CADTH Reimbursement Review
Chlormethine Gel (Ledaga)
Sponsor: Recordati Rare Diseases Canada Inc.
Therapeutic area: Mycosis fungoides-type cutaneous T-cell lymphoma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
A
adverse event
BSA
body surface area
CAILS
Composite Assessment of Index Lesion Severity
CLF
Cutaneous Lymphoma Foundation
CSPA
Canadian Skin Patient Alliance
CTCL
cutaneous T-cell lymphoma
CI
confidence interval
CR
complete response
EE
efficacy-evaluable
EMA
European Medicines Agency
HRQoL
health-related quality of life
ITT
intention-to-treat
LCT
large cell transformation
MF
mycosis fungoides
MF-CTCL
mycosis fungoides-type cutaneous T-cell lymphoma
MID
minimal important difference
NB-UVB
narrow band ultraviolet B
NM
nitrogen mustard
PR
partial response
PUVA
psoralen plus ultraviolet A
SDT
skin-directed therapy
SWAT
Severity-Weighted Assessment Tool
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Chlormethine gel (Ledaga), 160 mcg chlormethine per gram gel, in 60 g tubes, for topical application to the skin |
Indication | Proposed: For the topical treatment of MF-CTCL in adult patients |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | June 8, 2021 |
Sponsor | Recordati Rare Diseases Canada Inc. |
MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma; NOC = Notice of Compliance.
Introduction
Cutaneous T-cell lymphomas (CTCLs) are a group of rare non-Hodgkin lymphomas characterized by initial localization of malignant T-lymphocytes to the skin. The most common form among CTCLs is mycosis fungoides (MF), accounting for approximately 55% to 60% of cases.1 The incident rate of MF has remained relatively stable over the past 2 decades at about 5.6 per million persons. In Canada, 2,510 cases of MF-type CTCL (MF-CTCL) were documented from 1992 through 2010.2,3 The clinical presentation of MF is manifold. Early stages present with limited patches and plaques that are prone to misdiagnosis, and later stages are characterized by severe disease, presenting with tumours, ulcerations, and systemic involvement.1 The diagnosis of MF-CTCL is made with skin biopsy and is further confirmed with immunophenotyping and DNA analysis of the T-cell receptor gene rearrangement to define the clonal population.4 Lymph node biopsies may be performed at initial staging in patients with overt advanced disease or if nodes are enlarged on physical examination or imaging studies.1,4
Most treatments for MF-CTCL aim to relieve skin symptoms, and treatment strategy follows a stepwise stage-adapted approach.4,5 The majority of available treatments are rarely able to induce durable remission.6 Patients in early stages are primarily treated with skin-directed therapies (SDTs). Options include topical steroids, topical retinoids, and phototherapy; should patients relapse after remission, they receive further courses of the same or another SDT. Systemic therapy is mainly considered for patients with advanced disease and for refractory cutaneous disease.4,6 Given that MF-CTCL is a chronic condition, the overarching goal of treatment is to achieve remission with improvement or at least maintenance of quality of life and to decrease toxicity from treatment, as many patients cycle through different treatment options.1,4,5
Chlormethine (mechlorethamine, also referred to as nitrogen mustard [NM]) is an alkylating agent that received its initial approval in the US for the topical treatment of MF in 1949. Recently, based on the results of a pivotal phase II study, a commercial chlormethine hydrochloride 0.02% gel (Ledaga, or Valchlor in the US) was approved by the US FDA for the treatment of stage IA and stage IB MF-CTCL in patients who have received prior SDT.7
The objective of this review is to evaluate the efficacy and safety of ready-to-use 0.02% w/w chlormethine hydrochloride topical gel (Ledaga) for the treatment of adult patients with MF- CTCL.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One joint patient group submission was provided on behalf of 3 organizations: Lymphoma Canada, the Canadian Skin Patient Alliance (CSPA), and the Cutaneous Lymphoma Foundation (CLF).
Lymphoma Canada, with the collaboration and input of CSPA and CLF, conducted an online survey of cutaneous lymphoma patients from September 2020 to January 2021. Overall, 233 patients responded to the survey; of these, 210 (90%) patients were diagnosed with MF. Fifty-six (33%) patient respondents indicated they had experience with chlormethine gel.
Patients with MF report having visible patches or lesions, itchiness, pain or burning of the skin or lesions, plaques, and rash-like skin redness. The patients indicated that these symptoms negatively impact their quality of life and mental and emotional well-being. Furthermore, the patients reported that living with MF-CTCL has negatively impacted their personal image, family relationships, intimate relationships, and work.
The patients indicated that having a choice in treatment options was extremely important to them. The patients reported that they want treatments that result in longer survival, better quality of life, longer remission, fewer side effects, and easier and/or faster treatment application.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH noted that current treatments have limitations. Unmet needs include treatments that can be curative, easily accessible, and well tolerated. There is currently no ideal SDT. Topical corticosteroids are not curative, and it is unclear if they can prevent disease progression. Long-term use can cause side effects. Phototherapy may not be accessible to some patients, and it may cause skin atrophy and increase the risk of skin cancer. Topical chlormethine causes dermatitis and may not be tolerated, especially when large surface areas are involved. These treatments have efficacy ranging from 60% to 80%, depending on disease severity. Therefore, different treatment options may be required for refractory disease.
The clinical experts anticipated that it is unlikely that Ledaga will shift the current treatment paradigm as it is only supplied in small 60 g tubes and can only be used for the treatment of small surface areas because of its potential to cause skin irritation. However, it may be used to treat lesions refractory to topical corticosteroids or when phototherapy is not accessible or is ineffective. The clinical experts identified patients least likely to benefit from Ledaga as those with extensive disease (> 20% affected body surface area [BSA]) or those with tumours.
Clinician Group Input
The clinician group that provided input for this review was coordinated by Lymphoma Canada, a national not-for-profit organization for Canadian lymphoma and chronic lymphocytic leukemia patients. Five clinicians contributed to the clinician group responses.
The clinicians noted that the addition of effective topical treatment would be extremely useful in the treatment of patients with MF-CTCL. The goals of this topical therapy include disease control, symptom control, and improved quality of life. Importantly, for select skin sites such as the scalp and other hair-bearing areas, where the application of creams and ointments is difficult, having a gel product that can be applied would be especially useful in the treatment of these patients. Gel is stable and non-greasy, and a quick drying formulation ultimately allows for convenient, simple at-home administration, thereby encouraging compliance. This would reduce the severity of a patient’s symptoms, prevent disease progression, improve skin-related quality of life, and improve skin disease scores. Chlormethine is a standard and useful treatment, but currently is only rarely used because it is not always available, and not stable. This option is more convenient than light treatment (phototherapy or photochemotherapy) for patients who live far from a clinic. Considering the treatment goals described previously, the clinicians reported that patients who would benefit from this therapy include adult patients with stage IA to stage IIA of MF with less than 15% BSA involvement (stage IA and stage IIA < 10%; stage IB > 10%) and patients with select skin sites involved by MF (e.g., hair-bearing areas).
Drug Program Input
The main concern raised by the Provincial Advisory Group was the use of chlormethine ointment as a comparator to chlormethine gel in the pivotal trial. Chlormethine is not a funded or available treatment in most jurisdictions. In terms of place in therapy, in the pivotal trial, patients were required to have been treated with at least 1 prior SDT. The Provincial Advisory Group asked if this would apply to routine clinical care. The clinical experts consulted by CADTH noted that chlormethine would be used as second-line therapy to treat lesions refractory to topical corticosteroids, or when phototherapy is not feasible or is ineffective. Another question concerned the quantity of chlormethine gel dispensed and the quantity needed to treat skin lesions with the 60 g tube format of the drug. The clinical experts explained that patients with high skin burden require a higher quantity of the drug than those with low skin burden. For example, a patient with 5% affected BSA would require a 60 g tube of Ledaga approximately every month, whereas a patient with 50% affected BSA would require 1 60 g tube of Ledaga every 1 day to 2 days.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
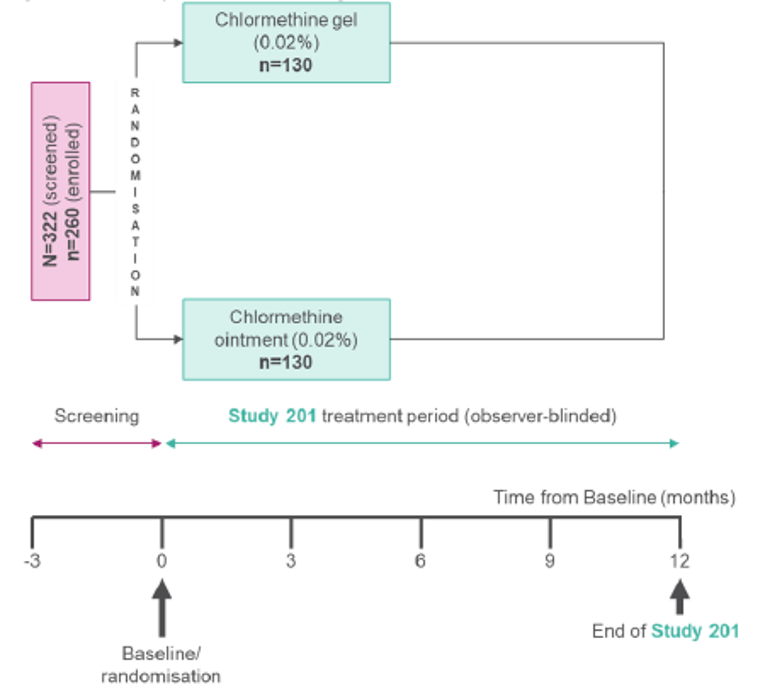
Study 201 (2005NMMF-201-US) was a randomized, controlled, observer-blinded, multi-centre trial conducted in 13 academic centres across the US that investigated the safety and efficacy of chlormethine hydrochloride 0.02% topical gel (Ledaga) for patients with early-stage MF-CTCL (May 2006 to August 2011). It was designed as a noninferiority trial comparing chlormethine hydrochloride 0.02% gel with chlormethine hydrochloride 0.02% compounded ointment over a 12-month period. Blocked randomization stratified by MF stage (stage IA versus stage IB and stage IIA) was performed; 260 patients with biopsy-confirmed stage I, or stage IIA (cutaneous only) MF-CTCL who had received at least 1 prior SDT for MF, were randomized 1:1 to receive treatment with chlormethine gel (n = 130) or chlormethine ointment (n = 130). All patients completed a washout period of MF-CTCL therapies for 4 weeks before initiating the trial treatments. After a 4-week washout period, patients in both treatment groups were instructed to apply the treatment once daily to specific lesions, or to the total skin surface depending on the extent of BSA coverage of the patients. The primary efficacy end point of Study 201 was response rate, defined as improvement of 50% or more in the patient’s Composite Assessment of Index Lesion Severity (CAILS) score from baseline. Response rate was assessed every month between month 1 and month 6, and every 2 months between month 7 and month 12. A patient was considered a responder if the response was maintained for at least 2 consecutive visits (or at least 28 days). The main secondary efficacy end point was response rate using the Severity-Weighted Assessment Tool (SWAT).
The majority of patients were between 18 years and 64 years of age (71.5% in the gel treatment arm and 66.2% in the ointment treatment arm). Overall, 59.2% of patients were male and 40.8% were female. In total, 54.2% of patients had stage IA disease at baseline and 44.2% of patients had stage IB disease at baseline; 2 patients in each treatment arm had stage IIA disease at baseline. The most common prior SDT was corticosteroids, used in 86% of patients in both treatment arms.
Efficacy Results
In the intention-to-treat (ITT) population, the confirmed response rate was higher for chlormethine gel than chlormethine ointment (58.5% versus 47.7%); 18 (13.8%) patients in the chlormethine gel treatment arm and 15 (11.5%) patients in the chlormethine ointment treatment arm achieved complete response (CR), meaning there was no evidence of disease with 100% improvement. The ratio of the response rate of gel to ointment was 1.23 (95% confidence interval [CI], 0.97 to 1.55), meeting the pre-specified criterion for noninferiority (≥ 0.75 for the lower bound of 95% CI). Based on SWAT response, the overall response rate was 46.9% and 46.2% for chlormethine gel and chlormethine ointment, respectively. The ratio of response rate was 1.02 (95% CI, 0.78 to 1.32). CR was observed in 9 (6.9%) patients in the chlormethine gel arm and 4 (3.1%) patients in the chlormethine ointment arm (Table 2).
Harms Results
During the trial period, 84.4% of patients treated with chlormethine gel and 90.6% of patients treated with chlormethine ointment experienced at least 1 AE. Most AEs in both treatment arms were skin-related; the most frequently reported AEs were dermatitis (skin irritation, 19.6%), pruritus (17.6%), and erythema (15.7%).8 The incidence of skin irritation was higher in the gel arm compared to the ointment arm (25.0% versus 14.2% [Table 2]). During the 12-month trial period and the additional 12-month follow-up period (in the extension trial Study 202), 20 nonmelanoma skin cancers were detected in 11 of 255 patients (4.3% of patients), which included 10 basal cell carcinomas (5 occurring in a treatment area), 9 squamous cell carcinomas (1 in a treatment area), and 1 Merkel cell carcinoma (not in a treatment area). Eight of these patients developed nonmelanoma skin cancer during treatment; 3 additional patients developed nonmelanoma skin cancer during the 1-year follow-up period.
Table 2: Summary of Key Results From Pivotal Trial of Ledaga — Study 201
Outcomes | Chlormethine gel n (%) | Chlormethine ointment n (%) | Ratio gel or ointment | 95% CI |
|---|---|---|---|---|
Efficacy | ||||
Response (CAILS) | ||||
ITT population, n | 130 | 130 | ||
Overall (CR + PR), n (%) | 76 (58.5) | 62 (47.7) | 1.226 | 0.97 to 1.55 |
CR | 18 (13.8) | 15 (11.5) | NA | NA |
PR | 58 (44.6) | 47 (36.2) | NA | NA |
EE population, n | 90 | 95 | ||
Overall (CR + PR), n (%) | 69 (76.7) | 56 (58.9) | 1.301 | 1.065 to 1.609 |
CR | 17 (18.9) | 14 (14.7) | NA | NA |
PR | 52 (57.8) | 42 (44.2) | NA | NA |
Response (SWAT) | ||||
ITT population | 130 | 130 | ||
Overall (CR + PR), n (%) | 61 (46.9) | 60 (46.2) | 1.017 | 0.783 to 1.321 |
CR | 9 (6.9) | 4 (3.1) | NA | NA |
PR | 52 (40.0) | 56 (43.1) | NA | NA |
EE population | 90 | 95 | ||
Overall (CR + PR), n (%) | 57 (63.3) | 53 (55.8) | 1.135 | 0.893 to 1.448 |
CR | 8 (8.9) | 4 (4.2) | NA | NA |
PR | 49 (54.4) | 49 (51.6) | NA | NA |
Harmsa | ||||
AEs | 108 (84.4) | 115 (90.6) | NA | NA |
SAEs | 14 (10.9) | 11 (8.7) | NA | NA |
WDAE | 28 (21.9) | 23 (18.1) | NA | NA |
Deathsb | 1 (0.8) | 0 (0.0) | NA | NA |
AE = adverse event; CAILS = Composite Assessment of Index Lesion Severity; CI = confidence interval; CR = complete response; EE = efficacy-evaluable; ITT = intention-to-treat; NA = not applicable; PR = partial response; SAE = serious adverse event; SWAT = Severity-Weighted Assessment Tool; WDAE = withdrawal due to adverse event.
aSafety analysis set.
bDeath not related to study treatment.
Source: Clinical Study Report for Study 201.9
Critical Appraisal
The choice of a comparator (chlormethine ointment) that is not part of standard of care in Canada limits the interpretation and applicability of results of the pivotal trial with respect to current treatment options. The clinical experts consulted for this report noted that the more appropriate comparator for the Canadian population would have been phototherapy, which is the current standard of care for this patient population. The sponsor has acknowledged this point and explains that an active comparator control group rather than a placebo control was considered necessary, given the long duration of randomized treatment needed to evaluate response, the known progressive nature of the disease, and the reported association between disease progression and increased mortality risk. Another key limitation related to data analysis is the handling of missing data, where any patient who did not achieve a documented response was counted as a nonresponder in the ITT population. Imputing patients as nonresponders may have different implications, either biasing estimates toward the null (given similar dropout rates in both treatment arms), which would result in conservative inference or, conversely, lead to the underestimation of the standard error and thus an anti-conservative inference. The ultimate impact of the approach to handling of missing data on the study conclusions is unclear.
One important end point that was not included in Study 201 was health-related quality of life (HRQoL). This outcome was identified by both the patient and clinician groups consulted for this report as an important outcome, given the considerable negative impact of the disease on patients’ quality of life. Although it may be reasonable to assume an association between key efficacy end points (CAILS and SWAT) with HRQoL, in the absence of such evidence from the clinical trial, it is unclear whether clinical response translates to improved quality of life for patients.
The indication and reimbursement request of chlormethine gel as topical treatment for MF-CTCL in adult patients is broader than the inclusion criteria of Study 201 with respect to disease stage (early stage: stage IA, stage IB, and stage IIA) and treatment history (previously treated with at least 1 SDT). Although the trial population consisted of treatment-experienced patients with primarily stage I disease (stage IA, stage IB), no relevant differences in efficacy and safety are expected. In terms of line of therapy, treatment decisions are based on several factors such as availability of different treatment options in different regions and settings. Ledaga is the only drug of its class available in Canada and would be considered mainly in second-line therapy after other SDTs, including phototherapy and topical steroids.
Other Relevant Evidence
Description of Studies
Study 202 was an open-label, single-arm extension study that evaluated the efficacy and safety of a higher concentration of chlormethine gel (0.04%). Patients in Study 201 who had not achieved CR based on CAILS on either the chlormethine hydrochloride 0.02% gel or chlormethine hydrochloride 0.02% ointment during the 12-month study period were eligible to enrol in Study 202. All patients who enrolled in the study received the higher strength of chlormethine hydrochloride gel (0.04%) for up to 7 months, and were followed and evaluated for AEs and skin cancers during the 7-month study treatment period and for 5 months thereafter. Of the 100 enrolled patients, 98 were treated in Study 202; |||||||||| patients completed the trial and |||||||||| patients permanently withdrew from the study.
Efficacy Results
CAILS responses at the end of Study 202, relative to the Study 201 baseline, showed an overall confirmed response rate of 75.5%; 12 (12.2%) patients achieved CR and 62 (63.3%) patients achieved partial response (PR). CAILS responses relative to the Study 202 baseline showed a confirmed response rate of 23.5%; 10 (10.2%) patients achieved CR and 13 (13.3%) patients had PR. Confirmed SWAT responses were reported in 20.4% of patients; 3 (3.1%) patients had CR and 17 (17.3%) patients had PR.
Harms Results
Overall, 71 (72.4%) patients in Study 202 had an AE and 6 (6.1%) patients had a serious AE. The most common AEs were skin irritation (11.2%), erythema (10.2%), and pruritus (6.1%). Lack of systemic exposure to chlormethine or its degradation product was confirmed in this study.
Critical Appraisal
Study 202 was originally conceived to gather safety data, including information on ongoing AEs from Study 201 as well as the extended time period to allow detection of nonmelanoma skin cancer in patients treated in Study 201. This objective was achieved and there were no major issues with the conduct of the study. The primary limitations of Study 202 were the open-label administration (similar to Study 201) and absence of a comparator group, limiting the utility of this evidence for the efficacy of chlormethine gel. However, the clinical experts consulted by CADTH noted that for patients who do not achieve an adequate response with chlormethine hydrochloride 0.02% gel and who do not have significant adverse reactions to chlormethine hydrochloride 0.02% gel, they would consider using the higher strength chlormethine hydrochloride (0.04%) in their clinical practice.
Conclusions
Clinical evidence from 1 trial shows that chlormethine gel relieves skin symptoms of early-stage MF-CTCL but the noninferiority comparison is relative to an alternative formulation of the treatment that is no longer used. Like other treatments currently available for MF-CTCL, chlormethine gel is not a disease-modifying treatment and will not affect progression of the underlying disease. Patient group and clinical expert input highlighted the need for alternative treatment options, given that most patients with early-stage MF-CTCL cycle through multiple rounds of treatments in different sequences. Although the ease of application can offer a convenient treatment option for patients with MF-CTCL, the absence of quality-of-life outcomes from the trial leaves an important gap in the evidence. Moreover, chlormethine gel is associated with skin-related adverse events (AEs), which will likely limit its use to patients with lesions covering less than 10% of BSA, and following initial treatment for early-stage MF-CTCL with current standard of care treatments, such as phototherapy and topical steroids and retinoids, given established efficacy and lower risk of skin reactions. The available evidence suggests that chlormethine gel may offer an additional treatment option for selected patients with early-stage MF-CTCL.
Introduction
Disease Background
CTCLs are a group of extranodal non-Hodgkin lymphomas that account for approximately 2% of all lymphomas.10 MF, the epidermotropic form of CTCL, is a low-grade lymphoma that generally has a slow course and often remains confined to the skin. Over time, there is a low risk (< 10%) of progression to the lymph nodes and internal organs. MF is the most common of the skin lymphomas, accounting for 60% of new CTCL cases. It typically affects old adults with a median age at diagnosis of 55 years to 60 years, with a male-to-female ratio of 1.6:1 to 2:1.11 Incidence of the disease has been stable since 1995, at approximately 5.6 per million persons.1 In Canada, 2,510 cases of MF-CTCL were documented from 1992 through 2010, representing 37.5% of CTCL cases.12 The annual national incidence of MF-CTCL was estimated at 4 cases per million individuals nationally and remained stable from 1992 to 2010. Interprovincial variability in incidence rates has been reported.2
MF is a highly symptomatic disease, with variable clinical presentation.1,4 It commonly begins with a non-specific scaly eruption that leads to the development of patches and/or plaques. With further progress, the disease advances with the formation of tumours, generalized erythroderma often with a leukemic phase (Sézary syndrome), and lymphadenopathy. Eventually, widespread visceral lymphoma may lead to death from the disease. The ulceration of tumours, with secondary infection with Staphylococcus aureus, Enterobacteriaceae, and Pseudomonas aeruginosa, is also a common cause of morbidity and death. The diagnosis of MF-CTCL is made with a skin biopsy and is further confirmed with immunophenotyping and DNA analysis of the T-cell receptor gene rearrangement to define the clonal population. Lymph node biopsies may be performed at initial staging in patients with overt advanced disease or if nodes are enlarged on physical examination or imaging studies.1,4
After diagnosis, the staging of MF-CTCL is assessed using different techniques, including a CT scan of the neck, chest, abdomen, and pelvis, a lymph node biopsy, and a morphological assessment of peripheral blood.4 Clinical staging of patients with MF is essential not only for the assessment of prognosis but also to guide decisions in management of the disease. The disease is classified using a CTCL-specific modification of the tumour, nodes, metastasis, blood classification system.11,13,14 Patients are classified based on the number and type of skin lesions they have, lymph node involvement, metastasis or visceral organ involvement, and peripheral blood involvement, resulting in a diagnosis of a disease stage from stage IA through to stage IVB.11 These stages can be grouped as early-stage disease (stage IA, stage IB, and stage IIA) and advanced-stage disease (stage IIB to stage IVB).11,15 Other histologic findings with possible prognostic importance (not accounted for by the tumour, nodes, metastasis, blood classification) include folliculotropism (the infiltration of hair follicles) and large cell transformation (LCT), which is more than 25% large cells in the dermal infiltrate.1 Epidemiological studies in Europe and the US indicate that more than 2-thirds of patients with MF- CTCL have early-stage disease at the time of diagnosis, despite patients with MF-CTCL commonly experiencing a delay in diagnosis of approximately 2 years.15-18 There are limited Canadian data on the incidence and prevalence of MF-CTCL by stage. However, these international data are in line with input from Canadian clinical experts, who reported that 66% to 95% of MF-CTCL patients in their practices have early-stage MF-CTCL (stage IA to stage IIA).2
The skin symptoms of MF-CTCL have a high burden to patients, negatively affecting their functional, emotional, and social well-being even in early stages of the disease. Patients with MF-CTCL can also experience immune-related comorbidities and are at increased risk of developing secondary malignancies, including Hodgkin lymphoma and acute leukemia. Some therapies for MF-CTCL (e.g., phototherapy) may further increase the risk of developing secondary malignancies (i.e., nonmelanoma skin cancers).19 The burden of MF-CTCL increases as disease progresses; studies have shown that patients with advanced-stage disease had worse overall HRQoL than patients with early-stage disease (stage IA to stage IIA).20-22 Overall survival as well as disease-specific survival decrease with advancing clinical stage while the risk of disease progression increases with advancing disease stage.13,17,20,23-26 Patients with stage IB disease have a twofold reduction in overall survival and a fourfold reduction in disease-specific survival compared with patients with stage IA disease.23,27,28 In treated patients, median survival with early-stage disease (stage IA, stage IB, and stage IIA) is reported as 35.5 years, 21.5 years, and 15.8 years, respectively.23 The prognosis for patients with MF-CTCL is worse when the condition is not limited to the skin at the time of initial diagnosis (stage IIB through stage IV). Median survival for late-stage disease (stage IIB, stage IIIA, and stage IIIB) is reported to be 4.7 years, 4.7 years, and 3.4 years, respectively, and decreases further for stage IV disease.23,29 The annual mortality rate for MF-CTCL has remained stable in Canada at approximately 0.4 deaths per million annually from 1992 to 2010.12
Standards of Therapy
Durable remission is uncommon in MF and patients are often treated with consecutive treatments until loss of response or intolerability; most treatments for MF-CTCL aim to relieve the skin symptoms. Treatment is guided by the patient’s disease stage as well as other disease characteristics, including presentation (patch and/or plaque) and percentage of BSA affected. The goals of treatment of patch and/or plaque disease without lymph node involvement (stage IA and stage IB), and those with enlarged but histologically uninvolved lymph nodes (stage IIA), is to achieve remission, relieve symptoms, and achieve cosmetic improvement while avoiding long-term treatment-related toxicities.4,5 For patients with stage IA, stage IB, or stage IIA disease, management relies on the applications of SDT. For later stages of the disease, systemic therapy is used to treat underlying disease, while SDTs may also be additionally used to continue managing the skin burden. SDTs include topical pharmacotherapies: topical corticosteroids, topical retinoids (tazarotene, bexarotene), chlormethine, carmustine, imiquimod, and non-pharmacotherapy treatments — primarily, phototherapy (narrow band ultraviolet B [NB-UVB] and psoralen plus ultraviolet A [PUVA]).1,4,5 Based on input from clinical experts consulted by CADTH, currently, SDT options in Canada are limited. For years, the mainstays of treatment have been corticosteroids, chlormethine, and phototherapy. Tazarotene and imiquimod have not been widely used in Canada and are not covered under public drug plans. Carmustine is not available in topical form, and chlormethine was used as an aqueous solution or a compounded ointment but this is no longer available. Topical corticosteroids are the most commonly used first-line treatment for limited (< 10% BSA) patch and/or plaque disease. Phototherapy, if accessible, is preferred for more extensive lesions (> 10% BSA). Systemic retinoids (alitretinoin or acitretin) or methotrexate may be added to the topical steroids and phototherapy to enhance response, if necessary. Chlormethine is used as second-line treatment for refractory lesions. In advanced-stage disease (stage IIB+), SDT has a limited adjunctive role; systemic chemotherapy or radiotherapy are the primary treatment options.
Drug Under Review
Chlormethine is a bifunctional alkylating agent that inhibits rapidly proliferating cells.30 Alkylation of DNA is the primary basis for the cytotoxic actions of chlormethine. Chlormethine binds to N7 positions in guanines via its reactive chloroethyl moieties, potentially binding also to N3 positions in adenines. The bifunctional nature of chlormethine along with its small molecular size allows it to form interstrand cross- links within DNA, by alkylation of guanine-N7 positions in opposite DNA strands. Monoadducts and intrastrand biadducts are also formed, but the formation of interstrand cross-links makes chlormethine a more effective tumour chemotherapeutic agent than monofunctional analogues. Unrepaired interstrand cross-links prevent the transcription, replication, and segregation of DNA, and ultimately cause cell death.2,30
Ledaga is a gel consisting of 0.016% w/w of mechlorethamine (equivalent to 0.02% chlormethine hydrochloride) in propylene glycol. The supplied packaging format is a tube containing 60 g of gel with 0.2 mg of chlormethine hydrochloride (equivalent to 160 mcg of chlormethine per g of gel).30 Ledaga is indicated in the treatment of patients with MF-CTCL. It is for topical application to the skin only and should be initiated under the supervision of a physician experienced in the treatment of MF-CTCL. A thin film of the gel is applied once daily to affected areas of the skin. Treatment with Ledaga should be stopped for any grade of skin ulceration or blistering, or moderately severe or severe dermatitis (e.g., marked skin redness with edema). Upon improvement, treatment with Ledaga can be restarted at a reduced frequency of once every 3 days. If reintroduction of treatment is tolerated for at least 1 week, the frequency of application can be increased to every other day for at least 1 week and then to once-daily application, if tolerated. The main contraindication is severe hypersensitivity to mechlorethamine.2,30
Ledaga (chlormethine gel 160 mcg per g) has a Health Canada indication for the topical treatment of stage IA and IB MF-CTCL in adult patients who have received prior skin-direct therapy. At the time that the CADTH systematic review protocol was established, Ledaga was under review by Health Canada with a proposed indication for the topical treatment of MF-CTCL in adult patients and the reimbursement request for Ledaga was consistent with the proposed indication. In the US, chlormethine gel was approved by the FDA as Valchlor in August 2013 for the topical treatment of stage IA and stage IB MF-CTCL in patients who had received prior SDT for MF.7 In Europe, it is designated as an orphan medicinal product by the Committee for Orphan Medicinal Products. The European Medicines Agency’s (EMA’s) Committee for Medicinal Products for Human Use approved Ledaga for the topical treatment of MF-CTCL in adult patients in December 2016.29
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Groups and Information Gathered
One joint patient group submission was provided on behalf of 3 organizations: Lymphoma Canada, the CSPA, and the CLF.
Lymphoma Canada’s mission is to empower the Canadian lymphoma community through support, advocacy, education, and research. They promote early detection, finding new and better treatments, helping patients equally access those treatments, learning about lymphoma’s causes through research, and finding a cure.
The CSPA’s mission is to promote skin health and improve the quality of life of Canadians living with skin diseases, conditions, and traumas. They advocate for better treatment options and provide education of issues affecting patients with skin conditions.
The CLF is focused on supporting people affected by cutaneous lymphoma. They aim to eliminate the burden of cutaneous lymphoma through promoting awareness and education, advancing patient care, and fostering research.
Lymphoma Canada, with the collaboration and input of the CSPA and CLF, conducted an online survey of cutaneous lymphoma patients, primarily MF patients, from September 14, 2020, until January 11, 2021. The survey was distributed and promoted to the constituents of all 3 patient group organizations. Overall, 233 patients responded to the survey; of these, 210 (90%) patients were diagnosed with MF. Patients were from Canada, the US, and Europe. Of the patients that provided demographic information, 15% were Canadian, 56% were female, and 55% were 60 years old or older.
Disease Experience
MF-CTCL can present in different ways, leading to challenges with diagnosis. Patients reported that they were initially diagnosed with eczema (36%), dermatitis (26%), psoriasis (18%), allergic reaction (10%), and other conditions before being diagnosed with MF-CTCL. Only 25% of patients were correctly diagnosed with MF-CTCL at presentation.
Patients with MF have visible patches or lesions (raised, scaly, or discoloured), itchiness, pain or burning of the skin or lesions, plaques (thick raised lesions), and rash-like skin redness. The majority of respondents reported that their disease had progressed since diagnosis, with more patches or raised plaques, or patches covering more of their body. These symptoms negatively impact the patients’ quality of life and mental and emotional well-being. Patients reported stress related to their diagnosis, anxiety, concerns regarding their body image or physical appearance, difficulty sleeping, feeling self-conscious or embarrassed, difficulty concentrating, financial concerns, and depression.
Patients reported that living with MF-CTCL has negatively impacted their personal image, family relationships, intimate relationships, and work. The following are quotes provided by patients regarding their experience with MF-CTCL:
“Prior to treatment the redness and scaly patches made me self-conscious of the appearance of my skin, especially when the disease progress to areas that were visible in summer clothes.”
“I worry that if my MF progresses beyond stage 1 that my common-law relationship will not last. Trying to apply the cortisone cream by myself is difficult as I can’t always see when new patches are coming out. Afraid to ask for help when home to apply the cream for fear of rejection or argument.”
“I can manage obligations but not without detailed, planned coordination. However, when an itch flare-up occurs, my favorite activities such as running are very uncomfortable.”
Experience With Treatment
Patient respondents reported experience with a variety of MF-CTCL treatments, including systemic therapies, radiation, light treatment, and topical drugs. The most commonly selected systemic therapies included methotrexate and bexarotene. Light treatments included UVB, UVA, and PUVA light therapy. Topical therapies included topical steroids, retinoids, and compounded NM.
In general, patients reported experiencing a range of side effects during and following their treatments: fatigue, itchiness, skin irritation or rash, skin pain or burning, skin discolouration, hair loss, nausea, peripheral neuropathy, and infections. Fatigue, hair loss, severe itchiness, skin burning, and pain were reported to be the most difficult to tolerate.
Patients additionally reported that the number of clinic visits, treatment-related fatigue, and length of time for treatment administration had a significant impact on their quality of life. Patients found that their treatments had a negative effect on their activities, work, and travel.
Patients indicated that they experienced challenges accessing treatments locally within their community, and long travel times had a negative impact on their quality of life. Patients reported that out-of-pocket costs, the cost of treatment, time off work, and travel costs had negative financial impact. The following are quotes from patients regarding their challenges accessing treatment:
“One hour travel required for treatment. Number of treating facilities seems limited. Have traveled as far as 100 miles one way for treatment.”
“[Hospital] isn’t close, but I prefer going there than a local place with no specialist. Traveling there takes time and a lot of money in tolls and parking fees.”
Fifty-six (33%) patient respondents indicated that they had experience with chlormethine gel (Ledaga). The majority of those patients (N = 51 out of 56, [91%]) who had experience with chlormethine gel treatment were from the US. Approximately 56% of patients received chlormethine gel treatment at the same time as light therapy, systemic therapy, and/or radiation. Patients reported that chlormethine gel managed their disease symptoms, including red skin patches, skin itchiness, skin ulcers, and skin pain. Approximately 20% of patients stopped treatment early due to side effects, which included itching, hyperpigmentation, skin blistering, and rash.
Overall, patients did not report a significant negative impact on their quality of life with chlormethine gel treatment, with 39% of patients reporting that their overall health and well-being was unchanged. However, 19% of patients reported great improvement and 32% of patients indicated that their overall health and well-being was somewhat improved by chlormethine gel treatment.
Patients reported that chlormethine gel treatment did not change their ability to exercise, work, and volunteer, spend time with family and friends, and complete activities of daily living. Patients reported some challenges related to travel because the chlormethine gel needs to be refrigerated. Most patients did not report financial challenges related to taking time off work or medication to manage side effects, although the cost of the chlormethine gel treatment did have a financial impact. Overall, 46% of patients indicated that they had a good-to-excellent experience with chlormethine gel treatment, and 74% would take the treatment again if it was an option for them. The following are quotes from patients regarding their experience with chlormethine gel:
“Ledaga has maintained the positive effect originally delivered from my PUVA treatment. I have been very stable, neither positive or negative reactions.”
“It is the only treatment I have had that has improved my skin at all.”
“Other than cost and difficulty to get in Canada, it was a game changer for me.”
Improved Outcomes
The majority of patients (80%) indicated that having a choice in treatment options was extremely important to them. Patients want treatments that result in longer survival, better quality of life, longer remission, fewer side effects, and easier and/or faster treatment application. Overall, 37% of patients would be willing to tolerate potential treatment side effects with a new treatment if their doctor recommended it while 50% were unsure, stating that it would depend on the type of side effect, duration, and cost-benefit ratio.
Clinician Input
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by clinical specialists with expertise in the diagnosis and management of MF-CTCL.
Unmet Needs
The clinical experts consulted by CADTH indicated that current SDT options are limited. Topical corticosteroids are the most commonly used first-line treatment for limited T1 (< 10% BSA) patch/plaque disease. Phototherapy, if accessible, is preferred for T2 (> 10% BSA) disease. Systemic retinoids (alitretinoin or acitretin) or methotrexate may be added to the topical steroids and phototherapy to enhance response, if necessary. Chlormethine is used as second-line treatment for refractory lesions. SDT has a limited adjunctive role in advanced-stage disease (stage IIB+). Systemic chemotherapy or radiotherapy is the primary treatment. Early-stage CTCL has an indolent course. It is unclear if SDT changes the natural history of the disease. The goal of SDT is symptomatic relief of pruritus, reduction in skin disease burden, cosmetic improvement, and possibly reduction in the rate of disease progression. For limited patch disease, observation without treatment is reasonable.
For early-stage MF-CTCL, the clinical experts reported that the goal of treatment is to relieve symptoms (itch, pain), improve quality of life, and prevent disease progression. Quality of life may be affected by physical or psychological impairments. Depending on the extent of the disease (< 10% versus > 10%, patch versus plaques, thin plaques versus thick plaques), symptoms and impact on quality of life vary from minimal to marked. An ideal SDT would clear the skin lesions, be curative or remittive rather than just suppressive, be well tolerated, and be easily accessible. Current treatments have limitations. Topical corticosteroid has a response rate of about 80% but is considered to be suppressive and not a remittive treatment. Long-term use is necessary and may cause skin atrophy. Long-term application to large surface areas may cause adrenal suppression and other systemic corticosteroid adverse effects. Phototherapy is preferred when large surface areas need to be treated. However, there may be sanctuary sites that cannot be easily exposed to the light and these areas may require supplemental topical therapy (corticosteroid or chlormethine). Phototherapy may not be available in some areas or patients may have to commute long distances to receive treatment. It may also increase the risk of skin cancers.
Based on the experts’ clinical experience with topical chlormethine (compounded ointment), it may be remittive, although studies are limited. It is often used for lesions refractory to corticosteroids and/or phototherapy. It may cause allergic or irritant contact dermatitis. Clinical experience suggests that Ledaga gel is more irritating than the compounded ointment; its use is therefore often limited to small areas (< 10% BSA).
The clinical experts noted that current treatments have limitations. Unmet needs include treatments that can be curative, easily accessible, and well tolerated. There is currently no ideal SDT. Topical corticosteroids are not curative. It is unclear if topical corticosteroids can prevent disease progression. Long-term use can cause side effects. Phototherapy may not be accessible to some patients. It may cause skin atrophy and increase the risk of skin cancer. Topical chlormethine causes dermatitis and may not be tolerated, especially when large surface areas are involved. These treatments have efficacy ranging from 60% to 80%, depending on disease severity. Therefore, different treatment options may be required for refractory disease.
Place in Therapy
The clinical experts consulted by CADTH anticipated that it is unlikely that Ledaga will shift the current treatment paradigm as it is only supplied in small 60 g tubes and can only be used for treatment of small surface areas because of its irritancy potential. Ledaga may be used as second-line treatment for lesions refractory to topical corticosteroids or when phototherapy is not accessible or is ineffective. It is unclear if Ledaga can prevent disease progression. Past treatments with chlormethine compounded ointment have shown that it can induce long-term remission in some patients.
Ledaga is only supplied in small 60 g tubes and can only be used for the treatment of small surface areas because of its irritancy.
Patient Population
The clinical experts anticipated that Ledaga may be used to treat lesions refractory to topical corticosteroids or when phototherapy is not accessible or is ineffective. It is best suited for these patients when the area that needs to be treated is limited (< 5% BSA). In most cases, Ledaga will not be used as first-line therapy. Patients will be treated with first-line corticosteroids or phototherapy. Ledaga will be considered for refractory lesions when the disease is limited (< 10% BSA, preferably < 5%; patch or plaque). Ledaga would not be suitable for patients with extensive disease (> 20% BSA) or those with tumours.
Assessing Response to Treatment
Per the clinical experts consulted by CADTH, treatment response is assessed clinically (the reduction of extent of disease, the flattening of lesions) and should not be difficult to determine. The outcomes used in clinical practice to assess response to treatment include the clearance of skin, the reduction of extent of disease, the flattening of lesions, the relief of symptoms, and improvement in quality of life. These also represent a clinically meaningful response to treatment. These outcomes are easy to assess clinically and are not expected to vary across physicians. Treatment response should be assessed at 3 months initially, and every 3 months to 6 months thereafter.
Discontinuing Treatment
Per the clinical experts, factors that should be considered when deciding to discontinue treatment include disease progression or lack of response after 6 months of treatment, as well as adverse effects such as irritation that are not ameliorated by treatment such as reducing application frequency, diluting medication, corticosteroid treatment, and so forth.
Prescribing Conditions
The clinical experts consulted by CADTH thought that diagnosis, treatment, and the monitoring of patients with MF-CTCL should be carried out at CTCL clinics with specialists knowledgeable in CTCL and its various treatments. As such, Ledaga should be administered under the direction of specialty CTCL clinic physicians.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. Lymphoma Canada, a national not-for-profit organization for Canadian lymphoma and chronic lymphocytic leukemia patients, coordinated the clinician group response. The feedback provided from 5 clinicians on Ledaga for the topical treatment of MF-CTCL in adult patients is summarized as follows.
Unmet Needs
According to the clinician group, the treatment that can be compared to Ledaga currently is compounded chlormethine ointment, which has limited availability in Canada. The paradigm of treatment for the MF-CTCL patient population is a prioritization of SDT for early-stage disease (stage IA to stage IIA). There is no gold standard treatment, and combination therapies have been beneficial. Chlormethine is positioned as a key therapy for early-stage skin limited disease (first-line treatment in other countries, second-line treatment in Canada). Chlormethine can be compounded into an alcoholic base, although ointment is what is generally used. However, very few pharmacies are capable of compounding it in either base. Furthermore, compounded ointments have limited stability. Additional comparisons include compounded bis-chloroethyl nitrosourea, which requires a regular blood test due to a non-negligible risk of bone marrow suppression and/or toxicity. Chlormethine directly results in apoptosis of malignant cells as well as the improvement of symptoms of itch and/or burning caused by MF. Other SDTs for early-stage MF (stage IA to stage IIA) have variable response rates and include topical steroids (first-line treatment), imiquimod (cost not covered for the treatment of MF), tazarotene gel (cost not covered for the treatment of MF), phototherapy (UVB, NB-UVB light), photochemotherapy (PUVA light), or external electron beam radiotherapy (used for unilesional disease).
The clinicians noted that the addition of effective topical treatment would be extremely useful in the treatment of patients. The goals of this topical therapy include disease control, symptom control, and improved quality of life. Importantly, for select skin sites such as scalp and other hair-bearing areas where the application of creams and ointments is difficult, having a gel product that can be applied would be especially useful in the treatment of these patients. Gel is stable, non-greasy, and quick drying, and ultimately allows for convenient, simple at-home administration, thereby encouraging compliance. This would reduce the severity of a patient’s symptoms, prevent disease progression, improve skin-related quality of life, and improve skin disease scores. Chlormethine is a standard and useful treatment, but currently is only rarely used because it is not always available, and not stable. Further, this option is more convenient than light treatment (phototherapy or photochemotherapy) for patients who live far from a clinic.
Considering the treatment goals described previously, the clinician group reported that patients who would benefit from this therapy include adult patients with stage IA to stage IIA of MF with less than 15% BSA involvement (stage IA and stage IIA < 10%; stage IB > 10%) and patients with select skin sites involved by MF (e.g., hair-bearing areas). MF is a chronic disease where patients often experience disease relapse. Hence, most patients throughout the course of their disease cycle through multiple treatments (topical steroids to retinoids to a combination of steroids and retinoids, to imiquimod, phototherapy, radiotherapy, and so forth). Chlormethine gel can be offered to patients who have failed or not tolerated at least 1 prior SDT (e.g., potent and ultrapotent topical steroids for 3 months or phototherapy for 30 treatments). This therapy will offer more choices for this population, and a stable gel formulation would be of particular benefit to patients with hairy areas involved (scalp, beard area), where the existing topical preparations (compounded creams or ointments) are difficult to apply.
Overall, the clinicians noted that given most patients are diagnosed in the early stage of the disease (stage IA to stage IIA) and that there are limited therapeutic options for early-stage disease, there is a need for additional effective topical treatment for MF-CTCL. Chlormethine gel represents an ideal therapy as it is stable, easy to apply at home, has low toxicity, requires no laboratory or blood test monitoring, and has few side effects. There is a need for formulations that are more convenient to apply since MF is a chronic disease.
Place in Therapy
In terms of how chlormethine gel would fit into the current treatment paradigm, the clinician group noted that treatment with chlormethine gel would be ideal for patients with MF-CTCL with less than 10% to 15% of BSA affected (stage IA to stage IIA) and with disease affecting hair-bearing areas. The clinician group anticipated that this would be a second-line therapy for patients who have failed topical steroids, but who are neither severe enough, nor progress quickly enough, to require systemic therapy. This drug could be used as monotherapy or in combination with other treatments with non-overlapping toxicities (e.g., topical steroids or topical retinoids such as tazarotene gel). Topical corticosteroids (for 3 months) and NB-UVB are considered the first-line treatments in patients with mild disease. For certain areas such as beard and scalp, there are no good first-line alternatives. Therefore, this topical agent could be used as a first-line agent in these locations. For other locations, chlormethine gel would be considered a second-line treatment, with the main alternative of UVB. If UVB was not available, chlormethine gel could be used after potent or ultrapotent topical steroids had failed.
The clinician group indicated that topical steroids could be administered again if chlormethine gel fails. This would be within the second-line treatment options. There are third-line and fourth-line treatments if second-line therapy fails. Frequently, multiple therapies are used that have synergistic beneficial effects, but different side effects. Progressive disease would require other treatment modalities (topical tazarotene, imiquimod for limited affected area [< 10% to 15% BSA], radiation, photochemotherapy, or systemic therapies with retinoids, methotrexate, extracorporeal photopheresis, and/or interferon for more extensive disease). If there is a response and relapse after treatment discontinuation, restarting treatment with chlormethine gel and a slower wean would be appropriate. For many patients, greater access to this therapy would displace UVB and other therapies, except for a short course of potent steroids and radiotherapy (for unilesional disease).
Patient Population
In terms of which patients would be best suited for treatment with chlormethine gel, the clinician group suggested it as second-line therapy for patients who have failed topical steroids and or phototherapy (or if phototherapy is not available or contraindicated) — specifically, patients with early-stage MF (stage IA to stage IIA). This treatment will be considered especially for patients affected with the disease in hair-bearing areas of the skin.
Regarding how patients best suited for treatment with chlormethine gel be identified, the clinician group explained that the diagnosis of early MF can be challenging as it is based on clinicopathologic correlation. Ideally, patients should be evaluated in a multidisciplinary clinic or by specialized dermatologists with a biopsy skin tissue reviewed by a specialized pathologist. Only patients with a pathologic confirmation in the early stages of the disease (stage IA to stage IIA) would be offered this therapy. It is likely that initial SDT would include topical steroids and/or phototherapy (unless phototherapy is not available or contraindicated — as in porphyria or solar urticaria patients). As such, chlormethine gel would likely be second-line therapy, and it is reasonable to consider that diagnosis would have been already properly established. The progression or lack of response of skin compartment is decided based on a clinical exam using a modified SWAT and visual activity score as well as the Dermatology Life Quality Index and Skindex-29 tool for pruritus assessment. There would not be any other considerations for selecting patients to receive this treatment. Patients may be less suited for this therapy if they have thick lesions, are erythrodermic, and with folliculotropic and/or syringotropic (i.e., deeper-seated) disease. Further, MF-CTCL patients in the advanced stages (≥ stage III) or tumour stage (stage IIB) and pediatric patients (< 18 years of age) would be least suitable for treatment with this therapy. There is no predictor of response except the occurrence of contact dermatitis to chlormethine gel, which is associated with a better clinical response and the thickness of plaques (thinner lesions exhibit better clinical response).
Assessing Response to Treatment
Per the clinician group, clinical improvement (defined as thinning of the plaques or disappearance at 3 months to 6 months after daily application begins) is generally used in clinical practice to determine whether a patient is responding to treatment. Pathologic confirmation of response is not required. Outcomes to determine patient response can include a modified SWAT and a visual activity score as well as the Dermatology Life Quality Index, and the Skindex-29 tool for pruritus assessment. Treatment should be continued daily for at least 6 months before declaring it as ineffective if no objective response is observed. If skin improvement is noted along with the resolution of plaques and/or patches, the treatment will be continued for 1 year, at which point the patient can be switched to a different therapy or this therapy (chlormethine gel) could be tapered to less frequent usage. Treatment response should be assessed every 3 months to 6 months for efficacy and safety. It may take more than 9 months to 12 months to achieve maximum clinical response.
Discontinuing Treatment
Per the clinician group, factors to consider when deciding to discontinue treatment include a lack of clinical response (or a loss of clinical response if previously responsive), and development of persistent and severe allergy or other prohibitive side effects. These include dermatitis (redness, skin breakdown) that interferes with the quality of life and is not responsive to dose decrease and topical steroids. Notably, the development of mild transient contact dermatitis at the site of the treated lesion corresponds with the improved clinical response of the malignant skin patch and/or plaque.
Prescribing Conditions
In terms of appropriate settings for patients with MF-CTCL to receive treatment, the clinician group suggested that patients attend a multidisciplinary clinic or specialist with an interest and/or expertise in this disease. This would include a hospital-based subspecialty clinic; however, any outpatient setting in specialized clinics or a community setting is appropriate for patients to receive treatment with chlormethine gel and be monitored while receiving treatment.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Jurisdictional implementation issues | |
Relevant comparators | |
Chlormethine ointment was used as a comparator to chlormethine gel in phase II of Study 201. Chlormethine is not a funded or available comparator for most jurisdictions. | This is a valid concern shared by clinical experts consulted for this report. An ideal comparator would have been one that is standard of care in Canada (e.g., phototherapy). |
Policy considerations for reimbursing the drug | |
Considerations for initiation of therapy | |
Is diagnosis of MF-CTCL confirmed with a skin biopsy or are there alternate methods of diagnosis? Should diagnosis be confirmed within a specific time frame before initiating treatment with chlormethine gel? | Diagnosis is confirmed with a skin biopsy. There is no specific time frame for initiating treatment. |
MF is the most common subtype of CTCL. Are there any other subtypes or variants of MF-CTCL that are eligible? | Some patients with Sezary symptoms could be considered for this treatment. |
In Study 201, patients were eligible if they had persistent or recurrent stage IA, stage IB, or stage IIA MF-CTCL without progression beyond stage IIA. The submitted funding request includes all stages. If there will be restrictions on eligibility based on stage in the CADTH recommendation, what would be the definitions for each stage? | Chlormethine gel would be considered for disease stages included in the trial (stage IA, stage IB, and some stage IIA), but not all stages of the disease. |
In Study 201, patients were required to have been treated with at least 1 prior SDT. Should patients be required to have been treated with at least 1 SDT before being eligible for chlormethine gel? | Chlormethine would be used as second-line therapy to treat lesions refractory to topical corticosteroids or when phototherapy is not accessible or ineffective. If there are no major contraindications to phototherapy or corticosteroids, these are typically used as first-line treatment. |
In Study 201, patients were required to have a 4-week washout period of treatment directed at the disease before initiating chlormethine gel. In practice, is a washout period required before starting chlormethine gel and, if so, for what duration? | A washout period is not needed before initiation of any treatment for MF. |
Are patients eligible for re-treatment at any time while off therapy? | Yes. |
Considerations for continuation or renewal of therapy | |
In Study 201, the CAILS and SWAT response criteria tools were used. Are these appropriate methods to evaluate benefit from/response to chlormethine gel? | The rating tools are appropriate for the trial but CAILS, in particular, is not commonly used in clinical practice to assess treatment response in patients with MF. |
Time to response in Study 201 was reported as a median of 26 weeks in the chlormethine gel treatment arm. What is the recommended frequency of treatment response assessment? | Treatment response is assessed every 2 months to 3 months. If the patient is not experiencing adverse reactions to the drug, treatment is continued for at least 6 months before a decision is made regarding efficacy. |
Considerations for discontinuation of therapy | |
How is response to chlormethine gel monitored? What are the definitions for response? Is treatment continued if some lesions respond and others do not respond? What are the criteria to determine treatment discontinuation of chlormethine gel? | Clinical improvement can include the following: complete or significant partial remission, reduction in the extent of the disease, thinning of the plaques or disappearance at 3 months to 6 months after daily application begins, and improvement in a patient’s quality of life. Pathologic confirmation of response is not required. Outcomes to determine patient response can include mSWAT and VAS as well as DLQI and the Skindex-29 tool for pruritus. The discontinuation of chlormethine gel is considered in the case of disease progression or lack of response after 6 months of treatment, or adverse effects such as irritation that is not ameliorated by treatment like reducing application frequency, dilution of medication, corticosteroid treatment, and so forth. |
Considerations for prescribing of therapy | |
How is quantity to be dispensed determined? Chlormethine gel is provided in a 60 g tube. The sponsor estimated similar treatment costs using a dose of 1.8 g topically per day per 30 days for patients with both low skin burden disease and high skin burden disease. How long does a 60 g supply last in patients with low skin burden vs. high skin burden? | Patients with high skin burden require a higher quantity of the drug than those with low skin burden. For a patient with 5% affected BSA, a 60 g tube may last 1 month, whereas for a patient with 50% affected BSA, a 60 g tube may last 1 day to 2 days. |
Special implementation issues | |
Generalizability | |
Are patients with Sézary syndrome (a subtype of CTCL) eligible for treatment with chlormethine gel if they have skin lesions? | Sézary syndrome usually involves larger lesions. Chlormethine is generally not appropriate to treat large lesions (higher percentage of BSA). |
Care provision issues | |
Are there any special precautions or PPE required for the patient or caregiver for the handling or administration of chlormethine gel? What safety measures should be in place for storing the opened product? | Patients must wash hands thoroughly with soap and water after handling or applying Ledaga. Caregivers must wear disposable nitrile gloves when applying Ledaga to patients and wash hands thoroughly with soap and water after removing gloves. Refrigerated storage is required once Ledaga is dispensed (before dispensing, it must be stored in the freezer at −25°C to −15°C). |
System and economic issues | |
The budge impact analysis may be underestimated both due to the number of patients and the volume of skin lesions requiring additional tubes. The sponsor estimated similar quantities of chlormethine gel required for both high skin burden disease vs. low skin burden disease categories. | The quantity of chlormethine gel required for the treatment of patients with MF is proportional to skin burden. Patients with higher skin burden require a higher quantity of the drug to treat lesions. |
BSA = body surface area; CAILS = Composite Assessment of Index Lesion Severity; CTCL = cutaneous T-cell lymphoma; DLQI = Dermatology Life Quality Index; MF = mycosis fungoides; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma; mSWAT = Modified Severity-Weighted Assessment Tool; PPE = personal protective equipment; SDT = skin-directed therapy; SWAT = Severity-Weighted Assessment Tool; VAS = visual activity score; vs. = versus.
Clinical Evidence
The clinical evidence included in the review of chlormethine hydrochloride 0.02% topical gel (Ledaga) is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as any studies that were selected according to a protocol established in advance. The second section includes an extension study. No indirect evidence (i.e., indirect treatment comparison) was submitted by the sponsor.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the efficacy and safety of ready-to-use 0.02% w/w chlormethine hydrochloride topical gel (Ledaga) for the treatment of adult patients with MF-CTCL
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 4. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans. Of note, the systematic review protocol presented below was established before the granting of a Notice of Compliance from Health Canada.
Table 4: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients (≥ 18 years of age) with MF-CTCL Subgroups:
|
Intervention | Ready-to-use 0.02% w/w chlormethine hydrochloride topical gel (Ledaga) |
Comparator |
|
Outcomes | Efficacy outcomes:
Patient-reported outcomes/HRQoLa Harms outcomes:
Notable harms:
|
Study designs | Published and unpublished RCTs |
AE = adverse event; HRQoL = health-related quality of life; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma; NB-UVB = narrow band ultraviolet B; PUVA = psoralen plus ultraviolet A; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus; WDAE = withdrawal due to adverse event.
aThese outcomes were identified as being of particular importance to patients in the input received by CADTH from patient groups.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.31
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. The search strategy comprised both controlled vocabulary, such as the US National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Ledaga, chlormethine, and cutaneous T-cell lymphoma. Clinical trials registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, the WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, the European Union Clinical Trials Register, and Canadian Cancer Trials.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategy.
The initial search was completed on January 26, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on June 10, 2021.
Grey literature was identified by searching relevant websites from the following sections of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.32 Included in the search were the websites of regulatory agencies (the US FDA and EMA). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 586 citations were identified; 582 were excluded, while 4 potentially relevant citations were retrieved for full-text screening.8,33-35 Three potentially relevant reports from other sources, including clinical practice guidelines and regulatory approval, were also identified.4,7,29 One study met the selection criteria and was included in this systematic review (Figure 1).8 The details of the included study (Study 201) are summarized in Table 5: Details of the Included Study. Excluded studies are listed in Appendix 2, Table 28. Other information relevant to this report was derived from additional sources, including the submission to CADTH and Health Canada, FDA, and EMA reports.7,29,36
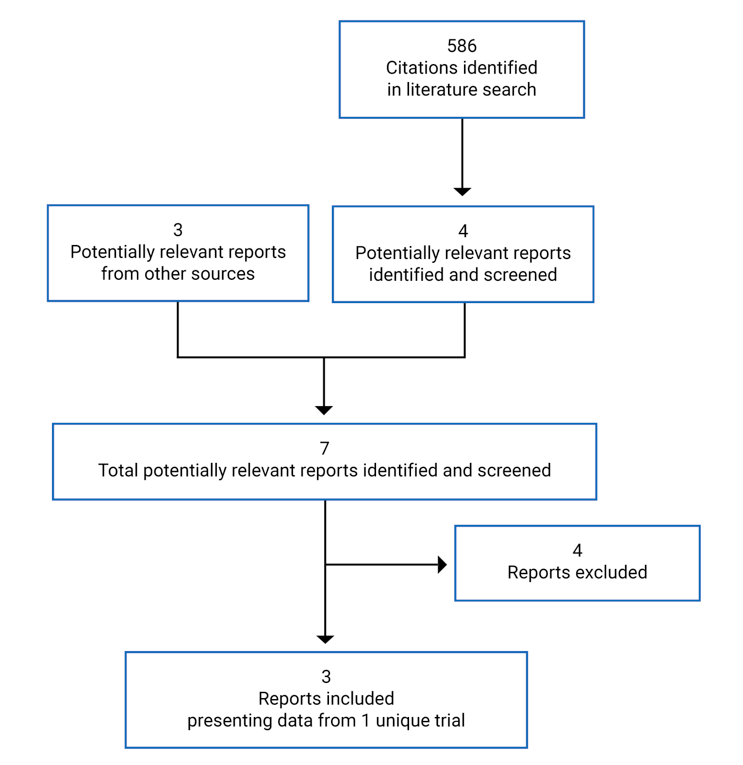
Table 5: Details of the Included Study
Criteria | Study 201 (2005NMMF-201-US) |
|---|---|
Design and population | |
Study design | Randomized, controlled, observer-blinded, multi-centre trial |
Locations | 13 academic centres in the US |
Study duration | May 2006 to July 2010 (plus August 2011 for extended 12-month follow-up) |
Randomized (N) | 260 (1:1) |
Inclusion criteria |
|
|
|
Drugs | |
Intervention | Topical 0.02% mechlorethamine hydrochloride in propylene glycol gel, applied once daily to specific lesions or to the total skin surface for up to 12 months |
Comparator(s) | Topical 0.02% mechlorethamine hydrochloride in petrolatum ointment (Aquaphor), applied once daily to specific lesions or to the total skin surface for up to 12 months |
Duration | |
Phase | |
Run-in | 4-week washout period |
Double-blind | 12 months |
Follow-up | 12 months |
Outcomes | |
Primary end point | Response rate using the CAILS |
Secondary and exploratory end points |
Safety and tolerability:
|
Notes | |
Publications | Lessin et al. (2013)8 |
AE = adverse event; BSA = body surface area; CAILS = Composite Assessment of Index Lesion Severity; CBC = complete blood count; MF = mycosis fungoides; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma; SDT = skin-directed therapy; SWAT = Severity-Weighted Assessment Tool.
Note: 3 additional reports were included (the Common Technical Document36 and regulatory review reports from the European Medicines Agency29 and the FDA7).
Source: Clinical Study Report for Study 201.9
Description of Study 201
Study 201 (NCT00168064) was a randomized, controlled, observer-blinded, multi-centre trial conducted in 13 academic centres across the US that investigated chlormethine/mechlorethamine hydrochloride 0.02% topical gel for patients with early-stage MF-CTCL (the study initiation date was May 8, 2006, and the study completion date was August 4, 2011). It was a noninferiority trial comparing 0.02% chlormethine hydrochloride gel with 0.02% chlormethine hydrochloride compounded ointment over a 12-month period (Figure 2). The sponsor states that chlormethine ointment was chosen as a comparator for Study 201 because its effectiveness and safety have been well established in a number of studies and historical use in real-world clinical practice. Although non-gel formulations of chlormethine were previously used in clinical practice, these formulations are no longer widely used due to issues associated with the formulation, including compound stability, accessibility (e.g., availability of compounding pharmacies), and the inconvenience of applying it to the skin (i.e., greasiness). The gel formulation was intended to overcome these formulation-based issues and improve patient adherence to treatment.2
Sample size: The final sample size for Study 201 was calculated with an assumed 68% response rate for the comparator arm in the efficacy-evaluable (EE) population. Assuming a 75% retention effect (a lower bound on the noninferiority margin of 0.75 based on the ratio of response rate), a power of 80%, a 95% CI for the estimate of the ratio, and a 25% non-evaluability rate, a sample size of approximately 125 patients per group was required.
Randomization: Prior to randomization, patients were stratified into 2 groups by MF stage (stage IA versus stage IB and stage IIA). Stratified, blocked randomization was performed by personnel in each site. The master list of randomization numbers with the corresponding study drug assignments was sent to the study sites where the site pharmacist was responsible for providing the correct study drug using the master list.9 Patients were screened for eligibility and randomized to treatment arms up to 90 days before the baseline visit, at which time disease status was reassessed. If disease status had changed from stage IA to stage IB or stage IIA, the patient was re-randomized. If the patient had progressed beyond stage IIA, they were withdrawn from the trial.37
Blinding: Investigators and other individuals involved with patient assessments were blinded to the assigned treatment. The study site personnel not involved with patient assessment were not blinded. Patients could not be blinded due to differences in the physical characteristics of the 2 treatments — 1 a clear, colourless, alcohol-based gel and the other a petrolatum-based (Aquaphor) formulation.
Treatment phase: All patients completed a washout period of MF-CTCL therapies for 4 weeks before initiating the trial treatments. After a 4-week washout period, patients in both treatment groups were instructed to apply the treatment once daily to specific lesions or to the total skin surface, depending on the extent of BSA coverage of the patients. Treatment was continued for 12 months unless disease progression, treatment-limiting toxicity, concomitant illness, or other changes in a patient’s health status necessitated the discontinuation of study treatment.2,8
Follow-up period and open-label extension trial: All patients who entered the study and received at least 1 dose of the study drug were evaluated during an additional 12 months (off-study) for more safety information, regardless of whether they completed the 12 months of study treatment or withdrew before the end of study for any reason. Follow-up visits occurred every 3 months and consisted of a targeted history, including any ongoing AEs, current treatment for MF, and the assessment of toxicity with special attention to nonmelanoma skin cancers. Additionally, during this 12-month follow-up period, patients who had not achieved a CR based on the primary efficacy outcome (CAILS) with either the chlormethine hydrochloride gel or chlormethine hydrochloride ointment (0.02%) were given the option to enrol in Study 202, an open-label 7-month extension study investigating a higher strength formulation of chlormethine hydrochloride gel (0.04%).2 Patients who did not enrol in Study 202 from the chlormethine gel arm (n = 37) or chlormethine ointment arm (n = 26) were able to begin any other therapy for MF-CTCL within the follow-up period, as deemed medically necessary by the principal investigator.2
Populations
Inclusion and Exclusion Criteria
A skin biopsy of a representative lesion obtained within the 90 days before study initiation and after a 4-week washout period was used to confirm diagnosis of MF-CTCL. Patients must not have used steroids for at least 4 weeks before the diagnostic skin biopsy. To be included in the study, patients had to:
have a diagnosis of stage I or stage IIA (cutaneous only) MF, without history of progression beyond stage IIA; patients with histologic variants, folliculotropic or syringotropic MF, or LCT were eligible
have had previous treatment with at least 1 SDT for MF, including PUVA, UVB, and/or corticosteroids
have laboratory values within the range of normal limits for the participating institution, unless they were deemed not clinically relevant by the principal investigator
be free of serious concurrent illness
for females and males of child-bearing potential, be using an effective means of contraception; females had to have a negative pregnancy test.
The main exclusion criteria were that patients:
were newly diagnosed with MF-CTCL with no prior therapy
had prior treatment with topical mechlorethamine within the past 2 years or topical carmustine (bis-chloroethyl nitrosourea)
had used topical or systemic therapies, including corticosteroids for MF, within 4 weeks of entry in the study
had radiation therapy within 1 year of study entry
were pregnant or breastfeeding
were patients with serious known concurrent medical illness or infection that could potentially present a safety risk or affect compliance with the requirements of the treatment program.
Baseline Characteristics
Of the 322 patients assessed for eligibility, 62 were excluded (53 did not meet inclusion criteria, 7 declined to participate, and 2 were excluded for other reasons). The remaining 260 patients were enrolled, stratified by their baseline MF stage (stage IA, n = 141 [54%]; stage IB and stage IIA, n = 119 [46%]) and randomized to receive treatment with chlormethine hydrochloride 0.02% gel (n = 130) or chlormethine hydrochloride 0.02% ointment (n = 130).
Baseline demographic and clinical characteristics of the 260 patients randomized into the trial are summarized in Table 6. Baseline characteristics were generally well balanced across the 2 treatment arms. The slight imbalance across MF-CTCL stages between the gel and ointment treatment arms was due to a protocol violation involving randomization at 1 study site, which is described in more detail later in the report. The median age was 58 years (range = 11 years to 88 years). The majority of patients were between 18 years and 64 years of age (71.5% in the gel treatment arm and 66.2% in the ointment treatment arm). Overall, 59.2% of patients were male and 40.8% were female. Overall, 54.2% of patients had stage IA disease and 44.2% of patients had stage IB disease at baseline; 2 patients in each treatment arm had stage IIA disease at baseline. There were 5 patients with folliculotropic MF, 1 patient with syringotropic MF,1 patient with LCT and 1 patient with folliculotropic MF and LCT changes in the study.2 The median percentage of BSA involvement at baseline was 8.0% (range = 1% to 61%) in the gel arm and 10.0% (range = 1% to 90%) in the ointment arm.
The median number of prior treatments was 2 (range = 1 to 12 treatments). The most common prior SDT was corticosteroids used in 86% of patients in both treatment arms.8
Table 6: Summary of Baseline Characteristics
Characteristic | Chlormethine gel (N = 130) | Chlormethine ointment (N = 130) |
|---|---|---|
Demographics | ||
Sex, N (%) | ||
Male | 77 (59.2) | 77 (59.2) |
Female | 53 (40.8) | 53 (40.8) |
Race/ethnicity, N (%) | ||
Caucasian | 97 (74.6) | 96 (73.8) |
Afro-American | 16 (12.3) | 19 (14.6) |
Other | 17 (13.1) | 15 (11.5) |
Age, years, N (%) | ||
< 18 | 0 (0.0) | 1 (0.8) |
18 to 64 | 93 (71.5) | 86 (66.2) |
65 to 74 | 29 (22.3) | 33 (25.4) |
≥ 75 | 8 (6.2) | 10 (7.7) |
Disease characteristics | ||
Time from initial diagnosis, N (%) | ||
< 6 months | 47 (36.2) | 45 (34.6) |
6 months to 1 year | 18 (13.8) | 22 (16.9) |
1 year to 2 years | 14 (10.8) | 13 (10.0) |
≥ 2 years | 51 (39.2) | 50 (38.5) |
Prior MF therapies, N (%)a | ||
Corticosteroids | 112 (86.1) | 113 (86.9) |
Phototherapy | 50 (38.5) | 53 (40.8) |
Targretin (bexarotene) | 23 (17.7) | 23 (17.7) |
Topical NM (> 2 years from study) | 16 (12.3) | 13 (10.0) |
Interferons | 3 (2.3) | 5 (3.8) |
Methotrexate | 3 (2.3) | 3 (2.3) |
Radiation | 3 (2.3) | 2 (1.5) |
Othera | 14 (10.8) | 34 (26.2) |
MF stage, N (%) | ||
Stratum 1: Stage IA | 76 (58.5) | 65 (50.0) |
Stratum 2 | 54 (41.5) | 65 (50.0) |
Stage IB | 52 (40.0) | 63 (48.5) |
Stage IIA | 2 (1.5) | 2 (1.5) |
Baseline CAILS score, mean (± SD) | 37.3 (17.54) | 37.4 (17.56) |
Median (range) | 34 (2 to 79) | 34 (6 to 87) |
Baseline SWAT score, mean (± SD) | 14.4 (15.87) | 19.2 (20.58) |
Median (range) | 9.0 (1 to 104) | 11.0 (1 to 104) |
Baseline percentage of BSA, mean (± SD) | 12.1 (11.78) | 16.6 (17.19) |
Median (range) | 8.0 (1 to 61) | 10.0 (1 to 90) |
BSA = body surface area; CAILS = Composite Assessment of Index Lesion Severity; MF = mycosis fungoides; NM = nitrogen mustard; SD = standard deviation; SWAT = Severity-Weighted Assessment Tool.
aPatients could have more than 1 prior therapy. “Other” includes primarily emollients, antibacterials, antifungals, and retinoids other than Targretin.
Source: Lessin et al. (2013)8 and Ledaga European Public Assessment Report.29
The baseline percentages of BSA according to the MF-CTCL stage in the chlormethine gel arm and the chlormethine ointment arm are presented in Table 7. These were largely similar between the 2 treatment arms: the median percentage of BSA was || for patients with stage IA in both the gel and ointment arms and |||| and |||| for patients in the gel arm and ointment arm, respectively.38
Table 7: Baseline Percentage of Body Surface Area by Baseline MF-CTCL Stage and Treatment Group — Intention-To-Treat Population
Baseline percentage of BSA | Chlormethine gel | Chlormethine ointment | All patients | ||||
|---|---|---|---|---|---|---|---|
MF stage IA (N = 76) | MF stage IB or stage IIA (N = 54) | Total (N = 130) | MF stage IA (N = 65) | MF stage IB or stage IIA (N = 65) | Total (N = 130) | N = 260 | |
N | 75 | 54 | 129 | 63 | 64 | 127 | 256 |
Mean (SD) | |||||| | |||||||||||||| | |||||||||||| | |||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Median | | | | | | | | | | | | | | |
Interquartile range (Q1, Q3) | |||||||||| | |||||||||||||| | |||||||||||| | |||||||| | |||||||||||||| | |||||||||||| | |||||||||||| |
Range (min., max.) | |||| | |||| | |||| | |||| | |||| | |||| | |||| |
BSA = body surface area; MF = mycosis fungoides; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma; max. = maximum; min. = minimum; Q1 = quartile 1; Q3 = quartile 3; SD = standard deviation.
Source: Sponsor’s responses to CADTH’s request for additional information.38
Interventions
The investigational treatment was mechlorethamine hydrochloride 0.02% in propylene glycol gel and the comparator treatment was chlormethine hydrochloride 0.02% compounded in Aquaphor ointment. Patients were instructed to apply a thin layer of gel or ointment to the affected skin at approximately the same time each day and not to wash it off for a minimum of 4 hours. Patients with stage IA disease were instructed to apply the treatment to all affected lesions. Patients who had either stage IB or stage IIA MF or those whose severity of new lesions after treatment initiation met criteria for progressive disease (≥ 25% worsening) could apply the treatment to the full body (except mucous membranes).29 Once-daily treatment was continued for up to 12 months unless disease progression, treatment-limiting toxicity, concomitant illness, or other changes in health status necessitated treatment discontinuation. The daily frequency of application was reduced for toxicity (e.g., every other day). If new lesions appeared in untreated areas, patients were converted from spot treatment to regional or whole-body treatment. Full body application was generally prescribed if the patient had either stage IB or stage IIA MF or the severity of new lesions developing after treatment initiation met the criteria for progressive disease (≥ 25% worsening). The final decision to treat specific lesions or the whole body was at the discretion of the investigator.8 Other therapies to treat MF were not allowed during the trial. Topical steroids (up to 1%) were permitted, but only on non-MF lesions.
Outcomes
A list of efficacy and safety end points identified in the CADTH review protocol that were assessed in Study 201 is provided in Table 9. These end points are further summarized as follows and in more detail in Appendix 4.
The primary efficacy end point of Study 201 was response rate, defined as improvement of 50% or more (i.e., CR or PR) in the patient’s CAILS score versus baseline. The response rate was measured at each study visit for up to 12 months of treatment. A patient was considered a responder if the response (CR or PR) was maintained for at least 2 consecutive visits (or at least 28 days). The CAILS requires scoring of up to 5 index lesions selected for assessment of efficacy: scaling, erythema, plaque elevation, and surface area. The sum of the scores for each of these categories and each of the 5 index lesions provides the total CAILS score.
The main secondary efficacy end point was response rate using the SWAT. This score is a determination of the weighted percentage involvement of total BSA and captures both the extent and severity of skin disease on a continuous scale; it is intended to provide an objective and quantitative measure of disease status. The SWAT score was determined by weighting BSA involvement for patches, plaques, and tumours, and summing the scores for each category. The SWAT score was the sum of (1 × patch percentage of BSA) + (2 × plaque percentage of BSA) + (3 × tumour per ulcer percentage of BSA).9
The CAILS and SWAT scores were calculated at baseline and at each study visit within the 12-month study period. Response was categorized using standard oncology criteria as follows:
CR: No evidence of disease — 100% improvement and a score of 0
PR: Partial but incomplete clearance (50% to < 100%); evidence of disease remains — a score of 50% or more in a reduction from the baseline score
Stable disease: Disease has not changed from baseline condition — a score of less than 50% in a reduction from the baseline score
Progressive disease: Disease is worse than at baseline evaluation by a score of 25% or more in an increase from the baseline score
Other secondary end points were as follows:
Total percentage BSA response rate: There was a change in the percentage of total BSA involved and a component of SWAT was used as a measure of the overall extent of cutaneous disease. To assess noninferiority with respect to the percentage of BSA, consistent with CAILS and SWAT, response was defined as an improvement of 50% or more from baseline in the percentage of BSA that is confirmed at the next visit in 28 days or later.
Time to response: Assessed by the CAILS score, this was defined as the time interval from the first day that the study drug was dispensed to the time of the first confirmed response.
Duration of response: Assessed by the CAILS score, this was defined as the time from the first evidence of response to the first assessment where the response was no longer apparent (≥ 25% increase from the baseline CAILS score).
Time to progression: This was the time from the first day study treatment was applied to the date that the first disease progression occurred (≥ 25% increase from the baseline CAILS score).
Safety Outcomes
All patients who received at least 1 dose of the study treatment were evaluated for safety outcomes. This included standard laboratory blood tests (chemistries and complete blood cell count, and differential cell count), physical examinations, and AE monitoring. Based on previous published data on the topical use of chlormethine in various formulations that suggest lack of toxicity due to systemic exposure to chlormethine, in Study 201, the initial list of potential adverse drug reactions was limited to AEs occurring in the skin and with an incidence of 2% or more (≥ 3 patients in either treatment group). The list was further contrasted with the findings in the published literature and taking into account the pharmacology of the drug and any reasonable causal relationships. Additionally, all non-skin AEs reported in more than 3 patients in the chlormethine gel group compared to the chlormethine ointment group were added to the list of potential adverse drug reactions.2
Toxicity was evaluated and graded according to the National Cancer Institute Common Toxicity Criteria of Adverse Events, version 3.0. AEs were classified by standardized Medical Dictionary for Regulatory Activities query and Medical Dictionary for Regulatory Activities preferred terms.
Treatment-limiting AEs: Grade 3 or grade 4 local dermal irritation that did not resolve to grade 2 or lower within 2 weeks off the study medication. In these cases, treatment frequency was reduced, or treatment was discontinued for up to a maximum of 4 weeks and treatment was resumed after irritation had improved to a grade 2 or lower. Therapies allowed for skin irritation included topical emollients and systemic antihistamines; topical corticosteroids were not permitted. Grade 3 or grade 4 local dermal irritation with a positive patch was considered allergic contact dermatitis but other manifestations were considered irritant contact dermatitis (Table 8).
Serious AEs: This is any AE that is fatal or life-threatening, is permanently disabling, requires or prolongs an inpatient’s hospitalization, or is a congenital anomaly, cancer, or overdose.
Death: All deaths were listed for all randomized and treated patients with the characteristics of the corresponding event that led to death.
Squamous cell carcinomas: Patients received follow-up and were evaluated for squamous cell carcinomas of the skin for an additional 12 months after receiving the study treatment.
Serum assays were collected from a subset of patients who agreed to have blood levels evaluated (on day 1 and at 4 weeks) to measure systemic absorption of chlormethine using high-performance liquid chromatography.
Table 8: Grading of Local Dermal Irritation
Grade | Defining clinical signs |
|---|---|
0 = No reaction | None |
1 = Mild | Definite pink or red colouration |
2 = Moderate | Increased redness, possible edema |
3 = Moderately severe | Very red, with edema, with or without vesiculation |
4 = Severe | Deep red, with swelling and edema, with or without signs of bullae formation and necrosis |
Source: Clinical Study Report for Study 201.9
Response and AEs were assessed every month between month 1 and month 6 and every 2 months between month 7 and month 12.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | Study 201 |
|---|---|
ORR | Confirmed response rate, CR, PR |
DOR | DOR |
Patient-reported outcomes/HRQoL | NR |
Harms outcomes AEs Death (while on treatment) AEs of interest:
|
|
AE = adverse event; CR = complete response; DOR = duration of response; HRQoL = health-related quality of life; NR = not reported; ORR = overall response rate; PR = partial response.
Statistical Analysis
This trial was designed as a noninferiority study. A noninferiority statistical end point was chosen to show that the gel formulation was statistically and clinically noninferior to the ointment formulation, since the 2 formulations are expected to have similar performance. Chlormethine gel was considered noninferior to chlormethine ointment if the lower limit of the 95% CI around the ratio of response rate (≥ 50% improvement in baseline CAILS score during the study period, confirmed at the next visit at least 4 weeks later) of the gel to the ointment was more than 0.75 in the ITT population. In response to CADTH’s request for additional information regarding the choice of a noninferiority margin of 0.75 in Study 201, the sponsor explained that at the time of Study 201, a single randomized placebo-controlled study in early-stage MF-CTCL had been published, which evaluated 43 patients on active treatment (Peldesine cream) and 46 patients on placebo, and which used a similar version of the CAILS score as in Study 201. In this study, the placebo response rate was 24% (95% CI, 12.6% to 38.8%).39 The estimated response rate of 68% for the control treatment arm in Study 201 greatly exceeded the established placebo response rate of 24% and its upper limit of the 95% CI. The chosen noninferiority margin was intended to ensure that the efficacy of chlormethine gel would be greater than the placebo response rate, assuming an effect size of 68% (i.e., that 0.75 × 68%, or 51%, was greater than a placebo response rate of 24%).40 The ratio of CAILS response rates along with its 95% confidence limits were estimated using the likelihood-based methods of Miettinen and Nurminen. The secondary end point, SWAT response, was analyzed using the same method as for CAILS response.
The total percentage of BSA changes from baseline to the final assessment was compared between the gel and ointment treatment groups using the patient’s initial value as a covariate. The time to response was assessed using Kaplan–Meier estimates of proportions of patients with CR or PR within the ITT population for each planned time point in the study. Patients not showing CR or PR sustained for at least 28 days were included in the analysis as censored observations at the time of their last assessment. The difference in time to confirmed response between the gel and ointment treatment groups was assessed using log rank test and a 95% CI of the difference in the Kaplan–Meier estimates of the proportions of patients responding at 12 months. For patients who showed CR or PR as assessed by CAILS, duration of response using Kaplan–Meier estimates of proportion of patients still responding (CR or PR) was estimated at 28-day intervals. The difference in the duration of response between the 2 treatment groups was assessed using log rank test and a 95% CI of the difference in the Kaplan–Meier estimates of the proportions of patients responding at 16 weeks. Similarly, Kaplan–Meier estimates of time to progression were calculated for each planned time point in the study up to and including 12 months, and the difference in time to progression between the 2 treatment groups was assessed using log rank test and a 95% CI of the difference in the Kaplan–Meier estimates of the proportions of patients with progression-free survival at 12 months in the 2 treatment groups.9 No adjustment for multiple comparisons was made for secondary end points for noninferiority comparisons.
Subgroup analyses were conducted using the same methods as with the main analyses and included analysis of CAILS overall response by age, sex, race, and baseline MF stage (stage IA versus stage IB or stage IIA). No interim analysis was planned or conducted.
Analysis Populations
All randomized patients were included in the ITT population. All patients who were treated for at least 6 months and had no significant protocol violations were included in the protocol-defined EE population. The safety population included all the patients who used any study medication.
Handling of Dropouts or Missing Data
For the primary end point, which was an improvement of 50% or more from baseline CAILS score confirmed at the next visit at least 4 weeks later, any patient randomized or treated who did not achieve a documented CR or PR was counted as a nonresponder for the ITT populations. Similarly, for the EE population, any patient included in the dataset who did not achieve a CR or PR was counted as a nonresponder. The same criteria were applied for the analyses of response based on the SWAT and the percentage of BSA. For the Kaplan–Meier analyses, patients who never had an event were censored as of their last available CAILS score. Those with no baseline CAILS score (patients who never received the study drug, n = 4) were excluded from the analyses. Patients with only a baseline CAILS score (i.e., no post-baseline assessment) were censored at time 0.9
Results
Patient Disposition
A total of 260 patients were enrolled, with 130 randomized to each treatment arm (ITT population); 255 patients (98.1%) received at least 1 application of the study drug (chlormethine gel [n = 128] or chlormethine ointment [n = 127]). A total of 75 patients enrolled (28.8%) were excluded from the EE dataset; 39 (15.0%) of the patients enrolled were excluded due to withdrawal for skin toxicity before month 6. The other 36 patients, including those from Site #7, comprised 13.8% of the patients enrolled. Sixty-two percent of patients in the gel arm and 66% of patients in the ointment arm completed the 12-month study. A total of 88 patients (47 in the gel arm and 41 in the ointment arm) discontinued or withdrew before completing 12 months of treatment (Table 10).
Study Details | Study 201 | |
|---|---|---|
Chlormethine gel | Chlormethine ointment | |
Screened | N = 322 | |
Randomized, N | 130 | 130 |
Discontinued from study, N (%) | 47 (36) | 41 (31) |
Reason for discontinuation, N (%) | ||
Treatment-limiting toxicity | 21 (16) | 16 (12.3) |
Other adverse events | 5 (3.8) | 6 (4.6) |
Lack of efficacy | 4 (3.1) | 4 (3.1) |
Subject’s best interest | 1 (0.77) | 0 (0) |
Concurrent illness | 4 (3.1) | 3 (2.3) |
Non-compliance | 2 (1.5) | 3 (2.3) |
Lost to follow-up | 4 (3.1) | 3 (2.3) |
Withdrew consent | 3 (2.3) | 3 (2.3) |
Other | 3 (2.3) | 3 (2.3) |
Completed 12 months of study treatment, N (%) | 81 (62) | 86 (66) |
ITT (all randomized patients), N | 130 | 130 |
EE (patients with no major protocol violations who were in study for 6 months), N | 90 | 95 |
SAS,a N | 128 | 127 |
EE = efficacy-evaluable; ITT = intention-to-treat; SAS = safety analysis set.
aSAS population consists of all patients who used any study medication.
Source: Lessin et al. (2013).8
Exposure to Study Treatments
Overall median exposure to study treatments was 51.9 weeks — 51.7 weeks for patients in the chlormethine gel treatment arm and 52.0 weeks for patients in the chlormethine ointment treatment arm. Overall, 82.7% of patients did not require any modifications to dosing frequency throughout the study period; 22.7% of patients in the chlormethine gel arm and 11.8% of patients in the chlormethine ointment arm required changes to dosing frequency of their study treatment. Forty-four (34.4%) patients in the chlormethine gel arm and 25 (19.7%) patients in the chlormethine ointment arm required a temporary suspension of the study treatment (Table 11).
Table 11: Patient Exposure by Treatment Group and Dose Reductions
Exposure (weeks) | Chlormethine gel (N = 128) n (%) | Chlormethine ointment (N = 127) n (%) | All patients (N = 255) n (%) |
|---|---|---|---|
N | 128 | 127 | 255 |
Mean (SD) | 39.3 (19.34) | 41.5 (17.60) | 40.4 (18.49) |
Median | 51.7 | 52.0 | 51.9 |
By range of weeks, n (%) | |||
> 0 to 4 | 5 (3.9) | 4 (3.1) | 9 (3.5) |
> 4 to 8 | 14 (10.9) | 7 (5.5) | 21 (8.2) |
> 8 to 12 | 7 (5.5) | 3 (2.4) | 10 (3.9) |
> 48 | 81 (63.3) | 84 (66.1) | 165 (64.7) |
The duration of exposure is from the date of study treatment first dispensed to date of last study treatment | |||
Reductions in dosing frequency: None | 99 (77.3) | 112 (88.2) | 211 (82.7) |
Any | 29 (22.7) | 15 (11.8) | 44 (17.3) |
1 reduction in dosing frequency | 21 (16.4) | 12 (9.4) | 33 (12.9) |
2 reductions in dosing frequency | 8 (6.3) | 3 (2.4) | 11 (4.3) |
Temporary suspensions: None | 84 (65.6) | 102 (80.3) | 186 (72.9) |
Any | 44 (34.4) | 25 (19.7) | 69 (27.1) |
Permanent suspension due to TLT/other AE: None | 102 (79.7) | 105 (82.7) | 207 (81.2) |
Any | 26 (20.3) | 22 (17.3) | 48 (18.8) |
AE = adverse event; SAS = safety analysis set; SD = standard deviation; TLT = treatment-limiting toxicity.
Note: SAS population.
Source: Ledaga European Public Assessment Report.29
Concomitant Therapy
One patient in the chlormethine ointment treatment arm was treated with UVB 3 days before the last visit but 2 weeks after the last application of the trial medication and subsequently withdrew from the study; the patient was included in the per-protocol EE analyses. The records of patients who had indicated use of corticosteroids as concomitant medication during the trial were reviewed. No patient met the criterion for a major protocol violation.29
Protocol Violations
There was an error in randomization at Site #7 where study treatment was assigned to 16 patients based on their MF stage and not the randomization list (i.e., the gel was dispensed to all patients in stratum 1 with stage IA disease and the ointment was dispensed to all patients in stratum 2 with stage IB or stage IIA disease). A total of 18 patients were accrued at this site: | stage IA patients on chlormethine gel, | stage IA patient on chlormethine ointment (1 of the last | patients enrolled and randomized), and | stage IB patients on chlormethine ointment. All 18 patients (6.9% of patients enrolled) from this study site (11 [8.5%] patients in the gel arm and 7 [5.4%] patients in the ointment arm) were considered as having a major protocol violation. When the error was discovered, the investigator was unblinded to treatment. The last 2 patients enrolled were assigned treatments based on their randomization schedule. Since the integrity of the randomization process at this site was compromised, additional analyses were introduced to evaluate the impact of this protocol violation. Analyses were performed for (1) the ITT population, including the Site #7 patients as assigned and treated (N = 260) and (2) the ITT population that included all patients randomized and assessed by a blinded observer, excluding Site #7 patients (N = 242). As a measure of sensitivity, the primary efficacy end point was also analyzed for all patients enrolled, including the Site #7 patients, as they should have been randomized (ITT with Site #7 as planned). The analyses showed that the protocol violation concerning a randomization error at 1 study site did not impact the determination of noninferiority on the overall response rate (see the Results section and Appendix 3).9
|||||||| patients (|||| consisting of |||||||||| patients in the gel arm and |||||||| patients in the ointment arm) had protocol violations defined as selection criteria not met. This included disease that had progressed beyond stage IIA at baseline (|||||| patients in the gel arm and |||||| patients in the ointment arm) and the use of prohibited concomitant medication (|||||||| patients in the gel arm and |||||| patients in the ointment arm).9,29
Efficacy
Primary Efficacy End Point
Confirmed CAILS Response Rate
In the ITT population, the confirmed response rate was numerically higher for chlormethine gel than for chlormethine ointment (58.5% versus 47.7%); 18 (13.8%) patients in the chlormethine gel and 15 (11.5%) patients in the chlormethine ointment treatment arm achieved CR. The ratio of the response rate of gel to ointment was 1.23 (95% CI, 0.97 to 1.55), meeting the pre-specified criterion for noninferiority (≥ 0.75 for the lower bound of 95% CI). Similarly, in the EE population, the confirmed response rate was higher for chlormethine gel than for chlormethine ointment (76.7% versus 58.9%); 17 (18.9%) patients in the chlormethine gel ointment treatment arm and 14 (14.7%) patients in the chlormethine ointment treatment arm achieved CR. The ratio of the response rate of gel to ointment was 1.30 (95% CI, 1.06 to 1.61). Detailed results for the primary efficacy outcome are presented in Table 12. The results of primary efficacy analyses in the ITT population, excluding Site #7 (the study site with the protocol violation involving randomization), were similar (see Appendix 3).9
Table 12: Confirmed CAILS Response Rate
Analysis set | Chlormethine gel | Chlormethine ointment | Ratio gel/ ointment | 95% CIa |
|---|---|---|---|---|
ITT | N = 130 | N = 130 | — | — |
Overall (CR + PR), n (%) | 76 (58.5) | 62 (47.7) | 1.226 | 0.97 to 1.55 |
CR | 18 (13.8) | 15 (11.5) | NA | NA |
PR | 58 (44.6) | 47 (36.2) | NA | NA |
No response | 54 (41.5) | 68 (52.3) | NA | NA |
Stable disease | 42 (32.3) | 61 (46.9) | NA | NA |
Progressive disease | 5 (3.8) | 3 (2.3) | NA | NA |
Unevaluableb | 7 (5.4) | 4 (3.1) | NA | NA |
EE | N = 90 | N = 95 | — | — |
Overall (CR + PR), n (%) | 69 (76.7) | 56 (58.9) | 1.301 | 1.065 to 1.609 |
CR | 17 (18.9) | 14 (14.7) | NA | NA |
PR | 52 (57.8) | 42 (44.2) | NA | NA |
No response | 21 (23.3) | 39 (41.1) | NA | NA |
Stable disease | 19 (21.1) | 39 (41.1) | NA | NA |
Progressive disease | 2 (2.2) | 0 (0.0) | NA | NA |
CAILS = Composite Assessment of Index Lesion Severity; CI = confidence interval; CR = complete response; EE = efficacy-evaluable; ITT = intention-to-treat; NA = not applicable; PR = partial response.
aEstimated using the likelihood-based methods of Miettinen and Nurminen.
b “Unevaluable” includes 5 patients who never received study drug and 6 patients who were withdrawn without any post-baseline assessment.
Source: Ledaga European Public Assessment Report.29
Secondary Efficacy End Points
Confirmed SWAT Response Rate
The results of the key secondary efficacy end point, SWAT, are presented in Table 13. In the ITT population, the overall response rate was 46.9% and 46.2% for chlormethine gel and chlormethine ointment, respectively. The ratio of response rate was 1.02 (95% CI, 0.78 to 1.32), which met the predefined criterion for noninferiority. CR was observed in 9 (6.9%) patients in the chlormethine gel arm and 4 (3.1%) patients in the chlormethine ointment arm.
Table 13: Confirmed SWAT Response Rate
Analysis set | Chlormethine gel | Chlormethine ointment | Ratio gel/ ointment | 95% CIa |
|---|---|---|---|---|
ITT | N = 130 | N = 130 | — | — |
Overall (CR + PR), n (%) | 61 (46.9) | 60 (46.2) | 1.017 | 0.783 to 1.321 |
CR | 9 (6.9) | 4 (3.1) | NA | NA |
PR | 52 (40.0) | 56 (43.1) | NA | NA |
No responses | 69 (53.1) | 70 (53.8) | NA | NA |
EE | N = 90 | N = 95 | — | — |
Overall (CR + PR), n (%) | 57 (63.3) | 53 (55.8) | 1.135 | 0.893 to 1.448 |
CR | 8 (8.9) | 4 (4.2) | NA | NA |
PR | 49 (54.4) | 49 (51.6) | NA | NA |
No responses | 33 (36.7) | 42 (44.2) | NA | NA |
CI = confidence interval; CR = complete response; EE = efficacy-evaluable; ITT = intention-to-treat; NA = not applicable; PR = partial response; SWAT = Severity-Weighted Assessment Tool.
aEstimated using the likelihood-based methods of Miettinen and Nurminen.
Source: Ledaga European Public Assessment Report.29
Total Percentage of BSA Response Rate (Extent of Cutaneous Disease)
For the ITT population, the BSA response rate was 44.6% for chlormethine gel and 43.1% for chlormethine ointment. The ratio of response rate for the percentage of BSA was 1.03 (95% CI, 0.78 to 1.36), meeting the protocol-defined criterion for noninferiority (Table 14).
Table 14: Total Percentage of Body Surface Area Response Rate
Percentage of BSA response | Chlormethine gel | Chlormethine ointment | Ratio of response | 95% CIa |
|---|---|---|---|---|
ITT | ||||
Responders, n (%) | 58 (44.6) | 56 (43.1) | 1.036 | 0.78 to 1.36 |
Nonresponders, n (%) | 72 (55.4) | 74 (56.9) | NA | NA |
EE | ||||
Responders, n (%) | 54 (60.0) | 50 (52.6) | 1.140 | 0.88 to 1.47 |
Nonresponders, n (%) | 36 (40.0) | 45 (47.4) | NA | NA |
BSA = body surface area; CI = confidence interval; EE = efficacy-evaluable; ITT = intention-to-treat; NA = not applicable.
aEstimated using the likelihood-based methods of Miettinen and Nurminen.
Source: Ledaga European Public Assessment Report.29
Time to First Confirmed Response
The estimated times to a 50% response were 26 weeks (95% CI, 21 weeks to 35 weeks) in the gel treatment arm and 42 weeks (95% CI, 29 weeks to 53 weeks) in the ointment treatment arm. The gel arm therefore reached a 50% response approximately 16 weeks sooner than the ointment arm. Approximately 46.2% of patients treated with gel achieved a confirmed response at 24 weeks versus 36.9% of patients treated with ointment. At 52 weeks, 76.2% of patients in the gel arm had achieved a CR, versus 56.2% of patients in the ointment arm (Figure 3).8
Figure 3: Time to First Confirmed Response Based on CAILS and Intention-To-Treat Population
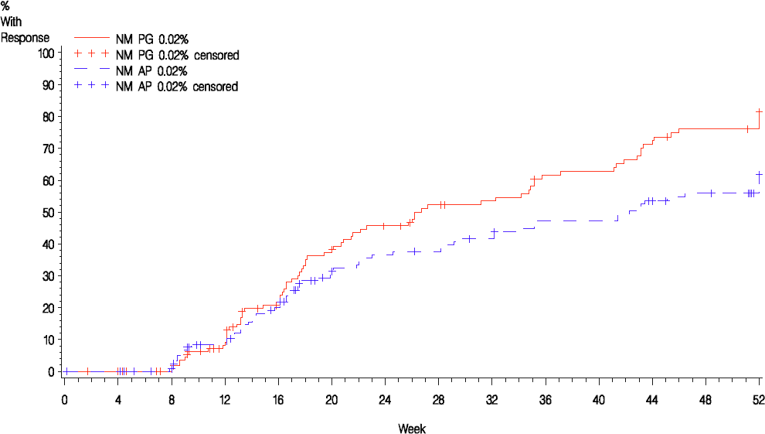
CAILS = Composite Assessment of Index Lesion Severity; NM AP = nitrogen mustard in Aquaphor ointment (chlormethine compounded ointment formulation); NM PG = nitrogen mustard in propylene glycol (chlormethine gel formulation).
Source: Ledaga European Public Assessment Report.29
Duration of Response
The duration of response (based on the CAILS score) in the ITT population was analyzed in patients who achieved a response (gel arm, n = 76, and ointment arm, n = 62 [Figure 4]). Based on the Kaplan–Meier analysis, small differences between the 2 treatment arms were observed (P = 0.48, log rank test).8 Further analysis estimated that at least 90% of responses (using the consensus guidelines) will be maintained for at least 10 months.8
Figure 4: Duration of Response Based on CAILS and Intention-To-Treat Population
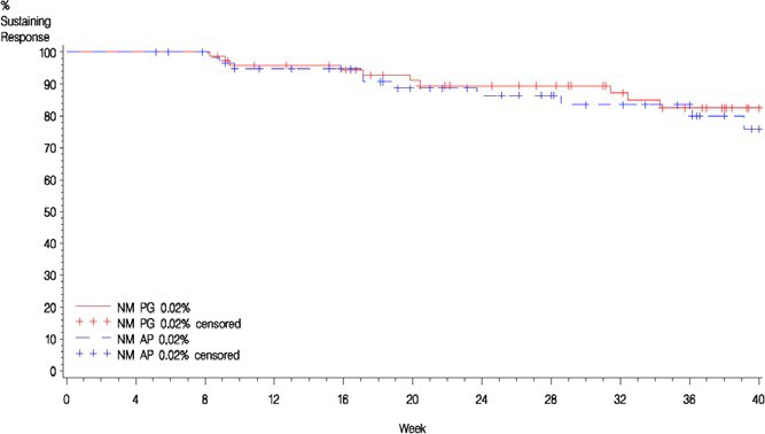
CAILS = Composite Assessment of Index Lesion Severity; NM AP = nitrogen mustard in Aquaphor ointment (chlormethine compounded ointment formulation); NM PG = nitrogen mustard in propylene glycol (chlormethine gel formulation).
Source: Ledaga European Public Assessment Report.29
Time to Progression
Fifteen patients randomized to the chlormethine gel arm and 10 patients randomized to the ointment arm had an increase of 25% or more from their baseline CAILS score at some time during the study (protocol-defined disease progression). However, the majority of patients remained on treatment and 7 of the patients in the gel arm who stayed on treatment achieved a confirmed response. Eight patients (5 patients in the gel arm and 3 patients in the ointment arm) met the criterion for progressive disease without influencing their T classification at the time of the last visit.8 There was little difference observed between the Kaplan–Meier curves (P = ||||, log rank test [Figure 5]).9 Approximately 90% of patients in both treatment arms never experienced an increase of 25% or more in their CAILS score during the study. This analysis only captured the time to the first instance of disease progression, which may not capture whether the patient will benefit from treatment if they continue treatment. Skin toxicity often occurring early in the treatment course may lead to an increase in the CAILS score.
Figure 5: Time to Progression Based on CAILS and Intention-To-Treat Population
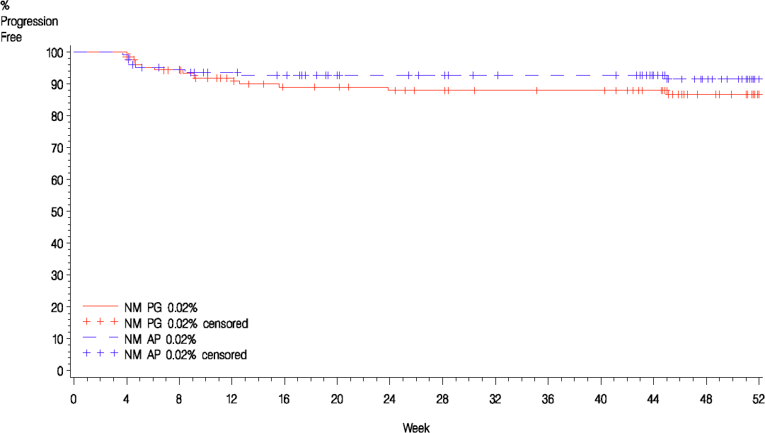
CAILS = Composite Assessment of Index Lesion Severity; NM AP = nitrogen mustard in Aquaphor ointment (chlormethine compounded ointment formulation); NM PG = nitrogen mustard in propylene glycol (chlormethine gel formulation).
Source: Ledaga European Public Assessment Report.29
Subgroup Analysis
The results of subgroup analysis by MF-CTCL stage (stratum 1 [stage IA, n = 141] and stratum 2 [stage IB and stage IIA, n = 119]) for CAILS responses are presented in Table 15. Response rate ratios (chlormethine gel versus chlormethine ointment) were consistent with the overall study results. In the ITT population, a 59.2% overall CAILS response rate for chlormethine gel versus 40.0% for chlormethine ointment was observed in stratum 1 (response rate ratio = 1.48; 95% CI, 1.05 to 22.14). In stratum 2, the overall CAILS response rate for chlormethine gel versus chlormethine ointment was 57.4% versus 55.4%, respectively (response rate ratio = 1.04; 95% CI, 0.75 to 1.43).
Table 15: Confirmed CAILS Responses by MF-CTCL Stage
CAILS response | Chlormethine gel | Chlormethine ointment | Ratio gel/ ointment | 95% CIa |
|---|---|---|---|---|
ITT | N = 130 | N = 130 | — | — |
MF-CTCL stage at baseline, n/N (%) | ||||
Stage IA | 45/76 (59.2) | 26/65 (40.0) | 1.480 | 1.053 to 2.135 |
Stage IB or stage IIA | 31/54 (57.4) | 36/65 (55.4) | 1.037 | 0.747 to 1.425 |
EE | N = 90 | N = 95 | — | — |
MF-CTCL stage at baseline, n/N (%) | ||||
Stage IA | 39/49 (79.6) | 23/41 (56.1) | 1.419 | 1.063 to 1.989 |
Stage IB or stage IIA | 30/41 (73.2) | 33/54 (61.1) | 1.197 | 0.892 to 1.604 |
CAILS = Composite Assessment of Index Lesion Severity; CI = confidence interval; EE = efficacy-evaluable; ITT = intention-to-treat; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma.
aEstimated using the likelihood-based methods of Miettinen and Nurminen.
Source: Ledaga European Public Assessment Report.29
Posthoc subgroup analyses of the SWAT response by MF-CTCL stage are presented in Table 16. These were largely consistent with the main analyses.
Table 16: SWAT Responses by MF-CTCL Stage
SWAT responses | Chlormethine gel | Chlormethine ointment | Ratio gel/ ointment | 95% CIa |
|---|---|---|---|---|
ITT | N = 130 | N = 130 | — | — |
MF-CTCL stage at baseline, % | ||||
Stage IA | 40.8 | 36.9 | 1.105 | 0.731 to 1.690 |
Stage IB, stage IIA | 55.6 | 55.4 | 1.003 | 0.718 to 1.386 |
EE | N = 95 | N = 95 | — | — |
MF-CTCL stage at baseline, % | ||||
Stage IA | 57.1 | 48.8 | 1.171 | 0.793 to 1.776 |
Stage IB, stage IIA | 70.7 | 61.1 | 1.157 | 0.854 to 1.559 |
CI = confidence interval; EE = efficacy-evaluable; ITT = intention-to-treat; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma; SWAT = Severity-Weighted Assessment Tool.
aDerived posthoc using the likelihood-based methods of Miettinen and Nurminen.
Source: Ledaga European Public Assessment Report.29
Posthoc subgroup analyses on the percentage of BSA response data were performed by MF stage. These posthoc analyses showed that the percentage of BSA response rates were numerically higher with chlormethine gel compared with chlormethine ointment in patients with stage IA compared with patients with stage IB or stage IIA in both the ITT and EE populations (Table 17).38
Table 17: Clinical Response of 50% or More Improvement in Skin Score by MF-CTCL Stage in Posthoc Analyses of Study 201 Data
Percentage of BSA | Chlormethine gel | Chlormethine ointment | P value |
|---|---|---|---|
ITT | N = 130 | N = 130 | — |
MF-CTCL stage at baseline, % | |||
Stage IA | | | | | | | | | | | | |
Stage IB, stage IIA | | | | | | | | | | | | |
EE | N = 95 | N = 95 | — |
MF-CTCL stage at baseline, % | |||
Stage IA | | | | | | | | | | | | |
Stage IB, stage IIA | | | | | | | | | | | | |
BSA = body surface area; EE = efficacy-evaluable; ITT = intention-to-treat; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma.
Source: Sponsor’s responses to CADTH’s request for additional information.38
Pre-specified subgroup analyses to assess treatment efficacy for the percentage of BSA at baseline and for the percentage of BSA by disease stage (stage IA versus stage IB and stage IIA MF-CTCL) were not performed. Pre-specified subgroup analyses based on other variables of interest identified in the CADTH protocol (i.e., patch versus plaque presentation, lymph node involvement, previous treatment) were also not performed.38
Harms
The safety data were consistent with the lack of systemic exposure to chlormethine or its degradation product. Clinical laboratory monitoring (carried out at baseline, at month 4, month 8, and month 12) and high-performance liquid chromatography assays (performed in 16 patients in the gel treatment arm carried out at 0 hours, 1 hour, 3 hours, and 6 hours after application on day 1 and at week 4) showed no detectable blood levels or evidence of systemic absorption of chlormethine.8
Adverse Events
Table 18 provides a summary of aggregate AE outcomes. During the trial period, 84.4% of patients treated with chlormethine gel and 90.6% of patients treated with chlormethine ointment experienced at least 1 AE. Most AEs in both treatment arms were skin-related; the most frequently reported AEs were dermatitis (skin irritation, 19.6%), pruritus (17.6%), and erythema (15.7%).8 The incidence of skin irritation was higher in the gel arm compared to the ointment arm (25.0% versus 14.2%). Skin-related AEs occurring in 5% or more of patients are summarized in (Table 19).
Serious Adverse Events
Serious AEs occurred in approximately 10% of patients in both groups and were recorded as skin and subcutaneous tissue disorders (1 patient in the ointment arm), cardiac disorders (1 patient in the gel arm and 4 patients in the ointment arm), respiratory disorders (3 patients in the gel arm and 1 patient in the ointment arm), and malignant neoplasms (1 patient in each arm).29
Withdrawals Due to Adverse Events
More patients in the chlormethine gel group discontinued treatment prematurely due to AEs than in the chlormethine ointment group (Table 18). Most withdrawals occurred within the first few months.8
Death
There was 1 death reported during the study and none during the 12-month follow-up period. The patient was diagnosed with metastatic cancer less than 2 months after the initiation of chlormethine gel and died on day 84 of the study.29
Table 18: Summary of All Adverse Events
Evaluation, n (%) | All patientsa (N = 255) n (%) | Chlormethine gel (N = 128) n (%) | Chlormethine ointment (N = 127) n (%) |
|---|---|---|---|
Patients with AEs | 223 (87.5) | 108 (84.4) | 115 (90.6) |
AEs | 988 | 505 | 483 |
Patients with drug-related AEs | 143 (56.1) | 79 (61.7) | 64 (50.4) |
Drug-related AEs | 366 | 206 | 160 |
Patients with SAEs | 25 (9.8) | 14 (10.9) | 11 (8.7) |
Patients who discontinued due to AEs | 51 (20.0) | 28 (21.9) | 23 (18.1) |
Patients who discontinued due to drug-related AEs | 49 (19.2) | 27 (21.1) | 22 (17.3) |
Deaths | 1 (0.4) | 1 (0.8) | 0 (0.0) |
AE = adverse event; SAE = serious adverse event; SAS = safety analysis set.
aSAS population.
Source: Clinical Study Report for Study 201.9
Table 19: Skin-Related Adverse Events Occurring in 5% or More of Patients
Adverse event | Chlormethine gel (N = 128) n (%) | Chlormethine ointment (N = 127) n (%) | Total (N = 255) |
|---|---|---|---|
Skin irritationa | 32 (25.0) | 18 (14.2) | 50 (19.6) |
Pruritus | 25 (19.5) | 20 (15.7) | 45 (17.6) |
Erythema | 22 (17.2) | 18 (14.2) | 40 (15.7) |
Contact dermatitis | 19 (14.8) | 19 (15.0) | 38 (14.9) |
Skin hyperpigmentation | 7 (5.5) | 9 (7.1) | 16 (6.3) |
Folliculitis | 7 (5.5) | 5 (3.9) | 12 (4.7) |
aP = 0.04 Fisher exact test.
Source: Lessin et al. (2013).8
Potential AEs by modified system organ class are presented in Table 20.
Table 20: Summary of Potential Adverse Events by Modified System Organ Class and Preferred Term, Recoded — Safety Analysis Set
Modified SOC Preferred term | Chlormethine gel (N = 128) n (%) | Chlormethine ointment (N = 127) n (%) | All patients (N = 255) n (%) |
|---|---|---|---|
Skin and subcutaneous tissue disorder AEs with an incidence of ≥ 2% patients in either treatment group | | | | | | | | | | | | |
Dermatitis | 70 (54.7) | 73 (57.5) | 143 (56.1) |
Pruritus | 26 (20.3) | 21 (16.5) | 47 (18.4) |
Skin infections | 15 (11.7) | 14 (11.0) | 29 (11.4) |
Skin hyperpigmentation | 7 (5.5) | 9 (7.1) | 16 (6.3) |
Skin ulcerating or blistering | 8 (6.3) | 5 (3.9) | 13 (5.1) |
Actinic keratosis | 5 (3.9) | 2 (1.6) | 7 (2.7) |
Non-skin AEs reported by ≥ 3 more patients in the chlormethine gel group vs. the chlormethine ointment group | |||
Gastrointestinal disorders | 6 (4.7) | 3 (2.4) | 9 (3.5) |
Nausea | 6 (4.7) | 3 (2.4) | 9 (3.5) |
Infections and infestations | 6 (4.7) | 3 (2.4) | 9 (3.5) |
Sinusitis | 6 (4.7) | 3 (2.4) | 9 (3.5) |
Musculoskeletal and connective tissue disorders | 5 (3.9) | 2 (1.6) | 7 (2.7) |
Back pain | 5 (3.9) | 2 (1.6) | 7 (2.7) |
Respiratory, thoracic, and mediastinal disorders | 6 (4.7) | 0 (0.0) | 6 (2.4) |
Dyspnea | 4 (3.1) | 0 (0.0) | 4 (1.6) |
Pneumonia | 3 (2.3) | 0 (0.0) | 3 (1.2) |
General disorders | 3 (2.3) | 0 (0.0) | 3 (1.2) |
Xerosis | 3 (2.3) | 0 (0.0) | 3 (1.2) |
AE = adverse event; SOC = system organ class.
Source: Clinical Summary Report for Ledaga.2
At the end of Study 201, | patients had | ongoing skin AEs, with a larger percentage occurring in the chlormethine gel group ( | AEs in | patients) than in the chlormethine ointment group ( | AEs in | patients). |||||||| of the |||||||| ongoing skin AEs resolved during the 12-month follow-up period. Of the ongoing skin AEs, resolution occurred in | of | (|||) AEs among patients treated with chlormethine gel and in | of | (|||) AEs among patients treated with chlormethine ointment during Study 201. Because || out of the |||||||||||| patients in the year of the follow-up were placed on other therapies for MF, analysis of ongoing AEs was confounded by possible drug-related AEs due to that therapy.
Notable Harms
Secondary Skin Cancers
During the 12-month trial period, and the additional 12-month follow-up period, 20 nonmelanoma skin cancers were detected in 11 (4.3%) patients (Table 21). These included 10 basal cell carcinomas (6 in a treatment area; 2 in the gel arm patients and 4 in the ointment arm), 9 squamous cell carcinomas (1 in a treatment area), and 1 Merkel cell carcinoma (not in a treatment area).8,29 Eight of these patients developed nonmelanoma skin cancer during treatment and 3 additional patients developed nonmelanoma skin cancer during the 1-year follow-up period. Three of these patients were treated only with chlormethine hydrochloride 0.02% gel, 7 were treated only with chlormethine hydrochloride 0.02% ointment, and 1 patient was treated with chlormethine ointment followed by 7 months of treatment with chlormethine hydrochloride 0.04% gel in Study 202. Five of these patients (2 treated with chlormethine hydrochloride 0.02% gel and 3 treated with chlormethine ointment) had a squamous cell carcinoma. It was concluded that the final data obtained from the 12-month follow-up do not indicate any increased risk of skin cancers with chlormethine hydrochloride 0.02% gel relative to chlormethine ointment.
Table 21: Occurrence of Nonmelanoma Skin Cancers
Tumour type | All patientsa (N = 255) n (%) | Chlormethine gel (N = 128) n (%) | Chlormethine ointment (N = 127) n (%) |
|---|---|---|---|
Any skin (nonmelanoma) malignancy | 11 (4.3) | 3 (2.3) | 7 (5.5) |
Basal cell carcinoma | 5 (2.0) | 1 (0.8) | 3 (2.4) |
Squamous cell carcinoma | 3 (1.2) | 1 (0.8) | 2 (1.6) |
Merkel cell carcinoma | 1 (0.4) | 0 (0.0) | 1 (0.8) |
Both basal cell carcinoma and squamous cell carcinoma | 2 (0.8) | 1 (0.8) | 1 (0.8) |
aIncludes 12-month follow-up period.
Source: Ledaga European Public Assessment Report.29
Critical Appraisal
Internal Validity
The objective of Study 201 was to assess the efficacy of chlormethine 0.02% gel compared to chlormethine 0.02% ointment in patients with stage I to stage IIA MF-CTCL. The design of Study 201 was suitable for determining the objective of noninferiority of chlormethine gel to the ointment formulation. However, the clinical experts consulted by CADTH noted that the more appropriate comparator for the Canadian population would have been phototherapy, which is the current standard of care for this patient population. An active comparator control group was used, given the long duration of randomized treatment needed to evaluate response, the known progressive nature of the disease, and the reported association between disease progression and increased mortality risk. A different formulation of chlormethine acceptable for home use was considered the best available option. At the time of the trial, the selected chlormethine 0.02% ointment corresponded to the current standard of care in the US and was considered to have an established efficacy and safety profile based on published data. It was acknowledged that chlormethine ointment had not been evaluated in controlled clinical trials and that the anticipated effect size on the primary end point selected for the study (CAILS) could not be exactly determined. The choice of the active comparator drug was discussed in detail in scientific advisory meetings with the UK’s Medicines and Health care products Regulatory Agency and the National Security Agency of Medicines and Health Products in France. Both agencies agreed that the use of the chlormethine ointment formulation represented the best option available to the sponsor under the circumstances.36 Reviewers for the FDA noted that single-arm studies have been performed in this disease setting with response rates ranging from 50% to 85% in single-arm studies for first-line treatment of early-stage MF. Information on second-line therapy, which is the setting for Study 201, is scarce.37 In addition, chlormethine is not a new treatment and is not intended to replace other SDT, which have their place in the MF treatment armamentarium. Rather, the aim of the trial was to establish the noninferiority of the gel to the compounded ointment to offer a more convenient application of topical chlormethine for patients.
The protocol-defined criterion for noninferiority was the lower limit of the 95% CI for the ratio of the overall response rate for chlormethine gel versus chlormethine ointment of 0.75 or more. The chosen noninferiority margin was selected to show that the efficacy of chlormethine gel would be greater than a historical placebo response rate. However, the clinical relevance of this approach of defining a noninferiority margin based on placebo response (versus active treatment response) is unclear. The sponsor acknowledges the potential methodological issues with a noninferiority approach in a situation where the expected magnitude of the effect of the comparator (chlormethine ointment) could not be based on data from controlled studies. The sponsor has previously explained that chlormethine ointment was considered to have an established efficacy of clinical relevance based on published data and ongoing clinical use. The noninferiority margin was deemed acceptable by the FDA, taking into account various factors including the well-established nature of the comparator, the likely lower response rates observed in a controlled trial than in open-label studies, historical case series, and feasibility of a controlled study in a rare disease.36 In regulatory approval reviews by the EMA and FDA, the design of Study 201 as a noninferiority study was considered to be acceptable for this application. The choice of noninferiority margin was not of major concern because, based on the results of the primary efficacy end point, the conclusion of noninferiority would have been reached with more conservative margins.29,37
Statistical power calculations were reported for Study 201 and enrolment exceeded the target sample size to demonstrate the noninferiority of chlormethine gel over the ointment formulation for the primary efficacy end point. Randomization was performed using an appropriate methodology with adequate allocation concealment. There was a protocol violation related to randomization at 1 site (Site #7). However, this issue was dealt with appropriately and additional analyses excluding this site were carried out to evaluate the impact of this protocol violation. In terms of blinding, this was a single-blinded (investigator-blinded) trial as the 2 chlormethine formulations differed in appearance and were dispensed in different containers (tube for gel and jar for ointment), making it impossible to blind patients. However, this is not expected to have biased the results as steps were taken to ensure the blinding of outcome assessors. For example, patients were instructed not to apply study medication before their clinical visit and to transport the study drug to and from visits in a bag that did not reveal the type of container they had been dispensed.
Stratification was based on a relevant prognostic factor (MF-CTCL stage). Patients were well balanced across the 2 treatment arms for age and other baseline characteristics, including prior MF therapy. One notable difference was the distribution of MF stage (stage IA versus stage IB and stage IIA), which was imbalanced between the gel arm (58.5% versus 41.5%) and the ointment arm (50% versus 50%), although the imbalance was primarily a result of the protocol violations for the single site previously mentioned. Subgroup analyses based on MF stage did not suggest differential response to treatment, as the CAILS response in both subgroups met the noninferiority threshold. However, the estimated treatment effect (CAILS response) for gel versus ointment was more pronounced in the stage IA subgroup (ratio of gel versus ointment = 1.48) compared to the stage IB and stage IIA subgroup (ratio of gel versus ointment = 1.037).
The primary and key secondary efficacy end points were assessed using CAILS and SWAT. These end points and several secondary end points (the percentage of BSA, the time to first confirmed response, the duration of response, and the time to progression) were considered acceptable per the clinical experts consulted by CADTH. The primary end point (CAILS), although not extensively validated, is considered an appropriate end point for MF-CTCL trials,29 and has been shown to correlate with the percentage of BSA, physician global assessment, and the time to complete remission during PUVA therapy. For this review, no information was identified regarding reliability, responsiveness, and minimal important difference (MID) of CAILS. Likewise, SWAT, 1 of the most widely used tools for skin scoring in MF performed by the investigator, captures both the extent and severity of skin disease and is used in clinical practice.41 Overall response as assessed by SWAT supplements the primary efficacy end point in the interpretation of the results as it contains direct assessment of the percentage of BSA for each MF-CTCL lesion. However, there is a paucity of information regarding SWAT’s reliability, responsiveness to change, or MID in the MF population (see Appendix 4 for detailed description of appraisal of outcome measures). Time to event analyses for the secondary efficacy end points were adequate. However, as the statistical reviewers for the FDA also noted, the CAILS time to progression results are difficult to interpret because CAILS time to progression was limited to the assessment of progression in index lesions, and progression in non-index lesions or new lesions were not captured.37 Overall, firm conclusions may be drawn only for the primary outcome (CAILS); results for secondary outcomes must be interpreted with caution due to the increased risk of type I error, since multiple comparisons (for noninferiority) were not accounted for in the analyses.
Patient disposition in Study 201 was thoroughly documented and well reported. The number of discontinuations or withdrawals from the trial were within the 25% proportion (at 6 months) assumed in the sponsor’s power calculations. The majority of exclusions in the EE dataset (75 patients) were due to the protocol deviation (randomization error at 1 study site, n = 18) and skin toxicity (n = 39). There did not appear to be important differences between the treatment arms regarding the reason for withdrawal from the study. One exception was treatment-limiting toxicity for which more patients discontinued in the gel treatment arm (n = 21) compared to the ointment treatment arm (n = 16). The incidence of skin irritation was higher in the gel arm. The clinical experts noted that this is not unexpected, as the emollient nature of chlormethine ointment may help reduce skin irritation.
While the ITT population provides an assessment of all patients enrolled, the EE population is an assessment of treatment effect in a population that is able to tolerate treatment (the EE population consisted of patients who remained on treatment ≥ 6 months). For the ITT population, any patient randomized and/or treated who did not achieve a documented response was counted as a nonresponder. Of note, the proportion of patients designated as nonresponders was lower in the EE population versus the ITT population (23% versus 41% in the gel arm and 41% versus 52% in the ointment arm). Imputing patients as nonresponders likely has 2 implications. First, since dropout was similar between the 2 treatment arms, it may bias estimates toward the null, which would result in conservative inference. This is supported by the difference in estimates between the ITT and EE populations, with the response rates being higher and with a higher estimated effect for the primary outcome in the EE dataset. Second, imputing patients as nonresponders assumes that more patients were observed than was the case, which can lead to underestimation of the standard error and narrower 95% CIs. Such bias can lead to anti-conservative inference. Thus, the ultimate impact of the approach to the handling of missing data on the study conclusions is unclear.
External Validity
In Study 201, the interventional drug (chlormethine gel) is compared to a drug (chlormethine ointment) that is not used in Canada. Therefore, the question of comparative efficacy and safety of chlormethine gel to current standards of care in Canada cannot be answered. However, the clinical experts consulted for this report considered the comparison reasonable, taking into account the feasibility of using other comparators and given the noninferiority design of the trial.
The inclusion criteria for Study 201 were reasonable, based on the intended patient population. The clinical experts consulted stated that the characteristics of the patient population were generally a good representation of the target population in their clinical practice. However, in Study 201, 256 patients (98.5%) had early-stage I (stage IA or stage IB) disease. This may not be entirely representative of clinical practice; while the majority of patients are diagnosed with early stages of MF-CTCL (at least two-thirds of patients), the trial was based almost exclusively on stage I disease (only 4 out of 260 patients had stage IIA disease). Therefore, in theory, the generalizability of the results beyond stage I disease is limited. The clinical experts consulted by CADTH noted that the requirement of at least 1 prior therapy was appropriate as it is reflective of routine care where treatments that include phototherapy, topical steroids, and topical retinoids are considered as first-line therapies for patients with early-stage MF-CTCL. The clinical experts noted that in routine practice, the percentage of BSA and patch versus plaque presentation constitute important factors in treatment decision-making. Chlormethine gel would be considered a treatment option for patients with an affected percentage of BSA of 10% to 15% or less, with primarily patch presentation. In Study 201, the mean percentage of BSA at baseline was approximately 12% in the gel arm and 15% in the ointment arm. Not reported, however, were data on treatment response based specifically on the percentage of BSA as well as AEs based on the percentage of BSA at baseline that were of interest to the clinical experts consulted for this review.
In terms of trial end points, the clinical experts consulted by CADTH noted that the rating tools used to measure primary efficacy outcome and the key secondary efficacy outcome (i.e., CAILS and SWAT) are used primarily in research settings and are not widely used in routine clinical practice to make decisions with respect to treatment efficacy. However, this should not limit the interpretation of findings and the applicability of results to clinical practice. One important end point that was not included in Study 201 was HRQoL. This outcome was identified by patient and clinician groups, as well as the clinical experts consulted, as a relevant outcome to assess in patients with MF-CTCL, given the considerable impact that the disease has on patients’ quality of life (e.g., visible patches and/or plaques, itching). The clinical experts acknowledged that it is reasonable to assume an association between key efficacy end points (CAILS and SWAT) and HRQoL. However, the clinical experts pointed out that some patients with lower SWAT scores may still have a poor HRQoL. Furthermore, HRQoL takes into account adverse effects of treatment; a patient with lower skin burden from the disease may be experiencing adverse reactions from the treatment, which can negatively impact their quality of life. In the absence of HRQoL data from the clinical trial, it is unclear whether response to treatment and resolution of symptoms translate to better quality of life for patients.
The indication and reimbursement request of chlormethine gel as topical treatment for MF-CTCL in adult patients is broader than the inclusion criteria of Study 201 with respect to disease stage (early stage: stage IA, stage IB, and stage IIA), and treatment history (previously treated with at least 1 SDT). Although the trial population consisted of treatment-experienced patients with primarily stage I disease (stage IA or stage IB), no relevant differences in efficacy and safety are expected. Reviewers for the FDA and EMA concluded that the safety and efficacy of Ledaga are considered established for treatment of patients at any stage of the disease. In terms of line of therapy, treatment decisions are based on several factors, such as the availability of different treatment options in different regions and settings. As noted earlier, Ledaga is the only drug of its class available in Canada and the clinical experts consulted by CADTH anticipated that it would be considered mainly in second-line treatment following phototherapy.
Indirect Evidence
No indirect treatment comparisons were submitted for this review.
Other Relevant Evidence
This section includes a submitted extension study provided in the submission to CADTH.
Extension Studies
Study 202 (Extension Study)
Methods
Study 202 was an open-label, single-arm extension study that evaluated the efficacy and safety of chlormethine 0.04% gel. Patients in Study 201 who had not achieved CR based on CAILS on either the chlormethine 0.02% hydrochloride gel or chlormethine hydrochloride 0.02% ointment during the 12-month study period were eligible to enrol in Study 202. All patients who enrolled into Study 202 received a higher strength of chlormethine gel (0.04%) for up to 7 months. Patients who entered Study 202 were followed and evaluated for AEs and skin cancers during the 7-month study treatment period and for 5 months thereafter (or the remainder of the 12-month safety follow-up period of Study 201, if treatment was discontinued prematurely).2,42
Populations
Patients were eligible for this extension study if they completed 12 months of treatment with chlormethine 0.02% hydrochloride gel or chlormethine ointment in Study 201 without reaching CR.
Interventions
Chlormethine hydrochloride 0.04% gel was applied once daily. Application frequency could be reduced for toxicity.
Outcomes
The primary efficacy end point was the same as for Study 201 (i.e., response rate defined as ≥ 50% improvement in CAILS of up to 5 lesions, confirmed ≥ 4 weeks later).42 The key secondary efficacy end point was response rate based on SWAT scores (i.e., response rate defined as ≥ 50% improvement from baseline in the SWAT score).
Statistical Analysis
Analyses were conducted using the safety analysis set (N = 98), which included all patients who received at least 1 application of chlormethine 0.04% gel.29 The CAILS responses for “prior index lesions” (i.e., index lesions that were used to assess efficacy in Study 201) were assessed, first, relative to the baseline scores of Study 201 and, second, relative to the baseline scores of Study 202. The CAILS responses for “all index lesions” (i.e., prior index lesions still present at baseline of Study 202 and new lesions that were identified as index lesions upon entry to Study 202 but were already present at baseline of Study 201) were assessed by comparison with the Study 202 baseline score only.29
Patient Disposition
Of the 100 enrolled patients, 98 were treated in Study 202. Of those, |||||||||| patients completed the trial and |||||||||||| patients permanently withdrew from the study (Table 22).
Table 22: Patient Disposition — Study 202
Patient disposition | Prior study (Study 201) treatment arm | Study 202 | |
|---|---|---|---|
Chlormethine 0.02% gel | Chlormethine 0.02% ointment | Chlormethine 0.04% gel (N = 98), n (%) | |
Consented | — | — | 100 |
Treated | 40 | 58 | 98 (100) |
Complete treatment | 37 | 48 | 85 (86.7) |
Permanently withdrawn from studya | 3 | 10 | 13 (13.3) |
Treatment-limiting toxicity | 0 | 2 | 2 (2.0) |
Other AE | 1 | 1 | 2 (2.0) |
Concurrent illness | 1 | 0 | 1 (1.0) |
Lack of efficacy | 0 | 3 | 3 (3.1) |
Non-compliance | 0 | 2 | 2 (2.0) |
Lost to follow-up | 0 | 1 | 1 (1.0) |
Otherb | 1 | 1 | 2 (2.0) |
AE = adverse event; CAILS = Composite Assessment of Index Lesion Severity.
aPatients were counted once under their primary reason for withdrawal.
bTwo patients were withdrawn for other reasons. One had initiated treatment with chlormethine 0.04% gel but had a CAILS score of 0 at the end of Study 201 with a subsequent biopsy that confirmed complete response. Another patient had a dispensing error at the month 6 visit.
Source: Ledaga European Public Assessment Report.29
Efficacy
Primary Efficacy End Point: The CAILS responses at the end of Study 202, relative to the Study 201 baseline, showed an overall confirmed response rate of 75.5%; 12.2% of patients achieved CR and 63.3% achieved PR (Table 23).29
The CAILS responses relative to the Study 202 baseline showed an overall confirmed response rate of 23.5% (95% CI, 15.9% to 32.5%); 10 (10.2%) patients achieved CR and 13 (13.3%) patients had PR.29 The CAILS responses for all index lesions were assessed by comparison with the Study 202 baseline score only; 26 (26.5%) patients achieved confirmed CAILS response from Study 202 baseline, including 6 (6.1%) patients showing a CR and 20 (20.4%) patients showing a PR (Table 24).29 In addition, 14 (14.3%) patients had their first response at final visit (unconfirmed response rate = 40.8%). By week 88, 33 (84.4%) patients who had previously received chlormethine hydrochloride 0.02% gel and 39 (67.9%) patients who had previously received chlormethine hydrochloride 0.02% ointment in Study 201 had responses over the course of these sequential studies.42
Table 23: CAILS Responses From Baseline of Study 201 for Prior Index Lesions — Study 202
CAILS outcome assessmenta | Chlormethine 0.04% gel (N = 98) |
|---|---|
Prior index lesions,b n (%) | |
Complete response | 12 (12.2) |
Partial response | 62 (63.3) |
Complete or partial unconfirmed response | 6 (6.1) |
Stable disease | 16 (16.3) |
Progressive disease | 2 (2.0) |
Unevaluable | 0 (0.0) |
Overall confirmed response rate, % (95% CI) | 75.5 (66.3 to 83.2) |
Overall response rate, % (95% CI) | 81.6 (73.1 to 88.3) |
CAILS = Composite Assessment of Index Lesion Severity; CI = confidence interval.
aResponses based on assessment of lesions compared to baseline of Study 201.
bIncludes only lesions identified as lesions in Study 201.
Source: Ledaga European Public Assessment Report.29
Table 24: CAILS Response From Baseline — Study 202
CAILS outcome assessmenta | Chlormethine 0.04% gel (N = 98) |
|---|---|
Prior index lesions,b n (%) | |
Complete response | 10 (10.2) |
Partial response | 13 (13.3) |
Complete or partial unconfirmed response | 13 (13.3) |
Stable disease | 49 (50.0) |
Progressive disease | 10 (10.2) |
Unevaluable | 3 (3.1) |
Overall confirmed response rate, % (95% CI) | 23.5 (15.9 to 32.5) |
Overall response rate, % (95% CI) | 36.7 (27.7 to 46.6) |
All index lesions,c n (%) | |
Complete response | 6 (6.1) |
Partial response | 20 (20.4) |
Complete or partial unconfirmed response | 14 (14.3) |
Stable disease | 52 (53.1) |
Progressive disease | 5 (5.1) |
Unevaluable | 1 (1.0) |
Overall confirmed response rate, % (95% CI) | 26.5 (18.6 to 35.9) |
Overall response rate, % (95% CI) | 40.8 (31.5 to 50.7) |
CAILS = Complete Assessment of Index Lesion Severity; CI = confidence interval.
aResponses based on assessment of lesions at baseline of Study 202.
bIncludes only lesions identified as index lesions in Study 201.
cIncludes all lesions identified as index lesions in Study 202.
Source: Ledaga European Public Assessment Report.29
Secondary Efficacy End Point: Confirmed SWAT responses were reported in 20.4% of patients; 3 (3.1%) patients had CR and 17 (17.3%) patients had PR (Table 25).29
Table 25: SWAT Response From Baseline — Study 202
SWAT assessmenta | Chlormethine 0.04% gel (N = 98) |
|---|---|
Comparison with baseline at entry to Study 202 | |
SWAT outcome assessment, n (%) | |
Complete response | 3 (3.1) |
Partial response | 17 (17.3) |
Stable disease | 60 (61.2) |
Progressive disease | 17 (17.3) |
Unevaluable | 1 (1.0) |
Overall confirmed response rate, % (95% CI) | 20.4 (13.4 to 29.2) |
Comparison with baseline at entry to Study 201 | |
SWAT outcome assessment, n (%) | |
Complete response | 4 (4.1) |
Partial response | 63 (64.3) |
Stable disease | 28 (28.6) |
Progressive disease | 3 (3.1) |
Unevaluable | 0 (0.0) |
Overall confirmed response rate, % (95% CI) | 68.4 (58.7 to 76.9) |
CI = confidence interval; SWAT = Severity-Weighted Assessment Tool.
aSWAT response from SWAT scores at the end of Study 202.
Source: Ledaga European Public Assessment Report.29
Harms
A summary of all AEs in Study 202 is presented in Table 26. Overall, 72.4% of patients in the trial had an AE and 6.1% of patients had a serious AE. The most common AEs were skin irritation (11.2%), erythema (10.2%), and pruritus (6.1%).42 There were no deaths during the study or within 30 days of stopping study treatment. One patient died due to metastatic lung cancer 6 months after premature discontinuation of study treatment, due to lung cancer.29 No measurable concentrations of chlormethine or its degradation product in blood collected 1 hour post-application on day 1 or after 2 months, 4 months, or 6 months of treatment were detected, confirming the lack of systemic exposure of chlormethine gel observed in Study 201.
Table 26: Summary of All Adverse Events — Study 202, Safety Analysis Set
Evaluation | Prior study (Study 201) treatment arm | Study 202 | |
|---|---|---|---|
Chlormethine gel (N = 40) n (%) | Chlormethine ointment (N = 58) n (%) | Chlormethine 0.04% gel (N = 98) n (%) | |
Patients with AE | 24 (60.0) | 47 (81.0) | 71 (72.4) |
Patients with SAE | 2 (5.0) | 4 (6.9) | 6 (6.1) |
Patients with AE leading to discontinuation of study treatment | 2 (5.0) | 3 (5.2) | 5 (5.1) |
Deaths occurring during study | 0 (0.0) | 0 (0.0) | 0 (0.0) |
AE = adverse event; SAE = serious adverse event.
Source: Ledaga European Public Assessment Report.29
Critical Appraisal
Study 202 is considered supportive only, as the strength of chlormethine gel is higher than the proposed reimbursement request.
Internal Validity: As with most long-term extension phase studies, the primary limitations of Study 202 were the open-label administration (similar to Study 201) and absence of a comparator group. Study 202 was originally conceived to gather safety data, including information on ongoing AEs from Study 201, as well as to extend the follow-up of patients from Study 201 to allow the detection of nonmelanoma skin cancer in patients treated in Study 201; in parallel, Study 202 was also to evaluate a higher concentration of chlormethine gel. This objective was achieved and there were no major issues with the conduct of the trial.
External Validity: The clinical experts noted that for patients who do not achieve an adequate response with chlormethine hydrochloride 0.02% gel and who do not have treatment-limiting adverse reactions to chlormethine hydrochloride 0.02% gel, they would consider using the higher strength chlormethine hydrochloride 0.04% gel in their clinical practice.
Discussion
Summary of Available Evidence
The evidence base for this review consists of 1 randomized controlled trial (Study 201) and an extension study (Study 202). Study 201 was a randomized, active comparator-controlled, observer-blinded, multi-centre trial of 260 previously treated patients with biopsy-confirmed stage I or stage IIA MF-CTCL. The trial was designed as a noninferiority study comparing the efficacy and safety of chlormethine hydrochloride 0.02% gel (n = 130) to chlormethine hydrochloride 0.02% ointment (n = 130). Given that the only difference between the 2 trial treatments was delivery formulation (with the same active ingredient), this was an acceptable study design to support the demonstration of noninferior clinical efficacy of chlormethine gel relative to the ointment formulation in the selected MF patient population. Chlormethine gel would be considered noninferior to the ointment formulation if the lower limit of the 95% CI around the ratio of the response rate of the gel to the ointment formulation (based on ≥ 50% improvement in the baseline CAILS score that was confirmed at the next visit ≥ 4 weeks later) was 0.75 or more. All affected areas (generally specific lesions for stage IA patients and the whole body for stage IB or stage IIA patients) were treated once daily for up to 12 months, with the frequency of application adjusted for toxicity. The primary end point was response, defined as improvement of 50% or more in baseline CAILS for 2 or more consecutive visits. Secondary end points included improvement of 50% or more in SWAT, the percentage of BSA, and the time to CAILS response. Outcome assessment was carried out every month until month 6 and every 2 months until month 12 (9 post-baseline study visits in total). The baseline characteristics were well balanced. Most patients were 18 years to 64 years of age, and had stage IA or stage IB disease with prior therapy consisting of corticosteroids and phototherapy. After completion of the trial, patients were followed-up off-study for an additional 12 months to gather additional safety data and assess the occurrence of squamous cell carcinoma. There were no major issues with the conduct of the study. However, the use of a comparator treatment that is not part of standard of care in Canada limits interpretation of the results. The extension study, Study 202, is considered supportive only, as the strength of chlormethine gel is higher than the proposed reimbursement request.
Interpretation of Results
Efficacy
The clinical trial of chlormethine hydrochloride 0.02% gel (Ledaga), Study 201, achieved its primary end point for noninferiority of gel versus ointment based on CAILS response. The CAILS response rate for chlormethine gel was 58.5% versus 47.7% for the ointment formulation, with a response rate ratio of 1.23 (95% CI, 0.97 to 1.55). The key secondary efficacy end points were consistent with the primary end point analyses and supported noninferiority, though these end points were not controlled for multiplicity for the noninferiority comparison. These included the SWAT response that showed a response rate of 46.9% in the chlormethine gel arm and 46.2% in the chlormethine ointment arm (ratio of response rate = 1.02; 95% CI, 0.78 to 1.32), and a percentage of BSA response that showed 44.6% and 43.1% response in the gel arm and ointment arm, respectively (ratio of response rate = 1.03; 95% CI, 0.78 to 1.36). The 2 chlormethine formulations used in the pivotal trial are considered comparable based on the known pharmacokinetics and other characteristics of the products, including the same active substance, strength, route of administration, and indication; they differ only in delivery formulation.29 The expected response rate of the ointment formulation is within the range of responses observed in previous uncontrolled studies of chlormethine/NM compounded formulations.6,43-45 Therefore, the differences observed between chlormethine gel and the ointment comparator in Study 201 are not considered clinically relevant and as such, the results are consistent with the 2 formulations having similar efficacy.29 Further evidence from the extension trial (Study 202) suggests that increasing the dose of chlormethine gel and extending treatment duration may result in a better chance of response when compared to baseline index lesions at the start of Study 201. However, it should be noted that when compared to index lesions at the start of Study 202, the proportion of patients with a PR decreased substantially.
Subgroup analyses of efficacy by MF stage showed that although response rate was higher in the gel arm compared to the ointment arm, the difference in response rates between the gel arm and ointment arm was numerically greater in stratum 1 (stage IA) compared to stratum 2 (stage IB and stage IIA). The CAILS response rate was 59.2% versus 40.0% in the gel arm versus ointment arm in stratum 1, and 57.4% versus 55.4% in stratum 2. A similar pattern was observed in subgroup analyses of secondary efficacy end points, SWAT response, and the percentage of BSA response. The higher response rate overall, and in earlier stages of disease (stage IA), may suggest that this group of patients may benefit more from treatment with chlormethine gel, though the results of the subgroup analysis must be interpreted with caution due to increased risk of type I error. This finding is also supported by the primary efficacy analyses of response based on SWAT (which includes the percentage of BSA as a component) and the percentage of BSA, both of which showed lower overall response rates compared to CAILS. This evidence from the clinical trial aligns with clinical practice where the percentage of BSA is an important factor in selecting patients who are more likely to benefit from treatment with chlormethine gel while avoiding excessive skin irritation. The clinical experts and the clinician group consulted by CADTH considered chlormethine gel as a treatment option primarily in patients with early-stage MF — those with less than 10% to 15% of BSA involved.
MF is a chronic condition that is generally considered incurable; the main aim of treatment is the remission of symptoms while improving or maintaining quality of life.1 Most patients eventually relapse or progress during treatment or after discontinuing treatment, and often cycle through several treatment options. As noted in a number of clinical practice guidelines in Europe and the US, the individual choice of the appropriate therapy can differ and will depend on clinical presentation and histologic characteristics (e.g., folliculotropism or LCT), as well as treatment availability.1,4 In their input to CADTH, both the patient and clinician groups emphasized that having a choice in treatment options was of great importance to them. The patient group indicated that their symptoms have a considerable negative impact on their quality of life and mental and emotional well-being. The patients reported that they want treatments that result in better quality of life, longer remission, fewer side effects, and more convenient application. Quality of life plays an important role in treatment decision-making and clinical management of MF. Given its established efficacy and ease of application, chlormethine in its ready-to-use gel formulation can offer an additional treatment option for patients with MF. However, the absence of HRQoL outcomes from the trial leaves an important gap in the evidence. Other limitations of the trial, including a protocol violation that led to imbalances in patient characteristics and imputation of patients as nonresponders, should be noted although they may not have had a major impact on the results. Other limitations of the evidence discussed in the preceding sections — including uncertainty about noninferiority margins, and using an active comparator that is not a standard of care treatment in Canada — may somewhat limit interpretation and application of the efficacy results from the trial.
Harms
The evidence regarding the safety of chlormethine gel is derived from Study 201 and Study 202 (extension study). More than half of the patients in both treatment arms experienced skin-related AEs, most commonly irritant dermatitis. The majority of skin-related AEs resolved during the observation period, even though most patients continued to receive other therapies for MF. There was no evidence of systemic exposure following topical application of chlormethine hydrochloride 0.02% gel or application with the higher strength 0.04% in the extension trial. During the clinical trial and the 12-month post-treatment follow-up, 4% of patients developed nonmelanoma skin cancers. Some of these occurred in patients who had received prior therapies known to cause nonmelanoma skin cancers. None of the nonmelanoma skin cancers observed were attributed specifically to chlormethine as they occurred in untreated areas, in patients with a history of skin cancers, or in patients who had received previous treatment with therapies known to increase the risk of skin cancers.46
The following skin-related AEs were deemed related to the topical use of chlormethine: dermatitis, pruritus, skin infections, skin hyperpigmentation, and skin ulcerating or blistering.2,30 Based on previous studies of topical chlormethine/NM, and the pharmacology and pharmacokinetics (i.e., lack of systemic absorption) of chlormethine, AEs not deemed related to topical chlormethine use included actinic keratosis (system organ class skin and subcutaneous tissue disorders); all but 1 patient who reported actinic keratosis as an AE had a medical history of actinic keratosis, squamous or basal cell carcinoma, or previous exposure to phototherapy. Xerosis (system organ class general disorders), a common clinical manifestation associated with MF-CTCL, is known to be an adverse reaction to total skin electron beam therapy, and the most common dermatosis of the skin by the age of 70 years. Xerosis was therefore not identified as an AE related to chlormethine gel. Non-skin AEs, including nausea, sinusitis, back pain, dyspnea, and pneumonia, were reported in more patients in the chlormethine treatment arm than in the chlormethine ointment arm. Given the lack of evidence of systemic exposure to chlormethine and the similar frequency of occurrence of these conditions in the general population, it was concluded that these were not related to chlormethine gel use in the trial.
Overall, the results of the trial with respect to safety are in line with previous uncontrolled studies of chlormethine/NM that reported no significant evidence of long-term toxicity or an increased risk of secondary skin cancer.6,43-45 The clinical experts consulted for this review noted that irritant dermatitis or skin irritation is a known AE of chlormethine and is relatively manageable in most patients. They also explained that the higher rate of skin irritation observed with the gel formulation (25.0% versus 14.2% in the ointment arm) is not unexpected since the emollient nature of the ointment helps decrease irritation. All relevant safety information and contraindications appear in the (draft) product monograph for Ledaga.30
Conclusions
Clinical evidence from 1 trial shows that chlormethine gel relieves skin symptoms of early-stage MF-CTCL but the noninferiority comparison is relative to an alternative formulation of the treatment that is no longer used. Like other treatments currently available for MF-CTCL, chlormethine gel is not a disease-modifying treatment and will not affect progression of the underlying disease. Patient group and clinical expert input highlighted the need for alternative treatment options given that most patients with early-stage MF-CTCL cycle through multiple rounds of treatments in different sequences. Although the ease of application can offer a convenient treatment option for patients with MF-CTCL, the absence of quality-of-life outcomes from the trial leaves an important gap in the evidence. Moreover, chlormethine gel is associated with skin-related AEs, which will likely limit its use to patients with lesions covering less than 10% BSA and following initial treatment for early-stage MF-CTCL with current standard of care treatments, such as phototherapy and topical steroids/retinoids, given established efficacy and lower risk of skin reactions. The available evidence suggests that chlormethine gel may offer an additional treatment option for selected patients with early-stage MF-CTCL.
References
1.Trautinger F, Eder J, Assaf C, et al. European Organisation for Research and Treatment of Cancer consensus recommendations for the treatment of mycosis fungoides/Sezary syndrome - Update 2017. Eur J Cancer. 2017;77:57-74. PubMed
2.Clinical Summary: Ledaga® (chlormethine gel) for mycosis fungoides-type cutaneous T-cell lymphoma (MF-CTCL) [internal sponsor's report]. Toronto (ON): Recordati Rare Diseases Canada; 2020.
3.Korgavkar K, Xiong M, Weinstock M. Changing incidence trends of cutaneous T-cell lymphoma. JAMA Dermatol. 2013;149(11):1295-1299. PubMed
4.Primary Cutaneous Lymphomas. Version 1.2021. NCCN Clinical Practice Guidelines in Oncology. Plymouth Meeting (PA): National Comprehensive Cancer Network (NCCN); 2020.
5.Hristov AC, Tejasvi T, Wilcox RA. Mycosis fungoides and Sezary syndrome: 2019 update on diagnosis, risk-stratification, and management. Am J Hematol. 2019;94(9):1027-1041. PubMed
6.Trautinger F, Knobler R, Willemze R, et al. EORTC consensus recommendations for the treatment of mycosis fungoides/Sezary syndrome. Eur J Cancer. 2006;42(8):1014-1030. PubMed
7.Center for Drug Evaluation Research. Drug approval package: Valchlor (mechlorethamine) gel. Company: Ceptaris Therapeutics. Application No.:202317. Approval date: 08/23/2013. Silver Spring (MD): U.S. Food and Drug Administration; 2013: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/202317Orig1s000TOC.cfm. Accessed 2021 Jan 31.
8.Lessin SR, Duvic M, Guitart J, et al. Topical chemotherapy in cutaneous T-cell lymphoma: positive results of a randomized, controlled, multicenter trial testing the efficacy and safety of a novel mechlorethamine, 0.02%, gel in mycosis fungoides. JAMA Dermatol. 2013;149(1):25-32. PubMed
9.Clinical Study Report 2005NMMF-201-US. A phase II pivotal trial to evaluate the safety and efficacy of nitrogen mustard (NM) 0.02% ointment formulations in patients with stage I or IIA mycosis fingoides (MF) [internal sponsor's report]. Malvern (PA): Yaupon Therapeutics; 2011.
10.Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105(10):3768-3785. PubMed
11.Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(6):1713-1722. PubMed
12.Ghazawi FM, Netchiporouk E, Rahme E, et al. Comprehensive analysis of cutaneous T-cell lymphoma (CTCL) incidence and mortality in Canada reveals changing trends and geographic clustering for this malignancy. Cancer. 2017;123(18):3550-3567. PubMed
13.Gilson D, Whittaker SJ, Child FJ, et al. British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br J Dermatol. 2019;180(3):496-526. PubMed
14.Bunn PA Jr, Lamberg SI. Report of the committee on staging and classification of cutaneous T-cell lymphomas. Cancer Treat Rep. 1979;63(4):725-728. PubMed
15.Talpur R, Singh L, Daulat S, et al. Long-term outcomes of 1,263 patients with mycosis fungoides and Sezary syndrome from 1982 to 2009. Clin Cancer Res. 2012;18(18):5051-5060. PubMed
16.Jawed SI, Myskowski PL, Horwitz S, Moskowitz A, Querfeld C. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sezary syndrome): part I. Diagnosis: clinical and histopathologic features and new molecular and biologic markers. J Am Acad Dermatol. 2014;70(2):205 e201-216; quiz 221-202.
17.Kim YH, Liu HL, Mraz-Gernhard S, Varghese A, Hoppe RT. Long-term outcome of 525 patients with mycosis fungoides and Sezary syndrome: clinical prognostic factors and risk for disease progression. Arch Dermatol. 2003;139(7):857-866. PubMed
18.Skov AG, Gniadecki R. Delay in the histopathologic diagnosis of mycosis fungoides. Acta Derm Venereol. 2015;95(4):472-475. PubMed
19.Hodak E, Lessin S, Friedland R. New insight into associated co-morbidities in patients with cutaneous T-cell lymphoma (mycosis fungoides). Acta Derm Venereol. 2013;93(4):5. PubMed
20.Demierre MF, Tien A, Miller D. Health-related quality-of-life assessment in patients with cutaneous T-cell lymphoma. Arch Dermatol. 2005;141(3):325-330. PubMed
21.Molloy K, Jonak C, Woei AJF, et al. Characteristics associated with significantly worse quality of life in mycosis fungoides/Sezary syndrome from the Prospective Cutaneous Lymphoma International Prognostic Index (PROCLIPI) study. Br J Dermatol. 2020;182(3):770-779. PubMed
22.Wright A, Wijeratne A, Hung T, et al. Prevalence and severity of pruritus and quality of life in patients with cutaneous T-cell lymphoma. J Pain Symptom Manage. 2013;45(1):114-119. PubMed
23.Agar NS, Wedgeworth E, Crichton S, et al. Survival outcomes and prognostic factors in mycosis fungoides/Sezary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. J Clin Oncol. 2010;28(31):4730-4739. PubMed
24.Scarisbrick JJ, Kim YH, Whittaker SJ, et al. Prognostic factors, prognostic indices and staging in mycosis fungoides and Sezary syndrome: where are we now? Br J Dermatol. 2014;170(6):1226-1236. PubMed
25.Scarisbrick JJ, Prince HM, Vermeer MH, et al. Cutaneous lymphoma international consortium study of outcome in advanced stages of mycosis fungoides and Sezary syndrome: effect of specific prognostic markers on survival and development of a prognostic model. J Clin Oncol. 2015;33(32):3766-3773. PubMed
26.Wilcox RA. Cutaneous B-cell lymphomas: 2016 update on diagnosis, risk-stratification, and management. Am J Hematol. 2016;91(10):1052-1055. PubMed
27.Quaglino P, Pimpinelli N, Berti E, et al. Time course, clinical pathways, and long-term hazards risk trends of disease progression in patients with classic mycosis fungoides: a multicenter, retrospective follow-up study from the Italian Group of Cutaneous Lymphomas. Cancer. 2012;118(23):5830-5839. PubMed
28.Smith A, Crouch S, Lax S, et al. Lymphoma incidence, survival and prevalence 2004-2014: sub-type analyses from the UK's Haematological Malignancy Research Network. Br J Cancer. 2015;112(9):1575-1584. PubMed
29.European Public Assessment report (EPAR): Ledaga. Amsterdam (NL): European Medicines Agency,; 2017: www.ema.europa.eu/en/documents/assessment-report/ledaga-epar-public-assessment-report_en.pdf. Accessed 2021 May 3.
30.PrLedaga® (chlormethine): 160 micrograms/gram topical gel [draft product monograph]. Toronto (ON): Ricordati Rare Diseases Canada; 2020 Apr 6.
31.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. Journal Clin Epidemiol. 2016;75:40-46. PubMed
32.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Jan 25.
33.Geskin LJ, Kim EJ, Angello JT, Kim YH. Evaluating the treatment patterns of chlormethine/mechlorethamine gel in patients with stage I-IIA mycosis fungoides: by-time reanalysis of a randomized controlled phase 2 study. Clin Lymphoma Myeloma Leuk. 2020;03:03.
34.Gilmore ES, Alexander-Savino CV, Chung CG, Poligone B. Evaluation and management of patients with early-stage mycosis fungoides who interrupt or discontinue topical mechlorethamine gel because of dermatitis. JAAD Case Rep. 2020;6(9):878-881. PubMed
35.Querfeld C, Geskin LJ, Kim EJ, et al. Lack of systemic absorption of topical mechlorethamine gel in patients with mycosis fungoides cutaneous T-cell lymphoma. J Invest Dermatol. 2021;08:08.
36.Drug Reimbursement Review sponsor submission: Ledaga (chlormethine): topical gel 160 micrograms/gram [internal sponsor's package]. Toronto (ON): Recordati Rare Diseases Canada; 2020 Dec 21.
37.Center for Drug Evaluation Research. Statistical review. Valchlor (mechlorethamine) gel. Company: Ceptaris Therapeutics. Application No.:202317. Approval date: 08/23/2013 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration; 2013: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/202317Orig1s000StatR.pdf. Accessed 2021 Jan 31.
38.Recordati Rare Diseases Canada response to March 16, 2021 drug reimbursement review request for additional information regarding Ledaga (chlormethine gel) for the treatment of T-cell lymphoma [internal additional sponsor's information]. Toronto (ON): Recordati Rare Diseases Canada; 2021.
39.Duvic M, Olsen EA, Omura GA, et al. A phase III, randomized, double-blind, placebo-controlled study of peldesine (BCX-34) cream as topical therapy for cutaneous T-cell lymphoma. J Am Acad Dermatol. 2001;44(6):940-947. PubMed
40.Recordati Rare Diseases Canada response to March 17, 2021 drug reimbursement review request for additional information regarding Ledaga (chlormethine gel) for the treatment of T-cell lymphoma [internal additional sponsor's information]. Toronto (ON): Recordati Rare Diseases Canada; 2021.
41.Stevens SR, Ke MS, Parry EJ, Mark J, Cooper KD. Quantifying skin disease burden in mycosis fungoides-type cutaneous T-cell lymphomas: the severity-weighted assessment tool (SWAT). Arch Dermatol. 2002;138(1):42-48. PubMed
42.Kim YH, Duvic M, Guitart J, Lessin S. Efficacy and safety of mechlorethamine (MCH) 0.04% gel in mycosis fungoides (MF) after treatment with topical MCH 0.02% [abstract]. J Clin Oncol. 2014;32(15 Suppl):9093.
43.Kim YH, Martinez G, Varghese A, Hoppe RT. Topical nitrogen mustard in the management of mycosis fungoides: update of the Stanford experience. Arch Dermatol. 2003;139(2):165-173. PubMed
44.Lindahl LM, Fenger-Gron M, Iversen L. Topical nitrogen mustard therapy in patients with mycosis fungoides or parapsoriasis. J Eur Acad Dermatol Venereol. 2013;27(2):163-168. PubMed
45.Lindahl LM, Fenger-Gron M, Iversen L. Secondary cancers, comorbidities and mortality associated with nitrogen mustard therapy in patients with mycosis fungoides: a 30-year population-based cohort study. Br J Dermatol. 2014;170(3):699-704. PubMed
46.Addendum 2 to Clinical Study Report 2005NMMF-201-US. A phase II pivotal trial to evaluate the safety and efficacy of nitrogen mustard (NM) 0.02% ointment formulations in patients with stage I or IIA mycosis fingoides (MF) [internal sponsor's report]. Malvern (PA): Ceptaris Therapeutics; 2012.
47.Olsen EA, Whittaker S, Kim YH, et al. Clinical end points and response criteria in mycosis fungoides and Sezary syndrome: a consensus statement of the International Society for Cutaneous Lymphomas, the United States Cutaneous Lymphoma Consortium, and the Cutaneous Lymphoma Task Force of the European Organisation for Research and Treatment of Cancer. J Clin Oncol. 2011;29(18):2598-2607. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: January 26, 2021
Alerts: Bi-weekly search updates until project completion
Study Types: All study types
Limits: Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ab | Abstract |
.dq. | Candidate term word |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.nm. | Name of substance word |
.ot. | Original title |
.pt | Publication type |
.rn | Registry number |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Database(s): Embase 1974 to 2021 January 21, Ovid MEDLINE(R) ALL 1946 to January 25, 2021
Search Strategy:
Mechlorethamine/
(chlormethine* or Ledaga* or Valchlor* or azotyperite or azotoyperite or azotoyperit or antimit or Caryolysine or cariolysine or cariolisin or Chlorethazine or Chlormethine or Chlormethinum or Cloramin or Clormetina or clearazide or chloroethazin or chlorethazine or chloramin or chloramine or Dichlor amine or Diethylamine or dimitan or dichloren or dema or EINECS 200-120-5 or EINECS 200-246-0 or Embichin or erasin or embikin or embikhine or embiquine or embichine or erasol or kloramin or karyolysine or ENT-25294 or ENT25294 or HN-2 or HN2 or HSDB 5083 or HSDB5083 or HSDB 7176 or HSDB7176 or Mechlorethamine or mebichloramine or Mecloretamina or methylchlorethamine or methylbischloroethylamine or Mitomen or mustargen or mustarnitrogen or mitoxine or mustine or mba hydrochloride or N-Methyl-lost or nitrogranulogen or nitromen or nitromin or nitrogen mustard* or nitrous yperite or nitol or nitrasin or onco cloramin or pliva* or NSC 762 or NSC762 or NSC-10107 or NSC10107 or NSC 128663 or NSC128663 or Stickstofflost or stickstoffsenfgas or Zagreb* or sk101 or sk 101 or T 1024 or T1024 or TL 146 or TL146 UN 2927 or UN2927 or c6866 or c 6866 or CCRIS 448 or CCRIS448 or AI3 16195 or AI316195 or NCI C56382 or NCI36582 or 50D9XSG0VR or L0MR697HHI).ti,ab,ot,kf,hw,nm,rn.
1 or 2
exp Lymphoma, T-Cell, cutaneous/
((t-cell* or tcell*) adj4 (leukem* or leukaem* or lymphom* or lymphoproliferative or neoplas* or malignan*) adj6 (cutaneous or skin)).ti,ab,kf.
CTCL.ti,ab,kf.
(mycosis fungoides or granuloma fungoides or granulomatous slack skin or Pagetoid Reticulos* or Woringer-Kolopp Disease or Ketron-Goodman disease).ti,ab,kf.
or/4-7
3 and 8
9 use medall
*Chlormethine/
(chlormethine* or Ledaga* or Valchlor* or azotyperite or azotoyperite or azotoyperit or antimit or Caryolysine or cariolysine or cariolisin or Chlorethazine or Chlormethine or Chlormethinum or Cloramin or Clormetina or clearazide or chloroethazin or chlorethazine or chloramin or chloramine or Dichlor amine or Diethylamine or dimitan or dichloren or dema or EINECS 200-120-5 or EINECS 200-246-0 or Embichin or erasin or embikin or embikhine or embiquine or embichine or erasol or kloramin or karyolysine or ENT-25294 or ENT25294 or HN-2 or HN2 or HSDB 5083 or HSDB5083 or HSDB 7176 or HSDB7176 or Mechlorethamine or mebichloramine or Mecloretamina or methylchlorethamine or methylbischloroethylamine or Mitomen or mustargen or mustarnitrogen or mitoxine or mustine or mba hydrochloride or N-Methyl-lost or nitrogranulogen or nitromen or nitromin or nitrogen mustard* or nitrous yperite or nitol or nitrasin or onco cloramin or pliva* or NSC 762 or NSC762 or NSC-10107 or NSC10107 or NSC 128663 or NSC128663 or Stickstofflost or stickstoffsenfgas or Zagreb* or sk101 or sk 101 or T 1024 or T1024 or TL 146 or TL146 UN 2927 or UN2927 or c6866 or c 6866 or CCRIS 448 or CCRIS448 or AI3 16195 or AI316195 or NCI C56382 or NCI36582 or 50D9XSG0VR or L0MR697HHI).ti,ab,kw,dq.
11 or 12
exp Cutaneous T cell lymphoma/
((t-cell* or tcell*) adj4 (leukem* or leukaem* or lymphom* or lymphoproliferative or neoplas* or malignan*) adj6 (cutaneous or skin)).ti,ab,kw,dq.
CTCL.ti,ab,kw,dq.
(mycosis fungoides or granuloma fungoides or granulomatous slack skin or Pagetoid Reticulos* or Woringer-Kolopp Disease or Ketron-Goodman Disease).ti,ab,kw,dq.
or/14-17
13 and 18
19 not (conference abstract or conference review).pt.
20 use oemezd
10 or 21
remove duplicates from 22
Clinical Trials Registries
ClinicalTrials.gov
Produced by the U.S. National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | chlormethine or mechlorethamine AND cutaneous T-cell lymphoma]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- chlormethine or mechlorethamine AND cutaneous T-cell lymphoma]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- chlormethine or mechlorethamine AND cutaneous T-cell lymphoma]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- chlormethine or mechlorethamine AND cutaneous T-cell lymphoma]
Canadian Cancer Trials
Produced by the Canadian Partnership Against Cancer Corporation. Targeted search used to capture registered clinical trials.
[Search terms -- chlormethine or mechlorethamine AND cutaneous T-cell lymphoma]
Grey Literature
Search dates: January 13-20, 2021
Keywords: Ledaga, Valchlor, chlormethine, mechlorethamine, cutaneious T-cell lymphoma
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Gilmore, E.S. et al.34 | Study design (case report) |
Querfeld, C. et al.35 | Study design (letter) |
Geskin, L.J. et al.33 | Posthoc reanalysis of Study 201 data |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Tables 28 and 29 show the results of efficacy analyses including and excluding NY (Site 7) following the protocol violation involving randomization at Site #7.
Table 29: Results for the Primary and Secondary Efficacy End Points
Chlormethine gel response rate | Chlormethine ointment response rate | Ratio response | 95% CI | |
|---|---|---|---|---|
Primary end point, % | ||||
CAILS | ||||
ITT including Site #7 (As Treated) | 58.5 | 47.7 | 1.226 | 0.974 to 1.552 |
ITT excluding Site #7 | 59.7 | 48.0 | 1.224 | 0.983 to 1.582 |
Site #7 as planned | 57.8 | 48.5 | 1.192 | 0.948 to 1.506 |
EE | 76.7 | 58.9 | 1.301 | 1.065 to 1.609 |
Secondary end points, % | ||||
SWAT | ||||
ITT including Site #7 | 46.9 | 46.2 | 1.017 | 0.783 to 1.321 |
ITT excluding Site #7 | 49.6 | 46.3 | 1.070 | 0.822 to 1.394 |
EE | 63.3 | 55.8 | 1.135 | 0.893 to 1.448 |
Percentage of BSA | ||||
ITT including Site #7 | 44.6 | 43.1 | 1.036 | 0.786 to 1.366 |
ITT excluding Site #7 | 47.1 | 43.1 | 1.092 | 0.826 to 1.446 |
EE | 60.0 | 52.6 | 1.140 | 0.883 to 1.478 |
BSA = body surface area; CAILS = Composite Assessment of Index Lesion Severity; CI = confidence interval; EE = efficacy-evaluable; ITT = intention-to-treat; SWAT = Severity-Weighted Assessment Tool.
Source: Clinical Study Report for Study 201.9
Table 30: CAILS Treatment Response, n (%) — ITT, Excluding Site #7
CAILS outcome | Chlormethine gel (N = 119) | Chlormethine ointment (N = 123) |
|---|---|---|
Response | 71 (59.7) | 59 (48.0) |
CR | 17 (14.3) | 14 (11.4) |
PR | 54 (45.4) | 45 (36.6) |
Nonresponse | 48 (40.3) | 64 (52.0) |
Stable disease | 36 (30.3) | 59 (48.0) |
Progressive disease | 5 (4.2) | 1 (0.8) |
Unevaluable | 7 (5.9) | 4 (3.3) |
CAILS = Composite Assessment of Index Lesion Severity; CR = complete response; ITT = intention-to-treat; PR = partial response.
Source: Clinical Study Report for Study 201.9
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
CAILS
SWAT
Findings
Table 31: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
CAILS | Skin scoring by physician | No information on the validity, reliability, or responsiveness was found. | Not identified. |
SWAT | Skin scoring by physician | Validity: Correlated with percentage total body surface area (r = 0.95, P < 0.001), physician global assessment (r = 0.60, P < 0.001), and time to complete remission during PUVA therapy. Reliability: No information found. Responsiveness: No information found. | Not identified. |
CAILS = Composite Assessment of Index Lesion Severity; MID = minimal important difference; SWAT = Severity-Weighted Assessment Tool.
Source: Clinical Study Report9 and Stevens et al. (2002).41
Composite Assessment of Index Lesion Severity
The CAILS is a method of index lesion scoring for patch and plaque disease performed by the investigator.9 The CAILS score was obtained by adding the severity score of each of the following symptoms for up to 5 index lesions: erythema, scaling, plaque elevation, and surface area.9 For each Index lesions severity is scored from 0 (none) to 8 (severe) for erythema and scaling, from 0 (no evidence of plaque above normal skin level) to 3 (marked elevation) for plaque elevation and 0 (no measurable area) to 18 (> 300 cm2) for surface area. Criteria for the severity scores for each symptom used in the pivotal Study 201 are detailed in Table 32. The CAILS score ranges from 0 to 185, with higher scores indicating increased skin symptom burden.
In the pivotal trial (Study 201), the sponsor defined a response as a reduction of 50% or more in the baseline CAILS score that is confirmed at the next visit in 4 weeks or later.
No information on the CAILS’s validity, reliability, responsiveness to change, or MID was found.
Table 32: Grading Scale for CAILS
Symptom | Severity score |
|---|---|
Scaling | 0 - No evidence of scaling on the lesion 1* 2 - Mild: Mainly fine scales; lesion partially covered 3* 4 - Moderate: Somewhat coarser scales; lesion partially covered 5* 6 - Severe: Coarse, thick scales; virtually all of the lesion covered; rough surface 7* 8 - Very severe: Coarse, very thick scales; all of the lesion covered; very rough surface |
Erythema | 0 - No evidence of erythema, possible brown hyperpigmentation 1* 2 - Mild: Light red lesion 3* 4 - Moderate: Red lesion 5* 6 - Severe: Very red lesion 7* 8 - Very severe: Extremely red lesion |
Plaque Elevation | 0- No evidence of plaque above normal skin level 1- Mild elevation 2- Moderate elevation 3 – Marked elevation |
Index Lesion Area | 0 - 0 cm2 (no measurable area) 1 - > 0 and ≤ 4 cm2 2 - > 4 and ≤ 10 cm2 3 - > 10 and ≤ 16 cm2 4 - > 16 and ≤ 25 cm2 5 - > 25 and ≤ 35 cm2 6 - > 35 and ≤ 45 cm2 7 - > 45 and ≤ 55 cm2 8 - > 55 and ≤ 70 cm2 9 - > 70 and ≤ 90 cm2 |
Index Lesion Area (continued) | 10 - > 90 and ≤ 110 cm2 11 - > 110 and ≤ 130 cm2 12 - > 130 and ≤ 155 cm2 13 - > 155 and ≤ 180 cm2 14 - > 180 and ≤ 210 cm2 15 - > 210 and ≤ 240 cm2 16 - > 240 and ≤ 270 cm2 17 - > 270 and ≤ 300 cm2 18 - > 300 cm2 |
*Intermediate intervals 1,3,5, and 7 are to serve as mid-points between the defined grades 0,2,4,6, and 8.
Source: Clinical Study Report.9
Severity-Weighted Assessment Tool
The SWAT is the most widely used tool for skin scoring in MF performed by the investigator.47 The SWAT captures the extent and severity of skin disease on a continuous numerical scale and provides a quantitative measure of disease status.41
The SWAT is derived by measuring each involved area as a percentage of total BSA and multiplying it by a severity-weighting factor41: 1 for patch disease; 2 for plaques; 3 for cutaneous tumours or ulceration (including fissuring). Patch disease is defined as a flat erythema and plaque disease is an elevated area. Tumours are dome-shaped nodular regions of more than 1 cm elevation.
The percent BSA (% BSA = 0% to 100%) affected by each of the 3 lesion types is measured. The patient’s palm is defined as 1% of that patient’s BSA, and the extent of disease involvement is determined as multiples of the patient’s palm area.36,41 Percentages of BSA are also assigned for 12 regions: 7% for head, 2% for neck, 13% for anterior trunk, 13% for posterior trunk, 5% for buttocks, 1% for genitalia, 8% for upper arms, 6% for forearms, 5% for hands, 19% for thighs, 14% for lower leg, and 7% for feet.9
The SWAT score is calculated by multiplying the sum of the BSA of each lesion type by the severity-weighting factor: SWAT = (patch percentage of BSA × 1) + (plaque percentage of BSA × 2) + (tumour or ulcer percentage of BSA × 3).9,41 The SWAT score ranges from 0 to 300, with higher scores indicating increased skin symptom burden.
A study conducted by Stevens et al. (2002) was done to develop and investigate the validity of the SWAT in 323 patients with MF more than 1,186 visits.41 The SWAT score correlated with percentage total BSA (r = 0.95, P < 0.001), physician global assessment (r = 0.60, P < 0.001), and time to complete remission during PUVA therapy (r = 0.80, P < 0.001). In this study, physician global assessment was rated on a scale from 0 (clear of disease) to 3 (severe). No additional information on the SWAT’s validity was found.
No information on the SWAT’s reliability, responsiveness to change, or MID was found.
Pharmacoeconomic Review
Abbreviations
BCNU
bis-chloroethyl nitrosourea
BIA
budget impact analysis
EQ-5D-3L
EQ-5D Three-Level
EQ-5D-5L
EQ-5D Five-Level
ICER
incremental cost-effectiveness ratio
MF-CTCL
mycosis fungoides-type cutaneous T-cell lymphoma
PUVA
psoralen plus ultraviolet A
QALY
quality-adjusted life-year
RCT
randomized controlled trial
SWAT
Severity-Weighted Assessment Tool
WTP
willingness-to-pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Chlormethine gel (Ledaga), 0.02% |
Submitted price | Chlormethine gel, 0.02%, 60 g tube: $2,710.38 |
Indication | Proposed: For the topical treatment of mycosis fungoides-type cutaneous T-cell lymphoma in adult patients |
Health Canada approval status | Under review (pre-NOC) |
Health Canada review pathway | Standard |
NOC date | June 8, 2021 |
Reimbursement request | As per indication |
Sponsor | Recordati Rare Diseases Canada Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult patients with MF-CTCL |
Treatment | Chlormethine gel |
Comparator | Phototherapy (consisting of PUVA and UVB) |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs |
Time horizon | Lifetime (44 years) |
Key data sources | Chlormethine gel informed by Study 201; Phototherapy informed by Phan et al. (2019) and Whittaker et al. (2012) |
Submitted results | Chlormethine gel is dominant (less costly [incremental costs = –$19,893] and more effective [incremental QALYs = 0.66]) compared to phototherapy. |
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma; PUVA = psoralen plus UV A; QALY = quality-adjusted life-year; SWAT = Severity-Weighted Assessment Tool; UVB = UV B.
Conclusions
The comparative clinical effects of chlormethine gel relative to phototherapy and other treatments for MF-CTCL are unknown. Based on the CADTH clinical review, chlormethine gel relieves skin symptoms of early-stage MF-CTCL; however, there is no direct evidence comparing chlormethine gel and phototherapy, and the sponsor was unable to conduct an indirect treatment comparison owing to a lack of data. The efficacy of chlormethine gel relative to phototherapy in the model was based on naive unadjusted comparisons, without adjustment or accounting for differences in patient characteristics, which introduces additional uncertainty.
Given the lack of comparative evidence, a CADTH base case could not be derived to estimate the cost-effectiveness of chlormethine gel compared with phototherapy. CADTH performed exploratory reanalyses, assuming confidence in the naive comparison of chlormethine gel and phototherapy. These reanalyses addressed limitations in the sponsor’s submission, including using a common source for phototherapy effectiveness estimates, revising the timing of response assessment for phototherapy, excluding costs associated with wound care, and increasing the daily dose of chlormethine gel. However, CADTH was unable to address the lack of head-to-head comparative clinical data for chlormethine gel and phototherapy, the impact of basing treatment response on a Severity-Weighted Assessment Tool (SWAT) score, the lack of data for the effectiveness of chlormethine gel among patients with late-stage disease, and uncertainty related to health state utility values. The validity and interpretability of the results are limited by the lack of comparative evidence.
In the CADTH exploratory analysis, chlormethine gel had a 0.2% probability of being cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per quality-adjusted life-year (QALY) (incremental cost-effectiveness ratio [ICER] of $358,310 per QALY gained compared with phototherapy). The key driver of the ICER was the cost of chlormethine gel acquisition. In a scenario analysis in which chlormethine gel was assumed to be used only by patients with early-stage disease (stage IA with < 10% skin involvement), chlormethine gel was associated with an ICER of $802,268 per QALY gained compared with phototherapy. The lack of comparative clinical evidence means that these results are highly uncertain and likely do not reflect the true clinical efficacy of chlormethine gel. Consequently, the cost-effectiveness of chlormethine gel compared to phototherapy is unknown within the indicated population.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Joint patient input was received on behalf of Lymphoma Canada, the Canadian Skin Patient Alliance, and the Cutaneous Lymphoma Foundation, which included 233 patient responses as part of an online survey (90% with mycosis fungoides). Respondents indicated that mycosis fungoides affects their work life, intimate and family relationships, and personal image, as well as their mental health (i.e., anxiety and/or worry). Respondents described experience with a variety of treatments, including systemic therapies, radiation, phototherapy, and topical drugs. Respondents who had experience with chlormethine gel indicated that it improved their disease symptoms, including red patches, itchiness, ulcers, and pain. Adverse events, including itching, hyperpigmentation, skin blistering, and rash, frequently led to discontinuation of chlormethine gel. Patients stated that treatments that improved survival, quality of life, and remission duration, with fewer side effects and easier and/or faster treatment application, were preferred.
Input from a group of 5 registered clinicians noted that currently available skin-directed therapies for early-stage disease (stage IA to stage IIA) include compounded mechlorethamine ointment (limited stability and availability across Canada), compounded bis-chloroethyl nitrosourea (BCNU), topical steroids, imiquimod, tazarotene gel, phototherapy, and external beam radiotherapy. The clinicians described limitations with the use of some treatments, including compounding and stability (i.e., mechlorethamine ointment and BCNU), adverse event monitoring (BCNU), availability (compounded mechlorethamine ointment), or coverage for mycosis fungoides (imiquimod, tazarotene gel). Clinicians indicated that they anticipated that chlormethine gel will provide an improved treatment application compared to current creams and ointments, possibly encouraging compliance and self-administration at home, and that a gel formulation would be of particular benefit to patients with involvement of hairy areas (e.g., scalp, bearded area), for which existing topical preparations are not suitable. Clinicians noted that mycosis fungoides is a chronic disease and that patients often experience disease relapse. Further, clinicians indicated that chlormethine gel would be most suitable as second-line treatment for patients who had failed or were intolerant to at least 1 prior skin-directed therapy (e.g., topical steroids and/or phototherapy) and who have stage IA to stage IIA disease and limited (e.g., 10% to 15%) body surface area involvement.
CADTH participating drug plans noted that the choice of comparator in the submitted pivotal trial (Study 201) may not be appropriate because chlormethine ointment is not currently funded or available in most jurisdictions. Further, the comparator in the economic model, phototherapy, is associated with barriers to access, including frequent appointments and restrictions to urban centres. Finally, drug plans noted that other topical treatments (e.g., carmustine, imiquimod) are currently funded. The drug plans also noted that the sponsor assumed similar treatment costs for both patients with either a low extent or high extent of body surface area involvement, which may potentially underestimate the resulting budget impact.
Several of these concerns were addressed in the sponsor’s model:
Treatment effectiveness is modelled in the sponsor’s submission in terms of modified SWAT score, which considers the extent of body surface area involvement and whether the lesions are patches, plaques, or tumours.
Grade 3 and grade 4 adverse events that occurred in at least 5% of trial participants were included in the sponsor’s model; however, these did not include the full range of adverse events considered important to patients or clinicians.
In addition, CADTH addressed some of these concerns as follows:
The cost-effectiveness of chlormethine gel in patients with less than 10% skin involvement was assessed in scenario analyses.
The dosage of chlormethine gel was based on the extent of body surface area involvement in scenario analyses.
CADTH was unable to address the following concerns raised from stakeholder input:
The impact of chlormethine gel on patient-important outcomes (quality of life, key symptoms, survival) is unknown.
The cost-effectiveness of chlormethine gel relative to carmustine and imiquimod could not be assessed owing to a lack of data.
The structure of the sponsor’s model did not permit the assessment of the cost-effectiveness of chlormethine gel as a second-line treatment after prior skin-directed therapy.
Economic Review
The current review is for chlormethine gel (Ledaga) for the topical treatment of mycosis fungoides-type cutaneous T-cell lymphoma (MF-CTCL) in adult patients.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing chlormethine gel in adult patients with MF-CTCL compared with phototherapy.1 The target population of the sponsor’s analysis reflects the proposed Health Canada indication. Key data inputs for chlormethine gel are derived from Study 201,2 which includes patients with early-stage disease (stage IA, stage IB, stage IIA). The sponsor assumed that phototherapy consists of psoralen plus UV A (PUVA) and UV B (UVB), with 21.8% of patients assumed to receive PUVA and the remainder to receive UVB.
Chlormethine gel is supplied as a 60 g tube, with a recommended application of “a thin film applied daily to the affected areas of the skin.”3 At the submitted price of $2,710.38 per 60 g tube, the sponsor calculated the monthly drug acquisition costs of chlormethine gel to be $2,475 per patient, assuming that 1.80 g of gel would be used daily based on the median daily dose in Study 201. For phototherapy, the sponsor calculated the monthly cost to be $89 per patient.
The clinical outcomes of interest were QALYs and life-years.1 The economic analysis was undertaken over a lifetime time horizon (44 years) from the perspective of the public health care payer. Discounting (1.5% per annum) was applied to both costs and outcomes.
Model Structure
The sponsor submitted a Markov model with health states related to disease stage (stage IA, stage IB/IIA, stage IIB+) and skin burden (low skin burden, high skin burden, reduced skin burden, no skin burden), as well as states related to the treatment of progressed disease (skin-directed therapy, systemic therapy) and death (Figure 1). Disease stage IA, stage IB, and stage IIA were assumed to reflect early-stage disease, and patients in these stages were assumed to receive skin-directed therapy (chlormethine gel or phototherapy). Stage IIB+ was assumed to reflect late-stage disease, and patients in this state were assumed to receive both skin-directed and systemic cancer therapies.1 Patients entered the model in either stage IA, stage IB/IIA, or stage IIB+, and were further distributed between the low skin burden and high skin burden health states on the basis of the percentage of body surface area or skin involvement (low skin burden: < 10% skin involvement; high skin burden: 10%–80% skin involvement). Patients in stage IA were assumed to be in the low skin burden state, and patients in stage IB and stage IIA were assumed to be in the high skin burden state. Patients in stage IIB+ were distributed between the low skin burden state and the high skin burden state based on the distribution in the Prospective Cutaneous Lymphoma International Prognostic Index (PROCLIPI) international registry (16% = low skin burden; 84% = high skin burden).1
Within the model, patients could progress through disease states (stage IA, stage IB/IIA, and stage IIB+), as well as move between skin burden states within a disease state (Figure 1). Once a patient progressed to a more advanced disease stage, they could not return to a less severe state. Movement between states was based on treatment response (see the following). Patients who progressed to a more advanced disease stage from a low skin burden state or high skin burden state were assumed to transition to the skin-directed therapy state or systemic therapy state, depending on whether they had initially received chlormethine gel or phototherapy. In the skin-directed therapy state, patients were rechallenged with skin-directed therapy, which was assumed to consist of chlormethine gel (for 80% of patients) or phototherapy (for 20% of patients). For patients who initially received phototherapy, patients whose disease progressed while in the low skin burden health state or high skin burden health state were assumed to transition directly to the systemic therapy health state rather than transitioning to the skin-directed therapy health state; these patients were assumed to receive pegylated interferon-alfa. Patients in the low skin burden state could transition to the reduced skin burden state or the no skin burden state, and those in the no skin burden state were assumed to receive watchful waiting. From the high skin burden state, patients could move either to the reduced skin burden state or to the skin-directed therapy or systemic therapy state (depending on the initial treatment received) if their disease progressed. Patients with stable disease were assumed to receive pegylated interferon-alfa therapy and to remain in their current skin burden health state. Patients could experience a relapse (i.e., skin symptoms that return following an initial treatment response) following either an initial partial response or complete response. Within the model, the sponsor assumed that patients would progress by a single disease stage (e.g., stage IA progresses to stage IB/IIA only), and patients could die from any state.
Transition between the low skin burden, high skin burden, reduced skin burden, and no skin burden health states was based on treatment response, which was assessed after 6 months of treatment for chlormethine gel and 13 weeks of treatment for phototherapy. Treatment response was assessed by use of the modified SWAT using observed data from Study 201. Patients with 100% improvement in their SWAT score from baseline were classified as having a complete response, while patients with 50% to 99% reduction in their SWAT score from baseline were classified as having a partial treatment response. Those with a reduction from baseline of less than 50% were classified as having stable disease, while patients whose SWAT score increased by 25% or more from baseline were classified as having progressive disease.2 The effectiveness of skin-directed therapy was assumed to be equivalent for patients in the same skin burden state, regardless of disease stage.
Model Inputs
The baseline characteristics in the model were aligned with those of the Study 201 patient population for age (median 55.7 years) and sex (59.2% male) and with the Prospective Cutaneous Lymphoma International Prognostic Index registry for the proportion of patients in each disease stage at baseline (stage IA = ||||%; stage IB/IIA = ||||%; stage IIB+ = ||||%).1,2 The sponsor incorporated a combination of patient-level data from Study 201 and results from the published literature to inform the transitions between health states, treatment response, relapse, and death. The sponsor estimated the probability of disease progression based on a retrospective analysis of progression-free survival that was based on patients in the Integrated Cancer Research (ICARSIS) database.4 For chlormethine gel, transitions between skin burden health states (low skin burden, high skin burden, reduced skin burden), skin-directed therapy, and systemic therapy were based on SWAT response rates from Study 201.2 For phototherapy, these transition probabilities were based on treatment response rates reported in a 2019 meta-analysis of phototherapy for the treatment of early mycosis fungoides (stage IA to stage IIA).5 For chlormethine gel, the probability of relapse after a partial response was based on data from Study 201, while the probability of relapse after a complete response was based on the probability of relapse among patients who had received topical nitrogen mustard.6 For phototherapy, the probability of a relapse after a partial response or complete response was based a randomized controlled trial (RCT) involving patients with stage IIA or stage IB MF-CTCL who received PUVA alone or PUVA plus bexarotene.7 The sponsor assumed that mortality for patients in stage IA is equal to the Canadian general population.8 The risk of death for patients in stage IB/IIA and in stage IIB+ additionally incorporated the median overall survival of patients in each disease stage.4
The sponsor’s model incorporated treatment-associated grade 3 or grade 4 adverse events occurring in at least 5% of participants in Study 201 for chlormethine gel2 and in an RCT of patients who received PUVA alone or PUVA plus bexarotene for phototherapy.7 For chlormethine gel, these included dermatitis contact, erythema, and skin irritation.2 Because no grade 3 or grade 4 adverse events were reported for at least 5% of patients who received phototherapy in the Whittaker et al. (2012) RCT,7 the sponsor assumed that the probability of an adverse event with phototherapy was 0%.
Health-related quality of life estimates were not collected as part of Study 201. In the model, the sponsor incorporated health state utility value estimates from a vignette study involving proxy respondents.9 In this study, EQ-5D Five-Level (EQ-5D-5L) utility estimates were indirectly elicited from clinicians based on theoretical patients with characteristics encompassing disease stage, SWAT score, skin burden, Eastern Cooperative Oncology Group score, and age at diagnosis. The sponsor mapped the EQ-5D-5L values to the EQ-5D Three-Level (EQ-5D-3L) using a mapping algorithm10 and UK preference weighting. Using the utility value assigned to each SWAT range from the patient vignettes, the sponsor calculated a weighted average utility for each health state. The sponsor assumed that the mean change in SWAT score for patients in the low skin burden and high skin burden states would be equivalent across early and advanced disease stages. The sponsor applied a utility decrement (0.03) for adverse events.11
The model included costs related to drugs (acquisition, administration), disease management (oncologist visits, dermatologist visits, nurse time, pharmacist time, CT and PET scans, laboratory monitoring tests, wound dressings, radiotherapy), adverse events, and end-of-life care.1 Drug acquisition costs for chlormethine gel were based on the sponsor’s submitted price,1 with the cost of other treatments obtained from the Ontario Exceptional Access Program,12 Ontario Drug Benefit Formulary,13 and previous CADTH submissions.14,15 Drug costs were calculated using an average weight of 76 kg and body surface area of 1.85 m2 where applicable. The cost of phototherapy was based on physician costs per treatment,16 with a mean of 13.04 and 10.87 PUVA and UVB sessions administered per month, respectively.17 No other costs associated with phototherapy were included. Systemic therapy (for patients with advanced-stage disease) was assumed to comprise brentuximab vedotin, gemcitabine, pegylated interferon-alfa, and extracorporeal photopheresis. Administration costs were included for phototherapy and systemic therapies.16 The cost of contact with health care professionals and testing (as part of disease management) was based on the Ontario Schedule of Benefits for Physician Services16 and the Ontario Schedule of Benefits for Laboratory Services,18 and the frequency of resource use was based on the opinion of clinical experts consulted by the sponsor. As part of disease management costs, the sponsor assumed patients would receive wound-care dressings for skin-related symptoms (1 each of small dressing, medium dressing, and large dressing per month), with the cost based on a CADTH review of vismodegib for basal cell carcinoma.19 End-of-life care costs were applied as a 1-time cost at the time of death.20 Adverse event costs were based on consultation with a dermatologist.16
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base case and scenario analyses). The deterministic and probabilistic results were similar; however, the incremental costs predicted by the probabilistic analyses were lower than in deterministic analyses. The probabilistic findings are presented as follows. Additional results from the sponsor’s submitted economic base case are presented in Table 8.
Base-Case Results
In the sponsor’s base-case analysis, chlormethine gel was dominant over phototherapy in that it was associated with lower costs (incremental costs = –$19,893) and higher QALYs (incremental QALYs = 0.66) compared with phototherapy over a 44-year horizon (Table 3). In the sponsor’s base case, chlormethine gel had an 80% probability of being the most cost-effective strategy at a WTP threshold of $50,000 per QALY.
Results were driven by the drug acquisition cost of chlormethine gel (incremental costs = $75,576) and the cost associated with monitoring and resource use (incremental costs = –$95,576) (Appendix 3, Table 8). The majority of QALYs gained with chlormethine hydrochloride gel were accrued by patients with stage IIA or stage IB disease (incremental QALYs = 0.41). At the end of the lifetime time horizon, 0% of patients receiving chlormethine hydrochloride gel and phototherapy remained alive.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. phototherapy ($/QALY) |
|---|---|---|---|---|---|
Phototherapy | 988,817 | Reference | 11.85 | Reference | Reference |
Chlormethine gel | 968,923 | –19,893 | 12.51 | 0.66 | Dominanta |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
aDominant indicates that a treatment is less costly and more effective (higher QALYs) than the reference.
Source: Sponsor’s Pharmacoeconomic Submission.1
Sensitivity and Scenario Analysis Results
The sponsor assessed the impact of several model parameters in probabilistic scenario analyses, including adopting alternative discount rates and time horizons, assuming a reduced frequency of wound dressings, and assuming that the amount of daily chlormethine gel usage would vary by disease stage (i.e., by extent of body surface area involvement). Chlormethine gel remained the dominant treatment in all scenarios except when a reduced number of wound-care administrations was applied, resulting in an ICER of $62,597 per QALY compared to phototherapy.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
The comparative efficacy of chlormethine gel with phototherapy is unknown. There is no direct evidence comparing chlormethine gel and phototherapy, and the sponsor was unable to conduct an indirect treatment comparison owing to a lack of data. The efficacy of chlormethine gel relative to phototherapy in the model was based on naive unadjusted comparisons, without adjustment or accounting for differences in patient characteristics. CADTH notes that, owing to the direct use of data from multiple sources, it is not possible to determine if any observed differences in effectiveness between the therapies are solely due to the treatment or, rather, due to bias or confounding factors (e.g., differences in study populations, definitions of outcomes, study designs).
For phototherapy inputs, the sponsor incorporated data from multiple sources; this introduces additional uncertainty. The majority of effectiveness inputs (transition between health states, rate of complete or partial response, rate of progressive disease) were based on a 2019 systematic review involving patients with stage IA, stage IB, or stage IIA mycosis fungoides (Phan et al. [2019]).5 The sponsor based the rate of relapse following a complete or partial response to phototherapy on data from a small RCT (Whittaker et al. [2012])7 of PUVA alone versus PUVA plus bexarotene in patients with stage IB/IIA disease, pooling the data from both treatment arms. As noted in the CADTH Clinical Review Report, Study 201 — the main source of data for chlormethine gel — enrolled patients with early-stage MF-CTCL.
CADTH was unable to address the lack of comparative data for chlormethine gel and phototherapy. Given the lack of comparative evidence, CADTH was unable to derive a CADTH base case. CADTH undertook exploratory analyses to correct the sponsor’s model using best available evidence. In the CADTH exploratory analyses, a common source was used for phototherapy effectiveness estimates (Phan et al. [2019]),5 with input data stratified based on disease stage. The impact of this change was assessed in sensitivity analyses.
The sponsor’s submission lacks face validity in reflecting the management of MF-CTCL in clinical practice. The target population in the sponsor’s submission is adult patients with MF-CTCL, which is in line with the proposed Health Canada indication. However, the clinical experts consulted by CADTH for this review noted that skin-directed therapy, including chlormethine gel, would typically be used in practice only for patients with less than 10% skin involvement. The clinical experts noted that chlormethine gel is difficult to tolerate for patients with greater skin involvement. The clinical experts consulted by CADTH also noted that, in practice, first-line treatment for MF-CTCL is phototherapy or topical steroids, and that chlormethine gel would be considered as a second-line treatment for lesions refractory to first-line treatment. The clinical experts also indicated that, for patients with low skin involvement (i.e., < 10%), phototherapy or topical steroids may be used initially to reduce the skin involvement to approximately 5% before chlormethine gel is used to treat the remaining lesions. The clinical experts additionally noted that chlormethine gel is not likely to be used in practice for patients with stage IIB+ disease and that these patients would be more likely to receive radiation treatment.
The sponsor assumed that response to treatment would be assessed after 6 months of treatment for chlormethine gel and after 13 weeks of treatment for phototherapy. The clinical experts consulted by CADTH indicated that response to treatment would be assessed after 6 months for both chlormethine gel and phototherapy. In the model, treatment response (complete or partial) was modelled based on a SWAT score, which considers the extent of body surface area involvement and whether the lesions are patches, plaques, or tumours. CADTH notes that, in Study 201, the primary outcome of treatment response was assessed by use of the Composite Assessment of Index Lesion Severity measure, while SWAT score was a secondary outcome. Clinical experts consulted by CADTH indicated that patient-reported improvements in quality of life would also be considered in treatment decisions.
In CADTH exploratory reanalysis, treatment response was assumed to be assessed after 6 months of treatment for both chlormethine gel and phototherapy. The cost-effectiveness of chlormethine gel in patients with early-stage disease (stage IA: < 10% skin involvement) was explored in scenario analyses. CADTH could not address the impact of basing treatment response on the Composite Assessment of Index Lesion Severity score owing to a lack of data.
The costs associated with wound care were overestimated. The sponsor assumed that patients would require wound dressings for their skin-related symptoms, and that they would require 1 dressing of each size (small = 5 cm to 10 cm × 5 cm to 10 cm; medium = 10 cm to 20 cm × 10 cm to 20 cm; large =3 20 cm × 20 cm) per month. The monthly cost of each dressing was assumed to be $1,186 (total monthly cost = $3,558). The sponsor based the monthly wound dressing cost on that reported in a CADTH review of vismodegib for basal cell carcinoma19; however, the wound dressing cost reported in the vismodegib review ($3,558) was the cost per 3-month period. Notably, the clinical expert consulted by CADTH indicated that wound-care dressings are rarely required for patients receiving skin-directed therapy and are not typically used in this population.
In CADTH exploratory analysis, costs related to wound care were removed. The impact of this assumption was explored in scenario analyses.
The daily use of chlormethine gel was underestimated. The sponsor assumed that patients would apply 1.8 g of chlormethine gel per day regardless of disease stage or extent of skin involvement, based on the median daily usage in Study 201. The daily usage in Study 201 was calculated based on the number of gel tubes returned across study visits, without accounting for participants who did not return tubes or who did not attend follow-up appointments, which may have led to an underestimate of drug usage. Further, this calculation was based on the assumption of a full year of treatment, not on the actual time on treatment. As noted in the Clinical Review Report, |% of patients in the chlormethine gel group completed 12 months of treatment in Study 201. Further, clinical experts consulted by CADTH indicated that it is unlikely that patients would apply the same amount of gel regardless of the disease stage or skin involvement. Based on individual patient data provided by the sponsor, the mean daily application of chlormethine gel in Study 201 was 2.21 g, with a maximum daily application of 10.40 g. An additional estimate of 2.8 g per day is available from the FDA product monograph21 based on Study 201; however, the sponsor was unable to clarify how this was calculated.
In the CADTH exploratory analysis, the median daily usage of chlormethine gel (1.8 g) was replaced with the mean daily usage (2.21 g), as mean values are preferred to medians for model inputs. The impact of alternative estimates of daily usage was explored in scenario analyses.
The efficacy of chlormethine gel in patients with advanced disease is uncertain. The clinical inputs for chlormethine gel were based on Study 201, which enrolled patients with early-stage MF-CTCL. In the pharmacoeconomic model, the sponsor assumed that the effectiveness of chlormethine gel observed in Study 201 for patients with early-stage disease would be equivalent in late-stage disease, based on the opinion of clinical experts consulted by the sponsor. No data were provided to support this assumption.
CADTH was unable to address the lack of data pertaining to patients with advanced-stage disease. The cost-effectiveness of chlormethine gel in this population is thus uncertain.
The impact of chlormethine gel on quality of life is uncertain. The impact of treatment with chlormethine gel on quality of life was not assessed in Study 201. To inform the economic model, the sponsor indirectly elicited utility values via a de novo vignette study9 involving clinician proxy respondents. The vignettes described patients with varying stages of disease (stage IA to stage IVB) and skin burden (represented by SWAT score). Seven clinicians in the UK were asked to rate, using the EQ-5D-5L proxy version, how they thought patients with MF-CTCL would rate their quality of life. The sponsor used a mapping approach10 to convert the EQ-5D-5L values to the EQ-5D-3L, and the preferences were valued by use of the UK tariffs, which may not reflect the preference of Canadian patients. Mapping utilities from EQ-5D-5L to EQ-5D-3L introduces additional uncertainty into the model, and the use of EQ-5D-3L utilities instead of EQ-5D-5L utilities was not justified by the sponsor.
The sponsor assumed a linear relationship between the SWAT score and quality of life. The clinical experts consulted by CADTH for this review indicated that treatment may affect the relationship between the SWAT score and quality of life, and that the relationship may not be linear. The relationship between SWAT and patient-reported quality of life has not been validated. The clinical experts also noted that quality of life assessments should consider the impact of treatment on quality of life, as well as whether the patient’s lesions are patches or plaques.
CADTH was unable to address this limitation owing to a lack of alternative health state utility values. Patient preferences for the model health states are thus uncertain.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (see Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients enrolled in Study 201 were assumed to be representative of patients in Canada who would be eligible for chlormethine gel. | Reasonable. Clinical experts consulted by CADTH indicated that the Study 201 trial participant characteristics were generally representative of patients with MF-CTCL. Study 201 enrolled patients who had received at least 1 previous skin-directed therapy, and clinical experts indicated that this is representative of how they would use chlormethine gel in their practice (i.e., as second-line treatment). |
Patients with more than 80% skin involvement were excluded from the sponsor’s model. | Reasonable. Patients with more than 80% skin involvement would be unlikely to receive a topical treatment in clinical practice. |
Costs associated with PUVA were assumed to consist of physician administration costs (code G470).16 | Uncertain. The cost of psoralen as part of PUVA was not considered in the sponsor’s model. Psoralen comprises about 1% of the cost of PUVA (Appendix 1). Owing to the low relative 28-day cost of psoralen compared to Ledaga (Appendix 1), the impact of this on the ICER is likely negligible. |
Phototherapy was assumed to consist of PUVA (received by 21.8% of patients) and UVB (received by 78.2% of patients). PUVA and UVB were assumed to have equivalent efficacy and safety. | The assumption of equivalent efficacy was deemed to be reasonable by the clinical experts consulted by CADTH for this review, although the relative usage of PUVA and UVB may vary by centre. In scenario analyses, CADTH explored the impact on the ICER of assuming that all patients receive either PUVA or UVB. |
Patients with stage IA disease would have similar mortality to the Canadian general population. | Reasonable. Clinical experts indicated that early-stage disease is not expected to affect life expectancy. |
The sponsor’s model included adverse events of3 grade 3 that occurred in at least 5% of patients for either comparator (dermatitis, erythema, skin irritation). Because no adverse events of3 grade 3 severity were reported by Whittaker et al. (2012),7 the sponsor assumed no adverse events would be experienced by patients who received phototherapy in the model. | Uncertain. The inclusion of only adverse events occurring in at least 5% of patients does not consider rare events that may be costly to treat. The frequency of adverse events was adopted from different sources (from Study 201 for chlormethine gel and from Whittaker et al. [2012]7 for phototherapy), without adjustment or accounting for differences in patient characteristics or treatment durations. The adverse events included in the model do not capture the range of adverse events deemed to be of special interest to clinicians or noted in the patient input received by CADTH for this review. Clinical experts indicated that notable harms of interest in this population include secondary skin cancers (e.g., squamous cell carcinoma), which were not considered in the sponsor’s model. As noted in the Clinical Review Report, skin malignancies were reported for 2.3% of patients who received chlormethine gel in Study 201 and serious adverse events were experienced by 10.9% of patients in the chlormethine gel group. |
MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma; PUVA = psoralen plus UV A; UVB = UV B.
CADTH Reanalyses of the Economic Evaluation
Several limitations with the sponsor’s submission could not be adequately addressed (i.e., lack of head-to-head comparative clinical data, lack of data to inform chlormethine gel efficacy in late-stage disease, and uncertainty related to health state utility values). The lack of comparative effectiveness evidence between chlormethine gel and phototherapy not only presents a fundamental problem for interpreting the results of the sponsor’s economic evaluation — since the utilities used to calculate QALYs are derived from the sponsor-submitted data — but also for conducting any reanalysis using the sponsor’s model. As a result, CADTH was unable to conduct any base-case reanalysis of the sponsor’s model, given that any estimate of incremental effectiveness would be misleading.
Exploratory and Scenario Analysis Results
In light of the lack of comparative clinical data for chlormethine gel and phototherapy, CADTH conducted exploratory reanalyses. Details of the exploratory analysis are presented in Appendix 4. In this analysis, chlormethine gel was associated with higher costs and higher QALYs than phototherapy over a 44-year horizon. There was a 0.2% probability that chlormethine gel is optimal compared to phototherapy at a WTP threshold of $50,000 per QALY. However, the validity and interpretability of the results are limited by the comparative evidence. An exploratory price reduction analysis suggested that the price of chlormethine gel would need to be reduced by 48% to become cost-effective at a WTP threshold of $50,000 per QALY; however, this value is based on a highly uncertain estimate of incremental effectiveness and may underestimate the true amount.
Several scenario and sensitivity analyses were conducted on the CADTH exploratory reanalysis. These scenario analyses explored the impact of the following model parameters and assumptions: the assumption that chlormethine gel would be used only for patients with stage IA (< 10% skin involvement), the assumption of a shorter duration of phototherapy, the assumption of a higher or lower daily dose of chlormethine gel, the assumption that the daily dose of chlormethine gel would be based on disease stage (i.e., higher usage among those with greater skin involvement), and the impact of including costs associated with wound care (Table 12). Of these, CADTH’s ICER most notably changed when it was assumed that chlormethine gel would be used only among patients with stage IA disease or when all patients receiving phototherapy were assumed to receive PUVA. In none of the scenario analyses did chlormethine gel become cost-effective compared to phototherapy.
Issues for Consideration
The clinical experts consulted by CADTH indicated that chlormethine gel would be considered primarily as second-line treatment following phototherapy; however, phototherapy may be inaccessible to some patients (e.g., those living in remote regions). For such patients, the clinical experts indicated that chlormethine gel may be considered as first-line therapy.
CADTH participating drug plans noted that carmustine and imiquimod could be considered relevant comparators for chlormethine gel; however, the clinical experts consulted by CADTH indicated that these treatments are not widely available or commonly used for this population. Hospital pharmacies may prefer commercial products over agents that need to be compounded owing to the potential for hazardous drug exposure.
Overall Conclusions
The comparative effects of chlormethine gel relative to phototherapy and other treatments for MF-CTCL are unknown. Based on the CADTH clinical review, chlormethine gel relieves skin symptoms of early-stage MF-CTCL but the pivotal trial, Study 201, compared chlormethine gel with a treatment that is no longer used in clinical practice. There is no direct evidence comparing chlormethine gel and phototherapy, and the sponsor was unable to conduct an indirect treatment comparison owing to a lack of data. The efficacy of chlormethine gel relative to phototherapy in the model was based on naive unadjusted comparisons, without adjustment or accounting for differences in patient characteristics, which introduces additional uncertainty. As such, the cost-effectiveness of chlormethine gel is unknown.
CADTH conducted exploratory reanalyses, which assumed confidence in the naive comparison of chlormethine gel and phototherapy. This exploratory reanalysis addressed several limitations in the sponsor’s submission, including using a common source for phototherapy effectiveness estimates, revising the timing of response assessment for phototherapy, excluding costs associated with wound care, and increasing the daily dose of chlormethine gel. CADTH was unable to address the lack of head-to-head comparative clinical data for chlormethine gel and phototherapy, the impact of basing treatment response on a SWAT score, the lack of data for the effectiveness of chlormethine gel among patients with advanced-stage disease, and uncertainty related to health state utility values.
In the CADTH exploratory reanalysis, chlormethine gel had a 0.2% probability of being cost-effective at a WTP threshold of $50,000 per QALY. A price reduction could not be estimated due to limitations within the clinical evidence. While the cost of chlormethine gel was the principal cost driver in the pharmacoeconomic analysis, the results of the sponsor’s base case suggested that the additional drug cost would be offset by the avoided costs of wound care. Clinical experts consulted by CADTH for this review indicated the inclusion of wound costs was inappropriate, given that wound care is rarely required by this patient population. The model was highly sensitive to this parameter, as the removal of wound-care costs alone resulted in a shift from chlormethine gel being cost saving (in the sponsor’s submission) to having an ICER well above a $50,000 WTP threshold.
Due to the limitations identified previously, most crucially the lack of comparative clinical efficacy evidence, the cost-effectiveness of chlormethine gel is unknown for this indication.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ledaga (chlormethine): topical gel 160 micrograms/gram. Toronto (ON): Recordati Rare Diseases Canada; 2021.
2.Clinical Study Report: 2005NMMF-201-US. A phase II pivotal trial to evaluate the safety and efficacy of nitrogen mustard (NM) 0.02% ointment formulations in patients wth stage I or IIA mycosis fungoides (MF) [internal sponsor's report]. Toronto (ON): Recordati Rare Diseases Canada; 2011 Jul 15.
3.PrLedaga® (chlormetine): 160 micrograms/gram topical gel [draft product monograph]. Toronto (ON): Recordati Rare Diseases Canada; 2020 Apr 6.
4.Agar NS, Wedgeworth E, Crichton S, et al. Survival outcomes and prognostic factors in mycosis fungoides/Sézary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer Staging Proposal. J Clin Oncol. 2010;28(31):4730-4739. PubMed
5.Phan K, Ramachandran V, Fassihi H, Sebaratnam DF. Comparison of narrowband UV-B with psoralen-UV-A phototherapy for patients with early-stage mycosis fungoides: a systematic review and meta-analysis. JAMA Dermatol. 2019;155(3):335-341. PubMed
6.Kim YH, Liu HL, Mraz-Gernhard S, Varghese A, Hoppe RT. Long-term outcome of 525 patients with mycosis fungoides and Sezary syndrome: clinical prognostic factors and risk for disease progression. Arch Dermatol. 2003;139(7):857-866. PubMed
7.Whittaker S, Ortiz P, Dummer R, et al. Efficacy and safety of bexarotene combined with psoralen-ultraviolet A (PUVA) compared with PUVA treatment alone in stage IB-IIA mycosis fungoides: final results from the EORTC Cutaneous Lymphoma Task Force phase III randomized clinical trial (NCT00056056). Br J Dermatol. 2012;167(3):678-687. PubMed
8.Table 13-10-0114-01 Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2021: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2021 Mar 02.
9.Scarisbrick J, Schmidt F, Turini MM, et al. PRO140 Health-related quality of life associated with mycosis fungoides-type cutaneous T-cell lymphoma patients: determination of utility values from a UK-based clinician questionnaire. Value Health. 2020;23:S715.
10.van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708-715. PubMed
11.Brentuximab vedotin for treating CD30-positive cutaneous T-cell lymphoma. London (UK): National Institute for Health and Care Excellence (NICE); 2019: https://www.nice.org.uk/guidance/ta577. Accessed 2021 Mar 03.
12.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 Mar 3.
13.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2020; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Apr 02.
14.pan-Canadian Oncology Drug Review final economic guidance report: pembrolizumab (Keytruda) non-small cell lung cancer. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/pcodr/pcodr_pembrolizumab_keytruda_nsclc_1stln_fn_egr.pdf. Accessed 2021 Mar 24.
15.pCODR Expert Review Committee (pERC) final recommendation: bentuximab vedotin (Adcetris). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pcodr/Reviews2020/10213BrentuximabVedotinpcALCLMF_fnRec_Post03Dec2020_final.pdf. Accessed 2021 Mar 24.
16.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2021 Mar 3.
17.Gilson D, Whittaker SJ, Child FJ, et al. British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br J Dermatol. 2019;180(3):496-526. PubMed
18.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2021 Mar 3.
19.pan-Canadian Oncology Drug Review final economic guidance report: vismodegib (Erivedge) for basal cell carcinoma. Ottawa (ON): CADTH; 2014: https://cadth.ca/sites/default/files/pcodr/pcodr-erivedge-bcc-fn-egr.pdf. Accessed 2021 Mar 24.
20.Walker H, Anderson M, Farahati F, et al. Resource use and costs of end-of-life/palliative care: Ontario adult cancer patients dying during 2002 and 2003. J Palliat Care. 2011;27(2):79-88. PubMed
21.Prescribing information: ValchlorTM. Silver Spring (MD): US Food and Drug Administration; 2013: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/202317lbl.pdf. Accessed 2021 Mar 26.
22.Cancer drug manual: carmustine monograph. Vancouver (BC): BC Cancer Agency; 2018: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Carmustine%20monograph.pdf. Accessed 2021 Mar 03.
23.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/. Accessed 2021 Jan 12.
24.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ledaga (chlormethine): topical gel 160 micrograms/gram. Toronto (ON): Recordati Rare Diseases Canada; 2021.
25.Sutherland G, Dinh Thy. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): Conference Board of Canada; 2017: http://innovativemedicines.ca/wp-content/uploads/2017/12/20170712-understanding-the-gap.pdf. Accessed 2021 Mar 5.
26.BC cancer benefit drug list: March 2021. Vancouver (BC): BC Cancer; 2021: http://www.bccancer.bc.ca/systemic-therapy-site/Documents/Policy%20and%20Forms/Benefit%20Drug%20List.pdf. Accessed 2021 Mar 5.
27.Ghazawi FM, Netchiporouk E, Rahme E, et al. Comprehensive analysis of cutaneous T-cell lymphoma (CTCL) incidence and mortality in Canada reveals changing trends and geographic clustering for this malignancy. Cancer. 2017;123(18):3550-3567. PubMed
28.Non-insured health benefits program: First Nations and Inuit Health Branch: Annual report 2018 to 2019. Ottawa (ON): Indigenous Services Canada; 2020: https://www.sac-isc.gc.ca/DAM/DAM-ISC-SAC/DAM-HLTH/STAGING/texte-text/nihb-Annual_Report_2018-19_1589921777815_eng.pdf. Accessed 2021 Mar 5.
29.Table 17-10-0005-01 Population estimates on July 1st, by age and sex. Ottawa (ON): Statistics Canada; 2021: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2021 Mar 5.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following tables have been deemed to be appropriate based on feedback from clinical expert(s) and CADTH participating drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the tables may not represent the actual costs to public drug plans.
Table 5: CADTH Cost Comparison Table for the Topical Treatment of Mycosis Fungoides-Type Cutaneous T-Cell Lymphoma
Treatment | Strength | Form | Price ($) | Price per gram ($) | Recommended dosage |
|---|---|---|---|---|---|
Chlormethine (Ledaga) | 160 mcg chlormethine per gram | 60 g tube topical gel | 2,710.3800a | 45.1730 | Thin film applied daily |
Topical steroids | |||||
Betamethasone valerate (generic) | 0.1% | 1 g cream | 0.0889 | 0.0889 | Thin layer applied daily to affected areas |
Antineoplastic agent | |||||
Carmustine (BiCNU) | 0.4%c | 100 mg powderb | 120.0400c | 1,200.4000 | No recommended daily dose. Use as directed by clinicians. |
Imiquimod Pump (generic) | 5% | 7.5 g cream | 325.7625 | 43.4349 | No recommended daily dose. Use as directed by clinicians. |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed April 2021), unless otherwise indicated, and do not include dispensing fees.
aSponsor-submitted price.1
bTopical preparation, compounded as per the BC Cancer Agency Manual for carmustine (100 mg carmustine in 25 g petrolatum).22
cWholesale price from Delta PA,23 end date 2015-02-13. Current price unknown. Does not include cost of petrolatum.
Table 6: CADTH Cost Comparison Table for Phototherapy Treatment of Mycosis Fungoides-Type Cutaneous T-Cell Lymphoma
Treatment | Strength | Form | Price ($) | Recommended dosage | Daily cost ($) | Average 28-day cycle cost ($) |
|---|---|---|---|---|---|---|
Methoxsalen | 10 mg | Capsule | 0.5580a | 20 mg on UVA therapy days | 0.03 to 0.50 | 1 |
UVA | NA | N/A | 7.85b | 2 to 3 times weekly, for up to 6 months | 2.24 to 3.36 | 63 to 94 |
PUVA (methoxsalen + UVA) | 2.27 to 3.41 | 64 to 96 | ||||
Narrow band UVB | NA | NA | 7.85b | 2 to 3 times weekly, for up to 6 months | 2.24 to 3.36 | 63 to 94 |
NA = not applicable; UV = ultraviolet.
aOntario Drug Benefit Formulary (accessed April 2021; does not include dispensing fees).13
bOntario Schedule of Benefits – Physician services: Code G470 ultraviolet light therapy.16
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The sponsor’s model assumes that patients with body surface area involvement up to 80% would receive chlormethine gel. Clinical experts consulted by CADTH indicated that chlormethine gel would be considered only for patients with low skin involvement (i.e., less than 10%) at disease early stages. The submission does not differentiate between first- and second-line use; however, clinicians indicated that chlormethine gel would be used in clinical practice as second-line treatment after first-line treatment with topical steroids or phototherapy. |
Model has been adequately programmed and has sufficient face validity | Yes | NA |
Model structure is adequate for decision problem | Yes | NA |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | NA |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | NA |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | NA |
NA = not applicable.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
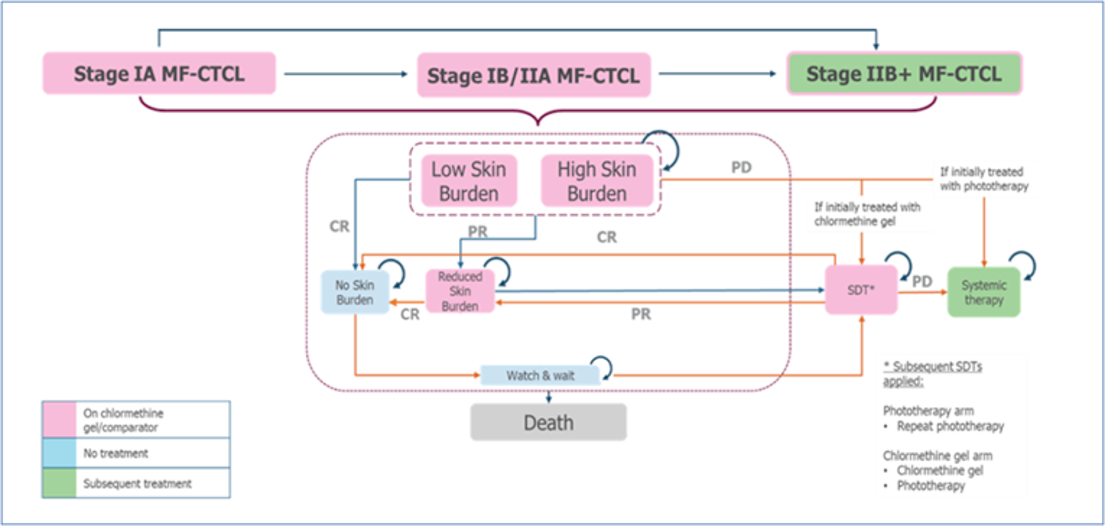
CR = complete response; MF-CTCL = mycosis fungoides cutaneous t-cell lymphoma; PD = progressive disease; PR = partial response; SDT = skin-directed therapy.
Source: Sponsor’s Pharmacoeconomic Submission.1
Detailed Results of the Sponsor’s Base Case
Table 8: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Drug | Chlormethine hydrochloride gel | Phototherapy | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 15.95 | 15.95 | 0.00 |
Discounted QALYs | |||
Total | 12.51 | 11.85 | 0.66 |
By health state | |||
Initial skin burden | 0.51 | 0.11 | 0.40 |
No skin burden | 4.00 | 2.02 | 1.98 |
Reduced skin burden | 4.51 | 0.93 | 3.58 |
Watch and wait | 0.87 | 1.85 | –0.98 |
Skin-directed therapy | 0.80 | 0.58 | 0.22 |
Systemic therapy | 1.87 | 6.36 | –4.49 |
By disease stage | |||
Stage IA | 6.97 | 6.83 | 0.14 |
Stage IIA/stage IB | 4.57 | 4.16 | 0.41 |
Stage IIB+ | 1.02 | 0.86 | 0.16 |
Discounted costs ($) | |||
Total | 968,923 | 988,817 | –19,894 |
Drug acquisition | 284,882 | 209,306 | 75,576 |
Advanced disease management | 119,923 | 119,923 | 0 |
Monitoring and resource use | 534,825 | 630,401 | –95,576 |
Adverse events | 107 | 0 | 107 |
End-of-life care | 29,186 | 29,186 | 0 |
ICER ($/QALY) | Dominant | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SDT = skin-directed treatment.
Source: Sponsor’s Pharmacoeconomic Submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Exploratory Reanalysis
Exploratory Reanalysis Results
In response to the lack of comparative clinical data for chlormethine gel and phototherapy, CADTH conducted exploratory reanalyses that addressed several other limitations within the model, as summarized in Table 9. Changes to model parameter values and assumptions were determined in consultation with clinical experts.
Table 9: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | None | None |
Changes to derive the CADTH exploratory analysis | ||
1. Rate of relapse after an initial complete or partial treatment response | Based on Whittaker et al. (2012)7 RCT | Based on Phan et al. (2019)5 systematic review |
2. Timing of response assessmenta | Chlormethine gel = 6 months; | Chlormethine gel = 6 months; |
3. Costs associated with wound care | Included | Excluded |
4. Daily dose of chlormethine gel | 1.8 g (median daily dose in Study 201) | 2.21 g (mean dose in Study 201) |
CADTH exploratory reanalysis | 1 + 2 + 3 + 4 | |
RCT = randomized controlled trial.
aPatients were assumed to receive initial treatment (chlormethine gel or phototherapy) until the time of response assessment.
CADTH undertook a stepped analysis, incorporating each change proposed in Table 9 to sponsor’s base case to highlight the impact of each change (Table 10; disaggregated results are presented in Table 11)
Table 10: Summary of the Stepped Analysis of the CADTH Exploratory Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Phototherapy | 988,817 | 11.85 | Reference |
Chlormethine gel | 968,923 | 12.51 | Dominant | |
CADTH reanalysis 1 | Phototherapy | 924,477 | 12.09 | Reference |
Chlormethine gel | 969,279 | 12.57 | 93,112 | |
CADTH reanalysis 2 | Phototherapy | 979,524 | 11.95 | Reference |
Chlormethine gel | 970,046 | 12.57 | Dominant | |
CADTH reanalysis 3 | Phototherapy | 403,356 | 11.83 | Reference |
Chlormethine gel | 478,572 | 12.50 | 112,241 | |
CADTH reanalysis 4 | Phototherapy | 991,905 | 11.87 | Reference |
Chlormethine gel | 1,019,244 | 12.53 | 41,428 | |
CADTH exploratory reanalysis (reanalysis 1 + 2 + 3 + 4) | Phototherapy | 375,784 | 12.13 | Reference |
Chlormethine gel | 525,931 | 12.55 | 358,310 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Reanalyses are based on publicly available prices of the comparator treatments.
Chlormethine gel was associated with higher costs (incremental = $150,146) and higher QALYs (incremental = 0.42) than phototherapy over a 44-year horizon. The ICER for chlormethine gel versus phototherapy was $358,310 per QALY. There is a 0.2% probability that chlormethine gel is optimal compared to phototherapy at a WTP threshold of $50,000 per QALY. The incremental QALYs with chlormethine gel treatment in the first year was –0.07, indicating that all of the incremental benefits with chlormethine gel were accrued in the post-trial period and were derived on the basis of extrapolated trial findings rather than observed benefit. The cost of chlormethine gel acquisition is a key driver of the ICER, representing 99.9% of the total incremental costs (Table 11).
Table 11: Disaggregated Summary of CADTH’s Exploratory Economic Evaluation Results
Drug | Chlormethine gel | Phototherapy | Incremental |
|---|---|---|---|
Discounted LYs | |||
Totala | 15.95 | 15.95 | 0.00 |
Discounted QALYs | |||
Total | 12.55 | 12.13 | 0.42 |
By health state | |||
Initial skin burden | 0.52 | 0.12 | 0.39 |
No skin burden | 4.01 | 3.30 | 0.71 |
Reduced skin burden | 4.52 | 0.75 | 3.77 |
Watch and wait | 0.87 | 1.78 | –0.92 |
Skin-directed therapy | 0.80 | 0.57 | 0.24 |
Systemic therapy | 1.88 | 5.60 | –3.72 |
By disease stage | |||
Stage IA | 7.02 | 6.94 | 0.08 |
Stage IIA/ stage IB | 4.57 | 4.27 | 0.30 |
Stage IIB+ | 1.01 | 0.92 | 0.09 |
Discounted costs ($) | |||
Total | 525,931 | 375,784 | 150,146 |
Drug acquisition | 333,412 | 183,374 | 150,039 |
Advanced disease management | 119,417 | 119,417 | 0 |
Monitoring and resource use | 43,710 | 43,710 | 0 |
Adverse events | 108 | 0 | 108 |
End-of-life care | 29,283 | 29,283 | 0 |
ICER ($/QALY) | 358,310 | ||
ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year.
aDeterministic. The sponsor’s model was not programmed to provide a probabilistic estimate of life-years.
Scenario Analyses
A set of scenario analyses were performed using the exploratory reanalysis base case. These analyses were performed to investigate the impact that critical assumptions had on cost-effectiveness, despite the limitations of the comparative clinical efficacy evidence. These scenario analyses explored the impact of the following model parameters and assumptions: assuming that chlormethine gel would be used only for patients with stage IA (< 10% skin involvement), assuming a shorter duration of phototherapy, assuming a higher or lower daily dose of chlormethine gel, assuming that the daily dose of chlormethine gel would be based on disease stage (i.e., higher usage among those with greater skin involvement), and including costs associated with wound care (Table 12). Of these, CADTH’s ICER most notably changed when it was assumed that chlormethine gel would be used only among patients with stage IA disease or when all patients receiving phototherapy were assumed to receive PUVA. In none of the scenario analyses did chlormethine gel become cost-effective compared to phototherapy.
Exploratory Scenario Analysis Results
Table 12: CADTH Exploratory Scenario Analyses
Scenario | CADTH exploratory reanalysis | CADTH exploratory scenario |
|---|---|---|
Scenario analyses | ||
1. Disease stage | Stage IA, stage IB/stage IIA, stage IIB+ | Stage IA only (< 10% skin involvement) |
2. Duration of phototherapy | 6 months | 3 months |
3. Chlormethine gel dose | 2.21 g daily | 2.8 g daily21 |
4. Chlormethine gel dose | As above | Based on disease stage (stage IA = 1.31 g; stage IB/stage IIA = 3.46 g daily; based on Study 201) |
5. Chlormethine gel dose | As above | 1.8 g daily, based on mean daily usage in Study 201 |
6. Wound-care costs | Excluded | Included (total monthly cost = $1,186)19 |
7. Phototherapy composition | 21.8% PUVA; 78.2% UVB | Assume all PUVA |
8. Phototherapy composition | As above | Assume all UVB |
9. Rate of relapse following an initial treatment response (phototherapy) | Based on Phan et al. (2019)5 systematic review | Based on Whittaker et al. (2012)7 RCT |
RCT = randomized controlled trial; UV = ultraviolet.
Table 13: Probabilistic Results of CADTH’s Exploratory Scenario Analyses
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
CADTH exploratory reanalysis | |||
Phototherapy | 375,784 | 12.13 | Reference |
Chlormethine gel | 525,931 | 12.55 | 358,310 |
Scenario 1: Relevant population assumed to be patients with stage IA disease only (< 10% BSA) | |||
Phototherapy | 305,148 | 18.68 | Reference |
Chlormethine gel | 532,208 | 18.96 | 802,268 |
Scenario 2: Duration of phototherapy assumed to be 3 months | |||
Phototherapy | 377,366 | 12.10 | Reference |
Chlormethine gel | 528,953 | 12.52 | 358,443 |
Scenario 3: Chlormethine gel dose assumed to be 2.81 g daily | |||
Phototherapy | 376,008 | 12.09 | Reference |
Chlormethine gel | 599,250 | 12.51 | 535,685 |
Scenario 4: Chlormethine gel dose based on disease stage | |||
Phototherapy | 374,793 | 12.13 | Reference |
Chlormethine gel | 544,242 | 12.55 | 399,460 |
Scenario 5: Chlormethine gel dose assumed to be 1.8 g daily | |||
Phototherapy | 376,967 | 12.14 | Reference |
Chlormethine gel | 477,609 | 12.56 | 237,309 |
Scenario 6: Costs associated with wound care includeda | |||
Phototherapy | 549,891 | 12.10 | Reference |
Chlormethine gel | 688,857 | 12.52 | 332,217 |
Scenario 7: Phototherapy assumed to be comprised solely of PUVA | |||
Phototherapy | 276,927 | 12.86 | Reference |
Chlormethine gel | 509,508 | 12.62 | Dominated |
Scenario 8: Phototherapy assumed to be comprised solely of UVB | |||
Phototherapy | 398,114 | 11.99 | Reference |
Chlormethine gel | 528,733 | 12.52 | 247,307 |
Scenario 9: Rate of relapse following an initial treatment response | |||
Phototherapy | 393,176 | 11.95 | Reference |
Chlormethine gel | 528,972 | 12.56 | 220,842 |
BSA = body surface area; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Reanalyses are based on publicly available prices of the comparator treatments.
aMonthly cost of wound care assumed to be $1,186.19
A price reduction analysis was performed based on the sponsor’s base case and CADTH’s exploratory reanalysis (Table 14). In the CADTH exploratory reanalysis, a price reduction of 48% would be required for chlormethine gel to be considered cost-effective at a WTP threshold of $50,000 per QALY. These estimates are likely to underestimate the true price reduction necessary.
Table 14: Exploratory CADTH Price Reduction Analyses
ICERs for chlormethine hydrochloride gel vs. phototherapy | ||
|---|---|---|
Price reduction | Sponsor base case | CADTH exploratory reanalysis |
No price reduction | Dominanta | 358,310 |
10% | NA | 277,200 |
20% | NA | 228,241 |
30% | NA | 166,639 |
40% | NA | 97,120 |
50% | NA | 33,174 |
ICER = incremental cost-effectiveness ratio; vs. = versus.
Note: Based on the publicly available prices of the comparator treatments.
aIn the sponsor’s base case, chlormethine gel was less costly and more effective (higher QALYs) than phototherapy.
Exploratory Scenario Analysis: Patients with < 10% Skin Involvement
The majority of incremental QALYs in the CADTH exploratory reanalysis gained with chlormethine gel were accrued by patients with stage IIA/stage IB disease (10%–80% skin involvement). Clinical experts consulted by CADTH for this review indicated, however, that chlormethine gel would not be considered for patients with more than 10% skin involvement. In a scenario analyses, CADTH explored the cost-effectiveness of chlormethine gel in patients with less than 10% skin involvement (stage IA disease). In this analysis, chlormethine gel was associated with an ICER of $802,268 per QALY gained compared with phototherapy.
An additional exploratory price reduction analysis was performed within this population; results are presented in Table 15. A price reduction of 58% would be required for chlormethine gel to be considered cost-effective at a WTP threshold of $50,000 per QALY in patients with stage IA disease.
Table 15: Exploratory Price Reduction Analyses – Stage IA Population
ICERs for chlormethine hydrochloride gel vs. phototherapy | ||
|---|---|---|
Price reduction | Sponsor base casea | CADTH reanalysis |
No price reduction | 18,338 | 802,268 |
10% | NA | 679,692 |
20% | NA | 560,244 |
30% | NA | 418,554 |
40% | NA | 296,059 |
50% | NA | 163,010 |
58% | NA | 44,444 |
ICER = incremental cost-effectiveness ratio; vs. = versus.
Note: Based on the publicly available prices of the comparator treatments.
aSponsor’s base case, with the population restricted to patients with stage IA disease.
Appendix 5: Submitted Budget Impact Assessment and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 16: CADTH Summary Findings from the Sponsor’s Budget Impact Assessment
Key Take-Aways of the Budget Impact Assessment |
|---|
|
Summary of Sponsor’s Budget Impact Assessment
The submitted budget impact analysis (BIA)24 assessed expected budgetary impact resulting from the introduction of chlormethine hydrochloride gel for the topical treatment of MF-CTCL in adults. The comparator to chlormethine gel was assumed to be phototherapy, and both treatments were assumed to be given on a background of topical steroids. The BIA was undertaken from the perspectives of Canadian public drug plans and Canadian public health care payers over a 3-year time horizon. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec), as well as the Non-Insured Health Benefits Program. Key inputs to the BIA are documented in Table 17.
The sponsor estimated the current population using an epidemiologic approach, with the estimated prevalence of MF-CTCL among Canadian adults used to estimate the total number eligible patients. The sponsor assumed that 52% of patients would have stage IA disease, 33% would have stage IB/IIA disease, and that 15% would have stage IIB+ disease, and that a proportion of patients in each stage would receive skin-directed therapy (stage IA = 80%; stage IB/stage IIA = 70%; stage IIB+ = 55%). The further sponsor assumed that 100% of patients would be eligible for public drug plan coverage in British Columbia, Alberta, Manitoba, Saskatchewan, and the NIHB. The proportion of patients eligible for the remaining jurisdiction was assumed range from 34.9% to 38.1% on the basis of the age distribution of MF-CTCL participants in Study 201 (< 65 = 71.5%; > 65 = 28.5%) and proportion of the population enrolled in public drug plans for each age group.25 The sponsor assumed that 0.5% of patients receive chlormethine gel in the reference scenario through Special Access Programs.26
The sponsor’s submission considered a reference scenario in which patients received phototherapy and a new drug scenario in which chlormethine gel was reimbursed. The cost of chlormethine gel was based on the sponsors submitted price ($2,710.38 per 60 g tube) and the median daily dose used in Study 201 (1.8 g daily; 11 tubes annually), for an estimated annual cost of $29,699. Patients were assumed to receive 39 phototherapy treatments during the analysis horizon (3 treatments weekly for 13 weeks), with an annual estimated cost $306, which was included in the public health care payer perspective only.16,17 The sponsor assumed that topical steroids would be applied as 1.8 g twice daily, with the cost based on the Ontario Drug Benefit Formulary13 price for clobetasol propionate (annual cost = $300). The uptake of chlormethine gel was assumed to be 4.7% in year 1, 14.0% in year 2, and 32.6% in year 3, with the market share of chlormethine gel assumed to be captured from patients who would otherwise receive phototherapy.
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate |
|---|---|
Target population | |
MF-CTCL prevalence | 0.0068%27 |
Proportion of MF-CTCL patients by disease stage | |
Stage IA | 52%a |
Stage IB/stage IIA | 33%a |
Stage IIB+ | 15%a |
Proportion who receive skin-directed treatment | |
Stage IA | 80%a |
Stage IB/stage IIA | 70%a |
Stage IIB+ | 55%a |
Population growth | |
Number of eligible patients (Y1/Y2/Y3) | 949 / 961 / 974 |
Market uptake (Y1/Y2/Y3) | |
Uptake (reference scenario) Chlormethine gel Psoralen plus ultraviolet A Ultraviolet B | 0.5%/0.5%/0.5% 21.7%/21.7%/21.7% 77.7%/77.7%/77.7% |
Uptake (new drug scenario) Chlormethine gel Psoralen plus ultraviolet A Ultraviolet B | 4.7%/14.0%/32.6% 20.8%/18.8%/14.7% 74.5%/67.2%/52.7% |
Annual cost of treatment (per patient) | |
Chlormethine gel Psoralen plus ultraviolet A Ultraviolet B Topical corticosteroids | $29,699 $306b $306b $300 |
MF-CTCL = mycosis fungoides cutaneous T-cell lymphoma; Y = year.
aClinical expert opinion.
bIncluded in the health care payer perspective only; cost reflects the fee per treatment based on the Ontario Schedule of Benefits for Physician Services (G470).16
Summary of the Sponsor’s BIA Results
The sponsor estimated the net 3-year budget impact to the public drug plans of introducing chlormethine gel for the treatment of MF-CTCL in adults to be $14,286,109 (year 1 = $1,162,340; year 2 = $3,839,084; year 3 = $9,284,685). The budget impact for the public health care payer was projected by the sponsor to be $14,744,821 over 3 years.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of patients eligible for chlormethine gel is uncertain. The prevalence of MF-CTCL (0.0068%) incorporated in the sponsor’s base case reflects the estimated prevalence in 2010 and is lower than the sponsor-estimated prevalence of MF-CTCL in 2020 (0.0096%). The estimated 2020 prevalence was used by the sponsor only in scenario analyses. As such, the current number of patients with MF-CTCL is likely underestimated in the sponsor’s base case.
The sponsor assumed that chlormethine gel would be used for patients with stage IA to stage IIB+ disease. As noted previously, clinical experts consulted by CADTH for this review indicated that chlormethine gel would typically be used only for patients with early-stage disease (stage IA) and less than 5%–10% skin involvement. The clinical experts also noted that chlormethine gel would be considered as a second-line treatment for lesions refractory to first-line phototherapy treatment. As such, chlormethine gel would not be expected to take market share from phototherapy.
The sponsor estimated the proportion of patients eligible for public drug plan coverage by use of the number of patients enrolled in public plans for each jurisdiction.25 It is more appropriate to use the proportion of patients eligible, rather than enrolled, as the market size will be determined by all eligible for public coverage, and the BIA should consider all patients eligible regardless of whether they are presently enrolled. Should chlormethine gel be reimbursed by public plans, it is assumed that all eligible patients for this treatment would enrol for public coverage.
o In CADTH’s reanalyses, the sponsor’s estimated prevalence of MF-CTCL in 2020 (0.0096%) was adopted, and the proportion of patients eligible for public drug plan coverage was used to determine the market size for chlormethine gel. Additionally, in scenario analysis, all patients were assumed to be covered for chlormethine gel regardless of age. If chlormethine gel becomes reimbursed under Exceptional Access Programs, then coverage would be expected to be provided to all patients regardless of age. Further scenario analyses explored the impact of assuming that chlormethine gel would be used only by patients with stage IA disease.
Costs related to chlormethine gel and phototherapy are underestimated: As noted in the Appraisal of the Sponsor’s Economic Evaluation section, the sponsor assumed that patients would apply 1.8 g of chlormethine gel per day, based on the median daily usage in Study 201. Based on individual data provided by the sponsor, the mean daily usage was 2.21 g in Study 201. An additional estimate of 2.8 g per day is available from the FDA product monograph21 based on Study 201. The sponsor further assumed that patients would use the same amount of chlormethine gel daily regardless of disease stage or the extent of body surface area involvement, which clinical experts indicated is unlikely.
The sponsor assumed that patients would receive 39 phototherapy treatments over the analysis horizon, consistent with 3 weekly visits over 13 weeks. Clinical experts consulted by CADTH indicated that phototherapy is typically received for 6 months. Additionally, the sponsor did not include the cost of psoralen treatment as part of PUVA.
To align the economic evaluation and the BIA, the mean dosage of chlormethine gel from Study 201 was adopted in the CADTH base case (2.21 g per day). The structure of the sponsor’s BIA model did not allow for different daily usage by disease stage. Scenario analyses explored the impact of higher daily usage based on the FDA monograph.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by using the number of patients eligible for public coverage, rather than enrolled, to estimate the percentage of patients who would be covered in each jurisdiction, adopting a mean daily dose of chlormethine gel of 2.21 g, and assuming a 6-month duration phototherapy (Table 18).
Table 18: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
None | None | None |
Changes to derive the CADTH base case | ||
1. Prevalence of MF-CTCL | The prevalence of MF-CTCL was estimated by the sponsor to be 0.0068% on the basis of cases diagnosed between 1992 and 201027 | The 2020 prevalence of MF-CTCL was estimated by the sponsor to be 0.0096% on the basis of prevalent cases in 2010 and the annual incidence and mortality of MF-CTCL27 |
2. Percentage of patients covered by public drug plans | Determined by the percentage of patients enrolled | Determined by the percentage of patients eligible for enrolment |
3. Daily dose of chlormethine gel | 1.8 g (median daily dose, Study 201) | 2.21 g (mean dose, Study 201) |
4. Duration of phototherapy | 13 weeks | 6 months |
CADTH base case | 1 + 2 + 3 + 4 | |
BIA = budget impact analysis; MF-CTCL = mycosis fungoides-type cutaneous T-cell lymphoma.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 19 and a more detailed breakdown is presented in Table 20.
In the CADTH reanalysis, the 3-year budget impact to the public drug plans of reimbursing chlormethine gel is estimated to be $30,313,481. The impact to the public health care payer is estimated to be $31,720,481 over the 3-year analysis horizon.
Table 19: Summary of the CADTH Reanalyses of the BIA
Scenario | 3-year total | |
|---|---|---|
Drug costs only ($) | Total costsa ($) | |
Submitted base case | 14,286,109 | 15,016,313 |
CADTH reanalysis 1 | 20,866,532 | 21,932,996 |
CADTH reanalysis 2 | 16,906,855 | 17,800,895 |
CADTH reanalysis 3 | 17,540,167 | 18,470,239 |
CADTH reanalysis 4 | 14,286,109 | 14,869,045 |
CADTH base case | 30,313,481 | 31,720,481 |
BIA = budget impact analysis.
Note: Reanalyses are based on publicly available prices of the comparator treatments.
aIncludes the cost of phototherapy, as well as administration, dispensing, and markup costs.
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 20.
Assumed 100% of MF-CTCL patients would be eligible for public coverage
Assumed usage of chlormethine gel by patients only with stage IA disease
Assumed a higher daily dose of chlormethine gel (2.8 g, based on the US FDA monograph)21
Reduced the price of chlormethine to the value in which it would be cost-effective at a $50,000 per QALY threshold (48%)
Table 20: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Annual (drug costs only) | 3-year total | |||
|---|---|---|---|---|---|---|
Year 1 | Year 2 | Year 3 | Drug costs only | Total costsa | ||
Sponsor’s base case | Reference | 434,952 | 440,987 | 447,107 | 1,323,046 | 2,789,250 |
New drug | 1,597,292 | 4,280,071 | 9,731,792 | 15,609,155 | 17,805,562 | |
Budget impact | 1,162,340 | 3,839,084 | 9,284,685 | 14,286,109 | 15,016,313 | |
CADTH base case | Reference | 751,724 | 767,591 | 783,458 | 2,302,773 | 6,306,507 |
New drug | 3,232,528 | 8,898,249 | 20,485,478 | 32,616,254 | 38,026,988 | |
Budget impact | 2,480,803 | 8,130,658 | 19,702,020 | 30,313,481 | 31,720,481 | |
CADTH scenario analysis 1: 100% eligibility | Reference | 922,159 | 941,625 | 961,090 | 2,824,874 | 6,910,908 |
New drug | 4,369,487 | 12,028,046 | 27,691,020 | 44,088,553 | 47,481,687 | |
Budget impact | 3,447,327 | 11,086,421 | 26,729,930 | 41,263,679 | 40,570,778 | |
CADTH scenario analysis 2: Stage IA only | Reference | 836,629 | 867,030 | 897,431 | 2,601,090 | 6,011,375 |
New drug | 3,351,670 | 9,302,338 | 21,694,655 | 34,348,662 | 37,225,841 | |
Budget impact | 2,515,041 | 8,435,308 | 20,797,224 | 31,747,572 | 31,214,466 | |
CADTH scenario analysis 3: higher daily dose of chlormethine gel | Reference | 823,046 | 840,420 | 857,795 | 2,521,261 | 5,540,497 |
New drug | 3,966,145 | 11,141,706 | 25,819,630 | 40,927,481 | 43,437,693 | |
Budget impact | 3,143,099 | 10,301,286 | 24,961,836 | 38,406,220 | 37,897,196 | |
CADTH scenario analysis 4: 48% price reduction | Reference | 623,490 | 636,646 | 649,803 | 1,909,940 | 4,929,176 |
New drug | 1,913,508 | 4,864,588 | 10,894,853 | 17,672,950 | 20,183,162 | |
Budget impact | 1,290,018 | 4,227,942 | 10,245,051 | 15,763,010 | 15,253,986 | |
BIA = budget impact analysis.
Note: Reanalyses are based on publicly available prices of the comparator treatments.
aIncludes the cost of phototherapy, as well as administration, dispensing, and markup costs.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.