CADTH Health Technology Review
Lenses and Spectacles to Prevent Myopia Worsening in Children
Rapid Review
Authors: Srabani Banerjee, Jennifer Horton
Abbreviations
CI
confidence interval
CrI
credible interval
D
dioptre
DIMS
defocus incorporated multiple segments
MD
mean difference
OK
orthokeratology
OR
odds ratio
RCT
randomized controlled trial
SMD
standardized mean difference
SVC
single-vision contact lens
SVL
single-vision lens
SVS
single-vision spectacle lens
Key Messages
A total of 5 relevant systematic reviews and 7 randomized controlled trials (RCTs) were identified.
Myopia progression and axial length elongation was less with omafilcon A (MiSight) contact lenses compared to single-vision lenses (1 RCT; statistical significance of difference was not reported).
Myopia progression and axial length elongation was less with defocus incorporated multiple segments spectacle lenses compared to single-vision spectacle lenses (1 RCT; the between-group difference was statistically significant).
Myopia progression was less with orthokeratology contact lenses compared to single-vision contact lenses or single-vision lenses (2 systematic reviews and 2 RCTs; between-group difference was statistically significant or statistical significance was not reported) and axial length elongation was less (5 systematic reviews and 2 RCTs; between-group difference was statistically significant or statistical significance was not reported).
Myopia progression and axial length elongation was less with multifocal lenses compared with single-vision contact lenses (1 systematic review and 2 RCTs; between-group difference was statistically significant).
Findings need to be interpreted in the light of limitations, such as limited quantity and quality of the included primary studies, limited information regarding adverse events, and lack of long-term data.
No economic evaluations reporting on the cost-effectiveness of these interventions were identified.
Context and Policy Issues
Myopia is also known as near-sightedness or short-sightedness. In myopia, the light rays entering the eye from distant objects are focused in front of the retina instead of on the surface of the retina as in the emmetropic (normal) eye, resulting in distant objects appearing blurred.1 Myopia occurs due to the cornea and/or lens being too curved, the length of the eyeball being too long, or a combination of these factors.1 It is a type of refractive error that is measured in terms of spherical equivalent. Myopia is defined as a spherical equivalent of less than 0 dioptres (D), clinically significant myopia as −1 D or less, and moderate or high myopia as less than −3 D.2 Myopic individuals may have anisomyopia (a difference of more than 1 D in refractive status between the eyes)3 or anisometropia (the eyes have different refractive powers).4 The prevalence of myopia increases throughout childhood. In the US, it is estimated that prevalence of myopia is 1% to 5% in preschool children, approximately 9% in school-aged children, and approximately 30% in adolescents.5 If left untreated, myopia will progress to high myopia.6 High levels of myopia are associated with ocular diseases such as glaucoma, macular degeneration, cataracts, and retinal detachment, and can lead to significant visual impairment.7-9
The prevalence of myopia has increased worldwide, and it is a global public health problem.10,11 It is estimated that by 2050 half of the world’s population will have myopia.1,12 It is important that progression of myopia is controlled to reduce the incidence of other detrimental eye conditions later on. Treatment options for controlling myopia include optical interventions (a variety of lenses) as well as pharmaceutical interventions (such as atropine and timolol drops).1 For children, spectacles are used typically as the initial treatment of myopia because they provide clear vision with few potential side effects.1 Contact lenses may be used but their use requires greater dexterity and responsibility.1 Lenses of various designs have been developed to control the progression of myopia. There appears to be lack of consensus regarding the use of the various lens types.13 To control the progression of myopia in children, there has been interest regarding the clinical effectiveness and cost-effectiveness of certain optical interventions, such as soft contact lenses (i.e., MiSight), defocus integrated multiple segments (DIMS) spectacle lenses, orthokeratology (OK), and multifocal contact lenses. The MiSight contact lens comprises a large central correction area surrounded by concentric zones of alternating distance and near power.8 The DIMS spectacle lens comprises a hexagonal central zone of distance refractive correction surrounded by an annular defocus zone with dense microlens segments of 3.5 D added.12 The OK lenses are specially designed and fitted contact lenses to temporarily reshape the cornea to improve vision. Most OK lenses are worn at night to reshape the front surface of the eye while the wearer is sleeping.14 The purpose of this report is to summarize the evidence regarding the clinical effectiveness and cost-effectiveness of specific optical interventions (e.g., soft contact lenses, such as MiSight; DIMS; OK; and multifocal contact lenses) for control of progression of myopia in children.
Research Questions
What is the clinical effectiveness of soft contact lenses (MiSight lenses) for the prevention of myopia worsening in children?
What is the clinical effectiveness of DIMS spectacle lenses for the prevention of myopia worsening in children?
What is the clinical effectiveness of OK for the prevention of myopia worsening in children?
What is the clinical effectiveness of multifocal contact lenses for the prevention of myopia worsening in children?
What is the cost-effectiveness of soft contact lenses (MiSight lenses) for the prevention of myopia worsening in children?
What is the cost-effectiveness of DIMS spectacle lenses for the prevention of myopia worsening in children?
What is the cost-effectiveness of OK for the prevention of myopia worsening in children?
What is the cost-effectiveness of multifocal contact lenses for the prevention of myopia worsening in children?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were pediatrics, myopia, and single-use and/or soft contact lenses, DIMS spectacles, OK, and multifocal contact lenses. When possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and February 2, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Children (under 18 years) with myopia in 1 or both eyes (or anisomyopia, or anisometropia if 1 or both eyes are myopic) |
Intervention | Q1 and Q5: Omafilcon A lenses (i.e., MiSight) in combination with atropine or alone Q2 and Q6: DIMS spectacle lens (i.e., Miyosmart) in combination with atropine or alone Q3 and Q7: OK (i.e., Ortho-K, OK, overnight vision correction, corneal refractive therapy, gentle vision shaping system) in combination with atropine or alone Q4and Q8: Multifocal contact lenses in combination with atropine or alone |
Comparator | Atropine eye drops; single-vision lens or spectacles |
Outcomes | Q1 to Q4: Myopia progression (i.e., change in the spherical equivalent and axial length), quality of life, medication side effects, risks of infection, medication adherence Q5 to Q8: Cost-effectiveness (e.g., quality-adjusted life-years, incremental cost-effectiveness) |
Study designs | Health technology assessments, systematic reviews, RCTs, and economic evaluations |
OK = orthokeratology; RCT = randomized controlled trial.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Systematic reviews that were captured by an included overview of systematic reviews were excluded. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. For question 2, primary studies that did not specifically report the intervention as DIMS spectacle lens were excluded. For question 4, primary studies that did not specifically report the intervention as multifocal or bifocal contact lens were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)15 for systematic reviews, the Questionnaire to Address the Relevance and Credibility of a Network Meta-Analysis16 for network meta-analyses (NMAs), and the Downs and Black checklist17 for randomized controlled trials (RCTs). Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
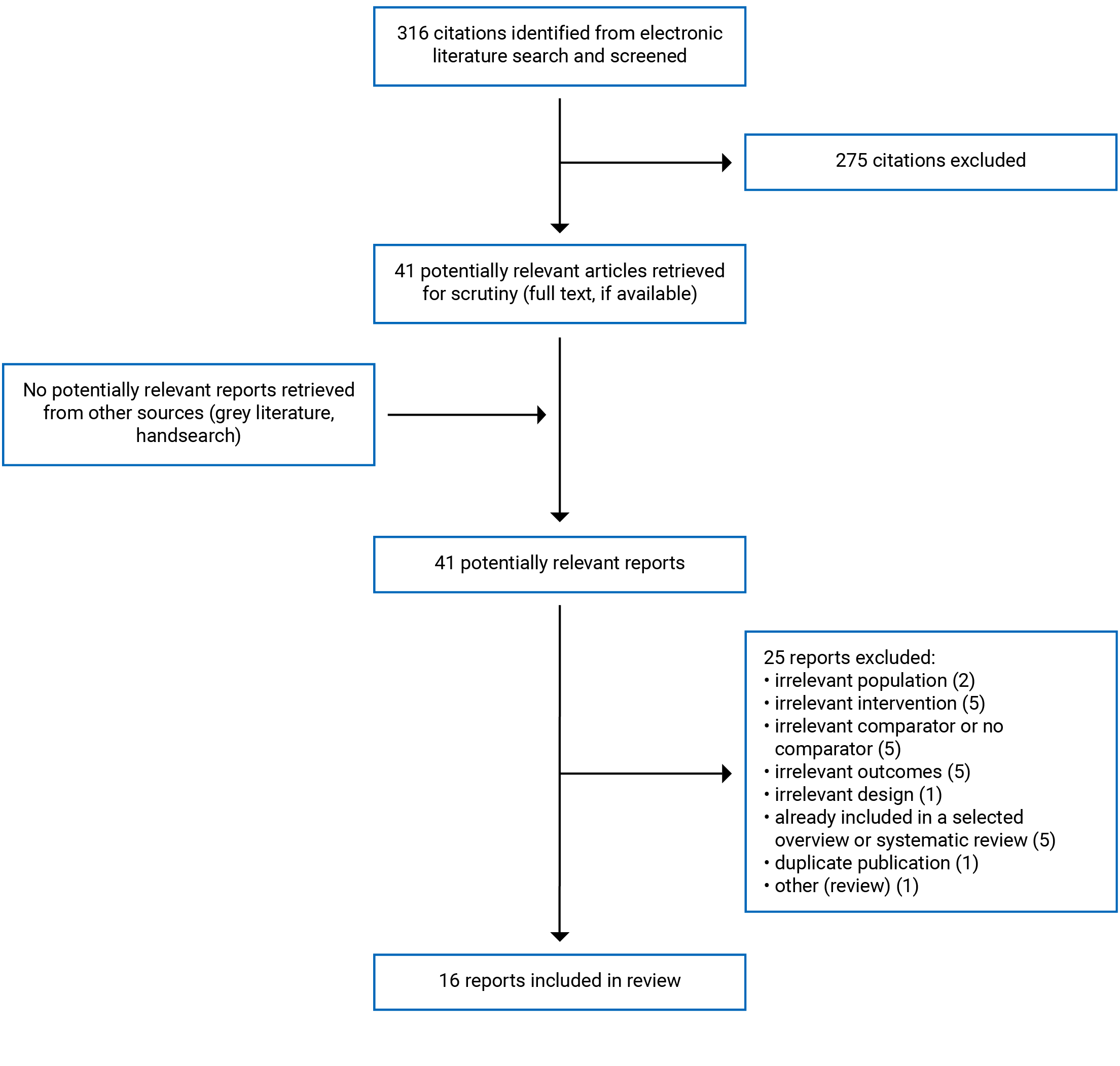
A total of 316 citations were identified in the literature search. Following screening of titles and abstracts, 275 citations were excluded and 41 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 25 publications were excluded for various reasons, and 16 publications met the inclusion criteria and were included in this report. These comprised 1 overview13 of systematic reviews, 4 systematic reviews,1,10,11,18 and 7 RCTs,6-9,12,19-24 of which 1 RCT was reported in 4 publications8,19,20,24 and 1 RCT was reported in 2 publications.12,21 No relevant economic evaluations were identified. Appendix 1 presents the PRISMA25 flow chart of the study selection.
Summary of Study Characteristics
One overview13 of systematic reviews, 4 systematic reviews1,10,11,18 and 7 RCTs,6-9,12,19-24 were identified. The overview13 and 1 systematic review1 had broader inclusion criteria than the current report and investigated optical as well as pharmaceutical interventions; therefore, only the subset of interventions relevant for this current report is presented here. One systematic review with an NMA10 was included in the selected overview13; however, the NMA results were not reported in the overview, so only the NMA results for this systematic review will be presented separately in this current report. Henceforth, the overview of systematic reviews and the systematic reviews will be referred to as systematic reviews in this report. The relevant primary studies in the included the systematic reviews are listed in Appendix 5. There was some overlap in the studies included in the systematic reviews; therefore, the findings from the systematic reviews are not exclusive. Of the 7 RCTs, 1 RCT had relevant information reported in 4 publications8,19,20,24 and 1 RCT had relevant information reported in 2 publications.12,21 Additional details regarding the characteristics of included publications are provided in Appendix 2 (Table 2 and Table 3).
Study Design
Of the 5 systematic reviews,1,10,11,13,18 3 systematic reviews1,11,13 included meta-analyses, 1 systematic review10 included an NMA, and 1 systematic review18 described results narratively. The number of relevant primary studies (RCTs or prospective or retrospective non-randomized studies) included in the systematic reviews1,11,13,18 ranged between 7 and 16. The systematic review10 with an NMA included a total of 30 RCTs; it appears all the RCTs were used for the NMA because there was no mention of a subset of RCTs being used, but it was not explicitly stated. The authors of the NMA presented a network diagram and conducted a Bayesian random-effects NMA. They estimated posterior densities of all unknown parameters using the Markov chain Monte Carlo method. As the objective of this NMA was different from that of the current report (i.e., to assess the effectiveness of different interventions, including several drug interventions, to slow the progression of myopia), the majority of the interventions of relevance for the current report were not included in the NMA. The latest date of the literature search for the systematic reviews ranged between December 2017 and February 2019. The systematic reviews were published between 2016 and 2020.
For the 7 included RCTs,6-9,12,21-24 both the investigator and patient were masked in 2 RCTs,7,9 the patient was masked but not the investigator in 1 RCT,21 and it was unclear if there was any masking in the remaining 4 RCTs.6,8,22,23 The RCTs were published between 2021 and 2020.
Country of Origin
In the 5 included systematic reviews, the first author was from the US in 2 systematic reviews,1,18 from China in 2 systematic reviews,10,11 and from Greece in 1 systematic review.13 In 4 systematic reviews,1,10,11,13 the countries in which the primary studies were conducted included China, Japan, Korea, East Asia, Australia, New Zealand, Spain, and the US. In 1 systematic review,18 the countries where the studies were conducted was not specified; instead, it was reported by ethnicity of the children. In this systematic review,18 the majority of the studies included Asian children.
Of the 7 included RCTs,6,7,9,12,20-23 4 RCTs6,21-23 were conducted in China, 2 RCTs7,20 were conducted in Spain, and 1 RCT9 in the US.
Patient Population
All 5 systematic reviews1,10,11,13,18 reported on children with myopia. In 4 systematic reviews,1,11,13,18 the numbers of children in the individual studies that were included in these systematic reviews ranged from 24 to 663. The ranges of mean ages were between 3 years and 17 years in 3 systematic reviews,1,11,18 and mean ages were less than 18 years in 1 systematic review.13 The spherical equivalent refraction of primary study participants was less than or equal to −0.25 D in 2 systematic reviews,1,13 between −0.5 D and −10.0 D in 1 systematic review,11 and between −0.5 D and −7.0 D in another systematic review.18 In the systematic review10 with an NMA, there were 5,387 children; the mean ages ranged between 8 years and 14 years, spherical equivalent refraction ranged between −1.1 D and −6.3 D, and axial length ranged between 24.1 mm and 25.4 mm.
All 7 selected RCTs6-9,21-23 reported on children with myopia. In the individual RCTs, the number of children ranged between 20 and 294, and the mean ages ranged between 10 years and 13 years. In 6 RCTs,7-9,21-23 the mean spherical equivalent refractions ranged between −2.0 D and −6.7 D, and in 1 RCT,6 the mean spherical equivalent refraction was not reported; however, the inclusion criteria indicated a range of −0.50 D to −6.00 D. In 6 RCTs,7-9,21-23 the mean axial lengths ranged between 24 mm and 26 mm, and in 1 RCT,6 the mean axial length was not reported.
Interventions and Comparators
Of the 5 systematic reviews,1,10,11,13,18 4 systematic reviews1,11,13,18 compared OK contact lenses versus single-vision spectacles (SVS),1,11,18 single-vision contact lenses (SVC),18 and single-vision lenses (SVL; when the lens was not specified as spectacle lens or contact lens)13; multifocal contact lenses versus SVL13; and bifocal contact lenses versus SVC.1,13 In the systematic review10 with an NMA, several optical and pharmaceutical interventions were compared.
Of the 7 selected RCTs,6-9,21-23 6 RCTs6-9,21,22 investigated MiSight contact lenses (MiS),8 DIMS spectacles,6,21 2 types of OK (OK1 and OK2 targeted for myopia reduction of 6.00 D and 4.00 D, respectively)22 multifocal contact lenses,7 and 2 types of multifocal contact lenses (high-add power multifocal contact lens [MF-Ch] and medium-add power multifocal contact lens [MF-Cm]).9 The comparators in these 6 RCTs were SVC7,9 and SVS.6,8,21,22 The remaining RCT23 compared OK with SVS, both with and without atropine. This RCT23 compared atropine plus OK, placebo plus OK, atropine plus SVS, and placebo plus SVS.
Outcomes
The outcomes reported in the selected 5 systematic reviews1,10,11,13,18 included refractive error (a measure of myopia progression),1,10,13,18 axial length,1,10,11,13,18 and adverse events.1,13 Follow-up ranged between 1 year to 5 years.
The outcomes reported in the selected RCTs6-9,21-23 included change in refractive error,7-9,21-23 change in axial length,7-9,21-23 adverse events,7-9,21,22 visual symptoms,6 quality of life,24 and acceptability of the intervention.6 Refractive error was expressed as spherical equivalent or spherical equivalent refraction and used as a measure to assess myopia progression. Follow-up ranged between 1 year and 3 years.
Summary of Critical Appraisal
An overview of the critical appraisal of the included publications is summarized below. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3 (Table 4 and Table 5).
Systematic Reviews
In the 5 selected systematic reviews,1,10,11,13,18 the objective and inclusion criteria were clearly stated, a literature search was conducted using multiple databases, the selection of articles was described and a flow chart presented, a list of the included primary studies was presented, and the characteristics of the included studies were described. In 4 systematic reviews1,10,11,13 the associated flow chart for article selection was presented but not presented in 1 systematic review.18 The list of excluded studies was presented in 2 systematic reviews,1,13 and not presented in 3 systematic reviews.10,11,18 Study selection and data extraction were done independently by 2 reviewers in 4 systematic reviews.1,10,11,13 In 1 systematic review,18 the article selection was done by 1 reviewer, and it was unclear if data extraction was done by 2 reviewers, hence potential for errors cannot be ruled out. Quality of the included studies was assessed in all 5 systematic reviews. In 2 systematic reviews, the Grading of Assessment, Development and Evaluation (GRADE) was used to determine the certainty of evidence.1,13 In the systematic review by Prousali et al.,13 the certainty of the evidence for the various outcomes was reported as very low, low, or moderate. In the systematic review by Walline et al.,1 the certainty of evidence for the various outcomes was reported as low or moderate. In the systematic review by Guan et al.,11 it was reported that the included studies had low risk of bias. In the systematic review by VanderVeen et al.,18 it was reported that the majority of the included studies were level II according to the Oxford Centre for Evidence-Based Medicine rating scale (i.e., in the middle level, between levels I and III; details presented in Table 4). In the systematic review by Huang et al.,10 which included an NMA, it was reported that the included studies were of low-to-moderate quality. Meta-analyses were conducted in 4 systematic reviews1,10,11,13,18 and were appropriate; a meta-analysis was not conducted in 1 systematic review,18 but the reason for not conducting it was not stated. In 4 systematic reviews,10,11,13,18 the authors reported that there were no conflicts of interest. In the remaining 1 systematic review,1 the authors declared their conflicts of interests and some authors had associations with industries interested in myopia control; therefore, the potential for bias cannot be ruled out.
NMA
Huang et al.10 conducted a Bayesian random-effects NMA. The authors did not present justification of their choice of the model; however, a random-effects model seemed appropriate considering the heterogeneity among the RCTs. Within-study randomization seemed to have been maintained. Node-splitting analyses were conducted for comparisons for which results for both direct and indirect comparison results were available, and there were no statistically significant inconsistencies. However, in the network structure, there were no closed loops for the intervention (OK) and comparator (atropine) that were relevant for the current report; therefore, consistency could not be ascertained for this comparison. Sensitivity analyses were conducted to explore uncertainty, removing studies that contributed to heterogeneity reduced the width of the credible intervals. In the NMA, the control group included both SVS and placebo, which is not a relevant comparator for our current report; it is possible that the inclusion of placebo in the comparator group would reduce the effectiveness of the comparator, biasing outcomes in favour of the intervention group. The number of RCTs included in the network structure for each of the outcomes was not explicitly stated.
RCTs
In the 7 selected RCTs,6-9,21-23 the objective, inclusion and exclusion criteria, patient characteristics, interventions, and outcomes were described. The method of randomization was described and was appropriate in 4 RCTs7-9,21 and was not described in 3 RCTs.6,22,23 In 2 RCTs7,9 both the investigator and the participants were masked. In 1 RCT21 the participants were masked but the investigator was not, and in 4 RCTs6,8,22,23 it was unclear if there was any masking. Although lack of masking has the potential of introducing detection and performances biases because the outcomes were mainly objective, this may not be a serious issue. Sample size calculations were undertaken in 5 RCTs,6-9,21 and the appropriate number of participants were recruited. In the remaining 2 RCTs,22,23 it was unclear if sample size calculations had been undertaken; however, as statistically significant differences (indicated by P values < 0.05) in outcomes were detected between the intervention and control groups, this may not be an issue. In the RCT by Lyu et al.,22 there were no discontinuations, and in the RCT by Walline et al.,9 the discontinuation in each treatment group was minimal (≤ 1%) therefore unlikely to introduce attrition bias. In the RCT by Zhao et al.,23 there was 6% discontinuation, but the discontinuations in the different groups were not reported separately; therefore, the direction of impact, if any, is unclear. In the remaining 4 RCTs,7,8,21 the discontinuation rates in the intervention and control groups were variable, and ranged between 10% and 24%; therefore, there is potential for attrition bias, but the direction of impact is unclear. The reasons for discontinuation were mainly loss to follow-up, unwillingness to wear glasses, or loss of motivation. In 4 RCTs, the authors reported that there were no conflicts of interest. In the remaining 3 RCTs,7-9 the conflicts of interest of the authors were declared, and some authors had associations with the manufacturers of lenses,9 the lenses used in the trial were provided by the manufacturer,7 or the trial was sponsored by the manufacturer but was reported not to have had any role in the conduct of the trial.8 Therefore, the potential for bias cannot be ruled out.
Summary of Findings
Main findings from the included publications are summarized below. Appendix 4 presents the main study findings and authors’ conclusions. There was some overlap in the primary studies that were included in the systematic reviews; the pooled estimates from separate reviews thus contain some of the same data. A citation matrix illustrating the degree of overlap is presented in Appendix 5. In some publications, the results were presented in terms of mean difference (MD) or standardized mean difference (SMD) and 95% confidence interval (CI); a 95% CI that included 0 indicated that the changes were not statistically significant. Also, in some publications, the results were presented in terms of odds ratio (OR) and 95% CI; a 95% CI that included 1 indicated that the changes were not statistically significant. In some publications, the 95% CI was not reported; instead, the P value was reported; P < 0.05 was considered a statistically significant change.
Clinical Effectiveness of Soft Contact Lenses (MiSight)
One RCT regarding soft contact lenses (MiSight) was identified; relevant information was reported in 3 publications.8,19,20
Refractive Error and Axial Length
Over 2 years, myopia progression (based on mean spherical equivalent values) was numerically less in the MiSight group compared to the SVS group (mean between-group difference = 0.29 D); the statistical significance of the between-group difference was not reported.8 Over 2 years there was less axial elongation in the MiSight group compared to the SVS group (mean between-group difference = 0.16 mm); the statistical significance of the between-group difference was not reported.8
After 2 years, a subset of 55 children was divided into 3 groups and followed for an additional year in an extension study of the RCT20 to investigate rebound effects. The 3 groups were children who continued with MiSight, children who stopped wearing MiSight in the third year and wore instead SVS, children who wore SVS and continued with SVS. The authors concluded that neither myopia progression nor axial length elongation were faster for the children who discontinued MiSight wear compared to those who continued with MiSight or those who continued with SVS (for myopia progression the statistical significance was not reported; for axial length elongation, P > 0.05).
Quality of Life
Quality of life was assessed using the Pediatric Error Refractive Profile questionnaire. At both 12 months and 24 months, the ratings with respect to appearance, satisfaction, effect on activities, handling, and peer perceptions were statistically significantly better for the MiSight group compared to the SVS group (P < 0.05), as was the total score.24
Adverse Effects
In the MiSight group, there was a significant increase in limbal hyperemia (P = 0.007), palpebral hyperemia (P = 0.05), and conjunctival staining (P < 0.0001) at 24-months compared to baseline values. In the SVS group, there were no significant changes in these variables. It was reported that there were no serious adverse events in with MiSight or SVS groups.19
Clinical Effectiveness of DIMS Spectacle Lenses
Two RCTs6,12,21 were identified that presented information on DIMS spectacle lenses. In the RCT by Lam et al., outcomes were reported in 2 publications.12,21
Refractive Error and Axial Length
In the RCT by Lam et al.,21 at 2 years follow-up, myopic progression (based on mean spherical equivalent refraction values) was statistically significantly less in the DIMS spectacles group compared to the SVS group (between-group difference = −0.55 D; SE = 0.09 D; P < 0.0001); a statistically significant improvement was also found at the 6-month and 1-year follow-ups.
In the RCT by Lam et al.,21 at 2 years follow-up, the axial length elongation was statistically significantly less in the DIMS spectacle group compared to the SVS group (between-group difference = 0.32 mm; SE = 0.04 mm; P < 0.0001); a statistically significant reduction was also found at the 6-month and 1-year follow-ups.
Adverse Events
The RCT by Lam et al.12 showed that over 2 years, there were no statistically significant differences in visual function changes between the DIMS spectacle group and the SVS group, and the authors concluded that DIMS spectacle wear did not lead to adverse events related to visual function when compared to SVS wear.
In the crossover RCT by Lu et al.,6 over a period of 1 week, 35% of the children complained of paracentral and peripheral blurred vision with DIMS spectacle wear, and none complained with SVS wear (P = 0.01). There were no statistically significant differences between DIMS and SVS in the number of complaints regarding the following symptoms: eyestrain, headache, dizziness, diplopia, nausea, photophobia, darkened vision field, colour change, ghosting images and metamorphopsia (P ranged from 0.342 to 1.000).
Clinical Effectiveness of OK
Five systematic reviews1,10,11,13,18 and 2 RCTs22,23 were identified that provided relevant information regarding OK contact lenses.
Refractive Error and Axial Length
For the comparison of refractive error with OK versus other lenses, the systematic review by Prousali et al.13 showed that over 2 years, the refractive error was statistically significantly improved with OK compared with SVC or SVL (MD = −0.66 D; 95% CI, −1.01 to −0.31); a statistically significant improvement was also found at the 1-year follow-up. VanderVeen et al.18 did not conduct a meta-analysis in their systematic review and presented results for each individual study separately. They reported that myopic progression was less with OK compared to spectacles or contact lenses (P values were generally not reported). The RCT by Lyu et al.22showed that over 2 years, there was no statistically significant difference in myopic progression between OK1 and OK2 (P = 0.12), and statistically significantly less myopic progression with both OK1 and OK2 compared to SVS (P < 0.05).
When evaluating refractive error with OK compared with atropine, the systematic review by VanderVeen et al.18 included 1 study that showed that myopic progression was statistically significantly less with OK compared to 0.125% atropine (P = 0.001). The systematic review by Prousali et al.13 included 1 study that showed that myopic progression was statistically significantly less with OK compared to 0.125% atropine (P = 0.001). In the RCT by Zhao et al.,23 at 1 month, the changes from baseline in refractive error (indicating improvement) were significant in both OK groups (atropine plus OK and placebo plus OK), but the changes in control SVS groups (atropine plus SVS and placebo plus SVS) were not (statistical significance was not reported).
For the comparison of OK versus other lenses, the systematic review by Prousali et al.13 showed that over 2 years, the axial length elongation was statistically significantly less with OK compared to SVC or SVL (MD = −0.27 mm; 95% CI, −0.31 to −0.23). The systematic review by Guan et al.11 showed that at 2 years or more, the axial length elongation was statistically significantly less with OK compared to SVS (SMD = −0.90 mm; 95% CI, −1.14 to −0.65); a statistically significant reduction was also found at the 1-year follow-up. The systematic review by Walline et al.1 showed that at the 2-year follow-up, the axial length elongation was statistically significantly less with OK compared to SVS (MD = −0.28 mm; 95% CI, −0.38 to −0.19). VanderVeen et al.18 did not conduct a meta-analysis in their systematic review and presented results for each individual study separately. They found that increase in axial length was generally less with OK compared to spectacles or contact lenses (statistical significance was not generally reported; when reported, P values ranged between < 0.001 and 0.02). The RCT by Lyu et al.22 showed that over 12 months, there was no statistically significant difference in axial length elongation between OK1 and OK2 (P = 0.46) and there was statistically significant reduction in axial length elongation with both OK1 and OK2 compared to SVS (P < 0.05).
To evaluate axial length with OK compared with atropine, VanderVeen et al.18 included 1 study that found that axial length increased less with OK compared to 0.125% atropine (statistical significance was not reported). In the RCT by Zhao et al.23 after 1 month, the axial length remained practically unchanged in the 2 OK groups (i.e., atropine plus OK and placebo plus OK) but increased in the SVS control groups (i.e., atropine plus SVS or placebo plus SVS) compared with baseline values (for differences between 1 month and baseline: P = 1.00 for both atropine plus OK and placebo plus OK; P < 0.05 for both atropine plus SVS and placebo plus SVS). The between-group differences in axial length change (from baseline to 1 month) were statistically significant for the OK groups compared to the control SVS groups (P < 0.001 for atropine plus OK versus atropine plus SVS, favouring atropine plus OK; P < 0.001 for placebo plus OK versus placebo plus SVS, favouring OK). The authors mentioned that the axial length remained unchanged in the atropine plus OK and placebo plus OK groups likely due to the changes in the central corneal thickness and subfoveal choroidal thickness, induced by OK lenses, which compensated for the actual growth of the eye.
Indirect evidence regarding axial length, as presented in the NMA by Huang et al.,10 showed that axial length elongation was statistically significantly less with OK compared with control (SVS and placebo) (the 95% credible interval did not include zero, indicating a statistically significant between-group difference). They also showed that there were no statistically significant differences in axial length elongation with OK compared with either high-dose, moderate-dose, or low-dose atropine (the 95% credible intervals included zero, indicating no statistically significant between-group differences).
Adverse Events
The systematic review by Prousali et al.13 found that mild corneal erosion was not statistically significantly different between OK and SVC or SVL (OR = 4.56; 95% CI, 0.49 to 42.25). In the systematic review by Walline et al.,1 it was reported that there were no serious adverse effects. In the RCT by Lyu et al.,22 the mean rate of corneal staining (detects cornea damage) was 28.97%, 13.06%, and 0.81% with OK1, OK2, and SVS, respectively. The risk of corneal staining was significantly higher in OK1 compared to OK2 (P < 0.05).
Clinical Effectiveness of Multifocal Contact Lenses
Two systematic reviews1,13 and 2 RCTs7,9 were identified that provided relevant information regarding multifocal or bifocal contact lenses.
Refractive Error and Axial Length
The systematic review by Prousali et al.13 showed that over 2 years, the refractive error was statistically significantly improved with multifocal contact lenses compared with SVL (MD = −0.50 D; 95% CI, −0.65 to −0.35 D); a statistically significant improvement was also found at 1-year follow-up. It also showed that over 2 years, the refractive error was statistically significantly improved with bifocal contact lenses compared to SVC (MD = −0.20 D; 95% CI, −0.38 to −0.02 D); a statistically significant improvement was also found at the 1-year follow-up. The systematic review by Walline et al.1 showed that over 1 year, the refractive error was not statistically significantly different with bifocal contact lenses compared with SVC (MD = 0.02 D; 95% CI, −0.06 to 0.47 D). The RCT by Garcia-del Valle et al.7 showed that at 1 year follow-up, the change in refractive error was statistically significantly improved with multifocal contact lenses compared with SVC (P = 0.02). The RCT by Walline et al.9 investigated 2 types of multifocal lenses (MF-Ch and MF-Cm). The RCT showed that at 3 years follow-up, the refractive error was statistically significantly improved with MF-Ch compared with SVC (MD = 0.45 D; 95% CI 0.25 to 0.66 D; P < 0.001). Also, at 3 years follow-up, the refractive error was not statistically significantly different with MF-Cm compared with SVC (MD, 0.16 D; 95% CI −0.01 to 0.33; P = 0.19).
The systematic review by Prousali et al.13 showed that over 2 years, the axial length elongation was statistically significantly less with multifocal contact lenses compared to SVL (MD = −0.13 mm; 95% CI, −0.20 to −0.06 mm); a statistically significant reduction was also found at 1-year follow-up. This systematic review also showed that over 2 years, the change in axial length was statistically significantly less with bifocal contact lenses compared to SVC (MD = −0.12 mm; 95% CI, −0.20 to −0.04 mm); statistically significantly less elongation was also found at 1-year follow-up. The systematic review by Walline et al.1 showed that at the 1-year follow-up, the change in axial length was statistically significantly less with bifocal contact lenses compared to SVC (MD = −0.11 mm; 95% CI, −0.14 to −0.08 mm). The RCT by Garcia-del Valle et al.7 showed that at the 1-year follow-up, the change in axial length was statistically significantly less with multifocal contact lenses compared with SVC (P = 0.03). The RCT by Walline et al.9 showed that at the 3-year follow-up, axial length elongation was statistically significantly less with MF-Ch compared with SVC (MD = −0.23 mm; 95% CI −0.30 to −0.17 mm; P < 0.001), but not statistically significantly different with MF-Cm compared with SVC (MD = −0.07 mm; 95% CI −0.16 to 0.03 mm; P = 0.15).
Adverse Effects
The systematic review by Prousali et al.13 showed that there was no statistically significant difference in discomfort or unwillingness to wear contact lenses between the bifocal contact lenses and SVC (OR = 0.95; 95% CI, 0.49 to 1.81). In the systematic review by Walline et al.,1 it was reported that there were no serious adverse effects with bifocal contact lenses or SVC. In the RCT by Garcia-del Valle et al.,7 it was reported that 1 or more adverse events (such as corneal neovascularization, conjunctival hyperaemia, micropapillary response, papillary conjunctivitis, and superficial punctate keratitis) occurred in 25.0% and 15.4% of children using multifocal contact lenses and SVC, respectively, although none of the adverse events were considered serious or unexpected. In the RCT by Walline et al.,9 the proportions of adverse events were 40.0% with MF-Ch, 22.9% with MF-Cm, and 37.1% with SVC. None of the adverse events were considered serious. The 3 most common adverse events were giant papillary conjunctivitis, infiltrative keratitis, and ocular allergies. There were no significant differences in these adverse events between the 3 groups.
Cost-Effectiveness of Soft Contact Lenses (MiSight)
No economic evaluation was identified regarding the cost-effectiveness of soft contact lenses (MiSight).
Cost-Effectiveness of DIMS Spectacle Lenses
No economic evaluation was identified regarding the cost-effectiveness of DIMS spectacle lenses.
Cost-Effectiveness of OK
No economic evaluation was identified regarding the cost-effectiveness of OK contact lenses.
Cost-Effectiveness of Multifocal Contact Lenses
No economic evaluation was identified regarding the cost-effectiveness of multifocal contact lenses.
Limitations
There is limited evidence regarding the clinical effectiveness of MiSight (1 RCT) and DIMS (2 RCTs). Although systematic reviews were identified that reported on multifocal lenses, the number of primary studies that provided evidence was limited in quantity for the various outcomes assessed (based on 1 to 5 studies [with majority being 1 or 2 studies], and of relatively small size [number of participants ranging from 20 to 300]).
In the selected systematic reviews, there was overlap of primary studies; therefore, the findings are not exclusive (i.e., in some instances, the same primary study was used in the meta-analyses in more than 1 systematic review). The systematic reviews were generally well conducted, but the quality of the included studies was variable, and the certainty of the evidence ranged between very low and moderate.
There was little information with respect to quality of life and adherence outcomes or evaluating atropine as a comparator. Reporting of adverse events was sparse. Most of the studies had a 2-year duration, hence long-term effects are not known and it is unclear if these interventions to control myopia progression in childhood will result in prevention of other eye conditions in adulthood.
Considering the limitations described, definitive conclusions about the clinical effectiveness of MiSight, DIMS, OK, and multifocal lenses are difficult. The majority of the studies were conducted in Asian countries; therefore, the generalization to the Canadian context is unclear.
No cost-effectiveness studies were identified regarding MiSight, DIMS, OK, or multifocal contact lenses.
Conclusions and Implications for Decision- or Policy-Making
Five relevant systematic reviews1,10,11,13,18 and 7 relevant RCTs (reported in 11 publications)6-9,12,19-24 were identified regarding the clinical effectiveness of certain lenses and spectacles (MiSight, DIMS, OK, and multifocal contact lenses) to prevent myopia worsening in children. No economic evaluations on the cost-effectiveness of these lenses and spectacles were identified.
One relevant RCT (reported in 3 publications)8,19,20 regarding soft contact lenses (MiSight) was identified. This RCT found that there was less axial length elongation and reduced myopia progression with MiSight contact lenses compared with SVS, and no serious adverse events in either group.
Two relevant RCTs (reported in 3 publications)6,12,21 regarding DIMS were identified. One RCT12,21 found statistically significant slowing of myopic progression and less axial length elongation with DIMS spectacles compared with SVS, and no statistically significant differences between the 2 interventions in adverse effects with respect to visual function.
Five relevant systematic reviews1,10,11,13,18 and 2 relevant RCTs22,23 regarding OK were identified. There was slowing of myopic progression with OK compared with SVC or SVL, with statistically significant between-group differences reported (1 systematic review13 and 1 RCT22) or with statistical significance of difference not reported (1 systematic review18 and 1 RCT23). There was slowing of axial length elongation with OK compared with SVC or SVL, with statistically significant between-group differences reported (4 systematic review,1,10,11,13 and 1 RCT22) or statistical significance of difference not reported (1 systematic review18 and 1 RCT23). With respect to adverse events, there was statistically significantly greater mild corneal erosion with OK compared to SVC or SVL (1 systematic review13), 1 case of infiltrative keratitis with OK (1 study that was included in the systematic review by VanderVeen et al.18), and greater risk of corneal staining (detects cornea damage) with OK compared to SVS (1 RCT22).
Two systematic reviews1,13 and 2 RCTs7,9 regarding multifocal or bifocal contact lenses were identified. There was slowing of myopic progression with multifocal contact lenses compared with SVC or SVL, with statistically significant between-group differences in (1 systematic review)13 and 2 RCTs7,9 There was no statistically significant difference in slowing of myopic progression with bifocal contact lenses compared to SVC (1 systematic review1). There was less axial length elongation with multifocal contact lenses compared with SVC or SVL, with a statistically significant between-group difference in 1 systematic review13 and 2 RCTs7,9). There was statistically significantly less axial elongation with bifocal contact lenses compared to SVC (1 systematic review1). Proportion of patients experiencing 1 or more adverse events was numerically higher with multifocal lenses compared to SVC (2 RCT7,9).
While the results of the included studies suggest that MiSight, DIMS, OK, and multifocal or bifocal lenses slow myopia progression and axial length elongation relative to SVC or SVL, these findings need to be interpreted in the light of limitations (such as limited quantity and quality of the included primary studies, limited information regarding adverse events, and lack of long-term data).
Despite the identification of several systematic reviews, a small number of primary studies (i.e., up to 5, typically 1 or 2) were included in each systematic review to address relevant outcomes, and there was overlap in the primary studies captured by each systematic review. Further research with large, well-designed studies investigating these lens types compared to single-vision contact lenses, spectacles, and atropine eye drops are needed to better understand their clinical effectiveness in controlling progression of myopia. Longer-term follow-up may reveal whether use of these lenses in childhood would impact the development of other ocular conditions in adulthood. Furthermore, to better assist with decision-making, economic evaluations regarding the cost-effectiveness of these outcomes need to be conducted.
References
1.Walline JJ, Lindsley KB, Vedula SS, et al. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2020;1:CD004916. PubMed
2.Holmstrom GE, Larsson EK. Development of Spherical Equivalent Refraction in Prematurely Born Children During the First 10 Years of Life. A Population-Based Study. Arch Ophthalmol. 2005;123(10):1404-1411. PubMed
3.Chen J, He JC, Chen Y, Xu J, Wu H, Wang F, Lu F, Jiang J. Interocular Difference of Peripheral Refraction in Anisomyopic Eyes of Schoolchildren. PLoS One. 2016;11(2):e0149110. PubMed
4.Strabismus. AAfPOa. Anisometropia. AAPOS Glossary 2020; https://aapos.org/glossary/anisometropia. Accessed 2021 Mar 21.
5.Coates DK, Paysee EA. Refractive Errors in Children. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2020. www.uptodate.com. Accessed 2021 Mar 21.
6.Lu Y, Lin Z, Wen L, et al. The Adaptation and Acceptance of Defocus Incorporated Multiple Segment Lens for Chinese Children. Am J Ophthalmol. 2020;211:207-216. PubMed
7.Garcia-Del Valle AM, Blazquez V, Gros-Otero J, et al. Efficacy and safety of a soft contact lens to control myopia progression. Clin Exp Optom. 2021;104(1):14-21. PubMed
8.Ruiz-Pomeda A, Perez-Sanchez B, Valls I, Prieto-Garrido FL, Gutierrez-Ortega R, Villa-Collar C. MiSight Assessment Study Spain (MASS). A 2-year randomized clinical trial. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):1011-1021. PubMed
9.Walline JJ, Walker MK, Mutti DO, et al. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA. 2020;324(6):571-580. PubMed
10.Huang J, Wen D, Wang Q, et al. Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Ophthalmology. 2016;123(4):697-708. PubMed
11.Guan M, Zhao W, Geng Y, et al. Changes in axial length after orthokeratology lens treatment for myopia: a meta-analysis. Int Ophthalmol. 2020;40(1):255-265. PubMed
12.Lam CSY, Tang WC, Qi H, et al. Effect of Defocus Incorporated Multiple Segments Spectacle Lens Wear on Visual Function in Myopic Chinese Children. Transl Vis Sci Technol. 2020;9(9):11. PubMed
13.Prousali E, Haidich AB, Fontalis A, Ziakas N, Brazitikos P, Mataftsi A. Efficacy and safety of interventions to control myopia progression in children: an overview of systematic reviews and meta-analyses. BMC Ophthalmol. 2019;19(1):106. PubMed
14.Mukamal R. What is orthokeratology? San Francisco (CA): American Academy of Ophthalmology; 2018. https://www.aao.org/eye-health/glasses-contacts/what-is-orthokeratology. Accessed 2021 Mar 21.
15.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
16.Jansen JP, Trikalinos T, Cappelleri JC, et al. Appendix A: Questionnaire to assess the relevance and credibility of a network meta-analysis. Value Health. 2014;17(2):Supplementary Material.
17.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
18.VanderVeen DK, Kraker RT, Pineles SL, et al. Use of Orthokeratology for the Prevention of Myopic Progression in Children: A Report by the American Academy of Ophthalmology. Ophthalmology. 2019;126(4):623-636. PubMed
19.Ruiz-Pomeda A, Perez-Sanchez B, Prieto-Garrido FL, Gutierrez-Ortega R, Villa-Collar C. MiSight Assessment Study Spain: Adverse Events, Tear Film Osmolarity, and Discontinuations. Eye Contact Lens. 2018;44 Suppl 2:S180-S186. PubMed
20.Ruiz-Pomeda A, Prieto-Garrido FL, Hernandez Verdejo JL, Villa-Collar C. Rebound Effect in the Misight Assessment Study Spain (Mass). Curr Eye Res. 2021:1-4. PubMed
21.Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020;104(3):363-368. PubMed
22.Lyu T, Wang L, Zhou L, Qin J, Ma H, Shi M. Regimen Study of High Myopia-Partial Reduction Orthokeratology. Eye Contact Lens. 2020;46(3):141-146. PubMed
23.Zhao W, Li Z, Hu Y, et al. Short-term effects of atropine combined with orthokeratology (ACO) on choroidal thickness. Contact Lens Anterior Eye. 2020;101348. PubMed
24.Pomeda AR, Perez-Sanchez B, Canadas Suarez MDP, Prieto Garrido FL, Gutierrez-Ortega R, Villa-Collar C. MiSight Assessment Study Spain: A Comparison of Vision-Related Quality-of-Life Measures Between MiSight Contact Lenses and Single-Vision Spectacles. Eye Contact Lens. 2018;44 Suppl 2:S99-S104. PubMed
25.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Prousali et al. (2019)13 Greece Funding: Co-funded by Greece and the European Union (European Social Fund). The authors reported that the funders had no role in the conduct of the study or writing of the manuscript. | Overview of systematic reviews This overview had broader inclusion criteria than the current report. It included a total of 18 systematic reviews of which10 were relevant for the current report. From these relevant systematic reviews,16 primary studies (RCT and cohort studies) were relevant for the current report. Inclusion criteria: Children and adolescents aged ≤ 18 years, spherical equivalent refraction ≤ −0.25 D, with or without astigmatism, and no ocular comorbidities; and studies investigating ocular and pharmaceutical interventions. Exclusion criteria: Surgical interventions for myopia Aim: To synthesize evidence reported in in systematic reviews on myopia control | Children with myopia N = ranged from 39 to 663 (for the relevant comparisons and outcomes reported in this current report) Age (years): < 18 | BF-C vs. SVC: concentric ring bifocal soft contact lenses vs. single-vision soft contact lenses MF-C vs. SVL (MF-C details: peripheral add multifocal soft contact lens). OK vs. SVL | Outcomes: Refractive error, axial length, and adverse events. Follow-up: Up to 2 years |
Guan et al. (2020)11. China Funding: Supported by a Yunnan Health Science and Technology Project grant | Systematic review with meta-analysis. It included 13 studies (RCTs, prospective and retrospective non-randomized studies); 7 studies were from China, 2 each from Japan and Spain, and 1 each from Korea and East Asia. The studies were published between 2011 and 2018. Inclusion criteria: Children < 18 years without organic lesions and only articles in English Exclusion criteria: Articles with duplicate data; abstracts, comments, reviews and case reports, and studies with individuals with other eye diseases Aim: To assess the effect of OK on axial length change compared with glasses | Children with myopia Number of children: Ranged between 29 and 271 Age (years): Ranged between 3 and 17 years Degree of myopia: Ranged between −0.5 D and −10.0 D The degree of astigmatism was under 2.00 D | OK vs. glasses In the included studies the comparator (glasses) was reported as spectacles or SVS. For this current report, glasses will be reported simply as SVS | Outcomes: Change in axial length Follow-up:1 year to 3 years |
Walline et al. (2020)1 US Funding: Supported by the National Eye Institute, National Institute of Health, US; and the National Institute of Health Research, UK | Systematic review with meta-analysis This systematic review had broader inclusion criteria than the current report. It included a total of 41 primary studies of which 8 RCTs (reported in 17 publications) were relevant for the current report. Of the 8 studies 4 were conducted in China, and 1 each in Australia, Japan, New Zealand, and the US. The studies were published between 2011 and 2018. Inclusion criteria: Trials that compared various interventions (spectacles, contact lenses, and pharmaceutical agents) with SVS, SVC, or placebo; or with each other. Exclusion criteria: Studies in which majority of the participants were above 18 years of age, and participants had less than −0.25 D spherical equivalent myopia at baseline. Aim: To assess the effects of interventions (spectacles, contact lenses and pharmaceutical agents) on controlling progression of myopia | Children with myopia BF-C vs. SVC comparison (4 studies):
OK vs. SVS comparison (4 studies):
Degree of myopia was not reported for the participants in the study. However, for each study the inclusion and exclusion criteria were reported. Presenting all the details is beyond the scope of this current report. Details of study characteristics can be found in the report by Walline et al.1 | BF-C vs. SVC OK vs. SVS | Outcomes: Change in refractive error, change in axial length, and adverse effects Follow-up: 1 year to 2 years |
VanderVeen et al. (2019)18 US Funding: Without commercial support by the American Academy of Ophthalmology | Systematic review It included a broader range of comparators than that relevant for the current report. Of the 13 studies included, 12 studies (RCTs, prospective and retrospective non-randomized studies) were relevant. Countries where the studies were conducted were not reported. The studies were published between 2011 and 2015. Inclusion criteria: Children aged 16 years or younger, RCT or non-randomized comparative studies, and individuals were followed up for at least 1 year. Exclusion criteria: Noncomparative studies, reviews, and commentaries Aim: To assess the effectiveness of OK in reducing myopic progression | Children with myopia. Number of children ranged between 32 and 282. Age ranged between 6 years and 11 years Myopia: −0.5 D to −7.0 D | OK vs. spectacles or contact lenses (11 studies) OK vs. 0.125% atropine (1 study) | Outcomes: Changes in axial length, and degree of myopic progression (refractive error) Follow-up: 1 year to 5 years |
Huang et al. (2016)10 China Funding: Government agencies. The funders had no role in the conduct of the research or preparation of the manuscript | Systematic reviewa with network meta-analysis. It included 30 RCTs (9 studies each from US and China, 4 studies from Singapore, 3 studies from Taiwan, 1 study each from Japan, Malay, Israel, Denmark and Finland). The studies were published between 1989 and 2014. Inclusion criteria: Children undergoing interventions for controlling progression of myopia, and treatment duration of at least 1 year Exclusion criteria: Patients aged > 18 years when enrolled in the trial, patients having < 0.25 D of spherical equivalent myopia at baseline, and studies that were non-randomized or noncomparative. Aim: To assess the effectiveness of different interventions to slow the progression of myopia | Children with myopia N = 5,387 children (5,422 eyes) In the individual primary studies: Number of eyes ranged between 48 and 484 Mean age (years) ranged between 8 and 14 Mean baseline refraction ranged between −1.1 D and −6.3 D Mean baseline axial length ranged between 24.1 mm and 25.4 mm | The network included the following interventions: atropine (3 separate groups: low, medium, and high concentrations), pirenzepine, cyclopentolate, timolol, more outdoor activities, OK, bifocal spectacle lenses, progressive addition spectacle lenses, prismatic bifocal spectacle lenses, peripheral defocus modifying contact lenses, peripheral defocusing modifying spectacle lenses, rigid gas-permeable contact lenses, soft contact lenses, under-corrected single-vision spectacle lenses, and SVS or placebo (i.e., SVS and placebo were grouped together).b | Outcomes: Change in refraction, and change in axial length Follow-up: 12 months to 36 months |
BF-C = bifocal contact lenses; D = dioptre; MF = multifocal; MF-C = multifocal contact lens; OK = orthokeratology; RCT = randomized controlled trial; SVC = single-vision contact lenses; SVL = single-vision lens; SVS single-vision spectacles.
aThis systematic review was included in the selected overview of systematic reviews by Prousali et al.13; therefore, only the relevant section of the network meta-analysis is considered in this current report.
bNote: only results of comparisons that are relevant for the current report are presented)
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Ruiz-Pomeda et al. (2018-2021)8,19,20,24 Spain Funding: Sponsored by Cooper Vision S.L. Spain. The authors reported that the sponsor had no role in the design or conduct of the study | RCT (blinding was not reported except that the researcher who examined patients had no access to the randomization schedule) The RCT was followed by an extension study with a subset of patients from the RCT. Setting: Novovision ophthalmic clinic and the Universidad Europea in Madrid. Inclusion criteria: Children aged 8 to 12 years, in good general health, low-to-moderate level of refractive error (0.75 to 4.00 D) and astigmatism (< 1.00 D). Exclusion criteria: Current or prior use of contact lenses, bifocal, progressive lenses or atropine or any other treatment to control myopia. History of corneal hypoesthesia, corneal ulcer, corneal infiltrates, or ocular infections. | Children with myopia N = 79 (46 in MiS, 33 in SVS) Age (years), mean (SD): 10.94 (1.24) in MiS, 10.12 (1.38) in SVS (P = 0.007) Spherical equivalent (D), mean (SD): −2.10 (0.91) in MiS, −1.75 (0.94) in SVS (P = 0.095) Axial length (mm), mean (SD): 24.11 (0.57) in MiS, 24.00 (0.86) in SVS (P = 0.525) Ethnicity: NR Extension study with a subset of 55 children divided into 3 groups (Mis-C, MiS-D, and SVS) according to further intervention used (see Intervention) Age (years), mean (SD): 12.9 (1.2) in MiS-C, 13.2 (1.2) in MiS-D, and 11.9 (1.3) in SVS (P = 0.0064) There were no significant differences among the 3 groups for axial length (P = 0.33) and spherical equivalent (P = 0.44) | MiS vs. SVS. MiS is made from a material that comprises 40% omafilcon A and 60% water After 24 months of follow-up, the children could freely choose the method of controlling myopia. In a subset of 55 children, 13 children continued with MiS (MiS-C group), 15 children stopped wearing MiS in the third year and wore instead SVS (MiS-D group) and 18 children wearing SVS continued with SVS in the third year (SVS group) | Outcomes: Spherical equivalent, axial length, QoL, adverse events Follow-up: 24 months. In the extension study, a subset of 55 children were assessed after the third year |
Garcia-del Valle et al. (2020)7 Spain Funding: Sponsored by Tiedra Farmaceutica S.L. (patent owner of the Esencia lens design). The authors reported that Tiedra Farmaceutica S.L. provided the contact lenses and maintenance solutions but no other financial support. | RCT, double masked (both investigator and patient were masked). Setting: 7 clinical centres in Spain Inclusion criteria: Children aged 7 years to 15 years with cycloplegic spherical autorefraction measurements between −0.50 D and −8.75 D, and visual acuity = 1, in good ocular and general health Exclusion criteria: Children with uncontrolled psychiatric or neurologic disorders | Children with myopia N = 70 (36 in MF-C group, and 34 in the SVC group); 58 completed the study (32 in MF-C group and 26 in SVC group) Characteristics were reported for the 58 children who completed the study, however for some characteristics the reported values did not always include the entire group. Age (years), mean (SD): 12.20 (2.22) in MF-C, and 11.3 (2.13) in SVC (P = 0.620) Objective cycloplegic spherical equivalent refraction (D), mean (SD): −2.80 (1.79) in MF-C and −3.31 (1.76) in SVC (P = 0.273) Axial length (mm), mean (SD): 24.54 (0.89) in MF-C and 24.48 (0.78) in SVC (P = 0.806) Ethnicity (ratio of Caucasian to Asian): 20:0 in MF-C and 18:1 in SVC | MF-C vs. SVC. MF-C: Esencia lens, a progressive multifocal and reverse geometry soft contact lens. SVC: Conventional soft contact lens | Outcomes: Spherical equivalent, axial length, adverse events Follow-up: 1 year |
China Funding: Sponsored by Hoya, Japan. In addition to financial support the sponsor provided the spectacle lenses and frames. | RCT (investigator unmasked; children and their parents masked) Setting: Center for Myopia Research at the Hong Kong Polytechnic University. Inclusion criteria: Children aged 8 years to 13 years, spherical equivalent refraction from −1.00 D to −5.00 D, astigmatism and anisometropia of 1.50 D or less Exclusion criteria: Strabismus and binocular vision abnormalities; ocular and systemic abnormalities; and prior experience of myopia control | Children with myopia N = 183 (93 in DIMS group, and 90 in the SVS group); 160 completed the study (79 in DIMS group and 81 in SVS group). Patient characteristics were reported for the 160 children who completed the study. Age (years), mean (SD): 10.20 (1.47) in DIMS and 10.00 (1.45) in SVS Objective cycloplegic spherical equivalent refraction (D), mean (SD): −2.97 (0.97) in DIMS and 2.76 (0.96) in SVS Axial length (mm), mean (SD): 24.7 (0.82) in DIMS and 24.60 (0.83) in SVS Ethnicity: NR | DIMS vs. SVS. DIMS are spectacle lens | Outcomes: Cycloplegic spherical equivalent refractiona and axial length; and adverse effects Follow-up: 24 months |
Lu et al. (2020)6 China Funding: Funds were received from the Hunan Provincial Science and Technology Department, China. Publication of the research was supported by Hoya Co, Japan. DIMS and SVS were provided by Hoya Co, Japan. | RCT, crossover study (unclear if there was any masking) Setting: NR Inclusion criteria: Children aged 7 years to 15 years, spherical equivalent refraction from −0.50 D to −6.00 D, astigmatism of ≤ 1.50 D Exclusion criteria: NR | Children with myopia. N = 20 Age (years), mean (SD): 10.80 (2.55) Objective cycloplegic spherical equivalent refraction (D): −0.05 to −6.00 according to inclusion criteria Axial length (mm): NR Ethnicity: NR (the authors reported that their aim was to assess the acceptability of DIMS in Chinese youth) | DIMS vs. SVS DIMS are spectacle lens | Outcomes: Visual symptoms, and acceptability of the intervention Follow-up: 1 week for DIMS and 1 week for SVS |
Lyu et al. (2020)22 China Funding: None | RCT (unclear if there was any masking) Setting: Henan Provincial Ete Hospital, China. Inclusion criteria: Children aged 8 years to 15 years, spherical equivalent refractive error in the range −6.00 D to −8.75 D, astigmatism < 1.50 D, and with no ocular or systematic disease that could cause impaired vision Exclusion criteria: NR | Children with high myopia N = 102; 34 in OK1 (target myopia reduction of 6.00 D) group, 34 in the OK2 (target myopia reduction of 4.00 D) group), and 34 in the control (SVS) group Patient characteristics were reported for 90 children (29 in OK1, 30 in OK2, and 31 in SVS) Age (years), mean (SD): 12.55 (1.90) in OK1, and 12.73 (1.86) in OK2, 12.55 (1.86) in SVS (P = 0.91) Spherical equivalent refractive error (D), mean (SD): −6.70 (0.67) in OK1, −6.76 (0.74) in OK2, and −6.56 (0.65) in SVS (P = 0.35) Axial length (mm), mean (SD): 25.80 (0.56) in OK1, 25.99 (0.68) in OK2, and 25.95 (0.66) in SVS (P = 0.18) Ethnicity: NR | OK1 vs. OK2 vs. SVS OK1 and OK2 are 2 types of contact lenses. OK1 and OK2 are targeted for myopia reduction by 6.00 D and 4.00 D, respectively | Outcomes: Spherical equivalent refractive error, axial length, and corneal staining Follow-up: 12 months |
Walline et al. (2020)9 US Funding: Grants from the National Institute of Health | RCT, double masked (investigator; and patient and guardian) Setting: 2 optometry schools located in the US Inclusion criteria: children aged 7 to 11 years, had myopia of −0.75 D to −5.00 D (spherical component by cycloplegic autorefraction), astigmatism less than 1.00 D cylinder Exclusion criteria: Those who had used for > 1 month; gas-permeable, soft bifocal, or orthokeratology contact lenses; > 1 month of myopia control (including atropine and bifocal spectacles); systemic issues that could affect myopia progression; or if using oral or ophthalmic steroids | Children with myopia N = 294 (98 in each of the 3 groups: MF-Ch,MF-Cm, SVC) For all 3 groups combined:
For the individual groups:
| MF-Ch vs. MF-Cm vs. SVC | Outcomes: Change in refractive error, change in eye length, and adverse events Follow-up: 3 years |
Zhao et al. (2020)23 China Funding: supported by the Fundamental Research funds of the State Key Laboratory of Ophthalmology, China. | RCT (unclear if there was any masking) Setting: Zhongshan Ophthalmic Center, Sun Yat-Sen University, China. Inclusion criteria: Children aged 8 to 12 years; spherical equivalent between −1.00 and −6.00 in both eyes, astigmatism ≤ 1.50 D; and normal intraocular pressure and binocular function Children who used spectacles for optical correction or remained uncorrected before enrolment were eligible. Exclusion criteria: Children with ocular pathology (e.g., strabismus, allergic conjunctivitis, dry eye), already undergoing other treatments to control myopic progression; having a condition that can impact vision development | Children with myopia N = 164; 154 completed study (39 in AOK, 42 in ASVS group, 36 in POK group, and 37 in PSVS group) Age (years), mean (SD): 10.23 (1.11) in AOK, 10.33 (1.65) in POK, 9.96 (1.03) in ASVS, and 9.73 (1.04) in PSVS (P = 0.154) Spherical equivalent refractive error (D), mean (SD): −3.12 (1.20) in AOK, −2.74 (1.06) in POK, −3.01 (1.22) in ASVS, and −3.25 (1.10) in PSVS (P = 0.272) Axial length (mm), mean (SD): 24.78 (0.98) in AOK, 24.69 (0.63) in POK, 24.90 (0.78) in ASVS, 24.86 (0.72) in PSVS (P = 0.648) Ethnicity: NR | AOK vs. POK vs. ASVS vs. PSVS Atropine when used was of 0.01% | Outcomes: Spherical equivalent refractive error, and axial length Follow-up: 1 month |
AOK = atropine plus orthokeratology, ASVS = atropine plus single-vision spectacles, D = dioptre; DIMS = Defocus Incorporated Multiple Segments; MF-C = multifocal contact lenses; MF-Ch = multifocal contact lenses (high add power); MF-Cm = multifocal contact lenses (medium add power); MiS = MiSight contact lenses; NR = not reported; OK = orthokeratology; POK = placebo plus orthokeratology; PSVS = placebo plus single-vision spectacles; QoL = quality of life; RCT = randomized controlled trial; SD = standard deviation; SVC = single-vision contact lenses; SVS = single-vision spectacle; vs. = versus.
aCycloplegic refraction measurement is a procedure to determine refractive error by temporarily relaxing the focusing muscles of the eye.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 215 and the ISPOR Questionnaire16
Strengths | Limitations | |
Prousali et al. (2019)13 | ||
|
| |
Guan et al. (2020)11 | ||
|
| |
Walline et al. (2020)1 | ||
|
| |
VanderVeen et al. (2019)18 | ||
|
| |
Huang et al. (2016)10 | ||
|
| |
NMA:
| NMA:
| |
GRADE Working Group grades of evidence | ||
High certainty | “Further research is very unlikely to change our confidence in the estimate of effect (p. 6).” | |
Moderate certainty | “Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate (p. 6).” | |
Low certainty | “Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate (p. 6).”1 | |
Grading based on rating scale developed by the Oxford Centre for Evidence-Based Medicine | “Level I rating to well-designed and well-conducted randomized clinical trials, a level II rating to well-designed case-control and cohort studies and lower-quality randomized studies, and a level III rating to comparative case series (p. 625).”18 | |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; BF-C = bifocal contact lenses; CRD = Centre for Reviews and Dissemination; DARE = Database of Abstracts of Reviews of Effects; GRADE = Grading of Recommendations Assessments, Development and Evaluation; HTA = Health Technology Assessment; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; MF-C = multifocal contact lenses; RCT = randomized controlled trial; ROBIS = risk of bias assessment tool for systematic reviews; vs = versus.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist17
Strengths | Limitations |
|
|
Garcia-del Valle et al. (2020)7 | |
|
|
|
|
Lu et al. (2020)6 | |
|
|
Lyu et al. (2020)22 | |
|
|
Walline et al. (2020)9 | |
|
|
Zhao et al. (2020)23 | |
|
|
ITT = intention-to-treat; MF-C = multifocal contact lenses; MF-Ch = multifocal contact lenses (high add power); MF-Cm = multifocal contact lenses (medium add power); MiSight = MiSight lenses; NR = not reported.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Included Systematic Reviews and Network Meta-Analyses
Prousali et al. (2019)13
Main Study Findings
OK versus SVC or SVL
Refractive error (D), MD (95% CI)
At 1 year, change in refractive error: −0.27 (−0.50 to −0.04), favouring OK (1 study, 39 children; I2 = NA)
At 2 years, change in refractive error: −0.66 (−1.01 to −0.31), favouring OK (1 study, 39 children; I2 = NA)
Axial length (mm), MD (95% CI)
At 1 year, change in axial length: −0.19 (−0.21 to −0.16), favouring OK (8 studies, 524 children; I2 = 0%)
At 2 years, change in axial length: −0.27 (−0.31 to −0.23), favouring OK (1 study, 128 children; I2 = NA)
Adverse events, OR (95% CI)
Mild corneal erosion: 4.56 (0.49 to 42.25); no statistically significant difference between OK and SVC or SVL (2 studies, 151 children; I2 = 0%)
Bifocal contact lenses versus SVC
Refractive error (D), MD (95% CI)
At 1 year, change in refractive error: −0.31 (−0.60 to −0.02), favouring bifocal contact lenses (3 studies, 264 children; I2 = 88%)
At 2 years, change in refractive error: −0.20 (−0.38 to −0.02), favouring bifocal contact lenses (1 study, 128 children; I2 = NA)
Axial length (mm), MD (95% CI)
At 1 year, change in axial length: −0.12 (−0.19 to −0.06), favouring bifocal contact lenses (3 studies, 264 children; I2 = 66%)
At 2 years, change in axial length: −0.12 (−0.20 to −0.04), favouring bifocal contact lenses (1 study, 128 children; I2 = NA)
Adverse events, OR (95% CI)
Contact lens related discomfort or unwillingness to wear contact lenses: 0.95 (0.49 to 1.81); no statistically significant difference between bifocal contact lenses and SVC (2 studies, 261 children; I2 = 0%)
Multifocal contact lenses versus SVL
Refractive error (D), MD (95% CI)
At 1 year, change in refractive error: −0.23 (−0.31 to −0.14), favouring multifocal contact lenses (5 studies, 294 children; I2 = 0%)
At 2 years, change in refractive error: −0.50 (−0.65 to −0.35), favouring multifocal contact lenses (2 studies, 99 children; I2 = 0%)
Axial length (mm)
At 1 year, change in axial length: −0.10 (−0.14 to −0.05), favouring multifocal contact lenses (5 studies, 294 children; I2 = 37%)
At 2 years, change in axial length: −0.13 (−0.20 to −0.06), favouring multifocal contact lenses (2 studies, 99 children; I2 = 0%)
Authors’ Conclusion
“Our data suggest that atropine followed by orthokeratology and novel multifocal soft contact lenses demonstrate efficacy in controlling myopic progression… It remains unclear if atropine or orthokeratology could lead to a permanent long-term effect on myopia control. Possible rebound effect upon treatment cessation should also be assessed for OK and multifocal lenses… Finally, systematic collection of evidence on safety issues is essential, as these treatments gradually enter routine practice all over the world (p. 15).”13
Guan et al. (2020)11
Main Study Findings
OK versus SVS
Axial length (mm), SMD (95% CI)
At 1 year, change in axial length: −0.86 (−1.15 to −0.57), favouring OK (10 studies; I2 = 70.4%)
At 2 years or longer, change in axial length: −0.90 (−1.14 to −0.65), favouring OK (9 studies; I2 = 50.4%)
Authors’ Conclusion
“In summary, OK lens treatment is more effective than wearing normal glasses to slow axial elongation during the early treatment of myopia in children. More studies with long-term follow-up data are expected to draw a precise conclusion for myopia treatment (p. 263).”11
Walline et al. (2020)1
Main Study Findings
OK versus SVS
Axial length (mm), MD (95% CI)
At 2 years, change in axial length: was −0.28 (−0.38 to −0.19), favouring OK (2 studies, 106 children, I2 = 0%)
The authors reported that the evidence was of moderate certainty (using GRADE)
A third study did not report sufficient data for analysis, hence was not included in the analysis
Refractive error (D)
The authors did not analyze the change in refractive error. The rationale was that as OK temporarily reduces myopia, their myopia control treatment effect can only be assessed by axial elongation measurements.
Adverse effects
No serious adverse effects were reported
Bifocal contact lenses versus SVC
Refractive error (D), MD (95% CI)
At 1 year, change in refractive error: 0.2 (−0.06 to 0.47), between-group difference not statistically significant (4 studies, 300 children; I2 = 85.7%)
The authors reported that the evidence was of low certainty (using GRADE)
Axial length (mm), MD (95% CI)
At 1 year, change in axial length: −0.11 (−0.14 to −0.08), favouring bifocal contact lenses (4 studies, 300 children; I2 = 66.8%)
The authors reported that the evidence was of low certainty (using GRADE)
Adverse effects
Of the 4 included studies, 1 study involving 40 children reported on adverse effects. In this study, 3 children in each group did not complete the follow-up; the authors reported that 4 children withdrew due to difficulty in handling contact lenses, 1 withdrew due to dislike with cycloplegia, and 1 withdrew due to negative publicity regarding contact lens solutions.
No serious adverse effects were reported.
Authors’ Conclusion
“Orthokeratology contact lenses, although not intended to modify refractive error, were more effective than SVLs [single-vision lenses] in slowing axial elongation (p. 2).”1
VanderVeen et al. (2019)18
Main Study Findings
OK versus standard spectacles or contact lenses
Refraction and axial length
The authors in their systematic review presented results for each individual study separately. They reported that myopic progression was less with OK compared to spectacles or contact lenses (P values were generally not reported). This systematic review18 also included 1 study that showed that myopic progression was statistically significantly less with OK compared to 0.125% atropine (P = 0.001).
The authors reported that OK typically reduced axial elongation by about 50% over a duration of 2 years; average axial length change values were approximately 0.3 mm for OK and 0.6 mm for control (standard spectacles or contact lenses). The increase in axial length was generally less with OK compared to spectacles or contact lenses (statistical significance was not generally reported; when reported, P values ranged between < 0.001 and 0.02). The authors also included 1 study that found that axial length increased less with OK compared to 0.125% atropine (statistical significance was not reported).
Compared to standard spectacles or contact lenses, with OK there was slower rate of axial elongation as measured by optical biometry and slower rate of myopic progression as measured by cycloplegic refractions. Several studies showed greater effect in the younger children (aged ≤ 9 years) compared to older children. The authors mentioned that though rates of myopic progression were statistically significantly slower with OK compared with standard spectacles and contact lenses, the clinical effects were small. However, they did not mention what is considered a clinically important effect.
Adverse events
In 1 included study, 1 case of infiltrative keratitis was reported in the OK group. The authors mentioned in their discussion that microbial keratitis was a major risk with contact lens wear in children (citing 3 references; publications that were not in their list of included studies).
OK versus 0.125% atropine nightly
This systematic review included 1 retrospective cohort study comparing OK with atropine
Refractive error
Myopic progression (D per year) was −0.28 ± 0.18 with OK and −0.34 ± 0.21 with atropine; statistically significantly less with OK compared to atropine (P = 0.001)
Axial length
The increase in axial length (mm per year) was 0.28 ± 0.08 with OK and 0.34 ± 0.09 with atropine statistically significantly less increase with OK compared to atropine (P < 0.001)
Note: Although numerical values were reported, the central tendency or spread was not specified.
Authors’ Conclusion
“Orthokeratology may be effective in slowing myopic progression for children and adolescents, with a potentially greater effect when initiated at an early age (6-8 years). Safety remains a concern because of the risk of potentially blinding microbial keratitis from contact lens wear (p. 623).”18
Huang et al. (2016)10
Main Study Findings
Note: this systematic review was included in the selected overview of systematic reviews by Prousali et al.13; therefore, only the relevant section of the network meta-analysis is considered in this current report.
Indirect comparisons (network meta-analysis) (only results relevant for this current report are presented here)
Change in refraction (D per year), MD (95% CrI)
High-dose atropine versus OK: not reported (NR)
Moderate-dose atropine versus OK: NR
Low-dose atropine versus OK: NR
OK versus SVS: NR
Change in axial length (mm per year), MD (95% CrI)
OK versus high-dose atropine: −0.07 (−0.16 to 0.02)
OK versus moderate-dose atropine: 0.00 (−0.12 to 0.12)
OK versus low-dose atropine: −0.07 (−0.19 to 0.05)
OK versus SVS: −0.15 (−0.22 to −0.08)
Authors’ Conclusion
“This network analysis indicates that a range of interventions can significantly reduce myopia progression when compared with single-vision spectacle lenses or placebo… In terms of axial length, atropine, orthokeratology, peripheral defocus modifying contact lenses, pirenzepine, and progressive addition spectacle lenses were effective (p. 697).”10
Summary of Findings of Included Primary Clinical Studies
Ruiz-Pomeda et al. (2018-2021)8,19,20,24
Main Study Findings
Outcomes over 2 years, in 74 children who completed the study (RCT)
Spherical equivalent values (D) at various times,8 mean (SD)
At baseline: −2.16 (0.94) for the MiS group; −1.75 (0.94) for the SVS group
At 12 months: −2.34 (1.05) for the MiS group; −2.18 (1.01) for the SVS group
At 24 months: −2.61 (1.20) for the MiS group; −2.48 (1.13) for the SVS group
Over 2 years, the mean myopic progression (based on spherical equivalent values) was 0.45 (CI, 0.27 to 0.64) D for the MiS group, and 0.74 (CI, 0.53 to 0.95) D for the SVS group. There was less myopic progression in the MiS group compared with the SVS group (mean between-group difference = 0.29 D).
Axial length (mm) at various times,8 mean (SD)
At baseline: 24.09 (0.55) for the MiS group; 24.00 (0.86) for the SVS group
At 12 months: 24.21 (0.58) for the MiS group; 24.24 (0.86) for the SVS group
At 24 months: 24.37 (0.59) for the MiS group; 24.45 (0.88) for the SVS group
Over 2 years, the total increase in axial length was 0.28 (CI, 0.20 to 0.37) mm in the MiS group, and 0.44 (CI, 0.35 to 0.54) mm in the SVS group. There was less axial elongation in the MiS group compared with the SVS group (mean between-group difference = 0.16 mm).
Quality of life (QoL)24
QoL was assessed using the Pediatric Error Refractive Profile questionnaire
Both at 12 months and 24 months, the ratings with respect to appearance, satisfaction, effect on activities, handling, and peer perceptions were statistically significantly better for the MiS group compared to the SVS group (P ranged from < 0.001 to 0.026), as was the total score.
At 12 months: total score was 79.41 for MiS group and 71.78 for SVS group (P = 0.018)
At 24 months: total score was 81.06 for MiS group and 70.74 for SVS group (P = 0.001)
Higher values indicate better QoL
Adverse events19
The authors reported that there were no serious or significant adverse effects in the MiS or SVS groups.
In 2 individuals in the MiS group, a unilateral foreign body was found attached to the cornea; however, there were no symptoms or reduction in best-corrected visual acuity. This was later resolved.
In both groups, 29 eyes (39%) had grade 2 bulbar hyperemia and peripheral roughness.
In the MiS group, there was significant increase in limbal hyperemia (P = 0.007), palpebral hyperemia (P = 0.05), and conjunctival staining (P = < 0.0001) at 24-months compared to baseline values. In the SVS group, there were no significant changes in these variables.
In both groups, there were no significant changes in bulbar hyperemia, corneal vascularization, palpebral roughness and corneal staining (P > 0.05).
In both groups, there were no significant changes in osmolarity data over the 24 months (P ≥ 0.05).
Outcomes in a subset of 55 children who were further assessed at the end of 3 years (extension study of the RCT)20
This subset comprised 13 children who continued with MiS (MiS-C group), 15 children who stopped wearing MiS in the third year and wore SVS (MiS-D group) instead, and 18 children who were wearing SVS and continued with SVS in the third year (SVS group).
It was reported that there were no significant differences in myopia progression based on the spherical equivalent values (D) among the 3 groups: mean (SD): −0.37 (0.44) in MiS-C group, −0.46 (0.39) in MiS-D group, and −0.55 (0.45) in SVS group; P value was not reported.
There were no significant differences in axial length (mm) among the 3 groups, mean (SD): 0.15 (0.11) in MiS-D, 0.22 (0.11) in MiS-D group, and 0.21 (0.10) in SVS group; P > 0.05.
Authors’ Conclusion
“MiSight contact lens wear reduces axial elongation and myopia progression in comparison to distance single-vision spectacles in children (p. 1011).”8
“MiSight CL wear for controlling myopia improves vision related quality of life in children when compared with spectacle wear (p. S99).”24
“No clinically serious events were observed in either group. Our results show that correct use of MiSight CLs is a safe option for myopia correction (p. S180).”19
“Over a one-year period, neither myopia progression nor eye growth was faster for the subjects who discontinued MiSight contact lens wear compared to those who continued to wear MiSight contact lenses or those who continued to wear single-vision spectacles, indicating no rebound effect with MiSight contact lenses for 2 years (p. 1).”20
Garcia-del Valle et al. (2020)7
Main Study Findings
Outcomes over 1 year, in 58 children who completed the study (RCT)
Changes (from baseline) in objective cycloplegic spherical equivalent refraction (D) at various times, mean (SD)
At 6 months: −0.25 (0.32) for the multifocal contact lens group, and −0.46 (0.53) for the SVC group; P = 0.10
At 12 months: −0.28 (0.35) for the multifocal contact lens group, and −0.57 (0.52) for the SVC group; P = 0.02
Changes (from baseline) in axial length (mm) at various times, mean (SD)
At 6 months: 0.07 (0.10) for the multifocal contact lens group, and 0.09 (0.10) for the SVC group; P = 0.66
At 12 months: 0.13 (0.12) for the multifocal contact lens group, and 0.22 (0.14) for the SVC group; P = 0.03
Both multifocal contact lens and SVC were reported to provide a high degree of comfort and good quality of vision, and there were no significant between-group differences; P > 0.05.
Adverse events
Proportion of patients with 1 or more adverse events (such as corneal neovascularization, conjunctival hyperaemia, micropapillary response, papillary conjunctivitis, and superficial punctate keratitis) was 25.0% in the multifocal contact lens group, and 15.4% in the SVC group. All adverse events were classified as non-serious, expected, treatment-related, and mild during contact lens use. No serious or unexpected adverse events were reported.
Authors’ Conclusion
“In summary, results from the analysis of the 12-month data of this clinical trial indicate that the Esencia SCL seems to be an efficacious option of control of myopia progression in myopic children, with similar visual performance and safety as with a conventional SCL. These results must be confirmed in the longer term, with a two-year follow-up or more (p. 7).”7
Note: Esencia SCL is the same as multifocal contact lens, and SCL is the same as SVC.
Main Study Findings
Outcomes over 2 years, in 160 children who completed the study (RCT)
Changes (from baseline) in cycloplegic spherical equivalent refraction (D) at various times, mean (SE)
At 6 months: −0.13 (0.03) for the DIMS group and −0.37 (0.04) for the SVS group; between-group difference = −0.24 (0.05; P < 0.0001)
At 12 months: −0.17 (0.05) for the DIMS group and −55 (0.04) for the SVS group; between-group difference = −0.38 (0.07; P < 0.0001)
At 24 months: −0.38 (0.06) for the DIMS group and −0.93 (0.06) for the SVS group; between-group difference = −0.38 (0.07; P < 0.0001); between-group difference = −0.55 (0.09; P < 0.0001).
Changes (from baseline) in axial length (mm) at various times, mean (SE)
At 6 months: 0.03 (0.01) for the DIMS group, and 0.20 (0.01) for the SVS group; between-group difference = 0.16 (0.02; P < 0.0001).
At 12 months: 0.11 (0.02) for the DIMS group, and 0.32 (0.02) for the SVS group; between-group difference = 0.21 (0.02; P < 0.0001).
At 24 months: 0.21 (0.02) for the DIMS group, and 0.53 (0.03) for the SVS group; between-group difference = 0.32 (0.04; P < 0.0001).
Adverse effects
Repeated measures analysis of variance with group as a factor, showed that there were no statistically significant differences in visual function changes between the DIMS and SVS groups (P > 0.05). This indicated that wearing of DIMS spectacles did not lead to adverse effects on visual function, when compared with wearing of SVS.
Authors’ Conclusion
“Daily wear of the DIMS lens significantly slowed myopia progression and axial elongation in myopic schoolchildren as compared with wearing SV spectacle lenses. They provided good vision while presenting simultaneous MD to the eyes. This intervention is simple to use and is the least invasive method compared with pharmacological or contact lens treatments. The DIMS spectacle lens offers an alternative treatment modality for myopia control (p. 367).”21
“In conclusion, DIMS lens wear had no adverse effect on the measured visual function. Further studies are needed to determine any effects occurring over longer periods of time (p. 1).”12
Lu et al. (2020)6
Main Study Findings
Outcomes over 1 week, in 20 children (RCT, crossover study)
Tolerance
It was reported that 35% (7 of 20) of the children complained of paracentral and peripheral blurred vision with DIMS, and none with SVS (P = 0.01).
There were no statistically significant differences between DIMS and SVS, in the number of complaints regarding symptoms: eyestrain, headache, dizziness, diplopia, nausea, photophobia, darkened vision field, colour change, ghosting images, and metamorphopsia (P ranged from 0.342 to 1.000).
Acceptability
All 20 children were willing to wear SVS, and 85% (17 of 20) of children were willing to wear DIMS. However, when they were informed that DIMS would slow down progression of myopia by 59%, then 90% were willing to wear DIMS.
Authors’ Conclusion
“Mid-peripheral vision through DIMS lenses was slightly affected compared with SV lenses. Otherwise, DIMS lenses received good tolerance and acceptance by Chinese children (p. 207).”6
Lyu et al. (2020)22
Main Study Findings
Outcomes at 12 months, in 87 children
Spherical equivalent refractive error (D), mean (SD)
At baseline: −6.698 (0.672) for the OK1 group, −6.763 (0.741) for the OK2 group, and −6.585 (0.650) for the SVS group
At 12 months: −1.078 (0.732) for the OK1 group, −3.075 (0.803) for the OK2 group, and −7.149 (0.664) for the SVS group
There was no statistically significant difference in progression of myopia between the OK1 and OK2 groups (P = 0.124). However, the between-group differences in myopia progression were statistically significant for both OK1 and OK2 groups compared to SVS group, favouring OK1 and OK2 (P < 0.05).
Axial length
At 12 months, the difference in elongation of axial length was not statistically significant between the OK1 and OK2 groups (P = 0.461). However, the between-group differences in axial length elongation were statistically significant for both OK1 and OK2 groups compared to SVS group, favouring OK1 and OK2 (P < 0.05).
Safety issues
Corneal staining (detects cornea damage): the mean rate of corneal staining was 28.97% in the OK1 group, 13.06% in the OK2 group and 0.81% in the SVS group. The risk of corneal staining was significantly higher in OK1 compared to OK2 (P < 0.05).
Authors’ Conclusion
“The two ortho-k regimens, target reduction of 6.00 D and target of 4.00 D, had similar effects in controlling the increase in axial length and refractive error in high-myopia children. However, subjects with a target myopia reduction of 6.00 D had a higher rate of corneal staining than in subjects with a target myopia reduction of 4.00 D (p. 141).”22
Walline et al. (2020)9
Main Study Findings
Outcomes over 3 years, in 292 (97 in MF-Ch, 98 in MF-Cm, and 97 in SVC) children who were included in the analysis (RCT)
Refractive error (D)
At baseline: mean = −2.30 (SD = 0.91) in the in MF-Ch group, mean = −2.46 (SD = 1.09) in the in MF-Cm group, and mean = −2.45 (SD = 0.96) in the SVC group
At 3 years: mean = −2.84 (SD = 1.22) in the MF-Ch group, mean = −3.32 (SD = 1.48) in the MF-Cm group, and mean = −3.46 (SD = 1.20) in the SVC group
For MF-Ch versus SVC: MD = 0.45 (95% CI, 0.25 to 0.66) favouring MF-Ch (P < 0.001)
For MF-Cm versus SVC: MD = 0.16 (95% CI, −0.01 to 0.33) with no significant difference between-group difference (P = 0.19)
For MF-Ch versus MF-Cm: MD = 0.29 (95% CI, 0.09 to 0.50) favouring MF-Ch (P = 0.01)
Eye length (mm)
At baseline: mean = 24.42 (SD = 0.75) in the in MF-Ch group, mean = 24.55 (SD = 0.84) in the in MF-Cm group, and mean = 24.43 (SD = 0.83) for the SVC group
At 3 years: mean = 24.81 (SD = 0.83) in the MF-Ch group, mean = 25.12 (SD = 0.97) in the MF-Cm group; mean = 25.08 (SD = 0.85) in the SVC group
For MF-Ch versus SVC: MD = −0.23 (95% CI, −0.30 to −0.17) favouring MF-Ch (P < 0.001)
For MF-Cm versus SVC: MD = −0.07 (95% CI, −0.16 to 0.03) no significant difference between group (P = 0.15)
For MF-Ch versus MF-Cm: MD = −0.16 (95% CI, −0.26 to −0.07) favouring MF-Ch (P = 0.002)
Adverse events
Proportion of adverse events was 40.0% in the in MF-Ch group, 22.9% in the MF-Cm group, and 37.1% in the SVC group.
None of the adverse events were serious or severe, or caused permanent discontinuation of wearing of contact lenses.
The 3 most common adverse events were giant papillary conjunctivitis, infiltrative keratitis, and ocular allergies. There were no significant differences in these adverse events between the 3 groups (P = 0.41).
Authors’ Conclusion
“Among children with myopia, treatment with high add power multifocal contact lenses significantly reduced the rate progression over 3 years compared with medium add power multifocal and single-vision contact lenses. However, further research is needed to understand the clinical importance of the observed differences (p. 578).”9
Zhao et al. (2020)23
Main Study Findings
Outcomes over 1 month, in 154 children who completed the study (RCT)
Note: For spherical equivalent refractive error, axial length, and choroidal thickness, when the 4 groups were compared together, independent sample 1-way ANOVA analyses were used. For pairwise comparison, the Bonferroni method was used for multiple comparisons.
Spherical equivalent refractive error (D), mean (SD)
At baseline: −3.12 (1.20) for the atropine plus OK group, −2.81 (0.96) for the placebo plus OK group, −3.01 (1.22) for the atropine plus SVS group, and −3.25 (1.10) for the placebo plus SVS group (P = 0.414)
At 1 month: −0.53 (1.16) for the atropine plus OK group, −0.77 (1.08) for the placebo plus OK group, −3.06 (1.21) for the atropine plus SVS group, and −3.29 (1.06) for the placebo plus SVS group (P < 0.001)
Change from baseline: 2.63 (1.03) for the atropine plus OK group, 2.15 (1.02) for the placebo plus OK group, −0.04 (0.23) for the atropine plus SVS group, and −0.04 (0.18) for the placebo plus SVS group (P < 0.001). The authors reported that the differences between baseline and 1 month were significant for both the atropine plus OK and placebo plus OK groups, but not in the atropine plus SVS and placebo plus SVS groups (however a measure of statistical significance was not reported).
Axial length (mm), mean (SD)
At baseline: 24.78 (0.98) for the atropine plus OK group, 24.69 (0.63) for the placebo plus OK group, 24.90 (0.78) for the atropine plus SVS group, and 24.86 (0.72) for the placebo plus SVS group (P = 0.648).
Change from baseline at 1 month: −0.01 (0.05) for the atropine plus OK group, −0.00 (0.03) for the placebo plus OK group, −0.04 (0.04) for the atropine plus SVS group, and −0.06 (0.06) for the placebo plus SVS group (P < 0.001). The differences between baseline and 1 month were statistically significant (P < 0.05) in both the atropine plus SVS and placebo plus SVS groups, but not statistically significant (P = 1.00) for both the atropine plus OK and placebo plus OK groups.
Subfoveal choroidal thickness (μm), mean (SD)
At baseline: 263.17 (46.55) for the atropine plus OK group, 266.74 (57.50) for the placebo plus OK group, 251.12 (44.76) for the atropine plus SVS group, and 258.05 (52.34) for the placebo plus SVS group (P = 0.443).
At 1 month: 277.28 (46.04) for the atropine plus OK group, 276.17 (59.10) for the placebo plus OK group, 256.61 (46.55) for the atropine plus SVS group, and 253.24 (50.67) for the placebo plus SVS group (P = 0.071).
Change from baseline: 14.12 (12.88) for the atropine plus OK group, 9.43 (9.14) for the placebo plus OK group, 5.49 (9.38) for the atropine plus SVS group, and −4.81 (9.93) for the placebo plus SVS group (P < 0.001).
Authors’ Conclusion
“In conclusion, the current study indicates that combination treatment with OK and atropine could induce a greater increase in ChT [choroidal thickness] than monotherapy with atropine, which might predict a better effect on childhood myopia control. This paper is a preliminary report of a longitudinal study, and future follow-up periods include 3 months, 6 months and every 3 months afterwards until 24 months. Additional results from this longitudinal study are required to determine the long-term effect of the combination of OK and atropine on ChT and its relationship with eye growth (p. 5-6).”23
Appendix 5: Overlap Between Included Systematic Reviews
Table 6: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Guan et al. (2020)11 | Walline et al. (2020)1 | Prousali et al. (2019)13 | VanderVeen et al. (2019)18 | Huang et al. (2016)10. |
Aller et al. Optometry Vis Sci. 2016, 93(4):344--52 | NA | Yes | Yes | NA | NA |
Aller and Wildoset. Ophthal Physiol optics. 2006: 26(Suppl 1):8-9 | NA | Yes | NA | NA | Yes |
Aller. 10th Int Myopia Conf. 2004 | NA | Yes | NA | NA | NA |
Anstice. Ophthalmology. 2011, 118(6): 1152-61 | NA | Yes | Yes | NA | Yes |
Chan et al. Cont Lens Anterior Eye. 2012, 35(4): 180-4 | NA | Yes | NA | Yes | NA |
Charm et al. Ophthalmology. 2015, 122(3):620–630. | Yes | NA | NA | NA | NA |
Charm and Cho. Cont Lens Anterior Eye. 2013, 36(4):164-70 | NA | Yes | NA | NA | NA |
Charm and Cho. Optometry VisSc. 2013, 90(6):530-9 | NA | Yes | Yes | Yes | Yes |
Charm and Cho. Cont Lens Anterior Eye. 2011, 34: S3 | NA | Yes | NA | NA | NA |
Chen et al. Invest Ophthalmol Vis Sci. 2013, 54(10):6510–6517 | Yes | NA | Yes | Yes | NA |
Chen et al. Optom Vis Sci. 2012;89: 1636-1640. | NA | NA | NA | Yes | NA |
Cheng et al. Optom Vis Sci. 2016, 93: 353-366 | NA | NA | Yes | NA | NA |
Cheung and Cho. Cont Lens Anterior Eye. 2016, 39(4):262–265 | Yes | Yes | NA | NA | NA |
Cheung and Cho. Invest Ophthamol Vis Sci. 2013,54(3):1613-5 | NA | Yes | NA | NA | NA |
Cho and Cheung. Cont Lens Anterior Eye. 2017, e 40(2):82–8 | Yes | NA | NA | NA | NA |
Cho and Cheung. Cont Lens Anterior Eye. 2017, 58(3): 1411-6 | NA | Yes | NA | NA | NA |
Cho and Cheung. Invest Ophthalmol Vis Sci. 2012, 53(11):7077–7085 | Yes | Yes | Yes | Yes | Yes |
Cho and Cheung. Cont Lens Anterior Eye. 2011, 34:S2-3. | NA | Yes | NA | NA | NA |
Cho et al. Curr Eye Res. 2005, 30: 71-80 | NA | NA | Yes | NA | NA |
Davis. Adv Ophthalmol Vis Syst. 2015;2 | NA | NA | NA | Yes | NA |
Downe and Lowe. Eye Contact Lens. 2013; 39:303-310. | NA | NA | NA | Yes | NA |
Fujikado et al. Clin Ophthalmol. 2014, 8: 1947-56 | NA | Yes | Yes | NA | NA |
Han. Eye Contact Lena. 2018, 44(4):268-71 | NA | Yes | NA | NA | NA |
He et al. BMC Ophthalmol. 2016, 16:126. | Yes | NA | NA | Yes | NA |
Hiraoka et al. Invest Ophthalmol Vis Sci. 2012, 53(7):3913–3919 | Yes | NA | Yes | Yes | NA |
Kakita et al. Invest Ophthalmol Vis Sci. 2011, 52(5):2170–2174 | Yes | NA | Yes | Yes | NA |
Lam et al. Br J Ophthalm. 2014, 98 (1): 40-5 | NA | Yes | Yes | NA | Yes |
Lam et al. Optometry Vis Sci. 2011, 88(3): 444-5 | NA | Yes | NA | NA | NA |
Lin et al. BMC Ophthalmol. 2014;14:40. | NA | NA | Yes | Yes | NA |
Paune. Biomed Res Int. 2015, 2015(D):507572 | Yes | NA | Yes | Yes | NA |
Na. Jpn J Ophthalmol. 2018, 62(3):327–334 | Yes | NA | NA | NA | NA |
Sankaridurg et al. Invest Ophthalmol Vis Sci. 2011, 52: 9362-9367 | NA | NA | Yes | NA | NA |
Santodomingo-Rubido et al. Curr Eye Res. 2017, 42(5):713–720 | Yes | NA | NA | NA | NA |
Santodomingo-Rubido et al. Invest Ophthalmol Vis Sci. 2012;53:5060-5065. | NA | NA | Yes | Yes | NA |
Swarbrick et al. Ophthalmology. 2015, 122(3):620–630 | Yes | NA | NA | NA | NA |
Walline et al. Optom Vis Sci. 2013, 90: 1207-1214 | NA | NA | Yes | NA | NA |
Zhu et al. BMC Ophthalmol. 2014, 14:141 | NA | NA | Yes | Yes | NA |
NA = not applicable.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca