CADTH Health Technology Review
Bupropion for Treatment-Resistant Depression
Rapid Review
Authors: Khai Tran, Sarah C. McGill, Jennifer Horton
Abbreviations
CI
confidence interval
ICER
incremental cost-effectiveness ratio
MAOI
monoamine oxidase inhibitor
MDD
major depressive disorder
NHB
net health benefit
QALY
quality-adjusted life-year
RCT
randomized controlled trial
RR
rate ratio
SNRI
serotonin-norepinephrine reuptake inhibitor
SR
sustained release
SSRI
selective serotonin reuptake inhibitor
STAR*D
Sequenced Treatment Alternatives to Relieve Depression
TCA
tricyclic antidepressant
TRD
treatment-resistant depression
VAST-D
Veterans Affairs Augmentation and Switching Treatments for Improving Depression Outcomes
WTP
willingness to pay
Key Messages
Switching to monotherapy after failure with a first antidepressant resulted in no significant difference in efficacy and tolerability among bupropion, sertraline, and venlafaxine.
In treatment-resistant depression, augmentation of previous treatment with bupropion did not result in significant differences in remission compared with switching to bupropion monotherapy, augmentation with aripiprazole, or augmentation with buspirone.
Switching to bupropion monotherapy or augmentation with bupropion was associated with significantly higher incidence of anxiety, decreased appetite, dry mouth, and increased blood pressure, but lower incidence of increased appetite, increased weight, somnolence, akathisia, and laboratory test abnormality compared to augmentation with aripiprazole.
Augmentation therapy with bupropion or aripiprazole may be a cost-effective option relative to switching to bupropion in treatment-resistant depression.
Among the monotherapies, switching to vortioxetine appeared to be the most cost-effective option relative to other medications such as agomelatine, bupropion, venlafaxine, or sertraline; bupropion, venlafaxine, and sertraline monotherapies were not significantly different from one another in terms of cost-effectiveness.
Context and Policy Issues
Major depressive disorder (MDD) is a common and disabling illness and 1 of the most common mood disorders. It affects the entire body and mind, leading to reductions in quality of life and significant costs to the health care sector and society.1 MDD is associated with a high risk of mortality with a relative risk of 1.81 compared with persons without depression.2 According to Statistics Canada’s 2012 Canadian Community Health Survey on Mental Health, it is estimated that 5.4% of the Canadian population aged 15 years and older have reported mood disorders in the previous 12 months, including 4.7% for major depression.1 A recent survey on COVID-19 and mental health during the last 3 months of 2020 found that 1 in 5 Canadians had a positive screening for at least 1 of the 3 mental disorders: MDD, generalized anxiety disorder, and post-traumatic stress disorder.3 MDD was the most prevalent mental disorder, with 15% Canadians screening positive with moderate or severe symptoms.3 A variety of antidepressant agents have been used for the treatment of patients with MDD including selective serotonin reuptake inhibitor (SSRI), serotonin-norepinephrine reuptake inhibitor (SNRI), tricyclic antidepressant (TCA), monoamine oxidase inhibitor (MAOI), glutamate antagonist, and atypical antidepressants such as bupropion.4 Despite advances in understanding the efficacy and safety of those pharmacological agents, 10% to 15% of patients do not respond to their first course of antidepressant pharmacotherapy, and 30% to 40% achieve only partial remission.5 After proper diagnosis and adequate treatment of MDD with antidepressants, individuals who are still nonresponders or partial responders are considered to have treatment-resistant depression (TRD). Although there is no universally accepted definition of TRD, approximately half of clinical trials required a minimum of 2 treatment failures to be considered TRD.6 The pharmacological options for treating TRD are not well-established and remain a challenge for physicians.7 Options for treatment of TRD include augmentation and switching of the initial antidepressant.7
Bupropion is an atypical antidepressant which inhibits the reuptake of noradrenaline and dopamine and has been used for treatment of MDD.8 It is generally well-tolerated but can cause weight loss and low rates of sexual dysfunction.8 However, its clinical effectiveness and cost-effectiveness in the treatment of TRD is less well understood. The current report aims to review the clinical effectiveness and cost-effectiveness of bupropion for the treatment of adults with TRD.
Research Questions
What is the clinical effectiveness of bupropion for the treatment of adults with TRD?
What is the cost‐effectiveness of bupropion for the treatment of adults with TRD?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and Embase via Ovid, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were bupropion and depression. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, network meta-analyses, or economic studies. Conference abstracts, comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and February 26, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Adults with TRD, with or without comorbid conditions |
Intervention | Bupropion, as a single ingredient, as primary or adjunct to other pharmaceutical therapy, all formulations and all routes of administration |
Comparator |
|
Outcomes | Q1: Clinical effectiveness (e.g., symptoms, mood stability, quality of life, cognitive function, functional outcomes, tachyphylaxis) and safety (e.g., misuse, abuse, side effects [e.g., sexual dysfunction], adverse events, morbidity, mortality) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year, cost per patient adverse event avoided, cost per clinical outcome) |
Study designs | Health technology assessment, systematic review, and economic evaluation |
MAOI = monoamine oxidase inhibitor; SNRI = serotonin-norepinephrine reuptake inhibitor; SSRI = selective serotonin reuptake inhibitor; TCA = tricyclic antidepressant.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2017. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)9 for systematic reviews, and the Drummond checklist10 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
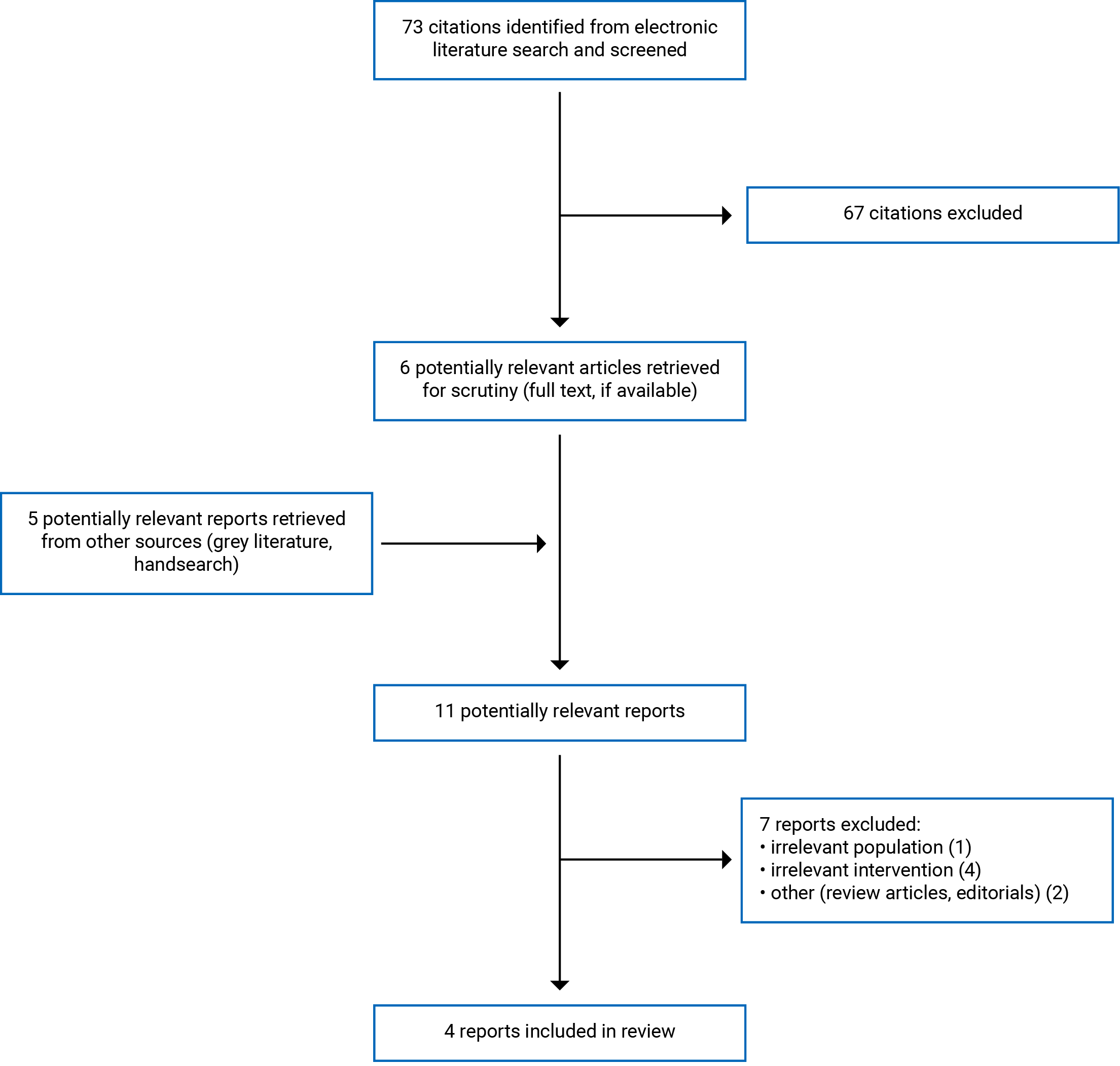
A total of 73 citations were identified in the literature search. Following screening of titles and abstracts, 67 citations were excluded and 6 potentially relevant reports from the electronic search were retrieved for full-text review. Five potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 7 publications were excluded for various reasons, and 4 publications met the inclusion criteria and were included in this report. These comprised 1 systematic review and 3 economic evaluations. Appendix 1 presents the PRISMA11 flow chart of the study selection.
Summary of Study Characteristics
The detailed characteristics of the included systematic review4 (Table 2) and economic studies12-14 (Table 3) are presented in Appendix 2.
Study Design
The included systematic review4 conducted a narrative synthesis on pharmacological treatments for patients with TRD. The systematic review included 71 randomized controlled trials (RCTs), of which 4 assessed bupropion. The literature search was performed from 2 main databases (i.e., PubMed and PsycINFO), with no search restrictions on the publication year or type. The quality of the included studies was not assessed. The 4 studies that assessed bupropion were 2 level 2 STAR*D (Sequenced Treatment Alternatives to Relieve Depression) RCTs,15,16 a VAST-D (Veterans Affairs Augmentation and Switching Treatments for Improving Depression Outcomes) RCT,17 and a cohort study by Lam and colleagues.18
Three economic studies12-14 were included: 2 were cost-utility studies12,14 and 1 was a cost-effectiveness study.13
The cost-utility analysis study by Yoon et al.12 was conducted using the efficacy and utility data of the VAST-D trial17 to compare the cost-utility of augmentation therapy versus monotherapy. The time horizon was 12 weeks. The study considered a health sector perspective for the primary analysis and included all mental health care costs (study drugs, outpatient mental health, and inpatient psychiatric care). Additional analyses also included a societal perspective which accounted for all other health care costs and costs borne by patients.
The other cost-utility analysis study by Soini et al.14 used the efficacy and utility data from the REVIVE trial19 and an indirect treatment comparison from a previous systematic review by Brignone et al. (2016)20 to compare the cost-utility of 5 different monotherapies after switching treatment in patients with MDD. The time horizon was 1 year. The base-case analysis was conducted from the Finnish health care payer’s perspective, considering all direct costs related to depression treatment and management. Additional analyses also included a societal approach that accounted for other costs, including patients’ productivity losses.
The cost-effectiveness analysis study by Singh et al.13 was conducted using the effectiveness data from the level 2 STAR*D trial15 to determine which of the switch options was more cost-effective. The analyses were carried out from the perspective of the US government as the payer and considering direct costs including drug costs, outpatient and emergency department visit costs, and hospitalization costs.
Country of Origin
The included systematic review was conducted by authors from the US.4 The included economic studies were conducted by authors from the US12,13 and Finland.14
Patient Population
The systematic review 4 included studies involving patients with MDD over the age of 18 who had failed to respond to at least 1 antidepressant. Sample sizes ranged from 32 to 1,522 patients. Details of patient characteristics were not described.
Patients in the cost-utility analysis study by Yoon et al.12 were treatment-resistant MDD patients (N = 1,522 veterans) who did not respond to initial pharmacologic treatment in the VAST-D trial.17 Patients were predominantly male (85%) with a mean age of 54 years. The mean duration of the current episode of MDD was 87 months. All patient baseline characteristics were balanced between treatment groups.
The other cost-utility analysis study by Soini et al.14 used patient data from the REVIVE trial19 and the indirect treatment comparison from a previous systematic review.20 Participants were patients with MDD who required second-line treatment after inadequate response to an SSRI or SNRI. Details of patient characteristics were not described.
The cost-effectiveness analysis study by Singh et al.13 used patient data from the level 2 STAR*D trial.15 Participants were outpatients (N = 727) with nonpsychotic MDD who did not respond to initial treatment with the SSRI citalopram or subsequent treatments. The mean age was 42 years and 41% were male. The mean duration of MDD was 17 years. All patient baseline characteristics were balanced between treatment groups.
Interventions and Comparators
The systematic review 4 narratively synthesized 4 studies involving bupropion.15-18 The first level 2 STAR-D trial published by Rush et al. (2006)15 compared switching to bupropion (n = 239), sertraline (n = 238), or venlafaxine (n = 250) in patients with MDD who had no remission of symptoms with the SSRI citalopram. The second level 2 STAR-D trial, which was published by Trivedi et al. (2006)16 compared augmenting citalopram with bupropion (n = 279) or augmenting citalopram with buspirone (n = 286) in patients who failed to respond to citalopram. The VAST-D trial by Mohamed et al. (2017)17 compared 3 treatment options in MDD patients who failed to respond to at least 1 antidepressant: switching to bupropion (n = 511), augmentation with bupropion (n = 506), or augmentation with aripiprazole (n = 505). The cohort study by Lam et al. (2004)18 compared bupropion monotherapy (n = 17), citalopram monotherapy (n = 12), or a combination of bupropion and citalopram (n = 32) in MDD patients who failed either bupropion or citalopram.
The cost-utility analysis study by Yoon et al.12 compared the cost-utility of 3 treatment options in the VAST-D trial17: augmenting antidepressant therapy with aripiprazole, augmenting antidepressant therapy with bupropion, and switching to bupropion over a 12-week acute treatment phase.
The cost-utility analysis study by Soini et al.14 assessed the cost-utility of vortioxetine compared with agomelatine, bupropion, sertraline, and venlafaxine over a 12-week treatment period.
The cost-effectiveness analysis study by Singh et al.13 compared the cost-effectiveness of 3 switching options in the level 2 STAR*D trial15: bupropion, sertraline, and venlafaxine over a 14-week treatment period.
Outcomes
The outcomes considered in the SR4 were remission, response, and adverse events. Definitions of outcomes were not provided.
The outcomes considered in the cost-utility analysis study by Yoon et al.12 were incremental cost-effectiveness ratio (ICER) for costs per remission and ICER for costs per quality-adjusted life-year (QALY) analyzed from the health sector perspective and societal perspective.
The main outcome in the cost-utility analysis study by Soini et al.14 was ICER per QALY gained analyzed from the Finnish health care payer’s perspective and societal perspective.
In the study by Singh et al.,13 the cost-effectiveness was calculated using the net health benefit (NHB) framework with the formula: NHB = (µEi – µCi) / λ, where µEi and µCi are the average effectiveness and costs, respectively, for treatment i, and λ is the amount of money for which there is a willingness to pay (WTP) per unit of effectiveness. WTP was assumed to be US$30,000 for remission or response over the duration of treatment. The treatment option with the highest NHB is considered to be the most cost-effective option.
Summary of Critical Appraisal
The detailed quality assessments of the included systematic review4 (Table 4) and economic studies12-14 (Table 5) are presented in Appendix 3.
The systematic review4 was explicit in its objective and inclusion criteria for the review, selection of study design for inclusion, and included a comprehensive literature search strategy. It was unclear if the study selection and data extraction was performed in duplicate. The quality of the included studies was not assessed. The systematic review did not report whether a protocol had been published before the conduct of the review. The systematic review also did not report the sources of funding of the studies included in their review nor provide a list of excluded studies. The included studies were narratively synthesized without describing the study characteristics. Conflicts of interest were declared. Overall, the systematic review was of poor methodological quality.
All 3 of the included economic studies clearly stated the objectives, the economic importance of the research questions, the rational for choosing the alternative comparators, the viewpoint of the analysis, and the type of economic evaluation that was conducted. However, none of the studies justified the choice of form of economic evaluation in relation to the questions addressed. For data collection, all 3 studies clearly stated the sources of utility and effectiveness estimates with details of the design and the findings of those studies, the primary outcome measures for the economic evaluation, the methods to value benefits, the methods for the estimation of quantities and unit costs, currency and price data, and details of the model used. The economic evaluations provided justification for the choice of model used and the key parameters on which it is based. For the analysis and interpretation of results, all 3 studies clearly stated time horizon of costs and benefits, details of statistical tests and confidence intervals, and the approach to sensitivity analysis. All studies provided justification for the choice of variables for sensitivity analysis, and the ranges over which the variables were varied. The conclusions in all studies were based on the data reported and were accompanied by the appropriate caveats. Overall, all 3 economic studies were of high methodological quality with respect to study design, data collection, and analysis and interpretation of results.
Summary of Findings
The main findings and authors’ conclusions of the systematic review4 and the economic evaluations12-14 are presented in Appendix 4.
Clinical Effectiveness of Bupropion for TRD
The clinical efficacy of bupropion as a switch medication compared with other antidepressants and as an augmentation strategy with another antidepressant was reviewed.
Switch to Another Antidepressant
The systematic review4 discussed the results of level 2 of the STAR*D study by Rush et al. (2006).15 In this trial, adult patients with MDD (N = 727) who had inadequately improved with the SSRI citalopram and agreed to switch were randomized to receive 1 of the following drugs for up to 14 weeks: bupropion (n = 239), sertraline (n = 238), or venlafaxine (n = 250). There were no significant differences in remission rates (21.3%, 17.6%, and 24.8%, respectively; P = 0.16) and response rates (26.1%, 26.7%, and 28.2%, respectively; P = 0.72) among switching drugs. There were also no significant differences among treatment groups in time to remission, time to response, and intolerability.
Augmentation Strategy
The systematic review4 discussed the results of 3 trials: the VAST-D trial,17 the cohort study by Lam et al. (2004),18 and level 2 of the STAR*D study by Trivedi et al. (2006).16
In the VAST-D trial,17 1,522 adult veterans who failed with at least 1 antidepressant were randomized to receive 1 of 3 options: switch to bupropion (switch-bupropion group, n = 511), augmentation of previous treatment with bupropion (augment-bupropion group, n = 506), or augmentation with the atypical antipsychotic drug aripiprazole (augment-aripiprazole group, n = 505) for 12 weeks. The remission rates for the 3 treatment groups were 22.3%, 26.9%, and 28.9%, respectively. There was no significant difference in the remission rates between the augment-bupropion group and the switch-bupropion group (rate ratio [RR] = 1.20; 95% confidence interval [CI], 0.97 to 1.50; P = 0.09). Augmentation with aripiprazole resulted in no significant difference in remission rates compared with augmentation with bupropion (RR = 1.08; 95% CI, 0.88 to 1.31; P = 0.47) but was significantly higher than the group that switched to bupropion (RR = 1.30; 95% CI, 1.05 to 1.60; P = 0.02). Cox regression analysis of time to remission showed no significant differences in cumulative remission when comparing between treatment groups. Response rate was significantly higher for the augment-aripiprazole group (74.3%) than for both the switch-bupropion group (62.4%; RR = 1.19; 95% CI 1.09 to 1.29; P < 0.001) and the augment-bupropion group (65.6%; RR = 1.13; 95% CI, 1.04 to 1.23; P = 0.003). There was no significant difference in response rate between the augment-bupropion group and the switch-bupropion group (RR = 1.05; 95% CI, 0.96 to 1.15; P = 0.29). During the 12-week study period, adverse events occurred significantly more frequently in the switch-bupropion group and the augment-bupropion group compared to the augment-aripiprazole group, such as anxiety (24.3%, 22.5%, and 16.6%, respectively; P = 0.007), decreased appetite (15.5%, 11.9%, and 7.9%, respectively; P = 0.001), dry mouth (10%, 7.1%, and 2.8%, respectively; P < 0.001), and increased blood pressure (1.2%, 1.2%, and 0, respectively; P = 0.03). Other adverse events occurred significantly less frequently in the switch-bupropion group and the augment-bupropion group compared to the augment-aripiprazole group such as increased appetite (7.4%, 8.7%, 16.0%; P < 0.001), increased weight (0.4%, 0.6%, 5.7%; P < 0.001), somnolence (7.2%, 7.9%, and 14.5%; P < 0.001), akathisia (4.3%, 5.3%, and 14.9%; P < 0.001), and laboratory test abnormality (2.7%, 3.8%, and 8.7%; P < 0.001).
The cohort study by Lam et al.18 compared the combination of bupropion plus citalopram (n = 32) with the switch monotherapy group (either bupropion [n = 17] or citalopram [n = 12]) in 61 patients who had failed either bupropion or citalopram. The combination group had a significantly higher remission rate (28%) than that of the switch monotherapy group (7%; P < 0.05). The frequency and severity of side effects were not significantly different between groups.
In level 2 of the STAR*D trial,16 565 adult patients with MDD who had inadequately improved with the SSRI citalopram were randomized to receive augmenting citalopram with bupropion (n = 279) or augmenting citalopram with buspirone (n = 286) for up to 14 weeks. There were no significant differences between groups in remission rate (29.7% versus 30.1%; P = 0.93) or in response rate (31.8% versus 26.9%; P = 0.21). The bupropion group had a significantly lower dropout rate (12.5%) than buspirone group (20.6%) due to intolerance (P < 0.009).
Cost-Effectiveness of Bupropion for TRD
The findings of the 3 included economic evaluations12-14 on the cost-effectiveness of bupropion relative to other treatment strategies were presented at the study level.
The cost-utility analysis by Yoon et al. (2018)12 was conducted as part of the VAST-D trial to compare the cost-effectiveness of 3 alternate treatments for TRD: switching to bupropion, augmentation with bupropion, and augmentation with aripiprazole. From the health care sector perspective, the ICER for cost per remission between augmentation with bupropion and switching to bupropion was –US$640 (95% CI, –US$5,770 to US$3,008) with 79.0% at the lower-right quadrant by bootstrapping analyses, indicating that bupropion augmentation was associated with lower costs and greater benefits. Bupropion augmentation strongly dominated bupropion switching. The ICER for cost per remission between aripiprazole augmentation and switching to bupropion was US$1,074 (95% CI, US$47 to US$5,022) with 97.9% at the upper-right quadrant by bootstrapping analyses, indicating greater costs and benefits. The ICER for cost per remission between aripiprazole augmentation and bupropion augmentation was US$5,094 (95% CI, –US$34,027 to US$32,774) with 75.6% at the upper-right quadrant by bootstrapping analyses, indicating greater costs and benefits. The cost-effectiveness acceptability curves comparing the cost-effectiveness of the treatments across a range of WTP values per remission showed that at a WTP of less than US$10,000, bupropion augmentation had higher probability of being more cost-effective than the other 2 strategies, whereas at a WTP greater than US$10,000, aripiprazole augmentation had 76% probability of being more cost-effective than the other strategies. When the ICER for cost was expressed per QALY from the health care sector perspective, only bupropion augmentation was more cost-effective than bupropion switching. From the societal perspective, the results were similar to those from the health care sector perspective that both the augmentation groups were more cost-effective relative to the switching to bupropion group, and aripiprazole augmentation was more cost-effective than bupropion augmentation.
The cost-utility analysis by Soini et al. (2017)14 compared the cost-effectiveness of vortioxetine switching relative to 4 other switching monotherapies (i.e., agomelatine, bupropion, venlafaxine, and sertraline) in MDD patients with inadequate response to SSRI or SNRI. The base-case analyses showed that vortioxetine treatment resulted in higher QALY and lower costs compared to all other comparators, including bupropion. The changes in QALY between vortioxetine and subsequent comparators (agomelatine, bupropion, sertraline, and venlafaxine) were 0.0134, 0.0166, 0.0250, and 0.0276, respectively. The changes in total direct costs between vortioxetine and subsequent comparators were –€223, –€128, –€110, and –€238, respectively. The changes in total indirect costs between vortioxetine and subsequent comparators were –€850, –€829, –€609, and –€1,152, respectively. The changes in total societal costs between vortioxetine and subsequent comparators were –€1,074, –€957, –€720, and –€1,390, respectively. Thus, vortioxetine was associated with a dominant ICER compared with all comparators (i.e., less costly and more effective), regardless of the perspective considered. Probabilistic sensitivity analyses showed that vortioxetine dominated all the comparators (dominant in > 72%), regardless of the WTP threshold.
The cost-effectiveness analysis by Singh et al. (2017)13 compared the cost-effectiveness of 3 switching monotherapies (bupropion, sertraline, and venlafaxine) following unsuccessful treatment with citalopram. The cost-effectiveness analyses were conducted by calculating the NHB, and the treatment with the highest NHB is the most cost-effective option. The NHB values expressed in terms of response with a WTP of US$30,000 per unit effectiveness for bupropion, sertraline, and venlafaxine were 0.1931 (95% CI, 0.1402 to 0.2499), 0.1909 (95% CI, 0.1316 to 0.2501), and 0.1992 (95% CI, 0.1442 to 0.2549), respectively. When expressed in term of remission, the values were 0.1896 (95% CI, 0.1324 to 0.2522), 0.1917 (95% CI, 0.1314 to 0.2525), and 0.1672 (95% CI, 0.1168 to 0.2204), respectively. Linear regression models showed no significant differences in NHB among treatments for either effectiveness (i.e., response or remission) measure.
Limitations
The systematic review4 analyzed the findings of 3 large RCTs and 1 small cohort study regarding the comparative clinical effectiveness and tolerability of antidepressants, including bupropion, for TRD. However, none of the trials had a placebo arm to control for spontaneous remission, making it difficult to ascertain which treatment strategy was effective due to pharmacological effects of the medication. There was a lack of standard definition of TRD among the included studies. Some studies included patients who were intolerable or had an inadequate response to the previous medication. It is also unclear whether participants in 1 study might be more treatment-resistant than those in the other study. The comparison of the efficacy of the medications between trials was difficult due to variation in rating scales, which may differ in sensitivity. Treatment durations of the included studies were short, ranging from 12 to 14 weeks, and there were no long-term follow-ups. Thus, the long-term efficacy and safety of the treatments remain unclear. Another limitation is the risk of publication bias that studies with insignificant results might not have been published. The findings might be of limited generalizability to the Canadian population and the real-world setting.
One of the limitations in the included economic evaluations12-14 was that the costs and benefits for treatment were limited to short time periods (i.e., up to 14 weeks). One economic evaluation14 extrapolated data to a 1-year time horizon, assuming the same rates of effectiveness for all treatments. The measures of quality of life for the estimation of utilities in 2 studies12,14 might not have been sensitive enough to show differences between treatment groups. It is unclear if the occurrence of adverse events of the treatment medications had an impact on quality of life, a self-reported assessment, and ultimately the QALY measurement. Health care utilization costs might not have been accurately measured due to an outpatient care setting. One study13 used the interactive voice response system to collect health care services utilization information, resulting in missing data for up to 68.5% of participants. One economic evaluation12 was based on a trial in which the rate of withdrawal during treatment (24.8%) and the follow-up period (51.9%) was relatively high. Therefore, multiple imputations and assumptions were made for missing outcome data.
Conclusions and Implications for Decision- or Policy-Making
One systematic review4 and 3 economic evaluations12-14 were included to address the comparative clinical effectiveness and cost-effectiveness of bupropion for the treatment of adults with TRD.
Clinical evidence suggests that switching to monotherapy after failure with a first antidepressant, such as the SSRI citalopram, resulted in no significant difference in efficacy and tolerability among bupropion, sertraline, and venlafaxine despite low remission and response rates. Augmentation of previous treatment with bupropion after failure with at least 1 antidepressant showed no significant differences in remission or response compared with switching to bupropion monotherapy. In addition, augmentation with bupropion was not associated with significant differences in remission compared with augmentation with aripiprazole or augmentation with buspirone. In terms of adverse events, switching to bupropion or augmentation with bupropion was associated with a significantly higher incidence of anxiety, decreased appetite, dry mouth, and increased blood pressure, and significantly lower incidence of increased appetite, increased weight, somnolence, akathisia, and laboratory test abnormality compared with augmentation with aripiprazole.
Cost-effectiveness evidence suggests that augmentation therapy with bupropion or aripiprazole may be a cost-effective option relative to switching to bupropion in TRD patients. Among switching monotherapies, vortioxetine appeared to be the most cost-effective option relative to other medications, such as agomelatine, bupropion, venlafaxine, or sertraline, whereas the switch options of bupropion, venlafaxine, and sertraline were not significantly different from one another in terms of cost-effectiveness. The findings were similar for both the health care payer’s perspective and societal perspective.
Given the limitations of the included studies, interpretations of the findings should be taken with caution. As no cost-effectiveness studies conducted in Canada were identified, the results of the included economic studies may be of limited generalizability to the Canadian context. Thus, a cost-effectiveness analysis of bupropion after treatment failure in MDD from a Canadian health care payer perspective is warranted.
References
1.Public Health Agency of Canada. What is Depression? 2016; https://www.canada.ca/en/public-health/services/chronic-diseases/mental-illness/what-depression.html. Accessed 2021 Mar 29.
2.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. PubMed
3.Statistics Canada. Survey on COVID-19 and mental health, September to December 2020. The Daily. 2021. https://www150.statcan.gc.ca/n1/daily-quotidien/210318/dq210318a-eng.htm. Accessed 2021 Mar 29.
4.Ruberto VL, Jha MK, Murrough JW. Pharmacological treatments for patients with treatment-resistant depression. Pharmaceuticals (Basel). 2020;13(6). PubMed
5.Thase ME, Rush AJ. When at first you don't succeed: sequential strategies for antidepressant nonresponders. J Clin Psychiatry. 1997;58 Suppl 13:23-29. PubMed
6.Brown S, Rittenbach K, Cheung S, McKean G, MacMaster FP, Clement F. Current and common definitions of treatment-resistant depression: findings from a systematic review and qualitative interviews. Can J Psychiatry. 2019;64(6):380-387. PubMed
7.Connolly KR, Thase ME. If at first you don't succeed: a review of the evidence for antidepressant augmentation, combination and switching strategies. Drugs. 2011;71(1):43-64. PubMed
8.Patel K, Allen S, Haque MN, Angelescu I, Baumeister D, Tracy DK. Bupropion: a systematic review and meta-analysis of effectiveness as an antidepressant. Ther. 2016;6(2):99-144. PubMed
9.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
10.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 Mar 29.
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Yoon J, Zisook S, Park A, Johnson GR, Scrymgeour A, Mohamed S. Comparing cost-effectiveness of aripiprazole augmentation with other “next-step” depression treatment strategies: A randomized clinical trial. J Clin Psychiatry. 2018;80(1):18. PubMed
13.Singh A, Brooks MM, Voorhees RE, et al. Cost-effective drug switch options after unsuccessful treatment with an SSRI for depression. Psychiatr Serv. 2017;68(1):81-87. PubMed
14.Soini E, Hallinen T, Brignone M, et al. Cost-utility analysis of vortioxetine versus agomelatine, bupropion SR, sertraline and venlafaxine XR after treatment switch in major depressive disorder in Finland. Expert Rev Pharmacoecon Outcomes Res. 2017;17(3):293-302. PubMed
15.Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med. 2006;354(12):1231-1242. PubMed
16.Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med. 2006;354(12):1243-1252. PubMed
17.Mohamed S, Johnson GR, Chen P, et al. Effect of antidepressant switching vs augmentation on remission among patients with major depressive disorder unresponsive to antidepressant treatment: the VAST-D randomized clinical trial. JAMA. 2017;318(2):132-145. PubMed
18.Lam RW, Hossie H, Solomons K, Yatham LN. Citalopram and bupropion-SR: combining versus switching in patients with treatment-resistant depression. J Clin Psychiatry. 2004;65(3):337-340. PubMed
19.Montgomery SA, Nielsen RZ, Poulsen LH, Häggström L. A randomised, double-blind study in adults with major depressive disorder with an inadequate response to a single course of selective serotonin reuptake inhibitor or serotonin-noradrenaline reuptake inhibitor treatment switched to vortioxetine or agomelatine. Hum Psychopharmacol. 2014;29(5):470-482. PubMed
20.Brignone M, Diamand F, Painchault C, Takyar S. Efficacy and tolerability of switching therapy to vortioxetine versus other antidepressants in patients with major depressive disorder. Curr Med Res Opin. 2016;32(2):351-366. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of the Included Systematic Review
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Ruberto et al. (2020)4 US Source of funding: Ehrenkranz Laboratory for Human Resilience and the Friedman Brain Institute | Objective: To identify effective pharmaco-therapeutic strategies currently available for patients with TRD. Total 71 RCTs were included in qualitative synthesis, of which 4 studies with bupropion were reviewed. Quality assessment tool: Quality of the included studies was not assessed. Databases: PubMed and PsycINFO. There were no search restrictions placed on the publication year or type. | Patients with MDD older than 18 years who had failed to respond to at least 1 antidepressant. Age range: 18 years to 80 years. Other detail characteristics of the included studies were not reported. | The level 2 of STAR*D study by Rush et al. (2006)15
The VAST-D study by Mohamed et al. (2017)17
Lam et al. (2004)18
| Outcomes:
|
MDD = major depressive disorder; RCT = randomized controlled trial; STAR*D = Sequenced Treatment Alternatives to Relieve Depression; TRD = treatment-resistant depression; VAST-D = the Veterans Affairs Augmentation and Switching Treatments for Improving Depression Outcomes.
Table 3: Characteristics of Included Economic Evaluations
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
Yoon et al. (2018)12 US Source of funding: Veterans Affairs Cooperative Studies Program of the Department of Veterans Affairs | Cost-utility analysis Time horizon: 12 weeks Perspective: Health sector and societal | Treatment-resistant MDD patients (1,511 veterans) who did not respond to initial pharmacologic treatment (VAST-D trial). Mean age: 54 years % male: 85 Median lifetime episode of depression: 3 Mean duration of current episode of MDD: 87 months | Switch to bupropion (n = 505) Augment with bupropion (n = 503) Augment with aripiprazole (n = 503) | Linear mixed models adjusted for baseline measures and treatment group ICER for costs per remission (the difference in costs between each treatment strategy vs. the other divided by the differences in remission rates) ICER for cost per QALY | The main effects of remission from depression, QALYs, costs, and other outcomes were estimated from the trial and administrative data collected at baseline and 12 weeks after randomization
| An ICER below WTP threshold per QALY (typically US$50,000 to US$100,000) leads to recommendation of treatment |
Singh et al. (2017)13 US Source of funding: Not reported | Cost-effectiveness analysis Time horizon: Duration of level 2 (secondary treatment, up to 14 weeks) Perspective: Government as payer | Outpatients (N = 727) with nonpsychotic MDD who did not respond to initial treatment with citalopram (SSRI) or subsequent treatments (STAR*D trial). Mean age: 42 years % male: 41 Mean number of episodes of major depression: 7.13 Mean duration of MDD: 17 years | Switch drugs:
| NHBa framework Bootstrapping method involved resampling costs and effects 1,000 times randomly with replacement (in a joint manner) to obtain estimates of NHB variability for each treatment option | The STAR*D trial (level 2) Effectiveness outcomes: Remission,b responsec Costs: antidepressant medications, other medications, and all health care facility utilization (e.g., outpatient and ED visit costs, and costs from bed days due to hospitalizations) All medication unit costs were obtained from RED BOOK. Health care facility costs were obtained from the Physician Fee Schedule or the Health care Cost and Utilization Project databases All costs were discounted at a 3% rate to year 2014 | WTP to be US$30,000 for remission or response Sensitivity analysis varied the WTP from US$10,000 to US$50,000 per effectiveness outcome (remission or response) |
Soini et al. (2017)14 Finland Source of funding: Oy H. Lundbeck Ab, Turku, Finland, and Lundbeck SAS, France | Cost-utility analysis Time horizon: 1 year Perspective: Finnish health care payer’s perspective and societal perspective | Patients with MDD who required second-line treatment after inadequate response to SSRI or SNRI. Detail characteristics were not reported | Switch drugs:
| Decision tree and Markov model structure ICER (as cost per QALY gained) | REVIVE trial and ITC findings of a systematic review Effectiveness outcomes: Remission,d recovery, relapse, switch, and time in remission Drug costs were obtained for the Pharmaceutical database of Finland and from the Finnish Medicines Tariff Direct medical costs: Psychiatrist visits, general practitioner visits, psychotherapist visits, and hospitalizations QoL (EQ-5D) data were from REVIVE trial applicable to the Finnish setting No discounting was applied due to the 1-year time horizon | WTP threshold of €50,000/QALY gained was considered |
ED = emergency department; EQ-5D = EuroQol 5-Dimensions; HAMD = Hamilton Depression Rating Scale; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; MDD = major depressive disorder; NHB = net health benefits; NR = not reported; QALY = quality-adjusted life-year; QIDS-C16 = Quick Inventory of Depressive Symptomatology-Clinician Rating; RCT = randomized controlled trial; SNRI = serotonin-norepinephrine reuptake inhibitor; SR = sustained release; SSRI = selective serotonin reuptake inhibitor; VA = Veterans Affairs; WTP = willingness to pay; XR = extended release.
aNHB = (µEi – µCi) / λ, where µEi and µCi are the average effectiveness and costs, respectively, for treatment i, and λ is the amount of money for which there is a WTP per unit of effectiveness. The treatment option with the highest NHB is considered to be the most cost-effective option.
bRemission was defined as a score of ≤ 5 on the QIDS-C16.
cResponse was defined as ≥ 50% reduction in baseline QIDS-C16 score and a QIDS-C16 score of > 5.
dRemission was defined as a Montgomery-Asberg Depression Rating Scale score ≤ 10 or a HAMD score ≤ 7.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 29
Item | Ruberto et al. (2020)4 |
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes – Population: Patients with MDD older than 18 years who had failed to respond to at least 1 antidepressant Intervention and comparator: Antidepressants, SGAs, lithium, thyroid hormone, lamotrigine, ketamine, and esketamine Outcome: Efficacy outcomes of the medications Design: RCT |
2. Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | No |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes – Only RCTs were included in the narrative synthesis |
4. Did the review authors use a comprehensive literature search strategy? | Probably yes – Two electronic databases (PubMed and PsycINFO) were searched for publications |
5. Did the review authors perform study selection in duplicate? | NR |
6. Did the review authors perform data extraction in duplicate? | NR |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | No |
8. Did the review authors describe the included studies in adequate detail? | No – Only the results were described in the qualitative analysis |
9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | No |
10. Did the review authors report on the sources of funding for the studies included in the review? | No |
11. If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? | NA |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | NA |
13. Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review? | NA |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | No |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | NA |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; NA = not applicable; NR = not reported; PICO = Population, Intervention, Comparator, Outcomes; RCT = randomized controlled trial; RoB = risk of bias; SGA = second-generation antipsychotic.
Table 5: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist10
Item | Yoon et al. (2018)12 | Singh et al. (2017)13 | Soini et al. (2017)14 |
Study design | |||
1. The research question is stated. | Yes – Compared the cost-effectiveness of 3 alternative treatments for depression. | Yes – To estimate the costs incurred during level 2 of the STAR*D trial. | Yes – To assess the cost-utility of vortioxetine vs. relevant comparator (agomelatine, bupropion SR, sertraline, and venlafaxine XR). |
2. The economic importance of the research question is stated. | Yes – Compared between augmentation and switching strategies. | Yes – To determine if 1 option was more cost-effective than the others (bupropion, sertraline, venlafaxine). | Yes – In the Finnish setting. |
3. The viewpoint(s) of the analysis are clearly stated and justified. | Yes – From the health care sector perspective. Additional analyses included societal perspective. | Yes – From the perspective of the government as the payer. | Yes – From the Finnish health care payer perspective. |
4. The rationale for choosing alternative programs or interventions compared is stated. | Yes – Aripiprazole is the most commonly prescribed atypical antipsychotic drug for MDD. Bupropion is a widely prescribed atypical antidepressant. | Yes – Based on the level 2 of the STAR*D trial. | Yes – Based on a previous systematic review. |
5. The alternatives being compared are clearly described. | Yes – Augmenting antidepressant therapy with aripiprazole was compared with augmenting antidepressant therapy with bupropion, and with switching to bupropion. | Yes – Based on the level 2 of the STAR*D trial. | Yes – Based on a previous systematic review. |
6. The form of economic evaluation used is stated. | Yes – Cost-utility | Yes – Cost-effectiveness | Yes – Cost-utility |
7. The choice of form of economic evaluation is justified in relation to the questions addressed. | NR | NR | NR |
Data collection | |||
8. The source(s) of effectiveness estimates used are stated. | Yes – Based on data from an RCT conducted in parallel. | Yes – Based on the level 2 of the STAR*D trial. | Yes – Based on a previous systematic review. |
9. Details of the design and results of effectiveness study are given (if based on a single study). | Yes – Based on data from an RCT conducted in parallel. | Yes – Based on the level 2 of the STAR*D trial. | Yes – Based on a previous systematic review. |
10. Details of the methods of synthesis or meta-analysis of estimates are given (if based on a synthesis of a number of effectiveness studies). | NA | NA | Yes – Based on a previous systematic review. |
11. The primary outcome measure(s) for the economic evaluation are clearly stated. | Yes – ICER for costs per remission, and ICER for costs per QALY. | Yes – The net health benefits. | Yes – ICER per QALY gained. |
12. Methods to value benefits are stated. | Yes – Difference in costs between each treatment strategy vs. the other divided by the differences in remission rates. | Yes – A formula was provided. | Yes – Cost per quality-adjusted life-year gained. |
13. Details of the subjects from whom valuations were obtained were given. | Yes – Based on data from an RCT conducted in parallel. | Yes – Based on the level 2 of the STAR*D trial. | Yes – Based on a previous systematic review. |
14. Productivity changes (if included) are reported separately. | Yes | NA | Yes |
15. The relevance of productivity changes to the study question is discussed. | Yes | NA | Yes |
16. Quantities of resource use are reported separately from their unit costs. | Yes | No | Yes |
17. Methods for the estimation of quantities and unit costs are described. | Yes – The main effects of remission from depression, QALYs, costs, and other outcomes were estimated from the trial and administrative data collected at baseline and 12 weeks after randomization. | Yes – All medication unit costs were obtained from RED BOOK. Health care facility costs were obtained from the Physician Fee Schedule or the Health care Cost and Utilization Project databases. | Yes – Drug costs were obtained for the Pharmaceutical database of Finland and from the Finnish Medicines Tariff. Direct medical costs such as psychiatrist visits, general practitioner visits, psychotherapist visits, and hospitalizations were based on Finnish clinical practice estimates. |
18. Currency and price data are recorded. | Yes – US currency | Yes – US currency | Yes – Euro currency |
19. Details of currency of price adjustments for inflation or currency conversion are given. | NA | NA | NA |
20. Details of any model used are given. | Yes – Linear mixed models adjusted for baseline measures and treatment group. | Yes – Linear regression models were used to estimate the effect of treatment on net health benefits. Details of models were not provided. Only references were given. | Yes – Decision tree and Markov model structure. |
21. The choice of model used and the key parameters on which it is based are justified. | Yes | Yes | Yes |
Analysis and interpretation of results | |||
22. Time horizon of costs and benefits is stated. | Yes – 12 weeks. | Yes – Costs during level 2 of the STAR*D trial (i.e., secondary treatment up to 14 weeks). | Yes – 1-year time horizon. |
23. The discount rate(s) is stated. | NA | Yes – 3% discounting rate for year 2014. | NA |
24. The choice of discount rate(s) is justified. | NA | No justification provided. | NA |
25. An explanation is given if costs and benefits are not discounted. | Yes – Short time horizon. | NA | Yes – Due to 1-year time horizon. |
26. Details of statistical tests and confidence intervals are given for stochastic data. | Yes – Using bootstrapping method. | Yes – Using bootstrapping method. | Yes |
27. The approach to sensitivity analysis is given. | Yes – Probabilistic sensitivity analysis. | Yes – Probabilistic sensitivity analysis. | Yes – Scenarios, deterministic and probabilistic sensitivity analyses. |
28. The choice of variables for sensitivity analysis is justified. | Yes – WTP thresholds. | Yes – WTP thresholds. | Yes – WTP thresholds. |
29. The ranges over which the variables are varied are justified. | Yes – WTP varied from US$0 to US$80,000 per effectiveness outcome (remission). | Yes – WTP varied from US$10,000 to US$50,000 per effectiveness outcome (remission or response). | Yes – WTP varied from €0 to €120,000 per effectiveness outcome. |
30. Relevant alternatives are compared. | Yes – Switch to bupropion, augment with bupropion. | Yes – Bupropion, sertraline, venlafaxine. | Yes – Agomelatine, bupropion SR, sertraline, and venlafaxine XR. |
31. Incremental analysis is reported. | Yes | No | Yes |
32. Major outcomes are presented in a disaggregated as well as aggregated form. | Yes | Yes | Yes |
33. The answer to the study question is given. | Yes | Yes | Yes |
34. Conclusions follow from the data reported. | Yes | Yes | Yes |
35. Conclusions are accompanied by the appropriate caveats. | Yes | Yes | Yes |
ICER = incremental cost-effectiveness ratio; MDD = major depressive disorder; NA = not applicable; NR = not reported; RCT = randomized controlled trial; SGA = second-generation antipsychotic; vs. versus; WTP = willingness to pay; XR = extended release.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings Included Systematic Review
Ruberto et al. (2020)4
Main Study Findings
Switch to another antidepressant
The level 2 of STAR*D study by Rush et al. (2006)
Adult patients with MDD (N = 727) who had inadequately improved with SSRI citalopram were randomized to receive 1 of the following drugs for up to 14 weeks: bupropion sustained release (SR) (n = 239), sertraline (n = 238), and venlafaxine extended release (XR) (n = 250)
Remission rates for bupropion, sertraline, and venlafaxine were 26.1%, 26.7%, and 28.2%, respectively (P = 0.16)
Response rates to bupropion, sertraline, and venlafaxine were 21.3%, 17.6%, and 24.8%, respectively (P = 0.72)
Time to remission (P = 0.93)
Time to response (P = 0.72)
Side effects and adverse events (tolerability): No significant difference between treatment groups.
Augmentation studies
The VAST-D study by Mohamed et al. (2017)
Adult veterans with MDD (N = 1,522) who failed to respond to at least 1 antidepressant were randomized to one of the 3 treatment options: switch to bupropion (switch-bupropion group, n = 511), augment current treatment with bupropion (augment-bupropion group, n = 506), augment with atypical antipsychotic aripiprazole (augment-aripiprazole group, n = 505) for 12 weeks (acute treatment phase) and up to 36 weeks for longer-term follow-up (continuation phase).
Remission rates at 12 weeks
Switch-bupropion group, augment-bupropion group, and augment-aripiprazole group: 22.3%, 26.9%, and 28.9%, respectively
Augment-aripiprazole group versus switch-bupropion group: RR = 1.30 (95% CI, 1.05 to 1.60; P = 0.02)
Augment-aripiprazole group versus augment-bupropion group: RR = 1.08 (95% CI, 0.88 to 1.31; P = 0.47)
Augment-bupropion group versus switch-bupropion group: RR = 1.20 (95% CI, 0.97 to 1.50; P = 0.09)
Cox regression analysis of time to remission
Augment-aripiprazole group versus switch group: hazard ratio (HR) = 1.28 (95% CI, 1.00 to 1.64; P = 0.05)
Augment-aripiprazole group versus augment-bupropion group: HR = 1.06 (95% CI, 0.84 to 1.35; P = 0.61)
Augment-bupropion group versus switch-bupropion group: HR = 1.15 (95% CI, 0.89 to 1.48; P = 0.27)
Response rates at 12 weeks
Switch-bupropion group, augment-bupropion group, and augment-aripiprazole group: 62.4%, 65.6%, and 74.3%, respectively
Augment-aripiprazole group versus switch-bupropion group: RR = 1.19 (95% CI, 1.09 to 1.29; P < 0.001)
Augment-aripiprazole group versus augment-bupropion group: RR = 1.13 (95% CI, 1.04 to 1.23; P = 0.003)
Augment-bupropion group versus switch-bupropion group: RR = 1.05 (95% CI, 0.96 to 1.15; P = 0.29)
Side effects and adverse events
Adverse events included anxiety (24.3%, 22.5%, and 16.6% for switch-bupropion, augment-bupropion, and augment-aripiprazole, respectively; P = 0.007), decreased appetite (15.5%, 11.9%, 7.9%, respectively; P = 0.001), dry mouth (10%, 7.1%, 2.8%, respectively; P < 0.001), and increased blood pressure (1.2%, 1.2%, 0, respectively; P = 0.03) which were significantly more frequent in the switch-bupropion group and the augment-bupropion group compared to the augment-aripiprazole group.
Adverse events included increased appetite (7.4%, 8.7%, and 16.0%, for switch-bupropion, augment-bupropion, and augment-aripiprazole, respectively; P < 0.001), increased weight (0.4%, 0.6%, 5.7%, respectively; P < 0.001), somnolence (7.2%, 7.9%, 14.5%, respectively; P < 0.001), akathisia (4.3%, 5.3%, 14.9%, respectively; P < 0.001), and laboratory test abnormality (2.7%, 3.8%, 8.7%, respectively; P < 0.001) were significantly more frequent in the augment-aripiprazole group compared to the other 2 bupropion groups.
Lam et al. (2004)
Patients with MDD (N = 61) who had failed either bupropion or citalopram were subjected to 3 treatment options: switching to bupropion monotherapy (n = 17), switching to citalopram monotherapy (n = 12), and combination of bupropion and citalopram (n = 32). Data of both monotherapy groups were combined as switch group (n = 29).
Remission rates of combination group versus switch group: 28% versus 7% (P < 0.05)
Side effects: No significant difference between treatment groups
The level 2 of STAR*D study by Trivedi et al. (2006)
Adult patients with MDD (N = 565) who had inadequately improved with SSRI citalopram were randomized to receive augmenting citalopram with bupropion (n = 279) or augmenting citalopram with buspirone (n = 286) for up to 14 weeks.
Remission rates for augmenting citalopram with bupropion group and augmenting citalopram with buspirone group were 29.7% and 30.1%, respectively (P = 0.93)
Response rates for augmenting citalopram with bupropion group and augmenting citalopram with buspirone group were 31.8% and 26.9%, respectively (P = 0.21)
Bupropion group had significantly lower dropout rate (12.5%) than buspirone group (20.6%) due to intolerance (P < 0.009).
Author’s Conclusion
“In conclusion, ketamine and esketamine appear to be effective medications for TRD. Specific SGAs, such as augmentation agents, are also effective for TRD. Lithium, T3, lamotrigine, and combining antidepressants, such as bupropion, mirtazapine, and TCAs, are also effective treatments for TRD. There is not enough research to conclude the efficacy of ziprasidone or T4. Very little comparative efficacy data between agents for TRD is available to inform treatment decisions. Clinicians should take a shared decision-making approach to take each patient’s predisposition and individual needs into consideration when choosing an antidepressant or augmentation agent (p. 17).”4
Summary of Findings of Included Economic Evaluations
Yoon et al. (2018)12
Main Study Findings
Based on VAST-D trial by Mohamed et al. (2017)
Switch-bupropion versus augment-bupropion versus augment-aripiprazole
Mental health care costs per patient for 12-week follow-up from the health care sector perspective, mean (95% CI)
Switch-bupropion: US$2,201 (US$1,617 to US$2,785)
Augment-bupropion: US$2,171 (US$1,597 to US$2,746)
Augment-aripiprazole: US$2,273 (US$1,696 to US$2,850)
Rates of remission from depression
Switch-bupropion: 0.22
Augment-bupropion: 0.27
Augment-aripiprazole: 0.29
ICER (95% CI) for cost per remission from the health care sector perspective
Augment-bupropion versus switch-bupropion: –US$640 (–US$5,770 to US$3,008); 79.0% at the lower-right quadrant by bootstrapping analyses, indicating lower costs and greater benefits. Bupropion augmentation strongly dominated bupropion switching.
Augment-aripiprazole versus switch-bupropion: $1,074 (US$47 to US$5,022); 97.9% at the upper-right quadrant by bootstrapping analyses, indicating greater costs and benefits.
Augment-aripiprazole versus augment-bupropion: $5,094 (–US$34,027 to US$32,774); 75.6% at the upper-right quadrant by bootstrapping analyses, indicating greater costs and benefits.
Cost-effectiveness acceptability curves comparing cost-effectiveness of the treatments across a range of WTP values per remission
At WTP less than US$10,000, bupropion augmentation had higher probability of being more cost-effective than the other 2 strategies.
At WTP greater than US$10,000, aripiprazole augmentation had 76% probability of being more cost-effective than the other 2 strategies.
At WTP greater than US$10,000, bupropion augmentation had 23% probability of being more cost-effective than the other 2 strategies.
ICER (95% CI) for cost per QALY from the health care sector perspective
Augment-bupropion versus switch-bupropion: US$29,039 (–US$185,604 to US$181,823)
Augment-aripiprazole versus switch-bupropion: US$468,126 (–US$425,881 to US$400,934)
Augment-aripiprazole versus augment-bupropion: US$85,817 (–US$483,214 to US$466,643)
Only bupropion augmentation was more cost-effective than bupropion switching.
Mental health care costs per patient for 12-week follow-up from societal perspective, mean (95% CI)
Switch-bupropion: US$6,650 (US$4,770 to US$8,531)
Augment-bupropion: US$7,281 (US$5,431 to US$9,131)
Augment-aripiprazole: US$6,894 (US$5,036 to US$8,752)
ICER (95% CI) for cost per remission from societal perspective
Augment-bupropion versus switch-bupropion: US$13,538 (–US$57,555 to $104,560)
Augment-aripiprazole versus switch-bupropion: US$3,669 (US$979 to US$15,890)
Augment-aripiprazole versus augment-bupropion: –US$19,473 (–US$117,762 to US$119,115)
Both augmentation groups were cost-effective relative to switching group. Aripiprazole augmentation was more cost-effective than bupropion augmentation.
ICER (95% CI) for cost per QALY from societal perspective
Augment-bupropion versus switch-bupropion: US$36,256 (–US$374,525 to US$291,251)
Augment-aripiprazole versus switch-bupropion: US$73,295 (–US$716,747 to US$655,476)
Augment-aripiprazole versus augment-bupropion: US$293,620 (–US$750,761 to US$748,494)
Only bupropion augmentation was more cost-effective than bupropion switching.
Author’s Conclusion
“Many patients with major depressive disorder who do not receive optimal benefit from their initial or subsequent treatment trial may benefit from augmentation therapy with aripiprazole or bupropion, and these treatments are cost-effective relative to switching to commonly prescribed antidepressant. Additional considerations should be given to side effects in selecting an augmentation therapy for nonresponsive depression (p. 7).”12
Singh et al. (2017)13
Main Study Findings
Based on level 2 of the STAR*D study by Rush et al. (2006)
Switch drugs: bupropion versus sertraline versus venlafaxine
Total drugs and health care costs per patient for 14 weeks follow-up from government payer perspective, mean (SD)
Bupropion: US$1,972.30 (1,628.60)
Sertraline: US$2,231.70 (3,247.90)
Venlafaxine: US$2,425.50 (2,175.50)
After adjusting for multiplicity, the pairwise comparisons showed no significant differences between average total costs for the drugs.
Effectiveness measured by response rates
Bupropion: 0.26
Sertraline: 0.27
Venlafaxine: 0.28
Effectiveness measured by remission rates
Bupropion: 0.26
Sertraline: 0.27
Venlafaxine: 0.25
NHBs expressed in term of response with WTP of US$30,000 per unit effectiveness, mean (95% CI)
Bupropion: 0.1931 (0.1402 to 0.2499)
Sertraline: 0.1909 (0.1316 to 0.2501)
Venlafaxine: 0.1992 (0.1442 to 0.2549)
NHBs expressed in term of remission with WTP of US$30,000 per unit effectiveness, mean (95% CI)
Bupropion: 0.1896 (0.1324 to 0.2522)
Sertraline: 0.1917 (0.1314 to 0.2525)
Venlafaxine: 0.1672 (0.1168 to 0.2204)
Linear regression models showed no significant differences in NHBs among treatment for either effectiveness (response or remission) measure.
Cost-effectiveness acceptability curves:
By response: the 3 curves overlapped (i.e., no differences)
By remission: venlafaxine appeared to be less cost-effective than other 2 drugs.
Author’s Conclusion
“After unsuccessful treatment with citalopram, the switch options of bupropion, sertraline, and venlafaxine were not significantly different from each other in terms of cost-effectiveness (p. 81).”13
Soini et al. (2017)14
Main Study Findings
Switch drugs: vortioxetine, agomelatine, bupropion, venlafaxine, sertraline
Rates of remission after 8 weeks
Vortioxetine: 0.41
Agomelatine: 0.30
Bupropion: 0.30
Venlafaxine: 0.33
Sertraline: 0.26
Total QALY for 1 year
Vortioxetine: 0.7523
Agomelatine: 0.7338; difference relative to vortioxetine = 0.0134
Bupropion: 0.7356; difference relative to vortioxetine = 0.0166
Venlafaxine: 0.7272; difference relative to vortioxetine = 0.0250
Sertraline: 0.7247; difference relative to vortioxetine = 0.0276
Total direct costs for 1 year
Vortioxetine: €2,833
Agomelatine: €3,056; difference relative to vortioxetine = –€223
Bupropion: €2,961; difference relative to vortioxetine = –€128
Venlafaxine: €2,943; difference relative to vortioxetine = –€110
Sertraline: €3,070; difference relative to vortioxetine = –€238
Total indirect costs for 1 year
Vortioxetine: €7,309
Agomelatine: €8,159; difference relative to vortioxetine = –€850
Bupropion: €8,138; difference relative to vortioxetine = –€829
Venlafaxine: €7,918; difference relative to vortioxetine = –€609
Sertraline: €8,461; difference relative to vortioxetine = –€1,152
Total societal costs for 1 year
Vortioxetine: €10,142
Agomelatine: €11,215; difference relative to vortioxetine = –€1,074
Bupropion: €11,099; difference relative to vortioxetine = –€957
Venlafaxine: €10,861; difference relative to vortioxetine = –€720
Sertraline: €11,531; difference relative to vortioxetine = –€1,390
Vortioxetine was associated with a dominant ICER compared with all comparators (i.e., less costly and more effective), regardless of the perspective considered.
Probabilistic sensitivity analyses with a threshold of €50,000 per QALY gained
At threshold of 0
Vortioxetine versus agomelatine: 97.0%
Vortioxetine versus bupropion: 74.7%
Vortioxetine versus venlafaxine: 71.8%
Vortioxetine versus sertraline: 92.8%
At threshold of €10,000
Vortioxetine versus agomelatine: 97.0%
Vortioxetine versus bupropion: 84.1%
Vortioxetine versus venlafaxine: 89.2%
Vortioxetine versus sertraline: 97.6%
At threshold of €20,000
Vortioxetine versus agomelatine: 97.0%
Vortioxetine versus bupropion: 86.6%
Vortioxetine versus venlafaxine: 93.8%
Vortioxetine versus sertraline: 98.6%
At threshold of €30,000
Vortioxetine versus agomelatine: 97.0%
Vortioxetine versus bupropion: 88.1%
Vortioxetine versus venlafaxine: 95.5%
Vortioxetine versus sertraline: 99.0%
At threshold of €50,000
Vortioxetine versus agomelatine: 97.1%
Vortioxetine versus bupropion: 89.5%
Vortioxetine versus venlafaxine: 96.8%
Vortioxetine versus sertraline: 99.3%
Vortioxetine dominated all comparators (i.e., more effective and cost less).
Author’s Conclusion
“This cost-utility analysis showed vortioxetine to be a good alternative for MDD patients switching therapy in Finland (p. 293).”14
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca