Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Olezarsen (Tryngolza)
Indication: As an adjunct to diet in adult patients for the treatment of familial chylomicronemia syndrome (FCS)
Sponsor: Theratechnologies Inc.
Final Recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Tryngolza?
Canada’s Drug Agency (CDA-AMC) recommends that Tryngolza be reimbursed by public drug plans for familial chylomicronemia syndrome (FCS).
Why Did CDA-AMC Recommend Reimbursement?
The Canadian Drug Expert Committee (CDEC) determined that Tryngolza demonstrates acceptable clinical value versus placebo in patients with FCS. This determination was enough for CDEC to recommend that Tryngolza be reimbursed. Given that Tryngolza is expected to be an adjunct to a low-fat diet, acceptable clinical value refers to added value versus diet alone.
Evidence from a clinical trial showed that Tryngolza given for 12 months improved triglyceride levels and the rate of acute pancreatitis in adult patients with FCS. Certainty in the results was moderate due to some imprecision because of small sample sizes given the rarity of FCS. Results from the trial about health-related quality of life (HRQoL) were inconclusive. Patients receiving Tryngolza had fewer adverse events (AEs) than patients receiving placebo, few patients discontinued treatment due to AEs, and no AEs of special interest were observed. Altogether, treatment with Tryngolza for 12 months was considered well-tolerated.
As there are no other therapies indicated for the treatment of FCS in Canada that are safe and effective in improving these outcomes, Tryngolza is expected to address some identified clinical needs that are not being met by treatment with diet alone.
Which Patients Are Eligible for Coverage?
Tryngolza should only be reimbursed for adult patients with FCS in line with the Health Canada indication.
What Are the Conditions for Reimbursement?
Tryngolza should only be reimbursed if patients are diagnosed with FCS based on genetic or clinical assessments, as detailed in Table 1, and if the cost of Tryngolza is reduced. Because FCS is a rare disease, initiation and management of therapy with Tryngolza should be managed by a specialist with expertise in treating FCS. The recommended period for initial reimbursement is 6 months, followed by annual renewals thereafter. Renewal is recommended to be based on an observation of clinical benefit, as demonstrated by a reduction in fasting triglyceride levels, and no signs of substantial disease worsening that would indicate poor or nonresponse to treatment (i.e., increased rate of acute pancreatitis as judged by the treating clinician).
Review Background
Disease background: FCS is a rare, serious, recessively inherited metabolic disorder in which the body’s metabolism does not break down fats correctly due to a deficiency in lipoprotein lipase function. Patients with FCS have severely elevated levels of triglycerides in their blood, causing a high risk for acute pancreatitis episodes, which can be painful and potentially life-threatening and can lead to long-term complications after repeated events. FCS is a rare disease with an estimated global prevalence of approximately 1 to 10 per million people, although it is more common in some regions of Quebec due to a genetic founder effect. Genetic testing is not comprehensive of all causative mutations for FCS and is not equitably accessible across Canada.
Indication and reimbursement request: Olezarsen (Tryngolza) has been approved by Health Canada for FCS in adults. The sponsor is seeking reimbursement for this patient population.
Drug under review: Olezarsen is an antisense oligonucleotide inhibitor of apolipoprotein CIII. It is available as a 0.8 mL (80 mg) autoinjector. The dosage recommended in the product monograph is 80 mg injected subcutaneously once monthly.
Treatment costs: At the submitted price of $41,000 per 0.8 mL autoinjector, the annual cost of olezarsen is expected to be $492,000 per patient, based on the Health Canada–recommended dosage.
Highlights of Input From Interested Parties
The patient group, the Canadian Organization for Rare Disorders, noted the following points regarding effects of the disease, unmet needs, and important outcomes:
Patients with FCS and their caregivers highlighted that severe dietary restrictions, life-threatening complications, acute pancreatitis episodes, and associated severe pain and hospitalizations contribute to a profound burden of illness on their quality of life. Some patients expressed feeling very isolated due to not being able to share meals with family, friends, or work colleagues. Patients also mentioned experiencing complications in their home and work lives because of disease-related flare-ups and highly restrictive lifestyle-based management.
Patients with FCS often experience delayed diagnoses or misdiagnoses due to the disease being rare and unknown among medical professionals, and because the disease can present with nonspecific symptoms such as recurrent abdominal pain, fatigue, malaise, and brain fog. Patients with late diagnoses described experiencing dismissal by medical professionals of their nonspecific symptoms (e.g., fatigue and stomach aches throughout their lives), ineffective treatments, and stigma from doctors due to being mistaken for a person with alcohol dependency and/or due to a lack of knowledge about this rare condition.
Patients with FCS have severely elevated fasting triglyceride levels that typically do not respond to conventional management strategies (e.g., lifestyle changes, diet, alcohol abstinence) or to pharmacologic therapies (e.g., statins and fibrates) because of the underlying mechanism of the disease. Because there are currently no available therapies for the treatment of FCS in Canada, many patients try off-label therapies with no supportive evidence for FCS that are known to be ineffective.
Patients with FCS and their caregivers highlighted that treatment goals include reduction of triglyceride levels with few side effects and prevention of future pancreatitis episodes. They also expressed a need for a therapy that has a minimally disruptive administration schedule and does not require travel for those living far from specialty centres. Patients would also like a therapy that allows them to relax dietary restrictions such that they could partake in social events without anxiety of severe medical consequences.
The clinician group (at the Lipid Clinic at Hamilton General Hospital in Ontario) and the clinical experts consulted by CDA-AMC noted the following points regarding unmet needs arising from the disease and the place in therapy for the drug under review:
FCS is a rare, serious, genetic disease that causes substantial morbidity and mortality and for which there are no approved therapies for management. Standard therapies for lowering triglyceride levels are known to be ineffective in FCS.
The primary treatment goal is to reduce fasting serum triglyceride levels, followed by the reduction in episodes of acute pancreatitis. Other secondary goals include the reduction of abdominal pain and other symptoms.
The participating public drug programs raised potential implementation issues related to considerations for initiation, discontinuation, and prescribing of therapy.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through with this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as 1 element contributing to a broader understanding of the condition and treatment under review.
Recommendation
With a vote of 14 in favour to 0 against, CDEC recommends that olezarsen be reimbursed for FCS only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Treatment with olezarsen as an adjunct to diet should be reimbursed when initiated in patients aged 18 years or older who are diagnosed with FCS. | Evidence from the Balance trial suggested that treatment with olezarsen resulted in a clinical benefit compared to placebo in adult patients with FCS. | Adherence to a low-fat diet: The clinical benefit of treatment with olezarsen was demonstrated in combination with a low-fat diet. According to input from the clinical experts, ongoing adherence to a strict low-fat diet is essential. |
2. Genetic testing must be conducted. 2.1. If genetic test results are positive, then diagnosis is confirmed and treatment with olezarsen can be initiated. 2.2. If after conducting genetic testing FCS is not confirmed, treatment with olezarsen can be initiated in patients with a clinical diagnosis of FCS based on a result of ≥ 45 on the NAFCS tool. 2.3. If both genetic test results and the NAFCS result are inconclusive or negative, treatment with olezarsen can be initiated in patients who meet all the following criteria: 2.3.1. persistent triglyceride levels ≥ 10 mmol/L despite treatment with prior triglyceride-lowering therapy 2.3.2. alcohol abstinence 2.3.3. adequate control of hemoglobin A1c levels 2.3.4. documented prior pancreatitis episode. | All patients in the Balance trial had genetically confirmed FCS. Due to the price of olezarsen and limited long-term evidence informing the safety and efficacy of treatment, genetic testing must be conducted to confirm the diagnosis. Genetic testing is not comprehensive of all possible causes of FCS. The NAFCS tool is a validated scale that may be used to inform a clinical diagnosis of FCS if needed. Though it is not commonly used in clinical practice, it has been validated to correlate with genetic diagnoses of FCS. If FCS is suspected but genetic test results and the NAFCS result are negative or inconclusive, the criteria suggested in reimbursement condition 2.3 are aligned with a clinical diagnosis based on clinical expert input. | Mitigating potential treatment delays: CDEC noted that initiation of treatment with olezarsen based on a clinical criteria diagnosis (reimbursement condition 2.2 or 2.3) may be considered when a delay in access to treatment is expected due to delays in obtaining the results of genetic testing. Of note, genetic testing should still be conducted before treatment initiation. Cost of genetic testing: Given the limited availability of genetic testing for FCS and the cost burden that implementation would place on public health care systems, CDEC recommends that the sponsor be required to cover the cost of these tests across Canada and to ensure its availability where needed. Prior therapy: Inadequate management of triglyceride levels with prior therapy is defined as triglyceride levels ≥ 10 mmol/L despite at least 6 months of a low-fat diet and prior treatment with standard lipid-lowering agents (e.g., statins or fibrates) for at least 1 week to 1 month. Hemoglobin A1c: Adequate control of hemoglobin A1c levels may vary between patients, but it generally can be considered a hemoglobin A1c measurement ≤ 8.5%. |
3. Duration of initial authorization is 6 months. | The primary outcome of the Balance trial was the percent change in fasting triglyceride levels from baseline at 6 months. Assessment at 6 months is consistent with clinical practice in Canada based on expert input. | Documentation at baseline: Fasting triglyceride levels and the annualized frequency of acute pancreatitis episodes should be documented at baseline before initiating treatment to inform the renewal criteria. |
Renewal | ||
4. Renewal after initial authorization and subsequent renewals should be assessed annually. | Annual assessments will help ensure the treatment is used for those benefiting from the therapy and would reduce the risk of unnecessary treatment. | — |
5. For renewal after initial and subsequent authorization, documentation of beneficial clinical effects is required when requesting continuation of reimbursement. Beneficial clinical effects are defined by all the following: 5.1. a reduction in triglyceride levels compared to baseline that is considered clinically meaningful according to the treating clinician 5.2. no substantial worsening of pancreatitis due to FCS according to the treating clinician. | The percent change in fasting triglyceride levels from baseline to month 12 was a secondary end point in the Balance trial. The percent change from baseline to month 12 in the olezarsen treatment group was an LS mean of –38.50% (95% CI, –58.19% to –18.82%). Based on clinical expert input, a reduction in triglyceride levels between 10% and 30% may be meaningful, but there is no defined threshold in patients with FCS. | Lifestyle and risk factor management: Adherence to a low-fat diet, alcohol abstinence, and management of other triglyceride-elevating conditions are crucial during treatment with olezarsen. Substantial worsening of pancreatitis: One of the most important goals of treatment for patients with FCS is to reduce the risk of acute pancreatitis. CDEC acknowledged that the frequency of acute pancreatitis events can be unpredictable and may vary between patients or over time. Therefore, substantial worsening of pancreatitis should be based on clinician judgment. |
Prescribing | ||
6. Olezarsen must be prescribed by specialists with qualifications and experience in the diagnosis and management of FCS (e.g., endocrinologists, cardiologists, lipidologists, medical biochemists, internal medicine specialists). | This is meant to ensure that olezarsen is prescribed for appropriate patients. FCS is a rare and serious condition requiring expertise in management. | Shared care models featuring virtual consultations and local monitoring may be appropriate approaches for patients with geographical challenges in accessing specialist facilities due to the scarcity of experts across Canada, especially outside Quebec. |
Pricing | ||
7. A reduction in price. | Using the CDA-AMC base-case analysis, the ICER for olezarsen plus SOC was $3,041,706 per QALY gained when compared with SOC alone in the indicated population. A band 4a price reduction would be required to achieve cost-effectiveness at a $50,000 per QALY threshold. A band 4a price reduction would be required to achieve cost-effectiveness at a $100,000 per QALY threshold. Exact price reductions at any given willingness-to-pay threshold can be found in the CDA-AMC Main Report and Supplemental Material documents. | — |
CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; CI = confidence interval; FCS = familial chylomicronemia syndrome; ICER = incremental cost-effectiveness ratio; LS = least squares; NAFCS = North American Familial Chylomicronemia Score; QALY = quality-adjusted life-year; SOC = standard of care.
aFor the statement regarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Clinical Value
Based on the totality of the clinical evidence, CDEC concluded that olezarsen demonstrates acceptable clinical value in patients with FCS.
Evidence from 1 phase III randomized controlled study (Balance, N = 66) demonstrated that treatment for 12 months with olezarsen 80 mg likely results in added clinical benefit for patients with FCS compared with placebo (both in combination with a low-fat diet) in fasting triglyceride levels and the rate of acute pancreatitis events. Between baseline and 12 months, the between-group difference in least squares mean change in fasting triglyceride levels was –59.39% (95% confidence interval, –90.66% to –28.12%), favouring olezarsen. In the olezarsen 80 mg group, 1 patient (4.5%) experienced 1 event of adjudicated acute pancreatitis, and in the placebo group, 7 patients (30.4%) experienced a total of 11 such events. No new safety signals were observed in the Balance study or in the open-label extension (OLE) study.
Patients and clinicians identified substantial unmet needs given that there are no approved therapies indicated for the treatment of FCS. The key unmet needs include a safe and tolerable therapy that can meaningfully reduce triglyceride levels and reduce the rate or prevent episodes of acute pancreatitis. CDEC concluded that olezarsen likely meets these needs, but the committee was unable to draw conclusions on HRQoL due to inconclusive results in the Balance study.
Additional information on the committee’s discussion about clinical value is provided in the Summary of Deliberation section.
Developing the Recommendation
The determination of acceptable clinical value was sufficient for CDEC to recommend reimbursement of olezarsen. As part of the deliberation on whether to recommend reimbursement, the committee also considered unmet clinical need, unmet nonclinical need, and health inequity. Information on this discussion is provided in the Unmet Clinical Need and the Distinct Social and Ethical Considerations domains in the Summary of Deliberation section.
Because CDEC recommended that olezarsen be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations, or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
CDEC considered all domains of value of the deliberative framework before developing its recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Appropriate comparators: There are no approved therapies for FCS. Placebo, in addition to a low-fat diet (≤ 20 g of fat per day), was an appropriate comparator for olezarsen as an adjunct to diet. Although many patients receive off-label therapies such as statins, omega-3s, and fibrates, these are not expected to be effective in lowering triglyceride levels or preventing pancreatitis in patients with FCS.
Efficacy versus placebo: Evidence from 1 phase III randomized controlled study (Balance, N = 66) demonstrated that treatment for 12 months with olezarsen 80 mg likely results in added clinical benefit for patients with FCS compared with placebo (both in combination with a low-fat diet) in fasting triglyceride levels and in the rate of acute pancreatitis events. Between baseline and 12 months, the between-group difference in least squares mean change in fasting triglyceride levels was –59.39% (95% CI, –90.66% to –28.12%), favouring olezarsen. In the group receiving olezarsen 80 mg, 1 patient (4.5%) experienced 1 event of adjudicated acute pancreatitis, and in the placebo group 7 patients (30.4%) experienced a total of 11 events. There was imprecision in the results for both outcomes (triglyceride levels and pancreatitis rate) resulting in moderate certainty in the conclusions. Uncertainty in the results for pancreatitis rate was also increased because of this being an uncommon event in a small population, and there were some between-group differences in baseline pancreatitis rates that could potentially raise the risk of bias. The HRQoL results of the Balance study did not report any meaningful difference versus placebo based on the FCS Symptoms and Impacts Scale.
Clinical importance of treatment effects: The committee concluded that the benefits of reducing triglyceride levels and reducing the rate of acute pancreatitis were likely clinically important in magnitude based on patient group input, clinician group input, and clinical expert input. There was uncertainty in both end points due to imprecision. For the outcome of acute pancreatitis, the magnitude of benefit is also uncertain because of the challenge of evaluating an uncommon event in a small patient population over a limited duration of time. The HRQoL results did not demonstrate a clinically important treatment effect.
Certainty of the evidence: The committee recognized that imprecision affected the certainty of the results. As FCS is a rare disease, the pivotal study and supportive studies each had small sample sizes. For all secondary end points in the pivotal study, there was an elevated risk of type I errors and the analyses were not controlled for multiplicity.
Tolerability: The committee discussed that AEs were less common in the olezarsen 80 mg group than the placebo group. It was also noted that patients treated with olezarsen 80 mg experienced fewer AEs and serious AEs than patients treated with placebo. No new safety signals were identified.
Clinical diagnoses: The committee heard that current clinical practice in the diagnosis of FCS is based on clinical gestalt and that specialists are required to diagnose FCS. The pivotal Balance study only included patients with genetically confirmed FCS. The Switch study was submitted to address the gap in the evidence regarding patients with clinical-only diagnoses, but the data are limited as only 4 of 24 patients had clinical-only diagnoses in the study. The clinical experts noted that based on their expert opinions and on prior trial experience with volanesorsen (which is not approved for use in Canada but has a similar mechanism of action as olezarsen), patients with or without genetic confirmation of FCS are not expected to differ in treatment response or prognosis. The committee deliberated on the initiation criteria for olezarsen given the expense associated with the drug and concluded that patients with a negative or inconclusive genetic test could qualify based on North American Familial Chylomicronemia Score (NAFCS) results. The NAFCS scale is a new but validated diagnostic scale for FCS that is currently not commonly used in clinical practice. Based on clinical expert input, the committee decided on a list of criteria that a patient with probable FCS could meet if both the genetic test and NAFCS results are inconclusive (refer to Table 1).
Long-term safety and efficacy: An ongoing, phase III, multicentre OLE of the Balance study was submitted as supportive evidence. All patients received olezarsen 80 mg during the OLE study and end points were evaluated for up to 12 months of treatment in the OLE study. Interim results did not reveal any additional safety concerns; however, the ability to draw conclusions from it was limited by few patients, interim data, and lack of a comparator group.
Renewal criteria: In consultation with the advising clinical expert, the committee discussed that renewal of reimbursement for olezarsen is appropriate in circumstances in which the triglyceride levels of the patient are meaningfully lower after receiving the therapy. The clinical expert estimated that clinicians may consider a reduction between 10% and 30% to be a minimal clinically important lowering of triglyceride levels; however, a specific threshold for adequate response is difficult to quantify in the absence of evidence. The committee also discussed that preventing or reducing the rate of acute pancreatitis events is a high priority, but that events may still occur during treatment with olezarsen for a variety of reasons. However, if there are signs of nonresponse to the therapy, including a lack of substantial lowering of triglyceride levels or an apparent worsening of the rate of pancreatitis, it would be appropriate to discontinue treatment.
Clinical value: Based on all the preceding considerations, the committee determined there was added clinical value associated with olezarsen as an adjunct to diet versus standard of care (SOC) (diet alone).
Unmet Clinical Need
Input on unmet clinical need: Patients with FCS and their caregivers identified a need for a safe and tolerable treatment that can effectively reduce the elevated serum triglyceride levels and acute pancreatitis risk associated with FCS. Clinician group input and clinical experts consulted by CDA-AMC for this review concurred that despite intensive lifestyle interventions and commonly used off-label pharmacotherapies (such as statins), substantial unmet needs persist. The clinician group input highlighted that there is a critical need for a targeted, well-tolerated, and effective treatment that can reduce chylomicron levels, prevent pancreatitis, improve daily symptoms, and reduce the overall burden on patients and caregivers.
Severity of the disease: The committee recognized the clinical expert input that FCS is a genetic, lifelong condition with which patients have severely elevated triglyceride levels and are at increased risk of recurring acute pancreatitis, which can be a serious, life-threatening event requiring hospitalization. The clinical experts highlighted that many patients have recurrent hospitalizations and that mortality associated with FCS is primarily related to multiorgan failure or other sequelae of pancreatitis. Despite adherence to a restrictive diet, patients may still experience recurrent pancreatitis and downstream complications of pancreatitis, which may include exocrine pancreatic insufficiency, type 3c diabetes, and chronic pancreatitis.
Availability of treatment options: There are no therapies indicated for the treatment of FCS in Canada. The clinical experts and clinician group input described that current management relies on an extremely restrictive diet of ≤ 20 g fat per day, but patients still experience symptoms, severely elevated triglyceride levels, and elevated risk of pancreatitis despite adherence to the diet. Off-label pharmacotherapies such as statins, fibrates, and omega-3 fatty acids are often used with little to no clinical benefit.
Significant unmet clinical need: Due to challenges with evidence generation associated with the rarity of FCS, the severity of the disease, and the lack of effective treatment options, CDEC considered there to be significant unmet need as described in the recommendation framework in the Procedures for Reimbursement Reviews.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: The committee acknowledged that the restrictive diet requiring ≤ 20 g dietary fat per day is difficult to adhere to and affects patients’ ability to participate in social events related to food, according to patient and clinician group inputs and the clinical experts consulted for this review. Patients also described facing stigma and a lack of understanding about the importance of this diet from family, friends, and work colleagues due to the rarity and lack of knowledge of FCS. The committee heard that patients frequently face stigma, delayed diagnoses, misdiagnoses (with more common conditions), and dismissal of nonspecific symptoms by medical professionals for the same reasons.
Significant unmet nonclinical need: The committee determined that there was a significant unmet nonclinical need but that olezarsen is not likely to address these needs because the drug is intended to be prescribed in conjunction with the low-fat diet and will not affect the knowledgeability of medical professionals or the general population about FCS.
Economic Considerations
Health effects of olezarsen versus relevant comparator: Olezarsen plus SOC is predicted to be associated with a gain of 1.15 life-years compared to SOC alone and may result in a gain of 1.42 quality-adjusted life-years (QALYs) compared to SOC. The survival benefit is predominantly driven by the number of acute pancreatitis events and their impact on mortality, which is uncertain.
Cost of olezarsen versus relevant comparators: Olezarsen plus SOC is predicted to be associated with higher costs to the health care system than SOC alone (incremental costs = $4,307,982), primarily driven by the drug acquisition cost of olezarsen.
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA-AMC base-case analysis estimated that the incremental cost-effectiveness ratio for olezarsen in adult patients with FCS was $3,041,706 per QALY gained when compared with SOC (Figure 1).
Figure 1: Estimate of the ICER Used by CDEC to Inform the Price Condition
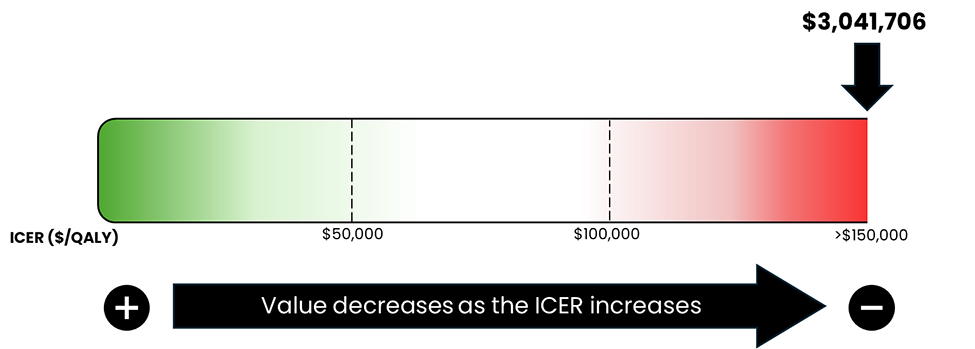
CDEC = Canadian Drug Expert Committee; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Certainty of the evidence: The estimated cost-effectiveness of olezarsen plus SOC compared to SOC is uncertain due to a lack of long-term data and uncertainty in the impact of treatment on the frequency and mortality risk of acute pancreatitis, which is a key driver of the survival benefit. If the survival benefit is not realized, the incremental cost-effectiveness ratio for olezarsen plus SOC compared to SOC alone will be higher than predicted in the CDA-AMC analysis.
Other considerations: The sponsor submitted an additional cost-effectiveness analysis adopting a societal perspective. In this analysis, the sponsor’s approach to estimating productivity and caregiver HRQoL outcomes was uncertain due to a lack of relevant data. As a result of the lack of evidence related to the impact of treatment for patients with FCS on these outcomes, CDA-AMC was unable to present an analysis from the societal perspective.
Impacts on Health Systems
Anticipated budget impact: CDA-AMC estimated that by year 3 of reimbursement, 48 patients would be eligible for olezarsen plus SOC; of them, 38 patients would be expected to receive olezarsen plus SOC. The estimated incremental budget impact of reimbursing olezarsen plus SOC is predicted to be approximately $50 million over the first 3 years. Because SOC costs are assumed to be $0, the entire incremental budget impact reflects expenditures on olezarsen (i.e., $50 million). The actual budget impact will depend on the market uptake of olezarsen.
Genetic testing and diagnoses: The committee discussed that FCS is a genetic disease with some known causative mutations in a suite of genes related to lipid metabolism. Based on clinical expert input, it is anticipated that approximately 20% of patients with FCS could have inconclusive genetic testing results due to causative mutations not captured by gene panels. The committee noted that genetic testing is not consistently available across jurisdictions in Canada and is primarily available through out-of-country testing. Currently, genetic testing may be publicly funded on a case-by-case basis or through out-of-pocket expenses, creating potential equity concerns. To ensure olezarsen is only provided to patients with confirmed FCS diagnoses, the committee discussed the need to ensure genetic testing is broadly available, and in cases with inconclusive test results, a clinical assessment is used.
Organizational implications: The committee discussed that if NAFCS results are required or strongly recommended for the reimbursement of olezarsen, clinicians managing patients with FCS may need to receive training on applying this scale.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project web page):
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor, as well as relevant ethical issues related to olezarsen (refer to the Main Report and Supplemental Material document)
the sponsor’s comments on the draft report and the CDA-AMC responses
patients' perspectives gathered by 1 patient group, the Canadian Organization for Rare Disorders (refer to the Patient and Clinician Group Input document)
input from a person with lived experience who delivered a brief presentation and answered questions from the committee (refer to the Person With Lived Experience section earlier in this document)
input from 1 clinician group, at the Lipid Clinic at Hamilton General Hospital (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 2 clinical experts and 2 panellists with expertise in the management of FCS consulted by CDA-AMC.
Special thanks: CDA-AMC extends special thanks to the individual who presented directly to CDEC and to the patient organizations supporting the community of those living with FCS, including the Canadian Organization for Rare Disorders, which includes Jida El Hajjar and Marie-Christine Boisclair.
General note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys to ensure lived experience perspectives are included and considered in Reimbursement Reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journeys with CDEC.
CDEC Information
Members of the Committee
Dr. Peter Jamieson (Chair), Dr. Kerry Mansell (Vice-Chair), Sally Bean, Daryl Bell, Dan Dunsky, Dr. Ran Goldman, Dr. Trudy Huyghebaert, Dr. Dennis Ko, Dr. Christine Leong, Dr. Alicia McCallum, Dr. Srinivas Murthy, Dr. Nicholas Myers, Dr. Krishnan Ramanathan, Dr. Marco Solmi, Carla Velastegui, Dr. Edward Xie, and Dr. Peter Zed.
Meeting date: December 17, 2025
Regrets: Two expert committee members did not attend.
Conflicts of interest: None
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.