CADTH Reimbursement Review
Osimertinib (Tagrisso)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
CCSN
Canadian Cancer Survivor Network
CI
confidence interval
CNS
central nervous system
CT
computed tomography
ctDNA
circulating tumour DNA
DFS
disease-free survival
EGFR
epidermal growth factor receptor
FAS
full analysis set
HR
hazard ratio
HRQoL
health-related quality of life
IDMC
independent data monitoring committee
L858R
sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21
L-DAC
Lung Cancer Drug Advisory Committee
LCC
Lung Cancer Canada
LHF
Lung Health Foundation
MCS
Mental Component Summary
MID
minimal important difference
NR
not reached
NSCLC
non–small cell lung cancer
OH-CCO
Ontario Health (Cancer Care Ontario)
OS
overall survival
PCS
Physical Component Summary
PFS
progression-free survival
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumors
SAE
serious adverse event
SF-36 v2
Short Form (36) Health Survey version 2
T790M
amino acid substitution from a threonine to a methionine at position 790 in EGFR
TKI
tyrosine kinase inhibitor
TTD
time to deterioration
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Osimertinib (Tagrisso), 40 mg and 80 mg tablets, oral |
Indication | As adjuvant therapy after tumour resection in patients with stage IB to stage IIIAa NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review, Project ORBIS |
NOC date | January 18, 2021 |
Sponsor | AstraZeneca Canada Inc. |
EGFR = epidermal growth factor receptor; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
aDisease stages according to the American Joint Committee on Cancer 7th edition staging system. Equivalent stages using the 8th edition are stage IIA to stage IIIB.
Introduction
Lung cancer is the most commonly diagnosed cancer and a leading cause of cancer deaths in Canada, with non–small cell lung cancer (NSCLC) accounting for approximately 88% of cases.1 Approximately half of all lung cancer cases in Canada are stage I to stage III at diagnosis,1 and one-third of NSCLC patients have operable disease.2 Overall, approximately 15% of Canadians with NSCLC have an epidermal growth factor receptor (EGFR) mutation.3-5
The goal of treatment for patients with stage IB to stage IIIA (American Joint Committee on Cancer [AJCC] 7th edition staging system) NSCLC is to cure the disease and primarily involves surgical resection of the tumour.2,6 After surgical resection, patients may receive adjuvant platinum-based chemotherapy.2,6,7 Four cycles of adjuvant chemotherapy are recommended for patients with stage II to stage IIIA disease and for high-risk patients with stage IB disease (e.g., tumours > 4 cm in diameter, nodal involvement, perineural or lymphovascular invasion, or disease spread through air spaces).2,7 Meta-analyses have estimated a 5-year overall survival (OS) benefit of approximately 4% to 5% with adjuvant platinum-based chemotherapy.8-10 However, not all patients receive post-operative adjuvant chemotherapy.11 Reasons may include that it was declined by the patient, comorbidities, complication or delay in surgery recovery, and poor performance status.11 Additionally, patients who receive adjuvant chemotherapy may not finish the planned number of cycles.11 Cisplatin-based chemotherapy is the preferred treatment in Canada, and carboplatin-based chemotherapy is used if there is a contraindication to cisplatin.2,7 Adjuvant radiotherapy after surgical resection is not routinely recommended.2,7 After adjuvant chemotherapy is complete, patients receive active surveillance, which includes CT scans every 3 months to 6 months for 2 years to 3 years, then annually thereafter.6,7
Osimertinib is an oral EGFR tyrosine kinase inhibitor (TKI) available in 40 mg and 80 mg tablets.12 The recommended dose is 80 mg taken once a day. Osimertinib is indicated as adjuvant therapy after tumour resection in patients with stage IB to stage IIIA (AJCC 7th edition) NSCLC whose tumours have EGFR exon 19 deletions or a sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21 (L858R). A validated test is required to identify EGFR mutation–positive status before treatment.12 Per the product monograph, patients in the adjuvant setting should receive treatment, until disease recurrence or unacceptable toxicity, for up to 3 years.
Osimertinib has been previously reviewed by CADTH for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR mutations, and for the treatment of patients with locally advanced or metastatic EGFR amino acid substitution from a threonine to a methionine at position 790 in EGFR (T790M) mutation–positive NSCLC who have progressed on or after EGFR TKI therapy.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of osimertinib (80 mg dose, oral) as adjuvant therapy after tumour resection in patients with stage IB to stage IIIA NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from the clinical experts consulted by CADTH for the purpose of this review.
Patient Input
CADTH received submissions from 4 patient groups for this review: the Canadian Cancer Survivor Network (CCSN), Lung Cancer Canada (LCC), Lung Health Foundation (LHF) (formerly Ontario Lung Association), and the CanCertainty Coalition (CanCertainty). The CCSN is a national network of patients, families, friends, community partners, and sponsors who promote the best standards of care regarding early diagnosis, timely treatment, follow-up care, support, survivorship, and quality of end-of-life care. LCC is a national charitable organization that provides resources for lung cancer education, patient support, research, and advocacy. The LHF is a charity that focuses on respiratory illness and lung health that provides programs and services to patients and health care providers, invests in lung research, and advocates for improved policies on lung health. CanCertainty is made up of more than 30 Canadian patient groups, cancer health charities, and caregiver organizations that, along with oncologists and cancer care professionals, work to improve the affordability and accessibility of cancer treatments. For their submissions, the CCSN and LCC conducted interviews with Canadian patients (n = 18 and n = 6, respectively) diagnosed with stage IB to stage IIIA NSCLC. The LHF conducted an online survey, for which they received responses from 11 patients with lung cancer and 2 family caregivers, and online focus groups that included 7 patients and 3 caregivers. CanCertainty developed its submission based on published reports relating to lung cancer statistics and Canadian drug coverage and on a past survey the group had conducted of more than 1,600 Nova Scotia residents from the general population.
The symptoms and challenges patients noted as being most significant were fatigue, shortness of breath, cough, difficulty fighting infection, and chest tightness. Other health issues that were mentioned included pain, wheezing, reduced appetite, weight loss, anxiety, and sadness. Patients reported that having lung cancer interfered with their daily lives and their ability to work, complete household chores, exercise, enjoy leisure activities, and socialize. Patients also noted the negative impact cancer had on taking day trips, thinking positively about the future, mental health, relationships with others, and time spent both managing symptoms and attending appointments.
The patients surveyed by the CCSN, LCC, and LHF identified improvements in the following outcomes as important: desire for a cure, delaying disease recurrence, limiting side effects, and maintaining quality of life. The CCSN felt that participants valued disease-free survival (DFS) and its association with improved quality of life. Patients from the LCC submission felt that new medications should not interfere with daily living and should allow individuals to maintain their independence at a level similar to what it was before having cancer. The LHF respondents also emphasized better management and reduction of symptoms along with improving quality of life—not just extension of life.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical panel reported that the current treatment for Canadian patients with surgically resected stage IB to stage IIIA (AJCC 7th edition), EGFR-mutated NSCLC is adjuvant chemotherapy followed by active surveillance or active surveillance alone. The goal of adjuvant treatment is to treat microscopic metastatic disease, reduce the risk of recurrence, and improve cure and OS rates. The clinical experts noted that while adjuvant chemotherapy is beneficial, recurrence rates are high in these patients. The clinical experts reported that when NSCLC recurs, it is typically in a setting where it is no longer curable and treatment intent is palliative. The clinical panel indicated that better treatments are needed to decrease disease recurrence and improve OS. In the absence of improved longevity, the clinical experts noted that another important outcome of adjuvant therapy may be to delay the presentation of advanced disease in a context where presenting with advanced disease has high morbidity (i.e., new brain metastasis). The clinical panel indicated that adjuvant therapy is not intended to improve symptoms.
The clinical panel reported that osimertinib would be indicated for all surgically resected stage IB to stage IIIA EGFR-mutated NSCLC patients for 3 years. The clinical panel indicated that osimertinib is not intended to replace adjuvant chemotherapy; osimertinib would be used after standard chemotherapy (if chemotherapy was indicated). The clinical panel noted that higher-risk patients who decline or are unfit to receive standard chemotherapy may be best suited to receive treatment with osimertinib. The panel also noted that patients with later-stage disease may have a larger benefit than those with earlier-stage disease. The clinical panel indicated that patients without an EGFR mutation (e.g., those with interstitial lung disease or cardiac dysfunction) or with intolerable toxicity to the drug would not be suitable for osimertinib. The clinical panel indicated that patients with stage IB disease may be less suitable for treatment because they may have a smaller benefit from adjuvant treatment and a higher cure rate from surgery, and may not want to commit to 3 years of osimertinib. The clinical panel noted there is no data on the efficacy of osimertinib in patients with resistance mutations.
The clinical panel thought that the frequency at which response to treatment is assessed should be at the clinician’s discretion. For follow-up and toxicity management, the clinical panel indicated that patients would have visits at 2 weeks and 4 weeks, blood work every 3 months, CT scans every 3 months to 6 months for the first 2 years, then CT scans annually for years 3 to 5. The members of the clinical panel indicated they would likely perform annual CT scans and visits after 5 years for additional follow-up. The clinical panel further indicated that treatment with osimertinib should be discontinued if the patient experiences disease recurrence or unacceptable toxicity.
Clinician Group Input
Input was received from 2 clinician groups: the Ontario Health (Cancer Care Ontario)’s Lung Cancer Drug Advisory Committee (OH-CCO’s L-DAC) and LCC. The OH-CCO’s L-DAC submission included input from 5 clinicians; the LCC submission included input from 16 clinicians. Input from the clinician groups was generally consistent with that of the clinical panel consulted by CADTH. The clinician groups indicated there is a need to improve DFS and OS in patients with resected, EGFR-mutated stage IB to stage IIIA NSCLC. The clinician groups agreed that osimertinib would not replace adjuvant chemotherapy. The clinician groups thought that patients who complete 3 years of adjuvant osimertinib and relapse at least 6 months following completion of therapy would be considered for re-treatment with osimertinib therapy for advanced or metastatic disease. Similar to the clinical panel, the clinician groups agreed that re-treatment with osimertinib in the advanced or metastatic setting after use in the adjuvant setting is a consideration, but data are not available to inform on re-treatment.
Drug Program Input
The drug programs noted that osimertinib has potential for drug–drug interactions, which could potentially increase pharmacy resource use. The drug programs also indicated that osimertinib adjuvant therapy may change the place in therapy of comparator drugs and the drugs reimbursed in subsequent lines. The drug plans reported that EGFR mutation testing is not reflexively completed for early-stage NSCLC across most Canadian jurisdictions; thus, expansion of testing would be required to identify eligible patients. Lastly, the drug programs expressed concerns that the budget impact may be substantial because the duration of therapy per patient is 3 years.
In response to the drug programs’ questions regarding when adjuvant chemotherapy would benefit patients that might be considered for osimertinib, the clinical panel indicated that osimertinib is not intended to replace adjuvant chemotherapy. The clinical panel thought that osimertinib would be used after standard adjuvant chemotherapy, if chemotherapy was indicated, to further reduce the risk of disease recurrence. The drug programs also asked whether patients who receive osimertinib in the adjuvant setting and experience disease relapse while off treatment would be eligible for re-treatment with osimertinib in the metastatic setting and, if so, what time frame after completion of adjuvant therapy would be appropriate to be eligible for re-treatment. The clinical experts indicated they would restart osimertinib if patients experienced disease relapse while off treatment after completing 3 years of adjuvant osimertinib. The clinical experts indicated they would rechallenge with osimertinib earlier than 12 months off treatment if a patient relapsed. The clinical experts suggested a 2-month to 3-month off-treatment interval based on clinical experience but noted that the first CT scan occurs at 6 months after treatment unless the patient experiences other symptoms indicating recurrence.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The systematic review of osimertinib included 1 ongoing phase III randomized controlled trial (RCT). The ADAURA trial (N = 682) is an ongoing international, multi-centre, phase III, double-blind, placebo-controlled RCT to investigate the efficacy and safety of osimertinib in patients with stage IB to stage IIIA NSCLC with a centrally confirmed common-sensitizing EGFR mutation (exon 19 deletion and/or exon 21 (L858R) substitution mutations, either alone or in combination with other EGFR mutations), who have undergone complete tumour resection, with or without post-operative adjuvant chemotherapy. Patients were randomized in a 1:1 ratio to either 80 mg osimertinib orally per day (n = 339) or matching placebo (n = 343). The primary outcome of the ADAURA trial is DFS by investigator assessment. Secondary outcomes are OS and health-related quality of life (HRQoL) assessed by the Short Form (36) Health Survey version 2 (SF-36 v2). The main HRQoL outcome measures of interest were time to deterioration (TTD) of the 2 summary scores, the Physical Component Summary (PCS) and the Mental Component Summary (MCS), in the stage II to stage IIIA population. Exploratory end points included central nervous system (CNS) DFS, disease recurrence rate, progression-free survival (PFS), time to next treatment, and TTD in PCS and MCS in the overall population (i.e., stage IB to stage IIIA).
The results from the ADAURA trial presented in this review are from an unplanned interim analysis with a data cut-off date of January 17, 2020. The study protocol and statistical analysis plan were amended to incorporate a multiple-testing procedure to account for the interim analysis, which controls the type I error for the end points of DFS and OS in the stage II to stage IIIA population and overall population.
Baseline characteristics were balanced between the treatment arms. In the overall population (stage IB to stage IIIA), the mean age of the patients was 62.1 years. The majority of patients had stage II to stage IIIA disease (68.3%), a WHO performance status of 0 (63.6%), adenocarcinoma histology type (96.5%), had undergone a lobectomy (95.3%), were Asian (63.6%), and female (70.1%). Most patients had received post-operative adjuvant chemotherapy (60.0%). Overall, 54.7% of patients had exon 19 deletions and 45.2% had exon 21 (L858R) substitution mutations.
Efficacy Results
As of the interim analysis, OS data were immature, per the sponsor’s assessment. Per the trial’s multiple-testing procedure, OS was formally tested in the stage II to stage IIIA population at the interim analysis. At the data cut-off date, 25 deaths had occurred in the stage II to stage IIIA patient population (5.3% maturity), comprising 8 deaths (3.4%) in the osimertinib arm and 17 deaths (7.2%) in the placebo arm. The hazard ratio (HR) was 0.40 (95% confidence interval [CI], 0.18 to 0.89; P = 0.0244), which did not reach statistical significance (P value < 0.0002 required). Since OS did not reach statistical significance in the primary stage II to stage IIIA population, OS in the overall population was not formally tested for statistical significance, per the multiple-testing procedure. A total of 29 patients (4.3%) in the overall population had died as of the interim analysis, comprising 9 patients (2.7%) in the osimertinib arm and 20 patients (5.8%) in the placebo arm. The HR was 0.48 (95% CI, 0.23 to 1.02).
The primary end point of DFS was met at the interim analysis. In the stage II to stage IIIA population, 26 patients (11.2%) in the osimertinib arm and 130 patients (54.9%) in the placebo arm had experienced a DFS event. The HR was 0.17 (95% CI, 0.12 to 0.23), which was statistically significant (P < 0.0001). In the overall population, 37 patients (10.9%) in the osimertinib arm and 159 patients (46.6%) in the placebo arm had experienced a DFS event. The HR was 0.20 (95% CI, 0.15 to 0.27), which was also statistically significant (P < 0.0001). The results of the pre-specified subgroup analyses were consistent with the primary analysis of DFS in showing a benefit of osimertinib (HR of < 0.4) for all subgroups. A post hoc exploratory analysis of DFS with disease recurrence in the CNS only suggested an improvement with osimertinib compared with placebo (HR = 0.14; 95% CI, 0.07 to 0.27).
As of the interim analysis, the disease recurrence rate was 10.9% in the osimertinib arm and 45.8% in the placebo arm. Data on PFS and time to next treatment were immature, per the sponsor’s assessment, and the comparisons for these end points were not controlled for multiple comparisons. As of the data cut-off date, 13 patients (3.8%) in the osimertinib arm and 46 patients (13.4%) in the placebo arm had experienced a PFS event. Thirty-one patients (9.1%) in the osimertinib arm and 134 patients (39.1%) in the placebo arm had experienced a first subsequent anti-cancer therapy or a death event. Of these events, 30 patients (96.8%) in the osimertinib arm and 125 patients (93.3%) in the placebo arm had received a subsequent anti-cancer treatment.
In the pre-specified TTD analyses of PCS and MCS in the stage II to stage IIIA population, comparisons were made without adjustment for multiple-comparison testing. For the PCS score, 58 patients (24.9%) in the osimertinib arm experienced confirmed deterioration by 3.1 points or greater or death compared with 39 patients (16.5%) in the placebo arm (HR = 1.43; 95% CI, 0.96 to 2.13). For the MCS score, 52 patients (22.3%) in the osimertinib arm and 52 patients (21.9) in the placebo arm experienced a confirmed deterioration by 3.8 points or greater or death (HR = 0.90; 95% CI, 0.61 to 1.33). The TTD in PCS and MCS scores in the overall population were analyzed as post hoc exploratory analyses and the results were consistent with the stage II to stage IIIA population.
Harms Results
A total of 329 patients (97.6%) in the osimertinib arm and 306 patients (89.2%) in the placebo arm experienced at least 1 treatment-emergent adverse event (AE) (any grade) as of the interim analysis. The most frequently reported AEs in the osimertinib and placebo arms were diarrhea (46.3% and 19.8%, respectively), paronychia (25.2% and 1.5%, respectively), dry skin (23.4% and 6.4%, respectively), pruritis (19.3% and 8.7%, respectively), and cough (18.4% and 16.6%, respectively).
In the ADAURA trial, 54 patients (16.0%) in the osimertinib arm and 42 patients (12.2%) in the placebo arm experienced a serious adverse event (SAE) as of the interim analysis. The most frequently reported SAEs in the osimertinib and placebo arms were pneumonia (1.5% and 1.2%, respectively), cataracts (0.9% and 0%, respectively), diarrhea (0.6% and 0%, respectively), acute kidney injury (0.6% and 0%, respectively), ureterolithiasis (0.6% and 0%, respectively), and femur fracture (0.6% and 0.3%, respectively).
Withdrawals specifically due to AEs were not reported. As of the data cut-off, a total of 33 patients (4.8%) had withdrawn from the ADAURA trial: 19 (5.6%) in the osimertinib arm and 14 (4.1%) in the placebo arm. Thirty-six patients (10.7%) in the osimertinib arm and 10 patients (2.9%) in the placebo arm had discontinued study treatment due to AEs. The most common AEs leading to treatment discontinuation in the osimertinib arm were interstitial lung disease (n = 8; 2.4%), diarrhea (n = 3; 0.9%), and decreased appetite (n = 3; 0.9%). The most common AE leading to treatment discontinuation in the placebo arm was decreased ejection fraction (n = 3; 0.9%).
A total of 29 patients (4.3%) had died as of the interim analysis: 9 patients (2.7%) in the osimertinib arm and 20 patients (5.8%) in the placebo arm.
Regarding notable harms, 8 patients (2.4%) experienced interstitial lung disease and 2 patients (0.6%) experienced pneumonitis in the osimertinib arm as of the interim analysis. No patients in the placebo arm experienced interstitial lung disease or pneumonitis. The frequency of cardiac disorder AEs was greater in the osimertinib arm compared with the placebo arm (11.0% versus 5.2%, respectively). In the osimertinib arm, 6.5% patients experienced QT interval prolongation compared with 1.2% in the placebo arm. Four patients (1.2%) in the osimertinib arm experienced congestive heart failure, cardiac failure, or left ventricular dysfunction compared with zero in the placebo arm. Four patients (1.2%) in the osimertinib arm experienced atrial fibrillation compared with 1 (0.3%) in the placebo arm; 6 patients (1.8%) in the osimertinib arm experienced an arrhythmia other than atrial fibrillation compared with zero in the placebo arm. Overall, 3 patients (0.4%) experienced keratitis: 2 (0.6%) in the osimertinib arm and 1 (0.3%) in the placebo arm. In the osimertinib arm, 70.6% experienced a skin or subcutaneous tissue disorder compared with 35.6% of patients in the placebo arm. The most common skin disorders in the osimertinib and placebo arms were paronychia (25.2% and 1.5%, respectively), dry skin (23.4% and 6.4%, respectively), pruritis (19.3% and 8.7%, respectively), and dermatitis acneiform (11.0% and 4.7%, respectively).
Table 2: Summary of Key Results From the ADAURA Trial
Results | Stage II to IIIA population | Overall population | ||
|---|---|---|---|---|
Osimertinib N = 233 | Placebo N = 237 | Osimertinib N = 339 | Placebo N = 343 | |
OS | ||||
Patients with events, n (%)a | 8 (3.4) | 17 (7.2) | 9 (2.7) | 20 (5.8) |
HR (95% CI)b,c | 0.40 (0.18 to 0.89) | 0.48 (0.23 to 1.02) | ||
Two-sided P valueb | 0.0244d | 0.0553e | ||
Median OS (95% CI), monthsf | NR (NR to NR) | NR (NR to NR) | NR (NR to NR) | 48.2 (48.2 to NR) |
DFS | ||||
Patients with events, n (%) | 26 (11.2) | 130 (54.9) | 37 (10.9) | 159 (46.4) |
Disease recurrencea | 26 (11.2) | 129 (54.4) | 37 (10.9) | 157 (45.8) |
Death | 0 | 1 (0.4) | 0 | 2 (0.6) |
Censored | 207 (88.8) | 107 (45.1) | 302 (89.1) | 184 (53.6) |
HR (95% CI)b,c | 0.17 (0.12 to 0.23) | 0.20 (0.15 to 0.27) | ||
Two-sided P valueb | < 0.0001 | < 0.0001 | ||
Median DFS (95% CI), monthsf | NR (38.8 to NR) | 19.6 (16.6 to 24.5) | NR (NR to NR) | 27.5 (22.0 to 35.0) |
CNS DFSg | ||||
Patients with events, n (%)a | 4 (1.7) | 32 (13.5) | 6 (1.8) | 39 (11.4) |
CNS recurrence | 3 (1.3) | 27 (11.4) | 4 (1.2) | 33 (9.6) |
Death | 1 (0.4) | 5 (2.1) | 2 (0.6) | 6 (1.7) |
Censored, n (%) | 229 (98.3) | 205 (86.5) | 333 (98.2) | 304 (88.6) |
HR (95% CI)b,c | 0.14 (0.07 to 0.27) | 0.18 (0.10 to 0.33) | ||
Two-sided P valueb,h | < 0.0001 | < 0.0001 | ||
Median DFS in CNS (95% CI), monthsf | NR (38.8 to NR) | NR (NR to NR) | NR (39.0 to NR) | 48.2 (NR to NR) |
Disease recurrence rate | ||||
Disease recurrence, n (%)a | 26 (11.2) | 129 (54.4) | 37 (10.9) | 157 (45.8) |
Local or regional only | 17 (7.3) | 48 (20.3) | 23 (6.8) | 61 (17.8) |
Distant only | 8 (3.4) | 67 (28.3) | 10 (2.9) | 78 (22.7) |
Local or regional and distant | 1 (0.4) | 14 (5.9) | 4 (1.2) | 18 (5.2) |
PFS | ||||
Patients with PFS events, n (%) | NR | NR | 13 (3.8) | 46 (13.4) |
HR (95% CI)b,c | NR | 0.24 (0.14 to 0.41) | ||
2-sided P valueb,h | NR | < 0.0001 | ||
Median PFS (95% CI), monthsf | NR | NR | NR (NR to NR) | 48.2 (NR to NR) |
Time to next treatment or death | ||||
Patients with events, n (%) | NR | NR | 31 (9.1) | 134 (39.1) |
Death | NR | NR | 1 (3.2) | 9 (6.7) |
First subsequent anti-cancer therapy | NR | NR | 30 (96.8) | 125 (93.3) |
Median time to next treatment or death (95% CI), monthsf | NR | NR | NR (NR to NR) | 39.8 (30.8 to NR) |
HR (95% CI)b,c | NR | 0.20 (0.14 to 0.27) | ||
2-sided P valueb,h | NR | < 0.0001 | ||
HRQoL by the SF-36 v2 (TTD in MCS and PCS)i | ||||
PCS | ||||
Patients with confirmed deterioration or death, n (%) | 58 (24.9) | 39 (16.5) | Not reported | Not reported |
Deterioration | 57 (24.5) | 37 (15.6) | Not reported | Not reported |
Death | 1 (0.4) | 2 (0.8) | Not reported | Not reported |
HR (95% CI)b,c | 1.43 (0.96 to 2.13) | 0.98 (0.82 to 1.67)g | ||
Two-sided P valueb,h | 0.0817 | NR | ||
Median deterioration-free survival (95% CI)f | NR (NR to NR) | NR (NR to NR) | NR | NR |
MCS | ||||
Patients with confirmed deterioration or death, n (%) | 52 (22.3) | 52 (21.9) | NR | NR |
Deterioration | 51 (21.9) | 49 (20.7) | NR | NR |
Death | 1 (0.4) | 3 (1.3) | NR d | NR |
HR (95% CI)b,c | 0.90 (0.61 to 1.33) | 0.98 (0.70 to 1.39)hg | ||
Two-sided P valueb,h | 0.5949 | NR | ||
Median deterioration-free survival (95% CI)f | 39.0 (NR to NR) | NR (NR to NR) | NR | NR |
Harms — safety population | ||||
N | NR | NR | 337 | 343 |
AEs, n (%) | 329 (97.6) | 306 (89.2) | ||
SAEs, n (%) | 54 (16.0) | 42 (12.2) | ||
Discontinued study treatment due to AEs, n (%) | 37 (11.0) | 10 (2.9) | ||
Deaths, n (%) | 9 (2.7) | 20 (5.8) | ||
Notable harms — safety population | ||||
N | NR | NR | 337 | 343 |
Interstitial lung disease, n (%) | 8 (2.4) | 0 | ||
Pneumonitis, n (%) | 2 (0.6) | 0 | ||
Cardiac disorders, n (%) | 37 (11.0) | 18 (5.2) | ||
QT interval prolongation | 22 (6.5) | 4 (1.2) | ||
Atrial fibrillation | 4 (1.2) | 1 (0.3) | ||
Arrhythmias (other than atrial fibrillation)j | 6 (1.8) | 0 | ||
Congestive heart failure, cardiac failure, left ventricular dysfunction | 4 (1.2) | 0 | ||
Cardiomyopathy | 2 (0.6) | 0 | ||
Myocardial infarction | 2 (0.6) | 0 | ||
Keratitis, n (%) | 2 (0.6) | 1 (0.3) | ||
Skin and subcutaneous tissue disorders, n (%) | 238 (70.6) | 122 (35.6) | ||
Dermatitis acneiform | 37 (11.0) | 16 (4.7) | ||
Dry skin | 79 (23.4) | 22 (6.4) | ||
Erythema multiforme | 1 (0.3) | 0 | ||
Paronychia | 85 (25.2) | 5 (1.5) | ||
Pruritus | 65 (19.3) | 30 (8.7) | ||
Rash | 27 (8.0) | 9 (2.6) | ||
Skin fissures | 19 (5.6) | 0 | ||
Stevens-Johnson syndrome | 0 | 0 | ||
AE = adverse event; CI = confidence interval; CNS = central nervous system; DFS = disease-free survival; HR = hazard ratio; HRQoL = health-related quality of life; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; MCS = Mental Component Summary; NR = not reached; OS = overall survival; PCS = Physical Component Summary; PFS = progression-free survival; SAE = serious adverse event; SF-36 v2 = Short Form (36) Health Survey version 2; TTD = time to deterioration.
aEvents that do not occur within 2 scheduled visits of the last evaluable assessment (or randomization) were censored and therefore excluded in the number of events.
bThe analysis was performed using a log-rank test stratified by stage (IB vs. II vs. IIIA), race (Asian vs. non-Asian), and mutation type (exon 19 deletions vs. L858R). Stratification factors were as recorded in the interactive voice response system.
cAn HR < 1 favours osimertinib. The HR and CI were obtained directly from the U- and V-statistics.
dTwo-sided significance level of 0.0002 required for the interim analysis of OS.
eDue to a failed test of a previous end point in the multiple-testing procedure, this P value cannot be interpreted for inference and should be considered descriptive.
fCalculated using the Kaplan-Meier method.
gPost hoc analysis.
hP value has not been controlled for multiple comparisons.
iThe TTD of HRQoL was defined as time from date of randomization to the date of worsening (change from baseline of ≤ −3.1 points for the PCS and ≤ −3.8 points for the MCS) confirmed at the subsequent assessment, or death (by any cause) in the absence of worsening, provided death occurred within 2 assessment visits of the last assessment where HRQoL could be evaluated and regardless whether the patient had withdrawn from randomized therapy or received another anti-cancer therapy before symptom deterioration. Patients with 2 missed visits before confirmed deterioration were censored at the last evaluable assessment before the 2 missed visits.
jIncludes supraventricular arrhythmia, sinus arrhythmia, supraventricular extrasystoles, and ventricular extrasystoles.
Source: Clinical Study Report,13 sponsor’s submission to CADTH.14
Critical Appraisal
The ADAURA trial was a double-blind RCT to minimize bias. Baseline characteristics were balanced between treatment arms and few randomized patients had been lost to follow-up as of the data cut-off. The interim analysis was not planned, and the trial is ongoing. A multiple-testing procedure was employed to control overall type I error at the 5% 2-sided level for the end points of DFS and OS, which was modified to account for the unplanned interim analyses. The primary end point was met at the interim analysis since the log-rank test for DFS in patients with stage II to stage IIIA disease met the pre-specified threshold for statistical significance. The log-rank test for DFS in the overall population also met statistical significance for this analysis. Due to early reporting of the study, data maturity is lower than planned at the interim analysis, per the sponsor. At the data cut-off date, the sponsor assessed the OS data to be immature. Furthermore, the comparison of OS in the stage II to stage IIIA population was not statistically significantly different between the treatment groups. Thus, at the time of this review, we cannot conclude that osimertinib confers an OS benefit compared with placebo. In addition, the data on time to next treatment and PFS are considered by the sponsor to be of limited clinical significance at the data cut-off of the interim analysis due to the immaturity of the data on patients who experienced a disease recurrence event, and comparisons for these end points were not controlled for multiple comparisons. The results did not support conclusions for an effect of osimertinib on PFS and time to next treatment, and any potential clinical benefit for these outcomes is associated with uncertainty due to the immaturity of the data and lack of control for type I error. Conclusions could not be drawn for the effect of osimertinib on HRQoL end points, as these end points were not adjusted for multiple comparisons. In addition, the majority of patients had not had the opportunity to receive the study treatment for the planned duration of 3 years.
The osimertinib dose and treatment regimen used in the ADAURA trial aligns with the Health Canada indication. The ADAURA trial included patients who had received standard-of-care adjuvant chemotherapy, which is commonly used in Canadian practice. This also aligns with the intended use of osimertinib in Canada, per the clinical experts consulted by CADTH and the clinician groups that provided input, both of which indicated that osimertinib is not intended to replace adjuvant chemotherapy. The clinical experts consulted by CADTH thought that the inclusion and exclusion criteria used in the trial were appropriate and generally reflected the characteristics of the intended patient population in Canada. However, the trial limited enrolment to patients with a WHO performance status of 0 to 1 and the clinical experts reported that many patients in their practice with resected stage IA to stage IIIB NSCLC have a performance status of 2. The clinical experts did not think that exclusion of patients with worse performance status limits the generalizability of the trial results. The proportion of Asian patients in the trial was higher than in the Canadian NSCLC population, per the clinical experts consulted by CADTH. In addition, the ADAURA trial reported a higher EGFR mutation–positive rate than currently seen in Canada, where EGFR genetic testing is routinely offered to patients with locally advanced disease that is not amenable to curative-intent therapy or who have metastatic NSCLC only.
Indirect Comparisons
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH or identified in the literature search.
Conclusions
One ongoing phase III, double-blind, placebo-controlled RCT (ADAURA) provided direct evidence regarding the safety and efficacy of osimertinib adjuvant therapy in adult patients with resected stage IB to stage IIIA (AJCC 7th edition) NSCLC. The trial included patients regardless of whether they had received standard adjuvant chemotherapy. The ADAURA trial met its primary end point at an unplanned interim analysis that showed a statistically significant difference in DFS in both the stage II to stage IIIA population and the overall population. This DFS benefit was consistently observed in all pre-specified subgroups. The results did not support conclusions for an effect of osimertinib on OS, PFS, or time to next treatment, and any potential clinical benefit for these outcomes is associated with uncertainty due to the immaturity of the data. Conclusions could not be drawn for the effect of osimertinib on HRQoL end points, as these end points were not adjusted for multiple comparisons. The majority of study participants reported treatment-emergent AEs. A greater proportion of patients in the osimertinib arm experienced an AE compared with the placebo arm. Interstitial lung disease, pneumonitis, cardiac disorders, and skin and subcutaneous tissue disorders were reported more frequently in the osimertinib arm. These AEs are consistent with the known safety profile of osimertinib. Keratitis was uncommon in both treatment arms. A greater number of patients in the osimertinib arm discontinued study treatment due to AEs and experienced an SAE. Overall, 4% of study participants had died as of the interim analysis.
Introduction
Disease Background
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer deaths in Canada.1 Survival from lung cancer of all stages and histologies is poor, with an overall 5-year net survival rate of 19%.1 In 2020, it was estimated there would be 29,800 new cases of lung cancer diagnosed and 21,200 deaths from lung cancer that year.1 It is estimated that 1 in 17 Canadians will die of lung cancer.15
Lung cancer is classified as either NSCLC or small cell lung cancer, with NSCLC accounting for approximately 88% of cases in Canada.1 NSCLC is further classified into 3 main histologic subtypes: adenocarcinoma, squamous cell carcinoma, and large-cell carcinoma. To determine a patient’s prognosis and treatment, NSCLC is staged using the AJCC staging criteria, which involves TNM (tumour, node, metastasis) classification of the disease based on the size and spread of the primary tumour (T), lymph node involvement (N) and occurrence of metastasis (M).16 Approximately half of all lung cancer cases in Canada are stage I to stage III at diagnosis.1 Early-stage (i.e., stage I to stage IIIA per the AJCC 7th edition) NSCLC is often asymptomatic.16,17 If patients do present with symptoms, they are often unspecific and difficult to directly attribute to a lung cancer diagnosis.17 The most common symptoms include unspecific cough, chest and shoulder pain, hemoptysis, weight loss, dyspnea, hoarseness, bone pain, and fever.17 Diagnostic procedures include imaging of the lungs, sputum cytology, and tissue biopsy.2 Approximately one-third of NSCLC patients have operable disease.2
Approximately 15% of Canadians with NSCLC have an EGFR–activating mutation in the region encoding the tyrosine kinase domain.3-5 EGFR mutations are more frequently observed in those who have never smoked, people of Asian ethnicity, patients with adenocarcinoma, and females.3,18 The most common EGFR mutations are exon 19 deletions and the exon 21 codon 858–point mutation (L858R).4,5
Standards of Therapy
The goal of treatment for patients with stage IB to stage IIIA NSCLC (per the AJCC 7th edition; the equivalent stages using the AJCC 8th edition are stage IIA to stage IIIB) is to cure the disease and primarily involves surgical resection of the tumour.2,6 After surgical resection, the majority of patients will receive 4 cycles of adjuvant platinum-based chemotherapy.2,6,7 Meta-analyses have estimated a 5-year OS benefit of approximately 4% to 5% with adjuvant platinum-based chemotherapy.8-10 Adjuvant chemotherapy is recommended for patients with stage II to stage IIIA disease and stage IB patients considered at high risk of relapse (e.g., tumours > 4 cm in diameter, nodal involvement, perineural or lymphovascular invasion, or disease spread through air spaces).2,7 However, not all patients receive post-operative adjuvant chemotherapy. A retrospective real-world study conducted in Europe, which included 831 patients with stage IB to stage IIIA NSCLC, found that 52% of patients did not receive adjuvant chemotherapy (15.1% of those with stage IB, 55.1% with stage II, and 71.4% of patients with stage IIIA received adjuvant chemotherapy).11 The most common reasons for not receiving adjuvant chemotherapy were that it was declined by the patient (12.6%), comorbidities (11.9%), complication or delay in surgery recovery (8.4%), and poor performance status (7.0%).11Additionally, approximately one-third of patients who received chemotherapy did not finish the planned number of cycles.11 In Canada, cisplatin-based chemotherapy is the preferred systemic treatment and carboplatin-based chemotherapy is used if there is a contraindication to cisplatin.2,7 Adjuvant radiotherapy after complete surgical resection is not routinely recommended.2,7 After adjuvant chemotherapy is complete, patients receive active surveillance, also known as “watch and wait,” which includes CT scans every 3 months to 6 months for 2 years to 3 years then annually thereafter until year 5.6,7
Drug
Osimertinib (Tagrisso) is an oral EGFR TKI available in 40 mg and 80 mg tablets.12 The recommended dose is 80 mg taken once a day. Osimertinib is a selective irreversible inhibitor of EGFR-sensitizing mutations and the T790M resistance mutation that has limited activity against wild-type EGFR (mutation-negative) NSCLC. Osimertinib is indicated as adjuvant therapy after tumour resection in patients with stage IB to stage IIIA (AJCC 7th edition) NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations. A validated test is required to identify EGFR mutation–positive status before treatment.12 Per the product monograph, patients in the adjuvant setting should receive treatment, until disease recurrence or unacceptable toxicity, for up to 3 years. Osimertinib underwent Health Canada priority review and was part of Project ORBIS.14 Health Canada issued a Notice of Compliance on January 18, 2021. The sponsor’s reimbursement request is per the Health Canada indication.
Osimertinib is also indicated for the first-line treatment of patients with locally advanced (not amenable to curative therapies) or metastatic NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations (either alone or in combination with other EGFR mutations).12 In addition, osimertinib is indicated for the treatment of patients with locally advanced or metastatic EGFR T790M mutation–positive NSCLC whose disease has progressed while on or after TKI therapy.12 For this latter indication, marketing authorization was based on results from a randomized phase III trial (AURA3) demonstrating that osimertinib was superior to platinum-doublet chemotherapy in prolonging PFS as assessed by investigator using Response Evaluation Criteria in Solid Tumors Version 1.1 (RECIST 1.1) guidelines.12 Osimertinib has been previously reviewed by CADTH for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR mutations and for the treatment of patients with locally advanced or metastatic EGFR T790M mutation–positive NSCLC whose disease has progressed while on or after EGFR TKI therapy.
Table 3: Key Characteristics of Osimertinib
Characteristic | Osimertinib |
|---|---|
Mechanism of action | Selective irreversible inhibitor of EGFR-sensitizing mutations and T790M resistance mutation that has limited activity against wild-type EGFR. |
Indicationa | As adjuvant therapy after tumour resection in patients with stage IB to stage IIIA NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations. |
Route of administration | Oral |
Recommended dose | 80 mg once a day |
Serious adverse effects or safety issues |
|
Other | A validated test is required to identify EGFR mutation–positive status in tumour tissue before treatment. |
EGFR = epidermal growth factor receptor; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NSCLC = non–small cell lung cancer; QTc = corrected QT interval.
aHealth Canada–approved indication.
Source: Product monograph,12 sponsor’s submission to CADTH.14
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Groups and Information Gathered
CADTH received 4 submissions from patient groups for the reimbursement review of osimertinib from the CCSN, LCC, LHF (formerly Ontario Lung Association), and CanCertainty. CCSN is a national network of patients, families, friends, community partners, and sponsors who promote the best standards of care regarding early diagnosis, timely treatment, follow-up care, support, survivorship, and quality of end-of-life care. LCC is a national charitable organization that provides resources for lung cancer education, patient support, research, and advocacy. LHF is a charity that focuses on respiratory illness and lung health that provides programs and services to patients and health care providers, invests in lung research, and advocates for improved policies on lung health. CanCertainty is made up of more than 30 Canadian patient groups, cancer health charities, and caregiver organizations who, along with oncologists and cancer care professionals, work to improve the affordability and accessibility of cancer treatments.
For its submission, the CCSN contracted help from Broadstreet Health Economics and Outcomes Research (an independent consultancy specializing in epidemiology and health economics) to conduct interviews with Canadian English-speaking patients who had been diagnosed with stage IB, stage II, or stage IIIA lung cancer (33%, 17%, and 50%, respectively). Interviews were approximately 45 minutes long, held over Zoom (teleconferencing platform), and took place between January 13 and February 8, 2021. Interview participants were found through the organization’s Right2Survive mailing list. The majority of the 18 participants were female (83%), ranged in age from 51 years to 85 years, and were from across the country: Atlantic region (22%), prairies (22%), central (50%), and west coast (6%).
LCC conducted interviews with 6 Canadian patients who had stage IB to stage IIIA EGFR mutation–positive NSCLC. Females made up 83% of respondents and ages ranged from 45 years to 69 years.
In February 2021, LHF released an online survey to which they received responses from 11 patients with lung cancer and 2 family caregivers. In April 2021, 3 focus groups were held over Zoom that were made up of 7 patients and 3 caregivers. Participants were from British Columbia, Alberta, Manitoba, Ontario, Quebec, New Brunswick, and Nova Scotia. A certified respiratory educator who works with LHF also provided input and reviewed sections related to disease experience, treatment, and outcomes.
CanCertainty developed its submission based on published reports relating to lung cancer statistics and Canadian drug coverage as well as a past survey (2017) the group had conducted of more than 1,600 randomly selected individuals from the general population of Nova Scotia.
Disease Experience
Patients who were interviewed for the CCSN submission expressed fear and concern over the low survival rate and the possibility that their tumour may be inoperable. One interviewee reflected, “I guess I was kind of desperate to think I was going to be okay and asked how things looked. And, she told me at the time that I had a 15 percent chance of surviving five years… it becomes such a psychological burden that, you know, I was looking at 15 people out of a 100 survive for five years. What’s the chance that I would be one of those 15?”
From the 23 LHF respondents, the symptoms and challenges patients noted as being most significant were fatigue (64%), shortness of breath (64%), cough (27%), difficulty fighting infection (27%), and chest tightness (18%). Other health issues that were mentioned include pain, wheezing, reduced appetite, weight loss, anxiety, and sadness. Patients responded that having lung cancer interfered with their daily lives and their ability to work (54%), complete household chores (40%), exercise (40%), enjoy leisure activities (36%), and socialize (29%). The submission also noted the negative impact cancer had on taking day trips, thinking positively about the future, mental health, relationships with others, and time spent both managing symptoms and attending appointments. To further illustrate this, the following quotes describe some of their experiences, “You never stop thinking about it,” “It can be so overwhelming,” and “I have a lot of anxiety and sadness now.” The LHF focus group discussed challenges that patients faced, such as a lack of support groups for those living with lung cancer compared with other cancers, feeling that there are limited treatment options, and not being able to access services close to home.
Experiences With Currently Available Treatments
Patients from the CCSN submission had previously received surgery (89%) and chemotherapy (56%) as cancer treatments. Although most reported that their surgery was successful, 1 patient responded that the cancer had metastasized before surgery while another was devastated with how their lifestyle changed due to reduced lung function as a result of the surgery. One participant interviewed also explained that they declined chemotherapy since it was not a guaranteed cure.
LCC described that the patient experience and burden of care with chemotherapy cited by patients in the current submission is consistent with that of other lung cancer treatment settings that have been discussed in previous LCC submissions to CADTH. Financial burden and additional strain on caregivers were other factors that patients considered when deciding on treatments. They also noted that patients who receive adjuvant chemotherapy may relapse, which demonstrates the need for therapies that are effective at preventing disease recurrence.
The LHF respondents reported trying the following treatments: gefitinib, entrectinib, Anoro Ellipta, Ventolin, Trelegy, Onbrez, Alvesco, amlodipine, Lyrica, and Breo. Respondents indicated these treatments were associated with side effects that included fatigue, diarrhea, nausea, appetite loss, weight loss, heart palpitations, face blistering or rash, headaches, and difficulty sleeping.
CanCertainty noted in its submission that reimbursement of oral cancer drugs is not equal across jurisdictions in Canada. As a result, patients who do not have adequate insurance may have to pay out-of-pocket for medication and/or apply to funding-assistance programs, which can take time and delay access to treatment. The group also considered that patients who do have private insurance they may still have co-pays, deductibles, and annual or lifetime caps that increase the financial burden on them and their families. CanCertainty suggested that, due to the differential drug coverage plans among provinces and territories, patients can face discrimination based on age, income, geography, and cancer type or treatment. From their survey of Nova Scotia residents, 60% of respondents stated they would consider leaving the province if they had to pay for cancer treatments and only 7% felt they could afford monthly drug costs exceeding $200. Furthermore, CanCertainty investigated the impact of “financial toxicity” that can result from out-of-pocket costs, lost income, and treatment-related expenses. CanCertainty indicated that those at greater risk of “financial toxicity” are patients who are young, have limited income, are uninsured or unemployed, have been recently diagnosed, or have more severe cancer. To mitigate the financial burden, CanCertainty noted that patients may delay or skip treatment, opt for less expensive alternatives, or avoid appointments.
Improved Outcomes
The patients surveyed by the CCSN, LCC, and LHF identified improvements in the following outcomes as important: desire for a cure, delaying disease recurrence, limiting side effects, and maintaining quality of life.
The CCSN felt that the participants valued DFS and its association with improved quality of life, and 72% of participants indicated they would be willing to take a medication that improved DFS without data on OS. One individual stated, “You can live a decent life without being cured of cancer if you can keep it stable or under control,” while another shared, “I would go for the quality over the quantity.” Patients also felt that being involved in the treatment decision-making process was very important along with having access to comprehensive information, either through their own research or their health care team.
In addition to the improved outcomes stated earlier, patients contributing to the LCC submission felt that new medications should not interfere with daily living and should allow individuals to maintain their independence at a level similar to what it was before having cancer. Further discussion around quality of life highlighted the value that patients and families placed on being able to return to work and regular life and on being productive.
The LHF respondents also emphasized better symptom reduction and management along with improving quality of life and not just extension of life. Other topics that came up were having access to information about lung cancer and to community-based support.
Experience With Drug Under Review
LCC interviewed 1 patient who had not yet started treatment, 4 who were currently receiving osimertinib, and 1 who had past experience with it; all of these patients were described as having stage IB to stage IIIA cancer. The setting (i.e., adjuvant or metastatic) where these patients received osimertinib was not reported in the submission. Patients were able to receive osimertinib through a special access program (n = 3), insurance (n = 2), or clinical trial (n = 1). Of the 5 who received the drug, the duration of treatment ranged from 1 month to 4 months. The single patient who was part of a clinical trial had to stop after 3 months due to pneumonitis. In general, patients were described as tolerating the medication well, allowing them to return to work full time and continue with their daily lives. Patients preferred an oral pill to receiving treatment intravenously and osimertinib was described as being “much better than chemotherapy.” LCC also noted that osimertinib could reduce the burden on caregivers, the need to travel for treatment, the time spent receiving treatment, and the burden on hospitals because treatment does not require occupying a chemotherapy chair. Patients described the following side effects while receiving treatment with osimertinib: rash on face and/or chest, pneumonitis (which resulted in discontinuing the drug), skin pustules (which were treated with cortisol and resolved), and mild nausea. According to LCC, if not for assistance enabling them to access the medication (e.g., special access programs, insurance, clinical trial), costs would be prohibitive for these patients. Furthermore, the patient group indicated that a diagnosis of later-stage early lung cancer appeared to influence patients to accept osimertinib more readily.
No patients interviewed or surveyed by the CCSN or LHF had experience with osimertinib at the time of the submission.
Companion Diagnostic Test
LCC noted that EGFR genetic testing is routine for later-stage lung cancer in many cancer centres across Canada and suggested it could be expanded to include earlier-stage cancers.
Additional Information
The CCSN highlighted the value of having treatments approved quickly by decision-makers, for instance, when only DFS information is known, and OS data are not yet available. The patients emphasized that treatment approval and improved access are both key to potentially offering the best chances of survival. The group also acknowledged that differential approval across jurisdictions is another hurdle to accessing medications.
LCC noted in its submission that early treatment could not only improve patients’ long-term outcomes and prevent progression to later-stage disease, but it may also alleviate pressures on patients, families, and the health care system.
CanCertainty emphasized the importance of equitable access to cancer medications for all Canadians. The group also raised concerns over the safety of take-home cancer drugs compared with those administered in clinics by trained health care professionals, particularly with regard to dosing, handling, limited monitoring or nonadherence, and toxicity.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the osimertinib review, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion is presented subsequently.
Unmet Needs
The clinical panel reported that current treatment for Canadian patients with surgically resected stage IB to stage IIIA (AJCC 7th edition), EGFR-mutated NSCLC is adjuvant chemotherapy followed by active surveillance or active surveillance alone. Adjuvant chemotherapy consists of 4 cycles of platinum-doublet chemotherapy (e.g., cisplatin plus vinorelbine, cisplatin plus pemetrexed). Adjuvant chemotherapy is offered to patients with good performance status and without other comorbidities that would contraindicate chemotherapy (e.g., recent myocardial infarction, neuropathy). In patients with stage IA (AJCC 7th edition) disease, active surveillance is offered to patients with a tumour size of less than 4 cm, whereas adjuvant chemotherapy is offered to those with a tumour size of 4 cm or greater. The clinical experts reported that cisplatin-based adjuvant chemotherapy can be challenging to administer because it requires adequate performance status and renal function. Cisplatin-based adjuvant chemotherapy also has substantial toxicity (e.g., chronic renal failure, future blood dyscrasias, neuropathy, hearing loss) and some patients are not candidates for it.
The clinical panel indicated that the goal of adjuvant treatment is to treat microscopic metastatic disease, reduce the risk of recurrence, improve cure rates, and improve OS. The clinicians noted they are not able to identify patients who are cured with surgery alone versus those who have microscopic residual disease; therefore, adjuvant chemotherapy is offered to all eligible patients. The clinical experts reported that adjuvant chemotherapy improves cure by approximately 5% to 15%, depending on disease stage. The members of the clinical panel indicated that, in their experience, approximately one-quarter to one-third of patients decline adjuvant chemotherapy because the patients consider this small clinical benefit to be not worth the toxicity associated with adjuvant chemotherapy treatment. Other patients are unfit for 4 cycles of chemotherapy.
The clinical experts noted that while adjuvant chemotherapy is beneficial, recurrence rates remain high in these patients. The clinical panel reported that many patients with resected lung cancer eventually relapse despite receiving adjuvant chemotherapy. The clinical experts reported that when NSCLC recurs, it is typically in a setting where the disease is no longer curable and treatment intent is considered palliative. The clinical experts estimated that greater than 50% to 60% of patients with resected stage IIIA NSCLC relapse with incurable disease. The clinical panel indicated that better treatments are needed to decrease disease recurrence and improve OS.
In the absence of improved survival, the clinical experts noted that other important outcomes of adjuvant therapy may be to delay the presentation of advanced disease, in the context where presenting with advanced disease has high morbidity (e.g., new brain metastasis). The clinical experts also noted that some patients may be cured with surgery; therefore, an ideal adjuvant therapy would have a minimal side effect profile and minimal risk from long-term complications. The clinical panel indicated that adjuvant therapy is not intended to improve symptoms.
Place in Therapy
The clinical panel thought that osimertinib would be indicated for 3 years for all patients with surgically resected stage IB to stage IIIA (AJCC 7th edition) EGFR-mutated NSCLC. The clinical experts estimated this would include approximately 15% to 20% of patients with lung cancer in Canada. The clinical panel indicated that osimertinib is not intended to replace adjuvant chemotherapy; rather, osimertinib would be used after standard chemotherapy (if chemotherapy was indicated). As such, the clinical panel thought that osimertinib likely would not cause a shift in the current treatment paradigm, except in patients with EGFR-mutated stage IB disease (tumour < 4 cm) where often only active surveillance is required after tumour resection. In this setting, the clinical panel thought that some clinicians might offer 3 years of adjuvant osimertinib only. In addition, osimertinib could be considered for patients who are unfit for adjuvant chemotherapy.
The clinical experts reported that, in their experience, most patients (approximately two-thirds to three-quarters) who are offered adjuvant chemotherapy will complete 4 cycles. However, the clinical experts thought that there is no reason that patients would need to complete all 4 cycles of chemotherapy before starting osimertinib, and that osimertinib could be offered to patients who receive fewer than 4 cycles (i.e., the clinical experts thought there is no required minimum number of cycles). The clinical panel also noted there is a small group of patients who would be eligible for osimertinib and who would not be offered chemotherapy (e.g., stage IB, unfit). The clinical experts reiterated that osimertinib is not a substitute for chemotherapy.
The clinical experts predicted that the use of osimertinib in the adjuvant setting would necessitate a change in the timing for EGFR genetic testing in NSCLC patients. In Canada, EGFR genetic testing is routinely done in patients with late-stage NSCLC. EGFR genetic testing often is not performed in patients with early-stage NSCLC due to the cost and the fact that it likely would not impact early care. The clinical panel noted that EGFR genetic testing availability varies by jurisdiction. The clinical panel noted there is a potential added cost to treatment if EGFR genetic testing occurs earlier in the treatment course. They noted that a subset of early-stage patients (e.g., stage IB) would be cured with resection and adjuvant chemotherapy and, thus, would never need testing for metastatic disease, which is when most testing occurs. The clinical panel noted that osimertinib is currently available in some jurisdictions through special access programs in the adjuvant setting for patients with stage IB to stage IIIA resected EGFR-mutated NSCLC.
Patient Population
The clinical panel indicated that patients who meet the eligibility criteria for the ADAURA trial (i.e., those with EGFR-mutated, resected, stage IB to stage IIIA NSCLC) would be suitable for treatment with osimertinib. The clinical panel thought that higher-risk patients who decline or are unfit to receive standard chemotherapy may be best suited to receive treatment with osimertinib. The panel also thought that patients with later-stage disease may receive a larger benefit with adjuvant osimertinib than those with earlier-stage disease.
The clinical panel indicated that patients without an EGFR mutation and those who have intolerable toxicity to the drug (e.g., interstitial lung disease or cardiac failure) would not be suitable for osimertinib. The clinical panel thought that patients with stage IB disease may be less suitable for treatment because they receive less clinical benefit from adjuvant treatment, experience a higher cure rate from surgery, and may not want to commit to 3 years of osimertinib. However, the clinical experts noted that, with the current treatment options, recurrence is approximately 25% in patients with stage IB disease. In addition, the clinical panel thought that patients with resistance mutations could be less suitable for treatment with osimertinib, but there are no data in that setting.
Assessing Response to Treatment
The clinical panel identified the following outcomes of interest when assessing response to osimertinib treatment: no disease recurrence, OS, DFS, and prevention of CNS metastases.
The clinical panel thought that the frequency at which treatment response is assessed should be at the clinician’s discretion. For follow-up and toxicity management, the members of the clinical panel indicated they would require visits at 2 weeks and 4 weeks, blood work every 3 months, CT scans every 3 months to 6 months for the first 2 years, and then CT scans annually for years 3 to 5. The clinical panel indicated they would likely perform annual CT scans and require visits after 5 years for additional follow-up.
Discontinuing Treatment
The clinical panel indicated that treatment with osimertinib should be discontinued if the patient experiences disease recurrence or unacceptable toxicity (e.g., SAEs or chronic AEs that do not respond to dose reduction). The clinical panel thought that patients whose disease progresses while on osimertinib would be discontinued and treated with platinum-doublet chemotherapy or be assessed for enrolment in a clinical trial.
Prescribing Conditions
The clinical panel indicated that osimertinib should be prescribed and monitored by medical oncologists, general practitioners of oncology, or nurse practitioners who have been trained in oncology. Patients would be treated in the outpatient community setting.
Additional Considerations
The clinical experts were uncertain about the time frame for re-treatment with osimertinib if a patient relapsed while off treatment (i.e., patient completed 3 years of osimertinib adjuvant therapy then experienced disease recurrence or relapsed with metastatic disease). They were also uncertain about defining an off-treatment interval (after completing 3 years of osimertinib adjuvant therapy) before restarting osimertinib due to the limited evidence available to inform on this issue. In patients who progress while off treatment with a treatment-free interval of 3 months or greater, the clinical experts indicated they would try rechallenging with osimertinib. In that situation, the clinical experts indicated they might re-biopsy the metastatic disease and look at genetic testing for a mechanism resistant to osimertinib. If there was no resistance, they would restart osimertinib treatment. The clinical panel noted that patients who restart treatment usually respond immediately (e.g., within 3 weeks), and this response can be observed clinically and/or with a chest X-ray rather than needing a CT scan. If the patient did not experience benefit after approximately 3 months of treatment, they would stop osimertinib. The clinical experts indicated they would be unlikely to use another TKI when rechallenging. The clinical experts also noted that, in their experience, patients with EGFR-mutated NSCLC do not respond well to immunotherapy (< 10% response rate); thus, they thought that immunotherapy is unlikely to be offered to these patients.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Input was received from 2 clinician groups on the reimbursement review of osimertinib as adjuvant therapy after tumour resection for the treatment of patients with stage IB to stage IIA NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations.
The OH-CCO’s L-DAC provides evidence-based clinical and health system guidance on drug-related issues in support of its mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. Information for this review was collected through joint discussions through emails. Four physicians (1 cardiothoracic surgeon and 3 medical oncologists) and 1 pharmacist provided input for this submission.
LCC is a national charitable organization that is a resource for lung cancer education, patient support, research, and advocacy. The organization is based in Toronto, Ontario and includes both regional and pan-Canadian initiatives. The organization is also a member of the Global Lung Cancer Coalition. Information for this submission was gathered through relevant published clinical data and expert evidence-based review among lung cancer medical oncologists across Canada. Sixteen physicians (14 medical oncologists and 2 pathologists) provided input for this submission.
Unmet Needs
The OH-CCO’s L-DAC noted that adjuvant chemotherapy is offered as standard therapy to patients with resected primary tumours greater than 4 cm or who have other high-risk features such as positive lymph nodes, invasion of the chest wall, or satellite nodules in the same lung or the ipsilateral lung. The clinician group added this includes most patients with stage IB to stage IIIA tumours, based on the AJCC 7th edition staging system, and equivalent stage IIA to stage IIIB tumours, per the 8th edition. LCC noted that in current Canadian practice, treatments for early-stage NSCLC do not differentiate between patients with and without EGFR mutations. Adjuvant platinum-doublet chemotherapy given after tumour resection typically consists of 4 cycles of treatment, with each cycle lasting 21 days for a total of 12 weeks of therapy.
LCC indicated that the primary goal of treatment for patients with stage IB to stage IIIA disease (AJCC 7th edition) is a cure, which is reflected in improvements in 5-year OS rates. Both clinician groups indicated that the goal of adjuvant therapy is to improve OS and HRQoL. The clinician groups thought that increasing DFS could translate into improved OS. The OH-CCO’s L-DAC added that in situations where recurrence is often symptomatic and unpredictable, improving DFS may improve HRQoL. Both groups also agreed that the side effects of adjuvant therapy should be minimal.
The OH-CCO’s L-DAC noted that despite adjuvant chemotherapy, the risk of disease recurrence and death remains high in patients with resected stage IIA to stage IIIB NSCLC. The clinician group reported that the 5-year OS rate ranges from 70% for stage IIA to 40% for stage IIIB. Similarly, LCC indicated that current therapies are inadequate to achieve high rates of cure and certain patient outcomes, particularly DFS and OS, remain poor despite adjuvant chemotherapy. In addition, the OH-CCO’s L-DAC noted that adjuvant chemotherapy is not used or accepted by a large portion of lung cancer patients and more than 30% of patients do not receive adjuvant chemotherapy. The clinician groups reported that while targeted therapies are routinely used in more advanced EGFR-mutated NSCLC, there are currently no targeted therapies available in the adjuvant setting.
The OH-CCO’s L-DAC reported that patients with EGFR-mutated NSCLC are often non-smokers and therefore would not be eligible for current screening programs for lung cancer; thus, these patients have a greater unmet need for an effective treatment. According to LCC, patients with stage II and stage IIIA NSCLC have the greatest unmet need, as their baseline DFS and OS rates are poorer than for patients with stage IB disease. Higher-risk individuals within the stage IB population (i.e., those with larger tumour sizes, perineural or lymphovascular invasion, or disease spread through air spaces) may also have an unmet need, even with adjuvant chemotherapy, and LCC believes that this subset of stage IB patients could benefit more from osimertinib compared with patients with stage IB disease without high-risk characteristics.
Place in Therapy
For patients with stage IB to stage II NSCLC, the standard treatment is complete surgical resection. A minority of patients with stage IB disease also have pathological findings indicating a high risk of relapse (e.g., larger tumours, lymphovascular or perineural invasion, or disease spread through air spaces) are offered adjuvant platinum-doublet chemotherapy. For patients with stage IIIA disease, if surgery is considered reasonable, neoadjuvant chemotherapy concurrent with radiation followed by complete surgical resection is typically offered. The OH-CCO’s L-DAC reported that adjuvant chemotherapy is routinely offered to patients with resected stage IIA to stage IIIB NSCLC, per the AJCC 8th edition. The clinician group added that patient uptake of adjuvant chemotherapy in stage IIA is lower than in stage IIB and stage III disease, and that patients with EGFR-mutated resected NSCLC are also offered adjuvant chemotherapy. The OH-CCO’s L-DAC commented that osimertinib would represent an additional treatment option for patients after adjuvant chemotherapy and those who do not receive adjuvant chemotherapy.
LCC thought that osimertinib should be added to the standard post-operative management of patients with resected stage IB to stage IIIA NSCLC disease carrying an eligible EGFR mutation. Both clinician groups thought that osimertinib should not be considered a replacement for adjuvant chemotherapy and that osimertinib would be used post adjuvant chemotherapy. LCC thought that adjuvant chemotherapy should be administered independent of the consideration of osimertinib, where appropriate.
LCC commented that 3 years of administration of an oral drug could change the current treatment paradigm because the only adjuvant treatment currently available is adjuvant chemotherapy, which is completed over approximately 3 months (4 treatment cycles). LCC indicated the impact on health care utilization might be modest because osimertinib is a home-based oral, low-toxicity drug.
With respect to sequencing, the OH-CCO’s L-DAC noted that osimertinib is currently used as first-line therapy for advanced or metastatic NSCLC. The clinician group noted that if patients received adjuvant osimertinib and relapse on treatment, they would not receive osimertinib for advanced or metastatic disease. For patients who complete 3 years of adjuvant osimertinib and relapse after a 6-month off-treatment interval, the clinician group thought these patients would be considered for re-treatment with osimertinib. Additionally, the clinician group noted that for patients who exhibit oligoprogression or, in some cases, “flare” (such as bone metastases after therapy) while on osimertinib, osimertinib would be expected to be continued.
Patient Population
The OH-CCO’s L-DAC noted that patients with resected stage IIA to stage IIIB NSCLC with exon 19 deletions or exon 21 (L858R) substitution EGFR mutations would be candidates for adjuvant osimertinib. LCC indicated that patients with a higher disease stage are more likely to benefit from adjuvant osimertinib, although patients with stage IB disease may also benefit.
Both clinician groups agreed that patients who do not carry EGFR mutations or who do not have surgically resected NSCLC would be least suitable for treatment with osimertinib. The OH-CCO’s L-DAC added that osimertinib is not indicated in patients with other types of EGFR mutations (i.e., who do not have exon 19 deletions or L858R-point mutation) or those with wild-type EGFR tumours.
Assessing Response to Treatment
The OH-CCO’s L-DAC indicated that a clinically meaningful response to adjuvant osimertinib therapy would be the absence of disease recurrence. Similarly, LCC indicated that DFS and OS are used to determine whether a patient is benefiting from adjuvant osimertinib in clinical practice.
Since adjuvant osimertinib therapy would be administered for 3 years, LCC thought that periodic follow-up for toxicity and disease recurrence is required. LCC commented that patients may have more frequent follow-up appointments (monthly to every 2 months) near the initiation of treatment, then less frequent follow-ups for up to every 6 months for the remainder of the treatment period. LCC noted that imaging scans at 3-month to 4-month intervals would be common near the beginning of the treatment period, followed by scans every 6 months or less frequently toward the end of adjuvant therapy. Similarly, the OH-CCO’s L-DAC thought that response to treatment should be assessed every 3 months near the initiation of therapy, and CT scans should be conducted at least every 6 months during the 3 years of osimertinib therapy to monitor for disease recurrence. LCC noted that patients with resected stage IB to stage IIIA NSCLC are generally followed up for at least 5 years postoperatively in current Canadian practice. LCC reported that with current treatments, recurrences of stage IB to stage IIIA NSCLC occur for most patients within 2 years to 3 years and OS typically requires a greater number of years of follow-up.
Discontinuing Treatment
Both clinician groups agreed the primary reason for drug discontinuation would be disease recurrence, intolerable toxicity, or completion of 3 years of adjuvant therapy.
Prescribing Conditions
The OH-CCO’s L-DAC indicated that adjuvant osimertinib therapy would be administered in the outpatient setting under the supervision of an oncologist. LCC indicated that adjuvant osimertinib is suitable in all oncology settings and is appropriate for treatment in the community setting, including in medical oncology outpatient clinics and the inpatient setting.
Additional Considerations
The OH-CCO’s L-DAC indicated that EGFR mutation testing should be reflexively performed on all patients newly diagnosed with non-squamous NSCLC so those with early-stage NSCLC who have eligible EGFR mutations might be readily identified. The clinician groups noted that an EGFR genetic testing infrastructure for patients with advanced or metastatic NSCLC has been set up across Canada. As a result, these groups think there will be no major infrastructure gaps when testing is expanded in the adjuvant setting, and there may be minimal-to-modest increases in costs. LCC noted that patients with other sensitizing EGFR mutations that are rarer than exon 19 deletions or exon 21 (L858R) substitution mutations may also benefit from osimertinib.
The LCC clinician group estimates that the total number of patients who will qualify for adjuvant osimertinib will range from 300 patients to 400 patients per year in the first few years, if osimertinib is reimbursed. The OH-CCO’s L-DAC reported that osimertinib is a generally well-tolerated therapy. LCC indicated that delaying or reducing disease recurrence has benefits to HRQoL, utilization of health care resources, economic loss of productivity, and overall costs to society.
The clinician groups indicated that re-treatment with osimertinib in the metastatic setting after completing adjuvant osimertinib therapy is a consideration, but data are not yet available to inform re-treatment. LCC suggested that with the lack of available data on re-treatment with osimertinib, it may be reasonable to consider allowing clinicians to re-treat with osimertinib at their discretion if they believe it will provide clinical benefit.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
The drug programs noted that osimertinib has the potential for drug–drug interactions, which could potentially increase pharmacy resource use. The drug programs also indicated that osimertinib adjuvant therapy may change the place in therapy of comparator drugs and drugs reimbursed in subsequent lines. The drug plans reported that EGFR genetic testing is not reflexively completed for early-stage NSCLC across most Canadian jurisdictions; thus, expansion of testing would be required to identify eligible patients. Lastly, the drug programs expressed concern that the budget impact may be substantial because the duration of therapy per patient is 3 years.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
In ADAURA, osimertinib demonstrated a DFS benefit in patients with or without post-operative adjuvant chemotherapy. When would adjuvant chemotherapy benefit patients who might be considered for osimertinib? Can the clinical experts clarify the eligible patient population based on the AJCC 8th edition staging system? | The clinical panel indicated that osimertinib is not intended to replace adjuvant chemotherapy. Osimertinib would be used after standard chemotherapy, if chemotherapy was indicated, to further reduce the risk of disease recurrence. Adjuvant chemotherapy is offered to patients with good performance status and tumours of ≥ 4 cm or nodal involvement. Osimertinib can also be considered for patients who are unfit for adjuvant chemotherapy. The reimbursement request is for stage IB to stage IIIA NSCLC using the AJCC 7th edition. The equivalent stages using the AJCC 8th edition are stage IIA to stage IIIB. |
The submitted economic model incorporated possible re-treatment with osimertinib in the metastatic setting if disease relapse occurred 48 months after the start of adjuvant osimertinib (e.g., 12 months elapsed since completion of adjuvant osimertinib). Should patients who receive osimertinib in the adjuvant setting and experience disease relapse off treatment be eligible for re-treatment with osimertinib in the metastatic setting? What time frame after the completion of adjuvant therapy is appropriate to be eligible for re-treatment? | The clinical experts indicated they would restart osimertinib if patients experienced disease relapse off treatment after completing 36 months of adjuvant osimertinib. The clinical experts indicated they would rechallenge with osimertinib earlier than 12 months off treatment if a patient relapsed. The clinical experts suggested a 2-month to 3-month off-treatment interval based on clinical experience but noted that the first CT scan occurs at 6 months after treatment unless the patient experiences other symptoms indicating recurrence. |
AJCC = American Joint Committee on Cancer; DFS = disease-free survival; NSCLC = non–small cell lung cancer.
Clinical Evidence
The clinical evidence included in the review of osimertinib is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. No indirect evidence, long-term extension studies, or other relevant studies were identified.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of osimertinib (80 mg dose, oral) as adjuvant therapy after tumour resection in patients with stage IB to stage IIIA NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Patients with stage IB to stage IIIAa NSCLC who have undergone tumour resection and whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations. Subgroups:
|
Intervention | Osimertinib (80 mg, oral, once daily) |
Comparators |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; CNS = central nervous system; DFS = disease-free survival; EGFR = epidermal growth factor receptor; HRQoL = health-related quality of life; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NSCLC = non–small cell lung cancer; OS = overall survival; QTc = corrected QT interval; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus; WDAE = withdrawal due to adverse event.
aDisease stages according to the American Joint Committee on Cancer 7th edition staging system. The equivalent stages using the 8th edition are stage IIA to stage IIIB.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.19
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) through Ovid and Embase (1974‒) through Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Tagrisso (osimertinib) and NSCLC. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, the WHO International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
Search filters were applied to limit retrieval to RCTs or controlled clinical trials. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on April 19, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Expert Review Committee (pERC) on August 11, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.20 Included in this search were the websites of regulatory agencies (the FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for network meta-analyses dealing with NSCLC was run in MEDLINE All (1946–) on April 16, 2021. No search limits were applied.
Findings From the Literature
A total of 5 reports presenting data from 1 unique study were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6.
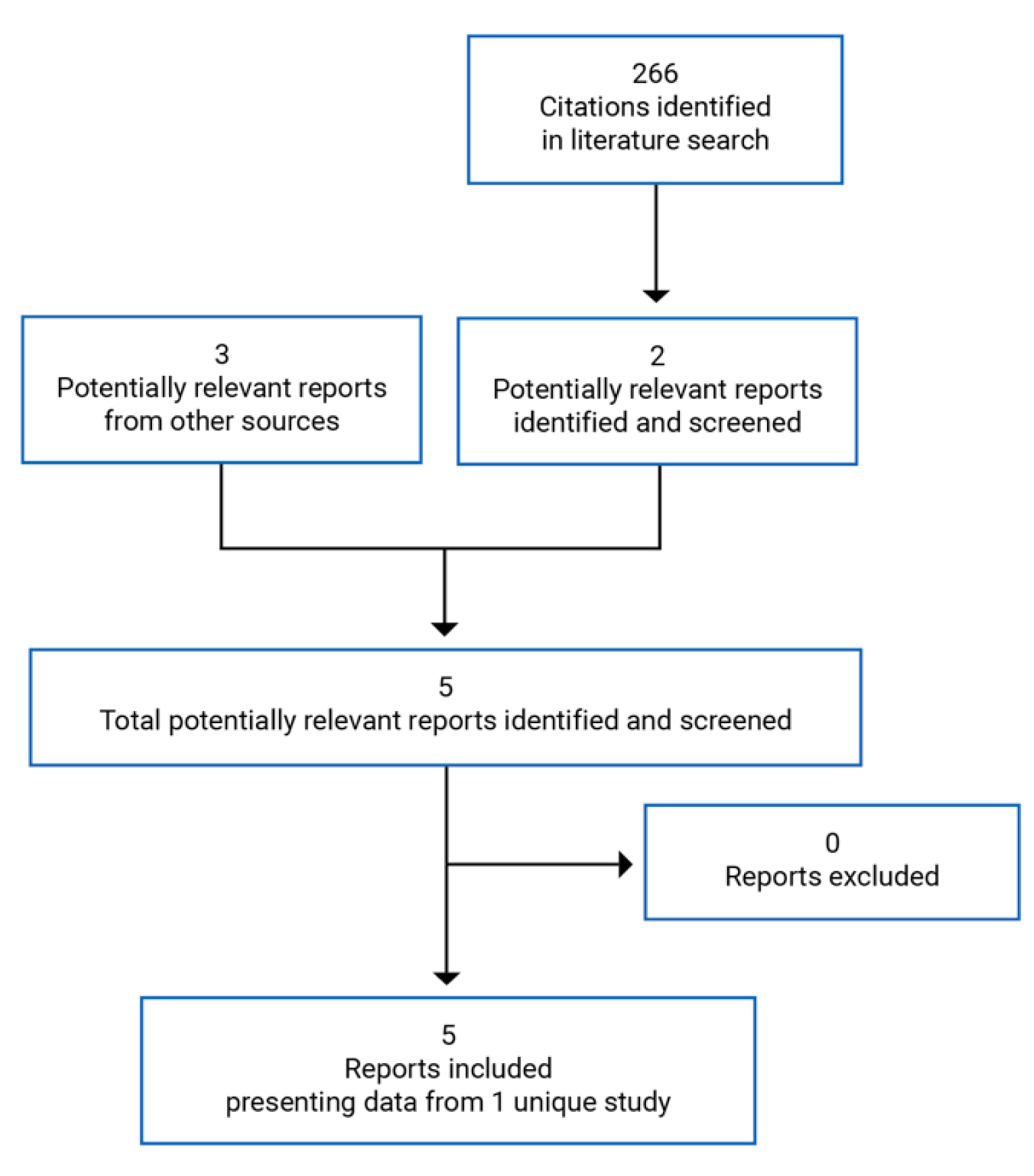
Table 6: Details of Included Studies
Detail | ADAURA |
|---|---|
Designs and populations | |
Study design | Phase III DB RCT |
Locations | 185 sites in 24 countries in Europe, Asia-Pacific, North America, and South America |
Patient randomization dates | November 2015 to February 2019 |
Randomized (N) | 682:
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | 80 mg osimertinib orally once daily |
Comparator(s) | Placebo orally once daily |
Duration | |
Phase | |
Run-in | 28 days |
Double-blind treatment | 3 years |
Follow-up | 5 years (planned) |
Outcomes | |
Primary end point | DFS by investigator assessment |
Secondary, safety, and exploratory end points | Secondary:
Safety:
Exploratory:
|
Notes | |
Publications | Wu et al. (2018)21 — trial protocol Wu et al. (2020)22 — interim analysis results |
AE = adverse event; AJCC = American Joint Committee on Cancer; cMET = hepatocyte growth factor receptor; ctDNA = circulating tumour DNA; DB = double blind; DFS = disease-free survival; ECG = electrocardiogram; EGFR = epidermal growth factor receptor; Ex19del = exon 19 deletions; HER2 = human epidermal growth factor receptor 2; HRQoL = health-related quality of life; ILD = interstitial lung disease; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; LVEF = left ventricular ejection fraction; MRD = minimal residual disease; NSCLC = non–small cell lung cancer; OS = overall survival; PFS = progression-free survival; PK = pharmacokinetic(s); QTc = corrected QT interval; RCT = randomized controlled trial; RNA = ribonucleic acid; SF-36 = Short Form (36) Health Survey; T790M = amino acid substitution from a threonine to a methionine at position 790 in EGFR; TNM = tumour, nodes, and metastases; ULN = upper limit of normal.
Note: 3 additional reports were included — Clinical Study Report,13 Health Canada reviewer’s report,23 and sponsor’s submission to CADTH.14
aTreatment could not commence within 4 weeks following surgery. No more than 10 weeks were to have elapsed between surgery and randomization for patients who did not receive adjuvant chemotherapy, and no more than 26 weeks were to have elapsed between surgery and randomization for patients who received adjuvant chemotherapy. Additionally, complete postoperative wound healing had to have occurred following any surgery and, for patients who received post-operative adjuvant platinum-based chemotherapy, a minimum of 2 weeks had to have elapsed (but no more than 10 weeks) from the last administered dose of chemotherapy to the date of randomization. Finally, at the time of starting study treatment, patients had to have recovered from all toxicities of prior therapy greater than grade 1 under the Common Terminology Criteria for Adverse Events (with the exception of alopecia) and grade 2 neuropathy related to prior platinum therapy.
bHistory of other malignancies, except adequately treated non-melanoma skin cancer, curatively treated in situ cancer, or other solid tumours curatively treated with no evidence of disease for > 5 years following the end of treatment and which, in the opinion of the treating physician, did not have a substantial risk of the prior malignancy recurring.
cIncluding heart failure, hypokalemia, congenital long QT syndrome, family history of long QT syndrome, or unexplained sudden death under 40 years of age in first-degree relatives, or any concomitant medication known to prolong the QT interval.
dInadequate bone marrow reserve or organ function as demonstrated by any of the following laboratory values: absolute neutrophil count < 1.5 × 109/L, platelet count < 100 × 109/L, hemoglobin < 90 g/L, alanine aminotransferase > 2.5 × ULN, aspartate aminotransferase > 2.5 × ULN, total bilirubin > 1.5 × ULN or > 3 × ULN in the presence of documented Gilbert syndrome (unconjugated hyperbilirubinemia), creatinine > 1.5 × ULN concurrent with creatinine clearance < 50 mL/min (measured or calculated by Cockcroft-Gault equation). Confirmation of creatinine clearance is required only when creatinine is > 1.5 × ULN.
Source: Clinical Study Report,13 Wu et al. (2018),21 Wu et al. (2020).22
Description of Studies
The ADAURA trial is an ongoing, international, multi-centre, phase III, double-blind, randomized, placebo-controlled trial.13 The objective of the trial is to assess the efficacy and safety of osimertinib versus placebo in patients with stage IB to stage IIIA NSCLC with a centrally confirmed, common-sensitizing EGFR mutation (exon 19 deletions and/or exon 21 [L858R] substitution mutations, either alone or in combination with other EGFR mutations) who have undergone complete tumour resection, with or without post-operative adjuvant chemotherapy. Patients were staged according to the 7th edition of the AJCC cancer staging manual. A total of 682 patients were randomized in a 1:1 ratio to osimertinib (80 mg oral, once daily) or matching placebo: 339 patients to the osimertinib arm and 343 to the placebo arm. Randomization was stratified by disease stage (stage IB versus II versus IIIA), mutation type (exon 19 deletions or L858R), and race (Asian or non-Asian). Patients were randomized from 185 sites in 24 countries in Europe, Asia-Pacific, North America, and South America. One site in Canada enrolled patients into the ADAURA trial. The study design of the ADAURA trial is summarized in Figure 2.
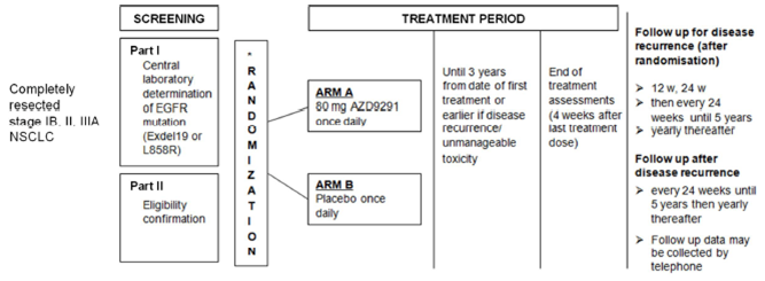
AZD9291 = osimertinib; EGFR = epidermal growth factor receptor; Exdel19 = exon 19 deletions; L858R = exon 21 L858R substitution mutation; NSCLC = non–small cell lung cancer; w = week.
Source: Clinical Study Report.13
To be eligible for the ADAURA trial, patients must have sufficiently recovered from surgery and completed any standard-of-care adjuvant chemotherapy (if applicable) before randomization. Patients must have been randomized within 10 weeks of complete surgical resection if adjuvant chemotherapy was not administered, or within 26 weeks if adjuvant chemotherapy (platinum-based doublet chemotherapy, maximum of 4 cycles) was administered. Patients were required to have a baseline CT scan (chest and abdomen, including liver and adrenal glands) following surgical resection and within 28 days before treatment initiation to confirm that disease was not present.
The ADAURA trial employed a 2-part screening period. In part 1, patients provided informed consent in writing for their tumour sample to be sent to the central laboratory for EGFR genetic testing. The EGFR mutation status of patients was prospectively tested by the central cobas EGFR mutation test (Roche Molecular Systems). A separate informed consent form was then required before any other study procedures were done. After patients signed this second informed consent form, eligibility for the trial was confirmed in part 2 of the screening. Patients received study treatment for 3 years or until they experienced disease recurrence or unmanageable toxicity.
The primary end point of the ADAURA trial is DFS by investigator assessment. Radiological assessments for disease recurrence were done at 12 weeks, 24 weeks, every 24 weeks until 5 years, and then annually. In the event of disease recurrence, imaging procedures were undertaken to capture all sites of NSCLC relapse. Treatments received by the patient after relapse were determined by the treating physician, and post-recurrence cancer treatments and procedures were recorded.
The ADAURA trial is ongoing. An interim analysis with a data cut-off date of January 17, 2020, was conducted. As of the interim analysis, a total of 3 protocol amendments had been implemented during the ADAURA trial. The first amendment (December 18, 2018) consisted of updates to provide clarity on study procedures and additional information. The second amendment (April 28, 2020) included an OS extension period and a new multiple-testing procedure to account for 2 unplanned interim analyses of DFS. This amendment also added an analysis of time to new brain lesions or death. The third amendment (June 23, 2020) was to update the multiple-testing procedure again for the testing of OS.
Populations
Inclusion and Exclusion Criteria
The ADAURA trial enrolled adult patients aged 18 years and older (20 years and older in Japan and Taiwan) with a diagnosis of NSCLC of predominately non-squamous histology and a WHO performance status of 0 or 1.13 Patients must have had complete surgical resection of the primary NSCLC and their cancer must have been postoperatively classified as stage IB, II, or IIIA (AJCC 7th edition). Confirmation by the central laboratory that the tumour harboured 1 of the 2 common EGFR mutations associated with EGFR TKI sensitivity (exon 19 deletions or L858R), either alone or in combination with other EGFR mutations, was required. Patients must have sufficiently recovered from surgery and completed adjuvant chemotherapy (if applicable) before randomization. Standard post-operative adjuvant chemotherapy consisting of a platinum-based doublet for 4 or fewer cycles was allowed. No more than 26 weeks or 10 weeks could elapse between surgery and randomization for patients who had or had not received adjuvant chemotherapy, respectively. Patients were excluded from the ADAURA trial if they had previous treatment with pre- or post-operative radiation therapy, preoperative chemotherapy, EGFR TKIs, and/or potent cytochrome P450 3A4 (CYP3A4) inducers.
Baseline Characteristics
The baseline characteristics of patients were balanced between treatment arms. In the overall population, the mean age of the patients was 62.1 years.13 The majority of patients had stage II to stage IIIA disease (68.3%), a WHO performance status of 0 (63.6%), adenocarcinoma histology type (96.5%), undergone a lobectomy (95.3%), and were Asian (63.6%) and female (70.1%). Most patients had received post-operative adjuvant chemotherapy (60.0%). Overall, 54.7% of patients had exon 19 deletions and 45.2% had exon 21 (L858R) substitution mutations.
Table 7: Summary of Baseline Characteristics in the ADAURA Trial — FAS
Characteristic | ADAURA | ||
|---|---|---|---|
Osimertinib (N = 339) | Placebo (N = 343) | Total (N = 682) | |
Age, years | |||
Mean (SD) | 62.5 (10.27) | 61.6 (10.46) | 62.1 (10.37) |
Median (minimum, maximum) | 64.0 (30, 86) | 62.0 (31, 82) | 63.0 (30, 86) |
Sex, n (%) | |||
Male | 109 (32.2) | 95 (27.7) | 204 (29.9) |
Female | 230 (67.8) | 248 (72.3) | 478 (70.1) |
Race, n (%) | |||
White | 122 (36.0) | 122 (35.6) | 244 (35.8) |
Asian | 216 (63.7) | 218 (63.6) | 434 (63.6) |
Other | 1 (0.3) | 2 (0.6) | 3 (0.4) |
Missing | 0 | 1 (0.3) | 1 (0.1) |
Ethnic group, n (%) | |||
Hispanic or Latino | 12 (3.5) | 9 (2.6) | 21 (3.1) |
Asian (other than Chinese or Japanese) | 78 (23.0) | 67 (19.5) | 145 (21.3) |
Chinese | 95 (28.0) | 100 (29.2) | 195 (28.6) |
Japanese | 46 (13.6) | 51 (14.9) | 97 (14.2) |
Other | 108 (31.9) | 116 (33.8) | 224 (32.8) |
BMI, kg/m2 | |||
Mean (SD) | 24.8 (4.29) | 24.9 (4.36) | 24.9 (4.32) |
Median (minimum, maximum) | 24.4 (15.1, 41.8) | 24.1 (16.6, 42.0) | 24.2 (15.1, 42.0) |
WHO performance status, n (%) | |||
0 | 216 (63.7) | 218 (63.6) | 434 (63.6) |
1 | 123 (36.3) | 125 (36.4) | 248 (36.4) |
AJCC stage at diagnosis, n (%)a | |||
IB | 107 (31.6) | 109 (31.8) | 216 (31.7) |
IIA | 86 (25.4) | 90 (26.2) | 176 (25.8) |
IIB | 29 (8.6) | 26 (7.6) | 55 (8.1) |
IIIA | 117 (34.5) | 118 (34.4) | 235 (34.5) |
EGFR mutations, n (%)b | |||
Exon 19 deletions | 185 (54.6) | 188 (54.8) | 373 (54.7) |
L858R | 153 (45.1)c | 155 (45.2) | 308 (45.2) |
Histology type, n (%) | |||
Adenocarcinoma | 326 (96.2) | 332 (96.8) | 658 (96.5) |
Acinar | 85 (25.1) | 82 (23.9) | 167 (24.5) |
Papillary, malignant | 43 (12.7) | 44 (12.8) | 87 (12.8) |
Malignant | 183 (54.0) | 188 (54.8) | 371 (54.4) |
Bronchiolo-alveolar | 11 (3.2) | 13 (3.8) | 24 (3.5) |
Solid with mucus formation | 4 (1.2) | 5 (1.5) | 9 (1.3) |
Non-adenocarcinoma | |||
Bronchial gland carcinoma (not otherwise specified) | 1 (0.3) | 2 (0.6) | 3 (0.4) |
Carcinoma, adenosquamous, malignant | 4 (1.2) | 5 (1.5) | 9 (1.3) |
Other | 8 (2.4) | 4 (1.2) | 12 (1.8) |
Lung cancer resection type, n (%) | |||
Lobectomy | 328 (96.8) | 322 (93.9) | 650 (95.3) |
Sleeve resection | 1 (0.3) | 3 (0.9) | 4 (0.6) |
Bilobectomy | 7 (2.1) | 8 (2.3) | 15 (2.2) |
Pneumonectomy | 3 (0.9) | 10 (2.9) | 13 (1.9) |
Post-operative adjuvant chemotherapy, n (%) | |||
Yes | 202 (59.6) | 207 (60.3) | 409 (60.0) |
No | 137 (40.4) | 136 (39.7) | 273 (40.0) |
AJCC = American Joint Committee on Cancer; BMI = body mass index; EGFR = epidermal growth factor receptor; Exdel19 = exon 19 deletions; FAS = full analysis set; IVRS = interactive voice response system; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; SD = standard deviation.
aData are derived from the electronic case report form and differ from the number of patients recorded with each disease stage in the IVRS.
bEGFR mutations identified by central cobas test. Patients can have more than 1 EGFR mutation. There were 10 patients who were mis-stratified in the IVRS. The data presented show numbers confirmed by prospective central testing.
cOne patient was negative for both mutations and was discontinued from the study before receiving osimertinib.
Source: Clinical Study Report.13
Interventions
Patients were randomized using an interactive voice response system to receive either osimertinib 80 mg orally once daily or matching placebo.13 Doses were to be taken approximately 24 hours apart and at the same time each day. Treatment continued until disease recurrence, a treatment discontinuation criterion was met (e.g., patient decision, unacceptable toxicity, AE, pregnancy), or until a maximum treatment duration of 3 years was reached.
Other anti-cancer therapies, investigational drugs, and radiotherapy were not permitted while the patient was receiving the study treatment. Pre-medication (including treatments for the management of diarrhea, nausea, and vomiting) was allowed after the first dose of the study drug. Other medication considered necessary for the safety and well-being of a patient could be given at the discretion of the investigator.
Outcomes
A list of the efficacy end points identified in the CADTH review protocol that were assessed in the ADAURA trial and included in this review is provided in Table 8.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | ADAURA trial end point | Definition | Included in the hierarchical multiple-testing procedure |
|---|---|---|---|
OS | Secondary | Time from the date of randomization until date of death due to any cause. | Yes |
DFS | Primary | Time from the date of randomization until the date of disease recurrence or death by any cause in the absence of recurrence. | Yes |
Disease recurrence rate | Exploratory | Proportion of patients who experienced disease recurrence from the date of randomization until the end of follow-up. | No |
Time to disease recurrence | Not reported | NA | NA |
Time to intracranial CNS metastases | Not reported | NA | NA |
PFS | Exploratory | Time from the date of randomization to the date of disease progression by investigator assessment per RECIST v1.1 criteria or death. | No |
Time to next treatment | Exploratory | Time from the date of randomization to the earlier of the date of first subsequent anti-cancer therapy or procedure start date following study drug discontinuation, or death. | No |
HRQoL by the SF-36 v2 (TTD in MCS and PCS) | Secondary in the stage II to stage IIIA population Exploratory in the overall population (i.e., stage IB to stage IIIA) | A 36-item, generic, self-reported questionnaire with a recall period of 28 days. It consists of 8 subscales and 2 component summary scores for physical and mental health (PCS and MCS). Subscale and summary scores range from 0 to 100, where a higher score indicates better HRQoL. | No |
CNS = central nervous system; DFS = disease-free survival; HRQoL = health-related quality of life; MCS = Mental Component Summary; NA = not applicable; OS = overall survival; PCS = Physical Component Summary; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors; SF-36 v2 = Short Form (36) Health Survey version 2; TTD = time to deterioration.
Source: Clinical Study Report.13
A detailed discussion and critical appraisal of DFS as a surrogate outcome measure for OS is provided in Appendix 3.
In the ADAURA trial, HRQoL was measured using the SF-36 v2 questionnaire. Specifically, the trial reported the TTD in the MCS and PCS of the SF-36 v2. The SF-36 v2 is an instrument for measuring a person’s general health status over the past 28 days. The SF-36 v2 includes 8 domains: Physical Functioning, Role-Physical, Vitality, General Health, Bodily Pain, Social Function, Role-Emotional, and Mental Health. SF-36 v2 results can be grouped into 2 summary scores, the PCS and the MCS. Final scores for each scale range from 0 to 100, with higher scores indicating better health. The minimal important differences (MIDs) for this instrument have not been established in patients with NSCLC. The MIDs from the general population are 2 points for the PCS and 3 points for the MCS. A detailed discussion and critical appraisal of the SF-36 v2 is provided in Appendix 3.
Statistical Analysis
Sample Size and Power Calculation
It was planned that approximately 700 patients would be randomized in a 1:1 ratio (osimertinib to placebo) to the ADAURA study.13 It was estimated that 3,200 patients would be screened to randomize 700 patients. The primary end point of the study is DFS based on investigator assessment and was assessed first in patients with stage II to stage IIIA disease (primary analysis population) and then the overall population (i.e., patients with stage IB to stage IIIA).
The ADAURA trial is event-driven. The primary analysis of DFS was planned to occur when approximately 247 disease recurrence events had been observed in approximately 490 patients in the stage IIA to stage IIIA patient population. If the true DFS HR for the comparison of osimertinib versus placebo in this patient population is 0.70, 247 disease recurrence events would provide 80% power to demonstrate a statistically significant difference in DFS at a 5% 2-sided significance level (translating to an improvement in median DFS from 40 months to 57 months, assuming DFS is exponentially distributed). Based on these assumptions, the minimum DFS HR that would be considered statistically significant (2-sided P < 0.05) is 0.78.
If the true DFS HR for the comparison of osimertinib versus placebo in the overall population (i.e., patients with stage IB to stage IIIA disease) is 0.70, then 317 disease recurrence events would provide approximately 90% power to demonstrate a statistically significant difference in DFS at a 4% 2-sided significance level (translating to an improvement in median DFS from 46 months to 66 months, assuming DFS is exponentially distributed). Based on these assumptions, the minimum DFS HR that would be considered statistically significant (2-sided P < 0.04) is 0.79.
At the time of the planned primary analysis of DFS, it was anticipated that approximately 195 OS events (28% maturity) would have occurred (assuming a median OS of 96 months for the placebo arm). If the true OS HR for the comparison of osimertinib versus placebo is 0.66, then 195 death events would provide approximately 80% power to demonstrate a statistically significant difference in OS between the treatment arms. Assuming 195 death events and a true OS HR of 0.85, there would be an approximately 90% chance of observing an HR of less than 1.02.
Assuming 28 months of nonlinear recruitment, the data cut-off for the primary analysis was estimated to occur approximately 68 months to 70 months after the first patient was randomized.12
Analyses, Multiple-Testing Procedure, and Alpha Spending
The primary end point of DFS and the secondary end point of OS were tested in the stage II to stage IIIA population (primary analysis population) and in the overall population (i.e., patients with stage IB to stage IIIA disease).13 To control the type I error at the 5% 2-sided level, a hierarchical multiple-testing procedure was employed across these end points (Figure 3). This procedure was added as an amendment to the study protocol and statistical analysis plan to account for the unplanned interim analysis. The multiple-testing procedure was ordered such that DFS in patients with stage II to stage IIIA disease was tested first using the full alpha. If statistical significance was shown for DFS in the stage II to stage IIIA population, DFS in the overall population would be tested. If the DFS results in both the stage II to stage IIIA population and the overall population were statistically significant, OS would then be assessed first in the stage II to stage IIIA population, and then in the overall population if statistical significance was reached in the stage II to stage IIIA population.
Figure 3: Multiple-Testing Procedure in the ADAURA Trial
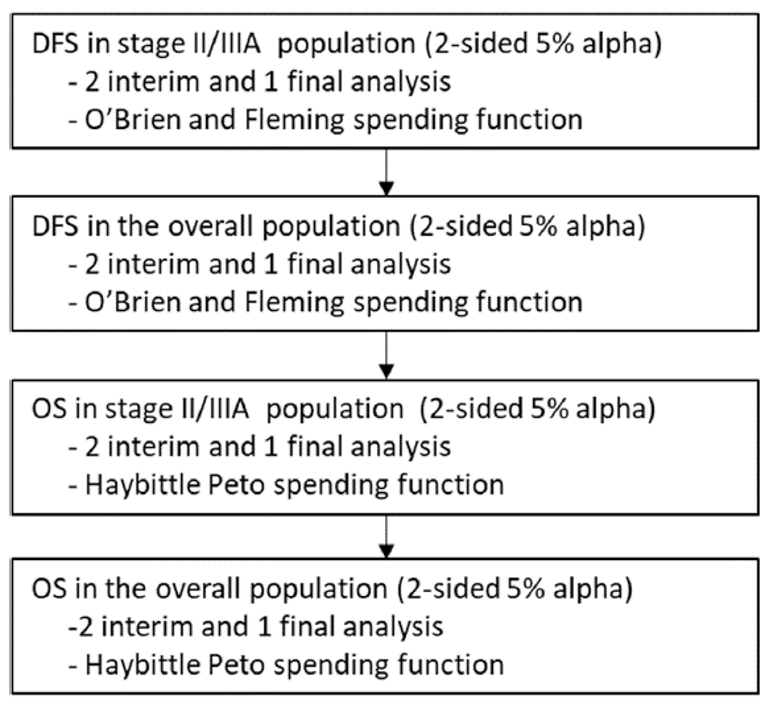
DFS = disease-free survival; OS = overall survival.
Source: ADAURA study protocol.12
In the original ADAURA trial protocol, a single, primary analysis of DFS was planned; a further analysis was to be performed only if there were fewer than 70 DFS events in the stage IB population. For the overall population analysis, it was estimated there would be approximately 317 DFS events in approximately 700 patients, with approximately 70 events in the stage IB subgroup. If, however, there were meaningfully fewer than 70 DFS events (defined as 63 DFS events or fewer) in the stage IB subgroup at the time of the primary analysis, additional follow-up of patients could be performed and a further analysis of DFS could be conducted when at least 70 DFS events were observed in the stage IB subgroup.
Regular independent data monitoring committee (IDMC) meetings took place during the study to monitor safety data, and a scheduled event-based futility analysis took place to support the sixth IDMC meeting in February 2019. After ruling out futility, the IDMC made an ad hoc request to evaluate key efficacy data (Kaplan-Meier curves for DFS and key recurrence data tables) at their seventh meeting, which was held on April 7, 2020, with a data cut-off date of January 17, 2020. Following the seventh IDMC meeting, the IDMC recommended that a full analysis of efficacy and safety be performed by the sponsor as soon as possible for public disclosure. The sponsor conducted the interim analysis, and the sponsor was unblinded at the time of this analysis. Patients and investigators remain blinded to individual treatment allocations, and the study is ongoing.
The unplanned interim analysis of DFS was conducted at the time of observing 156 DFS events in the stage II to stage IIIA population. The corresponding information fraction was 0.63, where the final number of events would have been 247. The interim analysis needed to be taken into account to control the type I error rate at 5% (2-sided) and the multiple-testing procedure was revised to the procedure depicted in Figure 3. The Lan-DeMets approach that approximates the O’Brien and Fleming spending function was used to maintain an overall 2-sided 5% type I error.
The ADAURA trial is ongoing. The sponsor plans to conduct the final analysis of OS when approximately 94 deaths have been observed in the stage II to stage IIIA population (approximately 20% maturity).
Analysis of Outcomes
All efficacy analyses were performed using the full analysis set (FAS), which included all randomized patients. The FAS included 2 populations: the overall population (i.e., patients with stage IB to stage IIIA disease) and the stage II to stage IIIA population. The primary analysis population is the stage II to stage IIIA population. Results of all statistical analyses were presented using a 95% CI and 2-sided P value.
The statistical analyses performed of the efficacy end points that were identified in the CADTH systematic review protocol are summarized in Table 9.
Primary Outcome
DFS was calculated as the time from the date of randomization until the date of disease recurrence or death by any cause in the absence of recurrence. Patients who were disease-free and alive at the time of the analysis were censored at the date of their last follow-up assessment. The DFS time was based on the scan (assessment) dates and not visit dates. The DFS rate at 2, 3, 4, and 5 years was defined as the proportion of patients alive and disease-free at 2, 3, 4, and 5 years, respectively, estimated from Kaplan-Meier plots of the primary end point of DFS at the time of the primary analysis.
DFS in the subset of patients with stage II to stage IIIA disease was analyzed using a log-rank test stratified by stage (II, IIIA), mutation type (exon 19 deletions, L858R), and race (Asian, non-Asian) for the generation of the P value and using the Breslow approach for handling ties. DFS in the overall population was analyzed using a log-rank test stratified by stage (IB, II, IIIA), mutation status (exon 19 deletions or L858R as confirmed by a central test) and race (Asian, non-Asian) for the generation of the P value and using the Breslow approach for handling ties. The HRs and CIs were obtained directly from the U- and V-statistics provided by the log-rank test and the LIFETEST procedure. Proportionality was assessed for the HR.
A Kaplan-Meier plot of DFS was presented by treatment arm.
Subgroup analyses were conducted by comparing DFS between treatment arms in the following groups of patients: stage (IB, II, IIIA), EGFR mutation status (positive or negative for exon 19 deletions or L858R), EGFR mutation type (exon 19 deletions, L858R) mutation detectable in plasma-derived circulating tumour DNA (ctDNA), pre-treatment T790M mutation status (positive, negative), race (Asian, non-Asian), adjuvant chemotherapy (yes, no), gender (male, female), age at randomization (< 65, ≥ 65), and smoking history (never, ever). No adjustment was made to the significance level for statistical testing since the subgroup analyses may only be supportive of the primary analysis of DFS. For each subgroup level, the HR and 95% CI were calculated from a single Cox proportional-hazards model that contained a term for treatment, the subgroup covariate of interest, and the treatment-by-subgroup interaction term. The HR was obtained from this model for each level of the subgroup.
DFS rates were derived using the same model used for the primary analysis of DFS. Kaplan-Meier plots were produced. Estimates of the DFS rate at 6 months, 12 months, 18 months, 24 months, 36 months, 48 months, and 60 months were obtained from the Kaplan-Meier plot and presented for each treatment arm.
Sensitivity analyses to assess for quantitative interactions, evaluation-time bias, and attrition bias were planned.14 The presence of quantitative interactions was assessed by means of an overall global interaction test. To assess possible evaluation-time bias that could occur if scans are not performed at the protocol-scheduled time points, the midpoint between the time of recurrence and the previous evaluable assessment was analyzed using a log-rank test stratified by stage, mutation status, and race. Possible attrition bias was assessed by repeating the primary DFS analysis such that the actual DFS times were included in the analysis, rather than the censored times of patients who had experienced recurrence or died in the absence of recurrence immediately following 2 or more non-evaluable assessments. In addition, patients who took subsequent therapy before recurrence or death were censored at their last evaluable assessment before taking the subsequent therapy.
DFS with disease recurrence in the CNS only was analyzed as a post hoc exploratory analysis.
The disease recurrence rates in the stage II to stage IIIA population and overall population were reported within the reporting of DFS events.
Secondary Outcomes
Overall Survival
OS was calculated as the time from the date of randomization until date of death due to any cause. Any patient not known to have died at the time of analysis was censored based on the last recorded date on which the patient was known to be alive. OS data were analyzed using the same methodology and model as for the analysis of DFS with the exception that the sensitivity, subgroup, and exploratory analyses were not performed.
A Kaplan-Meier plot of OS was presented by treatment group. The OS rate at 2, 3, 4, and 5 years was defined as the proportion of patients alive at 2, 3, 4, and 5 years, respectively, estimated from the Kaplan-Meier plot of OS.
HRQoL Assessed Using the SF-36
Patient-reported HRQoL was assessed using the SF-36 v2 questionnaire. The compliance with the SF-36 was summarized by visit. Compliance rates were calculated as the number of evaluable forms (i.e., a questionnaire with a completion date and at least 1 domain that is non-missing) divided by the number of expected forms (i.e., a questionnaire from a patient who has not died, is not lost to follow-up, or has not withdrawn from the study at the scheduled assessment time) multiplied by 100.
The absolute values and change from baseline were calculated for each of the 8 domain scores and for the PCS and MCS summary scores at each post-baseline assessment. The responses to each of the health domain scores and the 2 summary scores were also categorized as improved, worsened, or stable at each post-baseline assessment and reported as counts and proportions.
The primary HRQoL outcome measures were TTD of the 2 summary scores (PCS and MCS) in the stage II to stage IIIA population (pre-specified secondary end points). The TTD analyses in the stage IIA to stage IIIA population were analyzed using a log-rank test stratified by stage (II, IIIA), mutation type (exon 19 deletions, L858R) and race (Asian, non-Asian) using the Breslow approach for handling ties. The HRQoL end points were not included in the multiple testing procedures and thus these analyses were not controlled for multiple-comparison testing.
The TTD in PCS and MCS were analyzed in the overall population as a post hoc exploratory analysis.
Exploratory Outcomes
Progression-Free Survival
PFS was calculated as the time from the date of randomization to the date of disease progression or death. Patients alive and for whom disease progression had not been observed were censored at the last time known to be alive and without disease progression. Progression status at the time of analysis by treatment arm was categorized into radiological, symptomatic, other progression, or death, with reasons for censoring also summarized accordingly. PFS data were analyzed for the overall population using the same methodology and model as for the analysis of DFS with the exception that the sensitivity, subgroup, and exploratory analyses were not performed.
Time to Next Treatment
Time to next treatment was defined as the time from the date of randomization to the earlier of the date of first subsequent anti-cancer therapy or procedure start date following study drug discontinuation, or death. The time to next treatment was calculated for the overall population using the same methodology and model as for the analysis of DFS with the exception that the sensitivity, subgroup, and exploratory analyses were not performed.
Table 9: Statistical Analysis of Efficacy End Points — ADAURA Trial
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
OS |
| None | None |
DFS |
| None |
|
Disease recurrence rate | Counts and proportions reported for disease recurrence events | None | None |
Time to disease recurrence | NR | NR | NR |
Time to intracranial CNS metastases | NR | NR | NR |
PFS | Log-rank test stratified by stage, mutation, and race | None | None |
Time to next treatment | Log-rank test stratified by stage, mutation, and race | None | None |
HRQoL by the SF-36 v2 (TTD in the MCS and PCS) | Log-rank test stratified by stage, mutation, and race using the Breslow approach for handling ties | None | None |
CNS = central nervous system; DFS = disease-free survival; HRQoL = health-related quality of life; KM = Kaplan-Meier; MCS = Mental Component Summary; NR = not reported; OS = overall survival; PCS = Physical Component Summary; PFS = progression-free survival; SF-36 v2 = Short Form (36) Health Survey version 2; TTD = time to deterioration.
Source: Clinical Study Report.13
Analysis Populations
The FAS included all randomized patients and was used for all efficacy analyses. The FAS included 2 populations: the overall population (i.e., patients with stage IB to stage IIIA disease) and stage II to stage IIIA population. The stage II to stage IIIA population is considered the primary analysis population in the ADAURA trial. Treatment groups were compared based on randomized study treatment, regardless of the treatment received.
The safety analysis set consisted of all patients who received at least 1 dose of the study treatment.
Results
The results from the ADAURA trial presented in this report are from the unplanned interim analysis with a data cut-off date of January 17, 2020.
Patient Disposition
A summary of the disposition of patients in the ADAURA trial as of the interim analysis is included in Table 10. A total of 2,447 patients were screened for EGFR mutations. A total of 1,250 patients (51.1%) were EGFR mutation–negative; for 110 patients (4.5%), the EGFR status was not evaluable. A total of 239 patients (9.8%) did not sign the main informed consent form for further screening of eligibility (screening part 2). The reasons why patients did not sign the informed consent form were not reported. A total of 791 patients were identified as having EGFR mutation–positive disease and entered screening part 2, of which 109 (13.8%) were not randomized: 106 (97.2%) due to not meeting the eligibility criteria, and 3 (2.8%) due to patient decision. A total of 682 were randomized to receive osimertinib (n = 339) or placebo (n = 343). A total of 680 patients (99.7%) were treated: 337 patients (99.4%) in the osimertinib arm, and all 343 patients (100%) in the placebo arm.
As of the data cut-off for the interim analysis, 91.2% of patients in the osimertinib arm and 89.5% of patients in the placebo arm were ongoing in the ADAURA trial. A total of 92 patients (27.3%) in the osimertinib arm and 174 patients (50.7%) in the placebo arm had discontinued study treatment. The most common reasons for treatment discontinuation in the osimertinib arm were AEs (n = 36; 10.7%), patient decision (n = 30; 8.9%), and disease recurrence (n = 24; 7.1%). The most common reason for treatment discontinuation in the placebo arm was disease recurrence (n = 148; 43.1%).
Table 10: Patient Disposition — ADAURA Trial
Detail | Osimertinib | Placebo |
|---|---|---|
Screened — part 1, Na | 2,447 | |
EGFR mutation–positive, n (%)b | 1,087 (44.4) | |
EGFR mutation–negative, n (%) | 1,250 (51.1) | |
EGFR status not evaluable, n (%) | 110 (4.5) | |
Did not sign main study ICF to enter screening part 2, n (%) | 239 (9.8) | |
Screened — part 2, Nc | 791 | |
Not randomized, n (%) | 109 (13.8) | |
Eligibility criteria not fulfilled, n (%) | 106 (97.2) | |
Patient decision, n (%) | 3 (2.8) | |
Randomized, N | 339 | 343 |
Treated, N (%) | 337 (99.4) | 343 (100.0) |
Discontinued study treatment at DCO,d N (%) | 92 (27.3) | 174 (50.7) |
Patient decision | 30 (8.9) | 9 (2.6) |
Adverse events | 36 (10.7) | 10 (2.9) |
Severe non-compliance to CSP | 0 | 3 (0.9) |
Disease recurrence | 24 (7.1) | 148 (43.1) |
Other | 2 (0.6) | 4 (1.2) |
Ongoing study at DCO,d N (%) | 309 (91.2) | 307 (89.5) |
Terminated study at DCO,d N (%) | 30 (8.8) | 36 (10.5) |
Death | 8 (2.4) | 20 (5.8) |
Withdrawal by patient | 19 (5.6) | 14 (4.1) |
Lost to follow-up | 1 (0.3) | 2 (0.6) |
Other | 1 (0.3) | 0 |
Missing | 1 (0.3) | 0 |
FAS, N | 339 | 343 |
Overall population, N | 339 | 343 |
Stage II to stage IIIA population, N | 233 | 237 |
Safety, N | 337 | 343 |
CSP = clinical study procedure; DCO = data cut-off; EGFR = epidermal growth factor receptor; FAS = full analysis set; ICF = informed consent form.
aIn screening part 1, pre-screening informed consent was received to send tumour sample to central laboratory for EGFR mutation testing.
bEGFR mutation–positive included any EGFR mutation detected by the cobas test and was not limited to exon 19 deletions and L858R mutations.
cMain informed consent received. Eligibility confirmed at screening part 2.
dDCO date of January 17, 2020.
Source: Clinical Study Report.13
Exposure to Study Treatments
Exposure to study treatments as of the interim analysis is summarized in Table 11. Patients in the osimertinib arm had a longer median total exposure time to the study drug (22.5 months versus 18.7 months). As of the data cut-off date, 40 patients (12%) in the osimertinib arm and 33 patients (10%) in the placebo arm had completed 3 years of treatment.22
Table 11: Exposure to Study Treatments in the ADAURA Trial — Safety Population
Treatment duration | Osimertinib (N = 337) | Placebo (N = 343) |
|---|---|---|
Total exposure time, monthsa | ||
Mean (SD) | 21.7 (10.61) | 18.6 (10.71) |
Median (minimum, maximum) | 22.5 (0, 38) | 18.7 (0, 36) |
Total treatment years | 609.5 | 532.1 |
Actual exposure time, monthsb | ||
Mean (SD) | 21.5 (10.57) | 18.5 (10.68) |
Median (minimum, maximum) | 22.2 (0, 38) | 18.3 (0, 36) |
Total treatment years | 603.2 | 529.7 |
Actual cumulative exposure over time, n (%) | ||
≥ 1 day | 337 (100) | 343 (100) |
≥ 6 months | 294 (87.2) | 288 (84.0) |
≥ 12 months | 274 (81.3) | 223 (65.0) |
≥ 18 months | 221 (65.6) | 177 (51.6) |
≥ 24 months | 148 (43.9) | 117 (34.1) |
≥ 30 months | 88 (26.1) | 62 (18.1) |
≥ 36 monthsc | 8 (2.4) | 5 (1.5) |
SD = standard deviation.
aTotal exposure time = (last dose date where dose > 0 mg minus first dose date) plus 1, divided by 30.4375.
bActual exposure time = (last dose date where dose > 0 mg minus first dose date) plus 1, minus total duration of dose interruption (i.e., number of days with dose = 0 mg) divided by 30.4375.
cOne patient had 38 months of treatment based on the data calculated using exposure information. The patient discontinued the study and is no longer on treatment. The last date of exposure was not available, as the patient was lost to follow-up.
Source: Clinical Study Report.13
The dose interruptions and reductions that occurred in the ADAURA trial by treatment arm are summarized in Table 12. Overall, 54.3% of patients in the osimertinib arm and 41.7% of patients in the placebo arm had a dose interruption for any reason during the study, with a median duration of 8.0 days and 5.0 days, respectively. The most common reasons for dose interruptions were patients forgetting to take a dose (29.7% in the osimertinib arm, 31.5% in the placebo arm) and patients experiencing an AE (31.5% in the osimertinib arm, 10.5% in the placebo arm). The most common AEs leading to treatment interruption in the osimertinib arm were diarrhea (n = 13; 3.9%) and stomatitis (n = 8; 2.4%). In the placebo arm, the most common AEs leading to study treatment interruption were diarrhea (n = 4; 1.2%) and vomiting (n = 3; 0.9%).
In the osimertinib arm, 14.5% of patients had a dose reduction compared with 0.9% of patients in the placebo arm. The most common reason for dose reduction was an AE (13.6% in the osimertinib arm, 0.9% in the placebo arm). AEs leading to dose reductions in 1 or more patients in the osimertinib arm were stomatitis (n = 5; 1.5%), paronychia (n = 4; 1.2%), hypertension (n = 2; 0.6%), diarrhea (n = 2; 0.6%), nausea (n = 2; 0.6%), and QT interval prolonged (n = 2; 0.6%). No AE leading to a dose reduction was reported by more than 1 patient in the placebo arm.
Table 12: Summary of Treatment Interruptions and Dose Reductions — Safety Population
Detail | Osimertinib (N = 337) | Placebo (N = 343) |
|---|---|---|
Received planned starting dose, n (%) | 336 (99.7)a | 343 (100) |
Dose interruptions | ||
Patients with interruptions, n (%) | ||
Any | 183 (54.3) | 143 (41.7) |
1 | 79 (23.4) | 68 (19.8) |
> 2 | 104 (30.9) | 75 (21.9) |
Reason for interruption, n (%)b | ||
AEc | 106 (31.5) | 36 (10.5) |
Patient forgot to take dose | 100 (29.7) | 108 (31.5) |
Patient decision | 20 (5.9) | 12 (3.5) |
Laboratory abnormality not reported as an AE | 0 | 1 (0.3) |
Other | 12 (3.6) | 19 (5.5) |
Total number of any interruptions, n (%)d | 124 (36.8) | 59 (17.2) |
Median length of interruption (range), days | 8.0 (1 to 92) | 5.0 (1 to 83) |
Dose reductions | ||
Patients with any dose reduction, n (%) | 49 (14.5) | 3 (0.9) |
Reason for dose reduction, n (%) | ||
AE | 46 (13.6) | 3 (0.9) |
Other | 3 (0.9) | 0 |
AE = adverse event.
aOne patient did not receive osimertinib treatment on the day of randomization and so was recorded as having missed their planned starting dose. This patient started osimertinib 80 mg 9 days after the date of randomization.
bReasons for interruption are not mutually exclusive for patients with multiple interruptions, although reasons were counted only once per category.
cThe number of dose modifications due to AEs in this exposure summary differs from the number of AEs resulting in a dose modification due to the differences in data capture between the exposure and AE electronic case report forms. In the exposure summary, each dose modification action is taken into account; whereas, within the AE datasets, only the last action taken for an AE is recorded and summarized.
d“Any” is defined as the total number of patients with at least 1 dose interruption. The total number of interruptions excludes any interruptions where the patient forgot to take their dose.
Source: Clinical Study Report.13
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the CADTH review protocol are reported subsequently.
Overall Survival
The OS results from the ADAURA trial as of the interim analysis are summarized in Table 13. As of the data cut-off date, the sponsor considered the OS data to be immature. A total of 29 patients (4.3%) had died: 9 (2.7%) in the osimertinib arm and 20 (5.8%) in the placebo arm. Most patients were in survival follow-up (616 patients; 90.3%). This included 309 patients (91.2%) in the osimertinib arm and 307 patients (89.5%) in the placebo arm. The median follow-up for OS in the stage II to stage IIIA population was 26.1 months and 24.6 months in the osimertinib and placebo arms, respectively; the median follow-up for OS in the overall population was 26.1 months and 25.9 months in the osimertinib and placebo arms, respectively.
Per the multiple-testing procedure, OS was formally tested in patients with stage II to stage IIIA disease at the interim analysis. At the data cut-off, 25 deaths had occurred in the stage II to stage IIIA population (5.3% maturity of data), comprising 8 deaths (3.4%) in the osimertinib arm and 17 deaths (7.2%) in the placebo arm. The Kaplan-Meier plots of OS in the stage II to stage IIIA population are depicted in Figure 4. The HR was 0.40 (95% CI, 0.18 to 0.89; P = 0.0244), which did not reach statistical significance (P value < 0.0002 required).
Since OS did not reach statistical significance in the primary stage II to stage IIIA population, OS in the overall population was not formally tested for statistical significance per the multiple-testing procedure. The analysis of OS in the overall population should therefore be regarded as an exploratory analysis. The Kaplan-Meier plots of OS in the overall population are depicted in Figure 5. The HR was 0.48 (95% CI, 0.23 to 1.02). In the overall population, 9 patients (2.7%) in the osimertinib arm and 20 patients (5.8%) in the placebo arm had died.
Table 13: Overall Survival in the ADAURA Trial — FAS
Outcome | Stage II to IIIA population | Overall population | ||
|---|---|---|---|---|
Osimertinib (N = 233) | Placebo (N = 237) | Osimertinib (N = 339) | Placebo (N = 343) | |
Patient deaths, n (%)a | 8 (3.4) | 17 (7.2) | 9 (2.7) | 20 (5.8) |
HR (95% CI)b,c | 0.40 (0.18 to 0.89) | 0.48 (0.23 to 1.02) | ||
2-sided P valueb | 0.0244d | 0.0553e | ||
Median follow-up time for OS in all patients, months | 26.1 | 24.6 | 26.1 | 25.9 |
Median follow-up time for OS in censored patients, months | 26.1 | 25.2 | 26.1 | 26.5 |
Median OS (95% CI), monthsf | NR (NR to NR) | NR (NR to NR) | NR (NR to NR) | 48.2 (48.2 to NR) |
OS rate at 2 years (95% CI), %d | 100 (100 to 100) | 92.6 (87.6 to 95.6) | 99.6 (96.9 to 99.9) | 94.7 (91.4 to 96.8) |
OS rate at 3 years (95% CI), %d | 91.7 (82.4 to 96.2) | 89.0 (82.1 to 93.3) | 93.9 (87.4 to 97.1) | 91.8 (87.1 to 94.9) |
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NR = not reached; OS = overall survival.
aOS events that do not occur within 2 scheduled visits (plus visit window) of the last evaluable assessment (or randomization) are censored and therefore excluded in the number of events.
bThe analysis was performed using a log-rank test stratified by stage (IB vs. II vs. IIIA), race (Asian vs. non-Asian), and mutation type (exon 19 deletions vs. L858R). Stratification factors were as recorded in an interactive voice response system.
cAn HR of less than 1 favours osimertinib. The HR and CI were obtained directly from the U- and V-statistics.
dA 2-sided significance level of 0.0002 was required for the interim analysis of OS.
eDue to a failed test of a previous end point in the statistical testing hierarchy, this P value cannot be interpreted for inference and should be considered descriptive.
fCalculated using the Kaplan-Meier method.
Source: Clinical Study Report.13
Figure 4: Kaplan-Meier Plot of OS in the ADAURA Trial — FAS, Stage II to Stage IIIA Population
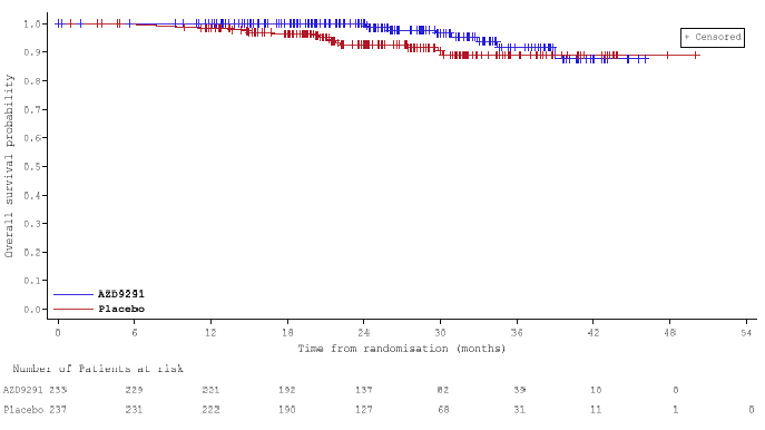
AZD9291 = osimertinib; FAS = full analysis set; OS = overall survival.
Source: Clinical Study Report.13
Figure 5: Kaplan-Meier Plot of OS in the ADAURA Trial — FAS, Overall Population
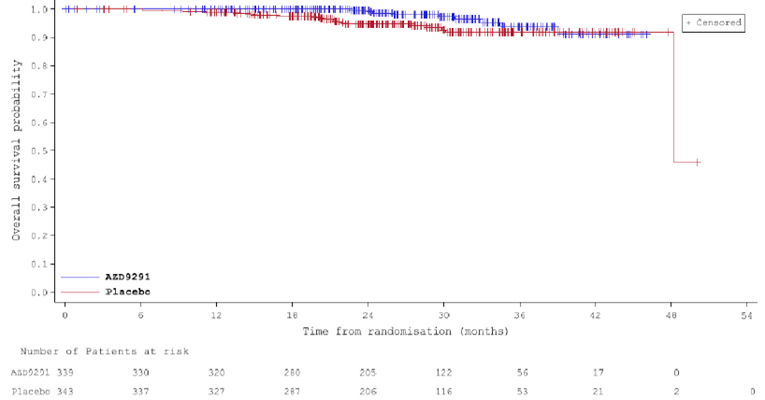
AZD9291 = osimertinib; FAS = full analysis set; OS = overall survival.
Source: Clinical Study Report.13
Disease-Free Survival
The DFS results from the ADAURA trial as of the interim analysis are summarized in Table 14. As of the data cut-off date, median follow-up time for DFS in the stage II to stage IIIA population was 22.1 months in the osimertinib arm and 14.9 months in the placebo arm. The median follow-up for DFS in the overall population was 22.1 months in the osimertinib arm compared with 16.6 months in the placebo arm.
In the stage II to stage IIIA population, 26 patients (11.2%) in the osimertinib arm and 130 patients (54.9%) in the placebo arm had experienced a DFS event. The Kaplan-Meier plots of DFS in the stage II to stage IIIA population are depicted in Figure 6. The HR was 0.17 (95% CI, 0.12 to 0.23), which was statistically significant (P < 0.0001). The Kaplan-Meier estimate of the median duration of DFS was not reached (NR) in the osimertinib arm (95% CI, 38.8 months to NR) compared with 19.6 months (95% CI, 16.6 to 24.5) in the placebo arm.
In the overall population, 37 patients (10.9%) in the osimertinib arm and 159 patients (46.6%) in the placebo arm had experienced a DFS event. The Kaplan-Meier plots of DFS in the overall population are depicted in Figure 7. The HR was 0.20 (95% CI, 0.15 to 0.27), which was statistically significant (P < 0.0001). The Kaplan-Meier estimate of the median duration of DFS was NR in the osimertinib arm (95% CI, NR to NR) compared with 27.5 months (95% CI, 22.0 to 35.0) in the placebo arm.
Table 14: DFS in the ADAURA Trial — FAS
Outcome | Stage II to IIIA population | Overall population | ||
|---|---|---|---|---|
Osimertinib (N = 233) | Placebo (N = 237) | Osimertinib (N = 339) | Placebo (N = 343) | |
Recurrence or death events, n (%) | ||||
Patients with events, n (%) | 26 (11.2) | 130 (54.9) | 37 (10.9) | 159 (46.4) |
Disease recurrencea | 26 (11.2) | 129 (54.4) | 37 (10.9) | 157 (45.8) |
Local or regional only | 17 (7.3) | 48 (20.3) | 23 (6.8) | 61 (17.8) |
Distant only | 8 (3.4) | 67 (28.3) | 10 (2.9) | 78 (22.7) |
Local or regional and distant | 1 (0.4) | 14 (5.9) | 4 (1.2) | 18 (5.2) |
Deathb | 0 | 1 (0.4) | 0 | 2 (0.6) |
Censored | 207 (88.8) | 107 (45.1) | 302 (89.1) | 184 (53.6) |
Alive and disease recurrence–free | 196 (84.1) | 100 (42.2) | 279 (82.3) | 175 (51.0) |
No evaluable assessments or no baseline data | 3 (1.3) | 4 (1.7) | 8 (2.4) | 4 (1.2) |
2 or more missed visits before recurrence or death | 0 | 1 (0.4) | 0 | 1 (0.3) |
Lost to follow-up | 0 | 1 (0.4) | 0 | 1 (0.3) |
Withdrawn consent | 8 (3.4) | 0 | 14 (4.1) | 0 |
Evidence of disease at study entry | 0 | 1 (0.4) | 1 (0.3) | 3 (0.9) |
HR (95% CI)c,d | 0.17 (0.12 to 0.23) | 0.20 (0.15 to 0.27) | ||
2-sided P valuec | < 0.0001 | < 0.0001 | ||
Median follow-up time for DFS in all patients, months | 22.1 | 14.9 | 22.1 | 16.6 |
Median follow-up time for DFS in censored patients, months | 22.1 | 21.9 | 22.1 | 22.1 |
Median and landmark DFS rate | ||||
Median DFS (95% CI), monthse | NR (38.8 to NR) | 19.6 (16.6 to 24.5) | NR (NR to NR) | 27.5 (22.0 to 35.0) |
DFS rate at 6 months (95% CI),e % | 99.1 (96.5 to 99.8) | 83.1 (77.6 to 87.3) | 99.1 (97.2 to 99.7) | 86.3 (82.1 to 89.5) |
DFS rate at 12 months (95% CI),e % | 97.2 (93.9 to 98.7) | 60.8 (54.1 to 66.8) | 97.4 (94.9 to 98.7) | 68.5 (63.2 to 73.2) |
DFS rate at 18 months (95% CI),e % | 90.9 (85.7 to 94.3) | 51.7 (44.8 to 58.2) | 91.6 (87.6 to 94.4) | 60.2 (54.6 to 65.4) |
DFS rate at 24 months (95% CI),e % | 89.5 (84.0 to 93.2) | 43.6 (36.5 to 50.6) | 89.1 (84.5 to 92.4) | 52.4 (46.4 to 58.1) |
DFS rate at 36 months (95% CI),e % | 78.3 (64.5 to 87.3) | 27.9 (18.9 to 37.6) | 78.9 (68.7 to 86.1) | 40.0 (32.1 to 47.8) |
CI = confidence interval; DFS = disease-free survival; FAS = full analysis set; HR = hazard ratio; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NR = not reached.
aDFS events that do not occur within 2 scheduled visits (plus visit window) of the last evaluable assessment (or randomization) are censored and therefore excluded in the number of events.
bDeath in the absence of disease recurrence, or death occurring within 2 visits of baseline where the patient has no evaluable assessments or no baseline data.
cThe analysis was performed using a log-rank test stratified by stage (IB vs. II vs. IIIA), race (Asian vs. non-Asian), and mutation type (exon 19 deletions vs. L858R). Stratification factors were as recorded in an interactive voice response system.
dAn HR of less than 1 favours osimertinib. The HR and CI were obtained directly from the U and V statistics.
eCalculated using the Kaplan-Meier method.
Source: Clinical Study Report.13
Figure 6: Kaplan-Meier Plot of DFS in the ADAURA Trial — FAS, Stage II to Stage IIIA Population
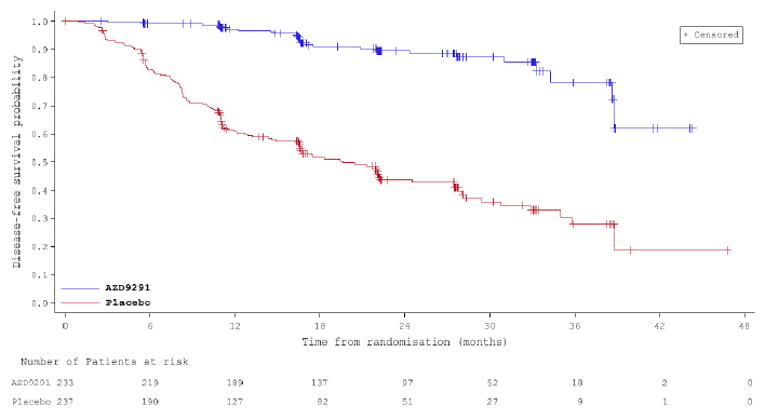
AZD9291 = osimertinib; DFS = disease-free survival; FAS = full analysis set.
Source: Clinical Study Report.13
Figure 7: Kaplan-Meier Plot of DFS in the ADAURA Trial — FAS, Overall Population

AZD9291 = osimertinib; DFS = disease-free survival; FAS = full analysis set.
Source: Clinical Study Report.13
Sensitivity analyses were performed in the stage II to stage IIIA population to assess evaluation-time bias, attrition bias, and the presence of quantitative interactions, and the results of these analyses are summarized in Appendix 2. There was no evidence of evaluation-time bias (Table 25) or attrition bias (Figure 15). The presence of quantitative interactions was assessed using an overall global interaction test, and the results of these tests are summarized in Table 26. These analyses indicated there was evidence of a quantitative interaction in EGFR mutation type (exon 19 deletions versus L858R) on DFS (P = 0.0132), suggesting that osimertinib showed a treatment benefit in both exon 19 deletions and L858R mutation subgroups, but with a difference in magnitude (significance level of 0.1).
The results of the pre-specified subgroup analyses of DFS are summarized in Table 15. Consistent with the FAS population, a benefit with osimertinib was consistently observed with an HR of less than 0.4 for all subgroups.
Table 15: Subgroup Analyses of DFS in the ADAURA Trial — FAS, Overall Population
Subgroup | Category | Treatment | N | Patients with events, n (%) | HR (95% CI)a,b |
|---|---|---|---|---|---|
Disease stage | IB | Osimertinib | 106 | 11 (10.4) | 0.39 (0.18 to 0.76) |
Placebo | 106 | 29 (27.4) | |||
II | Osimertinib | 118 | 11 (9.3) | 0.17 (0.08 to 0.31) | |
Placebo | 118 | 52 (44.1) | |||
IIIA | Osimertinib | 115 | 15 (13.0) | 0.12 (0.07 to 0.20) | |
Placebo | 119 | 78 (65.5) | |||
EGFR mutation typec | Ex19del | Osimertinib | 187 | 15 (8.0) | 0.12 (0.07 to 0.20) |
Placebo | 191 | 98 (51.3) | |||
L858R | Osimertinib | 152 | 22 (14.5) | 0.31 (0.18 to 0.49) | |
Placebo | 152 | 61 (40.1) | |||
Adjuvant chemotherapy | Yes | Osimertinib | 203 | 22 (10.8) | 0.16 (0.10 to 0.26) |
Placebo | 207 | 103 (49.8) | |||
No | Osimertinib | 136 | 15 (11.0) | 0.23 (0.13 to 0.40) | |
Placebo | 136 | 56 (41.2) | |||
Race | Asian | Osimertinib | 216 | 27 (12.5) | 0.21 (0.13 to 0.31) |
Placebo | 218 | 104 (47.7) | |||
Non-Asian | Osimertinib | 123 | 10 (8.1) | 0.15 (0.07 to 0.28) | |
Placebo | 125 | 55 (44.0) |
CI = confidence interval; DFS = disease-free survival; EGFR = epidermal growth factor receptor; Ex19del = exon 19 deletions; FAS = full analysis set; HR = hazard ratio; IVRS = interactive voice response system; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21.
aAn analysis of DFS by subgroups was conducted using a Cox proportional-hazards model that contained a term for treatment, the subgroup covariate of interest, and the treatment-by-subgroup interaction term.
bAn HR of less than 1 favours osimertinib.
cStratification factors were as recorded in an IVRS. Ten patients were mis-stratified by EGFR mutation type because the EGFR mutation status entered in the IVRS differed from the status confirmed by central prospective EGFR genetic testing.
Source: Clinical Study Report.13
A post hoc exploratory analysis of DFS with disease recurrence in the CNS only (determined by investigator assessment) was performed in the FAS, and the results are summarized in Table 16. In the overall population, 45 patients experienced disease recurrence in the CNS or death, with most events occurring in patients with stage II to stage IIIA disease (36 patients). Among all patients randomized to the osimertinib arm (overall population), 4 patients (1.2%) had recurrence in the CNS, corresponding to 10.8% of all recurrence events in this arm. In the placebo arm, 33 patients (9.6%) had recurrence in the CNS, corresponding to 21% of all recurrence events in this arm. The results suggested a benefit with osimertinib compared with placebo in CNS DFS, with an HR of 0.14 (95% CI, 0.07 to 0.27) for stage II to stage IIIA patients and an HR of 0.18 (95% CI, 0.10 to 0.33) for the overall population. In the stage II to stage IIIA population, the median CNS DFS was NR (95% CI, 38.8 to NR) and NR (95% CI, NR to NR) in the osimertinib and placebo arms, respectively. In the overall population, the median CNS DFS was NR in the osimertinib arm versus 48.2 months (95% CI, NR to NR) in the placebo arm.
Table 16: Summary of CNS DFS in the ADAURA Trial — FAS
Outcome | Stage II to IIIA population | Overall population | ||
|---|---|---|---|---|
Osimertinib (N = 233) | Placebo (N = 237) | Osimertinib (N = 339) | Placebo (N = 343) | |
Patients with events, n (%)a | 4 (1.7) | 32 (13.5) | 6 (1.8) | 39 (11.4) |
CNS recurrenceb | 3 (1.3) | 27 (11.4) | 4 (1.2) | 33 (9.6) |
Deathc | 1 (0.4) | 5 (2.1) | 2 (0.6) | 6 (1.7) |
Censored, n (%) | 229 (98.3) | 205 (86.5) | 333 (98.2) | 304 (88.6) |
HR (95% CI)d,e | 0.14 (0.07 to 0.27) | 0.18 (0.10 to 0.33) | ||
Median DFS in CNS (95% CI), months | NR (38.8 to NR) | NR (NR to NR) | NR (39.0 to NR) | 48.2 (NR to NR) |
CNS DFS rate at 6 months (95% CI), % | 100.0 (100.0 to 100.0) | 97.2 (93.9 to 98.7) | 100.0 (100.0 to 100.0) | 97.5 (95.0 to 98.7) |
CNS DFS rate at 12 months (95% CI), % | 99.5 (96.8 to 99.9) | 90.7 (85.5 to 94.0) | 99.7 (97.7 to 100.0) | 92.1 (88.4 to 94.7) |
CNS DFS rate at 18 months (95% CI), % | 98.8 (95.2 to 99.7) | 83.8 (76.7 to 88.9) | 99.2 (96.8 to 99.8) | 88.0 (83.2 to 91.5) |
CNS DFS rate at 24 months (95% CI), % | 98.8 (95.2 to 99.7) | 79.7 (71.7 to 85.7) | 98.0 (94.6 to 99.3) | 85.0 (79.6 to 89.1) |
CNS DFS rate at 36 months (95% CI), % | 98.8 (95.2 to 99.7) | 75.1 (64.5 to 83.0) | 98.0 (94.6 to 99.3) | 82.4 (75.6 to 87.5) |
CI = confidence interval; CNS = central nervous system; DFS = disease-free survival; FAS = full analysis set; HR = hazard ratio; NR = not reached.
aDFS events are defined as disease recurrence in the CNS or death. DFS events that do not occur within 2 scheduled visits (plus visit window) of the last evaluable assessment (or randomization) are censored and therefore excluded in the number of events.
bOne patient in the osimertinib arm and 1 patient in the placebo arm had CNS metastases at baseline. They were therefore censored at day 1 and are not counted in this table as having a CNS recurrence.
cDeath in the absence of CNS disease recurrence, or death occurring within 2 visits of baseline where the patient had no evaluable assessments or no baseline data.
dThe analysis was performed post hoc using an unstratified log-rank test due to low event counts in the strata combinations.
eAn HR < 1 favours osimertinib. The HR and CI were obtained directly from the U- and V-statistics.
Source: Clinical Study Report.13
Figure 8: Kaplan-Meier Plot of CNS DFS in the ADAURA Trial — FAS, Stage II to Stage IIIA Population
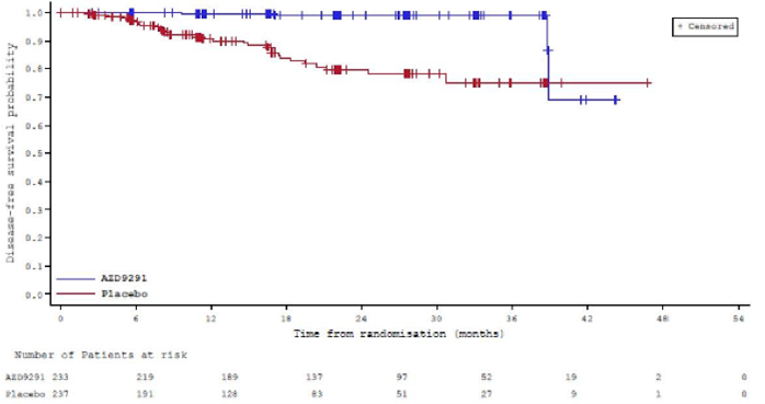
AZD9291 = osimertinib; CNS = central nervous system; DFS = disease-free survival; FAS = full analysis set.
Source: Clinical Study Report.13
Figure 9: Kaplan-Meier Plot of CNS DFS in the ADAURA Trial — FAS, Overall Population
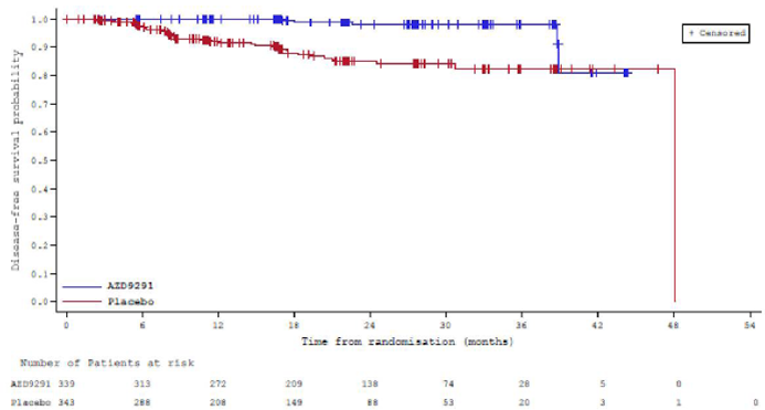
AZD9291 = osimertinib; CNS = central nervous system; DFS = disease-free survival; FAS = full analysis set.
Source: Clinical Study Report.13
Disease Recurrence Rate
A summary of disease recurrence in the overall population of the ADAURA trial is presented in Table 17. As of the data cut-off, 37 patients (10.9%) in the osimertinib arm and 157 patients (45.8%) in the placebo arm had experienced disease recurrence. In the osimertinib arm, disease recurrence was local or regional only in 23 patients (6.8%), distant in 10 patients (2.9%), and both distant and local or regional in 4 patients (1.2%). In the placebo arm, disease recurrence was local or regional only in 61 patients (17.8%), distant in 78 patients (22.7%), and both distant and local or regional in 18 patients (5.2%). The most common tumour-recurrence locations in the osimertinib and placebo arms were the lung (5.6% and 17.8%, respectively), lymph nodes (2.9% and 14.0%, respectively), CNS (1.5% and 9.9%, respectively), and bone (1.5% and 8.2%, respectively).
Table 17: Summary of Disease Recurrence in the ADAURA Trial — FAS, Overall Population
Detail | Osimertinib (N = 339) | Placebo (N = 343) |
|---|---|---|
Disease recurrence events, n (%) | 37 (10.9) | 157 (45.8) |
Local or regional only | 23 (6.8) | 61 (17.8) |
Distant only | 10 (2.9) | 78 (22.7) |
Distant and local or regional | 4 (1.2) | 18 (5.2) |
Tumour-recurrence location, n (%) | ||
Adrenal | 0 | 2 (0.6) |
Bone | 5 (1.5) | 28 (8.2) |
CNS | 5 (1.5) | 34 (9.9) |
Head and neck | 2 (0.6) | 3 (0.9) |
Liver | 3 (0.9) | 8 (2.3) |
Lung | 19 (5.6) | 61 (17.8) |
Peritoneum | 0 | 1 (0.3) |
Pleura | 0 | 12 (3.5) |
Renal | 1 (0.3) | 0 |
Pancreas | 0 | 1 (0.3) |
Lymph nodes | 10 (2.9) | 48 (14.0) |
Pleural effusion | 0 | 6 (1.7) |
Other | 0 | 1 (0.3) |
Missing | 0 | 1 (0.3) |
CNS = central nervous system; FAS = full analysis set.
Source: Clinical Study Report.13
Time to Disease Recurrence
Data on the time to disease recurrence were not reported in the ADAURA trial.
Time to Intracranial CNS Metastasis
Data on the time to intracranial CNS metastasis were not reported in the ADAURA trial.
Progression-Free Survival
Data on PFS determined by investigator assessment as of the interim analysis are summarized in Table 18, and the Kaplan-Meier plot is depicted in Figure 10. As of the interim analysis, the sponsor considered the PFS data to be immature. As of the data cut-off date, 13 patients (3.8%) in the osimertinib arm and 46 patients (13.4%) in the placebo arm had experienced a PFS event. The comparisons for this end point were not controlled for multiple comparisons.
Table 18: Progression-Free Survival in the ADAURA Trial — FAS, Overall Population
Detail | Osimertinib (N = 339) | Placebo (N = 343) |
|---|---|---|
Patients with PFS events, n (%) | 13 (3.8) | 46 (13.4) |
HR (95% CI)a,b | 0.24 (0.14 to 0.41) | |
2-sided P valuea,c | < 0.0001 | |
Median PFS (95% CI), monthsd | NR (NR to NR) | 48.2 (NR to NR) |
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NR = not reached; PFS = progression-free survival.
aThe analysis was performed using a log-rank test stratified by stage (IB vs. II vs. IIIA), race (Asian vs. non-Asian), and mutation type (exon 19 deletions vs. L858R). Stratification factors were as recorded in an interactive voice response system.
bAn HR of less than 1 favours osimertinib. The HR and CI were obtained directly from the U- and V-statistics.
cP value has not been controlled for multiple comparisons.
dCalculated using the Kaplan-Meier method.
Source: Clinical Study Report.13
Figure 10: Kaplan-Meier Plot of PFS in the ADAURA Trial — FAS, Overall Population
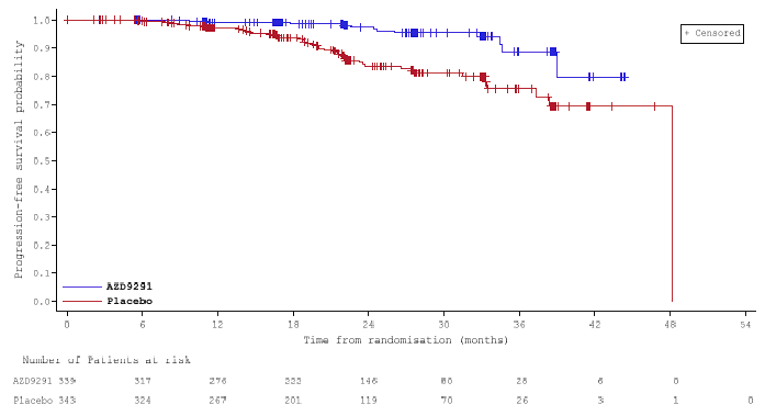
AZD9291 = osimertinib; FAS = full analysis set; PFS = progression-free survival.
Source: Clinical Study Report.13
Time to Next Treatment
Data on time to next treatment in the ADAURA trial as of the interim analysis are summarized in Table 19, and the Kaplan-Meier plot is depicted in Figure 11. As of the data cut-off date, the sponsor considered the time to next treatment data to be immature. The comparisons for this end point were not controlled for multiple comparisons.
As of the data cut-off date, 31 patients (9.1%) in the osimertinib arm and 134 patients (39.1%) in the placebo arm had experienced an event (death or first subsequent anti-cancer therapy). Of these events, 30 patients (96.8%) in the osimertinib arm and 125 patients (93.3%) in the placebo arm received a subsequent anti-cancer treatment. The HR was 0.20 (95% CI, 0.14 to 0.27).
The types of subsequent anti-cancer therapy received by patients are summarized in Table 20. The most commonly received type was TKIs (5.0% and 27.4% in the osimertinib and placebo arms, respectively). The most common TKIs were gefitinib (2.7% and 10.5% in the osimertinib and placebo arms, respectively), osimertinib (0.9% and 5.5% in the osimertinib and placebo arms, respectively), afatinib (0.6% and 4.4% in the osimertinib and placebo arms, respectively), and erlotinib (0.6% and 4.4% in the osimertinib and placebo arms, respectively).
Table 19: Time to Next Treatment in the ADAURA Trial — FAS, Overall Population
Detail | Osimertinib (N = 339) | Placebo (N = 343) |
|---|---|---|
Patients with events, n (%) | 31 (9.1) | 134 (39.1) |
Death | 1 (3.2) | 9 (6.7) |
First subsequent anti-cancer therapy | 30 (96.8) | 125 (93.3) |
Median time to next treatment or death (95% CI), monthsa | NR (NR to NR) | 39.8 (30.8 to NR) |
HR (95% CI)b,c | 0.20 (0.14 to 0.27) | |
2-sided P valueb,d | < 0.0001 | |
Time to next treatment or death rate at 2 years (95% CI), %a | 92.5 (88.7 to 95.1) | 60.8 (55.1 to 66.1) |
Time to next treatment or death rate at 3 years (95% CI), %a | 85.8 (78.7 to 90.7) | 56.3 (50.0 to 62.1) |
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NR = not reached.
aCalculated using the Kaplan-Meier method.
bThe analysis was performed using a log-rank test stratified by stage (IB vs. II vs. IIIA), race (Asian vs. non-Asian), and mutation type (exon 19 deletions vs. L858R). Stratification factors were as recorded in an interactive voice response system.
cAn HR of less than 1 favours osimertinib. The HR and CI were obtained directly from the U- and V-statistics.
dP value has not been controlled for multiple comparisons.
Source: Clinical Study Report.13
Figure 11: Kaplan-Meier Plot of Time to Next Treatment in the ADAURA Trial — FAS, Overall Population
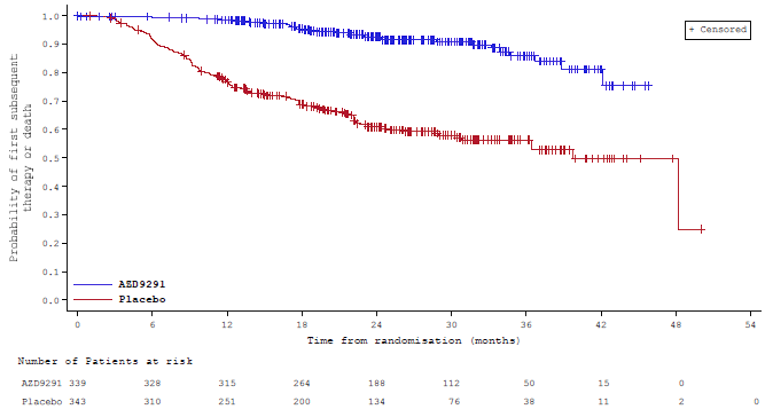
AZD9291 = osimertinib; FAS = full analysis set.
Source: Clinical Study Report.13
Table 20: Summary of type of First Subsequent Anti-Cancer Therapy — FAS, Overall Population
Type of first subsequent anti-cancer therapy | Osimertinib (N = 339) | Placebo (N = 343) |
|---|---|---|
Patients who received a subsequent anti-cancer therapy, n (%) | 31 (9.1) | 125 (36.4) |
Type of anti-cancer therapy, n (%) | ||
Bisphosphonates | 0 | 1 (0.3) |
Detoxifying drugs for antineoplastic treatment | 1 (0.3) | 0 |
Folic acid analogues | 5 (1.5) | 4 (1.2) |
Monoclonal antibodies | 3 (0.9) | 5 (1.5) |
Platinum compounds | 9 (2.7) | 8 (2.3) |
Tyrosine kinase inhibitors | 17 (5.0) | 94 (27.4) |
Afatinib (Gilotrif) | 2 (0.6) | 15 (4.4) |
Epitinib (HMPL-813) | 0 | 1 (0.3) |
Erlotinib (Tarceva) | 2 (0.6) | 15 (4.4) |
Gefitinib (Iressa) | 9 (2.7) | 36 (10.5) |
Icotinib (Conmana) | 1 (0.3) | 8 (2.3) |
Osimertinib (Tagrisso) | 3 (0.9) | 19 (5.5) |
Pyrimidine analogues | 3 (0.9) | 1 (0.3) |
Taxanes | 1 (0.3) | 5 (1.5) |
Unspecified herbal and traditional medicine | 0 | 2 (0.6) |
Vinca alkaloids and analogues | 0 | 1 (0.3) |
All other therapeutic products | 0 | 1 (0.3) |
Other plant alkaloids and natural products | 1 (0.3) | 0 |
Uncoded | 6 (1.8) | 22 (6.4) |
FAS = full analysis set.
Source: Clinical Study Report.13
Health-Related Quality of Life: SF-36 v2
The SF-36 v2 was used to measure HRQoL in the ADAURA trial. This generic instrument includes 8 domains that can be grouped into 2 summary scores, the PCS and MCS. The sponsor defined a clinically relevant change in PCS and MCS as 3.1 points or greater and 3.8 points or greater, respectively.12 The rationale for these MIDs was not reported by the sponsor. CADTH identified the MID in the general population as 2 points for the PCS score and 3 points for the MCS score (Appendix 3). No MID in patients with NSCLC was identified.
The compliance rates (i.e., the number of evaluable forms divided by the number of expected forms) for the SF-36 over time are depicted in Figure 12. In the overall population, compliance rates for SF-36 completion were greater than 90% in both treatment arms from baseline until week 144, with a reduction to 87.2% and 84.8% at week 156 in the osimertinib and placebo arms, respectively. However, the number of forms expected decreased over time in both treatment arms and included a small proportion of patients at later time points.
Figure 12: Compliance Rates for Completion of the SF-36 v2 in the ADAURA Trial — Overall Population
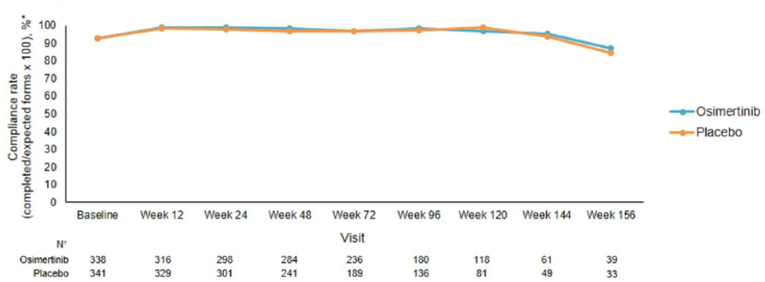
SF-36 v2 = Short Form (36) Health Survey version 2.
* Compliance rates were calculated as the number of evaluable forms (i.e., a questionnaire with a completion date and at least 1 domain that is non-missing) divided by the number of expected forms (i.e., a questionnaire from a patient who has not died, is not lost to follow-up, or has not withdrawn from the study at the scheduled assessment time) multiplied by 100.
† Number of expected forms.
Source: Sponsor’s submission to CADTH.14
In the overall population, the proportion of patients reporting improvements in the PCS of 3.1 points or greater over time increased in both the osimertinib and placebo arms from week 12 (29.9% versus 33.2%) to week 48 (41.0% versus 50.2%), declined transiently at week 72 (38.7% versus 50.0%), and then increased again at week 96 (43.0% versus 53.2%). In both the osimertinib and placebo arms, the proportion of patients reporting improvement in the MCS by 3.8 points or greater increased from week 12 (34.4% versus 41.5%) to week 48 (46.4% versus 49.3%), followed by a trend of decline to week 96 (37.0% versus 44.4%).
Table 21: Summary of Change From Baseline and Categories of Change for the SF-36 v2 PCS and MCS Scores — FAS, Overall Population
Treatment arm | Time point | N | Change from baseline | Categories of change, n (%)a | |||
|---|---|---|---|---|---|---|---|
Mean (SD) | Median (Q1, Q3) | Improved | Stable | Worsened | |||
PCS | |||||||
Osimertinib (N = 339) | Week 12 | 291 | 0.16 (6.34) | 0.32 (−3.89 to 4.26) | 87 (29.9) | 122 (41.9) | 82 (28.2) |
Week 24 | 274 | 0.88 (7.01) | 1.42 (−3.23 to 5.13) | 98 (35.8) | 104 (38.0) | 72 (26.3) | |
Week 48 | 261 | 1.36 (6.80) | 1.39 (−3.05 to 5.89) | 107 (41.0) | 89 (34.1) | 65 (24.9) | |
Week 72 | 212 | 1.88 (6.94) | 1.50 (−2.12 to 6.69) | 82 (38.7) | 88 (41.5) | 42 (19.8) | |
Week 96 | 165 | 1.15 (7.89) | 1.57 (−3.30 to 6.23) | 71 (43.0) | 52 (31.5) | 42 (25.5) | |
Week 120 | 105 | 1.85 (6.49) | 2.20 (−3.28 to 6.71) | 48 (45.7) | 29 (27.6) | 28 (26.7) | |
Week 144 | 51 | 2.98 (6.86) | 2.71 (−2.00 to 6.94) | 24 (47.1) | 20 (39.2) | 7 (13.7) | |
Week 156 | 30 | 3.55 (7.48) | 3.91 (−0.21 to 7.73) | 18 (60.0) | 6 (20.0) | 6 (20.0) | |
Treatment discontinuation | 66 | −1.85 (7.66) | −0.70 (−5.69 to 3.46) | 17 (25.8) | 22 (33.3) | 27 (40.9) | |
Placebo (N = 343) | Week 12 | 301 | 1.14 (6.08) | 0.79 (−2.54 to 4.56) | 100 (33.2) | 135 (44.9) | 66 (21.9) |
Week 24 | 275 | 1.94 (6.64) | 2.05 (−2.36 to 5.69) | 114 (41.5) | 102 (37.1) | 59 (21.5) | |
Week 48 | 219 | 2.80 (7.50) | 3.13 (−1.75 to 7.72) | 110 (50.2) | 63 (28.8) | 46 (21.0) | |
Week 72 | 172 | 3.38 (7.02) | 2.93 (−1.48 to 8.02) | 86 (50.0) | 54 (31.4) | 32 (18.6) | |
Week 96 | 124 | 3.59 (6.60) | 3.76 (−0.41 to 8.05) | 66 (53.2) | 38 (30.6) | 20 (16.1) | |
Week 120 | 76 | 3.15 (7.37) | 1.90 (−1.35 to 7.89) | 33 (43.4) | 31 (40.8) | 12 (15.8) | |
Week 144 | 42 | 3.00 (7.78) | 2.88 (−1.38 to 9.66) | 20 (47.6) | 16 (38.1) | 6 (14.3) | |
Week 156 | 24 | 3.22 (8.05) | 4.89 (0.28 to 8.28) | 13 (54.2) | 7 (29.2) | 4 (16.7) | |
Treatment discontinuation | 109 | −0.73 (7.70) | 0.20 (−4.75 to 4.69) | 34 (31.2) | 37 (33.9) | 38 (34.9) | |
MCS | |||||||
Osimertinib (N = 339) | Week 12 | 291 | 0.99 (8.07) | 1.25 (−4.01 to 6.43) | 100 (34.4) | 114 (39.2) | 77 (26.5) |
Week 24 | 274 | 1.33 (8.92) | 1.05 (−4.04 to 6.63) | 100 (36.5) | 104 (38.0) | 70 (25.5) | |
Week 48 | 261 | 2.79 (9.30) | 3.33 (−3.32 to 8.10) | 121 (46.4) | 79 (30.3) | 61 (23.4) | |
Week 72 | 212 | 1.35 (9.87) | 1.66 (−3.85 to 7.35) | 89 (42.0) | 70 (33.0) | 53 (25.0) | |
Week 96 | 165 | 2.06 (9.19) | 1.75 (−4.03 to 7.43) | 61 (37.0) | 61 (37.0) | 43 (26.1) | |
Week 120 | 105 | 0.69 (9.63) | 0.70 (−5.60 to 6.29) | 37 (35.2) | 39 (37.1) | 29 (27.6) | |
Week 144 | 51 | −2.69 (10.34) | −3.81 (−8.60 to 3.63) | 12 (23.5) | 13 (25.5) | 26 (51.0) | |
Week 156 | 30 | −0.18 (9.29) | 0.42 (−4.96 to 6.16) | 10 (33.3) | 11 (36.7) | 9 (30.0) | |
Treatment discontinuation | 66 | −2.03 (10.31) | −2.34 to (−6.44 to 4.01) | 17 (25.8) | 22 (33.3) | 27 (40.9) | |
Placebo (N = 343) | Week 12 | 301 | 2.60 (8.97) | 2.04 (−2.72 to 7.27) | 125 (41.5) | 114 (37.9) | 62 (20.6) |
Week 24 | 275 | 1.94 (10.15) | 1.74 (−4.18 to 7.24) | 114 (41.5) | 89 (32.4) | 72 (26.2) | |
Week 48 | 219 | 2.76 (9.14) | 3.43 (−2.85 to 9.32) | 108 (49.3) | 64 (29.2) | 47 (21.5) | |
Week 72 | 172 | 2.80 (9.06) | 3.18 (−1.99 to 9.10) | 80 (46.5) | 63 (36.6) | 29 (16.9) | |
Week 96 | 124 | 2.82 (9.93) | 1.72 (−2.31 to 9.09) | 55 (44.4) | 42 (33.9) | 27 (21.8) | |
Week 120 | 76 | 2.16 (9.35) | 2.29 (−3.81 to 7.31) | 33 (43.4) | 24 (31.6) | 19 (25.0) | |
Week 144 | 42 | 1.52 (9.97) | 3.93 (−2.90 to 7.42) | 21 (50.0) | 11 (26.2) | 10 (23.8) | |
Week 156 | 25 | 2.54 (11.40) | 5.85 (−0.62 to 8.00) | 14 (56.0) | 6 (24.0) | 5 (20.0) | |
Treatment discontinuation | 109 | −1.76 (11.83) | −1.20 (−9.00 to 4.44) | 32 (29.4) | 30 (27.5) | 47 (43.1) | |
FAS = full analysis set; MCS = Mental Component Summary; PCS = Physical Component Summary; Q1 = first quartile; Q3 = third quartile; SD = standard deviation; SF-36 v2 = Short Form (36) Health Survey version 2.
aCategory of change was considered improved if the change from baseline was an increase of ≥ 3.1 points for the PCS and ≥ 3.8 points for the MCS. Category of change was considered worsened if the change from baseline was a decrease of ≤ 3.1 points for the PCS and ≤ 3.8 points for the MCS. Otherwise, the category of change was considered stable.
Source: Clinical Study Report.13
A conference abstract included in the sponsor’s submission to CADTH reported a post hoc exploratory analysis of HRQoL that was conducted in the overall population.14 For this analysis, the SF-36 was scored using norm-based scoring relative to the 2009 US general population (mean ± standard deviation, 50 ± 10), resulting in t scores. Higher t scores indicate better health. The adjusted mean change in the SF-36 PCS and MCS t scores from baseline to week 96 are depicted in Figure 13.
Figure 13: Adjusted Mean Change From Baseline in SF-36 PCS and MCS T Scores Until Week 96 — FAS, Overall Population (Post Hoc Exploratory Analysis)
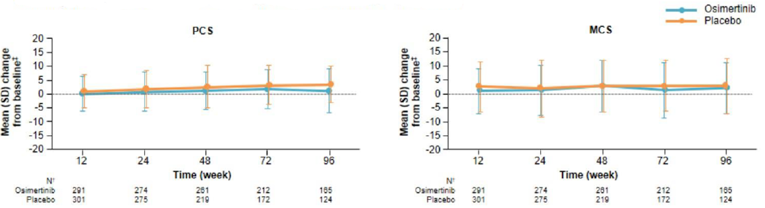
FAS = full analysis set; MCS = Mental Component Summary; PCS = Physical Component Summary; SD = standard deviation; SF-36 = Short Form (36) Health Survey.
Note: t scores were calculated through a linear transformation of 0 to 100 scores to a metric with a mean of 50 and an SD of 10 in the 2009 US general population. Higher t scores indicate better health.
Source: Sponsor’s submission to CADTH.14
The pre-specified TTD analyses of PCS and MCS scores were conducted in the stage II to stage IIIA population only, though these analyses were not adjusted for multiple comparisons. For the PCS score, 58 patients (24.9%) in the osimertinib arm experienced a confirmed deterioration of 3.1 points or greater or death compared with 39 patients (16.5%) in the placebo arm (HR = 1.43; 95% CI, 0.96 to 2.13; P = 0.0817). For the MCS score, 52 patients (22.3%) in the osimertinib arm and 52 patients (21.9%) in the placebo arm experienced a confirmed deterioration of 3.8 points or greater or death (HR = 0.90; 95% CI, 0.61 to 1.33; P = 0.5949). The results suggested no difference between groups in the TTD in either summary score.
Table 22: Summary of TTD in SF-36 v2 PCS and MCS Scores — FAS, Stage II to Stage IIIA Population (Per-Protocol Analysis)
Summary of TTD in SF-36 v2 scores | Osimertinib (N = 233) | Placebo (N = 237) |
|---|---|---|
PCS | ||
Patients with confirmed deterioration or death, n (%) | 58 (24.9) | 39 (16.5) |
Deterioration | 57 (24.5) | 37 (15.6) |
Death | 1 (0.4) | 2 (0.8) |
HR (95% CI)a,b | 1.43 (0.96 to 2.13) | |
2-sided P valuea,c | 0.0817 | |
Median deterioration-free survival (95% CI)d | NR (NR to NR) | NR (NR to NR) |
Proportion of patients who are deterioration-free (95% CI)d | ||
6 months | 78.5 (72.4 to 83.5) | 89.4 (84.4 to 92.8) |
12 months | 76.4 (70.0 to 81.6) | 82.1 (75.5 to 87.1) |
18 months | 74.4 (67.8 to 79.9) | 77.4 (69.8 to 83.4) |
24 months | 72.5 (65.5 to 78.4) | 75.9 (67.7 to 82.3) |
30 months | 70.0 (62.2 to 76.4) | 75.9 (67.7 to 82.3) |
MCS | ||
Patients with confirmed deterioration or death, n (%) | 52 (22.3) | 52 (21.9) |
Deterioration | 51 (21.9) | 49 (20.7) |
Death | 1 (0.4) | 3 (1.3) |
HR (95% CI)a,b | 0.90 (0.61 to 1.33) | |
2-sided P valuea,c | 0.5949 | |
Median deterioration-free survival (95% CI)d | 39.0 (NR to NR) | NR (NR to NR) |
Proportion of patients who are deterioration-free (95% CI)d | ||
6 months | 83.6 (77.9 to 88.0) | 81.1 (75.2 to 85.8) |
12 months | 80.9 (74.8 to 85.6) | 77.1 (70.4 to 82.4) |
18 months | 77.3 (70.6 to 82.7) | 73.4 (66.1 to 79.4) |
24 months | 74.5 (67.3 to 80.4) | 70.7 (62.5 to 77.4) |
30 months | 70.2 (60.9 to 77.8) | 70.7 (62.5 to 77.4) |
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; HRQoL = health-related quality of life; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; MCS = Mental Component Summary; NR = not reached; PCS = Physical Component Summary; SF-36 v2 = Short Form (36) Health Survey version 2; TTD = time to deterioration.
Note: TTD of HRQoL is defined as time from date of randomization to the date of worsening (change from baseline of ≤ −3.1 points for the PCS and ≤ −3.8 points for the MCS) confirmed at the subsequent assessment, or death (by any cause) in the absence of worsening, provided death occurs within 2 assessment visits of the last assessment where HRQoL could be evaluated and regardless of whether the patients withdraws from randomized therapy or receives another anti-cancer therapy before symptom deterioration. Patients with 2 missed visits before confirmed deterioration were censored at the last evaluable assessment before the 2 missed visits.
aThe analysis was performed using a log-rank test stratified by stage (IA vs. II vs. IIIA), race (Asian vs. non-Asian), and mutation type (exon 19 deletions vs. L858R). Stratification factors were as recorded in an interactive voice response system.
bAn HR of less than 1 favours osimertinib. The HR and CI were obtained directly from the U- and V-statistics.
cP value has not been controlled for multiple comparisons.
dCalculated using the Kaplan-Meier method.
Source: Clinical Study Report.13
A conference abstract included in the sponsor’s submission to CADTH included the results of post hoc exploratory analyses of TTD in PCS and MCS in the overall patient population (i.e., stage IB to stage IIIA).14 The TTD curves are depicted in Figure 14. The results of these analyses were consistent with the pre-specified analyses of TTD in the stage II to stage IIIA population for both the PCS score (HR = 0.98; 95% CI, 0.82 to 1.67) and the MCS score (HR = 0.98; 95% CI, 0.70 to 1.39).
Figure 14: TTD in SF-36 v2 PCS and MCS Scores — FAS, Overall Population (Post Hoc Exploratory Analysis)
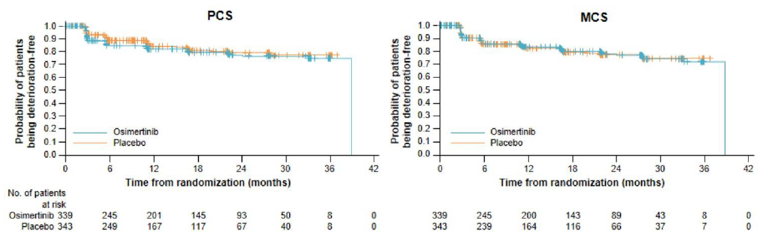
FAS = full analysis set; MCS = Mental Component Summary; PCS = Physical Component Summary; SD = standard deviation; SF-36 v2 = Short Form (36) Health Survey version 2; TTD = time to deterioration.
Note: Deterioration was defined as a change from baseline of ≤ −3.1 points for the PCS and ≤ −3.8 points for the MCS.
Source: Sponsor’s submission to CADTH.14
Harms
Only those harms identified in the CADTH review protocol are reported subsequently. See Table 23 for detailed harms data.
Adverse Events
As of the data cut-off date for the interim analysis, 97.6% of patients in the osimertinib arm and 89.2% of patients in the placebo arm experienced at least 1 treatment-emergent AE (any grade). The most frequently reported AEs in the osimertinib and placebo arms were diarrhea (46.3% and 19.8%, respectively), paronychia (25.2% and 1.5%, respectively), dry skin (23.4% and 6.4%, respectively), pruritis (19.3% and 8.7%, respectively), and cough (18.4% and 16.6%, respectively). Detailed data on AEs reported in 10% or more of patients in either treatment arm by grade is reported in Appendix 2 (Table 27).
Serious Adverse Events
In the ADAURA trial, 16.0% of patients in the osimertinib arm and 12.2% of patients in the placebo arm experienced an SAE as of the interim analysis. The most frequently reported SAEs in the osimertinib and placebo arms were pneumonia (1.5% and 1.2%, respectively), cataracts (0.9% and 0%, respectively), diarrhea (0.6% and 0%, respectively), acute kidney injury (0.6% and 0%, respectively), ureterolithiasis (0.6% and 0%, respectively), and femur fracture (0.6% and 0.3%, respectively).
Withdrawals Due to Adverse Events
Withdrawals from the ADAURA trial specifically due to AEs were not reported. As of the data cut-off for the interim analysis, a total of 33 patients (4.8%) had withdrawn from the trial: 19 (5.6%) in the osimertinib arm and 14 (4.1%) in the placebo arm.
As of the data cut-off date, 10.7% of patients in the osimertinib arm and 2.9% of patients in the placebo arm had discontinued study treatment due to AEs. The most common AEs leading to treatment discontinuation in the osimertinib arm were interstitial lung disease (n = 8; 2.4%), diarrhea (n = 3; 0.9%), and decreased appetite (n = 3; 0.9%). The most common AE leading to treatment discontinuation in the placebo arm was decreased ejection fraction (n = 3; 0.9%).
Mortality
As of the data cut-off date for the interim analysis, 9 patients (2.7%) in the osimertinib arm and 20 patients (5.8%) in the placebo arm had died. The majority of deaths were attributed to NSCLC (9 patients in the osimertinib arm, 18 patients in the placebo arm).
Notable Harms
In the osimertinib arm, 8 patients (2.4%) experienced interstitial lung disease and 2 patients (0.6%) experienced pneumonitis as of the interim analysis. No patients in the placebo arm experienced interstitial lung disease or pneumonitis.
Overall, the frequency of cardiac disorder AEs was greater in the osimertinib arm compared with the placebo arm (11.0% versus 5.2%). Twenty-two patients (6.5%) in the osimertinib arm and 4 patients (1.2%) in the placebo arm experienced QT interval prolongation. Four patients (1.2%) in the osimertinib arm experienced congestive heart failure, cardiac failure, or left ventricular dysfunction compared with none in the placebo arm. Four patients (1.2%) in the osimertinib arm experienced atrial fibrillation compared with 1 (0.3%) in the placebo arm; 6 patients (1.8%) in the osimertinib arm experienced an arrhythmia (other than atrial fibrillation) compared with none in the placebo arm.
Overall, 3 patients (0.4%) experienced keratitis: 2 (0.6%) in the osimertinib arm and 1 (0.3%) in the placebo arm.
Overall, 70.6% of patients in the osimertinib arm and 35.6% of patients in the placebo arm experienced a skin or subcutaneous tissue disorder AE. The most common skin disorders in the osimertinib and placebo arms were paronychia (25.2% and 1.5%, respectively), dry skin (23.4% and 6.4%, respectively), pruritis (19.3% and 8.7%, respectively), and dermatitis acneiform (11.0% and 4.7%, respectively). One patient in the osimertinib arm experienced erythema multiforme. No patients in the ADAURA trial experienced Stevens-Johnson syndrome.
Table 23: Summary of Harms in the ADAURA Trial — Safety Population
Harms | Osimertinib (N = 337) | Placebo (N = 343) |
|---|---|---|
Patients with ≥ 1 AE, n (%) | ||
n (%) | 329 (97.6) | 306 (89.2) |
Most common events, n (%)a | ||
Diarrhea | 156 (46.3) | 68 (19.8) |
Paronychia | 85 (25.2) | 5 (1.5) |
Dry skin | 79 (23.4) | 22 (6.4) |
Pruritis | 65 (19.3) | 30 (8.7) |
Cough | 62 (18.4) | 57 (16.6) |
Stomatitis | 59 (17.5) | 14 (4.1) |
Nasopharyngitis | 47 (13.9) | 35 (10.2) |
Upper respiratory tract infection | 45 (13.4) | 35 (10.2) |
Decreased appetite | 44 (13.1) | 13 (3.8) |
Mouth ulceration | 39 (11.6) | 8 (2.3) |
Dermatitis acneiform | 37 (11.0) | 16 (4.7) |
Patients with ≥ 1 SAE | ||
n (%) | 54 (16.0) | 42 (12.2) |
Most common events, n (%)b | ||
Pneumonia | 5 (1.5) | 4 (1.2) |
Cataracts | 3 (0.9) | 0 |
Diarrhea | 2 (0.6) | 0 |
Acute kidney injury | 2 (0.6) | 0 |
Ureterolithiasis | 2 (0.6) | 0 |
Femur fracture | 2 (0.6) | 1 (0.3) |
Patients who discontinued study treatment due to AEs | ||
n (%) | 37 (11.0) | 10 (2.9) |
Most common events, n (%)b | ||
Interstitial lung disease | 8 (2.4) | 0 |
Diarrhea | 3 (0.9) | 0 |
Decreased appetite | 3 (0.9) | 0 |
Dermatitis acneiform | 2 (0.6) | 0 |
Pruritus | 2 (0.6) | 0 |
Acute kidney injury | 2 (0.6) | 0 |
Fatigue | 2 (0.6) | 0 |
Ejection fraction decreased | 1 (0.3) | 3 (0.9) |
Deathsc | ||
n (%) | 9 (2.7) | 20 (5.8) |
Death related to disease under investigation only | 9 (2.7) | 18 (5.2) |
AE with outcome of death only | 0 | 0 |
Death related to disease and an AE with outcome of death | 0 | 1 (0.3) |
Other | 0 | 1 (0.3) |
Notable harms | ||
Interstitial lung disease, n (%) | 8 (2.4) | 0 |
Pneumonitis, n (%) | 2 (0.6) | 0 |
Cardiac disorders, n (%) | 37 (11.0) | 18 (5.2) |
QT interval prolongation | 22 (6.5) | 4 (1.2) |
Atrial fibrillation | 4 (1.2) | 1 (0.3) |
Arrhythmias (other than atrial fibrillation)d | 6 (1.8) | 0 |
Congestive heart failure, cardiac failure, left ventricular dysfunction | 4 (1.2) | 0 |
Cardiomyopathy | 2 (0.6) | 0 |
Myocardial infarction | 2 (0.6) | 0 |
Keratitis, n (%) | 2 (0.6) | 1 (0.3) |
Skin and subcutaneous tissue disorders, n (%) | 238 (70.6) | 122 (35.6) |
Dermatitis acneiform | 37 (11.0) | 16 (4.7) |
Dry skin | 79 (23.4) | 22 (6.4) |
Erythema multiforme | 1 (0.3) | 0 |
Paronychia | 85 (25.2) | 5 (1.5) |
Pruritus | 65 (19.3) | 30 (8.7) |
Rash | 27 (8.0) | 9 (2.6) |
Skin fissures | 19 (5.6) | 0 |
Stevens-Johnson syndrome | 0 | 0 |
AE = adverse event; SAE = serious adverse event.
aFrequency > 10% in either treatment arm.
bReported in ≥ 2 patients in either treatment arm.
cDeath related to disease under investigation was determined by the investigator.
dIncludes supraventricular arrhythmia, sinus arrhythmia, supraventricular extrasystoles, and ventricular extrasystoles.
Source: Clinical Study Report.13
Critical Appraisal
Internal Validity
The ADAURA trial was double blind to minimize bias. However, it is possible that the investigators and patients could have been unblinded due to the profile of AEs in the osimertinib arm. The primary outcome was DFS, which was assessed by the blinded investigators. Disease recurrence was not assessed by an independent central review committee. EGFR mutations were determined by a central laboratory. The enrolled sample size (N = 682 in overall population; N = 470 in stage II to stage IIIA population) was considered adequate.
Baseline characteristics were balanced between treatment arms and few randomized patients had been lost to follow-up as of the data cut-off date. However, a notable proportion of patients that tested positive for eligible EGFR mutations did not provide consent for further eligibility screening to participate in the trial. The reason(s) why these patients did not sign the main study informed consent form is unknown, and no information is available on how these patients compared with the study population in baseline characteristics. It is possible the exclusion of patients who did not sign the main informed consent form could have introduced selection bias.
Randomization was stratified by disease stage, EGFR mutation type, and race. Randomization was not stratified by prior adjuvant chemotherapy status, which was a subgroup that the clinical experts consulted by CADTH identified as important because adjuvant chemotherapy is known to confer an OS benefit in the patient population under review. However, the treatment arms were balanced with respect to the receipt of prior adjuvant chemotherapy and therefore adjuvant chemotherapy status would not bias the results in favour of either treatment arm. The ADAURA trial employed an intention-to-treat analysis, and efficacy outcomes were analyzed by the log-rank test stratified by disease stage, mutation, and race.
The interim analysis was not planned, and the trial is ongoing. The sponsor performed the interim analysis and was unblinded to treatment allocation at the time of this analysis. However, patients and investigators remain blinded to individual treatment allocations and the study is continuing. The primary end point was met at this interim analysis, since the DFS HR for patients with stage II to stage IIIA disease met statistical significance. The DFS HR for the overall population also met statistical significance at this time. A multiple-testing procedure was employed to control the overall type I error at the 5% 2-sided level for the end points of DFS and OS, which was modified to account for the unplanned interim analyses. At the reported interim analysis, formal statistical testing was done for DFS in the primary stage II to stage IIIA population and overall population, and for OS in the stage II to stage IIIA population, per the multiple-testing procedure. OS in the overall population was not formally tested for statistical significance per the multiple-testing procedure.
Due to the early reporting of the study, data maturity is lower than planned by the sponsor at the interim analysis. At the data cut-off date, the sponsor assessed the OS data to be immature, and assessed the data on time to next treatment and PFS to have limited clinical significance due to the immaturity of the data on patients who experienced a disease recurrence event. In addition, most patients have not had the opportunity to receive the planned study treatment duration of 3 years.
In the ADAURA trial, DFS was the primary outcome and OS was the key secondary outcome. DFS is a reasonable surrogate for OS in this treatment setting. Further details on DFS as a surrogate outcome measure for OS are available in Appendix 3. However, using DFS as an end point has disadvantages, such as including non-cancer deaths and having to balance the timing of assessments among treatment arms. The FDA guidelines recommend clearly defining the DFS end point and outlining the schedule for assessments, including an estimation of the treatment effect size and ensuring blinding of treatment assignments to help to reduce bias.24 In the ADAURA trial, DFS and the schedule of assessments were clearly defined and the trial was double blinded, so investigators were unaware of treatment assignments. The European Medicines Agency recommends that when DFS is the primary end point, OS should be the secondary end point, which was done in the ADAURA trial.25 The final analysis of OS data is planned to be conducted when approximately 94 deaths have been observed in the stage II to stage IIIA population (approximately 20% maturity); therefore, OS data are not yet available from the trial to assess whether the observed DFS benefit translates to a clinically meaningful OS benefit.
Subgroup analyses for DFS were specified a priori and based on stratification variables to maintain randomization. However, they were not adjusted for multiplicity and, therefore, were not considered supportive evidence. The analysis of CNS DFS was performed post hoc and, therefore, should also be considered an exploratory analysis.
The ADAURA trial used the SF-36 v2 to measure HRQoL. The SF-36 is a generic, self-reported health-assessment questionnaire that has been used in clinical trials to study the impact of chronic disease on HRQoL. The SF-36 has been previously validated for a variety of health states and diseases. However, the SF-36 has not been validated in patients with NSCLC and no MID for this population was identified in the literature by CADTH. The SF-36 is less sensitive and responsive to changes when compared with the disease-specific European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and its lung cancer–specific supplement (EORTC QLQ-L13). The clinical experts consulted by CADTH indicated it was appropriate to use a generic HRQoL instrument as opposed to a disease-specific instrument in this setting because patients with resected early-stage NSCLC are expected to have a lower symptom burden relative to patients with late-stage NSCLC. The threshold used by the sponsor to categorize change from baseline as improved, worsened, or stable for the PCS and MCS summary scores was greater than the MID identified in the literature by CADTH. The sponsor did not report its rationale for the MIDs used in its analysis of MCS and PCS. The TTD in MCS and PCS was analyzed as pre-specified secondary end points in the stage II to stage IIIA population only (i.e., patients —not in stage IB). The TTD in MCS and PCS analyses in the overall population were analyzed as an exploratory post hoc analysis and, thus, considered a supportive analysis only. Compliance rates for SF-36 v2 completion were high in both treatment arms. However, the number of expected forms decreased significantly at later time points. This is likely because the trial is ongoing and many patients had not yet reached the later time points, at which the SF-36 forms are collected (median duration of total treatment exposure was less than 2 years in both arms; 12% and 10% of patients in the osimertinib and placebo arms, respectively, had received 3 years of treatment as of the data cut-off date). The small number of patients contributing to the HRQoL analysis at later time points introduces uncertainty in estimates reported at these later time points.
External Validity
The dose and treatment regimen used in the ADAURA trial aligns with the Health Canada indication for osimertinib. However, due to the early reporting at the unplanned interim analysis, the majority of patients in the ADAURA trial had not yet received the recommended treatment duration of 3 years as of the data cut-off date. It is uncertain whether the results of the interim analysis are generalizable to a longer treatment duration of osimertinib (e.g., HRQoL, harms outcomes).
The comparator used in the ADAURA trial was placebo. Following tumour resection and adjuvant chemotherapy, Canadian patients with stage IB to stage IIIA (AJCC 7th edition) NSCLC receive active surveillance. Osimertinib will be the first drug to be used as adjuvant therapy following tumour resection (with or without prior adjuvant chemotherapy); therefore, it was appropriate that the ADAURA trial was placebo-controlled as opposed to active comparator–controlled.
The clinical experts consulted by CADTH thought that the inclusion and exclusion criteria used in the trial were appropriate and generally reflected the characteristics of the intended patient population in Canada. However, the ADAURA trial limited enrolment to patients with a WHO performance status of 0 to 1. The clinical experts noted that this criterion is common for clinical trials in NSCLC, but many patients in Canada with resected stage IA to stage IIIB NSCLC have a performance status of 2. The clinical experts indicated they did not believe the exclusion of patients with worse performance status from the ADAURA trial limits the generalizability of the results; however, the clinical experts did indicate that patients with a performance status of 3 or 4 would be unlikely to receive adjuvant treatment until their performance status improved.
The ADAURA trial included patients who had received standard-of-care adjuvant chemotherapy, which is commonly used in Canadian practice. This also aligns with the intended use for osimertinib in Canada, per the clinical experts consulted by CADTH and per the input from the clinician groups, both of which indicated that osimertinib is not intended to replace adjuvant chemotherapy.
The ADAURA trial enrolled patients with stage IB to stage IIIA disease according to the AJCC 7th edition staging system. The Health Canada indication aligns with the overall trial population (i.e., stage IB to stage IIIA). The primary analysis population in the ADAURA trial was stage II to stage IIIA (i.e., non-IB) patients, and results were reported for the overall population. The clinical experts consulted by CADTH noted that the proportion of patients enrolled in the ADUARA trial with stage IB disease was greater than they expected based on their clinical experience. However, the clinical experts noted that Canadian patients with stage IB disease may not be routinely referred to medical oncologists for adjuvant chemotherapy after surgical resection of their tumours.
In current Canadian practice, patients with early-stage NSCLC are not routinely tested for EGFR mutations. In the ADAURA trial, mutation status was determined by a central laboratory test only. It is unknown whether local laboratory testing would be sufficient, or if there could be discrepancies between results from central versus local laboratory tests, based on the trial data.
In the ADAURA trial, radiological assessments were performed more frequently in the trial than in clinical practice. The clinical experts reported that imaging is performed after surgery or after adjuvant chemotherapy every 4 months to 6 months for the first 2 years and annually thereafter until year 5 in regular clinical practice.
The majority of patients enrolled in the ADAURA trial were Asian. The proportion of Asian patients in the trial is higher than in the Canadian NSCLC population, per the clinical experts consulted by CADTH. However, the clinical experts noted that EGFR mutations are found more frequently in Asian patients. It is possible that the patient population with eligible EGFR mutations in Canada may also have a higher proportion of patients of Asian ethnicity. In addition, the majority of patients enrolled in the ADAURA trial were female. The clinical experts reported that this reflects their clinical experience, because EGFR mutations are more common in females.
The clinical experts noted that the ADAURA trial reported a higher EGFR mutation–positive rate than what is currently seen in Canada, where EGFR genetic testing is routinely offered only to patients with locally advanced or metastatic NSCLC. The clinical experts reported that, in their clinical experience, approximately 15% of Canadian patients test positive for EGFR mutations. The clinical experts noted that the higher rate of EGFR-positive genetic tests observed in the ADAURA trial was likely due to many of the study sites being in countries with larger Asian populations. The proportion of patients in Canada with early-stage NSCLC that are EGFR mutation–positive is unknown because testing is not routinely done in these patients. The EGFR mutation test–positivity rate seen in the ADAURA trial may or may not reflect the eligible patient population in Canada.
The patient advocacy groups that provided input for this review reported that patients value DFS and its association with improved quality of life. Common themes for improved outcomes reported by the patient groups also included desire for a cure, delaying disease recurrence, limiting side effects, and maintaining quality of life. This aligns with the outcomes of DFS and HRQoL assessed by the SF-36 v2 in the ADAURA trial.
The types of subsequent anti-cancer therapies received by patients in the ADAURA trial were generally consistent with current Canadian practice, per the clinical experts consulted by CADTH. The clinical experts noted that most patients in the ADAURA trial who received a subsequent anti-cancer therapy were treated with a TKI, which is consistent with current Canadian practice, although the type of TKIs available may vary across jurisdictions. Platinum-doublet chemotherapy also was received as a subsequent treatment by some ADAURA trial participants, which is used in Canadian practice per the clinical experts. However, the clinical experts indicated they would not use a monoclonal antibody in patients with an EGFR mutation.
Indirect Evidence
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH.
Discussion
Summary of Available Evidence
The systematic review of osimertinib included 1 ongoing phase III RCT. The ADAURA study (N = 682) is an international, multi-centre, phase III, double-blind, placebo-controlled RCT that investigated the efficacy and safety of osimertinib in patients with stage IB to stage IIIA NSCLC (AJCC 7th edition) with a centrally confirmed common-sensitizing EGFR mutation (exon 19 deletion and/or exon 21 [L858R] substitution mutations, either alone or in combination with other EGFR mutations), who have undergone complete tumour resection, with or without post-operative adjuvant chemotherapy. Patients were randomized in a 1:1 ratio to either 80 mg osimertinib orally per day (N = 339) or matching placebo (N = 343). The primary outcome of the ADAURA trial was DFS by investigator assessment. The secondary outcomes were OS and TTD in HRQoL as assessed by the SF-36 v2 summary scores (MCS and PCS) in the stage II to stage IIIA population. Exploratory outcomes included CNS DFS, disease recurrence rate, PFS, time to next treatment, and TTD in HRQoL by the SF-36 v2 summary scores (MCS and PCS) in the overall population (i.e., stage IB to stage IIIA). The ADAURA trial is ongoing, and study results are from an unplanned interim analysis.
Most patients enrolled in the ADAURA trial had stage II to stage IIIA disease, had a WHO performance status of 0, adenocarcinoma histology type, had undergone a lobectomy, had received post-operative adjuvant chemotherapy, and were Asian and female. The mean age of all patients was 62.1 years. Overall, 54.7% of patients had exon 19 deletions and 45.2% had exon 21 (L858R) substitution mutations.
No indirect treatment comparisons or other evidence were included in the sponsor’s submission to CADTH or identified in the literature search.
Interpretation of Results
Efficacy
The results from the ADAURA trial are from an early, unplanned analysis, which limits the interpretation of efficacy results for some outcomes (OS, PFS, time to next treatment, and HRQoL). While the primary analysis was planned to be conducted at 50% DFS data maturity, this early interim analysis was conducted at 33.2% DFS maturity. Furthermore, most patients had not yet received the recommended 3-year treatment duration at the time of the data cut-off date, with an average treatment duration of 21.7 months and 18.6 months in the osimertinib and placebo arms, respectively. The average duration of follow-up was approximately 2 years, and the clinical experts consulted by CADTH indicated that patients with resected early-stage NSCLC are typically followed for 5 years in standard clinical practice. These limitations contribute to the uncertainty regarding the efficacy of osimertinib with respect to outcomes other than DFS.
DFS was considered an important outcome by the clinical panel consulted by CADTH, clinician groups, and the patient advocacy groups that provided input for this review. The ADAURA trial met its primary end point of DFS at the unplanned interim analysis. Osimertinib demonstrated a statistically significant improvement in DFS compared with placebo in both the stage II to stage IIIA (primary analysis) population and the overall population. These results were considered clinically significant by the clinical panel consulted by CADTH and the clinician groups that provided input for this submission. Results of the pre-specified subgroup analyses were consistent with the primary analysis in showing a DFS benefit with osimertinib compared with placebo in all patient subgroups. The clinical experts thought that the results of the supportive subgroup analyses suggest the magnitude of benefit may be smaller in the stage IB population compared with patients with stage II and stage IIIA disease. Furthermore, the clinical experts also thought that the subgroup analyses indicated the magnitude of benefit is larger in the later-stage groups (i.e., II and IIIA), which the clinical experts indicated are at a higher risk of relapse. DFS with recurrence in the CNS only was analyzed post hoc. This exploratory analysis suggested there may be benefit in CNS DFS with osimertinib, although this is associated with uncertainty due to the small number of patients who had events. The clinical panel consulted by CADTH indicated that these results have clinical significance, since CNS metastases are associated with high morbidity; however, firm conclusions cannot be drawn based on these results due to the post hoc nature of the analysis.
The overall disease recurrence rate was lower in the osimertinib arm compared with the placebo arm. In the osimertinib arm, most disease recurrences were local or regional only and the most common sites of recurrence were in the lung and lymph nodes. In the placebo arm, most disease recurrences were distant only or the patients had disease recurrence at both distant and local or regional sites. The most common sites of disease recurrence in the placebo arm were in the lung, lymph nodes, CNS, and bone. The clinical experts consulted by CADTH indicated that the site of disease recurrence is clinically significant because local or regional disease has the potential to be cured, whereas patients with distant metastases cannot be cured.
The clinical panel consulted by CADTH and clinician groups indicated that OS was an equally or more important outcome compared with DFS. It was noted that the relative importance of DFS versus OS is controversial among clinicians who treat NSCLC, and it is uncertain whether benefits in DFS translate into benefits in OS or just delay the time to recurrence. The patient advocacy groups indicated that patients want to be cured but they also value DFS and its association with improved HRQoL. At the time of the data cut-off date for the interim analysis, the OS data were immature, per the sponsor’s assessment (4% of randomized patients had died). The comparison of OS in the stage II to stage IIIA population was not statistically significantly different between the treatment groups. Thus, at the time of this review, it cannot be concluded that osimertinib confers an OS benefit compared with placebo. However, the patients providing input on this submission indicated they value quicker access to treatment and therefore are willing to take osimertinib based on its DFS benefit and do not want to wait for mature OS data to become available. Data on PFS and time to next treatment are also immature, per the sponsor’s assessment. These outcomes were not included in the multiple-testing procedure; thus, the results for these end points are associated with substantial uncertainty and are limited in their statistical and clinical significance.
The patient advocacy groups that provided input for this review emphasized the importance of treatments maintaining HRQoL. Similarly, the clinical panel indicated that the impact of adjuvant osimertinib on HRQoL is important for deciding if the treatment is worthwhile to patients in this setting. HRQoL was measured by the SF-36 v2. The HRQoL end points of interest specified in the study protocol were TTD in the MCS and PCS scores in the stage II to stage IIIA population, which were analyzed as secondary end points but not adjusted for multiple comparisons. Therefore, limited conclusions can be drawn on the effect of osimertinib on HRQoL end points and the results should be considered only as supportive evidence for the primary results of DFS and OS. As of the interim analysis, a numerically greater proportion of patients with stage II to stage IIIA disease in the osimertinib arm experienced a confirmed deterioration in the PCS score of the SF-36 of 3.1 points or greater or death compared with the placebo arm. A numerically similar proportion of patients in each treatment arm experienced confirmed deterioration in the MCS score of the SF-36 greater than the MID or death. The TTD in MCS and PCS scores in the overall population, which aligns with the reimbursement request, were analyzed as a post hoc exploratory analysis and the results were consistent with the results observed in the stage II to stage IIIA population.
Harms
AEs were reported more frequently in the osimertinib arm compared with the placebo arm and most AEs were grade 1 to 2. The overall frequency of AEs in the placebo arm was higher than expected by the clinical experts consulted by CADTH. The most frequently reported AEs in the osimertinib arm were diarrhea, paronychia, dry skin, pruritis, cough, and stomatitis; the most frequently reported AEs in the placebo arm were diarrhea and cough. The incidence of cough in both treatment arms was higher than expected by the clinical experts consulted by CADTH. SAEs were reported more frequently in the osimertinib arm compared with the placebo arm. The most frequently reported SAEs were pneumonia, cataracts, diarrhea, acute kidney injury, ureterolithiasis, and femur fracture. As of the interim analysis, 9 patients (2.7%) in the osimertinib arm and 20 patients (5.8%) in the placebo arm had died. As of the interim analysis, more patients in the osimertinib arm had discontinued study treatment due to AEs compared with the placebo arm.
The product monograph for osimertinib contains warnings and precautions for interstitial lung disease and pneumonitis, QT interval prolongation, left ventricular dysfunction, and cardiomyopathy. Keratitis and skin disorders were also identified as harms of special interest by the clinical experts consulted by CADTH. Interstitial lung disease and pneumonitis occurred in a total of 3% of patients in the osimertinib arm, whereas no patients in the placebo arm experienced these AEs. Cardiac disorders occurred more frequently in the osimertinib arm, including QT interval prolongation. Two patients in the osimertinib arm experienced cardiomyopathy and no patients in either treatment arm experienced congestive heart failure. Keratitis occurred in a small number of patients in both treatment arms. Skin and subcutaneous tissue disorders occurred more frequently in the osimertinib arm compared with the placebo arm, which included dermatitis acneiform, dry skin, paronychia, pruritus, rash, and skin fissures. One patient in the osimertinib arm experienced erythema multiforme and no patients experienced Stevens-Johnson syndrome.
Although the safety data from the ADAURA trial are consistent with the known safety profile of osimertinib, the results are from an unplanned interim analysis and most patients in the ADAURA trial have not yet had the opportunity to receive the planned treatment duration of 3 years. As a result, evaluation of the harms associated with the planned 3-year treatment is limited by the data available at the time of this review.
Conclusions
One ongoing phase III, double-blind, placebo-controlled RCT (ADAURA) provided direct evidence regarding the safety and efficacy of osimertinib adjuvant therapy in adult patients with resected stage IB to stage IIIA (AJCC 7th edition) NSCLC. The trial included patients regardless of whether they had received standard adjuvant chemotherapy. Compared with placebo, patients treated with adjuvant osimertinib showed benefits in DFS. The ADAURA trial met its primary end point at an unplanned interim analysis that showed a statistically significant difference in DFS in both the stage II to stage IIIA population and overall population. This DFS benefit was consistently observed in all pre-specified subgroups. The results did not support conclusions for an effect of osimertinib on OS, PFS, and time to next treatment, and any potential clinical benefit for these outcomes is associated with uncertainty due to the immaturity of the data. Conclusions could not be drawn for the effect of osimertinib on HRQoL end points, as these end points were not adjusted for multiple comparisons. The majority of study participants reported treatment-emergent AEs. A greater proportion of patients in the osimertinib arm experienced an AE compared with the placebo arm. Interstitial lung disease, pneumonitis, cardiac disorders, and skin and subcutaneous tissue disorders were reported more frequently in the osimertinib arm. These AEs are consistent with the known safety profile of osimertinib. Keratitis was uncommon in both treatment arms. A greater number of patients in the osimertinib arm discontinued study treatment due to AEs or because they experienced an SAE. Overall, 4% of study participants had died as of the interim analysis.
References
1.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Toronto, ON: Canadian Cancer Society; 2020: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf?rev=15c66a0b05f5479e935b48035c70dca3&hash=3D51B0D0FB5C3F7E659F896D66495CE8. Accessed 2021 Apr 26.
2.BC Cancer. Lung. 2013; http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-guidelines/lung/lung#Management. Accessed 2021 Jun 3.
3.Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9):2892-2911. PubMed
4.Graham RP, Treece AL, Lindeman NI, et al. Worldwide Frequency of Commonly Detected EGFR Mutations. Arch Pathol Lab Med. 2018;142(2):163-167. PubMed
5.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. PubMed
6.National Comprehensive Cancer Network. Non-small cell lung cancer. (NCCN Clinical practice guidelines in oncology). Plymouth Meeting (PA): National Comprehensive Cancer Network; 2021.
7.Alberta Health Services. Non-small cell lung cancer stage III. (Clinical practice guideline LU-003). 2012: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lu003-nlscs-stage3.pdf. Accessed June 3, 2021.
8.Pignon J-P, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26(21):3552-3559. PubMed
9.Arriagada R, Auperin A, Burdett S, et al. Adjuvant chemotherapy, with or without postoperative radiotherapy, in operable non-small-cell lung cancer: two meta-analyses of individual patient data. Lancet. 2010;375(9722):1267-1277. PubMed
10.Artal Cortés Á, Calera Urquizu L, Hernando Cubero J. Adjuvant chemotherapy in non-small cell lung cancer: state-of-the-art. Translational lung cancer research. 2015;4(2):191-197. PubMed
11.Chouaid C, Danson S, Andreas S, et al. Adjuvant treatment patterns and outcomes in patients with stage IB-IIIA non-small cell lung cancer in France, Germany, and the United Kingdom based on the LuCaBIS burden of illness study. Lung Cancer. 2018;124:310-316. PubMed
12.Tagrisso (osimertinib tablets): 40 mg and 80 mg osimertinib as osimertinib mesylate Epidermal Growth Factor Receptor (EGFR) Tyrosine Kinase Inhibitor[product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Jan 15.
13.Clinical Study Report: D5164C00001. Phase III, double-blind, randomized, placebo-controlled multi-centre, study to assess the efficacy and safety of AZD9291 versus placebo, in patients with epidermal growth factor receptor mutation positive stage IB-IIIA non-small cell lung carcinoma, following complete tumour resection with or without adjuvant chemotherapy (ADAURA) [internal sponsor's report]. Cambridge (GB): AstraZeneca; 2020 Jul 31.
14.Drug Reimbursement Review sponsor submission: tagrisso (osimertinib), 40 mg and 80 mg osimertinib tablets[internal sponsor's package]. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Mar 24.
15.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019. Toronto, ON: Canadian Cancer Society; 2019: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-Cancer-Statistics-2019-EN.pdf?la=en&la=en. Accessed 2021 Apr 26.
16.Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The eighth edition lung cancer stage classification. Chest. 2017;151(1):193-203.
17.Birring SS, Peake MD. Symptoms and the early diagnosis of lung cancer. Thorax. 2005;60(4):268-269. PubMed
18.Ellis PM, Verma S, Sehdev S, Younus J, Leighl NB. Challenges to implementation of an epidermal growth factor receptor testing strategy for non-small-cell lung cancer in a publicly funded health care system. J Thorac Oncol. 2013;8(9):1136-1141. PubMed
19.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
20.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Jul 16.
21.Wu YL, Herbst RS, Mann H, Rukazenkov Y, Marotti M, Tsuboi M. ADAURA: phase III, double-blind, randomized study of osimertinib versus placebo in EGFR mutation-positive early-stage NSCLC after complete surgical resection. Clin Lung Cancer. 2018;19(4):e533-e536. PubMed
22.Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383(18):1711-1723. PubMed
23.Health Canada reviewer's report: Tagrisso (osimertinib mesylate) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: tagrisso (osimertinib), 40 mg and 80 mg osimertinib tablet. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Mar 24.
24.Clinical trial endpoints for the approval of cancer drugs and biologics. (Guidance for industry). Silver Spring (MD): U.S. Food and Drug Administration; 2018: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-trial-endpoints-approval-cancer-drugs-and-biologics. Accessed 2021 Apr 26.
25.Guideline on the clinical evaluation of anticancer medicinal products. London (GB): European Medicines Agency; 2019: https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-evaluation-anticancer-medicinal-products-man-revision-6_en.pdf. Accessed 2021 Apr 26.
26.Mauguen A, Pignon JP, Burdett S, et al. Surrogate endpoints for overall survival in chemotherapy and radiotherapy trials in operable and locally advanced lung cancer: a re-analysis of meta-analyses of individual patients' data. Lancet Oncol. 2013;14(7):619-626. PubMed
27.Savina M, Gourgou S, Italiano A, et al. Meta-analyses evaluating surrogate endpoints for overall survival in cancer randomized trials: A critical review. Crit Rev Oncol Hematol. 2018;123:21-41. PubMed
28.Fiteni F, Westeel V, Bonnetain F. Surrogate endpoints for overall survival in lung cancer trials: a review. Expert Rev Anticancer Ther. 2017;17(5):447-454. PubMed
29.Maruish ME. User's manual for the SF-36v2 health survey; 3rd edition. Lincoln (RD): Quality Metric Incorporated; 2011.
30.Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-483. PubMed
31.Jenkinson C, Stewart-Brown S, Petersen S, Paice C. Assessment of the SF-36 version 2 in the United Kingdom. J Epidemiol Community Health. 1999;53:46-50. PubMed
32.The Short-Form-36 health survey (Rand Corporation and John E. Ware Jr., 1990, revised 1996). Excerpt from Ian McDowell Measuring health: a guide to rating scales and questionnaires. New York (NY): Oxford University Press; 2006: http://www.med.uottawa.ca/courses/CMED6203/Index_notes/SF36%20fn%20.pdf. Accessed 2021 Apr 26.
33.Möller A, Sartipy U. Long-term health-related quality of life following surgery for lung cancer. Eur J Cardiothorac Surg. 2012;41(2):362-367. PubMed
34.Zhang L, Su Y, Hua Y, et al. Validation of EORTC QLQ-LC43 for Chinese patients with lung cancer. Lung Cancer. 2014;85(1):94-98. PubMed
35.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30a(5):635-642. PubMed
36.Pompili C, Brunelli A, Xiume F, et al. Prospective external convergence evaluation of two different quality-of-life instruments in lung resection patients. Eur J Cardiothorac Surg. 2011;40(1):99-105. PubMed
37.Chiu CC, Lee KT, Wang JJ, et al. Preoperative health-related quality of life predicts minimal clinically important difference and survival after surgical resection of hepatocellular carcinoma. J Clin Med. 2019;8(5). PubMed
38.Jayadevappa R, Malkowicz SB, Wittink M, Wein AJ, Chhatre S. Comparison of distribution- and anchor-based approaches to infer changes in health-related quality of life of prostate cancer survivors. Health Serv Res. 2012;47(5):1902-1925. PubMed
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: April 19, 2021
Alerts: Bi-weekly search updates until project completion
Search filters applied: Randomized controlled trials or controlled clinical trials
Limits
No publication date limits
No language limits
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq=# | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(tagrisso* or osimertinib* or AZD-9291 or AZD9291 or mereletinib* or AZ7550 or AZ-7550 or AZ5104 or AZ-5104 or 3C06JJ0Z2O or RDL94R2A16 or NI2ZUZ6F4O or 2DWZ6SE1E1 or Q27162944).ti,ab,ot,kf,hw,nm,rn.
1 use medall
*osimertinib/
(tagrisso* or osimertinib* or AZD-9291 or AZD9291 or mereletinib* or AZ7550 or AZ-7550 or AZ5104 or AZ-5104).ti,ab,kw,dq.
3 or 4
(conference abstract or conference review).pt.
5 not 6
7 use oemezd
2 or 8
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
"Randomized Controlled Trial (topic)"/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
"Controlled Clinical Trial (topic)"/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf,kw.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf,kw.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf,kw.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf,kw.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(pragmatic study or pragmatic studies).ti,ab,hw,kf,kw.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf,kw.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(phase adj3 (III or "3") adj3 (study or studies or trial*)).ti,hw,kf,kw.
or/10-40
9 and 41
remove duplicates from 42
Clinical Trials Registries
ClinicalTrials.gov
Produced by the U.S. National Library of Medicine. Targeted search used to capture registered clinical trials.
Search: Tagrisso (osimertinib) AND Non-small cell lung cancer (NSCLC)
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
Search terms: Tagrisso (osimertinib) AND Non-small cell lung cancer (NSCLC)
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search terms: Tagrisso (osimertinib) AND Non-small cell lung cancer (NSCLC)
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Search terms: Tagrisso (osimertinib) AND Non-small cell lung cancer (NSCLC)
Grey Literature
Search dates: April 13 to April 15, 2021
Keywords: (Tagrisso OR osimertinib OR AZD-9291) AND (Non-small cell lung cancer OR NSCLC)
Limits: No publication date limits
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Detailed Outcome Data
Note this appendix has not been copy-edited.
Table 25: Sensitivity Analysis of DFS for Evaluation-Time Bias — FAS, Stage II to Stage IIIA Population
Group | N | Patients with events, n (%) | Comparison between groupsa | |
|---|---|---|---|---|
HR (95% CI)b | 2-sided P value | |||
Osimertinib | 233 | 26 (11.2) | 0.17 (0.12 to 0.23) | < 0.0001 |
Placebo | 237 | 130 (54.9) | ||
CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; FAS = full analysis set.
a The analysis was performed using a log-rank test stratified by stage (II versus IIIA), race (Asian versus non-Asian), and mutation type (Ex19del versus L858R).
b An HR of less than 1 favours osimertinib. The HR and CI were obtained directly from the U and V statistics.
Source: Clinical Study Report.13
Table 26: Sensitivity Analysis of DFS for Quantitative Interactions — FAS, Stage II to Stage IIIA Population
Sensitivity analysis | Degrees of freedom | P valuea | If significant quantitative or qualitative |
|---|---|---|---|
Global test | — | 0.0609b | — |
EGFR mutation type (Ex19Del / L858R) | 1 | 0.0132 | Quantitativec |
DFS = disease-free survival; FAS = full analysis set.
a Likelihood ratio P values.
b Significance level for interaction test was 10%.
c Quantitative interaction is defined as treatment effects in same direction but of different magnitude.
Source: Clinical Study Report.13
Figure 15: Sensitivity Analysis of DFS for Attrition Bias — FAS, Stage II to Stage IIIA
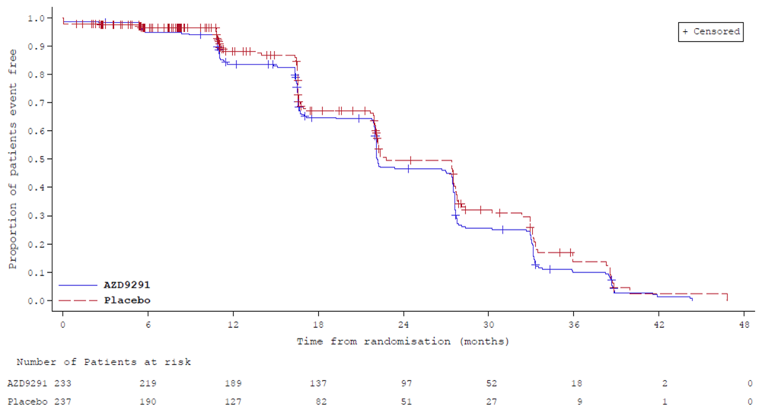
AZD9291 = osimertinib; DFS = disease-free survival; FAS = full analysis set.
Kaplan-Meier plot with censoring and event flags reversed from the primary DFS analysis.
Source: Clinical Study Report.13
Table 27: Adverse Events by Grade Reported in 10% or More of Patients in Either Arm of the ADAURA Trial — Safety Population
Adverse events | Osimertinib (N = 337) | Placebo (N = 343) | ||||
|---|---|---|---|---|---|---|
Any grade | Grade 1 to 2 | Grade ≥ 3 | Any grade | Grade 1 to 2 | Grade ≥ 3 | |
Diarrhea, n (%) | 156 (46.3) | 148 (43.9) | 8 (2.4) | 68 (19.8) | 67 (19.5) | 1 (0.3) |
Paronychia, n (%) | 85 (25.2) | 81 (24.0) | 4 (1.2) | 5 (1.5) | 5 (1.5) | 0 |
Dry skin, n (%) | 79 (23.4) | 78 (23.1) | 1 (0.3) | 22 (6.4) | 22 (6.4) | 0 |
Pruritis, n (%) | 65 (19.3) | 65 (19.3) | 0 | 30 (8.7) | 30 (8.7) | 0 |
Cough, n (%) | 62 (18.4) | 62 (18.4) | 0 | 57 (16.6) | 57 (16.6) | 0 |
Stomatitis, n (%) | 59 (17.5) | 53 (15.7) | 6 (1.8) | 14 (4.1) | 14 (4.1) | 0 |
Nasopharyngitis, n (%) | 47 (13.9) | 47 (13.9) | 0 | 35 (10.2) | 35 (10.2) | 0 |
Upper respiratory tract infection, n (%) | 45 (13.4) | 43 (12.8) | 2 (0.6) | 35 (10.2) | 35 (10.2) | 0 |
Decreased appetite, n (%) | 44 (13.1) | 42 (12.5) | 2 (0.6) | 13 (3.8) | 13 (3.8) | 0 |
Mouth ulceration, n (%) | 39 (11.6) | 39 (11.6) | 0 | 8 (2.3) | 8 (2.3) | 0 |
Dermatitis acneiform, n (%) | 37 (11.0) | 37 (11.0) | 0 | 16 (4.7) | 16 (4.7) | 0 |
Appendix 3: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
DFS as a surrogate outcome for OS
SF-36 v2
Findings
Table 28: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
DFS | A surrogate outcome for OS. | Validity and reliability were demonstrated in studies of patients with operable and locally advanced NSCLC treated with chemotherapy versus no chemotherapy and radiotherapy + chemotherapy versus only radiotherapy. No literature was identified that assessed DFS for responsiveness in populations with NSCLC. | Not identified in populations with NSCLC. |
SF-36 v2 | A 36-item, generic, self-reported questionnaire using a Likert-type scale. It has a recall period of 4 weeks and consists of 8 subscales and 2 component summaries for physical and mental health. Subscale and summary scores range from 0 to 100 where a higher score indicates better HRQoL. | The SF-36 has been previously validated for a variety of health states and diseases. Validity was demonstrated for some subscales, but the SF-36 was less sensitive and responsive to changes when compared with the disease-specific EORTC QLQ. | General population MID:
Not identified in populations with NSCLC. |
DFS = disease-free survival; EORTC QLQ = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; HRQoL = health-related quality of life; MCS = Mental Component Summary; MID = minimal important difference; NSCLC = non–small cell lung cancer; OS = overall survival; PCS = Physical Component Summary; SF-36 v2 = Short Form (36) Health Survey version 2.
Disease-Free Survival as a Surrogate Outcome for Overall Survival
DFS by investigator assessment was the primary outcome used to evaluate the efficacy of osimertinib compared with placebo in the ADAURA trial.13 Radiological assessments for disease recurrence were conducted at 12 weeks, 24 weeks, every 24 weeks until 5 years, and yearly thereafter. DFS was defined as the number of days from the date of randomization to the date of recurrence or death (by any cause) during study treatment (up to 3 years) or beyond treatment discontinuation according to the study plan.
In a guidance document assessing end points used in clinical trials for cancer drugs and biologics, the FDA noted the benefits and drawbacks to using DFS.24 Its advantages include being an objective measure based on quantitative assessment, being evaluable sooner, and needing a smaller sample size compared with studies using OS as an end point. Using DFS as an end point has its disadvantages such as including non-cancer deaths and having to balance the timing of assessments among treatment arms. For the traditional drug approval process (which is based on clinical benefit being demonstrated or the effect on a surrogate end point that is known to predict clinical benefit), DFS has been used in studies for breast cancer, colorectal cancer, gastrointestinal stromal tumours, melanoma, and renal cell carcinoma. The FDA guidelines also recommend clearly defining the end point, outlining the schedule for assessments, including an estimation of the treatment effect size and ensuring blinding of treatment assignments to help to reduce bias. The European Medicines Agency recommends that when DFS is the primary end point, OS should be the secondary end point.25
Mauguen et al. assessed meta-analyses investigating DFS as a surrogate for OS in operable and locally advanced NSCLC.26 In the adjuvant setting, 17 trials (N = 5,379 patients) evaluated chemotherapy versus no chemotherapy while another 7 studies (N = 2,247) assessed radiotherapy and chemotherapy versus just radiotherapy. Individual- and trial-level associations for DFS versus OS were ρ2 (95% CI = 0.83 (0.83 to 0.83) and R2 (95% CI) = 0.92 (0.88 to 0.95), respectively, for the chemotherapy/none studies. For the radio + chemotherapy/radiotherapy studies, ρ2 (95% CI) = 0.87 (0.87 to 0.87) and R2 (95% CI) = 0.99 (0.98 to 1.00). The 3-year DFS compared with the 5-year OS (R2 [95% CI]) were estimated to be 0.88 (0.83 to 0.93) and 0.96 (0.93 to 0.99) for the different adjuvant treatment types.26
Savina et al.27 reviewed meta-analyses evaluating surrogate end points for OS, one of which was the Mauguen et al.26 publication, and found that DFS was a good surrogate for studies investigating colon cancer, operable and locally advanced NSCLC, gastric cancer, and locally advanced head and neck cancer all of which were treated in an adjuvant setting with chemotherapy and/or radiotherapy. Based on the findings in the Mauguen et al.26 publication, Savina et al. concluded the strength of the associations were high as per the German Institute of Quality and Efficiency in Health Care (IQWiG) guidelines and excellent according to the Biomarker-Surrogate Evaluation Schema (BSES) guidelines.27 Fiteni et al. came to similar conclusions that the associations showed high reliability and correlation based on IQWiG guidelines and were valid surrogated end points for a specific disease and intervention class (i.e., level 2) according to the Fleming 4-level hierarchy.28
Also in the review, Mauguen et al. commented that surrogate end points are validated for specific therapies, and in the case of the ADAURA trial of osimertinib, a targeted EGFR-specific treatment, validation would need to be reassessed.26 The investigators also noted additional confounding factors, such as subsequent cancer therapies and treatment crossover in trials, that can impact OS.
Short Form (36) Health Survey Version 2
The SF-36 is a generic, self-reported health-assessment questionnaire that has been used in clinical trials to study the impact of chronic disease on HRQoL.29 There are 2 versions of the instrument, the original SF-3630 and SF-36 version 2 (SF-36 v2).29,31 Compared with the original SF-36, the SF-36 v2 contains minor changes to the original survey, including changes to: instructions (reduced ambiguity), questions and answers (better layout), item-level response choices (increased), cultural/language comparability (increased), and elimination of a response option from the items in the mental health and vitality subscales.29,31 The questionnaire consists of 36 items representing 8 subscales: Physical Functioning (PF; 10 items), Role-Physical (RP; 4 items), Bodily Pain (BP; 2 items), General Health (GH; 5 items), Vitality (VT; 4 items), Social Functioning (SF; 2 items), Role-Emotional (RE; 3 items), and Mental Health (MH; 5 items). The second question of the survey is a single item not used for scoring the 8 scales, but instead used to estimate the general health from a cross-sectional standpoint.32 The SF-36 has a recall period of 4 weeks and item response options are presented on a 3-point to 6-point, Likert-like scale.29,31 Each item is converted to a score ranging from 0 to 100 where a higher value indicates a more favourable health state and item scores are averaged together to create the 8 subscale scores. The SF-36 also provides 2 component summaries, the PCS and the MCS, which are created by aggregating the 8 subscales according to a scoring algorithm. The first 4 subscales (PF, RP, BP, and GH) belong to the PCS while the next 4 subscales (VT, SF, RE, and MH) make up the MCS. Like the individual items, the PCS, MCS, and 8 subscale scores are each measured from 0 to 100. The subscale and summary scores (PCS and MCS) are t scores standardized to a reference population with a mean of 50 and standard deviation of 10.29 Thus, a score of 50 on any scale would be at the average or norm of the reference and a score 10 points lower (i.e., 40) would be 1 standard deviation below the norm.
Möller and Sartipy (2011) conducted a prospective, population-based, cohort study of Swedish patients who had lung surgery and assessed HRQoL using the Swedish version of the SF-36.33 Overall, 166 patients completed the questionnaire before as well as 6 months and 2 years after lung surgery. In total, 69.9% of patients were reported as having stage I to III tumours, 23.5% had received adjuvant chemotherapy, and 4.2% had adjuvant radiotherapy. After 2 years, the patients were compared with an age- and sex-matched reference population. Mean (SD) PCS scores decreased from baseline to 6 months post operation and were similar at 2 years (47.4 [10.3], 41.1 [10.5], and 41.4 [11.6], respectively). The patient PCS score was lower at 2 years compared with the reference population (44.0 [3.9]; P = 0.013). Mean (SD) MCS scores increased for the same 3 timepoints from 40.5 [13.8] to 44.6 [12.6] at 6 months to 46.9 [12.2] at 2 years but were also lower than the reference population (50.6 [1.7]; P = 0.01).
In a 2014 study by Zhang et al., 317 Chinese patients with lung cancer were given the SF-36 and the EORTC QLQ-C30 and supplemental lung cancer–specific module (QLQ-L13).34 While the C30 measures HRQoL in relation to cancer, the LC13 focuses on symptoms and side effects specific to lung cancer and treatment, and both instruments have been validated.34,35 The 2 EORTC QLQs administered together were denoted as the LC43.34 Pearson’s correlation coefficients were calculated between the SF-36 and LC43 and were found to be highest among similar subscales such as 0.675 for PF on either questionnaire, 0.621 for PF of the SF-36 and role functioning of the LC43, 0.567 for both pain subscales, and 0.537 for SF on either questionnaire. Most of the other correlation coefficients were less than 0.5 which could be due to the SF-36 being a measure of general health and not being disease-specific like the LC43.
In a similar manner, Pompili et al. compared the SF-36 with the EORTC QLQ-C30 and LC13 in 33 patients with NSCLC who underwent pulmonary resection.36 The questionnaires were completed before and 3 months after the operation. When assessing the pre- and post-operative changes using Cohen effect size (ES), the investigators found that none of the SF-36 subscales showed a large and clinically meaningful effect (less than −0.8 or greater than 0.8). An average moderate ES (0.5 < |ES| < 0.79) was noted for the PCS and RP scores while all others ESs were small demonstrating limited responsiveness of the SF-36 to changes in patients with NSCLC who have had surgery. To assess convergent validity, correlation coefficients were calculated between the 2 questionnaires. Two subscales had correlations greater than 0.5: the SF of either instrument (0.55) along with the MH of the SF-36 and emotional functioning of the EORTC QLQ-C30 and LC13 (0.57). Again, these results show that the SF-36 may be less sensitive to health changes in patients with lung cancer and that the questionnaires measure different aspects of HRQoL.
For the general population, the SF-36 User’s Manual proposed the following MIDs: a change of 2 points on the PCS, and 3 points on the MCS.29 The manual also suggested the following minimal mean group differences, in terms of t score points, for SF-36 v2 individual subscale scores: PF, 3; RP, 3; BP, 3; GH, 2; VT, 2; SF, 3; RE, 4; and MH, 3. It should be noted that these MIDs were determined as appropriate for groups with mean t score ranges of 30 to 40; for higher t score ranges, values may be higher.29 Furthermore, the MIDs do not represent patient-derived scores. The MIDs for the SF-36 v2 are based on clinical and other non–patient-reported anchors.
Chiu et al. assessed 369 patients in Taiwan who received surgical resection for hepatocellular carcinoma to estimate a MID for the SF-36.37 Using a distribution-based method (one-half SD), they suggested 3.6 points for the PCS and 4.2 points for the MCS. In a separate study of 528 prostate cancer survivors, Jayadevappa estimated MIDs for individual items of the SF-36 using both distribution-based methods (one-half and one-third SD) and anchor-based methods (baseline global health and patient-reported symptoms).38 Mean MIDs using distribution-based methods ranged from 7.0 to 16.1 points while mean estimates from anchor-based methods ranged from 5.0 to 12.4 points. The low and high ends of the ranges were for the Mental Health and Role-Physical items, respectively.
No MID was identified from the literature specific to patients with NSCLC.
Pharmacoeconomic Review
Abbreviations
1L
first-line treatment
2L
second-line treatment
AE
adverse event
BIA
budget impact analysis
DF
disease-free
DFS
disease-free survival
DM
distant metastatic
EGFR
epidermal growth factor receptor
EGFRm
epidermal growth factor receptor–mutated
EQ-5D
Euro-Qol 5 dimensions
ICER
incremental cost-effectiveness ratio
LR
local or regional recurrence
L858R
sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21
NSCLC
non–small cell lung cancer
OS
overall survival
QALY
quality-adjusted life-year
RDI
relative dose intensity
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Osimertinib (Tagrisso), 40 mg and 80 mg tablets, oral |
Submitted price |
|
Indication | As adjuvant therapy after tumour resection in patients with stage IB to stage IIIANSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review, Project ORBIS |
NOC date | January 18, 2021 |
Reimbursement request | As per indication |
Sponsor | AstraZeneca Canada Inc. |
Submission history | Yes Indication: NSCLC
Indication: NSCLC (first-line treatment)
|
EGFR = epidermal growth factor receptor; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation |
|
Target population | Adult patients (aged ≥ 18 years) with completely resected, early-stage EGFR mutation–positive NSCLC |
Treatment | Osimertinib |
Comparator | Active surveillance consisting of no active treatment |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (38 years) |
Key data source | ADAURA trial, a randomized, double-blind, placebo-controlled, multi-centre phase III study evaluating the efficacy of osimertinib as adjuvant therapy following complete tumour resection with curative intent |
Submitted results | ICER = $35,811 per QALY (incremental costs = $114,513; incremental QALYs = 3.20) |
Key limitations |
|
CADTH reanalysis results |
|
1L DM = first-line treatment for distant metastatic disease; 2L DM = second-line treatment for distant metastatic disease; AE = adverse event; DF = disease-free; EGFR = epidermal growth factor receptor; ICER = incremental cost-effectiveness ratio; LR = local or regional recurrence; LY = life-year; NSCLC = non–small cell lung cancer; OS = overall survival; QALY = quality-adjusted life-year; RDI = relative dose intensity.
Conclusions
The CADTH clinical review found that compared with placebo, patients treated with osimertinib showed benefits in disease-free (DF) survival (DFS). However, the results did not support conclusions for an effect of osimertinib on OS, PFS, and time to next treatment, and any potential clinical benefit for these outcomes is associated with uncertainty due to the immaturity of the data.
CADTH undertook reanalyses to address limitations relating to uncertainty in long-term DF status and OS associated with adjuvant osimertinib, time-to-establish cure, subsequent therapies in local or regional recurrence (LR), local or regional disease management costs, radiotherapy and dialysis costs for progressed disease, health state utility values, relative dose intensities (RDIs), and transitions from second-line treatment for distant metastatic disease (2L DM) to death for patients not re-treated with osimertinib. Based on the CADTH reanalysis, the incremental cost-effectiveness ratio (ICER) for osimertinib relative to active surveillance was $328,026 per quality-adjusted life-year (QALY). A reduction of at least 82% in the price of osimertinib is required for osimertinib to achieve an ICER of $50,000 per QALY compared with active surveillance.
Crucially, the cost-effectiveness of osimertinib is contingent on long-term DFS and whether this translates into OS gains. The sponsor’s approach to model the link between DFS and OS is evidence-based and appropriately modelled; however, it lacks data to validate long-term DFS and OS for patients who receive osimertinib in the adjuvant setting. The CADTH clinical review concluded there is substantial uncertainty as to whether osimertinib will generate OS benefit in the adjuvant setting. Longer-term evidence is required to validate what the OS will be for patients taking osimertinib as adjuvant therapy. If relative to active surveillance, osimertinib only delays the rate at which disease progression occurs, then, based on optimistic OS benefits associated with DFS, a price reduction of 72% (log-logistic extrapolation) to 81% (Weibull extrapolation) may be sufficient to achieve cost-effectiveness at a threshold of $50,000 per QALY. If there is no OS benefit, the incremental QALYs generated from osimertinib are substantially less than the CADTH base-case estimate, requiring a price reduction of more than 95% to ensure cost-effectiveness. Conversely, if osimertinib leads to sustained long-term DFS and this translates into long-term overall survival (OS) benefits, then the cost-effectiveness of osimertinib is improved.
CADTH was unable to address limitations related to the model not explicitly incorporating a possibility of cure for patients with LR and incorporating only osimertinib-related adverse events (AEs) in the first month of treatment. Addressing these limitations would likely increase the ICER, making osimertinib less cost-effective. CADTH was unable to address the potential impacts of patients being on adjuvant chemotherapies before osimertinib. If efficacy is believed to be different among those who received prior chemotherapy, then this would have an impact on the cost-effectiveness conclusions. Finally, the impact of re-treatment with osimertinib is highly uncertain due to the lack of evidence as to when patients would be re-treated and how this might impact health outcomes.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from 4 Canadian-based patient groups: the Canadian Cancer Survivor Network (CCSN), Lung Cancer Canada (LCC), the Lung Health Foundation (LHF), and the CanCertainty Coalition (CanCertainty). The CCSN and LCC conducted patient interviews. LHF collected information through an online survey, with responses from 11 patients and 2 caregivers. The LHF also conducted 3 focus groups consisting of patients and caregivers. CanCertainty’s submission was based on published lung cancer statistical reports, Canadian drug coverage, and a past 2017 survey conducted by the group. Overall, patients’ disease experience was influenced by the physical symptoms associated with lung cancer (e.g., fatigue, shortness of breath, cough) and the impact of fear of low survival on their mental health and relationships with others. The patients who responded to the survey had experience with chemotherapy, with reports of side effects, including fatigue, nausea, and appetite loss, and reporting a fear of relapsing after adjuvant chemotherapy. Patients also reported having mostly successful experiences with surgery, apart from 1 respondent whose lifestyle was affected by their reduced lung function after resection. In terms of hopes for improved outcomes with a new therapy, patients expressed a desire for a cure, delayed disease recurrence, and for their quality of life to be maintained. Patients valued DFS with improved quality of life and medications that allow them to maintain their independence. Finally, patients expressed a desire for symptom reduction and management. Patients with experience using osimertinib reported mostly tolerating the medication well, along with some side effects; for 1 patient, side effects resulted in them discontinuing treatment after 4 months. It was also noted that EGFR genetic testing is not readily available until later stages, and an expansion to earlier stages would be helpful in this area.
Input from registered clinicians was received from 2 groups: LCC and the Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee. The clinician input noted that the current care pathway for patients is dependent on their stage after resection, with a minority of patients with stage IB disease offered adjuvant chemotherapy. Fit patients with stage II disease will be offered adjuvant chemotherapy. Patients with stage IIIA disease are offered adjuvant chemotherapy concurrent with radiation followed by complete resection. Some may be offered adjuvant chemotherapy after resection. Clinicians reported that improving OS and quality of life are the main expectations for treatment, but also noted that extending DF time, especially when recurrence is symptomatic, is also valuable. There was also an expressed desire to prevent recurrence. It was noted that osimertinib adjuvant treatment does not replace adjuvant chemotherapy but is an add-on to current care.
Drug plan input considered whether patients would be eligible for re-treatment with osimertinib in the metastatic setting if they had received it as adjuvant therapy. It was also noted that EGFR genetic testing would need to be expanded to identify those eligible for adjuvant osimertinib. Finally, the drug plans noted that, as the ADAURA trial data are immature, the time patients will spend on osimertinib is uncertain, leading to uncertainty in the 3-year budget impact.
Several of these concerns were addressed in the sponsor’s model:
DFS and health state utilities capturing lung cancer symptoms and quality of life were included.
AEs associated with osimertinib were included in the pharmacoeconomic analysis; chemotherapy-related AEs were not.
EGFR genetic testing costs for those receiving osimertinib were included in the analysis.
Patients who progress to distant metastatic disease more than 48 months after initiating osimertinib were eligible for re-treatment.
Time-to-treatment discontinuation extrapolations from the ADAURA trial were used to estimate the duration spent on therapy in the budget impact analysis (BIA).
In addition, CADTH addressed some of these concerns as follows:
incorporating adverse event disutility while remaining on treatment.
Economic Review
The current review is for osimertinib (Tagrisso) as adjuvant therapy for adult patients (aged ≥ 18 years) with stage IB to stage IIIA non–small cell lung cancer (NSCLC) whose tumours have EGFR exon 19 deletions or a sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21 (L858R substitution mutations).1
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of osimertinib adjuvant therapy after tumour resection in patients with stage IB to stage IIIA NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations, compared with active surveillance.1 Both osimertinib-treated and active-surveillance patients could have received adjuvant chemotherapy after resection. The model population comprised adult patients (aged ≥ 18 years) with completely resected, early-stage EGFR mutation–positive, NSCLC, which was aligned with the Health Canada indication.2
Osimertinib is available as a 40 mg or 80 mg tablet. The recommended dose of osimertinib adjuvant therapy is 80 mg orally once daily for up to 3 years or until disease recurrence or unacceptable toxicity.2 At the sponsor’s submitted price of $294.68 per 80 mg tablet, the annual cost of osimertinib adjuvant therapy would be $107,557 if patients remained on therapy for a full year. No drug-acquisition costs were modelled for active surveillance, which was assumed to consist of no active treatment.1 It was noted that some patients would receive adjuvant chemotherapy; however, as osimertinib is an add-on therapy, the cost of any adjuvant chemotherapies would be the same regardless of the decision to use osimertinib. Therefore, no adjuvant chemotherapy costs were applied in the model.
The clinical outcomes of interest were QALYs and life-years. The economic analysis was undertaken over a lifetime (38-year) time horizon from the perspective of a Canadian public health care payer. Discounting (1.5% per annum) was applied to both costs and outcomes.
Model Structure
The sponsor submitted a semi-Markov, multi-state model with 5 mutually exclusive health states with 1-month cycle lengths (4.35 weeks) (Figure 1). All patients begin in the DF health state, where they could remain DF or transition to LR or first-line treatment for distant metastatic disease (1L DM). People with LR could remain in the LR health state or transition to 1L DM. From 1L DM, patients could transition to 2L DM. Patients receiving 2L DM could only transition to death. Patients in any health state could transition to death starting in the first cycle. To incorporate time-varying probabilities in each state, the sponsor used tunnel states so that the probability of transitioning to another state was dependent on how long the patient had spent in a given health state. For example, if a patient spends 4 years in the DF state, the likelihood of them moving to LR and 1L DM falls dramatically, as a proportion of this patient’s cancer is assumed to be cured.
Model Inputs
The model’s baseline population characteristics and clinical efficacy parameters for the adjuvant treatment space were characterized by the ADAURA trial, a randomized, double-blind, placebo-controlled, multi-centre phase III study designed to evaluate the efficacy of osimertinib 80 mg once daily as adjuvant therapy following complete tumour resection with curative intent compared with placebo.3 The sponsor assumed that the ADAURA population (baseline characteristics: mean age = 62.1 years; proportion male = 30%)3 reflected the Canadian population.
Transition probabilities were derived using a variety of data sources, with data from the ADAURA trial being used to model transitions from the DF health state to LR and 1L DM health states.3 Data sources for all transitions are summarized in Table 10. The FLAURA trial, a phase III, double-blind, randomized trial comparing osimertinib with standard of care (either gefitinib or erlotinib) for the first-line treatment of locally advanced or metastatic NSCLC, was used to model transitions from the distant metastatic health states (1L DM to 2L DM and death; 2L DM to death).4 To model transitions from LR to 1L DM, the sponsor selected an “ADAURA-like” cohort of patients with completely resected EGFR-mutated (EGFRm) stage IA to stage IIIB NSCLC from CancerLinQ Discovery, an American database of electronic medical records.1,5
Parametric survival modelling was used to derive health state transition probabilities, with survival distributions being selected based on clinical plausibility of long-term projections, visual inspection of fit, and the Akaike information criterion and Bayesian information criterion.1 A competing-risks approach was taken when modelling transitions from the DF state, as the DF survival curve from ADAURA contained progression and death events. Survival distributions were then transformed into transition probabilities.
The sponsor incorporated a cure assumption for some patients in the DF health states. It was assumed that, among those receiving both adjuvant osimertinib and active surveillance alone, a proportion of patients who remain in the DF state after 4 years will be cured. Patients receiving active surveillance gradually transition to cure over 2 years, whereas this occurs over 5 years for patients who received osimertinib adjuvant treatment. This longer transition-to-cure period is to account for the 36 months patients received osimertinib, during which time no patients would transition to cure. A maximum cure point of 95% was used, meaning that 95% of patients would be assumed to be cured if they remain DF after year 5 and year 8 (for patients receiving active surveillance or osimertinib, respectively). At the point of cure, patients are no longer at risk of death or relapse due to lung cancer, so will have the same outcomes as the general Canadian population.
The model incorporated the possibility of exploring a treatment-waning effect after discontinuation of osimertinib adjuvant therapy. This was not included in the sponsor’s base case because of limited data availability after osimertinib discontinuation in the ADAURA trial.
Mortality among those in the DF state was assumed to be equal to that of the general Canadian population.1 For those in the LR state, mortality was modelled as that of the general Canadian population, with a standardized mortality ratio of 1.26 applied.6 For the distant metastatic states, the sponsor reported that mortality was derived from the time-to-treatment discontinuation data from the FLAURA trial.4 For 1L DM to death, the time-to-treatment discontinuation could not be lower than the risk of death in the LR state (i.e., it was superseded by general population mortality with a standardized mortality ratio of 1.26 applied).1
The grade 3 or greater AEs observed in the ADAURA trial were incorporated into the model with an associated cost and disutility.3 These are applied for the first month only to patients on treatment in the DF state; after 1 month, no additional AEs are applied.
Health state utility values were sourced from the literature. A Canadian study on patients with metastatic NSCLC receiving EGFR tyrosine kinase inhibitors was used. That study found a utility of 0.85 for people using osimertinib in the metastatic setting.7 The sponsor assumed that quality of life would not be worse in the DF setting and, therefore, assumed that the utility of those using osimertinib in the metastatic setting was representative of DF patients. For LR, it was assumed that the utilities would be equal to that of the DF state.1 Utilities for patients receiving 1L DM and 2L DM were sourced from a Canadian study of patients with EGFRm NSCLC.7 All utility values, along with the values examined in the sponsor’s scenario analyses, are in Table 11. Disutilities for AEs were sourced from the literature8,9 and incorporated as a single disutility as a 1-off in the first cycle.
Costs in the model included treatment-acquisition costs for adjuvant osimertinib and subsequent therapies, disease management, AEs, and EGFRm testing. Dosing for osimertinib adjuvant therapy was incorporated by multiplying the price per 80 mg tablet by the number of days in a model cycle (30.44 days) and multiplying that by an RDI of ||||, leading to per-cycle and annual costs of $8,870.55 and $106,082, respectively.1 Treatment costs for subsequent therapies were sourced from IQVIA. Patients who had not progressed 48 months after initiating osimertinib adjuvant therapy could be re-treated with osimertinib upon progression; those who progressed less than 48 months after initiation could not.1 The proportion of patients receiving subsequent therapies and the costs used in the sponsor’s analysis are presented in Table 12.
Disease management costs included those for routine monitoring and were based on real-world studies for LR and distant metastatic health states.10 DF disease management costs were based on a study by the sponsor using the Institute for Clinical Evaluative Sciences database.5 AE costs were sourced from the Ontario Case Costing Initiative and applied as a 1-time cost in cycle 1.11 EGFRm testing costs (sourced from a Cancer Care Ontario report5) were applied in cycle 1 for patients receiving osimertinib adjuvant therapy and when patients receiving active surveillance progressed to distant metastatic disease. The sponsor did not incorporate testing costs for those patients who are tested to assess eligibility for osimertinib but test negative.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,500 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently.
Base-Case Results
Osimertinib adjuvant therapy was associated with a gain of 3.20 QALYs at an additional cost of $114,513, resulting in an ICER of $35,811 compared with active surveillance. The vast majority of the QALY benefit was derived through the life extension occurring after the trial period. The sponsor reported that, compared with active surveillance, osimertinib alone was cost-effective at a willingness-to-pay threshold of $50,000 per QALY in 66.3% of iterations.1
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Total QALYs | Incremental LYs | Incremental QALYs | ICER vs. active surveillance ($/QALY) |
|---|---|---|---|---|---|---|---|
Active surveillance | 247,500 | Reference | 10.32 | 8.57 | Reference | Reference | Reference |
Osimertinib | 362,014 | 114,513 | 14.02 | 11.77 | 3.70 | 3.20 | 35,811 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters in probabilistic scenario analyses. When a shorter (15-year) time horizon was selected, the ICER increased to $64,911. All other scenario analyses resulted in ICERs below $50,000 per QALY.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The impact of osimertinib adjuvant therapy on long-term DFS and OS is uncertain. At 3 years, all patients will discontinue osimertinib. The sponsor’s DFS extrapolations assume a DFS benefit of osimertinib that is sustained indefinitely after osimertinib is discontinued (Figure 2). This results in patients who received osimertinib remaining in a DF state for, on average, an additional 6.23 years compared with those who received active surveillance alone. According to the clinical experts consulted by CADTH for this review, the impact of osimertinib adjuvant therapy on long-term DFS, especially once the 3-year treatment period is completed, is unknown. In addition, the experts indicated it is difficult to know the effect of adjuvant treatment once it is discontinued. If the impact of osimertinib is not sustained after discontinuation, the separation in the DFS curves may not be maintained indefinitely after completion of adjuvant therapy. This makes long-term extrapolation from the trial data challenging, as the trial data are not capturing the long-term impacts for those who discontinue osimertinib, which is 100% of patients after 3 years.
As information on OS in the trial was immature, rather than extrapolating OS based on the trial, the sponsor appropriately used a Markov model to predict long-term outcomes based on progression from the DF state. In the model, once a patient is no longer DF, their survival outcomes are worse. Therefore, the sponsor assumes that, by remaining DF, the probability of death is lower and that patients will live longer. The clinical experts consulted by CADTH felt this assumption was uncertain in the context of osimertinib. They noted it is uncertain whether benefits in DFS translate into benefits in OS, or just delay the time to recurrence. As per the evidence reviewed for this submission, there was no statistically significant evidence that suggested osimertinib conferred a survival benefit relative to active surveillance alone.
To address uncertainty in long-term DFS upon completion of 3 years of adjuvant therapy, in line with clinical expert opinion, the CADTH reanalyses for osimertinib used the Gompertz distribution to extrapolate transitions from DF to LR and DF to 1L DM (Figure 4). In those analyses, CADTH assumed that long-term outcomes are similar between osimertinib and active surveillance; therefore, the proportion of DF patients considered cured is the same in both arms.
To explore the uncertainty around long-term DFS and potential OS benefits, CADTH also ran several scenario analyses where the period of DF survival benefit associated with osimertinib was extended by using the Weibull extrapolations of DFS and, most optimistically, the log-logistic extrapolation, while assuming no difference in long-term cure rates. An additional scenario analysis was conducted that assumed osimertinib leads to a sustained DFS benefit translating into an increase in long-term cure rates.
The time-to-establish cure that was used may be underestimated. In the sponsor’s model, a cure assumption is applied wherein patients in the DF health state transition from being at risk of progression due to lung cancer to having no risk of disease progression and, therefore, having the same health outcomes as the general Canadian population. These transitions start to occur at year 4 in the model. Assuming that a proportion of patients in the DF state are cured is appropriate as, according to the clinical experts consulted for this review, the goal after tumour resection is cure. The clinical experts noted that in Canadian clinical practice, the time-to-establish cure is 5 years after adjuvant chemotherapy, indicating that the time-to-establish cure in the sponsor’s base case is faster than what is seen in clinical practice.
In addition to a proportion of DF patients transitioning to cure, the clinical experts consulted reported that some patients with LR could receive curative-intent treatment, meaning that cure may be possible for a proportion of patients in the LR state. Cure for patients in the LR state was not explicitly examined in the sponsor’s model, as all patients in LR remained at risk of progression to 1L DM.
The CADTH reanalyses adjusted the time to cure from 4 years to 5 years to align with current clinical practice. CADTH was unable to address the lack of incorporation of cure for patients with LR.
Subsequent treatments for LR were not aligned with Canadian clinical practice. In the sponsor’s model, when both osimertinib-treated and active-surveillance patients progress to LR, they may receive subsequent therapies at the frequencies specified in Table 12. According to the clinical experts consulted for this review, the proportion of patients receiving surgery or stereotactic body radiation therapy is much higher in the sponsor’s analysis than what would be expected in Canadian practice. The experts noted that most patients with LR will receive chemoradiotherapy, whereas only 36% of patients in the sponsor’s model receive chemoradiotherapy. It was also noted that the preferred and more commonly used chemoradiotherapy regimen in most Canadian jurisdictions is pemetrexed-cisplatin (CISPPEME) rather than the regime used in the sponsor’s model (etoposide-cisplatin).
The CADTH reanalyses adjusted the distribution of patients across subsequent therapies to align with Canadian clinical practice. These reanalyses also incorporated CISPPEME as the chemoradiotherapy regimen.
Annual disease management costs for the LR health state do not meet face validity. A breakdown of costs by category and overall health state costs are provided in Table 13.
There are several concerns using the disease management costs sourced from Seung et al. (2019).10 First, the costs were for all NSCLC patients rather than just those with EGFR mutations. Second, the population in Seung et al. (2019) may not be generalizable to the population that would receive osimertinib adjuvant therapy, as the ADAURA trial population had a lower median age than the costing study.3,10 Additionally, using the costs for patients with stage III unresectable disease to approximate LR disease management costs may not be appropriate because, as noted by the sponsor, some local recurrence may be resectable and, according to the clinical experts consulted by CADTH for this review, a proportion of patients with LR may be expected to achieve cure. Using costs from Seung et al. (2019) results in higher disease management costs for patients with LR compared with those with distant metastatic disease. According to the clinical experts consulted by CADTH for this review, while disease management costs among those with LR and DM may be similar, they are not expected to be higher, limiting the face validity of these cost estimates.
In addition, several of the cost categories used across health states may be inappropriate. For example, patients in both the DF and LR health states are assigned dialysis costs; however, according to experts, it is not expected that patients in these health states would require dialysis beyond that of the general population. Further, the radiotherapy costs observed in Seung et al. (2019) were applied to the total cancer clinic costs for the LR and DM health states; however, as radiotherapy had been costed as a subsequent therapy, this leads to double counting.
CADTH was unable to find a more appropriate costing source for patients with LR. So, to align with the experts’ feedback that LR costs may be similar to but not higher than costs for DM, the LR costs were set to equal those of DM in the CADTH reanalysis.
To avoid double counting, radiotherapy costs were removed from the total cancer clinic costs; dialysis costs were removed for patients who are DF or have LR, in keeping with the expert’s feedback.
AEs were assumed to occur only in the first month of treatment. AEs were incorporated in the sponsor’s model as a one-off cost and the disutility was applied only during the first cycle of the model. This approach would be appropriate if all AEs emerged within the first month of patients taking osimertinib, and if experiencing an AE caused all patients to discontinue treatment and, therefore, resulted in them no longer experiencing the AE. In the first model cycle, discontinuation for osimertinib is 0.028%, which is less than the overall percentage of osimertinib patients who discontinued treatment due to AEs in the ADAURA trial (11%). Further, patients in the trial continued to discontinue due to AEs after the first month of therapy.
CADTH was unable to account for an ongoing experience of AEs due to difficulties in determining the appropriate time frame during which AEs were experienced, since the trial is ongoing. If AEs are expected to occur beyond the first month of treatment, since AEs occurred in greater frequency in the osimertinib arm compared with active surveillance, this limitation favours osimertinib.
Health state utility values do not meet face validity. The sponsor populated the health state utility values based on the literature (see Table 11 for values and associated sources). DF utility values were based on a confidential retrospective cohort study of patients with metastatic EGFRm NSCLC. That study found a utility value of 0.85 for those with metastatic disease who were treated with osimertinib.5 While this study reports baseline characteristics, the approach used to derive utility values, including the source of the data and measurement methods, is not reported. Further, the resulting utility value, 0.85, is higher than age-specific utility norms (0.842 for those aged 60 to 64).12 According to the clinical experts consulted for this review, patients who are DF following a lung resection who are expected to experience long-term effects from surgery would be expected to have poorer health-related quality of life than that of the general population. This limits the face validity of the DF utility estimate used in the sponsor’s base case, as it suggests that patients receiving osimertinib have better quality of life than the general population.
Utilities for 1L DM, which were based on a retrospective cohort study of patients with EGFRm NSCLC disease treated in an outpatient setting, used the EuroQol 5-Dimensions questionnaire (EQ-5D) and were treatment-specific (0.815 for those receiving osimertinib and 0.756 for those receiving chemotherapy). According to the CADTH Guidelines for the Economic Evaluation of Health Technologies: Canada, treatment-specific utility values are not preferred; instead, it is more appropriate to assign a utility value for the 1L DM health state and then apply any treatment-specific AE-related disutilities, if applicable.7
The sponsor also derived utilities based on ADAURA and FLAURA trial data. The ADAURA trial assessed health-related quality of life using the Short Form (36) Health Survey, which was mapped to EQ-5D values using the UK tariff. Trial-based utility values are presented in Table 11. These values appear to have greater face validity, as the utility for DF is lower than that of the general Canadian population, aligning with clinical expert expectations. Additionally, the trial-based utilities for 1L DM are not treatment-specific and fall between the sponsor’s base-case estimates for those receiving osimertinib versus chemotherapy in 1L DM.
To align with clinical expert expectations of health-related quality of life, age-adjusted trial-based utilities were selected for the CADTH base case.
Time to re-treatment with osimertinib upon progression is uncertain. In the sponsor’s model, re-treatment with osimertinib in the metastatic setting was possible if treatment with osimertinib was successful in the adjuvant setting (i.e., patients do not progress during their 3 years on adjuvant therapy). The sponsor assumed patients may be re-treated with osimertinib if they remained DF for 4 years after initiating adjuvant therapy (i.e., re-treatment was permitted 1 year after successfully completing 3 years of adjuvant therapy). In discussion with clinical experts, there is considerable uncertainty regarding the time to re-treatment with osimertinib due to the limited evidence available. Clinician estimates on the minimum time to re-treatment ranged from re-treating as soon as 3 months to 1 year. The model assumes that patients who are re-treated with osimertinib in the 1L DM setting will have the same outcomes, regardless of whether they have previously received osimertinib in the adjuvant setting. This is highly uncertain and therefore limits the exploration of the impact of re-treatment on cost-effectiveness.
To explore the uncertainty surrounding the time to re-treatment, CADTH explored shortening the time to re-treatment with osimertinib to 3 months after completion of 3-year adjuvant therapy.
The transitions from 2L DM to death are not clinically valid. FLAURA trial data were used to model transitions from 2L DM to death based on whether the patient received osimertinib in the 1L DM setting. Currently, patients who progress to 1L DM will receive osimertinib. However, if osimertinib is administered in the adjuvant setting when patients progress to 1L DM, they may not be re-treated with osimertinib. To account for this, the sponsor assumed that patients who do not receive osimertinib in the 1L DM setting will have survival outcomes associated with the standard-of-care arm of the FLAURA trial. However, post-progression survival was better in the standard-of-care arm of the FLAURA trial, likely due to crossover, meaning that FLAURA patients receiving standard of care had the opportunity for treatment with osimertinib upon progression to 2L DM. This is something that would not be expected to occur in clinical practice.
In the CADTH base case, survival benefits in the FLAURA standard-of-care arm relative to osimertinib, potentially associated with treatment crossover, were removed.
The following limitations were identified but were not deemed key limitations:
The parameterization of uncertainty for osimertinib DFS is inappropriate. The sponsor did not effectively characterize uncertainty in their probabilistic analysis. The model requires the probability of transitioning from DF to LR or DM to be, at worst, equal for osimertinib relative to active surveillance. This assumption restricts the range of survival curves that could be sampled, thus preventing the full range from being considered. There is also likely a correlation between the DFS curves for osimertinib and active surveillance alone. By not incorporating this correlation, the model generates scenarios that likely bias in favour of osimertinib.
CADTH was unable to derive a solution for this limitation that would ensure that uncertainty was characterized properly for osimertinib DFS curves. In the CADTH base case, DFS curves for osimertinib were deterministic; however, the active-surveillance arm remained probabilistic, ensuring that some incremental uncertainty between the 2 treatment options was captured.
The incorporation of RDI is inappropriate. The sponsor incorporated an RDI of ||| for osimertinib adjuvant therapy based on the FLAURA trial. No RDI was reported in the ADAURA trial; therefore, whether this value is applicable in the adjuvant setting is uncertain. Additionally, although patients may miss a dose of osimertinib adjuvant treatment, this might not influence overall costs to public drug plans, as full drug claims will still be dispensed.
The CADTH reanalyses assumed an RDI of 1 for both osimertinib adjuvant therapy and all subsequent therapies.
The difference in cost-effectiveness between an adjuvant and a non-adjuvant setting is uncertain. In the sponsor’s model, there is no option to assess the cost-effectiveness of osimertinib among patients who had received adjuvant chemotherapy versus those who did not. CADTH notes that, as osimertinib is an add-on therapy, the incremental drug cost of osimertinib would be the same, regardless of whether the patient received adjuvant chemotherapy. However, the level of cost-effectiveness may be influenced by whether osimertinib has different efficacy for patients who receive adjuvant chemotherapy relative to those who do not. The CADTH clinical review subgroup analysis noted that the efficacy of osimertinib was similar in those who received adjuvant chemotherapy versus those who did not.
As CADTH could not explore the adjuvant chemotherapy subgroup within the sponsor’s model, the difference in cost-effectiveness of using osimertinib, among patients who received adjuvant chemotherapy versus those who did not, is uncertain.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation Not Noted as Limitations to the Submission
Sponsor’s key assumption | CADTH comment |
|---|---|
Mortality for those in the DF health state was assumed to be equal to that of the general Canadian population. | According to the clinical experts consulted for this review, patients in the DF state who undergo surgical resection of part of their lung may be at increased risk of mortality compared with the general population. However, there is limited evidence to suggest how much greater this increased risk of death might be. |
SMR of 1.26 used for LR to death. | Inappropriate. The 1.26 value is derived from the hazard of mortality due to carrying a BRCA mutation in the absence of melanoma and cancer of the breast, ovary, or prostate6 and is therefore not applicable to the disease area. However, as the clinical experts noted that the true SMR is uncertain and might be close to the SMR used by the sponsor, this assumption was not expected to influence model results. |
BRCA = breast cancer gene; DF = disease-free; LR = local or regional recurrence; SMR = standardized mortality ratio.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH reanalyses addressed several limitations within the economic model, which are summarized in Table 5. CADTH was unable to address the limitations regarding the cure of patients with LR, having AEs occur beyond the first month of treatment, and having the cost-effectiveness of osimertinib assessed according to the prior receipt of adjuvant chemotherapy.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
Drug costs | Included in PSA | Removed from PSA |
Gompertz curve | Included in PSA | Removed from PSA |
Changes to derive the CADTH base case | ||
1.Survival extrapolation: DF to LR | Generalized gamma | Gompertz + equal long-term cure |
2. Survival extrapolation: DF to 1L DM | Generalized gamma | Gompertz + equal long-term cure |
3. Time-to-establish cure | 4 years | 5 years |
4. Distribution and type of subsequent treatments for LR | 26.1% SBRT, 14.1% surgery and 19.6% BSC; 35.8% for chemoradiotherapy (cisplatin-etoposide) | 5% for SBRT, surgery and BSC; 80.6% for chemoradiotherapy (CISPPEMEb) |
5. LR costs | Higher than DM costs ($16,687 annually) | Equal to DM costs ($12,419 annually) |
6. Dialysis and radiotherapy costs for DF and LR | Included | Excluded |
7. Health state utility values | Literature-based (Table 11) | Trial-based (Table 11) and age-adjusted |
8.RDI | ||% | 100% |
9.Transitions from 2L DM to death for patients who do not receive osimertinib in the 1L DM setting | Incorporated survival benefits in the 2L DM state potentially associated with treatment crossover in the FLAURA trial | Removed survival benefits in the 2L DM state potentially associated with treatment crossover in the FLAURA trial |
CADTH base case | — | 1 + 2 + 3 + 4 + 5 + 6 + 7 + 8 + 9 |
1L DM = first-line treatment for distant metastatic disease; 2L = second-line treatment for distant metastatic disease; AE = adverse event; BSC = best supportive care; DF = disease-free; LR = local or regional recurrence; PSA = probabilistic sensitivity analysis; RDI = relative dose intensity; SBRT = stereotactic body radiation therapy.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or standard errors in probabilistic analyses) that are not identified as limitations.
bCISPPEME regimen: pemetrexed 500 mg/m2 + cisplatin 75 mg/m2 every 21 days for 3 cycles.13
The results of CADTH’s stepped analysis are presented in Table 6. CADTH’s base-case reanalysis demonstrates that, compared with active surveillance, adjuvant treatment with osimertinib is $165,781 more expensive and yields 0.51 greater QALYs, resulting in an ICER of $328,026 (Table 6). Changing the survival curve to extrapolate progression from DF to 1L DM resulted in the largest change to the sponsor’s base case. The majority (85%) of the total costs for osimertinib are treatment-acquisition costs. All of the QALY gain for osimertinib compared with standard of care occurs in the DF health state (Table 14). Of the total 8.11 QALYs associated with osimertinib treatment, 2.35 are accrued during the 3 years of adjuvant treatment. At a $50,000 per-QALY threshold, there is a 0% chance that osimertinib is cost-effective.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total LYs | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|---|
Sponsor’s base case (deterministic) | Active surveillance | 247,832 | 10.31 | 8.56 | Reference |
Osimertinib | 369,380 | 14.10 | 11.84 | 37,028 | |
CADTH reanalysis | |||||
1.DF to LR Gompertz | Active surveillance | 247,832 | 10.31 | 8.56 | Reference |
Osimertinib | 382,152 | 13.69 | 11.47 | 46,076 | |
2.DF to 1L DM Gompertz | Active surveillance | 247,832 | 10.31 | 8.56 | Reference |
Osimertinib | 380,020 | 12.19 | 10.16 | 82,371 | |
3.Time-to-establish cure = 5 years | Active surveillance | 258,802 | 9.99 | 8.28 | Reference |
Osimertinib | 384,584 | 13.71 | 11.50 | 39,100 | |
4.Distribution and type of subsequent treatments for LR | Active surveillance | 246,140 | 10.31 | 8.56 | Reference |
Osimertinib | 368,050 | 14.10 | 11.84 | 37,138 | |
5.LR disease management costs | Active surveillance | 243,997 | 10.31 | 8.56 | Reference |
Osimertinib | 366,435 | 14.10 | 11.84 | 37,300 | |
6.Removing dialysis costs | Active surveillance | 249,585 | 10.31 | 8.56 | Reference |
Osimertinib | 384,080 | 14.10 | 11.84 | 41,035 | |
7.HSUVs trial-based + age-adjusted | Active surveillance | 247,832 | 10.31 | 7.84 | Reference |
Osimertinib | 369,380 | 14.10 | 10.75 | 41,753 | |
8.RDI 1 | Active surveillance | 249,624 | 10.31 | 8.56 | Reference |
Osimertinib | 372,755 | 14.10 | 11.84 | 37,511 | |
9.2L DM to death based on FLAURA osimertinib arm | Active surveillance | 247,832 | 10.31 | 8.56 | Reference |
Osimertinib | 367,795 | 13.98 | 11.76 | 37,510 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7 + 8 + 9): deterministic | Active surveillance | 253,382 | 9.99 | 7.60 | Reference |
Osimertinib | 420,768 | 10.54 | 8.05 | 368,532 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7 + 8 + 9): probabilistic | Active surveillance | 253,304 | 10.00 | 7.60 | Reference |
Osimertinib | 419,085 | 10.62 | 8.11 | 328,026 | |
1L = first-line treatment for distant metastatic disease; 2L = second-line treatment for distant metastatic disease; DF = disease-free; HSUV = health state utility value; ICER = incremental cost-effectiveness ratio; LR = local or regional recurrence; LY = life-year; QALY = quality-adjusted life-year; RDI = relative dose intensity.
Note: Results of all steps are presented deterministically. The cumulative CADTH base case is presented probabilistically, as well.
Scenario Analysis Results
CADTH undertook price-reduction analyses in the CADTH base case (Table 7). These analyses demonstrated that a price reduction of 82% would be required for osimertinib to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY. CADTH noted that if the deterministic results were used, the price reduction required increases to 84%.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for osimertinib vs. active surveillance | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $35,811 | $328,026 |
10% | NA | $298,906 |
20% | NA | $263,816 |
30% | NA | $224,236 |
40% | NA | $193,735 |
50% | NA | $160,301 |
60% | NA | $124,027 |
70% | NA | $87,914 |
80% | NA | $53,248 |
90% | NA | $19,745 |
ICER = incremental cost-effectiveness ratio; NA = not applicable; vs. = versus.
To address remaining uncertainty regarding the parameterization of the model, CADTH conducted several scenario analyses. Full results are presented in Table 15. In a scenario analysis in which time to re-treatment is 3 months after completion of 3 years of adjuvant therapy, the ICER decreased slightly to $299,795. This is because more patients who received osimertinib as first-line treatment received it when they developed distant metastatic disease, and this improved their health outcomes. This scenario analysis is very limited due to uncertainty associated with health outcomes for patients re-treated with osimertinib. CADTH also conducted several reanalyses using alternative survival extrapolation choices for DF to 1L DM and DF to 2L DM. Figure 7 and Figure 9 present DFS and OS, respectively, for an analysis that used the Weibull extrapolation while assuming no long-term difference in cure. This extrapolation led to a lower ICER than in the CADTH base case ($282,166 per QALY gained). Under these assumptions, an 81% price reduction would be required to achieve an ICER below $50,000 per QALY.
Figure 8 and Figure 10 present DFS and OS, respectively, for an analysis that used the log-logistic extrapolation while also assuming no difference in long-term cure rates. While assuming no difference in long-term cure rates, this extrapolation led to the most optimistic DFS and OS outcomes and a lower ICER than in the CADTH base case ($197,367 per QALY gained). Under these assumptions, a 72% price reduction would be required to achieve an ICER below $50,000 per QALY.
CADTH also conducted a reanalysis that used a Weibull survival distribution to extrapolate long-term DFS while also assuming that osimertinib leads to sustained DFS benefits, with more patients achieving a cure (Figure 6). This leads to a lower ICER of $141,330 per QALY. However, according to the clinical experts, the likelihood of an increased long-term cure rate was deemed too uncertain based on current available evidence.
Issues for Consideration
Osimertinib has been previously reviewed by CADTH for the treatment of patients with locally advanced or metastatic NSCLC that is positive for the amino acid substitution from a threonine to a methionine at position 790 in EGFR (the EGFR T790M mutation) that has progressed on or after therapy with an EGFR tyrosine kinase inhibitor,14 and for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have other EGFR mutations.15 These reviews were at the same submitted price as this submission (i.e., $294.68 per 40 mg or 80 mg tablet). Both reviews received a recommendation for reimbursement with clinical criteria and/or conditions.14,15 These conditions included improvement of the cost-effectiveness of osimertinib.14,15
Availability of osimertinib as adjuvant therapy will require EGFRm testing in the post-resection period. Currently, this testing is typically done only upon progression to distant metastatic disease. As some post-resection patients may go on to be cured, this will result in an overall greater number of patients undergoing EGFRm testing to determine eligibility for osimertinib compared with the current testing paradigm. If testing costs $300 and prevalence is 15%, then it will cost $2,000 to find a patient eligible for treatment. Currently, testing costs are incurred when a patient has distant metastasis so the incremental cost of testing will be dependent on how many additional patients will be tested. If testing was not done in the DM setting, then the incremental cost of testing would be $2,000 per patient.
Overall Conclusions
The CADTH clinical review found that, compared with placebo, patients treated with osimertinib showed benefits in DFS. However, the results did not support conclusions for an effect of osimertinib on OS, PFS, and time to next treatment, and any potential clinical benefit for these outcomes is associated with uncertainty due to the immaturity of the data.
CADTH undertook reanalyses to address limitations relating to uncertainty in long-term DF status and OS associated with adjuvant osimertinib, time-to-establish cure, subsequent therapies in LR, local or regional disease management costs, radiotherapy and dialysis costs for progressed disease, health state utility values, RDIs, and transitions to death from 2L DM for patients not re-treated with osimertinib. Based on the CADTH reanalysis, the ICER for osimertinib relative to active surveillance was $328,026 per QALY. A reduction of at least 82% in the price of osimertinib is required for osimertinib to achieve an ICER of $50,000 per QALY compared with active surveillance.
Crucially, the cost-effectiveness of osimertinib is contingent on long-term DFS and whether this translates into OS gains. The sponsor’s approach to model the link between DFS and OS is evidence-based and appropriately modelled; however, it lacks data to validate long-term DFS and OS for patients who receive osimertinib in the adjuvant setting. The CADTH clinical review concluded there is substantial uncertainty as to whether osimertinib will generate OS benefit in the adjuvant setting. Longer-term evidence is required to validate what the OS will be for patients taking osimertinib as adjuvant therapy. If osimertinib only delays the rate at which disease progression occurs relative to active surveillance, then, based on optimistic OS benefits associated with DFS, a price reduction of 72% (log-logistic extrapolation) to 81% (Weibull extrapolation) may be sufficient to achieve cost-effectiveness at a $50,000 per-QALY threshold. Without any OS benefit, the incremental QALYs generated from osimertinib are substantially less than the CADTH base-case estimate, requiring a price reduction of more than 95% to ensure cost-effectiveness. Conversely, if osimertinib leads to sustained long-term DFS and this translates into long-term OS benefits, then the cost-effectiveness of osimertinib is improved.
In the model, after a patient moves from the DF state, all subsequent outcomes are generated from evidence outside of the trial due to the lack of follow-up data. Obtaining evidence from other sources is necessary and the sponsor has taken the correct approach in deriving sources of evidence. However, in the sponsor’s analysis, the majority (79%) of QALY gains are incurred after 3 years, which further increases the uncertainty of the cost-effectiveness conclusions.
CADTH was unable to address limitations relating to the model not incorporating a possibility of cure for some patients with LR, and related to having AEs occur only in the first month of treatment. Addressing these limitations would likely increase the ICER, making osimertinib less cost-effective. CADTH was unable to address the potential impacts of patients being on adjuvant chemotherapies before osimertinib. If efficacy is believed to be different among those who received prior chemotherapy, then this would have an impact on the conclusions regarding cost-effectiveness. Finally, the impact of re-treatment with osimertinib is highly uncertain due to the lack of evidence as to when patients would be re-treated and how this might impact health outcomes.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: tagrisso (osimertinib), 40 mg and 80 mg osimertinib tablets. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Mar 24.
2.Tagrisso (osimertinib tablets): 40 mg and 80 mg osimertinib as osimertinib mesylate Epidermal Growth Factor Receptor (EGFR) Tyrosine Kinase Inhibitor [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Jan 15.
3.Clinical Study Report: D5164C00001. Phase III, double-blind, randomized, placebo-controlled multi-centre, study to assess the efficacy and safety of AZD9291 versus placebo, in patients with epidermal growth factor receptor mutation positive stage IB-IIIA non-small cell lung carcinoma, following complete tumour resection with or without adjuvant chemotherapy (ADAURA) [internal sponsor's report]. Cambridge (GB): AstraZeneca; 2020 Jul 31.
4.Soria J-C, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N Engl J Med. 2017;378(2):113-125. PubMed
5.Drug Reimbursement Review sponsor submission: tagrisso (osimertinib), 40 mg and 80 mg osimertinib tablets [internal sponsor's package]. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Mar 24.
6.Mai PL, Chatterjee N, Hartge P, et al. Potential excess mortality in BRCA1/2 mutation carriers beyond breast, ovarian, prostate, and pancreatic cancers, and melanoma. PLoS One. 2009;4(3):e4812. PubMed
7.Jiang SX, Walton RN, Hueniken K, et al. Real-world health utility scores and toxicities to tyrosine kinase inhibitors in epidermal growth factor receptor mutated advanced non-small cell lung cancer. Cancer Med. 2019;8(18):7542-7555. PubMed
8.Nafees B, Lloyd AJ, Dewilde S, Rajan N, Lorenzo M. Health state utilities in non-small cell lung cancer: An international study. Asia Pac J Clin Oncol. 2017;13(5):e195-e203. PubMed
9.National Institute for Health and Care Excellence. Osimertinib for treating EGFR T790M mutation-positive advanced non-small-cell lung cancer. (Technology appraisal guidance TA653) 2020; https://www.nice.org.uk/guidance/ta653. Accessed 2021 Jun 8.
10.Seung SJ, Hurry M, Hassan S, Walton RN, Evans WK. Cost-of-illness study for non-small-cell lung cancer using real-world data. Curr Oncol. 2019;26(2):102-107. PubMed
11.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2021 Jun 8.
12.Guertin JR, Feeny D, Tarride J-E. Age-and sex-specific Canadian utility norms, based on the 2013–2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
13.CISPPEME Regimen: CISplatin-Pemetrexed. (Regiment monograph). Toronto (ON): Cancer Care Ontario: https://www.cancercareontario.ca/sites/ccocancercare/files/CISPPEME_LU_NSC_A.pdf. Accessed 2021 Jun 8.
14.CADTH pCODR Expert Review Committee (pERC) final recommendation: osimertinib (Tagrisso). Ottawa (ON): CADTH; 2017 May 4: https://www.cadth.ca/sites/default/files/pcodr/pcodr_osimertinib_tagrisso_nsclc_fn_rec.pdf. Accessed 2021 Jun 9.
15.CADTH pCODR Expert Review Committee (pERC) final recommendation: osimertinib (Tagrisso). Ottawa (ON): CADTH; 2019 Jan 4: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10137OsimertinibNSCLC_FnRec_2019-01-02_ChairApproved_Post_04Jan2019_final.pdf. Accessed 2021 Jun 9.
16.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 Jun 8.
17.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: tagrisso (osimertinib), 40 mg and 80 mg osimertinib tablets. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Mar 24.
18.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics-A 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-cancer-statistics-2020_special-report_EN.pdf?la=en&la=en. Accessed 2021 Apr 6.
19.Statistics Canada. Population estimates on July 1st, by age and sex. Table: 17-10-0005-01 2020; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501&pickMembers%5B0%5D=1.1&pickMembers%5B1%5D=2.1&cubeTimeFrame.startYear=2020&cubeTimeFrame.endYear=2020&referencePeriods=20200101%2C20200101. Accessed 2021 Jun 22.
20.Canadian Cancer Society. Cancerous tumours of the lung. [2021]; https://www.cancer.ca/en/cancer-information/cancer-type/lung/lung-cancer/cancerous-tumours/?region=on. Accessed 2021 May 12.
21.Canadian Partnership Against Cancer. Lung. Stage distribution. [2013]; https://www.systemperformance.ca/disease-sites/lung/stage-distribution/#!figures. Accessed 2021 May 12.
22.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. PubMed
23.Russo A, Franchina T, Ricciardi G, Battaglia A, Picciotto M, Adamo V. Heterogeneous responses to Epidermal Growth Factor Receptor (EGFR) tyrosine kinase inhibitors (TKIs) in patients with uncommon EGFR mutations: new insights and future perspectives in this complex clinical scenario. Int J Mol Sci. 2019;20(6). PubMed
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and, as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Adjuvant Therapies After Tumour Resection in Patients With Stage IB to Stage IIIA Non–Small Cell Lung Cancer
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cycle cost ($) |
|---|---|---|---|---|---|---|
Osimertinib (Tagrisso) | 40 mg 80 mg | Tablet | 294.6764 294.6764 | 80 mg once daily | 294.68 | 8,251 |
Note: All prices are from the Ontario Drug Benefit Formulary Exceptional Access Program (accessed May 2021), unless otherwise indicated, and do not include dispensing fees.16
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | Yes | CADTH agrees with the appropriateness of choosing a Markov model structure rather than a partition survival model. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Fixed costs were included in PSA. Many parameters varying by 10% rather than standard error. CADTH noted incorporation of uncertainty around DFS curves were biased due to imposed assumptions around cure and influence of comparator curves. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
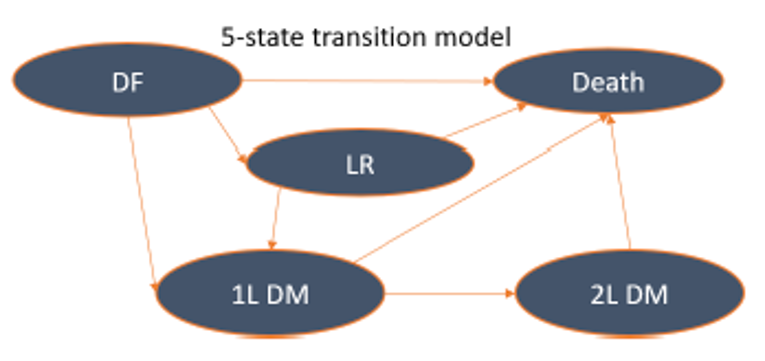
1L = first-line treatment; 2L = second-line treatment; DF = disease-free; DM = distant metastatic; LR = local or regional recurrence.
Source: Sponsor’s pharmacoeconomic submission.1
Table 10: Data Sources and Sponsor’s Distribution Choices for Health State Transitions
TP | Transition | Data source | Sponsor’s selected survival distribution |
|---|---|---|---|
TP1 | DF to LR | ADAURA | Generalized gamma |
TP2 | DF to 1L DM | ADAURA | Generalized gamma |
TP3 | DF to death | Canadian life tables | NA |
TP4 | LR to 1L DM | CancerLinQ ADAURA-like cohort | Lognormal |
TP5 | LR to death | Canadian life tables + SMR of 1.26 | NA |
TP6 | 1L DM to 2L DM | FLAURA | Weibull |
TP7 | 1L DM to death | FLAURA | Exponential |
TP8 | 2L DM to death | FLAURA | Weibull |
1L DM = first-line treatment for distant metastatic disease; 2L DM = second-line treatment for distant metastatic disease; DF = disease-free; LR = local or regional recurrence; NA = not applicable; TP = transition probability.
Table 11: Health State Utility Values
Health state | Sponsor’s base-case utility value | Trial-based utilities |
|---|---|---|
Disease-free | 0.85 (confidential quality of life study)5 | 0.8253 |
Local or regional recurrence | 0.85 (assumed same as DF) | 0.825 (Assumed same as DF) |
First-line distant metastatic | 0.815 (osimertinib) 0.756 (standard of care) (Jiang, 2019)7 | 0.7944 |
Second-line distant metastatic | 0.678 (Jiang, 2019)7 | 0.6404 |
Table 12: Subsequent Therapies Received by Health State and Initial Treatment in the DF State
Treatment | Percentage of patients receiving | Cost per cycle ($) |
|---|---|---|
Local/regional recurrence | ||
Chemoradiotherapy (platinum doublet chemotherapy consisting of etoposide + cisplatin for 2 cycles with or without 1 course of radiotherapy) | 35.8% | Chemo: 935.96 Radiotherapy: 3,355.70 |
Chemotherapy (cisplatin monotherapy) for 2 treatment cycles with or without 1 course of radiotherapy | 4.4% | 587.10 |
SBRT | 26.1% | 38,030.36 |
Surgery | 14.1% | 19,003.56 |
BSC alone (i.e., no anticancer therapy) | 19.6% | 0 |
Total | 100% | NA |
First-line distant metastatic recurrence | ||
Active surveillance patients & patients who progress to DM1 later than 48 months of osimertinib | ||
Osimertinib | 95% | 8,870.55 |
BSC | 5% | 0 |
Total | 100% | NA |
Osimertinib adjuvant patients to progress to DM1 before 48 months of osimertinib | ||
Cisplatin plus pemetrexed for up to 6 treatment cycles followed by maintenance pemetrexed monotherapy until progression | 29% | 5,988.80 Maintenance: 5,596.15 |
BSC | 71% | 0 |
Total | 100% | NA |
Second-line distant metastatic recurrence | ||
Active surveillance patients and patients who progress to 1L DM after 48 months of osimertinib | ||
Cisplatin plus pemetrexed for up to 6 treatment cycles followed by maintenance pemetrexed monotherapy until progression | 29% | 5,988.80 Maintenance: 5,596.15 |
BSC | 71% | 0 |
Total | 100% | NA |
Osimertinib adjuvant patients to progress to 1L DM before 48 months of Osimertinib | ||
Docetaxel | 31% | 2,318.02 |
BSC | 69% | 0 |
Total | 100% | NA |
1L DM = first-line treatment for distant metastatic disease; BSC = best supportive care; NA = not applicable.
Table 13: Health Care Resource Use and Disease Management Costs
Health care resource use | DFS ($) | Per year | |||||
|---|---|---|---|---|---|---|---|
Year 1 | Year 2 | Year 3 | Year 4 | Year 5+ | LR | 1LDM + 2L DM | |
Cancer clinic total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 5,390.55 | 2,562.76 |
Complex continuing care total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 763.18 | 640.71 |
Dialysis total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 194.87 | 194.87 |
Emergency department total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 368.63 | 293.35 |
Inpatient hospitalization total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 4,818.32 | 4,579.92 |
Laboratory (OHIP) total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 137.71 | 137.71 |
Non-physician (OHIP) total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 926.88 | 912.23 |
Outpatient total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 1,130.95 | 838.44 |
All OHIP Costs (GP + Spec + Shadow billing) | ||||| | ||||| | ||||| | ||||| | ||||| | 2,505.08 | 2,042.84 |
Rehabilitation (inpatient) total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 156.90 | 110.05 |
Same-day surgery total costs | ||||| | ||||| | ||||| | ||||| | ||||| | 294.39 | 106.58 |
Total cost per year | ||||| | ||||| | ||||| | ||||| | ||||| | 16,687.45 | 12,419.46 |
Total cost per cycle | ||||| | ||||| | ||||| | ||||| | ||||| | 1,390.62 | 1,034.96 |
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
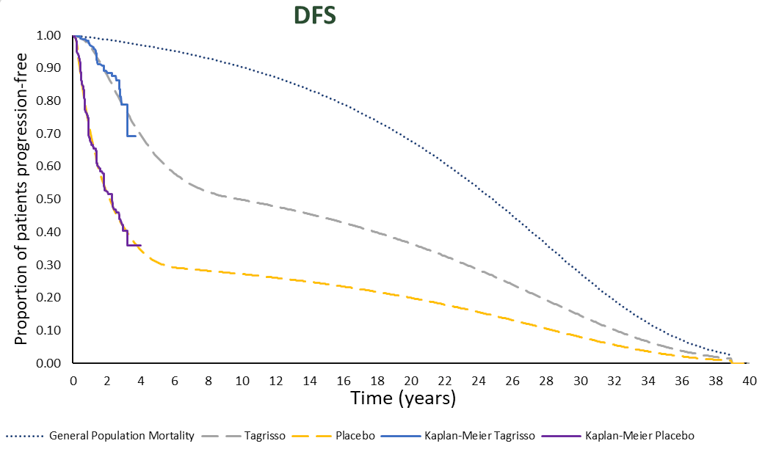
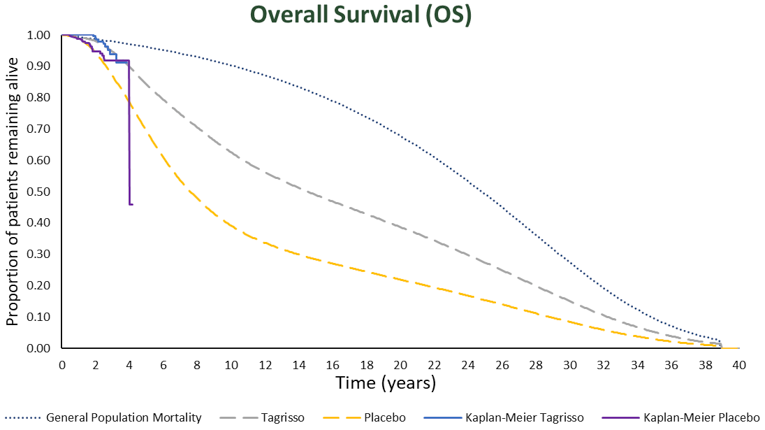
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Osimertinib | Active surveillance | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 10.62 | 10.00 | 0.62 |
DF | 7.83 | 6.57 | 1.26 |
LR | 0.91 | 0.95 | −0.04 |
1L DM | 0.97 | 1.56 | −0.60 |
2L DM | 0.91 | 0.92 | −0.01 |
Discounted QALYs | |||
Total | 8.11 | 7.60 | 0.51 |
DF | 6.11 | 5.09 | 1.02 |
LR | 0.71 | 0.75 | −0.03 |
1L DM | 0.74 | 1.21 | −0.47 |
2L DM | 0.55 | 0.56 | −0.01 |
AEs | −0.00018 | −0.0001 | −0.00017 |
Discounted costs ($) | |||
Total | 419,085 | 253,304 | 165,781 |
Acquisition | 357,899 | 189,033 | 168,865 |
Administration | 0 | 0 | 0 |
Disease management | 60,386 | 60,717 | −331 |
Other direct costs | 300 | 3,502 | −3,202 |
AEs | 501 | 52 | 449 |
ICER ($/QALY) | $328,026 | ||
1L = first-line treatment; 2L = second-line treatment; DF = disease-free; DM = distant metastatic; LR = local or regional recurrence; ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year.
Detailed Results of CADTH Base Case
Figure 4: Predicted Disease-Free Survival Outcomes Based on CADTH Reanalysis Parametric Survival Extrapolation Choices (Gompertz)
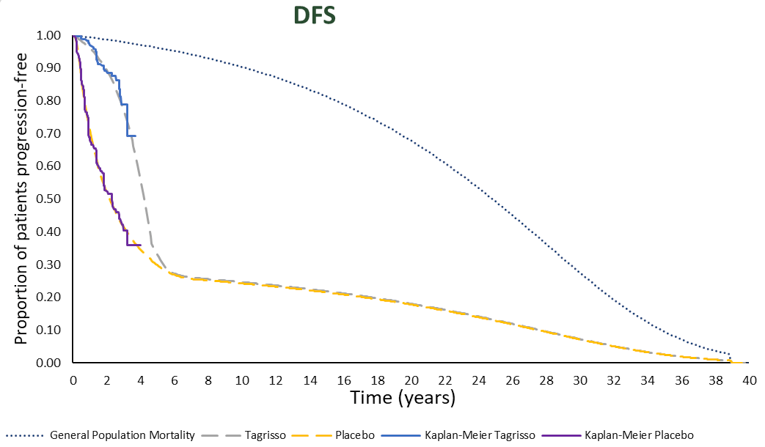
DFS = disease-free survival; PMH = Princess Margaret Hospital.
Figure 5: Predicted Overall Survival Outcomes Based on CADTH’s Parametric Survival Extrapolation Choices (Gompertz)
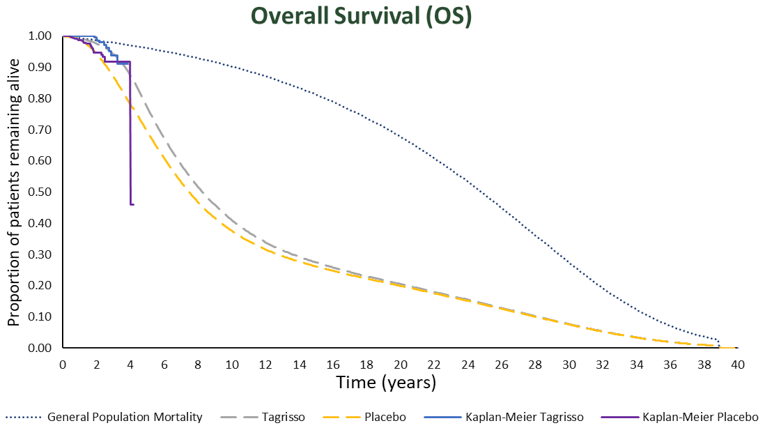
OS = overall survival; PMH = Princess Margaret Hospital.
Figure 6: Predicted Disease-Free Survival Outcomes Based on CADTH Scenario Reanalysis Using Weibull Function and Sustained DFS
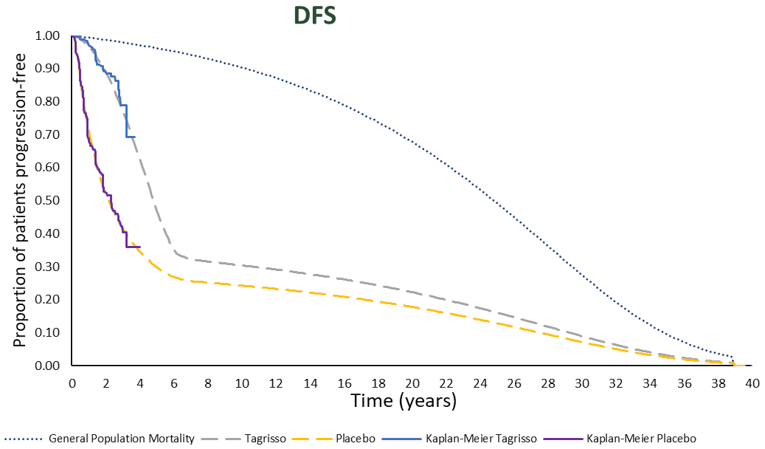
DFS = disease-free survival; PMH = Princess Margaret Hospital.
Figure 7: Predicted Disease-Free Survival Outcomes Based on CADTH Scenario Reanalysis Using Weibull and No Sustained DFS
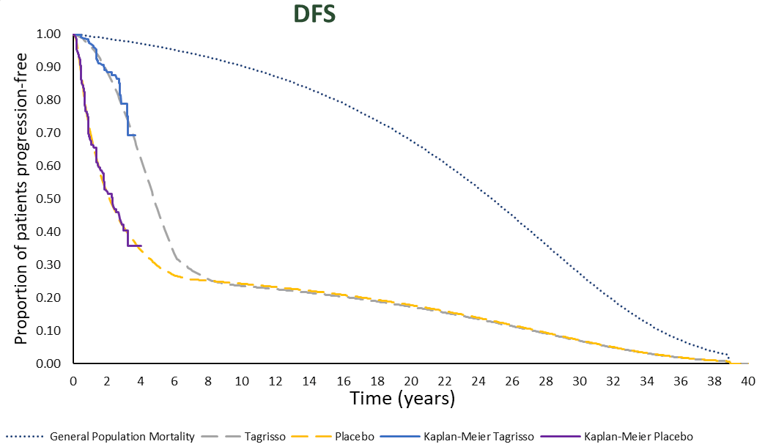
DFS = disease-free survival.
Figure 8: Predicted Disease-Free Survival Outcomes Based on CADTH Scenario Reanalysis Using Log-Logistic and No Sustained DFS
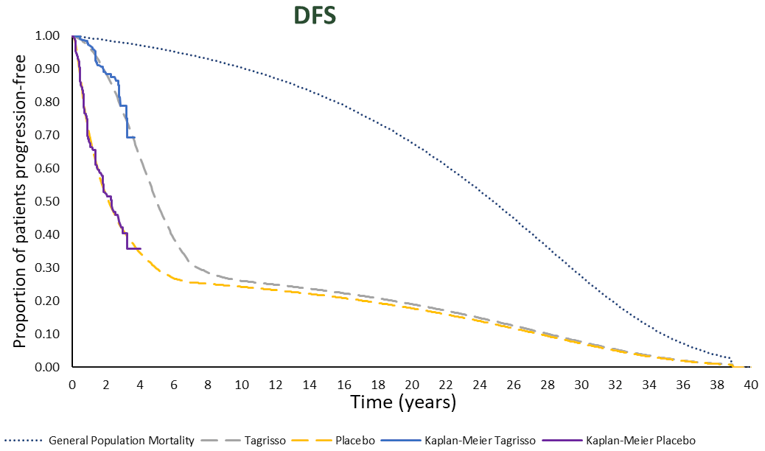
DFS = disease-free survival; PMH = Princess Margaret Hospital.
Figure 9: Predicted Overall Survival Outcomes Based on CADTH’s Scenario Reanalysis Using Weibull and No Sustained DFS
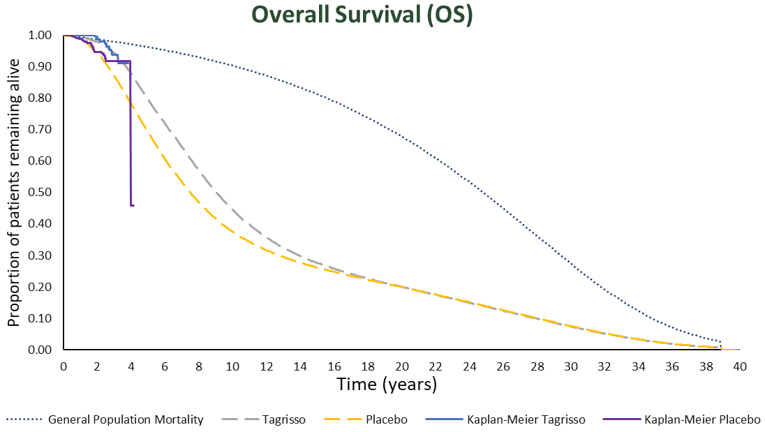
DFS = disease-free survival; OS = overall survival.
Figure 10: Predicted Overall Survival Outcomes Based on CADTH’s Scenario Reanalysis Using Log-Logistic and No Sustained DFS
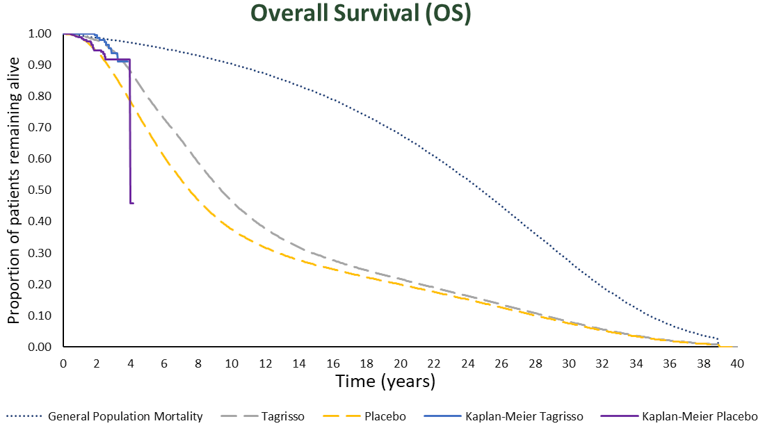
DFS = disease-free survival; OS = overall survival.
Scenario Analyses
Table 15: CADTH Scenario Analyses
Stepped analysis | Drug | Total costs ($) | Total LYs | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|---|
CADTH base case | Active surveillance | 253,304 | 10.00 | 7.60 | Reference |
Osimertinib | 419,085 | 10.62 | 8.11 | 328,026 | |
Weibull extrapolation for DF to LR and 1L DM- sustained DFS | Active surveillance | 253,753 | 9.99 | 7.59 | Reference |
Osimertinib | 414,516 | 11.43 | 8.73 | 141,330 | |
Three months to re-treatment | Active surveillance | 253,504 | 9.99 | 7.59 | Reference |
Osimertinib | 455,619 | 10.83 | 8.27 | 299,795 | |
Weibull extrapolation for DF to LR and 1L DM-no sustained DFSa | Active surveillance | 253,382 | 9.99 | 7.60 | Reference |
Osimertinib | 435,605 | 10.78 | 8.24 | 282,166 | |
Weibull extrapolation for DF to LR and 1L DM-no sustained DFS 81% price reductiona | Active surveillance | 123,616 | 9.99 | 7.60 | Reference |
Osimertinib | 154,787 | 10.78 | 8.24 | 48,268 | |
Log-logistic extrapolation for DF to LR and 1L DM-no sustained DFSa | Active surveillance | 253,382 | 9.99 | 7.60 | Reference |
Osimertinib | 429,419 | 11.10 | 8.49 | 197,367 | |
Log-logistic extrapolation for DF to LR and 1L DM-no sustained DFS 72% price reductiona | Active surveillance | 138,034 | 9.99 | 7.60 | Reference |
Osimertinib | 182,554 | 11.10 | 8.49 | 49,914 |
1L DM = first-line treatment for distant metastatic disease; DFS = disease-free survival; ICER = incremental cost-effectiveness ratio; LR = local or regional recurrence; LY = life-year; QALY = quality-adjusted life-year.
aBased on deterministic results due to uncertain specification of uncertainty around DFS.
Appendix 5: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 16: Summary of Key Take-Aways
Key Take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) estimating the budget impact of introducing osimertinib as adjuvant therapy after tumour resection in patients with stage IB to IIIA NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations.17 The BIA base case was undertaken from a publicly funded drug plan perspective considering only oral drug costs over a 3-year time horizon.17 Costs included that of adjuvant therapy and first-line treatments used among patients who progress. Osimertinib costs were calculated by incorporating an RDI of |||| and were based on the time patients spent on osimertinib and their likelihood of recurrence, calculated from the time-to-treatment discontinuation curves from the ADAURA trial.3 As costs of subsequent therapies were included, ADAURA trial DFS curves were used to determine the probabilities of recurrence in the adjuvant setting. Subsequent treatments were dependent on whether patients received osimertinib adjuvant or active surveillance alone, and, in the current scenario, the patient’s EGFRm status. Patients who had received osimertinib could not receive it as first-line therapy in the distant metastatic setting; those who had not and were EGFRm could.
The analytic framework, which used an epidemiology-based approach, leveraged data from multiple sources in the literature and assumptions based on clinical expert input to determine the estimated population size (Figure 11). The sponsor compared a reference scenario where osimertinib is not reimbursed as adjuvant therapy, with a new drug scenario, where osimertinib is funded as adjuvant therapy as per the Health Canada indication. Treatments available in the reference included active surveillance alone, which was assumed to consist of no active treatment, and treatments for recurrence. Key inputs to the BIA are documented in Table 18.
Figure 11: Sponsor’s Estimation of the Size of the Eligible Population
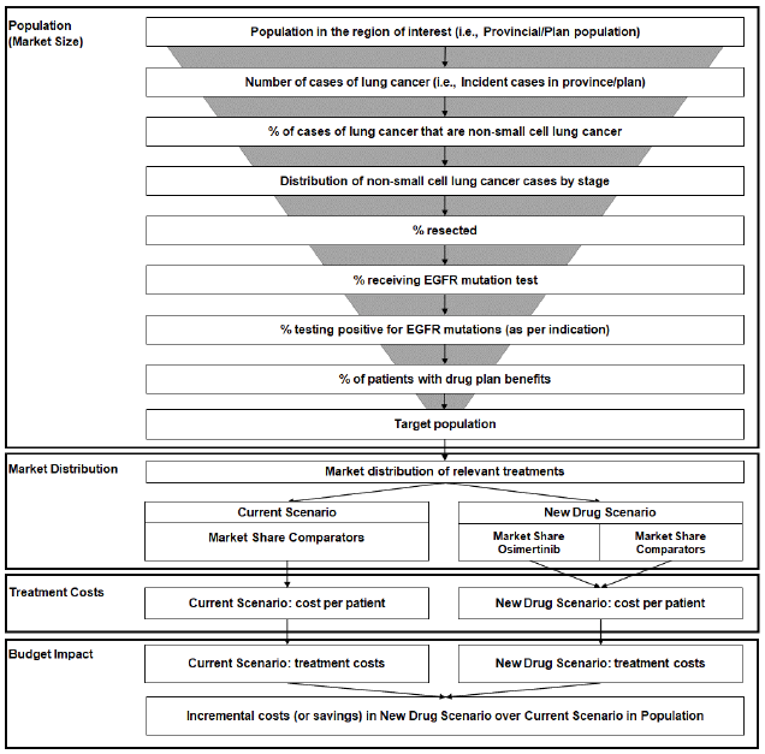
EGFR = epidermal growth factor receptor
Table 17: Age-Specific Incidence Rates of Lung Cancer
Age group | Adjusted number of incident cases per 100,000 |
|---|---|
0 to 44 | 1.124 |
45 to 54 | 27.282 |
55 to 64 | 111.173 |
65 to 74 | 276.605 |
75 to 84 | 418.739 |
85+ | 341.388 |
Source: Canadian Cancer Society.18
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Population size | Statistics Canada19 |
Incidence | See Table 17 |
Proportion NSCLC | 85.0%20 |
Distribution of cases by stage | 9.05%, 9.07%, and 12.63% stage IB, II, and IIIA, respectively21 |
Percent resected | 56.0%, 54.2%, and 13.7% stage IB, II, and IIIA, respectively5 |
Percent receiving EGFRm testing | |||% / |||% / |||% in year 1, 2, and 3, respectively |
Percent positive for EGFRm | 15%22 |
Percent with exon 19 deletion or exon 21 L858R | 90%23 |
Percent with public drug plan coverage | Jurisdiction-specific drug plan benefits (100% for patients 65+) |
Number of patients eligible for drug under review | 174 / 195 / 217 |
Market uptake (3 years) | |
Uptake (reference scenario) Active surveillance Osimertinib | 100% / 100% / 100% 0% / 0% / 0% |
Uptake (new drug scenario) Active surveillance Osimertinib | |||||||||||||||||||| |||||||||||||||||||| |
Cost of treatment (per patient) | |
Cost of treatment over 1 month Active surveillance Osimertinib | $0 $8,864.48 |
EGFRm = epidermal growth factor receptor–mutated; L858R = sensitizing mutation in the EGFR gene with substitution of a leucine with an arginine at position 858 in exon 21; NSCLC = non–small cell lung cancer.
Summary of the Sponsor’s BIA Results
The sponsor’ base case estimated the net budget impact of introducing osimertinib as adjuvant therapy after tumour resection in patients with stage IB-IIIA NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations to be $10,598,700 in year 1, $23,683,196 in year 2, and $40,278,125 in year 3 for a total budget impact over 3 years of $74,560,021.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The proportion of the population with resected disease that undergoes EGFRm testing is underestimated. The sponsor’s base case assumed that |||% / |||% / |||% of patients who undergo surgical resection will receive EGFRm testing in year 1, 2, and 3, respectively. According to the clinical experts consulted by CADTH for this review, if adjuvant osimertinib was funded and if EGFRm testing is available post-resection, all resected patients would be tested for EGFRm.
CADTH reanalyses assumed that 100% of the resected population would undergo EGFRm testing. To account for potential variation in testing rates, a scenario analysis assuming a testing rate of 90% was conducted.
The proportion of patients with distant metastatic disease who undergo EGFRm testing is underestimated. The sponsor assumed that 85% of patients with distant metastatic disease will undergo testing and have a valid result, based on clinician input. According to the clinical experts consulted by CADTH for this review, as it is important to establish EGFRm status in the metastatic setting as this influences treatment options and patient outcomes, they felt that not determining EGFRm status in 15% of DM patients was higher than expected in Canadian clinical practice.
CADTH reanalyses assumed 95% of patients undergo EGFRm testing, with 5% either not being tested or having an invalid result.
RDI implementation was inappropriate. The sponsor incorporated an RDI of |||% based on the FLAURA trial, which studied osimertinib in the metastatic setting. RDI was not reported based on the ADAURA clinical study report, and therefore this value could not be validated. It is unknown whether the RDI for osimertinib observed in the metastatic setting will apply to the adjuvant setting. Further, it is expected that pharmacies will dispense the full drug claim for patients, meaning that public payers will incur the full cost of the claim, regardless of patient adherence.
CADTH reanalyses assumed an RDI of 100%.
The uptake of osimertinib adjuvant is not aligned with clinical expert expectations. In the sponsor’s base case, it was assumed that ||||||||% of eligible patients would uptake osimertinib, should it become available. According to the clinical experts consulted by CADTH for this review, approximately 75% of patients are expected to initiate treatment upon osimertinib becoming available in the adjuvant setting.
In CADTH reanalysis, the proportion of eligible patients uptaking osimertinib in year 1 and year 2 was changed to 75% and 80%. Year 3 uptake remained unchanged from the sponsor’s base case.
The proportion of patients eligible for public coverage is uncertain. The sponsor’s base-case analysis used age and jurisdiction-specific public coverage rates for all medications. Intravenous oncology drugs are likely to be fully covered. Depending on the jurisdiction, oral oncology drugs may be fully reimbursed or may only be reimbursed by regular public drug plans, as assumed in the sponsor’s base case.
To address uncertainty regarding the proportion eligible for public drug plan coverage, CADTH assumed 100% coverage across jurisdictions and age as a scenario analysis.
The distribution of treatments for LR is not aligned with the pharmacoeconomic analysis. In the sponsor’s BIA, it was assumed that 32.5%, 17.5%, and 50% of those with LR will be treated using stereotactic body radiation therapy, resection, or chemoradiotherapy, respectively. This is not aligned with the sponsor’s LR estimates, nor the proportions receiving LR treatments used in CADTH pharmacoeconomic reanalyses.
CADTH assumed 5%, 5%, and 90% of patients with LR will receive stereotactic body radiation therapy, resection, and chemoradiotherapy, respectively.
Estimates of subsequent treatments in the reference scenario are potentially incorrect. Currently patients who progress to 1L DM will receive osimertinib if they are EGFRm positive. If osimertinib was to be used in the adjuvant setting this would reduce the number of patients who receive osimertinib in the 1L DM setting. As such, for some patients, osimertinib (new drug scenario) might not represent a net cost as patients would still receive osimertinib, at a later line of therapy. Due to lack of transparency and complexity with the sponsor's approach, it is unclear if the sponsor has correctly estimated the proposed reduction in the number of patients who receive osimertinib in the 1L DM setting. It would appear the sponsor has double counted the 15% EGFR positive estimate. Once to generate the cohort size for the BIA and then again to determine 1L DM eligibility. This would underestimate the number of patients currently eligible for osimertinib in the 1L DM setting.
Due to the complexity of the BIA model, CADTH was unable to address this limitation. If reference scenario costs are underestimated, then the budget impact of introducing osimertinib adjuvant therapy will be less than estimated in both the sponsor’s and CADTH’s reanalyses.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by assuming all patients in the new drug scenario will undergo EGFRm testing at the time of resection; assuming 95% of patients in the reference scenario who progress to DM will receive EGFRm testing and have a valid result, changing the RDI to 100%, increasing osimertinib uptake in year 1 and 2 and aligning the distribution of patients across subsequent therapies for LR with the pharmacoeconomic analysis. Table 19 notes the assumptions used by the sponsor in comparison to those used by CADTH in its reanalysis.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Percent undergoing EGFRm testing post-surgical resection in the new drug scenario | |||% / |||% / |||% | 100% / 100% / 100% |
2. Percent undergoing EGFRm testing and obtaining a valid result upon progression in the reference scenario | 85% | 95% |
3. Relative dose intensity | ||% | 100% |
4. Uptake of osimertinib in year 1 / 2 / 3 | ||||||||||||||||% | 75% / 80% / 85% |
5. Distribution of subsequent therapies for LR |
|
|
CADTH base case | 1 + 2 + 3 + 4 + 5 + 6 | |
EGFRm = epidermal growth factor receptor–mutated; LR = local or regional recurrence; SBRT = stereotactic body radiation therapy.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or SEs in probabilistic analyses) that are not identified as limitations.
Applying these changes increased the total 3-year budget impact to $130,498,368. The results of the CADTH stepwise reanalysis are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21.
Table 20: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 74,560,021 |
CADTH reanalysis 1: 100% EGFR testing | 116,644,434 |
CADTH reanalysis 2: % getting tested in DM setting | 74,280,699 |
CADTH reanalysis 3: RDI 100% | 75,391,056 |
CADTH reanalysis 4: Osimertinib uptake | 82,506,335 |
CADTH reanalysis 5: Distribution of subsequent therapies for LR | 74,555,423 |
CADTH base case | 130,498,368 |
BIA = budget impact analysis; EGFRm= epidermal growth factor receptor–mutated; DM = distant metastatic; LR = local or regional recurrence; RDI = relative dose intensity.
CADTH also conducted additional scenario analyses to address remaining uncertainty:
Assuming 90% of the resected population underwent EGFRm testing
Reduced the price of osimertinib to the value in which it would be cost-effective at a $50,000 per-QALY threshold (82%)
100% of the population is eligible for public coverage
Including EGFRm testing costs
Results of CADTH’s scenario analyses demonstrate that the estimated budget impact is highly sensitive to the size of the eligible population (Table 21). If 100% of patients have public coverage for osimertinib adjuvant therapy, the expected budget impact is estimated to be $148,039,604 over 3 years. While including EGFRm testing costs increased the overall budget impact, the impact of this change is small (< 2% change from CADTH base case). If the price of osimertinib was reduced by 82%, the 3-year budget impact is expected to be much lower at $23,492,813 over 3 years.
Table 21: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|
Submitted base case | Reference | $200,409 | $745,700 | $1,548,512 | $2,494,621 |
New drug | $10,799,110 | $24,428,896 | $41,826,637 | $77,054,642 | |
Budget impact | $10,598,700 | $23,683,196 | $40,278,125 | $74,560,021 | |
CADTH base case | Reference | $376,189 | $1,368,524 | $2,759,794 | $4,504,506 |
New drug | $22,099,644 | $44,734,304 | $68,168,926 | $135,002,874 | |
Budget impact | $21,723,455 | $43,365,781 | $65,409,131 | $130,498,368 | |
CADTH scenario analysis 1: 90% undergo EGFRm testing | Reference | $338,570 | $1,231,671 | $2,483,815 | $4,054,056 |
New drug | $19,889,680 | $40,260,874 | $61,352,033 | $121,502,587 | |
Budget impact | $19,551,110 | $39,029,203 | $58,868,218 | $117,448,531 | |
CADTH scenario analysis 2: 82% price reduction | Reference | $103,836 | $329,427 | $631,274 | $1,064,537 |
New drug | $4,017,891 | $8,137,412 | $12,402,047 | $24,557,350 | |
Budget impact | $3,914,056 | $7,807,985 | $11,770,772 | $23,492,813 | |
CADTH scenario analysis 3: 100% eligible for coverage | Reference | $427,573 | $1,554,528 | $3,130,455 | $5,112,556 |
New drug | $25,151,674 | $50,790,921 | $77,209,565 | $153,152,160 | |
Budget impact | $24,724,101 | $49,236,393 | $74,079,110 | $148,039,604 | |
CADTH scenario analysis 4: EGFRm testing costs included | Reference | $392,376 | $1,393,333 | $2,791,480 | $4,577,189 |
New drug | $22,835,287 | $45,490,607 | $68,946,284 | $137,272,178 | |
Budget impact | $22,442,911 | $44,097,274 | $66,154,804 | $132,694,989 |
BIA = budget impact analysis; EGFRm = epidermal growth factor receptor–mutated.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.