CADTH Horizon Scan
2022 Health Technology Trends to Watch: Top 10 List
Round Up
Authors
Jeff Mason, Francesca Brundisini, Shannon Hill, Diksha Kumar, and Tamara Rader
Contributors
The authors are grateful to CADTH staff Ashley Baddeley, Barbara Greenwood Dufour, Brandy Appleby, Jennifer Horton, Julie Boucher, Kathleen Burns, Kristen Moulton, Renata Axler, and Sinwan Basharat for their involvement in the project and/or their feedback on the content of this report.
Workshop Participants
The authors are grateful to the workshop participants for their time, expertise, and input into the final ranking of the list. Their participation, discussion, and insights (as well as the appearances of children and pets throughout the meeting) are greatly appreciated.
Working Group
The authors are grateful to the following individuals who formed the working group to develop the 2022 Health Technology Tends to Watch: Top 10 List. They provided project oversight and reviewed earlier versions of the draft report.
Robert Denton Bacigalupo, MSc
Policy Analyst, Health Technology Assessment
British Columbia Ministry of Health
Tanya Ewashko, MPH, BScPT
Senior Project Manager
Alberta Health Services
Michaela Knot
Accessibility Specialist
CNIB Foundation
Jay Shaw, PT, PhD
Assistant Professor
Department of Physical Therapy, University of Toronto
Mahadeo Sukhai, PhD
VP, Research & International Affairs and Chief Accessibility Officer
CNIB Foundation
Linda Wilhelm
President
The Canadian Arthritis Patient Alliance
Conflicts of Interest
No members declared any relevant conflicts of interest.
Key Messages
The 2022 Health Technology Trends to Watch list presents the top 10 technologies that have the potential to fundamentally shift the way health care is provided and accessed in Canada within the next 2 years. The list was developed with direction and insights from pan-Canadian stakeholders, which included patients, health care decision-makers, researchers, representatives from government agencies, and industry experts.
The Top 10 List includes technologies for remote care monitoring, artificial intelligence for public health, and portable dialysis machines, among others. These technologies have the potential to transform health systems and improve health outcomes. For example, they may allow for more convenient and improved access to screening, diagnosis, and treatments; provide more tailored approaches to care; and help facilitate more person-centred care.
Implementing these new and emerging technologies would cause varying levels of disruption; for example, some would require new training for health care providers, new frameworks for integrating the technologies into practice, and/or new infrastructure to address issues of equity, accessibility, and data privacy.
Introduction
CADTH’s Horizon Scanning Service identifies new and emerging technologies that are likely to have a significant impact on Canada’s health care system in the next 1 year to 3 years. Through regular monitoring of various health information resources, CADTH endeavours to support decision-makers by keeping them informed about promising technologies not yet available in Canada or not widely adopted by Canadian health care providers and health care organizations. In 2021, as an extension of its suite of horizon scanning products, CADTH published its first health technology trends to watch list. The 2021 list was developed through targeted literature searches combined with the knowledge and expertise of members of CADTH’s Horizon Scanning Service. Building on the 2021 list, CADTH aimed to incorporate the views of a wider network of stakeholders and experts to better reflect and anticipate the future of health care in Canada. Therefore, this 2022 Top 10 List was developed by collecting the views of people from across Canada about new and emerging health technologies and trends and prioritizing them using a consensus-based decision-making process adapted from the James Lind Alliance (JLA). For more details, refer to the Methods in Appendix 1.
Technologies considered for the list had to be new or emerging health technologies, including medical devices or diagnostic tests; medical, surgical, or dental procedures; and other non-drug clinical interventions. Emerging technology trends were also considered for the list, such as continuously growing technology areas with a good prospect of continuing development in the future. Drugs or technologies defined as drugs by Health Canada (such as most stem cell products) were excluded from consideration as were technologies or trends without direct patient-related outcomes (e.g., health human resources; heating, ventilation, and air conditioning systems).
Due to the interconnectedness of technologies, some items on the list may not fit into single categories. For example, voice recognition software may have an artificial intelligence (AI) component or a mobile app may be used for remote care. Technologies and trends were placed in categories where they fit “best,” recognizing that there may be some overlap. Moreover, although some technologies have only recently been developed or received regulatory approval, others are further along in the product life cycle and have begun to be introduced into clinical practice. However, all technologies included in the list have the potential to disrupt the practice of health care in Canada.
The 10 items presented in the final 2022 trends to watch list are listed in the order workshop participants prioritized as the most important (1 being the most important) technologies and trends for decision-makers in Canada’s health care system to consider over the next 2 years. The list represents the consensus priorities of health care providers, patients, industry representatives, and others with an interest in the future of health care in Canada. The list covers a range of new and emerging technologies relevant to different conditions, models of health care delivery, and tools used to improve patient care. The list was developed during the COVID-19 pandemic; therefore, some technologies reflect the changes in health care due to the pandemic. Other technologies represent the next generation of medical devices already in use but with newer features that could considerably change how, where, or by whom they are used. Finally, some technologies are emerging and reflect a potential future of health care in Canada. The list is not an endorsement of any specific technology mentioned — it is intended to be used for information purposes only.
Top 10 Health Technology Trends to Watch in 2022
1. Remote Diagnostics, Remote Monitoring, and Remote Care Management
Remote care refers to the delivery of care at a location and time that is convenient for all members within the circle of care. The proliferation and expansion of remote care technologies that allow for the diagnosis, monitoring, and management of patients outside of traditional health care settings may fundamentally shift the way health care is provided and the way people access health care in Canada. These technologies include synchronous (real-time) apps such as videoconferencing and asynchronous (store-and-forward) technologies such as digital pathology or digital dermatology tools. The importance and use of remote diagnostics, remote monitoring, and remote care management emerged throughout the COVID-19 pandemic (e.g., virtual emergency departments) and have begun to highlight the potential for these technologies to impact patient outcomes. Effective and efficient interventions may allow for more strategic resource allocation and health care utilization and diffusion through a more accessible and personalized approach to care and a general shift in the way society thinks about the delivery of health care.
Remote care technologies have the potential to expand access to health care across wider geographic areas, for example, by enabling people living in rural and remote areas to connect with specialists and specialty care otherwise unavailable to them without travel. These technologies may also help facilitate tailored management of chronic conditions, such as diabetes or heart failure, or change care pathways, for example, by allowing care to be provided by a broader group of health care professionals. Improved monitoring of chronic conditions may lead to improved patient outcomes in a less invasive manner. An additional benefit of being able to offer personalized care plans remotely is that it may be a more cost-effective solution for both individuals and the health system. However, the proliferation of these technologies does not come without challenges related to equity and implementation, such as bandwidth and connectivity, equitable design, and culturally appropriate care.
CADTH previously conducted an Health Technology Review that assessed the implementation of remote monitoring programs for the management of chronic heart failure, atrial fibrillation, hypertension, and cardiac rehabilitation for acute and chronic conditions. CADTH is also undertaking a Health Technology Assessment related to internet-delivered cognitive behavioural therapy for chronic non-cancer pain.
Examples of emerging remote care technologies and applications include:
Remote examination and diagnosis. This includes the use of connected devices to support remote examination and diagnosis in primary and specialty care.
Digital biomarkers for Alzheimer disease or dementia. Emerging tools to assess “digital biomarkers” that monitor hand and eye movements or changes in speech may allow clinicians to monitor changes or in diagnosing people with conditions such as Alzheimer disease or dementia.
2. Point-of-Care Testing
Point-of-care testing refers to testing outside of a centralized laboratory and has a variety of potential applications for screening and diagnosis. Common tests already in use include those used for blood glucose monitoring, home pregnancy tests, and assays for detecting infectious diseases. The onset of the COVID-19 pandemic also spurred substantial uptake of COVID-19 tests that can rapidly and accurately provide results at or near the point-of-care. This proliferation also led to an increased awareness about how such tests may be applied across different aspects of medicine. Their emergence and the integration of point-of-care testing is of importance to health care decision-making because it has the potential to ease demand on central laboratories, provide timely guidance about treatment decisions, and support public health efforts in disease control and surveillance. Many point-of-care tests can be performed without specialized training and in a variety of care settings, including primary and urgent care settings, non-clinical settings, and at home by end-users (self-testing). This flexibility allows for a higher degree of convenience for the end-user and potential cost-savings for health systems because point-of-care testing tends to be less expensive compared with laboratory testing.
Point-of-care testing is designed to be a relatively simple and convenient option; however, these tests may be more prone to user error and can be less accurate than standard laboratory testing. When used incorrectly, point-of-care testing may produce false results (both positive and negative) that can lead to health consequences for the individual and potentially others, as with infectious diseases. As a result, the current intended use of many point-of-care testing is to complement — not replace — central laboratory testing or to help triage people in critical care settings. Potential barriers that are important to consider for enabling expansion of point-of-care testing in different settings may include the need to facilitate interprofessional collaboration, determining the role of tests within clinical workflows, and ensuring equitable access.
Examples of emerging point-of-care testing in Canada include:
HIV rapid diagnostic tests. HIV rapid diagnostic tests for point-of-care testing and self-testing has emerged as an option to support in diagnosing HIV in point-of-care environments by either health professionals or the individual undergoing testing.
Hemoglobin testing for type 2 diabetes. Point-of-care glycated hemoglobin testing for diagnosing type 2 diabetes has shown to perform as well as laboratory testing. These testing devices can be used to identify people at risk of developing type 2 diabetes.
Evaluation of mild traumatic brain injuries. Biomarker-based point-of-care tests for the evaluation of mild traumatic brain injuries may contribute information to help health care professionals determine the need for imaging in those suspected of having a mild traumatic brain injury, avoiding unnecessary radiation exposure in others and saving health care resources.
3. Molecular and Genomic Testing
Molecular and genomic testing refers to medical tests that can detect individuals’ unique genetic and/or protein makeup to inform treatment and care. Molecular and genomic testing can be done for a variety of reasons including diagnostic testing, pre-symptomatic or predictive testing, newborn screening, and preimplantation testing of embryos before in vitro fertilization, and to inform treatment decisions. These testing strategies offer many benefits to clinical outcomes through early detection and diagnosis and progression monitoring, selecting treatments which can have a higher likelihood of treatment success, and avoiding adverse events. Molecular and genomic testing is increasingly being used for personalized medicine to provide cancer therapy based on a person’s individual genetic profile, leading to better clinical outcomes.
Although targeted molecular and genomic testing is already conducted for many conditions, emerging whole genome sequencing (or more commonly, sequencing of protein-coding regions) will be disruptive and transformative to the Canadian health care landscape. Developments are occurring in improved testing platforms, for both whole genome sequencing and assays for detecting specific mutations, and computational algorithms used to analyze genomic data to make predictions and assess risk profiles. Molecular and genomic testing has the potential to have a major impact on health care systems because the large amount of detailed patient data that would be collected and used to make precision medicine a routine part of health care in Canada. The proliferation of molecular and genomic testing will be associated with an increased demand for genetic counsellors and health care professionals to understand the implications of test results. For health care decision-makers, ongoing developments within molecular and genomic testing raise important considerations related to equitable access to testing, the implications of incidental findings for individuals and the health care system, the cost-benefit impact of testing, and Canada’s technological and data privacy infrastructure for housing large amounts of genomic data.
Emerging examples of molecular and genomic testing include:
Genome sequencing of children with medical complexity. Researchers and clinicians at the Hospital for Sick Children in Toronto are working to demonstrate the utility and effectiveness of whole genome sequencing as part of standard care for children with complex conditions to reduce diagnostic and treatment delays.
Population-level cancer screening. The Screen Project at Women’s College Hospital in Toronto is evaluating the benefits of providing BRCA1 and BRCA2 genetic testing to any person, irrespective of risk factors, and its effect on mortality rates due to cancers associated with mutations in those genes.
Diagnosing rare diseases. Early findings from a UK-based pilot study suggest that whole genome sequencing delivered though the National Health Service as part of routine care for children and families affected by rare conditions can help improve rates of diagnoses and favourably impact clinical outcomes.
4. Health Apps and Wearable Technologies (mHealth)
Mobile health apps are a growing field of digital health technologies, and are intended for the diagnosis, treatment, or prevention of health conditions or diseases. Mobile health apps can offer a variety of functions to support the health and well-being of people. Some of these functions include the ability to store and track health information, provide health education information, provide periodic reminders or motivational guidance, and use GPS tracking to direct or alert patients. Wearable technologies fall within the realm of mobile health technologies and are specific add-on devices or sensors that connect with smart phones or watches, tablets, and cloud-based computing systems to collect the wearer’s health data and health metrics. Wearable technologies can provide health status updates to both the patient and their health care provider in real time, which may facilitate more timely interventions and may improve resolution of data to inform treatments. Some of these technologies may facilitate health promotion or disease prevention if used by people autonomously (e.g., weight management or physical activity monitoring) or in a collaboration with a health care provider to oversee and monitor patient outcomes (e.g., chronic disease management). These devices may also provide a platform to deliver care to people who may face barriers to accessing care in traditional settings or who may face stigma when seeking care (e.g., mobile mental health apps).
Mobile health apps and technologies are likely to be disruptive to health care systems because they continue to proliferate and emerge within the health care landscape. If shown to be clinically effective, they may provide a novel approach for people to access and collect health information, increase patient involvement, and provide a new platform to improve access and convenience of care for certain conditions. Although the emergence of mobile health apps and wearable technologies has happened quickly and on a large scale (there are more than 350,000 health apps available for download), few of these apps have been designed for or reviewed and authorized for clinical use in Canada. For the majority of health apps that will not need authorization, alternative approaches for assessing quality may need to be considered. There is often little to no clinical evidence assessing the claims of different health apps; other issues related to their safety, data privacy, and equity will also be important to consider.
Examples of emerging mobile health apps and wearable technologies include:
Diabetes management. Developed by eHealth Innovation at the University Health Network in Toronto, bant is a mobile health app that provides glucose management feedback and offers management strategies for people living with diabetes.
Cardiovascular monitoring. Researchers have used wearable devices to track and monitor physiologic responses for people living with or at risk of developing heart conditions.
Mental health management. Ontario Shores Centre for Mental Health Sciences has compiled a collection of online tools and mobile health apps that target specific mental health conditions.
5. Companion Diagnostics
Companion diagnostic tests are an emerging health technology supporting the expansion of personalized medicine by assessing predictive biomarkers, such as genetic variation or protein expression in individuals to determine the safe and effective use of an associated therapy. Companion diagnostic tests are usually developed for a particular condition to assess for specific genetic mutations or biomarkers rather than sequencing the whole genome, which is substantially more costly. This targeted approach provides the capability to tailor therapies for a specific person and is important for the development of newer and potentially more effective interventions for certain health conditions. Emerging companion diagnostics that examine circulating tumour DNA or ctDNA (DNA fragments shed by tumours) within the bloodstream also provide a less invasive, quicker, and potentially safer alternative to assessing biomarkers compared with traditional tissue biopsies. Increasingly, targeted cancer therapies are being co-developed with companion diagnostics to better inform early detection and treatment decisions that can improve patient outcomes and reduce adverse effects.
Despite the proliferation of companion diagnostics, a barrier to adoption in Canada has been the disjointed reimbursement and delivery landscape of these devices and their associated therapies across health systems. This barrier to adoption may highlight the need for the development of health technology assessment frameworks in Canada to co-assess both emerging therapies and their associated diagnostic tests. Important areas to watch for companion diagnostics will be ongoing work evaluating the evidence on the real-world impact on patient outcomes, diagnostic accuracy of different devices, and cost-effectiveness analyses for health systems. CADTH developed guidance surrounding the economic evaluation specifically for companion diagnostics that considers the nuances with evaluating companion diagnostics in Canada.
Examples of emerging companion diagnostics technologies include:
Liquid biopsy testing. Follow It is a liquid biopsy panel that analyzes ctDNA in plasma samples. The assay is designed to detect cellular traces associated with multiple solid tumour types.
Cancer detection. FoundationOne CDx is a genomic profile test that detects genomic alterations often found in solid cancers. It can be used to detect different cancer types including but not limited to non–small cell lung cancers, colorectal cancer, breast cancer, ovarian cancer, and melanoma.
Pharmacogenetic testing for psychiatric disorders. Genecept Assay is a genetic test that aims to identify medications that are more likely to be safe and effective for individuals with various psychiatric disorders.
6. Voice Technology
Voice technology has many applications within the virtual care space, including conversational AI technology (e.g., chatbots) that act as voice assistants for health assessment, diagnostics, and companionship for patients. It can also play a key role in the administrative tasks often handled by health care providers through real-time charting, storing health care data, and communicating with other health professionals. Voice technology has the potential to provide an accessible platform for patients to interface with aspects of the health care system and drive efficiencies in areas of care that require a high volume of resources. By introducing new avenues for patients to access care or health information at home, these apps may transform the way that people navigate health care services and technologies. As a mechanism for therapeutics, voice technology has the potential to reduce barriers to communication and its natural interface may provide patients with a sense of comfort and familiarity. People with visual or mobility disabilities may also benefit from voice-activated health care applications.
However, the adoption of voice technology in the Canadian health care system has been relatively slow. Potential barriers to the implementation to voice technology in health care can be issues around data privacy, integration with patients’ health records, and the need for evidence to assess its clinical effectiveness, safety, and cost-effectiveness. Voice technology apps may also have limited accessibility among patients if they are designed with only English speakers in mind.
Specific emerging uses of voice technology include:
Diagnosis of neurogenerative conditions. Wearable devices with integrated speech recognition can detect semantic, syntactic, and acoustic voice features associated with conditions like mild cognitive impairment and Alzheimer disease, thereby aiding in early detection and diagnosis.
Symptom assessment. Ada is a mobile health companion app that integrates with home-based virtual assistant devices to assess the user’s health based on their indicated symptoms. The app combines the utility of a voice interface with an AI-based database to monitor personal health data and assist in proactive care.
Prehospital triaging. The Cardiology Heart Failure Clinic at McGill University Health Centre uses a COVID-19 screening tool that uses the Amazon Alexa voice assistant to screen patients.
7. Artificial Intelligence for Diagnostics and Public Health
Artificial intelligence is an umbrella term used to describe a variety of approaches (e.g., machine learning, natural language processing) that allow computer programs to perform tasks that have been traditionally done by humans. CADTH produced a Horizon Scan that provided an overview of clinical applications of AI, detailing its use in diagnosing cardiac conditions and promoting dermatological screening, among other use cases. In diagnostics, AI can be used in cancer screening (e.g., for quality assurance in breast cancer screening), pathology (e.g., to automatically grade tumours), and in critical care medicine (e.g., for the prediction and detection of sepsis). Automating or making informed predictions within certain settings can potentially increase efficiency of clinical workflows, reduce costs, reduce the time it takes to perform tasks and report findings, and free up costly and limited health human resources (e.g., specialized technicians or radiologists).
In the field of public health, AI may help improve disease surveillance, detection, and mitigation by facilitating analyses of large volumes of complex, multi-sourced data from around the world. By using AI to support health data collection, researchers can investigate new methods of assessing the effectiveness of public health interventions and informing targeted health promotion activities and disease incidence forecasts. Natural language processing, a subfield of AI, can be used to support evidence-based decision-making by enhancing public health surveillance systems with real-world evidence.
The adoption of AI in health care is disruptive because it will transform traditional approaches of clinical and health care decision-making, which can also introduce certain challenges. For example, there are concerns that some communities may be underrepresented in the data used to train AI algorithms, which could result in health disparities and discrimination, and exacerbate access and trust issues in the health care system, and worsen health-related outcomes. Continued proliferation of AI requires decision-makers to consider issues related to increasing transparency, ongoing assessment of its safety, and addressing ethical and equity concerns about the technology to improve trust among patients, caregivers, and health care providers.
Some emerging examples of AI include:
Radiology. XrAI is an AI radiology tool approved for use in Canada that uses deep learning to assist clinicians in interpreting chest X-rays. XrAI was recently deployed across Canada to confirm pneumonia and other respiratory symptoms associated with COVID-19.
Cancer diagnostics. CADTH has published several reports regarding AI applications for diagnostics, including AI for the classification of lung nodules and AI for the measurement of breast density.
Public health surveillance. An aggregation of epidemiological and digital trace data (e.g., from social media and news reports) was used to forecast the incidence of Zika virus infections during the 2016 Latin America outbreak.
8. Advanced Closed-Loop Insulin Pumps
Diabetes is a chronic condition that affects more than 3 million people in Canada, an estimated 9% to 10% of whom use insulin to manage their glucose levels and diabetes. Technological advances in insulin management for people living with type 1 diabetes have been developing over time, and emerging innovations may offer better methods of achieving stable glucose levels and, in the long-term, assist in reducing the risk of diabetes-related complications. In particular, advanced closed-loop insulin pumps are an important development within diabetes care because they use sensing technologies and AI algorithms to automatically adjust insulin in response to predicted glucose levels. This functionality can help support self-management and ensure glucose levels are within the target range for a longer period compared with other insulin management options. Real-time insulin administration eliminates the use of insulin injections, thus reducing the inconvenience of hands-on management for people living with type 1 diabetes.
By using closed-loop insulin pumps, people living with diabetes (and their caregivers) can participate in daily activities without the worry of severe hypoglycemia, which can be life-threatening. A reduction in long-term diabetes-related complications, such as cardiovascular disease, chronic renal failure, vision impairment, and amputation, may lead to decreased use of health care services associated with managing and treating those conditions. Advances in the technology have the potential to transform diabetes care. The innovations aim to improve the quality of life for people living with type 1 diabetes (and their caregivers) by offering greater flexibility around diabetes management and increasing the accessibility, functionality, and reliability of insulin delivery systems. Universal design principles should be a key consideration for the development of emerging closed-loop systems to ensure the technology is accessible to people with diverse needs.
CADTH completed a Health Technology Review on the clinical effectiveness, safety, budget impact, patient perspectives and experiences, and ethical issues associated with the first generation of hybrid closed-loop insulin delivery systems in Canada and developed recommendations for their use.
Some emerging changes in advanced closed-loop delivery systems include:
Innovative features of existing hybrid closed-loop systems including a pump with integrated blood glucose sensors to autocorrect insulin dosing and a system that uses predictive algorithms to adapt insulin delivery to reduce significant fluctuations in blood glucose levels.
Emerging advanced closed-loop insulin pumps may use fast-acting insulin analogues, integrate additional health metrics, and improve designs of previous systems.
9. Portable Dialysis Machines
End-stage renal disease affects thousands of people in Canada; national figures show more than 23,000 people received chronic dialysis in 2019. Although home-based dialysis is not a new technology, emerging portable dialysis machines present a new generation of devices that may provide people with kidney failure more options to access a home-based, point-of-care alternative to conventional dialysis at a hospital or clinic. These devices are smaller and more mobile than a hospital-based units or previous generation home machines. They take up less space and are less intrusive to home life. They also provide people with the option of undergoing treatment during waking or sleeping hours and the smaller profile allows for more flexibility in treatment location — potentially allowing people to perform dialysis while on vacation or in another location — improving autonomy and quality of life. With portable dialysis machines, people can allocate approximately 12 hours to dialysis a week at home, instead of spending 4 hours to 5 hours per hemodialysis session, 3 times a week, at a hospital or clinic. By reducing travel time and increasing treatment flexibility, people who do at-home dialysis typically have more energy, require fewer fluid and dietary restrictions, need fewer medications, and have overall better health outcomes.
This emerging technology is disruptive because it can transform care for end-stage renal disease and provide solutions to better support person-centred care. The COVID-19 pandemic also highlighted the need to provide more flexible treatment options. By changing how people with end-stage renal disease receive care, portable home options for dialysis can increase the autonomy of patients and their caregivers, and potentially reduce health care utilization and costs compared with conventional dialysis at a hospital or clinic by easing demand on hospitals and other facilities. Portable dialysis machines may also be useful in remote clinic settings with resource constraints.
Home-based hemodialysis was evaluated in CADTH’s Optimal Use Report on dialysis modalities for the treatment of end-stage kidney disease and found to be less costly compared with in-centre hemodialysis.
Examples of newer, more portable dialysis machines include:
Connected portable dialysis systems. The NxStage System One is a portable machine for home use available for sale in Canada. Identified in CADTH’s Horizon Scan on emerging portable hemodialysis systems, the device is connected with a tablet-based health app that collects and displays treatment data that can be shared with health care providers.
Customizable systems. Another machine discussed in the Horizon Scan is the Quanta SC+ system, which is not yet authorized in Canada. It is a compact and lightweight device that features digital health connectivity. Unlike other portable hemodialysis systems, Quanta claims the SC+ system delivers higher dialysate flow rates like those typically used in conventional 3-times-a-week prescriptions, which reduces the need for daily home treatments. Patients can also receive more frequent, longer, and gentler treatment sessions if that suits their needs.
10. Artificial Intelligence for Health Professionals
Another emerging application of AI within the health care system is to change the way health professionals approach patient consultations and develop treatment plans. A main functionality of AI in health care is the ability to store and analyze data in a way that could offer helpful predictions for health care delivery. This ability to make data-driven predictions can play a major role in health screening (e.g., cancer screening) by alerting health professionals to early signs of disease. AI for use by health professionals is likely to be disruptive because it could change how treatment decisions are made in real time and bring the technology to the people responsible for providing care or making decisions about care needs.
AI can also be beneficial in health care settings such as emergency care, critical care, and operating rooms where efficiencies and increased patient support are needed and can have direct implications on patient outcomes. An example of how AI may be implemented within the health care setting is through directing traffic within hospitals to allow for a more streamlined approach to providing and receiving care. Additionally, AI can be applied to identify novel and targeted treatments for a wide variety of conditions, which allows for more innovative and personalized approaches to patient care.
A CADTH Environmental Scan on AI and machine learning trends in mental health services indicated the use of these tools within the context of clinical practices in Canada is still quite limited. Kids Help Phone, which provides online and telephone crisis counselling and support to youth across Canada, uses AI to triage users. Further evidence is needed to assess the effectiveness of certain AI apps. Better data collection is necessary to build prediction models, such as those used to support decision-making for COVID-19. Additionally, trust in AI will need to be developed.
Some current and potential use cases of AI in health care delivery include:
Treatment plan design. AI-driven software developed by IBM Watson analyzes a patient’s medical record along with information from research to provide suggestions to the health care professional of possible treatment options that could be considered for the patient’s clinical context.
Critical care. CADTH’s Horizon Scan on clinical applications of AI encompasses several ways that AI can improve health care systems through machine learning algorithms, including its potential use in critical care settings. By predicting outcomes such as patient mortality and early onset of sepsis, AI tools can reduce the average length of stay in the intensive care unit and decrease health care utilization costs.
Mobile charting. Apps with integrated AI technology, such as Nuance DAX, can save time and allow medical information to be shared more conveniently among members of the patient care team. A performance report for the app states that patients were more satisfied with their consultations because they felt their provider was more engaged and less inundated with documentation.
Appendix 1: Methods
The JLA Priority Setting Partnership Process
The methods used to develop the 2022 Health Technology Trends to Watch list was broadly guided by JLA Priority Setting Partnership (PSP) process. The JLA’s principles align with CADTH’s priorities of equal involvement and inclusivity (e.g., balanced representation from patients, clinicians, and other CADTH stakeholders), transparency (e.g., visible audit trail of submitted technologies and trends, publication of interim documents), and a commitment to using and contributing to the evidence base (e.g., using technologies and trends to inform future CADTH products).
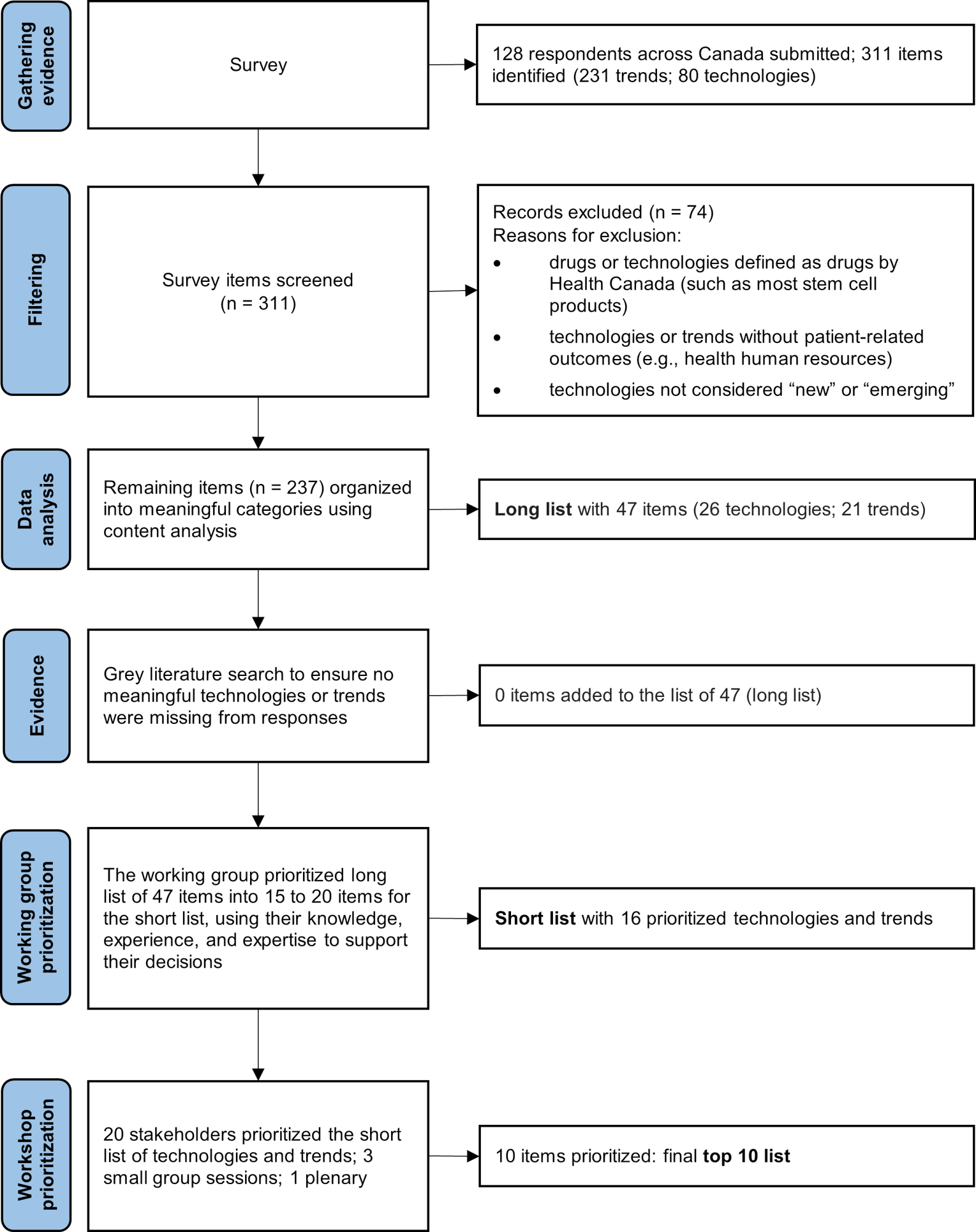
Adopting the principles of the JLA PSP process enabled the health care decision-makers, patients, clinicians, representatives from industry, academics, and CADTH researchers to work together to identify and rank emerging health technologies with the most potential to disrupt Canada's health care system in the next 2 years. The PSP process used a staged approach that developed a PSP working group, synthesized evidence from different sources, and used consensus building to identify and rank the final top 10 list of emerging health technologies to watch in 2022. Figure 1 illustrates steps of the JLA PSP process.
Figure 1: The James Lind Alliance Priority Setting Partnership Process Used to Develop the Top 10 List

Creating a Working Group
In July 2021, health care and technology innovation experts (external to CADTH) were contacted to form the working group. Six experts worked alongside CADTH staff to oversee and guide the priority setting process, and informed project decisions via monthly meetings. The working group also facilitated outreach and connections with stakeholders and championed the project through their networks. Finally, the external members of the working group developed a short list of technologies and trends to be considered for the final top 10 list. All external experts participated in at least 1 working group meeting, and all were offered an honorarium.
Gathering Evidence
An online exploratory survey was used to identify new and emerging health technologies that could potentially disrupt Canada’s health care system in the next 2 years. A 2-year time frame was selected to capture technologies that might be in late-stage development and could potentially impact the Canadian health system in the near future. The survey provided the following definitions for key terms, which are also used in the report:
Technology refers to any medical device or diagnostic test; any medical, surgical, or dental procedure; or any other non-drug clinical intervention. However, drugs or technologies defined as drugs by Health Canada (such as most stem cell products) were not considered for the list. Technologies or trends without direct patient-related outcomes (e.g., health human resources; heating, ventilation, and air conditioning systems) were also excluded.
A technology was considered new if it was in the phase of adoption when it has only been available for clinical use for 1 year to 2 years and typically in the launch or early post-marketing stage.
A technology was considered emerging if the health care system had not yet been adopted it, such as medical devices not yet available in the Canadian market, within 6 months of becoming available in Canada, or available in Canada but less than 10% diffused or localized to a few centres.
An existing technology with new indications could also be considered new or emerging.
Technology trend refers to a continuously growing technology area with a consistent direction of development and with a good prospect of continuing its development in the future.
Online Survey Content and Dissemination
The survey included 18 questions organized into 4 sections with a combination of both open-ended and close-ended questions. These sections asked about respondents’ views on future technological trends, the potential impact of those trends on health care systems in Canada, specific new and emerging technologies, and their potential for disruptiveness. The survey also asked about respondents’ demographic information and whether they would be interested in participating in the final prioritization workshop to be held in December 2021. The survey took approximately 20 minutes to complete; the full text of the survey questions is available.
The survey was reviewed by the working group and piloted by CADTH staff before distribution. The survey was disseminated to ensure responses from people with diverse experiences and a broad range of perspectives, although it did not aim to be representative of all health care stakeholders in Canada. The approach aimed to include people from different roles within health care systems, health technology stakeholders, and members of the public interested in the future of the Canadian health care system.
The web-based survey was developed using the SurveyMonkey platform and was distributed by CADTH's Implementation Support and Knowledge Mobilization (ISKM) team, CADTH's professional network, and networks of internal project teams. People were also engaged through CADTH’s social media channels, including CADTH’s Twitter (with more than 18,500 followers) and CADTH’s LinkedIn page (with close to 8,000 followers), and newsletter subscribers (approximately 8,000 people). The survey was distributed from September 7 to October 8, 2021, and was available in both English and French. It was recirculated to a list of additional respondents on October 11 and October 29, 2021. Responses received by November 4, 2021, were included in the analysis.
Profile of Survey Respondents
A total of 128 individuals who live or work in Canada completed the survey. All survey responses were in English except for 1 in French. Respondents were from a variety of roles, organizations, and agencies across Canada, including those working in government agencies, non-profit organizations (e.g., patient, family advisor, advocacy group representatives), academia, health care services (e.g., health care providers), teaching hospitals, research institutions, industry (e.g., medical technology company representatives), and professional associations. Figure 2 shows the proportions of the respondents based on their primary place of work or occupation affiliation.
Figure 2: Survey Respondents’ Primary Place of Work or Occupation Affiliation (N = 128).
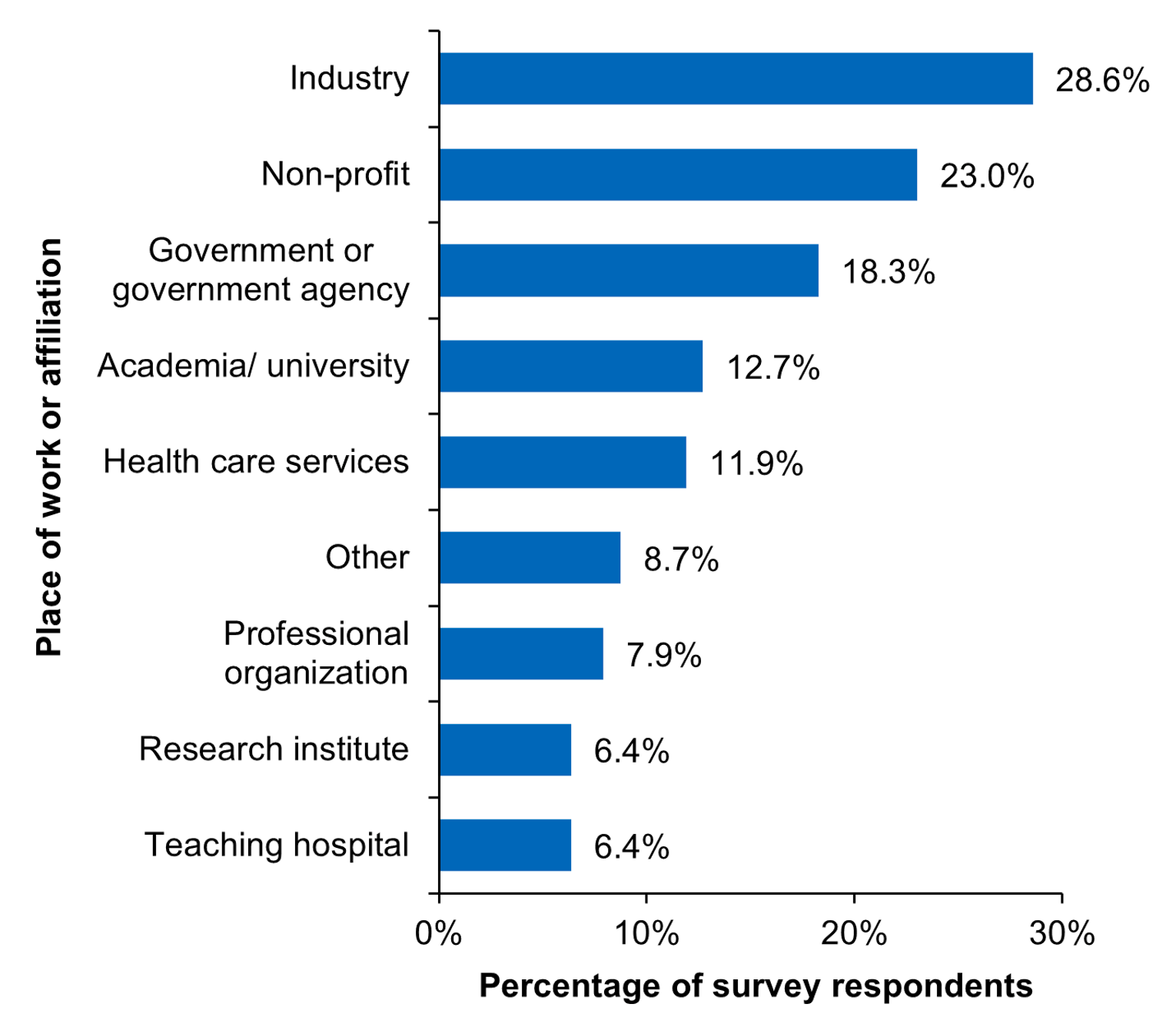
Note: Respondents could select more than 1 option; therefore, the total is more than 100%.
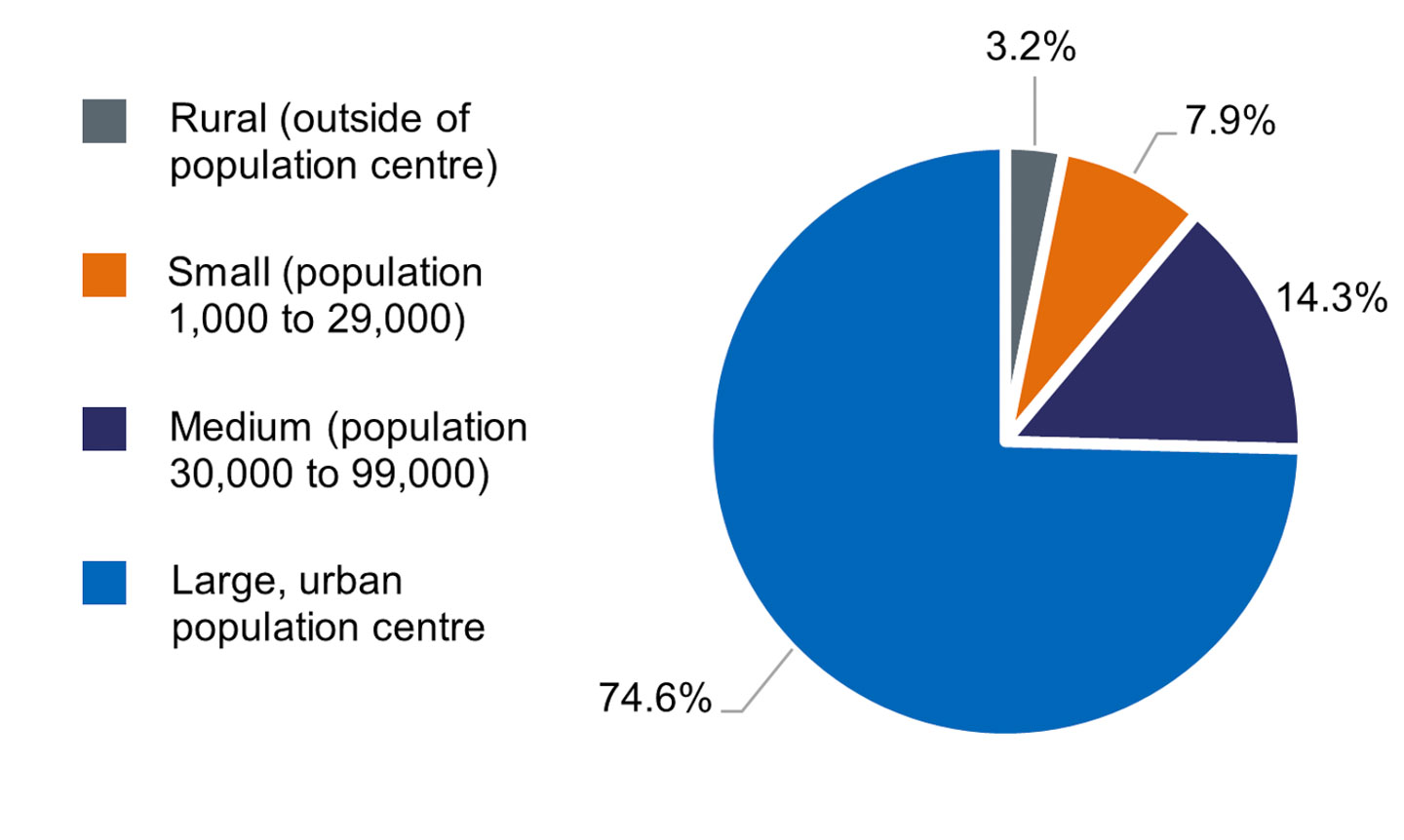
Most respondents were from Ontario, followed by Quebec, Alberta, Manitoba, British Columbia, New Brunswick, Prince Edward Island, Saskatchewan, Yukon, and Newfoundland and Labrador. No responses were collected from the Northwest Territories, Nova Scotia, and Nunavut (Figure 3). Of the 126 respondents who answered the question about their place of residence, the majority (74.6%) lived in large urban population centres (i.e., with a population of 100,000 or more). Few (3.2%) lived in rural areas (Figure 4).
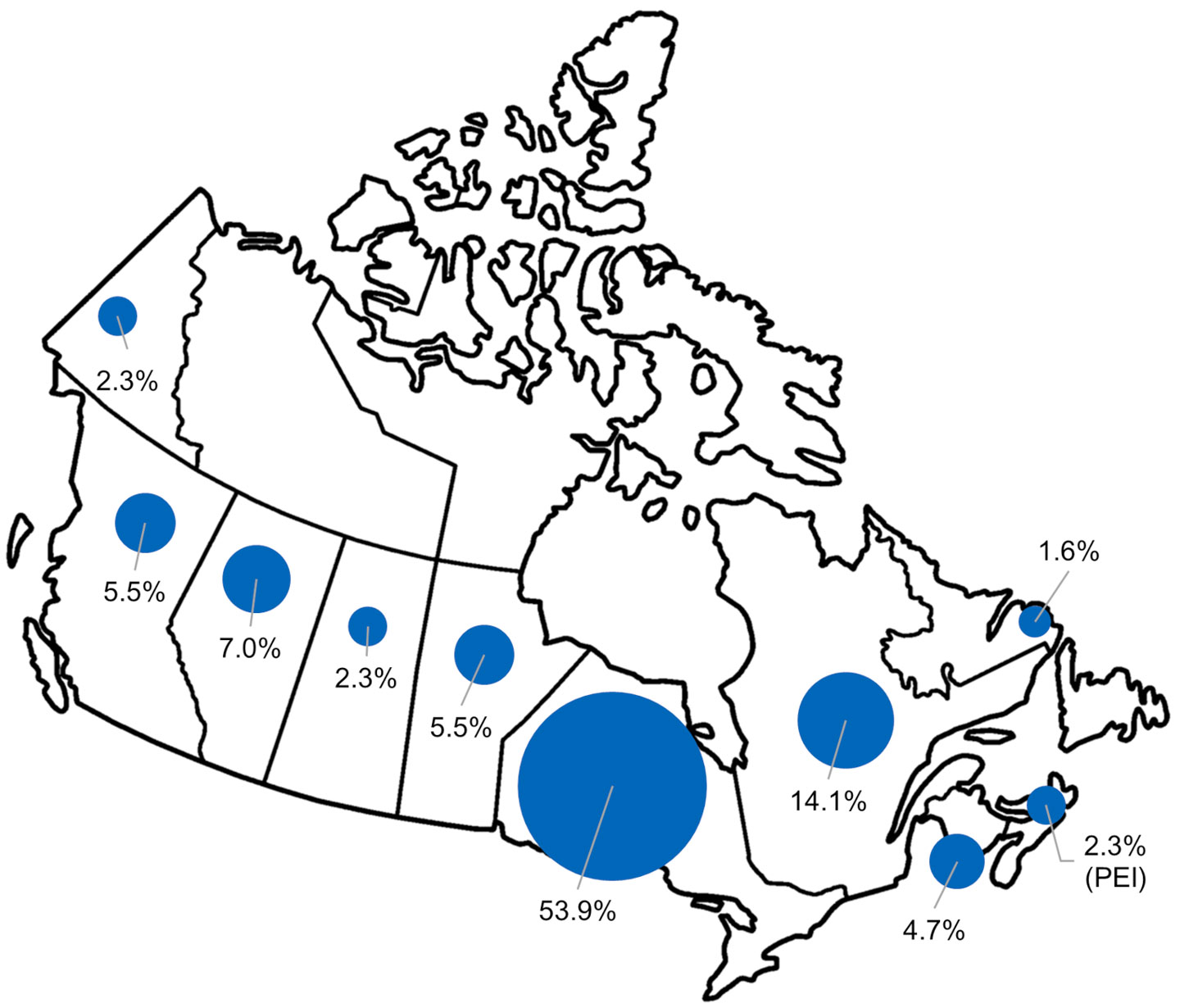
Figure 4: Survey Respondents’ Place of Residence or Location of Practice Based on Size of Population Centre (N = 126).
Summarizing Survey Responses
CADTH researchers reviewed all survey responses and removed out-of-scope items to create a long list of unique technologies and trends. The survey identified 311 technologies and trends of which 74 items were removed because they were considered out of scope. Technologies defined as drugs by Health Canada (such as most stem cell products), as well as technologies or trends without patient-related outcomes (e.g., health human resources or blockchain), and those not falling under our definition of “new” and “emerging” technology were removed. Trends such as real-world data, immunotherapy, gene therapy, and health systems–related responses were also removed.
Content analysis was used to organize the participants’ responses into meaningful technologies and trends categories. Three researchers independently sorted and coded the survey responses and regularly met with a third-party to resolve disagreements through discussion. A table was developed that listed the identified technologies and trends plus descriptions of their key characteristics, including their use cases, benefits and limitations, text excerpts from respondents’ answers, and the occupation profile of the respondent. Responses were not quantified because the sample was not intended to be representative. Survey responses were also used to inform summary descriptions about technologies and trends, their potential impact, and reasons for their disruptiveness to the Canadian health care system. The final long list included 47 items, of which 26 were technologies and 21 were technology trends.
Checking Evidence
A targeted grey literature search was used identify publicly available technology trends lists within 10 years to ensure no key technologies or trends were missed. The search was conducted on October 13, 2021, by searching sources listed in relevant sections of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist. Google was used to search for additional internet-based materials. No additional technologies and trends were identified from this search.
Setting Interim Priorities
From the long list of 47 technologies, the working group was tasked with narrowing down the list to 15 to 20 technologies and trends. The working group was provided a set of guiding questions about the innovative and disruptive nature of each item and a table summarizing the survey responses for each item. They used their own knowledge, experience, and expertise to support their decisions.
Based on their deliberation, the working group produced a short list of 16 technologies and trends. CADTH staff wrote descriptions about each of 16 items using information from the survey responses and supplemental searches. Additional items on the short list that did not make the top 10 list are presented in Appendix 2.
Workshop
The final prioritization workshop took place virtually on December 10, 2021. The workshop brought together 20 stakeholders to identify and prioritize the top 10 items from the short list of 16 technologies and trends. To ensure a balanced and diverse range of perspectives, workshop participants included people with lived experiences with health technologies, consumer advocates, health care professionals, government policy analysts, academic researchers, and industry representatives. Three members of the working group also participated in the workshop. Three CADTH staff members, including 1 who is an advisor with the JLA, facilitated the workshop sessions. The facilitators ensured that all participants were actively included in the discussion and that JLA’s principle of equal involvement was upheld. Another 21 individuals participated in the workshop as observers.
Before the workshop, participants were provided with a workshop guide, the 16-item short list with summaries about each technology and trend, and a participant priorities worksheet. Before attending the workshop, participants were asked to review and rank the technologies and trends in the short list using the participant priorities worksheet.
During the workshop, participants discussed the 16 technologies and trends on the short list; using a consensus-based approach, they ranked the order of their importance during 3 small group sessions and 1 plenary session. At the end of the workshop, participants reached consensus about the list and their ranking order for the 2022 Health Technology Trends to Watch: Top 10 List.
An overview of the selection process to develop the Top 10 List is provided in Appendix 3. The survey tool and the long list are also available. Additional materials related to the prioritization process and the workshop are available upon request via Requests@CADTH.ca.
Limitations
Some limitations to this research should be noted. The development of the Top 10 List was guided by the JLA PSP principles of equal involvement and inclusivity, transparency, and commitment to using and contributing to the evidence base. However, some aspects of the PSP process were modified to accommodate a shorter project timeline — 6 months instead of 12 months to 18 months typically required to conduct the JLA PSP process — and an online format was adopted to respect current COVID-19 safety measures.
The survey was a key tool used to obtain the views of a wide range of health care stakeholders in Canada. However, the survey sample was a limitation in the research design because it was not feasible or intended to be representative; rather, it aimed to capture insights from across the health technology landscape, including patients, health care providers, industry representatives, government officials, researchers, academics, and other people interested in the future of health care in Canada. The distribution and diversity of the respondents may not be fully representative of all health care stakeholders. In particular, there were no responses from the Northwest Territories, Nunavut, or Nova Scotia. The diversity and balance of perspectives of the working group members were intended to help reduce potential biases in the survey responses.
The categorization and clustering of individual technologies and trends can be difficult to place into discreet categories because there can be substantial overlap and interrelated innovations among different technologies and trends. Participants within both the working group and the final prioritization workshop had differing views about how to group certain technologies and trends. For example, some participants considered voice recognition technologies to be related to AI, whereas others considered it to be more related to mobile health care apps. Discussions within the project research team, the working group, and the workshop group helped to refine the categories; however, alternative grouping could be used in different contexts.
Appendix 2: Short List of Technologies and Trends Beyond the Top 10 List
These items are presented in the order in which they were ranked after the top 10 on the 16-item short list.
Augmented Reality and Virtual Reality
Augmented reality (AR) and virtual reality (VR) are emerging tools within the virtual care space. AR is the overlap of software-based graphics on top of real-world live images to enhance the experience, while VR provides software-based graphics that immerse the user in a different reality. Both AR and VR are beneficial for helping patients navigate the health care space and they can also be used in enhancing health professional training through stimulating and immersive environments. AR is also being explored for its applications in remote monitoring through integration with the smartphones, tablets, and other devices. Some of the applications for VR have been in mental health care, pain management, and palliative care. The use of AR and VR has offered cost-effective alternatives to different therapies, remote services, and training experiences for both the patient and health care provider.
Surgical Robots
A new generation of smaller, more specialized surgical robots have the potential to execute minimally invasive procedures less expensively and at greater speed and with greater accuracy than traditional surgical techniques. Robots are able to perform complicated and repetitive tasks, which are often susceptible to human error, without experiencing fatigue. Robotic assistance has increased in popularity for neurosurgical applications because surgeries involving the brain and spine require a high degree of technical proficiency. Broadly, surgical robots can aid in the diagnosis and treatment of neurologic disorders such as Alzheimer disease, Parkinson disease, strokes, aneurysms, degenerative diseases, and trauma to the spinal cord and brain. Specific procedures include stereotactic brain biopsies, stereoelectroencephalography for epilepsy treatment, spinal instrumentation, and neuroendovascular interventions. Bringing these technological advances into clinical practice may improve patient outcomes and also decrease wait times for surgery and length of hospital stays, should emerging evidence indicate so. Surgical robots may also help reduce health inequity by providing health care centres with staffing constraints the ability to perform complex neurosurgeries.
Transcatheter Heart Valves
Congenital heart defects, calcium buildup, high blood pressure, and a combination of other risk factors can contribute to heart valve impairments that can cause several cardiac conditions. With an aging population in Canada, degenerative heart valve conditions, such as aortic stenosis (in which the aortic valve narrows and constricts blood flow from the heart to the aorta), are a growing concern for health systems. Transcatheter heart valves are an emerging health technology that involves inserting a replacement valve through a catheter, which is a less invasive alternative to open heart procedures. For patients with different heart valve conditions who are at high risk of complications or fatality from surgery, transcatheter heart valves may provide a safer alternative to surgical repair or replacement procedures. The minimally invasive procedure may also reduce recovery times and length of hospital stays, which would have positive implications for health care systems. Assessing the cost-effectiveness of the procedure using real-world evidence and clinical trials will be important for informing future clinical use and health policy decisions about its availability.
Leadless Implantable Pulse Generators
Implantable leadless pulse generators are miniaturized cardiac electronic devices that, unlike traditional pacemakers, are powered by a small battery. The leadless pacemaker consists of a self-contained generator and electrode system; without wiring, it is 90% smaller than a transvenous pacemaker. These pulse generators are typically implanted directly into the right ventricle via a femoral vein transcatheter, which is a less invasive approach that does not require a chest incision or a visible subcutaneous generator pocket. Patients with permanent atrial fibrillation with bradycardia, bradycardia-tachycardia syndrome, or who infrequently require pacing are best suited for this type of pacemaker. Additionally, patients who have experienced an infection with a traditional transvenous pacemaker, or are at risk of developing one, may be better suited for a leadless device. Although leadless pulse generator batteries are expected to last over a decade, there are concerns regarding early-life battery failure in certain models.
UV Light Sterilization for Operating Rooms
Despite declining rates of infections in hospitals, health care–associated infections remain a challenge in Canada — up to 1 in 8 patients treated in intensive care units develop an infection. Antimicrobial resistance can exacerbate the harms of health care–associated infections and increase the risk of morbidity and mortality. UV sterilization is an emerging health technology that may be an effective adjunct to disinfection protocols used in both surgical operating rooms and patient rooms in hospitals. Devices using UV sterilization may help reduce the length of time needed to prepare and disinfect rooms after patient discharge by automating elements of cleaning protocols and limiting manual cleaning approaches, thereby improving clinical workflows. Safety features in emerging devices include sensors to ensure it is not activated while any person is present in the room and remote operation to prevent any UV exposure to health care staff or patients. Ongoing research examining the impact of UV sterilization on reducing health care–associated infections as well as operational considerations and potential cost-savings of emerging devices will be important to watch as hospitals begin to pilot different systems.
Bots and Digital Avatars
Robotics, specifically bots or digital avatars, can provide various methods of both formal and informal care. The benefits of including bots within health care include efficiency and enhancement of patient experiences. Bots can offer a wide range of technical support for health care providers. The design can be complex (e.g., using AI informed sensory technology to respond to human input) or basic depending on the use. Additionally, bots may relieve labour shortages within the health care system and may meet the need for increased care of an aging population. Bots can offer many practical health applications, including digital health care assistance, screening and triage, mental health care, and cardiovascular care.
Appendix 3: Overview of the Identification and Selection Process for Developing the Top 10 List
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca