CADTH Health Technology Review
Stereotactic Ablative Radiotherapy for the Treatment of Oligometastatic Cancer: A Clinical Review as Part of a Health Technology Assessment
This is the baseline clinical review for a living systematic review. Please see the CADTH project page to access the latest version of the report and for the version history
Clinical Review
Authors
Clinical Review
Dr. Chantelle C. Lachance, PhD, (CADTH) led the protocol development for the clinical review; screened and selected studies; extracted, critically appraised, and interpreted data; contributed to synthesis; wrote the clinical review; revised the review based on reviewers’ feedback; and provided final approval of the version of the report submitted for publication.
Dr. Khai Tran, PhD, (CADTH) assisted with protocol development for the clinical review; screened and selected studies; extracted, critically appraised, and interpreted data; contributed to synthesis; contributed to the preparation of the clinical review; and provided final approval of the version of the report submitted for publication.
Elizabeth Carson, MSc, (CADTH) contributed to protocol development for the clinical review; provided methodological oversight and support; provided critical review of the contents of the report; and provided final approval of the version of the report submitted for publication.
Dr. Joanne Kim, PhD, (CADTH) contributed to the study design during protocol development for the clinical review; provided methodological oversight and support; provided critical review of the contents of the report; and provided final approval of the version of the report submitted for publication.
Dr. David Palma, MD, MSc, PhD, FRCPC, (London Health Sciences Centre, Schulich School of Medicine & Dentistry, University of Western Ontario) provided clinical expert opinion throughout the duration of the review, helped interpret data, and reviewed draft reports.
Dr. Shaun Loewen, MD, PhD, FRCPC, (Tom Baker Cancer Centre, Cumming School of Medicine, University of Calgary) provided clinical expert opinion throughout the duration of the review, helped interpret data, and reviewed draft reports.
Patient Engagement
Tamara Rader, MLIS, (CADTH) led patient engagement activities, wrote the summary of those activities included in the report, and provided final approval to the version of the report submitted for publication.
Research Information Science
Danielle MacDougall, MLIS, (CADTH) designed and executed the literature search strategies, wrote the literature search methods section and appendix, and managed the report referencing.
Caitlyn Ford, MLIS, (CADTH) designed and executed draft literature search strategies and assisted with designing final search strategies.
Contributors
The authors are grateful to Michelle Clark, Program Officer, for her involvement in detailed scoping for this project; Diksha Kumar, for contributing to screening and selection of studies; Brit Cooper-Jones, for leading knowledge mobilization activities; Paula Murray, Project Management Officer, for project management support; David Kaunelis, Research Information Specialist – Methods, for his assistance with the literature search methodology; Dr. Matthew Bryan, Scientific Advisor, for statistical support; Dr. Laura Weeks, Director, Health Technology Assessment and Program Development, for her methodology support and project oversight; and Chris Kamel, Director, Health Technology Assessment and Rapid Response, for his feedback on the protocol for this report. Further, we would like to thank the patient volunteer who shared their insights into and experiences of oligometastatic cancer and treatment with stereotactic ablative body radiotherapy confidentially; and the stakeholders who submitted feedback on the draft report.
External Reviewer
Dr. Rathod kindly provided comments on a draft version of this report.
Dr. Shrinivas Rathod, MBBS, MD, FRCPC
CancerCare Manitoba, University of Manitoba
Winnipeg, Manitoba
Conflicts of Interest
There are no conflicts of interest to declare relevant to this report.
Abbreviations
3DCRT
3-dimensional conformal radiation therapy
ADT
androgen deprivation therapy
AE
adverse event
CI
confidence interval
CT
computerized tomography
CTCAE
Common Terminology Criteria for Adverse Events
ENRT
elective nodal radiotherapy
GRIPP2-SF
Guidance for Reporting Involvement of Patients and the Public (version 2) – Short Form
HR
hazard ratio
HTA
Health Technology Assessment
IQR
interquartile range
LC
lesional control
LSR
living systematic review
OS
overall survival
PFS
progression-free survival
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
QoL
quality of life
RCT
randomized controlled trial
RoB 2
Cochrane risk-of-bias tool for randomized trials
RoBANS
Risk of Bias Assessment Tool for Nonrandomized Studies
SABR
stereotactic ablative radiotherapy
SOC
standard of care
Section | Amendment | Rationale |
Decision problem | The decision problem was expanded beyond the elements related to the clinical review. | To reflect the scope of the entire Health Technology Assessment as described in the Scoping Brief.1 |
Research questions | The term “clinical effectiveness” replaced “clinical benefits” and the term “safety” replaced “clinical harms” in the phrasing of the 2 research questions. | To clarify the scope of information sought for each clinical research question. |
Literature search methods | For the baseline review, the WHO’s International Clinical Trials Registry Platform (ICTRP) search portal was removed from the search strategy. | The access portal was not working when the baseline review was being conducted (March to August 2020). |
Selection and eligibility criteria | The protocol stated that outcomes for question 2 are restricted to the AEs described in the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. For the baseline review and subsequent updates, all relevant studies reporting quantifiable AEs for both groups are included irrespective of the tools used. | To capture all AEs. |
The protocol stated that the progression-free survival and freedom-from-progression outcomes for question 1 included the time from randomization (or diagnosis for nonrandomized controlled trials) to any documented progression of disease at any site using RECIST. The lesional control outcome for question 1 was defined as time from randomization (or diagnosis for nonrandomized controlled trials) until radiological evidence of progression at the treated site or development of a previously unknown metastatic lesion using RECIST criteria. For the baseline review and subsequent updates, the restriction to the use of RECIST criteria for the definition of progression-free survival, freedom from progression, and lesional control outcomes is removed. | Progression-free survival and lesional control definitions varied among included studies and were not limited to RECIST criteria. No data were identified for the freedom-from-progression outcome for the baseline review; however, the protocol was amended to maintain a consistent approach for all progression-related outcomes for subsequent updates. | |
The protocol defined lesional control as time from randomization (or diagnosis for nonrandomized controlled trials) until radiological evidence of progression at the treated site or development of a previously unknown metastatic lesion. For the baseline review and subsequent updates, lesional control was redefined as the absence of progression in the lesions initially present at randomization or at diagnosis from nonrandomized controlled trials. | Based on clinical expert input that lesional control only concerns existing lesions and not new lesions. | |
The protocol stated that studies of patients with a history of widespread metastatic disease (i.e., patients with induced oligometastatic cancer) would be excluded based on clinical expert input indicating that the nature of their disease progression is clinically different than the intended oligometastatic population for this review. The protocol also stated that for studies with mixed populations (i.e., comprising both individuals who met and those who did not meet the eligibility criteria) that did not report results for the population of interest separately, those studies would be considered eligible if at least 80% of the population met the inclusion criteria. For the baseline review and subsequent updates, it was clarified that “induced metastatic cancer” included “induced oligoprogression and induced oligopersistence.” In addition, results were included only if 100% of the population met the inclusion criteria. | To clarify and ensure that the findings were relevant to the population of interest, based on further clinical expert input. | |
The protocol stated that if there were multiple publications fulfilling the inclusion criteria from the same study (i.e., same population), all publications that provided unique results (e.g., different outcomes or time points) would be included. For the baseline review and subsequent updates, all publications for each relevant study would be included, even if reporting the same results. | For comprehensiveness, as there were no pre-specified criteria to determine which citation should be included when reporting results described in multiple publications. | |
Data extraction | The protocol stated that Microsoft Excel and the SR management software DistillerSR2 would be used to facilitate data extraction. For the baseline review, only Microsoft Excel was used for data extraction. This change will also be made for the updates. | Microsoft Excel was sufficient for data extraction. |
The protocol stated that data from each included study would be extracted by 1 reviewer and checked for accuracy by a second reviewer. For the baseline review, all relevant study data were extracted independently by 2 reviewers and then compared and combined. Discrepancies were resolved through discussion until consensus was reached, involving a third reviewer and clinical experts when necessary. This change will also be made for the updates. | To further increase the methodological rigour. | |
Critical appraisal | For the baseline review and subsequent updates, an overall risk-of-bias judgment was made for each nonrandomized study assessed with RoBANS, as follows:
This was not specified in the protocol. | This was done to provide an overall risk-of-bias judgment for nonrandomized studies consistent with the planned approach to do this for RCTs. As the RoBANS guidance did not provide a specific approach for making study-level judgments, this was borrowed from the RoB 2 guidance for methodological consistency. |
For the baseline review and subsequent updates, the risk of bias was assessed for individual outcomes within individual studies (i.e., bias due to deviations from missing outcome data and measurement of the outcome in RCTs, outcome assessment, and incomplete outcome data in nonrandomized studies). This was not specified in the protocol. | To address sources of bias that may differ across outcomes within a single primary study. | |
Patient engagement | The protocol stated that a patient will be invited to reflect on their personal experiences with SABR treatment before protocol finalization and during drafting and upon completion of the final report. This was updated to specify patient involvement during drafting and completion of the baseline clinical review, and to add opportunities for involvement during clinical review updates as part of the LSR phase and upon transitioning the clinical review out of living mode. | To clarify the planned patient engagement activities for the baseline clinical review and throughout the LSR phase. |
Summary
Key Messages
Oligometastatic cancer (cancer with a limited number of metastases) represents an intermediate state between cancer confined to a single location in the body and cancer that has metastasized — or spread — widely.
One treatment option, for which there is growing interest, is stereotactic ablative radiotherapy, also known as SABR.
SABR precisely delivers a high dose of radiation to ablate tumours at specific sites while minimizing the radiation dose to surrounding normal tissues.
SABR may be used independently or alongside other treatment options in the management of oligometastatic cancer.
This CADTH clinical review evaluated the evidence regarding the clinical effectiveness and safety of SABR with or without standard of care (SOC) for people with oligometastatic cancer and found the following:
SABR in addition to SOC may offer a benefit in terms of overall survival (OS) and progression-free survival (PFS).
The findings for the effectiveness of SABR alone compared with SOC were mixed and deemed inconclusive.
There are insufficient data related to adverse events (AEs) at the present time to draw conclusions regarding the safety of SABR relative to SOC alternatives.
Note that this is the baseline report of a living systematic review (LSR) that is being updated every 3 months to ensure the findings remain up to date as new evidence emerges. Please refer to the CADTH project page for the latest version of the report and for the version history.
Abstract
Context and Decision Problem(s)
Oligometastatic cancer (cancer with a limited number of metastases) represents an intermediate state between cancer confined to a single location in the body and cancer that has metastasized — or spread — widely. Treatment options for oligometastatic cancer may include surgery, conventional radiotherapy, or systemic therapy, depending on factors such as the type, location, and ease of access of each lesion. SABR is an additional treatment option for which there is growing interest. SABR precisely delivers a high dose of radiation to ablate tumours at specific sites while minimizing the radiation dose to surrounding normal tissues. SABR may be used independently or alongside other treatment options in the management of oligometastatic cancer.
While interest in the use of SABR for oligometastatic cancer is high, there remain key questions. What is the clinical effectiveness and safety of SABR for patients with oligometastatic cancer? What would form appropriate patient selection criteria and what would be the optimal dose or regimen? What is the cost-effectiveness of SABR, and what are the key implementation considerations? The purpose of this CADTH Health Technology Assessment (HTA) was to address these questions, starting with a review of the clinical evidence, which is presented here.
Clinical Effectiveness and Safety Evidence
Because the evidence on SABR for oligometastatic cancer is rapidly evolving, CADTH is using a “living systematic review” (LSR) format for the clinical review. The status of the LSR is being updated every 3 months to ensure the findings reflect the latest up-to-date evidence on the topic.
CADTH compared SABR plus SOC with SOC alone, and compared SABR alone with SOC alone, for people with oligometastatic cancer. Outcomes identified as important by patient and clinical expert input were OS, PFS, and AEs. Additional outcomes of interest included freedom from progression, health-related quality of life (QoL), lesional control (LC), and systemic therapy use after treatment.
A total of 3 randomized controlled trials (RCTs) and 6 nonrandomized studies were identified. The findings suggested there may be OS and PFS benefits associated with SABR plus SOC compared with SOC alone. However, the findings from the studies comparing SABR alone with SOC were mixed and deemed inconclusive. With regard to AEs, there are limited available data to assess whether SABR with or without SOC is more or less harmful than SOC alone. There was a lack of literature identified to inform conclusions for other outcomes of interest.
Conclusions and Implications for Decision- or Policy-Making
The current clinical evidence suggests that SABR plus SOC may offer survival benefits for patients with oligometastatic cancer. To inform patient selection criteria, future research on the effectiveness of SABR in patients with different characteristics would clarify who might benefit most from this treatment. Evidence on the optimal regimen or dose of SABR for the treatment of oligometastases is also needed. Additional studies are expected to be identified during the LSR phase of this project. Finally, this clinical review represents 1 component among many that decision-makers will consider when making the decision about the expanded use of SABR in Canada. CADTH is currently undertaking an Environmental Scan of implementation considerations that will contribute to this HTA to further support decision-making.
Introduction
Background and Rationale
Cancer and Oligometastatic State
Cancer is the leading cause of death in Canada, comprising 30% of all death events.3 In 2020, there will be an estimated 225,800 new cancer cases and 83,300 deaths.3 Tumour metastasis is the main cause of cancer-related death.4-6 The development of metastases is a potential complication among patients with cancer.7 Metastasis occurs when cancer cells, originating from 1 part of the body, move from the place of origin (primary tumour) and spread to another location to form 1 or more tumours.4,7 The extent of systemic disease and the number, size, and location(s) of lesions can affect the overall prognosis for a patient.8
In 1995, Hellman and Weichselbaum first introduced the term oligometastatic state and proposed that the process of cancer metastasis occurs along a continuum — from localized to widespread metastatic disease.9,10 Oligometastases may represent a paradigm shift in the treatment intent for metastatic cancer: if a limited number of metastases can be treated, then the outcome may be curative.11 Hellman and Weichselbaum described 2 different clinical scenarios that would both be considered oligometastases “tumours early in the chain of progression with metastases limited in number and location;” and “patients with oligometastases who had widespread metastases that were mostly eradicated by systemic drugs, the chemotherapy having failed to destroy those remaining because of the number of tumour cells, the presence of drug-resistant cells, or the tumour foci being located in some pharmacologically privileged site.”9 Moreover, as these 2 classes of oligometastases represent different clinical scenarios, they are associated with different prognoses and may also require different treatments.12 Current definitions of oligometastatic disease in the literature are heterogeneous, although the European and American societies for radiotherapy and oncology recently published a consensus definition as 1 to 5 metastatic lesions, with control of the primary tumour being optional but where all metastatic sites must be safely treatable.13
Since the publication of this seminal paper by Hellman and Weichselbaum,9 the concept of oligometastasis has been generally accepted; however, specific criteria that define an oligometastatic state, such as the number of metastases and organ sites, are still unclear.12,14 Oligometastasis includes situations where the primary tumour is present, not present (i.e., removed), treated, or untreated; therefore, a patient can have oligometastases regardless of the state of the primary tumour.15 Moreover, patients can be described as having synchronous oligometastatic disease (maximum 6-month interval between the diagnosis of oligometastatic disease and the primary cancer diagnosis) and metachronous oligometastatic disease (more than a 6-month interval between the diagnosis of oligometastatic disease and the primary cancer diagnosis).12 Imaging is currently the most relevant diagnostic method for defining oligometastatic cancer, which is broadly understood as a limited number of metastatic lesions.12,16
Stereotactic Ablative Radiotherapy
Treatment options for patients presenting with oligometastatic cancer may include, but are not limited to, surgery, conventional radiotherapy, systemic therapy (e.g., chemotherapy, hormone therapy), observation, and ablative therapies such as cryoablation, microwave ablation, radiofrequency ablation, and SABR.11,17-19 SOC is variable according to the type of cancer. The notion of using targeted therapies such as surgery or radiation therapy to eliminate oligometastatic disease has been termed metastasis-directed therapy or local consolidative therapy.9,20,21 Metastasis-directed therapy has been shown to improve survival relative to SOC (observation or maintenance systemic therapy) in RCTs of patients with oligometastatic prostate cancer22 and non–small cell lung cancer.21 In those studies, the choice of surgery or radiation therapy, particularly SABR, was determined by the multidisciplinary team and patient characteristics. Though there are multiple treatment options within the class of metastasis-directed therapies, and surgical resection is considered the gold standard for the treatment of certain oligometastases (e.g., partial liver resection for metastases from colorectal cancer), SABR may be an alternative non-invasive treatment option for achieving LC.17
SABR, also known as stereotactic body radiation therapy (SBRT), is a method of precisely delivering high doses of radiation to ablate tumours at specific sites while sparing radiation dose to surrounding normal tissue.23-25 First developed in Sweden in the early 1990s,26 SABR builds on the treatment delivery paradigm used to treat brain tumours with intracranial stereotactic radiosurgery, but it targets tumours outside of the brain (e.g., lungs, liver, bone, and lymph nodes).23 SABR relies on an imaging component to map the treatment area using CT (CT) scans or MRI (MRI), tumour motion reduction, and reproducible patient set-up strategies (e.g., respiratory compression, body immobilization devices [e.g., alpha-cradle or vacuum-lock system]), and advanced radiotherapy-delivery techniques using conventional linear accelerators or novel precision delivery systems.23 Newer technology with the potential for application in this area includes C-arm S-band linear accelerator systems, robotic X-band CyberKnife, image-guided Gamma Knife Icon system, proton-based applications, and MR Linac.27,28 SABR is considered an alternative to surgical resection and is often the preferred option for patients with cancer that is medically inoperable. Treatment advantages include limited recovery time before resuming systemic therapy and the ability to treat areas with metastatic involvement that are either not surgically accessible or include more than 1 organ, or patients at high risk of post-operative complications.12
SABR in Canada
The availability of SABR has increased across Canada. In 2014, a survey of 41 Canadian radiotherapy centres reported that 5 provinces (British Columbia, Alberta, Manitoba, Ontario, Quebec) had centres with SABR capacity and substantial growth was expected.29 Currently, all provinces in Canada have SABR capability.30 SABR is also available in some northern centres (e.g., Northeast Cancer Centre in Ontario).31 Canadian centres are using SABR to treat primary tumours and oligometastases in different areas of the body, such as the lungs, liver, bone, and lymph nodes.29,32 However, there is variation in patient selection criteria for SABR treatment across radiotherapy centres, and not all centres offer SABR for the treatment of oligometastases.29
CADTH received input from Canadian jurisdictions that identified several common considerations regarding the use and implementation of SABR for oligometastatic cancer. There is a desire to determine the appropriate use of SABR across Canada regarding which patients should be treated with SABR to achieve the greatest benefit (e.g., location and number of metastases) and how those patients should be managed (e.g., radiation dose fractionation, treatment sites, immobilization methods, tumour-tracking methods, and image guidance strategies). Decision-makers are also seeking more information regarding the long-term outcomes of treatment with SABR. In addition to patient treatment and management, jurisdictions expressed interest in gathering information regarding the implementation of the technology, including how other jurisdictions have successfully operationalized the use of technology for oligometastatic cancer (e.g., billing codes, time to treatment, length of individual treatment sessions, staffing), and in a review of resource and infrastructure considerations (e.g., requirements for additional staff training, software, or equipment upgrades). An understanding of patients’ and clinicians’ perspectives (e.g., acceptability, feasibility) and ethical considerations (e.g., a shifting risk-benefit profile compared with standard care) will also become salient if expanded use of SABR is pursued. Equity issues relating to accessing SABR as a result of the specialized nature of therapy and its delivery in urban centres may also emerge. All of the jurisdictions that responded expressed an interest in an economic analysis of the expanded use of this technology.
Moreover, the use of SABR for the ablation of oligometastases is an active area of research. Specifically, a 2019 paper identified 64 ongoing studies examining SABR for oligometastatic cancer.33 In the summer of 2016, the National Health Service (UK) produced a policy document stating that it would not routinely commission SABR for oligometastatic cancer, given there was inconclusive evidence to support the provision of treatment.34 However, recently identified evidence has suggested the potential for improved health outcomes, such as OS and PFS, with the use of SABR for oligometastases.35 A CADTH HTA is warranted for critically reviewing the current evidence of SABR in the treatment of patients with oligometastatic cancer.
Decision Problem
Based on the context, jurisdictional feedback, and results of a detailed scoping exercise, the aim of a CADTH HTA on this topic was to inform the following decision problem:
Should the use of SABR be expanded to include the treatment of patients with oligometastatic cancer?
If so, what are the appropriate patient selection criteria?
If so, what is the optimal regimen or dose?
What is the value for money and affordability of SABR for oligometastatic cancers?
What are the main challenges to and enablers of the implementation of SABR in Canada?
Objective
The clinical evidence regarding SABR is still developing; therefore, a staged approach to this HTA was followed, as proposed in the Scoping Brief.1 CADTH first conducted a clinical review using systematic review methods to synthesize and critically appraise the current evidence of SABR for the treatment of patients with oligometastatic cancer. An Environmental Scan is also being conducted to explore considerations for the implementation of SABR for this purpose.
The scoping review did not identify any qualitative literature on the topics of oligometastatic cancer or SABR. Given the paucity of published evidence, engaging directly with patients who have experience with SABR is a more relevant method for capturing patients’ experiences with this health technology.
Similarly, the scoping review did not identify any literature reporting ethical considerations related to the use of SABR for the treatment of oligometastatic cancer. Ethical considerations were acknowledged and discussed among the broader review team, such as the potential to exacerbate existing equity considerations regarding access to cancer treatments, and the aforementioned challenges in defining an oligometastatic state. However, in consultation with ethics experts and in the absence of published literature, it was determined that a full ethical analysis would not be warranted.
As previously noted, jurisdictions have expressed an interest in an economic analysis of the expanded use of SABR for oligometastatic cancer. At the time of the protocol development in 2020, CADTH was aware of several Canadian groups conducting analyses addressing the economic considerations regarding the use of SABR for the treatment of oligometastatic cancer. To avoid duplication of effort, CADTH will monitor ongoing Canadian economic analyses and attempt to broker existing work to meet the economic evidence needs of stakeholders.
The objective of this report is to address the decision problem by assessing the clinical effectiveness and safety of SABR in the treatment of patients with oligometastatic cancer through a systematic review of the literature. As the clinical evidence regarding SABR is still developing and there are several ongoing clinical trials, CADTH will use an LSR approach to regularly update the review. The deliverable for this report is the baseline review of an LSR of the clinical evidence. The results of the Environmental Scan will be incorporated in the report upon subsequent updates to this review. An analytical framework (Figure 1) guiding the clinical review can be found in Appendix 1.
Research Questions
This clinical review addressed the following research questions:
What is the clinical effectiveness of SABR alone or in combination with other therapies for the treatment of patients, of any age, with oligometastatic cancer?
What is the safety of SABR alone or in combination with other therapies for the treatment of patients, of any age, with oligometastatic cancer?
Opportunities for Stakeholder Feedback
Stakeholders (i.e., clinicians, policy-makers, researchers, health associations) have been given the opportunity to provide feedback on the draft of the list of included studies and a draft report of the baseline clinical review. No unpublished data were identified as part of the feedback process. Additionally, CADTH will periodically (e.g., annually) seek input from decision-makers in Canadian jurisdictions to determine whether there is continued interest in this topic to inform whether to maintain or transition the review out of living mode.
Methods
The conduct of the clinical review was informed by a CADTH Rapid Response report,36 an informal scoping review of the existing literature (Scoping Brief),1 discussion with clinical experts, and patient engagement. A protocol37 was written a priori, using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Protocols (PRISMA-P)38 for guidance on clarity, transparency, and completeness, and the protocol was followed throughout the study process. Any deviations from the prospectively registered protocol were disclosed in the final report (Table 1: Protocol Amendments) and updates were made to the PROSPERO submission accordingly (registration number: CRD42020167767).
Study Design
This clinical review was designed as an LSR to answer research questions 1 and 2, enabling continual surveillance and updates to the analysis contingent on following a priori stopping rules (see Project Protocol37 for more details). The LSR model will allow for ongoing assessment of the clinical effectiveness and safety of SABR, and the incorporation of the results from several ongoing clinical trials identified during the scoping process with expected completion dates ranging from the year 2020 through 2029 as well as the results of any other relevant trials or studies that may be currently under way.
This review aims to comprehensively explore the clinical effectiveness and safety of SABR for oligometastatic cancer for different primary tumours and any metastatic sites amenable to SABR, as outlined in research questions 1 and 2. Specifically, CADTH decided to conduct an LSR in consideration of the methods outlined in the Cochrane Handbook for Systematic Reviews of Interventions.39
This report presents the baseline review for the LSR, which is in keeping with the same core methods and review steps as a standard systematic review. Thus, standard systematic review methods (e.g., screening, data extraction, risk-of-bias assessment) were followed. The clinical review is now considered in living mode with the publication of this baseline review. Details on the updating and ending of the LSR can be found in the protocol.37
Literature Search Methods
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist (www.cadth.ca/resources/finding-evidence/press).40 The complete search strategy is presented in Appendix 2.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) through Ovid, Embase (1974‒) through Ovid, and the Cochrane Central Register of Controlled Trials (CENTRAL) through Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were SABR and oligometastatic cancer. The following clinical trial registries were searched: the US National Institutes of Health’s clinicaltrials.gov, the Health Canada Clinical Trials Database, and the Canadian Cancer Trials Database.
No filters were applied to limit the retrieval by study type. Retrieval was limited to publications published between January 1, 1990 and March 20, 2020. Conference abstracts were excluded from the search results, though they were reviewed by clinical team members for forecasting purposes.
The initial search was completed on March 20, 2020. Monthly alerts were conducted until the end of the stakeholder feedback period for the baseline review (January 18, 2021). Since then, alerts are run every 3 months to support the LSR phase of the HTA. The clinical trial registries search was updated before the completion of the stakeholder feedback period for the baseline review. Following the completion of the baseline report, the clinical trial registries search will be updated every 6 months.
Grey literature (literature that is not commercially published) was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist (www.cadth.ca/grey-matters),41 which includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, systematic review repositories, patient-related groups, and professional associations. Google was used to search for additional internet-based materials. These searches were supplemented through contacts with experts, as appropriate. The grey literature search was updated before the completion of the stakeholder feedback period. Grey literature will be updated every 6 months during the LSR phase of the HTA. See Appendix 2 for more information on the grey literature search strategy.
Selection and Eligibility Criteria
Studies were included if they met the eligibility criteria, including the specific population, intervention, comparators, and outcomes (PICO), presented in Table 2. The inclusion criteria were informed by the CADTH Rapid Response report,36 the informal scoping review of the existing literature,1 patient engagement, and consultation with clinical experts.
Table 2: Selection Criteria for Clinical Review
Criteria | Description |
Population | Patients with oligometastatic cancer (i.e., limited metastatic lesions). No restrictions on age, sex, gender, ethnicity, comorbidities, location of primary cancer site, or length of time since diagnosed. Exclusions:
|
Interventions | Intervention(s) SABR of any dose or fractionation alone or in combination with 1 or more concurrent or neoadjuvant therapies, for example:
|
Comparators | Comparator(s) Standard of care (variable according to cancer type). For example: • surgery • conventional radiotherapy • chemotherapy • immunotherapy • hormone therapy • other ablative treatments, such as cryoablation and radiofrequency ablation • targeted therapy (e.g., targeting specific mutations, proteins) • no treatment |
Outcomes | Question 1 (clinical effectiveness):
Question 2 (safety):
|
Study Design(s) | Comparative study designs:
Exclusions:
|
Study Setting | Any setting |
Time Frame | 1990 to presenti |
Language | Studies published in English |
AE = adverse event; LC = lesional control; OS = overall survival; PFS = progression-free survival; SABR = stereotactic ablative radiotherapy.
aThese outcomes were identified as being of importance to a patient, based on the input received during an interview conducted by CADTH.
bOS: Time from randomization (or diagnosis for nonrandomized controlled trials) to death from any cause. OS is appropriate for this review, as it is generally based on objective and quantitative assessment.
cPFS: Time from randomization (or diagnosis for nonrandomized controlled trials) to any documented progression of disease at any site, appearance of new metastases, or death from any cause, whichever occurs first (follow-up: any length of time).
dFreedom from progression: Time from randomization (or diagnosis for nonrandomized controlled trials) to any documented progression of disease at any site or appearance of new metastases, whichever occurs first (follow-up: any length of time).
eHealth-related quality of life. All instruments measuring quality of life were considered; possible questionnaires included: Functional Assessment of Cancer Therapy–General (FACT-G), European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), MD Anderson Symptom Inventory for Lung Cancer (MDASI-LC).
fLC: The absence of progression in the lesions initially present at randomization (or at diagnosis for nonrandomized controlled trials).
gNonrandomized controlled trials are defined as a clinical trial in which the participants are not assigned by chance to different treatment groups. Participants may choose which group they want to be in, or they may be assigned to the groups by the researchers.42
hCohort studies are defined as studies in which participants are sampled based on exposure and in which outcomes are assessed in a follow-up. This is distinct from case series studies, in which participants are sampled based on the presence of an outcome, or of both an exposure and outcome, where absolute or relative risk cannot be calculated.43 Only study designs providing comparative evidence are eligible for inclusion.
iSABR was first developed in the early 1990s in Sweden,26 and the term oligometastatic state was first introduced by Hellman and Weichselbaum in 1995.9 Given this, only studies published after the year 1990 were included, which should include a complete list of relevant studies.
For this clinical review, the population of interest was patients with oligometastatic cancer, described by study authors as having limited metastatic lesions using terminology such as “oligo,” “limited,” or “few.” Studies that did not state clearly that the patient population was restricted to or included oligometastatic patients were excluded. Oligometastasis includes situations where the primary tumour is present, not present (i.e., removed), treated, or untreated.15 Since a participant can have oligometastases regardless of the state of the primary tumour, the status of the primary tumour was not part of the eligibility criteria.15 Moreover, this review included patients with an imaging-based diagnosis of a limited number of metastases identified at presentation or before initial therapy, or a limited number of metastases identified after initial therapy of the primary tumour, or a metastatic relapse of a limited number of metastases where initial metastatic sites are controlled or resolved, or a known metastatic site that responded to previous treatment (local treatment or systemic treatment or both) that showed interval growth (or regrowth) with or without a systemic-free interval.12,44-47 Studies of patients with a history of widespread metastatic disease (i.e., patients with induced oligometastatic cancer, including induced oligoprogression and induced oligopersistence) were excluded based on clinical expert input indicating that the nature of their disease progression is clinically different than the intended oligometastatic population for this review.12 Studies that included patients with a history of metastases but did not report enough detail to determine whether this represents a history of oligometastasis (i.e., limited or few metastases) versus a history of widespread metastatic disease were also excluded. Studies with mixed populations (i.e., comprising both individuals who met and those who did not meet the eligibility criteria) were considered eligible for inclusion if the results pertaining to the population of interest were reported separately.
The intervention of interest was SABR (synonym: SBRT), with or without 1 or more concurrent or neoadjuvant therapies. Stereotactic radiosurgery for brain-only metastases was excluded, as ablative therapy to the central nervous system is more clinically established and not the focal area of interest for this HTA.48 Studies of metastasis-directed therapy that did not report results specific to SABR were also excluded. For instances where the intervention was SABR in combination with 1 or more concurrent or neoadjuvant therapies, the study was eligible for inclusion if the comparator also included the same concurrent or neoadjuvant therapies to explore the true effects of SABR.
For the clinical effectiveness outcomes for research question 1, the data at all time points as reported in the included studies were included, but different time points were not combined. In cases where studies used more than 1 tool to assess health-related QoL, all data were included. The “systemic therapy use” outcomes were meant to explore whether there was a difference in the need for systemic therapy subsequent to treatment with SABR (e.g., in terms of the number of cycles or total duration of systemic therapy) compared with the use of systemic therapy in patients who do not receive SABR.
For the safety outcomes for research question 2, data that allowed for comparisons between the intervention and comparator groups were of interest and included, irrespective of the tools used to measure or describe the AEs (e.g., frequencies or prevalence of individual or grades of AEs [e.g., grades 1 to 2 versus grades 3 to 5] reported for each group were in scope, but non-quantifiable lists of AEs for both groups were not in scope).
If there were multiple publications fulfilling the inclusion criteria from the same study (i.e., same population), all publications were included; in those cases, data from multiple publications were extracted and discussed as 1 single study.
Study Selection
Study selection was conducted using the systematic review management software DistillerSR (Evidence Partners, Ottawa, Canada). Two reviewers independently screened titles and abstracts of all retrieved citations (i.e., literature searches of academic databases, clinical trial registries, grey literature searches, citations identified by clinical content experts, and stakeholder feedback) against the eligibility criteria (Table 2). Exclusion by both reviewers was required for a record to be excluded at the title and abstract level. Articles that were judged to be potentially relevant by at least 1 reviewer from their title or abstract were retrieved for full-text screening. The same 2 reviewers independently examined all full-text articles against the eligibility criteria and compared their included and excluded studies from the full-text review. Consensus was required for inclusion in the review. Discrepancies were resolved by discussion between the 2 reviewers, through the involvement of a third reviewer, or by consultation with a clinical expert as needed.
Studies identified via monthly database search alerts and semi-annual clinical trial registry and grey literature search alerts meeting the selection criteria of the review were incorporated into the analysis if they were identified before the end of the stakeholder feedback period for this baseline review. Since the stakeholder feedback period, database search alerts have been scheduled every 3 months, and clinical registry and grey literature search alerts will continue on a semi-annual basis, as part of the LSR protocol. Any studies identified after the stakeholder feedback period will be retained to be screened along with the next set of results from database search alerts (conducted every 3 months as part of the LSR process).
Lists of included studies and excluded studies were generated. The study selection process was documented in a PRISMA49 flow chart (Appendix 3).
Data Extraction
Reviewers used Microsoft Excel to document and tabulate all relevant information from the included studies. Using the data-extraction spreadsheet, 2 reviewers extracted data independently and then compared and combined their data. Discrepancies were resolved through discussion until consensus was reached; when necessary, a third reviewer or clinical experts were also involved.
The following relevant information was extracted, where available:
Study level: Description of publication (e.g., first author’s last name, title, publication year, journal), study characteristics (e.g., clinical trial registry identification number, trial acronym, objectives, study design, year of the conducted study, sample size, study setting, country of the conducted study, study funding source).
Patient level: Number of patients, age (mean, standard deviation), proportion of women or female patients (as reported by study authors), clinical situation of the diagnosis (e.g., limited metastases at presentation or before initial therapy, after therapy, relapse), number of metastases (mean, standard deviation), location of primary tumour site, status of primary tumour (e.g., treated versus untreated), previous treatment (e.g., for the primary tumour or for metastases), location(s) of metastases, number of metastases per metastatic site
Intervention level: type (SABR, co-intervention), dose, total duration of treatment, frequency of treatment (e.g., single dose, multiple fractions or treatment), equipment type (brand)
Comparator level: type (e.g., surgery, conventional radiotherapy, chemotherapy, immunotherapy, hormone therapy, other ablative treatment [cryoablation, radiofrequency ablation, and so forth], targeted therapy [e.g., targeting specific mutations, proteins], no treatment), dose, total duration of treatment, frequency of treatment (i.e., number of cycles), and equipment type (brand)
Outcome level: Description of outcomes (e.g., subgroup definition, measurement method, unit of measurement, length of follow-up), results, and conclusions of outcomes and subgroups of interest
Data were extracted for all relevant outcomes for this study at any duration of follow-up. Measures of treatment effects (e.g., risk ratios, odds ratios, or risk differences for dichotomous outcomes, mean differences or standardized mean differences for continuous outcomes, and hazard ratios [HRs] for survival outcomes), and any results of statistical tests reported on those measures were extracted. Data from figures were extracted if explicit numerical data were reported. No attempts were made to contact study authors, as no relevant data were deemed conflicting or missing and needed for meta-analyses, which were the 2 conditions pre-specified in the protocol for contacting the corresponding authors.37
As mentioned, if a study was reported in multiple publications and each publication provided unique results, data from these publications were extracted and discussed as 1 single study.
Critical Appraisal
The risk of bias of the primary studies was systematically evaluated using the methods described in version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2)50 and the Risk of Bias Assessment Tool for Nonrandomized Studies (RoBANS),51,52 including cohort studies.
The RoB 2 tool50 allowed for the assessment of 5 sources of bias or “domains”: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Each question within each domain was answered with a yes, probably yes, probably no, no, or no information. Afterwards, a judgment of “low risk of bias,” “high risk of bias,” or “some concerns” was assigned for each domain, with rationale for each decision included in the comments box field.50 An overall risk-of-bias judgment for each study was provided as “high risk of bias” if the study had at least 1 domain that was at “high risk of bias;” “some concerns” if the study had at least 1 domain that indicated “some concerns” but no domain that was at “high risk of bias;” or “low risk of bias” where the study had “low risk of bias” for all domains, as per the RoB guidance.50
The RoBANS tool51,52 allowed for the assessment of the risk of 5 types of bias across 8 domains: the possibility of the target group comparisons, target group selection, confounder, exposure measurement, blinding of assessors, outcome assessment, incomplete outcome data, and selective outcome reporting. For each item, a risk-of-bias judgment of “low,” “high,” or “unclear” was assigned with rationale for each decision included in the comments box field.51 An overall risk-of-bias judgment for each study was provided as “high risk of bias,” where the study had at least 1 domain that was at “high risk of bias;” “some concerns,” where the study had at least 1 domain that was “unclear” but no domain that was at “at high risk of bias;” or “low risk of bias,” where the study had “low risk of bias” for all domains. As the RoBANS guidance did not provide a specific approach for making study-level judgments, this was borrowed from the RoB 2 guidance for methodological consistency.
For sources of bias that may differ across outcomes within a single primary study (i.e., bias due to deviations from missing outcome data and measurement of the outcome in RCTs; outcome assessment and incomplete outcome data in nonrandomized studies), the risk of bias was assessed for individual outcomes within individual studies.
The risk-of-bias assessments of the included studies was performed by 1 reviewer and verified by a second reviewer. All disagreements were resolved through discussion between the 2 reviewers. The tools were used as a guide to evaluate the risk of bias in the included studies; additional insight beyond the items on the instruments has also been provided, when applicable. Summary scores were not calculated; rather, the strengths and limitations of each included study and how they affect the study findings were described narratively. Results of the risk-of-bias assessment were not used to exclude studies from this review.
Data Analysis and Synthesis
Narrative Synthesis
Narrative syntheses were performed. The narrative syntheses included presentation of study characteristics (e.g., the total number of studies included, study designs, publication years, countries in which the studies were conducted, and PICO elements, including dose) and findings within the main text and summary tables. All data analyses and narrative syntheses for this review were conducted separately for each outcome. Under each outcome, all intervention-comparator comparisons were grouped under 1 of 2 different categories — SABR plus SOC versus SOC alone and SABR alone versus SOC alone — which allowed us to summarize the effects of SABR alone or in combination with 1 or more concurrent therapies separately.
For assessing safety outcomes (research question 2), AEs were reported as described in each respective publication. In some studies, the number of patients experiencing an AE or complication was reported, whereas in other studies, the number of unique AEs or complications (i.e., events) was reported; in both cases, some individuals may have experienced more than 1 AE or complication.
The direction and size of any observed effects and any results of statistical tests that reported on those effects were summarized across studies, including an assessment of the likelihood of clinical benefit (i.e., research question 1, clinical effectiveness) or harm (i.e., research question 2, safety). If relevant statistical comparisons were not conducted in the primary studies, this was explicitly stated; the direction of findings was summarized subjectively where possible in the text (e.g., whether the outcome variable changed numerically over time or was numerically different between groups) and overall findings were described as “uncertain” or “unclear.”
The following subgroups were of interest for both narrative and quantitative syntheses for research question 1:
age
sex or gender
location of primary tumour site
number of metastases sites (e.g., number of metastatic locations; single [e.g., lung only] versus multiple sites [e.g., lung, kidney, adrenal])
number of metastases (e.g., total, regardless of metastatic location; 5 or fewer versus 3 or fewer metastases)
location of metastases (e.g., metastatic site specific [e.g., prostate only, lung only])
previous treatment of primary tumour (i.e., yes, no)
previous treatment of metastases (i.e., yes, no)
Any relevant data on these subgroups of interest were extracted and analyzed.
A narrative summary of the results of the critical appraisal for each included study was provided. Specifically, tables were developed to present the answers to the questions within the critical appraisal tools, along with a narrative description of the strengths and limitations of the included studies within the main text of the report to provide the reader with an overview of the quality of the literature.
Meta-Analysis
The possibility of conducting meta-analyses was considered for OS, PFS, and AE outcomes (i.e., the outcomes identified as most important by the interviewed patient and clinical experts consulted) and all subgroups of interest. Specifically, clinical, methodological, and statistical characteristics of the included studies were explored, in consultation with clinical and statistical experts, to determine if the data were sufficiently homogeneous for pooling. Meta-analyses were deemed inappropriate and not conducted, and the reasons for these decisions were documented.
Reporting of Findings
The systematic review was prepared in consideration of relevant reporting guidelines (i.e., PRISMA statement,53 Synthesis Without Meta-analysis [SWiM] guideline,54 and Guidance for Reporting Involvement of Patients and the Public – Short Form [GRIPP2-SF] reporting checklist55), and meets the criteria outlined in A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2) checklist.56
Patient Engagement
CADTH involves patients, patient families, and patient groups to improve the quality and relevance of our assessments, ensuring that those affected by the assessments have an opportunity to contribute to them. CADTH has adopted the CADTH Framework for Patient Engagement in Health Technology Assessment.57 The framework includes Standards for Patient Involvement in Individual Health Technology Assessments and is used to support and guide our activities involving patients. CADTH engaged 1 adult cancer patient who has lived experience with SABR treatment for their oligometastatic cancer.
Invitation to Participate and Consent
A person with SABR experience was identified through CADTH’s informal network of radiation oncologists. A CADTH patient engagement officer contacted potential participants by phone to explore their interest in becoming involved. The preliminary request described CADTH and the purpose and scope of this review, the purpose of the engagement, and the nature of the engagement activities. The patient engagement officer obtained this person’s informed consent.
Engagement Activities
The objective of patient engagement is to inform the research team about the experience of SABR and to raise considerations and perspectives that are not available in clinical trials. The purpose is not to analyze the views and comments of the patient; rather, the patient’s perspectives are used to help interpret the clinical evidence. A patient was and will be invited to reflect on their personal experiences at several time points during assessment, including:
before clinical protocol finalization
during drafting of the initial baseline clinical review
upon completion of the baseline clinical review
during the clinical review update(s) as part of the LSR phase
upon transitioning the clinical review out of living mode.
The patient perspectives gained through engagement helped ensure the relevance of outcomes of interest for the clinical assessment and added comments on other key concepts that were initially identified through prior scoping activities. The involvement of patients prompted the research team to consider the possible need to explore avenues of analysis that may have otherwise been missed or underdeveloped. The involvement of patients enabled the research team to consider the evidence alongside an understanding of the wider experiences of patients and caregivers.
Once preliminary findings of the initial baseline review were available, the participant was invited to be interviewed. The conversation explored the patient’s perceptions of key findings, including whether the findings were understandable, and whether they reflect personal experiences or understandings. Final conversations will be held with the participant upon completion of the final baseline clinical review. CADTH will share the key results of the full assessment and describe how engagement activities were used. A similar process for patient engagement will be followed during any updating of the clinical review during the LSR phase and when the clinical review transitions out of living mode.
Reporting
The reporting of this section follows the GRIPP2-SF reporting checklist.55
Results
Quantity of Research Available
A total of 2,859 citations were identified in the literature search. Following screening of titles and abstracts, 2,726 citations were excluded and 133 were retrieved for full-text review. An additional 10 potentially relevant reports were retrieved from other sources (i.e., search alerts). Of these 143 potentially relevant articles, 131 publications were excluded for various reasons, and 9 unique studies (3 RCTs and 6 nonrandomized studies) in 12 publications met the inclusion criteria and were included in this review. One RCT (i.e., SABR-COMET) had 3 publications,32,58,59 and 1 nonrandomized study had 2 publications.60,61 No unique studies that met the inclusion criteria were submitted by stakeholders. Nine studies in 12 publications were relevant to research question 1,32,58-68 and 6 studies in 8 publications were relevant to research question 2.32,58,62,63,66-68 The study selection process (Figure 2) is outlined in Appendix 3 using a PRISMA flow chart. Lists of included and excluded citations, with details describing the rationale for those excluded, are presented in Appendix 4 and Appendix 5, respectively. CADTH acknowledges that there are randomized trials of metastasis-directed therapy for oligometastatic cancer that are not limited to SABR. However, given the focus of this HTA on SABR specifically, studies of metastasis-directed therapy that did not report results specific to SABR were excluded and can be found in Appendix 5.
Heterogeneity and Decisions Regarding Meta-Analysis
The included studies were generally considered to be too heterogeneous in terms of clinical, methodological, or statistical characteristics to be pooled in meta-analyses for OS, PFS, and AE outcomes and for the subgroups of interest. In 1 instance, a meta-analysis might have been appropriate for 2 studies but was deemed unlikely to add any statistical value to the narrative synthesis, as the point estimates from those studies matched closely in their direction, magnitude, and statistical significance. Thus, findings for all outcomes were synthesized narratively for this baseline review. The complete list of relevant studies for each comparison and the detailed rationale for not conducting meta-analyses is found in Appendix 6. In brief, sources of heterogeneity included differences across the studies in:
different study designs (i.e., RCTs and nonrandomized studies needing to be analyzed separately, leading to a small numbers of studies)
data unavailability (e.g., 2 relevant studies for the comparison of interest, but HRs reported for only 1 study)
data variability (e.g., the AEs that were reported included different AE grades, treatment versus non–treatment-related AEs, or event data versus patient data)
discordant results (i.e., large variability in the direction, magnitude, and statistical significance of the results).
Study Characteristics
Additional details regarding the characteristics of included studies are provided in Appendix 7.
Study Design, Year of Publication, Sample Size, and Funding
Question 1: Clinical Effectiveness
Three RCTs (in 5 publications32,58,59,62,63) and 6 nonrandomized studies (1 prospective cohort study64 and 5 retrospective cohort studies in 6 publications60,61,65-68) were identified regarding the clinical effectiveness of SABR (with or without SOC) versus SOC comparators. These studies were published between 2013 and 2020. Figure 3 identifies the number of publications by study year.
The sample size of the included studies ranged from 26 to 506 patients (RCTs: 29 to 99 patients; nonrandomized studies: 26 to 506 patients). Of the included studies, 3 received public funding,32,58,59,63,66 1 disclosed that no financial support was provided to undertake the research,67 and 5 studies did not report the source of funding.60,61,64,65,68,69 No studies reported being sponsored by industry.
Question 2: Safety
Three RCTs (in 4 publications32,58,63,69) and 3 nonrandomized studies (all retrospective cohort studies66-68) were identified regarding the safety of SABR (with or without SOC) versus SOC comparators. These studies were published between 2016 and 2020 (Figure 3).
The sample size of the included studies ranged from 26 to 506 patients (RCTs: 29 to 99 patients; nonrandomized studies: 26 to 506 patients). Of the included studies, 3 received public funding,32,58,63,66 1 disclosed that no financial support was provided to undertake the research,67 and 2 did not report the source of funding.68,69
Country of Origin
Question 1: Clinical Effectiveness
Two RCTs were conducted in the US63,69 and 1 RCT (in 3 publications)32,58,59 was conducted at multiple institutions across Canada, the Netherlands, UK, and Australia. The nonrandomized studies were conducted in Turkey,65 the Netherlands,60,61,64 Italy,68 and China.67 One additional nonrandomized study66 was conducted across multiple institutions across Belgium, Italy, France, Switzerland, UK, and Spain.
Question 2: Safety
Two RCTs were conducted in the US63,69 and 1 RCT (in 2 publications)32,58 was conducted across multiple institutions across Canada, the Netherlands, UK, and Australia. The nonrandomized studies were conducted in China67 and Italy.68 One additional nonrandomized study66 was conducted across multiple institutions across Belgium, Italy, France, Switzerland, the UK, and Spain.
Patient Population
Question 1: Clinical Effectiveness
The median patient age ranged from 6366 to 7167 years, and males were more represented overall, given the prevalence of patients with primary prostate cancer in the included studies.
Consistent with our inclusion criteria, all studies included patients with oligometastatic cancer, as described by study authors as having limited metastatic lesions using terminology such as “oligo,” “limited,” or “few.”32,58-68 The location of the primary tumour and metastatic sites varied widely across studies and, in some cases, within a study (i.e., in a single study, the included population may have included patients with different primary tumour locations or metastatic sites).
Type of primary tumour included breast,32,58,64 lung,32,58-61,64,69,70 kidney,60,61,64 colorectal,32,58-61,67,68 prostate,32,58,59,63-66,70 sarcoma,60,61 and other (non-specified).32,58-61,64 Most studies included patients who had some previous treatment of the primary tumour (3 RCTs,32,58,59,62,63 6 nonrandomized studies60,61,64-68).
All studies allowed for up to 5 metastatic lesions per patient with the exception of 2 studies,63,67 which included patients with up to 3 metastatic lesions. Locations of the metastases included bone,32,58,59,63-65,69 lymph nodes,32,58,59,65-67,69 soft tissue,63,64 brain,32,58,59 nasopharynx,69 adrenal,32,58,59,69 lung,32,58-61,68,69 liver,32,58,59,64,69 and other.64 Of note, in the RCT (SABR-COMET) that included patients with brain metastases (n = 1 metastatic lesion in the SABR intervention group; n = 3 metastatic lesions in the control group), all of those patients also had metastases in locations other than the brain.32,58,59
Three nonrandomized studies60,61,67,68 included patients with metastasis to a single location in either the lung60,61,68 or liver.67 Six studies (3 RCTs,32,58,63,69 3 nonrandomized studies64-66) included patients with metastasis to multiple locations, 5 studies32,58,63-65,69 included patients with metastases in the bone and other sites, and 1 study66 had patients with metastases in the lymph nodes of the pelvic and extra-pelvic areas.
Seven studies included at least some patients who had received previous treatment for metastases32,58-61,64,66-69; the remaining 2 studies were unclear in their reporting of any history of treatment for oligometastases.63,65
Question 2: Safety
The median patient age ranged from approximately 6366 to 7167 years, and males were more represented overall, given the prevalence of patients with primary prostate cancer in the included studies.
All studies included patients with oligometastatic cancer.32,58,63,66-69 The location of the primary tumour and metastatic sites varied widely across studies and, in some cases, within a study. Types of primary tumour included breast,32,58 lung,32,58,69 colorectal,32,58,67,68 prostate,32,58,63,66 and other (non-specified).32,58 Three RCTs32,58,63,69 and 3 nonrandomized studies66-68 included patients who all had any previous treatment of the primary tumour. Two studies included patients with metastasis to a single location (i.e., lung metastases67,68); 3 studies included patients with metastasis in the bone and other sites, including lung, liver, brain, adrenal, mediastinum, axilla and nasopharynx32,58,63,69; and 1 study had patients with metastasis in the lymph nodes of pelvic and extra-pelvic areas.66 As noted previously, 4 patients in 1 RCT (SABR-COMET)32,58,59 with brain metastases (1 in the SABR group and 3 in the control group) also had metastases in locations other than the brain. Five studies included at least some patients who had previous treatment of metastases,32,58,66-69 and 2 studies were unclear in their reporting of any history of treatment for oligometastases.63,67
Interventions and Comparators
Question 1: Clinical Effectiveness
The intervention of interest was SABR of any dose or fractionation alone or in combination with 1 or more concurrent or neoadjuvant therapies (i.e., SABR alone or in combination with SOC). In the included studies, 5 examined SABR alone,60,61,63,64,67,68 2 examined SABR with systemic therapy,32,58,59,69 and 2 examined SABR with or without systemic therapy (i.e., hormonotherapy, androgen deprivation therapy [ADT]) at the discretion of the physician.65,66 The dose used when administering SABR was study-dependent and varied based on the protocol used in consideration of the location(s) of the targeted metastatic site(s), and the frequency and number of fractions per lesion per patient (see Appendix 7).
SABR was compared with SOC. The SOC comparators in the included studies comprised no therapy (i.e., observation),63 surgery,60,61,68 systemic therapy (i.e., maintenance chemotherapy),69 conventional radiotherapy (i.e., 3-dimensional conformal radiation therapy [3DCRT]),64,67 conventional radiotherapy (i.e., conventional fractionation radiotherapy or elective nodal radiotherapy [ENRT]) with or without systemic therapy (i.e., hormonotherapy, ADT) at the discretion of the physician,65,66 and palliative SOC.32,58,59 Specifically, palliative SOC offered to the SABR-COMET trial’s control group included systemic therapy and palliative (not radical) radiotherapy to alleviate symptoms or prevent anticipated complications of progression.32,58,59
For the 2 studies65,66 that had common treatments (i.e., systemic therapy) provided in both the intervention and control groups, the effects of those treatments were assumed to be the same in both groups, allowing the comparison of interest to distill down to SABR versus SOC for the sake of categorization in this review.
Question 2: Safety
Among 7 included studies, 4 examined SABR alone,63,67,68 2 examined SABR with systemic therapy,32,58,69 and 1 examined SABR with or without systemic therapy (i.e., ADT) at the discretion of the physician.66
The comparators included observation,63 surgery,68 systemic chemotherapy (i.e., maintenance chemotherapy),69 conventional radiotherapy (i.e., 3DCRT),67 a combination of radiotherapy with palliative intent and systemic therapy,32,58 and radiotherapy (i.e., ENRT) with or without systemic therapy (i.e., ADT) at the discretion of the physician.66
Outcomes
Question 1: Clinical Effectiveness
All studies captured at least 1 key outcome (i.e., OS, PFS) to answer this research question. Seven studies examined OS (2 RCTs,32,58,69 5 nonrandomized studies60,61,64,65,67,68), and 7 studies examined PFS (3 RCTs,32,58,63,69 4 nonrandomized studies60,61,64,65,68).
Additional outcomes of interest included health-related QoL (3 studies: 2 RCTs32,58,59,63 and 1 nonrandomized study64) and LC (2 studies: 1 RCT,32,58 1 nonrandomized study60,61). The 2 RCTs assessed health-related QoL using validated tools such as the Brief Pain Inventory (Short Form)63 and the Functional Assessment of Cancer Therapy–General (FACT-G).32,58,59 The nonrandomized study64 measured QoL using validated questionnaires: European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core 15 Palliative (QLQ-C15-PAL), Brief Pain Inventory, and the EuroQol 5-Dimensions questionnaire (EQ-5D). None of the included studies explored freedom from progression or systemic therapy use after treatment with SABR.
In the included studies, the length of follow-up was variable and also reported inconsistently (i.e., some studies reported total follow-up,58,60,61,63,65-67,69 and others reported follow-up separately for the intervention and comparator32,64,68). The shortest follow-up point for a key outcome was a median follow-up of 9.6 months (interquartile range [IQR], 2.4 to 30.2 months)69; the longest follow-up point was a median follow-up of 91 months (IQR, 69.6 to 117.6 months).61
Question 2: Safety
Six studies examined AEs (3 RCTs,32,58,63,69 3 nonrandomized studies66-68). The studies used version 3 or version 4 of the Common Terminology Criteria for Adverse Events (CTCAE) or the Radiation Therapy Oncology Group (RTOG) assessment tool to evaluate AEs for SABR compared with its comparators. Reporting on AEs varied among studies: 3 reported AE grades of 1 or higher,63,67,69 1 reported AE grades of 2 or higher,32,58 1 reported AE grades of 0 or higher,68 and 1 reported AE grades of 3 or higher.66
Critical Appraisal of Individual Studies
A summary of the critical appraisal for RCTs can be found in Table 3 and in Table 4 for nonrandomized studies. Appendix 8 presents details of the critical appraisal of both the included RCTs (Table 18) and nonrandomized studies (Table 19). Overall, each of the included studies exhibited some risk of bias, described subsequently.
Risk of Bias in RCTs
The risk of bias in 3 RCTs (from 5 publications32,58,59,63,69) was assessed with RoB 2 (Table 3).
For 2 of the included RCTs,32,58,59,63 there was a high risk of bias arising from the randomization process. Though both studies used a computerized random allocation sequence, no information was provided about whether the allocation sequence was concealed until participants were enrolled and assigned to the intervention.32,58,59,63 Moreover, some baseline differences between intervention groups may suggest a problem with the randomization process, although no statistical comparisons were conducted for them: in Phillips et al.,63 the control arm had a higher Gleason score (from the grading classification system that helps in evaluating the prognosis of patients with prostate cancer) and a higher proportion of patients in the intervention arm received prior ADT; in SABR-COMET,32,58,59 the intervention arm had a higher proportion of patients with prostate cancer. Generally, the methods described in the third RCT by Iyengar et al.69 were brief in nature, making the risk of bias for various categories uncertain; therefore, it is possible the risk of bias is higher or lower than what was reported (i.e., the quality of the reporting might have impacted the critical appraisal). Due to the lack of information provided by Iyengar and colleagues,69 there were some concerns of bias arising from the randomization process. Iyengar et al.69 did not provide details about whether the allocation sequence was random and, if so, concealed until participants were enrolled and assigned to the intervention groups. However, the authors reported no significant differences in baseline characteristics between the 2 arms, which might argue against there being any serious problem with the randomization process.69
There were some concerns of bias due to deviations from intended interventions for all 3 RCTs.32,58,59,63,69 All 3 RCTs were open-label studies, meaning both the participants and the individuals delivering the interventions were aware of the intervention assignments during the trial, which could have led to some deviations. However, although 1 patient from the control group in the SABR-COMET study32,58,59 withdrew consent for further follow-up to pursue SABR, this single deviation was unlikely to have affected the balance between the groups or the results due to the relatively large sample size. Similarly, Iyengar et al.69 reported that 2 patients crossed over from the control arm to the intervention arm, but these deviations were unlikely to have affected the interpretation of the results. For the other RCT,63 no information was provided about whether there were deviations from the intended intervention that arose because of the trial context.
The included RCTs32,58,59,63,69 used appropriate analyses to estimate the effect of intervention assignments using an intention-to-treat (ITT) analysis. For all outcomes of interest for all included RCTs,32,58,59,63,69 outcome data were available for all or nearly all participants randomized. Thus, there was a low risk of bias due to missing outcome data for all included RCTs.
The level of risk of bias in the measurement of the outcome depended on the RCT being assessed and the type of outcome explored, ranging from low risk to some concerns. Generally, the method of measurement and analysis for all included outcomes for all RCTs was likely appropriate (e.g., the Kaplan–Meier method was used to estimate survival outcomes, CTCAE was used to classify AEs, FACT-G was used to assess QoL).32,58,59,63,69 However, none of the studies reported having adjusted for multiplicity in their outcome measures, suggesting that the type I error rate might have been inflated if multiple testing was conducted. For 1 RCT, outcome assessors were aware of the intervention received by study participants63; however, this was unclear for the other 2 RCTs.32,58,59,69 However, it is unlikely that the measurement or ascertainment of the outcomes would have been different between the intervention groups.32,58,59,63,69 For outcomes that inherently have some subjectivity in the assessment (e.g., outcomes that involve assessment of a radiograph or clinical examination based on medical records, such as LC, AEs, and QoL outcomes), it is possible that the assessment of these outcomes could have been influenced by the knowledge of the intervention received.
There was a low risk of bias in the selective reporting of outcomes for the included RCTs,32,58,59,63,69 as data analyses and reported results were all in accordance with a pre-specified analysis plan indicated in the corresponding protocols.32,58,59,63,69
One RCT32,58,59 reported a similar median follow-up between the treatment arms, but the range was wider in the comparator arm. The other 2 RCTs63,69 reported only the median follow-up of the total population with a wide IQR, without providing follow-up details for each treatment arm. Therefore, it was unclear whether there was any difference in the follow-up duration between the treatment arms in those studies.
Overall risk-of-bias judgment revealed that 2 RCTs32,58,59,63 were considered to have an overall high risk of bias and 1 RCT69 as having some concerns of bias overall.
Table 3: Risk of Bias Summary — RCTs (Cochrane Risk of Bias Tool 250)
Author (year); relevant for research question(s) | Bias arising from the randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of the outcome | Bias in selection of the reported result | Overall risk-of-bias judgment |
Phillips et al. (2020)63 1, 2 | High risk | Some concerns | PFS: Low risk AEs: Low risk QoL: Low risk | PFS: Low risk AEs: Some concerns QoL: Some concerns | Low risk | High risk |
SABR-COMET Palma et al. (2019),32Palma et al. (2020),58Olson et al. (2019)59 | High risk | Some concerns | OS: Low risk PFS: Low risk AEs: Low risk LC: Low risk QoL: Low risk | OS: Low risk PFS: Low risk AEs: Some concerns LC: Low risk QoL: Some concerns | Low risk | High risk |
Iyengar et al. (2018)69 1, 2 | Some concerns | Some concerns | OS: Low risk PFS: Low risk AEs: Low risk | OS: Low risk PFS: Low risk AEs: Some concerns | Low risk | Some concerns |
AE = adverse event; LC = lesional control; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; QoL = quality of life.
Risk of Bias in Nonrandomized Studies
The risk of bias in 6 nonrandomized studies (from 7 publications)60,61,64-68 was assessed using RoBANS51,52 (Table 4).
The risk of selection bias from the domain related to the possibility of the target group comparisons varied between the included studies: 1 study was considered to be at low risk of bias because pertinent baseline characteristics were balanced between groups,67 and 4 studies were considered to be at high risk of bias because the intervention groups differed in some of the main baseline characteristics.60,61,64,66,68 For instance, 1 study60,61 had older patients (i.e., higher in median age) receiving SABR, 2 studies (in 3 publications)60,61,64 had higher proportions of patients in the SABR group who had received prior treatment for metastatic disease and had imbalances in the primary tumour location between groups, 1 study66 had a higher proportion of patients receiving adjuvant ADT in the comparator group compared with SABR, and 1 study68 had a higher proportion of patients in the SABR group who had been diagnosed with metastases at a later period compared with surgery. Given various differences in baseline characteristics, it is difficult to predict the direction of bias. The remaining study65 was considered to have an unclear risk of bias because the baseline characteristics were not reported for each group, preventing comparison.65
All nonrandomized studies were at low or unclear risk of selection bias for the target group selection domain. Studies were considered to be at low risk of bias when the participant recruitment strategy (e.g., standard of inclusion or exclusion, selection method) was the same for both groups.64,67,68 Studies were considered to have an unclear risk of bias when the participant recruitment strategy was not clearly described (e.g., unknown whether participants selected from different institutions were balanced between groups).60,61,65,66
All nonrandomized studies were at a low risk or unclear risk of selection bias due to confounders: low-risk studies confirmed confounders and considered them during the planning and analysis stages,60,61,64,66,68 and the studies with unclear risk of bias were not clear for at least 1 outcome if confounders were confirmed or considered during the planning and analysis stages.65,67
For all included nonrandomized studies,60,61,64-68 there was a low risk of performance bias (i.e., exposure measurement domain), since the data were obtained from medical records — and for reasons of detection bias (i.e., blinding of assessor’s domain) — as the main end points were time-to-event (survival) outcomes (i.e., objective outcomes).
For all outcomes of all included nonrandomized studies,60,61,64-68 the outcome assessment was probably appropriate (i.e., low risk of confirmation bias), since outcome data were confirmed with medical records. One study64 reported having adjusted for multiplicity but only for QoL outcome measures, and no other study reported having adjusted for multiplicity in its outcome measures, suggesting the type I error rate might have been inflated if multiple testing was conducted.
When considering attrition bias via the incomplete outcome data domain, 2 studies were at low risk of bias, given there were no missing data in the analysis of all reported outcomes,60,61,68 and 3 studies had an unclear risk of bias, as it was unclear whether all participant data were included in the analyses.65-67 One study64 had a low risk of attrition bias for OS and PFS outcomes (i.e., all data included in analyses), but a high risk of bias for pain response and QoL outcomes because not all patient data were included in the analyses for these outcomes (i.e., study authors excluded all patients with no pain at baseline).
One study had been publicly registered a priori (ClinicalTrials.gov NCT02356497; low risk of reporting bias).64 The remaining studies did not mention having or registering a protocol a priori; therefore, it is unclear whether there was any selective outcome reporting (i.e., reporting bias) for these studies.60,61,65-68
Regarding follow-up duration, 2 studies64,68 reported that the median follow-up in the intervention group was much shorter compared with that in the comparator group. Four studies60,61,65-67 reported the median follow-up of the total population. It was therefore unclear whether there was any difference in the duration of follow-up between the treatment arms in those studies.
Overall risk-of-bias judgment revealed that 4 studies60,61,64,66,68 were considered to have an overall high risk of bias and that 2 studies65,67 had some concerns of bias overall.
Table 4: Risk of Bias Summary — Nonrandomized Studies (RoBANS51,52)
Author (year); relevant for research question(s) | The possibility of the target group comparisons | Target group selection | Confounder | Exposure measurement | Blinding of assessors | Outcome assessment | Incomplete outcome data | Selective outcome reporting | Overall risk-of-bias judgment |
Risk of selection bias due to selection of inappropriate comparison target group | Risk of selection bias due to inappropriate intervention or inappropriate selection of exposure group or patient group | Risk of selection bias due to inappropriate confounder confirmation and consideration | Risk of performance bias due to inappropriate intervention or inappropriate exposure measurement | Risk of confirmation bias due to inappropriate blinding of assessors | Risk of confirmation bias due to inappropriate outcome assessment methods | Risk of attrition bias due to inappropriate handling of incomplete data | Risk of reporting bias due to selective outcome reporting | ||
Hurmuz et al. (2020)65 1 | Unclear | Unclear | Unclear | Low | Low | OS: Low PFS: Low | OS: Unclear PFS: Unclear | Unclear | Some concerns |
van de Ven et al. (2020)64 1 | High | Low | Low | Low | Low | OS: Low PFS: Low Pain response: Low QoL: Low | OS: Low PFS: Low Pain response: High QoL: High | Low | High risk |
De Bleser et al. (2019)66 1, 2 | High | Unclear | Low | Low | Low | AEs: Low | AEs: Unclear | Unclear | High risk |
He et al. (2018)67 1, 2 | Low | Low | Unclear | Low | Low | OS: Low AEs: Low | OS: Unclear AEs: Unclear | Unclear | Some concerns |
Filippi et al. (2016)68 1, 2 | High | Low | Low | Low | Low | OS: Low PFS: Low AEs: Low | OS: Low PFS: Low AEs: Low | Unclear | High risk |
Widder et al. (2013)60 and Lodeweges et al. (2017)61 1, 2 | High | Unclear | Low | Low | Low | OS: Low PFS: Low LC: Low | OS: Low PFS: Low LC: Low | Unclear | High risk |
AE = adverse event; LC = lesional control; OS = overall survival; PFS = progression-free survival; RoBANS = Risk of Bias Assessment Tool for Nonrandomized Studies; QoL = quality of life.
Data Analysis and Synthesis
Table 5 presents a high-level summary of the findings of the included studies on the clinical effectiveness and safety of SABR for the treatment of patients with oligometastatic cancer, which were grouped into 2 main comparisons (i.e., SABR + SOC versus SOC alone, and SABR versus SOC). Appendix 9 presents the main study findings with regard to OS (Table 20), PFS (Table 21), health-related QoL (Table 22, Table 23), and AEs (Table 24).
Due to the limited amount of available data, subgroup analyses were not possible.
Table 5: High-Level Summary of the Findings
Overarching comparison | Intervention vs. comparator | Effects by OUTCOME | ||||||
OS | PFS | FFP | HRQoL | LC | Systemic therapy use | AEs | ||
SABR + SOC vs. SOC (RCT) | Short-term F/U: NS Longer-term F/U: + | Short-term F/U: + Longer-term F/U: + | NR | NS | Short-term F/U: + Longer-term F/U: + | NR | Related AE grade ≥ 2 –; other NS | |
SABR + chemotherapy vs. chemotherapy69 | ? | + | NR | NR | NR | NR | ? | |
SABR vs. SOC (non-randomized study) | SABR vs. observation63 | NR | + | NR | NS | NR | NR | ? |
SABR ± hormonotherapy vs. conventional fractionation radiotherapy ± hormonotherapy65 | NS | + | NR | NR | NR | NR | NR | |
SABR vs. 3DCRT64 | + | + | NR | NS | NR | NR | NR | |
SABR ± ADT vs. ENRT ± ADT66 | NR | NR | NR | NR | NR | NR | + | |
SABR vs. 3DCRT67 | NS | NR | NR | NR | NR | NR | NS | |
SABR vs. various resections68 | NS | – | NR | NR | NR | NR | ? | |
NS | NS | NR | NR | NS | NR | NR | ||
+= intervention more favourable than comparator; – = intervention less favourable than comparator; ? = not compared statistically; 3DCRT = 3-dimensional conformal radiation therapy; ADT = androgen deprivation therapy; AE = adverse event; ENRT = elective nodal radiotherapy; FFP = free from progression; F/U = follow-up; LC = lesional control; NR = not measured or not reported; NS = not statistically significant; OS = overall survival; PFS = progression-free survival; PME = pulmonary metastasectomy; SABR = stereotactic ablative radiotherapy; SOC = standard of care; vs. = versus.
Question 1: Clinical Effectiveness
SABR With SOC Versus SOC Alone
Overall Survival
From 2 RCTs using ITT analyses,32,58,69 with an overall risk of bias of either high or with some concerns and considering multiple metastatic sites and up to 5 oligometastases in patients previously treated for their primary tumour, there is some evidence suggesting an OS benefit associated with SABR plus SOC compared with SOC alone (Table 6). The initial findings from the SABR-COMET RCT (N = 99 patients)32 found longer median OS and a lower HR for OS in the SABR plus systemic therapy (n = 66 patients) compared with systemic therapy (n = 33; i.e., systemic therapy with patients being allowed to receive radiotherapy with palliative intent) in patients with multiple primary tumour locations. The median OS was 41 months (95% confidence interval [CI], 26 to not reached) for SABR plus systemic therapy and 28 months (95%CI, 19 to 33) for systemic therapy alone. The unadjusted HR was 0.57 (95% CI, 0.30 to 1.10; P = 0.09) with a median follow-up of 26 months (IQR, 23 to 37) for SABR plus systemic therapy and 25 (IQR, 19 to 54) months for systemic therapy. A longer surveillance period (median follow-up for both arms was 51 months; IQR, 46 to 58 months) revealed a significant difference in OS in favour of SABR plus systemic therapy compared with systemic therapy alone (unadjusted HR was 0.47; 95% CI, 0.27 to 0.81; P = 0.006).58 the Iyengar et al. RCT69 of 29 patients with primary lung cancer provided limited OS findings for their study: for the SABR plus maintenance chemotherapy intervention arm (n = 14), median OS was not reached during the investigation period (i.e., more than half the patients were still alive); for the maintenance chemotherapy arm, median OS was nearly 1 year for patients who did not cross over (n = 13) and was 17 months for patients who crossed over to receive SABR at oligoprogression (n = 2). No HRs for OS were reported and the authors reported their study was not powered to show a statistical difference in survival.69 Both RCTs32,58,69 had patients who had been previously treated for their metastases.
Table 6: OS Comparing SABR With SOC Versus SOC
Study | Treatments (intervention vs. comparator); follow-up | Study characteristics | Death events; n | 2-year OS rate, % (95% CI) | 5-year OS rate, % (95% CI) | Median OS (95% CI); months | Unadjusted HR (95% CI) |
RCTs | |||||||
SABR-COMET | SABR + systemic therapy (n = 66) vs. systemic therapy (n = 33) Short-term F/U Median F/U (IQR):
Long-term F/U Median F/U (IQR): Total: 51 (46 to 58) months58 | Age, median (IQR):
% male:
Primary tumour location; Breast, colorectal, lung, prostate, and other (not described in publication) Met site: Multiple Number of mets: ≤ 5 Mets location: Adrenal, bone, liver, lung, other: • brain (3 lesions in control; 1 lesion in SABR + SOC)
Previous tx primary tumour: Yes Previous tx mets: Yes | Short-term F/U: 24 vs. 16 Long-term F/U: 35 vs. 24 | Short- and long-term F/U: NR | Short-term F/U: NR Long-term FU: 42.3 (28 to 56) vs. 17.7 (6 to 34) | Short-term F/U: 41 (26 to not reached) vs. 28 (19 to 33) Long-term F/U: 50 (29 to 83) vs. 28 (18 to 39) | Short-term F/U: 0.57 (0.30 to 1.10); P = 0.09 Long-term F/U: 0.47 (0.27 to 0.81); P = 0.006 |
Iyengar et al. (2018)69 | SABR + chemotherapy (n = 14) vs. chemotherapy (n = 15) Median F/U (IQR): Total: 9.6 (2.4 to 30.2) months | Age, median (IQR):
% male:
Primary tumour location: Lung Met site: Multiple Number of mets: ≤ 5 Mets location: Lung, adrenal, mediastinum, axilla, liver, nasopharynx, bone (rib, spine) Previous tx primary tumour: Yes Previous tx mets: Yes | NR | NR | NR | Not reached (NR) vs. about 1 year without crossover; 17 months with crossover (NR) | NR |
CI = confidence interval; F/U = follow-up; HR = hazard ratio; IQR = interquartile range; met = metastasis; mets = metastases; NR = not reported; OS = overall survival; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; SOC = standard of care; tx = treatment; vs. = versus.
Progression-Free Survival
In 2 RCTs,32,58,69 either at high risk of bias or with some concerns of bias overall, there is some early evidence to suggest that SABR plus systemic therapy may be more effective than systemic therapy alone for PFS32,58,69 (Table 7). Both RCTs32,58,69 included patients with multiple metastatic sites and a maximum of 5 oligometastases.
One RCT (SABR-COMET) with 2 publications32,58 reported a significant advantage in PFS for patients with multiple primary tumour locations who received SABR plus systemic therapy compared with systemic therapy alone. The initial findings from the SABR-COMET RCT32 found a significant PFS benefit for SABR plus systemic therapy compared with systemic therapy alone (unadjusted HR was 0.47; 95% CI, 0.30 to 0.76; P = 0.0012; median follow-up was 26 months [IQR, 23 to 37 months] for SABR plus systemic therapy; and 25 months [IQR, 19 to 54] for systemic therapy alone). A longer surveillance period (median follow-up for both arms was 51 months; IQR, 46 to 58 months) revealed similar PFS benefits in favour of SABR plus systemic therapy (unadjusted HR was 0.48; 95% CI, 0.31 to 0.76; P = 0.001).58 Another RCT by Iyengar et al.69 of patients with primary lung cancer also reported a significant PFS benefit for SABR plus maintenance chemotherapy compared with maintenance chemotherapy alone (unadjusted HR was 0.304; 95% CI, 0.113 to 0.815; P = 0.01). Both RCTs32,58,69 had patients whose primary tumour and metastases had been previously treated.
Table 7: PFS Comparing SABR With SOC Versus SOC
Study | Treatments (intervention vs. comparator); follow-up | Study characteristics | Progression events; n | 4-year PFS rate, % (95% CI) | 5-year PFS rate, % (95% CI) | Median PFS (95% CI); month | Unadjusted HR (95% CI) |
RCTs | |||||||
SABR-COMET | SABR + systemic therapy (n = 66) vs. systemic therapy alone (n = 33) Short-term F/U Median F/U (IQR):
Long-term F/U Median F/U (IQR): Total: 51 (46 to 58) months58 | Age, median (IQR):
% male:
Primary tumour location: Breast, colorectal, lung, prostate, and other Met site: Multiple Number of mets: ≤ 5 Mets location: Adrenal, bone, liver, lung, other:
Previous tx primary tumour: Yes Previous tx mets: Yes | Short-term F/U: 39 vs. 28 Long-term F/U: 45 vs. 29 | Short-term F/U: NR Long-term F/U: 21.6 (12 to 33) vs. 3.2 (0 to 14) | Short-term F/U: NR Long-term F/U: 17.3 (8 to 30) vs. 0 (NA) | 12 (6.9 to 30.4) vs. 6.0 (3.4 to 7.1) Long-term F/U: 11.6 (6.1 to 23.4) vs. 5.4 (3.2 to 6.8) | 0.47 (0.30 to 0.76); P = 0.0012 Long-term F/U: 0.48 (0.31 to 0.76); P = 0.001 |
Iyengar et al. (2018)69 | SABR + chemotherapy (n = 14) vs. chemotherapy alone (n = 15) Median F/U (IQR): Total: 9.6 (2.4 to 30.2) months | Age, median (IQR):
% male:
Primary tumour location: Lung Met site: Multiple Number of mets: ≤ 5 Mets location: Lung, adrenal, mediastinum, axilla, liver, nasopharynx, bone (rib, spine) Previous tx primary tumour: Yes Previous tx mets: Yes | 4 vs. 10 | NR | NR | 9.7 (NR) vs. 3.5 (NR) | 0.304 (0.113 to 0.815); P = 0.01 |
CI = confidence interval; F/U = follow-up; HR = hazard ratio; IQR = interquartile range; met = metastasis; mets = metastases; NR = not reported; PFS = progression-free survival; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; SOC = standard of care; tx = treatment; vs. = versus.
Freedom From Progression
None of the included studies explored freedom from progression. Consequently, no summary of evidence has been conducted.
Health-Related QoL
One RCT with 3 publications32,58,59 with an overall high risk of bias reported no significant differences between SABR plus systemic therapy and systemic therapy in health-related QoL outcomes (Table 8). The SABR-COMET study reported no significant differences between the 2 groups at 6 months in the patient-reported FACT-G outcome measure used to assess health-related QoL (FACT-G total, mean [standard deviation] for SABR plus systemic therapy: 82.6 [16.6] versus systemic therapy: 82.5 [16.4]; P = 0.99).32 There were also no significant differences between the 2 groups when examining subscales of the FACT-G tool at 6 months (i.e., physical, social, emotional, functional: P > 0.40 for all).32 The SABR-COMET trial also examined the same QoL outcome measures over 42 months and over 5 years.59 At both time points, no significant differences were found between the 2 groups (P values ranged from 0.17 to 0.98).58,59 Thus, the SABR-COMET study concluded SABR plus systemic therapy was not associated with a QoL detriment.32,58,59 This RCT32,58,59 included patients with multiple primary tumour locations and multiple metastatic sites with up to 5 oligometastases. Patients had been previously treated for their primary tumour and metastases.
Table 8: Health-Related QoL Comparing SABR With SOC Versus SOC Alone
Study | Study characteristics | Tool, follow-up, results |
SABR-COMET Palma et al. (2019),32 Palma et al. (2020),58 Olson et al. (2019)59 | Age, median (IQR):
% male:
Primary tumour location: Breast, colorectal, lung, prostate, and other Mets sites: Multiple Number of mets: ≤ 5 Mets location: Adrenal, bone, liver, lung, other:
Previous tx primary tumour: Yes Previous tx mets: Yes | QoL (tool: FACT-G; 4 subscales: physical well-being, social/family well-being, emotional well-being, and functional well-being) SABR plus systemic therapy vs. systemic therapy alone32
Total score:a 82.6 (16.6) vs. 82.5 (16.4); P = 0.99 Subscales: Physical: 22.4 (4.8) vs. 23.1 (4.9); P = 0.54 Functional: 19.4 (5.8) vs. 18.8 (7.0); P = 0.74 Emotional: 18.1 (5.1) vs. 18.3 (4.3); P = 0.87 Social: 22.8 (5.1) vs. 21.8 (6.3); P = 0.48 SABR plus systemic therapy vs. systemic therapy alone59
Subscales: Physical (P = 0.98) Functional (P = 0.59) Emotional (P = 0.82) Social (P = 0.17) SABR plus systemic therapy vs. systemic therapy alone58
Subscales: Physical (P = 0.72) Functional (P = 0.47) Emotional (P = 0.77) Social (P = 0.19) |
FACT-G = Functional Assessment of Cancer Therapy–General; met = metastasis; mets = metastases; IQR = interquartile range; QoL = quality of life; SABR = stereotactic ablative radiotherapy; SD = standard deviation; SOC = standard of care; tx = treatment.
aTotal score = sum of FACT‐G physical, social, emotional, and functional well‐being scores.
Lesional Control
Limited data from 1 RCT32,58 with an overall high risk of bias provided inconclusive evidence about LC to assess whether SABR plus SOC is more effective than SOC alone (Table 9).
The SABR-COMET RCT32,58 found improved crude LC rates for SABR plus systemic therapy compared with systemic therapy alone during initial follow-up (75% versus 49%; P = 0.0010; median follow-up: 26 [IQR, 23 to 37] months for SABR plus systemic therapy; 25 [IQR, 19 to 54] months for systemic therapy)32 and after longer surveillance (63% versus 46%; P = 0.039; median follow-up for both arms 51 [IQR, 46 to 58] months).58 HRs were not calculated for this outcome.32,58 This RCT32,58 included patients with multiple primary tumour locations and multiple metastatic sites with up to 5 oligometastases. Patients had been previously treated for their primary tumour and metastases.
Table 9: Lesional Control Comparing SABR With SOC Versus SOC
Study | Treatments (intervention vs. comparator) | Study characteristics | Crude LC rate, % (95% CI) |
RCTs | |||
SABR + systemic therapy (n = 66) vs. systemic therapy (n = 33) Short-term F/U Median F/U (IQR):
Long-term F/U Median F/U (IQR): Total: 51 (46 to 58) months58 | Age, median (IQR):
% male:
Primary tumour location: Breast, colorectal, lung, prostate, and other Met site: Multiple Number of mets: ≤ 5 Mets location: Adrenal, bone, liver, lung, other:
Previous tx primary tumour: Yes Previous tx mets: Yes | Short-term F/U: 75 (NR) vs. 49 (NR), P = 0.0010 Long-term F/U: 63 (NR) vs. 46 (NR), P = 0.039 | |
CI = confidence interval; F/U = follow-up; IQR = interquartile range; LC = lesional control; met = metastasis; mets = metastases; NR = not reported; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; tx = treatment; vs. = versus .
Systemic Therapy Use
None of the included studies explored systemic therapy use after treatment with SABR. Consequently, no summary of evidence has been conducted.
SABR Versus SOC
Overall Survival
Five nonrandomized studies60,61,64,65,67,68 at either high risk of bias or with some concerns of bias overall provided inconclusive evidence about OS to determine whether SABR is more effective than SOC (Table 10); 4 studies did not report any significant differences between SABR and SOC for OS measures reported (i.e., OS rates, unadjusted HRs, adjusted HRs),60,61,65,67,68 and 1 study found an OS benefit for SABR when compared with 3DCRT.64 None of the studies reported whether they performed a sample size calculation to obtain enough power to determine a statistical difference between groups for OS.
Hurmuz et al.65 found no OS benefit for SABR with or without hormonotherapy (n = 129) at 2 years compared with conventional fractionation radiotherapy with or without hormonotherapy (n = 47) in patients with controlled primary prostate cancer with multiple metastatic sites and a maximum of 5 oligometastases. As patients from both arms optionally received hormonotherapy, the comparison in this study was considered to be SABR versus conventional fractionation radiotherapy. The 2-year OS rate was 87.7% (95% CI not reported) for the SABR group compared with 87.3% (95% CI not reported) for the conventional fractionation radiotherapy group (P = 0.91; median follow-up for both arms was 22.9 [IQR, 3.3 to 77.8] months). No HRs were provided by this study.65
Filippi et al.68 compared SABR (n = 28) with surgery (n = 142) for lung oligometastases (up to 5 lesions) from previously controlled colorectal cancer and found no significant differences in OS between groups according to the unadjusted HR of 1.7 (95% CI, 0.84 to 3.43), and adjusted HR of 1.71 (95% CI, 0.82 to 3.54). This study was highly imbalanced in terms of numbers of patients in each cohort (i.e., n = 28 in the SABR group versus n = 142 in the surgery group), which was exacerbated by a higher proportion of patients who died (i.e., 36% versus 26%) and more patients lost to follow-up at 30 months (i.e., 7 versus 1) in the SABR group compared with the surgery group. That imbalance might have led to the large difference in median follow-up between the 2 groups (i.e., SABR: 27 [IQR, 16.1 to 71.7] months versus surgery: 45.8 [IQR, 13.6 to 107.1] months) and potentially to the large uncertainty in the HR estimates.
Furthermore, another nonrandomized study compared OS outcomes at both short- and long-term follow-up time points with SABR (n = 42) versus surgery (n = 68) in patients with multiple primary tumour locations that metastasized to the lung with up to 5 oligometastases.60,61 All patients had been previously treated for their primary tumour. The median short-term follow-up was 43 (IQR, 36 to 60) months60 and the median long-term follow-up was 91.2 (IQR, 69.6 to 117.6) months.61 Regardless of length of follow-up, no significant differences were found in OS between groups: the unadjusted HR for short-term follow-up was 0.79 (95% CI, 0.43 to 1.42); the adjusted HR for short-term follow-up was not reported. The unadjusted HR for long-term follow-up was 1.11 (0.70 to 1.75), and the adjusted HR for long-term follow-up was 0.76 (95% CI, 0.38 to 1.54).60,61
He et al.67 compared SABR (n = 11) with 3DCRT (n = 15) in patients with primary colorectal cancer that metastasized to the liver with up to 3 oligometastases. All patients had been previously treated for their primary tumour. With a median follow-up of 13 months across groups, the study67 did not find an OS benefit for SABR when compared with 3DCRT (unadjusted HR: 0.61; 95% CI, 0.23 to 1.65). No other results with statistical testing were reported.67
Van de ven and colleagues64 found an OS benefit for the SABR group (n = 65) compared with the 3DCRT group (n = 66; unadjusted HR: 0.44; 95% CI, 0.21 to 0.81) in patients with multiple primary tumour locations that metastasized to the bone and other locations with up to 5 oligometastases, despite a significantly shorter time of follow-up in the SABR group (i.e., patients in the SABR group had a median follow-up of 25 [IQR, 5 to 52] months, and patients in the 3DCRT group had a median follow-up 46 [IQR, 9 to 55] months).
Table 10: OS Comparing SABR Versus SOC
Study (year) | Treatments (intervention vs. comparator); follow-up | Study characteristics | Death events; n | OS rate, % (95% CI) | Median OS (95% CI); months | Unadjusted HR (95% CI) | Adj HR (95% CI) | ||||
1-year | 2-year | 3-year | 4-year | 5-year | |||||||
NRSs | |||||||||||
Hurmuz et al. (2020)65 | SABR ± hormonotherapy (n = 129) vs. conventional fractionation radiotherapy ± hormonotherapy (n = 47) Median F/U (IQR): Total: 22.9 (3.3 to 77.8) months | Age, median (range): 65 (42 to 84) years % male: 100 Primary tumour location: Prostate Met site: Multiple Number of mets: ≤ 5 Mets location: Bone or lymph node Previous tx primary tumour: Yes Previous tx mets: Unclear | NR | NR | 87.7 (NR) vs. 87.3 (NR); P = 0.91 | NR | NR | NR | NR | NR | NR |
van de Ven et al. (2020)64 | SABR (n = 65) vs. 3DCRT (n = 66) Median F/U (IQR):
| Age: 64.4 years (SABR); 68.3 years (3DCRT) % male: 51.4 Primary tumour location: Prostate, breast, lung, kidney, other (not clear in publication) Met site: Multiple Number of mets: ≤ 5 Mets location: Bone, other Previous tx primary tumour: Some patients Previous tx mets: Some patients |
| 85 (NR) vs. 65 (NR) | NR | NR | NR | NR | Not reached (NR) vs. 18 months (NR); P < 0.0001 | 0.44 (0.24 to 0.81); P = NR | NR |
He et al. (2018)67 | SABR (n = 11) vs. 3DCRT (n = 15) Median F/U: Total: 13 months | Age, median (IQR): 71 (45 to 87) years % male: 100 Primary tumour location: Colon and rectum Met site: Single Number of mets: ≤ 3 Mets location: Liver Previous tx primary tumour: Yes Previous tx mets: Some patients | NR | 68.2 (NR) vs. 55.8 (NR) | 40.9 (NR) vs. 16.0 (NR) | 20.5 (NR) vs. 0.0 (NR) | NR | NR | 20 (NR) vs. 14 (NR) | 0.61 (0.23 to 1.65); P = 0.323 | NR |
Filippi et al. (2016)68 | SABR (n = 28) vs. surgery (n = 142) Median F/U (IQR):
| Age, median (IQR):
% male:
Primary tumour location: Colon and rectum Met site: Single Number of mets: ≤ 5 Mets location: Lung Previous tx primary tumour: Yes Previous tx mets: For some patients | 10 vs. 37 | 89 (70 to 96) vs. 96 (92 to 99) | 77 (56 to 89) vs. 82 (74 to 87) | NR | NR | NR | NR | 1.7 (0.84 to 3.43); P = 0.139 | 1.71 (0.82 to 3.54); P = 0.149 |
Widder et al. (2013)60 and Lodeweges et al. (2017)61a | SABR (n = 42) vs. Surgery (PME) (n = 68) Short-term F/U: Median F/U (IQR) Total: 43 (36 to 60) months60 Long-term F/U: Median F/U (IQR) Total: 91.2 (69.6 to 117.6) months61 | Age, median (IQR):
% male:
Primary tumour location or type: Colorectal, lung sarcoma, kidney, other Met site: Single Number of mets: ≤ 5 Mets location: Lung Previous tx primary tumour: Yes Previous tx mets: For some patients | Short-term F/U: 17 vs. 35 Long-term F/U: NR | Short- and long-term F/U: 98 (84 to 100) vs. 87 (76 to 93) | Short- and long-term F/U: 86 (71 to 93) vs. 74 (61 to 82) | Short-term F/U: 60 (42 to 73) vs. 62 (49 to 73) Long-term F/U: 64 (48 to 77) vs. 63 (51 to 73) | Short-term F/U: 60 (42 to 73) vs. 47 (33 to 59) Long-term F/U: 57 (41 to 70) vs. 50 (38 to 61) | Short-term F/U: 49 (25 to 69) vs. 41 (27 to 54) Long-term F/U: 45 (30 to 59) vs. 41 (29 to 53) | Short- and long-term F/U: NR | Short-term F/U: 0.79 (0.43 to 1.42); P = 0.427 Long-term F/U: 1.11 (0.70 to 1.75); P = NR; NS | Short-term F/U: NR Long-term F/U: 0.76 (0.38 to 1.54); P = NR; NS |
3DCRT = 3-dimensional conformal radiation therapy; adj = adjusted; F/U = follow-up; HR = hazard ratio; IQR = interquartile range; met = metastasis; mets = metastases; NR = not reported; NRS = nonrandomized study; NS = non-significant; OS = overall survival; PME = pulmonary metastasectomy; SABR = stereotactic ablative radiotherapy; SOC = standard of care; tx = treatment; vs. = versus .
aOS rates at 6, 7 and 8 years for SABR vs. surgery (PME) were 35% (95% CI, 21% to 50%) vs. 37% (95% CI, 26% to 48%), 29% (95% CI, 16% to 44%) vs. 35% (95% CI, 24% to 46%), and 13% (95% CI, 3% to 30%) vs. 35% (95% CI, 24% to 46%), respectively.
Progression-Free Survival
Five studies (1 RCT,63 4 nonrandomized studies60,61,64,65,68) at either high risk of bias or with some concerns of bias overall explored PFS for patients receiving SABR or SOC to treat their oligometastatic cancer (Table 11). Overall, the results were mixed: 3 studies suggested SABR provides a PFS benefit compared with SOC,63-65 1 study reported SABR provides a worse prognosis in terms of PFS compared with SOC,68 and 1 study did not provide any statistical comparison between groups.60,61
One RCT compared SABR with observation in patients with previously controlled primary prostate cancer that metastasized to multiple sites (bone or soft tissue) with up to 3 oligometastases, and found a PFS benefit for the SABR group.63 The unadjusted HR was 0.3 (95% CI, 0.11 to 0.81; P = 0.002), with a median follow-up for both arms of 18.8 (IQR, 5.8 to 35.0) months.63
The nonrandomized study by Hurmuz et al.65 found a PFS benefit of SABR with or without hormonotherapy compared with conventional fractionation radiotherapy with or without hormonotherapy (adjusted HR: 0.26; 95% CI, 0.13 to 0.55; P < 0.001; median total follow-up: 22.9; 95% CI, 3.3 to 77.8 months) in patients with previously controlled primary prostate cancer that metastasized to multiple sites (bone or lymph node or both) with up to 5 oligometastases.
The nonrandomized study by van de Ven and colleagues64 reported a PFS benefit for SABR compared with 3DCRT in patients with multiple primary tumour locations and multiple metastatic sites with up to 5 oligometastases. The unadjusted HR was 0.63 (95% CI, 0.41 to 0.95), with a median follow-up of 25 (IQR, 5 to 52) months for the SABR group and 46 (IQR, 9 to 55) months for the 3DCRT group.64
One nonrandomized study reported SABR provides a worse prognosis in terms of PFS compared with surgery (adjusted HR: 2.78; 95% CI, 1.67 to 4.62; P < 0.001) in patients with previously controlled primary colorectal cancer that metastasized to the lung with up to 5 oligometastases.68 However, it should be noted that the study authors stated their PFS results were unreliable because different follow-up protocols were applied in the 2 cohorts.68
Finally, another nonrandomized study compared PFS outcomes at both short- (median follow-up 43 [IQR, 36 to 60] months)60 and long-term (91.2 [IQR, 69.6 to 117.6] months)61 follow-up time points for SABR (n = 42) versus surgery (n = 68) in patients with multiple primary tumour locations that metastasized to the lung with up to 5 oligometastases. The primary tumour in all patients had been previously treated. PFS rates provided for both groups in 1-year increments from 1 to 8 years suggested lower rates with SABR compared with surgery for metastases in the lung; however, without any statistical comparison, a conclusion could not be drawn.60,61 HRs were not calculated for any length of follow-up to determine the effect of SABR on PFS.60,61
Table 11: PFS Comparing SABR Versus SOC
Study (year) | Treatments (Intervention vs. Comparator) | Study characteristics | PFS rate, % (95% CI) | Median PFS (95% CI); month | Unadjusted HR (95% CI) | Adj HR (95% CI) | |||||
6-month | 1-year | 2-year | 3-year | 4-year | 5-year | ||||||
RCTs | |||||||||||
Phillips et al. (2020)63 | SABR (n = 36) vs. observation (n = 18) Median F/U (IQR): Total: 18.8 (5.8 to 35.0) months | Age, median (IQR):
% male: 100 Primary tumour location: Prostate Met site: Multiple Number of mets: ≤ 3 Mets location: Bone or soft issue Previous tx primary tumour: Yes Previous tx mets: Unclear | 19 (9.6 to 35.4) vs. 61 (38.5 to 79.6) | NR | NR | NR | NR | NR | Not reached (NR) vs. 5.8 (NR) | 0.3 (0.11 to 0.81); P = 0.002 | NR |
Non-RCTs | |||||||||||
Hurmuz et al. (2020)65 | SABR ± hormonotherapy (n = 129) vs. conventional fractionation radiotherapy ± hormonotherapy (n = 47) Median F/U (IQR): Total: 22.9 (3.3 to 77.8) months | Age, median (range): 65 (42 to 84) years % male: 100 Primary tumour location: Prostate Met site: Multiple Number of mets: ≤ 5 Mets location: Bone or lymph node or both Previous tx primary tumour: Yes Previous tx mets: Unclear | NR | 86.2 (NR) vs. 54.9 (NR); P < 0.001 | NR | NR | NR | NR | NR | NR | 0.26 (0.13 to 0.55); P < 0.001 |
van de Ven et al. (2020)64 | SABR (n = 65) vs. 3DCRT (n = 66) Median F/U (IQR):
| Age:
% male: 51.4 Primary tumour location: Prostate, breast, lung, kidney, other (not clear in publication) Met site: Multiple Number of mets: ≤ 5 Mets location: Bone, other Previous tx primary tumour: Some patients Previous tx mets: Some patients | NR | 54 (NR) vs. 19 (NR) | NR | NR | NR | NR | 12 (NR) vs. 5 (NR); P = 0.002 | 0.63 (0.41 to 0.95); P = NR | NR |
Filippi et al. (2016)68 | SABR; n = 28 vs. surgery; n = 142 Median F/U (IQR):
| Age, median (IQR):
% male:
Primary tumour location: Colon and rectum Met site: Single Number of mets: ≤ 5 Mets location: Lung Previous tx primary tumour: Yes Previous tx mets: For some patients | NR | NR | NR | NR | NR | NR | NR | 2.44 (1.51 to 3.94); P < 0.001 | 2.78 (1.67 to 4.62); P < 0.001 |
Widder et al. (2013)60 and Lodeweges et al. (2017)61a | SABR (n = 42) vs. surgery (PME) (n = 68) Short-term F/U Median F/U (IQR): Total: 43 (36 to 60) months60 Long-term F/U Median F/U (IQR): Total: 91.2 (69.6 to 117.6) months61 | Age, median (IQR):
% male:
Primary tumour location or type: Colorectal, lung, sarcoma, kidney, other Met site: Single Number of mets: ≤ 5 Mets location: Lung Previous tx primary tumour: Yes Previous tx mets: For some patients | Short- and long-term F/U: NR | Short-term F/U: 50 (34 to 64) vs. 54 (42 to 65) Long-term F/U: 49 (34 to 63) vs. 56 (43 to 66) | Short-term F/U: 21 (9 to 35) vs. 33 (22 to 45) Long-term F/U: 27 (14 to 41) vs. 35 (23 to 46) | Short-term F/U: 8 (2 to 22) vs. 22 (12 to 33) Long-term F/U: 18 (8 to 32) vs. 26 (16 to 36) | Short-term F/U: 8 (2 to 22) vs. 18 (9 to 30) Long-term F/U: 18 (8 to 32) vs. 23 (13 to 33) | Short-term F/U: NR Long-term F/U: 18 (8 to 32) vs. 20 (11 to 30) | Short- and long-term F/U: NR | Short- and long-term F/U: NR | Short- and long-term F/U: NR |
3DCRT = 3-dimensional conformal radiation therapy; adj = adjusted; F/U = follow-up; HR = hazard ratio; IQR = interquartile range; met = metastasis; mets = metastases; NR = not reported; NRS = nonrandomized study; PFS = progression-free survival; PME = pulmonary metastasectomy; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; SOC = standard of care; tx = treatment; vs. = versus .
aPFS rates at 6, 7, and 8 years for SABR vs. surgery (PME) for all time points were 18% (95% CI, 8% to 32%) vs. 20% (95% CI, 11% to 30%).
Freedom From Progression
None of the included studies explored freedom from progression. Consequently, no summary of evidence has been conducted.
Health-Related QoL
Two studies (1 RCT,63 1 nonrandomized study64) with an overall high risk of bias reported no significant differences between SABR versus SOC groups in the majority of health-related QoL outcomes (Table 12).
With no quantitative data reported, the RCT by Phillips and colleagues63 concluded there were no differences in Brief Pain Inventory (Short Form) scores between groups (i.e., SABR versus observation) in patients with previously controlled primary prostate cancer that metastasized to bone or soft tissue with up to 3 oligometastases.
The nonrandomized study by van de Ven et al.64 compared SABR with 3DCRT in patients with multiple primary tumour locations and multiple metastatic sites with up to 5 oligometastases and did not find any significant differences in pain response between treatment groups. The nonrandomized study authors also assessed additional pain variables, including complete response, partial response, pain progression, responders, median duration of pain response, ongoing pain response, and re-irradiation for pain recurrence or progression. At all assessed time points (3, 6, and 12 months), no significant differences were observed between the 2 groups with the exception of responders at 12 months (i.e., complete or partial response was achieved on at least 1 of the follow-up time points: SABR: 80%, n = 8; 3DCRT: 50%, n = 13; P = 0.04) and re-irradiation for pain recurrence or progression, where significantly more patients required re-irradiation for pain recurrence or progression after 3DCRT radiation therapy compared with SABR (SABR: 5%, n = 3; 3DCRT: 33.3%, n = 22; P < 0.05). It should be noted, however, the authors of this nonrandomized study excluded all patients with no pain at baseline for the assessment of pain response, which limited the number of patients for analysis and may have amplified the effect. Moreover, no significant differences between groups were found at follow-up for any QoL subscales. The physical functioning subscale appeared to be in favour of the SABR group (52-week follow-up: P = 0.04). However, the study considered P values of less than 0.01 to be statistically significant for mixed models in the QoL analyses.64 The median follow-up in the SABR group was 25 months (IQR, 5 to 52 months), which was notably shorter than the median follow-up of 46 months in the 3DCRT group (IQR, 9 to 55 months).64
Table 12: Health-Related QoL Comparing SABR Versus SOC
Study | Study characteristics | Tool, follow-up, results |
RCT | ||
Phillips et al. (2020)63 | Age, median (IQR):
% male: 100 Primary tumour location: Prostate Met site: Multiple Number of mets: ≤ 3 Mets location: Bone or soft issue Previous tx primary tumour: Yes Previous tx mets: Unclear | Tool: Brief Pain Inventory (Short Form) Median F/U (IQR): Total: 18.8 (5.8 to 35.0) months QoL results: “No differences in Brief Pain Inventory (Short Form) scores were observed between arms or within either arm across time.” (Data not shown.) |
NRS | ||
van de Ven et al. (2020)64 | Age:
% male: 51.4 Primary tumour location: Prostate, breast, lung, kidney, other Met site: Multiple Number of mets: ≤ 5 Mets location: Bone, other Previous tx primary tumour: Some patients Previous tx mets: Some patients | Tool or measure:
Median F/U (IQR):
Pain results Number of patients with pain at baseline:
Mean (SD) numeric rating scale scores at baseline:
Pain response:
Complete response:
Partial response:
Pain progression:
Intermediate responses plus stable responses:
Responders:
Median duration of pain response (range):
Ongoing pain response:
Re-irradiation for pain recurrence or progression:
QoL results (where P values of < 0.01 were considered statistically significant for mixed models):
|
3DCRT = 3-dimensional conformal radiation therapy; EORTC QLQ-BM22 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for Patients with Bone Metastasis 22; EORTC QLQ-C15-PAL = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative; EQ-5D = EuroQol 5-Dimensions questionnaire; FACT-G = Functional Assessment of Cancer Therapy–General; F/U = follow-up; IQR = interquartile range; met = metastasis; mets = metastases; NRS = nonrandomized study; QoL = quality of life; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; SBRT = stereotactic body radiotherapy; SOC = standard of care; tx = treatment.
Lesional Control
One nonrandomized study (from 2 publications)60,61 with an overall high risk of bias explored LC outcomes (Table 13). The study compared LC outcomes at both short- and long-term follow-up time points between SABR (n = 42) and surgery (n = 68) in patients with multiple primary tumour locations that metastasized to the lung with up to 5 oligometastases. The primary tumour in all patients had been previously treated. The median short-term follow-up was 43 (IQR, 36 to 60) months60 and the median long-term follow-up was 91.2 (IQR, 69.6 to 117.6) months.61 LC rates in 1-year increments from 1 to 8 years were numerically comparable between groups, without any statistical comparison. An unadjusted HR was calculated at long-term follow-up, which found no significant differences between groups; the unadjusted HR was 0.8 (95% CI, 0.24 to 2.65).61
Table 13: Lesional Control Comparing SABR Versus SOC
Study | Treatments (intervention vs. comparator) | Study characteristics | LC rate, % (95% CI) SABR vs. surgery | Median LC (95% CI); months | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | |||||
1-year | 2-year | 3-year | 4-year | 5-year | 6-year | ||||||
NRSs | |||||||||||
Widder et al. (2013)60 and Lodeweges et al. (2017)a,61 | SABR (n = 42) vs. surgery (PME) (n = 68) Short-term F/U Median F/U (IQR):
Long-term F/U Median F/U (IQR):
| Age, median (IQR):
% male:
Primary tumour location or type: Colorectal, sarcoma, lung, kidney, other Met site: Single Number of mets: ≤ 5 Mets location: Lung Previous tx primary tumour: Yes Previous tx mets: For some patients | Short-term F/U: 94 (79 to 99) vs. 93 (83 to 97) Long-term F/U: 95 (80 to 99) vs. 93 (83 to 97) | Short-term F/U: 94 (79 to 99) vs. 90 (78 to 96) Long-term F/U: 95 (80 to 99) vs. 91 (79 to 96) | Short-term F/U: 85 (55 to 96) vs. 83 (65 to 92) Long-term F/U: 90 (70 to 97) vs. 85 (70 to 93) | Short-term F/U: 85 (55 to 96) vs. 83 (65 to 92) Long-term F/U: 90 (70 to 97) vs. 85 (70 to 93) | Short-term F/U: NR Long-term F/U: 83 (57 to 94) vs. 81 (65 to 90) | Short-term F/U: NR Long-term F/U: 83 (57 to 94) vs. 81 (65 to 90) | Short- and long-term F/U: NR | Short-term F/U: NR Long-term F/U: 0.8 (0.24 to 2.65) | Short- and long-term F/U: NR |
adj = adjusted; CI = confidence interval; F/U = follow-up; HR = hazard ratio; IQR = interquartile range; LC = lesional control; met = metastasis; mets = metastases; NR = not reported; NRS = nonrandomized study; PME = pulmonary metastasectomy; SABR = stereotactic ablative radiotherapy; SOC = standard of care; tx = treatment; vs. = versus .
aRate of LC at 7 and 8 years for SABR and surgery (PME) at both time points was 83% (95% CI, 57% to 94%) vs. 81% (95% CI, 65% to 90).
Systemic Therapy Use
None of the included studies explored systemic therapy use after treatment with SABR; consequently, no summary of evidence has been conducted.
Question 2: Safety
SABR With SOC Versus SOC
Adverse Events
Two RCTs (from 3 publications)32,58,69 at either high risk of bias or with some concerns of bias overall monitored toxicity for patients who received either SABR plus SOC or SOC alone to treat their oligometastatic cancer (Table 14). Both studies used the CTCAE version 4.0 tool to assess AEs.32,58,69 Overall, it is unclear if there is a difference in AE incidence when comparing SABR with SOC to SOC alone.
Iyengar et al.69 compared SABR plus maintenance chemotherapy to maintenance chemotherapy alone in patients with a controlled primary lung tumour that metastasized to multiple locations with up to 5 oligometastases. This study provided AE frequencies for each group, separated according to AE grade, but did not report statistical findings. Despite this, the study authors concluded there were no differences in toxic effects between groups.69
The SABR-COMET RCT in 2 publications32,58 compared SABR plus systemic therapy to systemic therapy alone in patients with controlled primary tumours in multiple locations that metastasized to multiple sites with up to 5 oligometastases. Various toxicity comparisons were presented, including AEs (grade 2 or greater), treatment-related AEs (grade 2 or greater), death (grade 5), fatigue (grade 2 and grade 3), dyspnea (grade 2 and grade 3), and pain (grade 2 [any type, including muscle, bone, and other] and grade 3 [any type]). Results from SABR-COMET32,58 revealed that SABR plus systemic therapy was associated with a significantly higher rate of related AEs of grade 2 or greater compared with systemic therapy alone (29% versus 9%; P = 0.026), with an absolute increase of 20% (95% CI, 5 to 34). For all other AE comparisons, no significant differences between groups were found.32,58
Table 14: Adverse Events Comparing SABR With SOC Versus SOC
Study | Study characteristics | Tool, follow-up, results |
RCTs | ||
SABR-COMET | Age, median (IQR):
% male:
Primary tumour location: Breast, colorectal, lung, prostate, and other (not described in publication) Met site: Multiple Number of mets: ≤ 5 Mets location: Adrenal, bone, liver, lung, other:
Previous tx primary tumour: Yes Previous tx mets: Yes | Tool used to assess toxicity: CTCAE v4.0 Short-term F/U: Median F/U (IQR) — SABR + SOC: 26 (23 to 37) months; SOC: 25 (19 to 54) months32 Long-term F/U: Median F/U (IQR) — Total: 51 (46 to 58) months58 Results: Number of patients with AEs AE grade ≥ 2: SABR + SOC: 61% (n = 40) vs. SOC: 46% (n = 15); P = 0.15 Treatment-related AE grade ≥ 2: SABR + SOC: 29% (n = 19) vs. SOC: 9% (n = 3); P = 0.026 with an absolute increase of 20% (95% CI, 5 to 34) Death (grade 5): SABR + SOC: 4.5% (n = 3; radiation pneumonitis [n = 1], pulmonary abscess [n = 1], and subdural hemorrhage after surgery to repair a SABR-related perforated gastric ulcer [n = 1]) vs. SOC: 0% (n = 0); P = 0.55 Fatigue (grade 2): SABR + SOC: 6% (n = 4) vs. SOC: 6% (n = 2); P = 0.45 Fatigue (grade 3): SABR + SOC: 0% (n = 0) vs. SOC: 3% (n = 1); P = 0.45 Dyspnea (grade 2): SABR + SOC: 2% (n = 1) vs. SOC: 0% (n = 0); P = 1.00 Dyspnea (grade 3): SABR + SOC: 2% (n = 1) vs. SOC: 0% (n = 0); P = 1.00 Pain (any type, including muscle, bone, and other; grade 2): SABR + SOC: 8% (n = 5) vs. SOC: 0% (n = 0); P = 0.14 Pain (any type, including muscle, bone, and other; grade 3): SABR + SOC: 5% (n = 3) vs. SOC: 0% (n = 0); P = 0.14 |
Iyengar et al. (2018)69 | Age, median (IQR): • SABR + maintenance chemotherapy: 63.5 (51.0 to 78.0 years) • Maintenance chemotherapy: 70.0 (51.0 to 79.0) years % male: • SABR + maintenance chemotherapy: 64.3 • Maintenance chemotherapy: 73.3 Primary tumour location: Lung Met site: Multiple Number of mets: ≤ 5 Mets location: Lung, adrenal, mediastinum, axilla, liver, nasopharynx, bone (rib, spine) Previous tx primary tumour: Yes Previous tx mets: Yes | Tool used to assess toxicity: CTCAE v4.0 Median F/U (IQR) Total: 9.6 (2.4 to 30.2) months Toxicity results (number of events): • Grade 1 — SABR + maintenance: 13 vs. maintenance only: 17 • Grade 2 — SABR + maintenance: 5 vs. maintenance only: 5 • Grade 3 — SABR + maintenance: 4 vs. maintenance only: 2 • Grade 4 — SABR + maintenance: 0 vs. maintenance only: 1 • Grade 5 — SABR + maintenance: 3 vs. maintenance only: 6 |
AE = adverse event; CI = confidence interval; CTCAE = Common Terminology Criteria for Adverse Events; F/U = follow-up; IQR = interquartile range; met = metastasis; mets = metastases; NR = not reported; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; SOC = standard of care; tx = treatment; vs. = versus .
SABR Versus SOC
Adverse Events
Four studies (1 RCT,63 3 nonrandomized studies66-68) at a high risk of bias or with some concerns of bias overall monitored toxicity for patients who received either SABR or SOC to treat their oligometastatic cancer (Table 15). The majority of studies used the CTCAE63,66-68 or RTOG grading system66,67 to assess AEs. Overall, it is unclear if there is a difference in AE incidence when comparing SABR with SOC.
One RCT by Phillips et al. reported a larger number of grade 1 and 2 AEs at both 90-day and 180-day time points for the SABR group versus observation.63 Patients in this trial had controlled primary prostate cancer that metastasized to the bone or soft tissue with up to 3 oligometastases.
One nonrandomized study by De Bleser et al.66 compared SABR with or without ADT to ENRT with or without ADT in patients with controlled primary prostate cancer that metastasized to pelvic and extra-pelvic lymph nodes with up to 5 oligometastases. Three toxicity comparisons were presented, including early toxicity (all grades), late toxicity (all grades), and early and late toxicity (grade 3 or higher).66 Compared with ENRT, SABR was associated with a lower rate of AEs for all 3 comparisons (P < 0.05; median follow-up for both arms: 18.8 months; IQR, 5.8 to 35.0 months).66
One nonrandomized study by He et al.67 compared SABR with 3DCRT in patients with controlled primary colorectal cancer that metastasized to the liver with up to 3 oligometastases. The study found no differences between groups for the hepatic toxicity–inducing rate, though specific rates per group were not reported (P = 0.674). Between-group differences were descriptively reported for liver toxicity: the SABR group had 1 patient with a grade 1 or 2 AE and 1 patient with a grade 3 AE, and the 3DCRT group had 3 patients with a grade 1 or 2 AE and 2 patients with a grade 3 AE.67
One nonrandomized study by Filippi et al.68 did not conduct statistical testing to evaluate AEs with SABR compared with SOC. The study reported specific AEs with the number and proportion of patients in each grade, which precludes suitable comparison between groups; however, the study authors reported the SABR group had multiple grade 1 to 3 AEs and the surgery group reported 1 death. Patients in this study had primary colorectal cancer that metastasized to the lung with up to 5 oligometastases.
Table 15: Adverse Events Comparing SABR Versus SOC
Study | Study characteristics | Tool, follow-up, results |
RCTs | ||
Phillips et al. (2020)63 | Age, median (IQR):
% male: 100 Primary tumour location: Prostate Met site: Multiple Number of mets: ≤ 3 Mets location: Bone or soft issue Previous tx primary tumour: Yes Previous tx mets: Unclear | Tool used to assess toxicity: CTCAE v4.0 Median follow-up (IQR): Total: 36 (23 to 56) months Results: Number of patients with AEs New grade 1 AEs at 90 days: SABR: 29/36 (81%) vs. observation: 12/16 (75%) New grade 1 AEs at 180 days: SABR: 15/36 (42%) vs. observation: 3/11 (27%) New grade 2 AEs at 90 days: SABR: 3/36 (8%) vs. observation: 0/16 (0) New grade 2 AEs at 180 days: SABR: 2/36 (6%) vs. observation: 0/11 (0) Grade 3 or higher: None |
NRSs | ||
De Bleser et al. (2019)66 | Age (median, IQR):
Met site: Multiple Number of mets: ≤ 5 Mets location: Pelvic and extra-pelvic lymph nodes Previous tx primary tumour: Yes Previous tx mets: Some patients | Tool used to assess toxicity: CTCAE or RTOG grading system Median F/U (IQR): Total: 18.8 (5.8 to 35.0) months. Results: Number of patients with AEs
Early toxicity of all grades:
Late toxicity of all grades:
|
He et al. (2018)67 | Age, median (IQR): 71 (45 to 87) years % male: 100 Primary tumour location: Colon and rectum Met site: Single Number of mets: ≤ 3 Mets location: Liver Previous tx primary tumour: Yes Previous tx mets: Some patients | Tool used to assess toxicity: CTCAE v3.0 or RTOG Median F/U: Total: 13 months Liver toxicity results:
Hepatic toxicity–inducing rate: No difference between groups (P = 0.674) |
Filippi et al. (2016)68 | Age, median (IQR):
% male:
Primary tumour location: Colon and rectum Met site: Single Number of mets: ≤ 5 Mets location: Lung Previous tx primary tumour: Yes Previous tx mets: For some patients | Tool used to assess toxicity: CTCAE v3.0 Median F/U (IQR):
Results: SABR:
Surgery: Death: 0.7% (n = 1) within 30 days |
3DCRT = 3-dimensional conformal radiation therapy; AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; ENRT = elective nodal radiotherapy; F/U = follow-up; IQR = interquartile range; met = metastasis; mets = metastases; NRS = nonrandomized study; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; RTOG = Radiation Therapy Oncology Group; tx = treatment.
Patient Engagement
A patient collaborator was involved in the development of this project, from discussing the research question and outcomes in the protocol, to commenting on the draft findings, to being invited to provide feedback on the baseline clinical review.
The involvement of a patient collaborator enabled the research team to consider the evidence along with the wider experiences of patients and families when preparing the assessment. A deep discussion of clinical outcomes, particularly OS, PFS, and health-related QoL, revealed the goals of treatment with SABR. In CADTH’s conversations with the patient collaborator, the outcome that was discussed most by the patient was health-related QoL, including pain and fatigue, indicating the importance of remaining active and being able to return to work after treatment. The patient compared and contrasted the experience of having chemotherapy to treat the primary tumour versus SABR to treat the metastatic site and highlighted that SABR provided improved health-related QoL outcomes. A description of the patient collaborator’s rural location and distance to travel for treatment was noted. Patient group stakeholders (Canadian Partnership Against Cancer and Canadian Cancer Survivors Network) were invited to provide feedback on the clarity and relevance of the draft of the baseline clinical review.
Patient involvement was guided by the GRIPP2-SF reporting checklist and is reported in Table 25.55
Summary of Results
Three RCTs (from 5 publications32,58,59,62,63) and 6 nonrandomized studies (from 7 publications60,61,64-68) were identified that compared SABR alone or in combination with other SOC therapies with SOC alone for the treatment of patients with oligometastatic cancer. All 9 studies reported on clinical effectiveness. Three RCTs and 3 nonrandomized studies reported on AEs. For the included studies, SOC interventions comprised surgery, conventional radiotherapy, systemic therapy (i.e., chemotherapy, hormonotherapy, ADT), or no therapy (i.e., observation). The studies were grouped into 2 main comparisons (i.e., SABR with SOC versus SOC alone and SABR versus SOC). Key findings were narratively synthesized; no meta-analyses were conducted.
Regarding the clinical effectiveness of SABR plus SOC versus SOC alone, 2 RCTs (from 3 publications)32,58,69 provided some evidence that SABR plus SOC might be associated with OS and PFS benefits compared with SOC alone. The overall risk of bias of these studies was either high or with some concerns. Results from SABR-COMET32,58 showed longer median OS and lower HRs for OS in the SABR plus systemic therapy group, compared with systemic therapy alone, in both short- and long-term follow-ups. Likewise, the results from the Iyengar et al. RCT69 also suggested longer median OS in the SABR plus maintenance chemotherapy group compared with the maintenance chemotherapy alone group. Consistently, the available PFS data from 2 RCTs58,69,71 suggest that SABR plus SOC provides a significant PFS benefit compared with SOC alone. Considering patients with oligometastases have already had progression of their cancer via metastases, benefits in PFS may be of particular importance to this population; CADTH’s patient collaborator agreed with this suggestion. In terms of health-related QoL, 1 RCT found no significant differences between SABR plus systemic therapy versus systemic therapy alone in the overall mean of the FACT-G scores, or in any of the physical, social, functional, or emotional subscales.58,59 In terms of LC, 1 RCT32,58 found improved crude rates for SABR plus systemic therapy compared with systemic therapy alone in both the shorter- and longer-term follow-ups. The paucity of available evidence for health-related QoL and LC makes it difficult to provide definitive conclusions for those outcomes. None of the included studies explored freedom-from-progression outcomes or subsequent systemic therapy use.
Seven studies, comprising 1 RCT63 and 6 nonrandomized studies (from 7 publications),60,61,64-68 explored the clinical effectiveness of SABR versus SOC. The overall risk of bias of these studies was either high or with some concerns. The SOC comparator varied widely between studies and was dependent on the type of cancer being treated. SOC comparators included observation,63 3DCRT,64,65,67 conventional fractionation radiotherapy with or without hormonotherapy,65 ENRT with or without ADT,66 and surgery (various resections, pulmonary metastasectomy).60,61,68 Consideration for these differences in the comparator is warranted when interpreting the following narrative findings.
Five nonrandomized studies60,61,64,65,67,68 provided evidence suggesting that SABR may not be more effective than SOC for OS. Specifically, 1 nonrandomized study64 found that SABR was associated with a significantly longer median OS than 3DCRT, despite the shorter follow-up in the SABR group; however, the study authors attributed the OS benefit largely to selection bias demonstrated by imbalances in baseline characteristics between the 2 groups. The remaining 4 nonrandomized studies60,61,65,67,68 did not find significant differences in OS between SABR and SOC. Most of the nonrandomized studies likely had several limitations, such as incomplete control for confounding factors, immaturity in data, selection of patients as shown by differences in baseline characteristics between treatment groups, lack of power, and imbalances in sample sizes and differences in follow-up protocols between treatment groups. These preliminary findings from nonrandomized studies with potential limitations precluded a definitive conclusion regarding the clinical benefit of SABR alone compared with SOC alone in improving OS for patients with oligometastatic cancer.
In terms of PFS, 5 studies (1 RCT63 and 4 nonrandomized studies60,61,64,65,68) provided mixed results when comparing SABR with SOC. Three studies (1 RCT63 and 2 nonrandomized studies64,65) suggested SABR provided a PFS benefit compared with SOC alone (i.e., observation, hormonotherapy, or radiotherapy), 1 nonrandomized study68 suggested that SABR provided a worse prognosis in terms of PFS compared with surgery, and 1 nonrandomized study60,61 did not find any significant differences between SABR and surgery. Several of the limitations for OS in the nonrandomized studies indicated previously might also apply to PFS and, since PFS data do not always correlate with OS,72 the overall findings of PFS in the comparison of SABR versus SOC should be interpreted with caution. One RCT63 and 1 nonrandomized study64 explored health-related QoL outcomes and found no significant differences between groups (i.e., SABR versus observation,63 SABR versus 3DCRT64) in the majority of health-related QoL outcomes. One nonrandomized study (from 2 publications)60,61 investigated LC and found no differences in LC rates between SABR and pulmonary metastasectomy surgery at both short- and long-term follow-ups.60,61 None of the included studies explored outcomes related to freedom from progression or systemic therapy use.
The second clinical research question for this review aimed to determine the safety of SABR alone or in combination with other therapies for the treatment of patients with oligometastatic cancer compared with SOC alone. Results were narratively summarized by comparison (i.e., SABR plus SOC versus SOC alone, SABR versus SOC).
Two RCTs (from 3 publications)32,58,69 explored AEs for patients who received SABR plus systemic therapy or systemic therapy alone. For the SABR-COMET trial,32,58 SABR plus systemic therapy was associated with a significantly higher rate of treatment-related AEs of grade 2 or greater, without any significant differences for all other AE comparisons. The trial by Iyengar and colleagues69 did not statistically compare the AEs experienced by patients, but the study authors concluded there were no differences in toxic effects between SABR plus maintenance chemotherapy and maintenance chemotherapy alone.
Four studies (1 RCT,63 3 nonrandomized studies66-68) provided unclear evidence on whether SABR reduces AE incidence compared with SOC (i.e., observation, radiotherapy, or surgery). Two studies60,63,68 did not conduct statistical testing to determine whether rates of AEs were different between SABR and SOC groups. The nonrandomized study that explored SABR with or without ADT versus ENRT with or without ADT66 found that SABR was associated with a lower rate of AEs compared with ENRT. Finally, the nonrandomized study that compared SABR with 3DCRT67 did not find significant differences in hepatic toxicity–inducing rates between groups.
Discussion
Generalizability of Findings
This clinical review explores the clinical effectiveness and safety of SABR for any patients with oligometastatic cancer. There is currently no standardized definition of the oligometastatic state; therefore, CADTH used a definition for oligometastatic cancer informed by clinical experts and solicited stakeholder feedback on the included studies list for this review. For the purposes of this review, the population of interest was patients with oligometastatic cancer, described by study authors as having limited metastatic lesions using terminology such as “oligo,” “limited,” or “few,” including identification of de novo or repeat oligometastatic disease at any time during the patient’s course of treatment, irrespective of the status of the primary tumour. However, this definition may have excluded studies that other research groups may have deemed to involve oligometastatic cancer that did not meet our definition, and the results of this review may not be applicable to every interpretation of “oligometastatic cancer.” On the other hand, the other inclusion criteria were quite broad and allowed for the inclusion of diverse patient populations within the oligometastatic disease spectrum; comparative studies examining SABR for patients with oligometastatic cancer were included regardless of the location of primary tumour, location of metastases, number of metastases, or number of metastatic sites. This review excluded studies involving patients who had a history of widespread metastatic disease (i.e., induced oligometastatic disease); however, it is possible that a study included “oligometastatic” patients without additional information regarding previous widespread disease. For this review, it was assumed that patients had no history of widespread metastatic disease if this was not explicitly described in the study; in those cases, the studies may have included patients with a history of widespread metastatic disease that were unknowingly included in this review.
Oligometastatic disease is an umbrella term in the sense that patients can have different types of primary and metastatic location combinations and may have different clinical profiles. Different primary cancer types have different disease prognoses, making it difficult to assess transferability of findings between patient populations. This review did not identify any subgroup analysis for the subgroups of interest. Nevertheless, some of the findings were specific to primary lung cancer69 or primary prostate cancer,65,66 including up to 3 metastases,63,67 multiple metastatic sites32,58,59,63-66,69 or a single metastatic site such as lung60,61,68 or liver,67 patients with previous treatment of a primary tumour,32,58-61,63,65-68 or patients with previous treatment of metastases.32,58-61,64,66-69 In addition, while patients of any age were of interest for this review, all included studies evaluated adult patients, with a median age above 60 years in all treatment groups. Therefore, the results may not be applicable to pediatric patients or to younger adults with oligometastatic cancer.
For this review, 1 RCT (from 3 publications)32,58,59 was conducted at multiple institutions across Canada, the Netherlands, UK, and Australia. The remaining 8 studies60-68 were conducted outside of Canada. However, the majority of the evidence was from developed countries and, therefore, may be generalizable to the Canadian context.
CADTH engaged 1 patient with lived experience of oligometastatic cancer to inform the selection of important clinical outcomes and to provide the reviewers with some context for interpretation of the findings. The purpose of patient engagement is not to be representative of all Canadians, recognizing that individual patients have a diversity of experiences and perceptions related to oligometastatic cancer and its treatment. Comments and perspectives from our patient collaborator were not analyzed; rather, CADTH drew on patient perspectives and impressions to help better inform the work and help interpret the clinical evidence. Of note, the topic and research questions were already determined before engaging the patient collaborator. Possible limitations of this patient engagement were that our collaborator and other patient stakeholders were invited to participate within a set time frame and with a deadline for providing feedback. People need access to reliable technology and phone and internet service to participate; lack of such access could possibly exclude some voices.
Limitations
There are certain limitations to consider when reviewing the report, which are described subsequently.
Evidence Gaps
There were a number of gaps in the evidence identified for this review. Namely, there were relatively few studies identified for each intervention and comparator combination; 3 studies (2 RCTs32,58,59,69) evaluated SABR plus SOC versus SOC alone, and 8 studies (1 RCT63 and 7 nonrandomized studies60,61,64-68,70) evaluated SABR versus SOC. Within those comparison categories, the outcomes of interest for this review were often not reported by all of the included studies, further reducing the available evidence for comparison. Evidence for the AE outcomes in particular was very limited due to how the data were recorded (e.g., treatment-related versus non–treatment-related AEs, event data versus patient data, only selective grades reported). No data were identified from any study to report on freedom from progression and subsequent use of systemic therapy. In addition, subgroup analyses within studies were lacking; instead, studies were described with relevant patient characteristics only when presenting overall study results. There was no evidence identified to comment on the effectiveness or safety of SABR based on patient age, sex, or gender.
To be comprehensive, this review used broad inclusion criteria for SOC for metastatic cancer, which varies according to the type of primary cancer and metastatic site. This variety is reflected in the wide range of SOC comparators described in the included studies, which were narratively synthesized in the same manner without discerning the efficacy of 1 comparator over another (e.g., surgery versus observation). In addition, several studies broadly included patients with oligometastatic cancer that included multiple types of primary cancers and locations of oligometastases without presenting subgroup analyses of results by primary tumour or oligometastatic location. While results in the present work compare SABR with any type of SOC deemed appropriate for patients of a certain variation of oligometastatic cancer, there was not enough evidence identified in this review to truly discern whether certain cancer types or intervention combinations may benefit from SABR more than others. Similarly, the dose used when administering SABR was study-dependent and varied based on the protocol used in consideration of the location(s) of the targeted metastatic site(s), the frequency and number of fractions per lesion per patient, and complication risks to nearby normal tissue. Clinical experts engaged by CADTH have suggested that this is consistent with their experience in practice. Furthermore, the relationship between the size of the lesion(s) and dose may affect patient outcomes. For example, treating larger lesions may be associated with higher toxicities from treatment, and lower LC rates may be observed in situations where lower-dose prescriptions are used for patient safety. CADTH is unable to provide details on the optimal SABR regimen or dose, given the variation in the included studies. As SABR dose is dependent on many factors, it may be challenging to identify optimal SABR regimens or standardized doses that could be applicable across all oligometastatic cancers or patients.
Taken together, the limited amount of evidence identified combined with the variation in patient characteristics and outcome reporting across and within the included studies affected the ability to quantitatively synthesize findings and reflects a high degree of uncertainty in the findings to date. For this review, 9 studies (from 12 publications) were included. A 2019 paper identified 64 ongoing studies examining SABR for oligometastatic cancer.33 CADTH’s detailed scoping exercise and additional grey literature searches also identified a number of ongoing clinical trials.1 Thus, there is undoubtedly more evidence coming down the research pipeline in the near future that will likely add to our current evidence base to inform whether SABR should be used for patients with oligometastatic cancer and under what conditions (e.g., patient characteristics, dose). Regular updates of this baseline review are planned to capture additional and relevant studies in the form of a LSR.
Heterogeneity
There was substantial clinical, methodological, and statistical heterogeneity among the included studies preventing meta-analyses of the data. Specifically, sources of heterogeneity included differences in study design (i.e., RCT, nonrandomized study), data unavailability (e.g., 2 relevant studies for the comparison of interest, but HRs reported for 1 study), data variability (e.g., AE results included different AE grades reported, treatment-related versus non–treatment-related AEs, or event data versus patient data), and discordant results (i.e., large variability in the direction, magnitude, and statistical significance of the results). As discussed previously, there was variation in the patient characteristics within and across included studies (e.g., type of primary tumour, location of oligometastases) and types of treatment comprising SOC that contributed to the heterogeneity, which is also reflected by the inconsistent results in the narrative synthesis for some comparisons and outcomes.
Quality of Evidence
The included studies comprised both RCTs and nonrandomized studies (with the majority using a retrospective cohort study design). The risk of bias of the included studies ranged from high risk of bias to some concerns. All included RCTs were phase II trials with limitations in the randomization process and with relatively small sample sizes, although power calculations were performed. All of the included nonrandomized studies were susceptible to the risk of selection bias, reporting bias, and lack of power calculations. For feasibility reasons, only studies published in English were eligible for inclusion. It is acknowledged that there is a potential for language bias when language restrictions are used; however, there is also evidence for minimal impact of including studies published in other languages.73,74
Directions for Future Research
To facilitate decisions around appropriate patient selection and the optimal SABR regimen or dose, additional studies examining the clinical effectiveness and safety of SABR with detailed reporting of criteria for patient selection and dosing are required. Additional studies examining any clinical outcomes outlined in this review may also enable future meta-analyses of the data to provide more robust findings, as several of the comparisons could not be pooled due to the lack of available evidence (i.e., no HRs to pool). Specifically, the patient partner emphasized QoL as 1 of the central outcomes of interest, including breathing issues, fatigue, impact on physical activity, and being able to return to work after treatment. Some evidence was available regarding QoL (3 studies), mainly focusing on pain and less on physical functioning. Additional research regarding the interventions’ impact on QoL is warranted. Moreover, the patient collaborator described the distance to travel for treatment and the costs associated with travel, highlighting some practical considerations related to accessing SABR treatment. As SABR for the treatment of oligometastatic cancer is an active field of research, additional studies are expected to be identified upon updates of this baseline review during the LSR phase. Such updates may provide an opportunity to fill in gaps in the clinical evidence and strengthen the conclusions of this review.
Conclusions and Implications for Decision-Making
To CADTH’s knowledge, this is the first systematic review exploring the clinical effectiveness and safety of SABR for any patients with oligometastatic cancer (i.e., no restrictions on primary or metastatic locations). Key outcomes of interest included OS, PFS, and AEs, consistent with the opinions of our clinical experts and patient partner. Findings from the included studies suggested there may be OS and PFS benefits associated with SABR plus SOC compared with SOC alone. Findings from the included studies on OS and PFS for SABR alone versus SOC were mixed and deemed inconclusive, as the studies were generally limited by unadjusted baseline imbalances associated with the retrospective cohort study design and had small sample sizes and uncertainty around whether the survival data were mature. Few studies statistically compared AE data, making it unclear if SABR, with or without SOC, is more or less harmful than SOC alternatives for patients with oligometastases. There was a lack of literature identified to inform conclusions for other outcomes of interest, including freedom from progression, health-related QoL, LC, and use of systemic therapy after treatment, and for subgroups of interest (i.e., age, sex, gender, location of primary tumour site, number of metastases sites, number of metastases, location of metastases, previous treatment of primary tumour, and previous treatment of metastases). More comparative studies using rigorous methods, such as high-quality randomized trials with sufficient sample sizes and mature OS data, are required to reduce this uncertainty. Future research on the effectiveness of SABR in patients with different characteristics would clarify who might benefit most from this treatment, which would inform patient selection criteria. In addition, evidence on the optimal regimen or dose of SABR for treatment of oligometastases is still needed. Additional studies are expected to be identified during the LSR phase of this project, which will see routine monitoring for newly published literature and regular updating of this baseline review. Finally, this clinical review represents 1 component among many that decision-makers will consider when making the decision about the expanded use of SABR in Canada.
References
1.Stereotactic ablative body radiotherapy for the treatment of oligometastatic cancer. (CADTH scoping brief). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/pdf/ht0029-sabr-for-oligometastatic-cancer-scoping-brief.pdf. Accessed 2020 Feb 15.
2.Evidence Partners. DistillerSR [computer program]. Ottawa (ON): Evidence Partners; 2011.
3.Canadian Cancer Society. Cancer statistics at a glance. Cancer information 2020; https://www.cancer.ca/en/cancer-information/cancer-101/cancer-statistics-at-a-glance/?region=on. Accessed 2020 Aug 5.
4.Canadian Cancer Society. What is metastatic cancer? Metastatic cancer 2019; https://www.cancer.ca/en/cancer-information/cancer-type/metastatic-cancer/metastatic-cancer/?region=on. Accessed 2019 Dec 18.
5.Rankin EB, Giaccia AJ. Hypoxic control of metastasis. Science. 2016;352(6282):175-180. PubMed
6.Massague J, Obenauf AC. Metastatic colonization by circulating tumour cells. Nature. 2016;529(7586):298-306. PubMed
7.Fuentes R, Osorio D, Exposito Hernandez J, Simancas-Racines D, Martinez-Zapata MJ, Bonfill Cosp X. Surgery versus stereotactic radiotherapy for people with single or solitary brain metastasis. Cochrane Database Syst Rev. 2018;8:CD012086. PubMed
8.Algan O, Giem J, Young J, Ali I, Ahmad S, Hossain S. Comparison of doses received by the hippocampus in patients treated with single isocenter- vs multiple isocenter-based stereotactic radiation therapy to the brain for multiple brain metastases. Med Dosim. 2015;40(4):314-317. PubMed
9.Hellman S, Weichselbaum RR. Oligometastases. J Clin Oncol. 1995;13(1):8-10. PubMed
10.Takeda A, Sanuki N, Kunieda E. Role of stereotactic body radiotherapy for oligometastasis from colorectal cancer. World J Gastroenterol. 2014;20(15):4220-4229. PubMed
11.Reyes DK, Pienta KJ. The biology and treatment of oligometastatic cancer. Oncotarget. 2015;6(11):8491-8524. PubMed
12.Guckenberger M, Lievens Y, Bouma AB, et al. Characterisation and classification of oligometastatic disease: a European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer consensus recommendation. Lancet Oncol. 2020;21(1):e18-e28. PubMed
13.Lievens Y, Guckenberger M, Gomez D, et al. Defining oligometastatic disease from a radiation oncology perspective: an ESTRO-ASTRO consensus document. Radiother Oncol. 2020;148:157-166. PubMed
14.Milano MT, Vokes EE, West HJ, Salama JK. Oligometastatic non-small cell lung cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2017: www.uptodate.com. Accessed 2019 Aug 02.
15.Ashworth A, Senan S, Palma DA, et al. An individual patient data meta-analysis of outcomes and prognostic factors after treatment of oligometastatic non-small cell lung cancer. Int J Radiat Oncol Biol Phys. 2014;90(5 suppl 1):S4.
16.deSouza NM, Tempany CM. A risk-based approach to identifying oligometastatic disease on imaging. Int J Cancer. 2019;144(3):422-430. PubMed
17.Wild AT, Yamada Y. Treatment Options in Oligometastatic Disease: Stereotactic Body Radiation Therapy - Focus on Colorectal Cancer. Visc Med. 2017;33(1):54-61. PubMed
18.Ni Y, Ye X, Yang X, et al. Microwave ablation as local consolidative therapy for patients with extracranial oligometastatic EGFR-mutant non-small cell lung cancer without progression after first-line EGFR-TKIs treatment. J Cancer Res Clin Oncol. 2020;146(1):197-203. PubMed
19.Hiraki T, Kanazawa S. Lung radiofrequency ablation: potential as a therapy to oligometastasis and oligorecurrence. Pulm Med. 2012;2012:196173. PubMed
20.Ost P, Bossi A, Decaestecker K, et al. Metastasis-directed therapy of regional and distant recurrences after curative treatment of prostate cancer: a systematic review of the literature. Eur Urol. 2015;67(5):852-863. PubMed
21.Gomez DR, Tang C, Zhang J, et al. Local Consolidative Therapy Vs. Maintenance Therapy or Observation for Patients With Oligometastatic Non-Small-Cell Lung Cancer: Long-Term Results of a Multi-Institutional, Phase II, Randomized Study. J Clin Oncol. 2019;37(18):1558-1565. PubMed
22.Ost P, Reynders D, Decaestecker K, et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J Clin Oncol. 2018;36(5):446-453. PubMed
23.Buyyounouski MK, Price RA, Harris EE, et al. Stereotactic body radiotherapy for primary management of early-stage, low-to intermediate-risk prostate cancer: report of the American Society for Therapeutic Radiology and Oncology Emerging Technology Committee. Int J Radiat Oncol Biol Phys. 2010;76(5):1297-1304. PubMed
24.Velazquez S, Montero E, Rubio M, Ortiz M. An emerging method of faster stereotactic body radiation therapy through stereotactic multidampening. Int J Radiat Oncol Biol Phys. 2016;96(2 suppl 1):E651.
25.Krishnan MS, Shiloh R, Dougherty P, Whitehouse CM, Buckman A, Balboni TA. The TEACHH model: clinical utility of identifying patients living fewer than 2 months. Int J Radiat Oncol Biol Phys. 2016;96(2 suppl 1):S194.
26.Blomgren H, Lax I, Näslund I, Svanström R. Stereotactic high dose fraction radiation therapy of extracranial tumors using an accelerator: clinical experience of the first thirty-one patients. Acta Oncol. 1995;34(6):861-870. PubMed
27.Ma L, Wang L, Tseng CL, Sahgal A. Emerging technologies in stereotactic body radiotherapy. Chin Clin Oncol. 2017;6(suppl 2):S12. PubMed
28.Goddard LC, Brodin NP, Bodner WR, Garg MK, Tomé WA. Comparing photon and proton-based hypofractioned SBRT for prostate cancer accounting for robustness and realistic treatment deliverability. Br J Radiol. 2018;91(1085):20180010. PubMed
29.Lund CR, Cao JQ, Liu M, Olson R, Halperin R, Schellenberg D. The Distribution and Patterns of Practice of Stereotactic Ablative Body Radiotherapy in Canada. J Med Imaging Radiat Sci. 2014;45(1):8-15. PubMed
30.Loewen S. Personal communication. Calgary (AB): Tom Baker Cancer Centre; 2020 Feb 07.
31.Council of Academic Hospitals of Ontario (CAHO). Fewer treatments, better outcomes: HSN uses new form of radiation for elderly patients with lung cancer. http://caho-hospitals.com/fewer-treatments-better-outcomes-hsn-uses-new-form-of-radiation-for-elderly-patients-with-lung-cancer/. Accessed 2020 Feb 27.
32.Palma DA, Olson R, Harrow S, et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): a randomised, phase 2, open-label trial. Lancet. 2019;393(10185):2051-2058. PubMed
33.Al-Shafa F, Arifin AJ, Rodrigues GB, Palma DA, Louie AV. A Review of Ongoing Trials of Stereotactic Ablative Radiotherapy for Oligometastatic Cancers: Where Will the Evidence Lead? Front Oncol. 2019;9:543. PubMed
34.NHS England Specialised Services Clinical Reference Group for Radiotherapy. Clinical commissioning policy: the use of stereotactic ablative radiotherapy (SABR) in the treatment of oligometastatic disease. London (UK): NHS England; 2016: https://www.england.nhs.uk/wp-content/uploads/2018/07/Stereotactic-ablative-radiotherapy-as-a-treatment-option-for-patients-with-oligometastatic-disease.pdf. Accessed 2020 Feb 27.
35.Palma D, Olson R, Harrow S, et al. Stereotactic ablative radiation therapy for the comprehensive treatment of oligometastatic tumors (SABR-COMET): results of a randomized trial. Int J Radiat Oncol Biol Phys. 2018;102(3):S3-S4.
36.Stereotactic Body Radiotherapy for oligometastatic cancer: a review of clinical effectiveness and cost-effectiveness. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1071%20Stereotactic%20Body%20Radiotherapy%20Final.pdf. Accessed 2020 Nov 19.
37.Stereotactic ablative radiotherapy for the treatment of oligometastatic cancer. (CADTH health technology assesment - project protocol). Ottawa (ON)2020: https://cadth.ca/sites/default/files/pdf/ht0029-sabr-for-oligometastatic-cancer-clinical-protocol.pdf. Accessed 2020 Jul 31.
38.Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. PubMed
39.Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020). Chichester (UK): John Wiley & Sons; 2020: https://training.cochrane.org/cochrane-handbook-systematic-reviews-interventions. Accessed 2020 Nov 19.
40.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
41.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2020 Apr 27.
42.National Cancer Institute. NCI dictionary of cancer terms. 2019; https://www.cancer.gov/publications/dictionaries/cancer-terms/. Accessed 2019 Jan 30.
43.Dekkers OM, Egger M, Altman DG, Vandenbroucke JP. Distinguishing case series from cohort studies. Ann Intern Med. 2012;156(1 pt 1):37-40. PubMed
44.Laurie SA, Banerji S, Blais N, et al. Canadian consensus: oligoprogressive, pseudoprogressive, and oligometastatic non-small-cell lung cancer. Curr Oncol. 2019;26(1):e81-e93. PubMed
45.Weickhardt AJ, Scheier B, Burke JM, et al. Local ablative therapy of oligoprogressive disease prolongs disease control by tyrosine kinase inhibitors in oncogene-addicted non–small-cell lung cancer. J Thorac Oncol. 2012;7(12):1807-1814. PubMed
46.Kissel M, Martel-Lafay I, Lequesne J, et al. Stereotactic ablative radiotherapy and systemic treatments for extracerebral oligometastases, oligorecurrence, oligopersistence and oligoprogression from lung cancer. BMC Cancer. 2019;19(1):1237. PubMed
47.Niibe Y, Hayakawa K. Oligometastases and oligo-recurrence: the new era of cancer therapy. Jpn J Clin Oncol. 2010;40(2):107-111. PubMed
48.Linskey ME, Andrews DW, Asher AL, et al. The role of stereotactic radiosurgery in the management of patients with newly diagnosed brain metastases: a systematic review and evidence-based clinical practice guideline. J Neurooncol. 2010;96(1):45-68. PubMed
49.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
50.Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. PubMed
51.Kim SY, Park JE, Lee YJ, et al. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J Clin Epidemiol. 2013;66(4):408-414. PubMed
52.Kim SY, Lee YJ, Seo HJ, Park JE. Revision of clinical research literature classification tool and risk of bias assessment tool. Wonju (KR): Health Insurance Review & Assessment Service; 2013.
53.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. PubMed
54.Campbell M, McKenzie JE, Sowden A, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020;368:l6890. PubMed
55.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453. PubMed
56.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
57.CADTH framework for patient engagement in health technology assessment. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2021 Feb 09.
58.Palma DA, Olson R, Harrow S, et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J Clin Oncol. 2020;38(25):2830-2838. PubMed
59.Olson R, Senan S, Harrow S, et al. Quality of Life Outcomes After Stereotactic Ablative Radiation Therapy (SABR) Versus Standard of Care Treatments in the Oligometastatic Setting: A Secondary Analysis of the SABR-COMET Randomized Trial. Int J Radiat Oncol Biol Phys. 2019;105(5):943-947. PubMed
60.Widder J, Klinkenberg TJ, Ubbels JF, Wiegman EM, Groen HJ, Langendijk JA. Pulmonary oligometastases: metastasectomy or stereotactic ablative radiotherapy? Radiother Oncol. 2013;107(3):409-413. PubMed
61.Lodeweges JE, Klinkenberg TJ, Ubbels JF, Groen HJM, Langendijk JA, Widder J. Long-term Outcome of Surgery or Stereotactic Radiotherapy for Lung Oligometastases. J Thorac Oncol. 2017;12(9):1442-1445. PubMed
62.Iyengar P, Tumati V, Gerber D, et al. Consolidative radiotherapy for limited metastatic nonesmall cell lung cancer: A randomized phase 2 trial. Int J Radiat Oncol Biol Phys. 2017;99(5):1314.
63.Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020;6(5):650-659. PubMed
64.van de Ven S, van den Bongard D, Pielkenrood B, et al. Patient-Reported Outcomes of Oligometastatic Patients After Conventional or Stereotactic Radiation Therapy to Bone Metastases: An Analysis of the PRESENT Cohort. Int J Radiat Oncol Biol Phys. 2020;30:30. PubMed
65.Hurmuz P, Onal C, Ozyigit G, et al. Treatment outcomes of metastasis-directed treatment using (68)Ga-PSMA-PET/CT for oligometastatic or oligorecurrent prostate cancer: Turkish Society for Radiation Oncology group study (TROD 09-002). Strahlenther Onkol. 2020;196(11):1034-1043. PubMed
66.De Bleser E, Jereczek-Fossa BA, Pasquier D, et al. Metastasis-directed Therapy in Treating Nodal Oligorecurrent Prostate Cancer: A Multi-institutional Analysis Comparing the Outcome and Toxicity of Stereotactic Body Radiotherapy and Elective Nodal Radiotherapy. Eur Urol. 2019;76(6):732-739. PubMed
67.He Z, Chen G, Ouyang B, et al. Conformal radiation therapy or stereotactic body radiation therapy: Institutional experience in the management of colorectal liver metastases by radiation therapy. Technol Cancer Res Treat. 2018;17:1533033818816080.
68.Filippi AR, Guerrera F, Badellino S, et al. Exploratory Analysis on Overall Survival after Either Surgery or Stereotactic Radiotherapy for Lung Oligometastases from Colorectal Cancer. Clin Oncol (R Coll Radiol). 2016;28(8):505-512. PubMed
69.Iyengar P, Wardak Z, Gerber DE, et al. Consolidative Radiotherapy for Limited Metastatic Non-Small-Cell Lung Cancer: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2018;4(1):e173501. PubMed
70.Katoh N, Onishi H, Uchinami Y, et al. Real-Time Tumor-Tracking Radiotherapy and General Stereotactic Body Radiotherapy for Adrenal Metastasis in Patients With Oligometastasis. Technol Cancer Res Treat. 2018;17:1533033818809983. PubMed
71.Olson RA, Senan S, Harrow S, et al. Quality of Life Outcomes after Stereotactic Ablative Radiotherapy (SABR) vs. Standard of Care Palliative Treatments: A Secondary Analysis of the SABR-COMET Randomized Trial. Int J Radiat Oncol Biol Phys. 2019;105(1 suppl):S72-S73.
72.Davis S, Tappenden P, Cantrell A. A review of studies examining the relationship between progression-free survival and overall survival in advanced or metastatic cancer. London (UK): National Institute for Health and Care Excellence (NICE); 2012: https://www.ncbi.nlm.nih.gov/books/NBK425826/pdf/Bookshelf_NBK425826.pdf. Accessed 2020 Nov 19.
73.Morrison A, Polisena J, Husereau D, et al. The effect of English-language restriction on systematic review-based meta-analyses: a systematic review of empirical studies. Int J Technol Assess Health Care. 2012;28(2):138-144. PubMed
74.Nussbaumer-Streit B, Klerings I, Dobrescu AI, et al. Excluding non-English publications from evidence-syntheses did not change conclusions: a meta-epidemiological study. J Clin Epidemiol. 2020;118:42-54. PubMed
Appendix 1: Analytical Framework
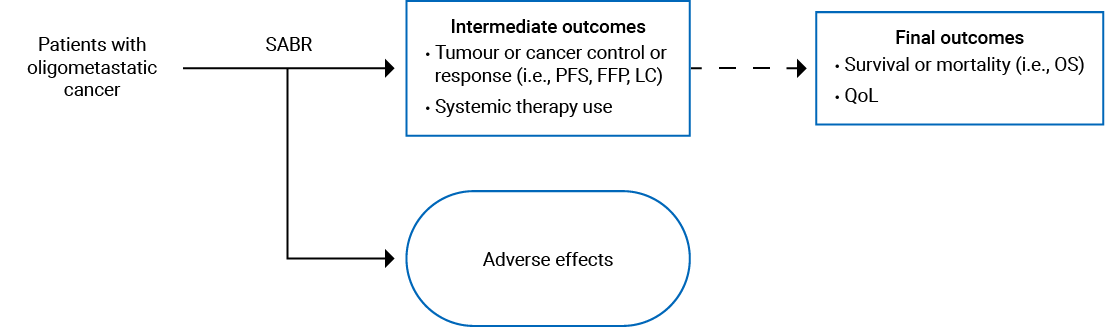
Appendix 2: Literature Search Methods
Clinical Literature Search
Overview
Interface: Ovid
Databases: MEDLINE All (1946-present), Embase (1974-present), Cochrane Central Register of Controlled Trials (CCTR)
Note: Subject headings have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: March 20, 2020
Alerts: Monthly search updates until project completion. After completion search alerts will occur every 3 months.
Study types: No publication type filters will be applied.
Limits: Publication date limit: 1990-present
Language limit: none
Conference abstracts: excluded
Syntax Guide
/ = At the end of a phrase, searches the phrase as a subject heading
MeSH = Medical Subject Heading
.fs = Floating subheading
Exp = Explode a subject heading
* = Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings
? = Truncation symbol for 1 or no characters only
adj# = Requires terms to be adjacent to each other within # number of words (in any order)
.ti = Title
.ab = Abstract
.kf = Author keyword heading word (MEDLINE)
.kw = Author keyword (Embase); keyword (CCTR)
.dq = Candidate term word (Embase)
.pt = Publication type
.my = Device index terms word (Embase)
.dv = Device trade name (Embase)
.dm = Device manufacturer (Embase)
freq = # = Requires terms to occur # number of times in the specified fields
medal = Ovid database code: MEDLINE All, 1946 to present, updated daily
oemezd = Ovid database code; Embase, 1974 to present, updated daily
cctr = Ovid database code; Cochrane Central Register of Controlled Trials
Multi-Database Strategy (Line Number and Search Strategy)
(exp radiotherapy/ or radiotherapy.fs.) and (stereo?ta* or stereo ta*).ti,ab,kf,kw.
((stereo?ta* or stereo ta*) adj5 (ablat* or body or lung* or liver* or spin*) adj5 (radiat* or radio therap* or radio?therap* or radio surg* or radiosur* or radio frequen* or radiofrequen* or proton* or photon*)).ti,ab,kf,kw.
((stereo?ta* or stereo ta* or intensity modulat* or linear accelerat*) adj4 (radiat* or radio therap* or radio?therap* or radio surg* or radiosur* or irradiation* or radio frequen* or radiofrequen* or proton* or photon*)).ti,ab,kf,kw.
((fraction* or ultra hypofraction* or ultrahypofraction* or hypofraction* or hyperfraction*) adj4 (radio therap* or radio?therap* or radio surg* or radiosur* or irradiation* or radio frequen* or radiofrequen* or proton* or photon*)).ti,ab,kf,kw.
((dynamic* or volumetric modulat*) adj5 (ARC or wave ARC* or waveARC*)).ti,ab,kf,kw.
(precision* adj5 deliver* adj5 system*).ti,ab,kf,kw.
(fraction* adj5 (stereo ta* or stereota*)).ti,ab,kf,kw.
(SRS* or SABR* or SBRT* or mdSBRT* or FSR or FSRT or LINAC* or DCA or VMAT or IMRS or IMPT or stereo tacic RT* or stereotacic RT* or stereo taxic RT* or stereotaxic RT* or systemSRBT*).ti,ab,kf,kw.
(xknife* or infinity* or novalis* or trilogy* or clinac* or accuray* or radixac* or cyberknife* or cyber knife* or synergy* or gammaknife* or gamma knife* or exactrac* or exac trac* or truebeam* or true beam* or MRLinac* or MR Linac* or eclipse* or rapid ARC* or rapidARC* or prefexion* or vero* or model u*2 or modellu* or modellc* or model c*2).ti,ab,kf,kw.
(integra or elekta* or varian or brainlab* or brain lab* or Mitsubishi Heavy*).ti,ab,kf,kw.
(versa*3 or precise*3 or edge*3).ti,kf,kw.
or/1-11
exp Neoplasm Metastasis/ and oligo*.ti,ab,kf,kw.
(oligomet* or oligoprogress* or oligorecur* or oligopersist* or oligofraction* or oligoclonal* or oligosynchron*).ti,ab,kf,kw.
(oligo* adj5 (meta* or progress* or recur* or persist* or fraction* or clonal* or synchron*)).ti,ab,kf,kw.
((tumour* or tumour* or cancer* or neoplasm* or carcinoma*) adj3 (migration* or spread*)).ti,ab,kf,kw.
((few* or limited* or advanced* or number*) adj2 (tumour* or tumour* or site* or metastases or spread or micrometastas*)).ti,ab,kf,kw.
((transitional or intermediate) adj5 (metasta* or micrometastas*)).ti,ab,kf,kw.
Limited Metastatic.ti,ab,kf,kw.
(secondary adj5 (tumour* or tumour* or lesion* or metastases or micrometastas*)).ti,ab,kf,kw.
or/13-20
12 and 21
22 use medall
22 use cctr
(exp radiosurgery/ or exp radiotherapy equipment/ or exp radiotherapy/ or radiotherapy.fs.) and (stereo?ta* or stereo ta*).ti,ab,kw,dq.
((stereo?ta* or stereo ta*) adj5 (ablat* or body or lung* or liver* or spin*) adj5 (radiat* or radio therap* or radio?therap* or radio surg* or radiosur* or radio frequen* or radiofrequen* or proton* or photon*)).ti,ab,kw,dq.
((stereo?ta* or stereo ta* or intensity modulat* or linear accelerat*) adj4 (radiat* or radio therap* or radio?therap* or radio surg* or radiosur* or irradiation* or radio frequen* or radiofrequen* or proton* or photon*)).ti,ab,kw,dq.
((fraction* or ultra hypofraction* or ultrahypofraction* or hypofraction* or hyperfraction*) adj4 (radio therap* or radio?therap* or radio surg* or radiosur* or irradiation* or radio frequen* or radiofrequen* or proton* or photon*)).ti,ab,kw,dq.
((dynamic* or volumetric modulat*) adj5 (ARC or wave ARC* or waveARC*)).ti,ab,kw,dq.
(precision* adj5 deliver* adj5 system*).ti,ab,kw,dq.
(fraction* adj5 (stereo ta* or stereota*)).ti,ab,kw,dq.
(SRS* or SABR* or SBRT* or mdSBRT* or FSR or FSRT or LINAC* or DCA or VMAT or IMRS or IMPT or stereo tacic RT* or stereotacic RT* or stereo taxic RT* or stereotaxic RT* or systemSBRT*).ti,ab,kw,dq.
(xknife* or infinity* or novalis* or trilogy* or clinac* or accuray* or radixac* or cyberknife* or cyber knife* or synergy* or gammaknife* or gamma knife* or exactrac* or exac trac* or truebeam* or true beam* or MRLinac* or MR Linac* or eclipse* or rapid ARC* or rapidARC* or prefexion* or vero* or model u*2 or modellu*or modellc* or model c*2).ti,ab,kw,dq,my,dv,dm.
(integra or elekta* or varian or brainlab* or brain lab* or Mitsubishi Heavy*).ti,ab,kw,dq,dv,dm.
(versa*3 or precise*3 or edge*3).ti,kw,dq,my,dv,dm.
or/25-35
exp metastasis/ and oligo*.ti,ab,kw,dq.
(oligomet* or oligoprogress* or oligorecur* or oligopersist* or oligofraction* or oligoclonal* or oligosynchron*).ti,ab,kw,dq.
(oligo* adj5 (meta* or progress* or recur* or persist* or fraction* or clonal* or synchron*)).ti,ab,kw,dq.
((tumour* or tumour* or cancer* or neoplasm* or carcinoma*) adj3 (migration* or spread*)).ti,ab,kw,dq.
((few* or limited* or advanced* or number*) adj2 (tumour* or tumour* or site* or metastases or spread or micrometastas*)).ti,ab,kw,dq.
((transitional or intermediate) adj5 (metasta* or micrometastas*)).ti,ab,kw,dq.
Limited Metastatic.ti,ab,kw,dq.
(secondary adj5 (tumour* or tumour* or lesion* or metastases or micrometastas*)).ti,ab,kw,dq.
or/37-44
36 and 45
46 use oemezd
47 not conference abstract.pt.
23 or 24 or 48
limit 49 to yr = 1990-current
remove duplicates from 50
Clinical Trial Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search terms will include - Stereotactic Ablative Radiotherapy (SABR) OR Stereotactic Radiosurgery (SRS) OR stereotactic body radiation therapy (SBRT) OR fractionated stereotactic radiotherapy (FSRT) OR LINAC OR XKnife OR Versa OR Infinity OR Precise OR Novalis Tx OR Trilogy OR Clinac OR Accuray Tomotherapy OR Radixac OR CyberKnife OR Synergy OR Gamma Knife Icon OR ExacTrac OR TrueBeam OR Edge OR Eclipse RapidArc OR Gamma Knife Model U OR Gamma Knife Model C OR Gamma Knife Prefexion]
Health Canada. Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms will include - Stereotactic Ablative Radiotherapy (SABR) OR Stereotactic Radiosurgery (SRS) OR stereotactic body radiation therapy (SBRT) OR fractionated stereotactic radiotherapy (FSRT) OR LINAC OR XKnife OR Versa OR Infinity OR Precise OR Novalis Tx OR Trilogy OR Clinac OR Accuray Tomotherapy OR Radixac OR CyberKnife OR Synergy OR Gamma Knife Icon OR ExacTrac OR TrueBeam OR Edge OR Eclipse RapidArc OR Gamma Knife Model U OR Gamma Knife Model C OR Gamma Knife Prefexion]
Canadian Cancer Trials
Produced by the Canadian Partnership Against Cancer Corporation. Targeted search used to capture registered clinical trials.
[Search terms will include - Stereotactic Ablative Radiotherapy (SABR) OR Stereotactic Radiosurgery (SRS) OR stereotactic body radiation therapy (SBRT) OR fractionated stereotactic radiotherapy (FSRT) OR LINAC OR XKnife OR Versa OR Infinity OR Precise OR Novalis Tx OR Trilogy OR Clinac OR Accuray Tomotherapy OR Radixac OR CyberKnife OR Synergy OR Gamma Knife Icon OR ExacTrac OR TrueBeam OR Edge OR Eclipse RapidArc OR Gamma Knife Model U OR Gamma Knife Model C OR Gamma Knife Prefexion]
Grey Literature
Dates for Search: April 27, 2020 to May 07, 2020
Keywords: Stereotactic Ablative Radiotherapy (SABR) OR Stereotactic Radiosurgery (SRS) OR stereotactic body radiation therapy (SBRT) OR fractionated stereotactic radiotherapy (FSRT) OR LINAC OR XKnife OR Versa OR Infinity OR Precise OR Novalis Tx OR Trilogy OR Clinac OR Accuray Tomotherapy OR Radixac OR CyberKnife OR Synergy OR Gamma Knife Icon OR ExacTrac OR TrueBeam OR Edge OR Eclipse RapidArc OR Gamma Knife Model U OR Gamma Knife Model C OR Gamma Knife Prefexion
Limits: Publication years: 1990-present
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trial Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 3: PRISMA Flow Chart of Selected Reports
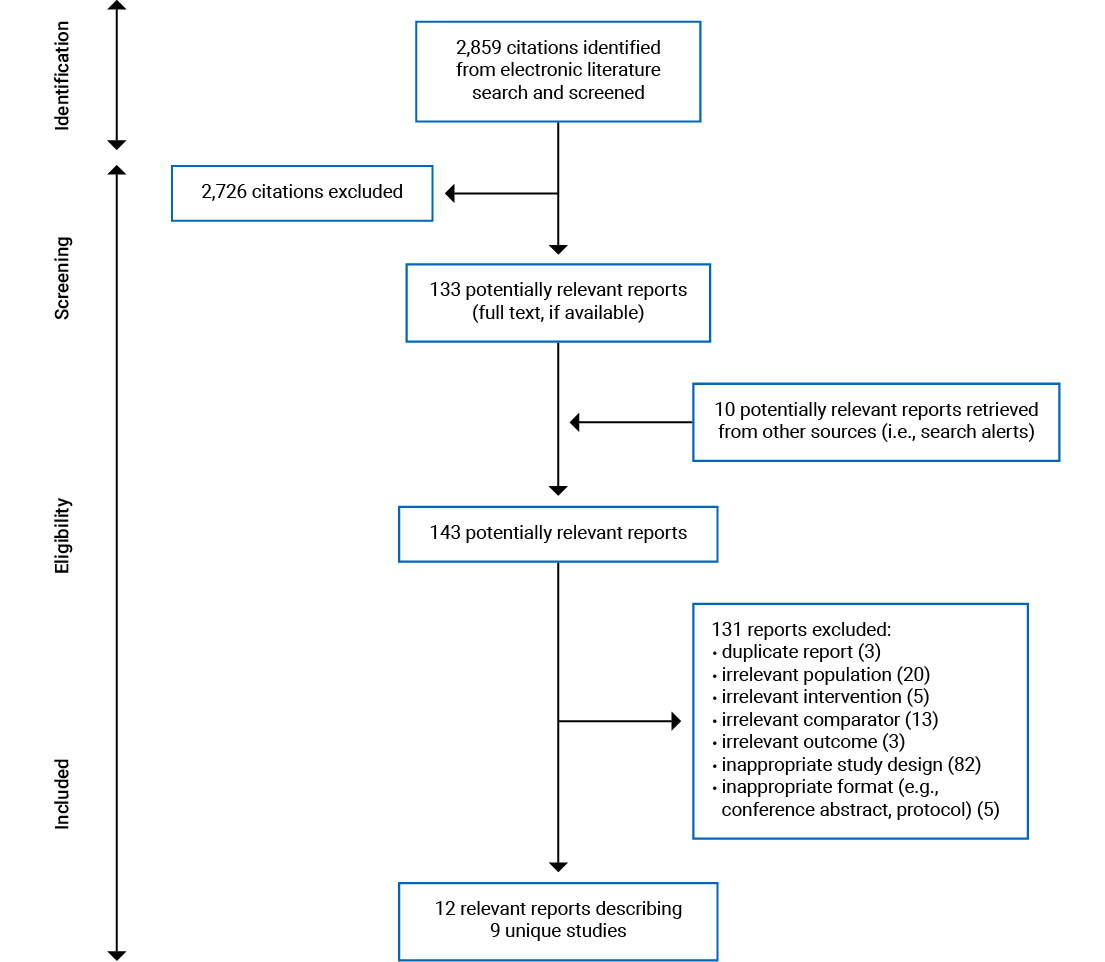
Appendix 4: List of Included Studies
1.Hurmuz P, Onal C, Ozyigit G, et al. Treatment outcomes of metastasis-directed treatment using (68)Ga-PSMA-PET/CT for oligometastatic or oligorecurrent prostate cancer: Turkish Society for Radiation Oncology group study (TROD 09-002). Strahlenther Onkol. 2020;196(11):1034-1043. PubMed
2.Palma DA, Olson R, Harrow S, et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J Clin Oncol. 2020;38(25):2830-2838. PubMed
3.Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020;6(5):650-659. PubMed
4.van de Ven S, van den Bongard D, Pielkenrood B, et al. Patient-Reported Outcomes of Oligometastatic Patients After Conventional or Stereotactic Radiation Therapy to Bone Metastases: An Analysis of the PRESENT Cohort. Int J Radiat Oncol Biol Phys. 2020;107(1):39-47. PubMed
5.De Bleser E, Jereczek-Fossa BA, Pasquier D, et al. Metastasis-directed Therapy in Treating Nodal Oligorecurrent Prostate Cancer: A Multi-institutional Analysis Comparing the Outcome and Toxicity of Stereotactic Body Radiotherapy and Elective Nodal Radiotherapy. Eur Urol. 2019;76(6):732-739. PubMed
6.Olson R, Senan S, Harrow S, et al. Quality of Life Outcomes After Stereotactic Ablative Radiation Therapy (SABR) Versus Standard of Care Treatments in the Oligometastatic Setting: A Secondary Analysis of the SABR-COMET Randomized Trial. Int J Radiat Oncol Biol Phys. 2019;105(5):943-947. PubMed
7.Palma DA, Olson R, Harrow S, et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): a randomised, phase 2, open-label trial. Lancet. 2019;393(10185):2051-2058. PubMed
8.He Z, Chen G, Ouyang B, et al. Conformal radiation therapy or stereotactic body radiation therapy: Institutional experience in the management of colorectal liver metastases by radiation therapy. Technol Cancer Res Treat. 2018;17.
9.Iyengar P, Wardak Z, Gerber DE, et al. Consolidative Radiotherapy for Limited Metastatic Non-Small-Cell Lung Cancer: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2018;4(1):e173501. PubMed
10.Lodeweges JE, Klinkenberg TJ, Ubbels JF, Groen HJM, Langendijk JA, Widder J. Long-term Outcome of Surgery or Stereotactic Radiotherapy for Lung Oligometastases. J Thorac Oncol. 2017;12(9):1442-1445. PubMed
11.Filippi AR, Guerrera F, Badellino S, et al. Exploratory Analysis on Overall Survival after Either Surgery or Stereotactic Radiotherapy for Lung Oligometastases from Colorectal Cancer. Clin Oncol (R Coll Radiol). 2016;28(8):505-512. PubMed
12.Widder J, Klinkenberg TJ, Ubbels JF, Wiegman EM, Groen HJ, Langendijk JA. Pulmonary oligometastases: metastasectomy or stereotactic ablative radiotherapy? Radiother Oncol. 2013;107(3):409-413. PubMed
Appendix 5: List of Excluded Studies and Reasons for Exclusion
Duplicate Report (n = 3)
1.McDonald F, Hanna GG. Oligoprogressive Oncogene-addicted Lung Tumours: Does Stereotactic Body Radiotherapy Have a Role? Introducing the HALT Trial. Clin Oncol (R Coll Radiol). 2018;30(1):1-4. PubMed
2.Trovo M, Furlan C, Polesel J, et al. Radical radiation therapy for oligometastatic breast cancer: Results of a prospective phase II trial. Radiother Oncol. 2018;126(1):177-180. PubMed
3.Kao J, Timmins J, Ozao-Choy J, Packer S. Effects of combined sunitinib and extracranial stereotactic radiotherapy on bone marrow hematopoiesis. Oncol Lett. 2016;12(3):2139-2144. PubMed
Irrelevant Population (n = 20)
1.Deek MP, Taparra K, Phillips R, et al. Metastasis-directed Therapy Prolongs Efficacy of Systemic Therapy and Improves Clinical Outcomes in Oligoprogressive Castration-resistant Prostate Cancer. Eur Urol Oncol. 2020. PubMed
2.Papadopoulos KP, Johnson ML, Lockhart AC, et al. First-In-Human Study of Cemiplimab Alone or In Combination with Radiotherapy and/or Low-dose Cyclophosphamide in Patients with Advanced Malignancies. Clin Cancer Res. 2020;26(5):1025-1033. PubMed
3.Schullian P, Putzer D, Laimer G, Levy E, Bale R. Feasibility, safety, and long-term efficacy of stereotactic radiofrequency ablation for tumors adjacent to the diaphragm in the hepatic dome: a case-control study. Eur Radiol. 2020;30(2):950-960. PubMed
4.Schullian P, Putzer D, Silva MA, Laimer G, Kolbitsch C, Bale R. Stereotactic Radiofrequency Ablation of Liver Tumors in Octogenarians. Front Oncol. 2019;9:929. PubMed
5.Shen PC, Chang WC, Lo CH, et al. Comparison of Stereotactic Body Radiation Therapy and Transarterial Chemoembolization for Unresectable Medium-Sized Hepatocellular Carcinoma. Int J Radiat Oncol Biol Phys. 2019;105(2):307-318. PubMed
6.Franzese C, Comito T, Clerici E, et al. Liver metastases from colorectal cancer: propensity score-based comparison of stereotactic body radiation therapy vs. microwave ablation. J Cancer Res Clin Oncol. 2018;144(9):1777-1783. PubMed
7.Ost P, Reynders D, Decaestecker K, et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J Clin Oncol. 2018;36(5):446-453. PubMed
8.Sapir E, Tao Y, Schipper MJ, et al. Stereotactic Body Radiation Therapy as an Alternative to Transarterial Chemoembolization for Hepatocellular Carcinoma. Int J Radiat Oncol Biol Phys. 2018;100(1):122-130. PubMed
9.Schulz D, Wirth M, Piontek G, et al. Improved overall survival in head and neck cancer patients after specific therapy of distant metastases. Eur Arch Otorhinolaryngol. 2018;275(5):1239-1247. PubMed
10.Sprave T, Verma V, Forster R, et al. Quality of Life Following Stereotactic Body Radiotherapy Versus Three-Dimensional Conformal Radiotherapy for Vertebral Metastases: Secondary Analysis of an Exploratory Phase II Randomized Trial. Anticancer Res. 2018;38(8):4961-4968. PubMed
11.Stenman M, Sinclair G, Paavola P, Wersall P, Harmenberg U, Lindskog M. Overall survival after stereotactic radiotherapy or surgical metastasectomy in oligometastatic renal cell carcinoma patients treated at 2 Swedish centres 2005-2014. Radiother Oncol. 2018;127(3):501-506. PubMed
12.Fleming C, Rimner A, Foster A, Woo KM, Zhang Z, Wu AJ. Palliative efficacy and local control of conventional radiotherapy for lung metastases. Ann. 2017;6(Suppl 1):S21-S27. PubMed
13.Moon SH, Cho KH, Lee CG, et al. IMRT vs. 2D-radiotherapy or 3D-conformal radiotherapy of nasopharyngeal carcinoma: Survival outcome in a Korean multi-institutional retrospective study (KROG 11-06). Strahlenther Onkol. 2016;192(6):377-385. PubMed
14.Reijneveld JC, Taphoorn MJB, Coens C, et al. Health-related quality of life in patients with high-risk low-grade glioma (EORTC 22033-26033): a randomised, open-label, phase 3 intergroup study. Lancet Oncol. 2016;17(11):1533-1542. PubMed
15.Jacob R, Turley F, Redden DT, et al. Adjuvant stereotactic body radiotherapy following transarterial chemoembolization in patients with non-resectable hepatocellular carcinoma tumours of >/= 3 cm. HPB (Oxford). 2015;17(2):140-149. PubMed
16.Langendijk H, Kaanders JH, Doornaert P, et al. POPART vs CPORT in squamous cell head and neck cancer: Results of a multicenter randomised study of the Dutch head and neck Study Group. Radiother Oncol. 2015;114:9-10.
17.Jiang Z, Wang Q, Yang G, et al. Optimized treatment with RF thermotherapy and immunotherapy combined with CyberKnife for advanced high-risk tumors: A clinical trial report. Biomed Rep. 2014;2(2):245-249. PubMed
18.Yu W, Tang L, Lin F, et al. Stereotactic radiosurgery, a potential alternative treatment for pulmonary metastases from osteosarcoma. Int J Oncol. 2014;44(4):1091-1098. PubMed
19.Choi BO, Choi IB, Jang HS, et al. Stereotactic body radiation therapy with or without transarterial chemoembolization for patients with primary hepatocellular carcinoma: preliminary analysis. BMC Cancer. 2008;8:351. PubMed
20.Guo J, Sun XN, Huang M. Evaluation of the efficacy for alternated treatment on primary liver cancer by interventional therapy in combination with fractionated stereotactic conformal radiotherapy. Chin J Clin Oncol. 2005;32(24):1418-1420.
Irrelevant Intervention (n = 5)
1.Chan OSH, Lam KC, Li JYC, et al. ATOM: A phase II study to assess efficacy of preemptive local ablative therapy to residual oligometastases of NSCLC after EGFR TKI. Lung Cancer. 2020;142:41-46. PubMed
2.Gomez DR, Tang C, Zhang J, et al. Local Consolidative Therapy Vs. Maintenance Therapy or Observation for Patients With Oligometastatic Non-Small-Cell Lung Cancer: Long-Term Results of a Multi-Institutional, Phase II, Randomized Study. J Clin Oncol. 2019;37(18):1558-1565. PubMed
3.Steuber T, Jilg C, Tennstedt P, et al. Standard of Care Versus Metastases-directed Therapy for PET-detected Nodal Oligorecurrent Prostate Cancer Following Multimodality Treatment: A Multi-institutional Case-control Study. Eur Urol Focus. 2019;5(6):1007-1013. PubMed
4.Chan OSH, Lee VHF, Mok TSK, Mo F, Chang ATY, Yeung RMW. The Role of Radiotherapy in Epidermal Growth Factor Receptor Mutation-positive Patients with Oligoprogression: A Matched-cohort Analysis. Clin Oncol (R Coll Radiol). 2017;29(9):568-575. PubMed
5.Roos DE, Turner SL, O'Brien PC, et al. Randomized trial of 8 Gy in 1 versus 20 Gy in 5 fractions of radiotherapy for neuropathic pain due to bone metastases (Trans-Tasman Radiation Oncology Group, TROG 96.05). Radiother Oncol. 2005;75(1):54-63. PubMed
Irrelevant Comparator (n = 13)
1.Franzese C, Comito T, Vigano L, et al. Liver Metastases-directed Therapy in the Management of Oligometastatic Breast Cancer. Clin Breast Cancer. 2020;20(6):480-486. PubMed
2.Kalinauskaite GG, Tinhofer, II, Kufeld MM, et al. Radiosurgery and fractionated stereotactic body radiotherapy for patients with lung oligometastases. BMC Cancer. 2020;20(1):404. PubMed
3.Desideri I, Francolini G, Scotti V, et al. Benefit of ablative versus palliative-only radiotherapy in combination with nivolumab in patients affected by metastatic kidney and lung cancer. Clin Transl Oncol. 2019;21(7):933-938. PubMed
4.Lepinoy A, Silva YE, Martin E, et al. Salvage extended field or involved field nodal irradiation in (18)F-fluorocholine PET/CT oligorecurrent nodal failures from prostate cancer. Eur J Nucl Med Mol Imaging. 2019;46(1):40-48. PubMed
5.Fanetti G, Marvaso G, Ciardo D, et al. Stereotactic body radiotherapy for castration-sensitive prostate cancer bone oligometastases. Med Oncol. 2018;35(5):75. PubMed
6.Frost N, Tessmer A, Schmittel A, et al. Local ablative treatment for synchronous single organ oligometastatic lung cancer-A propensity score analysis of 180 patients. Lung Cancer. 2018;125:164-173. PubMed
7.Katoh N, Onishi H, Uchinami Y, et al. Real-Time Tumor-Tracking Radiotherapy and General Stereotactic Body Radiotherapy for Adrenal Metastasis in Patients with Oligometastasis. Technol Cancer Res Treat. 2018;17:1533033818809983. PubMed
8.Mazzola R, Tebano U, Aiello D, et al. Increased efficacy of stereotactic ablative radiation therapy after bevacizumab in lung oligometastases from colon cancer. Tumori. 2018;104(6):423-428. PubMed
9.Sundahl N, Rottey S, Decaestecker K, et al. Phase 1 trial of pembrolizumab with SBRT in metastatic urothelial carcinoma. Radiother Oncol. 2018;127:S357-S358.
10.Sundahl N, De Wolf K, Rottey S, et al. A phase I/II trial of fixed-dose stereotactic body radiotherapy with sequential or concurrent pembrolizumab in metastatic urothelial carcinoma: evaluation of safety and clinical and immunologic response. J Transl Med. 2017;15(1):150. PubMed
11.Fleckenstein J, Petroff A, Schafers HJ, Wehler T, Schope J, Rube C. Long-term outcomes in radically treated synchronous vs. metachronous oligometastatic non-small-cell lung cancer. BMC Cancer. 2016;16:348. PubMed
12.Siva S, Kron T, Bressel M, et al. A randomised phase II trial of Stereotactic Ablative Fractionated radiotherapy versus Radiosurgery for Oligometastatic Neoplasia to the lung (TROG 13.01 SAFRON II). BMC Cancer. 2016;16:183. PubMed
13.Wang YS, Yang G, Wang YY, Yang JL, Yang K. Early efficacy of stereotactic body radiation therapy combined with adoptive immunotherapy for advanced malignancies. Mol Clin Oncol. 2013;1(5):925-929. PubMed
Irrelevant Outcome (n = 3)
1.Xue P, Wu Z, Wang K, Gao G, Zhuang M, Yan M. Oncological outcome of combining cytoreductive prostatectomy and metastasis-directed radiotherapy in patients with prostate cancer and bone oligometastases: A retrospective cohort study. Cancer Manag Res. 2020;12:8867-8873. PubMed
2.Bouman-Wammes EW, van Dodewaard-De Jong JM, Dahele M, et al. Benefits of Using Stereotactic Body Radiotherapy in Patients With Metachronous Oligometastases of Hormone-Sensitive Prostate Cancer Detected by [18F]fluoromethylcholine PET/CT. Clin Genitourin Cancer. 2017;15(5):e773-e782. PubMed
3.Youland RS, Blanchard ML, Dronca R, et al. Role of radiotherapy in extracranial metastatic malignant melanoma in the modern era. Clin Transl Radiat Oncol. 2017;6:25-30. PubMed
Inappropriate Study Design (n = 82)
1.Burkon P, Oberreiterova S, Kazda T, et al. Stereotactic Body Radiotherapy of Lymph Node Oligometastases. Klin Onkol. 2020;33(2):114-122. PubMed
2.Guo T, Ni J, Yang X, et al. Pattern of Recurrence Analysis in Metastatic EGFR-Mutant NSCLC Treated with Osimertinib: Implications for Consolidative Stereotactic Body Radiation Therapy. Int J Radiat Oncol Biol Phys. 2020;107(1):62-71. PubMed
3.Higa J, Wilenius K, Savino S, Larsen C, Scholz M, Vogelzang N. Real World Experience With Pembrolizumab in Recurrent or Advanced Prostate Cancer. Clin Genitourin Cancer. 2020;18(4):e397-e401. PubMed
4.Kim DW, Lee G, Lee H, et al. Stereotactic Body Radiation Therapy to a Splenic Metastasis in Oligoprogressive Non-small Cell Lung Cancer. Adv Radiat Oncol. 2020;5(3):516-521. PubMed
5.Marzec J, Becker J, Paulsen F, et al. (68)Ga-PSMA-PET/CT-directed IGRT/SBRT for oligometastases of recurrent prostate cancer after initial surgery. Acta Oncol. 2020;59(2):149-156. PubMed
6.Nikitas J, Roach M, Robinson C, et al. Treatment of oligometastatic lung cancer with brain metastases using stereotactic radiosurgery (SRS) and stereotactic body radiation therapy (SBRT). Clin Transl Radiat Oncol. 2020;21:32-35. PubMed
7.Pei S, Chen K, Yang Y, Chen L, Zhu X. A retrospective cohort study of low-dose intensity-modulated radiotherapy for unresectable liver metastases. J Int Med Res. 2020;48(4):300060519892382. PubMed
8.Thomas T. SABR improves outcomes in men with recurrent oligometastatic prostate cancer. Nat Rev Urol. 2020;17(5):256. PubMed
9.Agolli L. Stereotactic body radiation therapy could improve disease control in oligometastatic patients with renal cell carcinoma: do we need more evidence? Ann. 2019;7(Suppl 3):S105. PubMed
10.Augugliaro M, Marvaso G, Ciardo D, et al. Recurrent oligometastatic transitional cell bladder carcinoma: is there room for radiotherapy? Neoplasma. 2019;66(1):160-165. PubMed
11.Aujla KS, Katz AW, Singh DP, Okunieff P, Milano MT. Hypofractionated Stereotactic Radiotherapy for Non-breast or Prostate Cancer Oligometastases: A Tail of Survival Beyond 10 Years. Front Oncol. 2019;9:111. PubMed
12.Bashir U, Tree A, Mayer E, et al. Impact of Ga-68-PSMA PET/CT on management in prostate cancer patients with very early biochemical recurrence after radical prostatectomy. Eur J Nucl Med Mol Imaging. 2019;46(4):901-907. PubMed
13.Beckham TH, Imber BS, Simone CB, 2nd. Stereotactic body radiation therapy for oligometastatic renal cell carcinoma: improving outcomes in an otherwise radioresistant malignancy. Ann Transl Med. 2019;7(Suppl 3):S98. PubMed
14.Chia B, Landau D, Hanna G, Conibear J. Thoracic intervention and surgery to cure lung cancer: an overview of stereotactic ablative radiotherapy in early and oligometastatic lung cancer. J R Soc Med. 2019;112(8):334-340. PubMed
15.Giraud N, Abdiche S, Trouette R. Stereotactic irradiation in targeted therapy of oligometastatic oncogene-addicted (non-small-cell) lung cancer. Cancer Radiother. 2019;23(4):361. PubMed
16.Giraud N, Abdiche S, Trouette R. Stereotactic radiotherapy in targeted therapy treated oligo-metastatic oncogene-addicted (non-small-cell) lung cancer. Cancer Radiother. 2019;23(4):346-354. PubMed
17.Gomez-Iturriaga A, Casquero Ocio F, Ost P, et al. Outcomes after a first and/or second salvage treatment in patients with oligometastatic prostate cancer recurrence detected by (18-F) choline PET-CT. Eur J Cancer Care (Engl). 2019;28(5):e13093. PubMed
18.Jacobs CD, Palta M, Williamson H, et al. Hypofractionated Image-Guided Radiation Therapy With Simultaneous-Integrated Boost Technique for Limited Metastases: A Multi-Institutional Analysis. Front Oncol. 2019;9:469. PubMed
19.Kroeze SGC, Fritz C, Kaul D, et al. Stereotactic radiotherapy concurrent to immune or targeted therapy for oligometastatic NSCLC: Clinical scenarios affecting survival. Ann Oncol. 2019;30(Suppl 2):ii63.
20.Lohaus F, Zophel K, Lock S, et al. Can Local Ablative Radiotherapy Revert Castration-resistant Prostate Cancer to an Earlier Stage of Disease? Eur Urol. 2019;75(4):548-551. PubMed
21.Malik NH, Keilty DM, Louie AV. Stereotactic ablative radiotherapy versus metastasectomy for pulmonary metastases: guiding treatment in the oligometastatic era. J Thorac Dis. 2019;11(Suppl 9):S1333-S1335. PubMed
22.Marcu LG, Marcu D. The role of hypofractionated radiotherapy in the management of head and neck cancer - a modelling approach. J Theor Biol. 2019;482:109998. PubMed
23.Matsuo Y. Stereotactic body radiotherapy as an alternative to metastasectomy for pulmonary oligometastasis. J Thorac Dis. 2019;11(Suppl 9):S1420-S1422. PubMed
24.Qiu H, Katz AW, Milano MT. Stereotactic body radiation therapy versus metastasectomy for oligometastases. J Thorac Dis. 2019;11(4):1082-1084. PubMed
25.Rodrigues G, Yartsev S, Roberge D, et al. A Phase II Multi-institutional Clinical Trial Assessing Fractionated Simultaneous In-Field Boost Radiotherapy for Brain Oligometastases. Cureus. 2019;11(12):e6394. PubMed
26.Scorsetti M, Comito T, Franzese C, et al. Role of stereotactic body radiation therapy in the management of oligometastatic pancreatic cancer: single institution experience. Ann Oncol. 2019;30(Suppl 4):iv107.
27.Spencer K, Velikova G, Henry A, Westhoff P, Hall PT, van der Linden YM. Net Pain Relief After Palliative Radiation Therapy for Painful Bone Metastases: a Useful Measure to Reflect Response Duration? A Further Analysis of the Dutch Bone Metastasis Study. Int J Radiat Oncol Biol Phys. 2019;105(3):559-566. PubMed
28.Stintzing S, Einem JV, Fueweger C, Haidenberger A, Fedorov M, Muavcevic A. Long-term Survival in Patients Treated with a Robotic Radiosurgical Device for Liver Metastases. Cancer Res Treat. 2019;51(1):187-193. PubMed
29.Wegner RE, Abel S, Hasan S, Schumacher LY, Colonias A. Stereotactic Body Radiotherapy (SBRT) for Oligometastatic Lung Nodules: A Single Institution Series. Front Oncol. 2019;9:334. PubMed
30.Wujanto C, Vellayappan B, Siva S, et al. Stereotactic Body Radiotherapy for Oligometastatic Disease in Non-small Cell Lung Cancer. Front Oncol. 2019;9:1219. PubMed
31.SABR Combats Metastatic Disease. Cancer Discov. 2018;8(12):1501-1502. PubMed
32.He X, Zhang P, Li Z, et al. Curative-intent radiotherapy in patients with oligometastatic lesions from colorectal cancer: A single-center study. Medicine (Baltimore). 2018;97(40):e12601. PubMed
33.Korzets Ceder Y, Fenig E, Popvtzer A, et al. Stereotactic body radiotherapy for central lung tumors, yes we can! Radiat Oncol. 2018;13(1):77. PubMed
34.Luke JJ, Lemons JM, Karrison TG, et al. Safety and Clinical Activity of Pembrolizumab and Multisite Stereotactic Body Radiotherapy in Patients With Advanced Solid Tumors. J Clin Oncol. 2018;36(16):1611-1618. PubMed
35.McDonald F, Hanna GG. Oligoprogressive Oncogene-addicted Lung Tumours: Does Stereotactic Body Radiotherapy Have a Role? Introducing the HALT Trial. Clin Oncol (R Coll Radiol). 2018;30(1):1-4. PubMed
36.Trovo M, Furlan C, Polesel J, et al. Radical radiation therapy for oligometastatic breast cancer: Results of a prospective phase II trial. Radiother Oncol. 2018;126(1):177-180. PubMed
37.Verma V, Chang JY. Stereotactic ablative radiotherapy for oligometastatic non-small cell lung cancer. J Thorac Dis. 2018;10(1):21-24. PubMed
38.Zilli T, Ost P. Metastasis-directed therapy: a new standard for oligorecurrent prostate cancer? Oncotarget. 2018;9(76):34196-34197. PubMed
39.Bates JE, Milano MT. Prognostic significance of sites of extrathoracic metastasis in patients with non-small cell lung cancer. J Thorac Dis. 2017;9(7):1903-1910. PubMed
40.Conde-Moreno AJ, Herrando-Parreno G, Muelas-Soria R, et al. Whole-body diffusion-weighted magnetic resonance imaging (WB-DW-MRI) vs choline-positron emission tomography-computed tomography (choline-PET/CT) for selecting treatments in recurrent prostate cancer. Clin Transl Oncol. 2017;19(5):553-561. PubMed
41.Franceschini D, Cozzi L, De Rose F, et al. Role of stereotactic body radiation therapy for lung metastases from radio-resistant primary tumours. J Cancer Res Clin Oncol. 2017;143(7):1293-1299. PubMed
42.Gkika E, Adebahr S, Kirste S, et al. Stereotactic body radiotherapy (SBRT) in recurrent or oligometastatic pancreatic cancer: A toxicity review of simultaneous integrated protection (SIP) versus conventional SBRT. Strahlenther Onkol. 2017;193(6):433-443. PubMed
43.Habl G, Straube C, Duma MN, et al. Oligometastases from Prostate Cancer: Local treatment with stereotactic body radiotherapy (SBRT). Strahlenther Onkol. 2017;193(1 suppl 1):S69-S70. PubMed
44.Haidenberger A, Heidorn SC, Kremer N, Muacevic A, Furweger C. Robotic Radiosurgery for Adrenal Gland Metastases. Cureus. 2017;9(3):e1120. PubMed
45.Kim YT. Local Therapy for Pulmonary Oligometastases: Is SABR a New Champion? J Thorac Oncol. 2017;12(9):1335-1337. PubMed
46.Klement RJ, Guckenberger M, Alheid H, et al. Stereotactic body radiotherapy for oligo-metastatic liver disease - Influence of pre-treatment chemotherapy and histology on local tumor control. Radiother Oncol. 2017;123(2):227-233. PubMed
47.Koontz BF. Stereotactic Body Radiation Therapy for Oligometastatic Prostate Cancer: The Hunt for the Silver Bullet. Int J Radiat Oncol Biol Phys. 2017;99(4):761-763. PubMed
48.Kwint M, Walraven I, Burgers S, et al. Outcome of radical local treatment of non-small cell lung cancer patients with synchronous oligometastases. Lung Cancer. 2017;112:134-139. PubMed
49.Molina-Mata K, Navarro-Martin A, Martinez-Villacampa M, et al. Stereotactic body radiotherapy: A promising approach for colorectal lung oligometastases. Ann Oncol. 2017;28(suppl 3):iii117.
50.Niibe Y, Jingu K, Onishi H. Long-Term Outcome of Surgery or Stereotactic Radiotherapy for Lung Oligo-recurrence. J Thorac Oncol. 2017;12(11):e191. PubMed
51.Phillips R, Ost P, Tran PT. What role does stereotactic ablative radiotherapy have in advanced castrate-resistant prostate cancer? Future Oncol. 2017;13(24):2121-2124. PubMed
52.Ricardi U, Giaj Levra N, Badellino S, Alongi F. Role of consolidative stereotactic ablative radiotherapy in patients with oligometastatic non-small cell lung cancer. J Thorac Dis. 2017;9(8):2235-2237. PubMed
53.Effects of combined sunitinib and extracranial stereotactic radiotherapy on bone marrow hematopoiesis. Oncol Lett. 2016;12(3):2139-2144. PubMed
54.Ahmed KA, Caudell JJ, El-Haddad G, et al. Radiosensitivity Differences Between Liver Metastases Based on Primary Histology Suggest Implications for Clinical Outcomes After Stereotactic Body Radiation Therapy. Int J Radiat Oncol Biol Phys. 2016;95(5):1399-1404. PubMed
55.Anonymous. (P002) HER2 Status and Site of Metastases Predict Survival for Women Treated With Stereotactic Body Radiation Therapy/Stereotactic Radiosurgery (SBRT/SRS) for Oligometastases. Oncology (Williston Park). 2016;30 suppl:216533. PubMed
56.Hargreaves S, Comins C. Stereotactic Ablative Radiotherapy for Oligometastatic Disease: a Treatment in Search of Evidence - a Response. Clin Oncol (R Coll Radiol). 2016;28(8):503-504. PubMed
57.Hishida T, Yoshida J, Aokage K, Nagai K, Tsuboi M. Postoperative oligo-recurrence of non-small-cell lung cancer: clinical features and survival. Eur J Cardiothorac Surg. 2016;49(3):847-853. PubMed
58.Kropp LM, De Los Santos JF, McKee SB, Conry RM. Radiotherapy to Control Limited Melanoma Progression Following Ipilimumab. J Immunother. 2016;39(9):373-378. PubMed
59.Macbeth F, Treasure T. Stereotactic Ablative Radiotherapy for 'Oligometastases': a Treatment in Search of Evidence. Clin Oncol (R Coll Radiol). 2016;28(8):501-502. PubMed
60.Napieralska A, Miszczyk L, Stapor-Fudzinska M. CyberKnife stereotactic radiosurgery and stereotactic ablative radiation therapy of patients with prostate cancer bone metastases. Neoplasma. 2016;63(2):304-312. PubMed
61.Onesti CE, Iacono D, Angelini S, et al. Unexpected long survival of brain oligometastatic non-small cell lung cancer (NSCLC) treated with multimodal treatment: a single-center experience and review of the literature. Transl Lung Cancer Res. 2016;5(6):712-719. PubMed
62.Orecchia R, Surgo A, Muto M, et al. VERO® radiotherapy for low burden cancer: 789 patients with 957 lesions. Ecancermedicalscience. 2016;10:677. PubMed
63.Pasqualetti F, Panichi M, Sainato A, et al. [(18)F]Choline PET/CT and stereotactic body radiotherapy on treatment decision making of oligometastatic prostate cancer patients: preliminary results. Radiat Oncol. 2016;11:9. PubMed
64.Dearman C, van As N, Crellin A, Slevin N, Sharma RA. Surgery versus SABR for resectable non-small-cell lung cancer. Lancet Oncol. 2015;16(8):e373-e374. PubMed
65.Broomfield JA, Greenspoon JN, Swaminath A. Utilization of stereotactic ablative radiotherapy in the management of oligometastatic disease. Curr Oncol. 2014;21(3):115-117. PubMed
66.de Vin T, Engels B, Gevaert T, Storme G, De Ridder M. Stereotactic radiotherapy for oligometastatic cancer: a prognostic model for survival. Ann Oncol. 2014;25(2):467-471. PubMed
67.Kao J, Chen CT, Tong CC, et al. Concurrent sunitinib and stereotactic body radiotherapy for patients with oligometastases: final report of a prospective clinical trial. Target Oncol. 2014;9(2):145-153. PubMed
68.Corbin KS, Hellman S, Weichselbaum RR. Extracranial oligometastases: a subset of metastases curable with stereotactic radiotherapy. J Clin Oncol. 2013;31(11):1384-1390. PubMed
69.Lim CS, Grundy PL. Effectiveness and outcomes of surgery for cerebral metastases. Br J Neurosurg. 2013;27(5):654-657. PubMed
70.Onishi H, Ozaki M, Kuriyama K, et al. Stereotactic body radiotherapy for metachronous multisite oligo-recurrence: a long-surviving case with sequential oligo-recurrence in 4 different organs treated using locally radical radiotherapy and a review of the literature. Pulm Med. 2012;2012:713073. PubMed
71.Solanki AA, Weichselbaum RR, Appelbaum D, et al. The utility of FDG-PET for assessing outcomes in oligometastatic cancer patients treated with stereotactic body radiotherapy: a cohort study. Radiat Oncol. 2012;7:216. PubMed
72.Casamassima F, Masi L, Menichelli C, et al. Efficacy of eradicative radiotherapy for limited nodal metastases detected with choline PET scan in prostate cancer patients. Tumori. 2011;97(1):49-55. PubMed
73.de Jonge MJ, Dumez H, Kitzen JJ, et al. Phase I safety and pharmacokinetic study of SU-014813 in combination with docetaxel in patients with advanced solid tumours. Eur J Cancer. 2011;47(9):1328-1335. PubMed
74.Liao Z, Lin SH, Cox JD. Status of particle therapy for lung cancer. Acta Oncol. 2011;50(6):745-756. PubMed
75.Yap J. Giving oligometastases the best shot using stereotactic body radiosurgery with image guidance. How far is the cat out of the bag? J Gastrointest Oncol. 2010;1(1):5-6. PubMed
76.Ben-Josef E, Lawrence TS. Using a bigger hammer: the role of stereotactic body radiotherapy in the management of oligometastases. J Clin Oncol. 2009;27(10):1537-1539. PubMed
77.Christodouleas JP, Marks LB. Analysis of patients with oligometastases undergoing 2 or more curative-intent stereotactic radiotherapy courses: in regard to Milano et al. (Int J Radiat Oncol Biol Phys 2009;73:832-837). Int J Radiat Oncol Biol Phys. 2009;74(5):1628; author reply 1628-1629. PubMed
78.Norihisa Y, Nagata Y, Takayama K, et al. Stereotactic body radiotherapy for oligometastatic lung tumors. Int J Radiat Oncol Biol Phys. 2008;72(2):398-403. PubMed
79.Milker-Zabel S, Zabel A, Thilmann C, Schlegel W, Wannenmacher M, Debus J. Clinical results of retreatment of vertebral bone metastases by stereotactic conformal radiotherapy and intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys. 2003;55(1):162-167. PubMed
80.Eggert A, Ikegaki N, Kwiatkowski J, Zhao H, Brodeur GM, Himelstein BP. High-level expression of angiogenic factors is associated with advanced tumor stage in human neuroblastomas. Clin Cancer Res. 2000;6(5):1900-1908. PubMed
81.Chamberlain M, Kormanik P, Barba D, Fuller B, Smith D, Shea W. Stereotactic radiosurgery for metastatic brain tumors. Int J Oncol. 1996;8(3):617-624. PubMed
82.Bernstein M, Laperriere N, Glen J. Stereotactic high-activity brachytherapy for malignant intra-axial brain tumors. Status report as of March, 1995. Stereotact Funct Neurosurg. 1995;65(1-4):167-170. PubMed
Inappropriate Format (For Example, Conference Abstract, Protocol; n = 5):
1.Mattes MD, Eubank TD, Almubarak M, et al. Outcomes from a Phase II Clinical Trial Evaluating the Systemic (Abscopal) Response from the Addition of Local Radiation to Standard-of-Care Immunotherapy for Metastatic Non-Small Cell Lung Cancer. Int J Radiat Oncol Biol Phys. 2019;105(1):E519.
2.Luke JJ, Chmura SJ, Allred JB, et al. A randomized phase II study of anti-PD1 antibody [MK-3475 (Pembrolizumab)] alone versus anti-PD1 antibody plus stereotactic body radiation therapy in advanced merkel cell carcinoma (Alliance A091605). J Clin Oncol. 2018;36(15_suppl):TPS9599.
3.Senan S, Olson R, Harrow S, et al. Stereotactic ablative radiotherapy for oligometastatic cancers: Efficacy and toxicity results from the randomized SABR-COMET Trial. Ann Oncol. 2018;29(Supplement 9).
4.Chmura SJ, Winter KA, Salama JK, et al. NRG-BR002: a phase IIR/III trial of standard of care therapy with or without stereotactic body radiotherapy (SBRT) &/or surgical ablation for newly oligometastatic breast cancer. Cancer Res. 2017;77(4 Suppl):Abstract nr OT1-04-06.
5.Sidaway P. Lung Cancer: SABR effective against oligometastatic disease. Nat Rev Clin Oncol. 2017;14(12):712. PubMed
Appendix 6: Considerations for Meta-Analyses
Table 16: Rationale for Not Conducting Meta-Analysis
Outcome | Intervention | Comparator | Relevant studies | Meta-analysis appropriate? |
Question 1: Clinical Effectiveness | ||||
OS | SABR plus SOCa | SOC | RCTs: SABR-COMET: Palma et al. (2019)32 and Palma et al. (2020)58 Iyengar et al. (2018)69 | No: Data unavailability (i.e., HRs available for 1 of 2 studies) |
SABR | SOC | NRSs: Hurmuz et al. (2020)65 van de Ven et al. (2020)64 He et al. (2018)67 Filippi et al. (2016)68 Widder et al. (2013)60 and Lodeweges et al. (2017)61 | No: Discordant results (i.e., large variability in the direction, magnitude, and statistical significance of the results) | |
PFS | SABR plus SOC | SOC | RCTs: SABR-COMET: Palma et al. (2019)32 and Palma et al. (2020)58 Iyengar et al. (2018)69 | No: No statistical gain (i.e., point estimates similar in direction, magnitude, and statistical significance leading to no added value in pooling) |
SABR | SOC | RCT: Phillips et al. (2020)63 | No: One study | |
NRSs: Hurmuz et al. (2020)65 van de Ven et al. (2020)64 Filippi et al. (2016)68 | No: Data unavailability (i.e., HRs available for 2 studies) | |||
Question 2: Safety | ||||
AEs | SABR plus SOC | SOC | RCTs: SABR-COMET: Palma et al. (2019)32 and Palma et al. (2020)58 Iyengar et al. (2018)69 | No: Data variability (e.g., AEs included different AE grades reported, treatment vs. non–treatment-related AEs, or event data vs. patient data) |
SABR | SOC | RCT: Phillips et al. (2020)63 | No: One study | |
NRSs: De Bleser et al. (2019)66 He et al. (2018)67 Filippi et al. (2016)68 | No: Data variability (e.g., AEs included different AE grades reported, treatment vs. non–treatment-related AEs, or event data vs. patient data) | |||
AE = adverse event; HR = hazard ratio; NRS = nonrandomized study; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; SOC = standard of care.
aSOC may include surgery, conventional radiotherapy, chemotherapy, immunotherapy, hormonotherapy, other ablative treatment, targeted therapy, or no treatment (observation).
Appendix 7: Characteristics of Included Publications
Table 17: Characteristics of Included Primary Studies
Author (year); country; trial acronym (registry ID); source of funding | Study design, analytical approach, follow-up | Eligibility criteria | Sample size, patient characteristics | Intervention, comparator | Relevant for clinical research question(s); relevant outcomes measured |
RCTs | |||||
Phillips et al. (2020)63 US Trial acronym: ORIOLE (NCT02680587) Funding source: Nesbitt-McMaster Foundation, Ronald Rose and Joan Lazar, Movember Foundation, Prostate Cancer Foundation, and the NCI; SDW/DT and Shanahan Cancer Research Funds; NIH Director’s New Innovator Award; Virginia and D.K. Ludwig Fund for Cancer Research; CRK Faculty Scholar Fund; Transdisciplinary Integration of Population Science Program of Sidney Kimmel Cancer Center–Jefferson Health, and a Challenge Grant from the Prostate Cancer Foundation. | RCT, phase II, open-label, parallel trial from 3 US radiation treatment facilities affiliated within a university hospital. Two-sided Fisher exact test used for comparisons of progression events. The Kaplan–Meier method used to calculate PFS and the P values were calculated using the log-rank test. The Holm- Šidák method for multiple t-tests was used to compare Brief Pain Inventory responses (QoL outcome) between and within arms across time. All analysis was performed on an ITT basis. Median follow-up (IQR): Total: 18.8 (5.8 to 35.0) months. | Inclusion criteria: Adult patients (≥ 18 years of age) with recurrent hormone-sensitive prostate cancer and 1 to 3 asymptomatic metastatic tumours of the bone or soft tissue within the prior 6 months that are ≥ 5.0 cm on the largest axis or 250 cm2. Certain hematology values must have been within a certain range to qualify (PSA, testosterone, leukocytes, neutrophils). Primary tumours were treated with surgery or radiation or both. ADT was not allowed within 6 months of enrolment. Patients must have a life expectancy ≥ 12 months and an ECOG performance status ≤ 2. Locations of metastasis were bone or soft tissue. Exclusion criteria: Patients who previously received more than 3 years of ADT, received ADT in the prior 6 months, or developed castration-resistant disease; patients with spinal cord compression, suspected pulmonary or liver metastases > 10 mm in largest axis, and received other investigational drugs; patients with certain hematology values outside a specific range (serum creatinine, bilirubin, transaminases). | Total N = 54 Median age (IQR):
Sex, % male: 100.0 Number of metastases per patient: 1 to 3
| SABR (n = 36)
Observation (n = 18)
| Research questions: 1, 2 Outcomes Primary: progression events Secondary:
Definitions:
|
SABR-COMET Palma et al. (2019),32 Palma et al. (2020),58 and Olson et al. (2019)59 Canada, the Netherlands, UK, and Australia Trial acronym: SABR-COMET (NCT01446744) Funding source: Ontario Institute for Cancer Research and a London Regional Cancer Program Catalyst Grant. | RCT, phase II, open-label, parallel trial from 10 hospital centres. A chi-square test or Fisher exact test was used to compare differences in rates of grade 2 or higher toxicity and LC rate between groups. The Kaplan–Meier method were used to calculate OS and PFS, and the stratified log-rank test was used to compared differences. Hazard ratios were calculated using Cox regression adjusted for stratification. All analysis was performed on an ITT basis. Short-term follow-up Median follow-up (IQR):
Long-term follow-up Median follow-up (IQR):
| Inclusion criteria: Adult patients (≥ 18 years of age) with 1 to 5 metastases in total and a maximum of 3 metastases in any single organ system (e.g., lung, liver, brain, bone), with good ECOG performance status (score 0 to 1), and a life expectancy of at least 6 months. The primary tumour had to have been treated definitively by resection, radiofrequency ablation, or radiotherapy at least 3 months before enrolment with no progression at that site since definitive treatment. Locations of primary tumour were breast, colorectal, lung, prostate, and other. Location of metastases included adrenal, bone, liver, lung, and other (brain [3 lesions in systemic therapy; 1 lesion in SABR + systemic therapy], lymph nodes [1 lesion in control, 3 lesions in SABR + systemic therapy], and para-renal [1 in systemic therapy]). Metastases had to have been previously treated and controlled by resection, radiofrequency ablation, or radiotherapy. Exclusion criteria: Patients with serious comorbidities that preclude radiotherapy, metastasis in a femoral bone, hormone-sensitive disease, 1 to 3 brain metastases and no disease elsewhere, prior radiotherapy to a site requiring treatment, malignant pleural effusion, clinical or radiologic evidence of spinal cord compression OR tumour within 3 mm of spinal cord on MRI, dominant brain metastasis requiring surgical decompression, pregnancy, or lactation. | Total N = 99 Median age (IQR):
Sex, % male: Gender, % men:a
Number of metastases per patient:
| SABR + Systemic therapy (n = 66)
Systemic therapy (n = 33)
| Research questions: 1,32,58,59 232,58 Outcomes Primary: Secondary: Definitions:
|
Iyengar et al. (2018)69 US Trial acronym: NR (NCT02045446) Funding source: NR | RCT, phase II, open-label, parallel trial from a single institution. Survival analyses for PFS and OS were performed using Kaplan–Meier method. The log-rank test was used to test for difference between groups. All analysis was performed on an ITT basis. Median follow-up (IQR):
| Inclusion criteria: Adult patients (≥ 18 years of age) with a Karnofsky Performance Scale score of 70 + , with biopsy-proven metastatic lung (NSCLC; stage IV). Metastases allowed per patient were 1 to 5 lesions with no more than 3 sites in the liver or lung. Primary tumour (lung) had been treated with platinum-based chemotherapy, achieving stable disease or a partial response on imaging by RECIST. Locations of metastasis were lung, adrenal, mediastinum, axilla, liver, nasopharynx, bone (rib, spine). Exclusion criteria: Patients receiving first-line targeted therapy for EGFR-positive or ALK-positive lung (NSCLC); patients with previously irradiated primary disease progressed within 3 months of that treatment; patients with untreated or uncontrolled brain metastases or disease involving the gastrointestinal tract and skin. | Total N = 29 Median age (IQR):
Sex; % male
Number of metastases per patient:
| SABR + maintenance chemotherapy (n = 14)
Maintenance chemotherapy (n = 15)
| Research Questions: 1, 2 Outcomes Primary: PFS Secondary:
Definitions:
|
NRSs | |||||
Hurmuz et al. (2020)65 Turkey Trial acronym: TROG Funding source: NR | Retrospective cohort study from 10 institutions. The Kaplan–Meier method was used to calculate OS and PFS rates. Univariate analysis was performed via the log-rank test. Multivariate analyses were performed using the Cox proportional hazards model, using covariates with a P value of less than 0.05 in univariate analysis. Median follow-up (IQR):
| Inclusion criteria: Patients with biopsy-proven prostate cancer (treated between 2014 and 2019) and synchronous or metachronous bone or lymph node metastasis limited to ≤ 5 sites detected with 68Ga-PSMA-PET/CT and with a minimum of 3 months of follow-up after MDT. Patients included hormone-naive, hormone-sensitive, or castration-resistant disease; concurrent ADT or chemotherapy at the time of SBRT was allowed. Exclusion criteria: Patients with ECOG performance status of ≥ 2 and patients treated previously with radiotherapy to the same oligometastatic site. | Total N = 176 Median age (range):
Sex, % male: 100.0 Number of metastases per patient:
| SABR with or without hormonotherapy (n = 129)
Conventional RT with or without hormonotherapy (n = 47)
| Research question: 1 Outcomes
Definitions:
|
van de Ven et al. (2020)64 The Netherlands Trial acronym: PRESENT (NCT02356497) Funding source: NR | Prospective cohort study (subset of patients with oligometastatic disease from full PRESENT cohort) from single institution. Linear mixed models for repeated measures were used to compared QoL between groups. All QoL analyses were adjusted for primary tumour, WHO performance status, presence of non-bone metastases, number of metastases, whether all metastases were treated at baseline, and pain at baseline. Survival outcomes were assessed using the Kaplan–Meier method and were compared using the log-rank test. Median follow-up (IQR):
| Inclusion criteria: Adult patients (≥ 18 years of age) with either synchronous or metachronous oligometastatic disease (≤ 5 metastatic lesions within ≤ 3 different organs). Primary tumours were located at various sites (prostate, breast, lung [NSCLC], kidney, other). Some patients had received treatment of primary tumour and previous treatment of metastases. Locations of metastasis were bone and other. Exclusion criteria: NR | Total N = 131 Mean age:
Sex, % male:
Number of metastases per patient:
| SABR (n = 65)
3DCRT (n = 66)
| Research Question: 1 Outcomes
Definitions:
|
De Bleser et al. (2019)66 Belgium, Italy, France, Switzerland, UK, Spain Trial acronym: NA Funding source: NIHR | Retrospective cohort study from 15 centres in several European countries. The Fisher exact test was used for comparisons between treatment groups. Median follow-up (IQR):
| Inclusion criteria: Male adult patients (≥ 18 years of age) with hormone-sensitive nodal metachronous oligorecurrent prostate cancer (5 or fewer lymph nodes). Primary tumours were treated with local therapy (either radical prostatectomy, radiotherapy, or both). Some patients had previous treatment of metastases with ADT (39% in SBRT; 32% in ENRT). Locations of metastasis were pelvic lymph nodes, extra-pelvic lymph nodes, both (i.e., both regional [N1] and distant [M1a] included). Exclusion criteria: Patients with synchronous prostate relapse and bone or visceral metastasis at recurrence; patients having a testosterone level of < 50 ng/dL at the time of metastatic recurrence; patients with oligometastases at primary diagnosis. | Total N = 506 Median age (IQR):
Sex, % male: 100.0 Number of metastases per patient:
| SABR with or without ADT (n = 309)
ENRT with or without ADT (n = 197)
| Research Questions: 1, 2 Outcomes
Definition:
|
He et al. (2018)67 China Trial acronym: NA Funding source: None | Retrospective cohort study from a single institution. Chi-square test was used for comparisons between groups. Survival analyses for OS and LCS were performed using the Kaplan–Meier method for univariate analysis and Cox regression model for multivariate analysis. Median follow-up:
| Inclusion criteria: Adult patients (≥ 18 years of age) with colorectal cancer that had been treated with tumour radical resection, post-operative staging IIIA-C (N positive), normal liver function (Child-Pugh class A), and unsuitable for or unwilling to undergo surgical resection. Patients diagnosed with a limited number of metachronous liver metastases (≤ 3 metastatic lesions in the liver per patient). Exclusion criteria: Patients with tumour site exceeding 6 cm in diameter, more than 3 metastatic lesions in the liver, presence or metastatic sites other than liver, and tumour recurrence in the abdomen or pelvis. | Total N = 26 Median age (IQR):
Sex, % male:
Number of metastases per patient:
| SABR (n = 11)
3DCRT (n = 15)
| Research questions: 1, 2 Outcomes
Definitions:
|
Filippi et al. (2016)68 Italy Trial acronym: NA Funding source: NR | Retrospective cohort study from a single institution. Chi-square test, Fisher exact test, t-test, or Wilcoxon rank sum test were used to compared variables. The Kaplan–Meier method was used to calculate OS and PFS, which were compared using the log-rank test. Median follow-up (IQR):
| Inclusion criteria: Adult patients (≥ 18 years of age) with colorectal adenocarcinoma previously treated with radical surgery, both synchronous and metachronous lung metastases (1 to 5 lesions), controlled primary tumour or controlled extra-lung metastases by local therapies or previous systemic therapies. The maximum tumour diameter had to be ≤ 50 mm. Patients must have had adequate pulmonary function and an ECOG performance status of 0 to 1. Exclusion criteria: NR | Total N = 170 Median age (IQR):
Sex; % male:
Number of metastases per patient:
| SABR (n = 28)
Surgery (n = 142)
| Research questions: 1, 2 Outcomes
Definitions:
|
Widder et al. (2013)60 and Lodeweges et al. (2017)61 The Netherlands Trial acronym: NA Funding source: NR | Retrospective cohort study from a single institution. Survival times were estimated using the Kaplan–Meier method and differences were assessed using the log-rank test. Short-term follow-up Median follow-up (IQR):
Long-term follow-up Median follow-up (IQR):
| Inclusion criteria: Adult patients (≥ 18 years of age) with up to 5 pulmonary metastases from various types of primary tumour (colorectal, sarcoma, lung (NSCLC), kidney, other) previously treated by surgery or thermal ablation. Exclusion criteria: NR | Total N = 110 Median age (IQR):
Sex; % male:
Number of metastases per patient:
| SABR (n = 42)
Surgery (n = 68)
| Research question: 1 Outcomes
Definitions:
|
3DCRT = 3-dimensional conformal radiation therapy; ADT = androgen deprivation therapy; AE = adverse event; ALK = anaplastic lymphoma kinase; CT = CT; CTCAE = Common Terminology Criteria for Adverse Events; ECOG = Eastern Cooperative Oncology Group; EGFR = estimated glomerular filtration rate; ENRT = elective nodal radiotherapy; EORTC = European Organisation for Research and Treatment of Cancer; FACT-G = Functional Assessment of Cancer Therapy–General; Gy = gray; IG-VMAT = image-guided volumetric modulated arc therapy; IQR = interquartile range; ITT = intention to treat; LC = lesional control; LCS = local control survival; MDT = metastatic-directed therapy; MV = megavolt; MRI = MRI; N = node; NA = not applicable; NCI = National Cancer Institute; NIH = National Institutes of Health; NIHR = National Institute for Health Research; NR = not reported; NRS = nonrandomized study; NSCLC = non–small cell lung cancer; OS = overall survival; PET = PET; PFS = progression-free survival; PSA = prostate-specific antigen; PSMA = prostate-specific membrane antigen; QoL = quality of life; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria In Solid Tumors; RTOG = Radiation Therapy Oncology Group; SABR = stereotactic ablative radiotherapy; SOC = standard of care; VMAT = volumetric modulated arc therapy.
aReported gender as described in the publication.
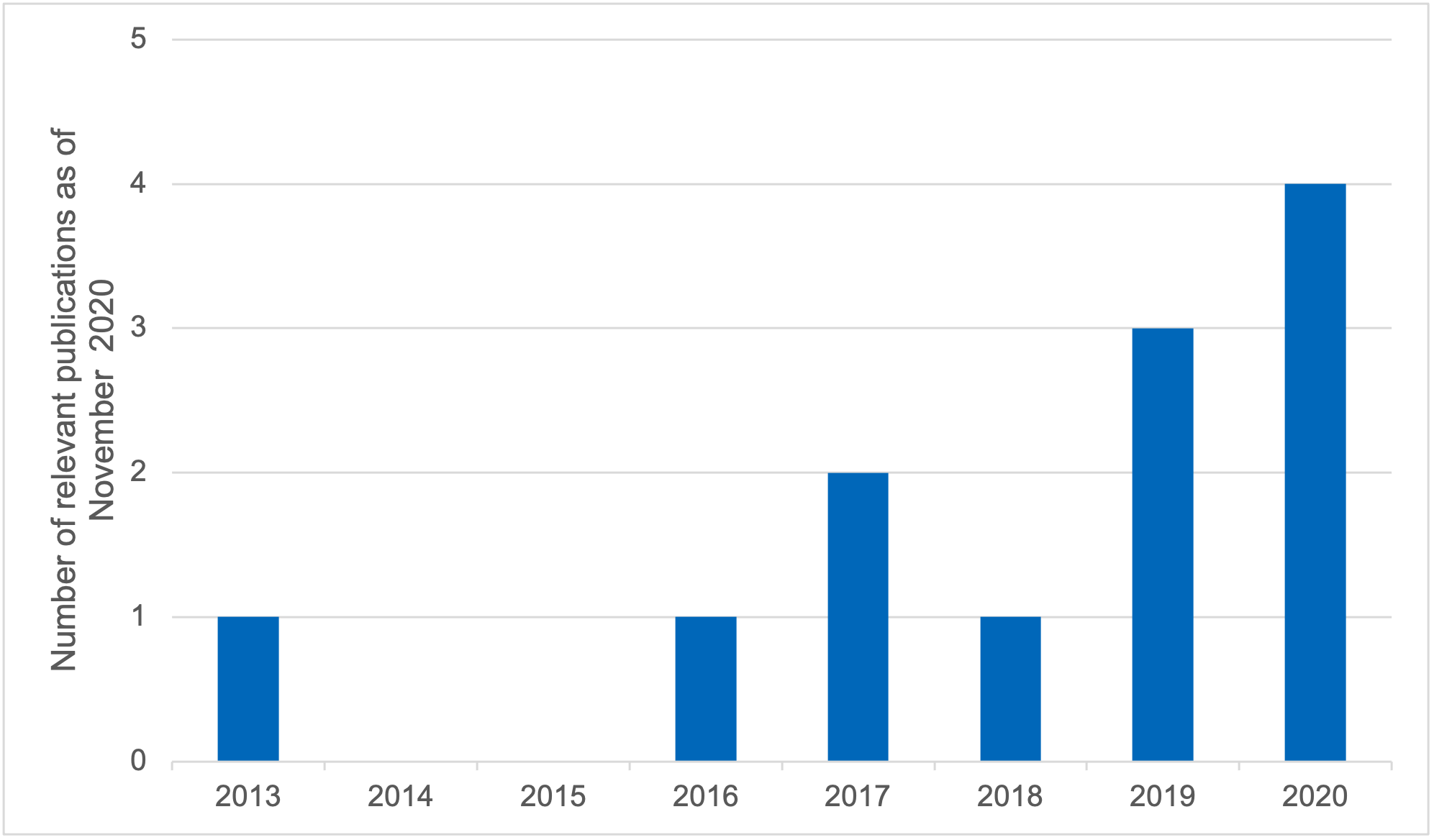
Appendix 8: Critical Appraisal of Included Studies
Table 18: Risk of Bias Among Randomized Controlled Trials (Cochrane Risk of Bias Tool 250)
Author (year); relevant for research question(s) | Bias arising from the randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of the outcome | Bias in selection of the reported result | Overall risk of bias |
Phillips et al. (2020)63 1, 2 | High risk 1.1 (Y). Allocation sequence random using an interactive web response system 1.2 (NI). No information about whether allocation sequence was concealed until participants were enrolled and assigned to intervention 1.3 (PY). The baseline differences between groups may suggest a problem with the randomization process (Gleason grade higher in the comparator arm vs. intervention arm; higher proportion of patients in intervention arm received prior ADT) (PY) | Some concerns 2.1 (Y). Participants were aware of their assigned intervention during the trial (open-label) 2.2 (Y). Carers and people delivering the intervention were aware of the participants’ assigned intervention during the trial (open-label) 2.3 (NI). No information about whether there were deviations from the intended intervention that arose because of the trial context 2.6 (Y). Appropriate analysis used to estimate the effect of assignment to intervention (ITT analysis) | PFS: Low risk AEs: Low risk QoL: Low risk Progression events: Low risk 3.1 (Y). Outcome data available for all, or nearly all, participants randomized | PFS: Low risk AEs: Some concerns QoL: Some concerns Progression events: Low risk 4.1 (PN). The method of measurement was probably not inappropriate (Kaplan–Meier method used to estimate PFS; CTCAE for AEs) 4.2 (PN). It is not likely that the measurement or ascertainment of the outcome had been different between intervention groups 4.3 (Y). Outcome assessors were aware of the intervention received by study participants 4.4 (PY). The assessment of the outcome probably could have been influenced by knowledge of the intervention received (can be some subjectivity for outcomes that involve assessment of a radiograph or clinical examination based on medical records, such as AE and QoL outcomes) 4.5 (PN). It is not likely that the assessment of the outcome was influenced by the knowledge of the intervention received (PN) | Low risk 5.1 (PY). Data that produced these results were probably analyzed in accordance with a pre-specified analysis plan The numerical result being assessed was not likely to have been selected, based on results from:
| High risk |
SABR-COMET Palma et al. (2019),32 Palma et al. (2020),58 Olson et al. (2019)59 | High risk 1.1 (Y). Allocation sequence randomized using a computer-generated randomization list with permuted blocks of 9 stratified by the number of metastases (1 to 3 vs. 4 to 5) 1.2 (NI). No information about whether allocation sequence was concealed until participants were enrolled and assigned to intervention 1.3 (PY). The baseline differences between groups may suggest a problem with the randomization process (intervention group had a preponderance of patients with prostate cancer and all the patients had 5 metastases) | Some concerns 2.1 (Y). Participants were aware of their assigned intervention during the trial (open label) 2.2 (Y). Carers and people delivering the intervention were aware of the participants’ assigned intervention during the trial (open label) 2.3 (PN). No major deviations from the intended intervention arose because of the trial context (1 patient from comparator group withdrew consent for further follow-up to pursue SABR)32 2.4 (PY). Probably no imbalance in deviations from intended intervention between groups 2.5 (NA).32 2.6 (Y). Appropriate analysis used to estimate the effect of assignment to intervention (ITT analysis) | OS: Low risk PFS: Low risk AEs: Low risk LC: Low risk QoL: Low risk 3.1 (Y) Outcome data available for all, or nearly all, participants randomized | OS: Low risk PFS: Low risk AEs: Some concerns LC: Low risk QoL: Some concerns 4.1 (PN). The method of measurement was probably not inappropriate (Kaplan–Meier method was used to estimate PFS and OS; CTCAE v.4 used to assess toxicity; FACT-G was used to assess QoL) 4.2 (PN). It is not likely that the measurement or ascertainment of the outcome had been different between intervention groups 4.3 (NI). No information about whether outcome assessors were aware of the intervention received by study participants 4.4 (PY). The assessment of the outcome probably could have been influenced by knowledge of the intervention received (can be some subjectivity for outcomes that involve assessment of a radiograph or clinical examination based on medical records, such as LC, AE, and QoL outcomes) 4.5 (PN). It is not likely that the assessment of the outcome was influenced by the knowledge of the intervention received | Low risk 5.1 (PY) Data that produced these results were probably analyzed in accordance with a pre-specified analysis plan The numerical result being assessed was not likely to have been selected, based on results from: • 5.2 (PN). Multiple eligible outcome measurements within the outcome domain or • 5.3 (PN). Multiple eligible analyses of the data (PN), based on the a priori protocol | High risk |
Iyengar et al. (2018)69 1, 2 | Some concerns 1.1 (NI). No information about whether allocation sequence was random 1.2 (NI). No information about whether allocation sequence was concealed until participants were enrolled and assigned to intervention 1.3 (N). The lack of baseline differences between groups does not suggest a problem with the randomization process | Some concerns 2.1 (Y). Participants were aware of their assigned intervention during the trial (open-label) 2.2 (Y). Carers and people delivering the intervention were aware of the participants’ assigned intervention during the trial (open-label) 2.3 (NI). No information about whether there were deviations from the intended intervention that arose because of the trial context (NI) 2.6 (Y). Appropriate analysis used to estimate the effect of assignment to intervention (ITT analysis) | OS: Low risk PFS: Low risk AEs: Low risk Progression events: Low risk 3.1 (Y) Outcome data available for all, or nearly all, of the randomized participants | OS: Low risk PFS: Low risk AEs: Some concerns Progression events: Some concerns 4.1 (PN). The method of measurement was probably not inappropriate (Kaplan–Meier method was used to estimate PFS and OS) 4.2 (PN). It is not likely that the measurement or ascertainment of the outcome been different between intervention groups 4.3 (NI). No information about whether outcome assessors were aware of the intervention received by study participants 4.4 (PY). The assessment of the outcome probably could have been influenced by knowledge of the intervention received (can be some subjectivity in the assessment of AE outcomes) 4.5 (PN). It is not likely that the assessment of the outcome was influenced by the knowledge of the intervention received | Low risk 5.1 (PY). Data that produced these results were probably analyzed in accordance with a pre-specified analysis plan The numerical result being assessed was not likely to have been selected, based on results from:
| Some concerns |
ADT = androgen deprivation therapy; AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events version 4.0; FACT-G = Functional Assessment of Cancer Therapy–General; ITT = intention to treat; N = no; NA = not applicable; NI = no information; OS = overall survival; PFS = progression-free survival; PN = probably no; PY = probably yes; QoL = quality of life; SABR = stereotactic ablative radiotherapy; Y = yes.
Table 19: Risk of Bias Among Nonrandomized Studies (RoBANS51,52)
Author (year); relevant for research question(s) | The possibility of the target group comparisons | Target group selection | Confounder | Exposure measurement | Blinding of assessors | Outcome assessment | Incomplete outcome data | Selective outcome reporting | Overall risk-of-bias judgment |
Selection bias due to selection of inappropriate comparison target group | Selection bias due to inappropriate intervention or inappropriate selection of exposure group or patient group | Selection bias due to inappropriate confounder confirmation and consideration | Performance bias due to inappropriate intervention or inappropriate exposure measurement | Confirmation bias due to inappropriate blinding of assessors | Confirmation bias due to inappropriate outcome assessment methods | Attrition bias due to inappropriate handling of incomplete data | Reporting bias due to selective outcome reporting | ||
Hurmuz et al. 202065 1 | Unclear; patient characteristics of each group were not reported individually | Unclear; unknown whether participants selected from the 10 centres were balanced between groups | Unclear; some confounders were adjusted for PFS, but not for OS | Low; data obtained from medical records | Low; main end points are time-to-event (survival) outcomes | OS: Low PFS: Low Local Progression: Low Outcomes confirmed with medical records | OS: Unclear PFS: Unclear Local Progression: Unclear Unclear if all participant data were included in the analyses | Unclear; no protocol to verify | Some concerns |
van de Ven et al. (2020)64 1 | High; groups differ in some of the main characteristics (age, type of metastases, pain) | Low; participant recruitment strategy (standards for inclusion and exclusion and selection method) was the same for both groups | Low; confounders were confirmed and considered during planning and analysis stages | Low; data were obtained from patient records | Low; main end points are time-to-event (survival) outcomes | OS: Low PFS: Low Pain response: Low QoL: Low Outcomes confirmed with medical records | OS: Low PFS: Low Pain response: High QoL: High Not all patient data used in the analysis of QoL (authors excluded all patients with no pain at baseline) | Low; registered protocol a priori with ClinicalTrials.gov (NCT02356497) | High risk |
De Bleser et al. (2019)66 | High; groups differ in some of the main characteristics (use of adjuvant ADT at the time of MDT) | Unclear; unknown whether participants selected from the 15 centres were balanced between groups | Low; confounders were confirmed and considered during planning and analysis stages | Low; data were obtained from patient records from multiple centres | Low; main end points are time-to-event (survival) outcomes | Local progressions: Low AEs: Low Outcomes likely confirmed with medical records | Local progressions: Unclear AEs: Unclear Unclear if all participant data were included in the analyses | Unclear; no protocol to verify | High risk |
He et al. (2018)67 1, 2 | Low; no statistical differences between groups in pre-treatment clinical characteristics | Low; participant recruitment strategy (standards for inclusion and exclusion and selection method) was the same for both groups | Unclear; unclear whether confounders were confirmed and considered during planning and analysis stages for OS outcome | Low; data were obtained from patient records | Low; main end points are time-to-event (survival) outcomes | OS: Low AEs: Low Outcomes likely confirmed with medical records | OS: Unclear AEs: Unclear Unclear if all participant data were included in the analyses | Unclear; no protocol to verify | Some concerns |
Filippi et al. (2016)68 1, 2 | High; groups differ in some of the main characteristics (age, period of treatment) | Low; participant recruitment strategy (standard inclusion and exclusion selection method) was the same for both groups | Low; confounders were confirmed and considered during planning and analysis stages | Low; data were obtained from patient records | Low; main end points are time-to-event (survival) outcomes | OS: Low PFS: Low AEs: Low Progressions: Low Outcomes confirmed with medical records | OS: Low PFS: Low AEs: Low Progressions: Low No missing data in the analyses of all outcomes | Unclear; no protocol to verify | High risk |
Widder et al. (2013)60 and Lodeweges et al. (2017)61 1, 2 | High; groups differ in some of the main characteristics (age, primary tumour, metastasis-free interval, prior chemotherapy) | Unclear; participant recruitment strategy (selection method) not clearly described | Low; confounders were confirmed and considered during planning and analysis stages | Low; data were obtained from patient records | Low; main end points are time-to-event (survival) outcomes | OS: Low PFS: Low LC: Low Outcomes likely confirmed with medical records | OS: Low PFS: Low LC: Low No missing data in the analyses of all outcomes | Unclear; no protocol to verify | High risk |
ADT = androgen deprivation therapy; AE = adverse event; LC = lesional control; MDT = metastatic-directed therapy; OS = overall survival; PFS = progression-free survival; RoBANS = Risk of Bias Assessment Tool for Nonrandomized Studies; QoL = quality of life.
Appendix 9: Main Study Findings
Author (year) | Treatments (Intervention vs. comparator) Follow-up | Death events; n | OS rate, % (95% CI) | Median OS (95% CI); months | Unadj HR (95% CI) | Adj HR (95% CI) | |||||
1-year | 2-year | 3-year | 4-year | 5-year | |||||||
RCTs | |||||||||||
SABR-COMET | SABR + systemic therapy (n = 66) vs. systemic therapy alone (n = 33) Short-term Median F/U (IQR):
Long-term Median F/U (IQR): Total: 51 (46 to 58) months58 | Short-term F/U: 24 vs. 16 Long-term F/U: 35 vs. 24 | Short- and long-term F/U: NR | Short- and long-term F/U: NR | Short- and long-term F/U: NR | Short- and long-term F/U: NR | Short-term F/U: NR Long-term F/U: 42.3 (28 to 56) vs. 17.7 (6 to 34) | Short-term F/U: 41 (26 to not reached) vs. 28 (19 to 33) Long-term F/U: 50 (29 to 83) vs. 28 (18 to 39) | Short-term F/U: 0.57 (0.30 to 1.10); P = 0.09 Long-term F/U: 0.47 (0.27 to 0.81); P = 0.006 | Short and long-term F/U: NR | |
Authors’ conclusions: “In patients with a controlled primary tumour and one to five oligometastases, SABR is associated with a 13-month increase in overall survival. With extended follow-up, the impact of SABR on OS was larger in magnitude than in the initial analysis and durable over time.”32 | |||||||||||
Iyengar et al. (2018)69 | SABR + chemotherapy (n = 14) vs. chemotherapy alone (n = 15) Median F/U (IQR): Total: 9.6 (2.4 to 30.2) months | NR | NR | NR | NR | NR | NR | Not reached (NR) vs. about 1 year without crossover; 17 months with crossover (NR) | NR | NR | |
Authors’ conclusions: “Median OS was not reached for the SABR plus maintenance chemotherapy arm, though the study was not powered to show a statistical difference in survival.”69 | |||||||||||
NRSs | |||||||||||
Hurmuz et al. (2020)65 | SABR ± hormonotherapy (n = 129) vs. conventional fractionation radiotherapy ± hormonotherapy (n = 47) Median F/U (IQR): Total: 22.9 (3.3 to 77.8) months | NR | NR | 87.7 (NR) vs. 87.3 (NR); P = 0.91 | NR | NR | NR | NR | NR | NR | |
Authors’ conclusions: “There was no significant difference in OS between patients treated with SBRT and conventional fractionation.”65 | |||||||||||
van de Ven et al. (2020)64 | SABR (n = 65) vs. 3DCRT (n = 66) Median F/U (IQR):
| 3 months: 2 vs. 5; 6 months: 4 vs. 13; 12 months: 6 vs. 20 | 85 (NR) vs. 65 (NR) | NR | NR | NR | NR | Not reached (NR) at 18 months; P < 0.0001 vs. NR | 0.44 (0.24 to 0.81); P = NR | NR | |
Authors’ conclusions: “OS survival rates were significantly better in the SBRT group, which is probably largely due to selection of patients, and confirmed by the differences in baseline between the two treatment groups.”64 | |||||||||||
He et al. (2018)67 | SABR (n = 11) vs. 3DCRT (n = 15) Median F/U: Total: 13 months | NR | 68.2 (NR) vs. 55.8 (NR) | 40.9 (NR) vs. 16.0 (NR) | 20.5 (NR) vs. 0.0 (NR) | NR | NR | 20 (NR) vs. 14 (NR) | 0.61 (0.23 to 1.65); P = 0.323 | NR | |
Authors’ conclusions: “The slightly better overall survival…in the stereotactic body radiation therapy group in comparison to the conformal radiation therapy group…is insignificant.”67 The authors acknowledged that the OS results might be affected by study’s limitations, i.e., small sample size, differences in study and patient characteristics between groups, and the lack chemotherapy after SABR or RTRT. | |||||||||||
Filippi et al. (2016)68 | SABR (n = 28) vs. surgery (n = 142) Median F/U (IQR):
| 10 vs. 37 | 89 (70 to 96) vs. 96 (92 to 99) | 77 (56 to 89) vs. 82 (74 to 87) | NR | NR | NR | NR | 1.7 (0.84 to 3.43); P = 0.139 | 1.71 (0.82 to 3.54); P = 0.149 | |
Authors’ conclusions: “Patients treated with SBRT for CRC lung oligometastases could achieve overall survival rates at 2 years comparable with surgery.”68 | |||||||||||
Widder et al. (2013)60 and Lodeweges et al. (2017)61a | SABR (n = 42) vs. surgery (PME) (n = 68) Short-term F/U: Median F/U (IQR): Total: 43 (36 to 60) months60 Long-term F/U: Median F/U (IQR): Total: 91.2 (69.6 to 117.6) months61 | Short-term F/U: 17 vs. 35 Long-term F/U: NR | Short- and long-term F/U: 98 (84 to 100) vs. 87 (76 to 93) | Short- and long-term F/U: 86 (71 to 93) vs. 74 (61 to 82) | Short-term F/U: 60 (42 to 73) vs. 62 (49 to 73) Long-term F/U: 64 (48 to 77) vs. 63 (51 to 73) | Short-term F/U: 60 (42 to 73) vs. 47 (33 to 59) Long-term F/U: 57 (41 to 70) vs. 50 (38 to 61) | Short-term F/U: 49 (25 to 69) vs. 41 (27 to 54) Long-term F/U: 45 (30 to 59) vs. 41 (29 to 53) | Short- and long-term F/U: NR | Short-term F/U: 0.79 (0.43 to 1.42); P = 0.427 Long-term F/U: 1.11 (0.70 to 1.75); P = NR; NS | Short-term F/U: NR Long-term F/U: 0.76 (0.38 to 1.54); P = NR; NS | |
Authors’ conclusions: “Although SABR was second choice after PME, survival after PME was not better than after SABR.”60 | |||||||||||
3DCRT = 3-dimensional conformal radiation therapy; adj = adjusted; CI = confidence interval; CRC = colorectal cancer; F/U = follow-up; HR = hazard ratio; IQR = interquartile range; NR = not reported; NS = non-significant; OS = overall survival; PME = pulmonary metastasectomy; RoBANS = Risk of Bias Assessment Tool for Nonrandomized Studies; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; SBRT = stereotactic body radiation therapy; unadj = unadjusted; vs. = versus .
aOS rates at 6, 7, and 8 years for SABR vs. surgery (PME) were 35% (95% CI, 21% to 50%) vs. 37% (95% CI, 26% to 48%), 29% (95% CI,16% to 44%) vs. 35% (95% CI, 24% to 46%), and 13% (95% CI, 3% to 30%) vs. 35% (95% CI, 24% to 46%), respectively.
Table 21: Progression-Free Survival
Author (year) | Treatments (intervention vs. comparator) Follow-up | Progression events; n | PFS rate, % (95% CI) | Median PFS (95% CI); months | Unadj HR (95% CI) | Adj HR (95% CI) | ||||||
6-month | 1-year | 2-year | 3-year | 4-year | 5-year | |||||||
RCTs | ||||||||||||
Phillips et al. (2020)63 | SABR (n = 36) vs. observation (n = 18) Median F/U (IQR): Total: 18.8 (5.8 to 35.0) months | 7 vs. 11; P = 0.005 | 19 (9.6 to 35.4) vs. 61 (38.5 to 79.6) | NR | NR | NR | NR | NR | Not reached (NR) vs. 5.8 (NR) | 0.3 (0.11 to 0.81); P = 0.002 | NR | |
Authors’ conclusions: “SABR is a safe and effective modality for metastases-directed therapy in oligometastatic prostate cancer that improves PFS compared with observation and results in a systemic adaptive immune response.”63 | ||||||||||||
SABR-COMET | SABR + systemic therapy (n = 66) vs. systemic therapy alone (n = 33) Short-term Median F/U (IQR):
Long-term Median F/U (IQR): Total: 51 (46 to 58) months58 | Short-term F/U: 39 vs. 28 Long-term F/U: 45 vs. 29 | Short- and long-term F/U: NR | Short- and long-term F/U: NR | Short- and long-term F/U: NR | Short- and long-term F/U: NR | Short-term F/U: NR Long-term F/U: 21.6 (12 to 33) vs. 3.2 (0 to 14) | Short-term F/U: NR Long-term F/U: 17.3 (8 to 30) vs. 0 (NA) | 12 (6.9 to 30.4) vs. 6.0 (3.4 to 7.1) Long-term F/U: 11.6 (6.1 to 23.4) vs. 5.4 (3.2 to 6.8) | 0.47 (0.30 to 0.76); P = 0.0012 Long-term F/U: 0.48 (0.31 to 0.76); P = 0.001 | Short- and long-term F/U: NR | |
Authors’ conclusions: “In patients with a controlled primary tumour and one to five oligometastases, SABR is associated with… a doubling of progression-free survival.”32 | ||||||||||||
Iyengar et al. (2018)69 | SABR + chemotherapy (n = 14) vs. chemotherapy (n = 15) Median F/U (IQR): Total: 9.6 (2.4 to 30.2) months | 4 vs. 10 | NR | NR | NR | NR | NR | NR | 9.7 (NR) vs. 3.5 (NR) | 0.304 (0.113 to 0.815); P = 0.01 | NR | |
Authors’ conclusions: “Consolidative SABR prior to maintenance chemotherapy appeared beneficial, nearly tripling PFS in patients with limited metastatic NSCLC compared with maintenance chemotherapy alone.”69 | ||||||||||||
NRSs | ||||||||||||
Hurmuz et al. (2020)65 | SABR ± hormonotherapy (n = 129) vs. conventional fractionation radiotherapy ± hormonotherapy (n = 47) Median F/U (IQR): Total: 22.9 (3.3 to 77.8) months | NR | NR | 86.2 (NR) vs. 54.9 (NR); P < 0.001 | NR | NR | NR | NR | NR | NR | 0.26 (0.13 to 0.55); P < 0.001 | |
Authors’ conclusions: “2-year PFS was significantly better in patients treated with SBRT to the oligometastatic site than those treated with conventional fractionation.”65 | ||||||||||||
van de Ven et al. (2020)64 | SABR (n = 65) vs. 3DCRT (n = 66) Median F/U (IQR):
| NR | NR | 54 (NR) vs. 19 (NR) | NR | NR | NR | NR | 12 (NR) vs. 5 (NR); P = 0.002 | 0.63 (0.41 to 0.95); P = NR | NR | |
Authors’ conclusions: “PFS survival rates were significantly better in the SBRT group, which is probably largely due to selection of patients, and confirmed by the differences in baseline between the 2 treatment groups.”64 | ||||||||||||
Filippi et al. (2016)68 | SABR (n = 28) vs. surgery (n = 142) Median F/U (IQR):
| 21 vs. 87 | NR | NR | NR | NR | NR | NR | NR | 2.44 (1.51 to 3.94); P < 0.001 | 2.78 (1.67 to 4.62); P < 0.001 | |
Authors’ conclusions: “…, both Kaplan-Meier functions and Cox models indicated a worse prognosis in terms of PFS for the SBRT cohort. However, much of this effect seems to be attributable to the more intensive follow-up protocol applied after SBRT.”68 | ||||||||||||
SABR (n = 42) vs. surgery (PME) (n = 68) Short-term Median F/U (IQR): Total: 43 (36 to 60) months60 Long-term Median F/U (IQR): Total: 91.2 (69.6 to 117.6) months61 | Short-term F/U: 32 vs. 51 Long-term F/U: NR | Short- and long-term F/U: NR | Short-term F/U: 50 (34 to 64) vs. 54 (42 to 65) Long-term F/U: 49 (34 to 63) vs. 56 (43 to 66) | Short-term F/U: 21 (9 to 35) vs. 33 (22 to 45) Long-term F/U: 27 (14 to 41) vs. 35 (23 to 46) | Short-term F/U: 8 (2 to 22) vs. 22 (12 to 33) Long-term F/U: 18 (8 to 32) vs. 26 (16 to 36) | Short-term F/U: 8 (2 to 22) vs. 18 (9 to 30) Long-term F/U: 18 (8 to 32) vs. 23 (13 to 33) | Short-term F/U: NR Long-term F/U: 18 (8 to 32) vs. 20 (11 to 30) | Short- and long-term F/U: NR | Short- and long-term F/U: NR | Short- and long-term F/U: NR | ||
Authors’ conclusions: No specific conclusion regarding PFS was provided. | ||||||||||||
3DCRT = 3-dimensional conformal radiation therapy; adj = adjusted; CI = confidence interval; ENRT = elective nodal radiotherapy; F/U = follow-up; HR = hazard ratio; IQR = interquartile range; NA = not applicable; NR = not reported; PFS = progression-free survival; PME = pulmonary metastasectomy; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; SBRT = stereotactic body radiation therapy; unadj = unadjusted; vs. = versus .
aPFS rates at 6, 7, and 8 years for SABR vs. surgery (PME) for all time points were 18% (95% CI, 8% to 32%) vs. 20% (95% CI, 11% to 30%).
Author (year); follow-up | Tools and definitions | Results |
RCTs | ||
Phillips et al. (2020)63 | QoL: Brief Pain Inventory (Short Form) | QoL: Data not provided |
Authors’ conclusions: “No differences in Brief Pain Inventory (Short Form) scores were observed between arms or within either arm across time.”63 | ||
SABR-COMET Palma et al. (2019),32 Palma et al. (2020),58 Olson et al. (2019)59 Short-term median F/U (IQR): Long-term median F/U (IQR): Total: 51 (46 to 58) months58 | QoL: FACT-G (4 subscales: physical well-being, social/family well-being, emotional well-being, and functional well-being) | QoL: SABR + systemic therapy vs. systemic therapy FACT-G at 6 months, mean (SD):a,32
FACT-G subscales, mean (SD):
FACT-G over 42 months59:
FACT-G over 5 years58
|
Authors’ conclusions: “There were no significant differences in overall mean FACT-G scores at 6 months, or in any of the physical, social, functional, or emotional QoL subscales.”32 “The use of SABR, compared with standard of care, was not associated with a QoL detriment. This suggests that broad QoL changes are due to underlying disease processes over time. Future research could further explore site- and tumour-specific QoL measures and their ability to detect more subtle changes over time and differences between treatment options. We believe this work supports future clinical trials that are histology and site specific.”59 “The long-term analysis of FACT-G scores over time are shown in Figure 3, with no differences in total QoL scores, or subscale score.”58 | ||
NRS | ||
van de Ven et al. (2020)64 Median F/U (IQR):
| Pain: Pain scores and response were assessed only in patients who reported pain at baseline Pain response: Defined according to international consensus criteria using NRS and Brief Pain Inventory scores; information on pain medication and daily oral morphine equivalent based on returned QoL questionnaires or gathered during follow-ups Partial response = a pain reduction of at least 2 points without an increase in analgesic use, or at least a 25% reduction in opioid use without an increase in pain score Complete response = a pain score of 0 without an increase in analgesic use Pain progression = an increase in pain score of 2 or more points above baseline with no change in analgesic use, or an increase in pain score of 1 point above baseline with an increase in analgesic use of 25% or more Stable pain = no change in pain score or analgesic use Intermediate response = all other responses that do not fit under partial response, complete response, pain progression, or stable pain Responders = complete or partial response was achieved on at least 1 of the follow-up time points Duration of pain response = time until pain progression, intermediate pain response, stable pain, or death Ongoing pain response = a continuous pain response (e.g., partial or complete) 1 year after treatment QoL tools (global, functional, and role scales) EORTC QLQ-BM22, EORTC QLQ-C15-PAL, Brief Pain Inventory, EQ-5D; validated tools used | Pain Number of patients with pain at baseline:
Mean (SD) NRS scores at baseline:
Pain response:
Complete response:
Partial response
Pain progression:
Intermediate responses + stable responses:
Responders:
Median duration of pain response (range):
Ongoing pain response:
Re-irradiation for pain recurrence or progression:
QoL (where P values of < 0.01 were considered statistically significant for mixed models)
|
Authors’ conclusions: “In patients with oligometastatic disease, SBRT to bone metastases did not improve pain response or QoL compared with 3DCRT. Reirradiation was less often needed in the SBRT group.”64 | ||
3DCRT = 3-dimensional conformal radiation therapy; EORTC QLQ-BM22 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for Patients with Bone Metastasis 22; EORTC QLQ-C15-PAL = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative; EQ-5D = EuroQol 5-Dimensions questionnaire; FACT-G = Functional Assessment of Cancer Therapy–General; F/U = follow-up; IQR = interquartile range; NRS = numeric rating scale; QoL = quality of life; SABR = stereotactic ablative radiotherapy.
aBaseline values were not reported numerically, but graphically instead.
Author (year) | Treatments (intervention vs. comparator); follow-up | Local progression events; n | Crude LC rate, % (95% CI) | LC rate, % (95% CI) | Median LC (95% CI); months | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | |||||
1-year | 2-year | 3-year | 4-year | 5-year | 6-year | |||||||
RCTs | ||||||||||||
SABR + systemic therapy (n = 66) vs. systemic therapy (n = 33) Short-term Median F/U (IQR):
Long-term Median F/U (IQR): Total: 51 (46 to 58) months58 | Short- and long-term F/U: NR | Short-term F/U: 75 (NR) vs. 49 (NR); P = 0∙0010 Long-term F/U: 63 (NR) vs. 46 (NR); P = 0.039 | NR | NR | NR | NR | NR | NR | NR | NR | NR | |
Authors’ conclusions: “The proportion of patients with lesional control (i.e., the absence of progression in the lesions initially present of randomization) was 49% (28 of 57 assessable lesions) in the control group and 75% (75 of 100 assessable lesions) in the SABR group (p=0.0010), represented by an absolute increase of 26% (95% CI 10–41)” (p. 2055).32 “The overall long-term LC rate, defined as the absence of progression in the lesions initially present at random assignment on the basis of RECIST version 1.1, was 46% (26 of 57 assessable lesions) in the control arm and 63% (65 of 104 assessable lesions in the SABR arm (P = .039), corresponding to an absolute increase of 17% (95% CI, 1% to 33%)” (p. 4).58 | ||||||||||||
Iyengar et al. (2018)69 | SABR + chemotherapy (n = 14) vs. chemotherapy (n = 15) Median F/U (IQR): Total: 9.6 (2.4 to 30.2) months | 0 vs. 7 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Authors’ conclusions: No specific conclusion provided. | ||||||||||||
NRSs | ||||||||||||
De Bleser et al. (2019)66 | SABR (n = 309) vs. ENRT (n = 197) Median F/U (IQR): Total: 36 (23 to 56) months | 50 vs. 9 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Authors’ conclusions: No specific conclusion provided. | ||||||||||||
Hurmuz et al. (2020)65 | SABR ± hormonotherapy; n = 129 vs. conventional fractionation radiotherapy ± hormonotherapy; n = 47 Median F/U (IQR): Total: 22.9 (3.3 to 77.8) months | 2 vs. 7 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Authors’ conclusions: No specific conclusion provided. | ||||||||||||
Filippi et al. (2016)68 | SABR (n = 28) vs. surgery (n = 142) Median F/U (IQR):
| 6 vs. 6 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Authors’ conclusions: No specific conclusion provided. | ||||||||||||
Widder et al. (2013)60 and Lodeweges et al. (2017)61a | SABR (n = 42) vs. surgery (PME) (n = 68) Short-term F/U Median F/U (IQR): Total: 43 (36 to 60) months60 Long-term F/U Median F/U (IQR): Total: 91.2 (69.6 to 117.6) months61 | Short- and long-term F/U: NR | NR | Short-term F/U: 94 (79 to 99) vs. 93 (83 to 97) Long-term F/U: 95 (80 to 99) vs. 93 (83 to 97) | Short-term F/U: 94 (79 to 99) vs. 90 (78 to 96) Long-term F/U: 95 (80 to 99) vs. 91 (79 to 96) | Short-term F/U: 85 (55 to 96) vs. 83 (65 to 92) Long-term F/U: 90 (70 to 97) vs. 85 (70 to 93) | Short-term F/U: 85 (55 to 96) vs. 83 (65 to 92) Long-term F/U: 90 (70 to 97) vs. 85 (70 to 93) | Short-term F/U: NR Long-term F/U: 83 (57 to 94) vs. 81 (65 to 90) | Short-term F/U: NR Long-term F/U: 83 (57 to 94) vs. 81 (65 to 90) | Short- and long-term F/U: NR | NR Long-term F/U: 0.8 (0.24 to 2.65) | Short- and long-term F/U: NR |
Authors’ conclusions: “Patterns of progressions and post-treatment management did not differ between SABR and PME” (p. 411).60 | ||||||||||||
CI = confidence interval; ENRT = elective nodal radiotherapy; F/U = follow-up; HR = hazard ratio; IQR = interquartile range; LC = lesional control; NR = not reported; PME = pulmonary metastasectomy; RCT = randomized controlled trial; SABR = stereotactic ablative radiotherapy; vs. = versus .
aLC rates at 7 and 8 years for SABR vs. surgery (PME) for both time points was 83% (95% CI, 57% to 94%) vs. 81% (95% CI, 65% to 90%).
Author (year); follow-up | Tools | Results |
RCTs | ||
Phillips et al. (2020)63 Median F/U (IQR): Total: 18.8 (5.8 to 35.0) months | CTCAE v4.0 | Number of patients with AEs New grade 1 AEs at 90 days:
New grade 1 AEs at 180 days:
New grade 2 AEs at 90 days:
New grade 2 AEs at 180 days:
Grade 3 or higher AEs: None |
Authors’ conclusions: “The adverse effects associated with SABR were mild and did not appear to affect quality of life.” | ||
SABR-COMET Palma et al. (2019),32 Palma et al. (2020)58 Short-term Median F/U (IQR):
Long-term Median F/U (IQR): Total: 51 (46 to 58) months58 | CTCAE v4.0 | Number of patients with AEs AE grade ≥ 2:
Treatment-related AE grade ≥ 2:
Death (grade 5):
Fatigue (grade 2):
Fatigue (grade 3):
Dyspnea (grade 2):
Dyspnea (grade 3):
Pain (any type, including muscle, bone, and other; grade 2)
Pain (any type, including muscle, bone, and other; grade 3)
|
Authors’ conclusions: “SABR was associated with an improvement in overall survival, meeting the primary end point of this trial, but 3 (4∙5%) of 66 patients in the SABR group had treatment-related death.”32; “There were no new safety signals, and SABR had no detrimental impact on QoL.”58 | ||
Iyengar et al. (2018)69 Median F/U (IQR): Total: 9.6 (2.4 to 30.2) months | CTCAE v4.0 | Toxicity (number of events) Grade 1:
Grade 2:
Grade 3:
Grade 4:
Grade 5:
|
Authors’ conclusions: “Consolidative SABR prior to maintenance chemotherapy appeared beneficial, nearly tripling PFS in patients with limited metastatic NSCLC compared with maintenance chemotherapy alone, with no difference in toxic effects.”69 | ||
NRSs | ||
De Bleser et al. (2019)66 Median F/U (IQR): Total: 36 (23 to 56) months | CTCAE or RTOG grading system | Number of patients with AEs Grade 3 or higher in both early and late toxicity
Early toxicity of all grades:
Late toxicity of all grades:
|
Authors’ conclusions: “ENRT reduces the number of nodal recurrences as compared with SBRT, however at higher toxicity.”66 | ||
He et al. (2018)67 Median F/U: Total: 13 months | CTCAE v3.0 or RTOG | Liver toxicity:
Hepatic toxicity–inducing rate:
|
Authors’ conclusions: “Non-invasive radiation therapy provides satisfactory survival benefit for limited colorectal cancer liver metastases without intolerable toxicity and is therefore especially suitable for those elderly patients with poor performance status.”67 | ||
Filippi et al. (2016)68 Median F/U (IQR):
| CTCAE v3.0 | Number of patients with AEs SABR:
Surgery:
|
Authors’ conclusions: No specific conclusions for AEs. | ||
3DCRT = 3-dimensional conformal radiation therapy; AE = adverse event; CI = confidence interval; CTCAE = Common Terminology Criteria for Adverse Events; ENRT = elective nodal radiotherapy; F/U = follow-up; IQR = interquartile range; NSCLC = non–small cell lung cancer; PFS = progression-free survival; QoL = quality of life; SABR = stereotactic ablative radiotherapy; RCT = randomized controlled trial; SBRT = stereotactic body radiotherapy; NRS = nonrandomized study; RTOG = Radiation Therapy Oncology Group.
Table 25: Patient and Public Involvement in CADTH’s SABR for the Treatment of Oligometastatic Cancer HTA
Topic | Item |
Aim | A patient with experience with SABR was involved in developing the protocol and commenting on the findings. This patient and other patient stakeholder groups (Canadian Partnership Against Cancer, Canadian, Canadian Cancer Survivor Network) were invited to provide feedback on the draft of the baseline clinical review. |
Methods | We engaged 1 patient with oligometastatic cancer (primary head and neck cancer with a lung metastasis) that was treated with SABR. An oncology trialist identified this individual as a patient collaborator. After giving informed consent, the patient collaborator discussed their experience of SABR treatment via teleconference and email communication. Once preliminary findings from the review were available, the patient was invited to give their perceptions of key findings, including whether the findings are understandable and if they reflect their experiences. |
Study results | In their discussions, the researchers were made aware of the importance of 3 outcomes in particular: overall survival, progression-free survival, and quality of life, especially with regard to breathing problems and fatigue. They mentioned that being able to exercise and be active was important to them. They mentioned satisfaction in being able to return to work after SABR treatment. The involvement of a patient prompted the research team to discuss which adverse effects of SABR were of concern to the patient collaborator. Pain and fatigue were mentioned and reported in the results, where available. Sharing these concerns allowed the research team to consider the evidence in the context of the wider experiences of patients and caregivers when preparing the assessment. |
Discussion and conclusions | Success of patient involvement in this report is related to several factors. First, the patient partners were briefed on the objectives of the project and their role. Second, they were supported by experienced patient engagement officers who can facilitate the use of their involvement with the research team. Established processes were put in place and our patient collaborator was offered compensation for their time to participate in the project. However, there were limitations. The topic and research questions were already determined before engaging the patient collaborator. Due to time constraints, our collaborator and other patient stakeholders were invited to participate within a set time frame and with a deadline for providing feedback. |
Reflections and critical perspective | Our patient collaborator was highly engaged in the conversation with researchers. They had clear opinions and concerns during the teleconference. They reported family-borne costs or burdens such as travel that was covered by private insurance. Although not within the scope of this report, the conversation of patient-borne costs and experiences of travelling for treatment helped the researchers appreciate the reality of receiving SABR treatment. Ethical and equity issues are sometimes revealed in the telling of their experiences. For example, our patient collaborator lived in a northern, rural location. It was 1,200 km to the largest cancer centre where the treatment plan was made and a PET scan performed. They were able to receive treatment 450 km from home at a regional cancer centre. They sometimes needed a family member to travel with them. They stayed in housing for patients and families located near the cancer centre for the duration of their treatment. Many of their costs were covered by their private insurance plan through work. These comments allowed the researchers to reflect on geographic barriers to accessing services, as well as additional patient considerations when travelling for treatment. Some limitations of our patient engagement are that people often have concerns that are not part of the project scope (e.g., accessing diagnosis, difficulty finding a knowledgeable health care provider), but the topic and question are already identified when the project begins. It can be difficult to identify a patient whose experience is similar to the population of interest. The time frame of the project makes it difficult for patients to participate fully, on terms that work for them (e.g., daytime teleconferences). People need access to reliable technology and phone and internet service to participate; lack of such access could possibly exclude some voices. |
HTA = Health Technology Assessment; PET = PET; SABR = stereotactic ablative radiotherapy.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.