CADTH Health Technology Review
Screening Tools for Chronic Post-Surgical Pain
Rapid Review
Authors: Charlotte Wells, Suzanne McCormack
Key Messages
Potentially relevant risk factors for the development of chronic post-surgical pain include genetics, pre-surgical pain (presence and severity), mental health, surgical techniques, type of surgery, and sex.
Tools to assess these factors may be useful for identifying patients at a higher risk of developing chronic pain post-surgery.
No relevant publications were identified demonstrating a benefit of using tools to assess the risk of chronic post-surgical pain development and improving patient outcomes. Therefore, no conclusions regarding clinical utility can be provided.
Context and Policy Issues
Chronic post-operative pain (or chronic post-surgical pain [CPSP]) is a potential long-term complication of surgical interventions. CPSP is generally defined as pain that develops after a surgical intervention, lasts greater than 2 months, interferes with quality of life, is a continuation of pain developed in the acute phase post-surgery, or develops after a period with no pain, localized to the surgical area, and is not caused by other factors.1 Prolonged post-operative pain can lead to high health care utilization and costs, poorer clinical outcomes for patients, and lower quality of life.2 Depending on which surgery is performed, the incidence of lasting chronic pain can be from 5% to 85%.3 In Ontario, chronic pain (in general) costs CA$1,742 per person in 2014 (approximately CA$10 billion per year). As CPSP is a common driver of the rates of chronic pain, CPSP contributes to a large portion of health care spending in Ontario, not including a patient’s direct or indirect out-of-pocket costs.1 Additionally, the development of CPSP is linked to higher rates of opioid consumption. Persistent opioid use is associated with higher mortality and morbidity, and patients taking opioids to help with CPSP still report moderate to severe pain, higher disability, and lower overall global health.4 As opioid use and misuse is a global epidemic, strategies to reduce the development of CPSP may lower the use of opioids for pain relief.
Risk factors for the development of CPSP can include pain before and after the operation (and severity of that pain), the type of surgery being performed, posttraumatic negative affect, and pain catastrophizing (i.e., exaggeration of a negative mental health state).1 In 1 systematic review examining factors related to the development of CPSP,5 preoperative factors that showed significant correlation with pain development were younger age (excluding pediatric patients), female sex, smoking, history of depressive or anxiety symptoms, sleep difficulties, higher body mass index, preoperative pain, and use of preoperative analgesia.6 Other suggested factors included genetics, length of surgery, and surgical techniques (e.g., type of surgical method, amount of trauma to area, and amount of tissue handling).7,8
It has been proposed that tools that are used to measure these factors may be applicable in both predicting patients who may develop chronic pain and in the prevention of chronic pain. Tools that can classify patients as a higher risk may help physicians tailor both treatment and preventive measures for these patients or may prompt them to provide more intensive care.
Validated tools to assess risk factors associated with CPSP include psychological assessments (e.g., Hospital Anxiety and Depression Scale,9 Pain Anxiety Symptoms Scale,10 Beck Depression Inventory,11 Amsterdam Preoperative Anxiety and Information Scale), pain catastrophizing (e.g., pain catastrophizing scale12), pain assessments (e.g., 6-factor risk model for CPSP13), and quality of life assessments (e.g., EuroQuol 5-Dimensions Questionnaire14). However, some models used to predict chronic pain can be narrow in that they do not include multiple surgical factors (e.g., laparoscopy versus open surgery) that can contribute to CPSP; specifically, they may not provide consistent definitions of psychosocial factors leading to CPSP and may not be fully validated in certain populations.15 Additionally, these models may be underpowered (lacking large datasets required for accuracy) and do not identify all the factors relevant to CPSP.15 With the goal of using validated tools for predicting the development of CPSP, it has been suggested that, if a patient is identified to be at high risk of developing CPSP, preventive measures could be taken. Some potential measures include providing preoperative analgesia, providing selective norepinephrine and serotonin reuptake inhibitors, using laparoscopic or less invasive surgery when possible, using regional anesthesia, and providing other pain-minimizing pharmaceuticals such as IV lidocaine, ketamine, or glucocorticoids.8
The objective of this report is to summarize evidence regarding the clinical utility of perioperative screening or prediction tools for preventing CPSP.
Research Question
What is the clinical utility of screening or prediction tools for the prevention of the progression of acute post-surgical pain to chronic postsurgical pain?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were chronic post-surgical pain and screening tools. No filters were applied to limit retrieval by study type. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2013 and December 7, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Surgical patients (any age) |
Intervention | Perioperative (i.e., preoperative, intraoperative, and post-operative) screening or prediction tools for risk factors associated with CPSP (e.g., pain-specific tools, psychological tools, health-related quality of life tools) Excluding the Minnesota Multiphasic Personality Inventory-2, Amsterdam Preoperative Anxiety and Information Scale, and quantitative sensory testing |
Comparator | Other screening tools, no screening |
Outcomes | Clinical benefits and harms of screening (e.g., development of or progression to CPSP, reduction in post-operative opioid usage or misuse, overdose and overdose-related harms, emergency room visits, hospitalization) |
Study Designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies |
CPSP = chronic post-surgical pain.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2013. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Studies examining relevant tools assessing risk factors for the development of chronic pain were excluded if clinical outcomes related to the benefits and harms of screening were not reported (e.g., if only diagnostic accuracy or prediction accuracy were reported).
Summary of Evidence
Quantity of Research Available
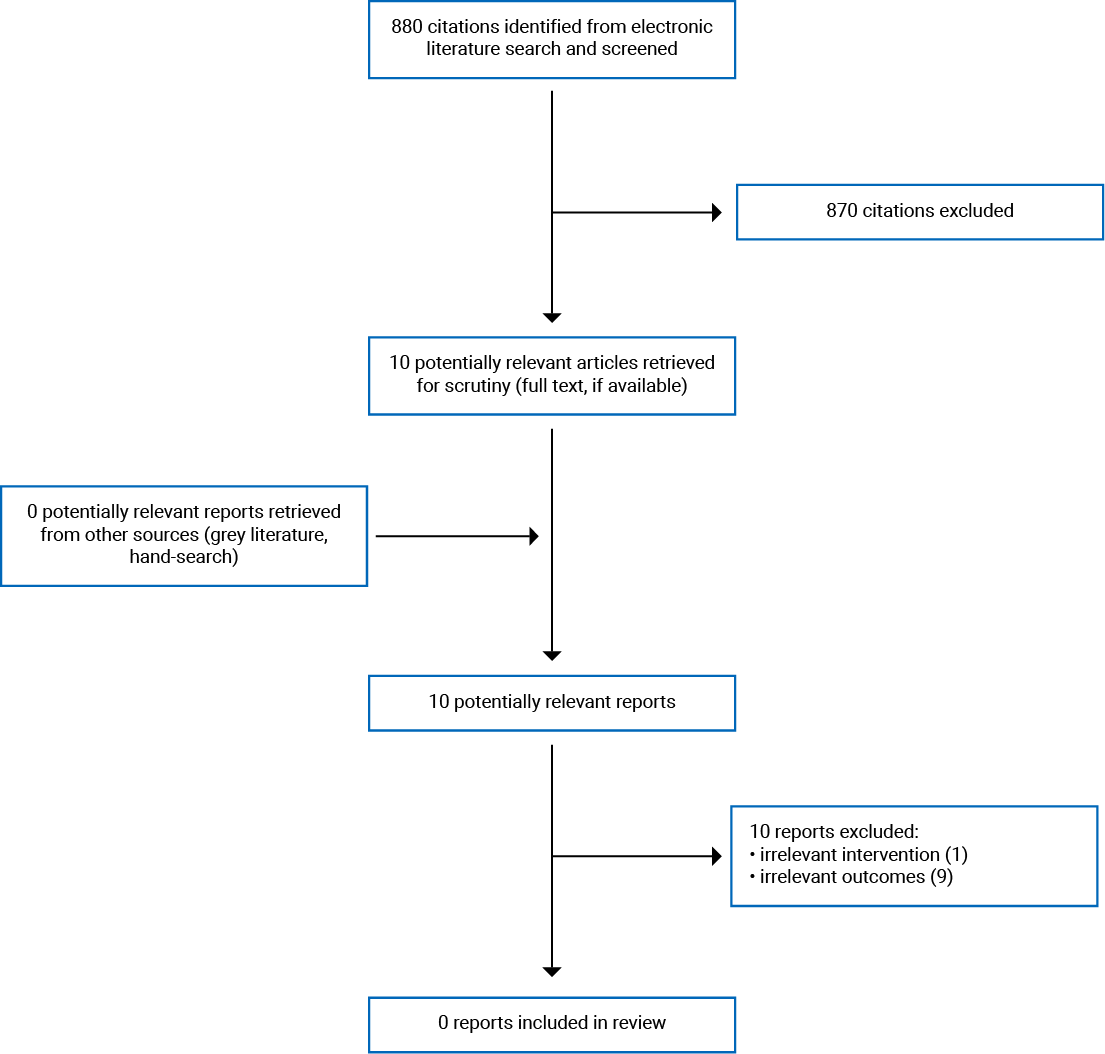
A total of 880 citations were identified in the literature search. Following the screening of titles and abstracts, 870 citations were excluded and 10 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 10 publications were excluded for various reasons and no publications met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA16 flow chart of the study selection.
Summary of Findings
Clinical Utility of Tools for Assessing the Risk of Chronic Post-Surgical Pain
No relevant publications were identified that examined the clinical utility of any tools for assessing the risk of chronic post-surgical pain development. Therefore, no summary can be provided.
Limitations
The major limitation of the body of evidence is the lack of patient-related clinical utility outcomes for preventing chronic post-surgical pain. For example, no studies were identified that examined a predictive tool that, when used, led to different care or clinical outcomes for patients.
Conclusions and Implications for Decision- or Policy-Making
Despite studies showing a potential link between some risk factors and CPSP, such as mental health state, pre-surgical pain, and pain catastrophizing,1 no evidence was identified regarding the clinical utility of tools that identify these risk factors to predict the progression to CPSP in patients assessed with those tools perioperatively.
While no relevant studies were identified for inclusion in this report, there are programs that attempt to classify patients at risk of CPSP and provide services accordingly. An example of a program used to attempt to prevent post-operative complications and chronic pain is the Transitional Pain Service at Toronto General Hospital.1 The service is an integrated and multidisciplinary team that provides treatment to patients who are at high risk of developing chronic pain post-surgery. Created in 2014, the goal is to prevent the development of CPSP, provide better access to care for patients after surgery, and minimize emergency room visits related to pain.17 Patients are assessed starting in the preoperative period by the acute pain service nurses for an individual risk of chronic pain. Referral criteria include presence of pre-surgical chronic pain, history of drug abuse, current use of opioids, presence of post-surgical pain, and current emotional distress.1 The patients deemed high risk for the development of CPSP are placed into the Transitional Pain Service and are offered psychological services (acceptance and commitment therapy), multimodal medication optimization, physical therapy, and acupuncture.1 Challenges in the implementation of the Transitional Pain Service included institutional acceptance when first delivering the program, the overwhelming numbers of referrals when the program was accepted, difficulty discharging patients (e.g., due to lack of primary care providers), and data security.1 Preliminary results show that the Transitional Pain Service may help with pain intensity and opioid use, but the specific comparisons in these studies were not relevant for this report.1
Chronic pain is a debilitating condition for many patients and is costly to both the health care system and the individual. Future research could focus on the development of an algorithm or tool to detect patients at high risk of developing CPSP and a measure of the utility of this tool (i.e., the “personal benefit” that a patient receives from an intervention, or the downstream clinical effects of using the tool). Future research could also focus on whether care decisions guided by assessment tools lead to better health outcomes for patients, such as improved quality of life.
References
1.Katz J, Weinrib AZ, Clarke H. Chronic postsurgical pain: From risk factor identification to multidisciplinary management at the Toronto General Hospital Transitional Pain Service. Can J Pain. 2019;3(2):49-58.
2.Correll D. Chronic postoperative pain: recent findings in understanding and management. F1000Res. 2017;6:1054-1054. Medline
3.Thapa P, Euasobhon P. Chronic postsurgical pain: current evidence for prevention and management. Korean J Pain. 2018;31(3):155-173. Medline
4.Huang A, Azam A, Segal S, et al. Chronic postsurgical pain and persistent opioid use following surgery: the need for a transitional pain service. Pain Manag. 2016;6(5):435-443. Medline
5.Yang MMH, Hartley RL, Leung AA, et al. Preoperative predictors of poor acute postoperative pain control: a systematic review and meta-analysis. BMJ Open. 2019;9(4):e025091. Medline
6.Schug SA, Bruce J. Risk stratification for the development of chronic postsurgical pain. Pain Rep. 2017;2(6):e627-e627. Medline
7.Bruce J, Quinlan J. Chronic Post Surgical Pain. Rev Pain. 2011;5(3):23-29. Medline
8.Al-Mahrezi A, Al-Shidhani A. Is Chronic Post-Surgical Pain Preventable? In: Shallik NA, ed. Pain Management in Special Circumstances. London: IntechOpen; 2018: https://www.intechopen.com/books/pain-management-in-special-circumstances/is-chronic-post-surgical-pain-preventable-.
9.Carreon LY, Jespersen AB, Støttrup CC, Hansen KH, Andersen MO. Is the Hospital Anxiety and Depression Scale Associated With Outcomes After Lumbar Spine Surgery? Global Spine J. 2020;10(3):266-271. Medline
10.McCracken LM, Zayfert C, Gross RT. The Pain Anxiety Symptoms Scale: development and validation of a scale to measure fear of pain. Pain. 1992;50(1):67-73. Medline
11.Marcolino JA, Mathias LA, Piccinini Filho L, Guaratini AA, Suzuki FM, Alli LA. Hospital Anxiety and Depression Scale: a study on the validation of the criteria and reliability on preoperative patients. Rev Bras Anestesiol. 2007;57(1):52-62. Medline
12.Sullivan MJL, Bishop SR, Pivik J. The Pain Catastrophizing Scale: Development and validation. Psychol Assess. 1995;7(4):524-532.
13.Montes A, Roca G, Cantillo J, Sabate S, Group GS. Presurgical risk model for chronic postsurgical pain based on 6 clinical predictors: a prospective external validation. Pain. 2020;161(11):2611-2618. Medline
14.Vartiainen P, Mäntyselkä P, Heiskanen T, et al. Validation of EQ-5D and 15D in the assessment of health-related quality of life in chronic pain. Pain. 2017;158(8). Medline
15.Fregoso G, Wang A, Tseng K, Wang J. Transition from Acute to Chronic Pain: Evaluating Risk for Chronic Postsurgical Pain. Pain physician. 2019;22(5):479-488. Medline
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
17.Mount Sinai Hospital. Transitional Pain Service. 2021; https://www.mountsinai.on.ca/care/pain-management-clinic/transitional-pain-service.
Appendix 1: Selection of Included Studies
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca