CADTH Reimbursement Review
Daunorubicin and Cytarabine Liposome (Vyxeos)
Sponsor: Jazz Pharmaceuticals Canada Inc.
Therapeutic area: Acute myeloid leukemia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
7 + 3
conventional (non-liposomal) cytarabine and daunorubicin
AE
adverse event
alloSCT
allogeneic stem cell transplantation
AML
acute myeloid leukemia
AML-MRC
acute myeloid leukemia with myelodysplasia-related changes
CI
confidence interval
CLSG
Canadian Leukemia Study Group
CMMoL
chronic myelomonocytic leukemia
CR
complete remission
CRi
complete remission with incomplete platelet or neutrophil recovery
DAC
Drug Advisory Committee
ECOG
Eastern Cooperative Oncology Group
EFS
event-free survival
FLAG-IDA
fludarabine + cytarabine + filgrastim + idarubicin
FLT3
FMS-like tyrosine kinase 3
G-CSF
granulate colony-stimulating factor
HMA
hypomethylating agent
HR
hazard ratio
HRQoL
health-related quality of life
HSCT
hematopoietic stem cell transplant
ICU
intensive care unit
ITT
intention-to-treat
LLSC
Leukemia and Lymphoma Society of Canada
MDS
myelodysplastic syndrome
MRD
measurable residual disease
NGS
next-generation sequencing
OH-CCO
Ontario Health (Cancer Care Ontario)
OR
odds ratio
SAE
serious adverse event
SD
standard deviation
t-AML
therapy-related acute myeloid leukemia
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Daunorubicin and cytarabine liposome for injection, 44 mg daunorubicin and 100 mg cytarabine per vial, IV infusion |
Indication | Treatment of adults with newly diagnosed therapy-related acute myeloid leukemia or AML with myelodysplasia-related changes |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | April 29, 2021 |
Sponsor | Jazz Pharmaceuticals Canada Inc. |
AML = acute myeloid leukemia; IV = intravenous; NOC = Notice of Compliance.
Introduction
Acute myeloid leukemia (AML) is a hematologic malignancy associated with clonal expansion of myeloid progenitor cells in the bone marrow and peripheral blood.1 Two subclassifications of AML — AML with myelodysplasia-related changes (AML-MRC) and therapy-related AML (t-AML) — represent high-risk subgroups.2 Acute myeloid leukemia and its associated subclassifications are uncommon cancers, representing approximately 1% of all cancer diagnoses. According to CADTH reviewer estimates based on Statistics Canada data, the incidence of new AML cases in Canada is 4.89 per 100,000 (for patients > 20 years of age),3 as noted in the CADTH Pharmacoeconomic Review Report. Diagnoses of AML-MRC and t-AML are more prevalent in elderly populations.4
The clinical experts consulted by CADTH for this review indicated that the prognosis for patients with t-AML or AML-MRC is poor. Patients with t-AML or AML-MRC are considered high-risk subpopulations of AML, and the disease is fatal if left untreated. Certain risk factors are associated with poorer prognosis, such as adverse genetic risk factors and lower overall patient fitness.5 Therapeutically, the ideal goal of treating t-AML or AML-MRC in sufficiently fit adults as a bridge to hematopoietic stem cell transplantation (HSCT) is improved overall survival. Transplantation is considered after a patient undergoes induction therapy (achieves a remission) and treatment may also include consolidation therapy.6 The clinical experts consulted by CADTH indicated that induction and consolidation for adult patients in Canada is typically performed using conventional (non-liposomal) cytarabine and daunorubicin (7 + 3) or, less commonly, fludarabine + cytarabine + filgrastim + idarubicin (FLAG-IDA). The clinical experts and patient groups consulted by CADTH for the purposes of this review indicated that response to these treatments is often limited, and less than half of patients treated with existing induction therapy will have an adequate response that permits moving on to HSCT.
The indication for daunorubicin and cytarabine liposome for injection is for the treatment of adults with newly diagnosed t-AML or AML-MRC. Liposomal daunorubicin and cytarabine is administered intravenously via a constant infusion and is intended to act as an induction and consolidation agent for patients with t-AML or AML-MRC. Dosing for first induction therapy is daunorubicin 44 mg/m2 and cytarabine 100 mg/m2 on days 1, 3, and 5. Dosing for second induction is daunorubicin 44 mg/m2 and cytarabine 100 mg/m2 on days 1 and 3. Dosing for consolidation therapy is daunorubicin 29 mg/m2 and cytarabine 65 mg/m2 on days 1 and 3.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of daunorubicin and cytarabine liposome for injection (44 mg daunorubicin and 100 mg cytarabine per vial) administered intravenously for the treatment of adults with newly diagnosed t-AML or AML-MRC.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Patient input was provided by the Leukemia and Lymphoma Society of Canada (LLSC) through an English- and French-language online survey from December 7, 2020, through January 24, 2021. Patients were asked to describe their experiences with treatment for AML. All of the 29 individuals who responded identified as patients living in Canada. No breakdown was provided on proportions of patients with AML-MRC or t-AML.
Patients reported how AML symptoms varied, from losing the ability to work, impacting social lives and relationships, fatigue, numbness, and a large number of detrimental effects on health. Many respondents indicated that they felt physically and socially isolated, and those who had completed therapy identified concerns about relapse.
Patients listed a physician recommendation as the most important factor when deciding on new treatments, followed by possible impacts on disease, quality of life, closeness to home, and outpatient treatment.
In general, respondents would prefer new therapies that have fewer side effects, are more holistic, help maintain their remission, are covered through drug plans, and are accessible closer to home. Patients were also interested in having more information on emerging therapies and being able to access all possible treatments in the future.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH for this review described how patients in this population are high-risk individuals with high unmet needs. Existing induction and consolidation therapies were described by the experts as not meeting the needs of all patients, resulting in many individuals not achieving remission and becoming ineligible for HSCT. The drug under review is intended to act at the same step of the clinical pathway in patients with AML-MRC or t-AML who are fit enough for induction therapy. Survival, as well as response to induction therapy, was highlighted as a key outcome of interest that may influence decisions regarding subsequent HSCT, which reported by the experts to confer a survival benefit.
Clinician Group Input
Two clinician groups provided input for this review, the Ontario Health (Cancer Care Ontario) (OH-CCO) Hematology Disease Site Drug Advisory Committee (DAC) and the Canadian Leukemia Study Group (CLSG). The clinical experts consulted by CADTH for this review and the clinician group agreed broadly on the patient populations of interest, their unmet needs, and the outcomes of importance in this population. The clinician groups indicated that the proposed product would act in a similar role and replace existing 7 + 3 therapy.
Drug Program Input
The drug program had questions about alternative therapies, as only evidence of liposomal daunorubicin and cytarabine relative to 7 + 3 was identified, whereas FLAG-IDA is used frequently in Canadian practice. No data were identified, and clinical experts were uncertain about the relative effects of liposomal daunorubicin and cytarabine versus FLAG-IDA.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
One study, Study 301, was identified and included in this review. Study 301 was a phase III, randomized, controlled, multi-centre, open-label, therapy-controlled clinical trial was identified and included in this review. Study 301 recruited 309 patients across 39 centres, 4 of which were based in Canada. Patients included those with t-AML or AML-MRC between 60 and 75 years of age. Patients were randomly assigned to either liposomal daunorubicin and cytarabine (N = 153) or 7 + 3 (N = 156).
The primary outcome was overall survival, and secondary end points included response, event-free survival (EFS), remission duration, and proportions of patients achieving HSCT. Response was defined as patients who achieved complete remission (CR) or complete remission with incomplete platelet or neutrophil recovery (CRi) during the treatment phase. CR was defined as bone marrow blasts of less than 5%, absence of blasts with Auer rods, absence of extramedullary disease, an absolute neutrophil count greater than 1.0 × 109/L (1,000/μL), a platelet count greater than 100 × 109/L (100,000/μL), and independence from red blood cell transfusions. CRi was defined as all CR criteria except for residual neutropenia (< 1.0 × 109/L [1,000/μL]) or thrombocytopenia (< 100 × 109/L [100,000/μL]). Event-free survival was defined as the time from study randomization to the date of induction treatment failure (persistent disease), relapse from CR or CRi, or death from any cause, whichever came first. Remission duration was measured from the date of achievement of a remission (CR or CRi) until the date of relapse or death from any cause. All outcomes that had formal statistical assessments were conducted using a 1-sided 0.025 hypothesis-testing cut-off alpha value.
Patients within this study had a mean age of 67.7 years (standard deviation [SD] = 4.14) and were predominantly male (61%). The most common AML subtype was AML-MRC with prior exposure to a hypomethylating agent (HMA) (34%). Seventy-two patients (50.3%) in the liposomal daunorubicin and cytarabine treatment group and 83 patients (56.8%) in the 7 + 3 treatment group had an unfavourable cytogenetic risk, while 64 patients (44.8%) in the liposomal daunorubicin and cytarabine treatment group and 58 patients (39.7%) in the 7 + 3 treatment group had an intermediate cytogenetic risk. The median duration of follow-up between treatment arms was similar, at 20.5 months for patients treated with liposomal daunorubicin and cytarabine and 21.22 months for patients treated with 7 + 3.
Efficacy Results
The primary outcome, overall survival, was assessed in 153 patients who were randomized to the liposomal daunorubicin and cytarabine treatment group and 156 patients who were randomized to the 7 + 3 treatment group (the intention-to-treat [ITT] population). The median overall survival in the liposomal daunorubicin and cytarabine treatment group was 9.56 months (95% confidence interval [Cl], 6.60 to 11.86), and in the 7 + 3 treatment group it was 5.95 months (95% CI, 4.99 to 7.75). In the 153 patients assigned to liposomal daunorubicin and cytarabine treatment, there were 104 events, and in the 156 patients assigned to 7 + 3 treatment there were 132 events. The liposomal daunorubicin and cytarabine treatment group was associated with a statistically significant improvement in overall survival when compared to patients who received 7 + 3 (hazard ratio [HR] = 0.69; 95% CI, 0.52 to 0.90; 1-sided log-rank test P = 0.003). At a 5-year follow-up, 18% of patients who received liposomal daunorubicin and cytarabine were alive versus 8% who received 7 + 3, with median overall survivals of 9.33 months and 5.95 months in the liposomal daunorubicin and cytarabine treatment and 7 + 3 treatment groups, respectively, resulting in an HR of 0.70 (95% CI, 0.55 to 0.91) in favour of liposomal daunorubicin and cytarabine.7 However, results from the 5-year follow-up are considered descriptive and should be interpreted with caution.
The median EFS was higher in the liposomal daunorubicin and cytarabine treatment group (2.53 months, 95% CI, 2.07 to 4.99) compared with the 7 + 3 treatment group (1.31 months; 95% CI, 1.08 to 1.64), resulting in a statistically significant HR of 0.74 (95% CI, 0.58 to 0.96; 1-sided log-rank test P = 0.011).
For response rates, 73 patients (47.7%) in the liposomal daunorubicin and cytarabine treatment group achieved a CR or CRi, as opposed to 52 patients (33.3%) in the 7 + 3 treatment group. The liposomal daunorubicin and cytarabine treatment group was associated with a statistically significantly higher response compared to the 7 + 3 treatment group (odds ratio [OR] = 1.77; 95% CI, 1.11 to 2.81; 1-sided P = 0.008).
No statistically significant difference was observed in remission duration in patients in the liposomal daunorubicin and cytarabine treatment group compared with the 7 + 3 treatment group. The median remission duration in the liposomal daunorubicin and cytarabine treatment group was 6.93 months (95% CI, 4.60 to 9.23) compared to 6.11 months (95% CI, 3.45 to 8.71) in the 7 + 3 treatment group (HR = 0.77; 95% CI, 0.47 to 1.26; 1-sided log-rank test P = 0.147).
The percentage of patients receiving an HSCT in the liposomal daunorubicin and cytarabine treatment group was 34%, as opposed to 25% in the 7 + 3 treatment group. No statistically significant difference was reported for the proportion of patients receiving HSCT when the liposomal daunorubicin and cytarabine treatment group was compared with the 7 + 3 treatment group (OR = 1.54, 95% CI, 0.92 to 2.56; 1-sided P = 0.049).
Health-related quality of life (HRQoL) was not assessed in Study 301.
Harms Results
All patients included in Study 301 experienced at least 1 adverse event (AE). Similarly, serious adverse events (SAEs) were comparatively common, with 59% of patients in the liposomal daunorubicin and cytarabine treatment group experiencing an SAE compared to 43% of patients in the 7 + 3 treatment group. The nature of SAEs was relatively consistent between treatment arms, although the incidence of sepsis in the liposomal daunorubicin and cytarabine treatment group (7.8%) was twice that in the 7 + 3 treatment group (3.3%).
Most harms of special interest were relatively evenly distributed between treatment arms, with the proportions of patients experiencing an event varying depending on the event of interest. For admission to an intensive care unit (ICU), a greater proportion of patients who received 7 + 3 (25.2%) were admitted compared to patients who received liposomal daunorubicin and cytarabine (18.3%). In contrast, ICU stays were longer for patients who received liposomal daunorubicin and cytarabine (mean ICU stay duration = 8.2 days; SD = 9.69) when compared with patients who received 7 + 3 (mean ICU stay duration = 6.9 days; SD = 4.85), although the median duration of ICU stays (6 days) was the same between treatment arms.
Table 2: Summary of Key Results From Study 301
Key result | Liposomal daunorubicin and cytarabine N = 153 | 7 + 3 N = 156 |
|---|---|---|
Overall survival, ITT populationa | ||
n events (%) | 104 (67.9) | 132 (84.6) |
Median overall survival in months (95% CI) | 9.56 (6.6 to 11.86) | 5.95 (4.99 to 7.75) |
HR (95% CI) | 0.69 (0.52 to 0.90) | |
P value (1-sided) | 0.003 | |
Proportion of patients with CR + CRi, ITT populationb | ||
n (%) | 73 (47.7) | 52 (33.3) |
OR (95% CI) | 1.77 (1.11 to 2.81) | |
P value (1-sided) | 0.008 | |
Proportion of patients with a CR, ITT populationb | ||
n (%) | 57 (37.3) | 40 (25.6) |
OR (95% CI) | 1.69 (1.03 to 2.78) | |
P value (1-sided) | 0.02 | |
Proportion of patients receiving a stem cell transplant, ITT populationb | ||
n (%) | 52 (34) | 39 (25) |
OR (95% CI) | 1.54 (0.92 to 2.56) | |
P value (1-sided) | 0.049 | |
Event-free survival, ITT populationa | ||
Median event-free survival in months (95% CI) | 2.53 (2.07 to 4.99) | 1.31 (1.08 to 1.64) |
HR (95% CI) | 0.74 (0.58 to 0.96) | |
P value (1-sided) | 0.011 | |
Remission duration, ITT populationa | ||
Remission duration in months (95% CI) | 6.93 (4.60 to 9.23) | 6.11 (3.45 to 8.71) |
HR (95% CI) | 0.77 (0.47 to 1.26) | |
P value (1-sided) | 0.147 | |
Harms, n (%), safety population | N = 153 | N = 151 |
Adverse events | 153 (100) | 151 (100) |
Serious adverse events | 90 (59) | 65 (43) |
Withdrawals from study treatment due to AEs | 3 (2) | 2 (1.3) |
Deaths | 106 (69.3) | 128 (84.8) |
Harms of special interest, n (%), safety population | ||
Cardiotoxicity | 0 (0) | 1 (0.7) |
Patients with grade 3 to 5 bleeding events | 18 (12) | 13 (8.6) |
Drug hypersensitivity | 1 (0.7) | 2 (1.3) |
Febrile neutropenia | 107 (70) | 108 (72) |
Sepsis | 14 (9.2) | 11 (7.3) |
Intensive care admission | 28 (18.3) | 38 (25.2) |
Hepatobiliary disorders (any grade) | 11 (7.2) | 7 (4.6) |
Acute renal failure | 12 (7.8) | 15 (9.9) |
7 + 3 = conventional cytarabine and daunorubicin; AE = adverse event; CI = confidence interval; CR = complete remission; CRi = complete remission with incomplete hematologic recovery; HR = hazard ratio; ITT = intention-to-treat; OR = odds ratio.
aStratified log-rank test (test for superiority, 1-sided alpha of 0.025).
bStratified Mantel-Haenszel test (test for superiority, 1-sided alpha of 0.025).
Source: Clinical Study Report for Study 301.8
Critical Appraisal
A dynamic balancing randomization algorithm was used in Study 301 to ensure that the assignment of treatments was balanced across all stratification factors. However, because it was an open-label trial, patients were aware of the treatment allocation following randomization. Therefore, the evaluation of AEs may be biased by treatment knowledge.
Overall, no differences were noted in dropout rates between treatment arms in Study 301. The identified statistical analyses were pre-specified and powered adequately. Many outcomes identified as being significant to patient and clinician groups were reported within the study, and outcomes used were similar to those used in other clinical trials and close to criteria routinely used in practice across Canada. The patient population recruited as representative of high-risk Canadian patients, and the associated response to conventional therapy (7 + 3) in terms of efficacy and safety outcomes was noted by clinical experts to be similar to what is observed in practice. As the trial population recruited only patients who were 60 to 75 years of age, there is uncertainty whether results from Study 301 are generalizable to younger or older patients who may be eligible for treatment with liposomal daunorubicin and cytarabine.
An important limitation of these findings is the lack of an HRQoL assessment. This was identified as an important outcome by the patient and clinician groups who provided input to CADTH for this submission; hence, the effect of liposomal daunorubicin and cytarabine on HRQoL is uncertain. Similarly, measurable residual disease (MRD) was noted to be an informative measure in determining post-transplantation survival; however, because MRD was not captured in Study 301, assessment of the comparative efficacy of liposomal daunorubicin and cytarabine relative to 7 + 3 is not possible for these outcomes.
Indirect Comparisons
No indirect comparison was performed for this review. A feasibility assessment was provided by the sponsor. Using a non-systematic literature review, the sponsor did not identify any studies that would be appropriate to analyze using indirect treatment comparison methods. Studies varied with regard to patient inclusion and exclusion criteria, and treatments provided were non-overlapping. An important limitation of this feasibility assessment is the non-systematic nature of the evidence-identification process, which was not described in sufficient detail to formally assess. As such, there is uncertainty as to whether all appropriate evidence has been identified for indirect comparisons.
Conclusions
Liposomal daunorubicin and cytarabine statistically significantly improved overall survival versus 7 + 3 in a single randomized controlled trial of adult patients with t-AML or AML-MRC. The difference between treatment groups was considered clinically meaningful by the clinical experts consulted by CADTH. Similarly, statistically significant improvements were noted in response rates and EFS. Although the proportion of patients receiving HSCT and the duration of remission in patients with CR or CRi were numerically higher in the liposomal daunorubicin and cytarabine treatment group relative to the 7 + 3 treatment group, the differences were not statistically significant. Adverse events, while frequently reported, were broadly similar across treatment groups, although proportionately higher numbers of SAEs were noted in patients receiving liposomal daunorubicin and cytarabine when compared to patients receiving 7 + 3. Relevant outcomes such as HRQoL were not assessed; hence, the effect of liposomal daunorubicin and cytarabine on HRQoL is uncertain. No direct or indirect evidence from comparisons against other induction regimens used in clinical practice within Canada was identified, and the comparative efficacy and safety of liposomal daunorubicin and cytarabine against other induction regimens such as FLAG-IDA are unknown.
Introduction
Disease Background
Acute myeloid leukemia is a hematologic malignancy associated with clonal expansion of myeloid progenitor cells in the bone marrow and peripheral blood.1 One such subclass of AML is known as AML with myelodysplasia-related changes.2 Another non-primary AML type, therapy-related AML, develops following exposure to cytotoxic chemotherapy or radiation. Estimates of the relative proportion of AML cases attributable to these subtypes varies from 25% of all AML diagnoses9 to 48%.10 Diagnosis of AML is made according to international criteria, such as the WHO classification system,11,12 typically by specialist physicians in hematology or medical oncology using a bone marrow aspirate and biopsy. Risk stratification is also informed by genetic assessment, typically a cytogenetic assessment, although next-generation sequencing (NGS) is an emerging topic of interest.13 The use of NGS is standard of care for risk stratification in some Canadian centres, and the American Society for Transplantation and Cellular Therapy advocates routine NGS for patients potentially eligible for transplant.14
Untreated, AML is fatal within 11 to 20 weeks.15 Patients with AML-MRC or t-AML are considered to have a worse prognosis when compared to patients with other subtypes of AML. In these patient cohorts, treated populations have an estimated median survival of 6 to 12 months,16 although survival can vary significantly based on factors such as genetic risk status, patient age, and patient fitness.5 Diagnoses of AML-MRC and t-AML are more prevalent in elderly populations.4 Patients who are older will more frequently have adverse genetic abnormalities and increased comorbidities that can limit therapeutic options.17 CADTH reviewers estimated the incidence of new AML cases in Canada to be 4.89 per 100,000, based on Statistics Canada data (for patients > 20 years of age),3 as noted in the CADTH Pharmacoeconomic Review Report. In Canada, the estimated median age at diagnosis of AML is 60 years,18 although global estimates place median age estimates for patients with AML-MRC to be 68 years.10
Standards of Therapy
For the purposes of this review, information on treatment of Canadian patients with t-AML or AML-MRC was gathered from Canadian clinicians. The information detailed in the following section is from this feedback.
Adult patients with newly diagnosed t-AML or AML-MRC are typically assessed for eligibility to undergo intensive induction therapy, eligibility for which is based on patient fitness. Patients who are more frail are often deemed ineligible for induction therapy. The panel noted that a precise age threshold is in itself insufficient to determine eligibility, although it is an influential feature of assessing fitness. No universal definition of fitness was noted by the panel. Patients who are too frail to receive induction therapy, or those who may have a personal preference to not receive induction therapy, are often offered alternative treatment strategies, such as azacitidine, low-dose cytarabine, or best supportive care.19
In Canada, adult patients with t-AML or AML-MRC who are fit enough to be treated with induction chemotherapy most frequently receive 7 + 3 treatment.6 This therapy consists of 3 days of daunorubicin or idarubicin, and 7 days of cytarabine by continuous infusion. Alternatively, patients may receive a combination of fludarabine, high-dose cytarabine, granulocyte colony-stimulating factor (G-CSF), and an idarubicin combination regimen known as FLAG-IDA. Induction therapy is provided intravenously in an inpatient setting and requires a skilled interprofessional team to monitor treatment, complications, and recovery. The goal of induction therapy is to achieve a complete response and to remain in remission. A complete response is the prerequisite to move forward with further cycles of consolidation chemotherapy and/or an HSCT.6 For patients not achieving an adequate hematologic response, consideration would be given to salvage therapy (which can include 7 + 3, FLAG-IDA, or similar drugs, de-escalation to less-intensive therapy, or enrolment in a clinical trial).
The primary goal of induction therapy is for the patient to have a disease response that would allow for an HSCT; assessment of complete remission (CR) post-induction is a critical response criterion for this population. The assessment typically occurs between 28 days and 35 days post-induction and includes an assessment of bone marrow and extramedullary disease and a complete blood count.19 Patients achieving CR or CRi may be evaluated further for HSCT eligibility. Patients who do not achieve CR or CRi may be eligible for other salvage therapy with a goal of reaching a treatment response that would allow for HSCT.
The clinical experts consulted by CADTH for this review indicated that MRD status is an emerging area of consideration for this patient population, although assessment methods have not yet been standardized. The panel noted that achievement of an MRD-free state may have significance with regard to survival post-HSCT, although this is an active topic of research. In long-term follow-up post-HSCT, relapse or failure events are most commonly encountered within the first 2 years.
Drug
The study drug, daunorubicin and cytarabine liposome (also known as CPX-351) is a lyophilized liposomal formulation of a fixed-dose combination of cytarabine and daunorubicin in a 5:1 molar ratio. Cytarabine is a cytidine analogue,20 and daunorubicin is an anthracycline antibiotic that intercalates between DNA base pairs.21 Liposomal daunorubicin and cytarabine is administered intravenously and the combination is intended to act as an induction and consolidation agent for patients with t-AML or AML-MRC. Dosing for first induction therapy is daunorubicin 44 mg/m2 and cytarabine 100 mg/m2 on days 1, 3, and 5. Dosing for the second induction is daunorubicin 44 mg/m2 and cytarabine 100 mg/m2 on days 1 and 3. Dosing for consolidation therapy is daunorubicin 29 mg/m2 and cytarabine 65 mg/m2 on day 1 and day 3.22
Liposomal daunorubicin and cytarabine is currently undergoing an expedited review at Health Canada. The requested reimbursement criteria align with the Health Canada indication. Jazz Pharmaceuticals Canada Inc., the sponsor, is requesting reimbursement for the treatment of adults with newly diagnosed t-AML or AML-MRC.23 A description of the key characteristics of commonly recommended drugs for these conditions is provided in Table 3.
Table 3: Key Characteristics of Liposomal Daunorubicin and Cytarabine, 7 + 3, and FLAG-IDA
Characteristic | Liposomal daunorubicin and cytarabine | 7 + 3 | FLAG-IDA |
|---|---|---|---|
Mechanism of action | Cytidine analogue + DNA intercalation | Cytidine analogue + DNA intercalation | Cytidine analogue + white blood cell growth factor + DNA intercalation |
Indicationa | Under consideration | Induction and maintenance of remission in acute leukemia in both adults and children | Induction and maintenance of remission in acute leukemia in both adults and children |
Route of administration | Intravenous | Intravenous | Subcutaneous (filgrastim), IV (cytarabine, idarubicin, fludarabine) |
Recommended dose (first induction) | 100 units/m2 by 90-minute IV infusion on days 1, 3, and 5 | Cytarabine at a dosage of 100 mg/m2/day on days 1 through 7 by continuous infusion, and daunorubicin at a dosage of 60 mg/m2/day on days 1, 2, and 3 | Filgrastim 300 mcg (days 1 to 4) Idarubicin 10 mg/m2 (days 1 to 2) Fludarabine 30 mg/m2 days (1 to 4) |
Serious adverse effects or safety issues | Myelosuppression Hypersensitivity reactions Hemorrhagic events Cardiotoxicity | Myelosuppression Hypersensitivity reactions Hemorrhagic events Cardiotoxicity | Myelosuppression Hypersensitivity reactions Hemorrhagic events Cardiotoxicity |
7 + 3 = conventional cytarabine and daunorubicin; FLAG-IDA = fludarabine + cytarabine + filgrastim + idarubicin.
aHealth Canada–approved indication.
Source: CADTH Reimbursement Review clinical experts, Clinical Study Report for Study 301,8 proposed Vyxeos product monograph,22 cytarabine product monograph,24 daunorubicin product monograph,25 idarubicin product monograph,26 Compendium of Pharmaceuticals and Specialties (electronic version),27 and Cancer Care Ontario.28
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Group(s) and Information Gathered
CADTH received 1 submission from the LLSC for this review. The LLSC’s mission is to cure leukemia, lymphoma, Hodgkin disease and myeloma, as well as improve the quality of life of Canadians affected by all of the 137 different types of blood cancer.
The LLSC gathered the information for this patient group submission through an online survey, available in both English and French, between December 7, 2020, and January 24, 2021. The survey, which was promoted through the group’s social media platforms and by email, asked patients about their experiences with treatments for AML. All of the 29 individuals who responded identified as patients and 5 reported receiving treatment with the drug under review (liposomal daunorubicin and cytarabine). Overall, 18 respondents identified as female, 10 as male, and 1 did not respond. All 29 respondents were living in Canada and from Ontario (n = 13), Quebec (n = 6), British Columbia (n = 6), and Alberta (n = 4). Ages ranged from 25 to 84 years, with 9 younger than 54 years, 9 between 55 years and 64 years, 9 between 65 years and 74 years, and 2 older than 75 years. No breakdown was provided on proportions of patients with AML-MRC or t-AML.
Disease Experience
When asked how AML symptoms affected their daily lives, responses varied, from being unable to exercise or work to impacting their social lives and relationships and causing a number of detrimental effects on their health. Patients reported being easily fatigued, losing vision in 1 eye, nausea, bruising, numbness or body aches, and being immunocompromized. Many of these symptoms left them feeling physically and/or socially isolated and in fear of relapse, leading to negative effects on their psychological well-being.
The following quotes illustrate patients’ experiences of living with AML:
“I no longer do many of the active activities I did before the AML like hiking and biking. I was also forced into early retirement. My dating life is over. I still tire easily.”
“Very straining on relationships. Difficult to make plans and look to the future.”
“Can’t return to work due to still being immunosuppressed post-stem cell transplant….”
“The initial year was absolutely overwhelming, in terms of treatment and expenses.”
Three respondents indicated that exercise and physical activity helped with their fatigue and other symptoms, with 1 reporting that “all of the symptoms are difficult, to be honest, but perhaps for me the easiest over time was recovering my energy. I used exercise.”
When asked how being diagnosed with AML affected the quality of life of their family and friends, respondents noted the additional burden it had, such as needing help with completing daily tasks, being worried about the patient’s health, and being uncertain about the future. One individual responded, “It affects those in your immediate household since they will most probably be your primary caregivers. However, anyone that is close to you will be affected as well.” Another added, “there is an element of fear for me and my family that it will return.” However, patients also described the support they received during their treatment and recovery, with 1 individual reflecting that “they worked hard to support me, visit me in hospital, take me to appointments, arrange food, etc.”
Experiences With Currently Available Treatments
After being diagnosed with AML, patients received the following treatments: chemotherapy (n = 24), stem cell or bone marrow transplant (n = 16), drug therapy (n = 6), radiation therapy (n = 5), and chimeric antigen receptor T-cell therapy (n = 1).
Respondents identified the following as common treatment side effects that had either a large or extremely large impact on their quality of life: hair loss (n = 17), weakness (n = 15), extreme fatigue (n = 14), diarrhea (n = 10), infections (n = 8), anemia (n = 8), mouth sores (n = 8), and nausea and vomiting (n = 7). These AEs affected their physical activity, anxiety, mental health and overall happiness, ability to eat, and social and educational development. Patients described their hardships:
“The Chemo, transplant, radiation and drug therapies are all hard on the body and short term, long term effects are tough as well. The worst part is that these therapies can cause other illnesses.”
“The most difficult experiences I had involved the stem cell transplant and the intensive chemotherapy. I became very ill and was hospitalized for several weeks. I would say that the other difficult experience was being diagnosed with AML and told I had one month to live, without treatment. I had hardly any symptoms and was absolutely shocked. We had to move to another city for treatment, as well.”
Feelings of isolation during hospitalization for stem cell transplants was another common issue among respondents.
When asked to consider positive experiences, many noted the support they received from medical staff, and a few were generally positive about the treatments. One patient described their experience: “Positive: first chemotherapy treatment, the availability of various medicine regimes, bone marrow transplant, and blood transfusions.” Another respondent shared, “Venetoclax treatment was way more tolerable and I was able to be more independent while on it. It got be [sic] into remission quickly and was able to get a transplant within 2 months.”
The LLSC survey asked patients if they faced any challenges with accessing treatments or health care services to which 15 individuals indicated they had generally positive experiences with the hospitals, health care providers, and speed of treatment. Six individuals recalled having negative experiences due to a long referral period with their physician, lack of treatment information, difficulty getting a room for consolidation therapy, having to receive treatment in another city or province, being away from their support system as a result of moving, and a general lack of psychological support.
Improved Outcomes
Patients listed physician recommendation as the most important factor when deciding on new treatments, followed by possible impact on disease, quality of life, closeness to home, and outpatient treatment.
In general, respondents would prefer new therapies that have fewer side effects, are more holistic, will help maintain their remission, are covered through drug plans, and are accessible closer to their home. Patients were also interested in more information on emerging therapies and being able to access all possible treatments in the future.
Experience With the Drug Under Review
Five respondents indicated they had received daunorubicin and cytarabine, although 1 individual did not respond to the rest of the survey questions for this section. One individual had received the medication through a special-access program, 2 stated their treatment was standard or routine while in the hospital, and 1 accessed the drug outside of their home province. Four individuals noted their experience was extremely difficult due to the move and the cost of travel, meals, and accommodations. Patients indicated that they accessed this drug because their doctor had recommended it, while 2 others stated they were unaware of other options. When asked about their experience with daunorubicin and cytarabine, the responses were generally positive: “A few minor setbacks but on the whole treatment was not as bad as I thought it would be” and “Got me into remission quickly.”
At least 1 of the 4 patients rated the following side effects as very serious: cough, rash, nausea, vomiting, mouth or throat sores, constipation, muscle pain, tiredness, breathing difficulties, headaches, decreased appetite, chills, and sleep problems. The patients considered many of the side effects manageable or were those they had not experienced.
When compared to other treatments they had received, 1 individual reported that daunorubicin and cytarabine had improved their quality of life, 2 neither agreed not disagreed, and 1 replied that it had not. One patient believed that treatment with this drug was significantly more challenging, another stated it was more challenging, and 2 were neutral about their experience. One individual reported that the treatment had extended their life, while another stated, “I found vyexos one of the harder chemos I've had.” The survey asked if respondents were willing to tolerate the side effects of daunorubicin and cytarabine, to which patients responded, “Any treatment was better than no treatment,” “It was the only treatment option offered so had no choice,” and “I wanted to live.”
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). In addition, as part of the daunorubicin and cytarabine liposome review, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, help identify and communicate situations with gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion follows.
Description of the Current Treatment Paradigm for the Disease
Currently, adult patients with newly diagnosed t-AML or AML-MRC are typically assessed for eligibility to undergo intensive induction therapy. Induction therapy eligibility is based upon patient fitness, and patients who are more frail are often deemed ineligible for induction therapy. The panel noted that a precise age threshold is in itself insufficient to determine eligibility, although it is an influential feature in assessing fitness. The panel identified no universal definition of fitness. Patients who are too frail to receive induction therapy, or those who may prefer not to receive induction therapy, are often offered alternative treatment strategies, such as azacitidine, low-dose cytarabine, or best supportive care.
In Canada, adult patients with t-AML or AML-MRC who are fit enough to be treated with induction chemotherapy most frequently receive 7 + 3. This therapy consists of 3 days of daunorubicin or idarubicin, and 7 days of cytarabine by continuous infusion. In some jurisdictions, the preferred regimen is a combination of fludarabine, high-dose cytarabine, G-CSF, and FLAG-IDA. Induction therapy is provided intravenously in an inpatient setting and requires a skilled interprofessional team to monitor treatment, complications, and recovery. The goal of induction therapy is to achieve CR and remain in remission. A CR is the prerequisite to move forward with further cycles of consolidation chemotherapy and/or a HSCT. For patients not achieving an adequate hematologic response, consideration would be given to salvage therapy (which could include FLAG-IDA, de-escalation to less-intensive therapy, or enrolment in a clinical trial).
Treatment Goals
The predominant goal of induction therapy is for the patient to achieve an appropriate response, typically CR, to allow for subsequent HSCT, as HSCT is considered a potentially curative option for this patient population, and is associated with improvements in overall survival. Panellists emphasized the importance of HSCT as a therapeutic goal for patients who undergo induction therapy. Eligibility for HSCT is based on response to induction, as assessed via international guidelines, such as the AML working group criteria.29 Physicians use CR or CRi as key indicators to determine HSCT eligibility. An emerging assessment criterion in AML is MRD, although this is not currently used widely in Canada for adult patients with AML, and methods for assessing MRD are currently heterogeneous. Patients are typically assessed for response between 28 and 35 days after initiation of induction. Complete response and achievement of a negative MRD status are both positive factors for subsequent HSCT success and associated overall survival for patients. Patient fitness is typically assessed alongside response to induction. Taken together, the goal of induction therapy is to minimize disease burden while retaining patient fitness for subsequent HSCT.
Unmet Needs
Patients with t-AML or AML-MRC are a high-risk subpopulation when compared to patients with de novo AML. In particular, patients older than 60 years, those with multiple comorbidities, and those deemed to be frail are considered more challenging to treat. Response to induction therapy in this population with current treatment options is suboptimal, resulting in lower HSCT rates when compared to patients with de novo AML. Survival outcomes are poorer for patients with t-AML or AML-MRC post-HSCT when compared to patients with de novo AML. Improving response to induction would therefore facilitate greater proportions of HSCT-eligible patients who could then enjoy the survival benefits this procedure provides. Few approved induction treatments exist for this patient population, and the most predominant therapy in Canada (7 + 3) has been in use for several decades. As a result, treatments that are better tolerated and come with better response to induction therapy are needed for adult patients with t-AML or AML-MRC.
Place in Therapy
The drug combination under review, daunorubicin and cytarabine liposome for injection, is intended to replace 7 + 3 or FLAG-IDA in the first-line induction treatment for this patient population. It acts on the underlying disease process through a mechanism similar to that of existing therapies. The clinical panel did not consider liposomal daunorubicin and cytarabine as an alternative second-line therapy following treatment with existing induction regimens. The panel indicated that, for patients receiving either 7 + 3 or FLAG-IDA who require consolidation, consolidation would generally consist of high-dose cytarabine with or without an anthracycline rather than changing to liposomal daunorubicin and cytarabine. The panel also noted that liposomal daunorubicin and cytarabine typically would not be considered for salvage treatment following induction failures. The administration of liposomal daunorubicin and cytarabine for injection would be in the same inpatient therapeutic setting for induction. Daunorubicin and cytarabine liposome for injection would not be considered a component of combination therapy at present, pending results of ongoing studies combining it with a number of novel agents.
Patient Population
Although age is a significant component in assessing eligibility for overall induction therapy, it was not an exclusive consideration for this process. Patients are assessed holistically for their general fitness using a number of clinician-led assessments in conjunction with patient age. Older patients between the ages of 60 years and 75 years in particular are a challenging subpopulation to treat, although patients younger than this with significant comorbidities or a lack of fitness may also be considered equally poor candidates for induction therapy.
Similar to patients with de novo AML, patients with t-AML or AML-MRC have poor prognosis if untreated, and rapid initiation of treatment is necessary. Diagnosis of t-AML or AML-MRC is straightforward. Timely cytogenetic and molecular assessment was identified as a potential barrier to therapy initiation. Genetic mutations, such as those in TP5330 or FMS-like tyrosine kinase 3 (FLT3) genes,31 are associated with a poorer predicted response to existing therapy and a worse prognosis. Multiple mutations are known in these and other genes relevant to prognosis, and testing requires screening for multiple mutations and mutation sites to assess status. The panel noted that complex interactions of genetic risk markers can create challenges for risk identification and turnaround times for tests. The use of NGS is also emerging as a tool for this patient population, yet turnaround time and harmonization of these methods remain challenges to the immediacy of treatment required in this population.
Mutation status may play a role in determining eligibility to undergo induction therapy. Additionally, some approved therapies, such as midostaurin, are available for patients with known FLT3 mutations. Timely initiation of therapy is critical post-diagnosis. Panellists noted it is possible to defer therapy for up to 5 days without adversely affecting outcomes in patients who are not acutely unwell. In instances where genetic status is not available within this window, it was noted that treatment can be initiated without genetic information. The panel noted that challenges surrounding genetic assessment can influence treatment decisions with existing regimens to the same degree as with daunorubicin-cytarabine liposome for injection.
Panellists noted that, although the principal trial population was older (60 to 75 years of age), they would not preclude patients outside of this age range for treatment with daunorubicin-cytarabine liposome. Younger patients with t-AML or AML-MRC treated with the drug combination under review are expected to respond similarly to older patients. The panel noted that, outside of general fitness and the genetic profile, limited data are available regarding specific prognostic or predictive factors for response to therapy. It was noted that most centres have similar, albeit unique, criteria for assessing HSCT eligibility. Liposomal daunorubicin and cytarabine was noted to be unlikely to expand the criteria for those eligible for induction therapy; patients who are fit enough for induction with existing regimens (7 + 3 or FLAG-IDA) would be equally eligible for liposomal daunorubicin and cytarabine treatment, but patients who are unfit for the traditional induction therapies would not be considered fit for liposomal daunorubicin and cytarabine.
Some patients with antecedent myelodysplastic syndrome before their AML-MRC diagnosis may have received therapy for this condition with HMAs. It was determined that prior treatment or lack of prior treatment with these drugs would not significantly influence the decision to treat with daunorubicin and cytarabine liposome.
Assessing Response to Treatment
The panel noted that the primary goal of induction therapy is for the patient to have a disease response that would allow for an HSCT; assessment of CR post-induction is a critical response criterion for this population. The assessment typically occurs between 28 and 35 days post-induction and includes an assessment of bone marrow, extramedullary disease, and a complete blood count. Patients achieving CR or CRi may be evaluated further for HSCT eligibility. Patients who do not achieve CR or CRi may be eligible for another salvage therapy, with a goal of reaching a treatment response that would allow for HSCT.
MRD status is an emerging area of consideration for this patient population, although assessment methods have yet to be standardized. The panel noted that achievement of an MRD-free state may have significance with regard to survival post-HSCT, although this is an active topic of research. For long-term follow-up post-HSCT, it was noted that relapse or failure events are most commonly encountered within the first 2 years.
Alongside improving overall survival and proportions of patients receiving HSCT, a key treatment goal is the improvement of patient HRQoL. No specific standardized and validated tool to assess HRQoL exists for this patient population. Instead, assessment of patient daily activities (e.g., ability to return to work), infection burden, and transfusion independence form part of this assessment.
Discontinuing Treatment
Treatment discontinuation is considered within the context of a lack of response following induction and consolidation, as well as due to toxicity of available therapies.
Prescribing Conditions
Patients within this population are typically cared for by a multidisciplinary team within larger hospital settings. Diagnosis is dependent on the input of hematopathologists to review bone marrow aspiration and biopsies, as well as input from laboratory specialties such as cytogenetics and molecular diagnostics. Administration of induction therapies, including liposomal daunorubicin and cytarabine for injection, is conducted under inpatient settings with close monitoring by specialists during and after infusion. Support from transfusion specialists may be required depending on patient status post-induction. The panel noted that consolidation therapy may be administered in less-stringent settings, such as an outpatient context, but these practices vary across Canada, depending on local capacity. Daunorubicin and cytarabine liposome for injection was described as stable only for short periods once a vial is prepared for patient infusion, necessitating close involvement of specialty pharmacy professionals.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Two clinician groups provided input on the reimbursement review of daunorubicin and cytarabine (Vyxeos) for the treatment of adults with newly diagnosed t-AML or AML-MRC.
The OH-CCO DAC provides evidence-based clinical and health-system guidance on drug-related issues in support of OH-CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. The input provided by OH-CCO DAC was discussed jointly at a DAC meeting.
The CLSG is a cross-Canada collective of physicians treating acute leukemia who are representative of physicians at all major leukemia centres in all provinces. The CLSG has noted its purpose is “to improve the diagnosis and treatment of leukemia in Canada, by identifying diagnosis and management best practices, promoting Canada-wide standards of care, fostering clinical and basic leukemia research, and improving new drug access.” The CLSG opinions gathered for this reimbursement review were through ongoing group discussions and polling of members, with input requested from other international experts as appropriate. The opinions from the CLSG members were then reviewed, edited, and approved by the full group.
Unmet Needs
The DAC noted that conventional 3 + 7 and FLAG-IDA are the current treatment options for these patients. In addition, the CLSG noted that both t-AML and AML associated with myelodysplastic syndrome (MDS) are broadly categorized as secondary AML and are associated with a poor prognosis. The CLSG added that there is no single standard of care for patients with secondary AML, and in younger adults (generally those younger than 75 years with acceptable performance status and minimal comorbidities), induction chemotherapy is used, with traditional 3 + 7. The CLSG also added that response rates are lower in this group than in de novo AML.
For patients who achieve remission with 3 + 7, the CLSG noted that consolidated with allogeneic stem cell transplantation (alloSCT) is considered with curative intent. For patients who are not candidates for induction therapy, or those who elect for a less-intensive treatment strategy given the toxicities and risks of 3 + 7 with relatively poor outcomes, the CLSG noted that azacitidine is often used. However, the CLSG also noted that, in this case, the aim of treatment with azacitidine is not curative but rather disease control, lessening symptom burden, and extending overall survival, and that evidence to support the use of an azacitidine strategy is minimal (subgroup analysis of other trials).
The most important treatment goals noted by OH-CCO DAC for this patient population were to prolong life, delay disease progression, improve quality of life, attain CR, and get patients to alloSCT. The CLSG added that the inclusion criterion for the clinical trial was adults younger than 75 years with minimal comorbidities, with traditional 3 + 7 used as a control arm. Therefore, CLSG concluded that the aim of the therapy under review would be the achievement of CR (defined as clearance of immature myeloblasts to less than 5% in the bone marrow with restoration of normal blood counts). Curative treatment intent would be for patients with CR after induction chemotherapy and those eligible for alloSCT. The CLSG noted that improvement in CR rates and higher rates of alloSCT would be expected to produce an improvement in overall survival. The CLSG added that the CR rate and rate of alloSCT are important end points for this patient population.
The CLSG noted that the only currently available treatments for this population are traditional induction chemotherapy (7 + 3) and azacitidine. The CLSG added that evidence supporting the use of these treatments in this population is lacking, and the available data suggest that response rates are lower and relapse rates are higher in this patient population than they are in patients with de novo AML. The DAC noted that this treatment improves outcomes in higher-risk patients (those with secondary AML or AML-MRC).
Both clinician groups agreed that patients with the greatest unmet need for intervention with daunorubicin and cytarabine are higher-risk patients (those with secondary AML or AML-MRC). The CLSG noted that secondary AML, by definition, is a subpopulation of AML patients (those with a history of MDS, MDS-related cytogenetic abnormalities, or AML with previous chemotherapy or radiation therapy for a previous malignancy). Secondary AML patients were described by the CLSG as patients with a clearly inferior prognosis, and in need of new therapies.
Place in Therapy
The OH-CCO DAC noted that the daunorubicin and cytarabine combination would replace conventional 7 + 3 and subsequent consolidation cycles. The group added that, although it has not been directly compared to FLAG-IDA, the combination may also replace FLAG-IDA in some cases. The CLSG added that the combination of daunorubicin and cytarabine would become the new first-line therapy for patients with secondary AML who are fit for intensive chemotherapy (usually under age 75 with minimal comorbidities and acceptable performance status). The CLSG added that daunorubicin and cytarabine would not be used in combination with other treatments, would be the first approved and available therapy for this high-risk population, and would result in a shift in the treatment paradigm.
Both clinician groups agreed that it would not be appropriate for patients to try other treatments before initiating treatment with daunorubicin and cytarabine, as the clinical trial study was designed for newly diagnosed AML patients.
For sequencing, the DAC noted that daunorubicin and cytarabine will replace currently available treatments in this population. The CLSG noted that, if the treatment fails, patients could potentially receive azacitidine treatment; however, it added that evidence for this situation is lacking. The CLSG indicated that gilteritinib may be an option for patients with an FLT3 mutation.
Patient Population
Both clinician groups agreed that, although the pivotal trial included older patients aged 60 to 75 years, the clinicians would not exclude younger patients who would otherwise meet eligibility criteria and in whom it would be reasonable to use daunorubicin and cytarabine. The CLSG added that the standard of care for populations younger than 60 years is the same as the standard used for the clinical trial (3 + 7 induction) which was shown to be inferior to daunorubicin and cytarabine.
The DAC noted that patients best suited for treatment should be identified by a clinical history and bone marrow biopsy. The CLSG anticipated no issues in identifying patients who will benefit the most as recognizing who will be eligible is straightforward. The CLSG added that misdiagnosis is unlikely to occur, given the concrete nature of the diagnosis.
The DAC noted that patients who are not candidates for induction treatment would be least suitable for treatment with daunorubicin and cytarabine. The CLSG pointed out that patients who do not have secondary AML should not receive this therapy and, although they would expect patients under 60 years of age with secondary AML to benefit, they were not specifically included in the trial.
Both clinician groups agreed that there was no predictive marker to identify patients who are most likely to exhibit a response to treatment and that all subgroups in the trial appeared to benefit. The CLSG advocated that all patients with secondary AML be considered candidates for daunorubicin and cytarabine.
Assessing Response to Treatment
A bone marrow aspirate to establish remission status was identified by OH-CCO DAC as an indicator of whether a patient is responding to treatment in clinical practice. The CLSG added that both the CR rate and rate of alloSCT are end points commonly used in clinical practice and as such align with outcomes in the trial. The CLSG noted that blood counts should be monitored frequently, particularly during the initial treatment cycle, and that indicators of response include improvement in blood counts, achievement of CR (less than 5% blasts in a cellular marrow), and transfusion independence.
Both clinician groups agreed that a meaningful response to treatment would be achieving CR. The CLSG added that the ability to proceed to potentially curative alloSCT, and as a result, a prolonging of overall survival and EFS, would be a goal of treatment. The CLSG indicated that the end points were all clear and would not vary by physician or jurisdiction.
OH-CCO DAC noted that, in the pivotal trial, day 14 bone marrow assessments were conducted to determine if additional doses of daunorubicin and cytarabine liposome are needed. The CLSG added that a bone marrow aspirate should be completed after count recovery from induction to determine remission status.
Discontinuing Treatment
OH-CCO DAC noted that treatment discontinuation should be based on the bone marrow result. The CLSG indicated that patients who do not achieve remission after induction chemotherapy would be ineligible for further treatment. The CLSG added that the study allowed for a second cycle of induction for those who had persistent disease at day 14 of treatment and that, while practice across Canada varies in this regard and many centres do not routinely perform a day 14 bone marrow aspirate, it is reasonable to consider a second cycle that follows the protocol. The CLSG felt that patients who achieve remission but then experience progression or a relapse during consolidation should not receive further therapy with daunorubicin and cytarabine. The group added that cytopenias are expected with this treatment and are not a reason to discontinue therapy.
Prescribing Conditions
Both clinician groups agreed that, because induction chemotherapy for AML is completed in hospital, inpatient administration would be needed due to high rates of complications, such as febrile neutropenia, mucositis, and substantial transfusion requirements. The CLSG noted that specialized hematology and/or leukemia clinics, either community-based or at academic centres, are appropriate settings and that treatment should be administered and supervised by a hematologist with expertise in managing acute leukemia patients and with experience in the use of these drugs. The OH-CCO’s DAC added that consolidation can be given in an outpatient setting if the centre has outpatient consolidation infrastructure in place.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert responses |
|---|---|
How does daunorubicin-cytarabine liposome for injection (Vyxeos) compare to FLAG-IDA? | The clinical experts noted that no evidence provided in the current materials provided evidence on this comparison. Anecdotally, it was noted that FLAG-IDA is considered to have a similar efficacy profile as 7 + 3 for some patients, although this is not a formal comparison from which comparative efficacy estimates can be made. |
Is cytarabine consolidation currently considered the standard of care? | The clinical experts indicated that typically, consolidation therapy typically consists of the same therapeutic regimen (in an alternative dose or schedule) used for induction. For example, 7 days of cytarabine and 3 days of daunorubicin induction would be followed by 5 days of cytarabine and 2 days of daunorubicin consolidation if indicated. High-dose cytarabine may also be considered within this context, and several approaches exist to administer high-dose cytarabine consolidation. |
How does daunorubicin-cytarabine liposome for injection (Vyxeos) compare to high-dose cytarabine consolidation? | The clinical experts indicated that the current data do not allow for an isolated comparison of this question. Patients within the trial were treated separately for induction and consolidation, and therefore determining how each performs in isolation for consolidation is currently not possible. |
Patients who are not eligible for intensive induction chemotherapy like 7 + 3 may receive azacitidine. How does azacitidine compare with daunorubicin and cytarabine liposome? | The clinical experts indicated that azacytidine with or without venetoclax is reserved for patients who are not candidates for induction therapy, and patients who are treated with azacitidine with or without venetoclax are different from those treated with 7 + 3, FLAG-IDA, or liposomal daunorubicin and cytarabine. |
What definition of t-AML or AML-MRC should be used to assist with implementation criteria? Patients were enrolled in the pivotal study (Study 301) if they met the following inclusion criteria:
| The clinical experts indicated that the criteria were representative of patients identified in practice, although it was highlighted that 1 criterion, 50% dysplasia in 2 or more lineages in de novo AML, can be used to identify a patient as having AML-MRC. Patients meeting this criterion, which was not specified, are not necessarily considered to be unique with respect to risk when compared to other patients with AML-MRC. |
In Study 301, patients were eligible to receive up to 2 cycles of consolidation. Are there any clinical scenarios where more than 2 cycles of consolidation are considered? | The clinical experts noted that more than 2 cycles of consolidation would be very rare. One hypothetical scenario identified was that of a patient who had completed their induction, but for operational reasons had a delay in receiving HSCT. |
In addition to the inclusion criteria mentioned above, patients had to be 60 to 75 years of age at the time of diagnosis of AML, and with ECOG performance status between 0 and 2. Would you treat patients with daunorubicin-cytarabine liposome for injection (Vyxeos)
| The clinical experts had the following responses to the following patient groups:
|
Do you expect that daunorubicin-cytarabine liposome for injection (Vyxeos) will be used off-label, for example, in patients with other AML subtypes and other lines of therapy? | The clinical experts noted it was unlikely that liposomal daunorubicin and cytarabine would be used in other AML subtypes. Receiving liposomal daunorubicin and cytarabine in another line of therapy was considered very unlikely. |
Would patients who are currently on 7 + 3 or FLAG-IDA be switched over to daunorubicin-cytarabine liposome (Vyxeos)? If this switch can happen, is there a cut-off point at which the switch can occur (e.g., can the switch in treatment be applied if the patient is already on consolidation?) | The clinical experts noted that this switch is unlikely in the majority of cases. For a small number of patients this may be relevant during the window for which compassionate-use ends and approval (if provided) is given. No specific cut-off point was identified. |
Is vial sharing feasible? Do you expect drug wastage? | The clinical experts noted that vial sharing was not considered possible, given that the half-life of the mixed product is short. In terms of operational characteristics, patients are typically seen and treated 1 at a time (as opposed to many patients being treated simultaneously in a clinic-style setting). As such, vial sharing is not considered feasible. |
7 + 3 = conventional cytarabine and daunorubicin; AML = acute myeloid leukemia; AML-MRC = acute myeloid leukemia with myelodysplasia-related changes; CNS = central nervous system; ECOG = Eastern Cooperative Oncology Group; FLAG-IDA = fludarabine + cytarabine + filgrastim + idarubicin; HSCT = hematopoietic stem cell transplant; MDS = myelodysplastic disorder; MPN = myeloproliferative neoplasms; t-AML = therapy-related acute myeloid leukemia.
Clinical Evidence
The clinical evidence included in the review of liposomal daunorubicin and cytarabine is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes an assessment of a feasibility assessment provided by the sponsor.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of daunorubicin and cytarabine liposome for injection (44 mg daunorubicin and 100 mg cytarabine per vial) administered intravenously for the treatment of adults with newly diagnosed t-AML or AML-MRC.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflected outcomes considered important to patients, clinicians, and drug plans.
The systematic review protocol was established before the granting of a Notice of Compliance from Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults with newly diagnosed t-AML or AML-MRC Subgroups:
|
Intervention | Daunorubicin and cytarabine liposome for injection administered intravenously Induction: daunorubicin 44 mg/m2 and cytarabine 100 mg/m2 administered intravenously over 90 minutes on days 1, 3, and 5 as the first course of induction therapy and on days 1 and 3 as the subsequent course of induction therapy, if needed (a subsequent cycle of induction may be administered 2 to 5 weeks after the first in patients who do not achieve remission and show no unacceptable toxicity) The first consolidation: 5 to 8 weeks after the start of the last induction; consolidation consists of daunorubicin 29 mg/m2 and cytarabine 65 mg/m2 administered intravenously over 90 minutes on days 1 and 3 as subsequent courses of consolidation therapy, if needed |
Comparator | 7 + 3 induction (3 days of daunorubicin or idarubicin and 7 days of cytarabine by continuous infusion) Combination of fludarabine, high-dose cytarabine, granulocyte colony-stimulating factor, and idarubicin combination regimen (FLAG-IDA) 7 + 3 combination + midostaurin |
Outcomes | Efficacy outcomes
Harms outcomes
Notable harms/harms of special interest
|
Study designs | Published phase III and IV randomized controlled trials |
7 + 3 = conventional cytarabine and daunorubicin; AE = adverse event; AML = acute myeloid leukemia; AML-MRC = acute myeloid leukemia with myelodysplasia-related changes; FLAG-IDA = fludarabine-cytarabine-filgrastim-idarubicin; MDS = myelodysplastic disorder; MPN = myeloproliferative neoplasms; PS = performance status; SAE = serious adverse event; t-AML = therapy-related acute myeloid leukemia; WDAE = withdrawal due to adverse event.
The literature search was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were acute myeloid leukemia and Vyxeos. Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
Search filters were applied to limit retrieval to randomized controlled trials or controlled clinical trials. Retrieval was not limited by publication date or by language. Where possible, retrieval was limited to the human population. Conference abstracts were excluded from the search results. Appendix 1 provides detailed search strategies.
The initial search was completed on February 22, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on June 10, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist. Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
In addition, the manufacturer of the drug was contacted for information regarding unpublished studies. Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
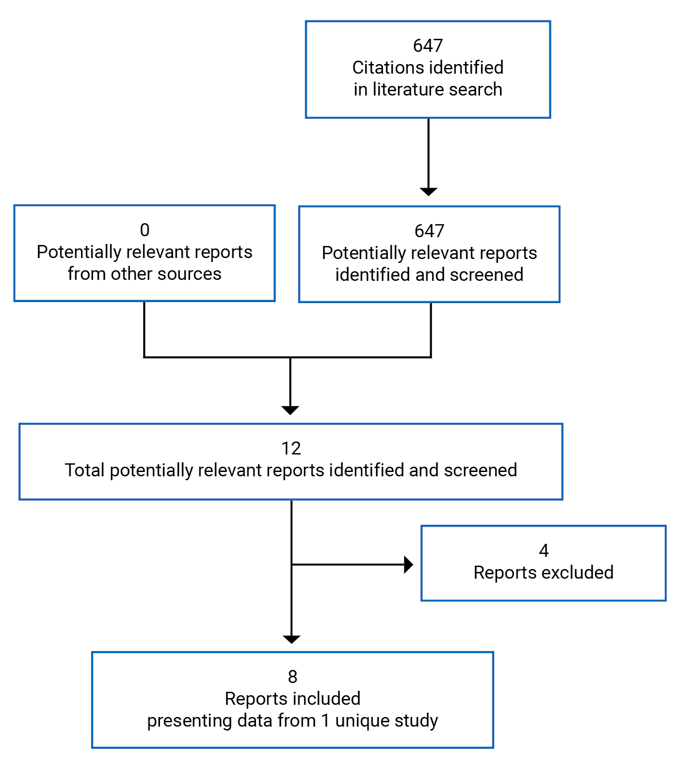
Findings From the Literature
One study was identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 2.
Detail | Description |
|---|---|
Designs and populations | |
Study design | Phase III, multi-centre, randomized, open-label, therapy-controlled trial |
Locations | 39 centres: 4 in Canada and 35 in the US |
Patient enrolment dates: | December 13, 2012 (first patient enrolled) December 31, 2015 (last patient completed primary end point) |
Randomized (N) | 309 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention |
|
Comparator(s) |
|
Duration | |
Phase | |
| 5 to 32 weeks |
| Up to 60 months after randomization |
Outcomes | |
Primary end point | Overall survival, measured from the date of randomization to death from any cause; patients not known to have died by the last follow-up were censored on the date they were last known to be alive; analysis was planned upon 236 observed events |
Secondary and exploratory end points | Secondary
|
Notes | |
Publications | Lancet et al. (2018)32 |
7 + 3 = conventional cytarabine and daunorubicin; AML = acute myeloid leukemia; CMMoL = chronic myelomonocytic leukemia; CPX-351 = liposomal daunorubicin and cytarabine in a fixed 5:1 molar ratio; CR = complete remission; CRi = complete remission with incomplete hematologic recovery; HSCT = hematopoietic stem cell transplantation; MDS = myelodysplastic syndrome; MPN = myeloproliferative neoplasm; t-AML = therapy-related acute myeloid leukemia.
Source: Lancet et al. (2018)32 and Clinical Study Report for Study 301.8
Description of Study
Study 301
Study 301 was a phase III randomized controlled, multi-centre, open-label, therapy-controlled clinical trial. In total, 301 patients were recruited across 39 centres, with 4 sites based in Canada. Patients were randomly assigned to be treated with either liposomal daunorubicin and cytarabine or 7 + 3, with stratification for age (age 60 to 69 years or age 70 to 75 years) and AML type (t-AML, MDS transformed to AML with prior HMA treatment, MDS transformed to AML without prior HMA treatment, chronic myelomonocytic leukemia [CMMoL] transformed to AML, and de novo AML with an MDS karyotype). Recruitment was initiated on December 13, 2012, and database lock occurred on December 31, 2015. One interim analysis was conducted upon full enrolment to review 60-day mortality to determine whether the study should continue if death rates were elevated, but a recommendation was not made to discontinue the study. Follow-ups for patients were planned for 5 years.
Populations
Inclusion and Exclusion Criteria
Study 301 recruited patients aged 60 years to 75 years with secondary AML of multiple subtypes. AML was defined according to WHO criteria, and the included subtypes were t-AML, MDS, CMMoL, or de novo AML with fluorescence in situ hybridization or cytogenetic changes linked to MDS. Patients were excluded if they had favourable cytogenetic features, or prior induction therapy for AML. A full list of inclusion and exclusion criteria is provided in Table 6.
Baseline Characteristics
A summary of patient baseline characteristics is provided in Table 7 for patients in the primary analysis (ITT) population. Patients enrolled in Study 301 had a mean age of 67.7 years and were predominantly male (61%); the most common AML subtype was AML-MRC. Most patients had unfavourable cytogenetic risk factors, with 39% of patients having an intermediate cytogenetic risk and 50% of patients were classified as unfavourable risk.
Patients were well matched with regards to stratification factors (age and AML subtype) and most other demographic features. There were minor differences in Eastern Cooperative Oncology Group (ECOG) performance status, with a higher proportion of patients with an ECOG performance status of 2 (worse performance) in the group receiving 7 + 3 compared to those receiving liposomal daunorubicin and cytarabine, although the reverse was true for an ECOG performance status of 0, with greater proportions identified in the 7 + 3 population. Distributions of specific genetic risk factors were well distributed between treatment arms. Associated peer-review publications noted that a greater proportion of patients who received 7 + 3 had an unfavourable cytogenetic risk (56.8%) when compared to those treated with liposomal daunorubicin and cytarabine.32 Overall, patients represented a high-risk population (as noted in the Clinician Input section) of secondary AML.
Table 7: Summary of Baseline Characteristics, ITT Population
Characteristic | Study 301 | |
|---|---|---|
Liposomal daunorubicin and cytarabine (N = 153) | 7 + 3 (N = 156) | |
Age (mean) | 67.8 | 67.7 |
60 to 69 years, n (%) | 96 (63) | 102 (65) |
70 to 75 years, n (%) | 57 (37) | 54 (35) |
Sex, n (%) | ||
Male | 94 (61) | 96 (62) |
Female | 59 (39) | 60 (38) |
Race, n (%) | ||
American Indian or Alaska Native | 1 (0.7) | 0 |
Asian | 6 (3.9) | 2 (1.3) |
Black or African American | 7 (4.6) | 6 (3.8) |
White | 128 (84) | 139 (89) |
Other | 11 (7.2) | 8 (5.1) |
Multiple | 0 | 1 (0.6) |
Weight (kg), median | 82.0 | 82.7 |
Height (cm), median | 170.2 | 170.2 |
Body surface areas (m2), median | 2.0 | 2.0 |
ECOG PS, n (%) | ||
0 | 37 (24) | 45 (29) |
1 | 101 (66) | 89 (57) |
2 | 15 (9.8) | 22 (14) |
≥ 3 | 0 | 0 |
Extramedullary disease, n (%) | 5 (3.3) | 5 (3.2) |
AML subtype, n (%) | ||
CMMoL | 11 (7.2) | 12 (7.7) |
de novo | 41 (27) | 37 (24) |
MDS with prior HMA | 50 (33) | 55 (35) |
MDS without prior HMA | 21 (14) | 19 (12) |
t-AML | 30 (20) | 33 (21) |
Genetic mutations, n (%) | ||
FLT3 | 22 (14.4) | 21 (13.5) |
NPM1 | 13 (8.5) | 12 (7.7) |
CEBPA | 12 (7.8) | 5 (3.2) |
7 + 3 = conventional cytarabine and daunorubicin; AML = acute myeloid leukemia; AML-MRC = acute myeloid leukemia with myelodysplasia-related changes; CEBPA = CCAAT/enhancer binding protein alpha; CMMoL = chronic myelomonocytic leukemia; CPX-351 = liposomal daunorubicin and cytarabine; ECOG = Eastern Cooperative Oncology Group; FLT3 = FMS-like tyrosine kinase 3; HMA = hypomethylating agent; MDS = myelodysplastic disorder; MPN = myeloproliferative neoplasms; NPM1 = nucleophosmin 1; PS = performance status; t-AML = therapy-related acute myeloid leukemia.
Source: Clinical Study Report for Study 301.8
Interventions
In Study 301, patients received either liposomal daunorubicin and cytarabine or 7 + 3.
Liposomal daunorubicin and cytarabine is a fixed combination of cytarabine and daunorubicin in a 5:1 molar ratio. Liposomal daunorubicin and cytarabine was provided as a sterile, pyrogen-free lyophilized formulation in single-use 50 mL glass vials. Each vial contained 100 units of liposomal daunorubicin and cytarabine, with each unit containing 1 mg cytarabine and 0.44 mg daunorubicin base in liposomes. After the appropriate number of vials was reconstituted, liposomal daunorubicin and cytarabine was then diluted in approximately 500 mL of either 0.9% sodium chloride injection or 5% dextrose injection.
Doses of 7 + 3 were administered via intravenous infusion, according to institutional guidelines. Cytarabine (100 mg/m2/day) was administered as a 7-day (for first induction) or 5-day (for second induction or consolidations) continuous intravenous infusion. Daunorubicin (60 mg/m2/day) was administered on days 1, 2, and 3 (for first induction) or days 1 and 2 (for second induction or consolidations) via intravenous (push) infusion of 15 minutes duration.
Dosing varied with both treatments, depending on whether they were used as a first induction, a second induction or as consolidation therapy according to the following dosing schedules.
For the first induction: Liposomal daunorubicin and cytarabine was administered at 100 units/m2 by 90-minute intravenous infusion on days 1, 3, 5.
The 7 + 3 control arm was administered as: cytarabine at a dosage of 100 mg/m2/day on days 1 through 7 by continuous infusion, and daunorubicin at a dosage of 60 mg/m2/day on days 1, 2, and 3.
If a second induction was administered: Liposomal daunorubicin and cytarabine was administered at 100 units/m2 by 90-minute intravenous infusion on days 1 and 3.
The 5 + 2 control arm was administered as: cytarabine at a dosage of 100 mg/m2/day on days 1 through 5 by continuous infusion and daunorubicin at a dosage of 60 mg/m2/day on days 1 and 2.
For consolidation therapy: Liposomal daunorubicin and cytarabine were administered at 65 units/m2 by 90-minute intravenous infusion on days 1 and 3.
The 5 + 2 control arm was administered as: cytarabine at a dosage of 100 mg/m2/day on days 1 through 5 by continuous infusion, and daunorubicin at a dosage of 60 mg/m2/day on days 1 and 2.
The trial was conducted in an open-label manner, as the colour of the reconstituted liposomal daunorubicin and cytarabine product and the differences between the dosing schedules of the treatment regimens rendered blinding impossible.
Concomitant medications were used by all participants within the study. The top 5 medication classes as concomitant medications in the safety analysis population were serotonin (5HT3) antagonists (142 patients [92.8%] in the liposomal daunorubicin and cytarabine treatment group, 136 patients [90.1%] in the 7 + 3 treatment group), triazole derivatives (132 patients [86.3%] in the liposomal daunorubicin and cytarabine treatment group and 125 patients [82.8%] in the 7 + 3 treatment group), glucocorticoids (127 patients [83.0%] in the liposomal daunorubicin and cytarabine treatment group and 128 patients [84.8%] in the 7 + 3 treatment group), nucleosides and nucleotides (excluding reverse transcriptase inhibitors) (127 patients [83.0%) in the liposomal daunorubicin and cytarabine treatment group and 126 patients [83.4%] in the 7 + 3 treatment group), and benzodiazepine derivatives (120 patients [78.4%] in the liposomal daunorubicin and cytarabine treatment group and 114 patients [75.5%] in the 7 + 3 treatment group).
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 8. These end points are further summarized in the following section.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | Study 301 |
|---|---|
Overall survival | Primary: Overall survival was measured from the date of randomization to death from any cause; patients not known to have died by the last follow-up were censored on the date they were last known to be alive |
Event-free survival | Secondary: Event-free survival was defined as the time from study randomization to the date of induction treatment failure (persistent disease), relapse from CR or CRi, or death from any cause, whichever came first; patients alive and not known to have any of these events were censored on the date they were last examined on study (i.e., patients who stopped receiving study-defined treatments and may have gone onto HSCT or salvage treatment) |
Complete remission | Secondary: Defined as bone marrow blasts < 5%; absence of blasts with Auer rods; absence of extramedullary disease; ANC > 1.0 × 109/L (1,000/μL); platelet count > 100 × 109/L (100,000/μL); independence from red cell transfusions |
Complete remission with incomplete hematologic response | Secondary: Defined using all the CR criteria except for residual neutropenia (< 1.0 × 109/L [1000/μL]) or thrombocytopenia (< 100 × 109/L [100,000/μL]) |
Best response | Secondary: Patients who complete the induction(s) with a response of CRi may be upgraded to a CR during or after consolidation if the patient’s peripheral blood counts meet the criteria for CR after declaration of a CRi; to upgrade a response to CR both peripheral blood and bone marrow assessment were not required on the same day but must have been obtained within a 14-day period of each other and all criteria for CR must have been met (within a 14-day period, must have had full recovery of peripheral blood counts, and have been leukemia-free) |
Treatment failure (used for remission duration and response) | For use in remission duration and response
|
Remission duration | Secondary (for patients with CR or CRi): Remission duration was measured from the date of achievement of a remission (CR/CRi) until the date of relapse or death from any cause; patients who did not relapse or die at last follow-up were censored on the date they were last examined; for patients, whose best response was upgraded from CRi to CR, the remission duration for CR + CRi analyses was calculated from the date of CRi to the date of relapse or death |
Stem cell transplant | Secondary: the number and percentage of patients transferred for HSCT after induction treatment was recorded |
Adverse events | Adverse events were defined according to Medical Dictionary for Regulatory Activities coding |
ANC = absolute neutrophil count; CR = complete remission; CRi = complete remission with incomplete hematologic response; HSCT = hematopoietic stem cell transplantation.
Source: Clinical Study Report for Study 301.8
Statistical Analysis
Overall Survival (Primary Outcome)
Power Calculation and Analysis
Study 301 was designed to enrol 300 participants, with a minimum of 270 patients planned for the primary end-point analysis based on a presumed consent withdrawal rate of 10%. The study power calculation was based on an assumption of exponential survival, a median survival of 0.526 years in the 7 + 3 treatment arm and 236 deaths (events) being required for final study analysis. Patient recruitment was considered to be uniform at 135 patients per year, with a total accrual period of 2 years and an additional follow-up of 1.2 years. Under these assumptions, the study would have a 93.7% power with a 1-sided alpha of 0.025 to detect an HR of 0.635 between 2 treatment groups. Effect-size assumptions are based on data from a phase II trial (Study 204). This primary analysis population formed the data submitted to CADTH for this review.
An interim analysis was planned and conducted upon full trial enrolment, to determine whether 60-day death rates were substantially higher in patients who received liposomal daunorubicin and cytarabine when compared to those who received 7 + 3. No type I error adjustment was made based on this interim analysis. This was due to the fact that a recommendation to cease the study based on this analysis would not imply rejection of the null hypothesis. No formal rules for the interim analysis with regard to specified stopping rules were reported.
The primary analysis was conducted in the ITT population, regardless of the actual treatment received. Comparative efficacy was assessed by a stratified log-rank test.33 Stratification factors included age (60 to 69 years or 70 to 75 years) and AML type (t-AML, MDS transformed to AML with prior HMA treatment, MDS transformed to AML without prior HMA treatment, CMMoL transformed to AML, and de novo AML with an MDS karyotype). The distribution of survival per arm was estimated using the Kaplan-Meier estimation.
A Cox proportional hazard regression analysis, stratified by age and AML type, was performed for prognostic associations with overall survival. Univariate Cox regression analyses were performed for the treatment arm alongside selected prognostic factors. The prognostic factors entered into this regression analysis were not pre-specified.
Imputation rules were used for overall survival analyses. If only the death year was known, and the last date the patient was alive was known, the patient’s last alive date was used as the death date. If the last alive date occurred in a previous year, the missing month and day were imputed as the first day and month of the year. If the year and month were known and the last alive date was in the same year and month as the death date, then the last alive date was used. If the last alive date was in a month before the death month, then the death day was imputed as the first day of the month.
Secondary Outcome Power Calculations and Analysis
Power calculations were provided for 2 secondary efficacy end points.
For EFS, sample size was based on data from a previous study (Study 204). In this study, the observed HR for EFS of the liposomal daunorubicin and cytarabine arm versus the 7 + 3 arm was 0.35 in the patient population with secondary AML. The observed median EFS in the 7 + 3 arm was 42 days. Using the 270 patients planned for Study 301 over a period of 2 years with a 1.2-year follow-up resulted in a greater than 99.9% power and a 1-sided alpha significance level of 0.025 to detect an HR of 0.35 between arms. These calculations assumed that the events were exponentially distributed.
Values for EFS and remission duration were analyzed in the same manner as those for overall survival.
For observed response rate (CR + CRi), data were from a phase II study (Study 204) in secondary AML patients. In this study, response was approximately 74% in the liposomal daunorubicin arm and 42% in the 7 + 3 arm. Using the 270 patients planned for Study 301 provided an estimated 99.99% power and a 1-sided alpha significance level of 0.025 to detect an absolute improvement of 32% in the liposomal daunorubicin and cytarabine arm. These calculations assumed that the responses were binomially distributed and that the response rate in the control arm (7 + 3) was 42%.
Analysis of response rate differences between arms were assessed using the Mantel-Haenszel test, with stratifications for age (60 to 69 years or 70 to 75 years) and AML type (t-AML, MDS transformed to AML with prior HMA treatment, MDS transformed to AML without prior HMA treatment, CMMoL transformed to AML, and de novo AML with an MDS karyotype).
Analysis of HSCT rates were performed following the analytical strategy defined by response rate.
A hierarchical testing procedure was implemented for testing the secondary end points of CR and CR + CRi to control type I error at 0.025 in the following order.
If the 1-sided P value is less than or equal to 0.025 for overall survival, then reject the null hypothesis and proceed to test CR.
If the 1-sided P value is less than or equal to 0.025 for CR, then reject the null hypothesis and proceed to test CR + CRi.
If the 1-sided P value is less than or equal to 0.025, reject the null hypothesis. Otherwise, the null hypothesis of best CR + CRi was not rejected.
Other outcomes were not adjusted for multiple statistical testing. No information on statistical analyses for a planned interim analysis were identified. Subgroup analyses were not assessed using formal statistical methodologies to generate P values.
Table 9: Statistical Analysis of Efficacy End Points
End point | Study 301 | ||
|---|---|---|---|
Statistical model | Adjustment factors | Sensitivity analyses | |
Overall survival (primary outcome) Event-free survival Remission duration (secondary outcomes) | Kaplan-Meier Stratified log-rank test (Mantel) Cox proportional hazards | Stratified analyses for age and AML type | For overall survival, censoring at time of transplant (with stratification of age and AML subtype) |
Response rate Best response rate Stem cell transplant rate | Stratified log-rank (Mantel-Haenszel) | Stratified analyses for age and AML type | NA |
AML = acute myeloid leukemia; NA = not applicable.
Source: Clinical Study Report for Study 301.8
Analysis Populations
The ITT population was defined as all 309 patients who were randomized in the study.
The safety analysis population excluded 5 patients who were assigned to 7 + 3 but did not receive a single dose of the study drug.
A per-protocol population excluded 29 patients (8 assigned to liposomal daunorubicin and cytarabine, 21 assigned to 7 + 3). In addition, 25 patients failed or met 1 or more inclusion or exclusion criteria, respectively (8 in the liposomal daunorubicin and cytarabine and 17 in the 7 + 3 treatment groups). Five patients in the 7 + 3 treatment group did not receive at least 1 dose of the assigned study agent.
In the morphologic leukemia-free state population, 64 patients (27 in the liposomal daunorubicin and cytarabine and 37 in the 7 + 3 treatment groups) were excluded: 21 in the liposomal daunorubicin and cytarabine and 22 in the 7 + 3 treatment groups because they did not have an evaluable day 14 bone marrow assessment.
Results
Patient Disposition
The disposition of patients in Study 301 is summarized in Table 10. In total, 309 patients were randomized within the trial, with 153 patients receiving liposomal daunorubicin and cytarabine and 156 patients receiving 7 + 3. A total of 149 screening failures were reported, with the top 5 reasons for failure being non-confirmation of t-AML or AML-MRC (43 patients), no AML diagnosis (30 patients), “other” (24 patients), prior induction therapy received (11 patients), and exposure to anthracycline over 368 mg/m2 daunorubicin (9 patients).
Treatment completion in patients treated with liposomal daunorubicin and cytarabine was 14%, as opposed to 6.4% in patients treated with 7 + 3. Several noticeable differences between the 2 treatment arms were identified for study withdrawal. Most of these differences related to therapeutic aims (e.g., transplantation and response criteria). Outside of clinical response, consent withdrawal was notably different (5.8% to those assigned 7 + 3 compared with 2.0% to those assigned liposomal daunorubicin and cytarabine). Similarly, the proportion of patients withdrawn for “other” reasons was mismatched between groups, with 5.9% in the liposomal daunorubicin and cytarabine population compared to 3.2% in the 7 + 3 population.
A summary of patient analysis populations is provided in Table 10. For the safety population, 5 participants (3.2%) in the 7 + 3 arm were excluded from this analysis population as they did not receive at least 1 dose of the study drug. By contrast, no patients in the liposomal daunorubicin and cytarabine arm were excluded from the safety analysis. In the per-protocol analysis population, 8 patients who received liposomal daunorubicin and cytarabine (5.2%) were excluded due to either failure to meet inclusion criteria or meeting exclusion criteria. In the 7 + 3 treatment arm, 21 patients (13.5%) were excluded from the per-protocol population. In the 7 + 3 arm, 5 participants (3.2%) in the 7 + 3 arm were excluded from the per-protocol population as they did not receive at least 1 dose of the study drug, and 17 patients (10.8%) were excluded as they did not meet the inclusion or exclusion criteria.
Median duration of follow-up was similar between groups in the ITT population, with a median follow-up time of 20.5 months for patients treated with liposomal daunorubicin and cytarabine and a median follow-up time of 21.22 months for patients treated with 7 + 3. At the end of the planned 5-year (60-month) study period, 18% of patients assigned to liposomal daunorubicin and cytarabine were alive versus 8% in the 7 + 3 treatment arm.7
Table 10: Patient Disposition and Study Populations
Disposition | Study 301 | |
|---|---|---|
Liposomal daunorubicin and cytarabine | 7+3 | |
Screened, N | 458 | |
Randomized, N | 153 | 156 |
Discontinued from study, n (%)a | 131 (85.6) | 146 (93.6) |
Reason for discontinuation,a n (%) | ||
Withdrew consent | 3 (2) | 9 (5.8) |
Death | 12 (7.8) | 17 (11) |
Unacceptable toxicity | 4 (2.6) | 2 (1.3) |
Illness, investigator discretion, or non-protocol therapy | 13 (8.5) | 17 (10.9) |
Lack of response | 49 (32) | 70 (45) |
Relapse after CR or CRi | 4 (2.6) | 5 (3.2) |
Transplant | 37 (24) | 21 (13) |
Other | 9 (5.9) | 5 (3.2) |
ITT, n (%) | 153 (100) | 156 (100) |
PP, n (%) | 145 (95) | 135 (87) |
Safety, n (%) | 153 (100) | 151 (97) |
7 + 3 = conventional cytarabine and daunorubicin; CR = complete response; CRi = complete response with incomplete hematologic recovery; ITT = intention-to-treat; PP = per-protocol.
aPatients were discontinued if they did not complete consolidation therapy, and discontinuations include patients with successful transplant.
Source: Clinical Study Report for Study 301.8
Exposure to Study Treatments
Five patients, all of whom were assigned 7 + 3 treatment, did not receive at least 1 dose of the assigned therapy. These patients were therefore excluded from the safety analysis population. The 5 patients who did not receive a dose of the study drug were noted to have withdrawn consent immediately after being randomized. Of the remaining patients in the safety population, 48 (31%) received a second induction of liposomal daunorubicin and cytarabine, and 51 patients (34%) received a second induction of 7 + 3.
For consolidation, 49 patients (32%) who received liposomal daunorubicin and cytarabine received a first consolidation round as opposed to 32 patients (21%) who received 7 + 3. Second consolidation was provided to 23 patients (15%) who were provided liposomal daunorubicin and cytarabine as opposed to 12 patients (7.9%) assigned to 7 + 3.
The median duration of treatment exposure was 19 days for patients randomized to liposomal daunorubicin and cytarabine and 10 days for those assigned to 7 + 3.
In the safety analysis population, all patients in both treatment groups reported receiving concomitant medications before entering the study. Ten patients reported prior anthracycline exposure (6 in the liposomal daunorubicin and cytarabine and 4 in the 7 + 3 treatment groups). No patient in the liposomal daunorubicin and cytarabine treatment group had an anthracycline exposure to greater than 300 mg/m2 daunorubicin equivalents, whereas 2 patients in the 7 + 3 treatment group reported exposure to greater than 300 mg/m2 daunorubicin equivalents.
Efficacy
Only efficacy outcomes and analyses of subgroups identified in the review protocol are reported.
Overall Survival
The primary outcome, overall survival, was assessed in 153 patients who were randomized to the liposomal daunorubicin and cytarabine treatment group and 156 patients who were randomized to the 7 + 3 treatment group (the ITT population). The median overall survival was 9.56 months (95% Cl, 6.60 to 11.86) in the liposomal daunorubicin and cytarabine treatment group and 5.95 months (95% CI, 4.99 to 7.75) in the 7 + 3 treatment group. The 153 patients assigned to liposomal daunorubicin and cytarabine treatment experienced 104 events, and the 156 patients assigned to 7 + 3 treatment experienced 132 events. The liposomal daunorubicin and cytarabine treatment group was associated with a statistically significant improvement in overall survival when compared to patients who received 7 + 3 (HR = 0.69; 95% CI, 0.52 to 0.90; 1-sided log-rank test P = 0.003). A Kaplan-Meier survival curve of this analysis is presented in Figure 2. At the 5-year follow-up, 18% of patients who received liposomal daunorubicin and cytarabine were alive versus 8% who received 7 + 3, with a median overall survival of 9.33 months and 5.95 months in the liposomal daunorubicin and cytarabine and 7 + 3 treatment groups, respectively, resulting in a HR of 0.70 (CI, 0.55 to 0.91) in favour of liposomal daunorubicin and cytarabine treatment group.7
Figure 2: Overall Survival, ITT Population
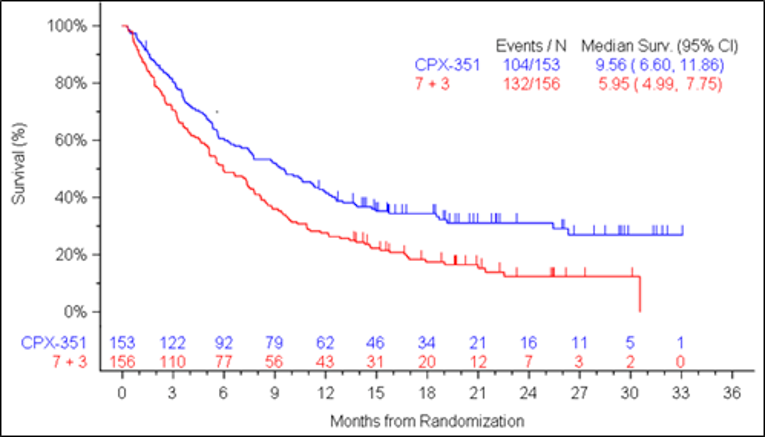
7 + 3 = conventional cytarabine and daunorubicin; CI = confidence interval; CPX-351 = liposomal daunorubicin and cytarabine; Surv. = survival.
Note: Numbers presented are for patients at risk.
Source: Clinical Study Report for Study 301.8
Overall Survival — Pre-Specified Sensitivity Analysis
A sensitivity analysis was undertaken to evaluate overall survival for 91 patients who received a transplant, landmarked at the time of transplantation. This analysis included 52 patients who received liposomal daunorubicin and cytarabine, and 39 patients treated with 7 + 3. The median survival duration post-transplant for patients in the 7 + 3 treatment group was 10.25 months (95% CI, 6.21 to 16.69) whereas patients who received liposomal daunorubicin and cytarabine had not reached an assessable median survival. A Kaplan-Meier analysis indicated that patients who received an HSCT in the liposomal daunorubicin and cytarabine treatment group had longer overall survival compared with patients in the 7 + 3 treatment group (HR = 0.46; 95% CI, 0.24 to 0.89; 1-sided P = 0.009). A follow-up analysis of the same population landmarked at the time of transplantation at 5 years demonstrated similar results. At this 5-year follow-up, the median overall survival duration for patients in the 7 + 3 treatment group was 10.25 months (95% CI, 6.21 to 16.69), whereas patients who received liposomal daunorubicin and cytarabine had not reached an assessable median overall survival. An updated 5-year Kaplan-Meier analysis indicated that patients who received an HSCT in the liposomal daunorubicin and cytarabine treatment group had longer overall survival than did patients in the 7 + 3 treatment group (HR = 0.51; 95% CI, 0.28 to 0.90).34
Data were identified for several subgroups of interest in peer-reviewed literature publications. For the following subgroups, no statistical comparison was undertaken and only HRs and associated 95% CIs are presented.32 When liposomal daunorubicin and cytarabine was compared to 7 + 3, the following HRs for overall survival were identified for patients with FLT3 wild-type (HR = 0.64; 95% CI, 0.47 to 0.87), FLT3 mutation–positive (HR = 0.76; 95% CI, 0.34 to 1.66), favourable or intermediate cytogenetic risk (HR = 0.64; 95% CI, 0.41 to 0.99), and unfavourable cytogenetic risk (HR = 0.73; 95% CI, 0.51 to 1.06). Kaplan-Meier survival curves for the population aged 60 to 69 years and those 70 to 75 years of age, along with a forest plot of subgroups, are provided in Figure 3. No subgroup data were identified by ECOG status, or by patients with specific concomitant therapies.
Figure 3: Subgroup Analyses for Overall Survival
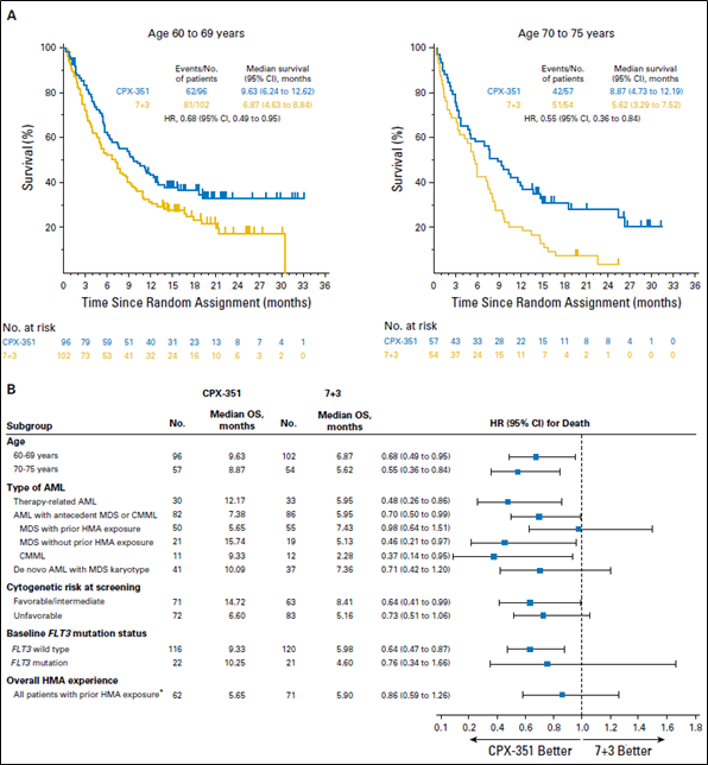
7 + 3 = conventional cytarabine and daunorubicin; CI = confidence interval; AML = acute myeloid leukemia; CMML = chronic myelomonocytic leukemia; CPX-351 = liposomal cytarabine and daunorubicin in a fixed 5:1 molar ratio; HMA = hypomethylating agent; HR = hazard ratio; MDS = myelodysplastic syndrome; ITT = intention-to-treat; OS = overall survival.
Note: Kaplan-Meier estimates are for overall survival by (A) age subgroup and (B) baseline patient characteristics.
* Includes patients in the pre-specified randomization strata of antecedent myelodysplastic syndrome with prior HMA exposure as well as patients in other strata (e.g., therapy-related AML and antecedent chronic myelomonocytic leukemia) who had previously received HMAs. Some patients received HMAs for therapy-related myelodysplastic syndrome, which then progressed to AML, and these patients may have been classified as having either therapy-related AML or antecedent myelodysplastic syndrome with prior HMA exposure.
Source: Lancet et al. (2018).32 Copyright © 2018 by the American Society of Clinical Oncology. Reprinted in accordance with CC BY-NC-ND 4.0.
Event-Free Survival
The median EFS was higher in the liposomal daunorubicin and cytarabine treatment group (2.53 months; 95% CI, 2.07 to 4.99) than in the 7 + 3 treatment group (1.31 months; 95% CI, 1.08 to 1.64), resulting in a statistically significant HR of 0.74 (95% CI, 0.58 to 0.96; 1-sided log-rank test P = 0.011). A Kaplan-Meier survival curve of this analysis is presented in Figure 4.
Figure 4: Event-Free Survival, ITT Population

7 + 3 = conventional cytarabine and daunorubicin; CI = confidence interval; CPX-351 = liposomal daunorubicin and cytarabine in a fixed 5:1 molar ratio; Surv. = survival.
Note: Numbers presented are for patients at risk.
Source: Clinical Study Report for Study 301.8
Data reported for several subgroups for EFS are summarized in Table 11. The directionality of the assessment measure favoured liposomal daunorubicin and cytarabine in each of the recorded subgroups. No subgroup data were identified by ECOG status, FLT3 mutation status, patients with myeloproliferative neoplasms, or patients with specific concomitant therapies.
Table 11: Subgroup Analyses for Event-Free Survival Results
Event-free survival result | Liposomal daunorubicin and cytarabine (N = 153) | 7 + 3 (N = 156) |
|---|---|---|
Subgroup of patients who were 60 to 69 years old | ||
N assessable | |||||||| | |||||||| |
Median EFS in months (95% CI) | |||||||| | |||||||| |
HR (95% CI) | |||||||| | |
P value | |||||||| | |
Subgroup of patients who were 70 to 75 years old | ||
N assessable | |||||||| | |||||||| |
Median EFS in months (95% CI) | |||||||| | |||||||| |
HR (95% CI) | |||||||| | |
P value | |||||||| | |
Subgroup of patients who were t-AML | ||
N assessable | |||||||| | |||||||| |
Median EFS in months (95% CI) | |||||||| | |||||||| |
HR (95% CI) | |||||||| | |
P value | |||||||| | |
7 + 3 = conventional cytarabine and daunorubicin; CI = confidence interval; EFS = event-free survival; HR = hazard ratio.
Source: Clinical Study Report for Study 301.8
Response
A secondary efficacy outcome, response (either CR or CRi) was assessed in 153 patients who were randomized to the liposomal daunorubicin and cytarabine treatment group and 156 patients who were randomized to the 7 + 3 treatment group (the ITT population). Seventy-three patients (47.7%) in the liposomal daunorubicin and cytarabine treatment group achieved CR or CRi, as opposed to 52 patients (33.3%) in the 7 + 3 treatment group. The liposomal daunorubicin and cytarabine treatment group was associated with a statistically significantly higher response compared to the 7 + 3 treatment group (OR = 1.77; 95% CI, 1.11 to 2.81; 1-sided P = 0.008).
Similarly, patients treated with liposomal daunorubicin and cytarabine demonstrated a statistically significant difference in CR alone when compared to patients who received 7 + 3 (OR = 1.69, 95% CI, 1.03 to 2.78; 1-sided P = 0.020). This was reflected in the CR rates, with 57 patients (37.3%) randomized to liposomal daunorubicin and cytarabine achieving CR, as opposed to 40 patients (25.6%) who were randomized to 7 + 3.
Data identified for several subgroups with regard to CR + CRi are summarized in Table 12. Other data were identified for several subgroups of interest in peer-reviewed publications. For several subgroups, no statistical comparison was undertaken and only HRs and associated 95% CIs are presented.32 When liposomal daunorubicin and cytarabine was compared to 7 + 3, the following odds ratios for CR + CRi were identified for patients in the following subgroups: FLT3 mutation–positive (OR = 6.86, 95% CI = 1.78 to 26.36), favourable or intermediate cytogenetic risk (OR = 1.26, 95% CI = 0.62 to 2.54), and unfavourable cytogenetic risk (OR = 2.79, 95% CI = 1.34 to 5.82). No subgroup data were identified for patients by baseline ECOG status, myeloproliferative neoplasm, or FLT3 wild-type mutation status.
Table 12: Subgroup Analyses for Response
Response | Liposomal daunorubicin and cytarabine (N = 153) | 7 + 3 (N = 156) |
|---|---|---|
Subgroup of patients who were 60 to 69 years old | ||
N assessable | 96 | 102 |
N with CR + CRi (%) | 48 (50) | 37 (36.3) |
OR (95% CI) | 1.76 (1.00 to 3.10) | |
P value | Not reported | |
Subgroup of patients who were 70 to 75 years old | ||
N assessable | 57 | 54 |
N with CR + CRi (%) | 25 (43.9) | 15 (27.8) |
OR (95% CI) | 2.03 (0.92 to 4.49) | |
P value | Not reported | |
Subgroup of patients with t-AML | ||
N assessable | 30 | 33 |
N with CR + CRi (%) | 14 (46.7) | 12 (36.4) |
OR (95% CI) | 1.53 (0.56 to 4.20) | |
P value | Not reported | |
Subgroup of patients who were FLT3 ITD mutation–positive | ||
N assessable | 22 | 21 |
N with CR + CRi (%) | 15 (68.2) | 5 (23.8) |
OR (95% CI) | 6.86 (1.78, 26.36) | |
P value | Not reported | |
7 + 3 = conventional cytarabine and daunorubicin; CI = confidence interval; CR = complete response; CRi = complete response with incomplete hematologic recovery; ITD = internal tandem duplication; OR = odds ratio; t-AML = therapy-related acute myeloid leukemia.
Source: Clinical Study Report for Study 301.8
Duration of Remission
A secondary efficacy outcome, remission duration (date of achievement of CR or CRi until the date of relapse or death from any cause) was assessed in 73 patients who received liposomal daunorubicin and cytarabine and 52 patients who received 7 + 3 (the ITT population). The median remission duration in the liposomal daunorubicin and cytarabine treatment group was 6.93 months (95% CI, 4.60 to 9.23) compared to of 6.11 months (95% CI, 3.45 to 8.71) in the 7 + 3 treatment group (HR = 0.77; 95% CI, 0.47 to 1.26; 1-sided log-rank test P = 0.147), indicating no statistically significant difference in remission duration between patients in the liposomal daunorubicin and cytarabine treatment group compared with the 7 + 3 treatment group. A Kaplan-Meier curve of this analysis is presented in Figure 5.
Subgroup analyses for remission duration was conducted by age and by t-AML status only (Table 13). The subgroup analyses did not favour any treatment group.
Figure 5: Remission Duration, ITT Population

7 + 3 = conventional cytarabine and daunorubicin; CI = confidence interval; CPX-351 = liposomal daunorubicin and cytarabine in a fixed 5:1 molar ratio.
Note: Numbers presented are for patients at risk.
Figure 5 was redacted.
Source: Clinical Study Report for Study 301.8
Table 13: Subgroup Analyses for Remission Duration for Study 301
Remission duration | Liposomal daunorubicin and cytarabine | 7 + 3 |
|---|---|---|
Subgroup of patients who were 60 to 69 years old | ||
Median remission duration in months (95% CI) | |||||||| | |||||||| |
HR (95% CI) | |||||||| | |
P value | |||||||| | |
Subgroup of patients who were 70 to 75 years old | ||
Median remission duration in months (95% CI) | |||||||| | |||||||| |
HR (95% CI) | |||||||| | |
P value | |||||||| | |
Subgroup of patients with t-AML | ||
Median remission duration in months (95% CI) | |||||||| | |||||||| |
HR (95% CI) | |||||||| | |
P value | |||||||| | |
7 + 3 = conventional cytarabine and daunorubicin; CI = confidence interval; HR = hazard ratio; t-AML = therapy-related acute myeloid leukemia.
Source: Clinical Study Report for Study 301.8
Stem Cell Transplantation
A secondary efficacy outcome, the proportion of patients receiving an HSCT, was assessed in 153 patients who were randomized to the liposomal daunorubicin and cytarabine treatment group and 156 patients who were randomized to the 7 + 3 treatment group (ITT population). The percentage of patients receiving an HSCT in the liposomal daunorubicin and cytarabine treatment group was 34%, as opposed to 25% in the 7 + 3 treatment group. No statistically significant difference was reported for the proportion of patients receiving HSCT when liposomal daunorubicin and cytarabine treatment group compared with the 7 + 3 treatment group (OR = 1.54, 95% CI, 0.92 to 2.56; 1-sided P = 0.049).
Subgroup analyses for number of patients who received HSCT was conducted by age and by t-AML status only. The liposomal daunorubicin and cytarabine treatment group was only favoured in the subgroup of patients who were 70 to 75 years old. No difference was reported for the other subgroup analyses conducted (Table 14).
Table 14: Subgroup Analyses for Patients Receiving a Stem Cell Transplant
Subgroup analysis | Liposomal daunorubicin and cytarabine (N = 153) | 7 + 3 (N = 156) |
|---|---|---|
Subgroup of patients who were 60 to 69 years old | ||
N assessable | 96 | 102 |
N with stem cell transplant (%) | 36 (37.5) | 33 (32.4) |
OR (95% CI) | 1.25 (0.70 to 2.25) | |
P value | Not reported | |
Subgroup of patients who were 70 to 75 years old | ||
N assessable | 57 | 54 |
N with stem cell transplant (%) | 16 (28.1) | 6 (11.1) |
OR (95% CI) | 3.12 (1.12 to 8.72) | |
P value | Not reported | |
Subgroup of patients who were t-AML | ||
N assessable | 30 | 33 |
N with stem cell transplant (%) | 11 (36.7) | 9 (27.3) |
OR (95% CI) | 1.54 (0.53 to 4.49) | |
P value | Not reported | |
7 + 3 = conventional cytarabine and daunorubicin; OR = odds ratio; t-AML = therapy-related acute myeloid leukemia.
Clinical Study Report for Study 301.8
Health-Related Quality of Life
Health-related quality of life was not assessed in Study 301.
Patient-Reported Symptoms
Patient-reported symptoms were not assessed in Study 301.
Transfusion Independence
In the safety analysis population, data were available for 153 patients who received liposomal daunorubicin and cytarabine and for 151 patients who received 7 + 3. All patients in both arms in this safety population received a transfusion, indicating no transfusion independence for patients within the study period.
Harms
Only those harms identified in the review protocol are discussed. Table 15 provides detailed harms data. The median duration of treatment exposure was 19 days for patients randomized to liposomal daunorubicin and cytarabine treatment, and 10 days for those randomized to 7 + 3 treatment.
Adverse Events
Overall, AEs were common in both treatment arms in Study 301, with every participant experiencing at least 1 AE (any grade). In particular, febrile neutropenia was noted in the majority of patients in each arm (70% of patients receiving liposomal daunorubicin and cytarabine and 72% of patients receiving 7 + 3). Several events were noted in 50% or more of the patients who received 7 + 3, including diarrhea (68%), nausea (55%), and peripheral edema (50%). No other events were noted in 50% or more of patients receiving liposomal daunorubicin and cytarabine. The incidence of AEs (any grade) that differed by more than 10% between treatment arms included those for diarrhea (46% in the liposomal daunorubicin and cytarabine treatment group versus 68% in the 7 + 3 treatment group), headaches (35% for the liposomal daunorubicin and cytarabine treatment group versus 25% in the 7 + 3 treatment group), and coughing (33% in the liposomal daunorubicin and cytarabine treatment group versus 22% in the 7 + 3 treatment group).
For grade 3 to 5 events, bacteremia occurred at a higher frequency in patients who received liposomal daunorubicin and cytarabine (9.8%) when compared to patients who received 7 + 3 (2%).
Serious Adverse Events
Serious adverse events were relatively common across the study, with a greater proportion of patients who received liposomal daunorubicin and cytarabine experiencing an SAE (59%) compared to 43% of patients who received 7 + 3. The nature of the SAEs was relatively consistent between treatment arms, although sepsis occurred in the liposomal daunorubicin and cytarabine arm (7.8%) at twice the frequency of that in the 7 + 3 arm (3.3%).
Withdrawals Due to Adverse Events
Few patients overall withdrew due to AEs. Three patients (2%) of those treated with liposomal daunorubicin and cytarabine withdrew due to AEs and 2 patients (1.3%) who were treated with 7 + 3 withdrew due to AEs. Of the 5 discontinuations due to an AE, 4 (80%) were due to cardiac complications and 1 was due to renal complications.
Mortality
A total of 106 deaths (69.3%) were reported for patients who received liposomal daunorubicin and cytarabine and 128 deaths (84.8%) in patients who received 7 + 3. Most deaths noted were due to disease progression. In terms of deaths relating to AEs, similar proportions were noted between study arms, with 15 deaths due to an AE (14.2%) for patients receiving liposomal daunorubicin and cytarabine and 19 deaths due to an AE (14.8%) for patients treated with 7 + 3. In total, 5 patients (3.9%) who received 7 + 3 died due to non-progressive disease with cancer-related organ failure, whereas no patients in the liposomal daunorubicin and cytarabine arm died due to non-progressive disease with cancer-related organ failure.
Harms of Special Interest
Harms of special interest (as defined by the study protocol and provided by Canadian clinicians consulted by CADTH) are listed in Table 15. Most harms of special interest were relatively evenly distributed between treatment arms, with the proportions of patients experiencing an event varying depending on the event of interest.
For ICU admission, a greater proportion of patients who received 7 + 3 were admitted to ICU (25.2%) compared with patients who received liposomal daunorubicin and cytarabine (18.3%). In contrast, the duration of ICU stays were longer for patients who received liposomal daunorubicin and cytarabine (mean ICU stay duration = 8.2 days; SD = 9.69) when compared to patients who received 7 + 3 (mean ICU stay duration = 6.9 days; SD = 4.85), although the median duration of ICU stays was the same (6 days) between treatment arms.
Table 15: Summary of Harms for Study 301
Harms | Liposomal daunorubicin and cytarabine N =153 | 7 + 3 N = 151 |
|---|---|---|
Patients with ≥ 1 adverse event | ||
n (%) | 153 (100) | 151 (100) |
Top 10 most common events, n (%) | ||
Febrile neutropenia | 107 (70) | 108 (72) |
Diarrhea | 70 (46) | 103 (68) |
Nausea | 75 (49) | 83 (55) |
Edema peripheral | 62 (41) | 76 (50) |
Constipation | 65 (42) | 60 (40) |
Decreased appetite | 50 (33) | 62 (41) |
Fatigue | 53 (35) | 53 (35) |
Headache | 53 (35) | 37 (25) |
Cough | 51 (33) | 33 (22) |
Chills | 41 (27) | 41 (27) |
Patients with grade 3 to 5 adverse events | ||
n (%) | 141 (92) | 137 (91) |
Top 10 most common events, n (%) | ||
Febrile neutropenia | 104 (68) | 107 (71) |
Pneumonia | 30 (20) | 22 (15) |
Hypoxia | 20 (13) | 23 (15) |
Hypertension | 16 (10) | 8 (5.3) |
Sepsis | 14 (9.2) | 11 (7.3) |
Respiratory failure | 11 (7.2) | 10 (6.6) |
Fatigue | 11 (7.2) | 9 (6.0) |
Bacteremia | 15 (9.8) | 3 (2.0) |
Hypotension | 9 (5.9) | 1 (0.7) |
Decreased ejection fraction | 8 (5.2) | 8 (5.3) |
Patients with ≥ 1 SAEs | ||
n (%) | 90 (59) | 65 (43) |
Most common events, n (%) | ||
Febrile neutropenia | 12 (7.8) | 8 (5.3) |
Respiratory failure | 11 (7.2) | 8 (5.3) |
Decreased ejection fraction | 9 (5.9) | 9 (6.0) |
Sepsis | 12 (7.8) | 5 (3.3) |
Pneumonia | 10 (6.5) | 6 (4.0) |
Disease progression | 6 (3.9) | 6 (4.0) |
Acute respiratory failure | 6 (3.9) | 3 (2.0) |
Patients who stopped treatment due to adverse events | ||
n (%) | 3 (2) | 2 (1.3) |
All safety discontinuation events, n (%) | ||
Cardiac failure | 1 (0.7) | 0 (0) |
Cardiomyopathy | 1 (0.7) | 0 (0) |
Ejection fraction decreased | 0 (0) | 2 (1.3) |
Renal failure acute | 1 (0.7) | 0 (0) |
Deaths | ||
n (%) | 106 (69.3) | 128 (84.8) |
Primary cause of death, n (%) | ||
Progressive leukemia | 65 (61.3) | 67 (52.3) |
Non-progressive disease, cancer-related organ failure | 0 (0) | 5 (3.9) |
Adverse event | 15 (14.2) | 19 (14.8) |
Unknown | 10 (9.4) | 15 (11.7) |
Other | 16 (15.1) | 22 (17.2) |
Harms of special interest, n (%) | ||
Cardiotoxicity | 0 (0) | 1 (0.7) |
Patients with grade 3 to 5 bleeding events | 18 (12) | 13 (8.6) |
Drug hypersensitivity | 1 (0.7) | 2 (1.3) |
Febrile neutropenia | 107 (70) | 108 (72) |
Sepsis | 14 (9.2) | 11 (7.3) |
Intensive care unit admission | 28 (18.3) | 38 (25.2) |
Hepatobiliary disorders (any grade) | 11 (7.2) | 7 (4.6) |
Acute renal failure | 12 (7.8) | 15 (9.9) |
7 + 3 = conventional cytarabine and daunorubicin.
Source: Clinical Study Report for Study 301.8
Critical Appraisal
Internal Validity
With regard to patient disposition and imbalances in Study 301, a mild discordance in the numbers of participants who withdrew consent was evident between the liposomal daunorubicin and cytarabine arm (2%) and the 7 + 3 arm (5.8%). The higher percentage of patients randomized to the 7 + 3 treatment group withdrawing consent could have been due to the open-label design, given that patients were aware of the treatment allocation following randomization.
Patient baseline characteristics were well distributed across treatment arms, with no significant discordance in potentially relevant prognostic factors. Marginal differences were noted in ECOG proportions between populations, with the 7 + 3 arm having a greater proportion of patients (14%) achieving an ECOG performance status of 2 when compared to liposomal daunorubicin and cytarabine patients (9.8%), but also higher proportions of patients with an ECOG performance status of 0 for patients assigned to 7 + 3 (29%) when compared to those assigned to liposomal daunorubicin and cytarabine (24%). It is uncertain whether these small discrepancies would have affected efficacy outcomes of interest.
Outcomes captured within the study were well defined and in concordance with similar clinical trials for patients in similar populations. The primary end point, overall survival, is not subject to interpretational bias and is well defined. No minimally important difference threshold is available for survival, although the difference in median survival times for the ITT population (9.56 in liposomal daunorubicin and cytarabine versus 5.95 in 7 + 3) is notable. Imputation for missing values in overall survival were well defined and uniform across treatment arms, and are based on a conservative estimate (i.e., taking shorter survival estimates for missing data). None of the provided data indicated a discordance in missing data between treatment arms. No obvious violation of the Cox proportional hazards assumption was identified in the primary analysis, although no statistical methods were used to assess the Cox proportional hazards assumption.
For the efficacy outcomes assessed (survival, EFS, response, duration of remission, and stem cell transplantation proportions), the direction of the effect was consistent. This was also the case in statistical testing of these outcomes, with the exception of duration of remission, which was not statistically significant. While overall survival was the listed primary outcome, evidence across multiple clinically relevant outcomes is beneficial in determining likely mechanisms for the observed survival differences.
The associated power calculations for the primary outcome were well aligned with what was observed in practice. The trial was powered to detect an HR of 0.635 at a 93.7% power, and an HR of 0.69 was observed. Subgroups described within this report were identified a priori and comparative statistical analyses were reserved only for secondary outcomes, which had pre-planned analytical criteria. However, analyses of remission duration, EFS, and patients transferred for HSCT after induction treatment were not adjusted for multiple comparisons; thus, the level of significance is inflated, and interpretation of results should take this into consideration.
For the secondary outcome of response, the associated power was predicated on 270 patients providing a 99.99% power to identify an absolute difference of 32% in the liposomal daunorubicin and cytarabine arm against a baseline control CR + CRi of 42%. The observed difference in effects was less than half of the anticipated difference (14.4%), and as such there was likely less statistical power than planned for this comparison.
The study sponsor provided several regression analyses for consideration. The prognostic factors to be entered into these regression analyses were not pre-specified.
Quality of life was not reported within this publication. Although no validated quality-of-life tool specific to this population is available, other general assessment measures may have been feasible within the population. As such, the associated influence of these treatments on patient quality of life is not possible to ascertain from the current study data. Similarly, data on MRD were not included, limiting conclusions on how this may influence post-induction treatment strategies.
The primary analysis (and other secondary/sensitivity analyses) for Study 301 used a 1-sided statistical test. The use of 1-sided statistical tests is not considered problematic by the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use if the associated alpha threshold is adjusted accordingly.35 Study 301 used an alpha threshold of 0.025, and the direction of effect was as planned (i.e., directionally favourable for liposomal daunorubicin and cytarabine). Because exploratory secondary outcomes demonstrated this directionality, the use of this analytical strategy is unlikely to be influential in the overall interpretation of these findings. In an associated peer-reviewed publication, 2-sided P values were reported for non-primary outcomes (response, EFS, and HSCT proportions) without pre-specification.32 All comparative efficacy assessments within this report are exclusively taken from the associated trial’s Clinical Study Report and are 1-sided, as defined in the original trial statistical analysis plan. No explanation is provided within the peer-reviewed literature as to why a 2-sided testing strategy was used for secondary outcomes.
Study 301 did not use a blinded study design due to the colour of the investigational product. Despite the potential for unblinded trials to introduce bias, this is unlikely to have influenced the primary outcome of overall survival, due to the objective nature of this assessment. Induction response (and associated EFS) may be potentially vulnerable to influence, although findings by an independent reviewer who assessed response criteria were used for induction response efficacy assessments. Independent and site investigators demonstrated good concordance on the assessment of CR (97.9% agreement), although the number was slightly lower for CRi (78.8% agreement).
External Validity
The clinical experts consulted by CADTH for this review indicated that patients enrolled in Study 301 were similar to the majority of patients seen in clinical practice. The included trial population consists exclusively of patients aged 60 to 75 years, a population that is more challenging to treat when compared to younger patient populations for the purposes of induction and subsequent HSCT. Interpreting the validity of the findings from Study 301 for younger or older patients who may be eligible for therapy may be challenging. While variability in routine practice with 7 + 3 was noted with regard to dose adjustments, the comparator intervention was considered to be sufficiently similar to what is delivered in many Canadian contexts. The clinical experts had noted that dose intensity may be adjusted depending on frailty, and that consolidation therapy would be reduced relative to induction therapy.
Due to a lack of indirect treatment comparisons (as described in the Indirect Evidence section), comparisons of therapy to FLAG-IDA, a routinely used induction and consolidation regimen, are unavailable. As such, comparisons of liposomal daunorubicin and cytarabine to FLAG-IDA cannot be appraised. No studies that included midostaurin-containing regimens as a comparator were identified, and therefore comparisons between liposomal daunorubicin and cytarabine cannot be made against these therapeutic approaches.
Outcome measures included within the trial are relevant to patients and physicians, covering survival, induction response and HSCT proportions. Data are missing on quality of life and MRD, both of which may be important to patients and physicians assessing this treatment.
Follow-up duration was sufficiently long to cover observed outcomes in the vast majority of included patients.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
A focused literature search for network meta-analyses dealing with AML was run in MEDLINE All (1946–) on February 23, 2021. No limits were applied to the search. This systematic review did not identify any indirect treatment comparisons that met the criteria for inclusion in this report. The sponsor provided a feasibility assessment, but no indirect treatment comparison.
Description of Feasibility Assessment
The sponsor provided a feasibility assessment that reviewed the appropriateness of conducting an indirect treatment comparison, either as a connected evidence network or using matching-adjusted indirect comparisons. The purpose of this assessment was to determine whether sufficient evidence existed to compare liposomal daunorubicin and cytarabine relative to FLAG-IDA. The feasibility assessment was based upon a non-systematic review of peer-reviewed literature as well as non–peer-reviewed materials, such as treatment guidelines and Health Canada approvals.
Outside of the sponsor’s trial (Study 301), 6 studies of relevance were identified, of which 4 were considered part of the feasibility assessment. Of the available studies, only a single FLAG-IDA study contained a shared 7 + 3 treatment that could be compared to Study 301. Other studies had disconnected evidence due to a single-arm design or the absence of a relevant 7 + 3 comparator. The review team assessed the study designs, inclusion and exclusion criteria, patient characteristics, and outcomes when compared to Study 301.
With regard to inclusion criteria, each comparator study allowed for mixed primary and secondary AML and 2 studies allowed for relapsed and/or refractory patients.
With regard to patient characteristics, several significant differences were noted between Study 301 and the available comparators. Where reported, proportions of patients with secondary AML (the population of interest for an indirect treatment comparison) varied from 8% to 100%. One included study did not report on AML subtype. When compared to Study 301, the average age was significantly younger in the available studies of interest, and 1 study included a proportion of pediatric patients. The ECOG status was only available for 1 comparator study, which reported a significantly greater proportion of patients who had an ECOG status of 0, and lower proportions of patients who had an ECOG status of 1 or 2 when compared to Study 301. For many covariates of interest, there was a significant degree of non-reporting, limiting comparisons.
Trials were broadly consistent with regard to definitions provided for outcomes. Only 1 comparator study provided outcomes stratified by AML type. Response rates and survival times differed notably between trials with shared treatment arms.
Critical Appraisal of Feasibility Assessment
The feasibility assessment had a significant lack of information regarding the search strategy used. The authors note that they searched “PubMed, Embase and MEDLINE,” but no search strategy was outlined for these databases. No criteria for population, intervention, control, and outcomes were provided for assessment of the inclusion and exclusion criteria. No list of study variables was provided to be extracted. Therefore, it is challenging to verify the completeness of the feasibility assessment and, as such, any judgment on whether any indirect treatment comparison methods are appropriate would be of limited value.
Discussion
Summary of Available Evidence
The evidence on the comparative efficacy and safety of liposomal daunorubicin and cytarabine was from 1 randomized controlled phase III clinical study. Study 301 assigned 309 patients aged 60 to 75 years with AML-MRC or t-AML to receive liposomal daunorubicin and cytarabine (N = 153) or 7 + 3 (N = 156). Patients in Study 301 were well balanced between treatment arms with respect to relevant patient baseline characteristics and treatment history. The primary outcome was overall survival, and secondary end points included EFS, response, remission duration, and proportions of patients achieving HSCT.
The main limitations of Study 301 pertain to the absence of an HRQoL assessment and the absence of data on MRD. As such, there is uncertainty regarding the influence of this therapy on HRQoL when compared to existing standards of care.
Interpretation of Results
Efficacy
Broadly, there was consistent evidence of statistically significant differences in overall survival for patients randomized to liposomal daunorubicin and cytarabine when compared to patients randomized to 7 + 3 in the ITT population. The median overall survival was 3.61 months longer in the liposomal daunorubicin and cytarabine treatment group than in the 7 + 3 treatment group.
Effect sizes and associated uncertainty varied across reviewed subgroups, although how much of this was due to smaller sample sizes is difficult to determine. For example, the analysis of overall survival of patients who had t-AML at baseline involved just 63 patients. As such, the associated statistical power may be lower than what is required to make judgments of subgroup effects. A formal statistical test was not performed for these subgroups and therefore no judgments concerning the significance of the observed effects are possible.
Secondary outcomes such as response (OR = 1.77; 95% CI, 1.11 to 2.81; 1-sided P = 0.008) and EFS (HR = 0.74; 95% CI, 0.58 to 0.96; 1-sided log-rank test P = 0.011) were also identified as having statistically significant differences in the ITT populations. These findings are supportive of those of the overall survival analysis, as these secondary outcomes are also associated with overall survival benefits.36 As with overall survival, exploratory results were provided (without statistical comparisons) for several subgroups of potential interest.
While the percentage of patients receiving an HSCT was numerically higher in the liposomal daunorubicin and cytarabine treatment group than in the 7 + 3 treatment group (34% versus 25%), no statistically significant difference was reported for the between-group difference (OR = 1.54; 95% CI, 0.92 to 2.56; 1-sided P = 0.049).
While the percentage of patients achieving CR or CRi was statistically significantly higher in the liposomal daunorubicin and cytarabine treatment group than in the 7 + 3 treatment group and the median remission duration in the liposomal daunorubicin and cytarabine treatment group was numerically higher in the liposomal daunorubicin and cytarabine treatment group than in the 7 + 3 treatment group (6.93 months versus 6.11 months), no statistically significant difference was reported for the between-group difference (HR = 0.77; 95% CI, 0.47 to 1.26; 1-sided log-rank test P = 0.147). One secondary outcome, remission duration, showed no statistically significant difference in the ITT population. The number of patients available for assessment limits the usefulness of this analysis. The assessable population was limited, as it was restricted to those who had a CR or CRi. In total, 125 patients could be assessed: 73 patients in the liposomal daunorubicin and cytarabine group and 52 patients in the 7 + 3 group. With this limitation in mind, it is possible that, while liposomal daunorubicin and cytarabine did have a favourable profile with regards to response rates and survival, it may not have an impact on the duration of remission.
Overall, potential biases or methodological issues with the included clinical trial reviewed raised few concerns. The clinical experts consulted by CADTH for this review indicated that patients enrolled in Study 301 were similar to the majority of patients seen in clinical practice. The patient populations were broadly similar across treatment arms, there was no evidence of discordant dropout rates, and the outcomes assessed were well defined.
An important limitation of these findings is the lack of an HRQoL assessment. This was noted to be an important outcome by the patient and clinician groups who provided input to CADTH on this submission, the effect of liposomal daunorubicin and cytarabine on HRQoL is uncertain. Similarly, MRD was noted to be an informative measure in determining post-transplantation survival; however, MRD was not captured in Study 301. As such, a meaningful assessment of the comparative efficacy of liposomal daunorubicin and cytarabine relative to 7 + 3 is not possible for these outcomes.
Efficacy outcome data were not available for all subgroups identified as potentially relevant in the clinical study protocol. As such, the efficacy of liposomal daunorubicin for subpopulations such as those with differing results in ECOG status, myeloproliferative neoplasm, and, in some outcomes, FLT3 mutation status, is uncertain.
In Canada, a proportion of adult patients with t-AML or AML-MRC may be treated with FLAG-IDA as an induction option. Based on the current evidence from this trial and the submitted indirect treatment comparison feasibility assessment, no formal assessment of liposomal daunorubicin and cytarabine can be made when compared to FLAG-IDA. Similarly, patients with FLT3 mutations may be treated with 7 + 3 and midostaurin. Patients with a positive FLT3 status were included in the current trial; however, assessing the comparative efficacy of liposomal daunorubicin and cytarabine against that of 7 + 3 with midostaurin is not possible based on the current evidence base.
Reasons for improved survival post-transplantation for patients who received liposomal daunorubicin and cytarabine when compared to patients who received 7 + 3 are unclear based on the current data. Median survival duration post-transplant for patients receiving 7 + 3 was 10.25 months (95% CI, 6.21 to 16.69), whereas patients who received liposomal daunorubicin and cytarabine had not reached an assessable median survival (HR = 0.46; 95% CI, 0.24 to 0.89; 1-sided P = 0.009). Post-transplant survival may be influenced by achievement of MRD status before transplantation,37 although it is not possible to formally assess this due to a lack of MRD data for this cohort. Similarly, improved patient fitness post-induction and pre-transplantation is associated with improved post-transplant survival38 although no formal assessment of post-induction fitness was made in this study. Both of these measures may be important in understanding patient responses to induction and the associated survival differences in patients who receive HSCT.
Harms
Adverse events were ubiquitous in the treatment arms of this study. Induction therapy is considered a highly intensive therapeutic option39 and, as evidenced by the high number of events (any grade) in the 7 + 3 arm, existing therapies also are associated with high AE rates. A numerically higher proportion of patients experiencing an SAE were treated with liposomal daunorubicin and cytarabine (59%) when compared to those treated with 7 + 3 (43%). Broadly, the types of events were comparable between treatment arms, with febrile neutropenia and gastrointestinal AEs the most commonly reported. The AEs reported within this trial across treatment arms aligned closely with the experiences of patients, as described in the patient group input for with this report.
The patient context of these therapies and the role of therapy is an important consideration when interpreting these findings. As highlighted in the clinician input, patients with these diseases often have poor survival, yet achieving a response and subsequent HSCT is associated with significant benefits to overall survival. Adverse events may have an influence on patient fitness, which is a key parameter when considering suitability for HSCT, but this was not measured within this trial and therefore cannot be considered in the context of therapy selection.
Due to a lack of a feasible indirect comparison or direct trial data, the comparative harms of alternative induction regimens such as FLAG-IDA and 7 + 3 with midostaurin could not be assessed.
Conclusions
Liposomal daunorubicin and cytarabine statistically significantly improved overall survival versus 7 + 3 in a single randomized controlled trial of adult patients with t-AML or AML-MRC. The difference between treatment groups was considered clinically meaningful based on input from the clinical experts consulted by CADTH. Similarly, statistically significant improvements were noted in response rates and EFS. Although the proportion of patients receiving HSCT and the duration of remission in patients with CR or CRi were numerically higher in the liposomal daunorubicin and cytarabine treatment group relative to the 7 + 3 treatment group, no statistically significant results were reported for the comparison between the treatment groups for these 2 outcomes. Adverse events, while frequent, were broadly similar across treatment groups, although proportionately more SAEs were noted in patients receiving liposomal daunorubicin and cytarabine when compared to patients who received 7 + 3. Because relevant outcomes such as HRQoL were not assessed, the effect of liposomal daunorubicin and cytarabine on HRQoL is uncertain. No direct or indirect evidence against other induction regimens used in clinical practice in Canada was identified; hence, the comparative efficacy and safety of liposomal daunorubicin and cytarabine against other induction regimens, such as FLAG-IDA, are unknown.
References
1.Saultz JN, Garzon R. Acute Myeloid Leukemia: A Concise Review. J Clin Med. 2016;5(3):33. PubMed
2.Hulegardh E, Nilsson C, Lazarevic V, et al. Characterization and prognostic features of secondary acute myeloid leukemia in a population-based setting: a report from the Swedish Acute Leukemia Registry. Am J Hematol. 2015;90(3):208-214. PubMed
3.Statistics Canada. Table 13-10-0111-01 Number and rates of new cases of primary cancer, by cancer type, age group and sex. 2021; https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1310011101. Accessed 2021 April 5.
4.Dombret H, Raffoux E, Gardin C. New insights in the management of elderly patients with acute myeloid leukemia. Current opinion in oncology. 2009;21(6):589-593. PubMed
5.Montalban Bravo G, Kanagal-Shamanna R, Sasaki K, et al. Outcomes of Patients with Acute Myeloid Leukemia (AML) with Myelodysplasia Related Changes (AML-MRC) Are Dependent on Diagnostic Criteria and Therapy. Blood. 2019;134(Supplement_1):1312-1312.
6.Brandwein JM, Zhu N, Kumar R, et al. Treatment of older patients with acute myeloid leukemia (AML): revised Canadian consensus guidelines. Am J Blood Res. 2017;7(4):30-40. PubMed
7.Lancet JE, Uy GL, Newell LF, et al. Five-year final results of a phase III study of CPX-351 versus 7+3 in older adults with newly diagnosed high-risk/secondary AML. 2020;38(15_suppl):7510-7510.
8.Clinical Study Report: Study CLTR0310-301 Phase III, Multicenter, Randomized, Trial of CPX-351 (Cytarabine: Daunorubicin)Liposome Injection versus Cytarabine and Daunorubicin in Patients 60 −75 years of age with Untreated High Risk (Secondary) AML [internal sponsor's report]. Ewing (NJ): Jazz Pharmaceuticals; 2017 Feb 24.
9.Kuykendall A, Duployez N, Boissel N, Lancet JE, Welch JS. Acute Myeloid Leukemia: The Good, the Bad, and the Ugly. 2018(38):555-573.
10.Arber DA, Erba HP. Diagnosis and Treatment of Patients With Acute Myeloid Leukemia With Myelodysplasia-Related Changes (AML-MRC). American Journal of Clinical Pathology. 2020;154(6):731-741. PubMed
11.Cazzola M. Introduction to a review series: the 2016 revision of the WHO classification of tumors of hematopoietic and lymphoid tissues. Blood. 2016;127(20):2361-2364. PubMed
12.Sabattini E, Bacci F, Sagramoso C, Pileri SA. WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: an overview. Pathologica. 2010;102(3):83-87. PubMed
13.Higgins A, Shah MV. Genetic and Genomic Landscape of Secondary and Therapy-Related Acute Myeloid Leukemia. Genes (Basel). 2020;11(7):749. PubMed
14.Mahmoudjafari Z, Alexander M, Roddy J, et al. American Society for Transplantation and Cellular Therapy Pharmacy Special Interest Group Position Statement on Pharmacy Practice Management and Clinical Management for COVID-19 in Hematopoietic Cell Transplantation and Cellular Therapy Patients in the United States. Biology of Blood and Marrow Transplantation. 2020;26(6):1043-1049. PubMed
15.Deschler B, Lübbert M. Acute myeloid leukemia: epidemiology and etiology. Cancer. 2006;107(9):2099-2107. PubMed
16.Hulegårdh E, Nilsson C, Lazarevic V, et al. Characterization and prognostic features of secondary acute myeloid leukemia in a population-based setting: A report from the Swedish Acute Leukemia Registry. 2015;90(3):208-214.
17.Brandwein JM, Geddes M, Kassis J, et al. Treatment of older patients with acute myeloid leukemia (AML): a Canadian consensus. Am J Blood Res. 2013;3(2):141-164. PubMed
18.Shysh AC, Nguyen LT, Guo M, Vaska M, Naugler C, Rashid-Kolvear F. The incidence of acute myeloid leukemia in Calgary, Alberta, Canada: a retrospective cohort study. BMC Public Health. 2017;18(1):94. PubMed
19.Sekeres MA, Guyatt G, Abel G, et al. American Society of Hematology 2020 guidelines for treating newly diagnosed acute myeloid leukemia in older adults. Blood Advances. 2020;4(15):3528-3549. PubMed
20.Shelton J, Lu X, Hollenbaugh JA, Cho JH, Amblard F, Schinazi RF. Metabolism, Biochemical Actions, and Chemical Synthesis of Anticancer Nucleosides, Nucleotides, and Base Analogs. Chem Rev. 2016;116(23):14379-14455. PubMed
21.Saleem T, Kasi A. Daunorubicin. StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
22.VYXEOS®Daunorubicin and cytarabine liposome for injection, Powder, 44 mg daunorubicin and 100 mg cytarabine per vial, intravenous infusion [product monograph]. Dublin: Jazz Pharmaceuticals Ireland Ltd; 2021.
23.Drug Reimbursement Review sponsor submission: VYXEOS® (daunorubicin and cytarabine, lyophilized liposome) [internal sponsor's package]. Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2021 Jan 21.
24.Cytarabine Injection 100 mg/mL (100 mg/mL, 1 g / 10 mL, 2 g / 20 mL) [product monograph]. Kirkland (QC): Pfizer Canada Inc.; 2017 Nov 6: https://pdf.hres.ca/dpd_pm/00042056.PDF. Accessed 2021 May 19.
25.Daunorubicin (Daunorubicin Hydrochloride) 20mg/Vial [product monograph]. 2017 Aug 2; https://pdf.hres.ca/dpd_pm/00040443.PDF. Accessed 2021 May 19.
26.Idarubicin (idarubicin hydrochloride injection 1 mg/mL) [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2021 Jan 18: https://pdf.hres.ca/dpd_pm/00059701.PDF. Accessed 2021 May 19.
27.e-CPS. Ottawa (ON): Canadian Pharmacists Association; 2020: https://www.e-therapeutics.ca/. Accessed 2020 March 03.
28.Cancer Care Ontario. Drug formulary: FLAG+IDA. 2019 May; https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/47971. Accessed 2021 May 19.
29.Cheson BD, Bennett JM, Kopecky KJ, et al. Revised Recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. Journal of Clinical Oncology. 2003;21(24):4642-4649. PubMed
30.Dutta S, Pregartner G, Rücker FG, et al. Functional Classification of TP53 Mutations in Acute Myeloid Leukemia. Cancers. 2020;12(3):637. PubMed
31.Daver N, Schlenk RF, Russell NH, Levis MJ. Targeting FLT3 mutations in AML: review of current knowledge and evidence. Leukemia. 2019;33(2):299-312. PubMed
32.Lancet JE, Uy GL, Cortes JE, et al. CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients With Newly Diagnosed Secondary Acute Myeloid Leukemia. Journal of Clinical Oncology. 2018;36(26):2684-2692. PubMed
33.Mantel N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer chemotherapy reports. 1966;50(3):163-170. PubMed
34.Lancet JE, Newell LF, Lin T, Hogge DE, et al. Five-Year Final Results of a Phase 3 Study of CPX-351 Versus 7+3 in Older Adults with Newly Diagnosed High-Risk/Secondary Acute Myeloid Leukemia (AML): Outcomes By Age Subgroup and Among Responders [abstract]. 62nd ASH Annual Meeting and Exposition Dec 5-8, 2020. 2020. https://ash.confex.com/ash/2020/webprogram/Paper136874.html. Accessed 2021 May 19.
35.Lewis JA. Statistical principles for clinical trials (ICH E9): an introductory note on an international guideline. 1999;18(15):1903-1942.
36.Maiti A, Kantarjian HM, Popat V, et al. Clinical value of event-free survival in acute myeloid leukemia. Blood Advances. 2020;4(8):1690-1699. PubMed
37.Czyz A, Nagler A. The Role of Measurable Residual Disease (MRD) in Hematopoietic Stem Cell Transplantation for Hematological Malignancies Focusing on Acute Leukemia. Int J Mol Sci. 2019;20(21):5362. PubMed
38.Chen EC, Garcia JS. Does patient fitness play a role in determining first-line treatment of acute myeloid leukemia? Hematology. 2020;2020(1):41-50. PubMed
39.Fernandez HF, Rowe JM. Induction therapy in acute myeloid leukemia: intensifying and targeting the approach. Curr Opin Hematol. 2010;17(2):79-84. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: February 22, 2021
Alerts: Bi-weekly search updates until project completion
Study types: randomized controlled trials; controlled clinical trials
Limits:
Humans
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for 1 character |
? | Truncation symbol for 1 or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multi-Database Strategy
Daunorubicin/ and Cytarabine/
(Vyxeos* or cpx 351 or cpx351).ti,ab,kf,ot,hw,rn,nm.
((daunorubicin* or daunomycin* or Cerubidine* or daunoblastin* or Rubidomycin* or daunoxome*) adj3 (cytarabine* or Cytosar* or cytosine arabinoside* or ara-C or Depocyt* or araC or arabinofuranosyl cytidine or alexan)).ti,ab,kf,ot,hw,rn,nm.
Daunorubicin/ and (cytarabine* or Cytosar* or cytosine arabinoside* or ara-C or Depocyt* or 04079A1RDZ or araC or arabinofuranosyl cytidine or alexan).ti,ab,kf,ot,hw,rn,nm.
Cytarabine/ and (daunorubicin* or daunomycin* or Cerubidine* or ZS7284E0ZP or daunoblastin* or Rubidomycin* or daunoxome*).ti,ab,kf,ot,hw,rn,nm.
(ZS7284E0ZP and 04079A1RDZ).ti,ab,kf,ot,hw,rn,nm.
or/1 to 6
exp Leukemia, Myeloid, Acute/
(AML or ANLL).ti,ab,kf.
(Acute adj5 (granulocytic* or myeloblastic* or myelocytic* or myelogenous* or myeloid* or nonlymphoblastic* or non-lymphoblastic* or nonlymphocytic* or non-lymphocytic* or basophilic* or eosinophilic* or erythroblastic* or megakaryoblastic* or monocytic* or megakaryocytic* or myelomonocytic*) adj5 (leukemia* or leukaemia*)).ti,ab,kf.
(erythroleukemia* or erythroleukaemia*).ti,ab,kf.
((mast-cell or promyelocytic*) adj3 (leukemia* or leukaemia*)).ti,ab,kf.
or/8 to 12
7 and 13
14 use medall
*cytarabine plus daunorubicin/
(Vyxeos* or cpx 351 or cpx351).ti,ab,kw,dq.
((daunorubicin* or daunomycin* or Cerubidine* or daunoblastin* or Rubidomycin* or daunoxome*) adj3 (cytarabine* or Cytosar* or cytosine arabinoside or ara-C or Depocyt* or araC or arabinofuranosyl cytidine or alexan)).ti,ab,kw,dq.
*Daunorubicin/ and (cytarabine* or Cytosar* or cytosine arabinoside* or ara-C or Depocyt* or araC or arabinofuranosyl cytidine or alexan).ti,ab,kw,dq.
*Cytarabine/ and (daunorubicin* or daunomycin* or Cerubidine* or daunoblastin* or Rubidomycin* or daunoxome*).ti,ab,kw,dq.
or/16 to 20
exp Acute myeloid leukemia/
(AML or ANLL).ti,ab,kw,dq.
(Acute adj5 (granulocytic* or myeloblastic* or myelocytic* or myelogenous* or myeloid* or nonlymphoblastic* or non-lymphoblastic* or nonlymphocytic* or non-lymphocytic* or basophilic* or eosinophilic* or erythroblastic* or megakaryoblastic* or monocytic* or megakaryocytic* or myelomonocytic*) adj5 (leukemia* or leukaemia*)).ti,ab,kw,dq.
(erythroleukemia* or erythroleukaemia*).ti,ab,kw,dq.
((mast-cell or promyelocytic*) adj3 (leukemia* or leukaemia*)).ti,ab,kw,dq.
or/22 to 26
21 and 27
28 use oemezd
15 or 29
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
“Randomized Controlled Trial (topic)”/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
“Controlled Clinical Trial (topic)”/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf,kw.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf,kw.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf,kw.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf,kw.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(pragmatic study or pragmatic studies).ti,ab,hw,kf,kw.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf,kw.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(phase adj3 (III or “3”) adj3 (study or studies or trial*)).ti,hw,kf,kw.
or/31 to 61
30 and 62
exp animals/
exp animal experimentation/ or exp animal experiment/
exp models animal/
nonhuman/
exp vertebrate/ or exp vertebrates/
or/64 to 68
exp humans/
exp human experimentation/ or exp human experiment/
or/70 to 71
69 not 72
63 not 73
74 not (conference abstract or conference review).pt.
remove duplicates from 75
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- (Daunorubicin AND Cytarabine) OR vyxeos OR “cpx 351” OR “cpx351”] – drug synonyms included in the search.
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- daunorubicin, cytarabine, Vyxeos, cpx-351 or cpx351]
EU Clinical Trials
Register: European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- daunorubicin, cytarabine, Vyxeos, cpx-351 or cpx351]
Grey Literature
Search dates: February 11 to 16, 2021
Keywords: daunorubicin, cytarabine, Vyxeos, cpx 351 or cpx351
Limits: None
Updated: Search updated before the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC).
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Villa KF, Ryan RJ, Chiarella M, Louie AC. Healthcare resource utilization in a phase 3 study of CPX-351 in patients with newly diagnosed high-risk/secondary acute myeloid leukemia. J Med Econ. 2020 Jul;23(7):714-720. doi: 10.1080/13696998.2020.1744613. Epub 2020 Apr 10. PMID: 32188326. | Outcomes – health care utilization |
Cortes J, Kantarjian H, Albitar M, Thomas D, Faderl S, Koller C, Garcia-Manero G, Giles F, Andreeff M, O'Brien S, Keating M, Estey E. A randomized trial of liposomal daunorubicin and cytarabine versus liposomal daunorubicin and topotecan with or without thalidomide as initial therapy for patients with poor prognosis acute myelogenous leukemia or myelodysplastic syndrome. Cancer. 2003 Mar 1;97(5):1234-41. doi: 10.1002/cncr.11180. PMID: 12599230. | Interventions – not in scope |
Issa GC, Kantarjian HM, Xiao L, Ning J, Alvarado Y, Borthakur G, Daver N, DiNardo CD, Jabbour E, Bose P, Jain N, Kadia TM, Naqvi K, Pemmaraju N, Takahashi K, Verstovsek S, Andreeff M, Kornblau SM, Estrov Z, Ferrajoli A, Garcia-Manero G, Ohanian M, Wierda WG, Ravandi F, Cortes JE. Phase II trial of CPX-351 in patients with acute myeloid leukemia at high risk for induction mortality. Leukemia. 2020 Nov;34(11):2914-2924. doi: 10.1038/s41375-020-0916-8. Epub 2020 Jun 16. PMID: 32546726. | Study design – phase II |
Lancet JE, Cortes JE, Hogge DE, Tallman MS, Kovacsovics TJ, Damon LE, Komrokji R, Solomon SR, Kolitz JE, Cooper M, Yeager AM, Louie AC, Feldman EJ. Phase 2 trial of CPX-351, a fixed 5:1 molar ratio of cytarabine/daunorubicin, vs cytarabine/daunorubicin in older adults with untreated AML. Blood. 2014 May 22;123(21):3239-46. doi: 10.1182/blood-2013-12-540971. Epub 2014 Mar 31. PMID: 24687088; PMCID: PMC4624448. | Study design – phase II |
Pharmacoeconomic Review
Abbreviations
7 + 3
7 days of conventional (non-liposomal) cytarabine and 3 days of daunorubicin
AE
adverse event
AML
acute myeloid leukemia
AML-MRC
acute myeloid leukemia with myelodysplasia-related changes
BSA
body surface area
EFS
event-free survival
FLAG-IDA
fludarabine + cytarabine + filgrastim + idarubicin
FLT-3
FMS-like tyrosine kinase 3
GVHD
graft-versus-host disease
HR
hazard ratio
HSCT
hematopoietic stem-cell transplant
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
QALY
quality-adjusted life-year
SAE
serious adverse event
t-AML
therapy-related acute myeloid leukemia
TTO
time trade-off
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Daunorubicin (44 mg) and cytarabine (100 mg) liposome (Vyxeos), vial for intravenous infusion |
Submitted price | Daunorubicin (44 mg/100 mL) and cytarabine (100 mg/100 mL) liposome: $7,774 per 100 mL vial |
Indication | Adults with newly diagnosed therapy-related AML or AML with myelodysplasia-related changes |
Health Canada approval status | Approved |
Health Canada review pathway | Priority review |
NOC date | April 29, 2021 |
Reimbursement request | As per indication |
Sponsor | Jazz Pharmaceuticals Canada Inc. |
Submission history | Previously reviewed: No |
AML = acute myeloid leukemia; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model (initiated with a decision tree) |
Target population | Adults with newly diagnosed therapy-related AML or AML with myelodysplasia-related changes |
Treatment | Liposomal daunorubicin and cytarabine |
Comparator | 7 + 3 (conventional 7 days of cytarabine plus 3 days of daunorubicin) |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs, LYs |
Time horizon | 15 years |
Key data source | Study 301 |
Submitted results | ICER = $85,832 per QALY (incremental costs: $76,418; incremental QALYs: 0.89) |
Key limitations |
|
| |
CADTH reanalysis results |
|
7 + 3 = 7 days of conventional (non-liposomal) cytarabine and 3 days of daunorubicin; AML = acute myeloid leukemia; HSCT = hematopoietic stem-cell transplant; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Conclusions
Based on the CADTH Clinical Review, liposomal daunorubicin and cytarabine treatment was associated with statistically significant improvements in overall survival, response rates, and event-free survival, and a greater (but not statistically significant) proportion of patients receiving hematopoietic stem-cell transplantation (HSCT) when compared to conventional (non-liposomal) cytarabine and daunorubicin (7 + 3).
CADTH undertook reanalyses to address limitations with the sponsor’s submission: alternative assumptions were made for the parametric overall survival curves used in the model; the health state utility value for post-HSCT remission was changed; the disutility associated with an induction and consolidation cycle of liposomal daunorubicin and cytarabine was changed; the percentage of patients anticipated to receive outpatient consolidation for liposomal daunorubicin and cytarabine was reduced; and the risk of post-HSCT mortality was increased. The results of the CADTH reanalysis aligned broadly with the sponsor’s submission. In the CADTH reanalysis, liposomal daunorubicin and cytarabine was more costly (incremental cost: $84,730), and more effective (incremental quality-adjusted life-years [QALYs]: 0.77) compared with 7 + 3, resulting in an incremental cost-effectiveness ratio (ICER) of $110,283 per QALY. A price reduction of at least 68% is needed for liposomal daunorubicin and cytarabine to be cost-effective compared to 7 + 3 at a threshold of $50,000 per QALY.
The choice of extrapolated overall survival curves for liposomal daunorubicin and cytarabine and 7 + 3 was a key driver in the economic analysis, and the sponsor’s use of separate curves according to response and transplant status increased the overall uncertainty around estimated comparative effectiveness. CADTH explored the impact of alternative parametric overall survival curves in scenario analyses and found that cost-effectiveness was sensitive to the chosen extrapolation function. Limitations with respect to the health state utility values and post-HSCT mortality assumptions for the indicated population generated additional uncertainty in the strength of the treatment effect when applied over a longer time horizon. These findings suggest that estimates for mean cost-effectiveness and price reduction are highly uncertain.
Due to the lack of comparative data, CADTH was unable to address the omission of relevant comparators from the pharmacoeconomic model, including fludarabine + cytarabine + filgrastim + idarubicin (FLAG-IDA) and 7 + 3 in combination with midostaurin for patients with an FMS-like tyrosine kinase 3 (FLT-3) mutation. As such, the cost-effectiveness of liposomal daunorubicin and cytarabine compared to other relevant comparators in Canada remains unknown.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process (specifically, information that pertains to the economic submission).
Patient input was received from the Leukemia and Lymphoma Society of Canada, collected through an online survey of Canadian patients who have received treatment for acute myeloid leukemia (AML). Patients’ responses focused on how AML symptoms affected their daily lives. Responses varied from being unable to exercise, being unable to work, diminished social lives and relationships, and several detrimental effects on their health. Patients brought up several negative aspects of the disease, including being easily fatigued, losing vision in 1 eye, nausea, bruising, numbness, or body aches. Patients emphasized treatment-related adverse events (AEs) from chemotherapy, transplant, radiation, and drug therapies, which included extreme fatigue, diarrhea, infections, anemia, mouth sores, nausea, and vomiting. Patients with experience taking the drug under review identified treatment-related side effects including cough, rash, nausea, vomiting, mouth or throat sores, constipation, muscle pain, tiredness, breathing difficulties, headache, decreased appetite, chills, and sleep problems. When compared to other treatments they had received, 1 individual reported that liposomal daunorubicin and cytarabine had improved their quality of life, 2 neither agreed not disagreed with that observation, and 1 indicated that it had not. Patients considered many of the side effects to be either manageable or effects they did not experience. When compared to other treatments they had received, there was variation among patients regarding whether liposomal daunorubicin and cytarabine improved their quality of life.
Registered clinician input was received from the Ontario Health (Cancer Care Ontario) Hematology Disease Site Drug Advisory Committee. Clinicians identified conventional 7 + 3 and FLAG-IDA as the current treatment paradigm for the disease. Clinicians stated that treatment with liposomal daunorubicin and cytarabine was expected to improve outcomes for higher-risk patients. Clinicians stated that patients with therapy-related acute myeloid leukemia (t-AML) and acute myeloid leukemia with myelodysplasia-related changes (AML-MRC) are at high risk and have the greatest unmet need of AML patients. Clinicians acknowledged that, although the pivotal trial included patients between the ages of 60 and 75 years, younger patients who would otherwise meet eligibility criteria may also receive the drug.
CADTH convened a panel of 4 clinical experts from across Canada to provide additional input related to unmet need, gaps in evidence, potential implementation challenges, and place in therapy for liposomal daunorubicin and cytarabine. Input from the clinical panel aligned with input from registered clinicians, with both identifying the relevant comparator (FLAG-IDA) and the relevance of treatment for patients less than 60 years of age who would otherwise be eligible for treatment. The panel also identified the relevance of next-generation sequencing (although challenges remain with turnaround time) in the patient population, the key treatment goals of survival, response, HSCT, and quality of life, and indicated that consolidation therapy may be administered in outpatient settings, although this would depend on local capacity.
Input from drug plans included questions related to relevant comparator agents, treatment administration costs, the potential for indication creep, and potential switching between drugs. Input from drug plans indicated that patients not eligible for intensive induction therapy may receive azacitidine, and that cytarabine consolidation is the current standard of care. Input also indicated that induction and/or consolidation therapy needs to be administered in an inpatient setting, which is not funded by drug programs in certain jurisdictions, and that there is a potential for indication creep in patients with other AML subtypes and other lines of therapy compared to what was studied in the clinical trial. Drug plans also identified a need to understand if patients receiving 7 + 3 or FLAG-IDA can be switched to daunorubicin and cytarabine, and if so, if there is a cut-off point at which the switch can occur.
The following concerns were addressed in the sponsor’s model:
inclusion of quality of life and cost impacts of AEs related to concerns identified by patients, including bacteremia, diarrhea, fatigue, and sepsis; the sponsor only included grade 3 to 4 AEs that occurred in more than 5% of any treatment arm in their model, and many treatment- and disease-related AEs identified by patients were not included in the model
a comparison of daunorubicin and cytarabine to 7 + 3 therapy as identified by clinicians as a key comparator
a scenario analysis that took a societal perspective, incorporating additional costs borne by patients.
In addition, CADTH addressed some of these concerns.
Patient input identified that patients found treatment with liposomal daunorubicin and cytarabine to be either neutral or more challenging compared to other treatments. CADTH revised the sponsor’s model for on-treatment disutilities for liposomal daunorubicin and cytarabine and 7 + 3 to be equal in the CADTH base case.
Clinician input identified that consolidation therapy (for liposomal daunorubicin and cytarabine and for conventional 7 + 3) may be administered in an outpatient setting depending on local capacity. CADTH removed the difference in the percentage of patients receiving outpatient consolidation therapy in the CADTH base case and explored an increase in the percentage of patients receiving outpatient consolidation therapy in a scenario analysis.
Drug plans identified that induction and consolidation therapy typically occur in an inpatient setting, which is not funded by drug programs in certain jurisdictions. CADTH revised the sponsor’s budget impact analysis to exclude treatment administered in hospital in the CADTH base case.
CADTH was unable to address 1 concern raised in stakeholder input. The economic model was not structured to include additional comparators relevant in Canadian clinical practice, including FLAG-IDA and 7 + 3 with midostaurin in patients with an FLT-3 mutation, or to assess the cost-effectiveness of liposomal daunorubicin and cytarabine in patients less than 60 or more than 75 years of age.
Economic Review
The current review is for liposomal daunorubicin and cytarabine (Vyxeos) for adults with newly diagnosed AML-MRC and t-AML.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of liposomal daunorubicin and cytarabine compared with 7 + 3 therapy (7 days cytarabine + 3 days of daunorubicin). The modelled population comprised adults with newly diagnosed t-AML or AML-MRC. This population aligns with the Health Canada–indicated population and reimbursement request.
Liposomal daunorubicin and cytarabine can be used in combination as induction therapy and as consolidation therapy. Cytarabine can be used in combination with other drugs for non-intensive and salvage therapy for the same patient population. Liposomal daunorubicin and cytarabine induction therapy is typically used as part of a sequence of treatments that can include stem-cell therapy, consolidation therapy, subsequent non-intensive therapy, and salvage therapy depending on patient characteristics and how patients respond to treatment. The sponsor’s submitted price of liposomal daunorubicin and cytarabine is $7,774 per vial. Each vial contains 44 mg of daunorubicin and 100 mg of cytarabine. After reconstitution, the solution contains 2.2 mg/mL of daunorubicin and 5 mg/mL of cytarabine equivalent to 100 units. Each pack size contains 1 vial, 2 vials, or 5 vials. The recommended dose of liposomal daunorubicin and cytarabine is 100 units/m2 of body surface area (BSA). The sponsor submitted 7 + 3 therapy (7 days of cytarabine plus 3 days of daunorubicin) as the current treatment paradigm. The sponsor stated that the first 4-week round of induction therapy with liposomal daunorubicin and cytarabine would cost $46,642 per patient. The second round of induction therapy and consolidation therapy would cost $31,094. The model accounted for wastage and was calculated by rounding up to the nearest complete vial for each treatment administration. The sponsor’s model included 1 or 2 rounds of induction therapy and 0 to 2 rounds of consolidation therapy.
The clinical outcomes estimated in the model were life-years and QALYs. The sponsor’s model took a public health care payer perspective, used a time horizon of 15 years, and used a discount rate of 1.5% applied to both costs and QALYs. The sponsor assumed an annual inflation rate of 2.07% to present costs in 2020 Canadian dollars.
Model Structure
The sponsor’s model consisted of a decision tree feeding into a partitioned survival model (Appendix 3: Figure 1, Figure 2). The decision tree contained decision nodes regarding the patient’s response to treatment (responder or nonresponder), the number of rounds of consolidation received (0, 1, or 2), and whether the patient received a stem-cell transplant (yes or no). The sponsor’s partitioned survival model had 3 health states: “event-free survival” (EFS), “progressed disease,” and “death.” The model consisted of patients who did not achieve remission on induction therapy, patients who received consolidation therapy, and patients who received stem-cell therapy. Each of these patient groups experienced distinct probabilities of being in each health state, determined by overall survival and EFS curves unique to each patient group. The percentage of patients in each health state in each of these groups is aggregated to capture the total number of patients in each health state. The sponsor’s model also included a time delay for the start of the overall survival and EFS curves for patients who achieved a response depending on the treatment received by patients (i.e., number of rounds of induction, consolidation, and transplant). This time shift delayed the start of overall survival and EFS parametric curves until transplant for patients with complete response and transplant, or to the last round of consolidation therapy for patients with complete response and no transplant. For patients who did not respond to treatment, there was no time shift of the curves, and overall survival and EFS started at time 0.
Model Inputs
Patient characteristics, including age, sex, AML type, and average BSA, were sourced from Study 301 (Lancet et al. [2018]),1 a phase III randomized controlled trial that compared liposomal daunorubicin and cytarabine with 7 + 3 therapy in patients aged 60 to 75 years with newly diagnosed secondary t-AML or AML-MRC.
The efficacy of the treatment and comparator were informed by data from the intention-to-treat population for Study 301.1 The sponsor performed logistic regression analyses to inform the transition probabilities within the decision tree portion of the model, and linear regression analyses to calculate the time delay in starting the overall survival and EFS parametric curves. Data from Study 301 was also used to inform the parametric survival methods that were applied separately for patients who: a) responded to treatment and received a transplant (i.e., post-transplant); b) responded to treatment and did not receive a transplant (i.e., post-consolidation); and c) did not respond to treatment (i.e., nonresponders). Given that the tail end of several of the Kaplan-Meier overall survival and EFS curves used in the sponsor’s model were based on a small number of observed patients, CADTH requested that the sponsor provide an updated model with reconstructed parametric curves using Kaplan-Meier curves that are right-hand censored when the number of patients was less than 5. The sponsor provided an updated model with the option of running a scenario analysis for post-HSCT and post-consolidation EFS based on right-censored Kaplan-Meier curves, noting that these were the only 2 curves in which the number of patients at risk in the trial went below 5 and for which there was a “notable change in survival between patient 5 and the end of follow-up.”2 General Canadian population mortality rates (age- and sex-specific) were used in the model; however, in any period and for any group for which the modelled overall survival suggested lower mortality than the general population, all-cause age- and gender-adjusted mortality from the Statistics Canada Life Table was used instead of the study-based estimate.3 Canadian clinical experts consulted by the sponsor were used to inform the second-line therapy options available as well as the proportion of use per option (e.g., the proportion of relapsing patient undergoing non-intensive therapy and the type of chemotherapy used for patients in Canada).1
Rates of AEs were sourced from Lancet et al. (2018)1; events with at least 5% frequency of occurrence in at least 1 treatment arm of the trial were included in the model. Feedback from clinical experts consulted by CADTH stated that visits to intensive-care units, dialysis, and renal failure were clinically relevant AEs and outcomes; therefore, CADTH requested that the sponsor provide an updated model that included these AEs (both probabilities of occurrence and costs). The sponsor provided an updated model that included the prevalence of renal failure based on rates reported in Lancet et al. (2018)1 and visits to intensive-care units based on a study by Villa et al. (2020)4 and assumed that all patients experiencing renal failure would require dialysis.
Quality-of-life data were not collected in Study 301. Utility values for health states, and disutilities due to treatment (induction, consolidation, and transplant) were sourced from a de novo utility elicitation study for AML patients in the UK.3 The utility elicitation study used a vignette-based time trade-off (TTO) approach that included 200 individuals from the UK general population; the mean age was 45.5 years and 49% were female. Twelve health states were described, each over a 1-year time horizon, with 1-month trading increments used during the interviews. Individuals were asked to choose between living for 1 year in the health state being described or for a shorter period in full health. Utility scores were determined based on the point of indecision. No separate disutilities for AEs were applied in the model; the sponsor assumed that AEs were included in the treatment-related utility decrements.5 Adverse events included in the treatment-specific states were based largely on the opinion of clinical experts. The authors indicated that the 1-year time horizon was selected to capture the utility impact of relatively brief events, to allow for use as utility decrements, and because they were deemed reasonable given the short life expectancy of patients.
Costs of the comparator treatment, 7 + 3 therapy, and subsequent therapies were sourced from the association québécoise des pharmaciens propriétaires, the McKesson platform, Alberta Health Services, or personal communications.3,6,7 Resource costs were sourced from the Ontario Schedule of Benefits.8 Adverse event and palliative care costs were sourced from the Health Data Branch of the Ontario Ministry of Health and Long-Term Care.9 All costs were adjusted for inflation to 2020 Canadian dollars using the Consumer Price Index.
Summary of Sponsor’s Economic Evaluation Results
The sponsor submitted probabilistic analyses for its base-case and scenario analyses using 5,000 and 200 model iterations, respectively. The sponsor presented deterministic results that align (within $1,000 per QALY) with its probabilistic results (Appendix 3).
Base-Case Results
The sponsor’s base-case results are presented in Table 3. The sponsor reported that the use of liposomal daunorubicin and cytarabine resulted in more QALYs compared with 7 + 3 (1.54 versus 0.65, respectively), with an incremental difference of 0.89 QALYs. The majority (approximately 73%) of the QALY gain was accrued in the post-progression health state. The use of liposomal daunorubicin and cytarabine resulted in greater costs than did 7 + 3 ($269,394 versus $192,976, respectively), with an incremental cost of $76,418. The ICER of liposomal daunorubicin and cytarabine compared to 7 + 3 was $85,832 per QALY gained. Disaggregated results are presented in Appendix 3. The submitted analysis is based on the publicly available prices of the comparator treatments.
At the end of the 15-year time horizon, 9% of patients on daunorubicin and cytarabine remained alive, while 1% of patients on 7 + 3 therapy remained alive.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER versus reference ($ per QALY) |
|---|---|---|---|---|---|
7 + 3 | 192,976 | Reference | 0.65 | Reference | Reference |
Liposomal daunorubicin and cytarabine | 269,394 | 76,418 | 1.54 | 0.89 | 85,832 |
7 + 3 = 7 days of conventional (non-liposomal) cytarabine and 3 days of daunorubicin; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.
Additional results from the sponsor’s submitted economic evaluation base case, including cost-effectiveness-analysis curves, are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor presented results for the full population and according to patient response (i.e., for 3 patient groups: responders and transplant, responders and non-transplant, and nonresponders). No subgroup analyses were presented based on AML subtype, age, Eastern Cooperative Oncology Group performance status, history of myeloproliferative neoplasms, combined myelodysplastic disorder and myeloproliferative neoplasms, or genetic risk factors. The sponsor conducted scenario analyses using a societal perspective and for a pre- and post-threshold period of 5 years (i.e., based on the 5-year data cut-off for Study 301), and undertook sensitivity analyses to explore the impact of various assumptions, including discount rate, inflation rate, time horizon, costing options, and hospitalization days. The sponsor-submitted sensitivity analyses that had the greatest impact on the ICER included time horizon (5 years = $166,732 per QALY; 10 years = $106,034 per QALY), extrapolation of post-HSCT overall survival for Vyxeos (Gompertz = $117,441 per QALY), extrapolation of post-HSCT overall survival for 7 + 3 (Gompertz = $110,403 per QALY), and extrapolation of nonresponder overall survival for both treatments (Gompertz = $105,995 per QALY).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Relevant comparators not included: The sponsor included 7 + 3 (3 days of daunorubicin and 7 days of cytarabine by continuous infusion) as the only comparator in the submitted model. Clinical experts consulted by CADTH indicated that relevant comparators for the population eligible for liposomal daunorubicin and cytarabine may also include 7 + 3, FLAG-IDA, or 7 + 3 + midostaurin (3 days of daunorubicin or idarubicin, and 7 days of cytarabine by continuous infusion) for patients with an FLT-3 mutation. The sponsor provided a feasibility assessment that reviewed the appropriateness of conducting an indirect treatment comparison (ITC) to compare liposomal daunorubicin and cytarabine to FLAG-IDA. The assessment found that an ITC of liposomal daunorubicin and cytarabine versus FLAG-IDA would not be appropriate. As noted in the Clinical Review Report, the feasibility assessment was limited by its non-systematic review of the literature, including a lack of reporting of the search strategy, inclusion and exclusion criteria, and data-extraction template. These limitations make it challenging to verify the completeness of the feasibility assessment and judge whether any ITC methods are appropriate. The cost-effectiveness of liposomal daunorubicin and cytarabine relative to these comparators is unknown. CADTH was unable to address this limitation due to the structure of the submitted model.
Uncertainty in the parametric OS and EFS curves: The sponsor’s use of a partitioned survival model, while appropriate for the decision question, introduces structural assumptions about the relationship between EFS and overall survival (i.e., non–mutually exclusive curves), for which adjustments could not be made in reanalysis. These assumptions introduce a post-progression survival bias that favours liposomal daunorubicin and cytarabine.
CADTH asked the sponsor to provide clinical evidence supporting an implied incremental post-event benefit of 0.64 QALYs for patients treated with liposomal daunorubicin and cytarabine. The sponsor submitted additional information to CADTH to substantiate this benefit. In reviewing this evidence, CADTH noted that the estimated benefit may be partially attributable to an increased proportion of partial response and the effect of HSCT among patients receiving liposomal daunorubicin and cytarabine (i.e., an improvement in patient response as a consequence of treatment) rather than being directly related to the clinical effectiveness of the drug. CADTH was not able to estimate the extent to which the post-EFS benefit estimated in the model was due to the clinical effect of liposomal daunorubicin and cytarabine, versus being due to the structural bias within the model. The extent to which cost-effectiveness was influenced by assumptions about the survival data was explored in scenario analysis.
The sponsor used fully parametric survival curves to extrapolate the trial data over the entire time horizon of the model, with separate curves for liposomal daunorubicin and cytarabine, 7 + 3, and each clinical pathway (i.e., by response and transplant status). The sponsor indicated that curve selection was based on statistical considerations (i.e., Akaike’s information criteria and Bayesian information criteria), graphical assessments of fit, and clinical plausibility. However, no pre-specified process was used for curve selection, even though curve selection is a key driver of the cost-effectiveness estimates. The use of separate curves for each clinical pathway and a weighted-average approach to generate overall aggregated overall survival and EFS curves also increases the number of required assumptions in the model and reduces the number of patients used to inform each of the separate parametric curves.
Log-normal curves were selected by the sponsor as the best-fitting curves for post-HSCT and post-consolidation overall survival (for liposomal daunorubicin and cytarabine and for 7 + 3) and a generalized gamma for overall survival for patients who do not achieve remission after induction. Clinical experts consulted by CADTH for this review indicated that all curves except the Weibull curve were considered plausible for this patient population based on survival estimates at years 1 and 2. Given the structural uncertainty of the curves for each patient population and treatment, CADTH selected alternative curves in the base-case and/or scenario analyses to equal the most conservative and clinically plausible estimates for overall survival.
CADTH used the sponsor’s assumptions for post-HSCT parametric overall survival curves in the base case and conducted a scenario analysis to assess the impact of assuming a Gompertz curve for 7 + 3.
CADTH used the log-logistic curves (for liposomal daunorubicin and cytarabine and 7 + 3) to estimate post-consolidation overall survival in the base case and conducted a scenario analysis using the sponsor’s assumptions (log-normal).
CADTH used the sponsor’s assumptions for the parametric overall survival curve for patients who did not achieve remission in the base case (generalized gamma) and conducted a scenario analysis to assess the impact of assuming a Gompertz curve.
Given the uncertainty in the tail end of the Kaplan-Meier curves used to predict the parametric overall survival and EFS curves, CADTH requested that the sponsor provide CADTH with updated parametric curves based on Kaplan-Meier curves censored at 5 patients. The sponsor revised its model to include the option of selecting alternative parametric post-HSCT and post-consolidation EFS curves based on Kaplan-Meier curves censored at 5 patients. The sponsor’s assumptions for parametric EFS curves were retained in the CADTH base case. CADTH conducted a scenario analysis using the parametric post-HSCT and post-consolidation EFS curves using Kaplan-Meier curves censored at 5 patients.
Uncertainty in appropriateness of utility estimates: Study 301 did not include of quality-of-life outcomes. The sponsor derived utility values from a vignette-based TTO study conducted in a UK general population.5 The use of direct methods for utility elicitation are highly dependent on the description of the health states and are likely to overestimate utility values.10 Furthermore, the derivation of utilities from a UK population may not reflect Canadian preferences. CADTH economic guidelines recommend that an indirect method of measurement based on a generic classification system be used for the reference case.11 The health state utility values for the post-transplant remission health state lacked face validity based on feedback from the clinical experts consulted for our review. This suggests that the utility in the post-transplant remission health state is likely to be less than that for the post-induction or consolidation remission health state. The utility values used in the sponsor’s reference case did not include potential complications that may occur post-transplant, such as graft-versus-host disease (GVHD), which would consequently overestimate the quality of life experienced by patients post-transplant. Additionally, given the limitations of the UK-based TTO study, and the findings from the CADTH Clinical Review suggesting that the AEs in the liposomal daunorubicin and cytarabine and the 7 + 3 groups were similar (although a proportionately higher numbers of serious adverse events [SAEs] were recorded with 7 + 3 patients), there is insufficient evidence to warrant the differential disutilities applied by the sponsor for treatment with 7 + 3 compared to liposomal daunorubicin and cytarabine. Finally, as noted in the CADTH Clinical Review, because Study 301 was an open-label trial, the evaluation of AEs — and therefore the estimation of their severity — may be biased by treatment knowledge.
CADTH revised the induction and consolidation treatment disutilities for liposomal daunorubicin and cytarabine and 7 + 3 to make them equal in the base case.
CADTH revised the post-transplant health state utility estimate to account for complications post-transplant using a weighted average of the 2 utility values reported for long-term follow-up after HSCT in Joshi et al. (2019).12 The average (0.609) was based on an assumption of a 58% incidence of GVHD, which was the same estimate that the sponsor used to calculate the costs associated with GVHD in the model.3
CADTH conducted a scenario analysis using the post-transplant remission health state utility value from the sponsor’s reference case.
Overestimate of the percentage of patients receiving outpatient consolidation therapy for liposomal daunorubicin and cytarabine: The sponsor assumed that 70% of patients receiving consolidation therapy with liposomal daunorubicin and cytarabine would receive it in an outpatient setting, compared to 40% of patients receiving consolidation with 7 + 3. According to the clinical experts consulted by CADTH for the review, it is anticipated that the percentage of patients receiving outpatient therapy is unlikely to differ between the 2 treatments. A higher percentage of patients receiving outpatient therapy for consolidation with liposomal daunorubicin and cytarabine overestimates the incremental quality of life and underestimate the costs associated with liposomal daunorubicin and cytarabine. The absolute percentage of patients likely to receive outpatient consolidation therapy is uncertain and likely to vary across centres. Clinical experts consulted by CADTH indicated that the percentage is likely to be at least 40% and may approach 60% to 70% in some centres.
CADTH set the percentage of patients receiving outpatient consolidation therapy for both liposomal daunorubicin and cytarabine and 7 + 3 to be equal (40%) in the base case.
CADTH conducted a scenario analysis using an estimate of 70% of patients receiving outpatient consolidation therapy for both liposomal daunorubicin and cytarabine and 7 + 3.
Underestimate of mortality risk post-HSCT: The sponsor assumed that patients receiving HSCT would experience the same background mortality as that of the general population. To assess the impact of post-transplant mortality on the results, the sponsor conducted a scenario analysis based on age-adjusted findings for the hazard ratio (HR) reported by Martin et al. (2010).13 The sponsor indicated that, although a previous appraisal by the National Institute for Health Care and Excellence had conducted a scenario analysis based on the HR of 4 to 9 reported in Martin et al. (2010), the HR was based on a population that was much younger than the patients modelled in the sponsor’s submission. As such, the sponsor used an HR of 2.3 (based on an HR of 2.25 for males and 2.5 for females weighted by the distribution of males and females in the trial population). However, given the relatively few included events involving older patient populations in Martin et al. (2010), this estimate remains uncertain,13 and could in fact be higher than the HR of 2.3 estimated by the sponsor. Underestimating overall survival post-transplant will overestimate the treatment benefit of liposomal daunorubicin and cytarabine given that a greater percentage of patients receiving liposomal daunorubicin and cytarabine proceed to transplant. The clinical experts consulted by CADTH indicated that a 4-fold increase in Canadian general mortality rates for patients’ post-transplant was reasonable.
As part of CADTH’s base-case analysis, a 4-fold increase in Canadian general mortality rates was used (rather than a 2-fold increase). The use of the sponsor’s mortality rate was explored in scenario analyses.
Appropriateness of the modelled patient population: The sponsor’s model was based on the characteristics of the patients included in Study 301, of whom 0.2% were less than 60 years of age. According to 2017 Statistics Canada data, 28% of patients diagnosed with AML were 20 to 59 years of age.14 The clinical experts consulted by CADTH indicated that there will likely be patients younger than 60 years of age for whom liposomal daunorubicin and cytarabine may be an option and these patients are not expected to have differential responses to treatment compared to patients aged older than 60 years; however, these patients were not included in Study 301.1 The cost-effectiveness of liposomal daunorubicin and cytarabine in patients younger than 60 years of age or older than 75 years of age who are otherwise eligible for treatment is unknown.
CADTH was unable to address this limitation in the model.
Missing relevant SAEs: The sponsor’s model included only grade 3 or 4 AEs that affected 5% or more of the patients receiving either liposomal daunorubicin and cytarabine or 7 + 3. As noted in the clinical review report, a greater proportion of patients receiving liposomal daunorubicin and cytarabine experienced an SAE (59%) compared to 43% of patients who received 7 + 3, which may result in an underestimate of AE costs that affect the predicted QALYs. As per CADTH guidelines, all relevant AEs should be included in the model.11
CADTH could not address this limitation due to the structure of the model.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (See Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
15-year time horizon | Uncertain: In the sponsor’s base case, approximately 9% of patients in the liposomal daunorubicin and cytarabine arm and 1% of patients in the 7 + 3 arm were alive at the end of the 15-year time horizon. Clinical experts consulted by CADTH stated that the majority of patients in the indicated population would be older than 60 years of age at the time of diagnosis and a 15-year time horizon may be an overestimate of the life expectancy of the modelled population. However, given that liposomal daunorubicin and cytarabine is indicated for all adults regardless of age, there may be patients for whom a longer time horizon may be warranted. CADTH guidelines indicate that the time horizon should be long enough to capture all potential differences in costs and outcomes associated with the interventions being compared. Given the uncertainty in the time horizon selected in the sponsor’s reference case, a scenario analysis was undertaken to explore the impact of a shorter (10 year) and a longer (30 year) time horizon. |
No vial sharing | Appropriate: The sponsor’s model accounted for wastage in both the liposomal daunorubicin and cytarabine arm and the 7 + 3 arm. Clinical experts consulted by CADTH stated that this was likely appropriate as no vial sharing is likely to occur in practice. The only exception to this was for azacitidine, with at least 1 jurisdiction indicating that vial sharing was possible. Wastage was not expected to have a noteworthy impact on the ICER estimates, and therefore no additional scenario analyses were undertaken by CADTH. |
Assumptions for second-line therapy | Uncertain: The sponsor calculated the total drug acquisition costs for second-line therapies by employing a weighted average of proportional use of each type of therapy based on input from key opinion leaders. Clinical experts consulted by CADTH indicated that the second-line therapies that the sponsor included in its model for patients who do not achieve remission post-induction (i.e., non-intensive low-dose chemotherapy [azacitidine and low-dose cytarabine] and for salvage therapy [NOVE-HiDAC and FLAG-IDA]) were appropriate; however, there is likely to be variation across centres in terms of the proportions of each used. |
Effect of time delay for overall survival and EFS curves | Unknown: The sponsor used linear regression models to estimate the number of weeks of delay in starting the overall survival and EFS curves to account for the time on treatment (i.e., receiving 1 or 2 rounds of induction, up to 2 rounds of consolidation, and transplant). Given the uncertain effects that the time delays have on the results, CADTH requested that the sponsor provide the results of a sensitivity analysis that reflect the impact of changes on the estimates for each of the 3 regression analyses. In response, the sponsor reported varying each of the covariates included in the regression equations using the upper and lower 95% confidence interval, which resulted in a range in ICERs of between $84,265 and $88,677 per QALY gained. The sponsor also reported the results of a sensitivity analysis that varied the overall mean time delay using the upper and lower confidence limits of the time to post-induction response, time from post-induction response to last consolidation treatment, and time from last consolidation treatment to HSCT. The ICER estimates varied from $84,856 to $89,537 per QALY gained. These analyses suggest that the ICER is robust to changes in time delay assumptions. CADTH did not vary the sponsor’s baseline values. |
Medical resources included | Appropriate: Clinical experts consulted by CADTH indicated that, in addition to the medical resources included by the sponsor in their submission, there may be additional resource use costs for cytogenetic and molecular testing, and CT scans; however, these resources are unlikely to differ between treatments. |
Price estimates for comparator drugs sourced from the AQPP price list | Not appropriate: The sponsor used prices from the 2020 AQPP price list to inform the pricing for some comparator and salvage therapies. CADTH’s preferred source for comparator drug prices are the schedules and formularies of Canadian ministries of health that are recipients of a CADTH reimbursement recommendation. CADTH revised the price estimates in the sponsor’s submission to reflect those from jurisdictions in Canada other than Quebec. |
7 + 3 = 7 days of conventional (non-liposomal) cytarabine and 3 days of daunorubicin; AQPP = Association québécoise des pharmaciens propriétaires; EFS = event-free survival; FLAG-IDA = fludarabine + cytarabine + filgrastim + idarubicin; HSCT = hematopoietic stem-cell transplant; ICER = incremental cost-effectiveness ratio; NOVE-HiDAC = mitoxantrone + etoposide + cytarabine; QALY = quality-adjusted life-year.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
To address limitations identified within the sponsor’s economic model, the CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (Table 5).
CADTH undertook a stepped analysis, incorporating each change proposed in Table 5 to the sponsor’s base case to highlight the impact of each change in Table 6.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
A. Revised drug prices for comparators, non-intensive therapy, and salvage therapy | Azacitidine: $6.4799 per mg Cytarabine: $0.0714 per mg Daunorubicin: $4.8500 per mg Fludarabine: $4.9788 per mg Idarubicin: $84.6200 per mg | Azacitidine: $5.9999 per mg Cytarabine: $0.15370 per mg Daunorubicin: $4.7500 per mg Fludarabine: $4.0076 per mg Idarubicin: $42.3040 per mg |
B. Remove inflation | 2.07% | 0% |
Changes to derive the CADTH base case | ||
1. Alternative choice for parametric curves for overall survival (post-consolidation) | Post-consolidation overall survival: Liposomal daunorubicin and cytarabine: Log-normal 7 + 3: log-normal Post-HSCT overall survival: As per sponsor’s assumptions Liposomal daunorubicin and cytarabine: Log-normal 7 + 3: log-normal Nonresponder overall survival: As per sponsor’s assumptions All patients: generalized Gamma | Post-consolidation overall survival: Liposomal daunorubicin and cytarabine: Log=logistic 7 + 3: log-logistic Post-HSCT overall survival: As per sponsor’s assumptions Liposomal daunorubicin and cytarabine: Log-normal 7 + 3: log-normal Nonresponder overall survival: As per sponsor’s assumptions All patients: generalized Gamma |
2. Reduction in health state utility post-transplant and equal treatment disutilities for liposomal daunorubicin and cytarabine and 7 + 3 | Health state utility for post-transplant: 0.859 (SE = 0.013) Disutility for induction cycle liposomal daunorubicin and cytarabine: 0.110 (SE = 0.044) Disutility for consolidation cycle liposomal daunorubicin and cytarabine (inpatient): 0.046 (SE = 0.042) Disutility for consolidation cycle liposomal daunorubicin and cytarabine (outpatient): 0.035 (SE = 0.042) | Health state utility for post-transplant: 0.609 (SE = 0.0258) Disutility for induction cycle liposomal daunorubicin and cytarabine: 0.155 (SE = 0.044) Disutility for consolidation cycle liposomal daunorubicin and cytarabine (inpatient): 0.113 (SE = 0.043) Disutility for consolidation cycle liposomal daunorubicin and cytarabine (outpatient): 0.102 (SE = 0.043) |
3. Reduction in the percentage of patients receiving outpatient consolidation for liposomal daunorubicin and cytarabine | Liposomal daunorubicin and cytarabine: 70% 7 + 3: 40% | Liposomal daunorubicin and cytarabine: 40% 7 + 3: 40% |
4. Increased risk of post-HSCT mortality | General population background mortality by age | 4-fold increase in risk of death post-transplant compared to the general population |
CADTH base case | — | Reanalysis 1 + 2 + 3 + 4 |
7 + 3 = 7 days of conventional (non-liposomal) cytarabine and 3 days of daunorubicin; SE = standard error.
In the CADTH base-case reanalysis, which used publicly available prices of the comparator treatments, liposomal daunorubicin and cytarabine was associated with an expected cost of $251,257 and 1.30 QALYs over a 10-year time horizon. When compared to 7 + 3, liposomal daunorubicin and cytarabine had an incremental cost of $84,730 and was associated with 0.77 incremental QALYs, resulting in an ICER of $110,283 per QALY. Liposomal daunorubicin and cytarabine had a 0.2% chance of being cost-effective at a cost-effectiveness threshold of $50,000 per QALY. Approximately 47% of the incremental QALYs (0.36) were gained in the extrapolated post-trial period. The majority (77%) of the incremental costs were a result of drug acquisition costs. Disaggregated results of CADTHs base-case reanalysis are reported in Table 11 and Table 12 (Appendix 4).
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALYs) |
|---|---|---|---|---|
Sponsor’s base case | 7 + 3 | 192,976 | 0.65 | Reference |
Liposomal daunorubicin and cytarabine | 269,394 | 1.54 | 85,832 | |
Sponsor’s corrected base case | 7 + 3 | 166,520 | 0.65 | Reference |
Liposomal daunorubicin and cytarabine | 245,548 | 1.54 | 88,804 | |
CADTH reanalysis 1 | 7 + 3 | 166,162 | 0.65 | Reference |
Liposomal daunorubicin and cytarabine | 245,152 | 1.52 | 90,801 | |
CADTH reanalysis 2 | 7 + 3 | 166,088 | 0.53 | Reference |
Liposomal daunorubicin and cytarabine | 245,168 | 1.39 | 92,787 | |
CADTH reanalysis 3 | 7 + 3 | 166,209 | 0.65 | Reference |
Liposomal daunorubicin and cytarabine | 250,861 | 1.54 | 94,896 | |
CADTH reanalysis 4 | 7 + 3 | 166,066 | 0.64 | Reference |
Liposomal daunorubicin and cytarabine | 245,564 | 1.46 | 97,212 | |
CADTH base-case (reanalysis 1 + 2 + 3 + 4) | 7 + 3 | 166,527 | 0.53 | Reference |
Liposomal daunorubicin and cytarabine | 251,257 | 1.30 | 110,283 |
7 + 3 = 7 days of conventional (non-liposomal) cytarabine and 3 days of daunorubicin; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
Price-reduction analyses were conducted using both the sponsor’s and CADTH’s base case (Table 7). Within the CADTH base case, a price reduction of at least 68% is needed for liposomal daunorubicin and cytarabine to be considered cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY.
CADTH also performed additional scenario analyses that included changes to the sponsor’s assumption for the extrapolated overall survival curve post-HSCT for patients receiving 7 + 3 and changes to the extrapolated overall survival curve for patients who do not achieve remission (Gompertz). These analyses used the sponsor’s assumptions for extrapolated curves for post-consolidation overall survival (log-normal), revised parametric EFS curves based on Kaplan-Meier curves right-censored at 5 patients, increased the percentage of patients in liposomal cytarabine and daunorubicin and 7 + 3 receiving outpatient consolidation therapy, used a 10-year time horizon, applied health state utilities based on an alternative peer-reviewed publication, and adjusted post-HSCT mortality to an HR of 2.3. The results of the CADTH scenario analyses are presented in Table 13. Alternative assumptions for the extrapolated overall survival curves (Gompertz curve for patients who did not achieve remission: $133,993 per QALY) and the time horizon (10-years: $129,181 per QALY) had the greatest impact on the results.
Table 7: CADTH Price Reduction Analyses
Price reduction | ICERs for liposomal daunorubicin and cytarabine versus 7 + 3 ($ per QALY) | |
|---|---|---|
Sponsor base case | CADTH reanalysis | |
No price reduction | $85,832 | $110,283 |
10% | $82,158 | $102,001 |
20% | $74,071 | $92,896 |
30% | $66,967 | $83,742 |
40% | $59,191 | $74,650 |
50% | $50,718 | $65,659 |
60% | $43,430 | $56,805 |
70% | $35,297 | $48,022 |
7 + 3 = 7 days of conventional (non-liposomal) cytarabine and 3 days of daunorubicin; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Issues for Consideration
Clinical experts consulted by CADTH indicated that there is variation across centres in Canada regarding the drugs, dosages, and schedules used for the comparator agents for patients with t-AML and AML-MRC. The sponsor assumed that 100 mg/m2/day of intravenous continuous infusion (200 mg/m2/day if ≥ 60 years) of cytarabine would be used for consolidation therapy on days 1 to 5 and daunorubicin 60 mg/m2 intravenous on days 1 and 2. However, clinicians in some centres may use 1,500 mg/m2/day (or 3,000 mg/m2/day for those aged < 60 years) of cytarabine on days 1, 3, and 5, and 45 mg/m2 on days 1 and 2. Induction therapy may also differ across centres, with some clinicians treating with idarubicin 12 mg/m2 instead of daunorubicin on days 1, 2, and 3, and some centres do not give a second induction. Efficacy data for alternative dosages and schedules for the comparator agents was not available.
The sponsor assumed that patients who do not achieve remission post-induction may receive non-intensive low-dose chemotherapy (azacitidine and low-dose cytarabine) and salvage therapy (mitoxantrone + etoposide + cytarabine and FLAG-IDA). Clinical experts consulted by CADTH indicated that there is also variation across centres in the use of these drugs; mitoxantrone + etoposide + cytarabine is not used in some centres, and granulocyte colony-stimulating factor may be omitted from FLAG-IDA in some cases. Azacitidine with venetoclax may also be used; however, this regimen is not publicly funded, and patients pay out of pocket. Furthermore, not all patients will opt for intensive chemotherapy, and best supportive care may be the primary treatment option for older, unfit patients, or patients with comorbidities.
The clinical panel convened by CADTH indicated that patients within this population are typically cared for by a multidisciplinary team within a larger hospital settings. Induction and/or consolidation should be administered in an inpatient setting, which is not funded by drug programs in certain jurisdictions. There is variation across centres in terms of the capacity to provide outpatient consolidation therapy.
The CADTH clinical review report protocol identified several subgroups of interest: age of less than 60 years, AML type, FLT-3 mutation, baseline Eastern Cooperative Oncology Group status, patients with myeloproliferative neoplasms, and concomitant therapeutic agents. The cost-effectiveness of liposomal daunorubicin and cytarabine compared to 7 + 3 in these specific subgroups is unknown.
Overall Conclusions
Based on the CADTH Clinical Review of Study 301, an induction and consolidation regimen with liposomal daunorubicin and cytarabine achieved statistically significant improvements in overall survival, response rates, and EFS, with a greater (non–statistically significant) proportion of patients receiving HSCT when compared to 7 + 3 and a median duration of follow-up of 20.5 months and 21.2 months, respectively. The choice of extrapolated overall survival curves for liposomal daunorubicin and cytarabine and 7 + 3 was a key driver in the economic analysis, and the sponsor’s use of separate curves according to response and transplant status increased the number of required assumptions in the model and associated uncertainty.
CADTH undertook reanalyses to address limitations with the sponsor’s submission, using alternative assumptions for the parametric overall survival curves used in the model; changes to the health state utility value for post-HSCT remission; changes to the disutility associated with an induction and consolidation cycle of liposomal daunorubicin and cytarabine; a reduced percentage of patients anticipated to receive outpatient consolidation for liposomal daunorubicin and cytarabine; and an increased risk of post-HSCT mortality. The cost-effectiveness results of the CADTH reanalysis aligned broadly with the sponsor’s base case: liposomal daunorubicin and cytarabine was more costly (incremental cost: $84,730), and more effective (incremental QALYs: 0.77) compared with 7 + 3, generating an ICER of $110,283 per QALY. Liposomal daunorubicin and cytarabine had a 0.2% chance of being cost-effective at a WTP threshold of $50,000 per QALY. A price reduction of at least 68% is needed for liposomal daunorubicin and cytarabine to be cost-effective compared to 7 + 3 at a threshold of $50,000.
The CADTH base-case results are associated with substantial uncertainty. First, 73% of the incremental QALYs estimated for liposomal daunorubicin and cytarabine compared with 7 + 3 occurred during the post-progression and post-trial extrapolation period, for which the results are limited by the structural limitations imposed by the parametric curves used. Additionally, while the clinical data suggest that there is a statistically significant difference in overall survival for patients receiving liposomal daunorubicin and cytarabine compared with 7 + 3 post-transplant, the limitations in the utility data available to inform the model and the uncertainty in post-HSCT survival for the indicated population generate uncertainty in the strength of the treatment effect when applied over a longer time horizon. Slightly less than half (47%) of incremental QALYs were gained during the extrapolated post-trial period within the model. Estimates of mean cost-effectiveness and the estimated price reduction are subject to the uncertainty in comparative effectiveness.
No data were available to compare the effectiveness of liposomal daunorubicin and cytarabine to that of other relevant comparators, including FLAG-IDA and 7 + 3 in combination with midostaurin (for patients with FLT-3 mutations), which limits the interpretation of the cost-effectiveness of liposomal daunorubicin and cytarabine in Canadian practice.
References
1.Lancet JE, Uy GL, Cortes JE, et al. CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients With Newly Diagnosed Secondary Acute Myeloid Leukemia. J Clin Oncol. 2018;36(26):2684-2692. PubMed
2.Sponsor's Response to Additional information request (Requested Mar 8 - Received Mar 16) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: VYXEOS® (daunorubicin and cytarabine, lyophilized liposome). Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2021.
3.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: VYXEOS® (daunorubicin and cytarabine, lyophilized liposome). Mississauga (ON): Jazz Pharmaceuticals Canada Inc; 2021 Jan 21.
4.Villa KF, Ryan RJ, Chiarella M, Louie AC. Healthcare resource utilization in a phase 3 study of CPX-351 in patients with newly diagnosed high-risk/secondary acute myeloid leukemia. Journal of Medical Economics. 2020;23(7):714-720. PubMed
5.Matza LS, Deger KA, Howell TA, et al. Health state utilities associated with treatment options for acute myeloid leukemia (AML). Journal of Medical Economics. 2019;22(6):567-576. PubMed
6.Alberta Health Care Insurance Plan: medical price list as of 31 March 2020. Edmonton (AB): Government of Alberta; 2020: https://open.alberta.ca/dataset/30add047-29c2-4fc7-83b5-a8ab78605cdd/resource/48d0dd0b-bb33-478d-a85c-85a86d4555ad/download/health-somb-medical-price-list-2020-03.pdf. Accessed 2021 May 19.
7.Association québécoise des pharmaciens propriétaires. AQPP - Mon pharmacien. 2021; https://www.monpharmacien.ca/en/aqpp/. Accessed 2021 May 19.
8.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2021 May 19.
9.Ontario Ministry of Health and Long Term Care. Health Data Branch Web Portal. 2021; https://hsim.health.gov.on.ca/hdbportal/. Accessed 2021 May 19.
10.Arnold D, Girling A, Stevens A, Lilford R. Comparison of direct and indirect methods of estimating health state utilities for resource allocation: review and empirical analysis. BMJ. 2009;339:b2688. PubMed
11.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/dv/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2021 May 19.
12.Joshi N, Hensen M, Patel S, Xu W, Lasch K, Stolk E. Health State Utilities for Acute Myeloid Leukaemia: A Time Trade-off Study. Pharmacoeconomics. 2019;37(1):85-92. PubMed
13.Martin PJ, Counts GW, Jr., Appelbaum FR, et al. Life expectancy in patients surviving more than 5 years after hematopoietic cell transplantation. J Clin Oncol. 2010;28(6):1011-1016. PubMed
14.Table 13-10-0111-01 Number and rates of new cases of primary cancer, by cancer type, age group and sex. https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1310011101. Accessed 2021 May 19.
15.Bank of Canada. Inflation calculator. 2021; https://www.bankofcanada.ca/rates/related/inflation-calculator/. Accessed 2021 May 19.
16.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 May 19.
Appendix 1: Cost Comparison Table
Table 8: CADTH Cost Comparison Table for Untreated High-Risk (Secondary) Acute Myeloid Leukemia
Treatment | Strength/ concentration | Form | Price | Recommended dosage | Average daily cost ($) | 28-day cycle cost ($) |
|---|---|---|---|---|---|---|
Daunorubicin and cytarabine liposome (Vyxeos) Induction and consolidationa | 44 mg / 100 mg per vial | Powder for IV infusion | 7,773.6200b | Daunorubicin 44 mg/m2, cytarabine 100 mg/m2 First induction: Days 1, 3, and 5 of a 28-day cycle. Second induction: Days 1 and 3 of a 28-day cycle. Consolidation: Daunorubicin 29 mg/m2, cytarabine 65 mg/m2; Days 1 and 3 of a 28-day cycle | 1,665.78 1,110.52 1,110.52 | 46,642 31,094 31,094 |
Induction Therapy (7+3 ± midostaurin) | ||||||
Cytarabine | 100 mg/mL (20 mL vial) 100 mg/mL (5mL vial) | Injectable solution | 306.5000 (15.3250 per mL) 76.85 (15.37 per mL) | 100 mg/m2/day continuous IV infusion days 1 to 7 (≥ 60 years of age) 200 mg/m2/day continuous IV infusion days 1 to 7 (< 60 years of age) | 19.21 | 538 |
Daunorubicin | 20 mg/20 mL vial 1 mg/mL (5 mL vial) | Powdered solution | 95.0000 (4.7500 per mg) 211.52 (42.304 per mL) | 60 mg/m2 IV days 1 to 3 | 61.07 | 1,710 |
Idarubicin | 5 mg/5 mL vial | IV solution | 211.5200 | 12mg/m2 days 1,2, 3 | 113.31 | 3,173 |
Midostaurin (Rydapt) | 25 mg | Capsule | 167.9248 | 50 mg twice daily on days 8 to 21 | 335.85 | 9,404 |
7 + 3 induction therapy (cytarabine 100 or 200 mg/m2 + daunorubicin 60 mg/m2) (daily and 28-day cycle costs): | 80.28 | 2,248 | ||||
7 + 3 induction therapy (cytarabine 200 mg/m2 + idarubicin 12 mg/m2) (daily and 28-day cycle costs) | 132.53 | 3,711 | ||||
7 + 3 induction therapy (cytarabine 100 or 200 mg/m2 + daunorubicin 60 mg/m2) + midostaurin (daily and 28-day cycle costs): | 416.13 | 11,652 | ||||
Consolidation therapy (7 + 3 or high-dose cytarabine ± midostaurin) | ||||||
Cytarabine | 100 mg/mL (20 mL vial) 100mg/mL (5mL vial) | Injectable solution | 306.5000 (15.3250 per mL) 76.85 (15.37 per mL) | 200 mg/m2 days 1 – 7 continuously 1,500 mg/m2 on days 1, 3, 5 for age ≥ 60 years and 3,000 mg/m2 on days 1, 3, 5 for age < 60 years High-dose cytarabine: 3,000 mg every 12 h on days 1, 3, and 5 | 19.21 49.40 to 90.57 181.15 | 538 1,383 to 2,536 5,072 |
Daunorubicin | 20 mg/20mL vial 1 mg/mL (5 mL vial) | IV powdered solution | 95.0000 (4.7500 per mg) 211.52 (42.304 per mL) | 60 mg/m2 days 1 to 2 45 mg/m2 days 1 and 2 | 37.32 30.54 | 1,045 855 |
Midostaurin (Rydapt) | 25 mg | Capsule | 167.9248 | 50 mg twice daily on days 8 to 21 | 335.85 | 9,404 |
7 + 3 consolidation therapy (cytarabine 1,500 mg/m2 + daunorubicin 45 mg/m2) (daily and 28-day cycle costs): | 79.94 | 2,238 | ||||
7 + 3 consolidation therapy (cytarabine 3,000 mg/m2 + daunorubicin 45 mg/m2) (daily and 28-day cycle costs): | 121.11 | 3,391 | ||||
High-dose cytarabine (3,000 mg every 12 h on days 1, 3, and 5) (daily and 28-day cycle costs) | 181.15 | 5,072 | ||||
High-dose Cytarabine (3,000 mg every 12 h on days 1, 3, and 5) (daily and 28-day cycle costs) + midostaurin: | 517.00 | 14,476 | ||||
FLAG-IDA (first-line or salvage therapy) | ||||||
G-CSF (filgrastim) | 0.480mg/1.6mL vial 0.30 mg/mL 1mL vial | IV solution IV solution | 281.8120 176.1330 | 0.3 mg days 1 to 5 of a 28-day cycle | 25.77 | 722 |
G-CSF (filgrastim) | 0.30 mg/0.5mL vial 0.48 mg/0.8mL pack 0.30 mg/mL pack 0.48 mg/0.8mL pack | Injectable solution | 144.3100 230.9000 144.3100 230.9017 | 0.3 mg days 1 to 5 of a 28-day cycle | 25.77 | 722 |
Idarubicin | 1 mg/mL vial | IV solution (5 mL vial) | 211.5200 (42.3040 per mL in 5mL vial) | 10 mg/m2 days 2 to 4 of a 28-day cycle | 90.6514 | 2,538 |
Fludarabine | 10 mg | Tablet | 40.0760c | 30 mg/m2 days 2 to 6 of a 28-day cycle | 42.94 | 1,202 |
Cytarabine | 100 mg/mL (20 mL vial) 100 mg/mL (5 mL vial) | Injectable solution | 306.5000 (15.3250 per mL) 76.85 (15.37 per mL) | 2,000 mg /m2 days 2 to 6 of a 28-day cycle | 99.07 | 3,065 |
FLAG-IDA Therapy (Daily and 28-day cycle costs): | 276.04 | 7,729 | ||||
Non-intensive chemotherapies (single agents) | ||||||
Azacitidine | 100 mg | Powdered suspension | 599.99 (5.9999 per mg) | 75 mg/m2 for days 1 to 7 in a 28-day cycle. | 300.00 | 8,400 |
Low-dose cytarabine | 100 mg/mL (20 mL vial) 100 mg/mL (5 mL vial) | Injectable solution | 306.5000 (15.3250 per mL) 76.85 (15.37 per mL) | 20 mg/m2 daily for 10 days of a 28-day cycle | 27.45 | 769 |
NOVE-HiDAC (salvage Therapy) | ||||||
Mitoxantrone | 2 mg/mL (10 mL vial) | IV solution | 63.0370 per mL vial | 12 mg/m2 for 5 days in a 28-day cycle | 22.51 | 630 |
Etoposide | 50 mg 20 mg/mL (5 mL vial) | Capsule IV solution | 41.5875c (15.0000 per mL) | 100 to 200 mg/m2 daily for 5 days in a 28-day cycle | 26.79 to 53.57 | 750 to 1,500 |
Cytarabine | 100 mg/mL (20 mL vial) 100 mg/mL (5mL vial) | Injectable solution | 306.5000 (15.3250 per mL) 76.85 (15.37 per mL) | 1,200 mg /m2 days 6 and 7 of a 28-day cycle | 27.45 | 769 |
NOVE-HiDAC (daily and 28-day cycle costs): | 76.75 | 2,149 | ||||
FLAG-IDA = fludarabine + cytarabine + filgrastim (G-CSF) + idarubicin; G-CSF = granulocyte colony-stimulating factor.
Note: All prices are from the IQVIA (accessed March 2021),15 unless otherwise indicated, and do not include dispensing fees. Assuming body surface area (BSA) of 1.81 m2. no vial sharing.
aConsolidation only for patients failing to achieve a response with the first induction cycle.3
bSponsor submitted price.3
cPrice from Ontario formulary (accessed March 2021).16
Note that this appendix has not been copy-edited.
The comparators presented in the table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The sponsor’s model was missing relevant comparators including FLAG-IDA and 7 + 3 in combination with midostaurin. Therefore, the cost-effectiveness of liposomal daunorubicin and cytarabine compared with the omitted comparators remains unknown. |
Model has been adequately programmed and has sufficient face validity | No | Due to the large number of regressions and statistical analysis preformed on the various subgroups (i.e., by response and transplant status), CADTH was unable to validate all the steps the sponsor took to reconstruct patient efficacy data. This reduced the model’s transparency. |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | The sponsor’s prices for the key comparator, 7 + 3, and some salvage and non-intensive chemotherapy regimens did not align with the prices reported in the IQVIA Delta PA database. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | The submission was generally well organized. |
7 + 3 = conventional (non-liposomal) cytarabine and daunorubicin; FLAG-IDA = fludarabine + cytarabine + filgrastim + idarubicin.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
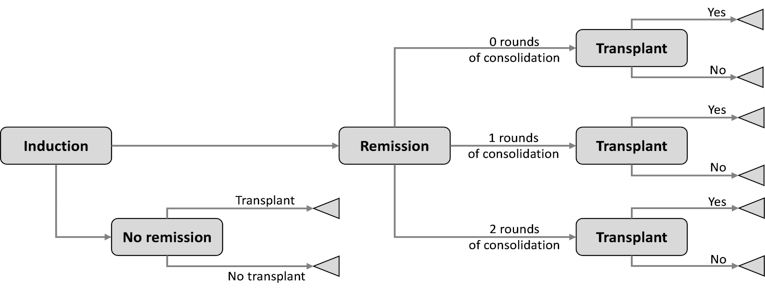
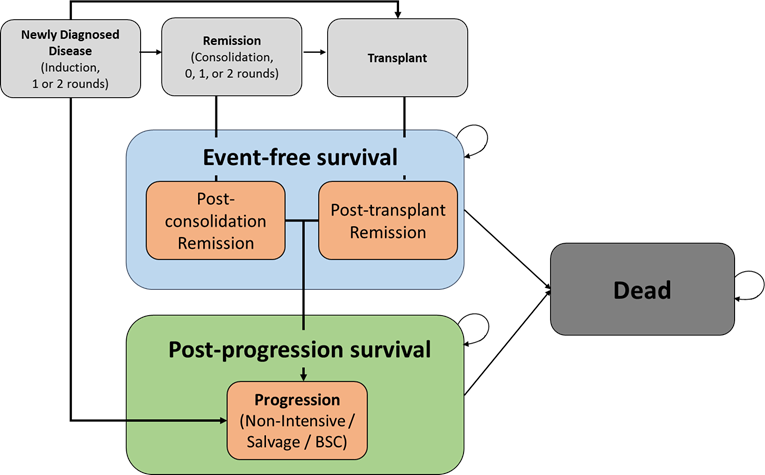
Table 10: Disaggregated Summary of Sponsor’s Submitted Economic Evaluation Results
Parameter | Liposomal daunorubicin and cytarabine | 7 + 3 | Incremental (liposomal daunorubicin and cytarabine versus 7 + 3) |
|---|---|---|---|
Discounted LYs | |||
Total LYs | 2.96 | 1.46 | 1.5 |
By health state | |||
Progression-free | 0.60 | 0.38 | 0.22 |
Post-progression | 2.36 | 1.08 | 1.28 |
Discounted QALYs | |||
Total QALYs | 1.54 | 0.65 | 0.89 |
By health state or data source | |||
Progression-free | 0.47 | 0.28 | 0.19 |
Post-progression | 1.30 | 0.66 | 0.64 |
Disutilities | −0.22 | −0.28 | 0.06 |
Discounted costs ($) | |||
Total | |||
Acquisition | 68,904 | 3,574 | 65,330 |
Administration | 74,755 | 73,521 | 1,234 |
Treatment monitoring | 2,769 | 3,326 | −557 |
Adverse events | 15,853 | 14,313 | 1,540 |
Transplant | 38,712 | 31,251 | 7,461 |
Remission post-consolidation and post-transplant | 3,079 | 1,877 | 1,202 |
Subsequent treatments | 56,310 | 55,256 | 1,054 |
End of life | 9,013 | 9,858 | −845 |
ICER ($ per QALY) (liposomal daunorubicin and cytarabine versus 7 + 3) | 85,832 | ||
7 + 3 = conventional (non-liposomal) cytarabine and daunorubicin; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year.
Figure 3: Cost-Effectiveness Acceptability Curve (Sponsor’s Base Case)
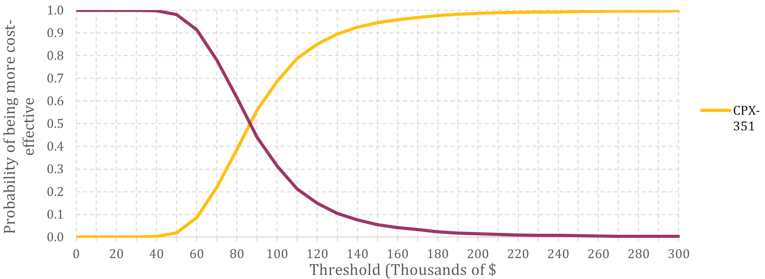
Source: Sponsor’s economic submission.3
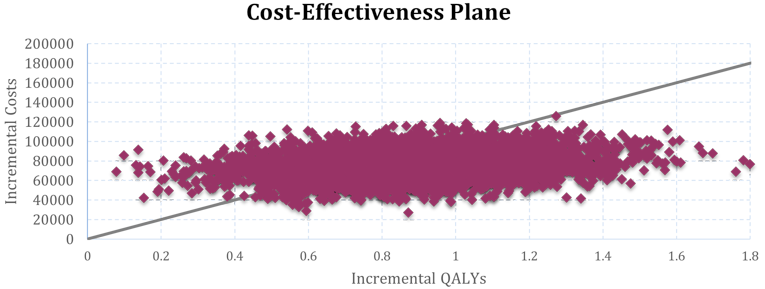
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 11: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Liposomal daunorubicin and cytarabine | 7 + 3 | Incremental (liposomal daunorubicin and cytarabine versus 7 + 3) |
|---|---|---|---|
Discounted LYs | |||
Total LYs | 2.78 | 1.45 | 1.33 |
By health state | |||
Progression-free | 0.54 | 0.31 | 0.23 |
Post-progression | 2.24 | 1.14 | 1.10 |
Discounted QALYs | |||
Total QALYs | 1.30 | 0.53 | 0.77 |
By health state or data source | |||
Progression-free | 0.34 | 0.19 | 0.15 |
Post-progression | 1.18 | 0.62 | 0.56 |
Disutilities | −0.22 | −0.28 | 0.06 |
Discounted costs ($) | |||
Total | 251,257 | 166,527 | 84,730 |
Acquisition | 68,877 | 3,576 | 65,301 |
Administration | 76,566 | 69,739 | 6,827 |
Treatment monitoring | 2,686 | 3,230 | −544 |
Adverse events | 15,032 | 13,578 | 1,454 |
Transplant | 36,674 | 29,784 | 6,890 |
Remission post-consolidation and post-transplant | 2,838 | 1,772 | 1,066 |
Subsequent treatments | 39,701 | 35,476 | 4,225 |
End of life | 8,883 | 9,373 | −490 |
ICER ($ per QALY) (liposomal daunorubicin and cytarabine versus 7 + 3) | 110,283 | ||
7 + 3 = conventional (non-liposomal) cytarabine and daunorubicin; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year.
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results: On-Trial and Post-Trial Period (143 Weeks = 33 Months)
Parameter | Liposomal daunorubicin and cytarabine | 7 + 3 | Incremental (liposomal daunorubicin and cytarabine versus 7 + 3) | |||
|---|---|---|---|---|---|---|
On-trial period | Post-trial period | On-trial period | Post-trial period | On-trial period | Post-trial period | |
Discounted LYs | ||||||
Total LYs | 1.81 | 1.01 | 1.16 | 0.30 | 0.65 | 0.71 |
By health state | ||||||
Progression-free | 0.53 | 0.01 | 0.30 | 0.01 | 0.23 | 0.00 |
Post-progression | 1.28 | 0.99 | 0.86 | 0.29 | 0.42 | 0.70 |
Discounted QALYs | ||||||
Total QALYs | 0.78 | 0.53 | 0.37 | 0.17 | 0.41 | 0.36 |
By health state | ||||||
Progression-free | 0.33 | 0.01 | 0.19 | 0.01 | 0.14 | 0 |
Post-progression | 0.68 | 0.52 | 0.46 | 0.16 | 0.22 | 0.36 |
Disutilities | −0.22 | 0 | −0.28 | 0 | 0.06 | 0 |
Discounted costs ($) | ||||||
Total Costs | ||||||
Acquisition | 68,877 | 0 | 3,576 | 0 | 65,301 | 0 |
Administration | 76,566 | 0 | 69,739 | 0 | 6,827 | 0 |
Treatment monitoring | 2,686 | 0 | 3,230 | 0 | −544 | 0 |
Adverse events | 15,032 | 0 | 13,578 | 0 | 1,454 | 0 |
Transplant | 36,674 | 0 | 29,784 | 0 | 6,890 | 0 |
Remission post-consolidation and post-transplant | 2,713 | 132 | 1,657 | 120 | 1,056 | 12 |
Subsequent treatments | 39,412 | 314 | 35,337 | 150 | 4,075 | 164 |
End of life | 7,667 | 8,908 | 1,252 | 488 | 6,415 | 8,420 |
ICER ($ per QALY) (liposomal daunorubicin and cytarabine versus 7 + 3) | On-trial period: $201,691/QALY; Post-trial period: $2,597/QALY | |||||
7 + 3 = 7 days of cytarabine plus 3 days of daunorubicin; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year.
Scenario Analyses
Table 13: Summary of the CADTH Scenario Analysis
Scenario | Drug | Sequential ICER ($ per QALY) | |
|---|---|---|---|
1 | Alternate assumption for parametric OS curve post-HSCT for patients receiving 7 + 3 (Gompertz) | 7 + 3 | Reference |
liposomal daunorubicin and cytarabine | 123,821 | ||
2 | Alternate assumption for parametric OS curve for patients who do not achieve remission (Gompertz) | 7 + 3 | Reference |
liposomal daunorubicin and cytarabine | 133,993 | ||
3 | Use sponsor’s assumptions for parametric curves for post-consolidation OS (Log-normal) | 7 + 3 | Reference |
liposomal daunorubicin and cytarabine | 108,226 | ||
4 | Revised parametric EFS curves based on KM curves right-censored at 5 patients | 7 + 3 | Reference |
liposomal daunorubicin and cytarabine | 111,048 | ||
5 | 70% of patients in liposomal daunorubicin and cytarabine and 7 + 3 receiving outpatient consolidation therapy | 7 + 3 | Reference |
liposomal daunorubicin and cytarabine | 102,829 | ||
6 | 10-year time horizon | 7 + 3 | Reference |
liposomal daunorubicin and cytarabine | 129,181 | ||
7 | Health state utilities and disutilities based on sponsor-provided study, Joshi et al., 2019 | 7 + 3 | Reference |
liposomal daunorubicin and cytarabine | 110,571 | ||
8 | Post-HSCT mortality HR of 2.3 | 7 + 3 | Reference |
liposomal daunorubicin and cytarabine | 103,963 | ||
7 + 3 = conventional (non-liposomal) cytarabine and daunorubicin; EFS = event-free survival; HR = hazard ratio; HSCT = hematopoietic stem-cell transplant; ICER = incremental cost-effectiveness ratio; KM = Kaplan-Meier; OS = overall survival; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the Budget Impact Analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) that compared the change in expenditure with the adoption of liposomal daunorubicin and cytarabine compared to a reference scenario where liposomal daunorubicin and cytarabine was not available. The BIA was modelled over a 3-year time period (2022 to 2024) and a baseline year (2021). The population of interest was adults with newly diagnosed t-AML or AML-MRC, which is in line with the proposed Health Canada indication and the sponsor’s reimbursement request. The reference scenario included the availability of 7 + 3 (daunorubicin and cytarabine) and the new drug scenario included the availability of liposomal daunorubicin and cytarabine. The BIA was undertaken from the public payer perspective for the Canadian setting (including inpatient and outpatient drug costs).
The sponsor used an epidemiologic, incidence-based approach to estimate the eligible population size as illustrated in Table 15.
Table 15: Sponsor's Estimation of the Size of the Eligible Population
Population | Baseline year | Year 1 | Year 2 | Year 3 |
|---|---|---|---|---|
Canadian population | ||||
18 years and over | 30,987,191 | 31,355,226 | 31,723,261 | 32,091,296 |
Quebec population | ||||
18 years and over | 6,981,985 | 7,034,434 | 7,086,883 | 7,139,331 |
Canadian population (excluding Quebec) | ||||
18 years and over | 24,005,206 | 24,320,792 | 24,636,379 | 24,951,965 |
Number of new cases of AML in adults (excluding Quebec)a | 989 | 1,002 | 1,015 | 1,028 |
Number of adult patients with t-AML(10%) | 99 | 100 | 102 | 103 |
Number of adult patients with AML-MRC (25%) | 247 | 251 | 254 | 257 |
Total number of adult patients with t-AML or AML-MRC | 346 | 351 | 355 | 360 |
Number of adult patients with t-AML and AML-MRC who are eligible for intensive chemotherapy (77%) | 267 | 270 | 274 | 277 |
AML-MRC = acute myeloid leukemia with myelodysplasia-related changes; t-AML = therapy-related acute myeloid leukemia.
aCalculated by multiplying 4.12 per 100,000 by the Canadian population excluding Quebec. The Canadian population for 2021 to 2024 was projected using linear extrapolation of Statistics Canada data from 2013 to 2019.
Key inputs to the BIA are documented in Table 16.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 270 / 274 / 277 |
Market uptake (3 years) | |
Uptake (reference scenario) 7 + 3 | 100% / 100% / 100% |
Uptake (new drug scenario) liposomal daunorubicin and cytarabine 7 + 3 | 25% / 35% / 45% 75% / 65% / 55% |
Cost of treatment (per patient) | |
Cost of treatment per 1L 28-day induction cycle liposomal daunorubicin and cytarabine 7 + 3a | $46,642 $1,846 |
7 + 3 = 7 days of cytarabine plus 3 days of daunorubicin; 1L = first-line.
aThe sponsor used a weighted price of cytarabine, assuming 37% of patients would be under the age of 60 and would thus receive double the dose of cytarabine as part of 7 + 3 therapy.
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor’s results suggested the introduction of liposomal daunorubicin and cytarabine would lead to a budget impact of $4,408,784 in year 1, $6,252,389 in year 2, and $8,141,761 in year 3 with a 3-year budgetary impact of $18,802,933.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Exclusion of relevant comparators: The sponsor conducted a BIA that excludes relevant comparator agents – including FLAG-IDA. Although a feasibility assessment was submitted by the sponsor to justify the exclusion of FLAG-IDA as a relevant comparator in the pharmacoeconomic model, the relevance of this comparator in estimating the potential budget impact of liposomal daunorubicin and cytarabine remains. The exclusion of FLAG-IDA limits the interpretation of the incremental budget impact of a new drug scenario with liposomal daunorubicin and cytarabine. The cost of FLAG-IDA is higher than to 7 + 3, therefore, it is expected that there would be a reduction in the incremental budget impact of a new drug scenario with liposomal daunorubicin and cytarabine.
CADTH could not address this limitation in the BIA reanalysis.
Inclusion of in-hospital drug costs: The sponsor’s analysis included drug costs regardless of whether they were administered in the inpatient or the outpatient setting. The CADTH base case must reflect a pan-Canadian (national) public drug program perspective (excluding Quebec), and therefore the costs of drugs that are administered in the inpatient setting should not be included in the reference case. The sponsor assumed that 6% and 0% of patients receiving a first consolidation and second consolidation cycle of 7 + 3, respectively would receive treatment in the outpatient setting and that 51% and 61% of patients receiving a first and second consolidation of liposomal daunorubicin and cytarabine, respectively, would receive treatment in the outpatient setting. Consequently, the inclusion of drug costs that are administered in the inpatient setting of are a substantial proportion of the costs – approximately 99% for 7 + 3 and 91% for liposomal daunorubicin and cytarabine.
CADTH revised the base case to exclude drug costs that are administered on an inpatient basis.
CADTH conducted a scenario analysis to consider a broader Canadian health care payer perspective to include the cost borne by the hospital setting and including the cost associated with drug administration.
Uncertainty in the derivation of eligible patient population: The sponsor assumed a homogenous group of individuals – i.e., Canadian population ≥ 18 years with a common 4.12 incidence rate, a 10% incidence of t-AML and 25% of AML-MRC, and that 77% of patients would be eligible for intensive chemotherapy regardless of age. The sponsor also assumed that the incidence cases would stay constant (4.12) over the 3 years. Clinical experts consulted by CADTH indicated that incidence rate is likely higher, although variable across jurisdictions in Canada. Statistics Canada data from 2017 estimated 1,075 new cases of AML in Canada (excluding Quebec) with an incidence rate ranging from 0.8 per 100,000 population for age 25 to 29 years old to a rate of 25.9 per 100,000 population for ages 90 years +.14 The assumptions made by the sponsor may underestimate the eligible patient population.
CADTH revised the base case incidence of new AML cases in Canada to 4.89/100,000 based on Statistics Canada data (for patients > 20 years of age) and conducted scenario analyses to assess the impact of the uncertainty in the percentage of patients with t-AML and AML-MRC, and the percentage of patients eligible for intensive chemotherapy.
CADTH could not account for different percentages of patients with t-AML and AML-MRC according to age group.
Uncertainty in estimated market share: The sponsor assumed market share estimates for liposomal daunorubicin and cytarabine of 25% in Year 1, 35% in Year 2 and 45% in Year 3. The clinical experts consulted for this review indicated that there is the potential for the market share to be much higher (i.e., approach 80%) by Year 3 compared to the sponsor’s estimate of 45%. The experts recognized that there may be variability across centres, including a potential preference for FLAG-IDA for first induction in younger patients, however, the sponsor’s estimates have the potential to underestimate the potential budget impact of liposomal daunorubicin and cytarabine.
CADTH conducted a scenario analysis to estimate the impact of increasing the market share assumptions in years 2 and 3 to 57.5% in year 2 and 80% in year 3.
Inappropriate drug cost estimates: The sponsor used a BSA of 2.0m2 in their BIA and used prices sourced from AQPP price list (Association québécoise des pharmaciens propriétaires, 2020) to inform the pricing for 7 + 3. Additionally, the clinical experts consulted by CADTH for the review indicated that they anticipate that the percentage of patients receiving outpatient consolidation therapy is unlikely to be different between the liposomal daunorubicin and cytarabine. CADTH revised the sponsor’s estimates to align with the pharmacoeconomic model.
CADTH revised the BSA to 1.81m2 and drug price estimates of cytarabine ($0.15370 per mg) and daunorubicin ($4.75 per mg) in the base case. CADTH also revised the percentage of patients receiving outpatient consolidation therapy (first and second consolidation) to be equal at 40% for liposomal daunorubicin and cytarabine and 7 + 3.
CADTH Reanalyses of the Budget Impact Analysis
Table 17: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. Revised drug prices for comparators | Cytarabine: $0.0714 per mg Daunorubicin: $4.8500 per mg | Cytarabine: $0.15370 per mg Daunorubicin: $4.7500 per mg |
2. Body surface area | 2.0 m2 | 1.81 m2 |
Changes to derive the CADTH base case | ||
1. Incidence of AML in Canada (excluding Quebec) | 4.12 per 100,000 | 4.89 per 100,000 |
2. Market share assumptions | Year 1: 25% Year 2: 35% Year 3: 45% | Year 1: 25% Year 2: 57.5% Year 3: 80% |
3. In-hospital drug costs | Include | Exclude |
4. Percentage of patients receiving outpatient consolidation therapy | 7 + 3 first consolidation: 6% outpatient 7 + 3 second consolidation: 0% outpatient CPX-351 first consolidation: 51% outpatient CPX-351 second consolidation: 61% outpatient | 7 + 3 first consolidation: 40% outpatient 7 + 3 second consolidation: 40% outpatient CPX-351 first consolidation: 40% outpatient CPX-351 second consolidation: 40% outpatient |
CADTH base case | 1 + 2 + 3 + 4 | |
AML = acute myeloid leukemia.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions, or standard errors in probabilistic analyses) that are not identified as limitations.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19.
Table 18: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $18,802,933 |
CADTH Corrections | $18,640,207 |
CADTH reanalysis 1 – increased incidence of AML | $22,123,935 |
CADTH reanalysis 2 – increase market share assumptions for years 2 and 3 | $28,902,492 |
CADTH reanalysis 3 – exclude inpatient treatment costs | $1,717,725 |
CADTH reanalysis 4 – percentage of patients receiving outpatient consolidation therapy | $18,640,207 |
CADTH base case | $2,352,109 |
AML = acute myeloid leukemia.
In the CADTH reanalyses, the estimated a budget impact for liposomal daunorubicin and cytarabine is $355,685 in year 1, $828,692 in year 2, $1,167,732 in year 3. After 3 years since entering the market, the total anticipated budget impact of liposomal daunorubicin and cytarabine is $2,352,109. If a price reduction of 68% is applied to liposomal daunorubicin and cytarabine, the 3-year budget impact is $702,896, and if a greater percentage of patients (70%) receive liposomal daunorubicin and cytarabine in an outpatient setting, the 3-year budget impact is $4,116,191. Based on the CADTH reanalysis, the inclusion of inpatient drug costs is an influential assumption of the model resulting in a 3-year budget impact of $34,304,171.
Table 19: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Scenario analysis | Scenario | Baseline year | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $677,906 | $686,818 | $695,730 | $704,642 | $2,087,190 |
New drug | $677,906 | $5,095,601 | $6,948,119 | $8,846,403 | $20,890,123 | |
Budget impact | $0 | $4,408,784 | $6,252,389 | $8,141,761 | $18,802,933 | |
CADTH base case | Reference | $43,705 | $44,279 | $44,854 | $45,429 | $134,562 |
New drug | $43,705 | $399,965 | $873,546 | $1,213,161 | $2,486,672 | |
Budget impact | $0 | $355,685 | $828,692 | $1,167,732 | $2,352,109 | |
CADTH scenario analysis: 68% price reduction | Reference | $43,705 | $44,279 | $44,854 | $45,429 | $134,562 |
New drug | $43,705 | $150,571 | $292,498 | $394,390 | $837,459 | |
Budget impact | $0 | $106,292 | $247,644 | $348,961 | $702,896 | |
CADTH scenario analysis: including inpatient treatment costs | Reference | $983,394 | $996,322 | $1,009,251 | $1,022,179 | $3,027,752 |
New drug | $983,394 | $6,183,792 | $13,095,250 | $18,052,882 | $37,331,923 | |
Budget impact | $0 | $5,187,470 | $12,085,999 | $17,030,703 | $34,304,171 | |
CADTH scenario analysis: 70% of patients receiving outpatient therapy for first and second consolidation | Reference | $76,484 | $77,489 | $78,495 | $79,500 | $235,484 |
New drug | $76,484 | $699,939 | $1,528,706 | $2,123,031 | $4,351,675 | |
Budget impact | $0 | $622,450 | $1,450,211 | $2,043,531 | $4,116,191 | |
CADTH scenario analysis: sponsor’s assumptions for percentage of patients receiving outpatient consolidation | Reference | $6,076 | $6,156 | $6,235 | $6,315 | $18,706 |
New drug | $6,076 | $484,189 | $1,119,980 | $1,575,722 | $3,179,891 | |
Budget impact | $0 | $478,034 | $1,113,744 | $1,569,406 | $3,161,184 | |
CADTH scenario analysis: Increase in cases of t-AML (by 20%) and AML-MRC (by 34%) | Reference | $67,430 | $68,317 | $69,203 | $70,090 | $207,610 |
New drug | $67,430 | $617,089 | $1,347,757 | $1,871,733 | $3,836,579 | |
Budget impact | $0 | $548,772 | $1,278,553 | $1,801,644 | $3,628,969 | |
CADTH scenario analysis: Increase in patients eligible for intensive chemotherapy (decrease 25%) | Reference | $32,779 | $33,210 | $33,641 | $34,071 | $100,922 |
New drug | $32,779 | $299,974 | $655,160 | $909,870 | $1,865,004 | |
Budget impact | $0 | $266,764 | $621,519 | $875,799 | $1,764,082 | |
CADTH scenario analysis: sponsor’s market share assumptions for years 2 and 3 (35% and 45%, respectively) | Reference | $43,705 | $44,279 | $44,854 | $45,429 | $134,562 |
New drug | $43,705 | $399,965 | $549,275 | $702,278 | $1,651,518 | |
Budget impact | $0 | $355,685 | $504,421 | $656,849 | $1,516,956 |
AML-MRC = acute myeloid leukemia with myelodysplasia-related changes; t-AML = therapy-related acute myeloid leukemia.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.