CADTH Health Technology Review
Workplace Electronic Health Promotion Campaigns for Tobacco Smoking Prevention or Cessation
Rapid Review
Authors: Daphne Hui, Monika Mierzwinski-Urban
Abbreviations
EHPC
electronic health promotion campaign
Key Messages
There is a lack of recent evidence regarding the cost-effectiveness of workplace electronic health promotion campaigns (EHPCs) for the prevention or cessation of tobacco smoking.
There is a need for well-designed economic evaluations to assess the cost-effectiveness of workplace EHPCs for the prevention or cessation of tobacco smoking.
Context and Policy Issues
Tobacco smoking is the leading preventable cause of mortality with chronic obstructive pulmonary disease, lung cancer, and atherosclerotic cardiovascular disease as the main causes of smoking-related mortality.1,2 Canadian data from 2019 (excluding the territories) estimated the daily smoking prevalence rate to be more than 5% with 3,160,100 individuals 12 years and older (across both males and females) reporting they smoke daily.3 Individuals who smoke accrue more health care costs compared to those who have never smoked, with the accrual increasing with age.4,5 For example, in Ontario, annual health care costs of an 80 year old who has never smoked versus an 80 year old who currently smokes were estimated to be $8,740 versus $19,583, respectively.5 In 2012, tobacco use in Canada resulted in $16.2 billion dollars in expenses related to health care, tobacco control law enforcement, fire damage, and lost production among manufacturers and the service industry.6 In the workplace, smoking may result in increased employee absenteeism (e.g., sick leave), as well as presenteeism and reduced employee productivity (i.e., being physically present at work but mentally distracted resulting in lower productivity).7
The addictiveness of nicotine is the principal barrier to smoking cessation with nicotine withdrawal symptoms including restlessness, insomnia, irritability, anxiety, concentration difficulties, mood changes (e.g., depression or dysphoria), increased appetite, and weight gain.1 Tobacco smoking cessation is facilitated by pharmacological and behavioural interventions. Combination interventions (pharmacological and behavioural) have been shown to increase the success of smoking cessation compared to single-intervention approaches (e.g., solely relying on pharmacological interventions).8,9 Pharmacological interventions administered as first-line include nicotine replacement therapy (alternative forms of nicotine, such as gum or patches, to relieve withdrawal) and non-nicotine therapy (drugs such as varenicline or bupropion).8,10 Behavioural interventions aim to provide education or support, or offer techniques to problem solve, cope, and manage stress; multiple behavioural interventions may be used simultaneously.11 Behavioural interventions are administered in-person or through electronic or technology-based media and may include the following: counselling through individual or group sessions conducted in-person or via telephone or videocalls; self-help resources in print (e.g., pamphlets) or digital form (e.g., audio, video, or PDFs); mobile applications (apps) that offer behavioural change techniques or useful information (e.g., pharmacotherapy facts); web-based interventions that provide access to tailored and interactive materials12; and use of text messaging to relay motivational messages, provide positive feedback, and facilitate behavioural changes.13
There has recently been an emergence of EHPCs, which aim to promote health and prevent disease by encouraging individuals to exercise healthy behaviours and they usually address behavioural risk factors such as tobacco use.14 In the workplace, EHPCs may include knowledge mobilization campaigns, strategies, or programs such as awareness messages delivered through corporate intranet, social media, emails, text messages, and self-directed online programs. For instance, Butt Out is a self-directed online smoking cessation program that was developed by the Centre for Addiction and Mental Health for individuals who smoke in the Canadian Armed Forces. EHPCs may help to promote health and well-being while supporting the prevention or cessation of tobacco smoking among employees.15 Literature has demonstrated the effectiveness of non-electronic smoking cessation interventions4,7,16; however, the effectiveness of electronic smoking cessation interventions has not been well-studied.7 Evaluating the cost-effectiveness of workplace EHPCs may help to inform decision-making regarding their implementation.
The purpose of this rapid review is to evaluate the cost-effectiveness of workplace EHPCs for the prevention or cessation of tobacco smoking. This report compliments a CADTH Summary of Abstracts report on the cost-effectiveness of workplace EHPCs for substance use, gambling, and gaming prevention.17
Research Question
What is the cost-effectiveness of workplace EHPCs for the prevention or cessation of tobacco smoking?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, PsycINFO, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were smoking cessation and the workplace. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, network meta-analyses, or economic studies. The search was also limited to English language documents published between January 1, 2016 and January 7, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Adults, in a workplace setting, with or without a tobacco smoking addiction |
Intervention | EHPCs for the prevention of, or cessation of, tobacco smoking. For example:
|
Comparator | EHPCs, with concurrent nicotine replacement therapy Nicotine replacement therapy alone No intervention |
Outcomes | Cost-effectiveness (e.g., cost per quitter, cost per life-year saved, cost per quality-adjusted life-year gained, cost per disability-adjusted life-year) |
Study designs | Economic evaluations and health technology assessments |
EHPC = electronic health promotion campaign.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016.
Summary of Evidence
Quantity of Research Available
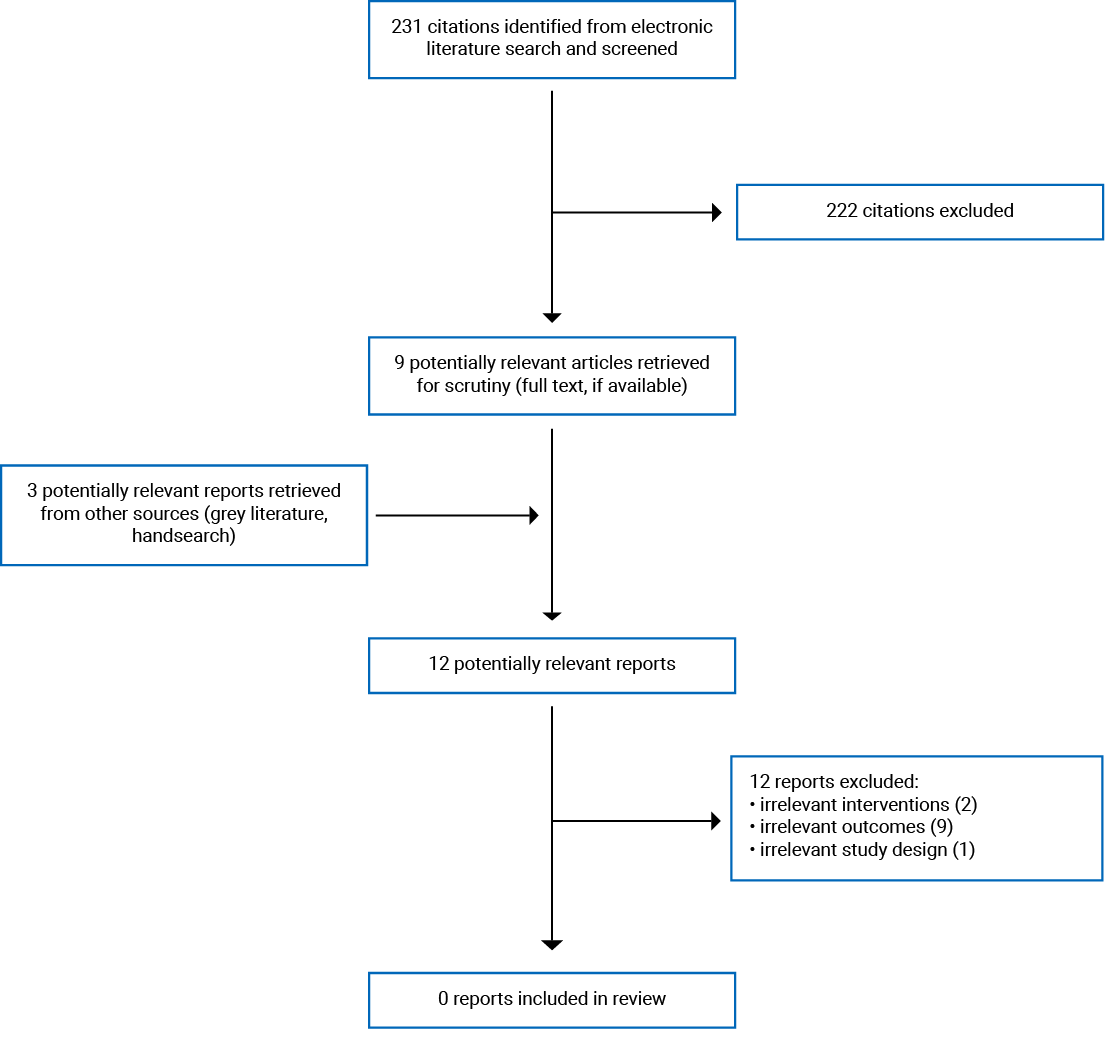
A total of 231 citations were identified in the literature search. Following screening of titles and abstracts, 222 citations were excluded and 9 potentially relevant reports from the electronic search were retrieved for full-text review. Three potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 12 publications were excluded for various reasons, and no publications met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA18 flow chart of the study selection. Additional references of potential interest are provided in Appendix 2.
Summary of Study Characteristics
No relevant literature (published between January 1, 2016 and January 7, 2021) was identified regarding the cost-effectiveness of workplace EHPCs for the prevention or cessation of tobacco smoking; therefore, no summary can be provided.
Limitations
No relevant literature was identified regarding the cost-effectiveness of workplace EHPCs for the prevention or cessation of tobacco smoking.
Conclusions and Implications for Decision or Policy-Making
No relevant literature was identified regarding the cost-effectiveness of workplace EHPCs for the prevention or cessation of tobacco smoking. Similarly, the authors of a 2020 systematic review of economic analyses evaluating workplace interventions for mental health and substance use (including smoking) only identified studies reporting the cost-effectiveness of pharmacotherapy and brief counselling for tobacco smoking cessation.7 Furthermore, in a 2020 economic evaluation of an in-person workplace smoking cessation intervention, the authors noted that there is limited evidence on the cost-effectiveness of smoking cessation programs in general, and in particular, to their knowledge, no economic evaluation from an employer’s perspective has been performed.16 Together, these findings highlight the absence of evidence regarding the cost-effectiveness of workplace EHPCs for the prevention or cessation of tobacco smoking. Future well-designed economic evaluations that assess the cost-effectiveness of workplace EHPCs for the prevention or cessation of tobacco smoking are needed and may help validate or refute the value and importance of these programs in the workplace.
References
1.Rigotti NA. Benefits and consequences of smoking cessation. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2020: www.uptodate.com. Accessed 2021 Feb 1.
2.Centers for Disease Control and Prevention (CDC). Smoking-attributable mortality, years of potential life lost, and productivity losses--United States, 2000-2004. MMWR Morb Mortal Wkly Rep. 2008;57(45):1226-1228. Medline
3.Statistics Canada. Health characteristics, annual estimates. Table: 13-10-0096-01 (formerly CANSIM 105-0508). 2021; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009601. Accessed 2021 Feb 1.
4.Ontario Agency for Health Protection and Promotion (Public Health Ontario), Berenbaum E, Keller-Olaman S, Watson K, Longo C. Economic benefits of smoking cessation interventions. Toronto (ON): Queen's Printer for Ontario; 2019: https://www.publichealthontario.ca/-/media/documents/r/2020/rapid-review-economic-benefits-smoking-cessation.pdf?la=en Accessed 2021 Jan 13.
5.Direct healthcare cost by smoking status among Ontario adults Toronto (ON): Ontario Tobacco Research Unit; 2018: https://otru.org/wp-content/uploads/2018/11/react_project_news_nov2018.pdf. Accessed 2021 Feb 1.
6.Dobrescu A, Bhandari A, Sutherland G, Dinh T. The costs of tobacco use in Canada, 2012. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/temp/90520846-5b6e-4299-bae3-24bb6a9b862c/9185_Costs-Tobacco-Use_RPT.pdf. Accessed 2021 Feb 1.
7.de Oliveira C, Cho E, Kavelaars R, et al. Economic analyses of mental health and substance use interventions in the workplace: a systematic literature review and narrative synthesis. Lancet Psychiatry. 2020;7(10):893-910. Medline
8.Rigotti NA. Overview of smoking cessation management in adults. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com/. Accessed 2021 Feb 1.
9.Stead LF, Koilpillai P, Fanshawe TR, Lancaster T. Combined pharmacotherapy and behavioural interventions for smoking cessation. Cochrane Database Syst Rev. 2016;3:CD008286. Medline
10.Rigotti NA. Treatment of tobacco use and dependence. N Engl J Med. 2002;346(7):506-512. Medline
11.Park ER. Behavioral approaches to smoking cessation. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2020: www.uptodate.com. Accessed 2021 Feb 1.
12.Civljak M, Stead LF, Hartmann-Boyce J, Sheikh A, Car J. Internet-based interventions for smoking cessation. Cochrane Database Syst Rev. 2013(7):CD007078. Medline
13.Whittaker R, McRobbie H, Bullen C, et al. Mobile phone text messaging and app-based interventions for smoking cessation. Cochrane Database Syst Rev. 2019;10(10):CD006611. Medline
14.World Health Organization. Health promotion and disease prevention through population-based interventions, including action to address social determinants and health inequity. 2021; http://www.emro.who.int/about-who/public-health-functions/health-promotion-disease-prevention.html. Accessed 2021 Jan 27.
15.Hartmann-Boyce J, Livingstone-Banks J, Ordóñez-Mena JM, et al. Behavioural interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev. 2021;1:CD013229. Medline
16.van den Brand FA, Nagelhout GE, Winkens B, et al. Cost-effectiveness and cost-utility analysis of a work-place smoking cessation intervention with and without financial incentives. Addiction. 2020;115(3):534-545. Medline
17.Workplace electronic health promotion campaigns for substance use, gambling, and gaming prevention (CADTH reference list: summary of abstracts). Ottawa (ON): CADTH; 2021: https://cadth.ca/workplace-electronic-health-promotion-campaigns-substance-use-gambling-and-gaming-prevention-cost. Accessed 2021 Feb 1.
18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
Alternative Interventions (in-person or non-electronic)
Peik S, Schimmel E, Hejazi S. Projected return on investment of a corporate global health programme. BMC Public Health. 2019 Nov 07;19(1):1476. Medline
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitus. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca