CADTH Health Technology Review
Tuberculosis Stigma and Racism, Colonialism, and Migration: A Rapid Qualitative Review
Rapid Review
Authors: Andrea Smith, Elijah Herington, Hannah Loshak
Key Messages
Current experiences of tuberculosis policy and care among Indigenous people are interpreted and understood in light of the past colonial violence and cultural genocide. The expressed reluctance to seek health care was often grounded in experiences of colonial violence and racism, pointing toward colonial and racist practice in health care as an important driver of tuberculosis stigma. The ongoing presence of anti-Indigenous racism in Canada’s health care systems underscores the ways that these worries are not confined to historical events but manifest in the interactions across individuals and systems today.
For tuberculosis stigma in the context of migration, tuberculosis policies and programs targeting migrant persons or racialized groups were seen as fuelling discriminatory and exclusionary views and practices toward these groups in the wider society and exacerbating tuberculosis stigma. Migrant detention centres were 1 of the sites where tuberculosis stigma was amplified through isolation when diagnosed. Further, the twining of immigration policy with tuberculosis policy led to worries among migrant persons about one’s tuberculosis status and its impact on one’s immigration status, and subsequently a reluctance to access health care. These findings ask us to consider the ways that tuberculosis policy, in concert with immigration policy, can generate tuberculosis stigma.
Tuberculosis stigma differs across contexts. It can be both a determinant of, and determined by, other forms of discrimination. Moreover, it requires close attention to the specific setting where tuberculosis stigma is sought to be addressed. The implications of this for tuberculosis policy and care are that a universal, one-size approach to addressing tuberculosis stigma is unlikely to be successful. Rather, program-specific approaches are likely needed that engage with questions as to how different forms of tuberculosis stigma play out in the context of care.
Cutting across this review findings were widespread experiences of racism in health care. These findings suggest that, in as much as tuberculosis stigma is a barrier to the uptake of tuberculosis screening and treatment, racism against Indigenous people and racialized migrants remains endemic in Canada’s health care system and may in some cases overshadow the role or experience of tuberculosis stigma. In light of these findings, and again, depending on the particular setting, engaging with anti-racist efforts and challenging white supremacy remain necessary and urgent.
Context and Policy Issues
The rate of active tuberculosis (TB) on the lands known as Canada is 1 of the lowest in the world.1 As “a social disease with a medical dimension,”2 it is well-recognized that success in eliminating TB is dependent not only upon medical treatment but upon addressing and remedying social inequalities and addressing these social determinants of health. Of the 1,796 cases of active TB reported in Canada in 2017, 72% were in people born outside of Canada and 17% were in Indigenous people.1 The disparities in the distribution of TB that these rates reveal must be understood in terms of structural conditions and social determinants of health, including poverty, inadequate housing and overcrowding, food insecurity, and access to health care.2
Stigma, as a social determinant of health, is of particular focus within TB policy and care. Underpinning TB elimination strategies in Canada is the expressed need to “[e]nd the stigma and discrimination associated with TB – the underlying social, cultural, and historical factors that lead to shame and silence around TB.”2 Viewing TB stigma as a social determinant of health highlights how TB stigma is “inextricably linked to an individual’s social positioning.”3 Within Canada, TB mostly afflicts Indigenous peoples and migrants. This highlights how other structural dimensions that shape social positioning — including colonialism, racism, and migration — are affected by and influence TB stigma.
The thrust of the attention on stigma around TB is that the shame associated with TB, and the fear of being isolated, is a barrier to the uptake of screening and treatment programs.2 The concept of health-related stigma and its intersection with other forms of identity-based discrimination are explored further in the 2019 annual report on the state of public health in Canada. Here, in the opening address, Chief Public Health Officer of Canada, Dr. Theresa Tam, describes how:
Stigma and discrimination towards persons with health conditions, such as mental illness, substance use disorders, and HIV, cannot be understood or treated separately from stigma related to other characteristics such as race, gender, sexual orientation, age, and income. These many forms of stigma, that intersect in complex ways, are very much present in our health system, driving those most in need from getting effective care and accessing services. It means that we, as health system leaders and practitioners, are contributing to negative health outcomes.(p. 5)4
A recent CADTH Policy Insights identified the importance of colonialism and stigma as affecting adherence to latent TB infection treatment.5 Stigma, which resulted in avoiding contact with health care systems and providers due to fear, was seen as part of Canada’s legacy of colonial TB policy toward Indigenous peoples, particularly in the North.5 From the 1940s to 1960s, Canada’s TB policy was to remove Indigenous children and adults from the north for treatment in sanatoria in the south. Many died and were never heard from again, with families still searching for their loved one’s graves.6 In 2019, the federal government issued an apology to the Inuit for these policies and practices, acknowledging them as colonial and as a destructive force in the lives of individuals, families, and communities, and as leaving a lasting impact to this day.7
For newcomers to Canada, the process of settlement is known to be highly disruptive and stressful.8 Migrants disproportionately work for low wages and in precarious jobs, and face additional challenges finding adequate housing — all of this in addition to language barriers and the process of acculturation. The socioeconomic position of migrants is attributable to the reactivation of latent TB infections.2
This CADTH Rapid Response aims to describe the ways that stigma interacts in relation to structural racism, colonialism, and migration that are particularly relevant to addressing TB in Canada. This specific focus aims not to diminish or negate other forms of discrimination and structural or social relations of power. Our aim is to further a broader understanding of how these particular forms of discrimination and systemic inequalities are shaped by and, in turn, shape stigma in TB policy and care.
Research Questions
How does stigma intersect with colonialism, racism, and migration in the context of tuberculosis policy and care?
What opportunities are there to address these intersections in the design, delivery, and offering of care for tuberculosis?
Methods
Key Assumptions
Several key assumptions guided the research team during the production and reporting of this review. These key assumptions served to orient us in our thinking around framing the research project and research question, the methods used, and the reporting of the results. We take these assumptions as orienting us toward ensuring our work is informative to the work of settler institutions and Canadian governments engaging in addressing racism and colonialism, and anti-migrant discrimination, in our health care systems, institutions, and practices. This review recognizes that any conversation around building health care services must begin with (and be maintained by) the meaningful participation, direction, and oversight (if not outright governance) of Indigenous peoples.
The public acknowledgement of and calls for justice and reconciliation around Canada’s legacy of colonial violence and cultural genocide9 toward Indigenous peoples inform the approach of this review. Several inquiries on Canada’s treatment of the Indigenous people have identified specific actions for health care systems and providers to move toward justice, including the “Calls to Action” of the Truth and Reconciliation Commission of Canada9 and the “Calls for Justice” from the National Inquiry into Missing and Murdered Indigenous Women and Girls.10 In particular, Call for Justice 7.110 (along with Call to Action 22)9 reminds all levels of health care institutions to:
…recognize that Indigenous Peoples – First Nations, Inuit, and Métis, including 2SLGBTQQIA people – are the experts in caring for and healing themselves, and that health and wellness services are most effective when they are designed and delivered by the Indigenous Peoples they are supposed to serve, in a manner consistent with and grounded in the practices, world views, cultures, languages, and values of the diverse Inuit, Métis, and First Nations communities they serve.10
We support the basic human rights of refugees and migrants by recognizing their need for access to basic services, including health care, as affirmed in the UN Global Compact for Safe, Orderly and Regular Migration.11 We see this as a driver to ensure that health care is accessible in one’s spoken language and provided in a culturally competent manner, and to address broader anti-migrant sentiment.
We take White supremacy and structural racism to be deeply entrenched in Canadian health care policy, systems, and institutions. Concepts of structural racism and systemic racism are often overlapping; we use the term structural racism to refer to:
A system in which public policies, institutional practices, cultural representations, and other norms work in various, often reinforcing ways to perpetuate racial group inequity. It identifies dimensions of our history and culture that have allowed privileges associated with “whiteness” and disadvantages associated with “color” to endure and adapt over time. Structural racism is not something that a few people or institutions choose to practice. Instead it has been a feature of the social, economic and political systems in which we all exist.12
We aim for this work to continue and support efforts to address and tackle White supremacy and racism in health care.
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and PsycINFO via Ovid, CINAHL via Ebsco, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were tuberculosis and stigma. Search filters were applied to limit retrieval to qualitative studies. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2010 and February 25, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Sample | People (living with TB and providing TB care), communities, and populations encountering stigma from TB, with specific attention to people living in the North, Inuit and Indigenous peoples, and refugees and new migrants |
Phenomenon of interest | Societal, group, and individual views of and experiences with stigma and TB, and the intersections between stigma and racism, colonialism, and settlement |
Design | Any qualitative design |
Evaluation | Conceptualizations, understandings and experiences of TB and stigma in the context of colonialism, racism and settlement; opportunities to address stigma and how it intersects with racism, colonialism, and settlement |
Research type | Primary qualitative studies |
TB = tuberculosis.
Exclusion Criteria
Articles were excluded if they did not meet the inclusion criteria outlined in Table 1, were duplicate publications (i.e., reporting on the same data and the same findings), or were published before 2010. Additionally, once we began to review the literature, we made the decision to exclude studies that focused on cultural knowledge, beliefs, and perceptions of TB. These studies were excluded, as they tended to place the problem of TB stigma as being due to a deficiency or defect because of the absence of knowledge or misinformation of TB, or because of wrongly held beliefs. While these studies may be insightful on the processes and experiences of TB stigma within particular communities, the focus of this review is on the tensions and pressures generated by structural processes of colonialism, racism, and settlement.
Qualitative evidence syntheses were not included but were used to identify additional, potentially eligible, publications.
Critical Appraisal of Individual Studies
The critical appraisal was conducted by the primary reviewer who followed Krefting’s13 approach for assessing trustworthiness in qualitative research. The trustworthiness of the study results was evaluated by asking questions around how the research methods shaped how the research team arrived at its findings or results. This was done with a particular focus on 4 guiding questions:
Were the study authors true to their participants (credibility)?
Does the analysis make sense in light of the data presented (confirmability)?
Is the analysis consistent across study findings (dependability)?
Is the analysis relevant to the research question of this review (transferability)?13
Results of the critical appraisal were used to understand the methodological and conceptual limitations of the included publications in specific relation to the research questions.
Data Analysis
The approach to data analysis was iterative and interpretive, drawing on the tenets of thematic synthesis14 and grounded theory,15 and involved multiple close readings of eligible studies, note-taking, and memoing, culminating in the construction of a synthetic analysis. The constant comparison method was used to compare notes and memos within and across studies. The synthetic analysis aimed to explore and understand the interplay between TB stigma and structural racism, colonialism, and migration, and was conducted by the primary reviewer. The primary reviewer oriented herself to the data analysis using the key assumptions and her understandings of colonialism as a process of systematic dispossession of Indigenous peoples’ lands by colonizing peoples through social, economic, and political processes that included cultural genocide16 and migration as a process of movement and displacement of peoples often due to social, economic, and political forces outside of their control.8 Concepts and experiences relating to racism, colonialism, migration, and TB stigma were used as sensitizing concepts to draw out insights from the primary studies.15
Analysis began by reading and rereading eligible studies multiple times, for which the primary reviewer made marginal notes on hard copies of the publications together with memos (in Word) to reflect preliminary thoughts, impressions, and insights related to the included studies. While many of the notes were descriptive and referred directly to the content of a single line or paragraph, others critiqued and drew upon various study components (e.g., design or method, positioning of study authors, commentary in the discussion section) to be used as part of a critical appraisal. The reviewer “coded” the data by underlining and bracketing lines or sections that seem particularly salient. Similar to the inductive logics of line-by-line and descriptive coding, this process allowed the reviewer to begin making connections throughout the empirical data found across the body of eligible studies.
These connections formed the basis of an outline of descriptive themes in Word and served as a skeleton for orienting and framing the synthetic analysis. At this stage, the primary reviewer formally turned toward the construction of a synthetic analysis. Drawing on the primary reviewer's growing familiarity with the dataset as built through (ongoing) iterative readings, the outline of themes was expanded and developed by returning to the primary reviewer’s memos and the original papers. Conversations with and reviews of written preliminary findings by the second reviewer helped focus and draw out the analysis and articulate connections within the data and across themes. Throughout the review process, we paid attention to the language and concepts employed by us and the primary researchers. We strived to use language and concepts that both did not obscure the social, material, and political relations in which TB is situated nor situate them as arising from individual or community faults. As a rapid review, analysis stopped when written synthetic findings were completed, which incorporated findings from the primary studies and provided information to answer the review’s research questions.
Summary of Included Literature
Quantity of Research Available
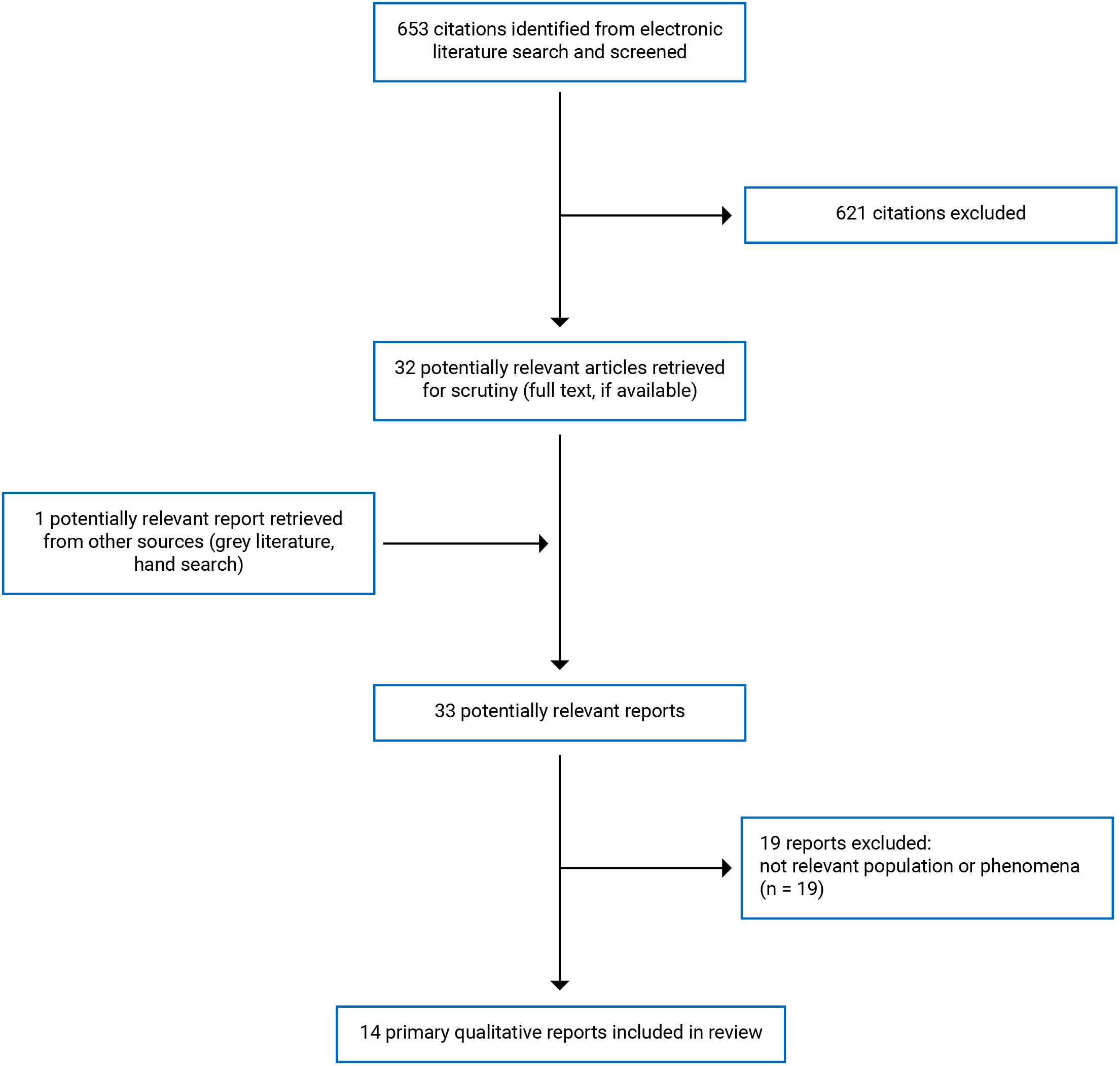
A total of 653 citations were identified in the literature search. Following screening of titles and abstracts, 621 citations were excluded and 32 potentially relevant reports from the electronic search were retrieved for full-text review. One additional publication was located through background scoping of the project. Of these 33 potentially relevant articles, 19 publications were excluded for various reasons and 13 studies reported in 14 publications met the inclusion criteria and were included in this report. One qualitative evidence synthesis was located and used to identify additional potentially eligible publications.17 Appendix 1 presents the PRISMA18 flow chart of the study selection.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications and their participants are provided in Appendix 2.
Study Design, Data Collection, and Method of Analysis
Four publications did not report the study design used.19-22 Three publications reported on the qualitative component of a mixed-methods study23-25 and 2 reported on both quantitative and qualitative components of a mixed method.26,27 One was a focused ethnography,28 one a qualitative description study,29 one used community-based participatory research methods,30 another relied on citizen panels (deliberative methods),31 and one was an interpretive phenomenology analysis.32
Six publications reporting on 5 studies collected data through interviews.21,23,25,28-30 Two publications collected data using interviews and focus groups19,22 and 1 used interviews with individuals and groups.24 Two publications collected data using focus groups20,26 and 1 publication collected data through community panels.31 One publication collected data using interviews and observations32 and another used interviews, focus groups, and observations.27
Two publications did not report a specific approach to data analysis.26,31 Five publications used thematic analysis as the method of data analysis19-21,27,32 and 2 others used a variation of thematic analysis. Content analysis was used to analyze data in 2 publications.29,30 One publication each used narrative analysis using social action,23 1 used a framework approach,28 and another used the constant comparative method.22
Location of Study
Six publications reporting on 5 studies were conducted in Canada.19,23,26,29,30,32 Three were in conducted in the UK.20,21,28 One publication was conducted in each of the following: the Netherlands,24 New Zealand,25 the US,22 and Australia.31 One cross-national comparison was conducted in the US and in Haiti.27
Study Participants and Study Objectives
Of the 3 studies reported in 4 publications that explored the experiences of Indigenous people, 2 included Indigenous people diagnosed with TB and living on- and off-reserve in Alberta, Saskatchewan, or Manitoba.23,29 One included Indigenous people who either had TB or had a close contact with someone who did and were living in Montreal, Canada,19 and another included Indigenous residents of a northern First Nations reserve who had experience (direct or through family members) of Canada’s TB programs including sanatoria. Two of these studies aimed to explore the experiences of colonialism in TB policy in Canada.23,30 One explored experiences of TB and barriers and facilitators to testing among Indigenous people living in an inner city19 and another aimed to understand how differences in community settings (urban, non-remote, remote, and isolated communities and reserves) affected the diagnosis of advanced TB among Indigenous peoples.29 In all these studies, stigma was not the main focus; rather, it was explored as a concept adjacent to health care access or returning to ones’ home community or arose in the findings.
Of the 9 publications that included migrant or immigrant participants, 4 included people seeking or granted asylum from African nations who had or were seen as at risk of having TB.(i.e., Eritrea,24 Sudan and South Sudan,31 Somalia;28 and African-born immigrants21). Two included staff of community-based organizations and health care providers caring for migrants from Africa who had or were seen as at risk of having TB.20,25 One publication included Haitians living in Haiti and living in Florida, US,27 and another included people with TB who were born outside of and were settling in Toronto, Canada.32 One publication included people who had emigrated from Vietnam31 and another from China.26
The research objectives across these studies varied. Three studies explicitly investigated TB stigma.21,24,27 One examined reasons for TB incidence among migrants.25 Four explored perspectives and experiences around TB policy and care within migrant communities.20,26,31,32 In those studies that did not explicitly investigate stigma in relation to migration and settlement, stigma was raised as a topic relating to experiences of TB by either researchers or participants.
One study explored TB stigma in US-born African-Americans who had TB or were at risk of TB.22 While not explored explicitly by the researchers, anti-Black racism was raised in the findings.
Summary of Critical Appraisal
The included studies ranged in quality, but overall the set of included studies were judged to be moderately to highly trustworthy.
Trustworthiness was judged to be moderate or high when researchers theoretically situated their inquiry, used methods to collect rich data (i.e., collected data from numerous participants, used multiple types of data, described reasons for stopping data collection), and described their findings clearly and with rich detail, appropriately supported by the data.
Given the centrality of the social determinants of health in TB, studies that framed the investigations solely in terms of an individual’s characteristics and lacked a structural view were found to be less trustworthy. For those studies exploring issues relating to stigma and migrants, and stigma and immigrants, several studies involved the use of community leaders as participants representing the experiences of migration, raised questions of who represents the community and who is excluded or missed in these accounts, and raised questions around the credibility and dependability of the analysis.
For the most part, studies did not offer definitions of stigma, while those that did tended to frame stigma in terms of the concept’s origins in describing an individual’s psychological experiences and perceptions. More recent structural conceptions,33,34 which are more consistent with social determinants of health, were less commonly employed. The absence of providing a definition of stigma was consistent with how stigma was not investigated as a substantial topic in and of its own right for most of the studies. Rather, it arose in the findings that explored knowledge, beliefs, and perceptions. These studies tended to explore stigma as something arising from people’s limited or inaccurate knowledge or understanding of TB. The limited use of structural conceptions of stigma, together with the emphasis on knowledge, beliefs, and perceptions, meant that socioeconomic and structural forces tended to be underexplored in relation to stigma, affecting the transferability of the studies to the questions of this review as a whole.
Results
TB Stigma and Colonialism in Canada
TB Policy as Colonial Policy and Its Legacy
Two studies focused specifically on the experiences of Canada’s TB policy toward Indigenous peoples from the 1940s to the 1960s;23,30 in another study,19 these experiences were drawn out during the interviews. Current experiences of TB policy and care among Indigenous peoples were interpreted and understood in light of the past colonial violence and cultural genocide, and participants drew on other forms of colonial violence, specifically residential schools, forced sterilization, and the 1960s scoops when describing their experiences with health care toward Indigenous peoples.19 In this way, the stigma around TB among Indigenous peoples was associated with the destructive forces of TB policy and the broader colonial entity that is Canada. TB, in some ways, was emblematic of colonization: “It’s almost like, some people say like it’s a White person’s disease that was brought in... to take out the First Nation’s people...”(p. 512)19
Indigenous participants’ stories described this history — the cumulative effect of Canada’s health care policy on TB in the 1940s to the 1960s — as very present in their lives and communities. Many who attended sanitoria or remember the TB policy as removal from their community to institutions where they were steeped in Western languages and practices, and cut off from their languages and practices, remain fearful of health care providers and institutions.23,30 While the purpose of this review is not to recount TB policy during this period, it is worth noting that the experiences described by those affected — directly and indirectly, and across generations — are experiences that echo the collective trauma of cultural genocide as enacted under residential schools.9 We, as settler researchers, see the importance of underscoring the traumatic effect of these experiences on individuals and communities to shield against dismissing this fear as unjustified or resulting from misconceptions.
As 1 Indigenous participant from a northern community recounted: “You know, ever since the trauma of being away for so long, I have learned to look after myself. I’ve learned to eat right to make sure I don’t go back to the sanitorium... When you go through a whole year like that institution, kind of unfriendly, you don’t want to go back there again. Now I take care of my health personally.” (p. 1596)30
Indigenous participants recounted different forms of stigma experienced upon returning home from sanitoria. Stigma was experienced based on physical appearance, as well as on ways of knowing, healing, and language. One Indigenous person described what happened to her brother when he came back from a sanitoria: “It was a very tough situation for the family because we, as siblings, rejected him because he looked like a White kid. He looked like a White kid because he was in a hospital with no sunshine. He was really white... Socially he became outcasted and ridiculed. The other kids called him ‘snowman’ because he was so white.”(p. 1595)30 Colonialism also manifests as displacing Indigenous ways of knowing and cultural healing practices. Traditional health practices and healers were not permitted within the sanitorium, lacking knowledge and appreciation (and respect) for Indigenous peoples and culture. Family, friends, and community healers were not able to travel to visit people once in the sanitoriums. Language was another way that assimilatory colonial practices were carried out, with English as the only spoken language. All these forms of stigma perpetuated a kind of structural violence.23 These accounts of being seen as an outsider by one’s own community as a result of being assimilated into settler culture due to being institutionalized at sanatoria highlight the way the TB stigma is intimately tied to colonization.
Silence is often associated with TB stigma, the silence being a reluctance to talk about TB because of the attending shame. In the case of those affected by TB and colonialism, Indigenous participants described not sharing the history with their children or families, or how their parents or grandparents did not share these stories with them.19 The researchers who present these findings note that, at the time of writing (2010), there was a broader public silence around TB policy toward Indigenous communities.19 This suggests that the silence may be not only because of the intergenerational trauma from these policies, but also because there was no public discourse in which these stories could fit. Since the article was published, public acknowledgement of the events from the 1940s to the 1960s, including Canadian Prime Minister Justin Trudeau’s apology, has changed; thus, it is possible these findings would differ today. However, we feel that recognizing this silence is important, as it is part of the stigma of colonial history itself in Canadian settler discourse around health policy.
Access to and Interactions With Heath Care
Indigenous participants’ accounts of seeking health care in the context of TB were filled with stories of racism, of discrimination, and of being dismissed.19,23,29 These stories were particularly prominent among those who were living in urban or off-reserve settings and who accessed mainstream health facilities (i.e., walk-in clinics and emergency departments), as opposed to care provided through targeted, inner-city, or Indigenous-run organizations (e.g., Friendship Centres). Indigenous participants described struggling to receive a TB diagnosis and noted that the process for receiving one often included repeat doctors’ visits and intensive self-advocacy.29 An Indigenous participant from an urban centre:
I went to the Medi-Centre... where I usually go, and I saw, I don’t know how many doctors there... my... sickness was progressing... I kept going and I even came to a point asking them if they can check my phlegm... I was terrified, so the doctors kept telling me that nothing was wrong with me. Finally, this 1 doctor, right away, before he examined me, he gave me a paper towel to cover my mouth. Right away, he knew. (p. 6)29
Others, particularly in urban centres, described how they felt like they were being judged as trying to abuse prescription medication. An Indigenous participant from an urban centre:
I kept going to the doctor. I kept going to walk-in clinics because... I just felt like I had the flu all the time, and then my doctor thought it was the flu and then of course I’d be taking Tylenol all the time and if I knew I was gonna run out by the weekend, I’d go to the walk-in clinic. And then they kinda looked at you, kind of funny-like, ‘Oh you know, you’re coming here for Tylenol.’(p. 6)29
Participants saw the failure to get a timely diagnosis of TB as an issue of justice. An Indigenous participant from an urban centre: “Somebody has to be reprimanded for misdiagnosing people... It’s probably other people it’s happened to... because you can’t go around misdiagnosing people...”(p. 7) 29 Indigenous persons’ descriptions of discrimination and dismissal of their health concerns were manifestations of anti-Indigenous racism.19,29 In this case, TB stigma was not raised as a concern or an experience. This suggests that the expectation of stigma around TB as a barrier may mask other, more salient forms of stigma in TB care.
While descriptions of diagnostic delays, even with repeated health care visits, and dismissive treatment existed in the accounts of people living in remote and isolated reserves, these experiences did not appear with the same frequency as those in urban settings. Rather, people referred to the importance of their positive relationships with nursing station staff in achieving quicker diagnoses.29 This was similar to the experiences of those who attended inner-city services or urban services that specifically attended to Indigenous persons.19,29 This is not to say that racism did not happen in other settings, nor that the care currently provided in remote and isolated reserves is culturally appropriate or meeting the needs of Indigenous peoples. Instead, it points us toward how endemic racism is in urban, non-targeted care.
Indigenous individuals who returned home after being diagnosed with TB described worries and experiences of having people avoid them, largely due to fears of being infected, because of their diagnosis.29 These worries and experiences caused individuals to hesitate to disclose their TB diagnoses to anyone other than those closest to them19,29 and were amplified by concerns about the confidentiality of the diagnoses due to the individuals being part of small, tight-knit, remote, or isolated communities where “people talk.”29(p. 9) At the same time, as articulated earlier, the reluctance to seek health care as expressed by many is often grounded in experiences of colonial violence and racism, and points toward colonial and racist practice in health care as an important driver of TB stigma. People feared being diagnosed because of fears around interacting with the health care system itself.19,30 The ongoing presence of anti-Indigenous racism in Canada’s health care systems underscores the ways that these worries are not confined to historical events but manifest in the interactions across individuals and systems, today.
Tuberculosis Stigma and Migration
Isolation and Migration
TB stigma, in the form of physical distance and isolation, is intimately related to the contagious nature of the condition.24,32 Isolation is an essential component of TB care strategies, but among migrants, forced isolation and detention exacerbated their socioeconomic vulnerability. Migrant participants shared their accounts of how their TB diagnoses and treatments resulted in them losing their jobs and housing.27,28,32
For those who had been sent to detention centres as part of their asylum-seeking and were diagnosed with TB, stigma played out while they were incarcerated.21,24 Migrant participants described how the stigma attached to a diagnosis of TB meant that those diagnosed were avoided and further isolated.21 One migrant participant in the UK recounted: “I was incarcerated... I was just left in my own room for several months. Those who were close to me were now shunning me. It was terrible. To tell you the truth, this was the worst experience I’ve ever had. Sometimes I cry just thinking about it.”(p. 47)21
Migrant participants living in tight-knit communities expressed worries about how TB stigma might lead to their isolation and hesitated to disclose their TB status to those around them.25,26 These experiences, and those described by Indigenous participants living in isolated northern communities, point to the ways that TB stigma as isolation can be particularly powerful when people are also excluded or isolated from (or viewed as outsiders to) the larger society.22,25 One TB program nurse in a US-born Black community in southeastern US describes the consequences of isolation as being social but also material:
[This town] is a very social and friendly community. If someone doesn’t have supper, they can go to someone else’s house down the street. If someone doesn’t have a car, someone will give them a ride. A lot of my patients are very poor; there are a lot of them that don’t work and they are used to being able to go to other people’s houses to do things. Eat or sleep, hang out. Some of them have been told you can’t come in here anymore because you have TB.22(p. 8)
As with Indigenous participants, TB stigma manifested in migrant participants' worries about being singled out.20,21,27 Migrant participants were concerned with how the design and provision of health care services could result in their TB status being disclosed. Some worried about how neighbours would see Direct Observation Therapy nurses visiting their home, which could make their TB known. 27 Additionally, TB clinics are often located in the same building as sexually transmitted infection and HIV clinics, compounding the stigma of TB. 27 In these ways, TB care can itself reinforce stigma.20,27 While these concerns are unlikely to be unique to migrants, in the context of the implications of isolation, the consequences of the lack of confidentiality or unwanted disclosure may be greater due to their marginalization.
Migration also meant isolation, as individual migrants were often alone. Nursing staff were described by migrant participants as enacting care in the form of kindness and helping overcome isolation by seeing migrants as connected, to inquiring about their lives: “Because, now, if someone has never even asked, to ask about, ‘how is your family back home? Have you communicated to them these days?’, then it means you are not concerned. What is your only concern is, am I taking your medication...”(p. 1074)32 Another way that nurses provided TB care in the form of kindness was through reducing stigma through body language. Nurses talked about how the practice of masking resulted in disclosure of TB status, but also created barriers to communication and connection. They then attended to their bodily positioning and placement: “If I’m going in, [to their house] I’m masking, they’re already alienated and the stigma attached, ‘ooh you’re dirty and nobody wants to touch you.’ I try not to do that with my body language when I meet them.”(p. 1074)32 While limited, these findings point toward the pivotal role of TB nursing staff in practising kindness in the context of migration and stigma.28,32
Anti-migrant Sentiment
Anti-migrant sentiments further alienated new migrants and asylum seekers, with migrant participants and those working with them sharing the palpable feeling that the broader public blamed migrants for bringing diseases to the new country.27,31,32 These sentiments led to, for instance, concerns about how TB screening and testing programs targeting migrants would be seen by the public, and that this might lead to further stigmatization of migrants and resistance to public funding for these programs.31 As 1 Haitian migrant participant put it: “The stigma of being responsible of spreading HIV in the U.S. has marked Haitians with a ‘stamp,’ and those who have TB think that if they state it openly they will be given the responsibility for bringing TB in the US as well.”27 Not pointing to particular countries or regions was seen as being important to avoid fuelling anti-migrant sentiments and to mitigate racism.31
African migrant participants described experiencing a double stigma, where TB was seen as a marker for HIV.21,24,25,27 “I think it’s linked to, as a saying, that sense of being picked on, you know, because I’m an African therefore I’ll have TB and I’m vulnerable to have every other disease. So I think there’s a sense of westerners labelling as well.”(p. 5)25 With this association, participants described being afraid of TB because of the HIV stigma rather than because of the stigma of TB. This points to the way that TB stigma is generated by HIV stigma in some contexts, but not all, as this did not play out in the case of Indigenous participants who saw TB and HIV as separate and unrelated.19
TB and Immigration Policy
Haitian migrants living in Florida described how TB, when detected during the immigration process, had very real consequences in the form of incarceration.27 This risk of incarceration in TB hospitals — which was compared to jail by migrant participants — led to people being fearful of a TB diagnosis.27 This example of stigma around TB out of fear of its treatment shares similarities to the ways Indigenous participants described fearing diagnosis, as previously described. It draws attention to the ways TB treatment and policy can fuel, if not generate, stigma for TB in particular settings; here, being those with a structural imbalance of power. Similarly, community organization staff described how the integration of TB policy with immigration policy meant that people would prioritize their immigration status and their ability to stay in the host country over their health.20,25 As one community worker described it: “An overstayer also will feel scared seeking for help because they know that if the doctor finds out that he or she’s an overstayer the doctor might call the immigration people to come and arrest him or her and deport him or her.”(p. 7)25
Similarly, discrimination based on their immigration status affected their ability to access health care for TB. A manager of a community-based organization put it this way: “But if they go to services and hit a brick wall because they’re not welcomed, if they’re asked for documents that are not essential, if they’re not really treated in a way that makes them feel like they ever want to come back, then that’s stopping access.”(p. 9)20 While this does not interact with TB stigma as such, it highlights the types of experiences faced by migrants in engaging with health care that are part and parcel of TB care. TB stigma, in this instance, does not even enter directly into the equation, as other forms of discrimination and social determinants of health (i.e., access to health care) are overbearing.
Limitations
There are several limitations relating to the way this research was undertaken and the set of included publications that influence the resulting understandings of the intersections between stigma around TB and forms of colonialism, racism, and migration.
The limited number of studies identified that directly explored TB stigma in relation to these forms of discrimination constrained our ability to engage with these intersections and ways of mitigating them. Those studies in which stigma emerged in the findings tended to undertheorize the TB stigma and use it to denote the fear of being isolated and less as a social determinant of health. The lack of data and conceptualization affected our ability to follow how these experiences are understood and shaped in and against other forms of discrimination across individuals, groups, and systems. No studies were found that addressed our second research question on interventions to address the interconnections between TB stigma and colonialism, racism, and migration. These limitations point to the general paucity of evidence around the topics under review.
We would also like to acknowledge that as settlers with White privilege, we made efforts to attend to the structures and relations — social, material, and economic — intertwined with TB stigma and discrimination. To that end, we explicitly avoided portrayals which place the cause of stigma within deficiencies of knowledge, attitudes, and beliefs of racialized and Indigenous people. While we worked toward being reflective and attuned to the concepts used in this report, we recognize that we may, however inadvertently, have reproduced White supremist and colonial visions of TB care.
Conclusions and Implications for Decision- or Policy-Making
Despite a limited number of included studies, which explicitly investigated TB stigma in the context of racism, colonialism, and migration, this review deepens our understanding of their complicated intersections.
For TB stigma in the context of colonialism, the history of TB policy is present in contemporary public health policy and care for TB among Indigenous communities. Moving forward would entail requiring institutions and individuals involved in TB programs and health care to reflect on how to develop programs that do not require removal of those with TB and would also ensure that anti-Indigenous racism is addressed in health care. Striving toward reconciliation with Indigenous communities in TB policy — indeed all policy — is necessary and of particular significance given the current crises with water, food security, and housing, which influence the incidence and prevalence of TB.2
For TB stigma in the context of migration, migration detention centres were 1 of the sites where TB stigma was amplified through isolation when a person was diagnosed with the disease. Further, the twining of immigration policy with TB policy led to worries among migrants about one’s TB status and its impact on one’s immigration status, and subsequently resulted in a migrant’s reluctance to access health care. TB policies and programs targeting migrants or racialized groups were seen as fuelling discriminatory and exclusionary views and practices toward these groups in the wider society, and exacerbating TB stigma. These findings ask us to consider the ways that TB policy, in concert with immigration policy, can generate TB stigma and anti-migrant sentiment.
The key findings are notable in several ways. First, they point clearly to the way that TB stigma is not a singular set of experiences or perceptions, but rather a dynamic and relational process, differing across contexts.27 In other words, there is not 1 way that TB stigma interacts with, for example, racism. In this review, looking at stigma across TB and other structural discriminatory or exclusionary practices, we see that TB stigma is shaped by colonialism and migration policies, but it also influences racism and anti-migration sentiment. This means being cognizant that TB stigma can both influence and be influenced by other forms of discrimination. Moreover, it requires close attention to the specific setting where TB stigma is sought to be addressed. The implications of this for TB policy and care are that a universal, 1-size approach to addressing TB stigma is unlikely to be successful. Rather, program-specific approaches that engage with questions as to how TB stigma plays out in the context of care are likely needed.
A recent CADTH report articulated the importance of disruption as a form of moving toward inclusive health care.35 As Herington writes, there is value in disrupting ideas of “the clinic as the privileged location of care. In this way, health care services are positioned as another piece of [sic] in the lives of peoples engaging with them and asks providers to become invested members of the communities they work in rather than providers external to these communities. Inclusion here, [sic] takes on a stance that asks how does service provision come to be included into the community rather than the community included into service provision.”(p. 18)35 While the CADTH report writes about inclusion, it relates in many ways to how TB stigma plays out. In the context of TB, this disruption might mean, for example, that public health practitioners and decision-makers consider how TB policy and care may itself generate and perpetuate TB stigma.
The notion of structural competency may be additionally helpful here. Developed in the field of medical education, structural competency looks toward bringing the structures that shape and influence clinical encounters into view.36 It asks health care providers to consider how a person engages with the world around them, how the structures — public transit, access to grocery stores, job security — can play out in clinical encounters. This is an explicit move away from the language of cultural competency, which is seen as placing too much of an emphasis on belief systems and being used to refer to ethnicity rather than focusing on structures (physical, systems, and bureaucratic) that shape stigma in practice.36 This lens may be of particular salience in the care for TB, as it draws attention away from TB stigma as internal and individual, and points instead toward the social determinants of TB and toward lack or precarity of employment, food insecurity, inadequate housing, and lack of access to appropriate health care.
Cutting across this review’s findings were widespread experiences of racism in health care. These findings suggest that in as much as TB stigma is a barrier to the uptake of TB screening and treatment, racism against Indigenous people and racialized migrants remains endemic in Canada’s health care system and may in some cases overshadow the role or experience of TB stigma. In light of these findings, and again, depending on the particular setting, engaging with anti-racist efforts and challenging White supremacy remain necessary and urgent.
References
1.Public Health Agency of Canada. Tuberculosis: monitoring. 2019; https://www.canada.ca/en/public-health/services/diseases/tuberculosis/surveillance.html. Accessed 2021 Apr 8.
2.The time is now - Chief Public Health Officer spotlight on eliminating tuberculosis in Canada. Ottawa (ON): Public Health Agency of Canada; 2018: https://www.canada.ca/content/dam/phac-aspc/documents/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/eliminating-tuberculosis/PHAC_18-086_TB_Report_E_forwebcoding.pdf. Accessed 2021 Mar 22.
3.Craig GM, Daftary A, Engel N, O'Driscoll S, Ioannaki A. Tuberculosis stigma as a social determinant of health: a systematic mapping review of research in low incidence countries. Int J Infect Dis. 2017;56:90-100. PubMed
4.Addressing stigma: towards a more inclusive health system. The Chief Public Health Officer's report on the state of public health in Canada 2019. Ottawa (ON): Public Health Agency of Canada; 2019: https://www.canada.ca/content/dam/phac-aspc/documents/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/addressing-stigma-what-we-heard/stigma-eng.pdf. Accessed 2020 Jul 13.
5.Supports to enhance adherence to the treatment of latent tuberculosis infection. (CADTH Policy Insights). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/supports-enhance-adherence-treatment-latent-tuberculosis-infection. Accessed 2021 Apr 8.
6.Beers R. Inuit describe 'bittersweet' experience at burial sites of lost loved ones in South. CBC News 2019; https://www.cbc.ca/news/canada/north/nanilavut-inuit-lost-loved-ones-1.5215116. Accessed 2021 Mar 29.
7.Prime Minister of Canada. Statement of apology on behalf of the Government of Canada to Inuit for the management of the tuberculosis epidemic from the 1940s-1960s. 2019: https://pm.gc.ca/en/news/speeches/2019/03/08/statement-apology-behalf-government-canada-inuit-management-tuberculosis. Accessed 2021 Mar 29.
8.Tuyisenge G, Goldenberg SM. COVID-19, structural racism, and migrant health in Canada. The Lancet. 2021;397(10275):650-652. PubMed
9.Truth and Reconciliation Commission of Canada: calls to action. Winnipeg (MB): Truth and Reconciliation Commission of Canada; 2012: http://trc.ca/assets/pdf/Calls_to_Action_English2.pdf. Accessed 2020 Jul 22.
10.The National Inquiry into Missing and Murdered Indigenous Women and Girls. Reclaiming power and place: the final report of the national inquiry into missing and murdered indigenous women and girls. Vol 1b. Ottawa (ON): Government of Canada; 2019: https://www.mmiwg-ffada.ca/wp-content/uploads/2019/06/Final_Report_Vol_1b.pdf. Accessed 2020 Jul 22.
11.Global compact for safe, orderly and regular migration: intergovernmentally negotiated and agreed outcome. Global Compact for Migration; 2018: https://refugeesmigrants.un.org/sites/default/files/180713_agreed_outcome_global_compact_for_migration.pdf. Accessed 2021 Apr 8.
12.Aspen Institute. 11 terms you should know to better understand structural racism. 2016: https://www.aspeninstitute.org/blog-posts/structural-racism-definition/. Accessed 2021 Apr 6.
13.Krefting L. Rigor in qualitative research: the assessment of trustworthiness. Am J Occup Ther. 1991;45(3):214-222. PubMed
14.Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45. PubMed
15.Charmaz K. Constructing grounded theory. Thousand Oaks (CA): Sage Publications Ltd; 2014.
16.Chrisjohn RD, Young S, Maraun M. The Circle Game: shadows and substance in the Indian Residential School experience in Canada. Penticton (BC): Theytus Books; 2003.
17.Abarca Tomas B, Pell C, Bueno Cavanillas A, Guillen Solvas J, Pool R, Roura M. Tuberculosis in migrant populations. A systematic review of the qualitative literature. PLoS One. 2013;8(12):e82440. PubMed
18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
19.Macdonald ME, Rigillo N, Brassard P. Urban aboriginal understandings and experiences of tuberculosis in Montreal, Quebec, Canada. Qual Health Res. 2010;20(4):506-523. PubMed
20.Berrocal-Almanza LC, Botticello J, Piotrowski H, et al. Engaging with civil society to improve access to LTBI screening for new migrants in England: a qualitative study. Int J Tuberc Lung Dis. 2019;23(5):563-570. PubMed
21.Chinouya MJ, Adeyanju O. A disease called stigma: the experience of stigma among African men with TB diagnosis in London. Public Health. 2017;145:45-50. PubMed
22.Royce RA, Colson PW, Woodsong C, et al. Tuberculosis knowledge, awareness, and stigma among African-Americans in three southeastern counties in the USA: a qualitative study of community perspectives. J Racial Ethn Health Disparities. 2017;4(1):47-58. PubMed
23.Komarnisky S, Hackett P, Abonyi S, Heffernan C, Long R. “Years ago”: reconciliation and First Nations narratives of tuberculosis in the Canadian Prairie Provinces. Critical Public Health. 2016;26(4):381-393.
24.Spruijt I, Haile DT, van den Hof S, et al. Knowledge, attitudes, beliefs, and stigma related to latent tuberculosis infection: a qualitative study among Eritreans in the Netherlands. BMC Public Health. 2020;20(1):1602. PubMed
25.Badu E, Mpofu C, Farvid P. Towards TB elimination in Aotearoa/New Zealand: key informant insights on the determinants of TB among African Migrants. Trop Med Infect Dis. 2018;3(2):22. PubMed
26.Gao J, Berry NS, Taylor D, Venners SA, Cook VJ, Mayhew M. Knowledge and perceptions of latent tuberculosis infection among Chinese immigrants in a Canadian urban centre. Int J Family Med. 2015;2015:546042. PubMed
27.Coreil J, Mayard G, Simpson KM, Lauzardo M, Zhu Y, Weiss M. Structural forces and the production of TB-related stigma among Haitians in two contexts. Soc Sci Med. 2010;71(8):1409-1417. PubMed
28.Gerrish K, Naisby A, Ismail M. Experiences of the diagnosis and management of tuberculosis: a focused ethnography of Somali patients and healthcare professionals in the UK. J Adv Nurs. 2013;69(10):2285-2294. PubMed
29.Mayan MJ, Gokiert RJ, Robinson T, et al. Community setting as a determinant of health for Indigenous peoples living in the Prairie provinces of Canada: high rates and advanced presentations of tuberculosis. Int Indig Policy J. 2019;10(2).
30.Moffatt J, Mayan M, Long R. Sanitoriums and the Canadian colonial legacy: the untold experiences of tuberculosis treatment. Qual Health Res. 2013;23(12):1591-1599. PubMed
31.Degeling C, Carter SM, Dale K, et al. Perspectives of Vietnamese, Sudanese and South Sudanese immigrants on targeting migrant communities for latent tuberculosis screening and treatment in low‐incidence settings: a report on two Victorian community panels. Health Expect. 2020;23(6):1431-1440. PubMed
32.Bender A, Andrews G, Peter E. Displacement and tuberculosis: recognition in nursing care. Health Place. 2010;16(6):1069-1076. PubMed
33.Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol. 2001;27(1):363-385.
34.Hatzenbuehler ML, Phelan JC, Link BG. Stigma as a fundamental cause of population health inequalities. Am J Public Health. 2013;103(5):813-821. PubMed
35.Building inclusive health care services: a rapid qualitative review. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://cadth.ca/building-inclusive-health-care-services-rapid-qualitative-review. Accessed 2021 Apr 8.
36.Metzl JM, Hansen H. Structural competency: theorizing a new medical engagement with stigma and inequality. Soc Sci Med. 2014;103:126-133. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications and Their Participants
Table 2: Characteristics of Included Publications and Their Participants
Author(year) country | Study objectives | Study setting | Description of study participants | Study design, method of data collection and analysis | Judgment on trustworthiness and transferability |
Studies on TB stigma among Indigenous peoples | |||||
Mayman et al. (2019) Canada29a | To understand how community setting may help explain the high rates and advanced presentations of TB among Indigenous peoples in the Prairie provinces | Indigenous peoples living in urban centres, non-remote, remote and isolated reserves in the Canadian Prairies (part of the Determinants of Tuberculosis Transmission project) | Indigenous persons living in the Prairie provinces who were aged 15 or older and diagnosed with culture-positive pulmonary TB (n = 56, but only 48 interviews used) | Qualitative description, semi-structured interviews, content analysis | Partially. Unclear if stigma arose in interviews or was prompted. Findings around stigma are centred around feelings of shame and exclusion, and not probed in more detail. No mention throughout of TB policy of the 1940s to 1960s, which points to its lack of taking historical context into account. Transferability to this review is limited by the focus on experiences of diagnosis. |
Komarnisky et al. (2016) Canada23a | To explore the implications of colonialism and health care on contemporary TB prevention, programming, and care | Indigenous peoples living in urban centres, non-remote communities, remote and isolated reserves in the Canadian Prairies (part of the Determinants of Tuberculosis Transmission project) | Indigenous persons living in the Prairie provinces who were aged 15 or older and diagnosed with culture-positive pulmonary TB and who described historical features of colonialism and TB policy when interviewed as part of the study (n = 20) | Qualitative component of a mixed-methods study, in-depth interviews, narrative analysis using social action | Mostly. Historically situated and oriented analysis. Questions of credibility centre around the secondary analysis of interviews (i.e., not collected for this particular research question). Transferability to this review is high, as it explores how colonial TB policy affects present daycare. |
Moffatt et al. (2013) Canada30 | To describe sanitoriums from the perspective of a First Nations reserve community in northern Canada and understand the sanitorium experience at a community level | A First Nations community (reserve) with a high incidence of TB | 15 Indigenous persons living on a First Nations reserve, 7 of whom had been taken to a sanitorium, 3 who had had a family member institutionalized there, and 1 who had been treated for TB in an outpatient setting; and 4 who had been taken to a sanitorium and had family members institutionalized in a sanitorium | Community-based participatory research design, semi-structured interviews, content analysis | Yes. Theoretically situated (historically and uses post-colonial theory) and demonstrated reflexivity throughout. Solid methods for data collection and analysis. Transferability to this review is high based on the review question and the setting. |
Macdonald et al. (2010) Canada19 | To explore the experiences of TB among Indigenous peoples living in Montreal, to understand its significance in their lives, as well as barriers and facilitators to testing and treatment | Native Friendship Centre of Montreal, Montreal, Canada (inner-city) | 27 self-reported Indigenous persons who either had TB (n = 19) or who had close contact with a person with active TB (n = 18) | NR, semi-structured interview and a focus group, thematic analysis | Yes. Historically framed and has an eye toward structural and colonial relations. Rich data collected and findings well-described. Highly transferable to this review in terms of research findings and setting. |
Studies on migrant populations | |||||
Degeling et al. (2020) Australia31 | To understand the perspectives of Vietnamese, Sudanese, and South Sudanese immigrants on options for LTBI screening and communication strategies | Victoria, Australia | Community panels formed of Vietnamese (n = 11) and Sudanese and South Sudanese community members (n = 9) | Community panel (deliberative method), deliberative panels, NR | Partially. Reliant on deliberative methods for data generation; lack of reporting on methods of analysis affect credibility. Transferability to this review is limited by the focus on preferences for types of TB testing and communication strategies. |
Spruijt et al. (2020) Netherlands24 | To describe the knowledge, attitudes, beliefs, and stigma associated with LTBI among Eritrean asylum seekers and refugees in the Netherlands | LTBI screening and treatment program for high-TB-risk migrant groups in the Netherlands | Eritrean asylum seekers living in asylum seeker centres (n = 42) and Eritrean refugees (n = 15) living in communities in the Netherlands who presented for LTBI screening and/or treatment | Qualitative component of a mixed-methods study, group interviews and semi-structured interviews, applied thematic approach | Partially. Study is focused on stigma as disconnected from the larger structural forces, affecting judgments around confirmability and dependability. Transferability to this review is limited by the study’s limited exploration of stigma in the context of structural forces. |
Berrocal-Almanza et al. (2019) UK20 | To gain insights from the community, community-based organizations, and public sector stakeholders on interventions that facilitate collaboration to improve health care outreach and delivery | LTBI program in England that offers testing and treatment to new entrant migrants from high-incidence countries and sub-Saharan Africa | Public health nurses (n = 3), physicians and public health epidemiologists (n = 4), political representatives (n = 1), managers and front-line worker from local community organization (n = 10), and individual community members (n = 3) | NR, focus groups, thematic analysis | Mostly. Study methods and findings are well-described and supported by the data, some concerns about the limited number of individual community members (reliance on community-based organization staff). Transferability to this review is slightly reduced by stigma being a finding as opposed to a direct focus of the study. |
Badu et al. (2018) New Zealand25 | To explore how individual, social, and structural factors may interact to influence TB incidence among African migrants to New Zealand | TB health professionals and support group for people living with TB who serve the African community | 9 participants who understood TB services and the African community, including health care providers (n = 4), community leaders (n = 4), and staff from a TB support organization (n = 1) | Qualitative component of a sequential mixed-methods study, semi-structured interviews, hybrid thematic analysis | Partially. Some questions around the dependability of findings because of the absence of reporting around reflexive practices. High-level themes are transferable to this review even with difference in immigration policy and health care systems. |
Chinouya and Adeyanju (2017) UK21 | To understand the meaning of stigma among African men with a previous TB diagnosis | Community-based organizations offering health-related support to African-born people in London | Black African-born men (n = 10) who had recovered from TB, lived in London, and could speak English 8 were unemployed, 3 had been in immigration detention centres All had been living in the UK for less than 15 years and all participants had been diagnosed with HIV following their TB diagnosis | NR, in-depth interviews, thematic analysis | Partially. Results are not thoroughly described and not always clear, leaving room for multiple interpretations, which affects credibility. Findings are transferable to this review even with the difference in immigration policy and health care systems. |
Gao et al. (2015) Canada26 | To document knowledge levels of patients in a TB clinic; identify Chinese immigrants’ knowledge and perceptions of LTBI; specify messages that would be most appropriate for LTBI education in this population; and identify the most appropriate format of health promotional material to address the specific needs of this population | Provincial TB clinics in the Greater Vancouver area | People who had immigrated to Canada from China more than 6 years ago (n = 6) and/or recent Chinese immigrants who came to Canada less than 6 years ago (n = 6) who had accessed services at the provincial TB clinic in the Greater Vancouver area (n = 12) | Mixed method study, focus groups, NR | Mostly. Appears to have collected very limited data to support findings around stigma and marginalization affecting credibility. Transferability to this review is limited by the focus on knowledge and perceptions, and the lack of a direct focus on stigma. |
Gerrish et al. (2013) UK28 | To explore experiences of the diagnosis and management of TB from the perspective of Somali patients and health care professionals involved in their care | TB care provided by general practitioners, TB physicians, TB specialist nurses, and health care specialist providers for migrants in an area with a large and established Somali population | Somali refugees (with status) who had received treatment for TB in the UK (n = 14) and health care practitioners with experience of caring for Somali TB patients (n = 18) | Focused ethnographic approach, interviews, framework approach | Partially. The study findings were superficial and left questions about explanations or details, there was limited supporting data in parts, which affected credibility. Transferability to this review is limited by stigma not being a direct focus of the review. |
Bender et al. (2010) Canada32 | To shed light on the experience of displacement as an integral aspect of understanding TB nurses’ relational work from an explicitly phenomenological stance | TB nurses providing services in a larger multicultural city including case management, DOT, and homeless teams | 9 female nurses, 8 of whom self-identified as White, who were born in Canada and for whom English was their first language 24 clients who had TB, 21 who were non‒Canadian-born, and 23 of whom did not speak English as a first language | Interpretive phenomenology, observations of visits between nurses and clients in homes, on the street, and in clinics, and open conversational interviews with nurses and clients; thematic analysis | Yes. Very theoretically situated study with richly described findings, which increased credibility and trustworthiness. High transferability to this review given the study setting (Toronto) and the focus on displacement. |
Coreil et al. (2010) US/Haiti27 | To investigate the influence of sociocultural context on TB-related stigma by comparing the components of perceived and anticipated stigma in an immigrant population with those found in the country of origin | Haitians living in South Florida and Haitians living in Léogâne commune, Haiti | Community residents (n = 95), TB health care providers (n = 72), TB patients (n = 126) | Mixed-methods, multi-phased study using the Explanatory Model Interview Catalogue; interviews, focus groups and observations (field work); thematic analysis | Yes. Study is theoretically situated and uses advanced methods to collect much, and multiple types, of data; used methods to ensure immersion in the data and practised reflexivity. Study findings transferable to this review keeping in mind differences in immigration policy and health care systems. |
Studies on health disparities among racialized persons | |||||
Royce et al. (2017) US22 | To examine TB perspectives among US-born African-Americans by investigating TB knowledge, awareness, beliefs, stigma, and health communication | 1 rural and 2 urban counties in the southeastern US with high morbidity due to disparities in TB | African-American patients with TB (n = 27); African-American patients with LTBI (n = 24); African-American patients at risk for TB because of HIV/AIDS, homelessness, or local TB outbreaks (n = 31); local community leaders (n = 20); and local TB program staff (n = 13) | NR, semi-structured interviews and focus groups, constant comparative method | Yes. Methods for the rich collection of data are well-described, as are the findings. Findings related to stigma are transferable to this review even with the difference in demographics, history, and health policy. |
LTBI = latent tuberculosis infection; DOT = Direct Observed Therapy; NR = not reported; TB = tuberculosis.
aMayman et al. (2019) and Komarnisky et al. (2016) use the same data but report on different findings.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein do not necessarily reflect the views of Health Canada, Canada’s provincial or territorial governments, other CADTH funders, or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to requests@cadth.ca