CADTH Health Technology Review
Stepped Care Models for Chronic Pain
Technology Review
Authors: Angela M. Barbara, Melissa Severn
Abbreviations
CBT
cognitive behaviour therapy
CINAHL
Cumulative Index to Nursing and Allied Health Literature
ESCAPE
Evaluation of Stepped Care for Chronic Pain
MeSH
Medical Subject Headings
NCCP
Non-cardiac chronic pain
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
RCT
randomized controlled trial
SCS
Stepped Care Strategy
SCM-PM
Stepped Care Model for Pain Management
Key Messages
CADTH included 6 reports describing the potential clinical benefits of 5 stepped care models for chronic pain in this review.
The randomized controlled trial of the stepped care model for patients who are overweight or obese with chronic pain due medial tibiofemoral osteoarthritis described the impact on pain remission, pain intensity, and function.
The before-after and retrospective cohort study of the Stepped Care Model of Pain Management described the effects on pain, quality of chronic pain care, pharmacotherapy use, and health care utilization in US veterans.
The before-after study of the biopsychosocial stepped care model for non-cardiac chest pain described the potential benefits on chest pain, depression, anxiety, quality of life, and health care use.
The prospective cohort study of the Stepped Care Strategy compared a cohort of patients who received stepped care strategy-consistent care for hip or knee pain due to osteoarthritis with a cohort who received stepped care strategy-inconsistent care and described the results on pain physical function, self-efficacy, active pain coping, and health care use.
The Evaluation of Stepped Care for Chronic Pain randomized controlled trial described the effects on pain, disability, and pharmacotherapy use in US veterans.
CADTH included 1 cost-effectiveness analysis that described the cost implications of a stepped care pathway for treating sciatica pain.
While all included models used a stepped care approach to chronic pain management, the models were customized, and the evaluation methods were heterogeneous.
Background
Chronic pain is generally defined as pain lasting for 3 months or longer or persisting beyond the time needed for normal tissue healing.1 It can affect the sufferer’s quality of life and can lead to substantial physical and psychological morbidity.2 One in 5 Canadians lives with chronic pain, and it is 1 of the most common reasons that Canadians seek medical attention. The economic burden is substantial.2 In 2019, between $15.1 and $17.2 billion in estimated direct costs were associated with managing chronic pain in Canada.3
Because chronic pain is difficult to cure, the goal of treatment is to control pain, maintain function, maximize coping, and prevent disability, and often involves a multidisciplinary pain management plan.1,4 CADTH conducted an Environmental Scan in 2021 to compile information on the models of care for chronic pain and chronic non-pain-related medical conditions being used in Canada and in other countries.5 One of the 3 priority models of care of interest in the Environmental Scan is the focus of the current review.
With stepped care, interventions that are used to manage chronic pain are organized into a series “steps” placed on a continuum from lowest to most intensive based on a variety of characteristics, including the facility’s level of care (e.g., primary, secondary, and tertiary care centres), type of care provider (e.g., education modules, workshops, individual therapies), treatment needs, patient effort, level of health care provider contact, and cost.6,7 Patients are initially offered the least intensive intervention that takes into account the nature, duration, severity and course of symptoms. Immediate access to this first level of care may meet the needs of a considerable portion of the chronic care population and has the potential to alleviate wait lists for patients who need higher levels of specialized care. The progression of symptoms and treatment outcomes are routinely monitored, and subsequent individual treatment efforts are adjusted and stepped up or down, until treatment goals are met.7,8 Figure 1 presents a simplified diagram of a stepped care.5
Figure 1: Simplified Diagram of a Stepped Care Model
Source: Brett K, MacDougall D. CADTH Health Technology Review Models of Care for Chronic Pain. Ottawa, ON: CADTH: https://www.cadth.ca/sites/default/files/es/ES0350%20_to%20Publishing%20Final.pdf. Accessed 2022 Mar 22.5
The CADTH Environmental Scan5 identified 4 stepped care models for chronic pain and 9 stepped models for other medical conditions (mental health and insomnia). The Environmental Scan also summarized the main categories of patient-related outcomes associated with models of care delivery for patients with chronic pain: pain (e.g., intensity and interference), psychosocial (e.g., coping, depression, anxiety, distress, and fear), function (e.g., disability and employment status), and health care use (e.g., prescription of any opioid, long-term opioid therapy, frequency of primary care visits, and number of visits to specialty health care services).
Stepped care programs have demonstrated clinical benefits for other conditions, such as depression and anxiety.9,10 In previous reviews of studies on stepped care models for chronic pain the authors reported positive results on pain, disability, general and physical health, depression, and anxiety.11,12 Preliminary findings from a 2020 report on the implementation of a stepped care program in Ottawa, Canada suggested that wait times for access to chronic pain programs may be considerably reduced with a stepped care approach.13 The current review aims to describe the available literature on the potential clinical benefits and harms of using stepped models for the management of chronic pain.
Stepped care models are designed to maximize the match between health care needs and interventions, while minimizing care costs.6 The cost-effectiveness of a stepped care model was shown in people with a depressive disorder in primary care.14,15 A 2010 economic evaluation16 explored the incremental benefit and incremental health services cost of a stepped care intervention in US veterans with chronic pain. The authors reported that the stepped care model resulted in more pain disability-free days compared with usual care. The stepped care group also had significantly higher costs than the usual care group, which the authors claimed were likely attributable to the cost of stepped care as well as changes in treatment due to its implementation.16 Another aim of the current review is to describe the available literature on potential cost implications of using stepped care models for the management of chronic pain.
Objectives
The key objectives of this CADTH review are as follows
Identify and summarize literature on the potential benefits and harms of stepped care models of care for chronic pain.
Identify and summarize literature on the potential cost implications of stepped care models of care for chronic pain.
The focus of this review is to summarize what literature exists on the clinical benefits, harms, and cost implications of stepped care models for chronic pain. Since chronic cancer pain and chronic non-cancer pain are distinct entities, as evidenced by unique clinical practice guidelines for each, this review focuses exclusively on chronic non-cancer pain.17,18 This review does neither includes a formal critical appraisal of the literature, nor is it a formal program evaluation. Thus, making conclusions or recommendations about the value of stepped care models for chronic pain are outside the scope of this review.
Research Questions
What literature describes the potential clinical benefits and harms of providing care using stepped care models for the management of people with chronic non-cancer pain?
What literature describes the potential cost implications of providing care using stepped care models for the management of people with chronic non-cancer pain?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycInfo, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were stepped care model and chronic pain. No filters were applied to limit the retrieval by study type. The search was limited to English language documents published between January 1, 2012 and April 1, 2022.
Selection Criteria
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text reports was based on the inclusion criteria presented in Table 1.
Chronic non-cancer pain and other disorders or diseases (e.g., mental health conditions, multiple sclerosis, and stroke) frequently occur together.19,20 Reports were included if the population included people with chronic non-cancer pain, regardless of the presence of other disorders or diseases. However, reports were excluded if the target population was people with the associated disorders or diseases only and there was no specific mention of addressing chronic pain jointly.
Criteria | Description |
|---|---|
Population | People (of any age) with chronic non-cancer pain in outpatient settings of publicly funded health care facilities |
Intervention | Care provided using stepped care models |
Type of information | Q1: Descriptions of potential clinical benefits (e.g., pain, physical function, sleep, social function, emotional and psychological functioning [e.g., anxiety, depression], health-related quality of life, changes in use of pharmacotherapy [e.g., opioids]) and harms (e.g., hospitalizations, substance use, adverse events) Q2: Descriptions of potential cost implications (e.g., budget impact, cost savings, economic benefits to individuals or health systems) |
Study designs | No restrictions on study design or type of report |
Search time frame | 10 years |
Synthesis Approach
Information from the relevant studies was extracted into tables and organized by objective by 1 reviewer. The information was then used to structure and inform the current review. Narrative summaries of the literature were presented separately for each stepped care model. Data were extracted on the model components and implementation; evaluation methods; and findings that related to potential clinical benefits and harms, and potential costs. The limitations of each study were also described, as reported by the study’s authors. No formal critical appraisal (e.g., risk of bias assessment) of the included studies was conducted.
Summary of Evidence
Quantity of Research Available
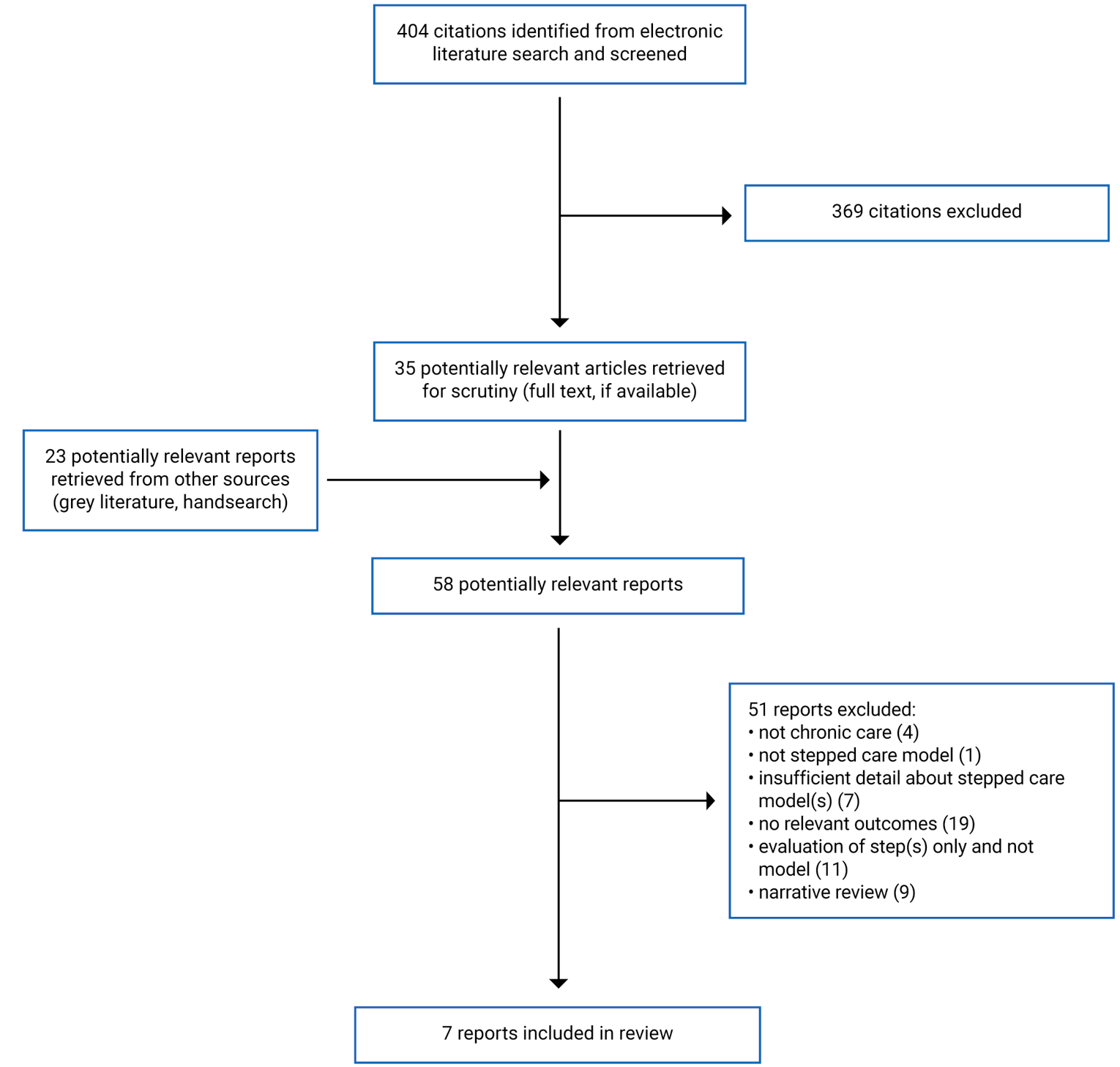
A total of 404 citations were identified in the literature search. Following screening of titles and abstracts, 369 citations were excluded, and 35 potentially relevant reports were retrieved for full-text review. An additional 23 potentially relevant reports were retrieved from the grey literature search for full-text review. Of the 58 potentially relevant reports, 51 were excluded. In total, 7 reports of 6 studies (2 randomized controlled trials [RCTs]21,22 and 4 non-randomized studies [1 prospective cohort,23 1 retrospective cohort,24 and 2 before-after studies],25,26evaluating 5 stepped care models and 1 report of 1 economic evaluation of a stepped treatment pathway27) were included. Figure 2 presents the PRISMA flow chart of the study selection.28
Reports of studies that evaluated 1 or more steps in the stepped care approach, rather than the implementation and evaluation of the stepped care model itself, were beyond the scope of this review and not included. A list of these reports is presented in Appendix 1.
Guidelines that made recommendations regarding the implementation of stepped care models for chronic pain were outside of the scope of this review but are listed as documents of potential interest in Appendix 2. Other reports of potential interest that were identified in the literature search but did not meet our inclusion criteria are also listed in Appendix 2.
Objective 1: Identify and Summarize Literature on the Potential Benefits and Harms of Stepped Care Models of Care for Chronic Pain
Six studies reporting on 5 stepped care models for chronic non-cancer pain21-26,29 were included in this review. Each study described the implementation, evaluation, and potential benefits of a specific stepped care model.
One of the studies21 described the potential harms of a stepped care model.
In the following sections, each stepped care model is presented. Details of the model components and implementation, evaluation methods, and relevant findings are presented in individual tables, and briefly summarized narratively. The limitations of each study as reported by the authors are also described. The models are presented in reverse chronological order of their publication dates (i.e., most recent publication is presented first).
Stepped Care Model in People With Excess Body Weight and Knee Osteoarthritis
One RCT evaluated a stepped care strategy for people aged 50 years and older with excess body weight and chronic pain due to medial tibiofemoral osteoarthritis.21 Characteristics of the stepped care model and RCT are presented in Table 2 and Table 3. Study participants in the intervention arm received stepped care. The first step in the model involved 18 weeks of a diet and exercise program. In the second step, patients in remission continued with diet and exercise. Disease remission was defined as symptomatic remission of pain plus decrease in disease activity and/or symptomatic remission of functional impairment, as assessed by the Patient Acceptable Symptom State. If remission was not achieved, participants were assigned to cognitive behavioural therapy (CBT), knee brace, or muscle strengthening for 12 weeks, depending on their clinical presentation for symptoms of depression and varus malalignment. The comparison group received education material about the management of knee osteoarthritis. The researchers who enrolled and assessed the study participants were blinded to group allocation. The participants, study coordinator, therapist delivering the strengthening exercises, and statistician were not blinded.21
Table 2: Characteristics of Stepped Care Model for People with Excess Body Weight and Knee Osteoarthritis21
Characteristic | Description |
|---|---|
Model, country | Stepped care model for people who are overweight or obese with chronic pain due to medial tibiofemoral osteoarthritis, Australia |
Model components | |
Step 1 | Diet and exercise regime (18 weeks) based on Healthy Weight for Life program
|
Step 2 | 1 of 4 treatments (12 weeks)
|
Implementation details | NR |
CBT = cognitive behavioural therapy; DASS 21 = Depression, Anxiety, and Stress Scale – 21 items; NR = not reported; PASS = Patient Acceptable Symptom State.
Table 3: Characteristics of RCT Evaluating the Stepped Care Model for People With Excess Body Weight and Knee Osteoarthritis21
Characteristic | Description |
|---|---|
Study design | RCT |
Setting | 1 hospital in Sydney, Australia |
Enrollment period | July 2015 to April 2017 |
Funding sources |
|
Inclusion criteria | Patients ≥ 50 years of age, BMI ≥ 28 kg/m2, radiographic evidence of predominantly medial tibiofemoral osteoarthritis, pain intensity ≥ 40 of 100 on VAS, scores above PASS cut-off value for patient global assessment of disease activity, functional impairment ≥ 31 of 100 on WOMAC function subscale |
Sample characteristics |
Comparison (educational pamphlets), N = 84
|
Relevant outcomes |
|
Follow-up | 32 weeks |
BMI = body mass index; DASS-21 = Depression, Anxiety, and Stress Scale – 21 items; PASS = Patient Acceptable Symptom State; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale; WOMAC = Western Ontario and McMaster Osteoarthritis Index.
The findings of the RCT are presented in Table 4. The study authors21 reported that the difference of 13% in disease remission in favour of the stepped care group was below the 25% difference rate that was initially estimated to make the intervention worthwhile for being implemented in clinical practice. Between-group (stepped care versus the comparison) differences in change from baseline for pain intensity, functional impairment, and depression were 3.3 (95% CI, −3.6 to 10.2), 6.0 (95% CI, 1.0 to 11.0), and −0.5 (95% CI, −3.7 to 2.6), respectively.
The study authors21 identified several limitations of the RCT. There was a higher dropout rate in the comparison group (19%) than the stepped care group (6%), which the authors suggested may have influenced the results. Treatment adherence, compliance, and fidelity were not assessed, and the authors were unable to determine if stepped care was not successful due to treatment nonadherence, noncompliance with study procedures, intervention not delivered as it was supposed to be delivered, or lack of effect.21
Table 4: Summary of Findings of an RCT Evaluating the Stepped Care Model for People With Excess Body Weight and Knee Osteoarthritis21
Outcome | Findings | |
|---|---|---|
Stepped care intervention n = 87 | Comparison group n = 84 | |
Disease remission, n (%) | 32 (39) | 18 (26) |
Between-group difference, % (95% CI) | 12.6 (−2.3 to 27.4) | |
P valuea | 0.10 | |
Pain intensity (VAS score) | ||
Baseline, mean (SD) | 61.0 (14.5) | 64.1 (16.4) |
32 weeks, mean (SD) | 40.0 (26.1) | 46.0 (23.6) |
Between-group difference in change from baseline, mean (95% CI) | 3.3 (−3.6 to 10.2) | |
P valueb | 0.35 | |
Functional impairment (WOMAC score) | ||
Baseline, mean (SD) | 50.8 (13.3) | 50.5 (12.3) |
32 weeks, mean (SD) | 30.4 (20.6) | 35.5 (18.9) |
Between-group difference in change from baseline, mean (95% CI) | 6.0 (1.0 to 11.0) | |
P valueb | 0.02 | |
Depression (DASS-21 score) | ||
Baseline, mean (SD) | 6.3 (6.8) | 6.1 (6.2) |
32 weeks, mean (SD) | 5.7 (6.4) | 5.9 (7.2) |
Between-group difference in change from baseline, mean (95% CI) | −0.5 (−3.7 to 2.6) | |
P valueb | 0.74 | |
Adverse events, n | 10 patients reported 13 adverse events:
| NR |
Serious adverse events, n | 0 | NR |
CI = confidence interval; DASS-21 = Depression, Anxiety, and Stress Scale – 21 items; NA = not applicable; NR = not reported; PASS = Patient Acceptable Symptom State; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale; WOMAC = Western Ontario and McMaster Osteoarthritis Index.
aTested via the 2-proportion Z-test.
bTested via independent t-test or Wilcoxon rank-sum test, as appropriate.
Additional analyses pre- and post- intervention were conducted in treatment subgroups at Step 2.21 The authors acknowledged that the sample size in each sub-treatment group was small and not powered to identify differences in outcomes between subgroups. The authors suggested that the lack of guidance provided to the participants allocated to the maintenance subgroup might have led to the worsening of symptoms observed during step 2 of the stepped care intervention.
The authors also claimed that they overestimated the disease remission rate in both stepped care and comparison groups, which impacted their sample size calculation. Finally, the trial authors stated that they did not conduct a cost-effectiveness analysis that would have assisted them in the decision to potentially implement the stepped care approach.21
Stepped Care Model for Pain Management (SCM-PM)
Two studies (1 uncontrolled before-after study25 and 1 retrospective cohort study24) reported on the Veterans Health Administration Stepped Care Model of Pain Management (SCM-PM), established in 2009 to bolster non-opioid, multimodal care for US veterans with chronic pain.24,25 The 3 steps in the model are based on levels of care: primary care, consultations with specialty care, and tertiary interdisciplinary care. The goal of the stepped care model was to change primary care providers’ behaviours and improve the process of care for people with chronic pain.24,25 Further details of the model are presented in Table 5.
The characteristics of both studies are presented in Table 6. The uncontrolled before-after study of 12 primary centres compared electronic health record data at 1 year before the implementation of SCM-PM for chronic pain with data at 1 year following the 3-year intervention.25 Participants included 25 primary care providers and their adult patients with chronic pain of any etiology. The patients were identified by a validated algorithm using available electronic health record data elements (e.g., diagnostic codes, pain scores, and prescribed medication). The retrospective cohort study24 compared a pain cohort treated according to SCM-PM with a non-pain cohort treated in the integrated veteran's health system over the same 5-year period.
Table 5: Characteristics of SCM-PM24,25
Characteristic | Description |
|---|---|
Model, country | Stepped Care Model of Pain Management, US |
Model components | |
Step 1 | Primary care:
|
Step 2 | Secondary consultation:
|
Step 3 | Tertiary interdisciplinary care:
|
Implementation details |
|
ECHO = Extension for Community Health Outcomes; EHR = electronic health record; PACT = patient-aligned care team; SCM-PM = Stepped Care Model for Pain Management.
Table 6: Characteristics of Studies Evaluating SCM-PM24,25
Characteristic | Description | |
|---|---|---|
Study design | Uncontrolled before-after study25 | Retrospective cohort study24 |
Setting | Community Health Care Centre, Inc, comprising 12 primary health centres at a multi-site community health centre in Connecticut, US | VA Connecticut Health Care System, comprising a tertiary hub with inpatient and outpatient facilities, another large outpatient facility, and 6 community-based outpatient clinics |
Study period | March 2010 to February 2015 | July 2008 to June 2013 |
Funding sources |
|
Medical Research Foundation:
|
Inclusion criteria | All primary care providers who were present during 3-year implementation of SCM-PM Adult patients with chronic pain under the care of the providers with ≥ 1 medical visit in previous year | Veteran patients receiving primary care through an integrated VA health system who had ≥ 1 visit with a documented pain intensity rating of moderate to severe over 5-year period (intervention group) Veteran patients seen in primary care with no indication of pain and veterans reporting only mild pain intensity (comparison group) |
Intervention | SCM-PM | SCM-PM (pain cohort) |
Comparison | NA | Non-pain cohort |
Sample characteristics | N = 25 primary care providers Female: 56% Medical doctor: 68% Advanced practice nurse practitioner: 32% Primary care providers’ patients: N = 3,357 patients at pre-intervention Age: 27% were aged 18 to 39 years; 57% were aged 40 to 59 years; and 16% were aged 60 years or older Female: 63% Medicaid insurance: 66% Medicare insurance 19% Private insurance 7% Uninsured 7% | Intervention (pain cohort), N = 31,286 Mean age: 62.6 years Female: 6.8% Mean maximum pain score: 6.5, on a scale of 0 (no pain) to 10 (worst pain imaginable) Comparison (non-pain cohort), N = NR Mean age: 68.9 years Female: 3.3% Mean maximum pain score: 0.3, on a scale of 0 (no pain) to 10 (worst pain imaginable) |
(continued) | N = 4,385 patients at post-intervention Age: 25% were aged 18 to 39 years; 56% were aged 40 to 59 years; and 18% were aged 60 years or older Female: 64% Medicaid insurance: 64% Medicare insurance 19% Private insurance 10% Uninsured 7% | |
Relevant outcomes |
|
|
Follow-up | 5 years (1 year before 3-year implementation and 1 year after implementation) | 5 years |
NA = not applicable; SCM-PM = Stepped Care Model for Pain Management; VA = Veterans Affairs.
The findings of the uncontrolled before-after study25 are presented in Table 7. The authors reported that implementation of SCM-PM was associated with improvements in provider's pain care documentation, pain treatment and pain follow-up. Referrals from primary care providers to behavioural health providers and chiropractic professionals increased and referrals to neurologic and orthopedic surgery decreased following implementation of SCM-PM. The study authors reported no decline in opioid prescribing. However, among patients receiving chronic opioid therapy, the use of opioid treatment agreements and urine drug screens increased by 27.3% and 22.6%, respectively.25
Table 7: Summary of Findings of an Uncontrolled Before-after Study Evaluating SCM-PM25
Outcome | Findings | ||
|---|---|---|---|
Pre-intervention | Post-intervention | P valuea | |
Pain care documentation (Pain Care Quality extraction tool), n (%) | N = 108 | N = 213 | — |
Documentation of pain | 69 (64) | 174 (81) | < 0.001 |
Source or cause of pain | 67 (62) | 158 (74) | 0.025 |
Functional assessment | 5 (5) | 42 (19) | < 0.001 |
Review of diagnostic tests | 6 (6) | 37 (17) | < 0.003 |
Treatment plan | 99 (92) | 209 (98) | 0.006 |
Pain medication ordered | 102 (94) | 182 (85) | 0.017 |
Pain consult ordered | 7 (7) | 60 (28) | < 0.001 |
Patient education | 16 (15) | 47 (22) | 0.121 |
Diagnostic imaging ordered | 25 (23) | 59 (28) | 0.379 |
Assessment of treatment effectiveness | 18 (17) | 83 (39) | < 0.001 |
Documented pain score, n (%) | N = 3,330 | N = 4,385 | — |
Pain score > 8 (scale NR), n (%) | 2,504 (75.2) | 3,245 (74.0) | 0.351 |
Opioid prescribing, n (%) | |||
Any opioid prescribed | 1,615 (48.5) | 1,943 (44.3) | 0.117 |
Chronic opioid therapy (≥ 90 days in 1 year) | 763 (22.9) | 921 (21.0) | 0.486 |
Health care visits | |||
Mean number of visits (SD) | 7.3 (14.37) | 6.83 (14.37) | 0.094 |
Patients with behavioural health visit, n (%) | 809 (24.3) | 1,276 (29.1) | 0.009 |
Pain referrals, n (%) | |||
Chiropractic | 3 (0.1) | 48 (1.1) | 0.008 |
Physical therapy | 480 (14.4) | 750 (17.1) | 0.508 |
Neurologic or orthopedic surgery | 663 (19.9) | 693 (15.8) | < 0.001 |
Rheumatology | 120 (3.6) | 136 (3.1) | 0.419 |
Health care use (for patients receiving chronic opioid therapy), n (%) | N = 1,309 | N = 1,230 | — |
Opioid treatment agreement | 360 (34) | 778 (61) | < 0.05 |
Urine drug screen | 680 (64) | 1,103 (87) | < 0.05 |
NR = not reported; SD = standard deviation.
aTested via multiple-group models that account for the clustering within provider.
The findings of the retrospective cohort study24 are presented in Table 8. The study authors reported that, within the pain cohort, long-term opioid treatment decreased over 5 years, while non-opioid prescriptions increased. The authors also reported that SCM-PM was associated with increased referrals by primary care providers for any consultations. Overall, the number of referrals to specialty services increased for the pain cohort, but little change was observed for those not in the pain cohort. The authors reported that the largest increases in the pain cohort were in referrals to physiotherapy and occupational therapy. Similarly, patient visits for any reason increased in the pain cohort, with the largest increases being in visits for mental health, clinical health psychology and physiotherapy. The study authors also reported that the proportion of veterans in the pain cohort receiving at least 1 non-opioid pain medication and at least 1 referral to a specialty care service increased from 24.5% in year 1 to 29% in year 5, which the authors considered receipt of multimodal pain care.24
Table 8: Summary of Findings of a Retrospective Cohort Study Evaluating SCM-PM24
Outcome | Findings | ||
|---|---|---|---|
Year 1a | Year 5b | P valuec | |
Pharmacotherapy use, % | |||
Long-term opioid therapy (> 90 days) | — | — | < 0.0001d |
Pain cohort | 4.2 | 3.3 | — |
Any non-opioid medication | — | — | < 0.0001 |
Pain cohort | 36.7 | 39.8 | — |
Non-pain cohort | 23.3 | 22.6 | — |
Sedative or hypnotic | — | — | < 0.0001 |
Pain cohort | 17.4 | 17.2 | — |
Non-pain cohort | 12.4 | 11.3 | — |
Topical analgesics | — | — | 0.0058 |
Pain cohort | 3.5 | 4.8 | — |
Non-pain cohort | 0.7 | 0.7 | — |
NSAIDs | — | — | < 0.0001 |
Pain cohort | 15.7 | 19.3 | — |
Non-pain cohort | 7.3 | 7.3 | — |
Antidepressant | — | — | < 0.0001 |
Pain cohort | 5.7 | 5.9 | — |
Non-pain cohort | 3.5 | 3.1 | — |
Anticonvulsant | — | — | < 0.0001 |
Pain cohort | 10.9 | 12.8 | — |
Non-pain cohort | 6.4 | 6.7 | — |
Referrals, % | |||
Any referral | — | — | < 0.0001 |
Pain cohort | 43.4 | 51.8 | — |
Non-pain cohort | 27.5 | 28.6 | — |
Mental health | — | — | 0.56 |
Pain cohort | 6.0 | 5.0 | — |
Non-pain cohort | 3.1 | 2.6 | — |
Physical therapy | — | — | < 0.0001 |
Pain cohort | 14.8 | 27.4 | — |
Non-pain cohort | 4.0 | 5.6 | — |
Occupational therapy | — | — | < 0.0001 |
Pain cohort | 5.2 | 11.0 | — |
Non-pain cohort | 1.9 | 2.2 | — |
Chiropractic | — | — | < 0.0001 |
Pain cohort | 1.4 | 3.2 | — |
Non-pain cohort | 0.3 | 0.5 | — |
Neurology | — | — | 0.002 |
Pain cohort | 10.3 | 10.7 | — |
Non-pain cohort | 3.4 | 3.0 | — |
Pain medicine | — | — | < 0.0001 |
Pain cohort | 3.2 | 3.8 | — |
Non-pain cohort | 0.2 | 0.4 | — |
Health care visits (≥ 1 visit by patient), % | |||
Any health care visit | — | — | < 0.0001 |
Pain cohort | 27.9 | 37.3 | — |
Non-pain cohort | 11.4 | 12.6% | — |
Mental health | — | — | < 0.0001 |
Pain cohort | 28.0 | 30.5 | — |
Non-pain cohort | 20.0 | 19.3 | — |
Clinical health psychology | — | — | < 0.0001 |
Pain cohort | 4.7 | 7.2 | — |
Non-pain cohort | 2.0 | 2.5 | — |
Physical therapy | — | — | < 0.0001 |
Pain cohort | 16.2 | 22.9 | — |
Non-pain cohort | 4.1 | 4.8 | — |
Occupational therapy | — | — | < 0.0001 |
Pain cohort | 5.6 | 10.0 | — |
Non-pain cohort | 2.0 | 2.3 | — |
Chiropractic | — | — | 0.0019 |
Pain cohort | 1.4 | 3.8 | — |
Non-pain cohort | 0.3 | 0.8 | — |
Neurology | — | — | < 0.0001 |
Pain cohort | 10.0 | 13.3 | — |
Non-pain cohort | 6.0 | 6.4 | — |
Pain medicine | — | — | < 0.0001 |
Pain cohort | 2.9 | 3.2 | — |
Non-pain cohort | 0.5 | 0.3 | — |
Multimodal care | — | — | < 0.0001 |
Pain cohort | 24.5 | 29.0 | — |
Non-pain cohort | 12.8 | 12.6 | — |
NSAID = nonsteroidal anti-inflammatory drug.
aSample sizes for year 1: Pain cohort, n = 11,601; non-pain cohort, n = 32,347.
bSample sized for year 5: Pain cohort, n = 15,099; non-pain cohort, n = 29,375.
cInteraction test via general estimating equations logit-linked, logistic regression models with robust variance estimation and intercept, controlling for patients nested within providers, and patient age and sex.
dChange over time in the pain cohort only.
Limitations were reported by the authors of both studies.24,25 In the uncontrolled before-after study,25 the authors acknowledged that the evaluation focused on process measures and did not include measures of patient outcomes other than pain scores. The interventions used in the study, such as templates and dashboards, were implemented agency-wide and could not be limited to selected practices. As such, randomization was not possible, limiting the ability to eliminate unmeasured confounders. Provider turnover, which ranged from 11% to 20% over the study period, also limited the number of health care providers included in the analysis.25
In the retrospective cohort study,24 the authors defined the pain cohort as veterans reporting moderate to severe pain during at least 1 outpatient primary care encounter. Neither did this definition distinguish presentations of acute versus chronic pain or include veterans with mild pain intensity, nor was information on pain-related diagnoses available. Also, some of the specialty pain care services included in the analyses provided services that extend beyond pain. Because the authors did not examine diagnoses associated with care in these settings, they were unable to conclude whether pain-specific care was delivered. Sedatives and/or hypnotics, antidepressants, and anticonvulsants are also commonly used for management of disorders other than pain. The data did not specify the diagnosis for the prescription. Furthermore, although the authors used a broad definition of 1 non-opioid pharmacological treatment and 1 nonpharmacological pain management service to represent multimodal pain care and guideline concordant care, details regarding veterans’ presenting problems and the services they received were not available and it was not possible to determine whether veterans were receiving appropriate services. Finally, because several changes were implemented at national, regional, and local levels, and changes were implemented throughout Veterans Health Administration Connecticut Health Care System, it was not possible to isolate what caused any specific change; rather, the authors were only able to examine temporal trends.24
Stepped Care Model for Non-Cardiac Chest Pain (NCCP)
One uncontrolled before-after study evaluated a pilot multidisciplinary biopsychosocial model with a stepped care approach that was set up in a cardiology outpatient clinic in London, UK for people with non-cardiac chest pain (NCCP).26 The model consisted of 3 steps: comprehensive physician and psychological assessment, low intensity CBT in the form of guided self-help delivered by a trained cardiac nurse or clinical psychologist, and high intensity CBT with a clinical psychologist. Details of the model are presented in Table 9.
The uncontrolled before-after study26 included 77 adult patients with NCCP occurring more than once per month. Patients were evaluated for chest pain and chest pain interference, beliefs about chest pain,26 depression, anxiety, quality of life, and health care use at baseline, then at 3- and 6-months after the initiation of treatment (post-treatment and follow-up beyond the end of treatment, respectively). The characteristics of the study are presented in Table 10.
Table 9: Characteristics of Stepped Care Model for NCCP26
Characteristic | Description |
|---|---|
Model, country | Stepped care approach for NCCP, UK |
Model components | |
Step 1 | Biopsychosocial assessment: in-depth assessment of chest pain by cardiologist and psychological factors by psychologist; medical therapy offered when appropriate (medical or referral to another medical services) |
Step 2 | Low intensity CBT: guided self-help, supported by a standardized booklet and audio CD, delivered in 30-minute sessions (up to 6 sessions available), 4 modules (mindful abdominal breathing, progressive muscle relaxation, increasing activity, cognitive therapy) |
Step 3 | High intensity CBT: additional information and support, delivered in 50-minute sessions (up to 8 sessions available), tailored treatment and additional aspects (such as psychoeducation about stress and specific psychosocial disorders, exploring beliefs, problem-solving and cognitive work, and behavioural activation for depression) |
Implementation details | Can be delivered by a cardiac nurse, clinical psychologist (trained in providing and supervising CBT), and a cardiologist, and integrated into any chest pain clinic |
CBT = cognitive behavioural therapy; CD = compact disc; NCCP = non-cardiac chest pain.
Table 10: Characteristics of Prospective Study Evaluating Stepped Care Model for NCCP26
Characteristic | Description |
|---|---|
Study design | Uncontrolled before-after study |
Setting | 1 chest pain clinic at a teaching hospital, London, UK |
Enrollment period | December 2011 to December 2012 |
Funding source | Guy's and St Thomas’ Charity |
Inclusion criteria | Adult patients with NCCP more than once per month for at least 3 months |
Sample characteristics | N = 77 patients at pre-intervention; 68 at post-intervention Mean age (SD): 50 (10.9) years, range 25 to 73 years Female: 54% Chest pain present > 6 months: 79% |
Relevant outcomes |
|
Follow-up | 6 months |
CSRI = Client Service Receipt Inventory; GAD7 = Generalized Anxiety Disorder 7-item Scale; NCCP = non-cardiac chest pain; PHQ9 = Patient Health Questionnaire 9; SD = standard deviation; WSAS = Work and Social Adjustment Scale.
The findings of the uncontrolled before-after study are presented in Table 11. The authors reported that the stepped care approach had large effects on chest pain post-intervention (3 months) and at 6 months compared to baseline (before the intervention), as indicated by reduced frequency of pain, improved chest pain interference and severity scores, and improved negative beliefs and/or convictions that chest pain is attributable to a cardiac cause. Depression and anxiety scores decreased at post-intervention and at 6 months compared to baseline, as did impact on daily life scores (i.e., less impairment). In addition, there was less use of numerous health care resources (e.g., general practitioner, emergency department, cardiologist, appointments, consultations) at 6 months following participation in the stepped care model.26
The study authors26 stated their limitations. There was no comparison group. The length of the intervention was not standardized, as treatment was tailored to each patient’s needs. Some participants, particularly those in the high intensity CBT group, continued to receive treatment after 3 months. Longer-term follow-up (e.g., 12 months) was not offered, which limited any claims about sustained improvement. There was no formal economic analysis, so the impact of the stepped care model on health care costs is uncertain.26
Table 11: Summary of Findings of an Uncontrolled Before-after Study Evaluating the Stepped Care Model for NCCP26
Outcome | Findings | |||
|---|---|---|---|---|
Pre-intervention, n = 77 | Post-intervention (3 months), n = 75 | Follow-up (6 months), n = 68 | P valuea | |
Pain frequency, % | — | — | — | < 0.001 |
Daily or more often | 44 | 13 | 7 | — |
Weekly | 39 | 28 | 19 | — |
Monthly | 17 | 20 | 25 | — |
Less than monthly | 0 | 39 | 49 | — |
Presence of pain, % | ||||
Do you have chest pain that bothers you? (Yes) | 100 | 73 | 65 | < 0.001 |
Scores on scale, mean (SD) | ||||
Severity of chest pain | 5.8 (2.5) | 4.0 (2.7) | 3.4 (2.4) | < 0.001 |
Interference of chest pain | 5.9 (2.2) | 3.2 (2.6) | 2.6 (2.1) | < 0.001 |
Negative beliefs | ||||
Chest pain is a heart attack | 5.6 (3.3) | 2.0 (2.1) | 1.9 (2.0) | < 0.001 |
Chest pain indicates a serious condition | 5.4 (3.2) | 2.2 (2.2) | 2.1 (2.2) | < 0.05 |
Depression (PHQ9 score) | 8.8 (7.2) | 5.4 5.8) | 4.4 (5.0) | < 0.05 |
Anxiety (GAD7 score) | 6.9 (6.0) | 4.6 (5.) | 3.6 (4.7) | < 0.05 |
Quality of life (WSAS score) | 10.4 (10.4) | 3.9 (7.5) | 2.5 (5.7) | < 0.001 |
Health care use (CSRI), n (%) | ||||
GP ≥ 3 visits | 47 (63) | NR | 30(47) | < 0.05 |
ED ≥ 1 visit | 21 (28) | NR | 5 (8) | < 0.05 |
Cardiologist ≥ 1 visit | 57 (63) | NR | 2 (3) | < 0.05 |
Other physician ≥ 1 visit | 25 (33) | NR | 19 (30) | < 0.05 |
Health care appointments, mean (SD) | 2.5 (1.1) | NR | 0.8 (1.2) | < 0.05 |
Consultations for chest pain, mean (SD) | 2.6 (3.1) | NR | 0.1 (0.5) | < 0.05 |
ED = emergency department; CSRI = Client Service Receipt Inventory; GAD7 = Generalized Anxiety Disorder 7-item Scale; GP = general practitioner; PHQ9 = Patient Health Questionnaire 9; SD = standard deviation; WSAS = Work and Social Adjustment Scale.
aTested via the Wilcoxon test for chest pain frequency and via paired t-tests for chest pain interference. For other outcomes, t-tests were used for normally-distributed data and Wilcoxon tests were used for proportions.
Stepped Care Strategy for Chronic Hip or Knee Pain (Beating osteoARThritis)
One prospective cohort study evaluated a multidisciplinary stepped care strategy (SCS), named Beating osteoARThritis, that was developed to improve the non-surgical care of people with chronic pain due to hip or knee osteoarthritis.23 The model and its implementation in general practices in Nijmegen, the Netherlands was also described in another separate publication.29 SCS aimed to support primary care providers and patients to achieve high-quality care by presenting the ideal sequence for care in a 3-step model. The first step includes modalities (e.g., education, lifestyle advice, and paracetamol), which should be offered to all patients or can be provided through self-care. The second and third steps include more advanced modalities (e.g., physical therapy, dietary therapy, and intra-articular injections) that can be provided if the previous options had not succeeded.23,29 Details of SCS are presented in Table 12.
Table 12: Characteristics of SCS23,29
Characteristic | Description |
|---|---|
Model, country | SCS, the Netherlands |
Model components | |
Step 1 |
|
Step 2 |
|
Step 3 |
|
Implementation details | A regional implementation advisory board, consisting of a patient representative and 9 experts representing the main disciplines involved in osteoarthritis care (2 GPs, 1 practice nurse, 1 physical therapist, 1 dietician, 1 rheumatologist, 1 orthopedic surgeon, 2 researchers) was set up to agree on implementation activities aligned to patients as well as different health care providers. The activities were based on previous implementation studies in related research fields and included: education and reminder material for patients; education outreach visits, education and reminder material, and multidisciplinary seminars for health care professionals. |
GP = general practitioner; NSAID = nonsteroidal anti-inflammatory drug; SCS = stepped care strategy.
The prospective cohort study23 compared a cohort of patients who received stepped care strategy-consistent (SCS-consistent) care for hip or knee pain due to osteoarthritis with a cohort who received SCS-inconsistent care over 2 years. Participants in the SCS-consistent group received the following: education and lifestyle advice during the study period, all advised step 1 modalities before any step-2 modality (if applicable), and all advised step 1 and step 2 modalities before any step 3 modality (if applicable). Further characteristics of the study are presented in Table 13.
Table 13: Characteristics of a Prospective Cohort Study Evaluating SCS23
Characteristic | Description |
|---|---|
Study design | Prospective cohort study |
Setting | 38 GP practices, Nijmegen, the Netherlands Rural practices: 61% Solo practices: 17% |
Study period | August 2010 to March 2013 |
Funding sources |
|
Inclusion criteria | Adult patients who visited their GP for a new episode of hip or knee complaints due to symptomatic hip or knee osteoarthritis |
Sample characteristics | N = 70 GPs Intervention (SCS-consistent care), N = 117 patients Mean age (SD) = 62 (10) years Female = 63% Pain location: hip = 54%, knee = 74% Duration of symptoms > 1 year: 76% Overweight (BMI > 25kg/m2): 65% Health insurance, with additional coverage: 95% Comparison (SCS-inconsistent care), N = 163 patients Mean age (SD): 65 (10) years Female: 62% Pain location: hip = 49%, knee = 80% Duration of symptoms > 1 year: 80% Overweight: 73% Health insurance, with additional coverage: 88% |
Relevant outcomes |
|
Follow-up | 2 years |
BMI = body mass index; GP = general practitioner; NSAID = nonsteroidal anti-inflammatory drug; SCS = stepped care strategy; SD = standard deviation; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index.
The authors of the prospective cohort reported23 that pain and physical function improved after receiving SCS-consistent care; whereas, the levels of self-efficacy and active pain coping did not differ after 2 years. The summary of findings for the SCS-consistent care group of the study is presented in Table 14.
The authors23 also reported that there were no differences between SCS-consistent and SCS-inconsistent care cohorts on scores for pain physical function, self-efficacy, or active pain coping, after adjusting for potential confounders. Seventeen percent of the patients in the SCS-consistent group and 18% in the SCS-inconsistent group received a surgical procedure within 2 years (P = 0.82). The summary of between-group findings is presented in Table 15.
Table 14: Summary of Findings of Cohort Study Evaluating SCS: Within Group Changes From Baseline in Intervention Group23
Outcome | Findings, n = 117 | |||
|---|---|---|---|---|
Baseline, mean (SD) | 24 months, mean (SD) | Change from baseline, mean (95% CI) | P valuea | |
Pain (WOMAC score) | 62 (22) | 70 (23) | 7.0 (4.2 to 9.8) | 0.00 |
Physical function (WOMAC score) | 64 (21) | 70 (23) | 5.6 (3.2 to 8.0) | 0.00 |
Self-efficacy (Dutch Self-Efficacy Scale) | 31 (5) | 31 (5) | 0.0 (−0.6 to 0.6) | 0.99 |
Active pain coping (Pain Coping Inventory) | 54 (12) | 52 (13) | −1.2 (−2.6 to 0.3) | 0.12 |
CI = confidence interval; SCS = Stepped Care Strategy; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index.
aTested via paired t-tests.
Table 15: Summary of Findings of Cohort Study Evaluating SCS: Between-Group Differences23,29
Outcome | Findings at 24 months | |||
|---|---|---|---|---|
SCS-consistent, Beta coefficient (95% CI) n = 117 | SCS-inconsistent, Beta coefficient (95% CI) n = 163 | Adjusted difference between groups (95% CI) a | P valuea | |
Pain (WOMAC score) | 3.6 (−0.6, 7.7) | 8.8 (4.9, 12.7) | −4.3 (−10.3 to 1.7) | 0.16 |
Physical function (WOMAC score) | 4.3 (0.42, 8.1) | 7.4 (4.0, 10.8) | −1.9 (−7.0, 3.1) | 0.45 |
Self-efficacy (Dutch Self-Efficacy Scale) | 0.6 (−0.3, 1.5) | −0.4 (−1.2, 0.4) | 0.6 (−8.3, 2.0) | 0.41 |
Active pain coping (Pain Coping Inventory) | −0.6 (−2.8, 1.6) | −1.6 (−3.6, 0.4) | 1.7 (−1.5, 4.9) | 0.30 |
CI = confidence interval; EHR = electronic health records; NA = not applicable; SCS = Stepped Care Strategy; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index.
aTested via generalized estimating equations analysis. The analyses were adjusted for age, number of comorbidities, additional insurance coverage, number of painful joints, general practitioner’s sex, and general practitioner’s attitude regarding the effectiveness of non-recommended non-surgical treatment modalities.
The authors23 noted several limitations of the prospective cohort study. Participants who received SCS-consistent care were younger, had fewer comorbidities and painful joints, and were more likely to have additional health care insurance; therefore SCS-inconsistent care may sometimes have been unavoidable or even preferable. The time frame of the study may have been too short to detect differences in pain, physical function, self-efficacy, and active pain coping. Lastly, the authors noted that an observational study, in contrast to an RCT, may not be the ideal design to evaluate SCS. Although baseline differences were adjusted in the analyses, unknown and not measured differences could not be adjusted for.23
Evaluation of Stepped Care for Chronic Pain (ESCAPE)
The Evaluation of Stepped Care for Chronic Pain (ESCAPE) RCT22 evaluated the effectiveness of a stepped care model involving 12 weeks of analgesic therapy optimization according to an algorithm coupled with pain self-management strategies (step 1) followed by 12 weeks of CBT (step 2) compared with usual care. US veterans of the Afghanistan and Iraq conflicts with chronic and disabling musculoskeletal pain were block randomized to the stepped care intervention or usual care. All baseline and follow-up assessments were conducted by a researcher who was blinded to the treatment allocation. Characteristics of the stepped care model and RCT are presented in Table 16 and Table 17.
Table 16: Characteristics of Model in ESCAPE22
Characteristic | Description |
|---|---|
Model, country | Evaluation of Stepped Care for Chronic Pain, US |
Model components | |
Step 1 | 12 weeks, with the aim of reducing pain intensity, encouraging activity, and providing education
|
Step 2 | 12 weeks
|
Implementation details |
|
CBT = cognitive behavioural therapy; ESCAPE = Evaluation of Stepped Care for Chronic Pain; NSAID = nonsteroidal anti-inflammatory drug;; VA = Veterans Affairs.
Table 17: Characteristics of ESCAPE RCT22
Characteristic | Description |
|---|---|
Study design | RCT |
Setting | 1 post-deployment clinic and 5 general medicine clinics at 1 VA medical centre, Indiana, US |
Enrollment period | Enrollment December 2007 to June 2011 |
Funding source | Merit Review grant from the VA Rehabilitation Research and Development |
Inclusion criteria | OEF/OIF/OND veteran patients with self-reported chronic pain (> 3 months’ duration) of the cervical or lumbar spine or an extremity (hip, knee, or shoulder), and if pain was at least moderately disabling (RMDQ score of ≥ 7) at the initial visit |
Sample characteristics | Intervention, N = 121 patients Mean age (SD): 36.4 (10.1) years Female: 9.9% Pain location: back = 52.9%, knee = 23.1%, neck = 8.3%, shoulder = 8.3%, hip = 7.4% Comparison (usual care), N = 120 Mean age (SD): 38.2 (10.5) years Female: 13.3% Pain location: back = 61.7%, knee = 20.0%, neck = 6.7%, shoulder = 5.8%, hip = 5.8% |
Relevant outcomes |
|
Follow-up | 9 months |
BPI = Brief Pain Inventory; CBT = cognitive behavioural therapy; ESCAPE = Evaluation of Stepped Care for Chronic Pain; GCPS = Graded Chronic Pain Scale; OEF = Operation Enduring Freedom; OIF = Operation Iraqi Freedom OND = Operation New Dawn; RCT = randomized controlled trial; RMDQ = Roland Morris Disability Scale; SD = standard deviation; VA = Veterans Affairs.
The findings of the RCT are presented in Table 18. The authors22 reported that the stepped care model led to improvements in the following pain outcomes compared to usual care: pain interference, pain severity, and pain-related disability. Patients in the stepped care group were more likely to demonstrate at least a 30% improvement in Roland Morris Disability Scale scores by 9 months (relative risk, 1.52 [95% CI, 1.22 to 1.99]; P < 0.001), with a number needed to treat of 7.5 for 30% improvement. Participants in the stepped care group received more analgesics at the end of step 1 (3 months) relative to what they were prescribed at baseline. However, at the study end (9 months), the authors reported that participants in stepped care were using more topical analgesics than those in the usual care group, and participants in the usual care group were receiving more tricyclic antidepressants than those in the stepped care group, but the authors stated they did not find a significant difference between groups in opioid use. The authors concluded that the stepped care model was effective in reducing pain-related outcomes in veterans with chronic musculoskeletal pain of the spine and extremities.22
Table 18: Summary of Findings of ESCAPE RCT22
Outcome | Stepped care, n = 121 | Usual care, n = 120 |
|---|---|---|
Pain interference (BPI score) | ||
Baseline, mean (SD) | 5.4 (2.1) | 5.4 (2.4) |
9 months, mean (SD) | 3.8 (2.6) | 4.5 (2.7) |
Change from baseline, mean (95% CI) | −1.7 (−2.1 to −1.3) | −0.9 (−1.2 to −0.05) |
Between-group difference, mean (95% CI) | −0.8 (−1.3 to −0.3) | |
P valuea | 0.003 | |
Pain severity (GCPS score) | ||
Baseline, mean (SD) | 67.3 (12.1) | 65.1 (15.2) |
9 months, mean (SD) | 56.9 (19.1) | 61.0 (19.3) |
Change from baseline, mean (95% CI) | −11.1 (−13.9 to −8.3) | −4.5 (−7.3 to −1.8) |
Between-group difference, mean (95% CI) | −6.6 (−10.5 to −2.7) | |
P valuea | 0.001 | |
Pain-related disability (RMDS score) | ||
Baseline, mean (SD) | 14.0 (4.3) | 13.7 (4.7) |
9 months, mean (SD) | 10.6 (6.3) | 12.1 (6.4) |
Change from baseline, mean (95% CI) | −3.7 (−4.5 to −2.8) | −1.7 (−2.6 to −0.9) |
Between-group difference, mean (95% CI) | −1.9 (−3.2 to −0.7) | |
P valuea | 0.002 | |
Pharmacotherapy use (EHR review), % | ||
Opioids | ||
Baseline | 34.7 | 44.2 |
9 months | 30.6 | 35.8 |
P value | 0.38 | |
Simple analgesics | ||
Baseline | 57.9 | 60 |
9 months | 45.5 | 47.5 |
P value | 0.74 | |
Topical analgesics | ||
Baseline | 1.7 | 1.7 |
9 months | 16.5 | 0.08 |
P value | 0.001 | |
Gabapentin | ||
Baseline | 5.8 | 19.2 |
9 months | 14.9 | 16.7 |
P value | 0.70 | |
Muscle relaxants | ||
Baseline | 17.4 | 15.8 |
9 months | 19 | 17.5 |
P value | 0.76 | |
Tricyclic antidepressants | ||
Baseline | 0.08 | 4.2 |
9 months | 0 | 4.2 |
P value | 0.023 | |
BPI = Brief Pain Inventory; CI = confidence interval; EHR = electronic health record; GCPS = Graded Chronic Pain Scale; RMDQ = Roland Morris Disability Scale; RCT = randomized controlled trial; SD = standard deviation.
aEstimates based on mixed-effect model with repeated measurements. Effect sizes are 0.26 for the BPI Pain Interference subscale, 0.21 for GCPS severity, and 0.24 for the RMDS.
bP value for between-group differences.
The authors22 identified key limitations of the ESCAPE trial. The participants were all recent US veterans with chronic musculoskeletal pain, and their results may not apply to veterans from other eras or to nonveterans. The RCT was conducted at a single medical centre. Single-centre RCTs have shown larger treatment effects than multicentre RCTs. The trial assessed a multimodal intervention and used a bundled approach to delivery. Finally, while the outcome assessors were blinded to the treatment allocation, the study participants were unblinded.22
Objective 2: Identify and Summarize Literature on the Potential Cost Implications of Stepped Care Models of Care for Chronic Pain
One economic evaluation27 was identified that described the cost implications of the stepped care approach. The study examined the relative cost-effectiveness of 3 pathways of treatment for sciatica pain. The stepped care pathway included 3 steps of increasing levels of complexity (initial, intermediate, and invasive therapies). The 2 comparison pathways were initial treatments in primary care only and immediate referral for surgery following initial treatments. The patient population was based on a systematic review that included studies of adult patients with sciatica or lumbar nerve root pain diagnosed clinically or confirmed by imaging, with a requirement for leg pain to be worse than back pain (i.e., to distinguish sciatica from nonspecific low back pain).27 To ensure consistency, the same population also formed the basis for the economic model. Further details of the cost-effectiveness study are presented in Table 19.
Table 19: Characteristics of Economic Evaluation27
Characteristic | Description |
|---|---|
Country | UK |
Intervention pathway | Stepped care approach Step 1: initial treatments — inactive control, usual care, education or advice, activity restriction, non-opioids, and opioids Step 2: intermediate treatments — manipulation, traction, passive and active physical therapy, alternative or non-traditional treatments (acupuncture), biologic drugs (provided in secondary care by multidisciplinary teams) Step 3 — invasive therapies epidural or nerve block, disk surgery |
Comparison pathways | Primary care only
|
Type of analysis | Cost-effectiveness analysis |
Funding source | UK National Institute for Health Research Health Technology Assessment program |
Perspective | UK National Health Service |
Time horizon | 12 months |
Population characteristics | Adult patients with sciatica or lumbar nerve root pain diagnosed clinically or confirmed by imaging. A requirement was that leg pain was worse than back pain. |
Approach |
|
Main outcomes (systematic review) |
|
Clinical and cost data |
|
Main assumptions |
|
NHS = National Health Service; SR = systematic review.
The results of the cost-effectiveness analysis27 are presented in Table 20. The incremental cost per patient with symptoms successfully resolved and the incremental cost per utility gained for a patient with sciatica pain managed through 1 of the 3 treatment pathways over a 12-month period were calculated. The study authors27 reported that the systematic review showed that no therapies can deliver 100% success. Their economic model similarly demonstrated that none of the strategies were 100% successful; however, the most successful regime in the stepped approach pathway was non-opioids, followed by biologic drugs, epidural and/or nerve block, and disk surgery. In the primary care pathway, the most successful regime was non-opioids. The pathway of immediate surgery was not cost-effective. The authors stated that the sensitivity analyses using the highest cost estimates resulted in comparable results. In terms of positive net benefit, the authors claimed that the stepped care approach would be regarded as cost-effective if the ceiling ratio for an additional unit of utility gain over 12 months was less than £5,100 and if the ceiling ratio for each additional success was less than £2,500.27
Table 20: Summary of Findings of the Economic Evaluation27
Main findings | Authors’ conclusion |
|---|---|
| “The stepped approaches to managing sciatica based on an initial treatment with non-opioids represent the most cost-effective regimens relative to direct referral to disk surgery, with positive net benefits emerging if the acceptable ceiling ratio for an additional unit of success was <£2500 with base-case costs and < £6000 if higher costs were applied to the model. The strategy of referring patients who fail initial treatments directly to disk surgery is unlikely to be cost-effective, with highly improbable reductions in cost and/or rates of success being required to elevate these regimens to the efficiency frontier. However, these findings remain tentative, and more research is required to develop the evidence base to inform more structurally appropriate economic models to inform decision-making and to determine patient preferences regarding treatment durations and extent of invasive treatments that would be acceptable.” (p. 1327) |
The authors described a number of limitations associated with the cost-effectiveness analysis.27 The time perspective was limited to a 12-month horizon, with no evidence available to inform the inclusion of relapse and recurrence within the model. The following were not considered in the analysis: issues relating to work and productivity, preferences of patients for symptom resolution and treatment duration, exploration from a personal social services perspective, and possible additional costs associated with disk surgery. The authors reported that the base-case assumption regarding ultimate failure having an additional 0 cost to the National Health Service was contentious, but lack of data and consensus limited the evaluation of alternatives. Because of the small number of relevant studies for some comparisons of treatment strategies, the authors warned that results should be interpreted with caution due to statistical heterogeneity (within pair-wise comparisons) and potential inconsistency (between pair-wise comparisons) with the network. The authors also claimed that inclusion of anti-inflammatory biologic drugs within their economic model could be seen as contentious. Finally, it was acknowledged that the nature of the economic model was simplistic and did not fully account for structural and parameter uncertainty and distributions.27
Limitations
The purpose of this CADTH custom report was to identify and describe the literature on the potential benefits and harms, and cost implications of stepped care models for chronic pain. This report was not a formal program evaluation, and no conclusions were formed. The literature was not critically appraised and the quality of the evidence from included publications is unknown.
The 5 stepped care models describing potential benefits21-26 were implemented in Australia, the Netherlands, US, and UK, where health care systems differ from those in Canada. The economic evaluation describing the cost implications of stepped care was conducted in the UK.27 Therefore, the applicability of their findings to the Canadian setting is unclear.
Conclusions
Six relevant studies describing the potential clinical benefits of 5 different stepped care models21-26 and 1 economic evaluation describing the cost implications of stepped care were included in this review. An RCT assessed a stepped care model for patients who are overweight or obese with chronic pain due medial tibiofemoral osteoarthritis (compared to a control group given educational booklets) and described the impact on pain remission, pain intensity and function, and adverse events.21 For the SCMP, a before-after study25 and a retrospective cohort study of a pain group versus and non-pain group24 described the effects of the stepped care model on pain, quality of chronic pain care, pharmacotherapy use, and health care utilization in US veterans.24,25 A before-after study of a biopsychosocial stepped care model for NCCP described the potential benefits on chest pain, depression, anxiety, quality of life, and health care use.26 A prospective cohort of SCS compared patients who received stepped care strategy-consistent care for hip or knee pain due to osteoarthritis with a cohort who received stepped care strategy-inconsistent care and described the results on pain physical function, self-efficacy, active pain coping and health care use.23 The ESCAPE RCT described the effects on pain, disability, and pharmacotherapy use in US veterans.22 All studies21,22,24-26 described at least some positive results for the clinical outcomes of interest. The authors of the economic evaluation27 reported that a stepped care pathway based on initial treatment with non-opioids may be cost-effective compared to direct referral to surgery.
References
1.Skelly A, Chou R, Dettori J, et al. Noninvasive nonpharmacological treatment for chronic pain: a systematic review. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018: https://www.ncbi.nlm.nih.gov/books/NBK556229/pdf/Bookshelf_NBK556229.pdf. Accessed 2022 Mar 21.
2.Canadian Pain Task Force. Chronic pain in Canada: laying a foundation for action. Ottawa (ON): Health Canada; 2019: https://physiotherapy.ca/sites/default/files/canadian_pain_task_force_june_2019_report_en.pdf. Accessed 2022 Mar 21.
3.Canadian Pain Task Force Report: May 2021. Ottawa: Health Canada; 2021: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2021.html. Accessed 2022 May 13.
4.Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Prepared by the International Association for the Study of Pain, Subcommittee on Taxonomy. Pain Suppl. 1986;3:S1-226. PubMed
5.Brett K, MacDougall D. CADTH Health Technology Review Models of Care for Chronic Pain. Ottawa, ON: CADTH; 2021: https://www.cadth.ca/sites/default/files/es/ES0350%20_to%20Publishing%20Final.pdf. Accessed 2022 Mar 22.
6.Duckworth MP, Iezzi T, Carlson GC. Chronic pain. Principle-based stepped care and brief psychotherapy for integrated care settings. Cham, Switzerland: Springer International Publishing/Springer Nature; Switzerland; 2018:129-142.
7.Mental Health Commission of Canada. Newfoundland and Labrador Stepped Care 2.0 e-mental health demonstration project. Ottawa: Health Canada; 2019: https://www.mentalhealthcommission.ca/wp-content/uploads/drupal/2019-09/emental_health_report_eng_0.pdf. Accessed 2022 May 13.
8.Meeuwissen JAC. The case for stepped care: Exploring the applicability and cost-utility of stepped-care strategies in the management of depression [dissertation]. Vrije Universiteit Amsterdam; 2018: https://research.vu.nl/en/publications/the-case-for-stepped-care-exploring-the-applicability-and-cost-ut. Accessed 2022 May 13.
9.van't Veer-Tazelaar PJ, van Marwijk HW, van Oppen P, et al. Stepped-care prevention of anxiety and depression in late life: a randomized controlled trial. Archives of general psychiatry. 2009;66(3):297-304. PubMed
10.Hunkeler EM, Katon W, Tang L, et al. Long term outcomes from the IMPACT randomised trial for depressed elderly patients in primary care. Bmj. 2006;332(7536):259-263. PubMed
11.Peterson K, Anderson J, Bourne D, Mackey K, Helfand M. Effectiveness of Models Used to Deliver Multimodal Care for Chronic Musculoskeletal Pain: a Rapid Evidence Review. J Gen Intern Med. 2018;33(Suppl 1):71-81. PubMed
12.Skelly AC, Chou R, Dettori JR, et al. Integrated and Comprehensive Pain Management Programs: Effectiveness and Harms. Rockville (MD): Agency for Healthcare Research and Quality; 2021: https://effectivehealthcare.ahrq.gov/products/integrated-pain-management/research. Accessed 2022 May 13.
13.Bell L, Cornish P, Gauthier R, et al. Implementation of the Ottawa Hospital Pain Clinic stepped care program: A preliminary report. Can J Pain. 2020;4(1):168-178. PubMed
14.Katon W, Russo J, Lin EH, et al. Cost-effectiveness of a multicondition collaborative care intervention: a randomized controlled trial. Archives of general psychiatry. 2012;69(5):506-514. PubMed
15.Simon GE, Katon WJ, Lin EH, et al. Cost-effectiveness of systematic depression treatment among people with diabetes mellitus. Archives of general psychiatry. 2007;64(1):65-72. PubMed
16.Dickinson KC, Sharma R, Duckart JP, Corson K, Gerrity MS, Dobscha SK. VA healthcare costs of a collaborative intervention for chronic pain in primary care. Medical care. 2010:38-44. PubMed
17.Busse JW, Craigie S, Juurlink DN, et al. Guideline for opioid therapy and chronic noncancer pain. CMAJ. 2017;189(18):E659-E666. PubMed
18.Sawhney M, Fletcher GG, Rice J, Watt-Watson J, Rawn T. Guidelines on management of pain in cancer and/or palliative care. Toronto (ON): Cancer Care Ontario; 2017: https://www.cancercareontario.ca/en/file/60576/download?token=u-u8pL3r.
19.Davis JA, Robinson RL, Le TK, Xie J. Incidence and impact of pain conditions and comorbid illnesses. J Pain Res. 2011;4:331-345. PubMed
20.Davis LL, Kroenke K, Monahan P, Kean J, Stump TE. The SPADE Symptom Cluster in Primary Care Patients With Chronic Pain. Clin J Pain. 2016;32(5):388-393. PubMed
21.Robbins SR, Melo LRS, Urban H, et al. Effectiveness of Stepped-Care Intervention in Overweight and Obese Patients With Medial Tibiofemoral Osteoarthritis: A Randomized Controlled Trial. Arthritis Care Res (Hoboken). 2021;73(4):520-530. PubMed
22.Bair MJ, Ang D, Wu J, et al. Evaluation of Stepped Care for Chronic Pain (ESCAPE) in Veterans of the Iraq and Afghanistan Conflicts: A Randomized Clinical Trial. JAMA Intern Med. 2015;175(5):682-689. PubMed
23.Smink AJ, van den Ende CH, Vliet Vlieland TP, et al. Effect of stepped care on health outcomes in patients with osteoarthritis: an observational study in Dutch general practice. Br J Gen Pract. 2014;64(626):e538-544. PubMed
24.Edmond SN, Moore BA, Dorflinger LM, et al. Project STEP: Implementing the Veterans Health Administration’s stepped care model of pain management. Pain Med. 2018;19(suppl_1):S30-S37. PubMed
25.Anderson DR, Zlateva I, Coman EN, Khatri K, Tian T, Kerns RD. Improving pain care through implementation of the Stepped Care Model at a multisite community health center. J Pain Res. 2016;9:1021-1029. PubMed
26.Chambers JB, Marks EM, Russell V, Hunter MS. A multidisciplinary, biopsychosocial treatment for non-cardiac chest pain. Int J Clin Pract. 2015;69(9):922-927. PubMed
27.Fitzsimmons D, Phillips CJ, Bennett H, et al. Cost-effectiveness of different strategies to manage patients with sciatica. Pain. 2014;155(7):1318-1327. PubMed
28.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
29.Smink AJ, Dekker J, Vliet Vlieland TP, et al. Health care use of patients with osteoarthritis of the hip or knee after implementation of a stepped-care strategy: an observational study. Arthritis Care Res (Hoboken). 2014;66(6):817-827. PubMed
30.Cosio D, Swaroop S. The use of mind-body medicine in chronic pain management: differential trends and session-by-session changes in anxiety. Journal of pain management & medicine. 2016;2(2).
31.Plagge JM, Lu MW, Lovejoy TI, Karl AI, Dobscha SK. Treatment of comorbid pain and PTSD in returning veterans: A collaborative approach utilizing behavioral activation. Pain Med. 2013;14(8):1164-1172. PubMed
32.Karp JF, Gao X, Wahed AS, et al. Effect of Problem-Solving Therapy Versus Supportive Management in Older Adults with Low Back Pain and Depression While on Antidepressant Pharmacotherapy. Am J Geriatr Psychiatry. 2018;26(7):765-777. PubMed
33.Matthias MS, Miech EJ, Myers LJ, Sargent C, Bair MJ. An expanded view of self-management: patients' perceptions of education and support in an intervention for chronic musculoskeletal pain. Pain Med. 2012;13(8):1018-1028. PubMed
34.Kroenke K, Krebs EE, Wu J, Yu Z, Chumbler NR, Bair MJ. Telecare collaborative management of chronic pain in primary care: a randomized clinical trial. Jama. 2014;312(3):240-248. PubMed
35.Tierce-Hazard S, Sadarangani T. Optimizing the primary care management of chronic pain through telecare. Journal of Clinical Outcomes Management. 2014;21(11):493-495.
36.Guilkey RE, Draucker CB, Wu J, Yu Z, Kroenke K. Acceptability of a telecare intervention for persistent musculoskeletal pain. J Telemed Telecare. 2018;24(1):44-50. PubMed
37.De Oliveira Silva D, Pazzinatto MF, Crossley KM, Azevedo FM, Barton CJ. Novel Stepped Care Approach to Provide Education and Exercise Therapy for Patellofemoral Pain: Feasibility Study. Journal of medical Internet research. 2020;22(7):e18584. PubMed
38.Skou ST, Roos EM. Good Life with osteoArthritis in Denmark (GLA: D™): evidence-based education and supervised neuromuscular exercise delivered by certified physiotherapists nationwide. BMC Musculoskelet Disord. 2017;18(1):1-13. PubMed
39.Rhon DI, Greenlee TA, Fritz JM. The Influence of a Guideline-Concordant Stepped Care Approach on Downstream Health Care Utilization in Patients with Spine and Shoulder Pain. Pain Med. 2019;20(3):476-485. PubMed
Appendix 1: Evaluations of Step(s) in Stepped Care Model
Note that this appendix has not been copy-edited.
Documents of studies that evaluated one or more steps in the stepped care approach, rather than the implementation and evaluation of the stepped care model itself, are outside the scope of this review and were not summarized in the review. Studies which evaluated components or steps that were part of the included stepped care models are briefly described in the following paragraphs.
Several studies evaluated individual interventions included in the stepped care model in NCCP and described potential clinical benefits. In brief, a retrospective cohort study assessed the impact of 10-week CBT intervention (compared to Acceptance and Commitment Therapy) as part of a stepped care model on pain severity and global distress in US veterans with chronic pain.30 An uncontrolled before-after study in US veterans with chronic pain and posttraumatic stress disorder assessed participation in a biopsychosocial evaluation plus up to 8 behavioural activation sessions on pain, mental health and quality of life.31 An RCT evaluated problem-solving compared to behavioural activation (both in addition to treatment with venlafaxine) as the second step in a stepped model for people 60 years of age and older with comorbid depression and low back pain.32
Several studies evaluated interventions included in ESCAPE and described potential clinical benefits. A qualitative study with 26 participants in the ESCAPE intervention group assessed the self-management education of step 2 in the model.33 An RCT examined the effectiveness34,35 and acceptability36 of a telecare intervention, which included nurse telephone contacts and was coupled with automated symptom monitoring, as part of the Stepped Care to Optimize pain Care Effectiveness (compared to usual care) for US veterans with chronic pain.
Two studies37,38 evaluated the delivery of education and exercise therapy interventions. An RCT37 assessed 12 weeks of physiotherapist-led (up to 8 sessions) education and exercise therapy delivered face-to-face versus telerehabilitation delivery in participants with chronic patellofemoral pain.37 An uncontrolled before-after study38 assessed education (2 to 3 sessions) and supervised exercises (twice weekly for 6 weeks) as the first step in a stepped care model for pain due to knee or hip osteoarthritis.
A retrospective cohort study compared 1-year downstream health care use and medical costs for patients with spine or shoulder pain who received manual therapy only compared to manual therapy and opioid prescriptions as the first step in a stepped care model.39
Appendix 2: Documents of Potential Interest
Note that this appendix has not been copy-edited.
Related CADTH Reports
Models of Care for Chronic Pain: CADTH Environmental Scan. Ottawa: CADTH; 2021. https://www.canjhealthtechnol.ca/index.php/cjht/article/download/es0350/es0350. Accessed 14 April 2022.
Tiered Care for Chronic Non-Malignant Pain: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines. Ottawa: CADTH; 2019. https://www.cadth.ca/tiered-care-chronic-non-malignant-pain-review-clinical-effectiveness-cost-effectiveness-and. Accessed 14 April 2022.
Development or Implementation of Stepped Care Model
Bell L, Cornish P, Gauthier R, et al. Implementation of the Ottawa Hospital Pain Clinic stepped care program: A preliminary report. Can J Pain. 2020;4(1):168-178. PubMed
Dorflinger L, Moore B, Goulet J, et al. A partnered approach to opioid management, guideline concordant care and the stepped care model of pain management. J Gen Intern Med. 2014;29 Suppl 4:870-876. PubMed
Egerton T, Hinman RS, Hunter DJ, et al. PARTNER: a service delivery model to implement optimal primary care management of people with knee osteoarthritis: description of development. BMJ Open. 2020;10(10):e040423. PubMed
Smink AJ, Dekker J, Vliet Vlieland TP, et al. Health care use of patients with osteoarthritis of the hip or knee after implementation of a stepped-care strategy: an observational study. Arthritis Care Res (Hoboken). 2014;66(6):817-827. PubMed
Systematic Reviews
Cochrane A, Higgins N, FitzGerald O, et al. Early interventions to promote work participation in people with regional musculoskeletal pain: A systematic review and meta-analysis. Clinical Rehabi. 2017;31(11):1466-1481. PubMed
Peterson K, Anderson J, Bourne D, Mackey K, Helfand M. Effectiveness of Models Used to Deliver Multimodal Care for Chronic Musculoskeletal Pain: A Rapid Evidence Review. J Gen Intern Med. 2018;33(Suppl 1):71-81. PubMed
Skelly AC, Chou R, Dettori JR, et al. Integrated and Comprehensive Pain Management Programs: Effectiveness and Harms. Rockville (MD): Agency for Healthcare Research and Quality; 2021: https://effectivehealthcare.ahrq.gov/products/integrated-pain-management/research Accessed 2022 May 13.
Scoping Review
Birnie KA, Pavlova M, Neville A, et al. Rapid Evidence and Gap Map of virtual care solutions across a stepped care continuum for youth with chronic pain and their families in response to the COVID-19 pandemic. Pain. 2021;162(11):2658-2668. PubMed
Guideline Documents
Doctors of BC. Improving Chronic Pain Management in BC. Last updated: June 2017. https://www.doctorsofbc.ca/sites/default/files/2017-07-improvingchronicpainmanagementinbc_id_113423.pdf. Accessed 14 April 2022.
The Dr. Robert Bree Collaborative. Collaborative Care for Chronic Pain Report and Recommendations; 2018. https://www.qualityhealth.org/bree/wp-content/uploads/sites/8/2018/11/Recommendations-Chronic-Pain-Draft-18-1031.pdf. Accessed 14 April 2022.
Faculty of Pain Medicine of the Royal College of Anaesthetists. Improving the Lives of People with Complex Chronic Pain: How to Commission Effective Pain Management Services in England; 2020. https://fpm.ac.uk/sites/fpm/files/documents/2020-06/Commissioning%20guidance%20draft%20design%20FINAL_0.pdf. Accessed 14 April 2022.
Interior Health Planning and Strategic Services. Interior Health’s Chronic Pain Strategy Recommendations and Actions for Consideration; 2012. https://www.interiorhealth.ca/sites/default/files/PDFS/ih-chronic-pain-strategy.pdf. Accessed 14 April 2022.
Kligler B, Bair MJ, Banerjea R, et al. Clinical Policy Recommendations from the VHA State-of-the-Art Conference on Non-Pharmacological Approaches to Chronic Musculoskeletal Pain. J Gen Intern Med. 2018;33(Suppl 1):16-23. PubMed
Ontario Health Quality. Chronic Pain Care for Adults, Adolescents, and Children; 2020. https://www.hqontario.ca/Portals/0/documents/evidence/quality-standards/qs-chronic-pain-quality-standard-en.pdf. Accessed 14 April 2022.
Luites JWH, Kuijer P, Hulshof CTJ, et al. The Dutch Multidisciplinary Occupational Health Guideline to Enhance Work Participation Among Low Back Pain and Lumbosacral Radicular Syndrome Patients. J Occup Rehabil. 2021 Jul 27. https://link.springer.com/content/pdf/10.1007/s10926-021-09993-4.pdf. Accessed 14 April 2022.
Conference Abstract
Clune H GW, Hren L. Applying the Stepped Care Model to Chronic Pain Management. Perm J. 2021;Nov(21).
Protocol
Fritz JM, Rhon DI, Teyhen DS, et al. A Sequential Multiple-Assignment Randomized Trial (SMART) for Stepped Care Management of Low Back Pain in the Military Health System: A Trial Protocol. Pain Med. 2020;21(Suppl 2):S73-S82. PubMed
Narrative Reviews
Barker S, Urbanek M, Penlington C. Psychological Interventions for Persistent Orofacial Pain. Prim Dent J. 2019;7(4):30-35. PubMed
Duckworth MP, Iezzi T, Carlson GC. Chronic pain. Principle-based stepped care and brief psychotherapy for integrated care settings. Cham, Switzerland: Springer International Publishing/Springer Nature; Switzerland; 2018:129-142.
Chronic Pain Among Service Members Using Administrative Data to Strengthen Research and Quality Improvement; 2021. https://www.rand.org/pubs/research_reports/RRA1160-1.html. Accessed 14 April 2022.
Gallagher RM. Advancing the Pain Agenda in the Veteran Population. Anesthesiol Clin. 2016;34(2):357-378. PubMed
Kongsted A, Kent P, Quicke JG, Skou ST, Hill JC. Risk-stratified and stepped models of care for back pain and osteoarthritis: are we heading towards a common model? Pain rep. 2020;5(5):e843. PubMed
Linton SJ, Nicholas M, Shaw W. Why wait to address high-risk cases of acute low back pain? A comparison of stepped, stratified, and matched care. Pain. 2018;159(12):2437-2441. PubMed
McCulloch Gallagher R, Sandbrink F. The Socioeconomic Burden of Pain From War. American Journal of Public Health. 2019;109(1):41-45. PubMed
Sharpe L. Psychosocial management of chronic pain in patients with rheumatoid arthritis: challenges and solutions. J Pain Res. 2016;9:137-146. PubMed
Speed TJ, Parekh V, Coe W, Antoine D. Comorbid chronic pain and opioid use disorder: literature review and potential treatment innovations. Int Rev Psychiatry. 2018;30(5):136-146. PubMed
U.S. Department of Veterans Affairs. Stepped-care and collaborative-care models for chronic musculoskeletal pain; 2018. https://www.research.va.gov/research_in_action/Stepped-care-and-collaborative-care-models-for-chronic-musculoskeletal-pain.cfm. Access 14 April 2022.
Acknowledgments: Allison Gates
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.