CADTH Reimbursement Review
Nivolumab (Opdivo)
Sponsor: Bristol-Myers Squibb Canada
Therapeutic area: Esophageal or gastroesophageal junction cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
CRT
chemoradiotherapy
CWC
Community Cancer Wellness program
DFS
disease-free survival
DMFS
distant metastasis-free survival
EAC
esophageal adenocarcinoma
EC
esophageal cancer
ECS
esophageal cancer subscale
ECOG PS
Eastern Cooperative Oncology Group Performance Status
ECOG PSR
Eastern Cooperative Oncology Group Performance Status Rating
EQ-5D-3L
EuroQol 5-Dimensions 3-Levels questionnaire
ESCC
esophageal squamous cell carcinoma
FACT-E
Functional Assessment of Cancer Therapy–Esophageal
FACT-G
Functional Assessment of Cancer Therapy–General
FACT-G7
Functional Assessment of Cancer Therapy–General 7 items
GEJC
gastroesophageal junction cancer
HR
hazard ratio
HRQoL
health-related quality of life
IKNL
Netherlands Comprehensive Cancer Organization
NCCN
National Comprehensive Cancer Network
OS
overall survival
pCR
pathological complete response
PD-1
programmed cell death protein 1
PD-L1
programmed cell death ligand 1
R0
complete resection
R1
positive circumferential, distal, or proximal margins
RPSLMC
Rush-Presbyterian-St Luke’s Medical Center
SAE
serious adverse event
VAS
visual analogue scale
ypT
pathologic tumour stage assessed after preoperative therapy
ypN
pathologic lymph node stage assessed after preoperative therapy
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo), 10 mg/mL, 40 mg, and 100 mg single-use vials for IV infusion |
Indication | For the adjuvant treatment of completely resected esophageal or gastroesophageal junction cancer in patients who have residual pathologic disease following prior neoadjuvant chemoradiotherapy |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Project ORBIS |
NOC date | July 2, 2021 |
Sponsor | Bristol Myers Squibb Canada |
NOC = Notice of Compliance.
Introduction
In Canada, esophageal cancer (EC) is ranked 19th among all cancer types based on incidence and 10th based on mortality.1 There are 2 dominant histological subtypes: esophageal adenocarcinoma (EAC), which begins in the glandular cells, and esophageal squamous cell carcinoma (ESCC), which begins in the squamous cells. Signs and symptoms of EC include dysphagia, weight loss, indigestion or heartburn, coughing, nausea, fatigue, and chest pain.2-4 As a result, patient quality of life is negatively affected.5 Clinically, EC is classified into stage I, stage II, stage III, and stage IV disease. Pathological primary tumour (T) stage is classified into T0, T1, T2, T3, and T4; pathological regional lymph node (N) stage is classified into N0, N1, N2, and N3; and distant metastasis (M) stage is classified as M0 and M1.6
The goal of treatment for EC and gastroesophageal junction cancer (GEJC) is curing the patient and, when that is not possible, delaying progression of disease, prolonging life, and improving or maintaining health-related quality of life (HRQoL). In Canada, provincial guidelines for EC recommend multimodality therapy consisting of neoadjuvant chemoradiotherapy (CRT) followed by resection (trimodality therapy) in patients with stage II or worse EC.4,7,8 Patients with GEJC can either be treated with trimodality therapy or perioperative chemotherapy with surgical resection. For patients with EC or GEJC undergoing trimodality therapy, no established adjuvant systemic treatments have been licensed. The standard of care for this population is surveillance.8,9 Given the high risk of recurrence for these patients, there is a significant urgent medical need for new, effective, and safe treatments for both EC and GEJC patients following neoadjuvant CRT and surgery.8,9
Nivolumab (Opdivo), for injection via IV infusion (10 mg/mL, 40 mg and 100 mg single-use vials) was approved by Health Canada in July 2021.10 Nivolumab is indicated for the adjuvant treatment of completely resected EC or GEJC in patients who do not achieve a pathologic complete response (pCR) following neoadjuvant CRT. The reimbursement request aligns with this Health Canada indication.
The objective of this clinical review is to review the beneficial and harmful effects of nivolumab for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following neoadjuvant CRT.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for patient and clinician input and from clinical experts consulted by CADTH for the purpose of this review. Issues identified by the Provincial Advisory Group that may affect clinician’s abilities to implement a recommendation are also summarized. The Stakeholder Perspectives Section provides more details.
Patient Input
One patient group, My Gut Feeling – Stomach Cancer Foundation of Canada, provided input for this review. The group, which includes patients with EC or GEJC, aims to support patients and caregivers by providing them with information, mentorship, and an advocacy platform. The information collected in this input was based on an international survey, which was conducted between June 29, 2021, and July 16, 2021, of 11 patients and 4 caregivers. Of the 15 participants, 1 patient who had surgically resected cancer and chemoradiation was treated with nivolumab.
Regarding clinical symptoms, patient respondents with EC or GEJC and caregiver respondents indicated that most symptoms experienced before diagnosis involved changes in appetite and pain. Other significant symptoms included weight loss, difficulty swallowing, nausea or vomiting, dumping syndrome, and reflux. Symptoms reported less often included bleeding, feeling a mass, ascites, bowel obstruction, food regurgitation, and shortness of breath. Respondents noted that these symptoms affected their day-to-day life.
Regarding current treatment, more than half (60%) of patient respondents agreed to some degree that current treatment helped them manage cancer symptoms. However, less than half (40%) of respondents were neutral or dissatisfied with their treatments. The patient group noted that physical, mental, social, financial, and occupational aspects of patients’ and caregivers’ lives often deteriorate as a result of diagnosis and treatment. All patients experienced at least 1 side effect from their therapies. Some side effects were well tolerated, but some led to hospitalization and/or delay in subsequent treatment.
One patient respondent accessed nivolumab through a hospital special access program. The patient indicated that a PET scan confirmed a lack of evidence of disease at 3 months following nivolumab therapy. The respondent did not experience any new side effects or exacerbation of side effects from surgery or chemoradiation, and he expressed strong satisfaction with improvement of quality of life.
Overall, the patient group indicated that there is an unmet need for the treatment of patient with EC or GEJC. The patient group strongly supported the use of nivolumab for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT. The patient group added that patients and caregivers should have equitable access to treatment options with the potential to improve quality and duration of life.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted for this review indicated that the treatment goals include improving disease-free survival (DFS), reducing adverse effects, improving or maintaining HRQoL, and improving overall survival (OS). There is currently no adjuvant therapy for patients with completely resected EC or GEJC who do not achieve a pCR to neoadjuvant CRT. Nivolumab is the first adjuvant therapy based on phase III evidence of a significant DFS benefit. The clinical experts agreed that nivolumab would represent a new standard of care for adjuvant therapy for patients who do not achieve a pCR following neoadjuvant CRT. As no other treatment is available for this population, it would not be appropriate to recommend that patients try other treatments before initiating treatment with nivolumab adjuvant therapy.
The clinical experts indicated that all patients who receive neoadjuvant CRT, esophagectomy with pathology showing no pCR should be assessed for adjuvant nivolumab treatment. Patients would need to have an adequate Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 or 1. Although not supported by clinical trial evidence, the experts agreed that the treatment can be extended to patients with an ECOG PS of 2. Patient should have no contraindication to nivolumab. The clinical experts indicated that nivolumab is contraindicated in patients with an ECOG PS of 3 or 4. According to the clinical experts, it is not possible to identify those patients who are most likely to benefit from treatment with nivolumab. The clinical experts noted that, based on criteria in the pivotal CheckMate 577 study, patients with positive circumferential, distal, or proximal margins (R1) would be excluded, and emphasized that the clinical management of R1 patients may be similar to patients with complete resection (R0) given the lack of available effective treatment options for R1 patients. The clinical experts indicated that, in clinical practice, clinicians may wish to administer nivolumab to R1 patients; however, they acknowledged that the expansion of nivolumab to R1 patients is out of the scope of this review.
Given that it is an adjuvant therapy, the clinical experts indicated that improved DFS is the desired outcome. Overall survival can be supportive. Scheduling CT scans every 3 to 6 months while on treatment can be used to determine if a patient has a recurrence and is therefore no longer benefiting from nivolumab.
The clinical experts indicated that nivolumab should continue for 17 cycles (with a maximum dose delay of 10 weeks as per the trial protocol) and be discontinued early if evidence confirms disease recurrence or unacceptable toxicity.
The clinical experts indicated that nivolumab should be prescribed at outpatient oncology clinics. Treatment should be supervised and delivered in institutions with staff trained in chemotherapy delivery.
According to the clinical experts, adjuvant treatment with nivolumab for this population represents a major advance in the care of EC and GEJC patients. There is no adjuvant treatment for this population, and nivolumab fills a major unmet need.
Clinician Group Input
The Ontario Health (Cancer Care Ontario) Gastrointestinal Drug Advisory Committee recognized the unmet needs in the current treatment algorithm for completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT and for whom the only option is post-operative surveillance. The clinician group indicated that this patient population has a high risk of recurrence that is associated with high mortality and poor quality of life. The clinician group indicated that patients should be offered nivolumab if they meet the eligibility criteria of the clinical trial and noted that outpatient chemotherapy-suite settings were appropriate treatment settings for patients. Prolonged life, delayed disease progression, reduced severity of symptoms, minimized adverse effects, and improved quality of life were identified as the most important goals of treatment. The clinician group also emphasized that toxicity and recurrence are factors that should be considered when deciding whether to discontinue treatment. Last, the clinician group described nivolumab as a new standard of care for this patient population.
Drug Program Input
The Provincial Advisory Group identified the following jurisdictional implementation issues: relevant comparators, consideration for initiation of therapy, consideration for discontinuation of therapy, generalizability, care provision, system issues, and economic considerations. The clinical experts consulted by CADTH weighed evidence from the CheckMate 577 study and other clinical considerations to provide responses to the Provincial Advisory Group’s drug program implementation questions. Table 4 provides more details.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
CheckMate 577 is an ongoing, phase III, randomized, double-blind, placebo-controlled, multi-centre, superiority study comparing nivolumab with placebo for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT.2
The trial was conducted in 170 sites in 29 countries (including Canada, the US, UK, Australia, and several European, South American, and Asian countries). Key characteristics of the study design are summarized in Table 6 and Figure 2.
The primary objective of study CheckMate 577 was to compare DFS associated with nivolumab treatment versus placebo in patients with completely resected EC or GEJC. The secondary objective was to compare OS in patients treated with nivolumab versus placebo. Main exploratory objectives included assessment of overall safety and tolerability, distant metastasis-free survival (DMFS), EuroQol 5-Dimensions 3-Levels questionnaire (EQ-5D-3L) index and visual analogue scale (VAS) scores, and patient cancer-related quality of life using the Functional Assessment of Cancer Therapy–Esophageal (FACT-E) questionnaire and selected components, such as the esophageal cancer subscale (ECS), Functional Assessment of Cancer Therapy–General (FACT-G), and Functional Assessment of Cancer Therapy–General 7 items (FACT-G7).
A total of 1,085 patients were screened, and 794 patients were randomized in a 2:1 ratio to receive nivolumab (n = 532) or placebo (n = 262). Randomization was done centrally using an interactive web response system. Randomization was stratified by the following 3 factors: histology (squamous versus adenocarcinoma), pathologic lymph node stage assessed after preoperative therapy (ypN) status (positive [≥ ypN1] versus negative [ypN0]) and tumour cell programmed cell death ligand 1 (PD-L1) status (≥ 1% versus < 1% or indeterminate or non-evaluable). The first patient was randomized on July 14, 2016, and the last patient was enrolled in August 2019. A total of 792 patients received at least 1 dose of nivolumab or placebo as assigned. While all patients in the nivolumab arm received at least 1 dose, 2 patients in the placebo arm did not receive the treatment.
Pre-specified interim analysis results (data cut-off date of July 3, 2020) for the primary outcome of DFS are provided in this submission. The sponsor indicated that the interim DFS result was considered final because the DFS interim analysis met pre-specified statistical significance criteria.3 The study is ongoing, with an estimated study completion date of October 11, 2025.
Efficacy Results
At the interim analysis as of database lock (July 3, 2020), nivolumab demonstrated a statistically significant and clinical meaningful improvement in DFS compared with placebo (hazard ratio [HR] = 0.69; 96.4% confidence interval [CI], 0.56 to 0.86; P value = 0.0003), which implies a 31% reduction in the risk of recurrence or death with nivolumab adjuvant treatment compared with placebo (the current standard of care, which is surveillance). The observed median DFS was twice as long in the nivolumab arm as in the placebo arm (22.41 months versus 11.04 months, respectively). The DFS rates at 6 months were higher in the nivolumab arm compared with the placebo arm (72.3% versus 63.4%, respectively, as shown in Table 2) In addition, the results from various subgroup analysis and sensitivity analysis were consistent with those of the primary analysis (Table 12 and Table 13).
As the secondary outcome, OS was not mature at the data cut-off and OS is therefore not available for this review.
Patient-reported and HRQoL outcomes were assessed as exploratory outcomes. Overall, the study found either no deterioration or maintenance from baseline in HRQoL with the treatment of nivolumab or placebo.
The improved benefit of nivolumab over placebo was also supported by DMFS results, as the median DMFS was numerically longer in the nivolumab arm than in the placebo arm (28.32 months versus 17.61 months), with an HR of 0.74 (95% CI, 0.60 to 0.92) (Table 2). However, DMFS was an exploratory outcome in the CheckMate 577 study.
Harms Results
Overall, the frequency of any grade of adverse events and serious adverse events (SAEs) were similar in both nivolumab and placebo arms. The most common adverse events |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Appendix 5). More patients treated with nivolumab experienced treatment-related adverse events and SAEs than patients treated with placebo2 |||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Appendix 5). Numerically, more patients discontinued from treatment due to adverse events or treatment-related adverse events in the nivolumab arm compared with the placebo arm. Notable adverse events including pneumonitis, myocarditis, and |||||||||||||||||||||||||||| were less than 5% in any arm. Pneumonitis and myocarditis were all-causality adverse events, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Overall, the clinical experts indicated that the nivolumab safety profile in this study was acceptable, manageable, and consistent with the known safety profile of nivolumab, and no additional safety signals were identified with adjuvant nivolumab monotherapy (Table 2, ||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2: Summary of Key Results from Pivotal and Protocol-Selected Studies
Outcomes | CheckMate 577 | |
|---|---|---|
Nivolumab (N = 532) | Placebo (N = 262) | |
DFS | ||
Events, n (%) | |||| | ||||| |
Median DFS (95% CI), monthsa | 22.41 (16.62 to 34.00) | 11.04 (8.34 to 14.32) |
HRb (||||||) or (||||||) | 0.69 |||||| or (||||||) | |
P valuec | 0.0003 | |
6-month DFS rates (95% CI), %a | 72.3 (68.2 to 76.0) | 63.4 (57.2 to 69.0) |
OSd | NE (NE to NE) | |
DMFS | ||
Events, n (%) | 218 (41.0) | 134 (51.1) |
Median DMFS (95% CI), monthsa | 28.32 (21.26 to NA) | 17.61 (12.45 to 25.40) |
HRb (95% CI) | 0.74 (0.60 to 0.92) | |
6-month DMFS rates (95% CI), %a | |||||| | |||||| |
Harms | ||
Patients with at least 1 AEe, n (%) | 510 (95.9) | 243 (93.5) |
Patients with at least 1 treatment-related AE, n (%) | 376 (70.7) | 119 (45.8) |
Patients with at least 1 SAE, n (%) | 158 (29.7) | 78 (30.0) |
Patients with at least 1 treatment-related SAE, n (%) | 40 (7.5) | 7 (2.7) |
Patients with an AE leading to discontinuation from the treatment, n (%) | 68 (12.8) | 20 (7.7) |
Patients with a treatment-related AE leading to discontinuation from treatment | 48 (9.0) | 8 (3.1) |
Deathf | |||||| | |||||| |
Notable harms or harms of special interestg | ||
Pneumonitis | |||||| | |||||| |
Myocarditis | |||||| | |||||| |
|||||| | |||||| | |||||| |
AE = adverse event; CI = confidence interval; DFS = disease-free survival; DMFS = distant metastasis-free survival; HR = hazard ratio; NA = not available; NE = not estimated; NR = not reported; SAE = serious adverse event.
aBased on Kaplan–Meier estimates.
bStratified Cox proportional hazards model. Hazard ratio was expressed as nivolumab over placebo. This model was stratified by programmed cell death ligand 1 status (≥ 1% vs. < 1% or indeterminate or non-evaluable), pathologic lymph node status (positive [≥ ypN1] vs. negative [ypN0]) and histology (squamous vs. adenocarcinoma).
cLog-rank test stratified by programmed cell death ligand 1 status (≥ 1% vs. < 1% or indeterminate or non-evaluable), pathologic lymph node status (positive [≥ ypN1] vs. negative [ypN0]) and histology (squamous vs. adenocarcinoma). Two-sided P values were from a stratified log-rank test. The boundary for statistical significance was a P value < 0.036. Additional accuracy for P value: 0.000339.
dThe study is ongoing. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
eReported as all-causality AE in the Clinical Study Report. All events occurred within 30 days of the last dose of study drug, unless otherwise indicated.
f||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
gNotable harms occurred within 100 days of last dose with or without immune-modulating medication. Pneumonitis and myocarditis were all-causality AEs, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Source: Clinical Study Report for CheckMate 577.2
Critical Appraisal
The included pivotal study (CheckMate 577) was a double-blinded and randomized placebo-controlled trial. Overall, it was well designed. Data for OS were not mature at the time of the data cut-off. However, according to the clinical experts consulted by CADTH for this review, DFS is a relevant and clinically important primary outcome for the adjuvant treatment in this population, considered to be meaningful, and likely to be correlated with OS in adjuvant treatment.
The patient-reported and HRQoL outcomes (ECS, FACT-E, FACT-G7, FACT-G, and ED-5D-3L) were assessed as exploratory outcomes. No formal statistical analysis compared the patient-reported and HRQoL outcomes between the 2 treatment arms. In addition, there is a potential risk of bias because of substantial missing data on these outcomes, and there may have been differential recall bias. Overall, the magnitude and direction of the impact of these missing data and the recall bias on the patient-reported and HRQoL outcomes are unknown. These patient-reported outcomes and HRQoL findings are therefore inconclusive.
No major generalizability issue was noted regarding the findings from the pivotal study.
Conclusions
One sponsor-submitted, ongoing, phase III, multinational, double-blind, randomized placebo-controlled trial is included in this review. Compared to placebo, adjuvant treatment with nivolumab (240 mg every 2 weeks by IV infusion for 16 weeks, followed by 480 mg every 4 weeks intravenously until disease progression or unacceptable toxicity, for a total treatment duration of 1 year) showed a statistically significant and clinically meaningful DFS benefit in the treatment of patients (≥ 18 years old) with completely resected EC or GEJC who have residual pathologic disease following prior neoadjuvant CRT. The safety profile of nivolumab in this study was consistent with the known safety profile of nivolumab, and no additional safety signals with adjuvant nivolumab therapy were identified in this study.
Introduction
Disease Background
In Canada, EC is ranked 19th among all cancer types based on incidence and 10th based on mortality.1 In 2020, it was estimated that a total of 2,400 Canadians would be diagnosed with EC and 2,300 Canadians would die from the disease.1 Esophageal cancer is among cancers with a high proportion of metastatic disease (stage IV) at first diagnosis (39.9%),5 and the 5-year survival rate for all ECs is a relatively low 15%.1 Later stages of EC are associated with poorer prognosis and survival.6 As EC progresses, the 5-year survival rate decreases from 47% for stages I and II to 25% for stage III and 5% for stage IV. The disease has the second-lowest survival rate among patients with cancer in Canada.7
Two dominant histological subtypes of EC are known: EAC, which begins in the glandular cells, and ESCC, which begins in the squamous cells.9,11 The former typically occurs in the distal esophagus and gastroesophageal junction.10 Based on 2012 epidemiology statistics for the US, the incidence rate of esophageal cancer was higher in males than in females. The male-to-female ratio of EC was 2.5 to 1 for ESCC and 6.5 to 1 for EAC.12 Although ESCC is the most common subtype diagnosed globally, EAC has become more predominant in Western countries.11 In Canada, the incidence of EAC has been increasing (10.9 cases per million in 1992 to 26.8 cases per million in 2010), while the incidence of ESCC has been declining (18.2 cases per million in 1992 to 14.7 cases per million in 2010).11 It is estimated that the incidence of EAC by 2026 would be 4.8 per 100,000 in men and 0.8 per 100,000 in women and the incidence of ESCC would be 1.3 per 100,000 in men and 0.6 per 100 women.13
Signs and symptoms of EC include dysphagia (difficulty swallowing), frequent choking on food, unexplained weight loss, indigestion or heartburn, coughing or hoarseness, nausea or vomiting, fatigue, and chest pain, pressure or burning.14-16 As a result, patient quality of life is negatively affected.17
The recommended diagnostic work-up includes an esophagogastroduodenoscopy with biopsy to establish the tumour’s location and histology, followed by a CT scan of the thorax, abdomen, and pelvis to further establish the tumour’s location, depth of penetration into the esophageal wall, invasion into adjacent structures, and involvement of regional and non-regional lymph nodes, and metastatic disease. To evaluate distant metastases, whole-body integrated fluorodeoxyglucose, PET scans, endoscopic ultrasound, and sometimes diagnostic laparoscopy are used.12 Blood laboratory test is also recommended to identify end organ dysfunction.16
Clinically, EC is classified into stage I, stage II, stage III, and stage IV disease. The tumour, node, and metastasis staging system of the combined American Joint Committee on Cancer and Union for International Cancer Control for EC is used universally. The primary tumour (T) stage is classified into T0 (negative, no evidence of primary tumour) and positive (T1, T2, T3 and T4); regional lymph node (N) stage is classified into N0 (negative, no regional lymph node metastasis) and positive (N1, N2, and N3); and distant metastasis (M) stage is classified as M0 (no distant metastasis) or M1 (distant metastasis).12
Both EC and GEJC are aggressive and associated with poor prognoses, and their incidence has increased in Canada for the last few decades.3,11 Patients with local and locoregional EC and GEJC tumours treated with neoadjuvant CRT and surgery (i.e., trimodality therapy) show clinical improvement compared with surgery alone. However, a substantial unmet medical need still exists in this specific population.18-20 Approximately 70% to 75% of patients were unable to achieve pCR after trimodality therapy and have a poorer prognosis compared with patients with pCR.21-25 The risk of disease recurrence following trimodality therapy remains high. Outcomes declined even further in patients with lymph node-positive disease.23 The 5-year OS rate was 52% for pCR patients and only 41% for non-pCR patients.3
Standards of Therapy
Canadian clinical management pathways for the curative treatment of resectable local advanced EC or GEJC are based on National Comprehensive Cancer Network (NCCN), American Society of Clinical Oncology, and European Society of Medical Oncology guidelines.9 In Canada, provincial guidelines for EC recommend multimodality therapy consisting of neoadjuvant CRT followed by resection (trimodality therapy) in patients with stage II or worse EC and GEJC.4,7,8 No established systemic treatments have been licensed for patients with EC or GEJC following neoadjuvant CRT and resection. The standard of care for this population has been surveillance.8,9 Active treatment can then be administered once the disease recurs and becomes advanced or metastatic. In this setting, any systemic treatment is palliative in nature. Given the high risk of recurrence for these patients, there is a significant urgent unmet medical need for new, effective, and safe adjuvant treatment in both EC and GEJC patients following neoadjuvant CRT and surgery.8,9
The clinical experts CADTH consulted for this review and the clinical group input indicated that the goals of treatment for these patients are to improve cure rates and, when that is not possible, to delay progression of disease, prolong life and improve or maintain HRQoL. The patient group indicated a need to access new and effective therapies that prolong overall survival, improve quality of life, and reduce disease symptoms, and have tolerable side effects.
Drug
Nivolumab (Opdivo), for injection by IV infusion (10 mg nivolumab /mL, 40 mg and 100 mg single-use vials) was approved by Health Canada in July 2021.26 It is indicated for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT (Table 3).
Binding of PD-L1 and programmed cell death ligand 2 to the programmed cell death protein 1 (PD-1) receptor on T cells inhibits T-cell anti-tumour immune response. Nivolumab is a human immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptors and blocks its interaction with PD-L1 and programmed cell death ligand 2, therefore blocking PD-1-pathway–mediated inhibition of T-cell antitumour immune responses and reactivating T-cell antitumour immune response.
The Health Canada–recommended dosage is 240 mg every 2 weeks or 480 mg every 4 weeks administered by IV infusion over 30 minute. After completing 16 weeks of therapy, the recommended dosage is 480 mg every 4 weeks until disease progression or unacceptable toxicity, for a total treatment duration of 1 year.26
Nivolumab should be administered under the supervision of physicians experienced in the treatment of cancer. It was previously approved by Health Canada26:
as adjuvant treatment of adult patients after complete resection of melanoma with regional lymph node involvement, in transit metastases/satellites without metastatic nodes, or distant metastases
as monotherapy for the treatment of hepatocellular carcinoma and classical Hodgkin lymphoma
as monotherapy or in combination with ipilimumab for the treatment of unresectable or metastatic melanoma, metastatic non–small cell lung cancer, metastatic renal cell carcinoma, and for the treatment of recurrent or metastatic squamous cell carcinoma of the head and neck in adults progressing on or after platinum-based therapy
in combination with ipilimumab for the treatment of unresectable malignant pleural mesothelioma, microsatellite instability-high/mismatch repair deficient metastatic colorectal cancer (Table 3).
Table 3: Key Characteristics of Nivolumab
Characteristic | Nivolumab |
|---|---|
Mechanism of action | Nivolumab is a human immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, releasing PD-1-pathway–mediated inhibition of the immune response, including the anti-tumour immune response |
Indicationa | For the adjuvant treatment of completely resected EC or GEJC cancer in patients who have residual pathologic disease following prior neoadjuvant chemoradiotherapy |
Route of administration | IV |
Recommended dose | 240 mg every 2 weeks or 480 mg every 4 weeks administered as IV infusion over 30 minute; after completing 16 weeks of therapy, administer as 480 mg every 4 weeks until disease progression or unacceptable toxicity for a total treatment duration of 1 year |
Serious adverse effects or safety issues | Pneumonitis, myocarditis, interstitial lung disease |
Other | Should be administered under the supervision of physicians experienced in the treatment of cancer |
EC = esophageal cancer; GEJC = gastroesophageal junction cancer; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1; PD-L2 = programmed cell death ligand 2.
aHealth Canada–approved indication
Source: Product monograph.26
The objective of this report is to review the beneficial and harmful effects of nivolumab for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT.
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
One patient group, My Gut Feeling – Stomach Cancer Foundation of Canada, provided input for this review. The patient group, which includes patients with EC or GEJC, aims to support patients and caregivers by providing them with information, mentorship, and an advocacy platform. The information collected in this input was based on an international survey, which was conducted between June 29, 2021, and July 16, 2021, with 11 patients and 4 caregivers. Of the 15 participants, 1 patient who had surgically resected cancer and chemoradiation was treated with nivolumab.
Regarding clinical symptoms, patient respondents with EC or GEJC and caregiver respondents indicated that, before diagnosis, the symptoms most often experienced were changes in appetite and pain. Other significant symptoms included weight loss, difficulty swallowing, nausea and vomiting, dumping syndrome, and reflux. Symptoms reported less often included bleeding, feeling a mass, ascites, bowel obstruction, food regurgitation, and shortness of breath. Respondents noted that these symptoms affected their day-to-day life.
Regarding current treatment, more than half (60%) of patient respondents agreed to some degree that current treatment helped them manage cancer symptoms. However, less than half (40%) of patient respondents were neutral or dissatisfied with their treatments. The patient group noted that many physical, mental, social, financial, and occupational aspects of patients’ and caregivers’ lives often deteriorated as a result of diagnosis and treatment. All patients experienced at least 1 side effect from their therapies. Some side effects were well tolerated, but some led to hospitalization and/or delays in the subsequent treatment.
One patient respondent accessed nivolumab through a hospital special access program. The patient respondent indicated that a PET scan confirmed a lack of evidence of disease at 3 months after nivolumab therapy. The respondent did not experience any new side effects or exacerbation of side effects he was having from surgery or chemoradiation, and he expressed strong satisfaction with improvement of quality of life.
Overall, the patient group indicated that there is an unmet need for the treatment of patient with EC or GEJC. The patient group strongly supports the use of nivolumab for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT. The patient group added that patients and caregivers should have equitable access to treatment options that have the potential to improve quality and duration of life.
The original patient group input is presented in Appendix 1.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of EC or GEJC.
Unmet Needs
The clinical experts CADTH consulted for this review indicated that there is currently no adjuvant therapy for patients with completely resected EC or GEJC patients who do not achieve a pCR to neoadjuvant CRT. This is an unmet need.
Place in Therapy
Nivolumab is the first adjuvant therapy based on phase III evidence that has demonstrated a significant DFS benefit. The clinical experts indicated that nivolumab would represent a new standard of care for adjuvant therapy for patients who do not achieve a pathologic complete response following neoadjuvant CRT. No other treatment is available for this population. It would not be appropriate to recommend that patients try other treatments before initiating treatment with nivolumab adjuvant therapy.
The most important goal of an adjuvant treatment is to improve the rate of cure. This trial uses DFS as its primary end point, which is appropriate for an adjuvant therapy RCT.
Patient Population
The clinical experts indicated that all patients who receive neoadjuvant CRT, esophagectomy with pathology showing no pCR should be assessed for adjuvant nivolumab treatment. Patients would need to have an adequate ECOG PS of 0 or 1. Although not supported by clinical trial evidence, the clinical experts support extension of treatment eligibility to select patients with an ECOG PS of 2. Patients should have no contraindication to nivolumab. The clinical experts indicated that there is no evidence to support the use of adjuvant nivolumab in patients with an ECOG PS of 3 or 4. According to the clinical experts, it is not possible to identify those patients who are most likely to exhibit benefit from treatment with nivolumab. The clinical experts noted that, based on the CheckMate 577 criteria, R1 patients would be excluded, and emphasized that the clinical management of R1 patients may be similar to that of R0 patients given the lack of available effective treatment options for R1 patients. The clinical experts noted that, in clinical practice, clinicians may wish to administer nivolumab to R1 patients; however, they acknowledged that expansion of nivolumab to R1 patients is out of the scope of this review.
Assessing Response to Treatment
Given that nivolumab is an adjuvant therapy, the clinical experts indicated that improved DFS is the desired outcome. Overall survival can be supportive. Scheduled CT scans every 3 to 6 months while on treatment can be used to determine if a patient has a recurrence and is therefore no longer benefiting from nivolumab. Improved DFS over placebo is considered a clinically meaningful response to treatment. According to the clinical experts, outside of a clinical trial, these patients do not undergo routine imaging for follow-up or surveillance. Follow-ups for clinical symptoms of relapse and investigations tend to be done at that time. Some clinicians may do bloodwork for ferritin or B12 to monitor for iron deficiency and other nutritional issues. Clinically, patients are not followed in the same way as they are in a clinical trial. The rationale for the differing approaches is that, because treatment for asymptomatic metastatic disease does not confer a survival benefit and likely will affect quality of life, it is better to first determine whether there are symptoms and then, if there is metastatic disease, treat at that point. This reduces the burden on the health care system by reducing the need for imaging.
The treatment goals include improving DFS, reducing the adverse effects (particularly long-term toxicity, given that it is a curative treatment), improving or maintaining HRQoL, and improving OS.
Discontinuing Treatment
The clinical experts indicated that administration of nivolumab should continue for 17 cycles (with a maximum dose delay of 10 weeks as per the trial protocol) and be discontinued early if evidence confirms disease recurrence or unacceptable toxicity.
Prescribing Conditions
The clinical experts indicated that nivolumab should be prescribed at outpatient oncology clinics. Treatment should be supervised and delivered in institutions by staff trained in chemotherapy delivery.
Additional Considerations
According to the clinical experts, adjuvant treatment with nivolumab for this population represents a major advance in the care of EC and GEJC patients. There is no adjuvant treatment for this population and nivolumab fills a major unmet need.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by 1 clinician group.
The Ontario Health (Cancer Care Ontario) Gastrointestinal Drug Advisory Committee recognized the unmet need in the current treatment algorithm for completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT and for whom the only option is post-operative surveillance. The clinician group indicated that this patient population has a high risk of recurrence that is associated with high mortality and poor quality of life. The clinician group indicated that patients should be offered nivolumab if they meet the eligibility criteria of the clinical trial and noted that outpatient chemotherapy-suite settings were appropriate treatment settings for patients. Prolonged life, delayed disease progression, reduced severity of symptoms, minimized adverse effects, and improved quality of life were identified as the most important goals of treatment. The clinician group also emphasized that toxicity and recurrence are factors that should be considered when deciding whether to discontinue treatment. Last, the clinician group described nivolumab as a new standard of care for this patient population.
The original clinician group input is presented in Appendix 2.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation.
Provincial Advisory Group implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Implementation considerations and issues | Clinical experts’ responses |
|---|---|
Relevant comparators | |
The comparator is appropriate as patients currently remain on active surveillance after neoadjuvant chemoradiation and surgery. | No response required. For CADTH pan-Canadian Oncology Drug Review Expert Review Committee consideration. |
Considerations for initiation of therapy | |
In CheckMate 577, patients were randomized to receive either nivolumab or placebo within 4 to 16 weeks after surgery. What is considered the maximum time frame following surgical resection to initiate nivolumab? | A significant benefit was observed for the nivolumab arm up to 16 weeks post-surgery. Although there are no data to support a maximum time, 16 weeks could be considered; it would also be reasonable for physician discretion to play a role in timing. |
The PAG noted that pembrolizumab for the first-line treatment of locally advanced unresectable or metastatic esophageal or esophagogastric junction cancer is also under CADTH review. The PAG emphasized that in other solid tumours (e.g., lung, melanoma), patients are eligible for downstream PD-1/PD-L1 inhibitors provided that disease recurrence (whether locoregional or distant) occurs more than 6 months from the last dose of an adjuvant PD-1/PD-L1 inhibitor. Can the same principle be applied in this setting? | Data for first-line therapy are only now emerging, as PD-1/PDL-1 inhibitors have only recently been added to the treatment algorithm for metastatic esophageal cancer. The clinical experts noted that the 6-month window for rechallenge or re-treatment is based on expert opinion as opposed to clinical trial data. While acknowledging the optimal treatment for patients who progress on or after single immunotherapy is not known, for consistency it would be reasonable to consider rechallenge or re-treatment if a patient relapsed after more than 6 months. |
Considerations for discontinuation of therapy | |
Although CheckMate 577 did not permit dose modifications due to toxicity, nivolumab could be interrupted or delayed for a maximum of 6 weeks during the first 16 weeks or for a maximum of 10 weeks during the remainder of the treatment period. If treatment interruptions occur, should the remainder of the doses be given even if it will take more than a year to deliver the treatments, provided there has been no disease progression in between? For example:
| The clinical experts noted that in both scenarios, a 5-month delay goes beyond the window of dose delay and therefore treatment should be discontinued. The clinical experts support treatment duration and delays as per the CheckMate 577 protocol for treatment duration and delays should be followed: patients are permitted to receive 52 weeks of nivolumab (as this allows for dose administration every 2 weeks or every 4 weeks) with a maximum delay of 10 weeks.) |
Consideration for prescribing therapy | |
The PAG noted that jurisdictions will implement weight-based dosing up to a cap, similar to other immunotherapy policies (i.e., nivolumab 3 mg/kg up to 240 mg every 2 weeks for the first 16 weeks followed by nivolumab 6 mg/kg up to 480 mg every 4 weeks beginning at week 17). | The PAG’s pragmatic weight-based dosing does offer a cap approach. The clinical experts note PAGs dosing approach for this indication is not supported by evidence from a phase III clinical trial. |
Generalizability | |
Eligibility criteria for CheckMate 577 included patients with an ECOG PS of 0 or 1. Patients with an ECOG PS greater than 1 were excluded from the trial. Can nivolumab use be extended to patients with an ECOG PS greater than 1? | Although not supported by clinical trial evidence, the clinical experts support extension to select patients with an ECOG PS of 2 is acceptable. |
The PAG noted that the current standard of care after surgery is surveillance. For patients who are already in active surveillance, is there a maximum time frame following surgical resection to allow such patients access to nivolumab? | As noted above, the clinical experts highlighted that although there is are no data to support a maximum time, 16 weeks could be considered;, it would also be reasonable for physician discretion to play a role in such decisions. |
Funding algorithm | |
The PAG noted that the current standard of care after surgery is surveillance and that pembrolizumab for the first-line treatment of locally advanced unresectable or metastatic esophageal or esophagogastric junction cancer is also under CADTH review. Do you expect that nivolumab would impact the treatment paradigm such that surveillance and subsequent lines of therapy (i.e., in the locally advanced unresectable or metastatic esophageal or esophagogastric junction setting) will be impacted? | Nivolumab would represent a new standard of care for adjuvant therapy for patients who do not achieve a pathologic complete response following neoadjuvant CRT, as nivolumab is the first adjuvant therapy based on phase III evidence that has demonstrated a significant DFS. It will affect the future paradigm if pembrolizumab and/or nivolumab is approved in the first-line metastatic patients who receive nivolumab in the adjuvant setting and progress or relapse within 6 months may not warrant re-treatment with a PD-1/PD-L1 inhibitor. |
System and economic Issues | |
The manufacturer estimates a 3-year pan-Canadian budget of $53.7 million. The market share uptake is predicted to be 50%, 65%, and 80% respectively, in years 1 to 3. The uptake is likely to be much more rapid because nivolumab will become the new standard of care for an aggressive disease that is associated with a high risk of recurrence. | Refer to the CADTH Pharmacoeconomic Report. |
DFS = disease-free survival; ECOG PS = Eastern Cooperative Oncology Group Performance Status; PAG = Provincial Advisory Group; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1.
Clinical Evidence
The clinical evidence included in this review of nivolumab is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor (if submitted) and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of nivolumab (10 mg nivolumab /mL, 40 mg and 100 mg single-use vials, IV infusion) for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Completely resected esophageal or gastroesophageal junction cancer patients who have residual pathologic disease following prior neoadjuvant CRT Subgroups
|
Intervention |
|
Comparators |
|
Outcomes | Efficacy outcomes
Harm outcomes
|
Study design | Published and unpublished phase III and IV randomized controlled trials |
AEs = adverse event; PD-L1 = programmed death ligand 1; SAE = serious adverse event; WDAE = withdrawal due to adverse event; ypN = pathologic lymph node stage assessed after preoperative therapy; ypT = pathologic tumour stage assessed after preoperative therapy.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies checklist.27
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Patient Headings), and keywords. The main search concepts were nivolumab for the adjuvant treatment of completely resected esophageal or gastroesophageal junction cancer. Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 3 provides detailed search strategies.
The initial search was completed on August 5, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on December 1, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.28 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 3 provides more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for network meta-analyses dealing with EC or GEJC was run in MEDLINE All (1946–) on August 5, 2021. No limits were applied to the search.
Findings From the Literature
One study (CheckMate 577)29 was identified from the literature for inclusion in the systematic review (Figure 1). The included study CheckMate 577 presented in 2 documents2,29 is summarized in Table 6. A list of excluded studies and reasons for exclusion is presented in Appendix 4.
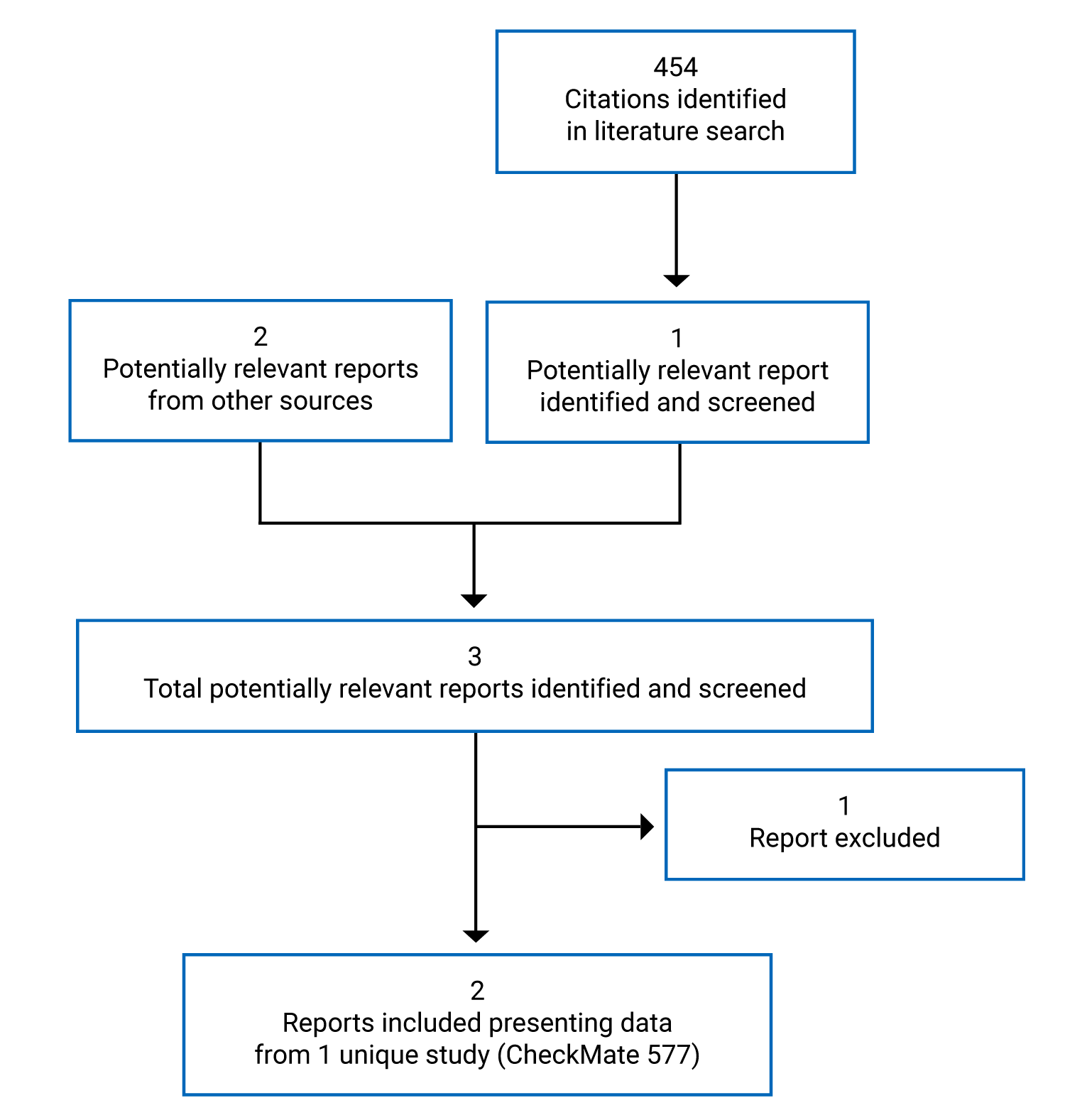
Table 6: Details of Included Studies
Study design | Description in the CheckMate 577 study |
|---|---|
Designs and populations | |
Study design | Double-blind, multi-centre, phase III, parallel, placebo-controlled randomized controlled trial |
Locations | 170 sites in 29 countries (Canada, the US, UK, and Australia, and 25 other countries in Europe, South America and Asia) |
Patient enrolment dates | July 2016 to August 2019a |
Randomized (N) | 794 |
Inclusion criteria | Target population:
|
Exclusion criteria |
|
Drugs | |
Intervention | Nivolumab 240 mg every 2 weeks IV infusion over 30 minute for 16 weeks, followed by 480 mg every 4 weeks intravenously until disease progression or unacceptable toxicity for a total treatment duration of 1 year |
Comparator(s) | Placebo IV infusion over 30 minutes with the same dosing schedule as nivolumab |
Duration | |
Phase | |
Run-in (screen) | |||||||||||||||||||||||| |
Double-blind | Up to 1 year |
Follow-up | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Outcomes | |
Primary end point | Disease-free survival |
Secondary and exploratory end points | Secondary
Exploratory
|
Notes | |
• The study is ongoing, with an estimated study completion date of October 11, 2025 • |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| •||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |
Publications | Kelly (2021)29 |
AJCC = American Joint Committee on Cancer; CRT = chemoradiotherapy; CTLA4 = cytotoxic T-lymphocyte-associated protein 4; DMFS = distant metastasis-free survival; EC = esophageal cancer; ECS = esophageal cancer subscale; EQ-5D-3L = EuroQol 5-Dimensions 3-Levels questionnaire; ESMO = European Society for Medical Oncology; FACT-E = Functional Assessment of Cancer Therapy–Esophageal; FACT-G7 = Functional Assessment of Cancer Therapy–General 7 items; F/U = follow-up; GEJ = gastroesophageal junction; GEJC = gastroesophageal junction cancer; NCCN = National Comprehensive Cancer Network; pCR = pathological complete response; PFS2 = progression-free survival after subsequent systemic therapy; PD-L1 = programmed death ligand 1; PD-L2 = programmed death ligand 2; Q = quarter; ypT1 = pathologic tumour stage 1; ypN1 = pathologic lymph node stage 1.12
Note: Two additional relevant reports or documents (Health Canada reviewer’s report30 and the sponsor’s submission3) are also included in the review.
aEnrolment period was approximately 37 months, from July 14, 2016, to August 2019. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Source: Clinical Study Report for CheckMate 577,2 submission,3 Kelly (2021),29 and the clinical trial registry.31
Description of Study
CheckMate 577 is an ongoing, phase III, randomized, double-blind, placebo-controlled, multi-centre superiority study comparing nivolumab with placebo for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT.2
The trial was conducted in 170 sites in 29 countries (Canada, the US, UK, Australia, and 25 other countries in Europe, South America, and Asia). The key characteristics of the study design are summarized in Table 6 and Figure 2.
The primary objective of this study was to compare DFS in patients with resected EC or GEJC who were treated with nivolumab versus those who received placebo. The secondary objective was to compare OS in the nivolumab arm versus the placebo arm. The main exploratory objectives were to assess the overall safety and tolerability of the study treatments and patient-reported outcomes including DMFS, EQ-5D-3L index and VAS, and patient’s cancer-related quality of life using the FACT-E questionnaire and selected components, including the ECS, FACT-G, and FACT-G7.
A total of 1,085 patients were screened, with 794 patients randomized in a 2:1 ratio to receive nivolumab (n = 532) or placebo (n = 262). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Randomization was stratified by the following 3 factors: histology (squamous versus adenocarcinoma), ypN (positive [≥ ypN1] versus negative [ypN0]) and tumour cell PD-L1 status (≥ 1% versus < 1% or indeterminate or non-evaluable). The first patient was randomized on July 14, 2016, and the last patient was enrolled in August 2019. A total of 792 patients received at least 1 dose of nivolumab or placebo as assigned. Two patients in the placebo arm did not receive the treatment.
Pre-specified interim analysis results (data cut-off date of July 3, 2020) for the primary outcome of DFS was provided in this submission. The sponsor indicated that the interim DFS results were considered final because the DFS interim analysis met the pre-specified statistical significance criteria.3
Figure 2: Study Design Schematic
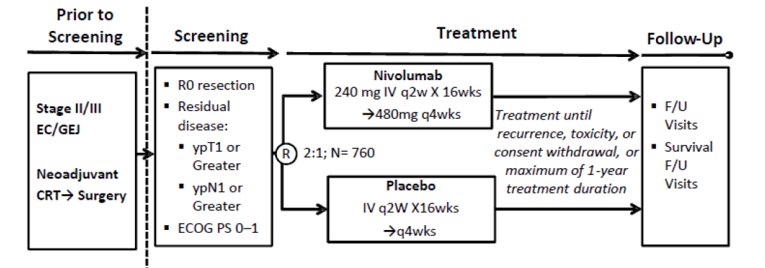
CRT = chemoradiotherapy; EC = esophageal cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; F/U = follow-up; GEJ = gastroesophageal junction cancer; IV = IV; q2w = every 2 weeks; q4w = every 4 weeks; R0 = complete resection; wks = weeks; ypT1 = pathologic tumour stage 1 assessed after pre-operative therapy; ypN1 = pathologic lymph node stage 1 assessed after pre-operative therapy.12
Source: Clinical Study Report for CheckMate 577.2
Populations
Inclusion and Exclusion Criteria
Eligible patients were adults (≥ 18 years old) with stage II or stage III EC and GEJC who completed neoadjuvant CRT followed by complete resection (R0), and were rendered free of disease (defined as no vital tumour present within 1 mm of the proximal, distal, or circumferential resection margins [R1]). Other key inclusion criteria were residual pathological disease (i.e., did not achieve pathological complete response to CRT) with a ypT of at least 1 or a ypN of 1 in the resected specimens, an ECOG PS score of 0 or 1, and a complete resection performed within 4 to 16 weeks before randomization. Disease-free status was to be documented by a complete physical examination and imaging studies (CT and/or MRI scan of chest and abdomen) within 4 weeks before randomization. The main exclusion criteria were patients with stage IV resectable EC or GEJC, and cervical esophageal carcinoma. Inclusion and exclusion criteria are described in more detail in Table 6.
Baseline Characteristics
Main baseline demographics and disease characteristics in all randomized patients are summarized in Table 7. All key baseline demographics and disease characteristics appeared to be balanced between the nivolumab and placebo arms, except for disease stage. The proportion of patients with stage III disease was slightly higher in the nivolumab arm (66.0%) than that in the placebo arm (62.2%). The proportion of patients with ypT1 was slightly higher in nivolumab arm (15.6%) than in the placebo arm (12.6%). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
The median age was 62.0 years (range = 26 to 86 years). Patients either had a baseline ECOG PS of 0 (58.4%) or 1 (41.6%). The majority of patients were male (84.5%) and White (81.6%). A total of 32.1% of patients were from US or Canada, 38.2% of patients were from Europe, 13.4% were from Asia, and 16.4% were from the rest of the world. Among the study population, 59.8% had EC, while 40.2 had GEJC at diagnosis, 64.7% had stage III disease, and 35.0% had stage II disease at initial diagnosis; 70.9% had histological confirmation of adenocarcinoma and 29.0% had squamous cell carcinoma; 93.7% had a positive tumour stage of at least ypT1 and 5.9% of patients had a negative tumour stage (ypT0); and 57.6% had a positive ypN and 42.3% of patients had a negative ypN. Baseline PD-L1 expression among patients was as follows: 71.8% with 1%, 16.2% with 1% or more, and 12.0% with indeterminate or non-evaluable expression. The majority (95%) of patients’ baseline PD-L1 status was determined from tumour tissues after completion of CRT, while 5% of patients’ baseline PD-L1 status was determined from the tumour tissues before CRT.
Table 7: Summary of Baseline Demographic and Disease Characteristics (All Randomized Patients)
Characteristic | Description in the CheckMate 5772 study | |
|---|---|---|
Nivolumab (N = 532) | Placebo (N = 262) | |
Age (years) | ||
Mean | 60.8 | 59.9 |
Median (minimum to maximum) | 62.0 (26 to 82) | 61.0 (26 to 86) |
< 65, n (%) | 333 (62.6) | 174 (66.4) |
≥ 65, n (%) | 199 (37.4) | 88 (33.6) |
Sex, n (%) | ||
Male | 449 (84.4) | 222 (84.7) |
Female | 83 (15.6) | 40 (15.3) |
Race, n (%) | ||
White | 432 (81.2) | 216 (82.4) |
Black or African-American | 7 (1.3) | 2 (0.8) |
Asian | 83 (15.6) | 34 (13.0) |
Other | 10 (1.9) | 7(2.7) |
Country by geographic region, n (%) | ||
|||||||||||||||||||| | |||||| | |||||| |
|||||||||||||||||||| | |||||| | |||||| |
Europe | 202 (38) | 101 (38.5) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||| | |||||| | |||||| |
|||||||||||||||||||| | |||||| | |||||| |
|||||| | |||||| | |||||| |
|||||||||||||||||||| | |||||| | |||||| |
Baseline ECOG PS, n (%) | ||
0 | 308 (57.9) | 156 (59.5) |
1 | 224 (42.1) | 106 (40.5) |
Disease at initial diagnosis, n (%) | ||
EC | 320 (60.2) | 155 (59.2) |
GEJC | 212 (39.8) | 107 (40.8) |
Disease stage at initial diagnosis, n (%) | ||
Stage I | 0 | 0 |
Stage II | 179 (33.6) | 99 (37.8) |
Stage III | 351 (66.0) | 163 (62.2) |
Stage IV | 0 | 0 |
Not reported | 2 (0.4) | 0 |
Disease at study entry, n (%) | ||
EC | 311 (58.5) | 151 (57.6) |
GEJC | 221 (41.5) | 111 (42.4) |
Histology, n (%) | ||
Adenocarcinoma | 376 (70.7) | 187 (71.4) |
Squamous cell carcinoma | 155 (29.1) | 75 (28.6) |
Other | 1 (0.2) | 0 |
Pathologic classification at study entry: tumour, n (%) | ||
YPT0 | 31 (5.8) | 16 (6.1) |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
Pathologic classification at study entry: nodes, n (%) | ||
YPN0 | 227 (42.7) | 109 (41.6) |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
Unknown | 0 | 1 (0.4) |
Time from complete resection to randomization, n (%) | ||
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
Baseline PD-L1 status based on a 1% cut off, n (%) | ||
≥ 1% | 89 (16.7) | 40 (15.3) |
< 1% | 374 (70.3) | 196 (74.8) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
EC = esophageal cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; GEJC = gastroesophageal junction cancer; PD-L1 = programmed death ligand 1; Q1 = quartile 1; Q3 = quartile 3; SD = standard deviation.
Source: Clinical Study Report for CheckMate 577.2
Interventions
Intervention/comparator: Patients received treatment with either nivolumab monotherapy (N = 532) or placebo (N = 260). Patients in the nivolumab arm received nivolumab 240 mg by IV infusion over 30 minutes every 2 weeks for 16 weeks (cycles 1 through 8) followed by nivolumab 480 mg IV infusion over 30 minutes every 4 weeks beginning at week 17 (2 weeks after the 8th dose, cycles 9 through 17) for a total duration of 1 year. Patients in the placebo arm received placebo by IV infusion over 30 minutes with the same dosing schedule as nivolumab. Treatment was continued until disease recurrence, unacceptable toxicity, or patient withdrawal of consent, with a maximum of 1-year total duration of study treatment. Nivolumab or placebo dose reductions were not permitted for the management of toxicities of individual patients. However, doses of nivolumab and placebo could be interrupted, delayed, or discontinued depending on how well the patient tolerated the treatment. Dosing visits were not skipped, only delayed. The maximum dose delay windows allowed were 42 days (6 weeks) during cycles 1 through 8 and 70 days (10 weeks) during cycles 9 through 17.2 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.3
Dose delays: A total of 226 (42.5%) patients treated with nivolumab and 113 (43.5%) patients treated with placebo experienced a dose delay. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Concomitant treatments: Immunosuppressive agents, immunosuppressive doses of systemic corticosteroids, and any concurrent anti-neoplastic therapy were prohibited during the treatment and follow-up phases (before recurrence) of the study. Patients were permitted to use topical, ocular, intra-articular, intranasal, and inhalational corticosteroids. Adrenal replacement doses of systemic corticosteroids were permitted.
Subsequent cancer therapy during the trial: Of the 532 patients in the nivolumab arm, 157 patients (29.5%) received subsequent therapy, including 123 patients (23.1%) who received subsequent chemotherapy. Of the 262 patients in the placebo arm, 111 (42.4%) received subsequent therapy, including 85 (32.4%) who received subsequent chemotherapy. The most common form of subsequent anticancer therapy was systemic therapy, which occurred in 125 patients (23.5%) in the nivolumab arm and 89 patients (34.0%) in the placebo arm.||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Table 24 in Appendix 5 provides more details.
Outcomes
A list of efficacy outcomes identified in the CADTH review protocol that were assessed in the CheckMate 577 study is presented in Table 8. A detailed discussion on the validity of the outcome measures is provided in Appendix 9.
The primary outcome of CheckMate 577 was DFS, which was defined as the time between the randomization date and the first date of recurrence or death from all causes, whichever occurred first. The secondary outcome was OS. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Distant metastasis-free survival, which was defined as the time between the date of randomization and the date of first distant recurrence or date of death from all causes, whichever occurred first, was an exploratory outcome. Patient-reported and HRQoL outcomes (i.e., EQ-5D-5L, FACT-E, ECS, FACT-G, and FACT-G7) and safety outcomes were also assessed as exploratory outcomes.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome | Summary of outcome in CheckMate 5772 | |
|---|---|---|
Efficacy | ||
DFSa | Primary | DFS was defined as the time between randomization date and first date of recurrence or death from all causes, whichever occurred first. Recurrence is defined as the appearance of 1 or more new lesions, which can be local, regional, or distant in location from the primary resected site (as revealed by imaging or pathology). For patients who remained alive and without recurrence, DFS was censored on the date of last evaluable disease assessment. As the primary definition, patients who started subsequent therapy (radiotherapy, surgery, or systemic therapy) or developed a second primary cancer without recurrence were censored on the last disease assessment date before the start of subsequent therapy or development of second primary cancer. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. |
OS | Secondary | OS is time between the date of randomization and the date of death. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
EQ-5D-3L | Exploratory | Overall health status was assessed using the EQ-5D-3L, which has 2 components: the descriptive system and the VAS. The instrument’s descriptive system consists of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 levels reflecting “no health problems” (level 1), “moderate health problems” (level 2), and “extreme health problems” (level 3). The VAS allows respondents to rate their own current health on a 100-point scale ranging from 0 (“worst imaginable”) to 100 (“best imaginable”) health state. |
FACT-E ECS FACT-G FACT-G7 | Exploratory | The FACT-E includes FACT-G and ECS, which provides a composite measure of general and targeted HRQoL. The 27-item FACT-G assesses symptoms and treatment-related effects affecting physical well-being (PWB; 7 items), social/family well-being (SWB; 7 items), emotional well-being (EWB; 6 items), and functional well-being (FWB; 7 items). The 17-item disease-specific ECS assesses concerns related to swallowing, vocalization, breathing, dry mouth, eating, disrupted sleep due to coughing, stomach pain, and weight loss. Each FACT-E item is rated on a 5-point scale ranging from 0 (not at all) to 4 (very much). Scores for the PWB, FWB, SWB, and EWB subscales can be combined to produce a FACT-G total. Seven of these items constitute the FACT-G7, an abbreviated version of the FACT-G that provides a rapid assessment of general HRQoL in cancer patients. |
DMFS | Exploratory | DMFS was defined as the time between the date of randomization and the date of first distant recurrence or date of death from all causes, whichever occurred first. The distant recurrence was |||||||||||||||||||||||||||||||||||||||||||||||||||||||||| determined by investigator. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. For patients who remained alive and distant recurrence-free, DMFS was censored on the date of last disease assessment ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. |
Harms | ||
Overall safety and tolerability | Exploratory | The assessment of safety was based on frequency of AEs, SAEs, AEs leading to discontinuation of study drug, AEs leading to dose modification (delay/reduction), Notable harms. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. |
AE = adverse event; CRF = case report form; DFS = disease-free survival; DMFS = distant metastasis-free survival; ECS = esophageal cancer subscale; EWB = emotional well-being; EQ-5D-3L = EuroQol 5-Dimensions 3-Levels questionnaire; FACT-E = Functional Assessment of Cancer Therapy–Esophageal; FACT-G = Functional Assessment of Cancer Therapy–General; FACT-G7 = Functional Assessment of Cancer Therapy–General 7 items; FWB = functional well-being; HRQoL = health-related quality of life; OS = overall survival; NR = not reported. PWB = physical well-being; SAE = serious adverse event; SWB = social/family well-being; VAS = visual analogue scale.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Clinical Study Report for CheckMate 577.2
Statistical Analysis
Primary Outcome
Power Calculation
The sample-size determination considered the comparison of the primary outcome of DFS and the secondary outcome of OS (data for OS were not mature for this review and OS is therefore not discussed in this report) between the 2 treatment arms. Disease-free survival was assumed to follow a piecewise exponential distribution, and the HR was modelled as piecewise HRs with ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, with an overall average HR of 0.72. According to the assumptions for DFS, the study required approximately 760 patients to be randomized in a 2:1 ratio to treatment with nivolumab or placebo. At least 440 DFS events were needed to achieve approximately 91% power to detect an average HR of 0.72 with a 2-sided alpha of 0.05. One interim analysis and 1 final analyses for DFS were planned. This sample-size determination accounted for 1 planned DFS interim analysis when at least 85.0% (374) of the DFS events would be observed. The final analysis of DFS was scheduled to take place at the point at which at least 440 DFS events had been observed.
Statistical Test or Model
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. DFS was compared between treatment arms using a 2-sided log rank test, stratified by the 3 randomization stratification factors (PD-L1 status: [≥ 1% versus < 1% or indeterminate or non-evaluable], ypN status (positive [≥ 1] versus negative [0]), and histology [squamous versus adenocarcinoma]). The HR for DFS with its corresponding alpha-adjusted 2-sided 96.4% CI was estimated via a stratified Cox model with the treatment arm as the only covariate in the model. Adjustment on the CI was based on the actual alpha level, which was based in turn on actual DFS events observed ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
One interim DFS analysis was scheduled to take place when at least 85% of all 440 DFS events (374 DFS events) had been observed. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Subgroup Analyses
The influences of baseline demographics and disease characteristics on the treatment effect among all randomized patients were examined by DFS hazard ratios (along with the 95% CIs) using an unstratified Cox model with the treatment arm as the only covariate in the model within each pre-specified subgroup.
||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Secondary Outcome
Overall survival was the secondary outcome of the CheckMate 577 study. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Other Exploratory Outcomes
Patient-reported and HRQoL outcomes, including EQ-5D-3L, ECS, FACT-E, FACT-G, and FACT-G7, were assessed as the exploratory outcomes. The mean scores and mean changes from baseline for these exploratory outcomes were summarized by treatment arm at each assessment time using descriptive statistics. No statistical analysis was performed to test between-group differences.
Safety Outcomes
Only descriptive statistics of safety were presented by treatment arm using version 23.0 of the Medical Dictionary of Regulatory Activities and version 4.0 of the National Cancer Institute Common Terminology Criteria for Adverse Events.
Table 9: Statistical Analysis of Efficacy Outcome for CheckMate 577
Outcome | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
DFS | DFS for each treatment arm was estimated and plotted using the Kaplan–Meier product-limit method. Median DFS was computed using the Kaplan–Meier estimate and a 95% CI for the median was computed based on a log-log transformation of the survivor function. | DFS was compared between treatment arms using a 2-sided log-rank test, stratified by the 3 randomization stratification factors (PD-L1 status: (≥ 1% vs. < 1% or indeterminate or non-evaluable), pathologic lymph node status (positive [≥ ypN1] vs. negative [ypN0]), and histology (squamous vs. adenocarcinoma). The HR for DFS with its corresponding alpha-adjusted 2-sided 96.4% CI was estimated via a stratified Cox model with treatment arm as the only covariate in the model. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; NR = not reported; PD-L1 = programmed death ligand 1; ypN = pathologic lymph node.
Source: Clinical Study Report for CheckMate 5772 and sponsor’s submission.3
Analysis Populations
The efficacy population in CheckMate 577 for the analysis of the primary outcome (DFS) was the intention-to-treat population (i.e., all randomized patients; Table 10).
Results
Patient Disposition
Patient disposition for the CheckMate 577 study is presented in Table 10. Of the 1,085 patients screened, 794 were randomized to receive nivolumab (n = 532) or placebo (n = 262). Of the 794 patients randomized, only 2 in the placebo arm did not receive their assigned treatment (1 requested to discontinue the study treatment and the other no longer met the study eligibility criteria).
At the time of the data cut-off date of July 3, 2020, a total of 742 patients (93.7%) discontinued treatment (n = 501 [94.2%] in the nivolumab arm and n = 241 [92.7%] in the placebo arm). The main reason for discontinuation of treatment was completed treatment (43.0% in the nivolumab arm and 38.1 in the placebo arm, respectively), followed by disease recurrence (28.0% and 43.5%, respectively) and adverse events (10.7% versus 3.1%, respectively). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
The efficacy (intention-to-treat) population included 794 patients, while the safety population included 792 patients.
Table 10: Patient Disposition for Checkmate 577
Category | Nivolumab (N = 532) | Placebo (N = 262) |
|---|---|---|
Screened, N | 1,085 | |
Randomized | 532 | 262 |
Patients treated, n (%)a | 532 (100.0) | 260 (99.2) |
Patients not treated, n (%)a | 0 | 2 (0.8) |
Reason for not being treated, n (%) | ||
Patient request to discontinue study treatment | 0 | 1 (0.4) |
Patient no longer meets study criteria | 0 | 1 (0.4) |
Patients continuing in the treatment period (%)b | 31 (5.8) | 19 (7.3) |
Patients not continuing in the treatment period (%)b | 501 (94.2) | 241 (92.7) |
Reason for not continuing in the treatment period, n (%)b | ||
Completed treatment | 229 (43.0) | 99 (38.1) |
Disease recurrence | 149 (28.0) | 113 (43.5) |
Study drug toxicity | 57 (10.7) | 8 (3.1) |
Death | 1 (0.2) | 0 |
Adverse event unrelated to study drug | 15 (2.8) | 9 (3.5) |
Patient request to discontinue study treatment | 30 (5.6) | 5 (1.9) |
Patient withdrew consent | 12 (2.3) | 4 (1.5) |
Lost to follow-up | 0 | 1 (0.4) |
Poor or non-compliance | 1 (0.2) | 0 |
Other | 7 (1.3) | 2 (0.8) |
|||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | | | | |
ITT, N | 532 | 262 |
PP, N | NA | NA |
Safety, N | 532 | 260 |
ITT = intention to treat; NA = not assessed; PP = per protocol.
aPercentages based on patients randomized.
bPercentages based on patients that were treated.
Source: Clinical Study Report for CheckMate 577.2
Exposure to Study Treatments
The median duration on therapy was similar between the nivolumab and placebo arms. As of the July 3, 2020, data cut-off date, the median treatment durations were 10.14 months (range = < 0.1 to 14.2) and 8.99 months (range = < 0.1 to 15) in the nivolumab and placebo arms, respectively. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Table 25 in Appendix 5 provides more details.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below. Appendix 5 provides more detailed efficacy data.
Disease-Free Survival
At the DFS interim analysis (in the intention-to-treat population) as of the July 3, 2020, data cut-off date, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. A total of 396 DFS events were observed (|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||). Nivolumab demonstrated a statistically significant improvement in DFS compared with placebo, with an HR of 0.69 (96.4% CI, 0.56 to 0.86; P value = 0.0003) (Table 11 and Figure 3).
The observed median DFS was longer in the nivolumab arm (22.41 months; 95% CI, 16.62 to 34.00) compared with the placebo arm (11.04 months; 95% CI, 8.34 to 14.32) (Table 11).
The DFS rates at 6 months were higher in the nivolumab arm (72.3%; 95% CI, 68.2 to 76.0) compared with the placebo arm (63.4%; 95% CI, 57.2 to 69.0) (Table 11).
As the DFS interim analysis met the pre-specified statistical significance criteria; it was considered the final analysis by the sponsor.3
Table 11: Overall Summary of Efficacy — ITT (All Randomized Patients)
Outcome | CheckMate 577 | |
|---|---|---|
Nivolumab (N = 532) | Placebo (N = 262) | |
Disease-free survival | ||
Events, n (%) | |||||||||||||||||| | |||||||||||||||||| |
Median DFS (95% CI), monthsa | 22.41 (16.62 to 34.00) | 11.04 (8.34 to 14.32) |
HRb (95% CI) or (96.4% CI) | 0.69 (0.56 to 0.85) or (0.56 to 0.86) | |
P valuec | 0.0003 | |
6-month DFS rates (95% CI), %a | 72.3 (68.2 to 76.0) | 63.4 (57.2 to 69.0) |
Overall survivald | NE (NE to NE) | |
DMFS | ||
Events, n (%) | |||||||||||||||||| | |||||||||||||||||| |
Median DMFS (95% CI), monthsa | 28.32 (21.26 to NA) | 17.61 (12.45 to 25.4) |
HRb (95% CI) | 0.74 (0.60 to 0.92) | |
6-month DMFS rates (95% CI), %a | |||||||||||||||||| | |||||||||||||||||| |
CI = confidence interval; DFS = disease-free survival; DMFS = distant metastasis-free survival; HR = hazard ratio; NA = not available; NE = not estimated; PD-L1 = programmed cell death ligand 1.
aBased on Kaplan–Meier estimates.
bStratified Cox proportional hazards model. Hazard ratio is nivolumab over placebo. This model was stratified by PD-L1 status (≥ 1% vs. < 1% or indeterminate or non-evaluable), pathologic lymph node status (positive [≥ ypN1] vs. negative [ypN0]) and histology (squamous vs. adenocarcinoma) as entered into the interactive response technology.
cLog-rank test stratified by PD-L1 status (≥ 1% vs. < 1% or indeterminate or non-evaluable), pathologic lymph node status (positive [≥ ypN1] vs. negative [ypN0]) and histology (squamous vs. adenocarcinoma). Twi-sided P values from stratified log-rank test. Boundary for statistical significance P value < 0.036. |||||||||||||||||||||||||||||||||||.
dThe study is ongoing. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Source: Clinical Study Report for CheckMate 577.2
Figure 3: Kaplan–Meier Plot of Disease-Free Survival (All Randomized Patients)
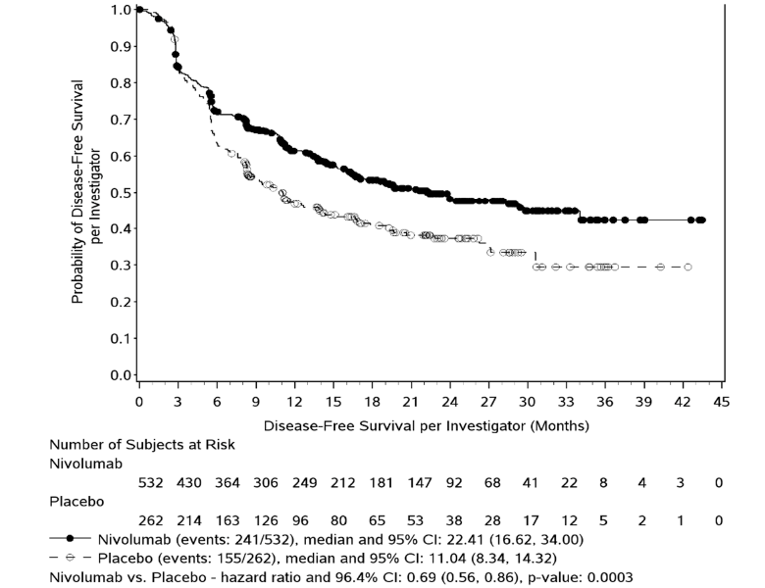
CI = confidence interval.
Source: Clinical Study Report for CheckMate 577.2
DFS Subgroup Analysis
In general, the pre-specified subgroup analyses for DFS were consistent with the DFS primary analysis results of an HR of < 1, with the exception of subgroups of patients 65 years of age and older, females, gastroesophageal junction cancer, ypT3/ypT4, ypN0, PD-L1 levels of 1% or greater, and indeterminate and non-evaluable, as well as stage II disease at initial diagnosis (Table 12, Figure 10, Figure 11 and Figure 12 in Appendix 5). The HRs were 0.61 (95% CI, 0.42 to 0.88) and 0.75 (95% CI, 0.59 to 0.96) in patients with squamous cell carcinoma and patients with adenocarcinoma, respectively; 0.67 (95% CI, 0.53 to 0.86) in positive (≥ ypN1) and 0.74 (95% CI, 0.51 to 1.06) in negative (ypN0) patients, respectively; and 0.75 (95% CI, 0.45 to 1.24) in patients with PD-L1 levels of 1% or greater and 0.73 (95% CI, 0.57 to 0.92) in patients with PD-L1 levels of less than 1%, respectively (Table 12).
Table 12: Disease-Free Survival Subgroups Analysis
Subgroup | CheckMate 577 | ||
|---|---|---|---|
Nivolumab (N = 532) | Placebo (N = 262) | HR (95% CI)b | |
Disease-free survivala | |||
Age, n/N (%) | |||
< 65 years | |||||||| | |||||||||||| | 0.65 (0.51 to 0.84) |
≥ 65 years | |||||| | |||||| | 0.80 (0.57 to 1.12) |
Sex, n/N (%) | |||
Male | |||||||||||||||||| | |||||||||||||||||| | 0.73 (0.59 to 0.91) |
Female | |||||||||||||||||| | |||||||||||||||||| | 0.59 (0.35 to 1.00) |
ECOG Performance Status, n/N (%) | |||
0 | |||||||| | |||||||||| | 0.73 (0.56 to 0.96) |
1 | |||||||| | |||||||||| | 0.66 (0.48 to 0.89) |
Histology, n/N (%) | |||
Adenocarcinoma | |||||||| | |||||||||||| | 0.75 (0.59 to 0.96) |
Squamous cell carcinoma | |||||| | |||||| | 0.61 (0.42 to 0.88) |
Primary tumour site, n/N (%) | |||
Esophagus | |||||||| | |||||||||| | 0.61 (0.47 to 0.78) |
Gastroesophageal junction cancer | |||||||| | |||||||||| | 0.87 (0.63 to 1.21) |
Pathological tumour status n/N (%) | |||
ypT0, | |||||||||||||||||| | |||||||||||||||||| | 0.35 (0.15 to 0.82) |
ypT1/ypT2 | |||||||||||||||||| | |||||||||||||||||| | 0.60 (0.44 to 0.83) |
ypT3/ypT4 | |||||||||||||||||| | |||||||||||||||||| | 0.84 (0.64 to 1.11) |
Unknown | |||||||||||||||||| | |||||||||||||||||| | NA |
Pathologic lymph node status, n/N (%) | |||
ypN0 | |||||||||||||||||| | |||||||||||||||||| | 0.74 (0.51 to 1.06) |
≥ ypN1 | |||||||||||||||||| | |||||||||||||||||| | 0.67 (0.53 to 0.86) |
|||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Baseline PD-L1 status, n/N(%) | |||
PD-L1 ≥ 1% | |||||||||||||||||| | |||||||||||||||||| | 0.75 (0.45 to 1.24) |
PD-L1 < 1% | |||||||||||||||||| | |||||||||||||||||| | 0.73 (0.57 to 0.92) |
Indeterminate or non-evaluable | |||||||||||||||||| | |||||||||||||||||| | 0.54 (0.27 to 1.05) |
Disease stage at initial diagnosis, n/N(%) | |||
Stage II | |||||||||||||||||| | |||||||||||||||||| | 0.72 (0.51 to 1.02) |
Stage III | |||||||||||||||||| | |||||||||||||||||| | 0.68 (0.53 to 0.88) |
|||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; NA = not analyzed; PD-L1 = programmed death ligand 1; ypT0–T4/ypN0 to N1 = pathologic tumour/lymph node stage assessed after preoperative neoadjuvant therapy.
aDisease-free survival per investigator in pre-defined subsets summary (all randomized patients).
bBased on a Kaplan–Meier estimate. Unstratified Cox proportional hazard model. The HR, nivolumab over placebo, is not computed for subset (except age and sex) category with fewer than 10 patients per treatment arm.
Source: Clinical Study Report for CheckMate 5772 and the sponsor’s submission.3
||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||| | |||||||||||| | |
|---|---|---|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
n/N (%) | |||||||||||||||||| | |||||||||||||||||| |
Median DFS (months)a (95% CI) | |||||||||||||||||| | |||||||||||||||||| |
HR (95% CI)/(96.4% CI) | |||||||||||||||||| | |
P valuec | |||||||||||||||||| | |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
n/N (%) | |||||||||||||||||| | |||||||||||||||||| |
Median DFS (months)a (95% CI) | |||||||||||||||||| | |||||||||||||||||| |
HR (95% CI)/(96.4% CI) | |||||||||||||||||| | |
P valuec | |||||||||||||||||| | |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
n/N (%) | |||||||||||||||||| | |||||||||||||||||| |
Median DFS (months)a (95% CI) | |||||||||||||||||| | |||||||||||||||||| |
HR (95% CI)/(96.4% CI) | |||||||||||||||||| | |
P valuec | |||||||||||||||||| | |
Source: Clinical Study Report for CheckMate 577.2
To further support a clinical benefit of adjuvant nivolumab, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Overall Survival
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Health-Related Quality of Life
Detailed findings for these patient-reported and HRQoL life outcomes (ECS, FACT-E, FACT-G7, FACT-G, and EQ-5D-3L) are summarized in Table 14. Additional data on the EQ-5D-3L by level are presented in Table 15. Patients in both arms appeared to experience no deterioration in HRQoL during the treatment period as measured by the ECS, FACT-E, FACT-G7, FACT-G, and EQ-5D-3L. The VAS and utility index scores for the EQ-5D-5L are presented in Figure 4 and Figure 5, respectively. These findings suggest that HRQoL is maintained during the treatment period.2
Outcome | N | Mean 95% CI | N | Mean 95% CI |
|---|---|---|---|---|
|||| | ||||
|||| | |||| | |||||||||||||||||||| | | | |||||||||||||| |
|||| | | | |||||||||||||||||| | | | |||||||||||||| |
|||| | | | |||||||||||||| | | | |||||||||| |
|||| | ||||
Baseline | |||| | |||||||||||||||||||||||||| | |||| | |||||||||||||||||||||| |
|||| | |||| | |||||||||||||||||||||||||||| | |||| | |||||||||||||||||||||| |
Change from baseline | |||| | |||||||||||||| | |||| | |||||||||||| |
|||||||||| | ||||
Baseline | |||| | |||||||||||||||||||| | |||| | |||||||||||||| |
|||| | |||| | |||||||||||||||||||| | |||| | |||||||||||||| |
Change from baseline | |||| | |||||||||||||| | |||| | |||||||| |
|||||||| | ||||
Baseline | |||| | |||||||||||||||||||| | |||| | |||||||||||||| |
|||| | |||| | |||||||||||||||||||| | |||| | |||||||||||||| |
Change from baseline | |||| | |||||||||||||| | |||| | |||||||||| |
|||||||| | ||||
Baseline | |||| | |||||||||||| | |||| | |||||| |
|||| | |||| | |||||||||||| | |||| | |||||||| |
Change from baseline | |||| | |||||||||| | |||| | |||||| |
|||||||||||||||||||||||||||||||||||| | ||||
Baseline | |||| | |||||||||||||||||||| | |||| | |||| |
|||| | |||| | |||||||||||||||||||| | |||| | |||| |
Change from baseline | |||| | |||||||||||||||||||||| | |||| | |||| |
Source: Clinical Study Report for CheckMate 577.2
Outcome | N | |||||| | |||||| | |||||| | N | |||||| | |||||| | |||||| |
|---|---|---|---|---|---|---|---|---|
|||||||||||||||||||||||||| | ||||||||
Baseline | | | |||||||||| | |||||| | ||| | | | |||||||||| | |||||| | ||| |
|||||| | | | |||||| | |||| | | | | | |||||| | ||| | | |
|||||||||||||||||||||||||||||| | ||||||||
Baseline | | | |||||||||| | |||| | ||| | | | |||||||||| | ||| | | |
|||||| | | | |||||| | ||| | | | | | |||||| | ||| | | |
|||||||||||||||||||||||||| | ||||||||
Baseline | | | |||||||||| | |||||||||| | |||| | | | |||||||||| | |||||| | ||| |
|||||| | | | |||||| | |||||| | | | | | |||||| | |||| | | |
|||||||||||||||||||||| | ||||||||
Baseline | | | |||||||||| | |||||||||| | ||| | | | |||||||||| | |||||||||| | ||| |
|||||| | | | |||||| | |||||| | ||| | | | |||||| | |||| | ||| |
|||||||||||||||||||||||||| | ||||||||
Baseline | | | |||||||||| | |||||||||| | ||| | | | |||||||||| | |||||| | | |
|||||| | | | |||||| | |||||| | ||| | | | |||||| | |||| | | |
Source: Clinical Study Report for CheckMate 577.2

Note: This figure has been redacted at the request of the sponsor.
Source: CheckMate Clinical Study Report for CheckMate 577.2

Note: This figure has been redacted at the request of the sponsor.
Source: Clinical Study Report for CheckMate 577.2
Distant Metastasis-free Survival
At the time of data cut-off (July 3, 2020), |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| The median DMFS was numerically longer in the nivolumab arm (28.32 months; 95% CI, 21.26 to not available) compared with the placebo arm (17.61 months; 95% CI, 12.45 to 25.40), with an HR of 0.74 (95% CI, 0.60 to 0.92) (Table 11 and Figure 6).
Figure 6: Kaplan–Meier Plot of Distant Metastasis-Free Survival (All Randomized Patients)
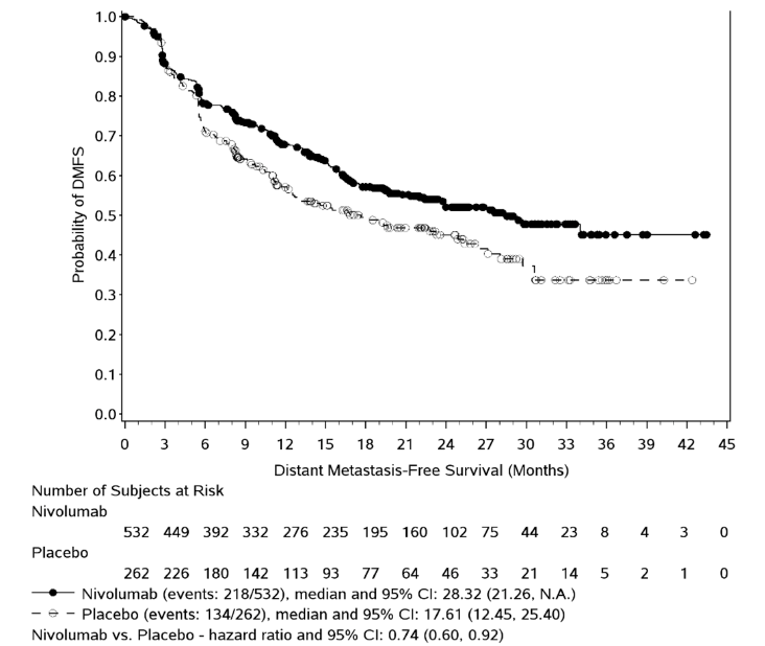
CI = confidence interval; NA = Not available.
Note: Statistical model for hazard ratio: stratified Cox proportional hazard model. Symbols represent censored observations.
Source: Clinical Study Report for CheckMate 577 for CheckMate 577.2
To further support clinical benefit of adjuvant nivolumab, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Symptom Severity
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Other Outcomes Not Assessed as a Clinical Outcome But Used in the Pharmacoeconomic Model
Time to Recurrence
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Harms
Only those harms identified in the review protocol are reported below. Table 16 provides more detailed data.
Adverse Events
A total of 95.9% of patients in the nivolumab arm and 93.5% of patients in the placebo arm experienced at least 1 adverse event, whereas a total of 34.4% of patients in the nivolumab arm and 32.3% patients in the placebo arm experienced an adverse event of grade 3 or worse. Table 16
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. More patients treated with nivolumab experienced treatment-related adverse events compared with patients in the placebo arm (70.7% versus 45.8%, respectively).2 Table 26 in Appendix 5).
Serious Adverse Events
A total of 29.7% of patients in nivolumab arm and 30.0% of patients in placebo arm experienced an SAE.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||). More patients treated with nivolumab experienced treatment-related adverse events compared with patients in the placebo arm (7.5% versus 2.7%)2 (Table 27 in Appendix 5).
Mortality
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Withdrawals Due to Adverse Events
All-causality adverse events leading to study drug discontinuation occurred in 12.8% of patients in the nivolumab arm versus 7.7% in the placebo arm. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Notable Harms
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 16: Summary of Harms in CheckMate 577
Adverse event | Nivolumab (N = 532) | Placebo (N = 260) | ||
|---|---|---|---|---|
Any grade | Grade 3 to 4 | Any grade | Grade 3 to 4 | |
Patients with at least 1 AE,a n (%) | 510 (95.9) | 183 (34.4) | 243 (93.5) | 84 (32.3) |
Patients with at least 1 treatment related AE, n (%) | 376 (70.7) | 71 (13.3) | 119 (45.8) | 15 (5.8) |
Patients with at least 1 SAE, n (%) | 158 (29.7) | 107 (20.1) | 78 (30.0) | 53 (20.4) |
Patients with at least 1 treatment-related SAE, n (%) | 40 (7.5) | 29 (5.5) | 7 (2.7) | 3 (1.2) |
Patients with AEs leading to DC from the treatment, n (%) | 68 (12.8) | 38 (7.1) | 20 (7.7) | 16 (6.2) |
Patients with a treatment-related AE leading to DC from the treatment | 48 (9.0) | 26 (4.9) | 8 (3.1) | 7 (2.7) |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | ||
|||||||||||||||||||||||| | ||||
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
AE = adverse event; DC = discontinuation; SAE = serious adverse event.
aReported as all-causality AE in the Clinical Study Report. All events occurred within 30 days of the last dose of study drug, unless otherwise indicated.
b||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Clinical Study Report for CheckMate 577.2
To further support a clinical benefit of adjuvant nivolumab, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Critical Appraisal
Internal Validity
The included pivotal study (CheckMate 577) was a well-designed, prospective, multi-centre, double-blind, randomized, parallel, placebo-controlled trial. The study used an appropriate randomization method (i.e., an interactive web response system), and the allocation concealment procedures were clearly described.
Overall, most of the demographic and baseline characteristics were well balanced between arms (Table 7). The key effect or prognostic factors, such as disease (EC versus GEJC), or histology (adenocarcinoma versus squamous cell carcinoma) were also well balanced between arms. Minor imbalances were observed between the 2 study arms in the proportion of patients with stage III disease, ||||||||||||, and patients with PD-L1 levels below 1%; however, the clinical experts consulted for this review stated that these minor imbalances would not likely have affected the comparative study results between the nivolumab and placebo groups.
According to the protocol, the time period between R0 and randomization should be 4 to 16 weeks. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. According to the clinical experts, this small percentage (balanced between arms) of the patients with potential protocol violations was unlikely to have affected the comparative clinical efficacy of nivolumab versus placebo. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. No impact on the comparative clinical efficacy of nivolumab versus the placebo was expected.
Use of immunosuppressive agents, immunosuppressive doses of systemic corticosteroids, and any concurrent antineoplastic therapy as a concomitant treatment was prohibited during the trial. Patients were only permitted the local use of corticosteroids (e.g., topical, ocular, intra-articular, intranasal, and inhalational corticosteroids). However, those local corticosteroids were unlikely to have affected the study efficacy results.
The primary outcome was DFS, which was defined as the time between randomization date and first date of recurrence or death from all causes. Recurrence was defined as the appearance of 1 or more new lesions, which can be local, regional, or distant in location from the primary resected site (as revealed by imaging or pathology). The efficacy measurement was therefore objective and not likely biased by the subsequent systematic therapy. Furthermore, the DFS primary analysis was estimated and plotted using a standard Kaplan–Meier product-limit method. Comparisons of DFS between treatment arms used a 2-sided log-rank test, stratified by the 3 randomization stratification factors (PD-L1 status, pathologic lymph node status, and histology of the cancer). The HR for DFS with its corresponding alpha-adjusted 2-sided CI of 96.4% was estimated by a stratified Cox model with the treatment arm as the only covariate in the model. In addition, various subgroup analysis and sensitivity analysis were supportive of the robustness of the primary analysis for DFS. The reported DFS results are considered final by the sponsor based on interim analysis according to pre-specified stopping criteria. Whether the actual final efficacy results would confirm the interim results remains unknown, although an additional |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Adjuvant nivolumab continued to demonstrate clinically meaningful efficacy versus placebo in patients following neoadjuvant CRT with this longer follow-up.34 Whether the DFS benefit can be transferred to a statistically significant and clinically meaningful OS benefit remains unknown.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Distant metastasis-free survival was assessed as an exploratory outcome. As the DMFS results were confounded by subsequent systematic therapy any interpretation should take this limitation into consideration.
The patient-reported and HRQoL outcomes (ECS, FACT-E, FACT-G7, FACT-G, and EQ-5D-3L) were assessed as exploratory outcomes. No formal statistical analysis was performed to compare the efficacy of the 2 treatment groups. There is a potential risk of bias because of substantial missing data on these outcomes. There also may have been differential recall bias. Overall, the magnitude and direction of the impact of these missing data and recall bias on the patient-reported and HRQoL outcomes are unknown.
Symptom reduction was identified as an outcome in the CADTH review protocol. The symptom severity was not assessed as a separate outcome in the pivotal CheckMate 577 study. However, the severity of symptoms such as pain was assessed in the EQ-5D-3L (Table 15) and ECS (Table 29 in Appendix 7).
External Validity
According to the clinical experts CADTH consulted for this review, the CheckMate 577 study population (completely resected EC or GEJC patients with residual pathologic disease following prior neoadjuvant CRT) is considered reflective of the requested reimbursement population. The following considerations are of importance regarding the external validity of CheckMate 577 study.
Population: Patients with clinical stage I disease were not included in the pivotal study. The clinical experts emphasized that, in clinical practice, most stage I patients would not receive chemoradiation; however, some patients may end up receiving chemoradiation and, in those rare instances, if a patient has residual disease afterward, it may be reasonable to administer nivolumab adjuvant treatment after R0.
Patients with an ECOG PS of 2 or greater were not included in the study. It is uncertain whether the finding can be generalized to patients with an ECOG PS of 2 or greater.
In the pivotal study, patients were eligible to receive either nivolumab or placebo if they had R0 or were surgically rendered free of disease with negative margins on resected specimens defined as no vital tumour present within 1 mm of the proximal, distal or circumferential resection margins. The clinical experts noted that, based on the CheckMate 577 criteria, R1 patients would be excluded, and emphasized that the clinical management of R1 patients may be similar to that of R0 patients, given the lack of available effective treatment options for R1 patients.
Intervention: The Health Canada–recommended dose is 240 mg every 2 weeks or 480 mg every 4 weeks administered as IV infusion over 30 minutes. After completing 16 weeks of therapy, the recommendation dosage is 480 mg every 4 weeks until disease progression or unacceptable toxicity for a total treatment duration of 1 year. In the pivotal CheckMate 577 study,2 nivolumab 480 mg every 4 weeks by IV infusion was not used as initial dose regime for the first 16 weeks. However, the sponsor indicated that, based on the clinical data from CheckMate 577,2 the predicted exposures of nivolumab between recommended dosing regimens and the flat exposure-response relationships in adjuvant EC or GEJC,3 the recommended nivolumab dosing regimen for treatment of EC or GEJC patients in an adjuvant setting is nivolumab 240 mg IV every 2 weeks or 480 mg IV every 4 weeks for 16 weeks, followed by 480 mg intravenously every 4 weeks up for to 1 year.3,26 In addition, the Health Canada reviewer’s report indicated that the dosing regimen for this proposed indication has been previously approved for Opdivo as a monotherapy with other indications.30
Outcome: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| The clinical experts indicated that the DFS interim results represent a clinically meaningful benefit for patients.
Setting: This study was a multinational, multi-centre trial. Among 170 sites in 29 countries that participated, 32.1% participants were from Canada or the US and 38.2% were from Europe.2 The clinical experts indicated that there is no concern that the findings from the pivotal study are not generalizable to Canadian clinical settings.
Indirect Comparisons
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search.
Other Relevant Evidence
Data from the Netherlands Comprehensive Cancer Organization (IKNL) nationwide registry dataset were used to inform the transition from post-recurrence to death as there are no OS data from CheckMate 577, and the IKNL data were applied to both nivolumab and comparator in the economic analysis. To use the IKNL registry dataset, the sponsor matched the CheckMate 577 population with patients diagnosed with esophageal and gastric cancer from the IKNL registry dataset. To facilitate the pharmacoeconomic analysis, a summary of the selection criteria for the IKNL nationwide registry dataset and appraisal of the comparability of the 2 populations (IKNL and CheckMate 577) were performed by CADTH and are provided in Appendix 8.
Discussion
Summary of Available Evidence
The CADTH clinical review report included input from patient groups, clinician groups, clinical experts, and drug programs, and a single pivotal, phase III, randomized controlled trial.
CheckMate 577 is a well-designed ongoing phase III, randomized, double-blind, placebo-controlled, multi-centre, superiority study comparing nivolumab to placebo for the treatment of completely resected EC or GEJC patients who have residual pathologic disease following prior neoadjuvant CRT. A total of 794 patients were randomized in a 2:1 ratio to receive nivolumab (n = 532) or placebo (n = 262). Patients were 18 years of age or older with stage II or III disease. Key baseline demographics and disease characteristics appeared to be balanced between the nivolumab and placebo arms. The primary outcome was DFS, which was defined as the time between randomization date and first date of recurrence or death from all causes, whichever occurred first. Recurrence was defined as the appearance of 1 or more new lesions, which could be local, regional, or distant in location from the primary resected site (as revealed by imaging or pathology). The OS was assessed as the secondary outcome. Other exploratory outcomes were patient-reported HRQoL (ECS, FACT-E, FACT-G7, FACT-G, and EQ-5D-3L) and DMFS, which was defined as the time between the date of randomization and the date of first distant recurrence or date of death from all causes, whichever occurred first. The distant recurrence ratio was determined by the investigator. Local or regional recurrence was not considered as an event for DMFS.
This is an ongoing study with interim results for the primary outcome of DFS. These interim results represented the final DFS analysis, with a data cut-off date of July 3, 2020.
Interpretation of Results
Efficacy
In Canada, EC is ranked 19th among all cancer types based on incidence and 10th based on mortality.1 It is among the cancers with a high proportion of metastatic (stage IV) disease at first diagnosis (39.9%),5 with a 5-year survival rate for all EC patients of 15%.1 Patient and caregiver respondents expressed the need for new and effective therapies that prolong OS, improve quality of life, reduce disease symptoms, and have tolerable side effects, given the poor and short survival rate for most patients with EC.
The clinical experts identified prolonged life and improved HRQoL as the goals of treatment. Similarly, the clinician groups identified prolonged life and improved or maintained HRQoL as the goals of treatment. Delaying progression of disease and ensuring adequate nutritional intake were additional goals of treatment identified by a clinical group.
The sponsor has proposed reimbursement criteria that are aligned with Health Canada’s indication for nivolumab for the treatment of completely resected EC or GEJC patients who have residual pathologic disease following prior neoadjuvant CRT. Disease-free survival is considered a standard and acceptable outcome measurement by regulatory agencies such as the FDA, Health Canada and Committee for Medicinal Products for Human Use for the population under review. In the pivotal study (CheckMate 577),2 nivolumab demonstrated a statistically significant clinical meaningful improvement in DFS compared with placebo (HR = 0.69; 96.4% CI, 0.56 to 0.86; P value = 0.0003), which implies a 31% reduction in the risk of recurrence or death with the adjuvant treatment compared with placebo (the current standard of care, which is surveillance). The observed median DFS was twice as long in the nivolumab arm as in the placebo arm (22.41 months versus 11.04 months, respectively). The DFS rates at 6 months were numerically higher in the nivolumab arm than in the placebo arm (72.3% versus 63.4%, respectively). In addition, results from various subgroup analysis and sensitivity analysis were largely consistent with the primary analysis, which supported the robustness of the benefit of nivolumab over placebo. The clinical experts consulted for this review indicated that the observed statistically significant DFS benefit in favour of nivolumab over placebo is clinically meaningful and impressive.
Data for OS were not mature at the data cut-off. However, the clinical expert indicated that the DFS is relevant, important, and clinical meaningful as a primary outcome for this review, as OS in this setting (adjuvant) could be biased by subsequent treatment. The goal of adjuvant treatment is to delay or prevent recurrence. While OS is generally considered a gold-standard outcome in oncology studies and reliably demonstrates clinical benefit,4 DFS is a clinically meaningful measurement of clinical benefit in the adjuvant setting and is likely to be correlated with OS in adjuvant treatment.
Patient-reported and HRQoL outcomes were identified as important outcomes for patients and were assessed as exploratory outcomes. Although significant improvement in quality of life was not expected with treatment for this population, overall, the evidence demonstrated that treatment with nivolumab or placebo was associated with maintenance (no deterioration) from baseline in HRQoL.
With regards to DMFS, the median DMFS was numerically longer in the nivolumab arm (28.32 months versus 17.61 months in the placebo arm) with a HR of 0.74 (95% CI, 0.60 to 0.92). Although it was an exploratory outcome, this supports the benefit of treatment with nivolumab compared with placebo.
The study included only patients with an ECOG PS of 0 or 1; as a result, the benefit and safety profile are unknown in those patients with an ECOG PS greater than 1. Although not supported by clinical trial evidence, the clinical experts supported extension of treatment to select patients with an ECOG PS of 2. Similarly, the clinical stage II disease was not included in the pivotal study. The clinical experts emphasized that, in clinical practice, some clinical stage I patients may end up receiving chemoradiation. Nivolumab adjuvant treatment may therefore be extended to stage I patients as long as such treatment is not contraindicated.
The Health Canada–approved indication for nivolumab is for adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT. In CheckMate 577, patients were eligible to receive either nivolumab or placebo if they had complete resection or were surgically rendered free of disease with negative margins on resected specimens defined as no vital tumour present within 1 mm of the proximal, distal, or circumferential resection margins. The clinical experts noted that, in clinical practice, clinicians may wish to administer nivolumab to R1 patients; however, they acknowledged that expansion of nivolumab to R1 patients is out of the scope of this review.
Overall, currently, there is no active treatment for this particular population (i.e., completely resected EC or GEJC patients who have residual pathologic disease following prior neoadjuvant CRT). The standard of care for this population is surveillance. Given the high unmet medical need and the risk of recurrence after CRT and resection in patients with residual pathologic disease, findings from CheckMate 577 support the use of nivolumab as a new standard of care in this setting (i.e., adjuvant treatment for patients with completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant CRT).
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Harms
The safety profile of nivolumab has been well established in previous clinical trials for the treatment of patients with gastroesophageal tumours.35-37 The frequency of any grade of adverse events and SAEs reported in nivolumab appeared similar to that in the placebo arm in the CheckMate 577 study. Numerically, more patients discontinued from treatment due to adverse events in the nivolumab arm compared with patients in the placebo arm. Notable adverse events (i.e., those of special interest to this review), including pneumonitis, myocarditis and ||||||||||||||||||||||||||||, were uncommon. Pneumonitis and myocarditis were all-causality adverse events |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Overall, the clinical experts indicated that the nivolumab safety profile observed in this study was acceptable, manageable, and consistent with the known safety profile of nivolumab. No additional safety signals were identified with adjuvant nivolumab monotherapy.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Conclusions
One sponsor-submitted, ongoing, phase III, multinational, double-blind, randomized, placebo-controlled trial is included in this review. Compared to placebo, adjuvant treatment with nivolumab (240 mg every 2 weeks by IV infusion for 16 weeks, followed by 480 mg every 4 weeks by IV infusion until disease progression or unacceptable toxicity, for a total treatment duration of 1 year) showed a statistically significant and clinically meaningful DFS benefit in the treatment of adult patients (≥ 18 years old) with completely resected EC or GEJC who have residual pathologic disease following prior neoadjuvant CRT. The safety profile of nivolumab in this study was consistent with the known safety profile of nivolumab, and no additional safety signals were identified with adjuvant nivolumab therapy in this study.
References
1.Canadian Cancer Society. Cancer-specific stats 2020. 2020: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2020-statistics/canadian-cancer-statistics/2020-resources/res-cancerstatistics-canadiancancerstatistics-2020_cancer-specific-stats.pdf?rev=a672053690e9493d921fe73453a749b4&hash=4F194657DA83EFC15ADB92A8E5ACBC5E&_ga=2.227709525.959122201.1629816912-819386897.1629816912&_gac=.28318798.1629816913.Cj0KCQjwsZKJBhC0ARIsAJ96n3Uwy2BFXiywbNxZBLIcGQTztDodij6BuYaB2TLpmVbvIvqa8qskgPwaAqyVEALw_wcB.
2.Clinical Study Report: CA209577. A Randomized, Multicenter, Double-Blind, Phase III Study of Adjuvant Nivolumab or Placebo in Subjects with Resected Esophageal, or Gastroesophageal Junction Cancer (CheckMate 577: CHECKpoint pathway and nivoluMAb clinical Trial Evaluation 577) [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2020 Oct 7.
3.Drug Reimbursement Review sponsor submission: Opdivo® (nivolumab) [internal sponsor's package]. Montreal: Bristol-Myers Squibb; 2021 Jul 7.
4.Oba K, Paoletti X, Bang YJ, et al. Role of Chemotherapy for Advanced/Recurrent Gastric Cancer: an Individual-Patient-Data Meta-Analysis. Eur J Cancer. 2013;49(7):1565-77. PubMed
5.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2018. Toronto: Canadian Cancer Society; 2018: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf. Accessed 2021 Nov 16.
6.BMS. Clinical dossier for nivolumab (OPDIVO™) for the adjuvant treatment of esophageal or gastroesophageal junction cancer. July 2021.
7.Thein HH, Jembere N, Thavorn K, et al. Estimates and predictors of health care costs of esophageal adenocarcinoma: a population-based cohort study. BMC Cancer. 2018;18(1):694. PubMed
8.Cattelan L, Ghazawi FM, Le M, et al. Epidemiologic trends and geographic distribution of esophageal cancer in Canada: A national population-based study. Cancer Medicine. 2020;9(1):401-417. PubMed
9.Canadian Cancer Society. Esophagael Cancer. 2021: https://www.cancer.ca/en/cancer-information/cancer-type/esophageal/esophageal-cancer/?region=o Accessed 2021 Nov 16.
10.Jain S, Dhingra S. Pathology of esophageal cancer and Barrett's esophagus. Ann Cardiothorac Surg. 2017;6(2):99-109. PubMed
11.Cattelan L. 2. Cattelan L, Ghazawi FM, Le M, et al. Epidemiologic trends and geographic distribution of esophageal cancer in Canada: A national population-based study. Cancer Med. 2020;9(1):401-417. 2020.
12.Saltzman JR, Gibson MK. Clinical manifestations, diagnosis, and staging of esophageal cancer Waltham (PA): UpToDate; 2020 Nov 16: www.uptodate.com.
13.Otterstatter MC, Brierley JD, De P, et al. Esophageal cancer in Canada: trends according to morphology and anatomical location. Canadian Journal of Gastroenterology. 2012;26(10):723-727. PubMed
14.Johns Hopkins Medicine. Warning Signs of Esophageal Cancer 2021; https://www.hopkinsmedicine.org/kimmel_cancer_center/cancers_we_treat/esophageal_cancer/warning-signs.html. Accessed 2021 Nov 16.
15.Mayo Clinic. Esophageal cancer: symptoms and causes. 2020; https://www.mayoclinic.org/diseasesconditions/esophageal-cancer/symptoms-causes/syc-20356084. Accessed 2021 Nov 16.
16.Esophageal Cancer. Edmonton: Cancer Care Alberta; 2021: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gi009-esophageal.pdf. Accessed 2021 Nov 16.
17.Smyth EC, Lagergren J, Fitzgerald RC, et al. Oesophageal cancer. Nat Rev Dis Primers. 2017;3:17048-17048. PubMed
18.Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11-20. PubMed
19.Macdonald JS, Smalley SR, Benedetti J, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med. 2001;345(10):725-30. PubMed
20.van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074-84. PubMed
21.Walsh TN, Noonan N, Hollywood D, et al. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med. 1996;335:462-7. PubMed
22.Depypere LP, Vervloet G, Lerut T, et al. ypT0N+: the unusual patient with pathological complete tumor response but with residual lymph node disease after neoadjuvant chemoradiation for esophageal cancer, what's up? J Thorac Dis. 2018;10(5):2771-8. PubMed
23.Reynolds JV, Muldoon C, Hollywood D, et al. Long-term outcomes following neoadjuvant chemoradiotherapy for esophageal cancer. Ann Surg. 2007;245(5):707-16. PubMed
24.van Meerten E, Muller K, Tilanus HW, et al. Neoadjuvant concurrent chemoradiation with weekly paclitaxel and carboplatin for patients with oesophageal cancer: a phase II study. Br J Cancer. 2006;94(10):1389 94.
25.Bosset JF, Gignoux M, Triboulet JP, et al. Chemoradiotherapy followed by surgery compared with surgery alone in squamous-cell cancer of the esophagus. N Engl J Med. 1997;337(3):161-67. PubMed
26.Opdivo® nivolumab for injection Intravenous Infusion, 10 mg nivolumab /mL 40 mg and 100 mg single-use vials [product monograph]. Montreal: Bristol-Myers Squibb Canada Co; 2021 Jul 6.
27.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
28.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Nov 16.
29.Kelly RJ, Ajani JA, Kuzdzal J, et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N Engl J Med. 2021;384(13):1191-1203. PubMed
30.Health Canada reviewer's report: Nivolumab (Opdivo) Montreal: Bristol-Myers Squibb Canada; 2021.
31.Bristol-Myers Squibb. An Investigational Immuno-therapy Study of Nivolumab or Placebo in Participants With Resected Esophageal or Gastroesophageal Junction Cancer (CheckMate 577) ClinicalTrials.gov Identifier: NCT02743494. Bethesda (MD): ClinicalTrials.gov; 2016 Apr 19 [last updated 2021 Jun 22]: https://clinicaltrials.gov/ct2/show/NCT02743494.
32.Greenwood, M. The errors of sampling of the survivorship tables, Reports on Public Health and Statistical Subjects, 33, Appendix 1, HMSO, London, 1926.
33.Klein, J. P. and Moeschberger, M. L. (1997), Survival Analysis: Techniques for Censored and Truncated Data, New York: Springer-Verlag.
34.Moehler M, Ajani JA, Kuzdzal J, et al. Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer following neoadjuvant chemoradiotherapy: 14-month follow-up of CheckMate 577. Presented at the ESMO Virtual Congress 2021, September 16–21.
35.Kang Y-K, Boku N, Satoh T, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017; 390: 2461-71. PubMed
36.Kato K, Cho BC, Takahashi M, et al. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 2019; 20: 1506-17. PubMed
37.Kudo T, Hamamoto Y, Kato K, et al. Nivolumab treatment for oesophageal squamous-cell carcinoma: an open-label, multicentre, phase 2 trial. Lancet Oncol 2017; 18: 631-9. PubMed
38.Clinical Study Report: ONO-4538-24/BMS CA209473 Phase III Study. A multicenter, randomized, open-label study in patients with esophageal cancer refractory or intolerant to combination therapy with fluoropyrimidine- and platinum-based drugs. [internal sponsor's report]. Osaka (Japan): Ono Pharmaceutical Co., Ltd; 2019 Mar 12.
39.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
40.EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
41.Doherty MK, Leung Y, Su J, et al. Health utility scores from EQ-5D and health-related quality of life in patients with esophageal cancer: a real-world cross-sectional study. Dis Esophagus. 2018;31(12). PubMed
42.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
43.FACIT. FACT-E. Functional Assessment of Cancer Therapy – Esophageal. 2021; https://www.facit.org/measures/FACT-E. Accessed 2021 Nov 16.
44.Darling G, Eton DT, Sulman J, Casson AG, Celia D. Validation of the functional assessment of cancer therapy esophageal cancer subscale. Cancer. 2006;107(4):854-863. PubMed
45.FACIT. FACT-G. Functional Assessment of Cancer Therapy - General. 2021; https://www.facit.org/measures/FACT-G. Accessed 2021 Nov 16.
46.Cella DF, Tulsky DS, Gray G, et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol. 1993;11(3):570-579. PubMed
47.Teckle P, McTaggart-Cowan H, Van der Hoek K, et al. Mapping the FACT-G cancer-specific quality of life instrument to the EQ-5D and SF-6D. Health Qual Life Outcomes. 2013;11:203. PubMed
48.Cella D, Hahn EA, Dineen K. Meaningful change in cancer-specific quality of life scores: differences between improvement and worsening. Qual Life Res. 2002;11(3):207-221. PubMed
49.Yost KJ, Eton DT. Combining distribution- and anchor-based approaches to determine minimally important differences: the FACIT experience. Eval Health Prof. 2005;28(2):172-191. PubMed
50.FACIT. FACT-G7. Functional Assessment of Cancer Therapy – General – 7 Item Version. 2021; https://www.facit.org/measures/FACT-G7. Accessed 2021 Nov 16.
51.Yanez B, Pearman T, Lis CG, Beaumont JL, Cella D. The FACT-G7: a rapid version of the functional assessment of cancer therapy-general (FACT-G) for monitoring symptoms and concerns in oncology practice and research. Ann Oncol. 2013;24(4):1073-1078. PubMed
52.Pearman T, Yanez B, Peipert J, Wortman K, Beaumont J, Cella D. Ambulatory cancer and US general population reference values and cutoff scores for the functional assessment of cancer therapy. Cancer. 2014;120(18):2902-2909. PubMed
Appendix 1: Patient Group Input
My Gut Feeling – Stomach Cancer Foundation of Canada
About Your Patient Group
My Gut Feeling – Stomach Cancer Foundation of Canada is the first non-profit organization in Canada, dedicated to providing support, awareness, education, information and advocacy to stomach cancer patients, survivors and caregivers. My Gut Feeling was founded by two stomach cancer survivors; although the organization was initially developed to help people affected by stomach cancer, people with gastroesophageal (GEJ) and esophageal cancer are included in our services and receive ongoing support. Our goals are to dispel misconceptions, to provide information on the day to day journey of being diagnosed, living with and surviving cancer, and to improve the quality of life, give a voice to patients and caregivers, and provide peer mentorship based on lived experience with cancer.
Information Gathering
In order to represent the patient and caregiver voice, My Gut Feeling - Stomach Cancer Foundation of Canada conducted an international survey to understand the perspective of patients and caregivers affected by esophageal and/or gastroesophageal (GEJ) cancer including experiences with current treatment and the novel immunotherapy under review. My Gut Feeling launched an online patient and caregiver survey between June 29th, 2021 to July 16, 2021. The survey link was posted on My Gut Feeling’s social media platforms (including Facebook, Instagram and Twitter). The survey was also shared in private online groups for patients with Esophageal Cancer, Lynch Syndrome and Stomach Cancer.
In total, fifteen people completed the survey, of those, eleven (73.3%) identified as patients and four as caregivers (26.7%). Specifically, 86.7% or respondents identified as female and 13.3% identified as male. Respondents were diagnosed across all ages ranging from 20 to 80 years old: 20-30 years (13.3%), 31-40 years (26.7%), 41-50 years (6.7%), 61 to 70 years (20%), and 71-80 years (6.7%). Data was gathered internationally with 53.3% of respondents residing in the United States, 40% in Canada and 6.7% in Australia. To ensure unbiased data collection, respondents were asked to refrain from using personal identifiers to preserve anonymity.
Disease Experience
Respondents included in this survey had a diagnosis of either esophageal and/or gastroesophageal (GEJ) cancer. The majority of respondents had adenocarcinoma (93.3%), the remainder had squamous cell carcinoma (6.7%). Of the respondents 66.7% were diagnosed with stage one to stage three cancer, 20% stage four; 13.3% were not aware or were not given their cancer stage. The majority of respondents did not have a distant spread, however, in those that had stage 4 disease, the primary areas of metastasis included the liver, lungs, and/or peritoneum.
Respondents commented that both the cancer itself and the treatments to control the cancer played a major impact on their daily living. Patients and caregivers were asked if any esophageal/GEJ
cancer-induced symptoms were experienced prior to diagnosis. All (100%) of respondents had experienced at least one symptom prior to being diagnosed. Changes in appetite (66.7%) and pain (66.7%) were the most reported symptoms. Other significant symptoms included weight loss (53.3%), difficulty swallowing (46.7%), nausea/vomiting (40%), dumping syndrome (33.3%), reflux (33.3%) bloodwork abnormalities (e.g. anemia, B12 deficiency, etc) (26.7%), blood clot (13.3%), chest pain (13.3%). Less reported symptoms included bleeding, feeling a mass, ascites, bowel obstruction, food regurgitation, shortness of breath (Figure 7). Respondents commented that these symptoms impacted their day to day life. One patient commented on the challenges of being diagnosed with cancer during the pandemic “it took a long time for me to get a diagnosis. I felt like I was going crazy because I knew something was wrong. My scope kept getting delayed because of COVID and for months I struggled with symptoms and not having answers”.
Figure 7: Patient and Caregiver Reported Symptoms Prior to Diagnosis With Esophageal or Gastroesophageal Cancer
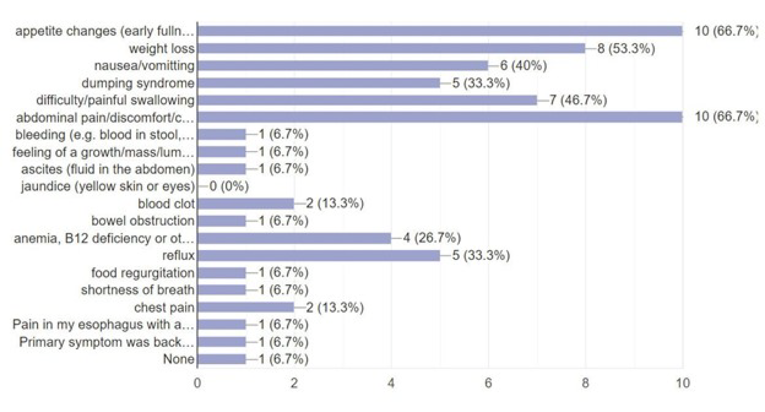
Most respondents felt that the cancer diagnosis had a significant impact on their quality of life (93.3%), only 6.7% felt it had a minimal impact and zero respondents felt that it did not impact their life. Areas affected were the ability to eat, work, social life, identity, personal image, physical health, mental health and finances. Both patients and caregivers were affected financially; many patients were unable to work and/or fulfill their family obligations. Barriers to work included post-treatment related physical changes, for example’ for example, one patient states: “I haven't been able to work much since I've had multiple incisions since I was diagnosed”; another patient had to quit her job since “Bathroom issues make it hard to work”. Mental health was a barrier to returning to work and family obligations, for example, one patient replied, “Lost a 100K + job, diagnosed with PTSD, difficulty with bowel control making employment extremely difficult.” Fear of recurrence prevented some from fulfilling their obligations: One patient said “why bother going back to work when this cancer can come back any day”. Receiving treatment forced patients and caregivers to experience job loss and financial strain. One caregiver had to... “quit my job and [become] separated from my family to help care for my dad”. Another patient replied that he had “Lost 2 months of wages for the surgery”. Treatment itself altered the quality and quantity of work. For example, one patient stated that “[cancer treatment] has slowed down my life a lot. I had to quit my 2nd part time job because of constant fatigue. I've used up all my sick days from my primary job on appointments and treatment days and now will soon have to use a donated sick day program as well as non-paid FMLA”. Familial obligations were also impacted. One mother wrote “it has been devastating. I am unable to work or even take care of my children. I feel like a bad mother”
The cancer diagnosis and its treatment impacted both physical and mental health in both the patient and caregiver respondents. Areas of physical and mental health included effects on stamina, ability to eat, body image, and impact on social life: One patient who underwent an esophagectomy responded that there was a global impact on her physical and mental health, stating “I feel tired, [and need] shorter meals, less social life, lost a lot of weight, compromised immune system”. Physical health had implications on body image for example one patient wrote that she “lost a bunch of weight, clothes don't fit, not as fit as I used to be. I feel weak and not like myself and I can't enjoy food as much as I used to”. One patient felt that he could no longer participate in activities that he enjoyed in the past because of treatment side effects stating, “I used to be involved in several theater groups as my hobbies and now can no longer do that because of fatigue and brain fog”. Overall, the cancer diagnosis and treatment itself impacted multiple aspects of patient and caregiver lives leading to a decline in mental and physical health and implications on wellbeing of the person diagnosed and family unit.
Experiences With Currently Available Treatments
Respondents reported that they had experience with a variety of treatment modalities. At the time of this survey 86.7% had received (or were in the process of receiving) some type of treatment and 13.3% had no treatment (or had completed treatment). Of those treated: 73.3% had surgery, 73.3% had chemotherapy, 40% had radiation alone, 6.7% had chemo-radiation, 26.7% had immunotherapy and 20% had alternative therapy. Respondents had experience with a variety of systemic treatments including CROSS (Carboplatin/paclitaxel), FOLFOX, Capecitabine, XELOX, FLOT, Herceptin, Pembrolizumab, Ramucirumab and Nivolumab. Participants were asked to rank how much they agreed with the statement that their current therp(ies) were able to manage cancer symptoms on a scale of 1 to 5. The majority of respondents (46.7) ranked this statement as a 5 or “strongly agreed”. The remainder of respondents rated the statement as 4 “agree” (13.4%), 3 “neither agree nor disagree” (20%), 2 “disagree” (6.7%) and 1 “strongly disagree” (13.3%) demonstrating that although current treatments appear to be effective for some people, there are still unmet needs in terms of cancer symptom control.
While current therapies appear to control some cancer symptomatology, current treatments have a variety of side effects impacting quality of life. All respondents identified at least one treatment related side effect with 100% reporting fatigue. Other common symptoms included nausea/vomiting (80%), diarrhea (73.3%), appetite changes (66.7%), constipation (66.7%), weight loss (60%), body ache (60%), hair loss (60%), taste changes (53.3%), abdominal pain (46.7%), brain fog (46.7%), sleep problems (46.7%), neuropathy (40%), dumping syndrome (40%). Less common symptoms included anemia (26.7%), mouth sores (26.7%), blood clot (13.3%), infection (13.3%), bloodwork abnormalities (13.3%), rash (6.7%), seizure (6.7%) hand-foot syndrome (6.7%), tachycardia (6.7%) (Figure 8). Respondents were able to leave additional comments regarding their treatment experiences. While surgical treatments were not individually assessed, respondents provided additional comments related to surgery alone. One patient stated that her most bothersome symptom was “the tube down my nose/throat while I was in the hospital [after surgery], the IV’s, and stomach pain when I ate too much after I was home from the surgery. While most (60%) were able to tolerate treatment, 13.3% had to stop treatment because of being hospitalized for an adverse event and 13.3% had to delay/skip their treatment due to toxicities. It is apparent from this survey that for the majority of respondents the currently available treatments had significant implications on quality of life.
Figure 8: Patient And Caregiver Reported Side Effects While on Treatment for Esophageal or Gastroesophageal Cancer
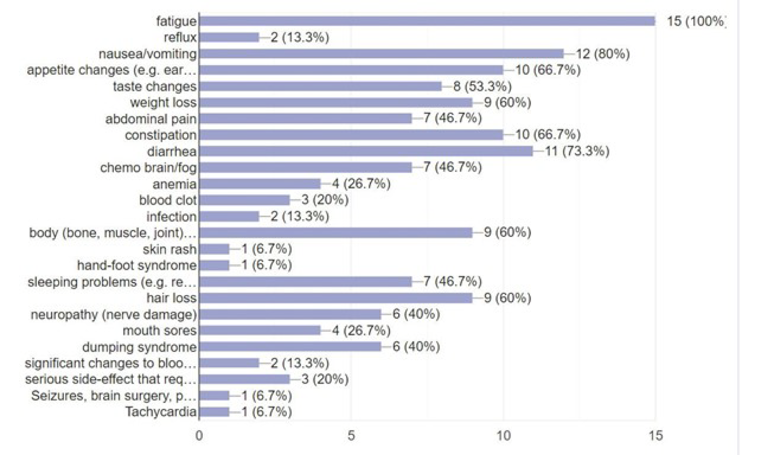
Improved Outcomes
When evaluating their treatment options, patients and caregivers considered multiple factors such as quality of life, treatment side effects, cost of treatment, convenience of treatment, duration of treatment and the survival benefits. Respondents recognized that treatments had trade-offs and each respondent placed a different value on these considerations based on their preferences. For example, when asked “how important is it for you that new therapies bring about improvement in quality of life”. Almost all respondents (93.3%) replied with a 10 (on a 0 to 10 scale) or “extremely important”. One patient wrote “I didn’t want to sit in a chemo chair all day and watch my life pass by” suggesting while cancer control is an important consideration, treatment comes at a cost to quality of life which may not be tolerable to all patients. Convenience of treatment was another consideration for patients and caregivers. For example, patients preferred an oral chemotherapy taken at home to an IV chemotherapy administered in a hospital. If chemotherapy was administered through IV, patients preferred less frequent infusions and less visits to the hospital. While our survey found that most people did not have to pay out of pocket for specific treatments, there were costs to having treatment: the cost to quality of life, cost of taking time off work, cost of travel to the hospital, cost to spending time with family and the cost to physical and mental health.
Another avenue to improve patient outcomes may be achieved through providing equal access to treatment access. Cost of treatment and availability of treatment depended on geographic location. Respondents received access to treatment through publicly funded healthcare, private insurance, drug access programs, personal savings or donations. Most respondents (86.7%) felt they did not have difficulties accessing treatment, however, 13.3% did report issues with access. Standard of care treatments such as surgery or chemotherapy were more accessible than novel therapies such as immunotherapy. For example, 40% of respondents required financial assistance from a pharmaceutical/biotech company and 30% received access to treatment through clinical trials. Most respondents were interested in discussing treatment options even if they were not covered by their current healthcare plan; 40% of respondents would be willing to pay for new therapies out of pocket with 33.3% maybe interested depending on the cost, 20% maybe interested depending on how much it would improve survival and 13.3% maybe interested depending on cost, improvement in survival, impact on quality of life and side effect profile (Figure 9).
Barriers to access identified included institutional and health care system barriers, limited availability of treatment and how quickly treatment could be accessed. One patient reported that he felt that “doctors were too busy to discuss options” citing limitations of the healthcare system. Another patient stated that access to treatment options depended on location since for her there were “no trials at my hospital”.
This year specifically, the already taxed healthcare system was strained and further limited access to care, specifically one patient cited “COVID” as causing a delay in getting surgery and his systemic therapy start dates. The other identified barrier to treatment was difficulty obtaining information and access to new therapies. Respondents expressed frustration that they were not informed about alternatives. One person replied that they “had to spend a long time researching the many options because doctors didn’t give me choices”. Many respondents felt that they wanted to know all their options upfront and felt that they needed to do their own research to get these options. Overall, participants were asked to rate the following statement on a 0 to 10 scale “How important is it to advocate for treatment options for esophageal and gastroesophageal cancer?”. The majority (93.3%) replied with a 10 or extremely important. While current treatments options may improve patient survival, there are clear limitations in available treatment options, access to new therapies and patient centered discussion regarding options. Patients and caregivers want more options to choose from so that they can make informed decisions based on their values and preferences.
Figure 9: Respondents Weighed Cost, Side-Effect Profile, Survival Benefit and Quality of Life Considerations When Considering Paying for Treatments
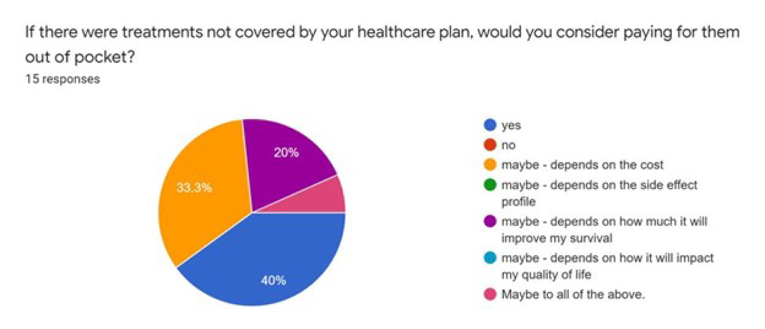
Experience With Drug Under Review
One patient had experience with the drug under review.This patient had surgically resected cancer and chemo-radiation. The drug was accessed via a hospital special access program. The patient was currently on Nivolumab at the time of the survey and had been on the drug for 3 months. When asked about the side-effect profile, they stated that they did not notice additional side effects since starting Nivolumab. They noted they did experience appetite changes (early fullness, lack of appetite), weight loss, difficulty swallowing, abdominal pain, nausea/vomiting, taste changes, body aches, hair loss, neuropathy, fatigue and constipation but felt that the addition of Nivolumab did not exacerbate these symptoms since they originally resulted from the surgery or chemo-radiation. When asked to rate the following statement: “Nivolumab has improved my quality of life”. The patient rated this as a 10 or “strongly agree”. The patient stated they were very satisfied with the drug because “3-months after surgery my PET scan showed NED [no evidence of disease]”. It appears that for this patient when he was presented with the option of additional therapy at no cost he did not have additional side effects and potentially had an impact on reducing recurrence. Although most patients were not treated directly with Nivolumab, our survey generated additional comments with respondents asking for more information about Nivolumab. This again demonstrates a need for patients and caregivers to have options and information on novel therapies that could improve the length and/or quality of life.
Companion Diagnostic Test
We did not ask questions related to companion diagnostic testing.
Anything Else? What we think from what we gathered.
Being diagnosed with any cancer is challenging. Esophageal and gastroesophageal cancer is rare in Canada with few treatment options. For those patients and caregivers impacted by this diagnosis, having options is important since it brings about a sense of control at a time when cancer strips the patient and family of their identity. This short survey administered by My Gut Feeling shows that there is an unmet patient and caregiver need to receive equitable access to therapies that may prolong life, reduce risk of recurrence and improve treatment tolerability. My Gut Feeling strongly supports the use of Nivolumab for the adjuvant treatment of resected esophageal or gastroesophageal junction cancer in patients who have residual pathologic disease following prior neoadjuvant chemoradiotherapy.
While only one respondent had direct experience with Nivolumab, it appears from his perspective that the drug did not cause him additional side effects but reduced his risk of recurrence making him satisfied with the decision to pursue this novel therapy.
Nivolumab is a good example of precision oncology. Our survey did not directly ask respondents about CPS testing, molecular profiling or MMR status and challenges with accessing this information.
However, targeted therapy is the future of oncology and there are subsets of esophageal and gastroesophageal cancer patients that can benefit from drugs such as Nivolumab. Surgery and chemo-radiation continues to be the gold standard of care for this population however these come at a great cost to physical and mental health. One patient writes My physical health was impacted immensely [by chemo-radiation and surgery]. My strength and energy level is a quarter of what it used to be”. Another wrote that she experienced “mental health implications, PTSD, panic attacks and feeling no control [during treatment]”. One patient described the impact that her diagnosis had on her caregiver: “Significant impact on my caregivers (my mental health issues, inability to gain weight etc). All of this was very much compounded by diagnosis and treatment occurring during Covid...My physical health has been affected as I am trying post surgery to recover from weight loss and muscle atrophy - I continue to try to be a very active person but increasing muscle will be very long term”.
Based on the objective research completed over a short time frame, the conclusion of My Gut Feeling - Stomach Cancer Foundation of Canada is to strongly support the use of Nivolumab for the adjuvant treatment of completely resected esophageal or gastroesophageal junction cancer in patients who have residual pathologic disease following prior neoadjuvant chemoradiotherapy (CRT). We believe that patients and caregivers should have equitable access to treatment options that have the potential to improve quality and duration of life. Patients and caregivers should have a choice in treatment options based on their own personal preferences without barriers to access. In the words of a patient: “A good quality of life is essential for esophageal patients. Even if overall survival is not dramatically improved, the quality of life improvement from this drug can bring significant advantages enabling them to spend more time with their families with the side effects of existing treatments”.
Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH CDR and pCODR programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No, My Gut Feeling independently completed this submission
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No, My Gut Feeling independently collected and analyzed data used for this submission
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 17: Companies That Provided Financial Payment to My Gut Feeling Over the Past 2 Years (Direct or Indirect Interest)
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
Eli Lily Canada Inc. | — | — | — | — |
Taiho Pharma Canada Inc. | — | — | X | X |
Bristol Myers Squibb | — | — | X | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Name: Ekaterina Kosyachkova
Position: Vice-Chair and Co-Founder
Patient Group: My Gut Feeling – Stomach Cancer Foundation of Canada
Date: July 29, 2021
Appendix 2: Clinician Group Input
Ontario Health (Cancer Care Ontario) Gastrointestinal Drug Advisory Committee
About Your Clinician Group
Please describe the purpose of your organization. Include a link to your website (if applicable).
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Please describe how you gathered the information included in the submission.
This input was jointly discussed at a DAC meeting.
Current treatments
Describe the current treatment paradigm for the disease
Focus on the Canadian context. Please include drug and non-drug treatments. Drugs without Health Canada approval for use in the management of the indication of interest may be relevant if they are routinely used in Canadian clinical practice. Are such treatments supported by clinical practice guidelines? Treatments available through special access programs are relevant. Do current treatments modify the underlying disease mechanism? Target symptoms?
Response: Currently there is no routine adjuvant treatment offered to these patients.
Treatment goals
What are the most important goals that an ideal treatment would address?
Examples: Prolong life, delay disease progression, improve lung function, prevent the need for organ transplant, prevent infection or transmission of disease, reduce loss of cognition, reduce the severity of symptoms, minimize adverse effects, improve health-related quality of life, increase the ability to maintain employment, maintain independence, reduce burden on caregivers.
Response
Prolong life
delay disease progression
reduce the severity of symptoms
minimize adverse effects
improve health-related quality of life
Treatment gaps (unmet needs)
Considering the treatment goals in Section 4, please describe goals (needs) that are not being met by currently available treatments.
Examples:
Not all patients respond to available treatments
Patients become refractory to current treatment options
No treatments are available to reverse the course of disease
No treatments are available to address key outcomes
Treatments are needed that are better tolerated
Treatment are needed to improve compliance
Formulations are needed to improve convenience
Response: Currently there is no adjuvant treatment for these patients
Which patients have the greatest unmet need for an intervention such as the drug under review?
Would these patients be considered a subpopulation or niche population? Describe characteristics of this patient population. Would the drug under review address the unmet need in this patient population?
Response: As per the study patient population
Place in therapy
How would the drug under review fit into the current treatment paradigm?
Is there a mechanism of action that would complement other available treatments, and would it be added to other treatments? Is the drug under review the first treatment approved that will address the underlying disease process rather than being a symptomatic management therapy? Would the drug under review be used as a first-line treatment, in combination with other treatments, or as a later (or last) line of treatment? Is the drug under review expected to cause a shift in the current treatment paradigm?
Response: Nivolumab will be an added post-operative therapy.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
If so, please describe which treatments should be tried, in what order, and include a brief rationale.
Response: No.
How would this drug affect the sequencing of therapies for the target condition?
If appropriate for this condition, please indicate which treatments would be given after the therapy has failed and specify whether this is a significant departure from the sequence employed in current practice. Would there be opportunity to treat patients with this same drug in a subsequent line of therapy? If so, according to what parameters?
Response: This could affect treatment decision at recurrence.
Which patients would be best suited for treatment with the drug under review?
Which patients are most likely to respond to treatment with the drug under review? Which patients are most in need of an intervention? Would this differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease)?
Response: All patients
How would patients best suited for treatment with the drug under review be identified?
Examples: Clinician examination or judgement, laboratory tests (specify), diagnostic tools (specify). Is the condition challenging to diagnose in routine clinical practice? Are there any issues related to diagnosis? (e.g., tests may not be widely available, tests may be available at a cost, uncertainty in testing, unclear whether a scale is accurate or the scale may be subjective, variability in expert opinion.) Is it likely that misdiagnosis occurs in clinical practice (e.g., underdiagnosis)? Should patients who are pre-symptomatic be treated considering the mechanism of action of the drug under review?
Response: No companion diagnostics required
Which patients would be least suitable for treatment with the drug under review?
Response: Patients should be offered nivolumab if they meet eligibility criteria of the clinical trial.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review? If so, how would these patients be identified?
Response: No
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response: NA
What would be considered a clinically meaningful response to treatment?
Examples:
Reduction in the frequency or severity of symptoms (provide specifics regarding changes in frequency, severity, and so forth)
Attainment of major motor milestones
Ability to perform activities of daily living
Improvement in symptoms
Stabilization (no deterioration) of symptoms
Consider the magnitude of the response to treatment. Is this likely to vary across physicians?
Response: NA
How often should treatment response be assessed?
Response: NA
What factors should be considered when deciding to discontinue treatment?
Examples:
Disease progression (specify; e.g., loss of lower limb mobility)
Certain adverse events occur (specify type, frequency, and severity)
Additional treatment becomes necessary (specify)
Response: Toxicity and recurrence
What settings are appropriate for treatment with the drug under review?
Examples: Community setting, hospital (outpatient clinic), specialty clinic
Response: Outpatient chemo suites
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review? If so, which specialties would be relevant?
Response: NA
Additional information
Is there any additional information you feel is pertinent to this review?
Response: This patient population has a high risk of recurrence associated with high rate of mortality and poor quality of life. Nivolumab demonstrated improvement in disease free survival and sets a new standard of care for this patient population.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Erin Kennedy
Position: Ontario Cancer Lead; surgeon
Date: 09-July-2021
Table 18: Conflict of Interest Declaration for Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Nothing to declare | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Jim Biagi
Position: Medical oncologist
Date: 09-July-2021
Table 19: Conflict of Interest Declaration for Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Nothing to declare | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Christine Brezden-Masley
Position: Medical Oncologist, Mount Sinai Hospital; Medical Director, Cancer Program for Sinai Health; Director, Marvelle Koffler Breast Centre, Mount Sinai Hospital; Senior Clinical Scientist, Lunenfeld-Tanenbaum Research Institute at Mount Sinai Hospital; Associate Professor of Medicine, University of Toronto
Date: 09-July-2021
Table 20: Conflict of Interest Declaration for Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Nothing to declare | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Tim Asmis
Position: Medical oncologist
Date: 9-July-2021
Table 21: Conflict of Interest Declaration for Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Nothing to declare | — | — | — | — |
Appendix 3: Literature Search Strategy
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–present)
Embase (1974–present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: August 5, 2021
Alerts: Bi-weekly search updates until project completion
Search filters applied: None
Limits: Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq=# | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multi-Database Strategy
# Searches
Nivolumab/
(opdivo* or nivolumab* or nivo or bms 936558 or bms936558 or cmab 819 or cmab819 or mdx 1106 or mdx1106 or ono 4538 or ono4538 or HSDB 8256 or HSDB8256 or GTPL 7335 or GTPL7335 or 31YO63LBSN).ti,ab,kf,ot,rn,nm.
1 or 2
exp Esophageal Neoplasms/
exp Esophagus/
(esophag* or gastroesophag* or oesophag* or cardioesophageal or cardiooesophageal or EG junction* or gastrooesophageal or GE junction*).ti,ab,kf.
((gastric* or GEJ or EGJ) adj2 (cancer* or neoplas* or tumo?r* or carcinoma* or adenocarcinoma* or squamous or malignan* or metast*)).ti,ab,kf.
or/4-7
3 and 8
9 use medall
*nivolumab/
(opdivo* or nivolumab* or nivo or bms 936558 or bms936558 or cmab 819 or cmab819 or mdx 1106 or mdx1106 or ono 4538 or ono4538 or HSDB 8256 or HSDB8256 or GTPL 7335 or GTPL7335).ti,ab,kw,dq.
11 or 12
exp Esophagus tumor/
exp Esophagus/
(esophag* or gastroesophag* or oesophag* or cardioesophageal or cardiooesophageal or EG junction* or gastrooesophageal or GE junction*).ti,ab,kw.
((gastric* or GEJ or EGJ) adj2 (cancer* or neoplas* or tumo?r* or carcinoma* or adenocarcinoma* or squamous or malignan* or metast*)).ti,ab,kw.
or/14-17
13 and 18
19 not (conference abstract or conference review).pt.
20 use oemezd
10 or 21
remove duplicates from 22
Clinical Trials Registries
ClinicalTrials.gov
Produced by the U.S. National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Opdivo OR nivolumab OR MDX 1106 OR MDX1106 OR BMS936558 OR BMS 936558 OR ONO4538 OR ONO 4538 OR HSDB 8256 OR HSDB8256 | esophageal OR esophagus OR gastroesophageal OR "gastro esophageal" OR gastric OR oesophagus OR oesophageal OR esophagogastric]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search -- Opdivo OR nivolumab OR MDX 1106 OR MDX1106 OR BMS936558 OR BMS 936558 OR ONO4538 OR ONO 4538 OR HSDB 8256 OR HSDB8256 | esophageal OR esophagus OR gastroesophageal OR "gastro esophageal" OR gastric OR oesophagus OR oesophageal OR esophagogastric]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search -- Opdivo OR nivolumab OR MDX 1106 OR MDX1106 OR BMS936558 OR BMS 936558 OR ONO4538 OR ONO 4538 OR HSDB 8256 OR HSDB8256 | esophageal OR esophagus OR gastroesophageal OR "gastro esophageal" OR gastric OR oesophagus OR oesophageal OR esophagogastric]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search -- Opdivo OR nivolumab OR MDX 1106 OR MDX1106 OR BMS936558 OR BMS 936558 OR ONO4538 OR ONO 4538 OR HSDB 8256 OR HSDB8256 | esophageal OR esophagus OR gastroesophageal OR "gastro esophageal" OR gastric OR oesophagus OR oesophageal OR esophagogastric]
Grey Literature
Search dates: July 14-19, 2021
Keywords: Opdivo, nivolumab, MDX 1106, MDX1106, BMS936558, BMS 936558, ONO4538, ONO 4538, HSDB 8256, HSDB8256 AND esophageal OR esophagus OR gastroesophageal OR "gastro esophageal" OR gastric OR oesophagus OR oesophageal OR esophagogastric
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals.
Appendix 4: Excluded Studies
Reference | Reason for exclusion |
|---|---|
ONO-4538 phase III study a multicenter, randomized, open-label study in patients with esophageal cancer refractory or intolerant to combination therapy with fluoropyrimidine- and platinum-based drugs (study protocol number: ono-4538-24/BMS CA209473)38 | Population and intervention not of interest |
Source: Sponsor’s submission3 and Clinical Study Report for CheckMate 577.38
Appendix 5: Detailed Outcome Data
Table 24: Subsequent Cancer Therapy (All Randomized Patients)
Subsequent cancer therapy | CheckMate 577 | |
|---|---|---|
Nivolumab (N = 532) | Placebo (N = 262) | |
Patients with any subsequent therapy, n (%)a | 157 (29.5) | 111 (42.4) |
Patients who received subsequent radiotherapy, n (%) | 43 (8.1) | 41 (15.6) |
Patients who received subsequent surgery, n (%) | 28 (5.3) | 20 (7.6) |
Patients who received systemic therapy, n (%) | 125 (23.5) | 89 (34.0) |
Immunotherapy | 4 (0.8) | 19 (7.3) |
|||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
|||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
Other systemic cancer therapy – chemotherapy | 123(23.1) | 85(32.4) |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
PD1 = programmed death 1 receptor; PD-L1 = program death-ligand 1; CTLA4 = cytotoxic T-lymphocyte associated protein 4; q2w = once every 2 weeks.
aPatient may have received more than one type of subsequent therapy. Subsequent therapy was defined as therapy started
Source: Clinical Study Report for CheckMate 577.2
Table 25: Summary of Exposure to Treatment, Safety Population
Study details | CheckMate 577 | |
|---|---|---|
Nivolumab (N = 532) | Placebo (N = 260) | |
||||||||||||||||||| | ||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
Relative dose intensity (%) | ||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
70% to < 90% | 67 (12.6) | NA |
50% to < 70% | 4 (0.8) | NA |
< 50% | 2 (0.4) | NA |
Duration of therapy (months) | ||
||||||||||||||||||| (minimum to maximum) | ||||||||||||||||||| (< 0.1 to 14.2) | ||||||||||||||||||| (< 0.1 to 15.0) |
Median | 10.14 | 8.99 |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
NA = not available; SD = standard deviation.
Source: Clinical Study Report for CheckMate 577.2



Table 26: Most Frequent Adverse Events (Any Grade)
Adverse events | CheckMate 577 | |
|---|---|---|
Nivolumab (N = 532) | Placebo (N = 260) | |
Overall Adverse events,a n (%) | 510 (95.9) | 243 (93.5) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
Treatment-related adverse events,b n (%) | 376 (70.7) | 119 (45.8) |
Most frequent treatment related adverse events (≥ 5% of patients in any arm), n(%) | ||
Fatigue | 90 (16.9) | 29 (11.2) |
Diarrhea | 88 (16.5) | 39 (15.0) |
Pruritus | 53 (10.0) | 9 (3.5) |
Rash | 52 (9.8) | 10 (3.8) |
Hypothyroidism | 50 (9.4) | 4 (1.5) |
Nausea | 47 (8.8) | 13 (5.0) |
Hyperthyroidism | 35 (6.6) | 1 (0.4) |
Arthralgia | 30 (5.6) | 4 (1.5) |
Increased aspartate aminotransferase | 29 (5.5) | 10 (3.8) |
Asthenia | 28 (5.3) | 4 (1.5) |
AE = adverse event; n = number of patients with events; N = number of patients included in the analysis.
aReported as all-causality adverse event in the Clinical Study Report. All adverse events occurred within 30 days of the last dose of study drug, unless otherwise indicated.
bReported as drug-related adverse event in the Clinical Study Report. All adverse events occurred within 30 days of the last dose of study drug, unless otherwise indicated.
Source: Clinical Study Report for CheckMate 577.2
Table 27: Serious Adverse Events (All Treated Patients)
Serious adverse events | CheckMate 577 | |||||
|---|---|---|---|---|---|---|
Nivolumab (N = 532) | Placebo (N = 260) | |||||
Any grade | Grade 3 to 4 | Grade 5 | Any grade | Grade 3 to 4 | Grade 5 | |
SAE | ||||||
Patients with ≥ 1 SAE,a n (%) | 158 (29.7) | 107 (20.1) | ||||||||||||||||||| | 78 (30.0) | 53 (20.4) | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
Treatment-related SAE | ||||||
Patients with a treatment-related SAE,b n (%) | 40 (7.5) | 29 (5.5) | 1 (0.2) | 7 (2.7) | 3 (1.2) | 0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
AE = adverse event; SAE = serious adverse event.
aReported as All-causality SAE in the Clinical Study Report. All SAEs occurred within 30 days of the last dose of study drug, unless otherwise indicated.
bReported as drug related SAE in the Clinical Study Report. All SAEs occurred within 30 days of the last dose of study drug, unless otherwise indicated.
Source: Clinical Study Report for CheckMate 577.2
Appendix 6: Redacted
Note that this appendix has been redacted at the request of the sponsor.

Appendix 7: Redacted
Note that this appendix has been redacted at the request of the sponsor.
Appendix 8: Real-World Evidence and CheckMate 577 — Summary and Comparison
Real-World Evidence and CheckMate 577 — Summary and Comparison
Data from the IKNL (Netherlands Comprehensive Cancer Organization) nationwide registry dataset were used to inform the transition from post-recurrence to death since there are no OS data from CheckMate 577 and are applied to both nivolumab and comparator in the economic analysis. In order to use the Netherlands IKNL registry dataset, the sponsor matched the CheckMate 577 population with patients diagnosed with esophageal and gastric cancer from the Netherlands IKNL registry dataset. As a result, a summary of the selection criteria for the IKNL nationwide registry dataset and appraisal of the comparability of the two populations (IKNL and CheckMate 577) are provided below.
CA209-77E is a retrospective study of patients diagnosed with esophageal and gastric cancer in the Netherlands, using the IKNL nationwide registry dataset. Matching process to align with CheckMate-577 population was applied to these patients. Briefly, data on all patients diagnosed with non-metastatic ESCC, EAC, GEJC and GC in 2015 and 2016 in the Netherlands and treated with curative intent were collected. Additional inclusion criteria applied were stage II or III disease (based on Union for International Cancer Control TNM version 7); preoperative, platinum-based CRT, then surgery; R0 resection; and residual pathological disease (i.e., non-pCR), with at least ypN1 or ypT1 in the pathology report for resected specimen. Lastly, patients should not have been treated with trastuzumab at early stage.
Table 28 highlights the baseline characteristics for comparison and matching purposes of CA209-77E pre-occurrence, CA209-77E post-occurrence and CheckMate-577.
Although the population described in IKNL (after matching for CheckMate 577) was considered to be the best match to the CheckMate 577 population and to the Canadian population, particularly considering the sparsity of published data for this indication, t was noted by the Clinical Review Team that despite the effort for alignment, there are some notable differences between the two populations. Firstly, evidence for PD-L1 status, exact composition of HER2 status, as well as information regarding smoking status is lacking in CA209-77E study. Secondly, there are no co-morbidity data reported from CheckMate 577. As well, clinical status as represented by ECOG PSR score, disease at diagnosis, and median weight show discrepancies. The clinical significance of these missing data and imbalance between the two population characteristics remains unknown as to what extent each of them exerts its effect on analyses of outcomes, such as recurrence, disease free survival, and mortality.
According to the clinician experts, the CA209-77E data, when matched to the CheckMate-577 study population based on the inclusion criteria above, are generalizable to the Canadian population with the esophageal and GEJ cancers in the absence of Canadian registry data. The clinician experts noted that distribution of EC and GEJC in CA209-77E and discrepancy in EC and GEJC between CA209-77E and CheckMate 577 (i.e., 93.6% of patients had EC and 6.4% of patients GEJC in CA209-77E compared to 59.8% of patients with EC and 40.2% of patients with GEJC in CheckMate-577) were potentially due to initial inclusion criteria differences between the two datasets and significantly less patients with GEJC captured in CA207-77E might have an impact on the recurrence rate depending on their Siewert classifications and/or stages. Nonetheless, in the absence of mature OS data for CheckMate 577 and Canadian registry data for recurrence, CA209-77E appeared to generalizable to the Canadian population with the esophageal and GEJ cancers.
Table 28: Population Comparison of CA209-77E Report 1C Pre-Recurrence, CA209-77E Report 1C Post-Recurrence, and CheckMate 577
Study details | CA209-77E Report 1C: pre-recurrence | CA209-77E Report 1C: post-recurrence | CheckMate 577 |
|---|---|---|---|
Ethnicities | Patients diagnosed with esophageal and gastric cancer in the Netherlands, using the IKNL nationwide registry dataset | Patients diagnosed with esophageal and gastric cancer in the Netherlands, using the IKNL nationwide registry dataset | Patients were enrolled at 170 sites in 29 countries (Argentina, Australia, Belgium, Brazil, Canada – 4.7%, China, Czech Republic, Denmark, France, Germany, Hong Kong, Hungary, Ireland, Israel, Italy, Japan, Mexico, Netherlands – 2.6%, Poland, Republic of Korea, Romania, Russian Federation, Singapore, Spain, Switzerland, Taiwan, Turkey, UK, and USA) |
Enrolment period | Diagnosed (ESCC/EAC/GEJC) and received treatment of curative intent 2015-2016 | Diagnosed (ESCC/EAC/GEJC) and received treatment of curative intent 2015-2016 | July 2016 to August 2019 |
Number of patients | The total sample size of the CM-577 aligned population is 718. | Any recurrence 359 | 1,085 subjects were enrolled, 794 subjects were randomized (532 to the nivolumab arm and 262 to the placebo arm) |
Inclusion criteria | ≥18 years of age at diagnosis | ≥18 years of age at diagnosis | ≥ 18 years of age |
Primary non-metastatic diagnosis of ESCC/EAC/GEJC | Primary non-metastatic diagnosis of ESCC/EAC/GEJC | Stage II or III (AJCC 7th edition) carcinoma of the esophagus or GEJ | |
Histologically confirmed predominant AC or SCC at the time of initial diagnosis | |||
Treated with curative intent. Received preoperative, platinum-based chemoradiotherapy, then surgery | Treated with curative intent. Received preoperative, platinum-based chemoradiotherapy, then surgery | Completed pre-op (neoadjuvant) CRT (consisting of platinum-based chemotherapy) followed by surgery prior to randomization. Chemotherapy and radiation regimens could be followed as local SoC per NCCN or ESMO guidelines | |
Received an R0 resection | Received an R0 resection | Complete resection (R0) performed in a window of 4 to 16 weeks prior to randomization. Should be surgically rendered free of disease with negative margins on resected specimens defined as no vital tumour present within 1 mm of the proximal, distal, or circumferential resection margins. | |
(continued) | Residual pathological disease (i.e., non-pCR), with at least ypN1 or ypT1 in the pathology report for resected specimen | Residual pathological disease (I.e., non-pCR), with at least ypN1 or ypT1 in the pathology report for resected specimen | Residual pathologic disease (non-pCR) of their EC or GEJC, with at least ypN1 or ypT1 listed in their pathology report |
NA | NA | Tumour cell PD-L1 status classification of ≥ 1%, < 1% or indeterminate/non-evaluable | |
ECOG PS 0–2 pre-occurrence | ECOG PS 0–4 post-occurrence | ECOG PS score 0 or 1 | |
NA | NA | Disease-free status documented by a complete physical examination and imaging studies within 4 weeks of randomization. Imaging studies must include CT/MRI scan of chest and abdomen. | |
Baseline characteristics | |||
Male, N (%) | 584 (81.3) | 300 (83.6) | 671 (84.5) |
Age (years), median, IQR | 65 (59 to 70) | 66 (60 to 71) | 62 (55 to 7) |
Race – White, N (%) | NA | 648 (81.6) | |
Comorbidities, N (%) | |||
0 | 206 (28.7) | 104 (29) | NR |
1 | 233 (32.5) | 109 (30.4) | NR |
≥ 2 | 241 (33.6) | 120 (33.4) | NR |
Unknown | 38 (5.3) | 26 (7.2) | NR |
ECOG PS, N (%) | |||
0 | 358 (49.9) | 46 (12.8) | 464 (58.4) |
1 | 255 (35.5) | 89 (24.8) | 330 (41.6) |
2 | 20 (2.8) | 32 (8.9) | 0 (0) |
3 | 0 (0) | 28 (7.8) | 0 (0) |
4 | 0 (0) | 5 (1.4) | 0 (0) |
Unknown | 85 (11.8) | 159 (44.3) | 0 (0) |
Weight, median (IQR) | 80 (70-91) | 73 (65-85) | 71.25 (60-83) |
Smoking, current/former | NA | NA | 561 (70.7) |
HER2 status, N (%) | |||
Positive | NAa | NA | 63 (7.9) |
Negative | NAa | NA | 207 (26.1) |
Unknown | NAa | NA | 2 (0.3) |
Not reported | NAa | NA | 522 (65.7) |
Disease at diagnosis, N (%) | |||
EC | 672 (93.6) | NA | 475 (59.8) |
GEJC | 46 (6.4) | NA | 319 (40.2) |
Treatment received after diagnosis, N (%) | |||
CRT | 697 (97.1) | NA | 794 (100) |
Esophagectomy | 711 (99) | NA | 703 (88.5) |
Total gastrectomy | 7 (1) | NA | 26 (3.3) |
Neoadjuvant | 718 (100) | NA | 792 (99.7) |
Neoadjuvant: carboplatin and paclitaxel (with radiation) | 703 (97.9) | NA | NR |
Neoadjuvant: carboplatin | NA | NA | 603 (75.9) |
Neoadjuvant: paclitaxel | NA | 599 (75.4) | |
Adjuvantb | 21 (2.9) | NA | 2 (0.3) |
AC = adenocarcinoma; AJCC = American Joint Committee on Cancer; CRT = chemoradiation therapy; EAC = esophageal adenocarcinoma; EC = esophageal cancer; ESCC = esophageal squamous cell carcinoma; ESMO = European Society of Medical Oncology; GEJC = gastroesophageal juncture cancer; HER2 = human epidermal growth factor receptor 2; INKL = Netherlands Comprehensive Cancer Organization; IQR = interquartile range; NA = not available; NCCN = National Comprehensive Cancer Network; non-pCR = non-pathologic complete response; NR = not reported; RT = radiation therapy; SCC = squamous cell carcinoma; SoC = standards of care;
aPatients with HER2 positive tumors were included, unless they received trastuzumab, in which case they were excluded
bCalculated differently. Direct comparison not possible.
Source: Clinical Study Report main, Clinical Study Report supplementary, Clinical Study Report protocol, CA209-77E main, CA209-77E supplementary.3
Appendix 9: Description and Appraisal of Outcome Measures
Aim
To describe the following outcome measures summarized in Table 29 and review their measurement properties (validity, reliability, responsiveness to change, and clinical relevance, i.e., MID):
Patient reported outcomes including the EQ-5D-3L and the FACT-E questionnaires, the latter’s selected ECS, and the FACT-G and FACT-G7, were reported in the pivotal trial (CheckMate 577)2 as exploratory end points.
Findings
Table 29: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EQ-5D-3L | A generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments | The validation of EQ-5D-3L is available across countries around the world and in various conditions.39,40 Validity: Strong correlation was observed between EQ-5D-3L and FACT-E total score (R = 0.73), as well as FACT-E subclass domains to varying degrees. Also, moderately strong correlation with ECOG scale (Spearman r = -0.65) and EQ-5D-3L HUS.41 Responsiveness: EQ-5D-3L HUS displayed a similar pattern as mean FACT-E and its subscale scores (P < 0.05 for time points studied). However, the ceiling effect was observed in the EQ-5D-3L HUS.41 | Unknown for esophageal cancer patient population For cancers (not including esophageal cancer)42: MID (UK): 0.10 to 0.12 based on PS range and 0.09 - 0.10 based on FACT-G score MID (US): 0.07 to 0.09 grouped by PS and 0.06 - 0.07 grouped by FACT-G score MIDs for VAS: 8 to 12 using PS and 7 to 10 using FACT-G quintiles |
FACT-E | An esophageal cancer-specific, preference-based HRQoL instrument with 5-point Likert type scale. Higher the score, better quality of life.43 FACT-E consists of 44 items in 5 subscale domains - physical, social/family, emotional, functional well-being, and ECS. FACT-E total scores and each subclass domain score, as well as FACT-G, ECS, TOI scores can be derived. | Overall, FACT-E is a reliable tool to measure HRQoL of esophageal cancer patients in any stage or severity with no reported ceiling effect. Validity: FACT-E overall scale, subscales, and aggregate scores demonstrated convergent and divergent validity compared with the EORTC QLQ 30 and OES 24.44 Reliability: Internal consistency (i.e., coefficient alpha) for all FACT-E | Not identified |
(continued) | subscales, total, and aggregate scores were >0.70 at both baseline and 3-7 days of follow-up.44 Responsiveness: FACT-E is responsive to changes in patient status over 3-4 months of standard therapies for esophageal cancer.44 | ||
ECS |
| Validity: Strong correlation between the overall ECS score, and the eating and swallowing indexes with the dysphagia (Spearman r > -0.80) and eating items (r > -0.72) from the OES 24 was demonstrated.44 Reliability: Both aggregate indexes derived from eating and swallowing items from the ECS had strong internal consistency (alpha > 0.80).44 Responsiveness: Overall ECS score demonstrated varying degrees of responsiveness depending on the sample population, i.e., differences in standards of therapies.44 | Not identified |
FACT-G | A cancer-specific, preference-based HRQoL instrument with 5-point Likert type scale that can be applied to a variety of tumour type. Higher the score, better quality of life.45 FACT-G consists of 27 items in 4 subscale domains – physical, social/family, emotional, and functional well-being. Total FACT-G score and individual subclass domain score is possible. In addition, the core measure can be supplemented with Additional Concerns subscales, which contain disease-, treatment-, or condition-specific items. | FACT-G is a well-studied HRQoL scoring measure that has been extensively validated by many groups. It is available in various languages.45 Validity: Convergent and divergent validity has been demonstrated compared to FLIC (Pearson r = 0.79), TMAS (r = −0.58), BriefPOMS (r = −0.65), ECOG 5-point PSR (r = −0.56), as well as shortened M-CSDS (r = 0.22). Construct validity, i.e., ability to differentiate clinical states, has been demonstrated based on stage of disease (I, II, III, IV), ECOG PSR (0, 1, 2, 3/4), and location of administration (indicating severity of condition or types of concerns).46 | For any cancer patient49: MID: for total FACT-G score: 3-7 points MIDs: for subclass domains PWB, EWB, SWB, FWB: 2-3 points. |
(continued) | Also, concurrent validity has been shown against EQ-5D (FACT-G overall score r = 0.649) and SF-6D (FACT-G overall score r = 0.714).47 Reliability: Internal consistency (coefficient alpha) of total FACT-G score was found to be 0.89. Test-retest reliability with 3-7 days of interval for total FACT-G score was shown to be 0.92.46 Responsiveness: FACT-G can clearly distinguish 3 groups patients whose clinical status changes can be mapped according to PSR category, i.e., declined PSR, improved PSR, or unchanged PSR (overall FACT-G score P = 0.002).46 FACT-G was also found to be able to capture patient-rated meaningful changes in clinical status over 2-3 months (overall FACT-G score P < 0.001).48 SWB subclass domain has been shown to be not sensitive or inconclusive.46,48 | ||
FACT-G7 | A cancer-specific, preference-based HRQoL instrument with 5-point Likert type scale that can be applied to any tumour type. Higher the score, better quality of life.50 A shortened, 7-item version of FACT-G to measure the most relevant symptoms and concerns ranked by cancer patients. FACT-G7 assesses 3 domains (physical, emotional, and functional well-being) in 7 questions:
| FACT-G7 mirrors FACT-G, which is well-studied HRQoL scoring measure that has been extensively validated by many groups. [2] Validity: FACT-G7 was highly correlated with the FACT-G total score (r = 0.89) moderately correlated with the EQ-5D (r = 0.60). Of all the subclass domains of FACT-G, SWB correlation was the weakest (r = 0.209). As for construct validity, FACT-G7 was able to successfully distinguish across ECOG PSR categories, with medium-to-large effect. Lastly, construct validity was ensured by incorporating patient and clinician output.51 Reliability: FACT-G7 showed good internal consistency for group comparisons in the NCCN cancer sample and the general US population sample with Cronbach’s | Based on US general adult population and cancer patients merged from 12 different studies52: MID: for total FACT-G7: 2-3 points |
(continued) |
| alphas of 0.74 and 0.80, respectively.51 Responsiveness: FACT-G7, and all subscales worsened with declining the ECOG PSR category and lower FACT-G7 scores were found with worsening disease status (P < 0.001; ES 0.11-0.73).52 |
BriefPOMS = Brief Profile of Mood States; ECOG = the Eastern Cooperative Oncology Group; ECS = esophageal cancer subscale; EORTC QLQ 30 = the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire 30; EQ-5D-3L = EuroQol 5-Dimensions 3-Levels questionnaire; FACT-E = Functional Assessment of Cancer Therapy–Esophageal; FACT-G = Functional Assessment of Cancer Therapy–General; FACT-G7 = Functional Assessment of Cancer Therapy–General 7 items; FLIC = Functional Living Index – Cancer; HRQoL = health-related quality of life; HUS = health utility scores; M-CSDS = Marlowe-Crown Social Desirability Scale; MID = minimal important difference; NCCN = the National Comprehensive Cancer Network; OES 24 = esophageal 24; PS = performance status; PSR = performance status rating; SF-6D = (EQ-5D) short form 6 dimension; SWB = social well-being; TMAS = Taylor Manifest Anxiety Scale; VAS = visual analogue scale.
EuroQol 5-Dimensions 3-Levels Questionnaire
The EQ-5D-3L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments.39,40 The first of two parts of the EQ-5D-3L is a descriptive system that classifies respondents (aged ≥ 12 years) into one of 243 distinct health states. The descriptive system consists of the following five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has three possible levels (1, 2, or 3) representing “no problems,” “some problems,” and “extreme problems.” respectively. Respondents are asked to choose one level that reflects their own health state for each of the five dimensions. A scoring function can be used to assign a value (EQ- 5D-3L index score) to self-reported health states from a set of population-based preference weights.39,40 The second part is a vertical, calibrated 20 cm VAS that has endpoints labeled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state,” respectively. Respondents are asked to rate their own health by drawing a line from an anchor box to the point on the VAS that best represents their own health on that day. Hence, the EQ-5D-3L produces three types of data for each respondent:
A profile indicating the extent of problems on each of the five dimensions represented by a 5-digit descriptor, such as 11121, 33211
A population preference-weighted health index score based on the descriptive system
A self-reported current health status based on the VAS that is used to assess the overall health of the respondent rather than selected dimensions of individuals’ health
The EQ-5D-3L index score is generated by applying a multi-attribute utility function to the descriptive system. Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK). The lowest possible overall score (corresponding to severe problems on all five attributes) varies depending on the utility function that is applied to the descriptive system (e.g., −0.59 for the UK algorithm and −0.109 for the US algorithm). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.
Validity
Doherty et al. analyzed 119 patients with histologically confirmed esophageal cancer and gastroesophageal junction cancer (Siewert I/II) of all disease stages at ambulatory clinics in a cross-sectional survey study and a real-world setting. Bivariate Spearman correlation and multivariable linear regression analyses characterized associations between the various FACT-E subscales, scales, and the FACT-E derived symptom complexes with EQ-5D-3L derived health utility scores (HUS). Strong correlation was observed between EQ-5D-3L and FACT-E (R = 0.73): the strongest correlation observed with the PWB subscale, followed in descending order by FWB, esophageal-specific symptoms, EWB, and SWB subscales. In addition, the association between FACT-E and EQ-5D-3L was maintained in a multivariable model (β of 0.0044, P < 0.001). Lastly, moderately strong correlation was also seen between a self-reported performance status based on the Eastern Co-operative Oncology Group (ECOG) scale (Spearman r = -0.65) and EQ-5D-3L HUS.41
Reliability
There is insufficient data to assess reliability of EQ-5D-3L in the setting of esophageal cancer.
Responsiveness
Doherty et al. analyzed the same sample in longitudinal follow-up surveys at baseline and predetermined subsequent visits, i.e., pre, during CRT, and post-treatment (within the first 6 months following definitive CRT or surgery), surveillance (more than 6 months from definitive treatment without relapse or progression), progression, and palliative chemotherapy. EQ-5D-3L HUS displayed a similar pattern as mean FACT-E and subscale scores, which dropped from baseline through treatment and recovered during post-treatment surveillance (P < 0.001), but with smaller differences (P = 0.07). In addition, the ceiling effect was observed in the EQ-5D-3L HUS. Briefly, among patients with stage II/III esophageal cancer, mean EQ-5D-3L HUS varied across disease states (P < 0.001), along with FACT-E and subscales (P < 0.001). Among patients with advanced disease, there was no significant difference between baseline and on-treatment total scores of EQ-5D-3L, but improved ECS scores were noted (P = 0.003). Overall, the observed differences in mean EQ-5D-3L HUS across cancer stages and disease states suggests some sensitivity to change in clinical circumstances.41
Clinical Relevance
There is insufficient information regarding the estimated MIDs for esophageal cancer.
Pickard et al. conducted a retrospective analysis on cross-sectional data collected from 534 cancer patients. A range of MIDs in EQ-5D index-based utility (UK and US) scores and VAS scores were estimated using both anchor-based (ECOG-PS and FACT-G total score-based quintiles) and distribution-based (0.5 standard deviation and standard error of the measure) approaches. Important differences in EQ-5D utility and VAS scores were similar for all cancers (not including esophageal cancer). For UK-utility scores, MID estimates based on PS ranged 0.10 - 0.12 and were 0.09 - 0.10 using FACT-G quintiles for all cancers (not including esophageal cancer). For US-utility scores, MIDs ranged 0.07 - 0.09 grouped by PS and when based on FACT-G quintiles, MIDs were 0.06 - 0.07 in all cancers (not including esophageal cancers). MIDs for VAS scores ranged from 8 to 12 (PS) and 7 to 10 (FACT-G quintiles).42
Other Considerations and Limitations
One limitation of the EQ-5D-3L was a significant ceiling effect, and left skew of the data, i.e., EQ-5D-3L may be more useful in a population with worse overall health status. Further, though EQ-5D-3L may be an adequate tool to summarize HRQoL, responsiveness to change may still be better captured using a more standard tool such as FACT-E.41 In addition, there is a lack of data for VAS to assess its validity in the setting of esophageal cancer.
Functional Assessment of Cancer Therapy–Esophageal and Esophageal Cancer Subclass
The FACT-E is a patient-reported, disease-specific, health-related quality-of-life measure that was developed to evaluate symptoms in esophageal cancer patients who are 18 years old and older. The FACT-E includes 44 items grouped into 5 subclass domains: (1) physical well-being (PWB), (2) social/family well-being (SWB), (3) emotional well-being (EWB), (4) functional well-being (FWB), and (5) esophageal cancer subscale (ECS). The ECS addresses concerns specific to patients with esophageal cancer such as eating, appetite, swallowing, pain, talking/communicating, mouth dryness, breathing difficulty, coughing, and weight loss. The questionnaire can be used to derive scores for FACT-E, FACT-G, and Trial Outcome Index (TOI). Briefly, the total FACT-E score is the sum of the ECS and the FACT-G scores. A TOI score, useful where the physical domains are of interest, can be computed by adding the PWB and FWB scores to the ECS score. All FACT-E items are rated on a 5-point Likert-type scale ranging from 0 = ‘‘not at all’’ to 4 = ‘‘very much’’. Negatively-worded items are reverse scored so that higher scores always represent better quality of life or less severe symptoms. Possible score ranges are PWB (0–28), FWB (0–28), SWB (0–28), EWB (0–24), ECS (0–68), TOI (0–124), swallowing index (0–20), eating index (0–12), FACT-G (0–108), and FACT-E (0–176).44 Patients recall their relevant experiences during the previous 7 days. The most recent version of FACT-E is v.4.43
Validity
The concurrent validity of FACT-E was assessed in 83 adult patients with esophageal cancer treated with surgery alone or neoadjuvant CRT and surgery in a prospective cohort study by comparing with the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ 30) and esophageal (OES 24). Spearman correlations (r) were used to determine the convergent and divergent validity of the FACT-E including the overall scale, subscales, and aggregate scores. The FACT-E demonstrated convergent and divergent validity compared with the EORTC QLQ 30 and OES 24. For example, a strong correlation between the PWB, FWB, EWB subscales of the FACT-E and the corresponding physical function, role function, and emotional function scales of the QLQ with r = 0.53, 0.58, and 0.67, respectively, was demonstrated. On the contrary, a weak correlation between EWB and the physical and role function scales of the QLQ with r = 0.22, 0.17, respectively, was observed. Furthermore, a strong correlation between the overall ECS score, and the eating and swallowing indexes with the dysphagia (r = -0.87, -0.80, -0.83) and eating items (r = -0.84, -0.82, -0.72) from the OES 24 was demonstrated. Overall, the scale shows a good concurrent validity when compared with another measure of conditions of cancer including esophageal cancer.44
Reliability
Test-retest reliability was determined 3- to 7-day interval after baseline. Coefficient alpha for all FACT-E subscales, total, and aggregate scores were > 0.70 at both baseline and follow-up. Also, both aggregate indexes derived from eating and swallowing items from the ECS had strong internal consistency (alpha > 0.80). Taken together, reliability of the FACT-E as represented by test-retest measure and internal consistency is acceptable.44
Responsiveness to Change
Paired sample t test and repeated measures analyses of variance (ANOVAs) were used to determine responsiveness to change in the FACT-E over 3 to 4 months. The clinical status changes were reflected in changes in FACT-E scores demonstrating responsiveness to change. For example, cohort A (N = 54) data showed that PWB decreased significantly (p = 0.006; ES = 0.4) over the study time interval, a result consistent with the expectations after major surgery, whereas EWB scores significantly improved (p = 0.001; ES = 0.35). The overall ECS score showed very little change over time, as many patients had almost regained their baseline level of well-being by 3 to4 months after surgery. Likewise, cohort B (N = 29) data showed that PWB (p = 0.000; ESs of adjacent means = 0.72, 1.75) and FWB (p = 0.000; ESs of adjacent means = 0.31, 0.77) scores declined significantly from baseline to week 7, but improved significantly by week 12 to 14, where there were no changes over time in the SWB and EWB scores. There was a significant improvement in overall ECS (p = 0.004; ESs of adjacent means = 0.20, 0.78) score from week 7 to week 12 to14. Therefore, the FACT-E is responsive to changes in patient status over the course of standard therapies for esophageal cancer.44
Clinical Relevance
There are no minimally important differences estimated for FACT-E.
Other Considerations and Limitations
The study population was divided into 2 groups, i.e., cohort A and cohort B, which further reduces the sample size. The initial validation in a group of surgical patients was done with cohort A (54 patients with histologically proven resectable squamous or adenocarcinoma of the esophagus or gastroesophageal junction). Then, further evaluation of responsiveness to change in clinical conditions was done in cohort B (29 patients with clinically staged locally advanced disease treated with neoadjuvant CRT before surgery: all ECOG 0-1) as well as cohort A. Therefore, statistical power and accuracy of results decreased.44
Functional Assessment of Cancer Therapy–General
The FACT-G is a self-administered, disease-specific, health-related quality-of-life measure for patients with any tumour type who are 18 years and older. The FACT-G is a 27-item instrument containing four subscales: Physical Well-Being (PWB; 7 items), Functional Well-Being (FWB; 7 items), Social Well-Being (SWB; 7 items), and emotional well-being (EWB; 6 items) on a 5-point Likert-type scale ranging from 0 (not at all) to 4 (very much) with a recall period of the past 7 days. Negatively worded items are reverse scored so that higher scores always represent better quality of life or less severe symptoms. Responses are summed to create a total FACT-G score and individual subscale scores. The highest possible score is 28 for the PWB, SWB, and FWB subscales, 24 for the EWB subscale, and 108 for the FACT-G total score.52 The core measure can be supplemented with Additional Concerns subscales, which contain disease-, treatment -, or condition-specific items. The most recent version of FACT-G is v.4.45
Validity
The assessment of convergent and discriminant validity was performed by Cella et al. in 316 patients with mixed cancer diagnoses. Convergent validity was evaluated by examining the association between scores of FACT-G v.2 and those of similar measures and divergent validity with dissimilar measures completed at the same time: high and low coefficient relations are expected, respectively. The Pearson correlation with Functional Living Index – Cancer (FLIC) was high (r = 0.79) as well as measures of mood distress (r FACT/ Taylor Manifest Anxiety Scale = −0.58; r FACT/BriefPOMS = -0.65). The correlation with activity level as measured by ECOG PS Rating (ECOG 5-point PSR) was moderately high (r = −0.56). On the contrary, the correlation with social desirability, as measured by shortened Marlowe-Crown Social Desirability Scale (M-CSDS) was low (r = 0.22), supporting divergent validity. Secondly, construct validity has been demonstrated by Cella et al. by sensitivity to differentiation. The total FACT-G score was able to differentiate patients according to stage of disease (I, II, III, IV), ECOG PSR (0, 1, 2, 3/4), and location of administration (Rush-Presbyterian-St Luke's Medical Center [RPSLMC]) inpatient indicating more severe conditions, RPSLMC outpatient indicating less severe conditions, Community Cancer Wellness program (CWC) which addresses social and emotional aspects of cancer). To be specific, FACT-G v.2 sensitivity to stage of disease was seen in the PWB (p < 0.01) and FWB (p < 0.0001) subscales, and the total score (p = 0.01). These scores were significantly lower in stage IV patients compared with stage I and II patients, reflecting poorer quality of life in physical (not social and emotional) areas. As for PSR, the total FACT-G v.2 score and all subscales were significantly higher (better) for patients with lower (better) PSR: PWB (p < 0.0001), FWB (p < 0.0001), SWB (p < 0.05), EWB (p < 0.0001). Total FACT-G v.2 score was higher for RPSLMC outpatients than those for RPSLMC inpatients and CWC participants (p < 0.0001). As expected, subscale scores for PWB and FWB were higher (p < 0.001) for RPSLMC outpatient than those for RPSLMC inpatient and CWC participants. Moreover, subscale scores for SWB and EWB were lower (p < 0.001) for CWC participants than either RPSLMC patients, reflecting the fact that patients were referred to CWC for social and emotional support.46
Another group confirmed concurrent validity of FACT-G v.4 by comparing it with EQ-5D (FACT-G overall score r = 0.649) and SF-6D (FACT-G overall score r = 0.714) in 367 patients with breast, colorectal, and lung cancer. As for correlation coefficients for subclasses of FACT-G v.4, PWB (EQ-5D r = 0.631; SF-6D r = 0.753) and FWB (EQ-5D r = 0.599; SF-6D r = 0.678) demonstrated high correlations with other selected preference-based measures, whereas EWB (EQ-5D r = 0.429; SF-6D r = 0.386) and SWB (EQ-5D r = 0.222; SF-6D r = 0.205) showed weak correlations.47
Reliability
Firstly, Cella et al. reported internal consistency (coefficient alpha) of each subscale and the total FACT-G v.2 score: PWB 0.82, FWB 0.80, SWB 0.69, EWB 0.74, and total FACT-G v.2 0.89. in 545 patients with mixed cancer diagnoses. Second, test-retest reliability was assessed in 60 outpatients with various cancer types with second administration of questionnaire 3-7 days later. Correlation coefficients for PWB = 0.88, FWB = 0.84, SWB = 0.82, EWB = 0.82, and total FACT-G score = 0.92.46
Responsiveness to Change
Cella et al. administered FACT-G v.2 to 104 patients currently receiving chemotherapy for advanced breast, lung, or colon cancer with follow-up period of 2 months. Multivariate analysis of variance confirmed a significant overall effect (p = 0.002), indicating that the FACT-G v.2 can clearly distinguish 3 groups patients whose clinical status changes can be mapped according to PSR category, i.e., declined PSR, improved PSR, or unchanged PSR. Results of the follow-up univariate tests indicate that the strongest responsiveness was observed in PWB (p < 0.001) and FWB (p < 0.01) subscales. Subscale EWB (p < 0.05) was somewhat sensitive to clinical change over time, however, SWB was not (p = N/A).46 Later study conducted by Cella et al. confirmed responsiveness of FACT-G v.3 in 308 cancer patients in the time interval of 2-3 months. Their findings based on one way analysis of variance support that FACT-G v.3 captured patient-rated meaningful changes in PWB (p < 0.001), FWB (p < 0.05), EWB (p < 0.005), and overall FACT-G v.3 (p < 0.001) scores over time; however, SWB (p > 0.05) remains inconclusive.48
Clinical Relevance
Yost et al. used a methodology that combined distribution- and anchor-based approaches to determine the MID for FACT-G. The range for meaningful differences for the total FACT-G score is 3-7 points. The range for meaningful differences for all four subscales (i.e., PWB, EWB, SWB, FWB) of FACT-G is 2-3 points.49
Other Considerations and Limitations
Different FACT-G versions were used in different studies. There is no sufficient information if different version significantly impacts assessment of validity, reliability, responsiveness, and clinical relevance (i.e., MID).
Functional Assessment of Cancer Therapy–General 7 Items
The FACT-G7 is a shortened, 7-item version of the FACT-G designed to capture the most relevant health-related quality-of-life issues to cancer patients who are 18 years old and older. The FACT-G7 can be used to rapidly assess top-rated symptoms and concerns by patients, such as fatigue and ability to enjoy life, for a broad spectrum of advanced cancers. There are 3 domains, i.e., Physical (PWB), emotional (EWB), and functional well-being (FWB). Each question is scored on a 5-point Likert-type scale, which ranges from 0 (not at all) to 4 (very much).50 Negatively-worded items are reverse scored so that higher scores always represent better quality of life or less severe symptoms.44 Only the overall FACT-G7 score can be calculated and it ranges from 0 to 28.51 The questionnaire is self-administered by patients who recall their experiences in the past 7 days. The most recent version of FACT-G7 is v.4.50
Validity
Firstly, Yanez et al. investigated concurrent validity, which was assessed by testing the strength of correlation between the FACT-G and FACT-G7 in oncology patients with advanced cancer (N = 533) from 11 diseases sites. The FACT-G7 was highly correlated with the FACT-G total score (Spearman correlation r = 0.89) and, with the exception of the SWB subscale (r = 0.29), moderately correlated with the PWB (r = 0.80), EWB (r = 0.62), and FWB (r = 0.82) subscales of the FACT-G (all P < 0.001). In addition, the FACT-G7 was moderately correlated with the EQ-5D (r = 0.60; P < 0.001) in the same study population. Secondly, the same study group tested construct validity and found that FACT-G7 was able to successfully distinguish across ECOG PSR categories, with medium-to-large effect sizes in the NCCN cancer sample (F statistic [2, 530] = 87.43; P < 0.001) and general population sample (F statistic [2, 1997] = 331.47, P < 0.001). Lastly, Yanez et al. ensured the content validity by developing indexes in the FACT-G7 by incorporating input from cancer patients and clinician experts in particular cancer types. Furthermore, while developing the indexes, the patients were encouraged to write in new symptoms and concerns that they felt were important. Taken together, concurrent, construct, and content validity has been demonstrated for the FACT-G7.51
Reliability
According to Yanez et al., internal consistency (i.e., Cronbach’s alphas) for the FACT-G7 is found to be acceptable (e.g.,> .70). To be more specific, the FACT-G7 showed good internal consistency for group comparisons in the NCCN cancer sample and the general US population sample with Cronbach’s alphas of 0.74 and 0.80, respectively.51
Responsiveness to Change
A sample of patients with cancer merged from 12 studies (N = 5,065) were analyzed Pearman et al. Multiple comparisons were adjusted for using a Tukey’s test. Within the adult cancer sample, scores on the FACT-G7, and all subscales worsened with declining the Eastern Cooperative Oncology Group Performance Status Rating (ECOG PSR) category and lower FACT-G7 scores were found with worsening disease status (p < 0.001; ES 0.11-0.73).52
Clinical Relevance
MID for FACT-G7 was derived by Pearman et al. Briefly, the range of observed 0.33 standard deviation and 1.0 standard error of the mean FACT-G7 score in their study was found to be from 1.83 to 2.57. This magnitude of change was closest to a combined ECOG PSR category of 2/3/4. Therefore, 2 to 3 points on the FACT-G7 score deemed meaningful differences in clinical status and patientive anchors.52
Pharmacoeconomic Review
Abbreviations
AE
adverse event
DFS
disease-free survival
EC
esophageal cancer
EQ-5D-3L
EuroQol 5-Dimensions 3-Levels questionnaire
FOLFOX
leucovorin plus 5-fluorouracil plus oxaliplatin
GEJC
gastroesophageal junction cancer
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
IKNL
Netherlands Comprehensive Cancer Organization
QALY
quality-adjusted life-year
TTR
time to recurrence
XELOX
capecitabine plus oxaliplatin
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo), IV infusion |
Submitted price | Nivolumab, 40 mg and 100 mg single-use vials:
|
Indication | Adjuvant treatment of completely resected esophageal or gastroesophageal junction cancer in patients who have residual pathologic disease following prior neoadjuvant chemoradiotherapy |
Health Canada approval status | NOC |
Health Canada review pathway | Other expedited pathway: Project ORBIS |
NOC date | July 2, 2021 |
Reimbursement request | As per indication |
Sponsor | Bristol-Myers Squibb Canada |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Completely resected patients with esophageal or gastroesophageal cancer who have residual pathologic disease following prior neoadjuvant chemoradiotherapy |
Treatment | Nivolumab |
Comparator | Surveillance (no systemic treatments) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | 30 years |
Key data sources | CheckMate 577 trial: transitions from pre-recurrence to post-recurrence based on DFS, pre-recurrence to death based on the risk of death among trial participants (up to 3 years) Netherlands Comprehensive Cancer Organization: transition from post-recurrence to death |
Submitted results | Nivolumab is associated with an ICER of $42,733 per QALY compared with surveillance (incremental costs: $71,474; incremental QALYs: 1.67) |
Key limitations |
|
CADTH reanalysis results |
|
DFS = disease-free survival; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Conclusions
Evidence from the interim analysis of the CheckMate 577 trial1 showed that nivolumab adjuvant treatment was associated with a clinically meaningful and statistically significant improvement in disease-free survival (DFS) compared to placebo in patients with esophageal cancer (EC) or gastroesophageal junction cancer (GEJC) who have residual pathologic disease following prior neoadjuvant chemoradiotherapy. The safety profile of nivolumab in this study was consistent with the known safety profile of nivolumab, and no additional safety signals with adjuvant nivolumab therapy were identified in this study. The patient-reported and health-related quality of life (HRQoL) outcomes (e.g., EuroQol 5-Dimensions 3-Levels questionnaire [EQ-5D-3L]) were assessed as exploratory outcomes, and there was a potential risk of bias because of substantial missing data on these outcomes during the trial follow-up period.
Although CADTH identified several limitations within the sponsor’s economic analysis, not all limitations could be addressed. CADTH made the following corrections to the sponsor’s model: the dosage regimens of subsequent chemotherapy were corrected, publicly listed prices for cisplatin, oxaliplatin, and leucovorin were used, standard errors of cost parameters without known variance to 20% of their mean values were increased, and the number of simulations was increased to 5,000 iterations. The CADTH base case assumed no vial sharing, used a flat dose of nivolumab, applied the same proportions of patients requiring subsequent chemotherapy to both nivolumab and surveillance arms, assigned a terminal-care cost to any patients who transitioned to death, and used 5 years as a cure time point.
CADTH’s base case resulted in a higher incremental cost-effectiveness ratio (ICER) of $79,241 per quality-adjusted life-year (QALY), compared with the sponsor’s $42,733 per QALY. Approximately 77% of the incremental QALYs and 6% of incremental costs came from the extrapolated period beyond the trial’s follow-up period. A price reduction of at least 36% in the current listed price would be required to ensure nivolumab is cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
The cost-effectiveness of nivolumab was sensitive to the assumed cure time point, followed by parametric models used to extrapolate DFS data. CADTH was unable to fully assess the methodological uncertainty associated with data used to derive the transition from pre-recurrence to death and post-recurrence utility values.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input from caregivers (N = 4) and patients (N = 11) with either esophageal and/or gastroesophageal cancer was received from My Gut Feeling – Stomach Cancer Foundation of Canada, collected via an online survey conducted from June 29, 2021, to July 16, 2021, in the US, Canada, and Australia. Of the participants, 93.3% had adenocarcinoma and 6.7% had squamous cell carcinoma, 66.7% were diagnosed with stage I to III cancer, 20% were diagnosed with stage IV cancer, and 13.3% were not aware of the diagnosed cancer stage. The participants reported that several symptoms of EC or GEJC can affect quality of life: changes in appetite, pain, weight loss, difficulty swallowing, nausea or vomiting, dumping syndrome, reflux, bloodwork abnormalities, blood clots, and chest pain. Cancer diagnosis also had a significant impact on quality of life, affecting the ability to eat, work, social life, identity, personal image, physical health, mental health, and finances. Current treatments include surgery, chemotherapy, radiation therapy, chemoradiation, immunotherapy, and alternative therapies. Systemic treatments included carboplatin plus paclitaxel (the subject of the Chemoradiotherapy for Esophageal Cancer followed by Surgery Study), leucovorin plus 5-fluorouracil plus oxaliplatin (FOLFOX), capecitabine, capecitabine plus oxaliplatin (XELOX), fluorouracil plus leucovorin plus oxaliplatin plus docetaxel (FLOT), herceptin, pembrolizumab, ramucirumab, and nivolumab. Most patients and caregivers reported improvement in symptoms of EC under standard of care with some common side effects, such as fatigue, nausea, appetite changes, constipation, weight loss, body ache, hair loss, taste changes, abdominal pain, brain fog, sleep problems, neuropathy, and dumping syndrome. Patients expressed a desire for new treatments that were more convenient (requiring less-frequent visits to the hospital) and accessible; 40% of respondents were willing to pay for new therapies out of pocket. One patient with surgically resected cancer and chemoradiation had direct experience with nivolumab through a hospital special access program. The patient did not report any exacerbated or additional side effects with its use. The patient reported improvement to quality of life and satisfaction with the decision to pursue nivolumab treatment to reduce the risk of recurrence.
Clinician input from the Ontario Health (Cancer Care Ontario) Gastrointestinal Drug Advisory Committee noted that there is an unmet need for routine adjuvant treatment to reduce the risk of recurrence in adults with completely resected EC or GEJC who have residual pathologic disease following prior neoadjuvant chemoradiotherapy. Treatment goals include prolonged life, delayed disease progression, reduced severity of symptoms, minimized adverse effects, and improved HRQoL. Clinicians noted that nivolumab would be added post-operatively in outpatient settings, such as chemotherapy suites, for all patients meeting the eligibility criteria, as described in the clinical trials. Clinicians added that nivolumab may affect treatment decisions at recurrence, and toxicity and recurrence may affect treatment continuation. Clinicians further noted that nivolumab may become a new standard of care, given its demonstrated improvement in DFS in a patient population that has a high risk of recurrence, high mortality rate, and poor quality of life.
The drug plans noted that jurisdictions will implement weight-based dosing up to a maximum dosage of 240 mg every 2 weeks for the first 16 weeks, followed by nivolumab 480 mg every 4 weeks beginning at week 17. The drug plans added that delayed treatment or treatment interruption in cases of toxicity may prolong nivolumab treatment past 1 year. The drug plans also anticipated a rapid market uptake of nivolumab, given that it may become a new standard of care for an aggressive disease with a high risk of recurrence.
The concern that clinical benefits be considered (i.e., delaying disease recurrence and fewer AEs associated with nivolumab) was addressed in the sponsor's economic model.
In addition, CADTH addressed the following concerns:
According to the drug plans, delayed treatment or interruption due to toxicity may extend nivolumab treatment beyond 1 year. Although the delay and interruption may not lead to an increased dose of nivolumab, CADTH took a conservative approach and assessed the impact of this concern by using DFS to represent the time to discontinuation in scenario analyses.
Nivolumab is funded using weight-based dosing in multiple jurisdictions. CADTH assessed the impact of this alternative dosing approach in scenario analyses.
CADTH was unable to address a concern raised in stakeholder input: a patient stated that their quality of life had improved due to nivolumab; however, the sponsor's model was unable to account for the impact of nivolumab on health utility values.
Economic Review
The current review is for nivolumab (Opdivo) for the adjuvant treatment of completely resected EC or GEJC in patients who have residual pathologic disease following prior neoadjuvant chemoradiotherapy.
Economic Evaluation
Summary of Sponsor's Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing costs and outcomes for nivolumab and surveillance (no systematic treatment) for the adjuvant treatment of completely resected EC or GEJC in patients with residual pathologic disease following prior neoadjuvant chemoradiotherapy. The modelled population was in line with the reimbursement request and Health Canada–approved indication.
Nivolumab is available as 40 mg and 100 mg single-use vials (10 mg/mL). According to the product monograph, the recommended dosage is 240 mg every 2 weeks or 480 mg every 4 weeks administered as an IV infusion over 30 minute.2 After completing 16 weeks of therapy, it is administered as 480 mg every 4 weeks until disease progression or unacceptable toxicity occurs, for a total treatment duration of 1 year. The cost of nivolumab is $782.22 for a 40 mg vial and $1,955.56 for a 100 mg vial, equating to a 28-day cost of $9,387. The sponsor assumed vial sharing and allowed 5% drug wastage in its drug-cost calculation. The sponsor’s analysis assumed that there was no treatment cost for those receiving surveillance.
The clinical outcomes were QALYs and life-years. The economic analysis was undertaken over a time horizon of 30 years from the perspective of a Canadian publicly funded health care system. Costs and QALYs were discounted at a rate of 1.5% per annum.
Model Structure
The sponsor submitted a Markov model with a cycle length of 1 month and the following health states: pre-recurrence, post-recurrence, and death (Appendix 3, Figure 1). All patients begin in the pre-recurrence health state, in which they can either remain, transition to death, or transition to the post-recurrence health state. Patients in the post-recurrence health state can remain or transition to death. All patients are assumed to receive treatments for up to 12 months or until disease progression or unacceptable toxicity. Upon discontinuation, the cost of treatment would no longer be incurred. Disease recurrence was defined as the appearance of 1 or more new lesions (local, regional, or distant in the location from the primary resected site, confirmed by imaging or a cytologic or pathological evaluation). The model incorporated a curative assumption, in which the risk of recurrence decreased to 0% after 3 years.
Model Inputs
The modelled population reflected the baseline patient characteristics of the enrolment population in the CheckMate 577 trial,1 a global, randomized, double-blind, placebo-controlled phase III trial that evaluates nivolumab as an adjuvant therapy in patients with GEJC. Approximately 1-third of the patients were from the US or Canada. The sponsor's model assumed a mean age of 60.5 years, a median weight of 71.25 kg, and a mean body surface area of 1.85 m2.
The transition from pre-recurrence to post-recurrence was informed by DFS curves obtained from the CheckMate 577 trial (data cut-off date of July 2020). The sponsor used flexible spline models to independently fit and extrapolate DFS curves for the nivolumab arm (splines odds with 2 knots) and surveillance arm (splines odds with 1 knot). The DFS curves were extrapolated until the point of cure (at 3 years). After 3 years, the sponsor’s model assumed that patients in the pre-recurrence health state who did not progress to the post-recurrence health state would not have a recurrence; they would therefore only transition from the pre-recurrence health state to death.
Transition from post-recurrence to death was assumed to be independent of treatment. This transition was informed by a real-world registry dataset from the Netherlands Comprehensive Cancer Organization (IKNL), due to immature overall survival data from the CheckMate 577 trial. The IKNL cohort was created to match the CheckMate 577 trial population in terms of tumour staging (stage II or III based on version 7 of the American Joint Committee on Cancer and the International Union for Cancer Control tumour-node-metastasis staging system), neoadjuvant therapy and surgery (required), resection status (R0 = resection required), and patients with residual pathological disease (non-pathological complete response). The sponsor also assumed that patients received the following subsequent treatments in the post-recurrence health state: cisplatin plus fluorouracil, FOLFOX, and XELOX. An exponential distribution was fit to the data to estimate the transition over the model time horizon. The transition from pre-recurrence to death was estimated from Canada-specific lifetables. The sponsor accounted for the higher mortality risk among participants of the CheckMate 577 trial by applying a hazard ratio of 4.26 to the Canadian all-cause mortality for up to 3 years, which is reflective of the length of the curative assumption.
The model accounted for adverse events (AEs) of grade 3 or higher that affected at least 5% of all study subjects enrolled in the CheckMate 577 trial.1 Health state–specific health utility values were based on an analysis of EQ-5D-3L data collected as part of the CheckMate 577 trial, which was derived using Canadian tariffs.3 The sponsor used a mixed-model approach to account for repeated EQ-5D-3L measurements per subject within a health state. Utility scores were further adjusted to reflect declining utility due to grade 3 to 4 AEs, which were obtained from the published literature.4,5
Costs included those for drugs (acquisition, administration, and subsequent treatments), disease management, AEs, and terminal care. Drug acquisition costs for each treatment were sourced from IQVIA Delta PA and the publicly available sources. Drug administration costs, including those associated with vial administration for IV therapies, were obtained from the Ontario Schedule of Benefits. Treatment dosing of subsequent treatments is based on the Cancer Care Ontario monographs for each treatment. The sponsor assumed that subsequent treatment is provided for 6.4 months, reflecting the median progression-free survival observed in the CheckMate 649 (6.9 months)6 and KEYNOTE-590 (5.8 months)7 trials. CheckMate 649 is a randomized, open-label, phase III trial evaluating nivolumab plus chemotherapy compared to chemotherapy alone as a first-line treatment for metastatic EC or GEJC, while KEYNOTE-590 is a randomized, double-blind, phase III study of cisplatin and 5-fluorouracil plus pembrolizumab compared to cisplatin and 5-fluorouracil plus placebo in patients with previously untreated advanced EC, GEJC, or esophageal adenocarcinoma.
The sponsor assigned disease management costs for pre-recurrence and post-recurrence health states. The resource use required per cycle was sourced from Canadian clinician opinion, while the unit costs were sourced from the Ontario Schedule of Benefits. The resources used for pre-recurrence consisted of monitoring patients in the adjuvant setting who received surveillance and were not managed with systemic treatment post-surgery. The model further assumed that disease management costs for pre-recurrence only incurred for the first 5 years; following those 5 years, it was assumed patients were no longer followed up if they maintained DFS. The post-recurrence disease management costs were applied throughout the model time horizon. A terminal-care cost was applied to patients who transitioned to the death health state up to the point of cure (3 years). The cost estimate was based on a study by Oliveria et al. (2016)8 that reported direct health care costs 12 months before death for EC patients in Ontario.
Summary of Sponsor's Economic Evaluation Results
All analyses were run probabilistically with 1,000 iterations. The deterministic and probabilistic results were similar, and the probabilistic findings are presented below.
Base-Case Results
In the sponsor's base-case analysis, nivolumab was associated with an ICER of $42,733 per QALY compared to surveillance over a 30-year time horizon (Table 3). At a willingness-to-pay threshold of $50,000 per QALY, the probability of nivolumab being cost-effective was 64.5%.
The main cost drivers were terminal care, followed by subsequent treatment and health state costs. At the end of the model time horizon (30 years), 10.2% of patients in the model were still alive.
A breakdown of the sponsor-submitted results for the base-case population by trial duration and extrapolated period shows that 83.9% of the expected QALY gains come from the time beyond the trial period.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. surveillance ($ per QALY) |
|---|---|---|---|---|---|
Surveillance | 47,520 | Reference | 5.80 | Reference | Reference |
Nivolumab | 118,994 | 71,474 | 7.48 | 1.68 | 42,733 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor's pharmacoeconomic submission.9
Sensitivity and Scenario Analysis Results
The sponsor performed scenario analyses by varying the time horizon, changing discount rates, varying cure points, using alternative parametric models for DFS curves, using an alternative definition of time to recurrence, changing drug wastage or nivolumab’s dosing assumption (i.e., weight-based versus flat dose), and using an alternative data source for post-recurrence survival. Key drivers of the cost-effectiveness results included a shorter time horizon of 10 years ($92,681 cost per QALY gained) and using a 5-year curative assumption ($56,442 cost per QALY gained).
CADTH Appraisal of the Sponsor's Economic Evaluation
CADTH identified several key limitations to the sponsor's analysis that have notable implications on the economic analysis:
Uncertainty in the long term survival benefits of nivolumab: Although the clinical experts agreed that DFS represents a clinically meaningful benefit for patients with EC or GEJC, the long-term extrapolation of DFS was highly uncertain given that the sponsor’s economic model was based on the results of interim analyses. Clinical experts consulted by CADTH noted that predicted DFS rates were not aligned with clinical expectations and were overestimated after 3 years.
Additional uncertainty was associated with the estimated survival benefits of nivolumab due to the sponsor's assumption regarding the curative assumption. The sponsor's model assumed that patients who were disease-free for a period of 3 years were cured; clinical experts consulted by CADTH disagreed with this assumption and suggested that a standard duration for the curative assumption was 5 years. The 3-year assumption used by the sponsor was also inconsistent with another assumption used in the model, which indicated that patients in pre-recurrence who maintained a disease-free status would only incur disease management costs for the first 5 years.
Additionally, CADTH identified limitations in using a specific data source for the transition probabilities from post-recurrence to death. The sponsor derived these transition probabilities from the real-world (IKNL) registry, due to immature overall survival data from the CheckMate 577 trial.1 While the sponsor attempted to align the IKNL registry data to the CheckMate 577 trial, the Clinical Review team identified notable differences between the 2 populations. Specifically, evidence on programmed cell death ligand 1 status, the exact composition of HER2 status, and smoking status were lacking in the IKNL registry, while no comorbidity data were reported from the CheckMate 577 trial. There were also discrepancies in clinical characteristics as represented by Eastern Cooperative Oncology Group Performance Status rating score, disease at diagnosis, and median weight between the 2 data sources. Given these observed discrepancies, transition probabilities from post-recurrence to death were highly uncertain because it was unclear whether transition probabilities estimated from the IKNL registry would reflect those derived from the participants of the CheckMate 577 trial.
Given the identified limitation, it was unclear whether the survival benefits estimated in the model were due to the efficacy of nivolumab or to the parameter and structural uncertainty within the model. CADTH attempted to address this concern, but the reanalysis was confined to the available data.
In the CADTH reanalysis, a 5-year curative assumption was used, as suggested by clinical experts consulted by CADTH. Additionally, CADTH replaced 2-knot spline odds used in the sponsor’s model to predict DFS data for nivolumab with a 2-knot spline hazard as this model led to predicted DFS in closer alignment with the clinical experts’ expectations. Further, the 2-knot spline hazard curve was adjusted to ensure DFS for nivolumab would not decline below that of surveillance in the event the curves crossed. Scenario analyses were performed to assess the impact of alternative parametric survival models extrapolating DFS rates. CADTH also assessed the uncertainty surrounding the transition probabilities from a post-recurrence health state to death by using an alternative data source.
High uncertainty regarding the time-to-recurrence (TTR) estimates: The sponsor used DFS data to estimate the transition from pre-recurrence to post-recurrence. The use of DFS results in double counting of death events and may introduce a survival benefit that favours nivolumab, as the risk of death was likely to be higher among patients in the surveillance arm. Although the sponsor used TTR data in 1 of the submitted scenario analyses and provided Kaplan–Meier curves, median values, and hazard ratios for TTR in response to CADTH's request, CADTH was unable to assess the validity of the TTR outcome because it was not submitted as part of the Clinical Study Report. It was unclear how this outcome was defined and measured.
CADTH was unable to fully assess the uncertainty associated with the TTR data but explored their use in a scenario analysis.
Inappropriate assumption regarding terminal-care cost: The sponsor obtained the terminal-care cost from a Canadian study conducted by Oliveria et al. (2016),8 which reported direct health care costs 12 months before death for EC patients in Ontario. While the data source was appropriate, the sponsor's approach, which applied a terminal-care cost to patients up to the point of cure (i.e., 3 years), may underestimate the total terminal-care cost. Terminal care captures the intensive services and palliative care required for this patient population before death; its cost should therefore be applied to all patients who transition to death, regardless of their cure status. Otherwise, downstream costs in people who have been cured are not correctly captured.
Due to the uncertainty regarding the cure time point, CADTH took a conservative approach to its base case and applied a terminal-care cost to all patients who transitioned to death.
Concerns about the uncertainty associated with health utility values: CADTH noted that the sponsor estimated pre-recurrence health utility by combining health utility data at the baseline visit with subsequent visits before the date of recurrence, but did not adjust for the baseline utility in regression analyses. Although economic data from randomized controlled trials usually rest on the assumption that baseline characteristics between the groups are well balanced, but there may be an imbalance in mean baseline utility between trial arms.1 This imbalance may cause misleading ICERs, as small changes in QALYs due to an imbalance in mean baseline utility may cause substantial variation in the ICERs.10 Further uncertainty in the health utility values comes from the small number of EQ-5D-3L measurements taken by the end of the trial. For nivolumab more than 500 patients were measured at baseline, but by week 53 this figure had dropped to just below 50 patients (for placebo it dropped from approximately 250 patients to 20).
CADTH also noted an additional limitation of the sponsor’s model was the inclusion of health utility decrements due to AEs. As the sponsor derived health utility values from the CheckMate 577 trial,1 these values likely accounted for AEs experienced by trial participants. Therefore, the model should remove disutilities due to AEs to avoid double counting.
CADTH was unable to account for the sponsor’s omission of baseline utility adjustment; however, the adjustment was estimated to have a minimal impact on the ICER because the sponsor's model assumed the same health utility values across treatment options. In the CADTH reanalysis, health utility decrements (i.e., disutilities) due to AEs were removed.
Inappropriate assumption regarding the dosage of nivolumab: The sponsor used a weight-based approach to calculate the cost of nivolumab. Clinical experts consulted by CADTH advised that it was more appropriate to use the dosage regimen indicated in a Health Canada–approved product monograph for drug-cost calculation.
In the CADTH reanalysis, a flat dose was used in place of weight-based dosing, as recommended by the product monograph (i.e., 240 mg every 2 weeks or 480 mg every 4 weeks; after completing 16 weeks of therapy, it is administered as 480 mg every 4 weeks until disease progression or unacceptable toxicity for a total treatment duration of 1 year).2
Two additional issues were identified but not considered to be key limitations:
CADTH identified a discrepancy between the model cycle length indicated in the sponsor's economic report and model. The report indicated that a cycle length of 28 days was used; however, a 30-day cycle length was used to derive the cost of nivolumab and transition probabilities in the economic model.
Given that 10.2% of patients in the model were still alive at the end of the model time horizon, CADTH considered it inappropriate to consider 30 years as a lifetime horizon. CADTH could not increase the time horizon in the reanalysis because the sponsor’s model set the maximum time horizon at 30 years.
Key assumptions made by the sponsor and appraised by CADTH are listed in Table 4.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor's key assumption | CADTH comment |
|---|---|
Patient characteristics (i.e., age, gender, weight, body surface area) from the CheckMate 577 trial were representative of a Canadian population. | The clinical experts consulted by CADTH agreed with this assumption. |
The proportions of patients who had disease recurrence and required subsequent chemotherapy were 23.1% and 32.4% for the nivolumab and surveillance arms, respectively. | Inappropriate. The clinical experts consulted by CADTH advised that the need for subsequent chemotherapy treatments should not depend on the type of first-line treatment. CADTH took a conservative approach, assuming that the proportion of the patients with disease recurrence who required subsequent chemotherapy and the types of chemotherapy in the surveillance arm were the same as those in the nivolumab arm. |
Patients who experienced disease recurrence were assumed to receive 3 main types of treatment consisting of cisplatin and 5-fluorouracil, folinic acid, fluorouracil, and oxaliplatin (FOLFOX) and capecitabine plus oxaliplatin. | The clinical experts consulted by CADTH suggested that patients who have the recurrent disease may also receive leucovorin plus fluorouracil plus irinotecan, or ramucirumab in combination with paclitaxel. However, this limitation was unlikely to affect the cost-effectiveness findings as the proportions of patients receiving these regimens are expected to be comparable across the treatment groups. |
The sponsor calculated the cost of FOLFOX based on the assumption that patients would receive 5-FU 2,400 mg/m2 IV continuous infusion over 24 hours every 2 weeks until disease progression. | Inappropriate. According to Ontario Health (Cancer Care Ontario), patients would receive 5-fluorouracil 400 mg/m2 by IV bolus in addition to a continuous infusion every 2 weeks until disease progression.11 |
The sponsor assumed that the risk of death among patients in the pre-recurrence health state was higher than that of the general Canadian population for up to 3 years. After 3 years, this risk of death was set to be equal to the age- and sex-specific all-cause mortality observed in the Canadian population. | Although this assumption may be acceptable, the cut-off point should be aligned with the curative assumption. In the CADTH reanalysis, a risk of death higher than that of the general Canadian population was applied to patients without recurrence for up to 5 years. |
The exponential distribution was used to predict the transition from post-recurrence to death. | CADTH noted that the exponential distribution did not fit the post-recurrence data well. The sponsor’s model was not flexible enough to test the impact of alternative survival models on the cost-effectiveness findings. However, the choice of survival model was unlikely to have a large impact on an ICER, as the model assumed that the transition from post-recurrence to death is independent of treatment. |
The sponsor’s model considered the following grade 3 to 4 AEs (which occurred in ≥ 5% of study subjects across all grades): fatigue, diarrhea, pruritus, rash, arthralgia, and increased aspartate aminotransferase. | Clinical experts consulted by CADTH noted that 2 clinically important AEs, pneumonitis and myocarditis, were not considered in the model. CADTH anticipates this limitation may have minimal impact on the cost-effectiveness of nivolumab, given the low incidence rate of these AEs. |
AE = adverse event; FOLFOX = leucovorin plus 5-fluorouracil plus oxaliplatin; ICER = incremental cost-effectiveness ratio.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Due to the immature overall survival and post-recurrence data, CADTH could not adequately address the resulting uncertainty. CADTH corrected the sponsor's model by adding 5-fluorouracil 400 mg/m2 IV bolus every 2 weeks to the FOLFOX regimen, correcting a dosage of capecitabine as part of XELOX (1,000 mg/m2 twice daily instead of 1,000 mg/m2 once daily), and using publicly listed prices for cisplatin, oxaliplatin and leucovorin. CADTH also increased standard errors of parameters without known variance (i.e., cost data), from 10% to 20% of their mean values for probabilistic analyses and increased the number of simulations to 5,000 iterations to align with common practices. CADTH’s base case assumed no vial sharing, used a flat dose of nivolumab, applied the same proportions of patients requiring subsequent chemotherapy to both nivolumab and surveillance arms, assigned a terminal-care cost to any patients who transitioned to death, used 5 years as a cure time point as suggested by clinical experts consulted by CADTH, and used an alternate survival model (a 2-knot spline hazard) to predict DFS for nivolumab. Table 5 and 6 detail the changes made to derive CADTH’s base case, and the summary results of the CADTH base case are presented in Table 7. Additional results are shown in Appendix 4.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor's value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor's base case | ||
1. Increase the number of simulations to 5,000 iterations | 1,000 | 5,000 |
2. Increase the variance for cost data with unknown standard error | 10% | 20% |
3. Correct unit costs and dosage for subsequent chemotherapy treatments | Cisplatin: $0.193 per mg Oxaliplatin: $0.726 per mg Leucovorin: $0.700 per mg FOLFOX: 5-fluorouracil 2,400 mg mg/m2 IV every 2 weeks | Cisplatin: $2.700 per mg Oxaliplatin: $0.725 per mg Leucovorin: $0.149 per mg FOLFOX: 5-fluorouracil 400 mg mg/m2 IV bolus every 2 weeks 5-fluorouracil 2,400 mg mg/m2 IV every 2 weeks |
Changes to derive the CADTH base case | ||
1. Vial sharing and drug wastage | Vial sharing with 5% drug wastage | No vial sharing with 5% drug wastage |
2. Dosing | Weight-based | Flat dose |
3. Utility decrement due to AEs | Included | Excluded |
4. Distribution of subsequent treatments | Nivolumab (%):
Surveillance (%):
| Nivolumab (%):
Surveillance (%):
|
5. Terminal-care cost | A terminal-care cost was applied for up to 3 years | A terminal-care cost was applied for all patient who transitions to death regardless of the cure status |
6. Time to cure | 3 years | 5 years |
7. Survival model for nivolumab DFS | Spline odds 2 knots | Spline hazard 2 knots |
CADTH base case | — | 1 + 2 + 3 + 4 + 5 + 6 + 7 |
CAPOX = capecitabine plus oxaliplatin; DFS = disease-free survival; FOLFOX = 5-fluorouracil + oxaliplatin + leucovorin.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Deterministic Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base casea | Surveillance | 47,520 | 5.80 | Reference |
Nivolumab | 118,994 | 7.48 | 42,733 | |
Sponsor’s correcteda base case | Surveillance | 46,559 | 5.82 | Reference |
Nivolumab | 118,433 | 7.48 | 43,185 | |
CADTH reanalysis 1 | Surveillance | 46,810 | 5.79 | Reference |
Nivolumab | 118,607 | 7.47 | 42,666 | |
CADTH reanalysis 2 | Surveillance | 46,810 | 5.79 | Reference |
Nivolumab | 128,178 | 7.47 | 48,353 | |
CADTH reanalysis 3 | Surveillance | 46,810 | 5.79 | Reference |
Nivolumab | 118,607 | 7.47 | 42,675 | |
CADTH reanalysis 4 | Surveillance | 46,281 | 5.79 | Reference |
Nivolumab | 118,607 | 7.47 | 42,980 | |
CADTH reanalysis 5 | Surveillance | 61,067 | 5.79 | Reference |
Nivolumab | 137,338 | 7.47 | 45,324 | |
CADTH reanalysis 6 | Surveillance | 52,947 | 5.11 | Reference |
Nivolumab | 132,752 | 6.42 | 60,821 | |
CADTH reanalysis 7 | Surveillance | 46,810 | 5.79 | Reference |
Nivolumab | 118,857 | 7.44 | 43,675 | |
CADTH base casea (1 through 7) | Surveillance | 62,340 | 5.14 | Reference |
Nivolumab | 150,351 | 6.25 | 79,241 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aBased on probabilistic results.
Results from CADTH's base case suggest that nivolumab was associated with higher costs ($88,011) and improved QALYs (1.11), with an ICER of $79,241 per QALY compared to surveillance. The estimated ICER was higher than the sponsor's base case, which is primarily due to the longer cure time point used (5 years versus 3 years). The probability that nivolumab is cost-effective was 20.9% at a willingness-to-pay threshold of $50,000 per QALY.
Table 7: Summary of the CADTH Reanalysis Results
Drug | Total costs ($) | Total QALYs | Total life-years | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor-corrected base case | ||||
Surveillance | 46,559 | 5.82 | 6.77 | Reference |
Nivolumab | 118,433 | 7.48 | 8.74 | 43,185 |
CADTH base case | ||||
Surveillance | 62,340 | 5.14 | 6.00 | Reference |
Nivolumab | 150,351 | 6.25 | 7.29 | 79,241 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years.
Scenario Analysis Results
Based on CADTH’s base case, scenario analyses were conducted. These analyses explored the impact of the following model parameters and assumptions: cure time points, alternative assumptions on TTR and the transitions from post-recurrence to death, treatment duration, dosing regimens of nivolumab, and parametric survival models to assess the uncertainty of DFS. The CADTH analyses also explored the impact of health utility values by replacing a post-recurrence utility of 0.801 used in the sponsor’s model with an alternative value of 0.795 shown in the sponsor’s supplementary EQ-5D-3L utility analysis report.
Results from scenario analyses (Appendix 4, Table 13) demonstrated that the cure time point was the key driver of the cost-effectiveness findings, followed by parametric models used to extrapolate DFS data. The ICERs increased from $48,615 per QALY (scenario 15, using a generalized gamma distribution to predict DFS for the surveillance group) to $157,295 per QALY (scenario 2, assuming a 10-year cure time point). The ICERs were also influenced by how treatment duration was estimated and the risk of death among patients in the pre-recurrence state. If DFS curves were used to reflect treatment duration for nivolumab (scenario 6), the ICER increased to $92,766 per QALY. Moreover, if patients in the pre-recurrence health status were to have a comparable risk of death to the participants of the CheckMate 577 trial (scenario 4), the ICER rose to $83,532 per QALY. Cost-effectiveness findings were found to be robust to changes in health utility values and transitions from post-recurrence to death.
Price-reduction analyses were not conducted on the sponsor's base case, given that the sponsor’s base case ICER for nivolumab was below a willingness-to-pay threshold of $50,000 per QALY. However, CADTH did undertake a price-reduction analysis based on the CADTH base case (Table 8). The results indicate that a price reduction of at least 36% is required for nivolumab to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Table 8: CADTH Price-Reduction Analyses
Analysis | ICERs for nivolumab vs. surveillance |
|---|---|
Price reduction | CADTH reanalysis |
No price reduction | $79,241 |
20% | $63,561 |
30% | $55,593 |
36% | $49,584 |
ICER = incremental cost-effectiveness ratio.
Issues for Consideration
Nivolumab alone or in combination with ipilimumab has previously been reviewed and approved with cost-effectiveness conditions for the following unrelated indications: unresectable malignant pleural mesothelioma in patients who have not received prior systemic therapy for the condition, metastatic or recurrent non–small cell lung cancer with no epidermal growth-factor receptor or anaplastic lymphoma kinase genomic tumour aberrations, adjuvant and unresectable or metastatic melanoma, untreated or previously treated metastatic renal cell carcinoma, and recurrent or metastatic squamous cell carcinoma of the head and neck in adults progressing on or after platinum-based therapy.
Overall Conclusions
Evidence from the interim analysis of the CheckMate 577 trial1 showed that, compared to placebo, nivolumab adjuvant treatment was associated with a clinically meaningful and statistically significant improvement in DFS in patients with EC or GEJC who have residual pathologic disease following prior neoadjuvant chemoradiotherapy. The safety profile of nivolumab in this study was consistent with the known safety profile of nivolumab, and no additional safety signals were identified with adjuvant nivolumab therapy in this study. The patient-reported and HRQoL outcomes (e.g., ED-5D-3L) were assessed as exploratory outcomes, and there was a potential risk of bias because of substantial missing data on these outcomes during the trial follow-up period.
CADTH identified several limitations within the sponsor's economic analysis, specifically the uncertainty associated with the use of interim DFS from the CheckMate 577 trial to represent the transition from pre-recurrence to recurrence; the use of an external data source to derive the transition from post-recurrence to death; the underestimating of terminal-care costs beyond 3 years; the inclusion of disutilities in addition to health state utilities, which likely results in double counting; and the assumption regarding a dosage regimen of nivolumab.
Although CADTH was unable to address all the limitations identified, it made several corrections and revisions to the sponsor's base case to derive the CADTH base case. CADTH corrected the 5-fluorouracil dosing used as part of the FOLFOX regimen and the capecitabine dosing as part of XELOX; used publicly listed prices for cisplatin, oxaliplatin, and leucovorin; increased standard errors of cost parameters without known variance to 20% of their mean values; and increased the number of simulations to 5,000 iterations. The CADTH base case assumed no vial sharing, used a flat dose of nivolumab, applied the same proportions of patients requiring subsequent chemotherapy to both nivolumab and surveillance arms, assigned a terminal-care cost to any patient who transitioned to death, used 5 years as a cure time point, and used a 2-knot spline hazard to predict DFS data for nivolumab. In addition, CADTH undertook further scenario analyses to explore the impact of alternative cure time points, differing parametric survival models for DFS, assumptions regarding the treatment duration, an assumption regarding the risk of death among patients without disease recurrence, and an alternate health utility value.
CADTH’s base case resulted in a higher ICER than the sponsor's base case ($79,241 per QALY versus the $42,733 per QALY used by the sponsor), and nivolumab was associated with higher costs and improved QALYs compared to surveillance. Approximately 77% of the incremental QALYs and 6% of incremental costs came from the extrapolated period beyond the trial’s follow-up period. A price reduction of at least 36% would be required to ensure nivolumab is cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
The cost-effectiveness of nivolumab was most sensitive to the assumption regarding the cure time point, followed by parametric models used to extrapolate DFS data, with ICERs ranging from $48,615 per QALY (scenario 15, using a generalized gamma distribution to predict DFS of the surveillance group) to $157,295 per QALY (scenario 2, assuming a 10-year cure time point). Cost-effectiveness findings were found to be robust to changes in health utility values and the transition from post-recurrence to death. However, CADTH was unable to fully assess the methodological uncertainty associated with the data used to derive the transition from pre-recurrence to death and post-recurrence utility.
References
1.Kelly RJ, Ajani JA, Kuzdzal J, et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N Engl J Med. 2021;384(13):1191-1203. PubMed
2.Opdivo® nivolumab for injection Intravenous Infusion, 10 mg nivolumab /mL 40 mg and 100 mg single-use vial [product monograph]. Montreal: Bristol-Myers Squibb Canada Co; 2021 Jul 6.
3.Bansback N, Tsuchiya A, Brazier J, Anis A. Canadian valuation of EQ-5D health states: preliminary value set and considerations for future valuation studies. PLoS One. 2012;7(2):e31115. PubMed
4.Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6:84. PubMed
5.National Institute for Health and Care Excellence. Ramucirumab for treating advanced gastric cancer or gastro-oesophageal junction adenocarcinoma previously treated with chemothreapy. 2016: https://www.nice.org.uk/guidance/ta378/resources/ramucirumab-for-treating-advanced-gastric-cancer-or-gastrooesophageal-junction-adenocarcinoma-previously-treated-with-chemotherapy-pdf-82602795958981. Accessed 2021 Nov 16.
6.Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398(10294):27-40. PubMed
7.Kato K S, Jong-Mu, Shad, Manish. . Pembrolizumab plus chemotherapy versus chemotherapy as a first-line therapy in patients with advanced esophageal cancer: the Phase 3 KEYNOTE-590 study. European Society of Medican Oncology (ESMO). 2020.
8.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
9.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Opdivo® (nivolumab) Montreal: Bristol-Myers Squibb; 2021 Jul 7.
10.Manca A HN, Sculpher M. . Estimating mean QALYs in trial-based cost-effectiveness analysis: the importance of controlling for baseline utility. . Health Econ. 2005:487-496. PubMed
11.Cancer Care Ontario: funded evidence-informed regimens. 2021; https://www.cancercareontario.ca/en/drugformulary/regimens.
12.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/.
13.Nova Scotia formulary. Halifax (NS): Nova Scotia Pharmacare; 2021 https://novascotia.ca/dhw/pharmacare/documents/formulary.pdf. Accessed 2021 Oct 6.
14.Government BC. BC PharmaCare formulary search. 2021; https://pharmacareformularysearch.gov.bc.ca.
15.Paclitaxel Injection USP Solution for Injection, 6 mg/mL [product monograph]. Kirkland, QC: Accord Healthcare Inc.; 2020 Sep 14: https://pdf.hres.ca/dpd_pm/00057982.PDF. Accessed 2021 Nov 16.
16.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Opdivo® (nivolumab) Montreal: Bristol-Myers Squibb; 2021 Jul 7.
17.Canadian Cancer Society. Canadian Cancer Statistics A 2018 special report on cancer incidence by stage. 2018; https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf. Accessed 2021 Nov 16.
18.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-E205. PubMed
19.Buas MF, Vaughan TL. Epidemiology and risk factors for gastroesophageal junction tumors: understanding the rising incidence of this disease. Semin Radiat Oncol. 2013;23(1):3-9. PubMed
20.van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074-2084. PubMed
21.Statistics Canada. Population estimates, quarterly Table: 17-10-0009-01. 2021; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000901&cubeT%20imeFrame.startMonth=01&cubeTimeFrame.startYear=2021&cubeTimeFrame.endM%20onth=04&cubeTimeFrame.endYear=2021&referencePeriods=20210101%2C2021040%201. Accessed 2021 Nov 16.
22.Statistics Canada. Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). 2019; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 2021 Sep 27.
23.Bank TW. Population growth (annual %) - Canada. 2021; https://data.worldbank.org/indicator/SP.POP.GROW?locations=CA. Accessed 2021 Nov 16.
24.Cisplatin injection BP Sterile solution 1 mg / mL (50 mg and 100 mg cisplatin per vial) [product monograph]. Kirkland (Québec): Pfizer Canada ULC 2018 Dec 7: https://pdf.hres.ca/dpd_pm/00048673.PDF. Accessed 2021 Nov 16.
25.Oxaliplatin Oxaliplatin Injection, Pfizer Standard 5 mg/mL oxaliplatin 50 mg / 10 mL, 100 mg / 20 mL, 200 mg / 40 mL [product monograph]. Kirkland (Québec): Pfizer Canada ULC; 2020 Jul 3: https://www.pfizer.ca/sites/default/files/202007/Oxaliplatin_PM_E_236783_2020.07.03.pdf. Accessed 2021 Nov 16.
26.Leucovorin calcium injection USP 10 mg/mL Sterile Solution [product monograph]. Kirkland (Québec): Pfizer Canada In; 2018 Jun 21: https://www.pfizer.ca/sites/default/files/201807/2018.06.21_Leucovorin_PM_E_215416.pdf. Accessed 2021 Nov 16. 27. Irinotecan hydrochloride injection USP (Irinotecan hydrochloride trihydrate) Sterile Solution 20 mg / mL (40 mg / 2 mL, 100 mg / 5 mL, 500 mg / 25 mL) [product monograph]. Kirkland (Québec): Pfizer Canada ULC; 2019 Mar 8: https://www.pfizer.ca/sites/default/files/201903/Irinotecan_HCL_USP_PM_E_224931_08Mar2019.pdf. Accessed 2021 Nov 16.
28.Teva-Capecitabine Capecitabine tablets 150 mg and 500 mg [product monograph]. Toronto: Teva Canada Limited; 2018 Jul 23: https://pdf.hres.ca/dpd_pm/00046666.PDF. Accessed 2021 Nov 16.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CADTH-participating drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 9: CADTH Cost Comparison Table for Adjuvant Treatment of Resected Esophageal or Gastroesophageal Junction Cancer
Treatment | Strength/ concentration | Form | Price per vial ($)a | Recommended dosage | Average daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Nivolumab (Opdivo) | 10 mg/mL | 4 mL 10 mL Vial for IV infusion | $782.2200 $1,955.5600 | 240 mg Q2W for 16 weeks, followed by 480 mg Q4W for 36 weeks 480 mg Q4W for 52 weeks | 335.24 | 9,387 |
IV = intravenous; Q2W = every 2 weeks; Q4W = every 4 weeks.
Note: Treatment with nivolumab is capped at 12 months.
aSponsor's submitted price for each dosage.
Table 10: CADTH Cost Comparison Table for Subsequent Treatment of Resected Esophageal or Gastroesophageal Junction Cancer
Treatment | Strength/ concentration | Form | Price per vial per mg ($) | Recommended dosage | Average daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Cisplatin-5-fluorouracil (CISPFU)a | ||||||
Cisplatin | 1 mg/mL | 50 mL 100 mL Vial for IV infusion | 135.0000 270.0000 | 80 mg/m2 Q3W or Q4W | 19.29 14.46 | 540 405 |
5-Fluorouracil | 50 mg / mL | 100 mL Vial for IV infusion | 160.9000b | 800 mg/m2/day on Days 1 to 5 or 1,000 mg/m2 on days 1 to 4 Q3W or Q4W | 11.03 8.27 | 309 232 |
CISPFU Q3W Or Q4W | 30.32 22.74 | 849 637 | ||||
Capecitabine-oxaliplatin (XELOX) | ||||||
Oxaliplatin | 5 mg/mL | 10 mL 20 mL 40 mL Vial for IV infusion | 36.2700 72.5400 145.0800 | 130 mg/m2 Q3W | 8.64 | 242 |
Capecitabine (Xeloda) | 150 mg 500 mg | Tablet | 0.4575 1.525 | 1,000 mg/m2 twice daily on Days 1 to 14 Q3W | 7.32 | 205 |
XELOX | 15.96 | 447 | ||||
Folinic Acid (Leucovorin)-Fluorouracil-Oxaliplatin (mFOLFOX) | ||||||
Oxaliplatin | 5 mg/mL | 10 mL 20 mL 40 mL Vial for IV infusion | 36.2700 72.5400 145.0800 | 85 mg/m2 Q2W | 10.36 | 290 |
Leucovorin | 10 mg/mL | 5 mL 50 mL Vial for IV infusion | 68.9400 74.4100c | 400 mg/m2 Q2W | 10.63 | 298 |
5-Fluorouracil | 50 mg/mL | 10 mL 100 mL Vial for IV infusion | 16.0900b 160.9000b | 400 mg/m2 IV bolus Q2W | 11.49 | 322 |
5-Fluorouracil | 50 mg/mL | 10 mL 100 mL Vial for IV infusion | 16.0900b 160.9000b | 2,400 mg/m2 IV continuous infusion Q2W | 11.49 | 322 |
mFOLFOX | 43.98 | 1,231 | ||||
Folinic Acid (Leucovorin)-Fluorouracil-Irinotecan (FOLFIRI) | ||||||
Irinotecan | 20 mg/mL | 2 mL 5 mL 25 mL Vial for IV infusion | 208.3400 8.1000 2,604.3750 | 180 mg/m2 Q2W | 2.31 | 65 |
Leucovorin | 10 mg/mL | 5 mL 50 mL Vial for IV infusion | 68.9400 74.4100c | 400 mg/m2 Q2W | 10.63 | 298 |
5-Fluorouracil | 50 mg/mL | 100 mL Vial for IV infusion | 160.9000b | 400 mg/m2 IV bolus Q2W | 11.49 | 322 |
5-Fluorouracil | 50 mg/mL | 100 mL Vial for IV infusion | 160.9000b | 2,400 mg/m2 IV continuous infusion Q2W | 11.49 | 322 |
FOLFIRI | 35.93 | 1,006 | ||||
Paclitaxel (weekly)-Ramucirumab (PACL(W)+RAMU) | ||||||
Ramucirumab | 10 mg/mL | 10 mL 50 mL Vial for IV solution | 620.0600 3,100.3000 | 8 mg/kg on Days 1 and 15 Q4W | 265.74 | 7,441 |
Paclitaxel | 6 mg/mL | 5 mL 16.7 mL 50 mL Injection for IV infusiond | 300.0000 1,249.1600 3,740.0000 | 80 mg/m2 on Days 1, 8 and 15 Q4W | 160.71 | 4,500 |
PACL(W)+RAMU | 426.45 | 11,941 | ||||
IV = intravenous; Q2W = every 2 weeks; Q3W = every 3 weeks, 5-FU = 5-fluorouracil.
Note: All prices are IQVIA Delta PA wholesale list prices12 (accessed July 2021), unless otherwise indicated, and do not include dispensing fees or markups. Wastage of excess medication in vials is included in costs. Recommended dosage is based on Cancer Care Ontario monograph formulary, unless otherwise indicated. For dosing that depends on weight or body surface area, CADTH assumed mean body weight of 71 kg and mean body surface area was 1.8 m2. Total cost estimates per regimen are based on the cheapest combination of the component drugs.
aMaximum 6 cycles of treatment due to cumulative cisplatin toxicity.11
bNova Scotia Formulary,13 as reported by IQVIA Delta PA (August 2021).
cBritish Columbia Formulary list price,14 as reported by IQVIA Delta PA (August 2021).
dPrice for 25 mL is available in IQVIA Delta PA but size is not listed on product monograph.15
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | CADTH identified errors in the drug-cost calculations. The sponsor’s model was not flexible to modify because some calculations, such as transition probabilities and drug costs, were hardcoded and not transparent. See CADTH appraisal section. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | CADTH identified limitations with the use of DFS data to represent time to recurrence, the use of an external data source to derive post-recurrence transition probabilities, and the omission of baseline utility data in the estimation of health state–specific utility. See CADTH appraisal section. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | The sponsor’s model did not provide alternate survival models to predict post-recurrence data. See CADTH appraisal section. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | There were discrepancies in the sponsor’s economic report and model regarding the cycle length. See CADTH appraisal section. |
DFS = disease-free survival.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
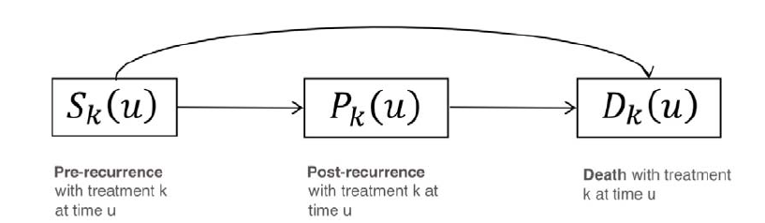
Figure 2: Predicted DFS Data From Parametric Survival Models — Nivolumab
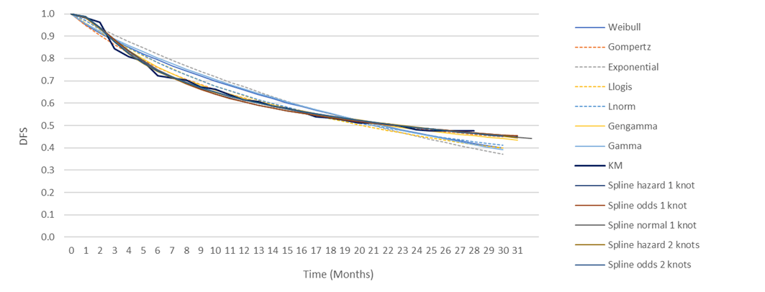
Source: Sponsor’s pharmacoeconomic submission.9
Figure 3: Predicted DFS Data From Parametric Survival Models — Surveillance
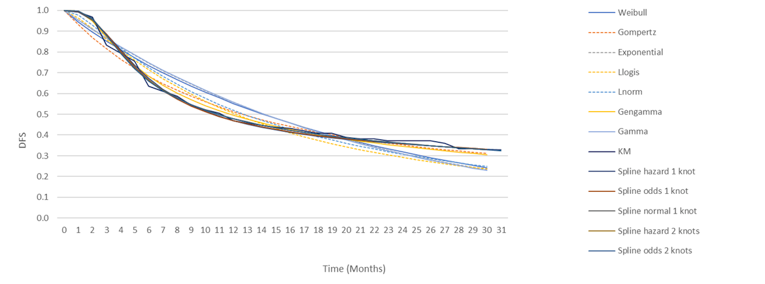
Source: Sponsor’s pharmacoeconomic submission.9

Detailed Results of the Sponsor’s Base Case
Figure 5: Results From the Sponsor’s Model Based on Time-to-Recurrence Data
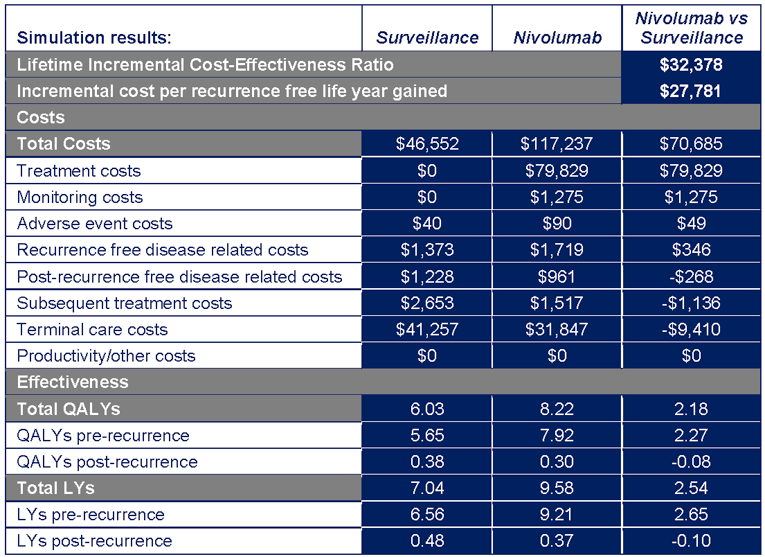
Source: Sponsor’s pharmacoeconomic submission.9
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Nivolumab | Surveillance | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 7.29 | 6.00 | 1.29 |
By health state or data source | |||
Pre-recurrence | 6.82 | 5.48 | 1.34 |
Post-recurrence | 0.47 | 0.52 | -0.05 |
Discounted QALYs | |||
Total | 6.25 | 5.14 | 1.11 |
By health state or data source | |||
Pre-recurrence | 5.88 | 4.73 | 1.15 |
Post-recurrence | 0.38 | 0.42 | -0.04 |
Discounted costs ($) | |||
Total | 150,351 | 62,340 | 88,011 |
Treatment cost | 88,544 | 0 | 88,544 |
Monitoring cost | 1,262 | 0 | 1,262 |
Adverse events cost | 90 | 40 | 49 |
Pre-recurrence health state cost | 2,291 | 1,843 | 449 |
Post-recurrence health state cost | 1,215 | 1,341 | -126 |
Subsequent treatment cost | 1,405 | 1,541 | -136 |
Terminal-care cost | 55,545 | 57,574 | -2,030 |
ICER ($/QALY) | 79,241 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
CADTH conducted several scenario analyses to assess the uncertainty surrounding the parameters used in the sponsor’s model. The analyses reveal that a parametric survival model used to predict DFS data was a key driver of the cost-effectiveness of nivolumab. Additionally, CADTH found that increased ICERs were associated with the longer duration used for a curative assumption, the longer time horizon at which a higher risk of death applied to all-cause mortality, the lower risk of transition from post-recurrence to death, the longer duration of nivolumab use, and the lower utility value for the post-recurrence health state. By contrast, smaller ICERs were associated with a shorter duration used for a curative assumption and the use of time-to-recurrence data to estimate the transition from pre-recurrence to recurrence.
Table 13: Summary of CADTH Scenario Analyses
Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|
Sponsor's corrected base case | |||
Surveillance | 46,559 | 5.82 | Reference |
Nivolumab | 118,433 | 7.48 | 43,185 |
CADTH’s base case | |||
Surveillance | 62,340 | 5.14 | Reference |
Nivolumab | 150,351 | 6.25 | 79,241 |
CADTH's scenario analysis 1: Assuming a 3-year cure time point | |||
Surveillance | 60,294 | 5.80 | Reference |
Nivolumab | 146,533 | 7.44 | 52,523 |
CADTH's scenario analysis 2: Assuming a 10-year cure time point | |||
Surveillance | 65,153 | 4.47 | Reference |
Nivolumab | 153,603 | 5.03 | 157,295 |
CADTH's scenario analysis 3: Using TTR to estimate the transition from pre-recurrence to recurrence | |||
Surveillance | 61,851 | 5.41 | Reference |
Nivolumab | 149,222 | 7.34 | 45,328 |
CADTH's scenario analysis 4: Applying the risk of death observed in participants of CheckMate 5771 to patients in the pre-recurrence state for 30 years | |||
Surveillance | 64,287 | 4.81 | Reference |
Nivolumab | 152,493 | 5.87 | 83,532 |
CADTH's scenario analysis 5: Using alternative data source to estimate the transition from post-recurrence to death (pooled data from CheckMate 649 and KEYNOTE-590 trials) | |||
Surveillance | 63,113 | 5.46 | Reference |
Nivolumab | 150,685 | 6.55 | 79,994 |
CADTH's scenario analysis 6: Using DFS to represent time-to-treatment discontinuation | |||
Surveillance | 62,574 | 5.16 | Reference |
Nivolumab | 164,581 | 6.26 | 92,766 |
CADTH scenario analysis 7: Reducing the number of treatment cycles of subsequent chemotherapy to 5.8 (median PFS reported in the KEYNOTE-590 trial) | |||
Surveillance | 62,251 | 5.13 | Reference |
Nivolumab | 150,004 | 6.26 | 77,611 |
CADTH scenario analysis 8: Assuming a weight-based dosing for nivolumab | |||
Surveillance | 62,536 | 5.14 | Reference |
Nivolumab | 140,726 | 6.26 | 69,704 |
CADTH scenario analysis 9: Using an alternative survival model to predict DFS of nivolumab – spline normal 1 knot | |||
Surveillance | 62,674 | 5.13 | Reference |
Nivolumab | 149,917 | 6.48 | 64,382 |
CADTH scenario analysis 10: Using an alternative survival model to predict DFS of nivolumab – spline odd 1 knot | |||
Surveillance | 62,408 | 5.13 | Reference |
Nivolumab | 149,097 | 6.73 | 53,997 |
CADTH scenario analysis 11: Using an alternative survival model to predict DFS of nivolumab – generalized gamma | |||
Surveillance | 62,612 | 5.12 | Reference |
Nivolumab | 151,041 | 6.28 | 75,975 |
CADTH scenario analysis 12: Using an alternative survival model to predict DFS of surveillance – spline normal 1 knot | |||
Surveillance | 62,993 | 4.94 | Reference |
Nivolumab | 150,361 | 6.25 | 66,658 |
CADTH scenario analysis 13: Using an alternative survival model to predict DFS of surveillance – spline odds 2 knotsa | |||
Surveillance | 63,078 | 4.94 | Reference |
Nivolumab | 150,778 | 6.42 | 58,664 |
CADTH scenario analysis 14: Using an alternative survival model to predict DFS of surveillance – spline hazard 2 knots | |||
Surveillance | 63,026 | 4.88 | Reference |
Nivolumab | 149,725 | 6.26 | 66,511 |
CADTH scenario analysis 15: Using an alternative survival model to predict DFS of surveillance – generalized gamma | |||
Surveillance | 64,130 | 4.49 | Reference |
Nivolumab | 150,219 | 6.26 | 48,615 |
CADTH scenario analysis 16: Using an alternative health utility value (0.795) obtained from the sponsor’s supplementary EQ-5D utility analysis report for the post-recurrence health state | |||
Surveillance | 62,486 | 5.13 | Reference |
Nivolumab | 150,254 | 6.25 | 78,554 |
DFS = disease-free survival; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aBased on deterministic results as a probabilistic analysis provided implausible results.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Takeaways
Key Takeaways of the Budget Impact Analysis |
|---|
|
Summary of Sponsor's Budget Impact Analysis
The sponsor’s submitted budget impact analysis (BIA)16 assessed the expected budgetary impact of introducing nivolumab for the adjuvant treatment of patients with completely resected EC or GEJC. The analysis was done from the perspective of the Canadian drug plans over a 3-year time horizon; the base year was assumed to be 2021 and the 3-year time horizon ran from 2022 to 2024. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec). Key inputs to the BIA are documented in Table 16.
The sponsor used a population-based approach, leveraging data from the Canadian Cancer Statistics17 and published literature,18-20 to estimate the number of incident patients eligible for treatment with nivolumab. Current standard of care includes surveillance alone, with no drug cost assumed under standard care. The sponsor assumed nivolumab captures a market share of || in year 1, || in year 2, and || in year 3 from surveillance.16 Eligible patients on nivolumab accrued the treatment cost of nivolumab for 7.58 months.1 Some patients were assumed to relapse; 23% of patients on nivolumab and 32% of patients under surveillance accrued the costs of subsequent chemotherapy.1 Subsequent systemic treatment includes FOLFOX, CISPFU and XELOX. The distribution of patients on subsequent chemotherapies differed following adjuvant nivolumab or surveillance. Among the patients previously on nivolumab who progressed and were treated with a subsequent therapy, 79.6% were treated with FOLFOX, 11.7% with CISPFU and 8.7% with XELOX. Among those on surveillance, the proportion of relapsed patients treated with FOLFOX was 78.8%, with CISPFU was 8.3% and with XELOX was 12.8%. The sponsor assumed patients were treated with CISPFU for 6 cycles, with FOLFOX for 13.914 cycles, and with XELOX for 9.276 cycles. Treatment costs were obtained from IQVIA Delta PA database,16 and the sponsor assumed weight-based dosing of nivolumab, and vial sharing with 5% wastage.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate |
|---|---|
Target population | |
Canadian population size (Year 1 / Year 2 / Year 3) | |
Annual population growth | 1.1%23 |
Incidence of EC (per 100,000 persons) | 6.518 |
Proportion with stage II disease (ESCC & EAC) | 14.0%17 |
Proportion with stage III disease (ESCC & EAC) | 23.3%17 |
Incidence of gastric cancer (per 100,000 persons) | 10.518 |
Proportion of patients with GEJC | 35.0%19 |
Proportion with stage II disease (GEJC) | 12.8%17 |
Proportion with stage III disease (GEJC) | 20.2%17 |
Proportion of patients eligible for surgery (ESCC & EAC and GEJC) | 80.0%16 |
Proportion of patients receiving neoadjuvant chemoradiotherapy ESCC & EAC GEJC | 87.5%16 50.0%16 |
Proportion achieving complete resection | 92.0%20 |
Proportion not achieving pathological complete response | 71.0%20 |
Proportion who are eligible for immunotherapy | 90.0%16 |
Number of patients eligible for drug under review (Year 1 / Year 2 / Year 3) | 379 / 383 / 38816 |
Market Uptake (Year 1 / Year 2 / Year 3) | |
Uptake (reference scenario) Surveillance | 100% / 100% / 100%16 |
Uptake (new drug scenario) Surveillance Nivolumab | |||||||||||||||||||||||16 |||||||||||||||||||||||16 |
Cost of 1L treatment (per patient) | |
Cost per treatment cycle (28 days) Nivolumaba | $8,80016 |
Cost of 2L treatment (per patient) | |
Cost of treatment course CISPFU XELOX FOLFOX | $53416 $25416 $77516 |
CISPFU = Cisplatin-5-fluorouracil, EAC = Esophageal adenocarcinoma, EC = Esophageal cancer, ESCC = Esophageal squamous cell carcinoma, FOLFOX = Folinic Acid (Leucovorin)-Fluorouracil-Oxaliplatin, GEJC = Gastroesophageal junction cancer, XELOX = Capecitabine-oxaliplatin, 1L = first line, 2L = second line.
aCost estimation assumed average weight of 71.25 kg, body surface area of 1.85 m2 and vial sharing with 5% drug wastage. Recommended dosage regimen of 213.75 mg administered every 2 weeks for 16 weeks (8 doses), followed by 428 mg nivolumab administered every 4 weeks beginning at week 17 (2 weeks after the eighth dose).
Summary of the Sponsor's Budget Impact Analysis Results
The sponsor estimated the 3-year budget impact to the public drug plans of introducing nivolumab for the adjuvant treatment of patients with completely resected EC or GEJC in adults to be $53,674,419 (Year 1: $13,589,515; Year 2: $17,860,699; Year 3: $22,224,205).
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor's analysis that have notable implications on the results of the BIA:
The number of individuals eligible for nivolumab treatment is underestimated: Given the Health Canada indication2 includes all patients with completely resected esophageal or gastroesophageal junction cancer who have residual pathological disease following prior neoadjuvant chemoradiotherapy, the sponsor underestimated the eligible market size for nivolumab by omitting patients with stage I cancer. According to the clinical experts consulted for this review by CADTH, some patients with stage I esophageal or gastroesophageal junction cancer may receive chemoradiation following surgery due to residual disease. Diagnosis of cancer stage is also imperfect in clinical practice. As such, a portion of the reimbursement population that would be eligible for nivolumab treatment is excluded from the sponsor’s estimated market size, which underestimates the budget impact. The clinical experts estimated the proportion of stage I cancer patients eligible for nivolumab treatment may be in the range of 5-10%.
In the CADTH reanalysis, the estimated market size included individuals with stage I esophageal (13.4%) and gastroesophageal junction cancer (14.7%) receiving neo-adjuvant chemoradiation therapy (10%) following surgery.17
Treatment acquisition costs of nivolumab is underestimated: The sponsor adopted weight-based dosing of nivolumab, a mean treatment duration of 7.58 months, and assumed vial sharing with 5% drug wastage in the calculation of treatment acquisition cost of nivolumab.17 The sponsor’s use of weight-based dosing, which equates to a dose of 213.75 mg every 2 weeks for 16 weeks followed by a dose of 428 mg every 4 weeks, underestimates the treatment cost of nivolumab and the budget impact of reimbursing nivolumab. The product monograph recommends a flat dose of 240 mg every 2 weeks or 480 mg every 4 weeks for 16 weeks, followed by 480 mg every 4 weeks, for a maximum treatment duration of one year.2 The product monograph also notes nivolumab is available as a single-use product.2 The sponsor’s approach to calculating nivolumab treatment cost does not align with the product monograph as well as input from clinical experts. The clinical experts consulted for this review by CADTH showed preference for adopting a flat dosing regimen in clinical practice as administered in the clinical trial, CheckMate 577.1 The public drug plans further noted treatment duration may be longer than one year in cases where treatment is interrupted or delayed due to toxicity, and clinical experts agreed with a maximum delay of 10 weeks. The sponsor’s adopted nivolumab treatment duration of 7.58 months1 underestimates treatment acquisition cost of nivolumab and the budget impact. Should treatment be interrupted or delayed, the treatment duration may be longer than one year, especially in cases of toxicity. CADTH reanalysis aligned assumptions in calculating nivolumab treatment costs with input from clinical experts, public plans, and the product monograph.2
In the CADTH reanalysis, nivolumab’s treatment cost was estimated based on a flat dosing strategy, a treatment duration of one year, and no vial sharing.2
Treatment acquisition costs of subsequent chemotherapies is underestimated: In the BIA, some patients were assumed to relapse and move to subsequent treatment with a systemic chemotherapy. The sponsor used the trial results from CheckMate 5771 to derive the proportion of patients taking FOLFOX, CISPFU and XELOX, which differed by treatment arm; 79.6% on FOLFOX, 11.7% on CISPFU and 8.7% on XELOX following adjuvant nivolumab, and 78.8% on FOLFOX, 8.3% on CISPFU and 12.8% on XELOX following surveillance. According to the clinical experts consulted for this review, there is no clinical reason for the proportion of patients on subsequent chemotherapies to differ following adjuvant nivolumab treatment or surveillance
The sponsor assumed vial sharing (no wastage) in estimating the treatment acquisition costs of these regimens. However, most of the components (cisplatin, oxaliplatin, leucovorin and irinotecan) in these treatment regimens are available as a single-use product, as noted in the respective monographs.24-27 Further, the sponsor’s estimation of FOLFOX treatment cost is missing a component of the regimen, in particular a 5-fluorouracil 400 mg/m2 IV bolus, and is based on an outdated unit price of leucovorin. The sponsor also significantly underestimated the treatment cost of XELOX. Capecitabine, a component of XELOX, is dispensed as 150 mg and 500 mg strength tablets28; however, the sponsor based the cycle cost of capecitabine on the total milligrams used to reach the recommended dosage, instead of the number of tablets, and disregarded drug wastage. As such, the sponsor’s approach and assumptions underestimated treatment acquisition cost of subsequent chemotherapies, which may influence the estimated budget impact if the distribution of patients on subsequent therapies differs by treatment arm. The clinical experts also noted other missing systematic chemotherapies relevant for this indication and patient population includes FOLFIRI and Ramucirumab + Paclitaxel. As such, not all relevant subsequent chemotherapies and costs are included, which may also impact the budget impact.
CADTH corrected FOLFOX treatment cost by including the cost of 400 mg/m2 5-fluorouracil IV bolus,11 and updating the unit price of leucovorin from $0.7000/mg16 to $0.1488/mg.12
CADTH corrected the treatment cost of XELOX by including drug wastage when estimating the cycle cost of capecitabine.
In the CADTH reanalysis, the distribution of patients on subsequent chemotherapies was assumed to be the same following adjuvant nivolumab or surveillance (i.e., 78.8% on FOLFOX, 8.3% on CISPFU and 12.8% on XELOX).
CADTH was unable to address the limitation on missing subsequent chemotherapies, FOLFIRI and Ramucirumab + Paclitaxel, because the proportion of patients on these regimens is uncertain. CADTH was also unable to address the limitation on vial sharing in estimating the cost of subsequent chemotherapies, owing to the structure of the budget impact model.
There is significant uncertainty in market share of nivolumab: The sponsor assumed nivolumab has a market share of || in year 1, |||||||||||| year 2 and |||||||||||| year 3. According to the clinical experts consulted for this review, given no adjuvant treatment for completely resected EG or GEJC currently exists in clinical practice, there is an unmet need in these patients. Further, there is limited access across Canada to current treatments such as esophagectomy and radiotherapy. The drug plans noted nivolumab may become the new standard of care if approved for funding, for an aggressive disease that is associated with a high risk of recurrence and mortality. Some patients may not be eligible for nivolumab treatment due to pre-existing immune conditions or deteriorated health, and a small minority may refuse treatment altogether. However, the clinical experts and drug plans anticipate a rapid market uptake of nivolumab, with a market share near 90%.
In the CADTH reanalysis, the market share of nivolumab was assumed to be 70% in year 1, and 90% in year 2 and 3.
CADTH Reanalyses of the Budget Impact Analysis
CADTH revised the sponsor’s base case by including patients with stage I esophageal or gastroesophageal junction cancer, assuming flat dosing of nivolumab, including drug wastage, extending treatment duration to 12 months, assuming a higher market share of nivolumab, and assuming no difference in the distribution of patients on subsequent chemotherapies.
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Unit price of leucovorin | $0.7000/mg | $0.1488/mg |
2. Missing component in FOLFOX treatment | 5-Fluorouracil 2,400 mg/m2 Oxaliplatin 85 mg/m2 Leucovorin 400 mg/m2 | 5-Fluorouracil 400 mg/m2 IV bolus11 5-Fluorouracil 2,400 mg/m2 Oxaliplatin 85 mg/m2 Leucovorin 400 mg/m2 |
3. Capecitabine in XELOX regimen | $79 per cycle | $158 per cycle |
Changes to derive the CADTH base case | ||
1. Estimated market size | Patients with esophageal or gastroesophageal junction cancer include: Stage II Stage III | Patients with esophageal or gastroesophageal junction cancer include: Stage I Stage II Stage III |
2. Nivolumab treatment | Weight-based dosing Treatment duration: 7.58 months Vial sharing: 5% wastage | Flat dosing Treatment duration: 12 months Vial sharing: No |
3. Market share of nivolumab (Year 1 / Year 2 / Year 3) | ||||||||||||||||||||||| | 70% / 90% / 90% |
4. Subsequent chemotherapies | The distribution of patients on subsequent chemotherapies differ following nivolumab treatment or surveillance | The distribution of patients on subsequent chemotherapies following nivolumab treatment or surveillance are the same (78.8% on FOLFOX, 8.3% on CISPFU, and 12.8% on XELOX) |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 | |
FOLFOX = Folinic Acid (Leucovorin)-Fluorouracil-Oxaliplatin, XELOX = Capecitabine-oxaliplatin
The results of the CADTH step-wise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18.
In the CADTH reanalysis, the 3-year budget impact of reimbursing nivolumab for adults with completely resected EC or GEJC increased to $122,873,802 (Year 1: $33,999,272; Year 2: $44,194,197; Year 3: $44,680,333).
CADTH also conducted additional scenario analyses to address remaining uncertainty in nivolumab dosing, using the CADTH base case. Results are provided in Table 18.
Assuming recommended dosage of nivolumab is based on weight
Price reduction of 36%
Nivolumab treatment duration of 7.58 months
Table 17: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total, $ |
|---|---|
Submitted base case, as provided | 53,674,419 |
CADTH correction 1 | 53,826,193 |
CADTH correction 2 | 53,665,552 |
CADTH correction 3 | 53,662,640 |
Sponsor’s base case, corrected | 53,805,548 |
Stepped analysis | |
CADTH reanalysis 1 | 56,593,746 |
CADTH reanalysis 2 | 91,192,160 |
CADTH reanalysis 3 | 68,925,696 |
CADTH reanalysis 4 | 53,806,831 |
CADTH base case (1+2+3+4) | 122,873,802 |
Table 18: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation), $ | Year 1, $ | Year 2, $ | Year 3, $ | Three-year total, $ |
|---|---|---|---|---|---|---|
Sponsor’s submitted base case | Reference | 1,085,378 | 1,097,317 | 1,109,387 | 1,121,591 | 4,413,673 |
New drug | 1,085,378 | 14,686,831 | 18,970,086 | 23,345,796 | 58,088,091 | |
Budget impact | 0 | 13,589,515 | 17,860,699 | 22,224,205 | 53,674,419 | |
Sponsor’s corrected base case | Reference | 841,009 | 850,260 | 859,613 | 869,069 | 3,419,950 |
New drug | 841,009 | 14,472,974 | 18,763,946 | 23,147,569 | 57,225,498 | |
Budget impact | 0 | 13,622,714 | 17,904,334 | 22,278,500 | 53,805,548 | |
CADTH base case | Reference | 884,590 | 894,320 | 904,158 | 914,104 | 3,597,172 |
New drug | 884,590 | 34,893,593 | 45,098,355 | 45,594,437 | 126,470,974 | |
Budget impact | 0 | 33,999,272 | 44,194,197 | 44,680,333 | 122,873,802 | |
CADTH scenario analysis 1: weight-based dosing | Reference | 884,590 | 894,320 | 904,158 | 914,104 | 3,597,172 |
New drug | 884,590 | 32,045,344 | 41,396,038 | 41,851,395 | 116,177,367 | |
Budget impact | 0 | 31,151,023 | 40,491,880 | 40,937,291 | 112,580,195 | |
CADTH scenario analysis 2: 36% price reduction | Reference | 884,590 | 894,320 | 904,158 | 914,104 | 3,597,172 |
New drug | 884,590 | 22,589,165 | 29,104,357 | 29,424,505 | 82,002,617 | |
Budget impact | 0 | 21,694,845 | 28,200,199 | 28,510,402 | 78,405,446 | |
CADTH scenario analysis 3: treatment duration | Reference | 884,590 | 894,320 | 904,158 | 914,104 | 3,597,172 |
New drug | 884,590 | 22,304,341 | 28,734,126 | 29,050,201 | 80,973,257 | |
Budget impact | 0 | 21,410,020 | 27,829,968 | 28,136,098 | 77,376,086 |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.