CADTH Health Technology Review
Autologous Hematopoietic Cell Transplant for Patients With Multiple Sclerosis
Rapid Review
Authors: Khai Tran, Hannah Loshak
Abbreviations
AE
adverse event
AHSCT
autologous hematopoietic stem cell transplantation
ALZ
alemtuzumab
ARR
annualized relapse rate
ASBMT
American Society for Blood and Marrow Transplantation
CI
confidence interval
CNS
central nervous system
DMT
disease-modifying therapy
EBMT
European Society for Blood and Marrow Transplantation
EDSS
Expanded Disability Status Scale
Gd
gadolinium
IR
incidence rate
MS
multiple sclerosis
MSFC
Multiple Sclerosis Functional Composite
MTX
mitoxantrone
NEDA
no evidence of disease activity
NRS
Neurologic Rating Scale
PML
progressive multifocal leukoencephalopathy
PPMS
primary-progressive multiple sclerosis
RCT
randomized controlled trial
RRMS
relapsing-remitting multiple sclerosis
SF-36 QoL
Short Form 36 (health survey) quality of life
SPMS
secondary-progressive multiple sclerosis
Key Messages
Evidence from 2 randomized controlled trials and 4 retrospective studies with limited methodological quality suggests that treatment with autologous hematopoietic stem cell transplantation was associated with significant improvement in clinical outcomes (e.g., disease progression, clinical relapse), MRI outcomes, the composite outcome “No Evidence of Disease Activity,” and quality of life compared to disease-modifying therapies.
Treatment with autologous hematopoietic stem cell transplantation was associated with no treatment-related mortality or life-threatening complications including progressive multifocal leukoencephalopathy. However, autologous hematopoietic stem cell transplantation was associated with expected short-term adverse events including febrile neutropenia, organ infections, sepsis, and viral reactivations; and long-term adverse events including the development of new autoimmune diseases, mainly thyroid disease.
Both identified guidelines recommend the use of autologous hematopoietic stem cell transplantation as standard of care for the treatment of highly active relapsing-remitting multiple sclerosis patients refractory to disease-modifying therapies and suggest that the treatment may be appropriate for progressive forms of multiple sclerosis with an active inflammatory component.
No cost-effectiveness studies were identified.
Context and Policy Issues
Multiple sclerosis (MS) is a chronic inflammatory autoimmune disorder of the central nervous system (CNS) that is more common in women than in men by a factor of approximately 3 to 1.1 One in every 400 Canadians live with MS and more than 4,000 people are diagnosed with MS every year.1
MS is heterogeneous in clinical course and can be classified into 4 subtypes: clinically isolated syndrome, relapsing-remitting MS (RRMS), primary-progressive MS (PPMS), and secondary-progressive MS (SPMS).2 Clinically isolated syndrome is a first episode of inflammation of the CNS that is a characteristic of MS but does not meet the criteria for the diagnosis of MS.2 The diagnosis of MS has been revised by the McDonald Criteria published in 2017 by the International Panel on the Diagnosis of Multiple Sclerosis.3 Biomarkers for MS on MRI are gadolinium (Gd)-enhancing lesions and new T2 or enlarging T2 lesions, which are indicators of ongoing CNS inflammation.4 Approximately 85% to 90% of MS patients have RRMS, which is characterized by clearly defined periods of neurologic symptoms (relapses) alternating with periods of partial or complete recovery (remissions).5 Relapses occur when the immune system attacks the myelin sheet of the nerve fibres, causing an acute inflammation of the CNS.5 Patients with RRMS will eventually transition to SPMS, which is characterized by a progressive worsening of neurologic function over time.2,6,7 Some patients develop PPMS, characterized by progressive disability from the onset of symptoms independent of relapses.2
There are currently more than a dozen of disease-modifying therapies (DMTs) for MS approved in Canada that are grouped into 3 categories: injectable medications (e.g., interferon beta-1a, interferon beta-1b, glatiramer acetate, ofatumumab, peginterferon beta-1a), oral medications (e.g., teriflunomide, fingolimod, cladribine, siponimod, dimethyl fumarate, ozanimod), and infused medications (e.g., alemtuzumab, ocrelizumab, natalizumab).8 These drugs have different mechanisms of action in modulating or suppressing the immune system, thereby reducing the disease activity and slowing down the rate of disability development.9 However, some patients with aggressive MS still show no improvement or have significant side effects after treatment with 1 or more approved DMTs.9
Autologous hematopoietic stem cell transplantation (AHSCT) may be considered as a suitable immune reconstitution therapy for some MS patients at the early stage of disease when the inflammation is predominant and the disability level is low.10 AHSCT has been used for the treatment of MS for more than 2 decades.10 With improving techniques and expertise of transplantation, together with properly selected patients, the efficacy and safety of AHSCT have improved over time.10 AHSCT procedures consists of 5 main stages such as mobilization of hematopoietic stem cells using growth factor and chemotherapy, collection of stem cells from peripheral blood, conditioning chemotherapy to suppress immune system, reinfusion of stem cells, and support with blood products and antibiotics as well as follow-up with regular blood tests and medication.11 The conditioning regimens are classified based on the grade of intensity: high intensity, intermediate intensity, and low intensity.10,12 The intermediate intensity is further divided into myeloablative and non-myeloablative, depending on the regimens, and have been used most commonly in MS.12 High-intensity regimens have been associated with serious adverse events (AEs), while low-intensity regimens have been less efficacious.12
The aim of this report is to review the clinical effectiveness and cost-effectiveness of AHSCT for the treatment of MS. The report also reviews the evidence-based guidelines regarding the use of AHSCT for MS. This report will support a CADTH Early Assessment Bulletin on MS.
Research Questions
What is the clinical effectiveness of AHSCT for treatment of MS?
What is the cost-effectiveness of AHSCT for treatment of MS?
What are the evidence-based guidelines regarding AHSCT for individuals with MS?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and Embase via Ovid, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were autologous hematopoietic cell transplant and MS. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or network meta-analyses, any types of clinical trials or observational studies, economic studies, or guidelines. Comments, newspaper articles, editorials, conference abstracts, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2015 and March 24, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Individuals with RRMS or other subtypes of MS |
Intervention | AHSCT also known as AHCT and formerly known as autologous bone marrow transplant |
Comparator | Q1 and Q2: Standard of care (e.g., DMT); different AHSCT regimen(s) (e.g., myeloablative vs. non-myeloablative). Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness: (e.g., disability, progression free survival, quality of life, pain; safety Q2: Cost-effectiveness Q3: Recommendations regarding treatment eligibility and suitability of candidates to receive AHSCT |
Study designs | HTA, SR, RCT, non-randomized studies, economic evaluations, evidence-based guidelines |
AHCT = autologous hematopoietic cell transplant; AHSCT = autologous hematopoietic stem cell transplant; DMT = disease-modifying therapy; HTA = health technology assessment; MS = multiple sclerosis; RCT = randomized controlled trial; RRMS = relapsing-remitting MS: SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or were published before 2015. Studies that involved allogenic donor stem cells or mesenchymal stem cells were excluded. Economic evaluations without conducting cost-effectiveness analysis were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: the Downs and Black checklist13 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research & Evaluation (AGREE) II instrument14 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
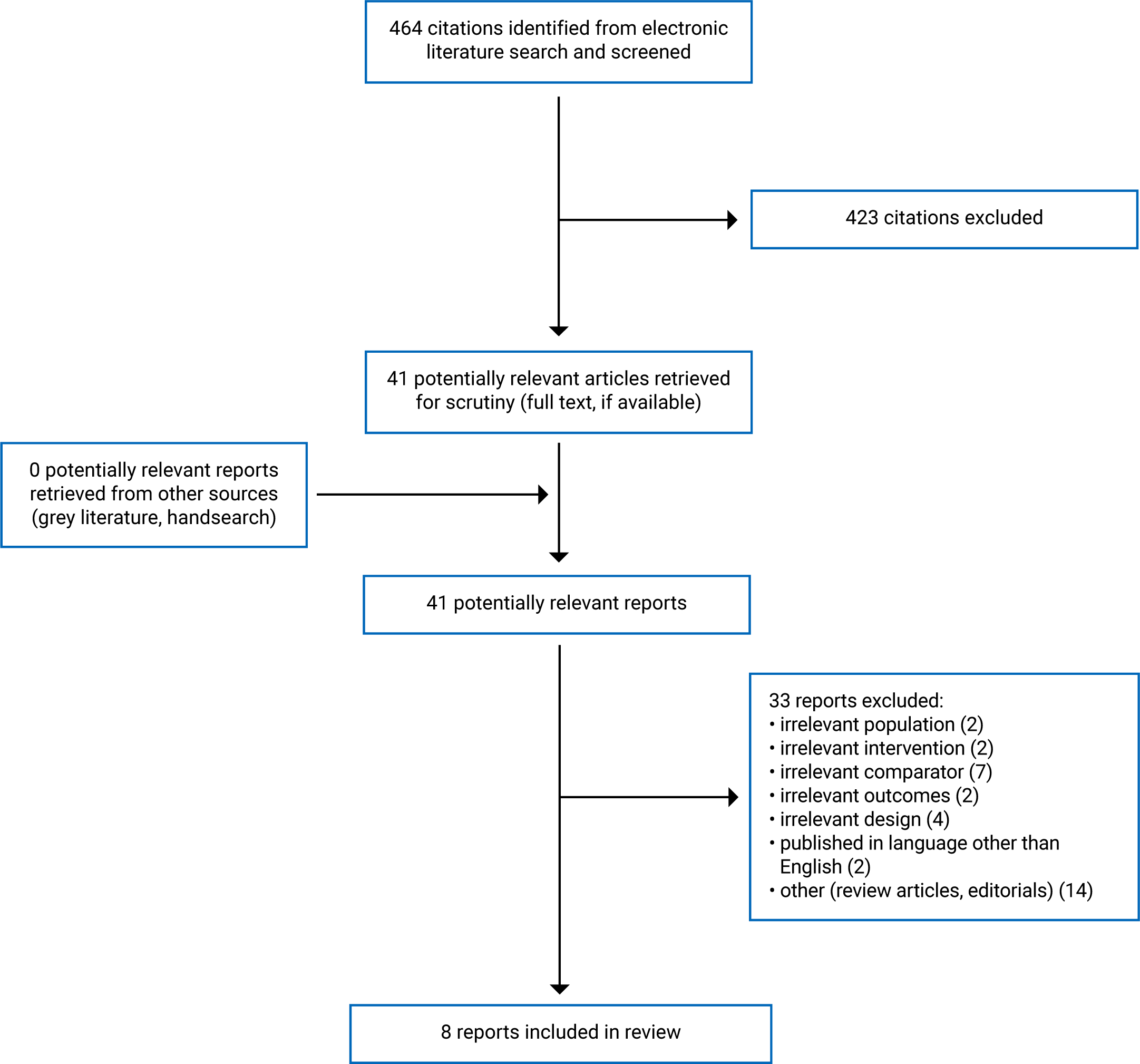
A total of 464 citations were identified in the literature search. Following the screening of titles and abstracts, 423 citations were excluded and 41 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 33 publications were excluded for various reasons and 8 publications met the inclusion criteria and were included in this report. These comprised 2 randomized controlled trials (RCTs), 4 non-randomized studies, and 2 evidence-based guidelines. Appendix 1 presents the PRISMA15 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The detailed characteristics of the included primary studies16-21 (Table 2) and the European Society for Blood and Marrow Transplantation (EBMT) guideline12 and the American Society for Blood and Marrow Transplantation (ASBMT)22 guideline (Table 3) are presented in Appendix 2.
Study Design
Of the 6 included primary studies, 2 were RCTs16,17 and 4 were retrospective cohort studies.18-21 Both RCTs (1 phase III16 and 1 phase II17) were open-label, multi-centre, parallel, 1:1 trials. Both reported sample size calculations to detect a clinically relevant treatment effect. The results in the phase III trial16 were analyzed using a per-protocol population and not the intention-to-treat population. Adjustment for multiple comparisons were not performed in both RCTs. None of the retrospective cohort studies reported a sample size calculation. One retrospective cohort study20 used multivariate analysis to account for differences in some baseline characteristics between groups, while the other 3 retrospective cohort studies18,19,21 did not identify and adjust for covariates in their analyses.
Both included guidelines12,22 were developed to update their previous guidelines on the recommendations of AHSCT on MS treatment. Evidence was identified from literature searches. The recommendations in both guidelines were developed by a panel of experts in AHSCT and MS. The EBMT guideline12 rated the evidence as I, II, or III based on the health benefits, side effects, and risks of AHSCT, as compared with non-cell transplant options. The strength of recommendations in the EBMT guideline12 were classified as S (standard of care), CO (clinical option), D (developmental), or GNR (generally not recommended) based on the level of evidence obtained. The ASBMT guideline22 did not rate the evidence or the strength of its recommendations. The method of recommendations development and evaluation was not clearly stated in the ASBMT guideline.22
Country of Origin
The included primary studies were conducted by authors from US,16 Italy,17,20,21 and Sweden.18,19 The included guidelines were conducted by authors from countries in Europe,12 and from the US and Canada.22
Patient Population
Patients in 416,19-21 out of 6 primary studies were exclusively RRMS. The phase II RCT17 included patients with progressive MS (67%) and RRMS (33%). One study18 had a patient population consisting mainly of RRMS with a small percentage of patients with PPMS (1.2%) and SPMS (6.1%). The sample sizes of 6 included studies ranged from 21 to 271. The mean age of patients in the included studies was approximately 35 years, with the percent of females ranging from 60% to 79%. The mean disease duration ranged from 6 to 11 years and the mean baseline Expanded Disability Status Scale (EDSS) score (which measures the progression or deterioration of MS) ranged from 2.5 to 6. The EDSS score ranges from 0 to 10 in 0.5-point increments from no neurologic disability (0) to worst neurologic disability (10).
The target populations in both guidelines12,22 are patients diagnosed with defined MS. The intended users of both guidelines are health care workers in the MS field working with transplant teams or considering the referral of patients.
Interventions and Comparators
AHSCT was the intervention in all the included studies classified as myeloablative17,18,20,21 or non-myeloablative,16,18,19 based on the conditioning regimens. The comparators were DMT,16,21 mitoxantrone (MTX),17 and alemtuzumab (ALZ).18-20
The intervention considered in the evidence-based guidelines12,22 was AHSCT for MS.
Outcomes
The outcomes considered in the included primary studies16-21 could be classified as clinical outcomes, MRI outcomes, and safety outcomes. The clinical outcomes consisted of disease progression (defined as an increase in EDSS score of at least 1 point on 2 evaluations 6 months apart after at least 1 year of treatment), clinical relapse (a neurologic symptom lasting more than 24 hours; not associated with infection, fever, or heat intolerance), the Neurologic Rating Scale (NRS; range 0 to 100 in 1-point increments from worst [0] to no [100] disability; minimal clinically important difference, 10), the Short Form-36 quality of life (SF-36 QoL; range, 1 to 100; higher scores indicate more favourable health state), and the Multiple Sclerosis Functional Composite (MSFC) score (which incorporates the timed 25-ft walk test, the Nine-Hole Peg Test [a measure of arm function], and the Paced Auditory Serial Addition Test [scored as the total number correct out of 60 possible, and data shown are % of correct answers]). The MRI outcomes were MRI T2-weighted lesion volume (reported as % change from baseline), new T2 MRI lesions, Gd-enhancing lesions on T1-weighted MRI. No evidence of disease activity (NEDA) was a composite outcome defined as no progression, no relapses, and no new or enlarging lesions on MRI. The safety outcomes included mortality, early AEs (within 100 days after treatment), late AEs (after 100 days of treatment), and serious AEs. The follow-up period was 3 years in 5 studies17-21 and 5 years in 1 study.16
Both guidelines12,22 considered the efficacy and safety outcomes of AHSCT in MS in the development of recommendations. The EBMT guideline12 also considered the resources implications and other issues relevant to the implementation of AHSCT.
Summary of Critical Appraisal
All included primary studies16-21 were explicit in reporting (i.e., clearly described the objective of the study, the main outcomes, the characteristics of the participants, the interventions, differences in baseline characteristics between groups, and the main findings of the study). All studies16-21 provided estimates of the random variability (e.g., standard deviation or 95% confidence interval) in the data of the main outcome and actual P values for main outcomes. As 2 RCTs16,17 and 4 retrospective cohort studies18-21 with relatively small sample sizes, it was not applicable to determine if the participants were representative of the entire population from which they were recruited. However, the treatment settings were representative of the treatment received by most of the patients. Both RCTs16,17 were open-label, as it was not possible to perform blinding of participants, personnel, or outcome assessors. Allocation concealment was not reported in the RCTs.16,17 Sample size was determined in both RCTs16,17 but not in the retrospective cohort studies.18-21 The intervention and comparator groups in all included studies had the same follow-up. Appropriate statistical tests were used to assess the main outcomes, which were accurately measured. Three18,19,21 of 4 retrospective cohort studies did not identify or conduct any adjustment for potential confounders in the analyses from which the main findings were drawn. The findings in those studies were therefore considered as crude and less reliable. Overall, all studies, except for the phase III RCT,16 were of limited methodological quality.
Both included guidelines12,22 were explicit in scope and purpose (i.e., objectives, health questions, and populations) and had clear presentation (i.e., specific and unambiguous recommendations, different options for management of the condition or health issue, and easy to find key recommendations). Regarding stakeholder involvement, the guidelines clearly defined target users and the development groups; however, it was unclear if the views and preferences of the MS populations were sought. For rigour of development, both guidelines12,22 did not report details of systematic searches for evidence, criteria for selecting evidence, and methods of formulating the recommendations. Both guidelines considered health benefits, side effects, and risks in formulating the recommendations, were peer-reviewed before publication, and provided a procedure for updating. For applicability, the EBMT guideline12 was explicit in terms of facilitators and barriers to application, advice and/or tools on how the recommendations can be put into practice, resource (cost) implications, and monitoring and or auditing criteria. For editorial independence, it was unclear if the funding bodies had any influence over the content of the guidelines. The competing interests of the guideline development group members were reported. Overall, both included guidelines appeared to be of acceptable methodological quality.
Summary of Findings
The main findings and authors’ conclusions of the primary studies16-21 (Table 6) and the recommendations of the guidelines12,22 (Table 7) are presented in Appendix 4.
Clinical Effectiveness of AHSCT
Disease Progression
In the phase III RCT,16 the proportions of patients with disease progression at 1, 3, and 5 years of follow-up were significantly lower in the AHSCT group (1.9%, 5.2%, and 9.7%, respectively) compared to those in the DMT group (24.5%, 62.5%, and 75.3%, respectively); P < 0.001. The median time to disease progression of the AHSCT group could not be calculated because of too few events and the median time to disease progression in the DMT group was 24 months (range, 18 to 48 months) (hazard ratio = 0.07; 95% confidence interval [CI], 0.02 to 0.24; P < 0.001). The between-group difference in mean change in EDSS score from baseline to 1 year was −1.7; 95% CI, −2.03 to −1.29; P < 0.001. The phase II RCT17 with a small sample size (N = 21) reported no significant difference between the AHSCT and MTX groups in the proportions of patients with disease progression, or in the EDSS change. The unobserved differences between groups in disease progression were likely due to the low power of this trial. A retrospective cohort study by Zhukovsky et al.19 found that the EDSS changes from baseline to 1, 2, and 3 years of follow-up in the AHSCT group showed significant improvement compared to those in the ALZ group (P < 0.0001). Another retrospective cohort study by Boffa et al.20 found that AHSCT promoted significant EDSS improvement compared with ALZ (P = 0.035). The proportion of patients with confirmed improvement in EDSS scores was significantly higher in the AHSCT group compared to the DMT groups (44.4% versus 6.1%; P = 0.013).21
Clinical Relapse
In the phase III RCT,16 the proportions of patients with clinical relapse in the AHSCT group were significantly lower compared to those in the DMT group at all time points of follow-up (P < 0.001). The annualized relapse rate (ARR) reported in the phase II RCT17 was significantly lower in the AHSCT group compared to the MTX group (0.19 versus 0.60; rate ratio = 0.36; 95% CI, 0.15 to 0.88; P = 0.026). A retrospective study by Zhukovsky et al.19 also reported a significantly lower ARR in the AHSCT group compared to the ALZ group (0.04 versus 0.1; P = 0.03). Similarly, 2 other retrospective cohort studies also showed a significantly lower ARR in the AHSCT group compared to the ALZ group (0.05 versus 0.35; P = 0.02)20 and to DMT (0.0 versus 0.67; P < 0.0001).21
Neurologic Rating Scale
In the phase III RCT,16 the mean change in NRS score from baseline to 1 year in the AHSCT group was + 8.8 (improved) and that in the DMT group was –1.6 (worsened). The between-group difference in mean change in NRS score was + 11.2; 95% CI, + 8.08 to + 14.29; P = 0.001, indicating significant improvement in favour of the AHSCT group compared to the DMT group.
SF-36 QoL
In the phase III RCT,16 the quality of life in the AHSCT group was improved ( + 19.5) but worsened in the DMT group (−3.4). The between-group difference in mean change in SF-36 QoL score from baseline to 1 year was + 23; 95% CI, + 17.6 to + 28.9; P < 0.001.
Multiple Sclerosis Functional Composite
In the phase III RCT,16 the mean change in MSFC score from baseline to 1 year in the AHSCT group was + 0.32 (improved) and in the DMT group was −0.31 (worsened). The between-group difference was + 0.51; 95% CI, + 0.28 to + 0.72; P < 0.001. There were significant improvements in the timed 25-feet walk and the 9-Hole Peg Test in the AHSCT group compared to the DMT group (P < 0.001). However, there was no significant difference in the Paced Auditory Serial Addition Test score between groups (P = 0.61).
MRI outcomes
In the phase III RCT,16 the mean change in MRI T2-weighted lesion volume from baseline to 1 year in the AHSCT group was −31.7% (improved) and in the DMT group was + 34.3% (worsened). The between-group difference was −66% (95% CI, −70.6 to −61.3); P < 0.001. The phase II RCT17 showed that the number of new T2 lesions over 4 years was significantly reduced in the AHSCT group compared to the MTX group (rate ratio = 0.21; 95% CI, 0.10 to 0.48; P = 0.00016). The result remained significant in all sensitivity analyses. No patients in the AHSCT group had Gd-enhancing lesions compared to 56% of the MTX patients, who had at least 1 Gd lesions during 4 years of follow-up (P = 0.029).17 A retrospective cohort study by Boffa et al.20 showed that AHSCT significantly reduced the risk of MRI activity compared to the ALZ (MRI-activity-free survival: 85% versus 59%; hazard ratio = 0.13; 95% CI, 0.03 to 0.59; P = 0.009).
No Evidence of Disease Activity
The post-hoc analysis of the phase III RCT16 showed that the proportions of patients reaching NEDA at 1, 3, and 5 years after randomization were significantly higher in the AHSCT group (98.1%, 90.3%, and 78.5%, respectively) compared to the DMT group (20.8%, 5.9%, and 3%, respectively); P > 0.001. Three retrospective cohort studies19-21 also found similar results in that the proportions of patients with NEDA were significantly higher in the AHSCT group compared to the ALZ group19,20 or DMT group21 at the end of follow-up.
Safety
Four studies16,17,19,21 reported no deaths occurring in either intervention group. One study18 reported 1 death in the AHSCT group due to suicide (incidence rate [IR] per 1,000 person-years = 1.7; 95% CI, 0.0 to 9.6) and 4 deaths in the ALZ group (2 suicides, 1 heart attack, 1 cytomegalovirus reactivation) (IR per 1,000 person-years = 8.6; 95% CI, 2.3 to 22.0).
The phase III RCT16 reported that no AHSCT patients developed Common Toxicity Criteria grade 4 nonhematopoietic toxicities such as myocardial infarction, embolism, dialysis, sepsis, or need for pressor support. There were also no patients in the AHSCT group transferred to intensive care units; or who received parenteral nutrition, surgery, or other disabling or potential life-threatening events. Of the 52 study participants in the AHSCT group, few patients had inpatient grade 3 AE infections: there was 1 case (1.9%) of Clostridium difficile diarrhea, 1 case (1.9%) of Escherichia coli urinary tract infection, and 1 case (1.9%) of culture-negative pneumonia. Post-transplantation infections were mainly upper respiratory tract infections that occurred in both groups (16 cases [31%] in AHSCT group and 15 cases [29%] in DMT group). There was no progressive multifocal leukoencephalopathy (PML) caused by John Cunningham virus infections in either group. The rate of infection per patient-year was 0.19 in the AHSCT group and 0.23 in the DMT group. No statistical comparison between groups was given.
In the phase II RCT,17 early adverse events (occurring < 100 days after treatment) associated with AHSCT included grade 3 AEs, which included febrile neutropenia, leukopenia, anemia, platelet count decrease, amenorrhea, leukopenia; and grade 4 AEs, which included leukopenia, anemia, and platelet count decrease. In the MTX group, grade 3 AEs that occurred included neutrophil count decrease, amenorrhea, leukopenia, and lymphocyte count decrease; and grade 4 AEs that occurred included neutrophil count decrease. Severe AEs that occurred in the AHSCT group were sepsis, prolonged hospitalization, systemic candidiasis, cytomegalovirus reactivation, and engraftment failure. None of the patients in the MTX group had severe AEs. All AEs in the AHSCT group were resolved without sequelae. The IR of these AEs and statistical comparisons between groups were not provided.
A retrospective cohort study by Alping et al.18 found that thyroid disease occurred more often for AHSCT (IR per 1,000 person-years = 34; 95% CI, 18 to 56) compared to the non-induction therapy group (natalizumab, dimethyl fumarate, rituximab, fingolimod) (IR = 5.3; 95% CI, 3.9 to 7.1), but less frequent than ALZ (IR = 109; 95% CI, 75 to 154). The non-thyroid autoimmune disease was rare, and the IRs were comparable between groups. The incidence of any infection was highest among the AHSCT group (IR = 275; 95% CI, 213 to 350) compared to ALZ group (IR = 56; 95% CI, 34 to 87) and the non-induction therapy group (IR = 52; 95% CI, 47 to 58), but dropped to the level near to the ALZ and the non-induction therapy groups within the first year. Common infections found after treatment with AHSCT and ALZ were herpes infections and bacterial sepsis. Systemic antibiotics were given to all patients after AHSCT and to most patients after ALZ. No cases of PML were detected.
A retrospective cohort study by Zhukovsky et al.19 reported that 70% of patients treated with AHSCT developed early Common Toxicity Criteria grade 3 AEs or higher in which febrile neutropenia (58%) was the most common. None of the patients in the ALZ group had grade 3 AEs or higher. Late grade 3 AEs occurred in 1 patient (1.4%) treated with AHSCT (Lyme neuroborreliosis) and 5 patients (6.7%) treated with ALZ (4 cases [5.3%] of immune mediated thrombocytopenia, 1 case [1.3%] of breast cancer). Thyroid disease was the most common autoimmune adverse event that occurred in both groups: 20% in the AHSCT group and 47% in the ALZ group; P = 0.005. Herpes zoster infection developed in 5.8% in the AHSCT group and 6.7% in the ALZ group as late infection.
A retrospective cohort study by Boffa et al.20 reported that serious infections including neutropenic fever (64%) and sepsis (32%) were commonly diagnosed as early AEs in the AHSCT group. Late AEs such as autoimmune disorders, especially thyroid disorders, were more common in the ALZ group (28%) compared to the AHSCT group (4%).
A retrospective cohort study by Mariottini et al.21 found no life-threatening complications including PML after AHSCT. All infections and viral reactivations occurred within 1 year from transplantation. One patient in the AHSCT group (9%) developed autoimmune thyroiditis.
Cost-Effectiveness of AHSCT
No comparative cost-effectiveness studies of AHSCT were identified; therefore, no summary can be provided.
Guidelines
The EBMT guideline12 recommends that AHSCT should be offered to patients with RRMS who have high clinical and MRI inflammatory disease activity despite the use of 1 or more lines of approved DMTs. Patients should be younger than 45 years, with a EDSS score of 5.5, at most, and have a disease duration of less than 10 years. The strength of recommendation was categorized as S (standard of care) based on level I evidence. The guideline recommends that AHSCT should be considered for patients with “aggressive” MS who develop severe disability in the previous 12 months, even before failing a full course of DMT. The guideline suggests that SPMS, PPMS, and MS pediatric patients with documented evident disability progression in the previous 12 months should be considered for AHSCT, preferably in a prospective clinical trial. The strength of these recommendations was categorized as CO based on level II evidence. Details of the levels of evidence and strengths of recommendation are presented in the footnotes of Table 3 in Appendix 2.
The ASBMT guideline22 endorses AHSCT as “standard of care, with clinical evidence available” for patients with relapsing forms of MS (such as RRMS or progressive MS) who are refractory to treatment and have prognostic factors indicating a high risk of disability. This includes a clinical relapse and MRI activity, despite treatment with high efficacy MDTs. The strength of recommendation and the level of evidence were not given.
Limitations
The evidence from this review was derived from the findings of 2 RCTs16,17 and 4 retrospective cohort studies18-21 with relatively small sample sizes. Both RCTs were open-label by design because of the nature of the interventions that might result in a high risk of performance and detection biases. The study design of the phase III RCT16 allowed DMT patients to cross over to receive AHSCT after 1 year of follow-up in the event of treatment failure, resulting in up to 61% of DMT patients crossing over and thus limiting accurate comparisons of longer-term outcomes between groups. Two newer potent monoclonal antibodies — ocrelizumab and ALZ — were not included in the DMT group because of their unavailability or a safety concern that may result in a higher efficacy of AHSCT than their comparators.16 The phase III RCT used a per-protocol population in its analysis, which did not account for patients who were lost to follow-up after treatment. Adjustment for multiple comparisons were not performed in both RCTs. The results of the retrospective non-randomized studies18-21 might be affected by selection bias because of the nature of the study design. None of the retrospective cohort studies reported sample size calculations. There were significant differences between groups in certain patient characteristics, such as age, disease duration, ARR, EDSS, MS type, and MRI activity at baseline. Patients in the ASHCT group were younger and had longer disease duration and higher disease activity compared to those in the control group. Three studies18,19,21 did not attempt to adjust for confounders in the analyses. As most patients in the included studies were of RRMS type, evidence for the clinical effectiveness of AHSCT on progressive MS remains to be determined. Both guidelines were limited in terms of rigour of development, as the details of systematic searches for evidence, criteria for selecting evidence, and methods of formulating the recommendations were not reported. However, the guidelines were the updated versions of their previous ones and were developed in Europe, the US, and Canada. Despite these limitations, all included studies showed profound effects of AHSCT in halting disease activity and preventing disability in RRMS patients. The findings of the clinical studies and the recommendations of the guidelines are likely to be applicable to the Canadian context.
Conclusions and Implications for Decision- or Policy-Making
Two RCTs16,17 and 4 retrospective cohort studies18-21 were included to address the clinical effectiveness of AHSCT in patients with MS. Two evidence-based guidelines12,22 on the use of AHSCT in MS were identified. No studies regarding the cost-effectiveness of AHSCT for MS were identified.
Compared to ALZ or other DMTs, patients in the AHSCT group had significant improvement in clinical outcomes including disease progression, clinical relapse, NRS, MSFC score, and NEDA. Patients treated with AHSCT also experienced improvement in quality of life and a decrease in MRI activity such as new T2 lesions and Gd-enhancing lesions. For safety, there was no treatment-related mortality or life-threatening complications including PML after treatment with AHSCT. The most common AEs in the first 100 days after AHSCT treatment were febrile neutropenia, organ infections, sepsis and viral reactivations (e.g., Epstein-Barr virus, cytomegalovirus, varicella-zoster virus). Long-term AEs included the development of new autoimmune diseases, mainly thyroid disease. Studies comparing different AHSCT conditioning regimens such as myeloablative and non-myeloablative were not identified. Thus, AHSCT appears to be efficacious with expected adverse events. Treatment with DMTs including ALZs and MTZ were also associated with high rates of infection. Thyroid disease occurred more frequent in the patients treated with ALZ compared to AHSCT patients. The identified guidelines recommend the use of AHSCT as standard of care for the treatment of highly active RRMS patients refractory to DMTs and suggest that the treatment may be appropriate for progressive forms of MS with an active inflammatory component. As the follow-up period was 3 years in most included studies, longer-term efficacy and safety data of AHSCT remain to be determined. The findings in this report should be interpreted with caution because of some limitations of the included studies (e.g., small sample sizes, and limited in study design). Future large and well-designed RCTs with inclusion of more recent and potent DMTs are warranted to further evaluate the role of AHSCT in MS with longer-term efficacy and safety data. Moreover, trials aiming at refining treatment procedure by comparing different conditioning regimens are also needed.
References
1.MS Society of Canada. Prevalence and incidence of MS in Canada and around the world. 2020; https://mssociety.ca/research-news/article/prevalence-and-incidence-of-ms-in-canada-and-around-the-world#:~:text=Canada%20continues%20to%20have%20one,MS%20%E2%80%93%201%20in%20every%20400. Accessed 2021 Apr 22.
2.National Multiple Sclerosis Society. Types of MS. 2020; https://www.nationalmssociety.org/What-is-MS/Types-of-MS. Accessed 2021 Apr 22.
3.Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162-173. PubMed
4.Barnett Y, Garber JY, Barnett MH. MRI biomarkers of disease progression in multiple sclerosis: old dog, new tricks? Quant Imaging Med Surg. 2020;10(2):527-532. PubMed
5.Multiple Sclerosis Society of Canada. Relapses and relapse management. 2017; https://mssociety.ca/library/document/XtQHJqhSi1CGjrzKMgeNUuAc5kBPv3Wy/original.pdf. Accessed 2021 Apr 22.
6.Manouchehrinia A, Beiki O, Hillert J. Clinical course of multiple sclerosis: a nationwide cohort study. Mult Scler. 2017;23(11):1488-1495. PubMed
7.Fambiatos A, Jokubaitis V, Horakova D, et al. Risk of secondary progressive multiple sclerosis: a longitudinal study. Mult Scler. 2020;26(1):79-90. PubMed
8.MS Society of Canada. Disease-modifying therapies. 2021; https://mssociety.ca/managing-ms/treatments/medications/disease-modifying-therapies-dmts. Accessed 2021 Apr 22.
9.Vargas DL, Tyor WR. Update on disease-modifying therapies for multiple sclerosis. J Investig Med. 2017;65(5):883-891. PubMed
10.Mariottini A, De Matteis E, Muraro PA. Haematopoietic stem cell transplantation for multiple sclerosis: current status. BioDrugs. 2020;34(3):307-325. PubMed
11.Jessop H, Farge D, Saccardi R, et al. General information for patients and carers considering haematopoietic stem cell transplantation (HSCT) for severe autoimmune diseases (ADs): a position statement from the EBMT Autoimmune Diseases Working Party (ADWP), the EBMT Nurses Group, the EBMT Patient, Family and Donor Committee and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Bone Marrow Transplant. 2019;54(7):933-942. PubMed
12.Sharrack B, Saccardi R, Alexander T, et al. Autologous haematopoietic stem cell transplantation and other cellular therapy in multiple sclerosis and immune-mediated neurological diseases: updated guidelines and recommendations from the EBMT Autoimmune Diseases Working Party (ADWP) and the Joint Accreditation Committee of EBMT and ISCT (JACIE). Bone Marrow Transplant. 2020;55(2):283-306. PubMed
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Apr 22.
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
16.Burt RK, Balabanov R, Burman J, et al. Effect of nonmyeloablative hematopoietic stem cell transplantation vs continued disease-modifying therapy on disease progression in patients with relapsing-remitting multiple sclerosis: a randomized clinical trial. JAMA. 2019;321(2):165-174. PubMed
17.Mancardi GL, Sormani MP, Gualandi F, et al. Autologous hematopoietic stem cell transplantation in multiple sclerosis: a phase II trial. Neurology. 2015;84(10):981-988. PubMed
18.Alping P, Burman J, Lycke J, Frisell T, Piehl F. Safety of alemtuzumab and autologous hematopoietic stem cell transplantation compared to noninduction therapies for multiple sclerosis. Neurology. 2021;96(11):e1574-e1584. PubMed
19.Zhukovsky C, Sandgren S, Silfverberg T, et al. Autologous haematopoietic stem cell transplantation compared with alemtuzumab for relapsing-remitting multiple sclerosis: an observational study. J Neurol Neurosurg Psychiatry. 2021;92(2):189-194. PubMed
20.Boffa G, Lapucci C, Sbragia E, et al. Aggressive multiple sclerosis: a single-centre, real-world treatment experience with autologous haematopoietic stem cell transplantation and alemtuzumab. Eur J Neurol. 2047;27(10):2047-2055.
21.Mariottini A, Innocenti C, Forci B, et al. Safety and efficacy of autologous hematopoietic stem-cell transplantation following natalizumab discontinuation in aggressive multiple sclerosis. Eur J Neurol. 2019;26(4):624-630. PubMed
22.Cohen JA, Baldassari LE, Atkins HL, et al. Autologous hematopoietic cell transplantation for treatment-refractory relapsing multiple sclerosis: position statement from the American Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant. 2019;25(5):845-854. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Burt et al., 201916 US Funding: No industry support or pharmaceutical support | Phase III, open-label, multicenter, parallel, 1:1 RCT Sample size determination: Yes ITT analysis: No Adjustment for multiple comparisons: No | Patients with RRMS (N = 110) Mean age, years:
% female:
Mean duration of disease, months:
Mean EDSS:
Mean number of Gd-enhancing lesions on MRI:
Mean MRI T2-weighted lesion volume, cm3
| Non-myeloablative HSCT (n = 55): DMT was discontinued and variable washout periods were observed before admission for HSCT. DMT (n = 55): Received an FDA-approved DMT of higher efficacy or a different class than the therapy taken at the time of randomization. Could also receive immune-modulating or immunosuppressive drugs. Ocrelizumab and alemtuzumab were excluded. Patients experiencing progression of disability after at least 1 year of treatment were allowed to cross over to receive HSCT. | Primary Outcome: Disease progression (an increase in EDSS score of at least 1 point on 2 evaluations 6 months apart after at least 1 year of treatment) Secondary Outcomes:
Post-hoc Outcomes:
Adverse events: Transplantation-related; hospitalizations; ED visits; infections; new medical problems Follow-up: 5 years |
Mancardi et al., 210517 Italy Funding: Italian Multiple Sclerosis Foundation | phase II, open-label, multicenter, parallel, 1:1 RCT Sample size determinations: Yes ITT analysis: Yes Adjustment for multiple comparison: No | Patients with a defined MS (secondary-progressive MS or RRMS) (N = 21) Mean age, years:
% female:
Median EDSS (range)
Mean disease duration (range), years:
| Myeloablative AHSCT (n = 9) MTX (n = 12): 20 mg every month for 6 months | Primary Outcomes:
Secondary Outcomes:
Safety:
Follow-up: 4 years |
Alping et al., 202118 Sweden Funding: Patient-Centered Outcomes Research Institute award. | Retrospective cohort study Sample size determination: No Adjustment for covariates: No | Patients with MS (mainly RRMS) (N = 271) Mean age, years: 34.0 % female: 65.0 Mean MS duration, years: 6.7 MS type, %:
Mean EDSS score: 3.1 | Both non-myeloablative and myeloablative AHSCT (n = 139) ALZ (n = 132) Matched non-induction therapies (Natalizumab, dimethyl fumarate, rituximab, fingolimod; n = 2,486) | Outcomes:
Follow-up: 3 years |
Zhukovsky et al., 202119 Sweden Funding: No industry support or pharmaceutical support | Retrospective cohort study Sample size determination: No Adjustment for covariates: No | Patients with RRMS treated with AHSCT or alemtuzumab from 1 January 2011 to 31 December 2018 (N = 144) Median age (IQR):
% female:
Mean duration of disease, years:
ARR 1 year before treatment:
Median EDSS (IQR):
Median ARMSS (IQR):
| Non-myeloablative AHSCT (n = 69) ALZ (n = 75): 60 mg over 5 days and a repeated dose of 36 mg over 3 days after 1 year. New courses of 36 mg were administered if clinical relapses and/or new MRI lesions occurred. | Primary Outcomes:
Secondary Outcomes:
Follow-up: 3 years |
Boffa et al., 202020 Italy Funding: Did not receive any funding support | Retrospective cohort study Sample size determination: No Adjustment for covariates: Yes | Patients with aggressive RRMS (multiple [≥ 2] relapses with incomplete resolution in the past year; > 2 MRI scans showing new or enlarging T2 lesions or Gd-enhancing lesions despite active treatment; or EDSS score ≥ 4 within 5 years of onset; no response to therapy with 1 or more DMTs for up to 1 year) (N = 57) Mean age, years:
% female:
Median EDSS (IQR):
Mean disease duration, years:
Mean ARR:
MRI activity, %:
Mean number of Gd-enhancing lesions:
Mean follow-up, months:
| Myeloablative AHSCT (n = 25) ALZ (n = 32): 12 mg per day on 5 consecutive days and the second of 12 mg per day on 3 consecutive days, 12 months apart. | Outcomes: Primary:
Secondary:
Follow-up: 3 years |
Mariottini et al., 201921 Italy Funding: Not reported | Retrospective cohort study | Patients with RRMS who discontinued from natalizumab after at least 6 administrations and with at least 6 months of follow-up (N = 55) Median age (IQR), years:
% female:
Median disease duration (IQR), years:
Median EDSS score (IQR):
| Myeloablative AHSCT (n = 11) DMT (n = 41): First-line (interferons, glatiramer acetate, dimethyl fumarate) or second-line (fingolimod, alemtuzumab, rituximab, cyclophosphamide, mitoxantrone) | Outcomes:
Follow-up: 3 years |
AE = adverse event; AHSCT = autologous hematopoietic stem cell transplantation; ALZ = alemtuzumab; ARMSS = age-related multiple sclerosis severity score; ARR = annualized relapse rate; CDI = confirmed disability improvement; CDW = confirmed disability worsening; DMT = disease-modifying therapy; EDSS = Expanded Disability Status Scale; FDA = FDA; Gd = gadolinium; HSCT = hematopoietic stem cell transplantation; IQR = interquartile range; IQR = interquartile range; ITT = intention-to-treat; MCID = minimal clinically important difference; MRI = MRI; MSFC = Multiple Sclerosis Functional Composite; MTX = mitoxantrone; MS = multiple sclerosis; NEDA = no evidence of disease activity; NRS = Neurologic Rating Scale; PASAT = Paced Auditory Serial Addition Test; PPMS = primary-progressive MS; QoL = quality of life; RCT = randomized controlled trial; RRMS = relapse-remitting multiple sclerosis; SF-36 = Short Form 36; SPMS = secondary-progressive MS.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
EBMT, Sharrack et al., 202012 | ||||||
Intended users: Transplant physicians, nurses, neurologists Target population: Not primarily targeted at patients, families, and non-specialist health professional carers | HSCT in MS and immune-mediated neurologic diseases | Efficacy and safety of AHSCT | Evidence was found from PubMed searches and recent EBMT congress presentations. Evidence selection and synthesis: Not reported | Evidence levels (I, II, III)a based on consideration of health benefits, side effects and risks, and balanced against non-HSCT options. Recommendationsb were classified as S, CO, D or GNR | Updated of its previous guidelines Recommendations were developed by clinicians, nurses, statisticians and data management persons, all with experience in HSCT. Each recommendation provides potential for auditing clinical practice. The guideline considers resource implications and other issues relevant to implementations of HSCT. | Published in peer-reviewed journal |
ASBMT, Cohen et al., 201922 | ||||||
Intended Users: Neurologists in treating MS and transplantation physicians with experience in AHSCT Target Population: Patients with MS | AHSCT in MS | Efficacy and safety of AHSCT in MS | Evidence identified from the Embase and Ovid MEDLINE databases. One author reviewed all search results. Evidence selection and synthesis: Not reported | Evidence quality assessment: None, just by consensus from a panel of experts (expert opinion) | Updated of its previous guidelines Recommendations were developed by a panel of experts in AHSCT and MS. | Published in peer-reviewed journal |
AHSCT = autologous hematopoietic stem cell transplantation; ASBMT = American Society for Blood and Marrow Transplantation; HSCT = Hematopoietic stem cell transplantation; EBMT = European Group for Blood and Marrow Transplantation; MS = multiple sclerosis; RCT = randomized controlled trial.
Note that this table has been formatted for accessibility but has not been copy-edited.
aLevels of evidence:
I: from at least on well-executed RCT.
II: from at least 1 well-designed clinical trial without randomization; cohort or case-controlled analytic studies (preferably from more than 1 centre); multiple time-series studies; or dramatic results from uncontrolled experiments.
III: from opinions of respected authorities based on clinical experience, descriptive studies, or reports from expert committees.
bRecommendations:
S: Standard of care – Indications categorized as S are reasonably well defined and results compare favourably (or are superior) to those of non-transplant treatment approaches.
CO: clinical option – The CO category applies to indications for which the results of small patient cohorts show efficacy and acceptable toxicity of the HSCT procedure, but confirmatory randomized studies are missing, often as a result of low patient numbers.
D: Developmental – Indications have been classified as D when the experience is limited, and additional research is needed to define the role of HSCT.
GNR = Generally not recommended – The GNR category comprises a variety of clinical scenarios in which the use of HSCT cannot be recommended to provide a clinical benefit to the patient, including early disease stages when results of conventional treatment do not normally justify the additional risk of a HSCT, very advanced forms of a disease in which the chance of success is so small that does not justify the risks for patient and donor, and indications in which the transplant modality may not be adequate for the characteristics of the disease.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist13
Item | Burt et al., 201916 | Mancardi et al., 201517 | Alping et al., 202118 | Zhukovsky et al., 202119 | Boffa et al., 202020 | Mariottini et al., 201921 |
Reporting | ||||||
1. Is the hypothesis/aim/objective of the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
2. Are the main outcomes to be measured clearly described in the Introduction or Methods section? | Yes | Yes | Yes | Yes | Yes | Yes |
3. Are the characteristics of the patients included in the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
4. Are the interventions of interest clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
5. Are the distributions of principal confounders in each group of subjects to be compared clearly described? | NA – RCT, characteristic balanced between groups | NA – RCT, characteristic balanced between groups | Yes | Yes | Yes | NA –characteristic balanced between groups |
6. Are the main findings of the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
7. Does the study provide estimates of the random variability in the data for the main outcomes? | Yes – 95% CI provided | Yes – 95% CI provided | Yes – 95% CI provided | Yes – 95% CI provided | Yes – 95% CI provided | Yes – interquartile range provided |
8. Have all important adverse events that may be a consequence of the intervention being reported? | Yes | Yes | Yes – mainly reported on safety data | Yes | Yes | Yes |
9. Have the characteristics of patients lost to follow-up been described? | No | NA – no patients lost to follow-up | NA – retrospective study | NA – retrospective study | NA – retrospective study | NA – retrospective study |
10. Have actual P values been reported (e.g., 0.035 rather than < 0.05) for the main outcomes except where the P value is less than 0.001? | Yes | Yes | Yes | Yes | Yes | Yes |
External validity | ||||||
11. Were the subjects asked to participate in the study representative of the entire population from which they were recruited? | Probably no – from 4 centres | No – small sample size | NA – retrospective study | NA – retrospective study | NA – retrospective study | NA – retrospective study |
12. Were the subjects who were prepared to participate representative of the entire population from which they were recruited? | Probably no – only 12% included | No | NA – retrospective study | NA – retrospective study | NA – retrospective study | NA – retrospective study |
13. Were the staff, places, and facilities where the patients were treated, representative of the treatment the majority of the patients receive? | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity – bias | ||||||
14. Was an attempt made to blind study subjects to the intervention they have received? | No – not possible | No – not possible | NA – retrospective study | NA – retrospective study | NA – retrospective study | NA – retrospective study |
15. Was an attempt made to blind those measuring the main outcomes of the intervention? | No – not possible | No – not possible | NA – retrospective study | NA – retrospective study | NA – retrospective study | NA – retrospective study |
16. If any of the results of the study were based on “data dredging”, was this made clear? | NA | NA | NA | NA | NA | NA |
17. In trials and cohort studies, so the analyses adjust for different lengths of follow-up of patients, or in case-control studies, is the time period between the intervention and outcome the same for cases and controls? | Yes | Yes | Yes | Yes | Yes | Yes |
18. Were the statistical tests used to assess the main outcomes appropriate? | Yes | Yes | Yes | Yes | Yes | Yes |
19. Was compliance with the intervention/s reliable? | NA | NA | NA | NA | NA | NA |
20. Were the main outcome measures used accurate (valid and reliable)? | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity – confounding (selection bias) | ||||||
21. Were the patients in different intervention groups (trials and cohort studies) or were the cases and controls (case-control studies) recruited from the same population? | Yes | Unclear | Yes – From the Swedish Multiple Sclerosis Register | Yes | Yes | Yes |
22. Were study subjects in different intervention groups (trial and cohort studies) or were the cases and controls (case-controls studies) recruited over the same period of time? | Yes – between 2005 to 2016 | Yes | Yes | Yes – between 1 January 2011 to 31 December 2018 | Unclear | Yes – between January 2010 to June 2016 |
23. Were study subjects randomized to intervention groups? | Yes | Yes | No | No | No | No |
24. Was the randomized intervention assignment concealed from both patients and health care staff until recruitment was complete and irrevocable? | Unclear | Unclear | NA | NA | NA | NA |
25. Was the adequate adjustment for confounding in the analyses from which the main findings were drawn? | NA – RCT | NA – RCT | No | No | Yes – multivariate analysis | No |
26. Were losses of patients to follow-up taken into account? | No – no ITT analysis | NA – all patients were follow-up | NA – retrospective study | NA – retrospective study | NA – retrospective study | NA – retrospective study |
27. Did the study have sufficient power to detect a clinically important effect where the P value for a difference being due to chance is less than 5%? | Yes – sample size determination | Yes – sample size determination | No – no sample size determination | No – no sample size determination | No – no sample size determination | No – no sample size determination |
ITT = intention-to-treat; NA = not applicable; RCT = randomized controlled trial.
Table 5: Strengths and Limitations of Guidelines Using AGREE II14
Item | EBMT, Sharrack et al., 202012 | ASBMT, Cohen et al., 201922 |
Domain 1: Scope and Purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder Involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: Rigour of Development | ||
7. Systematic methods were used to search for evidence. | NR | NR |
8. The criteria for selecting the evidence are clearly described. | NR | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | No |
10. The methods for formulating the recommendations are clearly described. | NR | NR |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Probably yes | Probably yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes |
Domain 4: Clarity of Presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | Yes | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes | No |
21. The guideline presents monitoring and/or auditing criteria. | Yes | No |
Domain 6: Editorial Independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ASBMT = American Society for Blood and Marrow Transplantation; EBMT = European Group for Blood and Marrow Transplantation; NR = not reported; NA = not applicable.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Summary of Findings of Included Primary Clinical Studies
Main study findings
Burt et al., 201916
Non-myeloablative hematopoietic stem cell therapy (HSCT) (n = 55) versus DMT (n = 55)
Primary end point
Disease progression (EDSS score increase of ≥ 1):
HSCT: 3 patients
DMT: 34 patients
Follow-up: median, 2 years; mean, 2.8 years
Median time to progression:
HSCT: not estimable due to too few events
DMT: 24 months (interquartile range [IQR], 18 to 48 months)
hazard ratio (HR) (95% CI) = 0.07 (0.02 to 0.24); P < 0.001
Proportion of patients with disease progression:
HSCT:
One year and 2 years: 1.92% (95% CI, 0.27 to 12.9)
Three years: 5.19% (95% CI, 1.26 to 20.1)
Four and 5 years: 9.71% (95% CI, 3.0 to 28.8)
DMT:
One year: 24.5% (95% CI, 14.7 to 39.1)
Two years: 54.5% (95% CI, 40.7 to 69.4)
Three years: 62.5% (95% CI, 48.3 to 76.7)
Four years: 71.2% (95% CI, 56.8 to 84.2)
Five years: 75.3% (95% CI, 60.4 to 87.8)
Secondary end points
Death:
HSCT: 0
DMT: 0
Relapse in the first year:
HSCT: 2%
DMT: 69%
Between-group difference: 78% (95% CI, 64 to 88); P < 0.001
Proportion of patients with relapse:
HSCT:
Six months: 0%
One year: 1.92% (95% CI, 0.27 to 12.9)
Two years: 7.69% (95% CI, 2.96 to 19.2)
Three years: 9.61% (95% CI, 4.1 to 22)
Four and 5 years: 15.4% (95% CI 8.01 to 28.4)
DMT:
Six months: 51.9% (39.9 to 65.6)
One year: 64.8% (95% CI, 52.2 to 77.2)
Two years: 72.2% (95% CI, 66 to 87.7)
Three and 4 years: 79.63% (95% CI, 68.1 to 89.1)
Five years: 85.2% (95% CI, 74.5 to 93.1)
Mean change in EDSS score from baseline to 1 year:
HSCT: –1.02 (improved)
DMT: + 0.67 (worsened)
Between-group difference: –1.7 (95% CI, –2.03 to –1.29); P < 0.001
Mean change in NRS score from baseline to 1 year:
HSCT: + 8.8 (improved)
DMT: –1.6 (worsened)
Between-group difference: + 11.2 (95% CI, + 8.08 to + 14.29); P = 0.001
Mean change in MRI T2-weighted lesion volume from baseline to 1 year:
HSCT: –31.7% (improved)
DMT: + 34.3% (worsened)
Between-group difference: –66% (95% CI, –70.6 to –61.3); P < 0.001
Mean change in timed 25-feet walk from baseline to 1 year:
HSCT: –0.5 second (improved)
DMT: + 1.3 second (worsened)
Between-group difference: –2.85 second (95% CI, –3.92 to –1.77); P < 0.001
Mean change in 9-Hole Peg Test from baseline to 1 year:
HSCT: –6.8 second (improved)
DMT: + 0.9 second (worsened)
Between-group difference: –8.03 second (95% CI, –11.3 to –4.76); P < 0.001
Mean change in Paced Auditory Serial Addition Test from baseline to 1 year:
HSCT: + 10.4% (improved)
DMT: + 10.2% (improved)
Between-group difference: + 0.22% (95% CI, –72.4 to + 72.9); P = 0.61
Mean change in MSFC score from baseline to 1 year:
HSCT: + 0.32 (improved)
DMT: –0.31 (worsened)
Between-group difference: + 0.51 (95% CI, + 0.28 to + 0.72); P < 0.001
Mean change in SF-36 quality of life score from baseline to 1 year:
HSCT: + 19.5 (improved)
DMT: –3.4 (worsened)
Between-group difference: + 23 (95% CI, + 17.6 to + 28.9); P < 0.001
Post-hoc analysis
Median time to first relapse:
HSCT: not estimable due to too few events
DMT: 6 months (IQR, 3 to 36 months)
HR (95% CI) = 0.097 (0.045 to 0.208); P < 0.001
Proportion with NEDA:
HSCT:
Six months and 1 year: 98.1% (95% CI, 87.4 to 99.7)
Two years: 93.3% (95% CI, 80.6 to 97.8)
Three years: 90.3% (95% CI, 75.9 to 96.3)
Four and 5 years: 78.5% (95% CI, 59.8 to 89.5)
- DMT:
Six months: 39.6% (95% CI, 26.6 to 52.39)
One year: 20.8% (95% CI, 11 to 32.5)
Two years: 11.9% (95% CI, 4.3 to 23.6)
Three years: 5.93 (95% CI, 1.17 to 16.6)
Four and 5 years: 2.97% (95% CI,0.24 to 12.8)
Outcomes of patients in the DMT groups who crossed over to HSCT:
For 5 years after transplantation, 31 patients crossed over from DMT to HSCT. There was significant improvement in EDSS scores, NRS scores, and T2-weighted lesion volume percentages.
The results of combined group (52 + 31 = 83 patients) who underwent HSCT were comparable with those for the HSCT group alone (n = 52 patients).
Adverse events:
- HSCT:
Median day of white blood cell engraftment (absolute neutrophil count > 1000/µL): 9 days
Hospital day: 10 days
No Common Toxicity Criteria grade 4 nonhematopoietic toxicity (e.g., myocardial infarction, embolism, dialysis, sepsis, or need for pressor support), transfer to intensive care unit, parenteral nutrition, surgery, or other disabling or potential life-threatening events.
Inpatient grade 3 toxicities infections: Clostridium difficile diarrhea (n = 1), Escherichia coli urinary tract infection (n = 1), culture-negative pneumonia (n = 1)
Post-transplantation infections: 16 upper respiratory tract infections (7 sinusitis, 2 bronchitis, 2 undefined pneumonia, 2 streptococcal pharyngitis, 1 influenza, 1 respiratory syncytial virus, 1 Mycoplasma pneumoniae), 6 urinary tract infections, 2 C difficile diarrhea, and 7 dermatomal varicella-zoster reactivations.
No early or late fungal, Pneumocystis jirovecci, cytomegalovirus, John Cunningham virus infections in either group.
- DMT:
Post-transplantation infections: 15 upper respiratory tract infections (6 sinusitis, 2 bronchitis, 2 influenza, 1 streptococcal pharyngitis, 1 undefined pneumonia, 1 Mycoplasma pneumoniae, 1 tooth abscess, and 1 otitis media), 8 urinary tract infections, and 2 varicella-zoster reactivations.
Rate of infection per patient per year:
HSCT: 0.19
DMT: 0.23
Author’s conclusion
“In this preliminary study of patients with relapsing-remitting MS, nonmyeloablative HSCT, compared to DMT, results in prolonged time to disease progression. Further research is needed to replicate these findings and to assess long-term outcomes and safety.”16 (p. 165)
Main study findings
Mancardi et al., 201517
Myeloablative AHSCT (n = 9) versus MTX (n = 12)
MRI outcomes for 17 patients (AHSCT [n = 8] versus MTX [n = 9]; lost 4 patients [1 in HSCT, 3 in MTX])
- New T2 lesions over 4 years:
AHSCT: Median = 2.5; mean = 2.75; range = 0 to 8
MTX: Median = 8; mean = 12.75; range = 2 to 34
Rate ratio (RR) (95% CI) = 0.21 (0.10 to 0.48); P = 0.00016
Worst case scenario: RR (95% CI) = 0.32 (0.16 to 0.66); P = 0.002
Best case scenario: RR (95% CI) = 0.19 (0.09 to 0.41); P < 0.0001
Adjusting for baseline Gd + lesions: RR (95% CI) = 0.19 (0.09 to 0.41); P < 0.0001
Using PP population: RR (95% CI) = 0.18 (0.06 to 0.52); P < 0.0001
Applying a mixed effects model with new T2 lesions on each MRI scan over time: RR (95% CI) = 0.28 (0.13 to 0.62); P = 0.002
Imputing the 4 missing patients as having 0 new T2 lesions: RR (95% CI) = 0.25 (0.05 to 0.74); P = 0.012
Imputing the 4 missing patients as having 35 new T2 lesions: RR (95% CI) = 0.34 (0.15 to 0.82); P = 0.016
Excluding 2 outliers in the MTX group: RR (95% CI) = 0.39 (0.22 to 0.69); P = 0.001
Gd + lesions during 4 years:
AHSCT: 0
MTX: 56% had at least 1 Gd + lesion; P = 0.029
Results did not change when adjusting for disease phase (relapsing-remitting versus progressive)
Clinical outcome, disability, and relapses for 20 out of 21 randomized patients (AHSCT [n = 9] versus MTX [n = 11])
ARR:
AHSCT: 0.19
MTX = 0.6
RR (95% CI) = 0.36 (0.15 to 0.88); P = 0.026
Progression at end of follow-up:
AHSCT: 57%
MTX = 48%; P = 0.50
EDSS change: No differences between groups at year 1, 2, 3 and 4
Safety (no statistical comparison)
Mortality: None was found in both groups
Early AEs:
AHSCT:
Grade 3: Febrile neutropenia, leukopenia, anemia, platelet count decrease, amenorrhea, leukopenia,
Grade 4: Leukopenia, anemia, platelet count decreased
MTX:
Grade 3: Neutrophil count decreased, amenorrhea, leukopenia, lymphocyte count decreased
Grade 4: Neutrophil count decreased
Severe AEs:
AHSCT: Sepsis, late engraftment, prolonged hospitalization, systemic candidiasis, cytomegalovirus (CMV) reactivation, engraftment failure.
MTX: None
Author’s conclusion
“Intense immunosuppression followed by AHSCT is significantly superior to MTX in reducing MRI activity in severe cases of MS. These results strongly support further phase III studies with primary clinical endpoints.”17 (p. 981)
Main study findings
Alping et al., 202118
Myeloablative AHSCT (n = 139) versus ALZ (n = 132) versus matched patients treated with non-induction therapies (Natalizumab, dimethyl fumarate, rituximab, fingolimod; n = 2,486)
Safety
Mortality:
AHSCT: 1 death (suicide); IR per 1,000 person-years (95% CI) = 1.7 (0.0 to 9.6)
ALZ: 4 deaths (2 suicides, 1 heart attack, 1 CMV reactivation); IR per 1,000 person-years (95% CI) = 8.6 (2.3 to 22.0)
Matched: 7 deaths; IR per 1,000 person-years (95% CI) = 0.7 (0.3 to 1.3)
Thyroid disease:
AHSCT: 14; IR per 1,000 person-years (95% CI) = 34 (18 to 56)
ALZ: 32; IR per 1,000 person-years (95% CI) = 109 (75 to 154)
Matched: 45; IR per 1,000 person-years (95% CI) = 5.3 (3.9 to 7.1)
Non-thyroid autoimmune disease:
AHSCT: 1; IR per 1,000 person-years (95% CI) = 2.6 (0.1 to 14.5)
ALZ: 1; IR per 1,000 person-years (95% CI) = 3.0 (0.1 to 16.8)
Matched: 28; IR per 1,000 person-years (95% CI) = 3.4 (2.3 to 4.9)
Any infection:
AHSCT: 66; IR per 1,000 person-years (95% CI) = 275 (213 to 350)
ALZ: 19; IR per 1,000 person-years (95% CI) = 56 (34 to 87)
Matched: 405; IR per 1,000 person-years (95% CI) = 52 (47 to 58)
The incidence of infection was highest immediately after AHSCT but dropped to a level closer to alemtuzumab and matched control groups.
Infection diagnosed ≥ 6 months from therapy initiation:
AHSCT: 35; IR per 1,000 person-years (95% CI) = 108 (75 to 150)
ALZ: 15; IR per 1,000 person-years (95% CI) = 53 (30 to 87)
Matched: 349; IR per 1,000 person-years (95% CI) = 51 (46 to 57)
Types of infections:
AHSCT: Varicella zoster, herpes infections, bacterial sepsis
ALZ: Varicella zoster, herpes infections, bacterial sepsis
Systemic antibiotics were given to all patients after AHSCT and to a majority of patients after ALZ.
Author’s conclusion
“We confirmed a higher incidence of thyroid disease in alemtuzumab- and, to a smaller extent, AHSCT-treated patients and found a higher incidence of infection for AHSCT compared to both alemtuzumab and noninduction therapies. The incidence of non-thyroid autoimmune disease was low for both therapies.”18 (p. e1574)
Main study findings
Zhukovsky et al., 202119
Non-myeloablative AHSCT (n = 69) versus ALZ (n = 75)
Primary end point
NEDA at 3 years:
AHSCT: 88% (95% CI, 80 to 97)
ALZ: 37% (95% CI, 26 to 52); P < 0.0001
Freedom from MRI events:
AHSCT: 93% (95% CI, 86 to 99)
ALZ: 55% (95% CI, 44 to 69); P < 0.0001
Freedom from clinical relapses:
AHSCT: 93% (95% CI, 86 to 100)
ALZ: 70% (95% CI, 59 to 83); P = 0.005
Freedom from confirmed disability worsening (CDW):
AHSCT: 97% (95% CI, 93 to 100)
ALZ: 82% (95% CI, 73 to 92); P = 0.02
Secondary end points
ARR:
AHSCT: 0.04
ALZ: 0.1; P = 0.03
Proportions of patients who improved, stable or worsened:
AHSCT: 57%, 41%, 1%
ALZ: 45%, 43%, 12%; P = 0.06
Median (IQR) EDSS change:
AHSCT:
One year: –1 (–1.5 to 0)
Two years: –1 (–2 to –0.5)
Three years: –1 (–2.5 to –0.5)
ALZ:
One year: 0 (–0.5 to 1.3); P < 0.0001
Two years: 0 (–0.5 to 0.5); P < 0.0001
Three years: 0 (–0.5 to 1); P < 0.0001
Early AEs (during the first 100 days) grade ≥ 3:
AHSCT: 48 of 69 (70%); febrile neutropenia (58%), hypokalemia (19%)
ALZ: none
Late AEs grade 3:
AHSCT: 1.4%; Lyme neuroborreliosis (n = 1)
ALZ: 6.7%; immune mediated thrombocytopenia (n = 4), breast cancer (n = 1)
Autoimmune AEs:
AHSCT: 14 (20%); thyroid disease (n = 13; 19%)
ALZ: 35 (47%); thyroid disease (n = 31; 41%)
Kaplan-Meier estimates of thyroid disease at 3 years (AHSCT: 21%; ALZ: 46%; P = 0.005)
Late infection:
AHSCT: 4 herpes zoster (5.8%)
ALZ: 5 herpes zoster (6.7%)
Mortality:
AHSCT: none
ALZ: none
Author’s conclusion
“In this observational cohort study, treatment with AHSCT was associated with a higher likelihood of maintaining ‘no evidence of disease activity’. Adverse events were more frequent with AHSCT in the first 100 days, but thereafter more common in patients treated with ALZ.”19 (p. 189)
Main study findings
Boffa et al., 202020
Myeloablative AHSCT (n = 25) versus ALZ (n = 32)
Primary end point
NEDA at the end of observation:
AHSCT: 75%
ALZ: 56%
HR (95% CI) = 0.27 (0.08 to 0.84); P = 0.023
Relapse-free survival:
AHSCT: 84%
ALZ: 69%
HR (95% CI) = 0.13 (0.02 to 0.63); P = 0.012
MRI-activity-free survival:
AHSCT: 85%
ALZ: 59%
HR (95% CI) = 0.13 (0.03 to 0.59); P = 0.009
CDW:
AHSCT: 88%
ALZ: 94%
HR (95% CI) = 0.25 (0.02 to 2.86); P = 0.263
Secondary outcomes
ARR at 12 months:
AHSCT: 0.0
ALZ: 0.17; P = 0.03
ARR at 24 months:
AHSCT: 0.1
ALZ: 0.09; NS
ARR at 36 months:
AHSCT: 0.05
ALZ: 0.35; P = 0.02
EDSS improvement: AHSCT promoted significant EDSS improvement compared with ALZ (P = 0.035)
Safety
Serious infusion associated reactions:
AHSCT: 8
ALZ: 1
Serious infectious AEs:
AHSCT: 24 (16 neutropenic fever, 8 sepsis)
ALZ: 3 (1 neutropenic fever, 2 pneumonia)
CMC reactivation:
AHSCT: 2
ALZ: 0
Herpes simplex virus 1:
AHSCT: 1
ALZ: 3
Varicella-zoster virus:
AHSCT: 1
ALZ: 0
Monoclonal gammopathy of undetermined significance:
AHSCT: 1
ALZ: 1
Autoimmune disorders
AHSCT: 3 (1 thyroid disorder, 1 myositis, 1 asthma)
ALZ: 14 (9 thyroid disorders, 2 autoimmune thrombocytopenia, 2 psoriasis, 1 asthma)
Author’s conclusion
“Alemtuzumab and AHSCT are effective treatment choices for aggressive multiple sclerosis. AHSCT seems to be superior to alemtuzumab in inducing complete disease control and on promoting short-term disability improvement.”20 (p. 2047)
Main study findings
Mariottini et al., 201921
Myeloablative AHSCT (n = 11) versus DMT (n = 41) in patients withdrew from natalizumab (NTZ) treatment
Safety/AEs after AHSCT
Mortality or life-threatening complications, including PML: none
Fever of unknown origin: 5
Epstein-Barr virus reactivation: 5
Gastrointestinal AEs: 4
Pneumonia: 3
Enteritis: 2
Oral mucositis: 2
CMV reactivation: 2
Urinary infection: 1
Varicella-zoster reactivation: 1
Cutaneous erythema: 1
Autoimmune thyroiditis: 1
NEDA at 3 years of follow-up:
AHSCT: 54.5%
DMT: 11.5%; P = 0.0212
ARR (clinical relapses):
AHSCT: 0.0
DMT: 0.67; P < 0.0001
Disability worsening:
AHSCT:
Median (IQR) EDSS scores at baseline: 3.25 (2.0 to 4.5)
Median (IQR) EDSS scores at 3 years follow-up: 3.75 (2.0 to 4.5)
DMT:
Median (IQR) EDSS scores at baseline: 2.0 (1.5 to 4.5)
Median (IQR) EDSS scores at 3 years follow-up: 4.25 (1.5 to 6.0)
Confirmed improvement of EDSS scores:
AHSCT: 44.4%
DMT: 6.1%; P = 0.013
Conversion to secondary-progressive MS:
AHSCT: 0
DMT: 4; P = 0.566
Author’s conclusion
“These data suggest that an aggressive therapy should be established after NTZ with the shortest possible washout period. AHSCT after 6 months from NTZ withdrawal appears to be safe.”21 (p. 624)
Table 6: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
EBMT, Sharrack et al., 202012 | |
Recommendations of AHSCT for MS:
| Level of evidence: I Strength of recommendation: S |
| Level of evidence: II Strength of recommendation: CO |
| Level of evidence: II Strength of recommendation: CO |
| Level of evidence: II Strength of recommendation: CO |
| Level of evidence: II Strength of recommendation: CO |
ASBMT, Cohen et al., 201922 | |
Position Statement: “The ASBMT Task Force recommends revising the recommended indication for AHCT in MS to ‘standard of care, clinical evidence available’, for patients with relapsing forms of MS (RRMS or progressive MS with superimposed activity) who have prognostic factors that indicate a high risk of future disability, including ongoing clinical relapse or MRI lesion activity despite treatment with available DMTs, especially if disease activity continues despite treatment with high-efficacy DMTs and/or worsening disability.”22 (p. 851) | None |
AHCT = autologous hematopoietic cell transplantation; AHSCT = autologous hematopoietic stem cell transplantation; ASBMT = American Society for Bone Marrow Transplantation; DMT = disease-modifying therapy; EDSS = Expanded Disability Status Scale; Gd = gadolinium; MRI = MRI; MS = multiple sclerosis; PPMS = primary-progressive MS; RRMS = relapsing-remitting MS; SPMS = secondary-progressive MS.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
1.Stem cell transplant for multiple sclerosis: clinical effectiveness, cost-effectiveness, and guidelines (CADTH Rapid response report: reference list). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RA1150%20Stem%20Cell%20Transplant%20for%20MS%20Final.pdf. Accessed 2021 Apr 22.
Additional References
2.Burt RK, Tappenden P, Han X, et al. Health economics and patient outcomes of hematopoietic stem cell transplantation versus disease-modifying therapies for relapsing remitting multiple sclerosis in the United States of America. Mult Scler Relat. 2020;45:102404. PubMed
3.Miller AE, Chitnis T, Cohen BA, et al. autologous hematopoietic stem cell transplant in multiple sclerosis: recommendations of the National Multiple Sclerosis Society. JAMA Neurol. 2021;78(2):241-246. PubMed
4.Laureys G, Willekens B, Vanopdenbosch L, et al. A Belgian consensus protocol for autologous hematopoietic stem cell transplantation in multiple sclerosis. Acta Neurol Belg. 2018;118(2):161-168. PubMed
5.Ge F, Lin H, Li Z, Chang T. Efficacy and safety of autologous hematopoietic stem-cell transplantation in multiple sclerosis: a systematic review and meta-analysis. Neurol Sci. 2019;40(3):479-487. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca