CADTH Health Technology Review
Onabotulinum Toxin A (Botox) for Spasticity in Patients With Acquired Brain Injury
Rapid Review
Authors: Yan Li, Aleksandra Grobelna
Abbreviations
BoNT
botulinum toxin
BoNT-A
botulinum toxin type A
NR
not reported
RCT
randomized controlled trial
SR
systematic review
TBI
traumatic brain injury
Key Messages
No relevant literature was identified regarding the clinical effectiveness or cost-effectiveness of onabotulinum toxin A (Botox) for reducing spasticity in patients with traumatic or non-traumatic–acquired brain injury.
Authors of 1 evidence-based guideline recommend the use of botulinum toxin (subtype and formulation not specified) for the treatment of spasticity associated with traumatic brain injury.
Context and Policy Issues
Acquired brain injury is an umbrella term that encompasses traumatic brain injuries (TBIs) and non-traumatic brain injuries.1 Approximately 150,000 Canadians will sustain an ABI on an annual basis.2 An ABI is damage to the brain that is not due to a congenital or degenerative disorder.1 Occurring after birth, ABI can be caused by a traumatic event or external force (e.g., motor vehicle accident, sports injury), or a non-traumatic event or internal factor (e.g., infection, tumour).1 Injury to the brain can result in temporary or permanent physical (e.g., movement issues, spasticity, chronic pain), cognitive (e.g., impaired speech, memory loss), and/or emotional (e.g., depression, anger issues) impairments.2
As 1 of the major physical impairments resulting from an ABI, muscle spasticity is often described as muscle over-activity and is characterized by ongoing muscle contractions that are partly due to a decrease in skeletal stretch reflex threshold.3 Occurring spontaneously or continuously, spasticity typically affects muscles in the neck and upper and lower limbs.3 Spasticity can result in a variety of musculoskeletal issues such as involuntary shaking, joint stiffness, muscle contracture, and limited range of movement.3 This debilitating condition may limit one’s ability to perform the activities of daily living, impact one’s quality of life, and require additional assistance from caregivers.3
The treatment of ABI-related spasticity can involve a combination of pharmacological and non-pharmacological interventions.3 Non-pharmacological options may include casting and splinting to maintain positioning, stretching and strengthening to improve control of spastic muscles, and/or transcutaneous electric nerve stimulation to help reduce pain.3 Pharmacological options can be administered systemically (e.g., oral baclofen, tizanidine, clonidine, dantrolene sodium) or locally (e.g., injection of botulinum toxin type A [BoNT-A], phenol, baclofen).3 Botulinum toxin (BoNT), a neurotoxic protein produced by Clostridium botulinum bacteria, exists in multiple subtypes (i.e., A to G) and formulations.4
BoNT-A intramuscular injection is used to treat spasticity by inhibiting the release of acetylcholine, a neurotransmitter involved in activating skeletal muscles.3 BoNT-A injections result in temporary local paresis (i.e., partial paralysis) and may help to improve pain.5 BoNT-A is approved for various indications (i.e., not exclusive to spasticity), and is available as 3 formulations in North America: onabotulinum toxin A (Botox), abobotulinum toxin A (Dysport), and incobotulinum toxin A (Xeomin).5 Due to different manufacturing processes and pharmacological activities, these 3 formulations are not considered interchangeable products.4 This report focuses on onabotulinum toxin A, which will be referred to herein as Botox — its brand name.
The body of evidence evaluating treatment options for spasticity after brain injury is limited in quality and quantity, and there is uncertainty regarding the clinical effectiveness of Botox for this population.3 Another 2021 CADTH rapid review report focused on the use of Botox for the treatment of spasticity associated with multiple sclerosis.6 The aim of this rapid review report is to summarize and critically appraise the relevant evidence on the clinical effectiveness, cost-effectiveness, and evidence-based guidelines regarding the use of Botox for the treatment of ABI-associated spasticity.
Research Questions
What is the clinical effectiveness of onabotulinum toxin A (Botox) for reducing spasticity in patients with acquired brain injury?
What is the cost-effectiveness of onabotulinum toxin A (Botox) for reducing spasticity in patients with acquired brain injury?
What are the evidence-based guidelines regarding the use of onabotulinum toxin A (Botox) for reducing spasticity in patients with acquired brain injury?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were onabotulinum toxin A/Botox and brain injury and/or spasticity. No filters were applied to limit the retrieval by study type. The search was also limited to English-language documents published between January 1, 2016 and February 26, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients (any age) with traumatic or non-traumatic acquired brain injury resulting in muscle spasticity, excluding brain injury due to stroke and excluding cerebral palsy (e.g., infants with a brain injury classified under cerebral palsy) Examples of included etiologies: motor vehicle accidents, falls, assaults, gunshot wounds, sports injuries, diffuse brain lesions, anoxia, tumours, aneurysm, vascular malformations, and infections of the brain |
Intervention | Onabotulinum toxin A (Botox) or botulinum toxin A (if onabotulinum toxin A is not specified) |
Comparator | Q1 and Q2: No treatment (e.g., before-and-after studies); standard care (e.g., physical therapy, dantrolene sodium, clonidine, baclofen [intrathecally or orally; Ozobax], tizanidine [Zanaflex], cyclobenzaprine [Flexeril], diazepam [Valium], surgery, serial casting, bracing, orthoses); and other botulinum toxin variants (e.g., incobotulinum toxin A [Xeomin], abobotulinum toxin A [Dysport]) Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., symptoms of spasticity, muscle tightness, quality of life, harms or safety, range of motion) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratios) Q3: Recommendations regarding the dose and use of onabotulinum toxin A for spasticity related to acquired brain injury |
Study designs | HTAs, SRs, RCTs, non-randomized studies, economic evaluations, evidence-based guidelines |
HTA = health technology assessment; Q = question; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews (SRs) were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)7 for SRs and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument8 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
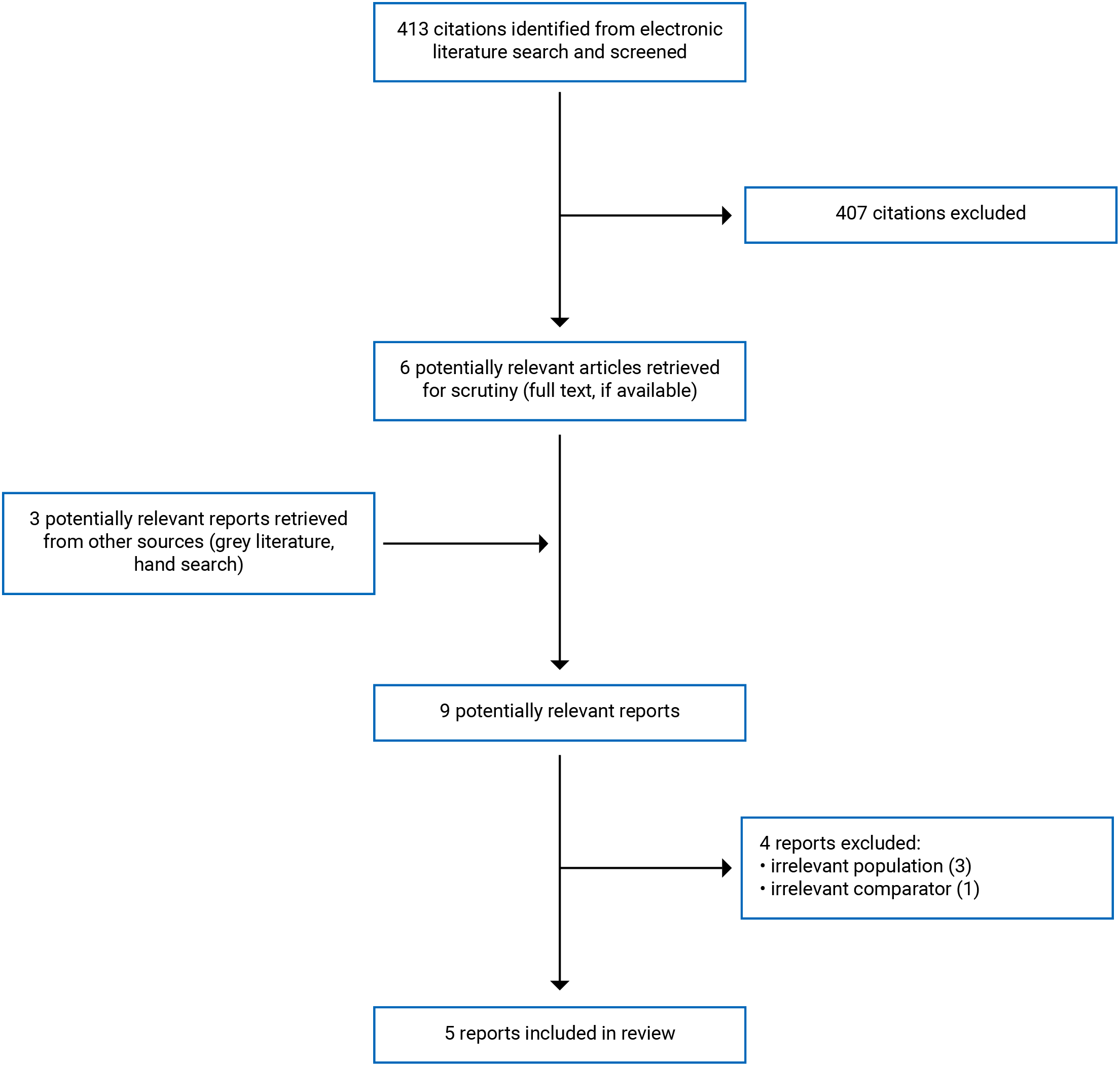
A total of 413 citations were identified in the literature search. Following the screening of titles and abstracts, 407 citations were excluded and 6 potentially relevant reports from the electronic search were retrieved for full-text review. Three potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 4 publications were excluded for various reasons and 5 publications met the inclusion criteria and were included in this report. These comprised 4 SRs and 1 evidence-based guideline. Appendix 1 presents the PRISMA9 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Four SRs3,5,10,11 and 1 evidence-based guideline12 were identified with relevance to the research questions and inclusion criteria of this report. All 4 included SRs had broader inclusion criteria than the present review. None of the included studies in the 4 SRs evaluated the comparison of interest for this report — namely, the clinical effectiveness or cost-effectiveness of Botox for reducing spasticity in patients with ABI.
Specifically, the SR authored by Dong et al. (2017)10 evaluated the use of any BoNT-A formulation (i.e., Botox, Dysport, and Xeomin) in adults with upper limb spasticity due to TBI or stroke and included randomized controlled trials (RCTs) published in English from database inception to September 10, 2016. The SR authored by Synnot et al. (2017)3 reviewed various pharmacological (e.g., BoNT-A that was not specific to Botox, baclofen) and non-pharmacological (e.g., casting, splinting) interventions in patients (any age) with TBI-related spasticity and included RCTs and crossover RCTs published in any language from database inception to June 2017. The SR authored by Baker and Pereira (2016)11 evaluated the use of BoNT-A (not specific to Botox) in adults with limb spasticity of any etiology and included RCTs published in English from 1989 to January 2015. Finally, the SR authored by Phadke et al. (2016)5 investigated the use of BoNT-A (not specific to Botox) in adults with focal spasticity of various etiologies (e.g., brain injury, stroke, cerebral palsy, multiple sclerosis) and included any study type (except for SRs) published in English from 1990 to 2013. Furthermore, this SR also assessed a Health Canada dataset containing adverse events reported from 2009 to 2013 related to Botox therapy used for spasticity of various unspecified etiologies.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Published in 2017, the included evidence-based guideline was developed by the University of Wisconsin’s UW Health and coauthored by 2 pharmacists.12 Professional backgrounds of the guideline workgroup members were not reported (NR). The recommendations were informed by literature searches on PubMed; however, search details such as key terms and search time frames were NR. The quality of evidence (i.e., very low, low, moderate, high) and strength of recommendations (i.e., strong, weak/conditional) were evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Recommendations were developed through a consensus process by incorporating evidence from the literature, expert opinion, and clinical experience. The draft recommendations were reviewed and approved by additional stakeholders or committees.
Country of Origin
The included guideline is meant to apply to the US, specifically to be used within the University of Wisconsin UW Health system.12
Patient Population
The target population covered by the included guideline consisted of adult and pediatric patients within the University of Wisconsin UW Health system, with a condition for which BoNT treatment may be appropriate.12 The intended users of this guideline are pharmacists, physicians, advanced practice providers, nurses, and individuals providing technical support for the purpose of screening for insurance coverage before the authorization of treatment.
Interventions and Comparators
The included guideline considered the use of BoNT (subtype and formulation not specified) as part of a documented rehabilitation and strengthening program.12
Outcomes
The outcomes considered in the guideline were sustained relief or reversal of conditions, prevention or delay of surgical or other invasive procedures, and a reduced effect of BoNT due to prolonged use.12
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
The 4 included SRs shared methodological strengths including clearly stated objectives, inclusion and exclusion criteria, key search terms, search time frames, comparators, and outcomes.3,5,10,11 Specific details regarding study populations (e.g., etiologies for spasticity) were reported in 3 SRs.3,5,10 The authors of these 3 SRs searched multiple databases and conducted grey literature searches, which decreases the risk of missing relevant, non-indexed studies.3,5,10 Details of study selection were explicitly stated and data extraction was conducted in duplicate in these 3 SRs, which decreases the risk of missing or inaccurate data and/or biased study selection.3,5,10 Furthermore, a list of included studies was provided and the characteristics of included studies were described in detail in these 3 SRs.3,5,10 Finally, authors of 2 SRs3,10 used appropriate tools to assess risk of bias, 2 SRs3,11 reported their sources of funding, and 3 SRs3,10,11 disclosed that there were no conflicts of interest.
The 4 included SRs shared methodological limitations including not providing justification for eligible study designs.3,5,10,11 Specific Botox formulations used in primary studies were clearly stated in 1 SR10 but not in the other 3 SRs.3,5,11 The use of an a priori study protocol, funding sources of included studies, and a list of excluded studies was reported in 1 SR3 but not in the other 3 SRs.5,10,11 While 1 SR3 did not restrict publication language, the authors of 3 SRs excluded non-English publications without providing the rationale.5,10,11 Authors of 1 SR10 did not report the sources of funding while in another SR,5 3 authors reported receiving funding from drug manufacturers (i.e., Botox and/or Xeomin). Additional limitations in the SR authored by Baker and Pereira (2016)11 included not conducting grey literature searches, not reporting the details of study selection and extraction, not providing a list of included studies or baseline characteristics (e.g., etiologies of spasticity) of participants, and not stating if a validated tool was used to assess for risk of bias.
Guideline
The included evidence-based guideline provided a clear description of the objectives, specified the target populations and users, presented monitoring criteria for the recommendations, described facilitators or barriers to their application, and provided tools for putting recommendations into practice.12 However, the views and preferences of the target population were not sought, details of the external review were NR, and procedures for guideline updates were NR. As the professional backgrounds of the guideline workgroup members and funding sources for developing this guideline were NR, it was unclear if the workgroup comprised all relevant professionals or if the guideline’s contents were influenced by external views. The recommendations were informed by literature searches in PubMed and the quality of evidence and strength of recommendation were ranked using the GRADE approach; however, further details (e.g., search dates, keywords) of the search strategy were NR. The link between the recommendations and the supporting evidence was unclear, as the relevant literature was not described in detail (e.g., BoNT subtype and formulation not specified). Furthermore, the recommendations regarding the use of BoNT for TBI did not specify the subtype or formulation. Although the guideline provides recommendations regarding usual doses of Botox for spasticity in general, recommendations for specific spasticity etiologies were not provided. Although a list of individuals who reviewed the guideline was provided, which consisted of professionals from multiple disciplines (e.g., anesthesia, surgery, pharmacy, neurology), it was unclear if these reviewers were external to the overall guideline development process.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Onabotulinum Toxin A for Spasticity in Patients With Acquired Brain Injury
No relevant evidence was identified regarding the clinical effectiveness of Botox for reducing spasticity in patients with ABI; therefore, no summary can be provided.
Cost-Effectiveness of Onabotulinum Toxin A for Spasticity in Patients With Acquired Brain Injury
No relevant evidence was identified regarding the cost-effectiveness of Botox for reducing spasticity in patients with ABI; therefore, no summary can be provided.
Guidelines
One identified evidence-based guideline12 addressed the use of BoNT for reducing spasticity in patients with ABI. This guideline recommends the use of BoNT (subtype and formulation NR) as part of a rehabilitation program for the treatment of TBI-related spasticity in the upper and lower extremities (strength of recommendation: strong; quality of evidence: high).12 Furthermore, this guideline recommends dosing Botox at 0.5 units to 20 units per kilogram (maximum dose: 400 units to 600 units) for treating adults and children with spasticity and non-cervical dystonia (specific etiologies of spasticity NR) (strength of recommendation and quality of evidence NR).12
Limitations
Limitations were identified in the critical appraisal (details in Appendix 3); however, additional limitations exist.
Overall, the body of evidence evaluating treatment options for ABI-related spasticity is limited in quality and quantity. All 4 included SRs had broader inclusion criteria than the present review because of mixed interventions and populations,5,10,11 or mixed interventions.3 The identified SRs combined studies investigating the use of various BoNT subtypes and formulations in patients with spasticity of differing etiologies; therefore, no direct evidence was available regarding the clinical effectiveness or cost-effectiveness of Botox for the treatment of ABI-associated spasticity. Furthermore, the recommendations from the identified evidence-based guideline were informed by publications that assessed various BoNT subtypes and formulations used in patients with spasticity from differing etiologies.12 Although this guideline is intended for use in adult and pediatric patients, it was unclear if the supporting evidence included pediatric populations. Because this guideline was developed by and intended for use in a hospital system in the US, with potentially different physician or patient care preferences and pharmacy formularies, the recommendations may not be generalizable to Canadian practice settings. Therefore, considering the limitations mentioned, the recommendations summarized in this report need to be interpreted with caution.
Conclusions and Implications for Decision- or Policy-Making
This report included 4 SRs3,5,10,11 regarding the clinical effectiveness of Botox for reducing spasticity in patients with ABI; however, these SRs did not contain primary studies relevant for this report. No relevant economic evaluations were identified regarding the cost-effectiveness of Botox for reducing spasticity in patients with ABI. One relevant evidence-based guideline12 was included regarding the use of Botox for the treatment of spasticity in patients with ABI. Specifically, the guideline recommends the use of BoNT for the treatment of TBI-related spasticity as part of a rehabilitation program (strong recommendation based on high-quality evidence); however, the guideline does not specify the BoNT subtype and formulation. Furthermore, this guideline recommends dosing Botox at 0.5 to 20 units per kilogram for patients with spasticity (strength of recommendation and quality of evidence NR); however, the etiologies for spasticity were not specified.12
The body of evidence was limited by the lack of evidence specific to the use of Botox for the treatment of spasticity related to ABI. The 4 SRs3,5,10,11 combined findings from studies that evaluated the clinical effectiveness of different BoNT subtypes and formulations in patients with spasticity due to various etiologies (e.g., brain injury, stroke, cerebral palsy, multiple sclerosis). Therefore, due to the different pharmacological activities of BoNT-A formulations (i.e., Botox, Dysport, and Xeomin are not interchangeable products), no direct evidence evaluating the use of Botox for ABI-related spasticity was identified. Indirect evidence from 1 SR10 suggested that BoNT-A (formulation not specified) improved muscle tone in patients with upper limb spasticity after a stroke or TBI (subgroup analysis NR for patients TBI). Indirect findings from 2 other SRs suggested there was inconclusive evidence regarding the clinical effectiveness of BoNT-A (formulation not specified) for spasticity associated with TBI3 or various etiologies including ABI.11
Further research investigating the clinical effectiveness and cost-effectiveness of Botox — particularly with controlled clinical trials with Canadian representation — would provide health care providers with an additional knowledge base to inform evidence-based guidance for the treatment of spasticity related to ABI.
References
1.Brain Injury Association of America. What is the difference between an acquired brain injury and a traumatic brain injury? 2021; https://www.biausa.org/brain-injury/about-brain-injury/nbiic/what-is-the-difference-between-an-acquired-brain-injury-and-a-traumatic-brain-injury. Accessed 2021 Mar 18.
2.Brain Injury Association of Durham Region. About brain injury. https://biad.ca/about-brain-injury/#:~:text=Each%20year%2C%20150%2C000%20Canadians%20suffer,in%20Canada%20every%203.5%20minutes. Accessed 2021 Mar 18.
3.Synnot A, Chau M, Pitt V, et al. Interventions for managing skeletal muscle spasticity following traumatic brain injury. Cochrane Database Syst Rev. 2017;11:CD008929. PubMed
4.Ferrari A, Manca M, Tugnoli V, Alberto L. Pharmacological differences and clinical implications of various botulinum toxin preparations: a critical appraisal. Funct Neurol. 2018;33(1):7-18. PubMed
5.Phadke CP, Balasubramanian CK, Holz A, Davidson C, Ismail F, Boulias C. Adverse clinical effects of botulinum toxin intramuscular injections for spasticity. Can J Neurol Sci. 2016;43(2):298-310. PubMed
6.Hui D, Argáez C. CADTH health technology review: onabotulinum toxin A (botox) for spasticity associated with multiple sclerosis. Can J Health Technol. 2021;1(3). https://cadth.ca/sites/default/files/rr/2021/RC1340%20Botox%20for%20MS%20Final.pdf. Accessed 2021 Mar 22.
7.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
8.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Mar 21.
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
10.Dong Y, Wu T, Hu X, Wang T. Efficacy and safety of botulinum toxin type A for upper limb spasticity after stroke or traumatic brain injury: a systematic review with meta-analysis and trial sequential analysis. Eur J Phys Rehabil Med. 2017;53(2):256-267. PubMed
11.Baker JA, Pereira G. The efficacy of botulinum toxin A for limb spasticity on improving activity restriction and quality of life: a systematic review and meta-analysis using the GRADE approach. Clin Rehabil. 2016;30(6):549-558. PubMed
12.Botulinum toxin - adult/pediatric - ambulatory clinical practice guideline. Madison (WI): University of Wisconsin Hospitals and Clinics Authority; 2017: https://www.uwhealth.org/cckm/cpg/medications/Botulinum-Toxin---Adult.Pediatric---Ambulatory-17.01.20.pdf. Accessed 2021 Mar 4.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Dong et al. (2017)10 China Funding Source: NR | Objective: To evaluate the clinical effectiveness of BoNT-A for upper limb spasticity Study design: SR with MA of RCTs Literature search strategy: The search was conducted in multiple databases for literature published in English from inception to September 10, 2016. Grey literature search for abstracts and conference proceedings was conducted Number of studies included: Of 22 included studies, none were relevant for this report Quality assessment tool: Cochrane risk of bias tool | Adult patients (age-specific criteria NR) with spasticity due to TBI or stroke | Eligible Intervention: BoNT-A Relevant Intervention: Botox Eligible Comparator: Placebo | Outcomes
|
Synnot et al. (2017)3 Australia Funding Source: Victoria Transport Accident Commission, Neurotrauma Evidence Translation Program, National Institute for Health Research | Objective: To evaluate the clinical effectiveness of various interventions (including BoNT-A) for treating spasticity Study design: SR of RCTs and crossover RCTs Literature search strategy: The search was conducted in multiple databases for literature published in any language from inception to June 2017. Grey literature search for clinical trials and references lists was conducted Number of studies included: Of 9 included studies, none were relevant for this report Quality assessment tool: Cochrane risk of bias tool | Patients (any age) with spasticity due TBI | Eligible Interventions: Any pharmacological (e.g., BoNT-A, baclofen, clonidine, dantrolene sodium, phenol) or non-pharmacological (e.g., casting, splinting, seating, stretching, transcutaneous electric nerve stimulation) intervention for the treatment of TBI-related spasticity Relevant Intervention: Botox Eligible Comparator: Placebo or another active intervention | Outcomes
Follow-up: Up to 1 year |
Baker and Pereira (2016)11 UK Funding Source: Australian National Health and Medical Research Council | Objective: To evaluate the clinical effectiveness of BoNT-A for limb spasticity Study design: SR with MA of RCTs Literature search strategy: The search was conducted in multiple databases for literature published in English from 1989 to January 2015. Grey literature search was not conducted Number of studies included: Of 25 included studies, none were relevant for this report Quality assessment tool: GRADE approach | Adult patients (age-specific criteria NR) with spasticity of any etiology, including patients with brain injury, stroke, cerebral palsy, MS | Eligible Intervention: BoNT-A Relevant Intervention: Possibly included Botox; however, this was unclear Eligible Comparator: Placebo/saline injection | Outcomes
Follow-up: NR |
Phadke et al. (2016)5 Canada Funding Source: NR | Objective: To review adverse events associated with BoNT-A used for focal spasticity Study design: SR of any study design except for SRs Literature search strategy: The search was conducted in multiple databases for literature published in English from 1990 to January 2013. Adverse events reported to Health Canada from 2009 to 2013 were included Number of studies included: Of 29 included studies, none were relevant for this report Quality assessment tool: Oxford Centre for Evidence-Based Medicine levels of evidence approach | Adults (> 18 years) with spasticity of various etiologies, including patients with brain injury, stroke, cerebral palsy, spinal cord injury, MS | Eligible Intervention: BoNT-A Relevant Intervention: Botox Eligible Comparator: NR | Clinical Outcomes:
Follow-up: NR |
AE = adverse event; BoNT = botulinum toxin; BoNT-A = botulinum toxin type A; GRADE = Grades of Recommendations Assessment, Development and Evaluation; MA = meta-analysis; MS = multiple sclerosis; NR = not reported; RCT = randomized controlled trial; SR = systematic review; TBI = traumatic brain injury.
Table 3: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
Botulinum Toxin – Adult/Pediatric – Ambulatory Clinical Practice Guideline (2017)12 | ||||||
Intended users or purposes: Pharmacists, physicians, advanced practice providers, nurses, technical support, and for the purpose of screening for insurance coverage before the authorization of treatment Target population: Adult and pediatric patients treated at UW Health with a condition for which BoNT may be appropriate | The guideline provided recommendations regarding the use of BoNT as first-, second-, or third-line therapy for conditions addressed in the guideline |
| Searches in PubMed were performed by guideline authors and workgroup members Expert opinion and clinical expertise were also sought | Evidence quality was assessed using the GRADE approach Quality of evidence:
| Recommendations were developed internally or adopted from external sources. Workgroup members discussed the evidence from the literature and expert experience, and finalized recommendations through a consensus process Strength of recommendations:
| The draft recommendations were reviewed and approved by other stakeholders or committees |
BoNT = botulinum toxin; GRADE = Grading of Recommendations Assessment, Development and Evaluation; UW Health = University of Wisconsin.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 27
Strengths | Limitations |
Dong et al. (2017)10 | |
|
|
Synnot et al. (2017)3 | |
|
|
Baker and Pereira (2016)11 | |
|
|
Phadke et al. (2016)5 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; BoNT-A = botulinum toxin type A; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NR = not reported; PICO = population, intervention, comparator, and outcome; RCT = randomized controlled trial; SR = systematic review.
Table 5: Strengths and Limitations of Guideline Using AGREE II8
Item | Botulinum Toxin — Adult/Pediatric — Ambulatory Clinical Practice Guideline (2017)12 |
Domain 1: Scope and Purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | No |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder Involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Unclear (Professions of guideline workgroup members were NR. The 2 guideline authors were pharmacists.) |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | No |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of Development | |
7. Systematic methods were used to search for evidence. | Unclear (Search dates, key terms, and study eligibility criteria were NR.) |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | No |
13. The guideline has been externally reviewed by experts before its publication. | Unclear (Reviewed by other stakeholders or committees but unclear if these bodies were external.) |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of Presentation | |
15. The recommendations are specific and unambiguous. | No (BoNT subtypes and formulations were NR. Furthermore, although Botox dosing was provided, the etiology of spasticity was NR.) |
16. The different options for management of the condition or health issue are clearly presented. | No |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Yes (Financial barriers were noted because of the high cost of BoNT.) |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes |
Domain 6: Editorial Independence | |
22. The views of the funding body have not influenced the content of the guideline. | NR (Funding sources were NR.) |
23. Competing interests of guideline development group members have been recorded and addressed. | No |
AGREE II = Appraisal of Guidelines for Research & Evaluation II; BoNT = botulinum toxin; NR = not reported.
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 6: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
Botulinum Toxin — Adult/Pediatric — Ambulatory Clinical Practice Guideline (2017)12 | |
Treatment of Upper and Lower Extremity Spasticity “BoNT should be offered to treat spasticity resulting from a stroke, traumatic or non-traumatic spinal cord injury, multiple sclerosis or other demyelinating disease of the central nervous system, traumatic brain injury or other central process with BoNT injections as a component of a documented rehabilitation and strengthening program (p.7).”12
Usual doses of Botox for spasticity and non-cervical dystonia (Adult and Pediatric Patients) “0.5 – 20 units/kg with a maximum dose of 400 – 600 units; initiate therapy at the lower end of the dose range (p.11).”12
| Recommendation strength: Strong Quality of evidence: High Recommendation strength: NR Quality of evidence: NR |
BoNT = botulinum toxin; BoNT-A = botulinum toxin type A; BoNT-B = botulinum toxin type B; NR = not reported.
Appendix 5: References of Potential Interest
Previous CADTH Reports
1.Hui D, Argáez C. CADTH health technology review: onabotulinum toxin A (botox) for spasticity associated with multiple sclerosis. Can J Health Technol. 2021;1(3). https://cadth.ca/sites/default/files/rr/2021/RC1340%20Botox%20for%20MS%20Final.pdf Accessed 2021 Mar 22.
2.Botulinum toxin for spasticity: clinical effectiveness and guidelines. CADTH Rapid response report: summary of abstracts. Ottawa (ON): CADTH; 2016: https://cadth.ca/sites/default/files/pdf/htis/apr-2016/RB0976%20Botulinum%20Toxin%20for%20Spasticity%20Final.pdf Accessed 2021 Mar 21.
Evidence-Based Guidelines
Mixed Population
3.Spasticity in adults: management using botulinum toxin. National guidelines 2018. London (GB): Royal College of Physicians; 2018: https://www.rcplondon.ac.uk/guidelines-policy/spasticity-adults-management-using-botulinum-toxin Accessed 2021 Mar 21.
4.Simpson DM, Hallett M, Ashman EJ, et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2016 May 10;86(19):1818-1826. PubMed
Non-Randomized Studies
No Comparator
5.Francisco GE, Bandari DS, Bavikatte G, et al. High clinician- and patient-reported satisfaction with individualized onabotulinumtoxinA treatment for spasticity across several etiologies from the ASPIRE study. Toxicon X. 2020 Sep;7:100040. PubMed
Mixed Population
6.Ghroubi S, Alila S, Elleuch W, Ayed HB, Mhiri C, Elleuch MH. Efficacy of botulinum toxin A for the treatment of hemiparesis in adults with chronic upper limb spasticity. Pan Afr Med J. 2020;35:55. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca