CADTH Reimbursement Review
Idecabtagene Vicleucel (Abecma)
Sponsor: Celgene Inc., a Bristol Myers Squibb Company
Therapeutic area: Multiple myeloma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Clinical Review
Abbreviations
AE
adverse event
AMT
antimyeloma therapy
BCMA
B-cell maturation antigen
CAR
chimeric antigen receptor
Cd
carfilzomib plus dexamethasone
CI
confidence interval
CMRG
Canadian Myeloma Research Group
CNS
central nervous system
CR
complete response
CRR
complete response rate
CRS
cytokine release syndrome
CyBorD
cyclophosphamide plus bortezomib plus dexamethasone
DAC
Drug Advisory Committee
DoR
duration of response
EHR
electronic health record
EMA
European Medicines Agency
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-MY20
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myeloma Module with 20 items
EQ-5D-5L
EuroQol 5-Dimensions 5-Levels questionnaire
EQ VAS
EuroQol Visual Analogue Scale
FLC
free light chain
HR
hazard ratio
HRQoL
health-related quality of life
ICU
intensive care unit
IMiD
immunomodulatory imide drug
IMWG
International Myeloma Working Group
IPTW
inverse probability treatment weighting
IRC
independent response committee
ITC
indirect treatment comparison
IV
intravenous
KM
Kaplan-Meier
MM
multiple myeloma
MRD
minimal residual disease
NE
not estimable
ORR
overall response rate
OS
overall survival
PAG
Provincial Advisory Group
PD
progressive disease
PFS
progression-free survival
PRO
patient-reported outcome
QoL
quality of life
RRMM
relapsed or refractory multiple myeloma
T0
baseline time point
TTP
time to progression
TTR
time to response
VAS
visual analogue scale
Vd
bortezomib plus dexamethasone
VGPR
very good partial response
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Idecabtagene vicleucel (Abecma), cell suspension in 1 or more patient-specific infusion bag(s); target dose of 450 × 106 CAR T cells, within a range of 275 × 106 to 520 × 106 CAR T cells; for IV infusion |
Indication | For the treatment of adult patients with multiple myeloma who have received at least 3 prior therapies, including an immunomodulatory drug, a proteasome inhibitor, and an anti-CD38 antibody, and who are refractory to their last treatment |
Reimbursement request | As per indication |
Health Canada approval status | NOC/c |
Health Canada review pathway | Priority review |
NOC date | May 26, 2021 |
Sponsor | Celgene Inc., a Bristol Myers Squibb Company |
CAR = chimeric antigen receptor; NOC = Notice of Compliance; NOC/c = Notice of Compliance with Conditions.
Introduction
Multiple myeloma (MM) is a malignant, clonal bone marrow plasma cell disorder that causes clinical features of renal failure, bone lesions, hypercalcemia, and bone marrow suppression. It results from excessive production of monoclonal proteins as well as direct tumour cell effects.1,2 Multiple myeloma is the second most common hematologic malignancy and represents approximately 1% of all cancers and roughly 10% to 15% of all hematologic malignancies. It primarily affects older individuals and is extremely rare in patients younger than 30 years old.3,4 In Canada, the median age at diagnosis is 70 years, with an average national incidence rate of 5.42 cases per 100,000 individuals per year, a steady rise in the annual rate of 0.96 cases per million individuals per year, and an estimated 3,400 new cases annually.1,5 At the provincial level, Quebec and Ontario have the highest MM incidence rates in Canada (5.82 cases per 100,000 individuals per year and 5.66 cases per 100,000 individuals per year, respectively). The mean national mortality rate in Canada stands at 3.57 deaths per 100,000 individuals per year.1 Patients are classified with relapsed or refractory multiple myeloma (RRMM) when there is a recurrence of disease after prior response on the basis of objective laboratory and radiological criteria.6 From there, patients begin moving to successive therapies as they advance in the course of the disease with further relapses and more lines of therapies.
The goal of treatment in patients with RRMM is to achieve disease control with acceptable toxicity and patient-defined health-related quality of life (HRQoL). Meeting this goal relies on effective systemic chemotherapy and supportive measures such as pain control, antibiotics, kyphoplasty, radiation therapy, dialysis, and psychosocial support. Although emerging options are increasingly available,7 no standard of care has been fully established and, despite advances, choosing an optimal strategy at relapse remains a challenge for clinicians. Currently, the options for patients with RRMM are second to fifth lines of therapies, which include several drugs. The sequencing of treatments depends largely on the type of response to previous therapies. Regimens commonly used in the Canadian landscape include combinations of daratumumab plus bortezomib plus dexamethasone, bortezomib plus dexamethasone (Vd), pomalidomide plus dexamethasone, and carfilzomib plus dexamethasone (Cd), each of which is used when there is resistance to lenalidomide. Regimens used when there is resistance to bortezomib-based therapies include combinations of daratumumab, lenalidomide, and dexamethasone; carfilzomib, lenalidomide, and dexamethasone; and lenalidomide and dexamethasone.7-9
Idecabtagene vicleucel is a cell therapy formed by chimeric antigen receptor (CAR)-positive T cells directed against the B-cell maturation antigen (BCMA). The indication is for the treatment of adult patients with MM who have received at least 3 prior therapies, including an immunomodulatory drug, a proteasome inhibitor, and an anti-CD38 antibody, and who are refractory to their last treatment. Idecabtagene vicleucel is provided as a single-dose, 1-time treatment in 1 or more patient-specific infusion bags containing a suspension of 275 × 106 to 520 × 106 CAR T cells. The target dose is 450 × 106 CAR T cells within a range of 275 × 106 to 520 × 106 CAR T cells. Pretreatment includes the use of lymphodepleting chemotherapy (LDC) with cyclophosphamide 300 mg/m2 IV and fludarabine 30 mg/m2 IV for 3 days. Idecabtagene vicleucel infusion is to be administered 2 days after completion of LDC. The objective of this report is to perform a systematic review of the beneficial and harmful effects of idecabtagene vicleucel for the treatment of adult patients with MM who have received at least 3 prior therapies, including an immunomodulatory drug, a proteasome inhibitor, and an anti-CD38 antibody.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Myeloma Canada submitted the patient input for this review. Founded in 2005, Myeloma Canada is the only national charitable organization created by and for Canadians affected by MM. The organization works to improve the lives of those affected by myeloma. Information from this input was gathered through a patient survey. The survey was accessed through email and social media from December 17, 2020, to January 4, 2021. A total of 388 individuals with myeloma responded to the survey.
Overall, patients described how myeloma, as part of their lives, affects major decisions for themselves and their family members. Patients who have been heavily treated expect new treatment options to provide prolonged remission, not having to be on their current treatment because they are in remission, better quality of life, better overall health, better control of myeloma symptoms, and fewer side effects. More than half of patients responding to the survey set optimistic expectations for new options such as CAR T-cell therapies. Among 6 patients with previous experience with a CAR T-cell therapy, 5 considered the intervention effective, and 3 stated that the burden of receiving it was tolerable, with decreased cognitive abilities and neutropenia as the most commonly described effects. “I’m still alive,” “so far in very, very good remission,” and “I would have otherwise run out of options” were some of the phrases obtained from the survey, along with some less-encouraging responses, such as “didn’t get the depth of response as we were hoping.”
The patient group highlighted that many Canadians are looking for new options for effective treatments, particularly when they reach the point of multiple treatments with remission and refractoriness to the available regimens. Patients were willing to trade some of the burdens of the new therapy as they assigned more value to outcomes such as prolonged survival and quality of life (QoL).
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH agreed that not all patients with MM respond to available treatments; most eventually become refractory to all treatment options. These patients have a short life expectancy, and their remaining life expectancy is often highly medicalized. Treatments are needed to control the disease and provide patients with a break from therapy. There are few options (other than palliative or supportive care) after the third and fourth line of therapy, leaving a major unmet need. The majority of CAR T-cell treatments are financially burdensome both at the level of the individual patient and the public budget.
In the current treatment paradigm, CAR T-cell therapies would be well positioned in the third line (current Canadian approval) and fourth line (older algorithms). The clinical experts noted that, when daratumumab, bortezomib, lenalidomide, and dexamethasone are approved as front-line treatments, CAR T cells could become a second-line option. The experts agreed that patients best suited for idecabtagene vicleucel treatment would be identified by following the inclusion and exclusion criteria from the study, together with an individual clinical assessment and judgment based on prior therapies, patient comorbidities, and fitness. Clear, transparent, and evidence-based recommendations will be important for decision-making. All standard diagnostic and baseline tests are available broadly in Canada.
The eligible population will be small because many patients already reach a palliation stage by the fourth line of treatment due to rapid disease progression, age, frailty, or toxicities from prior treatments. The eligible patients (i.e., those with a good performance status and those who have been previously treated with or are refractory to proteasome inhibitors, immunomodulatory imide drugs (IMIDs), and CD38 monoclonal antibodies) appear to be the most appropriate group with the greatest unmet need. Clinical experts stated that the patients best suited for this treatment would be those with an Eastern Cooperative Oncology Group (ECOG) status of 0 or 1, good organ status, and a willingness to travel (this therapy will not be offered in smaller centres). Those with relapsed or refractory disease should be prioritized first. Younger, fit patients with the least number of prior therapies (3 prior lines) are the most likely to benefit.
According to the experts consulted by CADTH, the patients least suitable for the treatment under review are those with a poor performance status, and those with other options available with a reasonable duration of disease control. Additionally, patients who are frail, elderly, have significant renal failure, neurologic disease, and an ECOG status of 2 or greater related to myeloma would not be suitable candidates for idecabtagene vicleucel treatment. The experts suggested that progression-free survival (PFS) longer than 6 months or overall survival (OS) for more than 1 year without life-threatening toxicities would be considered a clinically meaningful response to treatment.
The clinical experts consulted by CADTH agreed that idecabtagene vicleucel must be administered in a setting supervised by specialists trained in bone marrow transplant, a tertiary centre that is well-versed in complications related to stem cell transplant, or a centre that can accommodate phase I trials, with adequate intensive care, emergency, neurology, and infectious disease departments. They also agreed that a hematologist or an oncologist with specific experience in cellular therapy is required to diagnose, treat, and monitor patients who might receive idecabtagene vicleucel.
Clinician Group Input
Two clinician groups provided information for the reimbursement process: the Canadian Myeloma Research Group (CMRG), a charitable organization supported by myeloma physicians from 22 academic centres in Canada, and the Ontario Health (previously Cancer Care Ontario) Hematology Cancer Drug Advisory Committee (DAC), which provides evidence-based clinical and health system guidance on drug-related issues to provincial drug reimbursement programs and others.
Overall, both groups agreed with the clinical experts consulted by CADTH with respect to unmet needs in those whose life expectancy is limited (i.e., triple-class exposed patients) and both noted that only a few options are available for heavily treated patients with RRMM. The groups added that there is no sequencing information available beyond that used in the triple-class exposed population.
The clinician groups noted that, although no data are available to indicate which patients are most likely to exhibit a response, patients with good performance status, organ function, minimal or no comorbidities, robust blood counts, low tumour burden, and indolent disease are most likely to experience the best outcomes.
The clinician groups noted that the drug under review will be delivered at tertiary hospitals or transplant centres with expertise in cellular therapy. They added that idecabtagene vicleucel patients would require an inpatient bed for approximately 2 weeks (or longer if complications occur) and may require readmission.
Drug Program Input
The Provincial Advisory Group (PAG) provided questions considered important for decision-making.
Which patient (or disease) characteristics would be important in determining who should be treated with this therapy?
If capacity limitations exist, how to prioritize which patients should be offered idecabtagene vicleucel?
Do patients need to have disease considered refractory to an IMiD, proteasome inhibitor, and an anti-CD38 antibody to receive idecabtagene vicleucel?
It is important to discuss whether or not there should be re-treatment (provided data are scarce). The sponsor suggests idecabtagene vicleucel will be a single-dose, 1-time treatment, but re-treatment was allowed in the KarMMa trial. This would imply additional costs (i.e., due to cryopreservation, cell processing, tocilizumab, intensive care unit and hospital stays, etc.).
The clinical experts consulted by CADTH stated the characteristics of patients with MM who should receive idecabtagene vicleucel as above, to those with prior treatment with an IMiD, a proteasome inhibitor, or an anti-CD38 antibody. The only unresolved concern was the exact line of therapy to recommend when initiating CAR T-cell treatment. The clinical experts consulted by CADTH anticipated that prioritization of the therapy would rarely be a concern, in which case deliberations should be made on a case-by-case basis; the same conclusion was drawn for the re-treatment considerations.
PAG identified a possible issue with the prescription of idecabtagene vicleucel, specifically that access would be limited to jurisdictional capacity. Given that the sponsor plans to have 12 sites across Canada, out-of-province care may be needed for proper administration of the drug under review. Also, staff will need to be trained and specialized centres accredited by the sponsor, limiting the availability of clinics where the therapy can be provided.
PAG noted that there may be potential for “indication creep” to earlier lines of therapy. For example, triple-class exposure may occur in the first 2 lines of therapy, although the sponsor’s proposed indication does not establish a specific line of therapy. The clinical experts consulted by CADTH agreed that it would be important to establish the appropriate line of therapy for idecabtagene vicleucel (currently their recommendation was third or fourth) and which patient populations would be outside the scope of the reviewed indication. Furthermore, idecabtagene vicleucel may change the place in therapy of other (comparator) drugs and in subsequent lines as more data become available.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The KarMMa study (N = 140) was a phase II, open-label, multi-centre, single-arm trial conducted at 20 sites across Europe and North America, including 1 in Canada. Eligible patients were adults who had received at least 3 previous regimens for MM, including an immunomodulatory drug, a proteasome inhibitor, and an anti-CD38 antibody, and who had disease that was refractory to their last regimen (progression within 60 days after the last dose) according to International Myeloma Working Group (IMWG) criteria. The main objective of the study was to evaluate the efficacy, defined as the overall response rate (ORR), of idecabtagene vicleucel in patients with RRMM. Secondary objectives included the assessment of the safety of idecabtagene vicleucel and other measures of efficacy, such as the complete response rate (CRR), duration of response (DoR), time to response (TTR), time to progression (TTP), minimal residual disease (MRD)-negative status, OS, PFS, and HRQoL. Harms evaluated included adverse events (AEs), health care utilization, and others of special interest for this review, such as cytokine release syndrome (CRS), febrile neutropenia, and neurotoxicity.
All 140 enrolled patients underwent leukapheresis (i.e., drug manufacturing). If necessary, a bridging therapy (with corticosteroids, alkylating agents, IMiDs, proteasome inhibitors, and/or anti-CD38 antibodies alone or in combination) was provided while the idecabtagene vicleucel was manufactured but had to be stopped at least 14 days before LDC. All patients were required to undergo LDC with cyclophosphamide and fludarabine 5 days before infusion with idecabtagene vicleucel. Of the 140 patients enrolled, 128 received idecabtagene vicleucel infusion and were included as the idecabtagene vicleucel–treated population for the primary analysis of efficacy and safety. Patients received target doses of 150 × 106, 300 × 106, or 450 × 106 CAR T cells and were followed for at least 24 months and then asked to participate in a separate long-term follow-up study. The median age of the 140 enrolled patients was 60.5 years (range = 33 to 78), 82 (58.6%) were male, the median years since diagnosis was 6 years (range = 1 to 18), 46 (32.9%) were at high cytogenetic risk, and 131 (93.6%) had received a stem cell transplant.
Efficacy Results
The ORR, CRR, DoR, OS, and HRQoL were considered the most relevant outcomes by the clinical experts and clinician groups. In addition, patient groups considered improved HRQoL (e.g., fewer symptoms, higher functionality, and fewer side effects from treatments) to be highly valued outcomes.
At a median follow-up of 11.3 months, the KarMMa trial met its primary end point, achieving an ORR above the null hypothesis of 50% established in the protocol. The ORR in the population treated with idecabtagene vicleucel was 73.4% (95% confidence interval [CI], 65.8% to 81.1%; P < 0.0001) and 81.5% (95% CI, 68.6% to 90.7%) in the group with a target dose of 450 × 106 CAR T cells, respectively. Given that the test for ORR (the primary end point) was positive, the key secondary efficacy end point of CRR was tested against the null hypothesis of 10% or less — as prespecified — rejecting the null hypothesis, with 40 of 128 patients achieving a complete response equivalent to a CRR of 31.3% (95% CI, 23.2% to 39.3%; P < 0.0001), while in the group with a target dose of 450 × 106 CAR T cells, the CRR was 35.2% (95% CI, 22.7% to 49.4%). These values from the primary and key secondary end points were considered clinically meaningful by the clinical experts.
The DoR, TTR, and TTP were evaluated in the KarMMa trial as secondary end points. In the treated population, the median DoR was 10.6 months (95% CI, 9.0 to 11.3), the TTR was 1 month (range = 0.5 to 8.8), and the TTP was 8.9 months (95% CI, 6.0 to 11.6), while in the group with a target dose of 450 × 106 CAR T cells, the median DoR was 11.30 months (95% CI, 9.17 to 11.43) and the TTR was 1.0 months (range = 0.9 to 2.0); TTP was not assessed in the 450 × 106 CAR T cells group. Likewise, an MRD-negative status with a CR or better was observed in 31 of 128 patients (24.2%; 95% CI, 17.1% to 32.6%) treated with idecabtagene vicleucel, and in 13 of 54 of patients in the group with a target dose of 450 × 106 CAR T cells. Although these results may suggest a beneficial effect in patients treated with idecabtagene vicleucel and were considered likely to constitute a meaningful impact from the perspective of the clinical experts, none of these secondary end points were adjusted for multiplicity and should be interpreted with caution.
Both experts and patients considered OS an important and valued outcome and it is commonly used in clinical trials conducted in patients with MM. In the treated population, the observed median OS was 18.2 months (95% CI, 18.0 to not estimable [NE]), with 76% of individuals alive at 12 months; the clinical experts considered this a beneficial effect estimate for patients with the characteristics included in the KarMMa trial (i.e., those with a median of 6 years since diagnosis, with relapses, and who have been heavily treated). The OS was NE in patients in the group with a target dose of 450 × 106 CAR T cells. Similarly, based on the Kaplan–Meier (KM) estimates, the median PFS was 8.6 months (95% CI, 5.6 to 11.3), with 34% of patients event-free at 12 months in the idecabtagene vicleucel–treated group, and 11.3 months (95% CI, 8.8 to 12.4) in the group with a target dose of 450 × 106 CAR T cells, denoting a likely meaningful benefit for patients treated with idecabtagene vicleucel.
Outcomes involving HRQoL were frequently mentioned in the input submitted by patient groups and by clinician groups. Patients put a high value on decreasing symptoms, better physical functioning, less pain, and fewer side effects. Results of the KarMMa trial suggest that idecabtagene vicleucel treatment may be associated with improvements in the fatigue, pain, physical functioning, and global health/QoL subscales of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) by reaching points of meaningful clinical significance above the thresholds of probable benefit according to minimal important differences (MIDs) established in the literature. On average, no clinically meaningful deterioration in the EORTC QLQ-C30 cognitive functioning and the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myeloma Module with 20 items (EORTC QLQ-MY20) disease symptoms and side effects subscales were observed posttreatment. When addressing the EuroQol 5-Dimensions 5-Levels (EQ-5D-5L) subscales, no changes from baseline were observed. These findings appear to suggest that idecabtagene vicleucel treatment may be associated with improvements or stabilization in most primary HRQoL metrics. However, these results were observed over the first and middle part of the study follow-up, eventually decreasing to baseline levels, with added uncertainty due to imprecision (i.e., fewer patients at the end of the study) and the fact that all HRQoL outcomes in the KarMMa study were secondary end points assessed without adjustment for multiplicity.
Sensitivity analyses were based on whether the FDA or European Medicines Agency (EMA) rules for censoring DoR, TTP, and PFS outcomes were used; and on comparisons using an independent response committee (IRC) versus investigator adjudication of end points (for ORR, CRR, and TTP). Finally, scenarios were presented when analyzing the enrolled population against the population treated with idecabtagene vicleucel (for DoR, CRR, PFS, and OS). No notable differences from the primary effect estimates were observed for any of these outcomes using any of the sensitivity analyses.
Except for the ORR and CRR outcomes, no other secondary end points were considered in the adjustment for multiplicity and should be interpreted with caution.
In an updated data submission (cut-off date of January 14, 2020) with a median follow-up of 13.3 months,10 no significant changes were noted in the ORR, CRR, DoR, TTR, MRD, OS, or PFS. These updated results, described in Appendix 3, were not adjusted for alpha errors nor were they used for hypothesis testing.
Harms Results
AEs were reported in all 128 (100%) patients treated with idecabtagene vicleucel with. Most AEs, with the exception of hypogammaglobulinemia and infections, occurred within 8 weeks after infusion. The most commonly reported AEs were hematologic toxic effects, including neutropenia in 117 patients (91.4%), CRS in 107 patients (83.6%), anemia in 89 patients (69.5%), and thrombocytopenia in 81 patients (63.3%). A total of 86 patients (67.2%) had at least 1 serious adverse event (SAE). The most frequently reported SAEs (≥ 5% of patients) were CRS in 22 patients (17.2%), general physical health deterioration in 13 patients (10.2%), pneumonia in 11 patients (8.6%), and febrile neutropenia in 9 patients (7.0%).
Eight patients died after leukapheresis and before receiving idecabtagene vicleucel infusion: 5 patients (3.6%) died after leukapheresis and before starting LDC, while 3 patients (2.1%) died after starting LDC and before receiving idecabtagene vicleucel infusion. In the idecabtagene vicleucel–treated population as of the data cut-off date, 34 patients (26.6%) died on or after idecabtagene vicleucel infusion, with 24 of those death which were attributed to the malignant disease or complications due to the malignant disease under study.
Harms of special interest were identified according to the protocol for this review. Febrile neutropenia was present in 21 patients (16.4%) of the idecabtagene vicleucel–treated population. A total of 23 patients (18.0%) in the idecabtagene vicleucel–treated population had investigator-identified neurotoxicity on or after idecabtagene vicleucel infusion. Evidence of CRS on or after the idecabtagene vicleucel infusion was present in 107 patients (83.6%).
In an updated cut-off data submission (cut-off date: January 14, 2020),10 no differences in the number of patients with AEs were noted. Ten more deaths (44 [34.4%]) were reported at this cut-off date and 23 more cases of febrile neutropenia (for a total of 30 of 128 treated patients [16.3%]) were reported. The other harms of special interest were not significantly different at this cut-off date.
Table 2: Summary of Key Results From Pivotal and Protocol-Selected Studies
Result | Population treated with idecabtagene vicleucel Idecabtagene vicleucel (CAR T cells) target dose | |||
|---|---|---|---|---|
150 × 106 N = 4 | 300 × 106 N = 70 | 450 × 106 N = 54 | All doses N = 128 | |
Response or remission | ||||
Overall response rate (PR or better) | ||||
N (%) | 2 (50.0) | 48 (68.6) | 44 (81.5) | 94 (73.4) |
95% CIa | 6.8 to 93.2 | 56.4 to 79.1 | 68.6 to 90.7 | 65.8 to 81.1 |
P valueb | — | — | — | < 0.0001 |
Complete response rate (CR or better) | ||||
N (%) | 1 (25.0) | 20 (28.6) | 19 (35.2) | 40 (31.3) |
95% CIa | 0.6 to 80.6 | 18.4 to 40.6 | 22.7 to 49.4 | 23.2 to 39.3 |
P valueb | — | — | — | < 0.0001 |
Duration of responsec | ||||
N | 2 | 48 | 44 | 94 |
Censored, n (%) | 1 (50.0) | 15 (31.3) | 26 (59.1) | 42 (44.7) |
Progressed/died, n (%) | 1 (50.0) | 33 (68.8) | 18 (40.9) | 52 (55.3) |
Progressed | 1 (50.0) | 32 (66.7) | 18 (40.9) | 51 (54.3) |
Died without progression | 0 | 1 (2.1) | 0 | 1 (1.1) |
Median duration of response,d months (95% CI) | NE (2.79 to NE) | 9.92 (5.36 to 11.01) | 11.30 (9.17 to 11.43) | 10.58 (9.03 to 11.30) |
Time to response | ||||
N | 2 | 48 | 44 | 94 |
Median TTR,d months (minimum to maximum) | 1.0 (1.0 to 1.0) | 1.0 (0.5 to 8.8) | 1.0 (0.9 to 2.0) | 1.0 (0.5 to 8.8) |
Time to progressione | ||||
N | — | — | — | 128 |
Median, months (95% CI)f | — | — | — | 8.9 (6.0 to 11.6) |
MRD | ||||
Patients who achieved an MRD-negative status and at least CR,g N (%) | 1 (25.0) | 17 (24.3) | 13 (24.1) | 31 (24.2) |
95% CI | 0.6 to 80.6 | 14.8 to 36.0 | 13.5 to 37.6 | 17.1 to 32.6 |
Survival | ||||
Overall survival | ||||
|||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Medianf of overall survival time, months | ||||||||| | ||||||||| | ||||||||| | 18.2 |
95% CI | ||||||||| | ||||||||| | ||||||||| | 18.0 to NE |
Progression-free survivalh | ||||
||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Medianf of PFS time, months | 2.8 | 5.8 | 11.3 | 8.6 |
95% CI | 1.0 to NE | 4.2 to 8.9 | 8.8 to 12.4 | 5.6 to 11.3 |
Harms | ||||
||||||||||||||||||||||||||||| | — | — | — | ||||||||| |
|||||||||||||||||||||||| | — | — | — | ||||||||| |
||||||||||||||||||||||||||||||| | — | — | — | ||||||||| |
|||||||||||||||||||||||||||||||||||| | — | — | — | — |
||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | |||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Notable harms | ||||
Febrile neutropenia | ||||||||| | ||||||||| | ||||||||| | 21 (16.4) |
Cytokine release syndrome | ||||||||| | ||||||||| | ||||||||| | 107 (83.6) |
Investigator-identified neurotoxicity | ||||||||| | ||||||||| | ||||||||| | 23 (18.0) |
Replication-competent lentivirus | ||||||||| | ||||||||| | ||||||||| | 0 |
Hospital utilization – ICU admission | — | — | — | 25 (19.5) |
AE = adverse event; CAR = chimeric antigen receptor; CTCAE = Common Terminology Criteria for Adverse Events; CI = confidence interval; CR = complete response; HRQoL = health-related quality of life; ICU = intensive care unit; LDC = lymphodepleting chemotherapy; MRD = minimal residual disease; NE = not estimable; PFS = progression-free survival; PR = partial response; PT = preferred term; sCR = stringent complete response; SE = standard error; SOC = system organ class; TTP = time to progression; TTR = time to response.
aFor “Total” and “Enrolled population”: Wald CI; for individual target doses: Clopper-Pearson exact CI.
bP value from 1-sample binomial tests (normal approximation).
cApplying FDA censoring rules. The duration of response analysis is based on responders only, and therefore is the same for the idecabtagene vicleucel–treated population, enrolled population, and efficacy evaluable population, as responders in the 3 populations are the same (i.e., both patients enrolled but not treated with idecabtagene vicleucel and those treated with idecabtagene vicleucel but without baseline or post-baseline efficacy assessments were to be considered nonresponders). Data cut-off date of October 16, 2019.
dResponse is defined as achieving sCR, CR, very good partial response, or PR.
eTTP based on an independent response committee assessment, applying FDA censoring rules, idecabtagene vicleucel–treated population.
fBased on the Kaplan–Meier approach.
gUsing a 10-5 sensitivity level and next-generation sequencing.
hBased on an independent response committee review according to International Myeloma Working Group criteria for applying FDA censoring rules to an idecabtagene vicleucel–treated population.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Critical Appraisal
This single-arm, phase II study lacks a comparator group, which limits confidence in the effect estimates due to an increase in the risk of bias due to confounding fluctuations in health status, and unidentified prognostic factors that could affect subjectively assessed outcomes. The risk of attrition bias is low in the primary and key secondary end points, given that all patients in the population treated with idecabtagene vicleucel were included in the analysis. Outcomes regarding HRQoL were characterized by large amounts of missing data at baseline, with a significant proportion missing at a later time. Further, the open-label nature of the study design may introduce bias for patient-reported outcomes, such as HRQoL measures.
The only outcomes adjusted for multiplicity were the ORR and CR, and results of other secondary outcomes (DoR, TTR, TTP, MRD status, OS, PFS, and HRQoL) must therefore be interpreted with consideration for the risk of type I error.
It is unknown if bridging therapy interventions could affect the outcomes evaluated in these patients after they received idecabtagene vicleucel treatment.
Subgroups were planned a priori, but no formal subgroup effect tests were conducted due to the small number of patients and events (imprecision) expected.
The clinical variables and patient baseline characteristics from the KarMMa trial were generally representative of Canadian patients with RRMM who are refractory to IMiDs, proteasome inhibitors, and anti-CD38 drugs. The administration procedure of idecabtagene vicleucel will require additional actions (i.e., manufacturing, bridging therapies, and LDC); experts considered the administration procedure followed in the KarMMa study to be as anticipated in Canada.
Indirect Comparisons
Description of Studies
Two sponsor-submitted analyses are included that compare the information from the single-arm KarMMa study to observational evidence obtained from individual patient data or aggregated published data.
The first analysis (NDS-MM-003)12 is a comparison of the effects of idecabtagene vicleucel in the single-arm KarMMa study (MM-001) against other currently administered treatments for RRMM obtained from a set of real-world (RW) patient-level data collected from various sources, including databases and clinical sites from the US and Europe. To decrease the imbalances or differences in patients from the real-world evidence (RWE) when compared with the KarMMa population, propensity scores were created.
From the RWE databases, eligibility criteria were used to collect a first cohort of RRMM patients (eligible cohort) and a final cohort (matched cohort) of RRMM patients with the intention to use an estimated 2:1 matching of RW patients with RRMM to be compared with patients receiving idecabtagene vicleucel in the single-arm KarMMa study. Due to the strict criteria, fewer patients were available for the matched RRMM cohort, requiring a change in the statistical analysis. The investigators decided to use the eligible RRMM cohort for the main analysis, using a trimmed stabilized inverse probability treatment weighting (IPTW) method, leaving the matched-paired and untrimmed IPTW as supportive analyses.
The outcomes evaluated were the ORR, CRR, very good partial response (VGPR) rate, PFS, and OS. Baseline characteristics of the idecabtagene vicleucel arm and the RWE eligible RRMM cohort indicated an older population in the eligible RRMM cohort, with a higher risk of cytogenetic abnormalities, and fewer previous antimyeloma therapies. Prior to the IPTW adjustment, with the exception of age, the imbalance of the prognostic factors and prior treatments suggested the eligible RRMM cohort was a less heavily pretreated and less refractory population with a more favourable prognosis overall compared with the idecabtagene vicleucel cohort.
The second analysis is a sponsor-submitted matching-adjusted indirect comparison (MAIC)13 that compares the idecabtagene vicleucel–treated population from the KarMMa trial to aggregated data from a published RWE study (MAMMOTH). These analysis aim to provide a comparator arm, with adjustments for differences in baseline characteristics, prognostic factors, and effect modifiers, and produce an adjusted effect estimate for decision-makers and stakeholders, given the lack of a direct, head-to-head comparison of idecabtagene vicleucel to relevant comparators.
Efficacy Results
The NDS-MM-003 analysis included 128 patients from the original KarMMa trial (idecabtagene vicleucel–treated population) and compared them against 190 patients in the RWE databases (the eligible RRMM cohort) with similar eligibility criteria. The obtained ORR was lower in the eligible RRMM cohort compared with the idecabtagene vicleucel cohort (32.2% versus 76.4%; risk ratio (RR) = 2.4; 95% CI, 1.7 to 3.3; P < 0.0001).
In the eligible RRMM cohort, the median duration of follow-up for all treated patients (which includes duration up to death for patients who died and duration up to last date known alive for surviving patients), was 10.2 months (range = 0.2 to 24.0). In the idecabtagene vicleucel cohort, the median duration of follow-up after idecabtagene vicleucel infusion was 11.3 months (range = 0.2 to 18.6). These numbers were current as of the October 30, 2019, data cut-off date of the KarMMa study. After a median follow-up time of 15 months for all surviving patients in the eligible RRMM cohort, 55.8% of patients had died, while after a median follow-up time of ||||| |||| for all surviving patients in the idecabtagene vicleucel–treated cohort, ||||||% of patients had died. The median OS for RWE patients in the eligible RRMM cohort was 14.7 months (|||||||||) and ||||||||||||||||||||||||||||||| in the idecabtagene vicleucel cohort. A comparison of the 2 groups yielded an OS hazard ratio (HR) of (||||||||||||||||||||), favouring the idecabtagene vicleucel cohort compared with the eligible RRMM cohort treated with available therapy |||||||||||.
The median TTR for responders was 1.1 months (range = 0.2 to 8.6) in the eligible RRMM cohort versus 1.0 month (range = 0.5 to 8.8) in the idecabtagene vicleucel cohort. As of the data cut-off date, the median DoR was 9.0 months (95% CI, 7.5 to ||||||) for 30.5% of responders in the eligible RRMM cohort versus 11.0 months (95% CI, ||||||||||||) for 73.4% of responders in the idecabtagene vicleucel cohort. The HR for DoR was |||||||||||||||||. After a median follow-up time of |||||||||||||||| for all RW patients in the eligible RRMM cohort, ||||| of patients had a PFS event (progressive disease [PD] or death), while after a median follow-up time of 11.3 months for all patients in the idecabtagene vicleucel cohort, ||||| of patients had a PFS event. A comparison between the 2 groups yielded a PFS |||||||||||||||||||||||||||||||||||||||||||, favouring the idecabtagene vicleucel cohort compared with the eligible RRMM cohort treated with available therapy (||||||||||).
The analysis using MAIC yielded similar results. In the treated population, idecabtagene vicleucel was more efficacious than conventional care in terms of the ORR (odds ratio = |||||||||||||||||||||||||) and also in the population using the target dose of 450 × 106 CAR T cells. There was also a better PFS in the idecabtagene vicleucel–treated population compared with conventional care (HR = ||||||||||||||||||||||||||||||) and in patients receiving a target dose of 450 × 106 CAR T cells (|||||||||||||||||||||||||||||||), and longer OS, with the population treated with idecabtagene vicleucel performing better than conventional care in the MAMMOTH treated population in the adjusted MAIC (HR = ||||||||||||||||) and target dose (||||||||||||||||||||||||||||||||).
Harms Results
No harms data were provided in any of the analyses submitted.
Critical Appraisal
The NDS-MM-003 study has several limitations. The missing data from the databases throughout the process used to create the eligible cohort, which implies potential bias due to the need to rely on multiple imputation methods, increasing the uncertainty in effect estimates. Data were missing for a number of variables which would have been useful to include in the propensity scores. Although later addressed in the propensity score balancing, baseline differences in multiple variables observed between the RRMM cohort, the eligible RRMM cohort, and the idecabtagene vicleucel cohort (e.g., the presence of plasmacytoma or refractory status) suggest the possibility of other potentially unmeasured confounders, and the prospect that these can be unevenly distributed between groups without proper randomization. Prior to the IPTW adjustment, with the exception of age, the imbalance of the prognostic factors and prior treatments suggests the eligible RRMM cohort was a less heavily pretreated and a less refractory population with a more favourable prognosis overall compared with the idecabtagene vicleucel cohort. Differences that arose during study design and when combining patients across databases (i.e., selecting patients from different databases) may result in the introduction of clinical heterogeneity that cannot be accounted for in propensity score modelling. Furthermore, investigators used, in part, a data-driven approach; clinical relevance should be considered to select the covariates used in propensity score models.
Although the population from the eligible RRMM cohort is similar to the idecabtagene vicleucel cohort in several measures, generalizability of this and the matched final cohort, as well as the comparators, can be a concern in Canadian clinical practice due to the different and varied therapies included in the regimens provided. The availability of such regimens and drugs will vary depending on funding and feasibility for each province and territory. Only a fraction of the regimens evaluated as comparators in this indirect comparison were mentioned by clinical experts consulted by CADTH as being commonly used in clinical practice in Canada.
The second comparative analysis (a MAIC) was limited to study-level aggregated data from the full-text publication for MAMMOTH and compared to the KarMMa study. Although the unanchored MAIC had an appropriate rationale for comparing individual patient data from a single-arm study with aggregate published data, it is not clear if the underlying assumption of the unanchored MAIC that all effect modifiers and prognostic factors have been accounted for or if all of the relevant differences in patient characteristics were captured, as many identified prognostic elements were not reported on in MAMMOTH. Furthermore, the MAIC cannot address heterogeneity in study designs, with possible differences in outcome assessment and definitions (e.g., differences in setting and follow-up) that generate uncertainty. Potential violations of the proportionality assumption were observed in the time-to-event outcomes. The different treatments obtained in the MAMMOTH study also generate uncertainty about the generalizability of the results, particularly from the Canadian perspective, due to the fact that approximately a third of the comparators are not widely available in the different provinces and territories.
Conclusions
Evidence from the single-arm, open-label KarMMa-001 study suggests that the CAR T-cell therapy idecabtagene vicleucel at a target dose of 450 × 106 CAR T cells is associated with an induction of response, based on an ORR of 81.5% and a CRR of 35.2%. Results suggest that treatment with idecabtagene vicleucel may offer a benefit in terms of DoR, MRD, TTR, TTP, OS, and PFS, but none of these outcomes were controlled for multiplicity and all should be interpreted with consideration of type I error. The data for HRQoL outcomes were descriptive and could not be interpreted due to missing information. These effect estimates come from evidence with a risk of bias due to the lack of estimations from a comparison arm in a randomized design, and must be weighed against the observed undesirable effects, including AEs (such as CRS), the need for LDC, and bridging therapy. All patients treated with idecabtagene vicleucel reported at least 1 AE. The most commonly reported AEs were neutropenia, CRS, anemia, and thrombocytopenia.
Results of 2 indirect treatment comparisons (ITCs) of the population from the KarMMa study of individual patient observational (RWE) data and aggregated data from published studies add support for the beneficial effects observed in KarMMa, but also include a risk of bias due to inherent design differences in the bodies of evidence that cannot be adjusted for statistically, the potential impact of unmeasured and unaccounted-for prognostic factors and effect modifiers in the models, and undermined generalizability due to the inclusion of irrelevant comparators. Given the limitations of both ITCs and the absence of direct comparative evidence, any potential benefit of idecabtagene vicleucel over other treatment regimens used in this patient population remains unknown.
Introduction
Disease Background
Multiple myeloma is a malignant, clonal bone marrow plasma cell disorder that causes clinical features of renal failure, bone lesions, hypercalcemia, and bone marrow suppression resulting from excessive production of monoclonal proteins as well as direct tumour cell effects.1,2
The second most common of hematologic malignancies, MM represents approximately 1% of all cancers and roughly 10% to 15% of all hematologic malignancies. It primarily affects older individuals and is extremely rare in patients younger than 30 years old.3,4 Data from GLOBOCAN in 2012 estimated a global incidence of 114,000 patients and 80,000 deaths.14 In Canada, a recent epidemiological study1 found the median age at diagnosis was 70.07 years (standard deviation = 12.08), with an average national incidence rate of 5.42 cases per 100,000 individuals per year, a steady rise in the annual rate of 0.96 cases per million individuals per year, and an estimated 3,400 new cases annually.1,5 At the provincial level, Quebec and Ontario have the highest incidence rates of MM in Canada (5.82 and 5.66 cases per 100,000 individuals per year, respectively). The mean national mortality rate in Canada stands at 3.57 deaths per 100,000 individuals per year.1
An initial diagnosis of MM usually occurs when patients are referred to specialists by primary care physicians or by encountering nonspecific symptoms (fatigue, bone pain) and other incidental findings. The diagnosis of symptomatic MM (myeloma that necessitates treatment) is made based on IMWG recommendations.15 Specifically, the patient must have a clonal bone marrow plasma cell level of greater than 10% and exhibit any 1 of the following: hypercalcemia, renal insufficiency, anemia, bone lesions, or a clonal bone marrow plasma cell level of at least 60%. Additional indicators of MM include a serum free light chain (FLC) ratio of at least 100 or multiple focal lesions on MRI studies. In recent years, a global trend of marked improvement in 5-year survival rates has been reported in patients with MM. However, despite these advances in treatment and prognosis, MM remains highly fatal and relapses are common.16
Patients are considered to have RRMM when disease recurs after prior response as determined by objective laboratory and radiological criteria.6 From there, patients begin moving to successive therapies as they advance in their course of the disease with further relapses and more lines of therapies. In patients who experience relapse and progression despite receiving several therapies, outcomes are usually poor, with infrequent CRs, a median PFS of 3 to 4 months, and a median OS of 8 to 9 months.7
Standards of Therapy
The goal of treatment of RRMM is to achieve disease control with acceptable toxicity and sufficient patient-defined HRQoL. This goal is reliant on effective systemic chemotherapy and supportive measures (pain control, antibiotics, kyphoplasty, radiation therapy, dialysis, and psychosocial supports).
Initial therapy for patients with MM depends on their eligibility for a bone marrow transplant. For patients who are eligible for a transplant the current treatment includes cycles of induction with conventional chemotherapy, proteasome inhibitors, and a corticosteroid; for example, this phase includes cycles of a combination of cyclophosphamide, bortezomib, and dexamethasone (CyBorD), or IMiDs such as a combination of lenalidomide, bortezomib, and dexamethasone. The induction phase is followed by a harvest of stem cells in preparation for an autologous stem cell transplant. After the transplant, consolidation therapy may be warranted, followed by maintenance therapy, typically lenalidomide or bortezomib. In patients who are not eligible for transplant the options include a novel IMiD, or proteasome inhibitors and a steroid. These can include lenalidomide, CyBorD, or a combination of lenalidomide, bortezomib, and dexamethasone.
For patients with RRMM, although new options, including recently approved drugs such as daratumumab and isatuximab,7 are emerging and increasingly available, no standard of care has been fully established, and the choice of the optimal strategy at relapse remains a challenge for clinicians. Currently, the options for patients with RRMM are limited to second to fifth lines of therapies that include several drugs, and the sequencing of treatments depends largely on the type of response to previous therapies (i.e., previous response to lenalidomide- or bortezomib-based therapies such as CyBorD).
Regimens commonly used in the Canadian landscape include combinations of daratumumab, bortezomib and dexamethasone; Vd; pomalidomide and dexamethasone; and carfilzomib and dexamethasone, all of which are regimens used when there is resistance to lenalidomide. Also, regimens used when there is resistance to bortezomib-based therapies include combinations of daratumumab, lenalidomide and dexamethasone; carfilzomib, lenalidomide and dexamethasone; lenalidomide and dexamethasone.7-9
Drug
Chimeric antigen receptor T cells are modified T cells that express a CAR directed against specific antigens expressed only in tumours and not healthy tissues, potentially limiting toxicity. As these T cells are generated from autologous T cells collected from patients by leukapheresis, they represent an individualized therapeutic approach.17,18
Idecabtagene vicleucel is a cell therapy formed by CAR T cells directed against the BCMA. It is indicated for the treatment of adult patients with MM who have received at least 3 prior therapies, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody, and who are refractory to their last treatment. The reimbursement request from the sponsor is according to the indication. Idecabtagene vicleucel is provided as a single-dose, 1-time treatment in 1 or more patient-specific infusion bags. Each single infusion bag of idecabtagene vicleucel contains a suspension of 275 × 106 to 520 × 106 CAR T cells. The target dose is 450 × 106 CAR T cells within a range of 275 × 106 to 520 × 106 CAR T cells.19 Pretreatment includes the use of LDC with cyclophosphamide 300 mg/m2 IV and fludarabine 30 mg/m2 IV for 3 days. Idecabtagene vicleucel infusion is to be administered 2 days after completion of LDC. To minimize the risk of infusion reactions, acetaminophen (500 mg to 1,000 mg orally) and diphenhydramine 12.5 mg IV (or 25 mg to 50 mg orally), or another H1-antihistamine approximately 30 minutes to 60 minutes are administered before the idecabtagene vicleucel infusion. Patients should be monitored in a specialized treatment centre at least daily for 7 days following IV infusions for signs of CRS, which may be fatal or life-threatening, and neurologic toxicities, which may be severe or life-threatening and may occur concurrently with CRS, after CRS resolution, or in the absence of CRS.
Table 3 lists the main characteristics of idecabtagene vicleucel.
Table 3: Key Characteristics of Idecabtagene Vicleucel
Characteristic | Idecabtagene vicleucel |
|---|---|
Mechanism of action | A CAR T-cell therapy, i.e., a genetically modified autologous T-cell immunotherapy directed against cells expressing the B-cell maturation antigen, leveraging the patient’s immune response to tumour cells |
Indicationa | For the treatment of adult patients with multiple myeloma who have received at least 3 prior therapies, including an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 antibody, and who are refractory to their last treatment |
Route of administration | IV infusion |
Recommended dose | Idecabtagene vicleucel, (IV infusion target dose of 450 × 106 CAR T cells, within a range of 275 × 106 to 520 × 106 CAR T cells) |
Serious adverse effects or safety issues | Patients should be monitored in a specialized treatment centre at least daily for 7 days following IV infusions for signs of CRS, which may be fatal or life-threatening, and neurologic toxicities, which may be severe or life-threatening and may occur concurrently with CRS, after CRS resolution, or in the absence of CRS |
CAR = chimeric antigen receptor; CRS = cytokine release syndrome.
aHealth Canada–approved indication.
Source: Product monograph for idecabtagene vicleucel.19
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on input provided by patient groups.
About the Patient Groups and Information Gathered
Myeloma Canada submitted the patient input for this review. Founded in 2005, Myeloma Canada is the only national charitable organization created by and for Canadians affected by MM. The organization works to improve the lives of those affected by myeloma by empowering the community through awareness, education, and advocacy programs, and supporting clinical research to find the cure.
Information from this input was gathered through a patient survey. The survey was accessed through email and social media from December 17, 2020, to January 4, 2021. The 388 individuals with myeloma who responded to the survey were divided into 2 sets of patients. Subset 1, with 161 respondents from across Canada, did not have experience with the treatment under review. However, they did qualify to receive the treatment based on previous therapy regimens. Subset 2 consisted of 14 respondents who had received a CAR T-cell therapy. These 14 respondents were from Ontario (36%), Alberta (21%), British Columbia (21%), Quebec (14%) and Saskatchewan (7%).
Myeloma Canada received external help from Colucci Health to summarize the data and help prepare this report.
Disease Experience
When respondents were asked to rate on a scale of 1 to 4 (1 = “not important”; 5 = “very important”) how important it is for them to control various aspects of their myeloma, 70% of the respondents indicated that their major concern was control of infections, followed by kidney problems (56%) and mobility (51%). Other reported outcomes were neuropathy (pain, numbness, tingling, swelling, or muscle weakness), fatigue, and pain.
When asked, “Please rate on a scale of one to five (one is ‘not at all’, and five is ‘significant impact’), how much symptoms associated with myeloma impact or limit your day-to-day activities and quality of life (QoL),” the respondents (n = 315) indicated that their symptoms significantly affected their ability to travel (35%), work (26%) and exercise (21%).
The patient input indicated that myeloma is a relapsing-remitting cancer; it alternates between periods of symptoms and/or complications that need to be treated, and periods of remission that do not require treatment. Providing patients with an effective treatment and giving them a prolonged remission with limited side effects can play a major role in their well-being and allow patients to live a full and productive life.
Experiences With Currently Available Treatments
When asked, “If you are taking a treatment or were to consider taking treatment for your myeloma, how important is it to improve your overall QoL? Rate on a scale of one to five, one is ‘not important’ and five is ‘extremely important’,” 61% of the respondents (n = 288) expressed that it is extremely important, 30% felt it was very important, and 9% felt it was important. Additionally, 40% of the respondents (n = 315) visit a cancer centre once a month.
Respondents (n = 313) identified drug costs (35%), parking costs (33%), and lost income due to absence from work (29%) as their most significant financial implications. Other economic factors included travel costs, medical supply costs, accommodation costs, and drug administration fees.
Respondents were asked, “Do you need the support of a family member or caregiver to help you manage your myeloma or your treatment-related symptoms?” and 54% (n = 314) answered “yes.”
The respondents (n = 266) identified effective treatments, fewer side effects, and better QoL as the most important aspects when it came to treating their myeloma. The following are examples of respondents’ explanations of what they considered to be the most important aspects of treating their disease:
“Efficacy of the treatment for improved prognosis and ability to maintain similar quality and function of life activities.”
“Extending my life and having hope for treatments going forward and being pain free.”
“I would like to get off medications and as close to a long remission and cure as possible as I am a young myeloma patient.”
“It’s important that I am able to receive the most up-to-date treatment and have access to the best minds in the field. Considerations for my mental health and how best to maintain a positive outlook is also very important.”
“Being able to have a lifestyle rather than just a world revolving around treatment.”
“Minimizing side effects and portability or reduced frequency of time in hospital.”
Improved Outcomes
Respondents From Subset 1
Of 297 patients, 161 had received at least 3 prior therapies, including an IMiD such as thalidomide, lenalidomide (Revlimid), or pomalidomide (Pomalyst), a proteasome inhibitor such as bortezomib (Velcade), carfilzomib (Kyprolis), or ixazomib (Ninlaro), and an anti-CD38 antibody, either daratumumab (Darzalex) or isatuximab (Sarclisa).
Seventy-three percent (n = 117) of respondents answered “yes” to having previously heard of CAR T-cell immunotherapy, 23% answered “no,” and 4% did not know what CAR T-cell therapy was. Respondents from subset 1 were asked to select the statement that best fit their understanding of CAR T-cell immunotherapy from the following options: “I don’t know,” “T cells (T lymphocytes, which are special types of white blood cells) are first harvested from a cancer patient and then modified in a laboratory before they are reintroduced into the patient’s body intravenously,” “CAR T-cell immunotherapy involves genetically modified cells responsible for killing cancer cells,” “CAR T-cell immunotherapy is a new type of blood cancer treatment,” and “All of the above.”
Fifty-seven percent of the respondents (n = 161) answered correctly by selecting “all of the above.” Myeloma Canada interpreted these results to mean more than half of respondents had a concrete understanding of the CAR T-cell therapy process and how it differs from their current treatment regimens.
When respondents were asked what they believe to be the benefits of CAR T-cell immunotherapy compared to the type of treatment they are currently receiving or have already received, the majority (75%) of respondents (n = 118) replied that they believed they would receive all of the benefits listed in the survey. Namely, prolonged remission, not having to be on treatment because they are in remission, better QoL, better overall health, better control of myeloma symptoms, and fewer side effects.
Respondents (n = 155) were asked, “Considering that treatment options are becoming limited at this point in your myeloma journey, other than participating in clinical trials or another treatment, indicate what an estimated prolonged remission of 34.2 months means to you at this stage in your life.” A prolonged remission of 34.2 months was “extremely desirable” to 89 respondents, “very desirable” to 19 respondents, “desirable” to 16 respondents, “somewhat desirable” to 4 respondents, and 25 respondents did not know what it meant to them.
Myeloma Canada explained the treatment procedures and risks to the respondents as follows: “In some cases, the patient’s myeloma can progress during this time (i.e., the myeloma comes back) and the patient may require an additional (bridging) therapy. If this happens, the patient may no longer be eligible to proceed to the next step which is to receive their modified T cells. In this case, other treatment options are available and will be presented to the patient.” Respondents were asked to indicate, from a list, which sentence best reflects their sentiments about this kind of situation. Forty-six percent (n = 72) of the 156 respondents said they were not sure how it makes them feel and would like to discuss this situation further with their hematologist or oncologist. Twenty-three percent of respondents (n = 36) were willing to take the risk that their myeloma would return. Survey respondents reported that a loss of or decrease in cognitive abilities (66%) and loss of physical abilities and mobility (54%) were the most concerning CAR T-cell treatment side effects. Respondents were asked to rate side effects on a scale from 1 (most troublesome) to 5 (least troublesome). Among other concerning side effects reported by respondents were anemia, neutropenia, and thrombocytopenia.
When respondents (n = 151) were asked if they felt CAR T-cell immunotherapy could improve their health and well-being, 48% answered “yes,” 4% answered “no,” and 48% did not know. Additionally, 58% of respondents (n = 150) replied that they expected CAR T-cell immunotherapy could improve their long-term health outlook. When asked, “With what you know today, what treatment option would you consider first as your next treatment?,” 35% of the 151 respondents would choose CAR T-cell immunotherapy, 15% would choose another treatment suggested to them, 9% would choose a clinical trial, and 42% did not know what they would choose.
The following quotes express respondents’ feelings toward CAR T-cell immunotherapy:
“The potential of extending my life for shy of three years is much better than going through clinical trials that are only effective on average for 9 months.”
“The patient and caregiver are under a lot of stress try[ing] to adjust. Adjusting to travel, find[ing] accommodation, finding your way to the hospital, new doctors, having to go to more than one hospital. Unknown side effects. More medical expenses.”
“3 & a half years [of prolonged remission] is not that long.”
“I have been in four clinical trials. I would try another before I would consider CAR T-cell immunotherapy if I were eligible. I am 80 years old.”
Experience With Drug Under Review
Respondents From Subset 2
Fourteen respondents have been treated or are in the process of receiving a CAR T-cell immunotherapy to treat their myeloma. These respondents were asked which CAR T-cell therapy they received. Only 1 respondent received the treatment under review, 5answered they had received another CAR T-cell therapy, and 8 did not know which CAR T-cell therapy they had received. Myeloma Canada presented the data on all the patients who had received a CAR T-cell therapy, providing a directional perspective of this new therapy in an attempt to give CADTH a better understanding of the overall patient experience.
When respondents were asked, “How long ago did you receive your idecabtagene vicleucel CAR T-cell therapy?” 1 respondent answered, “less than three months ago,” 2 answered “between three and six months ago,” 1 answered “between six and 12 months ago,” 1 answered “over a year ago,” and 1 answered “over two or more years ago.” In addition, respondents (n = 6) were asked, based on their experience of the idecabtagene vicleucel CAR T-cell immunotherapy, how they would rate the effectiveness of this treatment in helping to control their myeloma. Among the 6 respondents, 1 answered it was “extremely effective,” 3 answered “very effective,” 1 answered “effective,” and 1 answered “not effective.”
Three of the 6 respondents answered that the overall side effects from idecabtagene vicleucel CAR T-cell immunotherapy were “very tolerable,” 2 answered they were “tolerable,” and 1 answered they were “somewhat tolerable.” Among the most frequent side effects seen in patients who participated in the idecabtagene vicleucel CAR T-cell immunotherapy trial, respondents (n = 6) reported neutropenia (n = 4) and decrease of cognitive abilities (n = 4) were the most bearable side effects. Other side effects considered most bearable by respondents were loss of physical abilities (n = 3), neuropathy (n = 3), pain (n = 3), muscle weakness (n = 3) and typical cold-like symptoms (n = 3).
Respondents were asked about the importance of not being on a treatment for their myeloma after idecabtagene vicleucel CAR T-cell immunotherapy, either for a prolonged or indeterminate period. Four of the 6 respondents answered it was “extremely important,” 1 answered “somewhat important,” and 1 answered, “not important.”
Five of the 6 respondents agreed that CAR T-cell therapy (idecabtagene vicleucel) met their expectations in treating myeloma. Quotes indicating respondents’ expectations included “I am so far in very, very good remission,” “I was in remission for about a year,” “Didn’t get depth of response as we were hoping,” “No more chemo!,” and “The required 2 weeks in hospital seemed very, very long.”
All 6 respondents agreed that CAR T-cell therapy (idecabtagene vicleucel) improved their long-term health outcomes. Three responded with “Yes, I’m still alive!,” “I would otherwise have run out of options, but more are now available,” and “I had it done 2 times and it gave me drug free time. I would do it again if they would allow me.”
Of the 6 respondents, 3 are still in remission, 1 indicated that their myeloma had just come back and they are about to start a new treatment soon, and 2 stated that their myeloma did come back and they are currently under a new treatment regimen.
Additional Information
Myeloma Canada highlighted that patients are looking for effective treatments. Given that no single treatment is effective for all myeloma patients, various treatment options must be available to improve patients’ prognoses and QoL. As represented in the patients’ responses, a CAR T-cell therapy can provide an important benefit for patients despite the number and severity of the side effects. Even though only a small number of respondents had experience with the treatment under review, about half of the respondents fit the criteria. For these patients, treatment options are becoming limited. Unfortunately, their lives depend on these treatment options because there is still no cure for myeloma.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process, providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy. In addition, as part of the idecabtagene vicleucel review, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, help identify and communicate situations in which there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, acquire further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion follows.
Unmet Needs
The clinical experts agreed that not all patients with MM respond to available treatments, and they eventually become refractory to all treatment options. These patients have a short life expectancy, and their remaining life is often highly medicalized. Treatments are needed to control the disease and provide patients with a break from therapy. The experts stated that there are few options after third- and fourth-line therapies, and the only standard options available after 3 therapies are palliation and supportive care. The majority of CAR T-cell treatments are financially burdensome either at the individual patient level or for the public health care system. Ideally, treatments should be affordable on a large scale.
Place in Therapy
The clinical experts consulted by CADTH acknowledged that idecabtagene vicleucel is a therapy with a different mechanism of action and therefore is appropriate for patients who have already been exposed to standard therapies and for whom continuing with standard therapies is not expected to have any further benefit. This treatment should only be given as monotherapy and not combined with other active agents. Formal clinical trials would be required to establish if this treatment can be complementary to other treatments. Based on current evidence, the clinical experts indicated that treatment should be used after patients become triple-exposed or double-refractory (i.e., following failure with or intolerance to lenalidomide and/or daratumumab and bortezomib-exposed). Treatment after patients become triple-exposed or double-refractory is inevitable as most other treatment options continue to be moved up into the front line. In the current treatment paradigm, CAR T-cell therapy would be well positioned in the third line (current Canadian approval) and fourth line. The clinical experts noted that, should daratumumab, bortezomib, lenalidomide, and dexamethasone be approved as a front-line therapy, CAR T cells could become a second-line option.
However, 1 of the clinical experts argued that it is unlikely CAR T cells will cause a shift in the current treatment paradigm as it is being considered as a last-line therapy, and it falls in line after current therapies. Given the toxicity of idecabtagene vicleucel, the expert stated that it is unlikely to move up in the treatment paradigm until more clinical trials are completed, and even then, only if superior efficacy compared with current standard therapies is demonstrated. The expert added that, while idecabtagene vicleucel may be tested in combination with other agents, those trials are far from complete.
Patient Population
The eligible population may be small because many patients already reach a palliative stage by fourth-line treatment due to rapid disease progression, age, or frailty and toxicities from prior treatments. Those patients who meet the inclusion criteria for the phase II trial would be the most appropriate and have the greatest unmet need. Patients with a good performance status and those who have been previously treated with or are refractory to proteosome inhibitors, IMiDs, and anti-CD38 monoclonal antibodies have an unmet need. Worse outcomes tend to occur if patients in rural communities forego important treatments just to stay closer to home and if patients with limited financial means are unable to pay for appropriate supportive care.
Clinical experts stated that the patients best suited for this treatment would be those with an ECOG status of 0 or 1, good organ status, and a willingness to travel (as this therapy will not be offered in smaller centres). Those with relapsed and refractory disease should be prioritized first. Younger, fit patients with the least number of prior therapies (3 prior lines) are most likely to benefit. Because idecabtagene vicleucel requires a certain level of fitness, the presence of comorbidities and fitness are important aspects to consider when determining whom to prioritize. Patients eligible for this novel therapy would need to fit as closely as possible the eligibility criteria of the phase II trial that is under review. If capacity limitations exist, then the relevant subgroups with the best response to this new agent should be assessed.
The clinical experts agreed that patients best suited for idecabtagene vicleucel would be identified using the inclusion and exclusion criteria from the study, and that clinical judgment should be based on prior therapies, patient comorbidities, and fitness. Clear, transparent, and evidence-based guidelines are important because capacity for treatment will likely be greater than the need. All standard diagnostic and baseline tests are available broadly in Canada. Once patients with relapsed or refractory disease are recognized, it is recommended that health regions and/or provinces form adjudication committees that can provide a recommendation about patient eligibility for this treatment to remove bias as to which patients may be eligible for this treatment.
Patients the least suitable for treatment with idecabtagene vicleucel would be those with a poor performance status and those with other options available with a reasonable duration of disease control. Additionally, patients who are frail, elderly, or have significant renal failure, neurologic disease, and an ECOG status of at least 2 related to myeloma would be the least suitable candidates for idecabtagene vicleucel. In general, the patients least suitable for treatment would be those who do not resemble the eligibility criteria of the pivotal trial under review.
Assessing Response to Treatment
The clinical experts agreed that a PFS of longer than 6 months and an OS of greater than 1 year without life-threatening toxicities would be clinically meaningful responses to treatment. They stated that the standard assessment of treatment response would be appropriate. Standard assessment would be conducted every month using serum protein electrophoresis or FLC testing for at least 1 year, after which assessments would be less frequent. However, there currently are no published data on re-treatment with this drug. Should published data indicate that re-treatment with this drug is efficacious, then it should be considered on a case-by-case basis when sufficient supplies of cryopreserved drugs are available.
Discontinuing Treatment
The clinical experts agreed that discontinuing CAR T-cell treatment is not applicable because once therapy is initiated, it is not able to be modified, stopped, or reversed. It is a 1-time infusion of cells; hence, discontinuation of treatment is difficult to perform as the effect is largely irreversible once administered. However, patients who become unwell before infusion may be deemed too sick to proceed with infusion.
Prescribing Conditions
Idecabtagene vicleucel must be administered in a setting supervised by specialists trained in bone marrow transplants, or a tertiary centre that is familiar with complications related to stem cell transplants or is able to accommodate phase I trials, with adequate ICU, emergency, neurology, and infectious disease departments. This will limit availability for some patients. In Canada these centres are those that are administering blood marrow transplants at institutions across the country accredited by Health Canada and the Foundation for the Accreditation of Cellular Therapy.
Clinical experts agreed that a specialist is required to diagnose, treat, and monitor patients who receive idecabtagene vicleucel. It would require a hematologist or oncologist with specific experience in cellular therapy; the majority of these experts would also have stem cell transplant experience.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Two clinician groups provided input on the reimbursement review of idecabtagene vicleucel for the treatment of adult patients with MM who have received at least 3 prior therapies, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody.
The CMRG is a charitable organization of myeloma physicians from 22 academic centres in Canada. The CMRG’s main purposes include conducting investigator-initiated academic clinical trials for myeloma patients, maintaining a national myeloma database, and generating consensus statements for myeloma management. The input provided to CADTH for the submission of idecabtagene vicleucel was drafted by the CMRG’s chief medical officer and sent to all members for input. The clinicians who agreed with and commented on the input were included as part of the input.
The Ontario Health Hematology Cancer DAC provides evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including provincial drug reimbursement programs and the systemic treatment program. For the review of idecabtagene vicleucel, the Ontario Health DAC collected information via email.
Unmet Needs
The Ontario Health Hematology Cancer DAC noted that the current treatment goal for patients is to prolong life, delay disease progression, and control disease. The CMRG added that controlling disease manifestations (bone destruction and pain, renal failure, hypercalcemia, and low blood counts), maintaining the control of the myeloma and its manifestations (PFS), minimizing adverse effects and caregiver burden, and optimizing QoL are current treatment goals.
The DAC noted that currently available treatments have low response rates and short durations of response. The CMRG added that myeloma remains incurable, and patients will eventually become refractory to all available agents. The CMRG also added that about 15% of patients have extremely aggressive disease at diagnosis and die within 1 to 2 years despite all therapies. In addition, the group noted that many patients will experience increasingly aggressive disease with time; at some point, patients succumb to their disease and often have a miserable QoL in the end stages. The CMRG noted that some treatments are not publicly funded despite Health Canada approval, and that in some instances only privately insured patients can access these potentially life-extending therapies, which poses an ethical challenge for patients, caregivers, and health care providers.
Patients with the greatest unmet need according to the DAC are those whose life expectancy is limited, including triple-exposed patients. The group noted that the drug under review would address this unmet need. However, according to the clinician groups, there may be challenges in delivering this drug in patients with comorbidities and low blood counts.
The CMRG added that the greatest unmet need is for patients who have failed therapy with proteasome inhibitors, IMiDs, and anti-CD38 monoclonal antibodies, as no effective therapy is available, and that the drug under review would address this unmet need.
Place in Therapy
Both the Ontario Health DAC and the CMRG noted that, as per the clinical trial, the drug under review would be most appropriate for patients who have been triple-exposed to MMRM therapies. The CMRG noted that the drug addresses the underlying malignancy and would be used in sequence after the other lines of therapy discussed earlier in this summary.
The DAC noted that there is insufficient information to determine whether it would be appropriate for patients to try other treatments before idecabtagene vicleucel. They cautioned that the risk of treating patients with other regimens such as Cd may result in organ dysfunction or treatment-related toxicities that could make the delivery of CAR T-cell therapy difficult. The CMRG added that no other effective drugs are available other than idecabtagene vicleucel in the fourth-line setting.
With respect to sequencing, the Ontario Health Hematology Cancer DAC noted that there is no sequencing information available other than that from the triple-exposed population. The CMRG added that, after failure of idecabtagene vicleucel, patients would most likely only be offered palliative radiotherapy and other supportive measures. The group noted that all effective and/or funded regimens have already been used. The CMRG added that many clinical trials of new immunotherapies exclude patients who have received anti-BCMA immunotherapy (such as idecabtagene vicleucel) from receiving another agent targeting BCMAs. Because BCMAs are the most common targets of new immunotherapeutic platforms, subsequent trial participation would be limited.
Patient Population
The Ontario Health DAC noted no information is available to identify the patient subgroups most likely to respond to treatment. The DAC added that the clinical trial recruited patients with a good performance status.
The CMRG noted that patients with other poor prognosis factors, such as extramedullary disease and experience with high-risk cytogenetics, do not fare significantly worse, and older age does not appear to be an exclusion factor. The group added that, from a practical point of view, patients whose disease is “progressing at a rate anticipated to allow them to remain stable and relatively well during the 4-5 week waiting time for CAR T-cell processing would be best suited for this treatment in order to avoid significant attrition.”
The DAC noted that patients best suited for the treatment should be identified through BCMA staining, which is not currently part of routine testing. They added that patients can be identified by applying routine criteria for myeloma relapse or progression. The CMRG added that identifying patients who should be treated with the drug under review will require careful matching of available resources with the potential numbers of patients with relapsed myeloma. Idecabtagene vicleucel patients would require an inpatient bed for approximately 2 weeks (or longer if complications occur) and may require readmission. The CMRG added that these patients require potentially expensive ancillary measures to treat CRS, neurotoxicity, and infections, and may need ICU support. Specialized training is required for staff, and each medical centre’s infrastructure and clinical pathways must be specific to meet the safety standards for treatment and follow-up. Appropriate guidelines need to be established.
The DAC noted that patient selection should align with the inclusion and exclusion criteria of the trial for treatment; those that do not align are least suited. The CMRG added that frail patients, those with rapidly proliferating disease, ongoing infection, and significant organ dysfunction, and patients with pre-existing pancytopenia would be least suitable for treatment with the drug under review.
The DAC added that no data are available to predict which patients are most likely to exhibit a response. However, the CMRG noted that patients with a good performance status and organ function, minimal or no comorbidities, robust blood counts, low tumour burden, and indolent disease are most likely to have the best outcomes. The CMRG added that, given the similar response and PFS rates in subset analysis of the clinical trials for the drug under review, it will likely be easier to develop exclusion criteria than inclusion criteria.
Assessing Response to Treatment
According to the Ontario Health DAC, outcomes that are used to assess whether a patient responding to treatment in clinical trials should be the standard myeloma response criteria. The CMRG added that responses are based on the monoclonal protein marker in the serum and/or urine, bone marrow biopsy, and in some instances imaging studies. The CMRG also added that these align with the criteria used in clinical trials and include the emerging parameter of marrow MRD.
To assess clinically meaningful responses, the DAC noted that at least a partial response (PR) should be present. As per myeloma response criteria, such responses include improvement in blood counts, improvement in end organ function (i.e., renal function), reduction in skeletal events (i.e., bone pain or fractures), and overall improvement in QoL. The CMRG noted that clinically meaningful responses usually correlate with at least a partial remission as defined by IMWG consensus criteria. The CMRG added that these include improvement in symptoms (cessation of bone destruction with less pain, fractures, and need for radiotherapy), energy levels, and ability to perform daily activities.
According to the DAC, assessment for responses should be conducted every 1 to 2 months. However, the CMRG noted that, in myeloma, responses are generally assessed every 2 to 3 months, depending on clinical stability.
Discontinuing Treatment
Both the Ontario Health DAC and the CMRG noted that discontinuation criteria for the treatment is not applicable as this is usually a single treatment.
Prescribing Conditions
The DAC noted that delivery of the drug under review will be at tertiary hospitals and transplant centres with expertise in cellular therapy. The CMRG added that this therapy is appropriate for a major medical facility with expertise in other cellular therapies for hematologic malignancies. The group noted that close interactions between a specialized inpatient service, an ICU familiar with immunosuppressed cancer patients, and an outpatient facility experienced in handling urgent hematologic problems are necessary. The CMRG noted that appropriate coordination with the emergency department to expedite care of patients recently discharged following treatment with the drug under review is also required.
Drug Program Input
Drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in the following section.
Jurisdictional Context
Relevant Comparators
The PAG noted that the choice of comparator in the submitted trial would need special consideration as there is no clear standard of care (i.e., when reaching the fourth line of therapy). The sponsor used several comparators based on the real-world NDS-MM-03 trial (i.e., pomalidomide plus dexamethasone, pomalidomide plus bortezomib plus dexamethasone, Cd, carfilzomib plus cyclophosphamide plus dexamethasone, Vd, and CyBorD). At this point, fourth-line treatment options would be cyclophosphamide plus dexamethasone, Vd, or CyBorD (which are funded by most jurisdictions). Although pomalidomide plus bortezomib plus dexamethasone was recently reviewed by CADTH with a reimbursement with conditions recommendation, it is not yet funded. Pomalidomide plus dexamethasone, Cd, and cyclophosphamide plus dexamethasone are typically not funded, although a few jurisdictions may consider them on a case-by-case basis. The clinical experts consulted by CADTH agreed with these assertions.
Policy Considerations for Reimbursing the Drug
Considerations for Initiation of Therapy
The PAG posed some questions related to decision-making, such as:
What patient (or disease) characteristics would be important in determining who should be treated with this therapy?
If capacity limitations exist, how should medical staff prioritize which patients are offered idecabtagene vicleucel?
Do patients need to have disease considered refractory to an IMiD, a proteasome inhibitor, and an anti-CD38 antibody to receive idecabtagene vicleucel?
The characteristics of patients who should receive idecabtagene vicleucel are described in the clinician input section of this report. The clinician groups also stated that any patient with prior treatments with IMiD, proteasome inhibitor, or anti-CD38 antibodies should be allowed to receive treatment with idecabtagene vicleucel. The only unresolved concern was the exact line of therapy to recommend when initiating CAR T-cell treatment, as many patients could be considered refractory at different lines of therapy (i.e., second to fifth lines). They also noted that prioritization of the therapy would be a rare concern and should be made on a case-by-case basis; the same conclusion was drawn for the re-treatment considerations.
Considerations for Prescribing
The PAG identified areas associated with prescribing idecabtagene vicleucel, most notably that access would be limited to jurisdictional capacity. Given that the sponsor plans to establish 12 sites across Canada, out-of-province care may be needed for proper administration of the drug under review. Also, specialized centres need to be trained and accredited by the sponsor, limiting the availability of clinics where the therapy can be provided. There is a high human resource burden to obtain and maintain certification (including developing various protocols and supporting yearly audits). Similarly, access and prolonged stay in (or near) specialized centres, particularly for patients from remote areas, are needed, as is the ability to coordinate patient care and product preparation with an external organization or manufacturer. Several manufacturers may provide CAR T-cell therapies and there is an administrative burden on specialized sites to manage various protocols and systems for preparation and delivery of each product type.
Special Implementation Issues
Generalizability
The PAG noted that there may be potential for “indication creep” to earlier lines of therapy if, for example, triple-class exposure occurs in the first 2 lines of therapy. The PAG noted that the current sponsor request is for the use of idecabtagene vicleucel after 3 prior therapies, and the provisional algorithm and the budget impact analysis includes a scenario to use idecabtagene vicleucel in a third-line setting. Although the economic submission is based primarily on the KarMMa trial (≥ 3 prior regimens), the sponsor included KarMMa-3 (inclusion criteria of at least 2 but no greater than 4 prior MM regimens). It was therefore considered important to establish what would be the line of therapy (e.g., third or fourth) for idecabtagene vicleucel and which patient populations would be outside the scope of the reviewed indication. Furthermore, idecabtagene vicleucel may change the place in therapy of other (comparator) drugs and in subsequent lines.
Care Provision Issues
The PAG highlighted the adjacent use of resources with idecabtagene vicleucel patients, including leukapheresis, cell processing, and use of bridging and LDC. The management of adverse effects will also require indirect costs for nursing, hospital beds, ICUs, and administration of tocilizumab to treat CRS.
The trial protocol required bridging therapy (e.g., daratumumab), which may not be publicly funded. Clinical experts consulted by CADTH agreed that it would be important to discuss the impact and feasibility of this strategy in real-world practice.
According to the experts, there will be no need for BCMA testing (which was an exploratory objective in the trial), although they agreed that there are few data on which to base decision-making with high certainty.
No items were identified by PAG in relation to considerations for renewal or discontinuation of idecabtagene vicleucel therapy.
Clinical Evidence
The clinical evidence included in the review of idecabtagene vicleucel is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the literature that met the selection criteria specified in the review. The third section is intended to include sponsor-submitted, long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review. No additional evidence was identified for this review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of idecabtagene vicleucel for the treatment of adult patients with MM who have received at least 3 prior therapies, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 4. Outcomes included in the CADTH review protocol reflect those considered to be important to patients, clinicians, and drug plans.
The systematic review protocol was established before the granting of a Notice of Compliance from Health Canada.
Table 4: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adult patients with multiple myeloma who have received at least 3 prior therapies, including an immunomodulatory agent, a proteasome inhibitor, and anti-CD38 antibodies Subgroups:
|
Intervention | Idecabtagene vicleucel, (IV infusion target dose of 450 × 106 CAR T cells, within a range of 150 × 106 to 540 × 106 CAR T cells) |
Comparators | Drug regimens used as palliative care:
|
Outcomes | Efficacy outcomes
Harms outcomes
|
Study design | Published and unpublished phase II, III, and IV RCTs |
AE = adverse event; ASCT = autologous stem cell transplant; BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; CR = complete response; CRS = cytokine release syndrome; cyclo = cyclophosphamide; DoR = duration of response; ECOG = Eastern Cooperative Oncology Group; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myeloma Module with 20 items; EQ-5D-5L = EuroQoL 5-Dimension 5-Levels questionnaire; HRQoL = health-related quality of life; ICANS = immune effector cell-associated neurotoxicity syndrome; ISS = International Staging System; IVIG = intravenous immunoglobulin; Kd = carfilzomib plus dexamethasone; KRd = carfilzomib plus lenalidomide plus dexamethasone; MRD = minimal residual disease; ORR = overall response rate; OS = overall survival; Pd = pomalidomide plus dexamethasone; PFS = progression-free survival; RCT = randomized controlled trial; Rd = lenalidomide plus dexamethasone; SAE = serious adverse event; TNT = time to next treatment; TTP = time to progression; TTR = time to response; Vd = bortezomib plus dexamethasone; WDAE = withdrawal due to adverse event.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies checklist (https://www.cadth.ca/resources/finding-evidence/press).20
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were idecabtagene vicleucel. Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, Canadian Partnership Against Cancer Corporation’s Canadian Cancer Trials, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on January 21, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on May 13, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist (https://www.cadth.ca/grey-matters).21 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Findings From the Literature
Of the 70 citations identified in the literature search, none were relevant according to the inclusion criteria and all were excluded, while 10 potentially relevant full-text reports from other sources were retrieved for scrutiny. One report describing 1 study is included in the CADTH systematic review. (Figure 1).
The included studies are summarized in Table 5. A list of excluded studies is presented in Appendix 2.
![Depicts the 70 citations identified in the literature search, none were relevant according to the inclusion criteria and all were excluded, while 10 potentially relevant full-text reports from other sources were retrieved for scrutiny. One report describing 1 study is included in the CADTH systematic review]](https://canjhealthtechnol.ca/index.php/cjht/article/download/pc0240r/version/251/493/1602/PG0240CL-fig01.png)
Table 5: Details of the Included Study — BB2121-MM-001 (KarMMa)
Detail | Description |
|---|---|
Designs and populations | |
Study design | Phase II, open-label, multi-centre, single-arm |
Locations | 20 sites (9 in the US, 1 in Canada, 2 in Spain, 2 in Italy, 3 in Germany, 2 in France, and 1 in Belgium) |
Patient enrolment dates | Date first patient enrolled: December 13, 2017 Date last patient enrolled: November 13, 2018 The study is ongoing for posttreatment follow-up |
Enrolled (N) | 140 patients |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Idecabtagene vicleucel, (IV infusion at a target dose of 150 × 106, 300 × 106, or 450 × 106 CAR T cells, within a dose range of 150 × 106 to 540 × 106 CAR T cells) |
Comparator(s) | No comparator arm included |
Duration | |
Phase | |
Pretreatment |
|
Treatment |
|
Posttreatment | 24 months (safety follow-up and efficacy assessment post–idecabtagene vicleucel infusion; re-treatment allowed) |
Outcomes | |
Primary end point | Overall response rate |
Secondary and exploratory end points | Secondary Complete response Time to response Duration of response Progression-free survival Time to progression Overall survival Safety Pharmacokinetics Immunogenicity Minimal residual disease Health-related quality of life: EORTC QLQ-C30; EQ-5D-5L; EORTC QLQ-MY20 Exploratory Biomarkers Participant experience with idecabtagene vicleucel Hospital resource utilization MRD using flow cytometry PFS on next regimen Time to progression on last prior regimen |
Notes | |
Publications | Munshi (2021)22 |
BCMA = B-cell maturation antigen; CNS = central nervous system; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-MY20 = Quality of Life Questionnaire Myeloma Module with 20 items; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; FLC = free light chain; HBV = hepatitis B virus; HCV = hepatitis C virus; INR = international normalized ratio; MRD = minimal residual disease; POEMS = polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, and skin changes; PPT = partial thromboplastin time; RRMM = relapsed or refractory multiple myeloma; TTP = time to progression; TTR = time to response.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Description of Studies
The KarMMa study was a phase II, open-label, multi-centre, single-arm trial conducted in 20 sites in the US, Spain, Italy, Germany, France, and Belgium, and 1 site in Canada. The study was run from January 3, 2018, when the first patient was enrolled, to the last data cut-off date of October 16, 2019. The main objective of the study was to evaluate the efficacy, defined as the ORR of idecabtagene vicleucel in patients with RRMM. Secondary objectives included the assessment of safety of idecabtagene vicleucel and other measures of efficacy and HRQoL, as described in Table 5. The study consisted of 3 periods:
pretreatment (screening, leukapheresis, and bridging therapy, if needed)
treatment (LDC and idecabtagene vicleucel infusion)
posttreatment (post–idecabtagene vicleucel infusion).
The overall design of the study in the pretreatment and treatment periods is depicted in Figure 2.
Figure 2: Pretreatment and Treatment of Patients During the Study
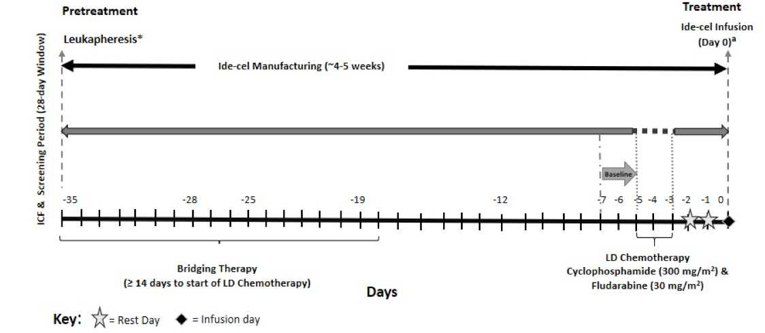
ICF = informed consent form; Ide-cel = idecabtagene vicleucel; LD = lymphodepletion.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
The pretreatment period consisted of the screening process, during which patients were evaluated for their suitability to enter the study. Patients who accepted and were enrolled underwent leukapheresis to enable idecabtagene vicleucel product generation, manufactured on a per-patient basis. At the clinical investigator’s discretion, patients could receive bridging therapy for myeloma control following leukapheresis while idecabtagene vicleucel was being manufactured, as long as the last dose of bridging therapy was administered at least 14 days before the initiation of LDC. Bridging therapies could include corticosteroids, alkylating agents, IMiDs, proteasome inhibitors, and/or anti-CD38 antibodies as single agents or in combination.
The treatment period began with the LDC. Patients who were eligible received a 3-day cycle of LDC with fludarabine and cyclophosphamide beginning 5 days before the target idecabtagene vicleucel infusion date. When LDC was completed, the idecabtagene vicleucel infusion was administered within a dose range of 150 × 106 to 540 × 106 CAR T cells per infusion. Before proceeding with idecabtagene vicleucel infusion, the patient’s clinical status must not have significantly worsened. The maximum dose (540 × 106 CAR T cells) was defined by the upper limit of 450 × 106 CAR T cells plus 20%. Patients were required to be hospitalized from the day of idecabtagene vicleucel infusion through day 14 post-infusion to monitor the risk of developing CRS and neurotoxicity.
After infusion with idecabtagene vicleucel, patients began the posttreatment period. In this safety phase, idecabtagene vicleucel expansion and persistence, HRQoL, myeloma response, disease status, and other end points were assessed at prespecified time intervals for all patients and will continue to be assessed for a minimum of 24 months from idecabtagene vicleucel infusion or until documented disease progression, whichever is longer. Patients with PD within 24 months of idecabtagene vicleucel infusion remain on the study and have select assessments collected until month 24. Patients who remain progression-free will have assessments collected for up to 5 years.
Re-treatment with a second infusion of idecabtagene vicleucel, including a second course of LDC, with or without bridging therapy, was allowed after disease progression if protocol-specified eligibility (inclusion and exclusion) criteria were met.
Amendments and Changes in the Conduct of the Study
Four protocol amendments were implemented during the conduction of the KarMMa study. The original protocol was amended 4 times before the data cut-off date of October 16, 2019. The first amendment modified the overall safety management plans in response to a then-recent SAE (a grade 4 neurotoxicity event) that occurred in the idecabtagene vicleucel phase I study. Amendment 2.0 was written to increase the idecabtagene vicleucel dose range, increase the sample size, modify the idecabtagene vicleucel overdose definition, and to incorporate feedback from health authorities. Amendment 3.0 provided further guidance on intercurrent illness or toxicity that is considered to place the subject at undue risk of proceeding to idecabtagene vicleucel infusion and for which idecabtagene vicleucel infusion should be delayed. Amendment 4.0 changed the MRD assessment by EuroFlow from a secondary objective and end point to an exploratory objective and end point. Specific points for the amendments to the protocol are summarized in Table 6.
Table 6: Summary of Protocol Amendments in the KarMMa trial
Amendment | Key changes to original protocol (as of August 25, 2017) |
|---|---|
Protocol Amendment 1.0 (November 9, 2017) | To modify the overall safety management plans in response to a then-recent serious adverse event (a grade 4 neurotoxicity event) that occurred in the idecabtagene vicleucel phase I study (CRB-401). Eligibility criteria were updated to exclude patients with a previous history of subarachnoid hemorrhage or other CNS bleed and patients on therapeutic anticoagulation due to the increased risk of coagulopathy and bleeding associated with CRS and neurotoxicity. In addition, Waldenstrom, POEMS, or clinically significant amyloidosis were added to the exclusion criteria. The exclusion criteria for defining adequate bone marrow function at screening was modified to an ANC < 1,000 cells/mm3 and a platelet count < 50,000 cells/mm3, with the requirement that those counts be achieved in the absence of growth factor or transfusion support. The overall safety monitoring plan was updated, including the addition of a required 14-day hospitalization after idecabtagene vicleucel infusion and twice-weekly visits during week 3 and week 4. |
Protocol Amendment 2.0 (June 14, 2018) | Written to 1) increase the idecabtagene vicleucel dose range, 2) increase the sample size, 3) modify the idecabtagene vicleucel overdose definition, and 4) incorporate feedback from health authorities. Significant changes included in this amendment are summarized as follows:
|
Protocol Amendment 3.0 (September 28, 2018) | Written in response to a death within 28 days of idecabtagene vicleucel infusion in Study MM-001, to provide further guidance on intercurrent illness or toxicity that is considered to place the subject at undue risk of proceeding to idecabtagene vicleucel infusion and for which idecabtagene vicleucel infusion should be delayed. Specific criteria were added to the idecabtagene vicleucel infusion procedures section of the protocol. |
Protocol Amendment 4.0 (||||||||||||||||||||||||||||||||||||||||) | Written primarily to change the MRD assessment by EuroFlow from a secondary objective and end point to an exploratory objective and end point. Other changes included:
|
ANC = absolute neutrophil count; BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; CNS = central nervous system; EMP = extramedullary plasmacytoma; MRD = minimal residual disease; POEMS = polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, and skin changes.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria of the KarMMa study are listed in Table 5. Briefly, the KarMMa study included patients with a diagnosis of RRMM who had received at least 3 prior antimyeloma therapy (AMT) regimens, were refractory to the last regimen received (defined as documented progressive disease during or within 60 days of completing treatment with the last antimyeloma drug regimen), and had been previously treated with an IMiD, a proteasome inhibitor, and an anti-CD38 antibody. Induction with or without a hematopoietic stem cell transplant and with or without maintenance therapy was considered a single regimen. Patients with solitary plasmacytomas, previous allogeneic stem cell transplant, relevant central nervous system (CNS) pathology, inadequate bone marrow function, and liver, renal, and other hematologically relevant conditions were excluded.
In addition, given that enrolled patients had RRMM and were refractory to their last line of therapy, it was expected that hematologic and organ function could worsen during the window between leukapheresis and initiation of LDC. To be eligible for LDC, antimyeloma bridging therapy must have been stopped 14 days before start of LDC, and patients were required to have adequate bone marrow, hepatic, and renal function, no infections or intercurrent illnesses, and adequate international normalized ratio and partial thromboplastin time.
Baseline Characteristics
Overall, key baseline characteristics of the enrolled population (n = 140) were broadly similar to those of the rest of the populations treated with idecabtagene vicleucel. Median ages in treatment groups were in a range of 54 years to 62 years, with a median of 60.5 years in the enrolled population; only a minority of all patients (3.6%) were in the group older 75 years of age. Most patients were male (58.6%) and White (80.7%), with similar distributions in the treated populations. The ECOG performance status was also similar between treatment populations, with the majority of patients established at an ECOG status of 1 (53.1% in the total population) and only 3 patients with a status of 3. All demographic and baseline characteristics for the enrolled population and the population treated with idecabtagene vicleucel are provided in Table 7.
The median duration of the disease was about 6 years in the enrolled and treated population, which is expected in patients with RRMM who have undergone several prior treatment regimens, according to the clinical experts consulted by CADTH. More than half of patients had been treated with 7 or more antimyeloma regimens, and more than 90% had received a stem cell transplant and radiation therapy. Most patients enrolled in the KarMMa study were double-refractory (in this case, more than 87% to an IMiD and proteasome inhibitor), and 26% of the enrolled population were penta-refractory. Most patients (> 85%) received bridging therapy while idecabtagene vicleucel was manufactured.
Table 7: Summary of Baseline Characteristics for the Enrolled Population and the Population Treated With Idecabtagene Vicleucel
Characteristic | Population treated with idecabtagene vicleucel Idecabtagene vicleucel (CAR T cells) target dose | Enrolled population N = 140 | |||
|---|---|---|---|---|---|
150 × 106 N = 4 | 300 × 106 N = 70 | 450 × 106 N = 54 | Total 150 × 106 to 450 × 106 N = 128 | ||
Age, years, median (minimum to maximum) | 54.0 (49 to 69) | 60.5 (33 to 76) | 62.0 (43 to 78) | 60.5 (33 to 78) | 60.5 (33 to 78) |
Age category, n (%) | |||||
< 65 years | 3 (75.0) | 47 (67.1) | 33 (61.1) | 83 (64.8) | 92 (65.7) |
≥ 65 years | 1 (25.0) | 23 (32.9) | 21 (38.9) | 45 (35.2) | 48 (34.3) |
< 75 years | 4 (100.0) | 69 (98.6) | 51 (94.4) | 124 (96.9) | 135 (96.4) |
≥ 75 years | 0 | 1 (1.4) | 3 (5.6) | 4 (3.1) | 5 (3.6) |
Sex, n (%) | |||||
Male | 4 (100.0) | 38 (54.3) | 34 (63.0) | 76 (59.4) | 82 (58.6) |
Female | 0 | 32 (45.7) | 20 (37.0) | 52 (40.6) | 58 (41.4) |
Race, n (%) | |||||
Asian | 0 | 3 (4.3) | 0 | 3 (2.3) | 3 (2.1) |
Black or African-American | 0 | 3 (4.3) | 3 (5.6) | 6 (4.7) | 8 (5.7) |
White | 4 (100.0) | 58 (82.9) | 41 (75.9) | 103 (80.5) | 113 (80.7) |
Unknown | 0 | 2 (2.9) | 8 (14.8) | 10 (7.8) | 10 (7.1) |
Other | 0 | 4 (5.7) | 2 (3.7) | 6 (4.7) | 6 (4.3) |
Ethnicity, n (%) | |||||
Hispanic or Latino | 0 | 7 (10.0) | 4 (7.4) | 11 (8.6) | 13 (9.3) |
Not Hispanic or Latino | 4 (100.0) | 58 (82.9) | 41 (75.9) | 103 (80.5) | 112 (80.0) |
Not reported | 0 | 1 (1.4) | 8 (14.8) | 9 (7.0) | 9 (6.4) |
Unknown | 0 | 4 (5.7) | 1 (1.9) | 5 (3.9) | 6 (4.3) |
Weight, kg, median (range) | 86.9 (69.4 to 96.5) | 76.1 (42.6 to 125.6) | 77.1 (48.0 to 106.1) | 76.3 (42.6 to 125.6) | 76.0 (42.6 to 125.6) |
ECOG performance status, n (%) | |||||
0 | 3 (75.0) | 31 (44.3) | 23 (42.6) | 57 (44.5) | 60 (42.9) |
1 | 1 (25.0) | 38 (54.3) | 29 (53.7) | 68 (53.1) | 77 (55.0) |
2a | 0 | 1 (1.4) | 2 (3.7) | 3 (2.3) | 3 (2.1) |
Time since initial diagnosis, years, median (range) | 9.5 (6.0 to 12.3) | 6.6 (1.7 to 17.9) | 5.8 (1.0 to 16.8) | 6.0 (1.0 to 17.9) | 6.0 (1.0 to 17.9) |
Presence of extramedullary plasmacytoma, n (%) | |||||
Yes | 0 | 34 (48.6) | 16 (29.6) | 50 (39.1) | 52 (37.1) |
No | 4 (100.0) | 36 (51.4) | 38 (70.4) | 78 (60.9) | 85 (60.7) |
Missing | 0 | 0 | 0 | 0 | 3 (2.1) |
|||||||||||||||||||||||||||||||||||||||| | |||||
| |||||| | |||||| | |||||| | |||||| | |||||| |
||||||||||||||||| | ||||||||||| | ||||||||||| | |||||||||| | ||||||||||| | |||||||||| |
Tumour burden (based on BM biopsy CD138+ plasma cell), n (%) | |||||
Low (< 50%) | 1 (25.0) | 33 (47.1) | 23 (42.6) | 57 (44.5) | 62 (44.3) |
High (≥ 50%) | 3 (75.0) | 34 (48.6) | 28 (51.9) | 65 (50.8) | 70 (50.0) |
Missing | 0 | 3 (4.3) | 3 (5.6) | 6 (4.7) | 8 (5.7) |
Tumour BCMA expression, n (%) | |||||
< 50% BCMA+ | 0 | 1 (1.4) | 2 (3.7) | 3 (2.3) | 3 (2.1) |
≥ 50% BCMA+ | 4 (100.0) | 60 (85.7) | 45 (83.3) | 109 (85.2) | 109 (77.9) |
Unknown | 0 | 9 (12.9) | 7 (13.0) | 16 (12.5) | 28 (20.0) |
R-ISS stage at baseline (derived),b n (%) | |||||
Stage I | 0 (0.0) | 12 (17.1) | 2 (3.7) | 14 (10.9) | 14 (10.0) |
Stage II | 3 (75.0) | 43 (61.4) | 44 (81.5) | 90 (70.3) | 97 (69.3) |
Stage III | 1 (25.0) | 12 (17.1) | 8 (14.8) | 21 (16.4) | 26 (18.6) |
Baseline cytogenetic risk,c n (%) | |||||
High riskd | 1 (25.0) | 20 (28.6) | 24 (44.4) | 45 (35.2) | 46 (32.9) |
Non–high risk | 3 (75.0) | 38 (54.3) | 25 (46.3) | 66 (51.6) | 73 (52.1) |
Not evaluable/missing | 0 | 12 (17.1) | 5 (9.3) | 17 (13.3) | 21 (15.0) |
Number of prior antimyeloma regimens,e median range) | 8.5 (4 to 12) | 6.0 (3 to 16) | 5.0 (3 to 13) | 6.0 (3 to 16) | 6.0 (3 to 17) |
Distribution of prior antimyeloma regimens, n (%) | |||||
3 | 0 | 8 (11.4) | 7 (13.0) | 15 (11.7) | 16 (11.4) |
4 | 1 (25.0) | 8 (11.4) | 10 (18.5) | 19 (14.8) | 20 (14.3) |
5 | 0 | 11 (15.7) | 11 (20.4) | 22 (17.2) | 23 (16.4) |
6 | 1 (25.0) | 12 (17.1) | 10 (18.5) | 23 (18.0) | 25 (17.9) |
≥ 7 | 2 (50.0) | 31 (44.3) | 16 (29.6) | 49 (38.3) | 56 (40.0) |
Prior stem cell transplant for MM,f n (%) | |||||
Yes | 4 (100.0) | 67 (95.7) | 49 (90.7) | 120 (93.8) | 131 (93.6) |
1 prior transplant | 1 (25.0) | 44 (62.9) | 31 (57.4) | 76 (59.4) | 82 (58.6) |
> 1 prior transplant | 3 (75.0) | 23 (32.9) | 18 (33.3) | 44 (34.4) | 49 (35.0) |
No | 0 | 3 (4.3) | 5 (9.3) | 8 (6.3) | 9 (6.4) |
Prior radiation therapies for MM, n (%) | 2 (50.0) | 45 (64.3) | 24 (44.4) | 71 (55.5) | 75 (53.6) |
Prior refractory status, n (%) | |||||
Immunomodulatory agent | 4 (100.0) | 70 (100.0) | 52 (96.3) | 126 (98.4) | 138 (98.6) |
Proteasome inhibitor | 4 (100.0) | 63 (90.0) | 49 (90.7) | 116 (90.6) | 126 (90.0) |
Anti-CD38 antibodies | 4 (100.0) | 66 (94.3) | 50 (92.6) | 120 (93.8) | 131 (93.6) |
Daratumumab | 3 (75.0) | 61 (87.1) | 45 (83.3) | 109 (85.2) | 120 (85.7) |
Immunomodulatory agent and PI (double-refractory) | 4 (100.0) | 63 (90.0) | 47 (87.0) | 114 (89.1) | 124 (88.6) |
Immunomodulatory agent, PI, and anti-CD38 antibodies (triple-refractory) | 4 (100.0) | 60 (85.7) | 44 (81.5) | 108 (84.4) | 117 (83.6) |
Penta-refractoryg | 1 (25.0) | 24 (34.3) | 8 (14.8) | 33 (25.8) | 37 (26.4) |
Any bridging therapies for MM, n (%) | 4 (100.0) | 61 (87.1) | 47 (87.0) | 112 (87.5) | 119 (85.0) |
Measurable disease at baseline,h n (%) | |||||
Yes | 4 (100.0) | 65 (92.9) | 53 (98.1) | 122 (95.3) | 122 (87.1) |
No | 0 | 5 (7.1) | 1 (1.9) | 6 (4.7) | 6 (4.3) |
Not available | 0 | 0 | 0 | 0 | 12 (8.6) |
BCMA = B-cell maturation antigen; BM = bone marrow; ECOG = Eastern Cooperative Oncology Group; LDC = lymphodepleting chemotherapy; MM = multiple myeloma; PI = proteasome inhibitor; PS = performance status; R-ISS = Revised International Staging System.
Note: Data cut-off date = October 16, 2019.
aThese patients had ECOG scores of less than 2 at screening for eligibility but subsequently deteriorated to ECOG scores of 2 at baseline before start of LDC.
bDerived R-ISS was calculated using baseline R-ISS stage, cytogenetic abnormality, and serum lactate dehydrogenase.
cBaseline cytogenetic abnormality was based on baseline cytogenetics from central laboratory if available. If a central laboratory was not available or was unknown, cytogenetics before screening was used.
dHigh-risk defined as deletion in chromosome 17p (del[17p]), translocation involving chromosomes 4 and 14 (t[4;14]), or translocation involving chromosomes 14 and 16 (t[14;16]).
eInduction with or without hematopoietic stem cell transplant and with or without maintenance therapy was considered a single regimen.
fPatients who had received a prior allogeneic stem cell transplant were excluded from the study per-protocol eligibility criteria and therefore all prior stem cell transplant information collected in the study was in reference to prior autologous stem cell transplantation.
gPenta-refractory is defined as refractory to all of lenalidomide, pomalidomide, bortezomib, carfilzomib, and daratumumab.
hMeasurable disease was determined by an independent response committee according to International Myeloma Working Group criteria.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Interventions
After informed consent was obtained and screening eligibility was met, patients were enrolled and underwent leukapheresis to enable production of idecabtagene vicleucel. Idecabtagene vicleucel was manufactured on a per-patient basis and there was expected variability in the number of CAR T cells that were manufactured for each patient. Patients who had a product manufacturing failure or a product manufactured with a dose of less than 150 × 106 CAR T cells could proceed to a second leukapheresis.
When necessary, patients could have received bridging therapy for myeloma disease control following leukapheresis while idecabtagene vicleucel was being manufactured (Figure 2). Bridging therapies could have included corticosteroids, alkylating agents, IMiDs, proteasome inhibitors, and/or anti-CD38 antibodies as single agents or in combination. The decision of whether or not to initiate bridging therapy, given patients’ expected rate of deterioration while idecabtagene vicleucel was being manufactured, was left to each respective investigator. Experimental agents and myeloma therapies to which the patient had not been previously exposed were not to be used as bridging therapy. Per-protocol, antimyeloma bridging therapies were stopped at least 14 days before the start of LDC.
The treatment period began with LDC. Eligible patients received a 3-day cycle of LDC with cyclophosphamide (300 mg/m2 IV infusion over 30 minutes) and fludarabine (30 mg/m2 IV infusion over 30 minutes administered immediately after cyclophosphamide) both at days −5, −4, and −3 of the study. After completing the LDC, patients were infused with idecabtagene vicleucel. Prior to proceeding with idecabtagene vicleucel infusion, the patient’s clinical status must not have significantly worsened (with worsening defined as having a suspected or active infection, fever unrelated to MM, requirement of supplemental oxygen, cardiac arrhythmia, hypotension, or other non-hematological disorder, or taking medications prohibited in the protocol).
The selection of the idecabtagene vicleucel dose range was informed by evolving data from the phase II (CRB-401, part A) study. Doses ranging from 50 × 106 to 800 × 106 CAR T cells were explored. Based on an overall benefit-risk assessment, a safety review committee recommended a dose range of 150 × 106 to 450 × 106 CAR T cells to evaluate dose expansion. Due to an updated manufacturing process for idecabtagene vicleucel, the selected dose range for initiation of the MM-001 study was modified to 150 × 106 to 300 × 106 CAR T cells, with the intent of treating 80 patients. After the initial 4 patients were treated at the target dose of 150 × 106 CAR T cells in the MM-001 study, subsequent patients were treated at the target dose of 300 × 106 CAR T cells. Based on an emerging dose-response relationship from the CRB-401 study and acceptable ongoing safety at both the 150 × 106 and 300 × 106 CAR T cells target dose levels in MM-001, the dose range in MM-001 was modified from 150 × 106 to 450 × 106 CAR T cells, along with expansion of the total sample size, with the intent of targeting the remaining patients at 450 × 106 CAR T cells. The maximum dose of idecabtagene vicleucel (540 × 106 CAR T cells) was defined by the upper limit of 450 × 106 CAR T cells plus 20%. The target dose was modified to 450 × 106 CAR T cells.
Patients were pre-medicated approximately 30 minutes before idecabtagene vicleucel infusion; these pre-medication included acetaminophen 650 mg orally and diphenhydramine 12.5 mg IV or 25 to 50 mg orally (or equivalent). Corticosteroids, as pre-medication, were not allowed.
Bridging therapy was considered for any patient, given their expected rate of deterioration, while idecabtagene vicleucel was being manufactured, based on the clinical judgment of the respective investigator. Bridging therapies could have included corticosteroids, alkylating agents, IMiDs, proteasome inhibitors, and/or anti-CD38 antibodies as single agents or in combination.
After idecabtagene vicleucel infusion, all patients were closely monitored for at least 14 days as inpatients for signs and symptoms of CRS or neurotoxicity post–idecabtagene vicleucel infusion. Tocilizumab was available at each site before infusion of each patient. Study sites had ICUs with the ability to manage CRS, neurotoxicity, and other potential complications.
Prohibited medications included systemic corticosteroids (unless used for CRS or neurotoxicity), any systemic MM therapy within 14 days before leukapheresis, any experimental agents for MM, bridging therapies not included in the protocol, any systemic MM therapy, including experimental agents, within 14 days of LDC, any concurrent chemotherapy, immunotherapy, biologic, experimental, or hormonal therapy following idecabtagene vicleucel infusion (posttreatment period) for treatment of MM before documentation of PD.
Subsequent AMTs were summarized for the idecabtagene vicleucel population and were also considered in the outcome time to subsequent AMT in the KarMMa study. In this instance, the idecabtagene vicleucel re-treatment (including LDC and bridging therapy) was not included as a subsequent AMT.
Patients were allowed to receive a second course of idecabtagene vicleucel (re-treatment) at the discretion of the clinical investigator, with or without bridging therapy (which had to be completed at least 14 days before the start of LDC), and if they fulfilled the following criteria:
At least 8 weeks since first idecabtagene vicleucel infusion
Best response to initial idecabtagene vicleucel infusion was stable disease or better, based on standard response criteria according to the IMWG uniform response criteria for MM
Evidence of disease progression according to IMWG criteria
No history of grade 4 CRS or neurotoxicity with prior idecabtagene vicleucel treatment
Eligibility criteria for enrolment continued to be met (except for patients with known CNS involvement with myeloma, inadequate bone marrow function, and those who received treatment with any gene therapy-based therapeutic for cancer or investigational cellular therapy or BCMA-targeted therapy)
Eligibility criteria for starting LDC continued to be met
Patients with progression of myeloma within the CNS who required whole-brain or directed cerebral radiotherapy (excluding palliative focal, minimally penetrating, radiotherapy to scalp or skull lesions) were not to receive idecabtagene vicleucel re-treatment infusion until a gap of at least 8 weeks from last radiotherapy treatment had been observed.
Re-treatment required the availability of enough cryopreserved idecabtagene vicleucel drug product for re-treatment, as remanufacture of idecabtagene vicleucel from cryopreserved peripheral blood mononuclear cells and repeat leukapheresis were not allowed. Re-treatment included a second course of LDC with or without bridging therapy.
Outcomes
The objective of the KarMMa study was to evaluate the effects of idecabtagene vicleucel on response and remission rates, survival, HRQoL, and safety in patients with RRMM. The primary objective was based on the ORR. The key secondary outcome was the CRR. Other outcomes of interest to this CADTH review encompassed in the secondary objectives of the study included DoR, TTR, PFS, TTP, PFS, OS, an MRD-negative status, and HRQoL. All these outcomes were evaluated up to a cut-off date of October 16, 2019, and all efficacy analyses were conducted using the population treated with idecabtagene vicleucel. Patients were evaluated for efficacy and harm outcomes monthly until month 6, then every 3 months for a minimum of 24 months post–idecabtagene vicleucel infusion or until PD, whichever was longer. A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial is provided in Table 8 and summarized in the following section. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | BB2121-MM-001 (KarMMa) |
|---|---|
Response or remission | |
Overall response rate | Primary |
Complete response rate | Key secondary |
Time to response | Secondary |
Duration of response | Secondary |
Time to progression | Secondary |
MRD-negative status | Secondary |
Survival | |
Progression-free survival | Secondary |
Overall survival | Secondary |
Health-related quality of life | |
EORTC QLQ-C30 | Secondary |
EQ-5D-5L | Secondary |
EORTC QLQ-MY20 | Secondary |
Safety and harms | |
AEs, SAEs, WDAEsa | Secondary |
Health care utilization | Exploratory |
AE = adverse event; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma with 20 items; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
aIncludes harms of special interest: febrile neutropenia, neurologic effects (i.e., immune effector cell-associated neurotoxicity syndrome), documented infections, replication-competent lentivirus, cytokine release syndrome, development of anti–chimeric antigen receptor antibody response, and mortality of any cause or treatment-related cause.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Response and Remission Rates
Response or remission rates identified as relevant by CADTH to this review were evaluated with the following end points3:
Overall response rate, defined as the percentage of patients who achieved a PR or better. To select the best response, the following order of response was used: stringent complete response (sCR) > CR > VGPR > PR > minimal response > stable disease > PD. The outcome was assessed by an IRC according to IMWG uniform response criteria for MM. The concordance and discordance between an IRC and investigator assessment were evaluated descriptively for subjects in each category of best overall response, and separately for responders with PR or better, VGPR or better, and a CR or better. Patients were evaluated for efficacy and harm outcomes monthly until month 6, then every 3 months for a minimum of 24 months post–idecabtagene vicleucel infusion or until PD, whichever was longer.
Complete response rate, defined as the percentage of patients who achieved a CR or sCR as assessed by an IRC according to IMWG uniform response criteria for MM. Patients were evaluated for efficacy and harm outcomes monthly until month 6, then every 3 months for a minimum of 24 months post–idecabtagene vicleucel infusion or until PD, whichever was longer.
Time to response, defined as the time from first idecabtagene vicleucel infusion to first documentation of response of a PR or better.
Duration of response, defined as the time from first documentation of response of PR or better to first documentation of disease progression or death from any cause, whichever occurred first. Censoring for DoR followed the censoring rules based on FDA23 and EMA24 guidance for cancer trials end points.
Time to progression, defined as the time from first idecabtagene vicleucel infusion to first documentation of PD. Censoring rules for TTP were similar to those for PFS, except that death was not considered as an event and was censored at the last response assessment date.
An MRD-negative status as revealed by next-generation sequencing, defined as the proportion of patients who achieved a CR or better and MRD-negative status at any time point within 3 months before achieving a CR or better until the time of PD or death (exclusive) (also referred to as MRD-negative status and ≥ CR), using a sensitivity of 10-5, based on the population treated with idecabtagene vicleucel.
Survival
Survival outcomes relevant to this review and assessed in the KarMMa study were:
Overall survival, defined as the time from first idecabtagene vicleucel infusion to time of death due to any cause. Patients who died on or before the data cut-off date were considered as having events on the date of death. Those who were alive or lost to follow-up were censored on the last date known alive. Those whose last date of follow-up confirmed they were alive at the data cut-off date were censored at the data cut-off date. If a patient was lost to follow-up and there was no contact after idecabtagene vicleucel infusion, the patient was censored at the idecabtagene vicleucel infusion date.
Progression-free survival, defined as the time from first idecabtagene vicleucel infusion to first documentation of PD or death due to any cause, whichever occurred first. Guidance from the FDA23 and EMA24 for cancer trials end points was applied, and PFS for the enrolled population was also examined.
Health-Related Quality of Life
Health-related quality of life is a patient-reported outcome (PRO) that was evaluated in the PRO population using recognized and validated tools that measure HRQoL in the oncology setting: the EORTC QLQ-C30, EORTC QLQ-MY20, and EQ-5D-5L scales.
The EORTC QLQ-C30 was measured in 121 patients from the KarMMa study. It is a generic cancer measure of HRQoL composed of both multi-item scales and single-item measures. The tool includes 5 functional scales (physical, role, emotional, cognitive, and social), 3 symptom scales (fatigue, nausea/vomiting, and pain), a global health/QoL scale, and 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). Each of the multi-item scales includes a different set of items and no item occurs in more than 1 scale. The EORTC QLQ-C30 employs week recall period of 1 week for all items and a 4-point scale for the functional and symptom scales and items with response categories of “not at all,” “a little,” “quite a bit,” and “very much.” The 2 items assessing global health/QoL utilize a 7-point scale ranging from 1 (“very poor”) to 7 (“excellent”),25 with higher scores on the functional and global scale indicating a higher response level. A higher score represents a high or healthy level of functioning and better HRQoL, but a high score for a symptom scale represents higher symptoms (worsening). The tool has demonstrated high reliability (internal consistency) with Cronbach alpha values greater than 0.80 for all 3 multi-item scales (ranging from 0.82 to 0.93). All 4 scales (including the single-item body image measure) had a test-retest reliability of 0.85 or greater.26 Construct and criterion validity of the EORTC QLQ-C30 are adequate, as well as a good responsiveness.27-30 Based on a mixed-methods study31 using a systematic review of the literature with clinician expert input, the MIDs for improvement and deterioration, respectively, were physical function (2 and −5), role function (6 and −7), cognitive function (3 and −1), emotional (6 and −3), social (3 and −6), fatigue (−4 and 5), pain (−5 and 3), nausea/vomiting (−3 and 5), financial (−3 and 2), and global QoL score (5 and −5). No studies assessing validity of the EORTC QLQ-C30 were found in patients from North America, which could affect the generalizability of the findings.
The EORTC QLQ-MY20 was evaluated in 120 patients in the KarMMa study. It includes a myeloma module to be administered alongside the core EORTC QLQ-C30. The EORTC QLQ-MY20 is a 20-item module intended for use among patients varying in disease stage and treatment modality. It is also 1 of the most widely used measures of HRQoL in patients with MM and in clinical trials of MM to assess treatment effect on HRQoL in conjunction with the EORTC QLQ-C30. The module included in this study is composed of 20 questions addressing 4 different domains of HRQoL that are important to patients with MM: 2 symptom scales (disease symptoms and side effects of treatment) and 2 functional scales (future perspective and body image). For the symptoms scales of the EORTC QLQ-MY20 (disease symptoms and side effects of treatment), a higher score indicates worsening of symptoms (higher symptom burden), while for the functional scales (future perspectives and body image), a higher score indicates a better level of functioning. The tool extension has appropriate internal consistency30 (Cronbach alpha values range from 0.77 to 0.80), validity, and responsiveness.32 The MIDs for the EORTC QLQ-MY20 were as follows: disease symptoms, −10 and + 10 points for improvement and deterioration, respectively; side effects of treatment, −10 and + 10 points for improvement and deterioration, respectively; body image, + 13 points and −13 for improvement and worsening, respectively; and future perspective (body image), + 9 and −9 points for improvement and deterioration, respectively.33
The EQ-5D-5L scale was evaluated in 120 patients. It is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments, including MM. A scoring function can be used to assign a value (index score) to self-reported health states from a set of population-based preference weights. The EuroQol Visual Analogue Scale (EQ VAS) has end points of 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state,” respectively. Respondents are asked to rate their own health by drawing a line from an anchor box to the point on the EQ VAS that best represents their own health on that day. Higher scores on the index and EQ VAS indicate better HRQoL. An MID of 0.08 for improvement and −0.10 for deterioration was defined by the sponsor and used in the KarMMa study based on recommendations from the published literature.31
Safety and Harms
Adverse events, SAEs, and withdrawals due to AEs were evaluated in the population treated with idecabtagene vicleucel, which included 128 patients who received idecabtagene vicleucel infusion. Data for all 140 patients who underwent leukapheresis (i.e., the enrolled population) were also included in select analyses. The report on the AEs considers those occurring in the period from LDC to immediately before the idecabtagene vicleucel infusion, which are reported as AEs related to LDC.
Health care utilization was considered in this review as a safety or harm outcome and was evaluated in the KarMMa study as an exploratory end point defined as the number of inpatient ICU days and standard care unit days.
Adverse events of special interest considered by CADTH were febrile neutropenia, neurologic effects, documented infections, replication-competent lentivirus events, development of anti-CAR antibody response, and the number of patients with CRS, all of which are evaluated in the KarMMa study.
Statistical Analysis
Sample Size
The sample size was calculated for the primary efficacy end point, ORR, based on a 1-sample binomial test with normal approximation. The null hypothesis was that the ORR (the proportion of patients with a PR or better based on all idecabtagene vicleucel–treated patients) is no more than 50%; the alternative hypothesis was that the ORR is greater than 50%, with a target ORR of 70%. The choice of a null hypothesis of 50% ORR was based on the observed clinical activity of the best available single-drug therapy in a heavily pretreated RRMM patient population. The calculated sample size was 119 idecabtagene vicleucel–treated patients. This number would have provided greater than 99% power at a 1-sided 0.025 alpha level. Assuming a dropout rate of 15% between the time of study enrolment and idecabtagene vicleucel infusion, a total of 140 patients were required to be enrolled.
Investigators planned the primary analysis for when all idecabtagene vicleucel–treated patients had sufficient follow-up. For the primary analysis, a minimum follow-up of 10 months after the last patient received idecabtagene vicleucel infusion (9 months from the time of the last patient’s first anticipated response) was considered sufficient. A data cut-off date of October 16, 2019, was planned for the primary analysis.
Statistical Tests and Analyses
Demographics, baseline characteristics, and medical history were summarized for the population treated with idecabtagene vicleucel. For the enrolled population, only demographics and baseline characteristics are presented. Continuous demographic and disease characteristics variables (e.g., age, time from diagnosis and number of prior regimens) at baseline were summarized using descriptive statistics, while categorical variables (e.g., age categories [< 65 and ≥ 65; < 75 and ≥ 75], sex, race, ECOG score, and Revised International Staging System stage) were summarized by frequency counts and percentages.
All efficacy analyses were conducted using the population treated with idecabtagene vicleucel. Supportive analyses of the primary (ORR), key secondary (CRR), and other secondary (PFS and OS) end points using the enrolled population were also conducted. Duration of response and TTR were measured on responders (i.e., patients who achieved a PR or better) and therefore were the same for the population treated with idecabtagene vicleucel, enrolled population, and efficacy evaluable population. The primary efficacy analysis was based on the IRC-adjudicated assessment according to IMWG uniform response criteria for MM in the population treated with idecabtagene vicleucel. There were no adjustments for multiple comparisons or procedure to control the type I error rate for the secondary outcomes beyond the assessment of the CR.
The end points were assessed as follows:
The ORR was calculated as the number of patients who achieved PR or better divided by the number of patients in the specific analysis population, using a 1-sample binomial test. The ORR was first tested against the null hypothesis of an ORR of no more than 50% at a 1-sided alpha level of 0.025. If the ORR test was significant, the CRR was to be subsequently tested against the null hypothesis of a CRR of no more than 10% at the same 1-sided alpha level of 0.025. The 2-sided Wald 95% CIs for all ORR values were calculated.
The CRR was tested against the null hypothesis of no more than 10% for the key secondary efficacy end point. It was calculated as the number of patients who achieved a CR or sCR divided by the number of patients in the specific analysis population. The CRR based on the IMWG criteria (i.e., CR and sCR) was calculated together with the 2-sided 95% CI. If the test for the ORR (primary end point) was positive, the CRR was to be tested against the null hypothesis of no more than 10% with a 1-sample binomial test using a stepdown approach to control the overall alpha level, which would remain at the 1-sided 0.025 level.
The DoR was analyzed (for responders only) using the KM method. Median DoR and the corresponding 95% CIs are provided. Censoring for DoR followed the censoring rules based on FDA23 and EMA24 guidance for cancer trials end points.
The TTR (assessed in responders only) was summarized using descriptive statistics.
The TTP censoring rules were similar to those for DoR, except that death was not considered an event and was censored at the last response assessment date. The TTP was summarized for the population treated with idecabtagene vicleucel using KM statistics; the KM approach was also applied to the median and 95% CI.
Progression-free survival was summarized for the population treated with idecabtagene vicleucel using KM statistics and a KM curve was used to depict the outcome. The median PFS along with the 2-sided 95% CI for the median was estimated. Censoring rules were likewise based on FDA23 and EMA24 guidance for cancer trials end points. Data for PFS in the enrolled population were also examined. For this analysis, the PFS was calculated from the date of enrolment (i.e., leukapheresis).
The MRD-negative rate was calculated and presented with the 95% CI. A 1-sample exact binomial test was performed for the MRD-negative rate as a descriptive analysis, with a null hypothesis of no more than 10% and an alternative hypothesis of greater than 10%.
Overall survival was analyzed for the population treated with idecabtagene vicleucel using the KM method. Median OS and the corresponding 95% CI are provided. Survival rates at specific time points and KM survival curves are also provided. Overall survival for the enrolled population was analyzed. For this analysis, the OS was calculated from the date of enrolment (i.e., leukapheresis). The censoring rules remained the same as for the analysis in the population treated with idecabtagene vicleucel. If the patient was lost to follow-up and there was no contact after enrolment, the patient was censored at the date of leukapheresis instead of the date of idecabtagene vicleucel infusion.
The PROs using HRQoL measures were evaluated with the EORTC QLQ-C30, EORTC QLQ-MY20, and EQ-5D-5L scales. The PRO end points of primary interest focused on the EORTC QLQ-C30 subscales of fatigue, pain, physical functioning, cognitive functioning, and global health/QoL. The EORTC QLQ-MY20 used the symptom subscales of disease symptoms and side effects. The EQ-5D-5L tool used the index and EQ VAS to depict the results. The analysis was descriptive and performed primarily to assess the total and subdomain scores on the primary PRO end points at each time point, describe the changes from baseline to each subsequent time point for the total and subdomain scores on the primary PRO end points, and evaluate the proportion of patients reaching the responder definitions in the changes from baseline to each subsequent time point for the total and subdomain scores on the primary PRO end points.
Subgroup Analysis
Prespecified subgroup analysis for the primary outcome were performed for subgroups in which an adequate number of patients were available to allow for meaningful interpretation of results. Analyses were performed for the following subgroups of interest to this review within the population treated with idecabtagene vicleucel:
age group 1: younger than 65 years, at least 65 years old; and age group 2: younger than 65 years, 65 to 69 years, 70 years and older
extramedullary plasmacytoma (yes, no)
number of prior AMT regimens per year (≤ 1, > 1)
revised International Staging System stage at baseline (I or II, III)
tumour BCMA expression (≥ 50%, < 50% BCMA+).
The ORR, CRR, and DoR were evaluated for each of the subgroups. Forest plots and 95% CIs were provided for the subgroup analyses of the ORR and CRR. Additional subgroup analyses could be explored as appropriate, but no other subgroups were analyzed a priori besides those already stated. No statistical test was performed to evaluate differences in effect estimates on these outcomes between subgroups.
Sensitivity Analyses
Alternate analyses were run for the outcome of PFS where the application of different guidance rules for censoring were applied using FDA and EMA rules.
Analysis Populations
Analysis populations included the enrolled population (all patients in the screened population who underwent leukapheresis), the population treated with idecabtagene vicleucel (all patients in the enrolled population who received idecabtagene vicleucel infusion), the population re-treated with idecabtagene vicleucel, (all patients who received idecabtagene vicleucel re-treatment), and the PRO analysis population (those who completed their baseline PRO questionnaires using HRQoL measures). Efficacy and safety analyses were evaluated in the population treated with idecabtagene vicleucel and in each idecabtagene vicleucel target dose group (i.e., 150 × 106, 300 × 106, and 450 × 106 CAR T cells).
Results
Patient Disposition
The KarMMa study screened 158 patients, of whom 18 failed to meet the eligibility criteria, as shown in Figure 3.
A total of 140 patients underwent leukapheresis and were included in the enrolled population. Of these, 128 patients received idecabtagene vicleucel infusion and were included in the idecabtagene vicleucel–treated population used for the primary analysis of efficacy and safety (Table 9).
Reasons for discontinuation for the pretreatment period (from leukapheresis to before LDC) and treatment period (from LDC to idecabtagene vicleucel infusion) for the enrolled population, and the posttreatment follow-up period for the population treated with idecabtagene vicleucel after initial idecabtagene vicleucel infusion are described. For re-treatment patients, discontinuation reasons are summarized separately.
Figure 3: Patient Disposition of Study BB2121-MM-001 (KarMMa)
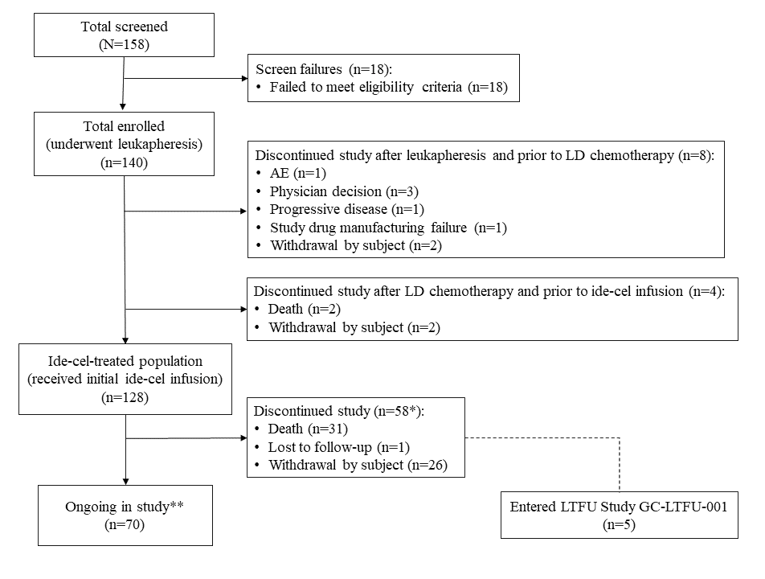
AE = adverse event, Ide-cel = idecabtagene vicleucel; LD = lymphodepleting; LTFU = lost to follow-up.
Note: Data cut-off date = October 16, 2019.
* Includes 41 patients who discontinued after initial idecabtagene vicleucel infusion without entering the re-treatment period and 17 patients who discontinued during the re-treatment period. The re-treatment period includes re-treatment screening, re-treatment baseline, re-treatment, and re-treatment follow-up.
** Includes 58 patients ongoing after initial idecabtagene vicleucel infusion without entering the re-treatment period and 12 patients ongoing after entering the re-treatment period. Patients ongoing in re-treatment follow-up include patients who were screened for re-treatment and have not discontinued the study as of the data cut-off date, regardless of whether or not the patient actually received idecabtagene vicleucel re-treatment.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
The majority of patients (91.4%) who underwent leukapheresis received the idecabtagene vicleucel infusion. Of the 12 patients who discontinued after leukapheresis, 8 did so before LDC. As of the October 16, 2019, cut-off date, 70 of the 128 idecabtagene vicleucel–treated patients (54.7%) were still participating in the study, including 58 (45.3%) ongoing after initial idecabtagene vicleucel infusion without entering the re-treatment period and 12 (9.4%) ongoing after entering the re-treatment period. Fifty-eight (45.3%) of the 128 idecabtagene vicleucel–treated patients discontinued the study, with 31 patients (24.2%) discontinuing due to death, 1 patient (0.8%) lost to follow-up, and 26 patients (20.3%) discontinuing due to withdrawal by subject. Although there were 26 withdrawals by patient, only 2 were censored for PFS due to discontinuing study without PD or death. The median time from leukapheresis to idecabtagene vicleucel product release was 32.0 days, from product release to idecabtagene vicleucel infusion the median time was 7.0 days, and from leukapheresis to idecabtagene vicleucel infusion it was 40.0 days.
Table 9: Patient Disposition in the BB2121-MM-001 (KarMMa) Trial
Disposition | BB2121-MM-001 (KarMMa) |
|---|---|
Screened, N | 158 |
Enrolled,a N (%) | 140 (88.6) |
Discontinued from study after leukapheresis and before LDC, N (%) | 8 (5.7) |
Reason for discontinuation, N (%) | |
Adverse events | 1 (0.7) |
Physician decision | 3 (2.1) |
Progressive disease | 1 (0.7) |
Study drug manufacturing failure | 1 (0.7) |
Withdrawal by patient | 2 (1.4) |
Discontinued from study after leukapheresis and before idecabtagene vicleucel infusion, N (%) | 4 |
Reason for discontinuation, N (%) | |
Death | 2 (1.4) |
Withdrawal by participant | 2 (1.4) |
Population treated with idecabtagene vicleucelb (N) | 128 |
Discontinued from study | 58 (45.3) |
Discontinued from study after idecabtagene vicleucel infusion, without entering re-treatment, N (%) | 41 (32.0) |
Population re-treated with idecabtagene vicleucel (N) | 27 |
Discontinued study during re-treatment period | 17 (13.3) |
PRO analysis populationc | |
EORTC QLQ-C30 EORTC QLQ-MY20 | 121 (86.4) 120 (85.7) |
Safety, N | 128 |
LDC = lymphodepleting chemotherapy; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myeloma Module with 20 items.
aThe enrolled population includes all patients in the screened population who underwent leukapheresis.
bThe idecabtagene vicleucel–treated population includes all patients in the enrolled population who received idecabtagene vicleucel infusion.
cThe patient-reported outcomes analysis population includes all patients who completed their baseline questionnaires and had at least 1 post-baseline patient-reported outcome measurement in the population treated with idecabtagene vicleucel.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
The disposition of patients who were re-treated after a first idecabtagene vicleucel administration is shown in Table 10.
Table 10: Patient Disposition of Re-treated Patients in the Population Treated With Idecabtagene Vicleucel
Disposition | Total, n (%) N = 128 |
|---|---|
Patients received idecabtagene vicleucel re-treatment, n (%) | 27 (21.1) |
|||||||||||||||||||||||||||||||||||||||||||||||| | |||||| |
||||||||||||||||||| | |||||||| |
|||||||||||||| | |||||| |
|||||||||||||| | |||||| |
|||||||||||||| | |||||| |
|||||||||||||||| | ||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||| |
||||||||||||||||||| | |||||| |
||||||||||| | |||||| |
||||||||||||||||||||| | |||||| |
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Exposure to Study Treatments
Lymphodepleting Chemotherapy
Of the 140 patients who were included and underwent leukapheresis, 132 received LDC, and of these 128 went on to receive the idecabtagene vicleucel infusion. Patient exposure to cyclophosphamide and fludarabine was consistent with the lymphodepletion treatment plan according to the protocol, and the number of patients and number of days dosed are supplied in Table 11.
Table 11: Administration of Lymphodepleting Chemotherapy in the Population Treated With Idecabtagene Vicleucel
Chemotherapy | Idecabtagene vicleucel (CAR T cells) target dose 150 × 106 to 450 × 106 N = 128 |
|---|---|
Patients who received LDC, n (%) | 128 (100.0) |
Patients who received LDC with adjusted dose, n (%) | 29 (22.7) |
Adjusted fludarabine, n (%) | 29 (22.7) |
Adjusted cyclophosphamide, n (%) | 0 |
Fludarabine | |
Number of days dosed | |
Mean (SD) | 3.0 (0.00) |
Median (minimum to maximum) | 3.0 (3.0 to 3.0) |
Cyclophosphamide | |
Number of days dosed | |
Mean (SD) | 3.0 (0.00) |
Median (minimum to maximum) | 3.0 (3.0 to 3.0) |
CAR = chimeric antigen receptor; LDC = lymphodepleting chemotherapy; SD = standard deviation.
Note: Data cut-off date: October 16, 2019.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Idecabtagene Vicleucel Infusion
Idecabtagene vicleucel was administered at planned target doses of 150 × 106, 300 × 106, or 450 × 106 CAR T cells per infusion. The median time from leukapheresis to idecabtagene vicleucel administration in the idecabtagene vicleucel–treated population was 40.0 days (range = 33 to 79). Seven of 128 patients (5.5%) were administered idecabtagene vicleucel more than 8 weeks (56 days) after leukapheresis and 12 of 128 patients (9.4%) were administered idecabtagene vicleucel within 5 weeks (35 days) of leukapheresis. One of the idecabtagene vicleucel–treated patients received a second leukapheresis due to manufacturing failure after the first leukapheresis. One patient did not receive idecabtagene vicleucel due to manufacturing failure.
Of the 128 patients who received idecabtagene vicleucel infusion, 4 (3.1%) had a target dose of 150 × 106 CAR T cells, 70 (54.7%) had a target dose of 300 × 106 CAR T cells, and 54 (42.2%) had a target dose of 450 × 106 CAR T cells. All idecabtagene vicleucel–treated patients received an actual dose between 150.5 × 106 and 518.4 × 106 CAR T cells, which was within the allowance of 20% over the target dose of 450 × 106 CAR T cells (i.e., less than 540 × 106 CAR T cells). The median actual dose received across all target dose levels was 315.3 × 106 CAR T cells. A total of 51 patients received an actual dose in excess of 450 × 106 CAR T cells; 4 patients received an actual dose of more than 500 × 106 CAR T cells. No patients had a dose interruption during idecabtagene vicleucel infusion.
Bridging Therapy
Bridging therapy was considered for a patient, given their expected rate of deterioration, while idecabtagene vicleucel was being manufactured, based on the clinical judgment of the respective investigator. Bridging therapies could have included corticosteroids, alkylating agents, IMiDs, proteasome inhibitors, and/or anti-CD38 antibodies as single agents or in combination. The majority of patients (87.5%) received bridging therapy for myeloma control during the idecabtagene vicleucel manufacturing period. The most commonly received bridging therapies were dexamethasone (70.3%), cyclophosphamide (36.7%), daratumumab (28.1%), carfilzomib (23.4%), bortezomib (19.5%), and pomalidomide (18.8%). The median duration of bridging therapy was 14.5 days (range = 1 to 33).
Subsequent Antimyeloma Therapies
The most commonly received (in ≥ 5% of patients) subsequent AMTs are shown in Table 12. Idecabtagene vicleucel re-treatment is not included as a subsequent therapy.
When considering the time to subsequent AMT in the population treated with idecabtagene vicleucel, idecabtagene vicleucel re-treatment (as well as bridging therapy for re-treatment and LDC before re-treatment) was counted as a subsequent AMT. As of the data cut-off date, 56 patients (43.8%) received a subsequent AMT (including idecabtagene vicleucel re-treatment, bridging AMT for re-treatment, or LDC before re-treatment). The KM estimate for median time to subsequent AMT was 13.2 months (95% CI, 10.9 to 15.1).
Table 12: Subsequent Antimyeloma Therapy Agents by Class That Were Received by at Least 5% of Patients in the Population Treated With Idecabtagene Vicleucel
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||| |||||||| |
|---|---|
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
|||||||||||||| | |||||||||| |
AMT = antimyeloma therapy; CAR = chimeric antigen receptor; WHO-DD = WHO Drug Dictionary.
Note: The table is sorted by descending frequency of drug class and then by descending frequency of preferred name within each class. Data cut-off date: October 16, 2019.
aIdecabtagene vicleucel re-treatment, which was received by 27 patients, is not included as a subsequent therapy in this summary.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below.
Data for cut-off dates of January 14, 2020, and April 7, 2020. are presented in Appendix 3.
Response and Remission Rates
Overall Response Rate
The primary efficacy end point was the ORR based on the IRC-adjudicated assessment of response. The ORR in the idecabtagene vicleucel–treated population was 73.4% (95% CI, 65.8 to 81.1; P < 0.0001). An ORR of 50.0% was observed at the target dose of 150 × 106 CAR T cells, 68.6% was observed at the target dose of 300 × 106 CAR T cells, and 81.5% was observed at the target dose of 450 × 106 CAR T cells. The results of this primary analysis in the population treated with idecabtagene vicleucel were consistent with those of the supportive analyses in the enrolled population. A total of 66 patients (51.6%; 95% CI, 42.9 to 60.2) achieved a VGPR or better.
A forest plot for ORRs for the idecabtagene vicleucel–treated population based on pre-planned subgroups, including those stated in the protocol for this review, is presented in Figure 22 in Appendix 3. The treatment effect for the ORR was generally consistent across subgroups, but appeared to be heterogeneous according to stage at diagnosis, based on the International Staging System stage. However, there is only a small number of patients in the stage III group and no a priori statistical tests were planned to provide definitive conclusions about any differences in subgroup effects.
Complete Response Rate
In the population treated with idecabtagene vicleucel, 40 patients out of 128 achieved a CR, equivalent to a CRR of 31.3% (95% CI, 23.2 to 39.3; P < 0.0001). A CR rate of 25.0% was observed at the target dose of 150 × 106 CAR T cells, 28.6% was observed at the target dose of 300 × 106 CAR T cells, and 35.2% was observed at the target dose of 450 × 106 CAR T cells. The results of this primary analysis of the CRR in the idecabtagene vicleucel–treated population were consistent with those of the supportive analyses in the enrolled population.
Duration of Response
The DoR analysis was based on responders only, and therefore was the same for the idecabtagene vicleucel–treated and enrolled population. A summary of DoR among responders based on an IRC assessment, applying FDA censoring rules, is presented in Table 13 and Table 14. As of the data cut-off date, 52 (55.3%) of 94 responders had progressed or died and 42 (44.7%) were censored. The KM estimate for median DoR among responders was 10.6 months (95% CI, 9.0 to 11.3). Based on KM estimates, ||||| of responders had responses lasting for at least 9 months, and ||||| of responders had responses lasting for 12 months or longer. The median DoR among responders was 9.9 months (95% CI, 5.4 to 11.0) at the target dose of 300 × 106 CAR T cells and 11.3 months (95% CI, 9.2 to 11.4) at the target dose of 450 × 106 CAR T cells. The median was NE at the target dose of 150 × 106 CAR T cells. A majority (59.1%) of responders at the target dose of 450 × 106 CAR T cells were still progression-free as of the data cut-off date.
Applying EMA censoring rules produced similar results when compared to applying the FDA rules. As of the data cut-off date, 54 (57.4%) of 94 responders had progressed or died and 40 (42.6%) were censored. The KM estimate for median DoR among responders was 10.5 months (95% CI, 8.0 to 11.3). Based on KM estimates, 60.5% of responders had responses lasting for at least 9 months, and 32.0% of responders had responses lasting for 12 months or longer.
Time to Response
The TTR was calculated as the time from idecabtagene vicleucel infusion to the first date of response (PR or better) and this analysis was based on responders only. A summary of TTR among responders based on the IRC assessment is presented in Table 13. As of the data cut-off date, the median TTR among patients who responded was 1.0 months (range = 0.5 to 8.8), which was the time of the first scheduled response assessment. Within 1 month after idecabtagene vicleucel infusion, 84.0% of responders achieved a first response. An additional |||||| of responders achieved a first response between 1 and 2 months after idecabtagene vicleucel infusion. The median TTR was 1.0 months for responders in each of the target dose groups.
Time to Progression
The TTP was defined as time from idecabtagene vicleucel infusion to the first documented progression. A summary of TTPs among responders based on the IRC assessment, applying FDA censoring rules, is presented in Table 13. The KM estimate for median TTP was 8.9 months (95% CI, 6.0 to 11.6). Based on KM estimates, 49.1% of patients remained event-free at 9 months and 35.5% of patients remained event-free at 12 months. Results produced by applying the EMA censoring rules were similar to those produced by applying FDA censoring rules; supportive analyses were also similar to primary analyses for this outcome.
Minimal Residual Disease–Negative Status
The primary analysis of MRD status was the proportion of patients who achieved a CR or better and MRD-negative status at any time point within 3 months before achieving a CR or better until the time of PD or death (referred to as MRD-negative status and a CR or better), based on the idecabtagene vicleucel–treated population and measurements using ne|t-generation sequencing with a sensitivity level of 10-5 nucleated cells. A summary of the primary analysis of MRD is presented in Table 13. As of the data cut-off date, 40 of 128 patients (31.3%) achieved a CR or better; 31 of 128 patients (24.2%) achieved an MRD-negative status and a CR or better (95% CI, 17.1 to 32.6), rejecting the null hypothesis of no more than 10% for this end point (P < 0.0001). The proportion of patients who achieved an MRD-negative status and a CR or better was 1 of 4 patients (25.0%) at the target dose of 150 × 106 CAR T cells, 17 of 70 patients (24.3%) at the target dose of 300 × 106 CAR T cells, and 13 of 54 patients (24.1%) at the target dose of 450 × 106 CAR T cells.
Table 13: Response and Remission Efficacy Outcomes — BB2121-MM-001 (KarMMa)
Outcome | Population treated with idecabtagene vicleucel Idecabtagene vicleucel (CAR T cells) target dose | Enrolled population N = 140 | |||
|---|---|---|---|---|---|
150 × 106 N = 4 | 300 × 106 N = 70 | 450 × 106 N = 54 | Total 150 × 106 to 450 × 106 N = 128 | ||
Overall response rate (PR or better) | |||||
N (%) | 2 (50.0) | 48 (68.6) | 44 (81.5) | 94 (73.4) | 94 (67.1) |
95% CIa | 6.8 to 93.2 | 56.4 to 79.1 | 68.6 to 90.7 | 65.8 to 81.1 | 59.4 to 74.9 |
P valueb | — | — | — | < 0.0001 | < 0.0001 |
CR rate (CR or better) | |||||
N (%) | 1 (25.0) | 20 (28.6) | 19 (35.2) | 40 (31.3) | 40 (28.6) |
95% CIa | 0.6 to 80.6 | 18.4 to 40.6 | 22.7 to 49.4 | 23.2 to 39.3 | 21.1 to 36.1 |
P valueb | — | — | — | < 0.0001 | < 0.0001 |
VGPR or better | |||||
N (%) | 2 (50.0) | 30 (42.9) | 34 (63.0) | 66 (51.6) | 66 (47.1) |
95% CIa | 6.8 to 93.2 | 31.1 to 55.3 | 48.7 to 75.7 | 42.9 to 60.2 | 38.9 to 55.4 |
Duration of responsec | |||||
N | 2 | 48 | 44 | 94 | — |
Censored, n (%) | 1 (50.0) | 15 (31.3) | 26 (59.1) | 42 (44.7) | — |
Progressed or died, n (%) | 1 (50.0) | 33 (68.8) | 18 (40.9) | 52 (55.3) | — |
Progressed | 1 (50.0) | 32 (66.7) | 18 (40.9) | 51 (54.3) | — |
Died without progression | 0 | 1 (2.1) | 0 | 1 (1.1) | — |
Median duration of response,d,e months | NE | 9.92 | 11.30 | 10.58 | — |
(95% CI) | (2.79 to NE) | (5.36 to 11.01) | (9.17 to 11.43) | (9.03 to 11.30) | — |
||||||||||||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
||||||||||||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
||||||||||||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
||||||||||||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
||||||||||||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Time to response | |||||
N | 2 | 48 | 44 | 94 | — |
Median TTR,d months (minimum to maximum) | 1.0 (1.0 to 1.0) | 1.0 (0.5 to 8.8) | 1.0 (0.9 to 2.0) | 1.0 (0.5 to 8.8) | — |
|||||||||||||||| | — | ||||
|||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
|||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
|||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Time to progressiong | |||||
|||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
|||||||||||||||||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
MRD | |||||
Patients who achieved MRD-negative status and at least CR,h N (%) | 1 (25.0) | 17 (24.3) | 13 (24.1) | 31 (24.2) | — |
95% CI | 0.6 to 80.6 | 14.8 to 36.0 | 13.5 to 37.6 | 17.1 to 32.6 | — |
CI = confidence interval; CR = complete response; HRQoL = health-related quality of life; MRD = minimal residual disease; NE = not estimable; PFS = progression-free survival; PR = partial response; sCR = stringent complete response; SE = standard error; TTR = time to response; VGPR = very good partial response.
Note: Data cut-off date: October 16, 2019
aFor “total” and “enrolled population”: Wald CI; for individual target doses: Clopper-Pearson exact CI.
bValue from a 1-sample binomial test (normal approximation).
cApplying FDA censoring rules. The duration of response analysis is based on responders only.
dResponse is defined as achieving sCR, CR, VGPR, or PR.
eKaplan-Meier estimates.
fA 3-day window was added to each month for months 1 to 8 and a 14-day window was added to each month from month 9 onward.
gThe TTP is based on an independent review committee assessment, applying FDA censoring rules, of the idecabtagene vicleucel–treated population.
hUsing 10-5 sensitivity level and next-generation sequencing.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11

Survival
Overall Survival
Overall survival for the idecabtagene vicleucel–treated population was defined as the time from idecabtagene vicleucel infusion to death due to any cause. For OS in the enrolled population, the OS was calculated from the date of enrolment (i.e., leukapheresis). A summary of OS in the population treated with idecabtagene vicleucel is presented in Table 14 and displayed in Figure 5. As of the data cut-off date, 34 patients (26.6%) had died. The KM estimate for the median OS was 18.2 months (95% CI, 18.0 to NE), with a median follow-up time for all surviving patients of 12.0 months. Based on KM estimates, 83.9% of patients were alive at 9 months and 76.9% of patients were alive at 12 months; 71.6% and 54.5% of patients were alive at 15 and 18 months, respectively. The median OS was 18.2 months (95% CI, 9.4 to 18.2) at the target dose of 150 × 106 CAR T cells. The median OS was NE (95% CI, 16.8 to NE) at the target dose of 300 × 106 CAR T cells, or at the target dose of 450 × 106 CAR T cells. Based on KM estimates, 78.6% and 76.8% of patients were alive at 12 months in the 300 × 106 and 450 × 106 CAR T cells target dose groups, respectively. In the enrolled population, as of the data cut-off date, 42 patients (30.0%) had died and the KM estimate for median OS was 19.3 months (95% CI, 17.94 to NE). Based on KM estimates, 81.3% of patients were alive at 9 months and 75.5% of patients were alive at 12 months; 67.3% and 61.8% of patients were alive at 15 months and 18 months, respectively.
Progression-Free Survival
Progression-free survival was defined as the time from idecabtagene vicleucel infusion to the first date of documented PD or death from any cause during the study, whichever occurred earlier. A summary of the PFS analysis in the population treated with idecabtagene vicleucel based on an IRC assessment, applying FDA censoring rules, is presented in Table 14 and displayed in Figure 6. As of the data cut-off date with a median PFS follow-up duration of 10.2 months (range = 0.03 to 18.3) for censored patients, 83 (64.8%) had a PFS event and 45 (35.2%) were censored. The KM estimate for median PFS was 8.6 months (95% CI, 5.6 to 11.3). Based on KM estimates, 47.4% of patients remained event-free at 9 months and 34.3% of patients remained event-free at 12 months. The median PFS was 5.8 months (95% CI, 4.2 to 8.9) at the target dose of 300 × 106 CAR T cells and 11.3 months (95% CI, 8.8 to 12.4), with 53.7% of patients progression-free at the target dose of 450 × 106 CAR T cells. The median PFS was 2.8 months (95% CI, 1.0 to NE) at the target dose of 150 × 106 CAR T cells, and 11.3 months (95% CI, 8.8, 12.4), with a slight majority of patients (53.7%) still progression-free, at the target dose of 450 × 106 CAR T cells. The most common reason for censoring was that patients were ongoing at the data cut-off date (39 patients; 30.5%). Two patients (1.6%) were censored due to discontinuing study without an event, 2 patients (1.6%) were censored due to taking anti-MM therapy before progression or death, and 2 patients (1.6%) were censored due to missing assessments. Analysis of the PFS using the EMA censoring rules produced results similar to those of the analysis using FDA censoring rules, with a median using the KM estimate of 8.2 months (95% CI 5.6 to 11.0).
Table 14: Survival Efficacy Outcomes — BB2121-MM-001 (KarMMa)
Outcome | Idecabtagene vicleucel–treated population Idecabtagene vicleucel (CAR T cells) target dose | |||
|---|---|---|---|---|
150 × 106 N = 4 | 300 × 106 N = 70 | 450 × 106 N = 54 | Total 150 × 106 to 450 × 106 N = 128 | |
Overall survival | ||||
Censored, n (%) | 2 (50.0) | 50 (71.4) | 42 (77.8) | 94 (73.4) |
Died, n (%) | 2 (50.0) | 20 (28.6) | 12 (22.2) | 34 (26.6) |
Mediana of overall survival time, months | 18.2 | NE | NE | 18.2 |
Median 95% CI | 9.4 to 18.2 | 16.8 to NE | NE to NE | 18.0 to NE |
3 months event-free, % (SE) | 100 (0.00) | 95.7 (2.44) | 92.6 (3.56) | 94.5 (2.02) |
6 months event-free, % (SE) | 100 (0.00) | 89. 6 (3.71) | 86.9 (4.61) | 88.8 (2.82) |
9 months event-free, % (SE) | 100 (0.00) | 86.6 (4.16) | 79.1 (5.62) | 83.9 (3.31) |
12 months event-free, % (SE) | 75.0 (21.65) | 78.6 (5.09) | 76.8 (5.92) | 76.9 (3.96) |
15 months event-free, % (SE) | 75.0 (21.65) | 72.7 (5.73) | — | 71.6 (4.72) |
18 months event-free, % (SE) | 75.0 (21.65) | 52.4 (13.0) | — | 54.5 (11.16) |
Progression-free survival | ||||
Censored, n (%) | 1 (25.0) | 15 (21.4) | 29 (53.7) | 45 (35.2) |
Progressed/died, n (%) | 3 (75.0) | 55 (78.6) | 25 (46.3) | 83 (64.8) |
Progressed | 3 (75.0) | 53 (75.7) | 23 (42.6) | 79 (61.7) |
Died without progression | 0 | 2 (2.9) | 2 (3.7) | 4 (3.1) |
Mediana of PFS time, months | 2.8 | 5.8 | 11.3 | 8.6 |
95% CI | 1.0 to NE | 4.2 to 8.9 | 8.8 to 12.4 | 5.6 to 11.3 |
3 months event-free % (SE) | 50.0 (25.00) | 71.3 (5.43) | 82.6 (5.27) | 75.3 (3.85) |
6 months event-free % (SE) | 25.0 (21.65) | 49.1 (6.05) | 70.8 (6.35) | 57.4 (4.45) |
9 months event-free % (SE) | 25.0 (21.65) | 37.2 (5.87) | 62.8 (6.77) | 47.4 (4.51) |
12 months event-free % (SE) | 25.0 (21.65) | 26.1 (5.42) | 49.0 (8.84) | 34.3 (4.84) |
||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
CAR = chimeric antigen receptor; CI = confidence interval; NE = not estimable; PFS = progression-free survival; SE = standard error.
Note: Data cut-off date: October 16, 2019
aMedian and 95% CI are based on the Kaplan-Meier approach.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11

||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This figure was redacted as per the sponsor request.

||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This figure was redacted as per the sponsor’s request
In an updated cut-off data submission (January 14, 2020)10 with a median follow-up of 13.3 months, no significant changes were noted in the ORR, CRR, DoR, TTR, MRD, OS, or PFS. These updated results are described in Appendix 3. As stated in the KarMMa 001 protocol, these data were not adjusted for alpha errors nor used for hypothesis testing. Also, data for cut-off dates of April 7, 2020, presented in Appendix 3, show no significant differences from the initial cut-off date analysis.
Intravenous Immunoglobin Replacement
Intravenous immunoglobin replacement was not assessed in the KarMMa study.
Health-Related Quality of Life
Health-related quality of life was evaluated with the EORTC QLQ-C30, the EORTC QLQ-MY20, and the EQ-5D-5L. Baseline levels for all 3 scales are shown in Table 15 and the changes from baseline for each measurement are presented in Figure 7 through Figure 15. These end points were considered descriptive in nature without adjustment for multiplicity, and were not evaluated as time-to-event outcomes.
European Organisation for Research and Treatment of Cancer QLQ-C30
Overall, based on data from the available patients described for this end point, a decrease in the fatigue subscale scores was observed in reference to the MID of −4 points from baseline to month 2, reaching a nadir at months 3, 4, 5, 6, and 9, and remaining below the MID for improvement at months 12 and 15 (Figure 7).
For the pain subscale, a similar direction in the scores described in the available population was observed, with an MID of −5 points from baseline to month 15. These changes in the score began at month 1 and reached a nadir by month 3. (Figure 8).
For the physical functioning subscale, an increase in mean scores from baseline of 2 points for the MID was reported beginning at month 1. The nadir was reached by month 2 and continued until month 12 (Figure 9). Cognitive functioning subscale scores generally demonstrated no change beyond or above the MID of 3 for improvement or −1 for deterioration, from baseline to month 15 (Figure 10).
Finally, an increase in global health/QoL subscale scores relative to the MID of 5 points from improvement began at month 2, reaching a nadir at months 4, 5, 6, and 9. The mean subscale score increases remained at months 12 and 15 (Figure 11).
European Organisation for Research and Treatment of Cancer QLQ-MY20
Small decreases crossing the MID reference of −10 points were observed in the disease symptoms subscale from baseline to months 3 through 15 posttreatment (Figure 12). A gradual increase in mean side effects subscale scores was observed from baseline to months 1 through 9 posttreatment; however, these increases did not go beyond the MID reference for deterioration of 10 points (Figure 13).
EuroQol 5-Dimensions 5-Levels Questionnaire
The EQ-5D-5L was measured using an index and the EQ VAS. For the index, a slight increase in mean scores was observed from baseline throughout follow-up, reaching a level above the MID, for an improvement of 0.08 beginning at month 2 (Figure 14). Beyond month 2, the index score remained relatively stable and marginally above the MID for improvement. For the EQ VAS, an increase in the MID in mean scores from baseline of 7 points was reported beginning at month 3 and at month 5 (Figure 15). Beyond month 5, the EQ VAS scores remained above the MID
Table 15: Health-Related Quality of Life Outcomes — Baseline Scores
HRQoL scale | Score |
|---|---|
EORTC QLQ-C30 | |
N | 121 |
Baseline scores, mean (SD) | |
Fatigue subscale | 39.3 (24.4) |
Pain subscale | 39.9 (28.2) |
Physical functioning subscale | 69.4 (25.2) |
Cognitive functioning subscale | 82.4 (20.6) |
Global health/QoL subscale | 60.7 (20.9) |
EORTC QLQ-MY20 | |
N | 120 |
Baseline scores, mean (SD) | |
Disease symptoms subscale | 32.5 (23.8) |
Side effects | 82.2 (14.8) |
EQ-5D-5L | |
N | 120 |
Baseline scores, mean (SD) | |
Index | 0.68 (0.25) |
EQ VAS | 68.0 (18.3) |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myeloma Module with 20 items; EQ-5D-5L = EuroQol 5 Dimensions 5-Levels questionnaire; EQ VAS = EuroQol Visual Analogue Scale; HRQoL = health-related quality of life; QoL = quality of life; SD = standard deviation.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Figure 7: Mean Change in Scores From Baseline on the EORTC QLQ-C30 Fatigue Subscale by Time Point
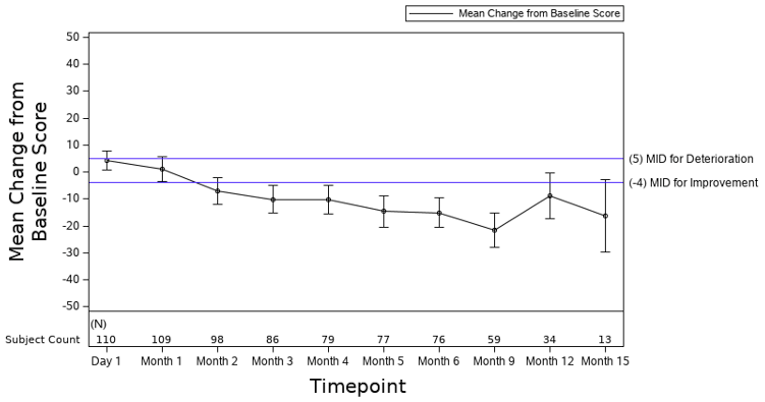
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LDC = lymphodepleting chemotherapy; MID = minimal important difference.
Note: Baseline defined as the last non-missing assessment on or before day of LDC. Error bars represent 95% confidence intervals. Data cut-off date: October 16, 2019.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Figure 8: Mean Change in Scores From Baseline on the EORTC QLQ-C30 Pain Subscale by Time Point
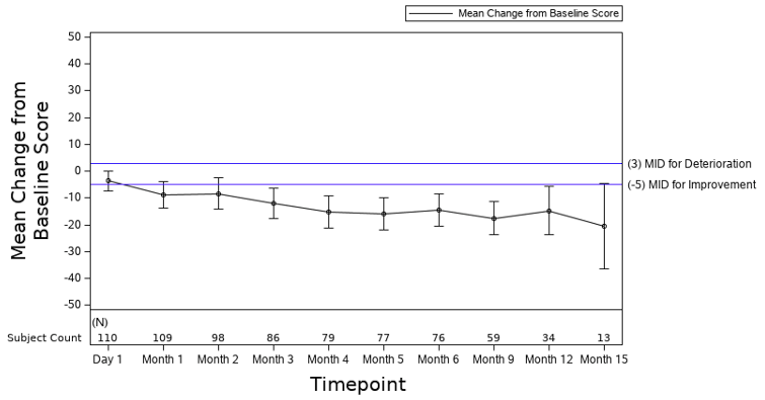
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LDC = lymphodepleting chemotherapy; MID = minimal important difference.
Note: Baseline defined as the last non-missing assessment on or before day of LDC. Error bars represent 95% confidence intervals. Data cut-off date: October 16, 2019.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Figure 9: Mean Change in Scores From Baseline on the EORTC QLQ-C30 Physical Functioning Subscale by Time Point
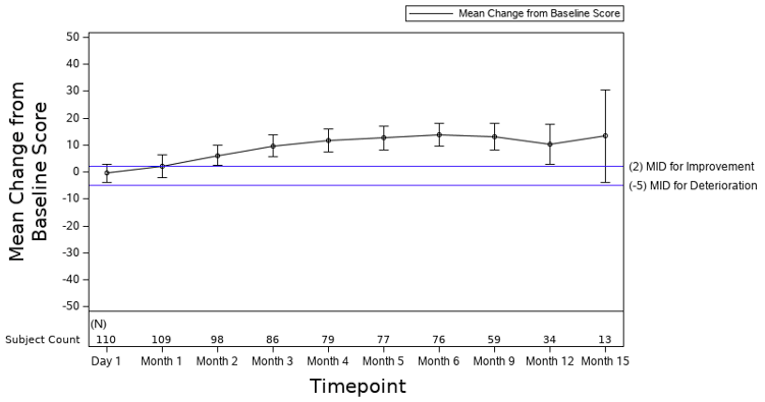
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LDC = lymphodepleting chemotherapy; MID = minimal important difference.
Note: Baseline defined as the last non-missing assessment on or before day of LDC. Error bars represent 95% confidence intervals. Data cut-off date: October 16, 2019.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Figure 10: Mean Change in Scores From Baseline on the EORTC QLQ-C30 Cognitive Functioning Subscale by Time Point
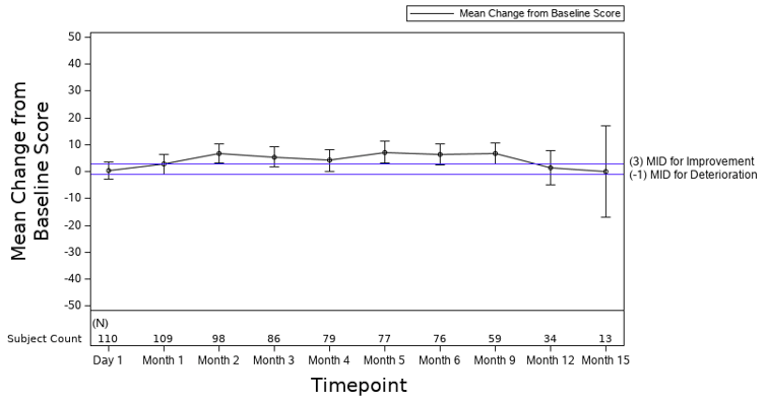
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer – Quality of Life C30 questionnaire; LDC = lymphodepleting chemotherapy; MID = minimal important difference.
Note: Baseline defined as the last non-missing assessment on or before day of LDC. Error bars represent 95% confidence intervals. Data cut-off date: October 16, 2019.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Figure 11: Mean Change in Scores From Baseline on the EORTC QLQ-C30 Global Health/QoL Subscale by Time Point
![The figure depicts the mean change from baseline in score of the EORTC QLA-C30 global health going from approximately −5 points at day 1 to 12 points at 6 months and then approximately 7 points at month 15. At month 3 it crosses the line of a minimally important difference of 5]](https://canjhealthtechnol.ca/index.php/cjht/article/download/pc0240r/version/251/493/1612/PG0240CL-fig11.png)
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LDC = lymphodepleting chemotherapy; MID = minimal important difference; QoL = quality of life.
Note: Baseline defined as the last non-missing assessment on or before day of LDC. Error bars represent 95% confidence intervals. Data cut-off date: October 16, 2019.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Figure 12: Mean Change in Scores From Baseline on the EORTC QLQ-MY20 Disease Symptoms Subscale by Time Point
![The figure depicts the mean change from baseline in score of the EORTC QLQ-MY20 going from approximately 0 points at day 1 to −13 points at 6 months and then approximately −15 points at month 15. At month 3 it crosses the line of a minimally important difference of −4]](https://canjhealthtechnol.ca/index.php/cjht/article/download/pc0240r/version/251/493/1613/PG0240CL-fig12.png)
EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myeloma Module with 20 items; LDC = lymphodepleting chemotherapy; MID = minimal important difference.
Note: Baseline defined as the last non-missing assessment on or before day of LDC. Error bars represent 95% confidence intervals. Data cut-off date: October 16, 2019.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11
Figure 13: Mean Change in Scores From Baseline on the EORTC QLQ-MY20 Side Effects Subscale by Time Point
![The figure depicts the mean change from baseline in score of the EORTC QLQ MY20 going from approximately −2 points at day 1 to 5 points at 6 months and then approximately 9 points at month 15. At month 3 it crosses the line of a minimally important difference of −4]](https://canjhealthtechnol.ca/index.php/cjht/article/download/pc0240r/version/251/493/1614/PG0240CL-fig13.png)
EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myeloma Module with 20 items; LDC = lymphodepleting chemotherapy; MID = minimal important difference.
Note: Baseline defined as the last non-missing assessment on or before day of LDC. Error bars represent 95% confidence intervals. Data cut-off date: October 16, 2019.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa).11

||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||11
Note: This figure has been redacted as per the sponsor’s request.

||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||
|||||||||||||||
Note: This figure has been redacted as per the sponsor’s request.
Harms
Harms identified in the protocol of this review are reported below. In the KarMMa trial, the primary safety analysis was based on the population treated with idecabtagene vicleucel, which included 128 patients who received an infusion of idecabtagene vicleucel. The safety evaluation included all safety data as of the data cut-off date of October 16, 2019. The median duration of follow-up after idecabtagene vicleucel infusion for all idecabtagene vicleucel–treated patients was 11.3 months (range = 0.2 to 18.6), and 17.8 months, 13.9 months, and 9.7 months in patients who received target doses of 150 × 106, 300 × 106, and 450 × 106 CAR T cells, respectively.
Table 16 provides detailed harms data. All data pertain to safety events occurring after the initial idecabtagene vicleucel administration; safety data during the re-treatment period are reported separately.
Adverse Events
All 128 patients treated with idecabtagene vicleucel reported grade 3 or 4 AEs occurring in 127 patients (99.2%). Most AEs, with the exception of hypogammaglobulinemia and infections, occurred within the first 8 weeks after infusion.
The most commonly reported AEs were hematologic toxic effects (Table 16), including neutropenia in 117 patients (91.4%), CRS in 107 patients (83.6%), anemia in 89 patients (69.5%), and thrombocytopenia in 81 patients (63.3%). Among patients with persistent grade 3 or grade 4 neutropenia (52 patients) or thrombocytopenia (62 patients) 1 month after infusion, the median time to recovery to grade 2 or lower was 1.9 months (range = 1.2 to 5.6) and 2.1 months (range = 1.2 to 13.8), respectively.
Serious Adverse Events
In the period on or after idecabtagene vicleucel infusion, 86 patients (67.2%) had at least 1 SAE. The most frequently reported SAEs (≥ 5% of patients) were CRS in 22 patients (17.2%), general physical health deterioration in 13 patients (10.2%), pneumonia in 11 (8.6%), and febrile neutropenia in 9 (7.0%). The frequencies of patients with SAEs were generally similar between the target dose subgroups, except for those who received a target dose of 450 × 106 CAR T cells, who had at least 5% higher frequencies of influenza when compared to the 300 × 106 CAR T cells group (5.6% versus 0% respectively), pyrexia (7.4% versus 1.4%), and basal cell carcinoma (7.4% versus 1.4%).
Mortality
Eight patients died after leukapheresis and before receiving idecabtagene vicleucel infusion: 5 patients (3.6%) died after leukapheresis and before starting LDC, and 3 patients (2.1%) died after starting LDC and before receiving idecabtagene vicleucel infusion. In 6 of these 8 patients, the death was classified as “death from malignant disease under study” or “complication due to malignant disease under study.” One of the other 2 deaths was categorized as “death from AE” due to acute respiratory failure, and the other as “death from other cause” due to an event coded as cerebral hemorrhage.
In total, in the population treated with idecabtagene vicleucel as of the data cut-off date, 34 patients (26.6%) died on or after idecabtagene vicleucel infusion, with 24 of these deaths attributed to the malignant disease under study or complications due to the malignant disease under study. The primary cause of death was attributed to “death from AE” in 6 patients (4.7%), including deaths due to bronchopulmonary aspergillosis, pneumonia cytomegaloviral, sepsis, gastrointestinal hemorrhage, CRS, and subdural hematoma (all occurring in 1 patient each, 0.8%).
Notable Harms
Harms of special interest were identified according to the protocol for this review. Febrile neutropenia was present in 21 patients (16.4%) in the population treated with idecabtagene vicleucel. For the outcome of neurotoxicity, a total of 23 patients (18.0%) in the idecabtagene vicleucel–treated population had investigator-identified neurotoxicity on or after idecabtagene vicleucel infusion. Psychiatric disorders included confusional states or anxiety (in 45 patients [35.2%]) and nervous system disorders (in 67 patients [52.3%]). The replication-competent lentivirus is a hypothetical complication occurring in patients receiving CAR T-cell therapies, but no cases were detected. Hospital utilization was measured with the number of ICU admissions, which 25 patients (19.5%) required. Infections or infestations were present in 88 patients (68.8%), most of which were upper respiratory infections (18 [14.1%]) and pneumonia (15 [11.7%]).
Cases of CRS on or after idecabtagene vicleucel infusion were reported in 107 patients (83.6%). The frequencies of patients with CRS-related AEs increased by target dose level: 50.0%, 75.7%, and 96.3% at the target doses of 150 × 106, 300 × 106, and 450 × 106 CAR T cells, respectively. The most frequent treatment for patients with CRS was tocilizumab (52%), followed by corticosteroids (14.8%), anakinra (1.6%), and siltuximab (0.8%). The majority of patients had CRS of grade 1 or 2 maximum severity (100 patients; 78.1%), while grade 3 or 4 maximum severity CRS was reported in 6 patients (4.7%). All CRS-related AEs occurred within the first 8 weeks after idecabtagene vicleucel infusion, with a median duration of all CRS cases of 5 days (range = 1 to 63 days).
Table 16: Adverse Events by System Organ Class and Preferred Term Reported for at Least 30% of Patients on or After Idecabtagene Vicleucel Infusion in the Population Treated With Idecabtagene Vicleucel
Adverse event | Idecabtagene vicleucel (CAR T cells) target dose, n (%) | |||
|---|---|---|---|---|
150 × 106 N = 4 | 300 × 106 N = 70 | 50 × 106 N = 54 | Total 150 × 106 to 450 × 106 N = 128 | |
Number of patients with ≥ 1 AE | 4 (100.0) | 70 (100.0) | 54 (100.0) | 128 (100.0) |
Blood and lymphatic system disorders | 4 (100.0) | 67 (95.7) | 53 (98.1) | 124 (96.9) |
Neutropenia | 4 (100.0) | 62 (88.6) | 51 (94.4) | 117 (91.4) |
Anemia | 4 (100.0) | 51 (72.9) | 34 (63.0) | 89 (69.5) |
Thrombocytopenia | 4 (100.0) | 42 (60.0) | 35 (64.8) | 81 (63.3) |
Leukopenia | 2 (50.0) | 34 (48.6) | 18 (33.3) | 54 (42.2) |
General disorders and administration site conditions | 4 (100.0) | 60 (85.7) | 37 (68.5) | 101 (78.9) |
Fatigue | 1 (25.0) | 28 (40.0) | 14 (25.9) | 43 (33.6) |
Pyrexia | 0 | 17 (24.3) | 15 (27.8) | 32 (25.0) |
Metabolism and nutrition disorders | 3 (75.0) | 57 (81.4) | 37 (68.5) | 97 (75.8) |
Hypokalemia | 1 (25.0) | 28 (40.0) | 16 (29.6) | 45 (35.2) |
Hypophosphatasemia | 0 | 24 (34.3) | 14 (25.9) | 38 (29.7) |
Hypocalcemia | 0 | 22 (31.4) | 12 (22.2) | 34 (26.6) |
Gastrointestinal disorders | 2 (50.0) | 55 (78.6) | 39 (72.2) | 96 (75.0) |
Diarrhea | 2 (50.0) | 23 (32.9) | 20 (37.0) | 45 (35.2) |
Nausea | 1 (25.0) | 20 (28.6) | 16 (29.6) | 37 (28.9) |
Infections and infestations | 3 (75.0) | 47 (67.1) | 38 (70.4) | 88 (68.8) |
Upper respiratory tract infection | 0 | 13 (18.6) | 5 (9.3) | 18 (14.1) |
Pneumonia | 0 | 8 (11.4) | 7 (13.0) | 15 (11.7) |
Musculoskeletal and connective tissue disorders | 3 (75.0) | 42 (60.0) | 28 (51.9) | 73 (57.0) |
Nervous system disorders | 2 (50.0) | 43 (61.4) | 22 (40.7) | 67 (52.3) |
Headache | 1 (25.0) | 19 (27.1) | 7 (13.0) | 27 (21.1) |
Dizziness | 1 (25.0) | 12 (17.1) | 4 (7.4) | 17 (13.3) |
Respiratory, thoracic and mediastinal disorders | 4 (100.0) | 42 (60.0) | 21 (38.9) | 67 (52.3) |
Cough | 3 (75.0) | 15 (21.4) | 8 (14.8) | 26 (20.3) |
Psychiatric disorders | 0 | 33 (47.1) | 12 (22.2) | 45 (35.2) |
Patients with ≥ 1 SAE (grade 3 or 4 CTCAE) | 4 (100.0) | 69 (98.6) | 54 (100.0) | 127 (99.2) |
Blood and lymphatic system disorders | 4 (100.0) | 67 (95.7) | 52 (96.3) | 123 (96.1) |
Neutropenia | 4 (100.0) | 59 (84.3) | 51 (94.4) | 114 (89.1) |
Anemia | 4 (100.0) | 42 (60.0) | 31 (57.4) | 77 (60.2) |
Thrombocytopenia | 3 (75.0) | 34 (48.6) | 30 (55.6) | 67 (52.3) |
Leukopenia | 2 (50.0) | 30 (42.9) | 18 (33.3) | 50 (39.1) |
Lymphopenia | 2 (50.0) | 19 (27.1) | 13 (24.1) | 34 (26.6) |
Febrile neutropenia | 2 (50.0) | 11 (15.7) | 7 (13.0) | 20 (15.6) |
Metabolism and nutrition disorders | 0 | 24 (34.3) | 15 (27.8) | 39 (30.5) |
Infections and infestations | 1 (25.0) | 14 (20.0) | 12 (22.2) | 27 (21.1) |
Pneumonia | 0 | 4 (5.7) | 4 (7.4) | 8 (6.3) |
Deathsa | ||||
Total number of deaths, n (%) | — | — | — | 34 (26.6) |
Death from malignant disease under study or complication due to malignant disease under study | — | — | — | 24 (18.8) |
Neoplasms benign, malignant, and unspecified (including cysts and polyps) | — | — | — | 21 (16.4) |
Plasma cell myeloma | — | — | — | 21 (16.4) |
Death from adverse events | — | — | — | 6 (4.7) |
Death from other causes | — | — | — | 4 (3.1) |
Notable harms | ||||
Febrile neutropenia | 2 (50.0) | 11 (15.7) | 8 (14.8) | 21 (16.4) |
Cytokine release syndrome | 2 (50.0) | 53 (75.7) | 52 (96.3) | 107 (83.6) |
Received tocilizumab for CRS, n (%) | 1 (25.0) | 30 (42.9) | 36 (66.7) | 67 (52.3) |
Received siltuximab for CRS, n (%) | 0 | 1 (1.4) | 0 | 1 (0.8) |
Received corticosteroids for CRS, n (%) | 0 | 7 (10.0) | 12 (22.2) | 19 (14.8) |
Received anakinra for CRS, n (%) | 0 | 1 (1.4) | 1 (1.9) | 2 (1.6) |
Investigator-identified neurotoxicity | 0 (0) | 12 (17.1) | 11 (20.4) | 23 (18.0) |
Replication-competent lentivirus | 0 | 0 | 0 | 0 |
Hospital utilization – ICU admission | — | — | — | 25 (19.5) |
AE = adverse event; CAR = chimeric antigen receptor; CRS = cytokine release syndrome; CTCAE = Common Terminology Criteria for Adverse Events; ICU = intensive care unit; LDC = lymphodepleting chemotherapy; PT = preferred term; SAE = serious adverse event; SOC = system organ class.
Note: Cases of CRS were graded using criteria from Lee (2014). Neurologic toxicity (broad) consists of all PTs within the primary or secondary SOCs of nervous system disorders and psychiatric disorders whereas neurologic toxicity (focused) consists of an ad hoc list of PTs.
aDeaths were not summarized for each of the idecabtagene vicleucel target dose groups.
Source: Clinical Study Report for BB2121-MM-001 (KarMMa) study.11
In an updated data submission (cut-off date: January 14, 2020),10 no differences in the number of patients with AEs were noted. Ten more deaths were reported at this cut-off date (44 [34.4%]) and 23 more cases of febrile neutropenia (a total of 30 of 128 treated patients [16.3%]) were reported. The other harms of special interest were not significantly different at this cut-off date. These results are described in Appendix 3.
Critical Appraisal
Internal Validity
The KarMMa study was a single-arm, open-label, phase II study. Limitations of the study stem from the single-arm design and lack of a comparator group, which reduce the confidence in the effect estimates due to an increase in the risk of bias associated with confounding fluctuations in health status, and unidentified prognostic factors, which could affect subjectively assessed outcomes. The open-label design may introduce bias and subjectivity when assessing HRQoL outcomes as it was not evaluated in a blinded fashion. The HRQoL outcomes were considered secondary end points and analyzed in smaller groups (N = 121). The use of well-validated measurement scales for assessing PROs were appropriate and may mitigate bias in the measurement of these outcomes.
Patients considered in the enrolled population (N = 140) and those included in the analyzed idecabtagene vicleucel–treated population (N = 128) were similar across different measures and outcomes, implying a low risk of bias due to differences in patients who withdrew from the study after enrolment. All patients in the population treated with idecabtagene vicleucel were analyzed, also suggesting a low risk of attrition bias and selection of participants into the cohort of treated patients. However, the number of patients included in the different target doses groups were dissimilar, mainly due to changes during the amendments in the study (Amendment 2.0), with small sample sizes in these individual groups (e.g., only 4 patients included in the 150 × 106 CAR T cells target dose group) which creates issues of imprecision in effect estimates in these groups. The patients from the 450 × 106 CAR T cells target dose group (n = 54) was similar overall in baseline and demographic characteristics. Similarly, the PROs (HRQoL outcomes) were not considered in a multiplicity adjustment, had significant amounts of missing data at baseline and a significant proportion missing at a later time, creating a potential for bias in those that remain and who may not be reflective of the overall population (i.e., those that died tend to have had a poorer HRQoL).
Investigators tested their primary efficacy end point, the ORR, against the null hypothesis of an ORR of less than 50% (i.e., a 50% improvement over daratumumab monotherapy) and if this was significant, the CRR would be tested against a null hypothesis of a CRR of less than 10% (a 10% improvement of idecabtagene vicleucel over daratumumab monotherapy). These historical values for the null hypothesis appear to be appropriate as they were obtained from recent clinical trials.
Bridging therapy for myeloma control following leukapheresis while idecabtagene vicleucel was being manufactured was used in the majority of patients (87.5%), and these included corticosteroids, alkylating agents, IMiDs, proteasome inhibitors, and/or anti-CD38 antibodies. Whether these interventions could have an effect on the outcomes evaluated in these patients after receiving idecabtagene vicleucel treatment is not known.
The prospective nature of the study defines the time of assigning and starting the intervention and the follow-up, which ameliorates any misclassification of variables and other measurements of different outcomes. Few deviations from the intended interventions were detected and all appeared to be properly reported. Deviations from the protocol occurred in 46 patients (35.9%) of the population treated with idecabtagene vicleucel and most were due to reporting errors. There were instances of missing data in the HRQoL, but there was adequate reporting of the censoring rules throughout the study according to FDA censoring rules for time-to-event outcomes (DoR, OS, and PFS).
Multiplicity was addressed only for the ORR and CR end points, using a stepdown procedure to control the family-wise type I error rate, testing first the primary end point of ORR, with the key secondary end point tested only if the test of primary efficacy end point was positive. The lack of multiplicity adjustments, (i.e., the type I error rate) for the other secondary and exploratory outcomes relevant to this report (DoR, TTR, TTP, MRD status, OS, PFS, and HRQoL) generates uncertainty due to the increased possibility of observing a chance association as causal.
Subgroups were planned a priori, but no formal subgroup effect tests were conducted due to the expected small number of patients and events (imprecision). Some subgroups were relatively small, producing relatively wide and imprecise CIs around the point estimates. Given the relatively small numbers of patients, it is unclear if they are representative of the larger population.
External Validity
According to input from the clinical experts, patients in the KarMMa trial were generally representative of those who are anticipated to receive idecabtagene vicleucel in the Canadian landscape (i.e., the population with RRMM of Canada) who have already received multiple lines of treatment but are usually considered in a health state to be able to receive the CAR T-cell therapy. Overall, the clinical variables and patient baseline characteristics from the KarMMa trial were similar to what would be expected to occur in clinical practice in patients who are already refractory to IMiD, proteasome inhibitors, and anti-CD38 drugs, including the performance status (Table 17).
The administration of idecabtagene vicleucel in the KarMMa study involves several additional actions to consider. First, the manufacturing process takes 4 to 5 weeks to complete, from the leukapheresis to the idecabtagene vicleucel infusion. Second, the use of bridging therapies requires treatments that are currently available in the Canadian clinical practice (i.e., corticosteroids, IMiD, proteasome inhibitors, and anti-CD38 antibodies). Third, LDC should be used in all patients before receiving idecabtagene vicleucel. These actions present further variables to consider in the feasibility and acceptability of the intervention as they would be a constant part of the new treatment. According to feedback from the clinical experts consulted by CADTH, these steps are necessary components of the idecabtagene vicleucel administration process and would be implemented in Canadian clinical practice.
Re-treatment of patients was allowed in the KarMMa study if they fulfilled specific clinical criteria, which included having enough cryopreserved material to produce another dose of idecabtagene vicleucel. This strategy is likely to be considered by physicians and patients receiving idecabtagene vicleucel. Complying with the eligibility criteria for re-treatment will be important for the applicability of this option.
Table 17: Assessment of Generalizability of Evidence for Idecabtagene Vicleucel
Domain | Factor | Evidence | CADTH assessment of generalizability |
|---|---|---|---|
Population | Patient with RRMM | Trial inclusion/exclusion criteria | The inclusion/exclusion criteria appeared to recruit the appropriate patient population. Some concerns exist regarding the number of patients who did not receive idecabtagene vicleucel after enrolment in the leukapheresis. |
Intervention | Idecabtagene vicleucel | Trial protocol | The target dose approved in Canada for idecabtagene vicleucel is 450 × 106 CAR T cells, within a range of 275 to 520 × 106 CAR T cells. This is reflective of the doses used in the KarMMa study. |
Comparator | Drug regimens used as palliative care in Canadian clinical practice, including:
| No comparator was used in the KarMMa study | There was no comparator in the KarMMa study. |
Outcomes | ORR, CRR, DoR, TTR, TTP, MRD, OS, PFS, HRQoL | Trial protocol | These outcomes are relevant to patients and clinicians and applicable in clinical practice. There was uncertainty in the HRQoL outcomes due to attrition of participants in the KarMMa study, affecting the generalizability of results, given that clinicians frequently use HRQoL scales in clinical practice. |
Setting | Inpatient cancer care | Trial sites | The administration of idecabtagene vicleucel requires a specialized unit and expert staff. This is in agreement with the settings that the trial used. |
CRR = complete response rate; cyclo = cyclophosphamide; DoR = duration of response; HRQoL = health-related quality of life; Kd = carfilzomib plus dexamethasone; KRd = carfilzomib plus lenalidomide plus dexamethasone; MRD = minimal residual disease; ORR = overall response rate; OS = overall survival; Pd = pomalidomide plus dexamethasone; PFS = progression-free survival; Rd = lenalidomide plus dexamethasone; RRMM = relapsed or refractory multiple myeloma; TTR = time to response; TTP = time to progression; Vd = bortezomib plus dexamethasone.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
This section summarizes and appraises indirect evidence comparing the relative efficacy and safety of idecabtagene vicleucel against relevant comparators.
One of the limitations of the KarMMa study is the lack of a comparator arm to evaluate the relative efficacy of idecabtagene vicleucel in patients with RRMM to standards of care.
Two sponsor-submitted analyses are included in this report. The first (NDS-MM-003)12 aims to evaluate the effect of idecabtagene vicleucel from the KarMMa study (MM-001), which has a single-arm design, and compare its results with the effectiveness of other currently administered treatments, using patient-level RWE collected from various sources in a comparable population (RRMM according to the inclusion and exclusion criteria of the KarMMa study). The second is a sponsor-submitted MAIC, which is described and evaluated in this section as a high-level critical appraisal.13
A supplemental literature search was conducted by CADTH to identify further ITCs of idecabtagene vicleucel in RRMM patients. A focused literature search for ITCs dealing with MM was run in MEDLINE All (1946–) on January 21, 2021. The search was limited to documents published between January 1, 2011, and January 21, 2021. Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer will be acquired. Reviewers made the final selection of studies to be included in the review, and differences were resolved through discussion. Based on this literature search conducted by CADTH, no additional ITCs were included in this review report.
Description of Indirect Evidence
The NDS-MM-003 study (or KarMMa-RW), which is included in this indirect evidence section, is a comparative study of a retrospective body of RWE (a synthesized cohort) obtained from multiple databases of patients using available MM treatments to be compared to the single-arm KarMMa trial population treated with idecabtagene vicleucel. Details about the population, interventions, outcomes, and study characteristics are described in Table 18.
Table 18: Study Methods for the Included Indirect Treatment Comparison
Domain | NDS-MM-003 (KarMMa-RW) |
|---|---|
Population | Patients with documented diagnosis of MM who have received a proteasome inhibitor, an IMiD, and an anti-CD38 antibody |
Intervention | Idecabtagene vicleucel at a target dose of 150 × 106 to 450 × 106 CAR T cells |
Comparator |
|
Outcomes |
|
Study design | Propensity score analysis of a cohort from a single-arm prospective trial against an eligible RRMM cohort (RWE). |
CAR = chimeric antigen receptor; CRR = complete response rate; IMiD = immunomodulatory imide drug; MM = multiple myeloma; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; RRMM = relapsed and refractory multiple myeloma; RWE = real-world evidence; VGPR = very good partial response.
Source: Sponsor-submitted indirect treatment comparison.12
Methods
Objectives
The primary objective of the study was to describe demographic and selected clinical characteristics of RW patients with RRMM who received at least 3 prior myeloma regimens, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody (RRMM cohort), and to describe demographics, disease characteristics, treatment patterns, and clinical outcomes of the RW cohort and for the cohort of RW patients who met eligibility criteria for the KarMMa study (the eligible RRMM cohort).
As a secondary objective, investigators aimed to assess the comparative effectiveness of patients treated with idecabtagene vicleucel in the KarMMa study (MM-001) versus external RW controls (the balanced RRMM cohort) using a propensity score analyses.
Data Selection and Collection Methods
The organization, selection, and flow of patients from databases to build the different cohorts used in the study are shown in Figure 16 and described in the following section.
RRMM Cohort
Patients were first identified from RW databases (“real-world patients”) based on broad inclusion and exclusion criteria. For inclusion, patients had to be at least 18 years of age at the time of MM diagnosis; have a documented diagnosis of MM; have received a proteasome inhibitor, an IMiD, and an anti-CD38 antibody; have received anti-CD38 antibody therapy on or after November 16, 2015 (daratumumab earliest FDA approval); have received at least 3 prior MM treatment regimens by September 30, 2018; and have undergone at least 2 consecutive cycles of treatment for each regimen, unless PD was the best response to the regimen. Induction with or without hematopoietic stem cell transplant and with or without maintenance therapy was considered a single regimen.
Patients were excluded if they had previous exposure to any BCMA-directed therapy or gene-modified therapy.
Eligible RRMM Cohort
The eligible RRMM cohort was generated from the RRMM cohort described earlier using the following criteria:
Additional inclusion criteria:
Refractory to the last regimen, with refractory defined as documented PD during or within 60 days (measured from the last dose) of completing treatment with the last regimen of AMT before study entry
Have measurable disease as measured by serum/urine M-protein and/or a serum FLC assay, including 1 of the following criteria:
serum M-protein greater or equal to 1.0 g/dL
urine M-protein greater or equal to 200 mg/24 hours
FLC level greater or equal to 10 mg/dL (100 mg/L) provided serum FLC ratio is abnormal
at least 1 documented disease assessment after the refractory condition or documented death.
Exclusion criteria:
ECOG status of at least 2 at baseline (T0, defined as the date that the RW subject became refractory to the last regimen)
Central nervous system involvement with MM
History or presence of clinically relevant pathology at the baseline time point (T0), including CNS (e.g., epilepsy, seizure, paresis, aphasia, stroke, severe brain injuries, dementia, Parkinson disease, cerebellar disease, organic brain syndrome, or psychosis), unresolved hepatic pathology, unresolved cardiac, pulmonary, pathology, and inadequate renal or bone marrow function
Current or prior viral infection with hepatitis B virus, hepatitis C virus, or HIV
Solitary plasmacytomas without other evidence of measurable disease
Active or history of plasma cell leukemia
Secondary malignancies requiring therapy.
Matched RRMM Cohort
The eligible RRMM cohort served as a selection pool of RW patients to construct the matched RRMM cohort, a smaller cohort with baseline characteristics similar to those of the idecabtagene vicleucel cohort. Due to the small sample size of the eligible RRMM cohort, only a subset of the idecabtagene vicleucel cohort was matched to this cohort. The original statistical analysis plan specified an estimated 2:1 matched RRMM cohort of patients to compare real-world and idecabtagene vicleucel patients. However, due to strict criteria, fewer patients were available for the matched RRMM cohort, requiring a change in the statistical analysis. Investigators therefore decided to use trimmed stabilized IPTW, leaving the matched-paired and untrimmed IPTW as supportive analyses.
Idecabtagene Vicleucel Cohort (MM-001 – KarMMa Study)
The KarMMa study, the main intervention arm for the NDS-MM-003 study, is fully described in this CADTH clinical review report. Briefly, it is an ongoing, open-label, single-arm, multi-centre, phase II study to evaluate the efficacy and safety of idecabtagene vicleucel in patients with RRMM. The primary analysis population from the KarMMa study consisted of the 128 patients in the idecabtagene vicleucel–treated population, which is defined as all patients in the enrolled population who received idecabtagene vicleucel infusion (hereafter referred to as the idecabtagene vicleucel cohort); all efficacy results reported for the idecabtagene vicleucel cohort are therefore a composite from patients across the target dose levels of 150 × 106 to 450 × 106 CAR T cells used to treat patients.
Baseline, Index Date, and Study Period Definition
Baseline (T0) for the eligible RRMM and matched RRMM cohorts was defined as the date that the RW subject became refractory to the last regimen, with refractory defined as documented PD during or within 60 days (measured from the last dose) of completing treatment with the last regimen of antimyeloma drug therapy before study entry.
Given that the RW subject met all eligibility criteria defined for each cohort, the index date or study day 1 was the start date of the first AMT after T0. For patients in the RRMM cohort, day 1 was defined as the start date of a new treatment regimen after receiving at least 2 consecutive cycles of a proteasome inhibitor, an IMiD, and an anti-CD38 antibody therapy regimen by September 30, 2018, provided that anti-CD38 antibody therapy was received on or after November 16, 2015. For both the eligible RRMM cohort and matched RRMM cohort, day 1 was the start date of a new AMT after the occurrence of a PD that occurred within 60 days of completing the last qualified AMT, which can be the fourth or later regimen started after meeting study eligibility criteria.
For the idecabtagene vicleucel cohort, the baseline value was defined as the last value on or before the first dose date on which LDC was administered. The index date or study day 1 was the start date of idecabtagene vicleucel infusion after T0.
Figure 16: Cohort Construction and Subject Selection in the KarMMa-RW Trial
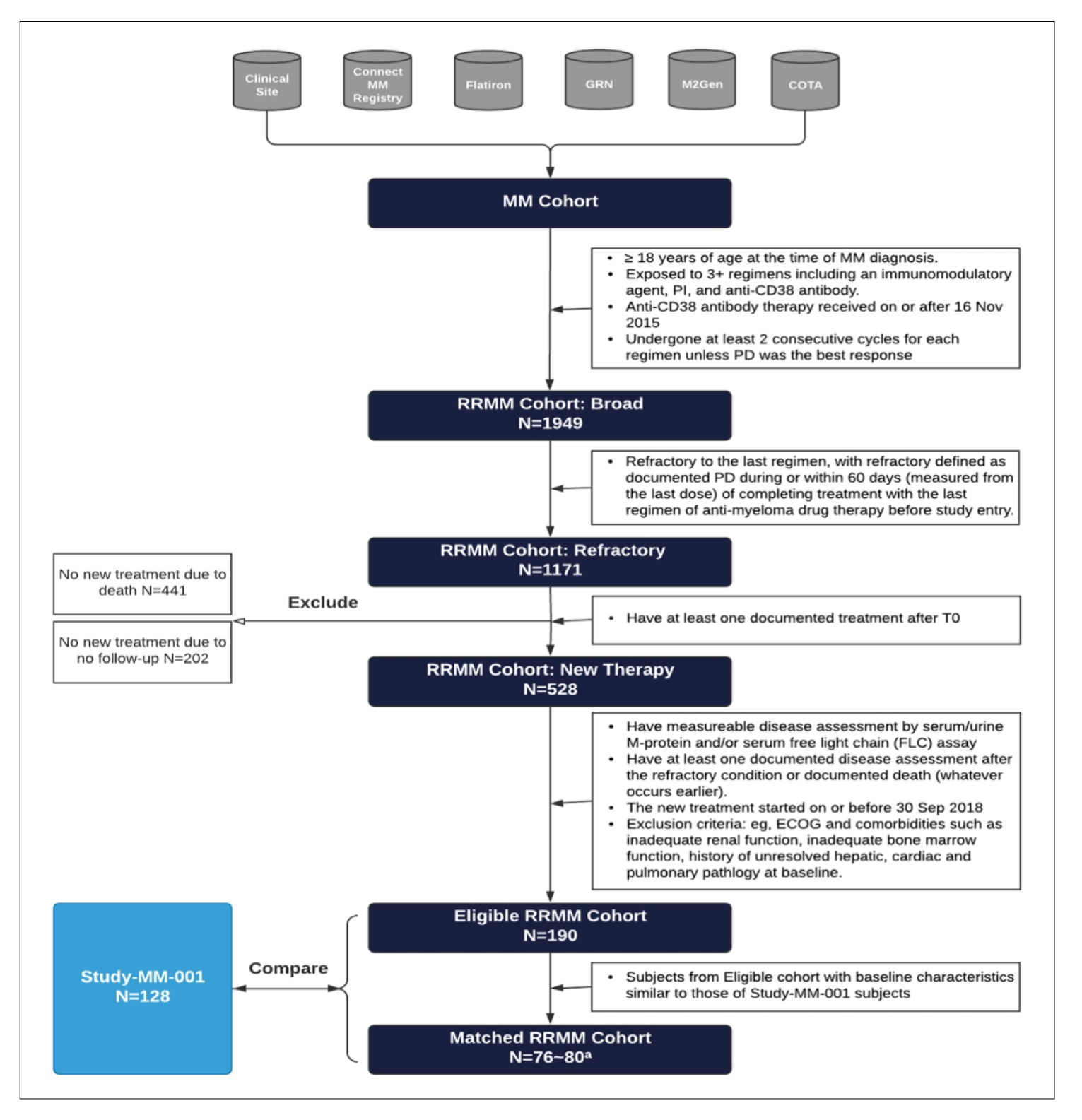
ECOG = Eastern Cooperative Oncology Group; GRN = Guardian Research Network; MM = multiple myeloma; PD = progressive disease; PI = proteasome inhibitor; RRMM = relapsed and refractory multiple myeloma; T0 = baseline time point.
a Numbers (minimum to maximum) of matched patients from 30 imputed datasets.
Source: Sponsor-submitted indirect treatment comparison.12
Data Sources
Real-world data for NDS-MM-003 were acquired from 3 types of sources: clinical sites, the Connect MM Registry, and external research database partners. All RW patient-level data collection was retrospective and did not change clinical practice or patient visit schedules. Each data source was responsible for ensuring data collection followed applicable national and local ethical, legal, and privacy regulations.
Clinical sites data were obtained through manual chart abstraction into the study electronic case report forms. Individual clinical sites consisted of academic centres representing primarily North America and Europe. Out of 30 sites that were approached, 14 were initiated and able to complete data collection. All data collection was captured by an external company using a data collection instrument specifically designed for the purpose of this study, with audits and quality checks performed throughout the process.
The Connect MM Registry is a multi-centre, prospective observational cohort study designed to explore the natural history and real-world management of patients with newly diagnosed MM. Treatment selections and disease response assessments are performed at the discretion of the treating physician in accordance with their usual care. The registry follows patients from approximately 200 sites in the US with experience in oncology and/or hematology trials and registries and an adequate number of patients with MM.
Several external research databases are included. First of these is the COTA-RWE database of de-identified (US Health Insurance Portability and Accountability Act–compliant) patient-level electronic health record (EHR) data from contributing US academic, for-profit, and community oncologist provider sites and hospital systems. Also included are the Flatiron Health database, a database of EHR data from cancer clinics and unstructured reports from physicians; the Guardian Research Network, a nationwide consortium of health systems in the US that harness clinical and molecular oncology de-identified patient EHR information; |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Data Collection, Integration, Quality Assurance, and Harmonization
Data from clinical sites were entered into a secure, internet-based electronic data-capture instrument by designated, trained personnel, with the principal investigator responsible for ensuring the accuracy and authenticity of the data.
Information from all sources was reformatted into a standardized study data model. Program and mapping specifications for variable transformations and derivations were created for each data element within each data source.
Upon receipt of raw data, a multi-stage quality control and validation protocol was initiated for each data source. The quality of raw data was evaluated through quantification of the magnitude and mechanism of missing data, density of laboratory results and clinical assessments, duplicated records, outliers, and extensive logic checks for time-related data points and those with dependencies. Upon completion of quality control and validation activities on the raw and integrated data, these data from multiple sources were pooled into a single dataset for harmonization.
End Points
The primary end point was the ORR, which was defined as the percentage of patients who achieved a PR or better. A PR was defined according to IMWG uniform response criteria for MM.3
Secondary end points included:
The VGPR rate, which was defined as the percentage of patients who achieved VGPR or better from the index date according to IMWG uniform response criteria for MM.
The CRR, which was defined as the percentage of patients who achieved CR or better according to IMWG uniform response criteria for MM. The assessment of this end point requires a bone marrow biopsy (also according to IMWG criteria), which is not typically performed in the routine care of RW patients, leading to limited data and the inability to assess CR for the RW population. The authors report this as “optional” and refer to analyses of VGPR or better to avoid underestimating response in the RW cohort.
The OS, which was defined as the time from index date to time of death due to any cause. Patients who did not die were to be censored at the last date known to be alive or a maximum follow-up time of ||| days, whichever occurred first.
The TTR, which was defined as the time from index date to first documentation of a response of PR or better in all patients responding.
The DoR, which was defined for responders as time from first response (PR or better) to PD or death from any cause, whichever occurred first; responders who did not progress or did not die were to be censored on the last adequate assessment date.
The PFS, which was defined as the time from index date to first documentation of PD or death due to any cause, whichever occurred first. Patients who did not have a PFS event were to be censored on the last adequate assessment date. Censoring rules based on EMA guidance for cancer trial end points were applied. Results using FDA censoring rules are also presented to assess any differences in both scenarios.23,24
Health care resource utilization, if available.
Analysis Methods
Descriptive analyses were performed to gain an understanding of the quality of the data collected and statistical distributions of characteristics of the RW patient cohorts. Continuous variables were described by the mean with standard deviation and 95% CI, median, upper, and lower quartiles, and maximum and minimum values. Categorical variables were reported as numbers and percentages with 95% CIs. Missing data were described in all summaries. For analysis comparing RW data with data from Study MM-001, a 2-sided P value of less than 0.05 was considered statistically significant without adjustment for multiplicity.
To enhance comparability between patients in the eligible RRMM cohort and in the idecabtagene vicleucel cohort (the KarMMa study), logistic regression was used to develop propensity scores, which were calculated on patient-level data to summarize the impact of covariates on treatment selection. These scores were then used by weighting individual patients (in the eligible RRMM cohort and the idecabtagene vicleucel cohort), IPTW, or through matching patients in these 2 cohorts to improve the balance of covariates and comparability between both groups. Authors used the propensity score trimmed stabilized IPTW method to enhance comparability of the baseline characteristics and weight the RW cohorts and the populations treated with idecabtagene vicleucel. These were achieved in 6 steps:
Step 1. Selection of covariates to include in multivariate logistic regression modelling: Prior to starting the initial analysis, variables for consideration in the propensity score analysis were selected based on clinical importance relating to outcome and disease severity based on the expertise of the study team with a further review by a team of 7 clinical experts, who elected and ranked the order of prognostic factors across studies using a structured approach as recommended by guidance from the National Institute for Health and Care Excellence. A score was generated for each subject using a logistic model and adding further potential prognostic factors for efficacy to be considered in the propensity score model using the demographic and baseline characteristics from the KarMMa study and the eligible RRMM population. Univariate logistic regression was used to identify potential covariates for the initial propensity score model. Any values missing for the candidate covariates were imputed via multiple imputation procedures. Covariates considered included age, sex, bone lesions, time from initial diagnosis, number of prior regimens, cytogenetic high or low risk, refractory to immunomodulatory agents, refractory to proteasome inhibitors, refractory to anti-CD38 antibody, and baseline laboratory tests (platelet, hemoglobin, albumin, and calcium). Covariates that were considered important clinical outcome predictors by the scientific steering committee (i.e., age, albumin and number of prior regimens) were forced into the model.
Step 2. Propensity score modelling: Once the covariates for the PS were calculated, 30 datasets were created (using multiple imputation of data when missing). Statistically significant variables (P values < 0.15) were included in the initial and/or full multivariate logistic regression to create a final propensity score model. This final model included age; baseline albumin; number of prior regimens; number of prior regimens/year; creatine clearance group; prior refractory to proteasome inhibitors, IMiDs, and anti-CD38 antibodies; bone lesions; and baseline calcium. A final propensity score for each imputed dataset and the stabilized IPTW were obtained and used to perform the balancing.
Step 3. Assessment of balance between cohorts: Assessment of balance in PS between cohorts was conducted through a side-by-side comparison of raw baseline data for the eligible RRMM and the idecabtagene vicleucel cohort versus the balanced IPTW eligible RRMM and KarMMa baseline data. For these comparisons, pooled standardized mean differences were computed using Rubin’s rules before and after balancing and a threshold of 0.2 to indicate potentially important imbalances (Table 20).
Step 4. Balancing methods and criteria: The balancing methodology used stabilized IPTW for the propensity score and greedy nearest-neighbour matching. The balancing originally anticipated that the eligible RRMM cohort would provide a 2:1 match for the idecabtagene vicleucel cohort, but both cohorts actually contained the same number of RW patients. The IPTW was chosen as the primary methodology, with a sensitivity analysis using the greedy nearest-neighbour matching (with a caliper width of 0.2 standard deviations of the logit of the propensity score). For 1:1 greedy nearest-neighbour matching, 1 subject in the RW cohort was matched with a single subject in the KarMMa study.
Step 5. Estimation of risk ratios and hazard ratios for each of the 30 datasets mentioned in step 2.
Step 6. Analysis with blinding (firewall) between the propensity score balancing process and the analysis of the post-baseline response and outcome data (blinded outcome assessors).
Because some imbalance remained between the 2 groups after propensity score balancing, doubly robust procedures, i.e., including the individual covariates from the initial propensity score model in addition to the IPTW in the analysis, were used to adjust for remaining unbalanced covariates for all the relevant comparisons. Due to the high degree of missing data (e.g., 46.8% of values in the RRMM eligible cohort were missing, as shown in Table 19), 30 separate datasets were generated using multiple imputation procedures and individual propensity scores were estimated within each dataset.
Several sensitivity analyses were conducted to assess the robustness of the primary analysis results. These included the use of the “greedy nearest-neighbour matching” (selected after a change in the statistical analysis plan, at which point the authors decided to use the IPTW as the primary methodology), analyses based on ECOG baseline data availability, and analyses using the enrolled population in the KarMMa study. Post hoc sensitivity analyses included those based on the European Union subgroup sensitivity analysis, which was used to contextualize the comparative evaluation of the primary outcome results within the European population, and a comparative analyses of the eligible RRMM cohort and the idecabtagene vicleucel–enrolled population for the ORR (primary end point) and VGPR.
The outcomes were reported as follows:
The ORR was tabulated, together with the 2-sided 95% CI; estimates for the analyses were then obtained using Rubin’s rule to combine the individual estimates from each dataset. Relative risk, 95% CI, and the P value from the relative risk regression or equivalent generalized linear model were presented. A doubly robust procedure was used, including the covariates still differentiating these groups obtained before unblinding assessors to outcome data, in addition to the IPTW.
The CR rate was tabulated with the 2-sided 95% CI and estimates for the analyses. The comparison of the eligible RRMM cohort to the idecabtagene vicleucel cohort was based on relative risk regression. Relative risk, 95% CI, and the P value from the generalized linear model were presented. A doubly robust procedure was used, including the covariates still differentiating these groups obtained before unblinding to outcome data.
Overall survival (defined as time from index date to death due to any cause with patients censored on the last-known alive date or the maximum follow-up time of ||| days) was assessed using a Cox proportional hazards model for the time to event with the associated HR and 95% CI and P values. Adjusted survival curves were used to depict differences in survival over time between the eligible RRMM and the idecabtagene vicleucel cohorts with the same statistics reported as in the IPTW comparison, adjusted for differences in baseline covariates obtained in the final propensity score model (i.e., age; baseline albumin; number of prior regimens; number of prior regimens per year; creatine clearance group; prior refractory to propensity scores, IMiDs, and anti-CD38 antibodies; bone lesions; and baseline calcium).
The TTR was summarized using descriptive statistics for the eligible RRMM cohort and the idecabtagene vicleucel cohort.
The DoR comparison was conducted using KM graphics, a Cox proportional hazards model, and the associated estimable group medians, HR with 95% CI and P value for differences. Survival plots and the associated statistics described earlier, adjusted for covariates (age; baseline albumin; number of prior regimens; number of prior regimens/year; creatine clearance group; prior refractory to proteasome inhibitors, IMiDs, and anti-CD38 antibodies; bone lesions; and baseline calcium), were used to compare DoR in the eligible RRMM cohort and the idecabtagene vicleucel cohort.
Progression-free survival was assessed in patients who had not progressed and were still alive according to EMA censoring rules (and presenting based on FDA rules) on the last adequate assessment date or at 730 days, whichever occurred first. A PFS comparison of the cohorts was conducted using KM graphics, Cox proportional hazards model, and the associated estimable group medians, HR with 95% CI, and P value for differences. Adjusted survival curves were used to depict differences in PFS over time between the eligible RRMM and the idecabtagene vicleucel cohorts with the same statistics reported as in the matched comparison, adjusted for differences in baseline covariates (i.e., age; baseline albumin; number of prior regimens; number of prior regimens/year; creatine clearance group; prior refractory to proteasome inhibitors, IMiDs, and anti-CD38 antibodies; bone lesions; and baseline calcium).
Results
Disposition
In total, 1,949 RW patients were included in the broad RRMM cohort, and of these, 1,171 were refractory to the last treatment regimen at baseline. Of the 1,171 patients in the refractory RRMM cohort, 643 did not receive a next-line treatment (441 due to death and 202 due to lack of follow-up data). This resulted in 528 patients in the RRMM cohort who received new therapy. Additional eligibility criteria similar to those of Study MM-001 were then applied, resulting in the selection of 190 RW patients for the eligible RRMM cohort.
For the KarMMa study, 140 patients underwent leukapheresis and were included in the enrolled population. Of these, 128 patients received idecabtagene vicleucel treatment and were included in the idecabtagene vicleucel cohort as the primary analysis population for comparison against the eligible RRMM cohort.
Baseline demographics and disease characteristics of the RRMM cohort, the eligible RRMM cohort, and the idecabtagene vicleucel population are presented in Table 19, while Table 20 lists the variables before and after balancing (using the trimmed stabilized IPTW method) of the eligible RRMM and idecabtagene vicleucel cohorts are shown.
Table 19: Baseline Demographics and Disease Characteristics
Parametera | RRMM cohort (N = 1,171) | Eligible RRMM cohort (N = 190) | KarMMa (Ide-cel) cohort (N = 128) |
|---|---|---|---|
Age at baseline (years) | |||
Median | 68.0 | 64.0 | 60.5 |
Minimum to maximum | 32.0 to 95.0 | 35.0 to 91.0 | 33.0 to 78.0 |
|||||||||||||||||| | |||
||||||||||| | ||||||||||| | ||||||||||| | ||||||||||| |
||||||||||| | ||||||||||| | ||||||||||| | ||||||||||| |
||||||||||| | ||||||||||| | ||||||||||| | ||||||||||| |
||||||||||| | ||||||||||| | ||||||||||| | ||||||||||| |
Sex, n (%) | |||
Male | 639 (54.6) | 111 (58.4) | 76 (59.4) |
Female | 532 (45.4) | 79 (41.6) | 52 (40.6) |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Ethnicity, n (%) | |||
||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
ECOG performance status, n (%) | |||
0 | 134 (11.4) | 29 (15.3) | 57 (44.5) |
1 | 328 (28.0) | 72 (37.9) | 68 (53.1) |
2 | 126 (10.8) | 0 (0.0) | 3 (2.3) |
3 | 28 (2.4) | 0 (0.0) | 0 (0.0) |
4 | 11 (0.9) | 0 (0.0) | 0 (0.0) |
Missing | 544 (46.5) | 89 (46.8) | 0 (0.0) |
Time from initial diagnosis (years) | |||
Median | 4.3 | 4.2 | 6.0 |
Minimum to maximum | 0.4 to 28.3 | 0.4 to 17.7 | 1.0 to 17.9 |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Baseline cytogenetic abnormalities high risk, n (%) | 352 (30.1) | 57 (30.0) | 45 (35.2) |
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Prior stem cell transplant for MM, n (%) | 679 (58.0) | 134 (70.5) | 120 (93.8) |
Number of prior antimyeloma regimens, median (minimum to maximum) | 5.0 (3.0 to 13.0) | 5.0 (3.0 to 12.0) | 6.0 (3.0 to 16.0) |
Prior relapse or refractory status, n (%) | |||
Immunomodulatory agent | 834 (71.2) | 142 (74.7) | 126 (98.4) |
Proteasome inhibitor | 746 (63.7) | 122 (64.2) | 116 (90.6) |
Anti-CD38 antibody | 956 (81.6) | 162 (85.3) | 120 (93.8) |
Immunomodulatory agent and PI (double-refractory) | 580 (49.5) | 102 (53.7) | 114 (89.1) |
Immunomodulatory agent, PI, and anti-CD38 antibody (triple-refractory) | 479 (40.9) | 82 (43.2) | 108 (84.4) |
Presence of plasmacytoma, n (%) | 143 (12.2) | 21 (11.1) | 50 (39.1) |
ECOG = Eastern Cooperative Oncology Group; Ide-cel = idecabtagene vicleucel; MM = multiple myeloma; PI = proteasome inhibitor; RRMM = relapsed or refractory multiple myeloma; RW = real-world; T0 = baseline time point.
aBaseline measurements for RW patients were collected after T0 and within 3 months of the subject becoming eligible, but before the start of the new regimen. Baseline measurements for the idecabtagene vicleucel cohort were collected before the start of idecabtagene vicleucel infusion.
bNot collected or reported = not collected, not reported, missing, or unknown.
cInternational Staging System values were calculated using baseline values of albumin and beta-2-microglobulin; unknown = missing or unknown.
Source: Sponsor-submitted indirect treatment comparison.12
Table 20: Summary of Covariate Balance Adjusted for Trimmed Stabilized IPTW of Eligible RRMM and Idecabtagene Vicleucel Cohorts
Parameter | KarMMa (N = 128) | Eligible RRMM (N = 190) | Standardized mean difference (KarMMa-eligible RRMM) | Balanced KarMMa (N = 128) | Balanced eligible RRMM (N = 190) | Standardized mean difference (KarMMa-eligible RRMM) |
|---|---|---|---|---|---|---|
Age, years | 59.8 | 64.5 | −0.5068 | 60.8 | 62.9 | −0.2189 |
Male, % | 60 | 60 | 0.0194 | 60 | 60 | −0.0753 |
Time since initial diagnosis, years | 6.9 | 4.9 | 0.5814 | 6.3 | 5.9 | 0.1289 |
Albumin serum (g/dL) | 3.7 | 3.6 | 0.2709 | 3.7 | 3.6 | 0.0712 |
Corrected calcium (mmol/L) | 3.0 | 2.4 | 0.4302 | 2.8 | 2.5 | 0.2693 |
Number of prior antimyeloma regimens | 5.6 | 4.8 | 0.5288 | 5.1 | 5.1 | 0.0611 |
Number of prior antimyeloma regimens per year | 1.2 | 1.3 | −0.1423 | 1.1 | 1.2 | −0.0770 |
Triple-class (IMiD agents, PIs, and mAbs) refractory status, % | 80 | 40 | 0.9491 | 60 | 60 | 0.1268 |
IMiD = immunomodulatory imide drug; IPTW = inverse probability treatment weighting; mAb = anti-CD38 monoclonal antibody; PI = proteasome inhibitor; RRMM = relapsed or refractory multiple myeloma.
Note: Multiple imputation procedures created 30 datasets and overall estimates were obtained using Rubin’s rules to combine the individual estimates. The stabilized IPTW was trimmed at the maximum of the minimum weight and the minimum of the maximum weight for the KarMMa cohort and the eligible RRMM cohort. A covariate was not included in the balancing if more than 30% of the data were missing for the eligible RRMM cohort. Means are presented for continuous variables and proportions are presented for categorical variables. The standardized mean difference was obtained from the KarMMa cohort minus the eligible RRMM cohort and used trimmed stabilized weights when combining the mean and standard deviation.
Source: Sponsor-submitted indirect treatment comparison.12
A total of 108 (56.8%) patients in the eligible RRMM cohort had discontinued from the study, all due to death. As of the October 30, 2019, data cut-off date, 58 patients (45.3%) in the idecabtagene vicleucel cohort had discontinued, with 31 patients (24.2%) discontinuing due to death, 26 (20.3%) discontinuing due to withdrawal by subject, and 1 (0.8) patient discontinuing due to lost to follow-up.
In the eligible RRMM cohort, the median duration of follow-up for all treated patients (which includes duration up to death for patients who died and duration up to last date known alive for surviving patients), was 10.2 months (range = 0.2 to 24.0). In the idecabtagene vicleucel cohort, the median duration of follow-up after idecabtagene vicleucel infusion was 11.3 months (range = 0.2 to 18.6). These numbers were current as of the October 30, 2019, data cut-off date of the KarMMa study.
The median follow-up duration for surviving patients (n = 82) was 15.0 months (range = 0.8 to 24.0) in the eligible RRMM cohort, while in the idecabtagene vicleucel–treated population (n = 94) the median was |||| months (range = |||||||||||||).
The most common regimens (i.e., those received by ≥ 5 patients) in the eligible RRMM cohort are listed in Table 21.
Table 21: Most Common Antimyeloma Treatment Regimens in Eligible RRMMa
Treatment regimen | Eligible RRMM, n (%) (N = 190) |
|---|---|
Carfilzomib, pomalidomide, and dexamethasone | 16 (8) |
Elotuzumab, lenalidomide, and dexamethasone | 10 (5) |
Carfilzomib, cyclophosphamide, and dexamethasone | 9 (5) |
Carfilzomib and dexamethasone | 5 (3) |
Cisplatin, cyclophosphamide, dexamethasone, and etoposide | 5 (3) |
Daratumumab, dexamethasone, and lenalidomide | 5 (3) |
Daratumumab, dexamethasone, and pomalidomide | 5 (3) |
Dexamethasone and pomalidomide | 5 (3) |
aIn 5 or more patients.
Source: Sponsor-submitted indirect treatment comparison.12
Results
Overall Response Rate
As of the data cut-off date, the ORR was lower in the eligible RRMM cohort compared with the idecabtagene vicleucel cohort (32.2% versus 76.4%; risk ratio = 2.4; 95% CI, 1.7 to 3.3; P < 0.0001). A summary of the ORR and VGPR-or-better rate adjusted for trimmed stabilized IPTW for patients in the eligible RRMM and idecabtagene vicleucel cohorts is presented in Table 22. Results of the ORR and VGPR-or-better rate from the supporting sensitivity analyses in the idecabtagene vicleucel–enrolled population were similar to those observed for the idecabtagene vicleucel–treated cohort used for the primary analysis.
The assessment of a CR according to IMWG criteria requires a bone marrow biopsy to be performed for patients. As a bone marrow biopsy is not typically performed in the routine care of RW patients, the CR rate was unable to be analyzed due to the limited availability of bone marrow biopsy results for the eligible RRMM cohort.
Responsea | KarMMa (N = 128) | Eligible RRMM (N = 190) |
|---|---|---|
ORR (95% CI), % | 76.4 (67.8 to 86.1) | 32.2 (24.4 to 42.3) |
RR (95% CI) | 2.4 (1.7 to 3.3) | |
P value | < 0.0001 | |
≥ VGPR (95% CI), % | |||||||||||||| |||||| | 13.7 (8.6 to 21.9) |
RR (95% CI) | 4.2 (||| to 7.2) | |
P value | < 0.0001 | |
CI = confidence interval; CR = complete response; IPTW = inverse probability treatment weighting; ORR = overall response rate; PR = partial response; RR = risk ratio; RRMM = relapsed or refractory multiple myeloma; VGPR = very good partial response.
aValues are derived for the KarMMa and eligible RRMM cohorts using a trimmed stabilized IPTW propensity score. The risk ratio, P value, and CI are based on a Poisson regression with robust error variance, adjusted for the unbalanced covariates in the propensity score model. The primary analysis used a log link function and stabilized IPTWs trimmed at the maximum of the minimum weight and the minimum of the maximum weight for the idecabtagene vicleucel cohort and eligible RRMM cohort.
Source: Sponsor-submitted indirect treatment comparsion.12
Overall Survival
After a median follow-up time of 15 months for all surviving patients in the eligible RRMM cohort, 55.8% of patients had died, while after a median follow-up time of ||| months for all surviving patients in the idecabtagene vicleucel cohort, a total of |||||| of patients had died (Figure 17). The median OS for RW patients in the eligible RRMM cohort was 14.7 months (95% CI, ||||||||||||||) and was |||||||||||| (95% CI = NE) in the idecabtagene vicleucel cohort. A comparison between the 2 groups yielded an HR for OS of ||||||||||||||||||||||||||||||||, favouring the idecabtagene vicleucel cohort compared with the eligible RRMM cohort treated with available therapy (P = |||||||).

||||||||||||||||||||||
|||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The figure was redacted as per the sponsor’s request.
Time to Response
As of the data cut-off date, the median TTR for responders was 1.1 months (range = 0.2 to 8.6) in the eligible RRMM cohort versus 1.0 month (range = 0.5 to 8.8) in the idecabtagene vicleucel cohort. As of the data cut-off date, the median DoR was 9.0 months (95% CI, 7.5 to ||||) in the eligible RRMM cohort versus ||| months (95% CI, ||||||||||||||) in the idecabtagene vicleucel cohort (Table 23).
Table 23: Time to Response and Duration of Response
Response | KarMMa (N = 128) | Eligible RRMM (N = 190) |
|---|---|---|
Number of responders, n (%) | 94 (73.4) | 58 (30.5) |
Time to response (months)a,b | ||
Median (minimum to maximum) | 1.0 (0.5 to 8.8) | 1.1 (0.2 to 8.6) |
Duration of response (months) | ||
Median (95% CI)c | ||||||||||| | 9.0 (7.5 to || |) |
HR (95% CI) d | ||||||||||| | |
|||||||| | ||||||||||| | |
CI = confidence interval; HR = hazard ratio; IPTW = inverse probability treatment weighting; RRMM = relapsed or refractory multiple myeloma.
aTime to response and duration of response analyses are based on responders only. For a summary of time to response categories, a 3-day window is added to each month for month 1 to month 8; and a 14-day window is added to month 9 and onward.
bOnly patients with a response of stringent complete response, complete response, very good partial response, or partial response were included in the analysis.
cThe median was based on the adjusted product-limit estimate with IPTW trimmed at the maximum of the minimum weight and the minimum of the maximum weight for the idecabtagene vicleucel cohort and the eligible RRMM cohort.
dThe hazard ratio and CI were based on a Cox model with study (eligible RRMM or idecabtagene vicleucel) cohorts as a term in the model and using IPTWs trimmed at the maximum of the minimum weight and the minimum of the maximum weight for idecabtagene vicleucel and eligible RRMM cohorts, as well as adjusted for unbalanced covariates used in the propensity score model.
Source: Sponsor-submitted indirect treatment comparsion.12
Progression-Free Survival
This evaluation was made based on EMA censoring rules; however, by using an FDA censoring scenario, the results were comparable. As of the data cut-off date, the median PFS adjusted by the trimmed stabilized IPTW for comparability was lower in the eligible RRMM cohort compared with the idecabtagene vicleucel cohort (3.5 months versus 11.1 months, respectively; Table 24).
Table 24: Time to Progression-Free Survival According to EMA Censoring Rules Adjusted for Trimmed Stabilized IPTW for Patients in the Eligible RRMM and Idecabtagene Vicleucel Cohorts
Parameter | KarMMa (N = 128) | Eligible RRMMa (N = 190) |
|---|---|---|
Progression-free survival | ||
Progressed or died (%) | ||||||||||| | ||||||||||| |
Censored (%) | ||||||||||| | ||||||||||| |
Progression-free survival time (months) | ||
Median (95% CI) b | ||||||||||| | ||||||||||| |
HR (95% CI) c | ||||||||||| | |
P value | ||||||||||| | |
CI = confidence interval; EMA = European Medicines Agency; HR = hazard ratio; IPTW = inverse probability treatment weighting; RRMM = relapsed or refractory multiple myeloma.
aThe index date for progression-free survival was the start of new therapy for members of the eligible RRMM cohort, and the infusion date for the idecabtagene vicleucel cohort.
bThe median of time to event was estimated using the adjusted product-limit estimate with IPTWs trimmed at the maximum of the minimum weight and the minimum of the maximum weight for idecabtagene vicleucel cohort and eligible RRMM cohort.
cThe hazard ratio and CI are based on a Cox model with study (eligible RRMM or idecabtagene vicleucel) cohort as a term in the model and using IPTWs trimmed at the maximum of the minimum weight and the minimum of the maximum weight for the idecabtagene vicleucel cohort and eligible RRMM cohort, as well as adjusted for unbalanced covariates.
Source: Sponsor-submitted indirect treatment comparsion.12
After a median follow-up time of || | months for all RW patients in the eligible RRMM cohort, || || of patients had a PFS event (PD or death), while after a median follow-up time of || | months for all patients in the idecabtagene vicleucel cohort, | ||| of patients had a PFS event. A comparison between the 2 groups yielded an HR for PFS of |||||||||||||||||||||||||||||||, favouring the idecabtagene vicleucel cohort compared with the eligible RRMM cohort treated with available therapy (||||||||||||; Figure 18).

||||||||||||||||||||||
|||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The figure was redacted as per the sponsor’s request.
An evaluation of the ORR outcomes by subgroup revealed that, for all subgroups evaluated, the results were consistent with the overall results for the ORR. In all subgroups in which the ORR was evaluated the benefit in the idecabtagene vicleucel cohort was maintained compared with the eligible RRMM cohort. The results were similar for the PFS outcome.
Critical Appraisal of NDS-MM-003
The NDS-MM-003 study compared a single-arm clinical trial (KarMMa) against a matched RRMM cohort from different databases and clinical sites. Investigators planned to achieve a balance of prognostic factors between these 2 groups for comparison purpose by using propensity score models. Due to the small sample size obtained from the databases (with important missingness of data), the investigators changed the methodology to restrict the primary analysis to an eligible RRMM cohort, and balanced factors between the eligible RRMM cohort and the idecabtagene vicleucel–treated population from the KarMMa study using the trimmed stabilized IPTW method, leaving the matched cohort evaluation as supportive analyses.
From the databases, the baseline disease characteristics were generally similar among RW patients from the different data sources. Patients from IQVIA, the Guardian Research Network, and M2GEN tended to be less heavily pretreated, with a lower number of prior antimyeloma regimens. Patients from IQVIA also had a lower degree of refractoriness to prior AMTs, as evidenced by a lower percentage of patients who were double-class or triple-class refractory.
The missing data from these databases throughout the process of creating the eligible cohort implies a potential bias due to the need to rely on multiple imputation methods. More than half of the data for a number of variables missing would have been important to include in the propensity scores. Multiple imputations of missing values made in generating the eligible RRMM cohort can increase the uncertainty in effect estimates. Furthermore, no methods were used to control the type I error rate across multiple outcomes, subgroups, or analyses.
Although later addressed in the propensity score balancing, baseline differences in multiple variables observed between the RRMM cohort, the eligible RRMM cohort, and the idecabtagene vicleucel cohort (e.g., the presence of plasmacytoma or refractory status) suggest the possibility of other unmeasured confounding factors, and the prospect that these can be unevenly distributed between groups without proper randomization. Prior to the IPTW adjustment, with the exception of age, the imbalance of the prognostic factors and prior treatments suggests the eligible RRMM cohort was a less heavily pretreated and less refractory population with a more favourable prognosis overall compared with the idecabtagene vicleucel cohort. Furthermore, differences in study designs and combining patients across databases (i.e., selecting patients from different databases) may introduce heterogeneity that cannot be accounted for in propensity score modelling. There is also the potential for differences in available covariates across databases, definitions of covariates, and outcome assessments due to practice variation across the regions and centres where the databases capture patients. Similarly, there is the potential for heterogenous assessment of end points when comparing an assessment by an IRC versus a clinician assessment as it was made in the KarMMa study.
Overall, 190 of the 1,171 patients of the RRMM cohort were included in the final set of eligible RRMM patients compared with the idecabtagene vicleucel cohort, which can be considered a significant reduction.
Further critical appraisal points include a lack of clarity regarding how the retrospective assessment of the IMWG for response was determined for the RWE cohorts (as opposed to the KarMMa study). Blinding of analysts to generate propensity scores occurred only for the first wave of analysis in this study, and a second wave of analysis was performed in an unblinded fashion, which can generate bias in outcome assessors. Clinical relevance should be considered to select the covariates used in propensity score models; investigators used, in part, a data-driven approach, which is not ideal. No data were available for health care resource utilization and drug exposure. It was not clear at what time points the interventions were available in the different databases; this can add generalizability issues, as rapidly changing practices mean some regimens may be outdated, introducing heterogeneity to the interventions.
Although the population from the eligible RRMM cohort is similar to the idecabtagene vicleucel cohort in several measures, generalizability of this and the matched final cohort as well as the comparisons can be a concern in the Canadian clinical practice due to the different and varied therapies included in the regimens provided. The availability of such regimens and drugs will vary depending on funding and feasibility for each province/territory. Only a fraction of the regimens evaluated as comparators in this indirect comparison were described by the clinical experts consulted by CADTH as commonly used in clinical practice in Canada. These regimens include pomalidomide plus dexamethasone, daratumumab plus dexamethasone plus lenalidomide, and Cd. The individual medications are approved in Canada. With regards to external validity, the RWE was derived mainly from retrospective databases within the US. It is likely a number of important differences between the US and Canada in the management of these patients would be expected to affect outcomes.
Summary
The NDS-MM-003 presented in this ITC section is a comparison of the patients from the single-arm, open-label KarMMa study who were treated with idecabtagene vicleucel (in a dose range of 150 × 106 to 450 × 106 CAR T cells) with a cohort of real-world RRMM patients obtained from different patient-level clinical sites or databases that function as the real-world comparison arm. Patients obtained from these cohorts of clinical sites and registries were selected to be similar to those in the KarMMa study, i.e., triple-class exposed to IMiD, proteasome inhibitors, and anti-CD38 antibodies. Authors of the study identified prognostic variables and adjusted for some of these using an IPTW methodology to make the groups more comparable. Due to a smaller-than-anticipated sample size, authors focused their comparison of the KarMMa trial and the eligible RRMM cohort using the trimmed stabilized IPTW method and presented the matched RRMM cohort comparison as supportive analysis.
The primary analysis focused on the ORR after adjustment of eligibility criteria, in which patients in the idecabtagene vicleucel cohort showed an improved ORR. Similarly, patients in the idecabtagene vicleucel arm had better PFS and OS after a median of 15 months of follow-up. No data on AEs, HRQoL, or health care resource utilization were provided.
While this propensity score analysis provides indirect evidence of the comparative effectiveness of idecabtagene vicleucel in patients who are refractory to multiple AMT, the evidence is limited by inherent design differences between the studies that cannot be adjusted for statistically, the potential impact of unmeasured and unaccounted-for prognostic factors and effect modifiers in the models, and reduced generalizability due to the inclusion of irrelevant comparators.
Other Relevant Indirect Treatment Comparisons
This section includes a sponsor-submitted ITC assessed as a high-level summary of information of the MAIC of efficacy outcomes based on the BB2121-MM-001 (KarMMa) and MAMMOTH studies.
Description of the Study
Based on the information from the KarMMa trial, which enrolled patients who have received at least 3 prior AMT regimens, been refractory to the last regimen received, and been previously treated with an IMiD, a proteasome inhibitor, and an anti-CD38 antibody, the authors of the study compare the effect of idecabtagene vicleucel single-arm trial data against independent data from observational studies (not funded by the sponsor) to provide further RWE for decision-makers and stakeholders. The largest such real-world study, MAMMOTH,34 was chosen by the authors as it evaluates conventional care in 275 patients with MM in US medical centres who were refractory to daratumumab or isatuximab, administered alone or in combination.
The current indirect comparison aimed to evaluate the comparative efficacy of idecabtagene vicleucel versus conventional care in terms of the ORR, as well as PFS and OS, for the treatment of patients with RRMM who have received 3 or more prior regimens, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody, using an unanchored MAIC of KarMMa and MAMMOTH.
The unanchored MAIC uses KarMMa data with a cut-off date of |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The median duration of follow-up after idecabtagene vicleucel infusion for all idecabtagene vicleucel–infused patients was |||||||||||||. This evidence on the clinical efficacy of idecabtagene vicleucel was obtained directly from the Clinical Study Report.
The authors of the unanchored MAIC performed a literature search that found 11 real-world studies, from which they selected MAMMOTH as the study with the largest sample size and available KM data.
MAMMOTH is a large, retrospective chart review of observational data of 275 RRMM patients from the US who are refractory to daratumumab or isatuximab, administered alone or in combination. Of these patients, 249 received a variety of regimens corresponding to conventional care following progression on anti-CD38 antibodies (treated population). The 249 patients in the treated population were categorized based on the individual conventional care regimens they received.
The following treatment groups correspond to the most common interventions received by patients in the NDS-MM-003 (RWE) study12 previously mentioned in this CADTH report, and which were selected by the investigators as the intervention subgroups:
daratumumab plus an IMiD (41 patients)
elotuzumab plus an IMiD (19 patients)
carfilzomib plus an alkylator (19 patients)
PACE-like (24 patients)
daratumumab plus a proteasome inhibitor (13 patients)
carfilzomib plus an IMiD (34 patients).
Data for the MAMMOTH study was extracted from its primary publication.34 MAMMOTH included patients who had received an anti-CD38 antibody therapy as their last line of treatment and were refractory to it. KarMMa restricted patients to those with an ECOG score of 0 or 1, while MAMMOTH did not have any ECOG restrictions.
The primary outcome, ORR, was defined in the KarMMa study using the IMWG criteria defined by the IRC, as well as in MAMMOTH, although in the latter study the ORR was calculated by combining the PR and better-than-VGPR rates. Definitions for PFS events were similar, and disease progression was defined based on IMWG response criteria in both studies. In the MAMMOTH study, PFS was measured as the onset of the next line of treatment in the treated population (PFS was not reported for the overall population). While OS was measured from either the time of leukapheresis (enrolled population) or the time of idecabtagene vicleucel infusion (infused population) in KarMMa, it was calculated from the time of PD on daratumumab or isatuximab for patients in MAMMOTH for all patient groups, and therefore includes a period of time during which the patient is untreated before they begin their next line of treatment.
Methods
This is an unanchored MAIC between idecabtagene vicleucel and mixed comparators using RWE from the MAMMOTH study. Because individual patient data for the comparator study (MAMMOTH) was not available, the analyses were limited to the study-level aggregate data from the publication.
Analyses were performed for the KarMMa populations (enrolled and infused populations as well as a target dose of 450 × 106 CAR T cells) versus the MAMMOTH treated population in terms of ORR, PFS, and OS. In MAMMOTH, the 249 patients in the treated population were categorized to 6 subgroups related to the interventions described earlier.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Efficacy Results
Patients in KarMMa tended to be younger than those in MAMMOTH, whereas the distribution of gender and race was similar in the 2 studies. Patients in KarMMa had the disease for a slightly longer time compared to MAMMOTH. In terms of prior treatment experience, patients in KarMMA and MAMMOTH had a median of 6 prior regimens versus 5 prior regimens, respectively. The proportions of patients refractory to bortezomib and those refractory to lenalidomide were also similar between the 2 studies, whereas a slightly higher percentage of patients were refractory to carfilzomib in KarMMa, as was the case for refractoriness to pomalidomide. Last, while the vast majority of patients had previously received autologous stem cell transplantation in KarMMa, the proportion of such patients was lower in MAMMOTH. Overall, patients were more refractory to prior treatments in KarMMa.
The KarMMa study included more heavily pretreated and refractory patients with a less-favourable prognosis compared with the MAMMOTH patients.
The authors mention effective sample size (EES) estimates in the enrolled and infused populations that were similar to existing ESS estimates in the literature, both in absolute terms and with respect to relative reductions (||||||||| for both the enrolled and infused populations when matched to the treated population in MAMMOTH). From literature evaluated by the authors, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
The baseline characteristics are presented in Table 25.
Table 25: Patient Baseline Characteristics in the KarMMa and MAMMOTH Studies
Patient characteristic | Description per level | KarMMa (idecabtagene vicleucel–treated) population | MAMMOTH | |
|---|---|---|---|---|
Treated population | Overall population | |||
Sample size | N | 128 | 249 | 275 |
Median age | years (range) | 60.5 (33 to 78) | 65 (27 to 90) | 65 (27 to 90) |
Sex | Male | 76 (59) | 135 (54) | 152 (55) |
Race | White | 103 (81) | 185 (74) | 202 (74) |
Black | 6 (5) | 38 (15) | 45 (16) | |
Hispanic | 19 (15) | 5 (2) | 6 (2) | |
Other | 19 (15) | 21 (8) | 22 (8) | |
Years from initial diagnosis | Median (range) | 6.0 (1.0 to 17.9) | 4.5 (0.4 to 19.4) | 4.5 (0.4 to 19.4) |
ISS stage at diagnosis | Stage I | 26 of 66 (39) | 63 of 212 (30) | 69 of 233 (30) |
Stage II | 22 of 66 (33) | 80 of 212 (38) | 84 of 233 (36) | |
Stage III | 18 of 66 (27) | 69 of 212 (33) | 80 of 233 (34) | |
Not evaluable | 62 | 37 | 42 | |
Exposure to prior antimyeloma regimens | Prior lines, median (range) | 6 (3 to 16) | 5 (2 to 17) | 5 (2 to 17) |
Refractoriness to prior regimens | Penta-refractory | 50 (39) | 63 (25) | 70 (25) |
Triple- or quadruple-refractory | 54 (42) | 134 (54) | 148 (54) | |
Prior ASCT | 120 (94) | 185 (74) | 198 (72) | |
High-risk cytogenetic assessment on most recent assessment | 45 of 111 (41) | 71 of 229 (31) | 80 of 255 (31) | |
ASCT = autologous stem cell transplantation; ISS = International Staging System.
Source: Sponsor-submitted indirect treatment comparison 2.13
Overall Response Rate
Idecabtagene vicleucel in the enrolled population was more efficacious than conventional care in terms of ORR, whether the analysis was naive or adjusted using the MAIC (||||||||||||||||||||||||||||||||||||||||||||||||). These results were consistent with the KarMMa infused population (||||||||||||||||||||||||||||||||||||||||||||||||||||||).

||||||||||||||||||||||
|||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The figure was redacted as per the sponsor’s request.
| ||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

|||||||||||||||||||||||||||||||||13
Note: This figure has been redacted as per the sponsor’s request.

|||||||||||||||||||||||||||||||||
Note: This figure has been redacted as per the sponsor’s request.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Harms Results
No data about harms were reported.
Critical Appraisal
This is an unanchored MAIC with an appropriate rationale for comparing individual patient data from a single-arm study with aggregate data from a published study to assess the effect of idecabtagene vicleucel treatment in a population with RRMM.
The approach to identification of prognostic factors and effect modifiers to include in the MAIC (i.e., a literature review designed to identify prognostic factors, a series of interviews with clinical experts, and an analysis described in this report from CADTH comparing MM-001 to MM-003) was appropriate. However, it is not clear if the underlying assumption of the unanchored MAIC that all effect modifiers and prognostic factors have been accounted for was accomplished. It is unclear whether all of the relevant differences in patient characteristics were captured (for both the effect modifiers and prognostic factors), as a number of identified prognostic elements were not reported in MAMMOTH. The ESS estimates for reduction were considered close to what is published in the literature related to oncology trials. For time-to-event outcomes (PFS and OS) the proportional hazards assumption was evaluated with resulting potential violations, and any HR should be interpreted with caution.
The MAIC cannot address heterogeneity in study designs. As a comparison between clinical trial data and RWE, differences in outcome assessments and definitions (e.g., differences in setting and follow-ups) can generate uncertainty. The analysis is limited to study-level aggregated data from the full-text publication for MAMMOTH and compared to the KarMMa study.
The different treatments obtained in the MAMMOTH study also generate uncertainty about the generalizability of the results, particularly from the Canadian perspective, due to the fact that approximately a third of the comparators are not widely available in the different provinces and territories.
Overall, beneficial effect estimates were observed in favour of idecabtagene vicleucel, although the certainty in these estimates remains unclear due to the observational nature of the evidence base, the possibility of residual confounding factors, heterogeneity, and risk of bias.
Discussion
Summary of Available Evidence
One clinical study was included in this report. The KarMMa study (N = 140) was a phase II, open-label, single-arm, prospective trial. Eligible patients were those who have received multiple previous treatments for RRMM, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody. A total of 128 patients received idecabtagene vicleucel target doses of 150 × 106, 300 × 106, or 450 × 106 CAR T cells. The primary end point was the ORR (a PR or better). The key secondary end point was a CR or better (comprising CR and sCR). Other secondary end points included DoR, TTR, TTP, MRD-negative status, survival outcomes (OS and PFS), and HRQoL.
In addition, 2 sponsor-submitted ITCs were included to provide indirect evidence of the comparative effectiveness of idecabtagene vicleucel to relevant treatment alternatives. The first is a propensity score analysis comparing the KarMMa trial MM-001 single-arm study to pooled RWE obtained from multiple clinical sites and registries from Europe and the US. The second ITC is a MAIC that compares the individual patient data from the KarMMa trial to aggregate-level data from a published RWE study that included multiple comparators. Both approaches aim at providing a comparator arm, with adjustment for differences in baseline characteristics, prognostic factors, and effect modifiers to produce an adjusted effect estimate for decision-makers and stakeholders, given the lack of a direct, head-to-head comparison of idecabtagene vicleucel to relevant comparators.
Interpretation of Results
Efficacy
The ORR, CRR, DoR, OS, and HRQoL were considered the most important outcomes from the perspective of clinical experts and clinician groups. In addition, patient groups considered improved HRQoL domains (fewer symptoms, higher functionality, and fewer side effects from treatments) to be highly valued outcomes.
At a median follow-up of 11.3 months, the KarMMa trial met its primary end point for the target dose of 450 × 106 CAR T cells, achieving an ORR of 81.5%, which was above the null hypothesis of 50% established in the protocol. Patients reached an ORR above this point in all target dose groups. Given that the test for the ORR (primary end point) was positive, the key secondary efficacy end point of the CRR was tested against the prespecified null hypothesis of 10% or lower. The result rejected the null hypothesis, with 35.2% of patients achieving a CR or better. Both these values from the primary and key secondary end points were considered clinically meaningful by the clinical experts.
The DoR, TTR, and TTP were evaluated in the KarMMa trial as secondary end points. With a median 10.6 months for DoR, 1 month for TTR, and 9 months for TTP, the results suggest a beneficial effect in patients treated with idecabtagene vicleucel and were considered by the clinical experts likely to represent a meaningful impact. Likewise, the MRD-negative status with a CR or better observed in a quarter of the patients treated with idecabtagene vicleucel was also supportive of a clinical benefit. However, none of these secondary end points were adjusted for multiplicity and all should be interpreted with caution.
Overall survival was considered by clinical experts and patients to be among the most valued outcomes used in clinical trials including those involving patients with MM. The observed median OS of 18.2 months, with 76% of individuals alive at 12 months, was considered by the clinical experts to be an overall beneficial effect estimate for patients with the characteristics included in the KarMMa trial (i.e., those with a median of 6 years since diagnosis, with relapses, and who have been heavily treated). Similarly, based on the KM estimates, the median PFS of 8.6 months, with 34% of patients event-free at 12 months, denoted a likely meaningful benefit for patients treated with idecabtagene vicleucel.
Health-related QoL outcomes were frequently mentioned in input from patient and clinician groups. Patients put a higher value on decreasing symptoms, improved physical functioning, less pain, and fewer side effects. In the KarMMa trial, idecabtagene vicleucel treatment was associated with improvements in the fatigue, pain, physical functioning, and global health/QoL subscales of the EORTC QLQ-C30 by reaching points of meaningful significance above the thresholds of probable benefit, according to MIDs established in the literature. On average, no clinically meaningful deterioration in the EORTC QLQ-C30 cognitive functioning and EORTC QLQ-MY20 disease symptoms and side effects subscales were observed posttreatment. With respect to the EQ-5D-5L subscales, no changes from baseline were observed in all subscales of this measurement. These findings suggest that idecabtagene vicleucel treatment is associated with improvements or stabilization in most primary HRQoL metrics. However, these results were observed over the first and middle parts of the study follow-up, eventually decreasing to baseline levels, with added uncertainty due to imprecision (i.e., fewer patients at the end of the study) and the fact that all HRQoL outcomes in the KarMMa study were secondary end points assessed without adjustment for multiplicity.
Evaluation of different scenarios (sensitivity analyses) in the analysis of the outcomes revealed no notable differences that had an impact on the final effect estimates. The investigator therefore obtained estimates based on whether the FDA or EMA rules for censoring were used (DoR, TTP, and PFS outcomes), or whether comparisons used IRC or investigator adjudication of end points (for ORR, CRR, and TTP). Finally, scenarios were presented comparing the enrolled population against the population treated with idecabtagene vicleucel (for DoR, CRR, PFS, and OS).
With the exception of the ORR and CR outcomes, no other secondary end points were considered in the adjustment for multiplicity, which should be interpreted with consideration of type I error.
Harms
All 128 patients treated with idecabtagene vicleucel (on or after the idecabtagene vicleucel infusion) reported AEs. The most common were neutropenia (91%), anemia (70%), and thrombocytopenia (63%); these were described in the patient group input as important but of low value when weighed against likely benefits, such as longer survival, remission, HRQoL, and reduced burden of symptoms. The clinical experts consulted by CADTH indicated that these AEs were expected, and the patient group provided similar input.
Serious AEs on or after idecabtagene vicleucel infusion were common (reported by almost two-thirds of patients) and comprised infections (pneumonia, sepsis), CRS, and blood disorders (febrile neutropenia, neutropenia, and thrombocytopenia).
Deaths on or after idecabtagene vicleucel infusion occurred in 34 patients as of the data cut-off date. Most deaths were attributed to the disease under study or complications attributed to the disease under study.
Among the notable harms established in this review protocol, CRS was common, as it was reported in 107 patients (84%). This was in accordance with the expectations from the clinical experts consulted by CADTH, who highlighted the need for treatment for this condition. Although CRS is manageable, it can impose extra costs and burdens on patients that must be weighed against the desirable effects of the therapy.
Neurotoxicity in the KarMMa trial was defined as investigator-identified neurotoxicity. These developed in 23 patients (18%), and included several signs and symptoms, such as a confusional state and encephalopathy. These symptoms and their frequency were important to both experts and patients.
No concerns were expressed over hospitalization rates or hospital utilization based on the number of patients admitted to ICUs during the study. Overall, the impact of the numbers of ICU admissions in the KarMMa trial was not an issue for patient groups or clinical experts.
No data on harms were provided from the RWE propensity score comparisons or ITC (MAIC) evaluated in this review.
Conclusions
Evidence from the single-arm, open-label KarMMa-001 study suggests that the CAR T-cell therapy idecabtagene vicleucel at a target dose of 450 × 106 CAR T cells is associated with an induction of response, based on an ORR of 81.5% and a CR of 35.2%. The results appear to indicate that treatment with idecabtagene vicleucel may offer a benefit in terms of DoR, MRD status, TTR, TTP, OS, and PFS, but none of these outcomes were controlled for multiplicity so the results should be interpreted with consideration of type I error. The data for HRQoL outcomes were descriptive and could not be interpreted due to missing data. These effect estimates come from evidence with risk of bias due to the lack of estimations from a comparison arm in a randomized design, and must be weighed against the observed undesirable effects, including AEs (such as CRS), the need for LDC, and bridging therapy. All patients treated with idecabtagene vicleucel reported at least 1 AE. The most commonly reported AEs were neutropenia, CRS, anemia, and thrombocytopenia.
Results of 2 indirect comparisons of the population from the KarMMa study to individual patient observational data (RWE) and aggregated data from published studies add support for the beneficial effects observed in KarMMa, but also include a risk of bias due to inherent design differences in the bodies of evidence that cannot be adjusted for statistically, the potential impact of unmeasured and unaccounted-for prognostic factors and effect modifiers in the models, and undermined generalizability by the inclusion of irrelevant comparators. Given the limitations of the 2 ITCs and the absence of direct comparative evidence, any potential benefit of idecabtagene vicleucel compared with other treatment regimens used in this patient population remains unknown.
References
1.Tsang M, Le M, Ghazawi FM, et al. Multiple myeloma epidemiology and patient geographic distribution in Canada: a population study. Cancer. 2019;125(14):2435-2444. PubMed
2.Rajkumar SV, Kumar S. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc. 2016;91(1):101-119. PubMed
3.Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328-e346. PubMed
4.Moreau P, San Miguel J, Ludwig H, et al. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24 Suppl 6:vi133-137. PubMed
5.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-E205. PubMed
6.Dimopoulos MA, Weisel K, Kaufman J, et al. A systematic literature review and network meta-analysis evaluating the efficacy of daratumumab-based regimens in patients with relapsed/refractory multiple myeloma. Indian J Hematol Blood Transfus. 2017;33 (1 Supplement 1):S2.
7.Mikhael J. Treatment options for triple-class refractory multiple myeloma. Clin Lymphoma Myeloma Leuk. 2020;20(1):1-7. PubMed
8.Mikhael J, Ismaila N, Cheung MC, et al. Treatment of multiple myeloma: ASCO and CCO joint clinical practice guideline. J Clin Oncol. 2019;37(14):1228-1263. PubMed
9.Moreau P, Kumar SK, San Miguel J, et al. Treatment of relapsed and refractory multiple myeloma: recommendations from the International Myeloma Working Group. Lancet Oncol. 2021;22(3):e105-e118. PubMed
10.Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration[internal sponsor's package]. St-Laurent (QC): Celgene Inc., a Bristol Myers Squibb company; 2020 Dec 16.
11.Clinical Study Report: Protocol BB2121-MM-001. A phase 2, multicenter study to determine the efficacy and safety of bb2121 in subjects with relapsed and refractory multiple myeloma [internal sponsor's report]. Summit (NJ): Celgene Corporation; 2017 Aug 25.
12.NDS-MM-003: A global, non-interventional, retrospective, multi-center study to generate real-world evidence of subjects with relapsed and refractory multiple myeloma with prior exposure to an anti-cd38 antibody [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration. Summit (NJ): Celgene Corporation; 2020 Mar 16.
13.A matching-adjusted indirect treatment comparison of efficacy outcomes based on BB2121-MM-001 (15+1) and MAMMOTH pivotal studies [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration. Saint Laurent (QC): Celgene Inc; 2020.
14.Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359-386. PubMed
15.Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-548. PubMed
16.Nijhof IS, van de Donk N, Zweegman S, Lokhorst HM. Current and new therapeutic strategies for relapsed and refractory multiple myeloma: an update. Drugs. 2018;78(1):19-37. PubMed
17.Kriegsmann K, Kriegsmann M, Cremer M, et al. Cell-based immunotherapy approaches for multiple myeloma. Br J Cancer. 2019;120(1):38-44. PubMed
18.Cohen AD. CAR T cells and other cellular therapies for multiple myeloma: 2018 update. Am Soc Clin Oncol Educ Book. 2018;38:e6-e15. PubMed
19.Abecma (idecabtagene vicleucel): cell suspension in one or more patient specific infusion bag(s), target dose of 450 x 106 CAR-positive T cells within a range of 275 to 520 x 106 CAR-positive T cells, for intravenous infusion [DRAFT product monograph]. St-Laurent (QC): Celgene Inc; 2021.
20.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
21.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2020 Jan 8.
22.Munshi NC, Anderson LD, Jr., Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705-716. PubMed
23.U.S. Food and Drug Administration (FDA). Clinical trials endpoints for the approval of cancer drugs and biologics: guidance for industry. 2018; https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-trial-endpoints-approval-cancer-drugs-and-biologics. Accessed 2021 Apr 26.
24.Appendix 1 to the guideline on the evaluation of anticancer medicinal products in man: methodological consideration for using progression-free survival (PFS) or disease-free survival (DFS) in confirmatory trials. Vol Amsterdam (NL): European Medicines Agency; 2013: https://www.ema.europa.eu/en/documents/scientific-guideline/appendix-1-guideline-evaluation-anticancer-medicinal-products-man-methodological-consideration-using_en.pdf. Accessed 2021 Apr 26.
25.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
26.Ahmadzadeh A, Yekaninejad MS, Saffari M, Pakpour AH, Aaronson NK. Reliability and validity of an Iranian version of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire for patients with multiple myeloma: the EORTC QLQ-MY20. Asian Pac J Cancer Prev. 2016;17(1):255-259. PubMed
27.Osborne TR, Ramsenthaler C, Siegert RJ, Edmonds PM, Schey SA, Higginson IJ. What issues matter most to people with multiple myeloma and how well are we measuring them? A systematic review of quality of life tools. Eur J Haematol. 2012;89(6):437-457. PubMed
28.Frick E, Borasio GD, Zehentner H, Fischer N, Bumeder I. Individual quality of life of patients undergoing autologous peripheral blood stem cell transplantation. Psychooncology. 2004;13(2):116-124. PubMed
29.Kvam AK, Fayers PM, Wisloff F. Responsiveness and minimal important score differences in quality-of-life questionnaires: a comparison of the EORTC QLQ-C30 cancer-specific questionnaire to the generic utility questionnaires EQ-5D and 15D in patients with multiple myeloma. Eur J Haematol. 2011;87(4):330-337. PubMed
30.Kontodimopoulos N, Samartzis A, Papadopoulos AA, Niakas D. Reliability and validity of the Greek QLQ-C30 and QLQ-MY20 for measuring quality of life in patients with multiple myeloma. ScientificWorldJournal. 2012;2012:842867. PubMed
31.Cocks K, King MT, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. PubMed
32.Cocks K, Cohen D, Wisloff F, et al. An international field study of the reliability and validity of a disease-specific questionnaire module (the QLQ-MY20) in assessing the quality of life of patients with multiple myeloma. Eur J Cancer. 2007;43(11):1670-1678. PubMed
33.Sully K, Trigg A, Bonner N, et al. Estimation of minimally important differences and responder definitions for EORTC QLQ-MY20 scores in multiple myeloma patients. Eur J Haematol. 2019;103(5):500-509. PubMed
34.Gandhi UH, Cornell RF, Lakshman A, et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia. 2019;33(9):2266-2275. PubMed
35.Landis JR, and Gary G. Koch. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. PubMed
36.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
37.Cohen J. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
38.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
39.Quality of life FAQs. Brussels (BE): EORTC.
40.Zhang L, Wang S, Xu J, et al. Etanercept as a new therapeutic option for cytokine release syndrome following chimeric antigen receptor T cell therapy. Exp Hematol Oncol. 2021;10(1):16. PubMed
41.Davda J, Kibet H, Achieng E, Atundo L, Komen T. Assessing the acceptability, reliability, and validity of the EORTC Quality of Life Questionnaire (QLQ-C30) in Kenyan cancer patients: a cross-sectional study. J Patient Rep Outcomes. 2021;5(1):4. PubMed
42.Kvam AK, Wisloff F, Fayers PM. Minimal important differences and response shift in health-related quality of life; a longitudinal study in patients with multiple myeloma. Health Qual Life Outcomes. 2010;8:79. PubMed
43.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
44.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644-650. PubMed
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–)
Embase (1974–)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: January 21, 2021
Alerts: Bi-weekly search updates until project completion
Study types: No search filters were applied
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
.ti | Title |
.ab | Abstract |
.dq | Candidate term word (Embase) |
.ot | Original title |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.yr | Publication year |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Search strategy
(Idecabtagene* or Abecma* or Ide-cel or bb 2121 or bb2121).ti,ab,kf,ot,hw,nm,rn.
(BCMA adj3 CAR T).ti,ab,kf.
1 or 2
3 use medall.
*idecabtagene vicleucel/
(Idecabtagene* or Abecma* or Ide-cel or bb 2121 or bb2121).ti,ab,kw,dq.
(BCMA adj3 CAR T).ti,ab,kw,dq.
or/5 to 7
8 use oemezd
10 not (conference review or conference abstract).pt
4 or 10
remove duplicates from 11
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | idecabtagene vicleucel or Abecma]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- idecabtagene vicleucel or Abecma]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- idecabtagene vicleucel or Abecma]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- idecabtagene vicleucel or Abecma]
Canadian Cancer Trials
Produced by the Canadian Partnership Against Cancer Corporation. Targeted search used to capture registered clinical trials.
[Search terms -- idecabtagene vicleucel or Abecma]
Grey Literature
Search dates: January 12 to 15, 2021
Keywords: idecabtagene Vicleucel, Abecma, multiple myeloma
Limits:
Updated: None
Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note this appendix has not been copy-edited
Reference | Reason for exclusion |
|---|---|
Munshi NC, Anderson Jr LD, Shah N, et al. Idecabtagene vicleucel (ide-cel; bb2121), a BCMA targeted CAR+T-cell therapy, in patients with relapsed and refractory multiple myeloma (RRMM): Initial KarMMa results. J Clin Oncol. 2020;38(15_suppl):8503-8503. | Abstract |
Delforge M, Miguel JS, Bertin KB, et al. Quality of life in patients with relapsed and refractory multiple myeloma treated with the BCMA-targeted CAR+T-cell therapy idecabtagene vicleucel (Ide-cel. BB2121): Results from the KarMMa trial. Braverman J. 06/12/20; 293491; EP1000 European Hematology Association (EHA). 2020. | Abstract |
Shah N, Delforge M, San Miguel JF, et al., Secondary Quality-of-Life Domains in Patients with Relapsed and Refractory Multiple Myeloma Treated with the BCMA-Directed CAR+T-Cell Therapy Idecabtagene Vicleucel (ide-cel; bb2121): Results from the KarMMa Clinical Trial. Blood (2020) 136 (Supplement 1): 28-29 | Abstract |
Raje NS, Siegel DS, Jagannath S, et al. Idecabtagene Vicleucel (ide-cel, bb2121) in Relapsed and Refractory Multiple Myeloma: Analyses of High-Risk Subgroups in the KarMMa Study. Blood (2020) 136 (Supplement 1): 16-17 | Abstract |
Berdeja J, Raje NS, Siegel DS, et al., Efficacy and Safety of Idecabtagene Vicleucel (ide-cel, bb2121) in Elderly Patients With Relapsed and Refractory Multiple Myeloma: KarMMa Subgroup Analysis. Blood (2020) 136 (Supplement 1): 16-17. | Abstract |
Shah N, Ayers D, Davies FE et al. A Matching-Adjusted Indirect Comparison of Efficacy Outcomes for Idecabtagene Vicleucel (ide-cel, bb2121), a BCMA-Directed CAR+T-Cell Therapy Versus Conventional Care in Triple-Class-Exposed Relapsed and Refractory Multiple Myeloma. Blood (2020) 136 (Supplement 1): 6-7. | Abstract |
Delforge M, Shah N, Rodriguez-Otero P et al. Health State Utility Valuation in Patients with Triple-Class-Exposed Relapsed and Refractory Multiple Myeloma Treated with the BCMA-Directed CAR+T-Cell Therapy, Idecabtagene Vicleucel (ide-cel, bb2121): Results from the Karmma Trial. Blood (2020) 136 (Supplement 1): 14-15 | Abstract |
An Efficacy and Safety Study of bb2121 in Patients With Relapsed and Refractory Multiple Myeloma and in Patients With High-Risk Multiple Myeloma (KarMMa-2) | Ongoing |
Delforge M, et al. KarMMa-3: A Phase 3 Study of Idecabtagene Vicleucel (ide-cel, bb2121), a BCMA Directed CAR+T-Cell Therapy Vs Standard Regimens in Relapsed and Refractory Multiple Myeloma. Blood (2020) 136 (Supplement 1): 24-25 | Ongoing and abstract preliminary results |
Appendix 3: Detailed Outcome Data
Note this appendix has not been copy-edited.

|||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||11
Note: This figure has been redacted as per the sponsor’s request.
Table 28: Summary of Key Results for Efficacy and Safety in the Population Treated With Idecabtagene Vicleucel — Data Cut-Off: January 14, 2020
Result | Idecabtagene vicleucel (CAR T cell) target dose | |||
|---|---|---|---|---|
150 × 106 N = 4 | 300 × 106 N = 70 | 450 × 106 N = 54 | Total 150 × 106 to 450 × 106 N = 128 | |
RESPONSE / REMISSION | ||||
Overall response rate (PR or better) | ||||
N (%) | 2 (50.0) | 48 (68.6) | 44 (81.5) | 94 (73.4) |
95% CIa | 6.8 to 93.2 | 56.4 to 79.1 | 68.6 to 90.7 | 65.8 to 81.1 |
CR rate (CR or better) | ||||
N (%) | 1 (25.0) | 20 (28.6) | 21 (38.9) | 42 (32.8) |
95% CIa | 0.6 to 80.6 | 18.4 to 40.6 | 25.9 to 53.1 | 24.7 to 40.9 |
Duration of response (≥ PR) (months)b,c, | ||||
N | 2 | 48 | 44 | 94 |
Censored, n (%) | 1 (50.0) | 12 (25.0) | 20 (45.5) | 42 (44.7) |
Progressed/died, n (%) | 1 (50.0) | 36 (75.0) | 24 (54.5) | 61 (64.9) |
Progressed | 1 (50.0) | 34 (70.8) | 24 (54.5) | 59 (62.8) |
Died without progression | 0 | 2 (4.2) | 0 | 2 (2.1) |
Median duration of response - months | NE | 9.92 | 11.30 | 10.7 |
(95%CI) | (2.79 to NE) | (5.36 to 11.01) | (10.3 to 11.43) | (9.03 to 11.30) |
Time to response | ||||
N | 2 | 48 | 44 | 94 |
Median TTR,d months (min, ma|) | 1.0 (1.0 to 1.0) | 1.0 (0.5 to 8.8) | 1.0 (0.9 to 2.0) | 1.0 (0.5 to 8.8) |
MRD | ||||
Patients who achieved MRD-negative status and at least CR g, N (%) | 1 (25.0) | 17 (24.3) | 15 (27.8) | 33 (25.8) |
95% CI | 0.6 to 80.6 | 14.8 to 36.0 | 16.5 to 41.6 | 18.5 to 34.3 |
SURVIVAL | ||||
Overall survival d | ||||
|||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
Median of overall survival time, months | ||||||||||||| | ||||||||||||| | ||||||||||||| | 19.4 |
95% CI | ||||||||||||| | ||||||||||||| | ||||||||||||| | 18.2 to NE |
Progression-free survivald | ||||
||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
Median of PFS time, months | 2.8 | 5.8 | 12.1 | 8.8 |
95% CI | 1.0 to NE | 4.2 to 8.9 | 8.8 to 12.3 | 5.6 to 11.6 |
HARMS | ||||
|||||||||||||||||||||||||||| | |||| | |||| | |||| | ||||||||||||| |
||||||||||||||||||||||||||||| | |||| | |||| | |||| | ||||||||||||| |
|||||||||||||||||||||||||||||||| | |||| | |||| | |||| | ||||||||||||| |
||||||||||||||||||||||||||||| | |||| | |||| | |||| | ||||||||||||| |
Common adverse events | ||||
|||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
Total number of deaths, n (%) | — | — | — | 44 (34.4) |
|||||||||||||||||||| ||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
Notable harms | ||||
Febrile neutropenia | |||| | |||| | |||| | 30 (16.3) |
Cytokine release syndrome | |||| | |||| | ||||||||||||| | 107 (83.6) |
iiNT | |||| | |||| | |||||||||||| | 23 (18.0) |
Replication-competent lentivirus | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
AE = adverse event; CAR = chimeric antigen receptor; CI = confidence interval; CR = complete response; CTCAE = Common Terminology Criteria for Adverse Events; iiNT = investigator-identified neurotoxicity; LDC = lymphodepleting chemotherapy; HRQoL = health-related quality of life; MRD = minimal residual disease; NE = not estimable; PFS = progression-free survival; PR = partial response; PT = preferred term; sCR = stringent complete response; SE = standard error; SOC = system organ class; TTP = time to progression.
aFor “Total” and “Enrolled population”: Wald CI; for individual target doses: Clopper-Pearson exact CI.
bThe TTR and DoR analyses were based on responders only, and therefore were the same for the ide-cel-treated population, enrolled population, and efficacy evaluable population, since responders in the 3 populations were the same (i.e., subjects enrolled but not treated with ide-cel and treated with ide-cel but without baseline or post-baseline efficacy assessments were to be considered nonresponders).
cFDA censoring rules were applied to DoR and PFS.
dMedian PFS and OS were measured from the day of infusion for the ide-cel-treated population and from the day of enrolment (i.e., leukapheresis) for the enrolled population. For PFS and OS, the median and corresponding 95% CI are based on the Kaplan-Meier approach.
Source: Amendment of Clinical Study Report for BB2121-MM-001 (KarMMa) study10 and global safety update cut-off date: January 14, 2020).10
||||||||||| | ||||||||||| | ||||||||||| | ||||||||||| | ||||||||||| |
|---|---|---|---|---|
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||
Table was redacted as per sponsor’s request.

|||||||||||||||||||||||||||||||||||||||||||||||
|||||||||
|||
|||||
||||||||||||||||||||.
Note: This figure has been redacted as per the sponsor’s request.

||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||
|||
|||||
||||||||||||||||||||.
Note: This figure has been redacted as per the sponsor’s request.

Appendix 4: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core30 (EORTC QLQ-C30)
EuroQol 5-Dimensions 5-Level questionnaire (EQ-5D-5L)
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myleoma Module with 20 items (EORTC QLQ-MY20)
Findings
A focused literature search was conducted to identify the psychometric properties and MID of each of the stated outcome measures.
The findings about validity, reliability, responsiveness, and MID of each outcome measure are summarized in Table 31.
Interpretation of the reliability and validity metrics were based on the following criteria:
Inter-rater reliability, kappa statistics (level of agreement)35:
less than 0 = poor agreement
0.00 to 0.21 = slight agreement
0.21 to 0.40 = fair agreement
0.41 to 0.60 = moderate agreement
0.61 to 0.8 = substantial
0.81 to 1.00 = almost perfect agreement
Internal consistency (Cronbach alpha) and test-retest reliability: ≥ 0.7 is considered acceptable.36
Validity; i.e., between-scale comparison (correlation coefficient, r)37:
less than or equal to 0.3 = weak
0.3 to ≤ 0.5 = moderate
greater than 0.5 = strong
Table 30: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | The EORTC QLQ-C30 is a standardized, patient self-administered questionnaire for evaluating the quality of life of patients with cancer. Consists of functional scales, 3 symptom scales, and 6 single-item scales. | Validity: All subscales shown to be impaired in MM patients compared to population norms. No correlation of any subscale with the SEIQoL‐Index suggesting independence. Reliability: The 5 functional scales reported an internal consistency greater than 0.7 except for cognitive function (alpha = 0.57). The global health status/HRQoL scale reported an internal consistency ranging from 0.82 to 0.93. All 4 scales (including the single-item body image measure) had test-retest reliability of 0.85 or greater. These are based on 2 studies in MM patients from Greek and Iranian populations. Responsiveness: Global QoL scale had statistically significant standardized response means (SRM) in MM patients who improved (SRM 0.32, P < 0.01) and deteriorated (SRM 0.57, P < 0.01). | Estimates for improvement and deterioration were, respectively: physical function (2, −5), role function (6, −7), cognitive function (3, −1), emotional (6, −3), social (3, −6), fatigue (−4, 5), pain (−5, 3), pain (−5, 3), nausea/vomiting (−3, 5), financial (−3, 2), and global QoL score (5, −5). |
EQ-5D-5L | Generic, preference-based HRQoL instrument, consisting of an index score and VAS scale score. The index score is based on 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. | Measurement properties of validity, reliability, and responsiveness not assessed in MM patients. | An absolute change of 0.08 to 0.10 points in the index score was important to MM patients.29 |
EORTC QLQ-MY20 | The QLQ-MY20 is a 20-item myeloma module intended for use among patients varying in disease stage and treatment modality. | Validity: Poor PS at baseline showed significant decrease in disease symptoms, side effects and body image subscales (P < 0.003) and approached significance for future perspective (P = 0.065).32 Reliability: Of the symptom scales; disease symptoms (alpha = 0.77) and side effects of treatment (alpha = 0.72). Future perspective was reported as an internal consistency of 0.80, body image was not assessed. Responsiveness: Disease symptoms and body image significantly decreased over time in these patients, and the side effects of treatment significantly increased. | :Disease Symptoms, −10 and + 10 points for improvement and deterioration, respectively; Side Effects of Treatment, −10 and + 10 points for improvement and deterioration, respectively; Body Image, + 13 points and −13 for improvement and worsening, respectively; and Future Perspective (body image) + 9 and −9 points for improvement and deterioration respectively.33 |
EORTC QLQ = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire; EQ-5D-5L = EuroQol 5-Dimensions 5-Level questionnaire; HRQoL = health-related quality of life; MID = minimal important difference; MM = multiple myeloma; PS = performance status; QoL = quality of life; SEIQoL = Schedule for the Evaluation of Individual Quality of Life; SRM = standardized response mean; VAS = visual analogue scale
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
Description
The EORTC QLQ-C30, is 1 of the most commonly used PRO measures in oncology clinical trials.38 It is a multi-dimensional, cancer-specific, evaluative measure of HRQoL. It was designed specifically for the purpose of assessing changes in participants’ HRQoL in clinical trials, in response to treatment.39 The core questionnaire of the EORTC QLQ-C30 consists of 30 questions that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item QoL scale, as outlined below.
Functional Scales (15 Questions)
Physical function (5)
Role function (2)
Cognitive function (2)
Emotional function (4)
Social function (2)
Symptom Scales (7 Questions)
Fatigue (3)
Pain (2)
Nausea and vomiting (2)
Single-Item Symptom Scales (6 Questions)
Dyspnea (1)
Insomnia (1)
Appetite loss (1)
Constipation (1)
Diarrhea (1)
Financial impact (1)
Global Quality of Life (2 Questions)
Global Quality of Life (2)
Scoring
Version 3.0, of the questionnaire, used in the 3 included trials in this report, is the most current version and has been in use since December of 1997.40 It is available in 90 different languages and is intended for use in adult populations only. Notably, the global QoL scale is also known as the Global Health Status, which was reported in the 3 trials and pooled analysis above.41
The EORTC QLQ-C30 uses a 1-week recall period in assessing function and symptoms. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4.40 For the 2 items that form the global quality of life scale, however, the response format is a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent).40
Raw scores for each scale are computed as the average of the items that contribute to a particular scale. This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of 1 unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better quality of life (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and quality of life scale would reflect an improvement. According to the EORTC QLQ-C30s scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least 1-half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.40
Validity
A total of 215 patients with MM were recruited from Imam Khomeini Hospital, Tehran. Patients were eligible for the study if they were 18 years of age or older, had been diagnosed with MM at least 1 month before study entry, and were able to read and speak Persian/Farsi. Patients who had a life expectancy of less than 3 months or had serious cognitive problems (as assessed by the Mini-Mental State Examination) were excluded from the study. Participating patients were asked to complete the EORTC QLQ-C30 3 times, at study entry, after 2 weeks, and again after 3 months.
Osborne et al., assessed the reported construct and criterion validity of the EORTC QLQ-C30. A systematic review was conducted to identify HRQoL tools validated for use in myeloma; identify issues important to HRQoL from the point of view of patients with myeloma; describe the measurement properties of each HRQoL tool; evaluate the content validity of HRQoL tools in terms of their ability to capture all issues important to patients and to explore the suitability of each HRQoL tool for use in different settings. From their systematic review of life tools, all subscales of those patients with MM were shown to be impaired compared to the general population. General QoL scales significantly improved with increasing time post‐HSCT. In MM patients, 67% and 43% of patients scored below the 10th percentile for physical functioning and global QoL subscales. Functional subscales and global QoL were found to be lower in MM than in general hematology. Pain, fatigue, physical and global QoL subscales in MM patients were able to discriminate those who improved versus stable or deteriorated. All subscales except single-item diarrhea discriminated between MM patients with different performance status and response status. There existed significant differences in global QoL or global health status between different treatment arms in trials for patients with MM.27 Additionally, there was no correlation of any subscale with the SEIQoL‐Index (individual QoL scale with patient‐nominated domains) suggesting independence.28
Kvam et al., reported the global QoL scale had statistically significant standardized response means in MM patients who improved (SRM 0.32, P < 0.01) and deteriorated (SRM 0.57, P < 0.01).29 Patients who improved had significantly (P < 0.01) higher scores at T2 in all 3 questionnaires. Patients who deteriorated reported lower scores at T2; however, for the 15D, the differences in score were not statistically significant.29
Reliability
Internal consistency reliability reported in the Tehran study was greater than 0.80 for all 3 multi-item scales (ranging from 0.82 to 0.93). All 4 scales (including the single-item body image measure) had test-retest reliability of 0.85 or greater. The disease symptoms scale had the highest test-retest reliability (ICC = 0.95).26
A sample of myeloma patients (N = 89) from 2 tertiary hospitals in Greece were surveyed with the QLQ-C30 and various demographic and disease related questions. Internal consistency of the QLQ-30 was assessed in this population. The 5 functional scales reported an internal consistency of greater than 0.7 except for cognitive function (alpha = 0.57). The global health status/HRQoL scale reported an internal consistency of 0.92. Of the symptom scales, fatigue (alpha = 0.89), nausea and vomiting (alpha = 0.74) and pain (alpha = 0.80) were assessed for internal consistency.30 Five symptom scales/items of the core QLQ-C30, that is, nausea/vomiting, appetite loss, constipation, diarrhea, and financial difficulties had high (> 50%) floor scores, implying a lack of these symptoms in this sample, but also suggest an underlying reduced discriminative ability. Conversely, no ceiling effects were observed on the core instrument despite 3 scales being close to the threshold value (role, cognitive, and social functioning).30
Responsiveness to Change
To assess responsiveness, Kvam et al., used the global rating of change (GRC) to identify whether patients have changed over time. A Wilcoxon signed-rank test for pair differences was used to calculate the significance of differences in the mean score changes between baseline (T1) and after 3 months (T2). Due to the small sample sizes in some of the GRC categories, data were pooled into the categories improved, unchanged, and deteriorated to yield sufficient numbers of cases in each category. “Improved” represented patients ‘who reported themselves as improved’ and similarly for deteriorated and unchanged patients. To assess the magnitude of the difference in scores between patients who improved ⁄ unchanged ⁄ deteriorated, standardized response means were calculated by dividing the mean score changes by the standard deviation (SD) of the change. This was compared against Cohen’s theory for interpreting the magnitude of mean differences in HRQoL scores, which suggests that a change of 0.20 represents a small change, 0.50 a moderate change, and > 0.80 a large change.29
In patients rating themselves as unchanged, mean score changes clustered around zero, and the SRMs were negligible. Patients who deteriorated reported lower scores at T2 compared with T1. The global QoL scale of the EORTC QLQ-C30 was the most responsive in deteriorating patients (SRM 0.57).29
Minimal Important Difference
One study42 assessed the MID of the EORTC QLQ-C30 by recruiting 239 patients with MM to complete the EORTC QLQ-C30 at baseline (T1) and after 3 months (T2). At T2, patients were asked if they had noticed any change in the domains pain, fatigue, physical function and global QoL. A combination anchor and distribution approach were used. The MIDs (absolute values) for patients rating themselves as improved was 6.2 for physical function, 14.7 for pain, 13.5 for fatigue and 7.6 for QoL. Patients reporting deterioration had MIDs (absolute values) of 8.6 for fatigue, 17.3 for pain, 12.8 for physical function, and 12.1 for QoL. However, there was considerable variation in the observed scores.
Another study used a systematic review of the literature and experts’ opinion to evaluate meaningful differences and magnitude of change31 in the QLQ C30 scores. In a meta-analysis of 118 relevant papers, authors estimated trivial, small, and medium size classes for meaningful change in the scales. These values were used in the KarMMa study using the lower threshold for small improvement and are presented in Table 31.
Table 31: Minimal Important Differences of EORTC QLQ-C30 Subscales
EORTC QLQ-C30 scales | MID for improvement | MID for deterioration |
|---|---|---|
Functional scales | ||
Physical function | 2 | −5 |
Role function | 6 | −7 |
Cognitive function | 3 | −1 |
Emotional function | 6 | −3 |
Social function | 3 | −6 |
Symptom scales | ||
Fatigue | −4 | 5 |
Pain | −5 | 3 |
Nausea and vomiting | −3 | 5 |
Single-Item symptom scales | ||
Dyspnea | −2 | 5 |
Insomnia | −5 | 2 |
Appetite loss | −7 | 2 |
Constipation | −4 | 5 |
Diarrhea | −3 | 5 |
Financial impact | −3 | 2 |
Global quality of life | ||
Global quality of life | 5 | −5 |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; MID = minimally important difference.
No studies assessing validity of the EORTC QLQ-C30 were found in patients from North America, which could affect the generalizability of the findings.
EuroQol 5-Dimensions 5-Levels Questionnaire
The EQ-5D-5L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments including MM. The EQ-5D-5L was developed by the EuroQol Group as an improvement to the EQ-5D 3- Level (EQ-5D-3L), to measure small and medium health changes and reduce ceiling effects. The instrument comprises 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: level 1 “no problems,” level 2 “slight problems,” level 3 “moderate problems,” level 4 “severe problems,” and level 5 “extreme problems” or “unable to perform.” A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state. The corresponding scoring of EQ-5D-5L health states is based on a scoring algorithm that is derived from preference data obtained from interviews using choice-based techniques (e.g., time trade-off) and discrete choice experiment tasks. The lowest score varies depending on the scoring algorithm used. The anchors are 0 (dead) and 1 (full health), however negative values are also allowed to represent health states that a society considers worse than death. As an example, a Canadian scoring algorithm results in a score of −0.148 for health state 55555 (worst health state). Another component of the EQ-5D-5L is a visual analogue scale (EQ VAS), which asks respondents to rate their health on a visual scale from 0 (worst health imaginable) to 100 (best health imaginable).43
The EQ-5D-5L has been extensively validated across countries around the world and in various conditions. However, the psychometric properties of the EQ-5D-5L have not been assessed in patients with MM, therefore its validity, reliability, and responsiveness to change have not been evaluated in this patient population of interest.
Minimal Important Difference
Kvam et al., used a combined distribution and anchor-based approach by using the whole set of scores at T1 and estimating the MIDs based on baseline SD for the whole sample. Cohen criteria for interpreting the absolute magnitude of a change were applied. From this analysis, an MID of 0.08 in MM patients who thought their QoL improved, and 0.10 in those who thought their QoL deteriorated.29
To estimate the MID values of the EQ-5D-5L for each country-specific scoring algorithm, a simulation-based approach based on instrument-defined single-level transitions has been used. The simulation-based instrument-defined generally accepted MID estimate (mean ± SD) for Canada is 0.056 ± 0.011.44
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Myeloma Module With 20 Items
The EORTC has developed a myeloma module referred to as QLQ-MY20, to be administered alongside the core QLQ-C30. The QLQ-MY20 is a 20-item myeloma module intended for use among patients varying in disease stage and treatment modality. The validity and reliability of QLQ-MY20 as MM-specific instrument has been demonstrated when used along with the QLQ-C30 in patients with MM. The module included in this study is composed of 20 questions addressing 4 different domains of HRQoL that are important to patients with MM: 2 symptom scales (i.e., disease symptoms and side effects of treatment) and 2 functional scales (i.e., future perspective and body image). Similar to the QLQ-C30, questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. Raw scores for each scale are computed as the average of the items that contribute to a particular scale. This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of 1 unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better quality of life (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and quality of life scale would reflect an improvement.
Validity and Responsiveness to Change
Cocks et al., assessed the validity and sensitivity of the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-MY20 questionnaire. Responsiveness analysis compared the baseline and follow-up scale scores for the 137 (57% of total) patients who achieved at least a PR. Multiple myeloma patients were recruited prospectively from ongoing or new clinical trials at the time of the study rather than setting up a separate questionnaire validation study. Trials had to be for newly diagnosed or relapsed/refractory MM patients with a minimum prognosis of 3 months. Maintenance therapy trials were not eligible. Questionnaires were issued to patients at the baseline for each trial (randomization or registration) according to the procedures for that trial. A panel reviewed each protocol and identified an appropriate follow-up time point for the field study QoL assessment, this had to be during treatment or within 4 weeks of completion of treatment and was 3 or 6 months from randomization for all protocols. Disease symptoms (P = 0.0001) and body image (P < 0.0001) significantly decreased over time in these patients, and the side effects of treatment significantly increased. The QLQ-MY20 scale scores for patients with performance status 0, 1 or 2 (number of patients, n = 200) were compared to those with performance status 3 or 4 (n = 25) at baseline. Three of the scales from the module: disease symptoms, side effects of treatment and body image showed evidence of a significant difference (P < 0.003) between the patient groups. The future perspective scale showed a trend toward a difference (P = 0.065).32
Reliability
A sample of MM patients (N = 89) from 2 tertiary hospitals in Greece were surveyed with the QLQ-MY20 and various demographic and disease related questions. Patients were approached during a scheduled visit to 1 of the hospitals. None had cancer metastases or severe comorbid conditions which could further compromise HRQoL. Internal consistency of the QLQ-MY20 was assessed in this population. Of the symptom scales, disease symptoms (alpha = 0.77) and side effects of treatment (Alpha = 0.72) demonstrated adequate (adequate measured at alpha = 0.70) internal consistency. Future perspective was reported as an internal consistency of 0.80, side effects of treatment at an internal consistency of 0.72, and disease symptoms at 0.77. Body image was not assessed.30
Minimal Important Difference
A mixed‐methods study by Sully et al., assessed MID scores of the MY20 using patient interviews that were conducted alongside an analysis of existing trial data. Data were pooled across 3 clinical trials: ASPIRE, ENDEAVOR, and CLARION. Each was a phase III, randomized, open‐label study comparing carfilzomib‐based regimens, with a primary end point of progression‐free survival (PFS) in patients with relapsed or refractory MM. Patients were eligible for entry into the pooled sample if they had completed the EORTC QLQ‐C30 or QLQ‐MY20 at baseline plus at least 1 other of the following time points: mid‐treatment or end of treatment. Twenty patient interviews were conducted.33
Two anchor‐based methods were applied, mirroring an approach in another pooled study of cancer patients. Potential anchors were identified by the authors reviewing the clinical trial protocols to identify measures available across the trials at mid‐treatment and end of treatment. Anchors were selected via review of the protocols and case report forms. Potential anchors were chosen if they were deemed to have conceptual overlap with any of the EORTC QLQ‐MY20 scales. Anchor‐based MIDs were estimated by calculating the mean change score of patients classified as improved and deteriorated according to anchor definitions. Patient‐reported anchors were the EORTC QLQ‐C30 global health/QoL scale and Functional Assessment of Cancer Therapy‐Gynecologic Oncology Group Neurotoxicity. Clinical anchor measures were the ECOG status, matched AEs, and peripheral neuropathy‐related AEs. Linear regression models were also fitted with EORTC QLQ‐MY20 score change as the outcome and a binary indicator of stable vs improved/worsened according to the anchor as a predictor, where the coefficient of this indicator was the MID estimate (incorporating the change score of stable patients). Diagnosis (newly diagnosed or relapsed) was accounted for in the model.
Based in the study by Sully et al., the recommended MIDs for the EORTC QLQ-MY20 were as follows: Disease Symptoms, −10 and + 10 points for improvement and deterioration, respectively; side effects of treatment, −10 and + 10 points for improvement and deterioration, respectively; Body Image, + 13 points and −13 for improvement and worsening, respectively; and future perspective (body image) + 9 and −9 points for improvement and deterioration respectively.33
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CAR
chimeric antigen receptor
CI
confidence interval
CRS
cytokine release syndrome
CyBorD
cyclophosphamide plus bortezomib plus dexamethasone
CyD
cyclophosphamide plus dexamethasone
ICER
incremental cost-effectiveness ratio
IMiD
immunomodulatory imide agent
ITC
indirect treatment comparison
KCyd
carfilzomib plus cyclophosphamide plus dexamethasone
LDC
lymphodepleting chemotherapy
MM
multiple myeloma
OS
overall survival
OSB
Ontario Schedule of Benefits
PCyd
pomalidomide plus cyclophosphamide plus dexamethasone
PD
progressive disease
PFS
progression-free survival
PVd
pomalidomide plus bortezomib plus dexamethasone
QALY
quality-adjusted life-year
RRMM
relapsed or refractory multiple myeloma
Vd
bortezomib plus dexamethasone
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Idecabtagene vicleucel (Abecma), given as a single IV infusion, target dose of 450 × 106 CAR-positive T cells, within a range of 275 × 106 to 520 × 106 CAR-positive T cells |
Submitted price | Idecabtagene vicleucel, target dose of 450 × 106 CAR T cells: $545,000 per IV infusion (in 1 or more patient-specific infusion bag(s), volume ranges from 10 mL to 100 mL per bag) |
Indication | For the treatment of adult patients with multiple myeloma who have received at least 3 prior therapies, including an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 antibody, and who are refractory to their last treatment |
Health Canada approval status | NoC/c |
Health Canada review pathway | Priority review |
NOC date | May 26, 2021 |
Reimbursement request | As per indication |
Sponsor | Celgene Inc., a Bristol Myers Squibb Company |
Submission history | Previously reviewed: No |
CAR = chimeric antigen receptor; NOC = Notice of Compliance; NOC/c = Notice of Compliance with Conditions.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adult patients with MM who have received at least 3 prior regimens, including regimens with an IMiD, a PI, and an anti-CD38 antibody, and who are refractory to their last treatment |
Treatment | Idecabtagene vicleucel |
Comparator | Conventional care, defined as a basket of chemotherapy regimens (efficacy and costs were based on a different definition of chemotherapy regimens) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (15 years) |
Key data source | Single-arm phase II KarMMa trial for idecabtagene vicleucel NDS-MM-003 retrospective registry for conventional care |
Submitted results | Base case: patients receiving the target dose in the KarMMa trial (n = 54)
Key scenario analyses
ICER = $334,059 per QALY |
Key limitations |
|
CADTH reanalysis results |
|
HR = hazard ratio; ICER = incremental cost-effectiveness ratio; IMiD = immunomodulatory agent; MM = multiple myeloma; OS = overall survival; PFS = progression-free survival; PI = proteasome inhibitor; QALY = quality-adjusted life-year; RWE = real-world evidence.
Conclusions
Results from the KarMMa study suggest that idecabtagene vicleucel between doses of 150 × 106 and 540 × 106 chimeric antigen receptor (CAR) T cells is associated with an induction of response in patients with multiple myeloma (MM) who have received at least 3 prior therapies and who are refractory to their last treatment, although interpretation of the results is challenging due to the lack of a comparison to a concurrent control arm and the study’s open-label design. Although the sponsor submitted an indirect treatment comparison (ITC), inherent design differences could not be adjusted for statistically and generalizability is of concern given the matched final cohort involved different and varied regimen therapies not reflective of Canadian clinical practice.
The CADTH review found that the sponsor’s base case included several major limitations that introduced significant uncertainties to the analysis of the cost-effectiveness of idecabtagene vicleucel. First, KarMMa was a phase II trial, and uncertainty remains regarding the efficacy of idecabtagene vicleucel. The efficacy of idecabtagene vicleucel is dependent on several implementation factors and it remains unclear if the implementation observed in the trial would reflect the Canadian setting. Because KarMMa was not a comparative study, relative effectiveness to conventional care was obtained by comparing the treated population from the KarMMa study to a patient cohort identified from several sites and database registries. Despite adjustment approaches to ensure comparability between the study populations, there is significant uncertainty on the relative efficacy of idecabtagene vicleucel and comparator treatments. Furthermore, although most of the incremental benefits in the model were accrued in the extrapolation period, overall survival (OS) data were immature in the KarMMa trial, introducing uncertainty in the extrapolation of efficacy.
The issues with the clinical data preclude a reasonable assessment of cost-effectiveness as there is no clear resolution to the identified uncertainties. As such, a CADTH base case could not be derived. Instead, CADTH undertook a series of exploratory reanalyses focused on the treated population, which indicated that the ICER of idecabtagene vicleucel was likely to be higher than that estimated by the sponsor. The ICERs were sensitive to different assumptions regarding relative efficacy. One set of CADTH exploratory reanalyses attempted to address some of the identified limitations by adjusting the distribution of regimens informing the cost of conventional care and removing treatment-specific utilities. When different combinations of possible efficacy scenarios were tested on top of these changes, the deterministic ICER for idecabtagene vicleucel was found to range from $286,142 to $1,276,217 per quality-adjusted life-year (QALY) compared with conventional care. However, majority (97.6% to 85.7%) of the incremental clinical benefits predicted by these scenarios were accrued beyond the trial observation period, for which there limited long-term evidence. Given the lack of robust information on the clinical effects of idecabtagene vicleucel compared with conventional care, the cost-effectiveness is unknown. A key cost driver is the acquisition cost of idecabtagene vicleucel.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from Myeloma Canada, which surveyed 388 patients with MM. Respondents identified the most important aspects of effective treatments as those providing fewer side effects and better quality of life. Respondents also identified drug costs, parking costs, and lost income due to absence from work as the most significant financial implications, and more than half of the respondents indicated that they have received help from a family member or caregiver. Of the survey respondents, 161 would be eligible for idecabtagene vicleucel (based on having received at least 3 prior therapies, including an immunomodulatory imide drug [IMiD], a proteasome inhibitor, and an anti-CD38 antibody) and half of these individuals were familiar with the CAR T-cell therapy process and how it differs from current treatment regimens. These patients believed that, compared to current therapies or those they have previously received, CAR T-cell therapy could prolong remission, eliminate the need for treatment during remission, improve quality of life, provide better control of symptoms, and result in fewer side effects. However, they were most concerned about side effects such as loss of or decrease in cognitive abilities and loss of physical abilities and mobility. Among the 14 patients who had previously received CAR T-cell treatment, only 1 had received the treatment under review. Most respondents found CAR T-cell therapies to be effective and the side effects to be tolerable.
Registered clinician input was received that identified pomalidomide or carfilzomib as current third-line therapies, while a regimen of bortezomib and steroids or the addition of cyclophosphamide to bortezomib plus dexamethasone (Vd) or steroids may be used as fourth-line therapy. The clinicians believed that idecabtagene vicleucel would be appropriate for triple-exposed relapsed or refractory multiple myeloma (RRMM) patients. Patient selection is required such that disease progression is at a rate that allows patients to remain stable and relatively well during the waiting time for cell processing (4 to 5 weeks). Patients with good performance status and organ function, minimal or no comorbidities, robust blood counts, low tumour burden, and indolent disease were identified to most likely demonstrate the best outcomes. Although it was noted that patients best suited for the treatment should be identified through B-cell maturation antigen staining (which is not currently part of routine testing), the clinicians added that patients can be identified using routine criteria for myeloma relapse or progression. Careful matching may be required to ensure those best suited receive treatment, given the extensive resources required to deliver this CAR T-cell therapy such as 2 weeks of inpatient hospital stay for treatment and resources to treat side effects (cytokine release syndrome [CRS] or neurotoxicity). Response to treatment should be based on standard myeloma response criteria.
Drug plans indicated that, among the conventional therapies in the comparator arm, only cyclophosphamide plus dexamethasone (CyD), Vd, and cyclophosphamide in combination with bortezomib plus dexamethasone (CyBorD) are currently funded in Canada by most jurisdictions. Pomalidomide in combination with bortezomib plus dexamethasone (PVd) is not yet funded and pomalidomide plus dexamethasone(Pd), carfilzomib plus dexamethasone (Kd), or carfilzomib plus cyclophosphamide plus dexamethasone (KCyD) are typically not funded except on a case-by-case basis. Specialized centres for the administration of idecabtagene vicleucel will be required that are trained and accredited by the sponsor, which would require a high human resource burden to maintain accreditation. Depending on the location of these specialized centres, drug plans noted that some patients may be required to go out of country or out of province for access. Potential travel expenses may be incurred by the public payer. In addition, drug plans noted that significant resources would be required for patient preparation, including leukapheresis, cell processing, and the use of bridging and lymphodepleting chemotherapy (LDC), and for the management of adverse effects. The bridging therapy studied in the trial (daratumumab) may not funded be publicly across all jurisdictions. The budget impact of idecabtagene vicleucel would depend on capacity, clinician interest, and place in therapy. There is a potential for indication creep to earlier lines of therapy if triple-class exposure occurs in the first 2 lines of therapy.
Several of these concerns were addressed in the sponsor’s model.
The economic model incorporated side effects and quality of life that are of concern to patients. Loss of physical abilities and mobility were accounted for within the model using the EuroQol 5-Dimensions 5-Levels questionnaire, in which both aspects are captured. The impact of grade 1 and grade 2 side effects as well as grade 3 and grade 4 CRS or neurotoxicity were accounted for within the model in terms of costs and disutilities.
Although the financial burden imposed by MM on patients was not considered in the base case, given the public health care payer perspective, indirect costs such as parking, caregiving, and productivity loss were addressed in a scenario analysis by the sponsor and CADTH.
The costs of health care resources associated with leukapheresis, bridging therapies, and LDC were captured in the submitted economic model. Bridging therapy assumed in the economic analysis (distribution within the model) included dexamethasone (70.3%), cyclophosphamide (36.7%), daratumumab (28.1%), carfilzomib (23.4%), bortezomib (19.5%), and pomalidomide (18.8%).
In addition, CADTH addressed some of these concerns as follows: revising the distribution of treatments within conventional care to reflect the currently funded therapies in Canada (i.e., CyD, Vd, CyBorD, and pomalidomide-based and carfilzomib-based regimens).
CADTH was unable to address the following concerns raised from stakeholder input:
Additional resources required to set up specialized centres were not captured in the economic analysis.
Expenses related to travel out of country or out of province were not included in the model.
The economic evaluation assumes no capacity constraints; the sponsor’s submitted budget impact analysis, to an extent, permits consideration of capacity constraint from a financial perspective.
Economic Review
The current review is for idecabtagene vicleucel (Abecma) for adult patients with MM who have received at least 3 prior therapies, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody, and who are refractory to their last treatment.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing idecabtagene vicleucel with conventional care in the treatment of adult patients with MM who have received at least 3 prior therapies, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody, and who are refractory to their last treatment, which is consistent with the Health Canada indication.1 Conventional care was defined as a distribution of chemotherapy regimens.2
The target dose of idecabtagene vicleucel is 450 × 106 CAR-positive T cells (range, 275 × 106 to 520 × 106), administered as a single IV infusion with a volume ranging from 10 mL to 100 mL.1 The submitted price of idecabtagene vicleucel is $545,000 per infusion,3 excluding the costs associated with leukapheresis, bridging therapies, and LDC. The treatment cost for conventional care was based on 8 Canadian therapies weighted by their anticipated use from a Canadian database, ONCO-CAPPS. This included: pomalidomide plus dexamethasone, PVd, pomalidomide plus cyclophosphamide plus dexamethasone (PCyd), carfilzomib plus dexamethasone, KCyd, Vd, CyBorD, and CyD (Table 13). Costs were calculated separately for each regimen and aggregated by taking a weighted average. The treatment costs for conventional care, as calculated by the sponsor, ranged from $10,166 for weeks 1 through 24 to $9,856 thereafter.2
The clinical outcomes of interest were QALYs and life-years. The analyses were conducted from the Canadian public health care payer perspective. The time horizon in the base case was 15 years, with a monthly cycle length and a 1.5% annual discount rate for costs and effects.2
Model Structure
A partitioned survival model was developed to capture all costs and outcomes associated with each modelled treatment. All patients entered the model in the progression-free survival (PFS) health state. In each cycle, patients could either remain in the PFS health state or transition to the progressive disease (PD) or death health state. The proportion of patients with PD or who died was derived based on areas under the survival curves. Specifically, OS was partitioned to estimate the proportion of patients in the PFS and PD states. The difference between the OS curve and the PFS curve was partitioned at each time point to estimate the proportion of patients in the PD health state.2
Model Inputs
The patients’ baseline characteristics, such as height and weight, were obtained from the enrolled population of individuals who underwent leukapheresis (n = 140) from the phase II single-arm KarMMa trial.4
Efficacy outcomes, modelled by PFS and OS, were obtained from KarMMa for the idecabtagene vicleucel arm (data cut-off at 13 months), and NDS-MM-003 for conventional care. Specifically, in the sponsor’s base case, the efficacy of idecabtagene vicleucel was based on patients who specifically received the target dose of 450 × 106 CAR T cells (target population; n = 54).2 The NDS-MM-003 study was a global, retrospective observational registry owned by the sponsor that assessed treatment patterns in real-world patients with RRMM.5 Within this registry, which is composed of several databases (detailed in the CADTH clinical review), more than 90 different combinations of regimens were included before matching. To estimate the comparative treatment effects, 190 patients within the registry were identified and selected for having met the key eligibility criteria of the KarMMa trial based on select baseline characteristics, including number of prior treatments, time since diagnosis, and refractoriness to carfilzomib, pomalidomide, bortezomib, and lenalidomide. Trimmed stabilized inverse probability of treatment weighting was then applied to patients from both populations (n = 190 in NDS-MM-003; n = 128 in the KarMMa trial’s treated population, i.e., those who received idecabtagene infusion) for balancing.5 To extrapolate comparative efficacy beyond the available trial data up to a 15-year time horizon, the log-normal function was chosen for PFS and the exponential function was chosen for OS for both idecabtagene vicleucel and conventional care, using Akaike’s information criteria or Bayesian information criteria values, visual inspection, and clinical plausibility.2 Scenario analyses were performed using alternate idecabtagene vicleucel populations in the KarMMa trial (i.e., enrolled population and treated population).2 In the model, adverse events (AEs) considered for idecabtagene vicleucel focused on grade 3 and grade 4 events occurring in more than 5% of patients and key grade 1 or grade 2 AEs (i.e., CRS and neurotoxicity) reported within the target population.2 Because no AEs were collected in NDS-MM-003, the same set of grade 3 and 4 AEs that were selected for the idecabtagene vicleucel arm of the model were selected and the rate of AE occurrence in the conventional care was informed by the literature.6-10
Treatment and health state–specific utility values were applied.2 The utility estimates for idecabtagene vicleucel were obtained from the KarMMa trial, which collected EuroQol 5-Dimensions 5-Levels data that were transformed with a Canadian preference weighting.11 The utility values used in the sponsor’s base case were informed from the utility estimates from the treated population instead of the target population as the sample size of the former was larger. The utility values for pre-progression health state were split to |||| in the first month and |||| after the first month for idecabtagene vicleucel to reflect the short-term side effects associated with infusions. The utility values of conventional care in the progression-free health state were assumed to be equivalent to the overall pre-progression utility values from the KarMMa trial for the treated population.11 The utility value of conventional care in the post-progression health state was derived from the literature.12 Disutilities associated with chemotherapy treatment administration (−0.02) and AEs were based on previous National Institute for Health and Care Excellence health technology assessments, published literature, or assumptions,13-16 with the duration of the AEs assumed to be the same across all treatments. A summary of the utility values and decrements used in the model is provided in Appendix 3 (Table 9).
Costs included those associated with drug acquisition (including subsequent treatment costs), administration, monitoring, AEs (1-time cost at cycle 1 for first-line treatment), additional resource use, and terminal care (1-time cost applied upon death). Drug acquisition costs were obtained primarily from the Ontario Drug Benefit Formulary,17 Ontario Exceptional Access Program,18 and previous CADTH Health Technology Assessments.19-21 Drug acquisition costs of idecabtagene vicleucel included the costs in the pre-treatment phase (leukapheresis: $2,625,22 bridging therapies: $9,011) and the treatment phase (LDC: $1,092, idecabtagene vicleucel: $545,0003). The drug costs for conventional care were based on weighting the 8 most commonly used regimens reported in the Canadian 2020 ONCO-CAPPS database.23 Subsequent therapies were assumed to be identical across treatment arms. Costs associated with treatment administration were captured for treatments administered intravenously or subcutaneously while the frequency of monitoring tests were based on the KarMMa trial, assuming monitoring frequency of testing would be the same across all modelled health states and between the treatment and comparator groups, with the exception of the tumour lysis syndrome/CRS panel, which would apply only to idecabtagene vicleucel (Table 10). Costs were obtained from a variety of sources, including the Ontario Schedule of Benefits (OSB),24 Ontario Schedule of Benefits for Laboratory Services,25 Canadian Institute for Health Information,26,27 or published literature.28,29 All costs related to AEs were based on direct costs for inpatient monitoring taken from the Ontario Case Costing Initiative, the OSB, or published literature.30,31 Resource costs such as hospitalizations not associated with AEs, concomitant drugs, hematologist visits, and surgical procedures for transfusions of red blood cells or platelets were also included based on published literature or the OSB.24,32
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (500 iterations for the base case and scenario analyses).2 The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section. The submitted analyses were based on publicly available prices of the comparator treatments.
Base-Case Results
In the sponsor’s base-case analysis, the ICER for idecabtagene vicleucel compared to conventional care was $216,606 per QALY. Specifically, idecabtagene vicleucel was associated with incremental costs of $581,489 and 2.68 additional QALYs compared to conventional care over a 15-year modelled time horizon. Disaggregated results are presented in Table 11 and Table 12; Appendix 3.2 The cost-effectiveness acceptability curves indicated that idecabtagene vicleucel had a 0% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY (Figure 2 in Appendix 3).2
Most of the incremental costs were attributable to the higher drug acquisition costs of idecabtagene vicleucel (Table 11). The major driver contributing to QALY gains for idecabtagene vicleucel occurred in the post-progression health state (Table 12). Furthermore, 94.2% of incremental QALYs were accrued beyond the 1-year trial observation period. By the end of the model duration (15 years), 99.99% patients on the conventional care had died compared to 93.13% patients on the idecabtagene vicleucel arm.2
Table 3: Summary of the Sponsor’s Economic Evaluation Results — Target Population
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. conventional care ($ per QALY) |
|---|---|---|---|---|---|
Conventional care | 122,604 | Reference | 1.13 | Reference | Reference |
Idecabtagene vicleucel | 704,093 | 581,489 | 3.81 | 2.68 | 216,606 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
Uncertainty was addressed probabilistically by changing the definition of the population cohort from the KarMMa trial (i.e., treated and enrolled), the OS distribution (Weibull), the population and the literature sources that inform treatment-specific utility weights, the comparator cost (100% PCyd or KCyd), the exclusion of certain cost categories (i.e., subsequent treatment, AEs, administrative, resource, and monitoring), and the body surface area or weight.2 The results were most sensitive to the definition of the population studied. The ICER increased by more than 50% if the cohort was defined as per the treated population (i.e., $318,107 per QALY) or enrolled population (i.e., $334,059 per QALY) within the KarMMa trial.2
The sponsor conducted a secondary analysis using data from the MAMMOTH study, a retrospective chart review in the US, to derive the comparative clinical efficacy of conventional care.33 Where MAMMOTH was used as the source to derive the comparative effectiveness of conventional care, the ICER for idecabtagene vicleucel compared to conventional care was $329,205 per QALY (i.e., additional costs of $562,553; 1.71 additional QALYs) compared to conventional care over a 15-year modelled time horizon.2
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Uncertainty in the clinical efficacy of idecabtagene vicleucel: The clinical efficacy of idecabtagene vicleucel, was informed from KarMMa, an open-label, single-arm phase II trial.4 There is uncertainty in the efficacy of idecabtagene vicleucel. The trial’s lack of a comparator arm increased the risk of bias in the estimation of treatment effects due to the potential for confounding, fluctuations in health status, and other unidentified prognostic variables. Protocol deviations also existed in the dose patients received that led to clinical estimates within the sponsor’s model, which was based on a small target dose group (n = 54).4 In addition, given the amount of missing data, this increases imprecision in the clinical outcomes. The efficacy of idecabtagene vicleucel is further dependent on several implementation factors, including the expected duration of the manufacturing process (the trial lasted for 4 to 5 weeks, from leukapheresis to idecabtagene vicleucel infusion), the use of bridging therapies, and the use of LDC. It remains unclear if the implementation in the trial will reflect real-world implementation in Canadian practice.
Unknown comparative effectiveness: As KarMMa was a non-comparative trial, relative effectiveness estimates were obtained from the NDS-MM-003 registry using propensity scores with inverse probability of treatment weighting to adjust variables.5 Although the propensity score method resulted in a balanced distribution between treatment and control groups, baseline differences in multiple variables were noted between the eligible RRMM cohort and the idecabtagene vicleucel cohort. Further uncertainty in the effect estimates remained because the data were obtained from observational groups without randomization and the effect of residual confounding (unmeasured and unaccounted prognostic factors and effect modifiers) remains unresolved. Inherent study design differences between the KarMMa trial and the NDS-MM-003 were also unaccounted for statistically. Multiple imputations of missing values were made to generate the eligible RRMM cohort from the NDS-MM-003 registry, which further increased the uncertainty in the effect estimates. Although the database contained 1,949 patients, only a small subset of patients were included in the final set of the eligible RRMM cohort that was used for comparison with the idecabtagene vicleucel cohort (n = 190).5 This introduces concerns with precision and generalizability. Furthermore, according to the CADTH clinical report, the generalizability of the regimens used in the matched cohort is of concern due to the different and varied therapies, some of which are not available in Canada. Although a scenario analysis was provided in which the efficacy of conventional care was based on a different ITC submitted by the sponsor (i.e., a matched adjusting indirect comparison) conducted against the MAMMOTH study,33 half of the regimens were either not funded for this line of therapy (daratumumab) or not available (PACE-like) in Canada, according to the clinical experts consulted by CADTH. As such, this alternative source was also deemed inappropriate to inform relative effectiveness. Together, there is significant uncertainty on the relative efficacy of idecabtagene vicleucel with comparator treatments.
CADTH was unable to address this limitation. CADTH conducted exploratory reanalyses over a plausible range of relative effectiveness scenarios. This included testing the upper and lower bounds of the 95% confidence intervals (CIs) of relative efficacy estimates derived from the sponsor’s submitted ITC.
Extrapolation of PFS and OS beyond study duration: The absolute and relative effectiveness on PFS and OS beyond the study duration (matched analysis was based on 13-month data cut-off for KarMMa) is not available and was extrapolated using mathematical models.2 The OS data in the treated population were immature given that the median OS was not reached at the time of the available data cut-off from the trial (||||% and ||||% of patients remained alive at 12 and 18 months, respectively).4 The appropriateness and quality of any extrapolation is dependent on the quantity of the available observed data. Closer to the data cut-off period, the number of patients at risk of death to inform survival decreased. With the smaller sample sizes, greater imprecision was introduced to the survival estimates at those time periods and in the extrapolation. The PFS data beyond the follow-up time was similarly uncertain given that more than ||||% of patients were censored at the median PFS follow-up duration.4 The parametric assumptions used in the sponsor’s base case (log-normal for PFS, exponential for OS)2 were deemed to be optimistic for the conventional care arm when validated by the CADTH clinical experts. When the sponsor’s PFS is examined alongside its selected OS curves, the extrapolations suggest that idecabtagene vicleucel is associated with a long-term post-progression survival benefit. This is not supported by the clinical evidence evaluated by CADTH nor does it align with the clinical experts’ feedback. The clinical experts indicated that they expect no residual survival benefit of idecabtagene vicleucel past progression and, once progressed, patients would be similar in terms of their expected survival.
The true long-term effectiveness (and relative effectiveness) remains unknown and CADTH was unable to fully address this limitation. Clinical experts expected OS at 5 years to be 0% given the severity of disease conditions in these patients. The gamma distribution, which may be a more plausible parametric assumption for the OS of conventional care, was selected by CADTH. Although this was the most conservative distribution available among those provided by the sponsor, CADTH clinical experts noted that the estimates produced from the gamma distribution remain optimistic, as 3% of patients were predicted to remain alive at 5 years. Given the lack of long-term data, the clinical experts noted that idecabtagene vicleucel outcomes may be similarly optimistic and considered the gamma distribution for the OS of idecabtagene vicleucel to be appropriate in the CADTH exploratory reanalyses. CADTH selected the gamma distribution to model PFS in conventional care and idecabtagene vicleucel as it provided the most conservative estimate.
Concerns with the choice of comparator: In the sponsor’s model, the comparator was defined as conventional care and was based on a pooled strategy of different treatment regimens. Costs were weighted based on 8 Canadian regimens claimed to be the most commonly prescribed for patients in lines of therapy equivalent to idecabtagene vicleucel, according to the ONCO-CAPPS database.23 However, CADTH’s clinical experts noted that 1 of these regimens (PVd) is currently under review and is not prescribed to patients for the same line of therapy in Canada. Furthermore, the distributions were found not to reflect Canadian practice patterns. The CADTH clinical experts indicated that pomalidomide plus dexamethasone is used more frequently while CyD is used less frequently in this patient group. Of further concern, the efficacy inputs for conventional care were informed by a different combination of oncology regimens found in the NDS-MM-003 database.5 Inconsistency exists in the definition of conventional care in terms of the treatments that informed costs and those that informed the efficacy inputs within the model. If multiple comparators may be relevant to the funding decision, individual treatment regimens should be considered on their own and all comparators should be assessed in a sequential analysis. The sponsor did not follow this approach.
CADTH could not address the issue of the use of a “basket of comparators” and could not evaluate the cost-effectiveness of idecabtagene vicleucel relative to individual oncology regimens. Given concerns with the composition of conventional care, CADTH revised the composition of the regimens in its exploratory reanalysis based on the feedback of CADTH clinical experts. This approach does not resolve the inconsistency arising from the fact that treatment costs for conventional care are based on a different composition of oncology regimens rather than the regimens that informed the efficacy inputs.
Application of treatment-specific utility weights: The model assumed a higher utility for idecabtagene vicleucel compared with conventional care for patients in the same health state (Table 9). The utility values for idecabtagene vicleucel in both health states (progression-free and PD) were drawn from the KarMMa trial,11 while the utility in the pre-progression health state for conventional care was assumed to be equivalent to the overall pre-progression utility values from the KarMMa trial.2 The utility values for conventional care in the PD health state were derived from the published literature.12 The use of treatment-specific utility values is contradictory to CADTH’s Guidelines for the Economic Evaluation of Health Technologies: Canada, which recommends that utilities should reflect the health states in the model.34 Differences by treatment should be transparently modelled and justified. Although the clinical experts consulted by CADTH agreed that patients on idecabtagene vicleucel may experience lower utility values immediately following infusion due to treatment administration and AEs, the utility in the pre-progression health state is expected to be similar for patients in the same health state, with the exception that utilities may be lower in the conventional care arm due to AEs and continued treatment administration. As the sponsor’s base case already incorporated disutilities due to chemotherapy treatment administration and AEs, there is little justification for applying treatment-specific utilities. This approach double-counts the disutility associated with these events. The clinical experts further noted that, once patients progressed, they are likely to have the same utility weight, regardless of prior treatment assignment. The application of treatment-specific utility weight favours idecabtagene vicleucel.
CADTH’s exploratory reanalyses set the health state–utility weights of both arms to be equal after the first month in the pre-progression health state to account for the utility impacts associated with the administration of CAR T-cell therapy. Specifically, the utility associated with the pre-progression health state was set to ||||||||||; reflecting the overall pre-progression utility value reported in the KarMMa trial for the treated population. Based on the clinical experts’ feedback that the post-progression utility weights were optimistic for idecabtagene vicleucel, the utility weight in the PD health state was based on the sponsor’s identified literature value (0.676).
Different patient populations informing model parameters: Three different populations were defined within the KarMMa trial: the target population, which reflected patients who specifically received the target dose of 450 × 106 CAR T cells (n = 54); the treated population, which reflected those who received idecabtagene vicleucel infusion across the varying doses (n = 128); and the enrolled population, which reflected all patients who underwent leukapheresis (n = 140).4 The sponsor’s base case included clinical parameters derived from different patient populations of the KarMMa trial. Data for PFS, OS, and AE were derived from the target dose population, while comparative efficacy and quality of life were derived from the treated population.2 This approach is inappropriate due to inconsistency within the model in terms of which population is being modelled.
As CADTH clinical experts suggested that not all patients would receive the target dose, exploratory reanalyses were performed in the treated population, as this population was considered to have better internal and external validity. Exploratory reanalyses on the target population were also provided, although cautious interpretation is required given concerns regarding inconsistencies in the patient population remain unaddressed in those reanalyses.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (See Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
The height and weight distribution of the KarMMa trial population were generalizable to Canadian patients with RRMM. | Uncertain but appears to be reasonable. Some costs were derived based on the patients’ weights, although these were not a main driver in the model. |
Idecabtagene vicleucel was assumed to not be a curative therapy. | Appropriate according to the clinical experts consulted by CADTH on this review. |
AE outcomes were based on the published literature and were assumed to represent AEs for the pooled regimens. Duration of AEs were assumed to be the same across idecabtagene vicleucel and conventional care. | Uncertain, although not a main driver in the model. |
AEs were costed separately and assumed to be independent events. | The inpatient monitoring costs for AEs were likely overestimated as they were costed separately, whereas it is possible that patients are treated for more than a single AE within a single hospitalization. However, this is not of concern given the model is not driven by AEs. |
Assumptions around subsequent treatment (i.e., the proportion of patients requiring subsequent treatment upon disease progression and the composition of subsequent treatment) were assumed to be the same for idecabtagene vicleucel and comparators. | Appropriate. According to the CADTH’s clinical experts, the subsequent treatment available to patients following progression is mostly palliative. |
The cost of in-hospital monitoring for idecabtagene vicleucel included post-infusion AE monitoring that was 14 days for grade 3 to grade 4 CRS/NT (9%) and 7 days for grade 1 to grade 2 CRS/NT (91%).2 | Uncertain. The KarMMa trial required 14 days of hospitalization post-infusion.4 CADTH clinical experts indicated that initial administration of CAR T-cell therapies may require 14 days of hospitalization. However, with experience, the duration of hospitalization may be reduced, according to the clinical experts consulted by CADTH, who noted that the duration of hospitalization has been reduced to an average of 7 days for other CAR T-cell therapies in Ontario. The duration of hospitalization was not a main driver in the model. |
All patients entering the model were assumed to receive treatment. | In the KarMMa trial, a proportion of patients who were enrolled (approximately 8.5%) did not receive an initial idecabtagene vicleucel infusion.4 The clinical experts noted that, with the initial roll-out, the proportion of patients not receiving CAR T-cell therapies will likely align with trial experience, although this proportion is expected to decrease over time, as experience would lead to better patient selection with respect to who is most suitable for treatment. CADTH conducted exploratory scenario reanalyses based on the enrolled population. |
AE = adverse event; CAR = chimeric antigen receptor; CRS = cytokine release syndrome; NT = neurotoxicity.
CADTH Reanalyses of the Economic Evaluation
Due to limitations with the submitted data and model, CADTH was unable to determine a base-case estimate for the cost-effectiveness of idecabtagene vicleucel compared to conventional care in Canada.
Corrections to Sponsor’s Base Case
CADTH identified the following issues with the submitted model, which was considered more appropriate as a corrected sponsor’s base case as opposed to CADTH reanalyses.
Incorrect administration costs: The administration costs for IV treatments were overestimated as the sponsor assumed that a physician visit for special single-drug or multi-drug therapy ($108.69) would be incurred for each administration.2 However, based on the Ontario Physician Schedule of Benefits, a physician visit for complex single-drug or multi-drug therapy ($75.00) would be more appropriate.24
This limitation had a minimal impact on the cost-effectiveness results and was corrected as part of the sponsor’s base case in Table 5.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. Incorrect administration cost | $108.69 | $75.00 |
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or SEs in probabilistic analyses, etc.) that are not identified as limitations.
CADTH-Corrected Sponsor’s Results
The results of the corrected sponsor’s model are presented in Table 6. The expected costs were lowered, although to a larger magnitude for the idecabtagene vicleucel arm. Nonetheless, CADTH’s corrections to the sponsor’s base case had minimal impact on the sponsor’s base case, resulting in a corrected ICER of $218,228 per QALY in the target population. In the corrected sponsor’s base case, 95.2% of incremental QALYs accrued beyond the trial observation period of 1 year.
Table 6: Corrected Sponsor’s Base Case — Target Population
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Conventional care | 122,604 | 1.13 | Reference |
Idecabtagene vicleucel | 704,093 | 3.81 | 216,606 | |
Sponsor’s corrected base case | Conventional care | 122,870 | 1.12 | Reference |
Idecabtagene vicleucel | 705,554 | 3.79 | 218,228 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CADTH’s Exploratory Analysis
CADTH could not address several limitations with the sponsor’s submission (i.e., lack of direct comparative evidence, uncertainty of the efficacy of idecabtagene vicleucel, and insufficient adjustment for known confounders). Due to the limitations with the available comparative clinical data and treatments available in the Canadian clinical setting, all CADTH reanalyses are considered exploratory.
CADTH conducted several exploratory reanalyses on the sponsor’s corrected base case, reflecting the treated population, as it was considered the most generalizable. These exploratory analyses evaluated the impact of the following model parameters and assumptions: varying the relative efficacy according to the 95% CI of the ITC estimates; providing an alternative parametric assumption for OS; revising the distribution of comparators that informed the costs of conventional care; and removing treatment-specific utility weights. The CADTH exploratory reanalyses were derived by making changes in model parameter values and assumptions in consultation with clinical experts. In addition, the following exploratory scenarios were considered: revisions to the clinical population modelled (i.e., target, enrolled), adoption of a societal perspective, and implementation of pay-for-performance reimbursement schemes.
CADTH’s Exploratory Reanalysis Results
The cost-effectiveness findings were most sensitive to different assumptions on relative efficacy. When changing the parametric assumption to the gamma distribution for both the PFS and OS curves, the ICER rose to $411,231 per QALY. In testing the upper and lower bounds of the 95% CI of the ITC estimates for PFS and OS, the deterministic ICER ranged from $225,885 to $483,904 per QALY. When combining the 2 scenarios, the deterministic ICER ranged from $240,526 to $1,000,835 per QALY. Other changes had less of an impact on the model.
One set of CADTH exploratory reanalyses attempted to address some of the identified limitations by adjusting the distribution of regimens informing the cost of conventional care and removing treatment-specific utilities alongside different combinations of plausible efficacy scenarios. In these reanalyses, the deterministic ICER ranged from $286,142 to $1,276,217 per QALY. Between 97.6% and 85.7% of the incremental QALYs were accrued beyond the 1-year trial observation period. The details of the cost-effectiveness of the various scenarios tested are listed in Table 15. Given the identified limitations, these results should be viewed as an exploration of inherent uncertainty.
In addition, exploratory analyses incorporating these changes were conducted in the enrolled population and target dose population. The enrolled population reflected a scenario in which plans only pay for treatment in those who receive infusion (91% in the KarMMa trial). However, cautious interpretation is required given the inconsistencies between model parameters in terms of the population informing these analyses.
CADTH also conducted scenarios on pay-for-performance schemes (i.e., pay for treatment in those who achieve PFS at 6 months or OS at 1 year) (Table 15) and price reduction analyses on 2 of the exploratory analyses (Table 16).
Issues for Consideration
Both the Provincial Advisory Group and the clinical expert panel noted a potential for idecabtagene vicleucel to be used in earlier lines of therapy if triple-class exposure occurs in the first 2 lines of therapy. The CADTH clinical experts also indicated that there may be a possibility of using idecabtagene vicleucel as early as the second line if patients are exposed to all 3 drug classes as part of their first-line treatment regimen for MM. This would increase the expected population size eligible for idecabtagene vicleucel and would be expected to increase the budget impact associated with idecabtagene vicleucel.
Capacity was not considered within the sponsor’s submitted economic evaluation (i.e., those eligible for treatment would not be delayed from receiving treatment and there would be no adverse clinical outcomes or additional costs arising from treatment delays due to capacity issues). Although it could be considered in the sponsor’s submitted budget impact analysis (BIA), the capacity was not reached in the sponsor’s or CADTH’s base case. Given the onboarding activities required before a site being eligible to treat patients with idecabtagene vicleucel and the number of planned sites,35 the availability of CAR T-cell therapy may be constrained by site capacity.
Idecabtagene vicleucel was issued a Notice of Compliance with Conditions at a recommended dose range of 275 × 106 to 520 × 106 CAR T cells, whereas the KarMMa trial provided patients with doses of idecabtagene vicleucel ranging from 150 × 106 to 540 × 106 CAR T cells. As the economic evaluation is based on the KarMMa trial, the treated and enrolled population in the economic analysis includes patients who received doses outside the Health Canada–approved dose range. CADTH was unable to evaluate the cost-effectiveness of idecabtagene vicleucel within the Health Canada–approved dose range given the lack of clinical information on the patients who received the Health Canada–approved dose range.
With respect to manufacturing failure, the KarMMa trial protocol stated that, in patients who had a manufacturing failure or a product with fewer than 150 × 106 CAR T cells, another attempt to manufacture the cells would be made. Within the trial, only 1 patient did not receive idecabtagene vicleucel due to manufacturing failure while another patient experienced manufacturing failure after leukapheresis, although the product was remanufactured and provided to this patient. It is unclear if manufacturing failure in the Canadian setting would differ from the rates observed in the trial and the implications on cost-effectiveness of idecabtagene vicleucel are uncertain.
Given the sponsor’s submitted implementation plan, not all provinces will have a site to provide idecabtagene vicleucel.35 For these jurisdictions, there will be a need to send patients out of province or out of country for treatment. Additional costs related to out-of-province or out-of-country treatment were not considered within the submitted model. Patients receiving treatment are required to be monitored for 7 days following infusion and need to be near the treatment centre in the first 4 weeks post-infusion.35 The sponsor’s patient support program is investigating whether to provide support to patients and caregivers with travel and lodging coordination.35 However, if travel expenses are instead funded by the public payer, this would increase the expected costs of idecabtagene vicleucel and result in a higher ICER estimate.
For a treatment site to be qualified to administer idecabtagene vicleucel, onboarding is required. This will include assessment and verification of apheresis facilities and procedures, assessment of information technology capabilities, training in CAR T-cell infusion and patient management, assessment of standard operating procedures in place, and training in patient enrolment, scheduling, and reimbursement. Each centre will also undergo product-specific training and preparation leading to risk-management-plan certification. The sponsor’s CAR T-cell service model includes the onboarding and post-onboarding phases.35
Re-treatment took place in 21% of the treated population in the KarMMa clinical trial.4 Re-treatment used previously cryopreserved idecabtagene vicleucel from the first treatment with a second course of LDC with or without bridging therapy. In addition to the costs associated with LDC and bridging therapy, re-treatment would require additional hospitalization and cryopreserving capacity if re-treatment is permitted. Although the additional health costs associated with re-treatment were not considered in the sponsor’s submitted economic analysis,2 such practice would be expected to increase the expected costs of idecabtagene vicleucel and result in an even higher ICER estimate.
Twelve patients (9%) in the trial discontinued the study after undergoing leukapheresis due to an AE, physician decision, PD, or death.4 According to the clinical experts consulted by CADTH, the proportion of patients who did not proceed to infusion following leukapheresis was generalizable to the Canadian setting in the initial roll-out, although this proportion is expected to lower as clinicians gain greater experience. When modelling the enrolled population, the sponsor’s submitted model incorporates both the cost of leukapheresis and further adjusts the drug acquisition to reflect only those who receive infusion of idecabtagene vicleucel.2 CADTH conducted a scenario analysis on the enrolled population with the same assumptions as the sponsors (Table 15).
Although the BIA assumes public drug programs will be paying for CAR T-cell therapies,36 it remains unclear who would be paying for this therapy. This may vary by jurisdiction.
Belantamab mafodotin is only available through compassionate access programs and the extent to which it is available to patients is uncertain. Regimens based on belantamab mafodotin were not included in the definition of conventional care, nor was idecabtagene vicleucel compared with belantamab mafodotin in the sponsor’s submitted economic model.
According to the clinical experts consulted by CADTH, several emerging CAR T-cell therapies for patients with MM are under development.37
Overall Conclusions
Results from the KarMMa study suggest that idecabtagene vicleucel between doses of 150 × 106 and 540 × 106 CAR T cells is associated with an induction of response among heavily pre-treated adult patients with MM who have received at least 3 prior therapies, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody, and who are refractory to their last treatment. However, interpretation of the results is challenging due to the lack of a comparison to a concurrent control arm and the open-label design. Although the sponsor submitted an ITC, inherent design differences could not be adjusted for statistically, the potential impact of unmeasured and unaccounted-for prognostic factors and effect modifiers in the models, and the small number of patients in the final set of eligible patients with RRMM used for a comparison with the idecabtagene vicleucel cohort resulted in imprecise effect estimates. Also, generalizability of this and the matched final cohort, as well as the comparisons, is not reflective of the Canadian clinical practice due to the different and varied therapies included in the regimens provided.
CADTH found that the sponsor’s base case included several major limitations that introduced significant uncertainties in the cost-effectiveness of idecabtagene vicleucel. First, KarMMa was a phase II trial, and uncertainty remains on the efficacy of idecabtagene vicleucel given the lack of a comparator arm and the amount of missing data. The efficacy of idecabtagene vicleucel is dependent on several implementation factors and it remains unclear if the implementation observed in the trial would reflect the Canadian setting. As KarMMa was not a comparative study, relative effectiveness to conventional care was obtained from an analysis comparing the treated population in the KarMMa study to a patient cohort identified from several sites and database registries. Despite adjustment approaches (i.e., propensity scores) to ensure comparability between the study populations, there is significant uncertainty about the relative efficacy of idecabtagene vicleucel with comparator treatments due to inherent design differences in the bodies of evidence that cannot be adjusted for statistically, the potential impact of unmeasured and unaccounted-for prognostic factors and effect modifiers in the models, and undermined generalizability due to the inclusion of irrelevant comparators. Furthermore, OS was immature in the KarMMa trial, introducing uncertainty in the extrapolation of efficacy; even though most of the incremental benefits in the model accrued in the extrapolation period.
The issues with the clinical data prohibit a reasonable assessment of cost-effectiveness as there is no clear resolution to the identified uncertainties. As such, a CADTH base case could not be derived. CADTH undertook a series of exploratory reanalyses focused on the treated population that indicated the ICER of idecabtagene vicleucel was likely to be higher than that estimated by the sponsor. The ICERs were sensitive to different assumptions regarding relative efficacy. One set of CADTH exploratory reanalyses attempted to address some of the identified limitations by adjusting the distribution of regimens, informing the cost of conventional care, and removing treatment-specific utilities. When different combinations of possible efficacy scenarios were tested on top of these changes, the deterministic ICER for idecabtagene vicleucel was found to range from $286,142 to $1,276,217 per QALY compared with conventional care. However, majority (97.6% to 85.7%) of the incremental clinical benefits predicted by these scenarios were accrued beyond the trial observation period, in which there is limited long-term evidence. Given the lack of robust information on the comparative clinical effects of idecabtagene vicleucel compared with conventional care, the cost-effectiveness is unknown. A key cost driver is the acquisition cost of idecabtagene vicleucel.
References
1.Abecma (idecabtagene vicleucel): cell suspension in one or more patient specific infusion bag(s), target dose of 450 x 106 CAR-positive T cells within a range of 275 to 520 x 106 CAR-positive T cells, for intravenous infusion [DRAFT product monograph]. St-Laurent (QC): Celgene Inc; 2021.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration. St-Laurent (QC): Celgene Inc., a Bristol Myers Squibb company; 2020 Dec 17.
3.Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration [internal sponsor's package]. St-Laurent (QC): Celgene Inc., a Bristol Myers Squibb company; 2020 Dec 16.
4.Munshi NC, Anderson LD, Jr., Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705-716. PubMed
5.NDS-MM-003: A global, non-interventional, retrospective, multi-center study to generate real-world evidence of subjects with relapsed and refractory multiple myeloma with prior exposure to an anti-cd38 antibody [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration. Summit (NJ): Celgene Corporation; 2020 Mar 16.
6.Baz RC, Martin TG, 3rd, Lin HY, et al. Randomized multicenter phase 2 study of pomalidomide, cyclophosphamide, and dexamethasone in relapsed refractory myeloma. Blood. 2016;127(21):2561-2568. PubMed
7.Miguel JS, Weisel K, Moreau P, et al. Pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone alone for patients with relapsed and refractory multiple myeloma (MM-003): a randomised, open-label, phase 3 trial. Lancet Oncol. 2013;14(11):1055-1066. PubMed
8.Reece DE, Trieu Y, Masih-Khan E, et al. Cyclophosphamide and bortezomib with prednisone or dexamethasone for the treatment of relapsed and refractory multiple myeloma. Clin Lymphoma Myeloma Leuk. 2016;16(7):387-394. PubMed
9.Trieu Y, Trudel S, Pond GR, et al. Weekly cyclophosphamide and alternate-day prednisone: an effective, convenient, and well-tolerated oral treatment for relapsed multiple myeloma after autologous stem cell transplantation. Mayo Clin Proc. 2005;80(12):1578-1582. PubMed
10.Dimopoulos MA, Goldschmidt H, Niesvizky R, et al. Carfilzomib or bortezomib in relapsed or refractory multiple myeloma (ENDEAVOR): an interim overall survival analysis of an open-label, randomised, phase 3 trial. Lancet Oncol. 2017;18(10):1327-1337. PubMed
11.Delforge M SN, Rodriguez-Otero P, Hari P, Braverman J, Trigg A, et al. Health state utility valuation in patients with triple-class-exposed relapsed and refractory multiple myeloma treated with the BCMA-directed CAR T cell therapy, idecabtagene vicleucel (ide-cel, bb2121): results from the karmma trial. Blood. 2020;136(Supplement 1):14-15.
12.Weisel K, Paner A, Engelhardt M, et al. Quality-of-life outcomes in patients with relapsed/refractory multiple myeloma treated with elotuzumab plus pomalidomide and dexamethasone: results from the phase 2 randomized eloquent-3 study. Blood. 2018;132(Supplement 1):2288-2288.
13.Health Quality Ontario. Continuous monitoring of glucose for type 1 diabetes: a health technology assessment. Ont Health Technol Assess Ser. 2018;18(2):1-160. PubMed
14.Lloyd A, Nafees B, Narewska J, Dewilde S, Watkins J. Health state utilities for metastatic breast cancer. Br J Cancer. 2006;95(6):683-690. PubMed
15.Matza LS, Cong Z, Chung K, et al. Utilities associated with subcutaneous injections and intravenous infusions for treatment of patients with bone metastases. Patient Prefer Adherence. 2013;7:855-865. PubMed
16.National Institute for Health and Care Excellence. Daratumumab monotherapy for treating relapsed and refractory multiple myeloma. (Technology appraisal guidance TA510) 2018; https://www.nice.org.uk/guidance/ta510. Accessed 2021 Apr 26.
17.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2020; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 March 01.
18.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2020: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 March 01.
19.CADTH pan-Canadian oncology drug review final economic guidance report: pomalidomide (Pomalyst) for multiple myeloma. Ottawa (ON): CADTH; 2014: https://cadth.ca/sites/default/files/pcodr/pcodr-pomalyst-mm-fn-egr.pdf. Accessed 2021 Apr 26.
20.CADTH pan-Canadian oncology drug review final economic guidance report: carfilzomib (Kyprolis) for multiple myeloma. Ottawa (ON): CADTH; 2017: https://cadth.ca/sites/default/files/pcodr/pcodr_carfilzomib_kyprolis_mm_rel_fn_egr.pdf.
21.CADTH pan-Canadian oncology drug review final economic guidance report: daratumumab (Darzalex) + Rd for newly diagnosed multiple myeloma. Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/pcodr/Reviews2020/10189DaratumumabNDMM_fnEGR_NOREDACTABBREV_Post05Mar2020_final.pdf. Accessed 2021 Apr 26.
22.Ellis K. Cost-effectiveness of chimeric antigen receptor T-cell therapy for treating large B-cell lymphoma patients in Canada. UWSpace 2019; https://uwspace.uwaterloo.ca/handle/10012/15515?show=full. Accessed 2021 Apr 26.
23.Oncology Continuous Audit of Patients and Prescriptions Syndicated (ONCO-CAPPS). Canadian multiple myeloma database. 2020.
24.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2021 March 01.
25.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2021 March 01.
26.DAD/HMDB inpatient hospitalizations: volumes, length of stay, and standardized rates (2018/2019). Ottawa (ON): Canadian Institute for Health Information; 2019.
27.Your health system: cost of a standard hospital stay. Ottawa (ON): Canadian Institute for Health Information; 2019: https://yourhealthsystem.cihi.ca/hsp/inbrief?lang=en#!/indicators/015/cost-of-a-standardhospital-stay/;mapC1;mapLevel2;/. Accessed 2021 Apr 26.
28.Hari P, Nguyen A, Pelletier C, McGarvey N, Gitlin M, Parikh K. Healthcare resource utilization and economic burden of cytokine release syndrome (CRS) and neurologic events (NE) in patients (pts) with relapsed/refractory multiple myeloma (RRMM) receiving idecabtagene vicleucel (ide-cel, bb2121) in KarMMa. J Clin Oncol. 2020;38(29 suppl):61.
29.Zheng B, Reardon PM, Fernando SM, et al. Costs and outcomes of patients admitted to the intensive care unit with cancer. J Intensive Care Med. 2021;36(2):203-210. PubMed
30.LeBlanc R, Hollmann S, Tay J. Canadian cost analysis comparing maintenance therapy with bortezomib versus lenalidomide for patients with multiple myeloma post autologous stem cell transplant. J Popul Ther Clin Pharmacol. 2016;23(1):e103-113. PubMed
31.Wehler E, Zhao Z, Pinar Bilir S, Munakata J, Barber B. Economic burden of toxicities associated with treating metastatic melanoma in eight countries. Eur J Health Econ. 2017;18(1):49-58. PubMed
32.Gaultney JG, Franken MG, Tan SS, et al. Real-world health care costs of relapsed/refractory multiple myeloma during the era of novel cancer agents. J Clin Pharm Ther. 2013;38(1):41-47. PubMed
33.A matching-adjusted indirect treatment comparison of efficacy outcomes based on BB2121-MM-001 (15+1) and MAMMOTH pivotal studies [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration. Saint Laurent (QC): Celgene Inc; 2020.
34.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/dv/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2021 March 15.
35.Implementation plan [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration. St-Laurent (QC): Celgene Inc., a Bristol Myers Squibb company; 2020 Dec 15.
36.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Abecma (idecabtagene vicleucel), single dose cell suspension for intravenous administration. St-Laurent (QC): Celgene Inc., a Bristol Myers Squibb company; 2020 Dec 15.
37.Wudhikarn K, Mailankody S, Smith EL. Future of CAR T cells in multiple myeloma. Hematology. 2020;2020(1):272-279. PubMed
38.Cancer Care Ontario Formulary. Pomalidomide, dexamethasone regimen. 2020.
39.Saskatchewan Drug Plan: search formulary. 2021; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2021 Feb 22, 1800.
40.Cancer Care Ontario Formulary. Cyclophosphamide, dexamethasone, pomalidomide. 2019.
41.Cancer Care Ontario Formulary. Lenalidomide, dexamethasone regimen. 2017.
42.Cancer Care Ontario Formulary. Carfilzomib, dexamethasone, lenalidomide regimen. 2019.
43.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/. Accessed 2021 Feb 22.
44.Cancer Care Ontario Formulary. Carfilzomib, dexamethasone regimen. 2019.
45.BC Cancer protocol summary for therapy of multiple myeloma using carfilzomib and dexamethasone with or without cyclophosphamide. Vancouver (BC): BC Cancer; 2018: http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Lymphoma-Myeloma/UMYCARDEX_Protocol.pdf. Accessed 2021 Apr 26.
46.Cancer Care Ontario Formulary. Bortezomib (with or without dexamethasone). 2019.
47.Cancer Care Ontario Formulary. Cyclophosphamide, bortezomib, dexamethasone. 2019.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and PAG. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CADTH Cost Comparison Table for Patients With Relapsed or Refractory Multiple Myeloma Who Have Received at Least 3 Prior Therapies
Treatment | Strength | Form | Price ($) | Recommended dosage | Cost per treatment course ($) | Course or annual cost ($) |
|---|---|---|---|---|---|---|
Idecabtagene vicleucel | Suspension of chimeric antigen reception (CAR) positive T cells in patient-specific infusion bag (volume = 10 mL to 100 mL) | Suspension for IV infusion | 545,000.0000a | 450 × 106 CAR-positive T cells (range: 275 to 520 × 106 CAR-positive T cells)b | 545,000 | 545,000 |
Regimens | ||||||
Pomalidomide + dexamethasone (Pd)c,d | ||||||
Pomalidomide | 1 mg 2 mg 3 mg 4 mg | Capsule | 500.0000e | 4 mg Days 1 to 21 | 10,500 | 136,875 |
Dexamethasone | 0.5 mg 0.75 mg 2 mg 4 mg | Tablet | 0.1564f 0.6763f 0.5530g 0.3046f | 20 to 40 mg, Days 1, 8, 15, 22 | 6 to 12 | 79 to 159 |
Pomalidomide + dexamethasone (Pd) | 10,506 to 10,512 | 136,954 to 137,034 | ||||
Cyclophosphamide + pomalidomide + dexamethasone (CycloPd)d,h | ||||||
Cyclophosphamide | 25 mg 50 mg | Tablet | 0.3520f 0.4740f | 400 mg: Days 1, 8, 15 | 11 | 148 |
Pomalidomide | 1 mg 2 mg 3 mg 4 mg | Capsule | 500.0000e | 4 mg Days 1 to 21 | 10,500 | 136,875 |
Dexamethasone | 0.5 mg 0.75 mg 2 mg 4 mg | Tablet | 0.1564f 0.6763f 0.5530g 0.3046f | 20 to 40 mg, Days 1, 8, 15, 22 | 6 to 12 | 79 to 159 |
Cyclophosphamide + pomalidomide + dexamethasone (CycloPd) | 10,506 to 10,521 | 137,103 to 137,182 | ||||
Lenalidomide + dexamethasone (Rd)d,i | ||||||
Lenalidomide | 2.5 mg 5 mg 10 mg 15 mg 20 mg 25 mg | Capsule | 329.5000e 340.0000e 361.0000e 382.0000e 403.0000e 424.0000e | 25 mg on Days 1 to 21 | 8,904 | 116,070 |
Dexamethasone | 0.5 mg 0.75 mg 2 mg 4 mg | Tablet | 0.1564f 0.6763f 0.5530g 0.3046f | 40 mg once on Days 1, 8, 15, 22 | 12 | 159 |
Lenalidomide + dexamethasone (Rd) | 8,916 | 116,229 | ||||
Carfilzomib + lenalidomide + dexamethasone (KRd)d,j,k | ||||||
Carfilzomib | 10 mg 30 mg 60 mg | Powder in vial | 255.5500l 766.6590l 1,533.330l | Cycle 1: 20 mg/m2 Days 1 and 2; 27 mg/m2 Days 8, 9, 15, 16 Cycles 2 to 12: 27 mg /m2 Days 1, 2, 8, 9, 15, 16 Cycles 13 to 18: 27 mg /m2 Days 1, 2, 15, 16 | Cycle 1: 8,178 Cycles 2 to 12: 9,200 Cycles 13 to 18: 6,133 | Year 1: 118,899 Year 2: 30,665 |
Lenalidomide | 2.5 mg 5 mg 10 mg 15 mg 20 mg 25 mg | Capsule | 329.5000e 340.0000e 361.0000e 382.0000e 403.0000e 424.0000e | 25 mg/day on Days 1 to 21 | 8,904 | 116,070 |
Dexamethasone | 0.5 mg 0.75 mg 2 mg 4 mg | Tablet | 0.1564f 0.6763f 0.5530g 0.3046f | 40 mg/day on Days 1, 8, 15, 22 | 12 | 159 |
Carfilzomib + lenalidomide + dexamethasone (KRd) | Cycle 1: 17,094 Cycles 2 to 12: 18,116 Cycles 13 to 18: 15,050 Cycles 19+: 8,916 | Year 1: 235,127 Year 2: 146,894 Year 3+: 116,229 | ||||
Carfilzomib + dexamethasone (Kd)d,k,m | ||||||
Carfilzomib | 10 mg 30 mg 60 mg | Powder in vial | 255.5500l 766.6590l 1,533.3300l | Cycle 1: 20 mg/m2 on Days 1, 2; 56 mg /m2 on Days 8, 9, 15, 16 Cycles 2+ 56 mg /m2 on Days 1, 2, 8, 9, 15, 16 | Cycle 1: 13,289 Cycle 2+: 16,866 | Year 1: 216,287 Year 2+: 219,864 |
Dexamethasone | 0.5 mg 0.75 mg 2 mg 4 mg | Tablet | 0.1564f 0.6763f 0.5530g 0.3046f | 20 mg /day, Days 1, 2, 8, 9, 15, 16, 22, 23 | 12 | 159 |
Carfilzomib + dexamethasone (Kd) | Cycle 1: 13,301 Cycle 2+: 16,879 | Year 1: 216,445 Year 2: 220,023 | ||||
Carfilzomib + cyclophosphamide + dexamethasone (KCyd)d,k,n | ||||||
Carfilzomib | 10 mg 30 mg 60 mg | Powder in vial | 255.5500l 766.6590l 1,533.330l | Cycle 1: 20 mg/m2 on Day 1; 70 mg/m2 on Days 8 and 15 Cycle 2+: 70 mg/m2 on Days 1, 8, 15 | Cycle 1: 7,667 Cycle 2+: 9,966 | Year 1: 127,620 Year 2+: 129,920 |
Cyclophosphamide | 25 mg 50 mg | Tablet | 0.3520f 0.4740f | 300 mg/m2 on Days 1, 8, 15 | 17 | 222 |
Dexamethasone | 0.5 mg 0.75 mg 2mg 4 mg | Tablet | 0.1564f 0.6763f 0.5530g 0.3046f | 40 mg on Days 1, 8,15 and 22 | 12 | 159 |
Carfilzomib + cyclophosphamide + dexamethasone (KCyd) | Cycle 1: 7,696 Cycle 2+: 9,996 | Year 1: 128,001 Year 2+: 130,301 | ||||
Bortezomib + dexamethasone (Vd)k,o | ||||||
Bortezomib | 2.5 mg (1 mg in 2.5 mg vial) | Vial for infusion | 1,001.73g | 1.3 mg /m2 on Days 1, 8, 15, 22 | 4,007 | 41,786 |
3.5 mg (1 mg in 10 mL vial) | 1,402.4199g | |||||
Dexamethasone | 0.5 mg 0.75 mg 2 mg 4 mg | Tablet | 0.1564f 0.6763f 0.5530g 0.3046f | 40 mg once weekly | 15 | 159 |
Bortezomib + dexamethasone (Vd) | 4,022 | 41,945 | ||||
Cyclophosphamide + bortezomib + dexamethasone (CyBord)d,p | ||||||
Cyclophosphamide | 25 mg 50 mg | Tab | 0.3520f 0.4740f | 300 mg /m2 on Days 1, 8, 15, 22 | 23 | 297 |
Bortezomib | 2.5 mg (1 mg in 2.5 mg vial) | Vial for infusion | 1,001.73g | 1.5 mg /m2 on Days 1, 8, 15, 22 | 5,610 | 73,126 |
3.5 mg (1 mg in 10 mL vial) | 1,402.4199g | |||||
Dexamethasone | 0.5 mg 0.75 mg 2 mg 4 mg | Tab | 0.1564f 0.6763f 0.5530g 0.3046f | Cycles 1 and 2: 40 mg on Days 1 to 4, 9 to 12, 17 to 20 Cycle 3+: 40 mg on Days 1, 8, 15, 22 | Cycles 1 and 2: 37 Cycle 3+: 12 | Year 1: 208 Year 2+: 159 |
Cyclophosphamide + bortezomib + dexamethasone (CyBord) | Cycle 1 and 2: 5,670 Cycles 3+: 5,645 | Year 1: 73,630 Year 2+: 73,582 | ||||
Cyclophosphamide + dexamethasone (Cydex)q | ||||||
Cyclophosphamide | 25 mg 50 mg | Tab | 0.3520f 0.4740f | 400 mg: Days 1, 8, 15 | 11 | 148 |
Dexamethasone | 0.5 mg 0.75 mg 2 mg 4 mg | Tab | 0.1564f 0.6763f 0.5530g 0.3046f | 20 to 40 mg, Days 1, 8, 15, 22 | 6 to 12 | 79 to 159 |
Cyclophosphamide + dexamethasone (Cydex) | 17 to 23 | 227 to 307 | ||||
Note: All prices are from the Ontario Drug Benefit Formulary (accessed September 21, 2020), unless otherwise indicated, and do not include dispensing fees.
aAs per the sponsor’s economic submission
bOne-time treatment cost
cPd CCO Regimen Monograph38
dPer 28-day treatment cycle
eObtained from the Ontario Exceptional Access Program18
fPrices are from the Ontario Drug Benefit Formulary (accessed February 22, 2020)17
gPrice obtained from the Saskatchewan Formulary39
hCycloPd regimen monograph40
iRd CCO Regimen Monograph41
jKRd CCO Regimen Monograph42
kAssumes body surface area = 1.85 m2
lObtained from IQVIA database43
mKd CCO Regimen Monograph44
nKCyd Regimen Monograph45
oVd CCO Regimen Monograph (Per 35-day treatment cycle: bortezomib twice weekly schedule, with dexamethasone once weekly)46
pCyBorD CCO Regimen Monograph47
qDue to several combinations, CyD is based on the CycloPd regimen monograph40
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing. | No | The comparator was a pooled strategy of regimens. Comparison with a specific regimen was therefore not possible. |
Model has been adequately programmed and has sufficient face validity. | No | The CADTH clinical experts indicated that the PFS and OS for both arms were overly optimistic. |
Model structure is adequate for decision problem. | Yes | No further comments. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis). | Yes | No further comments. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem. | Yes | No further comments. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details). | Yes | No further comments. |
OS = overall survival; PFS = progression-free survival.
Appendix 3: Additional Information on the Submitted Economic Evaluation
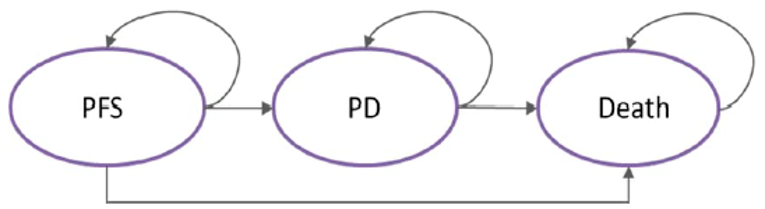
PD = progressed disease; PFD = progression free survival
Source: Sponsor’s pharmacoeconomic submission.2
Table 9: Utility and Disutility Values Used in the Sponsor’s Reference Case
Event | Utility value/decrement |
|---|---|
Health state | |
Idecabtagene vicleucel Pre-progression | ||||||||| (first month), ||||||||| |
Idecabtagene vicleucel Post-progression | ||||||||| |
Conventional Care Pre-progression | ||||||||| |
Conventional Care Post-progression | 0.676 |
Treatment administration disutility | |
Standard chemotherapy - agents with minor toxicity that require physician monitoring | −0.02 |
Each additional standard chemotherapy agent, other than initial agent | −0.02 |
Side effects disutility | |
Thrombocytopenia | −0.02 |
Anemia | −0.15 |
Neutropenia | −0.01 |
Fatigue | −0.01 |
Leukopenia | −0.01 |
Febrile neutropenia | −0.03 |
Diarrhea | −0.01 |
Lymphopenia | −0.01 |
CRS/NT | −0.23 |
CRS = cytokine release syndrome; NT = neurotoxicity
Source: Sponsor’s pharmacoeconomic submission2
Table 10: Monitoring Costs Associated With Each Treatment
Monitoring service | Unit cost | Monitoring Frequency (per cycle) | Source (cost; frequency) | |
|---|---|---|---|---|
Pre-progression | Post-progression | |||
Hematology panel | $7.92 | 1.00 | 1.00 | OSLS; KarMMa CSR |
Chemistry panel | $7.59 | 1.00 | 1.00 | OSLS; KarMMa CSR |
Coagulation panel | $7.98 | 0.08 | 0.08 | Harris et al. 2012, OSLS; KarMMa CSR |
Immunoglobulin (Igs) | $5.22 | 1.00 | 1.00 | OSLS; Assumption |
Electrophoresis, serum (including total protein) | $17.58 | 1.00 | 1.00 | OSLS; KarMMa CSR |
Urinalysis | $3.59 | 0.08 | 0.08 | OSLS; Assumption |
Gammopathy screen by immunoelectrophoresis or immunofixation (serum or urine) | $25.66 | 1.00 | 1.00 | OSLS; KarMMa CSR |
Computerized tomogram scan | $917.55 | 0.31 | 0.31 | OSB; KarMMa CSR |
Bone marrow biopsy and/or aspirate | $19.65 | 0.31 | 0.31 | OSLS; KarMMa CSR |
TLS/CRS panel* | $12.85 | 0.08 | 0.08 | OSLS72; KarMMa CSR |
*Only applies to patients treated with ide-cel.
Abbreviations: CRS = cytokine release syndrome; CSR = clinical study report; OSB = Ontario Schedule of Benefits; OSLS = Ontario Schedule of Benefits for Laboratory Services; TLS = tumour lysis syndrome
Source: Sponsor’s pharmacoeconomic submission.2
Detailed Results of the Sponsor’s Base Case
Table 11: Discounted Disaggregated Mean Costs for the Probabilistic Sponsor’s Reference Case Analysis — Target Population
Cost | Idecabtagene vicleucel | Conventional care | Incremental |
|---|---|---|---|
Pre-treatment costs | $13,320 | $0 | $13,320 |
Pre-progression costs | |||
Acquisition costs | $544,668 | $66,718 | $477,950 |
Administration costs | $1,214 | $1,398 | -$184 |
Monitoring costs | $4,725 | $2,350 | $2,375 |
AE costs | $30,623 | $5,986 | $24,637 |
Resource costs | $29,349 | $12,694 | $16,655 |
Post-progression costs | |||
Acquisition costs | $754 | $240 | $514 |
Administration costs | $0 | $0 | $0 |
Monitoring costs | $14,176 | $4,498 | $9,678 |
AE costs | $0 | $0 | $0 |
Resource costs | $61,357 | $24,288 | $37,069 |
Terminal care cost | $3,908 | $4,430 | -$522 |
Total costs | $704,093 | $122,604 | $581,489 |
Source: Sponsor’s pharmacoeconomic submission2
Table 12: Discounted Disaggregated Mean LYs and QALYs for the Probabilistic Sponsor’s Reference Case Analysis — Target Population
Parameter | Idecabtagene vicleucel | Conventional care | Incremental |
|---|---|---|---|
LYs | |||
Pre-progression | 1.61 | 0.55 | 1.06 |
Post-progression | 3.38 | 1.09 | 2.29 |
Total LYs | 4.99 | 1.64 | 3.35 |
QALYs | |||
Pre-progression | 1.33 | 0.44 | 0.89 |
Post-progression | 2.62 | 0.72 | 1.90 |
Adverse Event Decrements | −0.14 | −0.03 | −0.11 |
Total QALYs | 3.81 | 1.13 | 2.68 |
Source: Sponsor’s pharmacoeconomic submission2
Figure 2: Cost-Effectiveness Acceptability Curve — Target Population
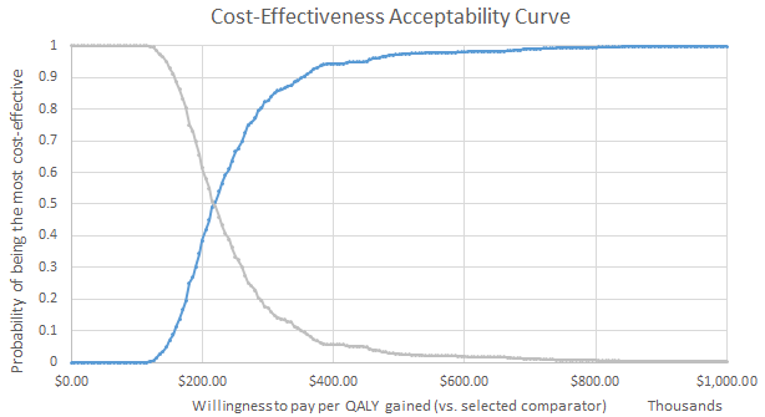
Source: Sponsor’s pharmacoeconomic submission.2
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Table 13: Chemotherapy Regimens Composing the Comparator and Associated Weighting
Regimen | Proportion used in sponsor’s model | Proportion used in CADTH base case |
|---|---|---|
Pd (Pomalidomide + Dexamethasone) | 6 | 50 |
PVd (Pomalidomide + Bortezomib + Dexamethasone) | 2 | 0 |
PCyd (Pomalidomide + Cyclophosphamide + Dexamethasone) | 25 | 25 |
KCyd (Carfilzomib + Cyclophosphamide + Dexamethasone) | 14 | 0 |
Kd (Carfilzomib + Dexamethasone) | 22 | 15 |
Vd (Bortezomib + Dexamethasone) | 2 | 3.3 |
CyBorD (Cyclophosphamide + Bortezomib + Dexamethasone) | 6 | 3.3 |
CyD (Cyclophosphamide + Dexamethasone) | 23 | 3.3 |
Results of Exploratory Analyses
Table 14: CADTH Revisions to the Sponsor’s Corrected Economic Evaluation for the Exploratory Analyses
Exploratory analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes in CADTH exploratory analyses | ||
A: Parametric assumption on PFS and OS | Idecabtagene vicleucel: Exponential for PFS and OS Conventional Care: Log-normal for PFS and Exponential for OS. | Gamma for all |
B: ITC estimates on PFS (deterministic) | ITC estimates | 95% CI on PFS |
C: ITC estimates on OS (deterministic) | ITC estimates | 95% CI on OS |
D: ITC estimates on PFS and OS (deterministic) | ITC estimates | 95% CI on PFS and OS |
E: Quality of Life | Idecabtagene vicleucel: |||||||||| (1 month) and |||||||||| pre-progression (month 2+), ||||||||| post-progression Conventional care: ||||||||| pre-progression, 0.676 post-progression | Idecabtagene vicleucel: ||||||||| (1 month) and ||||||||| pre-progression (month 2+); Conventional care: ||||||||| pre-progression Both: 0.676 post-progression |
F: conventional care cost (see Table 14) | Costs of 8 regimens from ONCO-CAPPS | Costs of 7 regimens used in Canada |
Table 15: CADTH Exploratory Analyses
Scenario | Treatment | Total costs ($)a | Total QALYsa | ICER ($ per QALY) Treated population unless specified |
|---|---|---|---|---|
Sponsor base case | Conventional care | 122,528 | 1.18 | Reference |
Idecabtagene vicleucel | 683,739 | 2.91 | 325,752 | |
Sponsor’s corrected base case | Conventional care | 121,865 | 1.18 | Reference |
Idecabtagene vicleucel | 682,830 | 2.93 | 321,358 | |
Exploratory analyses | ||||
A | Conventional care | 135,787 | 1.14 | Reference |
Idecabtagene vicleucel | 675,147 | 2.46 | 411,231 | |
B upper b | Conventional care | 168,112 | 1.23 | Reference |
Idecabtagene vicleucel | $682,036 | 2.90 | 307,213 | |
B lower b | Conventional care | 119,108 | 1.18 | Reference |
Idecabtagene vicleucel | $688,966 | 2.88 | 333,916 | |
C upper b | Conventional care | 150,571 | 1.44 | Reference |
Idecabtagene vicleucel | $712,620 | 3.80 | 238,357 | |
C lower b | Conventional care | 131,856 | 1.00 | Reference |
Idecabtagene vicleucel | $662,344 | 2.14 | 468,983 | |
D upper b | Conventional care | 180,649 | 1.47 | Reference |
Idecabtagene vicleucel | $708,524 | 3.83 | 225,885 | |
D lower b | Conventional care | 110,756 | 0.98 | Reference |
Idecabtagene vicleucel | $665,165 | 2.13 | 483,904 | |
A+D upper b | Conventional care | 150,398 | 1.45 | Reference |
Idecabtagene vicleucel | 708,237 | 3.77 | 240,526 | |
A+D lower b | Conventional care | 100,876 | 0.87 | Reference |
Idecabtagene vicleucel | 643,572 | 1.41 | 1,000,835 | |
E | Conventional care | 122,814 | 1.13 | Reference |
Idecabtagene vicleucel | 683,417 | 2.87 | 322,012 | |
F | Conventional care | 134,430 | 1.18 | Reference |
Idecabtagene vicleucel | 684,614 | 2.92 | 315,725 | |
A+E+F+D upper b | Conventional care | 164,711 | 1.44 | Reference |
Idecabtagene vicleucel | 708,237 | 3.34 | 286,142 | |
A+E+F+D lower b | Conventional care | 111,124 | 0.85 | Reference |
Idecabtagene vicleucel | 643,572 | 1.27 | 1,276,217 | |
Scenario by clinical trial populations | ||||
A+E+F+D upper b (enrolled population) | Conventional care | 164,003 | 1.43 | Reference |
Idecabtagene vicleucel | 653,428 | 3.10 | 292,899 | |
A+E+F+D lower b (enrolled population) | Conventional care | 110,761 | 0.84 | Reference |
Idecabtagene vicleucel | 596,890 | 1.28 | 1,104,828 | |
A+E+F+D upper b (target dose population) | Conventional care | 165,113 | 1.36 | Reference |
Idecabtagene vicleucel | 792,016 | 6.09 | 132,515 | |
A+E+F+D lower b (target dose population) | Conventional care | 110,271 | 0.81 | Reference |
Idecabtagene vicleucel | 629,055 | 0.89 | 6,548,874 | |
Societal perspective scenarios | ||||
A+E+F+D upper b | Conventional care | 220,492 | 1.44 | Reference |
Idecabtagene vicleucel | 798,576 | 3.34 | 304,335 | |
A+E+F+D lower b | Conventional care | 149,272 | 0.85 | Reference |
Idecabtagene vicleucel | 700,725 | 1.27 | 1,312,769 | |
Pay-for-performance scenarios | ||||
A+E+F+D upper (only in patient achieving PFS at 6 months = 63.05%) b | Conventional care | $220,492 | 1.44 | Reference |
Idecabtagene vicleucel | $624,176 | 3.34 | $212,522 | |
A+E+F+D lower (patient achieving PFS at 6 months = 63%)b | Conventional care | $111,124 | 0.85 | Reference |
Idecabtagene vicleucel | $441,922 | 1.27 | $792,885 | |
A+E+F+D upper (patients achieving OS at 1 year = 82%) b | Conventional care | $220,492 | 1.44 | Reference |
Idecabtagene vicleucel | $700,476 | 3.34 | $252,690 | |
A+E+F+D lower (patients achieving OS at 1 year = 72%) b | Conventional care | $111,124 | 0.85 | Reference |
Idecabtagene vicleucel | $490,972 | 1.27 | $910,452 | |
aResults reported for the treated population.
bCADTH exploratory analyses were conducted deterministically given that no probabilistic distributions could be defined around the upper and lower bounds of the 95% CI estimates.
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 16: CADTH Price Reduction Analyses — Treated Population
Price reduction | ICERs for idecabtagene vicleucel vs. conventional care ($ per QALY) | ||
|---|---|---|---|
Sponsor’s corrected base case ($ per QALY) | Exploratory analysis (A + E + F + D upper)a | Exploratory analysis (A + E + F + D lower)a | |
No price reduction | 321,358 | 286,142 | 1,276,217 |
20% | 266,593 | 228,758 | 1,014,956 |
40% | 202,920 | 171,375 | 753,696 |
60% | 137,819 | 113,991 | 492,435 |
80% | 73,650 | 56,608 | 231,174 |
83% | 64,529 | 48,000 | 191,985 |
90% | 42,337 | 27,916 | 100,544 |
94% | 29,421 | 16,439 | 48,292 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aThe CADTH price reduction analyses were conducted deterministically given that no probabilistic distributions could be defined around the upper and lower bounds of the 95% confidence interval estimates.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 17: Summary of Key Take-Aways
Key Take-Aways of the BIA |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
In the submitted BIA, the sponsor assessed the financial impact following the introduction of idecabtagene vicleucel for adults with MM who have received at least 3 prior therapies, including an immunomodulatory agent (IMiD), a proteasome inhibitor, and an anti-CD38 antibody. The sponsor’s base-case analysis was conducted from the perspective of the Canadian drug plans over a 3-year time horizon. In the reference scenario, the sponsor assumed that these patients would be eligible to receive Pd, PVd, PCyd, Kd, KCyd, Vd, CyBorD, CyD. In the new drug scenario, idecabtagene vicleucel was assumed to displace all treatments disproportionately.
The sponsor estimated the current population size using an epidemiological based approach, using prevalence to estimate the total number of pre-existing cases (Table 16). The sponsor estimated that approximately 30% of all prevalent cases between ages 20 and 79 were in the fourth (4L) or later lines of treatment (i.e., 10% in the 4L setting and 20% in the fifth or later line setting) and assumed that only patients with an ECOG status of 0 and 1 would be eligible for idecabtagene vicleucel. The sponsor further submitted a scenario analysis in which assumed idecabtagene vicleucel would be used as a third-line treatment.36
The sponsor’s base case was based on a drug plan perspective which only considered drug acquisition costs related to pre-treatment, treatment, subsequent treatment, and treatment for AEs. The Canadian public health care system perspective which further included treatment administration and monitoring costs, and AE costs was explored in a scenario analysis. Additionally, the sponsor assumed that none of the provincial capacity constraints for idecabtagene vicleucel were exceeded. The impact of a 20% reduction in provincial site capacity for CAR T-cell was explored in a scenario analysis.36
Key inputs to the BIA are documented in Table 18 and Table 19.
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as baseline / year 1 / year 2 / year 3 if appropriate) | |
|---|---|---|
Target population | ||
Prevalence (per 100,000) of multiple myeloma | 14.0 / 14.4 / 14.8 / 15.2 | |
Proportion of prevalent patients aged 20 to 79 years | 79% | |
Proportion of patients who are eligible to receive an active fourth-line treatment | 10 | |
Proportion of patients who are eligible to receive an active fifth-line (or later) treatment | 20% | |
Proportion receiving compassionate care/registered in clinical trial in fourth (or later) line | 18% | |
Proportion of fourth-line (or later) patients with an ECOG status (0 to 1) | 60% | |
Proportion of fourth-line patients who are triple-class exposed and eligible for idecabtagene vicleucel | ||||||||| % / ||||||||| % / ||||||||| % / ||||||||| % | |
Proportion of fifth-line (or later) patients who are triple-class exposed and eligible for idecabtagene vicleucel | ||||||||| % / ||||||||| % / ||||||||| % / ||||||||| % | |
Number of patients eligible for drug under review | 202 / 251 / 325 / 268 | |
Market uptake (3 years) | ||
Uptake (reference scenario) Pd PCyd PVd Kd KCyd Vd CyBorD CyD | ||||| %/ ||||| % / ||||| % ||||| % / |||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / |||||% ||||| % / ||||| % / ||||| % | |
Uptake (new drug scenario) Idecabtagene vicleucel Pd PCyd PVd Kd KCyd Vd CyBorD CyD | ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % ||||| % / ||||| % / ||||| % | |
Cost of treatment (per patient) | ||
Cost of drug based on median treatment duration of 3 monthsa Idecabtagene vicleucel Pd PCyd PVd Kd KCyd Vd CyBorD CyD | Pre-treatment cost $13,953.36 $0.00 $105.89 $41.75 $0.00 $141.06 $35.16 $279.57 $138.25 | Total acquisition $545,000.00 $36,392.61 $36,441.51 $53,177.03 $52,071.13 $52,144.38 $13,439.66 $16,533.83 $248.50 |
Key health care system costs CRS/NT | $16,994.04 | |
CyBorD = cyclophosphamide + bortezomib + dexamethasone; CyD = cyclophosphamide + dexamethasone; KCyd = carfilzomib + cyclophosphamide + dexamethasone; Kd = carfilzomib + dexamethasone; PCyd = pomalidomide + cyclophosphamide + dexamethasone; Pd = pomalidomide + dexamethasone; PVd = pomalidomide + bortezomib + dexamethasone; Vd = bortezomib + dexamethasone.
aIncludes wastage, mark-up, and dispensing fees.
Source: Sponsor’s submitted budget impact analysis.36
Summary of the Sponsor’s BIA Results
From the drug plan perspective, the incremental budget impact of reimbursing idecabtagene vicleucel for patients RRMM who have received at least 3 prior therapies, including an IMiD, a PI, and an anti-CD38 antibody is expected to be $10.67M in Year 1, $75.61M in Year 2, and $104.35M in Year 3 for a total 3-year budget impact of $190.63M. The sponsor additionally examined the 3-year budget impact from the Canadian publicly funded health care system perspective, which was $200.20M.36
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Use of idecabtagene vicleucel in the third-line (3L) treatment setting: As idecabtagene vicleucel would be administered to patients who had received at least 3 prior therapies, including an IMiD, a PI and an anti-CD38 antibody (i.e., triple-class exposed), the uptake of idecabtagene vicleucel was assumed in the fourth-line (4L) or later treatment settings. According to the clinical experts consulted by CADTH, idecabtagene vicleucel is most likely to be administered as early as in the 3L setting, and most patients would have been triple-class exposed by this time.
CADTH addressed this limitation by allowing patients to initiate treatment with idecabtagene vicleucel in the 3L setting rather than at the start of the 4L setting. As 1 clinical expert consulted by CADTH had a differing opinion from the others in that idecabtagene vicleucel would only be prescribed in the 4L+ setting, a scenario analysis assuming idecabtagene vicleucel would only be offered in the 4L+ setting.
Uncertainty regarding the number of patients eligible to receive idecabtagene vicleucel. The sponsor used an epidemiological approach to identify the patient population eligible to receive idecabtagene vicleucel which resulted in a total number of 251, 325, and 268 patients in Years 1, 2, and 3, respectively. The clinical experts consulted by CADTH indicated these numbers seemed lower than expected. CADTH’s clinical experts identified issues with the approach and assumptions taken to derive the size of the patient population. First, no age cut-off is likely to be applied for eligibility to CAR T-cell therapies although it would be reasonable to assume that most patients treated would be under the age of 80. Second, CADTH’s clinical experts indicated that patients with an ECOG ≥ 3 would be expected to receive compassionate care and therefore would have already been excluded when deriving the population size. By excluding patients who would receive compassionate care or who are registered in a clinical trial in the earlier step, there is no need to apply a subsequent filter to exclude patients based on ECOG status as this would introduce double-counting.
According to clinical experts’ feedback, CADTH addressed this limitation by changing the proportion of patients who would receive compassionate care or be registered in a clinical trial to 30% and removed the step for exclusion based on ECOG score. As there remains uncertainty to the population size eligible for idecabtagene vicleucel, CADTH conducted scenario analyses to explore the impact of increasing the population size by 10% and 25%, respectively.
Uncertainty in the uptake of idecabtagene vicleucel and how other regimens are displaced: The sponsor anticipated that idecabtagene vicleucel would capture ||||||||| %, ||||||||| %, and ||||||||| % of the market share distribution in Years 1, 2, and 3, displacing disproportionally the comparator regimens. However, CADTH’s clinical experts noted uncertainty in the uptake rate of idecabtagene vicleucel, especially in Year 1, and expected a higher uptake rate. Uncertainty was further raised regarding how idecabtagene vicleucel would displace existing regimens.
CADTH addressed this limitation by revising market share uptake of idecabtagene vicleucel in the new drug scenario to 15% in Year 1, 50% in Year 2, and 75% in Year 3 based on experts’ feedback and assumed equal displacement of the comparator regimens. To address the uncertainty around the uptake rate, CADTH conducted several scenario analyses varying different uptake of idecabtagene vicleucel. CADTH was unable to address the uncertainty to how idecabtagene vicleucel would displace existing regimens although this was not expected to have a large impact on the budget impact results.
Inaccurate representation of the comparator regimens and their market shares in the reference scenario. In the sponsor’s submitted BIA, regimens included in the reference case included Pd, PVd, PCyd, Kd, KCyd, Vd, CyBorD, and CyD. The sponsor assumed that, under the reference scenario, PCyd, CyD, Kd, and KCyd comprised the greatest patient share distribution (25%, 23%, 22%, and 14% respectively in the base year) while the remaining regimens captured smaller market shares over the 3-year time horizon. As noted above in the economic evaluation appraisal, the clinical experts consulted by CADTH indicated that the sponsor’s estimates do not reflect current Canadian clinical practice. Some regimens (i.e., PVd and KCyd) are not used in clinical practice.
CADTH addressed this limitation by revising the market shares of the treatments in the reference scenario to those indicated by the clinical experts (Table 13).
CADTH Reanalyses of the BIA
Changes made to the sponsor’s BIA as part of CADTH reanalysis are available in Table 19.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Calculation error in the Reference and New Therapy Scenario worksheets | Total budget impact did not sum to include the relevant costs for the selected perspective (i.e., cells Y94:Y99). e.g., Formula in cell Y94 “ = Y85” | Cells modified to include the selected costs based on analytical perspective. e.g., Formula in cell Y94 “= sum (K94:X94)” |
Changes to derive the CADTH base case | ||
1. Third-line setting | Excluded | Included |
2. Approach to derive market size | a. Proportion receiving compassionate care/registered in clinical trial in fourth-line (or later) = |||||| % b. Proportion of fourth-line (or later) patients with an ECOG status (0 to 1) = 60% | a. Proportion receiving compassionate care/registered in clinical trial in fourth-line (or later) = 30% b. Proportion of fourth-line (or later) patients with an ECOG status (0 to 2) = 100% |
3. Market share estimates in the new drug scenario (across Years 1 to 3) | Ide-cel: |||||| %/ |||||| %/ |||||| % | Ide-cel: 15% / 50% / 75% *Assumes equal displacement |
4. Market share estimates in the reference scenario (across Years 1 to 3) | See Table 13 | See Table 13 |
CADTH base case | — | Reanalyses 1 + 2 + 3 + 4 |
Abbreviations; Ide-cel = idecabtagene vicleucel; Pd = pomalidomide + dexamethasone; PVd = pomalidomide + bortezomib + dexamethasone; PCyd = pomalidomide + cyclophosphamide + dexamethasone; KCyd = carfilzomib + cyclophosphamide + dexamethasone; Kd = carfilzomib + dexamethasone; Vd = bortezomib + dexamethasone; CyBorD = cyclophosphamide + bortezomib + dexamethasone; CyD = cyclophosphamide + dexamethasone.
Applying these changes resulted in a slight increase in the budget impact under both the drug plan program and health care system perspectives. From the drug plan program perspective, 3-year total costs were estimated as $314.4M. The results of the CADTH stepwise reanalysis are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21.
Table 20: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total | |
|---|---|---|
Drug plan program perspective | Health care system perspective | |
Submitted base casea | $190,848,164 | $200,409,646 |
CADTH reanalysis 1 | $218,470,627 | $229,427,993 |
CADTH reanalysis 2 | $271,521,940 | $285,135,675 |
CADTH reanalysis 3 | $204,546,791 | $216,668,294 |
CADTH reanalysis 4 | $187,777,484 | $193,991,372 |
CADTH base case | $314,405,092 | $328,425,495 |
BIA = budget impact analysis.
aThe sponsor’s “Selected Population” is reported here as the base case, which used weighted averages for all inputs. The sponsor also conducted an “Aggregated pan-Canadian” analysis, which produced similar results but was produced by individually calculating and then summing individual jurisdictional results (with jurisdiction-specific inputs applied). The 3-year total budget impact of the “Aggregated pan-Canadian” analysis as reported by the sponsor, was $190,634,834 (drug plan perspective)
CADTH also conducted additional scenario analyses to address the remaining uncertainty regarding the potential size of the eligible population:
Applied a lower market share uptake for idecabtagene vicleucel using the |||||||||||||||||||||||||||||||| (8%, 45% and 75% in Years 1, 2, and 3 respectively).
Applied a higher market share uptake for idecabtagene vicleucel based on 1 expert feedback (20%, 50% and 75% in Years 1, 2, and 3 respectively).
Increased the number of patients eligible for idecabtagene vicleucel across Years 1 to 3 by (a) 10% and (b) 25%, respectively.
All patients (100%) receive dexamethasone as a bridging therapy.
Assumed there is a 20% capacity reduction than originally assumed by the sponsor.
Assumed that only patients in the fourth-line or later settings would be eligible to receive idecabtagene vicleucel.
Explored the impact of not paying idecabtagene vicleucel acquisition cost for patients who only undergo pre-treatment and do not receive subsequent infusion (9.1% of patients).
Assuming that 87.5% of patients received bridging therapy as per the proportion of patients in the KarMMa trial.
Applying an 83% reduction to the price of idecabtagene vicleucel (based on CADTH price reduction analysis) in which idecabtagene vicleucel would be cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained in 1 of the scenarios ($92,650).
Applying a 94% reduction to the price of idecabtagene vicleucel (based on CADTH price reduction analysis) in which idecabtagene vicleucel would be cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained in 1 of the scenarios ($32,700).
Table 21: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|
Submitted base case | Reference | $8,216,972 | $10,612,244 | $8,747,323 | $27,576,539 |
New drug | $18,895,866 | $86,324,244 | $113,204,593 | $218,424,703 | |
Budget impact | $10,678,893 | $75,712,000 | $104,457,271 | $190,848,164 | |
CADTH base case | Reference | $19,281,502 | $22,834,692 | $20,368,929 | $62,485,123 |
New drug | $47,269,806 | $148,690,976 | $180,929,432 | $376,890,214 | |
Budget impact | $27,988,304 | $125,856,284 | $160,560,504 | $314,405,092 | |
CADTH scenario analysis: Health Care Payer perspective | Reference | $24,500,931 | $29,060,597 | $25,857,020 | $79,418,549 |
New drug | $53,721,314 | $160,527,882 | $193,594,849 | $407,844,044 | |
Budget impact | $29,220,383 | $131,467,284 | $167,737,828 | $328,425,495 |
Table 22: CADTH Scenario Analyses
Scenario | Budget impact, by perspective | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|
CADTH base case | Drug plan program | $27,988,304 | $125,856,284 | $160,560,504 | $314,405,092 |
Health care system | $29,220,383 | $131,467,284 | $167,737,828 | $328,425,495 | |
CADTH scenario analysis: Low market share uptake of idecabtagene vicleucel | Drug plan program | $14,927,095 | $120,337,897 | $164,699,294 | $299,964,286 |
Health care system | $15,584,204 | $125,705,971 | $172,058,814 | $313,348,988 | |
CADTH scenario analysis: High market share uptake of idecabtagene vicleucel | Drug plan program | $37,317,738 | $121,191,567 | $164,059,042 | $322,568,347 |
Health care system | $38,960,510 | $126,597,221 | $171,390,376 | $336,948,107 | |
CADTH scenario analysis: Increased population size across Years 1 to 3 by 10% | Drug plan program | $30,787,134 | $135,712,859 | $166,912,331 | $333,412,324 |
Health care system | $32,142,421 | $141,757,757 | $174,369,270 | $348,269,449 | |
CADTH scenario analysis: Increased population size across Years 1 to 3 by 25% | Drug plan program | $34,985,380 | $149,972,940 | $174,159,891 | $359,118,211 |
Health care system | $36,525,478 | $156,645,585 | $181,935,878 | $375,106,941 | |
CADTH scenario analysis: all patients (100%) receive dexamethasone as bridging therapy | Drug plan program | $27,988,549 | $125,857,391 | $160,561,916 | $314,407,856 |
Health care system | $29,220,628 | $131,468,391 | $167,739,240 | $328,428,260 | |
CADTH scenario analysis: 20% capacity reductiona | Drug plan program | $27,988,304 | $125,856,284 | $160,560,504 | $314,405,092 |
Health care system | $29,220,383 | $131,467,284 | $167,737,828 | $328,425,495 | |
CADTH scenario analysis: patients in the fourth-line or later settings eligible to receive idecabtagene vicleucel | Drug plan program | $27,988,304 | $113,959,314 | $144,835,011 | $286,782,629 |
Health care system | $29,220,383 | $118,975,941 | $151,210,824 | $299,407,148 | |
CADTH scenario analysis: 9% of patients who receive all pre-treatments except for infusion | Drug plan program | $25,345,206 | $113,947,186 | $145,362,482 | $284,654,874 |
Health care system | $26,429,773 | $118,893,539 | $151,691,605 | $297,014,918 | |
CADTH scenario analysis: 87.5% of patients received bridging therapy as per KarMMa trial | Drug plan program | $27,918,699 | $125,542,664 | $160,160,271 | $313,621,633 |
Health care system | $29,149,430 | $131,147,592 | $167,329,846 | $327,626,868 | |
CADTH scenario analysis: Price of idecabtagene vicleucel reduced to $92,650 | Drug plan program | $3,715,343 | $16,488,772 | $20,989,076 | $41,193,191 |
Health care system | $4,947,422 | $22,099,772 | $28,166,401 | $55,213,595 | |
CADTH scenario analysis: Price of idecabtagene vicleucel reduced to $32,700 | Drug plan program | $498,445 | $1,994,282 | $2,491,658 | $4,984,385 |
Health care system | $1,730,524 | $7,605,282 | $9,668,983 | $19,004,789 | |
CADTH scenario analysis: 87.5% of patients received bridging therapy as per KarMMa trial | Drug plan program | $27,918,699 | $125,542,664 | $160,160,271 | $313,621,633 |
Health care system | $29,149,430 | $131,147,592 | $167,329,846 | $327,626,868 |
aThe total number of patients which can be treated with CAR T-cell therapies (i.e., capacity of health care system) when capacity is reduced by 20% is 177 patients in Year 1, 310 patients in Year 2, and 354 patients in Year 3.
bThe “Selected population” analysis is reported here as the base case. Inputs are based on weighted averages that are applied across all jurisdictions.
Ethics Review
Objective
The purpose of this report is to describe and summarize the ethical considerations raised explicitly in the literature associated with the use of idecabtagene vicleucel for the treatment of adult patients with multiple myeloma who have received at least 3 prior therapies, including an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 antibody.
Research Question
This report addresses the following research question:
What are the ethical considerations raised in the published literature relevant to the use of idecabtagene vicleucel for the treatment of adult patients with multiple myeloma who have received at least 3 prior therapies, including an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 antibody?
Methods
Data Collection: Review of Empirical and Normative Ethics Literature
A review of the empirical (i.e., focused on explaining “what is” through observation) and normative (i.e., focused on explaining “what ought to be” through argumentation) ethics literature was conducted to identify literature relevant to the identification of the potential ethical considerations related to the use of idecabtagene vicleucel.
Literature Search Methods
The search for literature identifying explicit ethical considerations was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.1 The search strategy is available on request.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid, Philosopher’s Index via Ovid, the Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCO, and Scopus. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were idecabtagene vicleucel or multiple myeloma or chimeric antigen receptor (CAR) T cell.
Search filters were applied to limit retrieval to citations related to empirical and normative ethical considerations. Retrieval was not limited by publication date or by language. The initial search was completed on December 8, 2020.
Literature Screening and Selection
The selection criteria can be found in Table 1.
Eligible reports were those published in English that explicitly identified normative or empirical ethical considerations related to the use of idecabtagene vicleucel. Descriptions of experiences of adult patients with multiple myeloma were sought as they related to the potential use of idecabtagene vicleucel. The following types of publications were included: primary or secondary research, normative analysis, opinion, commentary, books, or book chapters.
Criteria | Description |
|---|---|
Population | Adult patients with multiple myeloma who have received at least 3 prior therapies, including an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 antibody |
Interventions | Idecabtagene vicleucel or conventional care |
Context | Any health system |
Outcomes | Normative literature: provides normative analysis of an ethical consideration Empirical literature: provides empirical research directly addressing an ethical consideration |
Publication types | Primary or secondary research, normative analysis, opinion, commentary, book, or book chapter |
The selection of relevant literature proceeded in 2 stages. In the first stage, the title and abstracts of citations were screened for relevance by a single reviewer. Articles were categorized as “retrieve” or “do not retrieve,” according to the selection criteria outlined in Table 1, and the following criteria:
explicitly provides normative analysis (i.e., focused on explaining “what ought to be” through argumentation) of an ethical consideration arising in the use of idecabtagene vicleucel or CAR T-cell therapies more broadly, or from experiences of living with or being treated for multiple myeloma relevant to the indicated population
presents empirical research (i.e., focused on explaining “what is” through observation) directly addressing an ethical consideration arising in the use of use of idecabtagene vicleucel or CAR T-cell therapies more broadly, or from experiences of living with or being treated for multiple myeloma relevant to the indicated population
explicitly identifies, but does not investigate empirically, an ethical consideration arising from the use idecabtagene vicleucel or CAR T-cell therapies more broadly, or from experiences of living with or being treated for multiple myeloma relevant to the indicated population.
In the second stage, the full-text reports were reviewed by the same reviewer. Reports meeting these criteria were included in the review, and reports that did not meet these criteria were excluded. Members of the CADTH review team were consulted to resolve uncertainties related to eligibility of full-text reports.
Data Extraction
One reviewer extracted basic details on publication characteristics using a data extraction form. The following publication details were recorded: first author, article title, publication objectives, characteristics of study design and methodology, date of publication, country with which the first author is affiliated, and key findings identified related to ethical considerations.
Data Summary
One reviewer conducted 2 cycles of coding. In the initial coding phase, the publications were reviewed for ethical content. The Core Model 3.0 (Ethical Analysis Domain)2 questions deemed by European Network for Health Technology Assessment (EUnetHTA) as “critically important” were used as a guide to identify and categorize ethical considerations related to the use of idecabtagene vicleucel. The Core Model was chosen because it is a wide-ranging framework; the assessment questions in the domain are intended especially for identifying ethically relevant issues and conflicts.2 This guiding framework highlights the context of a technology and focuses on the following topics: benefit-harm balance; autonomy; respect for persons, justice, and equity; legislation; and ethical consequences of the health technology assessment.
Once identified, passages related to ethical content were coded using methods of qualitative description.3 Initial descriptive coding of the reports focused broadly on categories concerning what ethical considerations were described. Major themes and sub-codes were identified through repeated readings of the data.3 Once sub-codes emerged, they were deductively applied to all reports in the set and ethical content was summarized into the thematic categories. This review focused on ethical considerations relating specifically to the use of idecabtagene vicleucel. Other ethical considerations raised in the literature but not related to the use of idecabtagene vicleucel were outside of the scope of the current review and are not included in the summary.
Results
Description of Included Publications
A total of 1,548 citations were identified in the literature search. Following screening of titles and abstracts, 1,439 citations were excluded and 109 potentially relevant reports from the electronic search were retrieved for full-text review. Of these potentially relevant reports, 48 publications were excluded for various reasons (e.g., they did not explicitly describe ethical considerations related to the use of idecabtagene vicleucel or other therapies related to multiple myeloma (n = 43)4-46; they focused on the use of experimental or unapproved therapies (n = 3)47-49; or they were not in English (n = 2)50,51). A total of 61 publications met the inclusion criteria and were included in this report. Figure 1 presents the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) flow chart of the study selection process.
Details regarding the characteristics of the included publications are reported in Table 2. None of the included reports were directly on the topic of idecabtagene vicleucel for the treatment of adult patients with multiple myeloma. In all, 54 reports examined disparities in the incidence, treatment, and outcomes of multiple myeloma,52-105 3 examined questions of costs of novel therapies for multiple myeloma unrelated to the issue of disparities,106-108 and 7 reports examined disparities related to inclusion in clinical trials for multiple myeloma therapies.55,64,77,86,91,109,110 Three reports examined the balancing of risks and benefits of novel therapies for multiple myeloma given some limitations of the evidence base and the vulnerability of patient populations.46,94,101 Finally, single reports examined the decision-making capacity of older patients who may be eligible for novel therapies for multiple myeloma111 and the disposal of unused hematopoietic stem cell products.112
Key Ethics Considerations From the Literature
Disparities in Incidence, Treatment, and Outcomes of Multiple Myeloma
Multiple myeloma is marked by disparities in terms of incidence, treatment, and outcomes. Disparities in multiple myeloma incidence have been described with respect to race and ethnicity,53,55,59,63,67,77,80,95,105 socioeconomic status,63,80,82 and geography.53,80,105 For example, multiple myeloma incidence rates are reported as being double for African American populations compared with White populations in the US.80 However, some studies suggest that racial and ethnic disparities in incidence may be better explained by disparities in socioeconomic status.63 As 1 study suggests, differences in multiple myeloma incidence at different ages among different groups could affect the type of treatment received.55
Disparities in access to and receipt of multiple myeloma treatment (or similar treatments for other cancers) have been described with respect to age61,70,87,93,94; race and ethnicity55-58,61,64,65,68-74,76,77,91,92,98,99,102; socioeconomic status55,61,70,71,74,76,77,91; geography, proximity, or access to treatment centres55,61,64,76-78,101; insurance status61,70,76,77,89,91,97,101; and supply.101 For example, some studies have found that older age is associated with a lower likelihood of receiving some treatments61 or receiving any treatment at all.70,87 Some therapies for multiple myeloma have been found to used less frequently or later in racial and ethnic minority groups, even when equally beneficial and controlling for other factors, which may point to inequities related to referral patterns, sociodemographic factors, cultural beliefs, and other factors.55,61,69,72,77,91,98 However, some study authors note that disparities in access to treatments may be attenuated for autologous transplants because these are not dependent on finding suitable donors, as is the case for other forms of transplant (e.g., stem cell transplant).55 Much like disparities with incidence, there is some debate about whether racial and ethnic disparities in access to and receipt of multiple myeloma treatment are better explained in terms of socioeconomic factors.71,74,77,91 With respect to supply, some authors have argued that considerations of distributive and procedural justice may arise where the demand for CAR T-cell therapies exceeds manufacturing and administration capacities, which may be constrained by access to highly trained personnel and facilities capable of collecting, shipping, and handling cells, as well as administering the therapy.101
Finally, disparities in multiple myeloma outcomes have been described with respect to age53,55,66,79,81,87; race and ethnicity53-55,58,65,71,73,75,79-81,86,88,92,96; socioeconomic status52,66,71,75,80,83,85,86,88,96,100,103,104; geography, proximity, and access to treatment centres52,55,79,80,84,97; and insurance status.66,79,90 For example, 1 study found that patients aged 75 years of age and older had a significantly worse overall survival compared with younger age groups.53 Some authors suggest that although this may be due to differences in disease biology and therapeutic variability due to comorbidities in this age group, it may also reflect other factors, such as lack of social support systems, differences in insurance coverage, and difficulty in accessing health care facilities for injectable medications.53,55 In terms of racial and ethnic disparities in multiple myeloma outcomes, 1 American study, for example, showed that Asian patients had the best overall survival whereas Hispanic patients had the worst.55 Studies have also shown, for example, that African American patient populations had better outcomes than White patient populations overall in the US; however, relative survival rates have increased for White patient populations whereas there have been smaller, nonsignificant changes in relative survival rates for African American patient populations.55 Suggested causes for disparities in outcomes include the underutilization of some treatments among some racial and ethnic groups, as described previously.73 Despite some studies reporting evidence of racial and ethnic disparities in multiple myeloma outcomes, others have found no difference.60,62,66,69 Again, there is debate about whether any racial and ethnic disparities in outcomes are better explained by socioeconomic factors.72,75,86 One study found that receiving treatment at a specialized myeloma centre might overcome any differences in outcome secondary to race, socioeconomic status, or geography.55
Disparities Related to Inclusion in Clinical Trials for Multiple Myeloma Therapies
Some studies point to the poor representation of racial and ethnic minority groups in cancer clinical trials, including multiple myeloma trials,55,64,86,91,109,110 which some authors argue has led to limited understanding and elimination of racial and ethnic disparities for multiple myeloma.86 For instance, 1 analysis of 9 large national (US) Cooperative Group clinical trials in newly diagnosed multiple myeloma found that only 18% of trial participants were “non-White” and that enrolment of racial and ethnic minority groups actually decreased between 2002 and 2011.109 Other authors point to findings that racial and ethnic minority groups are more likely to be underinsured, obtain care at centres where clinical trials are less common, or present with significant underlying health conditions that render them ineligible for trial participation.91 One study found that the disparity in survival rates for multiple myeloma between rural and urban patients is minimized when patients are enrolled in clinical trials.77
Cost and Value of Novel Therapies for Multiple Myeloma
Some authors noted the high costs that are often associated with novel therapies for multiple myeloma and the related hesitancy that might exist to invest in those therapies.106-108
Balancing Risks and Benefits
One review highlighted the unique vulnerability of patients eligible for CAR T-cell therapy who may have few therapeutic options and who may be willing to pursue high-risk treatments if benefits are overstated or harms understated.101 The authors noted that there is no expert consensus concerning what constitutes an ethically justifiable or appropriate balance of risks and benefits when using axicabtagene ciloleucel, another CAR T-cell therapy, for the treatment of relapsed or refractory large B-cell lymphoma.101 Finding the right balance between under- and overtreating elderly patients was also raised by another study, which noted the difficulty in balancing longevity and quality of life when it comes to treatment options.94 One review emphasized that in this context it is important to recognize that patients are capable of making autonomous, rational decisions to pursue high-risk therapies.101
Decision-Making Capacity Among Older Patients
A single study exploring the frequency of medical decision-making incapacity among newly diagnosed older patients (≥ 65 years of age) with malignant lymphoma or multiple myeloma found that one-quarter of patients enrolled were judged as having some degree of decision-making incompetency due to higher levels of cognitive impairment and increasing age, and that physicians experienced difficulty performing competency assessments.111 The authors of the study noted that decision-making capacity to provide informed consent regarding treatment is essential among cancer patients.111
Storage, Usage, and Disposal of Autologous Tissues
One study found that there are discrepancies between the collection and storage of peripheral blood stem cells and their actual usage in subsequent autologous blood stem cell transplantation.112 Although potentially distinct from autologous CAR T cells collected for the purposes of idecabtagene vicleucel therapy, this study’s findings suggest that there may be significant efforts and costs associated with storage of unused transplant tissues, but that disposal of those tissues may raise legal and ethical questions.112 The authors suggested reviewing and adjusting existing patient information forms and consent forms to exclude incomplete or misleading information regarding tissue disposal or release for research purposes.112
Limitations
This review is limited by the lack of published literature examining ethical considerations relevant to the use of idecabtagene vicleucel for the treatment of adult patients with multiple myeloma. No published ethical analyses were retrieved on the topic of idecabtagene vicleucel.
The absence of published ethical analyses does not indicate that ethical considerations are not present because many of the ethical issues associated with the treatment of multiple myeloma, including the potential for disparities, are likely of relevance to idecabtagene vicleucel as well.
Finally, this review is limited to ethical considerations explicitly discussed in the published literature. Some of the results and insights raised relating to clinical benefits and costs might be discussed more comprehensively in the clinical and pharmacoeconomic review sections.
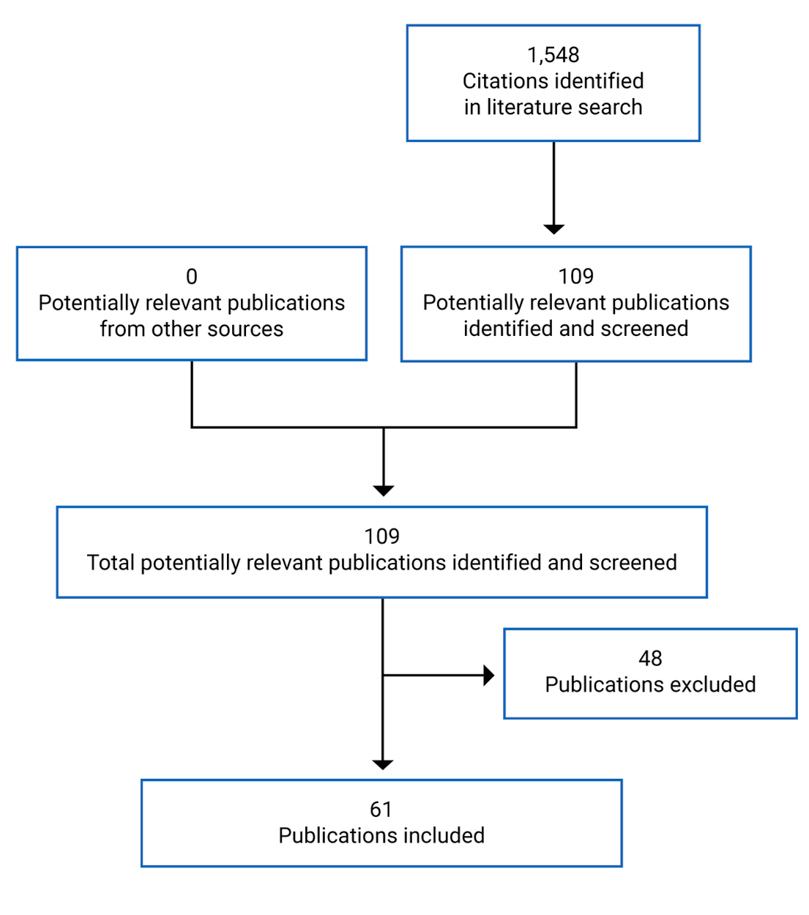
Table 2: Details of Included Publications
First author (year) | Country | Publication type | Objective | Key ethical considerations | Funding source |
|---|---|---|---|---|---|
Abou-Jawde (2006)52 | US | Retrospective analysis | To examine whether race, socioeconomic status, and distance travelled affect overall survival for African American patients with multiple myeloma. | Incidence and mortality of multiple myeloma in African American people was double that in White people; however, socioeconomic status, distance travelled, and race did not affect outcomes of patients with multiple myeloma if patients had access to specialized multidisciplinary myeloma centres. | The Pastore Foundation; the Myeloma Foundation of America |
Ailawadhi (2012)53 | US | Retrospective analysis | To evaluate ethnic disparities in multiple myeloma. | Older age at diagnosis was an independent predictor of decreased overall survival and myeloma-specific survival. Asian patients had the best median overall survival and myeloma-specific survival, whereas Hispanic patients had the worst median overall survival. These trends were more pronounced in patients older than 75 years. Cumulative survival benefit over successive years was highest among White patients and lowest among Asian patients. These disparities may be secondary to multifactorial causes that need to be explored and should be considered for optimal triaging of health care resources. | Not reported |
Ailawadhi (2014)59 | US | Retrospective analysis | To describe the incidence and impact of second primary malignancies among patients with multiple myeloma of different racial and ethnic subgroups. | The risk of developing second primary malignancies among patients with multiple myeloma is variable depending on the patient’s ethnic background. | Not reported |
Ailawadhi (2017a)55 | US | Review | To outline socioeconomic factors that have been reported in the context of multiple myeloma and the impact on health care economics. | Disparities have been found in terms of incidence, outcomes, access and/or treatment relative to age, race and/or ethnicity, socioeconomic status, geography, and insurance status. | Not reported |
Ailawadhi (2017b)56 | US | Retrospective analysis | To analyze the use of novel therapeutic agents and stem cell therapy during the first year after diagnosis of multiple myeloma across racial subgroups to better understand any patterns and explore any disparity that may help explain differences in survival. | Stem cell therapy use increased over time for all patients except African American patients. There was considerable variability in the use of multiple myeloma therapeutics with seeming inequity for racial and/or ethnic minority groups. These trends should be considered to eliminate disparities in drug access and use and achieve equitable benefit of therapeutic advances across all races. | Not reported |
Ailawadhi (2020)57 | US | Retrospective analysis | To analyze the association between race and treatment patterns and survival outcomes in multiple myeloma. | African American and White patients were found to have similar treatment patterns, suggesting that both groups had equal access to health care. | Celgene |
Ailawadhi (2019)58 | US | Retrospective analysis | To assess racial disparities in the treatment and outcomes among White, African American, and Hispanic patients with multiple myeloma. | Although overall survival rates were similar, African American and Hispanic patients may not be fully benefiting from the introduction of novel therapies because they receive these therapies later than White patients. | Celgene |
Ailawadhi (2019)54 | US | Retrospective analysis | To evaluate improvement in relative survival rates for young (≤ 40 years at the time of multiple myeloma diagnosis) and older (> 40 years at the time of multiple myeloma diagnosis) over time by race and/or ethnicity, specifically focusing on Hispanic patients with multiple myeloma. | Five- and 10-year relative survival rates improved significantly over time for all patients and older patients (> 40 years) by race. Relative survival rates for younger patients improved significantly for non-Hispanic White patients and non-Hispanic Black patients, but not for Hispanic patients. Findings suggest a lack of significant benefit in long-term outcomes for younger Hispanic patients with multiple myeloma over time. | Mayo Clinic |
Ailawadhi (2018)109 | US | Retrospective analysis | To evaluate the impact of patient race and/or ethnicity in pooled data from 9 large national cooperative group clinical trials in newly diagnosed multiple myeloma. | Among 2,896 patients enrolled over more than 2 decades, only 18% of patients were “non-White” and enrolment of racial and ethnic minority groups actually decreased in most recent years (2002 to 2011). African American patients were younger and had more frequent poor-risk markers, including anemia and increased lactate dehydrogenase. Hispanic patients had the smallest proportion of patients in trials using novel therapeutic agents. | National Cancer Institute, National Institutes of Health |
Ailawadhi (2018)102 | US | Retrospective analysis | To explore multiple myeloma care and racial disparities. | There was greater receipt of bortezomib and stem cell therapy among White and Black patients and higher receipt of immunomodulatory drugs among Hispanic and Asian patients. | Mayo Clinic |
Albain (2009)60 | US | Retrospective analysis | To determine whether racial disparities in survival exist among multiple cancer patients enrolled in consecutive trials conducted by the Southwest Oncology Group. | No statistically significant association between race and survival for lung cancer, colon cancer, lymphoma, leukemia, or myeloma was observed. | National Cancer Institute, National Institutes of Health |
Al-Hamadani (2014)61 | US | Retrospective analysis | To study the rate of upfront autologous hematopoietic cell transplantation use among 137,409 patients newly diagnosed with multiple myeloma between 1998 and 2010 in the US, and determine whether disparity exists among various sociodemographic and geographic subgroups. | In a multivariable analysis, patients with the following characteristics were the least likely to receive autologous stem cell transplantation: year of diagnosis from 1998 to 2003 before the era of novel agents, older age, Black race, Hispanic ethnicity, low level of education or annual household income, residence in a metro area, no or unknown medical insurance, treatment at a community cancer centre, and treatment facility located in the Northeast region. | Not reported |
Auner (2012)62 | UK | Retrospective analysis | To evaluate the characteristics and outcomes of all patients with multiple myeloma who underwent a first autologous stem cell transplantation at Hammersmith Hospital, later Imperial College Healthcare NHS Trust, over a 16-year period. | Patients from had similar progression-free survival and overall survival, which supports the notion that race should not affect decisions regarding autologous stem cell transplantation for multiple myeloma. | Not reported |
Baris (2000)63 | US | Population-based case-control study | To examine the relation between socioeconomic status and risk of multiple myeloma among Black and White people in the US. | The measured socioeconomic status–related factors account for a substantial amount of the Black vs. White differential in multiple myeloma incidence. | Not reported |
Bennett (2019)64 | US | Review | To review race and geographic location disparities for multiple myeloma. | Race and geographic disparities for multiple myeloma treatment exist. | Not reported |
Bhatnagar (2015)65 | US | Retrospective analysis | To evaluate experiences with White and Black patients with multiple myeloma who underwent autologous stem cell transplantation over a 13-year period to understand differences in disease biology (presentation and cytogenetics) and the impact of novel agents on survival. | Referral for transplant was significantly delayed in Black individuals. Overall survival from the time of transplant was similar for Black and White patients, but survival from the time of diagnosis was significantly longer among Black individuals. | Not reported |
CADTH (2019)101 | Canada | Review and ethical analysis | To identify and analyze ethical issues and considerations for the use of axicabtagene ciloleucel. | Several authors have drawn attention to the “hype” surrounding CAR T-cell therapy, which has been described by 1 author as a form of “experimental therapy” that blurs the line between research and clinical care. A primary ethical consideration for using axicabtagene ciloleucel, as with any therapy, is determining how to weigh therapeutic risks and benefits. There are several ethical considerations associated with using axicabtagene ciloleucel. Three commonly cited concerns include geographic constraints on access, supply constraints, and patient selection. The high cost of axicabtagene ciloleucel is commonly identified as an ethical challenge for individual patients, clinicians, treatment sites, and health system funders. Evidence gaps about safety and effectiveness underline the importance of informed consent processes and the need for clinical aids to assess patient-level risk and suitability for axicabtagene ciloleucel. | Not reported |
Costa (2015)68 | US | Retrospective analysis | To analyze the role of race and/or ethnicity, sex, and age-disparities in autologous hematopoietic cell transplantation utilization in the US. | Confirms the prior demonstration of profound underuse of autologous hematopoietic cell transplantation among Black patients with multiple myeloma. However, similar underuse was seen among Hispanic and Asian patients. | Not reported |
Costa (2016)66 | US | Retrospective analysis | To analyze the impact of marital status, insurance status, income, and race and/or ethnicity on the survival of younger patients diagnosed with multiple myeloma in the US. | Age, male sex, and 3 sociodemographic factors including marital status (other than married), insurance status (uninsured or Medicaid), and county-level income (lowest 2 quartiles) — but not race and/or ethnicity — were found to be associated with an increased risk of death. | Not reported |
Costa (2017)67 | US | Retrospective analysis | To analyze recent trends in multiple myeloma incidence and survival by age, race, and ethnicity in the US. | Multiple myeloma incidence increased significantly among non-Hispanic White and non-Hispanic Black men, but not among non-Hispanic Black women and Hispanic men and women. | Not reported |
Dennis (2020)69 | US | Retrospective review | To evaluate the use of triplet therapy and high-dose melphalan or stem cell transplantation across racial and/or ethnic groups. | Non-Hispanic White patients were 8 times as likely and Hispanic patients were 4 times as likely to receive a triplet regimen compared with non-Hispanic Black patients when adjusting for age, year of diagnosis, and comorbidities. There were no racial and/or ethnic differences with the use of triplet therapy for patients aged ≥ 65 years, and there were no differences in high-dose melphalan or stem cell transplantation (at 1 year or any time after diagnosis), regardless of age. | Not reported |
Duma (2018)110 | US | Retrospective analysis | To analyze the representation of racial and ethnic minority groups and elderly patients in multiple myeloma clinical trials. | Non-Hispanic White patients were more likely to be enrolled in clinical trials than non-Hispanic Black patients and Hispanic patients. | Not reported |
Fakhri (2018)70 | US | Retrospective analysis | To determine the variables that were independently associated with receipt of no treatment for older patients with newly diagnosed multiple myeloma. | Older age, poor performance indicators, comorbidities, African American race, and lower socioeconomic status, including enrolment in Medicaid, were significant factors associated with receipt of no systemic treatment. | Not reported |
Fiala (2020)74 | US | Retrospective analysis | To compare the relative use of bortezomib and lenalidomide in patients with newly diagnosed multiple myeloma, hypothesizing that the disparity between White and African American patients would be greater for lenalidomide because of its higher overall and out-of-pocket costs. | Bortezomib use was 31% less likely for African American patients compared with White patients. There was no statistically significant difference in lenalidomide use when other factors were controlled. These findings do not support the hypothesis that higher respective costs are the cause of the racial disparities in novel agent use for myeloma treatment. | Not reported |
Fiala (2017)73 | US | Retrospective analysis | To confirm previous findings regarding racial disparities in autologous stem cell transplantation use among patients with multiple myeloma in a nationally representative sample. | After controlling for overall health and potential access barriers, Black patients were found to be 37% less likely to undergo stem cell transplantation and 21% less likely to be treated with bortezomib. The underuse of these treatments was associated with a 12% increase in the hazard ratio for death among Black patients. | Not reported |
Fiala (2015)72 | US | Retrospective analysis | To determine if age at diagnosis, sex, socioeconomic status, primary insurance provider at diagnosis, and comorbidity score affected the racial disparities in stem cell transplantation use for treatment of multiple myeloma. | Racial disparities were observed between Black and White patients with multiple myeloma in stem cell therapy use, which was not fully accounted for by the covariates age, sex, socioeconomic status, insurance provider, and comorbidity score. | Not reported |
Fiala (2015)71 | US | Retrospective analysis | To analyze whether survival disparities between Black and White patients with multiple myeloma are related to socioeconomic status or race. | After controlling for race, age, year of diagnosis, severity of comorbidities, stem cell transplant use, and insurance provider, patients with low socioeconomic status had a 54% increase in mortality rate relative to patients with high socioeconomic status. Low socioeconomic status was independently associated with poorer overall survival in multiple myeloma. | Not reported |
Fillmore (2019)75 | US | Retrospective analysis | To investigate the impact of racial disparities on outcome in a large population of patients with multiple myeloma at Veterans Affairs hospitals with equal access to health care for all patients. | In the Veteran Affairs system, where there are no significant racial differences in the use of novel therapies or stem cell therapy in multiple myeloma, overall survival may be superior in African American patients, particularly in the younger population. With previous research in other health care systems that does demonstrate disparities, this study suggests disparity may be primarily due to socioeconomic factors. | VA Office of Research and Development Cooperative Studies Program; VA/National Cancer Institute Big Data–Scientist Training Enhancement Program; VA Merit Review Award; National Cancer Institute, National Institutes of Health |
Fonseca (2018)106 | Portugal | Commentary | To present data and assert that new drugs and associated expenses for multiple myeloma are of direct benefit to patients and society. | Aspirations of societal responsibility in terms of achieving lower health care costs via price controls or similar mechanisms are at odds with the primary responsibility of the physician: the patient. | Not reported |
Fuerst (2019)76 | US | Commentary | To communicate the results of a study led by Chamoun which was presented at a press briefing at the 2019 American Society of Clinical Oncology Annual Meeting. | Gender and race (Black or White) did not affect survival. Patients with a higher median regional income of US$46,000 or more had a 16% greater chance of survival than people with incomes less than US$46,000 per year. If patients received treatment in an academic institution, they had a 49% greater probability of survival. Patients with private insurance had a 59% greater probability of survival than those who were insured through Medicaid. Similarly, people with private insurance had a 62% greater probability of survival than those who had no insurance. For people aged 65 years and older, those who had private insurance also lived longer than those who had Medicare. | Not reported |
Ganguly (2019)77 | US | Review | To review certain aspects of disparities in multiple myeloma care, highlighting disparities among different racial and/or ethnic subgroups, rural-urban differences in the US, and global disparities at an international level. | Disparities have been described with regard to patient age, race and/or ethnicity, rural vs. urban residence, socioeconomic status, and insurance type, among other factors. Looking at the global picture of multiple myeloma care, there is substantial variability among different countries, primarily depending on the disparate availability of anti–multiple myeloma drugs and access to quality health care across the world, limiting the delivery of innovative therapeutic approaches at the individual patient level. The causes of these national and international disparities could be multifactorial, intricate, and difficult to isolate. | Not reported |
Hegney (2005)78 | Australia | Qualitative study | To report the experiences of 17 rural people from the regional city of Toowoomba who had been diagnosed with cancer and were required to travel to the capital city of Queensland (Brisbane) for radiotherapy. | At a time of stress, an increasing burden is placed on cancer clients and their families if they are required to travel for radiotherapy, which includes burdens related to the isolation of rural people who have to live in an unfamiliar environment at a time of great stress. | St. Andrew’s Toowoomba Hospital |
Hong (2016)103 | US | Retrospective analysis | To examine the association of socioeconomic status with outcomes in patients with myeloma after autologous hematopoietic cell transplantation. | There was no difference among socioeconomic status groups in overall survival, progression-free survival, nonrelapse mortality, or relapse in univariate and multivariable analysis. Similarly, socioeconomic status was not associated with survival in a subset analysis of 303 patients who had survived for 1 year after transplantation. | American Society of Hematology |
Intzes (2020)104 | Greece | Retrospective analysis | To determine the effect of socioeconomic status on survival in relation to the prognostic markers, multiple myeloma tumour burden at diagnosis, and patient access to new therapies. | Low socioeconomic status was found to be an independent poor prognostic survival factor, especially for elderly patients with multiple myeloma. | Not reported |
Jayakrishnan (2020)79 | US | Retrospective analysis | To explore the relationship between socioeconomic factors and outcomes for patients with multiple myeloma who were not considered for hematopoietic stem cell transplant in the first-line setting and how it varied over time. | Therapy enrolment in a multivariate model was significantly impacted by race and sex. Advanced age, earlier year of diagnosis, lack of insurance or Medicaid, and higher comorbidity were associated with poor survival, whereas female sex, non-Hispanic Black race, higher income, and treatment at an academic centre were associated with improved survival. | No funding |
Kamath (2020)80 | US | Retrospective analysis | To visualize variation in multiple myeloma incidence and mortality rates by race and/or ethnicity and geographic location and evaluate their correlation with neighbourhood-level population covariates within New York City. | Multiple myeloma incidence rates are double in African American individuals compared with White individuals. In New York City, strong neighbourhood-level correlations exist between incidence and mortality rates and high prevalence of residents of African ancestry, Latin American birth, daily sugary beverage and low fruit and vegetable consumption, and neighbourhood walkability. Higher multiple myeloma mortality also correlates with Hispanic ethnicity, obesity, diabetes, poverty, HIV/AIDS, air benzene concentration, and indoor pesticide use. | National Cancer Institute, National Institutes of Health |
Kaya (2012)81 | US | Retrospective analysis | To analyze the impact of age, race, and decade of treatment on overall survival in a critical population analysis of 40,000 patients with multiple myeloma. | Asian or Pacific Islander race was associated with improved overall survival. American Indian or Alaska Native race was associated with decreased overall survival. Multivariate analysis did not reveal statistically significant differences in overall survival between patients of White and Black race. Younger age (age < 65 years, and 65 to 75 years) was associated with improved overall survival compared with patients > 75 years of age. | Not reported |
Koessel (1996)82 | US | Population-based case-control study | To examine the risk of multiple myeloma in relation to socioeconomic status. | Risk among persons in the lowest quartile of scores was 63% higher than that among those in the highest quartile when the highest Nam-Powers score was used. Similar trends were evident for all 3 methods of classifying occupational history and for both Duncan and Nam-Power scores. The occupation-based scores were stronger predictors of risk than years of education. | Not reported |
Kristinsson (2009)83 | Sweden | Retrospective analysis | To assess the impact of socioeconomic status on survival in 2 large population-based cohorts of patients with acute myeloid leukemia and multiple myeloma diagnosed in Sweden between 1973 and 2005. | Socioeconomic status was significantly associated with survival in both acute myeloid leukemia and multiple myeloma. However, lower mortality was observed among the highest socioeconomic status group during more recent calendar periods. Differences in management, comorbidity, and lifestyle are likely factors to explain these findings. | Swedish Cancer Society; Stockholm County Council; Karolinska Institutet Foundations |
Krummradt (2020)112 | Germany | Retrospective analysis | To evaluate the storage and disposal practices and associated costs in 1,114 patients with multiple myeloma who underwent peripheral blood stem cells collection. | There are discrepancies between the collection yield and storage of peripheral blood stem cells collection harvests and their actual usage. This is associated with significant efforts and costs and disposal may raise legal and ethical questions. A careful review (and adjustment in terms of future policy) of existing patient information and consent forms is mandatory to exclude incomplete or misleading information regarding peripheral blood stem cells collection graft disposal or release for research purposes. | Not reported |
Landgren (2014)105 | US | Retrospective analysis | To define the prevalence and risk factors of monoclonal gammopathy of undetermined significance in a large cohort representative of the US population. | Monoclonal gammopathy of undetermined significance is significantly more common in Black patients, and more often has features associated with higher risk of progression to multiple myeloma. A strong geographic disparity in the prevalence of monoclonal gammopathy of undetermined significance between the North and Midwest vs. the South and West regions of the US was found, which has etiologic implications. | National Cancer Institute, National Institutes of Health; Intramural Program of the National Cancer Institute; the Jabbs Foundation; Henry J. Predolin Foundation |
Liu (2019)84 | US | Retrospective analysis | To explore disparities in hospital cost and in-hospital mortality among patients with multiple myeloma who received autologous hematopoietic cell transplantation. | Patients who received an autologous stem cell transplantation at very low-volume hospitals had significantly higher in-hospital mortality. Both geographic location and hospital type had impact on age- and gender-adjusted mortality rates and inflation-adjusted hospital cost. | Not reported |
Ludwig (2020)85 | Austria | Retrospective analysis | To analyze multiple myeloma incidence and mortality globally and the interrelations between health access and quality, economic resources, and patient empowerment. | The 1-mortality-to-indidence ratio varies between 9% and 64% and is closely related to myeloma incidence, health care access and quality index, patient empowerment, access to cancer drugs, and health care expenditures. | International Myeloma Foundation; Austrian Forum against Cancer |
Marinac (2020)86 | US | Review | To review racial disparities in multiple myeloma. | Comparisons of Black and White monoclonal gammopathy of undetermined significance patients and multiple myeloma patients suggest that differences in risk factors, biology, and clinical characteristics exist by race or ancestry, which may explain some of the observed disparity in multiple myeloma. However, poor accrual of Black monoclonal gammopathy of undetermined significance patients and multiple myeloma patients in clinical and epidemiological studies has limited our understanding of this disparity and hindered its elimination. Disparities in multiple myeloma survival also exist but appear to stem from inferior treatment use and access rather than underlying pathogenesis. | National Cancer Institute, National Institutes of Health; American Cancer Society; Stand Up To Cancer Dream Team Research Grant |
Mian (2020)87 | Canada | Retrospective analysis | To analyze disparities in treatment patterns and outcomes among younger and older adults with newly diagnosed multiple myeloma. | Although several improvements have been made, rates of no treatment and early mortality among patients not treated and those started on novel drugs remains a concern in older adults with newly diagnosed multiple myeloma. | Juravinski Cancer Centre Foundation; Institute for Clinical and Evaluative Sciences (ICES) |
Ojha (2007)88 | US | Commentary | To comment on a recently published study by Abou-Jawde et al. and specifically argue that the simultaneous analysis of correlated variables potentially over-controlled for the underlying mechanism and thus reduced the ability to observe separate effects of race, socioeconomic status, and distance travelled on survival among African American patients and Caucasians with multiple myeloma. | Previous studies have suggested a strong correlation between race and socioeconomic status with outcome for a variety of disorders. Distance travelled may be a function of race and socioeconomic status, which collectively serve as proxies for an underlying causal mechanism. | Not reported |
Olszewski (2018)89 | US | Retrospective analysis | To examine the association between prescription drug coverage, receipt of therapy, and survival among Medicare beneficiaries with myeloma. | Prescription drug coverage is associated with decreased use of classic cytotoxic chemotherapy and better survival among Medicare beneficiaries with myeloma, which suggests improved access to all existing treatment options. | Not reported |
Peña (2020)90 | Chile | Retrospective analysis | To describe clinical and survival characteristics of transplant-eligible patients with multiple myeloma in Latin America, with a special focus on differences between public and private health care facilities. | A great disparity in outcomes and survival between both groups was observed. Late diagnosis and low access to adequate frontline therapy and autologous stem cell transplantation in public institutions probably explain these differences. | Not reported |
Pepper (2018)107 | South Africa | Review | To review the implications of introducing cell and gene therapies into the health care sector in South Africa. | The authors asked whether South Africa should refrain from participation and simply be a bystander in the development of rapidly evolving and highly efficacious, albeit costly, new medicines. The answer was resoundingly negative. To refrain from participating in relevant research and innovative medical practice that, in time, may benefit all South Africans, merely because of current resource constraints, is not sensible or reasonable. | South African Medical Research Council |
Pierre (2020)91 | US | Review | To review opportunities to optimize care to decrease racial disparities for African American patients with multiple myeloma. | African American patients with multiple myeloma have a higher cost of treatment than Caucasian patients. For African American patients diagnosed with multiple myeloma, delays in time to diagnosis and treatment initiation have been associated with increased morbidity and mortality. Lenalidomide, an oral immunomodulatory agent used as a form of treatment for multiple myeloma, is underused in African American patients with multiple myeloma. African Americans diagnosed with multiple myeloma are still the least likely to receive a stem cell transplantation compared with other races and/or ethnicities. When controlling for variables including age, gender, socioeconomic status, insurance, and comorbidities, African American patients with multiple myeloma are also referred for consideration of a stem cell transplantation later in their disease course than Caucasian patients, despite having equal benefit from this key therapeutic modality. | Not reported |
Pierre (2020)91 (continued) | US | Review | To review opportunities to optimize care to decrease racial disparities for African American patients with multiple myeloma. | African American patients are underrepresented in clinical trials, including multiple myeloma trials. Racial and ethnic minority groups are more likely to be underinsured or obtain care at centres with minimally available clinical trials or present with significant underlying health conditions that can lead to ineligibility for trial participation. | Not reported |
Pulte (2014)92 | Germany and US | Retrospective analysis | To assess trends in survival and disease-related mortality for patients with myeloma based on US Surveillance, Epidemiology and End Results (SEER) data by ethnic group, including patients who are of non-Hispanic White, African American, Hispanic, Asian or Pacific Islander descent from 1998 to 2001 to 2006 to 2009. | Although survival increased greatly for non-Hispanic White patients with myeloma between 1998 and 2001 and between 2006 and 2009, smaller increases were observed for people of other ethnic groups. Persistent excess mortality was seen in African American and Hispanic patients with myeloma. Ethnic inequalities persisted or even increased from earlier periods to 2006 to 2009. The results suggest that ethnic minority groups may not have benefited from newer treatments to the same extent as non-Hispanic White patients have. | Not reported |
Puyade (2018)93 | France | Retrospective analysis | To investigate the relationships among age, adherence to guidelines in multiple myeloma, and overall survival. | There is less adherence to guidelines in multiple myeloma among older adults. Compliance to guidelines seems to be related to overall survival taking into account the main prognostic factors. Future guidelines should stress the point that age and frailty need to be taken into account in myeloma care. | Not reported |
Rosko (2017)94 | US | Commentary | To comment on finding the right balance between under- and overtreating elderly patients with myeloma. | Finding the balance between under- and overtreating elderly patients is 1 of the biggest challenges specific to them as a subgroup of patients with multiple myeloma. The balance between longevity and quality of life has not yet been established. | Not reported |
Silbert (2019)108 | US | Commentary | To examine whether and how to offer patients CAR T-cell therapy, and specifically to address value analysis and its application to CAR T-cell therapy, factors that might complicate equitable access to these drugs, and how much patients and families should be told about these therapies’ costs. | Although initial outcome projections show favourable cost-effectiveness, questions remain about whether there is equitable and just access to therapy. | Not reported |
Smith (2018)95 | US | Review | To analyze the biological determinants of multiple myeloma. | The observed disparity of incidence rates of multiple myeloma between patients of African descent and patients of European descent may be due to inherited susceptibility loci. | Not reported |
Sugano (2015)111 | Japan | Survey | To identify the frequency of decision-making incapacity among newly diagnosed older patients with hematological malignancy receiving first-line chemotherapy to examine factors associated with incapacity and assess physicians’ perceptions of patients’ decision-making incapacity. | Higher levels of cognitive impairment and increasing age were significantly associated with decision-making incapacity. Physicians experienced difficulty performing competency assessments. | Japanese Ministry of Health, Labour and Welfare; Japanese Ministry of Education, Culture, Sports, Science and Technology |
Sun (2018)96 | China | Retrospective analysis | To examine changes in the multiple myeloma survival rate from 1981 to 2010 using US SEER data by a period analysis and to show the influence of sex, age, race, and socioeconomic status on patient survival. | Survival for multiple myeloma improved each decade, with a larger increment in the last 2 decades, with a narrowing survival gap among races and a widening gap among socioeconomic status groups. | Not reported |
Tarin-Arzaga (2018)97 | Mexico | Retrospective analysis | To compare the outcomes of patients with newly diagnosed multiple myeloma with and without access to novel agents. | Stage at diagnosis, induction regimen, and autologous stem cell transplantation were found to be contributors to survival disparities between patients with multiple myeloma treated at public hospitals compared with private health systems in Mexico. | Not reported |
Verma (2008)98 | US | Retrospective analysis | To analyze the impact of race on outcomes of autologous transplantation in patients with multiple myeloma. | In a cohort of patients with myeloma who received autologous transplantation in an equal access health care system, there was comparable survival rates between African American patients and Caucasian patients, suggesting that the historical increased mortality for African American patients may be due to inequalities in access to care. | Not reported |
Waxman (2010)99 | US | Retrospective analysis | To analyze racial disparities in incidence and outcome in multiple myeloma. | This study found a younger age of onset among Black patients, better survival in Black patients between 1973 and 2005, and significant survival improvement in White patients over time, with smaller, nonsignificant change seen among Black patients, possibly due to unequal access to and/or disparate responsiveness to novel therapies. | National Cancer Institute, National Institutes of Health |
Xu (2020)100 | China | Retrospective analysis | To analyze education level as a predictor of survival in patients with multiple myeloma. | Low education levels may independently predict poor survival in patients with multiple myeloma in China. | Not reported |
References
1.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
2.EUnetHTA Joint Action 2 Work Package 8, HTA Core Model ® version 3.0 2016; www.htacoremodel.info/BrowseModel.aspx. Accessed 2020 Aug 20.
3.Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-340. PubMed
4.Owens GM. FDA Approvals in 2017 Represent a 21-Year High. American Health & Drug Benefits. 2018;11:18-20.
5.Balderas-Pena LM, Miranda-Ruvalcaba C, Robles-Espinoza AI, et al. Health-Related Quality of Life and Satisfaction With Health Care: Relation to Clinical Stage in Mexican Patients With Multiple Myeloma. Cancer Control. 2019;26(1):1073274819831281. PubMed
6.Belcher SM, Watkins Bruner D, Hofmeister CC, Kweon J, Meghani SH, Yeager KA. Characterizing Pain Experiences: African American Patients With Multiple Myeloma Taking Around-the-Clock Opioids. Clin J Oncol Nurs. 2020;24(5):538-546. PubMed
7.Benyounes A, Ma N, Kocoglu M, et al. Racial disparities in multiple myeloma patients with durable stringent complete response. Clin Lymphoma Myeloma Leuk. 2019;19:e287-e287.
8.Blue BJ, Luo S, Sanfilippo KM, et al. Race-based differences in routine cytogenetic profiles of patients with multiple myeloma. Br J Haematol. 2017;176(2):322-324. PubMed
9.Boyd KD, Ross FM, Chiecchio L, et al. Gender disparities in the tumor genetics and clinical outcome of multiple myeloma. Cancer Epidemiol Biomarkers Prev. 2011;20(8):1703-1707. PubMed
10.Bunce CM, Drayson MT. Dissecting racial disparities in multiple myeloma-clues from differential immunoglobulin levels. Blood Cancer J. 2020;10(4):44. PubMed
11.CADTH. Axicabtagene Ciloleucel for Large B-cell Lymphoma: Implementation and Ethics Project Protocol CADTH Optimal Use Report. 2019;9(1b).
12.CADTH. Tisagenlecleucel for B-Cell Acute Lymphoblastic Leukemia and Diffuse Large B-Cell Lymphoma — Project Protocol, Implementation and Ethics Section. CADTH Optimal Use Report. 2018;8(3b).
13.Cho Y-R, Yoo Y-S. Factors influencing supportive care needs of multiple myeloma patients treated with chemotherapy. Support Care Cancer. 2020;28(4):1783-1791. PubMed
14.Duffy TP. Physician assistance in dying: a subtler slippery slope. The Hastings Center report. 2014;44(2). PubMed
15.Dusetzina SB, Huskamp HA, Jazowski SA, et al. Oral Oncology Parity Laws, Medication Use, and Out-of-Pocket Spending for Patients With Blood Cancers. JNCI: Journal of the National Cancer Institute. 2020;112(10):1055-1062. PubMed
16.El Turabi A, Abel GA, Roland M, Lyratzopoulos G. Variation in reported experience of involvement in cancer treatment decision making: evidence from the National Cancer Patient Experience Survey. Br J Cancer. 2013;109(3):780-787. PubMed
17.Fifer SJ, Ho KA, Lybrand S, Axford LJ, Roach S. Alignment of preferences in the treatment of multiple myeloma - a discrete choice experiment of patient, carer, physician, and nurse preferences. BMC Cancer. 2020;20(1):546. PubMed
18.Greenberg AJ, Rajkumar SV. Elucidating disparities across racial and ethnic groups in multiple myeloma patients. Int J Hematol. 2012;95(4):453-454. PubMed
19.Greenberg AJ, Vachon CM, Rajkumar SV. Disparities in the prevalence, pathogenesis and progression of monoclonal gammopathy of undetermined significance and multiple myeloma between blacks and whites. Leukemia. 2012;26(4):609-614. PubMed
20.Hermann M, Kuhne F, Rohrmoser A, Preisler M, Goerling U, Letsch A. Perspectives of patients with multiple myeloma on accepting their prognosis-A qualitative interview study. Psycho Oncology. 2020;30:30. PubMed
21.Hoff L, Hermerén G. Identifying challenges to communicating with patients about their imminent death. J Clin Ethics. 2014;25(4):296-306. PubMed
22.Husson O, Thong MSY, Mols F, Oerlemans S, Kaptein AA, van de Poll-Franse LV. Illness perceptions in cancer survivors: what is the role of information provision? Psychooncology. 2013;22(3):490-498. PubMed
23.Kick L, Kirchner M, Schneider S. CRISPR-Cas9: From a bacterial immune system to genome-edited human cells in clinical trials. Bioengineered. 2017;8(3):280-286. PubMed
24.Kojovic B, Tariman JD. Decision Aids: Assisting Patients With Multiple Myeloma and Caregivers With Treatment Decision Making. Clin J Oncol Nurs. 2017;21(6):660-664. PubMed
25.Konstantinopoulos PA, Pantanowitz L, Dezube BJ, Konstantinopoulos PA, Pantanowitz L, Dezube BJ. Higher prevalence of monoclonal gammopathy of undetermined significance in African Americans than whites--the unknown role of underlying HIV infection. J Natl Med Assoc. 2006;98(11):1860-1861. PubMed
26.Kumar V, Alhaj-Moustafa M, Bojanini L, et al. Timeliness of Initial Therapy in Multiple Myeloma: Trends and Factors Affecting Patient Care. JCO Oncol Pract. 2020;16(4):e341-e349. PubMed
27.Kumar A, Mhaskar A, Vadaparampil S, Djulbegovic B, Quinn G. Fertility preservation and timing of cancer treatment. J Clin Oncol. 2009;27:e20629-e20629.
28.Lamers J, Hartmann M, Goldschmidt H, Brechtel A, Hillengass J, Herzog W. Psychosocial support in patients with multiple myeloma at time of diagnosis: who wants what? Psychooncology. 2013;22(10):2313-2320. PubMed
29.Lea CS, Bohra S, Moore T, Passwater C, Liles D. Exploring behaviors, treatment beliefs, and barriers to oral chemotherapy adherence among adult leukemia patients in a rural outpatient setting. BMC Res Notes. 2018;11(1):843. PubMed
30.McGaughey JW, Volpe RL. The Case: A Son's Refusal. Camb Q Healthc Ethics. 2010;19(4):530. PubMed
31.Mick J. The ethical dilemma of medical futility: the case of Mr. X. Clin J Oncol Nurs. 2005;9(5):611-616. PubMed
32.Minuk L, Sibbald R, Peng J, Bejaimal S, Chin-Yee I. Access to thalidomide for the treatment of multiple myeloma in Canada: physician behaviours and ethical implications. Curr. 2010;17(4):11-19. PubMed
33.Molassiotis A, Wilson B, Blair S, Howe T, Cavet J. Unmet supportive care needs, psychological well-being and quality of life in patients living with multiple myeloma and their partners. Psychooncology. 2011;20(1):88-97. PubMed
34.Mühlbacher AC, Nübling M, Mühlbacher AC, Nübling M. Analysis of physicians' perspectives versus patients' preferences: direct assessment and discrete choice experiments in the therapy of multiple myeloma. Eur J Health Econ. 2011;12(3):193-203. PubMed
35.Neelapu SS. Choosing treatment options in newly diagnosed patients with multiple myeloma. Community Oncol. 2009;6(2):55-58.
36.Nejati B, Lin CC, Aaronson NK, et al. Determinants of satisfactory patient communication and shared decision making in patients with multiple myeloma. Psychooncology. 2019;28(7):1490-1497. PubMed
37.Priscilla D, Hamidin A, Azhar MZ, Noorjan K, Salmiah MS, Bahariah K. The Socio-Demographic and Clinical Factors Associated with Quality of Life among Patients with Haematological Cancer in a Large Government Hospital in Malaysia. Malays J Med Sci. 2011;18(3):49-56. PubMed
38.Raje N, Faiman B, Harvey RD, et al. Identifying professional education gaps and barriers in multiple myeloma patient care: findings of the Managing Myeloma Continuing Educational Initiative Advisory Committee. Clin Lymphoma Myeloma Leuk. 2014;14(5):356-369. PubMed
39.Riva E, Schutz N, Pena C, et al. Significant differences in access to tests and treatments for multiple myeloma between public and private systems in Latin America. Results of a Latin American survey. GELAMM (Grupo de Estudio Latino Americano de Mieloma Multiple). Ann Hematol. 2020;99(5):1025-1030. PubMed
40.Saunders CL, Abel GA, Lyratzopoulos G. Inequalities in reported cancer patient experience by socio-demographic characteristic and cancer site: evidence from respondents to the English Cancer Patient Experience Survey. European Journal of Cancer Care. 2015;24(1):85-98. PubMed
41.Shi Q, Wang XS, Li G, et al. Racial/ethnic disparities in inflammatory gene single-nucleotide polymorphisms as predictors of a high risk for symptom burden in patients with multiple myeloma 1 year after diagnosis. Cancer. 2015;121(7):1138-1146. PubMed
42.Swanson JW, Van McCrary S. Doing All They Can: Physicians Who Deny Medical Futility. J Law Med Ethics. 1994;22(4):318-326. PubMed
43.Tariman JD, Doorenbos A, Schepp KG, Singhal S, Berry DL. Older adults newly diagnosed with symptomatic myeloma and treatment decision making. Oncol Nurs Forum. 2014;41(4):411-419. PubMed
44.VanValkenburg ME, Pruitt GI, Brill IK, et al. Family history of hematologic malignancies and risk of multiple myeloma: differences by race and clinical features. Cancer Causes Control. 2016;27(1):81-91. PubMed
45.Westrich K, Buelt L, Dubois RW. Why Value Framework Assessments Arrive at Different Conclusions: A Multiple Myeloma Case Study. J Manag Care Spec Pharm. 2017;23(6-a Suppl):S28-S33.
46.Atilla E, Kilic P, Gurman G. Cellular therapies: Day by day, all the way. Transfus Apher Sci. 2018;57(2):187-196. PubMed
47.Caplan AL, Teagarden JR, Kearns L, et al. Fair, just and compassionate: A pilot for making allocation decisions for patients requesting experimental drugs outside of clinical trials. J Med Ethics. 2018;44(11):761-767. PubMed
48.Daniels N, Sabin JE. Last chance therapies and managed care: pluralism, fair procedures, and legitimacy. Hastings Cent Rep. 1998;28(2):27-41. PubMed
49.Swisher KN. Insurance company forced to pay for autologous bone marrow transplant. Leonhardt v. Holden Business Forms Co. Journal of healthcare risk management: the journal of the American Society for Healthcare Risk Management. 1994;14(2):40-43.
50.Rial-Sebbag E, Chabannon C. [Chapter 6. Legal issues and for the health system of the development of a new class of innovative therapy in oncoimmunology: the “Car-T CellS”]. Journal International de Bioethique et Dethique des Sciences. 2018;29(2):113-128.
51.Viardot A. [Perspectives on CAR T-cell treatment]. Pathologe. 2020;28:28.
52.Abou-Jawde RM, Baz R, Walker E, et al. The role of race, socioeconomic status, and distance traveled on the outcome of African-American patients with multiple myeloma. Haematologica. 2006;91(10):1410-1413. PubMed
53.Ailawadhi S, Aldoss IT, Yang D, et al. Outcome disparities in multiple myeloma: a SEER-based comparative analysis of ethnic subgroups. Br J Haematol. 2012;158(1):91-98. PubMed
54.Ailawadhi S, Azzouqa AG, Hodge D, et al. Survival Trends in Young Patients With Multiple Myeloma: A Focus on Racial-Ethnic Minorities. Clin Lymphoma Myeloma Leuk. 2019;19(10):619-623. PubMed
55.Ailawadhi S, Bhatia K, Aulakh S, Meghji Z, Chanan-Khan A. Equal Treatment and Outcomes for Everyone with Multiple Myeloma: Are We There Yet? Curr Hematol Malig Rep. 2017;12(4):309-316. PubMed
56.Ailawadhi S, Frank RD, Advani P, et al. Racial disparity in utilization of therapeutic modalities among multiple myeloma patients: a SEER-medicare analysis. Cancer Med. 2017;6(12):2876-2885. PubMed
57.Ailawadhi S, Jagannath S, Lee HC, et al. Association between race and treatment patterns and survival outcomes in multiple myeloma: A Connect MM Registry analysis. Cancer (0008543X). 2020;126(19):4332-4340.
58.Ailawadhi S, Parikh K, Abouzaid S, et al. Racial disparities in treatment patterns and outcomes among patients with multiple myeloma: a SEER-Medicare analysis. Blood Adv. 2019;3(20):2986-2994. PubMed
59.Ailawadhi S, Swaika A, Razavi P, Yang D, Chanan-Khan A. Variable risk of second primary malignancy in multiple myeloma patients of different ethnic subgroups. Blood Cancer J. 2014;4:e243. PubMed
60.Albain KS, Unger JM, Crowley JJ, et al. Racial disparities in cancer survival among randomized clinical trials patients of the Southwest Oncology Group. JNCI: Journal of the National Cancer Institute. 2009;101(14):984-992. PubMed
61.Al-Hamadani M, Hashmi SK, Go RS. Use of autologous hematopoietic cell transplantation as initial therapy in multiple myeloma and the impact of socio-geo-demographic factors in the era of novel agents. Am J Hematol. 2014;89(8):825-830. PubMed
62.Auner HW, Pavlu J, Szydlo R, et al. Autologous haematopoietic stem cell transplantation in multiple myeloma patients from ethnic minority groups in an equal access healthcare system. Br J Haematol. 2012;157(1):125-127. PubMed
63.Baris D, Brown LM, Silverman DT, et al. Socioeconomic status and multiple myeloma among US blacks and whites. Am J Public Health. 2000;90(8):1277-1281. PubMed
64.Bennett C. Race & Geographic Location Create Disparities in Multiple Myeloma. Oncology Times. 2019;41:10-10.
65.Bhatnagar V, Wu Y, Goloubeva OG, et al. Disparities in black and white patients with multiple myeloma referred for autologous hematopoietic transplantation: a single center study. Cancer. 2015;121(7):1064-1070. PubMed
66.Costa LJ, Brill IK, Brown EE. Impact of marital status, insurance status, income, and race/ethnicity on the survival of younger patients diagnosed with multiple myeloma in the United States. Cancer. 2016;122(20):3183-3190. PubMed
67.Costa LJ, Brill IK, Omel J, Godby K, Kumar SK, Brown EE. Recent trends in multiple myeloma incidence and survival by age, race, and ethnicity in the United States. Blood Adv. 2017;1(4):282-287. PubMed
68.Costa LJ, Huang JX, Hari PN. Disparities in utilization of autologous hematopoietic cell transplantation for treatment of multiple myeloma. Biol Blood Marrow Transplant. 2015;21(4):701-706. PubMed
69.Dennis M, Maoz A, Cirstea D, Patel A, Lerner A, Sarosiek S. Treatment disparities in minority groups with multiple myeloma at a safety-net hospital. Leuk Lymphoma. 2020;61(10):2507-2510. PubMed
70.Fakhri B, Fiala MA, Tuchman SA, Wildes TM. Undertreatment of Older Patients With Newly Diagnosed Multiple Myeloma in the Era of Novel Therapies. Clin Lymphoma Myeloma Leuk. 2018;18(3):219-224. PubMed
71.Fiala MA, Finney JD, Liu J, et al. Socioeconomic status is independently associated with overall survival in patients with multiple myeloma. Leuk Lymphoma. 2015;56(9):2643-2649. PubMed
72.Fiala MA, Finney JD, Stockerl-Goldstein KE, et al. Re: Disparities in Utilization of Autologous Hematopoietic Cell Transplantation for Treatment of Multiple Myeloma. Biol Blood Marrow Transplant. 2015;21(7):1153-1154. PubMed
73.Fiala MA, Wildes TM. Racial disparities in treatment use for multiple myeloma. Cancer. 2017;123(9):1590-1596. PubMed
74.Fiala MA, Wildes TM, Vij R. Racial Disparities in the Utilization of Novel Agents for Frontline Treatment of Multiple Myeloma. Clin Lymphoma Myeloma Leuk. 2020;20(10):647-651. PubMed
75.Fillmore NR, Yellapragada SV, Ifeorah C, et al. With equal access, African American patients have superior survival compared to white patients with multiple myeloma: a VA study. Blood. 2019;133(24):2615-2618. PubMed
76.Fuerst ML. Socioeconomic Factors Predict Long-Term Survival in Multiple Myeloma. Oncology Times. 2019;41:14-14.
77.Ganguly S, Mailankody S, Ailawadhi S. Many Shades of Disparities in Myeloma Care. Am. 2019;39:519-529.
78.Hegney D, Pearce S, Rogers-Clark C, Martin-Mcdonald K, Buikstra E. Close, but still too far. The experience of Australian people with cancer commuting from a regional to a capital city for radiotherapy treatment. European Journal of Cancer Care. 2005;14(1):75-82. PubMed
79.Jayakrishnan TT, Bakalov V, Chahine Z, Lister J, Wegner RE, Sadashiv S. Disparities in the enrollment to systemic therapy and survival for patients with multiple myeloma. Hematol Oncol Stem Cell Ther. 2020;10:10. PubMed
80.Kamath GR, Renteria AS, Jagannath S, Gallagher EJ, Parekh S, Bickell NA. Where you live can impact your cancer risk: a look at multiple myeloma in New York City. Ann Epidemiol. 2020;48:43-50.e44. PubMed
81.Kaya H, Peressini B, Jawed I, et al. Impact of age, race and decade of treatment on overall survival in a critical population analysis of 40,000 multiple myeloma patients. Int J Hematol. 2012;95(1):64-70. PubMed
82.Koessel SL, Theis MK, Vaughan TL, et al. Socioeconomic status and the incidence of multiple myeloma. Epidemiology. 1996;7(1):4-8. PubMed
83.Kristinsson SY, Derolf AR, Edgren G, Dickman PW, Bjorkholm M. Socioeconomic differences in patient survival are increasing for acute myeloid leukemia and multiple myeloma in sweden. J Clin Oncol. 2009;27(12):2073-2080. PubMed
84.Liu Y, Han H, Shah G, et al. Significant Nationwide Variability in the Costs and Hospital Mortality Rates of Autologous Stem Cell Transplantation for Multiple Myeloma: An Analysis of the Nationwide Inpatient Sample Database. Biol Blood Marrow Transplant. 2019;25(1):41-46. PubMed
85.Ludwig H, Novis Durie S, Meckl A, Hinke A, Durie B. Multiple Myeloma Incidence and Mortality Around the Globe; Interrelations Between Health Access and Quality, Economic Resources, and Patient Empowerment. Oncologist. 2020;25:25. PubMed
86.Marinac CR, Ghobrial IM, Birmann BM, Soiffer J, Rebbeck TR. Dissecting racial disparities in multiple myeloma. Blood Cancer J. 2020;10(2):19. PubMed
87.Mian HS, Seow H, Wildes TM, et al. Disparities in treatment patterns and outcomes among younger and older adults with newly diagnosed multiple myeloma: A population-based study. J Geriatr Oncol. 2020;24:24. PubMed
88.Ojha RP, Prabhakar D, Evans E, Lowery K, Thertulien R, Fischbach LA. RE 10104: Abou-Jawde et al. The role of race, socioeconomic status, and distance traveled on the outcome of African-American patients with multiple myeloma. Haematologica 2006; 91: 1410-1413. Haematologica. 2007;92(4):e46. PubMed
89.Olszewski AJ, Dusetzina SB, Trivedi AN, Davidoff AJ. Prescription Drug Coverage and Outcomes of Myeloma Therapy Among Medicare Beneficiaries. J Clin Oncol. 2018;36(28):2879-2886. PubMed
90.Pena C, Riva E, Schutz N, et al. Different outcomes for transplant-eligible newly diagnosed multiple myeloma patients in Latin America according to the public versus private management: a GELAMM study. Leuk Lymphoma. 2020:1-8. PubMed
91.Pierre A, Williams TH. African American Patients With Multiple Myeloma: Optimizing Care to Decrease Racial Disparities. Clin J Oncol Nurs. 2020;24(4):439-443. PubMed
92.Pulte D, Redaniel MT, Brenner H, Jansen L, Jeffreys M. Recent improvement in survival of patients with multiple myeloma: variation by ethnicity. Leuk Lymphoma. 2014;55(5):1083-1089. PubMed
93.Puyade M, Defossez G, Guilhot F, Leleu X, Ingrand P. Age-related health care disparities in multiple myeloma. Hematol Oncol. 2018;36(1):224-231. PubMed
94.Rosko A, Giralt S, Mateos MV, Dispenzieri A. Myeloma in Elderly Patients: When Less Is More and More Is More. Am. 2017;37:575-585.
95.Smith CJ, Ambs S, Landgren O. Biological determinants of health disparities in multiple myeloma. Blood Cancer J. 2018;8(9):85. PubMed
96.Sun T, Wang S, Sun H, Wen J, An G, Li J. Improved survival in multiple myeloma, with a diminishing racial gap and a widening socioeconomic status gap over three decades. Leuk Lymphoma. 2018;59(1):49-58. PubMed
97.Tarin-Arzaga L, Arredondo-Campos D, Martinez-Pacheco V, et al. Impact of the affordability of novel agents in patients with multiple myeloma: Real-world data of current clinical practice in Mexico. Cancer. 2018;124(9):1946-1953. PubMed
98.Verma PS, Howard RS, Weiss BM. The impact of race on outcomes of autologous transplantation in patients with multiple myeloma. Am J Hematol. 2008;83(5):355-358. PubMed
99.Waxman AJ, Mink PJ, Devesa SS, et al. Racial disparities in incidence and outcome in multiple myeloma: a population-based study. Blood. 2010;116(25):5501-5506. PubMed
100.Xu L, Wang X, Pan X, et al. Education level as a predictor of survival in patients with multiple myeloma. BMC Cancer. 2020;20(1):737. PubMed
101.CADTH. Axicabtagene Ciloleucel for Large B-Cell Lymphoma: Ethics and Implementation Report. CADTH Optimal Use Report. 2019;9(1e).
102.Ailawadhi S, Frank RD, Sharma M, et al. Trends in multiple myeloma presentation, management, cost of care, and outcomes in the Medicare population: A comprehensive look at racial disparities. Cancer. 2018;124(8):1710-1721. PubMed
103.Hong S, Rybicki L, Abounader D, et al. Association of Socioeconomic Status with Outcomes of Autologous Hematopoietic Cell Transplantation for Multiple Myeloma. Biol Blood Marrow Transplant. 2016;22(6):1141-1144. PubMed
104.Intzes S, Symeonidou M, Zagoridis K, et al. Socioeconomic Status Is an Independent Prognostic Factor for Overall Survival in Patients With Multiple Myeloma: Real-World Data From a Cohort of 223 Patients. Clin Lymphoma Myeloma Leuk. 2020;20(10):704-711. PubMed
105.Landgren O, Graubard BI, Katzmann JA, et al. Racial disparities in the prevalence of monoclonal gammopathies: a population-based study of 12,482 persons from the National Health and Nutritional Examination Survey. Leukemia (08876924). 2014;28(7):1537-1542.
106.Fonseca VR, Romão VC, Agua‐Doce A, et al. The Ratio of Blood T Follicular Regulatory Cells to T Follicular Helper Cells Marks Ectopic Lymphoid Structure Formation While Activated Follicular Helper T Cells Indicate Disease Activity in Primary Sjögren's Syndrome. Arthritis & Rheumatology. 2018;70(5):774-784. PubMed
107.Pepper MS, Alessandrini M, Pope A, Van Staden W, Green RJ. Cell and gene therapies at the forefront of innovative medical care: Implications for South Africa. Samj, S. 2018;109(1):20-22.
108.Silbert S, Yanik GA, Shuman AG. How Should We Determine the Value of CAR T-Cell Therapy? AMA J Ethics. 2019;21(10):E844-851. PubMed
109.Ailawadhi S, Jacobus S, Sexton R, et al. Disease and outcome disparities in multiple myeloma: exploring the role of race/ethnicity in the Cooperative Group clinical trials. Blood Cancer J. 2018;8(7):67. PubMed
110.Duma N, Azam T, Riaz IB, Gonzalez‐Velez M, Ailawadhi S, Go R. Representation of Minorities and Elderly Patients in Multiple Myeloma Clinical Trials. Oncologist. 2018;23(9):1076-1078. PubMed
111.Sugano K, Okuyama T, Iida S, et al. Medical Decision-Making Incapacity among Newly Diagnosed Older Patients with Hematological Malignancy Receiving First Line Chemotherapy: A Cross-Sectional Study of Patients and Physicians. PLoS ONE [Electronic Resource]. 2015;10(8):e0136163. PubMed
112.Krummradt F, Sauer S, Pavel P, et al. Storage, Utilization, and Disposal of Hematopoietic Stem Cell Products in Patients with Multiple Myeloma. Biol Blood Marrow Transplant. 2020;26(9):1589-1596. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.