CADTH Reimbursement Review
Isatuximab (Sarclisa)
Sponsor: Sanofi Genzyme
Therapeutic area: Multiple myeloma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ASCO
American Society for Clinical Oncology
ASCT
autologous stem cell transplant
CCO
Cancer Care Ontario
CI
confidence interval
CMRG
Canadian Myeloma Research Group
CR
complete response
DOR
duration of response
DRd
daratumumab plus lenalidomide plus dexamethasone
DSU
Decision Support Unit
DVd
daratumumab plus bortezomib plus dexamethasone
ECOG
Eastern Cooperative Oncology Group
EORTC
European Organisation for Research and Treatment of Cancer
EQ-5D-5L
EuroQol 5-Dimensions 5-Levels
FLC
free light chain
HR
hazard ratio
HRQoL
health-related quality of life
IgA
immunoglobulin A
IgG
immunoglobulin G
IMWG
International Myeloma Working Group
IRC
independent review committee
IRT
interaction response technology
IsaKd
isatuximab plus carfilzomib plus dexamethasone
IsaPd
isatuximab plus pomalidomide plus dexamethasone
ISS
International Staging System
ITC
indirect treatment comparison
ITT
intention-to-treat population
IV
intravenous
Kd
carfilzomib plus dexamethasone
KRd
carfilzomib plus lenalidomide plus dexamethasone
MAIC
matching-adjusted indirect comparison
MM
multiple myeloma
MRD
minimal residual disease
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
OH-CCO DAC
Ontario Health Cancer Care Ontario Drug Assessment Committee
ORR
overall response rate
OS
overall survival
PD
progressive disease
PFS
progression-free survival
PR
partial response
QLQ-MY20
Quality of Life Multiple Myeloma Specific Module with 20 items
QLQ-C30
Quality of Life Cancer-Specific Questionnaire with 30 items
RCT
randomized controlled trial
R-ISS
Revised International Staging System
SAE
serious adverse event
sCR
stringent compete response
SCT
stem cell therapy
SD
standard deviation
TTR
time to response
VGPR
very good partial response
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Isatuximab (Sarclisa) 20 mg/mL IV infusion |
Indication | In combination with carfilzomib and dexamethasone for the treatment of adult patients with relapsed or refractory multiple myeloma who have received 1 to 3 prior lines of therapy |
Reimbursement request | In combination with carfilzomib and dexamethasone for the treatment of adult patients with relapsed or refractory multiple myeloma who have received 1 to 3 prior lines of therapy |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | September 3, 2021 |
Sponsor | Sanofi Genzyme, a division of Sanofi-Aventis Canada Inc. |
NOC = Notice of Compliance.
Introduction
Multiple myeloma (MM) is a blood cancer characterized by the uncontrolled growth of plasma cells. The abnormal plasma cells interfere with normal blood cell production and cause the overproduction of an abnormal antibody, the M protein. The abnormal plasma cells and M protein can damage bone marrow and renal tissue. According to the clinical experts consulted by CADTH, MM causes significant morbidity and mortality, including fractures, decreased blood cell counts, renal failure, and infections, among others. MM is a relapsing-remitting cancer, and there is no cure. According to GloboCan, in 2020, there were 3,186 new cases of MM diagnosed in Canada.1 The disease mainly affects older men,2 and the 5-year survival rate is 44%.3
According to the joint guidelines for treatment of MM published by Cancer Care Ontario (CCO) and American Society for Clinical Oncology (ASCO), patients with relapsed MM should be treated as soon as possible with at least 2 novel drugs (proteasome inhibitors, immunomodulators, or monoclonal antibodies), and treatment should continue until disease progression. They recommend that prior therapies be taken into consideration when choosing the first treatment at first relapse, stating that a monoclonal antibody–based regimen in combination with an immunomodulatory drug and/or proteasome inhibitor should be considered.4 According to the clinical experts consulted by CADTH for this review, the current treatment-sequencing algorithm in Canada is often based on the currently funded regimens, which are ultimately incorporated into the local guidelines. The overarching treatment goals are to maximize life expectancy and quality of life. According to the clinical experts consulted by CADTH, in MM, the best primary outcomes for evaluating a given line of treatment are progression-free survival (PFS), and overall survival (OS); health-related quality of life (HRQoL), harms, convenience, resource utilization, and caregiver burden are also relevant.
Isatuximab is administered as an IV infusion, at a dose of 10 mg/kg, in combination with carfilzomib and dexamethasone (IsaKd), for the treatment of patients with MM who have received 1 to 3 prior lines of therapy. Each treatment cycle is 28 days; in cycle 1, isatuximab is administered on days 1, 8, 15, and 22 (weekly), and, in cycle 2 and beyond, it is administered every 2 weeks. Treatment is continued until disease progression or unacceptable toxicity. The sponsor’s reimbursement request is consistent with the Health Canada indication.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of isatuximab 10 mg/kg IV infusion, in combination with carfilzomib and dexamethasone, for the treatment of patients with MM who have received 1 to 3 prior lines of therapy.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from the clinical expert consulted by CADTH for the purpose of this review.
Patient Input
Myeloma Canada submitted the patient input for this review. Myeloma Canada, founded in 2005, is the only national charitable organization created by and for Canadians affected by MM. The organization is driven to improve the lives of those affected by myeloma. Information from this input was gathered through a patient survey. The survey was accessed through email and social media from April 22, 2021, to May 9, 2021. A total of 208 individuals with myeloma responded to the survey.
Most patients surveyed indicated that having access to an effective treatment was very important, as was controlling symptoms such as infections, kidney problems, mobility, neuropathy, and fatigue. Patients described impacts on their abilities to perform day-to-day activities, such as working, travel, and exercise. Patients expect new treatment options to improve their quality of life, have maximum benefits with nondebilitating side effects, reduce their hospital visits, and achieve the longest remission possible in lieu of a cure. The patient group highlighted the importance of receiving information about emerging treatments and having timely access to these treatments. A copy of the patient input from Myeloma Canada is presented in Appendix 1.
Clinician Input
Input From Clinical Experts Consulted by CADTH
According to the clinical experts consulted by CADTH, newer treatments are needed that exhibit better control of MM and less toxicity. In particular, needs are not being met for patients who are refractory to certain drug classes, such as immunomodulators (lenalidomide) or proteasome inhibitors (bortezomib), and outcomes tend to be poor in these patients.
Isatuximab should be combined with other drugs that have unrelated mechanisms/toxicity profiles. Otherwise, it could be used in any line of therapy. For patients with 1 prior line of therapy, an isatuximab regimen could be particularly useful if they had not received a prior anti-CD38 drug. Whether there would be benefit for those previously treated with an CD38 antibody drug is unknown.
There is no established method for determining which patients would most or least benefit from treatment. A clinically significant response would be improved PFS with acceptable toxicity and quality of life. Response should be assessed before each treatment cycle and disease progression; unacceptable toxicity would warrant discontinuation of treatment. A copy of the input is presented in Appendix 2.
Clinician Group Input
Input was submitted by the Canadian Myeloma Research Group (CMRG) and the Ontario Health Cancer Care Ontario Hematology Cancer Drug Advisory Committee (OH-CCO DAC).
There were no notable differences between the input provided by the clinical experts consulted by CADTH on this review and that provided by the clinician groups.
The clinician groups did not specifically comment on their own experiences with IsaKd; however, they did note that they believed IsaKd would be useful in patients with relapse whose MM had progressed while they were receiving lenalidomide and/or bortezomib.
Drug Program Input
The Provincial Advisory Group identified jurisdictional implementation issues related to relevant comparators, considerations for initiation of therapy, considerations for prescribing of therapy, generalizability, considerations for a funding algorithm, care provision issues, and system and economic issues. The clinical experts consulted by CADTH weighed evidence from the IKEMA trial and other clinical considerations to provide responses to the Provincial Advisory Group’s implementation questions (Table 4).
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
The CADTH systematic review included 4 reports of 1 pivotal trial (IKEMA).5-8 No additional studies were identified from the literature. IKEMA is an ongoing, sponsor-funded, multinational (with Canadian sites) open-label randomized controlled trial (RCT) that randomized 302 adults (> 18 years) patients with relapsed and/or refractory MM and 1 to 3 prior lines of therapy, in a 3:2 manner, to either IsaKd or carfilzomib plus dexamethasone (Kd). Patients in the IsaKd group received isatuximab 10 mg/kg by IV infusion in 28-day cycles (weekly for first cycle, then biweekly thereafter) with carfilzomib 20 mg/m2, escalated to 56 mg/m2 IV days 1 to 2, 8 to 9, and 15 to 16, and dexamethasone 20 mg twice weekly, while patients in the Kd group received carfilzomib and dexamethasone at those same dosage regimens. Patients were treated until they experienced disease progression or unacceptable toxicity, or they decided to discontinue study treatment. Randomization was stratified by the number of prior lines of therapy (1 versus > 1) and the Revised International Staging System (R-ISS) score (I or II versus III versus not classified).
The primary outcome of the IKEMA trial was PFS, and the key secondary outcomes included overall response rate (ORR), very good partial response (VGPR) or better rate, duration of response (DOR), time to first response (TTR), minimal residual disease (MRD) negativity in patients with VGPR or better, as well as complete response (CR) rate, and OS. PFS, ORR, VGPR or better, and MRD negativity in patients with VGPR or better were included in the statistical testing hierarchy. HRQoL was assessed as an exploratory outcome. The findings in this report are from an interim analysis, which was planned to take place once 103 progression events had occurred (information fraction of 65%). Results for the final analysis, including OS data, are not expected until 2023. Harms including adverse events (AEs), serious adverse events (SAEs), and AEs of special interest, were also measured and reported.
Patients were an average of 63.1 years of age (standard deviation [SD] 9.9); 56% were men and 70.9% were White. The majority of patients had MM of the immunoglobulin G (IgG) subtype (67.9%) at diagnosis, followed by immunoglobulin A (IgA) (22.8%), and these percentages were similar to those observed at study entry (69.9% and 22.5%, respectively). The most common International Staging System (ISS) stage at study entry was stage I (53.0%), followed by stage II (31.1%) and stage III (15.2%). The majority of patients had relapsed and refractory MM (71.5%), while the remainder had relapsed MM (28.5%). The average number of prior regimens was 3.2 (SD 1.7), and the number of prior lines was 1.8 (SD 0.8). Patients were most commonly refractory to an immunomodulatory imide drug (45.0% of patients), followed by a proteasome inhibitor (33.1%) or both (20.5%).
Efficacy Results
The efficacy results for IKEMA are summarized in Table 2. PFS was the primary outcome of IKEMA, and, at the interim analysis (median follow-up of 20.73 months), median PFS was not reached in the IsaKd group and was 19.15 months (95% confidence interval [CI], 15.77 to not calculable) in the Kd group, for a stratified hazard ratio (HR) of 0.531 (99 CI, 0.318 to 0.889), and a P value for a stratified log-rank test of 0.0007. In the IsaKd group, 26.8% of patients had a PFS event, while, in the Kd group, 44.7% of patients had a PFS event. The results for sensitivity analyses performed for the primary outcome were consistent with the primary analysis, and planned subgroup analyses revealed consistent results across various subgroups of patients of interest for this review.
OS will be assessed at the end of study; therefore, no median OS data were available at the time of the interim analysis.
HRQoL was assessed using the European Organisation for Research and Treatment of Cancer Quality of Life of Cancer Patients questionnaire with 30 items (EORTC QLQ-C30), the EORTC MM module Quality of Life questionnaire with 20 items (QLQ-MY20), and the EuroQol 5-Dimensions 5-Levels (EQ-5D-5L) questionnaire. Interpretation of HRQoL data was limited by the large number of withdrawal from the study over time; however, generally, for the EORTC questionnaires, there was little change from baseline in HRQoL scores in the IsaKd group, and numerical increases from baseline over time were observed in the Kd group. An increase in score on these instruments indicates an improvement in HRQoL.
The ORR was assessed in all responders (patients achieving either a stringent complete response [sCR], CR, VGPR or partial response [PR]) and in patients achieving a VGPR or better. An sCR is defined as patients having a CR who also have normalized free light chain (FLC) ratio in the absence of bone marrow plasma cells when assessed by immunohistochemistry or immunofluorescence. The percentage of patients responding was 86.6% in the IsaKd group and 82.9% in the Kd group, and the between-group difference was not statistically significant (P = 0.1930). As this was the second outcome in the statistical hierarchy, testing was to have halted for subsequent outcomes, although the sponsor continued to conduct testing and report P values for descriptive purposes. The percentage of patients achieving a VGPR or better was 72.6% in the IsaKd group and 56.1% in the Kd group. No patients achieved an sCR, while 39.7% of patients in the IsaKd group and 27.6% of patients in the Kd group achieved a CR, and 33.0% and 28.5% of patients, respectively, achieved a VGPR. MRD negativity was achieved by 29.6% of patients in the IsaKd group and 13.0% of patients in the Kd group.
The median DOR was calculated based on 155 patients in the IsaKd group and 102 patients in the Kd group. The median DOR was not yet reached in either treatment group, and the HR was 0.425 (95% CI, 0.269 to 0.672). The median TTR was 1.08 months (95% CI, 1.05 to 1.12) in the IsaKd group and 1.12 months (95% CI, 1.05 to 1.18) in the Kd group, for a stratified HR of 1.143 (95% CI, 0.888 to 1.471).
Harms Results
A summary of the harms reported in the IKEMA trial is available in Table 2. There were 97.2% of patients in the IsaKd group and 95.9% of patients in the Kd group who had at least 1 AE, and 76.8% versus 67.2%, respectively, who had a grade 3 or greater AE, and 3.4% versus 3.3% who had a grade 5 AE. The most common AE in the IsaKd group was an infusion-related reaction, which occurred in 44.6% of patients in the IsaKd group and 3.3% of patients in the Kd group. Other common AEs (IsaKd versus Kd) included hypertension (36.7% versus 31.1%), diarrhea (36.2% versus 28.7%), upper respiratory tract infection (36.2% versus 23.8%), fatigue (28.2% versus 18.9%), and dyspnea (27.7% versus 21.3%). The most common grade 3 or greater AEs (IsaKd versus Kd) were hypertension (20.3% versus 19.7%) and pneumonia (16.4% versus 12.3%).
SAEs occurred in 59.3% of patients in the IsaKd group and 57.4% of patients in the Kd group. The most common SAE was pneumonia (IsaKd versus Kd, 18.1% versus 11.5%).
There were 8.5% of patients in the IsaKd group and 13.9% of patients in the Kd group who had an AE leading to definitive treatment discontinuation. One patient discontinued treatment of isatuximab due to an AE.
Among notable harms, respiratory tract infections occurred in 83.1% of patients in the IsaKd group and 73.8% of patients in the Kd group, and these were grade 3 or greater events in 32.2% versus 23.8% of patients, respectively. Cardiac disorders occurred in 7.3% of patients treated with IsaKd versus 5.7% of patients treated with Kd. Second primary malignancies (solid, non-skin) occurred in 2.8% versus 3.3% of patients in the IsaKd and Kd groups, respectively, and second primary malignancies (solid, skin) in 5.1% versus 2.5% of patients, respectively. There were no hematologic malignancies reported. Events of decreased neutrophil counts occurred in 54.8% of patients in the IsaKd group versus 43.4% of patients in the Kd group, and grade 3 or greater events occurred in 19.2% versus 7.4% of patients, respectively. Events of decreased platelet counts occurred in 94.4% of patients treated with IsaKd and 87.7% of patients treated with Kd, and these were grade 3 or greater events in 29.9% versus 23.8% of patients, respectively.
Table 2: Summary of Key Results From the IKEMA Trial
Outcome | IsaKd N = 179 | Kd N = 123 |
|---|---|---|
PFS | ||
Number (%) of events | 48 (26.8) | 55 (44.7) |
Number (%) of patients censored | 131 (73.2) | 68 (55.3) |
Kaplan–Meier estimates of PFS in months, median (95% CI) | Not reached | 19.15 (15.770 to NC) |
Stratifieda log-rank test P valueb | 0.0007 | |
Stratifieda HR (99% CI) | 0.531 (0.318 to 0.889) | |
Objective response | ||
Overall response | ||
Responders (sCR, CR, VGPR, or PR) | 155 (86.6) | 102 (82.9) |
95% CI estimated using Clopper-Pearson method | 0.8071 to 0.9122 | 0.7509 to 0.8911 |
Stratified CMH test P valuec vs. Kd | 0.1930 | |
VGPR or better | 130 (72.6) | 69 (56.1) |
95% CI estimated using Clopper-Pearson method | 0.6547 to 0.7901 | 0.4687 to 0.6503 |
Stratified CMH test P valuec,d vs. Kd | 0.0011 | |
Best overall response, n (%) | ||
sCR | 0 (0.0) | 0 (0.0) |
CR | 71 (39.7) | 34 (27.6) |
VGPR | 59 (33.0) | 35 (28.5) |
Biochemical CR but with missing bone marrow | 6 (3.4) | 7 (5.7) |
Near-CRe | 36 (20.1) | 13 (10.6) |
PR | 25 (14.0) | 33 (26.8) |
Minimal response | 4 (2.2) | 5 (4.1) |
Stable disease | 13 (7.3) | 6 (4.9) |
Non-PD | 1 (0.6) | 1 (0.8) |
PD | 2 (1.1) | 3 (2.4) |
Unconfirmed PD | 0 | 1 (0.8) |
Not evaluable/Not assessed | 4 (2.2) | 5 (4.1) |
Depth of response | ||
MRD negativity rate, n (%) | 53 (29.6) | 16 (13.0) |
95% CI by Clopper-Pearson | 0.2303 to 0.3688 | 0.0762 to 0.2026 |
Duration of response | N = 155 | N = 102 |
Number (%) of events | 33 (21.3) | 43 (42.2) |
Number (%) of patients censored | 122 (78.7) | 59 (57.8) |
Kaplan–Meier estimates of DOR in months, median (95% CI) | NC (NC to NC) | NC (14.752 to NC) |
Stratifieda HR (95% CI) | 0.425 (0.269 to 0.672) | |
Time to first response | ||
Number (%) of events | 155 (86.6) | 102 (82.9) |
Number (%) of patients censored | 24 (13.4) | 21 (17.1) |
Kaplan–Meier estimates of TTR in months, median (95% CI) | 1.08 (1.051 to 1.117) | 1.12 (1.051 to 1.183) |
Stratifieda HR (95% CI) vs. Kd | 1.143 (0.888 to 1.471) | |
Health resource utilization | ||
Not reported | Not reported | Not reported |
Harms | ||
Patients with at least one AE, n (%) | 172 (97.2) | 117 (95.9) |
Patients with at least one SAE, n (%) | 105 (59.3) | 70 (57.4) |
Patients with any TEAE leading to definitive treatment discontinuation, n (%) | 15 (8.5) | 17 (13.9) |
AE = adverse event; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; CR = complete response; DOR = duration of response; HR = hazard ratio; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; MRD = minimal residual disease; NC = not calculable; PD = progressive disease; PFS = progression-free survival; PR = partial response; SAE = serious adverse event; sCR = stringent complete response; TEAE = treatment-emergent adverse event; TTR = time to response; VGPR = very good partial response.
aStratified on number of prior lines of therapy (1 vs. > 1) and Revised International Staging System (R-ISS) stage (I or II vs. III vs. not classified) according to interactive response technology (IRT).
bOne-sided significance level is 0.005.
cStratified on randomization factors according to IRT. One-sided significance level is 0.025. Biochemical CR and Near-CR were assessed only for patients with confirmed VGPR as best overall response. Criteria for confirmation were not applied to Near-CR subcategory.
dThe statistical testing upon which these P values were based was conducted after failure of the hierarchy and therefore should not be used for drawing conclusions.
eAll criteria for a CR were met except that immunofixation remained positive.
Source: Clinical Study Report for IKEMA.7
Critical Appraisal
IKEMA was an open-label trial, and lack of blinding may have biased results, particularly for patient-reported outcomes such as HRQoL and for reporting of harms. Assessment of pathology was conducted by a blinded independent review committee (IRC) and therefore is unlikely to have been influenced by lack of blinding.
The results of the IKEMA trial were based on a planned interim analysis, with an information fraction of 65%; therefore, there is a risk of overestimation of the primary effect for PFS. However, given the statistically and clinically significant difference observed between the groups for PFS, the potential for overestimation is unlikely to have altered the conclusions.
Multiplicity was controlled for with the use of a hierarchical testing procedure; however, early failure of the hierarchy meant that statistical testing was conducted only on the primary and first secondary outcomes. This meant that there were several outcomes for which no inferences could be drawn about differences between groups. HRQoL was not included in the hierarchy, and differences between groups were not tested statistically; therefore, no conclusions could be drawn about this outcome.
The clinical experts consulted by CADTH noted that the patients included in the IKEMA trial were approximately 10 years younger and had a better Eastern Cooperative Oncology Group (ECOG) performance status than patients they would see diagnosed with MM, although this is a common occurrence in clinical trials, which tend to recruit younger, healthier patients. Otherwise, the baseline characteristics and the treatment regimens used in the trial were consistent with what 1 would expect to see in Canadian clinical practice.
Indirect Comparisons
Description of Studies
The sponsor conducted several indirect treatment comparisons (ITCs) that included fixed-effects network meta-analyses (NMAs) and matching-adjusted indirect comparisons (MAICs). A systematic review and feasibility assessment were done to identify studies to include in the ITCs. On that basis, it was determined that it was feasible to conduct an NMA including 8 studies (||||||||||) in a connected network that included IsaKd, and 4 separate MAICs based on individual-level data from the IKEMA trial and summary data from 2 studies. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Efficacy Results
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Harms Results
||||||||||||||||||||||||||||||||||||||||||||||||||||
Critical Appraisal
The trial populations included in the NMAs were relatively homogenous in age, ECOG performance status, race, and gender; however, there were some concerns from clinical experts regarding heterogeneity in the prior treatments received. Specifically, prior lenalidomide use is likely a large effect modifier that differs between trials and greatly increases the uncertainty in these findings. In addition, studies included in the network were conducted over a wide span of time, during which the treatment approach for MM has rapidly evolved. Thus, the time span of these trials may further introduce bias to the comparisons in the NMA. Sparsity of the network meant that only a fixed-effects model could be estimated, which limits the ability to detect and/or account for heterogeneity. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the MAICs, the assumption that all prognostic factors and effect modifiers were adequately adjusted for is unlikely to be the case. In general, the baseline characteristics differed across studies. Specifically, the variation in the prior treatments received may be a serious effect modifier, reflecting differences in care over the wide span of time during which the trials were conducted. Previous lenalidomide use was specifically noted as a likely effect modifier by 1 of the clinical experts, and prior treatment in general is an effect modifier. The choice of the matching factors was based on internal expert opinion (rather than a survey of clinical experts) and availability/completeness of data in the trials (which is inconsistent with the National Institute for Health and Care Excellence [NICE] Decision Support Unit [DSU] guidelines, which recommend the identification of key factors in the data). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||| The reported effective sample sizes, and the skewness or outliers apparent in the visualizations of the weight distributions, suggest that the results may be heavily influenced by a small subset of patients from the IKEMA trial. Generalizability may be an issue due to the small sample size remaining after the exclusions and matching — the remaining patients and weighted sample are unlikely to be representative of the entire patient population.
Conclusions
One multinational sponsor-funded open-label RCT, IKEMA, was included in the CADTH review. In a population of patients with relapsed and/or refractory MM with 1 to 3 prior lines of therapy, IsaKd exhibited a statistically significant and clinically meaningful improvement in PFS compared to Kd, which was the primary outcome of the trial. IKEMA is an ongoing study, and the analysis of OS is not yet available. IsaKd did not improve ORR, and no conclusions could be drawn regarding other outcomes such as MRD due to early failure of the statistical hierarchy. HRQoL data were collected; however, without a formal assessment of this outcome, no conclusions could be drawn from these data. Notable harms that may occur more frequently with IsaKd than with Kd include infusion reactions and pneumonia, although IKEMA was not powered to assess safety. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Introduction
Disease Background
MM is a blood cancer characterized by the uncontrolled growth of plasma cells. The abnormal plasma cells interfere with normal blood cell production and cause the overproduction of an abnormal antibody, the M protein. The abnormal plasma cells and M protein can damage bone marrow and renal tissue. According to the clinical experts consulted by CADTH, MM causes significant morbidity and mortality, including fractures, decreased blood cell counts, renal failure, and infections, among others. MM is a relapsing-remitting cancer, and there is no cure. According to GloboCan, in 2020, there were 3,186 new cases of MM diagnosed in Canada.1 This accounts for approximately 16.5% of all hematologic malignancies.9 The disease mainly affects older adults, with the majority of patients being diagnosed between the ages of 70 and 80, and there is a higher incidence in men.2 The 5-year survival rate is 44%.3 The diagnosis of symptomatic MM is made on the basis of the International Myeloma Working Group (IMWG) recommendations: documented clonal bone marrow cells greater than 10% and any 1 of the following: hypercalcemia, renal insufficiency, anemia, bone lesions, clonal bone marrow plasma cells 60% or more, serum involved/uninvolved FLC ratio 100 or more, or more than 1 focal lesion on MRI studies. With respect to prognosis, patients can be stratified into groups based on clinical and laboratory parameters.10 The IMWG defines high-risk cytogenetic features to include 1 or more of the following: fluorescence in situ hybridization–detected t(4;14), t(14;16), t(14;20), del(17p), or gain (1q); nonhyperdiploid karyotype, high-risk gene expression profile signature, and del(13) detected by conventional cytogenetics. In addition to cytogenetic risk factors, there are 2 other clinical features associated with aggressive disease: elevated lactate dehydrogenase and evidence of circulating plasma cells on routine peripheral smear examination (plasma cell leukemia).11 The R-ISS is a unified prognostic index that combines elements of tumour burden (i.e., ISS) and disease biology (presence of high-risk cytogenetic abnormalities or elevated lactate dehydrogenase).11
Standards of Therapy
According to the joint guidelines for treatment of MM published by CCO and ASCO, patients with relapsed MM should be treated as soon as possible with triple therapy, defined as a regimen with 2 novel drugs (proteasome inhibitors, immunomodulators, or monoclonal antibodies), and treatment should continue until disease progression.12 They recommend that prior therapies be taken into consideration when choosing the first treatment at first relapse, stating that a monoclonal antibody–based regimen in combination with an immunomodulatory drug and/or proteasome inhibitor should be considered. If an autologous stem cell transplant (ASCT) was not received after primary induction therapy, it should be offered to transplant-eligible patients. Repeat stem cell transplant (SCT) may be considered in relapsed MM if the PFS after first transplant is 18 months or more. In patients with genetic high-risk disease, a combination of a proteasome inhibitor, an immunomodulatory drug, and a steroid should be used initially, followed by 1 or 2 ASCTs, followed by proteasome inhibitor–based maintenance until progression.
According to the clinical experts consulted by CADTH, the current treatment-sequencing algorithm in Canada is often based on the currently funded regimens in provincial/territorial jurisdictions, which are ultimately incorporated into the local guidelines. The overarching treatment goals are to maximize life expectancy and quality of life. According to the clinical experts consulted by CADTH, in MM, the best primary outcome for evaluating a given line of treatment is likely PFS. OS, HRQoL, harms, convenience, resource utilization, and caregiver burden are also relevant.
Drug
Isatuximab is administered as an IV infusion, at a dose of 10 mg/kg, in combination with carfilzomib and dexamethasone, and has a Health Canada indication for the treatment of adult patients with relapsed or refractory MM who have received 1 to 3 prior lines of therapy. Each treatment cycle is 28 days; in cycle 1, isatuximab is administered on days 1, 8, 15, and 22 (weekly), and, in cycle 2 and beyond, it is administered every 2 weeks. Treatment is continued until disease progression or unacceptable toxicity. The sponsor’s reimbursement request is consistent with the Health Canada indication. IsaKd was submitted to CADTH before a NOC had been issued and was approved by Health Canada on September 13, 2021. Isatuximab is also indicated, in combination with pomalidomide and dexamethasone (IsaPd), for the treatment of patients with relapsed and refractory MM who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor. IsaPd was reviewed by CADTH for this indication and received a final CADTH pan-Canadian Oncology Drug Review Expert Committee recommendation for reimbursement on April 1, 2021.
Isatuximab is a monoclonal antibody that binds to a specific extracellular epitope of CD38, triggering mechanisms that result in the death of CD38-expressing tumour cells.13 CD38 is transmembrane glycoprotein with ectoenzymatic activity that is expressed in hematologic malignancies as well as other cell types and tissues. Isatuximab acts through IgG Fc-dependent mechanisms, including antibody-dependent cell-mediated cytotoxicity, antibody-dependent cellular phagocytosis, and complement-dependent cytotoxicity, and may also trigger death of tumour cells by inducing apoptosis through an Fc-independent mechanism.13 For further information on isatuximab and comparators, refer to Table 3.
Table 3: Key Characteristics of Isatuximab, Proteasome Inhibitors, Immunomodulatory Imide Drugs, and Daratumumab
Study details | Isatuximab | Proteasome inhibitors | Immunomodulatory imide drugs | Daratumumab |
|---|---|---|---|---|
Mechanism of action | Binds to a specific extracellular epitope of CD38, triggering mechanisms that result in the death of CD38-expressing tumour cells | Proteasome inhibition leads to accumulation of misfolded protein in ER, resulting in apoptosis; inhibits cell proliferation | Immunomodulatory and antineoplastic activity; inhibits proliferation and induces apoptosis of hematopoietic tumour cells | mAb targeting CD38 is overexpressed on tumour cells in hematologic malignancies; induces cell lysis via a variety of mechanisms, including ADCC, CDC, and ADCP |
Indicationa | In combination with carfilzomib and dexamethasone (IsaKd), for the treatment of patients with MM who have received at least one prior therapy In combination with pomalidomide and dexamethasone (IsaPd), for the treatment of patients with relapsed and refractory MM who have received at least 2 prior therapies, including lenalidomide and a PI | Carfilzomib: In combination with dexamethasone and daratumumab, or lenalidomide and dexamethasone (KRd), or dexamethasone alone (Kd), for patients relapsed MM who have received 1 to 3 prior lines of therapy Bortezomib: Part of combination therapy for previously untreated MM who are unsuitable for SCT Part of combination therapy for induction treatment of patients with previously untreated MM who are suitable for SCT Treatment of progressive MM in patients who have received at least one prior therapy and who have already undergone or are unsuitable for SCT | Lenalidomide: In combination with dexamethasone, for the treatment of MM patients who are not eligible for SCT Pomalidomide: In combination with dexamethasone and bortezomib for patients with MM who have received at least 1 prior treatment regimen that included lenalidomide In combination with dexamethasone for patients with MM for whom both bortezomib and lenalidomide have failed and who have received at least 2 prior regimens and demonstrated disease progression on the last regimen | In combination with lenalidomide and dexamethasone, or bortezomib, melphalan, and prednisone for newly diagnosed MM who are ineligible for ASCT In combination with lenalidomide and dexamethasone, or bortezomib and dexamethasone, for patients with MM who have received at least 1 prior therapy For treatment of patients with MM who have received at least 3 prior lines of therapy, including a PI and an immunomodulatory imide drug (IMiD) or who are refractory to both |
(continued) | Part of combination therapy for the treatment of patients with previously untreated mantle cell lymphoma who are unsuitable for SCT Treatment of patients with mantle cell lymphoma who have relapsed or were refractory to at least 1 prior therapy | |||
Route of administration | IV infusion | IV infusion | Oral | IV infusion |
Recommended dosage | 10 mg/kg weekly (days 1, 8, 15 and 22 of the 28-day cycle) for cycle 1 and every 2 weeks (days 1 and 15) for cycle 2 and beyond Treatment is repeated until disease progression or unacceptable toxicity | Carfilzomib: KRd twice weekly: 20 mg/m2 to start, then increase to 27 mg/m2 (10-minute infusion) Kd or DKd twice weekly: 20 mg/m2 to start, then increase to 56 mg/m2 (30-minute infusion) Kd once weekly: 20 mg/m2 to start, then increase to 70 mg/m2 (30-minute infusion) Treatment continued until disease progression or unacceptable toxicity Bortezomib: For MM, patients suitable for SCT In combination with other products used for MM, 1.3 mg/m2 IV twice weekly on days 1, 4, 8, and 11, followed by 20 day rest period | Pomalidomide: VPd: 4 mg once daily, days 1 to 14 of each 21-day cycle Lenalidomide: Rd: 25 mg/day, days 1 to 21 of 28-day cycle Treatment repeated until disease progression | DRd (4-week cycle): 16 mg/kg IV weekly, weeks 1 to 8; every 2 weeks, weeks 9 to 24; and every 4 weeks thereafter With bortezomib, melphalan, prednisone (6-week cycle): 16 mg/kg IV weekly, weeks 1 to 6; every 3 weeks, weeks 7 to 54; and every 4 weeks thereafter DVd (3-week cycle): 16 mg/kg IV weekly, weeks 1 to 9; every 3 weeks, weeks 10 to 24; every 4 weeks thereafter Treatment continued until disease progression |
(continued) | For patients not suitable for SCT In combination with melphalan and oral prednisone for 9 6-week cycles. Cycles 1 to 4: bortezomib twice weekly (days 1, 4, 8, 11, 22, 25, 29, 32); cycles 5 to 9: bortezomib once weekly (days 1, 8, 22 and 29) For relapsed MM: 1.3 mg/m2 twice weekly for 2 weeks followed by a 10-day rest period | |||
Serious adverse effects or safety issues | Neutropenia Infusion reactions Second primary malignancies | Carfilzomib: Infusion reactions TLS Infections Cardiac disorders Venous thrombosis Hypertension Hemorrhage Thrombocytopenia Hepatoxicity Hepatitis B reactivation Posterior reversible encephalopathy syndrome PML Acute renal failure Pulmonary toxicity | Both: Neutropenia Thrombocytopenia Infections DVT and PE Hepatoxicity Anaphylaxis Hepatitis B reactivation Severe rash (SJS, TEN, DRESS) TLS Teratogenic | Infusion reactions Neutropenia/ thrombocytopenia Infections Hepatitis B reactivation |
(continued) | Bortezomib: TLS Hemorrhage Hepatoxicity Posterior reversible encephalopathy syndrome PML Hypotension CHF Pericarditis QT prolongation Motor neuropathy Pulmonary toxicity Neutropenia | |||
Other | Pre-medication with dexamethasone, acetaminophen, H2 antagonist or proton pump inhibitor, and diphenhydramine is recommended to reduce risk and severity of infusion-related reactions | Pre-medication for carfilzomib recommended with dexamethasone (at least 30 minutes prior), to reduce incidence and severity of infusion reactions Antiviral prophylaxis should be considered before initiating bortezomib to prevent reactivation of herpes zoster | Antithrombotic prophylaxis recommended Only available under a controlled distribution program | Pre-medication with dexamethasone, antipyretics, and antihistamines is recommended; post-infusion (to prevent delayed infusion reactions), oral corticosteroid; antiviral prophylaxis should also be considered to prevent reactivation of herpes zoster |
ADCC = antibody-dependent cell-mediated toxicity; ADCP = antibody-dependent cellular phagocytosis; CDC = complement-dependent toxicity; CHF = congestive heart failure; DRESS = drug reaction with eosinophilia and systemic symptoms; DKd = daratumumab plus carfilzomib plus dexamethasone; DVT = deep vein thrombosis; ER = endoplasmic reticulum; H2 = histamine subtype 2 receptor; IMiD = immunomodulatory imide drug; IsaKd = isatuximab plus carfilzomib plus dexamethasone; IsaPd = isatuximab plus pomalidomide plus dexamethasone; Kd = isatuximab plus dexamethasone; KRd = isatuximab plus lenalidomide plus dexamethasone; mAb = monoclonal antibody; MM = multiple myeloma; PE = pulmonary embolism; PI = proteasome inhibitor; PML = progressive multifocal leukoencephalopathy; SCT = stem cell transplant; SJS = Stevens Johnson syndrome; TEN = toxic epidermal necrolysis; TLS = tumour lysis syndrome.
aHealth Canada–approved indication.
Source: e-CPS.14
Stakeholder Perspectives
Patient Group Input
Myeloma Canada submitted patient input for this review. Founded in 2005, Myeloma Canada is the only national charitable organization created by and for Canadians affected by MM. The organization is driven to improve the lives of those affected by MM. Information from this input was gathered through a patient survey, accessed through email and social media from April 22, 2021, to May 9, 2021. A total of 208 individuals with MM responded to the survey from all provinces, 1 territory (Yukon), and from outside Canada (1 response). Forty-eight responses were excluded because the respondents did not meet eligibility criteria, for a total of 160 included responses. Three respondents reported having received the treatment under review, 1 did not answer most questions regarding the treatment, and 1 was excluded due to mistaking the treatment under review for another treatment.
Most patients surveyed indicated that having access to an effective treatment was very important (96%). Other issues identified as important by patients included controlling symptoms such as infections (69%), kidney problems (57%), mobility problems (48%), neuropathy (42%), and fatigue (42%). Patients described impacts on their abilities to perform day-to-day activities, such as working, travel, and exercise. Patients expect new treatment options to improve their quality of life, have maximum benefits with nondebilitating side effects, reduce their hospital visits, and achieve the longest remission possible in lieu of a cure. One respondent who had had the treatment under review felt that the treatment was extremely effective, found the overall side effects to be tolerable, felt that their quality of life with the treatment was very good, and felt that the treatment improved their long-term health outlook. However, this respondent found the side effects of nausea/vomiting and thrombocytopenia to be completely intolerable. The patient group highlighted the importance of receiving information about emerging treatments and having timely access to these treatments. The patient input received from Myeloma Canada is presented in Appendix 2.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of MM.
Unmet Needs
The clinical experts consulted by CADTH on this review noted that MM remains an incurable disease, with significant impairment in HRQoL due both to the disease and treatments used to manage it. Newer treatments are needed that exhibit better control over the disease and less toxicity. Additionally, goals are not being met for patients who are refractory to certain classes of drugs (immunomodulators [specifically lenalidomide] or proteasome inhibitors [bortezomib]), and the clinical experts noted that outcomes tend to be particularly poor in these patients.
Place in Therapy
Isatuximab is an anti-CD38 monoclonal antibody, like daratumumab, and is likely best used in combination with other therapies with different mechanisms of action and toxicity profiles. Otherwise, it could be used in any line of therapy. For patients who have received 1 prior line of therapy, an isatuximab-containing regimen could be beneficial, particularly if they had not previously been treated with an anti-CD38 drug like daratumumab. Whether isatuximab is beneficial in patients previously treated with another anti-CD38 is unknown, as trials have not included patients previously treated with a monoclonal antibody.
Patient Population
Any myeloma patient who is suitable for treatment could benefit from isatuximab, and there are no established methods for determining patients who would not benefit. Patients whose disease is actively progressing or not responding to current treatment, or who are intolerant of their current therapy and are not yet adequately treated, could benefit from isatuximab.
The most likely approach to identifying patients who might best respond is clinical judgment. Pre-symptomatic patients should be treated, particularly if there is evidence of disease progression or lack of response to current or prior therapy. Patients who are dying would not be suitable for treatment with isatuximab. It is not possible to identify patients who are more likely to respond to isatuximab.
Assessing Response to Treatment
IMWG response criteria are used to determine whether a patient is responding to treatment. A clinically significant response to treatment is indicated by improved PFS, with acceptable drug toxicity and quality of life. Treatment response should be assessed before each treatment cycle.
Discontinuing Treatment
Disease progression or intolerable toxicity would warrant discontinuation of treatment.
Prescribing Conditions
The most appropriate setting for treatment with isatuximab, according to the clinical experts, is an outpatient systemic cancer therapy unit.
Additional Considerations
According to the clinical experts consulted by CADTH on this review, in Canada, first-line treatment of MM for transplant-eligible patients does not currently incorporate a CD38 antibody drug or carfilzomib except in clinical trials. In transplant-ineligible patients, first-line daratumumab plus lenalidomide plus dexamethasone (DRd) is not currently reimbursed, and, therefore, most patients in Canada have not received a monoclonal antibody in first-line treatment. In the second-line treatment setting, most patients are refractory to lenalidomide that has been given until disease progression, and many of the remaining patients are intolerant of lenalidomide. Therefore, a lenalidomide-free second-line regimen is needed. The most commonly used second-line options are daratumumab plus bortezomib plus dexamethasone (DVd) and Kd regimens, and DVd is often chosen as a means of providing a CD38 antibody drug to the patient, in which case Kd is deferred to third- or fourth-line treatment. DVd, although commonly used, is known to have poor outcomes for patients, as seen in the CASTOR trial (median PFS for DVd of 7.8 months to first relapse in patients refractory to lenalidomide).15 Real-world data from Canada also show poor outcomes for patients whose disease has progressed while they were receiving lenalidomide and who are then treated with DVd (median PFS of 11.47 months among patients progressing on lenalidomide maintenance following 1 line of treatment).16 Both DVd and Kd appear more effective than bortezomib plus dexamethasone in randomized trials, likely because of the addition of the CD38 antibody drug in DVd and because of a better-performing proteasome inhibitor in Kd. However, neither of these regimens typically leads to durable remission, and more effective treatments are needed. If the IsaKd regimen were available in Canada, it would be preferred over DVd or Kd due to superior efficacy and good tolerability. Regimens containing pomalidomide are often deferred for use following regimens based on carfilzomib. There are 2 reasons for this: patients refractory to lenalidomide who are not yet refractory to a proteasome inhibitor are thought to be more likely to benefit from a regimen based on a proteasome inhibitor regimen than 1 based on pomalidomide, and access to pomalidomide generally requires prior exposure to lenalidomide and a proteasome inhibitor exposure, although there is variation in this across jurisdictions arising from differences in funding.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups
Two clinician groups provided input for this review: OH-CCO DAC and the CMRG. OH-CCO DAC provides timely, evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program.
The CMRG is a charitable organization whose membership consists of physicians who treat MM affiliated with 22 major academic medical centres in Canada. The 3 main purposes of CMRG are to (1) conduct investigator-initiated academic clinical trials to improve the outcome for patients with MM; (2) maintain a national Myeloma Database, now consisting of more than 7,000 patients, to evaluate real-world patterns of treatment, outcomes, risk factors, and areas for future research in myeloma; and (3) generate consensus statements for MM management.
Unmet Needs
According to the CMRG, MM can cause significant mortality and morbidity, including fractures, decreased blood counts, renal failure, and infections, and these significantly affect patient quality of life. The most important goals of therapy are to ensure a high-quality and durable response to treatment (measured by response rates and PFS), which will delay disease-related complications and ultimately improve quality of life. The unmet needs include treatment for patients who become refractory to major classes of drug, specifically the immunomodulatory drugs (lenalidomide) and/or proteasome inhibitors (bortezomib). Patients refractory to these therapies tend to have poor outcomes overall. Many patients die before receiving subsequent lines of therapy. Therefore, there is a need to provide patients with optimal treatment to control the disease as early as possible in the disease course. According to OH-CCO DAC, patients who are not eligible for DRd have the greatest unmet need for an intervention such as IsaKd.
Place in Therapy
The CMRG believed that IsaKd is ideal for patients who have progressed after either a bortezomib- and/or lenalidomide-containing regimen. Among these patients, regimens containing CD38 antibody drugs are most commonly used at relapse as (1) they have a different mechanism of action from the drug previously received and (2) exposure to these drugs is required for future enrolment in clinical trials. Currently funded CD38 antibody regimens include DVd and DRd, and DVd is most commonly used second-line, as most patients progress on lenalidomide maintenance (ASCT eligible) or Rd (ASCT ineligible) in the first-line treatment setting. DVd is not optimal, however, as PFS is no more than 8 months in patients refractory to lenalidomide. Therefore, there remains an unmet need in optimizing regimens containing daratumumab in the post-lenalidomide setting, and further options are required. IsaKd would address the need of patients who have relapsed on lenalidomide and/or bortezomib. IsaKd would provide access to an CD38 antibody drug in this setting, along with a different proteasome inhibitor, which would be expected to replace and greatly improve upon current standard of care. Based on the ENDEAVOUR trial, carfilzomib is clearly superior to bortezomib in patients who have relapsed.17 OH-CCO DAC agreed that IsaKd would be an alternative treatment option for second-line treatment and beyond. This provides a monoclonal antibody treatment option for patients refractory to lenalidomide.
With respect to whether other therapies should be attempted before initiating IsaKd, CMRG noted that, in MM, it is important to use the best therapies up front, given the attrition seen with the disease. Additionally, the current standard of care, DVd, is suboptimal, with data showing poor efficacy in both clinical trials and real-world Canadian settings.16,18 OH-CCO DAC agreed it was not appropriate to recommend patients try other treatments before initiating treatment with IsaKd.
CMRG noted that sequencing would likely be affected by the approval of IsaKd, as it would most likely be used second-line in patients whose disease had progressed while they were receiving lenalidomide and/or proteasome inhibitors. Regimens containing daratumumab (DRd or DVd) or carfilzomib (isatuximab plus lenalidomide plus dexamethasone [KRd] or Kd) would likely not be used in further lines of treatment. The CMRG also noted that, if DRd is funded for first-line treatment of transplant-ineligible MM patients as per data from the ongoing phase III MAIA trial, IsaKd would likely no longer be used second-line.19 It would likely continue to have a role among transplant patients whose disease has progressed while receiving lenalidomide maintenance therapy, as they would not have been previously treated with a regimen containing an CD38 antibody drug. OH-CCO DAC agreed that, with respect to sequencing, the only option after IsaKd would be pomalidomide-based therapy.
Patient Population
In terms of which patients are best suited to IsaKd, CMRG noted that the PFS benefit was seen across most subgroups in the IKEMA trial. Patients least suited for IsaKd would be those with prior disease refractory to carfilzomib or previous CD38 antibody drugs, as they were excluded from IKEMA. They also noted emerging evidence suggesting that isatuximab given following therapy with daratumumab likely produces a poor response. The CMRG noted cardiovascular toxicity with carfilzomib is a concern; however, they also noted that IsaKd appeared to have a relatively favourable toxicity profile in IKEMA, although the reasons for this are unknown. As far as those most likely to benefit from treatment, the CMRG suggested patients with less advanced and less biologically aggressive disease would benefit the most, as is the case with all MM treatments. OH-CCO DAC believed that patients best suited to be treated with IsaKd are those who meet the eligibility criteria for the drug. They did not believe it is possible to identify those patients who are most likely to respond to the drug.
Assessing Response to Treatment
CMRG noted that the best ORR, quality of response (VGPR or complete remission), as well as durability of response (PFS) are outcomes used in clinical practice and clinical trials to assess response to treatment. MRD is becoming increasingly important in MM, given its concordance with OS. However, this end point is not routinely used as an indicator of response in Canadian clinical practice. A clinical meaningful response would be absence of progressive disease (PD) with minimal/tolerable side effects. Although deep (VGPR or better) and more sustained MRD-negative responses are ideal, any absence of PD provides a patient benefit, in that it minimizes myeloma-related end organ damage. This is particularly the case if relapse therapy is started when progression is documented by the usual parameters, but before severe myeloma-related organ damage has developed. In this setting, even stable disease may afford benefit. Almost all MM patients are followed continuously, with response assessed every 1 to 3 months with laboratory parameters (most commonly) and occasionally with advanced imaging and/or bone marrow biopsy (depending on the specific scenario). OH-CCO DAC stated that the usual MM response criteria would be sufficient to determine whether a patient is responding to therapy, and a clinically meaningful response would be indicated by improvement in myeloma parameters and in symptoms. They also noted that treatment response should be assessed every treatment cycle.
Discontinuing Treatment
Both clinician groups identified disease progression or intolerance to therapy despite dose reduction as the factors that should be considered when deciding to discontinue treatment with IsaKd.
Prescribing Conditions
The CMRG noted that MM is treated at many community and academic sites across Canada and that the drug is administered in specialized clinical spaces. Therefore, community-setting clinics, hospital outpatient clinics, and IV oncology drug administration facilities would all be appropriate treatment settings for IsaKd. According to OH-CCO DAC, IsaKd should be administered in outpatient chemotherapy suites.
Additional Considerations
OH-CCO DAC noted that IsaKd administration is associated with multiple visits to the chemotherapy suites, which may not be feasible for some patients.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
The trial included patients who had 1 to 3 prior lines of treatment. Should eligibility for isatuximab align with that of the trial? | The clinical experts agreed that eligibility for IsaKd should align with the IKEMA trial criteria; however, they noted there is no reason that patients who have > 3 prior lines could not access this therapy (assuming no prior exposure to CD38 antibody drugs). This should be taken into consideration since, as new therapies for MM become available, IsaKd may move further down in terms of line of therapy. It is unlikely there will be many patients with > 3 prior lines seen in clinical practice |
Do patients with high-risk cytogenetic results exhibit a distinct response to IsaKd, and should they be treated differently? | The clinical experts indicated that patients with high-risk cytogenetic results do not have a distinct response to IsaKd and therefore should not be treated differently. |
Considerations for prescribing therapy | |
There is increasing interest in weekly carfilzomib administration. Can the IKEMA trial data be generalized to use isatuximab with weekly carfilzomib-dexamethasone? | The clinical experts noted that carfilzomib is already being administered weekly for some patients, and there is some evidence to support this approach.20 This approach could benefit patients and the health care system, as less drug (if the dose remains the same, which may not be the case) and less chair time would be needed. |
If a component of the regimen has to be discontinued (e.g., carfilzomib, dexamethasone), should the regimen be discontinued altogether? | The clinical experts agreed that, if a component of the regimen must be discontinued, there is no reason to discontinue the remaining components of the regimen. |
Generalizability issues | |
Should the following patients be eligible for IsaKd?
| The clinical experts agreed that patients with an ECOG performance status of ≥ 2, those with primary refractory MM, those with serum free light chain measurable disease only, and those with known amyloidosis who also have MM should be eligible to receive IsaKd. They also added that patients with plasma cell leukemia should also be eligible. |
On a time-limited basis, should patients currently receiving carfilzomib-dexamethasone, whose disease has not yet progressed, be allowed to add isatuximab to their regimen? | Yes, the clinical experts agreed that patients currently receiving Kd, whose disease has not progressed, should be allowed to add isatuximab to their regimen. |
Funding algorithm | |
Which drugs may be preferred in which settings (or line of therapy):
| Second-line DRd or DVd vs. second-line IsaKd
Second-line IsaKd vs. third-line IsaPd
What evidence is available to support sequencing of isatuximab and daratumumab?
What evidence is available to support sequencing of IsaKd vs. IsaPd?
|
Care provision issues | |
Isatuximab is administered as a prolonged IV infusion, as per the product monograph. There is an ongoing clinical trial and there may be emerging data to administer a rapid infusion over 30 minutes if previous doses were tolerated. Can isatuximab be administered as a rapid infusion to minimize resource utilization and increase patient convenience? | The isatuximab schedule is busier than the daratumumab schedule (eventually daratumumab moves to a monthly administration schedule, but this is not the case with isatuximab). The clinical experts were not aware of available data on isatuximab administered as a rapid infusion and could not comment on its use in clinical practice. |
Additional comments (response not required):
| For consideration by pERC. |
System and economic issues | |
Additional comments (response not required):
| For consideration by pERC |
DRd = daratumumab plus lenalidomide plus dexamethasone; DVd = daratumumab plus bortezomib plus dexamethasone; ECOG = Eastern Cooperative Oncology Group; IsaKd = isatuximab plus carfilzomib plus dexamethasone; IsaPd = isatuximab plus pomalidomide plus dexamethasone; Kd = carfilzomib plus dexamethasone; KRd = isatuximab plus lenalidomide plus dexamethasone; MM = multiple myeloma; NaCl = sodium chloride.
Clinical Evidence
The clinical evidence included in the CADTH review of isatuximab is presented in 2 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section would normally include sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review. However, none were submitted by the sponsor or identified by the literature search.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of isatuximab 10 mg/kg in combination with carfilzomib and dexamethasone (IsaKd) for the treatment of adult patients with relapsed or refractory MM who have received 1 to 3 prior lines of therapy.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adult patients with MM who have received at least 1 prior therapy Subgroups:
|
Intervention | Isatuximab 10 mg/kg IV in combination with carfilzomib and dexamethasone, weekly for cycle 1 and every 2 weeks for cycle 2 and beyond. Each cycle is 28 days long. |
Comparators | Carfilzomib plus dexamethasone Pomalidomide plus dexamethasone Pomalidomide plus cyclophosphamide plus dexamethasone Daratumumab plus lenalidomide plus dexamethasone Carfilzomib plus lenalidomide plus dexamethasone Lenalidomide plus dexamethasone Daratumumab plus bortezomib plus dexamethasone Cyclophosphamide plus bortezomib plus dexamethasone Daratumumab plus pomalidomide plus dexamethasone Lenalidomide plus dexamethasone plus cyclophosphamide Pomalidomide plus bortezomib plus dexamethasone Isatuximab plus pomalidomide plus dexamethasone |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase III and IV RCTs |
AE = adverse event; IMWG = International Myeloma Working Group; ISS = International Staging System; MM = multiple myeloma; RCT = randomized controlled trial; R-ISS = Revised International Staging System; SAE = serious adverse events; WDAE = withdrawal due to adverse events.
aOutcomes identified as important to patients in input provided to CADTH.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.22
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was isatuximab (Sarclisa). Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on August 11, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on December 1, 2012.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.23 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings from the Literature
A total of 1 study was identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6.
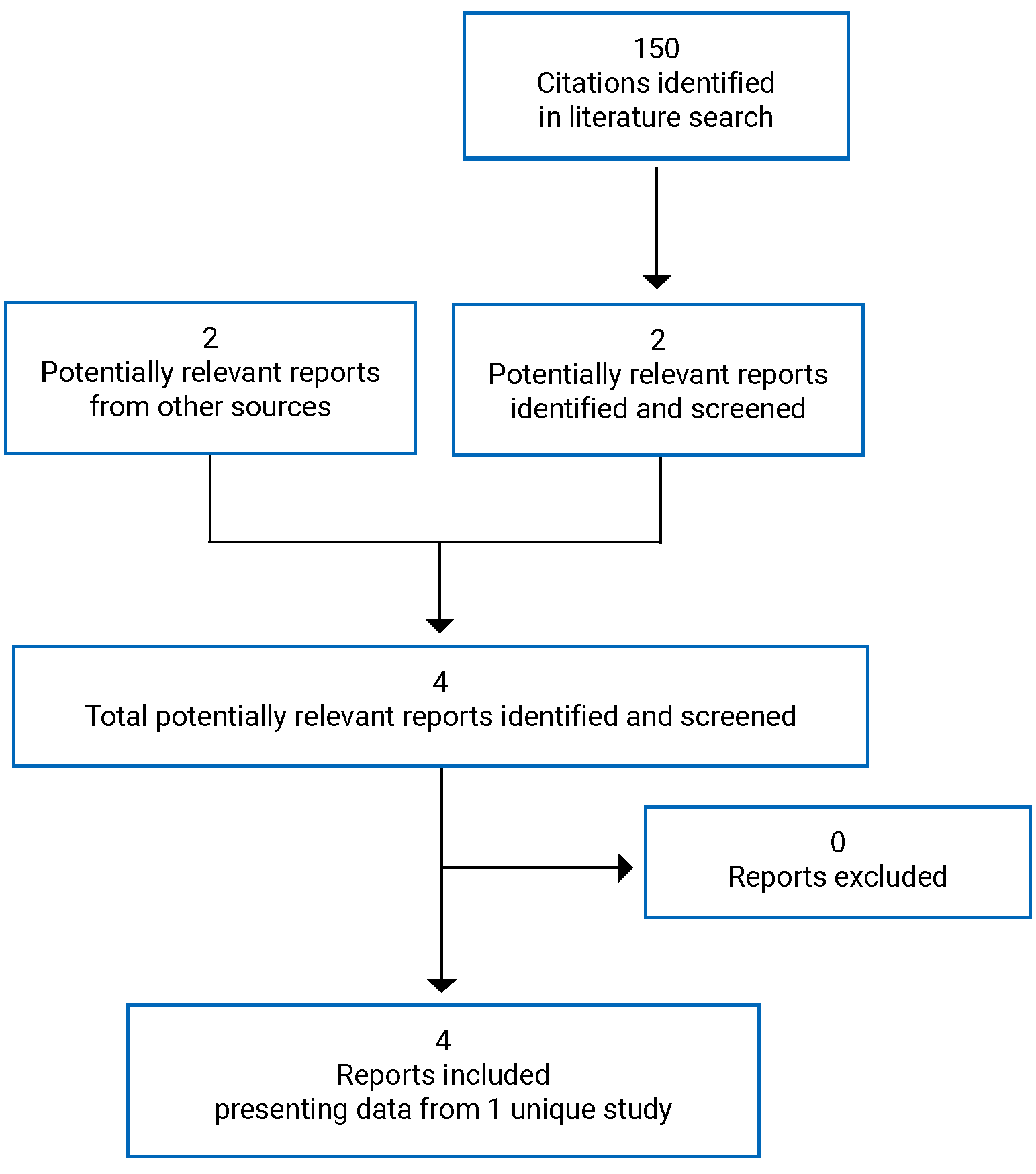
Table 6: Details of Included Study
Criteria | Description |
|---|---|
Design and populations | |
Study design | Phase III open-label RCT |
Locations | 69 sites (16 countries: Canada, US, Brazil, UK, Czech Republic, France, Greece, Hungary, Italy, Russia, Spain, Japan, South Korea, Australia, New Zealand, Turkey) |
Study period | Enrolment: October 25, 2017, to March 21, 2019 Data cut-off date: February 7, 2020 (interim analysis) |
Randomized (N) | 302 |
Inclusion criteria |
|
Exclusion criteria |
|
(continued) |
|
Drugs | |
Intervention |
|
Comparator(s) |
|
Phase and duration | |
Screening | 3 weeks |
Open label | Patients were treated until disease progression, unacceptable AE, or patient decision to stop the study treatment |
Follow-up | Every 3 months after last study treatment |
Outcome | |
Primary end point | PFS |
Other end points | Key secondary:
Other secondary: |
(continued) |
Exploratory:
Safety:
• Physical exam |
Notes | |
Publications | |
AE = adverse event; ALT = alanine aminotransferase; ANC = absolute neutrophil count; AST = aspartate aminotransferase; BCC = ; CHF = congestive heart failure; CR = complete response; DOR = duration of response; ECG = electrocardiogram; ECOG = Eastern Cooperative Oncology Group; FLC = free light chain; G-CSF = granulocyte colony-stimulating factor; HRQoL = health-related quality of life; LVEF = left ventricular ejection fraction; mAb = monoclonal antibody; MDRD = modified diet in renal disease; MI = myocardial infarction; MM = multiple myeloma; MR = minimal response; MRD = minimal residual disease; NCI CTCAE = National Cancer Institute Common Toxicity Criteria for Adverse Events; NYHA = New York Heart Association; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PFS2 = : PR = partial response; PS = performance status; RCT = randomized controlled trial; RRMM = relapsed or refractory multiple myeloma; SAE = serious adverse event; SCC = ; SCT = stem cell transplant; TIA = transient ischemic attack; TLS = tumour lysis syndrome; TTP = time to progression; ULN = upper limit of normal; VGPR = very good partial response.
aThe first infusion was initiated at 175 mg/hour and, in the absence of infusion reactions after 1 hour of infusion, the infusion rate was increased in 50 mg/hour increments every 30 minutes, to a maximum of 400 mg/hour. Subsequent infusions were initiated at 175 mg/hour and, in the absence of infusion reaction after 1 hour of infusion, the rate was increased by 100 mg/hour increments every 30 minutes, to a maximum of 400 mg/hour.
Source: Clinical Study Report for IKEMA7; sponsor’s submission to CADTH.8
Description of Study
One sponsor-funded multinational (16 countries, with 8 patients at Canadian sites) pivotal trial, IKEMA, was included in this CADTH review.5,7,8,24 The primary objective of IKEMA was to demonstrate the benefit of IsaKd in the prolongation of PFS using IMWG criteria. The key secondary efficacy objectives were to evaluate ORR, rate of VGPR or better, VGPR or better (IMWG criteria) with MRD negativity, CR rate (IMWG criteria), and OS. IKEMA is an ongoing phase III open-label RCT that randomized 302 patients with relapsed and/or refractory MM who had received 1 to 3 prior lines of therapy, in a 3:2 manner, to either IsaKd or Kd. Patients were treated until they experienced disease progression or unacceptable toxicity, or they decided to discontinue study treatment. Randomization was conducted using interactive response technology (IRT) and was stratified by number of prior lines of therapy (1 versus more than 1) and R-ISS score (I or II versus III versus not classified). The data cut-off for the interim analysis was 103 PFS events, which corresponded to a data cut-off date of February 7, 2020. By this time, the median duration of treatment exposure was 72.9 weeks (range 1 to 114 weeks) across the 2 treatment groups. The design of the IKEMA trial is depicted in Figure 2.
IKEMA included a 21-day screening period during which various baseline values were obtained and study eligibility was determined.
Figure 2: Design of IKEMA Trial
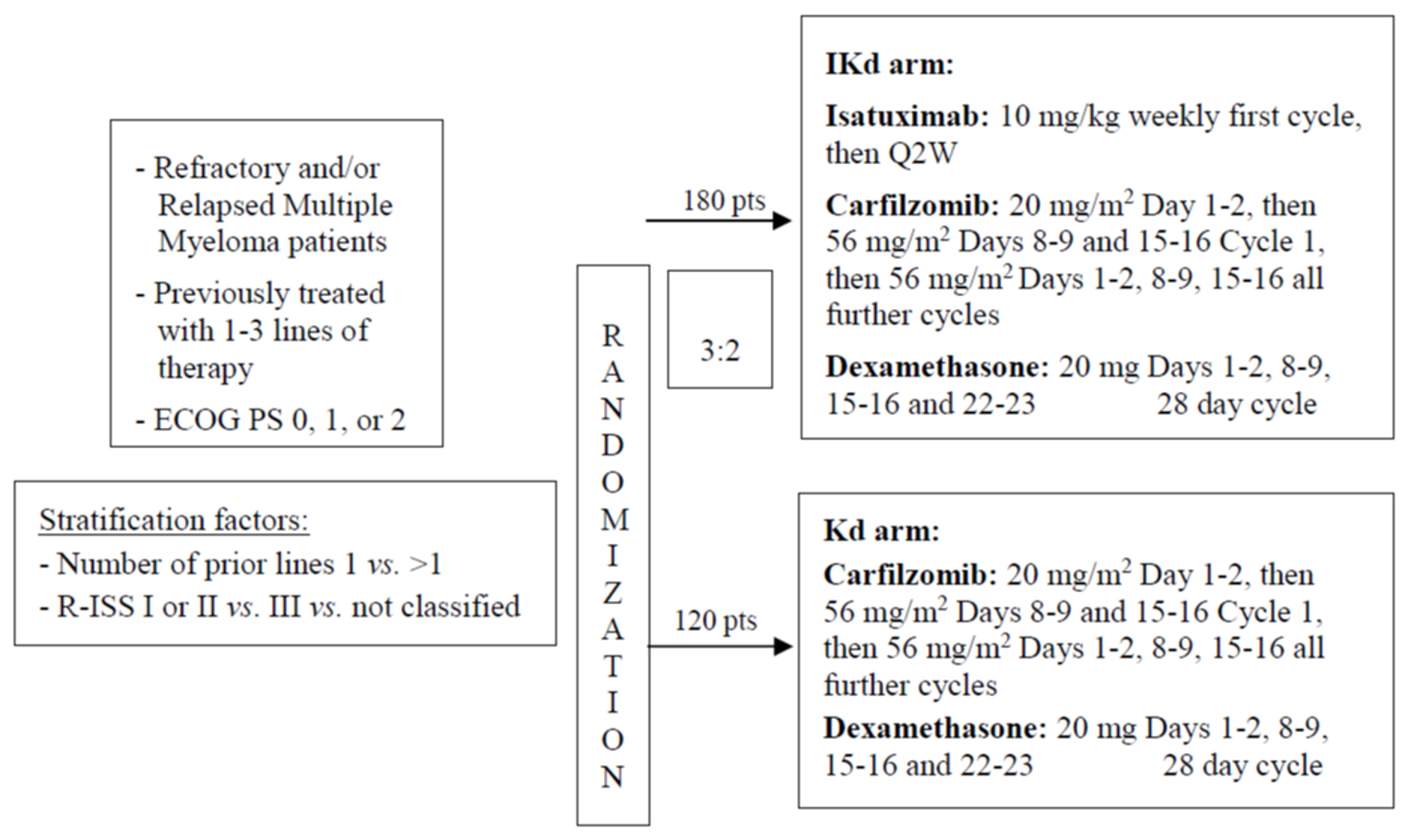
ECOG = Eastern Cooperative Oncology Group; IKd = isatuximab plus carfilzomib plus dexamethasone; Kd = isatuximab plus dexamethasone; PS = performance status; pt = patient; Q2W = every 2 weeks; R-ISS = Revised International Staging System.
Source: Clinical Study Report for IKEMA.7
Populations
Inclusion and Exclusion Criteria
To be included, patients had to have MM with measurable disease (by serum or urine M protein) and relapsed and/or refractory MM with at least 1 prior line of therapy and no more than 3 prior lines. Primary refractory patients (those who never achieved at least a minimal response with any treatment during their disease course) were excluded, as were those with serum FLC-measurable disease only and those with disease refractory to a prior CD38 monoclonal antibody drug (progression on or within 60 days after end of CD38 antibody treatment or failure to achieve at least a minimal response to treatment). Patients with an ECOG performance status more than 2 were also excluded.
Baseline Characteristics
Patients were an average of 63.1 years of age (SD 9.9); 56.0% were men and 70.9% were White (Table 7). The majority of patients had MM of the IgG subtype (67.9%) at diagnosis, followed by IgA (22.8%), and these percentages were similar to those observed at study entry (69.9% and 22.5%, respectively). The most common ISS stage at diagnosis was stage II (33.4%), followed by stage III (25.5%) and stage I (24.2%); stage was unknown in the remainder. At study entry, the most common stage was stage I (53.0%), followed by stage II (31.1%) and stage III (15.2%). Most patients had relapsed and refractory disease (71.5%), while the remainder had relapsed disease (28.5%). The average number of prior regimens was 3.2 (SD 1.7), and the number of prior treatment lines was 1.8 (SD 0.8). Patients were most commonly refractory to an immunomodulatory imide drug (45.0% of patients), followed by a proteasome inhibitor (33.1%) and both (20.5%).
There were some numerical differences between groups (IsaKd versus Kd) with respect to race (White 73.2% versus 67.5%), ISS stage at study entry (stage I: 49.7% versus 57.7%, stage II: 35.2% versus 25.2%), refractory status (relapsed and refractory: 68.2% versus 76.4%, relapsed: 31.8% versus 23.6%) and in the types of prior regimens used (alkylating antineoplastic drugs: 94.4% versus 82.1%; proteasome inhibitors: 92.7% versus 85.4%; immunomodulatory drugs: 76.0% versus 81.3%).
Table 7: Summary of Baseline Characteristics (Randomized Population)
IKEMA | ||
|---|---|---|
Characteristic | IsaKd N = 179 | Kd N = 123 |
Mean (SD) age, years | 63.3 (9.8) | 62.9 (10.0) |
Age group (years), n (%) | ||
< 65 | 88 (49.2) | 66 (53.7) |
≥ 65 to < 75 | 74 (41.3) | 47 (38.2) |
≥ 75 | 17 (9.5) | 10 (8.1) |
Female, n (%) | 78 (43.6) | 55 (44.7) |
Race, n (%) | ||
White | 131 (73.2) | 83 (67.5) |
Black/African descent | 5 (2.8) | 4 (3.3) |
Asian | 26 (14.5) | 24 (19.5) |
Multiple | 3 (1.7) | 0 |
Missing/not reported | 14 (7.8) | 12 (9.8) |
Time from initial diagnosis of MM to randomization, mean (SD) | 4.10 (3.02) | 4.25 (3.15) |
MM subtype at study entry, n (%) | ||
IgG | 126 (70.4) | 85 (69.1) |
IgA | 38 (21.2) | 30 (24.4) |
Other | 4 (2.2) | 1 (0.8) |
Kappa/lambda light chain only (urine) | 11 (6.2) | 7 (5.7) |
ECOG PS, n (%) | ||
0 or 1 | 168 (93.9) | 118 (95.9) |
> 1 | 11 (6.1) | 5 (4.1) |
ISS stage at study entry, n (%) | ||
Stage I | 89 (49.7) | 71 (57.7) |
Stage II | 63 (35.2) | 31 (25.2) |
Stage III | 26 (14.5) | 20 (16.3) |
Unknown | 1 (0.6) | 1 (0.8) |
R-ISS stage at study entry, n (%) | ||
Stage I | 45 (25.1) | 33 (26.8) |
Stage II | 110 (61.5) | 70 (56.9) |
Stage III | 16 (8.9) | 8 (6.5) |
Not classified | 8 (4.5) | 12 (9.8) |
Refractory status, n (%) | ||
Relapsed and refractory | 122 (68.2) | 94 (76.4) |
Primary refractory | 0 | 0 |
Relapsed | 57 (31.8) | 29 (23.6) |
Patients with soft tissue plasmacytoma as per eCRF, n (%) | 11 (6.2) | 13 (10.6) |
Patients with bone lesions as per eCRF, n (%) | 123 (69.1) | 90 (73.2) |
Cytogenetic risk as defined for R-ISS, n (%) | ||
High-risk cytogenetic abnormality | 42 (23.5) | 31 (25.2) |
Standard-risk cytogenetic abnormality | 114 (63.7) | 78 (63.4) |
Unknown or missing | 23 (12.8) | 14 (11.4) |
Number of abnormalities, n (%) | ||
No cytogenetic abnormality | 65 (36.3) | 43 (35.0) |
1 cytogenetic abnormality | 64 (35.8) | 41 (33.3) |
2 cytogenetic abnormalities | 21 (11.7) | 14 (11.4) |
3 cytogenetic abnormalities | 4 (2.2) | 5 (4.1) |
Unknown/missing | 25 (14.0) | 20 (16.3) |
Number of prior regimens | ||
Mean (SD) | 3.3 (1.8) | 3.1 (1.6) |
Number of prior regimens, n (%) | ||
1 | 29 (16.2) | 19 (15.4) |
2 | 32 (17.9) | 29 (23.6) |
3 | 44 (24.6) | 29 (23.6) |
4 | 38 (21.2) | 22 (17.9) |
5 | 16 (8.9) | 14 (11.4) |
6 | 13 (7.3) | 6 (4.9) |
> 6 | 7 (3.9) | 4 (3.3) |
Number of prior lines, mean (SD) | 1.8 (0.8) | 1.8 (0.9) |
Number of prior lines, n (%) | ||
1 | 79 (44.1) | 55 (44.7) |
2 | 64 (35.8) | 36 (29.3) |
3 | 33 (18.4) | 30 (24.4) |
> 3 | 3 (1.7) | 2 (1.6) |
Main prior antimyeloma therapies, n (%) | ||
Alkylating antineoplastic drugs | 169 (94.4) | 101 (82.1) |
Proteasome inhibitors | 166 (92.7) | 105 (85.4) |
Immunomodulatory imide drugs | 136 (76.0) | 100 (81.3) |
HDAC inhibitors | 1 (0.6) | 2 (1.6) |
Anthracyclins | 23 (12.8) | 14 (11.4) |
Corticosteroids | 179 (100) | 123 (100) |
Vinca alkaloids | 14 (7.8) | 9 (7.3) |
Monoclonal antibodies | 5 (2.8) | 1 (0.8) |
Daratumumab | 1 (0.6) | 0 (0.0) |
Elotuzumab | 4 (2.2) | 1 (0.8) |
ECOG PS = Eastern Cooperative Oncology Group performance status; eCRF = electronic case report form; HDAC = histone deacetylase; Ig = immunoglobulin; IsaKd = Isatuximab plus carfilzomib plus dexamethasone; ISS = International Staging System; Kd = carfilzomib plus dexamethasone; MM = multiple myeloma; R-ISS = Revised International Staging System; SD = standard deviation.
Source: Clinical Study Report for IKEMA.7
Interventions
Dexamethasone 20 mg was administered on days 1, 2, 8, 9, 15, 16, 22, and 23 in 28-day cycles, between 15 and 30 minutes (but no longer than 60 minutes) before isatuximab or at least 30 minutes before carfilzomib on days when there was no isatuximab administered. Dexamethasone was administered IV on the days that isatuximab and/or carfilzomib were administered and orally on the other days.
For each 28-day cycle, isatuximab was administered IV at a dose of 10 mg/kg on days 1, 8, 15, and 22 of cycle 1, then days 1 and 15 of subsequent cycles. The first infusion was initiated at 175 mg/hour; if there were no infusion reactions, this was increased in 50 mg/hour increments every 30 minutes to a maximum of 400 mg/hour. Subsequent infusions were initiated at 175 mg/hour but up-titrated after 1 hour by 100 mg/hour increments every 30 minutes to a maximum of 400 mg/hour.
After the patient was given appropriate hydration, carfilzomib was administered IV over 30 minutes at a dose of 20 mg/m2 on days 1 and 2 and 56 mg/m2 on days 8, 9, 15, and 16 of cycle 1 and days 1, 2, 8, 9, 15, and 16 of subsequent cycles if the patient did not experience any toxicities of grade 2 or higher, except in the case of noncomplicated hematologic toxicity related to treatment or resolved tumour lysis syndrome.
In the Kd group, dexamethasone was administered at the same dosage regimen as in the IsaKd group. However, it was given at least 30 minutes before administration of carfilzomib. Carfilzomib was administered as described previously.
Pre-medication was administered to prevent infusion-associated reactions to isatuximab and carfilzomib. Pre-medication consisted of oral acetaminophen (650 mg to 1,000 mg orally, 15 to 30 minutes before infusion), and IV ranitidine (50 mg IV or equivalent) and diphenhydramine (25 mg to 50 mg IV or equivalent), in addition to the IV dexamethasone, described previously. In countries with no IV formulation of diphenhydramine (or equivalent), an orally administered version was allowed and was administered 1 to 2 hours before isatuximab infusion. In cases where dexamethasone was prematurely discontinued and other study treatment was continued, pre-medication with methylprednisolone could be considered if infusion reaction pre-medication was needed. If a patient had not experienced an infusion reaction in 4 consecutive administrations of isatuximab, the investigator could consider whether specific pre-medication was necessary.
Concomitant therapy was permitted as long as it was necessary for patient welfare, unlikely to interfere with the study drugs, and not on the list of prohibited drugs. Antiviral prophylaxis, antibacterial prophylaxis, and thromboprophylaxis were given according to site/investigator practice and local labelling of carfilzomib. For patients who were hepatitis B virus carriers, prophylaxis with antivirals was considered. Combining dexamethasone with CYP3A inhibitors was avoided unless benefit outweighed risk of corticosteroid-related AEs, in which case patients were monitored for these AEs. Administration of granulocyte colony-stimulating factor was permitted for prophylactic use in patients experiencing recurring neutropenia or therapeutic use in patients with serious neutropenic complications, at the discretion of the investigator, consistent with the ASCO 2006 guidelines to decrease risk of neutropenia in patients with baseline extensive bone marrow involvement and/or low neutrophil count. Concomitant therapies that were prohibited included other antimyeloma therapies not specified in the protocol (although palliative radiotherapy was permitted for pain control); systemic corticosteroids (other than as part of the protocol-specified therapeutic regimen for treating hypersensitivity); as well as live vaccines, with the exception of routine vaccinations and influenza, pneumococcal, and Hemophilus influenzae vaccines, which were recommended.
Dose reductions, cycle delays, and/or dose omissions within a cycle were permitted when there were cases of toxicity associated with carfilzomib or dexamethasone. For isatuximab, dose reductions were not allowed, although dose interruptions, omissions, and delays were permitted. Specific guidance was provided for dose reductions due to various AEs. Once a dose of carfilzomib or dexamethasone was decreased, increase back to the previous dose was not permitted. Patients received the next cycle of study treatment after recovering from toxicity. Study treatment was discontinued if an AE persisted despite dose modifications or if any other AE occurred that, in the opinion of the investigator, warranted discontinuation. Other reasons why patients could be removed from the study included patient request and investigator determination that continuing in the study would be detrimental to the patient’s well-being (examples include disease progression, poor compliance with study protocol, and intercurrent illness).
Protocols were described for managing specific AEs. For infusion reactions, patients could be given diphenhydramine IV, methylprednisolone IV, IV fluids, vasopressors, oxygen, bronchodilators, and acetaminophen as per investigator judgment. Once a grade 2 infusion reaction leading to interruption had improved to grade 1 or better, the infusion was restarted at half the initial infusion rate, and, if symptoms did not recur after 30 minutes, the infusion rate could be increased in 50 mg/hour increments every 30 minute to a maximum of 400 mg/hour. Patients experiencing a grade 3 or 4 infusion reaction had causative study treatment permanently discontinued, and supportive therapy was administered. If it was not possible to determine which drug caused the infusion reaction, all study treatment was permanently discontinued. If a grade 3 or 4 infusion reaction occurred during isatuximab infusion, carfilzomib infusions were postponed by 1 day, and resumed if the infusion reaction improved to grade 1 or better.
The number of patients receiving subsequent antimyeloma therapy was also reported, with 26.3% of patients in the IsaKd group and 43.1% of patients in the Kd group receiving subsequent therapy, and the mean number of further regimens was 1.7 (SD 1.2) in the IsaKd group and 1.6 (SD 0.9) in the Kd group. The most frequent subsequent therapies (IsaKd versus Kd) were immunomodulatory imide drugs (83.0% versus 79.2% of subsequent regimens, the most common being pomalidomide [51.1% versus 39.6%] and lenalidomide [40.4% versus 43.4%]) and corticosteroids (80.9% versus 83.0%), followed by alkylating antineoplastic drugs (55.3% versus 39.6%), monoclonal antibodies (23.4% versus 54.7%; the most common being daratumumab [21.3% versus 47.2%]), and proteasome inhibitors (34.0% versus 20.8%; the most common being bortezomib [23.4% versus 17.0%]).
Outcomes
Table 8 provides a list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review. These end points are further summarized in this section. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 2.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | IKEMA | Place in statistical hierarchy |
|---|---|---|
PFS | Primary | First |
OS | Key secondary | Not in hierarchy |
HRQoL | Exploratory | Not in hierarchy |
Objective response | Key secondary | Second: ORR;a third: VGPR |
Depth of response (assessed by IMWG criteria) | Key secondary | Fourth (MRD negativity) |
Duration of response | Other secondary | Not in hierarchy |
Time to response | Other secondary | Not in hierarchy |
Health resource utilization | Not assessed | NA |
AEs | Safety outcome | Not in hierarchy |
SAEs | Safety outcome | Not in hierarchy |
AEs of special interest | Safety outcome | Not in hierarchy |
Infusion reactions | Safety outcome | Not in hierarchy |
AE = adverse event; HRQoL = health-related quality of life; IMWG = International Myeloma Working Group; MRD = minimal residual disease; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; SAE = serious adverse event; VGPR = very good partial response.
aHierarchy failed after ORR (second outcome).
Source: Clinical Study Report for IKEMA.7
Progression-Free Survival
The primary outcome was PFS, defined as the time from date of randomization to date of first documented PD (determined by the IRC) or death from any cause, whichever came first. If PD and death were not observed before the data cut-off date or date of initiation of further antimyeloma treatment, PFS was censored at the date of the last valid disease assessment not showing PD or the analysis cut-off date, whichever came first. Patients without an event and without any valid post-baseline assessment were censored at the date of randomization. Responses (including progression) were evaluated by a blinded IRC according to IMWG criteria using central laboratory results and central radiological review. Response and progression based on serum and/or urine M protein were confirmed by 2 consecutive assessments. Progression based on plasmacytomas or bone lesions did not require confirmation. For patients with measurable serum and/or urine M protein, PD was defined as at least 1 of the following (biologic criteria in 2 consecutive assessments):
25% or greater increase in serum M component from nadir (the absolute increase had to be 0.5 g/dL or more); serum M component increases of 1 g/dL or more in 2 consecutive assessments were sufficient to define relapse if starting M component was 5 g/dL or more; and/or
25% or greater increase in urine M component from nadir (the absolute increase had to be 200 mg/24 hours or more); and/or
definite development of new bone lesions or soft tissue extramedullary disease or an increase or 50% more from nadir in the sum of perpendicular diameters of existing soft tissue extramedullary disease lesions if there was more than 1 lesion or 50% or greater increase in the longest diameter of a previous soft tissue extramedullary disease lesion greater than 1 cm in short axis.
The date of the PD was defined as the earliest date that indicated PD (provided that PD was confirmed when required). An M protein assessment performed after the initiation of a further antimyeloma treatment was used to confirm PD. In addition, deaths due to PD within 45 days of the first documentation of PD (regardless of initiation of further therapies) were used to confirm PD. If a post-baseline disease assessment for response was determined to be “not evaluable” based on IMWG criteria, or the date of assessment was missing, the disease assessment was considered invalid. For a given time point not showing disease progression, if several examinations were performed on different dates, the date of the last valid assessment was the date of the latest examination. Clinical deterioration could also be considered progression in the primary analysis of PFS if the IRC considered that clinical data reported in the case report form supported clinical progression. In the case of hypercalcemia, a full disease assessment was performed to identify any measurable parameter of myeloma progression (e.g., serum and urine M protein, lytic lesions assessment, and plasmacytoma assessment), and potential alternative causes of hypercalcemia were ruled out. Progression was not diagnosed based on FLC progression only. If both serum and urine M protein were below the level of eligibility in the efficacy analyses performed on cycle 1, day 1, progression was assessed per IMWG response criteria.
Overall Survival
OS was a key secondary outcome and was defined as the time from date of randomization to death from any cause. OS was not assessed in the interim analysis but will be assessed in the final analysis, according to the statistical analysis plan.
Health-Related Quality of Life
HRQoL was assessed, and results were presented descriptively using 3 different instruments: the EORTC QLQ-C30, the EORTC QLQ-MY20, and the EQ-5D-5L. A more complete description is provided and the validity of these patient-reported outcomes is summarized in Appendix 4. Each of these instruments were completed by the patient on days 1 and 2 of each cycle, as well as at the end of treatment visit (30 days after the last treatment was administered) and 90 days (within 5 days) after administration of the last study treatment. The EORTC QLQ-C30 is a 30-item instrument, with 15 items related to function (physical, role, cognitive, emotional, social), 7 questions related to symptoms (7 questions), single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, diarrhea, financial impact), and 2 items related to global quality of life (QoL). All except global QoL are scored from 1 (“not at all”) to 4 (“very much”). Global QoL, also referred to as global health status, is scored on a scale from 1 (very poor) to 7 (excellent).25 The EORTC QLQ-MY20 is a module that was developed specifically for MM and consists of 20 items, 2 symptom scales (disease symptoms and side effects), and 2 functional scales (future perspective and body image).26 The questions are scored on the same 1 to 4 scale and responses are then converted to a standardized score that ranges from 0 to 100. The EQ-5D-5L consists of 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), and each dimension is rated on 5 levels, from level 1 (“no problems”) to level 5 (“extreme problems” or “unable to perform”).27 This rating is then converted, using an algorithm, to a scale from 0 (dead) to 1 (full health).28
Overall Response Rate
ORR, a key secondary outcome, was defined as the proportion of patients with sCR, CR, VGPR, and PR as best overall response, assessed by IRC using IMWG criteria, and was assessed at the time of the primary PFS analysis and/or the final PFS analysis. Bone marrow biopsy could have been performed for sCR assessment, per investigator decision. sCR was not defined in the study protocol; however, it is defined by the IMWG on their website as patients with a CR who also have a normalized FLC ratio in the absence of monoclonal bone marrow plasma cells when assessed by immunohistochemistry or immunofluorescence.29
Rate of VGPR or better was a key secondary outcome and was defined as the proportion of patients with an sCR, CR, or VGPR as their best overall response.
The CR rate was defined as the proportion of patients with sCR or CR as best overall response. Patients with demonstrated isatuximab interference were considered in the best overall response category, corresponding to the M protein assessment obtained without interference, when the antibody-capture interference assay was available. Antibodies that are used therapeutically can interfere with M protein assessment, because they can be detected by immunoelectrophoresis or immunofixation, making it difficult to determine whether the therapeutic antibody or the disease marker is being detected. Stable disease, non-PD, and PD were also reported. A patient was considered to have a non-PD response when they had no more measurable serum or urine M protein on cycle 1, day 1.
Depth of Response
The MRD negativity rate in patients with VGPR or better was a key secondary outcome. This was defined as the proportion of patients for whom MRD was negative at any time point after the first dose of study treatment. MRD status was assessed centrally by ClonoSEQ assay in bone marrow samples from patients who achieved VGPR or better, to determine the depth of response at the molecular level. The threshold for negativity was 10−5. MRD status was considered negative if at least 1 result of the assessment was negative in the patient; otherwise, the MRD was considered positive. Those in the intention-to-treat (ITT) population without MRD assessment were considered positive.
Bone marrow aspirates were collected at screening and at the time of VGPR or better for confirmation. Because bone marrow aspiration is an invasive procedure, guidance was provided to limit the number of bone marrow assessments. A maximum of 6 bone marrow assessments could be performed.
For patients with CR without previous documentation of VGPR:
The first bone marrow for MRD assessment was collected at time of confirmation of CR (i.e., at the second time point showing CR). If the patient was determined to be MRD-positive, another bone marrow sample was collected 3 months (3 cycles) later, to identify late negativity. A third sample may have been collected after another 3 months if the patient remained MRD-positive and was still being treated.
For patients with VGPR:
The first bone marrow assessment was performed when VGPR was confirmed at the second time point or at a later time point, as per investigator judgment, based on kinetics of M protein decrease and/or if a plateau phase was reached (defined as variation less than 20% over 12 weeks).
If MRD was positive at the first bone marrow assessment, a second assessment was performed 3 months later (3 cycles) to identify late negativity.
If MRD remained positive at the second bone marrow assessment, a third assessment was performed while the patient had VGPR; the timing to perform the third assessment could be postponed until CR was achieved.
If the patient had CR and was MRD-positive at the last bone marrow assessment performed during VGPR, a bone marrow assessment was performed to confirm CR.
If the patient had CR and the first bone marrow assessment was MRD-positive, the additional protocol-specified bone marrow assessment could be discussed with the patient.
Duration of Response
DOR was a secondary outcome, defined as the time from date of first IRC-determined response that was subsequently confirmed for patients achieving PR or better to the date of first documented PD determined by IRC, or death, whichever occurred first. DOR was censored at the date of last valid disease assessment not showing PD performed before initiation of a new antimyeloma treatment (if any) or the analysis cut-off date, whichever occurred first.
The observation period for safety variables was divided into the pre-treatment period (from signed informed consent up to first dose of study medication), the treatment period (time from first dose of study treatment until last dose of study treatment plus 30 days) and the post-treatment period (starting the day after the end of the treatment period up to the end of the study).
Adverse Events
AE data were collected from time of signed informed consent to 30 days following last administration of study treatment. All AEs were graded according to NCI CTCAE v4.03. Treatment-emergent AEs were defined as AEs that developed, worsened (according to investigator opinion), or became serious during this period.
Adverse Events of Special Interest
AEs of special interest included infusion reactions of grade 3 or greater, and reports of pregnancy (including female partners of male patients), and symptomatic overdose with the study treatment or noninvestigational medical products.
Statistical Analysis
Primary Outcome
Power Calculation
In determining sample size, the sponsor assumed a median PFS of 19 months in the Kd arm, that the IsaKd group would have an HR of 0.59 compared to the Kd group, and that, assuming proportional hazards, this was expected to correspond to an improvement in median PFS from 19 to 32 months. The sponsor cited the ENDEAVOUR study17 as a source for its PFS estimate of 19 months. The sponsor planned to perform a log-rank test at a 1-sided significance level of 2.5% and planned for a 3:2 randomization ratio, IsaKd to Kd, as well as an interim analysis for PFS when 65% of the PFS events had been observed. Based on these assumptions, a total of 159 events were needed to achieve 90% power, and 300 patients (180 in the IsaKd group and 120 in the Kd group) were needed to achieve the targeted number of PFS events. Assuming a uniform accrual of 19 patients per month, the final PFS cut-off date was expected to be approximately 36 months after the first patient was enrolled.
Statistical Test or Model
An O’Brien and Fleming alpha-spending function was used to obtain the nominal significance levels for the interim and final analyses of survival on PFS. The 1-sided nominal significance level to declare overwhelming efficacy when 103 PFS events (65% information fraction) were observed was 0.005 (corresponding to an HR of 0.59) and to declare superiority of IsaKd at the final analysis (159 events) was 0.023 (corresponding to a HR of 0.725). The stopping boundaries on the PFS end point at the interim analysis were calculated using the actual number of events.
The interim efficacy analysis was the comparison of PFS based on the IRC assessment in the IsaKd group versus the Kd group using a log-rank test procedure stratified by the stratification factors (i.e., R-ISS and number of previous lines of therapy). The nominal significance levels at the interim analysis were determined using an alpha-spending function to control the overall 1-sided type I error at 2.5%. The 1-sided nominal significance level to confirm superiority of IsaKd over Kd at the 65% information fraction (103 PFS events) was 0.005 (corresponding to a HR of 0.59). The HR and its CI were estimated using Cox proportional hazards model stratified using the stratification factors, as per IRT. PFS was analyzed using Kaplan–Meier estimates of the 25th, 50th, and 75th percentiles, and 95% CIs were constructed using a log-log transformation of the survival function and methods of Brookmeyer and Crowley. The interim analysis was conducted by an independent statistician under the supervision of the data monitoring committee. The data monitoring committee also reviewed secondary outcomes and safety data available at the time of the interim analysis.
Data Imputation Methods
If a post-baseline disease assessment of response was determined to be “not evaluable” based on IMWG criteria or the date of assessment was missing, the disease assessment was considered invalid.
There were no methods described for imputing missing data for efficacy outcomes.
Subgroup Analyses
The consistency of the results from the primary analysis was evaluated across predefined subgroups of patients. Subgroup analyses performed that were relevant to this review included PFS by previous treatment with a proteasome inhibitor (yes or no), previous treatment with immunomodulatory imide drugs (yes or no), previous treatment with a proteasome inhibitor and an immunomodulatory imide drug (yes or no), previous ASCT (yes or no), cytogenetic abnormality (del(17p), t(4;14), t(14;16)), ISS disease stage (stage I, II, or III), R-ISS score (stage I or II, III, or not classified), and number of prior lines of therapy (1 or more than 1). The latter 2 subgroups, R-ISS score, and prior lines of therapy were stratification factors.
For each subgroup, the treatment effect HR and its associated 95% CI were estimated using a nonstratified Cox proportional hazards model with terms for the factor, treatment, and their interaction. There does not appear to have been an accounting for multiplicity.
Multiplicity
Beginning with the primary outcome, testing on the subsequent secondary efficacy outcomes was conducted only if the null hypothesis was rejected for the previous outcome. The statistical testing hierarchy was PFS (primary outcome), then ORR, rate of VGPR or better, and MRD negativity rate. The CR rate was not tested for comparison, because the antibody-capture interference assay was not available. OS will be tested only at the end of the study.
Sensitivity Analyses
Sensitivity analyses of the primary outcome included (1) without censoring for further antimyeloma treatment; (2) using investigator assessment of response, including symptomatic deterioration; (3) using investigator assessment of response, ignoring symptomatic deterioration; (4) with initiation of further antimyeloma treatment considered as a PFS event; (5) with analysis based on scheduled assessment dates instead of actual assessment dates and with late PFS events censored; (6) an unstratified PFS analysis; and (7) a PFS analysis using stratification factors as per the eCRF.
Secondary Outcomes
For the key binary secondary end points, the significance levels at the interim and final analyses were determined using alpha-spending function specific to each end point, except if the information fraction was 100% at the interim analysis of PFS (i.e., information on binary secondary end points were available for every patient). For ORR and rate of VGPR or better, a Pocock-type boundary was used. For rates of CR and MRD negativity, the O’Brien-Fleming alpha-spending function was used. If the null hypothesis for any key efficacy end point was rejected at the interim PFS analysis, then any subsequent key efficacy end point was not tested until the final PFS analysis. CIs at (1 to 2 alpha) percent level (alpha being the adjusted 1-sided nominal significance level using the alpha-spending function specific to each outcome at final and interim analyses) were determined for ORR, rate of VGPR or better, CR rate (including sCR) and MRD negativity rate using the Clopper-Pearson method. Since the information fraction was 100% at the interim analysis, significance levels were 0.025 for all binary secondary outcomes. These outcomes were compared between treatment groups using the Cochran-Mantel-Haenszel test stratified by stratification factors, as entered in the IRT. A sensitivity analysis of key secondary outcomes (except MRD negativity rate) was performed using investigator assessment.
Analyses of “other” secondary outcomes was for descriptive purposes only, and any testing that was carried out was considered exploratory. Time-to-event outcomes were assessed using Kaplan–Meier methods. For HRQoL outcomes, a descriptive summary of results was provided at each visit, including end of treatment and an assessment performed 90 days after the last study treatment. Mean change from baseline was also provided, and data were reported for the safety population.
Table 9: Statistical Analysis of Efficacy End Points in the IKEMA Trial
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
PFS | Log-rank | Stratified by stratification factors (R-ISS scores, previous lines of therapy) | Without censoring for further antimyeloma treatment Using investigator assessment of response, including symptomatic deterioration Using investigator assessment of response, ignoring symptomatic deterioration Initiation of further antimyeloma treatment considered a PFS event Analysis based on scheduled assessment dates instead of actual dates, and with late PFS events censored Unstratified PFS analysis PFS analysis using stratification factors per eCRF |
ORR | CMH | Stratified by stratification factors (R-ISS scores, previous lines of therapy) | Using investigator assessed response |
VGPR or better | CMH | Stratified by stratification factors (R-ISS scores, previous lines of therapy) | Using investigator assessed response |
MRD negativity | CMH | Stratified by stratification factors (R-ISS scores, previous lines of therapy) | None |
CMH = Cochran-Mantel-Haenszel; MRD = minimal residual disease; ORR = overall response rate; PFS = progression-free survival; R-ISS = Revised International Staging System; VGPR = very good partial response.
Source: Clinical Study Report for IKEMA.7
Protocol Amendments
Notable protocol amendments included Amendment 3 (February 8, 2018), adding an objective to evaluate the rate of VGPR or better in patients who were MRD-negative (original outcome evaluated rate of CR in MRD-negative patients). The HR estimate and corresponding 95% CI was changed to HR and corresponding (1 to 2 alpha) percent level (alpha being the 1-sided nominal significance level: alpha = 0.023 at final analysis and 0.005 at PFS interim analysis). Amendment 3 also clarified that further antimyeloma therapies were collected until OS analysis and added delay for carfilzomib infusion if grade 3 to 4 infusion reactions occurred during the isatuximab infusion. Amendment 4 (July 2, 2018) allowed that, in the absence of radiological and M protein progression, if clinical and biologic data provided clear evidence of clinical progression, the IRC could consider clinical progression as a PFS event. Amendment 7 (November 13, 2019) changed censoring rules for the primary PFS analysis; the PFS definition was modified such that the date of initiation of further antimyeloma treatment was considered when determining the cut-off date for PFS.
Analysis Populations
The randomized population included all patients randomized into the study, regardless of whether they received study treatment. The ITT population is the randomized population, and patients were analyzed based on the treatment they were randomized to, regardless of whether they received any treatment or the treatment to which they were randomized. This was the primary population for all efficacy analyses. The safety population included all patients in the ITT population who received at least 1 dose of study drug, or a partial dose of study drug. This population was the primary population for analysis of all safety parameters, and analyses were based on the treatment actually received.
Results
Patient Disposition
A total of 341 patients were screened, and 302 of these patients were randomized into the study. The most common reason for screen failure (12 patients) was not having measurable disease (urine M protein ≥ 200 mg/24 hours or serum M protein ≥ 0.5 g/dL).
IKEMA is an ongoing trial, and 52.0% of IsaKd patients and 30.9% of Kd patients were still on treatment as of the most recent Clinical Study Report (Table 10). The data cut-off date for this interim analysis was February 7, 2020, corresponding to a median follow-up of 20.73 months. Of the remaining patients, 46.9% of those in the IsaKd group and 68.3% in the Kd group had “definitive treatment discontinuation.” The most common reason for discontinuation was progression of disease, affecting 29.1% and 39.8% of patients, respectively, followed by AEs, affecting 8.4% and 13.8% of patients, respectively.
IKEMA | ||
|---|---|---|
Characteristic | IsaKd | Kd |
Screened, N | 341 | |
Randomized, N | 179 | 123 |
Randomized and treated, n (%) | 177 (98.9) | 122 (99.2) |
Patients still on treatment, n (%) | 93 (52.0) | 38 (30.9) |
Patients with definitive treatment discontinuation,a n (%) | 84 (46.9) | 84 (68.3) |
Adverse event | 15 (8.4) | 17 (13.8) |
Progression of disease | 52 (29.1) | 49 (39.8) |
Poor compliance with protocol | 0 (0.0) | 0 (0.0) |
Withdrawal by patient | 11 (6.1) | 14 (11.4) |
Adverse event | 3 (1.7) | 5 (4.1) |
Study procedure | 1 (0.6) | 1 (0.8) |
Other | 7 (3.9) | 8 (6.5) |
Other | 6 (3.4) | 4 (3.3) |
Patients who discontinued at least one study drug, n (%) | 34 (19.2) | 5 (4.1) |
Adverse event | 34 (19.2) | 5 (4.1) |
Patients who discontinued carfilzomib, n (%) | 26 (14.7) | 1 (0.8) |
Patients who discontinued dexamethasone, n (%) | 11 (6.2) | 4 (3.3) |
Status at cut-off date,b n (%) | ||
Alive | 148 (82.7) | 98 (79.7) |
Death | 31 (17.3) | 25 (20.3) |
Analysis populations, n (%) | ||
Intention-to-treat population | 179 (100.0) | 123 (100.0) |
Safety | 177 (98.9) | 122 (99.2) |
Time from last contact to the data cut-off date | ||
≤ 2 weeks | 8 (4.5) | 19 (15.4) |
2 weeks and ≤ 1 month | 0 | 1 (0.8) |
> 1 month and ≤ 2 months | 0 | 0 |
> 2 months | 7 (3.9) | 3 (2.4) |
IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone.
aAll treatments discontinued.
bCut-off date for OS (February 7, 2020).
Source: Clinical Study Report for IKEMA.7
Protocol Deviations
The most common reason for protocol deviations was wrong stratum of randomization, which occurred in 7.3% of IsaKd patients and 16.3% of Kd patients. This was due to violations in number of prior lines (IsaKd: 2.8% versus Kd: 5.7%) and R-ISS stage (4.5% versus 10.6%, respectively).
Exposure to Study Treatments
The median duration of treatment exposure was 80.0 weeks (range 1 to 111 weeks) in the IsaKd arm and 61.4 weeks (range 1 to 114 weeks) in the Kd arm, and the median number of treatment cycles was 19.0 (range 1 to 27) and 14.5 (range 1 to 28), respectively. At least 1 cycle delay occurred in 70.1% of patients in the IsaKd group and 61.5% of patients in the Kd group, while 10.8% and 9.6% of cycles were delayed in each group, respectively. With isatuximab, the median relative dose intensity was 94.27% (range 66.7% to 108.2%), while, with carfilzomib, the median relative dose intensity in the IsaKd group was 91.18% and in the Kd group was 91.35%. With isatuximab, infusion interruptions occurred in 38.4% of patients, and in 1.4% of 5,715 infusions overall. Interruptions mainly occurred within the first 90 minutes of the first infusion. With carfilzomib, 35.0% of patients in the IsaKd group and 35.2% of patients in the Kd group had at least 1 dose reduction, and 71.2% and 72.1% of patients, respectively, had a dose omission. Dose interruptions of carfilzomib occurred in 4.0% of patients in the IsaKd group and 3.3% of patients in the Kd group.
Median duration of exposure to dexamethasone was 76.14 weeks (range 1 to 111 weeks) in the IsaKd group and 59.07 weeks (range 1 to 114 weeks) in the Kd group, and the median relative dose intensity of dexamethasone was 84.78% and 88.37% in each treatment group, respectively. With dexamethasone, dose delays occurred in 29.9% and 26.2% of patients in the IsaKd and Kd groups, respectively, and dose reductions in 43.5% and 38.5% of patients in the IsaKd and Kd groups, respectively, and dose omissions in 77.4% and 75.4% of IsaKd and Kd patients, respectively.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the CADTH review protocol are reported in this section. See Appendix 1 for detailed efficacy data. The median follow-up at the time of the interim analysis was 20.73 months, with a data cut-off of February 7, 2020.
Progression-Free Survival
PFS was the primary outcome of the IKEMA trial. At the interim analysis (median follow-up of 20.73 months), median PFS was not reached in the IsaKd group and was 19.15 months (95% CI, 15.77 to not calculable) in the Kd group, for a stratified HR of 0.531 (99% CI, 0.318 to 0.889) and a P value by log-rank test of P = 0.0007, well below the planned threshold for statistical significance of P = 0.005 (Table 11). At this time, 48 (26.8%) patients in the IsaKd group and 55 (44.7%) of patients in the Kd group had a PFS event (Figure 3).
Figure 3: Progression-Free Survival From IKEMA Trial
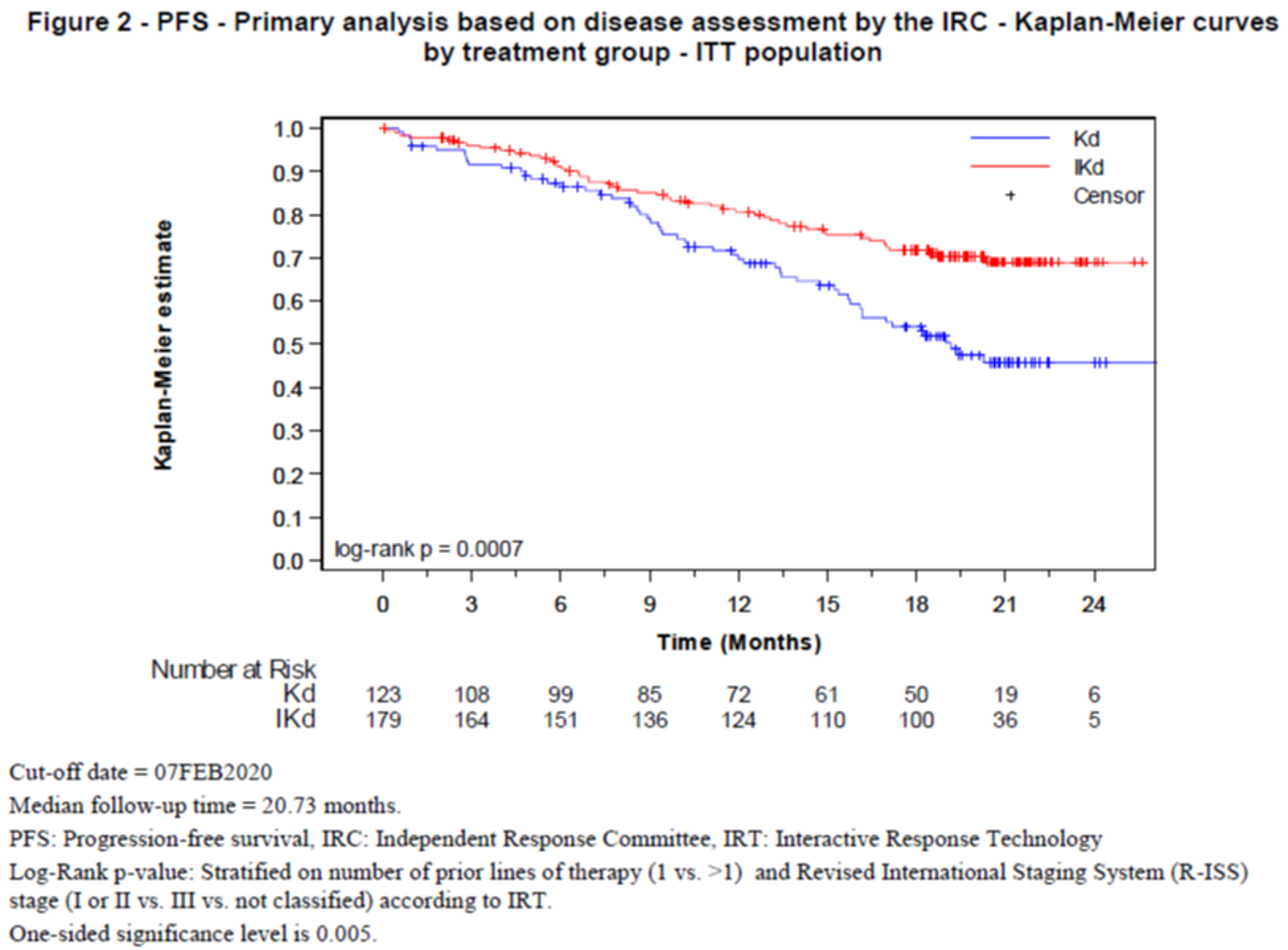
IKd = isatuximab plus carfilzomib plus dexamethasone; ITT = intention-to-treat; Kd = carfilzomib plus dexamethasone.
Source: Clinical Study Report for IKEMA.7
A number of sensitivity analyses of the primary outcome were performed, including per IRC without censoring for further antimyeloma treatment; per investigator, including symptomatic deterioration as an event; per investigator, ignoring symptomatic deterioration; per IRC, including initiation of further antimyeloma treatment as an event; per IRC stratified by stratification factors entered in the eCRF; and per IRC with censoring of progression or death occurring more than 8 weeks after last valid disease assessment. All results were consistent with that of the primary analysis.
Subgroup analyses for the primary outcome are summarized in Table 19, Appendix 3. Based on the interaction P values, there were no clear differences in response between subgroups of interest for this review.
Overall Survival
OS will be assessed at the end of the study; therefore, no data for median OS were reported at the time of the interim analysis. At the time of the interim analysis, after a median follow-up of 20.73 months at the data cut-off date, 31 (17.3%) patients had died in the IsaKd group and 25 had died (20.3%) in the Kd group.
Health-Related Quality of Life
HRQoL was assessed using the EORTC QLQ-C30, the EORTC QLQ-MY20, and the EQ-5D-5L instruments. Results were reported for change from baseline in each treatment group, but no statistical analyses were planned. Results from the EORTC QLQ-C30 global QoL scale are provided in Figure 4, and the results for the remainder of the EORTC QLQ-C30 scales and other questionnaires are available in Appendix 3, presented in graphs.
Compliance with filling out the EORTC QLQ-C30 was reported to be between 87.5% and 100% at each treatment cycle. Baseline scores were generally consistent between the treatment groups, although there were differences of up to 5 points for some subscales, including the EORTC QLQ-C30 global QoL scale. Mean changes from baseline in global QoL are presented in Figure 4. There was a considerable decline in patients sampled over time, largely due to attrition. Graphs in Appendix 3 provide an indication of the change in scores over time. Generally, there was little change from baseline in global QoL scores over time in the IsaKd group, while there were numerical increases from baseline over time in the Kd group. Increases in the global QoL score indicated an improvement in HRQoL. The threshold estimates for a small deterioration in the global health status is −5 to −10.
Figure 4: Mean Change From Baseline in EORTC QLQ-C30 Global QoL Scores Over Time
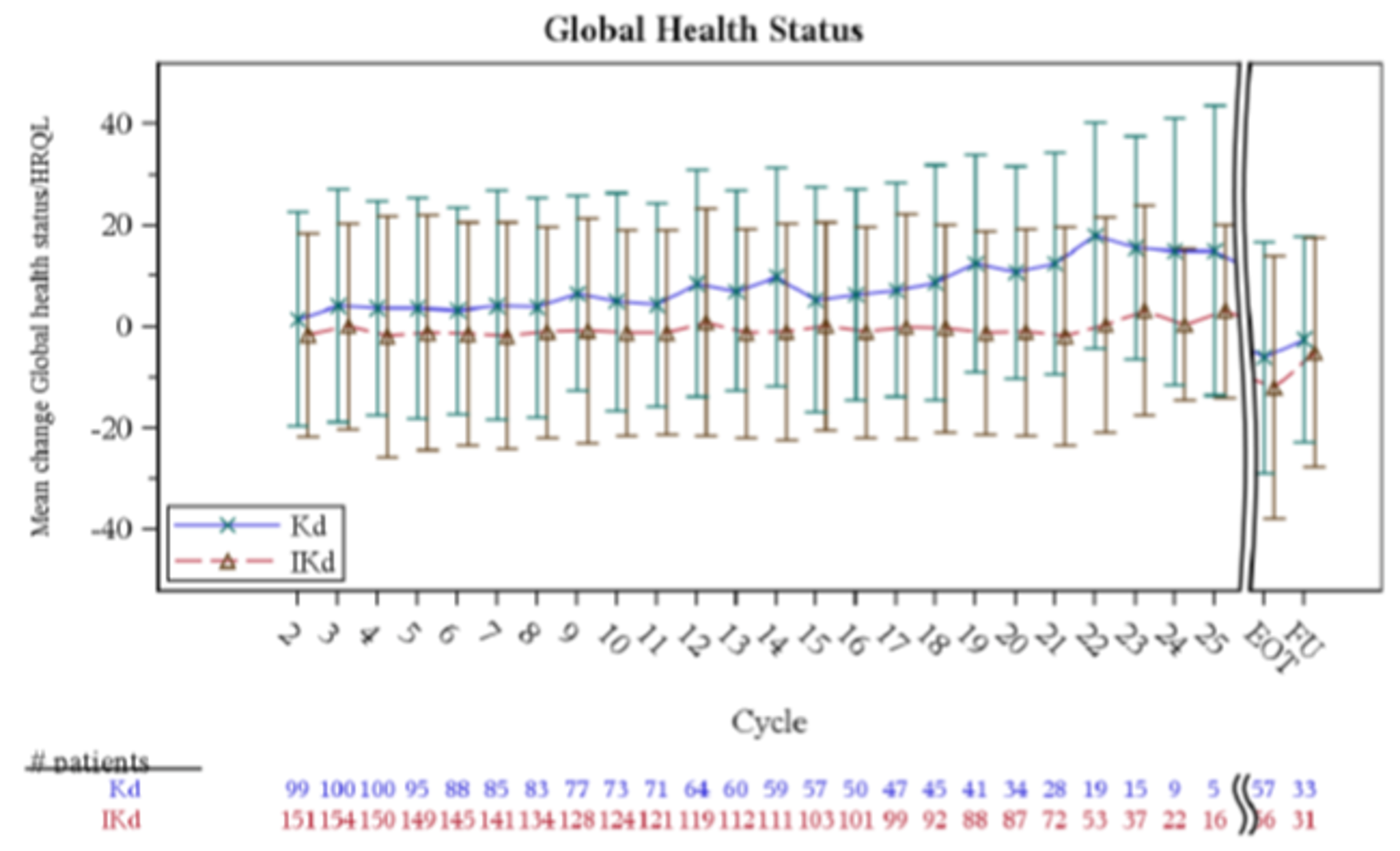
EORTC = European Organisation for Research and Treatment of Cancer; EOT = end of treatment; FU = follow = up; HRQoL = health-related quality of life; IKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; QLQ-C30 = Quality of Life Cancer-Specific Questionnaire with 30 items; QoL = quality of life.
Source: Clinical Study Report for IKEMA.7
Overall Response Rate
The ORR was assessed as 2 secondary outcomes, as responders (patients achieving either an sCR, CR, VGPR, or PR) and as patients achieving a VGPR or better, both by IRC assessment. The percentage of patients responding was 86.6% (95% CI, 0.8071 to 0.9122) in the IsaKd group and 82.9% (95% CI, 0.7509 to 0.8911) in the Kd group, and the difference between groups was not statistically significant (P = 0.1930) (Table 11). As this was the second outcome in the statistical hierarchy, testing was to have halted for subsequent outcomes; however, the sponsor continued to conduct testing and report P values for descriptive purposes. The percentage of patients achieving VGPR or better was 72.6% (95% CI, 0.6547 to 0.7901) in the IsaKd group and 56.1% (95% CI, 0.4687 to 0.6503) in the Kd group. No patients achieved an sCR, while 39.7% of patients in the IsaKd group and 27.6% of patients in the Kd group achieved a CR, and 33.0% and 28.5% of patients, respectively, achieved a VGPR. The results for ORR by investigator assessment were consistent with those conducted by the IRC.
Depth of Response
Bone marrow samples for the assessment of MRD were collected for patients with VGPR or better and included 78% and 74% of patients with at least 1 evaluable MRD sample in the IsaKd and Kd groups, respectively. MRD negativity (10−5 sensitivity level by central laboratory) was achieved by 29.6% of patients in the IsaKd group and 13.0% of patients in the Kd group (Table 11). At a sensitivity of 10−4, MRD negativity occurred in 40.2% and 24.4% of patients, respectively; and at a sensitivity of 10−6, 8.4% and 1.6% of patients, respectively.
Median Duration of Response
The median DOR was calculated based on 155 patients in the IsaKd group and 102 patients in the Kd group. The median DOR was not yet reached in either treatment group, and the HR was 0.425 (95% CI, 0.269 to 0.672) (Table 11).
Time to Response
The median TTR was 1.08 months (95% CI, 1.05 to 1.12) in the IsaKd group and 1.12 months (95% CI, 1.05 to 1.18) in the Kd group, for a stratified HR of 1.143 (95% CI, 0.888 to 1.471) (Table 11).
Health Resource Utilization
This outcome was not assessed.
IKEMA | ||
|---|---|---|
Outcome | IsaKd N = 179 | Kd N = 123 |
PFS | ||
Number (%) of events | 48 (26.8) | 55 (44.7) |
Number (%) of patients censored | 131 (73.2) | 68 (55.3) |
Kaplan–Meier estimates of PFS in months, median (95% CI) | Not reached | 19.15 (15.770 to NC) |
Stratifieda log-rank test P valueb | 0.0007 | |
Stratifieda HR (99% CI) | 0.531 (0.318 to 0.889) | |
OS | ||
Deaths, n (%) | 31 (17.3) | 25 (20.3) |
Median OS | Not reported | Not reported |
HRQoL | ||
Refer to graphs in Appendix 3 | ||
Objective response | ||
Overall response | ||
Responders (sCR, CR, VGPR, or PR) | 155 (86.6) | 102 (82.9) |
95% CI estimated using Clopper-Pearson method | 0.8071 to 0.9122 | 0.7509 to 0.8911 |
Stratified CMH test P valuec vs. Kd | 0.1930 | |
VGPR or better | 130 (72.6) | 69 (56.1) |
95% CI estimated using Clopper-Pearson method | 0.6547 to 0.7901 | 0.4687 to 0.6503 |
Stratified CMH test P valuec,d vs. Kd | 0.0011 | |
Best overall response, n (%) | ||
sCR | 0 (0.0) | 0 (0.0) |
CR | 71 (39.7) | 34 (27.6) |
VGPR | 59 (33.0) | 35 (28.5) |
Biochemical CR but with missing bone marrow | 6 (3.4) | 7 (5.7) |
Near-CRe | 36 (20.1) | 13 (10.6) |
PR | 25 (14.0) | 33 (26.8) |
Minimal response | 4 (2.2) | 5 (4.1) |
Stable disease | 13 (7.3) | 6 (4.9) |
Non-PD | 1 (0.6) | 1 (0.8) |
PD | 2 (1.1) | 3 (2.4) |
Unconfirmed PD | 0 | 1 (0.8) |
Not evaluable/not assessed | 4 (2.2) | 5 (4.1) |
Depth of response | ||
MRD negativity rate, n (%) | 53 (29.6) | 16 (13.0) |
95% CI by Clopper-Pearson | 0.2303 to 0.3688 | 0.0762 to 0.2026 |
Stratified CMH test P valuec,d vs. Kd | 0.0004 | |
Duration of response | N = 155 | N = 102 |
Number (%) of events | 33 (21.3) | 43 (42.2) |
Number (%) of patients censored | 122 (78.7) | 59 (57.8) |
Kaplan–Meier estimates of DOR in months, median (95% CI) | NC (NC to NC) | NC (14.752 to NC) |
Stratifieda HR (95% CI) | 0.425 (0.269 to 0.672) | |
Time to first response | ||
Number (%) of events | 155 (86.6) | 102 (82.9) |
Number (%) of patients censored | 24 (13.4) | 21 (17.1) |
Kaplan–Meier estimates of TTR in months, median (95% CI) | 1.08 (1.051 to 1.117) | 1.12 (1.051 to 1.183) |
Stratifieda HR (95% CI) vs. Kd | 1.143 (0.888 to 1.471) | |
Health resource utilization | ||
Not reported | Not reported | Not reported |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; CR = complete response; DOR = duration of response; HR = hazard ratio; HRQoL = health-related quality of life; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; MRD = minimal residual disease; NC = not calculable; PD = progressive disease; PR = partial response; sCR = stringent complete response; TTR = time to response; VGPR = very good partial response.
aStratified on number of prior lines of therapy (1 vs. > 1) and Revised International Staging System (R-ISS) stage (I or II vs. III vs. not classified) according to IRT.
bOne-sided significance level is 0.005.
cStratified on randomization factors according to IRT. One-sided significance level is 0.025. Biochemical CR and Near-CR were assessed only for patients with confirmed VGPR as BOR. Criteria for confirmation was not applied to Near-CR subcategory.
dThe statistical testing upon which these P values were based was conducted after failure of the hierarchy and therefore cannot be used for drawing conclusions.
eAll criteria for a CR were met except that immunofixation remained positive.
Source: Clinical Study Report for IKEMA.7
Harms
Only those harms identified in the CADTH review protocol are reported. Refer to Table 12 for detailed harms data.
Adverse Events
There were 97.2% of patients in the IsaKd group and 95.9% of patients in the Kd group who had at least 1 treatment-emergent AE; 76.8% versus 67.2%, respectively, who had at least a grade 3 AE; and 3.4% versus 3.3% who had a grade 5 AE (Table 12). The most common AE in the IsaKd group was infusion-related reaction, which occurred in 44.6% of patients in the IsaKd group and 3.3% of patients in the Kd group. Other common AEs, IsaKd versus Kd, were hypertension (36.7% versus 31.1%), diarrhea (36.2% versus 28.7%), upper respiratory tract infection (36.2% versus 23.8%), fatigue (28.2% versus 18.9%), and dyspnea (27.7% versus 21.3%). The most common AEs of grade 3 or higher were hypertension (IsaKd: 20.3% versus Kd: 19.7%) and pneumonia (IsaKd: 16.4% versus Kd: 12.3%).
Serious Adverse Events
SAEs occurred in 59.3% of patients in the IsaKd group and 57.4% of patients in the Kd group (Table 12). The most common SAE was pneumonia (IsaKd: 18.1% versus Kd: 11.5%).
Withdrawal Due to Adverse Events
There were 8.5% of patients in the IsaKd group and 13.9% of patients in the Kd group who had an AE leading to definitive treatment discontinuation, which was defined as discontinuing all treatments (Table 12). One patient discontinued isatuximab due to an AE. There were 14.7% of patients in the IsaKd group and 0.8% of patients in the Kd group who discontinued carfilzomib, and 6.2% of patients in the IsaKd group and 3.3% of patients in the Kd group who discontinued dexamethasone.
Notable Harms
Among notable harms, respiratory tract infections occurred in 83.1% of patients in the IsaKd group and 73.8% of patients in the Kd group, and these were grade 3 or greater events in 32.2% versus 23.8% of patients, respectively (Table 12). Cardiac disorders occurred in 7.3% of patients in the IsaKd group and 5.7% of patients in the Kd group; second primary malignancies (solid non-skin) in 2.8% versus 3.3% of patients, respectively; and second primary malignancies (solid, skin) in 5.1% versus 2.5% of patients, respectively. There were no hematologic malignancies reported in either treatment group. Events of decreased neutrophil count occurred in 54.8% of patients in the IsaKd group versus 43.4% of patients in the Kd group, and grade 3 or greater events occurred in 19.2% versus 7.4% of patients, respectively. Events of decreased platelet counts occurred in 94.4% of IsaKd patients and 87.7% of Kd patients, and these were grade 3 or greater events in 29.9% versus 23.8% of patients, respectively.
IKEMA | ||||
|---|---|---|---|---|
AEs | IsaKd N = 177 | Kd N = 122 | IsaKd N = 177 | Kd N = 122 |
Patients with at least one AE, n (%) | 172 (97.2) | 117 (95.9) | NA | NA |
Patients with any grade ≥ 3 AE, n (%) | 136 (76.8) | 82 (67.2) | NA | NA |
Patients with any grade 5 TEAE, n (%) | 6 (3.4) | 4 (3.3) | NA | NA |
Most frequent AE, ≥ 10% in any group, n (%) | Grade ≥ 3 AE | |||
Infusion-related reaction | 79 (44.6) | 4 (3.3) | 1 (0.6) | 0 |
Hypertension | 65 (36.7) | 38 (31.1) | 36 (20.3) | 24 (19.7) |
Diarrhea | 64 (36.2) | 35 (28.7) | 5 (2.8) | 3 (2.5) |
Upper respiratory tract infection | 64 (36.2) | 29 (23.8) | 6 (3.4) | 2 (1.6) |
Fatigue | 50 (28.2) | 23 (18.9) | 6 (3.4) | 1 (0.8) |
Dyspnea | 49 (27.7) | 26 (21.3) | 9 (5.1) | 1 (0.8) |
Insomnia | 42 (23.7) | 28 (23.0) | 9 (5.1) | 3 (2.5) |
Pneumonia | 42 (23.7) | 24 (19.7) | 29 (16.4) | 15 (12.3) |
Bronchitis | 40 (22.6) | 15 (12.3) | 4 (2.3) | 1 (0.8) |
Back pain | 39 (22.0) | 25 (20.5) | 3 (1.7) | 1 (0.8) |
Cough | 35 (19.8) | 17 (13.9) | 0 | 0 |
Asthenia | 32 (18.1) | 20 (16.4) | 3 (1.7) | 4 (3.3) |
Nasopharyngitis | 28 (15.8) | 14 (11.5) | 0 | 0 |
Nausea | 28 (15.8) | 20 (16.4) | 0 | 0 |
Vomiting | 27 (15.3) | 11 (9.0) | 2 (1.1) | 1 (0.8) |
Headache | 26 (14.7) | 21 (17.2) | 0 | 1 (0.8) |
Muscle spasms | 25 (14.1) | 19 (15.6) | 0 | 0 |
Peripheral sensory neuropathy | 25 (14.1) | 15 (12.3) | 0 | 1 (0.8) |
Edema, peripheral | 23 (13.0) | 21 (17.2) | 1 (0.6) | 0 |
Arthralgia | 22 (12.4) | 10 (8.2) | 3 (1.7) | 2 (1.6) |
Constipation | 22 (12.4) | 12 (9.8) | 1 (0.6) | 0 |
Fall | 20 (11.3) | 10 (8.2) | 3 (1.7) | 0 |
Pain in extremity | 19 (10.7) | 15 (12.3) | 0 | 1 (0.8) |
Influenza | 16 (9.0) | 17 (13.9) | 1 (0.6) | 5 (4.1) |
Pyrexia | 16 (9.0) | 18 (14.8) | 2 (1.1) | 0 |
SAEs | ||||
Patients with at least one SAE, n (%) | 105 (59.3) | 70 (57.4) | 94 (51.3) | 58 (47.5) |
Most common, ≥ 2% in any group | ||||
Pneumonia | 32 (18.1) | 14 (11.5) | 27 (15.3) | 14 (11.5) |
Lower respiratory tract infection | 7 (4.0) | 5 (4.1) | 7 (4.0) | 5 (4.1) |
Upper respiratory tract infection | 5 (2.8) | 2 (1.6) | 4 (2.3) | 1 (0.8) |
Respiratory tract infection | 4 (2.3) | 1 (0.8) | 2 (1.1) | 0 |
Viral upper respiratory tract infection | 4 (2.3) | 0 | 4 (2.3) | 0 |
Influenza | 1 (0.6) | 5 (4.1) | 1 (0.6) | 4 (3.3) |
Cardiac failure | 5 (2.8) | 2 (1.6) | 4 (2.3) | 2 (1.6) |
Deep vein thrombosis | 2 (1.1) | 3 (2.5) | 0 | 2 (1.6) |
Pathological fracture | 4 (2.3) | 1 (0.8) | 4 (2.3) | 0 |
Acute kidney injury | 3 (1.7) | 3 (2.5) | 2 (1.1) | 2 (1.6) |
Traumatic failure | 5 (2.8) | 2 (1.6) | 3 (1.7) | 2 (1.6) |
Withdrawal due to AEs | ||||
Patients with any TEAE leading to definitive treatment discontinuation | 15 (8.5) | 17 (13.9) | 11 (6.2) | 10 (8.2) |
Most common reason | ||||
Infections and infestations | 5 (2.8) | 6 (4.9) | 5 (2.8) | 5 (4.1) |
Pneumonia | 3 (1.7) | 4 (3.3) | 3 (1.7) | 3 (2.5) |
Patients with any TEAE leading to premature discontinuation of isatuximab | 1 (0.6) | 0 | 0 | 0 |
Most common reason | ||||
Infections and infestations | 1 (0.6) | 0 | 0 | 0 |
Patients with any TEAE leading to premature discontinuation of carfilzomib | 26 (14.7) | 1 (0.8) | 0 | 0 |
Most common reason | ||||
Cardiac disorders | 13 (7.3) | 0 | 7 (4.0) | 0 |
Cardiac failure | 5 (2.8) | 0 | 2 (1.1) | 0 |
Patients with any TEAE leading to premature discontinuation of dexamethasone | 11 (6.2) | 4 (3.3) | 6 (3.4) | 2 (1.6) |
Most common reason | ||||
Hypertension | 2 (1.1) | 1 (0.8) | 2 (1.1) | 1 (0.8) |
Notable harms, n (%) | Grade ≥ 3 AE | |||
Respiratory tract infections | 147 (83.1) | 90 (73.8) | 57 (32.2) | 29 (23.8) |
Upper respiratory tract infection | 64 (36.2) | 29 (23.8) | 6 (3.4) | 2 (1.6) |
Pneumonia | 42 (23.7) | 24 (19.7) | 29 (16.4) | 15 (12.3) |
Bronchitis | 40 (22.6) | 15 (12.3) | 4 (2.3) | 1 (0.8) |
Nasopharyngitis | 28 (15.8) | 14 (11.5) | 0 | 0 |
Influenza | 16 (9.0) | 17 (13.9) | 1 (0.6) | 5 (4.1) |
Lower respiratory tract infection | 16 (9.0) | 10 (8.2) | 7 (4.0) | 5 (4.1) |
Respiratory tract infection | 16 (9.0) | 8 (6.6) | 2 (1.1) | 0 |
Rhinitis | 10 (5.6) | 3 (2.5) | 0 | 0 |
Sinusitis | 9 (5.1) | 4 (3.3) | 1 (0.6) | 0 |
Cardiac disorders | 13 (7.3) | 7 (5.7) | 7 (4.0) | 4 (3.3) |
Cardiac failure | 8 (4.5) | 6 (4.9) | 4 (2.3) | 3 (2.5) |
Cardiac failure, congestive | 3 (1.7) | 0 | 1 (0.6) | 0 |
Cardiac failure, acute | 1 (0.6) | 0 | 1 (0.6) | 0 |
Cardiac failure, chronic | 1 (0.6) | 0 | 1 (0.6) | 0 |
Left ventricular failure | 0 | 1 (0.8) | 0 | 1 (0.8) |
Second primary malignancies, solid non-skin | 5 (2.8) | 4 (3.3) | 3 (1.7) | 3 (2.5) |
Second primary malignancies, solid skin | 9 (5.1) | 3 (2.5) | 1 (0.6) | 1 (0.8) |
Second primary malignancies, hematologic | 0 | 0 | 0 | 0 |
Neutrophil count decreased | 97 (54.8) | 53 (43.4) | 34 (19.2) | 9 (7.4) |
Platelet count decreased | 167 (94.4) | 107 (87.7) | 53 (29.9) | 29 (23.8) |
AE = adverse event; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; NA = not applicable; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Source: Clinical Study Report for IKEMA.7
Critical Appraisal
Internal Validity
The IKEMA trial appears to be a well-conducted study. It was planned with adequate power to meet the goals of the primary outcome (PFS), and enrolment targets were met, with a target enrolment of 300 patients and 302 patients randomized. The assumptions made when performing power calculations were based on a previous study30 and seemed reasonable. The randomization method appeared adequate, and randomization was stratified based on important prognostic factors in an effort to minimize important differences in baseline characteristics between groups. There were, however, some limitations and potential sources of bias, which are outlined in this section.
Results for the primary outcome were based on a pre-specified interim analysis (103 PFS events), which occurred at a 65% information fraction, relative to the planned final analysis (159 PFS events). As a result, there is a risk that the treatment effect for PFS has been overestimated. However, given the statistical and clinical significance of the difference observed between the IsaKd and Kd groups, this is likely not a major concern.
The included trial was open-label, and lack of blinding may bias results, particularly for patient-reported outcomes such as HRQoL. Objective clinical outcomes such as PFS and ORR are less likely to be influenced by lack of blinding. Reporting of harms may also be influenced by blinding, as patients may anticipate known adverse effects of IsaKd and thus may be more likely to report them when they do occur. Physician knowledge of their patient’s assigned treatment may also affect the way they manage their patient, and patient knowledge of their assigned treatment may make them more or less likely to remain in the study. Assessment of radiological and laboratory-related outcomes (such as ORR) was conducted by a blinded IRC, and therefore would not be subject to bias from lack of blinding.
Multiplicity was controlled for in the study by use of a hierarchical testing procedure. The hierarchy failed early (after the primary outcome). Therefore, as described in the protocol, testing should have stopped there. However, the sponsor continued to report P values for other outcomes in the hierarchy. The P values that were reported beyond the failure of the hierarchy should not be used to draw conclusions. Subgroup analyses were not adjusted for multiplicity and therefore should not be used to draw conclusions. Otherwise, subgroup analyses were planned a priori, and these included many of the subgroups included in the protocol for this review. Most subgroup results for PFS were consistent with the primary analysis results in favour of IsaKd, although some of these analyses were limited by small numbers.
There was a relatively large numerical difference between groups in patients discontinuing the trial early, with fewer discontinuations in the IsaKd group than the Kd group, and a large number of patients overall who discontinued. The largest number of these discontinuations were due to PD. This was expected, given that discontinuations due to PD were more frequent in the Kd group. A large difference in attrition between study groups can influence interpretation of harms outcomes, as the IsaKd group had longer exposure to study drug than the Kd group.
There does not appear to have been any accounting for missing data in analysis of efficacy outcomes such as ORR and patient-reported outcomes. For example, missing data for ORR are often counted as nonresponders. However, this procedure was not explicitly stated in the study protocol, although it was presumably followed. For best overall response, 2% of patient data in the IsaKd group and 4% in the Kd group were described as “not available/not assessed;” these patients do not appear to have been counted as responders, and this is appropriate.
There were some notable differences between groups in baseline characteristics. There were a larger percentage of White patients in the IsaKd group than in the Kd group (73.2% versus 67.5%) and a smaller percentage of Asian patients (14.5% versus 19.5%, respectively). It is unclear whether race plays a significant role in response to therapy in MM. A smaller percentage of IsaKd patients had MM at ISS stage I compared to Kd patients (49.7% versus 57.7%), and a larger percentage had MM at stage II (35.2% versus 25.2%). Although the percentage of patients with MM at R-ISS stage I was similar between IsaKd and Kd groups at baseline (25.1% versus 26.8%, respectively), there were more patients with MM at R-ISS stage II in the IsaKd group (61.5% versus 56.9%). Although R-ISS score was a stratification factor, the cut point was stage I or II versus III or not classified. Given that, in both cases, there were more patients with MM at stage II in the IsaKd group than in the Kd group, this could suggest that patients in the IsaKd had more advanced disease than those in the Kd group. However, the importance of this is unclear, although it could bias efficacy results against IsaKd. There were fewer patients in the IsaKd group than in the Kd group who had relapsed and refractory MM (68.2% versus 76.4%) and more patients who had relapsed MM (31.8% versus 23.6%). There were more patients in the IsaKd than in the Kd group who had 2 prior lines of therapy (35.8% versus 29.3%) and fewer who had 3 prior lines of therapy (18.4% versus 24.4%). Although the number of prior lines of therapy was a stratification factor, the cut point was 1 prior line of therapy versus more than 1 prior lines. A larger number of IsaKd than Kd patients had prior treatment with alkylating neoplastic drugs (94.4% versus 82.1%) and proteasome inhibitors (92.7% versus 85.4%), while fewer had been treated with immunomodulatory drugs (76.0% versus 81.3%).
External Validity
The IKEMA trial included all of the outcomes of most importance to patients. However, because the study is ongoing, OS data were not yet available (anticipated in 2023) and the difference in HRQoL outcomes between the groups was not formally assessed. The lack of formal assessment of HRQoL precludes any conclusions from being drawn about this important outcome, and this should therefore be considered an important limitation of this study. The lack of formal analysis of OS at this time should also be considered a limitation, given the importance of this outcome. PFS is considered a surrogate for OS, and the clinical experts consulted by CADTH believed it was an important outcome for patients and an appropriate primary outcome. The definition of PFS was changed after a late protocol amendment, adding that the date of initiation of subsequent myeloma treatment was censored. This change was requested by regulatory bodies and is therefore unlikely to have been influenced by investigator awareness of study data.
The clinical experts consulted by CADTH believed that the patients included in IKEMA were younger, on average, than the real-world patients they would be expecting to treat with IsaKd in routine clinical settings. The clinical experts noted that clinical trials in MM generally enrol patients who are younger and healthier. They also pointed out that the ECOG performance status in IKEMA is also better than 1 would expect to see in practice. Results from a planned subgroup analysis performed by the sponsor do not suggest that age affects response to IsaKd. Otherwise, the demographics and baseline disease characteristics seemed consistent with the patients the clinical experts would expect to receive the drug in Canadian clinical practice. Of the 302 patients included in the study, 8 patients were enrolled at Canadian sites.
The treatment regimens used in IKEMA appear consistent with what 1 would expect to see used in Canada, according to the clinical experts consulted by CADTH, and were aligned with the dosage in the Health Canada Product Monograph.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
Currently, the only head-to-head randomized comparison of IsaKd is the IKEMA trial. Since there are several other treatment options in this setting, it is important to obtain data on comparisons of IsaKd and the other treatment options. The sponsor submitted an ITC report in which an NMA and MAICs were conducted for the outcomes PFS, OS, and ORR.
In addition to the sponsor-submitted report, a literature search was conducted to determine whether there was any other indirect evidence available in the literature for IsaKd. A focused literature search for NMAs dealing with either isatuximab or MM was run in MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid on August 10, 2021, and updated on September 20, 2021. Conference abstracts were excluded. Study design filters were applied to limit the search to NMAs; no other limits were applied. Out of 92 publications, no relevant studies were identified that compared the treatment of interest in the patient population of interest.
Description of Indirect Comparisons
The sponsor-provided ITC report describes the NMA and MAICs that were performed. A systematic review and feasibility assessment were done to identify studies to include in the ITC, the eligibility criteria for which are summarized in Table 13. Briefly, it was determined that it was feasible to conduct an NMA including 8 studies (7 for PFS) in a connected network including IsaKd, and 4 separate MAICs based on individual-level data from the IKEMA trial and summary data from 2 studies.
Table 13: Study Selection Criteria and Methods for Indirect Treatment Comparisons
Parameter | Inclusion criteria | Exclusion criteria |
|---|---|---|
Population | Studies evaluating patients more than 18 years of age, diagnosed with RRMM (including Kahler disease, myelomatosis, plasma cell myeloma, and medullary plasmacytoma) with 1 to 3 prior lines of treatment were eligible for inclusion. Studies of mixed populations (for example, studies including patients with ≥ 1 prior line of treatment) were eligible only if outcomes were reported separately for patients with 1 to 3 prior lines of treatment or if 80% or more of the population was eligible. | Age < 18 years Treatment-naive patients only |
Intervention/ comparators | Studies that compare the following interventions (as single drugs or in combination) against each other, best supportive care, or placebo: | Any studies not including the interventions specified |
Comparators | Isatuximab Bortezomib Carfilzomib Daratumumab Dexamethasone Elotuzumab Ixazomib Lenalidomide Panobinostat Pomalidomide Thalidomide Melphalan Bendamustine Cyclophosphamide Prednisone Belantamab mafodotin Isatuximab + Pomalidomide + Dexamethasone Isatuximab + Carfilzomib + Dexamethasone Bendamustine + Thalidomide + Dexamethasone Bortezomib Bortezomib + Dexamethasone Bortezomib + Lenalidomide + Dexamethasone Bortezomib + Melphalan + Dexamethasone Bortezomib + Melphalan + Prednisone | — |
(continued) | Bortezomib + Pomalidomide + Dexamethasone Bortezomib + Thalidomide + Dexamethasone Carfilzomib + Dexamethasone Carfilzomib + Lenalidomide + Dexamethasone Carfilzomib + Pomalidomide + Dexamethasone Cyclophosphamide + Bortezomib + Dexamethasone Cyclophosphamide + Carfilzomib + Dexamethasone Cyclophosphamide + Lenalidomide + Dexamethasone Cyclophosphamide + Pomalidomide+ Dexamethasone Cyclophosphamide + Thalidomide + Dexamethasone Daratumumab + Bortezomib + Dexamethasone Elotuzumab + Bortezomib + Dexamethasone Daratumumab + Bortezomib + Dexamethasone+ Lenalidomide Daratumumab + Bortezomib + Dexamethasone+ Pomalidomide Daratumumab + Carfilzomib + Dexamethasone Daratumumab + Lenalidomide + Dexamethasone Daratumumab + Pomalidomide + Dexamethasone Daratumumab monotherapy Elotuzumab + Lenalidomide + Dexamethasone Elotuzumab + Pomalidomide + Dexamethasone Ixazomib + Lenalidomide + Dexamethasone Lenalidomide + Dexamethasone Lenalidomide + Melphalan + Prednisone Melphalan + Prednisone Panobinostat + Bortezomib + Dexamethasone Pomalidomide + Dexamethasone | |
Outcomes | Studies reporting at least one of the following: Progression-free survival Overall survival Time to progression MRD negativity rate Response: Complete response or stringent complete response Very good partial response Partial response Overall response rate Duration of response Time to response Time to best response Time on treatment Time to discontinuation Time to next treatment Adverse effects of treatment, specifically: Any grade 3 or higher adverse events Any serious adverse events Withdrawal due to AEs Infusion reactions Rate of infections Discontinuations: Overall treatment discontinuation Discontinuation due to AE Health-related quality of life outcomes and patient-reported outcome measures, including: EORTC QLQ-C30 EORTC QLQ-MY20 EQ-5D-5L/EQ-5D-3L Measures of patient satisfaction HRQoL EORTC QLQ-C30 EORTC QLQ-MY20 EQ-5D-5L/EQ-5D-3L Other patient satisfaction measures | — |
Study design | Randomized controlled trials (RCTs) | Phase I clinical trials, noncomparative, retrospective studies, observational studies, case reports Editorials, letters, comments SLRs and meta-analyses or article reviews |
Limits | English-language studies published in 2000 or later | Non-English-language studies published before 2000 |
AE = adverse event; EORTC = European Organisation for Research and Treatment of Cancer; MRD = minimal residual disease; QLQ-C30 = Quality of Life Cancer-Specific Questionnaire with 30 items; QLQ-MY20 = multiple myeloma module Quality of Life questionnaire with 20 items; RCT = randomized controlled trial; RRMM = relapsed or refractory multiple myeloma; SLR = systematic literature review.
Source: Sponsor-provided ITC report.
Methods of Indirect Treatment Comparisons
Objectives
The sponsor’s ITC aimed to compare the efficacy, as measured by PFS, OS, and ORR, among the following treatments for patients with RRMM:
Bortezomib + dexamethasone (Vd)
Bortezomib + pomalidomide + dexamethasone (VPd)
Cyclophosphamide + Kd (CKd)
Cyclophosphamide + Rd (CRd)
Cyclophosphamide + Vd (CVd)
Daratumumab + Kd (DKd)
Daratumumab + Vd (DVd)
Elotuzumab + Vd (EloVd)
IsaKd
Kd
Panobinostat + Vd (PanVd)
Study Selection Methods
The criteria used for inclusion and exclusion of studies in the systematic review are described in Table 14. The search was done in June 2020 using Ovid MEDLINE, Embase, CENTRAL, CDSR, DARE, Northern Light Life Sciences Conference Abstracts, Clinicaltrials.gov, NICE, CADTH, EMA, and FDA websites. In addition, the bibliographies of review articles and meta-analyses were reviewed to identify additional studies. An initial screening step was conducted by 2 reviewers independently, based on the titles and abstracts of the identified studies. If it could be determined from the abstract that the study did not match the eligibility criteria, then it was excluded. Otherwise, the studies proceeded to the full-text screening step. The full-text screen was done by 2 reviewers independently, and discrepancies were solved by a third reviewer.
Data extraction was done using a custom data extraction sheet in Excel by a primary reviewer, and an audit was performed by a second reviewer. Any disagreements between the 2 reviewers were adjudicated by a third reviewer. The risk of bias was assessed following the NICE criteria for assessment of risk of bias for RCTs. The study quality was used for descriptive purposes and not used to justify exclusion of studies.
The efficacy outcomes were PFS, OS, and ORR. For each study, the following were extracted: the outcome definition and how it was assessed, the unit of measurement, the number of individuals included in the analysis, the size of the estimated effect, and a measure of precision for each estimated effect.
For included studies, the risk of bias was assessed using the NICE criteria for assessment of risk of bias for RCTs. The assessment criteria were as follows:
Was the randomization method adequate?
Was the allocation adequately concealed?
Were the groups similar at the outset of the study in terms of prognostic factors; for example, severity of disease?
Were the care providers, participants, and outcome assessors blind to treatment allocation? If any of these people were not blind to treatment allocation, what might be the likely impact on the risk of bias (for each outcome)?
Were there any unexpected imbalances in dropouts between groups? If so, were they explained or adjusted for?
Was there any evidence that the authors measured more outcomes than they reported?
Did the analysis include an intention-to-treat analysis? If so, was this appropriate and were appropriate methods used to account for missing data?
Summary of Included Studies
A total of 11,635 records were assessed for eligibility; following this review, a total of 18 RCTs were included as eligible. The heterogeneity of the included trials was assessed according to the trial design, patient characteristics, and outcome data. All studies were determined to have low to medium risk of bias, and all but 2 studies were open-label design. Quality assessment was done systematically using a standardized set of criteria. Heterogeneity assessments and comparisons are summarized in Table 15. Inclusion and exclusion criteria were, in general, consistent across trials. All trials included patients with relapsed or refractory MM and at least 1 prior therapy. In general, patients could not have had prior treatment with the investigational drug or be refractory to the other drugs under study. Some variation was observed between trials, however, in the requirements for previous treatment, specifically lenalidomide and bortezomib. Many of the baseline characteristics were not reported among the trials, which makes it difficult to assess heterogeneity.
Four trials were excluded from the evidence network due to heterogeneity in the number of prior lines of treatment between them and the other trials. Of the remaining trials, 12 were in a connected network with sufficient data available for the NMA, while 4 were in a disconnected network. Of the 4 in the disconnected network, 2 were excluded from the MAICs, because of the inclusion of primary refractory patients in 1, and a sample size that was too small in the other.
Table 14: Assessment of Homogeneity for Indirect Treatment Comparisons
Study details | Description and handling of potential effect modifiers |
|---|---|
Study design | 16 trials were phase III, 2 trials were phase II, all but 2 studies were open-label. |
Location | 4 trials were single country; 1 was multi-country in Europe and North America; 10 were multi-country in Europe, North America, and Asia; 2 included South America; and 2 included South America and Africa. |
Clinical trial eligibility criteria | There was some variation in requirements for previous treatments. All trials had a minimum age of 18, and one trial had a maximum age of 75. Some variation in ECOG status, bone marrow function, and creatinine levels was observed but was not expected to contribute to heterogeneity. Four trials required previous treatment with lenalidomide; otherwise, the percentage who previously received the treatment varied from 5% to 48%. |
Dosage of comparators | Treatment duration in terms of the number of cycles and criteria for discontinuation varied among trials. |
Definitions of end points | The IMWG criteria were used for progression evaluation, with the exception of 1 trial which used EBMT, and 3 trials that did not report the criteria. |
Timing of end point evaluation or trial duration | Trials had a median follow-up ranging from 12 months to 60 months for PFS and OS. |
Withdrawal frequency | This was not reported directly, but the ITCs assessed whether the rates of dropout differed by treatment arm within each trial. |
EBMT = ; ECOG = Eastern Cooperative Oncology Group; IMWG = International Myeloma Working Group; ITC = indirect treatment comparison; OS = overall survival; PFS = progression-free survival.
Source: Sponsor-provided ITC report.
Network Meta-Analysis Methods
Separate NMA models were fit for PFS, OS, and ORR. The models were Bayesian fixed-effects mixed treatment comparisons, as recommended by the NICE DSU.31 These were used instead of random-effects models because the random-effects models did not converge due to sparsity in the network. The models were estimated using MCMC as implemented in JAGS and R software, using noninformative priors, 10,000 burn-in iterations, and 50,000 posterior iterations for 3 independent chains. Methods to assess convergence were not specified. For the PFS and OS outcomes, the analysis was based on HR estimates under the proportional hazards assumption and used normal likelihood models with a linear link to model the log HRs. For the ORR results, fixed-effects models with the binomial likelihood and logit link were used. In addition to the HRs, modelling of the time-to-event outcomes using fractional polynomials embedded within the normal likelihood and linear link functions on the log hazard scale was performed. This approach relaxed the proportional hazards assumption and allowed estimates of HRs to vary over follow-up time. Model fit was assessed using the deviance information criterion. One sensitivity analysis was performed in the ORR analysis by including trials that evaluated treatments in the second-line-only population.
Table 15: Network Meta-Analysis Methods
Analysis parameters | NMA |
|---|---|
ITC methods | Bayesian fixed-effects models |
Priors | Noninformative |
Assessment of model fit | Deviance information criteria |
Assessment of consistency | NA, no closed loops |
Assessment of convergence | Not reported |
Outcomes | PFS, OS, ORR |
Follow-up time points | Up to 48 months for PFS, up to 66 months for OS, best response during trial follow-up for ORR |
Construction of nodes | Based on distinct arms within each trial |
Sensitivity analyses | Fractional polynomials to assess sensitivity to the proportional hazards assumption; inclusion of second-line-only population |
Subgroup analysis | None reported |
Methods for pairwise meta-analysis | NA |
ITC = indirect treatment comparison; NA = not applicable; ORR = overall response rate; OS = overall survival; PFS = progression-free survival.
Source: Sponsor-provided study report.32
Network Meta-Analysis Results
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Figure 5: Evidence Network for PFS — Redacted

This figure has been redacted at the request of the sponsor.
Figure 6: Effect of IsaKd on PFS Relative to Other Treatments — Redacted

This figure has been redacted at the request of the sponsor.
Figure 7: Evidence Network for OS and ORR — Redacted

This figure has been redacted at the request of the sponsor.
Figure 8: Effect of IsaKd on OS Relative to Other Treatments — Redacted

This figure has been redacted at the request of the sponsor.
Figure 9: Effect of IsaKd on ORR Relative to Other Treatments — Redacted

This figure has been redacted at the request of the sponsor.
Matching-Adjusted Indirect Comparison Analysis Methods
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Matching-Adjusted Indirect Comparison Results
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 16: Results of Matching-Adjusted Indirect Comparisons — Redacted
|||||||||||||| | |||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||| | ||||
|---|---|---|---|---|---|---|---|
|||||||||||||| | |||||| |||||||||||| | |||||||||| | |||| | |||||||||||| | || | |||||||||||| | |||| |
|||||||| ||| | |||||||||||| | |||||||||| |||| | |||||| | |||||||||| |||| | |||||| | |||||||||| |||| | |||||| |
|||||||| ||| | |||||||||||| | |||||||||| |||| | |||||| | |||||||||| |||| | |||||| | |||||||||| |||| | |||||| |
|||||||||||||| |||||||||| | |||||||||||| | |||||||||| |||| | |||||||| | |||||||||| |||| | |||||| | |||||||||| |||| | |||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This table has been redacted at the request of the sponsor. The rest of the rows of the table have therefore been deleted.
Source: Sponsor-provided ITC report.35
Critical Appraisal of Indirect Treatment Comparisons
Network Meta-Analysis Critical Appraisal
The ITC methods and results, in general, were reported thoroughly and adequately for the purposes of this review, with some exceptions, as noted in this section. The study selection was pre-specified with clear criteria and conducted in a rigorous manner. Heterogeneity and risk of bias were assessed. The trial populations were relatively homogenous in age, ECOG status, race, and gender. However, there were some concerns from the clinical experts regarding heterogeneity in the prior treatments received. Specifically, prior lenalidomide use is likely a key effect modifier that differs between trials and greatly increases the uncertainty in the findings. In addition, studies included in the network were conducted over a wide span of time during which the treatment approach for MM has rapidly evolved. Thus, the time span of these trials may further introduce bias to the comparisons in the ITCs. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The study authors noted that results from fixed-effects models were reported, since results from random-effects models were considered unreliable or unstable. This was likely due to the sparsity of the network. So the fixed-effects approach was considered to be the only reasonable choice. However, the key assumption of fixed-effects models — that the true treatment effect is common in all studies comparing the same treatment — is unlikely to be plausible. Since the ITCs were based on sparse networks, in most cases, each direct comparison was supported by data from a single trial. For the most part, the network estimate is based solely on the indirect estimate (||||||||||||||||||||||). Typically, 1 benefit of a NMA is that it yields more precise estimates because it combines information from the direct and indirect estimates. This is not the case in the current NMAs, as many of the estimates are quite imprecise. Assessment of convergence for the NMA models was not described in the ITC report; however, the noted issues with the random-effects model would imply that some convergence assessment was done.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| The statistical methods for the NMA were appropriate given the limitations of the network. |||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Matching-Adjusted Indirect Comparison Critical Appraisal
In the MAICs, the unanchored nature of the comparison imposes the assumption that all prognostic factors and effect modifiers are adequately adjusted for, which is unlikely to be the case.36 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, and previous lenalidomide use, which was specifically noted as a likely effect modifier by 1 of the clinical experts, and prior treatment in general. As for the choice of the matching factors, it was based on internal expert opinion (rather than a survey of clinical experts) and availability and completeness of data in the trials (which is inconsistent with the NICE DSU guidelines, which recommend that all necessary factors be identified, regardless of availability in the data). Many of the matching factors were categorized or dichotomized, which discards information and may result in residual confounding and inadequate adjustment. |||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The reported effective sample sizes, and the skewness and outliers apparent in the visualizations of the weight distributions, suggest that the results may be heavily influenced by a small subset of patients from the IKEMA trial. Generalizability may be an issue due to the small sample size remaining after the exclusions and matching — the remaining patients and weighted sample are unlikely to be representative of the entire patient population.
Other Relevant Evidence
This section includes submitted long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review. There was no such evidence available for this review.
Discussion
Summary of Available Evidence
One ongoing, multinational (with 8 patients at Canadian sites), sponsor-funded open-label RCT, IKEMA, was included in the CADTH review. In IKEMA, 302 patients with relapsed or refractory MM and 1 to 3 prior lines of therapy were randomized in a 3:2 ratio to either IsaKd or Kd. Patients were treated until they experienced disease progression or unacceptable toxicity, or the patient decided to discontinue study treatment. Randomization was stratified by number of prior lines of therapy (1 versus > 1) and R-ISS score (I or II versus III versus not classified). The primary outcome was PFS, and key secondary outcomes included ORR, VGPR or better rate, MRD negativity in patients with VGPR or better, CR rate, and OS. All results presented were from a planned interim analysis, and results for OS are not expected until 2023. In addition to IKEMA, other evidence available included ITCs: a fixed-effects NMA that included 8 studies (7 for PFS) in a connected network including IsaKd, and 4 separate MAICs based on individual-level data from IKEMA and summary data from 2 studies. In total, IsaKd was compared to 10 other treatments for PFS and 11 other treatments for OS and for ORR. However, not all these comparators may be relevant to the Canadian context. There were limited data available for assessing HRQoL or safety. No other evidence was submitted by the sponsor or identified by the literature search conducted by CADTH, as there are no extension studies conducted to date.
In IKEMA, patients were an average of 63.1 years of age (SD 9.9), 56% were men, and 70.9% were White. The majority of patients had MM of the IgG subtype (67.9%) at diagnosis, followed by IgA (22.8%), and these percentages were similar to those observed at study entry (69.9% and 22.5%, respectively). The most common ISS stage at study entry was stage I (53.0%), followed by stage II (31.1%) and stage III (15.2%). The majority of patients had relapsed and refractory MM (71.5%), while the remainder had relapsed MM (28.5%). The average number of prior regimens was 3.2 (SD 1.7), and the number of prior lines was 1.8 (SD 0.8). Patients were most commonly refractory to an immunomodulatory imide drug (45.0% of patients), followed by a proteasome inhibitor (33.1%), or both (20.5%).
With respect to critical appraisal issues, IKEMA was an open-label trial, and lack of blinding may have biased results for patient-reported outcomes. Assessment of pathology was conducted by a blinded IRC; therefore, it is unlikely to have been biased as a result of the open-label design. The results of the trial are based on a planned interim analysis, with an information fraction of 65%; therefore, there is a risk of overestimation of the PFS benefit. This concern is mitigated somewhat by the statistically and clinically significant results observed for PFS. Early failure of the testing hierarchy meant that statistical testing was conducted only on the primary and first secondary outcome of ORR. HRQoL was not included in the statistical hierarchy, and, therefore, no conclusions should be drawn about these data. With respect to generalizability, the clinical experts consulted by CADTH noted that patients in IKEMA were younger than those they would expect to see diagnosed with MM in Canadian clinical practice.
Interpretation of Results
Efficacy
IsaKd improved PFS in comparison with Kd in patients with MM who had failed 1 to 3 prior lines of therapy, achieving the primary outcome of IKEMA. At the time of the interim analysis, 26.8% of patients in the IsaKd group and 44.7% of patients in the Kd had a PFS event, for a HR of 0.531 (95% CI, 0.318 to 0.889), and this was identified as being clinically significant by the clinical experts consulted by CADTH. PFS is a surrogate for OS, and OS data will not be available until the final analysis for IKEMA is completed in 2023. The PFS result was observed despite there being no statistically significant improvement in ORR, which was achieved in 86.6% of patients in the IsaKd group and 82.9% of patients in the Kd group. A CR was achieved in 39.7% of patients in the IsaKd group versus 27.6% of patients in the Kd group, and VGPR or better in 72.6% versus 56.1% of patients, respectively. The lack of improvement in ORR for IsaKd versus Kd is largely accounted for by PR responses, which were observed in 14.0% of patients in the IsaKd group and 26.8% of patients in the Kd group. The lack of statistical significance for ORR is particularly important, given that this was the first outcome tested in the statistical hierarchy after the primary outcome, and this early failure in the hierarchy meant that testing was to have halted. Therefore, no conclusions could be drawn about outcomes such as MRD, which is an important outcome in determining depth of response.
Between-group comparisons of HRQoL were not formally assessed in IKEMA. The lack of interpretable HRQoL data are an important limitation, given the significant impact of MM on HRQoL and the importance of this outcome to patients. In their input to CADTH, patients specifically noted renal issues, infections, issues with mobility, neuropathy, and fatigue as important to them. The clinical experts consulted by CADTH were also of the opinion that HRQoL is an important outcome to assess in these patients, as 2 key outcomes that indicate a positive response to treatment in a given patient are improved PFS and maintained or improved HRQoL.
IKEMA compared IsaKd to Kd, and this is an important and relevant comparator for this indication. Numerous other relevant comparators were identified in the systematic review protocol, for which data were lacking head-to-head comparisons. However, there is indirect evidence from an NMA and 4 MAICs submitted by the sponsor. |||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| However, these results must be interpreted with consideration to the limitations of the NMA. Specifically, there was uncertainty in these findings due to heterogeneity among included trials with respect to the number of prior lines and types of therapy, as well as due to the sparsity of the network, which limits the ability to account for observed heterogeneity or to conduct any sensitivity analyses. As noted, IsaKd did not improve ORR compared to Kd in IKEMA, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| It should be noted that the final analysis of OS from IKEMA will not be available until 2023. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| However, the limitations of the MAICs are much more significant than those of the NMA, since they involved unanchored comparisons that impose the assumption that all prognostic factors and effect modifiers are adequately adjusted for, which is unlikely to be the case. Consequently, there is a greater uncertainty in the results obtained from the MAICs. HRQoL was not assessed in the NMA or the MAICs; however, this was expected, given that this outcome was not formally assessed in IKEMA.
Harms
There were no clear differences in overall AEs or SAEs between the IsaKd and Kd groups in the IKEMA trial. However, there were some numerical differences in some notable harms. Infections, particularly pneumonia, were more common with IsaKd than Kd, and this was not surprising, considering that isatuximab has immunomodulatory effects. Daratumumab, another monoclonal antibody drug directed at CD38, is also known to cause an increased risk of infections.37 Safety outcomes were not included in the NMA provided by the sponsor, so neither direct nor indirect comparisons were available to inform whether the risk of pneumonia is higher, the same, or lower with isatuximab than with daratumumab or other comparators.
Infusion-associated reactions were a notable harm and were far more common in the IsaKd group than in the Kd group (44.6% versus 3.3% of patients, respectively). However, grade 3 or greater AEs were only reported in 1 patient in the IsaKd group and in none of the patients in the Kd group. The sponsor had a protocol for both prevention and treatment of infusion-associated reactions.
Other notable harms mentioned in the product monograph for isatuximab include cardiac toxicity, second primary malignancies, neutropenia, and thrombocytopenia. Much of the concern over cardiotoxicity likely originates from the carfilzomib component of IsaKd, which is known to have issues with cardiotoxicity.38 Proteasome inhibitors all have potential to cause cardiotoxicity as a core component of their mechanism of action. However, carfilzomib appears to accumulate in cardiac tissue in particularly high levels and thus may be the highest-risk drug in the class with respect to this safety issue.38 Cardiotoxicity is particularly concerning in this population, as patients are often elderly (> 65 years of age) and at higher baseline risk of cardiovascular disease. There was no clear and consistent indication in the IKEMA trial that the addition of isatuximab to Kd caused additional cardiac toxicity. SAEs of cardiac failure occurred in 2.8% of patients in the IsaKd group and 1.6% of patients in the Kd group, and grade 3 AEs of cardiac failure occurred in 2.3% of patients in the IsaKd group and 2.5% of patients in the Kd group. Treatment discontinuations of carfilzomib, specifically, were numerically more common in the IsaKd group than in the Kd group, and a large reason for this difference was cardiac disorders (7.3% versus 0, respectively). However, overall discontinuations of all study treatment were less common with IsaKd than with Kd (8.5% versus 13.9%, respectively), and there was no difference between the groups in discontinuations due to cardiac disorders. There were numerically more cases of neutropenia and thrombocytopenia with IsaKd than with Kd, although the significance of this is unclear, given that IKEMA was not powered to formally assess safety outcomes.
Harms were not assessed in the NMAs or the MAICs submitted to CADTH, and this should be considered a limitation of the indirect evidence. Therefore, the safety and tolerability of IsaKd relative to other regimens used in MM are unknown.
Conclusions
One multinational sponsor-funded open-label RCT, IKEMA, was included in the CADTH review. In a population of patients with relapsed or refractory MM with 1 to 3 prior lines of therapy, IsaKd exhibited a statistically significant and clinically meaningful improvement in PFS compared to Kd, which was the primary outcome of the trial. IKEMA is an ongoing study, and the analysis of OS is not yet available. IsaKd did not improve ORR, and no conclusions could be drawn regarding other outcomes such as MRD, due to early failure of the statistical hierarchy. HRQoL data were collected; however, without a formal assessment of this outcome, no conclusions could be drawn from these data. Notable harms that may occur more frequently with IsaKd than with Kd include infusion reactions and pneumonia, although IKEMA was not powered to assess safety. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
References
1.The Global Cancer Observatory. Canada: incidence, mortality and prevalence by cancer site. Lyon (France): Cancer Today; 2021: https://gco.iarc.fr/today/data/factsheets/populations/124-canada-fact-sheets.pdf. Accessed 2021 Oct 14.
2.Myeloma Canada. Multiple myeloma: incidence & prevalence in Canada. 2021; https://www.myelomacanada.ca/en/about-multiple-myeloma/what-is-myeloma-10/incidence-and-prevalence-in-canada. Accessed 2021 Sep 9.
3.Canadian Cancer Society. Survival statistics for multiple myeloma. 2021; https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/prognosis-and-survival/survival-statistics#:~:text=In%20Canada%2C%20the%205%2Dyear,for%20at%20least%205%20years. Accessed 2021 Sep 9.
4.Mikhael J, Richardson P, Usmani SZ, et al. A phase 1b study of isatuximab plus pomalidomide/dexamethasone in relapsed/refractory multiple myeloma. Blood. 2019;134(2):123-133. PubMed
5.Moreau P, Dimopoulos MA, Yong K, et al. Isatuximab plus carfilzomib/dexamethasone versus carfilzomib/dexamethasone in patients with relapsed/refractory multiple myeloma: IKEMA Phase III study design. Fut Oncol. 2020;16(2):4347-4358. PubMed
6.Moreau P, Hebraud B, Facon T, et al. Front-line daratumumab-VTd versus standard-of-care in ASCT-eligible multiple myeloma: matching-adjusted indirect comparison. Immunotherapy. 2021;13(2):143-154. PubMed
7.Clinical Study Report: EFC15246 (IKEMA). Randomized, open label, multicenter study assessing the clinical benefit of isatuximab combined with carfilzomib (Kyprolis®) and dexamethasone versus carfilzomib with dexamethasone in patients with relapsed and/or refractory multiple myeloma previously treated with 1 to 3 prior lines [internal sponsor's report]. Mississaugua (ON): Sanofi Genzyme; 2020.
8.Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), concentrate for solution for infusion (20mg/mL) [internal sponsor's package]. Mississaugua (ON): Sanofi Genzyme; 2021.
9.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-E205. PubMed
10.Laubach J, Garderet L, Mahindra A, et al. Management of relapsed multiple myeloma: recommendations of the International Myeloma Working Group. Leukemia. 2016;30(5):1005-1017. PubMed
11.Rajkumar SV. Multiple myeloma: 2020 update on diagnosis, risk‐stratification and management. Am J Hematol. 2020;95(5):548-567. PubMed
12.Mikhael J, Ismaila N, Cheung MC, et al. Treatment of multiple myeloma: ASCO and CCO joint clinical practice guideline. J Clin Oncol. 2019;37(14):1228-1263. PubMed
13.SarclisaTM (isatuximab for injections): concentrate for solution for infusion (20mg/mL) [product monograph]. Mississauga (ON): Sanofi Genzyme; 2020 Sep 13.
14.Canadian Pharmacists Association. e-CPS. 2021; https://www.e-therapeutics.ca. Accessed 2021 Oct 14.
15.Hungria V, Beksac M, Weisel KC, et al. Health-related quality of life maintained over time in patients with relapsed or refractory multiple myeloma treated with daratumumab in combination with bortezomib and dexamethasone: results from the phase III CASTOR trial. Br J Haematol. 2021;193(3):561-569. PubMed
16.Mian HS, Eisfeld C, Venner CP, et al. Efficacy of daratumumab containing regimens post lenalidomide maintenance in transplant eligible patients: Real-world experience from the Canadian Myeloma Research Group Database. Blood. 2020;136:26-27.
17.Dimopoulos MA, Goldschmidt H, Niesvizky R, et al. Carfilzomib or bortezomib in relapsed or refractory multiple myeloma (ENDEAVOR): an interim overall survival analysis of an open-label, randomised, phase 3 trial. Lancet Oncol. 2017;18(10):1327-1337. PubMed
18.Usmani SZ, Hoering A, Cavo M, et al. Clinical predictors of long-term survival in newly diagnosed transplant eligible multiple myeloma—an IMWG Research Project. Blood Cancer J. 2018;8(12):1-7. PubMed
19.Facon T, Kumar S, Plesner T, et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. NEJM. 2019;380(22):2104-2115. PubMed
20.Moreau P, Mateos MV, Berenson JR, et al. Once weekly versus twice weekly carfilzomib dosing in patients with relapsed and refractory multiple myeloma (A.R.R.O.W.): interim analysis results of a randomised, phase 3 study. Lancet Oncol. 2018;19(7):953-964. PubMed
21.Mikhael J, Belhadj-Merzoug K, Hulin C, et al. A phase 2 study of isatuximab monotherapy in patients with multiple myeloma who are refractory to daratumumab. Blood Cancer J. 2021;11(5):89. PubMed
22.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
23.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Aug 12.
24.Moreau P, Dimopoulos MA, Mikhael J, et al. Isatuximab, carfilzomib, and dexamethasone in relapsed multiple myeloma (IKEMA): a multicentre, open-label, randomised phase 3 trial. Lancet. 2021;397(10292):2361-2371. PubMed
25.Fayers PM, Aaronson NK, Bjordal K, et al. The EORTC QLQ-C30 Scoring Manual (3rd Edition). Brussels (BE): European Organisation for Research and Treatment of Cancer; 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2021 Nov 10.
26.Stead M, Brown J, Velikova G, et al. Development of an EORTC questionnaire module to be used in health-related quality-of-life assessment for patients with multiple myeloma. Br J Haematol. 1999;104(3):605-611. PubMed
27.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
28.EQ-5D-5L User Guide. Version 3. Rotterdam (Netherlands): EuroQol Research Foundation; 2019: https://euroqol.org/wp-content/uploads/2021/01/EQ-5D-5LUserguide-08-0421.pdf. Accessed 2021 Nov 10.
29.International Myeloma Foundation. International Myeloma Working Group (IMWG) Uniform Response Criteria for Multiple Myeloma. 2021; https://www.myeloma.org/resource-library/international-myeloma-working-group-imwg-uniform-response-criteria-multiple. Accessed 2021 Oct 14.
30.Dimopoulos MA, Moreau P, Palumbo A, et al. Carfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): a randomised, phase 3, open-label, multicentre study. Lancet Oncol. 2016;17(1):27-38. PubMed
31.Dias S, Welton NJ, Sutton AJ, Ades A. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. 2011.
32.Systematic literature review and network meta-analysis feasibility assessment of treatments for relapsed refractory multiple myeloma [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), concentrate for solution for infusion (20mg/mL). Mississaugua (ON): Sanofi Genzyme; 2021 Jul 6.
33.Bahlis NJ, Moreau P, Nahi H, et al. Daratumumab, lenalidomide, and dexamethasone (DRd) vs lenalidomide and dexamethasone (Rd) in relapsed or refractory multiple myeloma (RRMM): Efficacy and safety update (POLLUX). J Clin Oncol. 2017;35(15 suppl):8025.
34.Dimopoulos M, Wang M, Maisnar V, et al. Response and progression-free survival according to planned treatment duration in patients with relapsed multiple myeloma treated with carfilzomib, lenalidomide, and dexamethasone (KRd) versus lenalidomide and dexamethasone (Rd) in the phase III ASPIRE study. J Hematol Oncol. 2018;11(1):1-9. PubMed
35.Indirect comparisons of isatuximab and selected treatments for relapsed or refractory multiple myeloma [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), concentrate for solution for infusion (20mg/mL). Mississaugua (ON): Sanofi Genzyme; 2021 Jun 29.
36.Phillippo DM, Ades A, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submissions to NICE. Sheffield (UK): NICE Decision Support Unit, ScHARR, University of Sheffield; 2016: http://nicedsu.org.uk/wp-content/uploads/2017/05/Population-adjustment-TSD-FINAL.pdf.
37.Darzalex (daratumumab): concentrate for solution for infusion (20mg/mL) [product monograph]. Toronto (ON): Janssen Inc.; 2019 Oct 25: https://pdf.hres.ca/dpd_pm/00053751.PDF. Accessed 2021 Oct 14.
38.Wu P, Oren O, Gertz MA, Yang EH. Proteasome inhibitor-related cardiotoxicity: mechanisms, diagnosis, and management. Curr Oncol Rep. 2020;22:1-14. PubMed
39.Osborne TR, Ramsenthaler C, Siegert RJ, Edmonds PM, Schey SA, Higginson IJ. What issues matter most to people with multiple myeloma and how well are we measuring them? A systematic review of quality of life tools. Eur J Haematol. 2012;89(6):437-457. PubMed
40.Frick E, Borasio GD, Zehentner H, Fischer N, Bumeder I. Individual quality of life of patients undergoing autologous peripheral blood stem cell transplantation. Psychooncology. 2004;13(2):116-124. PubMed
41.Kontodimopoulos N, Samartzis A, Papadopoulos AA, Niakas D. Reliability and validity of the Greek QLQ-C30 and QLQ-MY20 for measuring quality of life in patients with multiple myeloma. ScientificWorldJournal. 2012;2012:842867. PubMed
42.Kvam AK, Fayers PM, Wisloff F. Responsiveness and minimal important score differences in quality-of-life questionnaires: a comparison of the EORTC QLQ-C30 cancer-specific questionnaire to the generic utility questionnaires EQ-5D and 15D in patients with multiple myeloma. Eur J Haematol. 2011;87(4):330-337. PubMed
43.Cocks K, King MT, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. PubMed
44.Cocks K, Cohen D, Wisloff F, et al. An international field study of the reliability and validity of a disease-specific questionnaire module (the QLQ-MY20) in assessing the quality of life of patients with multiple myeloma. Eur J Cancer. 2007;43(11):1670-1678. PubMed
45.Ahmadzadeh A, Yekaninejad MS, Saffari M, Pakpour AH, Aaronson NK. Reliability and validity of an Iranian version of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire for Patients with Multiple Myeloma: the EORTC QLQ-MY20. Asian Pacific Journal of Cancer Prevention: Apjcp. 2016;17(1):255-259. PubMed
46.Malta JS, Silveira LP, Drummond PLM, et al. Validity and reliability of the QLQ-MY20 module for assessing the health-related quality of life in Brazilians with multiple myeloma. Curr Med Res Opin. 2021;37(7):1163-1169. PubMed
47.Sully K, Trigg A, Bonner N, et al. Estimation of minimally important differences and responder definitions for EORTC QLQ-MY20 scores in multiple myeloma patients. Eur J Haematol. 2019;103(5):500-509. PubMed
48.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
49.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. JNCI: Journal of the National Cancer Institute. 1993;85(5):365-376. PubMed
50.EORTC Quality of Life. Questionnaires: Core. https://qol.eortc.org/core/. Accessed 2021 Aug 24.
51.Wettergren L, Sprangers M, Björkholm M, Langius‐Eklöf A. Quality of life before and one year following stem cell transplantation using an individualized and a standardized instrument. Psychooncology. 2008;17(4):338-346. PubMed
52.Strasser‐Weippl K, Ludwig H. Psychosocial QOL is an independent predictor of overall survival in newly diagnosed patients with multiple myeloma. Eur J Haematol. 2008;81(5):374-379. PubMed
53.Molassiotis A, Wilson B, Blair S, Howe T, Cavet J. Unmet supportive care needs, psychological well‐being and quality of life in patients living with multiple myeloma and their partners. Psychooncology. 2011;20(1):88-97. PubMed
54.Gulbrandsen N, Hjermstad MJ, Wisløff F, Group NMS. Interpretation of quality of life scores in multiple myeloma by comparison with a reference population and assessment of the clinical importance of score differences. Eur J Haematol. 2004;72(3):172-180. PubMed
55.Hensel M, Egerer G, Schneeweiss A, Goldschmidt H, Ho A. Quality of life and rehabilitation in social and professional life after autologous stem cell transplantation. Ann Oncol. 2002;13(2):209-217. PubMed
56.Kvam AK, Wisloff F, Fayers PM. Minimal important differences and response shift in health-related quality of life; a longitudinal study in patients with multiple myeloma. Health Qual Life Outcomes. 2010;8:79. PubMed
57.Wisloff F, Hjorth M. Health-related quality of life assessed before and during chemotherapy predicts for survival in multiple myeloma. Nordic Myeloma Study Group. Br J Haematol. 1997;97(1):29-37. PubMed
58.Sirohi B, Powles R, Lawrence D, et al. An open, randomized, controlled, phase II, single centre, two-period cross-over study to compare the quality of life and toxicity experienced on PEG interferon with interferon-α2b in patients with multiple myeloma maintained on a steady dose of interferon-α2b. Ann Oncol. 2007;18(8):1388-1394. PubMed
59.Lee SJ, Richardson PG, Sonneveld P, et al. Bortezomib is associated with better health‐related quality of life than high‐dose dexamethasone in patients with relapsed multiple myeloma: results from the APEX study. Br J Haematol. 2008;143(4):511-519. PubMed
60.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644-650. PubMed
61.Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649-656. PubMed
62.Stewart AK, Dimopoulos MA, Masszi T, et al. Health-related quality-of-life results from the open-label, randomized, phase III ASPIRE trial evaluating carfilzomib, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone in patients with relapsed multiple myeloma. J Clin Oncol. 2016;34(32):3921. PubMed
63.Facon T, Lee JH, Moreau P, et al. Phase 3 study (CLARION) of carfilzomib, melphalan, prednisone (KMP) v bortezomib, melphalan, prednisone (VMP) in newly diagnosed multiple myeloma (NDMM). Clinical Lymphoma, Myeloma and Leukemia. 2017;17(1):e26-e27.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: August 11, 2021.
Alerts: Biweekly search updates until project completion.
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits: Conference abstracts: excluded.
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ab | Abstract |
.dq | Candidate term word (Embase) |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.nm | Name of substance word (MEDLINE) |
.ot | Original title |
.pt | Publication type |
.rn | Registry number |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Sarclisa* or isatuximab* or SAR-650984 or SAR650984 or Hu-38SB19 or Hu38SB19 or R30772KCU0).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*isatuximab/
(Sarclisa* or isatuximab* or SAR-650984 or SAR650984 or Hu-38SB19 or Hu38SB19).ti,ab,kw,dq.
3 or 4
5 use oemezd
6 not (conference abstract or conference review).pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search terms – isatuximab, Sarclisa, SAR-650984, or SAR650984]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms – isatuximab, Sarclisa, SAR-650984, or SAR650984]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms – isatuximab, Sarclisa, SAR-650984, or SAR650984]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms – isatuximab, Sarclisa, SAR-650984, or SAR650984]
Grey Literature
Search dates: August 3 – 9, 2021
Keywords: multiple myeloma, isatuximab, Sarclisa, SAR-650984, or SAR650984
Limits: No limits
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
There were no studies excluded from the CADTH review.
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 18: Detailed Data on HRQoL — Redacted
|||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
|---|---|---|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | ||||||||||||||| |
||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This table has been redacted at the request of the sponsor. The rest of the rows of the table have therefore been deleted.
Source: Clinical Study Report for IKEMA.7
Figure 10: Mean Change From Baseline in EORTC QLQ-C30 Physical Functioning Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 11: Mean Change From Baseline in EORTC QLQ-C30 Role Functioning Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 12: Mean Change From Baseline in EORTC QLQ-C30 Cognitive Functioning Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 13: Mean Change From Baseline in EORTC QLQ-C30 Emotional Functioning Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 14: Mean Change From Baseline in EORTC QLQ-C30 Social Functioning Scale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 15: Mean Change From Baseline in EORTC QLQ-C30 Fatigue Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 16: Mean Change From Baseline in EORTC QLQ-C30 Physical Functioning Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 17: Mean Change From Baseline in EORTC QLQ-C30 Pain Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 18: Mean Change From Baseline in EORTC QLQ-C30 Dyspnea Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 19: Mean Change From Baseline in EORTC QLQ-C30 Insomnia Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 20: Mean Change From Baseline in EORTC QLQ-C30 Appetite Loss Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 21: Mean Change From Baseline in EORTC QLQ-C30 Constipation Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 22: Mean Change From Baseline in EORTC QLQ-C30 Diarrhea Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 23: Mean Change From Baseline in EORTC QLQ-C30 Financial Difficulties Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 24: Mean Change From Baseline in EORTC MY-20 Body Image Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 25: Mean Change From Baseline in EORTC MY-20 Future Perspective Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 26: Mean Change From Baseline in EORTC MY-20 Disease Symptoms Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 27: Mean Change From Baseline in EORTC MY-20 Side Effects of Treatment Subscale — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 28: Mean Change From Baseline in EQ-5D Health State Utility Index — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Figure 29: Mean Change From Baseline in EQ-5D VAS — Redacted

This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for IKEMA.7
Table 19: Subgroup Analyses for PFS — Redacted
|||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
|---|---|---|
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||||||||||||||| | ||
||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This table has been redacted at the request of the sponsor. The rest of the rows of the table have therefore been deleted.
Source: Clinical Study Report for IKEMA.7
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and minimally important difference [MID]):
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-C30 (EORTC QLQ-C30)
EuroQol 5-Dimensions 5-Level questionnaire (EQ-5D-5L)
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-MY20 (EORTC QLQ-MY20)
Findings
A focused literature search was conducted to identify the psychometric properties and the MID of each of the stated outcome measures.
The findings on reliability, validity, responsiveness, and the MID of each outcome measure are summarized in Table 20.
Table 20: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | The EORTC QLQ-C30 is a standardized, patient self-administered questionnaire for evaluating the health-related quality of life of patients with cancer. Consists of functional scales, 3 symptom scales, and 6 single-item scales. | Validity: All subscales shown to be impaired in MM patients compared to population norms.39 No correlation of any subscale with the SEIQoL‐Index, (an instrument which allows patients to select the 5 most important domains for their present QoL and measures their satisfaction in these domains) suggesting independence.40 Reliability: Internal consistency measured using Cronbach’s alpha in a study of MM patients: all 5 of the functional scales reported an α > 0.7 except for cognitive function (α = 0.57).41 Responsiveness: The Global HRQoL scale had SRM values in MM patients who improved (SRM 0.32) and deteriorated (SRM 0.57).42 | Threshold estimates for a small improvement (deterioration) across various cancer sites: Global Health Status GHS/QoL: 5 to 8 (-5 to -10) Function Subscales Cognitive: 3 to 7 (-1 to -7) Emotional: 6 to 9 (-3 to -12) Physical: 2 to 7 (-5 to -10) Role: 6 to 12 (-7 to -14) Social: 3 to 8 (-6 to -11) Symptom Subscalesa Fatigue: 4 to 9 (-5 to -10) Nausea/vomiting: 3 to 9 (-5 to -11) Pain: 5 to 9 (-3 to -11).43 |
EQ-5D-5L | Generic, preference-based, HRQoL measure consisting of 6 questions comprising 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and a VAS which records the subject’s self-rated health. | Responsiveness: SRM values for the EQ-5D-3L in MM patients who improved (SRM 0.43) and deteriorated (SRM 0.45).42 Measurement properties of validity, reliability have not been reported in MM patients. | For the EQ-5D-3L, an absolute change of 0.08 points for improvement and -0.10 points for deterioration in the index score was important to MM patients.42 |
EORTC QLQ-MY20 | A 20-item myeloma module intended for use among patients varying in disease stage and treatment modality. Contains 4 multi-item scales including: side effects, disease symptoms, body image, and future perspective. | Validity: Poor PS at baseline showed significant decrease in disease symptoms, side effects, and body image subscales (P = 0.0013) and approached significance for future perspective (P = 0.065). Convergent and divergent validity of disease symptom scale assessed with correlation coefficients of 0.771 and -0.386 for each, respectively.44 Reliability: Internal consistency ranging from 0.82 to 0.93 has been reported for the global health status/HRQoL scale.45 All 4 scales demonstrated test-retest reliability ≥ 0.85.45 Noted adequate internal consistency using Cronbach’s alpha for disease symptoms (α = 0.77) and side effects of treatment (α = 0.72).41 Future perspective was reported with an internal consistency of 0.80.41 Test-retest reliability was moderate to high with ICC values > 0.4 for all scales in a study in Brazil among MM patients.46 Responsiveness: Disease symptoms and body image significantly decreased over time in MM patients, and the side effects of treatment significantly increased.44 | Disease Symptoms: -10 for improvement and +10 points for deterioration. Side Effects of Treatment: -10 for improvement and +10 points deterioration. Body Image: +13 points for improvement and -13 for worsening. Future Perspective: +9 for improvement and -9 points deterioration.47 |
EORTC QLQ = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire; EQ-5D-5L = EuroQol 5-Dimensions 5-Level questionnaire; GHS = global health status; HRQoL = health-related quality of life; MID = minimal important difference; ICC = intraclass correlation coefficient; MM = multiple myeloma; PS = performance status; QoL = quality of life; SEIQoL = Schedule for the Evaluation of Individual Quality of Life; SRM = standardized response mean; VAS = visual analogue scale
aSymptom score directions were reversed to align with functioning scores (0 represents the worst possible scores and 100 represents the best)
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-C30
Description
The European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire-Core 30, or EORTC QLQ-C30, is one of the most commonly used patient-reported outcomes measures in oncology clinical trials.48 It is a multi-dimensional, cancer-specific, evaluative measure of HRQoL. The core questionnaire of the EORTC QLQ-C30 consists of 30 questions that are scored to create 6 multi-item functional scales, 2 multi-item symptom scales, 6 single-item symptom scales, and a 2-item quality of life (QoL) scale, as outlined in Table 21.25,49 Version 3.0 of the questionnaire, used in the included trial in this report, is the most current version. The questionnaire is available in more than 100 different languages and has been used in more than 3,000 studies.50
Table 21: Scales of EORTC QLQ-C30
Functional Scales (15 Questions) | Symptom Scales (7 Questions) | Single-Item Symptom Scales (6 Questions) | Global Quality of Life (2 Questions) |
|---|---|---|---|
Physical function (5) | Fatigue (3) | Dyspnea (1) | Global Quality of Life/Global Health Status (2) |
Role function (2) | Pain (2) | Insomnia (1) | NA |
Cognitive function (2) | Nausea and vomiting (2) | Appetite loss (1) | NA |
Emotional function (4) | NA | Constipation (1) | NA |
Social function (2) | NA | Diarrhea (1) | NA |
NA | NA | Financial impact (1) | NA |
Scoring
The EORTC QLQ-C30 uses a 1-week recall period in assessing function and symptoms. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4.25 For the 2 items that form the global QoL scale, however, the response format is a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent).
Raw scores for each scale are computed as the average of the items that contribute to a particular scale.25 This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of one unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better quality of life (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and QoL scale would reflect an improvement. According to the EORTC QLQ-C30’s scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least one-half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.
Validity
Osborne et al. (2012)39 assessed the reported construct and criterion validity of the EORTC QLQ-C30. A systematic review was conducted to identify HRQoL tools validated for use in MM; identify issues important to HRQoL from the point of view of patients with myeloma; describe the measurement properties of each HRQoL tool; evaluate the content validity of HRQoL tools in terms of their ability to capture all issues important to patients and to explore the suitability of each HRQoL tool for use in different settings. Results of the systematic review showed that all subscales of patients with MM were shown to be impaired compared to the general population.51-55 General QoL scales significantly improved with increasing time following hematopoietic SCT.55 Sixty-seven percent and 43% of patients scored below the 10th percentile for the physical functioning and global QoL subscales, respectively.54 Functional subscales and global QoL were found to be lower in MM than in general hematology populations.53 The subscales for pain, fatigue, physical and global QoL were able to discriminate between those who improved versus those who were stable/deteriorated.56 All subscales except the single-item diarrhea scale discriminated between MM patients with different performance status and response status.57 There were significant differences in global QoL between the different treatment arms in 2 examined trials of patients with MM.58,59 Additionally, there was no correlation of any subscale with the SEIQoL‐Index (an instrument which allows patients to select the 5 most important domains for their present QoL and measures their satisfaction in these domains) suggesting independence.40
Reliability
A sample of MM patients (n = 89) from 2 tertiary hospitals in Greece were surveyed with the EORTC QLQ-C30 and various demographic and disease-related questions.41 Internal consistency of the QLQ-C30 was assessed in this population. The 5 functional scales reported an internal consistency of greater than 0.7 (range, 0.77 to 0.90).7 except for cognitive function (α = 0.57). The global health status/HRQoL scale reported an internal consistency (α) of 0.92. Of the symptom scales, fatigue (α = 0.89), nausea and vomiting (α = 0.74) and pain (α = 0.80) were assessed for internal consistency, and all were considered acceptable. The 5 symptom scales/items of the core QLQ-C30, that is, nausea/vomiting, appetite loss, constipation, diarrhea, and financial difficulties suffered from high (> 50%) floor scores, implying a lack of these symptoms in this sample, but also suggesting an underlying reduced discriminative ability. Conversely, no ceiling effects were observed on the core instrument despite 3 scales being close to the threshold value (role, cognitive, and social functioning).
Responsiveness to Change
One study by Kvam et al. (2011)42 assessed HRQoL in patients with MM (n = 239) in Norway using the global health ⁄ QoL domains of the EORTC QLQ-C30. To assess responsiveness, the study used the global rating of change (GRC) to identify whether MM patients have changed over time. A Wilcoxon signed-rank test for pair differences was used to calculate the significance of differences in the mean score changes between baseline (T1) and after 3 months (T2). Due to the small sample sizes in some of the GRC categories, data were pooled into the categories improved, unchanged, and deteriorated to yield sufficient numbers of cases in each category. “Improved” represented patients ‘who reported themselves as improved’ and similarly for deteriorated and unchanged patients. To assess the magnitude of the difference in scores between patients who improved ⁄ unchanged ⁄ deteriorated, standardized response means (SRMs) were calculated by dividing the mean score changes by the SD of the change. This was compared against Cohen’s theory for interpreting the magnitude of mean differences in HRQoL scores, which suggests that a change of 0.20 represents a small change, 0.50 a moderate change, and > 0.80 a large change.
In patients rating themselves as unchanged, mean score changes clustered around 0, and the SRMs were negligible.42 MM patients who deteriorated reported lower global QoL scores at T2 compared with T1. The global QoL scale of the EORTC QLQ-C30 was the most responsive in deteriorating patients (SRM 0.57).
MID
A study43 examined 118 published studies on various types of cancer such as breast, lung, or head and neck as well as clinician expert input to evaluate meaningful differences and magnitude of change in the EORTC QLQ-C30 scores. A meta-analysis was conducted to estimate a weighted average change within each size class for large, medium, small, and trivial changes. Small changes indicated a subtle, clinically relevant change. The calculations or symptom subscales were reversed to achieve consistency in improvement or deteriorations over time across all scales. MIDs for improvement and deterioration for small changes in QoL are shown in Table 19.
One study56 assessed the MID of the EORTC QLQ-C30 by recruiting 239 patients with MM to complete the EORTC QLQ-C30 at baseline (T1) and after 3 months (T2). At T2, patients were asked if they had noticed any change in the domains pain, fatigue, physical function, and global QoL. The MID was determined using the mean score changes as observed by the patients stating improvement or deterioration for each domain. A combination anchor and distribution approach were used. The MIDs (SD) for patients rating themselves as improved was 6.2 (15.3) for physical function, -14.7 (35.9) for pain, -13.5 (24.7) for fatigue and 7.6 (23.7) for QoL. Patients reporting deterioration had MIDs (SD) of 8.6 (23.4) for fatigue, 17.3 (23.1) for pain, -12.8 (19.2) for physical function, and -12.1 (21.2) for QoL. However, there was considerable variation in the observed scores.
EuroQol 5-Dimensions 5-Levels Questionnaire
Description
The EQ-5D-5L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments including MM.27 The EQ-5D-5L was developed by the EuroQol Group as an improvement to the EQ-5D 3 level (EQ-5D-3L), to measure small and medium health changes and reduce ceiling effects. The instrument is comprised of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: level 1 “no problems,” level 2 “slight problems,” level 3 “moderate problems,” level 4 “severe problems,” and level 5 “extreme problems” or “unable to perform.”28 A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state.28 The corresponding scoring of EQ-5D-5L health states is based on a scoring algorithm that is derived from preference data obtained from interviews using choice-based techniques (e.g., time trade-off) and discrete choice experiment tasks. The lowest score varies depending on the scoring algorithm used. The anchors are 0 (dead) and 1 (full health), however negative values are also allowed to represent health states that a society considers worse than death. As an example, a Canadian scoring algorithm results in a score of -0.148 for health state 55555 (worst health state). Another component of the EQ-5D-5L is a visual analogue scale (VAS), which asks respondents to rate their health on a visual scale from 0 (worst health imaginable) to 100 (best health imaginable).27
The psychometric properties of the EQ-5D-5L have not been assessed in patients with MM; therefore, its validity and reliability have not been evaluated in this patient population of interest.
Responsiveness
Kvam et al. (2011)42 also assessed the responsiveness of the EQ-5D-3L using the aforementioned methods. The results found that the EQ-5D-3L was the most responsive among improved patients (SRM 0.43). The global QoL scale of the EQ-5D-3L for deteriorating patients had a SRM 0.45. The study also assessed the presence of floor and ceiling effects for EQ-5D-3L. A small floor or ceiling effect was defined as < 15% of patients attaining the worst and best health state and a serious effect was defined as > 15% of patients attaining these states. The results found small floor and ceiling effects for the EQ-5D-3L and noted that 10% of the patients achieved the maximum score (ceiling effect).
MID
Kvam et al. (2011)42 used both distribution and anchor-based approaches for the whole sample (n = 239) to determine MIDs for the EQ-5D-3L. The distribution-based approach was determined by multiplying the SDs at baseline and expected differences in scores associated with small (0.2), moderate (0.5), or large (0.8) changes as per Cohen’s criteria for interpreting the absolute magnitude of a change. From this analysis, using the small effect size as a value of MIDs, the expected MID score was 0.04 for the EQ-5D-3L. The anchor-based approach used the GRC as previously described as the anchor. From this analysis, an MID of 0.08 (95% CI: 0.04 to 0.12) in MM patients who thought their HRQoL improved, and -0.10 (95% CI: -0.16 to -0.04) in those who thought their HRQoL deteriorated.
To estimate the MID values of the EQ-5D-3L for each country-specific scoring algorithm, a simulation-based approach based on instrument-defined single-level transitions has been used. The simulation-based instrument-defined generally accepted MID estimate (mean ± SD) for Canada is 0.056 ± 0.011.60
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-MY20
Description
The questions in the QLQ-MY20 also have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4.26,46 Raw scores for each scale are computed as the average of the items that contribute to a particular scale. This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale.25 There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of one unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better quality of life (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and quality of life scale would reflect an improvement.41
Validity & Responsiveness to Change
A cross-sectional study in Brazil assessed the validity of the EORTC QLQ-MY20 questionnaire among 225 MM patients recruited from 3 clinics, more than 70% of which were more than the age of 60.46 Both convergent and divergent validity were assessed between the EORTC QLQ-C30 and QLQ-MY20 instruments using Spearman’s correlation coefficient. Correlation coefficients were defined as <0.4 for a weak correlation and ≥ 0.4 for a moderate to strong correlation. For convergent validity, a strong correlation was hypothesized between the 2 instruments’ symptom scales. For divergent validity, a weak correlation was hypothesized between the EORTC QLQ-C30 symptom scale and the QLQ-MY20 function scale. Results demonstrated a strong correlation for convergent validity and a weak correlation for divergent validity as hypothesized with correlation coefficients of 0.771 and -0.386 for each assessment, respectively.
Cocks et al. (2007)44 assessed the validity and sensitivity of the EORTC QLQ-MY20 questionnaire. MM patients were recruited prospectively from ongoing or new clinical trials at the time of the study rather than setting up a separate questionnaire validation study. Trials had to be for newly diagnosed or relapsed/refractory MM patients with a minimum prognosis of 3 months. Maintenance therapy trials were not eligible. Questionnaires were issued to patients at the baseline for each trial (randomization or registration) according to the procedures for that trial. A panel reviewed each protocol and identified an appropriate follow-up time point for the field study QoL assessment, this had to be during treatment or within 4 weeks of completion of treatment and was 3 or 6 months from randomization for all protocols. Responsiveness analysis compared the baseline and follow-up scale scores for the 137 (57% of total) patients who achieved at least a PR. The mean disease symptom score significantly decreased (a higher score indicates worse symptoms) from 31.9 (23.2) at baseline to 21.1 (18.7) at follow-up (p < 0.0001). The mean body image score significantly decreased over time (a higher score indicates better support/functioning) from 80.0 (29.8) at baseline to 63.2 (32.5) at follow-up (p < 0.0001). The EORTC QLQ-MY20 scale scores for patients with performance status 0, 1 or 2 (n = 200) were compared to those with performance status 3 or 4 (n = 25) at baseline. The performance status score is a measure of how disease impact’s a patient’s daily living abilities with a score ranging from 0 (“fully active”) to 5 (“dead”).61 Three of the scales from the module: disease symptoms, side effects of treatment and body image showed evidence of a significant difference (P = 0.0013) between the patient groups. The future perspective scale showed a trend toward a difference (p = 0.065).44
Reliability
In total, 215 patients with MM were recruited from Imam Khomeini Hospital, Tehran.45 Patients were eligible for the study if they were 18 years of age or older, had been diagnosed with MM at least one month prior to study entry, and were able to read and speak Persian/Farsi. Patients who had a life expectancy of less than 3 months or had serious cognitive problems (as assessed by the Mini-Mental State Examination) were excluded from the study. Participating patients were asked to complete the EORTC QLQ-MY20 3 times, at study entry, after 2 weeks, and again after 3 months. Internal consistency reliability reported was greater than 0.80 for all 3 multi-item scales (ranging from 0.82 to 0.93).45 All 4 scales (including the single-item body image measure) had test-retest reliability of 0.85 or greater. The disease symptoms scale had the highest test-retest reliability (ICC=0.95).
The aforementioned study46 in Brazil had a small sample of the studied population (n = 25) take the EORTC QLQ-MY20 at 2 time points (14 days apart) to measure test-retest reliability using intraclass correlation coefficient. ICC values between 0.6 and 0.8 were defined as satisfactory temporal stability and values > 0.8 suggested excellent temporal stability. Results found ICC values ranged from 0.41 to 0.79 for body image and diseases symptoms, respectively, indicating a moderate to high ability to create reproducible results. A sample of MM patients (n = 89) from 2 tertiary hospitals in Greece were surveyed with the EORTC QLQ-MY20 and various demographic and disease-related questions.41 Patients were approached during a scheduled visit to one of the hospitals. None were suffering from cancer metastases or severe comorbid conditions which could further compromise HRQoL. Internal consistency of the EORTC QLQ-MY20 was assessed in this population. Of the symptom scales, disease symptoms (α = 0.77) and side effects of treatment (α = 0.72) demonstrated adequate (adequate measured at α = 0.70) internal consistency. Future perspective was reported as an internal consistency of 0.80, side effects of treatment at an internal consistency of 0.72, and disease symptoms at 0.77. Body image was not assessed.
MID
A mixed‐methods study by Sully et al. (2019)47 assessed MID scores of the EORTC QLQ-MY20 using patient interviews that were conducted alongside an analysis of existing trial data. Data were pooled across 3 clinical trials: ASPIRE,62 ENDEAVOR,30 and CLARION63 (n = 2,147). Each was a phase III, randomized, open-label study comparing carfilzomib‐based regimens, with a primary end point of progression‐free survival (PFS) in patients with relapsed or refractory MM. Patients were eligible for entry into the pooled sample if they had completed the EORTC QLQ‐C30 or QLQ‐MY20 at baseline plus at least one other of the following time points: mid‐treatment (MT), or end of treatment (EOT). Twenty patient interviews were conducted.
Two anchor‐based methods were applied, mirroring an approach in another pooled study of cancer patients.47 Potential anchors were identified by the authors reviewing the clinical trial protocols to identify measures available across the trials at MT and EOT. Anchors were selected via review of the protocols and case report forms. Potential anchors were chosen if they were deemed to have conceptual overlap with any of the EORTC QLQ‐MY20 scales. Anchor‐based MIDs were estimated by calculating the mean change score of patients classified as improved and deteriorated according to anchor definitions. Patient‐reported anchors were the EORTC QLQ‐C30 Global Health Status/QoL scale and Functional Assessment of Cancer Therapy‐Gynecologic Oncology Group Neurotoxicity (FACT‐GOG‐Ntx). Clinical anchor measures were the Eastern Cooperative Oncology Group performance status (ECOG PS), matched adverse events (AEs) and peripheral neuropathy‐related AEs. Linear regression models were also fitted with EORTC QLQ‐MY20 score change as the outcome and a binary indicator of stable versus improved/worsened according to the anchor as a predictor, where the coefficient of this indicator was the MID estimate (incorporating the change score of stable patients). Diagnosis (newly diagnosed/relapsed) was accounted for in the model.47
Based on this mixed-method study, the recommended MIDs for the EORTC QLQ-MY20 were as follows: Disease Symptoms, -10 and +10 points for improvement and deterioration, respectively; Side Effects of Treatment, -10 and +10 points for improvement and deterioration, respectively; Body Image, +13 points and -13 for improvement and worsening, respectively; and Future Perspective (body image) +9 and -9 points for improvement and deterioration respectively.47
Pharmacoeconomic Review
Abbreviations
AE
adverse event
DRd
daratumumab plus lenalidomide plus dexamethasone
DVd
daratumumab plus bortezomib plus dexamethasone
EQ-5D
EuroQoL 5-Dimensions questionnaire
EQ-5D-5L
EuroQoL 5-Dimensions 5-Levels questionnaire
EQ-5D-3L
EuroQoL 5-Dimensions 3-Levels questionnaire
ICER
incremental cost-effectiveness ratio
IsaKd
isatuximab in combination with carfilzomib plus low-dose dexamethasone
IsaPd
isatuximab in combination with pomalidomide and dexamethasone
ITC
indirect treatment comparison
IV
intravenous
Kd
carfilzomib plus low-dose dexamethasone
KRd
carfilzomib plus lenalidomide plus dexamethasone
NMA
network meta-analysis
OS
overall survival
PCd
pomalidomide plus cyclophosphamide plus dexamethasone
Pd
pomalidomide plus dexamethasone
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
Rd
lenalidomide plus dexamethasone
RDI
relative dose intensity
TTD
time to treatment discontinuation
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Isatuximab (Sarclisa), solution for injection (20 mg/mL), 120 mg or 600 mg single-use vial |
Submitted price | Isatuximab, 6 mL (100 mg/5 mL), IV injection: $757.90 Isatuximab, 30 mL (500 mg/25 mL), IV injection: $3,789.49 |
Indication | For use in combination with carfilzomib and dexamethasone, for the treatment of adult patients with relapsed or refractory multiple myeloma who have received 1 to 3 prior lines of therapy |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | September 13, 2021 |
Reimbursement request | As per indication |
Sponsor | Sanofi Genzyme |
Submission history | Previously reviewed: Yes Indication: In combination with pomalidomide and dexamethasone, for the treatment of patients with relapsed or refractory multiple myeloma who have received at least 2 prior therapies including lenalidomide and a proteasome inhibitor. Recommendation date: April 1, 2020 Recommendation: Recommended with clinical criteria and/or conditions. |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model (PSM) |
Target population | Adults with relapsed or refractory multiple myeloma who have received 1 to 3 lines of prior therapy |
Treatment | Isatuximab in combination with carfilzomib and dexamethasone (IsaKd) |
Comparator | Carfilzomib plus dexamethasone (Kd) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (37 years) |
Key data source | IKEMA randomized controlled trial |
Submitted results | ICER = $141,824 per QALY (incremental costs = $588,809; incremental QALYs = 4.15) vs. Kd |
Key limitations |
|
CADTH reanalysis results |
|
AE = adverse event; DVd = daratumumab plus bortezomib plus dexamethasone; ICER = incremental cost-effectiveness ratio; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year; RDI = relative dose intensity; TTD = time to treatment discontinuation.
Conclusions
Isatuximab in combination with carfilzomib and dexamethasone (IsaKd) improves progression-free survival (PFS) relative to carfilzomib plus dexamethasone (Kd) among patients with multiple myeloma who have received 1 to 3 prior lines of therapy. However, its effects on quality of life and overall survival (OS) are uncertain, as are its comparative effects relative to other second- and later-line treatments for relapsed or refractory multiple myeloma.
The sponsor’s model predicts increased OS with IsaKd on the basis of OS data from the ongoing IKEMA trial. OS data from IKEMA trial are immature, and the extrapolation of short-term trial data over a 37-year horizon introduces considerable uncertainty. Further, whether the observed benefit in PFS in IKEMA will translate to an increase in OS is highly uncertain. Notably, OS is subject to confounding by the choice of subsequent treatment after disease progression, which was not considered in the sponsor’s model. CADTH was unable to address these limitations, and, given the limitations associated with the sponsor’s chosen model structure, a CADTH base case could not be derived to estimate the cost-effectiveness of IsaKd.
CADTH undertook exploratory reanalyses, within the constraints of the sponsor’s partitioned survival model (PSM). These reanalyses addressed some limitations in the sponsor’s submission, including correcting the price of bortezomib, adopting alternative parametric distributions for OS, using the IKEMA PFS hazard ratio to model the relationship between IsaKd and Kd, assuming correlation between PFS and time to treatment discontinuation (TTD), revising the utility values for PFS, including disutility values, and assuming that all patients receive the full dose of all drugs. CADTH was unable to address the limitations with the chosen modelling approach, the lack of head-to-head comparative clinical data for additional relevant comparators, the cost-effectiveness of IsaKd in relevant subgroups, lack of model transparency, and uncertainty associated with the use of subsequent therapy after disease progression. The validity and interpretability of the results are thus limited and should be viewed only as exploratory and likely underestimate the true incremental cost-effectiveness ratio (ICER).
In the CADTH reanalysis, IsaKd had a 0% probability of being cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per quality-adjusted life-years (QALYs) (ICER $1,588,632 per QALY gained compared with Kd). Cost-effectiveness could not be achieved even if the price of isatuximab was reduced by 100% (ICER falls to $437,022) due to the high cost and duration of use of adjunctive treatment. If isatuximab was $0, the budget impact of IsaKd would still be $28 million. If the cost of carfilzomib was reduced by 61%, isatuximab would still need a 100% price reduction for the combined IsaKd regimen to be considered cost-effective. However, this still assumes 100% of patients end up on subsequent therapy, an OS benefit exists, and proportional hazards hold. Relaxation of these assumptions would mean the price of carfilzomib has to be even lower for isatuximab to be considered cost-effective at a 100% price reduction. The key driver of the ICER was the acquisition cost of isatuximab and the extrapolation of OS from the IKEMA trial. In a scenario analysis in which no benefit in OS was assumed, IsaKd was associated with an ICER of $7,145,426 per QALY gained compared with Kd. The cost-effectiveness of IsaKd compared to other relevant and lower-cost comparator regimens is unknown, given the lack of robust evidence on its comparative effectiveness. Taking both points into consideration, the CADTH exploratory reanalysis likely underestimates the true ICER.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process (specifically, information that pertains to the economic submission).
Patient input was received from Myeloma Canada from patients with myeloma who had received at least 1 prior line of therapy, collected via online surveys. Patients described the impact on their ability to concentrate, work, travel, and exercise, as well as financial burden owing to drug costs, lost income due to absence from work, travel costs, and parking costs for medical appointments. Patients noted a desire for a treatment that extends remission, improves quality of life, and requires minimal visits to hospital for administration. Patients also expressed a desire for treatments that could control infections, kidney problems, neuropathy, and fatigue, and improve mobility. Respondents had experience with carfilzomib- and dexamethasone-containing regimens; adverse events (AEs) associated with treatment were noted to include neutropenia, thrombocytopenia, anemia, cardiac failure, hypertension, respiratory infections, vein thrombosis, renal failure, ocular disorders, diarrhea, nausea/vomiting, fatigue, shortness of breath, and infusion-related reactions. Of these, fatigue and diarrhea were noted to be the least tolerable AEs. Patients were concerned that treatment with isatuximab would be more difficult (i.e., travel, injection time) compared to current treatments. Of respondents with isatuximab experience, some noted that their quality of life was improved, although some noted that nausea/vomiting and thrombocytopenia were “completely intolerable.”
Clinician input received from the Canadian Myeloma Research Group noted that multiple myeloma is a noncurable disease, with limited treatment options among patients whose disease relapses after first-line treatment. After relapse, currently available treatments include regimens containing carfilzomib or daratumumab (second-line) or pomalidomide (third-line). Clinicians noted that the goal of therapy is a high-quality and durable response (response rates, PFS) that delays disease-related complications (e.g., decreased blood counts, renal failure, infections) and improves quality of life. Clinicians noted that there is an unmet treatment need for treatments for patients who become refractory to immunomodulatory drugs (lenalidomide) and/or proteosome inhibitors (bortezomib), and that it is important to provide patients with optimal treatment as early as possible in the disease course. At present, daratumumab plus bortezomib plus dexamethasone (DVd) is considered standard of care for second-line treatment in this population, although daratumumab plus lenalidomide plus dexamethasone (DRd) may also be used. Clinicians noted IsaKd may address an unmet need among patients whose disease has progressed on lenalidomide and/or bortezomib. Registered clinicians noted that the use of IsaKd as second-line treatment may affect subsequent line sequencing with carfilzomib-based regimens.
CADTH’s participating drug plans noted considerations related to relevant comparators and potential implementation factors. Drug plans noted that, at second-line, the most relevant comparators are lenalidomide plus dexamethasone (Rd), carfilzomib plus lenalidomide plus dexamethasone (KRd), DRd, and DVd; however, plans noted that reimbursement of isatuximab may change the place in therapy of some comparator drugs. Plans noted that Kd, the comparator in the sponsor’s economic evaluation, is most likely to be used as third-line therapy. Drug plans described concerns with drug wastage and noted that the combination of isatuximab and carfilzomib would increase the workload for pharmacy staff relative to other comparators. Plans noted that there is an ongoing clinical trial involving rapid IV (IV) infusion of isatuximab and highlighted that a rapid infusion would minimize resource utilization and increase convenience for patients compared with the monograph-recommended prolonged IV infusion.
Several of these concerns were addressed in the sponsor’s model:
PFS and quality of life were incorporated into the model.
Costs related to the treatment of grade 3 or greater AEs that occurred in at least 5% of trial participants were included; however, the impact of AEs on quality of life was not adequately addressed.
Drug wastage was assumed.
In addition, CADTH addressed some of these concerns as follows:
In CADTH reanalyses, disutilities related to AEs were incorporated.
CADTH was unable to address the following concerns raised from stakeholder input:
Although the sponsor provided a network meta-analysis (NMA) of IsaKd to some relevant comparators (e.g., DVd, DRd), the quality of the results was insufficient to support decision-making.
Treatment sequencing could not be addressed owing to the structure of the sponsor’s model.
The model did not include all AEs noted by patients.
Economic Review
The current review is for isatuximab (Sarclisa) for use in combination with carfilzomib and dexamethasone for the treatment of relapsed or refractory multiple myeloma in adult patients who have received 1 to 3 prior lines of therapy.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Isatuximab is indicated (in combination with carfilzomib plus dexamethasone [IsaKd]) for the treatment of relapsed or refractory multiple myeloma among adult patients who have received 1 to 3 prior lines of therapy.1 Isatuximab is additionally indicated in combination with pomalidomide and dexamethasone (IsaPd) for the treatment of relapsed or refractory multiple myeloma in patients who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor, and it has previously been reviewed by CADTH for this indication.2
The sponsor submitted a cost-utility analysis to assess the cost-effectiveness of IsaKd compared with carfilzomib plus dexamethasone (Kd) alone.3 The modelled population is consistent with the reimbursement request and is aligned with the IKEMA trial population, an ongoing phase III randomized controlled trial involving adults with relapsed or refractory multiple myeloma following 1 to 3 prior lines of therapy.
Isatuximab is supplied in single-use vials, at a submitted price of $757.90 per 6-mL vial or $3,789.49 per 30-mL vial. The recommended dose for isatuximab is 10 mg/kg body weight given as an IV infusion (weekly in the first 28-day cycle; biweekly in subsequent cycles) in combination with carfilzomib and dexamethasone “until disease progression or unacceptable toxicity.”1 Pre-medications (e.g., dexamethasone, acetaminophen, diphenhydramine) should be administered before administration of isatuximab. The dosage of carfilzomib and dexamethasone was based on the IKEMA trial (carfilzomib: 20 mg/m2 IV on days 1 and 2, then 56 mg/m2 IV on days 8, 9, 15, 16 of cycle 1; subsequent cycles 56 mg/m2 IV on days 1, 2, 8, 9, 15, 16; dexamethasone: 20 mg on day 1, 2, 8, 9, 15, 16, 22, 23 of each cycle). The sponsor’s calculated cost (including administration costs, relative dose intensity [RDI; based on the IKEMA trial], wastage) of IsaKd is $36,569 for the first 28-day cycle and $29,023 for subsequent cycles. Using similar assumptions, the sponsor estimated the cost of Kd at $9,212 for the first 28-day cycle and $18,412 for subsequent cycles.
The clinical outcomes of interest were QALYs and life-years. The economic analysis was undertaken over a lifetime horizon (37 years) from the perspective of a publicly funded health care payer. Costs and outcomes were discounted at a rate of 1.5% annually.
Model Structure
The sponsor submitted a PSM including 3 health states: pre-progression, post-progression, and death (Appendix 3).3 The modelled time cycle was 1 week. The proportion of patients who were progression-free, experienced disease progression, or dead at any time over the model’s time horizon was derived from nonmutually exclusive survival curves. Specifically, all patients entered the model in the pre-progression state; patients in this state were assumed to be stable or responding to therapy. The proportion of patients with progressed disease (i.e., in the post-progression state) was derived as the difference between the OS and PFS curves. PFS was modelled separately for patients on or off treatment. PFS in the IKEMA trial was defined as the time from randomization to the first documentation of disease progression according to the assessment of response by an independent response committee or death from any cause, whichever occurred first. Disease progression was based on the 2016 International Myeloma Working Group criteria, which defined progressive disease as an increase in serological markers (3 25% increase from baseline in serum M protein or urine M component), the appearance of new lesions, and/or 50% or greater increase in the size of existing lesions.4 TTD was based on extrapolated data from the IKEMA trial to identify the proportion of patients who were alive and who remained on treatment at any given point in time and was assumed to be independent of PFS. All patients whose disease progressed were assumed to receive subsequent treatment: those whose disease progressed while on IsaKd were assumed to receive pomalidomide plus cyclophosphamide plus dexamethasone (PCd), while patients whose disease progressed on Kd were assumed to receive DVd or PCd.
Model Inputs
The modelled cohort’s characteristics were based on the IKEMA trial (mean age 63.1 years; 56% men; body surface area 1.8 m2, mean weight 75.4 kg). Kaplan–Meier estimates of PFS, PFS while on treatment, TTD, and OS from the trial period were used to fit parametric survival curves to extrapolate the observed trial data (median follow-up 20.73 months) over the entire model time horizon (37 years) for IsaKd and Kd.3 Model selection was based on diagnostic plots (i.e., log-cumulative hazard plots, Schoenfeld residual plots), statistical fit (Akaike information criterion, Bayesian information criterion), visual assessment, and clinical expert opinion. Lognormal and Gompertz distributions were chosen by the sponsor for the long-term extrapolation of OS, PFS, and on-treatment PFS for IsaKd and Kd, respectively. For TTD, the sponsor chose the exponential distribution for both IsaKd and Kd. Treatment waning was not considered.
Health state utility values were based on EuroQol 5-Dimensions (EQ-5D) questionnaire data collected during the IKEMA trial and on pooled data for the IsaKd and Kd treatment groups. EQ-5D 5-Levels (EQ-5D-5L) data from IKEMA were valued using UK tariffs and were mapped to the EQ-5D 3-Levels (EQ-5D-3L).5 Within the pre-progression state, patients were assumed to have a higher utility while on treatment (||||) versus off treatment (||||). Utilities were adjusted for age and sex, and the utility values were capped by use of Canadian-specific utility estimates,6 such that the utility estimates from the IKEMA trial could not exceed general population utility values. Disutilities related to AEs were assumed to be captured as part of the EQ-5D-5L data collected during the IKEMA trial.3
The model included costs related to drug acquisition and administration, pre-medication (paracetamol, ranitidine, diphenhydramine), subsequent treatment after disease progression, supportive medications (granulocyte colony-stimulating factor, red blood cell transfusion, platelet transfusion), AEs, health care resource use in the pre-progression and post-progression health states, and terminal care costs. Drug acquisition costs for isatuximab were based on the sponsor’s submitted price,3 while the price of dexamethasone and carfilzomib was acquired from the Ontario Drug Benefit formulary7 and past CADTH pan-Canadian Oncology Drug Review reviews,8 respectively. Drug wastage was assumed in the sponsor’s base case, and the RDI for each treatment was based on the IKEMA trial. Administration costs were included for treatments administered orally, IV, or by subcutaneous/intramuscular injection.9 The cost of pre-medication was based on prices obtained from the Ontario Drug Benefit Formulary,7 with the dosage based on the schedule in the IKEMA trial. Costs for subsequent treatment were estimated as a 1-time cost that incorporated the distribution of patients receiving each drug and the expected treatment duration. Costs related to the treatment of grade 3 or greater AEs that occurred in at least 5% of patients in the IKEMA trial were included in the model; AEs were assumed to be treated via outpatient visits9 or in hospital.10 Health care resource use included costs related to medical visits (i.e., physician visits9) and monitoring (i.e., complete blood count, biochemistry11), with the resources used and the frequency based on clinical expert opinion.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations). The deterministic and probabilistic results were notably dissimilar, with the probabilistic ICER 28% higher than the deterministic ICER. CADTH felt this discrepancy was likely due to assumptions made by the sponsor, such as OS not exceeding that of the general population. However, due to unclear modelling practices, CADTH notes the probabilistic results in the sponsor’s analysis are highly uncertain. The probabilistic findings are presented in this section. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Base-Case Results
In the sponsor’s base-case analysis, IsaKd was associated with estimated costs of $1,170,887 and 8.20 QALYs over a 37-year time horizon. Treatment with IsaKd was both more costly and produced more QALYs than treatment with Kd alone (incremental costs: $558,809; incremental QALYs: 4.15), resulting in an ICER of $141,824 per QALY (Table 3). In the sponsor’s base case, IsaKd had an 0% probability of being the most cost-effective strategy at a WTP threshold of $50,000 per QALY.
Results were driven by the predicted differences in total life-years between IsaKd and Kd (incremental life-years: 5.70 years) and the increased drug acquisition costs associated with IsaKd (incremental costs: $560,672) (Appendix 3).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. KD ($/QALY) |
|---|---|---|---|---|---|
Kd | 582,079 | Reference | 4.05 | Reference | Reference |
IsaKd | 1,170,887 | 588,809 | 8.20 | 4.15 | 141,824 |
ICER = incremental cost-effectiveness ratio; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.3
Sensitivity and Scenario Analysis Results
The sponsor provided several scenario and sensitivity analyses, including adopting alternative time horizons, adopting alternative parametric curves for the extrapolation of OS and PFS (in combination), capping TTD at the time of PFS, adopting alternative discount rates, assuming no drug wastage, adopting treatment-specific health state utility values, and including additional comparators.
Several scenarios resulted in notable increases to the ICER, including adopting alternative parametric curves for the extrapolation of OS and PFS and adopting a shorter analysis time horizon. Notably, the sponsor’s model was highly sensitive to the parametric curve chosen for the extrapolation of OS and PFS (in combination), with an estimated 158% increase in the ICER (ICER for IsaKd: $366,000 per QALY versus Kd) compared to the base case, in which less optimistic parametric curves were chosen.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
Limitations associated with the sponsor’s chosen modelling approach. The sponsor submitted a PSM, in which treatment efficacy is represented by PFS and OS curves. PFS and OS model inputs were based on observations from the IKEMA trial (median follow-up: 20.73 months), which the sponsor extrapolated over model’s time horizon (37 years).3 The extrapolated estimates for IsaKd were highly variable across input parameters, dependent on the assumed statistical distribution. This is highlighted by the sponsor’s submitted scenario analyses, in which adopting alternative parametric distributions for the long-term extrapolation of OS and PFS resulted in a 158% increase in the ICER. As noted in the CADTH clinical review, the OS data from IKEMA are immature, which introduces considerable additional uncertainty in the long term extrapolation.
The sponsor’s base case predicts a survival advantage with IsaKd compared to Kd (incremental gain: 5.7 discounted life-years). The IKEMA trial was not powered to detect differences in survival between IsaKd and Kd, and the OS data are immature. Clinical experts consulted by CADTH noted that the maximum length of survival for this patient population is not expected to exceed 15 years. The sponsor’s chosen parametric distribution (lognormal) for the extrapolation of OS lacked face validity, in that the lognormal distribution predicted that approximately 24% of patients who receive IsaKd would remain alive 40 years after initiating treatment. Although the sponsor assumed that mortality probabilities would not be less than that of the age- and sex-matched general population, the use of lognormal distribution resulted in survival that was effectively equal to that of the general population after a period of time, which is unlikely for the indicated population.
PSMs assume independence between the PFS and OS survival functions (i.e., OS and PFS curves are extrapolated independently); however, this can result in implausible results (e.g., the PFS curve may intersect with the OS curve). CADTH notes that, when the most clinically plausible curves are chosen for OS and PFS for patients taking IsaKd, based on feedback from CADTH clinical experts, the PFS and OS curves intersect. Additionally, OS is susceptible to potential confounding that may not affect PFS (e.g., choice of subsequent treatments after disease progression).12 Such confounding may attenuate the OS effect in clinical practice, despite the presence of a statistically significant effect of treatment on PFS in a clinical trial. Clinical experts consulted by CADTH noted that the choice of subsequent therapies after IsaKd or Kd would be determined, at least in part, by prior treatment experience. Further, experts indicated that the survival of patients with multiple myeloma is likely to be affected by the receipt of a CD38 antibody drug (e.g., isatuximab, daratumumab) at any point during the disease course. While 80% of patients in the sponsor’s model were assumed to receive daratumumab as part of subsequent therapy after disease progression while on Kd, this was assumed to affect only costs (i.e., potential effects on survival were not considered). Further, clinical experts considered an incremental gain of approximately 6 life-years between patients who received IsaKd and Kd to be optimistic. Given the lack of long-term data and uncertainty associated with the extrapolated data, the external validity of the sponsor’s predicted survival benefit with IsaKd is highly uncertain. As a result, the predicted gain of life-years and QALYs associated with IsaKd relative to Kd should be interpreted with caution.
CADTH was unable to fully address the limitations associated with the chosen modelling approach, and the model calculations could not be fully validated. Given these limitations, a CADTH base case could not be derived. CADTH conducted exploratory reanalyses in which it adopted an alternative parametric distribution for IsaKd OS that clinical experts considered to be better aligned with the expected OS in this patient population. CADTH notes that, for IsaKd PFS, none of the extrapolated curves provided by the sponsor aligned with clinical expectations (i.e., predicted PFS was longer than the expected survival for the indicated population).
In CADTH reanalyses, IsaKd PFS was modelled by use of the hazard ratio observed in the IKEMA trial. This approach assumes proportional hazards over the patient’s lifetime, which overestimates the benefit seen in the trial and assumes no waning of effect. This therefore likely biases the results in favour of IsaKd.
Comparative effectiveness of IsaKd to relevant comparators is highly uncertain. The sponsor’s base case compared the cost-effectiveness of IsaKd to Kd, with the relative clinical effectiveness of IsaKd and Kd based on data from the IKEMA trial.3 As noted by the clinical experts consulted by CADTH for this review, treatment of multiple myeloma after first-line therapy is highly individualized and depends, at least in part, on prior treatments received. Relevant comparators after the first-line for patients with refractory multiple myeloma may include regimens containing daratumumab (e.g., DVd, DRd), as well as carfilzomib (e.g., KRd) or pomalidomide (e.g., pomalidomide plus dexamethasone [Pd], IsaPd). Clinical experts consulted by CADTH noted that DVd and Kd are commonly used as second-line treatments, as many patients’ myeloma is refractory to lenalidomide after first-line treatment (i.e., among those who received lenalidomide-containing regimens at first-line). As noted in the CADTH clinical review, no head-to-head trials of IsaKd and DVd or other clinically relevant regimens (beyond Kd) were identified.
The sponsor provided scenario analyses including DVd, KRd, and DRd as comparators. To inform OS and PFS for these analyses, the sponsor undertook indirect treatment comparisons (ITCs) including NMAs and match-adjusted treatment comparisons. As noted by the sponsor, the interpretation of the results is limited by heterogeneity among trials for key prognostic factors and issues with network connectivity. The sponsor further noted that “The hazard ratios generated from the NMA did not align with the expectations of consulted clinical experts and were deemed clinically implausible.”3 Clinical experts consulted by CADTH agreed that the interpretation of data from the sponsor’s ITC was limited by heterogeneity owing to differences in the number of prior lines of therapy and types of prior therapy among the included studies. As a result, there is substantial uncertainty with the interpretation of the clinical findings of the sponsor’s ITC and the submitted scenario analysis based on these data.
Given the lack of head-to-head evidence for IsaKd relative to other relevant comparators and the concerns with interpretation of the sponsor’s submitted comparative efficacy data, CADTH was unable to include additional comparators as part of its reanalyses or as part of scenario analyses. As a result, the cost-effectiveness of IsaKd compared to other relevant comparators remains unknown.
The model lacked flexibility to assess relevant subgroups. As previously noted, the choice of treatment depends, at least in part, on the number and type of prior treatments received. Clinical experts noted that, in Canadian clinical practice, IsaKd usage is most likely to be in the second-line setting among patients whose disease is refractory to lenalidomide. In the IKEMA trial, |||||||||% of patients had received 1 prior line of therapy, |||||||||% and |||||||||% had received 2 or 3 prior lines of therapy, respectively, and |||||||||% of patients were refractory to lenalidomide. Other clinically relevant subgroups include transplant-eligible and transplant-ineligible patients, which may confound the interpretation of OS. Notably, |||||||||% of IKEMA participants had previously received an autologous transplant.
CADTH could not assess the cost-effectiveness of IsaKd based on the number or type of prior treatments received, owing to the structure of the sponsor’s model. Similarly, CADTH could not evaluate the cost-effectiveness of IsaKd among patients who had or had not received a prior stem cell transplant. Consequently, the cost-effectiveness of IsaKd in such subgroups is unknown and, likewise, the cost-effectiveness in the full Health Canada population is highly uncertain, as none of this heterogeneity is considered. As per CADTH guidelines on economic evaluation, when there is considerable heterogeneity, a stratified analysis should be conducted.
Long-term extrapolation of TTD is uncertain: In the sponsor’s model, TTD and PFS were sampled from separate parametric distributions, such that there was no assumed correlation between treatment discontinuation and disease progression. The sponsor’s selected parametric survival distributions for TTD (i.e., exponential) predicted that patients who discontinue IsaKd will continue to incur benefit (i.e., remain progression-free) for a period of time after discontinuation (median TTD: 1.9 years; median PFS on treatment: 2.0 years; median overall PFS: 4.5 years). Clinical experts consulted by CADTH indicated that this prediction lacked face validity, in that patients who discontinue the full IsaKd regimen would be unlikely to remain progression-free for several years without additional therapy. The sponsor’s model additionally lacked face validity in that patients were assumed to discontinue all components of a regimen, which clinical experts noted was unlikely in clinical practice (i.e., if carfilzomib is discontinued, patients may remain on isatuximab and dexamethasone). Finally, the use of an exponential distribution to model treatment discontinuation implies that patients would discontinue treatment at a constant rate over the time horizon, which does not align with clinical expectations.
In the CADTH reanalyses, TTD was assumed to be correlated with PFS on the basis of clinical expert feedback. The relationship between PFS and TTD in the IKEMA trial was used to model the relationship between PFS and TTD over the analysis horizon (Appendix 3, Figure 2, Figure 3).
The impact of IsaKd on quality of life is uncertain. As noted in the CADTH clinical review, health-related quality of life was assessed in the IKEMA trial; however, no statistical analyses were undertaken. Further, CADTH identified several issues in the modelled utility estimates. First, the sponsor mapped EQ-5D-5L data collected in the IKEMA trial to EQ-5D-3L via a mapping function, which introduces uncertainty. Second, the utility values for patients in the PFS state on treatment (|||||||||) were higher than for patients in the PFS state off treatment (|||||||||). This lacks face validity, as, among patients in an identical PFS health state, patients on active treatment would be expected to have a lower quality of life than those who were off treatment due to the AEs associated with treatment; this issue was noted in the previous CADTH review of isatuximab.2 Third, the utilities applied for the post-progression state (i.e., reflecting progressed disease) are uncertain, as progression in the economic model was based on serological progression rather than clinical progression. As noted in the previous CADTH review of isatuximab, these types of progression may differ in terms of their impact on utility,2 which was not accounted for in the sponsor’s model. Fourth, patients whose disease has progressed and who receive subsequent treatment therapies may have a differing utility value compared to those who do not receive subsequent treatment, which was not accounted for in the sponsor’s model.
In CADTH reanalyses, CADTH assumed that patients in the PFS state would have the same health state utility value, regardless of whether they were on or off treatment. As noted previously, patients in the PFS state who are on active treatment would be expected to have lower quality of life than those off treatment owing to AEs. This is expected to be captured, at least in part, by the inclusion of AEs disutility values, which have been included in the CADTH reanalysis. In scenario analyses, CADTH explored the impact of alternative utility values based on nonmapped EQ-5D-5L values from the IKEMA trial. These values were higher than general population estimates, which limited their face validity. CADTH was unable to address potential differences in utilities between patients with serological progression compared to those with clinical disease progression, or differences in utilities depending on whether subsequent treatment is received after disease progression.
RDI may not correlate well with drug costs. In the calculation of drug costs, the sponsor incorporated the RDI for each drug observed in each arm of the IKEMA trial, which may not reflect clinical practice. In the IsaKd regimen, RDI was assumed to be |||||||||% for isatuximab. The sponsor did not state how RDI was calculated in the IKEMA trial; however, in IKEMA, dose adjustment (dose delay or dose omission) for isatuximab was permitted based on “individual patient tolerance,” while no dose reductions were allowed.4 CADTH notes that, based on the isatuximab product monograph, dose reductions are not recommended, although doses may be delayed (e.g., because of neutropenia).1 As a result, patients would still be expected to receive the recommended dosage of isatuximab, although on an altered schedule. However, in the sponsor’s model, the RDI was used to adjust the required amount of each drug, which inappropriately reduced the cost of isatuximab. Overall, without explicitly modelling dose delays and reductions for the patient population, the method of multiplying RDI by dose received is associated with substantial uncertainty, especially when viewed independently from discontinuation. As a result, the use of an RDI of less than 100% may inappropriately reduce the cost of isatuximab in the sponsor’s pharmacoeconomic model, which may bias the ICER in its favour.
In CADTH reanalyses, an RDI of 100% was adopted for all treatments.
Uncertainty about the impact of AEs. The sponsor incorporated costs related to grade 3 or greater AEs with an incidence of at least 5% as a 1-time cost in the pre-progression health state, based on the incidence in the IKEMA trial for IsaKd and Kd. The sponsor selected an arbitrary threshold to capture the impact of treatment-related AEs rather than selecting the most clinically meaningful AEs to include within the model. This may underestimate the impact of rare AEs. Serious infusion reactions, including severe anaphylactic reactions, have been observed after isatuximab administration.13 Further, the AEs included in the sponsor’s model do not capture the range of AEs deemed to be of special interest to clinicians (e.g., cardiac failure) or noted in the patient input (e.g., nausea/vomiting) received by CADTH for this review. Clinical experts further noted that the sponsor’s assumption that AEs would only occur only during the first month of treatment is inappropriate, as events such as infections or febrile neutropenia can occur during multiple treatment cycles.
The sponsor assumed that disutilities related to AEs would be captured as part of health state utility values. It is unlikely that the impact of AEs on quality of life would be adequately captured by EQ-5D values collected as part of the IKEMA trial, as the EQ-5D lacks specific domains that might be affected by AEs. Additionally, the EQ-5D was administered at set times during the trial and has a 1-day recall period, which is problematic in assessing the impact of AEs in clinical trials.14 Additionally, quality-of-life measurements in clinical trials are often missing in a way that is not random. Further, applying pooled utility weights to all treatments fails to account for differences in their respective safety profiles.
In CADTH reanalyses, disutility values provided by the sponsor were applied. CADTH notes, however, that these values were based on pooled EQ-5D values for all grade 3 or greater AEs in the IKEMA trial and, thus, do not account for the impact of individual AEs. CADTH was unable to address the frequency of AEs or the impact of rare AEs owing to a lack of data. The impact of AEs on the ICER is therefore uncertain.
Uncertainty related to subsequent treatment after disease progression. In the pharmacoeconomic model, the sponsor assumed that all patients whose disease progressed would receive subsequent treatment. Clinical experts consulted by CADTH for this review noted that, in practice, only approximately 50% to 75% of patients whose disease progresses on IsaKd would be likely to receive subsequent treatment (i.e., a proportion of patients will never receive a subsequent treatment after IsaKd). In a US retrospective cohort study, 21% to 57% of patients received only 1 line of therapy, depending on whether the patient had undergone an autologous stem cell transplant.15 CADTH notes that the assumption of 100% of patients receiving subsequent therapy is not aligned with assumptions made by the sponsor in its submitted budget impact analysis,16 in which approximately 29% of patients who receive second-line treatment were assumed to receive third- or later-line treatment.
In the pharmacoeconomic model, patients whose disease progressed while on IsaKd were assumed to receive PCd, while patients whose disease progressed on Kd were assumed to receive DVd (80% of patients) or PCd (20%). Subsequent treatment was assumed to affect costs only, while the effects of subsequent treatment on OS were not considered. Clinical experts consulted by CADTH noted that subsequent treatment is highly individualized and depends on previous treatments received. Further, as previously noted, patients who received daratumumab at any time during their disease course (i.e., as part of DVd) would be expected to receive clinical benefit from a CD38 antibody drug. As a result, the sponsor’s model lacks face validity, in that subsequent treatment was expected to impact costs only, and their impact on OS was not considered. CADTH additionally notes that the cost of subsequent therapy was based on the expected duration of subsequent treatment, based on a US-based analysis of drug utilization and expert input, and averaged for patients who received third-, fourth-, and fifth-line regimens that included the treatments of interest within the regimen. Whether this duration of subsequent treatment is applicable to the Canadian context is uncertain.
CADTH was unable to address uncertainty related to impact of subsequent treatments on the cost-effectiveness estimates, owing to the structure of the sponsor’s model and a lack of data. The sponsor’s model predicts $77,386 savings in subsequent therapy costs with IsaKd, which is unlikely. A scenario analysis was conducted in which 50% of patients were assumed to receive subsequent therapy.
Model lacked transparency. CADTH notes the that sponsor’s submission was overly complex, making simple validation checks very difficult. For example, there is duplication of key parameters across multiple sheets, making it unclear which parameter needs to be edited to implement a change. Likewise, the sponsor’s submitted model also included numerous IFERROR statements, which lead to situations in which the parameter value is over-written with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors. Probabilistic results of the sponsor’s model also lacked face validity when certain parametric survival curves were chosen. It was unclear how bootstrapped simulations used to characterize uncertainty around survival curves were generated and, therefore, the simulations could not be validated by CADTH.
CADTH was unable to address this limitation and notes that a thorough validation of the sponsor’s model was not possible.
Additional limitations were identified, but were not considered to be key limitations:
In the sponsor’s submission, the cost of branded bortezomib was included, despite the availability of a generic version. As previously noted, the sponsor assumed that, of patients whose disease progressed on Kd, 80% were assumed to receive DVd, while no patients whose disease progressed on IsaKd received DVd. The use of the price of branded bortezomib overestimates the cost of subsequent therapy for the Kd group, which biased the ICER in favour of IsaKd. However, given that the sponsor assumed that DVd was received for a maximum of 5.2 treatment cycles (28-day), this had little practical effect on the ICER.
In the CADTH reanalysis and scenario analyses, the generic price of bortezomib was used.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients enrolled in the IKEMA trial were assumed to be representative of patients in Canada who would be eligible for IsaKd (age 63.1 years, 56% men, 75.4 kg, body surface area 1.8 m2). | Reasonable, although clinical experts noted that the patients enrolled in IKEMA were generally younger than those with relapsed and/or refractory multiple myeloma in clinical practice. In Canada, the mean age at the time of multiple myeloma diagnosis is 70 years17 |
The dosage of carfilzomib was based on the IKEMA trial (carfilzomib: 20 mg/m2 IV on days 1 and 2, then 56 mg/m2 IV on days 8, 9, 15, 16 of cycle 1; subsequent cycles 56 mg/m2 IV on days 1, 2, 8, 9, 15, 16). | Reasonable, although the clinical experts consulted by CADTH indicated that, in clinical practice, carfilzomib may be administered weekly at the higher dose. This would be expected to have little effect on the ICER, as carfilzomib is administered as part of both IsaKd and Kd. Weekly carfilzomib administrations would increase resource use and patient visits to hospital. |
Duration of treatment effect on both therapies would last for the patient’s lifetime (i.e., no treatment waning). | Uncertain. As per CADTH economic guidelines, the impact of treatment effectiveness waning should be explored through scenario/sensitivity analyses. Clinical experts consulted by CADTH indicated that, for patients who remain on the full IsaKd regimen, the regimen’s effectiveness is likely to remain relatively constant over the treatment duration. Experts noted, however, that a proportion of patients may discontinue carfilzomib owing to toxicity (i.e., continue on isatuximab and dexamethasone). Among these patients, a waning of effectiveness is likely. CADTH was unable to explore the impact of partial regimen discontinuation owing to the structure of the sponsor’s model. |
Drug wastage was assumed (i.e., no vial sharing). | Uncertain. Isatuximab is supplied as a single-use vial; however, the clinical experts consulted by CADTH indicated that a combination of wastage and vial sharing would likely occur. The extent of sharing would likely depend on the practice centre (e.g., greater sharing may occur be at larger centres). |
ICER = incremental cost-effectiveness ratio; IsaKd = isatuximab plus carfilzomib plus dexamethasone; IV = IV; Kd = carfilzomib plus dexamethasone.
CADTH Reanalyses of the Economic Evaluation
Several limitations with the sponsor’s submission could not be adequately addressed due to structural or data limitations, including the notable limitations associated with the sponsor’s chosen modelling approach (i.e., PSM). Notably, the long-term extrapolation of OS is highly uncertain. CADTH was unable to address the lack of head-to-head comparative clinical data for additional relevant comparators (e.g., DVd), the cost-effectiveness of IsaKd in relevant subgroups, and uncertainty associated with the influence of subsequent therapy after disease progression on OS. As a result, CADTH was unable to conduct any base-case reanalysis of the sponsor’s model, given that any estimate of incremental effectiveness would be misleading.
Exploratory Results
CADTH undertook reanalyses that addressed limitations in the model, as summarized in Table 5. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Bortezomib price | $1,402.42 per 3.5 mg | $654.31 per 3.5 mg (IQVIA wholesale price, generic) |
Changes to derive the CADTH reanalysis | ||
1. Parametric distribution of OS | Based on extrapolated data from the IKEMA trial: Kd: Gompertz IsaKd: Lognormal | Based on extrapolated data from the IKEMA trial: Kd: Gompertz IsaKd: Gompertza |
2. Parametric distribution of PFS | Based on extrapolated data from the IKEMA trial: Kd: Gompertz IsaKd: Lognormal | Based on data from the IKEMA trial: Kd: Gompertz parametric distribution IsaKd: the OS hazard ratio (IsaKd v. Kd: 0.53) observed in the IKEMA trial was used to model the relationship between PFS for IsaKd and Kd |
3. Parametric distribution of TTD | Based on extrapolated data from the IKEMA trial: Kd: Exponential IsaKd: Exponential | Treatment discontinuation was assumed to correlated with PFS; the relationship between TTD and PFS in observed in the IKEMA trial was used to model this relationship over the model horizon (Appendix 4, Figures 2 and 3) |
4. Utility values for the PFS health state | PFS (on treatment): |||| PFS (off treatment): |||| | PFS (on treatment): |||| PFS (off treatment): |||| |
5. Disutility values | Not included | Included |
6. RDI | Based on the IKEMA trial. IsaKd Isatuximab: ||||% Carfilzomib: ||||% Dexamethasone: ||||% Kd Carfilzomib: ||||% Dexamethasone: ||||% | RDI was assumed to be 100% for all drugs in both regimens. |
CADTH exploratory reanalysis | Reanalysis 1 + 2 + 3 + 4 + 5 + 6 | |
IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; OS = overall survival; PFS = progression-free survival; RDI = relative dose intensity; TTD = time to treatment discontinuation.
aCADTH notes that implausible results were obtained when the sponsor’s model was run probabilistically with the Gompertz distribution selected for IsaKd OS. As a result, OS was assumed to be deterministic for both IsaKd and Kd in all CADTH reanalyses.
CADTH undertook a stepped analysis, incorporating each change proposed in Table 5 to sponsor’s base case to highlight the impact of each change (Table 6; disaggregated results are presented in Appendix 4, Table 11).
In CADTH’s exploratory reanalysis, IsaKd was associated with higher costs (incremental costs = $524,791) and higher QALYs (incremental QALYs = 0.30) than Kd over a 37-year horizon. The ICER for IsaKd versus Kd was $1,588,632 per QALY. There is a 0% probability that IsaKd is optimal compared to Kd at a WTP threshold of $50,000 per QALY. The incremental QALYs with IsaKd treatment in the first 2 years were 0.04, indicating that the majority of the incremental benefits were accrued in the post-trial period and were derived on the basis of extrapolated trial findings rather than observed benefit, suggesting that uncertainties in the extrapolation period remain key model drivers. The incremental gain in life-years with IsaKd compared with Kd were also key drivers of the ICER, along with drug acquisition costs for IsaKd, which represent 119% of the total incremental costs (Table 11).
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Kd | 597,332 | 2.85 | Reference |
IsaKd | 1,162,917 | 8.39 | 102,112 | |
Sponsor’s corrected base case | Kd | 583,204 | 2.85 | Reference |
IsaKd | 1,162,917 | 8.39 | 104,663 | |
CADTH reanalysis 1: OS extrapolation | Kd | 583,204 | 2.85 | Reference |
IsaKd | 1,136,625 | 3.21 | 1,535,282 | |
CADTH reanalysis 2: PFS extrapolation | Kd | 583,204 | 2.85 | Reference |
IsaKd | 1,162,917 | 8.20 | 108,286 | |
CADTH reanalysis 3: TTD extrapolation | Kd | 527,539 | 2.84 | Reference |
IsaKd | 2,473,919 | 8.45 | 347,062 | |
CADTH reanalysis 4: PFS utilities | Kd | 583,204 | 2.87 | Reference |
IsaKd | 1,162,917 | 8.59 | 101,221 | |
CADTH reanalysis 5: Disutilities | Kd | 583,204 | 2.84 | Reference |
IsaKd | 1,162,917 | 8.38 | 104,670 | |
CADTH reanalysis 6: RDI | Kd | 589,337 | 2.85 | Reference |
IsaKd | 1,216,894 | 8.39 | 113,300 | |
CADTH exploratory reanalysis (1 + 2 + 3 + 4 + 5 + 6) | Kd | 529,357 | 2.87 | Reference |
IsaKd | 998,299 | 3.17 | 1,588,632 |
ICER = incremental cost-effectiveness ratio; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; RDI = relative dose intensity; TTD = time to treatment discontinuation.
Note: Reanalyses are based on publicly available prices of the comparator treatments.
aIncluded values for the sponsor’s base case, sponsor’s corrected base case, and the CADTH reanalysis steps are based on the sponsor’s deterministic model. As noted in the Summary of the Sponsor’s Economic Evaluation, there were notable differences between the life-years (and hence QALYs and ICERs) predicted by the sponsor’s deterministic and probabilistic model. These differences were largely resolved in the CADTH reanalysis. Results of the CADTH exploratory reanalysis are based on probabilistic analyses.
Scenario Analysis Results
CADTH undertook a series of price reduction analyses on the price of isatuximab, based on the sponsor’s submitted base case and CADTH’s exploratory reanalysis. IsaKd is not cost-effective at a WTP threshold of $50,000 per QALY, even if isatuximab was offered at no cost (Table 7). CADTH undertook additional price reduction analyses of isatuximab while holding the price of carfilzomib constant at a 61% price reduction. Under this scenario, a 100% price reduction for isatuximab, combined with a greater than 61% price reduction for carfilzomib, would be required in order for IsaKd to be considered cost-effective within the $50,000 threshold when compared to Kd.
Table 7: CADTH Price Reduction Analyses
Analysis Isatuximab price reduction | ICERs for IsaKd vs. Kd ($/QALY) | ||
|---|---|---|---|
Sponsor base case | CADTH reanalysis (list price for carfilzomib unchanged) | CADTH reanalysis (assuming a 61% carfilzomib price reduction) | |
No price reduction | 141,824 | 1,588,632 | 1,207,043 |
10% | 132,651 | 1,473,471 | 1,091,882 |
20% | 123,479 | 1,358,310 | 976,721 |
30% | 114,307 | 1,243,149 | 861,560 |
40% | 105,135 | 1,127,988 | 746,399 |
50% | 95,963 | 1,012,827 | 631,238 |
60% | 86,791 | 897,666 | 516,077 |
70% | 77,618 | 782,505 | 400,916 |
80% | 68,446 | 667,344 | 285,755 |
90% | 59,274 | 552,183 | 170,594 |
99.9% | 50,193 | 437,022 | 55,433 |
ICER = incremental cost-effectiveness ratio; IsaKd = isatuximab in combination with carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; QALY = quality-adjusted life-year.
Note: Based on the publicly available prices of the comparator treatments.
Several scenario and sensitivity analyses of the CADTH exploratory reanalysis were conducted. These scenario analyses explored the impact of the following model parameters and assumptions:
Assumption of no survival difference between IsaKd and Kd.
Generalized gamma parametric distribution of OS for IsaKd.
Utility values for PFS and post-progression based on EQ-5D-5L data from the IKEMA trial.
Subsequent therapy received by 50% of patients with progressed disease.
The results of these analyses are presented in Table 13. The ICER is highly sensitive to OS. When OS was assumed to be equal for IsaKd and Kd, the ICER was $7,145,426 for IsaKd versus Kd.
Issues for Consideration
Clinical experts consulted by CADTH for this review indicated that, at present, IsaKd would most likely be used in the second-line treatment of multiple myeloma, especially for patients whose disease is refractory to lenalidomide. The experts noted, however, that this may change depending on the results of the ongoing phase III MAIA trial of the use of DRd in the first-line treatment of transplant-ineligible multiple myeloma.
The current submission is for the use of isatuximab in combination with carfilzomib and dexamethasone (IsaKd) for multiple myeloma in patients who have received 1 to 3 prior lines of therapy. Isatuximab is also indicated for use in combination with pomalidomide and dexamethasone (IsaPd) for patients with relapsed or refractory multiple myeloma who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor. IsaPd was previously reviewed by CADTH for this indication,2 and isatuximab is currently being considered for negotiation with the pan-Canadian Pharmaceutical Alliance for this indication.18
Generic submissions of pomalidomide and lenalidomide are currently under review by Health Canada, and the patent protection for carfilzomib ends in 2024. The introduction of generic formulations may result in a discounted cost of the branded drugs.
The use of isatuximab may be associated with the use of additional health care resources compared to currently available treatments. For example, additional health care resources may be required to manage infusion-related reactions or AEs related to isatuximab (e.g., neutropenia, thrombocytopenia, neuropathies).
Overall Conclusions
As noted in the CADTH clinical review, IsaKd improves PFS relative to Kd among patients with multiple myeloma who have received 1 to 3 prior lines of therapy. However, although health-related quality of life was assessed in IKEMA, no statistical analysis was undertaken by the sponsor, and the comparative effect of IsaKd on quality of life is uncertain. Further, OS data from the IKEMA trial are immature, and the extrapolation of short-term trial data over a 37-year horizon introduces considerable uncertainty. While the sponsor’s model predicts a survival benefit with IsaKd relative to Kd, this has not been shown in clinical studies; whether a benefit in PFS translates to an increase in OS is highly uncertain. CADTH also notes that the comparative effects of IsaKd relative to second- and later-line treatments other than Kd for relapsed or refractory multiple myeloma are uncertain owing to a lack of trial data and limitations with the sponsor’s ITC.
Given the limitations associated with the sponsor’s chosen model structure, a CADTH base case could not be derived to estimate the cost-effectiveness of IsaKd. The sponsor’s model predicts increased overall survival with IsaKd on the basis of immature OS data from the ongoing IKEMA trial; however, as previously noted, the long-term extrapolation of OS is highly uncertain. OS is also subject to potential confounding by the choice of subsequent treatment after disease progression, which was not considered in the sponsor’s model. CADTH undertook exploratory reanalyses, within the constraints of the sponsor’s PSM model, to address limitations in the sponsor’s submission, including correcting the price of bortezomib, adopting alternative parametric distributions for OS, adopting the IKEMA PFS hazard ratio to model the relationship between IsaKd and Kd, assuming correlation between PFS and TTD, revising the utility values for PFS, including disutility values, and assuming that all patients receive the full dose of all drugs. CADTH was unable to address the limitations with the chosen modelling approach, the lack of head-to-head comparative clinical data for additional relevant comparators, the cost-effectiveness of IsaKd in relevant subgroups, and uncertainty associated with the use of subsequent therapy after disease progression. The validity and interpretability of the results are thus limited, should be viewed as exploratory, and likely underestimate the true ICER.
In the CADTH reanalysis, IsaKd had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY (ICER $1,588,632 per QALY gained compared with Kd). Cost-effectiveness could not be achieved even if the price of isatuximab was reduced by 100% (ICER falls to $437,022) due to the high cost and duration of use of adjunctive treatment. If isatuximab was $0, the budget impact of IsaKd would still be $28 million. If the cost of carfilzomib was reduced by 61%, isatuximab would still need a 100% price reduction for the combined IsaKd regimen to be considered cost-effective. However, this still assumes 100% of patients end up on subsequent therapy, an OS benefit exists, and proportional hazards hold. Relaxation of these assumptions would mean the price of carfilzomib has to be even lower for isatuximab to be considered cost-effective at a 100% price reduction.
The results of the CADTH reanalyses were primarily driven by the acquisition cost of isatuximab and the predicted incremental gain in life-years over the model’s time horizon compared to Kd. In a scenario analysis in which no benefit in OS was assumed, IsaKd was associated with an ICER of $7,145,426 per QALY gained compared with Kd, highlighting the impact of uncertainty in OS on the ICER. The lack of long-term OS data and the potential confounding of OS by subsequent treatment mean that the results of the CADTH reanalysis are highly uncertain and may overestimate the true clinical efficacy of IsaKd. Consequently, the cost-effectiveness of IsaKd compared with Kd is highly uncertain. The cost-effectiveness of IsaKd compared to other relevant (and lower-cost) comparator regimens is unknown, given the lack of robust evidence on its comparative effectiveness. When these points are taken into consideration, the CADTH exploratory reanalysis likely underestimates the true ICER.
References
1.SarclisaTM (isatuximab for injections): concentrate for solution for infusion (20mg/mL) [product monograph]. Mississauga (ON): Sanofi Genzyme; 2020 Sep 13.
2.CADTH Drug Reimbursement Review: isatuximab (Sarclisa) for multiple myeloma (Sanofi Genzyme). Ottawa (ON): CADTH; 2021 Apr 1: https://cadth.ca/isatuximab-sarclisa-multiple-myeloma-details. Accessed 2021 Aug 20.
3.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), concentrate for solution for infusion (20mg/mL) [internal sponsor's package]. Mississaugua (ON): Sanofi Genzyme; 2021.
4.Clinical Study Report: EFC15246 (IKEMA). Randomized, open label, multicenter study assessing the clinical benefit of isatuximab combined with carfilzomib (Kyprolis®) and dexamethasone versus carfilzomib with dexamethasone in patients with relapsed and/or refractory multiple myeloma previously treated with 1 to 3 prior lines [internal sponsor's report]. Mississaugua (ON): Sanofi Genzyme; 2020.
5.van Hout B, Janssen MF, Feng Y-S, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708-715. PubMed
6.Guertin JR, Feeny D, Tarride J-E. Age- and sex-specific Canadian utility norms, based on the 2013–2014 Canadian Community Health Survey. Can Med Assoc J. 2018;190(6):E155. PubMed
7.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Oct 20.
8.Pan-Canadian Oncology Drug Review final economic guidance report: carfilzomib (Kyprolis) for multiple myeloma. 2016: https://www.cadth.ca/sites/default/files/pcodr/pcodr_carfilzomib_kyprolis_mm_fn_egr.pdf. Accessed 2021 Aug 23.
9.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2021 Oct 20.
10.Canadian Institute for Health Information. Patient cost estimator. 2021; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2021 Oct 20.
11.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2021 Oct 20.
12.Msaouel P, Grivas P, Zhang T. Adjuvant systemic therapies for patients with renal cell carcinoma: Choosing treatment based on patient-level characteristics. Eur Urol Oncol. 2021. PubMed
13.emc (Electronic Medicines Compendium). SARCLISA 20mg/mL concentrate for solution for infusion. 2021; https://www.medicines.org.uk/emc/product/11535/smpc#DOCREVISION. Accessed 2021 Oct 20.
14.Bansback N, Sun H, Guh DP, et al. Impact of the recall period on measuring health utilities for acute events. Health Econ. 2008;17(12):1413-1419. PubMed
15.Fonseca R, Usmani SZ, Mehra M, et al. Frontline treatment patterns and attrition rates by subsequent lines of therapy in patients with newly diagnosed multiple myeloma. BMC Cancer. 2020;20(1):1087. PubMed
16.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), concentrate for solution for infusion (20mg/mL) [internal sponsor's package]. Mississaugua (ON): Sanofi Genzyme; 2021.
17.Tsang M, Le M, Ghazawi FM, et al. Multiple myeloma epidemiology and patient geographic distribution in Canada: A population study. Cancer. 2019;125(14):2435-2444. PubMed
18.pan-Canadian Pharmaceutical Alliance. Sarclisa (isatuximab). 2021; https://www.pcpacanada.ca/negotiation/21444. Accessed 2021 Aug 25.
19.Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), concentrate for solution for infusion (20mg/mL) [internal sponsor's package]. Mississaugua (ON): Sanofi Genzyme; 2021.
20.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 Oct 20.
21.International Agency for Research on Cancer. Cancer Today: Data visualization tools for exploring the global cancer burden in 2018. 2018; https://gco.iarc.fr/today/home. Accessed 2021 Oct 20.
22.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019. Toronto: Canadian Cancer Society; 2019: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2019-statistics/canadian-cancer-statistics-2019-en.pdf. Accessed 2021 Sep 7.
23.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. Can Med Assoc J. 2020;192(9):E199. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Relapsed Multiple Myeloma
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Isatuximab + carfilzomib + dexamethasone (IsaKd) | ||||||
Isatuximab (Sarclisa)a | 20 mg/mL | 100 mg vial 500mg vial | 757.9000 3,789.4900 | Cycle 1: 10 mg/kg on days 1, 8, 15, 22 Cycle 2+: 10 mg/kg on days 1 and 15 | Cycle 1: 866 Cycle 2+: 433 | Cycle 1: 24,253 Cycle 2+: 12,126 |
Carfilzomib (Kyprolis) | 2 mg/mL | 10 mg 30 mg 60 mg Powder for IV infusion | 255.5500 766.6590 1,533.3300 | Cycle 1: 20 mg/m2 days 1, 2; 56 mg/m2 on days 8, 9, 15, 16 Cycles 2+: 56 mg/m2 on days 1, 2, 8, 9, 15, 16 | Cycle 1: 438 Cycle 2+: 548 | Cycle 1: 12,267 Cycle 2+: 15,333 |
Dexamethasone (generic) | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 20 mg on days 1, 2, 8, 9, 15, 16, 22, 23 | 0.44 | 12 |
IsaKd | Cycle 1: 1,305 Cycle 2+: 981 | Cycle 1: 36,532 Cycle 2+: 27,472 | ||||
Carfilzomib + dexamethasone (Kd) | ||||||
Carfilzomib (Kyprolis) | 2 mg/mL | 10 mg 30 mg 60 mg Powder for IV infusion | 255.5500 766.6590 1,533.3300 | Cycle 1: 20 mg/m2 on days 1, 2; 56 mg/m2 on days 8, 9, 15, 16 Cycles 2+: 56 mg /m2 on days 1, 2, 8, 9, 15, 16 | Cycle 1: 438 Cycle 2+: 548 | Cycle 1: 10,222 Cycle 2+: 15,333 |
Dexamethasone (generic) | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 20 mg on days 1, 2, 8, 9, 15, 16, 22, 23a | 0.44 | 12 |
Kd | Cycle 1: 439 Cycle 2+: 548 | Cycle 1: 12,279 Cycle 2+:15,345 | ||||
Lenalidomide plus dexamethasone (Rd) | ||||||
Lenalidomide (Revlimid) | 2.5 mg 5 mg 10 mg 15 mg 20 mg 25 mg | Cap | 329.5000 340.0000 361.0000 382.0000 403.0000 424.0000 | 25 mg on days 1 to 21 | 318 | 8,904 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 40 mg on days 1, 8, 15, 22 | 0.44 | 12 |
Rd | 318 | 8,916 | ||||
Pomalidomide plus dexamethasone (Pd) | ||||||
Pomalidomide (Pomalyst) | 1 mg 2 mg 3 mg 4 mg | Cap | 500.0000c | 4 mg on days 1 to 21 | 375 | 10,500 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 40 mg on days 1, 8, 15, and 22 | 0.44 | 12 |
Pd | 375 | 10,512 | ||||
Carfilzomib plus lenalidomide plus dexamethasone (KRd) | ||||||
Carfilzomib (Kyprolis) | 2 mg/mL | 10 mg 30 mg 60 mg Powder for IV infusion | 255.5500 766.6590 1,533.3300 | Cycle 1: 20 mg/m2 on days 1, 2; 27 mg/m2 on days 8, 9, 15, 16 Cycles 2 to 12: 27 mg /m2 on days 1, 2, 8, 9, 15, 16 Cycle 13 to 18: 27 mg/m2 on days 1, 2, 15, 16 | Cycle 1: 265 Cycle 2 to 12: 274 Cycle 13 to 18: 183 | Cycle 1: 7,155 Cycle 2 to 12: 7,667 Cycle 13 to 18: 5,111 |
Lenalidomide (Revlimid) | 2.5 mg 5 mg 10 mg 15 mg 20 mg 25 mg | Cap | 329.5000 340.0000 361.0000 382.0000 403.0000 424.0000 | 25 mg/d on days 1 to 21 | 318 | 8,904 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 40 mg on days 1, 8, 15, 22 | 0.44 | 12 |
KRd | Cycle 1: 574 Cycle 2 to 12: 592 Cycle 13 to 18: 501 | Cycle 1: 16,072 Cycle 2 to 12: 16,583 Cycle 13 to 18: 14,027 | ||||
Cyclophosphamide plus bortezomib plus dexamethasone (CyBorD) | ||||||
Cyclophosphamide | 25 mg 50 mg | Tab | 0.3545b 0.4773b | 300 mg/m2 on days 1, 8, 15, 22 | 0.75 | 21 |
Bortezomib (generic) | 3.5 mg | Powder in vial (for infusion) | 654.31 | 1.5 mg/m2 on days 1, 8,15, 22 | 93 | 2,617 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | Cycle 1 and 2: 40 mg on days 1 to 4, 9 to 12, 17 to 20 Cycles 3+: 40 mg on days 1, 8, 15, 22 | Cycle 1 to 2: 1.31 Cycle 3+: 0.44 | Cycle 1 to 2: 37 Cycle 3+: 12 |
CyBorD | Cycle 1 to 2: 96 Cycle 3+: 95 | Cycle 1 to 2: 2,675 Cycle 3+: 2,650 | ||||
Daratumumab plus bortezomib plus dexamethasone (DVd) | ||||||
Daratumumab (Darazalex) | 20 mg/mL | 5 mL vial 20 mL vial Concentrate solution for infusion | 598.0200 2,392.0800 | Cycle 1 to 3: 16 mg/kg on days 1, 8, 15 (21-day cycle) Cycle 4+: 16 mg/kg, on day 1 (21-day cycle for cycles 1 to 8, 28-day cycle for cycle 9+) | Cycle 1 to 3: 1,025 Cycle 4 to 8: 342 Cycle 9+: 256 | Cycle 1 to 3: 28,705 Cycle 4 to 8: 9,568 Cycle 9+: 7,176 |
Bortezomib | 3.5 mg | Powder in vial (for infusion) | 654.31 | Cycle 1 to 8: 1.3 mg/m2 days 1, 4, 8, 11 (21-day cycle); not administered past cycle 8 | Cycle 1 to 8: 125 | Cycle 1 to 8: 3,490 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | Cycle 1 to 8: 20 mg on days 1, 2, 4, 5, 8, 9, 11, 12 (21-day cycle); not administered past cycle 8 | Cycle 1 to 8: 0.58 | Cycle 1 to 8: 16 |
DVd | Cycle 1 to 3: 1,150 Cycle 4 to 8: 467 Cycle 9+: 256 | Cycle 1 to 3: 32,211 Cycle 4 to 8: 13,074 Cycle 9+: 7,176 | ||||
Daratumumab plus lenalidomide plus dexamethasone (DRd) | ||||||
Daratumumab | 20 mg/mL | 5 mL vial 20 mL vial Concentrate solution for infusion | 598.0200 2,392.0800 | Cycle 1 to 2: 16 mg/kg on days 1, 8, 15 Cycle 3 to 6: 16 mg/kg on days 1, 15 Cycles 7+: 16 mg/kg on day 1 | Cycle 1 to 2: 1,025 Cycle 3 to 6: 513 Cycle 7+: 256 | Cycle 1 to 2: 28,705 Cycle 3 to 6: 14,352 Cycle 7+: 7,176 |
Lenalidomide (Revlimid) | 2.5 mg 5 mg 10 mg 15 mg 20 mg 25 mg | Cap | 329.5000 340.0000 361.0000 382.0000 403.0000 424.0000 | 25 mg/d on days 1 to 21 | 318 | 8,904 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 40 mg on days 1, 8, 15, 22 | 0.44 | 12 |
DRd | Cycle 1 to 2: 1,344 Cycle 3 to 6: 831 Cycle 7+: 575 | Cycle 1 to 2: 37,621 Cycle 3 to 6: 23,269 Cycle 7+: 16,092 | ||||
Isatuximab plus pomalidomide plus dexamethasone (IsaPd) | ||||||
Isatuximab (Sarclisa) | 20 mg/mL | 6 mL vial 30 mL vial | 757.9000 3,789.4900 | Cycle 1: 10 mg/kg on days 1, 8, 15, 22 Cycle 2+: 10 mg/kg on days 1, 15 | Cycle 1: 866 Cycle 2+: 433 | Cycle 1: 24,253 Cycle 2+: 12,126 |
Pomalidomide (Pomalyst) | 1 mg 2 mg 3 mg 4 mg | Cap | 500.0000c | 4 mg on days 1 to 21 | 375 | 10,500 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 40 mg on days 1, 8, 15, 22 | 0.44 | 12 |
IsaPd | Cycle 1: 1,242 Cycle 2+: 809 | Cycle 1: 34,765 Cycle 2+: 22,639 | ||||
Lenalidomide plus cyclophosphamide plus dexamethasone (CRd) | ||||||
Lenalidomide (Revlimid) | 2.5 mg 5 mg 10 mg 15 mg 20 mg 25 mg | Cap | 329.5000 340.0000 361.0000 382.0000 403.0000 424.0000 | 25 mg/d on days 1 to 21 | 318 | 8,904 |
Cyclophosphamide | 25 mg 50 mg | Tab | 0.3545b 0.4773b | 300 mg/m2 on days 1, 8, 15 | 0.56 | 16 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 40 mg on days 1, 8, 15, 22 | 0.44 | 12 |
CRd | 319 | 8,932 | ||||
Pomalidomide plus bortezomib plus dexamethasone (PVd) | ||||||
Pomalidomide (Pomalyst) | 1 mg 2 mg 3 mg 4 mg | Cap | 500.0000c | 4 mg on days 1 to 14 (21-day cycle) | 333 | 9,333 |
Bortezomib (generic) | — | — | — | Cycles 1 to 8: 1.3 mg/m2 on days 1, 4, 8, 11 (21-day cycle) Cycles 9+: 1.3 mg/m2 on days 1, 8 (21-day cycle) | Cycle 1 to 8: 125 Cycle 9+:62 | Cycle 1 to 8: 3,490 Cycle 9+: 1,745 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | Cycle 1 to 8: 20 mg on days 1, 2, 4, 5, 8, 9, 11, 12 (21-day cycle) Cycles 9+: 20 mg on days 1, 2, 8, 9 (21-day cycle) | Cycle 1 to 8: 0.58 Cycle 9+: 0.29 | Cycle 1 to 8: 16 Cycle 9+: 8 |
PVd | Cycle 1 to 8: 459 Cycle 9+: 396 | Cycle 1 to 8: 12,839 Cycle 9+: 11,086 | ||||
Pomalidomide plus cyclophosphamide plus dexamethasone (PCd) | ||||||
Pomalidomide (Pomalyst) | 1 mg 2 mg 3 mg 4 mg | Cap | 500.0000c | 4 mg on days 1 to 21 | 375 | 10,500 |
Cyclophosphamide | 25 mg 50 mg | Tab | 0.3545b 0.4773b | 400 mg on days 1, 8, 15 | 0.41 | 11 |
Dexamethasone | 0.5 mg 4 mg | Tab | 0.1564b 0.3046b | 40 mg on days 1, 8, 15, 22 | 0.44 | 12 |
PCd | 376 | 10,524 | ||||
Note: All prices are from the Delta IQVIA database (accessed September 2021), unless otherwise indicated, and do not include dispensing fees. Recommended dosage is based on Cancer Care Ontario monographs, unless otherwise indicated. For dosing that depends on weight or body surface area, CADTH assumed 75.4 kg or 1.8 m2 based on the IKEMA trial. Total cost estimates per regimen are based on the cheapest combination of the component drugs, with wastage considered for single-use vials.
aIsatuximab price on the sponsor’s submission19; dosage based on the draft isatuximab product monograph, for use in combination with carfilzomib and dexamethasone.1
bOntario Drug Benefit Formulary.7
cOntario Exceptional Access Program.20
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Relevant interventions were not included as part of the economic analysis. The cost-effectiveness of these interventions against IsaPd remain unknown. The sponsor’s base case reflects a population of patients with exposure to 1 to 3 prior lines of therapy based on the IKEMA trial, while IsaKd is indicated for use beyond first-line (i.e., is not bounded by third-line therapy). Clinical experts consulted by CADTH noted that IsaKd is most likely to be used as second-line therapy at this time. |
Model has been adequately programmed and has sufficient face validity | No | The model includes numerous IFERROR statements. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors. Unclear how some simple calculations were derived, such as drug cost. |
Model structure is adequate for decision problem | No | A partitioned-free survival model was used which introduced structural constraints. A Markov model would have been more appropriate. Relevant subgroups (e.g., line of therapy, type of prior therapy) could not be considered. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | For some model parameters, the sponsor arbitrarily incorporated uncertainty using a standard deviation equal to +/−20% of the mean value (e.g., percentage of patients experiencing an adverse event, relative dose intensity, health care costs, adverse event costs), which does not reflect the true uncertainty around the model’s parameters possible values. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
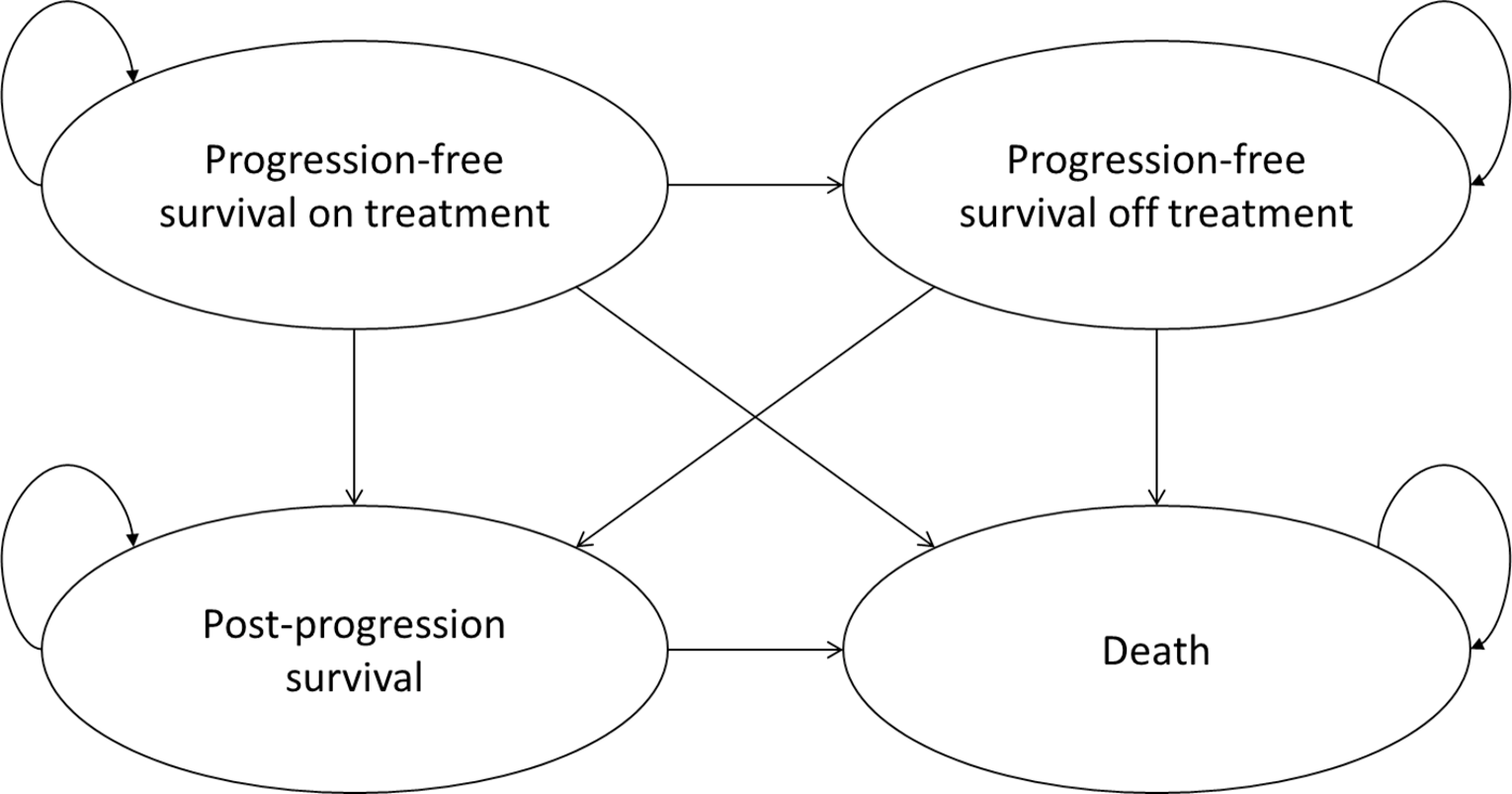
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | IsaKd | Kd | Incremental (v. Kd) |
|---|---|---|---|
Discounted LYs | |||
Progression-free | 7.81 | 1.85 | 5.96 |
Post-progression | 3.54 | 3.81 | −0.27 |
Total | 11.35 | 5.66 | 5.69 |
Discounted QALYs | |||
Progression-free | 5.76 | 1.41 | 4.35 |
Post-progression | 2.44 | 2.63 | −0.19 |
Total | 8.20 | 4.05 | 4.15 |
Discounted costs ($) | |||
Drug acquisition | 1,018,507 | 367,835 | 650,672 |
Administration | 21,871 | 12,753 | 9,118 |
Progression-free | 11,979 | 2,838 | 9,141 |
Post-progression | 5,416 | 5,729 | −313 |
Adverse events | 4,057 | 3,407 | 650 |
Subsequent therapy | 81,764 | 159,150 | −77,386 |
Terminal care | 27,294 | 30,368 | −3,074 |
Total | 1,170,887 | 582,079 | 588,808 |
ICER ($/QALY) | 141,824 | ||
ICER = incremental cost-effectiveness ratio; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission,3 probabilistic model. The results with the sponsor’s deterministic model were notably dissimilar, in that the ICER estimated with the probabilistic model was 28% higher than with the deterministic model.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Exploratory Reanalysis
Figure 2: Time to Treatment Discontinuation, Progression-Free Survival, and Overall Survival Curves Adopted in the CADTH Exploratory Reanalysis – IsaKd
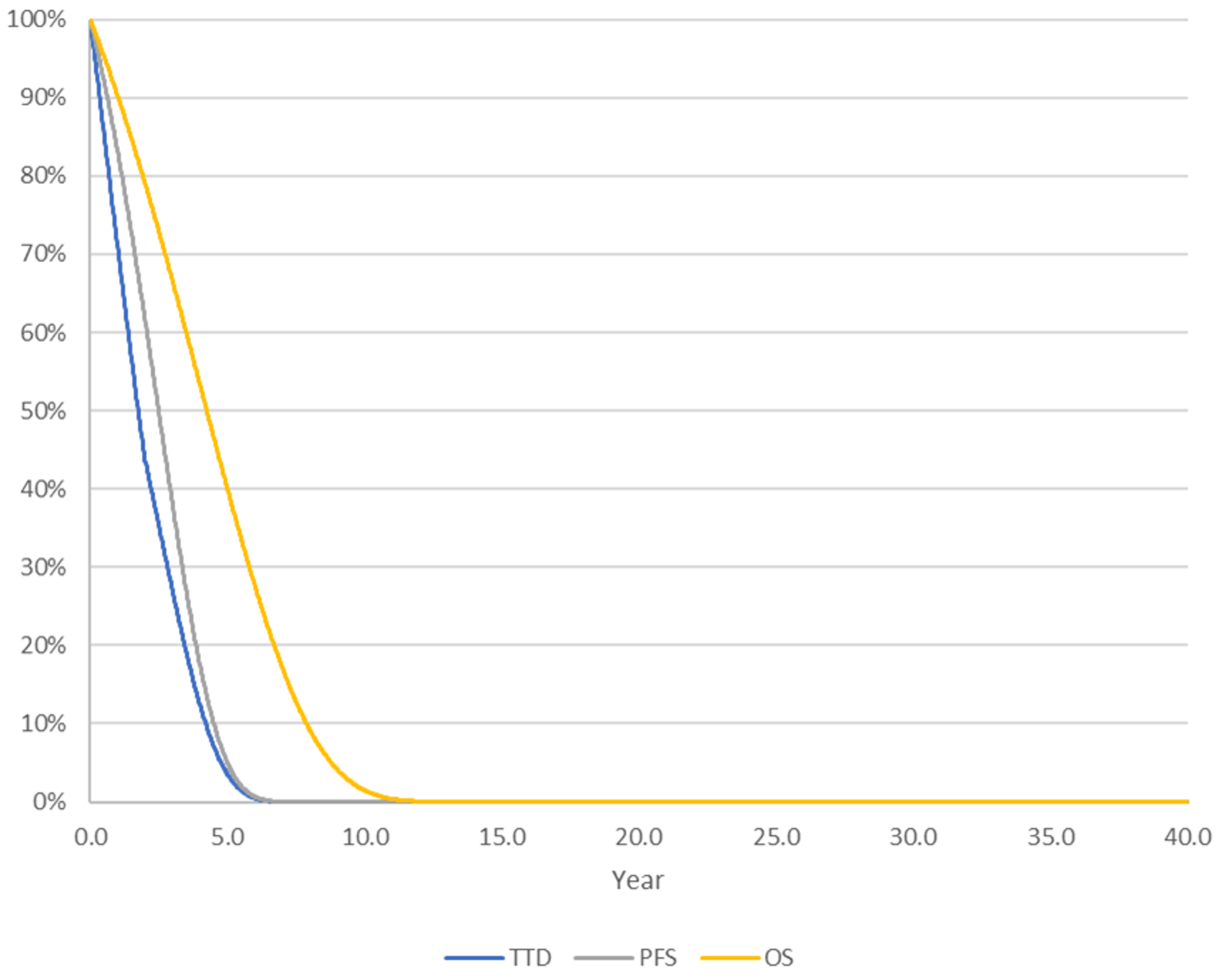
OS = overall survival; PFS = progression-free survival; TTD = time to treatment discontinuation.
Figure 3: Time to Treatment Discontinuation, Progression-Free Survival, and Overall Survival Curves Adopted in the CADTH Exploratory Reanalysis — Kd
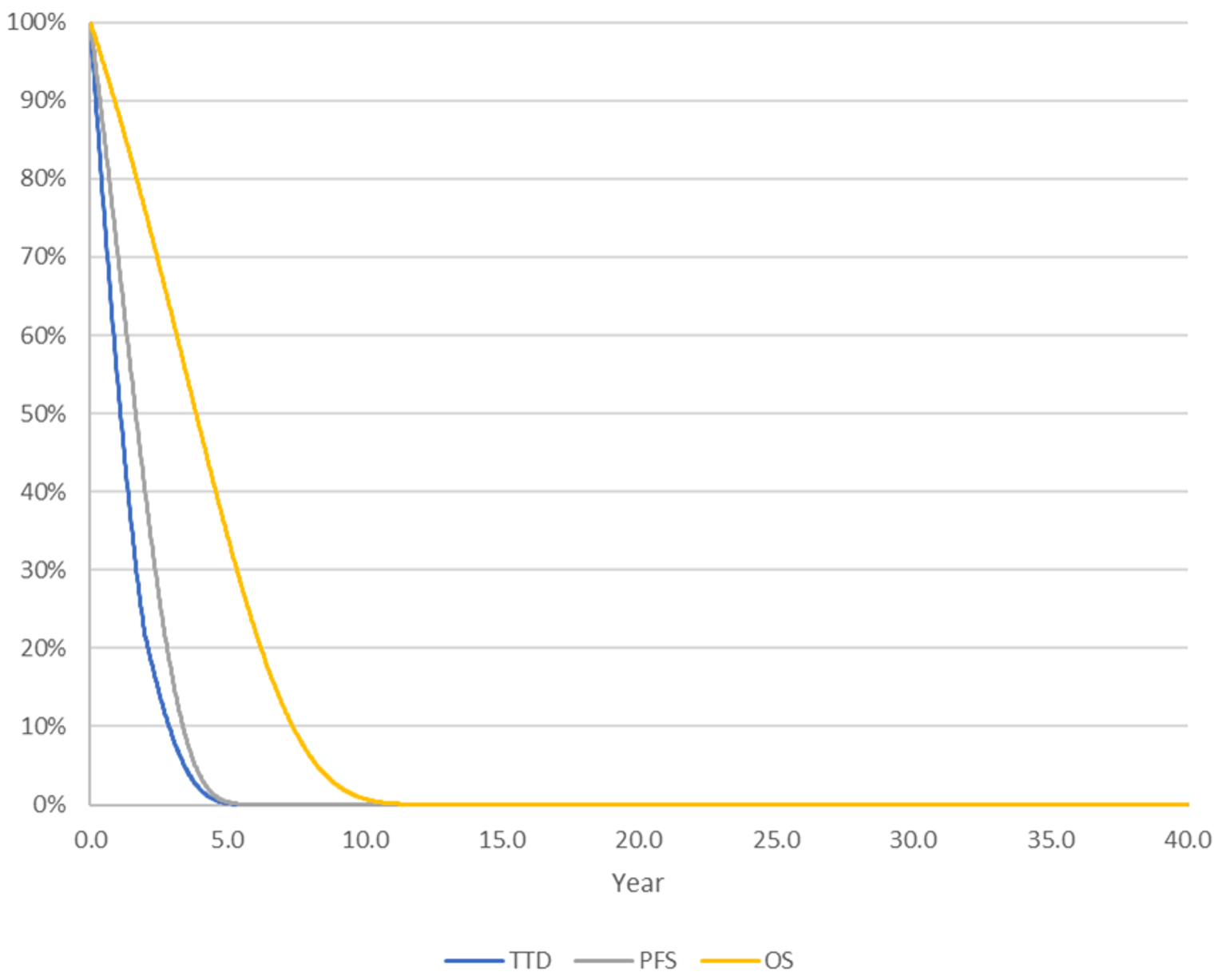
OS = overall survival; PFS = progression-free survival; TTD = time to treatment discontinuation.
Table 11: Disaggregated Summary of CADTH’s Exploratory Economic Evaluation Results
Parameter | IsaKd | Kd | Incremental (v. Kd) |
|---|---|---|---|
Discounted LYs | |||
Progression-free | 2.64 | 1.84 | 0.80 |
Post-progression | 1.59 | 2.07 | −0.47 |
Total | 4.24 | 3.91 | 0.33 |
Discounted QALYs | |||
Progression-free | 2.06 | 1.43 | 0.62 |
Post-progression | 1.11 | 1.44 | −0.33 |
Total | 3.17 | 2.87 | 0.30 |
Discounted costs ($) | |||
Drug acquisition | 856,467 | 331,677 | 524,791 |
Administration | 17,693 | 11,309 | 6,384 |
Progression-free | 4,071 | 2,833 | 1,238 |
Post-progression | 2,443 | 3,162 | −718 |
Adverse events | 4,057 | 3,407 | 650 |
Subsequent therapy | 82,416 | 145,657 | −63,241 |
Terminal care | 31,152 | 31,313 | −161 |
Total | 998,299 | 529,357 | 468,942 |
ICER ($/QALY) | 1,588,632 | ||
ICER = incremental cost-effectiveness ratio; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 12: CADTH Scenario Analyses
Outcomes | CADTH base case | CADTH scenario |
|---|---|---|
Scenario Analyses | ||
1. Overall survival | Based on extrapolated data from the IKEMA trial for IsaKd and Kd. Kd: Gompertz Isa Kd: Gompertz | Overall survival for IsaKd assumed to be equal to Kd (OS of IsaKd was set equal to the Gompertz OS parametric distribution for Kd). |
2. Overall survival | As above. | Kd: Gompertz IsaKd: Generalized Gamma |
3. Utility values | Based on mapped EQ-5D-3L values, derived from EQ-5D-5L values from the IKEMA trial. | EQ-5D-5L values from the IKEMA trial. |
4. Subsequent therapy | Received by 100% of patients with progressed disease.a | Subsequent therapy was assumed to be received by 50% of patients with progressed disease. |
IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; OS = overall survival; PFS = progression-free survival; RDI = relative dose intensity.
aCADTH notes that subsequent therapy was assumed to affect only costs (i.e., subsequent therapy was assumed by the sponsor to have no effect on OS).
Table 13: CADTH Scenario Analyses Results
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
CADTH base case | |||
Kd | 529,357 | 2.87 | Ref. |
IsaKd | 998,299 | 3.17 | 1,588,632 |
Scenario 1: Overall survival equal for IsaKd and Kd | |||
Kd | 533,673 | 2.87 | Ref. |
IsaKd | 973,698 | 2.93 | 7,145,426 |
Scenario 2: Greater overall survival for IsaKd | |||
Kd | 533,673 | 2.87 | Ref. |
IsaKd | 974,474 | 3.45 | 758,213 |
Scenario 3: Health state utility values (EQ-5D-5L) | |||
Kd | 533,673 | 3.14 | Ref. |
IsaKd | 974,040 | 3.44 | 1,450,241 |
Scenario 4: Subsequent therapy | |||
Kd | 454,018 | 2.87 | Ref. |
IsaKd | 932,772 | 3.16 | 1,650,082 |
ICER = incremental cost-effectiveness ratio; IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; QALY = quality-adjusted life-year; Ref. = reference.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Takeaways
Key Takeaways of the Budget Impact Analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the incremental budget impact of reimbursing isatuximab for use in combination with carfilzomib plus dexamethasone (IsaKd) for the treatment of relapsed/refractory multiple myeloma among patients who have received at least 1 prior therapy. The BIA was undertaken from the perspective of the Canadian public drug plans over a 3-year time horizon, and the sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec). Key inputs to the BIA are documented in Table 15.
The sponsor estimated the eligible population using an epidemiologic approach. In the reference scenario, patients were assumed to receive daratumumab plus lenalidomide plus dexamethasone (DRd), daratumumab plus bortezomib plus dexamethasone (DVd), carfilzomib plus dexamethasone (Kd) or carfilzomib plus lenalidomide plus dexamethasone (KRd). In the new-drug scenario, isatuximab was assumed to be reimbursed and prescribed as second- or later-line therapy as part of isatuximab plus carfilzomib plus dexamethasone (IsaKd). The sponsor estimated that IsaKd will displace the initiation of comparator regimens rather than interrupt the current use of comparators started before the introduction of isatuximab. In the second-line, isatuximab was estimated to capture |||||||||||||||||||||||||||| of market share in years 1, 2, and 3, respectively, with the majority of market share taken from DVd. In the third-line or later, IsaKd was assumed to take market share solely from daratumumab-containing regiments (i.e., DRd, DVd) and estimated to capture |||||||||||||||||||||||||| of the market share in years 1, 2, and 3, respectively.
In the sponsor’s base case, costs related to drug acquisition were captured, with dosing, RDI, days per cycle, and cycles of therapy based on published literature, product monographs, and information from a clinical trial database (not cited by the sponsor). The duration of treatment was based on the median duration of treatment in the IKEMA trial (IsaKd, Kd), POLLUX trial (DRd), CASTOR trial (DVd), and ASPIRE trial (KRd). The cost of isatuximab was based on the sponsors submitted price ($757.90 per 100 mg; $3,789.49 per 500 mg). Drug costs for carfilzomib and dexamethasone, and the components of comparator regimens, were obtained from “publicly available formularies and/or HTA recommendations, supplemented by information for the IQVIA DeltaPA database.”16 Costs related to dispensing, markup, administration, or subsequent therapy were not included.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (Year 1 / Year 2 / Year 3) |
|---|---|
Target population | |
pan-Canadian population | 30,219,724 / 30,645,252 / 31,077,047 |
Multiple myeloma prevalence (0.0267% / 0.0277% / 0.0287%)a | 8,062 / 8,475 / 8,910 |
Proportion who receive first-line treatment (95%) | 7,659 / 8,052 / 8,465 |
Proportion eligible for public drug plan coverage (100%) | 7,659 / 8,052 / 8,465 |
Proportion who receive second- or later-line therapy | |
Second-line: 25.5% / 24.7%/ 24.1% | 1,952 / 1,992 / 2,038 |
Third-line or later: 7.4% / 5.9% / 4.6% | 569 / 479 / 393 |
Proportion of patients initiating treatment | |
Second-line: 56.0% / 56.0% / 56.0% | 1,093 / 1,115 / 1,141 |
Third-line or later: 62.0% / 62.0% / 62.0% | 353 / 297 / 244 |
Market Uptake (3 years) | |
Uptake (reference scenario)b | |
IsaKd | 0% / 0% / 0% |
DRd | 58.2% / 59.4% / 60.8% |
DVd | 22.0% / 22.8% / 23.7% |
Kd | 10.2% / 9.4% / 8.5% |
KRd | 0.3% / 0.2% / 0.2% |
Pdc | 9.3% / 8.1% / 6.8% |
Uptake (new-drug scenario)b | |
IsaKd | ||||||||||||||||||||||||||||||||||||||||||||||||||| |
DRd | ||||||||||||||||||||||||||||||||||||||||||||||||||| |
DVd | ||||||||||||||||||||||||||||||||||||||||||||||||||| |
Kd | ||||||||||||||||||||||||||||||||||||||||||||||||||| |
KRd | ||||||||||||||||||||||||||||||||||||||||||||||||||| |
Pdc | ||||||||||||||||||||||||||||||||||||||||||||||||||| |
Total cost of treatment over the median treatment duration (per patient) | |
IsaKd | $587,605 |
DRd | $671,373 |
DVd | $206,846 |
Kd | $278,914 |
KRd | $371,943 |
Pd | $63,949 |
DRd = daratumumab + lenalidomide + dexamethasone; DVd = daratumumab + bortezomib + dexamethasone; IsaKd = isatuximab + carfilzomib + dexamethasone; Kd = carfilzomib + dexamethasone; KRd = carfilzomib + lenalidomide + dexamethasone; Pd = Pomalidomide plus dexamethasone.
aBased on a 5-year prevalence of 8,558 cases in 2018,21 to which the sponsor applied a 3.7% growth rate to derive the prevalence over the BIA analysis horizon.
bValues represent the pooled uptake across second-line and third-line and later treatment. Individual estimates were applied per line of treatment in the model.
cAssumed to be used as third-line and higher treatment only. The sponsor assumed that Pd market share would not be affected by the introduction of isatuximab for use in combination with carfilzomib plus dexamethasone.
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor estimated the net 3-year budget impact of reimbursing IsaKd as second-line treatment of relapsed/refractory multiple myeloma to be $91,781,801 (Year 1: $11,620,181; Year 2: $28,489,138; Year 3: $51,672,482). The net 3-year budget impact of reimbursing IsaKd as a third- or later-line therapy to be $7,196,972 (Year 1: $1,292,166; Year 2: $2,632,383; Year 3: $3,272,423). The budget impact for the full Health Canada indication was projected by the sponsor to be $98,978,773 over 3 years.
Under a health care payer perspective (i.e., including the cost of treating AEs), the estimated 3-year budget impact of reimbursing IsaKd as second- or later-line therapy was $99,067,490 (Year 1: $12,927,786; Year 2: $31,145,430; Year 3: $54,994,274).
Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of patients eligible for IsaKd is uncertain. The sponsor used an epidemiological approach to estimate the target population size, with the prevalence of multiple myeloma based on an estimated 5-year prevalence in 2018. The incidence of multiple myeloma in Canada is increasing over time, with incidence rates increasing by about 2.6% per year since 2007 per year among men and 0.6% per year among women since 1984.22 As such, a 5-year prevalence rate from 2018 may not reflect the true prevalence of multiple myeloma in Canada during the BIA analysis horizon. An estimated 3,400 people were newly diagnosed with multiple myeloma in 2020, with an age-standardized incidence rate of 7.8 per 100,000 people.23
In scenario analyses, CADTH explored the impact of a higher prevalence of multiple myeloma.
All relevant comparators were not considered. The sponsor’s BIA considered costs related to IsaKd, DRd, DVd, Kd, KRd. As shown in Table 8, there are additional relevant comparators that may be considered in this population, including IsaPd. The sponsor did not include IsaPd in the BIA as isatuximab is not currently publicly reimbursed. However, isatuximab received a conditional positive reimbursement recommendation from pERC in 2021 for use in IsaPd for patients relapsed and refractory multiple myeloma who have received at least 2 prior therapies including lenalidomide and a proteasome inhibitor,2 and isatuximab is currently under consideration for negotiation with the pan-Canadian Pharmaceutical Alliance for this indication.18 If isatuximab (as part of IsaPd) becomes publicly reimbursed during the 3-year BIA analysis horizon, it would be considered a relevant comparator should IsaKd be used as third or later-line treatment.
As noted by clinical experts consulted by CADTH for this review, the treatment of multiple myeloma after first-line therapy is highly individualized and depends, at least in part, on prior treatments received. Clinical experts indicated that the majority of usage of IsaKd is expected to be in the second-line among patients whose multiple myeloma is refractory to lenalidomide (i.e., those who received lenalidomide as part of first-line treatment). However, lenalidomide-containing regimens would be considered relevant comparators at the second-line among those whose multiple myeloma was not refractory to first-line lenalidomide. The sponsor’s BIA considers DRd (daratumumab plus lenalidomide plus dexamethasone) and KRd (carfilzomib plus lenalidomide plus dexamethasone) as a comparators, but other lenalidomide-containing regimens were not included (CRd, Rd) without justification.
CADTH was unable to consider the impact of including costs related to additional relevant treatment comparators, owing to the structure of the sponsor’s model and a lack of data (e.g., proportion of lenalidomide-refractory patients, eligible patients, market share).
Uncertainty regarding the uptake of IsaKd. The sponsor estimated that, in the second-line setting, the market share for isatuximab would be |||||||||||||||||in year 1, year 2, and year 3, respectively, and, in the third- and later-line setting, the market share for isatuximab would be ||||||||||||||||||||. The clinical experts consulted by CADTH for this review noted that this is likely an underestimate of the uptake of IsaKd, especially in the second-line setting. Clinical experts indicated that, of the patients not previously exposed to an anti-CD38 inhibitor, 75% would be expected to receive IsaKd as part of second-line therapy. CADTH notes that the sponsor’s BIA targets the use of IsaKd as second- later-line therapy, although the Health Canada indication for IsaKd is for patients with 1 to 3 prior lines of treatment (i.e., IsaKd is indicated as second to fourth line treatment). It is not clear from the sponsor’s model what proportion of patients in the BIA are assumed to receive IsaKd past fourth line treatment.
Owing to the structure of the sponsor’s BIA model, CADTH was unable to separately model the uptake of IsaKd among patients with previous exposure to an anti-CD38. CADTH explored the impact of higher isatuximab uptake in scenario analyses.
RDI is not well correlated with drug costs. As noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, the use of trial-based RDI may not reflect the use of cancer regimens in clinical practice. Within the IsaKd regimen in the IKEMA trial, RDI of isatuximab was | %. Based on the isatuximab product monograph, dosage reductions are not recommended, although doses may be delayed (e.g., because of neutropenia).1 Such patients would still be expected to receive the recommended dosage of isatuximab, although on an altered schedule. As such, the use of an RDI of less than 1 may inappropriately reduce the cost of isatuximab in the sponsor’s BIA.
In CADTH reanalyses, an RDI of 100% was adopted for all treatments.
Uncertainty regarding the duration of treatment. In the calculation of drug costs, the sponsor assumed that all patients would receive IsaKd for the median duration of treatment in the IKEMA trial (IsaKd: | months, Kd: | months). Similarly, the median duration of treatment for the other comparators was based on median treatment durations from clinical trials. Based on this assumption, in the sponsor’s BIA model assumes that all patients (with the exception of those taking DRd) would discontinue treatment by the start of year 3 of the BIA horizon (i.e., no drug costs are incurred in year 3). Based on parametric modelling used to inform the sponsor’s economic model for TTD, 33% of patients would be expected to remain on IsaKd 3 years after the initiation of treatment.
CADTH explored the impact of treatment duration in scenario analyses.
Misalignment of model inputs between the sponsor-submitted pharmacoeconomic and budget impact analyses. Despite the inclusion of drug costs related to pre-medication (paracetamol, ranitidine, diphenhydramine) in the cost-utility analysis, the sponsor excluded pre-medication costs from the submitted BIA. Pre-medication costs are relevant under the drug plan perspective and should be considered. Additionally, costs related to subsequent treatment after discontinuation of IsaKd and comparators were not considered in the BIA, despite these costs being relevant under the drug plan perspective. The exclusion of costs related to subsequent treatment lacks face validity, as clinical experts consulted by CADTH for this review noted that, in clinical practice, approximately 50%–75% of patients whose disease progresses on IsaKd would be likely to receive subsequent treatment.
CADTH incorporated pre-medication costs for isatuximab and daratumumab as part of the CADTH base case. CADTH was unable to consider costs related to subsequent treatment owing to the structure of the sponsor’s model and uncertainty regarding the duration and composition of subsequent treatments.
Additional limitations were identified, but were not considered to be key limitations. CADTH notes that the sponsor’s BIA included the cost of branded bortezomib, despite the availability of a generic version. The generic price of bortezomib was used in CADTH reanalyses.
CADTH Reanalyses of the Budget Impact Analysis
CADTH revised the sponsor’s base case by adopting the generic price of bortezomib, including pre-medication costs, and assuming an RDI of 100% for all drugs (Table 16).
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Bortezomib price | $1,402.42 per 3.5 mg | $654.31 per 3.5 mg (IQVIA wholesale price, Ontario) |
Changes to derive the CADTH base case | ||
1. Relative dose intensity | Based on the IKEMA trial for IsaKd and Kd. The RDI for other comparators was sourced from multiple clinical trials. | RDI was assumed to be 100% for all drugs in both regimens. |
2. Pre-medication costs | Excluded | Isatuximab: $1.30 per administrationa Daratumumab: $2.85 per administrationa |
CADTH base case | Reanalysis 1 + 2 | |
IsaKd = isatuximab plus carfilzomib plus dexamethasone; Kd = carfilzomib plus dexamethasone; RDI = relative dose intensity.
aAligned with pre-medication costs in the sponsor’s cost-utility analysis.3 Pre-medication for isatuximab was assumed to include paracetamol, ranitidine, and diphenhydramine. Pre-medication for daratumumab-containing regimes was assumed to include paracetamol, montelukast, famotidine, diphenhydramine
Applying these changes increased the total 3-year budget impact of reimbursing isatuximab for use in combination with carfilzomib plus dexamethasone (IsaKd) for the treatment of relapsed/refractory multiple myeloma. The results of the CADTH step-wise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18.
In the CADTH reanalysis, the 3-year budget impact of reimbursing isatuximab for use in combination with carfilzomib and dexamethasone for the treatment of relapsed/refractory multiple myeloma is estimated to be $117,104,492, with the majority of the costs incurred in the second-line setting.
Table 17: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | 98,978,773 |
Second-line | 91,781,801 |
Third+ line | 7,196,972 |
Corrected base case | 106,107,952 |
Second-line | 98,351,149 |
Third+ line | 7,756,804 |
CADTH reanalysis 1 | 117,254,626 |
CADTH reanalysis 2 | 105,938,725 |
CADTH base case | 117,104,492 |
Second-line | 108,613,687 |
Third+ line | 8,490,805 |
BIA = budget impact analysis.
Note: Reanalyses are based on publicly available prices of the comparator treatments.
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 18.
Assuming 10% higher prevalence of multiple myeloma
Assuming 25% higher uptake of IsaKd
Assuming that patients receive treatment for the full duration of the BIA analysis (exploratory to test the sensitivity of treatment duration on the budget impact)
Adopting a health care payer perspective (i.e., inclusion of costs related to the treatment of AEs [3 Grade 3], administration costs)
Adopting a 100% price reduction of isatuximab
Table 18: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 350,974,444 | 533,944,669 | 679,322,307 | 672,882,706 | 1,886,149,682 |
New drug | 350,974,444 | 546,857,016 | 710,443,827 | 727,827,611 | 1,985,128,455 | |
Budget impact | 0 | 12,912,347 | 31,121,521 | 54,944,905 | 98,978,773 | |
CADTH base case | Reference | 344,354,895 | 527,618,497 | 673,215,739 | 666,641,834 | 1,867,476,070 |
New drug | 344,354,895 | 543,399,425 | 709,504,184 | 731,676,953 | 1,984,580,562 | |
Budget impact | 0 | 15,780,928 | 36,288,445 | 65,035,119 | 117,104,492 | |
CADTH sensitivity analysis: Higher MM prevalence | Reference | 378,790,384 | 580,380,347 | 740,537,313 | 733,306,017 | 2,054,223,677 |
New drug | 378,790,384 | 597,739,368 | 780,454,602 | 804,844,648 | 2,183,038,618 | |
Budget impact | 0 | 17,359,021 | 39,917,289 | 71,538,631 | 128,814,941 | |
CADTH sensitivity analysis: Higher IsaKd uptake | Reference | 344,354,895 | 527,618,497 | 673,215,739 | 666,641,834 | 1,867,476,070 |
New drug | 344,354,895 | 547,373,912 | 718,626,277 | 747,953,404 | 2,013,953,593 | |
Budget impact | 0 | 19,755,415 | 45,410,538 | 81,311,570 | 146,477,523 | |
CADTH sensitivity analysis: Treatment duration | Reference | 344,354,895 | 554,722,643 | 756,795,232 | 753,177,598 | 2,064,695,474 |
New drug | 344,354,895 | 570,503,571 | 800,213,854 | 849,817,233 | 2,220,534,658 | |
Budget impact | 0 | 15,780,928 | 43,418,622 | 96,639,634 | 155,839,184 | |
CADTH sensitivity analysis: Health care payer perspective | Reference | 355,725,676 | 540,541,397 | 687,173,802 | 680,434,754 | 1,908,149,954 |
New drug | 355,725,676 | 556,785,885 | 724,572,332 | 747,495,522 | 2,028,853,738 | |
Budget impact | 0 | 16,244,487 | 37,398,530 | 67,060,767 | 120,703,784 | |
CADTH scenario analysis: 100% price reduction of isatuximab | Reference | 344,354,895 | 527,618,497 | 673,215,739 | 666,641,834 | 1,867,476,070 |
New drug | 344,354,895 | 530,389,966 | 683,294,900 | 681,689,827 | 1,895,374,692 | |
Budget impact | 0 | 2,771,469 | 10,079,161 | 15,047,993 | 27,898,622 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Myeloma Canada
About Myeloma Canada
See registration information www.myeloma.ca
Information Gathering
Over the years, Myeloma Canada has collected data on the impact of myeloma and its treatments on patients and caregivers, by conducting several patient and caregiver surveys. The compiled data are then presented to the Pan-Canadian Oncology Drug Review. Myeloma Canada is sharing patient input from one such survey regarding the combination of Sarclisa (isatuximab for injection) with carfilzomib (Kyprolis) and dexamethasone. Our survey was available from April 22nd to May 9, 2021, and was shared with patients across Canada, via email and social media. 208 patients answered the survey, from Alberta (26), British Columbia (27), Manitoba (6), New Brunswick (3), Newfoundland and Labrador (3), Nova Scotia (10), Ontario (86), Prince Edward Island (1), Quebec (38), Saskatchewan (5), Yukon (2), and (1) from outside of Canada. No patients from Nunavut or Northwest Territories responded, and a total of 48 did not meet the eligibility criteria thus their responses excluded from the report. Eligibility for the survey was determined by patients having received at least one prior line of therapy; eligible patients were then divided into 3 subsets based on the following criteria.
Subset 1: patients (15) had received the carfilzomib (Kyprolis) and dexamethasone combination only. Respondents of Subset 1 were from British Columbia (3), Ontario (7), Quebec (5). (Data specifically discussed in section 4)
Subset 2: all other eligible respondents who had no experience with the treatment combination under review, or carfilzomib (Kyprolis) and dexamethasone alone.
Subset 3: patients (3) who received the treatment under review. Respondents were from Ontario (1), Saskatchewan (1), and Québec (1). The respondent from Ontario did not respond to the majority of questions related to the treatment under review, and the respondent from Quebec was determined, based on their comments, to have confused the treatment combination under review, with another treatment and, did not receive isatuximab (for injection) with carfilzomib (Kyprolis) and dexamethasone, thus their results excluded from section 6. [Récidive au mois d’octobre 2020. Depuis octobre 2020, début d’un traitement avec Daratumumab, Velcade et dexamthasone. Je vais très bien !! » The Québec patient data’s removal was based on this comment.] (Data specifically discussed in section 6)
Disease Experience
Every day, 9 Canadians are diagnosed with myeloma. Despite its growing prevalence, the disease remains relatively unknown. To date there is no cure for myeloma. With myeloma, abnormal plasma cells (also known as myeloma cells) interfere with the production of normal healthy blood cells in the bone marrow and overproduce inactive clones of abnormal antibodies that can negatively affect different parts of the body such as the bones and kidneys. The cause(s) of myeloma remain unknown. Myeloma is what is known as a relapsing-remitting cancer; alternating between periods of remission that require no treatment, and symptomatic periods in which complications arise that require treatment, but it will ultimately always return to the latter.
When asked “How important it is for you to control various aspects of myeloma (Please rate on a scale of 1 ‘Not important,’ to 5 ‘Very important’)”, 158 eligible respondents identified the following symptoms as very important: infections (68.59%), kidney problems (56.69%), mobility (48.39%), neuropathy (42.04%), and fatigue (42.04%).
In answer to the question, “How important it is to you to have access to effective treatments for myeloma (Please rate on a scale of 1—Not important to 5—Very important)”, 96.25% (154) of respondents (160) selected “5—extremely important.”
When asked to “Rate on a scale of 1–5 (1 is ‘Not at all’, and 5 is ‘Significant impact’), how symptoms associated with myeloma impact or limit your day-to-day activities and quality of life.” 158 patient responses showed myeloma significantly impacted their ability to work (28.66%), to travel (25.95%), to concentrate (19.75%), and to exercise (19.62%) (Figure 1).
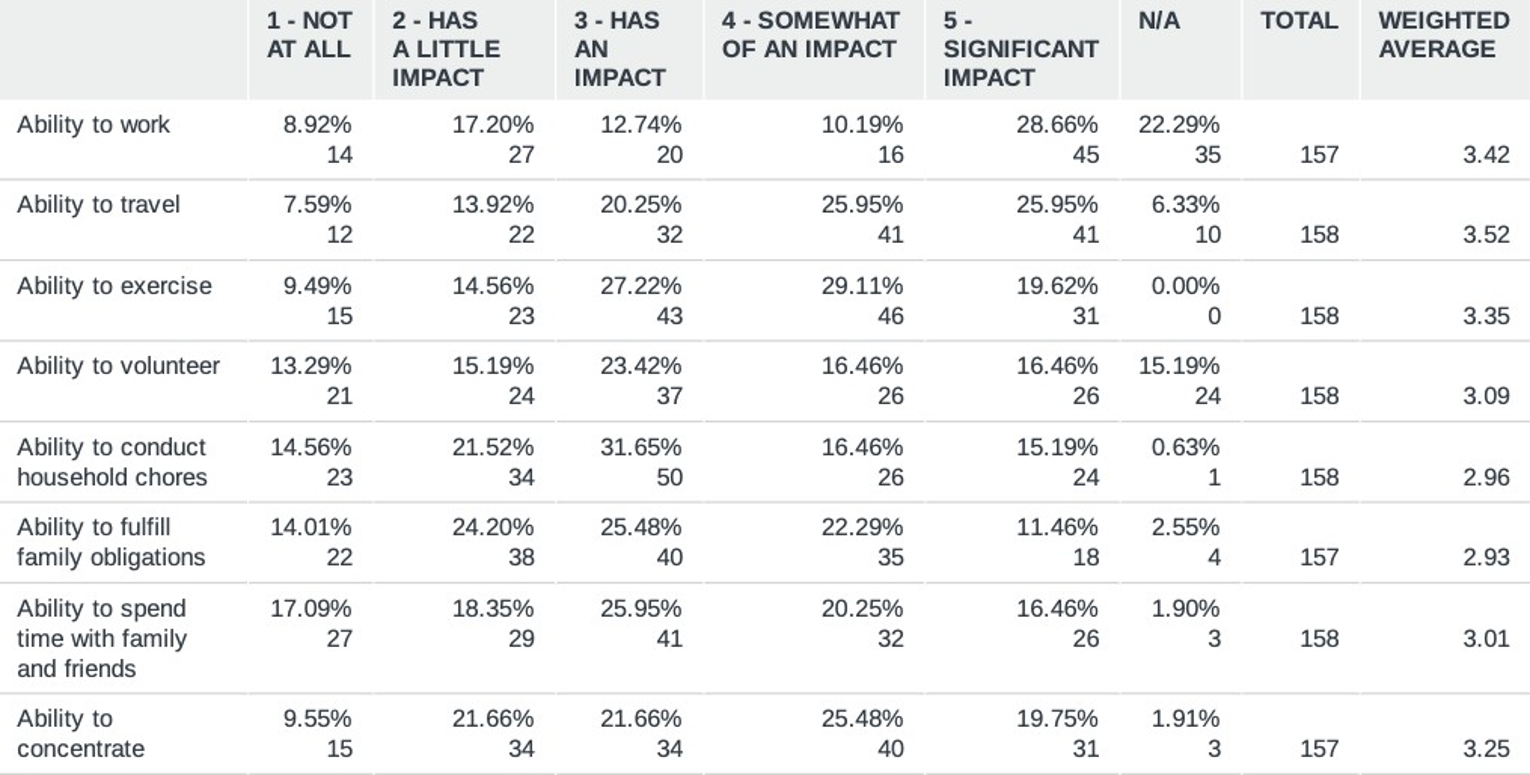
* This section presents data from all survey respondents: all three patient subsets combined.
Respondents (157) were asked, “What is the number one financial implication of your treatment,” and they identified: drug costs (14.65%), lost income due to absence from work (14.65%), and travel costs (10.19%) to be the most significant treatment-related financial implications they had experienced (Figure 2). 11.48% of patients selected ‘other’ and provided explanatory comments, a number of which expressed the desire to select multiple options listed. Here are a few comments provided: “While travel and parking costs have a limited financial implication, the critical financial implication is the costs of drugs. Without provincial coverage of the costs of drugs, they would essentially be inaccessible.”; “Lost great percentage of income from reduced insurances payments”; “My only expenses have been over the counter drugs that I need to control side effects from my myeloma drugs.”
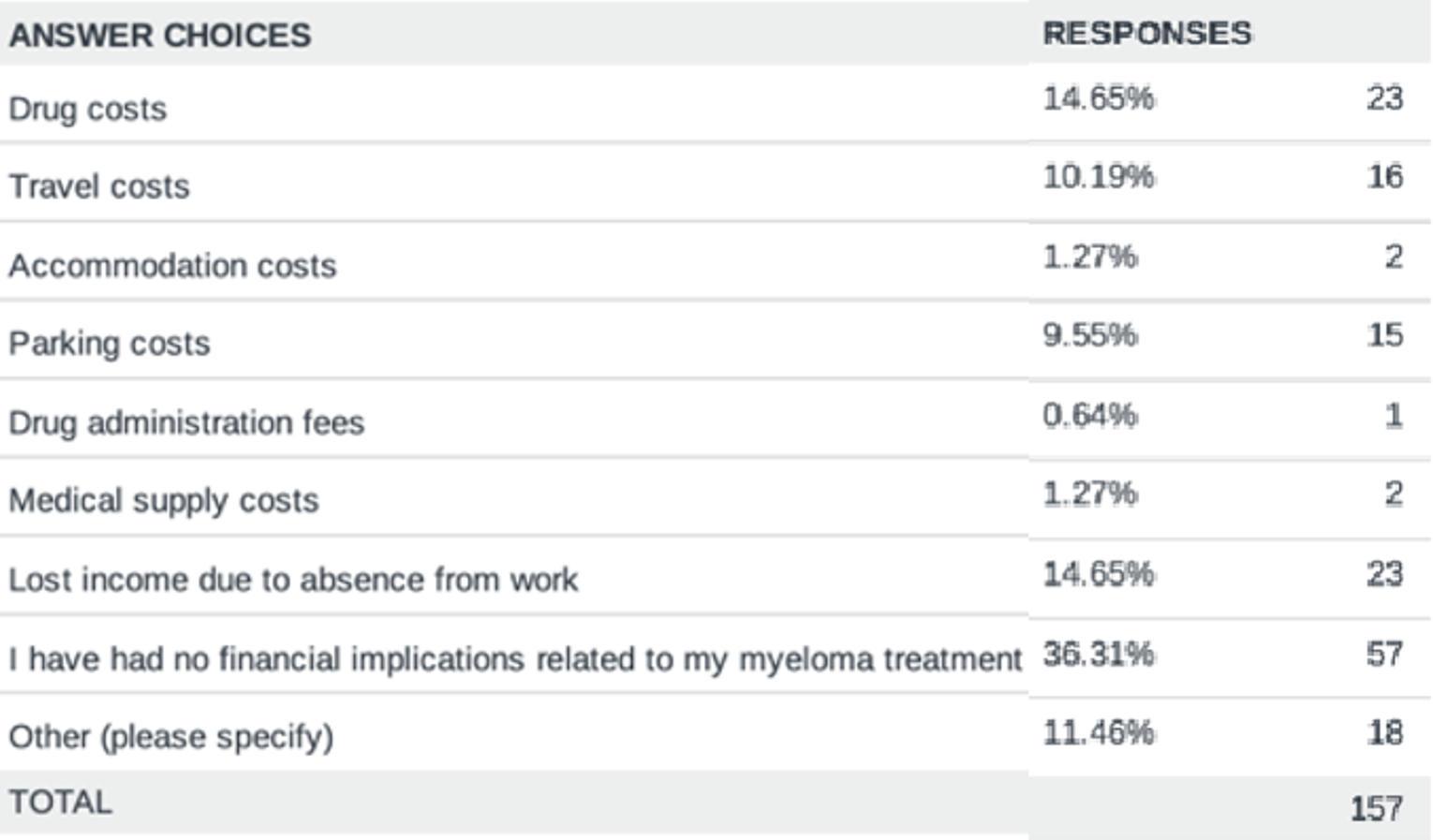
Experiences With Currently Available Treatments—Subset 1
When asked if and/or how their myeloma is currently being treated, of 15 respondents in Subset 1, 8 indicated they were receiving their third line of therapy, one was on their second line, one was under remission, and one patient’s myeloma had returned but they were not currently under treatment (Figure 3). Four patients did not respond to the question.
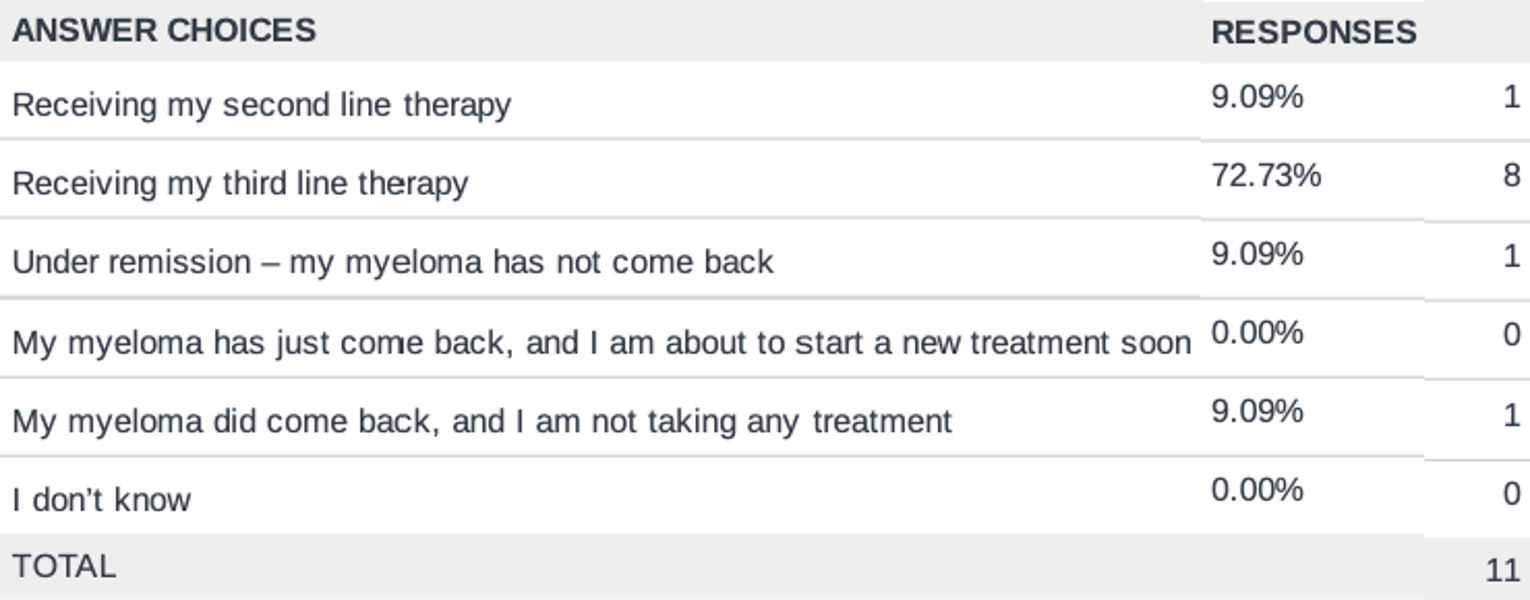
* This section presents data from solely from Subset 1.
It was inquired of patients (12), “How long have you been, or were previously on the treatment combination of carfilzomib (Kyprolis) and dexamethasone?”; 6 replied they were on the combination for 1–6 months, 4 said 7–12, 2 patients said 2–3 years, and 3 did not answer.
When asked “Have you progressed on lenalidomide (Revlimid) or bortezomib (Velcade) based regimens (or both) in your first-line setting?” 14 (of 15) answered yes, and 1 said no.
In response to the question, “Since taking the treatment combination of carfilzomib (Kyprolis) and dexamethasone, rate on a scale of 1–5 how symptoms associated with myeloma impact or limit your day-to-day activities and quality of life,” patients (12) indicated the most significant impact was upon their ability to work (6), exercise (5), and to conduct household chores (4) (Figure4).
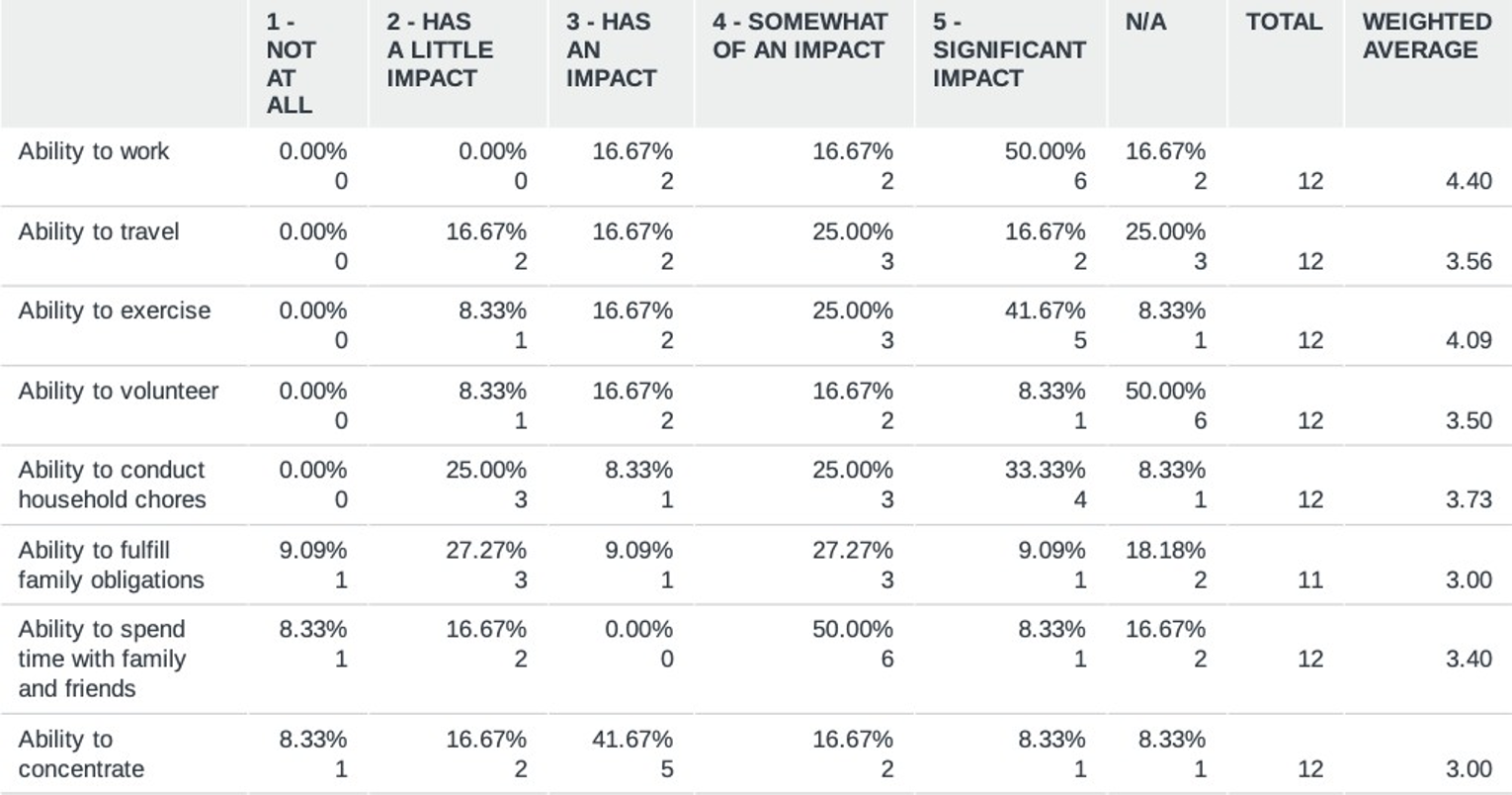
When asked, “How would you rate the common side effects that you have experienced with carfilzomib (Kyprolis) and dexamethasone?” 12 respondents indicated the least tolerable effects to be fatigue (6), and diarrhea (4); while the most tolerable were nausea/vomiting (7) neutropenia (5), and respiratory infections including pneumonia and bronchitis (5) (Figure 5).
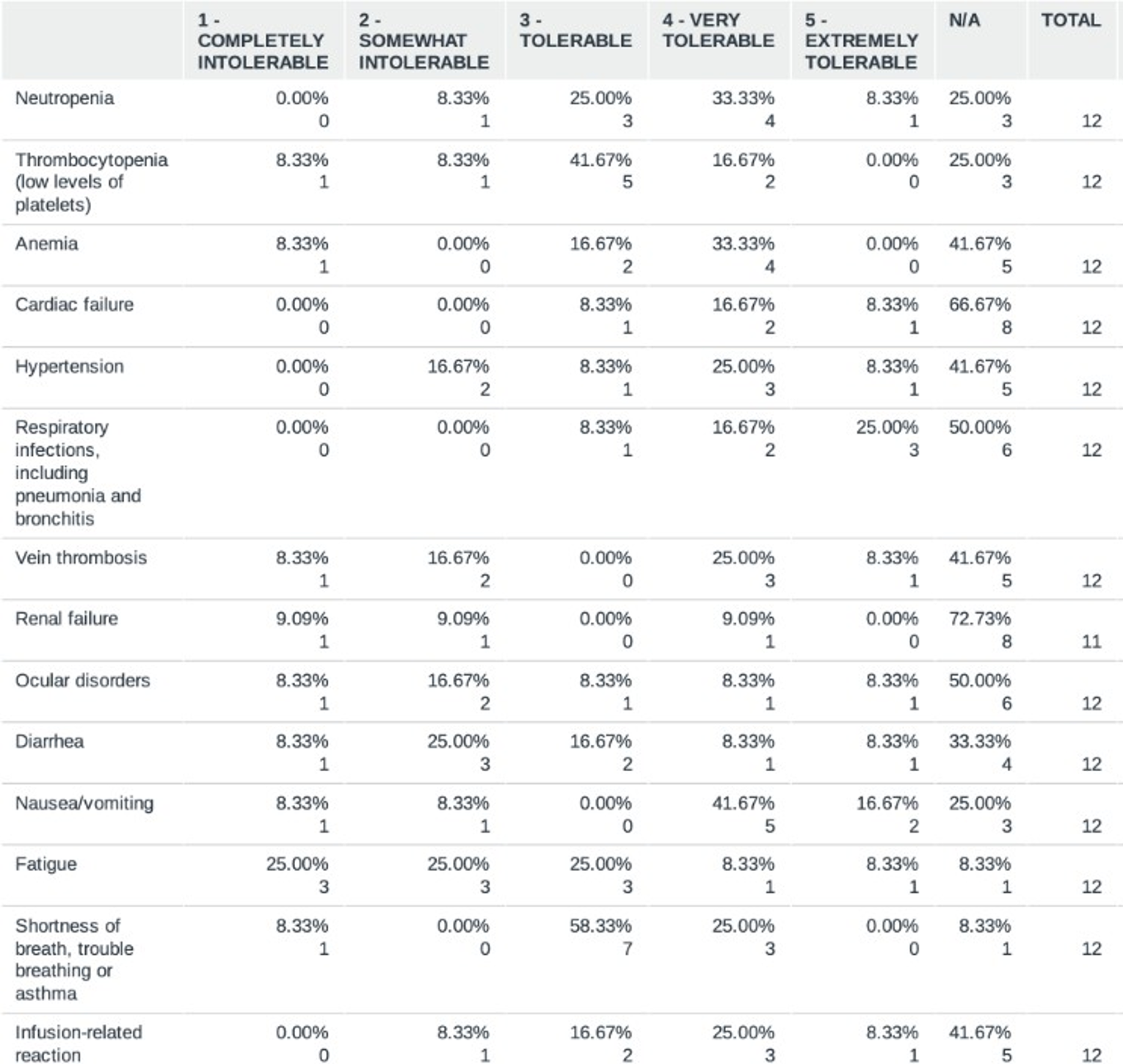
When asked, “Before taking carfilzomib (Kyprolis) with dexamethasone, what were your expectations of the treatment combination? Please rank from 1–7, 1 being the most important, 7 being least important.” Respondents (12) identified remission (3) and prolonged life (3) to be the most important, alongside disease control (2) and fewer side effects than other treatments (2) to a lesser extent.
Respondents (12) then indicated disease control (8), prolonged life (5), and enjoying and normal life (4) to be the expectations their treatment with carfilzomib (Kyprolis) and dexamethasone had best be fulfilled, though their responses show that to some degree, all listed expectations had been met (Figure 6).
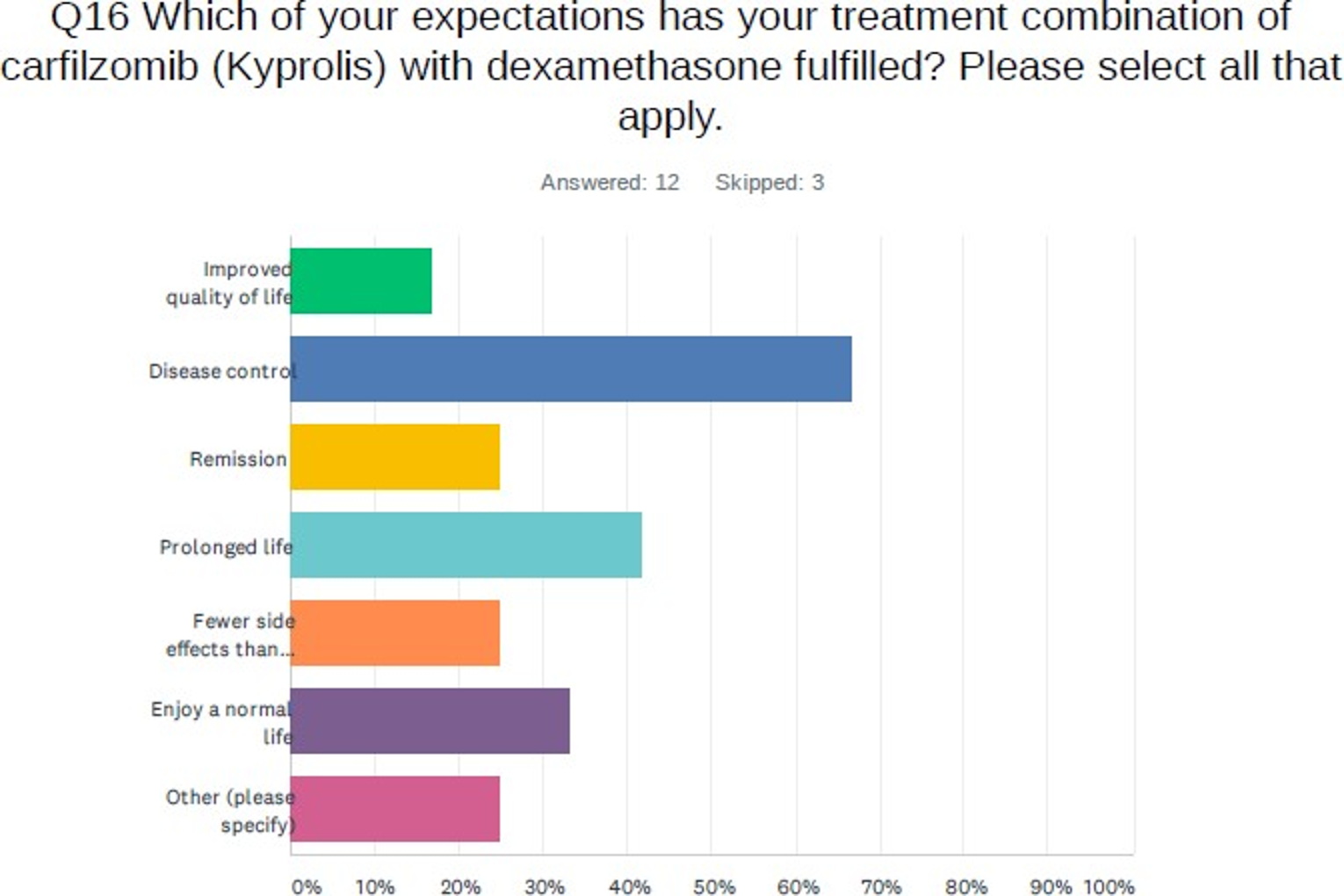
Improved Outcomes
To the question, “If you are taking a drug or were to consider taking a drug for your myeloma, how important is it that it improves your overall quality of life? (Rate on a scale from 1—Not important, to 5—Very important) 68.13% (109) of 160 respondents from all subsets felt it was ‘extremely important’ and 26.25% (42) answered, ‘very important.’
Patients in all subsets were asked, ’What treatment side effects are most important for you to avoid, please rank from 1 (most important to avoid) to 9 (least important to avoid)”.
Patients (2) from Subset 3 ranked insomnia (1), neuropathy (1), and pain (1) as ‘most important to avoid.’
Respondents from Subset 1 (15) indicated fatigue (4), pain (4), and infection (2), to be the most important to avoid.
Patients from Subset 2 (141) responded that the most important treatment side effects to avoid were infection (42), confusion (20), neuropathy (16) and pain (16).
When asked, ‘If you were eligible to receive the isatuximab (Sarclisa; for injection) with carfilzomib (Kyprolis) and dexamethasone, what do you believe the benefits would be for you, compared to the type of treatment you are currently receiving, or have already received?’ subset 1 respondents (12) expected to receive all benefits listed (7), and expected ‘prolonged remission—where myeloma is not present’ (6) (Figure 7).
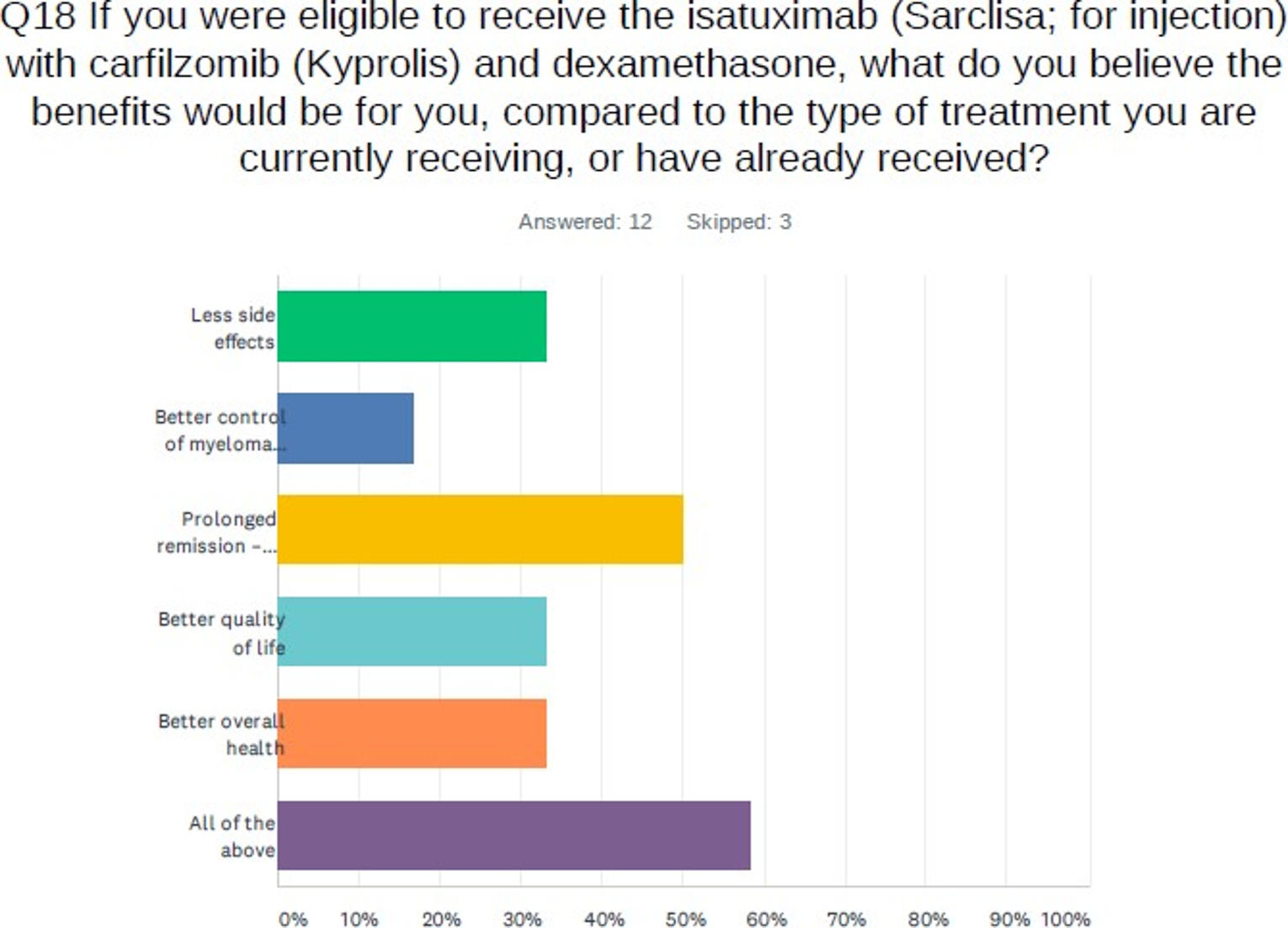
When asked, ‘If you were eligible to receive isatuximab (Sarclisa; for injection) with carfilzomib (Kyprolis) and dexamethasone, what do you think the disadvantages would be for you (compared to the type of treatment you are currently receiving, or have already received)?’ 8 respondents from Subset 1(12) answered, and thought these disadvantages would be, increased fatigue (4), decreased physical abilities (3), and difficulty of treatment (travel, injection time, etc.) (3). When asked, ’Do you feel that receiving isatuximab (Sarclisa; for injection) with carfilzomib (Kyprolis) and dexamethasone to treat your myeloma could improve your health and well-being?” among patients from Subset 1 (12) 3 said ‘yes,’ and 9 said they ‘did not know.’ No respondent said no.
Included in the survey for all 3 patient subsets, was the open-ended question, ‘What is important to you when it comes to treating your myeloma?’. Respondents most frequently mentioned effectiveness of treatment, quality of life, and achieving a long remission to be important to them. Some other responses of relevance are as follows: ‘Ability to access treatment without any payment other than my OHIP card’; ‘Access to latest technology’; ‘To have a lasting remission and not spend too much time in hospital for treatment.’; ‘Provide the ability to lead a nearly normal life with a minimal frequency of visits to doctors and the hospital’; ‘I would like to be well informed about consequences of treatment and be able to continue with a relatively decent quality of life while undergoing treatment.’; ‘Quality of life, how I feel during treatment and if I’m able to be with my family and friends. How long treatment will work.’
Experience with Drug Under Review—Subset 3
When asked to rate the effectiveness of isatuximab (Sarclisa) combined with carfilzomib (Kyprolis) and dexamethasone in controlling their myeloma, on a scale from 1 ‘Not effective’ to 5 ‘Extremely effective,’ one respondent felt it was ’5—extremely effective”.
To the question, “Did the administration of isatuximab (Sarclisa; for injection) (i.e., the way you took the treatment, by injection) have a negative effect on you?” one respondent indicated it did not have a negative effect upon them.
* This section presents results from Subset 3.
When it was enquired “Based on your personal experience with the combination of isatuximab (Sarclisa; for injection) with carfilzomib (Kyprolis) and dexamethasone, how would you rate the overall side effects? 1 is “Completely intolerable” and 5 is “Extremely tolerable”” one respondent replied “3—Tolerable.”
When asked, “How would you rate (on a scale from 1—Completely intolerable to 5—Extremely tolerable), the common side effects you have experienced with isatuximab (Sarclisa) in combination with carfilzomib (Kyprolis) and dexamethasone?” one respondent indicated that nausea/vomiting (1), and thrombocytopenia (1) were “completely intolerable.”
To the question “Did your myeloma treatment of isatuximab (Sarclisa) in combination with carfilzomib (Kyprolis) and dexamethasone improve your health and well-being” one respondent replied “yes.”
When asked “How would you rate your quality of life with isatuximab (Sarclisa) in combination with carfilzomib (Kyprolis) and dexamethasone’, on a scale from 1–5 (1 being “poor quality of life” and 5 being “excellent quality of life”)?”, one respondent said “4—very good.”
To the question “Did your myeloma treatment combination of isatuximab (Sarclisa) in combination with carfilzomib (Kyprolis) and dexamethasone improve your long-term health outlook,” one respondent said “yes.” When asked if isatuximab (Sarclisa) with carfilzomib (Kyprolis) and dexamethasone had met their expectations in treating their myeloma, one respondent said “yes.”
Anything Else?
Across subsets, when the opportunity was provided for patient comments, their responses frequently echoed similar sentiments. These are: desiring treatments to have maximum effectiveness but with non-debilitating side effects; to be minimally occupying their time with numerous visits to the hospital, and to ultimately achieve the longest remission possible for themselves (in lieu of a cure); all of which contribute to their (the patients’) abilities to lead a “normal” life (one of good quality). Patients also stated that receiving information and explanation about new and emerging treatments was important to them, as well as the timely provision of access to these treatments through government approval and coverage. These concerns are of particular significance considering (as detailed in section 4) the majority of Subset 1 patients (9 of 12 respondents) answered ‘I don’t know’ when asked if they would benefit from isatuximab (Sarclisa) in combination with carfilzomib (Kyprolis) and dexamethasone. Patients need a better understanding of their treatment options, and treatment sequencing, and they know it. There is no such thing as “one-treatment-fits-all” when it comes to treating myeloma. What works for one patient may not work for another, which is why each case must be assessed individually. As more and more treatment becomes available, it is important for patients to be able to chart, with their healthcare provider, the best action plan for them. This cannot be done without understanding their treatment options and their effects on their quality of life.
Patient Group Conflict of Interest Declaration for Myeloma Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it. No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it. No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Conflict of Interest Declaration for Myeloma Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen Canada Inc. | — | — | — | X |
Sanofi | — | — | — | X |
Janssen | — | — | — | X |
Bristol-Myers Squibb Canada Co. | — | — | — | X |
Celgene | — | — | — | X |
Takeda Canada Inc. | — | — | — | X |
Merck Canada Inc. | — | — | X | — |
Pfizer Canada | — | — | X | — |
Karyopharm Therapeutics | — | — | — | X |
Novartis | X | — | — | — |
GlaxoSmithKline Inc. | — | — | X | — |
Leo Pharma Inc. | — | X | — | — |
Rapid Novor Inc. | — | — | X | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Name: Martine Elias
Position: Executive Director
Patient Group: Myeloma Canada
Date: July 17, 2021
Clinician Group Input
Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
Please describe the purpose of your organization. Include a link to your website (if applicable).
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Please describe how you gathered the information included in the submission.
Discussed jointly via emails.
Current treatments
Describe the current treatment paradigm for the disease
Focus on the Canadian context. Please include drug and non-drug treatments. Drugs without Health Canada approval for use in the management of the indication of interest may be relevant if they are routinely used in Canadian clinical practice. Are such treatments supported by clinical practice guidelines? Treatments available through special access programs are relevant. Do current treatments modify the underlying disease mechanism? Target symptoms?
Response: Currently available treatment in patients who have received at least 1 prior line of treatment include: Daratumumab triplets, lenalidomide-based therapy, pomalidomide-based therapy, KRd, bortezomib retreatment, second autologous stem cell transplant.
Treatment goals
What are the most important goals that an ideal treatment would address?
Examples: Prolong life, delay disease progression, improve lung function, prevent the need for organ transplant, prevent infection or transmission of disease, reduce loss of cognition, reduce the severity of symptoms, minimize adverse effects, improve health-related quality of life, increase the ability to maintain employment, maintain independence, reduce burden on caregivers.
Response: Prolong life, delay disease progression, reduce symptom severity, improve QoL
Treatment gaps (unmet needs)
Considering the treatment goals in Section 4, please describe goals (needs) that are not being met by currently available treatments.
Examples: Not all patients respond to available treatments. Patients become refractory to current treatment options. No treatments are available to reverse the course of disease. No treatments are available to address key outcomes. Treatments are needed that are better tolerated. Treatment are needed to improve compliance. Formulations are needed to improve convenience
Response: IKd could be a better treatment alternative than DVd if would like to treat with proteasome inhibitor-based therapy in patients who relapsed/were refractory to IMiD-based treatment.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Would these patients be considered a subpopulation or niche population? Describe characteristics of this patient population. Would the drug under review address the unmet need in this patient population?
Response: Patients who are not eligible for DRd
Place in therapy
How would the drug under review fit into the current treatment paradigm?
Is there a mechanism of action that would complement other available treatments, and would it be added to other treatments? Is the drug under review the first treatment approved that will address the underlying disease process rather than being a symptomatic management therapy? Would the drug under review be used as a first-line treatment, in combination with other treatments, or as a later (or last) line of treatment? Is the drug under review expected to cause a shift in the current treatment paradigm?
Response: IKd will be an alternate treatment option for 2nd line of treatment and beyond. This gives a monoclonal antibody treatment option to lenalidomide-refractory patients
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
If so, please describe which treatments should be tried, in what order, and include a brief rationale.
Response: No
How would this drug affect the sequencing of therapies for the target condition?
If appropriate for this condition, please indicate which treatments would be given after the therapy has failed and specify whether this is a significant departure from the sequence employed in current practice.Would there be opportunity to treat patients with this same drug in a subsequent line of therapy? If so, according to what parameters?
Response: The only option after IKd will be pomalidomide-based therapy
Which patients would be best suited for treatment with the drug under review?
Which patients are most likely to respond to treatment with the drug under review? Which patients are most in need of an intervention? Would this differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease)?
Response: Patients who meet eligibility criteria would be suited for treatment with IKd
How would patients best suited for treatment with the drug under review be identified?
Examples: Clinician examination or judgement, laboratory tests (specify), diagnostic tools (specify) Is the condition challenging to diagnose in routine clinical practice? Are there any issues related to diagnosis? (e.g., tests may not be widely available, tests may be available at a cost, uncertainty in testing, unclear whether a scale is accurate or the scale may be subjective, variability in expert opinion.) Is it likely that misdiagnosis occurs in clinical practice (e.g., underdiagnosis)? Should patients who are pre-symptomatic be treated considering the mechanism of action of the drug under review?
Response: Through usual multiple myeloma diagnosis
Which patients would be least suitable for treatment with the drug under review?
Response: None.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
If so, how would these patients be identified?
Response: No.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response: Usual myeloma response criteria
What would be considered a clinically meaningful response to treatment?
Examples: Reduction in the frequency or severity of symptoms (provide specifics regarding changes in frequency, severity, and so forth), Attainment of major motor milestones, Ability to perform activities of daily living, Improvement in symptoms, Stabilization (no deterioration) of symptoms, Consider the magnitude of the response to treatment. Is this likely to vary across physicians?
Response: Improvement in myeloma parameters and improvement in symptoms
How often should treatment response be assessed?
Response: Every cycle
What factors should be considered when deciding to discontinue treatment?
Examples: Disease progression (specify; e.g., loss of lower limb mobility), Certain adverse events occur (specify type, frequency, and severity), Additional treatment becomes necessary (specify)
Response: Progression or intolerance despite dose reduction
What settings are appropriate for treatment with the drug under review?
Examples: Community setting, hospital (outpatient clinic), specialty clinic
Response: Outpatient chemo suites
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
If so, which specialties would be relevant?
Response: NA
Is there any additional information you feel is pertinent to this review?
Response: IKd administration is associated with multiple visits to the chemo suites which may not be feasible for some patients.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Tom Kouroukis
Position: Provincial Head – Complex Malignant Hematology (OH-CCO)
Date: 08-07-2021
Table 2: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Lee Mozessohn
Position: Hematologist/oncologist
Date: 05-08-2021
Table 3: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Canadian Myeloma Research Group
About Canadian Myeloma Research Group
Please describe the purpose of your organization. Include a link to your website (if applicable).
The Canadian Myeloma Research Group (CMRG), previously named the Myeloma Canada Research Network (MCRN), is a charitable organization whose membership consists of myeloma physicians from 22 major academic medical centres in Canada. The three main purposes of CMRG consist of: 1) conducting investigator-initiated academic clinical trials to improve the outcome of myeloma patients; 2) maintenance of a national Myeloma Database, now consisting of over 7000 patients, to evaluate real-word patterns of treatment, outcomes, risk factors and areas for future research in myeloma; and 3) generation of consensus statements for myeloma management.
Information Gathering
Please describe how you gathered the information included in the submission.
The information for this submission was gathered at our monthly meeting from other members. Subsequently the final draft has been further refined with the input of additional members and signed by them.
Current treatments
Describe the current treatment paradigm for the disease
Focus on the Canadian context. Please include drug and non-drug treatments. Drugs without Health Canada approval for use in the management of the indication of interest may be relevant if they are routinely used in Canadian clinical practice. Are such treatments supported by clinical practice guidelines? Treatments available through special access programs are relevant. Do current treatments modify the underlying disease mechanism? Target symptoms?
Response: Multiple Myeloma (MM) is a non-curable hematologic malignancy in which initial treatment stratification is based upon autologous stem cell transplantation eligibility. Patients eligible for stem cell transplant are treated with cyclophosphamide-bortezomib- dexamethasone followed by autologous stem cell and often lenalidomide maintenance. Patients ineligible for stem cell transplant are treated with either fixed duration bortezomib-containing regimen or lenalidomide based regimen until disease progression and/or toxicity.
In both groups at relapse, limited treated options exist which include a either daratumumab, carfilzomib orpomalidomide containing regimens which can be used in pre-specified combination based upon provincial drug funding programs (2nd line relapse: DRd, DVd, KRd, Kd; 3rd line: Pd)
Treatment goals
What are the most important goals that an ideal treatment would address?
Examples: Prolong life, delay disease progression, improve lung function, prevent the need for organ transplant, prevent infection or transmission of disease, reduce loss of cognition, reduce the severity of symptoms, minimize adverse effects, improve health-related quality of life, increase the ability to maintain employment, maintain independence, reduce burden on caregivers.
Response: Multiple myeloma both at diagnosis and at relapse can cause morbidity and mortality including fractures, decreased blood counts, renal failure, infections etc. This can have a significant impact on patient’s quality of life. The most important goals of myeloma therapy are to ensure there is a high quality and durable response to treatment (response rates and progression free survival) which will delay disease related complications and ultimately improve quality of life.
Treatment gaps (unmet needs)
Considering the treatment goals in Section 4, please describe goals (needs) that are not being met by currently available treatments.
Examples: Not all patients respond to available treatments. Patients become refractory to current treatment options. No treatments are available to reverse the course of disease. No treatments are available to address key outcomes. Treatments are needed that are better tolerated. Treatment are needed to improve compliance. Formulations are needed to improve convenience.
Response: Unmet treatment needs in this disease include patient who become refractory to major classes of drug specifically immunomodulatory drugs (lenalidomide) and/or proteosome inhibitors (bortezomib) [1].
Patient who are refractory to these agents have overall poor outcomes. Furthermore, we know that attrition is particularly important in MM and that many patients may die prior to receiving subsequent lines of treatment. Therefore, there is a need to provide patients with optimal treatment to control the disease as early as possible in the disease course.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Would these patients be considered a subpopulation or niche population? Describe characteristics of this patient population. Would the drug under review address the unmet need in this patient population?
Response
Isatuximab + Carfilzomib + Dex (IsaKd) is ideal therapy for a group of patients with significant unmet needs-- specifically, those individuals who have progressed after either a bortezomib and/or lenalidomide containing regimen. Among these patients, anti-CD38 containing regimens are most commonly used at relapse as 1) they have a different mechanism of action compared to the agents previously received by the patients and 2) exposure to these agents is required for future enrollment in clinical trials.
The current funded anti-CD38 regimens include daratumumab-bortezomib and dexamethasone (DVd) and daratumumab-lenalidomide-dexamethasone (DRd). As most patient progress on lenalidomide maintenance (ASCT eligible) or on lenalidomide-dexamethasone in the frontline setting (ASCT ineligible), the most commonly used treatment option for them is DVd in second line. This commonly used funded option is not optimal with a PFS of no more than 8 months in lenalidomide refractory population [2]. Thus, there remains an unmet need in optimizing the daratumumab-containing regimens in the post-lenalidomide setting and further options are required.
Place in therapy
How would the drug under review fit into the current treatment paradigm?
Is there a mechanism of action that would complement other available treatments, and would it be added to other treatments? Is the drug under review the first treatment approved that will address the underlying disease process rather than being a symptomatic management therapy? Would the drug under review be used as a first-line treatment, in combination with other treatments, or as a later (or last) line of treatment? Is the drug under review expected to cause a shift in the current treatment paradigm?
Response: The drug combination (IsaKd) under review would address the need of patients in relapse who have progressed on lenalidomide and/or bortezomib. Among these patients, as previously stated, our current funded options are suboptimal. IsaKd would provide access to anti-CD38 antibody therapy in this setting along with a different proteosome inhibitor which would be expected to replace and greatly improve upon the current standard of care. In fact, based on the ENDEAVOR trial, it is clear that carfilzomib is the superior PI compared to bortezomib in the relapsed setting (leading to its approval by CADTH and provincial funding).
This regimen (IsaKd) would cause an impact on subsequent line sequencing with carfilzomib-based regimens (Kd or KRd) as trials such as ASPIRE and ENDEAVOR which led to the approval of these regimens did not allow progression on previous carfilzomib. Similarly, IsaKd would also impact the sequencing of anti-CD38 based regimens (DRd or DVd) as the trials evaluating these therapies including POLLUX, CASTOR did not enroll patients that were progressing on anti-CD38.
Pomalidomide based regimens are less likely to be affected in sequencing.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
If so, please describe which treatments should be tried, in what order, and include a brief rationale.
Response: As mentioned above, attrition plays an important role in the treatment trajectory of myeloma; therefore, the best treatment options should ideally be used upfront. Additionally, our current standard of care DVd which is the most commonly used anti- CD38 containing regimen in second line is suboptimal with poor response rates both in trial as well as real-world Canadian data [2,3]. IsaKd would provide these patients with access to both an anti-CD38 as well as a more potent proteasome inhibitor and therefore would be optimal in this setting.
How would this drug affect the sequencing of therapies for the target condition?
If appropriate for this condition, please indicate which treatments would be given after the therapy has failed and specify whether this is a significant departure from the sequence employed in current practice. Would there be opportunity to treat patients with this same drug in a subsequent line of therapy? If so, according to what parameters?
Response: Sequencing will likely be impacted if this regimen is approved. If IsaKd is approved, it will most commonly be used in second line in patient progressing on lenalidomide and/or proteosome inhibitors. Subsequent use of funded daratumumab (DRd or DVd) or carfilzomib (KRd or Kd) containing regimens will likely not be utilized in further lines of treatment. As patient would be on IsaKd until disease progression or toxicity, it is unlikely patients would be re-treated with IsaKd in subsequent line of tx.
Once patients progress on IsaKd, pomalidomide based regimens would be most commonly used with the current funded regimen being Pomalidomide-dexamethasone +/- cyclophosphamide. (However, Isa+POM + dex would not be included as an option as prior therapy with IsaKd would result in anti-CD38 antibody refractoriness).
Additionally, if DRd is funded in first line for transplant ineligible MM patients as per the MAIA data, then sequencing will further be impacted for IsaKd. At that point, among transplant ineligible patient using DRd upfront, IsaKd would likely not be used in second line. IsaKd would still continue to have a role among transplant patients progressing on lenalidomide maintenance as they would have not been previously treated with an anti-CD38 antibody containing regimen.
Which patients would be best suited for treatment with the drug under review?
Which patients are most likely to respond to treatment with the drug under review? Which patients are most in need of an intervention? Would this differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease)?
Response: The IKEMMA trial, which tested IsaKd vs Kd was done in patients in one to three prior lines of treatment. The eligibility criteria were relatively generous for this type of study, particularly as patients with poor renal function were permitted (eGFR ≥ 15).
Patients with previous treatment to carfilzomib and an anti- CD38 were excluded. In the trial, the addition of Isa to Kd in the experimental arm significantly improved the primary end point of PFS (HR 0.53). This benefit was seen in most of the pre- specified subgroups, although a smaller treatment effect was observed in those with biologically aggressive disease and those progressing on lenalidomide.
How would patients best suited for treatment with the drug under review be identified?
Examples: Clinician examination or judgement, laboratory tests (specify), diagnostic tools (specify)Is the condition challenging to diagnose in routine clinical practice? Are there any issues related to diagnosis? (e.g., tests may not be widely available, tests may be available at a cost, uncertainty in testing, unclear whether a scale is accurate or the scale may be subjective, variability in expert opinion.) Is it likely that misdiagnosis occurs in clinical practice (e.g., underdiagnosis)? Should patients who are pre-symptomatic be treated considering the mechanism of action of the drug under review?
Response: Patient would be identified by biochemical or clinical relapse of MM based upon a combination of laboratory tests, imaging as well as clinician examination/judgement. Although patients with non- secretory MM, serum-free light chain measurable disease only and primary refractory myeloma were excluded in the trial, this regimen would also be expected to be effective and appropriate for that subgroup.
Which patients would be least suitable for treatment with the drug under review?
Response: Patient with prior refractory disease to carfilzomib or previous anti-CD38 would be less suitable for the treatment as they were excluded from the trial. Additionally, there is emerging evidence that Isatuximabpost-daratumumab likely produces poor response and therefore, this regimen may not be expected to provide the same degree of benefit vs Kd alone in those with previous refractory disease to anti-CD38.
Clinicians have been mindful about the potential for carfilzomib to cause cardiovascular toxicity in a small, but consistent, percent of treated patients, and discontinuation rates of this agent for adverse events have typically ranged from 15-25% in previous studies involving this agent. The IKEMA trial is notable in that the discontinuation rate for AEs with IKd was only 8% (versus 14% with Kd), and the incidence of fatal treatment-emergent AEs was only 3% (with both IKd and Kd). Although the precise factors contributing to the relatively favorable toxicity profile for IKd are not known, the findings are reassuring for its use in elderly patients who are prone to pre-existing cardiac issues.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
If so, how would these patients be identified?
Response: Almost all pre-specified groups benefited in the experimental arm (IsaKd) compared to Kd alone. Patients with less advanced and less biologically aggressive disease are the mostly likely to exhibit a response to the IKd regimen, as is the case with virtually all myeloma treatments. If feasible, initiation of relapse therapy before the disease burden becomes excessive, or before the disease has acquired more aggressive cytogenetic feature (such as del 17p or other secondary cytogenetic changes) may be one strategy to afford benefit to the most patients.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response: Both the overall response rate, quality of responses (very good partial response or complete remission) as well as the durability of response (progression free survival) are all outcomes which are used in both clinical practice, as well as clinical trials. The primary end point of the IKEMMA study was PFS which is a clinically relevant end point for patients. Minimal residual disease is increasingly become important in MM given its concordance with overall survival and although the IKEMMA study did include that as a secondary endpoint showing the increased rates of MRD negativity in in the experimental arm, this end point is not available routinely across Canada.
What would be considered a clinically meaningful response to treatment?
Examples: Reduction in the frequency or severity of symptoms (provide specifics regarding changes in frequency, severity, and so forth). Attainment of major motor milestones. Ability to perform activities of daily living. Improvement in symptoms. Stabilization (no deterioration) of symptoms.Consider the magnitude of the response to treatment. Is this likely to vary across physicians?
Response: A clinically meaningful response to treatment would be the absence of progressive disease with minimal/tolerable side effects. Even though deep (VGPR or better) and more so sustained MRD negative responses are ideal, any absence of progressive disease provides a patient benefit in ensuring that myeloma related end organ damage is minimal. This is particularly the case if relapse therapy is started when progression is documented by the usual parameters, but before severe myeloma-related organ damage has developed; in this setting, even stable disease may afford benefit. It is reassuring that, based on the submitted data, a substantial proportion of patients achieve at least PR if not the ideal endpoint of VGPR or better.
How often should treatment response be assessed?
Response: Almost all myeloma patients are followed continuously with treatment response being assessed every 1-3 months with most commonly laboratory parameters and occasionally with advanced imaging and/or bone marrow biopsy depending upon the specific scenario.
What factors should be considered when deciding to discontinue treatment?
Examples: Disease progression (specify; e.g., loss of lower limb mobility). Certain adverse events occur (specify type, frequency, and severity). Additional treatment becomes necessary (specify).
Response: Both disease response and toxicity should be considered when deciding to discontinue the drug. Progressive disease (biochemical or clinical) should be considered and would be an indication to discontinue or modify the treatment regimen. Similarly, treatment related toxicities and its impact of patient health-related QoL would also be an indication to discontinue or modify treatment.
What settings are appropriate for treatment with the drug under review?
Examples: Community setting, hospital (outpatient clinic), specialty clinic
Response: MM is treated at many communities and academic sites across the country. The drug is administered in specialized clinical spaces. Therefore, both community setting clinics, hospital outpatient clinics and intravenous oncology drug administration facilities would be appropriate setting for the drug under review.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
If so, which specialties would be relevant?
Response: N/A
Is there any additional information you feel is pertinent to this review?
Response: No
References
1. Moreau, P., Zamagni, E. & Mateos, MV. Treatment of patients with multiple myeloma progressing on frontline-therapy with lenalidomide. Blood Cancer J. 9, 38 (2019). https://doi.org/10.1038/s41408-019-0200-1.
2. Usmani, S. Z. et al. Efficacy of daratumumab in combination with standard of care regimens in lenalidomide-exposed or - refractory patients with relapsed/refractory multiple myeloma (RRMM): analysis of the castor, pollux, and MMY1001 studies. Blood 132, 3288 (2018).
3. Hira S Mian, Christine Eisfeld, Christopher P. Venner, Victor Jimenez-Zepeda, Cyrus Khandanpour, Arleigh McCurdy, Michael Sebag, Kevin W Song, Richard Leblanc, Esther Masih-Khan, Eshetu G Atenafu, Darrell J White, Julie Stakiw, Anthony Reiman, Martha L Louzada, Muhammad Aslam, Rami Kotb, Engin Gul, Donna E. Reece; Efficacy of Daratumumab Containing Regimens Post Lenalidomide Maintenance in Transplant Eligible Patients: Real-World Experience from the Canadian Myeloma Research Group Database. Blood 2020; 136 (Supplement 1): 26–27. doi: https://doi.org/10.1182/blood-2020-133372.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Hira Mian
Position: Assistant Professor
Date: 05-08-2021
Table 4: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Takeda, Jansen, BMS, Sanofi, Amgen, GSK (advisory board fees) | — | X | — | — |
Jansen Research Funding | — | — | — | X |
Declaration for Clinician 2
Name: Anette Hay
Position: Associate Professor, Queens University
Date: 05-08-2021
Table 5: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Mohammed Aljama
Position: Hematologist, JCC. Assistant Professor, Department of Oncology
Date: 05-08-2021
Table 6: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Donna Reece
Position: Chief Medical Officer, CMRG
Date: 05-08-2021
Table 7: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BMS/Celgene | — | — | X | — |
Janssen | — | — | X | — |
Amgen | — | — | X | — |
Sanofi | X | — | — | — |
GSK | X | — | — | — |
Takeda | X | — | — | — |
Declaration for Clinician 5
Name: Dr. Christopher Venner
Position: MD Hematology Tumor Group lead, Cross Cancer Institute, Edmonton, Alberta
Date: 05-08-2021
Table 8: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Celgene/BMS | X | — | — | — |
Takeda | X | — | — | — |
Janssen | X | — | — | — |
Amgen | X | — | — | — |
Sanofi | X | — | — | — |
GSK | X | — | — | — |
Declaration for Clinician 6
Name: Nicole Laferriere
Position: Hematologist/ Chief of Oncology
Date: 05-08-2021
Table 9: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astra Zeneca, AMGEN Canada, ROCHE, Abbvie, Sanofi Canada, Lundbeck, Janssen, Celgene, Teva Pharm, Novartis | X | — | — | — |
Declaration for Clinician 7
Name: Dr. Rami Kotb
Position: Hematologist, Oncologist, Cancer Care Manitoba
Date: 05-08-2021
Table 10: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BMS, Amgen, JNJ | — | X | — | — |
Takeda | X | — | — | — |
Sanofi, Merck, | — | — | — | X |
Karyopharm | — | — | — | X |
Declaration for Clinician 8
Name: Suzanne Trudel
Position: Oncologist
Date: 05-08-2021
Table 11: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 8
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Sanofi | X | — | — | — |
BMS | — | — | X | — |
Declaration for Clinician 9
Name: Kevin Song MD
Position: Hematologist, Vancouver General Hospital
Date: 05-08-2021
Table 12: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 9
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Bristol Myers Squibb | — | X | — | — |
Janssen | — | X | — | — |
Amgen | — | X | — | — |
Declaration for Clinician 10
Name: Dr. Julie Stakiw
Position: Oncologist
Date: 05-08-2021
Table 13: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 10
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Sanofi | X | — | — | — |
Declaration for Clinician 11
Name: Nizar Jacques Bahlis
Position: Associate Professor
Date: 05-08-2021
Table 14: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 11
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BMS | X | — | — | — |
Declaration for Clinician 12
Name: Darrell White
Position: Hematologist, Dalhousie University and QEII Health Sciences Centre
Date: 05-08-2021
Table 15: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 12
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BMS | — | X | — | — |
Janssen | — | — | X | — |
Declaration for Clinician 13
Name: Sindu Kanjeekal
Position: Hematologist/oncologist
Date: 05-08-2021
Table 16: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 13
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 14
Name: Dr. Anthony Reiman
Position: MD Oncologist
Date: 05-08-2021
Table 17: Conflict of Interest Declaration for Canadian Myeloma Research Group Clinician 14
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.