CADTH Health Technology Review
Codeine for Acute Pain Related to Caesarean Section
Rapid Review
Authors: Shannon Hill, Charlene Argáez
Abbreviations
C-section
Caesarian section
NSAID
nonsteroidal anti-inflammatory drug
RCT
randomized controlled trial
VAS
visual analogue scale
Key Messages
Caesarean section rates have increased over the past 3 decades. Caesarean section is often associated with acute post-operative abdominal pain and medications containing codeine have been used for pain management. There are concerns related to the use of codeine for this purpose, particularly regarding the potential for neonatal toxicity and opioid-related adverse events for the postpartum patient.
There is limited evidence regarding the clinical effectiveness of codeine, with or without acetaminophen or nonsteroidal anti-inflammatory drugs, in patients who have undergone Caesarean section. One randomized controlled trial found that codeine in combination with paracetamol (i.e., acetaminophen) provided better pain relief compared to paracetamol only or placebo in patients with high levels of post-Caesarean section pain. However, no difference in pain relief was observed between codeine in combination with paracetamol, paracetamol only, or placebo in patients with moderate levels of post-Caesarean section pain.
No evidence was found regarding the clinical effectiveness of codeine alone for acute pain in this specific population.
Context and Policy Issues
Caesarean section (C-section) is a method of birth through an incision in the abdominal wall and uterine wall.1,2 C-section rates have steadily increased worldwide in the last 3 decades.3 In Canada, C-section birth rates increased by approximately 50.8% from 1997 to 2016.3 C-section births may be planned or unplanned if there are complications that arise before birth or during labour.1 These complications may include an adverse position of the baby close to the due date, health conditions for the pregnant patient that may be worsened due to the stress of labour, chances of vertical transmission of a pre-existing infection to the baby, labour that is slow or stops completely, or signs of distress shown by the baby during labour.1,2 Hospital recovery after a C-section birth typically lasts 2 to 5 days; however, it may take weeks to months for a full recovery.1,2
Acute pain can be described as pain caused by something specific and does not last longer than 6 months.4 Acute pain in the abdominal region is common after a C-section birth, and pain medications containing codeine, alone or in combination with nonsteroidal anti-inflammatory drugs (NSAIDs), have been used in the past to subdue post-operative pain.5,6 Oral codeine is hepatically metabolized by the polymorphic CYP2D6 enzyme to a clinically active metabolite (i.e., morphine).7 Because of this metabolization process, oral codeine has the potential for drug interactions and adverse effects may be unpredictable due to interindividual differences in metabolism of codeine into morphine.7 In Canada, codeine-containing products are authorized to relieve pain or suppress cough; however, there may be safety issues with the use of codeine in postpartum patients.7-9 Specifically, in postpartum patients who are breastfeeding there is the potential for neonatal toxicity from prolonged codeine exposure,7,10,11 and there is the potential for central nervous system depression caused by opioid toxicity in both postpartum patients and breastfed babies.11 There are additional concerns with opioid use worldwide including inappropriate prescribing, opioid addiction and dependency, and opioid-related deaths, and Canada is the second-highest consumer of opioids.12 It is important to determine whether the clinical benefits of opioid use in patients who have undergone C-section outweigh the potential risks.
Four other CADTH reports have reviewed the clinical effectiveness of codeine with or without accompanying NSAIDs for acute pain related to osteoarthritis of the knee and hip,13 urological or general surgery,14 orthopedic surgery,15 and for acute pain in pediatric patients.16 The purpose of this report is to evaluate the clinical effectiveness of codeine with or without acetaminophen or other NSAIDs for patients with acute pain who have undergone C-section.
Research Questions
What is the clinical effectiveness of codeine for patients who underwent Caesarean section?
What is the clinical effectiveness of codeine with acetaminophen and/or a nonsteroidal anti-inflammatory drug for patients who underwent Caesarean section?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were codeine and C-section. No filters were applied to limit the retrieval to study type. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2011 and January 21, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients who underwent C-section with acute pain |
Intervention | Q1: Codeine alone Q2: Codeine with acetaminophen and/or an NSAID (e.g., acetylsalicylic acid, ibuprofen, naproxen) as single products or as combination drugs (e.g., codeine-acetaminophen-caffeine combination) |
Comparator | Other opioids (e.g., tramadol, oxycodone, morphine, hydromorphone, fentanyl), 1 or more non-opioid analgesics (e.g., acetaminophen, NSAID), other opioid combinations (e.g., oxycodone with acetaminophen), or placebo |
Outcomes | Clinical effectiveness (e.g., pain control, pain scales, health-related qualify of life), safety (e.g., overdose-related adverse events such as respiratory depression and liver toxicity, other adverse events such as constipation and risk of falls, dependence/addiction, hospitalizations, neonatal adverse events such as sleepiness and breathing difficulties in breastfed infants) |
Study Designs | HTAs, SRs, RCTs, non-randomized studies |
C-section = Caesarian section; HTA = health technology assessments; NSAID = nonsteroidal anti-inflammatory drug; Q = question; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or they were duplicate publications.
Critical Appraisal of Individual Studies
The included publication was critically appraised by 1 reviewer using the Downs and Black checklist17 as a guide. Summary scores were not calculated for the included study; rather, the strengths and limitations were described narratively.
Summary of Evidence
Quantity of Research Available
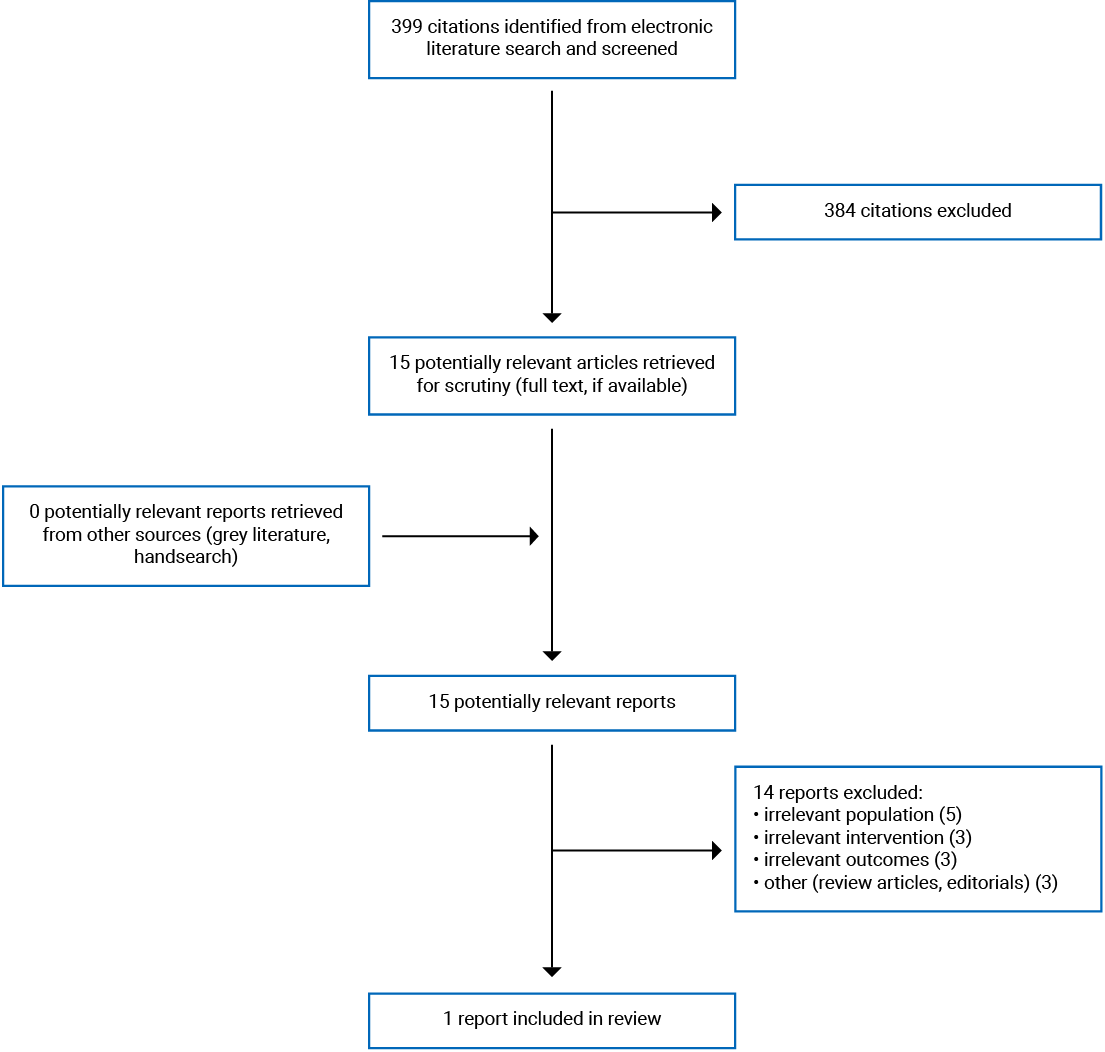
A total of 399 citations were identified in the literature search. Following the screening of titles and abstracts, 384 citations were excluded and 15 potentially relevant reports from the electronic search were retrieved for full-text review. Zero potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 14 publications were excluded for various reasons and 1 randomized controlled trial (RCT) met the inclusion criteria and was included in this report. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analysis, or PRISMA,18 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One RCT19 regarding the clinical effectiveness of codeine in combination with paracetamol (i.e., acetaminophen) for patients who underwent C-section was eligible for inclusion. Additional details regarding the characteristics of the included publication are provided in Appendix 2.
Study Design
One randomized, prospective, double-blind, single oral dose, parallel group study19 published in 1996 was included regarding the clinical effectiveness of codeine in combination with paracetamol for patients who underwent C-section.
Country of Origin
The included RCT19 was conducted in Norway.
Patient Population
The RCT19 recruited patients undergoing planned C-section surgery. Patients were included in the analysis if they reported moderate or strong pain intensity in the abdominal wound area at rest or with slight movement after surgery.19 Patients were grouped according to their pain levels at baseline for analysis as those with “strong baseline pain” or “moderate baseline pain.”
Interventions and Comparators
The RCT19 compared the use of submaximal paracetamol (800 mg) combined with a standard dose of codeine (60 mg) with maximally recommended paracetamol (1,000 mg) or placebo. The intervention and comparators were administered 1 or 2 days after patients underwent C-section surgery when oral medication was appropriate.19 The length of follow-up for patients included in the analysis was up to 6 hours after the intervention was initially administered.19
Outcomes
The relevant outcomes in the included RCT19 were differences in pain intensity and pain relief after treatment. Pain intensity and pain relief were measured at baseline and at 0.5, 1, 2, 3, 4, 5, and 6 hours after treatment. Pain intensity was measured using a visual analogue scale (VAS) from 0 mm (no pain) to 100 mm (unbearable pain). “Moderate pain” intensity was described as pain between 40 mm and 60 mm using the VAS. “Strong pain” intensity was described as pain over 60 mm using the VAS.19 Changes in pain intensity over time were reported as “time-weighted summed pain intensity differences” at 3 hours and 6 hours following treatment; however, how these values were calculated, and their clinical interpretation, was unclear.
Pain relief was measured using a 5-point verbal categorical scale from 0 (no relief) to 4 (total relief). “Time-weighted total pain relief” during the first 3 hours and 6 hours after treatment was reported as a measure of total pain relief over time; however, how these values were calculated, and their clinical interpretation, was unclear.
Summary of Critical Appraisal
The critical appraisal of the included RCT19 identified some strengths. The authors of the included RCT clearly described the aim, objective, inclusion and exclusion criteria, patient characteristics, process of randomization, intervention and comparators, and the main findings of the study. Additionally, the statistical analyses used to assess the main outcomes were appropriate and well-described, and patient adherence to the study intervention was likely reliable, as treatment was administered directly to patients post-C-section.19 Patients who were excluded from the analysis were reported and reasons for exclusion were provided that indicated that patient exclusion was unlikely to have systematically biased the results. Specifically, 17 out of 125 patients were excluded from the study before the opening of the randomization code and analyzing the effects (7, 6, and 4 from the codeine and paracetamol, paracetamol only, and placebo groups, respectively).19 Reasons for exclusion were: insufficient time elapsed since last analgesic medication and treatment, pain intensity at the time of treatment was less than the moderate threshold, and various other minor protocol violations.19
The critical appraisal of the included RCT19 also identified some limitations. These limitations included a lack of detail in the description of the recruitment process (e.g., where patients were recruited and the time period of recruitment), which may impact the external validity of the study.19 Additionally, patient eligibility was determined based on self-reported pain levels (i.e., moderate to strong pain) and the generalizability of the findings is unclear.19 It was unclear how the main outcomes (i.e., summed pain intensity differences and total pain relief) were calculated and it was not possible to evaluate their clinical relevance.
Additional details regarding the strengths and limitations of included publication are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Codeine in Combination With Paracetamol
Pain Intensity Difference
The included RCT19 measured the difference in pain intensity at 3 hours and 6 hours after treatment compared to baseline for patients who underwent C-section. Among patients who had strong pain at baseline, those who received codeine and paracetamol had a significantly greater reduction in pain intensity at 3 hours and 6 hours after treatment compared to those who received paracetamol alone or placebo.19 Among patients who had moderate pain at baseline, there were no significant differences between treatment groups in pain intensity from baseline to 3 hours or 6 hours after treatment.19 These findings suggest that codeine with paracetamol was better at reducing pain intensity compared to paracetamol only or placebo for patients with strong pain at baseline after undergoing C-section, but not in patients with moderate pain at baseline after undergoing C-section.19
Total Pain Relief
Total pain relief at 3 hours and 6 hours after treatment was also measured in the included RCT.19 Among patients who had strong pain at baseline, those who received codeine and paracetamol had significantly greater total pain relief at 3 hours and 6 hours after treatment compared to patients who received paracetamol only or placebo.19 Among patients who had moderate pain at baseline, those who received codeine and paracetamol had no significant difference in total pain relief at 3 hours and 6 hours after treatment compared to patients who received paracetamol only or placebo.19 The findings suggest that codeine with paracetamol provided the most pain relief compared to paracetamol only or placebo for patients who had strong pain at baseline after undergoing C-section, but not for patients with moderate pain at baseline after undergoing C-section.19
Adverse Events
The authors of the included RCT19 also provided findings on patient-reported adverse events. In total, 21 out of 125 patients reported adverse events of slight to moderate degrees.19 This included 10 patients who received codeine and paracetamol, 10 patients who received paracetamol only, and 1 patient who received the placebo.19 The reported adverse events included sweating, drowsiness, nausea, and dizziness. There were no significant differences in incidence or type of adverse events between intervention groups.19
Limitations
Only 1 study19 was included in this Rapid Response report. The study was published in 1996 and may have limited relevance to the current context. There is a lack of recent primary studies related to the use of codeine, alone or in combination with other NSAIDs, for the management of acute pain for patients who have undergone C-section. The included study also only provided follow-up for 6 hours after patients were given codeine and paracetamol, which does not provide any indication of the long-term implications related to codeine and paracetamol use for C-section patients or their babies. Additionally, the study compared codeine in combination with paracetamol to paracetamol alone or placebo; no evidence was found regarding the use of codeine alone for patients who underwent C-section.
Conclusions and Implications for Decision- or Policy-Making
This report provides a summary of the limited available evidence regarding the clinical effectiveness of codeine for patients with acute pain following C-section surgery. One relevant RCT19 was identified that compared the use of standard dose codeine plus submaximal paracetamol (i.e., acetaminophen) to maximally recommended paracetamol or a placebo for the management of acute pain in patients who underwent planned C-section surgery. Pain management was measured by pain intensity differences and total pain relief from baseline to up to 6 hours after treatment.19 Overall, the group that reported strong baseline pain and received codeine with paracetamol had a significantly greater reduction in pain intensity and significantly greater total pain relief compared to patients who received paracetamol only or placebo.19 There was no significant difference in pain intensity differences or total pain relief between treatments in patients who reported moderate pain at baseline. Additionally, 21 out of 125 patients within the study reported “slight to moderate” adverse events such as sweating, drowsiness, nausea, and dizziness.19 However, adverse events were not significantly difference between intervention groups.
The included RCT19 provided low-quality evidence regarding the clinical effectiveness of codeine plus paracetamol to manage acute pain in patients who underwent C-section; however, the findings were published in 1996 and may have limited applicability to the current health care context. The authors of the included RCT19 concluded that codeine plus paracetamol may be an effective treatment for severe acute pain in patients who underwent C-section, but current knowledge of opioid-related adverse events may also warrant consideration when selecting pain management options for this population in current practice.11,12
References
1.Healthwise. Caesarean section. 2019; https://www.healthlinkbc.ca/health-topics/tn8162. Accessed 2021 Feb 12.
2.Mount Sinai Hospital. Caesarean section. 2021; https://www.mountsinai.on.ca/care/cs. Accessed 2021 Feb 12.
3.Gu J, Karmakar-Hore S, Hogan ME, et al. Examining caesarean section rates in Canada using the modified Robson classification. J Obstet Gynaecol Can. 2020;42(6):757-765. Medline
4.Cleveland Clinic. Acute vs. chronic pain. 2020; https://my.clevelandclinic.org/health/articles/12051-acute-vs-chronic-pain. Accessed 2021 Feb 12.
5.Kelly LE, Chaudhry SA, Rieder MJ, et al. A clinical tool for reducing central nervous system depression among neonates exposed to codeine through breast milk. PLoS One. 2013;8(7):e70073. Medline
6.Niklasson B, Arnelo C, Ohman SG, Segerdahl M, Blanck A. Oral oxycodone for pain after caesarean section: a randomized comparison with nurse-administered IV morphine in a pragmatic study. Scand J Pain. 2015;7(1):17-24. Medline
7.Mariano ER. Management of acute perioperative pain. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2020: www.uptodate.com. Accessed 2021 Feb 22.
8.Health Canada. Prescription cough and cold products containing opioids and the risk of opioid use disorder in children and adolescents (< 18 years of age). 2020; https://healthycanadians.gc.ca/recall-alert-rappel-avis/hc-sc/2020/73741a-eng.php#:~:text=Currently%20in%20Canada%2C%20codeine%2Dcontaining,authorized%20for%20cough%20suppression%20only. Accessed 2021 Feb 18.
9.Health Canada. Non-prescription pain relief products containing codeine are not recommended for use in people under 18 years of age. 2020; https://healthycanadians.gc.ca/recall-alert-rappel-avis/hc-sc/2020/73635a-eng.php. Accessed 2021 Feb 18.
10.Juurlink DN, Gomes T, Guttmann A, et al. Postpartum maternal codeine therapy and the risk of adverse neonatal outcomes: a retrospective cohort study. Clin Toxicol. 2012;50(5):390-395. Medline
11.Canadian guideline for safe and effective use of opioids for chronic non-cancer pain. San Francisco (CA): National Opioid Use Guideline Group (NOUGG); 2010: https://nationalpaincentre.mcmaster.ca/documents/opioid_guideline_part_b_v5_6.pdf. Accessed 2021 Feb 18.
12.Centre for Addiction and Mental Health (CAMH). Canada needs national plan to combat opioid epidemic. 2021; https://www.camh.ca/en/camh-news-and-stories/canada-needs-national-plan-to-combat-opioid-epidemic. Accessed 2021 Feb 12.
13.Codeine for pain related to osteoarthritis of the knee and hip: a review of clinical effectiveness (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/pdf/htis/2020/RC1323%20Codeine%20for%20Osteoarthritis%20Pain%20Final.pdf. Accessed 2021 Feb 12.
14.Codeine for acute pain for urological or general surgery patients: a review of clinical effectiveness (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1201%20Codeine%20for%20Urological%20Pts%20Final.pdf. Accessed 2021 Feb 12.
15.Codeine for acute pain in patients undergoing orthopedic surgery: a review of clinical effectiveness (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1199%20Codeine%20for%20Orthopaedic%20Pts%20Final.pdf. Accessed 2021 Feb 12.
16.Codeine for pediatric patients with acute pain: a review of clinical effectiveness (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1200%20Codeine%20for%20Pediatric%20Patients%20Final.pdf. Accessed 2021 Feb 12.
17.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. Medline
18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
19.Bjune K, Stubhaug A, Dodgson MS, Breivik H. Additive analgesic effect of codeine and paracetamol can be detected in strong, but not moderate, pain after caesarean section. Baseline pain-intensity is a determinant of assay-sensitivity in a postoperative analgesic trial. Acta Anaesthesiol Scand. 1996;40(4):399-407. Medline
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design, setting, objective | Population characteristics | Intervention and comparator(s) | Clinical outcome(s), length of follow-up |
Bjune et al. (1996)19 Norway Funding Source: Weiders Farmasøytiske A/S | Study Design: Randomized prospective, double-blind, single oral dose, parallel group study Setting: Post-surgery, inpatient care Objective: To determine if submaximal paracetamol combined with a standard dose of codeine is at least as effective as maximally recommended paracetamol for pain relief after C-section | Inclusion criteria:Patients with moderate (40 mm ≤ VAS ≤ 60 mm) or strong (VAS ≥ 60 mm) pain intensity in the abdominal wound area were included on the first or second day after C-section, when oral medication was appropriate Exclusion criteria:Patients with severe preeclampsia; whose children were nursed in the NICU; known sensitivity to paracetamol or codeine; gestational pelvic pain; or on regular analgesic medication Total, n= 108a
| Intervention: Combination of paracetamol (800 mg) plus codeine (60 mg) Comparators: Paracetamol (1,000 mg) or placebo | Outcome: Pain intensity and pain relief Pain intensity was measured using a VAS from 0 (no pain) to 100 (unbearable pain); pain relief was measured using a 5-point verbal categorical scale from 0 (no relief) to 4 (total relief) Length of follow-up: Measurements were recorded at 0.5, 1, 2, 3, 4, 5, and 6 hours after treatment |
C-section = Caesarian section; N = number; NICU = neonatal intensive care unit; VAS = visual analogue scale.
aSeventeen out of 125 patients were excluded before the opening of the randomization code and analyzing of effects.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Clinical Study Using the Downs and Black checklist17
Strengths | Limitations |
Bjune et al. (1996)19 | |
|
|
C-section = Caesarian section; IQR = interquartile range.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Included Primary Clinical Study
Bjune et al. (1996)19
Main study findings
Median pain intensity difference for patients with strong baseline pain (VAS ≥ 60 mm) at 3 hours and 6 hours after initial drug intake
Paracetamol + codeine group (n = 21), median (interquartile range [IQR]):
Summed pain intensity differences at 3 hours (SPID3h) = 108 (27, 126)
Summed pain intensity differences at 6 hours (SPID6h) = 184 (84, 243)
Paracetamol group (n = 26), median (IQR):
SPID3h = 36 (12, 65)
SPID6h = 78 (30, 175)
Placebo group (n = 12), median (IQR):
SPID3h = −2.5 (−18, 3)
SPID6h = −7.5 (−42, 2.75)
P value for SPID3h outcome between groups:
All groups = 0.0002
Paracetamol + codeine vs. placebo group = 0.0002
Paracetamol + codeine vs. paracetamol group = 0.02
Paracetamol vs. placebo group = 0.005
P value for SPID6h outcome between groups:
All groups = 0.0004
Paracetamol + codeine vs. placebo group = 0.0007
Paracetamol + codeine vs. paracetamol group = 0.04
Paracetamol vs. placebo group = 0.002
Median pain intensity difference for patients with moderate baseline pain (40 mm ≤ VAS ≤ 60 mm) at 3 hours and 6 hours after initial drug intake
Paracetamol + codeine group (n = 23), median (IQR):
SPID3h = 24 (−11, 92)
SPID6h = 37 (−27, 132)
Paracetamol group (n = 17), median (IQR):
SPID3h = 29 (2, 64)
SPID6h = 60 (−18, 120)
Placebo group (n = 9), median (IQR):
SPID3h = 17 (6, 29)
SPID6h = 10 (1, 96)
P value for SPID3h outcome between groups:
All groups = NS
P value for SPID6h outcome between groups:
All groups = NS
Median total pain relief for patients with strong baseline pain (VAS ≥ 60mm) at 3 hours and 6 hours after initial drug intake
Paracetamol + codeine group (n = 21), median (IQR):
Total pain relief at 3 hours (TOTPAR3h) = 6.5 (4.5, 7.5)
Total pain relief at 6 hours (TOTPAR6h) = 10.5 (7.5, 11.5)
Paracetamol group (n = 26), median (IQR):
TOTPAR3h = 3.8 (1.5, 5.5)
TOTPAR6h = 6.4 (2.5, 13)
Placebo group (n = 12), median (IQR):
TOTPAR3h = 0 (0, 0.3)
TOTPAR6h = 0 (0, 0)
P value for TOTPAR3h outcome between groups:
All groups = 0.002
Paracetamol + codeine vs. placebo group = 0.001
Paracetamol + codeine vs. paracetamol group = 0.02
Paracetamol vs. placebo group = 0.003
P value for TOTPAR6h outcome between groups:
All groups = 0.002
Paracetamol + codeine vs. placebo group = 0.001
Paracetamol + codeine vs. paracetamol group = 0.4
Paracetamol vs. placebo group = 0.003
Median pain intensity difference for patients with moderate baseline pain (40 mm ≤ VAS ≤ 60mm) at 3 hours and 6 hours after initial drug intake
Paracetamol + codeine group (n = 23), median (IQR):
TOTPAR3h = 4 (1.5, 6.5)
TOTPAR6h = 6.5 (2, 12.5)
Paracetamol group (n = 17), median (IQR):
TOTPAR3h = 3 (1.5, 6.5)
TOTPAR6h = 8 (2, 11.5)
Placebo group (n = 9), median (IQR):
TOTPAR3h = 1.5 (1, 2)
TOTPAR6h = 1.5 (1, 8)
P value for TOTPAR3h outcome between groups:
All groups = NS
P value for TOTPAR6h outcome between groups:
All groups = NS
Adverse events
Paracetamol + codeine group (n = 50):
Reported side effect (n) = 10
Type of adverse effect (n):
Sweating = 7
Drowsiness = 2
Nausea = 2
Dizziness = 0
Paracetamol group (n = 50):
Reported side effect (n) = 10
Type of adverse effect (n):
Sweating = 8
Drowsiness = 3
Nausea = 1
Dizziness = 2
Placebo group (n = 25):
Reported side effect (n) = 1
Type of adverse effect (n):
Sweating = 1
Drowsiness = 0
Nausea = 0
Dizziness = 0
P value for all reported adverse events between groups was NS
Authors’ conclusion
“In conclusion, in patients with strong baseline pain (VAS>60 / 100) after Caesarean section, the combination of paracetamol 800 mg + codeine 60 mg was significantly superior to paracetamol 1000 mg, both of which were superior to placebo, in all efficacy variables of pain relief after Caesarean section. In patients with moderate baseline pain (40<VAS<60), there was no difference between the three study drugs in any of the efficacy variables (p. 406).”19
Appendix 5: References of Potential Interest
Previous CADTH Reports
1.Codeine for acute pain: a synopsis of the evidence. Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/codeine_actute_pain_evidence_synopsis.pdf. Accessed 2021 Feb 12.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca