CADTH Reimbursement Review
Andexanet Alfa (Ondexxya)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Reversal of FXa inhibitor anticoagulant effects
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
4F-PCC
4-factor prothrombin complex concentrate
AF
atrial fibrillation
ASD
absolute standardized difference
CanVECTOR
Canadian Venous Thromboembolism Research Network
CI
confidence interval
DOAC
direct oral anticoagulant
DVT
deep vein thrombosis
EAC
end point adjudication committee
eGFR
estimated glomerular filtration rate
EOB
end of bolus
ESS
effective sample size
FFP
fresh frozen plasma
FXa
factor Xa
GCS
Glasgow Coma Scale
GI
gastrointestinal
HHCS
Hartford HealthCare study
HR
hazard ratio
HRQoL
health-related quality of life
ICD-10
International Classification of Diseases, Tenth Revision
ICH
intracranial hemorrhage
ICU
intensive care unit
IPD
individual patient data
IPTW
inverse probability treatment weighting
IQR
interquartile range
ISTH
International Society on Thrombosis and Haemostasis
MID
minimal important difference
mRS
modified Rankin Scale
NICE
National Institute for Health and Care Excellence
NIHSS
National Institutes of Health Stroke Scale
OR
odds ratio
PCC
prothrombin complex concentrate
PE
pulmonary embolism
PSM
propensity score matching
RBC
red blood cell
RCT
randomized controlled trial
RWE
real-world evidence
SD
standard deviation
SLR
systematic literature review
TEAE
treatment-emergent adverse event
TFPI
tissue factor pathway inhibitor
VTE
venous thromboembolism
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Information on drug submitted for review | |
Drug product | Andexanet alfa (Ondexxya), 200 mg, powder for solution for infusion, IV infusion |
Sponsor | AstraZeneca Canada Inc. |
Indication | For adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding. |
Reimbursement request | As per indication |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC/c date | June 16, 2023 |
Recommended dose | Andexanet alfa is administered as an IV bolus, then as a continuous infusion.1
The recommended dosing is based on the specific FXa inhibitor, dose of FXa inhibitor, and time since the patient’s last dose of FXa inhibitor. |
FXa = factor Xa; NOC/c = Notice of Compliance with Conditions.
Introduction
Direct oral anticoagulants (DOACs), such as apixaban and rivaroxaban, are a class of anticoagulant commonly used for the prevention of stroke and embolisms in atrial fibrillation (AF) and venous thromboembolism (VTE).2,3 However, serious bleeding is a major risk associated with anticoagulant treatment and could manifest as gastrointestinal (GI) bleeding (30% to 45% risk), intracranial hemorrhage (ICH) (10% to 25%), and/or bleeding at a critical site (intraocular, pericardial, intraspinal, intra-articular).4-7 It is estimated that, in Canada, approximately 900,000 patients are on rivaroxaban or apixaban with an increase year over year of approximately 4%,8 and the annual risk of major bleeding is estimated to range from 2% to 4% in these patients.6,7,9 Factor Xa (FXa) inhibitor–related major bleeding events are associated with an increased risk of death; 30-day mortality estimates after FXa inhibitor–related major bleeding range from 9% to 45%.5,10-15
Reversal drugs for FXa inhibitors support the management of FXa inhibitor–related bleeding, in addition to cessation of anticoagulant therapy, initiation of resuscitation, application of local hemostatic measures, and administration of supporting therapy with blood products. To date, there is no available antidote in Canada to specifically reverse the anticoagulant effect of FXa inhibitors in the event of major bleeding. The usual care in the management of major bleeding associated with FXa inhibitors is the off-label use of prothrombin complex concentrate (PCC), a plasma-derived product that provides nonspecific supplementation of exogenous coagulation factors, although it does not directly reverse FXa inhibitor activity. Clinical trial evidence for PCC in treating FXa inhibitor–related bleeding is lacking and its use is primarily informed by the results of observational studies.16
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of andexanet alfa in adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to acute major bleeding, including life-threatening bleeds.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from the clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups, the Canadian Venous Thromboembolism Research Network (CanVECTOR) and the HeartLife Foundation, submitted input for this review. The input by CanVECTOR was informed by 33 interviews with patients with lived experience with VTE (deep vein thrombosis [DVT], n = 15; pulmonary embolism [PE], n = 6; both DVT and PE, n = 12) and varied treatment experience, including with warfarin, DOACs, and low-molecular-weight heparin.
According to the input by CanVECTOR, patients receiving treatment for VTE have to find a balance between the risk of another clot and managing the side effects of treatment. Patients expressed that bleeding is the most concerning potential side effect of VTE treatments and they may live with a fear of bleeding that can impact life choices and daily activities, quality of life, and mental health. The input noted that a variety of personal factors affect a patient’s treatment preferences. Many patients described the burden of treatment with warfarin (the inconvenience of blood monitoring, restrictions on diet and alcohol intake), or with low-molecular-weight heparin injections (pain, bruising, discomfort with self-injections) and some had later switched to a DOAC. The input noted fewer burdens with DOACs, but the lack of a reversal drug was mentioned by a few patients, for example, “However much I have my misgivings on Warfarin, it had one benefit. It was reversible. It had all the other things that were not attractive to it, but if you could make some of those things more attractive, or certainly if the new drug that would come on the market to replace or be an alternative to apixaban, if it had a reversibility aspect to it, I think would be attractive.” The HeartLife Foundation noted that the use of an FXa inhibitor can increase the risk of bleeding; as well, patients with heart failure may require invasive surgeries, which put them at risk of surgical bleeds. The group expressed a need for a treatment that can rapidly and effectively reverse the anticoagulant effect of an FXa inhibitor to prevent further bleeding and ensure the best possible outcome in patients who require urgent surgery or are experiencing life-threatening bleeds. This was echoed by the input from CanVECTOR, which highlighted that patients were concerned that the absence of a reversal drug for DOACs could prevent them from undergoing a surgery in case of an emergency: “If an accident happened and the surgery is almost immediate, a reversal agent can help me … [go] into the emergency surgery safely.” CanVECTOR also highlighted that some patients with a high risk of another clot will be prescribed blood thinners for the rest of their lives, and the experience could be daunting for a young person with decades of treatment ahead.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH noted there is an unmet need for a specific reversal drug for FXa inhibitor–related bleeding that can achieve rapid reversal of anticoagulation in patients with time-sensitive major bleeding. They also noted that PCC and blood products are not universally available in all clinical settings. As well, the risk of thrombosis carried by existing treatments is not well-characterized. The clinical experts expected that andexanet alfa would have the same place in therapy as PCC in the treatment of FXa inhibitor–related major bleeding. However, they were uncertain whether andexanet alfa or PCC should be the preferred therapy, and suggested this should be based on clinical presentation.
The clinical experts noted that patients receiving an FXa inhibitor who have major bleeding are potential candidates for andexanet alfa treatment. As well, patients who require emergency surgery while receiving an FXa inhibitor are also reasonable candidates in the clinical experts’ opinion, although the use of andexanet alfa was not studied in this patient population. The clinical experts noted that treatment candidates are identified based on clinical judgment with consideration of the patient’s clinical status (severity, bleed location, and response to nonspecific supportive measures) primarily, along with laboratory markers; clinicians in Canada most commonly use the International Society on Thrombosis and Hemostasis (ISTH) definition of major bleed. The clinical experts noted that patients with a minor bleed would not be suitable for andexanet alfa treatment since minor bleeds are expected to resolve on their own without the need for a reversal drug and with minimal patient harm.
The clinical experts noted that, in general, response to treatment is assessed based on hemostatic stability, hemostatic control (i.e., cessation of bleeding), need for blood transfusion, survival, and health-related quality of life (HRQoL). They considered it reasonable to allow prescribing by clinicians who have expertise in the management of acute major bleeds in a hospital setting. They noted that redosing with andexanet alfa is expected to be rare and should be done only in exceptional circumstances under the guidance of a transfusion medicine specialist, thrombosis physician, or hematologist, given the increased risk of thrombosis.
Clinician Group Input
The clinician group input was obtained from 5 clinician groups: Thrombosis Canada (represented by 2 clinicians), members of the Thrombosis and Anticoagulation Team at Dalhousie University (represented by 3 clinicians), faculty members at McMaster University in hematology and/or thromboembolism (represented by 5 clinicians), the Canadian Stroke Consortium (represented by 5 clinicians), and a journal club comprising local emergency department physicians in Peel Region (represented by 5 clinicians).
The clinician groups noted that current reversal treatments for bleeding associated with DOACs in patients who are receiving oral FXa inhibitors are nonspecific. The groups noted that PCCs, which are currently the treatment of choice for oral FXa reversal, have no effect on eliminating the active inhibitory action of oral FXa inhibitors and their use is considered off-label in the absence of robust clinical trial data supporting their efficacy or safety in this population. They noted that PCCs may promote a prothrombotic state and could potentially not be used safely in patients who have a history of heparin-induced thrombocytopenia or thrombosis, since a small amount of heparin may be present in PCC.
The clinician groups noted that andexanet alfa, being the only specific reversal drug available to patients who are on an FXa inhibitor, would be used as a first-line treatment in patients who require urgent anticoagulant reversal in the setting of serious, life-threatening bleeding or need for urgent surgery. One clinician group noted that PCCs would likely be used for an “average” patient who needs DOAC reversal, whereas andexanet alfa would be used in select patients with life-threatening bleeding that does not respond to supportive management (i.e., fluids, packed red blood cells [RBCs]), or patients with critical site bleeding (intracranial, spinal, pericardial) or in need of emergency (within 6 to 8 hours) or urgent (within 12 to 24 hours) surgery. They noted there is no established threshold for clinically significant hemostatic impairment and that most treatment centres do not have FXa inhibitor drug assays available, so treatment is usually considered based on the timing of the last dose, drug half-life, patient’s kidney or liver function, and examination findings (e.g., hypotension), radiographic findings (e.g., CT scans), and clinician judgment. They also noted that the patients who would be less suitable would be those who: last took their dose of FXa inhibitor more than 1 to 2 days ago (in the presence of normal renal function), have bleeding that is not life-threatening, or who can have their surgery delayed for 1 to 2 days after their last dose of an FXa inhibitor.
Outcomes to assess response to treatment deemed important by the clinician groups included: achievement of excellent or good hemostatic efficacy, thrombotic events, decreased mortality, decrease in hemoglobin or hematocrit by less than 20% compared with baseline, improvement of symptoms, reduction in hematoma expansion in ICH, survival to discharge, disability score on discharge, and measurement of anti-FXa levels before and after drug administration (not widely available). They noted that length of hospital stay may also be a surrogate marker. The clinical groups noted that criteria for discontinuation would include unexpected allergic or infusion reactions or thromboembolic events.
The clinical groups also supported the use of andexanet alfa in the hospital setting, including the emergency department, critical care unit, operating room, tertiary trauma centre, and stroke or neurosurgical referral centre, and administered by anesthesiologists or by surgical or other specialists such as those in emergency or internal medicine, depending on the site of the bleeding (e.g., neurologist or neurosurgeon for ICH, gastroenterologists for GI bleeding).
Drug Program Input
The drug programs expressed interest in understanding whether PCC is an appropriate comparator for andexanet alfa and the comparative efficacy and safety of andexanet alfa versus PCC, based on the submitted evidence. They also sought clinical expert input on the treatment approach for patients whose condition is not adequately managed by currently available treatments.
Other questions from the drug programs relate to: the initiation criteria, appropriateness of using andexanet alfa for edoxaban- and enoxaparin-related bleeding, sequencing of andexanet alfa relative to PCC, redosing, implementation issues related to idarucizumab, treatment eligibility in specific patient populations (pediatric patients, pregnant patients, and patients requiring emergency surgery in the absence of a life-threatening bleed), time required for reconstitution and administration of andexanet alfa relative to PCC, overdose management, requirement for laboratory tests for follow-up assessments, the logistics of dose assessment and accessing of drug products from transfusion medicine laboratories, assumptions of the pharmacoeconomic model, and drug utilization at the hospital level.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs. Refer to Table 4 for more details.
Clinical Evidence
Pivotal Studies and Randomized Controlled Trial Evidence
Description of Studies
One pivotal phase IIIb and IV, open-label, single-arm trial, ANNEXA-4 (N = 477),17 was included in the sponsor’s submission. The study assessed change in anti-FXa activity from baseline and whether hemostatic efficacy was reached with andexanet alfa treatment in adult patients with acute major bleeding while receiving FXa inhibitor treatment. Patients with features of severe ICH (i.e., Glasgow Coma Scale [GCS] score of less than 7 or an intracerebral hematoma volume above 60 cc) and those with an expected survival of less than 1 month were excluded from the study. Percent change from baseline in anti-FXa activity to on-treatment nadir and achievement of hemostatic efficacy at 12 hours postinfusion (coprimary end points), rebleeding, use of non–study-prescribed blood products and/or hemostatic drugs, RBC transfusion, change in neurologic status scores in patients with ICH (exploratory end points), and mortality (safety end point) were assessed. At baseline, patients (safety analysis set) had a mean age of 77.9 years (standard deviation [SD] = 10.66), with approximately half of them being male (54.3%) and the majority being white (86.8%). Most patients received apixaban (51.4%) or rivaroxaban (36.5%) anticoagulation and had an ICH (69.0%) or GI bleed (22.9%).
The sponsor submitted 2 pivotal phase III, double-blind, randomized controlled trials (RCTs), ANNEXA-A (N = 68) and ANNEXA-R (N = 80),18 comparing andexanet alfa and placebo with respect to the reversal of apixaban- (ANNEXA-A) or rivaroxaban-related (ANNEXA-R) anticoagulation in healthy volunteers; however, given that the study populations do not align with the indicated population for andexanet alfa, they were considered to have limited relevance to this review by the CADTH review team, in consultation with the clinical experts. Refer to the main body of the report for a brief summary of the study design and results.
Efficacy Results: ANNEXA-4
The efficacy end points that were noted to be important to patients and clinicians based on stakeholder input are summarized in Table 2.
All efficacy end points were assessed in the efficacy population except for rebleeding, use of non–study-prescribed blood products and hemostatic drugs, and RBC transfusion, which were assessed in the safety population. The efficacy population consisted of 347 of the 477 enrolled patients (73%) who met the ISTH-based criteria for bleeding severity and had baseline anti-FXa activity above the prespecified threshold (at least 75 ng/mL for apixaban- and rivaroxaban-treated patients, at least 40 ng/mL for edoxaban-treated patients, or at least 0.25 IU/mL for enoxaparin-treated patients). The safety population consisted of all 477 enrolled patients who received andexanet alfa treatment.
Table 2: Summary of Key Results From Pivotal Studies and RCT Evidence
Outcome | All patients |
|---|---|
Anti-FXa activity (efficacy population)a,b | |
Apixaban-treated patients, n | 172 |
Baseline (ng/mL), median (95% CI) | 146.9 (132.6 to 163.9) |
% change from baseline at on-treatment nadir (ng/mL),c,d median (95% CI) | −93.3 (−94.2 to −92.5) |
Rivaroxaban-treated patients, n | 130 |
Baseline, median (95% CI) | 213.5 (180.8 to 245.3) |
% change from baseline at on-treatment nadir (%),c,d median (95% CI) | −94.1 (−95.1 to −93.0) |
Hemostatic efficacy | |
Proportion of patients achieving “good” or “excellent” hemostatic efficacy at 12 hours after the EOIe (%) (95% CIf) | |
Efficacy population (N = 340) | 80.0 (75.3 to 84.1) |
P value | < 0.001 |
ICH subpopulation (N = 244) | 79.1 (73.5 to 84.0) |
High risk of hematoma expansion subgroup (N = 153) | 75.8 (68.2 to 82.4) |
Occurrence of rebleeding (safety population),g,h n/N (%) | 1/264 (0.4) |
Use of blood products and hemostatic drugs (safety populationh) | |
Patients who received 1 or more RBC transfusions by day 30, n/N (%) | 93/477 (19.5) |
95% CI of proportioni | 16.0 to 23.3 |
Use of non–study-prescribed blood products and/or hemostatic drugs, n/N (%)j | 118/477 (24.7) |
Clinical neurologic status (patients with ICH in efficacy populationb) | |
Modified Rankin Scale | |
Proportion of patients with modified Rankin Scale score of 0 to 2 (%) (95% CIi) | |
Baseline (n = 245) | 32.2 (26.4 to 38.5) |
1 hour (n = 146) | 22.6 (16.1 to 30.3) |
12 hour (n = 145) | 23.4 (16.8 to 31.2) |
Day 30 (n = 217) | 35.9 (29.6 to 42.7) |
National Institutes of Health Stroke Scalek | |
Baseline score, mean (SD) (n = 146) | 6.7 (6.33) |
Change from baseline in score, mean (SD) | |
1 hour (n = 139) | 0.4 (2.66) |
12 hour (n = 138) | 1.0 (3.58) |
Day 30 (n = 100) | −1.0 (4.96) |
Glasgow Coma Scalek | |
Baseline score, mean (SD) (n = 242) | 13.9 (1.72) |
Change from baseline in score, mean (SD) | |
1 hour (n = 141) | −0.4 (1.69) |
12 hour (n = 140) | −0.6 (2.06) |
Day 30 (n = 107) | 0.2 (2.23) |
Harms (safety population) | |
TEAEs, n (%) | 346 (72.5) |
Serious TEAEs, n (%) | 200 (41.9) |
Withdrawal from treatment due to TEAE, n (%) | 4 (0.8) |
Deaths, n (%) | 81 (17.0) |
Notable harms (safety population) | |
Thrombotic eventl | 50 (10.5) |
Infusion-related reaction | 2 (0.4) |
Neutralizing antibodies to FX, FXa, or andexanet alfa | 0 |
CI = confidence interval; EOI = end of infusion; FXa = factor Xa; GCS = Glasgow Coma Scale; ICH = intracranial hemorrhage; ISTH = International Society on Thrombosis and Hemostasis; NIHSS = National Institutes of Health Stroke Scale; RBC = red blood cell; RCT = randomized controlled trial; SD = standard deviation; TEAE = treatment-emergent adverse event.
Note: Outcomes summarized in this table were noted to be important to patients and clinicians based on input received from patient groups, clinician groups, and the clinical experts consulted by CADTH. Unless otherwise specified, safety data were presented by Medical Dictionary for Regulatory Activities (MedDRA) preferred term.
The details in the table were taken from the sponsor’s summary of clinical evidence.20
aResults were presented by FXa inhibitor received. Results of edoxaban- and enoxaparin-treated patients were not of interest to this review and, hence, not summarized.
bThe efficacy population consisted of 347 patients (73%) who met the ISTH-based criteria for bleeding severity and with baseline anti-FXa activity above the prespecified threshold (at least 75 ng/mL for apixaban- and rivaroxaban-treated patients, at least 40 ng/mL for edoxaban-treated patients, or at least 0.25 IU/mL for enoxaparin-treated patients). The safety population consisted of all 477 enrolled patients who received andexanet alfa treatment.
cThe on-treatment nadir was defined as the minimum value observed from the start of andexanet alfa administration (30 minutes after bolus) to 30 minutes before EOI. If results of both time points are missing, then it was equal to the baseline value.
fFor patients with missing values for nadir, change and percent change were imputed as zero. The 95% CI for the median was based on the distribution-free method.
eAchievement of hemostatic efficacy refers to patients with “excellent” or “good” hemostatic efficacy as adjudicated by the end point adjudication committee. Patients who were adjudicated as non-evaluable for clinical reasons were included in the efficacy population and considered as having “poor or none” hemostatic efficacy. Patients adjudicated as non-evaluable for administrative reasons (n = 7) were excluded.
fCI based on the exact binomial method.
gRebleeding was defined as recurrent bleeding from the same (or different) anatomic site in patients within 24 hours of initial andexanet alfa treatment and after achieving initial good or excellent hemostasis, as adjudicated by the end point adjudication committee.
hThe safety population consisted of all 477 enrolled patients who received andexanet alfa treatment.
iCI based on the Fischer exact method.
jRefers to the use of these treatments between the start of andexanet treatment and 12 hours after the EOI. They included platelets, 4-factor prothrombin complex concentrate, fresh frozen plasma, antithrombin III, human albumin, plasma, vitamin K, packed RBC transfusion, tranexamic acid, carbazochrome sodium sulfonate hydrate, phenylephrine, and other blood or coagulation treatments.
kNIHSS testing and the additional GCS assessments were not implemented until Protocol Amendment 4; therefore, the number of patients evaluated was lower for the baseline NIHSS and the later time points for GCS.
lAs adjudicated by the end point adjudication committee.
Source: ANNEXA-4 Clinical Study Report.19
Change From Baseline in Anti-FXa Activity (Coprimary End Point)
In the primary analysis, the median percent change from baseline in anti-FXa activity at on-treatment nadir (i.e., minimum value between end of bolus [EOB] and end of infusion) was −93.3% (95% confidence interval [CI], −94.2% to −92.5%) in apixaban-treated patients and −94.1% (95% CI, −95.1% to −93.0%) in rivaroxaban-treated patients in the efficacy population. A subgroup analysis showed results consistent with the primary analysis across bleed types; however, a subgroup analysis by estimated glomerular filtration rate (eGFR) is not available. Results in the safety population showed results consistent with the primary analyses.
Achievement of Hemostatic Efficacy (Coprimary End Point)
In the primary analysis of hemostatic efficacy, 80.0% (95% CI, 75.3% to 84.1%) of the efficacy population achieved “good” or “excellent” hemostatic efficacy. The lower bound of the 95% CI was greater than the predefined threshold of 50%, which is sufficient to reject the null hypothesis at the 0.05 level. Three sensitivity analyses were conducted to assess the effect of including patients rated as “non-evaluable for administrative reasons” among all patients with nonmissing baseline anti-FXa level, and in patients otherwise evaluable but with a baseline anti-FXa level below a prespecified threshold. The results of all sensitivity analyses and estimates within the subgroups of interest (by bleed type and eGFR) were consistent with the primary analysis.
The results of a hemostatic efficacy analysis in patients with ICH with a high risk of hematoma expansion (exploratory end point) were consistent with the whole ICH subpopulation as well as the efficacy population.
Rebleeding, Use of Non–Study-Prescribed Blood Products and Hemostatic Drugs, RBC Transfusion (Exploratory End Points)
In the safety population, rebleeding as adjudicated by the end point adjudication committee (EAC) occurred in 1 of 264 assessed patients (0.4%); 24.7% of patients received non–study-prescribed blood products and/or hemostatic drugs between the start of andexanet alfa treatment and 12 hours after the end of the infusion, and 19.5% (95% CI, 16.0% to 23.3%) of patients received RBC transfusion.
Modified Rankin Scale, National Institutes of Health Stroke Scale, and GCS Scores (Exploratory End Point)
The proportions of patients with ICH in the efficacy population who had a modified Rankin Scale (mRS) score of 0 to 2 at baseline, 1 hour posttreatment, 12 hours posttreatment, and at day 30 were 32.2% (95% CI, 26.4% to 38.5%), 22.6% (95% CI, 16.1% to 30.3%), 23.4% (95% CI, 16.8% to 31.2%), and 35.9% (95% CI, 29.6% to 42.7%), respectively.
The mean change from baseline in National Institutes of Health Stroke Scale (NIHSS) score at 1 hour posttreatment, 12 hours posttreatment, and day 30 was 0.4 (SD = 2.66), 1.0 (SD = 3.58), and −1.0 (SD = 4.96), respectively, in patients with ICH.
The mean change from baseline in GCS score 1 hour posttreatment, 12 hours posttreatment, and day 30 was −0.4 (SD = 1.69), −0.6 (SD = 2.06), and 0.2 (SD = 2.23), respectively, in patients with ICH.
Intensive Care Unit Admission, Hospital Length of Stay, and HRQoL (Other Outcomes of Interest to This Review)
Intensive care unit (ICU) admission and HRQoL were not measured. Length of hospital stay was not an efficacy outcome of the trials but the median was reported to be 10.9 days in the safety population.
Harms Results: ANNEXA-4
A summary of harms in the ANNEXA-4 trial is shown in Table 2.
A treatment-emergent adverse event (TEAE) was reported in 72.5% of patients, with the most common TEAEs being urinary traction infection (10.5%) and pneumonia (8.2%). Serious TEAEs were reported in 41.9% of patients, with the most common being pneumonia (4.2%), respiratory failure (2.5%), and ischemic stroke (2.1%). Four patients (0.8%) discontinued treatment due to TEAEs. Death occurred in 17.0% of patients.
A thromboembolic event was reported in 10.5% of patients, including cerebrovascular accident (4.6%), DVT (2.5%), myocardial infarction (1.9%), PE (1.0%), and transient ischemic attack (0.4%). Infusion-related reaction was reported in 2 patients (0.4%). There was no report of neutralizing antibodies to FX, FXa, or andexanet alfa.
Critical Appraisal: ANNEXA-4
An important limitation was the noncomparative study design, which precludes conclusions on whether any observed effect could be attributed to andexanet alfa alone due to the lack of consideration for potential confounders. The open-label study design could increase uncertainty in neurologic status outcomes (mRS, NIHSS, and GCS) due to potential reporting bias, given that these scales involve the subjective assessment of clinical parameters by the investigators, although the presence and extent of such bias could not be determined. All end points other than the coprimary end points were exploratory, which precludes definitive conclusions to be drawn from these analyses. Approximately 20% of patients were excluded from the primary efficacy analyses due to baseline anti-FXa activity below the prespecified threshold, and the impact of excluding such patients from neurologic status outcomes is unclear, since no sensitivity analyses were conducted. There is also potential attrition bias in neurologic status outcomes, given the large amount of missing data, although the direction and extent of bias are unclear.
The generalizability of the study population is limited due to the younger patient population and the exclusion of patients with severe ICH (GCS score less than 7, estimated intracerebral hematoma volume above 60 cc) and an expected survival of less than 1 month, which were suggestive of a study population with a better prognosis than in general clinical practice, based on clinical expert input. Patients without major bleeding but requiring FXa inhibitor reversal for emergency surgery, who are also expected to be reasonable candidates for andexanet alfa according to clinical expert input, were not included in the study; the treatment effects in these patients are unknown. According to the clinical experts, the coprimary end points were not as clinically relevant and meaningful to patients and clinicians compared with clinical outcomes, such as mortality, morbidity, and functional status, which were assessed as exploratory end points in the study. They noted that anti-FXa activity is not routinely measured in clinical practice during FXa inhibitor reversal treatment nor widely available; while hemostatic efficacy is a commonly measured outcome in clinical studies of reversal treatments for major bleeds, it is not a patient-important outcome. The absence of direct comparative evidence between andexanet alfa and PCC, the most relevant comparator for andexanet alfa per clinical expert input, represents a gap in evidence.
Studies Addressing Gaps in the Pivotal and RCT Evidence
Weighted Comparative Observational Evidence
Description of Studies
In the absence of direct comparative evidence between andexanet alfa and PCC, the sponsor submitted 3 published observational analyses assessing the comparative effect of andexanet alfa versus PCC in patients with major bleeding while receiving apixaban- or rivaroxaban-related anticoagulation, based on individual patient data (IPD) from the ANNEXA-4 trial and 3 observational cohort studies of PCC in real-world clinical practice, including the ORal ANticoagulant aGEnt-Associated Bleeding Events Reporting System (ORANGE) study, the Hartford Health care study (HHCS), and the German-Wide Multicenter Analysis of Oral Anticoagulant-Associated Intracerebral Hemorrhage Part Two (RETRACE-II) study.21-23
The analysis of the ANNEXA-4 trial versus the ORANGE study was conducted in patients with any bleed type using propensity score matching (PSM). The analysis of the ANNEXA-4 trial versus the HHCS was conducted in patients with ICH using propensity score overlap weighting. The analysis of the ANNEXA-4 trial versus the HHCS was conducted in patients with atraumatic ICH based on a propensity score model using the inverse probability treatment weighting (IPTW) approach. Outcomes assessed included 30-day mortality, in-hospital mortality, hemostatic efficacy (or hematoma expansion, which reflects failure to achieve hemostatic efficacy in ICH), mRS score at discharge or at day 30, and thrombotic event at day 5.
ANNEXA-4 Trial Versus ORANGE Study (Any Bleed Type)
The analysis included 322 patients in the andexanet alfa cohort from the ANNEXA-4 trial and the effective sample size (ESS) of the PCC cohort from the ORANGE study was 88 after PSM. Results of the 30-day mortality analysis estimated results in favour of andexanet alfa versus PCC in both the whole cohort (relative risk = 0.43; 95% CI, 0.29 to 0.63) and ICH cohort (relative risk = 0.31; 95% CI, 0.20 to 0.48). A reduced risk of 30-day mortality in the GI cohort (relative risk = 0.49; 95% CI, 0.21 to 1.16) and an increased risk with andexanet alfa in other bleeds (relative risk = 1.29; 95% CI, 0.17 to 9.55) were shown, but the results did not show a significant difference between the interventions. Harms were not assessed in this study.
ANNEXA-4 Trial Versus the HHCS (ICH Only)
The analysis included 107 patients in the andexanet alfa cohort from the ANNEXA-4 trial and 95 patients in the 4-factor PCC (4F-PCC) cohort from the HHCS. After weighting, results were in favour of andexanet alfa over 4F-PCC with respect to hemostatic efficacy (weighted odds ratio [OR] = 2.733; 95% CI, 1.163 to 6.421) and 30-day all-cause mortality (weighted OR = 0.355; 95% CI, 0.129 to 0.977). Thromboembolism occurred in 2 patients (1.9%) in the andexanet alfa cohort and 0 patients in the 4F-PCC cohort within 5 days posttreatment.
ANNEXA-4 Trial Versus the RETRACE-II Study (Atraumatic ICH Only)
In the subanalysis of patients receiving andexanet alfa (n = 85) or PCC (n = 73), after weighting, results were in favour of andexanet alfa over PCC with respect to hematoma expansion (risk ratio = 0.443; 95% CI, 0.223 to 0.878) but did not show a difference between the interventions in in-hospital mortality (hazard ratio = 0.852; 95% CI, 0.397 to 1.827) and mRS score at discharge or at 30 days (mean difference = −0.517; 95% CI, −1.146 to 0.113). Harms were not assessed in this study.
Critical Appraisal
Several important limitations were common to the 3 weighted comparative analyses that preclude drawing definitive conclusions regarding the comparative efficacy of andexanet alfa versus PCC. This includes a risk of selection bias for studies included in the analyses, given the absence of a systematic literature review (SLR) or the lack of reporting in SLR methods. Furthermore, there was evidence of heterogeneity in the inclusion and exclusion criteria between the included studies (e.g., definition of major bleeding, recent history of blood products, definition of ICH severity, recent history of thromboembolism, expected survival). There was also potential residual confounding due to inadequate adjustment for prognostic factors or treatment-effect modifiers; specifically, the studies were adjusted for covariates inconsistently and the resulting estimates varied widely. Lastly, the comparative efficacy of andexanet alfa and PCC for mental status, ICU admission, length of hospital stay, and HRQoL, all of which were of interest to the stakeholders, were not assessed.
Comparative Observational Evidence
Description of Studies
In the absence of direct comparative evidence between andexanet alfa and PCC, the sponsor submitted 6 studies summarizing the comparative evidence of andexanet alfa versus PCC in real-world clinical practice. All 6 studies were multicentre, retrospective hospital chart audits conducted in the US. The patient population for Coleman et al. (2021),24 Dobesh et al. (2022),25 Fermann et al. (2022),26 and Dobesh et al. (2023)27 were sourced from US Hospital Chart Audit, while the populations for Sutton et al. (2022)28 and Sutton et al. (2023)29 were sourced from US Department of Veterans Affairs databases. In all studies, data were captured from electronic medical records. The eligible patient population comprised adult patients aged 18 years and older hospitalized for FXa inhibitor–related bleeding. Patients were identified through electronic medical records using International Classification of Diseases, Tenth Revision (ICD-10) billing codes,24-27 or administrative claims and pharmacy dispensation information from the Veterans Affairs Informatics and Computing Infrastructure.28,29 Outcomes of interest were stratified by bleed type for each reversal or replacement agent (i.e., andexanet alfa and PCC) and included in-hospital mortality,24-27,29 in-hospital 30-day mortality,28 length of hospital stay,24,25,29 and ICU length of stay.24,25,29
Study sample size ranged from 255 to 4,395 patients. The average age of patients across the studies ranged from 65.0 years to 70.1 years. The most commonly used FXa inhibitors documented were apixaban (range, 40% to 84.0%) and rivaroxaban (range, 14.5% to 56%). Exposure to andexanet alfa ranged from 11.3% to 48.8% across the studies, while exposure to 4F-PCC ranged from 24.2% to 80.1%.
In-Hospital Morality
In-hospital mortality for those treated with andexanet alfa was 4% in Coleman et al. (2021), 6% in Dobesh et al. (2022) and (2023), and 10.6% in Sutton et al. (2022). In-hospital mortality for those treated with 4F-PCC was 10% in Coleman et al. (2021), 8% in Dobesh et al. (2022), 10.6% in Dobesh et al. (2023), and 25.3% in Sutton et al. (2022). In Coleman et al. (2021), in-hospital mortality was 11% in those treated with fresh frozen plasma (FFP). In Fermann et al. (2022), in-hospital mortality among patients treated with andexanet alfa was approximately 2.5% among patients with a GI bleed and ranged from 9.8% to 16.8% among patients with ICH; in patients treated with 4F-PCC, in-hospital mortality ranged from 3.2% to 6.0% among patients with a GI bleed and 14.5% to 24.0% in patients with ICH.
In the adjusted analysis performed by Dobesh et al. (2022), treatment with andexanet alfa was associated with a lower likelihood of death compared with treatment with 4F-PCC (OR = 0.69; 95% CI, 0.49 to 0.98). In Dobesh et al. (2023), treatment with andexanet alfa was also associated with a lower likelihood of in-hospital mortality compared with 4F-PCC across all bleeds (OR = 0.50; 95% CI, 0.39 to 0.65), GI bleeds (OR = 0.49; 95% CI, 0.29 to 0.81), and ICH (OR = 0.55; 95% CI, 0.39 to 0.76). In the adjusted analysis performed by Fermann et al. (2022), treatment with andexanet alfa was associated with lower odds of in-hospital mortality compared with treatment with 4F-PCC (OR = 0.67; 95% CI, 0.48 to 0.94). In Sutton et al. (2022), treatment with andexanet alfa was associated with a lower hazard of in-hospital mortality compared with treatment with 4F-PCC (hazard ratio [HR] = 0.31; 95% CI, 0.14 to 0.71).
30-Day Hospital Mortality
Thirty-day hospital mortality was explored in Sutton et al. (2022) only. The 30-day mortality rate was 20.0% and 32.4% in patients treated with andexanet alfa and 4F-PCC, respectively. Treatment with andexanet alfa was associated with a lower hazard of 30-day mortality compared with treatment with 4F-PCC (HR = 0.54; 95% CI, 0.30 to 0.98).
ICU Length of Stay
For patients who received andexanet alfa, the overall median ICU length of stay was 2 days (interquartile range [IQR] = 1 to 4) in Coleman et al. (2021), 2 days (IQR = 3) in Dobesh et al. (2022), and 1 day (IQR = 0 to 4) in Sutton et al. (2022). In Sutton et al. (2023), the mean lCU length of stay was 4.0 days (SD = 7.1). For patients who received 4F-PCC, the median ICU stay was 3 days (IQR = 2 to 5) in Coleman et al. (2021), 2 days (IQR = 3) in Dobesh et al. (2022), and 2 days (IQR = 0 to 5) in Sutton et al. (2022). In Sutton et al. (2023), the mean length of ICU stay was 5.0 days (SD = 8.6). In Coleman et al. (2021), the overall median ICU stay for patients who were treated with FFP was 3 days (IQR = 2 to 5).
Hospital Length of Stay
For patients who received andexanet alfa, the median hospital length of stay was 5 days (IQR = 3 to 6) in Coleman et al. (2021), 5 days (IQR = 5) in Dobesh et al. (2022), and 6 days (IQR = 3 to 10) in the Sutton et al. (2022) study. In Sutton et al. (2023), the mean length of stay was 11.3 days (SD = 22.8) while, in Fermann et al. (2022), the mean length of stay ranged from 6.4 (SD = 4.2) to 8.9 (SD = 6.2) days. For patients who received 4F-PCC, the median hospital stay was 5 days (IQR = 4 to 7) in Coleman et al. (2021), 5 days (IQR = 5) in Dobesh et al. (2022), and 7 days (IQR = 4 to 18) in Sutton et al. (2022). In Sutton et al. (2023), the mean length of hospital stay was 12.2 days (SD = 17.5) while, in Fermann et al. (2022), the mean length of hospital stay ranged from 6.3 (SD = 4.1) to 8.3 (SD = 6.2) days. In Coleman et al. (2021) the median length of hospital stay for patients who were treated with FFP was 5 days (IQR = 4 to 8).
Critical Appraisal
The nonrandomized comparison of the 6 real-world evidence (RWE) studies makes interpretation of the efficacy of andexanet alfa compared with 4F-PCC and other reversal or replacement agents challenging. The retrospective nature of the studies meant that data collection and entry were dependent on the personnel at each medical institution; thus, the quality and accuracy of data were dependent on the quality and accuracy of routine documentation. Moreover, the use of ICD-10 codes is associated with limitation for the purpose of clinical research.30,31 The influence of an important patient-level factor (e.g., advanced directives, thrombotic complications after administration of a reversal agent) — which could not be ascertained from medical records — on the treatment effect of andexanet alfa and 4F-PCC could not be ruled out. Although Dobesh et al. (2022), Dobesh et al. (2023), Fermann et al. (2022), and Sutton et al. (2022) employed covariate adjustment, there is a possibility of selection bias or residual confounding due to the nonrandomized nature of the study designs and a lack of any comprehensive literature to assess the relevant confounding variables. As a result, there is uncertainty around the comparative treatment effects of andexanet alfa compared with 4F-PCC due to selection bias and unmeasured and residual confounding that cannot be entirely ruled out.
Conclusions
One pivotal single-arm, open-label, phase IIIb and IV trial (ANNEXA-4) provided evidence regarding the efficacy and safety of andexanet alfa in the treatment of patients with acute major bleeding while receiving FXa anticoagulation. Results of clinically relevant outcomes, including 30-day mortality, neurologic status, rebleeding, need for blood products and hemostatic drugs, and length of hospital stay, were generally in line with the clinical experts’ clinical experience with PCC. Analyses of hemostatic efficacy and anti-FXa activity also lent support to the ability of andexanet alfa to achieve hemostasis and reduce the anticoagulant activity of FXa inhibitors. However, there was uncertainty in the magnitude of clinical benefit attributable to andexanet alfa, given the inherent limitations of a noncomparative study design. The generalizability of study findings was also limited by the younger study population compared with clinical practice, and the exclusion of patients with severe ICH and patients with expected survival of less than 1 month. Three weighted comparative observational studies and 6 comparative observational studies assessed the comparative efficacy of andexanet alfa versus PCC in real-world clinical practice; however, the results were inconclusive due to important methodological limitations (e.g., selection bias, inadequate adjustment for prognostic factors and effect modifiers) of these studies. The safety profile of andexanet alfa in the pivotal trial appeared to be consistent with PCC, per clinical expert input. One weighted comparative analysis suggested the frequency of thrombotic events was similarly low for both andexanet alfa and PCC within 5 days posttreatment, although results are uncertain due to the aforementioned limitations of the analysis.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of andexanet alfa 200 mg powder solution for IV infusion in adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to acute major bleeding.
Disease Background
The contents of this section were informed by materials submitted by the sponsor and clinical expert input. The following was summarized and validated by the CADTH review team.
DOACs, also known as non–vitamin K antagonist oral anticoagulants, are a class of anticoagulant that directly inhibit specific enzymes within the coagulation cascade.32,33 DOACs include oral FXa inhibitors (i.e., apixaban, rivaroxaban, edoxaban) that work by selectively blocking the active site of FXa. These drugs are used for a number of different indications, including the prevention of strokes and embolisms in individuals with AF and VTE.2,3 However, unanticipated, serious bleeding is a major risk associated with anticoagulant treatment that may occur spontaneously or following trauma, complications from invasive procedures, or other illnesses and conditions. It is estimated that, in Canada, approximately 900,000 patients are on rivaroxaban and apixaban, with an increase year over year of approximately 4%.8 According to the literature, FXa inhibitors consistently show that the annual risk of major bleeding ranges from 2% to 4%.6,7,9 Major FXa inhibitor–associated bleeds may occur in several critical sites, including intracranial, intraocular, pericardial, intraspinal, and intra-articular, or bleeding in the GI region. The most frequent type of major bleed related to FXa inhibitor use are GI bleeds, which account for 30% to 45% of all major bleeds, and ICHs, which account for between 10% to 25% of major bleeding events.4-7 FXa inhibitor–related major bleeding events are associated with an increased risk of death; in fact, 30-day mortality after FXa inhibitor–related major bleeding can range from 9% to 45%.5,10-15 In particular, a retrospective cohort study conducted in Ontario found that, in patients with ICH, 30-day mortality rates were approximately 34.7%.15 Alternative sources report that the 30-day mortality rate for ICH may be as high as 45%.10,13,14 The ARISTOTLE trial reported that all-cause mortality within 30 days of a GI bleed was approximately 9.2%,5 with additional trials from the US reporting 30-day mortality rates of approximately 14%.34 Major bleeds are managed through hemostatic measures or interventions to stop the bleed at its source, and additional supportive measures like fluid replacement or transfusion products can further help stabilize the patient.16,35 As anticoagulants exacerbate bleeding episodes, specific reversal drugs are required to stop the activity of the anticoagulant to further stabilize the patient or attempt to save the patient’s life.11,36 To date, there is no available antidote in Canada to specifically reverse the anticoagulant effects of FXa inhibitors in the event of major bleeding.
Several patient-specific risk factors have been identified that increase the risk for bleeding in patients receiving FXa inhibitors, including active or metastatic cancer, increasing age (e.g., > 65 years), genetic factors affecting vitamin K antagonist metabolism and antithrombotic effect, comorbidities (e.g., hypertension, diabetes, renal insufficiency, liver disease, chronic obstructive pulmonary disease, cardiomyopathy, peripheral vascular disease), concomitant medications (e.g., nonsteroidal anti-inflammatory drugs, antiplatelets), history of bleeding, previous stroke, recent surgery, thrombocytopenia, anemia, and alcohol abuse.11,12 Regrettably, some of these factors are expected to increase the use of FXa in Canada as the population ages, increasing the risk for thromboembolic conditions and thus the need for anticoagulation therapies. Recently, prescriptions for rivaroxaban and apixaban have increased in Canada following their addition to provincial formularies for stroke prevention in patients with AF.
Standards of Therapy
The contents of this section were informed by materials submitted by the sponsor and clinical expert input. The following was summarized and validated by the CADTH review team.
PCC, an off-label, plasma-derived, prohemostatic agent, is the usual care in Canada for managing major bleeding associated with FXa inhibitors. Clinical practice guidelines from bodies such as Thrombosis Canada, Canadian Cardiovascular Society, and Canadian Heart Rhythm Society support the use of PCC if a specific antidote is not available.16,37 The American College of Gastroenterology and Canadian Association of Gastroenterology have noted that the selective use of PCC may be clinically justifiable in some patients who have taken DOACs within the 24 hours preceding a life-threatening GI bleed; however, they could not recommend routine use of PCC for patients with GI bleeding receiving DOAC due to the uncertainty of the available evidence.38
PCC helps control bleeding by providing nonspecific supplementation of exogenous coagulation factors but does not directly reverse FXa inhibitor activity. Clinical trial evidence for PCC in treating FXa inhibitor–related bleeding is lacking and its use is primarily informed by results of small observational studies.16 Adjunctive use of anti-fibrinolytic treatment, most commonly tranexamic acid in Canada, may also be considered in managing FXa inhibitor–associated bleeding in select patients.16 None of the existing treatments have a specific mechanism of action targeting the reversal of FXa inhibitors.
In addition to PCC and adjunctive tranexamic treatments, major bleeding is managed by pausing anticoagulant therapy, initiating resuscitation, applying local hemostatic measures (including surgical measures), and administering supportive therapy with blood products (e.g., RBC, platelets, fibrinogen concentrate, cryoprecipitate, and plasma).16
The key goals of treatment in patients with an acute major bleed include improving survival, achieving hemodynamic stability, and avoiding thrombotic complications, according to the clinical experts consulted by CADTH. In patients with ICH, additional important treatment goals related to neurologic recovery are reducing morbidity and improving function, enabling an ability to return to independent living, and HRQoL. Avoidance of transfusion and ICU admission can also be patient-important outcomes.
Drug Under Review
The key characteristics of andexanet alfa and 4F-PCC for rapid reversal of anticoagulation are summarized in Table 3.
Andexanet alfa is a recombinant modified human FXa protein that lacks procoagulant or anticoagulant activity and acts as an antidote for apixaban and rivaroxaban by binding these FXa inhibitors in the plasma, thereby freeing endogenous FXa to resume its normal function in hemostasis.1 In addition to reversing the anticoagulant effect of drugs that target FXa, andexanet alfa binds to tissue factor pathway inhibitor (TFPI), an endogenous, naturally occurring anticoagulant that normally circulates in very low concentrations in plasma. TFPI binds reversibly to FXa, and the resulting TFPI–FXa complex inhibits the tissue factor–factor VIIa complex, which plays a key role in the activation of the tissue factor pathway, leading to thrombin generation. When andexanet alfa binds to TFPI, circulating TFPI concentrations are reduced, which may lead to increased thrombin generation.
This is the first review for andexanet alfa by CADTH. Andexanet alfa was granted a Health Canada Notice of Compliance with Conditions on June 16, 2023. The reimbursement request aligns with the Health Canada indication, which is for adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding. Andexanet alfa was approved by the FDA on May 3, 2018, for patients treated with rivaroxaban and apixaban when reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding.39 It was approved by the European Medicines Agency on April 26, 2019, and by the Medicines and Health care products Regulatory Agency in the UK on May 13, 2022, for the same indication. In its guidance issued on May 12, 2021, the National Institute for Health and Care Excellence (NICE) andexanet alfa is recommended as an option for reversing anticoagulation from apixaban or rivaroxaban in adults with life-threatening or uncontrolled bleeding only if the bleed is in the GI tract and the company supplying the andexanet alfa provides it according to a commercial arrangement. For ICH, NICE recommended that andexanet alfa be used only in research.
Andexanet alfa is administered as an IV bolus with a target rate of 30 mg/minute followed by continuous infusion for up to 120 minutes. Dosage is based on the specific oral FXa inhibitor, the dose, and the time since the patient’s last dose of the inhibitor.1 A low dose with an initial IV bolus of 400 mg and a follow-on infusion of 4 mg/minute for 120 minutes (480 mg) is indicated for a rivaroxaban dose of 10 mg or less, or an apixaban dose of 5 mg or less where the last dose was less than 8 hours ago or when the time of the last dose is unknown. A low dose is also indicated when the timing of the last dose was 8 hours or more, regardless of the last dose of the FXa inhibitor. A high dose with an initial IV bolus of 800 mg and a follow-on infusion of 8 mg/minute for 120 minutes (960 mg) is indicated for a rivaroxaban dose that is greater than 10 mg or unknown or an apixaban dose that is greater than 5 mg or unknown, where the last dose was less than 8 hours ago or unknown.1 The administration of andexanet alfa is to be conducted and/or monitored by a health care practitioner and, due to thromboembolic and ischemic risks, resumption of anticoagulant therapy should be considered as soon as medically appropriate after completion of treatment.1
Table 3: Key Characteristics of Andexanet Alfa and 4F-PCC
Detail | Andexanet alfa | 4F-PCC (Beriplex and Octaplex) |
|---|---|---|
Mechanism of action | Recombinant modified human FXa protein without procoagulant or anticoagulant activity that binds FXa inhibitors in the plasma, thereby freeing endogenous FXa to resume its normal function in hemostasis. | Plasma-derived product that provides nonspecific supplementation of coagulation factors containing pooled plasma products (i.e., factors II, VII, IX, and X).a |
Indicationb | For adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to acute life-threatening or uncontrolled bleeding. | Not approved (off-label use). |
Route of administration | IV infusion | IV infusion |
Recommended dose | Dosage is based on the specific oral FXa inhibitor, the dose of oral FXa inhibitor, and the time since the patient’s last dose of oral FXa inhibitor:
| 25 IU to 50 IU per kilogram of body weight or a fixed dose of 2,000 IU16 |
Serious adverse effects or safety issues |
| Thrombotic risk. |
4F-PCC = 4-factor prothrombin complex concentrate; DOAC = direct oral anticoagulant; FXa = factor Xa.
aNot a selective reversal agent and its effect is debatable in managing FXa inhibitor–related major bleeds with a lack of robust clinical and scientifically rigorous evidence.
bHealth Canada–approved indication.
Sources: Andexanet alfa product monograph (draft), Beriplex product monograph, Octaplex product monograph, and DOACs: Management of Bleeding (Thrombosis Canada).1,16,40,41
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient inputs received by CADTH have been included in the stakeholder section at the end of this report.
Two patient groups, CanVECTOR and the HeartLife Foundation, submitted input for this review. The input from CanVECTOR was informed by 33 interviews with patients with VTE lived experience (DVT, n = 15; PE, n = 6; both DVT and PE, n = 12) and varied treatment experience, including warfarin, DOACs, and low-molecular-weight heparin for anywhere from 1 to 6 months to long-term treatment (more than 3 years, n = 16).
According to the input by CanVECTOR, patients receiving treatment for a VTE have to find a balance between the risk of another clot and the actual or potential side effects of treatment. Patients expressed that bleeding is the most concerning potential side effect of VTE treatments and they may live with a fear of bleeding that can impact life choices and daily activities, quality of life, and mental health. The input noted that a variety of personal factors affect a patient’s treatment preferences. Many patients described the burden of treatment with warfarin (the inconvenience of blood monitoring, restrictions on diet and alcohol intake) or with low-molecular-weight heparin injections (pain, bruising, discomfort with self-injections), and some had later switched to a DOAC. The input noted there were fewer burdens described with DOACs, but the lack of a reversal drug was mentioned by a few patients, for example, “However much I have my misgivings on Warfarin, it had one benefit. It was reversible. It had all the other things that were not attractive to it, but if you could make some of those things more attractive, or certainly if the new drug that would come on the market to replace or be an alternative to apixaban, if it had a reversibility aspect to it, I think would be attractive.” The HeartLife Foundation noted that the use of an FXa inhibitor can increase the risk of bleeding; as well, patients with heart failure may require invasive surgeries, which put them at risk of surgical bleeds. The group expressed a need for a treatment that can rapidly and effectively reverse the anticoagulant effect of FXa inhibitors to prevent further bleeding and ensure the best possible outcome in patients who require urgent surgery or are experiencing life-threatening bleeds. This was echoed by the input by CanVECTOR, which highlighted that patients were concerned that the absence of a reversal drug for DOACs could prevent them from undergoing a surgery in case of an emergency: “If an accident happened and the surgery is almost immediate, a reversal agent can help me … [go] into the emergency surgery safely.” The CanVECTOR also highlighted that some patients with a high risk of another clot will be prescribed blood thinners for the rest of their lives, and the experience could be daunting for a young person with decades of treatment ahead.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of acute major bleeding in patients receiving an FXa inhibitor.
Unmet Needs
The clinical experts noted there is currently a lack of a specific reversal drug for FXa-related bleeding. They noted that currently available hemostatic agent (i.e., PCC) do not always achieve a rapid response; this can be a concern in patients with time-sensitive major bleeding, such as patients with bleeding within the central nervous system, high-risk GI bleeding, a trauma in need of urgent operative intervention and, in rare instances, patients with acute kidney injury who experience a prolonged anticoagulant effect from an FXa inhibitor. The clinical experts also noted that PCC and blood products are not universally available in all clinical settings. In addition, the risk of thrombosis with existing treatments is unclear, according to the clinical experts.
Place in Therapy
The clinical experts noted that andexanet alfa is a reversal drug specifically for FXa inhibitors and may act more rapidly than the other reversal agents currently available. The clinical experts anticipated that andexanet alfa would have the same place in therapy as PCC (i.e., as an alternative to PCC) in the treatment of acute major bleeding in patients receiving an FXa inhibitor; however, based on available evidence, it is unclear whether andexanet alfa or PCC should be the preferred therapy, and suggested this should be based on clinical presentation. The clinical experts noted that in addition to clinical evidence, practical factors such as treatment access (e.g., through hospital transfusion medicine laboratories versus hospital pharmacies) and cost could also affect which treatment is used; therefore, it is challenging to conclude with certainty whether andexanet alfa has the potential to cause a shift in the current treatment paradigm.
Patient Population
The clinical experts noted that patients receiving an FXa inhibitor who have acute major bleeding are potential candidates for andexanet alfa treatment. According to the clinical experts, such patient populations would most commonly include older patients who are compliant with their FXa inhibitor treatment and present to the emergency department with brisk nonvariceal upper GI bleeds or head trauma resulting in intracranial bleeding that is believed to be worsening or at risk of worsening. The clinical experts also noted that patients who are being treated with an FXa inhibitor and require urgent surgery (e.g., patients with a hip fracture who could benefit from early operative intervention) may also be candidates for andexanet alfa, although this patient population was not studied in the pivotal trial.
The clinical experts noted that the definition of major bleed by the ISTH42 is the 1 most commonly used by clinicians in Canada. According to the clinical experts, patients with major bleeding who require reversal of the anticoagulant effect of an FXa inhibitor would be identified in clinical practice primarily based on assessments of patients’ clinical status (severity, bleed location, and response to nonspecific supportive measures). Laboratory markers such as prothrombin time are not sensitive measures of anticoagulant activity; establishing when the last dose of anticoagulant was taken would be a more reliable indicator of whether anti-FXa activity is still present, according to the clinical experts. The clinical experts noted that FXa assays could help inform treatment decisions if done in a timely fashion (turnaround time of less than 1 hour); however, this is not realistic outside of a small number of treatment centres in Canada.
The clinical experts noted that patients with minor bleeding would not be suitable for andexanet alfa treatment since non-major bleeds are expected to resolve on their own without the need for a reversal agent and with minimal patient harm.
Assessing the Response to Treatment
The clinical experts noted that, in general, response to treatment is assessed based on hemostatic stability, hemostatic control (i.e., cessation of bleeding), need for blood transfusion, survival, and HRQoL. Stabilization of vital signs, improvement or normalization in laboratory markers (e.g., serial hemoglobin and lactate measures, coagulation profile), and cessation of bleeding (e.g., based on endoscopy findings) are typical indicators of achievement of hemostatic control, according to the clinical experts. The clinical experts noted that continuous monitoring of hemostatic control, transfusion needs, and survival is typically done for the first 72 hours after admission. An absence of thrombosis (ideally assessed at 5 days and 1 month posttreatment) and an improvement in HRQoL (ideally assessed at 1 month posttreatment) would also be indicative of a positive response to treatment, although the timing of the assessment could differ between patients.
Prescribing Considerations
The clinical experts noted that the vast majority of emergency department physicians would be comfortable prescribing andexanet alfa in consultation with a hematologist, thrombosis physician, or transfusion medicine specialist; however, the clinical experts indicated that access to any of these specialists is limited in remote and rural areas and that lack of such access could potentially be a barrier to the timely administration of a reversal drug in an emergency situation. Therefore, the clinical experts noted it may be reasonable to allow prescribing by clinicians who have expertise in the management of acute major bleeds.
The clinical experts noted it would be appropriate to prescribe andexanet alfa in a hospital setting (e.g., emergency department or an inpatient or operating room).
The clinical experts noted that redosing of a reversal treatment is rare in clinical practice, and the pharmacology of andexanet alfa suggests that redosing is not necessary. Redosing is associated with increased thrombotic risk and should be done only in exceptional circumstances under the guidance of a transfusion medicine specialist, thrombosis physician, or hematologist.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by the clinician groups. The full original clinician group inputs received by CADTH have been included in the stakeholder section at the end of this report.
Clinician group input was obtained from 5 clinician groups, including Thrombosis Canada (represented by 2 clinicians), members of the Thrombosis and Anticoagulation team at Dalhousie University (represented by 3 clinicians), faculty members at McMaster University in hematology and/or thromboembolism (represented by 5 clinicians), the Canadian Stroke Consortium (represented by 5 clinicians), and a journal club comprising local emergency medicine physicians in Peel Region (represented by 5 clinicians).
The clinician groups noted that PCC, which is currently the reversal treatment of choice for DOAC-related major bleeding, has a nonspecific mechanism of action and is an off-label drug with no robust clinical data supporting its efficacy or safety. They noted that PCC may promote a prothrombotic state and could potentially not be safely used in patients who have a history of heparin-induced thrombocytopenia or thrombosis, since a small amount of heparin may be present in PCC.
The clinician groups noted that andexanet alfa, being the only specific reversal treatment available to patients who are on an FXa inhibitor, would be used as a first-line treatment in patients who require urgent anticoagulant reversal in the setting of serious, life-threatening bleeding or a need for urgent surgery. One clinician group noted that PCCs would likely be used for an “average” patient who needs DOAC reversal, whereas andexanet alfa would be used in select patients with:
life-threatening bleeding that does not respond to supportive management (i.e., fluids, packed RBCs)
critical site bleeding (intracranial, spinal, pericardial)
a need for emergency (within 6 to 8 hours) or urgent (within 12 to 24 hours) surgery.
They noted there is no established threshold for clinically significant hemostatic impairment, and most centres do not have FXa inhibitor drug assays available, so treatment is usually considered based on the timing of the last dose, drug half-life, patient’s kidney or liver function, and examination findings (e.g., hypotension), radiographic findings (e.g., CT scans), and clinician judgment. They also noted that patients who would be less suitable would be those who took their last dose of FXa inhibitor more than 1 to 2 days ago (in the presence of normal renal function), who have bleeding that is not life-threatening, or whose surgery can be delayed for 1 to 2 days after their last dose of an FXa inhibitor.
Outcomes to assess response to treatment deemed important by the clinician groups included achievement of excellent or good hemostatic efficacy, thrombotic events, decreased mortality, decrease in hemoglobin or hematocrit by less than 20% compared with baseline, improvement in symptoms, reduction in hematoma expansion in ICH, survival to discharge, disability score on discharge, and measurement of anti-FXa levels before and after drug administration (not widely available). They noted that length of hospital stay may also be a surrogate marker. The clinical groups noted the criteria for discontinuation would include unexpected allergic or infusion reactions or thromboembolic events.
The clinical groups also supported the use of andexanet alfa in the hospital setting, including the emergency department, critical care unit, operating room, tertiary trauma centre, or stroke or neurosurgical referral centre, and administered by anesthesiologists or by surgical or other specialists such as those in emergency or internal medicine, depending on the site of the bleeding (e.g., neurologist or neurosurgeon for ICH, or gastroenterologists for GI bleeding).
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Comment: PCC is used off-label for the reversal treatment of bleeds related to apixaban and rivaroxaban (FXa inhibitors). Therefore, its current use for the reversal of FXa inhibition is off-label. The Thrombosis Canada guidelines acknowledge that PCCs are not selective reversal agents and their effect in managing FXa inhibitor–related major bleeds is debatable. However, in the Clinical Summary Report, the sponsor suggested that andexanet alfa is considered for the same indications for which PCC, tranexamic acid, or aminocaproic acid are considered. Pivotal clinical studies (ANNEXXA-4, ANNEXA-A, and ANNEXA-R) supporting effectiveness and safety are either a single-arm or placebo-controlled study. These studies do not provide evidence of comparative efficacy, effectiveness, or safety between andexanet alfa and currently available treatments for the reversal of anti-FXa–related major bleeds. | — |
Questions for CADTH review team | |
Are sponsor-supplied real-world evidence and weighted comparative observational studies appropriate to confirm better clinical outcomes compared with PCC? What does the clinical evidence suggest about comparative safety outcomes (e.g., thromboembolic event rate following treatment with PCC vs. andexanet alfa)? | The CADTH review team noted that evidence from the 3 weighted comparative observational studies and 6 comparative observational studies submitted by the sponsor suggested that andexanet alfa could reduce mortality, ICU admission, and length of hospital stay and was associated with a similarly low frequency of thrombosis compared with PCC in patients requiring reversal of anticoagulant effect during an acute major bleed; however, the important methodological limitations of these studies, including selection bias and residual confounding due to a lack of adjustment or an inadequate adjustment for prognostic factors and effect modifiers, preclude definitive conclusions about the comparative efficacy and harms of andexanet alfa and PCC. |
Would the CADTH review team or CPEC consider PCC an appropriate comparator of andexanet alfa even though PCC is used off-label for the same indication? | Off-label treatments that are currently reimbursed by public drug programs may be considered relevant comparators for the drug under review. The CADTH review team considers PCC to be a relevant comparator of andexanet alfa, based on input from the clinical experts. |
Question for clinical experts | |
The sponsor suggested that PCC’s off-label use leads to suboptimal care for the patients. Is there any evidence available to support this? | The clinical experts were not aware of any existing clinical evidence that shows that the use of PCC leads to suboptimal care in patients with major bleeding while receiving a DOAC. The clinical experts noted that the rates of thrombosis and mortality reported in meta-analyses of noncomparative studies of PCC in patients with major bleeding while receiving DOAC appeared to be similar to those reported in the ANNEXA-4 trial;43,44 however, the clinical experts acknowledge that the lack of comparative evidence between the interventions and the highly selected patient population in the ANNEXA-4 trial limit the conclusions that can be drawn. |
Comment: Andexanet alfa has the potential to replace the use of PCC, tranexamic acid, or aminocaproic acid. | The clinical experts noted that PCC and andexanet alfa are expected to have the same place in therapy for the management of major bleeding in patients receiving FXa inhibitors, while tranexamic and aminocaproic acid are considered to be adjunctive therapy. |
Questions for clinical experts | |
Are there any patients whose medical needs would not be managed by currently available treatments (i.e., PCC, tranexamic acid, or aminocaproic acid)? How are these patients managed? | The clinical experts noted that most patients with major bleeding could benefit from PCC treatment although, in some patients, the rapidity and extent of bleeding will result in poor clinical outcomes that might have been prevented with a more specific reversal agent. The clinical experts also noted there is a theoretical risk in using PCC in patients with a history of heparin-induced thrombocytopenia due to possible exacerbation of the disease, since a small amount of heparin may be present in PCC. The management strategy for these patients is either to focus on empiric therapies (tranexamic acid and transfusion) or prescribe PCC with close clinical and laboratory monitoring. In addition, the clinical experts noted there is a theoretical risk of inducing a prothrombotic state in patients with cirrhotic liver disease receiving higher doses of PCC; in that case, PCC may be given with close monitoring, weighing the risks of thrombosis vs. major bleeding. |
While PCC is available through the CBS PPRP formulary, is tranexamic acid or aminocaproic acid available readily for patients? | The clinical experts noted that tranexamic acid is widely available on hospital formularies, while aminocaproic acid is not, although its absence is unlikely to be a concern, since aminocaproic acid is not known to be more efficacious compared with tranexamic acid. |
Are we missing any other potential comparator drug? | The clinical experts considered PCC to be the most relevant comparator for andexanet alfa. They noted that adjunctive therapy, such as tranexamic acid, is prescribed on a case-by-case basis, generally only in cases of severe hemorrhage, considering that there is evidence suggesting that tranexamic acid can cause harm in patients with certain types of bleeding (e.g., GI, GU). No other relevant comparator was noted by the clinical experts. |
Considerations for initiation of therapy | |
Questions for CPEC | |
In the event of a criteria-based recommendation, a definition of major bleeds, minor bleeds, life-threatening bleeds, and so forth would be required. Which marker or criteria should be used to start therapy with andexanet alfa (e.g., major bleeding should be present to start treatment)? | For CPEC consideration. |
In the pivotal ANNEXA-4 study, bleeding due to other drugs of the same class (edoxaban, enoxaparin) was studied. Would patients with bleeding caused by these medications be eligible for andexanet alfa? | For CPEC consideration. |
Questions for clinical experts | |
Should patients use PCC, tranexamic acid, or aminocaproic acid before being made eligible for andexanet alfa? | The clinical experts noted there is currently no clinical evidence to inform which reversal agent of FXa inhibitors should be used first, although, in their opinion, if andexanet alfa is prohibitively expensive, it may be reasonable to prioritize the use of PCC. The clinical experts noted that tranexamic acid and aminocaproic acid are adjunctive therapies that may be used in addition to a reversal agent, although not all patients are eligible for these adjustive treatments due to concerns for thrombotic risk. |
If a patient has tried andexanet alfa and it does not control bleeding, would they be eligible for PCC or vice versa? | The clinical experts noted that while it may be reasonable to use an alternative reversal agent in patients who have ongoing life-threatening bleeding despite initial treatment, it is important to consider that both andexanet alfa and PCC have thrombotic risk, which is likely additive if used sequentially, and that recent use of PCC is currently an exclusion criterion for accessing andexanet alfa treatment in many jurisdictions. |
What eligibility is required for redosing of andexanet alfa? What is andexanet alfa’s safety and efficacy for redosing? | In the clinical experts’ experience, redosing of reversal agents is rare. The clinical experts expressed that redosing of andexanet alfa may not be necessary, based on its pharmacology, and it could result in an increased risk of thrombosis. They noted that redosing of andexanet alfa should only occur in exceptional circumstances under the guidance of a transfusion medicine specialist, thrombosis physician, or hematologist. |
Questions for CADTH review team and clinical experts | |
Is there a subset of patients who are likely to benefit the most from andexanet alfa or who are least likely to benefit? | The clinical experts noted that patients who receive anticoagulation treatment with apixaban or rivaroxaban and have either of the following are most likely to benefit from andexanet alfa treatment:
The clinical experts noted that patients whose last dose of FXa inhibitor was more than 24 hours ago and patients with a minor bleed would not be suitable for andexanet alfa treatment. The CADTH review team noted that the ANNEXA-4 trial was conducted in patients with acute major bleeding while receiving an FXa inhibitor treatment. Subgroup analyses were performed with respect to the coprimary end points of hemostatic efficacy and anti-FXa activity level; however, due to the limitations of the statistical analyses, no conclusion on subgroup effects can be drawn. |
Are there any patients taking apixaban or rivaroxaban who would not be candidates for andexanet or for whom PCC, tranexamic acid, or aminocaproic acid would be a reasonable first-line choice? | The clinical experts noted that most patients who have a life-threatening hemorrhage while receiving FXa anticoagulation treatment would be a potential candidate for andexanet alfa. However, there is a lack of clinical data on the use of andexanet alfa in pediatric patients; PCC would be considered the first-line reversal agent for these patients. |
Are there any situations in which PCC, tranexamic acid, or aminocaproic acid, and then andexanet alfa, could be used consecutively? For example, if PCC were given in an emergency situation before it was known that the patient was taking apixaban or rivaroxaban, would andexanet alfa ever be given after this was confirmed? | The clinical experts noted that in their clinical experience, redosing of PCC is uncommon, since most patients respond to a single dose of PCC. They noted that while it might be reasonable to consider andexanet alfa treatment in rare cases when patients experience ongoing bleeding and do not achieve hemostasis despite PCC treatment, doing so may increase thrombotic risk. |
Comment: While Praxbind (idarucizumab) is not the comparator or alternative for andexanet alfa, it is important to note that if andexanet alfa is listed, its access would be different than access to idarucizumab. Similar to andexanet alfa, idarucizumab replaces the use of PCC, but only for patients whose bleeding is due to Pradaxa (dabigatran). Understanding the current access to idarucizumab could potentially help inform the implementation of reimbursement criteria for andexanet alfa. | For CPEC consideration. |
Questions for the CADTH review team and clinical experts | |
How is idarucizumab made available to in-hospital patients? | According to the clinical experts, in Alberta, access to idarucizumab requires approval by a transfusion medicine specialist and the drug is dispensed from the pharmacy while, in Ontario, idarucizumab is a formulary drug dispensed from the pharmacy and can often be accessed in the emergency department, and approval from a transfusion medicine or other specialist is not required for drug access. |
Do hospitals implement any criteria for this drug? If so, are there any issues with the implementation of criteria in hospitals (including those with electronic and/or paper-based systems)? | According to an update provided by the Alberta Health Services Provincial Drugs and Therapeutics Committee in September,45 the restricted criteria for the use of idarucizumab in Alberta are as follows:
OR
The clinical experts were unaware of issues related to the implementation of such criteria in hospitals. |
While PCC is available without any criteria through CBS, are you aware of any hospital that has implemented criteria for PCC use? | One clinical expert noted they were unaware of any formal approval process required for PCC for hospitals within Alberta Health Services. The other clinical expert noted that in Ontario, some hospitals have implemented criteria for accessing PCC, and approval from a hematologist or thrombosis specialist is required. |
Did idarucizumab undergo a CADTH review? Are you able to provide a comparator reimbursement status for idarucizumab similar to the one provided for PCC? Should the criteria (if any) for idarucizumab and andexanet alfa be aligned? | CADTH has not completed a reimbursement review for idarucizumab and is unable to provide a summary of the reimbursement status of any idarucizumab comparators. |
Question for clinical experts | |
The safety and efficacy of andexanet alfa in patients with ICH with a GCS score of < 7 and an estimated intracerebral hematoma volume > 60 cc were unknown, since these patients were excluded from the ANNEXA-4 trial. Should patients with these characteristics be eligible for andexanet alfa treatment? | The clinical experts noted that a low GCS score and a large hematoma volume were indicative of severe ICH; patients with either of these features are generally less likely to benefit from reversal treatment compared with those who do not. The clinical experts noted it may be reasonable to exclude patients with an ICH from andexanet alfa treatment if they have a GCS score of < 7 and an intracerebral hematoma volume > 60 cc if clinicians felt that any treatment (including reversal and evacuation) would be futile in these patients. |
Generalizability | |
Questions for CPEC | |
Pediatric and pregnant populations were not included in the clinical trials. Would these groups be eligible for the treatment under consideration? | For CPEC consideration. |
For patients on apixaban or rivaroxaban who do not have life-threatening bleeding but require emergency surgery: Is there likely to be an indication creep and is this evidence-based? | For CPEC consideration. |
Care provision issues | |
Questions for clinical experts | |
Given andexanet alfa is used in an emergency (time-sensitive) situation, the duration of reconstitution (i.e., preparation) and administration is important. Does this drug require a longer or shorter time for reconstitution and administration compared with PCC? | The clinical experts noted that andexanet alfa requires more time for reconstitution compared with PCC, since it is a more viscous product. It may also have the potential to impact hospital workflow, given that it requires a bolus dose followed by an infusion, requiring programming of the IV pump. The setting where andexanet alfa is reconstituted could vary between hospitals (e.g., blood bank, bedside). However, the clinical experts noted that such differences are expected to have minimal impact on the clinical outcomes of patients. |
In cases where a patient has received an excessive amount of andexanet alfa, what is the potential risk of thromboembolic events or other adverse effects, and what measures can be taken to manage such risks? | The clinical experts noted that any reversal strategy carries thrombotic risk and in cases of inadvertent administration of an excess dose of andexanet alfa, no measures could reliably mitigate thrombotic risk. They noted that monitoring for thrombosis is important, and a management plan should be developed in consultation with a hematologist or transfusion medicine physician. |
Would any specific tests (e.g., FXa inhibitor level) be required after the administration of the first dose (or subsequent doses) of andexanet alfa to assess the efficacy and safety of the drug? | The clinical experts noted that clinical status and hemostasis are important clinical parameters to assess after administration of andexanet alfa. They noted that no specific laboratory test would be required for most patients receiving a reversal agent for anticoagulants although, for some patients who require emergency surgery, an anti-FXa assay may be performed to ensure the levels have fallen to a safe level to optimize the operative course. However, in most hospitals, anti-FXa levels have a long turnaround time (> 1 hour) and cannot be returned in time to inform the treatment decision, according to the clinical experts. |
Do you anticipate any issue if the drug is made available through blood banks (CBS PPRP formulary) rather than through hospital pharmacies (as for other “antidotes”)? | The clinical experts did not anticipate issues with accessing andexanet alfa through transfusion medicine laboratories; in fact, they thought it would provide more seamless access to treatment since access and support from hospital pharmacies could be limited outside of their usual operating hours. Based on the clinical experts’ experience, access to blood products is generally timely in most hospitals. |
Andexanet alfa dosage is based on the specific oral FXa inhibitor, the dose of the oral FXa inhibitor, and the time since the patient’s last dose of the oral FXa inhibitor. If andexanet alfa is listed, it will be available through the CBS PPRP formulary. This means it will be made available through hospital blood banks. Who will assess the appropriate dose before the drug is ordered in the hospital for a patient: the ordering physician, pharmacy, or blood bank staff? | The clinical experts noted that the dose of andexanet alfa is dependent on time since last drug ingestion, which would have been a part of the assessment by the treating physician. They felt that the dose of andexanet alfa would be determined by the treating physician in collaboration with a hematologist, thrombosis physician, or transfusion medicine specialist. |
System and economic issues | |
Questions for CADTH review team | |
In the pharmacoeconomic model, the proportion of major bleeding needed to be treated with the reversal agent and overall market size was estimated based on the ITC study (i.e., ORANGE, ANNEXA-4). Is this reasonable? | The clinical experts noted that the study population in the ANNEXA-4 trial is younger compared with clinical practice and it is reasonable to expect that younger patients would have better clinical outcomes. Additionally, the clinical experts noted that the proportion of major bleeding that needed to be treated with a reversal agent reported in the ORANGE study is low in comparison to their experience in clinical practice. Therefore, scenario analyses are performed in the budget impact analysis to explore the impact of a higher proportion of patients eligible for reversal agents. |
The number of patients on apixaban and rivaroxaban is calculated based on claims data from IQVIA. This calculation assumes patient numbers based on claims for receipt of direct oral anticoagulants, standardized number of days (appears to be 30 days) per claim, and persistence of treatment with a drug as a basis for estimating. How confident are we in this approach for calculating patient numbers? Is there any alternative way to derive patient numbers for estimating the budget impact analysis model? | The CADTH review team reached out to the sponsor to request additional information on the use of a claims-based approach to estimate the budget impact analysis. The sponsor noted that an epidemiologic-based approach was considered; however, due to the limited data on the prevalence of patients in Canada receiving treatment with apixaban and rivaroxaban, the number of patients in Canada using FXa inhibitors was indirectly estimated using IQVIA claims data. While a claims-based approach is not preferred for a budget impact analysis model, the sponsor provided an appropriate rationale for this approach. An alternative method to derive patient numbers was highlighted by the sponsor by using data from the UK, wherein 0.83% of the general population would receive some form of DOAC treatment. However, when this proportion was applied to the general population in Canada, the clinical experts consulted by the sponsor reported that this estimate is too high. |
There are 2 brands of PCC: Octaplex and Beriplex, which are available through the CBS PPRP formulary. These are the comparators for andexanet alfa and their prices are confidential. | This is a comment from the drug programs to inform CPEC deliberations. |
Question for clinical experts | |
Andexanet alfa, if made available, will come from the CBS PPRP formulary budget. This means hospital budgets will not be used for the procurement of this drug. If the drug becomes available, would hospitals have any incentive to ensure that less costly treatments are tried first? | The clinical experts noted that if it is made clear in the hospital protocol that the use of a reversal agent is dependent on patient eligibility, with the use of first-line treatments being the primary approach, it is unlikely that the source of funding will alter the careful stewardship of resources. However, 1 clinical expert noted that in their experience, some hospitals may not be as invested in ensuring proper utilization of drugs and/or blood products that are funded outside of their budget envelope. |
CBS = Canadian Blood Services; CPEC = Canadian Plasma Protein Product Expert Committee; DOAC = direct oral anticoagulant; FXa = factor Xa; GCS = Glasgow Coma Scale; GI = gastrointestinal; GU = genitourinary; ICH = intracranial hemorrhage; ICU = intensive care unit; ITC = indirect treatment comparison; PCC = prothrombin complex concentrate; PPRP = Plasma Protein and Related Products.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of andexanet alfa 200 mg powder for solution for IV infusion for rapid reversal of anticoagulation due to acute major bleeding, including life-threatening bleeds, in adult patients treated with FXa inhibitors (rivaroxaban or apixaban). The focus will be placed on comparing andexanet alfa with relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of andexanet alfa is presented in 2 sections, and CADTH’s critical appraisal of the evidence is included after each section. The first section includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second section includes additional studies that were considered by the sponsor to address important gaps in the pivotal and RCT evidence.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
Three pivotal studies (ANNEXA-4, ANNEXA-A, and ANNEXA-R)17,18
Three weighted comparative observational studies (a PSM analysis, a propensity score overlap–weighted analysis, and a propensity score-weighted analysis using IPTW)21-23
Six comparative observational studies: Coleman et al. (2021), Dobesh et al. (2022), Fermann et al. (2022), Dobesh et al. (2023), Sutton et al. (2022), Sutton et al. (2023).24-29
Pivotal Studies and RCT Evidence
The contents of this section were informed by materials submitted by the sponsor. The following was summarized and validated by the CADTH review team.
One pivotal study, ANNEXA-4,17 met the inclusion criteria for the systematic review conducted by the sponsor and was presented in this report. The sponsor submitted 2 additional pivotal trials of andexanet alfa conducted in healthy participants (ANNEXA-A and ANNEEXA-R),18 neither of which met the inclusion criteria for the sponsor’s systematic review. A brief summary of the ANNEXA-A and ANNEXA-R trials is also provided at the end of this section. The characteristics of the 3 pivotal studies are summarized in Table 5.
Table 5: Details of Pivotal Studies and RCT Evidence Identified by the Sponsor
Characteristics | ANNEXA-4 trial | ANNEXA-A trial | ANNEXA-R trial |
|---|---|---|---|
Designs and populations | |||
Study design | Phase IIIb and IV, multicentre, open label, single arm | Phase III, randomized, double blind, placebo controlled | Phase III, randomized, double blind, placebo controlled |
Locations | 85 sites: 26 in North America (including 2 in Canada), 49 in Europe, and 10 in Asia | 1 site in the US | 1 site in the US |
Patient enrolment dates |
|
|
|
Sample size (N) |
|
|
|
Key inclusion criteria |
|
| |
Key exclusion criteria |
|
| |
Drugs | |||
Intervention | Either high- or low-dose andexanet alfa based on the specific FXa inhibitor, dose of FXa inhibitor, and time since the patient’s last dose of FXa inhibitor:
| Andexanet alfa either as a 400 mg IV bolus (part 1), or as a 400 mg IV bolus followed by 4 mg/minute infusion for 120 minutes (part 2)k | Andexanet alfa either as an 800 mg IV bolus (part 1), or as an 800 mg IV bolus followed by 8 mg/minute infusion for 120 minutes (part 2)l |
Comparator(s) | None | Placebo either as an IV bolus (part 1), or as an IV bolus followed by IV continuous infusion (part 2)k | Placebo as an IV bolus (part 1), or as an IV bolus followed by IV continuous infusion (part 2)l |
Study duration | |||
Screening phase | < 1 day | ≤ 42 days | |
Treatment phase | < 1 day | 4 days | |
Safety follow-up phase | ≤ 30 days | ≤ 43 days | |
Outcomes | |||
Primary end point | Coprimary end points:
| % change from baseline in anti-FXa activity at the nadir following the bolus (part 1), or following the bolus and continuous infusion (part 2) | |
Secondary and exploratory end points | Secondary: none Exploratory:
| Secondary:
| |
Publication status | |||
Publications | Siegal et al. (2015)18 (NCT02207725, NCT02220725) | ||
DVT = deep vein thrombosis; EAC = end point adjudication committee; EOI = end of infusion; FXa = factor Xa; Hb = hemoglobin; ICH = intracranial hemorrhage; PCC = prothrombin complex concentrate; PE = pulmonary embolism; RCT = randomized controlled trial; VTE = venous thromboembolism.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.20
aFor example, severe hypotension, poor skin perfusion, mental confusion, or low urine output that could not be otherwise explained.
bThe dose of enoxaparin had to be at least 1 mg/kg/day.
cAs determined by the investigator based on medical history, full physical examination (including blood pressure and pulse rate measurement), 12-lead electrocardiogram, and clinical laboratory tests.
dFor example, controlled hypertension, noninsulin-dependent diabetes, osteoarthritis, hypothyroidism.
eUsing the Cockcroft-Gault equation.
fAs assessed by CT or MRI.
gIncluding venous thromboembolism (e.g., DVT, PE, cerebral venous thrombosis), myocardial infarction, including an isolated troponin level, disseminated intravascular coagulation, cerebral vascular accident, transient ischemic attack, unstable angina pectoris hospitalization, or severe peripheral vascular disease.
hAdministration of platelets or packed red blood cells was not an exclusion criterion.
iPatients with planned minimally invasive surgery or procedure (e.g., endoscopy, bronchoscopy, central line, bur hole) could be enrolled into the study.
jFor example, patients with a known or suspected hypercoagulable state, history of VTE, DVT, stroke, myocardial infarction, cancer (other than nonmelanoma skin cancer), atrial fibrillation, congestive heart failure, cardiomyopathy, phlebitis, lower extremity edema, major surgery or trauma within 2 months of study day −1, airplane travel ≥ 2 hours during 4 weeks before study day −1, or general immobility were excluded.
kPrior to initiation of andexanet alfa or placebo, patients received apixaban 5 mg orally every 12 hours for 3.5 days.
lPrior to initiation of andexanet alfa or placebo, patients received rivaroxaban 20 mg orally every 24 hours for 4 days.
Sources: Clinical Study Reports for the ANNEXA-4, ANNEXA-A, and ANNEXA-R trials.19,49,50
Description of ANNEXA-4 Trial
The ANNEXA-4 study was a phase IIIb and IV, multicentre, open-label, single-arm trial with primary objectives to demonstrate the decrease in anti-FXa activity following andexanet alfa treatment and to evaluate the hemostatic efficacy of andexanet alfa treatment in patients receiving an FXa inhibitor who are experiencing an acute major bleed (N = 477). The secondary objective was to assess the relationship between a decrease in anti-FXa activity and achievement of hemostatic efficacy in the study population. The study was conducted at 85 sites spread across North America (including 2 in Canada), Europe, and Asia. Patients were enrolled between April 2015 and March 2020 and consisted of 3 study periods: a screening period (day 1), where study eligibility was assessed; a treatment period (day 1), where all enrolled patients received andexanet alfa treatment (bolus followed by continuous infusion); and a safety evaluation period (day 1 to day 30), where patients were monitored for safety outcomes. The study design of ANNEXA-4 is presented in Figure 1.
Figure 1: ANNEXA-4 Study Design
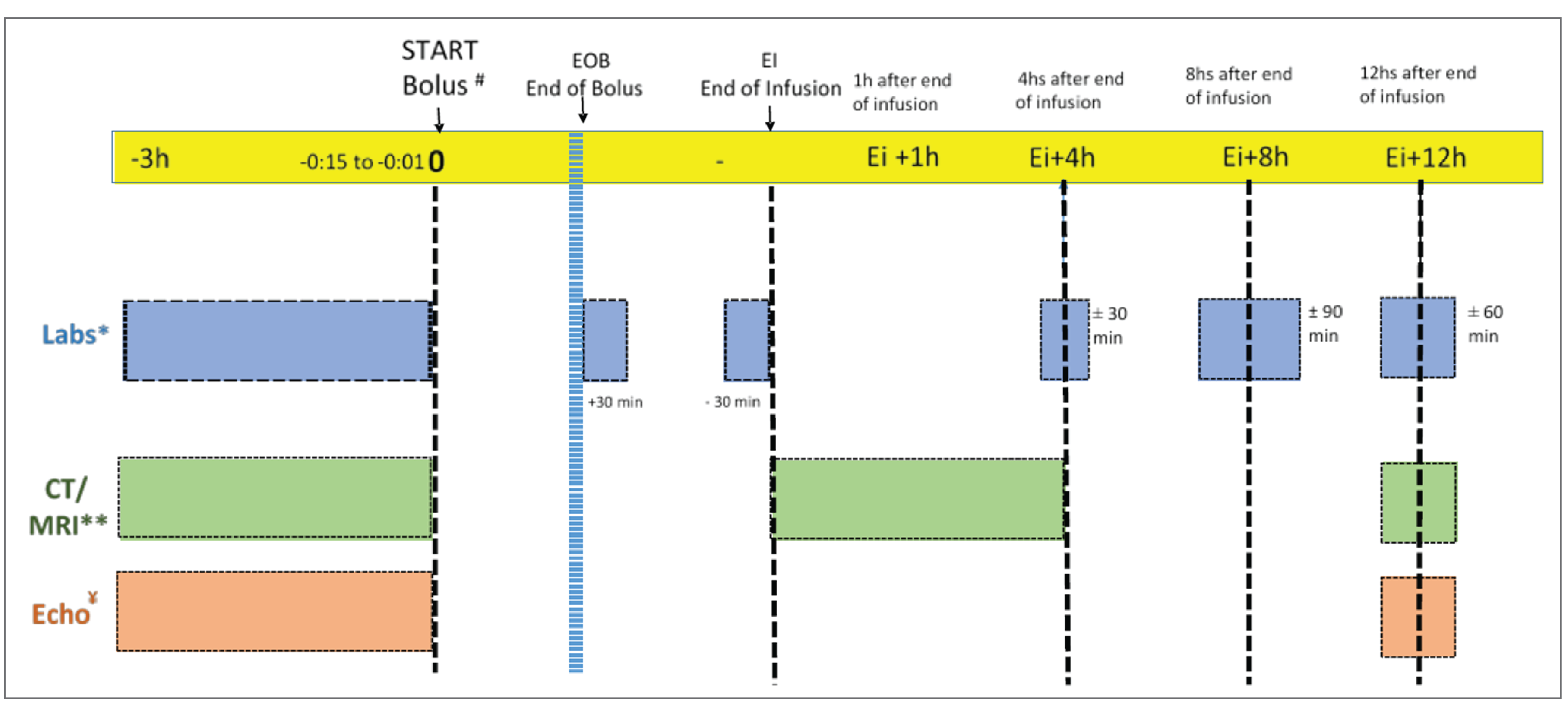
echo = echocardiogram; Ei = end of infusion; EOB = end of bolus; FXa = factor Xa; h = hour; ICH = intracranial hemorrhage; min = minutes.
Note: This figure outlines the study design in the treatment phase. The screening phase (not shown), which occurred just before the treatment phase, involved study eligibility assessments. The follow-up phase (not shown), which occurred after the treatment phase, involved safety monitoring for up to 30 days.
# Redosing procedures began before the start of the second bolus for measurement of anti-FXa activity.
** CT/MRI was required for ICH and intraspinal patients. The Ei + 1 hour scan (window Ei + 4 hours) is required for ICH only.
¥ Pericardial bleeds only.
Source: ANNEXA-4 Clinical Study Report.19
Population
Inclusion and Exclusion Criteria
The key inclusion and exclusion criteria of the ANNEXA-4 trial are presented in Table 5.
Eligible patients in the ANNEXA-4 trial were at least 18 years of age, presenting with acute major bleeding, and had (or were believed to have) received 1 of: apixaban, rivaroxaban, edoxaban, or enoxaparin within the past 18 hours.17 Acute major bleeding was defined (using the modified ISTH definition) as bleeding with 1 or more of the following features: potentially life-threatening bleeding with signs or symptoms of hemodynamic compromise, bleeding associated with a decrease in the hemoglobin level of at least 2 g/dL or a hemoglobin level of 8 g/dL or lower if baseline level was unavailable, or bleeding in a critical area or organ. Key exclusion criteria were planned surgery within 12 hours after andexanet alfa treatment (with the exception of minimally invasive procedures), ICH in a patient with a score of less than 7 on the GCS scale (scores range from 15 [normal] to 3 [deep coma]) or an estimated intracerebral hematoma volume of more than 60 cc, expected survival of less than 1 month, history of thrombotic event in the past 2 weeks, or use of a vitamin K antagonist, dabigatran, PCC, recombinant factor VIIa, whole blood, or plasma in the past 7 days.
Interventions
Patients in the ANNEXA-4 trial received either high-dose (800 mg bolus over approximately 15 to 30 minutes then 8 mg/minute continuous infusion for 120 minutes, i.e., 960 mg) or low-dose (400 mg bolus over approximately 15 to 30 minutes, then 4 mg/minute continuous infusion for 120 minutes, i.e., 480 mg) andexanet alfa in an inpatient setting based on the specific anticoagulant taken and the timing and amount of the last dose, as depicted in Table 6. If the timing of the last dose of FXa inhibitor was known, the start of the andexanet alfa bolus began within 18 hours following the last dose. If the timing of the last dose of FXa inhibitor was unknown, the andexanet alfa bolus began as soon as possible but no later than 3 hours after the completion of pretreatment procedures.
Platelet transfusions, systemic antifibrinolytic (e.g., aminocaproic acid and tranexamic acid), other systemic hemostatic agent, local hemostatic agents (e.g., microfibrillar collagen, chitosan-containing products), and topical vasoconstrictors were allowed. Packed RBC transfusions were allowed if the hemoglobin level was equal to or lower than 8.0 g/dL (plus or minus 1 g/dL). Procoagulant factor infusions (e.g., 3- or 4-factor PCC or activated PCC, recombinant factor VIIa) and whole blood were avoided until after the 12-hour hemostatic efficacy evaluation unless absolutely required, and the use of such blood products resulted in hemostatic efficacy with andexanet alfa being rated as “poor or none” for that patient. The use of anticoagulant and antiplatelet drugs was prohibited until after the 12-hour hemostatic efficacy evaluation.
One additional andexanet treatment was allowed in patients with rebleeding (i.e., recurrent bleeding from the same or another anatomic site, or new bleeding from a different anatomic site, within 24 hours of initial andexanet treatment and after achieving initial good or excellent hemostasis) based on predefined criteria, and investigators were required to document the clinical justification in the case report forms.
No blinding of patients, investigators, or study personnel took place in the trial, with the exception of the end point adjudication committee, which was blinded to all anti-FXa activity data during the adjudication process, and the core imaging laboratory that read the CT scans, which was blinded to anti-FXa activity data and the clinical outcomes for each patient.
Outcomes
A list of the efficacy end points assessed in this Clinical Review Report is provided in Table 7. Summarized end points are based on those included in the sponsor’s summary of clinical evidence as well as any identified as important to this review according to stakeholders, for example, the clinical experts, clinician groups, or patient groups.
Table 6: Andexanet Alfa Dosing Regimens — ANNEXA-4 Trial
FXa inhibitor | Last dose of FXa inhibitor | Timing of last dose of FXa inhibitor before initiation of andexanet alfa | |
|---|---|---|---|
< 8 hours or unknown | ≥ 8 hours | ||
Rivaroxaban | ≤ 10 mg | Low dose | Low dose |
> 10 mg or unknown | High dose | ||
Apixaban | ≤ 5 mg | Low dose | |
> 5 mg or unknown | High dose | ||
Enoxaparin | ≤ 40 mg | Low dose | |
> 40 mg or unknown | High dose | ||
Edoxaban | < 30 mg | Low dose | |
≥ 30 mg or unknown | High dose | ||
Unknown | Unknown | High dose | |
FXa = factor Xa.
Note: Low dose = 400 mg bolus plus 4 mg/minute continuous infusion for 120 minutes; high dose = 800 mg bolus plus 8 mg/minute continuous infusion for 120 minutes.
Source: ANNEXA-4 Clinical Study Report.19
Table 7: Outcomes Summarized From the ANNEXA-4 Trial
Outcome measure | Time point | ANNEXA-4 |
|---|---|---|
Anti-FXa activity | ||
% change from baseline in anti-FXa activity | At on-treatment nadira | Coprimaryb |
Hemostatic efficacy | ||
% patients with excellent or good hemostatic efficacy | At 12 hours after EOI | Coprimaryb |
Achievement of hemostatic efficacy in patients with ICH at high risk of hematoma expansion | At 12 hours after EOI | Exploratory |
Occurrence of rebleeding | 24 hours following andexanet alfa administration and after achieving initial good or excellent hemostasis | Exploratory |
Use of blood products and hemostatic drugs | ||
Use of non–study-prescribed blood products and/or hemostatic drugs | At 12 hours after EOI | Exploratory |
Number of RBC units transfused per patient | From start of bolus through 12 hours after EOI | Exploratory |
Proportion of patients receiving 1 or more RBC transfusions | From start of bolus through 12 hours after EOI | Exploratory |
Clinical neurologic status (patients with ICH only) | ||
Change from baseline in modified Rankin Scale | At 1 hour and 12 hours after EOI, and day 30 | Exploratory |
Change from baseline in National Institutes of Health Stroke Scale | At 1 hour and 12 hours after EOI, and day 30 | Exploratory |
Change from baseline in Glasgow Coma Scale | At 1 hour and 12 hours after EOI, and day 30 | Exploratory |
Other relevant outcomes not assessed in the studiesc | ||
ICU admission | NA | NA |
Hospital length of stay | NA | NAd |
HRQoL | NA | NA |
EOB = end of bolus; EOI = end of infusion; FXa = factor Xa; HRQoL = health-related quality of life; ICH = intracranial hemorrhage; ICU = intensive care unit; NA = not applicable; RBC = red blood cell.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.20
aThe on-treatment nadir was defined as the minimum value observed during treatment administration (i.e., minimum of EOB and EOI).
bStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
cAs per input from the clinical experts and clinician groups, ICU admission, length of stay in the hospital, and HRQoL are important outcomes to consider when assessing the efficacy of andexanet alfa; however, such outcomes were not measured as efficacy outcomes in the pivotal studies.
dHospital length of stay was not an efficacy end point, but it was reported in the Clinical Study Report.
Source: ANNEXA-4 Clinical Study Report.19
Efficacy Outcomes
Assessment time points included baseline; EOB; EOI; 1, 4, 8, 12, 18, 24, 48, and 72 hours after EOI; and day 30. Baseline measurement was defined as the last value obtained before the start of the andexanet alfa bolus.
Anti-FXa Activity
The percent change from baseline in anti-FXa activity to on-treatment nadir was the first coprimary efficacy end point. Anti-FXa activity was measured at baseline; EOB; EOI; and 4, 8, and 12 hours after EOI. On-treatment nadir was defined as the minimum value between EOB and EOI.
Anti-FXa activity refers to the concentration of an FXa inhibitor and was used in the study to assess the ability of andexanet alfa to reverse the anticoagulation effect of the FXa inhibitor. It was measured with a modified chromogenic assay at a central laboratory using plasma samples. As summarized in Table 8, no relevant studies assessing the psychometric properties and no established minimal important difference (MID) of anti-FXa activity were identified in the sponsor’s submission.
Hemostatic Efficacy
The proportion of patients with excellent or good hemostatic efficacy in stopping an ongoing major bleed at 12 hours from the EOI was the second coprimary end point in the ANNEXA-4 trial. The achievement of hemostatic efficacy in patients with ICH at high risk of hematoma expansion (i.e., the high-risk ICH population) was an exploratory efficacy end point. Hemostatic efficacy (“excellent,” “good,” “poor or none,” “not evaluable due to clinical reasons,” “not evaluable due to administrative reasons”) was adjudicated by the independent EAC that was blinded to anti-FXa activity levels based on predefined criteria. Patients who were adjudicated as non-evaluable for clinical reasons were included in the primary analysis of hemostatic efficacy, which was rated as “poor or none” in these patients. Patients who were adjudicated as non-evaluable due to administrative reasons (e.g., missing the 12-hour assessment due to investigator oversight, withdrawing consent before the 12-hour assessment) were excluded from the primary analysis.
According to the sponsor, the efficacy variable of “effective hemostasis” chosen in the study was an end point developed in collaboration with the FDA and agreed to by the European Medicines Agency’s Committee for Medicinal Products for Human Use as part of the scientific advice the sponsor received in 2014. The criteria for this end point were originally based on those used in the study by Sarode et al.,51 which was a registration trial for a reversal agent for warfarin-induced bleeding. The scoring system for effective hemostasis allows for the assessment of ICH, pericardial bleeding, intraspinal bleeding, and nonvisible bleeding based on objective measures, such as CT, MRI, echocardiogram, and corrected hemoglobin or hematocrit level. A description of the hemostatic efficacy rating system and psychometric properties are summarized in Table 8.
Rebleeding
The occurrence of rebleeding following andexanet alfa treatment was an exploratory efficacy end point. Rebleeding was defined as recurrent bleeding from the same (or different) anatomic site in patients within 24 hours of initial andexanet alfa treatment and after achieving initial good or excellent hemostasis. Rebleeding was adjudicated by the EAC.
Use of Blood Products and Hemostatic Drugs
The use of non–study-prescribed blood products and/or hemostatic drugs, the proportion of patients who received an RBC transfusion, and the number of RBC units transfused per patient from the start of the andexanet alfa bolus through 12 hours after the EOI were exploratory outcomes.
mRS, NIHSS, and GCS
The mRS, NIHSS, and GCS were evaluated for patients with ICH only as exploratory efficacy end points. The assessments were performed at baseline, at 1 hour, 12 post the end of andexanet alfa infusion, and at day 30 follow-up.
The mRS is a clinician-administered assessment that describes “global disability” after a stroke. The mRS scale score ranges from 0 (perfect health without symptoms) to 6 (death). A single point change on the scale is regarded as being clinically relevant, according to Broderick et al. (2017).52
The NIHSS is a clinician-administered rating scale for neurologic deficit and is composed of 11 items, each of which scores a specific ability between 0 and 4. For each item, a score of 0 typically indicates normal function in that ability, while a higher score is indicative of some level of impairment. The individual scores from each item are summed to calculate a patient’s total NIHSS. A score of 0, 1 to 4, 5 to 15, 16 to 20, or 21 to 42 indicates no stroke symptoms, minor stroke, moderate stroke, moderate to severe stroke, and severe stroke, respectively. A change of 2 points or more has been suggested as being clinically relevant, based on Harrison et al. (2013).53 In patients with an ICH following a treatment for thrombolysis or ischemic stroke, a change in 2 points or more in an individual parameter, or a change in 4 points or more overall, is considered clinically relevant.54
The GCS is a commonly used clinician-administered scale that describes the level of consciousness in all patients with acute medical conditions or trauma. In the trial, each patient was rated for all 3 GCS domains (i.e., eye opening, verbal response, and best motor response). The individual scores for each domain were summed to calculate a patient’s total GCS score. The maximum possible score was 15 (normal) and the minimum score was 3 (deep coma). No MID has been identified in patients with ICH.
ICU Admission, Length of Hospital Stay, and HRQoL
These outcomes were identified to be important to patients and clinicians based on stakeholder input; however, they were not assessed as efficacy end points in the pivotal trials. Hospital length of stay in the safety population was reported in the Clinical Study Report.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Detail | Conclusions about measurement properties |
|---|---|
Outcome measure: Anti-FXa activity | |
Anti-FXa activity refers to the concentration of FXa inhibitor in plasma as measured by an anti-FXa activity assay. Anti-FXa activity assays measure plasma heparin (UH and LMWH) levels and monitors anticoagulant therapy. Reference ranges for anti-FXa levels are dependent on the type and dose of the anticoagulant in use and the schedule and indication. | No relevant studies assessing the psychometric properties of anti-FXa activity were identified. Based on an exploratory analysis of the ANNEXA-4 study, there was no significant association between mortality and anti-FXa activity level at nadir in the overall andexanet alfa–treated patient population. MID: No established MID of anti-FXa activity was identified in the literature. |
Outcome measure: Hemostatic efficacy | |
Hemostatic efficacy is a clinical measure of blood clotting (hemostasis) as measured by hematoma volume observed by CT or MRI scans. In the ANNEXA-4 trial, hemostatic effectiveness is a binary assessment, i.e., effective or ineffective:
In terms of bleed location, hemostatic efficacy was defined in the ANNEXA-4 trial as follows:
| Validity: No relevant studies assessing the validity of hemostatic efficacy were identified. Based on data from 458 patients in the ANNEXA-4 study, a combined hemostatic efficacy rating of “excellent” or “good” was found to be correlated with lower mortality when compared with the combined rating of “poor or none.”17 Reliability: Using patient data from 3 anticoagulant-antidote studies (116 cases resulting in 464 assessments), method of agreement among 4 investigators was observed in 78.5% of assessments (Cohen kappa = 0.643; 95% CI, 0.575 to 0.694).55 Interobserver reliability was determined to be fair, with an overall agreement of 54.2% (Cohen kappa = 0.312).55 Responsiveness: No published studies examining the responsiveness of hemostasis efficacy were identified. MID: No established MID for hemostasis efficacy was identified in the literature. |
CI = confidence interval; EOI = end of infusion; FXa = factor Xa; ICH = intracranial hemorrhage; LMWH = low-molecular-weight heparin; MID = minimal important difference; RBC = red blood cell; UH = unfractionated heparin.
Statistical Analysis
A summary of the statistical analysis methods of the ANNEXA-4 trial is provided in Table 9.
Sample Size and Power Calculation
The study originally aimed to include 162 efficacy-evaluable patients, which would provide 80% power for detecting a response rate of 61% and a 95% CI completely above 50% with respect to the coprimary end point of effective hemostasis. The sample size was further increased to 250 based on the assumption that approximately 30% of the patients in the safety population would have a baseline anti-FXa activity of less than 75 ng/mL (or 0.25 IU/mL for patients receiving enoxaparin) and, thus, would not be included in the primary analysis, as well as the assumption that 5% of patients would not be evaluable for reasons unrelated to andexanet alfa. The final sample size was adjusted to 500 patients to allow enrolment of a minimum of 110 evaluable patients with ICH, as per a request from the FDA, and more patients receiving edoxaban or enoxaparin as well as patients of Japanese descent.
The sponsor noted that the threshold for a response rate of 50% was informed by unpublished observations at the April 2014 Cardiac Safety Research Consortium and by expert opinion noting that the ability to help 50% or more patients on FXa inhibitors with an acute bleed to achieve effective hemostasis would represent an important advancement relative to the current standard of care for such patients. The sponsor also noted that a 50% efficacy rate is similar to the lower bound of the 95% CI for effective hemostasis in the study by Sarode et al.,51 in which the same effective hemostasis end point was used in a population of vitamin K antagonist–treated patients with acute major bleeding.
Primary Efficacy End Points
Statistical Tests
The primary coprimary end point of percent change from baseline in anti-FXa activity was evaluated in the efficacy population using distribution-free 95% CIs for the median using the order statistics. If the CI for the median excluded 0, the first coprimary end point was considered to have been met.
The secondary coprimary end point of proportion of patients in the efficacy population with effective hemostasis (excellent or good) was considered met if the proportion was statistically significantly higher than 50% (at the 0.05 threshold). The significance test was calculated using the 1-sided exact binomial test.
Acknowledging the potential for error due to multiplicity in testing, a conclusion on the secondary coprimary end point (hemostatic efficacy) could be drawn only if the primary coprimary end point (percent change from baseline in anti-FXa activity) was met.
Handling of Missing Data
When both the EOB and EOI assessments of anti-FXa activity were missing, the maximum change was replaced with zero (i.e., no change from baseline) and the nadir was replaced with the baseline value (baseline observation carried forward). When either the EOB or EOI value were missing, the available sample was used for the imputation (last observation carried forward).
In the primary analysis of hemostatic efficacy, patients who were rated as “non-evaluable due to administrative reasons” were excluded and were considered to have experienced treatment failure.
Sensitivity and Subgroup Analyses
Sensitivity analyses were performed for both of the coprimary efficacy end points in patients who were otherwise efficacy-evaluable but who had a baseline anti-FXa level of less than 75 ng/mL for apixaban and rivaroxaban, less than 40 ng/mL for edoxaban, and less than 0.25 IU/mL for patients receiving enoxaparin. In addition, the primary efficacy analysis was performed for all patients in the safety population with a baseline anti-FXa level, including those below the evaluability threshold. For the coprimary end point of hemostatic efficacy, an additional sensitivity analysis was conducted in which all patient rated as “non-evaluable due to administrative reasons” were included and considered as having “poor or none” hemostatic efficacy.
Subgroup analyses were performed as exploratory analyses for the 2 coprimary end points. Two subgroups were of interest to this review based on input from the clinical experts consulted by CADTH: bleed type (GI, ICH, other) and renal function (eGFR of less than 50 mL/minute, eGFR of at least 50 mL/minute). No adjustment for type I error was made, nor was an interaction-by-subgroup test performed in the 2 subgroup analyses.
Secondary Efficacy End Points
There were no secondary efficacy end points in this study; however, a logistic regression model was used to estimate the OR of success of hemostatic efficacy (rated as excellent or good) by anti-FXa level activity as a covariate. This analysis was not believed by the CADTH review team to describe a meaningful effect, based on input from the clinical experts consulted by CADTH; therefore, the methods are not summarized in this report.
Exploratory Efficacy End Points
Occurrence of rebleeding, use of non–study-prescribed bleed products and/or hemostatic drugs, and change from baseline in NIHSS and GCS scores were analyzed using descriptive statistics. For the mRS analysis, the proportions of patients with an mRS score of 0 to 2 (i.e., qualified as success) and those with a score greater than 2 (i.e., qualified as failure) were presented at each assessment time point and the corresponding 95% Fisher exact CIs were presented. The proportion of patients who received an RBC transfusion and the Fisher exact 95% CI were presented. No quantitative analysis on the number of RBC units transfused per patient was reported.
Analysis Populations
The analysis populations of the ANNEXA-4 trial are summarized in Table 10.
Results
Patient Disposition
The patient disposition from the ANNEXA-4 trial is summarized in Table 11. The number of screening failures was not reported. In the ANNEXA-4 trial, 477 patients were enrolled, 17.2% of whom discontinued from the study, most commonly as a result of death (16.4%). The safety population consisted of all enrolled patients. The efficacy population consisted of 347 patients (72.7%). The most common reason for exclusion from the efficacy population was having a baseline anti-FXa level below the prespecified threshold (n = 94; 19.7%).
Table 9: Statistical Analysis of Efficacy End Points — ANNEXA-4 Trial
Testing hierarchy | End point | Statistical methods | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
1 | Percent change from baseline in anti-FXa activity (coprimary) |
|
|
|
2 | Proportion of patients with hemostatic efficacy at 12 hours after EOI (coprimary end point) |
|
|
|
NA | Achievement of hemostatic efficacy in patients with ICH at high risk of hematoma expansion (exploratory) | High-risk ICH population |
| NA |
NA | Occurrence of rebleeding (exploratory) |
| NA | NA |
NA | Number of RBC units transfused per patient (exploratory) | No quantitative analysis was reported | NA | NA |
NA | Proportion of patients receiving 1 or more RBC transfusion (exploratory) |
| NA | NA |
NA | Use of non–study-prescribed blood products and/or hemostatic drugs (exploratory) |
| NA | NA |
NA | Change from baseline in modified Rankin Scale (exploratory) |
| NA | NA |
NA | Change from baseline in National Institutes of Health Stroke Scale (exploratory) |
| Exclusion of patient from analysis if missing a value at baseline or 12 hours posttreatment | NA |
NA | Change from baseline in Glasgow Coma Scale (exploratory) |
| NA | NA |
BOCF = baseline observation carried forward; CI = confidence interval; EOB = end of bolus; EOI = end of infusion; FXa = factor Xa; ICH = intracranial hemorrhage; LOCF = last observation carried forward; NA = not applicable; RBC = red blood cell.
Note: No adjustment factors were applied to any of the analyses. The details in the table were taken from the sponsor’s summary of clinical evidence.20
aDescriptive statistics refers to, for example, mean (and standard deviation) or median (and range).
Source: ANNEXA-4 Clinical Study Report.19
Table 10: Analysis Populations — ANNEXA-4 Trial
Study | Population | Definition | Application |
|---|---|---|---|
ANNEXA-4 | Safety population | All patients treated who received any amount of andexanet alfa | Safety analyses: Analyzed by actual treatment received |
Efficacy population | All patients in the safety population who met all of the following criteria:
| Efficacy analyses: Performed by treatment assigned | |
High-risk ICH population | All patients in the efficacy population with an ICH with any of the following:
| Efficacy analyses: Performed by treatment assigned |
EAC = end point adjudication committee; FXa = factor Xa; Hb = hemoglobin; ICH = intracranial hemorrhage; ISTH = International Society on Thrombosis and Hemostasis.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.
aThe patients who met the ISTH-based bleeding inclusion criteria were those who had an acute overt major bleeding episode requiring urgent reversal of anticoagulation, which was defined as either: acute overt bleeding that is potentially life-threatening (e.g., with signs or symptoms of hemodynamic compromise); acute overt bleeding associated with a fall in Hb level by ≥ 2 g/dL, or an Hb ≤ 8 g/dL if no baseline Hb was available; or acute bleeding in a critical area or organ, such as a pericardial, intracranial, or intraspinal bleed.
Source: ANNEXA-4 Clinical Study Report.19
Table 11: Summary of Patient Disposition — ANNEXA-4 Trial
Patient disposition | ANNEXA-4 trial |
|---|---|
Screened, N | Not reported |
Enrolled, N | 477 |
Discontinued from study, n (%) | 82 (17.2) |
Reason for discontinuation, n (%) | |
Death | 78 (16.4) |
Early withdrawal | 2 (0.4)a |
Lost to follow-up | 1 (0.2) |
Withdrew consent | 1 (0.2)b |
Safety population, n (%) | 477 (100) |
Efficacy population, n (%) | 347 (72.7)c |
FXa = factor Xa.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.
aEarly withdrawal refers to patients who withdrew after day 1 and before day 30.
bWithdrawal of consent refers to patients who withdrew at hour 12.
cReasons for exclusion from the efficacy population in the ANNEXA-4 trial included patients who: had a baseline anti-FXa level below the efficacy threshold (i.e., baseline anti-FXa levels of < 75 ng/mL for apixaban and rivaroxaban, < 40 ng/mL for edoxaban, or < 0.25 IU/mL for enoxaparin) (n = 94), were missing a baseline anti-FXa level (n = 17), did not meet the clinical bleeding inclusion criteria (n = 14), did not meet the clinical bleeding inclusion criteria (refer to Table 4), or had a baseline anti-FXa level below the efficacy threshold (n = 5).
Source: ANNEXA-4 Clinical Study Report.19
Baseline Characteristics
A summary of baseline patient characteristics in the ANNEXA-4 trial is shown in Table 12. The baseline characteristics outlined in the table are limited to those that are most relevant to this review or were felt to impact the outcomes or interpretation of the study results.
The efficacy population had a mean age of 77.8 years (SD = 10.6). Fifty-three percent of patients were male. The majority of patients were white (86.5%). Most patients had a creatinine clearance of 30 mL/minute or above (84.7%) and received apixaban (49.6%) or rivaroxaban (37.5%). Bleeding was predominantly intracranial (71.2%) or GI (22.5%). Patients were hospitalized for a mean time of 3.4 hours (SD = not reported) before starting andexanet alfa treatment. At the time of informed consent for participation in the study, 76.9% of patients were in the emergency department and 15.9% of patients were in the ICU. No notable differences in the baseline characteristics were noted between the safety population and efficacy population.
Exposure to Study Treatments
In the ANNEXA-4 trial, 79.0% of the patients in the efficacy population received the low-dose regimen for andexanet alfa and 21.0% of patients received the high-dose regimen. The majority of patients (91.6%) completed andexanet alfa treatment without interruption, while others had study-drug interruptions (6.1%), modifications (1.4%), or a discontinuation (1.4%).
Table 12: Summary of Baseline Characteristics — ANNEXA-4 Trial
Characteristic | Safety population (N = 477) | Efficacy population (N = 347) |
|---|---|---|
Age (years), mean (SD) | 77.9 (10.7) | 77.8 (10.6) |
Male, n (%) | 259 (54.3) | 184 (53.0) |
Race, n (%) | ||
White | 414 (86.8) | 300 (86.5) |
Black or African American | 29 (6.1) | 21 (6.1) |
Other | 25 (5.2) | 20 (5.8) |
Missing | 9 (1.9) | 6 (1.7) |
Region, n (%) | ||
North America | 212 (44.4) | 152 (43.8) |
Europe | 248 (52.0) | 181 (52.2) |
Japan | 17 (3.6) | 14 (4.0) |
BMI (kg/m2), mean (SD) | 26.6 (5.6) | 26.6 (5.8) |
Creatinine clearance, n (%)a | ||
≥ 90 mL/minute | 91 (19.1) | 59 (17.0) |
≥ 60 and < 90 mL/minute | 137 (28.7) | 100 (28.8) |
30 to < 60 mL/minute | 180 (37.7) | 135 (38.9) |
< 30 mL/minute | 43 (9.0) | 34 (9.8) |
Missing data | 26 (5.5) | 19 (5.5) |
FXa inhibitor treatment, n (%) | ||
Apixaban | 245 (51.4) | 172 (49.6) |
Rivaroxaban | 174 (36.5) | 130 (37.5) |
Edoxaban | 36 (7.5) | 28 (8.1) |
Enoxaparin | 22 (4.6) | 17 (4.9) |
Bleed type, n (%) | ||
GI | 109 (22.9) | 78 (22.5) |
ICH | 329 (69.0) | 247 (71.2) |
Other | 39 (8.2) | 22 (6.3) |
Time from hospitalization to first dose of andexanet (hours), mean (SD) | 12.8 (53.1) | 11.6 (46.2) |
Location at time of informed consent, n (%) | ||
Emergency department | 364 (76.3) | 267 (76.9) |
Inpatient ward | 18 (3.8) | 13 (3.7) |
Intensive care unit | 78 (16.4) | 55 (15.9) |
Other | 17 (3.6) | 12 (3.5) |
BMI = body mass index; FXa = factor Xa; GI = gastrointestinal; ICH = intracranial hemorrhage; SD = standard deviation.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.
aCreatinine clearance was estimated according to the Cockcroft-Gault formula.
Source: ANNEXA-4 Clinical Study Report.19
Concomitant Medications
The use of concomitant medication, specifically coagulation factors, packed RBCs, non-RBC agents, and hemostatic agents, between the start of andexanet alfa bolus and 12 hours after EOI, was measured in the safety population and is summarized in Table 13. In the safety population, 24.7% received non–study-prescribed blood products and/or hemostatic drugs during this study period. The proportions of patients who received coagulation factor transfusions, hemostatic treatments, other coagulation products, or packed RBCs were 4.4%, 1.3%, 1.0%, and 20.3%, respectively.
Table 13: Concomitant Medications of Interest — ANNEXA-4 Trial (Safety Population)
Use of concomitant medications of interest (start of bolus to 12 hours after EOI), n (%) | ANNEXA-4 trial (N = 477) |
|---|---|
Coagulation factors, packed RBCs, non-RBC blood product, or hemostatic drug | 118 (24.7) |
Coagulation factor transfusion | 21 (4.4) |
Platelets | 16 (3.4) |
4-factor PCC | 3 (0.6) |
Fresh frozen plasma | 2 (0.4) |
Antithrombin III | 1 (0.2) |
Human albumin | 1 (0.2) |
Plasma | 1 (0.2) |
Vitamin K | 1 (0.2) |
Packed RBC transfusion | 97 (20.3) |
Hemostatic treatments | 6 (1.3) |
Tranexamic acid | 5 (1.0) |
Carbazochrome sodium sulfonate hydrate | 0 |
Phenylephrine | 1 (0.2) |
Other blood or coagulation treatment | 5 (1.0) |
EOI = end of infusion; PCC = prothrombin complex concentrate; RBC = red blood cell.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.
Source: ANNEXA-4 Clinical Study Report.19
Protocol Deviations
Major protocol deviations were reported in 59.1% of patients in the safety population. Major protocol deviations were most commonly related to missing or out-of-window laboratory data (35.4%) (e.g., anti-FXa data, hemoglobin level) and andexanet dosing (28.9%) (e.g., incorrect bolus or infusion rate, infusion dose, infusion started later than acceptable).
Efficacy
The efficacy results for the ANNEXA-4 trial are shown in Table 14, unless otherwise specified.
Anti-FXa Activity
Change From Baseline in Anti-FXa Activity (Coprimary End Point)
In the primary analysis, the median percent change from baseline in anti-FXa activity at on-treatment nadir (i.e., minimum value between EOB and EOI) in the efficacy population was −93.3% (95% CI, −94.2% to −92.5%) in apixaban-treated patients and −94.1% (95% CI, −95.1% to −93.0%) in rivaroxaban-treated patients. Subgroup analyses showed results consistent with the primary analysis across bleed types (ICH, GI, other bleeds) (Table 31 in Appendix 1); however, a subgroup analysis of eGFR level is not available.
A sensitivity analysis in patients who were otherwise efficacy-evaluable but who had a baseline anti-FXa level below the prespecified threshold (i.e., 75 ng/mL for apixaban and rivaroxaban, 40 ng/mL for edoxaban, and 0.25 IU/mL for enoxaparin) was planned but not performed. The results in the safety population (which included patients with low baseline anti-FXa levels) were consistent with the primary analyses, with a median percent change from baseline in anti-FXa activity at on-treatment nadir in apixaban-treated patients of −92.6% (95% CI, −93.1% to −91.9%) and −92.9% (95% CI, −93.7% to −90.7%) in rivaroxaban-treated patients.
Hemostatic Efficacy
Achievement of Hemostatic Efficacy (Coprimary End Point)
In the primary analysis of hemostatic efficacy, 80.0% (95% CI, 75.3 to 84.1) of the efficacy population achieved good or excellent hemostatic efficacy. The results of the 3 sensitivity analyses (which assessed the effect of including patients rated as “non-evaluable for administrative reasons” in the safety population with a baseline anti-FXa level, and in patients otherwise efficacy-evaluable but whose baseline anti-FXa level was below the prespecified threshold) were consistent with the primary analysis, as shown in Table 32 in Appendix 1. The results of the subgroup analyses were also consistent with the primary analysis across the 2 subgroups of interest (bleed type and eGFR), as shown in Figure 2 in Appendix 1.
Achievement of hemostatic efficacy in patients with ICH with a high risk of hematoma expansion (i.e., in the high-risk ICH population) was an exploratory end point. Results in the high-risk ICH population were consistent with the ICH subpopulation as well as the overall efficacy population.
Rebleeding (Exploratory End Point)
Of the 264 patients in the safety population after the implementation of Protocol Amendment 4 (when rebleeding was added as an exploratory outcome), rebleeding as adjudicated by the EAC (exploratory end point) occurred in 1 patient (0.4%).
Use of Blood Products and Hemostatic Drugs
Use of Non–Study-Prescribed Blood Products and Hemostatic Drugs (Exploratory End Point)
In the safety population, 24.7% received non–study-prescribed blood products and/or hemostatic drugs between the start of andexanet alfa treatment and 12 hours after the end of the infusion. The proportions of patients who received coagulation factor transfusion, hemostatic treatments, other coagulation products, and packed RBC transfusion were 4.4%, 1.3%, 1.0%, and 20.3%, respectively (Table 13).
Number of RBC Units Transfused (Exploratory End Point)
The number of RBC units transfused was recorded on the case report form; however, no quantitative analysis was conducted on the data.
Proportion of Patients Who Received 1 or More RBC Transfusions (Exploratory End Point)
In the safety population, 19.5% (95% CI, 16.0% to 23.3%) of patients received 1 or more RBC transfusions.
Clinical Neurologic Status in ICH Patients
Change From Baseline in mRS Score (Exploratory End Point)
The proportions of patients with ICH in the efficacy population who had an mRS score of 0 to 2 at baseline, 1 hour posttreatment, 12 hours posttreatment, and day 30 were 32.2% (95% CI, 26.4% to 38.5%), 22.6% (95% CI, 16.1% to 30.3%), 23.4% (95% CI, 16.8% to 31.2%), and 35.9% (95% CI, 29.6% to 42.7%), respectively.
Change From Baseline in NIHSS Score (Exploratory End Point)
The mean change from baseline in NIHSS score at 1 hour posttreatment, 12 hours posttreatment, and day 30 was 0.4 (SD = 2.66), 1.0 (SD = 3.58), and −1.0 (SD = 4.96), respectively, in the patients with ICH in the efficacy population.
Change From Baseline in GCS Score (Exploratory End Point)
The mean change from baseline in GCS score at 1 hour posttreatment, 12 hours posttreatment, and day 30 was −0.4 (SD = 1.69), −0.6 (SD = 2.06), and 0.2 (SD = 2.23), respectively, in the patients with ICH in the efficacy population.
ICU Admission, Hospital Length of Stay, HRQoL
ICU admission and duration and HRQoL were not measured in the ANNEXA-4 trial. Hospital length of stay was not an efficacy outcome in the trials but the median was reported to be 10.9 days in the safety population.
Table 14: Key Efficacy Results — ANNEXA-4 Trial
Outcome | All patients |
|---|---|
Anti-FXa activity (efficacy population)a | |
Apixaban-treated patients, n | 172 |
Baseline (ng/mL), median (95% CI) | 146.9 (132.6 to 163.9) |
Change from baseline at on-treatment nadir (ng/mL),b,c median (95% CI) | −136.2 (−148.1 to −121.3) |
% change from baseline at on-treatment nadir (%),b,c median (95% CI) | −93.3 (−94.2 to −92.5) |
Rivaroxaban-treated patients, n | 130 |
Baseline, median (95% CI) | 213.5 (180.8 to 245.3) |
Change from baseline at on-treatment nadir (ng/mL),b,c median (95% CI) | −175.3 (−197.6 to −149.9) |
% change from baseline at on-treatment nadir (%),b,c median (95% CI) | −94.1 (−95.1 to −93.0) |
Hemostatic efficacy | |
Proportion of patients achieving “good” or “excellent” hemostatic efficacy at 12 hours after the EOId (%) (95% CIe) | — |
Efficacy population (N = 340) | 80.0 (75.3 to 84.1) |
P value | < 0.001 |
ICH subpopulation (N = 244) | 79.1 (73.5 to 84.0) |
High risk of hematoma expansion subgroup (N = 153) | 75.8 (68.2 to 82.4) |
Low risk of hematoma expansion subgroup (N = 91) | 84.6 (75.5 to 91.3) |
Occurrence of rebleeding (safety population),f n/N (%) | 1/264 (0.4) |
Use of blood products and hemostatic drugs (safety population) | |
Patients who received 1 or more RBC transfusion by day 30, n/N (%) | 93/477 (19.5) |
95% CI of proportion of patients who received 1 or more RBC transfusion by day 30g | 16.0 to 23.3 |
Patients who received non–study-prescribed blood product and/or hemostatic drugs between the start of andexanet treatment and 12 hours after the EOI, n/N (%)h | 118/477 (24.7) |
Clinical neurologic status (patients with ICH in efficacy population) | |
Modified Rankin Scale | — |
Proportion of patients with a modified Rankin Scale score of 0 to 2 (%) (95% CIg) | — |
Baseline (n = 245) | 32.2 (26.4 to 38.5) |
At 1 hour (n = 146) posttreatment | 22.6 (16.1 to 30.3) |
At 12 hours (n = 145) posttreatment | 23.4 (16.8 to 31.2) |
At day 30 (n = 217) | 35.9 (29.6 to 42.7) |
NIHSSi | — |
Baseline score, mean (SD) (n = 146) | 6.7 (6.33) |
Change from baseline in score, mean (SD) | — |
At 1 hour (n = 139) posttreatment | 0.4 (2.66) |
At 12 hours (n = 138) posttreatment | 1.0 (3.58) |
At day 30 (n = 100) | −1.0 (4.96) |
Glasgow Coma Scalei | — |
Baseline score, mean (SD) (n = 242) | 13.9 (1.72) |
Change from baseline in score, mean (SD) | — |
At 1 hour (n = 141) posttreatment | −0.4 (1.69) |
At 12 hours (n = 140) posttreatment | −0.6 (2.06) |
At day 30 (n = 107) | 0.2 (2.23) |
CI = confidence interval; EOI = end of infusion; FXa = factor Xa; ICH = intracranial hemorrhage; NIHSS = National Institutes of Health Stroke Scale; RBC = red blood cell; SD = standard deviation.
Note: Outcomes summarized in this table were noted to be important to patients and clinicians based on input received from patient groups, clinician groups, and the clinical experts consulted by CADTH.
The details in the table were taken from the sponsor’s summary of clinical evidence.20
aResults were presented by FXa inhibitor received. Results of edoxaban- and enoxaparin-treated patients were not of interest to this review and, hence, not summarized.
bThe on-treatment nadir was defined as the minimum value observed from the start of andexanet alfa administration (30 minutes after bolus) to 30 minutes before EOI. If the results of both time points were missing, then it was equal to the baseline value.
cFor patients with missing values for nadir, change and percent change were imputed as zero. The 95% CI for the median was based on the distribution-free method.
dAchievement of hemostatic efficacy refers to patients with an “excellent” or “good” hemostatic efficacy result as adjudicated by the end point adjudication committee. Patients adjudicated as non-evaluable for clinical reasons are included in the efficacy population and were considered as having a “poor or none” hemostatic efficacy result. Patients adjudicated as non-evaluable for administrative reasons (n = 7) were excluded.
eCI based on the exact binomial method.
fRebleeding was defined as recurrent bleeding from the same (or different) anatomic site in patients within 24 hours of initial andexanet alfa treatment and after achieving initial good or excellent hemostasis, as adjudicated by the end point adjudication committee.
gCI based on the Fischer exact method.
hRefers to the use of these treatments between the start of andexanet treatment and 12 hours after the EOI. Treatments included platelets, 4-factor prothrombin complex concentrate, fresh frozen plasma, antithrombin III, human albumin, plasma, vitamin K, packed RBC transfusion, tranexamic acid, carbazochrome sodium sulfonate hydrate, phenylephrine, and other blood or coagulation treatments.
INIHSS testing and the additional Glasgow Coma Scale assessments were not implemented until Protocol Amendment 4; therefore, the number of patients evaluated was lower for the baseline NIHSS and the later time points for the Glasgow Coma Scale.
Source: ANNEXA-4 Clinical Study Report.19
Harms
A summary of harms in the ANNEXA-4 trial is shown in Table 15.
Adverse Events
A TEAE was reported in 72.5% of patients, with the most common TEAEs being urinary traction infection (10.5%) and pneumonia (8.2%).
Serious Adverse Events
Serious TEAEs were reported in 41.9% of patients, with the most common being pneumonia (4.2%), respiratory failure (2.5%), and ischemic stroke (2.1%).
Withdrawal Due to Adverse Events
Four patients (0.8%) discontinued treatment due to TEAEs (i.e., sudden death, cerebral vascular accident, acute myocardial infarction, and infusion-related reaction; 1 of each).
Mortality
Death occurred in 17.0% of patients. Cardiovascular and noncardiovascular-related deaths were reported in 12.8% and 3.1% of patients, respectively.
Notable Harms
Thromboembolic events were reported in 10.5% of patients, including cerebrovascular accident (4.6%), DVT (2.5%), myocardial infarction (1.9%), PE (1.0%), and transient ischemic attack (0.4%). Infusion-related reaction was reported in 2 patients (0.4%). There was no report of neutralizing antibodies to FX, FXa, or andexanet alfa.
Table 15: Summary of Harms — ANNEXA-4 Trial (Safety Population)
Harms | ANNEXA-4 trial (N = 477) |
|---|---|
TEAE, n (%) | |
Patients with ≥ 1 TEAE | 346 (72.5) |
Most common TEAEsa | |
Urinary tract infection | 50 (10.5) |
Pneumonia | 39 (8.2) |
Delirium | 21 (4.4) |
Hypotension | 19 (4.0) |
Pyrexia | 19 (4.0) |
Serious TEAE, n (%) | |
Patients with ≥ 1 serious TEAE | 200 (41.9) |
Most common serious TEAEsb | |
Pneumonia | 20 (4.2) |
Respiratory failure | 12 (2.5) |
Ischemic stroke | 10 (2.1) |
Patients who stopped treatment due to a TEAE, n (%) | |
Patients who stopped treatment due to adverse events | 4 (0.8) |
Sudden death | 1 (0.2) |
Cerebral vascular accident | 1 (0.2) |
Acute myocardial infarction | 1 (0.2) |
Infusion-related reaction | 1 (0.2) |
Death, n (%) | |
Patients who died | 81 (17.0)c,d |
Cardiovascular: Related to bleeding | 41 (8.6) |
Cardiovascular: Not related to bleeding | 20 (4.2) |
Noncardiovascular | 15 (3.1) |
Uncertain | 3 (0.6) |
Unknowne | 2 (0.4) |
Notable harm, n (%) | |
Thrombotic eventf | 50 (10.5) |
Cerebrovascular accident | 22 (4.6) |
Deep vein thrombosis | 12 (2.5) |
Myocardial infarction | 9 (1.9) |
Pulmonary embolism | 5 (1.0) |
Transient ischemic attack | 2 (0.4) |
Infusion-related reaction | 2 (0.4)g |
Neutralizing antibodies to FX, FXa, or andexanet alfa | 0 |
FX = factor X; FXa = factor Xa; TEAE = treatment-emergent adverse event.
Note: Unless otherwise specified, safety data were presented by MedDRA preferred term.
The details in the table were taken from the sponsor’s summary of clinical evidence.20
aPresent in ≥ 4% of patients in the ANNEXA-4 trial.
bPresent in ≥ 2% of patients.
cThe survival status of 6 patients could not be determined (3 patients were lost to follow-up, 1 patient withdrew early before study day 30, and 1 patient withdrew consent at hour 12); these patients are included in the analysis and considered to be still alive.
dThe reasons for the deaths that occurred during the 30-day safety follow-up period were adjudicated by the end point adjudication committee.
eRefers to the patients who were not adjudicated.
fAs adjudicated by the end point adjudication committee.
gOne patient experienced serious infusion-related reactions.
Source: ANNEXA-4 Clinical Study Report.19
Critical Appraisal
Internal Validity
The open-label single-arm design of the trial is a key limitation to interpreting the estimates of the study. The lack of randomization precludes conclusions on whether any observed effect could be attributed to andexanet alfa alone.56 Further, the open-label study design could increase uncertainty in neurologic status outcomes (mRS, NIHSS, and GCS) due to potential reporting bias, given that these scales involve subjective assessment of clinical parameters by the investigators. However, the presence and extent of such bias could not be determined from the trial data alone. The risk of bias due to the open-label design was low for objective outcomes, including anti-FXa activity, need for RBC transfusion (determined based on a study-defined, hemoglobin-based criterion), and need for other blood products and hemostatic drugs (administered as per institutional or local protocol). The concern was similarly low for hemostatic efficacy and rebleeding, which were adjudicated by an independent EAC that was blinded to anti-FXa activity levels of patients based on predefined criteria of objective measures (e.g., CT, MRI, echocardiogram, hemoglobin, hematocrit).
A large number of protocol deviations related to missing or out-of-window laboratory data (35.4%) and andexanet dosing (28.9%) was reported; however, it is unclear whether such deviations had any impact on the study findings.
The study was adequately powered to detect a response rate that has a 95% CI completely above a prespecified threshold of 50% with respect to the coprimary end point of effective hemostasis. The clinical experts consulted by CADTH noted that response rate could vary considerably by bleed type, although they considered the threshold of 50% assumed by the sponsor to be acceptable in the given study population. All end points other than the coprimary end points were exploratory, which preclude definitive conclusions to be drawn from these analyses. Subgroup analyses were performed on both coprimary end points; however, the findings should be considered exploratory due to the lack of sample size consideration, control for multiplicity, and treatment-by-subgroup interaction analysis.
The primary analyses of the coprimary end points were not assessed in the full trial population and instead were conducted in the efficacy population, including patients who had a baseline anti-FXa level above the prespecified threshold and who met the ISTH-based bleeding criteria for inclusion. A total of 130 of 477 enrolled patients (27.3%) were excluded from the efficacy population, most due to a baseline anti-FXa level below the prespecified threshold (19.7%). The sponsor noted that anti-FXa levels below the threshold are considered subtherapeutic and the exclusion of patients with such baseline anti-FXa levels from the efficacy population was to ensure that patients included in the analysis had at least therapeutic anti-FXa levels. The selection of patients with higher baseline anti-FXa levels introduces the potential for bias due to regression to the mean and likely produces an overestimation of the change in anti-FXa levels posttreatment.57 The impact of excluding such patients from the primary analysis of hemostatic efficacy was assessed in 2 sensitivity analyses (i.e., in otherwise efficacy-evaluable patients with a baseline anti-FXa level below the threshold, and in the safety population of patients with a baseline anti-FXa level), both of which showed results consistent with the primary analysis. No sensitivity analysis was conducted for the other end points studied in the efficacy population (i.e., mRS, NIHSS, GCS); therefore, the impact of excluding patients with a low baseline anti-FXa level from the primary analysis of these exploratory outcomes is unclear.
Study discontinuation occurred in 17.2% of patients, most commonly as a result of death. The baseline observation carried forward and last observation carried forward approaches that were used for imputation of missing data in the analysis of percent change from baseline in anti-FXa activity describe a hypothetical scenario in which patients would have survived to day 30. The target estimand is unclear, but these approaches likely produced a conservative estimate of percent change in anti-FXa activity that would be observed in clinical practice. There is uncertainty in the neurologic status outcomes, given that there were a lot of missing data at the posttreatment assessment time points (between 12.1% and 56.7% for the mRS and GCS analyses at all time points; 31.5% on day 30 for the NIHSS analysis). No data imputation was performed to account for the missing data. There is a risk of attrition bias, since the patients who remained in the trial were more likely to be those who had a better treatment response, although the magnitude of bias is unclear.
There is some evidence for the reliability of the hemostatic efficacy rating system, although evidence for validity and responsiveness was not identified. Exploratory analyses of the ANNEXA-4 trial suggested there was a correlation between achieving hemostatic efficacy and lower mortality, but not between anti-FXa activity and mortality in andexanet alfa–treated patients;17 however, these correlations do not describe a causal surrogate mechanism and can be largely explained by patients at high risk of death having poor prognostic factors. As noted in the FDA Guidance for Industry: Expedited Programs for Serious Conditions — Drugs and Biologics, evidence of pharmacological activity alone is insufficient to support a conclusion that a relationship of an effect on a surrogate end point to the effect on a clinical outcome is reasonably likely.58 Nonetheless, in the FDA Summary Basis for Regulatory Action for andexanet alfa, the FDA considered reduction of anti-FXa activity by andexanet alfa to be reasonably likely to predict clinical benefits in morbidity and mortality upon consideration of biological plausibility and the magnitude of anti-FXa activity reduction in the studies of healthy volunteers.39
External Validity
The clinical experts consulted by CADTH noted that the inclusion and exclusion criteria of the study in general align with the criteria for selecting candidates for reversal treatment of major bleeding related to FXa inhibition although, in their opinion, the exclusion of patients with a severe ICH (GCS score less than 7, estimated intracerebral hematoma volume above 60 cc) and an expected survival of less than 1 month could result in a study population with a better prognosis than seen in clinical practice. In addition, the clinical experts noted that the study population is younger compared with clinical practice, and it is reasonable to expect that younger patients would have better clinical outcomes. Patients without major bleeding but who require emergency surgery are also expected to be reasonable candidates for andexanet alfa, according to clinical expert input; however, such patients were not included in the study and the treatment effect within this population is unknown.
The dosing criteria of andexanet alfa in the study were consistent with the product monograph. The use of blood products and hemostatic drugs (e.g., RBC transfusion, antifibrinolytics) was generally in line with clinical practice, according to the clinical experts.
The clinical experts noted that while hemostatic efficacy, as assessed using modified ISTH criteria, is a commonly measured outcome in clinical trials of reversal agents for major bleeds, the criteria were adjudicated based on imaging and laboratory findings, which are not patient-important outcomes. The clinical experts expressed that the relevance of anti-FXa activity level is limited from a clinician’s perspective. They noted that anti-FXa level is not routinely measured in clinical practice and anti-FXa level is not a known surrogate marker for bleeding-related outcomes in patients receiving a DOAC. As such, this would favour interpretation of the results from the safety population rather than the efficacy population, which removed patients based on anti-FXa levels. The clinical experts noted that clinical outcomes such as mental and functional statuses and mortality are much more meaningful to patients and clinicians and have more weight in the overall assessment of treatment response. The neurologic status scales used in the study (i.e., GCS, NIHSS, mRS) are routinely conducted in clinical practice to assess the functional status of patients with an ICH and were considered to be relevant, per the clinical experts. The outcomes of interest to the clinical experts, which were not assessed, are ICU admission, hospital length of stay, and HRQoL; hence, the effect of andexanet alfa on these outcomes is unknown. The clinical experts considered the assessment time frame of hemostatic efficacy (12 hours postinfusion), neurologic status scales, and safety (up to 30 days for both) to be informative for describing the treatment effects of andexanet alfa.
This is the only phase III trial to date assessing the efficacy and safety of andexanet alfa in the reversal of an acute major bleed related to treatment with an FXa inhibitor. The absence of direct comparative evidence between andexanet alfa and PCC (the most relevant comparator for andexanet alfa, according to the clinical experts consulted by CADTH) represents a gap in the evidence.
Summary of ANNEXA-A and ANNEXA-R Trials
The CADTH review team, in consultation with the clinical experts, considered the relevance of the pivotal ANNEXA-A and ANNEXA-R trials to be limited, given that the study population does not align with the indicated population of andexanet alfa. The study design and findings are briefly summarized subsequently.
Description of Studies
ANNEXA-A and ANNEXA-R were similarly designed phase III, randomized, double-blind, placebo-controlled trials that aimed to compare andexanet alfa and placebo with respect to reversal of apixaban (ANNEXA-A trial) or rivaroxaban (ANNEXA-R trial) anticoagulation in healthy individuals aged 50 to 75 years with well-controlled, chronic, stable medical conditions who were not actively bleeding or at low risk of abnormal bleeding or thrombosis based on laboratory tests, risk factors, and medical history (ANNEXA-A trial, N = 68; ANNEXA-R trial, N = 80). Patients received either apixaban (ANNEXA-A trial) or rivaroxaban (ANNEXA-R trial) treatment for 4 days before being randomized to either andexanet alfa or placebo. Patients were divided into 2 cohorts (part 1 and part 2) that followed different dosing regimens for andexanet alfa (IV bolus only in part 1; bolus followed by continuous IV infusion in part 2). Note that the results of part 1 are not of interest to this review, since the dose in that cohort does not align with the recommended dose in the product monograph.
Results: Part 2
Efficacy
In part 2, the enrolled patients had a mean age of 59.4 (SD = 7.5) years in the ANNEXA-A trial and 57.3 (SD = 5.16) years in the ANNEXA-R trial. In both trials, the majority of patients were male and white.
The key efficacy results for part 2 of the trials are summarized in Table 16. In both trials, the analyses of the between-arm difference with respect to mean percent change from baseline in anti-FXa activity at nadir after the EOI (primary end point) and mean percent change from baseline in anti-FXa activity at nadir after the EOB (secondary end point) were both in favour of andexanet alfa. As well, all patients in the andexanet alfa arms and no patient in the placebo arms had at least an 80% reduction in anti-FXa activity from baseline at nadir after the EOI (secondary end point).
Harms
In the ANNEXA-A trial, a TEAE was reported in 10 patients (41.7%) in the andexanet alfa arm and 4 patients (50.0%) in the placebo arm. In the ANNEXA-R trial, a TEAE was reported in 11 patients (42.3%) in the andexanet arm and 6 patients (46.2%) in the placebo arm. There were no reports of any serious TEAEs or death in either trial. Study treatment discontinuation due to an adverse event was reported in 1 patient in each arm of the ANNEXA-A trial and in none of the patients in the ANNEXA-R trial. There were no reported deaths in either trial.
Table 16: Key Efficacy Results of ANNEXA-A and ANNEXA-R Trials — Part 2 (Efficacy Analysis Population)
Outcomes | ANNEXA-A trial (part 2) | ANNEXA-R trial (part 2) | ||
|---|---|---|---|---|
Andexanet alfa (N = 23) | Placebo (N = 8) | Andexanet alfa (N = 26) | Placebo (N = 13) | |
% change from baseline in anti-FXa activity | ||||
Patients contributing to the analyses, n (%) | 23 (100) | 8 (100) | 26 (100) | 13 (100) |
Baseline anti-FXa activity, mean (ng/mL) (SD) | 173.0 (50.5) | 191.7 (34.4) | 335.3 (91.0) | 317.2 (91.0) |
% change from baseline at nadir after the EOI,a mean (SD) | −92.3 (2.8) | −32.7 (5.6) | −96.7 (1.8) | −44.8 (11.7) |
Difference in meansb (95% CI) | −59.5 (−64.1 to −55.2) | −51.9 (−58.0 to −47.0) | ||
P valuec,d | < 0.0001 | < 0.0001 | ||
% change from baseline at the nadir after the EOB,e mean (SD) | −93.5 (1.5) | −16.7 (4.1) | −95.3 (1.6) | −23.6 (10.3) |
Difference in meansb (95% CI) | −77.1 (−80.0 to −74.0) | −74.5 (−78.9 to −64.5) | ||
P valuec,d | < 0.0001 | < 0.0001 | ||
Occurrence of ≥ 80% reduction in anti-FXa activity from baseline at nadira | ||||
Patients contributing to the analyses, n (%) | 23 (100) | 8 (100) | 26 (100) | 13 (100) |
≥ 80% reduction, n (%) | 23 (100) | 0 | 26 (100) | 0 |
P valued,f | < 0.0001 | < 0.0001 | ||
CI = confidence interval; EOB = end of bolus; EOI = end of infusion; FXa = factor Xa; SD = standard deviation.
Note: Baseline is the last assessment obtained before the bolus dose of andexanet alfa or placebo. Only patients with both a baseline and postbaseline assessment are presented in the table. The outcomes summarized in this table were noted to be important to patients and clinicians based on input received from patient groups, clinician groups, and the clinical experts consulted by CADTH.
The details in the table were taken from the sponsor’s summary of clinical evidence.20
aFor part 2, nadir after the EOI was defined as the smallest value for anti-FXa activity between the 110-minute time point (10 minutes before the end of the infusion) and the 5-minute time point after the completion of the infusion for each patient.
bBetween-arm difference was calculated using the Hodges-Lehman estimate of shift method.
cP value obtained from a 2-sided exact Wilcoxon rank sum test.
dThe end point has been adjusted for multiplicity.
eFor part 2, the nadir after the EOB was defined as the smaller value for anti-FXa activity at the + 2 minute or + 5 minute time point after the completion of the andexanet alfa bolus.
fComparison between arms was conducted using a Fisher exact test.
Sources: ANNEXA-A and ANNEXA-R Clinical Study Reports.49,50
Infusion-related reaction was reported in 4 patients (16.7%) in the andexanet alfa arm and 2 patients (25.0%) in the placebo arm in the ANNEXA-A trial, and none of the patients in the ANNEXA-R trial. There were no reported thromboembolic events or neutralizing antibodies to FX, FXa, or andexanet alfa in either trial.
Long-Term Extension Studies
No long-term extension studies were identified by the sponsor.
Indirect Evidence
No indirect evidence in the form of a network meta-analysis or matched-adjusted analysis were submitted for this review. Three weighted comparative analyses involving comparisons of IPD were submitted by the sponsor and are presented in the following section.
Studies Addressing Gaps in the Pivotal and RCT Evidence
The contents of this section were informed by materials submitted by the sponsor. The following was summarized and validated by the CADTH review team.
The sponsor identified 3 gaps in the pivotal and RCT evidence:
lack of comparative evidence versus the treatment used in current clinical practice (i.e., 4F-PCC)
lack of comparative evidence in the intended patient population
lack of evidence on health care resource use and mortality outcomes
To address these gaps, the sponsor submitted 3 studies presenting weighted comparative evidence for andexanet alfa in the pivotal trial (ANNEXA-4) versus PCC in real-world clinical practice, and 6 studies summarizing comparative observational evidence of andexanet alfa versus PCC in real-world clinical practice.
Weighted Comparative Observational Evidence: Andexanet Alfa in the Pivotal Trial Versus PCC in Real-World Clinical Practice
Description of Studies
Due to the lack of evidence from RCTs comparing andexanet alfa with PCC, the sponsor submitted 3 published observational analyses comparing IPD between the ANNEXA-4 trial and 3 external cohorts that recorded the use of PCC in real-world clinical practice, including the ORANGE study in the UK, the HHCS in the US, and the German-Wide Multicenter Analysis of Oral Anticoagulant-Associated Intracerebral Hemorrhage Part Two (RETRACE-II) study.21-23,59,60
All analyses were conducted in patients with major bleeding while receiving apixaban or rivaroxaban; in particular, patients with ICH in the analyses of the ANNEXA-4 trial versus the HHCS and the ANNEXA-4 trial versus the RETRACE-II study. Outcomes of interest to this review included 30-day mortality (included in all studies), hemostatic efficacy, thrombotic events (assessed in the analysis of the ANNEXA-4 trial versus the HHCS), and hematoma expansion, change in ICH lesion volume, 30-day in-hospital mortality, and mRS score (assessed in the analysis of the ANNEXA-4 trial versus the RETRACE-II study). PSM or weighting was used to adjust for potential confounding variables due to the absence of investigator control of treatment assignment in these studies. The key study design features and analysis methods of these studies are summarized in Table 17.
ANNEXA-4 Trial Versus the ORANGE Study
Objective
The objective of this study was to compare the effectiveness of andexanet alfa versus PCC in apixaban- or rivaroxaban-treated adults with a life-threatening or uncontrollable major bleeding event.
Study Selection: ANNEXA-4 Trial Versus the ORANGE Study
IPD from 2 sources were included in the sponsor’s study: the ANNEXA-4 trial and the ORANGE study, the latter of which enrolled patients receiving a range of treatments, including PCC. The ORANGE study was a 3-year (2013 to 2016) prospective cohort trial that collected information from multiple UK hospitals on adult patients who were admitted for a major bleeding episode while on an oral anticoagulant therapy. The results of the ANNEXA-4 trial were based on patients enrolled between April 2015 and May 2018.
Table 17: Key Study Design Features and Analysis Methods Used for Studies Submitted by the Sponsor
Characteristics | ANNEXA-4 trial vs. the ORANGE study | ANNEXA-4 trial vs. the HHCS | ANNEXA-4 trial vs. the RETRACE-II study |
|---|---|---|---|
Study design of the propensity score analysis | |||
Population | Apixaban- or rivaroxaban-treated adults with a life-threatening or uncontrollable major bleeding event | Apixaban- or rivaroxaban-treated adults hospitalized for an acute ICH episode | Apixaban- or rivaroxaban-treated adults hospitalized for ICH |
Intervention | Andexanet alfa (ANNEXA-4 trial) | ||
Comparator | PCC (ORANGE study) | 4F-PCC (HHCS) | Usual care comprised of treatment according to the physician’s discretion, primarily PCC (RETRACE-II) |
Outcome | 30-day mortality |
|
|
Study design of comparator trial | |||
Study design | ORANGE study: Prospective cohort study that collected information from multiple UK hospitals on the presentation and clinical outcomes of patients who were admitted for a major bleeding episode while on oral anticoagulant therapy | HHCS: Retrospective study using electronic health record data across the HHC system (consisting of 5 acute care hospitals in the northeastern US) to collect data on adults admitted for ICH and receiving 4F-PCC | RETRACE-II study: Observational cohort study that included patients with ICH during oral anticoagulation in Germany |
Patient recruitment time frame | 2013 to 2016 | December 1, 2016, to August 30, 2020 | January 2011 to December 2015 |
Analysis methods | |||
Analysis method | Propensity score matching analysis | Propensity score overlap–weighted analysis | Inverse propensity score–weighted analysis |
Covariates used for adjustment | Age, bleed site (ICH, GI bleed, other bleeds), medical history of AF, hypertension, diabetes, cancer, renal dysfunction, stroke, deep vein thrombosis, pulmonary embolism, coronary artery disease, transient ischemic attack | Age; sex; BMI; creatinine clearance; AF as the indication for oral anticoagulation; average SBP at admission (> 160 mm hg); medical history of HF, diabetes, MI, or stroke; concomitant antiplatelet use; time from index scan to reversal agent initiation; time from end of reversal agent administration to repeat scan; traumatic vs. spontaneous bleeding; infratentorial region involvement; single- vs. multi-compartment bleed; or bleeding in the intracerebral, intraventricular, subdural, or subarachnoid space on index scan and a bleed size > 10 mL in volume or 10 mm in thickness on index scan | Hematoma expansion analysis:c Prior use of antiplatelets, DOAC indication classified as “other,” initial ICH volume, Glasgow Coma Scale score, presence of infratentorial bleeding or intraventricular hemorrhage Mortality analysis:c Diastolic BP, history of diabetes, eGFR level, ICH score, Glasgow Coma Scale score, HAS-BLED score, presence of infratentorial bleeding or intraventricular hemorrhage mRS analysis:c SBP, history of dyslipidemia, eGFR level, ICH score, HAS-BLED score, CHA2DS2-VASc score, hemoglobin level |
Sensitivity analysis | Patients were matched by intracranial compartment: intracerebral, subarachnoid, and subdural bleeds in the ANNEXA-4 trial (no patients had epidural intracranial bleeds), and intracerebral, subarachnoid, subdural, or epidural bleeds in the ORANGE study | Attainment of hemostatic effectiveness (or lack thereof) for patients without a repeat scan within 24 hours was adjudicated based on clinical judgment by 2 independent investigators after a review of outcomes (e.g., need for unplanned surgery, subsequent administration of reversal agent, mortality) rather than being assumed to represent poor or no effectiveness | Sensitivity analyses included all covariates for propensity score model, patients with available baseline anti-FXa inhibitor levels or National Institutes of Health Stroke Scale values only, all follow-up radiographic measurements (independent of their time postbaseline), and time between initial and follow-up imaging |
Subgroup analysis | ICH, GI bleed, and other bleeds (non-ICH or GI) | Patients with only an intracerebral and/or intraventricular hemorrhage and available pre- and post-bleed scans | RETRACE-II study patients with PCC treatment |
4F-PCC = 4-factor prothrombin complex concentrate; AF = atrial fibrillation; BMI = body mass index; BP = blood pressure; DOAC = direct oral anticoagulant; eGFR = estimated glomerular filtration rate; FXa = factor Xa; GI = gastrointestinal; HF = heart failure; HHC = Hartford Health care; HHCS = Hartford Health care study; ICH = intracranial hemorrhage; MI = myocardial infraction; mRS = modified Rankin Scale; SBP = systolic blood pressure; vs. = versus.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.20
aThis outcome is not of interest to this review and the results have not been summarized in this report.
bResults for 30-day mortality since the analysis was done after failure of the statistical hierarchy (at 30-day in-hospital mortality).
cThese covariates were selected for inclusion from a list of predefined covariates based on predefined selection methods to include only the most important variable into the propensity score model. The list of predefined covariates considered for inclusion included age, gender, race, weight, body temperature, mean arterial pressure, systolic blood pressure, diastolic blood pressure, apixaban use, rivaroxaban use, reduce dose and last intake of DOAC, indication of DOAC, comorbidities (e.g., hypertension, diabetes dyslipidemia, prior myocardial infarction, congestive heart failure), laboratory values (hemoglobin, sodium, creatinine), Glasgow Coma Scale, National Institutes of Health Stroke Scale, ICH score, CHADS2 score, HAS-BLED score, initial intracranial hemorrhage volume, and presence of intraventricular hemorrhage and infratentorial bleeding.
Sources: Technical reports for the ANNEXA-4 trial vs. the ORANGE study and the ANNEXA trial vs. the RETRACE-II study,59,60 and Costa et al. (2022).22
The ORANGE trial was identified in an SLR and was included in the sponsor’s review because the population of PCC-treated patients had a distribution of bleed type and temporal concordance in recruitment time frame that was similar to the ANNEXA-4 trial, and the standard of care for anticoagulation treatment and reversal or replacement was comparable between the UK and the population of the ANNEXA-4 trial.
To increase comparability across the 2 study populations and reduce the potential heterogeneity of the treatment effects, only IPD from patients treated with rivaroxaban or apixaban and who had available data for all baseline characteristics of interest and 30-day mortality were included; in the ORANGE study, only IPD from patients treated with PCC were included. Thirty-day mortality was the primary outcome of interest in the analysis.
An assessment of similarity between the included studies is presented in Table 18.
Table 18: Assessment of Homogeneity for the ANNEXA-4 Trial Versus the ORANGE Study
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Treatment history | The ORANGE study included patients who received warfarin and direct anticoagulants (rivaroxaban, apixaban, and dabigatran), while the ANNEXA-4 trial included only patients who received an FXa inhibitor (rivaroxaban, apixaban, enoxaparin, or edoxaban). With the availability of patient-level data, it was possible to exclude treatments from the datasets to adjust the patient population included (rivaroxaban and apixaban only). |
Intervention and comparator | Patients in the ORANGE study received a variety of treatments, such as PCCs, tranexamic acid, blood transfusions, and combinations of these treatments; only patients treated with PCC were included in the weighted analysis. Patients in the ANNEXA-4 cohort received andexanet alfa. It is unclear whether the exposure to blood products and hemostatic treatments was similar between the study cohorts. |
Trial inclusion criteria | There were 2 key differences between the inclusion criteria used in each of the studies:
|
Trial exclusion criteria | No explicit exclusion criteria were noted in the ORANGE study. Exclusion criteria in the ANNEXA-4 trial included:
|
Period of patient enrolment | The time frames for recruitment began around 18 months earlier for the ORANGE study and ended 1 year later in the ANNEXA-4 trial (ORANGE study: October 2013 and August 2016; ANNEXA-4: April 2015 to May 2018) |
Study location | Study location was different between studies (ORANGE: UK; ANNEXA-4: North America, Europe, and Japan) |
FXa = factor Xa; GCS = Glasgow Coma Scale; PCC = prothrombin complex concentrate.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.20
Source: ANNEXA-4 trial vs. ORANGE study technical report.59
Analysis Methods: ANNEXA-4 Trial Versus ORANGE Study
A feasibility assessment was first performed among all patients in the patient cohort and in the ICH, GI bleed, and other major bleeds subgroups to determine whether PSM would be a numerically stable approach. A logistic regression model was used to contrast binary treatment assignment (andexanet alfa or PCC).61 The model covariates considered to be potential confounders for 30-day mortality and the treatment cohorts included: age, bleed site, and a medical history of AF, hypertension, diabetes, cancer, renal dysfunction, stroke, DVT, PE, coronary artery disease, or transient ischemic attack. A medical history of myocardial infarction or ischemic heart disease was expected to have an effect on 30-day mortality, but neither was included in the model due to insufficient data. Patients in the andexanet alfa group were matched to patients in the PCC group one-to-one using nearest-neighbour matching with replacement. The magnitude of the difference between the baseline characteristics of the 2 groups was calculated before and after matching to determine whether matching improved similarity. Balance between groups was considered successful if the absolute differences between the groups after matching were less than 10.62 Propensity scores were not trimmed, as there was overlap in all regions of the propensity score range.
Thirty-day mortality rates for patients receiving andexanet alfa or a PCC were calculated before and after PSM for each treatment group and each bleed type subgroup (ICH, GI bleed, and other major bleeds). Relative risk of 30-day mortality and 95% CIs were calculated for the 2 treatment groups after PSM adjustment. Lastly, because of potential differences in the severity of bleeds within the ICH subgroup, a sensitivity analysis was conducted where such patients were further matched by intracranial compartment: intracerebral, subarachnoid, and subdural bleeds in the ANNEXA-4 trial (no patients had epidural intracranial bleeds), and intracerebral, subarachnoid, subdural, and epidural bleeds in the ORANGE study.
Results: ANNEXA-4 Trial Versus ORANGE Study
After applying additional exclusion criteria to promote comparability between the studies, 322 of the 352 patients (91.5%) from the ANNEXA-4 trial and 145 of the 2,192 patients (6.6%) from the ORANGE study were included in the analysis.
The baseline patient characteristics before and after matching in the analysis of the ANNEXA-4 trial versus the ORANGE study are presented in Table 19 (whole cohort) and Table 33 in Appendix 1 (by bleed type subgroups). After matching, the ESS for the ORANGE cohort was reduced by 39.3%, from 145 to 88. There is no notable imbalance between the cohorts with respect to the covariates selected for inclusion in the propensity score model.
A notable reduction in the ESS of the ORANGE cohort was observed after matching across all bleed type subgroups (reduction ranged from 35.6% to 52.9%). Notable between-cohort differences in history of hypertension and cancer were consistently observed in all subgroups.
Table 19: Baseline Patient Characteristics for Whole Cohort, Before and After Matching — ANNEXA-4 Trial Versus ORANGE Study
Characteristic | ANNEXA-4 trial (AA) | ORANGE study (PCC) | Absolute difference between AA and PCC after propensity score matching | |
|---|---|---|---|---|
Before propensity score matching | After propensity score matching | |||
N | 322 | 145 | 88 | NA |
Age | 77.74 | 81.03 | 74.89 | 2.85 |
Patients with ICH (%) | 64.91 | 50.34 | 67.08 | −2.17 |
Patients with GI bleed (%) | 25.47 | 37.93 | 28.57 | −3.11 |
Patients with other bleeds (%) | 9.63 | 11.72 | 4.35 | 5.28 |
Medical history (%) | ||||
Stroke | 18.94 | 6.21 | 15.22 | 3.73 |
Coronary artery disease | 13.04 | 22.76 | 7.45 | 5.59 |
Transient ischemic attack | 7.45 | 24.14 | 7.14 | 0.31 |
Atrial fibrillation | 83.85 | 77.93 | 78.88 | 4.97 |
Hypertension | 78.26 | 55.86 | 72.67 | 5.59 |
Diabetes | 30.43 | 22.07 | 26.71 | 3.73 |
Renal dysfunction | 23.29 | 15.17 | 24.53 | −1.24 |
Cancer | 26.71 | 16.55 | 17.70 | 9.01 |
AA = andexanet alfa; GI = gastrointestinal; ICH = intracranial hemorrhage; PCC = prothrombin complex concentrate.
Note: The results of the ANNEXA-4 trial were based on patients enrolled between April 2015 and May 2018.
The details in the table were taken from the sponsor’s summary of clinical evidence.20
Source: ANNEXA-4 trial vs. ORANGE study technical report.59
Table 20 presents the 30-day mortality before and after PSM in the analysis of the ANNEXA-4 trial versus the ORANGE study in the whole cohort and by bleed type subgroup. The relative risk of 30-day mortality between the ANNEXA-4 cohort and the ORANGE cohort was 0.43 (95% CI, 0.29 to 0.63) in the whole cohort, 0.31 (95% CI, 0.20 to 0.48) in the ICH subgroup, and 0.49 (95% CI, 0.21 to 1.16) in the GI bleed subgroup. In the “other bleeds” subgroup, the relative risk was 1.29 (95% CI, 0.17 to 9.55), although it was based on a low sample size or ESS in both cohorts. Results for the sensitivity analyses, which included further matching by ICH bleed compartments (intracerebral, subarachnoid, and subdural or epidural hemorrhage), were similar to the primary analysis (whole cohort).
Table 20: 30-Day Mortality Before and After Matching — ANNEXA-4 Trial Versus ORANGE Study
Population | ANNEXA-4 trial (AA) | ORANGE study (PCC) | Relative risk (95% CI) between AA and PCC after propensity score matching | P value | |
|---|---|---|---|---|---|
Before propensity score matching | After propensity score matching | ||||
Whole cohort | |||||
N or ESS | N = 322 | N = 145 | ESS = 88 | NA | NA |
30-day mortality, % (95% CI) | 14.60 (10.72 to 18.47) | 31.72 (24.06 to 39.39) | 34.09 (23.99 to 44.19) | 0.43 (0.29 to 0.63) | < 0.001 |
ICH | |||||
N or ESS | N = 209 | N = 73 | ESS = 47 | NA | NA |
30-day mortality, % (95% CI) | 15.31 (10.39 to 20.23) | 42.47 (30.85 to 54.08) | 48.94 (34.10 to 63.77) | 0.31 (0.20 to 0.48) | < 0.001 |
GI bleed | |||||
N or ESS | N = 82 | N = 55 | ESS = 28 | NA | NA |
30-day mortality, % (95% CI) | 12.20 (4.96 to 19.43) | 21.82 (10.55 to 33.09) | 25.00 (7.90 to 42.10) | 0.49 (0.21 to 1.16) | 0.10 |
Other bleeds | |||||
N or ESS | N = 31 | N = 17 | ESS = 8 | NA | NA |
30-day mortality, % (95% CI) | 16.13 (2.42 to 29.84) | 17.65 (−2.56 to 37.85) | 12.50 (−17.06 to 42.06) | 1.29 (0.17 to 9.55) | NA |
AA = andexanet alfa; CI = confidence interval; ESS = effective sample size; GI = gastrointestinal; ICH = intracranial hemorrhage; NA = not applicable; PCC = prothrombin complex concentrate.
Note: Results of the ANNEXA-4 trial were based on patients enrolled between April 2015 and May 2018.
The details in the table were taken from the sponsor’s summary of clinical evidence.20
aRefers to the ESS of the PCC (ORANGE) cohort after propensity score matching.
Source: ANNEXA-4 trial vs. ORANGE study technical report.59
ANNEXA-4 Trial Versus the HHCS (Only Patients With ICH)
The objective of this study was to compare the effectiveness of andexanet alfa versus PCC in apixaban- or rivaroxaban-treated adults with ICH.
Study Selection
IPD from 2 sources were included in the propensity score overlap–weighting analysis: the ANNEXA-4 trial and the electronic health record data accessed across multiple acute care hospitals within a single health care system (Hartford Health care) in the northeastern US. The selection of the HHCS was not informed by an SLR.
To promote similarity among the patients from the 2 studies that were included in the analysis, the analysis included only patients experiencing an ICH while being treated with apixaban or rivaroxaban and whose ICH was managed with either andexanet alfa (from the ANNEXA-4 study) or 4F-PCC (from the HHCS data gathered from December 1, 2016, to August 30, 2020). In both studies, only adult patients admitted to a US hospital for a radiographically confirmed (CT or MRI) acute ICH, defined as a spontaneous or traumatic bleed in an intracerebral, subdural, or subarachnoid space, who had taken apixaban or rivaroxaban within 24 hours of the bleed were included in the analysis. Exclusion criteria for this analysis included a GCS score of less than 7 upon admission, an intracerebral bleed volume above 60 mL upon index CT or MRI scan, or planned surgery within 12 hours of the index scan.
An assessment of homogeneity between the ANNEXA-4 trial and the HHCS is presented in Table 21.
Table 21: Assessment of Homogeneity — ANNEXA-4 Trial Versus the HHCS
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Treatment history |
|
Intervention and comparator | Patients in the HHCS who received 4F-PCC were included in the weighted analysis. Patients in the ANNEXA-4 cohort received andexanet alfa. It is unclear whether the exposure to blood products and hemostatic treatments was similar between the study cohorts. |
Trial inclusion criteria | The ANNEXA-4 trial included patients with acute major bleeding requiring urgent reversal of anticoagulation; various bleed types (e.g., ICH, GI) were included. The weighted analysis included patients with acute ICH only from the ANNEXA-4 trial and HHCS datasets. |
Trial exclusion criteria | Exclusion criteria in the ANNEXA-4 trial included:
The analysis excluded patients who had GCS scores < 7 upon admission, hematoma volumes > 60 mL upon index CT or MRI scan, or planned surgery within 12 hours of index scan, to promote similarity between the study cohorts. |
Timing of end point evaluation | The assessment time frame of thromboembolic events was different between studies (HHCS: 5 days post reversal administration; ANNEXA-4 trial: up to day 30 post infusion). The weighted analysis of thromboembolic events was limited to the first 5 days posttreatment to account for the difference. |
Period of patient enrolment | The time frames for recruitment began around 20 months earlier for the ANNEXA-4 trial and ended 2 years later in the HHCS (HHCS: December 1, 2016, and August 30, 2020; ANNEXA-4: April 2015 to May 2018) |
Study location | The difference in study locations was noted (HHCS: US; ANNEXA-4 trial: North America, Europe, and Japan). Only patients recruited in the US were included in the weighted analysis. |
4F-PCC = 4-factor prothrombin complex concentrate; DNR = do not resuscitate; FXa = factor Xa; GCS = Glasgow Coma Scale; GI = gastrointestinal; HHCS = Hartford Health care study; ICH = intracranial hemorrhage; PCC = prothrombin complex concentrate.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.20
Source: Costa et al. (2022).22
Analysis Methods
Potential adjustment factors were identified based upon commonly used variables and accepted preselected risk factors for differential andexanet alfa or 4F-PCC exposure and development of the outcome of interest, including demographics, comorbidities, concurrent medications, ICH characteristics, vital signs, neurologic assessments, and laboratory values. The most impactful variables for inclusion in the propensity score model were selected if the variable was at least moderately associated with the outcome (absolute standardized difference [ASD] above 0.2) and not balanced between treatment cohorts, and less than 10% of data were missing. Propensity scores were calculated based on multivariable logistic regression.63 The covariates selected for inclusion in the propensity score model included baseline age; sex; BMI; creatinine clearance; AF as the indication for oral anticoagulation; average systolic blood pressures at admission (above 160 mm hg); medical history of heart failure, diabetes, myocardial infarction, or stroke; concomitant antiplatelet use; time from index scan to reversal agent initiation; time from end of reversal agent administration to repeat scan; traumatic versus spontaneous bleeding; infratentorial region involvement; single- versus multi-compartment bleeding; bleeding in the intracerebral, intraventricular, subdural, or subarachnoid space on index scan and a bleed size greater than 10 mL in volume or 10 mm in thickness on index scan. Since 100% of the patients in this study who received 4F-PCC were treated in the US, “country” could not be included in our propensity score model (nor weighted for). Consequently, estimated propensity scores were used to weight patients for analysis using an overlap-weighting approach. Overlap weighting assigned weights to patients that were proportional to their probability of belonging to the opposing treatment cohort.64,65 Propensity score model–eligible variables with less than 10% missing data had missing values imputed using a multiple imputation approach based on a fully conditional specification linear regression model utilizing all other available covariates and outcomes.66 ASDs were calculated for each variable before propensity score overlap weighting to illustrate the magnitude of the imbalance between cohorts at baseline (an ASD greater than 0.1 was considered to represent a relevant difference).63
The coprimary outcomes for this study were hemostatic effectiveness (“excellent” or “good” versus “poor or none”) and 30-day all-cause mortality. Occurrence of thrombotic events during the first 5 days after administration of the reversal agent was the secondary end point of interest in this review. Excellent or good hemostasis was defined as no greater than a 35% increase in hematoma size from index to the repeat scan taken approximately 12 hours after reversal administration. The repeat scan closest to 12 hours was utilized whenever possible. If no repeat scan was available within 12 hours (plus or minus 5 hours) of reversal administration, then the worst scan within 24 hours was used. If no repeat scan was available within 24 hours, the patient was assumed to have had poor hemostatic effectiveness. Patients whose index or repeat scan could not be accessed due to administrative reasons were excluded from this study. Adjudicated hemostatic effectiveness determinations from the ANNEXA-4 trial were used for all patients included in this study who received andexanet alfa. Patients who received 4F-PCC had their index and repeat scans read by 2 independent clinicians. Hemostatic effectiveness for patients who received 4F-PCC was then established based on the criteria for the ANNEXA-4 trial and after reaching investigator consensus. For the hemostatic effectiveness and mortality and thromboembolism outcomes, the propensity score overlap–weighted ORs were estimated with accompanying 95% CIs. Binomial (logit-link) generalized estimating equations using a robust sandwich estimator were used to calculate ORs.
A sensitivity analysis was performed in which attainment of hemostatic effectiveness (or lack thereof) for patients without a repeat scan within 24 hours was adjudicated based on the clinical judgment of 2 independent investigators after a review of outcomes (e.g., need for unplanned surgery, subsequent administration of reversal agent, mortality), rather than being assumed to represent poor or no effectiveness. Propensity scores were recalculated for the sensitivity analysis. A subgroup analysis restricted to patients with an intracerebral and/or intraventricular hemorrhage was also performed that evaluated the abovementioned outcomes and the absolute change in hematoma volume in millilitres from index to repeat scan. The subgroup analysis used propensity scores based on a logistic regression model, where total bleed volume in millilitres on index scan (continuous) was substituted for bleed sizes above 10 mL/mm. A propensity score overlap–weighted linear generalized estimating equation was used to determine the mean difference between andexanet alfa and 4F-PCC in hematoma volume from index to repeat scan.
Results
A total of 107 of 477 patients (22.4%) from the ANNEXA-4 trial and 95 of 385 patients (24.7%) from the HHCS were included in the analysis. Baseline characteristics before and after weighting in the analysis of the ANNEXA-4 trial versus the HHCS are presented in Table 22. Following propensity score overlap weighting, no notable imbalances were noted in any recorded covariates between the 2 cohorts.
Incidence of hemostatic efficacy, 30-day mortality, and thrombotic events within 5 days of reversal treatment is summarized in Table 23. After weighting, the adjusted OR between andexanet and 4F-PCC was 2.733 (95% CI, 1.163 to 6.421) with respect to achievement of excellent or good hemostatic efficacy, and 0.355 (95% CI, 0.129 to 0.977) with respect to 30-day mortality, both in favour of andexanet alfa. Thromboembolism occurred in 2 patients (1.9%) in the andexanet alfa cohort and 0 patients in the 4F-PCC cohort within 5 days of reversal agent administration.
Table 22: Baseline Patient Characteristics Before and After Propensity Score Overlap Weighting — ANNEXA-4 Trial Versus the HHCS
Characteristics | Before weighting | After weighting | ||
|---|---|---|---|---|
Andexanet alfa (N = 107) | 4F-PCC (N = 95) | Andexanet alfa (N = 107) | 4F-PCC (N = 95) | |
Demographics | ||||
Age (years), mean (SD) | 79 (8) | 77 (11) | 79 (8) | 79 (11) |
Male (%) | 49.5 | 52.6 | 49.6 | 49.6 |
Body mass index (kg/m2), mean (SD) | 27.19 (6.59) | 28.04 (5.75) | 27.81 (7.21) | 27.81 (5.71) |
Creatinine clearance (mL/minute), mean (SD) | 64.0 (28.3) | 72.8 (44.0) | 67.2 (29.6) | 67.2 (38.8) |
Systolic blood pressure > 160 mm hg (%) | 12.1 | 20.0 | 18.3 | 18.3 |
Glasgow Coma Scale score (SD)a | 14 (1) | 14 (2) | 14 (1) | 14 (2) |
Anticoagulant indication and medical history (%) | ||||
Anticoagulant indication, atrial fibrillation | 87.9 | 82.1 | 86.4 | 86.4 |
Medical history of: | ||||
Heart failure | 18.7 | 23.2 | 22.3 | 22.3 |
Diabetes | 28.0 | 27.4 | 28.7 | 28.7 |
Myocardial infarction | 12.1 | 8.4 | 9.4 | 9.4 |
Stroke | 21.5 | 24.2 | 24.0 | 24.0 |
Concomitant use of an antiplatelet | 33.6 | 24.2 | 24.2 | 24.2 |
Intracranial hemorrhage characteristics | ||||
Initial imaging to reversal start (hours), mean (SD) | 2.61 (1.79) | 2.07 (1.87) | 2.25 (1.56) | 2.25 (2.13) |
End of reversal to repeat imaging (hours), mean (SD) | 12.43 (1.14) | 8.12 (5.05) | 12.23 (1.07) | 12.23 (4.61) |
Traumatic onset (%) | 53.3 | 64.2 | 61.1 | 61.1 |
Infratentorial location (%) | 16.8 | 12.6 | 14.7 | 14.7 |
Size of bleed ≥ 10 mL or 10 mm (%) | 33.6 | 14.7 | 21.7 | 21.7 |
Single compartment bleed (%) | 77.6 | 85.3 | 78.3 | 78.3 |
Intracerebral and/or intraventricular bleed (%) | 59.8 | 48.4 | 53.3 | 53.3 |
Subdural bleed (%) | 32.7 | 40.0 | 38.4 | 38.4 |
Subarachnoid bleed (%) | 31.8 | 27.4 | 34.3 | 34.3 |
Reversal agent dosing (not included in the propensity score model) | ||||
Andexanet alfa | ||||
400 mg bolus + 440 mg infusion (%) | 96.3 | NA | 96.6 | NA |
800 mg bolus + 860 mg infusion (%) | 3.7 | NA | 3.4 | NA |
4F-PCC | ||||
25 units/kg infusion (%) | NA | 74.3 | NA | 79.3 |
50 units/kg infusion (%) | NA | 25.3 | NA | 20.7 |
4F-PCC = 4-factor prothrombin complex concentrate; ASD = absolute standardized difference; HHCS = Hartford Health care study; NA = not applicable; SD = standard deviation.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.20
Source: Costa et al. (2022).22
In the sensitivity analysis (wherein patients without a repeat scan within 24 hours had their hemostatic effectiveness adjudicated based on clinical judgment rather than being assumed to represent poor or no effectiveness), the OR in hemostatic efficacy between the ANNEXA-4 cohort and HHCS cohort was 2.19 (95% CI, 0.91 to 5.25).
In the subgroup analysis in patients with a single compartment intracerebral and/or intraventricular hemorrhage, the results for hemostatic effectiveness and 30-day mortality did not suggest a significant difference between the ANNEXA-4 cohort and the HHCS cohort in this subgroup, but estimates did favour andexanet alfa, with a weighted OR of 1.71 (95% CI, 0.36 to 8.11) for hemostatic efficacy and 0.22 (95% CI, 0.04 to 1.41) for 30-day mortality. There were no thromboembolic events within 5 days of reversal treatment administration in either treatment cohort.
Table 23: Comparative Hemostatic Efficacy, 30-Day Mortality, Thrombotic Events After Propensity Score Overlap Weighting — ANNEXA-4 Trial Versus the HHCS
Outcomes | Andexanet alfa (N = 107) weighted incidence, % (95% CI) | 4F-PCC (N = 95) weighted incidence, % (95% CI) | Weighted odds ratio (95% CI) |
|---|---|---|---|
Hemostatic effectiveness | 85.8 (77.7 to 91.8) | 68.1 (57.7 to 77.3) | 2.733 (1.163 to 6.421) |
30-day all-cause mortality | 7.9 (3.6 to 13.8) | 19.6 (12.1 to 24.0) | 0.355 (0.129 to 0.977) |
Thrombotic events within 5 days of reversal, n (%) | 2 (1.9) | 0 | NA |
4F-PCC = 4-factor prothrombin complex concentrate; CI = confidence interval; HHCS = Hartford Health care study; NA = not applicable.
Note: 30-day vascular mortality was an outcome of the study but was not of interest to this review and, thus, not summarized.
The details in the table were taken from the sponsor’s summary of clinical evidence.20
Source: Costa et al. (2022).22
ANNEXA-4 Trial Versus RETRACE-II Study (Only Patients With ICH)
The objective of this study was to compare the effectiveness of andexanet alfa versus PCC in apixaban- or rivaroxaban-treated adults with atraumatic ICH.
Study Selection
IPD from 2 sources were included in the propensity score analysis: the ANNEXA-4 trial and the RETRACE-II study, which is a multicentre retrospective cohort study of patients with ICH treated with oral anticoagulants at 19 tertiary care centres across Germany between January 2011 and December 2015. Selection of the RETRACE-II study was not informed by an SLR.
A subcohort of patients with atraumatic FXa inhibitor–related ICH was created from the ANNEXA-4 trial that included patients with bleeds in locations other than the parenchyma and excluded patients taking edoxaban. Patients from the RETRACE-II study who had been treated with dabigatran and patients with an ICH related to vitamin K antagonists were excluded. Further, patients were excluded if: their last intake of rivaroxaban or apixaban was more than 18 hours before admission, their ICH was secondary to trauma or hemorrhagic transformation of malignancies, their GCS score on admission was less than 7, their initial ICH volume was above 60 mL, or information about abnormal liver function or alcohol abuse was missing. Results of the ANNEXA-4 trial were based on patients enrolled between April 2015 and May 2018.
An assessment of homogeneity between the ANNEXA-4 trial and the RETRACE-II study is presented in Table 24.
Table 24: Assessment of Homogeneity — ANNEXA-4 Trial Versus RETRACE-II Study
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Treatment history | A difference in history of anticoagulation treatment was noted between the studies (ANNEXA-4 trial: rivaroxaban, apixaban, enoxaparin, and edoxaban; RETRACE-II study: warfarin and direct oral anticoagulants). Only patients receiving apixaban or rivaroxaban were included in the weighted analysis to account for the difference. |
Intervention and comparator | The RETRACE-II study included patients who received SoC for treatment of oral anticoagulant–associated bleeding, primarily PCC. Patients in the ANNEXA-4 cohort received andexanet alfa. It is unclear whether the exposure to blood products and hemostatic treatments was similar between the study cohorts. |
Trial inclusion criteria | The ANNEXA-4 trial included patients with acute major bleeding requiring urgent reversal of FXa anticoagulation; various bleed types (e.g., ICH, GI) were included. As well, enrolled patients received anticoagulation within 18 hours of andexanet alfa treatment. The RETRACE-II study included patients with ICH while receiving oral anticoagulation. The weighted analysis included only patients who had an ICH and received direct oral anticoagulation within 18 hours from both datasets to account for the difference between studies. |
Trial exclusion criteria | Exclusion criteria in the ANNEXA-4 trial included:
The RETRACE-II study had 1 exclusion criterion: ICH related to trauma, tumour, arteriovenous malformation, aneurysmal subarachnoid hemorrhage, acute thrombolysis, or other coagulopathies. The weighted analysis excluded patients with ICH due to trauma or tumour, a GCS score of < 7, or an ICH volume > 60 mL at baseline, to promote between-study similarity in the inclusion and exclusion criteria. In addition, patients with an abnormal liver function or alcohol abuse were excluded from the analysis. The sponsor noted that although these patients were not explicitly excluded in the ANNEXA-4 trial, no such patients were included in that study. Thus, the exclusion of these patients from the RETRACE-II study seemed necessary, as abnormal liver function or alcohol abuse may act as a confounder in the analyses. |
Timing of end point evaluation | The primary end points were 30-day mortality for the ANNEXA-4 cohort and 30-day in-hospital mortality for the RETRACE-II study. The difference in definition is due to the lack of follow-up of patients in the RETRACE-II cohort after hospital discharge. As a result, 30-day in-hospital mortality was considered the primary outcome in the weighted analysis. The functional outcome was based on the mRS at discharge in the RETRACE-II study and at day 30 in the ANNEXA-4 trial. |
Period of patient enrolment | There is an 8-month overlap in the recruitment time frames between studies (RETRACE-II study: January 2011 to December 2015; ANNEXA-4 trial: April 2015 to May 2018). |
Study location | A difference in study locations was noted (RETRACE-II study: Germany; ANNEXA-4 trial: North America, Europe, and Japan). |
GCS = Glasgow Coma Scale; GI = gastrointestinal; ICH = intracranial hemorrhage; mRS = modified Rankin Scale; PCC = prothrombin complex concentrate;
SoC = standard of care.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.20
Source: ANNEXA-4 trial vs. RETRACE-II study technical report.60
Analysis Methods
A collection of potential adjustment covariates included demographics, vital signs, type of DOACs and indication for oral anticoagulants, comorbidities, concomitant medications, laboratory values, and ICH disease characteristics. These variables were identified based on the largest available intersection of variables between both datasets. Only the most important variables that were at least moderately associated with the outcome and not balanced between treatment groups (ASD above 0.1) with less than 10% of data missing were included. A propensity score model was conducted using logistic regression analysis, with treatment as the dependent variable and the selected covariates as independent variables to model the probability of receiving each treatment. Propensity score–adjusted analyses were performed using the IPTW approach. Weights were stabilized by multiplying with the marginal probability of receiving treatment in the respective dataset. Distribution of weights in the treatment groups was evaluated in terms of mean, median, minimum, and maximum to identify indicators of outliers with subsequent trimming at a minimum of 0.1 and a maximum of 10. The balance of variables included in PSM was assessed by calculating the ASDs for the weighted cohorts.
The covariates included in the propensity score model were as follows:
Hematoma expansion analysis: Prior use of antiplatelets, DOAC indication classified as “other,” initial ICH volume, GCS score, presence of infratentorial bleeding, and presence of intraventricular hemorrhage.
Mortality analysis: Diastolic blood pressure, history of diabetes, eGFR level, ICH score, GCS score, HAS-BLED score, presence of infratentorial bleeding, and presence of intraventricular hemorrhage.
mRS analysis: Systolic blood pressure, history of dyslipidemia, eGFR level, ICH score, HAS-BLED score, CHA2DS2-VASc score, and hemoglobin level.
The primary outcome was defined as the proportion of patients with hematoma expansion 12 hours postbaseline in the ANNEXA-4 trial and at the first follow-up imaging in the RETRACE-II study. Hematoma expansion was defined as an increase in the ICH lesion volume of greater than 35% from baseline. Secondary outcomes of interest to this review included in-hospital mortality and functional outcome at discharge or at day 30. Data analyses to estimate treatment effects were performed as unadjusted analyses in the unweighted dataset and as IPTW analyses.
Inference of potential treatment effects was based on the weighted analyses. Hazard ratios for in-hospital mortality were estimated from IPTW Cox proportional hazard regression models. In these models, “person-time at risk” ended at the end of hospitalization, day 30, or death, whichever came first. Change in baseline hematoma volume was estimated using IPTW least squares means from a mixed model for repeated measures that included time, treatment, and time by treatment as independent variables.
Preplanned sensitivity analyses were conducted to evaluate the robustness of the analysis, including full PSM. Specifically, a sensitivity analysis was performed that included only patients treated with PCC in the “usual care” (standard of care) group. The sensitivity analyses included: all covariates for the propensity score model, patients with available baseline anti-FXa inhibitor levels or NIHSS values only, all follow-up radiographic measurements (independent of their time post baseline), and time between initial and follow-up imaging. A prespecified subgroup analysis was conducted for the subgroup of patients with PCC treatment in the RETRACE-II study. It was planned to address a secondary objective of 30-day mortality only if statistically significant superiority of andexanet alfa was observed for the primary outcome of 30-day in-hospital mortality (hierarchical testing). Finally, patients who died between hospital discharge and day 30 were assigned a value of 6 (death) in the ANNEXA-4 trial while, in the RETRACE-II study, these patients were analyzed using their mRS at discharge (which is necessarily less than 6). To address this, a sensitivity analysis was performed that used the last available assessment at hospital discharge (instead of a value of 6) in these patients.
Results
A total of 85 out of 352 patients (24.1%) from the ANNEXA-4 trial and 97 out of 168 patients (57.7%) from the RETRACE-II study were included in the analysis. Baseline characteristics (included in the propensity score model) before and after application of IPTW in the overall cohort are presented in Table 25. No notable imbalances were noted in these covariates between the cohorts after IPTW was applied.
The analysis estimates are summarized in Table 26. The relative risk of hematoma expansion between andexanet alfa and standard of care was estimated to be 0.40 (95% CI, 0.20 to 0.78) in favour of andexanet alfa. The estimated HR between andexanet alfa and standard of care for in-hospital mortality was 0.49 (95% CI, 0.24 to 1.04), the between-arm difference in mean mRS score at discharge was −0.47 (95% CI, −1.02 to 0.08), and the relative risk for an mRS score of 4 or above at discharge was 0.910 (95% CI, 0.728 to 1.138). Note that results of 30-day mortality were not reported because the study planned to only investigate 30-day mortality in detail if a significant effect was observed for in-hospital mortality during the first 30 days.
Table 25: Covariates Included in the Propensity Score Model, Before and After Application of IPTW — ANNEXA-4 Trial Versus the RETRACE-II Study
Variables | Before IPTW | After IPTW | |||
|---|---|---|---|---|---|
Andexanet | SoC | Andexanet | SoC | ASDa | |
Hematoma expansion analysis | |||||
Prior use of antiplatelets, n (%) | 24 (30.0) | 6 (9.1) | 16.2 (20.2) | 13.0 (19.4) | 0.019 |
DOAC indication classified as “other,” n (%) | 4 (5.0) | 2 (3.0) | 2.8 (3.5) | 1.6 (2.3) | 0.068 |
Mean initial ICH volume, cm3 (SD) | 13.37 (14.10) | 15.30 (15.05) | 15.40 (15.46) | 14.10 (15.31) | 0.085 |
Mean Glasgow Coma Scale (SD) | 13.47 (2.12) | 12.76 2.55) | 13.16 (2.26) | 13.00 (2.34) | 0.067 |
Infratentorial bleeding, n (%) | 16 (20.0) | 7 (10.4) | 14.1 (17.6) | 13.1 (19.6) | 0.051 |
Intraventricular hemorrhage, n (%) | 10 (12.5) | 29 (43.3) | 21.1 (26.4) | 17.6 (26.3) | 0.003 |
Mortality analysis | |||||
Mean diastolic BP, mm hg (SD) | 75.75 (20.67) | 89.84 (20.19) | 86.84 (28.39) | 83.36 (20.62) | 0.140 |
Diabetes, n (%) | 35 (41.2) | 32 (33.3) | 33.1 (39.0) | 37.5 (38.7) | 0.006 |
Mean eGFR, mL/minute (SD) | 66.27 (27.43) | 72.89 (26.95) | 68.29 (25.82) | 68.83 (26.45) | 0.020 |
Mean ICH score (SD) | 1.15 (1.02) | 1.44 (1.10) | 1.30 (1.05) | 1.27 (1.04) | 0.025 |
Mean Glasgow Coma Scale (SD) | 13.49 (2.09) | 12.99 (2.48) | 13.50 (2.02) | 13.31 (2.34) | 0.088 |
Mean HAS-BLED score (SD) | 2.69 (0.93) | 2.54 (0.95) | 2.63 (0.91) | 2.62 (0.99) | 0.012 |
Infratentorial bleeding, n (%) | 17 (20.0) | 11 (11.3) | 19.3 (22.7%) | 16.3 (16.8) | 0.150 |
Intraventricular hemorrhage, n (%) | 11 (12.9) | 38 (40.0) | 22.4 (26.3) | 25.5 (26.3) | 0.000 |
mRS analysis | |||||
Mean systolic BP (SD) | 145.66 (23.03) | 167.81 (34.11) | 155.39 (29.04) | 156.78 (33.63) | 0.044 |
Dyslipidemia, n (%) | 34 (50.0) | 32 (34.0) | 28.8 (42.4) | 39.5 (41.6) | 0.016 |
Mean hemoglobin (SD) | 13.16 (1.87) | 12.92 (2.41) | 13.25 (1.97) | 13.13 (2.45) | 0.054 |
Mean ICH score (SD) | 1.19 (1.03) | 1.45 (1.11) | 1.22 (0.95) | 1.29 (1.08) | 0.075 |
Mean HAS-BLED score (SD) | 2.66 (0.96) | 2.55 (0.96) | 2.55 (0.91) | 2.56 (1.00) | 0.008 |
Mean CHA2DS2-VASc score (SD) | 4.22 (1.46) | 4.40 (1.58) | 4.16 (1.45) | 4.30 (1.69) | 0.089 |
ASD = absolute standardized difference; BP = blood pressure; DOAC = direct oral anticoagulant; eGFR = estimated glomerular filtration rate; ICH = intracranial hemorrhage; IPTW = inverse probability treatment weighting; mRS = modified Rankin Scale; SD = standard deviation; SoC = standard of care.
Note: For categorical variables, P values were based on a chi-square test or Fisher exact test (50% or more of the cells have expected counts of less than 5).
The details in the table were taken from the sponsor’s summary of clinical evidence.20
aDifferences between treatment groups were reported as ASDs.
Source: ANNEXA-4 trial vs. RETRACE-II study technical report.60
Results of sensitivity analyses of in-hospital mortality, hematoma expansion, and proportion of patients with an mRS score of 4 or above at discharge were, in general, consistent with the primary analyses (Table 34), except for the sensitivity analysis of hematoma expansion (only patients from the ANNEXA-4 trial with a baseline NIHSS were included), which did not suggest a difference in hematoma change between andexanet alfa and PCC.
Table 26: Outcomes in the Overall Cohort — ANNEXA-4 Trial Versus the RETRACE-II Study
Outcome | Andexanet alfa | SoC | Andexanet alfa | SoC |
|---|---|---|---|---|
Unadjusted analysis | IPTW-adjusted analysis | |||
Hematoma expansiona | ||||
Patients with hematoma expansion,a n/N (%) | 11/80 (14) | 24/67 (36) | 10.0 (13) | 21.3 (32) |
Relative risk (95% CI) | 0.38 (0.20 to 0.73) | 0.40 (0.20 to 0.78) | ||
P value | 0.002 | 0.005 | ||
In-hospital mortality | ||||
n/N (%) | 14/85 (16.5) | 20/97 (20.6) | NR | NR |
Hazard ratio (95% CI) | 0.64 (0.32 to 1.28) | 0.49 (0.24 to 1.04) | ||
P value | 0.21 | 0.06 | ||
mRS at hospital discharge or day 30 | ||||
Number of patients in analysis | 68 | 95 | NR | NR |
mRS score at hospital discharge or day 30, mean (95% CI) | 3.82 (3.35 to 4.30) | 4.31 (4.02 to 4.59) | 3.75 (3.25 to 4.24) | 4.22 (3.91 to 4.52) |
Difference in means (95% CI) | −0.48 (−1.00 to 0.04) | −0.47 (−1.02 to 0.08) | ||
P value | 0.084 | 0.112 | ||
Patients with mRS ≥ 4, n (%) | 44 (64.7) | 69 (72.6) | 43.7 (64.3) | 67.1 (70.6) |
Relative risk (95% CI) | 0.891 (0.719 to 1.104) | 0.910 (0.728 to 1.138) | ||
P value | 0.2807 | 0.3992 | ||
CI = confidence interval; ICH = intracranial hemorrhage; IPTW = inverse probability of treatment weighting; mRS = modified Rankin Scale; SoC = standard of care.
Note: Results of 30-day mortality were not reported because the study plan was to investigate 30-day mortality in detail only if a significant effect was observed on in-hospital mortality during the first 30 days.
The details in the table were taken from the sponsor’s summary of clinical evidence.20
aHematoma expansion was defined as an increase in the initial ICH lesion volume of greater than 35%.
Source: ANNEXA-4 trial vs. RETRACE-II study technical report.60
The results for an a priori–defined subgroup analysis comparing patients treated with andexanet alfa (n = 85) with those treated with PCC (n = 73) are shown in Table 27. IPTW-adjusted analyses showed results consistent with the whole cohort (in favour of andexanet with respect to hematoma expansion, no difference between groups with respect to in-hospital mortality and mRS at discharge or 30 days).
Table 27: Subanalysis of Patients Receiving Andexanet Alfa or PCC — ANNEXA-4 Trial Versus RETRACE-II Study
End points | Unadjusted analysis | IPTW-adjusted analysis | ||
|---|---|---|---|---|
Treatment measure (95% CI) | P value | Treatment measure (95% CI) | P value | |
Hematoma expansiona,b | Risk ratio, 0.347 (0.183 to 0.659) | 0.001 | Risk ratio, 0.443 (0.223 to 0.878) | 0.017 |
In-hospital mortalityc | Hazard ratio, 0.800 (0.375 to 1.710) | 0.566 | Hazard ratio, 0.852 (0.397 to 1.827) | 0.680 |
mRS at discharge or 30 daysb | Mean difference, −0.331 (−0.908 to 0.246) | 0.261 | Mean difference, −0.517 (−1.146 to 0.113) | 0.110 |
CI = confidence interval; ICH = intracranial hemorrhage; IPTW = inverse probability of treatment weighting; mRS = modified Rankin Scale; PPC = prothrombin complex concentrate.
Note: The details in the table were taken from the sponsor’s summary of clinical evidence.20
aHematoma expansion was defined as an increase of the initial ICH lesion volume of greater than 35%.
bTreatment effect was estimated using the Cochrane-Mantel-Haenszel method.
cTreatment effect was estimated using Cox proportional hazard regression.
Source: ANNEXA-4 trial vs. RETRACE-II study technical report.60
Critical Appraisal
ANNEXA-4 Trial Versus ORANGE Study
The comparator ORANGE study was identified based on an SLR; however, it is unclear whether the SLR was conducted using appropriate study-selection methods (e.g., a priori selection criteria, duplicate independent reviewers for article screening and data extraction, risk of bias assessment) since there was no report on how the SLR was conducted. A justification for selecting the ORANGE study was provided by the sponsor; however, there was no mention of what other studies were identified in the literature search and the reasons for excluding them. Given the limited disclosure on how the SLR was conducted, it is unclear whether the ORANGE study was indeed systematically selected and, thus, there is a risk of selection bias.
Despite applying additional exclusion criteria to promote similarity among the patients included in the analyses, the analyses could not account for several differences with respect to the inclusion and exclusion criteria between studies. First, the definition of major bleeding differs between studies: in the ANNEXA-4 trial, patients with bleeding who had hemodynamic compromise were considered to have met the criteria for a major bleed, but this was not an inclusion criterion in the ORANGE study. Further, while the ANNEXA-4 trial required the bleed to be uncontrolled or life-threatening for enrolment, it was not a requirement in the ORANGE study, although the clinical experts consulted by CADTH commented that the sponsor’s assumption that PCC could be used as a proxy for the severity of the bleed (i.e., any patients who had received PCC were considered to have experienced a life-threatening or uncontrolled bleeding event) was reasonable. Second, patients who received a transfusion of RBCs or FFP were eligible for inclusion in the ORANGE study but not the ANNEXA-4 trial. The differences in these inclusion criteria could mean that the study population differed between the included studies, although it is unclear to what extent. Important differences in the exclusion criteria of the included studies were also not accounted for in the analysis, specifically, patients with an ICH who had a GCS score of less than 7, a hematoma volume above 60 cc, and an expected survival of less than 1 month, were excluded from the ANNEXA-4 trial but not from the ORANGE study. Since patients who meet such criteria typically have a worse prognosis than those who do not, as per input from the clinical experts, it is plausible that the patients in the ANNEXA-4 trial were generally healthier than those in the ORANGE study.
In addition to heterogeneity in the study population, there is some temporal discordance in patient recruitment between studies, and differences between the trials in the study site locations (UK only in the ORANGE study; North America, Europe, and Japan in the ANNEXA-4 trial). However, the impact of these differences on the study results is likely minimal, since the standard of care in these locations is not known to differ considerably during the study time frame, according to the clinical experts.
Covariates included in the propensity score model were balanced between the study cohorts after matching. However, differences in the baseline size or volume of bleeds, blood pressure reading, ventricular involvement for ICH, time from ICH symptoms to CT, medical history of ischemic heart disease and myocardial infarction — all of which were noted by the authors to be major determinants of mortality — were not adjusted for in the model due to insufficient data. Sex, weight, and creatinine clearance level were excluded from adjustment; however, they are considered by the clinical experts consulted by CADTH to be prognostic factors and were considered relevant in the other studies discussed. The lack of adjustment for these potential prognostic factors or treatment-effect modifiers could bias the estimated treatment effect due to unmeasured confounding across treatment groups. It is also unclear if there is any between-cohort difference in exposure to supportive treatments, such as blood transfusions and tranexamic acid, since such information was only available for the ANNEXA-4 cohort.
In the whole-cohort analysis, the ESS of the ORANGE cohort was notably reduced (by 39.3%) after matching, which suggests poor population overlap. Similarly, there was a notable reduction in the ESS of the ICH, GI bleed, and other bleed subgroups (by 35.6%, 49.1%, and 52.9%, respectively). A significant reduction in sample size can contribute to imprecision, increasing uncertainty of the results.
The study assessed 30-day mortality, which is an outcome that is important to patients and clinicians. The comparative efficacy of andexanet alfa and PCC in other relevant clinical outcomes such as mental and functional statuses, ICU admission, length of stay at hospital, and HRQoL were not investigated.
ANNEXA-4 Trial Versus the HHCS
The comparator trial, the HHCS, was not identified based on an SLR and justification for its selection was not provided. Thus, there is a risk of selection bias, given that studies included in the analysis were not identified using a systematic approach.
Patients were selected from the HHCS to mirror the inclusion criteria of the ANNEXA-4 trial; however, patients with an expected survival of less than 1 month and a history of thromboembolism in the past 2 weeks were not excluded from the HHCS, which could potentially result in a non-transportable patient cohort, with a better prognosis and lower risk of thrombosis in the HHCS compared with the ANNEXA-4 trial. Furthermore, anti-FXa assays were not available in most patients in the HHCS cohort, since obtaining these levels was not standard practice. As a result, anti-FXa levels could not be adjusted for or used to assess effectiveness in the present study, and it is not known whether the HHCS cohort and ANNEXA-4 cohort had similar levels of anticoagulation. Differential use of supportive treatments (e.g., RBC transfusion, antifibrinolytics) could also potentially impact clinical outcomes, although it is unclear what proportion of patients in the HHCS received these treatments. No significant between-study difference was identified with respect to outcome definition and assessment. There is a considerable overlap in study time frame between the ANNEXA-4 trial and the HHCS; as well, the ANNEXA-4 cohort included patients in the US only to reduce the potential for bias resulting from differences in standard of care across different countries between the HHCS and ANNEXA-4 cohorts.
Adjustment factors were selected from a list of commonly used variables and accepted preselected risk factors for differential andexanet alfa or 4F-PCC exposure, and the development of the outcome of interest was based on a multivariable analysis. Prespecified criteria were used to narrow down the covariates for inclusion in the propensity score model to those with the most impact on the effect estimates. No notable imbalance in the selected covariates was noted between the cohorts after weighting. The collection of variables included in the adjusted analysis agreed with those discussed by the clinical experts consulted. Nonetheless, there remains potential residual confounding from the less “impactful” covariates that were excluded from adjustment and the unmeasured heterogeneity of patient characteristics between the studies.
The results of the primary analysis of hemostatic efficacy and 30-day mortality were in favour of andexanet alfa; however, a sensitivity analysis of hemostatic efficacy that allows for adjudication of hemostatic efficacy in these patients based on clinical judgment (rather than assuming them to have “poor or none” hemostatic efficacy in the primary efficacy result) showed imprecise results. This leads to uncertainty in the ability to draw a conclusion on the relative effect of andexanet alfa and PCC with respect to hemostatic efficacy. As well, for both hemostatic efficacy and 30-day mortality outcomes, imprecision was similarly noted in the subgroup analyses of patients with an intracerebral and/or intraventricular hemorrhage.
It is noteworthy that change (and percent change) in ICH size from index scan and change in GCS score at 24 hours post reversal and at discharge were prespecified outcomes, in addition to the published outcomes, as per the study protocol. However, these outcomes were not published and no justification was provided; therefore, there is a risk of publication bias.
A limitation with respect to generalizability is that a low dose of 25 units/kg of 4F-PCC was used in the majority of patients (79.3%) in the HHCS cohort, which does not align with standard practice in Canada, according to the clinical experts consulted by CADTH. The clinical experts noted that a higher dose of PCC (minimum 2,000 unit per dose) is commonly used in Canada, and that the use of low-dose PCC has been shown to associate with worse clinical outcomes.
ANNEXA-4 Trial Versus RETRACE-II Study
Similar to the ANNEXA-4 trial versus HHCS analysis, there is a risk of selection bias, given that studies included in this analysis were not selected using a systematic approach.
The study applied additional exclusion criteria to promote heterogeneity in the patients included in the analysis although, unlike the ANNEXA-4 trial, patients with an expected survival of less than 1 month, recent history of thromboembolism, and planned surgery within 12 hours of admission were not excluded from the RETRACE-II study. The recruitment period and study locations differ between the studies (RETRACE-II study, January 2011 to December 2015 in Germany; ANNEXA-4 trial, April 2015 to March 2020 in the US, Europe, and Japan); however, the clinical experts noted that the standard of care has largely remained unchanged in this time frame and is not known to differ significantly between the countries where the studies took place. With respect to end point assessment, the time between the initial and follow-up imaging (at 12 hours posttreatment in the ANNEXA-4 trial; up to 36 hours posttreatment in the RETRACE-II study) and the mRS posttreatment assessment time point (at 30 days in the ANNEXA-4 trial; at discharge in the RETRACE-II study) were different between the studies, although the authors conducted descriptive analyses and linear regression analyses that suggested there was no meaningful relationship between the timing of these posttreatment assessments and the outcomes.
Prespecified criteria were used to identify the most important variable for inclusion in the propensity score model. Some variables were excluded from adjustment due to a low strength of association with the outcome or treatment assignment or due to having more than 10% of the data missing in 1 of the treatments groups, although the results of the sensitivity analyses of the full propensity score model were consistent with the primary analyses for all outcomes, increasing certainty of the findings. However, demographic data, such as age, sex, and weight, were not included in the adjustment model; therefore, there is a high risk of bias due to unmeasured confounding.
In both the whole-cohort analysis and PCC subgroup analysis, imprecision was evident in the point estimates (HR) of in-hospital mortality, with a wide 95% CI, which included the possibility of appreciable benefit and/or worse outcomes. This precludes any firm conclusion regarding the relative effect of andexanet alfa and standard of care (i.e., PCC) on in-hospital mortality. For the outcome of mRS after treatment, no baseline assessment was available in the RETRACE-II study. This limited the ability to control for potential baseline differences in this variable. However, other variables probably associated with the magnitude of mRS (e.g., ICH score, GCS score) were included in the propensity score model to work as a proxy for mRS at baseline.
Clinically relevant outcomes were assessed, including mRS (a measure of disability) and in-hospital mortality, while other outcomes that were of interest to stakeholders such as mental status, ICU admission, length of stay at hospital, and HRQoL were not.
Other Observational Evidence: Andexanet Alfa Versus PCC in Real-World Clinical Practice
The contents of this section were informed by materials submitted by the sponsor. The following was summarized and validated by the CADTH review team.
Description of Studies
The sponsor submitted 6 comparative observational studies comparing andexanet alfa with PCC in real-world clinical practice.24-29 The study design, inclusion and exclusion criteria, and outcomes of the 6 studies are summarized in Table 28.
Briefly, all 6 studies were multicentre, retrospective chart audits conducted in the US. The patient population for Coleman et al. (2021),24 Dobesh et al. (2022),25 Fermann et al. (2022),26 and Dobesh et al. (2023)27 were sourced from audits of US hospital charts, while the populations for Sutton et al. (2022)28 and Sutton et al. (2023)29 were sourced from US Veterans Affairs databases. In all studies, data were captured from electronic medical records. The eligible patient population comprised adult patients aged 18 years and older hospitalized for FXa inhibitor–related bleeding. Patients were identified through electronic medical records using ICD-10 billing codes,24-27 or administrative claims and pharmacy dispensation information from the Veterans Affairs Informatics and Computing Infrastructure.28,29 Fermann et al. (2022) estimated propensity scores using logistic regression to create inverse probability of treatment weights to balance the treatment groups with regards to potential confounders, and matching was conducted using full, nearest-neighbour matching.
Outcomes included in-hospital mortality,24-27,29 in-hospital 30-day mortality,28 length of hospital stay,24,25,29 and ICU length of stay.24,25,29
Coleman et al. (2022), Dobesh et al. (2022), Fermann et al. (2022), and Dobesh et al. (2023) provided descriptive analyses of results, stratified by bleed type for each reversal or replacement agent. The remaining studies presented results for each reversal or replacement agent, irrespective of bleed type. Across all studies, mortality outcomes were reported as counts (n) and frequency (%), and length-of-stay outcomes were reported as median days with IQR or mean days with SD. The Dobesh et al. (2022), Dobesh et al. (2023), and Fermann et al. (2022) studies also performed adjusted multivariate logistic regressions assessing the association between reversal or replacement agent and death. The Sutton et al. (2022) study conducted propensity score–weighted Cox models to explore the relationship between reversal or replacement agent and mortality. Of note, due the descriptive nature of most of the studies, the comparisons between andexanet alfa and PCC are descriptive in intent.
Table 28: Details of RWE Studies Addressing Gaps in Pivotal and RCT Evidence
Details | Coleman et al. (2021) | Dobesh et al. (2022) | Fermann et al. (2022) | Dobesh et al. (2023) | Sutton et al. (2022) | Sutton et al. (2023) |
|---|---|---|---|---|---|---|
Designs and populations | ||||||
Study design | Retrospective chart audit study | |||||
Data source | Audits of US hospital charts | US Veteran Affairs databases | ||||
Sites (N) | 45 | 184 | 182 | 354 | NA | NA |
Enrolled (N) | 3,030 | 2,830 | 2,451 | 4,395 | 255 | 1,005 |
Study period | ||||||
Start date | January 2016 | May 17, 2018 | May 17, 2018 | July 2018 | March 2014 | March 2014 |
End date | September 2019 | September 30, 2021 | September 30, 2021 | September 2022 | December 2020 | May 2022 |
Key inclusion criteria |
|
|
| |||
Key exclusion criteria | — | — | Any bleed type other than ICH or GI bleed | Treatment with both andexanet alfa and 4F-PCC for their bleeding event |
| |
Drugs | ||||||
Intervention |
|
|
| |||
Outcomes | ||||||
End points |
|
| In-hospital mortality | In-hospital mortality |
|
|
Notes | ||||||
Publications | Coleman et al. (2021)24 | Dobesh et al. (2022)25 | Fermann et al. (2022)26 | Dobesh et al. (2023)27 | Sutton et al. (2022)28 | Sutton et al. (2023)29 |
4F-PCC = 4-factor prothrombin complex concentrate; AF = atrial fibrillation; FXa = factor Xa; GI = gastrointestinal; ICD-10 = International Classification of Diseases, Tenth Revision; ICD-10-CM = International Classification of Diseases, Tenth Revision, Clinical Modification; ICH = intracranial hemorrhage; ICU = intensive care unit; LoS = length of stay; NA = not applicable; RCT = randomized controlled trial; RWE = real-world evidence; VT = venous thromboembolism.
aIn Dobesh et al. (2022), patients who were treated with both agents were categorized into the group for the reversal agent they received first. In Dobesh et al. (2023), patients treated with both andexanet alfa and 4F-PCC during the hospitalization for their bleeding event were excluded.
Sources: Coleman et al. (2021), Dobesh et al. (2022), Dobesh et al. (2023), Fermann et al. (2022), Sutton et al. (2022), and Sutton et al. (2023).24-29
Patient Population
Participant Characteristics
The study sample size ranged from 255 to 4,395 patients. The average age of patients across the studies ranged from 65.0 years to 70.1 years. The most commonly used FXa inhibitors documented were apixaban (40% to 84.0%) and rivaroxaban (14.5% to 56%); the other FXa inhibitors documented were enoxaparin (1% to 37.5%) and edoxaban (1% to 6%). Bleed types documented across the studies included GI (40% to 59.9%), ICH (11% to 32.0%), critical compartments (4% to 31%), and traumatic (1% to 11.0%). Across all studies, the reporting of bleed types was mutually exclusive.
Exposure to Interventions
Exposures
The exposure to reversal or replacement agents across the 6 studies is summarized in Table 29. Exposure to andexanet alfa ranged from 11.3% to 48.3% across the studies, while exposure to 4F-PCC ranged from 24.2% to 80.1%. Coleman et al. (2021) also documented the proportion of patients exposed to FFP (30.5%), other reversal or replacement therapies (26.2%) and no therapies (14.5%).24
Concomitant Medications
Concomitant use of reversal agents was reported in some studies.24,25,28,29 The most commonly used concomitant agent reported in the Dobesh et al. (2022) study included IV fluids (14% to 20%), vitamin K (10% to 17%), FFP (9% to 15%), and packed RBCs (8% to 10%). In the 2 Sutton et al. studies, the most commonly used concomitant reversal agents reported were RBCs (32.9% to 43.1%), vitamin K (10.6% to 44.1%), transfusion (8.2% to 15.9%), plasma (8.0% to 15.3%), and platelets (7.0% to 14.3%).28,29 While concomitant use of reversal agents was allowed in the Coleman et al. (2021) study such that the percentages of patients receiving reversal agents added to more than 100%, further details with respect to concomitant use were not reported.24
Table 29: Exposure to Reversal or Replacement Agents
Agent | Coleman et al. (2021) N = 3,030 | Dobesh et al. (2022) N = 2,830 | Fermann et al. (2022) N = 2,451 | Dobesh et al. (2023) N = 4,395 | Sutton et al. (2022) N = 255 | Sutton et al. (2023) N = 1,005 |
|---|---|---|---|---|---|---|
Treatment, n (%) | ||||||
Andexanet alfa | 343 (11.3) | 1,366 (48.3) | 1,196 (48.8) | 2,122 (48.3) | 85 (33.3) | 200 (19.9) |
4F-PCC | 733 (24.2) | 1,464 (51.7) | 1,255 (51.2) | 2,273 (51.7) | 170 (66.7) | 805 (80.1) |
FFP | 925 (30.5) | — | — | — | — | — |
Othera | 794 (26.2) | — | — | — | — | — |
No treatment | 438 (14.5) | — | — | — | — | — |
4F-PCC = 4-factor prothrombin complex concentrate; FFP = fresh frozen plasma; PCC = prothrombin complex concentrate.
aAll others: 3-factor PCC, recombinant factor VIIa, activated 4F-PCC, tranexamic acid, vitamin K.
Sources: Coleman et al. (2021),24 Dobesh et al. (2022);25 Dobesh et al. (2023),27 Fermann et al. (2022),26 Sutton et al. (2022),28 and Sutton et al. (2023).29
Results
Efficacy
Results for in-hospital mortality, 30-day hospital mortality, and hospital and ICU lengths of stay are summarized in Table 30.
In-Hospital Morality
In-hospital mortality for those treated with andexanet alfa was 4% in Coleman et al. (2021), 6% in Dobesh et al. (2022) and (2023), and 10.6% in Sutton et al. (2022). In-hospital mortality for those treated with 4F-PCC was 10% in Coleman et al. (2021), 8% in Dobesh et al. (2022), 10.6% in Dobesh et al. (2023), and 25.3% in Sutton et al. (2022). In Fermann et al. (2022), in-hospital mortality among patients treated with andexanet alfa was approximately 2.5% among patients with GI bleeds and ranged from 9.8% to 16.8% among patients with an ICH; in patients treated with 4F-PCC, in-hospital mortality ranged from 3.2% to 6.0% among patients with GI bleeds, and from 14.5% to 24.0% in patients with an ICH.
In the adjusted analysis performed by Dobesh et al. (2022), treatment with andexanet alfa was associated with a lower likelihood of death compared with treatment with 4F-PCC (OR = 0.69; 95% CI, 0.49 to 0.98). In Dobesh et al. (2023), treatment with andexanet alfa was also associated with a lower likelihood of in-hospital mortality compared with 4F-PCC across all bleeds (OR = 0.50; 95% CI, 0.39 to 0.65), GI bleeds (OR = 0.49; 95% CI, 0.29 to 0.81), and ICH (OR = 0.55; 95% CI, 0.39 to 0.76). In the adjusted analysis performed by Fermann et al. (2022), treatment with andexanet alfa was associated with lower odds of in-hospital mortality compared with treatment with 4F-PCC (OR = 0.67; 95% CI, 0.48 to 0.94). In Sutton et al. (2022), treatment with andexanet alfa was associated with a lower hazard of in-hospital mortality compared with treatment with 4F-PCC (HR = 0.31; 95% CI, 0.14 to 0.71).
30-Day In-Hospital Mortality
30-day in-hospital mortality was explored in Sutton et al. (2022) only. The 30-day mortality rate was 20.0% and 32.4% in patients treated with andexanet alfa and 4F-PCC, respectively. Treatment with andexanet alfa was associated with a lower hazard of 30-day mortality compared with treatment with 4F-PCC (HR = 0.54; 95% CI, 0.30 to 0.98).
ICU Length of Stay
For patients who received andexanet alfa, overall median ICU length of stay was 2 days (IQR = 1 to 4 days) in Coleman et al. (2021), 2 days (SD = 3) in Dobesh et al. (2022), and 1 day (IQR = 0 to 4 days) in Sutton et al. (2022). In Sutton et al. (2023), the mean ICU length of stay was 4.0 days (SD = 7.1). For patients who received 4F-PCC, the ICU stay was 3 days (IQR = 2 to 5) in Coleman et al. (2021), 2 days (IQR = 3) in Dobesh et al. (2022), and 2 days (IQR = 0 to 5) days in Sutton et al. In Sutton et al. (2023), the mean length of ICU stay was 5.0 days (SD = 8.6).
Hospital Length of Stay
For patients who received andexanet alfa, the median hospital stay was 5 days (IQR = 3 to 6) in Coleman et al. (2021), 5 days (SD = 5) in Dobesh et al. (2022), and 6 days (IQR = 3 to 10) in Sutton et al. (2022); and in Sutton et al. (2023), the mean length of stay was 11.3 days (SD = 22.8) while, in Fermann et al. (2022), the mean length of stay ranged from 6.4 days (SD = 4.2) to 8.9 days (SD = 6.2). For patients who received 4F-PCC, the median hospital stay was 5 days (IQR = 4 to 7) in Coleman et al. (2021), 5 (SD = 5) days in Dobesh et al. (2022), and 7 (IQR = 4 to 18) days in Sutton et al. (2022). In Sutton et al. (2023), the mean length of stay of hospital stay was 12.2 days (SD = 17.5), while in Fermann et al. (2022), the mean length of hospital stay ranged from 6.3 days (SD = 4.1) to 8.3 days (SD = 6.2).
Table 30: In-Hospital Mortality, 30-Day Hospital Mortality, and Hospital and ICU Lengths of Stay Reported Across the 6 RWE Studies
Study, study treatment, and bleed type | In-hospital mortality n (%) | 30-day hospital mortality n (%) | ICU LoS median (IQR) | Hospital LoS median (IQR) |
|---|---|---|---|---|
Coleman et al. (2021) | ||||
Andexanet alfa (n = 342) | ||||
All bleeds | 12 (4) | NE | 2.0 (1.04 to 4.0) | 5.0 (3.0 to 6.0) |
GI bleed | 2 (1) | NE | 2.0 (1.0 to 2.0) | 4.0 (3.0 to 5.0) |
ICH | 6 (9) | NE | 4.0 (3.0, 6.0) | 7.0 (6.0, 8.0) |
Critical component | 0 (0) | NE | 5.0 (4.0, 7.0) | 7.0 (6.0, 9.0) |
Traumatic | 4 (4) | NE | 2.0 (1.0, 3.5) | 5.0 (3.0, 6.0) |
Othera | 0 (0) | NE | NR | NR |
4F-PCC (n = 733) | ||||
All bleeds | 74 (10) | NE | 3.0 (2.0, 5.0) | 5.0 (4.0, 7.0) |
GI bleed | 12 (4) | NE | 2.0 (1.0, 3.0) | 4.0 (3.0, 5.0) |
ICH | 43 (25) | NE | 4.0 (3.0, 6.0) | 7.0 (4.0, 9.0) |
Critical component | 1 (4) | NE | 3.0 (2.0, 5.0) | 5.5 (4.0, 8.8) |
Traumatic | 16 (7) | NE | 3.0 (2.0, 5.0) | 6.0 (4.0, 8.0) |
Othera | 2 (10) | NE | NR | NR |
Dobesh et al. (2022) | ||||
Andexanet alfa (n = 1,288) | ||||
All bleeds | 78 (6) | NE | 2 (3)b | 5 (5)b |
ICH | 49 (14) | NE | 3 (4)b | 6 (6)b |
GI bleed | 21 (3) | NE | 2 (3)b | 4 (4) |
Critical component | 7 (4) | NE | 2 (2) | 4 (4) |
4F-PCC (n = 1,343) | ||||
All bleeds | 121 (8) | NE | 2 (3)b | 5 (5)b |
ICH | 78 (20) | NE | 3 (4)b | 6 (7)b |
GI bleed | 31 (4) | NE | 2 (3)b | 4 (5)b |
Critical component | 8 (5) | NE | 2 (4)b | 5 (6)b |
Fermann et al. (2022) | ||||
Andexanet alfa (n = 1,196) | ||||
ICH spontaneous | 16 (9.8) | NE | NE | 7.1 (4.6)c |
ICH traumatic | 33 (16.8) | NE | NE | 8.9 (6.2)c |
GI spontaneous | 17 (2.5) | NE | NE | 6.4 (4.2)c |
GI traumatic | 4 (2.4) | NE | NE | 7.1 (5.3)c |
4F-PCC (n = 1,244) | ||||
ICH spontaneous | 25 (14.5) | NE | NE | 7.9 (5.5)c |
ICH traumatic | 53 (24.0) | NE | NE | 8.3 (6.2)c |
GI spontaneous | 23 (3.2) | NE | NE | 6.3 (4.1)c |
GI traumatic | 8 (6.0) | NE | NE | 7.2 (5.0)c |
Dobesh et al. (2023) | ||||
Andexanet alfa (n = 2,122) | ||||
All bleeds | NR (6) | NE | NE | NE |
GI bleed | NR (2.5) | NE | NE | NE |
ICH | NR (12.6) | NE | NE | NE |
4F-PCC (n = 2,273) | ||||
All bleeds | NR (10.6) | NE | NE | NE |
GI bleed | NR (4.3) | NE | NE | NE |
ICH | NR (23.3) | NE | NE | NE |
Sutton et al. (2022) | ||||
Andexanet alfa (n = 85) | ||||
All bleeds | NR (10.6) | (20.0) | 1 (0 to 4)b,c | 6 (3 to 10)b,c |
4F-PCC (n = 170) | ||||
All bleeds | NR (25.3) | (32.4) | 2 (0 to 5)b,c | 7 (4 to 18)b,c |
Sutton et al. (2023) | ||||
Andexanet alfa (n = 200) | ||||
All bleeds | NE | NE | 4.0 (7.1)c | 11.3 (22.8)c |
4F-PCC (n = 805) | ||||
All bleeds | NE | NE | 5.0 (8.6)c | 12.2 (17.5)c |
4F-PCC = 4-factor prothrombin complex concentrate; FFP = fresh frozen plasma; GI = gastrointestinal; ICH = intracranial hemorrhage; ICU = intensive care unit; IQR = interquartile range; LoS = length of stay; NE = not evaluated; NR = not reported; RWE = real-world evidence; SD = standard deviation.
aOther bleeds were not included in the LoS analysis due to low sample size and variability of types of bleeds.
bLoS excluded mortality.
cPresented as mean and SD.
Sources: Coleman et al. (2021),24 Dobesh et al. (2022),25 Dobesh et al. (2023),27 Fermann et al. (2022),26 Sutton et al. (2022),28 and Sutton et al. (2023).29
Critical Appraisal
The nonrandomized comparison of the 6 RWE studies makes interpretation of the efficacy of andexanet alfa compared with 4F-PCC challenging. The retrospective nature of the studies meant that the quality and accuracy of data collection was dependent on the procedures of routine documentation at each institution. Moreover, the use of ICD-10 codes is associated with limitation for the purpose of clinical research.30,31 Although all 6 studies were multicentre studies, each medical centre may have distinct population characteristics and physician decision-making patterns. As a result, heterogeneity across the participating medical centres cannot be ruled out. Further, the point estimates varied between studies for both treatment groups, which increases the uncertainty that these comparisons are sufficient to provide evidence of efficacy. The influence of an important patient-level factor (e.g., advanced directives, thrombotic complications after reversal agent administration) — which could not be ascertained from the medical records — on the treatment effect of andexanet alfa and 4F-PCC could not be ruled out. Although Dobesh et al. (2022), Dobesh et al. (2023), Fermann et al. (2022), and Sutton et al. (2022) employed covariate adjustment and propensity weighting, there is a possibility of selection bias or residual confounding due to the nonrandomized nature of the study designs. As a result, there is uncertainty around the comparative treatment effects of andexanet alfa compared with 4F-PCC due to selection bias and unmeasured confounding that cannot be entirely ruled out.
Discussion
Summary of Available Evidence
This report summarizes the evidence for andexanet alfa in the reversal of the anticoagulant effect of anti-FXa inhibitors (apixaban and rivaroxaban) in patients with an acute major bleed based on 1 open-label single-arm trial, 2 RCTs, 3 weighted observational studies, and 6 comparative observation studies.
One pivotal trial, ANNEXA-4, met the inclusion criteria for the systematic review conducted by the sponsor. The ANNEXA-4 trial (N = 477) was a phase IIIb and IV, open-label, single-arm trial that aimed to demonstrate a decrease in anti-FXa activity and an increase in the achievement of hemostatic efficacy with andexanet alfa treatment in adult patients with acute major bleeding while receiving an FXa inhibitor treatment. Percent change from baseline in anti-FXa activity to on-treatment nadir and achievement of hemostatic efficacy at 12 hours postinfusion (coprimary end points), rebleeding, use of non–study-prescribed blood products and/or hemostatic drugs, RBC transfusion, change in neurologic status scores in patients with ICH (exploratory end points), and mortality (safety end point) were assessed. At baseline, patients (safety analysis set) had a mean age of 77.9 years (SD = 10.66), with approximately half of them being male and the majority being white. Most patients received apixaban (51.4%) or rivaroxaban (36.5%) anticoagulation and had an ICH (69.0%) or GI bleed (22.9%).
ANNEXA-A and ANNEXA-R were pivotal phase III, double-blind, RCTs comparing andexanet alfa and placebo with respect to the reversal of apixaban (ANNEXA-A trial) or rivaroxaban (ANNEXA-R trial) anticoagulation in healthy volunteers. Outcomes related to anti-FXa activity and harms are summarized in this report.
Given the lack of direct comparative evidence between andexanet alfa and PCC, the sponsor submitted 3 observational studies comparing andexanet alfa with real-world clinical practice using IPD from the ANNEXA-4 trial and external cohorts from the ORANGE study (all bleed types), the HHCS (ICH only), and the RETRACE-II study (atraumatic ICH only) using PSM or weighting. Thirty-day mortality, hemostatic efficacy, mRS, and thrombotic events were assessed. As well, 6 RWE comparisons of andexanet alfa and 4F-PCC data were submitted. All 6 studies were multicentre, retrospective chart audits conducted in the US and sourced from audits of US hospital charts and US Veterans Affairs databases. In-hospital mortality, in-hospital 30-day mortality, length of hospital stay, and ICU length of stay were assessed.
Interpretation of Results
Efficacy
In the ANNEXA-4 trial, the study-defined threshold for hemostatic efficacy at 12 hours after andexanet alfa infusion was achieved in the whole cohort (lower limit of the 95% CI above 50%), and across the subgroups of interest (bleed type and eGFR level). The clinical experts consulted by CADTH considered the results to be supportive of the efficacy of andexanet alfa, although they and the CADTH review team agreed it is difficult to determine whether the rate of hemostatic efficacy observed could be attributed to the effect of andexanet alfa alone, since potential confounding factors could not be accounted for in a noncomparative study. No conclusion could be drawn on subgroup effects (by bleed type and eGFR level) due to the lack of sample size consideration, control for multiplicity, and treatment-by-subgroup interaction analysis. Although hemostatic efficacy (adjudicated based on radiological and laboratory findings) is a common end point in clinical studies of reversal agents of anticoagulants, it is not a patient-important outcome.
Mortality and mental and functional statuses are considered to be more meaningful clinical outcomes to patients, clinicians, and the clinical experts consulted by CADTH. Thirty-day mortality was 17.0% in the study, which the clinical experts noted was in line with the mortality rate for PCC reported in the literature. Reduction in disability was assessed in patients with ICH using clinically relevant instruments, including the mRS, NIHSS, and GCS, which are neurologic scales for functional status, severity of stroke symptoms, and mental status, respectively. Results showed that the neurologic status of patients remained stable up to day 30. However, due to the exploratory nature of these neurologic outcomes, the large amount of missing data, and potential reporting bias associated with the open-label design, no definitive conclusion could be drawn. In addition, the analyses were conducted in the efficacy population, which excluded patients who had a baseline anti-FXa below a prespecified threshold and did not meet the bleeding inclusion criteria; the impact of such exclusion is unclear in the absence of sensitivity analyses in the intention-to-treat population (i.e., safety population). Other relevant outcomes, including occurrence of rebleeding, use of RBC transfusion and non–study-prescribed blood products and/or hemostatic drugs, and median length of stay at the hospital, in general, align with the clinical experts’ clinical experience with PCC.
The coprimary end point of percent change in anti-FXa activity from baseline at on-treatment nadir was met (the 95% CI for the median excluded 0). The reduction in the level of anti-FXa activity was more than 90% in rivaroxaban- and apixaban-treated patients. The clinical experts commented that this level of reduction aligned with their expectations, considering the mechanism of action for andexanet alfa is as a decoy protein for FXa inhibitors, although the clinical relevance of an anti-FXa assay is low in their opinion, since it is not routinely measured in clinical practice. The FDA considers reduction of anti-FXa activity by andexanet alfa to be reasonably likely to predict clinical benefits in morbidity and mortality in the indicated population, although there was some disagreement, since no evidence was provided for the mechanism of action beyond correlations. Anti-FXa activity–related end points were also assessed in the ANNEXA-A and ANNEXA-R trials, with the results favouring andexanet alfa compared with placebo; however, the results are not informative for the purpose of this review, given the trials were conducted in healthy volunteers with no major bleeding, as opposed to the indicated population.
It should be noted that the ANNEXA-4 study was conducted in a highly select population, excluding patients with severe ICH (GCS less than 7, estimated intracerebral hematoma volume above 60 cc) and those with an expected survival of less than 1 month. Patients were also generally younger compared with clinical practice, according to clinical expert input. These factors together suggest that the study population may have a better prognosis compared with patients in clinical practice, according to the clinical experts, limiting the generalizability of the study results. It is also unclear whether andexanet alfa could meet the unmet need expressed by the patient groups for a specific reversal agent for patients requiring emergency surgery while on FXa inhibitor treatment, since these patients, which the clinical experts noted were reasonable candidates for andexanet alfa, were not included in the study. ICU admission and HRQoL were important clinical outcomes, according to the clinical expert and clinician group input; however, they were not assessed in this study. Further, this study is the only clinical trial to date of patients experiencing acute major bleeding while receiving andexanet alfa; the absence of a direct comparison with PCC, the usual care for reversal of FXa inhibitor–related bleeding, represents a gap in the evidence.
In an effort to address this evidence gap, the sponsor submitted 3 weighted comparative observational studies, which suggested that andexanet alfa, compared with PCC, was associated with a lower rate of 30-day mortality in patients with ICH; a higher rate of hemostatic effectiveness in patients with ICH, including those related to atraumatic cause; and no difference in mRS at discharge or at 30 days in patients with ICH related to an atraumatic cause. However, these results are uncertain because of the important limitations they share. This includes potential bias in the study-selection process in the absence of an SLR or due to lack of transparency in the SLR methods used. As well, of the available information, there appeared to be heterogeneity in study designs and patient populations between studies that was not adequately accounted for, resulting in uncertainty in the comparative treatment-effect estimates.
Evidence from the 6 retrospective studies exploring the real-world effectiveness of andexanet alfa suggests that andexanet alfa, compared with PCC, was associated with lower 30-day mortality and shorter lengths of total hospital stay and ICU stay. However, the nonrandomized comparison of the 6 RWE studies makes the interpretation of the efficacy of andexanet alfa compared with 4F-PCC challenging. Again, the lack of an SLR makes it difficult to assess whether the studies selected are representative of the literature as a whole, or a select curated collection. Overall, there is uncertainty around the comparative treatment effects of andexanet alfa compared with 4F-PCC due to selection bias and unmeasured and residual confounding that cannot be entirely ruled out across the 6 studies.
The clinical experts noted to the CADTH team that some published meta-analyses of PCC and andexanet alfa for reversal of DOAC-related bleeding suggest there are similar mortality and thrombosis rates between them,43,44 although considering that they are naive comparisons, these estimated mortality results are also uncertain due to potential confounding.
Many of the limitations of the clinical evidence mentioned previously were similarly noted by NICE in its review of andexanet alfa. Its guidance document highlighted that there is uncertainty in the cost-effectiveness estimates, based on limitations of the clinical evidence, particularly with respect to the extent of the benefits in ICH of andexanet alfa in mortality and long-term disability. NICE therefore recommended andexanet alfa for routine use of reversal of anticoagulation in GI bleeding, but only in research of ICH. Note that a head-to-head comparison of andexanet alfa with usual care in patients with acute ICH is currently assessed in the ongoing phase IV randomized ANNEXA-I trial and results are forthcoming (estimated completion date is July 30, 2024).
Harms
In the ANNEXA-4 trial, 72.5% of patients experienced at least 1 TEAE and 41.9% of these were serious TEAEs at 30 days. Treatment discontinuation due to a TEAE was low, at 0.8%, and death was reported in 17.0% of patients. Thrombotic events were reported in 10.5% of patients. The clinical experts noted that, in general, there is a concern regarding the prothrombotic risk for reversal agents, which typically manifests as thrombosis within 24 hours after administration; however, they noted that, given results are based on a follow-up duration of 30 days, it is not possible to assess whether andexanet alfa has such properties and, given that other factors could also have influenced the thrombosis rate during this extended time frame. The clinical experts also noted that overall, without a control arm, it is challenging to determine whether the observed adverse events could be attributed to andexanet alfa alone. Nonetheless, the clinical experts did not have major concerns with the safety profile of andexanet alfa and noted that the thrombosis rate in this study was in line with that of PCC reported in the literature. The weighted comparative analysis between the reported thrombotic events in ANNEXA-4 and the HHCS suggested a similarly low frequency of thrombosis in both the andexanet alfa (1.9%) and PCC (0%) cohorts within 5 days posttreatment, although no conclusion can be drawn due to the aforementioned limitations of the study. Harms outcomes were not assessed across the 6 comparative observational studies comparing andexanet alfa with PCC in real-world clinical practice.
Conclusion
One pivotal single-arm, open-label, phase IIIb and IV trial (ANNEXA-4) provided evidence regarding the efficacy and safety of andexanet alfa in the treatment of patients with acute major bleeding while receiving FXa anticoagulation. Results of clinically relevant outcomes, including 30-day mortality, neurologic status, rebleeding, need for blood products and hemostatic drugs, and length of hospital stay, were generally in line with the clinical experts’ clinical experience with PCC. The analyses of hemostatic efficacy and anti-FXa activity also lent support to the ability of andexanet alfa to achieve hemostasis and reduce the anticoagulant activity of FXa inhibitors. However, there was uncertainty in the magnitude of the clinical benefit attributable to andexanet alfa, given the inherent limitations of the noncomparative study design. The generalizability of the study findings was also limited by the younger study population compared with clinical practice, and the exclusion of patients with a severe ICH and patients with an expected survival of less than 1 month. Three weighted comparative observational studies and 6 comparative observational studies assessed the comparative efficacy of andexanet alfa and PCC in real-world clinical practice; however, the results were inconclusive due to important methodological limitations (e.g., selection bias, inadequate adjustment for prognostic factors and effect modifiers) of these studies. The safety profile of andexanet alfa in the pivotal trial appeared to be consistent with PCC, as per clinical expert input. One weighted comparative analysis suggested the frequency of thrombotic events was similarly low for both andexanet alfa and PCC within 5 days posttreatment, although the results are uncertain due to the aforementioned limitations of the analysis.
References
1.PrOndexxya® (andexanet alfa): 200 mg powder for solution for intravenous infusion [product monograph]. Missisauga (ON): AstraZeneca Canada Inc; 2023 Jun 16.
2.PrXarelto® (rivaroxaban): 2.5 mg, 10 mg, 15 mg and 20 mg tablets [product monograph]. Mississauga (ON): Bayer Inc.; 2022 Jun 10.
3.PrEliquis® (apixaban) 2.5 mg and 5 mg tablets [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada Co.; 2019 Oct 7.
4.Beyer-Westendorf J, Förster K, Pannach S, et al. Rates, management, and outcome of rivaroxaban bleeding in daily care: results from the Dresden NOAC registry. Blood. 2014;124(6):955-962. PubMed
5.Held C, Hylek EM, Alexander JH, et al. Clinical outcomes and management associated with major bleeding in patients with atrial fibrillation treated with apixaban or warfarin: insights from the ARISTOTLE trial. Eur Heart J. 2015;36(20):1264-1272. PubMed
6.Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. PubMed
7.Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891. PubMed
8.PharmaStat Database. Apixaban and rivaroxaban claims, cost, units, and days data. Q3 2021-Q2 2022 [internal sponsor's report]. IQVIA; 2022.
9.Eikelboom JW, Connolly SJ, Bosch J, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med. 2017;377(14):1319-1330. PubMed
10.Xian Y, Zhang S, Inohara T, et al. Clinical characteristics and outcomes associated with oral anticoagulant use among patients hospitalized with intracerebral hemorrhage. JAMA Netw Open. 2021;4(2):e2037438. PubMed
11.Summers RL, Sterling SA. Emergent bleeding in patients receiving direct oral anticoagulants. Air Med J. 2016;35(3):148-155. PubMed
12.Qazi JZ, Schnitzer ME, Côté R, Martel MJ, Dorais M, Perreault S. Predicting major bleeding among hospitalized patients using oral anticoagulants for atrial fibrillation after discharge. PLoS One. 2021;16(3):e0246691. PubMed
13.Øie LR, Madsbu MA, Solheim O, et al. Functional outcome and survival following spontaneous intracerebral hemorrhage: a retrospective population-based study. Brain Behav. 2018;8(10):e01113. PubMed
14.Apostolaki-Hansson T, Ullberg T, Norrving B, Petersson J. Prognosis for intracerebral hemorrhage during ongoing oral anticoagulant treatment. Acta Neurol Scand. 2019;139(5):415-421. PubMed
15.Fernando SM, Qureshi D, Talarico R, et al. Intracerebral hemorrhage incidence, mortality, and association with oral anticoagulation use: a population study. Stroke. 2021;52(5):1673-1681. PubMed
16.DOACs: management of bleeding. Whitby (ON): Thrombosis Canada; 2021: https://thrombosiscanada.ca/wp-uploads/uploads/2021/11/23.-DOACs-Management-Bleeding_29November2021-1.pdf. Accessed 2023 May 2.
17.Milling TJ, Jr., Middeldorp S, Xu L, et al. Final study report of andexanet alfa for major bleeding with factor Xa inhibitors. Circulation. 2023. PubMed
18.Siegal DM, Curnutte JT, Connolly SJ, et al. Andexanet alfa for the reversal of factor Xa inhibitor activity. N Engl J Med. 2015;373(25):2413-2424. PubMed
19.Clinical Study Report 14-505 (ANNEXA-4). Prospective, open-label study of andexanet alfa in patients receiving a factor Xa inhibitor who have acute major bleeding (ANNEXA-4) [internal sponsor's report]. San Francisco (CA): Portola Pharmaceuticals, Inc.; 2020.
20.Sponsor's summary of clinical evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ondexxya (andexanet alfa) 200 mg powder for solution for intravenous infusion. Mississauga (ON): AstraZeneca Canada, Inc.; 2023 Mar 2.
21.Cohen AT, Lewis M, Connor A, et al. Thirty-day mortality with andexanet alfa compared with prothrombin complex concentrate therapy for life-threatening direct oral anticoagulant-related bleeding. J Am Coll Emerg Physicians Open. 2022;3(2):e12655. PubMed
22.Costa OS, Connolly SJ, Sharma M, et al. Andexanet alfa versus four-factor prothrombin complex concentrate for the reversal of apixaban- or rivaroxaban-associated intracranial hemorrhage: a propensity score-overlap weighted analysis. Crit Care. 2022;26(1):180. PubMed
23.Huttner HB, Gerner ST, Kuramatsu JB, et al. Hematoma expansion and clinical outcomes in patients with factor-Xa inhibitor-related atraumatic intracerebral hemorrhage treated within the ANNEXA-4 trial versus real-world usual care. Stroke. 2022;53(2):532-543. PubMed
24.Coleman CI, Dobesh PP, Danese S, Ulloa J, Lovelace B. Real-world management of oral factor Xa inhibitor-related bleeds with reversal or replacement agents including andexanet alfa and four-factor prothrombin complex concentrate: a multicenter study. Future Cardiol. 2021;17(1):127-135. PubMed
25.Dobesh PP, Coleman CI, Ulloa J, et al. Andexanet alfa is associated with a significant reduction in in-hospital mortality compared with 4F-pCC in a real-world analysis [abstract]. Presented at: International Society on Thrombosis and Haemostasis 2022 Congress; July 12, 2022; London (UK). 2022.
26.Fermann GJ, Dobesh PP, Danese M, et al. Andexanet alfa is associated with reduced in-hospital mortality compared with 4-factor prothrombin complex concentrate among patients with intracranial or gastrointestinal bleeding [abstract]. Presented at: ACEPT Scientific Assembly 2022; Oct 1-4, 2022; San Francisco (CA).
27.Dobesh PP, Coleman CI, Danese M, et al. Andexanet alfa is associated with lower in-hospital mortality compared with 4-factor prothrombin complex concentrate in patients with factor Xa inhibitor–related major bleeding [abstract]. Presented at: International Society on Thrombosis and Haemostasis 2023 Congress; June 24-28, 2023; Montreal (QC).
28.Sutton S, Maganoli J, Cummings T, Dettling T, Hardin J, Lovelace B. Real-world clinical outcomes among US veterans with oral Factor Xa inhibitor-related major bleeding treated with andexanet alfa or 4-factor prothrombin complex concentrate [abstract]. Presented at: Thrombosis & Hemostasis Summit of North America 2022; Aug 18, 2022; Chicago (IL).
29.Sutton S, Maganoli J, Cummings T, et al. Healthcare resource use among US veterans treated with andexanet alfa or 4-factor prothrombin complex concentrate for factor Xa inhibitor-related major bleeding [abstract]. Presented at: International Society on Thrombosis and Haemostasis 2023 Congress; June 24-28, 2023; Montreal (QC).
30.Mainor AJ, Morden NE, Smith J, Tomlin S, Skinner J. ICD-10 coding will challenge researchers: caution and collaboration may reduce measurement error and improve comparability over time. Med Care. 2019;57(7):e42-e46. PubMed
31.Crabb BT, Lyons A, Bale M, et al. Comparison of international classification of diseases and related health problems, tenth revision codes with electronic medical records among patients with symptoms of coronavirus disease 2019. JAMA Netw Open. 2020;3(8):e2017703. PubMed
32.Sikorska J, Uprichard J. Direct oral anticoagulants: a quick guide. Eur Cardiol. 2017;12(1):40-45. PubMed
33.Garcia D, Crowther M. Management of bleeding in patients receiving direct oral anticoagulants. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 Mar 20.
34.Milling TJ, Jr., Clark CL, Feronti C, et al. Management of Factor Xa inhibitor-associated life-threatening major hemorrhage: a retrospective multi-center analysis. Am J Emerg Med. 2018;36(3):396-402. PubMed
35.Canadian stroke best practices: management of spontaneous intracerebral hemorrhage. Toronto (ON): Heart & Stroke Foundation of Canada; 2020: https://www.strokebestpractices.ca/recommendations/management-of-intracerebral-hemorrhage/emergency-management-of-intracerebral-hemorrhage. Accessed 2022 Sep 2.
36.Milling TJ, Jr., Frontera J. Exploring indications for the use of direct oral anticoagulants and the associated risks of major bleeding. Am J Manag Care. 2017;23(4 Suppl):S67-s80. PubMed
37.Andrade JG, Aguilar M, Atzema C, et al. The 2020 Canadian Cardiovascular Society/Canadian Heart Rhythm Society comprehensive guidelines for the management of atrial fibrillation. Can J Cardiol. 2020;36(12):1847-1948. PubMed
38.Abraham NS, Barkun AN, Sauer BG, et al. American College of Gastroenterology-Canadian Association of Gastroenterology Clinical Practice Guideline: management of anticoagulants and antiplatelets during acute gastrointestinal bleeding and the periendoscopic period. Am J Gastroenterol. 2022;117(4):542-558. PubMed
39.Center for Biologics Evaluation and Research. Summary Basis for Regulatory Action. ANDEXXA (andexanet alfa) IV administration. Company: Astrazeneca. BLA 125586/0. Approval date: 05/03/2018 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2018: https://www.fda.gov/media/113954/download. Accessed 2023 Apr 12.
40.Beriplex® P/N 500 / Beriplex® P/N 1000 (human prothrombin complex): powder and solvent for solution for injection [product monograph]. Ottawa (ON): CSL Behring Canada, Inc; 2019 Oct 23: https://labeling.cslbehring.ca/PM/CA/Beriplex-PN/EN/Beriplex-PN-Product-Monograph.pdf. Accessed 2022 Sep 2.
41.Octaplex® (human prothrombin complex): powder and solvent for solution for injection [product monograph]. Toronto (ON): Octapharma Canada, Inc.; 2017 Nov 3: https://pdf.hres.ca/dpd_pm/00041970.PDF. Accessed 2022 Sep 2.
42.Schulman S, Kearon C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-694. PubMed
43.Piran S, Khatib R, Schulman S, et al. Management of direct factor Xa inhibitor-related major bleeding with prothrombin complex concentrate: a meta-analysis. Blood Adv. 2019;3(2):158-167. PubMed
44.Chaudhary R, Singh A, Chaudhary R, et al. Evaluation of direct oral anticoagulant reversal agents in intracranial hemorrhage: a systematic review and meta-analysis. JAMA Netw Open. 2022;5(11):e2240145. PubMed
45.Idarucizumab (Praxbind®) 2.5 g / 50 mL injection. DTC Update Suppl. 2016;Sept(Suppl 1).
46.Connolly SJ, Milling TJ, Jr., Eikelboom JW, et al. Andexanet alfa for acute major bleeding associated with factor Xa inhibitors. N Engl J Med. 2016;375(12):1131-1141. PubMed
47.Connolly SJ, Crowther M, Eikelboom JW, et al. Full study report of andexanet alfa for bleeding associated with factor Xa inhibitors. N Engl J Med. 2019;380(14):1326-1335. PubMed
48.Demchuk AM, Yue P, Zotova E, et al. Hemostatic efficacy and anti-FXa (factor Xa) reversal with andexanet alfa in intracranial hemorrhage: ANNEXA-4 substudy. Stroke. 2021;52(6):2096-2105. PubMed
49.Clinical Study Report 14-503 (ANNEXA-A). A phase 3 randomized, double-blind, placebo-controlled study in older subjects to assess safety and the reversal of apixaban anticoagulation with intravenously administered andexanet alfa [internal sponsor's report]. San Francisco (CA): Portola Pharmaceuticals, Inc.; 2015.
50.Clinical Study Report 14-504 (ANNEXA-R). A phase 3 randomized, double-blind, placebo-controlled study in older subjects to assess safety and the reversal of rivaroxaban anticoagulation with intravenously administered andexanet alfa [internal sponsor's report]. San Francisco (CA): Portola Pharmaceuticals, Inc.; 2015.
51.Sarode R, Milling TJ, Jr., Refaai MA, et al. Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized, plasma-controlled, phase IIIb study. Circulation. 2013;128(11):1234-1243. PubMed
52.Broderick JP, Adeoye O, Elm J. Evolution of the modified Rankin Scale and its use in future stroke trials. Stroke. 2017;48(7):2007-2012. PubMed
53.Harrison JK, McArthur KS, Quinn TJ. Assessment scales in stroke: clinimetric and clinical considerations. Clin Interv Aging. 2013;8:201-211. PubMed
54.von Kummer R, Broderick JP, Campbell BC, et al. The Heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke. 2015;46(10):2981-2986. PubMed
55.Abdoellakhan RA, Beyer-Westendorf J, Schulman S, Sarode R, Meijer K, Khorsand N. Method agreement analysis and interobserver reliability of the ISTH proposed definitions for effective hemostasis in management of major bleeding. J Thromb Haemost. 2019;17(3):499-506. PubMed
56.Evans SR. Clinical trial structures. J Exp Stroke Transl Med. 2010;3(1):8-18. PubMed
57.Barnett AG, van der Pols JC, Dobson AJ. Regression to the mean: what it is and how to deal with it. Int J Epidemiol. 2005;34(1):215-220. PubMed
58.Center for Drug Evaluation and Research. Guidance for industry: expedited programs for serious conditions – drugs and biologics. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2014: https://www.fda.gov/media/86377/download. Accessed 2023 May 17.
59.Propensity score matching technical report: andexanet alfa in the treatment of patients with a life threatnening or uncontrollable major bleeding event. [internal sponsor's report]. St. Albans (UK): Fiecon; 2020.
60.Andexanet alfa versus standard-of-care in patients with intracerebral hemorrhage due to oral anticoagulants: a propensity-score adjusted historical comparison of patients from ANNEXA4 and RETRACE II. Study Report. [internal sponsor's report]. Fort Mill (SC): Xcenda; 2019.
61.Caliendo M, Kopeinig S. Some practical guidance for the implementation of propensity score matching. J Econ Surv. 2008;22:31-72.
62.Mebazaa A, Parissis J, Porcher R, et al. Short-term survival by treatment among patients hospitalized with acute heart failure: the global ALARM-HF registry using propensity scoring methods. Intensive Care Med. 2011;37(2):290-301. PubMed
63.Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399-424. PubMed
64.Li F, Thomas LE, Li F. Addressing extreme propensity scores via the overlap weights. Am J Epidemiol. 2019;188(1):250-257. PubMed
65.Thomas LE, Li F, Pencina MJ. Overlap weighting: a propensity score method that mimics attributes of a randomized clinical trial. JAMA. 2020;323(23):2417-2418. PubMed
66.Sterne JA, White IR, Carlin JB, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393. PubMed
Appendix 1: Detailed Outcome Data
Table 31: Percent Change From Baseline in Anti-FXa Activity at On-Treatment Nadir by Bleed Type in the ANNEXA-4 Trial (Efficacy Population)
Subgroups | N | Baseline (ng/mL), median (95% CI) | Change from baseline at on-treatment nadir (ng/mL), median (95% CI) | Percent Change from baseline at on-treatment nadir (%), median (95% CI) |
|---|---|---|---|---|
Anti-FXa activity by bleed type | ||||
All apixaban-treated patients | 172 | 146.9 (132.6 to 163.9) | −136.2 (−148.1 to −121.3) | −93.3 (−94.2 to −92.5) |
GI bleed | 29 | 160.7 (147.3 to 254.3) | −148.1 (−183.9 to −127.0) | −91.5 (−93.9 to −87.9) |
ICH | 133 | 134.4 (118.0 to 161.5) | −125.2 (−146.5 to −109.7) | −93.7 (−94.5 to −92.9) |
Other bleed types | 10 | 157.2 (88.2 to 223.1) | −146.8 (−205.7 to −83.0) | −93.0 (−96.4 to −42.3) |
All rivaroxaban-treated patients | 130 | 213.5 (180.8 to 245.3) | −175.3 (−197.6 to −149.9) | −94.1 (−95.1 to −93.0) |
GI bleed | 40 | 245.1 (198.1 to 298.7) | −189.4 (−237.9 to −148.4) | −94.1 (−95.9 to −90.3) |
ICH | 81 | 198.1 (163.4 to 243.3) | −165.7 (−205.0 to −140.9) | −94.7 (−95.5 to −93.3) |
Other bleed types | 9 | 198.3 (107.2 to 389.1) | −176.7 (−269.5 to −72.2) | −89.1 (−94.3 to −79.8) |
CI = confidence interval; FXa = factor Xa; GI = gastrointestinal; ICH = intracranial hemorrhage.
Note this table has not been copy-edited.
Source: ANNEXA-4 Clinical Study Report.19
Table 32: Sensitivity Analyses of Hemostatic Efficacy in ANNEXA-4
Outcomes | Primary analysisa | Sensitivity Analyses | ||
|---|---|---|---|---|
Efficacy population - inclusion of patients rated as non-evaluable for administrative reasonsb | Safety population with baseline anti-FXa levelc | Patients who were otherwise efficacy-evaluable but with baseline anti-FXa level < 75 ng/mL (apixaban and rivaroxaban to treated patients only) | ||
Achievement of hemostatic efficacy at 12 hours from the EOIe | ||||
Patients contributed to the analysis, N | 340 | 347 | 456 | 79 |
Excellent or good, n (%) | 272 (80.0) | 272 (78.4) | 367 (80.5) | 65 (82.3) |
95% CI of proportion (%) | 75.3 to 84.1 | 73.7 to 82.6 | 76.5 to 84.0 | 72.1 to 90.0 |
CI = confidence interval; EOI = end of infusion; FXa = factor Xa.
aThe primary analysis was conducted in the efficacy population, which included all patients in the safety population who received any amount of andexanet, met clinical bleeding criteria, and had an anti-FXa level of ≥ 75 ng/mL for apixaban and rivaroxaban, ≥ 40 ng/mL for edoxaban, and ≥ 0.25 IU/mL for enoxaparin. Patients adjudicated as non-evaluable for administrative reasons were excluded.
bIn this sensitivity analysis, patients adjudicated as non-evaluable for administrative reasons (who were excluded from the primary analysis) were included and imputed as having “poor or none” hemostatic efficacy.
cPatients in the safety population with baseline anti-FXa level were included in this sensitivity analysis.
Note this table has not been copy-edited.
Source: ANNEXA-4 Clinical Study Report.19
Figure 2: Subgroup Analyses of Hemostatic Efficacy at 12 Hours After Andexanet Infusion in the ANNEXA-4 Trial (Efficacy Population)
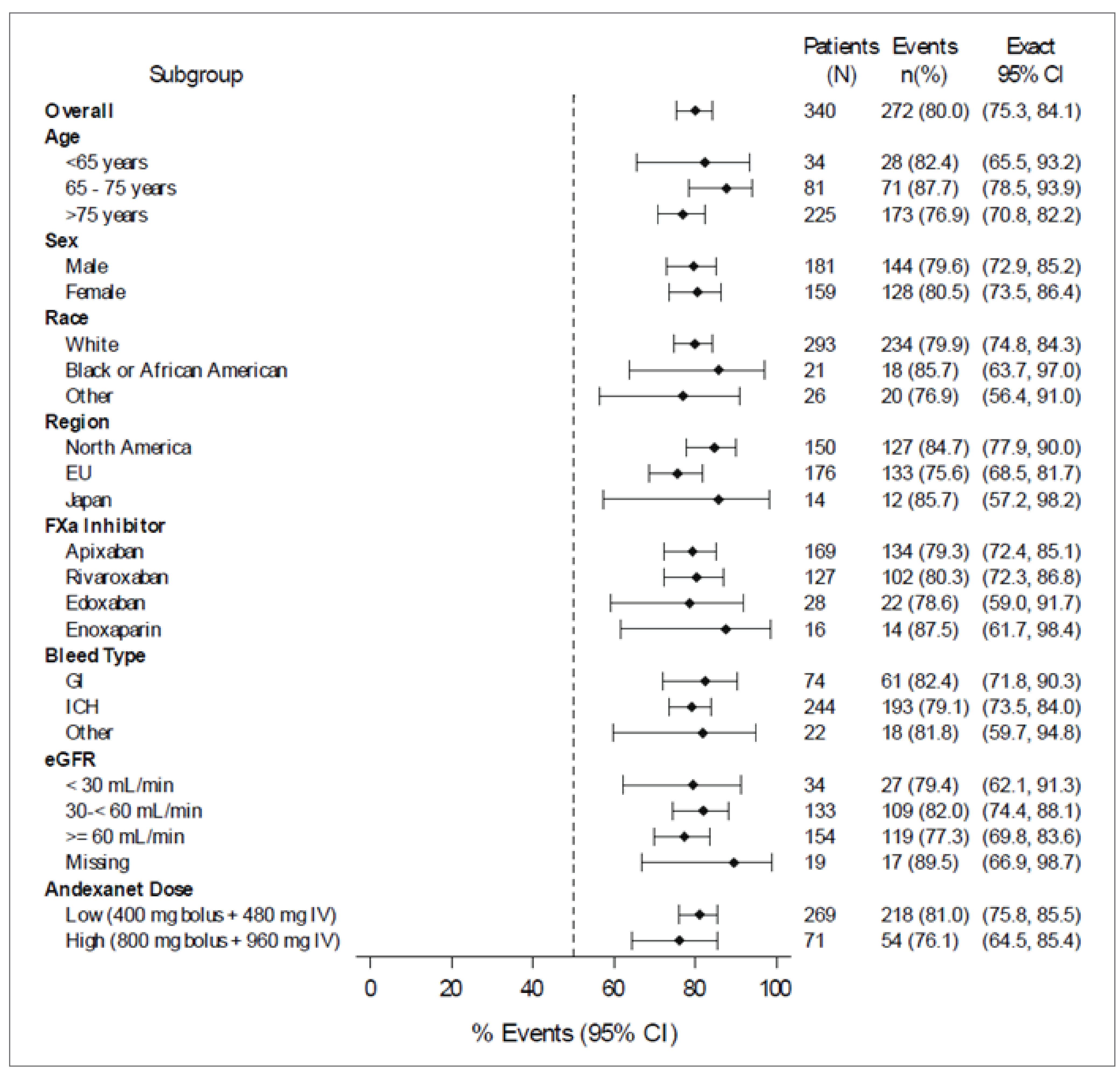
EU = Europe; CI = confidence interval; estimated glomerular filtration rate; GI = gastrointestinal; ICH = intracranial hemorrhage.
Note this figure has not been copy-edited.
Source: ANNEXA-4 Clinical Study Report.19
Table 33: Baseline Patient Characteristics by Bleed Type, Before and After Matching — ANNEXA-4 Trial Versus the ORANGE Study
Characteristic | ICH subgroup | GI bleed subgroup | Other bleeds subgroup | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
AA | PCC | Absolute difference between AA vs. PCC after PSM | AA | PCC | Absolute difference between AA vs. PCC after PSM | AA | PCC | Absolute difference between AA vs. PCC after PSM | ||||
Before PSM | After PSM | Before PSM | After PSM | Before PSM | After PSM | |||||||
N (or ESS) | 209 | 73 | (47) | NA | 82 | 55 | (28) | NA | 31 | 17 | (8) | NA |
Age | 79.67 | 80.34 | 80.55 | −0.87 | 75.62 | 81.71 | 75.51 | 0.11 | 70.29 | 81.76 | 73.06 | −2.77 |
Medical history (%) | ||||||||||||
Stroke | 21.05 | 4.11 | 34.45 | −13.40 | 17.07 | 5.45 | 9.76 | 7.31 | 9.68 | 17.65 | 3.23 | 6.45 |
CAD | 11.48 | 21.92 | 7.66 | 3.83 | 18.29 | 27.27 | 15.85 | 2.44 | 9.68 | 11.76 | 6.45 | 3.23 |
TIA | 7.66 | 23.29 | 4.31 | 3.35 | 6.10 | 25.45 | 3.66 | 2.44 | 9.68 | 23.53 | 6.45 | 3.23 |
AF | 89.00 | 82.19 | 89.00 | 0.00 | 75.61 | 74.55 | 67.07 | 8.54 | 70.97 | 70.59 | 93.55 | −22.58 |
Hypertension | 80.86 | 56.16 | 46.89 | −33.97 | 76.83 | 61.82 | 89.02 | −12.20 | 64.52 | 35.29 | 38.71 | 25.81 |
Diabetes | 32.54 | 21.92 | 46.89 | −14.35 | 31.71 | 23.64 | 21.95 | 9.76 | 12.90 | 17.65 | 6.45 | 6.45 |
RD | 19.62 | 8.22 | 3.35 | 16.27 | 32.93 | 23.64 | 32.93 | 0.00 | 22.58 | 17.65 | 12.90 | 9.68 |
Cancer | 25.84 | 10.96 | 14.35 | 11.49 | 25.61 | 25.45 | 14.63 | 10.98 | 35.48 | 11.76 | 51.61 | −16.13 |
AA = andexanet alfa; AF = atrial fibrillation; CAD = coronary artery disease; ESS = effective sample size; GI = gastrointestinal; ICH = intracranial hemorrhage; NA = not available; PCC = prothrombin complex concentrate; PSM = propensity score matching; RD = renal dysfunction; TIA = transient ischemic attack; vs. = versus.
Note this table has not been copy-edited.
Source: ANNEXA-4 trial vs. ORANGE study technical report.59
Table 34: Sensitivity Analyses for In-Hospital Mortality, Hematoma Expansion ≥ 35%, and Posttreatment mRS — ANNEXA-4 Trial Versus the RETRACE-II Study
Subgroups | In-hospital mortality HR (95% CI) | Hematoma expansion ≥ 35% RR (95% CI) | Posttreatment mRS RR (95% CI) |
|---|---|---|---|
Primary analysis | 0.49 (0.24 to 1.04) | 0.40 (0.201; 0.777) | 0.91 (0.73 to 1.14) |
Sensitivity analyses | |||
Full PS model | 0.62 (0.32 to 1.19) | 0.32 (0.16 to 0.63) | 0.86 (0.65 to 1.14) |
Baseline NIHSS available | 0.60 (0.25 to 1.44) | 0.50 (0.22 to 1.12) | 0.80 (0.57 to 1.11) |
All follow-up measurements available | NA | 0.38 (0.20 to 0.73) | NA |
Time between initial and follow-up imaging considered | NA | 0.40 (0.20 to 0.78) | NA |
Treatment with PCC | 0.85 (0.40 to 1.83) | 0.44 (0.22 to 0.88) | NA |
Baseline anti-FXa level available | 0.88 (0.36 to 2.16) | 0.40 (0.19 to 0.82) | NA |
Use last available mRS at discharge | NA | NA | 0.91 (0.73 to 1.14) |
CI = confidence interval; FXa = factor Xa; HR = hazard ratio; mRS = modified Rankin Scale; NA = not available; NIHSS = National Institutes of Health Stroke Scale; PCC = prothrombin complex concentrate; PS = propensity score; RR = relative risk.
Note this table has not been copy-edited.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CI
confidence interval
DOAC
direct oral anticoagulant
FXa
factor Xa
GI
gastrointestinal
ICER
incremental cost-effectiveness ratio
ICH
intracranial hemorrhage
ITC
indirect treatment comparison
mRS
modified Rankin Scale
PMPRB
Patented Medicine Prices Review Board
PCC
prothrombin complex concentrate
QALY
quality-adjusted life-year
RR
relative risk
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Andexanet alfa (Ondexxya), 200 mg powder for solution for IV infusion |
Submitted price | Andexanet alfa, 200 mg solution: $4,590.00 per 20 mL vial |
Indication | For adults treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding |
Health Canada approval status | NOC/c |
Health Canada review pathway | Standard review |
NOC/c date | June 18, 2023 |
Reimbursement request | As per indication |
Sponsor | AstraZeneca Canada Inc. |
Submission history | Previously reviewed: No |
FXa = factor Xa; NOC/c = Notice of Compliance with Conditions.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision tree plus a Markov model |
Target population | Adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding |
Treatment | Andexanet alfa (Ondexxya) |
Comparators | PCC, including human prothrombin complexes Beriplex and Octaplex |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (22 years) |
Key data source |
|
Submitted results | ICER = $43,891 per QALY gained (incremental costs of $43,634 with 0.994 additional QALYs) |
Key limitations |
|
CADTH reanalysis results |
|
CBS = Canadian Blood Services; CI = confidence interval; FXa = factor Xa; ICER = incremental cost-effectiveness ratio; ICH = intracranial hemorrhage; ITC = indirect treatment comparison; LY = life-year; mRS = modified Rankin Scale; PCC = prothrombin complex concentrate; PMPRB = Patented Medicine Prices Review Board; QALY = quality-adjusted life-year.
Conclusions
The CADTH Clinical Review of the 3 weighted comparative analyses (ANNEXA-4 trial versus the ORANGE study; ANNEXA-4 trial versus the Hartford Health care study; and the ANNEXA-4 trial versus the RETRACE-II study) found several limitations that prevented definitive conclusions regarding the comparative efficacy of andexanet alfa and prothrombin complex concentrate (PCC). CADTH’s appraisal of the indirect treatment comparisons (ITCs) found evidence of heterogeneity with the inclusion and exclusion criteria between studies (e.g., definition of major bleeding, recent history of blood product, intracranial hemorrhage [ICH] severity, recent history of thromboembolism, expected survival). Additional residual confounding due to inadequate adjustment for prognostic factors or treatment effect modifiers was also listed as a major limitation. As such, the clinical effectiveness of andexanet alfa compared with PCC is uncertain, both in the short-term (30 days) and long-term.
CADTH identified limitations in the sponsor’s economic analysis: overestimation of long-term survival for ICH patients prescribed andexanet alfa, inappropriate utilities reported for ICH patients who used andexanet alfa, underestimated relative risk (RR) of 30-day mortality, and lack of publicly available sources for the unit cost of PCC in Canada. To derive the CADTH base case, the following changes were made: applying equal modified Rankin Scale (mRS) distributions for both the andexanet alfa and PCC treatment groups and changing ICH long-term utilities for andexanet alfa to align with the PCC value (0.62). In the CADTH’s base case, a price reduction of at least 27% would be required to make andexanet alfa an optimal treatment option at a s (WTP) threshold of $50,000 per quality-adjusted life-year (QALY) gained. A scenario analysis conducted by CADTH demonstrated that the estimated incremental cost-effectiveness ratio (ICER) is highly sensitive to changes in the RR of 30-day mortality. Feedback obtained by CADTH from the clinical experts highlights that the 30-day mortality RR is likely higher (i.e., the difference between treatments is smaller) than what is reported in the sponsor submission. The true value of the ICER may be higher than the CADTH base case; as such, a further price reduction may therefore be warranted.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received input from 2 patient groups, the Canadian Venous Thromboembolism Research Network (CanVECTOR) and the HeartLife Foundation. The CanVECTOR input was collected through interviews (n = 33) with patients and caregivers in 7 countries with lived experience with venous thromboembolism (VTE). Of these 33 interviews, 8 were completed with patients in Canada. The HeartLife Foundation noted that the use of FXa inhibitor can increase the risk of bleeding and patients with heart failure may require invasive surgeries, which put them at risk of surgical bleeds. The group expressed a need for a treatment that can rapidly and effectively reverse the anticoagulant effect of FXa inhibitor to prevent further bleeding and ensure the best possible outcome in patients who require urgent surgery or are experiencing life-threatening bleeds. According to the CanVECTOR input, participants all had VTE and varied treatment experience; this included experience with warfarin, direct oral anticoagulants (DOACs), and low-molecular-weight heparin. Participants had been on treatment anywhere from 1 to 6 months to long-term (more than 3 years). A diverse group of participants was selected that included a mix of ages, education, and racial and gender identities. Several treatment options are available for VTE, and personal factors affect a patient’s treatment preferences. Generally, participants described the burden of treatment with warfarin and low-molecular-weight heparin to be higher than DOACs. Some patients started on warfarin or low-molecular-weight heparin and later switched to a DOAC. While treatment with DOACs was preferred by patients, a lack of reversal drugs available for DOACs was named as a concern and that the absence of reversal drugs could prevent patients from undergoing a surgery in the case of an emergency. No participants within the patient group had experience with andexanet alfa.
The clinician group input was obtained from 5 clinician groups: Thrombosis Canada (represented by 2 clinicians), members of the thrombosis and Anticoagulation Team at Dalhousie University (represented by 3 clinicians), faculty members at McMaster University in hematology and/or thromboembolism (represented by 4 clinicians), Canadian Stroke Consortium (represented by 5 clinicians), and a journal club comprising local emergency department physicians in the Peel Region (represented by 5 clinicians). The clinician groups note that PCCs have no effect on eliminating the active inhibitory action of oral factor Xa (FXa) inhibitors and while they are currently the treatment of choice, their use is considered off-label. One clinician group highlighted that there would be a clear division between the patients who would receive PCC versus andexanet alfa. The group noted that PCCs would likely be used for average cases requiring DOAC reversal and andexanet alfa would be used only in select patients (life-threatening bleeding that does not respond to supportive management, critical site bleeding, a need for emergent surgery). The clinicians noted that as most centres do not have FXa inhibitor drug assays available, treatment is considered based on the timing of the last dose or other factors, including examination findings, patient liver or kidney function, and clinician judgment. The groups supported the use of andexanet alfa by specialists and in the hospital setting. These settings included critical care units, operating rooms, trauma centres, stroke or neurosurgical referral centres, emergency departments.
The drug plan input received by CADTH noted concerns regarding the anticipated budget impact and sustainability. The drug plans requested input on the proportion of major bleeds that would need to be reversed with a reversal drug and the overall market size that was estimated based on the ITC of the ANNEXA-4 trial versus the ORANGE study. Additional concerns were noted on the use of claims data from IQVIA to determine the number of patients on apixaban and rivaroxaban. Lastly, the drug plans highlighted additional concerns with the implementation of andexanet alfa due to the costly unit price in comparison with PCC. The drug plans noted that a prioritization scheme that could be implemented in hospitals would be required.
Several of these concerns were addressed in the sponsor’s analysis and the CADTH reanalysis:
The feedback obtained by CADTH from the clinical experts suggests that the proportion of patients eligible for treatment with a reversal drug is reasonable; no additional findings in the literature have suggested otherwise.
The sponsor noted that an epidemiologically based approach was considered; however, due to the limited data on the prevalence of patients receiving treatment with apixaban and rivaroxaban in Canada, the number of patients using FXa inhibitors in Canada was estimated indirectly using IQVIA claims data.
Economic Review
The current review is for andexanet alfa (Ondexxya) for adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing andexanet alfa compared with PCC for the treatment of adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding.1 The modelled population aligned with the patients from the ANNEXA-4 trial on which the Health Canada indication was based. The reimbursement request is aligned with the Heath Canada–indicated population.2
Andexanet alfa is administered as an IV bolus with a target rate of 30 mg/minute, followed by continuous infusion with a target rate of 4 mg/minute to 8 mg/minute for up to 120 minutes. The recommended dose for andexanet alfa varies between 5 (low dose) to 9 (high dose) 200 mg vials, depending on the rivaroxaban or apixaban dose.3 The low dose of andexanet alfa comprises an initial IV bolus of 400 mg at a rate of 30 mg/minute, followed by a continuous IV infusion of 4 mg/minute for 120 minutes.3 The high dose of andexanet included an initial IV bolus of 800 mg at a rate of 30 mg/minute followed by a continuous IV infusion of 8 mg/minute for 120 minutes.3 To determine the average cost of andexanet alfa in the base case, the sponsor derived the proportion of patients receiving a low or high dose from the ANNEXA-4 pivotal study.2 The submitted price of andexanet alfa is $4,590 per 200 mg vial.1 Based on a mean patient weight of 77.8 kg, in alignment with the ANNEXA-4 trial, the average total treatment cost per patient is $26,787 (weighted cost for low dose = $18,153 and high dose = $8,634).2 Administration costs for andexanet alfa were sourced from the Ontario Schedule of Benefits, where andexanet alfa was considered a complex single-drug therapy with prolonged administration.4 Acute care costs were assumed to be equivalent to hospitalization costs associated with bleeding events and were sourced from the Canadian Institute for Health Information Patient Cost Estimator.5 Long-term costs for managing the health of bleed survivors were sourced from Canadian literature that assessed costs associated with each bleed.6-9 The associated cost of administration was $75.
At the time of the analysis, no specific reversal drugs were approved in Canada for the reversal of direct FXa inhibitors in adults with severe or life-threatening bleeding events.1 As such, the comparator used in the analysis was PCC and was used as a proxy for usual care. As human prothrombin complexes Beriplex and Octaplex are the only PCC products approved in Canada, PCC costing was based on the cost of these 2 products.1 The cost of PCC was calculated by weighting the cost of Beriplex and Octaplex by the percentage of patients who received each drug in the ORANGE study.10 As no Canadian list prices are published for PCC, unit costs were sourced from the median of available published list prices for PCC as specified by the Patented Medicine Prices Review Board (PMPRB) for assessing foreign prices of medications.11 The sponsor calculated an average weighted treatment cost of |||||| for PCC by using the percentage of patients who received each drug in the ORANGE study.12 The cost of administration was sourced from the Ontario Schedule of Benefits, where PCC is considered to be an agent with minor toxicity that may require monitoring.4 The associated cost of administration was $54.25 for PCC. Wastage was included in all cost calculations for both andexanet alfa and PCC.
The economic analysis was performed from the perspective of the Canadian publicly funded health care system. Costs and clinical outcomes (life-years and QALYs) were simulated over a model horizon of 22 years and discounted at an annual rate of 1.5%.
Model Structure
The sponsor submitted a combined decision tree and Markov model with a cycle length of 1 month to capture short- and long-term costs and health consequences associated with the use of andexanet alfa or PCC.1 The decision tree represented short-term survival (30 days) and was structured to represent the expected cohort of patients in Canada requiring rapid reversal of anticoagulation due to major bleeding, including: ICH, gastrointestinal (GI) bleeding, and intraspinal, intraocular, pericardial, and retroperitoneal bleeding. These bleeding sites requiring rapid reversal aligned with the inclusion criteria of the ANNEXA-4 study.2 Bleed survivors entered the Markov model in health states corresponding to the site of the bleeding. All survivors remained in their health state or transitioned into the death health state. Rebleeding was not included in the model, and it was assumed that all bleed survivors resumed anticoagulation therapy. A schematic of the sponsor’s model structure is available in Figure 1.
Model Inputs
The modelled population had baseline characteristics that were similar to the population enrolled in the ANNEXA-4 pivotal study.2 Patients had a mean body weight of 77.8 kg, and 53.1% of patients were male. The starting age in the model was 77.70 years, based on the mean age of trial participants.
In the sponsor’s model, as no head-to-head efficacy data were available for andexanet alfa compared with PCC, the comparative effectiveness in the base case was informed by an ITC. The ITC used patient-level data from the single-arm ANNEXA-4 pivotal trial and the ORANGE observational study to compare 30-day mortality rates.10 Functional outcomes were informed by an ITC by Huttner et al. (2022) that compared the distribution of functional outcomes following FXa inhibitor–associated ICH at 30 days or discharge.13 As adults treated with apixaban or rivaroxaban may experience major bleeding in several sites, the starting distribution of major bleed sites in the decision tree was informed by the ORANGE study and the proportions of patients experiencing a major bleed was matched with the ANNEXA-4 study.10 The 30-day mortality rates in patients who received andexanet alfa in the decision tree were derived using the propensity score–matched RR of all-cause 30-day mortality for andexanet alfa versus PCC.10 To estimate long-term mortality for ICH survivors in the Markov model, the sponsor used a study by Huybrechts et al. (2008), which provided long-term mortality estimates for 1,276 stroke survivors, measured with the mRS.14 The mRS distributions were redistributed to exclude death, as it was already captured in the 30-day decision tree. Long-term mortality estimates for severe GI bleed and other major bleeds in the Markov model were sourced from Friberg et al. (2007), which assessed the risk of death in a cohort of 3,824 patients with atrial fibrillation compared with a matched general population.15 The standardized mortality ratio (SMR) reported by the study was recalculated to a monthly SMR to determine the long-term survival of non-ICH patients with an uncontrolled bleeding event.15 Adverse events were not included in the economic analysis due to the low incidence of treatment-emergent adverse events in the ANNEXA-4 trial.
The decision tree component of the model incorporated utilities associated with acute, life-threatening, and uncontrollable bleeding events in the 30-day period following the major bleeding event. ICH utility scores were based on an EQ-5D health questionnaire sourced from the National Institute for Health and Care Excellence (NICE).16 A disutility was applied for non-ICH bleeds and was based on results from the Canadian Community Health Survey.17 Long-term utilities were incorporated into the Markov model component. For ICH survivors, long-term utility values were adjusted by mRS score and were derived from a published decision analytic model defining health state by mRS-defined ICH severity. For GI bleed survivors and pericardial bleed survivors, long-term utility was assumed to be the same as the utility for the general population in Canada. Disutilities for all other bleeds were derived from additional literature.18-20
Summary of Sponsor’s Economic Evaluation Results
The sponsor submitted a probabilistic analysis based on 2,500 model iterations. The deterministic and probabilistic results were similar. The deterministic findings are presented subsequently.
Base-Case Results
In the sponsor-submitted base case, andexanet alfa was associated with incremental costs of $43,634, incremental life-years of 1.249, and incremental QALYs of 0.994 in comparison with PCC, resulting in an ICER of $43,891 per QALY (Table 3). The probability of being cost-effective at a $50,000 per QALY WTP threshold was 76.9%.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|---|---|
PCC (usual care) | 52,054 | Reference | 3.772 | Reference | 2.771 | Reference | Reference |
Andexanet alfa | 95,688 | 43,634 | 5.021 | 1.249 | 3.765 | 0.994 | $43,891 |
ICER = incremental cost-effectiveness ratio; LY = life-year; PCC = prothrombin complex concentrate; QALY = quality-adjusted life-year
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted several sensitivity analyses involving short- and long-term utilities, 30-day mortality, and long-term care costs. When a value of 0.32 was used for long-term utility estimates for ICH bleeds, the resulting ICER was $57,723 per QALY gained.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Long-term survival for ICH survivors using andexanet alfa is overestimated: In its economic analysis, the sponsor used the results from the ANNEXA-4 trial versus the RETRACE-II study to inform the distribution of mRS scores in the ICH survivor clinical population. In this ITC, the 1-month baseline mRS scores for andexanet alfa and PCC were derived through propensity-score adjustment and resulted in differing mRS scores, with a higher proportion of the patients prescribed andexanet alfa remaining in the less severe mRS categories than patients prescribed PCC. Feedback obtained from the clinical experts consulted by CADTH highlighted that they did not expect a difference in survival or mRS distribution for patients prescribed andexanet alfa in comparison with PCC. The CADTH Clinical Review notes that the mean difference for mRS at discharge from the ANNEXA-4 trial versus the RETRACE-II study was not statistically significant (P value = 0.261 for unadjusted analysis and 0.110 for inverse probability of treatment weighting adjusted analysis), and that there is insufficient evidence to justify different mRS distributions between the 2 treatment groups. Additionally, CADTH’s clinical appraisal suggests a risk of bias due to unmeasured confounding, as demographic data such as age, sex, and weight were not included in the adjustment model.
Within the economic analysis, the sponsor also used differing utility values for ICH survivor health states between the andexanet alfa and PCC treatment groups, driven by the mRS distributions. As noted by the clinical experts and highlighted in the CADTH Clinical Review appraisal of the ANNEXA-4 trial versus the RETRACE-II study ITC, there is insufficient evidence to suggest mRS utilities will differ between treatments.
As part of the base case, in consultation with clinical experts, CADTH set mRS distributions as equal between andexanet alfa and PCC to inform ICH survival and long-term utilities.
Comparative clinical effectiveness of andexanet alfa is uncertain: In the absence of direct comparative evidence, the sponsor submitted an ITC using patient-level data from the single-arm ANNEXA-4 pivotal trial and the prospective ORANGE observational study to compare 30-day mortality rates. Based on this indirect evidence, the sponsor assumed a 30-day mortality RR of 0.43 (95% confidence interval [CI], 0.29 to 0.63) for andexanet alfa compared with PCC. To derive the RR, patients from the ORANGE study were matched based on baseline characteristics including age, bleed site, and medical history. Additional characteristics including sex, weight, and creatinine clearance were excluded from the adjustment, as the authors considered the characteristics to have no significant effect on 30-day mortality. However, the clinical experts consulted by CADTH highlighted that these characteristics are influential factors and were relevant in the other studies. The lack of adjustment for these treatment effect modifiers may result in confounding of the study results and may have led to an overestimation of comparative effectiveness, resulting in a bias that favours andexanet alfa.
The CADTH Clinical Review appraisal of the sponsor-submitted ITC notes that several limitations preclude definitive conclusions regarding the comparative efficacy of andexanet alfa and PCC. The Clinical Review highlighted a risk of selection bias for the studies that were included in the analysis, given the absence of a systematic literature review. Additionally, heterogeneity was found within the study population, with patients in the ANNEXA-4 trial generally presenting as healthier than those in the ORANGE study. In the pharmacoeconomic model, the RR for 30-day mortality was an important parameter in determining the cost-effectiveness of andexanet alfa. The estimate of the RR for 30-day mortality is highly uncertain.
CADTH could not address the potential bias in 30-day mortality in the reanalysis, as no other appropriate estimates were available. CADTH conducted a scenario analysis to explore the impact that this uncertainty has on cost-effectiveness. In consultation with the clinical experts, CADTH used the upper bound of the 95% CI (0.63) around the RR for 30-day mortality from the ANNEXA-4 trial versus the ORANGE study ITC.
Comparator pricing based on publicly available prices: The sponsor’s analysis estimated the cost of PCC using published list prices for Beriplex and Octaplex in the PMPRB basket of 11 comparator countries. Unit prices for Beriplex and Octaplex were available in only 2 and 3 of the 11 countries, respectively. Therefore, the price of PCC (Beriplex and Octaplex) does not reflect any confidential pricing that may have been negotiated by Canadian Blood Services (CBS). As such, the estimated drug acquisition costs for PCC are uncertain.
Due to confidentiality surrounding the negotiated price of PCC in Canada, CADTH was unable to address this limitation. To explore the potential impact of this uncertainty on the ICER, CADTH conducted a scenario analysis in which the drug price for PCC was reduced by an arbitrary 10%.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 5).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Resource usage for acute management was assumed to be the same between andexanet alfa and PCC. | Appropriate. According to the clinical experts consulted by CADTH, it is reasonable to expect the same resource usage between andexanet alfa and PCC. |
Only patients who received PCC in the ORANGE trial were included in the analysis. The patients were used as a proxy for severe or life-threatening bleeding. | Appropriate, according to the clinical experts consulted by CADTH. |
PCC = prothrombin complex concentrate.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH corrected the sponsor’s model by updating the acute care hospitalization costs for the reported bleed sites using the Canadian Institute for Health Information Patient Cost Estimator.5 CADTH used the same Case Mix Group (CMG) codes used in the sponsor submission to determine the acute care costs, including CMG 025 for ICH bleeds, CMG 254 for GI bleeds, and CMG 782 for all other bleeds. The difference in cost is highlighted in Table 6. Additionally, CADTH corrected the unit cost for apixaban to that reported in the Ontario Drug Benefit Formulary.21
The CADTH base case was derived by making changes in the model parameter values and assumptions, in consultation with the clinical experts. These changes include applying equal mRS distributions for both the andexanet alfa and PCC treatment groups and changing the ICH long-term utilities for andexanet alfa to be equal to the PCC value (0.62). Table 6 details the changes made to derive the CADTH reanalysis; the summary results of that reanalysis are presented in Table 7. The CADTH base-case results were broadly similar to the sponsor’s submitted base case. Treatment with andexanet alfa was more costly than PCC (incremental cost = $36,604) while improving overall survival (incremental life-year = 0.854) and quality-adjusted survival (incremental QALY = 0.592). The probability of being cost-effective at a $50,000 per QALY WTP threshold was 14.4%.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Acute care hospitalization costs by bleed site |
|
|
2. Apixaban cost | Unit cost: $1.2252 | Unit cost: $0.4084 |
Changes to derive the CADTH base case | ||
1. Equal mRS distributions for andexanet alfa and PCC | The sponsor assumed different mRS distributions between andexanet alfa and PCC, resulting in lower mRS states for patients using andexanet alfa. Distribution of mRS scores for PCC:
Distribution of mRS scores for andexanet alfa:
| Equal distribution to align with PCC. Distribution of mRS scores for PCC and andexanet alfa:
|
2. Equal ICH long-term utilities for andexanet alfa and PCC | Sponsor assumed different mRS distributions between andexanet alfa and PCC would result in varying long-term utilities for the ICH survivor andexanet alfa health state.
|
|
CADTH base case | — | Reanalysis 1 + 2 |
GI = gastrointestinal; ICH = intracranial hemorrhage; mRS = modified Rankin Scale; PCC = prothrombin complex concentrate.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total LYs | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|---|
Sponsor’s base case | PCC | 52,054 | 3.772 | 2.771 | Reference |
Andexanet alfa | 95,688 | 5.021 | 3.765 | 43,891 | |
Sponsor’s corrected base case | PCC | 49,060 | 3.772 | 2.771 | Reference |
Andexanet alfa | 92,009 | 5.021 | 3.765 | 43,202 | |
CADTH base case (reanalysis 1 + 2) | PCC | 48,996 | 3.762 | 2.763 | Reference |
Andexanet alfa | 85,600 | 4.616 | 3.355 | 61,865 |
ICER = incremental cost-effectiveness ratio; LY = life-year; mRS = modified Rankin Score; PCC = prothrombin complex concentrate; QALY = quality-adjusted life-year.
Note: Reanalysis 1 and 2 could not be completed as stepped analyses due to model settings. Altering a single setting in the model allowed for the mRS distributions and mRS utilities for andexanet alfa to be equal to PCC.
Scenario Analysis Results
CADTH undertook a price reduction analysis based on the sponsor’s base case and the CADTH reanalysis (Table 9). The results show that a price reduction of 27% is required for andexanet alfa to be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for andexanet alfa vs. PCC ($/QALY gained) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 43,891 | 62,027 |
10% | 41,127 | 57,472 |
20% | 38,356 | 52,939 |
27% | 35,586 | 49,785 |
30% | 32,815 | 48,406 |
ICER = incremental cost-effectiveness ratio; PCC = prothrombin complex concentrate; QALY = quality-adjusted life-year.
CADTH conducted a scenario analysis to explore the impact of changing the 30-day mortality RR for andexanet alfa. In this analysis, the mean estimate of 30-day survival was set to the upper bound of the 95% CI around the 0.63 RR reported in the ITC for the ANNEXA-4 trial versus the ORANGE study. In this scenario, the ICER increased to $85,235 per QALY gained (incremental costs = $32,687; incremental QALYs = 0.384) (results in Table 12). In the sponsor’s base case, the QALYs generated in the decision tree were 0.035 for andexanet alfa and 0.028 for PCC (incremental QALYs = 0.007). In the CADTH scenario analysis, the QALYs generated in the decision tree were 0.033 for andexanet alfa and 0.028 for PCC (incremental QALYs = 0.004).
Issues for Consideration
Andexanet alfa may be used outside of its indication: The feedback obtained from the clinical experts consulted by CADTH suggests that andexanet alfa may be used outside of its indication in clinical practice. The clinical experts explained that while the indication is limited to use on major bleeds due to the FXa inhibitors apixaban and rivaroxaban, major bleeds often occur in emergent care and patients may be prescribed andexanet alfa outside of a need for DOAC-related bleed reversals. This may lead to an increase in the incremental budgetary impact, as it was not accounted for in the budget impact analysis (BIA).
Division in treatment population for andexanet alfa in comparison with PCC: The feedback obtained from the clinical experts consulted by CADTH suggests that in clinical practice, andexanet alfa is expected to be prescribed for more emergent and severe cases, and PCC will continue to be used for other major bleeds. In the sponsor’s submission, it was assumed PCC and andexanet alfa could be used interchangeably. However, additional clinical input also highlighted that there would be a clear division between the patients, with PCC prescribed for average DOAC reversals and andexanet alfa prescribed for more severe cases. As the division between these patient groups was not reported in the trial, the incremental budgetary impact may be uncertain.
Overall Conclusions
The CADTH Clinical Review of the 3 weighted comparative analyses (ANNEXA-4 trial versus the ORANGE study, ANNEXA-4 versus the Hartford Health care study, and ANNEXA-4 versus the RETRACE-II study) found several limitations that prevented definitive conclusions regarding the comparative efficacy of andexanet alfa and PCC. CADTH’s appraisal of the ITCs found evidence of heterogeneity with the inclusion and exclusion criteria between studies (e.g., definition of major bleeding, recent history of blood product, ICH severity, recent history of thromboembolism, expected survival). Additional residual confounding due to inadequate adjustment for prognostic factors or treatment effect modifiers was also listed as a major limitation. As such, the clinical effectiveness of andexanet alfa compared with PCC is uncertain, both in the short-term (30 days) and long-term.
CADTH identified limitations in the sponsor’s economic analysis: overestimation of long-term survival for ICH patients prescribed andexanet alfa, inappropriate utilities reported for the ICH patients who used andexanet alfa, underestimated RR for 30-day mortality, and lack of publicly available sources for the unit cost of PCC in Canada. To derive the CADTH base case, the following changes were made: applying equal mRS distributions to both the andexanet alfa and PCC treatment groups and changing the ICH long-term utilities for andexanet alfa to align with the PCC value (0.62). In CADTH’s base case, a price reduction of at least 27% would be required to make andexanet alfa an optimal treatment option at a WTP threshold of $50,000 per QALY gained. A scenario analysis conducted by CADTH demonstrated that the estimated ICER is highly sensitive to changes in the RR for 30-day mortality. The feedback obtained by CADTH from the clinical experts highlights that the 30-day mortality RR is likely higher (i.e., the difference between treatments is smaller) than what is reported in the sponsor submission. The true value of the ICER may be higher than the CADTH base case; as such, a further price reduction may therefore be warranted.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ondexxya (andexanet alfa) 200 mg powder for solution for intravenous infusion. Mississauga (ON): AstraZeneca Canada, Inc.; 2023 Mar 2.
2.Clinical Study Report 14-505 (ANNEXA-4). Prospective, open-label study of andexanet alfa in patients receiving a factor Xa inhibitor who have acute major bleeding (ANNEXA-4) [internal sponsor's report]. San Francisco (CA): Portola Pharmaceuticals, Inc.; 2020.
3.PrOndexxya® (andexanet alfa): 200 mg powder for solution for intravenous infusion [product monograph]. Mississauaga (ON): AstraZeneca Canada, Inc; 2023 Jun 16.
4.Ontario schedule of benefits: physician services under the health insurance act (October 5, 2022 (effective December 1, 2022)). Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master_20221201.pdf. Accessed 2023 Mar 1.
5.Patient Cost Estimator. 2023; https://www.cihi.ca/en/patient-cost-estimator). Accessed 2023 Mar 1.
6.Mittmann N, Seung SJ, Hill MD, et al. Impact of disability status on ischemic stroke costs in Canada in the first year. Can J Neurol Sci. 2012;39(6):793-800. PubMed
7.Chan BC-F, Cadarette SM, Wodchis WP, Krahn MD, Mittmann N. The lifetime cost of spinal cord injury in Ontario, Canada: a population-based study from the perspective of the public health care payer. J Spinal Cord Med. 2019;42(2):184-193. PubMed
8.Persson J, Aronsson M, Holmegaard L, et al. Long-term QALY-weights among spouses of dependent and independent midlife stroke survivors. Qual Life Res. 2017;26:3059-3068. PubMed
9.Hogan M-E, Taddio A, Katz J, Shah V, Krahn M. Incremental health care costs for chronic pain in Ontario, Canada: a population-based matched cohort study of adolescents and adults using administrative data. Pain. 2016;157(8):1626-1633. PubMed
10.Cohen AT, Lewis M, Connor A, et al. Thirty‐day mortality with andexanet alfa compared with prothrombin complex concentrate therapy for life‐threatening direct oral anticoagulant‐related bleeding. J Am Coll Emerg Physicians Open. 2022;3(2):e12655. PubMed
11.Potential sources for foreign prices: PMPRB11. Ottawa (ON): Government of Canada; 2023: https://www.canada.ca/en/patented-medicine-prices-review/services/are-you-patentee/potential-sources-foreign-prices.html. Accessed 2023 Mar 1.
12.Green L, Tan J, Morris JK, et al. A three-year prospective study of the presentation and clinical outcomes of major bleeding episodes associated with oral anticoagulant use in the UK (ORANGE study). Haematologica. 2018;103(4):738. PubMed
13.Huttner HB, Gerner ST, Kuramatsu JB, et al. Hematoma expansion and clinical outcomes in patients with factor-Xa inhibitor–related atraumatic intracerebral hemorrhage treated within the ANNEXA-4 trial versus real-world usual care. Stroke. 2022;53(2):532-543. PubMed
14.Huybrechts KF, Caro JJ, Xenakis JJ, Vemmos KN. The prognostic value of the modified Rankin Scale score for long-term survival after first-ever stroke. Cerebrovasc Dis. 2008;26(4):381-387. PubMed
15.Friberg L, Hammar N, Pettersson H, Rosenqvist M. Increased mortality in paroxysmal atrial fibrillation: report from the Stockholm Cohort-Study of Atrial Fibrillation (SCAF). Eur Heart J. 2007;28(19):2346-2353. PubMed
16.Apixaban for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism. NICE technology appraisal guidance (TA341). London (UK): National Institute for Health and Care Excellence; 2023: https://www.nice.org.uk/guidance/ta341. Accessed 2023 Mar 1.
17.Guertin JR, Feeny D, Tarride J-E. Age-and sex-specific Canadian utility norms, based on the 2013–2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
18.Wittenborn JS, Clemons T, Regillo C, Rayess N, Kruger DL, Rein D. Economic evaluation of a home-based age-related macular degeneration monitoring system. JAMA Ophthalmol. 2017;135(5):452-459. PubMed
19.Matza LS, Chung K, Van Brunt K, et al. Health state utilities for skeletal-related events secondary to bone metastases. Eur J Health Econ. 2014;15:7-18. PubMed
20.Hogan M-E, Taddio A, Katz J, Shah V, Krahn M. Health utilities in people with chronic pain using a population-level survey and linked health care administrative data. Pain. 2017;158(3):408-416. PubMed
21.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Aug 1.
22.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ondexxya (andexanet alfa) 200 mg powder for solution for intravenous infusion. Mississauga (ON): AstraZeneca Canada, Inc.; 2023 Mar 2.
23.PharmaStat. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2023 Aug 1.
24.Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. PubMed
25.Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891. PubMed
26.Little DH, Sutradhar R, Cerasuolo JO, et al. Rates of rebleeding, thrombosis and mortality associated with resumption of anticoagulant therapy after anticoagulant-related bleeding. CMAJ. 2021;193(9):E304-E309. PubMed
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from the clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Adults Treated With FXa Inhibitors Resulting in Life-Threatening or Uncontrolled Bleeding
Treatment | Strength or concentration | Form | Price ($) | Recommended dose | Treatment cost ($) | Annual cost |
|---|---|---|---|---|---|---|
Andexanet alfa (Ondexxya) | 200 mg | Powder for IV infusion 20 mL vial | 4,590.0000a | Low dose: initial bolus of 400 mg then a follow-up IV infusion of 480 mg High dose: initial bolus of 800 mg then a follow-up IV infusion of 960 mg | Low dose: 22,950 High dose: 41,310 | 26,787b |
Prothrombin complex concentrates | ||||||
Human prothrombin complex (Beriplex) | 500 IU 1,000 IU | Powder for IV infusion 20 mL vial 40 mL vial | ||||||||||||||||| | 1,945 IUd | ||||| | ||||| |
Human prothrombin complex (Octaplex) | 500 IU 1,000 IU | Powder for IV infusion 20 mL vial 40 mL vial | ||||||||||||||||| | 1.750 IUd | ||||| | |
FXa = factor Xa.
Note: treatment cost assumes one reversal per patient per year.
aSponsor’s submitted price.22
bWeighted average of the low and high dose from the ANNEX trial.
cPrice from sponsor data on file. Cost data not available in formularies.
dDosing based on the ORANGE study using a patient weight of 77.80 kg.10
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
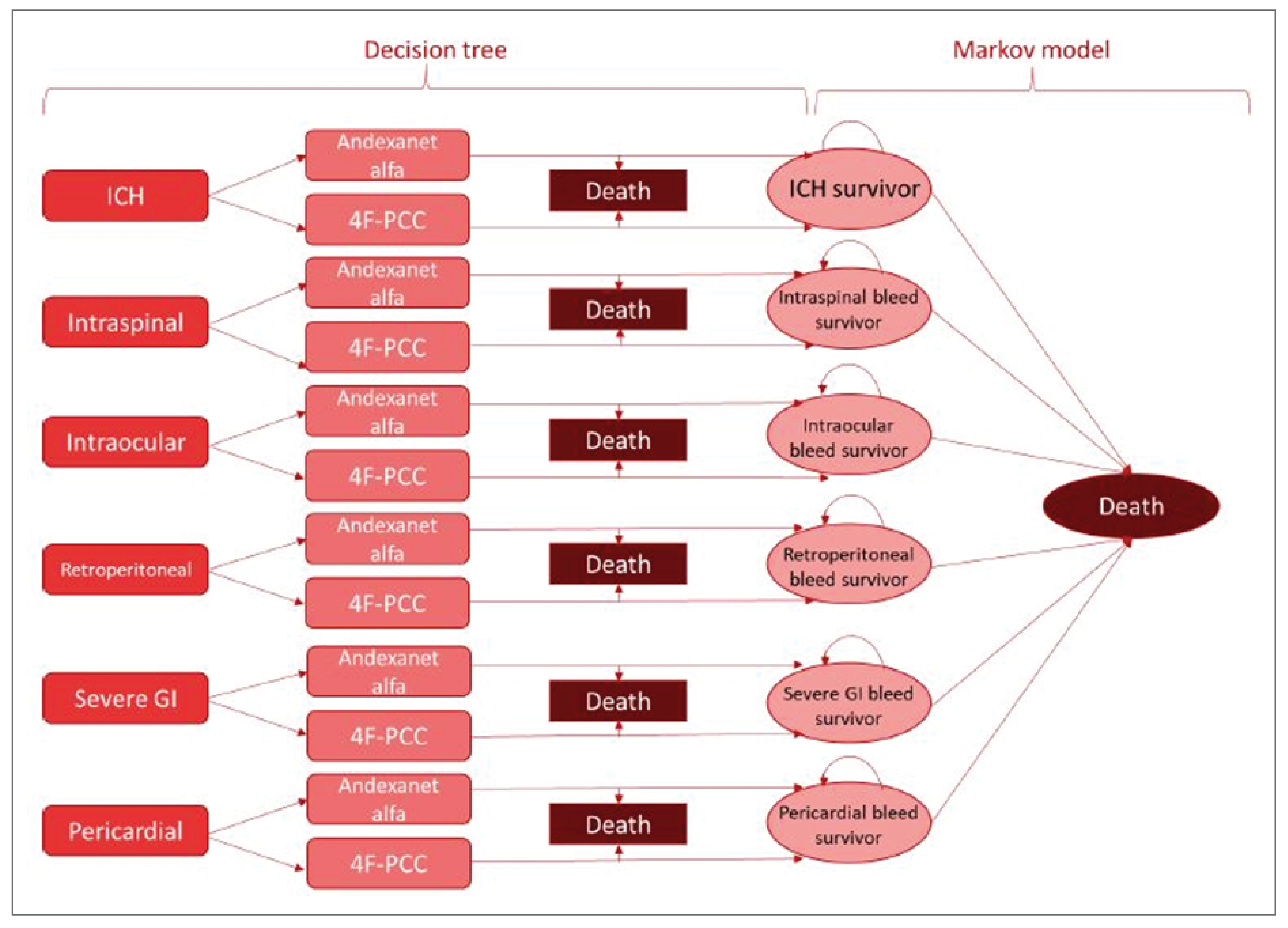
4F-PCC = 4-factor prothrombin complex concentrate; GI = gastrointestinal; ICH = intracranial hemorrhage.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Results of the Sponsor's Base Case
Parameter | Andexanet alfa | PCC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 5.021 | 3.772 | 1.249 |
ICH survivor | 1.623 | 0.794 | 0.829 |
Severe GI bleed survivor | 2.532 | 2.128 | 0.404 |
Pericardial bleed survivor | 0.104 | 0.096 | 0.008 |
Retroperitoneal bleed survivor | 0.104 | 0.096 | 0.008 |
Intraspinal bleed survivor | 0.329 | 0.329 | 0.000 |
Intraocular bleed survivor | 0.329 | 0.329 | 0.000 |
Discounted QALYs | |||
Total | 3.765 | 2.771 | 0.994 |
ICH survivor | 1.137 | 0.474 | 0.662 |
Severe GI bleed survivor | 2.001 | 1.682 | 0.320 |
Pericardial bleed survivor | 0.082 | 0.076 | 0.006 |
Retroperitoneal bleed survivor | 0.080 | 0.074 | 0.006 |
Intraspinal bleed survivor | 0.208 | 0.208 | 0.000 |
Intraocular bleed survivor | 0.257 | 0.257 | 0.000 |
Discounted costs ($) | |||
Total | 95,688 | 52,054 | 43,634 |
By health state | |||
ICH survivor | 52,146 | 23,768 | 28,377 |
Severe GI bleed survivor | 28,470 | 16,288 | 12,182 |
Intraspinal bleed survivor | 8,781 | 7,666 | 1,116 |
Intraocular bleed survivor | 4,099 | 2,983 | 1,116 |
Retroperitoneal bleed survivor | 1,102 | 680 | 422 |
Pericardial bleed survivor | 1,091 | 669 | 421 |
By resource | |||
Treatment cost | 26,862 | 1,498 | 25,364 |
Health state cost | 68,826 | 50,556 | 18,270 |
ICER ($/QALY) | 43,891 | ||
GI = gastrointestinal; ICER = incremental cost-effectiveness ratio; ICH = intracranial hemorrhage; LY = life-year; PCC = prothrombin complex concentrate; QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 11: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Andexanet alfa | PCC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 4.616 | 3.762 | 0.855 |
ICH survivor | 1.231 | 0.796 | 0.435 |
Severe GI bleed survivor | 2.530 | 2.125 | 0.405 |
Retroperitoneal bleed survivor | 0.106 | 0.098 | 0.008 |
Pericardial bleed survivor | 0.100 | 0.093 | 0.007 |
Intraspinal bleed survivor | 0.324 | 0.324 | 0.000 |
Intraocular bleed survivor | 0.325 | 0.325 | 0.000 |
Discounted QALYs | |||
Total | 3.355 | 2.763 | 0.592 |
ICH survivor | 0.736 | 0.476 | 0.260 |
Severe GI bleed survivor | 2.000 | 1.680 | 0.320 |
Retroperitoneal bleed survivor | 0.082 | 0.076 | 0.006 |
Pericardial bleed survivor | 0.079 | 0.073 | 0.006 |
Intraspinal bleed survivor | 0.205 | 0.205 | 0.000 |
Intraocular bleed survivor | 0.254 | 0.254 | 0.000 |
Discounted costs ($) | |||
Total | 85,600 | 48,996 | 36,604 |
By health state | |||
ICH survivor | 44,462 | 22,778 | 21,684 |
Severe GI bleed survivor | 26,783 | 14,836 | 11,947 |
Intraocular bleed survivor | 3,861 | 2,760 | 1,101 |
Intraspinal bleed survivor | 8,444 | 7,395 | 1,050 |
Retroperitoneal bleed survivor | 1,062 | 637 | 425 |
Pericardial bleed survivor | 988 | 590 | 398 |
By resource | |||
Treatment cost | 26,863 | 1,499 | 25,364 |
Health state cost | 58,738 | 47,497 | 11,240 |
ICER ($/QALY) | 61,865 | ||
GI = gastrointestinal; ICER = incremental cost-effectiveness ratio; ICH = intracranial hemorrhage; LY = life-year; PCC = prothrombin complex concentrate; QALY = quality-adjusted life-year.
Scenario Analyses
Table 12: Summary of CADTH Scenario Analysis
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
Sponsor’s corrected base case | |||
PCC | 49,060 | 2.771 | Reference |
Andexanet alfa | 92,009 | 3.765 | 43,202 |
CADTH base case | |||
PCC | 48,996 | 2.763 | Reference |
Andexanet alfa | 85,600 | 3.355 | 61,865 |
CADTH scenario analysis 1: Increasing 30-day mortality relative risk | |||
PCC | 49,060 | 2.771 | Reference |
Andexanet alfa | 81,747 | 3.155 | 85,235 |
CADTH scenario analysis 2: 10% price reduction of PCC | |||
PCC | 48,916 | 2.771 | Reference |
Andexanet alfa | 85,705 | 3.362 | 62,271 |
ICER = incremental cost-effectiveness ratio; PCC = prothrombin complex concentrate; QALY = quality-adjusted life-year.
Appendix 5: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 13: Summary of Key Takeaways
Key Takeaways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor-submitted BIA assessed the budgetary impact resulting from reimbursing andexanet alfa for the treatment of adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding.22 The BIA was conducted from the perspective of CBS over a 3-year horizon (2024 to 2027) with 2023 as the base year using a combination of a claims-based and epidemiological approach. The population size was derived using a claims-based approach by gathering IQVIA PharmaStat claims data for apixaban or rivaroxaban and was further narrowed epidemiologically to those experiencing a major bleed that would be eligible for reversal.23 Key inputs to the BIA are documented in Table 15.
The following key assumptions were made by the sponsor:
Historical claims data for apixaban and rivaroxaban were extracted from the IQVIA PharmaStat database for all CADTH-participating regions, regardless of payer (public versus private). Claims were standardized to 30 days using public and private historical days data for each jurisdiction, as available. Private days data were used as a proxy for the whole jurisdiction when no public days data were available. No claims data were available for Prince Edward Island; as such, Nova Scotia claims data were used as a proxy, adjusted for the population difference between Nova Scotia and Prince Edward Island.
The sponsor assumed 23.6% of all major bleeds are eligible to be treated with a reversal agent.
The sponsor assumed andexanet alfa would capture up to ||| of the market if reimbursed.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3, if appropriate) |
|---|---|
Target population | |
Patients on apixaban or rivaroxaban:
| |||||||||||||||||||| 2.1%24 |
Incidence of major bleeding:
Proportion treated with a reversal agent | 3.6%25 23.6% — |
Number of patients eligible for the drug under review | ||||| |||||| |||||| |
Market uptake (3 years) | |
Uptake (reference scenario):
| 100% / 100% / 100% |
Uptake (new-drug scenario):
| ||| |||| |||||||| |||| |||| ||| |||| |||||||| |||| |||| |
Cost of treatment (per patient) | |
Cost of treatment over course:
| $26,640 |||||| |
PCC = prothrombin complex concentrate.
aSponsor submitted IQVIA PharmaStat.
Summary of the Sponsor’s BIA Results
The sponsor’s base case reported that the reimbursement of andexanet alfa for the treatment of adult patients treated with FXa inhibitors (rivaroxaban or apixaban) when rapid reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding would result in an incremental budget impact of $15,952,349 in year 1, $34,389,366 in year 2, and $56,656,154 in year 3. The total 3-year incremental cost of $106,997,869. Sensitivity analyses were completed to (i) include an alternative proportion of patients eligible for reversal, (ii) adjust for pessimistic (−25%) and optimistic ( + 25%) market shares, and (ii) include an alternative low-dose/high-dose split. These sensitivity analyses impacted the 3-year incremental budget impact, which varied from $80,248,402 to $133,747,337.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Use of a claims-based approach to estimate market size introduces uncertainty with the anticipated budget impact of andexanet alfa: The sponsor estimated market size based on public claims data for patients using apixaban or rivaroxaban. While the sponsor did translate claims into the number of users, the sponsor assumes that all public claims for apixaban and rivaroxaban are at risk for major bleeding. Given the claims database does not specify the indication and the proportion of claims pertaining to use for other indications is unknown, using a claims-based approach to estimate market size introduces significant uncertainty in the estimated market size.
CADTH is unable to address this limitation due to the lack of literature on the pan-Canadian use of apixaban or rivaroxaban.
Proportion of patients treated with a reversal agent is uncertain: The sponsor’s submitted BIA assumed that 100% of patients with an ICH would require a reversal. However, the clinical expert feedback obtained by CADTH suggests that a low (< 7) Glasgow Coma Scale score and a large (> 60 cc) hematoma size are indicative of severe ICH bleeds and would not require reversal, as any means of treatment would be considered futile. Therefore, the proportion of patients with an ICH bleed eligible for reversal is overestimated. Additionally, the Little et al. (2001) study was used to determine the bleed type distribution.26 This study, however, focused on a population-based cohort of adults aged 66 years or older and thus more susceptible to bleeding, and results were based on 4 oral anticoagulants (apixaban, rivaroxaban, dabigatran, and warfarin). Given that apixaban and rivaroxaban have lower GI bleeding rates in comparison with warfarin, the bleed type distribution is uncertain.
To address this limitation, CADTH undertook a scenario analysis to explore the budgetary impact of reducing the proportion of patients treated with a reversal agent. Given that no alternative estimates were available, the CADTH scenario analysis used an arbitrary value of 18.6% (i.e., a 5% reduction in the size of the eligible population).
The price of drugs paid by CBS is uncertain: Due to the confidentiality of list prices for CBS products, both the sponsor’s and CADTH’s analyses are based on an estimation of the cost of PCC using published list prices for Beriplex and Octaplex in PMPRB basket of 11 comparator countries. Unit prices for Beriplex and Octaplex were only available in 2 and 3 of the 11 countries, respectively. In the sponsor’s base case, a median price was used of the published list prices.
To address this limitation, CADTH undertook a scenario analysis by using the lowest and highest list prices available in the PMPRB for Beriplex and Octaplex.
The market uptake of andexanet alfa is uncertain: The sponsor’s submitted BIA indicated that andexanet alfa would result in a market uptake of ||| in year 1, ||| in year 2, and ||| in year 3 based on internal sponsor market shares. However, CADTH obtained clinical expert feedback indicating that the market uptake of ||| in year 3 does not align with clinical expectations and indicated the sponsor likely overestimated andexanet alfa uptake. The clinical experts highlighted that while PCC is not indicated for the rapid reversal of anticoagulation due to life-threatening or uncontrolled bleeding in patients using FXa inhibitors (apixaban and rivaroxaban), clinicians are comfortable using PCC due to the robust published data and experience with the comparator. Additionally, the clinical experts reported uncertainty on the clinical efficacy of andexanet alfa in comparison with PCC and that the overestimation of the market share could be a result of the sponsor’s overestimation of the difference in benefit between PCC and andexanet alfa. CADTH clinical expert feedback deemed the sponsor’s estimate in year 1 and year 2 to be reasonable, but they indicated that the andexanet alfa market share would likely |||||| |||| by year 3.
To address this limitation, CADTH undertook a scenario analysis by revising the market share for andexanet alfa in the new-drug scenario to 25% in year 3.
CADTH Reanalyses of the BIA
Table 15: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH base case | ||
CADTH base case | No changes | |
CADTH did not undertake a base case reanalysis. Instead, CADTH explored the potential impact of several scenario analyses which included:
Using the lowest and highest PCC (Beriplex and Octaplex) list prices from the available PMPRB published prices.
||||||| |||||||| || || ||||||||| |||||||| || || ||||||||| |||||||| |||| || ||||||||| |||||||| || || ||||||||| |||||||| |||| || ||||||||||||||||| |||||||| || || |||||||| |||||||| || || ||||||||| |||||||| |||| ||||||| |||||||| || || ||||||||| |||||||| |||| || |||||||||. Assuming 25% market uptake of andexanet alfa in year 3, due to feedback obtained from clinical experts consulted by CADTH.
Assuming a lower proportion (18.6%) of patients treated with a reversal agent.
Exploring 100% of patients on low-dose andexanet alfa or high-dose andexanet alfa.
27% reduction in the price of andexanet alfa.
The results are presented in Table 18. The reimbursement of andexanet alfa was associated with a 3-year incremental budget impact of $106,997,869 in the base case. A price reduction of 27% reduces the budget impact, for a 3-year incremental budget impact of $76,452,748. In the first scenario analysis, using the lowest available pricing for PCC resulted in an increase of the budget impact, with a 3-year incremental budget impact of $108,452,021. Alternatively, the revised market uptake of andexanet alfa using feedback obtained from clinical experts consulted by CADTH resulted in a decrease, with a 3-year budget impact of $85,751,811. Similarly, reducing the proportion of patients treated with a reversal agent by 5% to a total of 18.6% resulted in a decrease in the 3-year budgetary impact, with a total of $84,366,966. When exploring the impact of the weight of low- or high-dose andexanet alfa, the fifth scenario highlights that 100% of patients on a low dose would result in a reduction in the 3-year budget impact for a total of $91,326,507. Alternatively, in the sixth scenario, altering the proportion of patients on a high dose to 100% results in a marked increase in budgetary impact, with a 3-year total of $169,293,482.
Table 16: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 0 | 914,253 | 1,970,907 | 3,247,051 | 6,132,211 |
New drug | 0 | 16,866,603 | 36,360,273 | 59,903,205 | 113,130,081 | |
Budget impact | 0 | 15,952,349 | 34,389,366 | 56,656,154 | 106,997,869 | |
CADTH scenario analysis 1: lowest list prices of PCC | Reference | 0 | 697,454 | 1,503,539 | 2,477,067 | 4,678,060 |
New drug | 0 | 16,866,603 | 36,360,273 | 59,903,205 | 113,130,081 | |
Budget impact | 0 | 16,169,149 | 34,856,733 | 57,426,138 | 108,452,021 | |
CADTH scenario analysis 2: highest list prices of PCC | Reference | 0 | 1,032,959 | 2,226,807 | 3,668,643 | 6,928,408 |
New drug | 0 | 16,866,603 | 36,360,273 | 59,903,205 | 113,130,081 | |
Budget impact | 0 | 15,891,605 | 34,258,415 | 56,440,415 | 106,201,672 | |
CADTH scenario analysis 3: revised market uptake | Reference | 0 | 914,253 | 1,970,907 | 2,029,407 | 4,914,567 |
New drug | 0 | 16,866,603 | 36,360,273 | 37,439,503 | 90,666,379 | |
Budget impact | 0 | 15,952,349 | 34,389,366 | 35,410,096 | 85,751,811 | |
CADTH scenario analysis 4: lower proportion treated with reversal agent | Reference | 0 | 720,882 | 1,554,044 | 2,560,274 | 4,835,200 |
New drug | 0 | 13,299,182 | 28,669,785 | 47,233,199 | 89,202,166 | |
Budget impact | 0 | 12,578,300 | 27,115,740 | 44,672,926 | 84,366,966 | |
CADTH scenario 5: 100% low-dose andexanet alfa | Reference | 0 | 914,253 | 1,970,907 | 3,247,051 | 6,132,211 |
New drug | 0 | 14,530,154 | 31,323,460 | 51,605,104 | 97,458,719 | |
Budget impact | 0 | 13,615,901 | 29,352,553 | 48,358,054 | 91,326,507 | |
CADTH scenario 6: 100% high-dose andexanet alfa | Reference | 0 | 914,253 | 1,970,907 | 3,247,051 | 6,132,211 |
New drug | 0 | 26,154,277 | 56,382,228 | 92,889,188 | 175,425,693 | |
Budget impact | 0 | 25,240,024 | 54,411,321 | 89,642,137 | 169,293,482 | |
CADTH scenario analysis 7: 27% price reduction for andexanet alfa | Reference | 0 | 914,253 | 1,970,907 | 3,247,051 | 6,132,211 |
New drug | 0 | 12,312,620 | 26,542,999 | 43,729,340 | 82,584,959 | |
Budget impact | 0 | 11,398,367 | 24,572,092 | 40,482,289 | 76,452,748 |
BIA = budget impact analysis; PCC = prothrombin complex concentrate.
Stakeholder Input
Patient Input
VTE-COS Patient Partners (Members of CanVECTOR)
About VTE-COS Patient Partners (Members of CanVECTOR)
The Canadian Venous Thromboembolism Research Network (CanVECTOR) is a team of researchers, patients, healthcare professionals, and students from across Canada who work together on developing research questions to improve the quality of care for all patients affected by Venous Thromboembolism Disease (venous blood clots, such as deep vein thrombosis, DVT and pulmonary embolism, PE). This involves: deciding which areas of patient care require new research (What question should we be asking), designing the way research is done (How can we answer the question), conducting research safely and fairly (Getting the answer), and sharing the results with patients, healthcare professionals, the general public or anyone who would benefit from the answer (Sharing the answer) (from CanVECTOR Patient Partners platform).
The input included here is provided by two patient partners with the CanVECTOR network (Carol West, patient partner platform co-lead; Suzanne Dubois, patient representative on the Scientific Steering Committee) who are KT Ambassadors on an ongoing CIHR-funded research project called VTE-COS. (Establishing an International Core Outcome Set for Clinical Trials of Interventions for Venous Thromboembolism). The purpose of this project is to involve patients, caregivers, researchers, clinicians, and other stakeholders to decide together on the best outcomes for venous thromboembolism (VTE) studies. This includes input from international groups to develop a core outcome set that is applicable worldwide. A related patient-led OSSU-funded project aims to empower patient ambassadors (Carol West and Suzanne Dubois) to advocate for outcomes that are important to patients “Empowering patient ambassadors to champion research outcomes that are a priority for people who have lived experience with venous thromboembolism”.
Information Gathering
One of the steps of the VTE-COS project was to hold interviews with patients or caregivers with VTE lived experience to identify outcomes that are meaningful to them. Thirty-three interviews have been completed with patients in seven countries, including eight from Canada. Participants all had VTE (DVT = 15, PE = 6, both DVT and PE = 12) and varied treatment experience, including warfarin, DOACs, and low molecular weight heparin, for anywhere from 1-6 months to long-term treatment (over 3 years = 16). We aimed to interview a diverse group and there is a mix of ages, education, racial identify and gender identity (results not yet published are available upon request).
Disease Experience
Living with VTE and treatment to reduce the risk of a future blood clot means finding a balance between the risk of another clot and actual or potential side effects. For patients, bleeding is the most concerning potential side effect of treatment. Even if a patient has not experienced serious bleeding, they may live with a fear of bleeding that can impact life choices and daily activities, quality of life, and mental health.
Experiences With Currently Available Treatments
There are several options available for treating VTE and a variety of personal factors that affect a patient’s treatment preferences. Many patients who participated in the VTE-COS study described the burden of treatment with warfarin (the inconvenience of blood monitoring, restrictions on diet or alcohol intake), or with LMWH injections (pain, bruising, discomfort with self-injections). Some patients had started on warfarin or LMWH initially and later switched to a DOAC. There were fewer burdens described with DOACs, but the lack of a reversal agent was mentioned by a few patients. It’s important to consider that some patients with a high risk of another clot will be prescribed blood thinners for the rest of their lives. For a young person with decades of treatment ahead of them this can be daunting.
“So, switching to Rivaroxaban, it really decreased my concerns. Because with INR, as you know, I had to watch for my food. Whenever I travel, I came, I should try to balance against the INR. So, it was really hectic.”
“I would say the priority is the convenience, because it really does affect your life.”
“Like taking Warfarin, the INRs, that was really hard when I had an infant. How do you make that work, right?”
Describing injections:
“At the start, I probably cried every morning taking them. Now that I’m used to taking them, I know where the spots are that don't really hurt putting them in.”
“So, however much I have my misgivings on Warfarin, Warfarin had one benefit. It was reversible. It had all the other things that were not attractive to it, but if you could make some of those things more attractive, or certainly if the new drug that would come on the market to replace or be an alternative to Apixaban, if it had a reversibility aspect to it, I think would be attractive.”
“Because in every other respect at the moment, I’m on a solid state on this drug, other than we may revisit the dose depending on how the next year of nose bleeds happens. But the reversibility aspect, certainly as I get older, and if you get other ailments, or other things, and you worry about doing that emergency ride in an ambulance to the hospital, and the medical professionals can’t do anything surgical to you for at least 24 hours from the time you took that last pill, well, there is consequences to that. And at the moment, I’m relatively healthy. I’m not dwelling on it. But certainly, as I will get older, it will be potentially a thing that will have me re-look at my choice of medication.”
“If an accident happened and the surgery is almost immediate, a reversal agent can help me with it to be going into the emergency surgery safely… Rivaroxaban, as I understand, whilst I can stop for one day, it does not have a reversal agent like warfarin which has vitamin K.”
Improved Outcomes
The results of VTE-COS study will describe all the outcomes of VTE treatments that patients feel are important. Specifically, with respect to bleeding, some patients said they were not concerned about bleeding, but others described fear and changes to their daily lives to avoid the risk of bleeding.
“I’m definitely worried that I’ll have a bleed that can’t be treated, like there will be long-term permanent effects from that, specifically like a brain bleed concerns me a lot.”
“Only that I'm guiding myself not to have wounds, not to cut myself because of that, so that my blood will not gush out like that. I'm guiding myself not to cut any part of my body at all.”
“I was terrified. I did not sleep for that month, I sat up every night, waiting for the bleed…. And I spend every day terrified I’ll bleed again…”
“Yes, I am much more afraid now when I cook, it's all stupid, but to say to me that I should not cut myself…”
“I have a little hemorrhoid, and I suddenly thought to myself, I think this was you know just the very start of anticoagulation. Oh, my goodness, you know, if that hemorrhoid starts bleeding, you know, I'm prone to bleed out, or whatever, you know, obviously I didn't know anything at that point, I just thought that any bleeding might not stop.”
Experience With Drug Under Review
Not applicable.
Companion Diagnostic Test
Not applicable.
Anything Else?
We are not advocating for or against a treatment. Our intent is to communicate about outcomes and concerns described by patients who have lived experience with VTE.
Conflict of Interest Declaration — VTE-COS Patient Partners (members of CanVECTOR)
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Nicole Langlois, Project Manager, VTE-COS; Senior Research Associate, Ottawa Hospital Research Institute; Manager of Clinical Research, CanVECTOR
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
The VTE-COS Research Team was involved in data collection (participant interviews) and analysis of the transcripts from the interviews.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for VTE-COS Patient Partners (Members of CanVECTOR)
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca (to the CanVECTOR network) | — | — | X | — |
HeartLife Foundation
About HeartLife Foundation
An estimated 750,000 people are currently living with heart failure in Canada (Heart & Stroke Foundation, 2022). In their 2022 Report on the health of Canadians, the Heart & Stroke Foundation estimates that 100,000 Canadians are diagnosed with heart failure each year and this number is on the rise. Heart failure costs the Canadian healthcare system more than $2.8 Billion dollars per year – with the majority of those dollars being spent on acute care. Research has shown that effective patient engagement improves clinical outcomes, prevents hospitalizations, increases patient self-efficacy for managing their condition, and overall quality of life. Despite these findings, few organizations currently exist to help heart failure patients self-manage their condition, provide education and support for patients and families, and advocate for access to care and innovative treatments. The HeartLife Foundation was created in response to this need.
The HeartLife Foundation is a patient-driven charity whose mission is to transform the quality of life for people living with heart failure by engaging, educating, and empowering a global community to create lasting solutions and build healthier lives. HeartLife
Foundation is Canada’s first – and only – national patient-led Heart Failure organization. We are a Federal Charity aimed at raising public awareness of Heart Failure, engaging patients, families, and caregivers to provide education and support, facilitate access to the latest research, innovations, and treatments, and advocate better care for all.
Founded in June 2016 by Dr. Jillianne Code, a heart failure survivor and heart transplant recipient, and Mr. Marc Bains, a heart failure survivor and heart transplant recipient, HeartLife aims to drive healthcare innovation and transformation by adding patient voices to the heart failure conversation. In collaboration with Dr. Sean Virani, one of Canada’s leading heart failure specialists and promoter of patient and family centred care, we endeavour to ensure that there is an open dialogue including patients as partners with healthcare providers, government, and industry across Canada. Our members are all patients along the heart failure continuum, their families and caregivers.
Vision: To create a better everyday life for people living with heart failure.
Mission: The HeartLife Foundation is a patient-driven charity whose mission is to transform the quality of life for people living with heart failure by engaging, educating, and empowering a global community to create lasting solutions and build healthier lives.
Website: www.heartlife.ca
Information Gathering
Review of study material and online literature.
Disease Experience
Heart failure is a common and growing cardiovascular condition in Canada that affects 750,000 people and results in 100,000 new diagnoses each year. Heart failure is an epidemic and can be caused by anything that damages the heart. While there is no cure for heart failure, medical therapies and lifestyle changes can help manage the condition. Access to care, medical therapies, and support services vary from region to region. Patients with heart failure experience physical, social, and emotional challenges and require daily monitoring and adherence to control their symptoms. Heart failure is commonly associated with comorbidities, anxiety, depression, cognitive decline, and negative impacts on mental health.
HF is commonly associated with Atrial Fibrillation, LVAD’s and Heart Transplant, all which require invasive surgeries. As more people are surviving heart failure, there is a greater need for advanced therapies, increasing the risk of complications from surgical bleeds.
Lives of patients with HF and their family carers dramatically change upon initial diagnoses. People with heart failure experience a wide range of physical, social and emotional challenges. Individual can be born with the disease, develop it throughout their adult lives, or be diagnosed in their later years. Symptoms of heart failure vary among patients. It is a condition that requires daily monitoring, adherence and vigilance on the part of the patient in order to control the delicate balance of symptoms. These symptoms include shortness of breath, extreme fatigue, low blood pressure, dizziness, edema and bloating. Many patients also have palpitations and arrhythmia resulting in the need for ICD’s or Pacemakers. Heart Failure is commonly associated with a variety of comorbidities, anxiety, depression, a decline in cognitive ability, and can have a negative impact on mental health.
Experiences With Currently Available Treatments
There are currently two drugs approved by the US FDA that can be used to reverse the anticoagulant effects of Factor Xa inhibitors: Andexanet alfa and Ciraparantag. Both drugs have been shown to be effective in rapidly reversing the anticoagulant effects of Factor Xa inhibitors and reducing the risk of bleeding in patients who require urgent surgery or are experiencing life-threatening bleeding.
The reversal of FXa (Factor Xa) inhibitor anticoagulants is important in emergency situations where patients taking these medications require urgent surgery or experience life-threatening bleeding. FXa inhibitors, such as rivaroxaban and apixaban, work by inhibiting the activity of Factor Xa, which is a key component of the coagulation cascade. However, this inhibition can increase the risk of bleeding, and in some cases, bleeding can become severe and potentially life-threatening. In these situations, prompt and effective reversal of the anticoagulant effect is critical to prevent further bleeding and ensure the best possible outcome for the patient.
Several reversal agents are available for FXa inhibitors, including andexanet alfa, which has been approved by regulatory authorities for use in the United States and Europe.
Improved Outcomes
The reversal of FXa inhibitor anticoagulants can help patients in emergency situations where they require urgent surgery or are experiencing life-threatening bleeding. FXa inhibitors work by inhibiting the activity of Factor Xa, a key component of the coagulation cascade, and as a result, can increase the risk of bleeding. In some cases, bleeding can be severe and potentially life-threatening, and therefore prompt and effective reversal of the anticoagulant effect is critical to prevent further bleeding and ensure the best possible outcome for the patient. Reversal of FXa inhibitors can also allow for the administration of other medications or interventions that may be needed to control bleeding or manage the underlying condition. In addition, reversal agents can help reduce the need for blood transfusions, which can be associated with various risks and complications. Overall, the reversal of FXa inhibitors can play an important role in improving patient outcomes and reducing the risks associated with anticoagulant therapy for people living with heart failure.
Experience With Drug Under Review
HeartLife did not speak to patients who had experience with the drug under review.
Companion Diagnostic Test
Not applicable.
Anything Else?
Andexanet alfa is a reversal agent used to reverse the anticoagulant effects of Factor Xa inhibitors, such as apixaban and rivaroxaban. The benefits of andexanet alfa include:
Rapid reversal of anticoagulation: Andexanet alfa works quickly to reverse the anticoagulant effect of Factor Xa inhibitors, which can be important in emergency situations where rapid control of bleeding is necessary.
Effective in restoring hemostasis: Studies have shown that andexanet alfa is effective in restoring hemostasis, or the ability of blood to clot, in patients taking Factor Xa inhibitors.
Reduced risk of bleeding: Reversal of Factor Xa inhibitors with andexanet alfa can help reduce the risk of bleeding, including life-threatening bleeding.
Allows for other interventions: Reversal of anticoagulation with andexanet alfa can allow for the administration of other medications or interventions that may be needed to control bleeding or manage the underlying condition.
Improved patient outcomes: By rapidly and effectively reversing the anticoagulant effects of Factor Xa inhibitors, andexanet alfa can improve patient outcomes and reduce the risks associated with anticoagulant therapy.
Overall, andexanet alfa is an important tool for managing patients taking Factor Xa inhibitors who require urgent surgery such as ICD’s, LVAD’s, and Heart Transplant or are experiencing life-threatening bleeding.
Conflict of Interest Declaration — HeartLife Foundation
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for HeartLife Foundation
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BI | — | — | — | X |
AZ | — | — | — | X |
Novartis | — | — | X | — |
BMS | — | — | X | — |
Bayer | — | — | X | — |
Servier | — | X | — | — |
Clinician Input
Canadian Stroke Consortium
About Canadian Stroke Consortium
The Canadian Stroke Consortium (CSC) is Canada’s national organization for stroke neurologists, neurointerventionalists and stroke professionals. The CSC is a member organization of the Canadian Neurological Sciences Federation (CNSF), encompassing health care practitioners and providers in multiple neurological specialties. We are involved in stroke research, clinical care, and advocacy for treatment and advancement of new and emerging therapies for stroke in Canada, a field which includes the use of both factor Xa inhibitors and intracerebral hemorrhage (ICH). Further details about our organization can be found at www.strokeconsortium.ca.
Information Gathering
Members of the Canadian Stroke Consortium have been involved in clinical trials and research programs using andexanet alfa and other therapies for reversal of hemorrhagic complications of direct oral anticoagulants, and have also been involved in the development of clinical guidelines for the use of these medications and the management of intracerebral hemorrhage, including the Heart and Stroke Foundation of Canada Stroke Best Practice Guidelines (www.strokebestpractices.ca). The information used in this submission reflects the expertise of our group as well as reviews of the current status of the literature and best practice recommendations for the management of acute intracerebral hemorrhage, including that secondary to the use of anticoagulants such as factor Xa inhibitors.
Current Treatments and Treatment Goals
In the Canadian context, current practice patterns vary for patients who present to hospital with acute intracerebral bleeding while on anticoagulation therapy with factor Xa inhibitors (apixaban, edoxaban, and rivaroxaban). This is in part due to the absence of availability for widespread use of andexanet alfa, a specific antidote to reverse anticoagulation with these agents, combined with the lack of good evidence of efficacy with empiric use of other non-specific reversal agents, such as 4-factor prothrombin complex concentrate. Of note, while empiric use of 4-factor prothrombin complex concentrate is recommended in practice guidelines for use in patients with acute ICH associated with factor-Xa inhibitors, this remains an off-label indication of use for 4F-PCC.
Acute ICH is associated with high rates of morbidity and mortality, particularly when associated with anticoagulation use including factor Xa inhibitors. A well-known yet modifiable risk factor associated with poor outcomes in these patients is the final hematoma volume. Furthermore, it is also well-known that following the initial hematoma, patients, particularly those on anticoagulation therapy including factor Xa-inhibitors, are at risk of a secondary increase in hematoma volume (also known as hematoma expansion) in the hours following the index event. Consequently, the overall treatment goal is to rapidly reverse and revert the coagulation status of ICH patients in order to prevent or minimise the risk of hematoma expansion. The availability of a specific and targeted anti-factor Xa reversal agent may expedite reversal of anticoagulation status of acute ICH and ultimately decrease the risk of hematoma expansion as a means to improve clinical outcomes, including reduction in death and disability, in these patients.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Currently, there is no targeted and specific reversal agents for anti-factor Xa inhibitors that can be administered in a timely fashion to decrease the risk of hematoma expansion in acute ICH. Furthermore, despite empiric use of non-specific reversal agents (such as 4-F-PCC), there is a lack of established benefit of their use for acute ICH associated with factor Xa inhibitors. As such, there is an immense gap in treatment for patients who use factor Xa inhibitors with intracerebral hemorrhage, and clinicians currently must use therapies that have no established clinical benefit, potentially leading to poorer outcomes.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Given the emergent nature of acute ICH management, administration of andexanet alfa cannot be a complementary or add-on treatment but rather a first-line agent.
Indeed, results of the phase 3/4 open-label ANNEXA-4 study showed that use of andexanet alfa as a first-line agent in patients with acute bleeding events including acute ICH (70% of the cohort), was associated with a rapid and sustained decrease anti-Xa activity levels following bolus administration along with good or excellent hemostasis efficacy occurring in 80% of patients (Stroke 2021; 52:2096-2105). This should be considered in the context of an absence of other specific therapies for reversal of factor Xa inhibitors; therefore, andexanet-alfa would be the first and only clinically proven therapy to date for this condition and would be a first-line therapy for patients with bleeding associated with factor Xa inhibitors.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
This therapy would be most appropriate for patients presenting with life threatening hemorrhage, including intracerebral hemorrhage, who are taking factor Xa inhibitors for indications such as prevention of cardioembolism from atrial fibrillation, or for the prevention of venous thromboembolism. This includes a large proportion of Canadian patients with atrial fibrillation, who rely on these medications for prevention of ischemic stroke, but who would be at risk of development of ICh as a result and who, until now, do not have a specific therapy available to block the action of factor Xa inhibitors in an acute situation. Eligible patients would be those who have been diagnosed with intracerebral hemorrhage on CT scan in the emergency department and who are found to have a history of use of factor Xa-inhibitors; eligibility would be determined on the basis of historical exposure to the medication, and patients would be monitored for clinical response as a stabilization in the size of the hematoma, which is currently done through clinical and radiological monitoring and which would be continued, similar to patients given idarucizumab for ICH in the context of direct thrombin inhibitors.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
As an emergent treatment, the response to andexanet alfa would be defined initially as reduction in hematoma expansion in ICH, which is typically measured with CT scan or MRI 6-24 hours after the initial presentation. Expansion of hematoma size is a risk factor for poor outcome in ICH, and patients with larger expansion of ICH have increased risk of mortality and disability following ICH. Even a 1 ml reduction in ICH growth can have an impact on long term outcome (Neurology 2006 Apr 25;66(8):1175-81).
What factors should be considered when deciding to discontinue treatment with the drug under review?
Andexanet alfa would be used only in the hyperacute phase on initial presentation; following treatment with a bolus dose and a two-hour infusion of drug, there would be no further therapy indicated for most patients.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Andexanet alfa would be provided in the emergency department to patients presenting with acute ICH. Monitoring would be provided by the use of neuroimaging which is standard-of-care therapy for this condition and would be used under the supervision of a stroke neurologist or emergency room physician with appropriate input from hematologists.
Additional Information
It should be pointed out that andexanet alfa is approved by the United States Food and Drug Administration for this indication, and any approval by Health Canada would be bringing Canadian practice in line with established standards of clinical care for ICH in other jurisdictions.
Conflict of Interest Declarations — Canadian Stroke Consortium
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Dylan Blacquiere
Position: Assistant Professor of Medicine (Neurology), University of Ottawa
Date: 27-03-2023
Table 3: COI Declaration for Canadian Stroke Consortium — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Roche Canada | X | — | — | — |
Declaration for Clinician 2
Name: Laura Gioia
Position: Assistant Professor of Medicine (Neurology), Université de Montréal
Date: 27-03-2023
Table 4: COI Declaration for Canadian Stroke Consortium — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca Canada | X | — | — | — |
BMS Pfizer | X | — | — | — |
Declaration for Clinician 3
Name: Dariush Dowlatshahi
Position: Professor of Medicine (Neurology), University of Ottawa
Date: 27-03-2023
Table 5: COI Declaration for Canadian Stroke Consortium — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca Canada | X | — | — | — |
Declaration for Clinician 4
Name: Andrew Demchuk
Position: Professor of Medicine, University of Calgary
Date: 26-03-2023
Table 6: COI Declaration for Canadian Stroke Consortium — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca Canada | — | X | — | — |
Declaration for Clinician 5
Name: Ghazela Basir
Position: Assistant Professor of Medicine (Neurology), University of Ottawa
Date: 27-03-2023
Table 7: COI Declaration for Canadian Stroke Consortium — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
McMaster University Faculty in Hematology/Thromboembolism
About McMaster University Faculty in Hematology/Thromboembolism
We are clinicians and clinician-scientists working at McMaster University-affiliated hospitals in Hamilton (Hamilton General Hospital, Juravinski Hospital, St. Joseph’s Healthcare), specializing in adult thrombosis medicine and, in particular, have considerable clinical experience dealing with anticoagulant-associated bleeding and need for urgent anticoagulant reversal in the setting of major (serious) bleeding or need for surgery. Collectively, we manage patients as part of stand-alone Thrombosis Clinical Services in which most, if not all, of anticoagulant-related bleeds and/or reversal are assessed by our service. We manage a considerable number of patients, on average 10-12 per week, who require DOAC reversal because of life-threatening bleeding or need for urgent surgery.
Information Gathering
The response herein is based on (a) our clinical experience in managing patients with anticoagulant and, specifically, direct oral anticoagulant (DOAC)-associated bleeding, coupled with (b) our knowledge of related literature. We have not been involved in clinical trials relating to anticoagulant reversal, nor do we have financial COIs with entities that manufacture anticoagulant reversal products (PCCs, idarucizumab, andexanet-a).
Current Treatments and Treatment Goals
In Canada, the only DOAC-specific reversal agent is idarucizumab, which can only be administered for patients who are receiving dabigatran, a DOAC that is not widely used (subjectively, we estimate in 5-10% of all DOAC users). For the vast majority of DOAC users, who are receiving a factor Xa (fXa) inhibitor (apixaban, edoxaban, rivaroxaban) there are only non-specific prohemostatic treatment options, comprising chiefly the 4-factor prothrombin complex concentrates (PCCs). It seems logical and clinically sensible that if there is a reversal agent available for warfarin (PCCs) and dabigatran (idarucizumab), such a reversal agent should be also available for oral fXa inhibitors, especially when these are, by far, the most commonly used anticoagulants.
The management of DOAC-associated bleeding, as with warfarin-associated anticoagulant bleeding, is anchored on non-drug supportive care that includes fluid administration, transfusion of packed red cells and invasive interventions (e.g., endoscopy for gastrointestinal bleeding). Although many DOAC-associated bleeds (subjective estimate is >50%) can be managed with supportive measures, DOAC-specific reversal agents would have benefit in patients with life-threatening bleeding (e.g., associated with cardiovascular collapse) or bleeding at a critical site (e.g., intracranial, spinal, pericardial).
Clinical practice guidelines support the use of DOAC-specific reversal agents (idarucizumab for dabigatran, andexanet-a for oral factor Xa inhibitors) in situations of life-threatening or critical site bleeding. Refs: Cuker A, et al. Am J Hematol 2019;94:697-709; Levy J, et al. J Thromb Haemost 2016;14:623-7; Milling T, et al. Am J Emerg Med 2020;38:1890-1903.
Current treatments for DOAC-associated bleeding in patients who are receiving oral factor Xa inhibitors (apixaban, edoxaban, rivaroxaban) are non-specific and, in some respects, counter-intuitive. Thus, PCCs which are currently the treatment of choice for oral fXa reversal has no effect on eliminating the anticoagulant. Instead PCCs act to increase factors II, VII, IX and X to supra-physiologic levels and, in doing so, potentially overwhelming the inhibitory effect of apixaban/edoxaban/rivaroxaban on factor Xa. In such patients, levels of factors II, VII, IX and X are within normal limits and adding more of these coagulation factors (with PCCs) does not eliminate the active inhibitory action of oral fXa inhibitors and may promote a prothrombotic state. Moreover, there is limited high-quality prospective data to support the efficacy and safety of PCCs. Refs: Kimpton M, et al. Hematology Am Soc Hematol Educ Program 2019;2019:204-208.
For patients who require urgent anticoagulant reversal, the ideal treatment would directly eliminate the anticoagulant action in a drug-specific manner. Thus, PCCs are effective for warfarin-associated bleeding because they directly replace the vitamin K-dependent coagulation factors (II, VII, IX and X) whose levels have been depleted by warfarin action. Similarly, dabigatran and andexanet-a would eliminate the anticoagulant effect of dabigatran and oral fXa inhibitors, respectively.
The use of anticoagulant reversal agents, comprising PCCs, idarucizumab and andexanet-a, have been shown to rapidly reverse the anticoagulant effect of warfarin, dabigatran and oral fXa inhibitors, respectively, but evidence is lacking for all of these agents that their administration affects mortality or serious morbidity. The outcomes measured in these two-arm or single-arm trials are primarily laboratory based, reflecting anticoagulant reversal, and secondary outcomes include subjective assessment (by the treating clinician) of site-specific hemostasis in the setting of major bleeding or need for urgent surgery. Emerging evidence suggests that anticoagulant reversal in patients with intracranial hemorrhage limits hematoma expansion, with the potential to improve neurological functional outcomes in such patients.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Although PCCs and idarucizumab are available for the management of warfarin- and dabigatran-associated bleeding, respectively, such availability is lacking for andexanet-a, which is the specific reversal agent for the most commonly used anticoagulants: apixaban (Eliquis – now generic), edoxaban (Lixiana), and rivaroxaban (Xarelto – now generic). This, in our view, represents an important missed opportunity to ensure clinicians have options for fXa reversal such that clinicians do not have to rely solely on one agent (PCC) that is non-specific, and which may have a prothrombotic effect by increasing coagulation factor levels II, VII, IX and X) to supra-physiologic levels.
In the domain of anticoagulant reversal, clinicians need to have DOAC-specific reversal agents available as a treatment option, especially for bleeding at critical sites (intracranial, spinal, pericardial) and to enable emergency/urgent surgery to safely proceed.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The mechanism of action of andexanet-a is specific to anticoagulants that inhibit factor Xa since andexanet-a acts a decoy molecule to competitively bind to factor Xa (without inactivation), thereby rendering it inaccessible to factor Xa inhibitors. This mechanism of action has applications to reversing all anticoagulants that work through fXa inhibition, whether parenteral agents (low-molecular-weight heparins or fondaparinux) or oral agents (apixaban, edoxaban, rivaroxaban), the latter of which are most widely used.
The drug under review (andexanet-a) would be the first treatment that is specific for the reversal of anticoagulants that act through fXa inhibition. It would be used as a first-line treatment in selected patients who require urgent anticoagulant reversal in the setting of serious, life-threatening bleeding or need for urgent surgery. The drug under review would not be considered for patient’s intolerant to other anticoagulant reversal strategies but would offer clinicians the option of a specific reversal agent for selected clinical circumstances.
If the drug under review becomes available for clinical use, it is expected to shift Canadian practice algorithms and guidance documents (e.g., by Thrombosis Canada – www.thrombosiscanada.ca) so it is included as a treatment option for DOAC reversal. It is expected that its availability will shift management from administering non-specific reversal agents (PCCs), although the extent of this shift is likely to be partial. Stated differently, we expect PCCs to be used for an ‘average’ patient who needs DOAC reversal whereas andexanet-a will be used in selected patients with (a) life-threatening bleeding that does not respond to supportive management (i.e., fluids, packed red cells), (b) critical site bleeding (intracranial, spinal, pericardial), and (c) a need for emergency (within 6-8 hours) or urgent (within 12-24 hours) surgery.
The initial treatment of anticoagulant/DOAC-associated bleeding always encompasses supportive measures; however, such supportive measures are likely to be ineffective for certain types of bleeds (e.g., intracranial) and will not be relevant to patients who are not bleeding but need anticoagulant/DOAC reversal for an emergency/urgent surgery.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
As mentioned previously, andexanet-a would be most suitable for patients who are receiving an oral fXa inhibitor (apixaban, edoxaban, rivaroxaban) and (a) have life-threatening bleeding that does not respond to initial supportive measures (fluids, pRBCs), (b) have bleeding at a critical site (intracranial, spinal, pericardial) that can lead to mortality or serious long-term morbidity, and (c) require an emergency (within 6-8 hours) or urgent (within 12-24 hours) surgery.
The decision as to whether to administer andexanet-a is a clinical decision that takes into account (a) the location and severity of the bleed, (b) the time since the last known dose of DOAC (although this is often not known), and (c) potential for improvement, accounting for patient comorbidities and goals of care. There is no widely-available and rapidly accessible laboratory test that can be used to inform this clinical decision as there are no DOAC-specific coagulation tests (as with the INR for warfarin-treated patients) that can be used as DOAC-specific tests (DOAC-calibrated anti-factor Xa levels) are not widely available and interpretation of the DOAC level is problematic. Moreover, routinely-available coagulation tests (INR, aPTT, TT), do not reliably reflect DOAC levels.
Response to treatment has been demonstrated with DOAC reversal agents using laboratory-based evidence for DOAC reversal in the case of dabigatran (normalized dilute thrombin time) and in the case of oral fXa inhibitors (normalized anti-factor Xa levels) that have been shown to occur within minutes after DOAC reversal administration, whether with idarucizumab or andexanet-a.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The principal outcome used to assess the response to andexanet-a is laboratory, namely measurement of anti-factor Xa levels before and after drug administration. However, as noted previously, such measurement testing is not widely available, and clinicians need to rely also on evidence of clinical stabilization of bleeding or intra- and post-operative surgical site hemostasis. In the seminal studies that investigated andexanet-a, both outcomes were measured, demonstrating a rapid and sustained effect on reduction and normalization of anti-factor Xa levels, and also demonstrating (subjectively) stabilization of hemostasis. These studies were not designed or powered to demonstrate improvements in mortality or morbidity (nor were other studies investigating idarucizumab or PCCs). In all studies, laboratory parameters (INR, dilute thrombin time, anti-fXa levels) were the primary outcome to assess efficacy.
What factors should be considered when deciding to discontinue treatment with the drug under review?
This issue does not apply to the product under review since it is administered as a one-time treatment for a short interval (2-4 hour infusion).
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
As mentioned above, the settings in which the product under review would be administered are patients with (a) life-threatening bleeding that does not respond to supportive management (i.e., fluids, packed red cells), (b) critical site bleeding (intracranial, spinal, pericardial), and (c) a need for emergency (within 6-8 hours) or urgent (within 12-24 hours) surgery.
The setting for its administration would be, typically, in the emergency department, intensive care unit or in-hospital ward.
The clinicians responsible for its administration would be emergency room, critical care, and medical-surgical specialists. In many hospitals, administration of this agent (as with use of PCCs and idarucizumab) would require approval by a specialist thrombosis or hematology service. Ideally, criteria for administration would be developed to reflect the expected case-mix at a particular hospital, for example, for tertiary trauma centers and stroke/neurosurgical referral centers.
Additional Information
No additional comments.
Conflict of Interest Declarations — McMaster University Faculty in Hematology/Thromboembolism
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: James D. Douketis MD, FRCPC, FCAHS
Position: Staff Physician, GIM and Thromboembolism Services, St. Joseph’s Healthcare Hamilton, Professor of Medicine, McMaster University
Date: 20-03-2023
Table 8: COI Declaration for McMaster University Faculty in Hematology/Thromboembolism — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Pfizer | X | — | — | — |
Leo Pharma | X | — | — | — |
Servier | X | — | — | — |
Fresenius-Kabi | X | — | — | — |
Note: No direct financial or other in-kind indirect financial compensation by companies for the product being assessed, andexanet-a, nor have any participation in any clinical trials or other studies involving this product.
Declaration for Clinician 2
Name: Dr. Rick Ikesaka
Position: Staff Physician, Hematology and Thromboembolism Services. St. Joseph’s Healthcare Hamilton, Assistant Professor of Medicine, McMaster University
Date: 24-03-2023
Table 9: COI Declaration for McMaster University Faculty in Hematology/Thromboembolism — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Alfonso Iorio
Position: Staff, Thrombosis Service, Juravinski Hospital, Division of Hematology, HHS and Chair, Department of Health Research Methods, Evidence, and Impact, McMaster University
Date: 20-03-2023
Table 10: COI Declaration for McMaster University Faculty in Hematology/Thromboembolism — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Lori Linkins
Position: Staff Physician, JH Thrombosis Service, Associate Professor of Medicine, McMaster University
Date: 21-03-2023
Table 11: COI Declaration for McMaster University Faculty in Hematology/Thromboembolism — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Dr. Siraj Mithoowani
Position: Hematology and Thromboembolism, St. Joseph’s Healthcare, Assistant Professor of Medicine, McMaster University
Date: March 24, 2023
Table 12: COI Declaration for McMaster University Faculty in Hematology/Thromboembolism — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Dalhousie University Thrombosis and Anticoagulation Team
About Dalhousie University Thrombosis and Anticoagulation Team
They physicians creating this submission are members of the Thrombosis and Anticoagulation Team at Dalhousie University and Nova Scotia Health. Drs. Shivakumar and Kelly are members of the Division of Hematology, and Dr. Tran is a member of the Division of General Internal Medicine.
Information Gathering
The information in this submission is taken from publicly available publications and guidelines, as well as our own local experience.
Current Treatments and Treatment Goals
In Canada, there are currently no antidotes for the direct Xa inhibitors. Currently, patients with life threatening bleeding or who require an urgent operation who are taking a direct Xa inhibitor have no targeted or specific therapy. Current treatment algorithms would include:
Local hemostatic control
Cessation of the anticoagulant
Replacement of blood products including transfusion of packed red blood cells, platelets, fresh frozen plasma, or cryoprecipitate, and in some cases activation of the Massive Transfusion protocol
Use of adjunct medications such as tranexamic acid
Prothrombin complex concentrates if life threatening bleeding
These are not targeted treatments and there is no clinical data to suggest efficacy or safety in this population.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There are no available antidotes for FXa inhibitors. Andexanet alfa is the only targeted antidote for the FXa inhibitors. It directly affects the FXa inhibitors by the way of acting as a decoy protein. This is targeted therapy and has been shown to clearly reduce the in vitro anticoagulant effect of the FXa inhibitors. The large cohort study also found acceptable bleeding rates.
The other option that has reports of being used in patients who are on FXa inhibitors and are bleeding is prothrombin complex concentrate (PCC). This product is intended to reverse patients who are on vitamin K antagonists (VKAs), such as warfarin. VKAs work by reducing the levels of factors II, VII, IX, and X. PCC reverses this by providing these factors, which mechanistically is very logical. Using PCC or coagulation factor replacement for an inhibitor of a coagulation factor is not targeted therapy and is not as logical. In addition, other coagulation factors are being added, which may increase the thrombotic risk unnecessarily. The other potential risk associated with PCC is that there are small amounts of heparin present. Patients who have a history of heparin-induced thrombocytopenia and thrombosis (HITT) would not be able to safely have this product. There is no such concern with andexanet alfa.
There are no published, randomized comparisons between andexanet alfa and PCC. Patients who would require an antidote to FXa inhibitors would be those that are experiencing life-threatening bleeding, life-altering bleeding (e.g. intracranial hemorrhage that could result in permanent disability) or require emergency surgery. The currently available treatment (PCC) would not specifically the mechanism of FXa inhibitors, and thus, may not be improving outcomes in these very sick patients.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Andexanet alfa would be the only treatment (and thus, first line treatment) targeted to patients who are on a FXa inhibitor and are experiencing bleeding or require emergent surgery. Andexanet alfa would be the only medication used in this setting due to the mechanisms described in the answer to 4.1. Thus, it would not make sense to have andexanet alfa be a second line treatment or to follow/combine andexanet alfa with other treatments, such as PCC. If approved, the treatment paradigm would shift to using andexanet alfa.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients who would require an antidote to FXa inhibitors would be those that are experiencing life-threatening bleeding, life-altering bleeding (e.g., intracranial hemorrhage that could result in permanent disability), or require emergency surgery, where there would not be time to wait for the FXa inhibitor’s levels to decrease to those acceptable for surgery. These patients would be quite clear clinically, based on examination findings (such as hypotension in the setting of bleeding), radiographic findings (such as hemorrhage size on CT head), or by surgeon judgment.
Patients that would be less suitable to the use of andexanet alfa would be those who last took their FXa inhibitor more than 1-2 days ago (in the presence of normal renal function), who have bleeding that is not life-threatening (e.g., normal blood pressure and heart rate), or those that can have surgery delayed for 1-2 days after their last dose of FXa inhibitor.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Andexanet alpha is used for patients when rapid reversal of anticoagulation is needed due to acute major bleeding, including life-threatening bleeds. A clinically meaningful response to therapy would be excellent or good hemostatic efficacy 12h after infusion. This could be assessed by various imaging modalities depending on the site of initial bleeding, or by a decrease in visible bleeding. Other outcomes that could be used to assess response include a decrease in Hemoglobin or Hematocrit by <20% as compared to baseline. Other important responses would be improvement of symptoms, decreased mortality.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Reasons to discontinue treatment with Andexanet alpha may include infusion reaction, or thromboembolic events. Symptoms of potential infusion reaction can range from urticaria, flushing, or diaphoresis. Most events were defined as non-serious or mild at a rate of about 18%. Over 90% of individuals who had a reaction did not require treatment. There has been reports of thromboembolic events including cerebrovascular accident, transient ischemia attack, pulmonary embolism, deep vein thrombosis, and/or acute myocardial infarction. The median time to a thrombotic event was 7 days.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Andexanet alpha is used for patients when rapid reversal of anticoagulation is needed due to acute major bleeding, including life-threatening bleeds. The use of this medication would be appropriate in the hospital setting including emergency department, critical care unit, or operating room. Specialties that would be relevant in administering Andexanet alpha would include Emergency medicine, Internal medicine (Critical care, Internal medicine, Hematology), anesthesia, and surgical specialists.
Additional Information
Not applicable.
Conflict of Interest Declarations — Dalhousie University Thrombosis and Anticoagulation Team
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Sudeep Shivakumar
Position: Head, Division of Hematology
Date: 26-Mar-2023
Table 13: COI Declaration for Dalhousie University Thrombosis and Anticoagulation Team — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca | X | — | — | — |
Declaration for Clinician 2
Name: Erica Kelly
Position: Hematologist, Division of Hematology
Date: 26-Mar-2023
Table 14: COI Declaration for Dalhousie University Thrombosis and Anticoagulation Team — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Allen Tran
Position: Internist, Division of General Internal Medicine
Date: 26-Mar-2023
Table 15: COI Declaration for Dalhousie University Thrombosis and Anticoagulation Team — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Thrombosis Canada
About Thrombosis Canada
For over 30 years, Thrombosis Canada (www.thrombosiscanada.ca) has been supporting healthcare professionals in sharing expertise to enable improved thrombosis care. From its beginnings as the Thrombosis Interest Group (TIG), led by Dr. Graham Turpie, it has grown in number of members, in the diversity of professions involved in supporting the mission, and in its impact on care. Our diverse membership includes thrombosis experts from across Canada many of whom are also considered to be global experts.
The development of up-to-date clinical guides, tools, patient materials, and resources has resulted in Thrombosis Canada becoming a driving force in improving the care of patients with or at risk for thrombosis. This is demonstrated by the yearly increases in the use of our Apps and website by individuals across Canada and internationally. The influence of our materials is also evident in the widespread feedback that we receive from users and others who reach out to us for updates when new evidence becomes available and in the number of organizations that reference our website and materials. Furthermore, our clinical guides are increasingly considered as Canadian standards of care in the areas of thrombosis and antithrombotic management.
The tools and resources that we produce are central components of our knowledge translation initiatives. We now look to ensuring that all potential users are aware of Thrombosis Canada and the valuable resources that we have to offer. It is our belief that, by increasing awareness and use of our resources, we will continue to improve the care of patients with or at risk for thrombosis. We also strive to expand the education provided to both healthcare providers and patients consistent with our vision. Where appropriate, we also endeavor to work with the community to ensure that patients have access to medications that will improve outcomes based upon research evidence.
Our vision is to improve the health of all Canadians by eliminating morbidity and mortality related to thrombotic disease.
Information Gathering
We obtained information from thrombosis experts who manage and research anticoagulant-related bleeding, and people with lived experience of anticoagulation. Patient input was obtained through an open survey of patients on anticoagulants or their caregivers. The survey was developed by an independent team of experts and persons with lived experience from across Canada. The team convened to develop the survey questions, review the draft survey individually and provide recommendations for any changes. The survey was hosted and fielded by an independent organization, Environics Research, in both English and French. Environics distributed the survey to their patient panel and shared a link with Thrombosis Canada for distribution and promotion. Survey responses were gathered from December 12, 2022, to February 6, 2023.
Current Treatments and Treatment Goals
Oral anticoagulants (OACs) including factor Xa inhibitors are used widely to prevent and treat cardiovascular diseases, such as stroke in patients with atrial fibrillation (AF) and venous thromboembolism (VTE). More than 40 million prescriptions for OACs are written annually in North America, including over 7 million in Canada. AF, the most common indication for their use, is associated with a 5-fold increase in the risk of ischemic stroke and affects an estimated 350,000 Canadians. Without OACs, the annual risk of ischemic stroke in AF is approximately 5%; OACs reduce the risk by about 65%. As the second most common cardiovascular disease, approximately 1-2 per 1000 persons per year will receive VTE diagnoses, and the risk of VTE increases with age. Given population aging, AF and VTE and their complications are expected to represent an even greater health problem within Canada and worldwide.
Anticoagulants are the most common cause of medication-related serious harm, in terms of emergency department visits, hospitalizations, and fatalities. Bleeding is the main complication of anticoagulation that limits its use. About 2% to 4% of patients receiving OACs experience major bleeding annually, and another 10% experience clinically relevant non-major bleeding for which they seek medical attention. Bleeding complications increase the short-term risk of death by 35-fold for intracranial bleeding and 5-fold for extracranial bleeding. Patients with OAC-related major bleeding have 30-day mortality rates up to ~10% to 40% (depending on the site of bleeding) emphasizing the need for management strategies to improve outcomes. Bleeding cessation is a clinical priority for OAC-treated patients experiencing severe bleeding complications. Reversal of anticoagulant effect is a key part of managing serious anticoagulant-related bleeding complications in conjunction with supportive measures and procedural intervention.
There are currently no agents available in Canada that reverse the anticoagulant effect of factor Xa inhibitor anticoagulants. In the absence of a specific reversal agent, and based on limited data guiding its use, 4-factor prothrombin complex concentrate (4F-PCC) is used (off-label) as a non-specific hemostatic therapy for factor Xa inhibitor treated patients with serious bleeding complications. The National Advisory Council on Blood and Blood Products Recommendations for use of Prothrombin Complex Concentrates in Canada endorses the use of 4F-PCC when specific reversal agents (e.g. andexanet alfa) are not available as follows: “Specific reversal agents for direct factor Xa inhibitors (including rivaroxaban, apixaban, and edoxaban), such as andexanet alfa, should be used, if available” (https://nacblood.ca). Other guidance from major professional societies has similar recommendations (e.g., American College of Cardiology, American Heart Association/American Stroke Association, Anticoagulation Forum).
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There are currently no approved therapies that have been shown to reverse the anticoagulant effect of factor Xa inhibitor anticoagulants. In the absence of reversal agents, 4F-PCC is used off-label to aid hemostasis in factor Xa inhibitor treated patients with serious bleeding by supplying exogenous coagulation factors. 4F-PCC contains plasma-derived inactive vitamin K–dependent coagulation factors. The effect of 4F-PCC on laboratory indices of DOAC anticoagulant effect has been studied in in vivo/ex vivo experiments, animal models, human volunteers, showing conflicting and, at best, modest effects on coagulation tests. Single-arm observational studies of factor Xa inhibitor-treated patients with major bleeding who received 4F-PCC in routine clinical practice have also been reported. Although rates of “hemostatic efficacy/effectiveness” are ~70% to 80% in these studies, rates of mortality up to ~30% and thromboembolism up to 10% are also reported. Given the lack of control group and other methodological limitations in these studies, the incremental benefit and harm of 4F-PCC in this setting are highly uncertain.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Andexanet alfa is a modified human factor Xa variant that reverses the anticoagulant effect of factor Xa inhibitor anticoagulants. There are no other available treatments that reverse factor Xa inhibitors. Judicious use of andexanet (e.g., via institutional protocols) will ensure that it is administered to patients who are most likely to benefit including those with (i) severe/life-threatening acute bleeding, and (ii) suspected or proven clinically significant levels of anticoagulant. Use of andexanet as a first line therapy for patients with serious factor Xa inhibitor associated bleeding is endorsed by The National Advisory Council on Blood and Blood Products Recommendations for use of Prothrombin Complex Concentrates in Canada when specific reversal agents (e.g., andexanet alfa) similar to guidance from other organizations and professional societies (e.g., American College of Cardiology, American Heart Association/American Stroke Association, Anticoagulation Forum).
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Candidates for andexanet are patients receiving factor Xa inhibitors (apixaban, rivaroxaban or edoxaban) who present with severe bleeding complications (e.g., life, limb or organ threatening) in whom clinically significant levels of drug are likely present. The presence of clinically significant drug levels can be assessed clinically based on the timing of the last dose in conjunction with estimated drug clearance (drug half-life and kidney/liver function) or based on a calibrated anti-Xa activity assay. Because there is no established threshold for clinically significant hemostatic impairment and most centers do not have factor Xa inhibitor drug levels available (at all, or with sufficiently rapid turnaround time for emergencies) treatment is usually considered based on the timing of the last dose, drug half-life and the patient’s kidney/liver function. Patients with non-serious bleeding are not suitable for andexanet.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Patients presenting with severe bleeding complications are managed in hospital. In clinical practice, the type of monitoring and outcomes depend on the specific site of bleeding (e.g. gastrointestinal bleeding versus intracranial bleeding). In clinical studies, “hemostatic efficacy” of andexanet and 4F-PCC (i.e. cessation of bleeding) has been determined according to site-specific and somewhat variable criteria that have not been prospectively validated. This includes clinical assessment, laboratory testing, and imaging investigations. Thrombotic events and mortality are also key outcomes monitored in clinical practice and reported in clinical studies.
What factors should be considered when deciding to discontinue treatment with the drug under review?
The drug under review is administered as an intravenous bolus followed by a 2-hour infusion. Therefore, given the limited duration of treatment, criteria for discontinuation are not relevant other than unexpected allergic reactions.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
As eligible patients (i.e., those with severe bleeding complications) will be managed in the emergency department and/or hospital, it is not appropriate for outpatient clinic use. Andexanet is likely to be administered in an acute care setting (e.g., emergency department) by an emergency department physician. Depending on the site of bleeding, specialists may be involved in the management of these patients (e.g., neurology/neurosurgery for intracranial hemorrhage, gastroenterologists for gastrointestinal bleeding, surgeons for other types of bleeding) but their involvement should not delay the administration of andexanet for immediately life-threatening bleeding.
Additional Information
To assess net clinical benefit of treatments for severe acute bleeding, both the risks of bleeding and thrombosis should be considered. While underlying thrombosis risk is an important consideration, during active serious bleeding the benefit of treatments to ameliorate ongoing bleeding likely outweighs theoretical harms of thrombosis. Patients with serious anticoagulant-related bleeding are at increased risk of thrombosis due to underlying pro-thrombotic conditions, anticoagulant withdrawal, activation of endogenous hemostatic mechanisms to stop bleeding, surgeries/procedures, and prolonged hospitalization. However, these risk factors for thrombosis should not preclude the administration of anticoagulant reversal strategies for patients with actual serious bleeding. Post-bleed assessments and resumption of anticoagulation after bleeding cessation are important for mitigating thrombotic events. For example, in the ANNEXA-4 study, thrombotic events occurred only among patients who had not yet resumed any anticoagulation.
As discussed above, patients with anticoagulant-related serious bleeding are at risk of thrombosis. In a randomized trial of prothrombin complex concentrate (PCC) versus plasma for major warfarin-associated bleeding (Sarode et al, 2013), the rate of thrombotic events was similar among patients treated with plasma (6.4%) compared to those treated with PCC (7.8%). It is important to acknowledge that studies evaluating reversal strategies (idarucizumab, andexanet) or PCC for patients with direct oral anticoagulant (DOAC)-related major bleeding lacked a control arm which limits our understanding about the potential incremental harms of these treatments. The reported rate of thrombotic events among anticoagulant-treated patients with major bleeding appear similar regardless of whether they were treated with plasma, PCC, idarucizumab, or andexanet alfa (about 4% to 10%). Although these reports may suggest some variability in the frequency of thrombotic events, these results should be interpreted with caution as these studies evaluated different treatments and cannot be compared head-to-head due to significant methodological differences (e.g., study design, population, outcomes, data collection, etc.). Cohort studies that retrospectively evaluated outcomes after administration of PCC for factor Xa inhibitor bleeding in routine clinical practice did not have standardized follow-up or assessments and are at risk of ascertainment bias. Further, the rate of thrombosis is influenced by mortality which is a competing event. For example, in one cohort of patients treated with PCC for factor Xa inhibitor associated bleeding, the rate of thrombosis was 4% while the mortality rate was 32% within 30 days.
In our recent patient survey outlined above, 305 individuals responded to the survey (57% female), of whom two-thirds answered on their own behalf while one-third answered as a caregiver. Most respondents (84%) were between 18 and 64 years of age and were taking an anticoagulant for venous thromboembolism (53%), atrial fibrillation (36%) or mechanical heart valve (21%). Among 214 individuals taking oral anticoagulants, 79 (37%) were receiving warfarin, 73 (34%) were receiving apixaban, and 61 (29%) were receiving rivaroxaban. Almost one quarter (23%) of respondents indicated that they had experienced major (serious) bleeding while taking an anticoagulant and of those,15% never restarted their anticoagulant. Almost half (47%) experienced minor bleeding while on an anticoagulant. Although respondents were generally comfortable taking anticoagulation, 75% indicated that they would feel more comfortable if they knew a reversal agent could be used for major bleeding about which 44% indicated was a concern.
Conflict of Interest Declarations — Thrombosis Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
Environics Research.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Thrombosis Canada has received grants from AstraZeneca who have direct interest in the drug under review.
Declaration for Clinician 1
Name: Deborah Siegal
Position: Hematologist (Thrombosis) The Ottawa Hospital; Associate Professor, Department of Medicine and School of Epidemiology and Public Health, University of Ottawa; Associate Scientist, Ottawa Hospital Research Institute
Date: 24-Mar-2023
Table 16: COI Declaration for Thrombosis Canada — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | X | — | — | — |
BMS-Pfizer | X | — | — | — |
Roche | X | — | — | — |
Servier | X | — | — | — |
Honorarium paid indirectly to institute.
Declaration for Clinician 2
Name: David Airdire
Position: Executive Director, Thrombosis Canada
Date: 24-03-2023
Table 17: COI Declaration for Thrombosis Canada — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
ER Journal Club, GTA
About ER Journal Club, GTA
Journal club comprising of local ER physicians in Peel region.
Information Gathering
Literature search for articles, and product monograph, EUSEM projects
Current Treatments and Treatment Goals
As the chair of the journal club, I was invited to speak at the European Emergency Congress, where I was pleasantly surprised to hear that this product was already available and in use, and the preliminary experience there thus far. We have been awaiting it for a long time in Canada. With the rise and essential takeover of DOAC anticoagulants replacing Warfarin (when indicated), has caused a void in the treatment algorithm of major bleeds, and clinically significant non major bleeds. While Dabigatran has a reversal agent available, the rest of the direct oral anticoagulants do not have a specific reversal agent to treat these major bleeds. This really handicaps us in the ER as we are the first line of physicians who see and treat the major bleeds in a 24/7 active department. While we use other nonspecific treatments, these do not have any specific action against these new DOAC drugs.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
As mentioned above, most patients do not respond to the general treatments, including tranexamic acid, or PCC/activated PCC. Even surgical treatment, if indicated, is often delayed as surgeons have to be called into hospital for these emergencies. Lifesaving and disability decreasing treatment options are required and a specific reversal agent such as Andexanet Alfa would be very helpful in treating our major bleed patients on the DOAC drugs.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Major bleeds or clinically significant non major bleeds that are not amenable for surgical/procedural intervention or where these intervention/s may be significantly delayed. It would be used to stop bleeds, and in some cases to temporize and stabilize the patients for definitive treatment.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients on Apixaban or Rivaroxaban with major bleeds presenting to the ER. Of note, the majority of patients on anticoagulation are on one of these 2 medications. Not indicated for patients on warfarin, on Dabigatran or not on anticoagulation.
Also, in patients who are on these medications who need unplanned emergent surgery or invasive procedures, this may be necessary to perform the procedure without causing excessive bleeding.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
This will vary to a large degree on the bleeding site. Obviously, mortality, survival to discharge, disability score on discharge are all objective parameters. Even OT assessments of ADL, mobility, speech, functioning are long term outcome measures. In the ER, the measures will be to be able to stabilize the patient, stop the bleed, or at least reduce the severity of the bleeding source. In cases of an intracerebral hemorrhage a quick administration of a reversal agent could mean the difference between life and death to a previously fully functioning patient. Major GI bleeds would also be helped, and the outcome measure would be to get them to OR or GI suite for surgical intervention and definitive treatment and decreasing rate of mortality or amount of disability. Length of stays in hospital may also be a surrogate marker.
What factors should be considered when deciding to discontinue treatment with the drug under review?
This is typically given only to reverse the DOAC. It would not be continued.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
I believe we can discuss with a hematologist on call in Emergency situations to get an approval on phone once we have discussed the case. Also, we suggest monitoring for the first year or 2 to ensure appropriate utilization of this product.
Additional Information
We are desperate to have these in the ER departments across Canada for all our patients who are on Rivaroxaban or Apixaban who present with major ongoing bleeds that compromise their life/limb/future disability.
Conflict of Interest Declarations — ER Journal Club, GTA
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Indraneel Ghosh
Position: Emergency Physician
Date: 27-03-2023
Table 18: COI Declaration for ER Journal Club, GTA — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS-Pfizer | X | — | — | — |
Servier | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Brent Andruko
Position: Emergency Physician
Date: 14-03-2023
Table 19: COI Declaration for ER Journal Club, GTA — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS-Pfizer | X | — | — | — |
Servier | X | — | — | — |
Declaration for Clinician 3
Name: Dr. Daniel Shogilev
Position: Emergency Physician
Date: 14-03-2023
Table 20: COI Declaration for ER Journal Club, GTA — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS-Pfizer | X | — | — | — |
Servier | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Zafar Ahmad
Position: Emergency Physician
Date: 14-03-2023
Table 21: COI Declaration for ER Journal Club, GTA — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS-Pfizer | X | — | — | — |
Servier | X | — | — | — |
Declaration for Clinician 5
Name: Dr. Thomas Campbell
Position: Emergency Physician
Date: 14-03-2023
Table 22: COI Declaration for ER Journal Club, GTA — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS-Pfizer | X | — | — | — |
Servier | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.