CADTH Reimbursement Review
Brexucabtagene Autoleucel (Tecartus)
Sponsor: Gilead Sciences Canada, Inc.
Therapeutic area: Mantle cell lymphoma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Clinical Review
Abbreviations
AE
adverse event
BOR
best objective response
BTK
Bruton tyrosine kinase
CAR
chimeric antigen receptor
CCO
Cancer Care Ontario
CI
confidence interval
CNS
central nervous system
CR
complete response
CRS
cytokine release syndrome
DOR
duration of response
DSMB
data and safety monitoring board
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EQ-5D
EuroQol 5-Dimensions questionnaire
EQ VAS
EuroQol Visual Analogue Scale
FAS
full analysis set
HR
hazard ratio
HRQoL
health-related quality of life
hyper-CVAD
cyclophosphamide, vincristine, doxorubicin, and dexamethasone alternating with high-dose methotrexate and cytarabine
IAS
inferential analysis set
ICU
intensive care unit
ITC
indirect treatment comparison
IWG
International Working Group
MAIC
matching-adjusted indirect comparison
MCL
mantle cell lymphoma
MIPI
Mantle Cell Lymphoma International Prognostic Index
mITT
modified intention to treat
ORR
objective response rate
OS
overall survival
PAG
Provincial Advisory Group
PFS
progression-free survival
PR
partial response
R-BAC
rituximab, bendamustine, and cytarabine
R-CHOP
rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone
R-DHA
rituximab, dexamethasone, and cytarabine
R-DHAP
rituximab, dexamethasone, cytarabine, and cisplatin
R-iBVD
rituximab, bendamustine, bortezomib, and dexamethasone
R/R
relapsed or refractory
SAE
serious adverse event
SCT
stem cell transplant
TEAE
treatment-emergent adverse event
VR-CAP
bortezomib, rituximab, cyclophosphamide, doxorubicin, and prednisone
WBC
white blood cell
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Brexucabtagene autoleucel (Tecartus) cell suspension in a patient-specific single infusion bag for IV use at a target dose of 2 × 106 chimeric antigen receptor T cells per kilogram |
Indication | TECARTUS is a CD19-directed genetically modified autologous T-cell immunotherapy indicated for:
|
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | June 8, 2021 |
Sponsor | Gilead Sciences Canada, Inc. |
NOC = Notice of Compliance.
Introduction
Mantle cell lymphoma (MCL) is an aggressive subtype of B-cell non-Hodgkin lymphoma that develops in the outer edge of a lymph node (i.e., the mantle zone) and is defined by the overexpression of cyclin D1 due to translocation (11;14)(q13;q32), making up less than 10% of all non-Hodgkin lymphoma diagnoses.1-7 Mantle cell lymphoma primarily affects men and is usually diagnosed in patients older than 60 years.5,6 Canadian-specific incidence and prevalence estimates of MCL are limited; however, it is estimated that 500 to 600 new cases of MCL are diagnosed each year.8,9 Patients are most often diagnosed with advanced stage disease, showing generalized lymphadenopathy and extranodal involvement of the blood, bone marrow, spleen, and gastrointestinal tract, resulting in swollen painless lymph nodes, headache, weakness, loss of appetite, nausea and/or vomiting, abdominal pain or bloating, fatigue, and general B symptoms including fever, weight loss, and night sweats.4,5 Diagnosis is confirmed by lymph node or bone marrow biopsy with immunohistochemistry or flow cytometry showing the presence of B-cell surface markers (CD20, CD19, CD5), cyclin D1 protein overexpression, t(11;14) translocation, or overexpression of the SOX11 transcription factor.2,4,8
Despite frequent diagnoses at the advanced stage, front-line treatments are generally associated with high response rates (objective response rate [ORR] = 95%; complete response [CR] = 53%) and extension of survival10-14; however, most patients will eventually relapse and require further therapy, generally with shorter periods of remission for each subsequent line of therapy.15 Front-line treatment consists of chemoimmunotherapy with a rituximab-containing regimen (rituximab, dexamethasone, and cytarabine [R-DHA]; rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone [R-CHOP] or rituximab, dexamethasone, cytarabine, and cisplatin [R-DHAP]; Nordic regimen; cyclophosphamide, vincristine, doxorubicin, and dexamethasone alternating with high-dose methotrexate and cytarabine [hyper-CVAD] plus rituximab; rituximab, bendamustine, and cytarabine [R-BAC]; bortezomib, rituximab, cyclophosphamide, doxorubicin, and prednisone [VR-CAP]; or bendamustine plus rituximab), followed by autologous stem cell transplant (SCT) in younger, fit patients. In patients not fit for SCT, chemoimmunotherapy and rituximab maintenance are the only treatment options in the first line.16 There is no established standard of care for patients in the relapsed or refractory (R/R) setting, and treatment options are based on prior therapies and response to treatment.9 Further treatment options for patients who experience a short response to prior treatment include additional chemoimmunotherapy or a Bruton tyrosine kinase (BTK) inhibitor or ibrutinib or acalabrutinib.16 Response to BTK inhibitors is associated with decreased efficacy in patients who have received more prior lines of therapy. Following failure of BTK inhibitors in the second line, treatment options consist of re-treatment with previously unused chemoimmunotherapy, BTK inhibitor, or palliative care.16
Brexucabtagene autoleucel (Tecartus) is a single-dose, autologous T-cell product manufactured from patients’ individual leukapheresis material. Brexucabtagene autoleucel was submitted as a priority review for a new drug (cell therapy) with pre–Notice of Compliance status (Notice of Compliance received on June 8, 2021). The objective of this report was to perform a systematic review of the beneficial and harmful effects of brexucabtagene autoleucel cell suspension in a patient-specific single infusion bag for IV infusion, with a target of 2 × 106 chimeric antigen receptor (CAR) T cells per kilogram per the Health Canada indication for the treatment of adult patients with R/R MCL after 2 or more lines of systemic therapy including a BTK inhibitor
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One patient group, Lymphoma Canada, provided input for the review of brexucabtagene autoleucel, based on information gathered through an anonymous online survey of patients with MCL that was circulated between October 2020 and January 2021. Thirty-three patients provided input on their experience with MCL.
Patients reported that the symptoms of MCL — such as enlarged lymph nodes, fatigue, gastrointestinal symptoms, aches and pains, and high or low white blood cell (WBC) count — had the greatest impact on their quality of life and affected their ability to travel, exercise, concentrate, perform daily activities like household chores, and perform regular duties like work or volunteering. Patients’ mental and emotional well-being was negatively impacted, and many patients experienced stress, anxiety or worry, and difficulty sleeping.
All patients surveyed rated faster remission and longer life as the most important outcomes for a new therapy. Other important outcomes included control of disease and symptoms, improved quality of life, and improved blood counts. Having choice in their treatment selection was rated as very important, with a large majority of patients agreeing that there is a need for more effective therapy options.
Most patients would accept a treatment with known and potentially serious adverse effects if it was recommended by their doctor. The majority of patients were willing to tolerate adverse effects of a new treatment if they were short-term.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Clinical experts came to the consensus that at the time of relapse or failure of BTK inhibitor, patients have a short duration of response and a poor life expectancy of around 6 months, and therefore new treatments that provide durable responses are needed for this population. The experts agree that the population eligible for treatment with brexucabtagene autoleucel would be small and would reflect the inclusion criteria of patients in the pivotal trial. Brexucabtagene autoleucel would be used post-ibrutinib or in those who are intolerant of ibrutinib. This would also include anyone with a suboptimal response to ibrutinib or acalabrutinib. Clinical experts agreed that if a patient starting BTK inhibitor therapy is a potential candidate for brexucabtagene autoleucel, this should be considered early, as once response to BTK inhibitors is lost, patients will rapidly deteriorate. Experts agreed that R/R MCL patients who have previously received chemoimmunotherapy and a BTK inhibitor and have a suitable Eastern Cooperative Oncology Group Performance Status (ECOG PS) (0 to 2) and adequate organ function would be readily available to receive this treatment, with no specific subgroups that would likely benefit more at this time.
Clinical experts agree that patients eligible for treatment would be identified by the treating specialist in hematology or oncology at the time of first relapse of MCL and that patients should be prioritized based on individual need, with those progressing on BTK inhibitors being higher need than those currently stable or responding to BTK inhibitor treatment. Experts believe that the least suitable patients for brexucabtagene autoleucel would be patients with a very high disease burden that is rapidly progressing and those who cannot tolerate further chemoimmunotherapy therapy, those with a poor performance status, and those with multiple comorbidities.
The clinical experts noted that in clinical practice, a combination of clinical exam, bloodwork (complete blood count and lactate dehydrogenase), and imaging (CT/PET) would be used to assess response to therapy, and response would be followed up post-infusion at 1 month and 3 months, and then as needed. Given that brexucabtagene autoleucel is a single-dose treatment, clinical experts stated that discontinuation is not possible, and any patients for whom the drug has been manufactured but who experience rapid decline would not receive treatment.
Clinician Group Input
Two physician groups provided input for this submission: the Ontario Health (Cancer Care Ontario [CCO]) Hematology Disease Site Drug Advisory Committee and a group of 7 lymphoma experts in Canada whose input was coordinated by Lymphoma Canada.
The experts noted that the current data support the role of this therapy as a single agent in patients treated with multiple therapies who have disease progression following primary chemoimmunotherapy and BTK inhibitor therapy. Brexucabtagene autoleucel would replace treatment options in the third line or later, including palliative chemotherapy; intensive chemotherapy or experimental treatments for select patients; or SCT in young, fit patients.
Drug Program Input
The Provincial Advisory Group (PAG) provided questions considered important for decision-making:
Are there specific subgroups of patients with R/R MCL who are more or less likely to benefit from brexucabtagene autoleucel?
If there is limited capacity to offer this treatment, how would you prioritize which patients should be offered brexucabtagene autoleucel? How would you select which ones should be treated in Canada versus out of country?
Is there evidence to support re-treatment with brexucabtagene autoleucel for R/R MCL if a patient responds then subsequently relapses or if the initial response is suboptimal?
PAG seeks guidance on the provision of brexucabtagene autoleucel in patients whose central nervous system (CNS) lymphoma or viral infection is being actively treated.
The clinical experts consulted by CADTH stated that the characteristics of patients who should receive brexucabtagene autoleucel align with the approved indication. With regard to capacity, the clinical experts stated that patients would likely remain treated in their home province, but, for those who want to receive treatment elsewhere, the decision would be made on a case-by-case basis. PAG identified a potential time-limited need to cover brexucabtagene autoleucel in patients who are on other therapies for R/R MCL, including immunochemotherapies and salvage chemotherapy, and would like confirmation that patients who are doing well on these therapies should not be switched to CAR T-cell therapy. If switching is an option, PAG would like to understand under what circumstances it would be preferred as opposed to waiting until disease progression. The clinical experts consulted by CADTH stated that there are currently no data available to suggest re-treatment or sequencing of treatment for brexucabtagene autoleucel; however, switching would not be warranted unless there was disease progression on a patient’s current therapy.
PAG noted the potential for “indication creep” in the use of brexucabtagene autoleucel in first-line treatment for MCL and in B-cell non-Hodgkin lymphomas or leukemias for which CAR T-cell therapy is not available. PAG also noted there may be creep to patients who have stable disease or partial response (PR) to prior therapies or who are at high risk of early relapse. Since the Health Canada–approved indication includes prior BTK inhibitor therapy as a requirement, treating patients who have not received this prior therapy would be considered indication creep. Experts agreed that indication creep is a possibility; however, there is currently no evidence for treatment in patients who are BTK inhibitor naive, and the place in therapy may change as more data become available.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
The ZUMA-2 study was a phase II, multi-centre, single-arm, open-label study evaluating the efficacy and safety of brexucabtagene autoleucel at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram (with a maximum dose of 2 × 108 anti-CD19 CAR T cells for patients more than 100 kg) in patients with R/R MCL whose disease had progressed on anthracycline- or bendamustine-containing chemotherapy, an anti-CD20 antibody, and a BTK inhibitor (ibrutinib and/or acalabrutinib). Eligible patients were adults (≥ 18 years) with pathologically confirmed MCL and documentation of either cyclin D1 overexpression or presence of t(11;14) that is relapsed or refractory, as defined by disease progression after the last regimen, or failure to achieve PR or CR to the last regimen. Patients should have received up to 5 prior treatment regimens that must have included all of the following: anthracycline or bendamustine-containing chemotherapy, anti-CD20 antibody, and ibrutinib or acalabrutinib. The primary objective of the ZUMA-2 study was ORR, defined as a CR or PR using central assessment per the Lugano classification.17 Key secondary outcomes included best objective response (BOR), duration of response (DOR), progression-free survival (PFS), overall survival (OS), and health-related quality of life (HRQoL). Harms evaluated included adverse events (AEs), including those of special interest to this review, such as cytokine release syndrome (CRS) and neurologic AEs.18
Seventy-four patients were enrolled and leukapheresed. Sixty-nine patients received lymphodepleting chemotherapy, and 68 patients received brexucabtagene autoleucel, making up the modified intention-to-treat (mITT) and safety populations. Of the patients who received brexucabtagene autoleucel, 38% received bridging therapy. The most commonly administered bridging therapies were ibrutinib (n = 14 [21%]) and dexamethasone (n = 12 [18%]). Patients in the full analysis set (FAS) were leukapheresed a median of 16.0 days (range = 5 days to 274 days) after study screening, and the median time from screening to leukapheresis was also 16.0 days (range = 5 days to 274 days). The median time from leukapheresis to administration of brexucabtagene autoleucel was 27.0 days (range = 19 days to 134 days).18
The median age of included patients was 65.0 years (range = 38 years to 79 years), and the majority of patients were male (84%) and White (93%). Fifty-five patients (81%) had received 3 or more prior regimens. Twenty-nine patients (43%) relapsed after prior autologous SCT; the remaining patients had either relapsed after their last therapy for MCL (n = 12 [18%]) or were refractory to their last therapy for MCL (n = 27 [40%]).
Efficacy Results
The ORR in the inferential analysis set (IAS) at the primary data cut-off (July 24, 2019) was 93% (95% confidence interval [CI], 83.8% to 98.2%), which was significantly higher than the pre-specified historical control rate of 25% (P < 0.0001), and the CR rate was 67% (95% CI, 53.3% to 78.3%). As of the December 31, 2019, data cut-off, the ORR was 92% (95% CI, 81.6% to 97.2%), which was also higher than the historical control (P < 0.0001), and the proportion of patients with CR was 67% (95% CI, 53.3% to 78.3%). The median time to CR or PR using the Lugano classification was 1.0 month (range = 0.8 months to 3.1 months), and the median time to achieve a CR was 3.0 months (range = 0.9 months to 9.3 months).
As of the July 24, 2019, data cut-off, and with a median follow-up time for DOR of 8.6 months, the median DOR was not reached (95% CI, 8.6 months to not estimable). At the December 31, 2019, data cut-off, with a median follow-up time for DOR of 14.1 months, the median DOR was also not reached (95% CI, 13.6 months to not estimable).
As of the July 24, 2019, data cut-off (12.3 months follow-up), the median PFS in the IAS was not reached (95% CI, 9.2 to not estimable). Kaplan–Meier estimates of PFS rates at 6 months and 12 months were 77.0% and 60.9%, respectively. As of the updated analysis, the median PFS was also not reached (95% CI, 9.6 to not estimable), with a median follow-up of 16.8 months.
The median OS was not reached (95% CI, 24.0 to not estimable) as of the July 24, 2019, data cut-off (12.3 months follow-up). The OS rates at 6 and 12 months were 86.7% and 83.2%, respectively. At the December 31, 2019, data cut-off, the median OS was not reached (95% CI, not estimable to not estimable), and the OS rates at 6 and 12 months were identical to those at the primary data cut-off.
Harms Results
At least 1 treatment-emergent adverse event (TEAE) was reported in all patients in the safety analysis set, of which 99% had AEs that were Grade 3 or higher. Eleven patients (16%) had Grade 3 TEAEs, 52 patients (76%) had Grade 4 TEAEs, and 4 patients (6%) had Grade 5 TEAEs. The most common Grade 3 or higher AEs were anemia and decreased neutrophil count (50%) and decreased WBC count (40%).
Serious AEs were recorded for 68% of patients. The most common serious AEs (SAEs)were encephalopathy and pyrexia (22% each), followed by hypotension (16%). The most common Grade 3 or higher SAEs were encephalopathy (18%) and hypotension and hypoxia (12% each). Two patients had Grade 5 SAEs of B-cell lymphoma and died due to disease progression. In general, the incidence of SAEs was slightly lower in the updated analysis. The most common Grade 3 or higher SAEs were encephalopathy (16%), pneumonia (which increased to 13% from 7%), and hypotension (12%).
As of the December 31, 2019, data cut-off, 18 patients had died: 16 (24%) due to progressive disease and 2 related to AEs (organizing pneumonia and staphylococcal bacteremia, both deemed related to lymphodepleting chemotherapy). Most deaths occurred more than 3 months after brexucabtagene autoleucel infusion (14 of 18 deaths).
Notable harms identified in the protocol of this review were CRS, which was reported in 62 patients (91%). The most common Grade 3 or higher CRS symptoms were hypotension (25%), hypoxia (19%), and pyrexia (11%). The median time to onset of CRS was 2 days following brexucabtagene autoleucel infusion, and it lasted a median of 11 days (range = 1 day to 50 days). As of the July 24, 2019, data cut-off, CRS had resolved in all 62 patients.
Neurologic AEs of any grade occurred in 43 patients (63%). The most common Grade 3 or higher neurologic events were encephalopathy (19%), confusional state (12%), and aphasia (4%). Twenty-two patients (32%) had serious neurologic events of any grade; 18% were Grade 3, and 9% were Grade 4.
The median onset of a neurologic event following brexucabtagene autoleucel infusion was 7 days. In patients whose neurologic AEs had resolved, the median duration was 12 days (range = 1 day to 567 days). As of the July 24, 2019, data cut-off, neurologic events had resolved in all but 6 patients.
Table 2: Summary of Key Results From Pivotal and Protocol Selected Studies
Key Results | ZUMA-2 | |
|---|---|---|
July 24, 2019, DCO | December 31, 2019, DCO | |
Clinical response outcomes (IAS, N = 60) | ||
Patients with objective response (CR + PR), n (%) 95% CI (Clopper-Pearson method) 95% CI (Wilson method) 95% CI (Agresti-Coull method) 95% CI (Modified Jeffrey method) | 56 (93) 83.8 to 98.2 84.1 to 97.4 83.6 to 97.8 84.9 to 97.7 | 55 (92) 81.6 to 97.2 NR NR NR |
P value of exact test for ORR ≤ 25% | < 0.0001 | < 0.0001 |
CR, n (%) 95% CI (Clopper-Pearson method) | 40 (67) 53.3 to 78.3 | 40 (67) 53.3 to 78.3 |
PR, n (%) 95% CI (Clopper-Pearson method) | 16 (27) 16.1 to 39.7 | 15 (25) 14.7 to 37.9 |
Stable disease, n (%) 95% CI (Clopper-Pearson method) | 2 (3) 0.4 to 11.5 | 2 (3) 0.4 to 11.5 |
Progressive disease, n (%) 95% CI (Clopper-Pearson method) | 2 (3) 0.4 to 11.5 | 2 (3) 0.4 to 11.5 |
DOR (IAS, N = 60) | ||
Patients with objective response, n (%) | 56 (93) | 55 (92) |
Median DOR (95% CI) | Not reached (8.6 to NE) | Not reached (13.6 to NE) |
PFS (IAS, N = 60) | ||
Median PFS (95% CI) | Not reached (9.2 to NE) | Not reached (9.6 to NE) |
PFS rate, % (95% CI) 6 months 12 months | 77 (64 to 86) 61 (45 to 74) | 77 (63 to 86) 62 (48 to 74) |
OS (IAS, N = 60) | ||
Median OS (95% CI) | Not reached (24.0 to NE) | Not reached (NE to NE) |
OS rate, % (95% CI) 6 months 12 months | 87 (75 to 93) 83 (71 to 91) | 87 (75 to 93) 83 (71 to 91) |
Harms, n (%) (safety analysis set, N = 68) | ||
Patients with ≥ 1 TEAE, n (%) Grade 3 Grade 4 Grade 5 | 68 (100) 11 (16) 52 (76) 4 (6) | 68 (100) 11 (16) 51 (75) 5 (7) |
Patients with ≥ 1 serious TEAE, n (%) Grade 3 Grade 4 Grade 5 | 46 (68) 20 (29) 13 (19) 4 (6) | 48 (71) 21 (31) 13 (19) 4 (6) |
Deaths, n (%) Progressive disease AE Other | 16 (24) 13 (19) 2 (3) 1 (1) | 18 (26) 16 (24) 2 (3) 0 (0) |
Notable harms | ||
Any CRS, n (%) | 62 (91) | 62 (91) |
Any neurologic event, n (%) | 43 (63) | 43 (63) |
AE = adverse event; CI = confidence interval; CR = complete response; CRS = cytokine release syndrome; DCO = data cut-off; DOR = duration of response; IAS = inferential analysis set; NE = not estimable; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; TEAE = treatment-emergent adverse event.
Source: ZUMA-2 Clinical Study Report18; ZUMA-2 Updated Analysis.19
Critical Appraisal
The ZUMA-2 study was a single-arm study that lacked a comparator arm, which increases the risk of bias in the estimation of treatment effects due to the potential for confounding related to placebo response, fluctuations in health status, and other unidentified prognostic factors that could affect subjectively assessed outcomes. The use of well-validated measurement scales for assessing patient-reported outcomes was appropriate and might ameliorate bias in the measurement of these outcomes; however, it does not remove the potential for bias related to lack of comparison. The follow-up time was considered appropriate for assessing response to treatment; however, it was noted to be immature for survival outcomes.
Primarily, the ZUMA-2 study did not include any Canadian patients. According to the panel of clinical experts, the eligibility criteria based on absolute neutrophil counts, platelet counts, and absolute lymphocyte counts were believed to be higher than would be seen in the general population. Moreover, they noted that the majority of patients had an ECOG PS of 0 (65%), indicating a healthier population, and only 10% of patients had bulky disease at baseline. Lastly, only 38% of patients received bridging therapy in preparation for brexucabtagene autoleucel infusion, which the experts believed to be low. Together, it is unclear whether the included population was healthier than would be typically seen in these patients in clinical practice; thus, generalizability of the results to the typical Canadian population may be limited.
Indirect Comparisons
Description of Studies
The sponsor submitted a matching-adjusted indirect comparison (MAIC) that compared the efficacy of brexucabtagene autoleucel to standard of care treatments in terms of OS, PFS, and tumour response outcomes. The analysis was informed by a systematic literature review that identified 9 uncontrolled, mainly retrospective, open-label studies that provided outcome data in patients with R/R MCL who received treatment following BTK inhibitor therapy (N = 12 to 73; median follow-up range = 3.2 months to 38 months). The subsequent therapies reported in the trials included lenalidomide-based treatments, venetoclax, R-BAC or rituximab in combination with bendamustine, bortezomib, and dexamethasone (R-iBVD), and mixed treatments (various chemo-immunotherapies or systemic therapies).
For the MAIC, a logistic propensity score model was used to estimate patient weights for the ZUMA-2 trial, so that the weighted mean baseline characteristics of the ZUMA-2 patients (FAS N = 74) matched the pooled mean characteristics of the standard of care studies. Pairwise indirect comparisons were then conducted using the weighted ZUMA-2 data and pooled outcome data for standard of care studies (n = 2 to 8).
Efficacy Results
The primary MAIC analyses for OS reported a hazard ratio (HR) of 0.18 (95% CI, 0.09 to 0.38; effective sample size = 36.2), a PFS HR of ||, (95% CI, ||||||||||||; effective sample size = 16.3), and an objective response odds ratio of 7.91 (95% CI, 2.35 to 26.62; effective sample size = 29.5).
Harms Results
The sponsor-submitted MAIC did not assess safety outcomes for brexucabtagene autoleucel.
Critical Appraisal
The key limitation of the MAIC is the assumption that absolute outcomes can be predicted from the covariates included in the model (i.e., that every effect modifier and prognostic factor are accounted for).20 This assumption is largely considered impossible to meet, and the failure of this assumption leads to an unknown amount of bias in the unanchored estimate.20 For the sponsor-submitted indirect treatment comparisons (ITCs), some prognostic factors were excluded from the model or may have been incompletely specified due to missing data from the clinical trials. The effective sample size was small for all outcomes (16 to 36), which suggests poor population overlap and unstable estimates. The results for the tumour response outcome lacked precision and showed wide 95% CIs. Uncertainty in the results of the unanchored MAIC are compounded by the inclusion of lower quality comparator trials and clinical heterogeneity across studies. Due to the limitations of the ITC, no conclusions on the comparative efficacy of brexucabtagene autoleucel can be drawn from the MAIC.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH.
Conclusions
Evidence from the single-arm, open-label ZUMA-2 trial suggests that CAR T-cell therapy with brexucabtagene autoleucel at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram is associated with statistically significant rates of objective response relative to a historical control. Moreover, brexucabtagene autoleucel was associated with substantial improvements in survival (PFS and OS) and improved HRQoL over 6 months, which are outcomes that patients have identified as relevant. The results of the ZUMA-2 trial may potentially be biased due to the inability to control for confounding and the unblinded assessment of subjective outcomes. As well, the included population may be more fit than the general Canadian population with MCL who would be eligible for treatment, which could limit the generalizability of the results. The observed benefits of brexucabtagene autoleucel also need to be weighed against the associated harms, including serious CRS and neurologic AEs, which result in further intensive care unit (ICU) admission. Data on long-term outcomes of therapy with brexucabtagene autoleucel are needed.
Given the lack of head-to-head studies for brexucabtagene autoleucel, the sponsor submitted an unanchored MAIC that provided indirect evidence of the efficacy of brexucabtagene autoleucel compared with standard of care therapies in patients with R/R MCL. However, due to limitations of the MAIC analysis methods, inclusion of lower quality comparator trials, clinical heterogeneity between studies, lack of complete covariate data to inform the patient weights, and poor population overlap, no conclusions can be drawn from the MAIC.
Introduction
Disease Background
Mantle cell lymphoma is an aggressive subtype of B-cell non-Hodgkin lymphoma that develops in the outer edge of a lymph node (i.e., the mantle zone) and is defined by the overexpression of cyclin D1 due to translocation (11;14)(q13;q32) in approximately 85% of patients.1-5 In Western countries, MCL makes up less than 10% of all non-Hodgkin lymphoma diagnoses.2-4,6,7 The annual incidence of MCL is approximately 0.5 per 100,000 people.3,21,22 In Canada, there are approximately 500 to 600 new cases of MCL diagnosed each year,8,9 occurring more frequently in men (3:1), and it is usually diagnosed in patients aged 60 to 70 years.5,6
The exact underlying cause of MCL is unknown. The molecular hallmark of MCL is the chromosomal translocation t(11;14)(q13;q32), which transposes the CCND1 gene at 11q13 to the immunoglobulin heavy chain of chromosome 14q32, leading to cyclin D1 overexpression. However, the transcription factor sex-determining region, Y-box 11 (SOX11), may be used as a diagnostic marker for the rare cases of MCL that are cyclin D1 negative.3,23,24 Mutations of TP53 are also associated with aggressive disease and poor outcomes in MCL.16,25 WHO recognizes 2 types of MCL: (a) nodal MCL (80% to 90% of cases) with unmutated immunoglobulin heavy chain, SOX11 overexpression, and nodal and extranodal involvement, which is generally more aggressive, and (b) non-nodal leukemic MCL (10% to 20% of cases) with mutated immunoglobulin heavy chain, no SOX11 mutation, increased WBC count, and splenomegaly, which typically has a more indolent behaviour.2,26
Generally, patients with MCL have multiple symptoms involving lymph nodes throughout the body, which include generalized lymphadenopathy and extranodal involvement of the blood, bone marrow, spleen, and gastrointestinal tract, resulting in non-specific symptoms including swollen painless lymph nodes, headache, weakness, loss of appetite, nausea and/or vomiting, abdominal pain or bloating, fatigue, and general B symptoms including fever, weight loss, and night sweats.4,5 Often, patients with early stages of the disease are asymptomatic, and MCL is usually diagnosed in later stages of the disease, which are characterized by an aggressive clinical course and a poor prognosis. Additional complications from MCL progression include cytopenias (neutropenia, anemia, and thrombocytopenia), and gastrointestinal, pulmonary, and CNS complications.2
Diagnosis of MCL is suspected by a hematologist or hematopathologist through the initial workup and laboratory assessments (complete blood count, serum lactate dehydrogenase) and imaging (PET/CT scans) and is confirmed by lymph node or bone marrow biopsy with immunohistochemistry or flow cytometry showing the presence of B-cell surface markers (CD20, CD19, CD5), cyclin D1 protein overexpression, t(11;14) translocation, or overexpression of the SOX11 transcription factor.2,4,8 No specific risk factors or predispositions have been identified.2 However, MCL has been associated with Borrelia infection, living or working on farmhouses, familial MCL, and autoimmune diseases.27-30
The Mantle Cell Lymphoma International Prognostic Index (MIPI) is used to determine prognosis and treatment plans in MCL patients, incorporating scores for age, performance status, normalized lactate dehydrogenase level, and WBC counts, which influence MCL prognosis (Table 3). Patients are assigned to a low-risk, intermediate-risk, or high-risk category based on the cumulative number of points assigned to the individual’s prognostic factors. Patients with 0 to 3 points are considered to be at low risk, patients with 4 to 5 points are intermediate risk, and patients with 6 to 11 points are high risk.4 A modification of the MIPI also includes the Ki-67 proliferative index.3,4
Table 3: Simplified MIPI Index
Points per prognostic factor | Age | ECOG PS | LDH levels | WBC count, 109/L |
|---|---|---|---|---|
0 | < 50 | 0 to 1 | < 0.67 | < 6.70 |
1 | 50 to 59 | 0.67 to 0.99 | 6.70 to 9.99 | |
2 | 60 to 69 | 2 to 4 | 1.00 to 1.49 | 10.00 to 14.99 |
3 | ≥ 70 | ≥ 1.50 | ≥ 15.00 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; LDH = lactate dehydrogenase; MIPI = Mantle Cell Lymphoma International Prognostic Index; WBC = white blood cell.
Source: Leukemia and Lymphoma Society.4
The advent of newer therapies has improved outcomes in the MCL population. From onset of the disease, the estimated median OS is 2.4 years to 4.25 years, while in patients with R/R MCL, the median OS is 1 year to 2 years.9,31
Quality of life in MCL is scarcely reported in published literature.32 Aside from the general psychological distress associated with a cancer diagnosis, symptoms are often associated with reduced quality of life, particularly difficulty with daily activities, and the resulting burden of B symptoms. Respondents to an unpublished survey indicated that anxiety and/or depression, fatigue, gastrointestinal symptoms, aches and pains, and blood cell counts were the symptoms that had the greatest impact on their lives, interfering with their ability to work, travel, exercise, and perform day-to-day activities.
Standards of Therapy
Mantle cell lymphoma is incurable with standard treatment for advanced disease, which is guided by the patient’s age and comorbidities. Patients are often diagnosed with advanced disease, which has a more aggressive clinical course and is associated with poor prognosis.2,7 Despite this, front-line treatments in MCL are generally associated with high response rates (ORR = 95%; CR = 53%) and extension of survival.10-14
Younger, fit patients are treated with aggressive induction chemoimmunotherapy, followed by autologous SCT and rituximab maintenance.9,16 Preferred chemoimmunotherapy options include16:
R-DHA (rituximab, dexamethasone, and cytarabine) + platinum chemotherapy (carboplatin, cisplatin, or oxaliplatin)
alternating R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) and R-DHAP (rituximab, dexamethasone, cytarabine, and cisplatin)
the Nordic regimen (rituximab plus cyclophosphamide, vincristine, doxorubicin, and prednisone, alternating with rituximab plus high-dose cytarabine)
hyper-CVAD (cyclophosphamide, vincristine, doxorubicin, and dexamethasone alternating with high-dose methotrexate and cytarabine) + rituximab
bendamustine + rituximab.
Older, less fit patients who are not appropriate for SCT are typically treated with chemoimmunotherapy and rituximab maintenance. Less aggressive chemoimmunotherapy options include bendamustine plus rituximab, VR-CAP, R-CHOP, lenalidomide plus rituximab, and R-BAC, followed by maintenance rituximab until progression or intolerance.16
Although initial treatment strategies achieve high response rates, most patients will eventually relapse and require further therapy, which generally results in shorter periods of remission with each subsequent line of therapy.15 There is no established standard of care for patients in the R/R setting, and treatment options are based on prior therapies and response to treatment.9 Further treatment options for patients that experienced a short response to prior treatment include additional chemoimmunotherapy or a BTK inhibitor or ibrutinib or acalabrutinib.16 Ibrutinib is the only BTK inhibitor publicly funded in Canada for MCL.15 However, response to BTK inhibitors is associated with decreased efficacy in patients who have received more prior lines of therapy.15,33,34 Following failure of BTK inhibitors in the second line, treatment options consist of re-treatment with previously unused chemoimmunotherapy, BTK inhibitor, or palliative care, with poor median survival of 1 year or less.35-40
Drug
Brexucabtagene autoleucel (Tecartus, also KTE-X19) is an autologous T-cell product manufactured from leukapheresis and administered after lymphodepleting chemotherapy, and optional bridging therapy, as a single-dose treatment in a patient-specific infusion bag, containing a suspension of anti-CD19 CAR T cells at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram.
Brexucabtagene autoleucel is a CD19-directed genetically modified autologous T-cell immunotherapy that targets CD19-expressing cancer cells and normal B cells. Anti-CD19 CAR T cells engage with CD19-expressing cells, and co-stimulatory domains CD28 and CD3-zeta activate downstream signalling cascades that lead to T-cell activation, proliferation, acquisition of effector functions, and secretion of inflammatory cytokines and chemokines, leading to the killing of CD19-expressing cells.41
The drug under review has not been previously reviewed by CADTH and was submitted as a priority review for a new drug (cell therapy) as pre–Notice of Compliance status. The Health Canada Notice of Compliance was received on June 8, 2021. Brexucabtagene autoleucel has already been approved for use by the FDA under accelerated approval based on ORR and durability of response for the treatment of adult patients with R/R MCL42 and is currently under review by the National Institute for Health and Care Excellence. The submitted indication for review is identical to the Health Canada indication: treatment of adult patients with R/R MCL after 2 or more lines of systemic therapy including a BTK inhibitor.43 The main characteristics of brexucabtagene autoleucel are summarized in Table 4.
Table 4: Key Characteristics of Brexucabtagene Autoleucel
Characteristic | Description |
|---|---|
Mechanism of action | Brexucabtagene autoleucel is a CAR T-cell therapy that binds to CD19-expressing cancer cells and normal B cells. Following anti-CD19 CAR T-cell engagement with CD19-expressing target cells, the CD28 and CD3-zeta co-stimulatory domains activate downstream signalling cascades that lead to T-cell activation, proliferation, acquisition of effector functions, and secretion of inflammatory cytokines and chemokines. This sequence of events leads to the killing of CD19-expressing cells. |
Indication | Treatment of adult patients with R/R MCL after 2 or more lines of systemic therapy including a BTK inhibitor. |
Route of administration | Single IV infusion. |
Recommended dosea | Brexucabtagene autoleucel: IV infusion target dose of 2.0 × 106 CAR T cells per kilogram body weight (range = 1 × 106 to 2 × 106 CAR T cells per kilogram) with a maximum of 2.0 × 108 CAR T cells. |
Serious adverse effects or safety issues | Due to the risks associated with Tecartus, delay of lymphodepleting chemotherapy and Tecartus treatment should be considered if the patient has 1 or more of the following: CRS including life-threatening reactions; active uncontrolled infection or inflammatory disorders; active GVHD or unresolved serious adverse reactions from prior therapies; or neurologic adverse reactions, including life-threatening reactions concurrently or independently of CRS. |
BTK = Bruton tyrosine kinase; CAR = chimeric antigen receptor; CRS = cytokine release syndrome; GVHD = graft-vs.-host disease; MCL = mantle cell lymphoma; R/R = relapsed or refractory.
aIt should be ensured that 4 doses of tocilizumab and access to emergency equipment are available before infusion and during the recovery period.
Source: ZUMA-2 Clinical Study Report18; Brexucabtagene autoleucel product monograph.41
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Groups and Information Gathered
One patient group, Lymphoma Canada, provided input for the review of brexucabtagene autoleucel. Lymphoma Canada is a national Canadian registered charity whose mandate is to empower the lymphoma community through education, support, advocacy, and research. It collaborates with patients, caregivers, health care professionals, and other organizations and stakeholders to promote early detection, find new and better treatments for lymphoma patients, help patients access those treatments, learn about the causes of lymphoma, and find a cure (www.lymphoma.ca).
The information submitted was gathered through an anonymous online survey of patients with MCL that was circulated between October 2020 and January 2021 using Lymphoma Canada’s email contact database, social media, US and Canadian cancer society message boards, physician specialists, and international lymphoma organizations’ contacts. Thirty-three patients provided input on their experience with MCL, including 1 US patient who had received brexucabtagene autoleucel therapy. Of the 25 patients who provided demographic data, 24 were from Canada (15 male and 9 female patients). All patients were over 44 years of age (age range 45 to 54 years: 5 patients; 55 to 64 years: 6 patients; 65 to 74 years: 11 patients; 75 to 84 years: 2 patients).
Disease Experience
The symptoms that patients experience due to MCL are variable and can change over time as the disease progresses. Respondents reported that enlarged lymph nodes (63% of patients), fatigue (75%), gastrointestinal symptoms (50%), aches and pains (68%), and high or low WBC count (50%) impacted their current quality of life. Patients with MCL stated that their symptoms had the greatest impact on their ability to travel, exercise, concentrate, perform daily activities like household chores, and perform regular duties like work or volunteering.
Receiving a diagnosis of MCL negatively impacted patients’ mental and emotional well-being. All respondents (N = 33) rated that 1 or more symptoms affected their quality of life, including stress of diagnosis (88%), anxiety or worry (79%), and difficulty sleeping (33%). As years pass from a patient’s MCL diagnosis, different mental and emotional aspects related to their disease may impact their quality of life, but anxiety, stress, and difficulty sleeping remained the most common issues among respondents.
As described by 1 patient: “I am extremely fortunate to have indolent MCL, but it can be difficult managing the anxiety of never knowing when or if I become sick and how aggressive my disease will be if I convert. It’s like living with a bomb sometimes.”
Experience With Treatment
Of the 25 respondents who provided information about their experience with MCL treatments, 76% required immediate treatment, while 24% remained in watch-and-wait status. Of the 25 respondents, 29% received more than 1 line of treatment following MCL relapse. The most commonly reported first-line treatment (44% of respondents) was the chemoimmunotherapy regimen R-CHOP, with 36% of patients receiving SCT. Of those who received more than 1 line of treatment, most received BTK inhibitors such as acalabrutinib or clinical trial drugs.
The most commonly reported adverse effects of MCL treatments included fatigue, hair loss, thrombocytopenia, diarrhea, nausea, anemia, neutropenia, confusion or memory loss, mouth sores, cough, skin rash or itching, constipation, and infections. Most patients (15 of 25 respondents) found fatigue, nausea, vomiting, hair loss, and neurocognitive effects such as brain fog or headaches were the most difficult adverse effects to tolerate. When asked about the impact of different aspects of their treatment on daily living, respondents noted that treatment-related fatigue, the duration of infusions, infusion reactions, and other late adverse effects of treatment had the most significant impact on their quality of life.
Treatment also had a financial impact on patients, with 36% reporting having to miss work, and 24% experiencing financial burdens related to drug costs.
One patient from the US, aged 65 to 74 years, had experience with brexucabtagene autoleucel through a clinical trial. This patient reported not being prepared for the numerous tests involved in determining treatment eligibility; however, the patient was moderately prepared and understood the various steps of CAR T-cell treatment, including the blood extraction process, wait times between extraction and infusion, the potential need for bridging therapy, and post-infusion monitoring. The patient experienced adverse effects of neutropenia, thrombocytopenia, and anemia, but was not admitted to the hospital for management of these adverse effects, and these adverse effects did not last for longer than 2 months post-treatment. The treatment burden (e.g., number of clinic visits, CAR T-cell extraction and infusion, adverse effect management, and travel and related costs) and emotional impact (e.g., worry or concern over potential adverse effects or the possibility of relapse) were rated as having a minor negative impact on this patient’s quality of life. Overall, the patient rated their experience with this treatment as positive.
Improved Outcomes
All patients surveyed rated faster remission and longer life as the most important outcomes for a new therapy. Other important outcomes included control of disease and symptoms (79%), improved quality of life (58%), and improved blood counts (58%). The majority of patients (58%) were willing to tolerate adverse effects of a new treatment if they were short-term, while the remaining respondents were unsure. Most patients (78%) would accept a treatment with known and potentially serious adverse effects if it was recommended by their doctor. Having choice in their treatment selection was rated as very important, with a large majority of patients (88%) agreeing that there is a need for more effective therapy options.
As described by 1 patient: “My great concern is that I am running out of treatment options. If I am to live, I need more options. It's really that simple.”
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). In addition, as part of the brexucabtagene autoleucel review, a panel of 3 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion is presented below.
Unmet Needs
There is currently no curative option readily available in this patient population. The clinical experts agreed that at the time of relapse or failure of BTK inhibitor, patients have a short DOR and a poor life expectancy. Once patients stop second-line ibrutinib or acalabrutinib, life expectancy is around 6 months, so new treatments are needed for this population. Treatments are needed to control the disease and provide patients with a durable response, as a substantial number of patients will not respond to chemoimmunotherapy at this point.
Place in Therapy
This therapy best fits into treatment of relapsed MCL. Clinical experts noted that it is important that patients are treated with chemoimmunotherapy at diagnosis, followed by autologous SCT (if eligible) and maintenance rituximab, as patients can have long durations of remission after initial therapy. Therapy with BTK inhibitors only works for a limited time period, and brexucabtagene autoleucel would be used after ibrutinib or acalabrutinib or in those who are intolerant of ibrutinib or acalabrutinib. This would also include anyone with a suboptimal response to ibrutinib or acalabrutinib. Clinical experts agreed that if a patient starting BTK inhibitor therapy is a potential candidate for brexucabtagene autoleucel, this should be considered early as once response to BTK inhibitors is lost, patients rapidly deteriorate. One clinical expert noted that given the cost of ibrutinib, if the intention is to give brexucabtagene autoleucel, it does not seem logical to continue BTK inhibitor therapy beyond what is necessary. It would not make sense for brexucabtagene autoleucel to be reserved for patients who are intolerant of other therapies. Treatment with brexucabtagene autoleucel would result in increased surveillance in real-world practice, with increased monitoring of any signs of relapse to ensure that patients rapidly receive treatment with brexucabtagene autoleucel.
Patient Population
In line with the clinical trial, the clinical experts considered ideal patients to be those with R/R MCL who have previously received chemoimmunotherapy and a BTK inhibitor. Moreover, patients should have a suitable ECOG PS (0 to 2) and adequate organ function. Experts noted that patients with a p53 mutation tend to have poor outcomes and may benefit the most in terms of improvement of survival.
Patients eligible for treatment would be identified by the treating specialist in hematology or oncology at the time of first relapse of MCL. Clinical experts agree that patients should be prioritized based on individual need, with those progressing on BTK inhibitors being higher need than those currently stable and/or responding to BTK inhibitor treatment. It was noted by all the clinical experts that this would be a limited number of patients, and prioritization for treatment within Canada compared to out of country is not of concern. One clinician noted that there will be patients who refuse to accept treatment due to travel requirements. Moreover, manufacturing capacity and COVID-19 implications play a role in whether patients would be willing to accept treatment within their province, out of province, or out of country.
The least suitable patients for brexucabtagene autoleucel were thought to be patients with a very high disease burden that is rapidly progressing and those who cannot tolerate further chemoimmunotherapy therapy, those with a poor performance status, and those with multiple comorbidities. In line with the trial, patients with cardiac or CNS disease were excluded; however, 1 clinical expert noted that perhaps if these comorbid conditions were controlled, the patients could be considered. In addition to the clinical aspects that render patients ineligible, clinical experts noted that patients without a caregiver, patients who cannot or do not want to travel to receive treatment, and patients who will not survive longer than 4 weeks to 8 weeks are unlikely to receive treatment with brexucabtagene autoleucel.
Assessing Response to Treatment
The clinical experts noted that in clinical practice, a combination of clinical exam, bloodwork (complete blood count and lactate dehydrogenase), and imaging (CT/PET) would be used to assess response to therapy. Unlike clinical trials, imaging may not be as frequent after initial response to therapy has been documented, as it typically does not change disease management. Clinical experts also noted that repeat bone marrow biopsy or measurement of minimal residual disease is not common practice in MCL. Typically, patients would be followed up with at 1 month, at 2 months, and then as needed until best response to treatment is determined.
More data are currently needed to determine which patients are more likely to exhibit a response; however, experts did note that patient factors, including performance status and organ function, are generally known to influence response to treatment. No subgroup data from the trial provide insight to this.
Discontinuing Treatment
Clinical experts agreed that discontinuing treatment for CAR T-cell therapy is not applicable as it is a 1-time treatment, and once the therapy is initiated, it is not able to be stopped. However, patients who become unwell before infusion, or those who experience rapid clinical decline, may be deemed unable to proceed with infusion. However, this would be considered before treatment with brexucabtagene autoleucel.
Clinical experts agreed that there was no evidence of re-treatment for brexucabtagene autoleucel at present.
Prescribing Conditions
Clinical experts agree that brexucabtagene autoleucel must be administered in a setting supervised by specialists such as a hematologist and, possibly, a transplant hematologist to determine the use of CAR T-cell therapy versus allogeneic SCT. Experts noted that such a setting may consist of academic or tertiary centres that already deliver cellular therapies (bone marrow transplant) with the ability to provide urgent intensive care and on-call neurology. At this time, treatment should only be conducted in a centre that offers transplantation to ensure that standard operating procedures and a multi-disciplinary team are available. One expert noted that there is some evidence that the treatment can be conducted in the outpatient setting, assuming that outpatient after-hour care is available (i.e., an assessment and infusion clinic in addition to a 24-hour emergency department).
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Two physician groups provided input for this submission: the Ontario Health (CCO) Hematology Disease Site Drug Advisory Committee and a group of lymphoma experts in Canada whose input was coordinated by Lymphoma Canada.
Cancer Care Ontario’s (CCO’s) Drug Advisory Committee provides timely evidence-based clinical health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program.
Lymphoma Canada, a national not-for-profit organization for Canadian lymphoma and chronic lymphocytic leukemia patients, coordinated the group clinician response from leading experts in lymphoma across Canada.
The information submitted was based on joint discussions at a CCO Drug Advisory Committee meeting and based on collated clinician responses to the template questions based on research results, clinical experience, and understanding of patient needs and challenges.
Unmet Needs
For patients who have failed multiple lines of therapy, clinicians may attempt to access unfunded targeted therapies or enrol patients in clinical trials. Allogeneic SCT has been employed for younger patients, who typically have disease progression following primary chemoimmunotherapy and BTK inhibitor therapy. However, clinical experts stated that this intensive approach is only available to the minority of patients who have a donor and are of an appropriate age and fitness. Palliative chemotherapy may be the only option for some patients.
Clinical experts agree that there is an unmet need for effective treatments that produce clinical responses and remission and may prolong life in patients with R/R MCL. Existing options benefit only a fraction of patients (35% to 75%) and typically do not offer durable responses (approximately 6 months to 18 months). Many of these treatments must be administered indefinitely, and toxicities may adversely affect quality of life. For example, lenalidomide may cause fatigue, gastrointestinal upset, and cytopenia, which predispose patients to infections. Venetoclax also is associated with some toxicities, including early tumour lysis syndrome. Unfortunately, the median survival in this population is quite short post–ibrutinib failure, typically between 4 months and 6 months. Patients with p53 mutation have an average PFS of 4 months, versus 12 months in patients without the p53 mutation.
Place in Therapy
Brexucabtagene autoleucel is a novel patient-specific targeted therapy that augments the immune system’s ability to control the cancer. The experts noted that the current data support the role of this therapy as a single agent in patients treated with multiple prior lines of therapy who have disease progression following primary chemoimmunotherapy and BTK inhibitor therapy. Brexucabtagene autoleucel would replace treatment options in the third line or later, including palliative chemotherapy; intensive chemotherapy or experimental treatments for select patients; or SCT in young, fit patients.
Clinical trials to determine the efficacy and toxicity of brexucabtagene autoleucel when administered earlier in the disease course are required to support earlier integration in the treatment pathway. To date, this therapy has not been evaluated against standard front-line approaches or in a large cohort of BTK inhibitor–naive patients. The population of MCL patients who are typically treated from an exclusively palliative approach, who may be older and frail, is not expected to change if CAR T-cell therapy is available.
Patient Population
The experts noted that brexucabtagene autoleucel should be reserved for patients who have progressed after having received standard chemoimmunotherapy and BTK inhibitor therapy (unless these are contraindicated). Progression would be identified by the treating hematologist or oncologist by standard clinical testing (imaging, laboratory findings). Candidates for brexucabtagene autoleucel therapy would include patients who are younger (although age is not a specific criterion), without comorbidity, and with good performance and fitness status. In addition, patients must express CD19, but this is almost universal in MCL, and patients must have adequate numbers of circulating T lymphocytes to allow generation of CAR T-cell product.
The experts identified patients least suitable for treatment with brexucabtagene autoleucel as including those whose disease could not be controlled in the short-term to allow them to proceed to CAR T-cell therapy. Experts noted that patients with comorbid illnesses that may increase their risk of sepsis, cytokine release–related complications, or neurologic complications immediately after the T-cell reinfusion may be less suitable for this treatment. Such comorbidities could include difficult to manage diabetes or diabetic complications, chronic renal failure with impairments of creatinine clearance or on dialysis, or significant symptomatic cardiomyopathies. Patients with obvious uncontrolled infections would not be acceptable candidates. Patients with active CNS lymphoma may not be good candidates unless the disease is controlled and stable.
Currently, it is not possible to identify patients who are most likely to exhibit a response to treatment.
Assessing Response to Treatment
Clinically meaningful results to therapy as stated by the clinical experts include stabilization of disease or objective response to therapy. These responses would usually be associated with improvement in constitutional or organ-related symptoms. Success with this treatment should ensure improved quality of life and independence in the activities of daily living. Durable responses would be important, given the logistical difficulties and expense of treatment.
Standard clinical parameters, including those obtained through CT scans and possibly PET scans, would be used to document clinical response and remission. Bloodwork and assessments of organ function and the hematologic profile would also be important. Response to treatment should be assessed radiologically post-treatment and several months again post-treatment. Ongoing imaging may be dependent on symptoms and the results of the previous testing, clinical findings, and laboratory results.
Discontinuing Treatment
Progression of disease or a recurrence of symptomatology would indicate treatment failure. It would be appropriate to consider initiating a new treatment at that time. As a single infusion therapy, the main question around discontinuation would be for patients who have disease control issues before T-cell infusion.
Prescribing Conditions
Experts agree that patients who would be candidates for this therapy would be identified by the treating hematologist or oncologist and that treatment should be administered in a tertiary referral cancer centre that has experience and infrastructure for cell therapies or autologous SCT. Currently, this would be centres with CAR T-cell experience, which typically would be regional academic transplant programs.
Additional Considerations
It was noted by experts that tocilizumab may be required to manage CRS in some patients. Also, bridging chemotherapy may be needed for some patients to control the disease before proceeding with brexucabtagene autoleucel.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Questions for clinical expert input | |
What is the anticipated optimal place in therapy for brexucabtagene autoleucel in R/R MCL? | Brexucabtagene autoleucel therapy best fits into treatment of relapsed MCL following failure of a BTK inhibitor. Brexucabtagene autoleucel would mostly be used after second-line treatment or after ibrutinib. The US indication is for R/R MCL and does not include the requirement for ibrutinib. In the trial, most patients received brexucabtagene autoleucel treatment following ibrutinib, except for those who were intolerant or contraindicated. |
Are there specific subgroups of patients with R/R MCL who are more or less likely to benefit from brexucabtagene autoleucel? | Patients who are more likely to benefit from treatment with brexucabtagene autoleucel are those with good organ function and performance status. Experts stated that the ZUMA-2 trial did not show improvements or differences for any specific subgroups; however, it is known that there is a difference in prognosis for some of the evaluated subgroups. Additionally, experts agreed that higher risk, p53-mutated patients might be able to have access to the treatment earlier; however, there is no evidence for this. |
Should all available therapies be exhausted before considering use of brexucabtagene autoleucel for treatment of R/R MCL? If so, can the specific therapies be specified? | It is important that patients are treated with chemoimmunotherapy at diagnosis, followed by autologous SCT (if eligible) and maintenance rituximab. This should not be altered due to potential eligibility for brexucabtagene autoleucel at time of relapse because patients can have long durations of remission after initial therapy. |
Is there evidence to support re-treatment with brexucabtagene autoleucel for R/R MCL if a patient responds then subsequently relapses, or if the initial response is suboptimal? | No, there is no evidence to support re-treatment at this time. |
For which therapies is there evidence for use upon progression after CAR T-cell therapy? | There is no evidence for any therapies following brexucabtagene autoleucel. Patients would be treated palliatively or on a clinical trial. |
Would this therapy be used instead of SCT? | At this point, for the transplant-eligible, younger patient, autologous SCT would still be the preferred first-line approach; however, approval and funding of brexucabtagene autoleucel will likely result in this therapy being given before consideration of allogeneic SCT. Brexucabtagene autoleucel is likely to replace allogeneic SCT or come before allogeneic SCT as a bridge to transplant for R/R MCL. |
If there is limited capacity to offer this treatment, how would you prioritize which patients should be offered brexucabtagene autoleucel? How would you select which ones should be treated in Canada vs. out of country? | There likely will not be a large proportion of patients eligible for this treatment; however, those progressing on BTK inhibitors are of the highest need. In general, it is believed there is capacity to manage the few MCL patients who need this treatment within Canada; however, the manufacturing capacity is uncertain, and the current COVID-19 pandemic has resulted in patients being treated out of country more often. There are patients who will refuse to travel outside the country to receive therapy, and there will be patients who will not get the therapy if it is unable to be delivered in their province. |
Eligible patient population | |
Are patients who are not able to use BTK inhibitors due to contraindication or intolerance eligible for treatment? | As per the trial, yes, these patients would be eligible for treatment with brexucabtagene autoleucel. |
Does effectiveness of brexucabtagene autoleucel differ in patients experienced with bortezomib, lenalidomide, autologous SCT, or allogeneic SCT? | The trial does not show evidence for this; however, it is not believed that there would be any difference between these patients. |
Under what circumstances would switching to CAR T-cell therapy be preferred as opposed to waiting until disease progression? | If patients are responding to current treatment, switching would not be necessary. Switching would be warranted in patients who were beginning to show signs of relapsing following BTK inhibitor therapy. Patients would be monitored more frequently with more frequent imaging to estimate the best time to switch to brexucabtagene autoleucel. |
The ZUMA-2 trial excluded patients with current or prior CNS lymphoma or HIV, HCV, or HBV infection. PAG seeks guidance on the provision of brexucabtagene autoleucel in patients whose CNS lymphoma or viral infection is being actively treated. | As per the trial, these patients were excluded from treatment; however, patients with CNS disease that is under treatment or controlled should not be excluded from consideration for brexucabtagene autoleucel. |
Implementation factors | |
Can patients who cannot tolerate fludarabine still be considered for brexucabtagene autoleucel therapy if alternate lymphodepleting therapies can be offered? | Patients may be offered a bendamustine regimen as opposed to a fludarabine regimen if the latter is unable to be tolerated. |
PAG noted that hospital admission is advised and seeks guidance on the feasibility of implementing this therapy for outpatients after the week-long hospitalization. | There is some evidence that treatment can be conducted in the outpatient setting, assuming that outpatient after-hour care is available (i.e., an assessment and infusion clinic in addition to a 24-hour emergency department). |
Additional information | |
What conditions indicate the use of ibrutinib as a bridge to stabilize disease, during CAR T-cell manufacturing, and selection of alternative therapies (e.g., corticosteroids) for bridging? | It is possible to identify patients who are starting to relapse, but it would be ideal to maintain them on BTK inhibitor therapy in the hope that they will maintain control of their disease. However, it is known that if BTK inhibitors are stopped too early there can be explosion of the disease. |
What treatment options are available after failure of brexucabtagene autoleucel? | There are no therapies with evidence for use upon progression of CAR T-cell therapies. Patients will likely be treated in clinical trial or with chemotherapies. A small number could respond to chemotherapy and be eligible for allogeneic SCT. Most will be treated palliatively with a poor prognosis. |
Should there be any re-treatment if CAR T cells are still detectable in circulation? | There is no evidence to support re-treatment with brexucabtagene autoleucel in a patient who has previously received this therapy. |
BTK = Bruton tyrosine kinase; CAR = chimeric antigen receptor; CNS = central nervous system; HBV = hepatitis B; HCV = hepatitis C; MCL = mantle cell lymphoma; PAG = Provincial Advisory Group; R/R = relapsed or refractory; SCT = stem cell transplant.
Clinical Evidence
The clinical evidence included in the review of brexucabtagene autoleucel is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review: Pivotal and Protocol Selected Studies
Objectives
To perform a systematic review of the beneficial and harmful effects of brexucabtagene autoleucel cell suspension in a patient-specific single infusion bag for IV infusion, with a target of 2 × 106 CAR T cells per kilogram, for the treatment of adult patients with R/R MCL previously treated with a BTK inhibitor.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Of note, the systematic review protocol presented below was established before the granting of a Notice of Compliance from Health Canada.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults with R/R MCL previously treated with a BTK inhibitor. Subgroups:
|
Intervention | Brexucabtagene autoleucel cell suspension in a patient-specific single infusion bag for IV use at a target dose of 2 × 106 CAR T cells per kilogram |
Comparator | Bendamustine ± rituximab Bortezomib ± rituximab PEPC ± rituximab Lenalidomide ± rituximab Venetoclax R-CHOP VR-CAP R-BAC R-CVP |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
| Published and unpublished phase II, III, and IV RCTs |
AE = adverse event; BTK = Bruton tyrosine kinase; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HRQoL = health-related quality of life; ICU = intensive care unit; IVIG = IV immunoglobulin; MCL = mantle cell lymphoma; OS = overall survival; PEPC = prednisone, etoposide, procarbazine, and cyclophosphamide; PFS = progression-free survival; R-BAC = rituximab, bendamustine, and cytarabine; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; RCT = randomized controlled trial; R-CVP = rituximab, cyclophosphamide, vincristine, and prednisone; R/R = relapsed or refractory; SAE = serious adverse event; TEAE = treatment-emergent adverse event; VR-CAP = bortezomib, rituximab, cyclophosphamide, doxorubicin, and prednisone.
Note: Health-related quality of life and improvement in cancer-related symptoms are noted as outcomes important to patients.
The literature search was performed by an information specialist using a peer-reviewed search strategy according to the PRESS (Peer Review of Electronic Search Strategies) checklist (https://www.cadth.ca/resources/finding-evidence/press).
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings) and keywords. The main search concept was brexucabtagene autoleucel. Clinical trial registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, Canadian Partnership Against Cancer Corporation’s Canadian Cancer Trials, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on January 25, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on May 13, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist (https://www.cadth.ca/grey-matters).44 Included in this search were the websites of regulatory agencies (the FDA and the European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
Findings From the Literature
Thirty-three studies were identified from the literature for inclusion in the systematic review, while 9 potentially relevant reports from other sources were retrieved for scrutiny (Figure 1). In total, 1 report from 1 study was included in the review.
The included study is summarized in Table 7. A list of excluded studies is presented in Appendix 2.
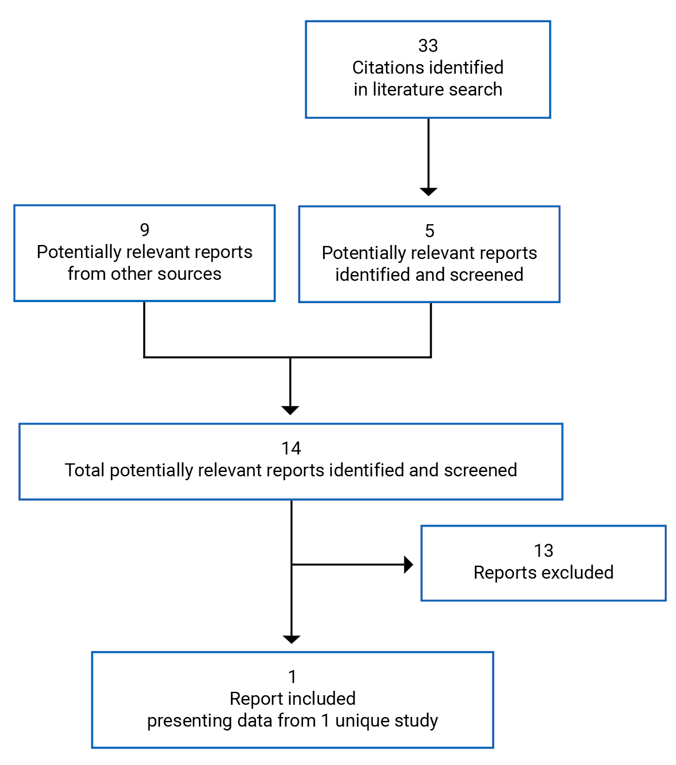
Table 7: Details of Included Studies
ZUMA-2 | |
|---|---|
Designs and populations | |
Study design | Phase II, multi-centre, open-label study |
Locations | France, Germany, the Netherlands, and the US |
Patient enrolment dates | May 16, 2016, to April 16, 2019 |
Enrolled (N) | 91 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Cohort 1: Brexucabtagene autoleucel at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram, with a maximum dose of 2 × 108 anti-CD19 CAR T cells for patients ≥ 100 kg as a single bag for IV infusion Cohort 2: Brexucabtagene autoleucel at a target dose of 0.5 × 106 anti-CD19 CAR T cells per kilogram, with a maximum dose of 0.5 × 108 anti-CD19 CAR T cells for patients ≥ 100 kg as a single bag for IV infusion |
Comparator(s) | Single-arm design (no comparator) |
Duration | |
Phase | Phase II |
Treatment conditioning | Lymphodepleting chemotherapy consisting of fludarabine 30 mg/m2/day and cyclophosphamide 500 mg/m2/day administered for 3 days. If deemed necessary by study investigators, bridging therapy was administered after leukapheresis and was completed at least 5 days before the initiation of lymphodepleting chemotherapy. |
Treatment period | Single infusion at the start of the study period |
Follow-up | Continues for each enrolled patient until approximately 15 years after the last patient had been treated with brexucabtagene autoleucel |
Outcomes | |
Primary end point | The primary efficacy end point was the ORR, defined as the incidence of CR or PR using central assessment by PET/CT scan. ORR was assessed at baseline, after bridging therapy and before lymphodepleting chemotherapy, 4 weeks after brexucabtagene autoleucel infusion, followed by every 3 months or at sign of disease progression. |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Notes | |
Publications | Wang et al. (2020)45 |
AE = adverse event; ALT = alanine aminotransferase; ANC = absolute neutrophil count; AST = aspartate aminotransferase; BOR = best objective response; CAR = chimeric antigen receptor; CNS = central nervous system; CR = complete response; CRS = cytokine release syndrome; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; EQ VAS = EuroQol Visual Analogue Scale; MCL = mantle cell lymphoma; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; SCT = stem cell transplant; ULN = upper limit of normal.
Source: ZUMA-2 Clinical Study Report.18
Description of Studies
One study met the inclusion criteria for this review. The ZUMA-2 study was a phase II, multi-centre, open-label study evaluating the efficacy and safety of brexucabtagene autoleucel (KTE-X19) in patients with R/R MCL whose disease had progressed on anthracycline- or bendamustine-containing chemotherapy, an anti-CD20 antibody, and a BTK inhibitor (ibrutinib and/or acalabrutinib).
ZUMA-2 was an open-label trial. Patients were assigned a unique patient identification number used to identify the patient throughout the study; it was used on all study documentation related to the patient. The study schema for the ZUMA-2 trial is shown in Figure 2.
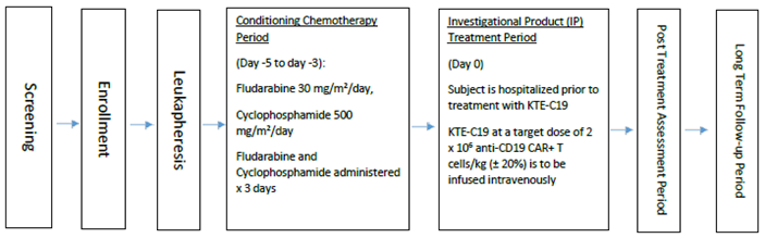
This study was conducted at 33 centres in the US, France, the Netherlands, and Germany. No Canadian sites were included.
Key eligibility criteria for the ZUMA-2 trial are summarized in Table 7. Eligible patients included adults diagnosed with R/R MCL who had received prior chemoimmunotherapy, anti-CD20 monoclonal antibody, and a BTK inhibitor. Patients were excluded if they had any measurable CNS disease or a history of allogeneic SCT or autologous SCT within 6 weeks of the planned infusion.18
Two cohorts were included in the ZUMA-2 trial to evaluate the efficacy of brexucabtagene autoleucel: Cohort 1, which aimed to treat up to 90 patients with a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram, and Cohort 2, which aimed to treat up to 40 patients with brexucabtagene autoleucel at a target dose of 0.5 × 106 anti-CD19 CAR T cells per kilogram, a 4-fold lower dose of brexucabtagene autoleucel. For the purposes of this report, we will only focus on Cohort 1, for whom the target dose of brexucabtagene autoleucel specified in the systematic review protocol (Table 6) was evaluated, which is the target dose in the funding request. Ninety-one patients were enrolled in the ZUMA-2 study: 74 patients in Cohort 1 at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram, and 17 patients in Cohort 2. Sixty-eight patients in Cohort 1 were treated with brexucabtagene autoleucel.18
The last observation and data cut-off for the ZUMA-2 trial was July 24, 2019, representing a median follow-up of 12.3 months (range = 7.0 months to 32.3 months) for the primary efficacy analysis.18,45 An updated analysis as of December 31, 2019 was provided, representing a median follow-up of 17.5 months (range = 12.3 months to 37.6 months).19,46
Populations
Inclusion and Exclusion Criteria
Eligible patients were adults (≥ 18 years) who were required to have pathologically confirmed MCL — with documentation of either cyclin D1 overexpression or presence of t(11;14) — that is relapsed or refractory, as defined by disease progression after the last regimen, or failure to achieve a PR or CR to the last regimen. Patients were required to have had prior treatment with up to 5 regimens that included all of the following: anthracycline or bendamustine-containing chemotherapy, anti-CD20 antibody, and ibrutinib or acalabrutinib. The original protocol did not specify the requirement for prior BTK inhibitors, and the inclusion criteria were modified at the June 22, 2018, protocol amendment to include ibrutinib and acalabrutinib as required prior therapies in all prospective patients. Therapy with a BTK inhibitor was not required to be the last line of therapy before trial entry, and patients were not required to have disease that was refractory to BTK inhibitor therapy. Additional inclusion criteria were an ECOG PS of 0 or 1, absolute neutrophil count greater than or equal to 1,000/μL, platelet count greater than or equal to 75,000/μL, absolute lymphocyte count greater than or equal to 100/μL, and adequate renal, hepatic, pulmonary, and cardiac function.18
Key exclusion criteria were a history of allogeneic SCT or autologous SCT within 6 weeks of study drug infusion. Patients were also excluded if they had detectable cerebrospinal fluid malignant cells or brain metastases, or a history of CNS lymphoma, cerebrospinal fluid malignant cells, or brain metastases; a history or presence of CNS disorders or any autoimmune disease with CNS involvement; or a history of myocardial infarction, cardiac angioplasty or stenting, unstable angina, active arrhythmias, or other clinically significant cardiac disease within 12 months before enrolment.18
Baseline Characteristics
The baseline and demographic characteristics of the ZUMA-2 trial are summarized in Table 8 for patients included in the safety analysis or mITT set, which included 68 patients. The median age of included patients was 65.0 years (range = 38 years to 79 years), and the majority of patients were male (84%), and the majority were White (93%). The majority of patients were from the US (91%), with 3, 2, and 1 patients from France, the Netherlands, and Germany, respectively.18
The majority of patients had classical MCL subtypes (n = 40 [59%]). Seventeen patients (25%) had blastoid MCL, while 4 (6%) had the classical MCL subtype of pleomorphic MCL. Based on the simplified MIPI, 28 patients (41%) were classified as low risk, 29 patients (43%) were classified as intermediate risk, and 9 patients (13%) were classified as high risk. Among the 49 patients with evaluable samples, the median percentage of tumour cells expressing Ki-67 was 65.0% (range = 1% to 95%), and 47 of patients (69%) had confirmed CD19 positivity.18
Fifty-five patients in Cohort 1 (81%) received 3 or more prior regimens. Twenty-nine patients (43%) relapsed after prior autologous SCT; the remaining patients had either relapsed after their last therapy for MCL (12 [18%]) or were refractory to their last therapy for MCL (27 [40%]). Per the protocol, all patients had received an anti-CD20 antibody and a BTK inhibitor. Forty-two treated patients (62%) had disease that did not respond to BTK inhibitor therapy (primary refractory disease), and 18 (26%) had a relapse after having an initial response while receiving BTK inhibitor therapy.18
Other prior treatments included anthracycline-based therapy (49 [72%]), bendamustine (37 [54%]), proteasome inhibitors (25 [37%]), and lenalidomide (19 [28%]).18
Table 8: Summary of Baseline Characteristics: mITT or Safety Analysis Set
Characteristic | ZUMA-2 (N = 68) |
|---|---|
Age Median (range) Mean (SD) < 65 years ≥ 65 years | 65.0 (38 to 79) 63.2 (7.9) 29 (43) 39 (57) |
Sex, n (%) Male Female | 57 (84) 11 (16) |
ECOG PS, n (%) 0 1 | 44 (65) 24 (35) |
Morphologic characteristics, n (%) Diffuse MCL Blastoid MCL Pleomorphic MCL | 20 (29) 17 (25) 4 (6) |
Ki-67 (%) IHC by central laboratory n Median (range) Mean (SD) | 49 65.0 (1 to 95) 57.1 (27.0) |
CD19 IHC positive by central laboratory, n (%) Yes No Not available | 47 (69) 4 (6) 17 (25) |
s-MIPI, n (%) Low risk Intermediate risk High risk Missing | 28 (41) 29 (43) 9 (13) 2 (3) |
Bulky disease, n (%) Yes No | 7 (10) 61 (90) |
LDH relative to upper limit, n (%) LDH < 0.67 ULN 0.67 ULN ≤ LDH < ULN ULN ≤ LDH < 1.5 ULN 1.5 ULN ≤ LDH Missing | 16 (24) 24 (35) 15 (22) 11 (16) 2 (3) |
Received bridging therapy, n (%) Yes No | 25 (37) 43 (63) |
Relapsed or refractory disease, n (%) Relapsed after autologous SCT Refractory to last MCL therapy Relapsed after last MCL therapy | 29 (43) 27 (40) 12 (18) |
Number of prior regimens Mean (SD) Median (range) 1, n (%) 2, n (%) 3, n (%) 4, n (%) 5, n (%) | 3.3 (1.0) 3.0 (1 to 5) 1 (1) 12 (18) 30 (44) 14 (21) 11 (16) |
Prior autologous SCT, n (%) Yes No | 29 (43) 39 (57) |
Prior BTK inhibitor therapy,a n (%) Ibrutinib Acalabrutinib | 58 (85) 16 (24) |
Disease that relapsed or was refractory to BTK inhibitor therapy, n (%) Refractory to BTK inhibitor therapy Relapse during BTK inhibitor therapy Relapse after BTK inhibitor therapy | 42 (62) 18 (26) 5 (7) |
BTK = Bruton tyrosine kinase; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IHC = immunohistochemistry; LDH = lactate dehydrogenase; MCL = mantle cell lymphoma; mITT = modified intent-to-treat; SCT = stem cell transplant; SD = standard deviation; s-MIPI = simplified Mantle Cell Lymphoma International Prognostic Index; ULN = upper limit of normal.
aSix patients (9%) received both ibrutinib and acalabrutinib.
Source: ZUMA-2 Clinical Study Report18; Wang et al. (2020).45
Interventions
Leukapheresis
All patients underwent leukapheresis to obtain leukocytes for the manufacturing of brexucabtagene autoleucel. A minimum of 12 L to 15 L of leukapheresis material was processed, with a goal of obtaining approximately 5 × 109 to 10 × 109 mononuclear cells.18
Bridging Therapy
If necessary, and at the discretion of the investigator, bridging therapy was considered for any patient, and particularly for patients with high disease burden at screening. Bridging therapy was administered after leukapheresis and was completed at least 5 days before the initiation of lymphodepleting chemotherapy. It was not intended for treatment purposes, only to ensure that a patient remained eligible for the brexucabtagene autoleucel infusion. The following bridging therapy regimens were permitted: dexamethasone 20 mg to 40 mg or equivalent orally or IV daily for 1 day to 4 days, ibrutinib at a dose of 560 mg daily or most recent dose if there had been a dose adjustment, or acalabrutinib 100 mg every 12 hours or most recent dose if there had been a dose adjustment.18
Conditioning Chemotherapy
Conditioning (lymphodepleting) chemotherapy consisting of fludarabine at a dose of 30 mg/m2/day and cyclophosphamide at a dose of 500 mg/m2/day was administered for 3 days on days −5, −4, and −3 to induce lymphocyte depletion. Lymphodepleting chemotherapy was supplied by the investigative site and to commence only when the brexucabtagene autoleucel was manufactured and available at the administrative site.18
Brexucabtagene Autoleucel
The ZUMA-2 study evaluated 2 doses of brexucabtagene autoleucel, an autologous T-cell product manufactured from individual patients’ leukapheresis material. Patients in Cohort 1 were to receive a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram, with a maximum dose of 2 × 108 anti-CD19 CAR T cells for patients 100 kg or more. Patients in Cohort 2 were to receive a target dose of 0.5 × 106 anti-CD19 CAR T cells per kilogram, with a maximum dose of 0.5 × 108 anti-CD19 CAR T cells for patients 100 kg or more.18 As previously stated, only the patients from Cohort 1 are of interest to this review.
The individual, patient-specific product in single-use infusion bags was cryopreserved and returned to the treatment facility in a liquid nitrogen dry shipper. The product was kept frozen until the patient was ready for treatment and stored in the bag in the vapour phase of liquid nitrogen. Patients were to receive a single IV infusion of brexucabtagene autoleucel on day 0, after receiving the 3-day lymphodepleting chemotherapy regimen on day –5 through day –3, with a 2-day rest period between the completion of lymphodepleting chemotherapy and the brexucabtagene autoleucel infusion. The volume of brexucabtagene autoleucel infused, the thaw start and stop times, and the brexucabtagene autoleucel administration start and stop times were recorded. The following medications were administered 1 hour before infusion: acetaminophen 650 mg, and diphenhydramine 12.5 mg to 25 mg IV or 25 mg orally. If the patient did not meet the criteria for infusion, the administration of brexucabtagene autoleucel was to be delayed until the events resolved. If the infusion was delayed by more than 2 weeks, the lymphodepleting chemotherapy was to be repeated. Patients were hospitalized for treatment with brexucabtagene autoleucel and were to remain in the hospital for a minimum of 7 days after treatment, unless a longer stay was required. Patients who achieved a PR or CR had the option to receive a second course of lymphodepleting chemotherapy and brexucabtagene autoleucel if their disease subsequently progressed more than 3 months after the initial brexucabtagene autoleucel infusion, provided that the relapse was confirmed to be CD19 positive.18
Concomitant Medications
Investigators could prescribe medications or treatments deemed necessary to provide adequate supportive care, including prophylactic antimicrobials, growth factor support, and routine anti-emetic prophylaxis. Targeted concomitant medications consisting of gamma globulin, immunosuppressives, anti-infective drugs, and vaccinations were to be recorded for 24 months or until disease progression, whichever occurred first.18
Corticosteroid therapy at a pharmacologic dose (≥ 5 mg/day of prednisone or equivalent doses of other corticosteroids) and other immunosuppressive drugs were to be avoided for 7 days before leukapheresis and 5 days before the brexucabtagene autoleucel infusion, unless these treatments were used for bridging therapy, and were also to be avoided for 3 months after brexucabtagene autoleucel infusion, unless used to manage brexucabtagene autoleucel–related toxicities. Other medications that could interfere with the evaluation of brexucabtagene autoleucel, such as nonsteroidal anti-inflammatory agents, were also to be avoided for the same period unless medically necessary. Treatment for the patient’s lymphoma other than what was defined or allowed in the protocol, such as chemotherapy, immunotherapy, targeted agents, radiation, high-dose corticosteroids, and other investigational agents, was prohibited except as needed for treatment of disease progression after brexucabtagene autoleucel infusion.18
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized in the sections that follow. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 3.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | ZUMA-2 |
|---|---|
ORR | Primary efficacy end point |
BOR | Secondary efficacy end point |
DOR | Secondary efficacy end point |
PFS | Secondary efficacy end point |
OS | Secondary efficacy end point |
HRQoL (EQ-5D) | Secondary efficacy end point |
Safety | Secondary efficacy end point |
Incidence of SCT after treatment with brexucabtagene autoleucel in the inferential analysis set | Exploratory efficacy end point |
Response to re-treatment with brexucabtagene autoleucel | Exploratory efficacy end point |
BOR = best objective response; DOR = duration of response; EQ-5D = EuroQol 5-Dimensions questionnaire; HRQoL = health-related quality of life; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; SCT = stem cell transplant.
Source: ZUMA-2 Clinical Study Report.18
Objective Response Rate
The primary efficacy end point was the ORR, defined as the incidence of CR or PR using central assessment per the Lugano classification. The original protocol had a primary end point of ORR per investigator assessment, which was amended to the Lugano classification based on independent radiological review on November 13, 2017. To maintain consistency, all subsequent patients enrolled in Cohort 1 were assessed by the investigators per the International Working Group (IWG) 2007 criteria as a secondary outcome. Patients were to have their first PET/CT scan to assess for disease 4 weeks after infusion of brexucabtagene autoleucel. Scans were repeated every 3 months, and as needed for patients who displayed symptoms suggestive of disease progression. Evaluations of bone marrow were also needed to confirm CR.17,18
Best Objective Response
Incidence of BOR (CR, PR, stable disease, progressive disease, and not evaluable) were calculated using central assessment per the Lugano classification,17 and investigator assessment per the IWG 2007 criteria.18,47
Duration of Response
Duration of response was evaluated only for patients who had an objective response (CR or PR) and was defined as the time from the first objective response to disease progression or death, using disease assessments (central and investigator assessment).18
Progression-Free Survival
Progression-free survival was defined as the time from the date of brexucabtagene autoleucel infusion to the date of disease progression or death from any cause using both central assessment and investigator assessment. In the FAS, PFS was defined as the time from the enrolment date to the date of disease progression or death from any cause.18
Overall Survival
Overall survival was defined as the time from the date of brexucabtagene autoleucel infusion to the date of death from any cause. In the FAS, OS was defined as the time from enrolment to the date of death from any cause.18
Health-Related Quality of Life: EuroQol 5-Dimensions Questionnaire
Patients’ HRQoL was assessed using the EuroQol 5-Dimensions questionnaire (EQ-5D) at screening (for baseline scores), week 4 (± 3 days), month 3 (± 1 week), and month 6 (during the long-term follow-up period) before any other assessments or procedures were performed. The EQ-5D was added to the schedule of assessments following a protocol amendment on August 23, 2016.18 For each health dimension in the EQ-5D, patients were instructed to select the severity level (no problems, slight problems, moderate problems, severe problems, or extreme problems) that best described their health status on the day that the questionnaire was administered. The EQ-5D also included the EuroQol Visual Analogue Scale (EQ VAS), in which patients rated their overall health status from 0 (representing “the worst health you can imagine”) to 100 (representing “the best health you can imagine”).18 A detailed discussion and critical appraisal of the EQ-5D measure is provided in Appendix 3.
Safety
Patients underwent safety assessments throughout the study. Investigators were to report all AEs and SAEs that occurred from enrolment through 3 months after brexucabtagene autoleucel infusion. Targeted AEs (e.g., neurologic, hematological, infections, autoimmune disorders, and secondary malignancies) were monitored and reported for 24 months after the brexucabtagene autoleucel infusion or until disease progression, whichever occurred first. All AEs were considered treatment emergent, defined as having had an onset on or after the brexucabtagene autoleucel infusion. Investigators were to identify CRS as a syndrome via case report form that was specifically designed to record CRS and to grade its severity according to a modification of the grading system proposed by Lee and colleagues.48 All SAEs were reported from screening to 3 months after infusion with brexucabtagene autoleucel. Adverse events were investigator reported and were coded with the Medical Dictionary for Regulatory Activities, version 22.0, and the severity of AEs was graded using Common Terminology Criteria for Adverse Events, version 4.03. Cytokine release syndrome, neurologic AEs, cytopenias, infections, and hypogammaglobulinemia were of special interest in the ZUMA-2 trial protocol.18
Statistical Analysis
Sample Size and Power Calculation
Up to approximately 130 patients with R/R MCL were enrolled and treated in 2 cohorts. Cohort 1 was to include at least 60, and up to approximately 80, patients who received brexucabtagene autoleucel at a dose of 2 × 106 anti-CD19 CAR T cells per kilogram (an additional 10 patients were treated with axicabtagene ciloleucel; these patients are reported separately from the results of ZUMA-2, as per the protocol amendment on June 22, 2018). The same protocol amendment clarified that the primary analysis was conducted after 60 patients in Cohort 1 were treated with brexucabtagene autoleucel and had the opportunity to be assessed for response 6 months after the week 4 disease assessment. A sample size of 60 patients in Cohort 1 had at least 96% power to distinguish between an active therapy with a true response rate of 50% or higher and a therapy with an ORR of 25% or less, with a 1-sided alpha level of 0.025.18
Interim and Final Analyses
Four interim analyses were performed for Cohort 1 and were reviewed by an independent data and the safety monitoring board (DSMB). The interim analyses for Cohort 1 included18:
Interim analysis 1, conducted after 10 patients in this cohort had been treated with anti-CD19 CAR T cells and had had the opportunity to be followed for 30 days. The DSMB reviewed these data for safety only.
Interim analysis 2, conducted after 20 patients in this cohort had had the opportunity to be evaluated for response 3 months after treatment with anti-CD19 CAR T cells. The DSMB reviewed these data for safety and futility and made study conduct recommendations based on the risk versus benefit of anti-CD19 CAR T-cell treatment. A rho (parameter = 0.30) beta spending function was used to allocate the beta level between the futility analysis at Cohort 1, interim analysis 2, and the primary efficacy analysis. The nonbinding futility boundary for this interim analysis would have been reached if no more than 5 of the 20 patients achieved a response. The criteria for futility were not met, and the DSMB recommended that the study continue.
Interim analysis 3, reviewed by manufacturer to assess the accumulating data of efficacy and safety. This analysis was performed after 38 patients in Cohort 1 had had the opportunity to be evaluated for response 6 months after the anti-CD19 CAR T-cell infusion.
Interim analysis 4, which occurred after 44 patients in this cohort had had the opportunity to be followed for 30 days after the anti-CD19 CAR T-cell infusion. The DSMB reviewed these data for safety only and focused on the first 6 patients treated with brexucabtagene autoleucel when enrolment in this cohort resumed in June 2018.
Two data cut-off analyses were included in this report. The original data cut-off date for the ZUMA-2 trial was July 24, 2019, representing a median follow-up of 12.3 months.18 The updated analysis data cut-off date was December 31, 2019, representing a median follow-up of 16.8 months.19 No additional patients were enrolled between the first and second data cut-offs, and the second data cut-off solely represents a longer follow-up time.
Primary End Point Analysis
Originally, Cohort 1 was designated as the nonpivotal cohort (November 13, 2017, protocol amendment), which was subsequently changed as the primary end point of ORR was updated to be based on the Lugano classification by an independent radiology review. In the fifth protocol amendment on June 22, 2018, it was clarified that Cohort 1 was again the pivotal cohort, and the primary analysis would be conducted after 60 patients treated with brexucabtagene autoleucel had been evaluated for response 6 months after their week 4 disease assessment (IAS).
The primary efficacy end point of ZUMA-2 was ORR, defined as the incidence of CR or PR using central assessment per the Lugano classification,17 which was updated from investigator review using the 2007 IWG criteria as of the November 13, 2017, protocol amendment.18 Confidence intervals for the ORR were calculated using the Clopper-Pearson method (an exact interval), Wilson method (sensitivity analysis), Agresti-Coull method (sensitivity analysis), and modified Jeffrey method (sensitivity analysis). Originally, the protocol’s hypothesis was that the response rate was greater than 20%.43 The protocol amendment as of June 22, 2018, specified that the hypothesis was that brexucabtagene autoleucel ORR using central assessment would be significantly higher than the pre-specified historical control rate of 25%, derived from 2 retrospective studies.35,37 This hypothesis was tested in the IAS of Cohort 1 at the 1-sided significance level of 0.025 using an exact binomial test.18 The primary end point of the study was not controlled for multiple comparisons.
Secondary End Point Analysis
For consistency before the protocol amendment, ORR was also calculated using investigator assessment and the 2007 IWG criteria. Incidence of BOR was calculated using the same methods used for ORR, with CR, PR, stable disease, progressive disease, and not evaluable as best response to treatment per the Lugano classification by central assessment and investigator assessment per the 2007 IWG criteria. Secondary outcomes were not tested against the historical control nor were they controlled for type I error. Concordance between central and investigator assessments were conducted for ORR and BOR using a kappa statistic and 2-sided 95% CI.18
Duration of response estimates were determined using the Kaplan–Meier approach and derived using disease assessments (per central and investigator assessment). The DOR for patients who had a new anticancer therapy (including SCT) was censored at the last evaluable disease assessment date before the initiation of the new anticancer therapy. The follow-up time for DOR was estimated using the reverse Kaplan–Meier approach described by Schemper and Smith (1996).49 A sensitivity analysis of DOR was conducted in which disease assessments obtained after SCT (for patients who received an SCT while in a brexucabtagene autoleucel–induced response) were used in the derivation of DOR.18
Kaplan–Meier plots, estimates, and 2-sided 95% CIs were generated for PFS, and the proportion of patients alive and progression-free at 3-month intervals was estimated. The number of patients censored and the reasons for censoring were summarized. Patients who were alive as of the data cut-off date and who had not met criteria for progression were censored at their last evaluable disease assessment date. Patients who went on to receive a new anticancer therapy (including SCT) while in response were censored at their last evaluable disease assessment date before receiving the anticancer therapy. A sensitivity analysis was conducted in which disease assessments obtained after SCT (for patients who received an SCT while in a brexucabtagene autoleucel–induced response) were included in the derivation of PFS.18
For OS, patients who had not died by the data cut-off date were censored at the last date they were known to be alive or at the data cut-off date, whichever was earlier.18
EQ-5D and EQ VAS scores were summarized at baseline and at each post-treatment visit using descriptive statistics.
Safety analyses included all the patients who had received treatment and were summarized using descriptive statistics.
Secondary and exploratory end points of the study were not controlled for multiplicity.
Subgroup Analyses
A priori subgroup analyses of the ORR, DOR, PFS, and OS were conducted for the following baseline covariates. Subgroups were analyzed to evaluate the robustness and consistency of treatment effects found overall.
ECOG PS at baseline
Age at baseline (< 65 years, ≥ 65 years)
Sex
Race
R/R subgroup
Morphologic characteristics
Ki-67 index
CD19 +
t(11;14)
Cyclin D1 overexpression
Disease stage and extent
s-MIPI
Number of prior regimens
Prior BTK inhibitors
Prior therapy regimens
Tumour burden
Analysis Populations
The following analysis populations were defined in ZUMA-218:
The FAS, which included all enrolled patients that underwent leukapheresis (n = 74). This analysis set was used for the summary of patient disposition, as well as for analyses of ORR and other key efficacy end points (BOR, DOR, PFS, and OS).
The IAS, which consisted of the first 60 patients treated with brexucabtagene autoleucel in Cohort 1 who had had the opportunity to be evaluated for response 6 months after the week 4 disease assessment after brexucabtagene autoleucel infusion. This analysis set was used for efficacy analyses in Cohort 1 and the hypothesis testing of the primary end point ORR at the time of the primary analysis (n = 60).
The safety analysis set and mITT analysis sets, which were identical and included all patients treated with any dose of brexucabtagene autoleucel (n = 68).
Results
Patient Disposition
ZUMA-2 was a single-arm, open-label, phase II clinical trial. Table 10 summarizes the disposition of enrolled patients. Seventy-four patients were enrolled and leukapheresed in Cohort 1 of ZUMA-2. In the FAS, brexucabtagene autoleucel was successfully manufactured for 96% of patients. Sixty-nine patients (93%) received lymphodepleting chemotherapy, and 68 patients (92%) received brexucabtagene autoleucel, making up the mITT and safety populations. One patient was not treated with brexucabtagene autoleucel after receiving lymphodepleting chemotherapy due to ongoing active atrial fibrillation. Of the patients who received brexucabtagene autoleucel, 38% received bridging therapy. As of the July 24, 2019, data cut-off, the median potential follow-up time (calculated as the time from KTE-X19 infusion to the data cut-off date) from the brexucabtagene autoleucel infusion was 11.6 months (range = 1.9 months to 32.3 months) in the FAS (12.3 months in the IAS), and 16 of the 68 patients who received brexucabtagene autoleucel had died: 14 due to progressive disease, and 2 due to AEs (organizing pneumonia and staphylococcal bacteremia).18
As of the December 31, 2019, data cut-off, the median potential follow-up time from brexucabtagene autoleucel infusion was 16.8 months in the FAS, and 18 patients (24%) had died.19
Patients in the FAS were leukapheresed a median of 16.0 days (range = 5 days to 274 days) after study screening, and the median time from screening to leukapheresis was also 16.0 days (range = 5 days to 274 days). The median time to from leukapheresis to administration of brexucabtagene autoleucel was 27.0 days (range = 19 days to 134 days). As per the study protocol, patients were to remain in hospital for at least 7 days following brexucabtagene autoleucel infusion. The mean duration of hospitalization was 21.2 days (SD: 14.9) (median = 15 days; range = 8 days to 87 days).18
Table 10: Patient Disposition: FAS
Patient disposition | ZUMA-2 (FAS) | |
|---|---|---|
July 24, 2019 DCO | December 31, 2019 DCO | |
Screened, N | 97 | |
Enrolled, N (%) | 74 | |
mITT, N | 68 | |
Safety, N | 68 | |
Patients enrolled and received bridging therapy, n (%) | 28 (38) | |
Patients treated with lymphodepleting chemotherapy, n (%) | 69 (93) | |
Patients treated with brexucabtagene autoleucel, n (%) | 68 (92) | |
Patients treated with brexucabtagene autoleucel and received bridging therapy, n (%) | 25 (34) | |
Primary reason for ending study for patients treated with brexucabtagene autoleucel, n (%) Death Full consent withdrawal | 16 (22) 0 | || || |
Primary reason for ending study for patients not treated with brexucabtagene autoleucel, n (%) Death Full consent withdrawal Other | 4 (6) 1 (1) 1 (1) | |
Potential follow-up time from brexucabtagene autoleucel infusion (month)a Mean (SD) Median (range) | 16.4 (9.7) 11.6 (1.9 to 32.3) | |||||||||||| |||||||||||||| |
Actual follow-up time from brexucabtagene autoleucel infusion (month)b Mean (SD) Median (range) | 13.7 (9.6) 10.3 (1.2 to 32.3) | |||||| |||||||||||||| |
Patients with ≥ 1 month potential follow-up, n (%) | 68 (100) | | |
Patients with ≥ 3 months potential follow-up, n (%) | 64 (94) | | |
Patients with ≥ 6 months potential follow-up, n (%) | 60 (88) | | |
Patients with ≥ 9 months potential follow-up, n (%) | 47 (69) | |||||||||||| |
Patients with ≥ 12 months potential follow-up, n (%) | 32 (47) | |||||||||||| |
Patients with ≥ 15 months potential follow-up, n (%) | 28 (41) | |||||||||||| |
Patients with ≥ 18 months potential follow-up, n (%) | 28 (41) | |||||||||||| |
Patients with ≥ 24 months potential follow-up, n (%) | 28 (41) | |||||||||||| |
Patients with ≥ 30 months potential follow-up, n (%) | 2 (3) | |||||||||||| |
DCO = data cut-off; FAS = full analysis set; mITT = modified intention to treat; SD = standard deviation.
Note: No new patients were enrolled following the primary data cut-off of July 24, 2019.
aPotential follow-up time is calculated as the time from brexucabtagene autoleucel infusion to the data cut-off date.
bActual follow-up time from brexucabtagene autoleucel infusion is calculated as time from first dose of brexucabtagene autoleucel to date of death or the last date known alive.
Source: ZUMA-2 Clinical Study Report18; ZUMA-2 updated analysis.19
Exposure to Study Treatments
Exposure to study treatments is summarized in Table 11. Bridging therapy was administered to patients at the discretion of the treating investigator. A total of 25 patients (37%) received bridging therapy. The most commonly administered bridging therapies were ibrutinib (n = 14 [21%]) and dexamethasone (n = 12 [18%]).18
All patients received the planned total body surface area–adjusted dose of cyclophosphamide (1,500 mg/m2), and patients received a median total body surface area–adjusted dose of fludarabine of 90 mg/m2 (range = 69 mg/m2 to 90 mg/m2). One patient received a total body surface area–adjusted dose of fludarabine that was reduced to 69 mg/m2 due to elevated creatinine. All other patients received within 10% of the planned total dose.18
The median weight-adjusted dose of brexucabtagene autoleucel was 2.0 × 106 anti-CD19 CAR T cells per kilogram. Two patients did not receive within 10% of the target dose, 1 of whom had progressive disease soon after leukapheresis and received a dose of 0.6 × 106 in lieu of being leukapheresed a second time. This patient was not among the first 60 patients to be treated with brexucabtagene autoleucel and, therefore, was not included the IAS.18
Table 11: Exposure to Study Treatments: Safety Analysis Set — DCO July 24, 2019
Exposure to study treatments | ZUMA-2 (N = 68) |
|---|---|
Lymphodepleting chemotherapy | |
Cyclophosphamide, total BSA-adjusted dose, mg/m2 Mean (SD) Median (range) Patients who received ± 10% planned total dose, n (%) | 1,500.0 (0.0) 1,500.0 (1,500.0 to 1,500.0) 68 (100) |
Fludarabine, total BSA-adjusted dose, mg/m2 Mean (SD) Median (range) Patients who received ± 10% planned total dose, n (%) | 89.7 (2.5) 90.0 (69.0 to 90.0) 67 (99) |
Bridging therapy | |
Patients with any bridging therapy, n (%) Ibrutinib Dexamethasone Acalabrutinib Methylprednisolone Patients with both BTK inhibitor and corticosteroid, n (%) Ibrutinib and corticosteroid AcaIabrutinib and corticosteroid | 25 (37) 14 (21) 12 (18) 5 (7) 2 (3) 6 (9) 4 (6) 2 (3) |
Brexucabtagene autoleucel | |
Weight-adjusted brexucabtagene autoleucel dose received, × 106 anti-CD19 CAR T cells per kilogram Mean (SD) Median (range) | 2.0 (0.2) 2.0 (0.6 to 2.0) |
Total number of anti-CD19 CAR T cells, × 106 Mean (SD) Median (range) | 158.6 (30.1) 160.5 (51.8 to 202.0) |
Total number of T cells infused, × 106 Mean (SD) Median (range) | 291.5 (95.6) 260.6 (143.2 to 579.4) |
Patients who received ± 10% planned total dose, n (%) | 66 (97) |
BSA = body surface area; BTK = Bruton tyrosine kinase; CAR = chimeric antigen receptor; DCO = data cut-off; SD = standard deviation.
Source: ZUMA-2 Clinical Study Report.18
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below.
Primary Efficacy End Point(s)
ORR Using Central Assessment: Primary Analysis Data Cut-Off — July 24, 2019
The ZUMA-2 trial met its primary efficacy end point of ORR per central assessment in the IAS. A summary of ORR results in the IAS and FAS is included in Table 12. The ORR in the IAS was 93% (95% CI, 83.8% to 98.2%) versus the pre-specified historical control rate of 25% (P < 0.0001), and the CR rate was 67% (95% CI, 53.3% to 78.3%). Twenty-four patients (57%) who initially had PR or stable disease went on to achieve a CR after a median of 2.2 months (range = 1.8 months to 8.3 months).18
In the FAS, the ORR was higher than the pre-specified historical control rate at 85% (95% CI, 75.0% to 92.3%), with a CR rate of 59% (95% CI, 47.4% to 70.7%).18
ORR Using Central Assessment: Updated Analysis Data Cut-Off — December 31, 2019
As of the longer-term data cut-off, with a median follow-up of 16.8 months (FAS), 55 patients (92%) in the IAS achieved an ORR (Table 12), which differed from the primary analysis (93%) due to a change in the disease response assessment for 1 patient. As with the primary analysis, the 92% ORR observed in the IAS and || ORR in the FAS were significantly higher than the pre-specified historical control rate of 25%.19
Table 12: Summary of Best Objective Response Using Central Assessment per Lugano Classification: IAS and FAS
Response per Lugano classification | July 24, 2019, DCO | December 31, 2019, DCO | ||
|---|---|---|---|---|
IAS (N = 60) | FAS (N = 74) | IAS (N = 60) | FAS (N = 74) | |
Patients with objective response (CR + PR), n (%) 95% CI (Clopper-Pearson method) 95% CI (Wilson method) 95% CI (Agresti-Coull method) 95% CI (modified Jeffrey method) | 56 (93) 83.8 to 98.2 84.1 to 97.4 83.6 to 97.8 84.9 to 97.7 | 63 (85) 75.0 to 92.3 75.3 to 91.5 75.1 to 91.7 75.8 to 91.8 | 55 (92) 81.6 to 97.2 NR NR NR | |||| ||||| |||| |||| |||| |
P value of exact test for ORR ≤ 25% | < 0.0001 | < 0.0001 | < 0.0001 | |||| |
CR, n (%) 95% CI (Clopper-Pearson method) | 40 (67) 53.3 to 78.3 | 44 (59) 47.4 to 70.7 | 40 (67) 53.3 to 78.3 | | |||||| |
PR, n (%) 95% CI (Clopper-Pearson method) | 16 (27) 16.1 to 39.7 | 19 (26) 16.2 to 37.2 | 15 (25) 14.7 to 37.9 | | |||||| |
Stable disease, n (%) 95% CI (Clopper-Pearson method) | 2 (3) 0.4 to 11.5 | 3 (4) 0.8 to 11.4 | 2 (3) 0.4 to 11.5 | |||| |||| |
Progressive disease, n (%) 95% CI (Clopper-Pearson method) | 2 (3) 0.4 to 11.5 | 2 (3) 0.3 to 9.4 | 2 (3) 0.4 to 11.5 | |||| |||| |
CI = confidence interval; CR = complete response; DCO = data cut-off; FAS = full analysis set; IAS = inferential analysis set; NR = not reported; ORR = objective response rate; PR = partial response.
Note: P values for ORR are not adjusted for type I error rate.
Source: ZUMA-2 Clinical Study Report18; ZUMA-2 updated analysis.19
Subgroup Analysis: Primary Analysis Data Cut-Off — July 24, 2019
Subgroups of interest outlined in the review protocol (Table 6) for ORR in the IAS are summarized in Table 13. Across all subgroups of interest, the ORRs ranged from 80% to 100%, compared with the ORR of 93% that was observed for all patients.18
Subgroup Analysis: Updated Analysis Data Cut-Off — December 31, 2019
Subgroup data for the IAS as of the December 31, 2019, data cut-off were consistent with the results observed for subsets in the primary analysis.19
Table 13: Subgroup Analysis of ORR Using Central Assessment per Lugano Classification: IAS — DCO July 24, 2019
Subgroup | Objective response rate | |
|---|---|---|
n | ORR (95% CI) | |
Age < 65 years (N = 28) ≥ 65 years (N = 32) | 26 30 | 0.93 (0.76 to 0.99) 0.94 (0.79 to 0.99) |
ECOG PS 0 (N = 39) 1 (N = 21) | 37 19 | 0.95 (0.83 to 0.99) 0.90 (0.70 to 0.99) |
Disease morphology Pleomorphic MCL (N = 4) Blastoid MCL (N = 14) | 4 13 | 1.00 (0.40 to 1.00) 0.93 (0.66 to 1.00) |
Disease status Relapsed after autologous SCT (N = 26) Relapsed after last MCL therapy (N = 10) Refractory to last MCL therapy (N = 24) | 24 10 22 | 0.92 (0.75 to 0.99) 1.00 (0.69 to 1.00) 0.92 (0.73 to 0.99) |
Bulky disease Yes (N = 5) No (N = 55) | 4 52 | 0.80 (0.28 to 0.99) 0.95 (0.85 to 0.99) |
Ki-67 (%) indexa < median (N = 21) ≥ median (N = 25) < 30% (N = 8) ≥ 30% (N = 38) < 50% (N = 14) ≥ 50% (N = 32) | 20 24 8 36 14 30 | 0.95 (0.76 to 1.00) 0.96 (0.80 to 1.00) 1.00 (0.63 to 1.00) 0.95 (0.82 to 0.99) 1.00 (0.77 to 1.00) 0.94 (0.79 to 0.99) |
CD19 positive Yes (N = 44) No (N = 3) | 42 3 | 0.95 (0.85 to 0.99) 1.00 (0.29 to 1.00) |
Number of prior treatments 1 (N = 0) 2 to 3 (N = 40) ≥ 4 (N = 20) | 0 38 18 | NA 0.95 (0.83 to 0.99) 0.90 (0.68 to 0.99) |
CI = confidence interval; DCO = data cut-off; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IAS = inferential analysis set; MCL = mantle cell lymphoma; NA = not applicable; ORR = objective response rate; SCT = stem cell transplant.
aThe median percentage of tumour cells expressing Ki-67 was 65%.
Source: ZUMA-2 Clinical Study Report.18
Secondary Efficacy End Points
ORR Using Investigator Assessment: Primary Analysis Data Cut-Off — July 24, 2019
In the IAS, the ORR using the investigators’ assessment of response per IWG 2007 criteria was 88% (95% CI, 77.4% to 95.2%), and the CR rate was 70% (95% CI, 56.8% to 81.2%).18
DOR: Primary Analysis Data Cut-Off — July 24, 2019
Duration of response in the IAS and FAS is summarized in Table 14. The median time to CR or PR using the Lugano classification was 1.0 month (range = 0.8 months to 3.1 months), and the median time to achieve a CR was 3.0 months (range = 0.9 months to 9.3 months). As of the July 24, 2019, data cut-off and a median follow-up time for DOR of 8.6 months (reverse Kaplan–Meier approach), the median DOR was not reached. Thirty-nine patients (65%) were censored due to ongoing response, receipt of non-SCT anticancer therapy or allogeneic SCT, and consent withdrawal. Among those who were not censored, 14 patients (25%) had disease progression and 3 patients (5%) died. The median DOR was not reached in the 40 patients who achieved a CR, as 52% of patients had an ongoing CR, and only 7 patients had disease progression. For the 16 patients who achieved a PR, the median DOR was 2.2 months (95% CI, 1.4 months to not estimable). Six patients were censored: 3 (5% of the IAS) had an ongoing PR, 2 started a non-SCT anticancer therapy, and 1 withdrew consent. Of those not censored, 7 patients had disease progression and 3 patients died.18
In the FAS, the median DOR was not reached with a median follow-up of 8.1 months (Table 14). Forty-five patients (71%) were censored: 39 (53%) in the FAS had an ongoing response (62% of patients with objective response), 3 started a non-SCT anticancer therapy, 2 had an allogeneic SCT, and 1 withdrew consent. Of the 18 patients who experienced progression or death, 15 had disease progression and 3 died.18
Table 14: DOR Using Central Assessment per Lugano Classification in Patients With OR, CR, and PR: IAS and FAS — DCO July 24, 2019
Response per Lugano classification | IAS (N = 60) | FAS (N = 74) | ||
|---|---|---|---|---|
OR (N = 56) | CR (N = 40) | PR (N = 16) | OR (N = 63) | |
Event, n (%) Disease progression Death | 17 (30) 14 (25) 3 (5) | 7 (18) 7 (18) NR | 10 (63) 7 (44) 3 (19) | 18 (29) 15 (24) 3 (5) |
Censored, n (%) Response ongoing, n (%) SCT, n (%) Started non-SCT new ACT, n (%) Withdrawal of consent or lost to follow-up, n (%) | 39 (70) 34 (61) 1 (2) 3 (5) 1 (2) | 33 (83) 31 (78) 1 (3) 1 (3) NR | 6 (38) 3 (19) NR 2 (13) 1 (6) | 45 (71) 39 (62) 2 (3) 3 (5) 1 (2) |
Median DOR, months (95% CI) | Not reached (8.6 to NE) | Not reached (13.6 to NE) | 2.2 (1.4 to NE) | Not reached (8.6 to NE) |
Event-free rate by KM estimation, % (95% CI) 3 months 6 months 9 months 12 months 15 months 18 months | 85.1 (72.3 to 92.2) 76.6 (62.4 to 86.1) 64.0 (46.9 to 76.9) 64.0 (46.9 to 76.9) 59.7 (41.8 to 73.8) 59.7 (41.8 to 73.8) | 100.0 (NE to NE) 94.0 (77.9 to 98.5) 76.2 (53.4 to 88.9) 76.2 (53.4 to 88.9) 69.9 (45.3 to 85.0) 69.9 (45.3 to 85.0) | 42.3 (16.6 to 66.3) 25.4 (6.4 to 50.5) 25.4 (6.4 to 50.5) 25.4 (6.4 to 50.5) 25.4 (6.4 to 50.5) 25.4 (6.4 to 50.5) | 84.4 (72.0 to 91.6) 76.0 (62.0 to 85.4) 63.5 (46.6 to 76.3) 63.5 (46.6 to 76.3) 59.3 (41.5 to 73.2) 59.3 (41.5 to 73.2) |
ACT = anticancer therapy; CI = confidence interval; CR = complete response; DCO = data cut-off; DOR = duration of response; FAS = full analysis set; IAS = inferential analysis set; KM = Kaplan–Meier; NE = not estimable; NR = not reported; OR = objective response; PR = partial response; SCT = stem cell transplant.
Source: ZUMA-2 Clinical Study Report.18
Sensitivity analysis of DOR was conducted in patients who received an allogeneic or autologous SCT while in response and were censored at their last evaluable disease assessment date after SCT. As of the July 24, 2019, data cut-off, 1 patient had received an allogeneic SCT while in remission induced by brexucabtagene autoleucel. Excluding this patient, and with a median follow-up of 8.6 months, the median DOR was not reached. Thirty-eight patients were censored compared to the 39 censored in the primary analysis: 34 (57%) had an ongoing response, 3 started a non-SCT anticancer therapy, and 1 withdrew consent.18
DOR: Updated Analysis Data Cut-Off — December 31, 2019
With a median follow-up time for DOR of 14.1 months, the median DOR was still not reached (95% CI, 13.6 months to not estimable), and the proportion of responders remaining in response at 6 months and 12 months was 77.2% and 65.6%, respectively. In patients who achieved a CR, the median DOR was still not reached (95% CI, 14.4 to not estimable), with a median follow-up time of 13.8 months (95% CI, 11.4 months to 26.5 months). Similarly, in the FAS, the median DOR was |||||||||||| (95% CI, ||||||||||||||||||||||) after 13.8 months follow-up (Table 15), and the proportion of responders remaining in response was similar to that of the IAS.19
Table 15: DOR Using Central Assessment per Lugano Classification in Patients With OR and CR: IAS and FAS — DCO December 31, 2019
Response per Lugano classification | IAS (N = 60) | FAS (N = 74) | |
|---|---|---|---|
Patients with OR (N = 55) | Patients with CR (N = 40) | Patients with OR (N = 62) | |
Event, n (%) | 21 (38) | 10 (25) | |||| |
Disease progression | 18 (33) | 10 (25) | |||| |
Death | 3 (5) | NR | |||| |
Censored, n (%) | 34 (62) | 30 (75) | |||| |
Response ongoing, n (%) | 29 (53) | 28 (70) | |||| |
SCT, n (%) | 1 (2) | 1 (3) | | |
Started non-SCT new ACT, n (%) | 3 (5) | 1 (3) | |||| |
Withdrawal of consent or lost to follow-up, n (%) | 1 (2) | NR | |||| |
Median DOR, months (95% CI) | Not reached (13.6 to NE) | Not reached (14.4 to NE) | ||||||| ||| |
Event-free rate by KM estimation, % (95% CI): 3 months 6 months 9 months 12 months 15 months 18 months 21 months 24 months 27 months 30 months 33 months | 84.9 (72.1 to 92.2) 77.2 (63.4 to 86.4) 67.6 (53.1 to 78.4) 65.6 (51.1 to 76.8) 58.6 (42.5 to 71.7) 58.6 (42.5 to 71.7) 58.6 (42.5 to 71.7) 58.6 (42.5 to 71.7) 58.6 (42.5 to 71.7) 52.7 (34.5 to 68.1) 52.7 (34.5 to 68.1) | 100.0 (NE to NE) 94.9 (81.0 to 98.7) 82.1 (66.0 to 91.0) 79.5 (63.1 to 89.2) 69.7 (49.3 to 83.2) 69.7 (49.3 to 83.2) 69.7 (49.3 to 83.2) 69.7 (49.3 to 83.2) 69.7 (49.3 to 83.2) 69.7 (49.3 to 83.2) 69.7 (49.3 to 83.2) | |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |
ACT = anticancer therapy; CI = confidence interval; CR = complete response; DCO = data cut-off; DOR = duration of response; FAS = full analysis set; IAS = inferential analysis set; KM = Kaplan–Meier; NE = not estimable; NR = not reported; OR = objective response; SCT = stem cell transplant.
Source: ZUMA-2 updated analysis.19
PFS: Primary Analysis Data Cut-Off — July 24, 2019
Results of PFS for the IAS and FAS are summarized in Table 16. As of the July 24, 2019, data cut-off (12.3 months follow-up), the median PFS in the IAS was not reached (9.2 to not estimable) (Figure 3a). Kaplan–Meier estimates of PFS rates at 6 months, 12 months, and 24 months were 77.0%, 60.9%, and 56.9%, respectively. In the FAS, the median PFS was not reached (9.9 to not estimable) and the 6-month, 12-month, and 24-month PFS rates were 75.2%, 55.6%, and 51.9%, respectively.18
Sensitivity analysis of PFS was conducted for patients who received an allogeneic or autologous SCT while in response and were censored at their last evaluable disease assessment date after SCT. As of the July 24, 2019, data cut-off, 1 patient had received an allogeneic SCT while in a brexucabtagene autoleucel–induced remission and was censored from the analysis. Similar to the overall IAS, the median PFS in the remaining patients was not reached with a median follow-up of 12.3 months, and the 6-month and 12-month PFS rate estimates were 77.2% and 59.4%.18
PFS: Updated Analysis Data Cut-Off — December 31, 2019
Results of PFS for the IAS and FAS as of the December 31, 2019, data cut-off are summarized in Table 16. As of the updated analysis, the median PFS in the IAS was still not reached (95% CI, 9.6 to not estimable; Figure 3b), and the Kaplan–Meier estimates of PFS rate at 6 months and 12 months were similar to those at the primary data cut-off, at 76.8% and 62.2%, respectively. The 24-month and 33-month PFS rate estimates were 55.5% and 50.5%, respectively.
In the FAS, the median PFS was ||||||||||||, and the 6-month,12-month, 24-month, and 33-month PFS rates were ||||||||||||||||||||||||||||||||||||||, respectively.19
Table 16: PFS Using Central Assessment per Lugano Classification
PFS | July 24, 2019, DCO | December 31, 2019, DCO | ||
|---|---|---|---|---|
IAS (N = 60)a | FAS (N = 74)b | IAS (N = 60)a | FAS (N = 74)b | |
Event, n (%) Disease progression Death | 20 (33) 17 (28) 3 (5) | 27 (36) 18 (24) 9 (12) | 24 (40) 21 (35) 3 (5) | |||| |||| |||| |
Censored, n (%) Response/stable disease ongoing Started non-SCT new ACT SCT Withdrawal of consent or lost to follow-up No disease assessment | 40 (67) 34 (57) 4 (7) 1 (2) 1 (2) NR | 47 (64) 39 (53) 4 (5) 2 (3) 1 (1) 1 (1) | 36 (60) 29 (48) 4 (7) 1 (2) 1 (2) 1 (2) | |||| |||| |||| |||| |||| |||| |
Median PFS, months (95% CI) | Not reached (9.2 to NE) | Not reached (9.9 to NE) | Not reached (9.6 to NE) | |||| |||| |
PFS rate by KM estimation, % (95% CI) 3 months 6 months 9 months 12 months 15 months 18 months 21 months 24 months 27 months 30 months 33 months 36 months | 86.2 (74.3 to 92.8) 77.0 (63.6 to 85.9) 70.4 (56.1 to 80.8) 60.9 (44.7 to 73.7) 56.9 (39.8 to 70.8) 56.9 (39.8 to 70.8) 56.9 (39.8 to 70.8) 56.9 (39.8 to 70.8) NR NR NR NR | 87.6 (77.5 to 93.3) 75.2 (63.0 to 83.8) 64.1 (50.7 to 74.7) 55.6 (40.8 to 68.1) 55.6 (40.8 to 68.1) 51.9 (36.4 to 65.3) 51.9 (36.4 to 65.3) 51.9 (36.4 to 65.3) NR NR NR NR | 85.9 (73.8 to 92.7) 76.8 (63.4 to 85.8) 71.3 (57.5 to 81.4) 62.2 (48.1 to 73.5) 59.2 (44.6 to 71.2) 55.5 (40.0 to 68.5) 55.5 (40.0 to 68.5) 55.5 (40.0 to 68.5) 55.5 (40.0 to 68.5) 50.5 (33.6 to 65.2) 50.5 (33.6 to 65.2) NR | |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |
ACT = anticancer therapy; CI = confidence interval; DCO = data cut-off; FAS = full analysis set; IAS = inferential analysis set; KM = Kaplan–Meier; NE = not estimable; NR = not reported; PFS = progression-free survival; SCT = stem cell transplant.
aProgression-free survival was defined as the time from the date of the brexucabtagene autoleucel infusion to the date of disease progression or death from any cause. Patients not meeting the criteria by the analysis data cut-off date were censored at their last evaluable disease assessment date before the data cut-off date or new ACT (including SCT) start date, whichever was earlier.
bProgression-free survival was defined as the time from the date of enrolment (i.e., date of leukapheresis) to the date of disease progression or death from any cause.
Source: ZUMA-2 Clinical Study Report18; ZUMA-2 updated analysis.19
Figure 3: PFS Using Central Assessment per Lugano Classification: IAS
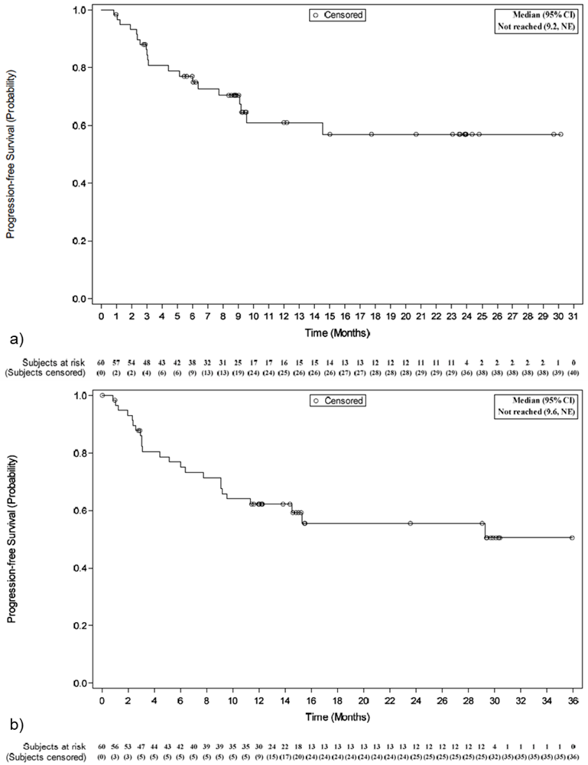
CI = confidence interval; IAS = inferential analysis set; NE = not estimable; PFS = progression-free survival.
Note: (a) Kaplan–Meier curve of PFS on the July 24, 2019, data cut-off; (b) Kaplan–Meier curve of PFS on the December 31, 2019, data cut-off.
Source: ZUMA-2 Clinical Study Report18; ZUMA-2 updated analysis.19
Progression-free survival rate estimates for patients in the IAS with CR and PR are summarized in Table 17. As of the July 24, 2019, data cut-off, the PFS rates at 6 months, 12 months, and 24 months were 100%, 76.6%, and 70.2% in patients with CR, and the median PFS was not reached (95% CI, 14.5 to not estimable). Among patients who achieved a PR, the PFS rate estimates at 6 months and 12 months were each 25.9%, and the median PFS was 3.1 months (95% CI, 2.3 to not estimable).18
As of the December 31, 2019, data cut-off, the median PFS was not reached for patients who achieved a CR (95% CI, 15.3 months to not estimable) and was identical to the median PFS reported for patients with PR in the primary analysis.19
Table 17: PFS in Patients With a CR or PR Using Central Assessment per Lugano Classification: IAS — Data Cut-Off July 24, 2019
PFS per Lugano classification | IAS (N = 60) | |
|---|---|---|
Patients with CR (N = 40) | Patients with PR (N = 16) | |
Event, n (%) Disease progression Death | 7 (18) 7 (18) NR | 10 (63) 7 (44) 3 (19) |
Censored, n (%) Response ongoing or stable disease, n (%) SCT, n (%) Started non-SCT new anticancer therapy, n (%) Withdrawal of consent or lost to follow-up, n (%) | 33 (83) 31 (78) 1 (3) 1 (3) NR | 6 (38) 3 (19) NR 2 (13) 1 (6) |
Median PFS, months (95% CI) | Not reached (14.5 to NE) | 3.1 (2.3 to NE) |
PFS rate by KM estimation, % (95% CI) 3 months 6 months 9 months 12 months 15 months 18 months 21 months 24 months | 100.0 (NE to NE) 100.0 (NE to NE) 90.7 (73.7 to 96.9) 76.6 (54.0 to 89.1) 70.2 (45.7 to 85.2) 70.2 (45.7 to 85.2) 70.2 (45.7 to 85.2) 70.2 (45.7 to 85.2) | 59.3 (30.7 to 79.3) 25.9 (6.6 to 51.1) 25.9 (6.6 to 51.1) 25.9 (6.6 to 51.1) 25.9 (6.6 to 51.1) 25.9 (6.6 to 51.1) 25.9 (6.6 to 51.1) NR |
CI = confidence interval; CR = complete response; IAS = inferential analysis set; KM = Kaplan–Meier; NE = not estimable; NR = not reported; PFS = progression-free survival; PR = partial response; SCT = stem cell transplant.
Source: ZUMA-2 Clinical Study Report.18
Subgroup Analysis: Primary Analysis Data Cut-Off — July 24, 2019
Subgroups of interest outlined in the review protocol (Table 6) of the IAS for PFS are summarized in Table 18. Across subgroups of interest to the review, the PFS rate ranged from 69% to 100%, which was comparable to the 77% PFS rate observed for the overall IAS population.18
Table 18: Subgroup Analysis of PFS Rate at Month 6 Using Central Assessment per Lugano Classification: IAS — DCO July 24, 2019
Subgroup | n | PFS rate (95% CI) |
|---|---|---|
Age < 65 years (N = 28) ≥ 65 years (N = 32) | 18 20 | 0.77 (0.55 to 0.89) 0.77 (0.58 to 0.88) |
ECOG PS 0 (N = 39) 1 (N = 21) | 24 14 | 0.74 (0.57 to 0.85) 0.83 (0.56 to 0.94) |
Disease morphology Pleomorphic MCL (N = 4) Blastoid MCL (N = 14) | 3 8 | 0.75 (0.13 to 0.96) 0.69 (0.36 to 0.87) |
Disease status Relapsed after autologous SCT (N = 26) Relapsed after last MCL therapy (N = 10) Refractory to last MCL therapy (N = 24) | 15 8 15 | 0.72 (0.50 to 0.85) 0.90 (0.47 to 0.99) 0.76 (0.52 to 0.90) |
Bulky disease Yes (N = 5) No (N = 55) | 2 36 | 0.75 (0.13 to 0.96) 0.77 (0.63 to 0.86) |
Ki-67 (%) indexa < median (N = 21) ≥ median (N = 25) < 30% (N = 8) ≥ 30% (N = 38) < 50% (N = 14) ≥ 50% (N = 32) | 14 19 6 27 10 23 | 0.76 (0.52 to 0.89) 0.88 (0.67 to 0.96) 0.88 (0.39 to 0.98) 0.81 (0.65 to 0.91) 0.79 (0.47 to 0.93) 0.84 (0.66 to 0.93) |
CD19 positive Yes (N = 44) No (N = 3) | 30 3 | 0.79 (0.64 to 0.94) 1.00 (NE to NE) |
Number of prior treatments 1 (N = 0) 2 to 3 (N = 40) ≥ 4 (N = 20) | 0 27 11 | 0 0.79 (0.62 to 0.89) 0.73 (0.46 to 0.88) |
CI = confidence interval; DCO = data cut-off; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IAS = inferential analysis set; MCL = mantle cell lymphoma; NE = not estimable; PFS = progression-free survival; SCT = stem cell transplant.
aThe median percentage of tumour cells expressing Ki-67 was 65%.
Source: ZUMA-2 Clinical Study Report.18
OS: Primary Analysis Data Cut-Off — July 24, 2019
Overall survival results for the IAS and FAS are summarized in Table 19. As of the July 24, 2019, data cut-off (12.3 months follow-up), the median OS was not reached (95% CI, 24.0 to not estimable) (Figure 4a) in the IAS, and the OS rates at 6 months, 12 months, and 24 months were 86.7%, 83.2%, and 66%, respectively. In the FAS, the 6-month, 12-month, and 24-month OS rates were 83.2%, 77.1%, and 64.3%, and the median OS was not reached (95% CI, 21.1 to not estimable) (Figure 4b).18
OS: Updated Analysis Data Cut-Off — December 31, 2019
Results of OS for the IAS and FAS as of the December 31, 2019, data cut-off are summarized in Table 19. As of the updated analysis, the median OS in the IAS was still not reached (Figure 4c), and the Kaplan–Meier estimates of OS at 6 months and 12 months were 86.7% and 83.3% and in the 24-month and 36-month estimates were 68.8%. These were comparable to the estimates in the primary analysis. In the FAS, the median OS was also ||||||||||||, and based on Kaplan–Meier estimates, the survival rate was |||||||||||||||||||||||||||||||||||||||||| at 6 months, 12 months, 24 months, and 36 months, respectively.19
Table 19: Overall Survival: IAS and FAS
OS | July 24, 2019, DCO | December 31, 2019, DCO | ||
|---|---|---|---|---|
IAS (N = 60)a | FAS (N = 74)b | IAS (N = 60)a | FAS (N = 74)b | |
Dead, n (%) Alive, n (%) | 15 (25) 45 (75) | 21 (28) 53 (72) | 16 (27) 44 (73) | | | |
Median OS, months (95% CI) | Not reached (24.0 to NE) | Not reached (21.1 to NE) | Not reached (NE to NE) | |||||||| |||||| |
OS rate by KM estimation, % (95% CI) 3 months 6 months 9 months 12 months 15 months 18 months 21 months 24 months 27 months 30 months 33 months 36 months | 95.0 (85.3 to 98.4) 86.7 (75.1 to 93.1) 83.2 (71.0 to 90.6) 83.2 (71.0 to 90.6) 72.9 (56.4 to 84.0) 72.9 (56.4 to 84.0) 69.4 (52.2 to 81.5) 66.0 (48.2 to 78.9) NR NR NR NR | 91.8 (82.7 to 96.2) 83.2 (72.3 to 90.1) 77.1 (65.3 to 85.3) 77.1 (65.3 to 85.3) 67.5 (52.1 to 78.9) 67.5 (52.1 to 78.9) 67.5 (52.1 to 78.9) 64.3 (48.3 to 76.4) NR NR NR NR | 95.0 (85.3 to 98.4) 86.7 (75.1 to 93.1) 83.3 (71.2 to 90.7) 83.3 (71.2 to 90.7) 76.0 (62.8 to 85.1) 76.0 (62.8 to 85.1) 72.4 (57.5 to 82.8) 68.8 (52.7 to 80.3) 68.8 (52.7 to 80.3) 68.8 (52.7 to 80.3) 68.8 (52.7 to 80.3) 68.8 (52.7 to 80.3) | |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |
CI = confidence interval; DCO = data cut-off; FAS = full analysis set; IAS = inferential analysis set; KM = Kaplan–Meier; NE = not estimable; NR = not reported; OS = overall survival.
aOverall survival is defined as the time from the date of the brexucabtagene autoleucel infusion to the date of death from any cause. Patients who were alive by the analysis data cut-off were censored at their last contact date before the data cut-off, with the exception that patients known to be alive or determined to have died after the data cut-off were censored at the data cut-off.
bOverall survival is defined as the time from the enrolment date to the date of death from any cause. Patients who were alive at the analysis data cut-off were censored at their last contact date before the data cut-off, with the exception that patients known to be alive or determined to have died after the data cut-off were censored at the data cut-off.
Source: ZUMA-2 Clinical Study Report18; ZUMA-2 updated analysis.19
Figure 4: OS Kaplan–Meier Estimates: IAS and FAS
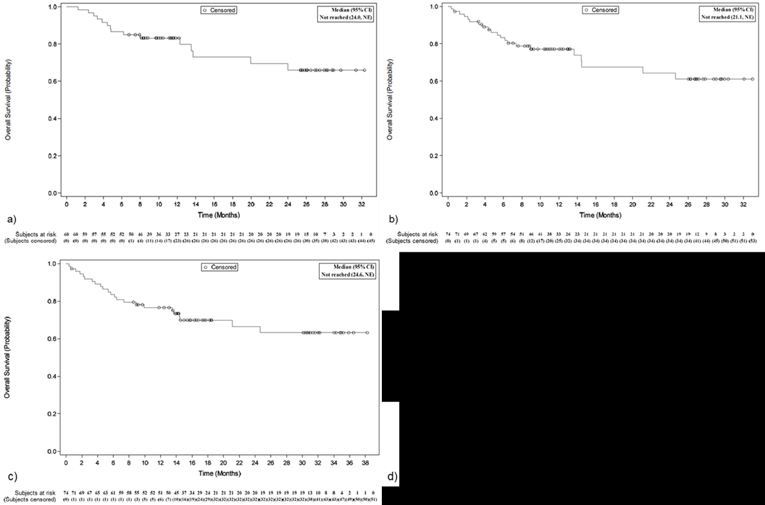
CI = confidence interval; FAS = full analysis set; IAS = inferential analysis set; NE = not estimable; OS = overall survival.
Note: (a) OS in the IAS (data cut-off July 24, 2019); (b) OS in the FAS (data cut-off July 24, 2019); (c) OS in the IAS (data cut-off December 31, 2019); (d) OS in the FAS (data cut-off December 31, 2019).
Source: ZUMA-2 Clinical Study Report18; ZUMA-2 updated analysis.19
Overall survival rate estimates for patients in the IAS with a BOR of CR and PR are summarized in Table 20. Among patients who achieved a CR, OS rate estimates at 6 months and 12 months were 100% and 97.2%, and the median OS was not reached. Among patients who achieved a PR, OS rate estimates at 6 months and 12 months were 62.5% and 56.3%, and the median OS was 19.9 months (3.8 months to not estimable).18
As of the December 31, 2019, data cut-off, the median OS for patients in the IAS with a CR was not reached and the median OS for patients with a PR was 12.6 months (95% CI, 3.3 months to not estimable). In the FAS, the median OS for patients with a CR was not reached and the median OS for patients with a PR was 13.5 months (95% CI, 5.4 months to not estimable).19
Table 20: OS in Patients with a Best Objective Response of CR or PR Using Central Assessment per Lugano Classification: IAS — DCO July 24, 2019
OS | IAS (N = 60) | |
|---|---|---|
Patients with CR (N = 40) | Patients with PR (N = 16) | |
Dead, n (%) Alive, n (%) | 4 (10) 36 (90) | 8 (50) 8 (50) |
Median OS, months (95% CI) | Not reached (NE to NE) | 19.9 (3.8 to NE) |
OS rate by KM estimation, % (95% CI) 3 months 6 months 9 months 12 months 15 months 18 months 21 months 24 months | 100.0 (NE to NE) 100.0 (NE to NE) 97.2 (81.9 to 99.6) 97.2 (81.9 to 99.6) 85.8 (60.5 to 95.4) 85.8 (60.5 to 95.4) 85.8 (60.5 to 95.4) 80.1 (54.0 to 92.3) | 87.5 (58.6 to 96.7) 62.5 (34.9 to 81.1) 56.3 (29.5 to 76.2) 56.3 (29.5 to 76.2) 56.3 (29.5 to 76.2) 56.3 (29.5 to 76.2) 46.9 (20.4 to 69.7) 46.9 (20.4 to 69.7) |
CI = confidence interval; CR = complete response; DCO = data cut-off; IAS = inferential analysis set; KM = Kaplan–Meier; NE = not estimable; OS = overall survival; PR = partial response.
Source: ZUMA-2 Clinical Study Report.18
Subgroup Analysis
Subgroups of interest outlined in the review protocol (Table 6) of the IAS for OS are summarized in Table 21. At the July 24, 2019, data cut-off, patients had a median follow-up of 12.3 months, and 53% of patients had at least 12 months of follow-up. Across evaluable subgroups of interest, the OS rate at month 12 (where the OS rate could be estimated) ranged from 71% to 100%, which was comparable to the 83% rate for the overall IAS population.18
Table 21: Subgroup Analysis of OS Rate at Month 12: IAS — DCO July 24, 2019
Subgroup | n | OS rate (95% CI) |
|---|---|---|
Age < 65 years (N = 28) ≥ 65 years (N = 32) | 11 16 | 0.78 (0.58 to 0.90) 0.88 (0.70 to 0.95) |
ECOG PS 0 (N = 39) 1 (N = 21) | 16 11 | 0.84 (0.69 to 0.93) 0.81 (0.57 to 0.92) |
Disease morphology Pleomorphic MCL (N = 4) Blastoid MCL (N = 14) | 3 4 | 1.00 (NE to NE) 0.71 (0.41 to 0.88) |
Disease status Relapsed after autologous SCT (N = 26) Relapsed after last MCL therapy (N = 10) Refractory to last MCL therapy (N = 24) | 9 5 13 | 0.81 (0.60 to 0.92) 0.90 (0.47 to 0.99) 0.83 (0.61 to 0.93) |
Bulky disease Yes (N = 5) No (N = 55) | 4 23 | 1.00 (NE to NE) 0.82 (0.69 to 0.90) |
Ki-67 (%) indexa < median (N = 21) ≥ median (N = 25) < 30% (N = 8) ≥ 30% (N = 38) < 50% (N = 14) ≥ 50% (N = 32) | 12 11 4 19 7 16 | 0.90 (0.67 to 0.98) 0.88 (0.67 to 0.96) 0.88 (0.39 to 0.98) 0.89 (0.74 to 0.96) 0.86 (0.54 to 0.96) 0.91 (0.74 to 0.97) |
CD19 positive Yes (N = 44) No (N = 3) | 21 2 | 0.86 (0.72 to 0.94) 1.00 (NE to NE) |
Number of prior treatments 1 (N = 0) 2 to 3 (N = 40) ≥ 4 (N = 20) | 0 17 10 | 0 0.87 (0.72 to 0.95) 0.75 (0.50 to 0.89) |
CI = confidence interval; DCO = data cut-off; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IAS = inferential analysis set; MCL = mantle cell lymphoma; NE = not estimable; OS = overall survival; SCT = stem cell transplant.
aThe median percentage of tumour cells expressing Ki-67 was 65%.
Source: ZUMA-2 Clinical Study Report.18
Health-Related Quality of Life
A summary of the proportion of patients in the safety analysis set (N = 68) who completed the questionnaire for each of the 5 domains of the EQ-5D is shown in Table 22. A total of 62 patients (91%) completed the questionnaire at study screening. The majority of responses were available at baseline or screening, with 66% to 95% of patients reporting no health problems on any of the 5 domains, with the highest percentages of no health problems observed for self-care (95%), mobility (85%), and usual activity (82%).18
The proportion of patients reporting severe health problems generally increased through week 4, and the largest decrease in percentage points of patients reporting no health problems between screening and week 4 was observed in the usual activities domain (39 percentage points), with increases in slight and moderate problems doing usual activities of 10 and 17 percentage points, respectively. Conversely, by month 3, increases of up to 26 percentage points were seen from week 4, and increases in the proportion of patients reporting no health problems increased at 3-month and 6-month assessments, demonstrating an improved HRQoL over time.18 Given the limited number of questionnaire respondents at longer follow-up durations, trends in HRQoL relative to earlier time points cannot be interpreted.
The median EQ VAS score was 85.0 (range = 45 to 100) at screening, which decreased to 78.0 (range = 38 to 100) at week 4, followed by higher median scores at month 3 (83.0; range = 40 to 100) and month 6 (90.0; range = 20 to 100). The proportion of patients with a decrease of 10% or more in EQ VAS scores relative to screening was 50% at week 4, 29% by month 3, and 12% by month 6,18 suggesting that HRQoL decreases following infusion but improves over time. Inferences on the trend for improvement in HRQoL over time cannot be made given the decrease in the number of respondents at longer time points (65 at screening versus 42 at 6 months).
Table 22: EQ-5D-5L Evaluation Summary by Level and Visit: Safety Analysis Set, N = 68 — DCO July 24, 2019
EQ-5D dimension | Screening | Week 4 | Month 3 | Month 6 |
|---|---|---|---|---|
Mobility, n No problems walking Slight problems walking Moderate problems walking Severe problems walking Unable to walk Patient with deterioration from screening | 62 53 (85) 7 (11) 2 (3) 0 (0) 0 (0) NA | 51 25 (49) 17 (33) 3 (6) 4 (8) 2 (4) 21 (41) | 54 37 (69) 10 (19) 4 (7) 2 (4) 1 (2) 13 (24) | 40 30 (75) 5 (13) 3 (8) 2 (5) 0 (0) 8 (20) |
Self-care, n No problems washing or dressing Slight problems washing or dressing Moderate problems washing or dressing Severe problems washing or dressing Unable to wash or dress Patient with deterioration from screening | 62 59 (95) 2 (3) 1 (2) 0 (0) 0 (0) NA | 52 35 (67) 9 (17) 2 (4) 4 (8) 2 (4) 16 (31) | 54 45 (83) 6 (11) 2 (4) 1 (2) 0 (0) 9 (17) | 40 37 (93) 1 (3) 0 (0) 2 (5) 0 (0) 3 (8) |
Usual activity, n No problems doing usual activities Slight problems doing usual activities Moderate problems doing usual activities Severe problems doing usual activities Unable to do usual activities Patient with deterioration from screening | 65 53 (82) 9 (14) 3 (5) 0 (0) 0 (0) NA | 51 22 (43) 12 (24) 11 (22) 3 (6) 3 (6) 25 (49) | 55 38 (69) 9 (16) 4 (7) 2 (4) 2 (4) 13 (24) | 41 30 (73) 7 (17) 3 (7) 0 (0) 1 (2) 8 (20) |
Pain/discomfort, n No pain or discomfort Slight pain or discomfort Moderate pain or discomfort Severe pain or discomfort Extreme pain or discomfort Patient with deterioration from screening | 65 43 (66) 14 (22) 6 (9) 2 (3) 0 (0) NA | 54 34 (63) 10 (19) 10 (19) 0 (0) 0 (0) 9 (17) | 55 33 (60) 9 (16) 10 (18) 2 (4) 1 (2) 13 (24) | 42 28 (67) 9 (21) 4 (10) 1 (2) 0 (0) 5 (12) |
Anxiety/depression, n Not anxious or depressed Slightly anxious or depressed Moderately anxious or depressed Severely anxious or depressed Extremely anxious or depressed Patient with deterioration from screening | 65 49 (75) 13 (20) 3 (5) 0 (0) 0 (0) NA | 54 36 (67) 14 (26) 3 (6) 0 (0) 0 (0) 11 (20) | 55 38 (69) 12 (22) 5 (9) 0 (0) 0 (0) 12 (22) | 42 26 (62) 11 (26) 5 (12) 0 (0) 0 (0) 10 (24) |
EQ VAS, n Mean (SD) Median (range) EQ VAS reduced by ≥ 10% from screening, n (%) | 65 82.0 (15.4) 85.0 (45 to 100) NA | 52 74.5 (15.6) 78.0 (38 to 100) 26 (50) | 55 80.1 (15.6) 83.0 (40 to 100) 16 (29) | 42 84.8 (17.5) 90.0 (20 to 100) 5 (12) |
DCO = data cut-off; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; EQ VAS = EuroQol Visual Analogue Scale; NA = not applicable; SD = standard deviation.
Note: Values are n (%) unless otherwise specified. Missing assessments are not included in the summary. Percentages are based on the number of patients with a non-missing assessment of a EuroQol dimension at each visit unless otherwise specified. Deterioration of a EuroQol dimension means the dimension worsened by at least 1 level from screening. The EQ VAS ranges from 0 to 100, with a higher score indicating a better health state.
Source: ZUMA-2 Clinical Study Report.18
Harms
Adverse Events
AEs: Primary Analysis Data Cut-Off — July 24, 2019
At least 1 TEAE was reported in all patients, of which 67 (99%) had AEs that were Grade 3 or higher. In the IAS, 11 patients (16%) had Grade 3 TEAEs, 52 patients (76%) had Grade 4 TEAEs, and 4 patients (6%) had Grade 5 TEAEs. The most common Grade 3 or higher AEs were anemia and decreased neutrophil count (50%) and decreased WBC count (39%). The most common AEs by preferred term were pyrexia (94%), anemia (68%), and decreased platelet count (53%); these AEs are summarized in Table 23.
Table 23: Incidence of AEs Occurring in at Least 15% of Patients: Safety Analysis Set, N = 68 — DCO July 24, 2019
MedDRA preferred term, n (%) | Any grade | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|
Pyrexia | 64 (94) | 41 (60) | 9 (13) | 0 (0) |
Anemia | 46 (68) | 12 (18) | 34 (50) | 0 (0) |
Platelet count decreased | 36 (53) | 3 (4) | 9 (13) | 17 (25) |
Hypotension | 35 (51) | 16 (24) | 13 (19) | 2 (3) |
Neutrophil count decreased | 35 (51) | 1 (1) | 5 (7) | 29 (43) |
Chills | 28 (41) | 11 (16) | 0 (0) | 0 (0) |
WBC count decreased | 27 (40) | 0 (0) | 5 (7) | 22 (32) |
Hypoxia | 26 (38) | 10 (15) | 8 (12) | 6 (9) |
Cough | 25 (37) | 11 (16) | 0 (0) | 0 (0) |
Hypophosphatemia | 25 (37) | 8 (12) | 15 (22) | 0 (0) |
Neutropenia | 25 (37) | 2 (3) | 5 (7) | 18 (26) |
Fatigue | 24 (35) | 13 (19) | 1 (1) | 0 (0) |
Headache | 24 (35) | 8 (12) | 1 (1) | 0 (0) |
Tremor | 24 (35) | 5 (7) | 0 (0) | 0 (0) |
Hypoalbuminemia | 23 (34) | 17 (25) | 1 (1) | 0 (0) |
Hyponatremia | 22 (32) | 0 (0) | 7 (10) | 0 (0) |
Nausea | 22 (32) | 10 (15) | 1 (1) | 0 (0) |
ALT increased | 21 (31) | 2 (3) | 5 (7) | 1 (1) |
Encephalopathy | 21 (31) | 3 (4) | 7 (10) | 6 (9) |
Hypokalemia | 21 (31) | 4 (6) | 3 (4) | 2 (3) |
Tachycardia | 21 (31) | 7 (10) | 0 (0) | 0 (0) |
Constipation | 20 (29) | 2 (3) | 0 (0) | 0 (0) |
Hypocalcemia | 19 (28) | 8 (12) | 3 (4) | 1 (1) |
Diarrhea | 18 (26) | 5 (7) | 2 (3) | 0 (0) |
Thrombocytopenia | 16 (24) | 3 (4) | 2 (3) | 9 (13) |
Peripheral edema | 15 (22) | 7 (10) | 0 (0) | 0 (0) |
AST increased | 14 (21) | 1 (1) | 7 (10) | 0 (0) |
Confusional state | 14 (21) | 3 (4) | 8 (12) | 0 (0) |
Decreased appetite | 14 (21) | 8 (12) | 0 (0) | 0 (0) |
Hyperglycemia | 14 (21) | 5 (7) | 4 (6) | 0 (0) |
Hypertension | 14 (21) | 4 (6) | 9 (13) | 0 (0) |
Asthenia | 13 (19) | 3 (4) | 1 (1) | 0 (0) |
Dyspnea | 13 (19) | 5 (7) | 1 (1) | 1 (1) |
Insomnia | 12 (18) | 4 (6) | 0 (0) | 0 (0) |
Pleural effusion | 12 (18) | 5 (7) | 2 (3) | 1 (1) |
Anxiety | 10 (15) | 5 (7) | 0 (0) | 0 (0) |
Aphasia | 10 (15) | 4 (6) | 3 (4) | 0 (0) |
Dizziness | 10 (15) | 2 (3) | 2 (3) | 0 (0) |
Hypogammaglobulinemia | 10 (15) | 8 (12) | 1 (1) | 0 (0) |
Hypomagnesemia | 10 (15) | 0 (0) | 0 (0) | 0 (0) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; DCO = data cut-off; MedDRA = Medical Dictionary for Regulatory Activities; WBC = white blood cell.
Note: Preferred terms are sorted in descending order of total frequency in the “Any grade” column. Treatment-emergent AE is defined as any AE with onset on or after the brexucabtagene autoleucel infusion. Adverse events that occurred on or after re-treatment are not included. Adverse events are coded using MedDRA, version 22.0, and graded per Common Terminology Criteria for Adverse Events, version 4.03.
Source: ZUMA-2 Clinical Study Report.18
Adverse events related to brexucabtagene autoleucel that occurred in at least 15% of patients are listed in Table 24. A total of 21 patients (31%) had brexucabtagene autoleucel–related AEs that were Grade 3, and 32 patients (47%) had such AEs that were Grade 4. The most common brexucabtagene autoleucel–related AEs that were Grade 3 or higher were decreased WBC count (31%), anemia (28%), and decreased neutrophil count (26%).18
Table 24: Incidence of Grade 2 to 4 Brexucabtagene Autoleucel–Related AEs Occurring in at Least 15% of Patients: Safety Analysis Set, N = 68 — DCO July 24, 2019
Preferred term, n (%) | Any | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|
Patients with any brexucabtagene autoleucel–related AE | 66 (97) | 10 (15) | 21 (31) | 32 (47) |
Pyrexia | 63 (93) | 40 (59) | 8 (12) | 0 (0) |
Hypotension | 35 (51) | 16 (24) | 14 (21) | 1 (1) |
Chills | 26 (38) | 11 (16) | 0 (0) | 0 (0) |
Tremor | 25 (37) | 5 (7) | 0 (0) | 0 (0) |
Anemia | 24 (35) | 5 (7) | 19 (28) | 0 (0) |
Hypoxia | 24 (35) | 10 (15) | 9 (13) | 4 (6) |
White blood cell count decreased | 22 (32) | 1 (1) | 4 (6) | 17 (25) |
Encephalopathy | 21 (31) | 3 (4) | 7 (10) | 6 (9) |
Tachycardia | 21 (31) | 6 (9) | 0 (0) | 0 (0) |
Fatigue | 20 (29) | 10 (15) | 1 (1) | 0 (0) |
Neutrophil count decreased | 20 (29) | 2 (3) | 3 (4) | 15 (22) |
Platelet count decreased | 19 (28) | 4 (6) | 4 (6) | 6 (9) |
Hypoalbuminemia | 18 (26) | 16 (24) | 0 (0) | 0 (0) |
ALT increased | 17 (25) | 1 (1) | 5 (7) | 1 (1) |
Headache | 17 (25) | 8 (12) | 1 (1) | 0 (0) |
Hypophosphatemia | 17 (25) | 5 (7) | 12 (18) | 0 (0) |
Hyponatremia | 16 (24) | 0 (0) | 4 (6) | 0 (0) |
Confusional state | 14 (21) | 3 (4) | 8 (12) | 0 (0) |
Nausea | 14 (21) | 8 (12) | 0 (0) | 0 (0) |
Cough | 13 (19) | 7 (10) | 0 (0) | 0 (0) |
AST increased | 12 (18) | 1 (1) | 7 (10) | 0 (0) |
Diarrhea | 11 (16) | 2 (3) | 2 (3) | 0 (0) |
Dyspnea | 11 (16) | 5 (7) | 1 (1) | 0 (0) |
Hypocalcemia | 11 (16) | 5 (7) | 1 (1) | 1 (1) |
Neutropenia | 11 (16) | 1 (1) | 2 (3) | 8 (12) |
Asthenia | 10 (15) | 2 (3) | 1 (1) | 0 (0) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; DCO = data cut-off.
Note: Preferred terms are sorted in descending order of total frequency in the “Any” column. Adverse events are coded using Medical Dictionary for Regulatory Activities, version 22.0, and graded per Common Terminology Criteria for Adverse Events, version 4.03.
Source: ZUMA-2 Clinical Study Report.18
AEs: Updated Analysis Data Cut-Off — December 31, 2019
Treatment-emergent AEs as of the December 31, 2019, data cut-off are summarized in Table 25. In the updated analysis, the most common Grade 3 or higher AEs were slightly higher than the primary analysis and included decreased neutrophil count (||), anemia (||), and decreased WBC count (||). The most common Grade 5 AEs by preferred term in the updated analysis included B-cell lymphoma ( | ), staphylococcal bacteremia (||), and organizing pneumonia (||).19
Table 25: Incidence of Grade 3 or Higher TEAEs Occurring in at Least 15% of Patients by Preferred Term and Grade: Safety Analysis Set, N = 68 — DCO December 31, 2019
Preferred term, n (%) | Any ≥ Grade 3 | Grade 3 | Grade 4 | Grade 5 |
|---|---|---|---|---|
Patients with any Grade 3 or higher TEAE | | | | | | | | |
Neutrophil count decreased | | | | | | | | |
Anemia | | | | | | | | |
White blood cell count decreased | | | | | | | | |
Platelet count decreased | | | | | | | | |
Neutropenia | | | | | | | | |
Hypophosphatemia | | | | | | | | |
Hypotension | | | | | | | | |
Hypoxia | | | | | | | | |
Encephalopathy | | | | | | | | |
Thrombocytopenia | | | | | | | | |
Leukopenia | | | | | | | | |
Pyrexia | | | | | | | | |
DCO = data cut-off; TEAE = treatment-emergent adverse event.
Note: Preferred terms are sorted in descending order of total frequency in the “Any ≥ Grade 3” column. Treatment-emergent AE is defined as any AE with onset on or after the brexucabtagene autoleucel infusion. Adverse events that occurred on or after re-treatment are not included. Adverse events are coded using Medical Dictionary for Regulatory Activities, version 22.0, and graded per Common Terminology Criteria for Adverse Events, version 4.03.
Source: ZUMA-2 updated analysis.19
Serious Adverse Events
SAEs: Primary Analysis Data Cut-Off — July 24, 2019
Serious AEs occurring in greater than or equal to 5% of patients in the safety analysis set of the ZUMA-2 trial are summarized in Table 26. Serious AEs were recorded for 68% of patients. The most common SAEs were encephalopathy and pyrexia (22% each), followed by hypotension (16%). The most common Grade 3 or higher SAEs were encephalopathy (18%) and hypotension and hypoxia (12% each). Two patients had Grade 5 SAEs of B-cell lymphoma, and these patients died due to disease progression.18
Table 26: SAEs by Grade in at Least 5% of Patients: Safety Analysis Set, N = 68 — DCO July 24, 2019
MedDRA preferred term, n (%) | ZUMA-2 (N = 68) | ||||
|---|---|---|---|---|---|
Any | Grade 2 | Grade 3 | Grade 4 | Grade 5 | |
Patients with any serious TEAE | 46 (68) | 7 (10) | 20 (29) | 13 (19) | 4 (6) |
Encephalopathy | 15 (22) | 1 (1) | 6 (9) | 6 (9) | 0 (0) |
Pyrexia | 15 (22) | 5 (7) | 3 (4) | 0 (0) | 0 (0) |
Hypotension | 11 (16) | 3 (4) | 6 (9) | 2 (3) | 0 (0) |
Hypoxia | 8 (12) | 0 (0) | 4 (6) | 4 (6) | 0 (0) |
Acute kidney injury | 5 (7) | 0 (0) | 1 (1) | 4 (6) | 0 (0) |
Confusional state | 5 (7) | 0 (0) | 5 (7) | 0 (0) | 0 (0) |
Pneumonia | 5 (7) | 0 (0) | 5 (7) | 0 (0) | 0 (0) |
Anemia | 4 (6) | 0 (0) | 4 (6) | 0 (0) | 0 (0) |
Respiratory failure | 4 (6) | 0 (0) | 0 (0) | 4 (6) | 0 (0) |
Sepsis | 4 (6) | 0 (0) | 1 (1) | 3 (4) | 0 (0) |
DCO = data cut-off; MedDRA = Medical Dictionary for Regulatory Activities; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Note: Preferred terms are sorted in descending order of total frequency in the “Any” column. Treatment-emergent AE is defined as any AE with onset on or after the brexucabtagene autoleucel infusion. Adverse events that occurred on or after re-treatment are not included. Adverse events are coded using MedDRA, version 22.0, and graded per Common Terminology Criteria for Adverse Events, version 4.03.
Source: ZUMA-2 Clinical Study Report.18
SAEs: Updated Analysis Data Cut-Off — December 31, 2019
The incidence of SAEs in the updated analysis is summarized in Table 27. Grade 3, Grade 4, and Grade 5 SAEs were observed in ||, ||, and 6% of patients, respectively. Similar to the primary analysis, the most common SAEs in the current analysis were pyrexia (||), encephalopathy (||), and hypotension (||), although incidence was slightly lower. The most common Grade 3 or higher SAEs in the current analysis were encephalopathy (||); pneumonia, which increased to || from ||; and hypotension (||).19
Table 27: SAEs by Grade in at Least 5% of Patients in the Updated Analysis: Safety Analysis Set, N = 68 — DCO December 31, 2019
MedDRA preferred term, n (%) | ZUMA-2 (N = 68) | ||||
|---|---|---|---|---|---|
Any | Grade 2 | Grade 3 | Grade 4 | Grade 5 | |
Patients with any serious TEAE | | | | | | | | | | |
Pyrexia | | | | | | | | | | |
Encephalopathy | | | | | | | | | | |
Hypotension | | | | | | | | | | |
Pneumonia | | | | | || | | | | |
Hypoxia | | | | | | | | | | |
Acute kidney injury | | | | | | | | | | |
Confusional state | | | | | | | | | | |
Anemia | | | | | | | | | | |
Respiratory failure | | | | | | | | | | |
Sepsis | | | | | | | | | | |
DCO = data cut-off; MedDRA = Medical Dictionary for Regulatory Activities; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Note: Preferred terms are sorted in descending order of total frequency in the “Any” column. Adverse events are coded using MedDRA, version 22.1, and graded per Common Terminology Criteria for Adverse Events, version 4.03.
Source: ZUMA-2 updated analysis.19
Mortality
As of the July 24, 2019, data cut-off, 16 patients (24%) had died, of whom 13 (19%) died due to progressive disease, 2 (3%) died due to AEs (organizing pneumonia and staphylococcal bacteremia, both deemed related to lymphodepleting chemotherapy), and 1 (1%) was listed as “other” as the cause of death was unknown; this was later changed to “progressive disease.” The majority of deaths occurred more than 3 months after brexucabtagene autoleucel infusion (12 of 16 deaths).18
Two additional deaths occurred between the primary analysis and the updated data cut-off of December 31, 2019, for a total of 18 deaths (26%). The 2 additional deaths were attributed to progressive disease (n = 16 [24%]) and occurred more than 3 months after infusion.19
Notable Harms/AEs of Special Interest
Cytokine Release Syndrome
Cytokine release syndrome and symptoms by preferred term are summarized in Table 28 and were all considered to be related to treatment with brexucabtagene autoleucel. Sixty-two patients (91%) had CRS, of which the majority were Grade 2 (47%). No patient had Grade 5 CRS. The most common CRS symptoms of any grade were pyrexia (100%), hypotension (56%), and hypoxia (37%). The most common Grade 3 or higher CRS symptoms were also hypotension (25%), hypoxia (19%), and pyrexia (11%). The median time to onset of CRS was 2 days after the brexucabtagene autoleucel infusion, with a median duration of 11 days (range = 1 day to 50 days). As of the July 24, 2019, data cut-off, CRS had resolved in all 62 patients.18
As of the December 31, 2019, data cut-off, no additional CRS symptoms had occurred.19
Table 28: Incidence of CRS in at Least 5% of Patients: Safety Analysis Set, N = 68 — DCO July 24, 2019
MedDRA preferred term, n (%) | ZUMA-2 (N = 68) | ||||
|---|---|---|---|---|---|
Any | Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
Patients with CRSa | 62 (91) | 20 (29) | 32 (47) | 8 (12) | 2 (3) |
CRS preferred termb | |||||
Pyrexia | 62 (100) | 15 (24) | 40 (65) | 7 (11) | 0 (0) |
Hypotension | 35 (56) | 4 (6) | 16 (26) | 14 (23) | 1 (2) |
Hypoxia | 23 (37) | 1 (2) | 10 (16) | 8 (13) | 4 (6) |
Chills | 21 (34) | 12 (19) | 9 (15) | 0 (0) | 0 (0) |
Tachycardia | 16 (26) | 11 (18) | 5 (8) | 0 (0) | 0 (0) |
Headache | 15 (24) | 7 (11) | 8 (13) | 0 (0) | 0 (0) |
ALT increased | 10 (16) | 5 (8) | 1 (2) | 3 (5) | 1 (2) |
AST increased | 9 (15) | 4 (6) | 0 (0) | 5 (8) | 0 (0) |
Fatigue | 9 (15) | 6 (10) | 2 (3) | 1 (2) | 0 (0) |
Nausea | 9 (15) | 5 (8) | 4 (6) | 0 (0) | 0 (0) |
Diarrhea | 6 (10) | 5 (8) | 0 (0) | 1 (2) | 0 (0) |
Sinus tachycardia | 6 (10) | 4 (6) | 2 (3) | 0 (0) | 0 (0) |
Dyspnea | 4 (6) | 1 (2) | 2 (3) | 1 (2) | 0 (0) |
Atrial fibrillation | 3 (5) | 2 (3) | 1 (2) | 0 (0) | 0 (0) |
Malaise | 3 (5) | 2 (3) | 1 (2) | 0 (0) | 0 (0) |
Myalgia | 3 (5) | 3 (5) | 0 (0) | 0 (0) | 0 (0) |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; CRS = cytokine release syndrome; DCO = data cut-off; MedDRA = Medical Dictionary for Regulatory Activities.
Note: Preferred terms are sorted in descending order of total frequency in the “Any” column. Adverse events are coded using MedDRA, version 22.0, and graded per Common Terminology Criteria for Adverse Events, version 4.03.
aOverall CRS is graded per the revised grading system proposed by Lee et al. (2014).48 The percentages are calculated using the total number of patients in the safety analysis set as the denominator.
bIndividual CRS symptoms are graded per Common Terminology Criteria for Adverse Events, version 4.03. Percentages are calculated using the number of patients with any treatment-emergent CRS of any grade as the denominator.
Source: ZUMA-2 Clinical Study Report.18
Neurologic AEs
Table 29 summarizes neurologic events in the safety analysis set. Forty-three patients (63%) had at least 1 neurologic event of any grade. The most frequently occurring neurologic events were Grade 3 (22%), while 6 patients (9%) had Grade 4 neurologic events, and no patients had a Grade 5 neurologic event. The most common neurologic events of any grade were tremor (35%), encephalopathy (31%), and confusional state (21%). The most common Grade 3 or higher neurologic events were encephalopathy (19%), confusional state (12%), and aphasia (4%). A total of 22 patients (32%) had serious neurologic events of any grade; 18% were Grade 3, and 9% were Grade 4. The most common serious neurologic event was encephalopathy (22%), followed by confusional state (7%) and aphasia (4%).
The median onset of a neurologic event following brexucabtagene autoleucel infusion was 7 days, and in patients whose neurologic events had resolved, the duration of neurologic events was a median of 12 days (range = 1 day to 567 days). Three patients had neurologic events beyond 200 days that were attributed to lymphodepleting chemotherapy and brexucabtagene autoleucel. As of the July 24, 2019, data cut-off, neurologic events had resolved in all but 6 patients. Neurologic events for 2 of these patients had not resolved at the time of death: 1 patient had Grade 2 nonserious agitation (deemed related to brexucabtagene autoleucel) and Grade 3 serious confusional state (deemed related to lymphodepleting chemotherapy and brexucabtagene autoleucel), and 1 patient had Grade 2 nonserious hyperesthesia. Ongoing neurologic events for the remaining 4 patients were Grade 1 or Grade 2.18
No additional neurologic events occurred between the primary analysis and the December 31, 2019, data cut-off, and no changes occurred in the most common neurologic events of any grade. The median time to resolution remained the same between data cut-offs; however, the mean time to resolution of neurologic events was 61.9 days in the updated analysis compared to 53.1 days in the primary analysis.19
Table 29: Incidence of Neurologic Events in at Least 5% of Patients: Safety Analysis Set, N = 68 — DCO July 24, 2019
MedDRA preferred term, n (%) | ZUMA-2 (N = 68) | ||||
|---|---|---|---|---|---|
Any | Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
Patients with any neurologic event | 43 (63) | 13 (19) | 9 (13) | 15 (22) | 6 (9) |
Tremor | 24 (35) | 19 (28) | 5 (7) | 0 (0) | 0 (0) |
Encephalopathy | 21 (31) | 5 (7) | 3 (4) | 7 (10) | 6 (9) |
Confusional state | 14 (21) | 3 (4) | 3 (4) | 8 (12) | 0 (0) |
Aphasia | 10 (15) | 3 (4) | 4 (6) | 3 (4) | 0 (0) |
Somnolence | 8 (12) | 4 (6) | 2 (3) | 2 (3) | 0 (0) |
Lethargy | 7 (10) | 1 (1) | 6 (9) | 0 (0) | 0 (0) |
Agitation | 5 (7) | 1 (1) | 3 (4) | 1 (1) | 0 (0) |
Disturbance in attention | 5 (7) | 3 (4) | 2 (3) | 0 (0) | 0 (0) |
Memory Impairment | 5 (7) | 2 (3) | 2 (3) | 1 (1) | 0 (0) |
Seizure | 4 (6) | 2 (3) | 1 (1) | 1 (1) | 0 (0) |
DCO = data cut-off; MedDRA = Medical Dictionary for Regulatory Activities.
Note: Preferred terms are sorted in descending order of total frequency in the “Any” column. Adverse events are coded using MedDRA, version 22.0, and graded per Common Terminology Criteria for Adverse Events, version 4.03. Percentages are calculated using the total number of patients in the treatment group as the denominator.
Source: ZUMA-2 Clinical Study Report.18
Other Harms Outcomes
Immunoglobulins were included as concomitant medications regardless of whether they were administered before or after the hospital discharge date following treatment with brexucabtagene autoleucel. A total of 22 patients (32%) were treated with immunoglobulins.18
Hypogammaglobulinemia was a TEAE of interest in the ZUMA-2 trial. As of the July 24, 2019, data cut-off, 13 patients (19%) in the safety analysis set had hypogammaglobulinemia, of which 11 (16%) were considered Grade 2 and the majority occurred in patients 65 years and older (8 [21%]).18 There were no additional cases of hypogammaglobulinemia as of the updated analysis.19
Critical Appraisal
Internal Validity
ZUMA-2 was the only individual study included in the review and is the only prospective clinical trial in the R/R MCL setting post–BTK inhibitor treatment. This phase II, multi-centre, single-arm trial aimed to assess the efficacy and safety of brexucabtagene autoleucel in the treatment of R/R MCL when patients have progressed on prior chemotherapy, anti-CD20 antibody, and BTK inhibitor therapy. The following points were noted in the appraisal of the internal validity of the ZUMA-2 trial.
As a single-arm study, the ZUMA-2 trial lacks a comparator arm, which increases the risk of bias in the estimation of treatment effects due to the potential for confounding related to placebo response, fluctuations in health status, and other unidentified prognostic factors that could affect subjectively assessed outcomes. The open-label, single-arm design can increase the risk of bias in reporting of outcomes that are subjective in measurement and interpretation, such as response, HRQoL, and AEs. Outcomes such as mortality are less likely to be affected. The risk of bias due to the open-label design may be unavoidable given the rarity of the indication and unmet need in a population where larger head-to-head randomized controlled trials are not methodologically or ethically feasible. The potential for this bias was also reduced by using an independent central assessment for key study outcomes such as ORR, DOR, and PFS.
The primary end point of the ZUMA-2 trial was ORR per central assessment using the Lugano classification. The original study protocol used the primary end point of ORR based on investigator assessment using IWG 2007 criteria, which was changed to the Lugano classification by independent radiology review at the fourth protocol amendment on November 13, 2017. For the clinical response outcome of ORR, a historical control of 25% was applied as of the June 22, 2018, protocol amendment based on 2 retrospective studies published before the ZUMA-2 protocol (2015 and 2016), which demonstrated that patients with R/R MCL who had 3 or more prior lines of therapy before receiving the BTK inhibitors had ORRs to salvage therapy of approximately 25%. The ZUMA-2 study demonstrated an overall ORR of 93% (95% CI, 83.8% to 98.2%), which was significantly superior to the historical control. While the lower limit of the CI was significantly higher than the historical control rate, clinical experts consulted by CADTH noted that the 25% rate is largely underestimated, which has the potential to bias the comparison of the results in favour of brexucabtagene autoleucel. However, the expected response with standard of care would be dependent on how many prior lines of therapy have been received and so may be variable. Objective response and CR were also analyzed using investigator assessment. The concordance rate demonstrated agreement between investigator assessment and central assessment, with concordance rates of 95% (κ = 0.70; 95% CI, 0.39 to 1.00) and 90% (κ = 0.77; 95% CI, 0.60 to 0.94) for ORR and CR, respectively. The Lugano classification is preferred in B-cell lymphomas compared to the IWG 2007 criteria50; however, it is unclear what impact the use of IWG 2007 criteria in the investigator assessment compared to the Lugano classification may have had on the direction or magnitude of results.
Health-related quality of life outcomes were not considered in a multiplicity adjustment and had significant missing data at later time points (i.e., 6 months), impacting the interpretability of trends over time and creating potential for bias in those that remain; the outcomes may therefore not be reflective of the overall population (i.e., patients who did not continue to complete assessments or who died tended to have poorer HRQoL). Therefore, the suggestion that HRQoL improves over time cannot be made. Also, no index scores for the EQ-5D were provided, and as such the net treatment effect across domains could not be captured.
Follow-up time (both potential and actual) as of the primary data cut-off was considered appropriate for assessing response and safety outcomes associated with brexucabtagene autoleucel. As per the protocol amendment on June 22, 2018, the primary analysis of the ZUMA-2 study was performed when 60 patients had been followed for 6 months after their 4-week assessment for ORR. However, the short median follow-up for the primary data cut-off of 11.6 months and 12.3 months in the FAS and IAS, respectively, was considered insufficient and immature for key survival outcomes of PFS and OS. It was acknowledged, however, that the median PFS and median OS were not reached in the IAS with 12.3 months or 16.8 months of follow-up and were considered impressive according to the clinical experts consulted by CADTH given the stage of disease and typical survival rates seen in this population.
Subgroups were defined a priori and were considered of clinical interest according to the experts consulted for this review. The subgroups were analyzed to evaluate the robustness and consistency of treatment effects found overall. However, many of the specific subgroups had limited sample sizes, for which results were imprecise, as reflected by the wider CIs, limiting the interpretability of the results. Furthermore, some subgroups (notably Ki-67 index and CD19 positivity) only reflected subpopulations of the overall study population, as there were missing data for certain covariates at baseline. The Ki-67 index is a known prognostic factor in MCL, and it has previously been shown that patients with Ki-67 greater than 50% have lower ORRs and CR rates.51 The Ki-67 index was evaluated in 3 ways (one of which was data driven using a median split rather than clinically relevant thresholds). It is unclear whether the analysis of patients with greater than or less than 30% or 50% thresholds were specified a priori, and the rationale for these cut-offs was unclear.
External Validity
The inclusion and exclusion criteria of ZUMA-2 aimed to enrol patients who have received second-line or later therapy for R/R MCL with prior treatments consisting of chemotherapy, anti-CD20 antibody, and BTK inhibitor therapy. There was a lack of Canadian sites in the ZUMA-2 trial, as well as no Canadian patients included in the trial. All co-interventions were readily available in Canadian clinical practice, and while there is no clear reason to assume major differences in the standards of practice and the patient population between the US and Canada, the lack of representation of Canadian patients could potentially reduce the generalizability to Canadian settings if practice variation exists. Brexucabtagene autoleucel was successfully manufactured for 96% of patients. The majority of patients in the ZUMA-2 trial received the target dose per the Health Canada indication (N = 66 [97%]). It is uncertain whether the time to infusion shown in the trial (median 27 days from leukapheresis) reflects what would be seen in the real world.
The outcomes used to inform the efficacy are clinically meaningful to the assessment of improvements in survival and are reflective of clinical practice in Canada. Despite the relevance of the efficacy end points to clinicians and patients, HRQoL — an outcome of particular importance to patients — was only assessed using the EQ-5D, which may not fully capture the impact of symptoms and treatment in R/R MCL.
The included population required patients to have an absolute neutrophil count greater than or equal to 1,000/μL, a platelet count greater than or equal to 75,000/μL, and an absolute lymphocyte count greater than or equal to 100/μL, which the clinical experts believed to be high; they noted that patients in a clinical setting would likely have lower counts than this, potentially impacting generalizability. They also noted that the ZUMA-2 trial population may represent a population that is generally healthier than would be found in clinical practice settings. As part of the inclusion criteria, patients were excluded if they had evidence of CNS lymphoma, or active CNS disease, and a history of significant cardiac disease. The clinical experts consulted by CADTH believed that should these aspects be under control, then these patients would also be eligible for treatment with brexucabtagene autoleucel.
Overall, the demographic and baseline characteristics of the included population generally reflect Canadian practice; however, the clinical expert panel noted that the ECOG PS of included patients may be lower than is seen in clinical practice, as 65% had an ECOG PS of 0, and they expect more ECOG PS 2 patients in the real world. Additionally, they noted that only 10% of patients had bulky disease at baseline, which given the disease stage and line of therapy, they would expect to be higher. Lastly, the proportion of patients who received bridging therapy was only 38%, which clinical experts considered to be low; they expected a higher proportion to require this. Together, although the ZUMA-2 population was reflective of the funding request and included R/R MCL patients who had failed BTK inhibitors, the selected patients may represent a less sick population and may not be generalizable to the typical Canadian patient at this stage of the disease.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to provide an appraisal and summary of indirect evidence for brexucabtagene autoleucel versus other therapies in patients with R/R MCL. A review of indirect evidence was undertaken due to the lack of comparative clinical trials for brexucabtagene autoleucel.
A focused literature search for ITCs dealing with MCL was run in MEDLINE All (1946–) on January 25, 2021. No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Articles were screened by 1 researcher for ITCs that met the patient, intervention, comparator, and outcome criteria listed in Table 6. In addition, the sponsor-submitted ITC was reviewed.
The literature search identified 5 articles, but none evaluated the efficacy or safety of brexucabtagene autoleucel in patients with MCL. The sponsor-submitted ITC, which was used to inform the pharmacoeconomic model, was appraised and summarized.43
Description of Indirect Comparison
The sponsor submitted a MAIC that compared the efficacy of brexucabtagene autoleucel to standard of care treatments in patients with R/R MCL who had previously been treated with BTK inhibitors.43
Methods of ITC
Objectives
The sponsor-submitted report had 2 objectives. The first was to conduct a systematic review and meta-analysis of studies to obtain estimates of the absolute treatment effects for OS, PFS, and tumour response of interventions considered standard of care for the treatment of R/R MCL after BTK inhibitor therapy. The second objective was to conduct a MAIC to estimate the relative treatment effects for brexucabtagene autoleucel versus standard of care treatments in patients with R/R MCL who had previously been treated with BTK inhibitors.
Study Selection Methods
The meta-analysis and ITC were informed by a systematic literature review conducted in 2018, with updates performed in 2019 and 2020. The study selection criteria and review methods have been summarized in Table 30. The population included in the literature review was broader than the population of interest for the ITC, and only studies that provided data for patients with R/R MCL who had received BTK inhibitor therapy (either the full study population or subgroup analysis) were included in the ITC.
Table 30: Study Selection Criteria and Methods for Sponsor-Submitted Systemic Literature Review
Item | Criteria |
|---|---|
Population | Adults with relapsed or refractory MCL who received at least 1 previous line of therapy |
Intervention | Any intervention for the treatment of relapsed or refractory MCL, including best supportive care |
Comparator | Any comparator for the treatment of relapsed or refractory MCL, including best supportive care |
Outcome | Overall survival or progression-free survival (reported as Kaplan–Meier curves) Best objective response: incidence of complete or partial response, stable disease, progressive disease, or unevaluable as best response to treatment Duration of response or duration of remission Time to response Safety: incidence of adverse events and clinically significant changes in laboratory values |
Study design | Controlled, prospective clinical trials (phase II or higher) Long-term follow-up studies (e.g., open-label extension studies) Prospective or retrospective observational cohort studies Systematic reviews (including meta-analyses) |
Publication characteristics | English language |
Exclusion criteria | Case reports, commentaries or letters, post hoc or secondary analyses, non-systemic reviews |
Databases searched | MEDLINE, Embase, Cochrane Library up to January 2020 Conference proceedings (2016 to 2020) Clinical trial registries Reference lists of relevant systematic reviews or meta-analyses Grey literature including websites of regulatory and HTA agencies |
Selection process | Independent screening of titles and abstracts (stage 1) and then full-text articles (stage 2) by 2 reviewers based on predefined criteria; consultation with a third reviewer to resolve disagreements |
Data extraction process | NR |
Quality assessment | NR |
HTA = health technology assessment; MCL = mantle cell lymphoma; NR = not reported.
Source: Additional information provided by the sponsor.52
ITC Analysis Methods
A feasibility assessment was conducted to review the standard of care studies identified in the systematic literature review. Its objective was to evaluate if the distribution of treatment, outcomes, study, and patient characteristics that may affect treatment response were sufficiently similar to permit pooling of the standard of care studies and if these characteristics were comparable to the ZUMA-2 trial of brexucabtagene autoleucel. The primary outcomes of interest were OS and PFS, and secondary outcomes were tumour response (objective response, CR, or PR). Only standard of care studies that reported outcome data for the target population that were suitable for meta-analysis were included.
Meta-Analysis of Standard of Care Studies
Data from the standard of care studies were pooled to obtain estimates of the absolute treatment effects for OS, PFS, and tumour response. For survival outcomes, Kaplan–Meier curves for OS or PFS, or individual patient data that could be used to construct the Kaplan–Meier curve, were required for pooling. Data from the Kaplan–Meier curves were digitized using Digitizelt software, and the number of patients at risk over time was extracted. Survival and censoring times for each study were created based on an algorithm proposed by Guyot et al.53 Commonly used survival distributions (i.e., exponential, log-normal, log-logistic, Weibull, Gompertz, gamma, and generalized gamma) were fitted to the reconstructed individual patient data from each study, and the best-fitting distribution was selected based on the Akaike information criterion and visual inspection of the fitted and observed survival data. The model parameter estimates for OS and PFS for each trial were then pooled using a Bayesian multivariate meta-analysis model (modified methods based on Achana et al. [2014]54). Bayesian models were run using 2 chains, with the first iterations discarded as burn-in (number of iterations not specified). No information was provided on prior distributions or model convergence diagnostics. Fixed- and random-effects models were used to estimate the pooled treatment effects, and the deviance information criterion was used to select the best-fitting model. Five sensitivity analyses were conducted for OS that excluded trials based on differences in the intervention or outcome definition (see Table 31 for details). No sensitivity analyses were conducted for PFS.
The meta-analysis of tumour response outcomes was based on the proportion of patients reporting objective response, CR, or PR in the standard of care studies. A frequentist generalized linear mixed model was used to estimate the pooled response rate outcomes. Both fixed- and random-effects models were estimated. Between-study statistical heterogeneity was assessed based on I2 values, where values greater than 50% were considered high heterogeneity and where random-effects models were preferred. Six sensitivity analyses were conducted for tumour response outcomes (see Table 31 for details). Clinical heterogeneity was assessed through the feasibility study.
The mean baseline patient characteristics of the standard of care studies were pooled as a weighted average.
Table 31: MAIC Analysis Methods
Method | Survival outcomes | Tumour response outcomes |
|---|---|---|
ITC methods | Unanchored MAIC:
Naive (unadjusted) ITC | Unanchored MAIC:
Naive (unadjusted) ITC |
Covariates used for propensity score weighting | 1. Number of prior therapies 2. Prior autologous SCT 3. Duration of prior BTK inhibitor therapy 4. Response to prior BTK inhibitor therapy 5. Blastoid morphology 6. Ki-67 (≥ 30%, ≥ 50%) | 1. Number of prior therapies 2. Prior autologous SCT 3. Duration of prior BTK inhibitor therapy 4. Response to prior BTK inhibitor therapy 5. Blastoid morphology 6. Ki-67 (≥ 30%, ≥ 50%) |
Outcomes | OS, PFS | ORR, complete response, partial response |
Follow-up time points | Up to 39 months | Up to 39 months |
Construction of nodes | Various SOC treatments and doses pooled into 1 survival function | Various SOC treatments and doses pooled into 1 treatment estimate |
Population | ZUMA-2 FAS population (N = 74); IAS (N = 60); safety (N = 68) including data up to December 2019 | ZUMA-2 FAS population (N = 74); IAS (N = 60); safety (N = 68) including data up to December 2019 |
Sensitivity analyses | OS: mixed treatments (n = 2); mixed treatments or venetoclax (n = 3); mixed treatments or R-BAC (n = 3); studies with survival time t = 0 from start of subsequent treatment (n = 3); studies with survival time t = 0 from start of subsequent treatment excluding venetoclax (n = 2) | All mixed treatment studies that reported ORR (n = 5); all sensitivity analyses reported for OS |
BTK = Bruton tyrosine kinase; CI = confidence interval; FAS = full analysis set; HR = hazard ratio; IAS = inferential analysis set; IPD = individual patient data; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; OR = objective response; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; R-BAC = rituximab, bendamustine, and cytarabine; SCT = stem cell transplant; SOC = standard of care.
Source: Sponsor’s submission to CADTH.43
Naive ITC and MAIC
The use of unanchored MAIC methods to conduct the ITC were necessary, as the single-arm design of ZUMA-2 precluded the use of other anchored ITC methods. The ITC’s authors stated that since there is no standard therapeutic approach for patients who have relapsed following BTK inhibitor therapy, comparison to a control group that included various subsequent treatments was justified.
For the MAIC, a logistic propensity score model was used to estimate patient weights for the ZUMA-2 trial so that the weighted baseline mean characteristics of ZUMA-2 matched the pooled mean characteristics of the standard of care studies (Table 31). Covariates used for weighting were identified based on a literature review and input from clinical experts on prognostic factors in patients with R/R MCL. From the literature search, the following variables were identified to be prognostic based on univariate or multivariate Cox regression models: number of prior therapies, duration of prior BTK inhibitor therapy, response to prior BTK inhibitor therapy (ORR), MIPI, ECOG PS, bulky disease, primary refractory disease and lactate dehydrogenase. These variables, and all other baseline characteristics reported in the trials, were reviewed and ranked by clinical experts from the sponsor, and 12 variables were selected (number of prior therapies, prior autologous SCT, duration of prior BTK inhibitor therapy, response to BTK inhibitor therapy, MIPI, blastoid morphology, Ki-67 (≥ 30%, ≥ 50%), disease stage, prior ibrutinib therapy, male sex, extranodal disease, and bone marrow involvement). This list of covariates was validated by experts from the UK and Canada. After reviewing the results of initial analyses that were based on the full list of covariates, a decision was made to include only the 6 most relevant characteristics, as the ITC’s authors stated this “led to more conservative and clinically plausible results while also giving a higher effective sample size.”43 Key opinion leaders were consulted, and the following covariates (in rank order) were included in the final propensity score model: number of prior therapies; prior autologous SCT; duration of prior BTK inhibitor therapy; response to prior BTK inhibitor therapy; blastoid morphology: and Ki-67 (≥ 30%, ≥ 50%). All but 1 of the standard of care studies were missing baseline data for at least 1 key characteristic used to determine patient weights in the MAIC: 3 studies were missing data for 2 covariates, 3 studies were missing data for 3 or 4 covariates, and 1 study was missing data for 6 covariates. To address the missing baseline data, a number of assumptions were made. The weighted average for specific characteristics was assumed to apply to any trials that were missing that parameter. For 3 trials where the population of interest was a subgroup and only the overall study population characteristics were reported, it was assumed that the overall population characteristics (i.e., the characteristics of those who did or did not receive therapy post–BTK inhibitor therapy) were representative of patients who had received subsequent therapy. Not all studies reported baseline characteristics at the start of subsequent therapy (e.g., at diagnosis or at start of BTK inhibitor therapy). It was assumed that the differences in the time of measurement did not have an impact on prognosis.
For OS and PFS, the same parametric survival function used in the meta-analysis was fitted to the weighted individual patient data from ZUMA-2, and the best-fitting model was determined based on the Akaike information criterion. The best-fitting parametric survival models for the weighted brexucabtagene autoleucel data and the pooled standard of care studies were then pooled in a pairwise indirect comparison to provide an estimate of the relative treatment effects of brexucabtagene autoleucel versus standard of care therapy. Results were reported as the average HR and 95% CI. For the tumour response outcomes, treatment effects were estimated for the weighted ZUMA-2 data versus pooled standard of care data using weighted contingency table methods and reported as odds ratios and 95% CIs.
The sponsor-submitted report also includes a naive ITC that compared unadjusted data from ZUMA-2 to the pooled outcomes from the standard of care studies.
For the ITC, follow-up time was truncated at 39 months, which was the longest follow-up time available for the ZUMA-2 study. The mean survival was defined as the area under the curve of the survival function from 0 months to 39 months. Based on the December 2019 update in the ZUMA-2 study, the median potential follow-up time was 21.7 months (from infusion to data cut-off). Overall, 88% of patients had completed 12 months of potential follow-up time, 41% had completed 24 months, 41% had completed 30 months, and 2 had completed 36 months.19 Three ZUMA-2 populations were estimated: the FAS (N = 74), the IAS (N = 60), and the safety set (N = 68). Effective sample size and baseline characteristics before and after weighting were reported for each scenario. The analyses were conducted using R software (version 3.6.1; meta, metaphor, and flexsurv packages), with Markov chain Monte Carlo methods implemented using JAGS software (version 4.3.0).
Results of ITC
Summary of Included Studies
Fifteen studies in patients with R/R MCL post–BTK inhibitor therapy were identified in the systematic review. Two studies were excluded due to small sample size (≤ 5 patients), and 1 was excluded as it evaluated ibrutinib as bridging therapy, which was not an intervention of interest.
The feasibility assessment included the ZUMA-2 trial and 11 other studies of standard of care treatments that were identified in the literature review. Based on the feasibility assessment, 2 trials were excluded from the meta-analysis because patients had received CAR T-cell therapy, which was not considered standard of care, and 1 trial was excluded in which there was substantial overlap between the patients enrolled with another study38 included in the analysis. Thus, 9 trials were included in the ITC (Table 32). The trials comprised 7 retrospective observational studies,35,36,38-40,55,56 a single arm from a randomized controlled trial,57 and ZUMA-2, which was a prospective uncontrolled phase II clinical trial.45 One study was available only as a poster, and thus limited data were available.56 Another study was published as a letter to the editor.55 All other studies were published in full text. Individual patient data were available for the ZUMA-2 study.
Across the 9 included studies, the sample size ranged from 12% to 73% of patients who had received subsequent therapy following BTK inhibitor treatment. The median number of prior therapies that patients had received for MCL ranged from 2 to 4. In the standard of care studies, the proportion of patients who stopped BTK inhibitor therapy due to progression ranged from 40% to 100%, and in 5 studies, 6% to 25% of patients stopped due to intolerance. For 4 studies, the subsequent therapies included mixed treatments, which consisted of various chemoimmunotherapies or systemic therapies (see Table 32). In the other 4 trials, the subsequent therapies included lenalidomide-based treatments, venetoclax, R-BAC, or R-iBVD, each reported in 1 study.
The median age of patients was 65 years for the ZUMA-2 trial and ranged from 63 years to 71 years in the other studies. Patients were predominantly male (standard of care: range = 72% to 85%; ZUMA-2: 84%). The proportion of patients with blastoid morphology ranged from 12% to 31% in the standard of care studies (not reported for 3 trials), compared with 25% for the ZUMA-2 study. In the ZUMA-2 trial, 88% of patients had Ki-67 greater than 30%, and in the standard of care studies that percentage ranged from 63% to 92% (not reported for 4 studies). For 3 trials,36,56,57 the population of interest consisted of a subgroup of the overall study population, and no baseline patient characteristics were reported for these patients.
Four standard of care trials provided OS outcome data,35,38,40,55 2 trials reported PFS data,40,55 and 8 trials35,36,38-40,55-57 reported tumour response outcome data that were suitable for analysis.
In the ZUMA-2 trial, survival outcomes were defined as the time from the date of brexucabtagene autoleucel infusion or leukapheresis to the date of death from any cause (OS), or until disease progression or death from any cause (PFS). Definitions of OS and PFS varied across the standard of care studies. One trial38 defined OS from the date of last ibrutinib infusion until death or date of last follow-up, and 2 studies35,40 defined survival from the start of subsequent therapy until death from any cause or the date last known to be alive. One study reported that OS and PFS were “calculated in the standard fashion,” from the start of subsequent therapy.55
Tumour response outcomes were based on the Lugano classification in 3 studies40,45,55 and the IWG definition in 4 studies35,36,39,57 (classification system not reported in 2 studies38,56). Tumour response outcomes were investigator-assessed in all the standard of care studies. Although the ZUMA-2 study reported both centrally adjudicated response (Lugano) and investigator-assessed tumour response outcomes, only central adjudication results were included in the MAIC. The definition of study baseline also varied for studies reporting only tumour response outcomes. The baseline was the start of BTK inhibitor therapy in Dreyling et al. (2016)57 and Epperla et al. (2017),36 whereas baseline was the start of subsequent therapy for Wang et al. (2017)39 and Regny et al. (2019).56
Table 32: Summary of Studies Included in the ITC
Study, study design, enrolment period | N (% subsequent treatment)a | Subsequent treatment post–BTK inhibitor | Median follow-up (range) | Region (study type) | Age in years, median (range) Male, % | Prior therapies, median (range) ECOG PS 0 or 1 (%) |
|---|---|---|---|---|---|---|
Studies reporting survival outcomes | ||||||
ZUMA-245 Single-arm trial 2015 to ongoing | 68 (100) | Brexucabtagene autoleucel 2 × 106 anti-CD19 CAR T cells per kilogram (n = 68) | 14.8 months (1.2 to 37.6) from CAR T-cell infusion | US, Europe (MC) | Age: 65 (38 to 79) Male: 84% | 3 (1 to 5) PS: 100 |
Jain et al. (2018)38 Retrospective 2011 to 2017 | 41 (88) | Salvage treatments (n = 36): R-hyperCVAD (n = 6), radiochemotherapy (n = 6), bendamustine-based (n = 5), lenalidomide-based (n = 4), bortezomib-based (n = 3), R-CHOP (n = 3), radiation alone (n = 3), R-ESHAP with allogenic SCT (n = 1), lenalidomide + rituximab + proteasome inhibitor (n = 2), phosphoinositide 3-kinase inhibitor (n = 1), miscellaneous (n = 2) | 38 months from end of BTK inhibitor therapy | US (SS) | Age: 69 (35 to 86) Male: NR | 3 (1 to 11) PS: NR |
Martin et al. (2016)35 Retrospective NR | 114 (64) | Subsequent treatments (n = 73): rituximab, 53%; lenalidomide, 26%; cytarabine, 18%; bendamustine, 16%; bortezomib, 10%; anthracycline, 7%; phosphoinositide 3-kinase inhibitor, 5% | NR | Europe, US (MC) | Age: 68 (46 to 85) Male: 75% | 3 (0 to 10) PS: NR |
Eyre et al. (2019)55,b Retrospective 2016 to 2018 | 20 (100) | Venetoclax (n = 20) | 3.2 months (0.5 to 13.1) from start of subsequent treatment | UK (MC) | Age: 69 (43 to 84) Male: 85% | 3 (2 to 5) PS: 55 |
McCulloch et al. (2020)40 Retrospective 2015 to 2019 | 36 (100) | R-BAC (n = 36) | 18 months (6 to 24) from start of subsequent therapy | Europe (MC) | Age: 66 (43 to 81) Male: 81% | 2 (1 to 6) PS: 80 |
Studies reporting tumour response outcomes only | ||||||
Dreyling et al. (2016)57,c RCT 2012 to 2013 | 139 (29) | Subsequent treatments (n = 40): rituximab (n = 21), bendamustine (n = 15), cyclophosphamide (n = 12) | NR | Europe, Latin America, Asia (MC) | 67 (IQR = 11) Male: 72% | 2 (1 to 9) PS: 99 |
Epperla et al. (2017)36,c Retrospective 2013 to 2015 | 97 (30) | Subsequent treatments (n = 29): bortezomib‐based (n = 10), lenalidomide‐based (n = 12), bendamustine‐based (n = 6) | NR | US (MC) | Age at diagnosis: 63 (39 to 87) Male: 82% | 2 (1 to 8) PS: 86 |
Wang et al. (2017)39 Retrospective 2009 to 2016 | 58 (100) | Lenalidomide monotherapy (n = 13), lenalidomide plus rituximab (n = 11), other lenalidomide combinations (n = 34) | NR | UK, US (MC) | Age: 71 (50 to 89) Male: 76% | 4 (1 to 13) PS: 48 |
Regny et al. (2019)56,c,d Retrospective 2016 to 2019 | 12 (100) | R-iBVD (n = 12) | 21.2 months | France (MC) | Age: 69 (40 to 91) Male: NR | NR PS: NR |
BTK = Bruton tyrosine kinase; CAR = chimeric antigen receptor; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IQR = interquartile range; ITC = indirect treatment comparison; MC = multi-centre; NR = not reported; R-BAC = rituximab, bendamustine, and cytarabine; R-CHOP = rituximab in combination with cyclophosphamide, doxorubicin, vincristine, and prednisolone; RCT = randomized controlled trial; R-ESHAP = rituximab in combination with etoposide, methylprednisolone, cytarabine, and cisplatin; R-hyperCVAD = rituximab in combination with hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone alternating with methotrexate and cytarabine; R-iBVD = rituximab in combination with bendamustine, bortezomib, and dexamethasone; SCT = stem cell transplant; SS = single centre.
aN represents the number of patients who discontinued BTK inhibitor and the percentage in parentheses represents the proportion of those patients who subsequently received treatment.
bStudy data based on letters to editor.
cOutcomes reported for the subgroup of patients who had received treatments post–BTK inhibitor therapy. Baseline characteristics are reported for the overall study population, which included patients with and without prior BTK inhibitor therapy.
dStudy data based on European Hematology Association poster.
Source: Sponsor’s submission to CADTH.43
Results
Table 33 includes a summary of the results of the meta-analysis of survival outcomes for the standard of care studies. For both OS and PFS, the random-effects models showed better fit than fixed-effects models, based on the deviance information criterion. The median OS was 9.3 months (95% CI, 7.4 months to 11.6 months) and the mean OS was 15.4 months (95% CI, 12.2 months to 18.9 months) for the analyses that included all 4 standard of care studies. The point estimate for the median OS ranged from 8.0 months to 10.3 months, and the mean OS ranged from 14.0 months to 16.1 months across the sensitivity analyses conducted (Table 33).
The estimate of the 1-year survival rate was 42% (95% CI, 34% to 49%), and 2-year survival was 22% (95% CI, 15% to 28%), based on the random-effects meta-analysis of the 4 standard of care studies (primary analysis). Across the other sensitivity analyses, the 1-year survival rate ranged from 38% to 45% and the 2-year survival rate ranged from 19% to 23%.
The median PFS was 6.6 months (95% CI, 4.6 to 9.3), and the mean PFS was 11.3 months (95% CI, 7.3 to 16.3), based on pooled data from 2 standard of care studies. The PFS rate was 30% (95% CI, 19% to 42%) at 1 year and 14% (95% CI, 6% to 23%) at 2 years.
Table 33: Random-Effects Meta-Analysis of Overall Survival or Progression-Free Survival for Standard of Care Treatment Studies
Scenarios | Median (95% CI) | Mean (95% CI) |
|---|---|---|
OS | OS, months | OS, months |
All studies reporting OS KM curves (4 studies) (primary analysis) | 9.3 (7.4 to 11.6) | 15.4 (12.2 to 18.9) |
Studies with mixed treatments (2 studies) | 8.8 (6.7 to 11.6) | 15.4 (11.6 to 19.5) |
Studies with mixed treatments or venetoclax (3 studies) | 8.0 (6.0 to 10.5) | 14.7 (11.0 to 18.7) |
Studies with mixed treatments or R-BAC (3 studies)a | 10.3 (8.3 to 12.7) | 16.1 (12.8 to 19.6) |
Studies with survival time t = 0 from start of subsequent treatment (3 studies) | 8.1 (6.1 to 10.6) | 14.0 (10.4 to 18.1) |
Studies with survival time t = 0 from start of subsequent treatment, excluding venetoclax (2 studies) | 9.0 (7.0 to 11.5) | 14.5 (10.8 to 18.6) |
PFS | PFS, months | PFS, months |
All studies reporting PFS KM curves (2 studies) | 6.6 (4.6 to 9.3) | 11.3 (7.3 to 16.3) |
CI = confidence interval; KM = Kaplan–Meier; OS = overall survival; PFS = progression-free survival; R-BAC = rituximab, bendamustine, and cytarabine.
Note: Based on log-normal random-effects model.
aData used to inform the pharmacoeconomic model.
Source: Sponsor’s submission to CADTH.43
For the tumour response outcomes, the meta-analysis of all standards of care studies reported an ORR of 42% (95% CI, 27% to 59%), a CR of 21% (95% CI, 11% to 38%), and a PR of 19% (95% CI, 13% to 38%) (random-effects model; Table 34). Results varied across the 7 sensitivity analyses conducted, with ORR point estimates (random effects) that ranged from 26% to 56%, depending on which studies were included in the analyses. The majority of analyses showed high heterogeneity, with 14 of 24 analyses reporting I2 values greater than 50% (range = 0% to 93%).
Table 34: Meta-Analysis of Tumour Response Outcomes for Standard of Care Treatment Studies
Scenarios | Model | Pooled ORR, % (95% CI) | Pooled CR, % (95% CI) | Pooled PR, % (95% CI) |
|---|---|---|---|---|
Primary analysis | ||||
All studies reporting ORR (8 studies) | FE | 38 (33 to 43) | 21 (17 to 27)a | 19 (14 to 24)a |
RE | 42 (27 to 59) | 21 (11 to 38)a | 19 (13 to 38)a | |
I2 | 84% | 81% | 49% | |
Sensitivity analyses | ||||
All studies reporting ORR: mixed treatments only (5 studies) | RE | 28 (23 to 34) | 13 (7 to 21)b,c | 14 (10 to 21)b |
All studies reporting OS and ORR data (4 studies) | RE | 48 (23 to 73)d | 23 (9 to 48)d | 18 (11 to 29)d |
OS studies: mixed treatments (2 studies) | RE | 26 (18 to 35) | 12 (5 to 27)d | 13 (6 to 26)c |
OS studies: mixed treatments or venetoclax (3 studies) | RE | 33 (21 to 47)d | 14 (7 to 25)c | 17 (8 to 33)d |
OS studies: mixed treatments or R-BAC (3 studies) | RE | 45 (17 to 78)d | 24 (7 to 58)d | 16 (10 to 24) |
OS studies with survival time t = 0 from start of subsequent treatment (3 studies) | RE | 55 (25 to 82)d | 23 (6 to 58)d | 22 (15 to 30) |
OS studies with survival time t = 0 from start of subsequent treatment, excluding venetoclax (2 studies) | RE | 56 (15 to 90)d | 25 (4 to 75)d | 19 (13 to 28) |
CI = confidence interval; CR = complete response; FE = fixed effects; ORR = objective response rate; OS = overall survival; PR = partial response; R-BAC = rituximab, bendamustine, and cytarabine; RE = random effects.
aAnalysis included data from 6 studies.
bAnalysis included data from 3 studies.
cI2 values 25% to 49%.
dI2 values greater than or equal to 50% (high heterogeneity).
Source: Sponsor’s submission to CADTH.43
Matching-Adjusted ITC
Only the results that included the FAS population of the ZUMA-2 study have been summarized in this report. The FAS population may be considered a more conservative estimate as it includes all patients eligible for CAR T-cell therapy who underwent leukapheresis (i.e., those who did and did not receive brexucabtagene autoleucel). In Table 35, the baseline characteristics of the ZUMA-2 FAS population have been summarized for the primary analyses of OS, PFS, and ORR, showing the differences before and after weighting to match the standard of care studies. After weighting, the studies appear to be well balanced for the 6 characteristics that were included in the propensity model (marked in bold in Table 35); however, a number of differences between the brexucabtagene autoleucel and comparator studies are evident in other characteristics that were identified as prognostic factors for OS in MCL (e.g., MIPI risk level and extranodal involvement, and prior ibrutinib BTK inhibitor therapy). Effective sample size was substantially reduced from 74 patients to 36.2 (OS), 16.3 (PFS), and 29.5 (objective response) for the primary analyses, which suggests there were important differences between patients included in the ZUMA-2 and standard of care studies.
Table 35: Baseline Patient Characteristics of ZUMA-2 (FAS) Before and After Matching to the Comparator Studies
Characteristic | Observed ZUMA-2 | OS scenario: all studies | PFS scenario: all studies | ORR scenario: all studies | |||
|---|---|---|---|---|---|---|---|
N = 74 | Pooled SOC (4 studies) | Weighted ZUMA-2 ESS = 36.2 | Pooled SOC (2 studies) | Weighted ZUMA-2 ESS = 16.3 | Pooled SOC (8 studies) | Weighted ZUMA-2 ESS = 29.5 | |
Number of prior treatments | 3.3 | 2.8 | 2.8 | 2.4 | 2.4 | 2.6 | 2.6 |
Proportion of patients with: | |||||||
Prior autologous SCT | 0.42 | 0.23 | 0.23 | 0.38 | 0.38 | 0.29 | 0.29 |
Prior BTK inhibitor duration > SOC mediana | Variesb | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
Prior BTK inhibitor ORR | 0.38 | 0.55 | 0.55 | 0.63 | 0.63 | 0.59 | 0.59 |
Ki-67 ≥ 30% | 0.58 | 0.74 | 0.74 | 0.82 | 0.82 | 0.77 | 0.77 |
Ki-67 ≥ 50% | 0.50 | 0.49 | 0.49 | 0.46 | 0.46 | 0.49 | 0.49 |
Blastoid morphology | 0.26 | 0.25 | 0.25 | 0.21 | 0.21 | 0.19 | 0.19 |
MIPI low | 0.4 | 0.15 | 0.32 | 0.20 | 0.30 | 0.26 | 0.31 |
MIPI intermediate | 0.42 | 0.27 | 0.40 | 0.23 | 0.34 | 0.35 | 0.41 |
Stage III | 0.11 | 0.10 | 0.10 | 0.10 | 0.09 | 0.11 | 0.10 |
Stage IV | 0.87 | 0.88 | 0.89 | 0.85 | 0.90 | 0.84 | 0.90 |
Prior BTK inhibitor: ibrutinib | 0.84 | 0.96 | 0.87 | 0.88 | 0.85 | 0.98 | 0.88 |
Male | 0.84 | 0.77 | 0.73 | 0.82 | 0.63 | 0.77 | 0.70 |
Extranodal | 0.58 | 0.85 | 0.55 | 0.85 | 0.50 | 0.63 | 0.51 |
Bone marrow involvement | 0.57 | 0.60 | 0.64 | 0.60 | 0.69 | 0.60 | 0.66 |
BTK = Bruton tyrosine kinase; ESS = effective sample size; FAS = full analysis set; MIPI = Mantle Cell Lymphoma International Prognostic Index; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; SCT = stem cell transplant; SOC = standard of care.
Note: Items in bold were included in the propensity score model for matching.
aMatched on > pooled SOC median duration of each scenario.
bZUMA-2 proportions vary depending on pooled SOC median duration of each scenario on median of each scenario.
Source: Sponsor’s submission to CADTH.43
The observed and weighted OS curves for the FAS population of the ZUMA-2 trial are shown in Figure 5. Weighted data are shifted toward better survival. The effective sample size of the weighted survival function was 36 patients at the start of follow-up, and after 21 months the curve is predicted based on 9 or fewer patients. Figure 6 shows the fitted parametric survival curve for the weighted brexucabtagene autoleucel data versus pooled standard of care studies for OS. The pairwise indirect comparison reported an average HR of 0.18 (95% CI, 0.09 to 0.38) for the primary analysis, which included all standard of care studies (n = 4 trials). Table 36 reports the results of the unadjusted (naive) and MAIC sensitivity analyses for OS, which show that the point estimates and 95% CI consistently favour brexucabtagene autoleucel over standard of care treatments. The effective sample size for brexucabtagene autoleucel ranged from 18.9 patients to 40.8 patients, depending on which standard of care studies the ZUMA-2 data were matched to.
Figure 5: Unadjusted and Matching-Adjusted Kaplan–Meier Curves for Overall Survival With Brexucabtagene Autoleucel: ZUMA-2 FAS
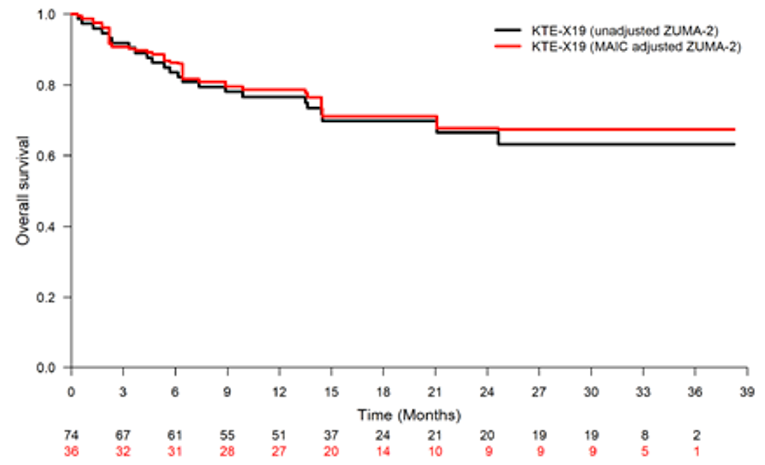
FAS = full analysis set; KTE-X19 = brexucabtagene autoleucel; MAIC = matching-adjusted indirect comparison.
Note: Matched to all studies reporting overall survival Kaplan–Meier curves.
Source: Sponsor’s submission to CADTH.43
Figure 6: MAIC Parametric Survival Curve for Overall Survival: Brexucabtagene Autoleucel Versus Standard of Care — ZUMA-2 FAS
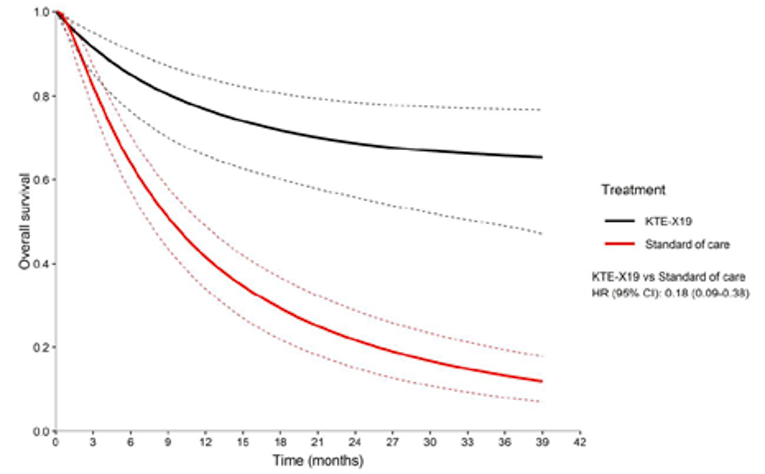
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; KTE-X19 = brexucabtagene autoleucel; MAIC = matching-adjusted indirect comparison.
Note: Matched to all studies reporting overall survival Kaplan–Meier curves.
Source: Sponsor’s submission to CADTH.43
Table 36: ITC of Overall Survival for Brexucabtagene Autoleucel Versus Standard of Care Treatments
Analyses | Brexucabtagene autoleucel (FAS) | SOC (pooled) | Brexucabtagene autoleucel vs. SOC | |
|---|---|---|---|---|
N or ESS | Mean OS,a months (95% CI) | Mean OS,a months (95% CI) | OS HRb (95% CI) | |
Unadjusted ITC | ||||
All studies reporting OS KM curves (4 studies) | 74 | 28 (23.7 to 31.3) | 14.1 (11.7 to 16.4) | 0.22 (0.11 to 0.43) |
MAIC | ||||
All studies reporting OS KM curves (4 studies) | 36.2 | 29.0 (24.7 to 32.1) | 14.1 (11.7 to 16.4) | 0.18 (0.09 to 0.38) |
Studies with mixed treatments (2 studies) | 40.8 | 28.5 (24.2 to 31.7) | 13.9 (11.2, 16.5) | 0.19 (0.10 to 0.39) |
Studies with mixed treatments or venetoclax (3 studies) | 38.6 | 28.8 (24.6 to 31.9) | 13.3 (10.6 to 15.8) | 0.18 (0.09 to 0.36) |
Studies with mixed treatments or R-BAC (3 studies) | 38.5 | 28.7 (24.5 to 31.9) | 14.8 (12.4 to 17.1) | 0.20 (0.10 to 0.40) |
Studies with survival time t = 0 from start of subsequent treatment (3 studies) | 18.9 | 30.2 (26.0 to 33.1) | 12.9 (10.3 to 15.6) | 0.15 (0.07 to 0.31) |
Studies with survival time t = 0 from start of subsequent treatment, excluding venetoclax (2 studies) | 27.7 | 30.7 (26.4 to 33.5) | 13.5 (10.9 to 16.1) | 0.19 (0.12 to 0.33) |
CI = confidence interval; ESS = effective sample size; FAS = full analysis set; HR = hazard ratio; ITC = indirect treatment comparison; KM = Kaplan–Meier; MAIC = matching-adjusted indirect comparison; OS = overall survival; R-BAC = rituximab, bendamustine, and cytarabine; SOC = standard of care; vs. = versus .
aMean OS is defined as the area under the curve of the survival function from 0 months to 39 months (based on either Gompertz or log-normal models).
bAverage HRs are based on hazard functions from 0 months to 39 months.
Source: Sponsor’s submission to CADTH.43
The unadjusted and matching-adjusted Kaplan–Meier curves for PFS for the ZUMA-2 intention-to-treat population are shown in Figure 7. The weighted data are shifted toward better survival up to 15 months, after which there is a substantial drop off of the survival curve and the effective sample size is reduced to 2.
The PFS MAIC for brexucabtagene autoleucel versus pooled standard of care studies (n = 2 studies) is shown in Figure 8 (average HR of || (95% CI, ||||||||||||). For this analysis, the effective sample size was 16.3. The average HR for the unadjusted (naive) ITC was || (95% CI, ||||||||||||) (Table 37).
Figure 7: Unadjusted and Matching-Adjusted Kaplan-Meier Curves for Progression-Free Survival with Brexucabtagene Autoleucel (ZUMA-2 FAS) Redacted

Source: Sponsor’s submission to CADTH.43
Figure 8: MAIC Parametric Survival Curve for Progression-Free Survival: Brexucabtagene Autoleucel Versus Standard of Care — ZUMA-2 FAS
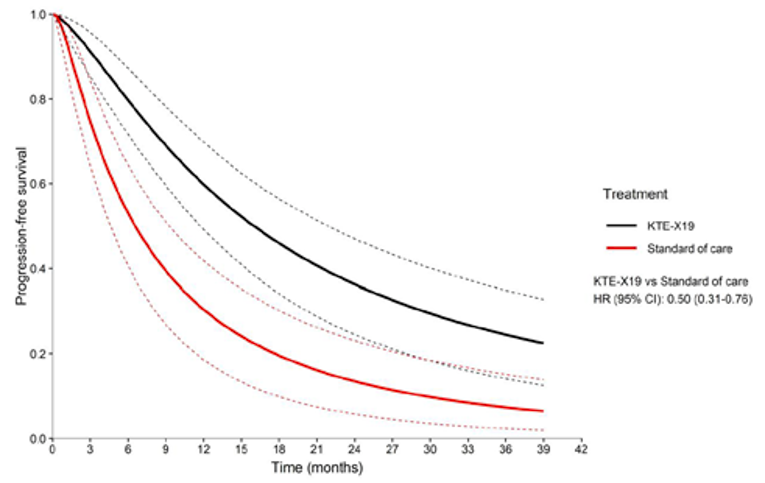
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; KTE-X19 = brexucabtagene autoleucel; MAIC = matching-adjusted indirect comparison.
Note: Matched to 2 studies reporting progression-free survival Kaplan–Meier curves.
Source: Sponsor’s submission to CADTH.43
Table 37: ITC of Progression-Free Survival for Brexucabtagene Autoleucel Versus Standard of Care Treatments
Analyses | Brexucabtagene autoleucel (FAS) | SOC (pooled) | Brexucabtagene autoleucel vs. SOC | |
|---|---|---|---|---|
N or ESS | Mean PFS,a months (95% CI) | Mean PFS,a months (95% CI) | PFS HRb (95% CI) | |
Unadjusted ITC | ||||
All studies reporting PFS KM curves (2 studies) | 74 | |||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||||| |
MAIC | ||||
All studies reporting PFS KM curves (2 studies) | 16.3 | |||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||||| |
CI = confidence interval; ESS = effective sample size; FAS = full analysis set; HR = hazard ratio; ITC = indirect treatment comparison; KM = Kaplan–Meier; MAIC = matching-adjusted indirect comparison; PFS = progression-free survival; SOC = standard of care; vs. = versus .
aMean PFS is defined as the area under the curve of the survival function from 0 months to 39 months (based on log-normal model).
bAverage HRs are based on hazard functions from 0 months to 39 months.
Source: Sponsor’s submission to CADTH.43
Table 38 provides a summary of the unadjusted ITC and MAIC results for ORR, CR, and PR outcomes. The effective sample size for the weighted ZUMA-2 data was 29.5 for objective response and 39.8 for CR and PR based on the primary analyses, which included all standard of care studies. Across the sensitivity analyses, the effective sample size ranged from 18.9 to 40.8, which suggests there were important differences between the populations enrolled in ZUMA-2 versus the comparator studies. The sensitivity analyses also show that the absolute treatment effects for the standard of care studies varied, with the ORR ranging from 25.7% to 55.5%, depending on which trials were included in the analysis.
The odds ratio of objective response was 7.91 (95% CI, 2.35 to 26.62) for brexucabtagene autoleucel versus standard of care therapy based on the MAIC primary analysis (pooled data for 8 studies) (Table 38). The odds ratio of CR was 5.91 (95% CI, 2.09 to 16.66) and of PR was 1.37 (95% CI, 0.57 to 3.29) based on the primary MAIC analyses. The point estimates for ORR and CR varied across the sensitivity analyses and showed wide 95% CIs. For the MAIC of PR, all analyses reported 95% CIs that included the null value of 1.0.
Table 38: ITC of Objective Response Rate for Brexucabtagene Autoleucel Versus Standard of Care Treatments
Analyses | Brexucabtagene autoleucel (FAS), % | SOC (pooled), % (95% CI) | Brexucabtagene autoleucel vs. SOC, odds ratio (95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|---|
ORR | CR | PR | ORR | CR | PR | ORR | CR | PR | |
Unadjusted ITC | |||||||||
All studies reporting ORR (8 studies) | 83.8 N = 74 | 59.5 N = 74 | 24.3 N = 74 | 42.3 (27.4 to 58.7) | 21.1 (10.6 to 37.8)a | 19.4 (12.8 to 28.3)a | 7.06 (2.85 to 17.45) | 5.47 (2.14 to 14.01) | 1.33 (0.65 to 2.76) |
MAIC | |||||||||
All studies reporting ORR (8 studies) (primary analysis) | 85.3 ESS = 29.5 | 61.3 ESS = 39.8 | 24.9 ESS = 39.8 | 42.3 (27.4 to 58.7) | 21.1 (10.6 to 37.8)a | 19.4 (12.8 to 28.3)a | 7.91 (2.35 to 26.62) | 5.91 (2.09 to 16.66) | 1.37 (0.57 to 3.29) |
Studies reporting ORR: mixed treatments only (5 studies) | 86.1 ESS = 31 | 58.1 ESS = 40.8 | 27.3 ESS = 40.8 | 28.0 (22.6 to 34.0) | 12.8 (7.4 to 21.2)b | 14.4 (9.8 to 20.5)b | 15.91 (5.53 to 45.74) | 9.49 (3.98 to 22.64) | 2.23 (0.99 to 5.04) |
All studies reporting OS KM curves (4 studies)c | 84.9 ESS = 36.2 | 63.7 ESS = 36.2 | 21.1 ESS = 36.2 | 47.6 (23.3 to 73.1) | 23.0 (8.7 to 48.1) | 18.1 (10.7 to 28.9) | 6.19 (1.49 to 25.70) | 5.90 (1.57 to 22.13) | 1.21 (0.44 to 3.31) |
Studies reporting OS: mixed treatments (2 studies)c | 83.8 ESS = 40.8 | 61 ESS = 40.8 | 22.8 ESS = 40.8 | 25.7 (18.4 to 34.7) | 12.4 (5.2 to 26.7) | 12.6 (5.6 to 25.8) | 14.93 (5.85 to 38.08) | 11.09 (3.55 to 34.66) | 2.05 (0.65 to 6.44) |
Studies reporting OS: mixed treatments or venetoclax (3 studies)c | 84.9 ESS = 38.6 | 61.4 ESS = 38.6 | 23.5 ESS = 38.6 | 32.5 (20.6 to 47.2) | 14.0 (7.1 to 25.5) | 16.7 (7.6 to 32.8) | 11.67 (3.98 to 34.22) | 9.82 (3.65 to 26.40) | 1.53 (0.48 to 4.90) |
Studies reporting OS: mixed treatments or R-BAC (3 studies)c | 84.1 ESS = 38.5 | 63.9 ESS = 38.5 | 20.1 ESS = 38.5 | 45.4 (16.6 to 77.6) | 24.2 (6.9 to 57.8) | 15.6 (9.6 to 24.3) | 6.34 (1.20 to 33.61) | 5.56 (1.12 to 27.59) | 1.36 (0.52 to 3.58) |
Studies reporting OS: survival time t = 0 from start of subsequent treatment (3 studies)c | 88.8 ESS = 18.9 | 65.5 ESS = 18.9 | 23.3 ESS = 18.9 | 55.1 (24.8 to 82.0) | 23.2 (6.2 to 57.9) | 21.7 (15.4 to 29.6) | 6.48 (0.93 to 45.20) | 6.27 (1.05 to 37.43) | 1.10 (0.35 to 3.45) |
Studies reporting OS: survival time t = 0 from start of subsequent treatment, excluding venetoclax (2 studies)c | 89.1 ESS = 27.7 | 75.2 ESS = 27.7 | 13.8 ESS = 27.7 | 55.5 (15.2 to 89.7) | 25.3 (3.7 to 75.0) | 19.3 (12.9 to 27.8) | 6.53 (0.67 to 63.68) | 8.99 (0.86 to 94.15) | 0.67 (0.21 to 2.19) |
CI = confidence interval; CR = complete response; ESS = effective sample size; FAS = full analysis set; ITC = indirect treatment comparison; KM = Kaplan–Meier; MAIC = matching-adjusted indirect comparison; ORR = objective response rate; OS = overall survival; PR = partial response; R-BAC = rituximab, bendamustine, and cytarabine; SOC = standard of care.
aAnalysis includes 6 studies.
bAnalysis includes 3 studies.
cOnly included studies that reported both overall survival KM curve and ORR.
Source: Sponsor’s submission to CADTH.43
Critical Appraisal of ITC
The meta-analysis and ITC were based on a systematic literature search that included a search of multiple databases, conference proceedings, clinical trial registries, and regulatory and health technology assessment agency websites. Screening was conducted based on standard methods, with studies selected independently in duplicate, according to pre-specific criteria. The literature search included a broad population of patients with MCL (all with R/R disease), with additional screening to identify studies that reported outcomes for patients after BTK inhibitor therapy. Although only English language articles were included, the likelihood that relevant trials were missed was thought to be low. No information was provided on the process used to extract data, and there was no quality assessment of the included studies. The lack of quality assessment is an important limitation, considering all studies may have higher risk of bias given that all were open-label uncontrolled studies (including 7 retrospective studies) with small sample sizes (12 to 73 patients).
The sponsor-submitted report included a description of the characteristics of the included studies and evaluated heterogeneity across trials. Several important differences were noted between trials in the study designs, populations, interventions, outcomes, and follow-up duration that could not be accounted for in the meta-analysis or the ITC. As described previously, there were differences in the start time of survival follow-up, with some studies starting at the time of subsequent therapy and others starting at an earlier time point. Median follow-up duration ranged from 3.2 months to 38 months. Only the ZUMA-2 study reported tumour response data based on central adjudication, which may be less susceptible to bias than investigator-rated outcomes. However, this is a potential source of heterogeneity, as all other studies were based on investigator-assessed tumour response. No sensitivity analyses were conducted using investigator-assessed outcomes from ZUMA-2. Variation in absolute tumour response rates were observed between studies, and the majority of the meta-analyses detected high statistical heterogeneity, with I2 values greater than 50%. The use of pooled comparator data that included several different interventions was justified by the study’s authors, based on the lack of standard treatments for patients with R/R MCL post–BTK inhibitor therapy. This, however, is a potential source of heterogeneity that could not be addressed through sensitivity analyses or other means. Moreover, not all treatments included in the analysis were relevant to the Canadian context.
The reporting of the conduct of the meta-analysis and ITC were clear and appear to follow accepted methods to generate individual patient data from published Kaplan–Meier plots,53 to select the best-fitting parametric survival function for each study,58 and to conduct the meta-analysis.54 The ITC’s authors searched the literature and consulted with clinical experts to identify potential prognostic factors or effect modifiers in patients with R/R MCL and derived patient weights using a logistic propensity score model, which was consistent with recommended technical guidance methods.20 The key limitation of the MAIC is inherent to unanchored indirect comparisons, which assume that absolute outcomes can be predicted from the covariates (i.e., that all effect modifiers and prognostic factors are accounted for in the model).20 This assumption is largely considered impossible to meet according to the National Institute for Health and Care Excellence Decision Support Unit technical guidance report on the methods for population-adjusted indirect comparisons.20 In the sponsor-submitted MAIC, not all the identified prognostic factors were included in the model used to derive patients weights, and the decision to exclude some factors was made after examining the results of preliminary analyses. As noted in Table 35, there were imbalances between brexucabtagene autoleucel and the comparator studies in some of these excluded prognostic factors (e.g., MIPI risk level, extranodal involvement, and prior ibrutinib BTK inhibitor therapy). Individual patient data from ZUMA-2 were weighted to match pooled patient characteristic data from the standard of care studies, which had several limitations. All but 2 of the comparator studies were conducted retrospectively and were therefore based on previously collected data, which provides no opportunity to prospectively gather covariate or outcome data in a standard systematic manner. Seven of the 8 standard of care studies were missing data for at least 1 baseline characteristic identified as a key prognostic factor, with 4 studies missing 3 or more of the 6 key prognostic factors used to determine patient weights. To address the missing data, the authors of the ITC assumed that the weighted average of the available data was representative of other studies’ missing data, which may not be valid. Due to the missing, excluded, or imbalanced characteristics between treatments, it appears that the foundational assumption of an unanchored MAIC (that all effect modifiers and prognostic factors are included in the model) has not been met. According to the National Institute for Health and Care Excellence Decision Support Unit technical guidance, “failure of this assumption leads to an unknown amount of bias in the unanchored estimate.”20
When conducting a MAIC, the inclusion criteria for the index study should be the same or broader than for the comparator study. It is unclear if this requirement was met, as it is likely that the standard of care studies included some patients who would not be eligible for brexucabtagene autoleucel. For example, the proportion of patients with an ECOG PS of 0 or 1 was low in 2 studies (48% to 55%) and ranged from 80% to 99% in 3 other studies (not reported in 3 trials), compared to 100% of patients in the ZUMA-2 study. Differences between the populations enrolled in the ZUMA-2 trial and the standard of care studies were evident given the substantial reduction in effective sample size for the weighted data. This is particularly an issue for PFS (effective sample size 16), and for later time points in the OS matched curve, which were informed by fewer than 10 patients. The small effective sample size suggests that the weights are highly variable due to poor population overlap, and as a result, the estimates may be unstable. The sponsor’s economic analysis noted limitations with the results of the MAIC due to the small effective sample size and stated that the weighted Kaplan–Meier curves for OS and PFS cross, which reduced the face validity of the matched curves.43
Uncertainty in the results of the unanchored MAIC are compounded by the inclusion of lower quality comparator trials and substantial clinical heterogeneity across all studies. The median follow-up duration varied across trials and was as short as 3.2 months. For the ZUMA-2 study, only 41% of patients had 30 months of follow-up. Thus, outcomes for later time points may be informed by few patients, which adds to the uncertainty. The tumour response outcomes showed high statistical heterogeneity across the standard of care studies, and the results from the MAIC lacked precision, showing wide 95% CIs.
The results of naive ITCs were provided for comparative purposes, but given the major limitations of this type of analysis, which does not control for any differences in prognostic factors or effect modifiers between studies, the results should be interpreted with extreme caution.
No indirect evidence was available for the comparative safety or impact on HRQoL of brexucabtagene autoleucel versus standard of care. Due to the limitations of the sponsor-submitted MAIC, no conclusions can be drawn about the comparative efficacy of brexucabtagene autoleucel in terms of OS, PFS, or tumour response outcomes.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH.
Discussion
Summary of Available Evidence
One pivotal study was included in this report. The ZUMA-2 trial was a phase II, single-arm, multi-centre, open-label study. It is the only prospective clinical trial in the R/R MCL post–BTK inhibitor setting. A total of 74 patients with R/R MCL whose disease had progressed on anthracycline- or bendamustine-containing chemotherapy, an anti-CD20 antibody, and a BTK inhibitor (ibrutinib and/or acalabrutinib) were leukapheresed, with 68 receiving treatment with brexucabtagene autoleucel at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram. The primary end point included the percentage of patients with an objective response (CR or PR) as assessed by the independent review committee, with key secondary outcomes of DOR, PFS, OS, and HRQoL.
The sponsor submitted a MAIC that compared the efficacy of brexucabtagene autoleucel to standard of care treatments in terms of OS, PFS, and tumour response outcomes. The analysis was informed by a systematic literature review that identified 9 uncontrolled, mainly retrospective, open-label studies that provided outcome data in patients with R/R MCL who received treatment following BTK inhibitor therapy (N = 12 to 73; median follow-up ranged from 3.2 months to 38 months). The subsequent therapies reported in the trials included lenalidomide-based treatments, venetoclax, R-BAC or R-iBVD, and mixed treatments (various chemoimmunotherapies or systemic therapies).
Interpretation of Results
Efficacy
With a median follow-up of 12.3 months, the primary end point of the study was met, as the ORR was significantly greater than the pre-specified historical control of 25% at 93% (95% CI, 83.8% to 98.2%; P < 0.0001) in the IAS. With 16.8 months follow-up, the ORR was also significantly greater than the historical control at 92% (95% CI, 81.6% to 97.2%). Of patients with ORR, 67% of patients achieved CR at both the July 24, 2019, and December 31, 2019, data cut-offs. According to the clinical experts consulted by CADTH, the historical control of 25% was thought to be low; however, the lower limit of the 95% CI for ORR would have potentially exceeded higher margins, given that it was 81.6%. Clinical experts noted that the proportion of patients achieving CR is clinically relevant given the population and stage of disease. Patients in the IAS achieved CR or PR at 1.0 month (range = 0.8 months to 3.1 months) post-treatment, and the median time to achieve CR was 3.0 months (range = 0.9 months to 9.3 months). The median DOR was not reached with 8.6 months of follow-up, as 57% of patients had ongoing response.
The median PFS and OS were not reached with 12.3 months of follow-up (95% CI, 9.2 to not estimable, and 95% CI, 24.0 to not estimable, respectively). At the December 31, 2019, data cut-off, the median PFS and OS were also not reached (95% CI, 9.6 to not estimable, and 95% CI, not estimable to not estimable, respectively). In the 16 patients who experienced PR, the median OS was 19.9 months (95% CI, 3.8 to not estimable), which was noted by the experts to be particularly long and not a typical benefit seen in these patients. With 12.3 months and 16.8 months of follow-up, 16 and 18 patients died, respectively. Overall, the deaths due to progressive disease were low compared to current treatments and within this population, with 15 patients dying due to disease progression. Subgroup analysis was conducted for all efficacy end points in pre-specified baseline covariates; however, the purpose was to check for consistency of results. The small sample size and the missing data for many covariates limits the interpretability of results.
While efficacy results for ORR and survival outcomes are clinically meaningful, the short duration of follow-up produces immature survival results; however, as noted by the clinical experts consulted by CADTH, survival in patients who have previously received or failed BTK inhibitor therapy is typically around 6 months, and the results of the ZUMA-2 trial exceed the typical life expectancy in these patients.
The proportion of patients experiencing moderate-to-severe health problems increased in the first month following infusion with brexucabtagene autoleucel for all EQ-5D subscales. Longitudinal changes in HRQoL are unable to be interpreted due to the decreasing numbers of patients reporting for HRQoL assessments over time. Overall, the median EQ VAS score improved by 5 points, from 85.0 to 90.0, from screening to month 6 and by 12 points from 78.0 at week 4 to 90.0 at 6 months, suggesting an immediate decrease followed by improvements in HRQoL after treatment with brexucabtagene autoleucel. An improvement of 7 to 12 points on the EQ VAS in patients with advanced cancer is considered a clinically meaningful difference59; however, given the missing data at later time points, interpretations in change over time are unable to be made.
For the MAIC, a logistic propensity score model was used to estimate patient weights for the ZUMA-2 trial so that the weighted mean baseline characteristics of the ZUMA-2 patients (FAS N = 74) matched the pooled mean characteristics of the standard of care studies. Pairwise indirect comparisons were then conducted using the weighted ZUMA-2 data and pooled outcome data for standard of care studies (n = 2 to 8). The primary MAIC analyses for OS reported an HR of 0.18 (95% CI, 0.09 to 0.38; effective sample size = 36.2), a PFS HR of || (95% CI, ||||||||||||; effective sample size = 16.3), and an objective response odds ratio of 7.91 (95% CI, 2.35 to 26.62; effective sample size = 29.5).
The key limitation of the MAIC is inherent in unanchored indirect comparisons, which assume that absolute outcomes can be predicted from the covariates included in the model (i.e., that every effect modifier and prognostic factor are accounted for).20 This assumption is largely considered impossible to meet, and failure of this assumption leads to an unknown amount of bias in the unanchored estimate.20 For the sponsor-submitted ITC, some prognostic factors were excluded from the model or may have been incompletely specified due to missing data from the clinical trials. The effective sample size was small for all outcomes (16 to 36), which suggests poor population overlap and unstable estimates. The results for the tumour response outcome lacked precision and showed wide 95% CIs. Uncertainty in the results of the unanchored MAIC are compounded by the inclusion of lower quality comparator trials and clinical heterogeneity across studies. Due to the limitations of the ITC, no conclusions about the comparative efficacy of brexucabtagene autoleucel can be drawn from the MAIC.
Harms
Serious TEAEs occurred in 68% of patients, with 29%, 19%, and 6% experiencing Grade 3, 4, and 5 serious TEAEs, respectively. Clinical experts noted that treatment with brexucabtagene autoleucel is accompanied by concerns about toxic effects including CRS and neurologic AEs. Cytokine release syndrome was seen in 92% of patients, with a median time to onset of 2 days and a median duration of 11 days. All patients recovered from CRS symptoms at 12.3 months follow-up. It was noted by clinical experts that the overall rate of CRS was high and that the most important symptoms were those that were Grade 3 (12%), Grade 4 (3%), or Grade 5 (0%), as these typically result in admission to the ICU.
Neurologic AEs occurred in 63% of patients, with a median onset of 7 days and a median time to resolution of 12 days (mean of 53.1 days) in patients whose events had resolved. The most common Grade 3 or higher neurologic events were encephalopathy (19%), confusional state (12%), and aphasia (4%). Neurologic AEs Grade 3 or higher occurred in approximately 30% of patients (22% Grade 3, 9% Grade 4). Clinicians noted that this proportion was high and that these patients would require ICU admission on top of the mandatory 7-day stay post-infusion.
Clinicians and provincial drug plan groups mentioned the need for prolonged IV immunoglobin following CAR T-cell administration, which is in limited supply in Canada and associated with increased human and physical resource use. Of the patients, 32% were treated with immunoglobulins in the ZUMA-2 study, which is important to note in the implementation of this treatment.
The concerns surrounding the harms of brexucabtagene autoleucel are to be weighed against the benefits related to survival and speed of remission, as these were noted to be important to the patient groups consulted.
The sponsor-submitted MAIC did not assess safety outcomes for brexucabtagene autoleucel.
Other Considerations
In terms of the intervention, preparation for treatment with brexucabtagene autoleucel requires several steps, including the use of bridging therapies and lymphodepleting chemotherapy, which yield further variables to consider in the feasibility and appropriateness of brexucabtagene autoleucel. These would be a constant part of the new treatment process and cannot be discounted in the implementation of brexucabtagene autoleucel; however, multiple treatment options do exist in Canada for these steps. It was noted that no new administrative qualifications will be necessary for Yescarta-authorized centres to administer brexucabtagene autoleucel, and all treatment centres that have completed the site qualifications will be able to administer brexucabtagene autoleucel; however, an impact assessment and associated training will be provided to these sites.
Conclusions
Evidence from the single-arm, open-label ZUMA-2 trial suggests that CAR T-cell therapy with brexucabtagene autoleucel at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram is associated with statistically significant rates of objective response and has a clinically important impact on CR and DOR. Moreover, brexucabtagene autoleucel was associated with substantial increases in the important survival outcomes of PFS and OS, which patients have identified as being of critical importance. Although the results of the ZUMA-2 trial suggested an improved HRQoL over 6 months, these results are uninterpretable over time due to the missing assessments. The benefits from the ZUMA-2 trial may be associated with a risk of bias due to the single-arm, open-label design, as well as an overall belief that the included population was more fit than the general Canadian population. These benefits also need to be weighed against the associated harms, including serious CRS and neurologic AEs that result in further ICU admission. Data on long-term outcomes of therapy with brexucabtagene autoleucel are needed.
Given the lack of head-to-head studies for brexucabtagene autoleucel, the sponsor submitted an unanchored MAIC that provided indirect evidence of the efficacy of brexucabtagene autoleucel compared with standard of care therapies in patients with R/R MCL. However, due to limitations of MAIC analysis methods, inclusion of lower quality comparator trials, clinical heterogeneity between studies, lack of complete covariate data to inform the patient weights, and poor population overlap, no conclusions can be drawn from the MAIC.
References
1.Schieber M, Gordon LI, Karmali R. Current overview and treatment of mantle cell lymphoma. F1000Res. 2018;7:F1000 Faculty Rev-1136.
2.Jain P, Wang M. Mantle cell lymphoma: 2019 update on the diagnosis, pathogenesis, prognostication, and management. American Journal of Hematology. 2019;94(6):710-725. PubMed
3.Cheah CY, Seymour JF, Wang ML. Mantle Cell Lymphoma. J Clin Oncol. 2016;34(11):1256-1269. PubMed
4.Leukemia & Lymphoma Society. Mantle Cell Lymphoma Facts. 2019: https://www.lls.org/sites/default/files/file_assets/FS4_MCL_Facts_Rev.pdf. Accessed 2021 Apr 22.
5.National Organization for Rare Disorders. Mantle Cell Lymphoma. 2021; https://rarediseases.org/rare-diseases/mantle-cell-lymphoma/. Accessed 2021 Apr 22.
6.Klener P. Advances in Molecular Biology and Targeted Therapy of Mantle Cell Lymphoma. Int J Mol Sci. 2019;20(18):4417. PubMed
7.Cohen JB, Zain JM, Kahl BS. Current Approaches to Mantle Cell Lymphoma: Diagnosis, Prognosis, and Therapies. American Society of Clinical Oncology Educational Book. 2017(37):512-525. PubMed
8.pan-Canadian Oncology Drug Review. Final Clinical Guidance Report. Ibrutinib (Imbruvica) for Mantle Cell Lymphoma. 2016: https://www.cadth.ca/sites/default/files/pcodr/pcodr_ibrutinib_imbruvica_mcl_fn_cgr.pdf. Accessed 2021 Apr 22.
9.Owen C, Berinstein NL, Christofides A, Sehn LH. Review of Bruton tyrosine kinase inhibitors for the treatment of relapsed or refractory mantle cell lymphoma. Curr Oncol. 2019;26(2):e233-e240. PubMed
10.Flinn IW, van der Jagt R, Kahl BS, et al. Randomized trial of bendamustine-rituximab or R-CHOP/R-CVP in first-line treatment of indolent NHL or MCL: the BRIGHT study. Blood. 2014;123(19):2944-2952. PubMed
11.Kluin-Nelemans HC, Hoster E, Hermine O, et al. Treatment of Older Patients with Mantle-Cell Lymphoma. N Engl J Med. 2012;367(6):520-531. PubMed
12.Lenz G, Dreyling M, Hoster E, et al. Immunochemotherapy With Rituximab and Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone Significantly Improves Response and Time to Treatment Failure, But Not Long-Term Outcome in Patients With Previously Untreated Mantle Cell Lymphoma: Results of a Prospective Randomized Trial of the German Low Grade Lymphoma Study Group (GLSG). J Clin Oncol. 2005;23(9):1984-1992. PubMed
13.Robak T, Huang H, Jin J, et al. Bortezomib-Based Therapy for Newly Diagnosed Mantle-Cell Lymphoma. N Engl J Med. 2015;372(10):944-953. PubMed
14.Hermine O, Hoster E, Walewski J, et al. Addition of high-dose cytarabine to immunochemotherapy before autologous stem-cell transplantation in patients aged 65 years or younger with mantle cell lymphoma (MCL Younger): a randomised, open-label, phase 3 trial of the European Mantle Cell Lymphoma Network. Lancet (London, England). 2016;388(10044):565-575. PubMed
15.Wang ML, Rule S, Martin P, et al. Targeting BTK with ibrutinib in relapsed or refractory mantle-cell lymphoma. The New England journal of medicine. 2013;369(6):507-516. PubMed
16.NCCN Clinical Practice Guidelines in Oncology. B-cell lymphomas. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2020 Aug 13.
17.Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2014;32(27):3059-3068. PubMed
18.Clinical Study Report: KTE-C19-102 A Phase 2 Multicenter Study Evaluating the Efficacy of KTE-X19 in Subjects with Relapsed/Refractory Mantle Cell Lymphoma (ZUMA-2) [internal sponsor's report]. Santa Monica (CA): Kite Pharma, Inc.; 2019 Nov 14.
19.Clinical Study Report: Summary of ZUMA-2 update analysis (data cut off 31 December 2019). A Phase 2 Multicenter Study Evaluating the Efficacy of KTE-X19 in Subjects with Relapsed/Refractory Mantle Cell Lymphoma (ZUMA-2) [internal sponsor's report]. Santa Monica (CA): Kite Pharma, Inc.; 2020 Oct 2.
20.Phillippo DM, Ades, A.E., Dias, S., Palmer, S., Abrams, K.R., Welton, N.J. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submission to NICE. 2016: http://www.nicedsu.org.uk/wp-content/uploads/2017/05/Population-adjustment-TSD-FINAL.pdf. Accessed 2021 Mar 8.
21.Zhou Y, Wang H, Fang W, et al. Incidence trends of mantle cell lymphoma in the United States between 1992 and 2004. Cancer. 2008;113(4):791-798. PubMed
22.Lynch DT AU. Mantle Cell Lymphoma. [updated 2020 Aug 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan - . Available from: https://www.ncbi.nlm.nih.gov/books/NBK536985/. Accessed 2021 Apr 21.
23.Jares P, Colomer D, Campo E. Molecular pathogenesis of mantle cell lymphoma. J Clin Invest. 2012;122(10):3416-3423. PubMed
24.Narurkar R, Alkayem M, Liu D. SOX11 is a biomarker for cyclin D1-negative mantle cell lymphoma. Biomarker Research. 2016;4(1):6. PubMed
25.Eskelund CW, Dahl C, Hansen JW, et al. TP53 mutations identify younger mantle cell lymphoma patients who do not benefit from intensive chemoimmunotherapy. Blood. 2017;130(17):1903-1910. PubMed
26.Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375-2390. PubMed
27.Schöllkopf C, Melbye M, Munksgaard L, et al. Borrelia infection and risk of non-Hodgkin lymphoma. Blood. 2008;111(12):5524-5529. PubMed
28.Smedby KE, Sampson JN, Turner JJ, et al. Medical history, lifestyle, family history, and occupational risk factors for mantle cell lymphoma: the InterLymph Non-Hodgkin Lymphoma Subtypes Project. J Natl Cancer Inst Monogr. 2014;2014(48):76-86. PubMed
29.Wang SS, Slager SL, Brennan P, et al. Family history of hematopoietic malignancies and risk of non-Hodgkin lymphoma (NHL): a pooled analysis of 10 211 cases and 11 905 controls from the International Lymphoma Epidemiology Consortium (InterLymph). Blood. 2007;109(8):3479-3488. PubMed
30.Smedby KE, Hjalgrim H, Askling J, et al. Autoimmune and Chronic Inflammatory Disorders and Risk of Non-Hodgkin Lymphoma by Subtype. JNCI: Journal of the National Cancer Institute. 2006;98(1):51-60. PubMed
31.Kumar A, Sha F, Toure A, et al. Patterns of survival in patients with recurrent mantle cell lymphoma in the modern era: progressive shortening in response duration and survival after each relapse. Blood Cancer J. 2019;9(6):50-50. PubMed
32.Monga N, Garside J, Davids MS, et al. Systematic Literature Review of Economic Evaluations, Costs/Resource Use, and Quality of Life in Patients with Mantle Cell Lymphoma. PharmacoEconomics - Open. 2020. PubMed
33.Rule S, Dreyling M, Goy A, et al. Outcomes in 370 patients with mantle cell lymphoma treated with ibrutinib: a pooled analysis from three open-label studies. Br J Haematol. 2017;179(3):430-438. PubMed
34.Rule S, Dreyling M, Goy A, et al. Ibrutinib for the treatment of relapsed/refractory mantle cell lymphoma: extended 3.5-year follow up from a pooled analysis. Haematologica. 2019;104(5):e211-e214. PubMed
35.Martin P, Maddocks K, Leonard JP, et al. Postibrutinib outcomes in patients with mantle cell lymphoma. Blood. 2016;127(12):1559-1563. PubMed
36.Epperla N, Hamadani M, Cashen AF, et al. Predictive factors and outcomes for ibrutinib therapy in relapsed/refractory mantle cell lymphoma-a “real world” study. Hematological oncology. 2017;35(4):528-535. PubMed
37.Cheah CY, Chihara D, Romaguera JE, et al. Patients with mantle cell lymphoma failing ibrutinib are unlikely to respond to salvage chemotherapy and have poor outcomes. Ann Oncol. 2015;26(6):1175-1179. PubMed
38.Jain P, Kanagal-Shamanna R, Zhang S, et al. Long-term outcomes and mutation profiling of patients with mantle cell lymphoma (MCL) who discontinued ibrutinib. Br J Haematol. 2018;183(4):578-587. PubMed
39.Wang M, Schuster SJ, Phillips T, et al. Observational study of lenalidomide in patients with mantle cell lymphoma who relapsed/progressed after or were refractory/intolerant to ibrutinib (MCL-004). Journal of hematology & oncology. 2017;10(1):171. PubMed
40.McCulloch R, Visco C, Eyre TA, et al. Efficacy of R-BAC in relapsed, refractory mantle cell lymphoma post BTK inhibitor therapy. Br J Haematol. 2020;189(4):684-688. PubMed
41.Tecartus™ Brexucabtagene autoleucel: Cell suspension in patient-specific single infusion bag, target of 2 × 106 chimeric antigen receptor (CAR)-positive viable T cells per kg body weight with a maximum of 2 × 108 CAR-positive viable T cells, for intravenous infusion [product monograph]. Mississauga: Gilead Sciences Canada, Inc.; 2020 Dec 7.
42.Tecartus (brexucabtagene autoleucel) [FDA approval package]. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2021 Mar 18: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/tecartus-brexucabtagene-autoleucel Accessed 2021 Apr 22.
43.Drug Reimbursement Review sponsor submission: Tecartus™ (brexucabtagene autoleucel), suspension for intravenous infusion [internal sponsor's package]. Mississauga: Gilead Sciences Canada, Inc.; 2020 Dec 18.
44.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Apr 22.
45.Wang M, Munoz J, Goy A, et al. KTE-X19 CAR T-Cell Therapy in Relapsed or Refractory Mantle-Cell Lymphoma. N Engl J Med. 2020;382(14):1331-1342. PubMed
46.Wang M, Munoz J, Goy AH, et al. One-Year Follow-up of ZUMA-2, the Multicenter, Registrational Study of KTE-X19 in Patients with Relapsed/Refractory Mantle Cell Lymphoma. Blood. 2020;136(Supplement 1):20-22.
47.Cheson BD, Pfistner B, Juweid ME, et al. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25(5):579-586. PubMed
48.Lee DW, Gardner R, Porter DL, et al. Current concepts in the diagnosis and management of cytokine release syndrome. Blood. 2014;124(2):188-195. PubMed
49.Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials. 1996;17(4):343-346. PubMed
50.CADTH. Axicabtagene Ciloleucel for Large B-Cell Lymphoma: Clinical Report. 2019: https://www.cadth.ca/sites/default/files/pdf/car-t/ct0002-clinical-report-redacted.pdf. Accessed 2021 Apr 21.
51.Wang ML, Lee H, Chuang H, et al. Ibrutinib in combination with rituximab in relapsed or refractory mantle cell lymphoma: a single-centre, open-label, phase 2 trial. Lancet Oncol. 2016;17(1):48-56. PubMed
52.Gilead Sciences Canada response to February 26, 2021 DRR request for additional information regarding brexucabtagene autoleucel DRR review [internal additional sponsor's information]. Mississauga (ON): Gilead Sciences Canada, Inc.; 2021.
53.Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC medical research methodology. 2012;12:9. PubMed
54.Achana FA, Cooper NJ, Bujkiewicz S, et al. Network meta-analysis of multiple outcome measures accounting for borrowing of information across outcomes. BMC medical research methodology. 2014;14:92. PubMed
55.Eyre TA, Walter HS, Iyengar S, et al. Efficacy of venetoclax monotherapy in patients with relapsed, refractory mantle cell lymphoma after Bruton tyrosine kinase inhibitor therapy. Haematologica. 2019;104(2):e68-e71. PubMed
56.Regny C, Oberic L, guillaume M, et al. Clinical efficacy of the RiBVD regimen for refractory/relapsed (R/R) mantle cell lymphoma (MCL) patients: A retrospective study of the LYSA Group: PF482. HemaSphere. 2019;3:193.
57.Dreyling M, Jurczak W, Jerkeman M, et al. Ibrutinib versus temsirolimus in patients with relapsed or refractory mantle-cell lymphoma: an international, randomised, open-label, phase 3 study. Lancet (London, England). 2016;387(10020):770-778. PubMed
58.Latimer NR. Survival analysis for economic evaluations alongside clinical trials--extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med Decis Making. 2013;33(6):743-754. PubMed
59.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70-70. PubMed
60.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
61.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
62.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Medical care. 2016;54(1):98-105. PubMed
63.Herdman M, Kerr C, Pavesi M, et al. Testing the validity and responsiveness of a new cancer-specific health utility measure (FACT-8D) in relapsed/refractory mantle cell lymphoma, and comparison to EQ-5D-5L. Journal of Patientreported Outcomes. 2020;4(1):22. PubMed
64.Richardson J, Iezzi A, Khan MA, Chen G, Maxwell A. Measuring the Sensitivity and Construct Validity of 6 Utility Instruments in 7 Disease Areas. Med Decis Making. 2016;36(2):147-159. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
Embase 1974 to present
MEDLINE Daily and MEDLINE 1946 to present
MEDLINE In-Process and Other Non-Indexed Citations
Note: Patient headings have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: December 9, 2019
Alerts: Weekly search updates until May 20, 2020
Study types: No search filters were applied
Limits:
No date or language limits were used
Conference abstracts were excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a patient heading |
MeSH | Medical Patient Heading |
.fs | Floating subheading |
exp | Explode a patient heading |
* | Before a word, indicates that the marked patient heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for 1 character |
? | Truncation symbol for 1 or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes patient headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase); |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multi-Database Strategy
(Tecartus* or brexucabtagene* or BREXUCABTAGENE AUTOLEUCEL or KTEX19 or 4MD2J2T8SJ).ti,ab,kf,ot,hw,rn,nm.
1 use medall
brexucabtagene Autoleucel/
(Tecartus* or brexucabtagene* or BREXUCABTAGENE AUTOLEUCEL or KTEX19).ti,ab,kw,dq.
3 or 4
5 use oemezd
6 not (conference abstract or conference review).pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Tecartus OR Brexucabtagene OR BREXUCABTAGENE AUTOLEUCEL OR KTEX19]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- Tecartus OR Brexucabtagene OR BREXUCABTAGENE AUTOLEUCEL OR KTEX19]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- Tecartus OR Brexucabtagene OR BREXUCABTAGENE AUTOLEUCEL OR KTEX19]
EU Clinical Trials
Register European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- Tecartus OR Brexucabtagene OR BREXUCABTAGENE AUTOLEUCEL OR KTEX19]
Canadian Cancer Trials
Produced by the Canadian Partnership Against Cancer Corporation. Targeted search used to capture registered clinical trials.
[Search terms -- Tecartus OR Brexucabtagene OR BREXUCABTAGENE AUTOLEUCEL OR KTEX19]
Grey Literature
Search dates: January 12, 2021 – January 19, 2021
Keywords: Tecartus OR Brexucabtagene OR BREXUCABTAGENE AUTOLEUCEL OR KTEX19 OR mantle cell lymphoma
Limits:
Updated: None
Search updated before CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) meeting
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)f
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for Exclusion |
|---|---|
Jain P, Nastoupil L, Westin J, et al. Outcomes and management of patients with mantle cell lymphoma after progression on brexucabtagene autoleucel therapy. Br J Haematol. 2021 Jan;192(2):e38-e42. | Study design |
Reagan PM, Friedberg JW. Axicabtagene ciloleucel and brexucabtagene autoleucel in relapsed and refractory diffuse large B cell and mantle cell lymphomas. Fut Oncol. 2021 Jan 15;15:15. | Review article |
Romero D. BREXUCABTAGENE AUTOLEUCEL active in MCL. Nat Rev Clin Oncol. 2020 06;17(6):336. | Review article |
Wang M, Jain P, Chi TL, et al. Management of a patient with mantle cell lymphoma who developed severe neurotoxicity after chimeric antigen receptor T-cell therapy in ZUMA-2. Journal for Immunotherapy of Cancer. 2020 Oct;8(2). | Study design (case report) |
Appendix 3: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the European Quality of Life 5 Dimension 5 Level (EQ-5D-5L) outcome measures and review its measurement properties (validity, reliability, responsiveness to change, and minimal important difference [MID]):
Findings
Table 41: Summary of Outcome Measures and their Measurement Properties
Outcome measure | Type | Conclusions about Measurement Properties | MID |
|---|---|---|---|
EQ-5D-5L | Generic, preference-based measure of HRQoL | Validity In patients with relapsed MCL showed good construct validity based on known groups approach and convergence with other disease specific HRQoL instruments Reliability No data Responsiveness Good responsiveness in patients with MCL | Canadian population: 0.037 for the health state index score60 Patients with advanced cancer: 7 to 12 for the VAS59 |
HRQoL = health-related quality of life; MID = minimal important difference; VAS = visual analogue scale.
The EQ-5D-5L was developed by the EuroQol Group as an improvement to the EQ-5D-3L to measure small and medium health changes and reduce ceiling effects.61 The patient reported instrument comprises 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: level 1 “no problems,” level 2 “slight problems,” level 3 “moderate problems,” level 4 “severe problems,” and level 5 “extreme problems” or “unable to perform.”61 A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state. The corresponding scoring of EQ-5D-5L health states is based on a scoring algorithm that is derived from preference data obtained from interviews using choice-based techniques (e.g., time trade-off) and discrete choice experiment tasks.61 The lowest and highest score varies depending on the scoring algorithm used. The anchors are 0 (dead) and 1 (full health); however, negative values are also allowed to represent health states that a population considers worse than death. For the economic model of brexucabtagene autoleucel the Canadian scoring algorithm was applied with scores that range from −0.148 for health state 55555 (worst health state) to 0.949 for health state 11111 (best health state). This range was derived from the time trade-off valuation tasks of 1,073 participants from the Canadian scoring function derivation study who valued the best health state as less than full health.62 However, the upper anchor point, full health, for the EQ-5D-5L index is typically set at 1.0, regardless. Another component of the EQ-5D-5L is a visual analogue scale (EQ VAS), which asks respondents to rate their health on that day using a visual scale from 0 (worst health imaginable) to 100 (best health imaginable).61
Data from a clinical trial of 132 patients with relapsed MCL was used to assess the validity and responsiveness of the EQ-5D-5L.63 Convergent validity was assessed by testing a priori hypotheses about the strength of correlation with other instruments that measured similar constructs. The EQ-5D-5L showed good convergent validity, reporting moderate correlation with the EQ VAS (r = 0.50) and strong correlation with Functional Assessment of Cancer Therapy (FACT) lymphoma specific subscale (r = 0.60) and FACT lymphoma total score, Trial Outcome Index (TOI) (r = 0.70). The EQ-5D-5L was able to discriminate between known groups based on presence or absence of lymphoma symptoms, ECOG performance score, and MIPI, showing statistically significantly differences between groups in the mean index scores. The index score showed good responsiveness, reporting an effect size of 0.67 for improvement and 0.80 for worsening based on the FACT lymphoma subscale.63
Richardson et al.64 examined various instruments, including the EQ-5D-5L, in respondents who were healthy and who had a chronic disease (i.e., arthritis, asthma, cancer, depression, diabetes, hearing loss, and heart disease) through an online survey in Australia, Canada, Germany, Norway, the UK, and the US (total N = 7,933; cancer N = 772). For discriminant validity, the mean EQ-5D-5L differed between healthy respondents and respondents with a chronic disease (0.88 in healthy, 0.18 in patients with cancer [standard deviation not reported]). For construct validity, the EQ-5D-5L was strongly correlated with the physical component of the SF-36 in cancer patients (r = 0.66), moderately correlated with the psychosocial content of the mental component of the SF-36, the Capabilities Instrument, and the Subjective Well-Being Instrument of the UK Office of National Statistics (r = 0.50), and moderately correlated with preference measures of VAS and time trade-off on own health state (r = 0.43).64
McClure et al. (2017) obtained the minimal important difference (MID) for the EQ-5D-5L by calculating the average absolute difference between the index score of the baseline health state and the index score of all single-level transitions from the baseline state.60 A single-level transition was defined as a change in a single dimension to the next worse/better level, while holding all other dimensions constant. Such single-level transitions across all 3,125 health states were averaged to arrive at MIDs for various countries, by applying country-specific scoring algorithms. For Canada, transitions between levels 3 and 4 were excluded from the average to form a constant distribution of MID values across the range of baseline scores. This analysis resulted in a Canadian-specific MID of 0.037.60 No estimates of the MID were identified for patients with MCL.
Pickard et al.(2007) estimated the MID of the EQ-5D VAS based on cross-sectional data collected from 534 patients with advanced (stage III or IV) cancer of the bladder, brain, breast, colon or rectum, head or neck, liver or pancreas, kidney, lung, lymphoma, ovary, or prostate.59 Using both anchor-based and distribution-based methods, estimates of the MID for the EQ-5D VAS ranged from 8 to 12 based on the ECOG performance status, and from 7 to 10 based on FACT QoL questionnaire quintiles.59
Pharmacoeconomic Review
Abbreviations
BSC
best supportive care
BTK
Bruton tyrosine kinase
CAR
chimeric antigen receptor
CI
confidence interval
ICER
incremental cost-effectiveness ratio
ICU
intensive care unit
IVIG
intravenous immunoglobin
MAIC
matching-adjusted indirect comparison
MCL
mantle cell lymphoma
OS
overall survival
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
R-BAC
rituximab, bendamustine, and cytarabine
R/R
relapsed or refractory
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Brexucabtagene Autoleucel (Tecartus), infusion bag for single IV infusion |
Submitted price | Brexucabtagene autoleucel: $533,523 per administration |
Indication | For the treatment of adult patients with relapsed or refractory mantle cell lymphoma (MCL) after 2 or more lines of systemic therapy including a Bruton’s tyrosine kinase (BTK) inhibitor. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | June 8, 2021 |
Reimbursement request | As per indication |
Sponsor | Gilead Sciences Canada, Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival mixture-cure model |
Target population | Patients with relapsed or refractory MCL whose disease progressed after treatment with anthracycline or bendamustine therapy, an anti-CD20 antibody, and a BTK inhibitor (ibrutinib and/or acalabrutinib), which reflects the population in the ZUMA-2 trial and aligns with the proposed Health Canada indication |
Treatment | Brexucabtagene autoleucel |
Comparator | BSC, defined as a blended comparator including several therapy options |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs; LYs |
Time horizon | Lifetime (50 years) |
Key data sources | ZUMA-2 phase II clinical trial was used to inform efficacy and safety inputs for brexucabtagene autoleucel; data from a sponsor-commissioned meta-analysis were used to inform efficacy of BSC |
Submitted results | ICER for brexucabtagene autoleucel therapy vs. BSC = $89,557 per QALY (incremental costs = $628,322; incremental QALYs = 7.02) |
Key limitations |
|
CADTH reanalysis results |
|
BSC = best supportive care; BTK = Bruton tyrosine kinase; ICER = incremental cost-effectiveness ratio; IVIG = IV immunoglobin; LY = life-year; MAIC = matching-adjusted indirect comparison; MCL = mantle cell lymphoma; PSM = partitioned survival model; QALY = quality-adjusted life-year.
Conclusions
Evidence from the ZUMA-2 trial suggests that brexucabtagene autoleucel is associated with improvements in outcomes relevant to both patients and clinicians (progression-free survival [PFS], overall survival [OS], and health-related quality of life over 6 months) relative to a historical control. However, there are important caveats with these findings given the inability to control for confounding and the high amount of censoring, which may inhibit the interpretation of the results. CADTH also noted that the data were not mature at last follow-up and identified concerns regarding the generalizability of the trial population to the Canadian setting. Due to the lack of head-to-head studies for brexucabtagene autoleucel, the sponsor submitted an unanchored matching-adjusted indirect comparison (MAIC) as indirect evidence of the clinical efficacy of brexucabtagene autoleucel compared with standard of care therapies in patients with relapsed or refractory (R/R) mantle cell lymphoma (MCL). However, due to several identified limitations, no conclusions can be drawn about the comparative clinical effectiveness of brexucabtagene autoleucel.
CADTH identified several major limitations with the sponsor’s submission to CADTH that introduced significant uncertainty in the cost-effectiveness of brexucabtagene autoleucel. In addition to the aforementioned limitations with the comparative effectiveness evidence and limitations with the clinical trial data for brexucabtagene autoleucel, the sponsor’s use of a naive comparison to assess the relative effectiveness of brexucabtagene autoleucel to best supportive care (BSC) in the economic evaluation, and the incorporation of a “cure” component, likely overestimated the benefit of brexucabtagene autoleucel. Additionally, the exclusion of relevant costs associated with brexucabtagene autoleucel underestimated the total cost of treatment. As such, the incremental cost-effectiveness ratio (ICER) is likely higher than the estimate submitted within the sponsor’s base case.
The considerable uncertainty around the clinical effectiveness evidence inhibits interpretation of the cost-effectiveness of brexucabtagene autoleucel. As such, CADTH could not determine a base-case estimate. CADTH undertook a series of exploratory analyses, most of which indicated that the ICER was higher than the sponsor’s estimate. The ICER was highly sensitive to the modelling approach and effectiveness assumptions. When CADTH removed the mixture-cure model and combined this with the “weighted” data from the MAIC, or a shorter time horizon to better reflect the currently available data, the ICER for brexucabtagene autoleucel compared with BSC ranged from $308,000 per quality-adjusted life-year (QALY) to $388,000 per QALY. Given the lack of robust comparative clinical data, the cost-effectiveness of brexucabtagene autoleucel is unknown.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
One patient group, Lymphoma Canada, provided input for the review of brexucabtagene autoleucel. This Canadian charity distributed an online survey to patients with MCL through email, social media, cancer message boards, and physician outreach. Of the 33 patients that responded, 24 patients were Canadian and 1 patient had experience with the therapy under review. Current treatments included chemoimmunotherapy and stem cell transplantation. Patients reported that treatment-related fatigue, infusion duration, and infusion reactions had the most significant impact on their quality of life and that their most important outcomes for a new therapy were disease control and improved quality of life. The 1 patient experienced with brexucabtagene autoleucel reported not being prepared for the numerous tests involved in determining treatment eligibility. The patient also experienced adverse effects of neutropenia, thrombocytopenia, and anemia but felt the treatment burden was minor and, overall, the therapy was positive.
Two registered clinician group inputs were received: from the Ontario Health Hematology Disease Site Drug Advisory Committee and a group of lymphoma experts whose input was coordinated by Lymphoma Canada. Clinicians stated that there is an unmet need for effective treatments that produce durable response; many patients do not benefit from current treatment options, and some experience unacceptable toxicities. Stem cell transplantation is available for a minority of patients, with palliative chemotherapy being the only option for some patients. Clinical experts noted that brexucabtagene autoleucel should be reserved for patients who have progressed after receiving standard chemoimmunotherapy and Bruton tyrosine kinase (BTK) inhibitor therapy in the third line of treatment or later.
The drug plans highlighted a number of implementation considerations for brexucabtagene: significant resource use for patient preparation, including leukapheresis and fludarabine-based conditioning chemotherapy; the use of bridging therapy with ibrutinib; substantial resources required for monitoring and treatment of adverse events (nursing, hospital beds, clinic visits, supporting therapies such as tocilizumab); the requirement for specialized centres in which the therapy can be administered; a high human resource burden to obtain and maintain site certification; issues with access and prolonged stay at or near specialized centres for patients from remote areas; and the relocation and interprovincial travel required for some patients.
Several of these concerns were addressed in the sponsor’s model:
Adverse events, including those noted by the patient group, were incorporated in the sponsor’s economic model for patients receiving brexucabtagene autoleucel.
Bridging therapy was included in the pharmacoeconomic model and budget impact analysis.
In addition, CADTH addressed some of these concerns as follows:
CADTH undertook reanalyses to consider alternate cost assumptions for bridging therapy, leukapheresis, and other costs not incorporated into the sponsor’s base case (e.g., IV immunoglobin [IVIG]).
CADTH was unable to address the following concerns raised from stakeholder input:
Adverse events were not included in the comparator arm for patients receiving BSC.
The sponsor did not present a scenario analysis from the societal perspective.
CADTH-participating drug plans identified several implementation considerations, including the requirement for specialized centres to administer the therapy and the need to maintain site certification. CADTH explores these and other implementation concerns, as detailed in the Issues for Consideration section.
CADTH-participating drug plans also noted that travel and costs associated with travel were of concern if patients were not located near a specialized centre equipped to administer brexucabtagene autoleucel.
Economic Review
The current review is for brexucabtagene autoleucel for patients with R/R MCL after treatment with a BTK inhibitor.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing brexucabtagene autoleucel with BSC, defined as a blended comparator including several therapy options, for the treatment of adult patients with MCL previously treated with a BTK inhibitor. The blended comparator BSC comprised the following therapies: rituximab (68.2%), bendamustine (57.4%), bortezomib (5.5%), and anthracycline (7.3%). Lenalidomide was added to the blended comparator in a scenario analysis. The reimbursement population aligns with the Health Canada–indicated population.
Brexucabtagene autoleucel is available as an infusion bag containing a suspension of anti-CD19 chimeric antigen receptor (CAR)–positive T cells in approximately 68 mL. The target dose of brexucabtagene autoleucel is 2 × 106 CAR-positive viable T cells per kilogram body weight (range = 1 × 106 – 2 × 106 CAR-positive viable T cells per kilogram), with a maximum of 2 × 108 CAR-positive viable T cells for patients 100 kg and above, administered as a single IV infusion.1 The sponsor’s submitted price for brexucabtagene autoleucel is $533,523 per infusion, not including costs associated with pre- and post-infusion management (i.e., leukapheresis, bridging therapy, conditioning chemotherapy).2 This is assumed to be a 1-time-only cost. Wastage was not considered for brexucabtagene autoleucel, nor was a cost assumed for re-administration of the therapy. The comparator for this analysis was a blended comparator of potential treatments that were deemed relevant to the patient population based on the sponsor’s interviews with expert clinicians and a meta-analysis based on values from the literature. The comparator, defined as BSC, comprised rituximab (68.2%), bendamustine (57.4%), bortezomib (5.5%), and anthracycline (7.3%). The cost calculation for this was a weighted average of the blended comparator and included physician services for the outpatient administration of the chemotherapy.2 Costs are presented for each therapy, at a particular dose, but the actual cost used in the reference case of the model (in a specific cycle) is not reported.
The outcomes of interest were QALYs and life-years. The analysis takes the perspective of a third-party payer (i.e., the health care system). The time horizon in the base case was specified by the sponsor as a lifetime horizon (50 years). The discount rate for costs and outcomes was 1.5% annually.2
Model Structure
The model takes the form of a partitioned survival mixture-cure model with 3 model states (pre-progression, post-progression, and death) (see Figure 1).2 All patients entered the model in the pre-progression health state, and after each 1-month cycle, patients could either remain in the pre-progression health state or transition to the post-progression or death health states. The proportion of patients in each state at any point in time was based on direct modelling of OS and PFS curves, which the sponsor extrapolated over the time horizon of the analysis using parametric methods. The difference between the OS curve and the PFS curve was partitioned at each time point to estimate the proportion of patients in the progressed disease health state. As the state transition approach considers OS to be dependent on PFS, which the sponsor considered was not in line with the expectation for this treatment, the sponsor incorporated a cure component for patients whose disease does not progress before a certain point in time and who may be considered “functionally cured” (i.e., experiencing long-term remission and survival). This time point is referred to as the “cure point,” which was set at 5 years in the base-case analysis. The sponsor’s model also presented an approach considering just the partitioned survival model (PSM), without the cure component.
Model Inputs
The patients’ baseline characteristics, such as weight, body surface area, and prior treatment, were obtained from the full analysis dataset of the ZUMA-2 trial (n = 74).2 These patients were predominantly male (85%), with a mean age of 63.7 years, a mean body weight of 81.8 kg, and a mean body surface area of 1.98 m2. All patients had previously received an anthracycline or bendamustine, a BTK inhibitor, and an anti-CD20 agent.
The key efficacy data used to inform the model were obtained from the single-arm ZUMA-2 clinical trial for brexucabtagene autoleucel at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram in patients with MCL. ZUMA-2 reported a complete response rate of 67% (95% confidence interval [CI], 53% to 78%) for brexucabtagene autoleucel, with the response being achieved in a median time to initial response of 1 month (range = 0.8 months to 3.1 months) and a median time to complete response of 3 months (range = 0.9 months to 9.3 months). The modelling of OS and PFS for brexucabtagene autoleucel was based on patient-level data collected by the December 2019 data cut-off of ZUMA-2.
The key data used to inform BSC within the model were obtained from a sponsor-commissioned meta-analysis of 4 published retrospective studies3-6 (OS) and 2 retrospective studies3,4 (PFS) in conjunction with qualitative interviews with clinical experts for BSC.2,7 These 4 studies included between 11 patients and 73 patients who had received subsequent MCL therapy and who had typically failed prior ibrutinib or acalabrutinib therapy. The median duration of follow-up ranged from 3.2 months to 38 months. The subsequent treatments in these studies differed, ranging from a broad mix of treatments (e.g., various chemo-immunotherapies or systemic treatments) to specific comparators (i.e., venetoclax, or rituximab, bendamustine, and cytarabine [R-BAC]). Baseline characteristics differed between studies. The sponsor did not include any studies that used venetoclax within the BSC treatments in the base-case analysis as it was thought not to be representative of the Canadian setting. The base-case analyses of OS included 3 studies3,5,6 in which BSC for R/R MCL patients consisted of chemo-immunotherapies, systemic treatments, or R-BAC. The base-case analyses of PFS used 1 study3 in which R-BAC was used. A MAIC was performed using individual patient data from ZUMA-2 and aggregate data from the aforementioned published studies for BSC. A logistic propensity score model was used to estimate weights for the ZUMA-2 individual patient data to align the baseline characteristics (i.e., Ki-67 levels, response to and duration of prior BTK inhibitor therapy, blastoid morphology, number of prior therapies, prior autologous stem cell transplant) with the BSC studies, after which outcomes for brexucabtagene autoleucel were predicted for the population receiving BSC. Various parametric survival functions were fitted to the unadjusted and adjusted ZUMA-2 individual patient data.8 The best-fitting models for the 2 treatment “arms” (i.e., brexucabtagene autoleucel and BSC) were then synthesized in a pairwise meta-analysis to estimate the relative treatment effects of brexucabtagene autoleucel and BSC. According to the model selection process, the best-fitting model was log-normal, with random effects for OS. The median OS was estimated to be 9.3 months (95% CI, 7.4 to 11.6). For PFS, based on a log-normal random-effects model, the median PFS was estimated to be 6.6 months (95% CI, 4.6 to 9.3). The base case used an exponential mixture-cure model for both OS and PFS based on the Akaike information criterion and the Bayesian information criterion, with a 5-year cure point included.7
Adverse events only occurred in the brexucabtagene autoleucel arm of the model and were treated as “one-off” costs and disutilities in the first model cycle where the patient received treatment. Adverse events were not considered as part of the BSC arm of the model.
Health-related quality of life data were collected alongside ZUMA-2 and assessed using the EuroQol 5-Dimensions questionnaire. These data were incorporated into the model appropriately using Canadian tariffs. However, due to the lack of data for post-progression and the estimated pre-progression utility from the ZUMA-2 being greater than the associated pre-progression utility value for long-term survivors taken from the literature, utility values were identified from the National Institute for Health and Care Excellence review of ibrutinib in patients with R/R MCL.9 The same utilities, by health state, were used for brexucabtagene autoleucel and BSC.
The costs for brexucabtagene autoleucel included in the model were the costs of leukapheresis, conditioning chemotherapy, bridging therapy, acquisition costs, and cell infusion and monitoring. All costs associated with brexucabtagene autoleucel were assumed to be incurred in the first model cycle. A cost of $1,343.98 for apheresis was used and was based on the cost of stem cell apheresis from a study of autologous stem cell transplantation in patients with multiple myeloma.10 For the purpose of ensuring patients would remain eligible for brexucabtagene autoleucel, bridging therapy was assumed to be used by 36.8% of patients in the model based on ZUMA-2. This consisted of IV ibrutinib (560 mg daily) and oral dexamethasone (40 mg daily for 4 days). Furthermore, all patients were assumed to receive conditioning chemotherapy before CAR T-cell infusion, which consisted of low-dose 500 mg/m2 cyclophosphamide and 30 mg/m2 fludarabine each for 3 days; unit costs were obtained from a prior CADTH pan-Canadian Oncology Drug Review report.11 Infusion of brexucabtagene autoleucel and subsequent monitoring were assumed to incur the cost of an elective hospitalization of $1,527 for approximately 21 days based on ZUMA-2, along with a per day intensive care unit (ICU) cost of $8,054 in 22.7% of patients. BSC regimens were included as a blended comparator including rituximab (68.2%), bendamustine (57.4%), bortezomib (5.5%), and anthracycline (7.3%), the costs of which were derived from various sources, including the Ontario Exceptional Access Program formulary12 and various CADTH pan-Canadian Oncology Drug Review reports. Administration costs were included for BSC and conditioning chemotherapy, derived from the Ontario Ministry of Health and Long-Term Care Schedule of Benefits for Physician Services.13 Further resource use costs were associated with the various health states. For the progression-free health state, these costs included those associated with active disease management, such as drug costs, physician and laboratory visits, and radiological tests. In the post-progression health state, patients continue to incur costs associated with medical management of the condition, in addition to palliative care costs, estimated to be $34,038 at the time of death.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically, with 1,000 iterations for the base-case and scenario analyses. The sponsor reported both probabilistic and deterministic results in their analysis, and the results are similar. The probabilistic findings are reported below.
Base-Case Results
In the sponsor’s base-case analysis, the results indicated that treatment with brexucabtagene autoleucel was associated with higher incremental costs ($628,322) and greater incremental effects (QALYs = 7.02) over the 50-year (i.e., lifetime) time horizon, resulting in an ICER of $89,557 per QALY gained. Disaggregated results are provided in Table 10 in Appendix 3. The sponsor’s cost-effectiveness acceptability curve indicated that brexucabtagene autoleucel had a 0% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Importantly, given the duration of the clinical trial observation period and the model time horizon, it is likely that most QALYs in the brexucabtagene autoleucel arm of the model were gained outside of what was observed in the clinical trial (i.e., extrapolated period); however, the extent of this could not be elucidated given the sponsor’s model structure and programming. These additional QALYs, which comprise the incremental gain between brexucabtagene autoleucel and BSC, largely influence the ICER of $89,957, as shown in Table 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs, $ | Incremental costs, $ | Total QALYs | Incremental QALYs | ICER, $/QALY |
|---|---|---|---|---|---|
Best supportive carea | 65,168 | Reference | 1.318 | Reference | Reference |
Brexucabtagene autoleucel | 693,490 | 628,322 | 8.334 | 7.02 | 89,557 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aBest supportive care is assumed to be a combination of rituximab, bendamustine, lenalidomide, bortezomib, and anthracycline based on a literature-based meta-analysis.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor reported a series of univariate scenario analyses in their pharmacoeconomic report to assess the impact of alternate assumptions regarding the time horizon, health state utilities, discount rate, parametric functions for OS and PFS for brexucabtagene autoleucel and BSC, the mixture-cure model, the comparative data used to inform the model, the ZUMA-2 trial population, and treatments included as part of BSC.
The key assumption driving the ICER was the estimation of survival, particularly “cured” survival, and the associated QALYs in the comparator arm, resulting in an ICER below $100,000 per QALY gained (based on the sponsor’s submitted analysis). The QALY gain was largely driven by the extrapolated OS and PFS curves, which were assumed to use parametric distributions for extrapolation (exponential).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
Uncertainty in the clinical efficacy of brexucabtagene autoleucel. The ZUMA-2 trial, which was used to inform the efficacy of brexucabtagene autoleucel, was a phase II trial that consisted of 74 patients, enrolled between October 2016 and April 2019. The open-label, single-arm design can increase the risk of bias in reporting of outcomes that are subjective in measurement and in interpretation, such as response. As of July 2019, the median follow-up time was 12.3 months; however, based on the most recent data cut-off (December 2019), the median potential follow-up was 16.8 months. As of the July 2019 data cut-off, 71% of patients in the full analysis set (used to inform the economic evaluation) had been censored. This small sample, the short duration of follow-up, and the high amount of censoring in the trial result in considerable uncertainty regarding the treatment effect.
The benefit provided by brexucabtagene autoleucel beyond study duration is not available and is based on extrapolation. The appropriateness and quality of any extrapolation is dependent on the quantity of observed data available. As noted in the CADTH Clinical Review Report, although follow-up time was considered appropriate to assess response to treatment, it was considered to be immature for assessing survival outcomes. Given the extent of censoring, the plateaus observed in the Kaplan–Meier curves cannot be interpreted as providing robust evidence to support brexucabtagene autoleucel as a curative therapy. As such, the clinical experts consulted by CADTH could not conclude that brexucabtagene autoleucel is a curative therapy. Thus, the incorporation of the mixture-cure component may overestimate the benefit associated with brexucabtagene autoleucel.
Finally, the clinical experts consulted by CADTH noted that the patients included in the ZUMA-2 trial were likely more fit than the patient population expected to receive brexucabtagene autoleucel in Canada.
CADTH was unable to address limitations pertaining to the efficacy of brexucabtagene autoleucel within the base-case analysis given the lack of alternate data available. CADTH conducted exploratory analyses that altered the assumed parametric distribution used for the extrapolation of OS and PFS in the brexucabtagene autoleucel arm of the sponsor’s economic model, excluded the mixture-cure component from the sponsor’s model, and used a shorter time horizon to assess the impact of these parameters on the cost-effectiveness of brexucabtagene autoleucel. CADTH could not address concerns regarding the generalizability of the population studied in ZUMA-2 to the expected population in the Canadian setting.
Unknown comparative effectiveness. ZUMA-2 was a phase II trial without a comparator. Effectiveness for the comparator (BSC) was derived from a sponsor-commissioned meta-analysis of published studies. Since the population included in the meta-analysis differed from the ZUMA-2 population, the sponsor commissioned a MAIC to assign weights to individual patient data from ZUMA-2 to match the BSC patient characteristics of the meta-analysis assisted by clinical expert opinion. This reduced the effective sample size for brexucabtagene autoleucel to 36 for OS and 16 for PFS. Due to the limitations associated with sample size, and the crossing of the OS and PFS curves that was observed, the sponsor used the unweighted (i.e., naive) comparison within the base case. The use of a naive comparison is subject to very strong, untestable assumptions, such as the concept of conditional constancy, which — given the aforementioned issues apparent within the MAIC — introduces substantial uncertainty into the determination of comparative effectiveness and the magnitude of any relative efficacy benefits associated with brexucabtagene autoleucel. The CADTH Clinical Report noted that the main limitation of the MAIC is inherent to all unanchored indirect comparisons, which assume that absolute outcomes can be predicted from the covariates included in the model (i.e., every effect modifier and prognostic factor are accounted for).14 This assumption is largely considered impossible to meet, and failure of this assumption leads to an unknown amount of bias in the unanchored estimate. This uncertainty is compounded due to the quality of the trials included in the submitted MAIC, particularly the heterogeneity among trials, the lack of data to calculate patients’ weights, and the poor overlap among trial populations.
CADTH was unable to address this limitation given the available data and how the data were used to inform the model (i.e., hard coded). CADTH incorporated an exploratory analysis in which the “weighted” results for brexucabtagene autoleucel, based on the MAIC, were used.
Underestimation of costs associated with bridging therapy and leukapheresis. The sponsor assumed that approximately 37% of patients would undergo bridging therapy based on data from the ZUMA-2 trial. Based on feedback from the clinical experts consulted by CADTH, this is likely to be an underestimate of the true percentage, with the expectation that approximately 50% to 70% of patients receiving brexucabtagene autoleucel are likely to receive bridging therapy. Furthermore, CADTH clinical expert feedback noted that the bridging therapy would be received for between 6 weeks to 8 weeks before receiving brexucabtagene autoleucel (i.e., determination of eligibility for CAR T-cell therapy) as opposed to 4 days as suggested by the sponsor. CADTH also noted that the cost of leukapheresis was taken from a dated study by Holbro et al. (2013)10; a more recent study by Ellis (2019)15 exploring the cost-effectiveness of CAR T-cell therapy in Ontario reported updated cost information.
CADTH corrected these components of the model to align with Canadian clinical expert feedback and updated data sources.
Concerns with the modelled comparator. In the sponsor’s model, the comparator, BSC, was defined as a blended comparator comprising currently available treatments. Costs were weighted based on patient numbers receiving those regimens in the meta-analysis, which were then adjusted based on clinical expert feedback received by the sponsor. CADTH noted that the efficacy inputs for conventional care were informed by a different combination of oncology regimens coming from the sponsor’s meta-analysis compared to the treatments that informed costs. Furthermore, feedback suggested that, of the components included in the sponsor’s analysis, bendamustine plus rituximab is likely to be the primary comparator in Canadian practice. The clinical experts consulted by CADTH noted that relevant comparators existed that were not considered by the sponsor, including R-BAC, which was used to inform the comparative efficacy. However, the clinical experts agreed that there is no standard of care in this setting. When multiple comparators may be relevant to the funding decision, individual treatment regimens should further be considered on their own, and all comparators should be assessed in a sequential analysis. This was not conducted by the sponsor.
CADTH reanalyses could not address the issue of a blended comparator and could not evaluate the cost-effectiveness of brexucabtagene autoleucel relative to individual treatment regimens. Given the feedback on the primary potential comparator, CADTH undertook an exploratory analysis assuming 100% of the costs were based on a combination of bendamustine plus rituximab. However, this approach does not resolve the inconsistency noted above regarding the fact that treatment costs for conventional care are based on a different composition of oncology regimens than the regimens that informed efficacy inputs.
Additional costs associated with CAR T-cell therapy not being considered in the model. The sponsor assumed that no patients received conditioning chemotherapy in the submitted base case, which was considered a large underestimate. Furthermore, feedback from the clinical experts consulted by CADTH noted that the sponsor failed to consider the upfront costs of assessment of CAR T-cell eligibility, which would include costs associated with MRIs, PET scans, bone marrow tranplants, lumbar punctures, bloodwork, and more. Should brexucabtagene autoleucel be reimbursed, clinical experts consulted by CADTH expected this assessment cost would be incurred by all patients with MCL who were refractory to BTK inhibitor therapy (regardless of whether they went on to receive brexucabtagene autoleucel). Additionally, the sponsor failed to consider the cost of IVIG within the submitted analysis. Clinical experts consulted by CADTH expected there to be significant cost associated with IVIG.
Given the model structure, CADTH was unable to incorporate the additional cost of testing for eligibility within the economic evaluation or to appropriately incorporate the cost of IVIG for patients receiving brexucabtagene autoleucel. CADTH undertook exploratory analyses that noted the small impact of conditioning chemotherapy on the modelled results (consisting of low-dose 500 mg/m2 cyclophosphamide and 30 mg/m2 fludarabine each for 3 days). While the model precluded CADTH from incorporating IVIG, a crude calculation suggests an additional cost of $2,048.70 per patient every 4 weeks for 1 year to 2 years, resulting in an additional cost of between $26,600 and $53,200 (see Appendix 5 for assumptions regarding IVIG use).
Utility values being associated with uncertainty. The sponsor incorporated values based on the published literature, as there were validity concerns regarding the values collected within the ZUMA-2 trial. These values assumed a higher utility score for patients in pre-progression who were considered “functionally cured.” This assumption was considered to be associated with uncertainty, given the clinical feedback that it was unclear based on the available evidence whether this was a curative treatment.
CADTH undertook an exploratory analysis in which the utility values for pre-progression were the same, regardless of assumed “cure” state.
Limited model transparency. The sponsor’s model trace was associated with limited transparency as, although patients were traced through the health states within the model, QALYs were applied subsequently within the VBA code in the Excel model. As such, CADTH was unable to easily determine the amount of incremental QALYs observed in the trial period compared with the incremental QALYs estimated based on the extrapolation beyond the trial period.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (see Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients are assumed to stay in hospital for 21.2 days post-infusion, in line with the ZUMA-2 protocol, and 22.7% of those days are assumed to be spent in ICU as in the NICE axicabtagene ciloleucel 2018 analysis.16 | Uncertain. Clinical experts consulted by CADTH stated that most patients would require some form of follow-up monitoring for 1 month to 2 months after CAR T-cell therapy. The clinical experts specifically noted that grade 2 to 4 ICANS were a significant consideration in CAR T-cell therapy, often resulting in an additional ICU stay. |
For disutilities that could not be identified, a disutility equal to the maximum of the identified non-CRS adverse event disutilities was assumed. This approach has been previously used in a NICE submission for the CAR T-cell therapy axicabtagene ciloleucel. | This approach seems appropriate. |
Health state utilities are assumed to be the same regardless of treatment and to only differ by health state (different utilities for pre-progression < 60 months, pre-progression cured, and progressed). | This seems to reflect available data. The data for health state utilities in the sponsor’s reference case were taken from the ZUMA-2 trial. |
CAR = chimeric antigen receptor; CRS = cytokine release syndrome; ICANS = immune effector cell–associated neurotoxicity syndrome; ICU = intensive care unit; NICE = National Institute for Health and Care Excellence.
CADTH Reanalyses of the Economic Evaluation
Given the uncertainty associated with the comparative treatment effects and the limitations with the modelling approach, CADTH could not estimate a base-case estimate for brexucabtagene autoleucel compared to BSC in the Canadian setting.
Corrections to Sponsor’s Base Case
CADTH identified the following issues with the submitted model, which were considered more appropriate as a corrected sponsor’s base case as opposed to CADTH reanalyses.
Incorrect leukapheresis costs. The sponsor’s cost of leukapheresis was taken from a dated study by Holbro et al. (2013).10 A more recent study by Ellis (2019)15 exploring the cost-effectiveness of CAR T-cell therapy in Ontario reported updated cost information, which was considered more appropriate.
Underestimated bridging therapy costs. The proportion of patients receiving bridging therapy and the duration was informed by the ZUMA-2 trial. As noted in the CADTH Clinical Review Report, the ZUMA-2 trial was considered to represent a healthier population than is likely to be treated in Canadian practice. Feedback from clinical experts consulted by CADTH noted that this greatly underestimated the use and costs associated with bridging therapy and provided alternate estimates for the Canadian setting.
These components had minimal impact on the cost-effectiveness results and were corrected as part of the sponsor’s base case in Table 5.
Table 5: CADTH Corrections to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. Incorrect leukapheresis cost | $1,344 | $2,625 |
2. Underestimate of bridging therapy use and duration | 37% use Duration of 4 days | 70% use Duration of 56 days |
Corrected base case | 1 + 2 | |
aCorrections are minor errors (e.g., transcription errors between report and model or misapplication of information).
Corrected Sponsor’s Base-Case Results
The results of the corrected sponsor’s model are presented in Table 6. The expected costs were slightly increased for patients receiving brexucabtagene autoleucel. Nonetheless, CADTH’s corrections to the sponsor’s base case had minimal impact on the sponsor’s base case, resulting in a corrected ICER of $91,559 per QALY.
Table 6: Summary Results of the Sponsor’s Corrected Base Case
Stepped analysis | Drug | Total costs, $ | Total QALYs | ICER, $/QALY |
|---|---|---|---|---|
Sponsor’s base case | Best supportive carea | 65,168 | 1.318 | Reference |
Brexucabtagene autoleucel | 693,490 | 8.334 | 89,557 | |
Correction 1 | Best supportive carea | 65,289 | 1.317 | Reference |
Brexucabtagene autoleucel | 694,555 | 8.331 | 89,726 | |
Correction 2 | Best supportive carea | 65,242 | 1.319 | Reference |
Brexucabtagene autoleucel | 705,085 | 8.346 | 91,064 | |
Sponsor’s corrected base case (1 + 2) | Best supportive carea | 65,703 | 1.320 | Reference |
Brexucabtagene autoleucel | 705,729 | 8.330 | 91,559 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aBest supportive care is assumed to be a combination of rituximab, bendamustine, lenalidomide, bortezomib, and anthracycline based on a literature-based meta-analysis.
CADTH Exploratory Analysis
CADTH could not address several key limitations associated with the sponsor’s economic evaluation, namely the lack of robust comparative effectiveness data and the uncertainty associated with the efficacy of brexucabtagene autoleucel. Due to these limitations, all reanalyses subsequently undertaken by CADTH are considered exploratory.
CADTH conducted a series of reanalyses to evaluate the impact of alternate cost assumptions (considering alternate costs for the comparator), alternate efficacy assumptions (using results for brexucabtagene autoleucel that were weighted based on the population observed in the meta-analysis, using alternate parametric distributions for OS and PFS, and assuming that utility in pre-progression is the same regardless of “cure” status), and alternate assumptions regarding the modelling approach (use of the PSM without the mixture-cure component, decreasing the time horizon).
Exploratory Analysis Results
The cost-effectiveness findings were most sensitive to efficacy and modelling assumptions. When using the “weighted” data for brexucabtagene autoleucel based on the MAIC, the ICER rose to $104,570 per QALY. When removing the mixture-cure component of the model and using the PSM, the ICER increased to $318,429 per QALY. When assessing shorter time horizons to minimize uncertainty in the long term effects and present results that may be useful for potential payment plan considerations, the ICER ranged from $189,827 per QALY (10 years) to $422,416 per QALY (5 years).
When combining the scenarios of the “weighted” brexucabtagene autoleucel data and the PSM without the mixture-cure component, the ICER increased to $308,034 per QALY. When combining the scenarios of the PSM without the mixture-cure component and a time horizon reduced to 10 years, the ICER increased to $388,880 per QALY. The details of the cost-effectiveness of the various scenarios tested are listed in Table 11, and results are provided in Table 12. Given the limitations previously identified, these results should be viewed as an exploration of the inherent uncertainty in the clinical data that underpin the economic evaluation.
Issues for Consideration
The evidence for the effectiveness of this therapy is still in its early stages, and evidence is emerging about the rate of complications, the duration of treatment effect, and what comprises follow-up for patients receiving brexucabtagene autoleucel. Furthermore, with a potentially curative therapy, there would be an expectation that patients with MCL will live a longer life, and as such, will incur additional costs to the health system. This would likely lead to an increase in the ICER for brexucabtagene autoleucel.
Travel costs for patients (and their families) and the requirement for time spent away from work were not included in the sponsor’s base case, given the perspective required for submissions to CADTH. The sponsor’s implementation plan indicated that not all provinces and territories will have a site to provide brexucabtagene autoleucel.17 For these jurisdictions, there will be a need for patients to travel out of province or out of country for treatment. Travel costs were not considered in the economic submission. Furthermore, it was noted by clinical experts that some provinces do not even have capacity to assess patients’ eligibility for CAR T-cell therapy, which would result in substantial out-of-pocket costs for patients travelling out of province to meet the eligibility requirements. The sponsor’s implementation plan suggests that patients not living within 2 hours or 200 km of a site may be offered support via a patient support program. If such a support program is not operationalizable and travel expenses (e.g., travel, lodging, booking) are absorbed by the patient or public payer, this would increase the expected costs of brexucabtagene autoleucel and result in a higher ICER estimate. Disparities in funding and treatment access may vary depending on the province or territory, and the requirement for access to a tertiary care centre for delivery of brexucabtagene autoleucel may have equity of access implications, which were not substantively considered in the economic submission.
The sponsor’s implementation plan indicated the manufacturing process took, on average, 16 days from leukapheresis to the time brexucabtagene autoleucel is ready to be infused back into the patient.17 Issues pertaining to the manufacturing are important to the successful delivery of CAR T-cell therapies.18 Moreover, manufacturing failure may occur due to an inadequate number of T cells in the apheresed product, poor selection of T cells on day 0 of manufacturing, irreversibly impaired T cells (i.e., no response to stimulation in culture), microbial contamination, equipment-related cell loss, high endotoxin level, or accidents. Approximately 4% of patients enrolled in the ZUMA-2 trial experienced manufacturing failure. Manufacturing failure is likely to increase the ICER because patients may require creation of an additional dose of brexucabtagene autoleucel and/or experience disease progression that needs intensive formal and informal care.
The sponsor’s implementation plan suggested that the sponsor has the capacity to produce therapy for approximately 4,000 patients per year, although it is unclear whether this estimate is Canada specific.17 The sponsor did not consider potential capacity constraints within the submitted economic evaluation, not just due to challenges in the process of creating the therapy but also in terms of a site being able to provide the therapy (i.e., those considered eligible for treatment would not have adverse clinical outcomes or additional costs arising from treatment delays due to capacity issues). Given the onboarding activities required before a site being eligible to treat patients with brexucabtagene autoleucel (e.g., training and certification) and the number of planned sites, the availability of CAR T-cell therapy may be constrained by site capacity and impact the efficacy and success of the administration of brexucabtagene autoleucel.
In ZUMA-2, patients treated with brexucabtagene autoleucel who achieved partial or complete response had the option to receive a second course of conditioning chemotherapy and brexucabtagene autoleucel if their disease subsequently progressed within 3 months after the initial brexucabtagene autoleucel infusion, provided that the relapse was confirmed to be CD19 positive. As noted in the CADTH Clinical Report, re-treatment took place in 2 of the 74 treated patients in the ZUMA-2 trial (3%). The CADTH review team could not identify whether re-treatment used the same brexucabtagene autoleucel as the original treatment or whether a new dose had to be created, or whether these patients received bridging therapy. Although the clinical experts consulted by CADTH indicated that there is evidence to suggest that a subsequent dose of brexucabtagene autoleucel would be effective, if patients were re-treated this would likely result in a higher ICER for brexucabtagene autoleucel.
Although the budget impact analysis assumes public drug programs will be paying for CAR T-cell therapy, it remains unclear who would be paying for this therapy. This may vary by jurisdiction.
Overall Conclusions
Results from the single-arm, open-label ZUMA-2 trial suggest that brexucabtagene autoleucel at a target dose of 2 × 106 anti-CD19 CAR T cells per kilogram is associated with statistically significant rates of objective response, relative to a historical control, and substantial improvements in survival (PFS and OS) and improved health-related quality of life over 6 months, which are outcomes that patients have identified as clinically relevant. However, there are limitations — given the inability to control for confounding and the unblinded assessment of subjective outcomes — that may inhibit the interpretation of the results. Given the lack of head-to-head studies for brexucabtagene autoleucel, the sponsor submitted an unanchored MAIC that provided indirect evidence of the efficacy of brexucabtagene autoleucel compared with standard of care therapies in patients with R/R MCL. However, due to several identified limitations (e.g., MAIC methods, inclusion of lower quality comparator trials, clinical heterogeneity between studies), no conclusions can be drawn about the comparative clinical effectiveness of Brexucabtagene autoleucel.
CADTH found that the sponsor’s submission to CADTH included several major limitations that introduced significant uncertainties in the cost-effectiveness of brexucabtagene autoleucel. The ZUMA-2 trial was a phase II trial, and uncertainty remains regarding the true absolute efficacy of brexucabtagene autoleucel given the small number of patients and the short follow-up duration. As ZUMA-2 was not a comparative study, the sponsor conducted a MAIC to compare brexucabtagene autoleucel with currently available treatments (BSC). The sponsor noted the differences in the patient populations, which reduced the small sample size and resulted in estimates that did not meet face validity. As such, the relative clinical effectiveness to BSC was estimated using a naive indirect comparison of data from ZUMA-2 with a sponsor-commissioned meta-analysis of 3 studies, which were used to inform efficacy of BSC. However, given the limitations associated with the strong assumptions required for a naive comparison, the appropriateness of this comparison is highly uncertain. As such, little is known about the comparative clinical effectiveness of brexucabtagene autoleucel compared with BSC. Furthermore, although follow-up time at the available data cut-off in the trial was considered appropriate to assess response to treatment, it was noted to be immature for assessing survival outcomes, introducing great uncertainty in the extrapolation of the efficacy of brexucabtagene autoleucel beyond the currently available follow-up period from ZUMA-2.
The sponsor’s base case results appear overly optimistic in terms of the overall and incremental benefit associated with brexucabtagene autoleucel, resulting in considerable uncertainty around the clinical effectiveness and cost-effectiveness of brexucabtagene autoleucel. This uncertainty is largely due to the limitations with the clinical trial and the lack of comparative effectiveness evidence. Based on CADTH’s exploratory analyses using the information available, the ICER could be greater than $300,000 per QALY, without taking into account additional costs associated with brexucabtagene autoleucel that could not be incorporated and would further increase the ICER.
References
1.Tecartus Brexucabtagene autoleucel Cell suspension in patient-specific single infusion bag, target of 2 × 106 chimeric antigen receptor (CAR)-positive viable T cells per kg body weight with a maximum of 2 × 108 CAR-positive viable T cells, for intravenous infusion [product monograph]. Santa Monica (CA): Kite Pharma Inc.; 2020 Dec 7.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Bexucabtagene autoleucel. Mississauga (ON): Gilead Sciences Inc., Canada; 2020.
3.McCulloch R, Visco C, Eyre T, al. E. Efficacy of R-BAC in relapsed, refractory mantle cell lymphoma post BTK inhibitor therapy. British journal of haematology. 2020;189:684-688. PubMed
4.Eyre T, Follows G, Hodson A, al. E. Efficacy of venetoclax monotherapy in patients with relapsed, refractory mantle cell lymphoma after Bruton tyrosine kinase inhibitor therapy. Haematologica. 2019;104:e71. PubMed
5.Jain P, Kanagal-Shamanna R, Zhang S, al. E. Long-term outcomes and mutation profiling of patients with mantle cell lymphoma (MCL) who discontinued ibrutinib. Br J Haematol. 2018;183:578-587. PubMed
6.Martin P, Maddocks K, Leonard J, al. E. Postibrutinib outcomes in patients with mantle cell lymphoma. Blood. 2016;127:1559-1563. PubMed
7.Updated Meta-Analysis and Indirect Comparison of Interventions for Relapsed or Refractory Mantle Cell Lymphoma Previously Treated with Bruton Tyrosine Kinase Inhibitors [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Brexucabtagene autoleucel. Mississauga (ON): Gilead Sciences Inc., Canada; 2020.
8.Survival analysis of the 12 months data cut: ZUMA-2 trial for KTE-X19 in Relapsed/Refractory Mantle Cell Lymphoma [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Brexucabtagene autoleucel. York (UK): Pharmerit International; 2020.
9.NICE. Ibrutinib for treating relapsed or refractory mantle cell lymphoma. 2018: https://www.nice.org.uk/guidance/ta502/resources/ibrutinib-for-treating-relapsed-or-refractory-mantle-cell-lymphoma-pdf-82606716182725. Accessed March 25, 2021.
10.Holbro A, Ahmad I, Cohen S, al. E. Safety and cost-effectiveness of outpatient autologous stem cell transplantation in patients with multiple myeloma. Biology of Blood and Marrow Transplantation. 2013;19:547-551. PubMed
11.CADTH. pCODR final economic guidance report - ibrutinib for mantle cell lymphoma. 2016: https://www.cadth.ca/imbruvica-mantle-cell-lymphoma-relapsedrefractory. Accessed March 25, 2021.
12.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2020: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed March 25, 2021.
13.Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed March 25, 2021.
14.Phillippo D, Ades A, Dias S, Palmer S, Abrams K, Welton N. NICE DSU Technical support document 18: methods for population-adjusted indirect comparisons in submission to NICE. 2016. Accessed March 8, 2021.
15.Ellis K. Cost-effectiveness of Chimeric Antigen Receptor T-cell therapy for treating Large B-cell lymphoma patients in Canada. 2019: https://uwspace.uwaterloo.ca/bitstream/handle/10012/15515/Ellis_Kristina.pdf?sequence=3&isAllowed=y. Accessed March 24, 2021.
16.NICE. Axicabtagene ciloleucel for treating diffuse large B-cell lymphoma and primary mediastinal B-cell lymphoma after 2 or more systemic therapies [ID1115]. 2018.
17.Implementation planning for cell or gene therapy [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Bexucabtagene autoleucel. Mississauga (ON): Gilead Sciences Inc., Canada; 2020.
18.Roddie C, O'Reilly M, Pinto J, Vispute K, Lowdell M. Manufacturing chimeric antigen receptor T cells: issues and challenges. Cytotherapy. 2019;21(3):327-340. PubMed
19.Robak T, Jin J, Pylypenko H, et al. Frontline bortezomib, rituximab, cyclophosphamide, doxorubicin, and prednisone (VR-CAP) versus rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) in transplantation-ineligible patients with newly diagnosed mantle cell lymphoma: final overall survival results of a randomised, open-label, phase 3 study. Lancet Oncol. 2018;19:1449-1458. PubMed
20.Flinn I, van der Jagt R, Kahl B, et al. Randomized trial of bendamustine-rituximab or R-CHOP/R-CVP in first-line treatment of indolent NHL or MCL: the BRIGHT study. Blood. 2014;123:2944-2952. PubMed
21.Lamm W, Kaufman H, Raderer M, et al. Bortezomib combined with rituximab and dexamethasone is an active regimen for patients with relapsed and chemotherapy-refractory mantle cell lymphoma. Haematologica. 2011;96:1008-1014. PubMed
22.Visco C, Chiappella A, Nassi L, et al. Rituximab, bendamustine, and low-dose cytarabine as induction therapy in elderly patients with mantle cell lymphoma: a multicentre, phase 2 trial from Fondazione Italiana Linfomi. Lancet Haematol. 2017;4(1):e15-e23. PubMed
23.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/.
24.Clinical Study Report: A Phase 2 Multicenter Study Evaluating the Efficacy of KTE-X19 in Subjects with Relapsed/Refractory Mantle Cell Lymphoma (ZUMA-2) [internal sponsor's report]. Santa Monica (CA): Kite Pharma, Inc.; 2019 Nov 14.
25.CADTH. pCODR Final economic guidance report: daratumumab (Darzalex)+VMP for multiple myeloma. 2019; https://cadth.ca/sites/default/files/pcodr/Reviews2019/10148Daratumumab%2BVMPforMM_fnEGR_NOREDACT-ABBREV_Post_29Aug2019_final.pdf.
26.CADTH. pCODR final economic guidance report venetoclax (venclexta) rituximab for chronic lymphocytic leukemia. 2019. https://cadth.ca/sites/default/files/pcodr/Reviews2019/10162VenetoclaxRituximabCLL_fnEGR_NOREDACT-ABBREV_31May2019_final.pdf.
27.CADTH. pCODR Final Economic Guidance Report for Gemtuzumab Ozogamicin (Mylotarg) for Acute Myeloid Leukemia. 2020: https://cadth.ca/sites/default/files/pcodr/Reviews2020/10190GemtuzumabOzogamicinAML_fnEGR_NOREDACT-ABBREV_Post02Apr2020_final.pdf.
28.Coleman M, Martin P, Ruan J, et al. Prednisone, etoposide, procarbazine, and cyclophosphamide (PEP-C) oral combination chemotherapy regimen for recurring/refractory lymphoma: low-dose metronomic, multidrug therapy. Cancer. 2008;15(112):2228-2232. PubMed
29.Ruan J, Martin P, Coleman M, et al. Durable responses with the metronomic regimen RT-PEPC in elderly patients with recurrent mantle cell lymphoma. Cancer. 2010;116(11):2655-2664. PubMed
30.Forstpointner R, Unterhalt M, Dreyling M, et al. Maintenance therapy with rituximab leads to significant prolongation of response duration after salvage therapy with a combination of rituximab, fludarabine, cyclophosphamide, and mitoxantrone (R-FCM) in patients with recurring and refractory follicular and mantle cell lymphomas: results of a prospective randomized study of the German Low Grade Lymphoma Study Group (GLSG). Blood. 2006;108:4003-4008. PubMed
31.Ruan J, Martin P, Shah B, et al. Lenalidomide plus Rituximab as Initial Treatment for Mantle-Cell Lymphoma. NEJM. 2015;373:1835-1844. PubMed
32.Davids MS, Roberts A, Seymour J, et al. Phase I First-in-Human Study of Venetoclax in Patients With Relapsed or Refractory Non-Hodgkin Lymphoma. Journal of Clinical Oncology. 2017;35(8):826-833. PubMed
33.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Bexucabtagene autoleucel. Mississauga (ON): Gilead Sciences Inc., Canada; 2020.
34.Statistics Canada. Population estimates on July 1st 2019. 2019; https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1710000501.
35.Blackhouse G, Gaebel K, Xie F, et al. Cost-utility of intravenous immunoglobulin (IVIG) compared with corticosteroids for the treatment of chronic inflammatory demyelinating polyneuropathy (CIDP) in Canada. Cost Eff Resour Alloc. 2010;8:14. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CADTH Cost Comparison Table for adult patients with relapsed or refractory mantle cell lymphoma previously treated with a BTK inhibitor
Treatment | Strength / Concentration | Forma | Priceb | Recommended dosage | Daily cost | 28-day cost |
|---|---|---|---|---|---|---|
Brexucabtagene autoleucel | 2*106 CAR + viable T cells per kg body weight (range: 1 × 106 – 2 × 106 CAR-positive viable T cells/kg), to a maximum of 2*108 cells | Cell suspension in patient-specific single infusion bag | $533,523.1000c | One-time dosed | NA | NA |
R-CHOP19 | ||||||
Cyclophosphamide | 20 mg/mL | Powder for IV infusion 500 mg 1,000 mg | $91.3100 $165.5200 | 750 mg/m2 every 3 weeks | $12.23 | $342 |
Doxorubicin | 2 mg/mL | IV infusion 5 mL 25 mL 100 mL | $50.4500 $252.2500 $973.0000 | 50 mg/m2 every 3 weeks | $24.02 | $673 |
Prednisone | 5 mg 50 mg | Tablet | $0.0220e $0.1735 | 100 mg/m2 5 times per 3 weeks | $0.17 | $5 |
Rituximab | 10 mg/mL | IV infusion 10 mL 50 mL | $482.3050f $2,411.5400 | 375 mg/m2 every 3 weeks | $183.74 | $5,145 |
Vincristine | 1 mg/mL | IV infusion | $30.6000 | 1.4 mg/m2 to 2 mg every 3 weeks | $2.91 | $82 |
R-CHOP regimen | $223.07 | $6,246 | ||||
VR-CAP19 | ||||||
Bortezomib | 1 mg/mL | Powder for IV infusion 3.5 mg | $1,402.4200 g | 1.3 mg/m2 4 times per 3 weeks | $267.13 | $7,480 |
Cyclophosphamide | 20 mg/mL | Powder for IV infusion 500 mg 1,000 mg | $91.3100 $165.5200 | 750 mg/m2 every 3 weeks | $12.23 | $342 |
Doxorubicin | 2 mg/mL | IV infusion 5 mL 25 mL 100 mL | $50.4500 $252.2500 $973.0000 | 50 mg/m2 every 3 weeks | $24.02 | $673 |
Prednisone | 5 mg 50 mg | Tablet | $0.0220e $0.1735 | 100 mg/m2 5 times per 3 weeks | $0.17 | $5 |
Rituximab | 10 mg/mL | IV infusion 10 mL 50 mL | $482.3050f $2,411.5400 | 375 mg/m2 every 3 weeks | $183.74 | $5,145 |
VR-CAP regimen | $487.28 | $13,644 | ||||
R-CVP20 | ||||||
Cyclophosphamide | 20 mg/mL | Powder for IV infusion 500 mg 1,000 mg | $91.3100 $165.5200 | 750 to 1,000 mg/m2 every 3 weeks | $12.23 to $15.76 | $342 to $441 |
Prednisone | 5 mg 50 mg | Tablet | $0.0220e $0.1735 | 100 mg/m2 5 times per 3 weeks | $0.17 | $5 |
Rituximab | 10 mg/mL | IV infusion 10 mL 50 mL | $482.3050f $2,411.5400 | 375 mg/m2 every 3 weeks | $183.74 | $5,145 |
Vincristine | 1 mg/mL | IV infusion | $30.6000 | 1.4 mg/m2 to 2 mg every 3 weeks | $2.91 | $82 |
R-CVP regimen | $199.05 to $202.58 | $5,573 to $5,672 | ||||
Bortezomib + Dexamethasone + Rituximab21 | ||||||
Bortezomib | 1 mg/mL | Powder for IV infusion 3.5 mg | $1,402.4200g | 1.3 mg/m2 4 times per 3 weeks | $267.13 | $7,480 |
Dexamethasone | 0.5 mg 4 mg | Tablet | $0.1564e $0.3046 | 40 mg 4 times per 3 weeks | $0.58 | $16 |
Rituximab | 10 mg/mL | IV infusion 10 mL 50 mL | $482.3050f $2,411.5400 | 375 mg/m2 every 3 weeks | $183.74 | $5,145 |
Bortezomib + dexamethasone + rituximab regimen | $451.44 | $12,640 | ||||
R-BAC22 | ||||||
Bendamustine | 5 mg/mL | Powder for IV infusion 25 mg 100 mg | $312.5000h $1,250.0000 | 70 mg/m2 twice per 4 weeks | $133.93 | $3,750 |
Cytarabine | 100 mg/mL | IV infusion 1 mL 5 mL 10 mL 20 mL | $5.0900i $76.8500 $153.2500 $306.5000 | 500 mg/m2 3 times per 4 weeks | $16.42 | $460 |
Rituximab | 10 mg/mL | IV infusion 10 mL 50 mL | $482.3050f $2,411.5400 | 375 mg/m2 every 4 weeks | $137.80 | $3,858 |
R-BAC regimen | $288.15 | $8,068 | ||||
Bendamustine + Rituximab20 | ||||||
Bendamustine | 5 mg/mL | Powder for IV infusion 25 mg 100 mg | $312.5000h $1,250.0000 | 90 mg/m2 twice per 4 weeks | $178.57 | $5,000 |
Rituximab | 10 mg/mL | IV infusion 10 mL 50 mL | $482.3050f $2,411.5400 | 375 mg/m2 every 4 weeks | $137.80 | $3,858 |
Bendamustine + rituximab regimen | $316.37 | $8,858 | ||||
BTK = Bruton’s tyrosine kinase; CAR + = chimeric antigen receptor positive.
Note: All prices are from the IQVIA Delta PA database (accessed January and February 2021),23 unless otherwise indicated, and do not include dispensing fees. Daily and 28-day costs were calculated assuming a body surface area of 1.98 m2 from ZUMA-2.24 Vial sharing was only assumed for those drugs in which the product monograph specifically stated it was possible.
aIf supplied in a form other than a tablet, the size of the product is noted.
bThe price listed is the price per tablet, vial, or vial of powder.
cSponsor submitted price.2
dBrexucabtagene autoleucel is delivered as a 1-time dose. Daily and annual costs were not calculated.
eOntario Drug Benefit formulary (accessed February 2021).13
fOntario Exceptional Access Program formulary (accessed February 2021).12
gpCODR Final Economic Guidance Report for Daratumumab (Darzalex) for Multiple Myeloma.25
hpCODR Final Economic Guidance Report for Venetoclax (Venclexta) Rituximab for Chronic Lymphocytic Leukemia.26
ipCODR Final Economic Guidance Report for Gemtuzumab Ozogamicin (Mylotarg) for Acute Myeloid Leukemia.27
Table 8: CADTH Cost Comparison Table for other therapies for relapsed or refractory mantle cell lymphoma
Treatment | Strength/ Concentration | Forma | Priceb | Recommended dosage | Daily cost | 28-day cost |
|---|---|---|---|---|---|---|
Brexucabtagene autoleucel | 2*106 CAR + viable T cells per kg body weight to a maximum of 2*108 cells | Cell suspension in patient-specific single infusion bag | $533,523.1000c | One-time dosed | NA | NA |
Cyclophosphamide | 25 mg 50 mg | Tablet | $0.3520 $0.4740 | 50 mg daily | $0.47 | $13 |
Etoposide | 50 mg | Capsule | $41.5875 | 50 mg daily | $41.59 | $1,164 |
Prednisone | 5 mg 50 mg | Tablet | $0.0220 $0.1735 | 20 mg daily | $0.09 | $2 |
Procarbazine | 50 mg | Capsule | $56.7958 | 50 mg daily | $56.80 | $1,590 |
Rituximab | 10 mg/mL | IV infusion 10 mL 50 mL | $482.3050e $2,411.5400 | 375 mg/m2 4 times per 16 weeks | $137.80 | $3,858 |
PEPC regimen28 | $98.95 | $2,770 | ||||
$236.75 | $6,629 | |||||
Lenalidomide ± rituximab31 | ||||||
Lenalidomide | 2.5 mg | Capsule | $329.5000e | 20 to 25 mg daily for 3 weeks, followed by 1 week off | $1,977.00 to $2,471.25 | $55,356 to $69,195 |
Rituximab | 10 mg/mL | IV infusion 10 mL 50 mL | $482.3050e $2,411.5400 | Initiation: 375 mg/m2 weekly for 4 weeks Subsequent: 375 mg/m2 every 8 weeks | $551.21 $68.90 | $15,434 $1,929 |
Lenalidomide + rituximab regimen | $2,045.90 to $3,022.46 | $57,285 to $84,629 | ||||
Venetoclax monotherapy32 | ||||||
Venetoclax | 10 mg 50 mg 100 mg | Tablet | $7.0000e $35.0000 $70.0000 | 200 to 1,200 mg daily | $140.00 to $840.00 | $3,920 to $23,520 |
CAR + = chimeric antigen receptor positive.
Note: All prices are from the Ontario Drug Benefit formulary (accessed February 2021),13 unless otherwise indicated, and do not include dispensing fees. Daily and 28-day costs were calculated assuming a body surface area of 1.98 m2 from ZUMA-2.24 Vial sharing was only assumed for those drugs in which the product monograph specifically stated it was possible.
aIf supplied in a form other than a tablet, the size of the product is noted.
bThe price listed is the price per tablet, vial, or vial of powder.
cSponsor submitted price.2
dBrexucabtagene autoleucel is delivered as a 1-time dose. Daily and annual costs were not calculated.
eOntario Exceptional Access Program formulary (accessed February 2021).12
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The primary comparator used consists of a ‘basket’ of various chemotherapies which may not reflect the individual jurisdictions’ preferences for treatment of r/r MCL. |
Model has been adequately programmed and has sufficient face validity | No | The use of a partitioned survival model may limit the validity of the results, particularly as these models tend to overpredict benefits in the post-progression phase. The estimated incremental QALYs in the reference case analysis appears to be high: 7 incremental QALYs (3 in the post-progression phase) seems optimistic in an older patient population with relapsed/refractory cancer. |
Model structure is adequate for decision problem | No | The model is overly simplistic in dealing with a relapsed/refractory cancer. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | None |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | None |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The submitted model and report were not fully aligned in terms of the information reported to be included in the base case and the information actually included in the base case. Furthermore, the report and model were presented in a way that made them difficult to interpret. |
QALYs = quality-adjusted life-years; r/r MCL = relapsed or refractory mantle cell lymphoma.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
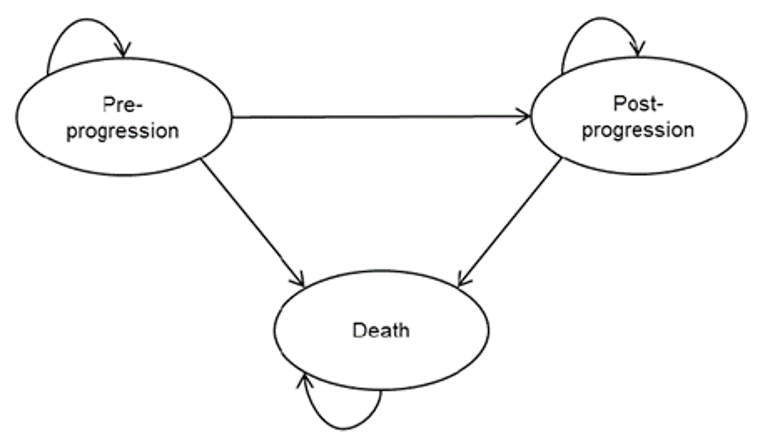
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Brexucabtagene autoleucel | BSC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.26 | 1.72 | 9.54 |
Pre-progression | 7.94 | 1.51 | 6.42 |
Post-progression | 3.32 | 0.21 | 3.12 |
Discounted QALYs | |||
Total | 8.33 | 1.32 | 7.02 |
Pre-progression, pre-cure point | 1.97 | 1.04 | 0.93 |
Pre-progression, post-cure point | 4.25 | 0.14 | 4.11 |
Post-progression | 2.15 | 0.14 | 2.01 |
Adverse events | −0.04 | 0.00 | −0.04 |
Discounted costs ($) | |||
Total | 693,490 | 65,168 | 628,322 |
Treatment-related costs | 599,386 | 27,688 | 571,698 |
Drug acquisition | 533,523 | 26,975 | 506,548 |
Apheresis | 1,344 | 0 | 1,344 |
Drug administration | 185 | 713 | −528 |
Conditioning chemotherapy | 646 | 0 | 646 |
Bridging therapy | 222 | 0 | 222 |
Hospitalization | 63,466 | 0 | 63,466 |
Disease management costs | 54,073 | 4,000 | 50,073 |
Pre-progression | 3,262 | 882 | 2,380 |
Post-progression | 50,811 | 3,118 | 47,693 |
Other costs | 40,032 | 33,480 | 6,552 |
End of life care | 28,652 | 33,480 | −4,828 |
Adverse events | 11,380 | 0 | 11,380 |
ICER ($/QALY) | 89,557 | ||
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic evaluation2
Figure 2: Cost-effectiveness plane for brexucabtagene autoleucel compared with BSC
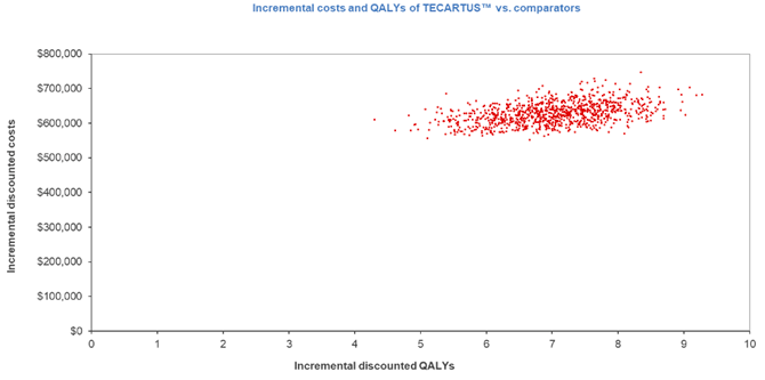
Source: Sponsor’s pharmacoeconomic evaluation2
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Exploratory Analyses
Table 11: Summary of CADTH Exploratory Analyses
Exploratory analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Cost implications | ||
1. Altering the proportion of delivered therapy in the BSC arm of the model | 68.2% of patients received rituximab, the most common component | This was altered so that patients received 100% rituximab + bendamustine to illustrate the impact |
Efficacy considerations | ||
2. Alternate dataset for brexucabtagene | Unweighted data from ZUMA-2 | Weighted data from ZUMA-2 |
3. Altering the parametric distribution used for the data extrapolation of OS and PFS for brexucabtagene | Exponential distribution | Weibull distribution |
4. Altering the parametric distribution used for the data extrapolation of OS and PFS for brexucabtagene | Exponential distribution | Log-normal distribution |
5. Alternate utility value assumptions | Utility for pre-progressed (not cured) = 0.780 Utility for pre-progressed (not cured) = 0.785 | Utility for pre-progressed (not cured) = 0.780 Utility for pre-progressed (not cured) = 0.780 |
6. Re-treatment | 0% | 3% (2 of 74 patients in ZUMA-2 required re-treatment) |
Modelling approach | ||
7. Modelling approach | PSMCM with 5-year cure point | Traditional PSM approacha |
8. Time horizon potentially excessively long | Lifetime (50 years) | Shortened to 5 years to better approximate a time that reflects the trial results and may be considered for payment schedules |
9. Time horizon potentially excessively long | Lifetime (50 years) | Shortened to 10 years to better approximate a time that reflects the trial results and may be considered for payment schedules |
BSC = best supportive care; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; PSMCM = partitioned survival mixture-cure model.
aThe PSM had been programmed to differentiate utilities at 5 years. To fully assess the PSM approach, the time to cure point was increased to 50 years.
Table 12: Summary of the CADTH Reanalysis Results
Scenario | Treatment | Total costs | Total QALYs | ICER vs. BSC |
|---|---|---|---|---|
Sponsor submitted base case | ||||
Sponsor’s base case | BSC | $65,168 | 1.318 | Reference |
Brexucabtagene autoleucel | $693,490 | 8.334 | 89,557 | |
Corrected base case | ||||
Sponsor’s base case | BSC | 65,703 | 1.320 | Reference |
Brexucabtagene autoleucel | 705,729 | 8.330 | 91,559 | |
CADTH exploratory analyses | ||||
CADTH exploratory analysis 1 | BSC | 77,710 | 1.318 | Reference |
Brexucabtagene autoleucel | 704,394 | 8.292 | 89,852 | |
CADTH exploratory analysis 2 | BSC | 65,203 | 1.319 | Reference |
Brexucabtagene autoleucel | 778,410 | 8.139 | 104,570 | |
CADTH exploratory analysis 3 | BSC | 65,686 | 1.320 | Reference |
Brexucabtagene autoleucel | 698,427 | 8.494 | 88,201 | |
CADTH exploratory analysis 4 | BSC | 65,277 | 1.317 | Reference |
Brexucabtagene autoleucel | 703,597 | 8.242 | 92,178 | |
CADTH exploratory analysis 5 | BSC | 65,167 | 1.318 | Reference |
Brexucabtagene autoleucel | 704,649 | 8.287 | 91,762 | |
CADTH exploratory analysis 6 | BSC | 64,891 | 1.313 | Reference |
Brexucabtagene autoleucel | 718,247 | 8.274 | 93,727 | |
CADTH exploratory analysis 7 | BSC | 64,867 | 1.323 | Reference |
Brexucabtagene autoleucel | 690,950 | 3.289 | 318,429 | |
CADTH exploratory analysis 8 | BSC | 61,247 | 1.016 | Reference |
Brexucabtagene autoleucel | 649,379 | 2.498 | 422,416 | |
CADTH exploratory analysis 9 | BSC | 64,832 | 1.250 | Reference |
Brexucabtagene autoleucel | 665,719 | 4.415 | 189,827 | |
Combined analysis 1 (2 + 7) | BSC | 64,635 | 1.328 | Reference |
Brexucabtagene autoleucel | 696,537 | 3.380 | 308,034 | |
Combined analysis 2 (7 + 9) | BSC | 64,251 | 1.263 | Reference |
Brexucabtagene autoleucel | 678,740 | 2.843 | 388,880 | |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years; vs. = versus .
Table 13: CADTH Price Reduction Analyses
Scenario | ICERs for brexucabtagene autoleucel vs. best supportive care ($ / QALY) | ||
|---|---|---|---|
Price reduction | Sponsor base case | CADTH corrected analysis | CADTH combined analysis 1 |
No price reduction | 89,557 | 91,559 | 308,034 |
10% | 82,134 | 83,431 | 283,069 |
20% | 74,533 | 75,916 | 255,321 |
30% | 66,933 | 68,375 | 229,148 |
40% | 59,332 | 60,931 | 204,209 |
50% | 51,731 | 53,360 | 177,544 |
60% | 43,690 | 45,528 | 152,148 |
70% | 36,172 | 37,886 | 126,371 |
80% | 28,391 | 29,949 | 100,488 |
90% | 21,050 | 22,741 | 73,691 |
99% | 14,013 | 15,854 | 50,235 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years; vs. = versus .
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: CADTH Summary Findings from the Sponsor’s Budget Impact Analysis
Key Take-Aways of the Budget Impact Analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) assessed the introduction of brexucabtagene autoleucel for the treatment of R/R MCL following treatment with a BTK inhibitor. The analysis was derived using an epidemiology-based approach over a 3-year time horizon, with a base year (assumed to be 2021). The analysis provides results from both a drug plan (drug acquisition costs only) and health care perspective (additionally mark-ups/dispensing fees, cost of health care resources, and drug administration costs). A summary of the sponsor’s derivation of the eligible population size is presented in Figure 3.
Figure 3: Sponsor’s Estimation of the Size of the Eligible Population
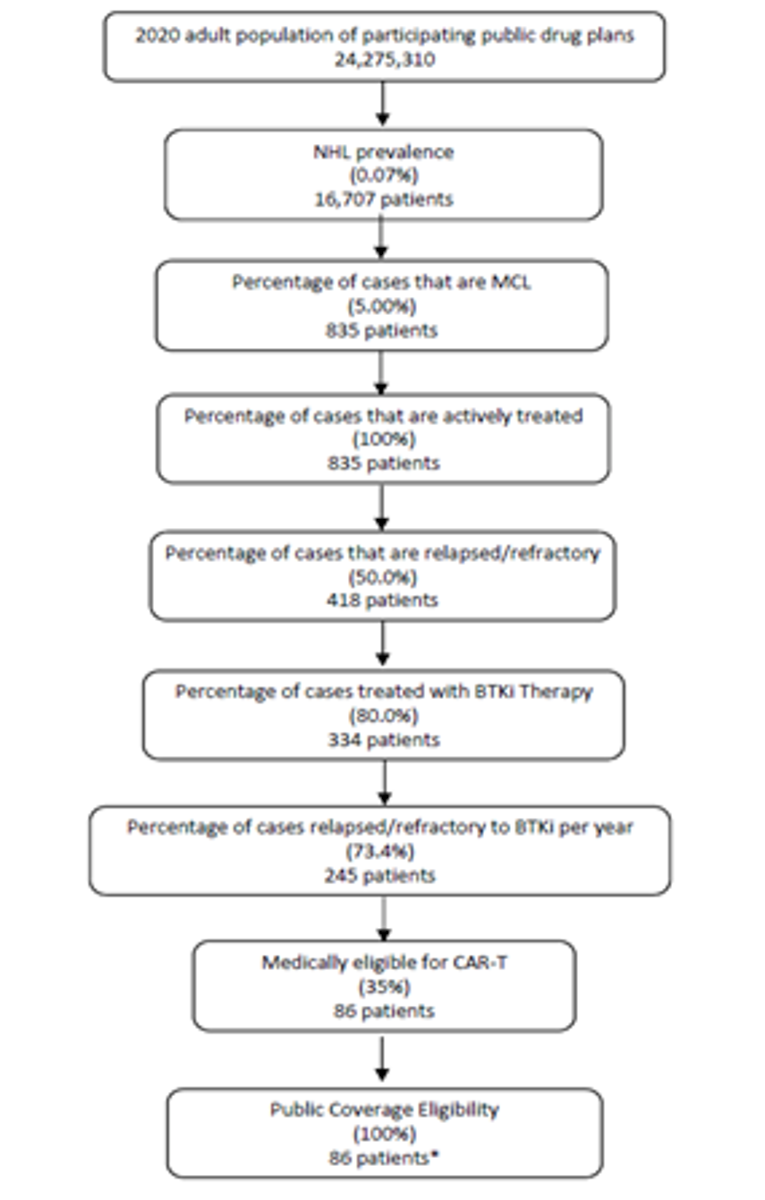
Source: Sponsor’s budget impact analysis.33
The main comparator for this analysis is BSC which was incorporated as a blended comparator including rituximab, bendamustine, lenalidomide, bortezomib, and doxorubicin. The reference case scenario included BSC as the only available treatment(s), while the new drug scenario included brexucabtagene autoleucel and BSC as the available treatments. Key inputs to the BIA are documented in Table 15.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
Annual population growth rate | 1.35%34 |
Number of patients eligible for brexucabtagene autoleucel | 87 / 88 / 89 |
Market Uptake (3 years) | |
Uptake (reference scenario) Brexucabtagene autoleucel BSC | 0% / 0% / 0% 100% / 100% / 100% |
Uptake (new drug scenario) Brexucabtagene autoleucel BSC | | % / | % / | % | % / | % / | % |
Cost of annual treatment in Ontario (per patient) | |
Brexucabtagene autoleucel | |
Drug cost Brexucabtagene autoleucel Conditioning fludarabine Conditioning cyclophosphamide Administration cost | $533,523.10 $908.82 $154.62 $815.90 |
Additional costs of care Apheresis Hospitalization cost for administration Bridging therapy Additional medical resource use CRS (Grade 2-4) CRS requiring tocilizumab usage | $1,343.98 $63,758.81 $579.15 $3,268.57 $10,106.25 $2,013.81 |
BSC | |
Drug cost Rituximab Bendamustine Lenalidomide Bortezomib Doxorubicin Administration cost | $15,799.80 $12,925.04 $0.00 $0.00 $791.05 $667.52 |
Additional costs of care Additional medical resource use | $946.73 |
BSC = best supportive care; CRS = cytokine release syndrome.
Note: Costs are presented for Ontario as a reference only and may differ by jurisdiction due to mark-ups and dispensing fees.
Summary of the Sponsor’s BIA Results
Based on the sponsor’s analysis, from a drug plan perspective the estimated budget impact of funding brexucabtagene autoleucel for MCL is $2,997,575 in year 1, $16,085,664 in year 2, and $20,303,229 in year 3, for a 3-year total of $39,386,468. From a health care system perspective, the expected budget impact is $3,464,707 in year 1, $18,592,382 in year 2, and $23,467,170 in year 3, for a 3-year total of $45,524,260.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Underestimation of the proportion of patients requiring bridging therapy and treatment duration: The sponsor assumed that bridging therapy would be used by 36.8% of patients based on ZUMA-2, and that this would consist of 560 mg/m2 daily of ibrutinib and 40 mg/m2 of dexamethasone daily, each for 4 days.24 Clinical experts consulted by CADTH noted that the proportion was most likely an underestimate and that the majority of patients awaiting CAR T-cell therapy would require bridging therapy to control their lymphoma. Furthermore, it was noted that bridging therapy would likely be required for up to 8 weeks (56 days) rather than 4 days, from the moment of determination of CAR T-cell therapy eligibility to the time of the cell infusion.
As part of the base case CADTH increased the proportion of patients requiring bridging therapy to 50% based on clinical expert feedback, and explored higher percentages (i.e., 70%) in a scenario analysis. As part of the base case CADTH increased the duration of bridging therapy from 4 days to 56 days.
Incorrect leukapheresis costs: The sponsor’s cost of leukapheresis was taken from a dated study by Holbro et al. 2013.10 A more recent study by Ellis et al. 201915 exploring the cost-effectiveness of CAR T-cell therapy in Ontario reported more recent cost information, which was considered more appropriate.
As part of the base case, CADTH updated the cost of leukapheresis.
Uncertainty around market share assumptions: The sponsor assumed market capture rates of | %, | %, and | % for brexucabtagene autoleucel in year 1, 2, and 3. Clinical experts consulted by CADTH expressed uncertainty around the estimates, particularly in years 2 and 3. It was noted that in medically eligible patients (e.g., clinical assessment of age, organ function, fitness) with MCL refractory to BTK inhibitor the market capture rate should be close to 100%. However, it was also stated that infrastructure limitations in some jurisdictions would make it difficult for patients to access brexucabtagene autoleucel, thus lowering the market capture rate.
CADTH performed scenario analyses on the market shares of brexucabtagene autoleucel which involved increasing or decreasing the market shares by 25% in all years
Uncertainty involving follow-up and monitoring costs: The sponsor assumed the infusion of and monitoring after brexucabtagene autoleucel would involve an elective hospitalization with a mean length of stay of 21.2 days as per ZUMA-2 and that, furthermore, a proportion of patients (22.7%) would require monitoring within an intensive care unit and would incur an additional ICU cost.24 Clinical experts consulted by CADTH stated that most patients would require some form of follow-up monitoring for 1 to 2 months following CAR T-cell therapy. Resources associated with this monitoring include but are not limited to electrolyte disturbances requiring infusions, filgrastim injections, red blood cell transfusions, daily nurse calls, weekly physician visits, and hospital readmission with further in-patient stays. The clinical experts were uncertain whether the sponsor’s assumptions about follow-up costs were adequate to capture this additional resource use, but noted that grade 2 to 4 ICANS (immune effector cell–associated neurotoxicity syndrome) were a significant consideration in CAR T-cell therapy often resulting in an ICU stay.
CADTH attempted to perform a scenario analysis in which the proportion of patients requiring ICU care was increased to 30%. However, this was not possible within the sponsor’s model as the follow-up hospitalization cost ($63,759) was hard coded into the model and was not able to be modified. This scenario analysis would have likely increased the budget impact as more patients would be requiring an ICU stay and incurring the extra cost.
Failure to consider the cost of IV immunoglobulin (IVIG): The sponsor failed to consider the cost of IVIG in their analysis from the health care system perspective. Clinical experts consulted by CADTH expected there to be significant cost associated with IVIG and estimated that 30% to 40% of patients receiving brexucabtagene autoleucel would require 1 to 2 years of therapy.
CADTH performed a scenario analysis which included IVIG costs. Specifically, it was assumed that 35% of patients would receive IVIG at a dose of 0.4g/kg every 4 weeks for 1 year, based on clinical expert input. An average patient weight of 81.8 kg from ZUMA-2 was used,24 and cost inputs for IVIG were derived from Blackhouse (2010).35
Failure to consider the upfront costs associated with CAR T-cell assessment: The sponsor failed to consider the upfront costs of assessment of CAR T-cell therapy eligibility, which would include costs associated with MRIs, PET scans, bone marrows, lumbar punctures, bloodwork, and more. Should brexucabtagene autoleucel be reimbursed, clinical experts consulted by CADTH expected that this assessment cost would be incurred by all patients with MCL who were refractory to BTK inhibitor therapy (approximately 245 per year, Figure 1). While the exact expense for assessment is uncertain, these costs represent additional resource use that would only occur in a world in which brexucabtagene autoleucel is available. While some of these scans and procedures are already performed, their use and frequency are expected to increase if brexucabtagene autoleucel were available as a treatment option.
CADTH performed scenario analyses in which an assessment cost of $5,000 and $8,000 was applied to all patients with MCL who were refractory to BTK inhibitor therapy. This cost was applied to the brexucabtagene autoleucel treatment arm only.
CADTH Reanalyses of the BIA
CADTH conducted 2 revisions as part of the base case by increasing both the duration of and proportion of patients receiving bridging therapy.
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | None | None |
Changes to derive the CADTH base case | ||
1. Increased duration of bridging therapy | 4 days | 56 days |
2. Increased proportion of patients requiring bridging therapy | 36.8% | 70% |
3. Updated cost of leukapheresis | $1,344 | $2,625 |
CADTH base case | — | Reanalysis 1 + 2 + 3 |
The results of the CADTH step-wise reanalysis are presented in summary format in Table 17 and more detailed breakdowns for the drug plan and health care perspective are presented in Table 18 and Table 19, respectively.
Based on the CADTH base case, the expected budget impact of funding brexucabtagene autoleucel for the treatment of relapsed/refractory MCL from a drug plan perspective was unchanged from the sponsor’s base case. From a health care system perspective, the expected budget impact estimated from the CADTH base case was $3,534,362 in year 1, $18,966,166 in year 2, and $23,938,956 in year 3, for a 3-year total of $46,439,484.
Scenario analyses were conducted involving proportion of patients on bridging therapy, the market shares of brexucabtagene, and the inclusion of IVIG or upfront assessment costs. From a drug plan perspective, the results of these scenario analyses ranged from $29,539,851 to $49,233,085 over 3 years, with the only changes coming from the scenario analysis involving market shares. From a health care system perspective, the results of the scenario analyses ranged from $34,829,613 to $58,049,356. The results from a health care system perspective were sensitive to market share assumptions and the inclusion of upfront assessment costs.
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total (drug plan) | Three-year total (health care system) |
|---|---|---|
Submitted base case | $39,386,468 | $45,524,260 |
CADTH reanalysis 1 – increased duration of bridging therapy | $39,386,468 | $46,112,340 |
CADTH reanalysis 2 – increased proportion of patients on bridging therapy | $39,386,468 | $45,540,486 |
CADTH reanalysis 3 – increased cost of leukapheresis | $39,386,468 | $45,624,236 |
CADTH base case | $39,386,468 | $46,439,484 |
BIA = budget impact analysis.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA (drug plan)
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $2,566,142 | $2,605,637 | $2,645,773 | $2,686,558 | $7,937,968 |
New drug | $2,566,142 | $5,603,212 | $18,731,437 | $22,989,787 | $47,324,436 | |
Budget impact | $0 | $2,997,575 | $16,085,664 | $20,303,229 | $39,386,468 | |
CADTH base case | Reference | $2,566,142 | $2,605,637 | $2,645,773 | $2,686,558 | $7,937,968 |
New drug | $2,566,142 | $5,603,212 | $18,731,437 | $22,989,787 | $47,324,436 | |
Budget impact | $0 | $2,997,575 | $16,085,664 | $20,303,229 | $39,386,468 | |
CADTH scenario analysis 1: 70% patients require bridging therapy | Reference | $2,566,142 | $2,605,637 | $2,645,773 | $2,686,558 | $7,937,968 |
New drug | $2,566,142 | $5,603,212 | $18,731,437 | $22,989,787 | $47,324,436 | |
Budget impact | $0 | $2,997,575 | $16,085,664 | $20,303,229 | $39,386,468 | |
CADTH scenario analysis 2a: increase brex market shares 25% | Reference | $2,566,142 | $2,605,637 | $2,645,773 | $2,686,558 | $7,937,968 |
New drug | $2,566,142 | $6,352,606 | $22,752,853 | $28,065,594 | $57,171,053 | |
Budget impact | $0 | $3,746,969 | $20,107,080 | $25,379,036 | $49,233,085 | |
CADTH scenario analysis 2b: decrease brex market shares 25% | Reference | $2,566,142 | $2,605,637 | $2,645,773 | $2,686,558 | $7,937,968 |
New drug | $2,566,142 | $4,853,818 | $14,710,021 | $17,913,980 | $37,477,819 | |
Budget impact | $0 | $2,248,181 | $12,064,248 | $15,227,422 | $29,539,851 | |
CADTH scenario analysis 3: include IVIG costs | Reference | $2,566,142 | $2,605,637 | $2,645,773 | $2,686,558 | $7,937,968 |
New drug | $2,566,142 | $5,603,212 | $18,731,437 | $22,989,787 | $47,324,436 | |
Budget impact | $0 | $2,997,575 | $16,085,664 | $20,303,229 | $39,386,468 | |
CADTH scenario analysis 4a: $5,000 assessment cost | Reference | $2,566,142 | $2,605,637 | $2,645,773 | $2,686,558 | $7,937,968 |
New drug | $2,566,142 | $5,603,212 | $18,731,437 | $22,989,787 | $47,324,436 | |
Budget impact | $0 | $2,997,575 | $16,085,664 | $20,303,229 | $39,386,468 | |
CADTH scenario analysis 4b: $8,000 assessment cost | Reference | $2,566,142 | $2,605,637 | $2,645,773 | $2,686,558 | $7,937,968 |
New drug | $2,566,142 | $5,603,212 | $18,731,437 | $22,989,787 | $47,324,436 | |
Budget impact | $0 | $2,997,575 | $16,085,664 | $20,303,229 | $39,386,468 |
BIA = budget impact analysis; brex = brexucabtagene autoleucel; ICU = intensive care unit; IVIG = IV immunoglobulin.
Table 19: Detailed Breakdown of the CADTH Reanalyses of the BIA (health care system)
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $2,850,578 | $2,894,497 | $2,939,129 | $2,984,485 | $8,818,111 |
New drug | $2,850,578 | $6,359,204 | $21,531,511 | $26,451,655 | $54,342,371 | |
Budget impact | $0 | $3,464,707 | $18,592,382 | $23,467,170 | $45,524,260 | |
CADTH base case | Reference | $2,850,578 | $2,894,497 | $2,939,129 | $2,984,485 | $8,818,111 |
New drug | $2,850,578 | $6,428,859 | $21,905,295 | $26,923,441 | $55,257,596 | |
Budget impact | $0 | $3,534,362 | $18,966,166 | $23,938,956 | $46,439,484 | |
CADTH scenario analysis 1: 70% patients require bridging therapy | Reference | $2,850,578 | $2,894,497 | $2,939,129 | $2,984,485 | $8,818,111 |
New drug | $2,850,578 | $6,455,055 | $22,045,867 | $27,100,869 | $55,601,790 | |
Budget impact | $0 | $3,560,558 | $19,106,737 | $24,116,384 | $46,783,679 | |
CADTH scenario analysis 2a: increase brex market shares 25% | Reference | $2,850,578 | $2,894,497 | $2,939,129 | $2,984,485 | $8,818,111 |
New drug | $2,850,578 | $7,312,450 | $26,646,837 | $32,908,180 | $66,867,467 | |
Budget impact | $0 | $4,417,953 | $23,707,708 | $29,923,695 | $58,049,356 | |
CADTH scenario analysis 2b: decrease brex market shares 25% | Reference | $2,850,578 | $2,894,497 | $2,939,129 | $2,984,485 | $8,818,111 |
New drug | $2,850,578 | $5,545,269 | $17,163,754 | $20,938,702 | $43,647,725 | |
Budget impact | $0 | $2,650,772 | $14,224,625 | $17,954,217 | $34,829,613 | |
CADTH scenario analysis 3: include IVIG costs | Reference | $2,850,578 | $2,894,497 | $2,939,129 | $2,984,485 | $8,818,111 |
New drug | $2,850,578 | $6,484,227 | $22,202,409 | $27,298,455 | $55,985,090 | |
Budget impact | $0 | $3,589,729 | $19,263,279 | $24,313,970 | $47,166,979 | |
CADTH scenario analysis 4a: $5,000 assessment cost | Reference | $2,850,578 | $2,894,497 | $2,939,129 | $2,984,485 | $8,818,111 |
New drug | $2,850,578 | $7,654,547 | $23,147,582 | $28,182,553 | $58,984,681 | |
Budget impact | $0 | $4,760,049 | $20,208,453 | $25,198,068 | $50,166,570 | |
CADTH scenario analysis 4b: $8,000 assessment cost | Reference | $2,850,578 | $2,894,497 | $2,939,129 | $2,984,485 | $8,818,111 |
New drug | $2,850,578 | $8,389,959 | $23,892,954 | $28,938,019 | $61,220,933 | |
Budget impact | $0 | $5,495,462 | $20,953,825 | $25,953,534 | $52,402,821 |
BIA = budget impact analysis; brex = brexucabtagene autoleucel; ICU = intensive care unit; IVIG = IV immunoglobulin.
Ethics Review
Abbreviations
CAR T-cell
chimeric antigen receptor T-cell
MCL
mantle cell lymphoma
Objective
The purpose of this report is to describe and summarize the ethical considerations raised explicitly in the literature associated with the use of brexucabtagene autoleucel for the treatment of adult patients with relapsed or refractory mantle cell lymphoma (MCL) who have received treatment with a Bruton’s tyrosine kinase inhibitor.
Research Question
This report addresses the following research question:
What are the ethical considerations raised in the published literature relevant to the use of brexucabtagene autoleucel for the treatment of adult patients with relapsed or refractory mantle cell lymphoma who have received treatment with a Bruton’s tyrosine kinase inhibitor?
Methods
Data Collection: Review of Empirical and Normative Ethics Literature
A review of the empirical (i.e., focused on explaining what is through observation) and normative (i.e., focused on explaining what ought to be through argumentation) ethics literature was conducted to identify literature relevant to the identification of the potential ethical considerations related to the use of brexucabtagene autoleucel.
Literature Search Methods
The search for literature identifying explicit ethical considerations was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist (https://www.cadth.ca/resources/finding-evidence/press).1 The search strategy is available on request.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid, the Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCO, Philosopher’s Index via Ovid, and Scopus. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were CAR-T or mantle cell lymphoma and brexucabtagene autoleucel.
Search filters were applied to limit retrieval to citations related to empirical and normative ethical considerations. Retrieval was not limited by publication date or language limits. The initial search was completed on December 8, 2020.
Literature Screening and Selection
The selection criteria can be found in Table 1.
Eligible reports were those published in English that explicitly identify normative or empirical ethical considerations relating to the use of brexucabtagene autoleucel. Descriptions of experiences of adult patients with relapsed or refractory MCL were also sought as they related to the potential use of brexucabtagene autoleucel. The following types of publications were included: primary or secondary research, normative analysis, opinion, commentary, books, or book chapters.
Criteria | Description |
|---|---|
Population | Adult patients with relapsed or refractory (r/r) mantle cell lymphoma (MCL) |
Interventions | Brexucabtagene autoleucel or standard of care/best supportive care |
Context | Any health system |
Outcomes | Normative literature: provides normative analysis of an ethical consideration Empirical literature: provides empirical research directly addressing an ethical consideration |
Publication types | Primary or secondary research, normative analysis, opinion, commentary, book, or book chapter |
The selection of relevant literature proceeded in 2 stages. In the first stage, the title and abstracts of citations were screened for relevance by a single reviewer. Articles were categorized as “retrieve” or “do not retrieve,” according to the selection criteria outlined in Table 1, and the following criteria:
Explicitly provides normative analysis (i.e., focused on explaining what ought to be through argumentation) of an ethical consideration arising in the use of brexucabtagene autoleucel or CAR T-cell therapies more broadly, or from experiences of living with or being treated for relapsed or refractory MCL relevant to the indicated population.
Presents empirical research (i.e., focused on explaining what is through observation) directly addressing an ethical consideration arising in the use of brexucabtagene autoleucel or CAR T-cell therapies more broadly, or from experiences of living with or being treated for relapsed or refractory MCL relevant to the indicated population.
Explicitly identifies, but does not investigate empirically, an ethical consideration arising from the use of brexucabtagene autoleucel or CAR T-cell therapies more broadly, or from experiences of living with or being treated for relapsed or refractory MCL relevant to the indicated population.
In the second stage, the full-text reports were reviewed by the same reviewer. Reports meeting the above criteria were included in the review, and reports that did not meet these criteria were excluded. Members of the CADTH review team were consulted to resolve uncertainties related to eligibility of full-text reports.
Data Extraction
One reviewer extracted basic details on publication characteristics using a data extraction form. The following publication details were recorded: first author, article title, publication objectives, characteristics of study design and methodology, date of publication, country with which the first author is affiliated, and key findings identified related to ethical considerations.
Data Summary
One reviewer conducted 2 cycles of coding. In the initial coding phase, the publications were reviewed for ethical content. The Core Model 3.0 (Ethical Analysis Domain)2 questions deemed by EUnetHTA as “critically important” were used as a guide to identify and categorize ethical considerations related to the use of brexucabtagene autoleucel. The Core Model was chosen because it is a wide-ranging framework; the assessment questions in the domain are intended especially for identifying ethically relevant issues and conflicts.2 This guiding framework highlights the context of a technology and focuses on the following topics: benefit-harm balance, autonomy, respect for persons, justice and equity, legislation, and ethical consequences of the health technology assessment.
Once identified, passages related to ethical content were coded using methods of qualitative description.3 Initial descriptive coding of the reports focused broadly on categories concerning what ethical considerations were described. Major themes and sub-codes were identified through repeated readings of the data.3 Once sub-codes emerged, they were deductively applied to all reports in the set and ethical content was summarized into the thematic categories. This review focused on ethical considerations relating specifically to the use of brexucabtagene autoleucel. Other ethical considerations raised in the literature but not related to the use of brexucabtagene autoleucel were outside of the scope of the current review and are not included in the summary.
Results
Description of Included Publications
A total of 865 citations were identified in the literature search. Following screening of titles and abstracts, 846 citations were excluded and 18 potentially relevant reports from the electronic search were retrieved for full-text review. Of these potentially relevant reports, 9 publications were excluded for various reasons (e.g., they did not explicitly describe ethical considerations related to the use of brexucabtagene autoleucel or treatment of MCL [N = 9]4-11; or they were not in English [N = 1]12). 9 publications met the inclusion criteria and were included in this report. Figure 1 presents the PRISMA flow diagram of the study selection process.
Details regarding the characteristics of the included publications are reported in Table 2. None of the included reports was directly on the topic of brexucabtagene autoleucel for the treatment of adult patients with relapsed or refractory MCL. Five reports examined disparities in MCL incidence and outcomes,13-17 2 reports examined questions of cost and value of novel therapies for MCL,18,19 1 report examined the balancing of risks and benefits of novel CAR T-cell therapies given some limitations of the evidence base and the vulnerability of patient populations,20 and 1 report explored whether it is ethically appropriate for the family and physician of a patient who lacks decision-making capacity to choose a treatment for malignant lymphoma despite the refusals of the incapacitated patient when there is significant uncertainty regarding outcomes.21
Key Ethics Considerations from the Literature
Disparities in MCL Incidence and Outcomes
Multiple studies have found age, gender, and racial disparities in MCL incidence and outcomes.13-17 For example, 1 study found that over the period of 1992 to 2009, MCL incidence increased at a faster rate in males (199.04% increase) than in females (53.19%), and that incidence rates increased 153.08% in Whites compared to 30.59% in Blacks, 85.92% in Hispanics, and 96.39% in Asians/Pacific Islanders.13 As another example, 1 study found that racial disparities in non-Hodgkin lymphoma survival exist but rapidly decrease from diagnosis for highly curable subtypes of non-Hodgkin lymphomas (i.e., Burkitt's lymphoma and diffuse large B-cell lymphoma), which the study authors suggest supports the hypothesis that such disparities are largely mediated by access to effective upfront therapy.15 However, among patients with MCL, these authors found that Black patients showed an unexpected advantage in terms of net survival that was not evident at diagnosis but increased over time.15 Some report the causes of these disparities to not be fully understood,13,17 though some suggest that gender-based disparities may be partly the result of different occupational hazards,14 and that racial disparities are often ascribed to inequities in access to health care resources and socioeconomic status.15 One study concluded that as a result of these findings, age, in addition to race, ethnicity and gender, needs to be carefully considered by groups developing treatments for MCL.13
Additionally, 1 study found that Hispanic ethnicity, private insurance, and treatment at an academic centre were associated with better overall survival; whereas, Black race was associated inferior overall survival despite more frequent treatment at academic cancer centres.16 The study noted that racial and ethnic disparities in overall survival could be explained independent of insurance and socioeconomic status, and suggested that these treatment pattern data could be used to elucidate new targets for improving access to care and health outcomes for rare cancers.16
Finally, 1 study suggested that because age is an important factor affecting treatment regimen selection and that intensive treatment regimens are most commonly recommended for healthier and younger patients due to better tolerance, their findings that MCL incidence in the elderly has been increasing suggests that drug development for MCL should focus more on the elderly population.14
Cost and Value of Novel Therapies for MCL
Some authors noted the high costs that are often associated with novel CAR T-cell therapies and the related hesitancy that might exist to invest in those therapies.18,19
Balancing Risks and Benefits
One review highlighted the unique vulnerability of patients eligible for CAR T-cell therapy who may have few therapeutic options and who may be willing to pursue high-risk treatments if benefits are overstated or harms understated.20 The authors noted that there is no expert consensus concerning what constitutes an ethically justifiable or appropriate balance of risks and benefits when using axicabtagene ciloleucel, another CAR T-cell therapy, for the treatment of relapsed or refractory large B-cell lymphoma. The study review emphasized that in this context it is important to recognize that patients are capable of making autonomous, rational decisions to pursue high-risk therapies.
Decision-Making Capacity
One study explored, through a hypothetical case, whether it is ethically appropriate for the family and physician of a patient who lacks decision-making capacity to choose a treatment for malignant lymphoma despite the refusals of the incapacitated patient when there is significant uncertainty regarding outcomes.21 Citing considerations of respect for patient dignity and the protection of human rights, the authors argue that in the absence of an advance directive, it would not be ethically permissible to override the (incapable) treatment refusals of a patient who lacks decision-making capacity due to diseases like dementia, as doing so would fail to appreciate that such a refusal is rooted in the patient’s feelings, which should be respected, and that dementia is a condition that will continue to worsen even if the malignant lymphoma improves. The authors argue that in such situations, overriding patient treatment refusal should be regarded as an exception, rather than a standard course of action, especially in the case where refusal is explicit, consistent, and stable.
Limitations
This review is limited by the lack of published literature examining ethical considerations relevant to the use of brexucabtagene autoleucel for the treatment of adult patients with relapsed or refractory MCL. No published ethical analyses were retrieved on the topics of brexucabtagene autoleucel or relapsed or refractory MCL.
The absence of published ethical analyses does not indicate that ethical considerations are not present, as many of the ethical issues associated with the treatment of MCL, including the potential for disparities, are likely of relevance to brexucabtagene autoleucel as well.
Finally, this review is limited to ethical considerations explicitly discussed in the published literature. Some of the results and insights raised relating to clinical benefits and costs might be discussed more comprehensively in the clinical and pharmacoeconomic review sections.
References
1.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. Journal of clinical epidemiology. 2016;75:40-46. PubMed
2.EUnetHTA Joint Action 2 Work Package 8, HTA Core Model ® version 3.0 www.htacoremodel.info/BrowseModel.aspx. Published 2016. Accessed 2020 Aug 20.
3.Sandelowski M. Whatever happened to qualitative description? Research in nursing & health. 2000;23(4):334-340. PubMed
4.Ansell P, Simpson J, Lightfoot T, et al. Non-Hodgkin lymphoma and autoimmunity: does gender matter? Int J Cancer. 2011;129(2):460-466. PubMed
5.Atilla E, Kilic P, Gurman G. Cellular therapies: Day by day, all the way. Transfus Apheresis Sci. 2018;57(2):187-196. PubMed
6.Daniels N, Sabin JE. Last chance therapies and managed care: pluralism, fair procedures, and legitimacy. Hastings Center Report. 1998;28(2):27-41. PubMed
7.Horrobin DF. Are large clinical trials in rapidly lethal diseases usually unethical? Lancet. 2003;361(9358):695-697. PubMed
8.Kick L, Kirchner M, Schneider S. CRISPR-Cas9: From a bacterial immune system to genome-edited human cells in clinical trials. Bioengineered. 2017;8(3):280-286. PubMed
9.Rial-Sebbag E, Chabannon C. [Chapter 6. Legal issues and for the health system of the development of a new class of innovative therapy in oncoimmunology: the “Car-T CellS”]. Journal International de Bioethique et Dethique des Sciences. 2018;29(2):113-128.
10.CADTH. Tisagenlecleucel for B-Cell Acute Lymphoblastic Leukemia and Diffuse Large B-Cell Lymphoma — Project Protocol, Implementation and Ethics Section. In: (CADTH optimal use report; vol.8, no.3b). Ottawa: CADTH; 2018: https://cadth.ca/sites/default/files/pdf/OP0538_Tisagenlecleucel_for_B-Cell_Protocol.pdf. Accessed 2021 Apr 21.
11.CADTH. Axicabtagene Ciloleucel for Large B-cell Lymphoma: Implementation and Ethics Project Protocol. In: (CADTH optimal use report; vol.9, no.1b). Ottawa: CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/ct0002-axi-cel-for-dlbcl-implementation-and-ethics-protocol.pdf. Accessed 2021 Apr 21.
12.Viardot A. [Perspectives on CAR T-cell treatment]. Pathologe. 2020;28:28.
13.Aschebrook-Kilfoy B, Caces DB, Ollberding NJ, Smith SM, Chiu BC. An upward trend in the age-specific incidence patterns for mantle cell lymphoma in the USA. Leuk Lymphoma. 2013;54(8):1677-1683. PubMed
14.Fu S, Wang M, Lairson DR, Li R, Zhao B, Du XL. Trends and variations in mantle cell lymphoma incidence from 1995 to 2013: A comparative study between Texas and National SEER areas. Oncotarget. 2017;8(68):112516-112529. PubMed
15.Migdady Y, Salhab M, Dang NH, Markham MJ, Olszewski AJ. Disparities in conditional net survival among non-Hodgkin lymphoma survivors: a population-based analysis. Leuk Lymphoma. 2016;57(3):676-684. PubMed
16.Shah NN, Xi Y, Liu Y, et al. Racial and Socioeconomic Disparities in Mantle Cell Lymphoma. Clin Lymphoma Myeloma Leuk. 2019;19(6):e312-e320. PubMed
17.Wang Y, Ma S. Racial differences in mantle cell lymphoma in the United States. BMC Cancer. 2014;14(1):764-764. PubMed
18.Pepper MS, Alessandrini M, Pope A, Van Staden W, Green RJ. Cell and gene therapies at the forefront of innovative medical care: Implications for South Africa. Samj, S. 2018;109(1):20-22.
19.Silbert S, Yanik GA, Shuman AG. How Should We Determine the Value of CAR T-Cell Therapy? AMA J Ethics. 2019;21(10):E844-851. PubMed
20.CADTH. Axicabtagene Ciloleucel for Large B-Cell Lymphoma: Ethics and Implementation Report. In: (CADTH Optimal Use Report; vol. 9, no.1e). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/car-t/ct0002-ipe-report.pdf. Accessed 2021 Apr 21.
21.Ishimoto H, Masaki S, Asai A. Should an Incapacitated Patient's Refusal of Treatment Be Respected? Discussion of a Hypothetical Case. Eubios: Journal of Asian and International Bioethics July. 2015;25(4):112-119.
Appendix 1: Selection of Included Studies
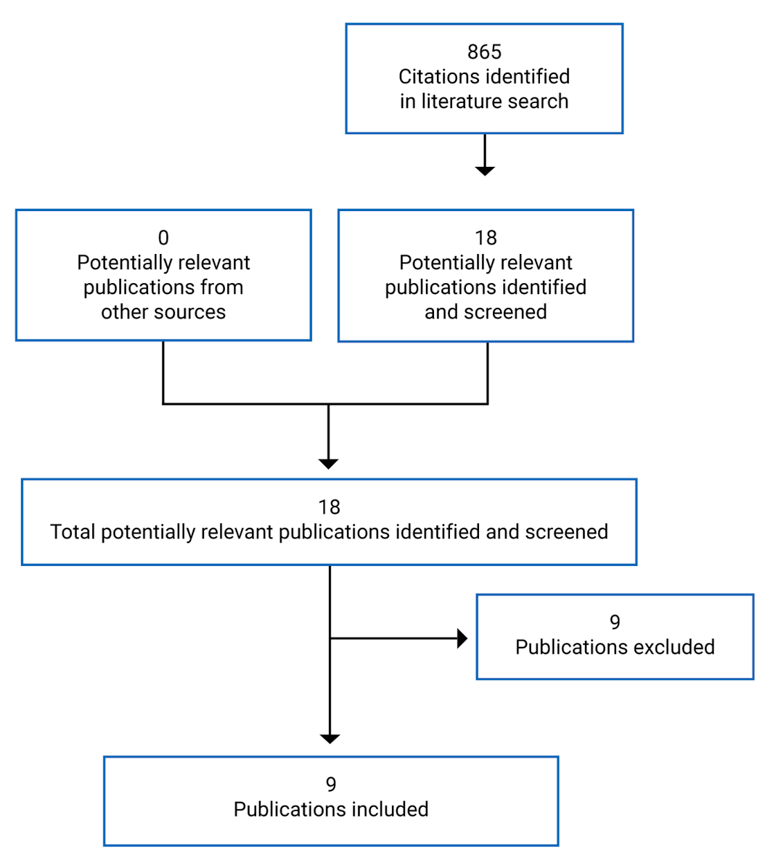
Appendix 2: Details of Included Studies
Note that this appendix was not copy-edited.
Table 2: Details of Included Publications
First author, year | Country | Publication type | Objective | Key ethical considerations | Funding source |
|---|---|---|---|---|---|
Aschebrook-Kilfoy, 201313 | US | Retrospective analysis | To analyze US population-based age-specific data for MCL. | Over the period of 1992-2009, MCL incidence increased at a faster rate in males (199.04% increase) than in females (53.19% increase). Over the period of 1992-2009, MCL incidence rates increased 153.08% in Whites compared to 30.59% in Blacks, 85.92% in Hispanics, and 96.39% in Asians/Pacific Islanders. The causes of these disparities are unknown. Age, in addition to race, ethnicity and gender, needs to be carefully considered by groups developing MCL treatments. | National Cancer Institute, National Institutes of Health |
CADTH, 201920 | Canada | Review and ethical analysis | To identify and analyze ethical issues and considerations for the use of axicabtagene ciloleucel. | Several authors have drawn attention to the “hype” surrounding CAR T-cell therapy, which has been described by 1 author as a form of “experimental therapy” that blurs the line between research and clinical care. A primary ethical consideration for implementing axicabtagene ciloleucel, as with any therapy, is determining how to weigh therapeutic risks and benefits. | Not reported |
CADTH, 201920 | There are several ethical considerations associated with accessing axicabtagene ciloleucel. Three commonly cited access concerns include geographic constraints on access, supply constraints, and patient selection. The high cost of axicabtagene ciloleucel is commonly identified as an ethical challenge for individual patients, clinicians, treatment sites, and health system funders. Evidence gaps about safety and effectiveness underline the importance of informed consent processes, on 1 hand, and the need for clinical aids to assess patient-level risk and suitability for axicabtagene ciloleucel, on the other hand. | ||||
Fu, 201714 | US | Retrospective analysis | To update the temporal trends and variations of MCL incidence in the US National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) areas and compare them with counterpart data in Texas from 1995 to 2013, and to evaluate variations in MCL incidence by age, gender, race, ethnicity and tumour stage. | Age is an important factor affecting treatment regimen selection. Intensive treatment regimens are most commonly recommended for healthier and younger patients due to better tolerance. MCL incidence in the elderly has been increasing. Drug development for MCL should focus more on the elderly population. | None |
Ishimoto, 201521 | Japan | Ethical analysis | To discuss whether or not an incapacitated patient’s refusal of treatment should be respected. | The authors argue that medical interventions should not be imposed upon the patient in the discussed scenario, and that forced treatments should be regarded as exceptions, rather than a standard course of action. | Not reported |
Migdady, 201615 | US | Retrospective analysis | To compare conditional survival in common non-Hodgkin lymphoma subtypes of varying malignant behaviour and to identify factors that retain prognostic effect on long-term disparities in survival. | Racial disparities in survival exist but rapidly decrease from diagnosis for highly curable subtypes of non-Hodgkin lymphomas, which the study authors suggest supports the hypothesis that such disparities are largely mediated by access to effective upfront therapy. However, among patients with MCL, these authors found that Black patients showed an unexpected advantage in terms of net survival that was not evident at diagnosis but increased over time. | Not reported |
Pepper, 201818 | South Africa | Review | To review the implications of introducing cell and gene therapies into the health care sector in South Africa. | The authors ask whether South Africa should refrain from participation and simply be a bystander in the development of rapidly evolving and highly efficacious, albeit costly, new medicines. They argue that the answer is a resounding negative. To refrain from participation in relevant research and innovative medical practice that, in time, may benefit all South Africans, merely because of current resource constraints, is not sensible or reasonable. | South African Medical Research Council |
Shah, 201916 | US | Retrospective analysis | To examine the effect of race and socioeconomic status on patients with MCL. | Hispanic ethnicity, private insurance, and treatment at an academic centre were associated with better overall survival, whereas Black race was associated inferior overall survival despite more frequent treatment at academic cancer centres. Racial and ethnic disparities in overall survival race and ethnicity could be explained independent of insurance and socioeconomic status. These treatment pattern data could be used to elucidate new targets for improving access to care and health outcomes for rare cancers. | National Institutes of Health |
Silbert, 201919 | US | Commentary | To examine whether and how to offer patients CAR T-cell therapy, and specifically to address: value analysis and its application to CAR T-cell therapy; factors that might complicate equitable access to these drugs; and how much patients and families should be told about these therapies’ costs. | Although initial outcome projections show favourable cost-effectiveness, questions remain with respect to whether there is equitable and just access to therapy. | Not reported |
Wang, 201417 | US | Retrospective analysis | To compare non-Hispanic Whites, Hispanic Whites, Blacks, and Asians/Pacific Islanders in multiple aspects of MCL. | Racial differences exist among MCL patients in the US in terms of patients’ characteristics, incidence, and survival. | National Cancer Institute, National Institutes of Health |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Patient to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be patient to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.