CADTH Health Technology Review
Treatment Sequences of Androgen Receptor–Targeted Agents for Prostate Cancer
Rapid Review
Authors: Khai Tran, Sarah McGill
Abbreviations
AA
abiraterone acetate
ADT
androgen deprivation therapy
ARTA
androgen receptor–targeted agent
CI
confidence interval
CRPC
castration-resistant prostate cancer
CSPC
castration-sensitive prostate cancer
CTX
cabazitaxel
DTX
docetaxel
ENZ
enzalutamide
HR
hazard ratio
IQR
interquartile range
LPD
life-prolonging drug
mCRPC
metastatic castration-resistant prostate cancer
OR
odds ratio
OS
overall survival
PFS
progression-free survival
PSA
prostate-specific antigen
RR
rate ratio
SR
systematic review
Key Messages
No evidence was found on the treatment sequences of androgen receptor–targeted agents in patients with castration-sensitive prostate cancer.
Evidence from retrospective studies, including those within a systematic review, suggests that sequential treatment of abiraterone followed by enzalutamide is more favourable than enzalutamide followed by abiraterone in improving clinical outcomes such as response rate and progression-free survival, but not overall survival, in patients with castration-resistant prostate cancer.
Evidence from a retrospective study suggests that docetaxel-containing treatment sequences with androgen receptor–targeted agents may improve progression-free survival compared to sequential therapy with androgen receptor–targeted agents alone in patients with castration-resistant prostate cancer.
Evidence from a retrospective study did not reveal differences in clinical outcomes of patients with castration-resistant prostate cancer treated with sequential androgen receptor–targeted agents with or without interposed chemotherapy or radium-223.
These findings were in line with those observed in a 2019 CADTH report.1 However, the findings should be interpreted with caution due to low-quality evidence.
No comparative cost-effectiveness studies were identified.
Context and Policy Issues
Prostate cancer is the most common cancer among men in Canada.2 Approximately 1 in 9 Canadian men will be diagnosed with prostate cancer in their lifetime.2 If prostate cancer is detected early, the survival rate is close to 100%; however, 3 of 4 men will die if the cancer is detected late.2 The death rate from prostate cancer has dropped by 50% since 1994.2
In the early development of prostate cancer, cancer cells require androgens to grow; therefore, the cancer at this stage is called castration-sensitive prostate cancer (CSPC).3 Androgen deprivation therapies (ADTs) are treatments that reduce androgen production by the testicles through a surgical procedure or gonadotropin-releasing hormone agonists or antagonists.3 However, patients treated with an ADT that blocks androgen production eventually become resistant, meaning that the cancer can progress even when the levels of androgens in the body are very low or undetectable.3 The cancer at this stage is termed castration-resistant prostate cancer (CRPC). Alternative hormone therapies for prostate cancer include treatments that block the action of androgens or their synthesis.3 Blocking the action of androgens can be achieved by using an androgen receptor blocker, such as enzalutamide (ENZ), apalutamide, or darolutamide, which competes with androgens for binding to androgen receptors, inhibiting the action of androgens in stimulating cancer cell growth.3 Abiraterone acetate (AA) is an androgen biosynthesis inhibitor that blocks the enzyme CYP17.3 Both AA and ENZ are androgen receptor–targeted agents (ARTAs). Various treatment options for CRPC include complete blocking of androgen action using ENZ + ADT, complete inhibition of androgen production using AA and ADT, immunotherapy using a cell-based immunotherapy named Sipuleucel-T, chemotherapy using taxanes such as docetaxel (DTX) or cabazitaxel (CTX), radiopharmaceutical radium-223, and sequential therapies among ARTAs and taxanes.4
A recent CADTH report1 identified weak evidence on 4 sets of comparative sequences of ARTA in the treatment of patients with metastatic CRPC. These were ENZ-to-ENZ + AA versus ENZ-to-AA, AA-to-ENZ versus ENZ-to-AA, ARTA-to-ARTA versus ARTA-to-taxane (DTX or CTX), and ARTA-to-ARTA versus ARTA-to-taxane-to-ARTA. It was found that AA had modest benefit in patients with metastatic CRPC (mCRPC) who progressed after treatment with ENZ, and the combination of ENZ + AA given as second-line therapy was not indicated because of observed adverse effects. The AA-to-ENZ sequence provided better clinical outcomes than the ENZ-to-AA sequence in mCRPC patients. After ARTA therapy, patients with mCRPC who received second-line taxane therapy achieved higher response rates compared with second-line ARTA. There was no difference in efficacy between ARTA-to-ARTA and ARTA-to-taxane-to-ARTA. No comparative cost-effectiveness studies were identified in the previous CADTH report.1
The aim of this report is to update and extend the previous report by reviewing the comparative clinical effectiveness and cost-effectiveness of varying treatment sequences of ARTA in patients with prostate cancer, including CSPC and CRPC with or without metastasis.
Research Questions
What is the comparative clinical effectiveness of various treatment sequences of ARTAs in patients with prostate cancer?
What is the comparative cost-effectiveness of various treatment sequences of ARTAs in patients with prostate cancer?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international health technology assessment database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Part of the search is an update of a literature search strategy developed for a previous CADTH report1 on ARTA drugs for CRPC. The initial search was limited to English-language documents published between January 1, 2014, and May 10, 2019. For the current report, database searches were rerun on February 1, 2021, to capture any articles published since the initial search date. The search of major health technology agencies was also updated to include documents published since May 2019.
An additional search was conducted with the main search concepts of ARTAs (including berdazimer sodium, ralaniten acetate, enzalutamide, apalutamide, abiraterone, darolutamide, Proxalutamide, and seviteronel) and CSPC. The additional search was also limited to English-language documents published between January 1, 2017 and February 1, 2021. Search filters were applied to limit retrieval to health technology assessments, systematic reviews (SRs), meta-analyses, or network meta-analyses, randomized controlled trials, controlled clinical trials, or any other type of clinical trial, and economic studies. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients with prostate cancer (non-metastatic or metastatic, castration-sensitive or castration-resistant, hormone-sensitive or hormone-resistant) |
Intervention | Treatment sequences of at least 2 ARTAs (e.g., enzalutamide, apalutamide, abiraterone combined with prednisone, darolutamide) with or without ADT in combination and with or without chemotherapy |
Comparator | Other ARTA sequences (e.g., ARTA followed by another ARTA, ARTA followed by chemotherapy followed by ARTA), sequences with only 1 ARTA (e.g., ARTA followed by chemotherapy), chemotherapy alone (e.g., docetaxel, cabazitaxel), or radioisotope alone (e.g., radium-223) |
Outcomes | Q1: Clinical effectiveness (e.g., progression-free survival, overall survival, response rate, quality of life, time to prostate-specific antigen progression); adverse events; discontinuation Q2: Cost-effectiveness (e.g., quality-adjusted life-year, incremental cost-effectiveness ratio) |
Study designs | HTA, SR, RCT, non-randomized study, and economic evaluation |
ADT = androgen deprivation therapy; ARTA = androgen receptor–targeted agent, HTA = health technology assessment; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2017. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs or if they were included in the recent CADTH report.1
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)5 for SRs, and the Downs and Black checklist6 for non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
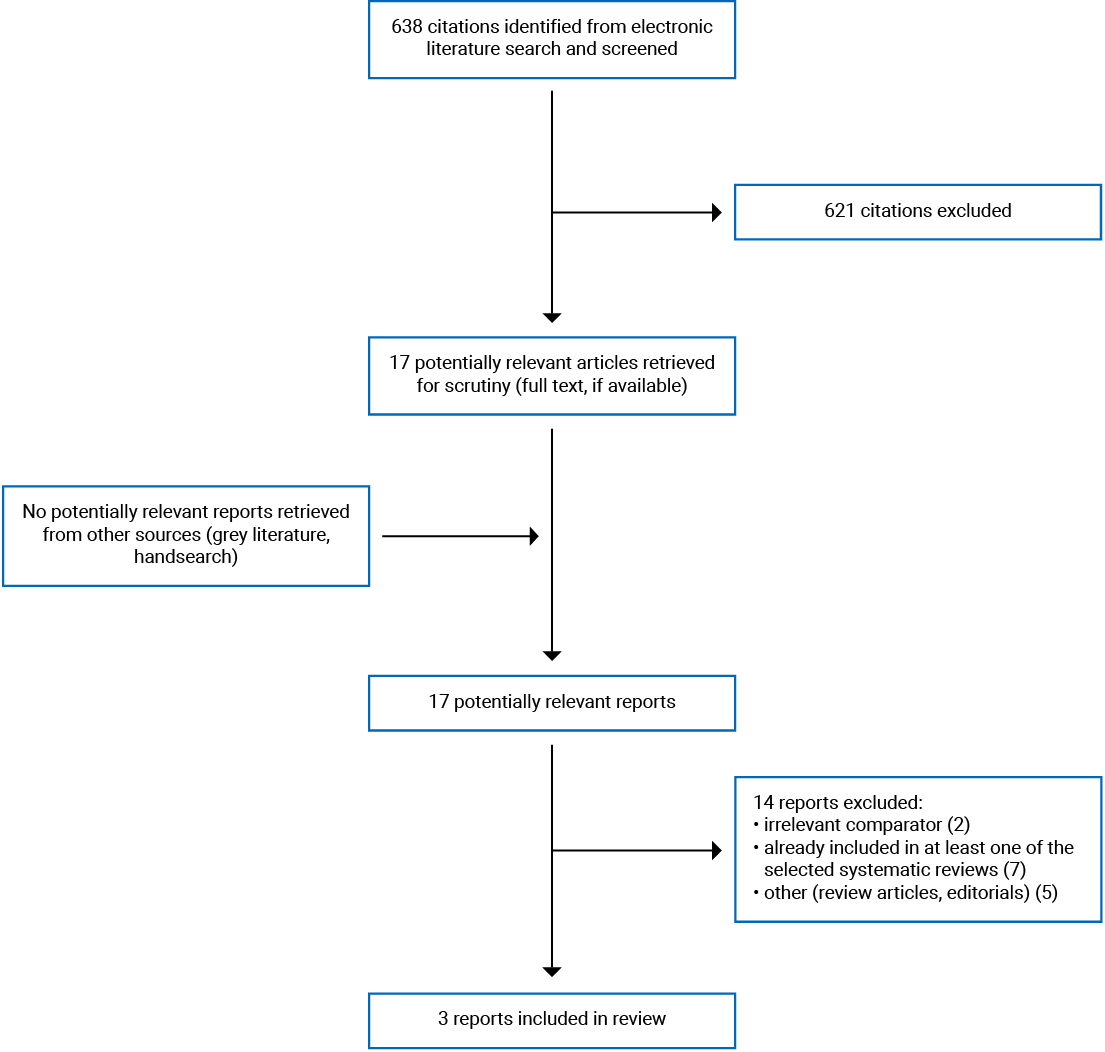
A total of 638 citations were identified in the literature search. Following screening of titles and abstracts, 621 citations were excluded and 17 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 14 publications were excluded for various reasons, and 3 publications met the inclusion criteria and were included in this report. These comprised 1 SR and 2 non-randomized studies. Appendix 1 presents the PRISMA7 flow chart of the study selection.
Summary of Study Characteristics
The detailed characteristics of the included SR8 (Table 2) and primary studies9,10 (Table 3) are presented in Appendix 2.
Study Design
The included SR8 included 10 studies (9 retrospective and 1 prospective), 8 of which were included in the meta-analysis. Of the included studies in this SR, 5 retrospective studies had been identified in the previous CADTH report.1 The literature search was performed from 4 main databases from database inception to December 2019. The quality of the included studies was assessed using the Newcastle-Ottawa Scale. This instrument contains 8 items within 3 domains, with a total maximum score of 9 (4 points for Selection, 2 points for Comparability, and 3 points for Outcomes).11 Random-effects and fixed-effects model meta-analyses were used to provide the summary estimates. Publication bias was assessed using funnel plots.
Both of the included primary studies9,10 were retrospective in design: 1 was a medical record review9 and the other was a registry review.10 One study9 used propensity score matching to minimize selection bias from potential confounders. The other study10 addressed confounders by excluding patients with missing data from the multivariate analysis.
Country of Origin
The included SR8 was conducted by authors from various countries including Canada. The primary studies were conducted by authors from Japan9 and the Netherlands.10
Patient Population
The SR8 included studies involving CRPC patients treated with sequential therapy of 2 ARTA agents: AA and ENZ. Patients’ median ages ranged from 62 years to 78 years. Most patients had a Gleason score of 8 of less, meaning their cancers were likely to spread more rapidly.12 Sample sizes of the included studies ranged from 35 to 255 patients, with a total of 1,096 patients.
The retrospective medical record review study9 included 315 DTX/ARTA-naïve CRPC patients who were treated with first-line ARTA (i.e., AA or ENZ) or DTX followed by second-line DTX or ARTA. Patients’ ages ranged from 67 years to 82 years, and approximately half of the patients had a Gleason score of 9 or greater.
The retrospective registry review study10 included 273 CRPC patients who were treated with a first-line ARTA such as AA + prednisone (P) or ENZ followed by a second-line ARTA such as ENZ or AA + P (ARTA-to-ARTA) or a first-line ARTA followed by a life-prolonging drug (LPD) such as DTX, CTX, or Ra-223 followed by an ARTA (ARTA-to-LPD-to-ARTA). Patients’ ages ranged from 50 years to 90 years, and approximately half of the patients had a Gleason score of between 8 and 10.
Interventions and Comparators
The SR8 compared the effect of ARTA sequential therapy and had 2 groups of patients: those treated with AA followed by ENZ (AA-to-ENZ) and those treated with ENZ followed by AA (ENZ-to-AA).
The retrospective medical record review study9 compared the effect of ARTA (AA or ENZ) sequential therapy with DTX-containing sequential therapy. There were 2 main groups of patients: those treated with ARTA followed by ARTA (ARTA-to-ARTA), and those treated with ARTA followed by DTX (ARTA-to-DTX) or DTX followed by ARTA (DTX-to-ARTA). The study also conducted subgroup analysis of AA-to-ENZ versus ENZ-to-AA.
The retrospective registry review study10 had 2 main groups of patients: ARTA-to-ARTA and ARTA-to-LPD-to-ARTA. The ARTA could be either AA + P or ENZ. If patients were treated with AA + P as the first ARTA treatment sequence then the second ARTA sequence was ENZ (AA + P-to-ENZ) or vice versa (ENZ-to-AA + P). The study also conducted subgroup analysis of AA + P-to-ENZ versus ENZ-to-AA + P.
Outcomes
Clinical outcomes considered in the SR8 were combined progression-free survival (PFS), prostate-specific antigen (PSA) PFS (PSA-PFS), overall survival (OS), and PSA response rate. Definitions of the outcomes were not provided in the SR.
The primary outcome in the retrospective medical record review study9 was OS, which was defined as the period from the start of first-line treatment after resistance to castration to death of any cause. The secondary outcome was PFS, which was defined as the period from the start of first-line treatment after resistance to castration to progression on second-line treatment. The diagnosis of progression in this study was largely based on PSA progression, but not based on radiographic or clinical assessment. It was therefore classified as PSA-PFS.
The retrospective registry review study10 considered PSA response to ARTA2 as the primary outcome, which was defined as a PSA decline of 50% or greater from baseline. The secondary outcome in this study was treatment duration, which was calculated as the interval between start and stop of the second ARTA.
Summary of Critical Appraisal
The detailed quality assessments of the included SR8 (Table 4) and primary studies9,10 (Table 5) are presented in Appendix 3.
The included SR8 was explicit in its objective and inclusion criteria for the review, selection of study design for inclusion, and comprehensive literature search strategy. It was unclear if the study selection was performed in duplicate; however, 2 reviewers independently extracted and assessed the quality of the included studies. The SR did not report whether or not a protocol had been published before the conduct of the review. The SR did not report the sources of funding of the studies included in their review nor provide a list of excluded studies. The SR described the characteristics of the included studies in adequate detail, used appropriate techniques to assess the quality of the included studies (i.e., the Newcastle-Ottawa Scale), used appropriate methods to combine the results (i.e., fixed-effects or random-effects model meta-analyses). The authors did not perform subgroup analyses based on the quality of the included studies nor account for the risk of bias in individual studies when interpreting or discussing the results. Publication bias was assessed using funnel plots. The authors declared that they had no conflict of interest for conducting the review. Overall, the included SR was of acceptable methodological quality.
In terms of reporting, both of the included retrospective studies9,10 clearly described the objectives, the main outcomes measured, the characteristics of the included patients, and the main findings. However, treatment dosage of the interventions was not reported, and adverse events were not considered as outcomes. In terms of external validity, it was unclear if the participants in both studies were representative of the entire populations from which they were selected. In terms of internal validity, there was a risk of selection bias as both studies had a retrospective design and the method of selection was not clearly described. Both studies used appropriate statistical methods in the analyses, and potential confounders were controlled using appropriate approaches. In both studies, the sample sizes were not based on power calculations; therefore, it remains unclear if the studies were adequately powered to detect clinically meaningful differences. Overall, the methodological quality of the included primary studies was considered low.
Summary of Findings
Clinical Effectiveness of Treatment Sequences of ARTA
The main findings and authors’ conclusions of the SR8 and the primary clinical studies9,10 are presented in Appendix 4.
Combined PFS
The meta-analysis of data from 4 studies in the SR8 showed that the sequential treatment of AA-to-ENZ was significantly associated with better combined PFS in patients with CRPC compared with ENZ-to-AA. The overall pooled hazard ratio (HR) was 0.62 (95% confidence interval [CI], 0.49 to 0.78; P < 0.001).
PSA-PFS
The meta-analysis data from 3 studies (1 RCT and 2 retrospective studies) in the SR8 showed that the sequential treatment of AA-to-ENZ was significantly associated with better PSA-PFS in patients with CRPC compared with ENZ-to-AA. The overall pooled HR was 0.48 (95% CI, 0.36 to 0.61; P < 0.001).
The retrospective medical record review study9 found that sequential treatment of ARTA-to-ARTA was associated with significantly shorter PSA-PFS compared with DTX-containing sequential therapy (i.e., DTX-to-ARTA or ARTA-to-DTX). Median PFS values were 13.7 and 18.9 months, respectively (HR = 1.65; 95% CI, 1.23 to 2.17; P < 0.001). Analysis of the propensity score–matched cohort also revealed that PSA-PFS was significantly shorter in the ARTA-to-ARTA group compared with the DTX-containing group (median PFS: 12.9 months versus 21.6 months; HR = 1.70; 95% CI, 1.16 to 2.48; P = 0.07). Subgroup analysis showed that the significant difference was mainly attributed by the difference between ARTA-to-ARTA and DTX-to-ARTA (median PFS: 13.7 months versus 22.7 months; HR = 1.92; 95% CI, 1.42 to 2.60; P < 0.001), but not between ARTA-to-ARTA and ARTA-to-DTX (median PFS: 13.7 months versus 15.6 months; HR = 1.15; 95% CI, 0.81 to 1.62; P = 0.435). Subgroup analysis also showed no significant difference in PFS between AA-to-ENZ and ENZ-to-AA groups (median PFS: 14.3 months versus 12.4 months; HR = 0.92; 95% CI, 0.59 to 1.44; P = 0.724).
OS
The meta-analysis data from 5 studies in the SR8 showed that the sequential treatment of AA-to-ENZ was not significantly associated with better OS in patients with CRPC compared with ENZ-to-AA. The overall pooled HR was 0.77 (95% CI, 0.59 to 1.01; P = 0.055).
The retrospective medical record review study9 found no significant difference in OS between the ARTA-to-ARTA group and the DTX-containing group (median OS: 34.6 months versus 38.7 months; HR = 1.05; 95% CI, 0.74 to 1.50; P = 0.781). Results in the propensity score–matched cohort also revealed no significant difference in OS between groups (median OS: 37.9 months versus 45.5 months; HR = 1.10; 95% CI, 0.68 to 1.79; P = 0.701). Subgroup analysis also showed no difference in OS between ARTA-to-ARTA and DTX-to-ARTA (median OS: 34.6 months versus 43.5 months; HR = 1.24; 95% CI, 0.84 to 1.81; P = 0.28) or between ARTA-to-ARTA and ARTA-to-DTX (median OS: 34.6 months versus 24.2 months; HR = 0.71; 95% CI, 0.45 to 1.13; P = 0.150). There was also no significant difference in OS between AA-to-ENZ and ENZ-to-AA groups (median OS: 31.9 months versus 42.0 months; HR = 0.62; 95% CI, 0.33 to 1.14; P = 0.123).
PSA Response Rate
The meta-analysis of data from 6 studies in the SR8 showed that the PSA response rate of ENZ as the first ARTA agent in ENZ-to-AA sequential therapy was significantly higher than AA as the first ARTA agent in AA-to-ENZ (response rate: 57.3% versus 46.7%; rate ratio [RR] = 1.31; 95% CI, 1.08 to 1.58; P = 0.025). The meta-analysis of data from 7 studies showed that the PSA response rate of AA as the second ARTA agent in the ENZ-to-AA group was also significantly lower than ENZ as second ARTA agent in AA-to-ENZ group (response rate: 8.2% versus 28.9%; RR = 0.30; 95% CI, 0.19 to 0.46; P < 0.001). When both agents were considered together, the pooled PSA response rates from 4 studies were significantly lower with the ENZ-to-AA compared with AA-to-ENZ sequence (response rate: 4.2% versus 23.5%; RR = 0.21; 95% CI, 0.09 to 0.47; P < 0.001).
The retrospective registry review study10 found no significant difference in PSA response rates of second ARTA between the ARTA-to-ARTA and ARTA-to-LPD-to-ARTA sequences in the overall cohort (20% versus 18%; P = 0.297). When 30% of patients were excluded from multivariate binary logistic regression analysis due to missing PSA response of second ARTA, the results showed no significant difference in the PSA response rate of the second ARTA between the ARTA-to-ARTA and ARTA-to-LPD-to-ARTA sequences (OR = 0.890; P = 0.89). Subgroup analysis also showed no significant difference in the PSA response rates of ARTA between the AA + P-to-ENZ and ENZ-to-AA + P sequences (23% versus 14%; P = 0.159).
Treatment Duration
The retrospective registry review study10 found that the median treatment durations of the second ARTA in the ARTA-to-ARTA and ARTA-to-LPD-to-ARTA sequences were 3.2 months (interquartile range [IQR], 1.9 to 7.5) and 3.2 months (IQR, 1.8 to 5.9; P = 0.04), respectively. Subgroup analysis showed no significant difference in the second ARTA treatment duration between AA + P-to-ENZ (3.2 months; IQR, 1.9 to 5.9) and ENZ-to-AA + P sequence (3.2 months; IQR, 1.8 to 7.3).
Cost-Effectiveness of Treatment Sequences of ARTA
No comparative cost-effectiveness studies of different treatment sequences of ARTA in patients with prostate cancer were identified; therefore, no summary can be provided.
Limitations
Although the included SR8 was well conducted, its included primary studies had several limitations. Most of the studies included in the analysis had a retrospective design, which has a high risk of selection bias. Heterogeneity in patient characteristics existed among the included studies. The proportion of patients with visceral metastases (range = 2.4% to 77.8%) and the follow-up times (range = 13.5 months to 56 months) varied widely among studies. Although the statistical heterogeneity was not significant in the pooled analyses as judged by the chi-square and I2 statistics, the clinical heterogeneity varied among studies which could affect the findings. Seven of 10 included studies were from Japan, thus limiting the generalizability of the findings to other populations. However, the findings may be applicable to the Canadian context because 2 of the included studies in the SR were from Canada and the US, and those findings were similar to those of the pooled analyses.
The results of the 2 retrospective non-randomized studies9,10 could have been affected by selection bias due to the nature of the study design. In addition, certain patient characteristics were imbalanced between groups. In the retrospective medical record review study,9 there were significant differences in baseline characteristics between groups, such as median age, proportion of patients who had a history of definitive therapy, serum PSA level, presence of pain, and visceral metastases. In the retrospective registry review study,10 significant differences in baseline characteristics between groups were median age, visceral metastases, laboratory values, and time of switching between ARTA. Although propensity score matching and multivariate analysis were performed to reduce the effect of selection bias, residual confounders may have not been excluded. Sample sizes were not based on power calculations; therefore, the lack of significant differences in the results between groups may be caused by insufficient sample sizes. Data on treatment decisions were not captured, and the known patient and disease characteristics may play a role in treatment selection by attending physicians, thus having great influence on the findings. Treatment-related adverse events were not reported, therefore the comparative safety among treatment sequences was unclear.
Conclusions and Implications for Decision- or Policy-Making
One SR8 and 2 retrospective non-randomized studies9,10 were included to address the comparative clinical effectiveness of various treatment sequences of ARTA in patients with prostate cancer. All patients in the included studies had CRPC, most of which were metastatic. No studies regarding the comparative cost-effectiveness of treatment sequences of ARTA in patients with prostate cancer were identified.
Three sets of comparative sequences of ARTA in the treatment of patients with mCRPC were identified: AA-to-ENZ versus ENZ-to-AA, ARTA-to-ARTA versus DTX-combined (i.e., ARTA-to-DTX or DTX-to-ARTA), and ARTA-to-ARTA versus ARTA-to-LPD (i.e., DTX, CTX, or Ra-223)-to-ARTA. Results from the SR8 suggested that sequential treatment of AA-to-ENZ may offer survival benefits such as combined PFS and PSA-PFS for patients with CRPC compared with the ENZ-to-AA sequence. However, significant differences between groups was not seen in OS. PSA response rates to both first and second ARTA agents were significantly higher in patients treated with an AA-to-ENZ sequence than an ENZ-to-AA sequence. Results from a retrospective study9 suggested that a DTX-combined treatment sequence may improve PFS, but not OS, compared with an ARTA-to-ARTA sequence in DTX/ARTA-naïve CRPC patients. Results from another retrospective study10 showed no difference between sequential ARTA therapies with or without interposed LPD (i.e., DTX, CTX, or Ra-223).
The findings in this updated report were in line with those in the previous CADTH report.1 First, an AA-to-ENZ sequence appeared to be more favourable than an ENZ-to-AA sequence in patients with mCRPC regarding improved clinical outcomes, such as combined PFS, time to PSA progression, and PSA response rate, but not for OS. Second, an ARTA-to-taxane (i.e., DTX or CTX) sequence appeared to be more effective than an ARTA-to-ARTA treatment sequence in patients with chemotherapy-naïve mCRPC regarding improved clinical outcomes such as combined PFS, time to PSA progression, and PSA response rate. Third, no differences were observed between ARTA-to-ARTA and ARTA-to-taxane-to-ARTA with respect to PSA response rate and time to PSA progression. Considering the limitations, including the retrospective nature of the included studies, collective findings in this report and the previous report1 should be interpreted with caution.
References
1.Androgen receptor targeted agents for castration resistant prostate cancer: a review of clinical effectiveness and cost-effectiveness (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1127%20ARTA%20for%20mCRPC%20Final.pdf. Accessed 2021 Feb 2.
2.Canadian Cancer Society. About prostate cancer: statistics. 2020; https://www.prostatecancer.ca/prostate-cancer/about-prostate-cancer/statistics. Accessed 2021 Mar 2.
3.National Cancer Institute. Hormone therapy for prostate cancer. 2019; https://www.cancer.gov/types/prostate/prostate-hormone-therapy-fact-sheet. Accessed 2021 Mar 2.
4.Moussa M, Papatsoris A, Abou Chakra M, Sryropoulou D, Dellis A. Pharmacotherapeutic strategies for castrate-resistant prostate cancer. Expert Opin Pharmacother. 2020;21(12):1431-1448. Medline
5.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. Medline
6.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. Medline
7.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
8.Mori K, Miura N, Mostafaei H, et al. Sequential therapy of abiraterone and enzalutamide in castration-resistant prostate cancer: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2020;23(4):539-548. Medline
9.Naito Y, Kato M, Kawanishi H, et al. The clinical benefit of sequential therapy with androgen receptor axis-targeted agents alone in patients with castration-resistant prostate cancer: a propensity score-matched comparison study. Prostate. 2020;80(15):1373-1380. Medline
10.Kuppen MCP, Westgeest HM, van den Eertwegh AJM, et al. Real-world outcomes of sequential androgen-receptor targeting therapies with or without interposed life-prolonging drugs in metastatic castration-resistant prostate cancer: results from the Dutch Castration-resistant Prostate Cancer Registry. Eur Urol Oncol. 2019. Medline
11.Gierish JM, Beadles C, Shapiro A, et al. Appendix B: Newcastle-Ottawa scale coding manual for cohort studies. In: Health disparities in quality indicators of healthcare among adults with mental illness. Washington (DC): Department of Veterans Affairs (US); 2014: https://www.ncbi.nlm.nih.gov/books/NBK299087/#:~:text=The%20Newcastle%2DOttawa%20Scale%20quality,and%203%20points%20for%20Outcomes. Accessed 2021 Mar 2.
12.American Society of Clinical Oncology (ASCO). Prostate cancer: stages and grades. 2020; https://www.cancer.net/cancer-types/prostate-cancer/stages-and-grades. Accessed 2021 Mar 2.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Review and Meta-Analysis
First author, publication year, country, funding | Study designs and numbers of primary studies included | Patient characteristics | Interventions and comparators | Clinical outcomes, length of follow-up |
Mori et al. (2020)8 Country: International collaboration including Canada Source of funding: NR | Objective: To assess the prognostic value of sequential therapy of AA and ENZ in patients with CRPC. Total 10 studies (9 retrospective and 1 prospective studies) Quality assessment tool: Newcastle-Ottawa Scale Databases: PubMed, Web of Science, Cochrane Library, and Scopus databases from their dates of inception to December 2019 Data analysis: Random effects meta-analysis | Patients with CRPC (N = 1,096) Median age: 62 to 78 years Group proportions:
Mean baseline PSA (ng/mL):
Proportion with Gleason score ≥ 8:
mCRPC rate:
Visceral metastasis rate:
| AA-to-ENZ vs. ENZ-to-AA |
Median follow-up: 13.5 to 56 months Outcomes definition: NR |
AA = abiraterone acetate; CRPC = castration-resistant prostate cancer; ENZ = enzalutamide; m = metastatic; NR = not reported; OS = overall survival; PFS = progression-free survival; PSA = prostate-specific antigen; vs. = versus.
Table 3: Characteristics of Included Primary Clinical Studies
First author, publication year, country, funding | Study design and analysis | Patient characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Naito et al. (2020)9 Country: Japan Source of funding: NR | Retrospective (medical record review) study Statistical analysis: Kaplan-Meier method to estimate OS and PFS; propensity score matching to minimize selection bias from potential confounders. Sample size calculation: No | Patients were diagnosed with adenocarcinoma by prostate needle biopsy, and all patients progressed to CRPC Patients were treated with first-line ARTA (i.e., AA or ENZ) or DTX. After first line failed, patients were treated with DTX or ARTA Two groups:
Median age (IQR), years:
ECOG PS ≥ 1, %
Median PSA (IQR), ng/mL:
mCRPC, %
Gleason score ≥ 9, %
|
Dosage: NR | Primary outcome: OS (defined as the period from the start of first-line treatment after resistance to castration to death of any cause) Secondary outcome: PFS (defined as the period from the start of first-line treatment after resistance to castration to progression on second-line treatment) Disease progression was defined as PSA elevation and/or radiographic progression (according to the Prostate Cancer Working Group 3 criteria) and/or clinical progression including exacerbation of prostate cancer-related symptoms. Median follow-up (IQR) of the overall cohort: 36.6 (22.6 to 72.4) months |
Median duration of response to primary ADT (IQR), months
History of definitive therapy, %
DTX-combined: 33.5; P = 0.005 | ||||
Kuppen et al. (2019)10 Country: the Netherlands Source of funding: Sanofi-Aventis | Retrospective (registry review) study Statistical analysis: Appropriate statistical methods used; confounders were addressed by excluding patients with missing data from the multivariate binary logistic regression analyses. Sample size calculation: No | Patients with mCRPC from 20 Dutch hospitals (N = 273) Patients were treated with first-line ARTA (i.e., AA + P or ENZ) followed by second-line ARTA (i.e., ENZ or AA + P), or sequential treatment of LPD (i.e., DTX, CTX, or Ra-223) and ARTA Two groups of treatment:
Median age (IQR), years:
ECOG PS ≥ 1, %
Gleason score 8 to 10, %
|
Dosage: NR | Primary outcome: PSA response of ARTA2 (defined as a ≥ 50% PSA decline from baseline) Secondary outcome: Treatment duration (the interval between the start and stop of ARTA2) Median follow-up (IQR) of ARTA2: 8.4 (0.3 to 35.8) months |
Median PSA (IQR), mcg/L
Visceral metastasis, %
Hemoglobin, mmol/L
ARTA1-to-LPD-to-ARTA2: 6.9; P < 0.01 |
AA = abiraterone acetate; ARTA = androgen receptor–targeted agent; CTX = cabazitaxel; DTX = docetaxel; ECOG PS = Eastern Cooperative Oncology Group performance status; ENZ = enzalutamide; IQR = interquartile range; LPD = life-prolonging drug (i.e., DTX, CTX, or Ra-223); OS = overall survival; NR = not reported; P = prednisone; PFS = progression-free survival; Ra-223 = radium-223.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Quality Assessment of the Systematic Review Using the AMSTAR 2 Checklist5
Item | Mori et al. (2020)8 |
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes – the study clearly described its objective and inclusion exclusion criteria |
2. Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | Unclear – it was unclear if a protocol had been established before conducting the review |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes – non-randomized observational, randomized, or cohort studies were included if they investigated CRPC patients treated with sequential ARTA |
4. Did the review authors use a comprehensive literature search strategy? | Yes – 4 databases were used |
5. Did the review authors perform study selection in duplicate? | Unclear – not reported |
6. Did the review authors perform data extraction in duplicate? | Yes – 2 reviewed authors independently extracted the data; discrepancies were resolved by consensus with a third author |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | No |
8. Did the review authors describe the included studies in adequate detail? | Yes – patients’ characteristics were described in adequate detail |
9. Did the review authors use a satisfactory technique for assessing the RoB in individual studies that were included in the review? | Yes – the Newcastle-Ottawa Scale was used to assess the quality of the included studies |
10. Did the review authors report on the sources of funding for the studies included in the review? | No |
11. If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? | Yes – fixed effects or random effects models were used for meta-analysis depending on the heterogeneity determined by I2 statistics |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | No – the authors did not perform subgroup analysis based on quality of include studies |
13. Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review? | No – the authors did not include RoB in included studies when interpreting/discussing the results |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Yes – I2 values were provided for statistical heterogeneity |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | Yes – funnel plots were used to assess publication bias |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes – the authors declared that they had no conflict of interest |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ARTA = androgen receptor–targeted agent; CRPC = castration-resistant prostate cancer; PICO = Population, Intervention, Comparator, Outcomes; RoB = risk of bias.
Table 5: Quality Assessment of Clinical Studies Using the Downs and Black checklist6
Item | Naito et al. (2020)9 | Kuppen et al. (2019)10 |
Reporting | ||
1. Is the hypothesis/aim/objective of the study clearly described? | Yes – the study compared sequential therapy of ARTA for treatment of CRPC patients | Yes – the study compared sequential therapy of ARTA with or without life-prolonging drugs for treatment of metastatic CRPC patients |
2. Are the main outcomes to be measured clearly described in the Introduction or Methods section? | Yes – outcomes were well described in the Methods section | Yes – outcomes were well described in the Methods section |
3. Are the characteristics of the patients included in the study clearly described? | Yes | Yes |
4. Are the interventions of interest clearly described? | No – dosage and duration of treatment were not provided | No – dosage and duration of treatment were not provided |
5. Are the distributions of principal confounders in each group of subjects to be compared clearly described? | Yes – propensity score–matched cohort was used to minimize selection bias from possible confounders | Yes – list of potential confounders was provided, and multivariate analysis was used to account for potential confounders |
6. Are the main findings of the study clearly described? | Yes | Yes |
7. Does the study provide estimates of the random variability in the data for the main outcomes? | Yes – 95% CI was provided | No – no standard error, standard deviation, or confidence interval was reported |
8. Have all important adverse events that may be a consequence of the intervention being reported? | No – the study did not consider adverse events as outcomes | No – the study did not consider adverse events as outcomes |
9. Have the characteristics of patients lost to follow-up been described? | NA – retrospective design | NA – retrospective study |
10. Have actual probability values been reported (e.g., 0.035 rather than < 0.05) for the main outcomes except where the probability value is less than 0.001? | Yes – actual P values were reported | Yes – actual P values were reported |
External validity | ||
11. Were the subjects asked to participate in the study representative of the entire population from which they were recruited? | Unclear – patients were retrospectively selected from 7 hospitals | Unclear – patients were retrospectively selected from 20 hospitals |
12. Were the subjects who were prepared to participate representative of the entire population from which they were recruited? | Unclear – patients were selected from 7 hospitals | Unclear – patients were retrospectively selected from 20 hospitals |
13. Were the staff, places, and facilities where the patients were treated, representative of the treatment the majority of the patients receive? | Yes – treatment was conducted in hospitals | Yes – treatment was conducted in hospitals |
Internal validity – bias | ||
14. Was an attempt made to blind study subjects to the intervention they have received? | NA – retrospective design | NA – retrospective study |
15. Was an attempt made to blind those measuring the main outcomes of the intervention? | NA – retrospective design | NA – retrospective study |
16. If any of the results of the study were based on “data dredging,” was this made clear? | NA – retrospective design | NA – retrospective study |
17. In trials and cohort studies, so the analyses adjust for different lengths of follow-up of patients, or in case-control studies, is the time period between the intervention and outcome the same for cases and controls? | NA – retrospective design | NA – retrospective study |
18. Were the statistical tests used to assess the main outcomes appropriate? | Yes | Yes |
19. Was compliance with the intervention/s reliable? | NA – treatment was carried out in hospital | NA – treatment was carried out in hospital |
20. Were the main outcome measures used accurate (valid and reliable)? | Yes | Yes |
Internal validity – confounding (selection bias) | ||
21. Were the patients in different intervention groups (trials and cohort studies) or were the cases and controls (case-control studies) recruited from the same population? | Unclear – both groups were recruited from 7 hospitals) | Unclear – both groups were recruited from 20 hospitals |
22. Were study subjects in different intervention groups (trial and cohort studies) or were the cases and controls (case-controls studies) recruited over the same period of time? | Yes – between January 2009 and December 2019 | Yes – between January 1, 2010, and December 31, 2015 |
23. Were study subjects randomized to intervention groups? | NA – retrospective design | NA – retrospective design |
24. Was the randomized intervention assignment concealed from both patients and health care staff until recruitment was complete and irrevocable? | NA – retrospective design | NA – retrospective study |
25. Was the adequate adjustment for confounding in the analyses from which the main findings were drawn? | Yes – propensity score–matched cohort was used to minimize selection bias from possible confounders | Yes – multivariate binary logistic regression was used |
26. Were losses of patients to follow-up taken into account? | NA – retrospective design | NA – retrospective study |
27. Did the study have sufficient power to detect a clinically important effect where the probability value for a difference being due to chance is less than 5%? | Unclear – sample size calculation was not performed | Unclear – sample size calculation was not performed |
ARTA = androgen receptor–targeted agent; CI = confidence interval; CRPC = castration-resistant prostate cancer; NA = not applicable.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of the Included Systematic Review
Mori et al. (2020)8
Main Study Findings
AA-to-ENZ versus ENZ-to-AA
Combined PFS (4 studies; N = 395)
AA-to-ENZ was significantly associated with better combined PFS in CRPC
Pooled HR (95% CI) = 0.62 (0.49 to 0.78); I2 = 51.5%; P < 0.001
No significant heterogeneity
PSA-PFS (3 studies; N = 337)
AA-to-ENZ was significantly associated with better combined PSA-PFS in CRPC
Pooled HR (95% CI) = 0.48 (0.36 to 0.61); I2 = 58.3%; P < 0.001
No significant heterogeneity
OS (5 studies; N = 430)
ARTA treatment sequence was not significantly associated with OS in CRPC
Pooled HR (95% CI) = 0.77 (0.59 to 1.01); I2 = 0.0%; P = 0.055
No significant heterogeneity
PSA response rate of first ARTA agent (6 studies; N = 460)
46.7% in AA-to-ENZ and 57.3% in ENZ-to-AA
ENZ-to-AA was significantly associated with better PSA response rate of first ARTA agent in CRPC
RR (95% CI) = 1.31 (1.08 to 1.58); I2 = 0.8%; P = 0.025
No significant heterogeneity
PSA response rate of second ARTA agent (7 studies; N = 606)
28.9% in AA-to-ENZ and 8.2% in ENZ-to-AA
AA-to-ENZ was significantly associated with better PSA response rate of second ARTA agent in CRPC
RR (95% CI) = 0.30 (0.19 to 0.46); I2 = 21.2%; P < 0.001
No significant heterogeneity
PSA response rate of both first and second ARTA agents (4 studies; N = 355)
23.5% in AA-to-ENZ and 4.2% in ENZ-to-AA
AA-to-ENZ was significantly associated with better PSA response rate of both first and second ARTA agents in CRPC
RR (95% CI) = 0.21 (0.09 to 0.47); I2 = 0.0%; P < 0.001
No significant heterogeneity
Authors’ Conclusion
“AA-to-ENZ sequential therapy in patients with CRPC was associated with better PFS, PSA-PFS, and PSA response rates. Regardless of sequencing, response to drug therapy was transient for both AA and ENZ when either agent was used as a secondary therapy. Despite this, treatment sequencing is important to achieve the maximum possible benefit from available drugs in CRPC (p. 539).”8
Summary of Findings of Included Primary Clinical Studies
Naito et al. (2020)9
Main Study Findings
ARTA-to-ARTA (n = 106) versus DTX-combined (i.e., DTX-to-ARTA or ARTA-to-DTX) (n = 209)
OS in the overall cohort
No significant difference between ARTA-to-ARTA and DTX-combined groups
Median OS: 34.6 versus 38.7 months
HR (95% CI) = 1.05 (0.74 to 1.50); P = 0.781
OS in the propensity score–matched cohort
No significant difference between ARTA-to-ARTA (n = 78) and DTX-combined groups (n = 78)
Median OS: 37.9 versus 45.4 months
HR (95% CI) = 1.10 (0.68 to 1.79); P = 0.701
OS in the subset analysis (ARTA-to-ARTA [n = 106] versus DTX-to-ARTA [n = 138])
No significant difference between ARTA-to-ARTA and DTX-to-ARTA groups
Median OS: 34.6 versus 43.5 months
HR (95% CI) = 1.24 (0.84 to 1.81); P = 0.28
OS in the subset analysis (ARTA-to-ARTA [n = 106] versus ARTA-to-DTX [n = 71])
No significant difference between ARTA-to-ARTA and ARTA-to-DTX groups
Median OS: 34.6 versus 24.2 months
HR (95% CI) = 0.71 (0.45 to 1.13); P = 0.15
OS in the subset analysis (AA-to-ENZ [n = 54] versus ENZ-to-AA [n = 52])
No significant difference between AA-to-ENZ and ENZ-to-AA groups
Median OS: 31.9 versus 42.0 months
HR (95% CI) = 0.62 (0.33 to 1.14); P = 0.123
PSA-PFS in the overall cohort
ARTA-to-ARTA group was associated with significantly shorter PFS than DTX-combined group
Median PFS: 13.7 versus 18.9 months
HR (95% CI) = 1.65 (1.23 to 2.17); P < 0.001
PSA-PFS in the propensity score–matched cohort
ARTA-to-ARTA group (n = 78) was associated with significantly shorter PFS than DTX-combined group (n = 78)
Median PFS: 12.9 versus 21.6 months
HR (95% CI) = 1.70 (1.16 to 2.48); P = 0.007
PSA-PFS in the subset analysis (ARTA-to-ARTA [n = 106] versus DTX-to-ARTA [n = 138])
ARTA-to-ARTA group was associated with significantly shorter PFS than DTX-to-ARTA groups
Median PFS: 13.7 versus 22.7 months
HR (95% CI) = 1.92 (1.42 to 2.60); P < 0.001
PSA-PFS in the subset analysis (ARTA-to-ARTA [n = 106] versus ARTA-to-DTX [n = 71])
No significant difference between ARTA-to-ARTA and ARTA-to-DTX groups
Median PFS: 13.7 versus 15.6 months
HR (95% CI) = 1.15 (0.81 to 1.62); P = 0.435
PSA-PFS in the subset analysis (AA-to-ENZ [n = 54] versus ENZ-to-AA [n = 52])
No significant difference between AA-to-ENZ and ENZ-to-AA groups
Median PFS: 14.3 versus 12.4 months
HR (95% CI) = 0.92 (0.59 to 1.44); P = 0.724
Authors’ Conclusion
“In conclusion, there was no difference in OS outcomes between ARTA-to-ARTA and DTX-combined sequential therapy, while DTX-combined sequential therapy had better PFS outcomes. These data indicate that there are certain patients who will benefit from ARTA-to-ARTA sequential therapy in a daily clinical setting. It is expected that research on additional clinical and molecular predictors of treatment response will be performed (p. 1379).”9
Kuppen et al. (2019)10
Main Study Findings
ARTA1-to-ARTA2 (n = 148) versus ARTA1-to-LPD-to-ARTA2 (n = 125)
PSA response rate of ARTA2 in the overall cohort
No significant differences between ARTA1-to-ARTA2 and ARTA1-to-LPD-to-ARTA2 groups
20% versus 18%; P = 0.297
PSA response rate of ARTA2 from multivariate binary logistic regression analysis
No significant differences between ARTA1-to-ARTA2 and ARTA1-to-LPD-to-ARTA2 groups
OR = 0.890; P = 0.89
PSA response rate of ARTA2 different subgroups
No significant differences between AA + P-to-ENZ and ENZ-to-AA + P subgroups
23% versus 14%; P = 0.159
Treatment duration of ARTA2 in the overall cohort
At the end of follow-up, 9% of patients in ARTA1-to-ARTA2 group and 3% of patients in ARTA1-to-LPD-to-ARTA2 group were still on treatment
Median (IQR): 3.2 (1.9 to 7.5) versus 3.2 (1.8 to 5.9) months; P = 0.042
Treatment duration of ARTA2 in different subgroups
No significant differences between AA + P-to-ENZ and ENZ-to-AA + P subgroups
Median (IQR): 3.2 (1.9 to 5.9) versus 3.2 (1.8 to 7.3) months; P = 0.158
Authors’ Conclusion
“The effect of ARTA2 seems to be low, with a low PSA response rate and a short treatment duration irrespective of interposed chemotherapy or radium-223 (p. 2).”10
“We observed no differences in outcomes of patients treated with sequential abiraterone acetate plus prednisone and enzalutamide with or without interposed chemotherapy or radium-223 (p. 2).”10
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca