) SoR: A (strong recommendation) |
SIGN (2011)17 | |
Recommendation “Low-dose oral corticosteroids can be used in combination with DMARD therapy for short term relief of signs and symptoms, and in the medium to long term to minimize radiological damage (p. 9).”17 A Cochrane review of RCTs suggested that low-dose corticosteroids were effective in the short-term relief of symptoms compared to NSAIDs and minimized radiographical damage in the medium- to long-term. An additional Cochrane review found that corticosteroids in combination with DMARDs reduced the rate of progression for RA. | Quality of Evidence: A (please refer to Table 2 for description of GRADE) |
Recommendation “Methotrexate and sulfasalazine are the DMARDs of choice due to their more favourable efficacy and toxicity profiles (p. 10).”17 “DMARD therapy should be sustained in patients with early RA to control the signs and symptoms of disease (p. 10).”17 Evidence from an SR suggested that the efficacy of MTX was similar to other common csDMARDs including LEF and SSZ, but HCQ was less effective. Additional evidence from 2 RCTs suggested sustained use of DMARD therapy was necessary because of relapse symptoms and signs occurring with therapy withdrawal. | Quality of Evidence: A Quality of Evidence: B |
Recommendation “A combination DMARD strategy, rather than sequential monotherapy, should be considered in patients with an inadequate response to initial DMARD therapy (p. 11).”17 An SR of 3 RCTs suggested that combination therapy was more effective than sequential monotherapy in overall RA improvement and the reduction in progression. MTX was the most common DMARD in combination therapy. | Quality of Evidence: A |
ACR = American College of Rheumatology; bDMARD = biologic disease-modifying antirheumatic drug; CRA = Canadian Rheumatology Association; csDMARD = conventional synthetic disease-modifying antirheumatic drug; DMARD = disease-modifying antirheumatic drug; EULAR = European League Against Rheumatism; GC = glucocorticoids; GRADE = Grading of Recommendations Assessment, Development and Evaluation; HCQ = hydroxychloroquine; IL-6 = interleukin 6; JAK = Janus kinase; LEF = leflunomide; LoA = level of agreement; LoE = level of evidence; MTX = methotrexate; NICE = National Institute for Health and Care Excellence; NR = not reported; NSAID = nonsteroidal anti-inflammatory drug; QoL = quality of life; RA = rheumatoid arthritis; RCT = randomized controlled trial; SIGN = Scottish Intercollegiate Guidelines Network; SoR = strength of recommendation; SR = systematic review; SSZ = sulfasalazine; TNF = tumour necrosis factor; TNFi = tumour necrosis factor inhibitor; tsDMARD = targeted synthetic disease-modifying antirheumatic drug.
aLevel 1 studies refer to SRs of RCTs, individual RCTs, and “all or none” studies.
bLevel 5 evidence refers to expert opinion without explicit critical appraisal.
cLevel 2 studies refer to SRs of cohort studies, individual cohort studies, or “outcomes” research and ecological studies.
dLevel 3 studies refer to SRs of case-control studies and individual case-control studies.
eThe American College of Rheumatology uses the term “DMARD” to describe conventional synthetic DMARD therapy.
Appendix 5: References of Potential Interest
Previous CADTH Reports
1.Leflunomide for the management of rheumatoid arthritis: Comparative clinical effectiveness. (CADTH Rapid Response report: Reference list) Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/2019/RA0999%20Leflunomide%20for%20RA%20Final.pdf
Accessed 2021 Apr 27.
2.Drugs for the management of rheumatoid arthritis: Clinical evaluation. (CADTH HealthTechnology Assessment report no. 146). Ottawa (ON): CADTH; 2018: https://cadth.ca/sites/default/files/pdf/HT0010_RA_Report.pdf
Accessed 2021 Apr 27.
3.Conventional synthetic disease-modifying antirheumatic drugs for adults with moderate to severe rheumatoid arthritis: Clinical effectiveness. (CADTH Rapid Response report: Reference list) Ottawa (ON): CADTH; 2018: https://cadth.ca/sites/default/files/pdf/htis/2018/RA0956%20csDMARDs%20for%20RA%20v.pdf
Accessed 2021 Apr 27.
Review Articles
4.Padjen I, Crnogaj MR, Anic B. Conventional disease-modifying agents in rheumatoid arthritis - a review of their current use and role in treatment algorithms. Reumatologia. 2020;58(6):390-400. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca