CADTH Health Technology Review
Bupropion for Major Depressive Disorder or Persistent Depressive Disorder (Dysthymia)
Rapid Review
Authors: Erika MacDonald, Jennifer Horton
Abbreviations
AHRQ
Agency for Healthcare Research and Quality
HAM-D
Hamilton Depression Rating Scale
MADRS
Montgomery-Åsberg Depression Scale
MDD
major depressive disorder
RCT
randomized controlled trial
SNRI
serotonin-norepinephrine reuptake inhibitor
SR
sustained release
SSRI
selective serotonin reuptake inhibitor
STAR*D
Sequenced Treatment Alternatives to Relieve Depression
XL
extended release (buproprion)
XR
extended release (venlafaxine)
Key Messages
Direct and indirect evidence from 6 systematic reviews did not demonstrate a difference in treatment response or remission rates, or functional outcomes, with bupropion as compared to other antidepressants in adults with major depressive disorder.
Direct and indirect evidence from 5 systematic reviews did not demonstrate a difference in overall adverse events, overall withdrawals, or withdrawals due to adverse events apart from a possible decreased risk of withdrawal due to adverse events with vortioxetine in a single indirect comparison.
Direct and indirect evidence from 2 systematic reviews supports that the risk of sexual dysfunction may be lower with bupropion than other antidepressants (escitalopram, paroxetine, sertraline, and fluoxetine), while 1 systematic review showed no significant difference in sexual function scores between bupropion and venlafaxine.
There is limited evidence supporting the cost-effectiveness of bupropion to augment citalopram, and dominance of vortioxetine compared to bupropion, for major depressive disorder with inadequate response to initial therapy.
There is a lack evidence surrounding the comparative clinical or cost-effectiveness of bupropion in dysthymia.
Context and Policy Issues
Major depressive disorder (MDD) has a high disease burden in Canada. It was estimated that in 2012, the lifetime prevalence in Canada was 9.9%, and more than 1.5 million Canadians aged 15 or older experienced a major depressive episode that year.1 In Ontario, Canada’s largest province, the total burden of MDD as measured in health-adjusted life-years has been estimated to be greater than the breast, colorectal, lung, and prostate cancers combined.2 MDD is diagnosed with the occurrence of at least 1 major depressive episode. An episode is defined as a period of at least 2 weeks in which 5 or more of the following symptoms are experienced: anhedonia, depressed mood, psychomotor retardation or agitation, poor concentration, sleep disturbances, thoughts of worthlessness or guilt, recurrent thoughts of death or suicide, and weight or appetite changes. In contrast, dysthymia is a form of persistent depressive disorder lasting 2 or more years, with at least 2 of the following 6 symptoms: appetite changes, hopelessness, low energy, sleep disturbances, poor concentration, and poor self-esteem.3
Guidelines from the Canadian Network for Mood and Anxiety Treatments recommend second-generation antidepressants as first-line therapy for patients with a major depressive episode of moderate or great severity.4 These include selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), agomelatine, bupropion, mirtazapine, and vortioxetine. The guidelines additionally recommend that physician expertise, as well as patients’ preferences and perceptions, should guide the selection of the antidepressant drug: patient and medication factors (including efficacy, tolerability, drug interactions, convenience, cost, and availability) should be taken into consideration for an individualized approach. Treatment should generally be continued for 6 to 9 months and for 2 years or more in the presence of risk factors for recurrence. These include frequent, chronic, severe, or difficult-to-treat episodes, the presence of other psychiatric or medical conditions, and the presence of residual symptoms.4
Bupropion, a dopamine and norepinephrine reuptake inhibitor, is marketed in 2 formulations in Canada: sustained release (SR) and extended release (the XL form).5,6 Bupropion is indicated for symptomatic relief of MDD, prevention of seasonal major depressive episodes, as well as smoking cessation.6 Seizures are a dose-related adverse effect of bupropion, occurring in clinical trials with an incidence of 0.1%. When crushed or dissolved and injected or inhaled, cases of seizures and death have been reported.6 The most common adverse events occurring with an incidence of greater than 5% in clinical trials are dry mouth, nausea, constipation, insomnia, dizziness, anxiety, and decreased appetite.6,7 Bupropion is structurally related to amphetamine, and can have mild stimulating effects; this may increase the potential for abuse.5,8
The objective of this report is to summarize the evidence regarding the comparative clinical and cost-effectiveness of bupropion for MDD and dysthymia.
Research Questions
What is the clinical effectiveness of bupropion for the treatment of adults with major depressive disorder or persistent depressive disorder (dysthymia)?
What is the cost‐effectiveness of bupropion for the treatment of adults with major depressive disorder or persistent depressive disorder (dysthymia)?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, PsycINFO, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were bupropion and major depressive disorder. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, and meta-analyses, or network meta-analyses; and economic studies. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2011 and March 9, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Adults with major depressive disorder or persistent depressive disorder (dysthymia), with or without comorbid conditions |
Intervention | Bupropion, as a single ingredient, as primary therapy, or as an adjunct to other pharmaceutical therapy; all formulations and all routes of administration |
Comparator |
|
Outcomes | Q1: Clinical effectiveness (e.g., symptoms, mood stability, quality of life, cognitive function, functional outcomes, tachyphylaxis) and safety (e.g., misuse, abuse, side effects [e.g., sexual dysfunction], adverse events, morbidity, mortality) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year, cost per patient adverse event avoided, cost per clinical outcome) |
Study designs | HTAs, SRs, economic evaluations |
HTA = health technology assessment; Q = question; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2011. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)9 for systematic reviews, the “Questionnaire to assess the relevance and credibility of a network meta-analysis” for network meta-analyses,10 and the Drummond checklist11 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
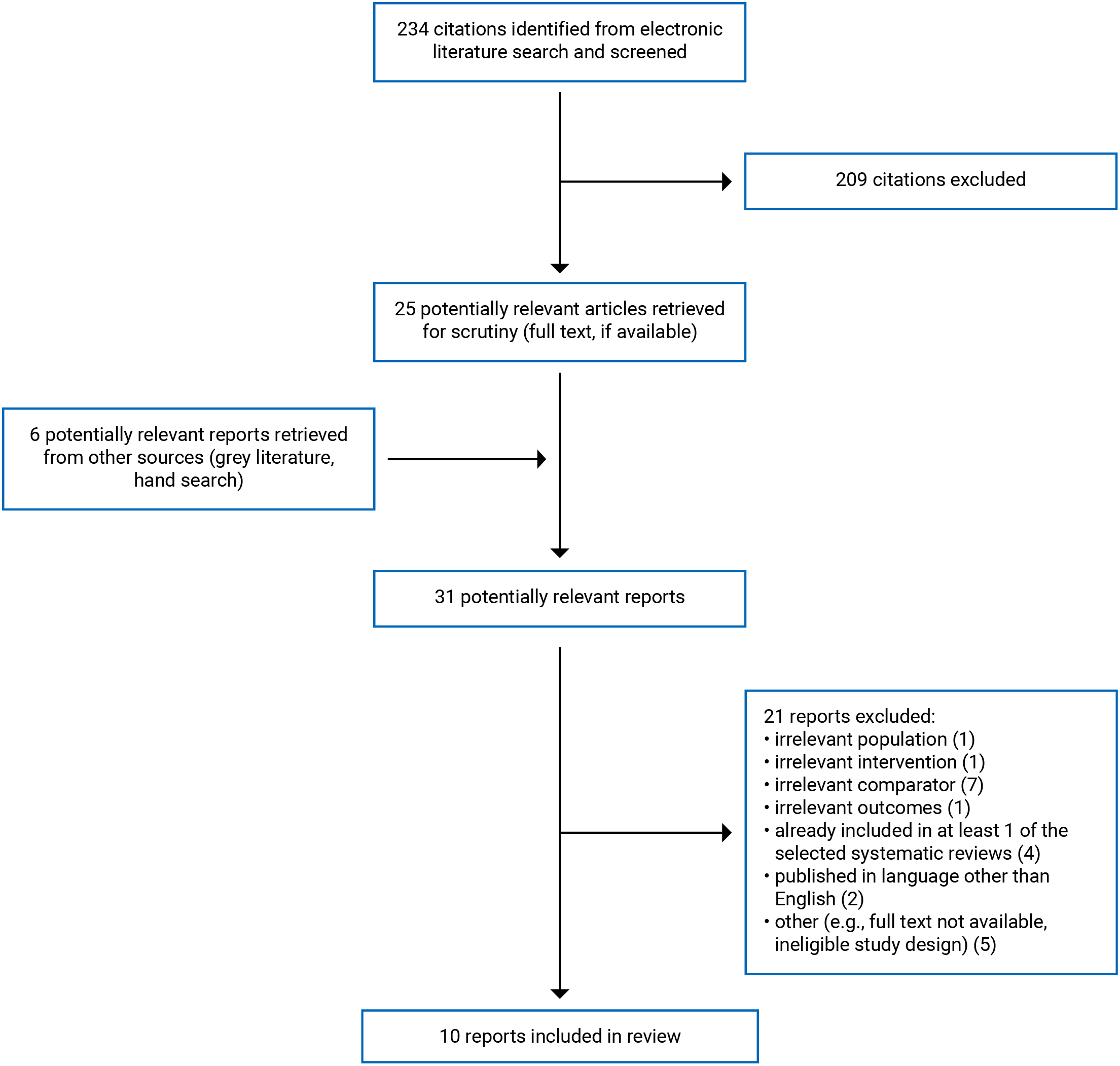
A total of 234 citations were identified in the literature search. Following the screening of titles and abstracts, 209 citations were excluded and 25 potentially relevant reports from the electronic search were retrieved for full-text review. Six potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 31 potentially relevant articles, 21 publications were excluded for various reasons and 10 publications met the inclusion criteria and were included in this report. These comprised 8 systematic reviews and 2 economic evaluations. Appendix 1 presents the PRISMA12 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Systematic Reviews
Of the 8 included systematic reviews,13-20 only 1 was not broader in scope than the present review;18 the others included comparisons of bupropion to placebo or non-pharmacologic interventions, in addition to the comparisons of relevance to this review. Patel et al. (2016) included patients with other types of mood disorders in addition to MDD and dysthymia.14
Regarding more specific populations, Brignone et al. (2016) and Zhou et al. (2015) specifically assessed patients with MDD not responding to SNRI or SSRI treatment.15,16 Sobieraj et al. (2019) aimed to assess adverse effects in adults with MDD aged 65 and older; 19 randomized controlled trials (RCTs) and 2 observational studies were included, and none were relevant to the present review.13 A single included RCT in Sobieraj et al. (2019) assessed bupropion in comparison to placebo only. Randomized and non-randomized comparative studies were eligible for inclusion, with a search date of May 2018.13
Only the characteristics and results in the subset of studies relevant to this report will be discussed throughout the remainder of this report.
Economic Evaluations
Two economic evaluations were included.21,22 Olgiati et al. (2013) performed a cost-utility analysis in a simulated trial of outpatients with inadequate response to initial therapy, primarily based on the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial.22 Soini et al. (2017) assessed the cost-utility of vortioxetine compared to bupropion SR, venlafaxine extended release (XR), and sertraline in patients with inadequate response to SSRI or SNRI therapy. Only the comparison of bupropion to vortioxetine is relevant to the present review.22
Study Design
Systematic Reviews
Of the 7 included systematic reviews with primary studies of relevance to this report, 5 included a network meta-analysis15-17,19,20 and 2 performed meta-analyses with direct comparisons of relevance.18,19
The search date in Cao et al. (2021)20 was December 2019. Forty-two RCTs in adults with MDD reporting Sheehan Disability Scale scores met inclusion criteria for the systematic review and 2 were relevant to the present review. Additional relevant indirect comparisons were made in the network meta-analysis. Details of the statistical analysis model were not provided, apart from the use of a random-effects analysis.
The search time frame of Brignone et al. (2016) was January 1980 to March 2014.15 Twenty-seven RCTs in patients with MDD not responding to SSRI or SNRI treatment met the inclusion criteria and 3 of those were included in the network meta-analysis. A single RCT was relevant to the present review. Although the single relevant RCT overlaps with the more comprehensive Gartlehner et al. (2011)19 systematic review that was also included in this report, additional relevant indirect comparisons were made in the network meta-analysis performed by Brignone et al. (2016).15 Bucher’s method was used to make simple adjusted indirect comparisons using risk differences from the primary studies.
Patel et al. (2016) had a search date of March 2015.14 This systematic review included 51 RCTs assessing the effectiveness of bupropion as an antidepressant, 15 of which were of relevance to this review. Twelve of these RCTs overlap with other systematic reviews in this report. Although a meta-analysis of bupropion versus placebo was performed, results relevant to this report were not statistically pooled and were described narratively.
The search time frame for Zhou et al. (2015) was 1970 to December 2013.16 This systematic review included 48 RCTs assessing 11 augmentation agents in treatment-resistant depression compared to placebo and each other. A single RCT assessing bupropion versus risperidone was included within this systematic review and relevant indirect comparisons of bupropion to other drugs were also performed in the network meta-analysis. The network meta-analysis used a Bayesian approach and random-effects model. Inconsistency was estimated by assessing differences between direct and indirect estimates, where available. A number of sensitivity analyses were performed considering clinical and methodological variables.
The search time frame for Reichenpfader et al. (2014) was 1980 to October 2012.17 Fifty-eight RCTs and 5 observational studies were included, with 37 RCTs included in a network meta-analysis. This systematic review aimed specifically to assess the association of second-generation antidepressants and sexual dysfunction in adults with MDD. Six individual RCTs with direct comparisons relevant to this report were included in the systematic review and network meta-analysis. The 6 RCTs with comparisons of relevance to this review overlap fully with Gartlehner et al. (2011),19 which is a more comprehensive systematic review. However, a network meta-analysis that incorporated indirect evidence for the sexual dysfunction outcome was additionally performed in Reichenpfader et al. (2014) and it was therefore still included in this report; the 6 relevant RCTs to this report were included in the network. Bayesian mixed-treatment comparisons were performed using Markov chain Monte Carlo methods to compute indirect comparisons. A random-effects model and non-informative prior distributions were used. Convergence was verified and sensitivity analyses were performed according to the method of assessment of sexual dysfunction.
The search time frame for Maneeton et al. (2013) was 1985 to February 2013.18 This systematic review included 3 RCTs comparing venlafaxine XR and bupropion XL and results were pooled in a random-effects meta-analysis.
Gartlehner et al. (2011) updated a 2007 comparative effectiveness review by the Agency for Healthcare Research and Quality (AHRQ) assessing the effectiveness of second-generation antidepressants for the treatment of depression in adults.19 Head-to-head and placebo-controlled RCTs were included, as well as meta-analyses and observational studies in the absence of other evidence. Of the 238 studies included, 12 RCTs were of relevance to this review, 9 of which specifically assessed sexual dysfunction. Meta-analyses of RCTs using a random-effects model were reported. Indirect mixed-treatment comparisons using Bayesian methods were performed when there were fewer than 3 head-to-head trials available for a given drug comparison, including 12 indirect comparisons involving bupropion for the response rate outcome. For indirect treatment comparisons, a random-effects model was conducted with software that used Markov chain Monte Carlo techniques. A vague prior distribution with a large range was used for the model, convergence was verified, and sensitivity analyses were performed to include studies rated by review authors as poor quality because of the high risk of bias.
A table depicting an overlap of relevant RCTs included within the systematic reviews is provided in Appendix 5. Only RCTs providing direct evidence of relevance to this report were included in the overlap table. For network meta-analyses incorporating evidence from placebo-controlled RCTs to provide indirect comparisons, the placebo-controlled RCTs in the network are not included in the overlap table, as they are not directly relevant to this report.
Economic Evaluations
In the cost-utility analyses by both Soini et al. (2017)22 and Olgiati et al. (2013),21 a Markov model was used. Health states in the Soini et al. analysis included remission, relapse, and recovery; whereas the Olgiati et al. (2013) analysis included acute depression (or non-remission, or relapse; all were assigned the same utility score), remission, and dropout. The time horizon in Soini et al. was 1 year, whereas in Olgiati et al. it was 26 weeks. A payer’s perspective was used for the base-case analysis in Soini et al. and an additional analysis using a societal approach was performed. The perspective was not explicitly stated in Olgiati et al. In Soini et al., the 2 main sources of efficacy data were a systematic review and a network meta-analysis by 1 of the same authors, as well as a single vortioxetine RCT. In Olgiati et al., clinical data were obtained from the STAR*D trial, as well as other RCTs and observational studies; methods for determining which evidence to use to inform the model were not described. Costs considered in Soini et al. include Finnish drug costs (pharmaceutical database in Finland and the Finnish medicines tariff), as well as direct costs of visits and hospitalizations based on Finnish data. Olgiati et al. considered medication costs in the US, as well as outpatient visit costs according to WHO data. In both evaluations, utility scores were obtained from a prior study. Soini et al. additionally used unpublished data from Lundbeck SAS to obtain utility scores. Several assumptions were made in Soini et al. about adverse events and the related management of patients, as described in Appendix 2.
Country of Origin
Systematic Reviews
Of the systematic reviews, 1 each was from researchers in the UK,14 the US,19 France,15 Austria,17 and Thailand;18 and 2 were from China.16,20
Economic Evaluations
The Soini et al. evaluation was conducted by researchers in, and was relevant, to Finland.22 The Olgiati et al. evaluation was conducted by researchers in Italy, but cost data were relevant to the US and results were presented in US dollars.21
Patient Population
Systematic Reviews
Brignone et al. (2016)15 included adults aged 18 years or older with MDD, dysthymia, or subsyndromal depression, receiving SSRI or SNRI at the time of study entry and classified as having failed treatment or having had inadequate response. The single relevant RCT from this systematic review, which was also included within Gartlehner et al. (2011),19 compared bupropion, sertraline, and venlafaxine, and included 727 patients with a mean age 41.8 (58.7% of which were female), and with a mean baseline Hamilton Depression Rating Scale (HAM-D) score of 18.9.15 A HAM-D score between 17 and 24 is generally considered moderate in severity, whereas higher than 24 is severe.23
In 4 of the systematic reviews, summary characteristics for the population of interest were not provided, but population characteristics were reported for each individual relevant study.14,17,19,20 Patel et al. (2016),14 Reichenpfader et al. (2014),17 and Cao et al. (2021)20 included adults aged 18 years and older with MDD; Gartlehner et al. (2011) included adults with MDD or dysthymia.19
Zhou et al. (2015) included adults with treatment-resistant depression.16 RCTs in patients with serious concomitant medical illness were excluded. A single RCT of 20 patients was relevant to this report and population characteristics were not reported separately for the RCT of relevance to this review.
Maneeton et al. (2013) included adults aged 18 to 65 years with MDD.18 In the 3 included RCTs comparing bupropion XL to venlafaxine XR, 65.6% were female. The mean age in the bupropion group was 41.83; it was 41.62 in the venlafaxine group.
Economic Evaluations
In Soini et al. (2017),22 the population was not specifically described; however, efficacy data were based primarily on a systematic review included within the present report.15 The population of interest was adults with MDD with inadequate response to SSRI or SNRI therapy.
In Olgiati et al. (2013), the study cohort was based on approximately 3,000 STAR*D trial participants aged 18 years to 75 years (mean 40.8 years) with MDD, with a HAM-D score of 14 or greater; 64% were women.21
Interventions and Comparators
Systematic Reviews
In Cao et al. (2021), bupropion SR was compared to escitalopram in 1 of the RCTs with a direct comparison of interest, and to venlafaxine in another. Additional comparisons to 11 other antidepressants were reported in the network meta-analysis.20
In Brignone et al. (2016),15 the single relevant RCT comparing bupropion SR at a dose of 200 mg to 400 mg per day to venlafaxine, sertraline, or placebo for 14 weeks was also included in Gartlehner et al. (2011);19 however, indirect comparison analyses to vortioxetine and agomelatine were also reported in the systematic review by Brignone et al.15
Patel et al. (2016)14 included studies of bupropion at any dose or formulation, including as augmentation strategy, compared to placebo or active comparator. Doses of bupropion and comparator for the 15 relevant RCTs were provided; however, the formulation of bupropion used was not clearly described. Relevant comparators included escitalopram, sertraline, fluoxetine, paroxetine, venlafaxine, duloxetine, trazodone, and nortriptyline.
In the single RCT relevant to this review included in Zhou et al. (2015), bupropion was compared to risperidone in 20 patients. Details on dosing, duration, or formulation were not provided. Trials that compared the continuation of the original drug with an augmentation drug that lacked a placebo augmentation were excluded from this systematic review.16
Reichenpfader et al. (2014) included RCTs of 13 second-generation antidepressants: bupropion, citalopram, desvenlafaxine, duloxetine, escitalopram, fluoxetine, fluvoxamine, mirtazapine, nefazodone, paroxetine, sertraline, trazodone, and venlafaxine. These interventions were compared with each other or versus placebo. Indirect comparisons of bupropion to citalopram, duloxetine, escitalopram, fluoxetine, fluvoxamine, mirtazapine, nefazodone, paroxetine, sertraline, and venlafaxine were made in the network meta-analysis. Details on dose and formulation was described for each individual study. The 6 RCTs with direct comparisons of relevance to this report compared bupropion SR or XL to sertraline, fluoxetine, or escitalopram.17
In the 3 included RCTs in Maneeton et al. (2013), bupropion XL at a dose of 150 mg per day to 450 mg per day was compared to venlafaxine 75 mg per day to 225 mg per day. Included studies were 14 weeks to 16 weeks duration.18
In Gartlehner et al. (2011), bupropion was compared to other second-generation antidepressants: citalopram, desvenlafaxine, duloxetine, escitalopram, fluoxetine, fluvoxamine, mirtazapine, nefazodone, paroxetine, sertraline, trazodone, or venlafaxine in the 12 relevant RCTs. Details on dose and formulation were described for each individual study.19
Economic Evaluations
Soini et al. (2017) compared bupropion SR 150 mg per day to 400 mg per day to vortioxetine at mean dose 15.7 mg per day for weeks 1 to 8, followed by 16.47 mg per day in the maintenance phase.22 Olgiati et al. (2013) compared the continuation of citalopram after an initial 13 weeks of treatment to augmentation with bupropion (mean dose 267 mg per day) or a switch to venlafaxine or sertraline for the next 13 weeks. The relevant comparison of interest was the continuation of citalopram versus augmentation with bupropion.21
Outcomes
Systematic Reviews
Patel et al. (2016), Zhou et al. (2015), Maneeton et al. (2013), and Gartlehner et al. (2011) assessed treatment response, defined as the percentage of patients whose scores on the HAM-D or Montgomery-Åsberg Depression Scale (MADRS) decreased by 50% or more.14,16,18,19 Patel et al. (2016), Brignone et al. (2016), and Maneeton et al. (2013) assessed remission;14,15,18 Brignone et al. (2016) and Maneeton et al. defined remission as a HAM-D score of 7 or less, or a MADRS score of 10 or less. Remission was not specifically defined in Patel et al. Gartlehner et al. defined remission according to what was reported by the authors of the primary studies.19 Maneeton et al. additionally assessed change in the aforementioned depression rating scale scores; a decrease in score reflects improvement.18 Cao et al. (2021) assessed mean change in the Sheehan Disability Scale — a self-reported functional impairment score ranging from 0 to 30, with higher scores indicating improved functioning.20
Zhou et al. (2015), Brignone et al. (2016), Maneeton et al. (2013), and Gartlehner et al. (2011) assessed tolerability (withdrawals due to adverse effects),15,16,18,19 and Zhou et al. and Maneeton et al. assessed acceptability (all-cause discontinuation). Reichenpfader et al. (2014) and Gartlehner et al. specifically assessed sexual dysfunction, as reported in included studies.17,19 Reichenpfader et al. noted that the methods of adverse events reporting, as well as the determination of sexual dysfunction, varied widely among the included studies: “Specific methods included prospective, systematically monitored and validated instruments to measure sexual function, rating scales, or structured clinical interviews to diagnose sexual dysfunction. Additionally, study authors relied on adverse events gathered by spontaneous patient reports, or using open questions or generic checklists by clinicians.” (p.5)17 Maneeton et al. did not specify sexual functioning as an outcome of interest in the systematic review eligibility criteria, but as all 3 included studies additionally reported on Changes in Sexual Functioning Questionnaire scores, these pooled results were also presented.18 Gartlehner et al. additionally assessed the following safety outcomes: overall adverse events, serious adverse events, specific adverse events or withdrawals because of specific adverse events, including: hyponatremia, seizures, suicide, hepatoxicity, weight gain, gastrointestinal symptoms, sexual side effects, and others.19
Economic Evaluations
Both Soini et al. (2017)22 and Olgiati et al. (2013)21 reported incremental quality-adjusted life-years, incremental costs, and incremental cost-effectiveness ratios.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
All of the reviews had a clear research objective.15-20 Zhou et al. (2015),16 Sobieraj et al. (2019),13 and Cao et al. (2021)20 contained explicit statements that the methods were established a priori and a protocol was available for Sobieraj et al. and Cao et al. In the other included systematic reviews, lack of predefined methods could introduce potential for bias if methods were established or adjusted after the start of the systematic review. A comprehensive literature search strategy was described in all except Brignone et al. (2016);15 therefore, it is possible that not all relevant studies were included. Study selection was performed in duplicate for all except Patel et al. (2016)14 and Cao et al.20 Data extraction was not performed in duplicate for Patel et al.,14 Zhou et al.,16 or Cao et al.20 and it was not clear whether duplicate data extraction was performed in Brignone et al. (2016).15
Population characteristics for individual included studies were not provided for Zhou et al.16 or Sobieraj et al.13
A risk of bias assessment of included studies was not performed in Patel et al.14 All other included systematic reviews used appropriate methods for assessing risk of bias and 5 appropriately considered study quality in their conclusions.13,16-19 The systematic review by Brignone et al. was authored by employees of the manufacturer of vortioxetine.15
Appropriate statistical methods were adequately described for systematic reviews with meta-analysis or network meta-analysis,13,16-19 apart from Cao et al.20 and Brignone et al.15 With respect to network meta-analysis methods, Zhou et al. (2015),16 Reichenpfader et al. (2014),17 and Gartlehner et al. (2011)19 described the network meta-analysis model in detail; they performed assessments of heterogeneity and consistency, and multiple sensitivity analyses. The type of model used was noted by Brignone et al.;15 however, further details were not described, such as the use of a random or fixed-effects analysis. A connected network was formed; however, there were no closed loops and therefore consistency could not have been assessed. Several relevant comparators were not assessed within the 3 RCTs included within the meta-analysis; multiple RCTs meeting eligibility for the systematic review were excluded from the network meta-analysis due to heterogeneity. Possible heterogeneity of studies included in the network meta-analysis was not described.15 Cao et al.20 did not state the type of statistical analysis used for the network meta-analysis apart from use of a random-effects model. Assessment of heterogeneity and consistency using a network forest plot was performed.
All reported potential conflicts of interest of the review authors except for Gartlehner et al.19
Economic Evaluations
In both Soini et al. (2017)22 and Olgiati et al. (2013),21 sources of effectiveness estimates, outcome measures, methods to value benefits, and estimate costs were stated and described. The models were well-described and the variables included in the sensitivity analyses were justified. Key assumptions were noted in Soini et al., and they appeared appropriate. Incremental cost-effectiveness ratios with 95% confidence intervals were reported in both, although the 95% confidence interval was not provided for the specific comparison of relevance to this report in Olgiati et al. A clear research question and viewpoint were included in Soini et al. but not in Olgiati et al. A comprehensive literature search to inform estimates of clinical effectiveness was not performed in Olgiati et al., whereas Soini et al. used a systematic review published by the same authors (i.e., Brignone et al. (2016),15 which is also included in this report). In both economic evaluations, the rationale for interventions and comparisons chosen was provided. Although the sources from which the utility values were obtained were referenced, there was no specific description of the population from which they came. The conclusions aligned appropriately with the results in Olgiati et al. Soini et al. did not address the lack of other relevant comparators (for example, other SSRIs in additional to sertraline and duloxetine) in their conclusions. Soini et al. was funded by and authored by employees of the manufacturer of vortioxetine.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Bupropion
No analyses or results relevant to the present review were included in Sobieraj et al. (2019).13
As noted in the Study Design section of this report, there was some overlap in the primary studies that were included in the systematic reviews. The pooled estimates from separate reviews thus contain some of the same data. A citation matrix illustrating the degree of overlap is presented in Appendix 5. Only primary studies that provided direct evidence relevant to the present review are included in the citation matrix. Additional placebo-controlled RCTs contributing to indirect evidence in network meta-analyses may also be overlapping in the reported network meta-analysis results presented in 5 included systematic reviews15-17,19,20 but are not included in the citation matrix.
Treatment Response and Remission
In Brignone et al. (2016), indirect comparisons in a network meta-analysis suggested an improved remission rate (based on HAM-D or MADRS scores) with vortioxetine compared to bupropion, but the difference was not statistically significant.15
Patel et al. (2016)14 presented results from 3 unique, relevant RCTs narratively (a total of 15 included RCTs were relevant to this review but 12 were also captured by Gartlehner et al. (2011).19 In summary, significant differences in response or remission for bupropion versus escitalopram, sertraline, fluoxetine, paroxetine, venlafaxine, duloxetine, trazodone, or nortriptyline were not observed, whether as combination or monotherapy. Specifically, for the 3 unique RCTs captured by this systematic review, there were no significant differences in response or remission rates, or HAM-D scores, when comparing bupropion with duloxetine, paroxetine, or nortryptiline.14
In Zhou et al. (2015), indirect comparisons for the outcome of response rate were reported in the network meta-analysis; no differences between bupropion and lamotrigine, lithium, olanzapine, quetiapine, risperidone, or aripiprazole were statistically significant and 95% credible intervals were wide.16
In Maneeton et al. (2013), mean change in depression scores, response rates, and remission rates was not statistically significantly different with bupropion versus venlafaxine based on a meta-analysis.18
In Gartlehner et al. (2011), results did not change from their 2007 review with this update; no differences in efficacy between second-generation antidepressants were found in patients with MDD, including no differences in response rates between bupropion and alternatives reported based on mixed-treatment comparison analyses. Strength of evidence was judged to be moderate by the systematic review authors. There was additionally moderate strength of evidence supporting no difference in efficacy between antidepressants in people with MDD and accompanying anxiety. This conclusion was based on 14 trials, including 1 study that was relevant to this report that compared bupropion SR with sertraline; for this study, response rates, remission rates, and improvement in anxiety scores were not different between treatment groups, although P values were not reported. Evidence was deemed by systematic review authors to be inadequate to draw conclusions about comparative effectiveness of antidepressants in dysthymia.19
Functional Outcomes
Cao et al. (2021) found no statistically significant differences in mean Sheehan Disability Scale scores with bupropion compared to 13 other antidepressants in the network meta-analysis.20
Sexual Dysfunction
In Reichenpfader et al. (2014), the network meta-analysis found statistically significantly lower odds of sexual dysfunction with bupropion than escitalopram, paroxetine, and sertraline. Odds ratios were also numerically lower for comparisons to citalopram, duloxetine, fluoxetine, and venlafaxine but higher compared to mirtazapine and nefazodone; however, these differences were not statistically significant and 95% credible intervals were wide.17
In Maneeton et al. (2013), differences in pooled mean change scores measuring sexual dysfunction were numerically lower in favour of bupropion compared with venlafaxine; however, this was not statistically significant.18
In a meta-analysis reported by Gartlehner et al. (2011), bupropion was associated with a statistically significantly higher rate of sexual satisfaction than fluoxetine, paroxetine, and sertraline. The results of additional studies of sexual dysfunction identified by Gartlehner et al. (2011) comparing bupropion with escitalopram, fluoxetine, or paroxetine were consistent with these meta-analysis findings. Strength of evidence was rated as high for that outcome.19
Other Safety Outcomes
In Brignone et al. (2016), the risk of withdrawals was significantly lower with vortioxetine as compared to bupropion.15
Results of the single relevant RCT in Zhou et al. (2015) were not described in detail; acceptability (all-cause discontinuation) was reported as occurring in 0 of 10 participants for bupropion and 1 of 10 with risperidone. Odds ratios for additional indirect comparisons between bupropion and lamotrigine, lithium, olanzapine, quetiapine, risperidone, or aripiprazole for outcomes of acceptability (all-cause discontinuation) and tolerability (discontinuation due to adverse events) were reported in the network meta-analysis; no differences were statistically significant and 95% credible intervals were wide.16
In the meta-analysis by Maneeton et al. (2013), overall discontinuation was not statistically significantly different with bupropion versus venlafaxine. Discontinuation due to adverse events was numerically lower in favour of bupropion; however, the difference was not statistically significant.18
In Gartlehner et al. (2011), results did not change from their 2007 review with this update; no other differences in safety between bupropion and other second-generation antidepressants were found in patients with MDD. Strength of evidence was judged to be moderate by systematic review authors.19
Cost-Effectiveness of Bupropion
In Soini et al. (2017), the base case demonstrated that vortioxetine was dominant in comparison to bupropion SR (i.e., less costly and more effective). The probability that vortioxetine was cost-effective at €0 per quality-adjusted life-year gained was 74.7% and €50,000 per quality-adjusted life-year gained was 89.5%.22
In Olgiati et al. (2013), the cost-utility analysis found an incremental cost-effectiveness ratio of $15,458 in favour of augmentation with bupropion compared with the continuation of citalopram in patients with insufficient response to 13 weeks of citalopram. Uncertainty around this estimate (i.e., the 95% confidence interval) was not provided. The intervention was considered to be cost-effective using the specified cost-effectiveness threshold of US$47,193. Investigators concluded that the cost-utility analysis supports a benefit for modifying citalopram therapy (either by augmenting with bupropion or switching to venlafaxine or sertraline) if there is insufficient response within 13 weeks.21
Limitations
No relevant evidence surrounding the effectiveness of bupropion in dysthymia was identified and there was little available evidence regarding the effectiveness of bupropion in patients with MDD and comorbid conditions like anxiety. Most estimates of the effectiveness of bupropion in MDD lacked precision (95% confidence intervals and credible intervals were wide) and several were based on indirect comparisons.
For the outcome of sexual dysfunction in which statistically significantly lower risk with bupropion compared to SSRIs was identified in 2 systematic reviews, 1 systematic review rated the strength of evidence as high,19 whereas the other that performed a network meta-analysis based on many of the same studies rated it as low “because of the indirect nature of the comparisons, the often wide credible intervals, and the high variation in magnitude of outcome.”17
There was a lack of long-term safety and efficacy studies in the identified systematic reviews.
Available economic evaluations21,22 were not done in the Canadian context, were specifically for patients with MDD with inadequate response to SSRI or SNRI treatment, and assessed a limited number of comparisons of relevance.
Conclusions and Implications for Decision- or Policy-Making
Eight systematic reviews13-20 and 2 economic evaluations21,22 comparing bupropion to other pharmacologic interventions for MDD or dysthymia were identified.
Seven systematic reviews14-20 included a total of 23 RCTs with direct comparisons of relevance to this report; 1 systematic review13 had no RCTs of relevance. The most comprehensive systematic review regarding the number of outcomes, populations, and comparisons of interest was published in 2011 at the AHRQ by Gartlehner et al.19 This systematic review did not find any of the second-generation antidepressants (which include bupropion) to be superior overall in efficacy or safety for the treatment of MDD;19 these results were consistent in the more recent included systematic reviews. Bupropion was, however, associated with a significantly lower risk of sexual dysfunction than several SSRIs (escitalopram, paroxetine, sertraline, and fluoxetine).19 The more recent systematic review and network meta-analysis of moderate quality assessing sexual dysfunction, published in 2014, also found that the risk of sexual dysfunction for people living with MDD was significantly lower with bupropion than escitalopram, paroxetine, and sertraline.17 Among the included systematic reviews, long-term clinical effectiveness data for bupropion in MDD was lacking and no evidence surrounding the effectiveness of bupropion in dysthymia, as compared to other pharmacologic treatments, was identified.
Regarding cost-effectiveness, a cost-utility analysis comparing continuation of citalopram in non-responders to augmentation with bupropion found that bupropion was a cost-effective intervention.21 Another cost-utility analysis funded by the manufacturer of vortioxetine found vortioxetine to be dominant, as compared to bupropion in patients not responsive to SNRI or SSRI treatment.22 The ability to draw firm conclusions regarding the cost-effectiveness of bupropion is limited owing to lack of cost-effectiveness evidence specific to the Canadian context and inclusion of a limited number of comparators in the available studies.
None of the studies included in this report addressed the potential for misuse and abuse of bupropion; however, potential for abuse and misuse has previously been identified as a potential issue.8 A 2010 CADTH Health Technology Inquiry Service report identified 3 case reports on bupropion abuse and misuse.24 A more recent systematic review, not meeting population eligibility criteria for the present report, found evidence of potential for a lower risk of misuse of bupropion than that of other commonly abused stimulants.25
A 2015 CADTH Rapid Response report aimed to summarize the effectiveness of antidepressants, including bupropion, in older adults. Limited evidence surrounding comparative effectiveness of antidepressants in adults 65 and older was noted and this is consistent with the present report.26
A CADTH Focused Critical Appraisal of a 2018 systematic review and network meta-analysis27 was published in 2020.28 The study was therefore not additionally included in the present review. The findings of this report are consistent with the comprehensive, high-quality network meta-analysis by Cipriani et al.27 that was described in the focused critical appraisal.28 In that systematic review and network meta-analysis, a total of 522 RCTs assessing antidepressants as monotherapy versus other antidepressants or placebo were included; 33 RCTs compared bupropion to placebo or another antidepressant in adults with MDD. Trials in which 20% or more of patients had treatment-resistant depression were excluded. For the outcomes of acceptability (dropout rate) and efficacy (response rate), the only statistically significant difference noted for bupropion was improved response as compared to reboxetine and trazodone; however, evidence was of low quality for both of those comparisons.27
Regarding future research, RCTs assessing the effectiveness of bupropion for dysthymia compared to other active interventions and placebo would reduce uncertainty. The long-term effectiveness of bupropion in MDD also remains uncertain, as well as effectiveness within specific subgroups of patients with MDD.
References
1.Patten SB, Williams JV, Lavorato DH, Wang JL, McDonald K, Bulloch AG. Descriptive epidemiology of major depressive disorder in Canada in 2012. Can J Psychiatry. 2015;60(1):23-30. PubMed
2.Ratnasingham S, Cairney J, Manson H, Rehm J, Lin E, Kurdyak P. The burden of mental illness and addiction in ontario. Can J Psychiatry. 2013;58(9):529-537. PubMed
3.Coryell W. Unipolar depression in adults: Course of illness. In: Post T, ed. UpToDate. Waltham (MA): Wolters Kluwer; 2020: www.uptodate.com. Accessed 2021 Apr 13.
4.Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments. Can J Psychiatry. 2016;61(9):540-560. PubMed
5.Hirsch M, Birnbaum RJ. Atypical antidepressants: Pharmacology, administration and side effects. In: Post T, ed. UpToDate. Waltham (MA): WoltersKluwer; 2020: www.uptodate.com. Accessed 2021 Apr 13.
6.Product Monograph. Wellbutrin XL. Bupropion Hydrochloride Extended-Release Tablets, USP 150 mg and 300 mg Antidepressant Laval (QC): Valiant Canada LP; 2020.
7.Product Monograph. Zyban. Bupropion Hydrochloride 150 mg Sustained Release Tablets Manufacturer’s Standard Smoking Cessation Aid. Laval (QC): Valiant Canada LP; 2020.
8.Stall N, Godwin J, Juurlink D. Bupropion abuse and overdose. CMAJ. 2014;186(13):1015. PubMed
9.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. https://www.bmj.com/content/bmj/358/bmj.j4008.full.pdf. Accessed 2021 Apr 13. PubMed
10.Berger ML, Martin BC, Husereau D, et al. A questionnaire to assess the relevance and credibility of observational studies to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):143-156. PubMed
11.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 Apr 13.
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Sobieraj DM, Martinez BK, Hernandez AV, et al. Adverse Effects of Pharmacologic Treatments of Major Depression in Older Adults. J Am Geriatr Soc. 2019;67(8):1571-1581. PubMed
14.Patel K, Allen S, Haque MN, Angelescu I, Baumeister D, Tracy DK. Bupropion: a systematic review and meta-analysis of effectiveness as an antidepressant. Ther Adv Psychopharmacol. 2016;6(2):99-144. PubMed
15.Brignone M, Diamand F, Painchault C, Takyar S. Efficacy and tolerability of switching therapy to vortioxetine versus other antidepressants in patients with major depressive disorder. Curr Med Res Opin. 2016;32(2):351-366. PubMed
16.Zhou X, Ravindran AV, Qin B, et al. Comparative efficacy, acceptability, and tolerability of augmentation agents in treatment-resistant depression: systematic review and network meta-analysis. J Clin Psychiatry. 2015;76(4):e487-498. PubMed
17.Reichenpfader U, Gartlehner G, Morgan LC, et al. Sexual dysfunction associated with second-generation antidepressants in patients with major depressive disorder: results from a systematic review with network meta-analysis. Drug Saf. 2014;37(1):19-31. PubMed
18.Maneeton N, Maneeton B, Eurviriyanukul K, Srisurapanont M. Efficacy, tolerability, and acceptability of bupropion for major depressive disorder: a meta-analysis of randomized-controlled trials comparison with venlafaxine. Drug Des Devel Ther. 2013;7:1053-1062. PubMed
19.Gartlehner G, Hansen RA, Morgan LC, et al. Second-Generation Antidepressants in the Pharmacologic Treatment of Adult Depression: An Update of the 2007 Comparative Effectiveness Review. Rockville (MD): Agency for Healthcare Research and Quality (US) 2011: https://www.ncbi.nlm.nih.gov/books/NBK83442/. Accessed 2021 Apr 13.
20.Cao B, Xu L, Wang D, et al. Comparative Efficacy of Pharmacological Treatments on Measures of Self -Rated Functional Outcomes Using the Sheehan Disability Scale in Patients with Major Depressive Disorder: A Systematic Review and Network Meta-analysis. CNS Spectrums. 2021. PubMed
21.Olgiati P, Bajo E, Bigelli M, Montgomery S, Serretti A. Challenging sequential approach to treatment resistant depression: Cost-utility analysis based on the Sequenced Treatment Alternatives to Relieve Depression (STAR(*)D) trial. Eur Neuropsychopharmacol. 2013;23(12):1739-1746. PubMed
22.Soini E, Hallinen T, Brignone M, et al. Cost-utility analysis of vortioxetine versus agomelatine, bupropion SR, sertraline and venlafaxine XR after treatment switch in major depressive disorder in Finland. Expert rev. 2017;17(3):293-302.
23.Zimmerman M, Martinez JH, Young D, Chelminski I, Dalrymple K. Severity classification on the Hamilton Depression Rating Scale. J Affect Disord. 2013;150(2):384-388. PubMed
24.CADTH. Bupropion for Depressive Illness: Abuse Potential and Clinical Practice Guidelines. Health Technology Inquiry Service. Ottawa (ON): CADTH; 2010: https://www.cadth.ca/sites/default/files/pdf/htis/oct-2010/K0265_Bupropion_Abuse_Potential_htis-1-5.pdf. Accessed 2021 Apr 13.
25.Naglich AC, Brown ES, Adinoff B. Systematic review of preclinical, clinical, and post-marketing evidence of bupropion misuse potential. Am J Drug Alcohol Abuse. 2019;45(4):341-354. PubMed
26.CADTH. Antidepressants in Elderly Patients with Major and Minor Depression: A Review of Clinical Effectiveness and Guidelines. Rapid Response. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/pdf/htis/aug-2015/RC0688%20Antidepressants%20in%20the%20Eldery%20Final.pdf. Accessed 2021 Apr 13.
27.Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357-1366. PubMed
28.CADTH. Drugs for major depressive disorder. Technology Review: Focused Critical Appraisal. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/hta-he/he0022-major-depressive-disorder-critical-appraisal.pdf. Accessed 2021 Apr 13.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Cao et al. (2021), China20 Funding: Startup Foundation for Talents from Southwest University | Systematic review 42 RCTs included; 2 relevant to the present review | Summary characteristics of population in relevant studies not described Baseline characteristics reported descriptively by study Inclusion criteria: adults with MDD | Eligible interventions included pharmacological treatments for MDD, comparison not specified The 2 RCTs of relevance compared bupropion to escitalopram and venlafaxine XR | Functional outcome: Mean difference in Sheehan Disability Scale |
Sobieraj et al. (2019), US13 Funding: AHRQ–Agency for Health Research and Quality | Systematic review 19 RCTs and 2 observational studies included None relevant to the present review | Inclusion criteria: Age 65 years and older with MDD, non-acute setting | SSRIs (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline), SNRIs (desvenlafaxine, duloxetine, levomilnacipran, milnacipran, and venlafaxine), and other antidepressants (bupropion, mirtazapine, trazodone, vilazodone, and vortioxetine) Comparators: as aforementioned, and additionally TCAs or MAOIs | Overall adverse events, bleeding, blood pressure, cognitive measures, electrocardiogram-related outcomes, emergency department visits, falls, fractures, hospitalizations, mortality, seizures, serious adverse events, suicide/suicide attempt, suicidal thoughts, SIADH or hyponatremia, weight changes, or number of subjects who withdrew from the study due to an adverse event Length of follow-up not specified |
Brignone et al. (2016), France15 Funding: Lundbeck SAS, the manufacturer of vortioxetine | Systematic review 27 RCTs met the inclusion criteria for the review, 3 were included in the network meta-analysis, 1 RCT was relevant to this report | Inclusion criteria: Adults 18 years or older with MDD, dysthymia, or subsyndromal depression, with inadequate response, receiving SSRI or SNRI at the time of entry into the study Inadequate response defined as failure to reduce depression rating scores by at least 50% From a relevant RCT comparing bupropion, sertraline, and venlafaxine (n = 727): mean age 41.8 58.7% female Mean HAM-D 18.9 | Interventions: fluoxetine, citalopram, fluvoxamine, sertraline, paroxetine, escitalopram, duloxetine, venlafaxine desvenlafaxine, milnacipran, phenelzine, tranylcypromine, moclobemide, doxepin, clomipramine, amitriptyline, desipramine, trimipramine, imipramine, protriptyline, maprotiline, agomelatine, mianserin, reboxetine, trazodone, mirtazapine, nefazodone, bupropion, vortioxetine, vilazodone; cognitive behavioural therapy, interpersonal therapy, and other psychotherapies; light therapy, exercise, and complementary and alternative medicine therapies Comparator: placebo, any of the included interventions administered as monotherapy, any non-pharmacological therapy, change in dose or duration of the same SSRI or SNRI The interventions and comparators for the relevant included RCT: bupropion SR 200 mg to 400 mg per day; venlafaxine XR 37.5 mg to 375 mg per day; sertraline 50 mg to 200 mg per day; placebo | Remission, defined as a HAM-D of 7 or less or a MADRS of 10 or less Tolerability defined as the number of patients in each treatment group who withdrew before completion of the study due to adverse events Study duration of 14 weeks in the included relevant RCT; 6 and 8 weeks duration for the other 2 that were included in the analysis |
Patel et al. (2016), UK14 Funding: none received | Systematic review 51 studies included 15 relevant RCTs included | Summary characteristics of population in relevant studies not described Baseline characteristics reported descriptively by study Inclusion criteria: adults 18 years and older with diagnosis of MDD, bipolar affective disorder, seasonal affective disorder, dysthymia, or postnatal (post-partum) depression (as defined by DSM-V or ICD-10, or previous versions of these diagnostic manuals) were included | Bupropion, any dose or formulation, including as augmentation therapy versus placebo or any active comparator Doses reported descriptively for the 15 relevant RCTs; formulation not consistently described | Studies evaluating efficacy using validated scales were eligible for inclusion: HAM-D, MADRS, IDS |
Zhou et al. (2015), China16 Funding: the National Basic Research Program of China | 48 RCTs 1 relevant RCT (n = 20) included | Baseline characteristics not reported separately for the RCT relevant to this review Inclusion criteria: Adults with treatment-resistant MDD, in acute phase MDD diagnosed according to standardized diagnostic criteria Treatment resistance defined as 1 treatment failure and failed at least 1 first-line treatment during current episode | Aripiprazole, bupropion, buspirone, lamotrigine, lithium, methylphenidate, olanzapine, pindolol, quetiapine, risperidone, and thyroid hormone Comparison: vs. each other or placebo The interventions and comparators for the relevant included RCT: bupropion vs. risperidone (dose and duration not described) | Treatment response (reduction of at least 50% in depression scale from baseline to post-treatment, including HAM-D, MADRS, or others) Acceptability (all-cause discontinuation) Tolerability (terminated study due to adverse effects) Length of follow-up not reported; between 2 and 14 weeks |
Reichenpfader et al. (2014), Austria17 Funding: AHRQ–Agency for Healthcare Research and Quality | 58 RCTs and 5 observational studies; 37 in NMA 6 RCTs relevant to this report | Summary characteristics of population in relevant studies not described Baseline characteristics reported separately by study Inclusion criteria: adult inpatients and outpatients with MDD | Bupropion, citalopram, desvenlafaxine, duloxetine, escitalopram, fluoxetine, fluvoxamine, mirtazapine, nefazodone, paroxetine, sertraline, trazodone, and venlafaxine Comparison: vs. each other or placebo; indirect comparisons performed in the NMA | Adverse effect of sexual dysfunction Studies of at least 6 weeks’ duration were included |
Maneeton et al. (2013), Thailand18 Funding: None received | 3 double-blind RCTs | Patients with MDD 18 years to 65 years of age 65.6% female Mean age for: Bupropion XL: 41.83 Venlafaxine XR: 41.62 | Bupropion 150 mg/day to 450 mg/day vs. venlafaxine 75 mg/day to 225 mg/day | Remission, response, overall discontinuation, and discontinuation due to adverse events Changes in sexual functioning questionnaire Included studies were 14 weeks to 16 weeks duration |
Gartlehner et al. (2011), US19 Funding: AHRQ–Agency for Healthcare Research and Quality | 248 studies: included meta-analyses, RCTs; comparative observational studies were included in absence of RCTs; 12 RCTs relevant to this report | Summary characteristics of population in relevant studies not described Baseline characteristics reported separately by study Inclusion criteria: adults with depressive disorders (MDD, dysthymia, subsyndromal depression) | Second-generation antidepressants compared to each other or placebo: bupropion, citalopram, desvenlafaxine, duloxetine, escitalopram, fluoxetine, fluvoxamine, mirtazapine, nefazodone, paroxetine, sertraline, trazodone, or venlafaxine in the 12 relevant RCTs Details on dose and formulation was described for each individual study | Maintenance of remission, response and remission for recurrent depression, safety and tolerability (overall adverse events, withdrawals because of adverse events, serious adverse events, specific adverse events or withdrawals because of specific adverse events, including: hyponatremia, seizures, suicide, hepatoxicity, weight gain, gastrointestinal symptoms, sexual side effects, others) Follow-up of at least 6 weeks |
DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, fifth edition; HAM-D = Hamilton Depression Rating Scale; ICD-10-CM = International Statistical Classification of Diseases and Related Health Problems; IDS = Inventory for Depressive Symptomology; MADRS = Montgomery–Åsberg Depression Rating Scale; MAOI = monoamine oxidase inhibitor; MDD = major depressive disorder; NMA = network meta-analysis; RCT = randomized controlled trial; SIADH = syndrome of inappropriate antidiuretic hormone; SR= sustained release; SSRI = selective serotonin reuptake inhibitor; TCA = tricyclic antidepressant; vs. = versus; XR = extended release
Table 3: Characteristics of Included Economic Evaluations
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
Soini et al. (2017), Finland22 Funding: Oy H. Lundbeck Ab, Turku, Finland, and Lundbeck SAS, France, the manufacturer of vortioxetine | Cost-utility analysis, 1 year Perspective: payer’s perspective (additional sensitivity analysis from societal perspective) | Population characteristics not provided Adult patients with MDD experiencing inadequate response with SSRI or SNRI | Bupropion SR 150 mg/day to 400 mg/day, vortioxetine (mean dose 15.7mg/day weeks 1 to 8, 16.47 mg/day in maintenance phase) Additional comparisons of vortioxetine to agomelatine and venlafaxine were not relevant to the present review | Markov model Health states: remission, relapse, and recovery | Cost data: Pharmaceutical database in Finland and the Finnish medicines tariff Utility data: previous publication and unpublished data from internal Lundbeck report Clinical data: REVIVE trial and a previously published systematic review with ITC analysis | Patients assumed to continue treatment for 6 months if no long-term AEs 20% of patients switched treatment during maintenance phase if long-term AE occurred Same relapse rate for all treatments AEs were independent AEs lasted 1 month No distribution around management of AEs was considered |
Olgiati et al. (2013), Italy21 Funding: None received | Cost-utility analysis, 26 weeks Perspective not stated; analyzed costs for drug acquisition and delivery, and visits in outpatient services | STAR*D trial participants: Mean age 40.8 years 64% Women Number of episodes: mean 6.0 Length of illness: mean 15.5 years Length of current episode: mean 24.6 months | Citalopram + bupropion (150 mg/day to 300 mg/day, mean 267mg) vs. citalopram (mean 41.7 mg/day) | Markov model Health states: acute depression (or non-remission, or relapse; all were assigned the same utility score), remission, and dropout | Cost data: Drug prices from Red Book; cost of outpatient care based on WHO data Utility data: single publication Clinical data: primarily from the STAR*D trial; RCTs and observational studies | None noted |
AE = adverse event; ITC = indirect treatment comparison; MDD = major depressive disorder; RCT = randomized controlled trial; SSRI = selective serotonin reuptake inhibitor; SNRI = serotonin-norepinephrine reuptake inhibitor; SR = sustained release; STAR*D = Sequenced Treatment Alternatives to Relieve Depression.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 2 Tool and the ISPOR Questionnaire
Strengths | Limitations |
Cao et al. (2021)20 | |
|
|
Sobieraj et al. (2019)13 | |
|
|
Brignone et al. (2016)15 | |
|
|
Patel et al. (2016)14 | |
|
|
Zhou et al. (2015)16 | |
|
|
Reichenpfader et al. (2014)17 | |
|
|
Maneeton et al. (2013)18 | |
|
|
Gartlehner et al. (2011)19 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; SSRI= selective serotonin reuptake inhibitor.
Note: This table relates to the AMSTAR 29 tool and ISPOR10 questionnaire; links can be found in the References section.
Table 5: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist
Strengths | Limitations |
Soini et al. (2017)22 | |
|
|
Olgiati et al. (2013)21 | |
|
|
Note: See Drummond Checklist reference.11
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings Included Systematic Reviews and Network Meta-Analyses
Cao et al. (2021)20
Main Study Findings
Results from network meta-analysis (NMA) of 42 randomized controlled trials (RCTs)
Sheehan Disability Scale, mean difference (95% confidence interval [CI]):
quetiapine versus (vs) bupropion: −0.45 (−4.19 to 3.29)
agomelatine vs bupropion: 0.13 (−2.12 to 2.37)
vortioxetine vs bupropion: 0.14 (−1.96 to 2.24)
bupropion vs desvenlafaxine: 0.25 (−2.09 to 2.59)
bupropion vs duloxetine: 1.14 (−1.08 to 3.36)
bupropion vs levomilacepam: 0.91 (−1.45 to 3.26)
bupropion vs venlafaxine: 0.66 (−1.48 to 2.76)
bupropion vs escitalopram: 0.17 (−2.12 to 2.45)
bupropion vs fluoxetine: −1.72 (−4.77 to 1.33)
bupropion vs paroxetine: 1.09 (−1.33 to 3.51)
bupropion vs sertraline: −0.12 (−3.07 to 2.83)
bupropion vs amitriptyline: −0.12 (−4.68 to 4.44)
Note: Negative value favours the first intervention.
Authors’ Conclusion
“Our results indicate that there may be differences across antidepressant agents and classes with respect to self-reported functional outcomes. Validation and replication of these findings in large scale RCTs are warranted. Our research results will be clinically useful for guiding psychiatrists in treating patients with MDD [major depressive disorder] and functional impairment.”(p.1)
No specific conclusions regarding bupropion were stated.
Sobieraj et al. (2019)13
Main Study Findings
No primary studies relevant to the present review were included.
Brignone et al. (2016)15
Main Study Findings
Results from NMA of 3 RCTs for the comparison of vortioxetine vs bupropion
Remission, increased with vortioxetine: risk difference −10.70% (95% CI, −27.8 to 6.4)
Withdrawals, decreased with vortioxetine: risk difference 18.3% (95% CI, 6.4 to 30.1)
Authors’ Conclusion
“Indirect comparisons showed that remission rates with vortioxetine are numerically higher than with other antidepressants in this patient group. The analysis suggests that vortioxetine is a relevant therapeutic alternative in patients who experience inadequate response to prior SSRI/SNRI [Selective serotonin reuptake inhibitor/serotonin-norepinephrine reuptake inhibitor] monotherapy. This study also provides a platform for further economic and clinical evaluations for switch interventions in patients with MDD.”(p. 363)
Patel et al. (2016)14
Main Study Findings
Results from 3 individual RCTs (that were not overlapping with Gartlehner et al. (2011)19)
Bupropion (300 mg/day) vs duloxetine (120 mg/day), 6 weeks:
Response: bupropion 71.4%, duloxetine 64%
Remission: bupropion 38.1%, duloxetine 32%
Differences were not statistically significant.
Bupropion vs paroxetine, 8 weeks:
Hamilton Depression Rating Scale (HAM-D) scores in favour of paroxetine (P = 0.002)
Values were not reported.
Bupropion vs nortriptyline, 6 weeks:
Response: bupropion 40%, nortriptyline 48%
P value was not reported; groups were noted to be comparable.
Authors’ Conclusion
“Methodologically more robust trials support the superiority of bupropion over placebo, and most head-to-head antidepressant trials showed an equivalent effectiveness, though some of these are hindered by a lack of a placebo arm. Most work on the coprescribing of bupropion with another antidepressant supports an additional effect, though many are open-label trials. Several large multi-medication trials, most notably STAR*D [Sequenced Treatment Alternatives to Relieve Depression], also support a therapeutic role for bupropion; in general, it demonstrated similar effectiveness to other medications, though this literature highlights the generally low response rates in refractory cohorts. Effectiveness has been shown in ‘other’ populations, though there is an overall dearth of research. Bupropion is generally well tolerated, it has very low rates of sexual dysfunction, and is more likely to cause weight loss than gain. Our findings support the use of bupropion as a sole or coprescribed antidepressant, particularly if weight gain or sexual dysfunction are, or are likely to be, significant problems. However there are notable gaps in the literature, including less information on treatment naïve and first presentation depression, particularly when one considers the ever-reducing rates of response in more refractory illness. There are some data to support bupropion targeting specific symptoms, but insufficient information to reliably inform such prescribing, and it remains uncertain whether bupropion pharmacodynamically truly augments other drugs.”(p. 99)
Zhou et al. (2015)16
Main Study Findings
Results from NMA of 48 RCTs:
Response rate, odds ratio (OR) (95% credible interval [CrI])
bupropion vs lamotrigine 1.24 (0.44 to 2.80)
bupropion vs lithium 1.01 (0.38 to 2.19)
bupropion vs olanzapine 0.99 (0.46 to 1.84)
bupropion vs quetiapine 0.72 (0.33 to 1.26)
bupropion vs risperidone 0.93 (0.44 to 1.77)
aripiprazole vs bupropion 1.49 (0.70 to 2.66)
All-cause discontinuation, OR (95% CrI)
lamotrigine vs bupropion 1.42 (0.32 to 3.92)
lithium vs bupropion 0.84 (0.25 to 2.07)
olanzapine vs bupropion 0.90 (0.28 to 2.10)
quetiapine vs bupropion 1.07 (0.37 to 2.51)
risperidone vs bupropion 0.85 (0.27 to 1.99)
bupropion vs aripiprazole 1.61 (0.54 to 4.18)
Discontinuation due to adverse effects, OR (95% CrI)
lamotrigine vs bupropion 1.68 (0.22 to 5.92)
lithium vs bupropion 0.65 (0.13 to 2.10)
olanzapine vs bupropion 0.44 (0.09 to 1.38)
quetiapine vs bupropion 0.39 (0.09 to 1.21)
risperidone vs bupropion 0.59 (0.08 to 2.03)
bupropion vs aripiprazole 2.90 (0.54 to 9.48)
Note: A value > 1 denotes higher frequency for the first drug.
Authors’ Conclusion
“Quetiapine and aripiprazole appear to be the best evidence-based options for augmentation therapy in adult treatment resistant depression (TRD) patients, but clinicians should interpret these findings cautiously in light of evidence of potential treatment-related adverse effects. More head-to-head and longer-term RCTs are required to strengthen the evidence regarding augmentation therapy for TRD (including potential moderators of response), and further development and validation of new augmentation agents with greater efficacy, acceptability and tolerability are still needed.”(p. e496)
Reichenpfader et al. (2014)17
Main Study Findings
Results from NMA of 37 RCTs:
Sexual dysfunction, OR (95%CrI) vs bupropion
citalopram 2.94 (0.81 to 7.90)
duloxetine 2.21 (0.88 to 4.67)
escitalopram 3.08 (1.27 to 6.45)
fluoxetine 1.02 (0.42 to 2.11)
fluvoxamine 1.35 (0.24 to 4.44)
mirtazapine 0.82 (0.20 to 2.29)
nefazodone 0.45 (0.10 to 1.29)
paroxetine 3.56 (1.45 to 7.38)
sertraline 2.21 (1.07 to 4.12)
venlafaxine 1.30 (0.47 to 2.93)
Note: A value > 1 denotes higher frequency than bupropion.
Authors’ Conclusion
“Based on the findings of this review using data from RCTs and observational studies on adverse events and second-generation antidepressants, the comparative risk of sexual dysfunction associated with a specific antidepressant cannot be precisely determined. Nevertheless, we observed three main patterns in our network meta-analysis with bupropion having a statistically significantly lower risk of sexual dysfunction than some other second generation antidepressant, and both escitalopram, and paroxetine showing a statistically significantly higher risk of sexual dysfunction than some other second generation antidepressant.”(p. 11)
Maneeton et al. (2013)18
Main Study Findings
Results from meta-analysis of 3 RCTs for the comparison of bupropion vs venlafaxine:
Change in depression scores: standardized mean difference (SMD) 0.05 (95% CI, –0.16 to 0.26)
Response: relative risk (RR) 0.92 (95% CI, 0.79 to 1.08)
Remission: RR 0.97 (95% CI, 0.75 to 1.24)
Overall discontinuation: RR 1.00 (95% CI, 0.80 to 1.26)
Discontinuation rate due to adverse events: RR 0.69 (95% CI, 0.44 to 1.10)
Note: A value > 1 denotes higher frequency with bupropion.
Mean change in Changes in Sexual Functioning Questionnaire scores: weighted mean difference 1.35 (95% CI, –0.04 to 2.75)
In favour of bupropion, not statistically significant.
Note: Significant statistical heterogeneity was observed for depression score, response, and remission.
Authors’ Conclusion
“According to the findings provided from these three RCTs, bupropion XL was as effective as venlafaxine XR for adult MDD patients. The equivalent dropout rate due to adverse events indicates the comparable tolerability of both active agents. Based on the overall discontinuation rates, which took into account both the efficacious benefit and risk from adverse events, these agents appeared to have comparable acceptability. Based on the Changes in Sexual Functioning Questionnaire scores, a trend indicated that bupropion is less likely to cause treatment-emergent sexual dysfunction. However, these outcomes should be considered as initial findings. Further well-defined clinical trials in this field should be conducted to confirm these findings. Additionally, further systemic reviews of bupropion in the treatment of MDD compared with other antidepressants, including SSRIs, may be useful.”(p. 1060)
Gartlehner et al. (2011)19
Main Study Findings
Patients With MDD
Response rate OR, mixed-treatment comparisons analysis:
citalopram vs bupropion 0.37 (95% CrI, 0.1 to 3.03)
escitalopram vs bupropion 0.74 (95% CrI, 0.50 to 1.06)
fluoxetine vs bupropion 1.11 (95% CrI, 0.81 to 1.48)
fluvoxamine vs bupropion 0.44 (95% CrI, 0.13 to 2.82)
paroxetine vs bupropion 0.93 (95% CrI, 0.65 to 1.28)
sertraline vs bupropion 0.90 (95% CrI, 0.66 to 1.20)
desvenlafaxine vs bupropion 0.89 (95% CrI, 0.58 to 1.31)
mirtazapine vs bupropion 0.74 (95% CrI, 0.46 to 1.26)
venlafaxine vs bupropion 0.78 (95% CrI, 0.53 to 1.10)
duloxetine vs bupropion 0.99 (95% CrI, 0.69 to 1.37)
bupropion vs nefazodone 1.20 (95% CrI, 0.66 to 2.00)
bupropion vs trazodone 0.92 (95% CrI, 0.54 to 1.47)
A value < 1 favours the first drug.
Overall discontinuation RR, meta-analysis:
bupropion vs SSRIs 0.86 (95% CI, 0.73 to 1.01)
In favour of bupropion.
Discontinuation due to adverse events RR, meta-analysis:
bupropion vs SSRIs 1.08 (95% CI, 0.53 to 2.18)
In favour of bupropion.
Sexual satisfaction RR, meta-analysis:
bupropion vs SSRIs (fluoxetine, paroxetine, sertraline) 1.28 (95% CI, 1.16 to 1.41); results reported from a prior meta-analysis of 5 RCTs; results presented from 3 additional RCTs (comparing bupropion with escitalopram, fluoxetine, or paroxetine) published since that meta-analysis were consistent)
In favour of bupropion.
Note: See Table 47 of the systematic review for characteristics and results of individual comparative studies of bupropion with SSRIs for sexual dysfunction outcomes.
Patients With MDD and Anxiety
Results from 1 RCT relevant to this report that compared bupropion SR with sertraline over 16 weeks in 248 patients with MDD, some with high anxiety (HAM-D score ≥ 19)
Response rate, high anxiety subgroup: bupropion vs sertraline “approximately 70 percent in each group” (p. 81), P value not reported
Remission rate, high anxiety subgroup: bupropion vs sertraline “approximately 70 percent in each group” (p. 81), P value not reported
Anxiety reduction (mean change in HAM-D score), high anxiety subgroup: bupropion (−10.0) vs sertraline (−9.7), P value not reported
Authors’ Conclusion
“Our findings indicate that the existing evidence does not warrant the choice of one second-generation antidepressant over another based on greater efficacy and effectiveness. Differences with respect to onset of action and adverse events may be taken into consideration for the choice of a medication.”(p. v)
Summary of Findings of Included Economic Evaluations
Soini et al. (2017)22
Main Study Findings
Vortioxetine vs bupropion
Incremental quality-adjusted life-years (QALYs): 0.0166
Incremental direct costs: –€128
Incremental indirect costs: –€829
Incremental societal costs: –€957
Probability that vortioxetine is cost-effective versus bupropion SR at the given cost-effectiveness threshold:
€0/QALY = 74.7%
€10,000/QALY 84.1%
€20,000/QALY 86.6%
€30,000/QALY 88.1%
€50,000/QALY 89.5%
Authors’ Conclusion
“The results of these cost-utility analyses suggest that vortioxetine should be the dominant strategy when switching antidepressants is needed in the treatment of patients with MDD. The greater effectiveness associated with vortioxetine is an important driver for the cost savings and quality of life gains accrued with vortioxetine. The results were robust based on several sensitivity analyses. According to the literature and Finnish clinical experience, there is an unmet need for new safe and effective treatment for patients who were switched from their initial AD [antidepressant] treatment. Vortioxetine provides a good alternative for this patient group in Finland.”(p.301)
Olgiati et al. (2013)21
Main Study Findings
Remission probability: 47.5% with augmentation of citalopram with bupropion vs 34.6% with continuation of citalopram (number needed to treat = 7.7)
ICER: $15,458
Incremental QALYs: 0.008
Incremental cost: $124.44
Sensitivity analyses around these estimates were not performed.
Bupropion augmentation was cost-effective at the specified threshold of US $47,193.
Authors’ Conclusion
“The results of this cost-utility analysis are consistent with current guidelines suggesting that antidepressant treatment should be modified after 3 months of insufficient response. However there might be less advantage for this approach than generally acknowledged, and it is necessary to combine symptomatic improvement, quality of life and costs to demonstrate its dominance over continuing with first-line treatment.”(Page 1745)
Appendix 5: Overlap Between Included Systematic Reviews
Table 6: Overlap in Relevant RCTs Between Included Systematic Reviews
Primary study citation | Cao et al. (2021)20 | Brignone et al. (2016)15 | Patel et al. (2016)14 | Zhou et al. (2015)16 | Reichenpfader et al. (2014)17 | Maneeton et al. (2013)18 | Gartlehner et al. (2011)19 |
Soczynska JK, et al. Psychiatry Research. 2014;220:245-50. | X | — | — | — | — | — | — |
Rush AJ, et al. N Engl J Med. 2006;354:1231-42. | — | X | — | — | — | — | X |
Shelton RC, et al. Neuropsychopharmacology. 2006;30(suppl 1):S238. | — | — | — | X | — | — | — |
Thase ME, et al. J Clin Psycopharmacol. 2006;26(5):482-488. | — | — | X | — | — | X | — |
Hewett K, et al. J Psychopharmacol (Oxford). 2009;23(5):531-538. | — | — | X | — | — | X | — |
Hewett K, et al. J Psychopharmacol (Oxford). 2010;24(8):1209-1216. | X | — | X | — | — | X | — |
Grunebaum M et al. Neuropsychopharmacology. 2012;37:697-706. | — | — | X | — | — | — | — |
Rosso et al. J Affect Dis. 2012;136(1-2)172-176. | — | — | X | — | — | — | — |
Masco et al. Curr Ther Res Clin Exp. 1994;55:851-63. | — | — | X | — | — | — | — |
Coleman CC, et al. Clin ther. 2001;23(7):1040-58. | — | — | X | — | X | — | X |
Feighner JP, et al. J Clin Psychiatry. 1991;52(8):329-35. | — | — | X | — | X | — | X |
Kennedy SH, et al. Can J Psychiatry. 2006;51(4):234-42. | — | — | X | — | — | — | X |
Coleman CC et al. Ann Clin Psychiatry. 1999;11(4):205-15. | — | — | X | — | X | — | X |
Croft H, et al. Clin ther. 1999. 21(4):643-58. | — | — | X | — | X | — | X |
Kavoussi RJ et al. J Clin Psychiatry. 1997;58(12):532-7. | — | — | X | — | — | — | X |
Rush AJ et al. Neuropsychopharmacol. 2001;25(1):131-8. | — | — | X | — | — | — | X |
Clayton AH, et al. Clin Psychiatry 2006;67(5):136-46. | — | — | X | — | X | — | X |
Segraves RT, et al. J Clin Psychopharmacol. 2000;20(2):122-8. | — | — | — | — | X | — | X |
Weihs KL, et al. J Clin Psychiatry. 2000;61(3):196-202. | — | — | — | — | — | — | X |
Doraiswamy et al. Am J Geriatr Psychiatry. 2001;9(4):423-8. | — | — | — | — | — | — | X |
Rush AJ, et al. Am J Psychiatry. 2006;163(11):1905-17. (STAR*D) | — | — | X | — | — | — | X |
Trivedi MH, et al. N Engl J Med. 2006;354(12):1243-52.(STAR*D) | — | — | — | — | — | — | X |
Weisler RH, et al. J Clin Psychopharmacol. 1994;14(3):170-9. | — | — | — | — | — | — | X |
Note: X indicates the primary study was included within the systematic review; — indicates the primary study was not included within the systematic review.
Appendix 6: References of Potential Interest
Previous CADTH Reports
1.Use of Bupropion in Patients with Depression and the Associated Risk of Seizures: Safety. Ottawa: CADTH; 2010 Apr. (CADTH Rapid Response). https://cadth.ca/sites/default/files/pdf/htis/apr-2010/L0171_bupropion_risk_seizure_htis-L2.pdf Accessed 2021 Apr 13.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca