CADTH Health Technology Review
Stellate Ganglion Block for the Treatment of Post-Traumatic Stress Disorder, Depression, and Anxiety
Rapid Review
Authors: Yan Li, Hannah Loshak
Abbreviations
CAPS
Clinician-Administered PTSD Scale
DoD
Department of Defense
DSM-4
Diagnostic and Statistical Manual of Mental Disorders, fourth edition
NR
not reported
PCL
PTSD Checklist
PTSD
post-traumatic stress disorder
RCT
randomized controlled trial
SGB
stellate ganglion block
SR
systematic review
VA
US Department of Veteran Affairs
Key Messages
The evidence regarding the clinical effectiveness of stellate ganglion block for the treatment of post-traumatic stress disorder was mixed. A randomized controlled trial included in a systematic review did not detect significant differences in post-traumatic stress disorder symptoms in the stellate ganglion block versus sham groups, while another randomized controlled trial did detect significantly greater improvements in symptoms between these groups. Furthermore, the second randomized controlled trial detected significantly greater improvements in depression, anxiety, and distress, but not in pain and mental and physical functioning for participants receiving stellate ganglion block compared to sham.
Authors of the randomized controlled trial included in the systematic review did not detect significant differences in rates of adverse events between groups. Of the 6 adverse events reported in the second randomized controlled trial, 3 were deemed related to stellate ganglion block treatment (injection site pain, self-resolving bradycardia, and temporary laryngeal irritation); the statistical analysis was not reported.
Authors of 1 evidence-based guideline were unable to provide recommendations for or against the use of stellate ganglion block for the treatment of post-traumatic stress disorder because of insufficient evidence.
No relevant literature or guidelines regarding the clinical effectiveness or use of stellate ganglion block for the treatment of depression or anxiety were identified.
Context and Policy Issues
Post-traumatic stress disorder (PTSD) can develop after exposure to a traumatic event related to combat or any life-threatening experience. 1 Common symptoms of PTSD may include recurring nightmares, loss of interest in activities, inability to feel pleasure, difficulty concentrating, and insomnia. 2 Subsequently, PTSD is a debilitating condition that is linked to reduced quality of life, depression, and anxiety. 1 According to a CAMH paper published in 2018, 3 the lifetime prevalence rate of PTSD for Canadians in general is approximately 9%, whereas 29% of police officers surveyed from 2 Canadian police departments were in the diagnostic range for PTSD. Furthermore, according to a Veteran Affairs Canada article published in 2019, up to about 10% of war zone Veterans will exhibit PTSD. 4
Treatments for PTSD typically involve psychotherapy and/or pharmacotherapy.1 Various forms of psychotherapy may be used such as exposure-based therapy, cognitive behavioural therapy, and stress inoculation training.1 Pharmacological treatment options may include antidepressants (e.g., selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors), antipsychotic drugs, mood stabilizers, and/or other agents.1 However, success rates of PTSD treatments are generally variable, with remission rates that range from 30% to 40%.1 Thus, alternative therapies such as stellate ganglion block (SGB) are being evaluated for the treatment of PTSD.
As part of the sympathetic nervous system, the stellate ganglion is collection of nerves located between the sixth (C6) and seventh (C7) cervical vertebrae.1 SGB is an outpatient procedure involving clinicians injecting a local anesthetic (e.g., ropivacaine 0.5%) to the stellate ganglion, which inhibits nerve impulses to the head, neck, and upper extremities.1 Since the stellate ganglion is connected to the amygdala — a brain region postulated to be abnormally activated in PTSD — SGB has been evaluated as a treatment modality for PTSD. However, its mechanism of action in ameliorating PTSD symptoms is not entirely elucidated.1 Furthermore, SGB has also been assessed for the treatment of anxiety and depression.2,3
The aim of this report is to summarize and critically appraise the relevant evidence regarding the clinical effectiveness and evidence-based guidelines regarding the use of SGB for the treatment of PTSD, depression, or anxiety. Another CADTH report focused on the clinical evidence and guidelines for the use of SGB for the treatment of acute or chronic pain in the head, neck, or upper extremities.4
Research Questions
What is the clinical effectiveness of stellate ganglion block for the treatment of post-traumatic stress disorder?
What is the clinical effectiveness of stellate ganglion block for the treatment of depression or anxiety?
What are the evidence-based clinical practice guidelines regarding the use of stellate ganglion block for the treatment of post-traumatic stress disorder, depression, or anxiety?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE via OVID, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were stellate ganglion block and anxiety, depression, or PTSD. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016 and January 21, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Q1and Q3: Individuals (any age) with PTSD Q2 and Q3: Individuals (any age) with depression (any type) or an anxiety disorder |
Intervention | Stellate ganglion block (i.e., anesthetic [any kind] injection into the stellate ganglion) |
Comparators | Q1 and Q2: Standard or usual treatment for PTSD (e.g., pharmacological, psychological therapies); placebo; no treatment (safety outcomes only) Q2: Standard or usual treatments for depression and anxiety (e.g., pharmacological, psychological therapies); placebo; no treatment (safety outcomes only) Q3: Not applicable |
Outcomes | Q1 and Q2: Clinical benefits and harms (e.g., remission of PTSD, PTSD symptoms, anxiety, depression, functional status, quality of life, hematoma, accidental injection of anesthetic into wrong space [e.g., intravascular, brachial plexus], allergic response, muscle spasm, infection) Q3: Recommendations regarding best practices (e.g., treatment protocols, who should be treated, counter indications for treatment) |
Study Designs | HTAs, SRs, RCTs, non-randomized studies, evidence-based guidelines |
HTA = health technology assessment; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Single-arm studies of SGB that reported safety outcomes were included, whereas single-arm studies with other clinical effectiveness outcomes that did not report safety outcomes were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)5 for SRs, the Downs and Black checklist6 for randomized controlled trials (RCT), and the Appraisal of Guidelines for Research & Evaluation (AGREE) II instrument7 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
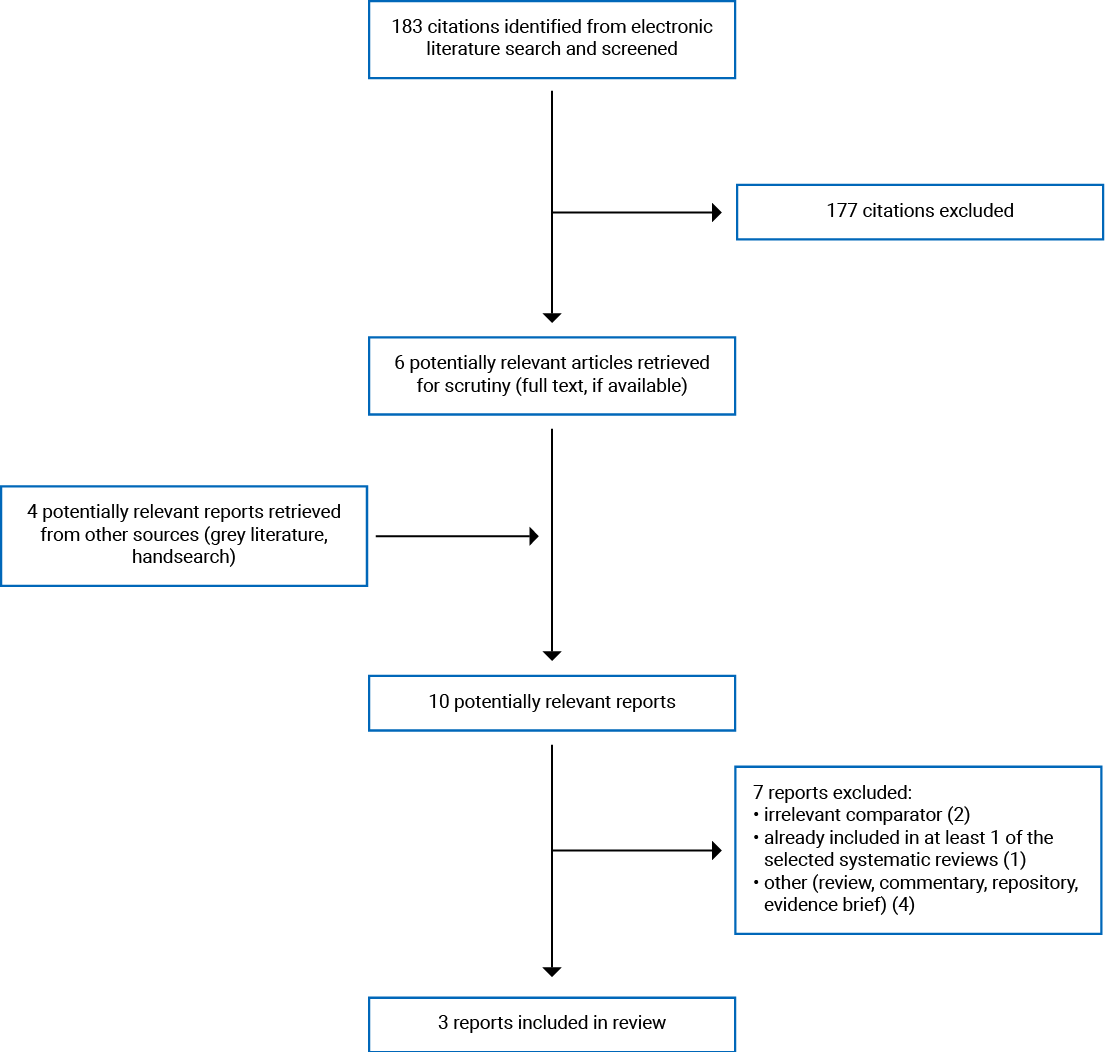
A total of 183 citations were identified in the literature search. Following the screening of titles and abstracts, 177 citations were excluded and 6 potentially relevant reports from the electronic search were retrieved for full-text review. Four potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 7 publications were excluded for various reasons and 3 publications met the inclusion criteria and were included in this report. These comprised 1 SR, 1 RCT, and 1 evidence-based guideline. Appendix 1 presents the PRISMA8 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One SR,1 1 RCT,9 and 1 evidence-based guideline10 were identified with relevance to the research questions and inclusion criteria of this report. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Published in 2017, the identified SR1 included 1 primary study, which was a sham-controlled RCT, where participants and assessors were blinded. Authors of this SR limited their search to English publications and the time frame from inception (earliest available date) to February 7, 2017. Systematic searches were conducted in various databases (i.e., MEDLINE, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, CINAHL, PsychINFO, and PILOTS).
One primary study published in 2020 was included in this report.9 The authors conducted a sham-controlled RCT, where participants and research coordinators were blinded.
The included evidence-based guideline, developed by the US Department of Veterans Affairs (VA) and the US Department of Defense (DoD), was published in 2017.10 This guideline was informed by systematic searches conducted in various databases (i.e., Cochrane Database of Systematic Reviews, Embase, Health Technology Assessment Database, MEDLINE, PILOTS, PsychINFO, and PubMed), with a search time frame from 2009 to March 2016. The quality of the evidence (ranging from high to very low quality) and strength of recommendations (ranging from “strong for” to “strong against”) were assessed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. The VA/DoD Work Group produced recommendations based on a consensus process.
Country of Origin
The first author of the included SR1 and primary RCT9 were from the US. The VA/DoD guideline is meant to apply to the US.
Patient Population
The identified SR included adult Veterans with PTSD.1 The included primary study recruited 42 primarily limited-duty male military personnel with both combat and noncombat PTSD (specific demographic data and comorbid conditions not reported [NR]).
The relevant primary RCT recruited 113 active-duty military members with PTSD receiving care at 1 of 3 US military hospitals (comorbid conditions NR).9 The mean age was 37.3 years and 11.5% were female.
The target population covered by the VA/DoD guideline was VA and DoD patients with PTSD or acute stress disorder.10 The intended users of this guideline are health care providers caring for patients within VA and DoD populations.
Interventions and Comparators
The SR sought primary studies that compared SGB versus any other treatment with any follow-up duration.1 The included primary study compared 2 rounds of ultrasound-guided SGB using 5 mL of ropivacaine 0.5% versus an inactive sham procedure using normal saline injected at the fifth (C5) or sixth (C6) cervical vertebrae on the right side of the neck.
The primary RCT compared 2 rounds of ultrasound-guided SGB using 7 mL to 10 mL of ropivacaine 0.5% versus an inactive sham procedure using normal saline injected at C6 on the right side of the neck.9
The VA/DoD guideline considered the overall management (i.e., diagnosis, treatment, and follow-up) of PTSD and related conditions.10 Recommendations relevant for this report pertained to the use of SGB.
Outcomes
The relevant outcomes from the identified SR included clinically significant improvements in PTSD symptoms defined by ≥ 15-point decrease in the Clinician-Administered PTSD Scale (CAPS-4) score, which is the Clinically-Administered PTSD Stress Scale for the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-4), ≥ 10-point decrease in the PTSD Checklist for DSM-4 (PCL-4) score, or ≥ 30% improvement in CAPS-4 or PCL-4.1 The authors did not specify which of the 3 versions (i.e., military, civilian, or specific) of PCL-4 was used in their assessment. Furthermore, related adverse events were reported. Considered as a gold standard assessment tool for PTSD, the CAPS-4 interview was performed by a technician using DSM-4 criteria for 17 PTSD symptoms, with higher scores indicating greater symptom severity (minimum and maximum score NR).2 PCL-4 is a self-administered assessment tool to measure PTSD symptoms as per DSM-4, with higher scores indicating greater symptom severity (minimum and maximum score NR).2 Outcomes were measured at 1 week and 1 month after the first and second injection, while participants were followed up for 3 months after their last injection.
The primary outcome for the identified RCT was CAPS total symptom severity score using the fifth edition of DSM (CAPS-5). The reported secondary outcomes included symptom severity scores on the PCL using the fifth edition of DSM (PCL-5) and the PCL-civilian version using the DSM-4 (PCL-C-IV), depression (Patient Health Questionnaire-9), anxiety (GAD-7 for generalized anxiety disorder, 7-item scale), distress (K-6 Kessler psychological distress scale), pain (numerical pain scale), and physical and mental functioning (SF-12).9 CAPS-5 is a 30-item structured interview, with scores ranging from 0 (lowest symptom severity) to 80 (highest symptom severity). With revised wording to reflect additional PTSD symptoms in DSM-5 versus DSM-4, the updated CAPS-5 scale prompts the respondent to focus on a single traumatic event versus up to 3 events in CAPS-4.11 PCL-5 is a 20-item self-administered assessment tool to measure 20 PTSD symptoms as per DSM-5, with scores ranging from 0 (lowest symptom severity) to 80 (highest symptom severity). With updated wording to reflect additional PTSD symptoms in DSM-5 versus DSM-4 and a revised rating scale of 0 to 4 versus 1 to 5, PCL-5 can be used to assess military and non-military populations.12 PCL-C-IV is a 17-item, self-administered assessment tool to measure 17 PTSD symptoms as per DSM-4, with scores ranging from 17 (lowest symptom severity) to 85 (highest symptom severity).9 Depression was measured using the Patient Health Questionnaire-9, with scores ranging from 0 (no depression symptoms) to 27 (highest depression level). Anxiety was measured using the GAD-7, with scores ranging from 0 (no anxiety symptoms) to 21 (highest anxiety level). Psychological distress was measured using the K-6 distress scale, with scores ranging from 0 (no distress) to 24 (highest distress level). Pain, which may present concurrently with PTSD, was measured using a numerical pain scale, with scores ranging from 0 (no pain) to 10 (worst possible pain). Physical and mental functioning was measured using the SF-12, with 8 domains (4 domains constituting physical health and 4 domains constituting mental health). Although score ranges were NR for the SF-12, lower scores indicated greater symptom severity. Furthermore, the Cohen’s d effect size was calculated for all primary and secondary outcomes. Related adverse events were presented without statistical analysis. Participants were followed up for 8 weeks.
The relevant outcomes from the VA/DoD guideline included patient health outcomes, quality of life, complications, and comorbidities.10
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Review
As per AMSTAR II criteria,5 the included SR was generally well-conducted, with clearly stated objectives, inclusion and exclusion criteria, and key search terms. The SR authors followed an a priori study protocol, provided search strategies, searched multiple databases, provided justification for included study designs, and provided a list of included and excluded studies.1 Furthermore, details of study selection were explicitly stated and data extraction was conducted in duplicate, which decreases the risk of missing or inaccurate data and/or biased study selection. A grey literature search was conducted, which decreases the risk of missing relevant, non-indexed studies. The SR authors disclosed their funding source and that there were no conflicts of interest.
There were methodological limitations in the identified SR and the included evidence.1 Justification was NR for restricting publication language to English. The authors graded the strength of the evidence using the Agency for Healthcare Research and Quality Methods Guide for Effectiveness and Comparative Effectiveness Reviews, but the grades were NR. Although assessed, the SR authors were unable to rule out publication bias in the included evidence. Because the included primary study was conducted in the US, the findings may not be generalizable to the Canadian setting. Furthermore, the findings may not be generalizable to non-Veteran populations. While 7 mL of ropivacaine 0.5% is a commonly used dose for SGB, 5 mL was used without justification in the included RCT in the SR. Needle placement was at C5 or C6 even though the stellate ganglion is typically located at C6 to C7. These factors may have resulted in more treatment failure and less symptom improvement. Additionally, many participants were in the process of disability evaluation, so there may also have been financial incentives to claim treatment failure. Although participants and assessors were blinded, clinicians administering the injections were not blinded to the interventions. Furthermore, the use of normal saline as a sham control may have been inadequate in blinding the participants, as those receiving SGB would have experienced Horner syndrome (i.e., eye droop). The absence of Horner syndrome and knowledge that they have received the sham treatment may have influenced participants’ responses to outcomes scales. Outcomes were measured up to 1 month after a participant’s last injection, so it is unclear if the study results would be generalizable to the long-term effects of SGB.
Randomized Controlled Trial
For methodological strengths, the identified RCT: 1) had clearly stated objectives, inclusion and exclusion criteria, interventions, outcome measures, and main findings; 2) used blinding of participants and research coordinators to help reduce bias; 3) planned data analyses at the outset of the study; 4) conducted a sample size calculation; 5) specified the time period over which patients were recruited; and 6) discussed potential adverse events relating to the interventions.9
This RCT had some methodological limitations.9 Although statistical tests were appropriately used and estimates of random variability were reported, P values were reported for some comparisons. Apart from their assigned treatment, characteristics of patients lost to follow-up were NR. Because the study was conducted in the US, the findings may not be generalizable to the Canadian setting. Furthermore, the findings may not be generalizable to non-Veteran populations. Although participants and assessors were blinded, clinicians administering the injections were not blinded to the interventions. The use of normal saline as a sham control may have been inadequate in blinding the participants, as those receiving SGB would have experienced Horner syndrome. Participants were followed for a total of 8 weeks, so the long-term effects of SGB are unclear.
Evidence-Based Guideline
The VA/DoD guideline provided a clear description of the objectives, specified the target populations and users, sought the views and preferences of the target population, provided unambiguous and easily identifiable recommendations, presented monitoring criteria for the recommendations, described facilitators or barriers to their application, provided tools for putting recommendations into practice, reported details of external review, and explicitly described procedures for guideline updates.10 The VA/DoD Work Group comprised experts from multidisciplinary areas and the views of the funding sources did not appear to have influenced the guideline’s contents. The supporting evidence, together with the quality of evidence used to inform the recommendations, were provided.
Summary of Findings
The overall findings of the included studies and guideline are subsequently below. One SR,1 1 primary RCT,9 and 1 evidence-based guideline10 met the inclusion criteria for this report. Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Stellate Ganglion Block for the Treatment of Post-Traumatic Stress Disorder
Evidence regarding the clinical effectiveness of SGB for the treatment of PTSD was available from 1 SR1 and 1 primary RCT.9
Clinically Administered Posttraumatic Stress Disorder Scale
The identified SR1 included 1 RCT published in 2016, which compared the effect of 2 rounds of SGB with 5 mL of 0.5% ropivacaine versus a sham procedure with normal saline in 42 US active or retired military participants with PTSD. At 1 week, at 1 month after the first injection, and 1at month after the second injection, the mean decrease in CAPS-4 score for the SGB group neither met the criteria for clinically significant improvement (i.e., ≥ 15-point decrease and ≥ 30% improvement) nor were significantly different from the sham group. At 1 week after the second injection, the mean decrease in CAPS-4 score for the SGB group met the first criterion for clinically significant improvement (i.e., ≥ 15-point decrease) but did not meet the second criterion (i.e., ≥ 30% improvement) and was not significantly different from the sham group.
In the identified primary study, Rae Olmsted et al. conducted an RCT comparing the effect of 2 rounds of SGB with 7 mL to 10 mL of 0.5% ropivacaine versus a sham procedure with normal saline in 113 US active-duty military members (age-specific criteria NR) with PTSD.9 Compared to the sham procedure, SGB injections resulted in significantly greater improvements in CAPS-5 total symptom severity score at 8 weeks. The authors did not specify thresholds for clinically significant improvements.
Post-traumatic Stress Disorder Checklist
In the RCT included in the identified SR,1 at 1 week and 1 month after the first and second injection, the mean decrease in the PCL-4 score for the SGB group neither met the criteria for clinically significant improvement (i.e., ≥ 10-point decrease and ≥ 30% improvement) nor was significantly different from the sham group.
In the identified primary study, SGB injections resulted in significantly greater improvements in PCL-5 and PCL-C-IV scores at 8 weeks compared to the sham procedure.9 The authors did not specify thresholds for clinically significant improvements.
Other Related Effectiveness Outcomes
Other related effectiveness outcomes including PCL-C-IV score, depression, anxiety, distress, pain, and mental and physical functioning were provided in the identified RCT.9 Compared to the sham procedure, SGB injections resulted in significantly greater improvements in depression, anxiety, and distress at 8 weeks of follow-up. However, no significant difference was detected in the mean change in pain and mental and physical functioning between the 2 groups. The authors did not specify thresholds for clinically significant improvements on any scale.
Adverse Events
In the RCT included in the identified SR,1 10 adverse events (8 in the SGB group and 2 in the sham group) were observed that were deemed related or possibly related to treatment. No significant difference was reported in the rate of adverse events between the SGB (12%) and sham (13%) groups. Complication rates were calculated based on the total number of injections for the SGB (70 injections) and sham (15 injections) group. Adverse events included injection site pain (incidence NR for either group) and self-resolving prolonged eye drooping (1 in SGB, 0 in sham group).
Six adverse events (none serious) were reported in the identified RCT (statistical analysis NR).9 In the SGB group, 2 events were unrelated and 3 events were related or possibly related to treatment (i.e., injection site pain, self-resolving bradycardia, and temporary laryngeal irritation). One adverse event was reported in the sham group and deemed unrelated to treatment.
Clinical Effectiveness of Stellate Ganglion Block for the Treatment of Depression or Anxiety
No relevant evidence regarding the clinical effectiveness of SGB for the treatment of depression or anxiety independent of PTSD was identified; therefore, no summary can be provided.
Evidence-Based Guidelines
One identified evidence-based guideline10 addressed the use of SGB in the treatment of VA and DoD patients with PTSD. The recommendations in the VA/DoD guideline were informed by an SR conducted by the VA/DoD Work Group. However, because of insufficient evidence, no recommendations for or against the use of SGB for PTSD were provided (strength of recommendation: not applicable; quality of evidence: NR).
No relevant guidelines regarding the use of SGB for the treatment of depression or anxiety were identified; therefore, no summary can be provided.
Limitations
Limitations were identified in the critical appraisal (details in Appendix 3); however, additional limitations exist.
Overall, there was a limited quantity (i.e., 1 RCT in an SR1 and 1 additional RCT9) of evidence regarding the clinical effectiveness of SGB for the treatment of PTSD. Likewise, 1 evidence-based guideline was identified that could not provide a recommendation for or against the use of SGB for PTSD because of insufficient evidence. As the study participants in the included literature were from military populations, the findings may not be generalizable to non-military populations.1,9 Furthermore, no relevant literature or evidence-based guidelines regarding the clinical effectiveness or use of SGB for the treatment of depression or anxiety were identified. Overall, considering the limitations mentioned, the findings and recommendations summarized in this report need to be interpreted with caution.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 1 SR1 (containing 1 relevant RCT) and 1 RCT9 regarding the clinical effectiveness of SGB for the treatment of PTSD. Specifically, both studies compared ropivacaine 0.5% with sham injections. Furthermore, 1 evidence-based guideline was identified regarding the use of SGB for the treatment of PTSD.10 No relevant literature or evidence-based guidelines regarding the clinical effectiveness or use of SGB for the treatment of depression or anxiety were identified.
The identified literature revealed mixed conclusions regarding the clinical effectiveness of SGB for the treatment of PTSD.1,9 Specifically, in the RCT included in the identified SR,1 participants receiving SGB did not experience clinically significant improvements in CAPS-4 or PCL-4 scores at 1 week and 1 month after either of 2 injections, with the exception of clinically significant improvements in CAPS-4 scores at 1 week after the second injection. However, no significant differences in CAPS-4 or PCL-4 improvements were detected between the SGB and sham group throughout the study (i.e., at 1 week and 1 month after the first and second injection). Furthermore, between the 2 groups, there was no significant difference in the rate of adverse events, which included injection site pain (incidence NR) and self-resolving prolonged eye drooping (1 in the SGB group). In the identified primary RCT,9 2 rounds of SGB resulted in significantly greater improvements in CAPS-5, PCL-5, PCL-C-IV score, depression, anxiety, and distress at 8 weeks compared to sham. However, the authors did not specify if these improvements were clinically meaningful and no significant differences in pain and mental and physical functioning improvements were detected between the 2 groups. Six adverse events (5 in the SGB and 1 in sham groups) were reported, with 3 deemed related to SGB treatment (injection site pain, self-resolving bradycardia, and temporary laryngeal irritation) (statistical analysis NR). It is important to note the differences between the 2 RCTs such as different SGB doses, injection sites, and follow-up durations;1,9it is possible that these differences may have contributed to the discrepant conclusions between studies.
Authors of the VA/DoD evidence-based guideline were not able to make recommendations for or against the use of SGB for PTSD because of insufficient evidence.10
The included literature shared some limitations such as the unblinding of clinicians administering the injections and relatively short follow-up durations.1,9 As the study participants in the included literature were from military populations, the findings may not be generalizable to non-military populations.1,9 Additionally, the limitations of the overall body of evidence (e.g., limited number of primary studies, SRs and RCTs conducted outside of Canada) should be considered when interpreting the findings of this report
Further research investigating the clinical effectiveness of SGB — particularly with controlled clinical trials with Canadian military, paramilitary, or Veterans representation and extended follow-up durations — would provide health care providers with an additional knowledge base and evidence-based guidance for the treatment of PTSD, depression, or anxiety.
References
1.Peterson K, Bourne D, Anderson J, Mackey K, Helfand M. Effectiveness of stellate ganglion block for treatment of Posttraumatic Stress Disorder (PTSD). Washington (DC): Department of Veterans Affairs; 2017: https://www.hsrd.research.va.gov/publications/esp/ganglionblock.pdf. Accessed 2021 Feb 19.
2.Hanling SR, Hickey A, Lesnik I, et al. Stellate ganglion block for the treatment of Posttraumatic Stress Disorder: a randomized, double-blind, controlled trial. Reg Anesth Pain Med. 2016;41(4):494-500. Medline
3.Lynch JH, Mulvaney SW, Kim EH, de Leeuw JB, Schroeder MJ, Kane SF. Effect of stellate ganglion block on specific symptom clusters for treatment of Post-Traumatic Stress Disorder. Mil Med. 2016;181(9):1135-1141. Medline
4.Stellate ganglion block for the treatment of pain. (CADTH reference list). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/rr/2021/RA1162%20SGB%20Pain%20Final.pdf. Accessed 2021 Feb 9.
5.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. Medline
6.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. Medline
7.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Feb 19.
8.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
9.Rae Olmsted KL, Bartoszek M, Mulvaney S, et al. Effect of stellate ganglion block treatment on Posttraumatic Stress Disorder symptoms: a randomized clinical trial. JAMA Psychiatry. 2020;77(2):130-138. Medline
10.Clinical practice guideline for the management of Posttraumatic Stress Disorder and Acute Stress Disorder. Washington (DC): Department of Veterans Affairs, Department of Defense; 2017: https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal012418.pdf. Accessed 2021 Jan 27.
11.U.S. Department of Veterans Affairs. Clinician-administered PTSD scale for DSM-5 (CAPS-5). 2021; https://www.ptsd.va.gov/professional/assessment/adult-int/caps.asp. Accessed 2021 Feb 19.
12.U.S. Department of Veterans Affairs. PTSD checklist for DSM-5 (PCL-5). 2021; https://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp. Accessed 2021 Feb 19.
13.CAMH. Posttraumatic Stress Disorder. 2021; https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/posttraumatic-stress-disorder. Accessed 2021 Feb 9.
14.Police mental health: a discussion paper. Toronto (ON): CAMH; 2018: https://www.camh.ca/-/media/files/pdfs---public-policy-submissions/police-mental-health-discussion-paper-oct2018-pdf.pdf?la=en&hash=B47D58B5ACBE4678A90907E3A600BB447EE134BF. Accessed 2021 Feb 9.
15.Veterans Affairs Canada. Post-traumatic stress disorder (PTSD) and war-related stress. 2019; https://www.veterans.gc.ca/eng/health-support/mental-health-and-wellness/understanding-mental-health/ptsd-warstress#Item5-2. Accessed 2021 Feb 9.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Peterson et al. (2017)1 US Funding Source: Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Quality Enhancement Research Initiative | Objective: To evaluate the clinical effectiveness of SGB for PTSD and determine Veteran subgroups most likely to benefit Study design: SR of SRs, RCTs, or concurrently controlled cohort studies Literature search strategy: The search was conducted in MEDLINE, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, CINAHL, PsychINFO, and PILOTS for literature published in English from inception (earliest available date to February 7, 2017 A grey literature search was conducted for reference lists and unpublished literature Number of studies included: 1 RCT was identified and is relevant for this report Quality assessment tool: Quality of evidence evaluated using criteria established by DERP and the AHRQ Methods Guide for Effectiveness and Comparative Effectiveness Reviews | Eligible Population: Adult Veterans with PTSD Relevant Population: N = 42 (primarily male military participants) | Eligible Intervention: SGB (dose-specific criteria NR) Relevant Intervention: SGB with 5 mL of 0.5% ropivacaine (N = 27) Eligible Comparator: Any comparator Relevant Comparator: Sham with normal saline (N = 15) | Outcomes:
Follow-up: Any follow-up duration |
AHRQ = Agency for Healthcare Research and Quality; CAPS-4 = Clinician-Administered PTSD Scale for DSM-4; CINAHL = Cumulative Index to Nursing and Allied Health Literature; DERP = Drug Effectiveness Review Project; NR = not reported; PCL-4 = PTSD Checklist for DSM-4; PILOTS = Published International Literature on Traumatic Stress; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; SGB = stellate ganglion block; SR = systematic review.
Table 3: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Randomized controlled trial | ||||
Rae Olmsted et al. (2020)9 US Funding Source: Office of the Assistant Secretary of Defense for Health Affairs through the Defense Medical Research and Development Program | Study design: Randomized controlled trial Setting: 3 US military hospitals with Interdisciplinary Pain Management Centers Objective: To compare the clinical effectiveness of SGB vs. sham for PTSD | Active-duty military members (age-specific inclusion criteria NR) with PTSD Number of patients: N = 113 Mean age [SD] (years): 37.3 [6.7] % female: 11.5% | Intervention: SGB with 7 mL to 10 mL of 0.5% ropivacaine (N = 74) Comparator: Sham with normal saline (N = 39) | Outcomes:
|
CAPS-5 = Clinician-Administered PTSD Scale for DSM-5; K-6 scale = Kessler Psychological Distress scale; NR = not reported; PHQ-9 = Patient Health Questionnaire 9 items; PCL = PTSD Checklist; PCL-5 = PTSD Checklist for DSM-5; PCL-C-IV = PTSD‒Civilian Version; PTSD = post-traumatic stress disorder; SD = standard deviation; SF-12 = 12-item short-form survey; SGB = stellate ganglion block; TSSS = total symptom severity scores; vs. = versus.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
US Department of Veteran Affairs and Department of Defense (2017)10 | ||||||
Intended users: Health care providers caring for patients within VA and DoD populations Target population: VA and DoD patients with PTSD or acute stress disorder | The guideline provided recommendations regarding the management (i.e., diagnosis, treatment, and follow-up) of PTSD and related conditions. Recommendations relevant for this report pertained to the use of SGB. | Patient health outcomes, quality of life, complications, comorbidities | Literature searches were conducted in the Cochrane Database of Systematic Reviews, Embase, Health Technology Assessment Database, MEDLINE, PILOTS, PsychINFO, and PubMed for literature published in English from 2009 to March 2016. A grey literature search was conducted for Evidence Synthesis Program reports. | Evidence quality was assessed using the GRADE approach. Quality of evidence:
| The VA/DoD Work Group produced recommendations based on scientific evidence and stakeholder input through a consensus process. Strength of recommendation:
| The Work Group held a patient focus group to solicit feedback. Furthermore, the draft guideline was reviewed by internal and external peer reviewers. |
DoD = Department of Defense; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; PTSD = post-traumatic stress disorder; SGB = stellate ganglion block; VA = Veterans Affairs.
Appendix 3: Critical Appraisal of Included Publications
Table 5: Strengths and Limitations of Systematic Review Using AMSTAR 28
Strengths | Limitations |
Peterson et al. (2017)1 | |
|
|
AHRQ = Agency for Healthcare Research and Quality; AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CINAHL = Cumulative Index to Nursing and Allied Health Literature; PICO = Population, Interventions, Comparator, and Outcomes; PILOTS = Published International Literature on Traumatic Stress.
Table 6: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist6
Strengths | Limitations |
Randomized controlled trial | |
Rae Olmsted et al. (2020)9 | |
|
|
Table 7: Strengths and Limitations of Guideline Using AGREE II7
Item | US VA/DoD (2017)10 |
Domain 1: Scope and Purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder Involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of Development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of Presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes |
Domain 6: Editorial Independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research &Evaluation II; DoD = Department of Defense; VA = Veterans Affairs.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Included Systematic Review
Peterson et al. (2017)1
Main study findings
SR included 1 RCT published in 2016 comparing the effect of 2 rounds of ultrasound-guided SGB with 5 mL of 0.5% ropivacaine vs. a sham procedure with normal saline in 42 active adult or retired military participants with both combat and noncombat PTSD.
Mean change from baseline in CAPS-4 score
First Injection
One week after: −12.7 (14.7% improvement) (SGB) vs. −11.3 (sham)
One month after: −6.6 (SGB) vs. −8.8 (sham)
No significant difference between SGB and sham at both time points
Second Injection
One week after: −17.8 (21.2% improvement) (SGB) vs. −9 (sham)
One month after: −7.5 (SGB) vs. −4.3 (sham)
No significant difference between SGB and sham at both time points
Mean change from baseline in PCL-4 score
First Injection
One week after: −3.6 (5.4% improvement) (SGB) vs. −4.1 (sham)
One month after: −2.0 (SGB) vs. −2.4 (sham)
No significant difference between SGB and sham at both time points
Second Injection
One week after: −7.9 (12.1% improvement) (SGB) vs. −4.6 (sham)
One month after: −6.5 (SGB) vs. −6.3 (sham)
No significant difference between SGB and sham at both time points
Note: Mean % improvement reported for some outcomes. P values NR.
Adverse Events
Eight (SGB group) and 2 (sham group) adverse events were deemed as “related” or “possibly related” to treatment, resulting in a 12% and 13% complication rate in the SGB and sham group, respectively (no significant difference; P value NR)
Complications included injection site pain (incidence NR for either groups) and self-resolving prolonged eye drooping (1 in SGB, 0 in sham group) (specifics of other adverse events NR)
Authors’ conclusion
“The main finding of this RCT was that at one week and one month after the first round of treatment, the magnitude of mean reduction in PTSD symptoms for SGB and sham neither met the proposed criteria for clinical relevance nor were different between groups, regardless of whether they were measured based on the Clinically-Administered PTSD Scale (CAPS) or the PTSD Checklist (PCL) (Table 1). In the subset of patients who received a second round of SGB or sham, the SBG group reached a clinically significant reduction after one week based on the CAPS, but not the PCL, but again there were no significant differences between SGB and sham (p. 9).”1
Summary of Findings of Included Randomized Controlled Trial
Rae Olmsted et al. (2020)9
Main study findings
RCT comparing the effect of 2 rounds of ultrasound-guided SGB with 7 mL to 10 mL of 0.5% ropivacaine vs. a sham procedure with normal saline in 113 active-duty military members (age-specific criteria NR) with PTSD. All outcomes were measured at baseline and at 8 weeks.
CAPS-5 Total Symptom Severity Scores
Adjusted mean change of −12.6 (95% confidence interval [CI], −15.5 to −9.7) for SGB treatment vs. −6.1 (95% CI, −9.8 to −2.3) sham treatment (P = 0.01)
Effect size (SD) = 0.56 (0.09) (95% CI, 0.38 to 0.73)
PCL-5
Adjusted mean change (SD) of −12.63 (14.34) for SGB treatment vs. −5.16 (13.99) sham treatment
Effect size (SD) = 0.53 (0.20) (95% CI, 0.14 to 0.91)
PCL-C-IV
Adjusted mean change (SD) of −11.45 (13.40) for SGB treatment vs. −4.30 (14.17) sham treatment
Effect size (SD) = 0.52 (0.20) (95% CI, 0.14 to 0.91)
Depression (Patient Health Questionnaire-9 items)
Adjusted mean change (SD) of −4.11 (5.55) for SGB treatment vs. −0.92 (4.78) sham treatment
Effect size (SD) = 0.60 (0.20) (95% CI, 0.21 to 0.99)
Anxiety (Generalized Anxiety Disorder 7-item scale)
Adjusted mean change (SD) of −4.42 (5.80) for SGB treatment vs. −1.22 (4.93) sham treatment
Effect size (SD) = 0.58 (0.20) (95% CI, 0.19 to 0.97)
Distress (Kessler psychological distress scale)
Adjusted mean change (SD) of −2.52 (4.86) for SGB treatment vs. −0.16 (4.59) sham treatment
Effect size (SD) = 0.49 (0.20) (95% CI, 0.11 to 0.88)
Pain
Adjusted mean change (SD) of −0.56 (1.65) for SGB treatment vs. −0.03 (1.44) sham treatment
Effect size (SD) = 0.34 (0.20) (95% CI, −0.04 to 0.72)
Short-Form Survey health questionnaire
Mental functioning
Adjusted mean change (SD) of 1.74 (7.58) for SGB treatment vs. −0.66 (7.21) sham treatment
Effect size (SD) = −0.32 (0.20) (95% CI, −0.71 to 0.06)
Physical functioning
Adjusted mean change (SD) of 2.56 (8.15) for SGB treatment vs. −0.37 (7.02) sham treatment
Effect size (SD) = −0.38 (0.20) (95% CI, −0.76 to 0.01)
Note: P values reported for some outcomes.
Adverse Events
Of the 6 adverse events, none were serious
SGB group: 5 adverse events
2 events deemed “definitely related” to treatment (i.e., injection site pain and self-resolving bradycardia)
1 event deemed “possibly related” (i.e., temporary laryngeal irritation)
2 events deemed as “definitely unrelated”
Sham group: 1 adverse event, which was deemed “definitely unrelated”
Statistical analysis NR
Authors’ conclusion
“In this trial of active-duty service members with PTSD symptoms (at a clinical threshold and subthreshold), 2 SGB treatments 2 weeks apart were effective in reducing CAPS-5 total symptom severity scores over 8 weeks. The mild-moderate baseline level of PTSD symptom severity and short follow-up time limit the generalizability of these findings, but the study suggests that SGB merits further trials as a PTSD treatment adjunct. (p. 4).”9
Table 8: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
US Department of Veterans Affairs and Department of Defense (2017)10 | |
“There is insufficient evidence to recommend for or against the following somatic therapies: repetitive transcranial magnetic stimulation (rTMS), electroconvulsive therapy (ECT), hyperbaric oxygen therapy (HBOT), stellate ganglion block (SGB), or vagal nerve stimulation (VNS). (p. 65).”10
| Recommendation strength: NA Quality of evidence: NR |
DoD = Department of Defense; NA = not applicable; NR = not reported; SR = systematic review; VA = Veterans Affairs.
Appendix 5: References of Potential Interest
Review Article
Summers MR, Nevin RL. Stellate ganglion block in the treatment of Post-traumatic stress disorder: a review of historical and recent literature. Pain Pract. 2017;17(4):546-553. Medline
Non-Randomized Studies – Single-Arm Studies Without Safety Outcomes
Lynch JH, Mulvaney SW, Kim EH, de Leeuw JB, Schroeder MJ, Kane SF. Effect of stellate ganglion block on specific symptom clusters for treatment of Post-Traumatic stress Disorder. Mil Med. 2016;181(9):1135-1141. Medline
Odosso RJ, Petta L. The efficacy of the stellate ganglion block as a treatment modality for Posttraumatic stress Disorder among active duty combat veterans: a pilot program evaluation. Mil Med. 2020;26:26.[online ahead of print] Medline
Additional References
Lynch JH. Stellate ganglion block treats posttraumatic stress: An example of precision mental health. Brain Behav. 2020;10(11):e01807. Medline
Pacific Northwest Evidence-based Practice Center, O'Neil M, Cheney T, et al. Pharmacologic and nonpharmacologic treatments for Posttraumatic Stress Disorder: an update of the PTSD-repository evidence base. (Comparative effectiveness report no. 235). Rockville (MD): Agency for Healthcare Research and Quality; 2020: https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/cer-235-pharma-nonpharm-ptsd-update-report.pdf. Accessed 2021 Feb 19.
Psychological Health Center of Excellence. Psych health evidence briefs: stellate ganglion block for posttraumatic stress disorder; 2017: https://pdhealth.mil/sites/default/files/images/docs/Stellate%20Ganglion%20Block%20for%20PTSD_508.pdf. Accessed 2021 Feb 19.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca