CADTH Health Technology Review
Remote Monitoring Programs for Cardiac Conditions
PROSPERO Registration Number:
Realist Review: CRD42021229271
Perspectives and Experiences Review: CRD42020211271
Health Technology Assessment
Authors
Realist Review
Alexander Clark and Bailey Sousa led the Realist Review; screened and selected studies; extracted, tabulated, critically appraised, and interpreted data; wrote the Realist Review; revised the review based on reviewers’ feedback; and provided final approval to the version of the report submitted for publication.
Perspectives and Experiences Review
Andrea Smith led the protocol development for the Perspectives and Experiences Review; screened, selected, and critically appraised included studies; constructed the synthetic analysis and wrote the review; revised the review based on reviewers’ comments; and provided final approval to the version of the report submitted for publication. She also participated in patient engagement and stakeholder consultation activities.
Ethical Issues Analysis
Duncan Steele led the protocol development for the ethics analysis, including revisions according to reviewers’ feedback. Additionally, he screened and selected articles retrieved by the ethics search according to eligibility criteria, thematized relevant content according to core values, wrote the report; and revised the report based on reviewers’ comments. He provided final approval of the version submitted for publication.
Patient Engagement
Tamara Rader led patient engagement activities and wrote the summary of those activities included in the report. She also reviewed the protocol and drafts of the patients’ Perspectives and Experiences Review and provided final approval to the version of the report submitted for publication.
Research Information Services
Danielle MacDougall designed the database search strategies for all sections of the report, executed the search strategies, completed grey literature searches, maintained search alerts, prepared the search methods and appendix, and provided final approval to the version of the report submitted for publication.
David Kaunelis peer-reviewed the search strategies, assisted with report referencing, and approved the final version of the report submitted for publication.
Program Development
Jeff Mason developed the project plan, contributed to the coordination of the review, authored the introduction, and contributed to the writing of the Discussion as well as the Conclusions and Implications for Policy-Making sections of the report. He approved the final version of the report submitted for publication.
Jonathan Harris contributed to the writing of the Discussion as well as the Conclusions and Implications for Policy-Making sections of the report and provided final approval to the version of the report submitted for publication.
Contributors
The authors would like to acknowledge:
Saleema Allana, Karice Hyun, Annette Peart, and Rhianna (Anna) Penfold for their contributions in conducting the Realist Review.
Gino De Angelis for providing project oversight and coordination throughout the planning, conduct, and reporting of the clinical review, including providing methodological input and critically reviewing drafts of the protocol and final report
Deirdre DeJean for providing methodological input for the Perspectives and Experiences Review and for critically reviewing drafts of the protocols and drafts of the ethical issues analysis and the Perspectives and Experiences Review
Brit Cooper-Jones for formulating the key messages for broader public understanding of CADTH’s assessment on remote monitoring
Paula Murray for providing project management support.
The authors would also like to thank the external stakeholders who submitted feedback on the draft report.
External Reviewers
These individuals kindly provided comments on a draft version of this report.
Krisan Palmer, RN
Regional Telehealth Director and Clinical Lead
Horizon Health Network, Saint John, New Brunswick
Olivia Magwood, MPH, PhD(c)
Research Associate
Bruyère Research Institute
Ottawa, Ontario
Conflicts of Interest
Duncan Steele disclosed a financial interest (i.e., stocks) in UnitedHealth Group. No other authors declared conflicts of interest.
Abbreviations
CASP
Critical Appraisal Skills Programme
CINAHL
Cumulative Index to Nursing and Allied Health Literature
EUnetHTA
European Network for Health Technology Assessment
HTA
health technology assessment
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PRISMA-P
Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols
RAMESES
Realist And Meta-narrative Evidence Syntheses: Evolving Standards
SPIDER
Sample, Phenomenon of Interest, Design, Evaluation, Research type
Section | Amendment | Page | Rationale |
|---|---|---|---|
Realist Review literature search methods (Addendum, vol. 10, no. 2a) | WHO’s International Clinical Trials Registry Platform search portal was removed from the search strategy. | 8 | Access portal was not working at the time the grey literature search was conducted. |
Realist Review literature search methods (Addendum, vol. 10, no. 2a) | Regular alerts were conducted; however, citations were not screened or included in the analysis of the final report. | 8 | Time constraints related to the project deadline prevented this. Given the large number of included studies, it was unlikely that additional studies identified in the alerts would have changed the overall conclusions of the Realist Review. |
Realist Review screening and study selection (Addendum, vol. 10, no. 2a) | The DistillerSR AI tool was not used to automatically check any references for inclusion; this was done by the project team. | 10 | To better ensure accuracy. |
Realist Review data extraction (Addendum, vol 10., no. 2a) | Authors were not contacted for missing data. | 11 | Time constraints related to the project deadline prevented this. |
Realist Review synthesis (Addendum, vol. 10, no. 2a) | The panel of experts was not involved in synthesis stage 2. | 13 | Time constraints related to the project deadline prevented this. |
Ethics Review literature search methods (vol. 10, no. 2a) | The Philosopher’s Index database and Scopus database were added to the Ethics Review literature search. | 18 | The Philosopher’s Index database was acquired after protocol was published. Scopus was added to round out literature search. |
Perspectives and Experiences Review (vol. 10, no. 2a) | NVivo 11 was not used for coding and data management. | 15 | The number of included studies did not require software for data management. |
Opportunities for stakeholder feedback | Stakeholders were not provided the opportunity to comment on a list of included studies. | 23 | Time constraints related to the project deadline prevented this. Stakeholders were instead encouraged to comment on the list of included of studies while the draft report was posted for stakeholder feedback. |
Stakeholder consultation | Stakeholder consultations were not conducted. | 20 | Process not anticipated to provide novel information not already captured during the review. Stakeholders were invited to provide feedback through the stakeholder feedback process. |
Key Messages
Remote monitoring is a type of telehealth whereby health care is delivered to patients outside traditional settings by allowing health data to be exchanged between patients and health care providers using telecommunication techniques (e.g., video conferencing) or stand-alone devices (e.g., portable heart rate monitors). The goals of remote monitoring centre around promoting home-based self-management to improve patient outcomes and/or reduce health system usage.
CADTH’s Health Technology Assessment included the following analyses:
A Realist Review: This sought to identify key perceived or actual mechanisms of remote monitoring programs. Substantial evidence was available regarding the use of remote monitoring programs for heart failure (n = 64) and cardiac rehabilitation (n = 23), limited evidence was available for atrial fibrillation (n = 4), and none was available for hypertension.
A Perspectives and Experiences Review: This thematic synthesis of primary qualitative research sought to understand and describe peoples’ experiences with and perspectives on remote monitoring programs for cardiac conditions. CADTH also engaged patients and caregivers directly in a patient engagement section.
An Ethics Review: This sought to identify and reflect upon key ethical issues that should be considered when contemplating the implementation of remote monitoring programs.
Overall, the vast majority of sampled patients, caregivers, and health professionals consistently found or perceived remote monitoring programs across different cardiac conditions to be easy to use and beneficial to health.
Remote monitoring programs may be an attractive adjunct as opposed to an alternative to existing health professionals and services.
Although remote monitoring programs may ultimately reduce avoidable hospitalizations, they may increase net costs and workload during set-up and operational phases without careful pathway design and expectations management.
More research is needed to identify the costs and cost-effectiveness of remote monitoring programs across chronic cardiac conditions.
Abstract
Context and Decision Problem
Remote monitoring is a type of telehealth whereby health care is delivered to patients outside traditional settings by allowing health data to be exchanged between patients and health care providers using telecommunication technologies (e.g., video conferencing) or stand-alone devices (e.g., portable heart rate monitors). The goals of using remote monitoring centre around promoting home-based self-management to improve patient outcomes or reduce health system usage. These outcomes are, in turn, theorized to enable patients to continue living at home and in the community.
Remote monitoring programs offer a potentially compelling alternative and supplement to traditional face-to-face health care for people in Canada with chronic cardiac conditions. Prior to the COVID-19 pandemic, remote monitoring for cardiac conditions was being studied in a number of projects and jurisdictions across the country. Since the COVID-19 pandemic began, interest in, demand for, and use of virtual care for patients with cardiac conditions (which includes remote monitoring) has increased. Jurisdictions across Canada have announced new funding for programs and clinician groups have produced guidance to support the implementation of patient care at a distance.
Based on jurisdictional feedback gathered by CADTH, the stage of diffusion of remote monitoring programs for people with cardiac conditions varies across the country. As such, while there is broad interest in the topic, the needs of each jurisdiction vary greatly. There is also uncertainty about which patients would benefit from participation in remote monitoring programs. Jurisdictions are faced with the question, how should remote monitoring programs for patients living in rural, remote, and urban settings be implemented? One driver behind this problem is a desire to provide care to patients in their homes or communities, minimizing the need for patients to travel or be transported from their homes to the hospital.
Realist Review
Methods
A Realist Review was conducted to identify key perceived or actual mechanisms of remote monitoring programs for adult persons living with a chronic cardiac condition or post-cardiac event, or persons who care for those living with a chronic cardiac condition or post-cardiac event. To be included, studies had to contain data or themes reasonably interpreted as relating to program mechanisms.
Results
Remote monitoring programs across cardiac conditions were consistently found or perceived by the vast majority of sampled patients, caregivers, and health professionals (often 80% to 90%) to be easy to use and beneficial to health.
Across all conditions sampled, in terms of the key mechanisms, adequate program technology was necessary but insufficient to foster positive outcomes. To ensure program effectiveness, technology had to integrate well with patients’ daily life patterns and homes, and promote understanding in patients not only of their condition but also of their personal health status. The main issues around technological uptake related far less to general fears about the technology than to frustrations around common but technically straightforward issues; notably, unstable connectivity of devices and poor battery life.
For cardiac rehabilitation, programs were seen to focus predominantly on promoting healthy lifestyle behaviours, with the capacity of technology to facilitate these outcomes being dependent on their ability to integrate with patients’ life patterns. Programs were most effective when motivated patients received highly individualized program content and components and leveraged existing strengths in relationships between health care providers and patients.
Patient experiences of heart failure were far more ambiguous, and programs were seen to provide vital support for daily ongoing self-care and knowledge. Programs tended to be more complex; nevertheless, the programs were most effective when technological aspects of programs were easy to use, supported adequately, and, crucially, were highly unobtrusive in patients’ lives. Similar to cardiac rehabilitation programs, heart failure programs were viewed as adjuncts to, not replacements for, traditional face-to-face health care provision; however, unlike cardiac rehabilitation programs, remote monitoring programs for heart failure provided more useful knowledge to interpret symptoms and guide self-care daily.
Evidence regarding atrial fibrillation programs was scant but ease of technological use guided patients’ uptake of platforms and was also seen to complement face-to-face health care.
Perspectives and Experiences Review
A thematic synthesis of primary qualitative research was conducted to understand and describe peoples’ experiences with and perspectives on remote monitoring programs for chronic cardiac conditions and cardiac rehabilitation.
Ideas around age and technological literacy were commonly raised by people living with cardiac conditions as a reason for being disinterested or unable to participate in remote monitoring programs. When people encountered technological challenges, they expressed being discouraged from adopting and using remote monitoring. Having informal caregivers, particularly adult children, who could help troubleshoot the technologies helped them overcome these hurdles. Sometimes the challenges were not with the use of the technologies but with the physical installation of the equipment itself, which meant finding the space and having the necessary connections, which was not always easy or possible, depending on peoples’ housing arrangements. These findings point to opportunities to develop programs that account for and anticipate potential challenges and provide the needed level of support and technological options that facilitate engagement with remote monitoring technologies.
Many people living with chronic cardiac conditions articulated an openness to taking greater responsibility for their own health through self-management. This required people living with cardiac conditions to make connections between their measurements and their behaviours over time. The self-management of medication required more guidance and support from health care providers in order for people with chronic cardiac conditions to become confident in changing their dosages or medications. Remote monitoring played a critical role as an external motivation for their self-management as it required them to be accountable and provided them with reminders. Once they discontinued remote monitoring programs, people described struggling with or giving up on monitoring their condition and lifestyle changes. These findings highlight the need for programs to provide adequate time to facilitate the process of self-management as well as the potential for longer-term technologies to support motivation and provide reminders.
People saw remote monitoring programs as a means of providing security through being watched, particularly for those with heart failure, and a way of accessing health care and fostering a closer connection between providers and patients. Providers and patients alike appreciated the ways that remote monitoring programs fostered people living with cardiac conditions to be more involved in their care. These findings suggest that remote monitoring was not an addendum to care but was experienced as a model of providing health care for patients with chronic cardiac conditions.
Providers’ experiences and expectations with remote monitoring embodied views of remote monitoring as both taking time and reducing time. Remote monitoring was seen by providers as increasing the amount of time needed due to the increased number and length of consultations. On the other hand, providers described remote monitoring programs as saving time because of the ability to identify and address health concerns early. Workload, particularly caseload, was raised by nurses as a concern when programs underestimated or did not allow for adequate time for consultations. When remote monitoring programs were not technically or organizationally integrated into health care delivery, they presented challenges to providers. These findings reveal opportunities to maximize the success of remote monitoring programs by taking the number and length of patient consultations into account and ensuring appropriate integration, particularly with electronic health records, within health care systems.
Ethics Review
Methods
An ethical analysis was conducted, building from a literature review of articles with either explicit normative analysis of ethical issues arising in the use of remote monitoring, whether for the treatment of the conditions of interest or more generally, or empirical research that included ethical issues arising in the use of remote monitoring.
Results
The goals of remote monitoring programs are not always clear. For decision-makers to implement their program with a good chance of success, they should pause to assess what gaps exist in current care and what options exist to meet those needs (technological, human resource, transportation, others). This assessment should occur with the inclusion of the voices and perspectives of those who will be most impacted by the decision, and who will also play a key role in the uptake and success of the program. That should likely include patients (especially lower-income, non-White, non-male ones, who are less likely to be represented at decision tables), their informal caregivers, such as family members and spouses who often play central and critical roles, as well as general practitioners and cardiac teams.
Remote monitoring programs are often framed as a solution to provide care to patients in their own homes or communities, and to increase their access to high-quality services. Unfortunately, there is limited evidence about the effectiveness of various components of remote monitoring programs. These evidence gaps are most notable with rural or remote, racialized and Indigenous people, and people of low socioeconomic status.
Remote monitoring programs are not necessarily a solution to health access challenges. Attention should be paid to what costs are borne by patients or their families in the target population(s) and subgroups. What may be a small expense to some patients and their families could be an impossible barrier to others (e.g., transportation to clinic, internet provider at home).
Programs that involve private third-party technology raise concerns around privacy and informed consent. User agreements between patients and a third party may be challenging because the risks to themselves and their genetic relatives from their health and other information may not be clear or reasonably known. If such legal agreements are a requirement for patients to receive care, this raises concerns about freedom of choice.
Conclusions and Implications for Policy-Making
From a program design standpoint, the incorporation of highly individualized clinical information via feedback data to the patient on their condition and progress can maximize the effectiveness of remote monitoring programs for heart failure, atrial fibrillation, and cardiac rehabilitation. Program benefits were dependent on the program integrating well with each individual patient’s context: their daily habits and life patterns. Future remote monitoring programs for cardiac conditions should not only use technology appropriately and efficiently but also be sufficiently adaptive to different patients’ needs and designed to adapt to different patients’ home settings.
Limited evidence on remote monitoring programs delivered in rural or remote settings is significant from a public policy standpoint, given common assertions that these programs increase access to specialist care in rural and remote populations. Similarly, the gap in evidence around the perspectives, experiences, and needs of family and other informal caregivers is also significant. Decision-makers should consider the additional work and costs to patients and caregivers associated with remote monitoring programs. Further evaluation is needed to better understand the effectiveness of remote monitoring programs for cardiac conditions in predominantly rural or remote populations, and the impacts on family and informal caregivers.
There is little evidence on the potential moderating effects of patient age, sex and/or gender, race and/or ethnicity, and income on program usage and effectiveness. More emphasis should be placed on understanding the experiences of those who may be marginalized and/or have poorer access to technologies, including reliable high-speed internet, and who may experience discrimination in the health system. For Canadian decision-makers interested in understanding how remote monitoring programs could complement the care of First Nations, Inuit, and Métis patients, no component of this report identified evidence that included Indigenous people or was concerned with indigeneity. This evidence gap emphasizes the need for decision-makers to ensure that the voices of people who are often excluded or marginalized are included when designing, implementing, and evaluating remote monitoring programs.
Remote monitoring programs may be an attractive adjunct as opposed to an alternative to existing health professionals and services. Although programs may ultimately reduce avoidable hospitalization, there is a strong likelihood that without careful pathway design and expectations management, remote monitoring programs may increase net costs and workload for host providers during set-up and operational phases. More research is needed to identify the costs and cost-effectiveness of remote monitoring programs across chronic cardiac conditions.
Introduction and Rationale
Remote monitoring (also known as remote patient monitoring or remote patient management) is a type of telehealth whereby health care is delivered to patients outside traditional settings by allowing health data to be exchanged between patients and health care providers using telecommunication technologies (e.g., video conferencing) or stand-alone devices (e.g., portable heart rate monitors).1,2 Canada Health Infoway has defined remote monitoring as “the delivery of [health care] to patients outside of conventional settings enabled by a technological application or device.”1 The stated goals of using remote monitoring in clinical practice centre around promoting home-based self-management to improve patient outcomes or reduce health system usage.3 Self-management strategies typically aim to improve diet and cholesterol levels, exercise levels, knowledge of the patient’s health condition, confidence to stay at home, patient satisfaction, and quality of life. These outcomes are, in turn, theorized to lead to improved patient outcomes over time and to enable patients to continue living at home and in the community.3
At its core, remote monitoring relies on the use of telecommunication technology for the transmission of health data between patients and health care providers.2 Examples of health data that may be transmitted include readings of physiologic activity such as oxygen saturation levels and cardiac rhythm or patient observations such as mental status and medication intake. For example, for patients with hypertension, blood pressure readings could be transmitted to evaluate treatment effectiveness and adherence. For the purposes of this HTA, CADTH considers a remote monitoring program to be a formal, organized offering from a health authority or health care organization that may employ a variety of technologies (e.g., video conferencing, blood pressure monitors, online portals) to collect and transmit patient data. This contrasts with the one-off use of remote monitoring devices (e.g., personal electrocardiogram devices) that may be used or prescribed by an individual clinician or clinician group.
Remote monitoring programs offer a potentially compelling alternative and supplement to traditional face-to-face health care for people in Canada with chronic cardiac conditions. The current base of trials evaluating remote monitoring programs continues to grow, but the type of evidence that these trials generate is often too general to be especially useful for local planning and implementation. This not only hampers local service design but also potentially harms patients and increases system-wide costs by failing to realize the potential of different remote monitoring techniques for different contexts.4,5
This situation should not, however, lead to the rejection of remote monitoring for the large population of people in Canada with cardiac conditions. Trials over the past 20 years continue to indicate that remote monitoring programs for cardiac conditions are generally effective.4,6,7 For example, programs for patients with a variety of cardiac conditions have been shown by randomized trials and meta-analyses to be effective at reducing adverse events (notably hospitalization) and improving quality of life8-10 and have, for more than a decade, been found in systematic reviews to have comparable effects to site-based programs.10 That said, beyond these positive effects, the actual components of the remote monitoring programs remain poorly described in the vast majority of published trials4,11 and meta-analyses.12 Reviewing the body of remote monitoring programs for heart failure, this tendency has been said to contribute to a policy-maker’s nightmare due to the evidence being vast, fragmented, heterogeneous, of variable quality, and with no clear answers to the question of what technologies, supported by what service infrastructure, to provide for whom.
Those charged with designing or adapting remote monitoring programs for specific settings therefore lack an evidence base that is sufficiently specific to inform their decisions. More research is still needed to unpack which components of remote monitoring programs matter most in different contexts for different populations.
Remote Monitoring for People With Cardiac Conditions
In Canada, the number of people with heart failure is increasing annually, with more than 600,000 people currently living with the condition and more than 50,000 new cases diagnosed each year.13,14 An estimated 350,000 Canadians live with atrial fibrillation,15 and more than 5.4 million Canadians have hypertension.16 Although many Canadians with cardiovascular disease would benefit from cardiac rehabilitation, only an estimated 10% to 30% have access to such programs.17,18
Remote monitoring for people living with cardiac conditions has been proposed as a means of detecting health issues earlier while also reducing the need for routine office visits, emergency department visits, and hospital admissions.19,20 Remote monitoring also aims to help patients maintain independence and remain in their home or community, which may be particularly relevant for patients living in rural or remote locations.18,19,21,22 For conditions like hypertension, dozens of home monitors are readily available to patients.23 Elsewhere in the remote monitoring space, several companies have drawn media and health care provider attention to low-cost, direct-to-consumer devices that are capable of monitoring heart rate, heart rhythm, and blood pressure at home.24-27 Large telehealth providers have also emerged to support care for cardiac patients.28,29 However, there remains uncertainty and gaps in the evidence surrounding the use of remote monitoring.30 Remote monitoring also raises concerns about patient privacy and data security because of its reliance on data and internet connections.18,22
Based on a comparison of various program objectives and characteristics, including duration,3 remote monitoring programs for people with cardiac conditions tend to be of 2 general forms: those that are without a pre-specified duration (e.g., ongoing monitoring) and those that are of a pre-set duration (between 4 weeks and 6 months). Remote monitoring programs of a shorter duration are designed to help patients improve their self-management, with the goal that improvements will last beyond the duration of the program. Ongoing remote monitoring programs are also designed to support self-management and can have the additional objective of improving the continuity of care through improved communication between care providers and patients.
Program activities can vary widely within remote monitoring programs for people with cardiac conditions. In general, they include processes that collect and transmit patient data, which is then evaluated and triggers a form of intervention.1 Data collection and transmission varies by what is collected, how it is collected (e.g., by a device or by the person living with a cardiac condition), how it is transmitted, and when it is transmitted (e.g., frequency). The data, once received, can be evaluated by a health care provider or program staff, a third party, or an algorithm. Interventions vary in how they are provided and their scope, which can include medication adjustments, prompts to support a healthy diet, increased physical activity, and smoking cessation, or advice to seek in-person care.
The severity of patients’ conditions is important when considering remote monitoring programs for people with cardiac conditions.24 This may be because, for remote monitoring programs to reduce health care utilization and to offset the expense of operating remote monitoring programs, it may be important to enrol patients who are at moderate or high risk of emergency department visits or hospitalization rather than enrol healthier patients.24 Hence, many large-scale programs typically describe contact with health care services (e.g., 1 or more emergency department visits) as eligibility criteria.3,24
Improved self-management of patients with chronic cardiac conditions through remote monitoring has been viewed as a means of reducing resource utilization across health care systems — including pre-hospital, emergency, acute care, and long-term care settings. These reductions in health care utilization are seen as both freeing up staff time (reducing pressures on health systems) and creating an opportunity for cost savings.3
Jurisdictions have expressed interest in an assessment of remote monitoring that explores the following patient groups: heart failure, atrial fibrillation, hypertension, and people eligible for cardiac rehabilitation.
Jurisdictions also expressed interest in an assessment of remote monitoring that includes rural, remote, and urban populations. CADTH’s Implementation Support and Knowledge Mobilization team indicated there is variability of cardiac care available to patients across the country, depending on the type of community in which they live. Therefore, remote monitoring programs may also have different impacts on patients in rural, remote, or urban settings.
Remote Monitoring Programs in Canada
Remote monitoring takes on particular salience in a geographically large country such as Canada, as it enables the delivery of health care outside of health care institutions and thus to patients who live remotely or rurally. In Canada, before the COVID-19 pandemic, remote monitoring of cardiac conditions was being studied in a number of projects and jurisdictions.1,18,21,22,29,31,32 In 2018, the Newfoundland and Labrador Centre for Applied Health Research completed an environmental scan that identified remote monitoring programs for chronic conditions in place across Canada and selected international jurisdictions to “inform the implementation and evaluation of [remote monitoring] for those living with chronic disease in remote and rural [Newfoundland and Labrador].”3 The authors identified 22 remote monitoring programs (or initiatives) active in the previous 5 years, 11 of which were in Canada and enrolled people with cardiac conditions. Of these 11 Canadian remote monitoring programs, some enrolled more than 1 type of patient group:
8 were available to people with heart failure
2 were open to people with hypertension and 1 for pulmonary hypertension
1 was for cardiac rehabilitation
2 were available to all people with chronic diseases
1 was open to all people in the province with a provincial health card.
These 11 remote monitoring programs were available to residents of British Columbia, Newfoundland and Labrador, New Brunswick, Ontario, Prince Edward Island, and Quebec. The scan also identified an additional 10 pilot remote monitoring programs or ongoing research studies from Canada. The environmental scan did not discuss barriers or facilitators to implementation, nor did it evaluate the remote monitoring programs identified.
Since the COVID-19 pandemic began, interest in, demand for, and use of virtual care for patients with cardiac conditions (which includes remote monitoring) has increased and research into the pandemic’s impact on the delivery of cardiac care is beginning to emerge.33-37 Jurisdictions across Canada, such as British Columbia, Ontario, and Saskatchewan, announced new funding for programs (both pilot projects and ongoing funding) and clinician groups, such as the Canadian Cardiovascular Society, produced guidance to support the implementation of patient care (e.g., virtual cardiac rehabilitation) at a distance.38-41
Based on jurisdictional feedback, the stage of diffusion of remote monitoring programs for people with cardiac conditions varies across the country. Some jurisdictions, such as New Brunswick, have well-established programs serving many different patient groups. Others, such as Manitoba and Saskatchewan, are just beginning to explore implementing remote monitoring programs for patients with cardiac conditions. As such, while there is broad interest in the topic, the needs of each jurisdiction vary greatly, depending on the level of adoption of remote monitoring technologies. There is also uncertainty about which patients would benefit from participation in remote monitoring programs. Because of existing work, jurisdictions indicated that additional assessment of remote monitoring programs for patients with implanted cardiac devices, such as implantable cardioverter-defibrillators, is not needed at this time.
Decision Problem
According to some jurisdictions, the implementation of remote monitoring technologies is not a question of if it will happen; rather, it is a question of when and how it will happen. Because of this (and the varied stages of diffusion), jurisdictions are faced with the question, how should remote monitoring programs for patients living in rural, remote, and urban settings be implemented? The driver behind this problem appears to be a desire — from policy-makers, patients, and health care providers alike — to provide care to patients in their homes or communities, minimizing the need for patients to travel or be transported from their homes to the hospital.
Objective
The purpose of this HTA is to address the decision problem through a series of analyses, including a Realist Review of remote monitoring programs for cardiac conditions; a qualitative evidence synthesis of the perspectives and experiences of those participating in remote monitoring programs for cardiac conditions, including patients, informal caregivers, and health care providers; and an analysis of ethical considerations. These analyses were informed by the results of a CADTH Environmental Scan of remote monitoring programs for cardiac conditions in Canada.42
Research Questions
The proposed HTA will address the decision problem by exploring the following research questions:
Realist Review
What aspects of remote monitoring programs for chronic cardiac conditions or post-cardiac events influence patient and system-level outcomes, for whom, in what circumstances, to what extent, and why?
Perspectives and Experiences Review
For people living with a chronic cardiac condition or post-cardiac event, what are their expectations of, experiences with, and perspectives on remote monitoring programs?
What are their families’ and care providers’ expectations of, experiences with, and perspectives on remote monitoring programs?
How do people living with a chronic cardiac condition or post-cardiac event, their families, and their care providers experience and understand:
how to adopt and use remote monitoring technologies?
how remote monitoring programs move health care into peoples’ places of residence and what is the impact of this shift on the families of people living with a chronic cardiac condition or post-cardiac event?
the changes in roles and responsibilities that can accompany remote monitoring programs and what the impact of this shift is on the families of people living with a chronic cardiac condition or post-cardiac event?
how and when remote monitoring programs are seen as working or as not working?
Ethics Review
What are the ethical issues related to the implementation of remote monitoring programs?
How might these issues be addressed in rural, remote, and urban settings?
Methods
To inform the conduct of this HTA, a preliminary scoping review of the existing literature — including HTAs and systematic reviews — was conducted. A protocol was written a priori, using appropriate reporting guidelines (e.g., the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols ([PRISMA-P]) for guidance on clarity and completeness. These guidelines were followed throughout the study process. Any deviations from the protocol were disclosed in this final report and updates were made to the PROSPERO submission accordingly (Realist Review: CRD42021229271; Perspectives and Experiences Review: CRD42020211271).43,44
A Realist Review was conducted to identify key perceived or actual mechanisms of remote monitoring programs for adult persons living with a chronic cardiac condition or post-cardiac event, or persons who care for those living with a chronic cardiac condition or post-cardiac event (see Realist Review section for further details). For the Perspectives and Experiences Review, a qualitative evidence synthesis of primary qualitative research was conducted to understand and describe peoples’ experience with and perspectives on remote monitoring programs for chronic cardiac conditions and cardiac rehabilitation (see Perspectives and Experiences Review section for further details). For the Ethics Review, a bioethical analysis was conducted to identify and reflect upon key ethical issues when considering remote monitoring programs for adult persons living with a chronic cardiac condition or a post-cardiac event, or their carers (see Ethics Review section for further details).
Opportunities for Stakeholder Feedback
Stakeholders were given the opportunity to provide feedback on the draft report, and the recommendations, if applicable.
Realist Review
Research Question(s)
To inform decisions about how remote monitoring programs can work most effectively, the research question underlying this review is:
What aspects of remote monitoring programs for chronic cardiac conditions or post-cardiac events influence patient and system-level outcomes, for whom, in what circumstances, to what extent, and why?
Key Messages
Remote monitoring programs are known to generally improve life quality and expectancy in patients with chronic cardiac conditions, but little is known about how programs should vary by context or the mechanisms moderating interventions effects, or how these mechanisms vary by context. This Realist Review sought to identify studies providing insights into the main mechanisms of effect of different kinds of remote monitoring programs and to examine how context influenced these mechanisms and outcomes.
Although the review identified only 1 dedicated realist evaluation, a sizable number of studies were identified that contained data on remote monitoring program mechanisms and/or contexts in studies examining programs for patients with heart failure (n = 64) and for cardiac rehabilitation (n = 23). A small number of studies (n = 4) addressed atrial fibrillation. No studies were identified focused on hypertension.
Remote monitoring programs across all the cardiac conditions were consistently seen by the vast majority of sampled patients, caregivers, and health professionals in studies to contribute to positive remote monitoring health outcomes, particularly in psychosocial and behavioural outcomes.
However, in terms of the key mechanisms and context explaining outcomes from studies, adequate program technology — while necessary — was insufficient to foster positive outcomes. Central to the positive effects of programs were mechanism-context synergies associated with the technology integrating well with patients’ daily life patterns and homes, and promoting understanding in patients not only of their condition but also of their personal health status. The main issues around technological uptake related far less to general fears about the technology than to frustrations around common but technically straightforward issues; notably, challenges around unstable connectivity of devices and poor battery life.
For cardiac rehabilitation remote monitoring programs, programs were seen to focus predominantly on promoting healthy lifestyle behaviours with the capacity of technology to facilitate these outcomes being dependent on their ability to integrate with patients’ life patterns. Programs were most effective when motivated patients received highly individualized program content and components and leveraged existing strengths in relationships between health care providers and patients.
Patient experiences of heart failure were far more ambiguous, and programs were seen to provide vital support for daily ongoing self-care. The remote monitoring programs tended to be more complex; nevertheless, the programs were also most effective when the technological aspects of programs were easy to use, supported adequately, and, crucially, highly unobtrusive in patients’ lives. Similar to cardiac rehabilitation programs, the remote monitoring programs for heart failure were viewed as complementary rather than as replacements for traditional face-to-face health care provision. However, unlike cardiac rehabilitation programs, remote monitoring programs for heart failure were seen to provide more useful knowledge to interpret symptoms and guide self-care daily.
While evidence regarding atrial fibrillation programs was scant, there was some evidence here that ease of technological use guided patients’ uptake of platforms and was also seen to complement face-to-face health care. This was key for atrial fibrillation, given remote monitoring was seen to function to prevent relatively low-probability, although potentially high-risk, arrhythmia.
Methods
This Realist Review has been developed from an addendum44 to the main HTA protocol.43 The protocol was drafted ensuring attention to elements described in the Realist And Meta-narrative Evidence Syntheses: Evolving Standards (RAMESES) publication standards, as appropriate.45 The protocol is registered with PROSPERO (CRD42021229271).
Study Design
A Realist Review was conducted to examine what works for whom, and when and why it works concerning remote monitoring programs for treatment and support of chronic cardiac conditions or cardiac rehabilitation.46 For the purpose of this review, a chronic cardiac condition is defined as a physician-confirmed diagnosis of heart failure, hypertension, or atrial fibrillation. Realist reviews are appropriate for assessing how and why various aspects of complex interventions work, for whom, in what contexts, and to what extent.46 Knowledge from a Realist Review provides useful and nuanced guidance for decision-makers in different contexts to inform local service design decisions.46 This can, for example, better ensure that interventions to promote health and self-care of chronic disease have more consistent benefits across different patients and settings.47 Accordingly, findings from realist reviews supplement and complement evidence from other methods (notably randomized trials and meta-analyses), which provide broad but less specific and useful evidence for decision-makers.4,5 While such methods convey that a health services intervention may generally work,6 the generic nature of this evidence fails to convey the influence on intervention outcomes of where the program is provided (context), how it influences outcomes (mechanisms), and what about the intervention promotes effectiveness (components).48
As an approach, realist reviews are grounded in the realist evaluation method,49 which has its roots in critical realist philosophy50 and complexity-driven methods and theory.51 These approaches share a rejection of research and theory that assume or imply that interventions such as policies, programs, or strategies involving behaviours influence outcomes in orderly, linear, law-like ways (e.g., intervention A leads to benefit B in population C).52 Instead, causality between the intervention and its effects is seen to be contingent on the effects of multiple factors — for example, related to patients, programs, and places — interacting to generate changes in outcomes.47 Under this contingent approach to causality, even small changes in 1 element of intervention design (such as a component or subcomponent, or a characteristic of context) could generate large changes in a primary outcome.53
Realist approaches to evaluation and review have profound implications for how health service interventions are conceptualized and researched. Accordingly, realist reviews focus less on making a judgment of the truth of a linear causal relation between 2 single variables (i.e., does x cause y?), and more on the complex ways in which x can cause y under conditions a, b, and so on.46 As such, Realist Review methods can be used to tease out the mechanisms and contextual factors that enable interventions to lead to desired outcomes and can identify key circumstances under which a complex intervention can fail or lead to unintended outcomes.46 This generative approach accounts for why interventions that ostensibly have the same components of design can have markedly different outcomes in different contexts49 or, in randomized trials of disease management interventions, why the benefits of affirmative trials are often not replicated or scaled over time in different trials.6 Realist approaches view such variations as inevitable consequences of complexity54 rather than weaknesses in interventions or study design, related to intervention design, provision, implementation, or fidelity.11
Realist review aligns well with remote monitoring programs for chronic cardiac conditions because these interventions can be termed complex interventions due to the number and type of interactions between intervention components. This includes monitoring program components, the context(s) in which programs are provided, the technology program(s) used, the theory guiding design and content, and the frequency and intensity of monitoring.54,55 Furthermore, program components can be conceived to be multi-faceted and interactive rather than singular and isolated,53 with intervention effects understood to be generated from interactions not only between these components but also between these components and certain aspects of patients and the context of the intervention.54 As such, realist approaches are highly suited to examining and explaining the effects of remote monitoring programs for chronic cardiac conditions.56
Yet, crucially, the existing evidence base has tended to leave the modifying influence of program components, context, and mechanisms unexplored and unacknowledged. See examples in cardiac rehabilitation,6,57 atrial fibrillation,58 and heart failure.6,59-61 This neglects and harms evidence quality,11 reduces its usefulness to decision-makers,62 and ultimately fails to fully realize the benefits to cardiac patients in different settings of promising remote monitoring programs.47
Specifically, therefore, this Realist Review explicates how context moderates the mechanisms of interventions to influence outcomes. Accordingly, the review assesses why remote monitoring programs for chronic cardiac conditions do or do not work in different contexts or circumstances, for different stakeholders, with different patient populations, and for different purposes. This was done by exploring the influence on intervention effects and effectiveness of aspects and interactions of intervention mechanisms, with a particular focus on how mechanisms are influenced by aspects of intervention contexts, components, and recipients (including patient characteristics) in published accounts of interventions for the most common chronic cardiac conditions addressed by health services: heart failure, hypertension, cardiac rehabilitation, and atrial fibrillation.
Research Methods
This Realist Review primarily followed Pawson’s (2005)46 realist review methods, drawing on an interpretive approach to synthesis63 that has been used successfully in a past Realist Review to identify the influence of mechanisms and context on remote and provider-based heart failure disease management interventions.61,64 These approaches mirror those of systematic reviews of intervention effects (e.g., incorporating systematic and comprehensive searches, quality appraisal, and synthesis of findings) with some modifications to ensure efficiency and accounting for scoping work that has already been conducted and a defined HTA timeline, while reflecting the realist underpinning of the approach. Although the steps are described sequentially, in practice they were overlapping and iterative, responding to results as they emerged. The final results are reported using the RAMESES guidelines45 for the reporting of realist evaluations.
The primary goal of the Realist Review was to consider how the effects of remote monitoring programs are influenced by aspects of context and intervention components via the influence of these key factors on perceived or actual intervention mechanisms. The realist synthesis identified studies using a comprehensive and detailed systematic search of published accounts of the mechanisms of remote monitoring programs for the most common programs offered for management, behavioural change, and self-care of cardiac conditions. Programs to be reviewed were for patients with a primary diagnosis (and reason for program referral) for heart failure, cardiac rehabilitation, atrial fibrillation, and hypertension, but could involve patients, family caregivers (e.g., partners, significant others), and health professionals. To explore the influence of program mechanisms with aspects of context, components, and patient characteristics on outcomes, this approach — as with other approaches to theory-building from qualitative data — generates findings that move beyond description to present a new interpretation of published literature. This can offer additional insight into the phenomena of remote monitoring programs.46 An example is Clark et al. (2016).64
Due to an anticipated lack of realist evaluations of remote monitoring programs for patients with chronic cardiac conditions, this review did not incorporate an extensive initial scoping of the literature or theory development as an integral part of the review, unlike other realist reviews.43 However, those contributing to the development of questions drew on their knowledge of remote monitoring programs in this patient population, and the inclusion criteria and search were designed to ensure they included relevant documents. This reflects RAMESES publication standards for realist synthesis45 because the search approach recognizes that the quality of a search in a realist synthesis depends on the “relevance and robustness of particular data for the purposes of answering a specific question” (p. 8).45 Relevance refers to the ability of data to contribute to the development of testing of theory around the research question,45 while rigour refers to the credibility and trustworthiness of these data.45 Accordingly, the search sought data that could be of reasonable use to theory-building around program mechanisms — extending to those from qualitative and mixed-method studies, quantitative-process data, and grey literature, including program reports. All can conceivably contribute to “different ways of identifying and elucidating program theories” (p. 9).45 As the number of documents identified in the search was large, the selection and appraisal stages were done in parallel with the synthesis stage.45
Literature Search Methods
The literature search to support this Realist Review was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.65 The complete search strategy is presented in Appendix 1.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid, Embase (1974‒) via Ovid, APA PsycINFO (1806‒) via Ovid, the Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCO, and Scopus. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were chronic cardiac conditions, cardiac rehabilitation, and remote monitoring. Clinical trials registries were searched: the National Institutes of Health’s clinicaltrials.gov, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was limited to English- and French-language documents published between January 1, 2010, and November 11, 2020. Conference abstracts were excluded from the search results.
The initial search was completed on November 11, 2020. Regular alerts updated the database literature searches until the initiation of the stakeholder feedback period. The clinical trials registries search was updated before the stakeholder feedback period was completed. Due to time constraints related to the project deadline, citations found through alerts were not screened or included in the analysis of the final report.
Grey literature (literature that is not commercially published) was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist.66 This includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, systematic review repositories, patient-related groups, and professional associations. Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of key papers and through contacts with experts and industry, as appropriate. The grey literature search was updated before the completion of the stakeholder feedback period. See Appendix 1 for more information on the grey literature search strategy.
Selection and Eligibility Criteria
The study eligibility criteria can be found in Table 2 using the Sample, Phenomenon of Interest, Design, Evaluation, Research type (SPIDER) tool.67
Table 2: Selection Criteria for Realist Review Question
Criteria | Description |
|---|---|
Sample | Adult persons living with a chronic cardiac condition (defined as physician-confirmed diagnosis of heart failure, hypertension, or atrial fibrillation) or a post-cardiac event (i.e., myocardial infarction, cardiac surgery, heart transplant, or angioplasty) in cardiac rehabilitation or a similar secondary prevention disease management program, and persons who care for those living with a chronic cardiac condition or post-cardiac event (e.g., partners, family, health care providers). |
Phenomena of interest | Perceived or actual mechanisms of remote monitoring programs defined as formal remote monitoring offered by a health care organization, including programs of both pre-specified duration and non–pre-specified duration set in primary, home, tertiary, community, or long-term care-based intervention/service in rural, remote, and urban areas. |
Design | Studies containing data or themes, which could be reasonably interpreted as relating to program mechanisms. |
Evaluation | Perspectives, experiences, or program-related data for people living with a chronic cardiac condition or post-cardiac event who engaged with remote monitoring programsa and for those involved in their care. |
Research type | Qualitative, mixed-method, or quantitative studies reporting primary data or dedicated themes extractable for chronic cardiac study populations reported in English. |
aThis was for the management of patients with relevant cardiovascular conditions, not for the diagnosis or detection of cardiovascular conditions.
Articles were excluded if they did not meet the selection criteria outlined in Table 2, did not contain data extractable specifically for chronic cardiac conditions or post-cardiac events, addressed single, one-off, or ad hoc remote monitoring techniques, or addressed hypertension associated with pregnancy. The review did not include studies published before January 1, 2010.
The approach to mechanisms proposed is important because mechanisms are defined poorly, narrowly, or not at all in many past realist reviews.68 Nevertheless, these serve the vital explanatory function of accounting for why particular programs have the effects they do. In short, mechanisms “explain why the relationships come about… (and) establish what goes on in the system that connects its various inputs and outputs” (p. 1).68 This definition reflects Pawson and Tilley’s (1997)49 original program-focused approach in which “mechanisms describe what it is about programs and interventions that bring about any effects…as the workings of a clock (mechanisms) cannot be seen but drive the patterned movements of the hands” (p. 23).49 As such, in this review, mechanisms are defined as referring to the “underlying entities, processes, or…structures which operate in particular contexts to generate outcomes of interest” (p. 372).69
This definition of mechanisms is inclusive, credible (reflecting past approaches to defining mechanisms),69 and ultimately useful. In short, it provides a fruitful basis for identifying how remote monitoring programs could be adapted for different settings. However, it is not straightforward in that mechanisms of programs may not be directly observable (though they can be inferred),69 readily measurable (though they can be captured via qualitative data), or objective (though they can be perceived).48 Furthermore, in health services interventions, research into mechanisms remains rudimentary and challenging — with mechanisms being defined, conceived, and researched in many different, often vague, ways — or lacking in any systematic definition at all.48 That said, the presence and influence of mechanisms on outcomes can be inferred from both dedicated realist evaluations (i.e., studies collecting primary data using variations of realist evaluation) and studies using other methods that contain qualitative or quantitative data on mechanisms,45 including studies of mechanisms and context in health services for cardiac conditions.64
For many years, systematic reviews demonstrated that context was comparatively neglected in published accounts of realist evaluations.69 This is a major weakness because the moderating effects of context on mechanisms are a core tenet of realist evaluation49 and do appear to influence outcomes and mechanisms in health service programs for cardiac conditions.61 Given the relatively small number of existing published realist evaluations, it is unrealistic to identify clearly delineated, almost mathematical context-mechanism-outcome synergies as envisaged by some theorists68 working in realist evaluation. However, as with mechanisms, the influence of context on mechanisms can be inferred for complex interventions for cardiac conditions from realist evaluations and qualitative, quantitative, and mixed-method studies.45,61 As such, the review search focused on published accounts of mechanisms but in the identified studies, we explored instances in which context has been found to moderate these mechanisms.
Study Selection
Due to the high number of articles the search identified during the preliminary search stage (level 1), 4 reviewers working in 2 dyads independently screened titles and abstracts in DistillerSR70 against the predetermined inclusion criteria (Table 2). If the reviewers could not judge that the articles were clearly relevant from the titles and abstracts alone, full-text copies of articles were obtained for more detailed screening (level 2). The reviewers in each dyad compared their chosen included and excluded studies; disagreements were recorded and discussed with a fifth reviewer (a project leader) until a consensus was reached on selection.
A pilot exercise was undertaken between the 4 reviewers to test the screening procedures and inclusion criteria with a cohort of 5 randomly selected papers. A project leader checked the accuracy and consistency of the reviewers’ screening and selection decisions. Feedback was provided to reviewers throughout the screening process.
Data Extraction
Data extraction was performed by the project leaders. For each study included in the review (from levels 1 and 2), 1 project leader performed data extraction using a standardized data extraction template within DistillerSR.70 For each included study, the second project leader checked the data extraction for completeness and accuracy. Omissions or disagreements were recorded and discussed by the 2 project leaders and resolved by consensus.
The data extraction template was developed by 1 project leader within DistillerSR,70 using a form developed for a previously funded Realist Review of disease management interventions for heart failure64 as a guide. Where possible, categorical fields were used. The extraction template was pilot tested by the second project leader using 3 randomly selected articles. Amendments from the pilot extraction stage were made before commencing extraction for the full review.
For each included study, the following details were extracted, and missing data were noted:
publication title
first author
full citation
main focus (heart failure, atrial fibrillation, hypertension, cardiac rehabilitation)
program recipient(s) (patient, caregiver, health professional, other)
method category (qualitative, quantitative, mixed, unclear)
qualitative (general, grounded theory, ethnography, critical, experiential, other)
quantitative (survey, trial, case control, cohort, other)
country of setting
inclusion criteria
population studied (inpatient, outpatient, community)
sex of sample (male or female)
mean age
recruitment method (volunteer, snowball, purposive, random, other)
data collection method (face-to-face interview, telephone interview, online interview, focus group, measurement, other)
remote monitoring components (telemonitoring, home telehealth, data transfer, other)
remote monitoring adjuncts (home visit, clinical visit, none)
data transfer (electrocardiogram, blood pressure, heart rate, body weight).
Data pertaining to mechanisms (including possible variations by context) in the form of verbatim data or themes were cut and pasted from published studies into a field in DistillerSR.70 For qualitative studies, data were derived from themes or data relating to mechanisms, while for quantitative or mixed-method studies, primary numerical data were extracted from each study that was interpreted as giving insight into underlying mechanisms. In deciding whether data or themes were pertinent to the synthesis, project leaders considered if the identified data offered an explanatory account of what was going on between the intervention(s) and its outcomes (stage 1 synthesis as follows). As such, data or themes were not necessarily specifically labelled as pertaining to mechanisms in study reports, but reasonably interpreted as pertaining to mechanisms of remote monitoring aspects of interventions for cardiac conditions to be included.
Critical Appraisal
Realist reviews should report the overall strengths of evidence supporting the explanatory insights that emerged.45 Consequently, to assess the merits of the research, the project leaders appraised the quality of each included study using the appropriate quality appraisal tools from the Centre for Evidence-Based Medicine (University of Oxford) for qualitative and quantitative studies (Critical Appraisal Skills Programme [CASP])71 and the Mixed Methods Appraisal Tool for mixed-method studies.72 These tools are narrative-based (i.e., they do not compute a quality score). The quality of each study was categorized independently as low, moderate, or high using the appropriate CASP tool of quality appraisal, with project leaders resolving disagreements until a consensus was reached. The papers were screened against quality criteria but not excluded based on quality, given long and ongoing disagreement over the use of quality criteria to appraise research.73 Each project leader acted as a primary quality appraiser for half of the finalized cohort of included studies and as the second check for the other project leader. Disagreements in critical appraisal were discussed and resolved by consensus.
Data Analysis and Synthesis
Data synthesis was carried out by the 2 project leaders. The approach to analysis and synthesis used was employed in a previous Realist Review into the mechanisms of disease management interventions for heart failure.64 As was the case with this past review, qualitative and quantitative data are useful in understanding mechanisms of remote monitoring interventions. Consequently, both types of data were synthesized. Though necessary, this is challenging because the synthesis of qualitative and quantitative research together remains relatively new; also, mechanisms usually have to be inferred or interpreted from these data as opposed to being clearly labelled in studies.69 To address these challenges, a combination of established approaches to identify main mechanisms was used: the realist synthesis approach46 and meta-ethnography.63
Stage 1
Each project leader read each study in the final cohort to identify or infer the main mechanisms in the studies and extract data as described previously. These mechanisms were those for which data could reasonably be interpreted as speaking to the presence of the influence of mechanisms. Two types of data were extracted: qualitative data relating to mechanisms and quantitative data that yield clues of underlying mechanisms.74 For qualitative studies, data were derived from themes or data interpreted reasonably as relating to mechanisms (even if not overtly labelled as such in studies). As per guidance for the systematic review of mechanisms, in a manner similar to meta-synthesis,63 the project leader extracted the same words and terms as the original studies as much as is possible when extracting these subjective data around mechanisms.46 For quantitative studies, primary numerical data were extracted from each study that is interpreted as giving insights into underlying mechanisms with a narrative “qualitized” account of what these data refer to. In the qualitative and quantitative studies, data and themes were extracted related to mechanisms, irrespective of whether these data are self-identified by authors to constitute mechanisms. This is normal in realist evaluation when mechanisms are theorized or inferred from data.75
Stage 2 (Second-Order Coding)
After data were extracted for each included study, each project leader examined the initial mechanisms and study descriptions identified during stage 1 and, using the meta-ethnography method, met to discuss emerging main mechanisms from the stage 1 synthesis that existed across studies. Using conceptual mindmaps,76 findings were translated and synthesized for both the qualitative and quantitative data into a core set of qualitative data about the nature of the main mechanisms more common or influential across studies, as well as how aspects of context influenced these mechanisms (recorded in Matrix 1). Studies were re-read in light of this emerging interpretive account and re-organized or interpreted as necessary via reflection, refutation, and clarification in a process of theory refinement. Hence, as per meta-ethnography,63 data from different types of studies were triangulated and interpretations were applied to the extracted data across the studies. The approach to theory development was discursive, with emerging themes and theorizations discussed extensively and resolved by consensus.
A matrix (Matrix 2) was used to organize data on mechanisms and study details for this stage; separate sections recorded mechanisms linked to key factors, such as, but not restricted to, sex, age, and disease type or severity, and were analyzed by the project leaders independently.
Stage 3 (Synthesis)
As with Noblit and Hare (1988),63 the project leaders generated the final synthesis account with an interpretive analysis77 of Matrix 2 to generate an account of the main mechanisms acting in each type of intervention and a description of how each is affected by context and populations. This synthesis is presented in the Results section.
Rigour and Methodological Uniformity
Although the data on mechanisms are heterogeneous and potentially difficult to identify, meta-ethnography was also used to identify mechanisms using primary qualitative and quantitative data, and it is well-suited for examining the mechanisms of interventions for cardiac conditions — an effort for which literature is not primarily grounded in the social sciences.48
Results
Quantity of Research Available
A total of 13,747 citations were identified in the literature search. Following screening of titles and abstracts, 13,461 citations were excluded and 286 potentially eligible reports from the electronic search were retrieved for full-text review. Of these, 195 publications did not meet the eligibility criteria and were excluded. A total of 91 studies,78-168 reported in 91 publications, met the inclusion criteria and were included in this report. Twenty-three studies focused on cardiac rehabilitation populations,78-100 64 on heart failure,101-164 and 4 on atrial fibrillation populations.165-168 No studies were identified addressing hypertension in the chronic cardiac populations. The study selection process is outlined in Appendix 2 using a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)169 diagram (Figure 1). Lists of included and excluded citations, with details describing the rationale for those excluded, are presented in Appendix 2, Table 9 and Table 10, respectively.
Study Characteristics
The studies included a total of 13,165 patients (8,697 males and 4,468 females; mean age = 66.35 years, standard deviation = 8.14 years), 72 caregivers, and 841 health professionals. Additional details regarding the characteristics of included publications and their participants are provided in Appendix 2.
Data were derived from a rich mix of qualitative (n = 23), quantitative (n = 54), and mixed-method (n = 14) studies. While the majority of studies were carried out in the US and UK, 9 studies recruited samples from Canada.79,82,108,111,123,127,134,137,164 Two studies were conducted in more than 1 country.128,145 Two studies recruited participants exclusively from rural areas,80,96 both in Australia. The review included 2 studies that only recruited women as participants,95, 118 whereas there were no studies that only recruited men.
Summary of Critical Appraisal
As per the RAMESES reporting guidelines,45 it is important to identify the characteristics of the documents included in the review. Only 1 study included was a realist evaluation,113 but all documents included in this review contained empirical data pertaining to mechanisms or contexts of remote monitoring programs that were published in full papers in commercial journals. Based on the volume of data and study designs, 3 out of 91 studies (3.29%) had high quality of data on mechanisms, 25 studies (27.47%) had medium quality of data on mechanisms, and 63 studies (69.23%) had low quality of data on mechanisms. Details by study are presented in Appendix 2, Table 10.
Data Synthesis
Cardiac Rehabilitation Remote Monitoring Programs
The second largest proportion of studies was identified for patients with various forms of atherosclerotic cardiovascular disease,78-100 defined as patients with a chronic cardiac condition after a cardiac event and/or in relation to a cardiac rehabilitation or secondary prevention program (collectively termed “cardiac rehabilitation programs” henceforth).
Patient Views of Outcomes: Health Behavioural Change
Across the studies, the remote monitoring programs for cardiac rehabilitation were seen to be focused on health behavioural change,78,79,82,88-90 with few participants focusing on benefits for self-care.82,86 Conversely, the lack of acknowledgement in programs even linking death to heart disease was cited as a problem.88
Generally, positive accounts of the benefits of programs were far more dominant and common than negative or harm-focused data and themes. There was a strong and consistent sense from patient users of the beneficial effects of programs on their general health78,82-84,87 and motivation to maintain their general health.78,82-84,87 These outcomes included:
Mainly, such benefits were invoked more generally but they were also invoked in relation to particular aspects of the interventions, such as text messaging78 or using pedometers.81 The programs could foster a sense of hope that recovery and a healthier life was possible.83,88
In terms of possible harms, no evidence of concerns over low safety of engaging in remote monitoring programs were raised in the studies. Indeed, high safety was seen to be an asset for some remote monitoring programs,82,84 with attendant levels of personal vulnerability being notably low.79,82-86
Based on this inclusive approach to what constitutes outcomes, the following key mechanisms-context synergies were the ones most predominantly associated with improvement in mechanisms.
In terms of access, remote monitoring programs were seen to be absolutely79,90,91 and relatively78,92 more accessible and to continue longer87 than face-to-face alternative programs. This led participants to having strong positivity regarding remote monitoring programs — for example, via having a sense of being lucky,83 being a priority,89 or having greater access to health professionals.89,90 These advantages were seen to hold despite individual variations in familiarity and prowess with the technical aspects of programs.
Key Mechanism and Context: Patients
Good Technology but Still Must Fit With My Life: The benefits of these remote monitoring programs for cardiac rehabilitation gained most value only when programs integrated well with facets of users’ own life context — that is, their daily life patterns, work, and aspirations. Remote programs were seen to more easily offer more life convenience and flexibility than traditional onsite programs.79,82,85,90 The remote monitoring programs were seen to take less time away from daily life patterns,82,83,90 require less disruptive transport,94 and also support users to integrate personal travel into their life82,83 while also leaving them feeling more connected to their community82 and broader social roles.94 As such, effective programs facilitated patients’ ability to feel more connected but less grounded by the requirements of the program.
Despite the programs studied often incorporating a range of heart and activity monitoring components (commonly blood pressure, heart rate, and physical activity monitoring), challenges, concerns, and resistance around the remote monitoring technology was comparatively rare across the studies, including those specifically reporting on technical satisfaction.93,95 Programs with more components could even be found to be positive.96
In terms of common technical difficulties, the most commonly cited difficulties with the technology related to aspects of connectivity rather than the programs or content per se, with signal disruption between devices91,93 and shortness of battery life91,93 being the most common issues consistently identified. No technical aspects of the remote monitoring programs were consistently found to be burdensome or otherwise contribute to negative outcomes. Generally, instances or reports of technical failures were rare in the studies — 70% to 80% of patients reported having no technical problems.93,95
Overall, technology was seen to promote effective cardiac rehabilitation.78 Across the different studies, there was evidence of users deriving benefit from the full range of components of remote monitoring programs. For example, text messaging was seen to keep users engaged,78,87,92 while videos of expert health professionals discussing heart disease78,84 promoted knowledge and confidence via feeling well informed. The information provided on the programs was particularly valued when it was not a generic web page92 but was tailored to be understandable,78 detailed,78 and then trustworthy.78 Likewise, feedback that was understandable was linked to behavioural change.98 Wearables and blood pressure monitoring devices were perceived to be comfortable and easy to use.91,98 Pedometers were noted to be useful in fostering in users a valuable and immediate sense of their progress.81
The Power of Individualization and Necessity of Motivation: Programs were most effective when they were perceived to provide highly tailored or individualized content for each patient. There was a consistent sense across studies that remote monitoring technologies could not only incorporate a high degree of individualization for each patient in terms of content and feedback, but that this was seen to be a central aspect to program benefits. For example, programs were seen to be able to be and stay responsive to participants’ highly personal and individual goals,80,81,85,88,91 and able to adapt to variability88 and to the individual’s progression over time.91
Individualization could be increased via technological and interpersonal aspects of the programs — notably, via the provision of personalized health data to users on performance,84 the tailoring of information to specific levels of understanding,88 or follow-up with in-person health professional consultations to supplement the remote monitoring programs.80
While there was a prevailing sense that remote monitoring would benefit most cardiac patients,78-84,86,87 benefits were seen to be contingent on a number of contextual patient-related factors. Irrespective of individualization, successful patients were seen to possess sufficient self-motivation,83 seriousness,83 and honesty.83 They had to have sufficient time82 and commitment86 to work with the remote monitoring technology.
Harnessing Health Professional Relationships, Ignoring Patient Relationships: Instead of seeing the remote monitoring program as being distinct from patient care, patients perceived that programs fostered higher-quality and quicker connections to their own health professional multidisciplinary team.89,90 Programs contributed to closer relationships with health professionals involved in their rehabilitation and/or preventive care79,83 — a connection that was also cited as a reciprocal benefit by professionals79,81,89 as augmenting the care they could provide.
Conversely, the most consistently cited negative aspect of remote monitoring programs was the lack of incorporation of or exposure to other patients in the remote monitoring programs,78,84,85,88,91 though other studies overtly disagreed with this, seeing lack of interactions as an advantage.90 Other patients were seen to provide valuable sources of social camaraderie via shared experience,78 social interactions,84 and social comparisons78 and functioning.99 The lack of this relational aspect in remote monitoring programs was seen to compromise program effectiveness.78,84,90,99
Context in Cardiac Rehabilitation Programs: No Influence of Demographic Factors
Few studies examined sex and gender effects specifically. In relation to sex and intersectionality, while cardiac disease burden and symptoms were found to be higher in women,100 sex was not found to influence outcomes.87 No studies explored the influence of race or Indigenous status on program use or effects. Older adults were seen to potentially need more support for the use of remote monitoring programs.78
Age was found to be an actual barrier to remote monitoring program use in some studies78,83,86,92 but not others.87,91 These findings were based on cultural assumptions about technology familiarity being higher in younger people.78,83 Other patient-related barriers identified as inhibiting positive outcomes were related to the lower likelihood of older patients choosing remote monitoring programs over face-to-face options,78,86,92 lower access in those of lower education,86 income,86 and physical activity.86
Heart Failure Remote Monitoring Programs
The largest proportion of studies of remote monitoring programs meeting the inclusion criteria focused on heart failure populations.101-164 Similar to cardiac rehabilitation programs, data or themes in the studies of remote monitoring programs for heart failure did not indicate that the ultimate outcomes of programs were to lengthen life or reduce avoidable hospitalization. However, in contrast to cardiac rehabilitation programs, self-care due to heart failure was predominantly viewed as the key goal of programs — with program quality being primarily appraised or viewed around this outcome in many studies.101-114 Only 1 included study noted that patients addressed or even mentioned death as a possible heart failure outcome.115
Patient Views of Outcomes: Heart Failure Self-Care
Programs were perceived in a large number of the studies to have a consistent and meaningful positive impact on a range of facets seen to be pertinent to or congruent with effective heart failure self-care. For example, in addition to being generally effective,102,103,105,116,162 the remote monitoring programs for heart failure were seen by patients to improve:
These effects could be sustained over the long term.107,119
In addition to these outcomes, benefits could be more process-related and subtle, such as fostering a new-founded realization of the real daily connection between self-care behaviours and consequential daily symptoms112,123,163 — behaviour was recognized to directly influence biology and symptoms. Other effects extended to various psychological and social aspects, such as a higher sense of personal accountability,106,123 control,123 empowerment,123 and motivation103,112,123,126 to self-manage heart failure. That said, expectations regarding how much the programs improved self-care could be high and unmet.152
Professionals’ Views of Outcomes: Disease Management and Health Systems
The remote monitoring programs were seen by health professionals as making faster and more responsive heart failure care possible for worsening symptoms,109,123,124,127,128 and allowing professionals to focus their clinical consultations on key areas.106,108 Patients also perceived the remote monitoring programs as improving links to health professionals via providing “live” access to their personal health data101,129 and a range of care improvements, including assessment,123 communication,106 and clinical decision-making. Commentary on rural settings was restricted to programs being seen to promote cheaper and easier access for rural patients (who needed to travel further to outpatient clinics).123
Although the patient benefits were not directly questioned by the health professional accounts, health professionals across a number of studies (notably nurses) cited a number of unintended negative consequences of programs on their wider work and capacity. These negative consequences included the workload around the remote monitoring technology set-up in patients’ homes,106,130 increased general work flow accruing from program alerts and follow-ups,108,127,128,130,131 and, paradoxically, a higher sense of ongoing responsibility for patients who were at home.124,131 Additionally, programs were seen by professionals to foster higher dependence and expectations in patients around health professional support.106 As a monitoring tool that complemented, but did not replace professionals’ support,130,132 programs were seen to contribute to inadequate remuneration for heart failure care provision.127 Although only 1 study was a realist evaluation,113 the studies presented insights into a number of intervention mechanisms (Table 3).
Key Mechanism and Context: Health Providers
Remote Monitoring Programs Work in Tandem With Physical Care Settings and Teams: In contrast to the cardiac rehabilitation programs, recipients of the heart failure programs saw the programs as being complementary rather than a replacement for care from health professionals.104-106,108,118,120,123,127,129,133-136,163 This could be related to improving health professional access to their personal data,101,129 and the constancy of the reassurance that the professionals were potentially at hand if needed.106,109,123,133,136 As such, the programs functioned within rather than outside of relationships between patients with heart failure and their health professional team.101,120,130,135-137,163 Furthermore, the remote monitoring programs added value to the patient-professional dyad via providing new opportunities for individualized care, more dialogue, and detailed feedback between patients and their professionals:101,106,113,123
It tends to eliminate one of the biggest problems of being sick and that’s a sense of isolation, because I know that there’s regular (ongoing) contact. So, if I’m not feeling well, I know I’m going to be getting a phone call and it seems to me that’s worth gold” (Patient #2) (p. 4).123
The influence of this was also apparent when low patient usage of programs occurred when the anticipated increase in contact with health professionals did not subsequently occur.136
Notably, these consolidated connections with health professionals did not reduce patient views of their own personal responsibility for managing their condition112,113,133 — even when health professionals were seen to have primary responsibility for managing the heart failure.106 As such, the remote monitoring programs were seen by patients to add value to the contributions of health professionals for patients by leveraging the quality and benefits of existing relationships between patients and their health professional team,104-106,108,118,134,135 including physicians.120,129,163 This was associated directly with increased security104,123 and a reassuring sense of surveillance123 by the professionals.
From the perspectives of professionals, the leveraging of programs with their care had a range of positive benefits. These included increasing the overall speed of professionals’ responsiveness,134 providing health professionals with better access to individual patient data on vital signs,123,129 focusing patient-professional discussions,110,135 increasing professionals’ involvement with family caregivers,120,136 reducing family caregiver anxiety,123,138 improving knowledge deficits,128,138 and reducing overall disease burden for patients.139
In contrast, remote monitoring programs were seen by health professionals to require high levels of the capacity of health systems to set up and implement. Health professionals could view remote monitoring programs as causing major disruptions to their work in terms of ensuring adequate monitoring of patient data,106,108,124,127,128,150 initial work in program set-up with individual patients,130 and ongoing difficulties around performing patient assessment remotely outside of the direct physical presence of patients.135,150 Fear was also expressed over inadequate remuneration for professionals in their handling of alerts.127,150
Key Mechanism and Context: Patients
Technology Must Be Easy and Accessible, Yet Unobtrusive for Me: In studies involving systematic measurement, there was a consensus that the remote monitoring programs studied were valuable and easy to use for 80% to 90% of patients.107,109,116,129,131,132,140 Similarly, there was a strong and prevailing sense that the various remote monitoring program technologies — though diverse — were generally easy to use.106,107,109,110,113-115,118,129,131-133,141-143,163 This ease was directly linked to higher subsequent usage in some studies,127,162 with smartphones identified as the preferred main access to the program.120,162 This ease contributed to lower anxiety124 and to normalizing personal health data.115 Set-up processes in patients’ homes that were well supported were particularly valued103,143,144 and fostered motivation for self-care when they consisted of simple steps,103,143,144 but reduced usage when they were seen to be technically complicated.136
Most of the difficulties with the technologies in the programs cited by patients related to aspects of the technology malfunctioning or failing to accommodate patients’ needs, as opposed to the content or components of the programs being seen as irrelevant or unhelpful. The technology could be seen by patients as obtrusive113 or unsuitable for technical novices.104,141 This placed a heavy dependency on the availability of adequate technical support, which was seen by patients to be essential for programs to work well and was strongly linked to usage by patients112,113,124,127,132 and professionals.144
As with the cardiac rehabilitation programs, the most challenging technological aspect of programs related to poor connectivity between equipment (notably from peripherals to smartphones),106,112,113,132,140,145-147 which inhibited data transfer.132,143,148 Caregivers often had to help resolve these problems.104,109,127,147,148 In addition to being technically troublesome, these glitches reduced patient motivation to use the remote monitoring programs.133 Reactions to technology of remote monitoring programs, while broadly very positive, could be mixed. Thus, device alerts could be interpreted as both helpful108,138 but annoying when frequently false.110,149
Conversely, system problems related to devices that were too noisy106,108 or screens that were too big106,113 and, thus, intrusive in the home setting. The realist evaluation in the studies reviewed identified that perceived intrusiveness could be the overriding determinant of subsequent patient use.110 In contrast, some patients with poor sight identified that screens were too small;127,144 these concerns were shared by health professionals.150
Other common problems cited included the high financial cost of broadband internet connections needed for equipment,106,144,162 the low battery life of devices,113,145 too many device alerts,123 inaccurate results,101,141,149 poor telephone mobility coverage,163 lack of readily accessible technical support for patients,113,140,163 installation or interfaces that were difficult,144,148 and calibration and connection issues.112,136,151 Problems also arose when patients attempted to use their own equipment134 or caregivers also used equipment in the remote monitoring program.141,149 While these technical issues could be seen to be more minor in significance, even a single factor that was not readily “fixable” (unlike a poor connection) could dramatically reduce perceived usability and patient usage. For example, when a single screen was seen to be too big for the home, this single facet was seen to constitute a major barrier in the home setting.113
Programs Must Integrate Into My Daily Life: The remote monitoring programs were seen to be beneficial because they facilitated the integration of health data and behaviours with daily life patterns around patients’ homes,101,104,112,118,123,133,164 perhaps reflecting the greater ubiquity of technology via smartphones with daily life in the 21st century. For example, patients would integrate daily weight monitoring on scales with their other set morning routines.133
Programs Must Help Me to Understand My Condition: Heart failure was often confusing for patients,104 or for those who had low foundational or prior knowledge.101, 113, 126 This lack of knowledge of heart failure was noted in the single realist evaluation to be a key mechanism affecting decreased usage of programs.113 Accordingly, to help make sense of their syndrome, patients strongly valued personal feedback in the form of data on their personal daily health status.103,106,113,118,123,131,136 Feedback was seen variously as promoting self-care behaviours,103,113 a sense of each patient’s normal data patterns,101 and a greater sense of progress over time.106,118,136 This individualized information was valued far more than general information on heart failure.118 Moreover, concerns about data security relating to data exchange of their health data were found to be very low.127
At times, patients lacked sufficient knowledge to interpret data on the programs104,136 (e.g., linking weight gain to their diet rather than heart failure)136 or cited insufficient knowledge in how to use programs with confidence and without fear,106,144 or understand how the data presented linked back to aspects of their heart failure.133,136 Cognitive difficulties were cited as a barrier in only 1 study.145 Some components could be used less often — for example, blood pressure if patients did not consider themselves hypertensive127 — or past knowledge of aspects of self-care was very low, such as the need for sodium restriction.123 Prior experience in using particular components, such as blood pressure monitoring devices or electronic weight scales, could increase usage.127
Context: Sex and Gender, Age, Ethnicity, Rural Effects, and Caregivers
Data on aspects of context were comparatively low across the studies. Patient sex121,125,153 and ethnicity were identified to have no effect on outcomes121,153,154 — although Black patients had poor health at heart failure hospitalization154 and tended to have symptoms at a younger age.141 Gender norms were cited in relation to male patients being more adept at handling technical complications with the remote monitoring programs via their past experiences in fixing electronic devices.101
Age profiles of patients did appear to be influential with mixed results, suggesting age had both negative effects on outcomes101,137,155 and no effects.121,126,153 Explanations offered for difficulties associated with age focused on how age influenced self-care — some studies indicated that age did not influence technology usage,101 or had a negative effect due to fear of technology linked to age,126,144 or general poorer health.143
Commentary on rural settings was restricted to programs being seen to promote cheaper and easier access for rural patients (who needed to travel further to outpatient clinics).123
The type of heart failure (e.g., heart failure with preserved ejection fraction versus reduced or mid-range ejection fraction) was not found to influence remote monitoring program outcomes160 but there was mixed evidence on the influence of heart failure severity on usage. Improvements in self-care were found to be higher in patients with poorer self-care at baseline161 — symptomatic New York Heart Association Class III heart failure participants were more likely to engage in self-care161 but were less confident in doing so.120 This relationship between heart function and use151 and effectiveness was not found in other studies.153 Mental health status (notably depression109,143,156 and anxiety156) was overtly linked to aspects of program usage, being associated with worse symptoms,112 and with depressive symptoms being linked to worse outcomes.109,156
Socioeconomic status was found to increase the likelihood of hospital admission during programs in some studies157 but not others.158 Concerns about the high costs of remote monitoring programs to patients were noted by some patients144 and were linked to lower use of remote monitoring programs.162 Higher levels of education obtained were associated with higher confidence in using remote monitoring devices and higher subsequent usage rates.120
Importantly, receiving remote monitoring care could be seen as being in total isolation to previous interactions with the health system related to heart failure. Previous heart failure admission was associated with improved program outcomes, with patients having received basic education on heart failure while in hospital109 or at subsequent outpatient visits.155
In terms of other factors, the size of the health care setting offering remote monitoring programs was not found to influence outcomes,153 although programs offered in primary care or ambulatory settings were noted to have higher patient adherence.159 Recommendations from health professionals for patients to use remote monitoring programs were seen to be especially influential in promoting the use of remote monitoring programs.162
Notably, few studies included or explored how caregivers functioned around remote monitoring programs. Health professionals did cite that family caregivers were a vital complement to them around remote monitoring programs and should be actively involved in discussing care plans.150 Very few studies addressed outcomes or impacts of the remote monitoring programs on family caregivers, with a small number identifying positive impacts on reduced caregiver anxiety124 and short-term benefits.150
Atrial Fibrillation Disease Management Programs
The number of studies examining remote monitoring for atrial fibrillation was much smaller than that of heart failure or cardiac rehabilitation remote monitoring programs. While, increasingly, technologies are being developed to monitor people for atrial fibrillation using apps and smartphones, only 4 studies165-168 were identified that examined aspects of mechanisms that constituted remote monitoring programs and incorporated data exchange.
In terms of outcomes, the purpose of the programs was not well understood by patients,166 although there was a more general sense that the programs were helpful in terms of health.165,166 Devices were found to be useful in terms of identifying instances of arrhythmia166 and providing prompts for medications166 or health care consultation appointments.166 Participants reported high confidence that programs would be helpful to them in future165,166 by, for example, identifying future arrhythmia166,167 and knowledge of new medications,166 and allowing a means to record their own individualized history of arrhythmia.166
Key Mechanism and Context: Patients
Ease of Use Leads to Enthusiasm: As with the heart failure programs, interfacing and using the atrial fibrillation programs was judged to be easy by the vast majority of patient participants across the studies.165-168 Health professionals shared this high satisfaction.168 Similarly, most participants reported high enthusiasm to use similar programs in the future.165 Setting up systems to measure heart rate was identified as difficult by most participants in some studies.166 Compared to heart failure programs, the purpose of the atrial fibrillation programs was considerably less well understood by patients,166 perhaps due to a pervading general lack of seeing atrial fibrillation management as a primary life goal.165-168 While data were scant, the most significant concerns about the remote monitoring programs for arrhythmia relate to their ability to accommodate patients of different needs, etiology, and history.166
Technology: Leverages Patient Consultations: As with the heart failure programs, health professionals viewed the atrial fibrillation remote monitoring programs in the context of broader care — in this instance, viewing the atrial fibrillation programs as reducing the time burdens on them to personally perform tasks related to monitoring.168 This was seen to promote their capacity to provide more comprehensive and individualized care.168
No influence of context was examined in the papers containing data on mechanisms of atrial fibrillation programs.165-168
Strengths and Limitations
Because of its strong focus on harnessing patient perspectives as users of programs, this review addresses an enduring, yet key, weakness associated with the underutilization of telehealth: the absence of patient users in informing the design and content of programs.170
While this review was executed using quality standards for realist synthesis45 and identified a number of key mechanisms and contextual considerations for future work, as with all reviews, it was constrained by the quality and design of the component studies. The overall quality of the included studies should be used to inform overall conclusions from the review, including recommendations for future research. Due to logistical constraints, the review only contained existing work published in English and French.
The volume of studies examining context and mechanisms together in the same individual studies was confined to 1 realist evaluation.113 As such, like past reviews into telehealth interventions for chronic disease populations,171 this review predominantly included studies using various methods that contained data on mechanisms or contexts.
In terms of future research priorities, more realist evaluations of remote monitoring programs for chronic cardiac conditions are needed. Where possible, study populations should include participants from the wide range of different rural and Indigenous communities.
In terms of other weaknesses, the studies consisted predominantly of evaluations of remote monitoring programs from high-income countries with more widespread availability of faster internet services for the remote monitoring programs. Similar programs may not be viable in countries or regions without such infrastructure. The predominant focus of studies on evaluating programs may have contributed to the overwhelmingly positive patient perspectives on programs in terms of ease of use and actual or potential benefits. In contrast, studies examining remote monitoring programs as part of routine care, such as via observational studies, were absent.
Only 1 study examined rural settings or populations only.123 More studies of remote monitoring programs in Canada and beyond are needed to develop and evaluate remote monitoring programs for remote and rural settings.
Summary of Results
This Realist Review addressed how remote monitoring programs for various chronic cardiac conditions worked to promote changes in outcomes.
The key mechanisms and contexts described for remote monitoring programs in this review (Table 3) indicate that remote monitoring programs across cardiac conditions are consistently seen by the vast majority of sampled patients, caregivers, and health professionals in studies to contribute to positive remote monitoring program outcomes, particularly in psychosocial and behavioural outcomes.
However, in terms of the key mechanisms and contexts explaining outcomes from studies, adequate program technology was necessary but insufficient to foster positive outcomes. Central to the positive effects of programs were mechanism-context synergies associated with the technology integrating well with patients’ daily life patterns and home, and promoting understanding in patients not only of their condition but also of their personal health status. Framed in terms of “fit,” the central role in effective programs of adequate integration of programs with patients’ context concurs with previous realist reviews of telehealth interventions for chronic conditions.172 This also aligns with recent reviews into heart failure self-care, which point to the influence on outcomes of patient context61 and daily life habits.173,174
Across the chronic cardiac conditions, programs were perceived by large proportions of those studied (often 80% to 90% of participants) to be easy to use and beneficial to health-related behaviours, psychosocial well-being, and outcomes. These effects, particularly on psychosocial outcomes associated with self-efficacy, mirror other past realist reviews of mechanisms of telehealth interventions for chronic disease populations.171 This is particularly notable given that a past meta-analysis of 65 studies has found that self-efficacy is the strongest wellness determinant of heart failure self-care behaviours175 and should be addressed in interventions for chronic cardiac populations176 or exercise promotion.177
Table 3: Key Mechanism-Context Synergies Across Studies
Key mechanism-context factors | |||
|---|---|---|---|
Stakeholder group | Cardiac rehabilitation programs | Heart failure programs | Atrial fibrillation programs |
Patients | Good technology but still must fit with my life | Technology must be easy, accessible, supported yet unobtrusive | Ease of use drives enthusiasm |
The power of individualization and necessity of motivation | Programs must integrate to my daily life | Technology leverages patient consultations | |
Programs must help me to understand my condition | |||
Professionals | Remote monitoring programs work in tandem with physical care settings and teams | ||
Patients and professionals | Harness health professional relationships, don’t ignore patient relationships | ||
There was also enduring and consistent consensus across the studies that remote monitoring programs were safe. These perceptions of benefit and safety concur with objective data from recent, more general effectiveness-focused systematic reviews of trials of remote monitoring programs for cardiac rehabilitation178 and heart failure,179 and meta-reviews of technology-based programs for diabetes.179, 180 Collectively, this evidence suggests that remote monitoring programs are a useful alternative to facility-based programs for chronic cardiac conditions.
As remote monitoring programs and similar telehealth interventions remain comparatively underutilized in health care settings,170 the psychosocial and convenience benefits of remote monitoring programs identified by this and other realist reviews172 should be interpreted in the context of 30 years of research, which has identified that access to facility-based disease management and rehabilitation services for cardiac patients is low, and may be most challenging for patients most in need of support, notably: women,181 patients with low income,182 Indigenous communities,183,184 people living in rural settings,185,186 or those who, because of intersectionality, experience multiple forms of marginalization.187 Remote monitoring programs may be a particularly attractive alternative to facility-based programs, given that past interventions to increase usage of these facility-based services have proven ineffective,188 and this review identified no strong or consistent negative effects of age, sex, ethnicity, or social status on remote monitoring program usage.
While programs were viewed as being easy to use and the most frequently reported technical glitches with programs were minor (i.e., poor connectivity and short battery life of devices), both patients and professionals indicated that to be effective, remote monitoring programs must have accessible and helpful technical support. This was a key finding of the single realist evaluation in the cohort of studies reviewed.113
Further, instead of being viewed by patients as being entirely separate care programs per se, remote monitoring programs across the conditions were viewed as extensions of, rather than replacements for, health professionals and facility-based care. As such, instead of replacing direct patient care, remote monitoring programs across chronic conditions consolidated existing patient-provider relationships and provided opportunities for more efficient and effective facility-based care consultations. This had the most significant implications for heart failure remote monitoring programs, for which care (by self, caregivers, or professionals) is notably complex, multi-faceted, and frequent.189 Consequently, the heart failure remote monitoring programs were also seen to incur considerable additional technical and care work for health care providers overseeing set-up and support for the remote monitoring programs. This finding questions approaches to remote monitoring programs for chronic cardiac conditions that categorize telehealth interventions as non-relational and “cold” compared to the supposed “warmth” of face-to-face clinical consultations.4,189 Indeed, the relational elements of remote monitoring programs is evident in existing realist reviews of trials of electronic, mobile, and telehealth tools for chronic disease in which professionals remain the dominant and more active agent in remote monitoring programs compared to patients.171 Future remote monitoring programs need to address how to re-balance this, improving design to better ensure that patients take a more active and frequent role in care.
Perspectives and Experiences Review
This section addresses the following research questions:
For people living with a chronic cardiac condition or post-cardiac event, what are their expectations of, experiences with, and perspectives on remote monitoring programs? What are their families’ and care providers’ expectations of, experiences with, and perspectives on remote monitoring programs?
To ensure the relevance of the analysis to this HTA, a set of secondary research questions was used to guide and focus the analysis on particular features of the use of remote monitoring programs:
How do people living with a chronic cardiac condition or post-cardiac event, their families, and their care providers experience and understand:
how to adopt and use remote monitoring programs?
how remote monitoring programs move health care into peoples’ places of residence and the impact of this shift on the families of people living with a chronic cardiac condition or post-cardiac event?
the changes in roles and responsibilities that can accompany remote monitoring programs and the impact of this shift on the families of people living with a chronic cardiac condition or post-cardiac event?
how and when remote monitoring programs are seen as working or not working?
Study Design
A qualitative evidence synthesis of primary qualitative research was conducted to understand and describe peoples’ experience with and perspectives on remote monitoring programs for chronic cardiac conditions and cardiac rehabilitation. Included publications were synthesized using thematic synthesis.190 The primary goal of this review was to consider how remote monitoring plays out in the lives of those who engage with it, and its impact on their lives, their roles and social relations, and their health care.
Literature Search Methods
The search for literature exploring perspectives and experiences was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.65 The complete search strategy is presented in Appendix 1.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid, CINAHL via EBSCO, and Scopus. Duplicates were removed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH, and keywords. The main search concepts were chronic cardiac conditions, cardiac rehabilitation, and remote monitoring.
CADTH-developed search filters were applied to limit retrieval to qualitative studies. Retrieval was not limited by publication date but was limited to English- or French-language documents.
The initial search was completed on August 26, 2020. Regular alerts updated the search until the publication of the final report.
Grey literature (literature that is not commercially published) was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist.66 This includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, systematic review repositories, patient-related groups, and professional associations. Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of key papers and through contacts with experts and industry, as appropriate. See Appendix 1 for more information on the grey literature search strategy.
Selection Criteria
Selected publications were primary English-language qualitative studies. For the purpose of this review, qualitative studies are those that use both qualitative data collection methods (e.g., documents, interviews, or participant observation) and qualitative data analysis methods (e.g., constant comparative method, content analysis). Studies that use surveys as a method of data collection were excluded.
Studies with multiple publications using the same dataset were included if they reported on distinct research questions. Table 4 describes the selection criteria used, built using the SPIDER criteria for framing qualitative evidence synthesis research questions.67
Table 4: Selection Criteria Using SPIDER
Criteria | Description |
|---|---|
Sample | Adult persons living with a chronic cardiac condition (i.e., heart failure, hypertension, or atrial fibrillation) or a post-cardiac event (i.e., myocardial infarction, cardiac surgery, heart transplant, or angioplasty); persons who care for those living with a chronic cardiac condition or post-cardiac event (e.g., partners, family, health care providers) |
Phenomena of interest | Remote monitoring programs for people living with a chronic cardiac condition or post-cardiac event that are delivered by health care systems (i.e., primary care clinics, specialist clinics, outpatient care, community health clinics, or long-term care facilities), and what they do, how they work, what it means for them to work, for whom they work, what is required for them to work; how people with chronic cardiac conditions engage with remote monitoring programs, and what is required for them to do so? What are the consequences of doing so on their understanding of their condition, their self-management, their health care and home, and social relationships and changes in roles (impact on friends, family, shifts from family member to caregiver)? |
Design | Qualitative studies of any design (e.g., phenomenology, grounded theory, qualitative description) |
Evaluation | Expectations, experiences, understandings, social relations, and perspectives of people living with a chronic cardiac condition or post-cardiac event and who engaged with remote monitoring programs, and of those involved in their care |
Research type | Primary qualitative studies using qualitative methods for both data collection and data analysis |
SPIDER = Sample, Phenomenon of Interest, Design, Evaluation, Research type.67
Publications reporting on remote monitoring programs that include people living with a chronic cardiac condition or post-cardiac event and those living with other health conditions (e.g., chronic obstructive pulmonary disease, diabetes) were included even if there was no separate reporting by cardiac conditions. Publications reporting on programs monitoring people with hypertension associated with pregnancy were excluded. Publications that were case reports, editorials, or commentaries or non–full-text publications (i.e., abstracts) were excluded.
Title and abstract screening involved 2 reviewers experienced with qualitative syntheses who assessed titles and abstracts of potentially eligible publications in DistillerSR.70 At the first level of screening, reviewers excluded citations based on title and abstract that were assessed as being not qualitative. At the second level of screening, they assessed citations for eligibility based on whether publications were about remote monitoring and adults with chronic cardiac conditions or those eligible for rehabilitation for an acute cardiac event. The reviewers conducted duplicate full-text screening and differing judgments about publication inclusion were resolved through discussion. Appendix 2, Figure 2 documents study selection using a PRISMA flow diagram.191
Data Extraction
One reviewer extracted data describing study and participant characteristics for each included publication, using electronic data extraction forms. Data extraction forms were built a priori to capture key study and participant characteristics; they are reported in Appendix 2, Table 11 (and summarized narratively).
Critical Appraisal
The process of critical appraisal was conducted to support qualitative reviewers’ understandings of the rigour of the included publications and relevance to this review. The primary reviewer assessed the quality of included publications and followed Krefting’s192 interpretation of Lincoln and Guba’s193 approach to assessing trustworthiness in quality research. The appraisal was guided by 3 primary questions intended to assess if and how a study demonstrated that it collected rich data, conducted a rigorous analysis, and incorporated reflexive practices leading to robust results that were useful for the objectives of this review: Is it credible? Is it trustworthy? Are the results transferable?192 The 10 items of the CASP Qualitative Checklist71 were used as prompts to engage with questions of credibility, trustworthiness, and transferability.
The primary reviewer conducted the appraisal. The second reviewer explored the primary reviewer’s assessment of the literature on key issues around credibility, trustworthiness and dependability, and transferability through conversation and a review of the Table of Quality Appraisal. Disagreements on the appraisal were resolved through conversation. Results of the critical appraisal were not used to exclude studies from this review, but instead to understand the methodological and conceptual limitations of the included publications in specific relation to this review. In particular, the process of critical appraisal informed the analysis in terms of the limits of what the available empirical research can tell us about peoples’ engagement with remote monitoring and the transferability of the results to the research questions and Canadian contexts.
The results of the critical appraisal were reported as a narrative summary and in the Table of Quality Appraisal, which document key issues around the credibility, trustworthiness, and transferability of each of the included studies.
Data Analysis
Descriptive Analysis
A descriptive analysis of study characteristics was conducted. The results are presented in tabular form and are accompanied by a narrative summary. The purpose of the descriptive analysis was to describe the set of included studies and understand the range of types of programs, participants, methods, and data that informed the synthesis.
Data Synthesis
The primary qualitative reviewer conducted the analysis, while the role of the second reviewer was to ensure that the concepts, findings, and their connections made sense, to probe and explore other configurations and relationships in the analysis and the data, and to ensure the review and its findings remained relevant to the decision problem this HTA seeks to address.
The analysis followed the principles of thematic synthesis, which draws on meta-ethnography and grounded theory.190,194 It involves 3 stages of formal coding procedures: (1) open coding, (2) descriptive coding, and (3) the development of analytic findings.190 These inductive coding practices draw heavily from grounded theory, and use the constant comparison method in which codes and data are compared across codes and within and across publications. From meta-ethnography, thematic synthesis borrows the concept of reciprocal translation where, in the first and second stage of coding, the process of coding and sorting “like with like” works to translate findings across studies.
Open and descriptive coding was conducted by the primary reviewer by reading and re-reading included studies and making marginal notes and memos (on the full-text PDFs and in Word) to capture initial observations, reflections, and disconnections and/or connections within the individual study and the set of included studies. The reviewer coded the data by highlighting and bracketing lines or sections that were annotated. Marginal notes were at first largely descriptive of the findings and referred directly to a single line or paragraph, but also included analytic notes that were an evaluation of or reflection on the findings or methods. Similar to the inductive logic of line-by-line and descriptive coding, this process allowed the reviewer to begin making connections across and within the data presented by the set of included studies.
The reviewer mapped emergent concepts as they related to the primary and secondary research questions using concept mapping techniques of diagramming. Preliminary and evolving analyses were brought to the second review and lead authors of other sections of this HTA for discussion and reflection, to identify potential overlaps in findings across the HTA, to continue to ensure that the analysis was responding to the scope and questions of this section and the HTA, and to foster reflexive practices among the team.
Based on these discussions, a refined concept map of key findings and their connections was developed that served as the basis of the analytic synthesis. Analytic synthesis is the development of constructs and categories that are interpretations of the data and descriptive findings. To develop analytic themes, further memoing and diagramming was used to assemble and sort the previously established descriptive findings, going back to the data to further develop the relationship between themes and codes, in keeping with the iterative nature of qualitative analysis. The purpose of this third stage of coding is interpretation — a new synthesis or interpretation of the existing published data in relation to the research question. Analytical synthesis stopped once findings and their relationships were well described, and no additional descriptive or interpretive insights arose from further analysis or coding of the included studies.
Reflexivity
Reflexivity is an epistemological principle and methodological approach in qualitative research that recognizes the role of the researcher as instrument. Reflexive practices and techniques are those that allow for and facilitate making researchers’ observations and interpretations transparent and explicit versus implicit and unacknowledged. This study employed the reflexive practices of memoing and frequent dialogue between the 2 qualitative reviewers and other members of the HTA team to probe and position reviewers in relation to the analysis. Further, the qualitative reviewers explored possible alternative interpretations of the findings to triangulate them with additional empirical sources (e.g., published qualitative reviews) and patient engagement activities to identify possible alternate concepts, connections, and interpretations.
Results
Quantity of Research Available
A total of 978 citations were identified in the literature search. Following screening of titles and abstracts, 924 citations were excluded and 54 potentially eligible reports from the electronic search were retrieved for full-text review. Of these, 24 publications did not meet the eligibility criteria and were excluded. A total of 27 studies, reported in 30 publications, met the inclusion criteria and were included in this report. Additional details are reported in Figure 2 (Appendix 2).
Descriptive Analysis
Additional details regarding the characteristics of the included publications and their participants are provided in Appendix 2, Table 11.
Methods of Data Collection and Analysis
Of the 30 included publications, 1 each was described as using community-based action research,141 multi-level qualitive study design,195 interpretive phenomenological analysis,130 descriptive qualitative with a phenomenographic approach,133 phenomenological-hermeneutic approach,90 and qualitative explorative approach.196 Two publications each were reported as using a qualitative descriptive design and197,198 grounded theory,199,200 and 2 publications from the same study used qualitative process design.201,202 The remaining 18 publications did not report the study design used.83,85,101,106,112,123,203-214
Semi-structured interviews were used as the primary method of data collection by 20 of the included publications.83,85,90,101,106,112,123,133,197,198,200-203,205-207,210,211,214 Five used both focus groups and interviews,130,204,208,209,213 and 3 publications used focus groups alone to collect data.141,199,212 One publication used audio- or video-recorded consultations between providers and patients196 and another used observations, documents, and interviews.195
Thematic analysis was used in 10of the included publications.83,85,197,198,201,204,210-213 Three publications reported using content analysis.123,205,209 Three publications each reported using grounded theory.199,200,208 Two publications each reported using constant comparison,101,214 a phenomenological approach,90,133 a framework approach,106,207 and deductive analysis.112,203 One publication each reported using grounded theory and thematic analysis,195 thematic analysis and constant comparison,202 category analysis,206 interpretive phenomenological analysis,130 and interaction analysis.196 One study did not report the method of data analysis used.141
Location of Study
Fourteen publications reported studies conducted in the UK.83,85,101,106,130,198,201,202,204,206-208,212,214 Six publications reported studies conducted in Sweden,112,133,196,200,205,211 4 in Canada,123,195,197,210 and 3 each in the US.141,203,209 One publication each reported on a study conducted in Malaysia,213 Finland,199 and Denmark.90
Description of Remote Monitoring Programs
Ten of the publications reported on remote monitoring programs for heart failure,101,106,112,123,133,141,203,205,206,209 and 6 publications reported on programs that included heart failure and other chronic conditions (e.g., chronic obstructive pulmonary disease, diabetes).130,195,200,204,207,208 These programs tended to measure weight, blood pressure, and pulse, and administered daily symptom questionnaires and transmitted data to a health care provider such as a telehealth nurse for monitoring, with the objective of preventing exacerbations of participants’ condition and hospitalizations.
Five publications reported on remote cardiac rehabilitation programs.83,85,90,197,199 These programs tended to include physical activity and health promotion education sessions virtually and collected self-reported data on diet and activity levels, to help promote a return to healthy activity and heart-health lifestyle choices.
Nine publications reported on remote monitoring programs for hypertension.196,198,201,202,210-214 These programs tended to be delivered by primary care providers or clinics and were used to adjust medications to address participants’ uncontrolled hypertension.
Description of Participants
For the purposes of narrative summary, participant descriptions were sorted into 4 categories: adults living with a chronic cardiac condition or eligible for cardiac rehabilitation; family members or informal carers for people living with a chronic cardiac condition or post-cardiac event; health care providers (e.g., nurses, general practitioners, cardiologists, health assistants) and decision-makers (e.g., hospital or health system managers); and public and patient stakeholders (e.g., patient engagement, public involvement, or advisory committee members).
Seventeen publications included people living with cardiac conditions or who were eligible for cardiac rehabilitation.83,85,90,101,112,133,197,199-203,209-211,213,214 Five publications included adults living with cardiac conditions and health care providers.106,123,196,198,204 One publication each included public and patient stakeholders and adults living with cardiac conditions141 and 2 publications included adults living with cardiac conditions and their spouses or informal carers.205,208
Three publications included health care providers,130,206,212 1 publication included adults living with cardiac conditions, health care providers, and decision-makers,195 and 1 included health care providers and stakeholders.207
Summary of Critical Appraisal
Overall, the studies were assessed to be moderately trustworthy. Additional details about the results of the critical appraisal can be found in Table 12 (Appendix 2).
Credibility was affected primarily by data collection and analysis strategies that included a priori assumptions, leading interview questions, limited ability to collect rich data, and raised questions about the coherence or adequacy of the description of findings. The majority of studies with the research objective of exploring experience and perspectives of people engaging with remote monitoring tended to operationalize this as a focus on barriers or facilitators to, and the acceptability of, remote monitoring programs. This narrowing of experiences and perspectives through lines of questioning tended to result in analyses that were superficial in their probing around the breadth of people’s experiences of remote monitoring. A few studies included participants who opted not to participate, which increased their credibility.
The dependability of the findings of the included studies was often undermined by the lack of reporting around the relationship of the authors to participants and no discussion of reflexive practices or the role of the research team. This led the reviewers to judge in these cases that the raw data presented were trustworthy, but not the findings per se.
Given the heterogeneity in remote monitoring interventions and this review’s orientation toward programs more broadly, the assessment of transferability focused less on issues of generalizability from intervention types and context and more on the objectives of the review. Transferability was sometimes lessened by the limited focus of many of the included studies on the acceptability of remote monitoring interventions. While these provided information on peoples’ views on whether they would accept, adopt, and/or use remote monitoring, they were not relevant to perspectives and experiences more broadly.
A final issue affecting the trustworthiness of the set of included studies was that most of the included studies recruited people who either started or completed a remote monitoring program as part of a trial or pilot study. Important differences between people who participated in the qualitative studies of remote monitoring studies (versus programs) raised concerns about representativeness of the findings across people with chronic cardiac conditions.
Data Synthesis
Adopting, Using, and Participating in Remote Monitoring and Cardiac Rehabilitation: The Perspectives of People Living With Cardiac Conditions
Peoples’ Perception of Their Technological Literacy Shaped Their Willingness to Adopt and Use Remote Monitoring and Cardiac Rehabilitation
Individuals’ views of their own low technological literacy and limited experiences using mobile phones, the internet, and computer technologies arose as a common response as to why they chose to not engage with remote monitoring programs or cardiac rehabilitation.85,197,199,203,205,208,213 This finding raises the possibility that those with high technological literacy would be more likely to adopt and use remote monitoring technologies, yet this was only limitedly described by participants adopting remote monitoring.203 It is possible that high levels of technological literacy may not act as a facilitator in the same way that low levels of technological literacy are evoked as a barrier to remote monitoring programs.
Where technological literacy was described by participants living with chronic conditions as a barrier to engaging with or successfully adopting remote monitoring, they often attributed it to their advanced age or being from another generation.85,197,199,203,205,208,213 Participants voiced these attitudes in ways such as: “[t]he thing is, you know, our age group, all of this is new technology and we haven’t done anything, and not the newer generation, they are going to be on it like a dirty shirt” (p. 10).197 This points to the way that assumptions around age and technological literacy are connected to peoples’ views of the desirability of engaging with remote monitoring programs.
Some seniors expressed that, beyond not knowing how, it was that they did not want to use mobile phones, the internet, or computers.199,205,208 However, in some cases, they saw non-computer devices such as a digital pen or health diary as acceptable.205 This suggests that differences in the technologies used in remote monitoring programs can accommodate a range of technological literacy and abilities.
Problems With the Technologies Discouraged People From Adopting and Using Remote Monitoring, Although Informal Caregivers Sometimes Helped to Overcome Them
When encountered, problems with the monitoring equipment were described by people as deterring them from continuing to participate in monitoring.133,197,208
Participants articulated being fatigued and frustrated when the way their remote monitoring equipment worked was not as consistent as expected.133,197 When equipment provided unreliable readings, inaccurate readings, or false alarms, participants found monitoring disruptive and stressful.85,208 Sometimes, technical challenges were a function of the monitoring equipment itself; for example, using displays with a small font that made it challenging for those with limited sight or small controls that were difficult for people with motor control symptoms, such as those with Parkinson disease.141,195 These challenges became even more insurmountable where language barriers were not accounted for.195,208
This led some to withdraw from monitoring programs or not participate.133,208 For others, the ability to call on informal caregivers, particularly adult children, to troubleshoot equipment problems helped them overcome technological challenges and continue participating in remote monitoring.85,101,112,133,195,197
Installing Equipment Required Finding the Space and Having the Necessary Connections, Which Was Not Always Easy or Possible
Depending on the type of connection required and the size of the equipment, people described finding a location for the equipment as being challenging, particularly when the equipment required a location with both a phone jack and electrical outlet.85,106,141,209
Large and bulky equipment was difficult to place in their homes, due to space limitations.106,203,209 For some participants, the equipment ended up being in a bedroom, which was not their preference.209 This deterred people at times from participating, as 1 participant with heart failure articulated:
[The equipment] wasn’t working at all… And the next thing you know he [equipment support staff] comes in and he says, “you can’t do without the…phone line,” and so I said to him, “It is somewhat of an aggravation, you must take it back”… I couldn’t, you know, have too many wires here and all this, you know. I said to myself, “why should I have it?” (p. 6).208
Although not widespread, some people with chronic cardiac conditions did report incurring out-of-pocket costs for participating in remote monitoring programs; for example, for broadband cable installation.106 These costs may be more substantial than reported given that many of the included studies were trials or pilots versus routinely delivered programs.
People to Learn How to Make Taking Measurements a Routine, Which Was Particularly Challenging for Those With Busy, Active Lives or Who Travelled
A crucial first step in adopting and using remote monitoring was finding ways to make the taking of measurements routine.101,112,133,202,209,213 People described being fearful of forgetting and found it challenging to remember to take daily measurements using the equipment.133,202,209 Many described that it took effort to do so, and time to develop their own strategies (e.g., taking measurements upon first waking) for making it a habit. Family members, particularly cohabitating partners, could help them remember.112
For those who were able to do so, travelling presented a particular challenge, with having to both bring along the equipment and keep their routines.112,213 Those using mobile phone-based monitoring systems reported enjoying the portability of it as they could continue to travel.123 People described that having to work full-time or being busy in the evenings made it difficult.202,213 It was unclear whether this was because of the logistics of taking measurements and/or time constraints per se, or if it was that the effort of remote monitoring had to be balanced out with other priorities. People balanced the challenges of making it routine with their perceptions of how the intervention would benefit them,202 suggesting that peoples’ ability and willingness to invest in the energy to make a routine involves multiple considerations, including, but not limited to, logistics. For some, they found it a role that they did not want to take on as it was too time consuming; as 1 participant expressed, they “did not want to be a nurse.”208
Engaging With Remote Monitoring Could Challenge One’s Identity and Sense of Self
For some, rather than fostering independence (one of the purported goals of remote monitoring), remote monitoring was experienced as increasing dependency for those who needed help to complete daily measurements because they were too ill.208
Respondents identified it as being for the sick or for those who had no one at home.203,208 The idea of being watched was interpreted as being a form of dependence, and as undermining their sense of independence in their own form of self-management.208 It was seen as relegating them to their home, as keeping them indoors versus out and about. and as interfering with other values and priorities in life.208 Where participants did not identify as being someone who they thought programs were for, they decided that remote monitoring was not for them.203,208
Remote Monitoring Programs and Understandings and Experiences of Self-Management
The Benefit of Self-Management Was Often Framed by People Living With Chronic Cardiac Conditions as a Process of Becoming Aware, Making Connections, and Feeling Responsible for Their Health
Remote monitoring programs involved people measuring and recording their bodies and symptoms. Participants living with chronic cardiac conditions described how the act of remote monitoring and taking measurements drew their attention toward their bodies both as measured and experienced (observed and felt).101,123,205 For some, this attention to their bodies and its changes was a source of anxiety and stress, particularly for those who thought high readings were indicative of an underlying serious health issue.112,123,133,202 As 1 participant with heart failure described, “I am a little frightened to step up on the scale. If I have gone up [in weight,] it will be fluid in the body and that can change rapidly” (p. 4).133 These worries are tied with how the act of measurement could contrast with peoples’ perceptions of their health and their bodies.
Listening to the body through the act of measurement was seen by participants as enabling them to make connections between their behaviours and lifestyle (e.g., diet, exercise, medications, stress) and their measurements or observations.112,123,198,200,202,204,211 One participant described how they saw it: “If you eat something that is very salty, for example, you go straight up… The next day you see that you have put on more weight, because it’s liquid that you store” (p. 451).112 Some described that living with the constant surveillance of remote monitoring was difficult.123 Remote monitoring challenged them as the need to measure and monitor their behaviour left them bounded, and they wanted “to enjoy life once in a while.”123
Acquiring insight into and about the connections between one’s behaviours and one’s measurements and body was a process that took time: time to make observations, for patterns to emerge, and to learn.101,112,204,209 Self-management, as a process, was about gaining understanding and control over these connections, bounded by the relationship and interactions between participants and their equipment. It was through interacting with remote monitoring over time that people learned the connections between their measurements, bodies, and behaviour.
Responsibility, in this way, was individualized: “It [remote monitoring program] taught you how to take care of yourself and do it on your own, because nobody else is gonna do it for you” (p. 220).209 As a form of self-management, it meant taking responsibility for and coping with or managing ones’ symptoms independently.112,133,209,211 Take, for instance, the following explanation relayed by someone living with heart failure about coping with breathlessness:
If I do feel ill, I can go on that and I can look at my own readings, rather than to start what you would call — having what you would call — going into a panic mode where your breathing would get, um, very difficult and you would, you start to panic, so then you would be ringing an ambulance, and now I can go on the machine and I can look at the readings and say, well, this is OK, this isn’t that bad, I don’t need to phone an ambulance, I just need to calm myself down (p. 314).204
These benefits were not seen or expressed by those whose measurements213 or health conditions were stable,200,214 or who had already been collecting and monitoring their own measurements,133,203 or who could not see a change in their health,205 even with lifestyle changes or medication changes.202 For some, it became a bother — repetitious, monotonous, boring: “It was just kind of the same old thing everyday, and I just got kind of bored with it I guess” (p. 221).209
Taking Responsibility for Self-Management of Medication Was Seen by People Living With Chronic Cardiac Conditions as Requiring More Guidance From Health Care Providers to Learn and Become Confident in Changing Doses or Medications
Overall, people described an openness to taking greater responsibility for their cardiac condition through remote monitoring; however, some participants expressed reservations about the demands that self-management of medication put on them.106,202,213,214 Some were happy to take instructions, but would not self-administer diuretics upon a weight increase.101 Some did not take the advice either, instead deferring to their own sense of their body or condition: “It’s difficult with the weight because sometimes I’ve had people phoning up and saying: ‘take an extra diuretic’ ...but I always go by the fact that I can see my veins and everything here and when I was ill I couldn’t because of the fluid” (p. 2450).101 Others described that they felt it was their doctor’s role214 or worried about potential side effects or contraindications, which led them to want to speak to their doctor before changing their medications.201 When they took an out-of-range reading but did not get input from their health care provider, or they lacked certainty in what course of action to take, they were reticent to make any medication changes.202,213
Others thought that they were following medication plans rather than adjusting their medication. Framing it this way continued to place a responsibility on the physician for prescribing, and they were just following the doctor’s advice: “I mean, it isn’t as though I’m taking an initiative in deciding what to take and what extra to take. It’s only… it’s still basically up to the doctor, isn’t it…” (p. 4).214 It was a matter of learning and gaining confidence through remote monitoring that led them to adjust their medications:
[T]he doctors kept saying to me that you can self-medicate with fluid tablets. And I would think “oh no [laugh], I don’t know what I’m doing here, so I’m not going to do that…” But then the [telemonitoring staff] at the other end said take another fluid tablet… And then gradually, I started to realise that when I felt unwell I was able to think “oh, you know, take another tablet or half a tablet” (p. 137).106
Remote Monitoring Was Seen as an External Motivation for Self-Management Requiring Accountability and Providing Reminders: Once Discontinued, People Struggled to Continue Implementing Lifestyle Changes
There was a strongly expressed view held by participants that remote monitoring supported them to self-manage by being an external motivation.83,85,133,205,209 This manifested through people using remote monitoring, and appreciating the reminders and the need to submit a record of their activity (whether diet or exercise): “It motivates you to think ohh I’ve got to get up and do 30 minutes exercise today. Because I’ve got to go up and fill the diary in. It’s motivating” (p. 437).83
As a source of reminders and requiring accountability, remote monitoring was seen as sustaining motivation for self-management: “You know I had stents four years ago, and you start off with the best of intentions, but nobody looks over your shoulder and you peter out. At this time, I felt this is a nifty program… somebody’s watching it and I better do it. Keeps you honest, keeps you focused” (p. 9).197 Here, being watched meant providing a sense of having to be accountable for one’s choices and behaviours.
In this light, it is not surprising that people shared that the patterns and habits built during remote monitoring programs of fixed duration were difficult to continue afterwards. Many expressed their desire or intention to purchase their own home monitoring equipment or their desire that the program would be extended.101,133,141,197,205,209
Expectations and Experiences of Remote Monitoring as More Than Self-Management
Remote Monitoring as Providing a Sense of Security by Being Watched and Cared For
A common thread among accounts of people who used remote monitoring was a feeling of security in that they were being watched.106,112,123,133,197,200,202,203,205,211 Expressions of this sense of security were most prominent among those with heart failure, likely a result of the nature of the condition (its variability and the panic associated with breathlessness) and program objectives (preventing exacerbations and keeping patients stable). Being watched meant that, as 1 participant with chronic heart failure described it, “I know if there’s something wrong, they are going to pick it up right away… if something goes wrong, they’ll phone me. [It’s a] safety net” (p. 137).106 The feeling of security experienced by people and their informal caregivers was described as being particularly present for those who did not have ready access to a primary care provider.207 On the other hand, those who felt they were already watched by caregivers chose not to participate.203 Those with heart failure described that they needed to be able to access health care services for unscheduled health care needs, drawing on their past experiences of seeking care for their symptoms.101
With this perception of being watched came a feeling of reassurance that one was being cared for.106,123,133 Care was felt as a form of concern and attention from health care providers that was embedded in remote monitoring: “[i]t gives the sort of reassurance that Big Brother’s watching me and even perhaps they can look after me” (p. 136).106
Remote monitoring was described by providers as enabling them to be able to care for patients more frequently and watch them more closely:106,211,212 “It allows us to look at patients every single day, as opposed to, at the moment, seeing people, maybe every four, six, or twelve weeks, depending on the patient, so you get a much better picture of their daily condition… things get picked up a lot quicker” (p. 136).106 However, some providers (nurses) expressed worries about social isolation being reinforced or not identified:
[I]f you get them to the clinic or a group session or we were visiting, we could identify social isolation. And perhaps day centres, things like that. So it can mask I think social isolation. This patient was crying out that I just wanted the human touch back... Just talking about things to someone and not to a box makes (sic) difference... because it’s (telehealth equipment) not a person, is it? (p. 5).130
This remark draws out how providers, when caring for their cardiac patients, attend to other social factors that relate to their patient’s heart condition that may not be able to be observed in the context of remote monitoring.
Remote Monitoring as Facilitating Access to Health Care and Fostering Closer Connections Between Patients and Providers
People who use remote monitoring described valuing it for the ways it provided them access to health care.195,197,200,208 This was both the convenience of being able to access health care without travel,123,195,197,208 and the ability to connect with their health care provider when they felt they needed it. As 1 participant described it, “When one was discharged from the hospital there never used to be real follow-up… You felt like you were being dropped off a cliff…[Telehomecare] provided a sense of security, because you were in contact with someone who could help you, versus having to make an appointment with your family physician, and get there, and back” (p. 8).195
Remote monitoring was described by participants as enabling them to have closer contact with those health care providers with whom they had pre-established relationships.123,133,205,211 As mentioned previously, it also facilitated access for some participants to health care providers, particularly for those who did not have a primary care provider.207 In some cases, people living with a chronic condition built new relationships with telehealth nurses, which they appreciated.101,195 Seeing remote monitoring as facilitating access to health care was also expressed by health care providers.195
Peoples’ sense of satisfaction with their existing health care services affected their desire to engage with remote monitoring programs.203,208 Those who described already having access to care when they sought it and who privileged their face-to-face and established relationships with providers did not see remote monitoring as offering them anything of value and chose to not participate.208 For those who had experienced instability in their care, such as transitioning between specialists or settings, they viewed being offered remote monitoring as further interrupting and destabilizing their care.208 Those who felt they did not need access to additional care (i.e., their condition was stable and they felt they had the tools and skills to manage at home) did not express interest in using remote monitoring for their heart condition.203
This suggests that expectations around remote monitoring programs are intimately intertwined with what one expects of health care services more generally, and how one negotiates care seeking. These views on remote monitoring as a way of accessing health care draw attention to how programs are seen and experienced by participants as part and parcel of health care as opposed to a supplemental program or technology.
Remote Monitoring as a Model of Care
Providers and patients alike appreciated the ways that remote monitoring programs fostered people living with cardiac conditions to be more involved in their care by, for example, having focused questions about medications and symptoms and readings for their consultations.101,196,197,201,211,215 In this light, remote monitoring is part of facilitating the provision of treatment and care of chronic heart conditions during scheduled visits and routine care as opposed to a stand-alone intervention. Ambiguity about whether remote monitoring was a new technology or clinical tool, or a new model of delivering care, was described as a barrier for adoption by providers because of the uncertainty it evoked.207
People living with chronic cardiac conditions saw remote monitoring as saving their general practitioners’ time, recognizing the pressures facing health care:201 “You can go in loaded with evidence, ‘I’ve been doing this’ and ‘I’m on the BP study’ and if they’re aware of it they’ll go ‘ah, better listen to this bloke.’ I’ve collated, then it’s going to save the doctor time and save me a lot of trouble as well. And improve me, which is important” (p. 10).201
Providers’ experiences and expectations with remote monitoring embodied views of remote monitoring as both taking time and reducing time.212 Taking time related to concerns around the increased time due to increased consultations,201,212 the time required to look at submitted data in preparation for consultations,211 and the consultations themselves taking more time.211 On the other hand, they were described as saving time,211,212 particularly in the long term, due to the increased efficiency they afford (being able to capture health concerns early and once patients were successfully self-managing). Remote monitoring programs were seen by providers as being a good use of time, even if it took more time: “[s]o it may increase workload, but in a good way, because it might mean that we visit them earlier and, but we are, you know, we are in the business of preventing admissions to hospital. So the workload is a correct way of our time, it’s the correct use, that’s fine, absolutely fine” (p. 5).130
Gains were also thought to be made as providers expressed that remote monitoring offered an opportunity to see more patients:207,212 “We are being asked to see more patients with no additional resources…How can we release a little bit of our capacity? Because our capacity is at absolute maximum all the time… I think telehealth helps from that point of view” (p. 331).207 However, those delivering remote monitoring programs described that expectations about volume needed to be tempered: “They say when you do health coaching your phone call should only last 7 min in order to maintain a caseload of 60 people… Well… it’s just not feasible when you’ve got some of the clientele we have” (p. 9).195 Many providers relayed experiences and concerns around an increase in workload in their descriptions of delivering remote monitoring programs.123,130,195,198,206,212 This increase in workload was attributed to a number of factors, including the increased number of patient contacts from those who were being monitored remotely;130,195,198,212 the need for rapid decision-making and responding to alerts, which interrupted work flow;123,198 and increased administrative duties on top of increased length of time and number of patient contacts.195
Additionally, remote monitoring programs were described by providers as changing the way they worked196 and how they consulted (increased use of telephone, non–face-to-face methods).198 As 1 provider commented, “It’s an organizational shift that we’re going to need to make at some stage soon anyway. I’ve been doing it [emails to help patients self-manage] for a number of years but we haven’t had a proper system set up… It’s undoubtedly much more time efficient”(p. 8).212 This highlights the general view that remote monitoring holds positive benefits, but those need to be implemented and integrated into the system for benefits to be realized.
Lack of integration in health care (organizationally and technically) of remote monitoring presented challenges for providers.130,206,211 Specifically, the lack of interoperability between remote monitoring systems and electronic health records increased workload for clinicians who had to enter data twice and worried about the ability to provide effective care when data were not accessible or available to the attending clinician.106,123,198,206,207,211
Condition-Specific Findings
People Enrolled in Cardiac Rehabilitation Programs Had Overlapping but Different Experiences Than Those Engaged in Remote Monitoring for Chronic Cardiac Conditions
While findings relating to technological literacy and the process of learning and adopting self-management skills and behaviours were shared across remote monitoring and cardiac rehabilitation programs, some findings were unique to remote cardiac rehabilitation.
Participants of remote cardiac rehabilitation programs appreciated the accessibility and convenience of being able to participate at home and not having to travel, particularly those living in rural or small urban areas without cardiac rehabilitation centres.197 The ability to do the program individually as opposed to as a group90 and on their own time was welcomed by many.85,90,197
Likely as a function of the patient population eligible for cardiac rehabilitation, issues with scheduling and finding time to balance participating (particularly exercising) with employment and family responsibilities were described by participants.83,85,90 Weather could also affect participants’ ability to engage in physical activity.83,85 “It was the wrong time of the year I mean if it had been another 6 weeks from now, it was all that awful weather so I was trying to walk around in the ice and snow and goodness know what, and it was cold” (p. 438).83 This is relevant for Canadian contexts.
The programs were at times asking for a large-scale shift in participants’ lifestyle (e.g., starting a new routine of physical activity, changes in types of foods eaten), which some experienced as a challenge.83,85,90 Some described that the expectations, particularly those relating to the exercise programs, were too high,83,85 or that their advanced age or other health conditions made it difficult for them to complete the activities.83,85 A mismatch between how people saw themselves and their lifestyle before an acute cardiac event and the expectations and lifestyle changes demanded by rehabilitation were described as affecting participants’ motivation for lifestyle change.83,90 Participants who frequently engaged in physical activity before remote rehabilitation were often motivated to meet the demands of the program. Participants who felt their level of physical activity was appropriately conducive to a healthy life sometimes but were asked to increase it experienced the increased demands as too great.90 Part of this was how people considered the investment of participating in cardiac rehabilitation in the context of their full life, that is, the ways they are willing to prioritize future health above other facets of their life.208 It also points to the ways that remote monitoring programs, as externally imposed expectations about one’s health and behaviour. can be in conflict with one’s own internal perception of their health and behaviour.
Variations in the Measurement of Blood Pressure Motivated and Complicated Remote Monitoring for Hypertension
More than other forms of monitoring, it took time for people using remote monitoring for hypertension to learn and be confident in taking blood pressure measurements.210,214 People with high blood pressure expressed worries around whether they were measuring their blood pressure correctly,201,210,214 or if readings were representative given they fluctuated throughout the day,201, 202 and could be lower at home than at the clinic.202,213,214 At the same time, taking blood pressure readings at home felt more accurate to participants because it was a more relaxed environment than at the clinic.198,214 Variation in views on and comfort with taking blood pressure readings was described as being influenced by peoples’ understandings of their blood pressure210,214 and length of time engaging with remote monitoring intervention.214
Health care providers worried about making their patients who lived with hypertension anxious or obsessed with measuring blood pressure, with the view that they could become immobilized due to worries when readings are high.198,211,212,214
These findings point to the ways that for hypertension, the experience of taking measurements at home may run against expectations of doing so. This suggests that there is a role for time to learn and acclimatize to the act of taking measurements that ought to be accounted for in the design of remote monitoring programs.
Summary of Results
Peoples’ perception of their technological literacy shaped their willingness to adopt and use remote monitoring and cardiac rehabilitation. Ideas around age and technological literacy were commonly invoked by people living with cardiac conditions as a reason for being disinterested or unable to participate in remote monitoring programs. When people encountered technological challenges, they expressed being discouraged from adopting and using remote monitoring. Having informal caregivers, particularly adult children, who could help troubleshoot the technologies helped them overcome these hurdles. Sometimes, the challenges were not with the use of the technologies but with the physical installation of the equipment itself, which meant finding the space and having the necessary connections. This was not always easy or possible, depending on peoples’ housing arrangements. These findings point to opportunities to develop programs that account for and anticipate potential challenges and provide the needed level of support and technological options that facilitate engagement with remote monitoring technologies.
Time was important in people’s experiences of the benefits of increasing self-management of their cardiac conditions through remote monitoring programs. It took time, and creative strategies, for people to learn how to weave measurement-taking into their daily lives, particularly for those who lived busy, active lives or who travelled. People living with cardiac conditions pointed to how they made connections between monitoring their condition and their behaviours related to diet, exercise and activity levels, and medication-taking, and this learning was a process of reflection and life experience that occurred over time. Self-management of medication was experienced by people with cardiac conditions as a process as well, requiring more guidance and support from health care providers to learn and become confident in changing doses or medications. Taken together, these findings point to the importance of considering the length of time or duration of remote monitoring programs to enable people to integrate measuring into their lives and to learn how to self-manage and take responsibility for their cardiac conditions from the process. The information provided by the included studies did not allow for detailed consideration of how systemic or structural inequalities affected how people living with chronic conditions engaged with remote monitoring — for example, by gender, for racialized people, or people living under conditions of poverty. One of the objectives of many remote monitoring programs is to facilitate people to self-manage their cardiac conditions, so this omission becomes of particular importance. For instance, self-management and behavioural changes necessitate access to resources (individual, community and societal) to support making choices that prioritized health. Findings around the lack of space may point to the ways that people, particularly seniors and those who are unable to work or are on a fixed income, may experience inadequate or precarious housing. The omission of the lenses of the social determinants of health means that the accounts provided here are unlikely to speak to the breadth of challenges people face when responsibility is individualized.
An openness to taking greater responsibility for their own health in the form of self-management was articulated by many. This was contrasted by accounts that remote monitoring was needed as an external motivation for their self-management, as it required them to be accountable and provided them with reminders. Once they discontinued remote monitoring programs, people described struggling with or giving up on monitoring their condition and implementing lifestyle changes. This draws into question the role of various mechanisms by which people find remote monitoring supports their self-management; that is, whether the process of learning and making connections and changing behaviour can happen in the absence of external mechanisms of accountability and reminders.
There are multiple expectations of remote programs in terms of what it provides individuals living with chronic cardiac conditions, the people providing care for them, and the health care systems in which they are situated. For many people using it (providers and patients), it is not just a technology that facilitates self-management. People expected and valued remote monitoring programs as a means of providing security through being watched, particularly for those with heart failure, and a way of accessing health care and fostering a closer connection between providers and patients. These point to the ways in which remote monitoring was not an addendum to care but a model of caring for patients with chronic cardiac conditions. As a model or an approach to care, this means the benefits of using remote monitoring are integral to its sustained use and it being integrated into peoples’ routine care.
While this review aimed to provide information on remote monitoring programs from the perspectives of family members and informal carers, few studies provided information from their perspective. The absence of information means that how family and informal carers experience remote monitoring, particularly the accompanied shift in responsibility to self-management, leaves unanswered questions around how it might require them to engage further in the care of their family members enrolled in remote monitoring. Similarly, whether remote monitoring programs lessen the burden of travelling to in-person medical appointments with family members remains unexplored. Additionally, while this review paid attention to differences between conditions, limitations in the reporting of the health condition of participants, particularly disease severity, left unanswered questions about how disease severity affects people’s expectations and experiences of remote monitoring.
Ethics Review
Background
The purpose of this analysis is to identify and reflect upon key ethical issues that should be considered when contemplating remote monitoring programs. The audience for this analysis is the decision-makers considering implementation or expansion of remote monitoring programs. Occasionally, questions are noted that cannot be answered in the current analysis because the HTA report lacks the fine-grained contextual information of the specific program, target population, and so forth. These guiding questions are intended to support decision-makers in their unique jurisdictions. Although other sections of this report broadly touch upon ethical dimensions, the aim of this analysis is to make such issues explicit and to identify additional ones that may be relevant to decisions in this context.
There are 2 central questions to consider when analyzing remote monitoring programs for managing chronic heart failure, atrial fibrillation, hypertension, and cardiac rehabilitation for acute and chronic conditions from an ethics lens:
What are the ethical issues related to the implementation of remote monitoring programs?
How might these issues be addressed in rural, remote, and urban settings?
Inquiry
The scope of remote monitoring programs is quite broad. The ethics analysis in this HTA report is directed toward decision-makers considering questions at the level of implementing remote monitoring programs, rather than toward individual clinicians facing the question of whether to prescribe a given remote monitoring technology at an individual patient level.
Notably, and somewhat uniquely in the HTA context, this HTA report does not include a review of clinical or economic evidence. Ethics as a domain of HTA often asks the following as foundational questions: What effect is a technology aiming to achieve, who benefits from it, and is that a worthwhile use of resources compared to other possible options? Therefore, consideration of clinical benefits will still form an important focus of this Ethics Review section, although in more general terms than a typical HTA.
Based on a review of the available literature, the following major themes were identified (drawn from the ethical analysis domain of the European Network for Health Technology Assessment [EUnetHTA] HTA Core Model)216 and are examined as follows.
Guiding Values
How is value and the corresponding success of remote monitoring programs defined?
What is important, what is valued, and by whom?
Are there value tensions?
Balance of Benefits and Harms
What are the known and estimated benefits and harms for patients when implementing or not implementing the technology?
What are the benefits and harms of remote monitoring programs for patients, informal caregivers, professionals, and organizations?
Are there any absences of evidence that are ethically consequential?
Justice and Equity
Are there factors that could prevent a group or person from gaining access to remote monitoring programs?
How does the implementation of remote monitoring programs affect the distribution of health care resources?
Patient Autonomy
Does the implementation or use of remote monitoring programs limit or affect patients’ capacities or possibilities to exercise their autonomy?
Professional Autonomy
How do remote monitoring programs limit or affect clinicians’ capacities to exercise their autonomy as professionals?
Privacy and Confidentiality
What risks do remote monitoring programs pose for patients’ privacy and confidentiality?
Data Collection: Review of Empirical and Normative Bioethics Literature
The literature review identified both explicit and implicit ethics content for the specific conditions in relation to remote monitoring programs. It also identified some ethical analyses of telehealth technologies in general, and the nature of patients’ relationships with these and their health care providers.
Literature Search Methods
The search for literature identifying explicit ethical considerations was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.65 The search strategy is available on request.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid, the Philosopher’s Index via Ovid, Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCO, and Scopus. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the US National Library of Medicine’s MeSH, and keywords. The main search concepts were chronic cardiac conditions, cardiac rehabilitation, and remote monitoring.
CADTH-developed search filters were applied to limit retrieval to citations related to empirical and normative ethical considerations. Retrieval was not limited by publication date but was limited to English- or French-language documents. The initial search was completed on August 28, 2020. Regular alerts updated the search until the publication of the final report.
Grey literature (literature that is not commercially published) was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist.66 This includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, systematic review repositories, patient-related groups, and professional associations. Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of key papers and through contacts with experts and industry, as appropriate. See Appendix 1 for more information on the grey literature search strategy.
Selection Criteria
The selection of relevant literature proceeded in 2 stages. In the first stage, the title and abstracts of citations were screened for relevance independently by a single reviewer. Articles were categorized as “retrieve” or “do not retrieve” according to the following criteria:
Explicitly provides normative analysis of an ethical issue arising in the use of remote monitoring, whether for the treatment of the conditions of interest or more generally.
Presents empirical research directly addressing an ethical issue arising in the use of remote monitoring.
The goal in a review of bioethics literature is to canvass what arises as an ethical issue from a broad range of relevant perspectives. As such, the quality of normative analysis does not figure in the article selection criteria; any identification of an issue by the public, patients, health care providers, researchers, or policy-makers is of interest, whether presented through rigorous ethical argumentation or not. For example, academic ethicists may focus on certain issues because these relate to theoretical trends in their discipline, while an opinion piece by a clinical or policy leader or a patient experience may bring to the fore ethical questions that are neglected by academic ethicists but are highly pertinent to the assessment of the technology in the relevant context. Despite the different standards of normative argumentation for each kind of report, the importance of the issues raised cannot be assessed solely by these standards and so literature cannot be excluded based on methodological standards.
In the second stage, the full-text reports were reviewed by a single reviewer with ethics expertise. Reports meeting the aforementioned criteria were included in the analysis.
Data Extraction and Abstraction Strategy
The ethical issues identified, values described, and solutions proposed in the literature were evaluated using the methods of ethical (applied philosophical) analysis. This included applying standards of logical consistency and rigour in argumentation, particularly where specific implications are identified and specific solutions advocated; responsiveness to important values of health care and health care policy in the field in which the technology is proposed for implementation; adequacy to the context for which the technology is being considered; and the representation of perspectives from diverse relevant communities, particularly attending to the possibility of the neglect of marginalized and vulnerable populations.
Stakeholders’ Perspectives
Relevant stakeholder perspectives were included via the literature review and the Perspectives and Experiences Review and patient engagement. These sources included patients of varying socioeconomic backgrounds; family members who provide informal care; health care providers, including physicians and nurses; and health systems perspectives. This review focuses on these populations. Some populations and perspectives may be absent not through intentional omission but because there is a lack of health research centred on them (e.g., rural and/or low-income patients, others) or because their perspectives in terms of values are not explicit (e.g., what is important to private industry).
Analysis
What Are the Ethical Issues Related to Remote Monitoring Programs?
Guiding Values
At the core of making an ethically justified decision is this question: What is important and to whom? Another way of framing this is to ask: What values are you trying to achieve through your decision? Answers that are often defaulted to as truisms include “good outcomes” or “efficiencies.” Those are reasonable aims but necessarily raise deeper questions of what values actually underpin them. Efficiency for what aim? Good outcomes in terms of social connectedness or reducing a person’s pain or overall lower hospitalization rates are all important outcomes. How to make sense of values that are in tension is a complex question, with more than 1 right answer, but beyond the scope of this report. It is something that decision-makers should work through for the sake of a successful remote monitoring program.
How is Value and the Corresponding Success of Remote Monitoring Programs Defined?
This is not a question only for the context of remote monitoring programs. It applies to any complex decision-making context that involves many stakeholders with different power who will be impacted by the results. As noted in the seminal work of Bent Flyvbjerg,217 parties with power have significant control over which evidence, perspective and/or voices are given consideration, and so effectively have control over what is seen as the rational basis of a good decision.
Without diving more deeply into decision sciences, the takeaway for decision-makers, who likely have authority and power over remote monitoring program decisions, is to reflect on who is empowered to define what is important. This definition of value is what will be measured to assess the success of the program. Although it can add to the challenges of decision-making in the front end, it may lead in the longer term to a more successful program, both in terms of implementation and of having impacts that are most important to those impacted.
What Is Important, What Is Valued, and by Whom?
Table 5 lists values that were named explicitly and implicitly by the groups and individuals involved in the research (both researchers and research participants) around remote monitoring programs.
Table 5: Summary of Ethics Analysis
Group | Description of the ethical issue |
|---|---|
Patients |
|
Informal caregivers |
|
Health care providers |
|
System level (including health systems, private industry, public research) |
|
Are There Value Tensions?
Looking at what is an incomplete list in Table 5, it seems self-evident there are and will be differences and tensions between what is important within and across these broad stakeholder groups.
The literature search revealed 1 value tension concerning different values around surveillance by health professionals of patients that is noteworthy and somewhat unique to remote monitoring programs. First, some patients noted the increased sense of safety they felt based on their understanding of how they would be monitored.106,115 Living with these cardiac conditions was anxiety provoking, and many patients noted their incomplete understanding of the conditions or what symptoms should provoke action (like seeking emergency care) or not. Remote monitoring technology was felt by some to mean a health professional was monitoring their data, or at least that their data would be available to doctors and nurses at the hospital if needed.115 Depending on the remote monitoring program, this was sometimes in tension with the program’s objectives. In other words, health professionals were not necessarily actively monitoring patients. Nor was information necessarily available and accessible quickly if a patient presented to a hospital. The objective of many, likely most, remote monitoring technologies is not to create a direct stream of data from each patient’s monitoring technology to a health professional 24/7. Anecdotally, patients commonly perceive the “health system” as a singular organization. However, it is more often a complex matrix of actors and systems that work more or less well together as patients move along their journey of care. It can be a surprise, then, when the data collected by the team at one’s cardiac clinic is not readily on-hand when a person presents themselves at an emergency department or even their general practitioner’s clinic.
The preceding example represents in part a mismatch of expectations and understandings and could be overlooked by decision-makers as something to resolve through clearer education materials for patients, and so forth. However, they also represent a more foundational disconnect that will not be rectified simply by telling patients more clearly or more often what to expect from their remote monitoring program. It also seems to be a disconnect between at least 3 parties (possibly more) about what is important, to whom, and how to implement and measure its success.
The example also points toward the tensions that can be inherent to a remote monitoring program because different stakeholder groups and individuals within those groups may hold sometimes incompatible values. For the patient in this rough example, they may value having access to health professionals who will understand their unique condition (based on collected remote monitoring data), and so can better and more quickly respond to any important fluctuations or emergencies, to keep them alive and living well. For providers in this example, they may value that using remote monitoring is more likely to get their patient access and longitudinal support from a specialist. If they are accountable for the remote monitoring program, they might also value its efficiency if it means they can provide services to more patients through fewer in-person appointments, or they may not value it because their workload increases in monitoring more patients or through increased caseloads that do not reduce their workloads. At a health authority level, the program may be valued because it is shown or predicted to reduce hospitalizations (also valued by most patients!) and other benchmarks that may signal good outcomes for the patients in the remote monitoring program, as well as other patients who may benefit from those acute care bed spaces and other resources that may be freed up.
Balance of Benefits and Harms
What Are the Known and Estimated Benefits and Harms for Patients When Implementing or Not Implementing the Technology?
This HTA report does not address clinical benefits and harms through a clinical effectiveness section or a cost section. Therefore, the evidence required to make a rigorous ethics analysis of benefits and harms is not available. However, this weighing of harms and benefits is likely a question of central importance to decision-makers who would have information about the condition(s) being targeted, their status quo, the remote monitoring program option(s) being considered, their patient population(s), their workforce, and so forth. In the final section on addressing ethical considerations, some guidance is provided for decision-makers on how to ensure consideration of benefits and harms are brought into their decisions. The evidence identified through the ethics literature review is incorporated and discussed in the following sections.
Are There Any Ethical Obstacles for Evidence That Are Ethically Consequential?
Because the scope of this assessment did not include an investigation of clinical effectiveness, it is difficult to fully identify obstacles in collecting evidence that are ethically consequential. Few of the studies in the literature review included patients from what could form the target population for a remote monitoring program: rural and remote groups, and populations with low socioeconomic status and other structural conditions correlated to higher rates of the diseases under investigation. This gap in evidence may also imply that the distribution of remote monitoring programs is not equitable or, at the very least, does not reach these populations. No literature explicitly drew this conclusion, so it can only be inferred as a possibility, but it is one that decision-makers should take into consideration. If a jurisdiction considers these or other populations who are not represented in research to be the target of their program, decision-makers might consider a co-designed program with representative patients (and providers), and a phased implementation with regular review before any adjustments and scaling up.
Most of the studies identified in the literature review centred on specialists and less often on patients, and very few examined the family physicians or informal caregivers who are often patients’ most intimate and consistent connections to the health system.
Justice and Equity
Are There Factors That Could Prevent a Group or Person From Gaining Access to a Remote Monitoring Program?
Remote monitoring programs are sometimes promoted or pursued as a means to improve access for patients living outside of urban centres or who experience structural constraints. These constraints may include lower numbers of health professionals or specialists, fewer specialized centres of care, and/or fewer means of transport to access them.
A remote monitoring program is not a fix-all for distributive justice concerns. Decisions about how it is implemented and what is considered within or outside of scope may have a greater impact on overall equity than any remote monitoring program alone. What should decision-makers consider?
In itself, a remote monitoring technology will not transport a patient home from hospital post-surgery, carry heavy equipment into their home if the patient is unable, set up and then learn to operate any programs or equipment, or pay for an internet provider. All of these aspects and others might be necessary for a patient to experience the benefits of a particular remote monitoring technology. As reported through the patient engagement consultations, informal caregivers (in this case, spouses) were a critical component to learning how to operate and set up remote monitoring equipment for patients after surgeries. Likewise, being able to travel to and from appointments and having somewhere affordable to sleep (for the patient or informal caregivers) on trips from rural to urban areas were a critical component to a successful health outcome.
Attention should be paid to the costs borne by patients or their families within the target population and its subgroups. What may be a small expense to some patients and their informal caregivers could be an impossible barrier to others. In the Canadian health care system, care is intended to be distributed equitably — based on one’s need and not one’s ability to pay. Therefore, assumptions about whether a patient has an internet connection, or a phone line, may significantly impact whether they will benefit from, or be burdened by, remote monitoring (see the Perspectives and Experiences Review). Decision-makers may be tempted by programs where patients are encouraged to purchase their own technology, sometimes known colloquially as “bring your own device.” This may be attractive because of reduced program budget costs or patient familiarity with their pre-existing devices. However, it should be approached with caution by decision-makers. It may create a de facto 2-tier program where either wealthier patients have better devices (and correspondingly potentially better outcomes), or additional barriers are created, and less wealthy patients have wait lists or limited access to a small supply of shared or cumbersome technologies (and correspondingly potentially worse outcomes).
Although technology is sometimes presented as the key ingredient to improved experiences and outcomes for patients, the “wraparound” supports provided by health professionals, including at cardiac centres and also in the community, are all critical to patient-centred definitions of success. These also include informal caregivers such as family members and neighbours or support networks, as well as general infrastructure like transportation and telecommunications. They should be considered as part of any decision-making around implementing a remote monitoring program. A lack in any of these components may be easily overcome by patients with personal means, who can pay out-of-pocket for transportation to access care, an at-home paid caregiver, telecommunications, and so forth. Decisions regarding remote monitoring that do not account for these gaps and private costs risk deepening inequities for populations where cardiac challenges are already borne predominantly by those with less means (see the Realist Review).
Rush et al.227 found in their mixed-method study of rural patients with atrial fibrillation in the Interior of British Columbia that on referral to a cardiologist or electrophysiologist in a larger centre, some older patients “will just say no” due to physical and financial reasons. Their physicians also noted their own reluctance to have patients travel unless absolutely necessary because of both the burden and the mixed quality in outcomes.227 The siloing of family physicians and cardiologists or cardiology teams was another concern named as relevant.227 Rural family physicians noted that when their patients did see specialists, they seldom had long-term follow-up, even when a treatment failed. They also noted their concern with referring complex patients who would return with complicated multi-drug regimens that were difficult for cognitively declining patients to manage or were in conflict with other recommendations.227
This underscores the complex structures (e.g., interprofessional and physician relationships) and challenges (e.g., transportation) that technology alone is unlikely to solve. It also adds weight to the overarching theme of the ethics section; that is, the importance of asking what is important, to whom, what gaps exist that remote monitoring programs (or other program changes) could meet, and whose ends would it support?
How Does Implementation of a Remote Monitoring Program Affect the Distribution of Health Care Resources?
It is possible that as funding and human resources are committed to a remote monitoring program, there may be pressures to transition patients into the new program and away from the existing one. This raises a number of important questions for decision-makers:
What evidence of benefits and harms exists for your population, and how will the impacts be evaluated at regular intervals to ensure intended outcomes and avoid harms?
What will be done to support individuals and populations who have structural barriers to using the technology — for example, being unable to afford or acquire internet or phone lines? Will decision-makers ensure equitable access through more traditional (non-remote monitoring) means, or allow the scope of the program to include budgeting for these structural constraints that are sometimes considered non–health care-related constraints?
In cases when these larger scope needs are not met, a program risks exacerbating inequitable health care. As Bauer notes in the context of telemedical services, the “digital divide” of unavailability of or inaccessibility to information technologies is a health care justice problem.228 Wealthier patients may receive the best health services, while poorer patients or ones with other socially determined health gaps may be left out of scope, no longer fitting the new requirements to receive care. As Bauer notes again, it creates the potential for “the well off and educated [to] have access to medical information and services that the poor and uneducated will not” (p. 249).228 This becomes more concerning in the context of cardiac conditions because of the intersectional nature of them.
For some patients and providers, a remote monitoring program may lead to better value, according to their definitions. For others, it may lead to negative consequences. This does not mean there is equivalency — that some will win, some will lose. Instead, it is a call to action for decision-makers to ensure they are not creating situations where the circumstances of the worst-off patients will be made even worse or that these patients will be inequitably left out. This may raise the question that if, on the other hand, the goal of decision-makers is centred on cost and resource savings above other values, could it conceivably have this outcome? That is a question that is somewhat context dependent. However, the Realist Review found the following:
As the remote monitoring programs were viewed as being an attractive adjunct as opposed to an alternative to existing health professionals and services, although programs may ultimately reduce avoidable hospitalization (for example for heart failure decompensation), there is a strong likelihood that without careful pathway design and expectations management, remote monitoring programs may increase net costs and workload for host providers during set up and operational phases. This aligns with systematic review of evidence from clinical trials pointing to ongoing uncertainty regarding the cost-effectiveness of remote monitoring programs for cardiac rehabilitation229 and heart failure populations.230 The small number of existing studies with cost-analyses fail to calculate full program costs230 and present very wide estimates.229 More research is needed to identify the costs and cost-effectiveness of remote monitoring programs across chronic cardiac conditions.
Decision-makers would be prudent to conduct a careful analysis of costs and other resource requirements (both internal and borne by patients) of their specific programs before wide-scale implementation.
Patient Autonomy
Does the Implementation or Use of a Remote Monitoring Program Limit or Affect Patients’ Capacities or Possibilities to Exercise Their Autonomy?
Respect for patient autonomy is a core principle of health care and is about enabling what is important to a patient to guide their life as much as possible. In the context of remote monitoring programs, there are 2 main themes reflected in the literature: patient values and informed consent.
Patient Values
Health care systems, particularly when publicly funded, prioritize the value of benefiting patients. This benefit differs, depending on the patient’s goals and conditions, but often includes some of the following: curing illness, reducing suffering, and maintaining or increasing the ability to flourish using one’s mental and physical capacities.
The more common understanding of the principle of respect for patient autonomy holds that patient values should guide their care as much as possible, within the bounds of what is possible, at a clinical and individual care-planning level. However, it also provides normative guidance at an organizational level of health program and system planning. At this level, respect for patient autonomy posits that what is important to patients should inform decision-makers as to what is possible; in other words, what types of programs achieve the goals of patients, and therefore should get funded.
At a system level, there are many patients with potentially different goals that may or may not be addressed through a remote monitoring program. Further complication occurs if the funding of multiple programs is being considered, and patients with a cardiac condition considered herein are only 1 group among many. That level of resource allocation and priority setting is beyond the scope of this analysis. However, it is worth noting that regardless of which level of decision is being made, patients’ values should be sought to guide and inform what is made possible through those decisions.
Informed Consent
To exercise their autonomy, and have their autonomy respected, it is essential for patients to genuinely know the potential benefits and risks or burdens of a decision before entering into it. This is even more critical in contexts with a fiduciary relationship such as when a health professional or health system has knowledge (or “known unknowns”) about the risks of harm to a patient.
The context of remote monitoring programs can present unique challenges to achieving informed consent. The use of software and applications are sometimes bound by legal user agreements between the owner of the technology or intellectual property and the user and/or patient.221 If a patient is required to relinquish legal rights or allow use of their private health or lifestyle information to access care, this is concerning. This concern may be mitigated by a health program retaining control over patient information, or by careful contracting between a jurisdiction and the third-party provider rather than allowing user agreements between third parties and patients.
An argument could be made that health professionals sometimes require patients to take certain actions, such as exercise or dietary changes, before being considered for a course of treatment that depends on those preceding actions, and that a user agreement is similar. However, this is critically different in at least 2 ways:
One is an agreement within a health system, which is bound and accountable to professional colleges, as well as provincial and federal laws. This power over accountability is much less clear and direct if the agents are operating under non-Canadian contexts. Consider the power a provincial college of physicians and surgeons has over a physician who sells patients’ personal health information without consent compared to an international corporation operating under international trade law.
For it to be ethically justified to require preceding actions by a patient before they will be granted access to a health program for which they have a health need, these actions must be necessary for the successful treatment of the condition. Signing a user agreement that carries the potential for exposing a patient and/or their genetic relatives to potential harms through the commodification of their health or other information is obviously not necessary for successful treatment.
In a health care setting, it is the responsibility and accountability of various actors, often a most responsible care provider, to understand the potential harms and benefits of any procedure for which they receive patient consent to action. With complex and potentially unclear or changing programs, it may be difficult to know the potential harms that could result from a patient consenting to a private software agreement.
Decision-makers considering remote monitoring programs should pay careful attention to enabling and ensuring genuinely informed consent. The following from Jusob et al.225 outlines the bounds succinctly:
Informed consent gives patients appropriate knowledge of what data are being collected, how they are stored and used, what rights they have to the data, and what the potential risks of disclosure could be. However, technological literacy limits users’ understanding of the true threats and advantages of technology. Because of the limitation of some users regarding technological literacy, it is necessary to develop mHealth systems that allow patients added control over their data such as, what data are collected and who has permission to access it (p. 250).
Professional Autonomy
How Do Remote Monitoring Programs Limit or Affect Clinicians’ Capacities to Exercise Their Autonomy as Professionals?
Technology design shapes and directs, to varying degrees, what choices are made. This carries normative weight because it can, whether intentionally or unintentionally designed, impact a care provider’s autonomy. The argument in favour of “choice architecture” is that designers can help to ensure that good or at least better decisions are made by users. There is some logic to this; designers may have the opportunity to program the standard of care, consult with experts, and so on. In the context of remote monitoring programs, this could mean that the standard of care for patients may be improved. However, it deserves some due care in choosing the program. As noted in Klugman et al.,221 “when a system provides information to a clinician, the setting of ‘defaults’ represents a powerful and often overlooked way of shaping behavior” (p. 40). What alerts are provided, for what thresholds, and regarding what data, as well as their frequency, can all shape how a care provider acts. If these defaults are difficult or complex to change, or their impacts are unnoticed, this can have unintended consequences on the patient and even the care provider. This again underscores the importance of carefully considering what is important, to whom, and how best to achieve the desired outcomes before implementing a remote monitoring program. For better or worse, remote monitoring programs could result in a reduction or truncation of professional autonomy. In the complexity of clinical care, and the complexity of deciding what is best or valuable, this should be carefully considered by decision-makers.
Privacy and Confidentiality
What Risks Do Remote Monitoring Programs Pose for Patients’ Privacy and Confidentiality?
Privacy overlaps with considerations around patient autonomy and consent (i.e., freedom to make choices about one’s life without interference or coercion). Considerations around structural coercion (e.g., having to accept an invasion of privacy in the terms of use for a technology), or unwanted use of one’s personal health and lifestyle information, have been covered in the preceding section concerning patient autonomy.
In the Canadian cardiac context, home visits by health care providers are not the predominant interaction between patient and provider. However, it is correctly noted by Bauer223 that where technology replaces the need for home visits, this can increase the physical privacy of patients and informal caregivers in their homes.
Users of remote monitoring programs face numerous potential risks related to how their health information is used. A summary drawing from Mittelstadt231 and Knorr et al.232 includes:
health and life insurance companies seeking health or lifestyle information that is not normally part of their regulated review procedures, impacting access for patients
discrimination in hiring practices by potential employers, or the monitoring of existing employees’ performance or work absenteeism
data intelligence companies who commodify demographic information
law enforcement in many ways; Klugman et al.221 note at least 1 example of law enforcement seeking pacemaker location data.
Some of these risks can be outlined in consent forms, but many are somewhat unprecedented as technology progresses. The profit motives driving some of these privacy risks are not entirely understood by decision-makers, health professionals, or patients. Therefore, informed consent processes may be critically incomplete. Furthermore, as noted already, consent cannot be genuine if it is the only option for access to the standard of care and so is necessarily coercive: consent or suffer potential health consequences.
Applications such as WhatsApp are noted as being increasingly used by health professionals.233 Although this falls outside the scope of the remote monitoring programs considered in this HTA, decision-makers should be wary of what guidance for private non-health applications is given to health professionals and also what unintended impacts may be created as a remote monitoring program is rolled out. Do health professionals know what privacy risks exist for patients if using unofficial email services, unencrypted information transfers, or private messaging applications? Does the remote monitoring have a challenging communication interface that might incentivize patients or professionals to shift toward using unapproved applications with potential privacy risks, and so forth?
There are technical concerns around informational privacy that focus on encryption methods for data and risks of breaches through computer hacking.225, 234 For an extended discussion and outline of relevant privacy frameworks such as Generally Accepted Privacy Principles, Privacy by Design, and Organisation for Economic Co-operation and Development standards, see Jusob et al.225
Decision-makers considering a specific remote monitoring program or technology should, if they have access, look to their jurisdiction’s privacy office, research ethics board, and compliance office and health law team for additional support.
How Might These Issues Be Addressed in Rural, Remote, and Urban Settings?
HTA reports generally compare a new technology against the status quo or a comparable intervention. In this case, the broad scope of technologies being reviewed (rather than, for example, a new technology being compared against the existing standard of care) and the focus on implementation decisions (rather than effectiveness) require that the ethical analysis be broad as well. Jurisdictions considering a remote monitoring program may wish to frame their decision-making based on the EUnetHTA Core Model216 of considering the ethics of their specific context, and borrowing from the analysis in the preceding sections:
What are the symptoms and burden of disease or condition for the patients?
What are the known and assumed benefits and harms for patients when implementing or not implementing the technology?
What are the known and assumed benefits and harms for relatives, other patients, care providers, the health system, and society?
In the evidence being used, what are the consequences of the choice of end points, cut-off values, and comparators and/or controls in the studies and/or assessments?
Are there problems related to the data or the assumptions in the economic evaluation?
What gaps or pressures exist in current care delivery in our context? Is it a lack of skilled clinicians, a lack of access for patients, issues in quality of care for patients, not enough service hours to respond to the needs of your population, a desire by clinicians or others to be or appear innovative, a drive to cut costs or to allocate budget most effectively and efficiently, and so forth? And, it follows, what type of program may address those gaps or pressures?
In the remote monitoring context, there are numerous stakeholders with various values that are not always compatible. For decision-makers, this should raise the question of what values and/or whose values should take priority when there is a misalignment. Working through this type of context is complex. The preceding ethics analysis is intended to support decision-makers in applying a values-based lens to their decisions.
Patient Engagement
Overview
CADTH involves patients, families, and patient groups to improve the quality and relevance of our assessments, ensuring that those affected by the assessments have an opportunity to contribute to them. CADTH has adopted the CADTH Framework for Patient Engagement in Health Technology Assessment.235 The framework includes standards for patient involvement in individual assessments and is used to support and guide our activities involving patient collaborators in this Realist Review. Engagement activities occur alongside a review of qualitative studies on perspectives and experiences, including those of patients, and consideration of patient-important outcomes in the clinical review. CADTH engaged 4 patients and 3 caregivers (spouses) with experience of remote monitoring during cardiac rehabilitation and for heart failure care to explore how patients interact with the technology used in monitoring, to identify challenges using the technology, and to confirm treatment outcomes that held meaning for patients and their families. Patient insights helped refine the protocol and interpret the overall findings of the assessment.
Methods
Invitation to Participate
People with lived experience were identified through CADTH’s connections to health care staff operating remote monitoring programs in New Brunswick and with the Canadian Cardiovascular Society, which recommended the HeartLife Foundation. A CADTH patient engagement officer contacted potential participants by email to explore their interest in becoming involved. The preliminary request included the purpose and scope of this project, the purpose of engagement, and the nature of engagement activities. The patient engagement officer obtained the person’s informed consent to share their lived experiences with remote monitoring with CADTH staff. Patient collaborators are recognized and thanked in the report’s Acknowledgements. Collaborators were also offered honorarium for their time and effort.
Engagement Activities
Persons with experience of remote monitoring reflected on if and how the assessment goals and findings resonated with their own personal experiences at several time points during assessment, including:
prior to protocol finalization
during drafting of the initial reviews
upon completion of the final report during the feedback period.
Patients’ insights gained through engagement processes were used to ensure relevance and to provide commentary on themes emerging from the qualitative Perspectives and Experiences Review, and to discuss other key concepts to inform the discussion section. The questions and subsequent discussion with the patient group representatives helped to clarify the technology under review and comment on the relevance of the findings to Canadian patients and families.
The involvement of patient collaborators enabled the research team to consider the evidence alongside an understanding of the wider experiences of patients and family caregivers. The patient and caregiver collaborators were able to identify goals of monitoring from their viewpoint, and to discuss the realities of life with a cardiac condition that requires monitoring.
The patient collaborators and other relevant stakeholders were invited to provide feedback to the report during the stakeholder feedback period. Through conversation and formal reporting, CADTH will clarify the key results of the full assessment and describe how engagement activities were used.
Reporting
The reporting of this section followed the GRIPP2 Short Form reporting checklist.236
Table 6: Patient and Caregiver Involvement in Remote Monitoring Programs for Cardiac Conditions
Section and topic | Item | Reported on page |
|---|---|---|
Aim | Four patients and 3 informal caregivers (spouses) with experience of remote monitoring were involved in developing the protocol and commenting on outcomes important to patients and families affected by cardiac conditions requiring monitoring. | 67 |
Methods | We engaged 3 patients and their informal caregivers (spouses) who underwent remote monitoring during cardiac rehabilitation. We engaged 1 patient with experience of heart failure before transplant. After giving informed consent, the patient and caregiver collaborators discussed their experience of remote monitoring via teleconference with CADTH researchers and in email communication. An honorarium was offered to all patient and caregiver collaborators for participating in teleconferences and to review a summary of their discussion. These collaborators were invited to provide stakeholder feedback on the draft of the full Health Technology Assessment and the recommendations report. | 42, 63, 67 |
Engagement results | The researchers were made aware of the importance of several considerations. Care for the whole person: Remote monitoring helps to track physical symptoms, but heart failure is more than just looking for exacerbations. It is a complex, chronic condition that needs social support and psychological support, and coordination among different health care providers. Meeting the needs of the whole person may be a challenge with remote monitoring if it fails to consider non-medical aspects of the patient experience. Support for caregivers: Informal caregivers sometimes assume the burden and responsibility of participating in remote monitoring, and in arranging the home as a place where health care is delivered. Coordination: The importance of the primary care doctor, cardiologist, pharmacist, dietitian, and staff of the remote monitoring program all having real-time access to the necessary information to avoid delays in care was shared by families. Confidence and trust: We heard that it is important for people to have reliable equipment, be able to easily reach their health care practitioner, and be reassured that a specialist would be consulted if necessary during remote monitoring. Own space and pace: From a practical standpoint, patients and caregivers appreciated being in their own environment, getting care at their own pace, and reducing the time and expense of driving to appointments. Ethical and equity: Having an internet connection at home or a cell phone data plan is necessary for participating in remote monitoring. Good communication skills and the ability to troubleshoot problems is necessary and sometimes falls to the informal caregiver if the patient is ill or is experiencing disability. Sharing these concerns allowed the research team to consider the evidence in the context of the wider experiences of patients and caregivers when preparing the assessment. | 11, 44, 47, 55 |
Discussion and conclusions | The success of patient involvement in this report is related to several factors. First, the patient collaborators and their families were briefed on the objectives of the project and their role. Second, they were supported by an experienced patient engagement officer who helped integrate their involvement with the research team. Established processes were in place, and our patient collaborators were offered compensation for their time to participate in the project. However, there were limitations. The topic and research questions were already determined before engaging patient collaborators. The Realist Review was conducted after the engagement had taken place, so the researchers relied only on the notes from those interactions, rather than discussing directly with the patient and caregiver collaborators. | 57, 68, 69 |
Reflections or critical perspective | Our patient collaborators were highly engaged in their conversations with researchers. They had clear opinions and concerns that they were able to express during the teleconferences. CADTH researchers listened openly and asked questions to help them link their roles in the assessment to the insights provided by the collaborators. Researchers understood the meaningfulness of the project for patients and caregivers. Some limitations of our patient engagement were that people often have concerns that are not part of the project scope (such as the need for peer support, or the quality of written education materials) but the topic and question are already identified when the project begins. The assessment was delayed more than once in 2020 and 2021, which made it harder for collaborators to remain motivated to stay involved than if there had been a fixed time frame. Stakeholders, including patient groups and patient collaborators, were invited to participate within a set time frame, and with a deadline for providing feedback. The time frame of the project can sometimes make it difficult for patients to participate fully, on terms that work for them (e.g., daytime teleconferences). As with remote monitoring itself, people need access to reliable technology, phone, and internet to collaborate with CADTH, which would possibly exclude some voices. | 51 |
Discussion
The evidence assessed across this report is intended to answer questions about how to best implement remote monitoring programs for cardiac conditions (i.e., heart failure, atrial fibrillation, and hypertension) and cardiac rehabilitation. It also assessed evidence with the intent of providing clarity about who could benefit most from such programs, particularly in relation to the ability of patients to receive care in their home or community while minimizing the need for travel, regardless of whether that home is in a rural, remote, or urban setting.
Overall, the evidence found in this HTA focuses primarily on remote monitoring programs for people with heart failure (see the Realist Review, Perspectives and Experiences Review, and Ethics Review). All sections of this HTA also found some evidence on remote monitoring programs for people participating in cardiac rehabilitation. Less evidence was found for both remote monitoring programs for people with atrial fibrillation (see the Realist Review and Ethics Review) and remote monitoring programs for people with hypertension (see the Perspective and Experiences Review and Ethics Review).
Enabling Optimal Use of Remote Monitoring Programs
An Environmental Scan of Canadian remote monitoring programs for cardiac conditions conducted by CADTH to inform the analyses in this review identified operational barriers and facilitators that may contribute to the successful implementation and maintenance of these programs.42 Common barriers identified by respondents included resourcing and funding limitations and cultural and language barriers. Common facilitators identified by respondents included patient engagement and clinician buy-in.
Successfully designing, implementing, and maintaining remote monitoring programs is enabled by a variety of intertwined technical, organizational, and human factors. This review found that, to be most effective, remote monitoring platform technologies must be highly functional and easy to use, incorporate individualized data feedback, and integrate smoothly with patients’ homes and routines, including physical design, network access, and compatibility with other in-home technologies. Although evidence from the Realist Review suggests that the most common technical glitches associated with remote monitoring technologies are relatively minor (i.e., network connectivity issues, battery life), patients and professionals cited the availability of accessible and helpful technical support as key to ensuring program effectiveness. Other factors identified as key to successful technology adoption included device portability and size, and accessibility factors, including options for those with visual or auditory impairments, and functionality and access to technical support in a variety of languages.
Evidence suggests that the ability to tailor programs to the needs of individual patients and informal caregivers is important for program success. For the examined indications, remote monitoring may require considerable learning of self-management techniques and routines on the part of patients and family or informal caregivers, which requires both time and support from the care team. Support from the care team may be particularly important in helping patients work through differences in their perceptions of their own health, when medication adjustments were required, or for conditions like hypertension where there can be considerable fluctuation in measurements.
This HTA found that, in addition to the patient, remote monitoring technologies should address the needs of family and other informal caregivers. Technologies should support caregiver contributions to patient care and address caregivers’ needs for adequate information and support. The Perspectives and Experiences Review identified a conspicuous absence of published evidence on the experiences of family and other informal caregivers, who are often directly implicated in the work of monitoring and providing care, and in the patient’s lifestyle changes.
A notable finding of this report is that although remote monitoring is sometimes conceived of as a replacement to or as an adjunct to regular care (whether in-person or inpatient), both patients and health professionals tend to experience it as complementary or synergistic and as a value-added component of overall care. For this reason, it should not be assumed that implementation of remote monitoring platforms will reduce clinicians’ ongoing workload or decrease patients’ expectations of health providers. For example, in heart failure, remote monitoring platforms appear to increase clinical workload. Evidence from the Perspectives and Experiences Review suggests that integration is key, and that efforts should be made to ensure that remote monitoring activities and data derived from them are integrated into clinical workflows and existing information systems. Remote monitoring may shift care from acute and specialist settings to primary care, which has implications for primary care providers. Additionally, evidence suggests that when implementing remote monitoring programs that serve rural and remote populations with limited access to specialist care, care coordination may pose a challenge. For example, patients who have been discharged from a tertiary centre with a remote monitoring device may experience issues with care coordination between the tertiary centre and local health providers when they seek follow-up care in their own communities.
A key finding of the Ethics Review is that the end goals of remote monitoring programs are not always clear or shared by all who deliver or access the programs. Program administrators, for example, may view remote monitoring programs as a means of reducing costs and finding efficiencies by reducing in-person consultations or acute care admissions. Health professionals involved in the delivery of remote monitoring programs, however, may experience the programs as increasing their workload without a corresponding increase in care quality for their patients. Prior to implementing remote monitoring programs, decision-makers should pause to assess what gaps exist in current care, and what options, including remote monitoring, may exist to meet those needs. This includes examining the needs, concerns, problems, and solutions for treatment and management of the target conditions, with all relevant stakeholders (patients, family and informal caregivers, primary care, and cardiac care teams) at the table.
While this review did not include an analysis of the costs of implementing and maintaining remote monitoring programs, it is important that decision-makers understand they also cannot assume these programs will lower health systems costs as is often believed. For example, a recent analysis seeking to understand the impact of changes in public coverage of remote monitoring services in the US during the COVID-19 pandemic found large cost increases observed during the rapid and sweeping expansion of remote monitoring may only account for a fraction of the potential market for these technologies and it is unclear how these services may persist beyond the pandemic.237
Who May or May Not Benefit
Understanding that patients and care providers view remote monitoring programs for cardiac conditions as a complementary and additional component of care (and thus potentially not cost or time neutral or cost or time saving), knowing which patients, in which settings, stand to benefit most from these programs becomes an important consideration. This review identified several gaps in the evidence that could make decision-making around patient selection for, and enrolment in, remote monitoring programs challenging.
As observed in the Ethics Review, remote monitoring programs are often framed as a solution for providing care to patients in their homes or communities and as a way to increase patient access to high-quality services. Overall, this review found that the research on remote monitoring programs for cardiac conditions focused predominantly on urban settings, with few studies seeking to understand how patients living in rural, remote, or isolated communities could benefit from these programs.
In addition to a limited scope in contexts of care, this review found the evidence for remote monitoring programs focused on narrow patient samples (i.e., patients in higher income countries) with little evidence about how characteristics such as patient age, sex or gender, income, and race or ethnicity may impact the use and effectiveness of remote monitoring programs. The Realist Review also found little consideration for how these intersecting identities could potentially impact the success of remote monitoring programs. For Canadian decision-makers interested in understanding how remote monitoring programs could complement the care of First Nations, Inuit, and Métis patients, no component of this review identified evidence that included Indigenous people or was concerned with indigeneity.
As discussed in the Patient Engagement section of this report, informal caregivers provide important supports to patients participating in remote monitoring programs for cardiac conditions. Families who collaborated with CADTH on this report shared that informal caregivers (the spouse) carried the main responsibility and burden for remote monitoring in the home. Caregivers learned to use the device, arranged for it to be connected, and made sure it was connected properly. Informal caregivers communicated with the nurse and, in the case of cardiac rehabilitation, arranged for the monitor to be returned after the monitoring period was over. Despite this, the Perspectives and Experiences Review found a conspicuous absence of information about how the lives of family and household members are affected by the presence, use, and demands of remote monitoring in their homes. This knowledge gap was also identified in the Realist Review and the Ethics Review.
That these evidence gaps exist may be surprising to some readers, given a growing body of literature examining the possible impact different lived experiences and identities have on patient outcomes in both the cardiac and chronic conditions spaces.182,187,238,239 As noted in the Ethics Review, including the voices of people who are often excluded or marginalized in this research in the decision-making concerning the design and implementation of remote monitoring programs could help to understand the gaps and barriers that actually exist for these groups and help find the best options to address their health care needs (which may or may not include remote monitoring). These evidence gaps also raise questions about the expectations placed on patients and informal caregivers and who may be left out or left behind by remote monitoring programs. If remote monitoring programs work best for people who are motivated to participate and make behavioural changes, have self-efficacy, and are able to raise questions about self-management (see the Perspectives and Experiences Review and Realist Review sections), are these expectations realistic, and when are they not? For example, if remote monitoring programs work best for those most able to make “healthy choices” (e.g., having access to healthy food, the ability to afford it, and a place and time to cook) while people affected by social determinants of health are less likely to benefit, what can be done to improve outcomes in these groups (e.g., putting supports in place, linking to community organizations)?
Conclusions and Implications for Policy-Making
In terms of implications for care decision-makers, the Realist Review draws attention to the importance of particular components of remote monitoring program design. The incorporation of highly individualized clinical information via feedback data to the patient on their condition and progress can maximize the effectiveness of remote monitoring programs for heart failure, atrial fibrillation, and cardiac rehabilitation. This aligns with past meta-analysis of trials of facility-based cardiac rehabilitation programs240 showing that the individualization of components and content for each patient is a prime objective determinant of program effectiveness. It also concurs with more recent evidence that, to be effective, remote monitoring-type programs for diabetes180 should incorporate individualized information and data feedback to patients.
That said, irrespective of the technical proficiency of programs, program benefits were dependent on the programs integrating well with each individual patient’s context: their daily habits and life patterns. Consequently, future remote monitoring programs for cardiac conditions cannot only be technically proficient but must also be sufficiently adaptive to different patients’ needs. Program designs must have sufficient flexibility to adapt to different patients’ home settings.
Additionally, decision-makers should consider the perhaps less obvious additional work and costs associated with effective remote monitoring programs. There was no evidence that any one demographic group consistently had challenges using the remote monitoring programs studied. However, while the most frequently reported technical glitches with programs were minor (i.e., poor connectivity and short battery life of devices), both patients and professionals indicated that to be effective, remote monitoring programs must have accessible and helpful technical support. Design and funding of remote monitoring programs must therefore ensure that adequate capacity for technical support is in place for a wide range of minor and more major technical issues.
The fact that there was limited evidence on remote monitoring programs delivered in rural or remote settings is significant from a public policy standpoint and is surprising given common assertions that these programs increase access to specialist care in rural and remote populations. Similarly, the gap in evidence around the perspectives, experiences, and needs of family and other informal caregivers is also significant, given the key role caregivers play in supporting remote monitoring patients. Further evaluation is needed to better understand the effectiveness of remote monitoring programs for cardiac conditions in predominantly rural or remote populations, and the impacts on family and informal caregivers. Such evaluation could also be used to support the development of Canadian guidelines for remote monitoring of cardiac conditions (noted as lacking in CADTH’s 2021 Environmental Scan).42
As noted in the Discussion section, little evidence was found on potential moderating effects of patient age, sex or gender, race or ethnicity, and income on program usage and effectiveness. More emphasis should be placed on understanding the experiences of those who may be marginalized and/or have poorer access to technologies, including reliable high-speed internet, and who may experience discrimination in the health system. For Canadian decision-makers interested in understanding how remote monitoring programs could complement the care of First Nations, Inuit, and Métis patients, no component of this report identified evidence that included Indigenous people or was concerned with indigeneity. This evidence gap emphasizes the need for decision-makers to ensure that the voices of people who are often excluded or marginalized are included when designing, implementing, and evaluating remote monitoring programs.
While not considered in the literature reviewed for this report, for policy-makers in jurisdictions where individuals access specialist cardiac care outside their province or territory of residence, limits on cross-jurisdictional practice created by professional licensure and credentialing requirements may also create a barrier to accessing remote monitoring.241, 242
Finally, remote monitoring programs may be an attractive adjunct as opposed to an alternative to existing health professionals and services. Although programs may ultimately reduce avoidable hospitalization (e.g., for heart failure decompensation), there is a strong likelihood that without careful pathway design and expectations management, remote monitoring programs may increase net costs and workload for host providers during set-up and operational phases. This aligns with the systematic review of evidence from clinical trials pointing to ongoing uncertainty regarding the cost-effectiveness of remote monitoring programs for cardiac rehabilitation229 and heart failure populations.230 The small number of existing studies with cost analyses fail to calculate full program costs230 and present very wide estimates.229 More research is needed to identify the costs and cost-effectiveness of remote monitoring programs across chronic cardiac conditions.
References
1.Connecting patients with providers: a pan-Canadian study on remote patient monitoring. Toronto (ON): Canada Health Infoway; 2014: https://www.infoway-inforoute.ca/en/component/edocman/1918-rpm-benefits-evaluation-study-full-report-final/view-document?Itemid=0. Accessed 2019 Jun 22.
2.Care Innovations. What is telehealth? What is remote patient monitoring? How are they different? https://news.careinnovations.com/blog/what-is-telehealth-what-is-remote-patient-monitoring-how-are-they-different. Accessed 2020 Sep 22.
3.Mackey S, Bornstein S. Remote patient monitoring: a jurisdictional scan. St. John's (NL): Newfoundland & Labrador Centre for Applied Health Research (NLCAHR); 2018: https://www.nlcahr.mun.ca/CHRSP/Remote_Patient_Monitoring_SEPT_2018.pdf. Accessed 2019 Jun 22.
4.Greenhalgh T, A'Court C, Shaw S. Understanding heart failure; explaining telehealth - a hermeneutic systematic review. BMC Cardiovasc Disord. 2017;17(1):156. PubMed
5.Pawson R. The science of evaluation: a realist manifesto. London (UK): Sage Publications Ltd; 2013.
6.Clark AM, Thompson DR. What heart failure programme works best? Wrong question, wrong assumptions. Eur J Heart Fail. 2010;12(12):1271-1273. PubMed
7.Kalogirou F, Forsyth F, Kyriakou M, Mantle R, Deaton C. Heart failure disease management: a systematic review of effectiveness in heart failure with preserved ejection fraction. ESC Heart Fail. 2020;7(1):194-212. PubMed
8.Jin K, Khonsari S, Gallagher R, et al. Telehealth interventions for the secondary prevention of coronary heart disease: a systematic review and meta-analysis. Eur J Cardiovasc Nurs. 2019;18(4):260-271. PubMed
9.Neubeck L, Redfern J, Fernandez R, Briffa T, Bauman A, Freedman SB. Telehealth interventions for the secondary prevention of coronary heart disease: a systematic review. Eur J Cardiovasc Prev Rehabil. 2009;16(3):281-289. PubMed
10.Clark AM, Hartling L, Vandermeer B, Lissel SL, McAlister FA. Secondary prevention programmes for coronary heart disease: a meta-regression showing the merits of shorter, generalist, primary care-based interventions. Eur J Cardiovasc Prev Rehabil. 2007;14(4):538-546. PubMed
11.Clark AM, Savard LA, Thompson DR. What is the strength of evidence for heart failure disease-management programs? J Am Coll Cardiol. 2009;54(5):397-401. PubMed
12.Savard LA, Thompson DR, Clark AM. A meta-review of evidence on heart failure disease management programs: the challenges of describing and synthesizing evidence on complex interventions. Trials. 2011;12:194. PubMed
13.The burden of heart failure: 2016 report of the health of Canadians. Ottawa (ON): Heart and Stroke Foundation; 2016: https://www.heartandstroke.ca/-/media/pdf-files/canada/2017-heart-month/heartandstroke-reportonhealth-2016.ashx?la=en&hash=0478377DB7CF08A281E0D94B22BED6CD093C76DB. Accessed 2020 Sep 22.
14.Heart disease in Canada: highlights from the Canadian Chronic Disease Surveillance System. Ottawa (ON): Public Health Agency of Canada; 2017: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/heart-disease-canada-fact-sheet.html. Accessed 2020 Sep 22.
15.Heart and Stroke Foundation of Canada. Atrial fibrillation: what is atrial fibrillation? https://www.heartandstroke.ca/heart/conditions/atrial-fibrillation. Accessed 2018 Oct 5.
16.Statistics Canada. Table 13-10-0096-09 High blood pressure, by age group. 2018; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009609. Accessed 2020 Sep 22.
17.Grace SL, Bennett S, Ardern CI, Clark AM. Cardiac rehabilitation series: Canada. Prog Cardiovasc Dis. 2014;56(5):530-535. PubMed
18.Lear SA, Banner-Lukaris D. The use of the internet to deliver cardiac rehabilitation remotely to patients with cardiovascular disease: report of the “Virtual” Cardiac Rehabilitation Program. Burnaby (BC): Simon Fraser University; 2014: https://www.infoway-inforoute.ca/en/component/edocman/2111-the-use-of-the-internet-to-deliver-cardiac-rehabilitation-remotely-to-patients-with-cardiovascular-disease/view-document?Itemid=0. Accessed 2020 Jun 22.
19.Medical Advisory Secretariat, Ministry of Health and Long Term Care. Remote monitoring of implantable cardioverter-defibrillators, cardiac resynchronization therapy, and permanent pacemakers: a health technology assessment. Ont Health Technol Assess Ser. 2018;18(7):1-199. https://www.hqontario.ca/Portals/0/documents/evidence/reports/hta-remote-monitoring-of-implantable-cardioverter-en.pdf. Accessed 2020 Sep 23. PubMed
20.Yee R, Verma A, Beardsall M, Fraser J, Philippon F, Exner DV. Canadian Cardiovascular Society/Canadian Heart Rhythm Society joint position statement on the use of remote monitoring for cardiovascular implantable electronic device follow-up. Can J Cardiol. 2013;29(6):644-651. PubMed
21.Ontario telemedicine network telehomecare deployment project: phase 2 - remote patient monitoring RPM-05B - benefits evaluation report. Toronto (ON): Canada Health Infoway; 2016: https://www.infoway-inforoute.ca/en/component/edocman/3176-ontario-telemedicine-network-telehomecare-deployment-project-phase-2-remote-patient-monitoring/view-document?Itemid=0. Accessed 2020 Sep 22.
22.Buhler H. Interior Health Cardiac Home Monitoring Project – Phase II: 2016- 2018. Benefits Evaluation Report. Kelowna (BC): Interior Health; 2018: https://www.infoway-inforoute.ca/en/component/edocman/3550-interior-health-cardiac-home-monitoring-project-phase-ii-2016-2018/view-document?Itemid=0. Accessed 2020 Sep 22.
23.Hypertension Canada. Blood pressure devices: blood pressure devices recommended by Hypertension Canada. 2018; https://hypertension.ca/hypertension-and-you/managing-hypertension/measuring-blood-pressure/devices/. Accessed 2020 Sep 22.
24.AliveCor. Kardiamobile. 20202; https://www.alivecor.com/kardiamobile. Accessed 2020 Sep 23.
25.FibriCheck. Home Page. 2018; https://fibricheck.com/. Accessed 2020 Sep 22.
26.Apple. Apple Watch Series 4: Health. 2018; https://www.apple.com/ca/apple-watch-series-4/health/. Accessed 2018 Oct 30.
27.Cloud Dx. Pulsewave Health Monitor. 2018; https://www.clouddx.com/#/pulsewavedevice. Accessed 2020 Sep 22.
28.TELUS Health. Home Health Monitoring (HHM). 2018; https://www.telushealth.co/health-solutions/patient-and-consumer-health-platforms/products/home-health-monitoring/. Accessed 2020 Sep 22.
29.Second Opinion Telemedicine Solutions Inc. Horizon Health Network New Brunswick. 2017; https://www.sotelemed.com/portfolio/horizon.html. Accessed 2020 Sep 22.
30.Ezekowitz JA, O'Meara E, McDonald MA, et al. 2017 Comprehensive update of the Canadian Cardiovascular Society guidelines for the management of heart failure. Can J Cardiol. 2017;33(11):1342-1433. PubMed
31.Remote patient monitoring project: Canada Health Infoway - benefits evaluation report. Charlottetown (PE): Health PEI; 2017: https://www.infoway-inforoute.ca/en/component/edocman/3476-remote-patient-monitoring-project-prince-edward-island/view-document?Itemid=0. Accessed 2020 Sep 23.
32.Zeidenberg J. ‘Tricorder’ enables patients to diagnose 15 illnesses. Thornhill (ON): Canadian Healthcare Technology; 2015: https://www.canhealth.com/2015/02/27/tricorder-enables-patients-to-diagnose-15-illnesses/. Accessed 2020 Sep 22.
33.Virtual care resources during COVID-19. Toronto (ON): Canada Health Infoway; 2021: https://www.infoway-inforoute.ca/en/resource-centre/virtual-care. Accessed 2021 Apr 06.
34.Cardiac Arrhythmia Network of Canada (CANet). Doctors repurposing medical devices and apps for COVID-19 2021; https://canet-nce.ca/doctors-repurposing-medical-devices-and-apps-for-covid-19. Accessed 2021 Apr 06.
35.Marzolini S, Ghisi GLM, Hebert AA, Ahden S, Oh P. Cardiac Rehabilitation in Canada During COVID-19. CJC Open. 2021;3(2):152-158. PubMed
36.UHN Foundation. Surge in remote monitoring for cardiac patients due to COVID-19. 2020: https://tgwhf.ca/stories/surge-in-remote-monitoring-for-cardiac-patients-due-to-covid-19. Accessed 2021 Aug 05.
37.Virani SA, Clarke B, Ducharme A, et al. Optimizing access to heart failure care in Canada during the COVID-19 pandemic. Can J Cardiol. 2020;36(7):1148-1151. PubMed
38.Saskatchewan expands virtual visits and introduces home health monitoring. Toronto (ON): Canada Health Infoway; 2020: https://www.infoway-inforoute.ca/en/solutions/rapid-response-to-covid-19/5266-solutions/rapid-response-to-covid-19/8575-saskatchewan-expands-virtual-visits-and-introduces-home-health-monitoring. Accessed 2021 Apr 06.
39.$3.3. million in funding will support virtual health care across British Columbia during COVID-19 and beyond. Toronto (ON): Canada Health Infoway; 2020: https://www.infoway-inforoute.ca/en/solutions/rapid-response-to-covid-19/5266-solutions/rapid-response-to-covid-19/8670-3-3-million-in-funding-will-support-virtual-health-care-across-british-columbia-during-covid-19-and-beyond. Accessed 2021 Apr 06.
40.The new “Virtual Reality”: practical approaches to the delivery of cardiac rehabilitation care during the COVID-19 crisis: guidance from the CSS COVID-19 Rapid Response Team. Ottawa (ON): Canadian Cardiovascular Society; 2020: https://ccs.ca/app/uploads/2020/12/Cardiac_Rehab_In_Covid_v2.4_Final_17_May_313.pdf. Accessed 2021 Apr 06.
41.OntarioMD. OntarioMD partners on remote patient monitoring pilot that yields benefits for high-risk patients in northern Ontario. 2021: https://www.ontariomd.ca/pages/ontariomd-partners-on-remote-patient-monitoring-pilot-that-yields-benefits-for-high-risk-patients-in-northern-ontario-.aspx. Accessed 2021 Apr 06.
42.Hill S, Li KX, MacDougall D. Remote monitoring programs for cardiac conditions in Canada. (CADTH environmental scan vol. 1, no. 3). Ottawa (ON): CADTH; 2021: https://cadth.ca/sites/default/files/es/ES0345%20Remote%20Monitoring%20-%20Final.pdf. Accessed 2021 May 03.
43.Remote monitoring programs for cardiac conditions — project protocol. (CADTH health technology assessment - project protocol). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/ou-tr/op0549-remote-monitoring-cardiac-conditions-protocol.pdf. Accessed 2021 Apr 06.
44.Addendum to Remote monitoring programs for cardiac conditions — project protocol. (CADTH health technology assessment - project protocol). Ottawa (ON): CADTH; 2021: https://cadth.ca/sites/default/files/ou-tr/op0549-rm-for-cardiac-conditions-realist-review-protocol.pdf. Accessed 2021 Apr 06.
45.Wong G, Greenhalgh T, Westhorp G, Buckingham J, Pawson R. RAMESES publication standards: realist syntheses. BMC Med. 2013;11(1):21. PubMed
46.Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist review--a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy. 2005;10 Suppl 1:21-34. PubMed
47.Clark AM, Redfern J, Thompson DR, Briffa T. More data, better data or improved evidence translation: what will improve cardiovascular outcomes? Int J Cardiol. 2012;155(3):347-349. PubMed
48.Clark AM, Thirsk LM, Wiens KS, Ski CF, Thompson DR. How to research the mechanisms of non-pharmacological cardiac interventions. Int J Cardiol. 2015;201:457-461. PubMed
49.Pawson R, Tilley N. Realistic evaluation. London (UK): Sage Publications Ltd; 1997.
50.Bhaskar R. The possibility of naturalism: a philosophical critique of the contemporary human sciences. New York (NY): Routledge; 2014.
51.Byrne DS. Complexity theory and the social sciences: an introduction. New York (NY): Routledge; 1998.
52.Clark AM, Lissel SL, Davis C. Complex critical realism: tenets and application in nursing research. ANS Adv Nurs Sci. 2008;31(4):E67-79. PubMed
53.Clark AM. What are the components of complex interventions in healthcare? Theorizing approaches to parts, powers and the whole intervention. Soc Sci Med. 2013;93:185-193. PubMed
54.Craig P, Dieppe P, Macintyre S, et al. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655. PubMed
55.Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008;27(3):379-387. PubMed
56.Allana S, Clark A. Applying meta-theory to qualitative and mixed-methods research. Int J Qual Methods. 2018;17(1):1609406918790042.
57.Thompson DR, Ski CF, Clark AM. Cardiac rehabilitation and secondary prevention: wrong terms, aims, models and outcomes? Eur J Prev Cardiol. 2019;26(9):995-997. PubMed
58.Clark AM, Hsu ZY. Addressing the growing burden of atrial fibrillation: evidence, sustainability and accessibility more important than territory. Eur J Prev Cardiol. 2012;19(5):1089-1090. PubMed
59.Thompson DR, Clark AM. Heart failure disease management interventions: time for a reappraisal. Eur J Heart Fail. 2020;22(4):578-580. PubMed
60.Thompson DR, Ski CF, Clark AM. Transitional care interventions for heart failure: what are the mechanisms? Am J Med. 2019;132(3):278-280. PubMed
61.Strachan PH, Currie K, Harkness K, Spaling M, Clark AM. Context matters in heart failure self-care: a qualitative systematic review. J Card Fail. 2014;20(6):448-455. PubMed
62.Clark AM, Thompson DR. Telemedicine and remote management of heart failure. Lancet. 2011;378(9806):e9; author reply e10. PubMed
63.Noblit GW, Hare RD. Meta-ethnography: synthesizing qualitative studies. London (UK): SAGE Publications, Inc; 1998.
64.Clark AM, Wiens KS, Banner D, et al. A systematic review of the main mechanisms of heart failure disease management interventions. Heart. 2016;102(9):707-711. PubMed
65.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
66.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2020 Nov 23.
67.Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res. 2012;22(10):1435-1443. PubMed
68.Dalkin SM, Greenhalgh J, Jones D, Cunningham B, Lhussier M. What's in a mechanism? Development of a key concept in realist evaluation. Implement Sci. 2015;10(1):49. PubMed
69.Astbury B, Leeuw FL. Unpacking black boxes: mechanisms and theory building in evaluation. Am J Eval. 2010;31(3):363-381.
70.Evidence Partners. DistillerSR [computer program]. Ottawa (ON): Evidence Partners; 2011-.
71.CASP Qualitative checklist. Oxford (UK): CASP UK; 2018: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf. Accessed 2020 Oct 18.
72.Hong QN, Fàbregues S, Bartlett G, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34(4):285-291.
73.Barbour RS. Checklists for improving rigour in qualitative research: a case of the tail wagging the dog? BMJ. 2001;322(7294):1115-1117. PubMed
74.Ron A. Regression analysis and the philosophy of social science. J Crit Realism. 2002;1(1):119-142.
75.Pawson R. Does Megan’s Law work? A theory-driven systematic review: working paper 8. London (UK): ESRC UK Centre for Evidence Based Policy and Practice, Queen Mary, University of London; 2002. Accessed 2020 Nov 13.
76.Wheeldon J, Faubert J. Framing experience: concept maps, mind maps, and data collection in qualitative research. Int J Qual Methods. 2009;8(3):68-83.
77.Dixon-Woods M, Agarwal S, Young B, Jones D, Sutton A. Integrative Approaches to Qualitative and Quantitative Evidence. London (UK): Health Development Agency; 2004.
78.Pfaeffli L, Maddison R, Whittaker R, et al. A mHealth cardiac rehabilitation exercise intervention: findings from content development studies. BMC Cardiovasc Disord. 2012;12:36. PubMed
79.Lear SA, Singer J, Banner-Lukaris D, et al. Randomized trial of a virtual cardiac rehabilitation program delivered at a distance via the Internet. Circ Cardiovasc Qual Outcomes. 2014;7(6):952-959. PubMed
80.Frohmader TJ, Lin F, Chaboyer W. Patient perceptions of nurse mentors facilitating the Aussie Heart Guide: a home-based cardiac rehabilitation programme for rural patients. Nurs Open. 2016;3(1):41-50. PubMed
81.Thorup CB, Gronkjaer M, Spindler H, et al. Pedometer use and self-determined motivation for walking in a cardiac telerehabilitation program: a qualitative study. BMC Sports Sci Med Rehabil. 2016;8:24. PubMed
82.Banner D, Lear S, Kandola D, et al. The experiences of patients undertaking a 'virtual' cardiac rehabilitation program. Stud Health Technol Inform. 2015;209:9-14. PubMed
83.Devi R, Carpenter C, Powell J, Singh S. Exploring the experience of using a web-based cardiac rehabilitation programme in a primary care angina population: a qualitative study. Int J Ther Rehabil. 2014;21(9):434-440.
84.Dinesen B, Nielsen G, Andreasen JJ, Spindler H. Integration of rehabilitation activities into everyday life through telerehabilitation: qualitative study of cardiac patients and their partners. J Med Internet Res. 2019;21(4):e13281. PubMed
85.O'Shea O, Woods C, McDermott L, et al. A qualitative exploration of cardiovascular disease patients' views and experiences with an eHealth cardiac rehabilitation intervention: the PATHway Project. PLoS One. 2020;15(7):e0235274. PubMed
86.Fang JY, Li JL, Li ZH, et al. Attitudes towards acceptance of an innovative home-based and remote sensing rehabilitation protocol among cardiovascular patients in Shantou, China. J Geriatr Cardiol. 2016;13(4):326-332. PubMed
87.Dorje T, Zhao G, Tso K, et al. Smartphone and social media-based cardiac rehabilitation and secondary prevention in China (SMART-CR/SP): a parallel-group, single-blind, randomised controlled trial. Lancet Digit Health. 2019;1(7):e363-e374. PubMed
88.Higgins RO, Rogerson M, Murphy BM, et al. Cardiac rehabilitation online pilot: extending reach of cardiac rehabilitation. J Cardiovasc Nurs. 2017;32(1):7-13. PubMed
89.Forman DE, LaFond K, Panch T, Allsup K, Manning K, Sattelmair J. Utility and efficacy of a smartphone application to enhance the learning and behavior goals of traditional cardiac rehabilitation: a feasibility study. J Cardiopulm Rehabil Prev. 2014;34(5):327-334. PubMed
90.Knudsen MV, Laustsen S, Petersen AK, Hjortdal VE, Angel S. Experience of cardiac tele-rehabilitation: analysis of patient narratives. Disabil Rehabil. 2021;43(3):370-377. PubMed
91.Rawstorn JC, Gant N, Rolleston A, et al. End users want alternative intervention delivery models: usability and acceptability of the REMOTE-CR Exercise-Based Cardiac Telerehabilitation Program. Arch Phys Med Rehabil. 2018;99(11):2373-2377. PubMed
92.Buys R, Claes J, Walsh D, et al. Cardiac patients show high interest in technology enabled cardiovascular rehabilitation. BMC Med Inform Decis Mak. 2016;16:95. PubMed
93.Worringham C, Rojek A, Stewart I. Development and feasibility of a smartphone, ECG and GPS based system for remotely monitoring exercise in cardiac rehabilitation. PLoS One. 2011;6(2):e14669. PubMed
94.Grover DB, Alexander JL. Patient attitudes toward telemedicine-delivered cardiac rehabilitation. Rehabil Nurs. 2019;44(6):358-363. PubMed
95.Sengupta A, Beckie T, Dutta K, Dey A, Chellappan S. A mobile health intervention system for women with coronary heart disease: usability study. JMIR Form Res. 2020;4(6):e16420. PubMed
96.Theodoulou E, Tirimacco R, Dollman J, Duncan M, Coote E, Ferrar KE. Preferences and attitudes to mobile phone and Internet-based cardiac rehabilitation maintenance programs in rural Australia. Aust J Rural Health. 2019;27(2):179-180. PubMed
97.Widmer RJ, Senecal C, Allison TG, Lopez-Jimenez F, Lerman LO, Lerman A. Dose-response effect of a digital health intervention during cardiac rehabilitation: subanalysis of randomized controlled trial. J Med Internet Res. 2020;22(2):e13055. PubMed
98.Ammenwerth E, Woess S, Baumgartner C, et al. Evaluation of an integrated telemonitoring surveillance system in patients with coronary heart disease. Methods Inf Med. 2015;54(5):388-397. PubMed
99.Piotrowicz E, Stepnowska M, Leszczynska-Iwanicka K, et al. Quality of life in heart failure patients undergoing home-based telerehabilitation versus outpatient rehabilitation--a randomized controlled study. Eur J Cardiovasc Nurs. 2015;14(3):256-263. PubMed
100.Zimmerman L, Barnason S, Hertzog M, et al. Gender differences in recovery outcomes after an early recovery symptom management intervention. Heart Lung. 2011;40(5):429-439. PubMed
101.Riley JP, Gabe JP, Cowie MR. Does telemonitoring in heart failure empower patients for self-care? A qualitative study. J Clin Nurs. 2013;22(17-18):2444-2455. PubMed
102.Sohn S, Helms TM, Pelleter JT, Muller A, Krottinger AI, Schoffski O. Costs and benefits of personalized healthcare for patients with chronic heart failure in the care and education program “Telemedicine for the Heart”. Telemed J E Health. 2012;18(3):198-204. PubMed
103.Davis C, Bender M, Smith T, Broad J. Feasibility and acute care utilization outcomes of a post-acute transitional telemonitoring program for underserved chronic disease patients. Telemed J E Health. 2015;21(9):705-713. PubMed
104.Chantler T, Paton C, Velardo C, et al. Creating connections - the development of a mobile-health monitoring system for heart failure: qualitative findings from a usability cohort study. Digit Health. 2016;2:2055207616671461. PubMed
105.Lefler LL, Rhoads SJ, Harris M, et al. Evaluating the use of mobile health technology in older adults with heart failure: mixed-methods study. JMIR Aging. 2018;1(2):e12178. PubMed
106.Fairbrother P, Ure J, Hanley J, et al. Telemonitoring for chronic heart failure: the views of patients and healthcare professionals - a qualitative study. J Clin Nurs. 2014;23(1-2):132-144. PubMed
107.Rahimi K, Velardo C, Triantafyllidis A, et al. A user-centred home monitoring and self-management system for patients with heart failure: a multicentre cohort study. Eur Heart J Qual Care Clin Outcomes. 2015;1(2):66-71. PubMed
108.Seto E, Morita PP, Tomkun J, et al. Implementation of a heart failure telemonitoring system in home care nursing: feasibility study. JMIR Med Inform. 2019;7(3):e11722. PubMed
109.Prescher S, Deckwart O, Winkler S, Koehler K, Honold M, Koehler F. Telemedical care: feasibility and perception of the patients and physicians: a survey-based acceptance analysis of the Telemedical Interventional Monitoring in Heart Failure (TIM-HF) trial. Eur J Prev Cardiol. 2013;20(2 Suppl):18-24. PubMed
110.Zan S, Agboola S, Moore SA, Parks KA, Kvedar JC, Jethwani K. Patient engagement with a mobile web-based telemonitoring system for heart failure self-management: a pilot study. JMIR Mhealth Uhealth. 2015;3(2):e33. PubMed
111.Jaana M, Sherrard H, Pare G. A prospective evaluation of telemonitoring use by seniors with chronic heart failure: adoption, self-care, and empowerment. Health Informatics J. 2019;25(4):1800-1814. PubMed
112.Hagglund E, Stromberg A, Hagerman I, Lynga P. Theory testing of patient perspectives using a mobile health technology system in heart failure self-care. J Cardiovasc Nurs. 2019;34(6):448-453. PubMed
113.Bartlett YK, Haywood A, Bentley CL, et al. The SMART personalised self-management system for congestive heart failure: results of a realist evaluation. BMC Med Inform Decis Mak. 2014;14:109. PubMed
114.Silva-Cardoso J, Moreira E, Lopes I, et al. SmartBEAT: a smartphone-based heart failure telemonitoring solution. MEDICON 2019: XV Mediterranean Conference on Medical and Biological Engineering and Computing – MEDICON 2019. 2019;76:1369-1376.
115.Hall AK, Dodd V, Harris A, McArthur K, Dacso C, Colton LM. Heart failure patients' perceptions and use of technology to manage disease symptoms. Telemed J E Health. 2014;20(4):324-331. PubMed
116.Ammenwerth E, Modre-Osprian R, Fetz B, et al. HerzMobil, an integrated and collaborative telemonitoring-based disease management program for patients with heart failure: a feasibility study paving the way to routine care. JMIR Cardio. 2018;2(1):e11. PubMed
117.Boyne JJ, Vrijhoef HJ, Spreeuwenberg M, et al. Effects of tailored telemonitoring on heart failure patients' knowledge, self-care, self-efficacy and adherence: a randomized controlled trial. Eur J Cardiovasc Nurs. 2014;13(3):243-252. PubMed
118.Woods LS, Duff J, Roehrer E, Walker K, Cummings E. Patients' experiences of using a consumer mHealth app for self-management of heart failure: mixed-methods study. JMIR Hum Factors. 2019;6(2):e13009. PubMed
119.Domingues FB, Clausell N, Aliti GB, Dominguez DR, Rabelo ER. Education and telephone monitoring by nurses of patients with heart failure: randomized clinical trial. Arq Bras Cardiol. 2011;96(3):233-239. PubMed
120.Albert NM, Dinesen B, Spindler H, et al. Factors associated with telemonitoring use among patients with chronic heart failure. J Telemed Telecare. 2017;23(2):283-291. PubMed
121.Caban PL. The use of home telemonitoring for heart failure management among Hispanics, non-Hispanic Blacks, and non-Hispanic Whites. Home Healthc Now. 2019;37(6):345-349. PubMed
122.Melin M, Hagglund E, Ullman B, Persson H, Hagerman I. Effects of a tablet computer on self-care, quality of life, and knowledge: a randomized clinical trial. J Cardiovasc Nurs. 2018;33(4):336-343. PubMed
123.Seto E, Leonard KJ, Cafazzo JA, Barnsley J, Masino C, Ross HJ. Perceptions and experiences of heart failure patients and clinicians on the use of mobile phone-based telemonitoring. J Med Internet Res. 2012;14(1):e25. PubMed
124.Liljeroos M, Thylen I, Stromberg A. Patients' and nurses' experiences and perceptions of remote monitoring of implantable cardiac defibrillators in heart failure: cross-sectional, descriptive, mixed methods study. J Med Internet Res. 2020;22(9):e19550. PubMed
125.Evangelista LS, Lee JA, Moore AA, et al. Examining the effects of remote monitoring systems on activation, self-care, and quality of life in older patients with chronic heart failure. J Cardiovasc Nurs. 2015;30(1):51-57. PubMed
126.Jiang J, Zhu Q, Zheng Y, Zhu Y, Li Y, Huo Y. Perceptions and acceptance of mHealth in patients with cardiovascular diseases: a cross-sectional study. JMIR Mhealth Uhealth. 2019;7(2):e10117. PubMed
127.Seto E, Leonard KJ, Masino C, Cafazzo JA, Barnsley J, Ross HJ. Attitudes of heart failure patients and health care providers towards mobile phone-based remote monitoring. J Med Internet Res. 2010;12(4):e55. PubMed
128.Kato NP, Johansson P, Okada I, et al. Heart failure telemonitoring in Japan and Sweden: a cross-sectional survey. J Med Internet Res. 2015;17(11):e258. PubMed
129.Browning SV, Clark RC, Poff RM, Todd D. Telehealth monitoring: a smart investment for home care patients with heart failure? Home Healthc Nurse. 2011;29(6):368-374. PubMed
130.Sharma U, Clarke M. Nurses' and community support workers' experience of telehealth: a longitudinal case study. BMC Health Serv Res. 2014;14:164. PubMed
131.Vuorinen AL, Leppanen J, Kaijanranta H, et al. Use of home telemonitoring to support multidisciplinary care of heart failure patients in Finland: randomized controlled trial. J Med Internet Res. 2014;16(12):e282. PubMed
132.Papoutsi C, A'Court C, Wherton J, Shaw S, Greenhalgh T. Explaining the mixed findings of a randomised controlled trial of telehealth with centralised remote support for heart failure: multi-site qualitative study using the NASSS framework. Trials. 2020;21(1):891. PubMed
133.Lynga P, Fridlund B, Langius-Eklof A, Bohm K. Perceptions of transmission of body weight and telemonitoring in patients with heart failure? Int J Qual Stud Health Well-being. 2013;8:21524. PubMed
134.Ware P, Ross HJ, Cafazzo JA, Laporte A, Gordon K, Seto E. User-centered adaptation of an existing heart failure telemonitoring program to ensure sustainability and scalability: qualitative study. JMIR Cardio. 2018;2(2):e11466. PubMed
135.Heckemann B, Wolf A, Ali L, Sonntag SM, Ekman I. Discovering untapped relationship potential with patients in telehealth: a qualitative interview study. BMJ Open. 2016;6(3):e009750. PubMed
136.Johnston G, Weatherburn G. Automated weight monitoring in chronic heart failure: the excluded majority. J Telemed Telecare. 2010;16(4):190-192. PubMed
137.Nguyen L, Keshavjee K, Archer N, Patterson C, Gwadry-Sridhar F, Demers C. Barriers to technology use among older heart failure individuals in managing their symptoms after hospital discharge. Int J Med Inform. 2017;105:136-142. PubMed
138.Piette JD, Striplin D, Marinec N, et al. A mobile health intervention supporting heart failure patients and their informal caregivers: a randomized comparative effectiveness trial. J Med Internet Res. 2015;17(6):e142. PubMed
139.Chiang LC, Chen WC, Dai YT, Ho YL. The effectiveness of telehealth care on caregiver burden, mastery of stress, and family function among family caregivers of heart failure patients: a quasi-experimental study. Int J Nurs Stud. 2012;49(10):1230-1242. PubMed
140.Triantafyllidis A, Velardo C, Chantler T, et al. A personalised mobile-based home monitoring system for heart failure: the SUPPORT-HF Study. Int J Med Inform. 2015;84(10):743-753. PubMed
141.Pekmezaris R, Schwartz RM, Taylor TN, et al. A qualitative analysis to optimize a telemonitoring intervention for heart failure patients from disparity communities. BMC Med Inform Decis Mak. 2016;16:75. PubMed
142.Finkelstein J, Wood J. Implementing home telemanagement of congestive heart failure using Xbox gaming platform. Annu Int Conf IEEE Eng Med Biol Soc. 2011;2011:3158-3163. PubMed
143.Svagard I, Austad HO, Seeberg T, et al. A usability study of a mobile monitoring system for congestive heart failure patients. Stud Health Technol Inform. 2014;205:528-532. PubMed
144.Cajita MI, Hodgson NA, Lam KW, Yoo S, Han HR. Facilitators of and barriers to mHealth adoption in older adults with heart failure. Comput Inform Nurs. 2018;36(8):376-382. PubMed
145.Stut W, Deighan C, Armitage W, Clark M, Cleland JG, Jaarsma T. Design and usage of the HeartCycle education and coaching program for patients with heart failure. JMIR Res Protoc. 2014;3(4):e72. PubMed
146.Dang S, Karanam C, Gomez-Orozco C, Gomez-Marin O. Mobile phone intervention for heart failure in a minority urban county hospital population: usability and patient perspectives. Telemed J E Health. 2017;23(7):544-554. PubMed
147.Dadosky A, Overbeck H, Barbetta L, et al. Telemanagement of heart failure patients across the post-acute care continuum. Telemed J E Health. 2018;24(5):360-366. PubMed
148.Varon C, Alao M, Minter J, et al. Telehealth on heart failure: results of the Recap project. J Telemed Telecare. 2015;21(6):340-347. PubMed
149.Radhakrishna K, Bowles K, Zettek-Sumner A. Contributors to frequent telehealth alerts including false alerts for patients with heart failure: a mixed methods exploration. Appl Clin Inform. 2013;4(4):465-475. PubMed
150.Portz JD, Ford KL, Elsbernd K, et al. “I like the idea of it...but probably wouldn't use it” - health care provider perspectives on heart failure mHealth: qualitative study. JMIR Cardio. 2020;4(1):e18101. PubMed
151.Gardner CL, Flanagan MC, Franklin C, et al. Electronic physiologic and subjective data acquisition in home-dwelling heart failure patients: an assessment of patient use and perception of usability. Int J Med Inform. 2016;93:42-48. PubMed
152.de Vries AE, van der Wal MH, Nieuwenhuis MM, et al. Health professionals' expectations versus experiences of internet-based telemonitoring: survey among heart failure clinics. J Med Internet Res. 2013;15(1):e4. PubMed
153.Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in patients with heart failure. N Engl J Med. 2010;363(24):2301-2309. PubMed
154.Qian F, Parzynski CS, Chaudhry SI, et al. Racial differences in heart failure outcomes: evidence from the Tele-HF Trial (Telemonitoring to Improve Heart Failure Outcomes). JACC Heart Fail. 2015;3(7):531-538. PubMed
155.Kao DP, Lindenfeld J, Macaulay D, et al. Impact of a telehealth and care management program on all-cause mortality and healthcare utilization in patients with heart failure. Telemed J E Health. 2016;22(1):2-11. PubMed
156.Radhakrishnan K, Jacelon CS, Bigelow C, Roche JP, Marquard JL, Bowles KH. Association of comorbidities with home care service utilization of patients with heart failure while receiving telehealth. J Cardiovasc Nurs. 2013;28(3):216-227. PubMed
157.Bikdeli B, Wayda B, Bao H, et al. Place of residence and outcomes of patients with heart failure: analysis from the telemonitoring to improve heart failure outcomes trial. Circ Cardiovasc Qual Outcomes. 2014;7(5):749-756. PubMed
158.Galinier M, Roubille F, Berdague P, et al. Telemonitoring versus standard care in heart failure: a randomised multicentre trial. Eur J Heart Fail. 2020;22(6):985-994. PubMed
159.Guzman-Clark JR, van Servellen G, Chang B, Mentes J, Hahn TJ. Predictors and outcomes of early adherence to the use of a home telehealth device by older veterans with heart failure. Telemed J E Health. 2013;19(3):217-223. PubMed
160.Jimenez-Marrero S, Yun S, Cainzos-Achirica M, et al. Impact of telemedicine on the clinical outcomes and healthcare costs of patients with chronic heart failure and mid-range or preserved ejection fraction managed in a multidisciplinary chronic heart failure programme: a sub-analysis of the iCOR randomized trial. J Telemed Telecare. 2020;26(1-2):64-72. PubMed
161.Lycholip E, Thon Aamodt I, Lie I, et al. The dynamics of self-care in the course of heart failure management: data from the IN TOUCH study. Patient Prefer Adherence. 2018;12:1113-1122. PubMed
162.Cajita MI, Hodgson NA, Budhathoki C, Han HR. Intention to use mHealth in older adults with heart failure. J Cardiovasc Nurs. 2017;32(6):E1-E7. PubMed
163.Alnosayan N, Chatterjee S, Alluhaidan A, Lee E, Houston Feenstra L. Design and usability of a heart failure mHealth system: a pilot study. JMIR Hum Factors. 2017;4(1):e9. PubMed
164.Ware P, Dorai M, Ross HJ, et al. Patient adherence to a mobile phone-based heart failure telemonitoring program: a longitudinal mixed-methods study. JMIR Mhealth Uhealth. 2019;7(2):e13259. PubMed
165.Magnani JW, Schlusser CL, Kimani E, Rollman BL, Paasche-Orlow MK, Bickmore TW. The Atrial Fibrillation Health Literacy Information Technology System: Pilot Assessment. JMIR Cardio. 2017;1(2):e7. PubMed
166.Hirschey J, Bane S, Mansour M, et al. Evaluating the usability and usefulness of a mobile app for atrial fibrillation using qualitative methods: exploratory pilot study. JMIR Hum Factors. 2018;5(1):e13. PubMed
167.Guhl E, Althouse AD, Pusateri AM, et al. The Atrial Fibrillation Health Literacy Information Technology Trial: pilot trial of a mobile health app for atrial fibrillation. JMIR Cardio. 2020;4(1):e17162. PubMed
168.Jiang J, Gu X, Cheng CD, et al. The Hospital-Community-Family-Based Telemedicine (HCFT-AF) program for integrative management of patients with atrial fibrillation: pilot feasibility study. JMIR Mhealth Uhealth. 2020;8(10):e22137. PubMed
169.Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. PubMed
170.Standing C, Standing S, McDermott M-L, Gururajan R, Kiani Mavi R. The paradoxes of telehealth: a review of the literature 2000-2015. Syst Res Behav Sci. 2018;35(1):90-101.
171.Parker S, Prince A, Thomas L, et al. Electronic, mobile and telehealth tools for vulnerable patients with chronic disease: a systematic review and realist synthesis. BMJ Open. 2018;8(8):e019192. PubMed
172.Vassilev I, Rowsell A, Pope C, et al. Assessing the implementability of telehealth interventions for self-management support: a realist review. Implement Sci. 2015;10:59. PubMed
173.Angus JE, Dale CM, Nielsen LS, et al. Gender matters in cardiac rehabilitation and diabetes: using Bourdieu's concepts. Soc Sci Med. 2018;200:44-51. PubMed
174.Jaarsma T, Cameron J, Riegel B, Stromberg A. Factors related to self-care in heart failure patients according to the middle-range theory of self-care of chronic illness: a literature update. Curr Heart Fail Rep. 2017;14(2):71-77. PubMed
175.Kessing D, Denollet J, Widdershoven J, Kupper N. Psychological determinants of heart failure self-care: systematic review and meta-analysis. Psychosom Med. 2016;78(4):412-431. PubMed
176.Rajati F, Sadeghi M, Feizi A, Sharifirad G, Hasandokht T, Mostafavi F. Self-efficacy strategies to improve exercise in patients with heart failure: a systematic review. ARYA Atheroscler. 2014;10(6):319-333. PubMed
177.Higgins TJ, Middleton KR, Winner L, Janelle CM. Physical activity interventions differentially affect exercise task and barrier self-efficacy: a meta-analysis. Health Psychol. 2014;33(8):891-903. PubMed
178.Batalik L, Filakova K, Batalikova K, Dosbaba F. Remotely monitored telerehabilitation for cardiac patients: a review of the current situation. World J Clin Cases. 2020;8(10):1818-1831. PubMed
179.Bashi N, Karunanithi M, Fatehi F, Ding H, Walters D. Remote monitoring of patients with heart failure: an overview of systematic reviews. J Med Internet Res. 2017;19(1):e18. PubMed
180.Greenwood DA, Gee PM, Fatkin KJ, Peeples M. A systematic review of reviews evaluating technology-enabled diabetes self-management education and support. J Diabetes Sci Technol. 2017;11(5):1015-1027. PubMed
181.Supervia M, Medina-Inojosa JR, Yeung C, et al. Cardiac rehabilitation for women: a systematic review of barriers and solutions. Mayo Clin Proc. 2017;92(4):565-577. PubMed
182.Clark AM, DesMeules M, Luo W, Duncan AS, Wielgosz A. Socioeconomic status and cardiovascular disease: risks and implications for care. Nat Rev Cardiol. 2009;6(11):712-722. PubMed
183.Reading J. Confronting the growing crisis of cardiovascular disease and heart health among Aboriginal Peoples in Canada. Can J Cardiol. 2015;31(9):1077-1080. PubMed
184.Prince SA, McDonnell LA, Turek MA, et al. The state of affairs for cardiovascular health research in Indigenous women in Canada: a scoping review. Can J Cardiol. 2018;34(4):437-449. PubMed
185.Field PE, Franklin RC, Barker RN, Ring I, Leggat PA. Cardiac rehabilitation services for people in rural and remote areas: an integrative literature review. Rural Remote Health. 2018;18(4):4738. PubMed
186.McAlister FA, Youngson E, Kaul P. Patients with heart failure readmitted to the original hospital have better outcomes than those readmitted elsewhere. J Am Heart Assoc. 2017;6(5):e004892. PubMed
187.Allana S, Thompson DR, Ski CF, Clark AM. Intersectionality in heart failure self-care: ignorance is not an option. J Cardiovasc Nurs. 2020;35(3):231-233. PubMed
188.Pio CSA, Chaves G, Davies P, Taylor R, Grace S. Interventions to promote patient utilization of cardiac rehabilitation: cochrane systematic review and meta-analysis. J Clin Med. 2019;8(2):189. PubMed
189.Clark AM, Spaling M, Harkness K, et al. Determinants of effective heart failure self-care: a systematic review of patients' and caregivers' perceptions. Heart. 2014;100(9):716-721. PubMed
190.Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45. PubMed
191.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
192.Krefting L. Rigor in qualitative research: the assessment of trustworthiness. Am J Occup Ther. 1991;45(3):214-222. PubMed
193.Lincoln YS, Guba EG. Naturalistic inquiry. Thousand Oaks (CA): SAGE Publishing; 1985.
194.Booth A, Noyes J, Flemming K, et al. Guidance on choosing qualitative evidence synthesis methods for use in health technology assessments of complex interventions. Bremen (DE): Integrate-HTA; 2016: https://www.integrate-hta.eu/wp-content/uploads/2016/02/Guidance-on-choosing-qualitative-evidence-synthesis-methods-for-use-in-HTA-of-complex-interventions.pdf. Accessed 2021 Apr 20.
195.Hunting G, Shahid N, Sahakyan Y, et al. A multi-level qualitative analysis of Telehomecare in Ontario: challenges and opportunities. BMC Health Serv Res. 2015;15:544. PubMed
196.Bengtsson U, Kjellgren K, Hallberg I, Lundin M, Makitalo A. Patient contributions during primary care consultations for hypertension after self-reporting via a mobile phone self-management support system. Scand J Prim Health Care. 2018;36(1):70-79. PubMed
197.Banner D, Kandola D, Bates J, et al. Patient experiences of undertaking a virtual cardiac rehabilitation program. Can J Cardiovasc Nurs. 2019;29(2):6-14.
198.Hanley J, Ure J, Pagliari C, Sheikh A, McKinstry B. Experiences of patients and professionals participating in the HITS home blood pressure telemonitoring trial: a qualitative study. BMJ Open. 2013;3(5). PubMed
199.Anttila MR, Kivisto H, Piirainen A, et al. Cardiac rehabilitees' technology experiences before remote rehabilitation: qualitative study using a grounded theory approach. J Med Internet Res. 2019;21(2):e10985. PubMed
200.Barenfeld E, Ali L, Wallstrom S, Fors A, Ekman I. Becoming more of an insider: a grounded theory study on patients' experience of a person-centred e-health intervention. PLoS One. 2020;15(11):e0241801. PubMed
201.Bradbury K, Morton K, Band R, et al. Using the Person-Based Approach to optimise a digital intervention for the management of hypertension. PLoS One. 2018;13(5):e0196868. PubMed
202.Morton K, Dennison L, Bradbury K, et al. Qualitative process study to explore the perceived burdens and benefits of a digital intervention for self-managing high blood pressure in Primary Care in the UK. BMJ Open. 2018;8(5):e020843. PubMed
203.Woo K, Dowding DW. Decision-making factors associated with telehealth adoption by patients with heart failure at home: a qualitative study. Comput Inform Nurs. 2020;38(4):204-214. PubMed
204.Bond CS, Worswick L. Self management and telehealth: lessons learnt from the evaluation of a Dorset telehealth program. Patient. 2015;8(4):311-316. PubMed
205.Lind L, Karlsson D. Telehealth for “the digital illiterate”--elderly heart failure patients experiences. Stud Health Technol Inform. 2014;205:353-357. PubMed
206.Odeh B, Kayyali R, Nabhani-Gebara S, Philip N. Implementing a telehealth service: nurses' perceptions and experiences. Br J Nurs. 2014;23(21):1133-1137. PubMed
207.Taylor J, Coates E, Brewster L, Mountain G, Wessels B, Hawley MS. Examining the use of telehealth in community nursing: identifying the factors affecting frontline staff acceptance and telehealth adoption. J Adv Nurs. 2015;71(2):326-337. PubMed
208.Sanders C, Rogers A, Bowen R, et al. Exploring barriers to participation and adoption of telehealth and telecare within the Whole System Demonstrator trial: a qualitative study. BMC Health Serv Res. 2012;12:220. PubMed
209.LaFramboise LM, Woster J, Yager A, Yates BC. A technological life buoy: patient perceptions of the Health Buddy. J Cardiovasc Nurs. 2009;24(3):216-224. PubMed
210.Albrecht L, Wood PW, Fradette M, et al. Usability and acceptability of a home blood pressure telemonitoring device among community-dwelling senior citizens with hypertension: qualitative study. JMIR Aging. 2018;1(2):e10975. PubMed
211.Hallberg I, Ranerup A, Bengtsson U, Kjellgren K. Experiences, expectations and challenges of an interactive mobile phone-based system to support self-management of hypertension: patients' and professionals' perspectives. Patient Prefer Adherence. 2018;12:467-476. PubMed
212.Bradbury K, Morton K, Band R, et al. Understanding how primary care practitioners perceive an online intervention for the management of hypertension. BMC Med Inform Decis Mak. 2017;17(1):5. PubMed
213.Abdullah A, Liew SM, Hanafi NS, et al. What influences patients' acceptance of a blood pressure telemonitoring service in primary care? A qualitative study. Patient Prefer Adherence. 2016;10:99-106. PubMed
214.Jones MI, Greenfield SM, Bray EP, et al. Patients' experiences of self-monitoring blood pressure and self-titration of medication: the TASMINH2 trial qualitative study. Br J Gen Pract. 2012;62(595):e135-142. PubMed
215.Hanley J, Pinnock H, Paterson M, McKinstry B. Implementing telemonitoring in primary care: learning from a large qualitative dataset gathered during a series of studies. BMC Fam Pract. 2018;19(1):118. PubMed
216.EUnetHTA joint action 2, work package 8. HTA Core Model ® version 3.0. Diemen (NL): EUnetHTA; 2016: http://www.corehta.info/model/HTACoreModel3.0.pdf. Accessed 2021 May 11.
217.Flyvbjerg B. Rationality and power: democracy in practice. Chicago (IL): University of Chicago Press; 1998.
218.May C, Harrison R, Finch T, MacFarlane A, Mair F, Wallace P. Understanding the normalization of telemedicine services through qualitative evaluation. J Am Med Inform Assoc. 2003;10(6):596-604. PubMed
219.Jones L, Grech C. The patient experience of remote telemonitoring for heart failure in the rural setting: a literature review. Contemp Nurse. 2016;52(2-3):230-243. PubMed
220.Pols J. Towards an empirical ethics in care: relations with technologies in health care. Med Health Care Philos. 2015;18(1):81-90. PubMed
221.Klugman CM, Dunn LB, Schwartz J, Cohen IG. The ethics of smart pills and self-acting devices: autonomy, truth-telling, and trust at the dawn of digital medicine. Am J Bioeth. 2018;18(9):38-47. PubMed
222.Rush KL, Hatt L, Gorman N, Janicki L, Polasek P, Shay M. Planning telehealth for older adults with atrial fibrillation in rural communities: understanding stakeholder perspectives. Clin Nurs Res. 2019;28(2):130-149. PubMed
223.Bauer KA. Home-based telemedicine: a survey of ethical issues. Camb Q Healthc Ethics. 2001;10(2):137-146. PubMed
224.Acheampong F, Vimarlund V. Chapter 12: innovating healthcare through remote monitoring: effects and business model. Health care delivery and clinical science: concepts, methodologies, tools, and applications. Hershey (PA): IGI Global; 2017:247-268.
225.Jusob FR, George C, Mapp G. Exploring the need for a suitable privacy framework for mHealth when managing chronic diseases. J Reli Intell Environ. 2017;3(4):243-256.
226.Kwan V, Hagen G, Noel M, Dobson K, Yeates K. Healthcare at your fingertips: the professional ethics of smartphone health-monitoring applications. Ethics Behav. 2017;27(8):615-631.
227.Rush KL, Burton L, Van Der Merwe F, Hatt L, Galloway C. Atrial fibrillation care in rural communities: a mixed methods study of physician and patient perspectives. BMC Fam Pract. 2019;20(1):144. PubMed
228.Bauer K. Distributive justice and rural healthcare: a case for e-health. Int J Appl Philos. 2003;17(2):241-252. PubMed
229.Shields GE, Wells A, Doherty P, Heagerty A, Buck D, Davies LM. Cost-effectiveness of cardiac rehabilitation: a systematic review. Heart. 2018;104(17):1403-1410. PubMed
230.Michaud TL, Zhou J, McCarthy MA, Siahpush M, Su D. Costs of home-based telemedicine programs: a systematic review. Int J Technol Assess Health Care. 2018;34(4):410-418. PubMed
231.Mittelstadt B. Ethics of the health-related internet of things: a narrative review. Ethics Info Tech. 2017;19(3):157-175.
232.Knorr K, Aspinall D, Wolters M. On the privacy, security and safety of blood pressure and diabetes apps. In: Federrath H, Gollmann D, eds. ICT Systems Security and Privacy Protection. 30th IFIP TC 11 International Conference, SEC 2015, Hamburg, Germany, May 26-28. Vol 455. Berlin (DE): Springer; 2015:571-584.
233.Barrios V, Cosin-Sales J, Bravo M, et al. Telemedicine consultation for the clinical cardiologists in the era of COVID-19: present and future. Consensus document of the Spanish Society of Cardiology. Rev Esp Cardiol. 2020;73(11):910-918. PubMed
234.Nordgren A. Privacy by design in personal health monitoring. Health Care Anal. 2015;23(2):148-164. PubMed
235.CADTH framework for patient engagement in health technology assessment. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2021 Feb 09.
236.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res Involv Engagem. 2017;3:13. PubMed
237.Mecklai K, Smith N, Stern AD, Kramer DB. Remote patient monitoring - overdue or overused? N Engl J Med. 2021;384(15):1384-1386. PubMed
238.Hardman R, Begg S, Spelten E. What impact do chronic disease self-management support interventions have on health inequity gaps related to socioeconomic status: a systematic review. BMC Health Serv Res. 2020;20(1):150. PubMed
239.Schrage B, Lund LH, Benson L, et al. Lower socioeconomic status predicts higher mortality and morbidity in patients with heart failure. Heart. 2021;107(3):229-236. PubMed
240.Clark AM, McAlister FA, Hartling L, Vandermeer B, University of Alberta Evidence-based Practice Centre. Randomized trials of secondary prevention programs in coronary artery disease: a systematic review. (Technology assessment). Rockville (MD): Agency for Healthcare Research and Quality; 2005: https://www.cms.gov/Medicare/Coverage/DeterminationProcess/Downloads/id31TA.pdf. Accessed 2021 May 05.
241.Inter-jurisdictional medical licensing to support telemedicine. (CADTH policy brief). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/hta-he/cadth-policy-brief-interjurisdictional-licensing-final.pdf. Accessed 2021 Aug 09.
242.The Virtual Care Task Force. Virtual care: recommendations for scaling up virtual medical services. Ottawa (ON): Canadian Medical Association (CMA); 2020: https://www.cma.ca/sites/default/files/pdf/virtual-care/ReportoftheVirtualCareTaskForce.pdf. Accessed 2021 Aug 09.
Appendix 1: Literature Search Strategy
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Realist Review Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Embase (1974-present)
APA PyscInfo (1806-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: November 11, 2020
Alerts: Monthly search updates until the end of the completion of stakeholder feedback period.
Study types: No filters were applied to limit the retrieval by study type.
Limits
Publication date limit: 2010-present
Humans
Language limit: English- and French-language
Conference abstracts: excluded
Table 7: Syntax Guide — Realist Review Literature Search
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ab | Abstract |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.id | Key concepts (PyscINFO) |
.pt | Publication type |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
pysh | Ovid database code: APA PsycInfo 1806 to present, updated weekly |
Multi-Database Strategy
exp heart failure/
((heart or cardiac* or cardio* or myocardi* or diastolic* or systolic* or paroxysmal*) adj5 (failure* or edema* or edema* or decompensation* or dyspnea* or asthma* or chronic* or insufficien*)).ti,ab,kf.
((preserved ejection* or reduced ejection*) adj5 fraction*).ti,ab,kf.
(congestive heart* adj5 disease*).ti,ab,kf.
((cardio renal* or cardiorenal* or reno cardiac* or renocardiac*) adj5 syndrome*).ti,ab,kf.
exp Hypertension/
(hypertension* or ((high* or elevat*) adj5 (blood pressure* or bloodpressure* or diastolic pressure* or systolic pressure*))).ti,ab,kf.
exp Arrhythmias, Cardiac/
(arrhythmia* or dysrhythmia* or bradycardia* or bradyarrhythmia* or tachycardia* or tachyarrhythmia*).ti,ab,kf.
((irregular* or slow* or rapid* or fast or junctional*) adj3 (heartbeat* or heart beat* or rhythm*)).ti,ab,kf.
((atrial or auricular or ventricular) adj5 (fibrillation* or flutter*)).ti,ab,kf.
((heart rhythm* or cardiac rhythm*) adj5 disorder*).ti,ab,kf.
(premature adj3 (atrial or ventricular or junctional or cardiac) adj3 (contraction* or complex*)).ti,ab,kf.
((accelerat* or junctional*) adj5 rhythm*).ti,ab,kf.
(extra beats or heart block or heart blocks or AV block or AV blocks).ti,ab,kf.
Coronary Artery Disease/
(atherosclerosis or atheroscleroses or arteriosclerosis or arterioscleroses or (coronary adj5 disease*)).ti,ab,kf.
(hard* adj3 arter*).ti,ab,kf.
(plaque adj4 build*).ti,ab,kf.
Cardiac Rehabilitation/
((cardiac* or cardio* or heart*) adj5 (rehab* or conditioning*)).ti,ab,kf.
or/1 to 21
exp telemedicine/ or exp Telemetry/ or exp Videoconferencing/ or exp computer communication networks/ or Mobile Applications/
(teleconsult* or telemonitor* or RPC or RPM or telemetry or telemetric* or telepatholog* or teleradialogue* or videoconference* or video conference* or asynchron* or ((remote or tele or virtual or rural or urban) adj5 (consult* or monitor* or checkin or check in or pathol* or radialogue*))).ti,ab,kf.
(telehealth* or telemed* or telecommunicat* or tele communicat* or e health* or ehealth* or m health* or mhealth* or e consult* or econsult* or telecar* or HBPMTM or ((tele or mobile or virtual) adj5 (health* or med* or care or caring or visit or visits or appointment*))).ti,ab,kf.
(telerehab* or ((remote* or tele* or virtual*) adj5 rehab*)).ti,ab,kf.
(telemed* or tele med* or telehealth* or tele health* or telerehab* or tele rehab* or telecar* or tele car* or e health* or ehealth or m Health* or mHealth* or e consult* or econsult*).jw.
or/23 to 27
22 and 28
29 use medall
exp heart failure/
((heart or cardiac* or cardio* or myocardi* or diastolic* or systolic* or paroxysmal*) adj5 (failure* or edema* or edema* or decompensation* or dyspnea* or asthma* or chronic* or insufficien*)).ti,ab,kw,dq.
((preserved ejection* or reduced ejection*) adj5 fraction*).ti,ab,kw,dq.
(congestive heart* adj5 disease*).ti,ab,kw,dq.
((cardio renal* or cardiorenal* or reno cardiac* or renocardiac*) adj5 syndrome*).ti,ab,kw,dq.
exp hypertension/
(hypertension* or ((high* or elevat*) adj5 (blood pressure* or bloodpressure* or diastolic pressure* or systolic pressure*))).ti,ab,kw,dq.
exp heart arrhythmia/
(arrhythmia* or dysrhythmia* or bradycardia* or bradyarrhythmia* or tachycardia* or tachyarrhythmia*).ti,ab,kw,dq.
((irregular* or slow* or rapid* or fast or junctional*) adj3 (heartbeat* or heart beat* or rhythm*)).ti,ab,kw,dq.
((atrial or auricular or ventricular) adj5 (fibrillation* or flutter*)).ti,ab,kw,dq.
((heart rhythm* or cardiac rhythm*) adj5 disorder*).ti,ab,kw,dq.
(premature adj3 (atrial or ventricular or junctional or cardiac) adj3 (contraction* or complex*)).ti,ab,kw,dq.
((accelerat* or junctional*) adj5 rhythm*).ti,ab,kw,dq.
(extra beats or heart block or heart blocks or AV block or AV blocks).ti,ab,kw,dq.
exp coronary artery disease/
(atherosclerosis or atheroscleroses or arteriosclerosis or arterioscleroses or (coronary adj5 disease*)).ti,ab,kw,dq.
(hard* adj3 arter*).ti,ab,kw,dq.
(plaque adj4 build*).ti,ab,kw,dq.
heart rehabilitation/
((cardiac* or cardio* or heart*) adj5 (rehab* or conditioning*)).ti,ab,kw,dq.
or/31 to 51
telehealth/ or telemedicine/ or telecardiology/ or telenursing/ or teleconsultation/ or telediagnosis/ or telemonitoring/ or telepathology/ or teleradiology/ or telerehabilitation/ or teletherapy/ or telemetry/ or remote sensing/ or telephone telemetry/ or videoconferencing/ or exp computer network/ or exp internet/ or social media/ or mobile application/
(teleconsult* or telemonitor* or RPC or RPM or telemetry or telemetric* or telepatholog* or teleradialogue* or videoconference* or video conference* or asynchron* or ((remote or tele or virtual or rural or urban) adj5 (consult* or monitor* or checkin or check in or pathol* or radialogue*))).ti,ab,kw,dq.
(telehealth* or telemed* or telecommunicat* or tele communicat* or e health* or ehealth* or m health* or mhealth* or e consult* or econsult* or telecar* or HBPMTM or ((tele or mobile or virtual) adj5 (health* or med* or care or caring or visit or visits or appointment*))).ti,ab,kw,dq.
(telerehab* or ((remote* or tele* or virtual*) adj5 rehab*)).ti,ab,kw,dq.
(telemed* or tele med* or telehealth* or tele health* or telerehab* or tele rehab* or telecar* or tele car* or e health* or ehealth or m Health* or mHealth* or e consult* or econsult*).jx.
or/53 to 57
52 and 58
59 use oemezd
60 not conference abstract.pt.
exp heart/ and failure/
((heart or cardiac* or cardio* or myocardi* or diastolic* or systolic* or paroxysmal*) adj5 (failure* or edema* or edema* or decompensation* or dyspnea* or asthma* or chronic* or insufficien*)).ti,ab,id.
((preserved ejection* or reduced ejection*) adj5 fraction*).ti,ab,id.
(congestive heart* adj5 disease*).ti,ab,id.
((cardio renal* or cardiorenal* or reno cardiac* or renocardiac*) adj5 syndrome*).ti,ab,id.
exp Hypertension/ or exp Blood Pressure/
(hypertension* or ((high* or elevat*) adj5 (blood pressure* or bloodpressure* or diastolic pressure* or systolic pressure*))).ti,ab,id.
exp “Arrhythmias (Heart)”/
(arrhythmia* or dysrhythmia* or bradycardia* or bradyarrhythmia* or tachycardia* or tachyarrhythmia*).ti,ab,id.
((irregular* or slow* or rapid* or fast or junctional*) adj3 (heartbeat* or heart beat* or rhythm*)).ti,ab,id.
((atrial or auricular or ventricular) adj5 (fibrillation* or flutter*)).ti,ab,id.
((heart rhythm* or cardiac rhythm*) adj5 disorder*).ti,ab,id.
(premature adj3 (atrial or ventricular or junctional or cardiac) adj3 (contraction* or complex*)).ti,ab,id.
((accelerat* or junctional*) adj5 rhythm*).ti,ab,id.
(extra beats or heart block or heart blocks or AV block or AV blocks).ti,ab,id.
Heart Disorders/
(atherosclerosis or atheroscleroses or arteriosclerosis or arterioscleroses or (coronary adj5 disease*)).ti,ab,id.
(hard* adj3 arter*).ti,ab,id.
(plaque adj4 build*).ti,ab,id.
exp heart/ and (rehabilitation/ or physical therapy/)
((cardiac* or cardio* or heart*) adj5 (rehab* or conditioning*)).ti,ab,id.
or/62 to 82
telemedicine/ or online therapy/ or exp teleconferencing/ or teleconsultation/ or telerehabilitation/ or Telemetry/ or computer mediated communication/ or internet/ or internet usage/ or online social networks/ or “smartphone use”/ or mobile applications/ or digital interventions/
(teleconsult* or telemonitor* or RPC or RPM or telemetry or telemetric* or telepatholog* or teleradialogue* or videoconference* or video conference* or asynchron* or ((remote or tele or virtual or rural or urban) adj5 (consult* or monitor* or checkin or check in or pathol* or radialogue*))).ti,ab,id.
(telehealth* or telemed* or telecommunicat* or tele communicat* or e health* or ehealth* or m health* or mhealth* or e consult* or econsult* or telecar* or HBPMTM or ((tele or mobile or virtual) adj5 (health* or med* or care or caring or visit or visits or appointment*))).ti,ab,id.
(telerehab* or ((remote* or tele* or virtual*) adj5 rehab*)).ti,ab,id.
(telemed* or tele med* or telehealth* or tele health* or telerehab* or tele rehab* or telecar* or tele car* or e health* or ehealth or m Health* or mHealth* or e consult* or econsult*).jx.
or/84 to 88
83 and 89
90 use psyh
30 or 61 or 91
limit 92 to yr = 2010-current
limit 93 to (english or french)
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | (remote monitoring OR remote consultation OR remote check-in) AND (heart failure OR atrial fibrillation OR hypertension OR cardiac rehabilitation)]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- [remote monitoring, remote consultation, remote check-in]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- (remote monitoring OR remote consultation OR remote check-in) AND (heart failure OR atrial fibrillation OR hypertension OR cardiac rehabilitation)]
Other Databases
CINAHL
Same MeSH, keywords, and limits used as per MEDLINE search, excluding study types and human restrictions. Syntax adjusted for EBSCO platform, including the addition of CINAHL headings. The search strategy is available on request.
Scopus
Same MeSH, keywords, and limits used as per MEDLINE search, excluding study types and human restrictions. Syntax adjusted for Scopus platform. The search strategy is available on request.
Perspectives and Experiences Review Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: August 26, 2020
Alerts: Monthly search updates until the completion of stakeholder feedback period
Study types: Qualitative studies
Limits
Publication date limit: no limit
Humans
Language limit: English- and French-language
Table 8: Syntax Guide — Perspectives and Experiences Review Literature Search
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
? | Truncation symbol for 1 or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ab | Abstract |
.kf | Author keyword heading word (MEDLINE) |
.pt | Publication type |
.jw | Journal title word (MEDLINE) |
Ovid Medline Database Strategy
exp heart failure/
((heart or cardiac* or cardio* or myocardi* or diastolic* or systolic* or paroxysmal*) adj5 (failure* or edema* or edema* or decompensation* or dyspnea* or asthma* or chronic*)).ti,ab,kf.
((preserved ejection* or reduced ejection*) adj5 fraction*).ti,ab,kf.
(congestive heart* adj5 disease*).ti,ab,kf.
((cardio renal* or cardiorenal* or reno cardiac* or renocardiac*) adj5 syndrome*).ti,ab,kf.
exp Hypertension/
(hypertension* or ((high* or elevat*) adj5 (blood pressure* or bloodpressure* or diastolic pressure* or systolic pressure*))).ti,ab,kf.
exp Arrhythmias, Cardiac/
(arrhythmia* or dysrhythmia* or bradycardia* or bradyarrhythmia* or tachycardia* or tachyarrhythmia*).ti,ab,kf.
((irregular* or slow* or rapid* or fast or junctional*) adj3 (heartbeat* or heart beat* or rhythm*)).ti,ab,kf.
((atrial or auricular or ventricular) adj5 (fibrillation* or flutter*)).ti,ab,kf.
((heart rhythm* or cardiac rhythm*) adj5 disorder*).ti,ab,kf.
(premature adj3 (atrial or ventricular or junctional or cardiac) adj3 (contraction* or complex*)).ti,ab,kf.
((accelerat* or junctional*) adj5 rhythm*).ti,ab,kf.
(extra beats or heart block or heart blocks or AV block or AV blocks).ti,ab,kf.
Coronary Artery Disease/
(atherosclerosis or atheroscleroses or arteriosclerosis or arterioscleroses or (coronary adj5 disease*)).ti,ab,kf.
(hard* adj3 arter*).ti,ab,kf.
(plaque adj4 build*).ti,ab,kf.
Cardiac Rehabilitation/
((cardiac* or cardio* or heart*) adj5 (rehab* or conditioning*)).ti,ab,kf.
or/1 to 21
exp telemedicine/ or exp Videoconferencing/ or exp computer communication networks/
(teleconsult* or telemonitor* or RPC or RPM or telemetry or telemetric* or telepatholog* or teleradialogue* or videoconference* or video conference* or asynchron* or ((remote or tele or virtual or rural or urban) adj5 (consult* or monitor* or checkin or check in or pathol* or radialogue*))).ti,ab,kf.
(telehealth* or telemed* or telecommunicat* or tele communicat* or e health* or ehealth* or m health* or mhealth* or e consult* or econsult* or telecar* or HBPMTM or ((tele or mobile or virtual) adj5 (health* or med* or care or caring or visit or visits or appointment*))).ti,ab,kf.
(telerehab* or ((remote* or tele* or virtual*) adj5 rehab*)).ti,ab,kf.
(telemed* or tele med* or telehealth* or tele health* or telerehab* or tele rehab* or telecar* or tele car* or e health* or ehealth or m Health* or mHealth* or e consult* or econsult*).jw.
or/23 to 27
exp Empirical Research/ or Interviews as Topic/ or Personal Narratives as Topic/ or Focus Groups/ or exp Narration/ or Nursing Methodology Research/ or Narrative Medicine/
(Interview or Personal Narrative).pt.
interview*.ti,ab,kf.
qualitative.ti,ab,kf,jw.
(theme* or thematic).ti,ab,kf.
ethnological research.ti,ab,kf.
ethnograph*.ti,ab,kf.
ethnomedicine.ti,ab,kf.
ethnonursing.ti,ab,kf.
phenomenol*.ti,ab,kf.
(grounded adj (theor* or study or studies or research or analys?s)).ti,ab,kf.
life stor*.ti,ab,kf.
(emic or etic or hermeneutic* or heuristic* or semiotic*).ti,ab,kf.
(data adj1 saturat$).ti,ab,kf.
participant observ*.ti,ab,kf.
(social construct* or postmodern* or post-structural* or post structural* or poststructural* or post modern* or post-modern*).ti,ab,kf.
(action research or cooperative inquir* or co operative inquir* or co-operative inquir*).ti,ab,kf.
(humanistic or existential or experiential or paradigm*).ti,ab,kf.
(field adj (study or studies or research or work)).ti,ab,kf.
(human science or social science).ti,ab,kf.
biographical method.ti,ab,kf.
theoretical sampl*.ti,ab,kf.
((purpos* adj4 sampl*) or (focus adj group*)).ti,ab,kf.
(open-ended or narrative* or textual or texts or semi-structured).ti,ab,kf.
(life world* or life-world* or conversation analys?s or personal experience* or theoretical saturation).ti,ab,kf.
((lived or life) adj experience*).ti,ab,kf.
cluster sampl*.ti,ab,kf.
observational method*.ti,ab,kf.
content analysis.ti,ab,kf.
(constant adj (comparative or comparison)).ti,ab,kf.
((discourse* or discurs*) adj3 analys?s).ti,ab,kf.
(heidegger* or colaizzi* or spiegelberg* or merleau* or husserl* or foucault* or ricoeur or glaser*).ti,ab,kf.
(van adj manen*).ti,ab,kf.
(van adj kaam*).ti,ab,kf.
(corbin* adj2 strauss*).ti,ab,kf.
or/29 to 63
22 and 28 and 64
limit 65 to (english or french)
Other Databases
CINAHL
Same MeSH, keywords, and limits used as per MEDLINE search, excluding study types and human restrictions. Syntax adjusted for EBSCO platform, including the addition of CINAHL headings. The search strategy is available on request.
Scopus
Same MeSH, keywords, and limits used as per MEDLINE search, excluding study types and human restrictions. Syntax adjusted for Scopus platform. The search strategy is available on request.
Grey Literature
Search dates: November 27, 2020 – December 04, 2020
Keywords: [(remote monitoring OR remote consultation OR remote check-in) AND (heart failure OR atrial fibrillation OR hypertension OR cardiac rehabilitation)]
Limits: no limits
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Clinical Trials Registries
Databases (free)
Internet Search
Open Access Journals
The complete search archive of sites consulted for this report is available on request.
Appendix 2: Large Tables and Figures
Note that this appendix has not been copy-edited.
Realist Review
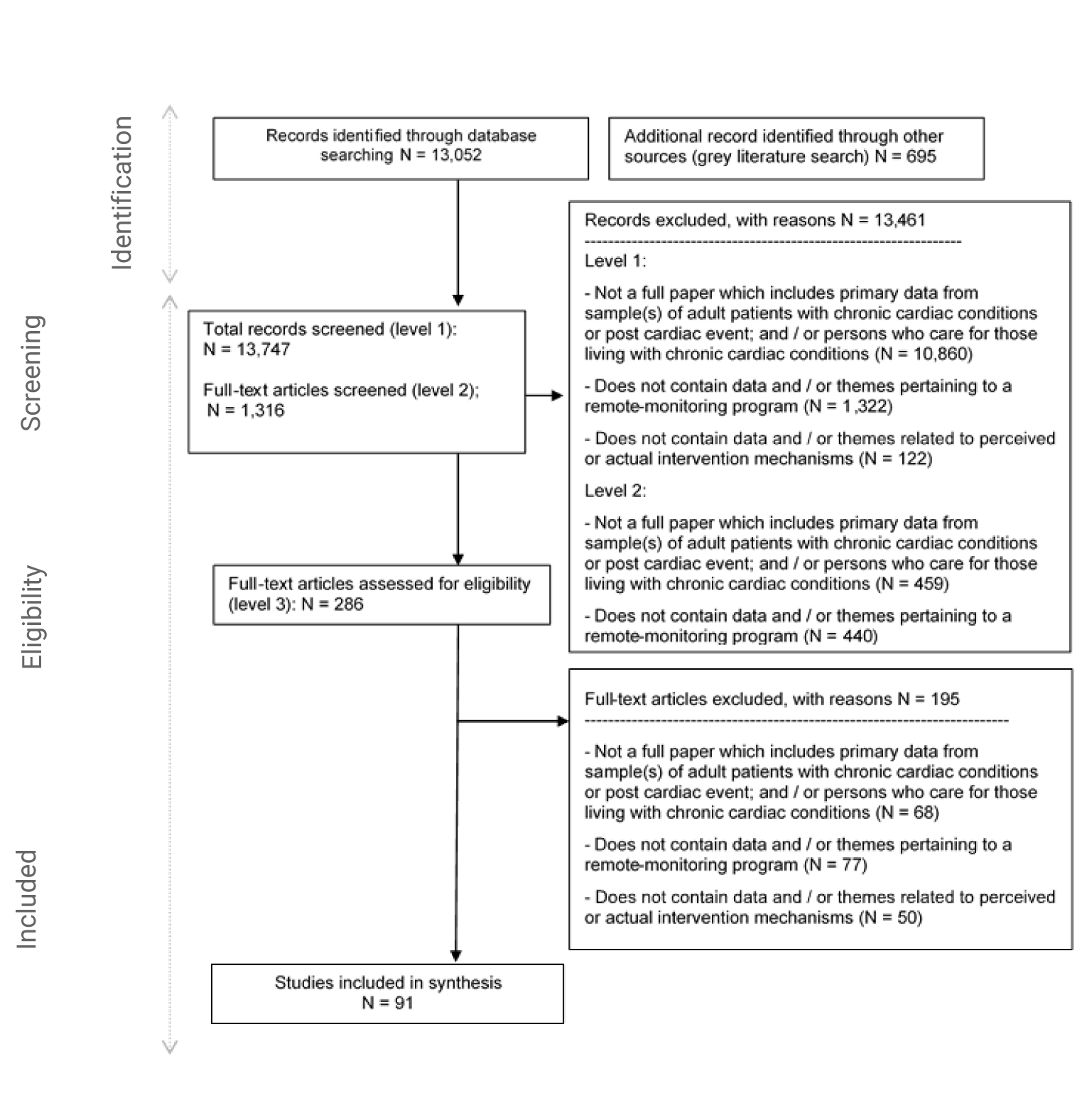
Table 9: Study Characteristics of Included Studies — Realist Review
Author | Condition | Country | Method | Design | Participant (mean age) | Caregiver/ profs |
|---|---|---|---|---|---|---|
Albert et al. (2017)120 | HF | US, Denmark | Quant | Survey; Cohort | 142 m / 64 f (64 years) | |
Alnosayan et al. (2017)163 | HF | US | MM | MM | 5 m / 3 f (62 years) | 13 Profs |
Ammenworth et al. (2015)98 | CR | Austria | Quant | Survey; NRE | 24 m / 1 f (63 years) | |
Ammenworth et al. (2018)116 | HF | Austria | Quant | NRE | 23 m / 5 f (67 years) | |
Banner et al. (2015)82 | CR | Canada | Qual | MM | 22 m / NS f | |
Bartlett et al. (2014)113 | HF | UK | Qual | Realist evaluation | NS | |
Bikedeli et al. (2014)157 | HF | US | Quant | Survey; RT | 903 m / 654 f (61 years) | |
Boyne et al. (2014)117 | HF | The Netherlands | Quant | Survey; RT | 226 m / 156 f (71 years) | |
Browning et al. (2011)129 | HF | US | Quant | NRE | 9 m / 15 f (79 years) | |
Buys et al. (2016)92 | CR | Belgium | Quant | Survey | 298 m / 12 f (62 years) | |
Caban (2019)121 | HF | US | Quant | Cohort | 40 m / 98 f (79 years) | |
Cajita et al. (2017)162 | HF | US | Quant | Survey | 95 m / 34 f (71 years) | |
Cajita et al. (2018)144 | HF | US | Qual | Gen qual | 7 m / 3 f (NS years) | |
Chantler et al. (2016)104 | HF | UK | MM | Survey; Gen qual | 37 m / 21 f (77 years) | |
Chaudhry et al. (2010)153 | HF | US | Quant | RT | 958 m / 695 f (61 years) | |
Chiang et al. (2012)139 | HF | Taiwan | Quant | NRE | 0 | 30 Caregivers |
Dadosky et al. (2018)147 | HF | US | Quant | RT | 110 m / 36 f | |
Dang et al. (2017)146 | HF | US | MM | NRE | 28 m / 14 f (53 years) | |
Davis et al. (2015)103 | HF | US | Quant | Cohort | 58 m / 60 f (64 years) | |
Devi et al. (2014)83 | CR | UK | Qual | Gen qual | 12 m / 4 f (66 years) | |
de Vries et al. (2013)152 | HF | Quant | Survey | 89 Clinics | ||
Dinesen et al. (2019)84 | CR | Denmark | Qual | Gen qual | 9 m / 5 f | 13 Caregivers |
Domingues et al. (2010)84 | HF | Brazil | Quant | RT | 68 m / 43 f (63 years) | |
Dorje et al. (2019)87 | CR | China | Quant | RT | 254 m / 58 f (61 years) | |
Evangelista et al. (2015)125 | HF | US | Quant | NRE | 11 f (73 years) | |
Fairbrother et al. (2014)106 | HF | UK | Qual | 7 m / 11 f (75 years) | ||
Fang et al. (2016)86 | CR | China | MM | MM | 116 m / 34 f (63 years) | |
Finkelstein and Wood (2011)142 | HF | US | Quant | NRE | 4 m / 6 f (43 years) | |
Forman et al. (2014)89 | CR | US | Quant | Cohort | 20 m / 6 f (59 years) | 3 profs |
Frohmader et al. (2016)80 | CR | Australia | Qual | Gen qual | 7 m / 6 f (59 years) | |
Galinier et al. (2020)158 | HF | France | Quant | RT | 677 m / 260 f (70 years) | |
Gardner et al. (2016)151 | HF | US | Quant | Survey | 28 m / 11 f (68 years) | |
Guhl et al. (2020)167 | AF | US | RCT | NRE | 87 m / 92 f (72 years) | |
Grover and Alexander (2019)94 | CR | US | Quant | Cohort | 12 m / 8 f (71 years) | |
Guzman-Clark et al. (2013)159 | HF | US | Quant | NRE | 240 m / 8 f (76 years) | |
Hagglund et al. (2019)112 | HF | Sweden | Qual | Grounded theory | 11 m / 6 f (75 years) | |
Hall et al. (2014)115 | HF | US | Qual | Gen qual | 10 m / 5 f (65 years) | |
Heckemann et al. (2016)135 | HF | The Netherlands | Qual | Gen qual | 20 Profs | |
Higgins et al. (2017)88 | CR | Australia | MM | NRE | 17 m / 4 f (62 years) | |
Hirschey et al. (2018)166 | AF | US | MM | MM | 7 m / 5 f (59 years) | |
Jaana et al. (2019)111 | HF | Canada | Quant | Survey | 16 m / 7 f (72 years) | |
Jiang et al. (2019)126 | HF | China | Quant | Survey | 124 m / 107 f (NS years) | |
Jiang et al. (2020)168 | AF | China | Quant | NRE | 38 m / 35 f (69 years) | |
Jimenez-Marrero et al. (2020)160 | HF | Spain | Quant | RT | 95 m / 87 f (77 years) | |
Johnston (2010)136 | HF | UK | Qual | Gen qual | 14 m / NS f (NS years) | 4 Profs; 10 Caregivers |
Kao et al. (2016)155 | HF | US | Quant | Cohort | 353 m / 268 f (69 years) | |
Kato et al. (2015)128 | HF | Japan, Sweden | Quant | Survey | 498 Profs | |
Knudsen et al. (2019)90 | CR | Denmark | Qual | Phen / exper | 7 m / 0 f (58 years) | |
Lear et al. (2014)79 | CR | Canada | Quant | RT | 56 m / 12 f (58 years) | |
Lefler et al. (2018)105 | HF | US | MM | MM | 16 m / 12 f (NS years) | |
Liljeroos et al. (2020)124 | HF | Sweden | MM | MM | 138 m / 37 f (70 years) | 30 Profs |
Lycholip et al. (2018)161 | HF | Sweden | Quant | RT | 83 m / 35 f (69 years) | |
Lynga et al. (2013)133 | HF | Sweden | Qual | Phen / exper | 15 m / 5 f (74 years) | |
Magnani et al. (2017)165 | AF | US | Quant | NRE | 19 m / 12 f (68 years) | |
Melin et al. (2018)122 | HF | Sweden | Quant | RT | 56 m / 26 f (75 years) | |
Nguyen et al. (2017)137 | HF | Canada | MM | Survey; Gen qual | 12 m / 6 f (75 years) | 10 Caregivers |
O’Shea et al. (2020)85 | CR | Ireland, Belgium | Qual | Gen qual | 34 m / 10 f (61 years) | |
Papoutsi et al. (2020)132 | HF | UK | Qual | Gen qual | NS | 3 Caregivers; 22 Profs |
Pekmezaris et al. (2016)141 | HF | US | Qual | Gen qual | 2 Caregivers; 18 Profs | |
Piette et al. (2015)138 | HF | US | Quant | RT | 329 m / 2 f (68 years) | |
Piotrowicz et al. (2015)99 | CR | Poland | Quant | RT | 180 m / 12 f (58 years) | |
Portz et al. (2020)150 | HF | US | Qual | Gen qual | 20 Profs | |
Prescher et al. (2013)109 | HF | Germany | Quant | Survey | 228 total (NS years) | 102 Profs |
Qian et al. (2015)154 | HF | US | Quant | Survey; RT | 820 m / 607 f (60 years) | |
Radhakrishna et al. (2013)149 | HF | US | MM | MM | 39 m / 44 f (83 years) | |
Radhakrishnan et al. (2013)156 | HF | US | Quant | Cohort | 184 m / 221 f (NS years) | |
Rahimi et al. (2015)107 | HF | UK | MM | MM | 34 m / 18 f (77 years) | |
Rawstorn et al. (2018)91 | CR | New Zealand | Quant | RT | 69 m / 13 f (61 years) | |
Riley et al. (2013)101 | HF | UK | Qual | Gen qual | 11 m / 5 f (74 years) | |
Sengupta et al. (2020)95 | CR | US | Quant | Survey | 0 m / 10 f (64 years) | |
Seto et al. (2010)127 | HF | Canada | Quant | MM | 74 m / 20 f (55 years) | 16 Profs |
Seto et al. (2012)123 | HF | Canada | Qual | Gen qual | 18 m / 4 f (57 years) | 5 Profs |
Seto et al. (2019)108 | HF | Canada | Quant | NRE | 4 m / 2 f (59 years) | NS Profs |
Sharma et al. (2014)130 | HF | UK | Qual | Gen qual | 25 Profs | |
Silva-Cardoso et al. (2020)114 | HF | Portugal | Quant | NRE | 7 m / 3 f (68 years) | |
Sohn et al. (2013)102 | HF | Germany | Quant | Econ anal | 233 m / 48 f (65 years) | |
Stut et al. (2014)145 | HF | UK, Germany, Spain | Quant | Survey | 97 m / 26 f (66 years) | |
Svagard et al. (2014)143 | HF | Norway | MM | Survey | 5 (total) | 4 Profs |
Theodoulou et al. (2019)96 | CR | Australia | Quant | Survey | 52 m / 24 f (69 years) | |
Thorup et al. (2016)81 | CR | Denmark | Qual | Gen qual | 8 m / 4 f (62 years) | 22 Profs |
Triantafyllidis et al. (2015)140 | HF | UK | Quant | NRE | 17 m / 9 f (72 years) | NS Caregivers |
Varon et al. (2015)148 | HF | Belgium | MM | Survey; RT | 288 m / 123 f (89 years) | |
Vuorinen et al. (2014)131 | HF | Finland | RCT | RT | 78 m / 16 f (58 years) | NS Profs |
Ware et al. (2018)134 | HF | Canada | Qual | Gen qual | 17 m / 6 f (60 years) | 4 Profs |
Ware et al. (2019)164 | HF | Canada | MM | MM | 184 m / 48 f (58 years) | |
Widmer et al. (2020)97 | CR | US | Quant | RCT | 48 m / 13 f (61 years) | |
Woods et al. (2019)118 | HF | Australia | MM | MM | 8 m / 0 f (69 years) | |
Worringham et al. (2011)93 | CR | Australia | Quant | NRE | 6 m / 1 f (54 years) | |
Zan et al. (2015)110 | HF | US | Quant | NRE | 29 m / 12 f (53 years) | |
Zimmerman et al. (2011)100 | CR | US | Quant | Survey; RT | 192 m / 40 f (72 years) |
HF = heart failure; CR = cardiac rehabilitation; AF = atrial fibrillation; MM = mixed methods; RTC = randomized control trial; RT = Randomized trial; NRE = non-randomized evaluation; f = female; m = male; NS = not specified
Table 10: Critical Assessment of Study Quality — Realist Review
Author | Study quality |
|---|---|
Albert et al. (2017)120 | Low |
Alnosayan et al. (2017)163 | Low |
Ammenworth et al. (2015)98 | Low |
Ammenworth et al. (2018)116 | Low |
Banner et al. (2015)82 | Low |
Bartlett et al. (2014)113 | High |
Bikedeli et al. (2014)157 | Medium |
Boyne et al. (2014)117 | Medium |
Browning et al. (2011)129 | Low |
Buys et al. (2016)92 | Low |
Caban (2019)121 | Low |
Cajita et al. (2017)162 | Low |
Cajita et al. (2018)144 | Medium |
Chantler et al. (2016)104 | Low |
Chaudhry et al. (2010)153 | Low |
Chiang et al. (2012)139 | Low |
Dadosky et al. (2018)147 | Low |
Dang et al. (2017)146 | Low |
Davis et al. (2015)103 | Low |
Devi et al. (2014)83 | Medium |
de Vries et al. (2013)152 | Low |
Dinesen et al. (2019)84 | Medium |
Domingues et al. (2010)84 | Low |
Dorje et al. (2019)87 | Medium |
Evangelista et al. (2015)125 | Low |
Fairbrother et al. (2014)106 | Medium |
Fang et al. (2016)86 | Low |
Finkelstein and Wood (2011)142 | Medium |
Forman et al. (2014)89 | Low |
Frohmader et al. (2016)80 | Low |
Galinier et al. (2020)158 | Low |
Gardner et al. (2016)151 | Low |
Guhl et al. (2020)167 | Low |
Grover and Alexander (2019)94 | Low |
Guzman-Clark et al. (2013)159 | Low |
Hagglund et al. (2019)112 | Medium |
Hall et al. (2014)115 | Medium |
Heckemann et al. (2016)135 | Medium |
Higgins et al. (2017)88 | Low |
Hirschey et al. (2018)166 | Low |
Jaana et al. (2019)111 | Low |
Jiang et al. (2019)126 | Low |
Jiang et al. (2020)168 | Low |
Jimenez-Marrero et al. (2020)160 | Low |
Johnston (2010)136 | Low |
Kao et al. (2016)155 | Low |
Kato et al. (2015)128 | Low |
Knudsen et al. (2019)90 | Low |
Lear et al. (2014)79 | Low |
Lefler et al. (2018)105 | Low |
Liljeroos et al. (2020)124 | Medium |
Lycholip et al. (2018)161 | Low |
Lynga et al. (2013)133 | Medium |
Magnani et al. (2017)165 | Low |
Melin et al. (2018)122 | Low |
Nguyen et al. (2017)137 | Medium |
O’Shea et al. (2020)85 | High |
Papoutsi et al. (2020)132 | High |
Pekmezaris et al. (2016)141 | Medium |
Piette et al. (2015)138 | Low |
Piotrowicz et al. (2015)99 | Low |
Portz et al. (2020)150 | Medium |
Prescher et al. (2013)109 | Low |
Qian et al. (2015)154 | Low |
Radhakrishna et al. (2013)149 | Low |
Radhakrishnan et al. (2013)156 | Low |
Rahimi et al. (2015)107 | Low |
Rawstorn et al. (2018)91 | Low |
Riley et al. (2013)101 | Medium |
Sengupta et al. (2020)95 | Medium |
Seto et al. (2010)127 | Medium |
Seto et al. (2012)123 | Medium |
Seto et al. (2019)108 | Medium |
Sharma et al. (2014)130 | Low |
Silva-Cardoso et al. (2020)114 | Low |
Sohn et al. (2013)102 | Low |
Stut et al. (2014)145 | Low |
Svagard et al. (2014)143 | Low |
Theodoulou et al. (2019)96 | Low |
Thorup et al. (2016)81 | Medium |
Triantafyllidis et al. (2015)140 | Low |
Varon et al. (2015)148 | Low |
Vuorinen et al. (2014)131 | Low |
Ware et al. (2018)134 | Low |
Ware et al. (2019)164 | Medium |
Widmer et al. (2020)97 | Medium |
Woods et al. (2019)118 | Low |
Worringham et al. (2011)93 | Low |
Zan et al. (2015)110 | Medium |
Zimmerman et al. (2011)100 | Low |
Perspectives and Experiences Review
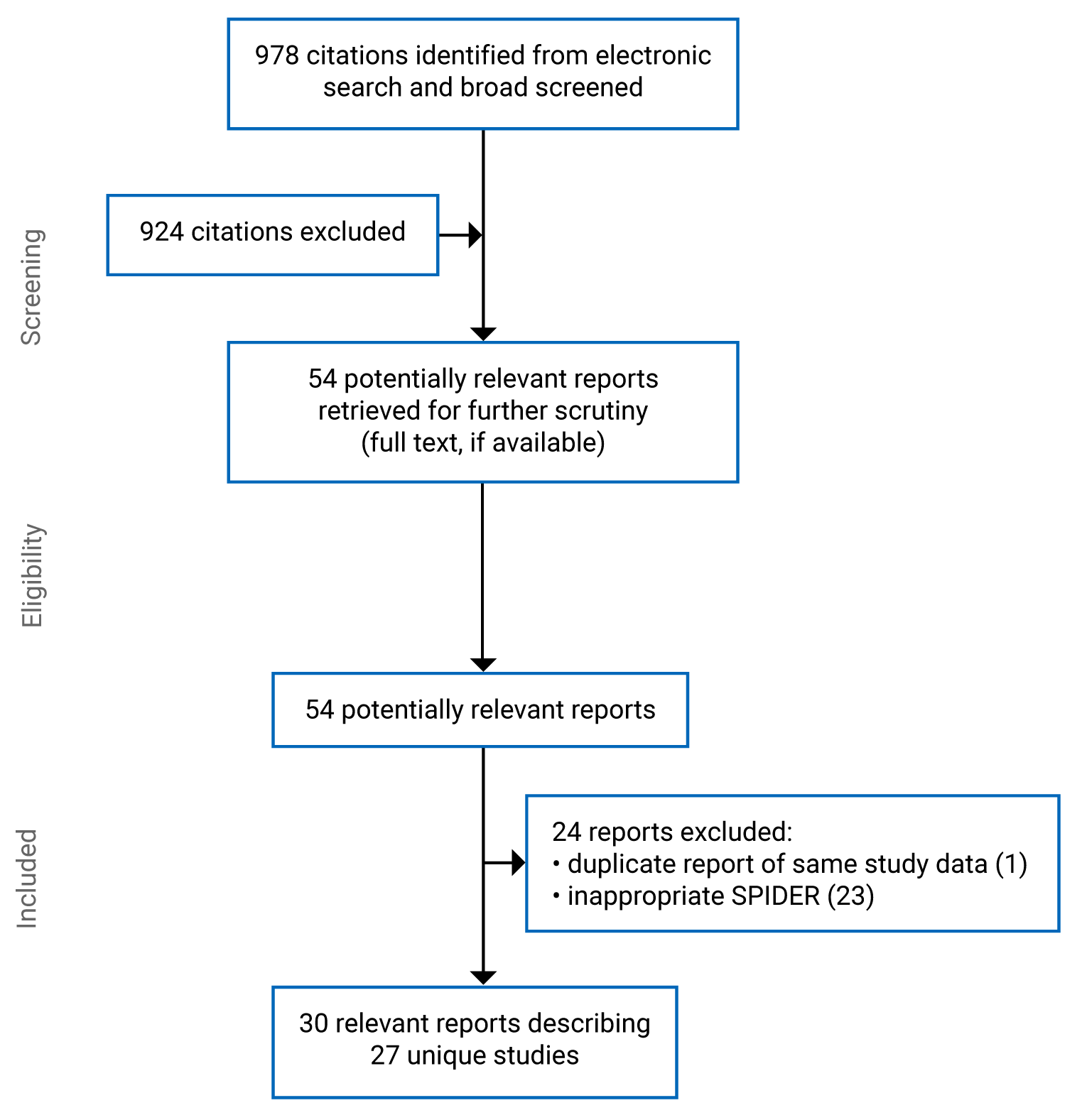
Table 11: Characteristics of Included Studies and Their Participants
First author (publication year), country | Funding | Study objectives | Description of remote monitoring program | Description and number of participants (type of participants, condition, age, gender/sex) | Study design, method of data collection, method of data analysis |
|---|---|---|---|---|---|
Studies on heart failure | |||||
Barenfeld, (2020) Sweden200 | Swedish Heart and Lund Foundation, Swedish Research Council, The Centre for Person-Centred Care at the University of Gothenburg, Hjalmar Svensson Foundation | To explore the experiences of a person-centred e-health intervention in patients diagnosed with COPD or HF | PROTECT intervention which included person-centred telephone conversations with a dedicated health professional, and access to an interactive digital platform including self-ratings, personal notes, and a health plan |
| Grounded theory; semi-structured interviews; grounded theory |
Woo (2020), US203 | National Institute of Nursing Research | To explore factors associated with patients’ decision to adopt telehealth at home |
|
|
|
Hagglund (2019), Sweden112 | No funding to disclose | To test whether 3 phases of the self-care process (self-care maintenance, symptom perception, and self-care management) could be validated in the experiences of persons with heart failure using an mHealth tool | mHealth System Optiloog that uses a tablet to connect to a scale and recommends titration of the dose of diuretics and provided daily tips for lifestyle maintenance for heart failure |
|
|
Pekmezaris (2016), US141 | Patient-Centered Outcomes Research Institute | To adopt a home telemonitoring program using a collaborative approach of community engagement in a population of Black and Hispanic HF patients from disparity communities | A trial of an interactive video monitoring system that transmitted daily vital sign monitoring (blood pressure, oxygen saturation rate, weight and pulse/heart rate) to their providers |
|
|
Bond (2015), UK204 | Dorset Clinical Commissioning Group | To conduct a qualitative evaluation of a local telehealth program | A telehealth system that monitored blood pressure, weight, temperature, and oxygen saturation levels and a tablet style computer, which relayed information to the HCP |
|
|
Hunting (2015), Canada195 | Ontario Ministry of Health and Long-term Care | To explore facilitators and barriers to Telehomecare implementation and adoption across 5 levels: technology, patients, providers, organizations, and structures | A 6-month long Telehomecare program to increase the self-management and monitor patients with COPD and HF, involving the daily transmission of weight, blood pressure, oxygen levels, and answers to a daily questionnaire monitored by a Telehomecare nurse and weekly coaching sessions |
|
|
Taylor (2015), UK207 | Assisted Living Innovation Platform, Technology Strategy Board and Economic and Social Research Council | To analyze staff accounts of using telehealth in everyday practice to examine acceptance and adoption over time | Remote monitoring programs for patients with COPD and HF who live in the community |
|
|
Lind (2014), Sweden205 | European Regional Development Fund, Swedish ICT Research, and the New Tools for Health Program | To explore patients’ and spouses’ experiences using a telemonitoring system, the Health Diary | A telehealth trial using a digital pen technology to enable the participation of the those with low digital literacy. The pen captures patients’ daily reports on shortness of breath, medications, weight, and other measures including a free text to the provider. |
|
|
Odeh (2014), UK206 | NR | To elicit nurse’s perceptions of a telehealth services with a primary care trust and barrier to implementing the service | A remote monitoring system that measured weight, oxygen saturation, temperature, and questions about symptoms. Data were transmitted to a monitoring centre, evaluated, and triaged if they need to be passed on to the practice nurse. |
|
|
Sharma (2014), UK130 | NR | To explore how the introduction of telehealth into health care can be experienced as disruptive by nurses and community support workers | A telehealth program being expanded for patients with asthma, diabetes, COPD, and HF that collected blood glucose, weight, blood pressure, oxygen saturation, and heart rate and transmitted it to a clinical team |
|
|
Fairbrother (2014), UK106 | Scottish Centre for Telehealth and Telecare | To explore the views of patients and professionals participating in the telemonitoring service | A telemonitoring service that used the Intel Health Guide that enabled patients to undertake a daily self-assessment of symptoms using an online touch screen questionnaire and measured pulse, oxygen saturation, blood pressure, and weight. Information was transmitted to specialist HF nurses. Additional education content supported self-management. |
|
|
Lynga (2013), Sweden133 | Reported no funding to disclose | To explore and describe patients’ perceptions of transmission of body weight as part of a telemedicine RCT | A telemedicine RCT where people with HF who were recently hospitalized were given an electronic scale that automatically transmitted their weight to an HF clinic and a clinician followed up with a patient and increased their diuretics as appropriate |
|
|
Riley (2012), UK101 | National Institute of Health Research: Research for Patient Benefit, England | To explore the extent to which telemonitoring in patients with heart failure empowers them to self-care | A telemonitoring program for HF that used a home monitoring system to measure weight, blood pressure and pulse, and a daily symptom questions transmitted to a cardiac nurse for review |
|
|
Sanders (2012), UK208 | Department of Health | To explore barriers to participation and adoption of telehealth or telecare from those who declined to participate or withdrew from the trial | Telehealth intervention involved daily monitoring of blood pressure, blood glucose, oxygen level, weight, and peak flow which were uploaded to a monitoring centre |
|
|
Seto (2012), Canada123 | Toronto General Hospital Foundation and the Natural Sciences and Engineering Research Council of Canada Strategic Research Network Grant | To provide in-depth insight into the effects of telemonitoring on self-care and clinical management, and to determine the features that enable successful heart failure telemonitoring | A telemonitoring program that enabled patients to take weight, blood pressure, and weekly single-lead ECGs, and to answer daily symptom questions on a mobile phone. Alerts were sent to a cardiologist’s mobile phone. |
|
|
LaFramboise (2009), US209 | NR | To discover perceptions about ease of use, efficacy, and difficulties encountered by who used an in-home telehealth communication device, the Health Buddy | A study using a telemonitoring device, the Health Buddy, which enabled patients to respond to a 7-question daily symptom questionnaire and provided lifestyle health tips transmitted to an HCP |
|
|
Studies on cardiac rehabilitation | |||||
O’Shea (2020), UK85 | European Union’s Horizon 2020 Framework Programme for Research and Innovation | To explore participants’ views and experiences of using the PATHway system, an eHealth cardiac rehabilitation intervention | A trial of a home-based, technology-enabled complex behaviour change intervention that provided regular exercises sessions to enable people to manage their CVD |
|
|
Anttila (2019), Finland199 | NR; no conflict of interest to declar | To explore rehabilitees’ experiences and attitudes toward technology before participating in a trial of a 12 months of remote rehabilitation | 12-month long remote rehabilitation program |
|
|
Banner (2019), Canada197 | Heart and Stroke Foundation of BC and Yukon and Canada Health Infoway | To examine patient experiences of a virtual cardiac rehabilitation program | A 4-month program designed to imitate a standard hospital-based cardiac rehabilitation program following an acute cardiac event. It included scheduled 1:1 chats with a nurse case manager, exercise specialist and dietician, weekly education sessions, and weekly measurement of blood pressure, heart rate, and weight. |
|
|
Knudsen (2019), Denmark90 | Novo Nordisk Foundation, Danish Nurses’ Organization Research Foundation, Aarhus University Graduate School of Health | To explore patients’ experiences of tele-rehabilitation and the perceived gains of taking part in a study on a tele-rehabilitation program | A 12-week telerehabilitation program including weekly monitoring of blood pressure and weight, and heart rate during 3x week exercise session. All measures were transferred from a smartphone application to a website where patients could comment on their results. |
|
|
Devi (2014), UK83 | National Institute for Health Reseach | To explore patients’ experiences of using a new web-based cardiac rehabilitation program as part of a trial | A 6-week web-based cardiac rehabilitation program delivered through a password protected internet site that included an exercise dairy and support from cardiac rehabilitation nurses |
|
|
Studies on high blood pressure | |||||
Albrecht (2018), Canada210 | Canadian Institutes of Health Research and Alberta Innovates Health Solutions | To examine the usability and acceptability of a home blood pressure telemonitoring device among senior citizens as part of a trial | A telemonitoring device where subjects took their blood pressure 4 times per day and reviewed by the case manager |
|
|
Bengtsson (2018), Sweden196** | University of Gothenburg Centre for Person-Centered Care | To explore and describe the structure, topic initiation, and patients’ contributions in follow-up consultations after the intervention study | An 8-week mobile phone-based system for supporting the self-management of hypertension in primary care that includes daily symptom questionnaire, home BP and pulse measurement, weekly motivational messages, graphical feedback to patients and providers of their symptom reports and BP |
|
|
Bradbury (2018), UK201* | National Institute for Health Research Programme Grants for Applied Research Programme | To describe how to use the Person-Based Approach to optimize a digital intervention for patients with hypertension | HOME BP, a web-based digital intervention that enabled participants to monitor their BP at home and make changes to their medications (dose and type) as recommended by their primary care providers. Optional lifestyle change modules were available. Two structured encounters with a nurse or health assistant (Supporters) were also part of the intervention. |
|
|
Hallberg (2018), Sweden211** | University of Gothenburg and Centre for Person-Centered Care | To explore patients’ and professionals’ experiences of and expectations for an interactive mobile phone-based system to support self-management of hypertension | An 8-week mobile phone-based system for supporting the self-management of hypertension in primary care that includes daily symptom questionnaire, home BP and pulse measurement, weekly motivational messages, graphical feedback to patients and providers of their symptom reports and BP |
|
|
Morton (2018), UK202* | National Institute for Health Research Programme Grants for Applied Research Programme | To understand the perceived burdens and benefits for patients using a digital self-management intervention for reducing high blood pressure | HOME BP, a web-based digital intervention that enabled participants to monitor their BP at home and make changes to their medications (dose and type) as recommended by their primary care providers. Optional lifestyle change modules were available. Two structured encounters with a nurse or health assistant (Supporters) were also part of the intervention. |
|
|
Bradbury (2017), UK212* | National Institute of Health Research | To examine how practice staff perceived the HOME BP intervention, and how acceptable and feasible the intervention might be to implement in practice and what further modifications using the Person-Based Approach to optimize the intervention | HOME BP, a telemonitoring program, with a Prescriber’s guide for GPs and nurse prescribes to efficiently prescribe medications for hypertension based on home blood pressure readings with the aim of reducing clinical inertia. A Supporters Guide provided information to provide nurses and health care assistants to provide 2 standardized support appointments for patients. |
|
|
Abdullah (2016), Malaya213 | University Malaya Research Fund | To explore patients’ acceptance of a blood pressure telemonitoring service delivered in primary care based on the technology acceptance model | A study of a BP telemonitoring service for primary care patients with uncontrolled hypertension using a digital blood pressure and pulse oximeter |
|
|
Hanley (2013), UK198 | BUPA Foundation, High Blood Pressure Foundation, and NHS Lothian | To identify factors facilitating or hindering the effectiveness of an intervention for home telemonitoring for blood pressure and those likely to influence its potential translation to routine practice | A trial of blood pressure monitoring in 6 primary care practices that measured blood pressure and transmitted data to their primary care provider for review for medication or lifestyle change |
|
|
Jones (2012), UK214 | Department of Health Policy Research Programme | To explore patients’ views of self-monitoring blood pressure and self-titration of antihypertensive medication | A trial of a self-monitoring intervention in primary care for patients with blood pressure who measured their blood pressure daily for 1 week each month. Data were transmitted to the research team, and readers were coded as normal, raised, or high and were advised to contact their GP if readings were high or low. Multiple consecutive out-of-range readings could trigger a medication change. |
|
|
NR = not reported; COPD = chronic obstructive pulmonary disease; HF = heart failure; HCP = health care providers; RCT = randomized control trial
*Bradbury (2018),201 Morton (2018)202 and Bradbury (2017)212 all report on different data from a series of studies of an intervention called HOME BP
**Bengtsson (2018)196 and Hallberg (2018)211 report on different data from the same study.
Table 12: Critical Appraisal of Included Studies
First author, publication year | Is the study credible? | Is the study trustworthy? (dependable, confirmable) | Is the study transferable? |
|---|---|---|---|
Studies on heart failure | |||
Barenfeld (2020)200 | Yes. Uses purposeful sampling and collects rich data. Analysis is described in thick detail and supporting quotes are provided. Hierarchical nature of themes is developed and displayed visually. | Yes. Multiple points demonstrating reflexivity, including the use of patient partners. | Yes. The study objectives, sample, and intervention are all transferable to this review. |
Woo (2020)203 | Partially. Semi-structured interviews with a guide collected data from participants who included both those who started the remote monitoring program and those who did not and were conducted until saturation was reached. Interviews were noticeably short (11-24 minute). A deductive analysis is presented, appropriately supported by the data, but as such, it is not a comprehensive exploration of decision-making around using remote monitoring for heart failure as is the study objective. | Yes. Multiple researchers involved, describe using audit trails, memoing, and data analysis and reflexive techniques that would facilitate the trustworthiness of the analysis. | Yes. The study objectives, sample, and intervention are all transferable to this review. |
Hagglund (2019)112 | Partially. Semi-structured interviews were conducted and lasted 20-60 minute, enabling rich data to be collected. Analysis was largely deductive, and themes were high-level descriptive topics. Theme were supported by the data. Appropriate for theory testing as the objective for their study, but the theory is linear and does not account for temporal interplay between phases of self-care, nor detailed description of the process as experienced by someone over time. | Partially. Multiple researchers involved but approaches to reflexivity not described. Trust the findings, at a high-level, as they do not account for those who are sickest or busy (acknowledged by authors). | Partially. The sample and intervention are all transferable to this review. The research question is highly relevant, but the deductive focus on validating the theory inhibits the broader situating of self-care and remote monitoring as a process. |
Pekmezaris (2016)141 | Partially. The focus was on the technology use by non-users and users. The small number of users (n = 4) whose views were explored through focus groups did not permit the collection of rich data. The presented analysis is more like minutes of the focus groups vs. an analysis, although data are presented. | Partially. Dependability was threatened by the small number of user participants (n = 4) and the data collection methods that did not enable the collection of rich data. | Partially. The intervention is transferable to the review, but the transferability of the findings are limited by their highly descriptive nature and the focus on modifying the trial. |
Bond (2015)204 | Partially. Strength of the evaluation is in interviewing both users and providers. Patients are interviewed upon initiation and at 3 months which would allow for a more nuanced analysis, yet interviews are very short (~ 10 minute). The reporting of results are heavily data driven and the findings lack description – trust the data, but the analysis is weak. | Partially. Details on the recruitment of providers are poorly reported. Data provided to support findings, but very thin. Opportunities to explore changes in experiences over time not used, which would be relevant to the evaluation. | Yes. The study objectives, sample, and intervention are all transferable to this review. |
Hunting (2015)195 | Yes. The study uses a mulit-level approach to exploring the implementation of a remote monitoring program for HF and COPD. Findings are thoroughly described and supported by multiple types of data. | Yes. Authors triangulate data and findings across data and participant types. | Yes. The study objectives, sample (setting is Ontario, Canada), and intervention (Telehomecare) are all highly transferable to this review. |
Taylor (2015)207 | Yes. 105 interviews were conducted (most face-to-face) with a median interview time was 45 minutes, using an interview topic guide that was piloted and refined iteratively. Data analysis involved multiple iterations and authors discuss how they were reflexive to their relationship with the data collection sites. Findings are richly described higher order observations supported by data. | Yes. A series of site-specific workshops were held to share findings and refine the issues identified at each site. | Yes. The study objectives, intervention, and sample are all relevant to this review. |
Fairbrother (2014)106 | Yes. Semi-structured interviews using interview guides were conducted, and the authors report taking field notes after interviews to support their analysis. The analysis uses both data sources which supports the development of their findings. | Partially. One concern lies in the low number of included providers (n = 5) and the lack of reporting of their characteristics), which might mean that divergent findings were not identified. | Yes. The study objective, intervention, and sample are all relevant to this review. |
Lind (2014)205 | No. Poor reporting of recruitment, low number of respondents, making it difficult to know who is included. Data does not support interpretation of the findings and are thinly described. | Partially. Issues with credibility and poor reporting make the reviewer trust the data but not the findings. | Partially. Relevant focus (on digital literacy) and comparable intervention and setting. Concerns around quality limit transferability. |
Odeh (2014)206 | No. Data were from 7 nurses collected by email which did not allow for the collection of rich data. This is reflected in the thin analysis. | Partially. The lack of breadth in respondents and thin analysis suggest that the data can be trusted by not the findings. | Partially. The study objectives, sample, and intervention are relevant, but concerns relating to quality limit transferability. |
Sharma (2014)130 | Partially. Seems really guided by the assumptions of the objective and does not appear to explore divergent cases (as in how disruption did not occur or was resolved). Data collection using focus groups and interviews at multiple time points is a strength. Description of results is short. | Partially. The description of the findings are supported by data and appear trustworthy, except where their credibility is questionable through the exclusion of divergent perspectives. The role of the researcher is not described and appears the analysis was conducted solely by 1 person. | Partially. Concerns with credibility and dependability limit transferability. |
Lynga (2013)133 | Partially. Narrow focus on transmission of body weight, interview questions narrow for the objective. Analysis is moderate, with data presented but some categories are weaker than others. | Partially. Different interpretations of categories (types of patients) leave a lack of clarity around their trustworthiness – trust the data, not the themes. | Partially. Narrowly focused on the transmission of body weight not monitoring per se. |
Riley (2012)101 | Yes. In-depth interviews at 2 time points using a guide and lasted ~ 40 minutes. A detailed analysis is presented, and well support by data. There are a couple of parts (variation by gender, sex and comorbidities) that are told, not shown. | Yes. Using data at 2 time points, using a team approach to analyzing the data support the trustworthiness of the findings. | Yes. The intervention, population, and study objectives are all relevant to this review. |
Sanders (2012)208 | Yes. This study uses multiple sources of information (observation, interviews). Iterative conducted of in-depth interviews and data analysis. Analysis is reported with thick detail, includes divergent cases, and supported by data. | Yes. The authors use multiple data sources and describe a team approach to building the analysis. | Yes. While the population is not limited to chronic cardiac conditions (HF), the study focus on non-users and the intervention is highly relevant to this review. |
Seto (2012)123 | Partially. The authors describe why they stopped collecting data, and attempted to elicit divergent views and experiences through in-depth interviews. The findings are overall well described, although methods are not well-reported. | Partially. Limited reporting of methods makes assessment challenging – no discussion of the role of the researchers. | Partially. Population includes other chronic conditions, limited to heart failure. |
LaFramboise (2009)209 | Partially. Unclear how many people were interviewed vs. who participated in focus groups. Assumptions built into questions, and research nurses conducted interviews. No examination of harms/negatives. Some themes overlap (ease of use and difficulties) in ways that are unexplored. | Partially. Data described and attempts made to explore dropouts (not just users). | Yes. Population, technology, and study objectives are relevant to this review. |
Studies on cardiac rehabilitation | |||
O’Shea (2020)85 | Partially. Data were collected using interviews lasting on average 23 minutes. The analysis is very focused on the specific elements of the PATHway program (rehab) and is largely data driven. | Partially. No discussion about reflexivity, or of relationships of authors to participants. Multiple authors were involved in the analysis improving trustworthiness. | Partially. The study focus is on the specific experience with components of the intervention, vs. the program experience more broadly, limiting transferability. |
Antilla (2019)199 | Yes. Focus group data with participants to explore their views of technology generally, but not specific to the types of technologies that were to be used in the rehabilitation program (not described). Variation is reported by interest in technology, and no gender or age analysis, the later seems quite important given assumptions around technology and age. Results are well described and supported by the data. | Partially. No discussion of how data and analysis were conducted iteratively, and no discussion about the decision to stop collecting and analyzing data. No discussion of reflexivity. | Partially. Not relevant to experiences of remote monitoring or rehab per se but to views of technology among people eligible for cardiac rehabilitation. |
Banner (2019)197 | Yes. Used purposive sampling to capture people who had high and low engagement in the program. Collected rich data, and a richly described findings supported by data. | Yes. Methods of analysis are well described, and multiple researchers were involved. | Yes. Highly relevant – conducted in Canada (BC). |
Knudsen (2019)90 | Partially. In-depth interviews were conducted using an interview guide. The analysis is theoretical but findings are not fully supported by the data. | Partially. All male sample, limits dependability to other genders. The researchers describe how they co-produced the analysis is good detail. | Partially. Issues with credibility and dependability limit transferability. |
Devi (2014)83 | Partially. Focused on general satisfaction with the program and takes peoples’ views at face value. Findings are poorly developed and categorized as barriers and facilitators without exploring the overlap. | Partially. Included patients who had completed and did not complete the trial. Limited description of the methods affects the ability to assess trustworthiness as it who is involved in the analysis is not reported. | Partially. The intervention is solely web-based (no monitoring) which affects its relevance to the |
Studies on high blood pressure | |||
Albrecht (2018)210 | Partially. In-depth interviews on user acceptability. Concerns regarding credibility come from the limited number of participants, and no description is any form of saturation was reached – unclear if the authors’ data were able to really build patterns and connection among their categories. | Partially. The lack of length of time in which participants engaged with the program is a concern (one week). Limited reporting of the methods of data analysis and who was involved, and no comments about reflexivity, raises further questions around dependability. | Yes. Even given concerns with credibility and dependability, study provides relevant information and was additionally conducted in Canada (AB). |
Bengtsson (2018)196 | Yes. The study uses audio and video recordings of consultations between patients and physicians at the end of the intervention, and describes using an analytic method appropriate for the research objectives. The analysis is well described and supported by the data. | Yes. A detailed description of the methods of data analysis and strategies employed to ensure accuracy in describing the structure of the consultations are offered. | Partially. The research focus is on the dynamics of the consultations, and as such, is less relevant to this review. |
Bradbury (2018)201* | Yes. Uses multiple time points for data collection, and recruited people enrolled in the intervention and those who were not interested in participating. Iterative data collection and analysis was used to modify the intervention, this is described in through detail. | Yes. The collection of multiple interviews and longitudinal data increase the dependability of the findings. | Partially. The research focus is on the process of modifying the intervention, not on the modifications themselves, limiting the relevance of the findings to this review. |
Hallberg (2018)211 | Yes. Semi-structured in-depth interviews with 20 patients and 7 providers using an interview guide. Interviews were ~ 45 minute in length and were analyzed using thematic analysis. The resulting analysis is described in detail and is supported by the data. | Yes. The full research team played a role in the analysis, and coded and recoded their data. | Yes. The research focus, intervention, and context are transferable to this review. |
Morton (2018)202* | Yes. Semi-structured in-depth interviews with 35 patients allowed for collection of rich data. Recruited people who participated in the intervention and those who did not (received usual care). Presents a strong analysis, nice and rich, that makes very good use of data | Yes. Analysis was supported by the full research team, and emergent findings were brought to patient and public involvement representatives involved in the RCT. | Yes. The research focus, intervention, and context are transferable to this review. |
Bradbury (2017)212* | Yes. Recruitment is well described and captures a range of providers who used the intervention. The resultant analysis is well described, supported by the data, and included attention to deviant cases. | Yes. Describes the role of team members in conducting the analysis, methods of data analysis well described | Partially. The focus of the research is on the specifics of the training guides for the particular intervention, which make the findings is less relevant to this review. |
Abdullah (2016)213 | Partially. It is unclear how long participants had been using the service which would affect their experiences and ideas around acceptability. The focus on acceptability itself is narrow, and the resultant analysis is limited and thin. | Partially. The superficial focus on acceptability means that the overall findings are dependable, but do not likely capture the full breadth of the phenomenon of acceptability. | Partially. The focus on acceptability is only partially relevant to this review. |
Hanley (2013)198 | Yes. Good detail around sampling strategy and conduct of semi-interviews to collect breadth of participants and data. Analysis presents divergent cases and is supported by data. | Yes. Describes the role of researchers and demonstrates reflexivity. | Yes. Relevant objectives, intervention, sample. |
Jones (2012)214 | Partially. Collected data using semi-structured interviews that were between 30 and 60 minutes and were analyzed from 23 patients. Did not intentionally recruit family members, people were just present during interviews. Limited description of the methods of analysis, analysis is highly descriptive and is supported by the data. | Partially. No description of reflexivity or role of researchers. | Yes. The intervention, population, and study objectives are all relevant to this review. |
*Bradbury (2018),201 Morton (2018)202 and Bradbury (2017)212 all report on different data from a series of studies of an intervention called HOME BP
**Bengtsson (2018)196 and Hallberg (2018)211 report on different data from the same study.
Appendix 3: List of Included Studies — Realist Review
1.Pfaeffli L, Maddison R, Whittaker R, et al. A mHealth cardiac rehabilitation exercise intervention: findings from content development studies. BMC Cardiovasc Disord 2012; 12: 1-9. PubMed
2.Lear SA, Singer J, Banner-Lukaris D, et al. Randomized trial of a virtual cardiac rehabilitation program delivered at a distance via the Internet. Circ Cardiovasc Qual Outcomes 2014;7(6):952-59. doi: PubMed
3.Frohmader TJ, Lin F, Chaboyer W. Patient perceptions of nurse mentors facilitating the Aussie Heart Guide: A home-based cardiac rehabilitation programme for rural patients. Nurs Open 2016;3(1):41-50. PubMed
4.Thorup CB, Gronkjaer M, Spindler H, et al. Pedometer use and self-determined motivation for walking in a cardiac telerehabilitation program: a qualitative study. BMC Sports Sci Med Rehabil 2016;8:24-24. PubMed
5.Banner D, Lear S, Kandola D, et al. The experiences of patients undertaking a 'virtual' cardiac rehabilitation program. Stud Health Technol Inform 2015;209:9-14. PubMed
6.Devi R, Carpenter C, Powell J, et al. Exploring the experience of using a web-based cardiac rehabilitation programme in a primary care angina population: a qualitative study. Int J Ther Rehabil 2014;21(9):434-40. 10.12968/ijtr.2014.21.9.434
7.Dinesen B, Nielsen G, Andreasen JJ, et al. Integration of Rehabilitation Activities Into Everyday Life Through Telerehabilitation: Qualitative Study of Cardiac Patients and Their Partners. J Med Internet Res 2019;21(4):e13281-e81. PubMed
8.O'Shea O, Woods C, McDermott L, et al. A qualitative exploration of cardiovascular disease patients' views and experiences with an eHealth cardiac rehabilitation intervention: The PATHway Project. PLoS ONE 2020;15(7):e0235274-e74. PubMed
9.Fang JY, Li JL, Li ZH, et al. Attitudes towards acceptance of an innovative home-based and remote sensing rehabilitation protocol among cardiovascular patients in Shantou, China. J Geriatr Cardiol 2016;13(4):326-32. PubMed
10.Dorje T, Zhao G, Tso K, et al. Smartphone and social media-based cardiac rehabilitation and secondary prevention in China (SMART-CR/CR): a parallel-group, single-blind, randomised controlled trial. Lancet Digit Health 2019;1(7):e363-e74. PubMed
11.Higgins RO, Rogerson M, Murphy BM, et al. Cardiac Rehabilitation Online Pilot: Extending Reach of Cardiac Rehabilitation. J Cardiovas Nurs 2017;32(1):7-13. PubMed
12.Forman DE, LaFond K, Panch T, et al. Utility and efficacy of a smartphone application to enhance the learning and behavior goals of traditional cardiac rehabilitation: a feasibility study. J Cardiopulm Rehabil Prev 2014;34(5):327-34. PubMed
13.Knudsen MV, Laustsen S, Petersen AK, et al. Experience of cardiac tele-rehabilitation: analysis of patient narratives. Disabil Rehabil 2019:1-8. PubMed
14.Rawstorn JC, Gant N, Rolleston A, et al. End Users Want Alternative Intervention Delivery Models: Usability and Acceptability of the REMOTE-CR Exercise-Based Cardiac Telerehabilitation Program. Arch Phys Med Rehabil 2018;99(11):2373-77. PubMed
15.Buys R, Claes J, Walsh D, et al. Cardiac patients show high interest in technology enabled cardiovascular rehabilitation. BMC Med Inform Decis Mak 2016;16:95-95. PubMed
16.Worringham C, Rojek A, Stewart I. Development and feasibility of a smartphone, ECG and GPS based system for remotely monitoring exercise in cardiac rehabilitation. PLoS ONE 2011;6(2):e14669-e69. PubMed
17.Grover DB, Alexander JL. Patient Attitudes Toward Telemedicine-Delivered Cardiac Rehabilitation. Rehabil Nurs J 2019;44(6):358-63. PubMed
18.Sengupta A, Beckie T, Dutta K, et al. A Mobile Health Intervention System for Women With Coronary Heart Disease: Usability Study. JMIR Form Res 2020;4(6):e16420-e20. PubMed
19.Theodoulou E, Tirimacco R, Dollman J, et al. Preferences and attitudes to mobile phone and Internet-based cardiac rehabilitation maintenance programs in rural Australia. Aus J Rural Health 2019;27(2):179-80. PubMed
20.Widmer RJ, Senecal C, Allison TG, et al. Dose-Response Effect of a Digital Health Intervention During Cardiac Rehabilitation: Subanalysis of Randomized Controlled Trial. J Med Internet Res 2020;22(2):e13055-e55. PubMed
21.Ammenwerth E, Woess S, Baumgartner C, et al. Evaluation of an Integrated Telemonitoring Surveillance System in Patients with Coronary Heart Disease. Methods Inform Med 2015;54(5):388-97. PubMed
22.Piotrowicz E, Stepnowska M, Leszczyńska-Iwanicka K, et al. Quality of life in heart failure patients undergoing home-based telerehabilitation versus outpatient rehabilitation – a randomized controlled study. Eur J Cardiovasc Nurs 2015;14(3):256-63. 10.1177/1474515114537023PubMed
23.Zimmerman L, Barnason S, Hertzog M, et al. Gender differences in recovery outcomes after an early recovery symptom management intervention. Heart Lung 2011;40(5):429-39. PubMed
24.Riley JP, Gabe JP, Cowie MR. Does telemonitoring in heart failure empower patients for self-care? A qualitative study. J Clin Nurs 2013;22(17-18):2444-55. PubMed
25.Sohn S, Helms TM, Pelleter JT, et al. Costs and benefits of personalized healthcare for patients with chronic heart failure in the care and education program “Telemedicine for the Heart”. Telemed J E Health 2012;18(3):198-204. PubMed
26.Davis C, Bender M, Smith T, et al. Feasibility and Acute Care Utilization Outcomes of a Post-Acute Transitional Telemonitoring Program for Underserved Chronic Disease Patients. Telemed J E Health 2015;21(9):705-13. PubMed
27.Chantler T, Paton C, Velardo C, et al. Creating connections - the development of a mobile-health monitoring system for heart failure: Qualitative findings from a usability cohort study. Digit Health 2016;2:2055207616671461-61. PubMed
28.Lefler LL, Rhoads SJ, Harris M, et al. Evaluating the Use of Mobile Health Technology in Older Adults With Heart Failure: Mixed-Methods Study. JMIR Aging 2018;1(2):e12178-e78. PubMed
29.Fairbrother P, Ure J, Hanley J, et al. Telemonitoring for chronic heart failure: the views of patients and healthcare professionals - a qualitative study. J Clin Nurs 2014;23(1-2):132-44. PubMed
30.Rahimi K, Velardo C, Triantafyllidis A, et al. A user-centred home monitoring and self-management system for patients with heart failure: A multicentre cohort study. Eur Heart J Qual Care Clin Outcomes 2015;1(2):66-71. PubMed
31.Seto E, Morita PP, Tomkun J, et al. Implementation of a Heart Failure Telemonitoring System in Home Care Nursing: Feasibility Study. JMIR Med Inform 2019;7(3):e11722-e22. PubMed
32.Prescher S, Deckwart O, Winkler S, et al. Telemedical care: feasibility and perception of the patients and physicians: a survey-based acceptance analysis of the Telemedical Interventional Monitoring in Heart Failure (TIM-HF) trial. Eur J Prev Cardiol 2013;20(2 Suppl):18-24. PubMed
33.Zan S, Agboola S, Moore SA, et al. Patient engagement with a mobile web-based telemonitoring system for heart failure self-management: a pilot study. JMIR MHealth UHealth 2015;3(2):e33-e33. PubMed
34.Jaana M, Sherrard H, Pare G. A prospective evaluation of telemonitoring use by seniors with chronic heart failure: Adoption, self-care, and empowerment. Health Inform J 2019;25(4):1800-14. PubMed
35.Hagglund E, Stromberg A, Hagerman I, Lynga P. Theory Testing of Patient Perspectives Using a Mobile Health Technology System in Heart Failure Self-care. J Cardiovas Nurs 2019; 34(6): 448-53. PubMed
36.Bartlett YK, Haywood A, Bentley CL, et al. The SMART personalised self-management system for congestive heart failure: results of a realist evaluation. BMC Med Inform Decis Mak 2014;14:109-09. PubMed
37.Silva-Cardoso J, Moreira E, Lopes I, et al. SmartBEAT: a smartphone-based heart failure telemonitoring solution. MEDICON 2019: XV Mediterranean Conference on Medical and Biological Engineering and Computing – MEDICON 2019. 2019;76:1369-1376.
38.Hall AK, Dodd V, Harris A, et al. Heart failure patients' perceptions and use of technology to manage disease symptoms. Telemed J E Health 2014;20(4):324-31. PubMed
39.Ammenwerth E, Modre-Osprian R, Fetz B, et al. HerzMobil, an Integrated and Collaborative Telemonitoring-Based Disease Management Program for Patients With Heart Failure: A Feasibility Study Paving the Way to Routine Care. JMIR Cardio 2018;2(1):e11-e11. PubMed
40.Boyne JJ, Vrijhoef HJ, Spreeuwenberg M, et al. Effects of tailored telemonitoring on heart failure patients' knowledge, self-care, self-efficacy and adherence: a randomized controlled trial. Eur J Cardiovas Nurs 2014;13(3):243-52. PubMed
41.Woods LS, Duff J, Roehrer E, et al. Patients' Experiences of Using a Consumer mHealth App for Self-Management of Heart Failure: Mixed-Methods Study. JMIR Hum Factors 2019;6(2):e13009-e09. PubMed
42.Domingues FB, Clausell N, Aliti GB, et al. Education and telephone monitoring by nurses of patients with heart failure: Randomized clinical trial. Arq Bras Cardiol 2011;96(3):233-39. PubMed
43.Albert NM, Dinesen B, Spindler H, et al. Factors associated with telemonitoring use among patients with chronic heart failure. J Telemed Telecare 2017;23(2):283-91. PubMed
44.Caban PL. The Use of Home Telemonitoring for Heart Failure Management Among Hispanics, Non-Hispanic Blacks, and Non-Hispanic Whites. Home Health Now 2019;37(6):345-49. PubMed
45.Melin M, Hagglund E, Ullman B, et al. Effects of a Tablet Computer on Self-care, Quality of Life, and Knowledge: A Randomized Clinical Trial. J Cardiovas Nurs 2018;33(4):336-43. PubMed
46.Seto E, Leonard KJ, Cafazzo JA, et al. Perceptions and experiences of heart failure patients and clinicians on the use of mobile phone-based telemonitoring. J Med Internet Res 2012;14(1):e25-e25. PubMed
47.Liljeroos M, Thylen I, Stromberg A. Patients' and Nurses' Experiences and Perceptions of Remote Monitoring of Implantable Cardiac Defibrillators in Heart Failure: Cross-Sectional, Descriptive, Mixed Methods Study. J Med Internet Res. 2020;22(9):e19550-e50. PubMed
48.Evangelista LS, Lee JA, Moore AA, et al. Examining the effects of remote monitoring systems on activation, self-care, and quality of life in older patients with chronic heart failure. J Cardiovas Nurs 2015;30(1):51-57. PubMed
49.Jiang J, Zhu Q, Zheng Y, et al. Perceptions and Acceptance of mHealth in Patients With Cardiovascular Diseases: A Cross-Sectional Study. JMIR MHealth UHealth 2019;7(2):e10117-e17. PubMed
50.Seto E, Leonard KJ, Masino C, et al. Attitudes of heart failure patients and health care providers towards mobile phone-based remote monitoring. J Med Internet Res 2010;12(4):e55-e55. PubMed
51.Kato NP, Johansson P, Okada I, et al. Heart Failure Telemonitoring in Japan and Sweden: A Cross-Sectional Survey. J Med Internet Res 2015;17(11):e258-e58. PubMed
52.Browning SV, Clark RC, Poff RM, et al. Telehealth monitoring: a smart investment for home care patients with heart failure? Home Healthc Nurs 2011;29(6):368-74. PubMed
53.Sharma U, Clarke M. Nurses' and community support workers' experience of telehealth: a longitudinal case study. BMC Health Serv Res 2014;14:164-64. PubMed
54.Vuorinen AL, Leppanen J, Kaijanranta H, et al. Use of home telemonitoring to support multidisciplinary care of heart failure patients in Finland: randomized controlled trial. J Med Internet Res 2014;16(12):e282-e82. PubMed
55.Papoutsi C, A'Court C, Wherton J, et al. Explaining the mixed findings of a randomised controlled trial of telehealth with centralised remote support for heart failure: multi-site qualitative study using the NASSS framework. Trials 2020;21(1):891-91. PubMed
56.Lynga P, Fridlund B, Langius-Eklof A, et al. Perceptions of transmission of body weight and telemonitoring in patients with heart failure? Int J Qual Stud Health Well-being 2013;8:21524-24. PubMed
57.Ware P, Ross HJ, Cafazzo JA, et al. User-Centered Adaptation of an Existing Heart Failure Telemonitoring Program to Ensure Sustainability and Scalability: Qualitative Study. JMIR Cardio 2018;2(2):e11466-e66. PubMed
58.Heckemann B, Wolf A, Ali L, et al. Discovering untapped relationship potential with patients in telehealth: a qualitative interview study. BMJ Open 2016;6(3):e009750-e50. PubMed
59.Johnston G, Weatherburn G. Automated weight monitoring in chronic heart failure: the excluded majority. J Telemed Telecare 2010;16(4):190-92. PubMed
60.Nguyen L, Keshavjee K, Archer N, et al. Barriers to technology use among older heart failure individuals in managing their symptoms after hospital discharge. Int J Med Inform 2017;105:136-42. PubMed
61.Piette JD, Striplin D, Marinec N, et al. A Mobile Health Intervention Supporting Heart Failure Patients and Their Informal Caregivers: A Randomized Comparative Effectiveness Trial. J Med Internet Res 2015;17(6):e142-e42. PubMed
62.Chiang LC, Chen WC, Dai YT, et al. The effectiveness of telehealth care on caregiver burden, mastery of stress, and family function among family caregivers of heart failure patients: a quasi-experimental study. Int J Nurs Stud 2012;49(10):1230-42. PubMed
63.Triantafyllidis A, Velardo C, Chantler T, et al. A personalised mobile-based home monitoring system for heart failure: The SUPPORT-HF Study. Int J Med Inform 2015;84(10):743-53. PubMed
64.Pekmezaris R, Schwartz RM, Taylor TN, et al. A qualitative analysis to optimize a telemonitoring intervention for heart failure patients from disparity communities. BMC Med Inform Decis Mak 2016;16:75-75. PubMed
65.Finkelstein J, Wood J. Implementing home telemanagement of congestive heart failure using Xbox gaming platform. Annual International Conference Of The IEEE Engineering In Medicine And Biology Society 2011;2011:3158-63.
66.Svagard I, Austad HO, Seeberg T, et al. A usability study of a mobile monitoring system for congestive heart failure patients. Stud Health Technol Inform 2014;205:528-32. PubMed
67.Cajita MI, Hodgson NA, Lam KW, et al. Facilitators of and Barriers to mHealth Adoption in Older Adults With Heart Failure. Compu Inform Nurs 2018;36(8):376-82. PubMed
68.Stut W, Deighan C, Armitage W, et al. Design and Usage of the HeartCycle Education and Coaching Program for Patients With Heart Failure. JMIR Res Protoc 2014;3(4):e72-e72. PubMed
69.Dang S, Karanam C, Gomez-Orozco C, et al. Mobile Phone Intervention for Heart Failure in a Minority Urban County Hospital Population: Usability and Patient Perspectives. Telemed J E Health 2017;23(7):544-54. PubMed
70.Dadosky A, Overbeck H, Barbetta L, et al. Telemanagement of Heart Failure Patients Across the Post-Acute Care Continuum. Telemed J E Health 2018;24(5):360-66. PubMed
71.Varon C, Alao M, Minter J, et al. Telehealth on heart failure: results of the Recap project. J Telemed Telecare 2015;21(6):340-47. PubMed
72.Radhakrishna K, Bowles K, Zettek-Sumner A. Contributors to frequent telehealth alerts including false alerts for patients with heart failure: a mixed methods exploration. App Clin Inform 2013;4(4):465-75. PubMed
73.Portz JD, Ford KL, Elsbernd K, et al. “I Like the Idea of It...But Probably Wouldn't Use It” - Health Care Provider Perspectives on Heart Failure mHealth: Qualitative Study. JMIR Cardio 2020;4(1):e18101-e01. PubMed
74.Gardner CL, Flanagan MC, Franklin C, et al. Electronic physiologic and subjective data acquisition in home-dwelling heart failure patients: An assessment of patient use and perception of usability. Int J Med Inform 2016;93:42-48. PubMed
75.de Vries AE, van der Wal MH, Nieuwenhuis MM, et al. Health professionals' expectations versus experiences of internet-based telemonitoring: survey among heart failure clinics. J Med Internet Res 2013;15(1):e4-e4. PubMed
76.Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in patients with heart failure. N Eng J Med 2010;363(24):2301-09. PubMed
77.Qian F, Parzynski CS, Chaudhry SI, et al. Racial Differences in Heart Failure Outcomes: Evidence From the Tele-HF Trial (Telemonitoring to Improve Heart Failure Outcomes). JACC Heart Failure 2015;3(7):531-38. PubMed
78.Kao DP, Lindenfeld J, Macaulay D, et al. Impact of a Telehealth and Care Management Program on All-Cause Mortality and Healthcare Utilization in Patients with Heart Failure. Telemed J E Health 2016;22(1):2-11. PubMed
79.Radhakrishnan K, Jacelon CS, Bigelow C, et al. Association of comorbidities with home care service utilization of patients with heart failure while receiving telehealth. J Cardiovas Nurs 2013;28(3):216-27. PubMed
80.Bikdeli B, Wayda B, Bao H, et al. Place of residence and outcomes of patients with heart failure: analysis from the telemonitoring to improve heart failure outcomes trial. Circ Cardiovasc Qual Outcomes 2014;7(5):749-56. PubMed
81.Galinier M, Roubille F, Berdague P, et al. Telemonitoring versus standard care in heart failure: a randomised multicentre trial. Eur J Heart Fail 2020;22(6):985-94. PubMed
82.Guzman-Clark JR, van Servellen G, Chang B, et al. Predictors and outcomes of early adherence to the use of a home telehealth device by older veterans with heart failure. Telemed J E Health 2013;19(3):217-23. PubMed
83.Jimenez-Marrero S, Yun S, Cainzos-Achirica M, et al. Impact of telemedicine on the clinical outcomes and healthcare costs of patients with chronic heart failure and mid-range or preserved ejection fraction managed in a multidisciplinary chronic heart failure programme: A sub-analysis of the iCOR randomized. J Telemed Telecare 2020;26(1-2):64-72. PubMed
84.Lycholip E, Thon Aamodt I, Lie I, et al. The dynamics of self-care in the course of heart failure management: data from the IN TOUCH study. Patient Prefer Adherence 2018;12:1113-22. PubMed
85.Cajita MI, Hodgson NA, Budhathoki C, et al. Intention to Use mHealth in Older Adults With Heart Failure. J Cardiovas Nurs 2017;32(6):E1-E7. PubMed
86.Alnosayan N, Chatterjee S, Alluhaidan A, et al. Design and Usability of a Heart Failure mHealth System: A Pilot Study. JMIR Hum Factors 2017;4(1):e9-e9. PubMed
87.Ware P, Dorai M, Ross HJ, et al. Patient Adherence to a Mobile Phone-Based Heart Failure Telemonitoring Program: A Longitudinal Mixed-Methods Study. JMIR MHealth UHealth 2019;7(2):e13259-e59. PubMed
88.Magnani JW, Schlusser CL, Kimani E, et al. The Atrial Fibrillation Health Literacy Information Technology System: Pilot Assessment. JMIR Cardio 2017;1(2):e7-e7. PubMed
89.Hirschey J, Bane S, Mansour M, et al. Evaluating the Usability and Usefulness of a Mobile App for Atrial Fibrillation Using Qualitative Methods: Exploratory Pilot Study. JMIR Hum Factors 2018;5(1):e13-e13. PubMed
90.Guhl E, Althouse AD, Pusateri AM, et al. The Atrial Fibrillation Health Literacy Information Technology Trial: Pilot Trial of a Mobile Health App for Atrial Fibrillation. JMIR Cardio LB - Ovid 2020;4(1):e17162-e62.
91.Jiang J, Gu X, Cheng CD, et al. The Hospital-Community-Family-Based Telemedicine (HCFT-AF) Program for Integrative Management of Patients With Atrial Fibrillation: Pilot Feasibility Study. JMIR MHealth UHealth 2020;8(10):e22137-e37. PubMed
Appendix 4: List of Excluded Studies and Reasons for Exclusion — Realist Review
The citations provided in this list are studies that were excluded after full-text review by 2 independent reviewers as part of this review.
Not a full paper which includes primary data from sample(s) of adult patients with chronic cardiac conditions or post-cardiac event; and/or persons who care for those living with chronic cardiac conditions:
1.Brohman K, Addas S, Dixon J, Pinsonneault A. Cascading feedback: A longitudinal study of a feedback ecosystem for telemonitoring patients with chronic disease. MIS Quart Manage Inf Syst. 2020;44(1):421-450.
2.Buis LR, Roberson DN, Kadri R, et al. Understanding the Feasibility, Acceptability, and Efficacy of a Clinical Pharmacist-led Mobile Approach (BPTrack) to Hypertension Management: Mixed Methods Pilot Study. J Med Internet Res. 2020;22(8):e19882. PubMed
3.Caceres BA, Hickey KT, Bakken SB, et al. Mobile Electrocardiogram Monitoring and Health-Related Quality of Life in Patients With Atrial Fibrillation: Findings From the iPhone Helping Evaluate Atrial Fibrillation Rhythm Through Technology (iHEART) Study. J Cardiovasc Nurs. 2020;35(4):327-336. PubMed
4.Chiwanza F, Irwin Y, Dowse R. Acceptance of ambulatory blood pressure monitoring in a semi-rural population in South Africa. Health Sa Gesondheid. 2020;25:1336. PubMed
5.Maciag A, Mitkowski P, Mazurek M, et al. Patient perspective and safety of remote monitoring of implantable cardioverter-defibrillators in the Polish Nationwide Multicenter Registry: Medtronic “CareLink” network evaluation. Kardiol Pol. 2020;14:14. PubMed
6.McBride CM, Morrissey EC, Molloy GJ. Patients' Experiences of Using Smartphone Apps to Support Self-Management and Improve Medication Adherence in Hypertension: Qualitative Study. JMIR Mhealth Uhealth. 2020;8(10):e17470. PubMed
7.Merks P, Religioni U, Arciszewska K, Pankiewicz W, Jaguszewski M, Vaillancourt R. Usability testing and satisfaction of “The Patient Access”: A mobile health application for patients with venous thromboembolic disease. A pilot study. Cardiol J. 2020;11:11. PubMed
8.Mustonen E, Horhammer I, Absetz P, et al. Eight-year post-trial follow-up of health care and long-term care costs of tele-based health coaching. Health Serv Res. 2020;55(2):211-217. PubMed
9.Shang-Lin C, Chien-Lung S, Liang-Cheng C, Yi-Pang L, Chueh-Ho L, Chia-Huei L. Effectiveness of a Home-Based Telehealth Exercise Training Program for Patients With Cardiometabolic Multimorbidity: A Randomized Controlled Trial. J Cardiovasc Nurs. 2020;35(5):491-501. PubMed
10.Srivatsa UN, Joy KC, Zhang XJ, Fan D, Oesterle A, Birgersdotter-Green U. Patient Perception of the Remote Versus Clinic Visits for Interrogation of Implantable Cardioverter Defibrillators. Crit Pathw Cardiol. 2020:22-25. PubMed
11.van der Velden RMJ, Hermans ANL, Pluymaekers NAHA, et al. Coordination of a remote mHealth infrastructure for atrial fibrillation management during COVID-19 and beyond: TeleCheck-AF. International J Care Coordination. 2020.
12.Walter C, Fischer F, Hanke JS, et al. Infrastructural needs and expected benefits of telemonitoring in left ventricular assist device therapy: Results of a qualitative study using expert interviews and focus group discussions with patients. Int J Artif Organs. 2020;43(6):385-392. PubMed
13.Banner D, Kandola D, Bates J, et al. Patient experiences of Undertaking a Virtual cardiac rehabilitation Program. Can J Cardiovasc Nurs. 2019;29(2):6-14.
14.Grant S, Hodgkinson J, Schwartz C, et al. Using mHealth for the management of hypertension in UK primary care: an embedded qualitative study of the TASMINH4 randomised controlled trial. Br J Gen Pract. 2019;69(686):e612-e620. PubMed
15.Hart D, Hopman WM, Hammond S, Redfearn DP. Augmenting Atrial Fibrillation Care After an Emergency Department Visit: Implementing Telephone Practice. J Nurs Care Qual. 2019;34(4):337-339. PubMed
16.Keane C, McClelland S, Gallagher J, et al. The Heart Failure Virtual Consultation - a powerful tool for the delivery of specialist care and the democratization of knowledge in the community. Eur J Heart Fail. 2019;21(2):255-256. PubMed
17.Shaughnessy K. The effect of telehealth on 30-day readmissions in medicare beneficiaries following isolated coronary artery bypass graft surgery. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2019;80(5-B(E).
18.Beran M, Asche SE, Bergdall AR, et al. Key components of success in a randomized trial of blood pressure telemonitoring with medication therapy management pharmacists. Journal of the American Pharmacists Association: JAPhA. 2018;58(6):614-621. PubMed
19.Bernocchi P, Vitacca M, La Rovere MT, et al. Home-based telerehabilitation in older patients with chronic obstructive pulmonary disease and heart failure: a randomised controlled trial. Age Ageing. 2018;47(1):82-88. PubMed
20.Blixen C, Sajatovic M, Moore DJ, et al. Patient Participation in the Development of a Customized M-Health Intervention to Improve Medication Adherence in Poorly Adherent Individuals with Bipolar Disorder (BD) and Hypertension (HTN). Int. 2018;4(1):25-35. PubMed
21.Bradbury K, Morton K, Band R, et al. Using the Person-Based Approach to optimise a digital intervention for the management of hypertension. PLoS ONE [Electronic Resource]. 2018;13(5):e0196868. PubMed
22.Jancin B. Home telemonitoring for heart failure cuts mortality. Chest Physician. 2018;13(12):31-31.
23.Ting Y, Pei Z, Chengzhong X, Zijing P, Yongfei W, Liang Z. Exploring distinct trajectories of use of telehealth devices among adults with hypertension: a latent class growth analysis approach. International Journal of Integrated Care (IJIC). 2018;18:1-2.
24.Yan M, Or C. Factors in the 4-week Acceptance of a Computer-Based, Chronic Disease Self-Monitoring System in Patients with Type 2 Diabetes Mellitus and/or Hypertension. Telemed J E Health. 2018;24(2):121-129. PubMed
25.Caban PL. Effect of Home Telemonitoring on Heart Failure Hospital Readmissions Among Adult Hispanics. Effect of Home Telemonitoring on Heart Failure Hospital Readmissions Among Adult Hispanics. 2017:1-1.
26.Crundall-Goode A, Goode KM, Clark AL. What impact do anxiety, depression, perceived control and technology capability have on whether patients with chronic heart failure take-up or continue to use home tele-monitoring services? Study design of ADaPT-HF. Eur J Cardiovasc Nurs. 2017;16(4):283-289. PubMed
27.Haynes SC, Kim KK. A mobile system for the improvement of heart failure management: Evaluation of a prototype. AMIA Annu Symp Proc. 2017;2017:839-848. PubMed
28.Lundin M, Makitalo A. Co-designing technologies in the context of hypertension care: Negotiating participation and technology use in design meetings. Inform Health Soc Care. 2017;42(1):18-31. PubMed
29.Mirk SM, Wegrzyn NM. Apps for Health-Related Education in Pharmacy Practice: Needs Assessment Survey Among Patients Within a Large Metropolitan Area. JMIR Res Protoc. 2017;6(7):e133. PubMed
30.Nichols M, Sarfo FS, Singh A, et al. Assessing Mobile Health Capacity and Task Shifting Strategies to Improve Hypertension Among Ghanaian Stroke Survivors. Am J Med Sci. 2017;354(6):573-580. PubMed
31.Thies K, Anderson D, Cramer B. Lack of Adoption of a Mobile App to Support Patient Self-Management of Diabetes and Hypertension in a Federally Qualified Health Center: Interview Analysis of Staff and Patients in a Failed Randomized Trial. JMIR Hum Factors. 2017;4(4):e24. PubMed
32.Yeo KJ, Handayani L, Satria H, Lee SH, Yap CK. Barriers and challenges to telecardiology adoption in Malaysia context. Int J Electr Comput Eng. 2017;7(1):260-265.
33.Abdullah A, Liew SM, Hanafi NS, et al. What influences patients' acceptance of a blood pressure telemonitoring service in primary care? A qualitative study. Patient Prefer Adherence. 2016;10:99-106. PubMed
34.Cunanan KM, Carlin BP, Peterson KA. A practical Bayesian stepped wedge design for community-based cluster-randomized clinical trials: The British Columbia Telehealth Trial. Clin. 2016;13(6):641-650. PubMed
35.Lee JA, Evangelista LS, Moore AA, et al. Feasibility Study of a Mobile Health Intervention for Older Adults on Oral Anticoagulation Therapy. Gerontol. 2016;2:2333721416672970. PubMed
36.Murga N, Romo M, Castro P, et al. Deploying telemonitoring services in an integrated care model. International Journal of Integrated Care (IJIC). 2016;16(6):1-3.
37.Prescott E, Meindersma EP, van der Velde AE, et al. A EUropean study on effectiveness and sustainability of current Cardiac Rehabilitation programmes in the Elderly: Design of the EU-CaRE randomised controlled trial. European Journal of Preventive Cardiology. 2016;23(2 suppl):27-40. PubMed
38.Schonenberg H, Pauws S, Chouvarda I, et al. What does it take to make integrated care work? International Journal of Integrated Care (IJIC). 2016;16(6):1-3.
39.Sokoreli I, De Massari D, Pauws SC, et al. Effectiveness of telehealth for heart failure management in routine practice. International Journal of Integrated Care (IJIC). 2016;16(5 Supplement):1-2.
40.Lear SA, Singer J, Banner-Lukaris D, et al. Improving access to cardiac rehabilitation using the internet: a randomized trial. Stud Health Technol Inform. 2015;209:58-66. PubMed
41.Siebermair J, Clauss S, Martens E, et al. Remote monitoring of implantable cardioverter-defibrillators. Problems and implications using a telemonitoring system. Herz. 2015;40 Suppl 2:110-118. PubMed
42.Taylor J, Coates E, Brewster L, Mountain G, Wessels B, Hawley MS. Examining the use of telehealth in community nursing: identifying the factors affecting frontline staff acceptance and telehealth adoption. J Adv Nurs. 2015;71(2):326-337. PubMed
43.Kang Y. Patient-related characteristics associated with rehospitalization in Medicare recipients with heart failure receiving telehomecare, University of Pennsylvania; 2014.
44.Laurent G, Amara W, Mansourati J, et al. Role of patient education in the perception and acceptance of home monitoring after recent implantation of cardioverter defibrillators: the EDUCAT study. Arch Cardiovasc Dis. 2014;107(10):508-518. PubMed
45.Lind L, Karlsson D. Telehealth for “the digital illiterate”--elderly heart failure patients experiences. Stud Health Technol Inform. 2014;205:353-357. PubMed
46.Morichelli L, Porfili A, Quarta L, Sassi A, Ricci RP. Implantable cardioverter defibrillator remote monitoring is well accepted and easy to use during long-term follow-up. J Interv Card Electrophysiol. 2014;41(3):203-209. PubMed
47.Odeh B, Philips N, Kayyali R, et al. 4 ACCEPTABILITY OF TELEHEALTH BY ELDERLY PATIENTS. Age Ageing. 2014;43(suppl_1):i1-i1.
48.Prescher S, Deckwart O, Koehler K, et al. Will telemonitoring be adopted by patients with chronic heart failure?: Analysis of the adherence of the TIM-HF study. Dtsch Med Wochenschr. 2014;139(16):829-834. PubMed
49.Willemse E, Adriaenssens J, Dilles T, Remmen R. Do telemonitoring projects of heart failure fit the Chronic Care Model? Int J Integr Care. 2014;14:e023. PubMed
50.Bardsley M, Steventon A, Doll H. Impact of telehealth on general practice contacts: findings from the whole systems demonstrator cluster randomised trial. BMC Health Serv Res. 2013;13:395. PubMed
51.Chen MJ, Chen KY, Chiang SJ, et al. A telehealth service model for the treatment of hypertension. J Telemed Telecare. 2013;19(5):238-241. PubMed
52.McCarthy D. University of California, San Francisco Medical Center: Reducing Readmissions Through Heart Failure Care Management: Part I...Reprinted with permission of The Commonwealth Fund at www.commonwealthfund.org. Care Management. 2013;19(3):12-19.
53.Papavasileiou LP, Forleo GB, Panattoni G, et al. Work burden with remote monitoring of implantable cardioverter defibrillator: is it time for reimbursement policies? J Cardiovasc Med. 2013;14(2):114-119. PubMed
54.Park LG. The Efficacy of Mobile Technology to Promote Medication Adherence, University of California, San Francisco; 2013.
55.Piette JD, Gregor MA, Share D, et al. Improving Heart Failure Self-Management Support by Actively Engaging Out-of-Home Caregivers: Results of a Feasibility Study. Congest Heart Fail. 2013;14(1). PubMed
56.Elwyn G, Hardisty AR, Peirce SC, et al. Detecting deterioration in patients with chronic disease using telemonitoring: navigating the 'trough of disillusionment'. J Eval Clin Pract. 2012;18(4):896-903. PubMed
57.Furukawa T, Maggi R, Bertolone C, et al. Effectiveness of remote monitoring in the management of syncope and palpitations. Europace. 2011;13(3):431-437. PubMed
58.Mattera JA. Patients' adoption and adherence to a heart failure telemonitoring intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2012;72(9-B).
59.Or CK, Karsh BT, Severtson DJ, Burke LJ, Brown RL, Brennan PF. Factors affecting home care patients' acceptance of a web-based interactive self-management technology. J Am Med Inform Assoc. 2011;18(1):51-59. PubMed
60.Radhakrishnan K. Characteristics of patients on telehealth that influence their heart failure outcomes in the home-care setting, University of Massachusetts Amherst; 2011.
61.Cardozo L, Steinberg J. Telemedicine for recently discharged older patients. Telemed J E Health. 2010;16(1):49-55. PubMed
62.Liu J-J. Pervasive telemonitoring for patients living with chronic heart failure: A quantitative study of telemedicine acceptance. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2010;70(9-B).
63.Maric B, Kaan A, Araki Y, Ignaszewski A, Lear SA. The use of the Internet to remotely monitor patients with heart failure. Telemed J E Health. 2010;16(1):26-33. PubMed
64.McManus RJ, Mant J, Bray EP, et al. Telemonitoring and self-management in the control of hypertension (TASMINH2): a randomised controlled trial. Lancet. 2010;376(9736):163-172. PubMed
65.Morey SA, Barg-Walkow LH, Rogers WA. Managing heart failure on the Go: Usability issues with mHealth apps for older adults. 2017.
Does not contain data and / or themes pertaining to a remote-monitoring program:
66.Chen YW, Wei J, Chen HL, Cheng CH, Hou IC. Developing a Heart Transplantation Self-Management Support Mobile Health App in Taiwan: Qualitative Study. JMIR Mhealth Uhealth. 2020;8(8):e18999. PubMed
67.Ding EY, Svennberg E, Wurster C, et al. Survey of current perspectives on consumer-available digital health devices for detecting atrial fibrillation. Cardiovasc Digit Health J. 2020;1(1):21-29. PubMed
68.Guo Y, Lane DA, Wang L, et al. Mobile Health Technology to Improve Care for Patients With Atrial Fibrillation. J Am Coll Cardiol. 2020;75(13):1523-1534. PubMed
69.Hu PT, Hilow H, Patel D, et al. Use of virtual visits for the care of the arrhythmia patient. Heart Rhythm. 2020;17(10):1779-1783. PubMed
70.Ip J, Jaffe B, Castellani M, Sheikh A, Castellani C, Ip R. Accuracy of arrhythmia detection in implantable cardiac monitors: A prospective randomized clinical trial comparing Reveal LINQ and Confirm Rx. Pacing Clin Electrophysiol. 2020;24:24. PubMed
71.Laustsen S, Oestergaard LG, van Tulder M, Hjortdal VE, Petersen AK. Telemonitored exercise-based cardiac rehabilitation improves physical capacity and health-related quality of life. J Telemed Telecare. 2020;26(1-2):36-44. PubMed
72.Mullens W, Sharif F, Dupont M, Rothman AMK, Wijns W. Digital health care solution for proactive heart failure management with the Cordella Heart Failure System: results of the SIRONA first-in-human study. Eur J Heart Fail. 2020;31:31. PubMed
73.Ollitrault P, Jacon P, Auquier N, et al. Atrial fibrillation detection by the subcutaneous defibrillator: real-world clinical performances and implications from a multicentre study. Europace. 2020;22(11):1628-1634. PubMed
74.Park LG, Ng F, J KS, Elnaggar A, Villero O. Perceptions and experiences of using mobile technology for medication adherence among older adults with coronary heart disease: A qualitative study. Digit Health. 2020;6:2055207620926844. PubMed
75.Pedraza LL, Moraes JRW, Rabelo-Silva ER. Development and testing of a text messaging (SMS) monitoring software application for acute decompensated heart failure patients. Rev Lat Am Enfermagem. 2020;28:e3301. PubMed
76.Shaw SE, Seuren LM, Wherton J, et al. Video Consultations Between Patients and Clinicians in Diabetes, Cancer, and Heart Failure Services: Linguistic Ethnographic Study of Video-Mediated Interaction. J Med Internet Res. 2020;22(5):e18378. PubMed
77.Treskes RW, van Winden LAM, van Keulen N, et al. Effect of Smartphone-Enabled Health Monitoring Devices vs Regular Follow-up on Blood Pressure Control Among Patients After Myocardial Infarction: A Randomized Clinical Trial. JAMA netw. 2020;3(4):e202165.
78.Wali S, Keshavjee K, Nguyen L, Mbuagbaw L, Demers C. Using an Electronic App to Promote Home-Based Self-Care in Older Patients With Heart Failure: Qualitative Study on Patient and Informal Caregiver Challenges. JMIR Cardio. 2020;4(1):e15885. PubMed
79.Woo K, Dowding DW. Decision-making Factors Associated With Telehealth Adoption by Patients With Heart Failure at Home: A Qualitative Study. CIN: Computers, Informatics, Nursing. 2020;38(4):204-214. PubMed
80.Akyar I, Dionne-Odom JN, Bakitas MA. Using Patients and Their Caregivers Feedback to Develop ENABLE CHF-PC: An Early Palliative Care Intervention for Advanced Heart Failure. J Palliat Care. 2019;34(2):103-110. PubMed
81.Baik D, Reading M, Jia H, Grossman LV, Masterson Creber R. Measuring health status and symptom burden using a web-based mHealth application in patients with heart failure. Eur J Cardiovasc Nurs. 2019;18(4):325-331. PubMed
82.Haldane V, Tan YG, Teo KWQ, et al. Perspectives on Acceptance and Use of a Mobile Health Intervention for the Prevention of Atherosclerotic Cardiovascular Disease in Singapore: Mixed-Methods Study. JMIR Mhealth Uhealth. 2019;7(3):e11108. PubMed
83.Hwang R, Morris NR, Mandrusiak A, et al. Cost-Utility Analysis of Home-Based Telerehabilitation Compared With Centre-Based Rehabilitation in Patients With Heart Failure. Heart Lung Circ. 2019;28(12):1795-1803. PubMed
84.Johansson P, Jaarsma T, Andersson G, Lundgren J. The impact of internet-based cognitive behavioral therapy and depressive symptoms on self-care behavior in patients with heart failure. A secondary analysis of a randomised controlled trial. Int J Nurs Stud. 2019:103454. PubMed
85.Kim YJ, Radloff JC, Crane PA, Bolin LP. Rehabilitation intervention for individuals with heart failure and fatigue to reduce fatigue impact: A feasibility study. Ann Rehabil Med. 2019;43(6):686-699. PubMed
86.Koshy AN, Ko J, Sajeev JK, et al. Evaluating patient attitudes and barriers towards smart technology for cardiac monitoring: Results from a prospective multicentre study. BMJ Innovations. 2019.
87.Reid RD, Aitken DA, Mullen KA, et al. Automated Telephone Follow-up for Smoking Cessation in Smokers with Coronary Heart Disease: A Randomized Controlled Trial. Nicotine and Tobacco Research. 2019;21(8):1051-1057. PubMed
88.Shariful Islam SM, Chow CK, Redfern J, et al. Effect of text messaging on depression in patients with coronary heart disease: a substudy analysis from the TEXT ME randomised controlled trial. BMJ Open. 2019;9(2):e022637. PubMed
89.Tarte VP, Amirehsani KA. Perceptions of Mobile Technology for Heart Failure Education and Self-Management Among Middle-Aged and Older Adults. J Gerontol Nurs. 2019;45(11):30-38. PubMed
90.Ten Eyck L, MacLeod S, Hawkins K, Guimont R, Hartley S. The Impact of a Heart Failure Management Program in a Medicare Advantage Population. Popul Health Manag. 2019;22(2):153-161. PubMed
91.Albrecht L, Wood PW, Fradette M, et al. Usability and Acceptability of a Home Blood Pressure Telemonitoring Device Among Community-Dwelling Senior Citizens With Hypertension: Qualitative Study. JMIR Aging. 2018;1(2):e10975. PubMed
92.Argha A, Savkin A, Liaw ST, Celler BG. Effect of Seasonal Variation on Clinical Outcome in Patients with Chronic Conditions: Analysis of the Commonwealth Scientific and Industrial Research Organization (CSIRO) National Telehealth Trial. JMIR Med Inform. 2018;6(1):e16. PubMed
93.Boyde M, Rankin J, Whitty JA, et al. Patient preferences for the delivery of cardiac rehabilitation. Patient Educ Couns. 2018;101(12):2162-2169. PubMed
94.Celano CM, Freedman ME, Beale EE, Gomez-Bernal F, Huffman JC. A Positive Psychology Intervention to Promote Health Behaviors in Heart Failure: A Proof-of-Concept Trial. JNMD. 2018;206(10):800-808. PubMed
95.Desteghe L, Vijgen J, Koopman P, et al. Telemonitoring-based feedback improves adherence to non-vitamin K antagonist oral anticoagulants intake in patients with atrial fibrillation. Eur Heart J. 2018;39(16):1394-1403. PubMed
96.Harzand A, Witbrodt B, Davis-Watts ML, et al. Feasibility of a Smartphone-enabled Cardiac Rehabilitation Program in Male Veterans With Previous Clinical Evidence of Coronary Heart Disease. Am J Cardiol. 2018;122(9):1471-1476. PubMed
97.Lundgren J, Johansson P, Jaarsma T, Andersson G, Karner Kohler A. Patient Experiences of Web-Based Cognitive Behavioral Therapy for Heart Failure and Depression: Qualitative Study. J Med Internet Res. 2018;20(9):e10302. PubMed
98.Nishii N, Miyoshi A, Kubo M, et al. Analysis of arrhythmic events is useful to detect lead failure earlier in patients followed by remote monitoring. J Cardiovasc Electrophysiol. 2018;29(3):463-470. PubMed
99.Palmisano P, Guerra F, Ammendola E, et al. Physical Activity Measured by Implanted Devices Predicts Atrial Arrhythmias and Patient Outcome: Results of IMPLANTED (Italian Multicentre Observational Registry on Patients With Implantable Devices Remotely Monitored). J Am Heart Assoc. 2018;7(5):24. PubMed
100.Reading M, Baik D, Beauchemin M, Hickey KT, Merrill JA. Factors Influencing Sustained Engagement with ECG Self-Monitoring: Perspectives from Patients and Health Care Providers. Appl Clin Inform. 2018;9(4):772-781. PubMed
101.Rohani Ghahari R, Holden RJ, Flanagan ME, et al. Using cardiac implantable electronic device data to facilitate health decision making: A design study. Int J Ind Ergon. 2018;64:143-154.
102.Saran T, Owoc J, Bojar I. Use of the ipaq questionnaire in the form of a mobile application in monitoring physical activity of patients with cardiovascular diseases. Ann Agric Environ Med. 2018;25(3):395-402. PubMed
103.Brewer LC, Kaihoi B, Schaepe K, et al. Patient-perceived acceptability of a virtual world-based cardiac rehabilitation program. Digit Health. 2017;3:2055207617705548. PubMed
104.Cornet VP, Daley CN, Srinivas P, Holden RJ. User-Centered Evaluations with Older Adults: Testing the Usability of a Mobile Health System for Heart Failure Self-Management. Proc. 2017;61(1):6-10. PubMed
105.Deighan C, Michalova L, Pagliari C, Elliott J, Taylor L, Ranaldi H. The Digital Heart Manual: A pilot study of an innovative cardiac rehabilitation programme developed for and with users. Patient Educ Couns. 2017;100(8):1598-1607. PubMed
106.Ghanbari H, Ansari S, Ghannam M, et al. Feasibility and usability of a mobile application to assess symptoms and affect in patients with atrial fibrillation: A pilot study. Journal of Atrial Fibrillation. 2017;10(2). PubMed
107.Hargreaves S, Hawley MS, Haywood A, Enderby PM. Informing the Design of “Lifestyle Monitoring” Technology for the Detection of Health Deterioration in Long-Term Conditions: A Qualitative Study of People Living With Heart Failure. J Med Internet Res. 2017;19(6):e231. PubMed
108.Mertens A, Becker S, Theis S, et al. Mobile technology improves therapy-adherence rates in elderly patients undergoing rehabilitation—A crossover design study. Vol 4822017:295-308.
109.Saba S, Adelstein E, Wold N, Stein K, Jones P. Influence of patients' age at implantation on mortality and defibrillator shocks. Europace. 2017;19(5):802-807. PubMed
110.van Engen-Verheul MM, Peek N, Haafkens JA, et al. What is needed to implement a web-based audit and feedback intervention with outreach visits to improve care quality: A concept mapping study among cardiac rehabilitation teams. Int J Med Inform. 2017;97:76-85. PubMed
111.Aranki D, Kurillo G, Yan P, Liebovitz DM, Bajcsy R. Real-Time Tele-Monitoring of Patients with Chronic Heart-Failure Using a Smartphone: Lessons Learned. IEEE Trans Affective Comput. 2016;7(3):206-219.
112.Burtch J. Telephonic Transitional Care Intervention to Reduce 30-Day Hospital Readmission Rates in Adults with Heart Failure. Telephonic Transitional Care Intervention to Reduce 30-day Hospital Readmission Rates in Adults with Heart Failure. 2016:1-1.
113.Doorenbos AZ, Levy WC, Curtis JR, Dougherty CM. An Intervention to Enhance Goals-of-Care Communication Between Heart Failure Patients and Heart Failure Providers. J Pain Symptom Manage. 2016;52(3):353-360. PubMed
114.Gude WT, van Engen-Verheul MM, van der Veer SN, et al. Effect of a web-based audit and feedback intervention with outreach visits on the clinical performance of multidisciplinary teams: a cluster-randomized trial in cardiac rehabilitation. Implement Sci. 2016;11(1):160. PubMed
115.Hale TM, Jethwani K, Kandola MS, Saldana F, Kvedar JC. A Remote Medication Monitoring System for Chronic Heart Failure Patients to Reduce Readmissions: A Two-Arm Randomized Pilot Study. J Med Internet Res. 2016;18(5):e91. PubMed
116.Krumholz HM, Chaudhry SI, Spertus JA, Mattera JA, Hodshon B, Herrin J. Do Non-Clinical Factors Improve Prediction of Readmission Risk?: Results From the Tele-HF Study. JACC Heart Fail. 2016;4(1):12-20. PubMed
117.Lind L, Carlgren G, Karlsson D. Old-and With Severe Heart Failure: Telemonitoring by Using Digital Pen Technology in Specialized Homecare: System Description, Implementation, and Early Results. CIN: Computers, Informatics, Nursing. 2016;34(8):360-368. PubMed
118.Wakefield B, Pham K, Scherubel M. Usability Evaluation of a Web-Based Symptom Monitoring Application for Heart Failure. West J Nurs Res. 2015;37(7):922-934. PubMed
119.Maddison R, Pfaeffli L, Stewart R, et al. The HEART Mobile Phone Trial: The Partial Mediating Effects of Self-Efficacy on Physical Activity among Cardiac Patients. Front. 2014;2:56. PubMed
120.Davidson KW, Bigger JT, Burg MM, et al. Centralized, stepped, patient preference-based treatment for patients with post-acute coronary syndrome depression: CODIACS vanguard randomized controlled trial. JAMA Internal Medicine. 2013;173(11):997-1004. PubMed
121.Radhakrishnan K, Bowles K, Hanlon A, Topaz M, Chittams J. A retrospective study on patient characteristics and telehealth alerts indicative of key medical events for heart failure patients at a home health agency. Telemed J E Health. 2013;19(9):664-670. PubMed
122.Shah H, Mezu U, Patel D, et al. Mechanisms of inappropriate defibrillator therapy in a modern cohort of remotely monitored patients. Pacing Clin Electrophysiol. 2013;36(5):547-552. PubMed
123.Singh S, Bansal M, Maheshwari P, et al. American society of echocardiography: Remote echocardiography with web-based assessments for referrals at a distance (ASE-REWARD) study. J Am Soc Echocardiogr. 2013;26(3):221-233. PubMed
124.Zai AH, Ronquillo JG, Nieves R, Chueh HC, Kvedar JC, Jethwani K. Assessing hospital readmission risk factors in heart failure patients enrolled in a telemonitoring program. Int J Telemed Appl. 2013;2013:305819. PubMed
125.Boyne JJ, Vrijhoef HJ, Crijns HJ, et al. Tailored telemonitoring in patients with heart failure: results of a multicentre randomized controlled trial. Eur J Heart Fail. 2012;14(7):791-801. PubMed
126.Grant RW, Pandiscio JC, Pajolek H, et al. Implementation of a web-based tool for patient medication self-management: the Medication Self-titration Evaluation Programme (Med-STEP) for blood pressure control. Inform Prim Care. 2012;20(1):57-67. PubMed
127.Goebel B, Luthardt E, Schmidt-Winter C, et al. Echocardiographic evaluation of left ventricular filling pressures validated against an implantable left ventricular pressure monitoring system. Echocardiography. 2011;28(6):619-625. PubMed
128.Huffman JC, Mastromauro CA, Boehm JK, et al. Development of a positive psychology intervention for patients with acute cardiovascular disease. Heart Int. 2011;6(2):e14. PubMed
129.Morak J, Kumpusch H, Hayn D, et al. Near Field Communication-based telemonitoring with integrated ECG recordings. Appl Clin Inform. 2011;2(4):481-498. PubMed
130.Powell BD, Cha YM, Asirvatham SJ, et al. Implantable cardioverter defibrillator electrogram adjudication for device registries: methodology and observations from ALTITUDE. Pacing Clin Electrophysiol. 2011;34(8):1003-1012. PubMed
131.Eakin E, Reeves M, Winkler E, Lawler S, Owen N. Maintenance of Physical Activity and Dietary Change Following a Telephone-Delivered Intervention. Health Psychol. 2010;29(6):566-573. PubMed
132.Furber S, Butler L, Phongsavan P, Mark A, Bauman A. Randomised controlled trial of a pedometer-based telephone intervention to increase physical activity among cardiac patients not attending cardiac rehabilitation. Patient Educ Couns. 2010;80(2):212-218. PubMed
133.Hickey KT, Reiffel J, Sciacca RR, et al. The Utility of Ambulatory Electrocardiographic Monitoring for Detecting Silent Arrhythmias and Clarifying Symptom Mechanism in an Urban Elderly Population with Heart Failure and Hypertension: Clinical Implications. Journal of Atrial Fibrillation. 2010;3(1):193. PubMed
134.Richardson CR, Buis LR, Janney AW, et al. An online community improves adherence in an internet-mediated walking program. Part 1: results of a randomized controlled trial. J Med Internet Res. 2010;12(4):e71. PubMed
135.Fischer S, Wünsche BC, Cameron L, et al. Web-based visualisations supporting rehabilitation of heart failure patients by promoting behavioural change. 2011.
136.Lowndes BR, Finnie D, Hathaway J, et al. Iterative implementation of a remote cardiac patient monitoring device using qualitative analysis and human factors engineering. 2017.
137.Orsama AL, Kaijanranta H, Leppänen J, Lvhteenmvki J, Partanen L, Heliö T. Profiling remotely monitored patients with adherence parameters. 2012.
Does not contain data and / or themes related to perceived or actual intervention mechanisms:
138.Boodoo C, Zhang Q, Ross HJ, Alba AC, Laporte A, Seto E. Evaluation of a Heart Failure Telemonitoring Program Through a Microsimulation Model: Cost-Utility Analysis. J Med Internet Res. 2020;22(10):e18917. PubMed
139.De Canniere H, Corradi F, Smeets CJP, et al. Wearable Monitoring and Interpretable Machine Learning Can Objectively Track Progression in Patients during Cardiac Rehabilitation. Sensors (Basel). 2020;20(12):26. PubMed
140.Ding H, Jayasena R, Chen SH, et al. The Effects of Telemonitoring on Patient Compliance With Self-Management Recommendations and Outcomes of the Innovative Telemonitoring Enhanced Care Program for Chronic Heart Failure: Randomized Controlled Trial. J Med Internet Res. 2020;22(7):e17559. PubMed
141.Guzman-Clark J, Yefimova M, Farmer MM, et al. Home Telehealth Technologies for Heart Failure: An Examination of Adherence Among Veterans. J Gerontol Nurs. 2020;46(7):26-34. PubMed
142.Kramer F, Butler J, Shah SJ, et al. Real-Life Multimarker Monitoring in Patients with Heart Failure: Continuous Remote Monitoring of Mobility and Patient-Reported Outcomes as Digital End Points in Future Heart-Failure Trials. Digit. 2020;4(2):45-59. PubMed
143.Leng Chow W, Aung CYK, Tong SC, et al. Effectiveness of telemonitoring-enhanced support over structured telephone support in reducing heart failure-related healthcare utilization in a multi-ethnic Asian setting. J Telemed Telecare. 2020;26(6):332-340. PubMed
144.Lopez-Villegas A, Catalan-Matamoros D, Peiro S, Lappegard KT, Lopez-Liria R. Cost-utility analysis of telemonitoring versus conventional hospital-based follow-up of patients with pacemakers. The NORDLAND randomized clinical trial. PLoS One. 2020;15 (1) (no pagination)(e0226188).
145.Margolis KL, Dehmer SP, Sperl-Hillen J, et al. Cardiovascular Events and Costs With Home Blood Pressure Telemonitoring and Pharmacist Management for Uncontrolled Hypertension. Hypertension. 2020;76(4):1097-1103. PubMed
146.Nabutovsky I, Nachshon A, Klempfner R, Shapiro Y, Tesler R. Digital Cardiac Rehabilitation Programs: The Future of Patient-Centered Medicine. Telemed J E Health. 2020;26(1):34-41. PubMed
147.Reading Turchioe M, Grossman LV, Baik D, et al. Older Adults Can Successfully Monitor Symptoms Using an Inclusively Designed Mobile Application. J Am Geriatr Soc. 2020;68(6):1313-1318. PubMed
148.Ruschel KB, Rados DR, Furtado MV, et al. Transition of care of stable ischaemic heart disease patients from tertiary to primary care with telemedicine support: Randomized noninferiority clinical trial. J Telemed Telecare. 2020:1357633X20906648.
149.Shaughnessy K, White KA, Murphy M, Crowell NA, Anderson KM. The effect of remote patient monitoring on discharge outcomes in post-coronary artery bypass graft surgery patients. J Am Assoc Nurse Pract. 2020;06:06.
150.Son YJ, Oh S, Kim EY. Patients' needs and perspectives for using mobile phone interventions to improve heart failure self-care: A qualitative study. J Adv Nurs. 2020;76(9):2380-2390. PubMed
151.Yanicelli LM, Goy CB, Gonzalez VDC, Palacios GN, Martinez EC, Herrera MC. Non-invasive home telemonitoring system for heart failure patients: A randomized clinical trial. J Telemed Telecare. 2020:1357633X19899261.
152.Zakeri R, Morgan JM, Phillips P, et al. Impact of remote monitoring on clinical outcomes for patients with heart failure and atrial fibrillation: results from the REM-HF trial. Eur J Heart Fail. 2020;22(3):543-553. PubMed
153.Park C, Otobo E, Ullman J, et al. Impact on Readmission Reduction Among Heart Failure Patients Using Digital Health Monitoring: Feasibility and Adoptability Study. JMIR Med Inform. 2019;7(4):e13353. PubMed
154.Jaana M, Sherrard H. Rural-Urban Comparison of Telehome Monitoring for Patients with Chronic Heart Failure. Telemed J E Health. 2019;25(2):101-108. PubMed
155.Snoek JA, Meindersma EP, Prins LF, et al. The sustained effects of extending cardiac rehabilitation with a six-month telemonitoring and telecoaching programme on fitness, quality of life, cardiovascular risk factors and care utilisation in CAD patients: The TeleCaRe study. J Telemed Telecare. 2019:1357633X19885793.
156.Berrios-Thomas S, Engel R, McCall J, Rosen D. Assessing Knowledge Regarding Managing Congestive Health Failure Symptoms: Differences in Patient and Professional Scores. J Patient Exp. 2018;5(4):289-295. PubMed
157.Dinesen B, Spindler H. The Use of Telerehabilitation Technologies for Cardiac Patients to Improve Rehabilitation Activities and Unify Organizations: Qualitative Study. JMIR Rehabil Assist Technol. 2018;5(2):e10758. PubMed
158.Duan YP, Liang W, Guo L, Wienert J, Si GY, Lippke S. Evaluation of a Web-Based Intervention for Multiple Health Behavior Changes in Patients With Coronary Heart Disease in Home-Based Rehabilitation: Pilot Randomized Controlled Trial. J Med Internet Res. 2018;20(11):e12052. PubMed
159.Grustam AS, Severens JL, De Massari D, Buyukkaramikli N, Koymans R, Vrijhoef HJM. Cost-Effectiveness Analysis in Telehealth: A Comparison between Home Telemonitoring, Nurse Telephone Support, and Usual Care in Chronic Heart Failure Management. Value Health. 2018;21(7):772-782. PubMed
160.Evangelista LS, Ghasemzadeh H, Lee JA, Fallahzadeh R, Sarrafzadeh M, Moser DK. Predicting adherence to use of remote health monitoring systems in a cohort of patients with chronic heart failure. Technol Health Care. 2017;25(3):425-433. PubMed
161.Gallagher BD, Moise N, Haerizadeh M, Ye S, Medina V, Kronish IM. Telemonitoring Adherence to Medications in Heart Failure Patients (TEAM-HF): A Pilot Randomized Clinical Trial. J Card Fail. 2017;23(4):345-349. PubMed
162.Hwang R, Mandrusiak A, Morris NR, Peters R, Korczyk D, Russell T. Assessing functional exercise capacity using telehealth: Is it valid and reliable in patients with chronic heart failure? J Telemed Telecare. 2017;23(2):225-232. PubMed
163.Bikmoradi A, Masmouei B, Ghomeisi M, Roshanaei G. Impact of Tele-nursing on adherence to treatment plan in discharged patients after coronary artery bypass graft surgery: A quasi-experimental study in Iran. Int J Med Inform. 2016;86:43-48. PubMed
164.Dario C, Luisotto E, Dal Pozzo E, et al. Assessment of Patients' Perception of Telemedicine Services Using the Service User Technology Acceptability Questionnaire. Int J Integr Care. 2016;16(2):13. PubMed
165.Du L, Dong P, Jia J, et al. Impacts of intensive follow-up on the long-term prognosis of percutaneous coronary intervention in acute coronary syndrome patients - A single center prospective randomized controlled study in a Chinese population. European Journal of Preventive Cardiology. 2016;23(10):1077-1085. PubMed
166.Evans J, Papadopoulos A, Silvers CT, et al. Remote Health Monitoring for Older Adults and Those with Heart Failure: Adherence and System Usability. Telemed J E Health. 2016;22(6):480-488. PubMed
167.Kidholm K, Rasmussen MK, Andreasen JJ, et al. Cost-Utility Analysis of a Cardiac Telerehabilitation Program: The Teledialog Project. Telemed J E Health. 2016;22(7):553-563. PubMed
168.Rosen D, McCall JD, Primack BA. Telehealth Protocol to Prevent Readmission Among High-Risk Patients With Congestive Heart Failure. Am J Med. 2017;130(11):1326-1330. PubMed
169.Lowres N, Redfern J, Freedman SB, et al. Choice of Health Options in prevention of Cardiovascular Events for people with Atrial Fibrillation (CHOICE-AF): A pilot study. Eur J Cardiovasc Nurs. 2016;15(1):39-46. PubMed
170.Mertens A, Brandl C, Miron-Shatz T, et al. A mobile application improves therapy-adherence rates in elderly patients undergoing rehabilitation: A crossover design study comparing documentation via iPad with paper-based control. Medicine. 2016;95(36):e4446. PubMed
171.Radhakrishnan K, Toprac P, O'Hair M, et al. Interactive Digital e-Health Game for Heart Failure Self-Management: A Feasibility Study. Games health j. 2016;5(6):366-374. PubMed
172.Ritchie CS, Houston TK, Richman JS, et al. The E-Coach technology-assisted care transition system: a pragmatic randomized trial. Transl Behav Med. 2016;6(3):428-437. PubMed
173.Rosen D, Berrios-Thomas S, Engel RJ. Increasing self-knowledge: Utilizing tele-coaching for patients with congestive heart failure. Soc Work Health Care. 2016;55(9):711-719. PubMed
174.Williams C, Wan TT. A remote monitoring program evaluation: a retrospective study. J Eval Clin Pract. 2016;22(6):978-984. PubMed
175.Sangster J, Furber S, Allman-Farinelli M, et al. Effectiveness of a pedometer-based telephone coaching program on weight and physical activity for people referred to a cardiac rehabilitation program: a randomized controlled trial. J Cardiopulm Rehabil Prev. 2015;35(2):124-129. PubMed
176.Agboola S, Jethwani K, Khateeb K, Moore S, Kvedar J. Heart failure remote monitoring: evidence from the retrospective evaluation of a real-world remote monitoring program. J Med Internet Res. 2015;17(4):e101. PubMed
177.Evangelista LS, Moser DK, Lee JA, et al. Examining Older Adults' Perceptions of Usability and Acceptability of Remote Monitoring Systems to Manage Chronic Heart Failure. Gerontol. 2015;1:2333721415618050. PubMed
178.Villani A, Malfatto G, Compare A, et al. Clinical and psychological telemonitoring and telecare of high risk heart failure patients. J Telemed Telecare. 2014;20(8):468-475. PubMed
179.Boyne JJ, Vrijhoef HJ. Implementing telemonitoring in heart failure care: barriers from the perspectives of patients, healthcare professionals and healthcare organizations. Curr Heart Fail Rep. 2013;10(3):254-261. PubMed
180.Kraal JJ, Peek N, van den Akker-Van Marle ME, Kemps HM. Effects and costs of home-based training with telemonitoring guidance in low to moderate risk patients entering cardiac rehabilitation: The FIT@Home study. BMC Cardiovasc Disord. 2013;13:82. PubMed
181.Radhakrishnan K, Jacelon CS, Bigelow C, Roche J, Marquard J, Bowles KH. Use of a homecare electronic health record to find associations between patient characteristics and re-hospitalizations in patients with heart failure using telehealth. J Telemed Telecare. 2013;19(2):107-112. PubMed
182.Bernocchi P, Scalvini S, Tridico C, et al. Healthcare continuity from hospital to territory in Lombardy: TELEMACO project. Am J Manag Care. 2012;18(3):e101-108. PubMed
183.Domingo M, Lupon J, Gonzalez B, et al. Evaluation of a telemedicine system for heart failure patients: feasibility, acceptance rate, satisfaction and changes in patient behavior: results from the CARME (CAtalan Remote Management Evaluation) study. Eur J Cardiovasc Nurs. 2012;11(4):410-418. PubMed
184.Gund A, Lindecrantz K, Schaufelberger M, Patel H, Sjoqvist BA. Attitudes among healthcare professionals towards ICT and home follow-up in chronic heart failure care. BMC Med Inform Decis Mak. 2012;12:138. PubMed
185.Radhakrishnan K, Jacelon C, Roche J. Perceptions on the use of telehealth by homecare nurses and patients with heart failure: A mixed method study. Home Health Care Management & Practice. 2012;24(4):175-181.
186.Seto E, Leonard KJ, Cafazzo JA, Barnsley J, Masino C, Ross HJ. Mobile phone-based telemonitoring for heart failure management: a randomized controlled trial. J Med Internet Res. 2012;14(1):e31. PubMed
187.Anand IS, Greenberg BH, Fogoros RN, Libbus I, Katra RP, Music I. Design of the Multi-Sensor Monitoring in Congestive Heart Failure (MUSIC) study: prospective trial to assess the utility of continuous wireless physiologic monitoring in heart failure. J Card Fail. 2011;17(1):11-16. PubMed
188.Andersen T, Bjorn P, Kensing F, Moll J. Designing for collaborative interpretation in telemonitoring: re-introducing patients as diagnostic agents. Int J Med Inform. 2011;80(8):e112-126. PubMed
189.Ando K, Koyama J, Abe Y, et al. Feasibility evaluation of a remote monitoring system for implantable cardiac devices in Japan: A prospective analysis. Int Heart J. 2011;52(1):39-43. PubMed
190.Bowles KH, Hanlon AL, Glick HA, et al. Clinical effectiveness, access to, and satisfaction with care using a telehomecare substitution intervention: a randomized controlled trial. Int J Telemed Appl. 2011;2011:540138. PubMed
191.Driscoll A, Worrall-Carter L, Hare DL, et al. Evidence-based chronic heart-failure management programmes: Reality or myth? BMJ Quality and Safety. 2011;20(1):31-37. PubMed
192.Korzeniowska-Kubacka I, Dobraszkiewicz-Wasilewska B, Bilinska M, Rydzewska E, Piotrowicz R. Two models of early cardiac rehabilitation in male patients after myocardial infarction with preserved left ventricular function: comparison of standard out-patient versus hybrid training programmes. Kardiol Pol. 2011;69(3):220-226. PubMed
193.Nolan RP, Upshur RE, Lynn H, et al. Therapeutic benefit of preventive telehealth counseling in the Community Outreach Heart Health and Risk Reduction Trial. Am J Cardiol. 2011;107(5):690-696. PubMed
194.Triantafyllidis A, Velardo C, Shah SA, et al. Supporting heart failure patients through personalized mobile health monitoring. 2015.
195.Varon C, Alao M, Minter J, et al. Effect of telehealth on self-care behavior of heart failure patients. 2014.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matter of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.