Drugs, Health Technologies, Health Systems
Reimbursement Review
Lemborexant (Dayvigo)
Sponsor: Eisai Limited
Therapeutic area: Insomnia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AHI
Apnea-Hypopnea Index
ASO
Alzheimer Society of Ontario
CBT-I
cognitive behavioural therapy for insomnia
CDA-AMC
Canada’s Drug Agency
CDEC
Canadian Drug Expert Committee
CI
confidence interval
CID
chronic insomnia disorder
CrI
credible interval
DORA
dual orexin receptor antagonist
DSM
Diagnostic and Statistical Manual of Mental Disorders
DSM-5
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
DSM-5-TR
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision
FSS
Fatigue Severity Scale
GI Society
Gastrointestinal Society
ICD-10
International Classification of Diseases, 10th Revision
ICSD-3
International Classification of Sleep Disorders, Third Edition
ITC
indirect treatment comparison
ISI
Insomnia Severity Index
LEM5
lemborexant 5 mg
LEM10
lemborexant 10 mg
LPS
latency to persistent sleep
LSM
least squares mean
MDSC
Mood Disorders Society of Canada
MID
minimal important difference
MVA
motor vehicle accident
NMA
network meta-analysis
OR
odds ratio
PBO
placebo
PGI
Patient Global Impression
RCT
randomized controlled trial
REM
rapid eye movement
RR
risk ratio
SAE
serious adverse event
SD
standard deviation
sSOL
subjective sleep onset latency
sWASO
subjective wake after sleep onset
TEAE
treatment-emergent adverse event
WASO
wake after sleep onset
WASO2H
wake after sleep onset in the second half of the night
Executive Summary
An overview of the submission details for lemborexant is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug (product) | Lemborexant (Dayvigo), 5 mg film-coated tablet and 10 mg film-coated tablet, oral |
Sponsor | Eisai Limited |
Health Canada indication | The treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance. |
Reimbursement request | For the treatment of insomnia in adults diagnosed according to the most recent version of the Diagnostic and Statistical Manual of Mental Disorders (DSM) referring to chronic insomnia disorder. |
Submission type | Resubmission |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 4, 2020 |
Recommended dosage | The recommended dose of lemborexant is 5 mg, taken no more than once per night and within a few minutes before going to bed, with ≥ 7 hours remaining before the planned time of awakening. The dose may be increased to the maximum recommended dose of 10 mg based on clinical response and tolerability. |
DSM = Diagnostic and Statistical Manual of Mental Disorders; NOC = Notice of Compliance.
Source: Product monograph for lemborexant.1
Introduction
Submission History and Rationale for Resubmission
In 2022, the sponsor filed the initial submission of lemborexant (project website), a dual orexin receptor antagonist (DORA), for consideration by the Canadian Drug Expert Committee (CDEC). The reimbursement request was the same as the Health Canada indication, which was “for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.” In 2023, CDEC reviewed the initial submission and recommended that lemborexant not be reimbursed by public drug plans. In the current Reimbursement Review, the sponsor filed a resubmission for lemborexant (project website) with a new reimbursement request that narrowed the target population from patients with insomnia to patients with chronic insomnia disorder (CID), diagnosed according to the most recent version of the Diagnostic and Statistical Manual of Mental Disorders (DSM). The sponsor also submitted new evidence to address gaps identified by CDEC.
The rationale of the 2023 CDEC recommendation against the reimbursement of lemborexant for the treatment of insomnia characterized by difficulties with sleep onset and/or sleep maintenance included the following points:
It was unclear whether lemborexant would address the needs identified as important to patients, including uninterrupted and restorative sleep, more effective treatment options, fewer side effects, and long-term treatment effectiveness.
Although 2 randomized, controlled, double-blind, phase III trials in adults with insomnia (the SUNRISE 1 trial [N = 1,006] and the SUNRISE 2 trial [N = 971]) showed that treatment with lemborexant resulted in statistically significant improvements in measures of sleep onset, sleep maintenance, and sleep efficiency compared with placebo (PBO), it remained uncertain whether the magnitude of the treatment effect was clinically meaningful for multiple outcomes due to variability in results, missing data, lack of control for multiplicity, lack of an estimated minimal important difference (MID), or the MID not being met.
It is unknown whether lemborexant had a beneficial effect on outcomes that were important to patients, including stress, anxiety, productivity, or relationships, because this was not assessed in the SUNRISE 1 or SUNRISE 2 trials.
Further evidence was needed to address key concerns associated with pharmacological treatment of insomnia, including somnolence, risk of falls, and dependence (i.e., rebound insomnia). In the pivotal SUNRISE 1 and SUNRISE 2 trials, rates of somnolence were higher among patients receiving lemborexant than among patients receiving comparators. The number of events for falls were small in the SUNRISE 1 and SUNRISE 2 trials. The rates of rebound insomnia and withdrawal symptoms or dependence were lower for lemborexant than for zolpidem in the SUNRISE 1 trial; however, the results had limitations such as missing data, and the differences between groups were not statistically tested.
Extended-release zolpidem was the active comparator used in the SUNRISE 1 trial, and PBO served as the control in the SUNRISE 2 trial. CDEC determined that extended-release zolpidem was not a comparator relevant to clinical practice in Canada because it was not used in Canada at the time of CDEC consideration (i.e., January 2023). There was no direct evidence comparing the efficacy and safety of lemborexant relative to other drugs commonly used to treat insomnia in clinical practice in Canada. The indirect evidence comparing lemborexant to other treatments was uncertain due to numerous limitations, precluding definitive conclusions. Based on the direct and indirect evidence available at the time, CDEC was not able to draw conclusions on how the efficacy or safety profile of lemborexant would compare to other drugs.
CDEC noted that the pivotal SUNRISE 1 and SUNRISE 2 trials included an enriched study population, in which the treatment effects observed might be larger than what would be observed in clinical practice. In addition, the generalizability of the results from the trials to patients excluded from the studies was considered uncertain.
CDEC noted that duration of treatment with lemborexant was 30 days in the SUNRISE 1 trial and up to 12 months in the SUNRISE 2 trial; therefore, data on long-term effectiveness and safety are limited to this time frame. Furthermore, CDEC noted that the safety demonstrated in the clinical trials may not always be generalizable to real-world practice.
To address some of the limitations and gaps in the evidence identified by CDEC, in the present resubmission the sponsor submitted additional data obtained from real-world settings. The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of lemborexant (Dayvigo), 5 mg film-coated tablet and 10 mg film-coated tablet, taken orally, in the treatment of patients with insomnia.
Disease Background and Standard of Therapy
CID, referred to as insomnia disorder in the DSM Fifth Edition (DSM-5), is defined as difficulties with sleep onset and/or sleep maintenance, with symptoms lasting for 3 nights or more per week for at least 3 months and being present despite adequate conditions for sleep.2 According to the clinical experts consulted by the review team, the DSM-5 Text Revision (DSM-5-TR) is the most recent version of the DSM. The clinical experts noted that in clinical practice, other classification systems, such as the International Classification of Sleep Disorders, Third Edition (ICSD-3) and the International Classification of Diseases, 10th Revision (ICD-10), are also used to diagnose CID. The clinical experts also noted that despite the terms used to describe CID being different among these classification systems (e.g., the DSM-5-TR used the term “insomnia disorder,” while ICSD-3 used “chronic insomnia disorder”), there were no major concerns regarding the difference, because these classification systems capture the key feature of CID, which is the duration of symptoms lasting at least 3 months. Several factors have been shown to be associated with an increased risk of insomnia, including older age, female sex, family history of insomnia, previous episode of insomnia, tendency to wake up more easily from sleep, tendency for increased sleep disturbances when faced with stressful events, as well as psychiatric and psychological factors (e.g., anxiety, depression, increased daytime stress reactivity).3 Many comorbidities, such as depression, anxiety, hypertension, chronic pain, pulmonary disease, obstructive sleep apnea, and substance use disorders, can coexist with CID and be worsened by CID.4 CID has a negative impact on patients’ health, stress levels, daytime functioning, productivity at work, academic performance, social interactions and romantic relationships, safety, and quality of life.4-6 The global prevalence of insomnia varies, ranging from 79% in Brazil to 23.2% in Western Europe.4 In Canada, the estimated prevalence of chronic insomnia based on the DSM-5 diagnostic criteria was 16.3% (95% confidence interval [CI], 15.1% to 17.6%), obtained via phone interviews conducted from April to October 2023 with 4,037 adults.7
The clinical experts consulted by the Canada’s Drug Agency (CDA-AMC) review team noted that the goals of treatment for CID include improved sleep initiation and maintenance, improvement of terminal insomnia and overall leading to restorative sleep, improved quality of sleep, as well as improved subjective wakefulness or function during the day. Cognitive behavioural therapy for insomnia (CBT-I) is considered the first-line treatment for chronic insomnia by expert consensus in Canada (i.e., the 2024 consensus for the management of CID in Canada),8 international clinical practice guidelines (e.g., the European Sleep Research Society 2023 update),9 and the clinical experts consulted by the review team. However, people do not always undergo CBT-I, either because it is not readily available or because there are barriers to accessing it (e.g., cost, lack of sleep behavioural specialists).10-13 CBT-I alone may also not be successful in some people. Thus, pharmacological therapy may be considered as an alternative. According to the clinical experts consulted by the review team, CBT-I and pharmacotherapy can be used concurrently or sequentially. There are currently no approved or recommended pharmacological treatments indicated for CID available through public drug plans in Canada. According to the clinical experts consulted by the review team, some of the currently used pharmacotherapeutic options in Canada include trazodone (an atypical antidepressant, commonly used off label), Z-drugs (e.g., zopiclone), antipsychotics (used off label), and benzodiazepines (either indicated for short-term insomnia or used off label). The 2024 consensus for the management of chronic insomnia in Canada pointed out that DORAs might have benefits that outweigh the risks of long-term use;8 however, no DORAs are publicly reimbursed for CID in Canada at the time of this review.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the CDA-AMC call for input and from the clinical expert(s) consulted for this review.
Patient Input
Input for this review was submitted by 4 patient groups: Migraine Canada, the Alzheimer Society of Ontario (ASO), the Mood Disorders Society of Canada (MDSC), and the Gastrointestinal Society (GI Society). Migraine Canada gathered information through 3 surveys for adults in Canada with migraine and sleep challenges or insomnia: a 2021 quality of life survey (N = 1,165), a 2022 national online survey for those with experience taking lemborexant (N = 220), and a 2024 national survey of patients who live with migraine and experience sleep issues or insomnia (N = 177). ASO gathered information through a review of published literature as well as semistructured interviews with patients with insomnia and clinicians with experience in this field. MDSC gathered information through a 2021 survey for individuals in Canada with sleep and mental health challenges (N = 1,200), a 2024 survey of patients with migraine and insomnia prepared by Migraine Canada (N = 142), and interviews with patients with insomnia (N = 8) and clinicians with experience in this field (N = 2). The GI Society gathered information through focused discussions with health care providers and researchers and 1 interview with a patient currently taking lemborexant.
Patient groups emphasized that chronic insomnia is a debilitating condition, arising from a wide range of factors, that impacts nearly all aspects of life and results in substantial societal cost. Patient groups highlighted that sleep deprivation compromises physical, mental, and emotional health; impairs daily functioning and productivity; and strains personal relationships. According to patient groups, insomnia is often associated with feelings of hopelessness, emotional instability, and chronic fatigue, diminishing patients’ ability to engage in work, relationships, and self-care.
Regarding CBT-1, patient groups reported limited access, lack of awareness or referrals, and variable effectiveness. Pharmacologic options often include benzodiazepines, nonbenzodiazepine hypnotics, barbiturates, and off-label use of antidepressants and antipsychotics. In the Migraine Canada survey, commonly used medications included zopiclone (27% of patients who responded to the survey), trazodone (27%), gabapentin (24%), and benzodiazepines (17%). However, adverse effects such as grogginess, withdrawal symptoms, weight gain, and mood disturbances associated with the use of these medications were frequently reported. Additionally, the potential for dependency with currently available treatments was reported by the patient groups as highly concerning for patients and physicians.
Generally, patients who had experience with lemborexant noted improved daily alertness, work performance, and relationship stability, with minimal grogginess or concerns about dependency. The most common adverse effect reported by these patients was vivid dreams or nightmares, which were described by some as milder than with other medications.
Patients strongly value nonaddictive, well-tolerated treatments that support both sleep initiation and maintenance, without residual sedation, to improve daytime functioning and quality of life. For patients with migraines, reducing the frequency and severity of attacks and improving sleep are key treatment goals.
In general, the patient group input submitted for the resubmission of lemborexant is aligned with the patient group input for the initial submission of lemborexant, despite the different areas of focus and interest. For the initial submission, CDA-AMC received input from MDSC, Migraine Canada, and Menopause Chicks. Patient group input from the initial submission highlighted that patients need treatment to address several important outcomes, including uninterrupted and restorative sleep, greater access to treatment, more effective treatment options, long-term treatment effectiveness, fewer side effects, less stress and anxiety, improved productivity, and improved relationships with family members and colleagues.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts consulted by the CDA-AMC review team noted that the goals of treatment are improved sleep initiation and maintenance, improvement of terminal insomnia and overall leading to restorative sleep, improved quality of sleep, and improved subjective wakefulness or function during the day. The clinical experts noted that the major unmet need is for effective pharmacological treatments with minimal side effects, including long-term side effects (particularly development of tolerance), and with low potential for addiction.
According to the clinical experts consulted by the CDA-AMC review team, the mechanism of action of DORAs (i.e., counteracting inappropriate wakefulness at night) is considered fundamentally different from any other pharmacologic drug on the market for the treatment of insomnia or CID. The clinical experts noted that DORAs will likely shift the treatment paradigm and become a first-line drug for the treatment of CID in the absence of other comorbidities and in patients with comorbid insomnia and sleep apnea, given its lack of effect on breathing patterns. The experts noted that DORAs may take up to 8 weeks to be fully effective. The experts highlighted that, based on their mechanism of action, DORAs such as lemborexant have the potential to address the root cause of CID, unlike other drugs used for insomnia.
The clinical experts consulted by the CDA-AMC review team noted that, in general, most people with insomnia may be candidates for treatment with lemborexant except for those who are younger than 18 years and those who are pregnant or nursing or have severe hepatic impairment, narcolepsy, or idiopathic hypersomnia. According to the clinical experts, people who might be more eligible for treatment with lemborexant include those with insomnia and a history of anxiety or trauma (frequently troubled by inappropriate wakefulness at night due to hyperarousal), older adults with insomnia disorder, and people with a history of addiction issues and insomnia disorder. The clinical experts noted that people who would not be eligible for treatment with lemborexant include those with narcolepsy or intolerance to the drug. The clinical experts noted that diagnosis of CID is primarily clinical. A polysomnography study can be done in certain cases (e.g., clinical suspicion of comorbid obstructive sleep apnea or another sleep disorder), and brief questionnaires can be used (e.g., Insomnia Severity Index [ISI], Sleep Condition Indicator), although they are not used routinely in clinical care.
According to the clinical experts consulted by the CDA-AMC review team, to assess their response to treatment, patients are asked generally if their symptoms have improved (e.g., whether they are sleeping better and/or longer and are feeling refreshed) and if they feel better about their daytime functioning. The clinical experts noted that objective tests or sleep diaries are not generally used, and beyond patients’ subjective descriptions, the following outcomes can be used to determine an adequate treatment response: sleep latency less than 30 minutes, sleep efficiency greater than 90%, improved functional outcome in the day (e.g., less groggy, more energy), improved mood or anxiety, improved performance at work or school, decreased irritability or emotionality, improvement in other symptoms (e.g., pain, overall improvement in subjective well-being, improved continuity of sleep at night, less wake after sleep onset [WASO]). The clinical experts noted that treatment response is most frequently assessed 1 to 3 months after treatment initiation but that there is a wide variability in the frequency of assessment.
According to the clinical experts consulted by the review team, lemborexant should be discontinued in cases of allergy to lemborexant, lack of treatment response (may need to use for ≥ 3 months to adequately assess the treatment effects on total sleep time and sleep efficiency), or side effects that are intolerable or unacceptable for patients (e.g., rapid eye movement [REM] intrusion phenomena, daytime sedation, nocturnal parasomnia behaviours).
The clinical experts consulted by the review team noted that clinicians in several fields (e.g., family physicians, psychiatrists, internal medicine specialists, neurologists) may use lemborexant to treat patients. According to the clinical experts, sleep specialists are usually not required to diagnose, treat, or monitor patients who might receive lemborexant unless a comorbid sleep condition (e.g., comorbid insomnia and sleep apnea) is suspected.
The input from the clinical experts on the resubmission for lemborexant is overall aligned with the input from the clinical experts for the initial submission of lemborexant.
Clinician Group Input
Input for this review was submitted by 8 clinician groups: addiction medicine specialists (8 health care providers), the Cardiometabolic Patient Clinician Group (12 health care providers), the Depression and Anxiety Clinician Group (5 health care providers), the Primary Care Clinician Group (24 health care providers), the Alberta Psychiatrists (11 health care providers), the Chronic Insomnia Clinician Group (17 health care providers), the Aging Patients Clinician Group (13 health care providers), and the Women’s Health Clinician Group (4 health care providers). These groups represent a broad range of health care providers across Canada, including psychiatrists, family physicians, internists, and specialists in addiction, mental health, women’s health, and geriatric care. Information included in the input was informed by clinical experience and gathered through advisory board meetings, focused discussions, and email correspondence.
The clinician groups highlighted the current treatment paradigm for chronic insomnia in Canada, which mainly includes nonpharmacologic therapies (e.g., CBT-I), pharmacologic treatments (e.g., benzodiazepines, Z-drugs, DORAs, antidepressants, atypical antipsychotics), and other nonprescriptive or over-the-counter treatments (e.g., melatonin, alcohol, cannabis, antihistamines, natural health products). According to the clinician groups, the currently available pharmacotherapies primarily promote sedation and alleviate the symptoms of chronic insomnia without addressing the underlying disease mechanism and are associated with notable side effects, such as next-day impairment, memory and motor issues, weight gain, dependence, and cardiac arrhythmias.
In alignment with the clinical experts consulted by the review team, the clinician groups agreed that the treatment goals for chronic insomnia should include improving sleep quality and continuity, enhancing daytime functioning, and minimizing adverse and sedative effects, and the groups supported the use of lemborexant as a first-line pharmacologic treatment for chronic insomnia. The clinician groups noted that, if reimbursed, lemborexant would lead to a shift in the current treatment paradigm.
The clinician groups noted that most patients aged 18 years or older with insomnia would be candidates for treatment with lemborexant. The Chronic Insomnia Clinician Group and the Primary Care Clinician Group noted that patients aged younger than 18 years or older adolescents may also be eligible to receive lemborexant. The Primary Care Clinician Group also noted that patients with insomnia who are pregnant may receive lemborexant, whereas the clinical experts consulted by the review team considered these patients ineligible. According to the input from the clinician groups, less eligible candidates for treatment with lemborexant included those with narcolepsy or those who respond well to the short-term use of existing therapies. Lemborexant may also be less effective in individuals with low treatment adherence or whose insomnia has been refractory to many previous treatments, because the clinician groups noted that there was evidence of possible reduced efficacy in these patients.
The clinician groups emphasized that patient-reported outcomes are key to evaluating treatment response, including perceived sleep quality (e.g., restful sleep, reduced nighttime awakenings), next-day functioning (e.g., alertness, reduced brain fog), and overall quality of life. Some clinician groups noted that standardized tools like the ISI or the Epworth Sleepiness Scale might be used to evaluate changes in sleep to determine treatment response and that objective markers, such as reduced time to sleep onset, fewer awakenings, improved sleep consolidation, and reduced need to nap, were useful in evaluating response.
The clinician groups noted that, in general, discontinuation of lemborexant should be based on joint patient-physician decisions, weighing the benefit with the potential risks. Discontinuation of lemborexant may be considered in cases of treatment inefficacy, patient preference, unacceptable adverse effects, or initiation of a sedating medication for another condition (e.g., antidepressant to treat depression). While lemborexant is expected to produce rapid sleep benefits, the clinician groups noted that it may take 2 to 4 weeks for lemborexant to show full effects, a shorter estimated time than that provided by the clinical experts consulted by the CDA-AMC review team (i.e., 4 to 8 weeks). The clinician groups noted that ongoing consistent use of lemborexant is required until patients experience several weeks to months of sustained remission to reduce the risk of recurrence.
The clinician groups noted that lemborexant could be administered in inpatient and outpatient settings, including emergency departments, long-term care facilities, clinics, hospitals, and patients’ homes. The clinician groups noted that lemborexant does not require a specialized setting or specialist to initiate treatment and monitor response because it is easy and safe to prescribe, with no titration needed and minimal risk of adverse effects, overdose, or dependency. The groups noted that family physicians and specialists could prescribe and monitor lemborexant treatment and that, in some jurisdictions, pharmacists would also be authorized to prescribe lemborexant to patients.
Clinician groups with first-hand experience prescribing lemborexant reported that it has significantly improved the treatment of chronic insomnia, allowing for earlier, more effective intervention, especially in patients with complex medical and psychiatric comorbidities. However, the clinician groups noted that cost remains a major barrier for patients using public drug plans, who often struggle to afford lemborexant without sacrificing other essentials or relying on family support.
All clinician groups expressed a favourable position on lemborexant. In addition, the Chronic Insomnia Clinician Group provided further input on the 2023 CDEC recommendation against the reimbursement of lemborexant for the treatment of insomnia characterized by difficulties with sleep onset and/or sleep maintenance, which has been summarized in the main body of the Clinical Review report.
The input from the clinician groups for the resubmission of lemborexant is overall aligned with the input from the clinician groups for the initial submission of lemborexant.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process. The following items were identified as key factors that could potentially impact the implementation of a recommendation of lemborexant:
relevant comparators
considerations for initiation of therapy
considerations for continuation or renewal of therapy
considerations for discontinuation of therapy
generalizability
systemic and economic issues.
The clinical experts consulted by the CDA-AMC review team provided input on the potential implementation issues raised by the drug programs; these issues and the clinical expert responses are presented in Table 3.
Evidence for the Resubmission
Two retrospective observational studies (Juday et al.14 and Hirata et al.15) from the real-world setting are included in this review and appraised by the review team.
Juday et al. Study
In the Juday et al.14 study, eligible patients were adults who had been diagnosed with insomnia, had at least 1 pharmacy claim for an insomnia medication of interest, had visited a health care system in the United States during the 6 months after the index date, and had no evidence of falls, hip fractures, or traumatic brain injuries for 6 months before the index date. Patients were required to have been exposed to 1 of the following insomnia medications: lemborexant, trazodone, zolpidem, or benzodiazepines (as a class). The primary outcome was the proportion of patients who experienced at least 1 fall during the 6-month follow-up period. After propensity score matching, there were 716 patients in each group, and the mean patient age was 54 years. About 62% and 38% of the patients were female and male, respectively. The most common comorbidities were anxiety disorders (35%), hypertension (34%), and mood disorders (24%).
Results
Risk of Falls in Patients Aged 18 Years and Older
In the 6-month follow-up period, 7.82% of patients in the lemborexant group, 9.92% in the zolpidem group, 9.22% in the trazodone group, and 13.83% in the benzodiazepine group had at least 1 fall recorded. Absolute between-group differences with 95% CIs were not provided. Compared to lemborexant, the risk ratio (RR) of falls was 1.179 (95% CI, 0.838 to 1.657) for trazodone, 1.268 (95% CI, 0.907 to 1.772) for zolpidem, and 1.768 (95% CI, 1.295 to 2.413) for benzodiazepines as a class.
Risk of Falls in Patients Aged 65 Years and Older
In the 6-month follow-up period, 8.54% of patients in the lemborexant group, 10.98% in the zolpidem group, 10.37% in the trazodone group, and 16.46% in the benzodiazepine group had at least 1 fall recorded. Absolute between-group differences with 95% CIs were not provided. Compared to lemborexant, the RR of falls was 1.214 (95% CI, 0.619 to 2.381) for trazodone, 1.286 (95% CI, 0.662 to 2.498) for zolpidem, and 1.929 (95% CI, 1.050 to 3.543) for benzodiazepines as a class.
Critical Appraisal
The reporting of the study did not adhere fully to the Guidance for Reporting Real-World Evidence.16 Risk of bias due to exposure misclassification is possible because the classification relied on the first pharmacy claim in the identification period, which does not consider adherence, discontinuation, switching of treatments, or concomitant use of other insomnia drugs during follow-up. There is a risk of bias in the selection of patients into the study due to the inclusion of patients who may have been using insomnia medications for some time before entering the study. Falls that occur early in treatment that might have caused patients to stop taking the drug would be missed.17 The issue is compounded by excluding patients with prior falls (in the past 6 months), resulting in patients at higher risk of falls being underrepresented in the sample. The inclusion requirement of at least 1 encounter with a health care system during follow-up may have excluded multiple patients who experienced a fall but did not report it or were not hospitalized for it, patients who died, and an unknown proportion of patients without the outcome of falls, and these patients may differ systematically across groups. Risk of bias due to outcome misclassification is possible due to substantial variation among clinicians in the level of detail recorded in their medical notes. The outcome definition included ICD-10 codes for various injuries, which obscured the true relationship between treatment exposures and fall risk. Propensity score matching was used to balance potential confounding variables between the lemborexant cohort and comparator cohorts. Although the propensity score matching was successful, residual confounding likely remains because relevant confounders such as treatment history, duration, intensity (dose), and time since diagnosis were not considered. Missing data were not imputed; missing data on race and ethnicity were classified as “unknown.” The authors did not describe how other categories of missing data were handled, which precluded full meaningful adjustment for some variables. Limitations to generalizability included the focus on data from patients in 50 large US health care organizations, which underrepresents patients without insurance or smaller practices; the insomnia definition being broader than the CID DSM criteria (includes acute insomnia); the lack of description of the doses of lemborexant and comparator insomnia medications used; and recurrent falls not being captured, which does not allow for the full impact on fall risk to be assessed.
Hirata et al. Study
In the Hirata et al.15 study, eligible patients were those aged 20 years or older admitted to 1 of 8 hospitals in Japan during the study period. The patients had been exposed to 1 of the following hypnotic medication groups at the time of admission: benzodiazepines, Z-drugs, suvorexant, lemborexant, ramelteon, or other hypnotics. The outcome of interest was the occurrence of in-hospital falls. Of the 150,278 patients, 390 (0.3%) were exposed to lemborexant. In the full population, the median age was 70 years (range, 58 years to 79 years), and 46.9% and 53.1% of the patients were female and male, respectively. The patients were classified into the fall group (n = 3,458) and the nonfall group (n = 146,820).
Results
Odds of In-Hospital Falls
Between patients who used the medication versus patients that did not use the medication, the odds ratio (OR) for falls was 1.188 (95% CI, 0.774 to 1.825) for lemborexant, 1.255 (95% CI, 1.118 to 1.409) for benzodiazepines, and 1.293 (95% CI, 1.118 to 1.496) for Z-drugs.
Critical Appraisal
The reporting of the study did not adhere fully to the Guidance for Reporting Real-World Evidence,16 and the aim of this pilot study was not to draw causal inferences. Instead, the study examined the association between hypnotic medication use and in-hospital falls. Medication exposure was ascertained using pharmacy records, but the time period during which exposure was ascertained and the actual time period of exposure before admission was not described in the study. Risk of bias due to misclassification of exposed or unexposed status is possible because the status was assigned without consideration of adherence, discontinuation, or switching of treatments occurring before hospitalization or during follow-up. There is a risk of bias in the selection of patients into the study because the limited reporting does not suggest that inclusion was limited to patients who recently started taking the relevant drugs. This means that patients may have been using insomnia medications for some time before entering the study. Falls that occurred early in treatment that might have caused patients to stop the drug would be missed, and the patients remaining on the treatments are likely to be those at lower risk of falls.17 Although there is a lack of clarity in the publication, it appears that exposure status was collected up to the day after admission. The time before the index date should have been classified as unexposed, but it is unclear whether this occurred. Some risk of immortal time bias (i.e., a follow-up interval in which the outcome could not occur because of the exposure definition) is possible,18 but the risk could be small because the time before the index date represents a single day of potentially misclassified exposure time. The potential for bias due to outcome misclassification could not be fully ascertained due to lack of reporting on the fall outcome description and its validation. A multivariable logistic regression model was used to adjust for several potentially confounding variables; empirical evaluation of the model performance (balance of confounders) was not possible.19 Residual confounding is likely to remain given that some relevant confounding variables were not considered, such as the presence of insomnia, insomnia treatment history, treatment duration and intensity (dose), and length of hospital stay (follow-up). Missing data were not imputed, which precluded full meaningful adjustment for some variables. Limitations to generalizability included the focus on inpatients, who were not required to be affected by insomnia; the setting being predominantly rural hospitals in Japan; the lack of description of the dose of lemborexant used; and the lack of direct comparative estimates versus other relevant treatments.
Conclusions
In the resubmission for lemborexant, CDA-AMC reviewed 2 retrospective cohort studies (Juday et al. [2022]14 and Hirata et al. [2024]15), which investigated the risk of falls associated with lemborexant in real-world outpatient and in-hospital settings, respectively. The results from the Juday et al. (2022) study suggested that the risk of falls over a 6-month follow-up period was lower with lemborexant than with benzodiazepines as a class both among adults with insomnia aged 18 years and older and in the subgroup of patients aged 65 years and older. Point estimates for comparisons between lemborexant and trazodone and between lemborexant and zolpidem were also suggestive of a lower risk of falls with lemborexant, but these estimates were inconclusive due to imprecision (i.e., the CIs crossed the null). Direct comparisons with other relevant treatments were not provided. The CDA-AMC review team acknowledges the value of the evidence from the observational studies, which provided insights into the risk of falls associated with lemborexant in real-world settings. However, this evidence was subject to uncertainty due to a number of internal and external validity concerns. No new evidence on the comparative efficacy or other potential harms of lemborexant was included in this review. Therefore, most gaps identified by CDEC in the initial review remain to be addressed. The new reimbursement request aligns with the inclusion criteria of the SUNRISE trials. Consequently, the previously submitted evidence was not reappraised by the review team. There remains a lack of clarity about whether lemborexant provides a preferable balance of benefits and harms compared to other treatments used for chronic insomnia.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of lemborexant (Dayvigo), 5 mg film-coated tablet and 10 mg film-coated tablet, taken orally, in the treatment of patients with insomnia.
Submission History
In 2022, the sponsor filed the initial submission of lemborexant (project website), a DORA, for consideration by CDEC. The reimbursement request was the same as the Health Canada indication, which was “for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.” In 2023, CDEC reviewed the initial submission and recommended that lemborexant not be reimbursed by public drug plans for the reimbursement request.
In the present resubmission, the sponsor changed its reimbursement request for lemborexant (project website) to the following: for the treatment of insomnia in adults diagnosed according to the most recent version of the DSM referring to CID.
Basis of Resubmission
The rationale of the 2023 CDEC recommendation against the reimbursement of lemborexant for the treatment of insomnia characterized by difficulties with sleep onset and/or sleep maintenance was as follows:
It was unclear whether lemborexant would address the needs identified as important to patients, including uninterrupted and restorative sleep, more effective treatment options, fewer side effects, and long-term treatment effectiveness.
Although 2 randomized, controlled, double-blind, phase III trials (SUNRISE 1 [N = 1,006] and SUNRISE 2 [N = 971]) in adults with insomnia showed that treatment with lemborexant resulted in statistically significant improvements in measures of sleep onset, sleep maintenance, and sleep efficiency compared with PBO, it remained uncertain whether the magnitude of the treatment effect was clinically meaningful for multiple outcomes due to variability in the results, missing data, lack of control for multiplicity, lack of an estimated MID, or the MID not being met.
It is unknown whether lemborexant had a beneficial effect on the outcomes important to patients, including stress, anxiety, productivity, or relationships, because these outcomes were not assessed in the SUNRISE 1 and SUNRISE 2 trials.
Further evidence is needed to address key concerns associated with the pharmacological treatment of insomnia, including somnolence, risk of falls, and dependence (i.e., rebound insomnia). In the pivotal SUNRISE 1 and SUNRISE 2 trials, the rates of somnolence were higher among patients receiving lemborexant than among patients receiving comparators. The number of events for falls was small in the SUNRISE 1 and SUNRISE 2 trials. The rates of rebound insomnia and withdrawal symptoms or dependence were lower for lemborexant than for zolpidem in the SUNRISE 1 trial; however, the results had limitations such as missing data, and the differences between groups were not statistically tested.
Extended-release zolpidem was the active comparator used in the SUNRISE 1 trial, and PBO served as the control in the SUNRISE 2 trial. CDEC determined that extended-release zolpidem was not a comparator relevant to clinical practice in Canada because it was not used in Canada at the time of CDEC consideration (January 2023). There was no direct evidence comparing the efficacy and safety of lemborexant relative to other drugs commonly used to treat insomnia in clinical practice in Canada. The indirect evidence comparing lemborexant to other treatments was uncertain due to numerous limitations, precluding definitive conclusions. Based on the direct and indirect evidence available at the time, CDEC was not able to draw conclusions on how the efficacy or safety profile of lemborexant would compare to other drugs.
CDEC noted that the pivotal SUNRISE 1 and SUNRISE 2 trials included an enriched study population, in which the treatment effects observed might be larger than would be observed in clinical practice. In addition, the generalizability of the results from the trials to patients excluded from the studies was considered uncertain.
CDEC noted that the duration of treatment with lemborexant was 30 days in the SUNRISE 1 trial and up to 12 months in the SUNRISE 2 trial. Therefore, data on the long-term effectiveness and safety of lemborexant are limited to this time frame. Furthermore, CDEC noted that the safety demonstrated in the clinical trials may not always be generalizable to real-world practice.
In the present resubmission, the sponsor submitted additional evidence on lemborexant that was developed in real-world settings. The review team screened this evidence and retained for further synthesis and appraisal any comparative studies that could potentially address the gaps in the evidence identified by CDEC.
The sponsor also submitted a new reimbursement request for the resubmission, which narrowed the target population from patients with insomnia to patients with CID diagnosed according to the most recent version of the DSM. This target population is aligned with the inclusion criteria of the SUNRISE trials.
Disease Background
The contents within this section have been informed by materials submitted by the sponsor and by clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
Insomnia is a common patient-reported sleep-wake condition characterized by difficulties in initiating sleep at bedtime, frequent or prolonged awakenings, or early morning awakening with an inability to return to sleep, despite adequate opportunity for sleep.4,7 Insomnia can occur on a situational, recurrent, or chronic basis.20 CID, referred to as insomnia disorder in the DSM-5, is defined as difficulties with sleep onset and/or sleep maintenance, with symptoms lasting for 3 nights or more per week for at least 3 months and being present despite adequate conditions for sleep.2 According to the clinical experts consulted by the review team, the DSM-5-TR is the most recent version of the DSM. The clinical experts consulted by the review team noted that in clinical practice, other classification systems, such as the ICSD-3 and the ICD-10, are also used to diagnose CID. The clinical experts also noted that despite the terms used to describe CID differing among these classification systems (e.g., the DSM-5-TR used the term “insomnia disorder,” while ICSD-3 used “chronic insomnia disorder”), there were no major concerns about the difference because these classification systems capture the key feature of CID, which is that the duration of symptoms is at least 3 months.
Several factors have been shown to be associated with an increased risk of insomnia, including older age, female sex, family history of insomnia, previous episode of insomnia, tendency to wake up more easily from sleep, tendency for increased sleep disturbances when faced with stressful events, and psychiatric and psychological factors (e.g., anxiety, depression, increased daytime stress reactivity).3 Many comorbidities, such as depression, anxiety, hypertension, chronic pain, cardiovascular disorder, trauma, pulmonary disease, obstructive sleep apnea, and substance use disorders, can coexist with CID and be worsened by CID.4 CID has a negative impact on patients’ health, stress levels, daytime functioning, productivity at work, academic performance, social interactions and romantic relationships, safety, and quality of life.4-6
The global prevalence of insomnia varies, ranging from 79% in Brazil to 23.2% in Western Europe.4 In Canada, the estimated prevalence of chronic insomnia based on the DSM-5 diagnostic criteria was 16.3% (95% CI, 15.1% to 17.6%), obtained via phone interviews conducted from April to October 2023 among 4,037 adults.7
Standards of Therapy
The contents within this section have been informed by materials submitted by the sponsor and by clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
According to the clinical experts consulted by the review team, the goals of treatment for CID include improved sleep initiation and maintenance, improvement of terminal insomnia and overall leading to restorative sleep, improved quality of sleep, and improved subjective wakefulness or function during the day. CBT-I is considered the first-line treatment for chronic insomnia by expert consensus in Canada (i.e., the 2024 consensus for the management of CID in Canada),8 international clinical practice guidelines (e.g., the European Sleep Research Society 2023 update),9 and the clinical experts consulted by the CDA-AMC review team.
The best results for CBT-I are achieved through individual face-to-face sessions.21 However, patients do not always undergo CBT-I, either because it is not readily available or because there are barriers to accessing it (e.g., cost, lack of sleep behavioural specialists).10-13 CBT-I alone may also not be successful in some patients. Thus, pharmacological therapy may be considered as an alternative to CBT-I or alongside CBT-I. The goals of concurrent treatment with CBT-I and pharmacological therapy are to prevent dependence on medication and successful use of CBT-I to improve insomnia symptoms and seek resolution.22 The recommended approach is to initiate CBT-I before or concurrent with medication; after the initial phase, medication should be discontinued while continuing CBT-I.22
There are currently no approved or recommended pharmacological treatments indicated for CID available through public drug plans in Canada. According to the clinical experts consulted by the CDA-AMC review team, CBT-I and pharmacotherapy can be adopted concurrently or sequentially, and some of the currently used pharmacotherapeutic options in Canada include trazodone (an atypical antidepressant, commonly used off label), Z-drugs (e.g., zopiclone), antipsychotics (used off label), and benzodiazepines (either indicated for short-term insomnia or used off label). The 2024 consensus for the management of CID in Canada states that long-term data on the efficacy of these pharmacotherapeutic options are lacking and that these pharmacotherapies are generally considered for short-term management.8 The 2024 consensus further pointed out that DORAs might have benefits that outweigh the risks for long-term use;8 however, no DORAs are publicly reimbursed for CID in Canada at the time of this review.
Drug Under Review
The key characteristics of lemborexant (Dayvigo) are summarized in Table 2, along with those of other relevant treatments available for insomnia.
Lemborexant is a competitive antagonist of both orexin receptor 1 and orexin receptor 2, with a higher affinity for orexin receptor 2. The orexin neuropeptide signalling system is a central promoter of wakefulness and blocking the binding of wake-promoting neuropeptides orexin A and orexin B to orexin receptor 1 and orexin receptor 2 is thought to suppress wake drive.1
Lemborexant was approved by Health Canada in 2020 “for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.”1 Lemborexant is available in 5 mg and 10 mg tablets, taken orally once per night within a few minutes before going to bed, with at least 7 hours before planned awakening time. The recommended dose is 5 mg once per night, although the dose may be increased to the maximum recommended dose of 10 mg based on clinical response and tolerability.
Lemborexant was initially reviewed by CDA-AMC in 2022, and the sponsor’s reimbursement request was the same as the Health Canada–approved indication. This initial review received a “do not reimburse” recommendation. In this resubmission, the sponsor is requesting reimbursement for the treatment of insomnia in adults diagnosed according to the most recent version of the DSM referring to CID.
Table 2: Key Characteristics of Lemborexant and Relevant Comparators
Drug | Mechanism of action | Indicationa | Route of administration | Recommended dosage | Serious adverse effects of safety issues | Notes |
|---|---|---|---|---|---|---|
Lemborexant | Competitive antagonist of OX1R and OX2R. Blocking the binding of wake-promoting neuropeptides orexin A and orexin B to receptors (OX1R and OX2R) is thought to suppress wake drive. | For the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance. | Oral | Five mg once per night taken within a few minutes before going to bed with at least 7 hours before planned awakening time. Dose may be increased to 10 mg based on response and tolerability. |
| NA |
Z-drugs | GABA A receptor–positive modulator presumed to exert its therapeutic effects through binding the benzodiazepine site of an alpha-1 subunit containing GABA A receptors, increasing the frequency of chloride channel opening, resulting in the inhibition of neuronal excitation | For short-term (usually not exceeding 7 to 10 days) use for treatment and symptomatic relief of insomnia characterized by difficulty in falling asleep, frequent nocturnal awakenings and/or early morning awakenings where disturbed sleep results in impaired daytime functioning. | Oral, sublingual | Varies by drug. Indicated for short-term use (usually not exceeding 7 to 10 days) |
| Drugs: zopiclone |
Benzodiazepines | Depressants of the CNS, believed to enhance or facilitate the effects of the inhibitory neurotransmitter GABA and act as agonists at the benzodiazepine receptor sites | Temazepam, triazolam, flurazepam: For the symptomatic relief of transient and short-term insomnia characterized by difficulty in falling asleep, frequent nocturnal awakenings and/or early morning awakenings. Nitrazepam: Short-term treatment and symptomatic relief of insomnia characterized by difficulty in falling asleep, frequent nocturnal awakenings, and/or early morning awakenings. | Oral | Varies by drug Treatment should usually not exceed 7 to 10 consecutive days. |
| Drugs indicated for insomnia: temazepam, triazolam, flurazepam, nitrazepam Drugs not indicated for insomnia: alprazolam, bromazepam, clonazepam, diazepam, lorazepam, oxazepam, chlordiazepoxide, clobazam |
Antidepressants | Unclear in humans | Not approved for insomnia. | Oral | Varies by drug |
| Drugs: trazodone, amitriptyline, mirtazapine |
Antipsychotics | Interact with a broad range of neurotransmitter receptors with direct and indirect effects | Not approved for insomnia. | Oral | Varies by drug |
| Drugs: quetiapine, olanzapine, others |
CNS = central nervous system; GABA = gamma-aminobutyric acid; NA = not applicable; OX1R = orexin receptor 1; OX2R = orexin receptor 2; QTc = corrected QT.
aHealth Canada–approved indications.
Sources: Lemborexant product monograph;23 zopiclone product monograph;24 alprazolam product monograph;25 bromazepam product monograph;26 clonazepam product monograph;27 diazepam product monograph;28 flurazepam product monograph;29 lorazepam product monograph;30 nitrazepam product monograph;31 oxazepam product monograph;32 temazepam product monograph;33 triazolam product monograph;34 chlordiazepoxide product monograph;35 clobazam product monograph;36 amitriptyline product monograph;37 mirtazapine product monograph;38 trazodone product monograph;39 quetiapine product monograph.40
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups.
Input for this review was submitted by 4 patient groups: Migraine Canada, ASO, MDSC, and the GI Society. Migraine Canada is a national, federally recognized charity focused on education, support, and awareness about the impact of migraine. Migraine Canada gathered information through 3 surveys for adults in Canada with migraine and sleep challenges or insomnia: a 2021 quality of life survey (N = 1,165), a 2022 national online survey for those with experience taking lemborexant (N = 220), and a 2024 national survey of patients who live with migraine and experience sleep issues or insomnia (N = 177). ASO is a provincial federation of 26 frontline health and community support service providers across Ontario, affiliated with the national Alzheimer Society. ASO gathered information through a review of published literature as well as semistructured interviews with patients with insomnia and clinicians with experience in this field. MDSC is a national mental health organization representing individuals with mental health challenges. MDSC gathered information through a 2021 survey for individuals in Canada with sleep and mental health challenges (N = 1,200), a 2024 survey of patients with migraine and insomnia prepared by Migraine Canada (N = 142), and interviews with patients with insomnia (N = 8) and clinicians with experience in this field (N = 2). The GI Society is a national charity committed to improving the lives of people with gastrointestinal and liver conditions by supporting research, advocating for patient health care access, and promoting gastrointestinal and liver health. The GI Society gathered information through focused discussions with health care providers and researchers and 1 interview with a patient currently taking lemborexant.
Patient groups emphasized that chronic insomnia is a debilitating condition, arising from a wide range of factors, that impacts nearly all aspects of life and results in a substantial societal cost. According to Migraine Canada, insomnia commonly co-occurs with migraines. The GI Society highlighted the link between gastrointestinal diseases and disorders and insomnia, citing recent survey results that indicate that approximately 56% of patients with inflammatory bowel disease have difficulty sleeping or insomnia. ASO noted that individuals with lower socioeconomic status are more likely to experience poor sleep due to irregular work hours, unsafe environments, stress, health behaviours, or comorbidities. ASO also highlighted that patients with dementia frequently experience insomnia, worsening cognitive and functional impairments. Patient groups highlighted that sleep deprivation compromises physical, mental, and emotional health; impairs daily functioning and productivity; and strains personal relationships. According to patient groups, insomnia is often associated with feelings of hopelessness, emotional instability, and chronic fatigue, which diminish people’s ability to engage in work, relationships, and self-care. Up to 40% of people with insomnia report coexisting mental health conditions, such as anxiety, depression, or bipolar disorder; depression is present in up to 90% of cases. A negative feedback loop often develops, with insomnia worsening mental health and vice versa. If left untreated, insomnia is associated with increased risks of mood disorders, cognitive decline, type 2 diabetes, cardiovascular and metabolic conditions, substance misuse, and suicide.
CBT-I is considered the first-line treatment for insomnia by several national and international expert bodies; however, patient groups reported limited access to CBT-I, lack of awareness or referrals, and variable effectiveness. Many patients initially self-manage their insomnia using over-the-counter treatments (e.g., antihistamines, melatonin, magnesium, analgesics, natural health products) and lifestyle changes (e.g., reducing caffeine or screen time). Pharmacologic options often include benzodiazepines, nonbenzodiazepine hypnotics, barbiturates, and off-label use of antidepressants and antipsychotics. In the survey by Migraine Canada, commonly used hypnotic medications included zopiclone (27% of patients who responded to the survey), trazodone (27%), gabapentin (24%), and benzodiazepines (17%). However, frequently reported adverse effects associated with the use of these medications included grogginess, withdrawal symptoms, weight gain, and mood disturbances. Additionally, the potential for dependency with currently available treatments was reported by the patient groups as highly concerning for patients and physicians, with 1 patient describing the discontinuation process as more distressing than their insomnia. The patient groups noted that current treatments often address only sleep initiation, without improving sleep quality or continuity, and are only meant for short-term use (7 to 10 days).
Twenty patients from the 2024 Migraine Canada survey, 6 patients interviewed by MDSC, and 1 patient with achalasia interviewed by the GI Society reported experience with lemborexant. Patients accessed lemborexant through private insurance (57% of patients who responded to the survey; 67% of patients who were interviewed), through out-of-pocket payment (29% of patients who responded to the survey; 17% of patients who were interviewed), or as a sample through health care providers (5% of patients who responded to the survey). Generally, patients noted improved daily alertness, work performance, and relationship stability, with minimal grogginess or concerns about dependency. Of the 20 patients who responded to the survey with experience taking lemborexant, 60% experienced some or substantial improvement in sleep or insomnia, 50% reported no adverse effects, 20% experienced mild adverse effects (including nightmares), and 15% discontinued use (including due to cost). Similarly, patients who were interviewed by MDSC described a rapid onset of action (often within 1 day) and substantial improvements in both sleep initiation and duration, with some reporting they could fall asleep within 20 minutes and sleep 6 to 7 hours per night. Two patients interviewed by MDSC reported reduced anxiety around sleep. One patient interviewed by MDSC found lemborexant less effective than previous treatments but preferred it because they felt it was a safer treatment option. The most common adverse effect reported by these patients was vivid dreams or nightmares, which were described by some as milder than with other medications. The patient interviewed by the GI Society with achalasia, a rare disorder resulting in chronic vomiting, heartburn, and coughing, had been sleeping upright to control gastroesophageal symptoms and reduce nighttime attacks. After 1 year taking lemborexant, this patient reported substantial improvement in REM sleep and had not experienced any adverse effects.
Patients strongly value nonaddictive, well-tolerated treatments that support both sleep initiation and maintenance, without residual sedation, to improve daytime functioning and quality of life. For patients with migraines, reducing the frequency and severity of attacks alongside improving sleep is a key treatment goal.
In general, the patient group input for the resubmission of lemborexant is aligned with the patient group input for the initial submission of lemborexant (from MDSC, Migraine Canada, and Menopause Chicks). The patient group input for the initial submission highlighted that patients are in need of a treatment to address several important outcomes, including uninterrupted and restorative sleep, greater access to treatment, more effective treatment options, long-term treatment effectiveness, fewer side effects, less stress and anxiety, improved productivity, and improved relationships with family members and colleagues.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of the clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of insomnia, as well as experience with the prescription of lemborexant and the management of patients using this drug.
Unmet Needs
The clinical experts consulted by the CDA-AMC review team noted that the treatment goals for CID include improved sleep initiation and maintenance, improvement of terminal insomnia and overall leading to restorative sleep, improved quality of sleep, and improved subjective wakefulness or function during the day.
According to the clinical experts consulted by the CDA-AMC review team, while CBT-I may address many factors contributing to insomnia, patients have insufficient access to, funds for, knowledge of, and confidence in this treatment modality; the latter 2 barriers may also even be experienced by health care providers. The clinical experts noted that pharmacological therapies may enhance sleep onset and raise the arousal threshold, yet they tend to have many side effects, including daytime sedation, fall risk, and potentially addiction, tolerance, and other problems (i.e., each drug has a different combination of side effects). As a result, according to the clinical experts, the main unmet need is for effective pharmacological treatments that have minimal side effects, including long-term side effects (particularly development of tolerance), and with low potential for addiction.
The clinical experts noted the constraints of current insomnia pharmacotherapy in Canada, with prescribers having to contend with a choice of off-label therapies, potentially unsafe drugs, or drugs not reimbursed by public drug plans.
Place in Therapy
According to the clinical experts consulted by the CDA-AMC review team, the mechanism of action of DORAs (i.e., counteracting inappropriate wakefulness at night) is considered fundamentally different from any other pharmacologic drug on the market for the treatment of insomnia or CID. The clinical experts noted that DORAs will likely shift the treatment paradigm and become a first-line drug for the treatment of CID in the absence of other comorbidities and in patients with comorbid insomnia and sleep apnea, given its lack of effect on breathing patterns. The clinical experts noted that other treatments might be chosen over DORAs in patients with a history of experiencing allergy or side effects to DORAs, in patients with narcolepsy, in patients who have concomitant depression or pain syndromes, when there is a drug-drug interaction, or due to cost. The experts highlighted that, based on their mechanism of action, DORAs such as lemborexant have the potential to address the root cause of CID, unlike other drugs used for insomnia.
Patient Population
The clinical experts consulted by the review team noted that most patients with insomnia may be candidates for lemborexant except for those who are younger than 18 years and those who are pregnant or nursing or who have severe hepatic impairment, narcolepsy, or idiopathic hypersomnia.
According to the clinical experts consulted by the review team, patients for whom treatment with lemborexant might be more suitable include those with insomnia and a history of anxiety or trauma (frequently troubled by inappropriate wakefulness at night due to hyperarousal), older adults with insomnia disorder, and those with a history of addiction issues and insomnia disorder. The clinical experts noted that patients for whom lemborexant would not be suitable include those with narcolepsy or intolerance to the drug.
The clinical experts consulted by the review team noted that diagnosis of CID is primarily clinical. According to the clinical experts, a polysomnography study can be done in certain cases (e.g., clinical suspicion of comorbid obstructive sleep apnea or another sleep disorder), and brief questionnaires can be used (e.g., ISI or Epworth Sleepiness Scale), but these tools are not used routinely in clinical care.
Assessing the Response to Treatment
According to the clinical experts consulted by the review team, to assess the response to treatment, patients are asked generally if their symptoms have improved (e.g., whether they are sleeping better and/or longer and feeling refreshed) and if they feel better about their daytime functioning.
The clinical experts consulted by the review team noted that objective tests or sleep diaries are not generally used. According to the clinical experts, beyond patients’ subjective descriptions, the following outcomes can be used to determine an adequate treatment response: sleep latency less than 30 minutes, sleep efficiency greater than 90%, improved functional outcome in the day (e.g., less groggy, more energy), improved mood or anxiety, improved performance at work or school, decreased irritability or emotionality, improvement in other symptoms (e.g., pain, subjective well-being, continuity of sleep at night, WASO).
The clinical experts noted that treatment response is most frequently assessed 1 to 3 months after treatment initiation but that there is a wide variability in the frequency of assessment.
Discontinuing Treatment
According to the clinical experts consulted by the review team, lemborexant should be discontinued due to allergy to lemborexant, when there is a lack of treatment response (may need ≥ 3 months to adequately assess the treatment effects on total sleep time and sleep efficiency), or when there are side effects that are intolerable or unacceptable for patients (e.g., REM intrusion phenomena, daytime sedation, nocturnal parasomnia behaviours). Based on patient experience using lemborexant, the clinical experts noted that it might take weeks (e.g., 4 to 8 weeks) for a DORA, including lemborexant, to show optimal treatment effects; some patients might not feel any effect in the first few days after treatment initiation.
Prescribing Considerations
The clinical experts consulted by the review team noted that clinicians in several fields (e.g., family physicians, psychiatrists, internal medicine specialists, neurologists) may use lemborexant to treat patients. According to the clinical experts, sleep specialists are usually not required to diagnose, treat, or monitor patients who might receive lemborexant unless a comorbid sleep condition (e.g., comorbid insomnia and sleep apnea) is suspected.
Input from the clinical experts for the resubmission of lemborexant is overall aligned with the input from the clinical experts for the initial submission of lemborexant.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups.
Input for this review was submitted by 8 clinician groups: addiction medicine specialists (8 health care providers), the Cardiometabolic Patient Clinician Group (12 health care providers), the Depression and Anxiety Clinician Group (5 health care providers), the Primary Care Clinician Group (24 health care providers), the Alberta Psychiatrists (11 health care providers), the Chronic Insomnia Clinician Group (17 health care providers), the Aging Patients Clinician Group (13 health care providers), and the Women’s Health Clinician Group (4 health care providers). These groups represent a broad range of health care providers across Canada, including psychiatrists, family physicians, internists, and specialists in addiction, mental health, women’s health, and geriatric care. The information included in the input was informed by clinical experience and gathered through advisory board meetings, focused discussions, and email correspondence.
The clinician groups highlighted the current treatment paradigm for chronic insomnia in Canada, which mainly includes nonpharmacologic therapies (e.g., CBT-I), pharmacologic treatments (e.g., benzodiazepines, Z-drugs, DORAs, antidepressants, atypical antipsychotics), and other nonprescriptive or over-the-counter treatments (e.g., melatonin, alcohol, cannabis, antihistamines, natural health products). The clinician groups noted that, although considered as first-line treatment for insomnia, CBT-I is not widely available or funded in Canada. According to the clinician groups, the currently available pharmacotherapies primarily promote sedation and alleviate the symptoms of chronic insomnia without addressing the underlying disease mechanism and are associated with notable side effects, such as next-day impairment, memory and motor issues, weight gain, dependence, and cardiac arrhythmias.
In alignment with the clinical experts consulted by the CDA-AMC review team, the clinician groups agreed that the treatment goals for chronic insomnia should include improving sleep quality and continuity, enhancing daytime functioning, and minimizing adverse and sedative effects. An ideal treatment would have a rapid onset of action, improve sleep architecture and reduce nighttime awakenings, be nonaddictive and safe for long-term use, and be accessible and well tolerated across a wide range of patients. The clinician groups supported the use of lemborexant as a first-line pharmacologic treatment for chronic insomnia and noted that if reimbursed, lemborexant would lead to a shift in the current treatment paradigm.
The clinician groups noted that lemborexant is suitable for most patients aged 18 years or older with insomnia, including those with comorbid psychiatric disorders and various nonpsychiatric medical conditions. The Chronic Insomnia Clinician Group and the Primary Care Clinician Group noted that patients aged younger than 18 years or older adolescents may also be eligible to receive lemborexant. The Primary Care Clinician Group also noted that patients with insomnia who are pregnant could receive lemborexant, whereas the clinical experts consulted by the review team considered that these patients would be ineligible. The patients identified by the clinician groups as likely to benefit from lemborexant included older patients (including those with comorbidities); patients with chronic insomnia who are unable to access CBT-I or whose chronic insomnia persists after receiving CBT-I; patients for whom prior treatment with currently available drugs such as Z-drugs or benzodiazepine receptor agonists has failed; patients who have developed a high tolerance to, or are unable to tolerate, these drugs; shift workers; patients who require high daytime functioning (e.g., health care professionals, drivers, first responders); patients with a history of addiction; patients with metabolic risk factors (e.g., obesity, prediabetes, hypertension) or issues (e.g., cardiometabolic issues); patients who were perimenopausal, menopausal, and postmenopausal with insomnia; and patients with sleep apnea. Based on the input from the clinician groups, patients for whom lemborexant is less suitable included those with narcolepsy or those who respond well to short-term use of existing therapies. Lemborexant may also be less effective in individuals who have low treatment adherence or whose insomnia has been refractory to many previous treatments, because the clinician groups noted that there was evidence of possible reduced efficacy in these patients.
The clinician groups emphasized that patient-reported outcomes are key to evaluating treatment response, including perceived sleep quality (e.g., restful sleep, reduced nighttime awakenings), next-day functioning (e.g., alertness, reduced brain fog), and overall quality of life. Some clinician groups noted that standardized tools like the ISI or the Epworth Sleepiness Scale might be used to evaluate changes in sleep to determine treatment response and that objective markers, such as reduced time to sleep onset, fewer awakenings, improved sleep consolidation, and reduced need to nap, were useful in evaluating response. Some clinician groups considered improvements in metabolic health (e.g., reductions in insulin resistance, obesity-related comorbidities, diabetes, and cardiovascular risk) as potentially meaningful indirect indicators of treatment response. Clinician groups suggested the following comparative safety measures in hospital and long-term care settings: monitoring rates of falls, delirium, and complications among older patients.
The clinician groups noted that, in general, discontinuation of lemborexant should be based on joint patient-physician decisions, weighing the benefit of discontinuation against the potential risks. Discontinuation of lemborexant may be considered in cases of insufficient efficacy, patient preference, unacceptable adverse effects, or initiation of a sedating medication for another condition (e.g., antidepressant to treat depression). Input from the Alberta Psychiatrists suggested that use of moderate or strong CYP3A inhibitors may also warrant discontinuation of lemborexant or closer monitoring. The Chronic Insomnia Clinician Group reported that some patients were able to discontinue lemborexant after 2 to 3 months without experiencing a recurrence, suggesting that, for some, treatment may not be indefinite. Based on their experience in using lemborexant — which has no empirical evidence to support its use — the clinical experts consulted by the review team noted that 1 year after successful use of lemborexant could be a reasonable time point to explore the possibility of discontinuing lemborexant. While lemborexant is expected to produce rapid sleep benefits, the clinician groups noted that it may take 2 to 4 weeks for lemborexant to show full effects, an estimate of time shorter than that provided by the clinical experts consulted by the review team (i.e., 4 to 8 weeks). The clinician groups noted that ongoing consistent use of lemborexant is required until patients experience several weeks to months of sustained remission to reduce the risk of recurrence.
The clinician groups noted that lemborexant could be administered in inpatient and outpatient settings, including emergency departments, long-term care facilities, clinics, hospitals, and patients’ homes. The clinician groups noted that lemborexant does not require a specialized setting or a specialist to initiate treatment and monitor response because it is easy and safe to prescribe, with no titration needed and minimal risk of adverse effects, overdose, or dependency. The groups noted that family physicians and specialists could prescribe and monitor lemborexant treatment and that, in some jurisdictions, pharmacists would also be authorized to prescribe lemborexant to patients.
Clinician groups with first-hand experience prescribing lemborexant reported that it has significantly improved the treatment of chronic insomnia, allowing for earlier, more effective intervention, especially in patients with complex medical and psychiatric comorbidities. Lemborexant was consistently described as safer than existing options, particularly for older adults and those with dementia, with observed improvements in memory, balance, and restorative sleep. It was noted to improve full sleep architecture, including REM and non-REM sleep, and to reduce the risk of postoperative delirium. The clinicians reported meaningful improvements in patients with coexisting depression, anxiety, bipolar disorder, obsessive-compulsive disorder, and substance use disorders. Lemborexant helped reduce distress, stabilize mood, and improve daytime function and, in many cases, led to full remission of insomnia after several months. Some patients noted improvements via sleep trackers, and others reported reduced use of alcohol and cannabis. The clinician groups noted that lemborexant enabled successful tapering and discontinuation of long-term Z-drug and benzodiazepine use, even in patients who had been taking high doses for years, without escalating to other sedatives. The clinician groups also noted that lemborexant helped patients avoid more toxic treatments and self-medication. The clinician groups emphasized that patients consistently expressed high satisfaction, citing fast sleep onset, no morning sedation, and ease of use. Many patients had described the effects as life-changing, restoring quality of life, function, and a sense of normalcy. The clinicians noted that such positive feedback was not common in psychiatric care. However, the clinician groups noted that cost remains a major barrier for patients with public drug plans, who often struggle to afford lemborexant without sacrificing other essentials or relying on family support.
While all the clinician groups expressed a favourable position on lemborexant, the Chronic Insomnia Clinician Group provided further input on the 2023 CDEC recommendation against the reimbursement of lemborexant for the treatment of insomnia characterized by difficulties with sleep onset and/or sleep maintenance, which are summarized as follows.
The Chronic Insomnia Clinician Group noted that CDEC’s interpretation of clinical meaningfulness may benefit from additional context. The clinician group acknowledged the general challenge of defining MIDs in insomnia, especially because many widely used treatments in Canada lack robust data from randomized controlled trials (RCTs). The clinician group outlined that the ISI score is commonly used to indicate clinically meaningful change (i.e., a score ≥ 7) and symptom remission (i.e., a total ISI score < 8) and noted that both criteria were met in the lemborexant trials.
The Chronic Insomnia Clinician Group noted that the generalizability to patients with comorbid conditions may have been overstated. The clinician group noted that trial participants had mild depression, anxiety, or sleep apnea and that treatment effects were consistent across these subgroups. The clinician group noted that the clinical experts consulted by CDA-AMC confirmed that the trial populations reflected real-world practice in Canada, yet this was not clearly reflected in the conclusions. The clinicians noted that the lemborexant trials represent some of the most generalizable RCT evidence in the field.
Regarding comparative evidence, the Chronic Insomnia Clinician Group noted that direct head-to-head trials are uncommon for insomnia treatments. The clinician group noted that it was reasonable to instead consider the overall mechanism of action of lemborexant and its favourable safety profile, particularly in the broader context of known risks associated with Z-drugs and benzodiazepines, including falls, cognitive impairment, and dependency. The clinician group emphasized that lemborexant has not shown similar safety concerns and highlighted findings from both clinical trials and real-world settings suggesting low potential for abuse, absence of withdrawal or rebound insomnia, and improved tolerability overall. The clinician group noted that zolpidem and zopiclone are comparable clinically because they are of the same drug class and have a shared mechanism of action.
The Chronic Insomnia Clinician Group noted that while long-term evidence in insomnia is limited overall, the 12-month data for lemborexant is considered robust, informative, and longer than the data that exist for many approved treatments. The clinician group noted that while the previous Clinical Review report questions whether lemborexant meets long-term patient needs, it also recognizes that the safety and efficacy profile aligns with patient priorities like uninterrupted sleep, improved function, and reduced side effects, an area of inconsistency. The clinicians noted that a 2-week duration of follow-up after discontinuation would be sufficient to detect signals of physical dependence and emphasized that lemborexant showed no evidence of potential for abuse across 3 nonclinical studies, had no receptor binding associated with addiction risk, and demonstrated low rates of adverse events (AEs) related to misuse or diversion during clinical development.
While nonpharmacological approaches like CBT-I remain an important first-line strategy, the Chronic Insomnia Clinician Group emphasized that pharmacotherapy is often necessary in real-world practice, particularly given the high rates of nonresponse, limited access, and poor uptake among patients with comorbidities associated with CBT-I. In these situations, lemborexant has offered a well-tolerated and effective alternative, helping reduce reliance on currently available medications that are often associated with greater risks. The clinician group shared that lemborexant has become a valuable tool in their treatment approach, with many observing transformative outcomes.
The Chronic Insomnia Clinician Group highlighted lemborexant as an important addition to their treatment options, allowing earlier intervention, reduced reliance on sedatives, and better patient outcomes. They shared examples of meaningful improvements in quality of life and mental health. While acknowledging that it is not suitable for all patients, the clinician group views lemborexant as a safer alternative where existing options are limited. The clinician group expressed concern that a lack of public coverage may push patients experiencing vulnerability toward less safe, off-label treatments. The clinician group felt that broader access to lemborexant would support both clinical practice and public health goals.
While providing novel insights derived from experience with the drug, the input from the clinician groups for the resubmission of lemborexant is overall aligned with the input from the clinician groups for the initial submission of lemborexant.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions from the drug programs and the corresponding responses from the clinical experts consulted for this review are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The sponsor notes the following:
Benzodiazepines, the antidepressants cited by the sponsor, and quetiapine are open benefits on most public drug plans. The funding status of zopiclone is not consistent across plans (open benefit for several; restricted benefit for some; not a benefit for some). It is unclear whether most health ministries across Canada provide funding for CBT-I or how accessible it is (although mysleepwell.ca [a website affiliated with Dalhousie University] provides recommendations for free apps and websites to enable broad access). Daridorexant is currently under review by CDA-AMC for CID and is not publicly reimbursed. | This is a comment from the drug plans to inform CDEC deliberations. According to the clinical experts consulted by the review team, most health ministries in Canada do not provide funding for CBT-I. |
Considerations for initiation of therapy | |
An inclusion criterion for the pivotal trials was an ISI score ≥ 13 (SUNRISE 1 trial) or ≥ 15 (SUNRISE 2 trial).
| The clinical experts consulted by the review team noted that no tools, including ISI, are routinely used in clinical practice in Canada. ISI may be used in select settings or for research purposes. Neither clinical expert consulted by the review team supports using improvement in ISI score as a reimbursement initiation criterion. According to the clinical experts, given the subjective nature of the ISI, the improvement in ISI score could be exaggerated for the purpose of reimbursement. |
It seems like either publicly funded or free, self-directed CBT-I may be accessible to a large proportion of individuals with CID.
| The clinical experts consulted by the review team disagreed with the statement that “either publicly funded or free, self-directed CBT-I may be accessible to a large proportion of individuals with CID.” In contrast, the clinical experts noted that CBT-I is likely unavailable to a large proportion of patients with CID. Neither clinical expert consulted by the review team supports patients with CID being required to receive CBT-I before being eligible for lemborexant. While acknowledging that CBT-I should be viewed as a first-line therapy, the clinical experts noted that eligibility for lemborexant should not be based on the prior use of CBT-I because there are many patients with CID who may not have access to CBT-I, whose phenotype of insomnia does not respond well to CBT-I, who need a combination therapy of CBT-I and pharmacologic drug(s), or who are unable to read and write. |
It is expected that a CDA-AMC recommendation will be issued for daridorexant before lemborexant is rereviewed by CDEC. Consider alignment with the initiation criteria, renewal criteria, discontinuation criteria, and prescribing criteria for daridorexant, as applicable or appropriate. | This is a comment from the drug plans to inform CDEC deliberations. |
Considerations for continuation or renewal of therapy | |
| The clinical experts consulted by the review team noted that no tools or objective end points (e.g., data from polysomnography or wearable sleep trackers) are routinely used in clinical practice to assess treatment response. Insomnia is routinely screened and monitored based on clinical subjective assessment, such as patient-reported sleep history (i.e., difficulties initiating and or maintaining sleep, daytime function, frequency and severity of symptoms). According to the clinical experts, it is hard to quantify the level of improvement in clinical practice, and the extent of improvement in sleep is determined by individual patients. The clinical experts consulted noted that in research settings, there are ways (e.g., questionnaires or survey data and, in some cases, polysomnography or actigraphy data) to quantify the level of improvement, but none of these are used commonly in clinical practice. According to the clinical experts, 1 to 3 months would be reasonable time points to assess treatment response. |
Considerations for discontinuation of therapy | |
Should treatment discontinuation be attempted at any time point after successful use? If so, under what circumstances? | The clinical experts noted that the circumstances that would inform the discontinuation of lemborexant after successful initiation in patients with CID are heterogeneous. Attempts could be made to discontinue lemborexant and see if initial symptoms return in patients whose sleep has been improved by lemborexant when other contexts surrounding the patients are stable, for example patients who have not had recent major depressive episodes that could trigger or worsen the sleep disorder. According to the clinical experts, based on their experience in using lemborexant, which has no empirical evidence to support its use, 1 year after successful use of lemborexant could be a reasonable time point to explore the possibility of discontinuing lemborexant. The clinical experts consulted by the review team further noted some potential challenges and barriers. Many of the patients with insomnia who go to sleep specialists do not have family doctors, raising the concern about who will reassess patients for discontinuation. |
Generalizability | |
The pivotal trials had numerous exclusion criteria.
| According to the clinical experts, patients aged younger than 18 years and patients with narcolepsy, idiopathic hypersomnia, or severe hepatic impairment should not be eligible for lemborexant. |
System and economic issues | |
The submitted budget impact analysis found that, at the submitted price, reimbursement of lemborexant is associated with an expected cumulative 3-year incremental budget impact of $64.1 million. Sensitivity analyses demonstrated that the 3-year incremental budget impact may vary from $48.1 million to $80.1 million. | This is a comment from the drug plans to inform CDEC deliberations. |
CBT-I = cognitive behavioural therapy for insomnia; CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; CID = chronic insomnia disorder; ISI = Insomnia Severity Index.
Evidence for the Resubmission
The objective of this Clinical Review report is to review and critically appraise new evidence submitted by the sponsor on the beneficial and harmful effects of lemborexant, 5 mg film-coated tablet and 10 mg film-coated tablet, taken orally, in the treatment of patients with insomnia. The focus will be placed on the new evidence submitted for the resubmission and how any evidence gap(s) identified by CDEC during the initial submission were addressed in the evidence. According to the sponsor, RCT and indirect evidence remains unchanged from the initial submission and new evidence consists of observational studies. Inclusion criteria and patient populations from previously submitted pivotal trials are aligned with the new reimbursement request (i.e., patients with CID). Consequently, no reappraisal of the evidence was conducted. The executive summary of the Clinical Report of the initial submission can be found in Appendix 1.
Included Studies
After assessing the studies submitted by the sponsor, the CDA-AMC review team included and appraised 2 studies that could potentially address some of the gaps identified by CDEC:
a retrospective observational study conducted by Juday et al.14
a retrospective observational study conducted by Hirata et al.15
Details of the excluded studies, including the rationale for exclusion, are shown in Appendix 2.
Description of Studies
The details of the real-world studies submitted by the sponsor for the resubmission are shown in Table 4.
Table 4: Details of the Real-World Studies Submitted by the Sponsor for the Resubmission
Detail | Juday et al.14 | Hirata et al.15 |
|---|---|---|
Designs and populations | ||
Funding source | Eisai Inc. | Japan Society for the Promotion of Science KAKENHI (grant number JP21H03166) |
Primary objective | To compare the 6-month fall rate among individuals who had insomnia treatment with lemborexant, trazodone, zolpidem, and benzodiazepines as a class | To examine the association between in-hospital falls and various hypnotic medications (e.g., benzodiazepines, Z-drugs, suvorexant, lemborexant, ramelteon, other hypnotics) |
Study design | Retrospective cohort study (unpublished) | Subanalysis of an unpublished multicentre retrospective cohort study |
Study location | 50 large health care organizations in the US | 8 hospitals in Japan |
Setting or data source | Electronic health records |
|
Observation period | January 1, 2020, to January 30, 2022 (6-month follow-up) | April 1, 2018, to March 31, 2021 (in-hospital follow-up of unreported duration) |
Number of patients or patient records | Propensity score-matched sample size for each of the cohorts was 716 patients | 150,278 patients (Fall group: 3,458; nonfall group: 146,820) |
Key inclusion criteria |
|
|
Key exclusion criteria | None | NR |
Drugs | ||
Intervention or exposures | At least 1 prescription for lemborexant, trazodone, zolpidem, or benzodiazepines | Patients were defined by the type of hypnotic medications prescribed at admission, including lemborexant, suvorexant, ramelteon, benzodiazepines, Z-drugs, and other hypnotics |
Outcomes | ||
Primary end point | 6-month fall rate | Occurrence of in-hospital falls |
Secondary end points | Incremental costs | NA |
Publications | ||
Publications | Juday et al. (2023)41 (poster) Clinical Study Report provided by the sponsor | Hirata et al. (2024)15 |
ICD-10 = International Classification of Diseases, 10th Revision; NA = not applicable; NR = not reported.
Sources: Juday et al;14 Hirata et al.15
Juday et al. Study
Populations
Eligible patients were adults who were diagnosed with insomnia, had at least 1 pharmacy claim for an insomnia medication of interest, visited a health care system during the 6 months after the index date, and had no evidence of falls, hip fractures, or traumatic brain injuries for 6 months before the index date. The date of the earliest prescription was labelled as the index date. No exclusion criteria were specified by Juday et al.14
Interventions or Exposures
Patients were required to be exposed to 1 of the following insomnia medications during the patient identification period (i.e., between June 1, 2020, and December 31, 2021): lemborexant, trazodone, zolpidem, or benzodiazepines (as a class). Classification of exposure was based on the first pharmacy claim occurring during the identification period.
Outcomes
The primary outcome was the proportion of patients with at least 1 fall during the 6-month follow-up period. Fall incidents were defined as having any falls, hip fractures, or traumatic brain injuries reported at a medical encounter, diagnosed with the ICD-10 codes and captured in medical claims. If an individual had multiple falls, only the first event was captured.
Statistical Analysis
Baseline characteristics were summarized using descriptive statistics. Patient counts and percentages were reported for categorical variables. Means and standard deviations (SDs) were reported for continuous variables. No imputation was performed for missing data, and patients with missing race or ethnicity data were assigned to the category of “unknown.”
To balance baseline confounders across treatment groups, 1:1 propensity score matching was implemented to match patients taking trazodone, zolpidem, and benzodiazepines (as a class) to the lemborexant group. Covariates used in the matching included age, sex, race, ethnicity, and common comorbidities. A greedy nearest neighbour-matching algorithm was used for the propensity score matching. Individual patients could only be matched once. A caliper of 0.2 SD of the logit of the propensity score was applied. A standardized mean difference of less than 0.1 was used to identify a balanced match.
Outcomes were evaluated on the patient population after propensity score matching. The primary analysis included patients aged 18 years and older, and an additional analysis included only patients aged 65 years and older. Matched pairwise comparisons were conducted, with lemborexant chosen as the reference for all comparisons to estimate the percentage of patients with at least 1 fall and corresponding RRs and 95% CIs.
Results
Demographic and Clinical Characteristics Before Propensity Score Matching
The demographic and clinical characteristics used for propensity score matching in patients aged 18 years and older and in patients aged 65 years and older are presented in Table 5 and Table 6, respectively.
Before propensity score matching in patients aged 18 years and older (Table 5), the distribution of demographic characteristics was generally balanced across groups. Imbalance was observed in clinical characteristics: a smaller percentage of patients in the lemborexant group had some comorbidities — such as hypertensive diseases, type 2 diabetes mellitus, mood (affective) disorders — than in other groups.
Before propensity score matching in patients aged 65 years and older (Table 6), there was a lower proportion of female patients (and a higher proportion of male patients) in the lemborexant group than in the other groups. The percentage of patients with comorbidities such as hypertensive diseases, type 2 diabetes mellitus, and pain not otherwise classified was smaller in the lemborexant group than in other groups (e.g., the benzodiazepines group, the trazodone group).
Table 5: Demographic and Clinical Characteristics of Patients Aged 18 Years and Older in the Juday et al. Study Before Propensity Score Matching
Characteristic | Benzodiazepines | Trazodone | Zolpidem | Lemborexant | ||||
|---|---|---|---|---|---|---|---|---|
N | % | N | % | N | % | N | % | |
Patients | 473,972 | 100.0 | 263,630 | 100.0 | 150,041 | 100.0 | 716 | 100.0 |
Demographic characteristics | ||||||||
Age at index date (years), mean (SD) | ████ | ████ | ████ | ████ | ||||
Sex | ||||||||
Female | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Male | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Race | ||||||||
American Indian or Alaska Native | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Asian | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Black or African American | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Native Hawaiian or Other Pacific Islander | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Unknown | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
White | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Ethnicity | ||||||||
Hispanic or Latino | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Not Hispanic or Latino | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Unknown | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Clinical characteristics | ||||||||
Hypertensive diseases | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Type 2 diabetes mellitus | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Mood (affective) disorders | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Anxiety, dissociative, stress-related, somatoform, and other nonpsychotic mental disorders | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Alzheimer disease | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Unspecified dementia | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Dementia in other diseases classified elsewhere | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Vascular dementia | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Pain, unspecified | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Pain in joint | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Mental and behavioural disorders due to psychoactive substance use | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Pain, not elsewhere classified | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
SD = standard deviation.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Source: Juday et al. Clinical Study Report.14
Table 6: Demographic and Clinical Characteristics of Patients Aged 65 Years and Older in the Juday et al. Study Before Propensity Score Matching
Characteristic | Benzodiazepines | Trazodone | Zolpidem | Lemborexant | ||||
|---|---|---|---|---|---|---|---|---|
N | % | N | % | N | % | N | % | |
Patients | 162,283 | 100.0 | 86,653 | 100.0 | 54,736 | 100.0 | 164 | 100.0 |
Demographic characteristics | ||||||||
Age at index date (years), mean (SD) | ████ | ████ | ████ | ████ | ||||
Sex | ||||||||
Female | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Male | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Race | ||||||||
American Indian or Alaska Native | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Asian | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Black or African American | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Native Hawaiian or Other Pacific Islander | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Unknown | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
White | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Ethnicity | ||||||||
Hispanic or Latino | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Not Hispanic or Latino | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Unknown | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Clinical characteristics | ||||||||
Hypertensive diseases | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Type 2 diabetes mellitus | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Mood (affective) disorders | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Anxiety or dissociative, stress-related, somatoform, and other nonpsychotic mental disorders | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Alzheimer disease | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Unspecified dementia | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Dementia in other diseases classified elsewhere | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Vascular dementia | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Pain, unspecified | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Pain in joint | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Mental and behavioural disorders due to psychoactive substance use | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
Pain, not elsewhere classified | ██ | ██ | ██ | ██ | ██ | ██ | ██ | ██ |
SD = standard deviation.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Source: Juday et al. Clinical Study Report.14
Demographic and Clinical Characteristics After Propensity Score Matching
The demographic and clinical characteristics after propensity score matching in patients aged 18 years and older and in patients aged 65 years and older are presented in Table 7 and Table 8, respectively. All characteristics had a standardized mean difference of less than 0.10.
After propensity score matching in patients 18 years and older (Table 7) and in patients 65 years and older (Table 8), the distribution of demographic and clinical characteristics was generally balanced between the reference group (i.e., the lemborexant group) and other treatment groups.
Table 7: Demographic and Clinical Characteristics of Patients Aged 18 Years and Older in the Juday et al. Study After Propensity Score Matching
Characteristic | Lemborexant (reference) | Benzodiazepines | SMD | Trazodone | SMD | Zolpidem | SMD | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
N | % | N | % | N | % | N | % | ||||
Patients | 716 | 100 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Demographic characteristics | |||||||||||
Age at index date (years), mean (SD) | 53.8 (14.6) | █ | █ | █ | █ | █ | █ | ||||
Sex | |||||||||||
Female | █ | 61.5 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Male | █ | 38.5 | █ | █ | █ | █ | █ | █ | |||
Race | |||||||||||
American Indian or Alaska Native | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Asian | █ | █ | █ | █ | █ | █ | █ | █ | |||
Black or African American | █ | █ | █ | █ | █ | █ | █ | █ | |||
Native Hawaiian or Other Pacific Islander | █ | █ | █ | █ | █ | █ | █ | █ | |||
Unknown | █ | █ | █ | █ | █ | █ | █ | █ | |||
White | █ | 78.2 | █ | █ | █ | █ | █ | █ | |||
Ethnicity | |||||||||||
Hispanic or Latino | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Not Hispanic or Latino | █ | 77.2 | █ | █ | █ | █ | █ | █ | |||
Unknown | █ | █ | █ | █ | █ | █ | █ | █ | |||
Clinical characteristics | |||||||||||
Hypertensive diseases | █ | 34.1 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Type 2 diabetes mellitus | █ | 13.3 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Mood (affective) disorders | █ | 23.6 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Anxiety, dissociative, stress-related, somatoform, and other nonpsychotic mental disorders | █ | 34.5 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Alzheimer disease | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Unspecified dementia | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Dementia in other diseases classified elsewhere | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Vascular dementia | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Pain, unspecified | █ | 4.9 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Pain in joint | █ | 15.9 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Mental and behavioural disorders due to psychoactive substance use | █ | 6.8 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Pain, not elsewhere classified | █ | 11.0 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
SD = standard deviation; SMD = standardized mean difference.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Source: Juday et al. Clinical Study Report.14
Table 8: Demographic and Clinical Characteristics of Patients Aged 65 Years and Older in the Juday et al. Study After Propensity Score Matching
Characteristic | Lemborexant (reference) | Benzodiazepines (as a class) | SMD | Trazodone | SMD | Zolpidem | SMD | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
N | % | N | % | N | % | N | % | ||||
Patients | 164 | 100 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Demographic characteristics | |||||||||||
Age at index date (years), mean (SD) | 73.0 (6.0) | █ | █ | █ | █ | █ | █ | ||||
Sex | |||||||||||
Female | █ | 52.4 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Male | █ | 47.6 | █ | █ | █ | █ | █ | █ | |||
Race | |||||||||||
American Indian or Alaska Native | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Asian | █ | █ | █ | █ | █ | █ | █ | █ | |||
Black or African American | █ | █ | █ | █ | █ | █ | █ | █ | |||
Native Hawaiian or Other Pacific Islander | — | — | — | — | — | — | — | — | |||
Unknown | █ | █ | █ | █ | █ | █ | █ | █ | |||
White | █ | 82.9 | █ | █ | █ | █ | █ | █ | |||
Ethnicity | |||||||||||
Hispanic or Latino | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Not Hispanic or Latino | █ | 83.5 | █ | █ | █ | █ | █ | █ | |||
Unknown | █ | █ | █ | █ | █ | █ | █ | █ | |||
Clinical characteristics | |||||||||||
Hypertensive diseases | █ | 53.0 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Type 2 diabetes mellitus | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Mood (affective) disorders | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Anxiety, dissociative, stress-related, somatoform, and other nonpsychotic mental disorders | █ | 28.0 | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Alzheimer disease | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Unspecified dementia | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Dementia in other diseases classified elsewhere | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Vascular dementia | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Pain, unspecified | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Pain in joint | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Mental and behavioural disorders due to psychoactive substance use | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
Pain, not elsewhere classified | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ | █ |
SD = standard deviation; SMD = standardized mean difference.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Source: Juday et al. Clinical Study Report.14
Outcome: Risk of Falls in Patients Aged 18 Years and Older
The results relating to risk of falls in patients aged 18 years and older are shown in Table 9. In the 6-month follow-up period, 7.82% of patients in the lemborexant group, 9.92% in the zolpidem group, 9.22% in the trazodone group, and 13.83% in the benzodiazepine group had at least 1 fall recorded. Absolute between-group differences with 95% CIs were not provided. Compared to lemborexant, the RR of falls was 1.179 (95% CI, 0.838 to 1.657) for trazodone, 1.268 (95% CI, 0.907 to 1.772) for zolpidem, and 1.768 (95% CI, 1.295 to 2.413) for benzodiazepines as a class.
Table 9: Risk of Falls in Patients Aged 18 Years and Older in the Juday et al. Study
Drug vs. reference | 6-month fall rate | RR (95% CI) |
|---|---|---|
Trazodone vs. lemborexant | 9.22% vs. 7.82% | 1.179 (0.838 to 1.657) |
Zolpidem vs. lemborexant | 9.92% vs. 7.82% | 1.268 (0.907 to 1.772) |
Benzodiazepines (as a class) vs. lemborexant | 13.83% vs. 7.82% | 1.768 (1.295 to 2.413) |
CI = confidence interval; RR = risk ratio; vs. = versus.
Source: Juday et al. Clinical Study Report.14
Outcome: Risk of Falls in Patients Aged 65 Years and Older
The results relating to the risk of falls in patients aged 65 years and older are shown in Table 10. In the 6-month follow-up period, 8.54% of patients in the lemborexant group, 10.98% in the zolpidem group, 10.37% in the trazodone group, and 16.46% in the benzodiazepine group had at least 1 fall recorded. Absolute between-group differences with 95% CIs were not provided. Compared to lemborexant, the RR of falls was 1.214 (95% CI, 0.619 to 2.381) for trazodone, 1.286 (95% CI, 0.662 to 2.498) for zolpidem, and 1.929 (95% CI, 1.050 to 3.543) for benzodiazepines as a class.
Table 10: Risk of Falls in Patients Aged 65 Years and Older in the Juday et al. Study
Drug vs. reference | 6-month fall rate | RR (95% CI) |
|---|---|---|
Trazodone vs. lemborexant | 10.37% vs. 8.54% | 1.214 (0.619 to 2.381) |
Zolpidem vs. lemborexant | 10.98% vs. 8.54% | 1.286 (0.662 to 2.498) |
Benzodiazepines (as a class) vs. lemborexant | 16.46% vs. 8.54% | 1.929 (1.050 to 3.543) |
CI = confidence interval; RR = risk ratio; vs. = versus.
Source: Juday et al. Clinical Study Report.14
Critical Appraisal
Internal Validity
The Guidance for Reporting Real-World Evidence16 forms the foundation for transparent reporting of real-world evidence studies; adherence facilitates appraisal by CDA-AMC.42 The study by Juday et al. did not report the following: a predefined protocol; justification of the use of data from the US and proposed generalizability to the context in Canada; how potentially confounding variables were selected; quality of the data specifications (access, cleaning); data sources, including the data dictionary that provides information on the validity of relevant variables; between-group absolute effect estimates with CIs.
The first pharmacy claim during the identification period was used to assign patients to exposure groups. Misclassification of exposure is possible if a prescription for a current treatment was not filled during this period, if treatment discontinuation or switching occurred during follow-up, and/or if there was concomitant exposure to more than 1 treatment. The clinical experts consulted by the review team confirmed that the treatments may be used short term and/or intermittently. Information on the extent of drug exposure (i.e., dose, duration of treatment) was not reported and may differ across groups, precluding any inference about dose-harm relationships. The intention-to-treat perspective used does not consider adherence, discontinuation, or switching of treatments. Instead, any exposure is considered to result in a permanent increase in fall risk, which may not be plausible. Consideration of an on-treatment exposure definition may have been preferred to address these issues, particularly when evaluating harms.43 Nondifferential exposure misclassification may result in bias toward the null.
There is a risk of bias in the selection of patients into the study due to the inclusion of patients undergoing treatment and who have not experienced falls in the past 6 months, and the conditioning on events occurring during follow-up. The inclusion of these patients results in misalignment between the start of the intervention and the follow-up. The clinical experts consulted by the review team noted that the risk of falls may be highest early in treatment. However, patients undergoing treatment are survivors of AEs such as falls occurring during the early phase of treatment (i.e., early events are missed).17 The issue is compounded by excluding patients with prior falls (past 6 months), resulting in patients at higher risk of falls being underrepresented. Falls may therefore be underestimated in all groups. If the group composition differed with respect to treatment initiation, then the effect estimates will be biased. The inclusion requirement of at least 1 encounter with a health care system during follow-up means that patients who died are excluded, as are those who had a fall that did not result in a health care visit and patients without an encounter. It is plausible that the probability of a follow-up encounter is related to both treatment group and outcome, resulting in a risk of bias of unpredictable direction.
The study authors used ICD-10 codes to capture falls. There was no mention of validation of the codes used to classify the outcome, and the authors indicate that there may be substantial variation among clinicians about the level of detail recorded in their clinical notes. Events may have been missed, resulting in risk of bias due to misclassification of the outcome. Additionally, falls that did not result in an encounter with a health care system are unaccounted for, even though these may be clinically meaningful. The outcome definition included codes for hip fracture and traumatic brain injury. The clinical experts consulted by the review team confirmed that these fractures can result from mechanisms other than falls. The inclusion of other injuries obscures the true relationship between the drug exposures and the fall risk.
The authors appropriately controlled for several potential confounding variables, and the propensity score matching was successful. The selection of variables for confounding adjustment was not described. The baseline characteristics suggest that patients in the lemborexant group had fewer comorbidities at baseline than the patients in the other groups before matching. It is uncertain whether propensity score matching allowed for the normalization of all health characteristics (including those that are unreported) across groups. The clinical experts consulted by the review team also noted that lemborexant and the comparators might be used in different phases of treatment and for different clinical presentations. Several potential confounding variables were not considered, including the type of insomnia (acute or chronic) and its severity, as well as patients experiencing frailty, multimorbidity, living in isolation, limitations in activities of daily living, lower body weakness, gait imbalance, and visual impairments, and patients taking other medications that may impact fall risk.44-46 Treatment history, duration and intensity (dose), and time since insomnia diagnosis were not considered. Missing data precluded full meaningful adjustment for some variables. Therefore, residual confounding likely remains, though no evaluation of its extent or direction were reported.
The study did not report the effect size it was powered to detect. Further, propensity score matching to the lemborexant group (which was the smallest) resulted in substantial reductions in the sample size for analysis. Estimates of the difference between groups in the risk of falls was affected by imprecision, particularly for comparisons of lemborexant with trazodone and lemborexant with zolpidem, where the 95% CIs crossed the null. This should not be interpreted as “no difference”; instead, the CIs suggest the possibility that lemborexant is favoured or that there is little to no important difference between groups. In the absence of CIs for the absolute between-group differences being reported, it is difficult to judge whether the lower bound of the CI includes the potential for a clinically important increase in the risk of falls with lemborexant compared to zolpidem. The wider CIs for the analysis including patients aged 65 years and older introduces important uncertainty because they include the potential that either lemborexant or the comparator are favoured. There was no prespecified protocol for the study. A statistical analysis plan was supplied, but its prespecification could not be confirmed. There is therefore an increased risk that the reported results are selected from multiple analyses of the data, based on a favourable direction, magnitude, or statistical significance of the effect estimates.
External Validity
There are some limitations to generalizing the findings from this study to the requested reimbursement population. Patients with various types of insomnia and those without falls in the past 6 months are included in the study. Generalizability to the indicated population (i.e., patients with CID as defined in the DSM), patients with prior falls, and those with fewer health care system encounters is not known. Patients with comorbidities were not excluded in the study, which enhances generalizability to the real-world population of patients with insomnia and other health conditions, as indicated by the clinical experts consulted for this review. The propensity score matching resulted in a large reduction in sample size among the comparator groups, and relevant portions of the population may have been excluded. Full appraisal was not possible because the characteristics of patients who were unmatched were not provided. The data source was the US TriNetX Dataworks; the clinical experts consulted by the review team did not express serious concerns, but differences between health care systems in the US and Canada might reduce generalizability to the context in Canada. Patients were from 50 large health organizations; it is unclear if the results are generalizable to patients from the US who are uninsured or from smaller practices.
It is not clear whether patients in the study were taking the indicated dose of lemborexant and the comparators, nor whether the drugs were taken continuously. Zolpidem was included, but it is not publicly reimbursed in Canada, and the clinical experts consulted by the review team confirmed that it is rarely used. Zopiclone is used in Canada and has a comparable mechanism of action, but CDEC noted that the pharmacokinetic profiles are not identical, which precludes direct extrapolation of the comparison of zolpidem to zopiclone.11 Benzodiazepines were grouped for analysis; however, the clinical experts consulted by the review team noted that the fall risk might not be similar for those with longer versus shorter mechanisms of action. Therefore, the comparison might not be generalizable to individual benzodiazepines.
The outcome was defined to capture falls requiring contact with a health care system. The first fall was recorded, and recurrent falls are not captured. The clinical experts consulted by the review team indicated that information on recurrent falls may be useful to understand the full comparative safety risk of lemborexant versus other drugs used for chronic insomnia. Longer follow-up may have helped to understand the full impact of the included drugs on the risk of falls.
Hirata et al. Study
Populations
Eligible patients were those aged 20 years or older admitted to 1 of 8 hospitals in Japan during the study period (i.e., between April 1, 2018, and March 31, 2021).
Interventions and Exposures
Patients were exposed to 1 of the following hypnotic medication groups at the time of admission: benzodiazepines, Z-drugs, suvorexant, lemborexant, ramelteon, or other hypnotics. Data on the prescription of hypnotic medications were collected from drug pharmacy records up to the day after admission.
Outcomes
The outcome of interest was the occurrence of in-hospital falls; only the first fall was counted.
Statistical Analysis
Patient data, including background information such as age, sex, underlying conditions, and the occurrence of in-hospital falls, were extracted from the patients’ medical records.
All categories of hypnotic medications and background factors were included in the analysis of in-hospital falls. A Spearman correlation coefficient of less than 0.5 was used as a cut-off for low collinearity among variables.
For highly collinear pairs, 1 of the variables was selected as a covariate. The method of selection was not further described. A multivariate logistic regression analysis was applied to estimate ORs for in-hospital falls, after adjusting for the following covariates: other insomnia drugs, hospital, age, sex, emergency admission, Bedriddenness Rank, Cognitive Function Score, emergency transportation, referral letter, care level, consciousness disturbance, use of walking aids, admitting department, independence of ground-level walking, dysphagia, urinary frequency, diabetes mellitus, history of stroke, lower limb paralysis, Parkinson syndrome, ophthalmic diseases, visual impairment, alcoholism, surgical operation during hospital stay, rehabilitation, antipsychotic medication, and history of falls.
Results
Baseline Characteristics
Of the 150,278 patients included in the study, the median age was 70 years (range, 58 years to 79 years); 46.9% were females and 53.1% were males, respectively; 13,271 (8.8%) used benzodiazepine hypnotics; 5,634 (3.7%) used Z-drugs; 2,130 (1.4%) used ramelteon, 2,777 (1.8%) used suvorexant; 390 (0.3%) used lemborexant; and 102 (0.1%) used other medications. The patients’ Bedriddenness Rank most commonly corresponded to “normal” or “independence/autonomy” (44.4% of patients); 16.9% of patients had to remain in their homes, 9.0% had to remain seated, and 16.9% had to remain in bed (the remaining 12.9% had missing data). The patients’ Cognitive Function Score was most commonly “normal” (75.9% of patients); 11.8% had some degree of cognitive impairment, and 12.3% had missing data.
Outcome: Odds of In-Hospital Falls
Between patients who used the medication versus patients who did not use the medication, the OR for falls was 1.188 (95% CI, 0.774 to 1.825; P = 0.431) for lemborexant, 1.255 (95% CI, 1.118 to 1.409; P < 0.001) for benzodiazepine hypnotics, 1.293 (95% CI, 1.118 to 1.496, P = 0.001) for Z-drugs, 1.087 (95% CI, 0.891 to 1.329; P = 0.412) for ramelteon, 1.139 (95% CI, 0.947 to 1.369; P = 0.167) for suvorexant, and 1.261 (95% CI, 0.452 to 3.522; P = 0.658) for other drugs.
Critical Appraisal
Internal Validity
The study by Hirata et al. (2024)15 did not report the following: justification of the use of data not from Canada or proposed generalizability to the context in Canada; a predefined protocol; clear information on the inclusion criteria; information on the study periods (e.g., lookback windows, start of follow-up); how potentially confounding variables were selected; details of the quality of the data specifications (access, cleaning); data sources, including the data dictionary that provides information on the validity of relevant variables; a clear definition of the outcome variable; or between-group absolute effect estimates with CIs.
Exposure was determined using pharmacy records up to the day after hospital admission. The study did not clearly describe the time period during which exposure was ascertained (i.e., how long it might have extended before admission). Misclassification of exposed or unexposed status is possible due to treatment nonadherence, discontinuation, or switching occurring before hospitalization or during follow-up. The clinical experts consulted by the review team confirmed that the treatments may be used short term and/or intermittently. The study did not report information on the extent of drug exposure (i.e., dose or duration of treatment), which could differ across groups, precluding any inference about dose-harm relationships. The intention-to-treat approach used does not consider adherence, discontinuation, treatment switching, or concomitant use of other hypnotic drugs during follow-up. Instead, it assumes that any exposure permanently increases in-hospital fall risk, which may not be plausible. Consideration of an on-treatment exposure definition may have been preferred to address these issues, particularly when evaluating harms.43 Nondifferential exposure misclassification could bias results toward the null.
There may be a risk of bias in selecting patients into the study because the limited reporting does not suggest that inclusion was limited to patients who recently started taking the relevant drugs. The likely inclusion of patients undergoing treatment results in misalignment between the start of the intervention and the follow-up. These patients are survivors of AEs, including falls, that occur during the early phase of treatment. These falls are missed, and the patients remaining on the treatments are likely to be those at lower risk of falls.17 The clinical experts consulted by the review team noted that the risk of falls may be highest in the early phase of treatment. In-hospital falls may therefore be underestimated in all treatment groups, which could result in a bias toward the null in the comparison of lemborexant to “no lemborexant.” Exposure status was collected up to the day after admission, and the start of follow-up was not reported. The time before the index date (start of lemborexant or another drug) should have been classified as unexposed. Without information to confirm this, there is some risk of immortal time bias (i.e., a follow-up interval in which the outcome could not occur because of the exposure definition) favouring the lemborexant group.18 The impact of this particular source of bias may be small because it involves only 1 misclassified day of follow-up among certain patients.
The in-hospital fall outcome was not described in the publication, which indicates only that this information was collected from medical records. Therefore, the validity and reliability of the outcome collection process could not be verified. It is unclear whether information on falls would be consistently captured in medical records by various clinicians. As such, there is a potential for bias due to exposure misclassification. However, the potential extent and direction cannot be ascertained due to the limited reporting.
The aim of this pilot study was not to draw causal inferences but, instead, to explore associations between various factors and the odds of in-hospital falls. There is a risk of confounding by indication, because the comparison of interest is to “no lemborexant,” applying to a group of patients who are likely to differ systematically from those who take lemborexant; patients whose data are classified as “no lemborexant” might not be affected by insomnia and likely are at different risk of the outcome.47,48 Nevertheless, a multivariable logistic regression model was used to adjust for several potentially confounding variables. This is a valid approach, but confounding adjustment would have been strengthened by using propensity score methods. Within the regression approach, specification of the outcome model occurs with knowledge of the outcome (i.e., there is no separation of the design and analysis as there would be in a randomized trial), which may introduce bias, and the performance of the model (i.e., balance of confounders) cannot be empirically checked.19 It is not clear how the variables in the model were chosen beyond removing highly collinear pairs. Some potentially relevant variables were not considered, which means residual confounding likely remains. These variables included the presence and type of insomnia, fall prevention measures, other medications that may impact fall risk (e.g., antihypertensives), drug-drug interactions, or polypharmacy. Treatment history, treatment duration and intensity (dose), possible synergistic effects arising from concomitant use of other hypnotic medications, and length of hospital stay (follow-up) were also not considered. Missing data (classified as “unknown”) precluded full meaningful adjustment for some variables. No evaluation of the extent or direction of residual confounding was reported.
Despite the large sample size, few (0.3%) of the patients who were included were classified as being exposed to lemborexant, and among these patients only 25 outcome events were reported. As a result, the odds of in-hospital falls were estimated with imprecision (i.e., a wide CI). This imprecision should not be interpreted as no difference. Instead, it represents uncertainty in the result, such that there is a possibility that lemborexant either increases or decreases the odds of in-hospital falls compared to “no lemborexant.” There was no evidence of a predefined protocol or statistical analysis plan. There is therefore an increased risk that the reported results are selected from multiple analyses of the data, based on a favourable direction, magnitude, or statistical significance of the effect estimates.
External Validity
There are some limitations to generalizing the findings from this study to the requested reimbursement population. The patients in the study may not have been affected by chronic insomnia because this was not an inclusion criterion. Therefore, the relevance of the comparisons to the indicated population is not fully clear. Additionally, although patients aged 20 years and older were eligible, the patients who were included reflect a predominantly older adult population, and the clinical experts consulted by the review team also noted that they would expect a higher proportion of female patients in practice. As a result, generalizability to the full eligible population in Canada may be reduced. The population under study was not highly selected and had no explicit exclusions, which is a strength of this real-world study compared with RCTs.
This study was conducted in several hospitals in Japan, with 6 of the 8 facilities located in rural prefectures. The clinical experts consulted by the review team suggested that differences in ethnicity are not likely to substantially impact the results; however, they expressed concerns about generalizing results from the primarily rural health care system in Japan to health care systems in Canada. The authors used the Bedriddenness Rank and the Cognitive Function Score, which are public activities of daily living scales developed by Japan’s Ministry of Health, Labour and Welfare, as variables in the regression model. Given that these scales were developed and validated in Japan, they provide internal validity, but not external validity in international contexts. Additionally, patients who were hospitalized are likely to differ substantially from outpatients receiving lemborexant targeted by the present submission. It is not possible to confidently extrapolate the findings to these patients.
It is not clear whether the patients in the study were taking the indicated dose of lemborexant and the comparators, nor whether the drugs were taken continuously. The clinical experts consulted by the review team noted that the array of drugs used in the study differed from what would be expected in Canada. Suvorexant and ramelteon are not currently available in Canada, and some Z-drugs are not widely used; conversely, trazodone use is not reported in the study, although it may be accounted for in the “others” category. Regardless, the study compared lemborexant to “no lemborexant” after controlling for the effect of other drugs, and no direct comparisons to other relevant treatments were provided, nor can they be made with the present data. At most, data on other drugs in this study may be viewed as positive or negative controls for an association with in-hospital falls, with the same methodological limitations.
The study captured the occurrence of the first in-hospital fall, and recurrent falls are not captured. The clinical experts consulted by the review team indicated that information on recurrent falls may be useful to understand the full impact of lemborexant on fall risk.
Discussion
Summary of Available Evidence
Two retrospective observational studies (Juday et al. and Hirata et al.) from real-world settings are included in this review and appraised by the CDA-AMC review team.
In the Juday et al.14 study, eligible patients were adults who had been diagnosed with insomnia, had at least 1 pharmacy claim for an insomnia medication of interest, had visited a health care system during the 6 months after the index date, and had no evidence of falls, hip fractures, or traumatic brain injuries for 6 months before the index date. Patients were required to have been exposed to 1 of the following insomnia medications: lemborexant, trazodone, zolpidem, or benzodiazepines (as a class). The primary outcome was the proportion of patients with at least 1 fall during the 6-month follow-up period. After propensity score matching, there were 716 patients in each group, and the mean patient age was 54 years. About 62% and 38% of the patients were female and male, respectively. The most common comorbidities were anxiety disorders (35%), hypertension (34%), and mood disorders (24%).
In the Hirata et al. study,15 eligible patients were those aged 20 years or older admitted to 1 of 8 hospitals in Japan during the study period. The patients were exposed to 1 of the following hypnotic medication groups at the time of admission: benzodiazepines, Z-drugs, suvorexant, lemborexant, ramelteon, or other hypnotics. The outcome of interest was the occurrence of in-hospital falls. Of the 150,278 patients, 390 (0.3%) were exposed to lemborexant. In the full population, the median patient age was 70 years (range, 58 years to 79 years), and 46.9% and 53.1% of patients were female and male, respectively. The patients were classified into the fall group (n = 3,458) and the nonfall group (n = 146,820). A limited set of other characteristics of these patients was reported.
Interpretation of Results
In the 2023 recommendation against the reimbursement of lemborexant for the treatment of insomnia characterized by difficulties with sleep onset and/or sleep maintenance, CDEC noted a number of limitations in the available evidence. Among these, CDEC stated that further evidence was needed to address 1 of the key concerns associated with pharmacological treatment of insomnia — risk of falls — given that the number of fall events was small in the pivotal SUNRISE 1 and SUNRISE 2 trials. Additionally, CDEC noted that the safety demonstrated in the pivotal trials might not always be generalizable to real-world practice. In this resubmission, the Juday et al. study and the Hirata et al. study provided evidence on the risk of falls associated with lemborexant in the real-world outpatient and in-hospital settings. In the previous submission, CDEC also noted that the duration of treatment with lemborexant was 30 days in the SUNRISE 1 trial and up to 12 months in the SUNRISE 2 trial; therefore, data on long-term safety were needed . However, in the resubmission, neither the Juday et al. study nor the Hirata et al. study could address this evidence gap because they did not report the duration of treatment with lemborexant.
In the Juday et al. study, the absolute between-group difference (with 95% CI) in the proportion of patients with falls in the 6-month follow-up was not reported for patients aged 18 years and older (primary analysis) or patients aged 65 years and older (additional analysis). In patients aged 18 years and older, there was a rough estimate of a 1% absolute decrease in the proportion of patients with falls with lemborexant compared to trazodone, a rough estimate of 2% absolute decrease compared to zolpidem, and a rough estimate of 6% absolute decrease compared to benzodiazepines. In patients aged 65 years and older, there was an estimate of a 2% absolute decrease in the proportion of patients with falls with lemborexant compared to trazodone or zolpidem and an estimate of an 8% absolute decrease compared to benzodiazepines. According to the clinical experts consulted by the CDA-AMC review team, a magnitude of decrease of 2% or more in absolute terms is clinically meaningful at a population level. However, this evidence was affected by several concerns for internal validity and external validity. Internal validity concerns included the potential for selection bias, the inclusion of patients undergoing treatment with no prior falls (leading to missed AEs occurring early in treatment and a population considered to be lower risk), potential misclassification of exposures and outcomes, and residual confounding. External validity concerns included that the definition of insomnia was broader than the reimbursement request, the doses of insomnia treatments used were unreported, and all data were from a select population in the US. The clinical experts consulted by the review team commented that the occurrence of falls requiring contact with a health care system was notably high in all groups and that the differential between the full population and patients aged 65 years and older was smaller than would be expected in practice. This is likely related to the outcome definition including events other than falls and the exclusion of an unknown proportion of the population without events due to requiring a health care visit during follow-up for inclusion in the study. Additionally, there was important imprecision in the comparison of the lemborexant group to the trazodone group (95% CI, 0.838 to 1.657) or the zolpidem group (95% CI, 0.907 to 1.772), partially due to the small sample of patients taking lemborexant (n = 716), suggesting a possibility that lemborexant was associated with either decreased risk of falls or little to no clinically important difference compared to trazodone and zolpidem. Without CIs for the absolute effects, it is not clear whether the lower bound of the CI would include a clinically important increase in the risk of falls with lemborexant compared to zolpidem. Only the RR for the comparison between the lemborexant group and the benzodiazepines group is statistically significant (95% CI, 1.295 to 2.413). However, individual benzodiazepines with different half-lives may have different fall risks; therefore, the effect might not be generalizable to all benzodiazepines. These limitations made it not possible to definitively attribute the fall risk estimated in the study to the individual treatments. Comparisons to other drugs commonly used to treat chronic insomnia in Canada were not available in this study.
The Hirata et al. study investigated the relationship between lemborexant received at admission and in-hospital falls. The study did not report the percentage of patients with falls, only the relative effect measure (i.e., OR). The findings showed that the OR for in-hospital falls was 1.188 (95% CI, 0.774 to 1.825; P = 0.431) for lemborexant, 1.255 (95% CI, 1.118 to 1.409; P < 0.001) for benzodiazepines, and 1.293 (95% CI, 1.118 to 1.496; P = 0.001) for Z-drugs between patients who used the medication versus patients who did not use the medication. No absolute effects were reported, which limits clinical interpretation of the findings. This evidence was affected by several concerns for internal validity and external validity. Internal validity concerns included the likely inclusion of patients undergoing treatment (leading to missed AEs occurring early in treatment and a population considered to be lower risk), some potential for time-related bias, potential misclassification of exposures and outcomes, and residual confounding. External validity concerns included the presence of chronic insomnia not being an inclusion criterion, unreported doses of insomnia treatments, the use of the Bedriddenness Rank and the Cognitive Function Score developed and validated in Japan, and all data being from inpatients in Japan. There were relatively few patients classified as those who received lemborexant and a small number of events, resulting in 95% CIs that are imprecise, suggesting the potential for lemborexant (versus no lemborexant) to be associated with either increased or decreased odds of in-hospital falls. These limitations made it impossible to definitively attribute the estimated odds of in-hospital falls to the individual treatments. Additionally, there were no direct comparisons between the treatments investigated in the study, and comparisons with other drugs commonly used to treat chronic insomnia in Canada were not available.
Other Considerations
In the initial submission of lemborexant in 2022, the reimbursement request was the same as the Health Canada indication: “for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.” In the present resubmission for lemborexant, the reimbursement request has changed to “for the treatment of insomnia in adults diagnosed according to the most recent version of the DSM referring to CID.” In the initial submission, the pivotal SUNRISE 1 and SUNRISE 2 trials both included patients with insomnia disorder diagnosed according to the DSM-5. The CDA-AMC review team did not identify any additional concerns about the generalization of the findings from the SUNRISE 1 and SUNRISE 2 trials to the population described in the revised reimbursement request.
Conclusion
In the resubmission for lemborexant, CDA-AMC reviewed 2 retrospective cohort studies (Juday et al. [2022] and Hirata et al. [2024]), which investigated the risk of falls associated with lemborexant in real-world outpatient and in-hospital settings, respectively. The results from the Juday et al. (2022) study suggested that the risk of falls over a 6-month follow-up period was lower with lemborexant than with benzodiazepines as a class both among adults with insomnia aged 18 years and older and in the subgroup of patients aged 65 years and older. Point estimates for comparisons between lemborexant and trazodone and between lemborexant and zolpidem were also suggestive of a lower risk of falls with lemborexant, but these estimates were inconclusive due to imprecision (i.e., the CIs crossed the null). Direct comparisons with other relevant treatments were not provided. The CDA-AMC review team acknowledges the value of the evidence from the observational studies, which provided insights into the risk of falls associated with lemborexant in real-world settings. However, this evidence was subject to uncertainty due to a number of internal and external validity concerns. No new evidence on the comparative efficacy or other potential harms of lemborexant was included in this review. Therefore, most gaps identified by CDEC in the initial review remain to be addressed. The new reimbursement request aligns with the inclusion criteria of the SUNRISE trials. Consequently, the previously submitted evidence was not reappraised by the review team. There remains a lack of clarity about whether lemborexant provides a preferable balance of benefits and harms compared to other treatments used for chronic insomnia.
References
1.Eisai Inc. Lemborexant (Dayvigo), 5 mg film-coated tablet and 10 mg film-coated tablet, oral [product monograph]. Jan 30, 2025.
2.Diagnostic and statistical manual of mental disorders: DSM-5™, 5th ed. American Psychiatric Publishing; 2013.
3.Benca R. Post TW, ed. Risk factors, comorbidities, and consequences of insomnia in adults. UpToDate; 2025. Accessed April 11, 2025. https://www.uptodate.com
4.McNamara S, Spurling BC, Bollu PC. Chronic Insomnia. StatPearls Publishing; 2025. Accessed May 2, 2025. https://www.ncbi.nlm.nih.gov/books/NBK526136/
5.Skobic I, Pezza M, Howe G, Haynes PL. Examining insomnia disorder and stress generation among individuals who have experienced involuntary job loss. J Psychosom Res. 2024;177:111585. doi: 10.1016/j.jpsychores.2023.111585 PubMed
6.Cernadas Curotto P, Sterpenich V, Sander D, Favez N, Rimmele U, Klimecki O. Quarreling After a Sleepless Night: Preliminary Evidence of the Impact of Sleep Deprivation on Interpersonal Conflict. Affect Sci. 2022;3(2):341-352. doi: 10.1007/s42761-021-00076-4 PubMed
7.Morin CM, Vezina-Im LA, Chen SJ, et al. Prevalence of insomnia and use of sleep aids among adults in Canada. Sleep Med. 2024;124:338-345. doi: 10.1016/j.sleep.2024.09.044 PubMed
8.Morin CM, Khullar A, Robillard R, et al. Delphi consensus recommendations for the management of chronic insomnia in Canada. Sleep Med. 2024;124:598-605. doi: 10.1016/j.sleep.2024.09.038 PubMed
9.Riemann D, Espie CA, Altena E, et al. The European Insomnia Guideline: An update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035. doi: 10.1111/jsr.14035 PubMed
10.Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(2):307-349. doi: 10.5664/jcsm.6470 PubMed
11.CADTH Reimbursement Review: Lemborexant (Dayvigo). Can J Health Technol. 2023;3(4). doi:10.51731/cjht.2023.624
12.Clinical Evaluation of Interventions for the Management of Insomnia: A Review of Reviews. CADTH; 2020. Accessed March 17, 2025. https://www.cda-amc.ca/sites/default/files/pdf/op0527_insomnia_clinical-evaluation-corrected.pdf
13.Lessard S, Chow WK, Cook SE, Lessard G, Khullar A. Insomnia Management in Primary Care: Outcomes from a Canadian National Survey Reveal Challenges and Opportunities to Improve Clinical Practice. Canadian Journal of Medicine. 2024;0(0):88-104. doi: 10.33844/cjm.2024.6041
14.Eisai Inc. Clinical Study Report: Retrospective Cohort Study Comparing Risk of Falls and Associated Incremental Costs Among Adults Treated With Specific Insomnia Medications [internal sponsor's report]. Sept 30, 2022.
15.Hirata R, Katsuki NE, Shimada H, et al. The Administration of Lemborexant at Admission is Not Associated with Inpatient Falls: A Multicenter Retrospective Observational Study. Int J Gen Med. 2024;17:1139-1144. doi: 10.2147/IJGM.S452278 PubMed
16.Guidance for Reporting Real-World Evidence. CADTH; 2023. Accessed June 20, 2025. https://www.cda-amc.ca/sites/default/files/RWE/MG0020/MG0020-RWE-Guidance-Report-Secured.pdf
17.Ray WA. Evaluating medication effects outside of clinical trials: new-user designs. Am J Epidemiol. 2003;158(9):915-20. doi: 10.1093/aje/kwg231 PubMed
18.Suissa S. Immortal time bias in pharmaco-epidemiology. Am J Epidemiol. 2008;167(4):492-9. doi: 10.1093/aje/kwm324 PubMed
19.Webster-Clark M, Sturmer T, Wang T, et al. Using propensity scores to estimate effects of treatment initiation decisions: State of the science. Stat Med. 2021;40(7):1718-1735. doi: 10.1002/sim.8866 PubMed
20.Morin CM, Benca R. Chronic insomnia. Lancet. 2012;379(9821):1129-41. doi: 10.1016/S0140-6736(11)60750-2 PubMed
21.Lancee J, van Straten A, Morina N, Kaldo V, Kamphuis JH. Guided Online or Face-to-Face Cognitive Behavioral Treatment for Insomnia: A Randomized Wait-List Controlled Trial. Sleep. 2016;39(1):183-91. doi: 10.5665/sleep.5344 PubMed
22.Alberta Medical Association. Assessment to Management of Adult Insomnia: Clinical Practice Guideline. 2015. Accessed March 17, 2025. https://www.albertadoctors.org/media/v51b22o2/adult-insomnia-guideline.pdf
23.Dayvigo (Lemborexant) [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=99675
24.Zopiclone [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=75747
25.Alprazolam [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=11803
26.Bromazepam [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=19056
27.Clonazepam [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=19063
28.Diazepam [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=2657
29.Dalmane (flurazepam) [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=4697
30.Lorazepam [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=6295
31.Nitrazepam [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=69245
32.Oxazepam [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=3463
33.Apotex Inc. Temazepam (temazepam): 15 mg and 30 mg capsules USP [product monograph]. 2020. Updated December 7, 2020. Accessed May 9, 2022. https://pdf.hres.ca/dpd_pm/00059186.PDF
34.Triazolam[productmonograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=9575
35.Chlordiazepoxide [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=4279
36.Clobazam [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=68625
37.Amitriptyline [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=96853
38.Mirtazapine [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=77206
39.Trazodone [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=102666
40.Quetiapine [product monograph] [sponsor supplied reference]. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=87337
41.Juday TR, Jang SR, Lundwall C, Pappadopulos E, Wickwire EM. Retrospective Cohort Study Comparing Risk of Falls Among Adults Treated with Specific Insomnia Medications [sponsor supplied reference]. presented at: Academy of Managed Care Pharmacy (AMCP) Annual Meeting; 2023; San Antonio, TX, USA.
42.Methods Guide for Health Technology Assessment. CDA-AMC; 2025. Accessed June 20, 2025. https://www.cda-amc.ca/sites/default/files/MG%20Methods/MG0030-Quantitative-Methods-Manual-Line-Numbered.pdf
43.National Institute for Health and Care Excellence. NICE real-world evidence framework. 2022. Accessed June 20, 2025. https://www.nice.org.uk/corporate/ecd9/chapter/overview
44.BC Guidelines. Fall Prevention: Risk Assessment and Management for Community-Dwelling Older Adults. 2023. Accessed June 13, 2025. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/fall-prevention
45.Ghossein N, Kang M, Lakhkar AD. Anticholinergic Medications. StatPearls Publishing; 2023. Accessed June 13, 2025. https://www.ncbi.nlm.nih.gov/books/NBK555893/
46.Centers for Disease Control and Prevention. Fact Sheet: Medications Linked to Falls. 2017. Accessed June 13, 2025. https://www.cdc.gov/steadi/media/pdfs/STEADI-FactSheet-MedsLinkedtoFalls-508.pdf
47.D'Arcy M, Sturmer T, Lund JL. The importance and implications of comparator selection in pharmacoepidemiologic research. Curr Epidemiol Rep. 2018;5(3):272-283. doi: 10.1007/s40471-018-0155-y PubMed
48.Lund JL, Richardson DB, Sturmer T. The active comparator, new user study design in pharmacoepidemiology: historical foundations and contemporary application. Curr Epidemiol Rep. 2015;2(4):221-228. doi: 10.1007/s40471-015-0053-5 PubMed
49.Eisai Limited. Drug Reimbursement Review sponsor submission: Dayvigo (lemborexant), 5 mg and 10 mg oral tablets [internal sponsor's package]. 2022.
50.Brasure M, MacDonald R, Fuchs E, et al. AHRQ Comparative Effectiveness Reviews: Management of Insomnia Disorder [sponsor supplied reference]. Agency for Healthcare Research and Quality (US); 2015.
51.Alberta Medical Association. Clinical Practice Guideline: assessment to management of adult insomnia. 2015. Accessed May 9, 2022. https://top.albertadoctors.org/CPGs/Lists/CPGDocumentList/Adult-Insomnia-CPG.pdf
52.Chaput JP, Yau J, Rao DP, Morin CM. Prevalence of insomnia for Canadians aged 6 to 79. Health Rep. 2018;29(12):16-20. PubMed
53.Health Canada. Summary basis of decision (SBD) for Dayvigo. 2021. Accessed May 9, 2022. https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?lang=en&linkID=SBD00529
54.Morin CM, Jarrin DC, Ivers H, Merette C, LeBlanc M, Savard J. Incidence, Persistence, and Remission Rates of Insomnia Over 5 Years. JAMA Netw Open. 2020;3(11):e2018782. doi: 10.1001/jamanetworkopen.2020.18782 PubMed
55.LeBlanc M, Merette C, Savard J, Ivers H, Baillargeon L, Morin CM. Incidence and risk factors of insomnia in a population-based sample. Sleep. 2009;32(8):1027-37. doi: 10.1093/sleep/32.8.1027 PubMed
56.Daley M, Morin CM, LeBlanc M, Grégoire JP, Savard J. The economic burden of insomnia: direct and indirect costs for individuals with insomnia syndrome, insomnia symptoms, and good sleepers. Sleep. 2009;32(1):55-64. PubMed
57.Summary of reports: interventions for insomnia disorder. CADTH; 2018. Accessed May 9, 2022. https://www.cadth.ca/sites/default/files/pdf/insomnia_summary_e.pdf
58.Neubauer DN. Post TW, ed. Pharmacotherapy for insomnia in adults. UpToDate. Accessed Mar 15, 2022. http://www.uptodate.com
59.Eisai Limited. Health Canada reviewer's report: Dayvigo (lemborexant) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dayvigo (lemborexant), 5 mg and 10 mg oral tablets. 2020.
60.Drake C, Yardley J, Pinner K, Lenderking W, Savva Y, Moline M. Perception of Lemborexant Effectiveness as Assessed by the Patient Global Impression- Insomnia Questionnaire (unpublished) [sponsor supplied reference].
61.Eisai Limited. Periodic Safety Update Report for Lemborexant (time period: between Dec 20, 2021 and Jun 19, 2022) [sponsor supplied reference]. 2022.
62.De Crescenzo F, D'Alo GL, Ostinelli EG, et al. Comparative effects of pharmacological interventions for the acute and long-term management of insomnia disorder in adults: a systematic review and network meta-analysis. Lancet. 2022;400(10347):170-184. doi: 10.1016/S0140-6736(22)00878-9 PubMed
63.Eisai Inc. Clinical Study Report: E2006-G000-304. SUNRISE 1. A multicenter, randomized, double-blind, placebo-controlled, active comparator, parallel-group study of the efficacy and safety of lemborexant in subjects 55 years and older with insomnia disorder [internal sponsor's report]. 2018.
64.Eisai Inc. Clinical Study Report: E2006-G000-303. SUNRISE 2. A long-term multicenter, randomized, double-blind, controlled, parallel-group study of the safety and efficacy of lemborexant in subjects with insomnia disorder [internal sponsor's report]. 2018.
65.Eisai Limited. Dayvigo (lemborexant): 5 mg, 10 mg oral tablet [product monograph]. Nov 3, 2020.
66.McElroy H, O'Leary B, Adena M, Campbell R, Monfared AAT, Meier G. Comparative efficacy of lemborexant and other insomnia treatments: a network meta-analysis. J Manag Care Spec Pharm. 2021;27(9):1296-1308. doi: 10.18553/jmcp.2021.21011 PubMed
67.Henmi R, Nakamura T, Mashimoto M, Takase F, Ozone M. Preventive Effects of Ramelteon, Suvorexant, and Lemborexant on Delirium in Hospitalized Patients With Physical Disease: A Retrospective Cohort Study. J Clin Psychopharmacol. 2024;44(4):369-377. doi: 10.1097/JCP.0000000000001876 PubMed
68.Horikoshi S, Miura I, Suzuki Y, et al. Switching to lemborexant for the management of insomnia in mental disorders: the SLIM study. J Clin Sleep Med. 2023;19(10):1753-1758. doi: 10.5664/jcsm.10668 PubMed
69.Katsuta N, Takahashi K, Kurosawa Y, et al. Safety and real-world efficacy of lemborexant in the treatment of comorbid insomnia. Sleep Med X. 2023;5:100070. doi: 10.1016/j.sleepx.2023.100070 PubMed
70.Mishima K, Fujimoto K, Endo A, Ishii M. Safety and Efficacy of Lemborexant in Insomnia Patients: Results of a Postmarketing Observational Study of Dayvigo((R)) Tablets. Drugs R D. 2024;24(2):211-226. doi: 10.1007/s40268-024-00462-w PubMed
71.Miyata S, Iwamoto K, Okada I, et al. Assessing the Real-World, Long-Term Impact of Lemborexant on Sleep Quality in a Home-Based Clinical Study. Nat Sci Sleep. 2024;16:291-303. doi: 10.2147/NSS.S448871 PubMed
72.Moline ML, Cheng JY, Durgin C, et al. Abuse Potential Similarities Between Hypnotic Classes: Real-World Data [sponsor supplied reference]. presented at: Annual Scientific Meeting of the College on Problems of Drug Dependence (CPDD); 2023; Denver, CO, USA.
73.Ozone M, Hirota S, Ariyoshi Y, et al. Efficacy and Safety of Transitioning to Lemborexant from Z-drug, Suvorexant, and Ramelteon in Japanese Insomnia Patients: An Open-label, Multicenter Study. Adv Ther. 2024;41(4):1728-1745. doi: 10.1007/s12325-024-02811-2 PubMed
74.Tanaka-Mizuno S, Fujimoto K, Mishima K, et al. Evaluation of prescribing patterns of switching to and add-on lemborexant in patients treated with hypnotic medication: a nationwide claims database study in Japan. Expert Opin Pharmacother. 2024;25(12):1707-1716. doi: 10.1080/14656566.2024.2392018 PubMed
Appendix 1: Executive Summary of the Initial Submission of Lemborexant
Please note that this appendix has not been copy-edited.
Appendix 1 was taken verbatim from the previous 2022 CADTH report from the initial submission of lemborexant (project website).
An overview of the submission details for the drug under review is provided in Table 11.
Table 11: Background Information of Initial Submission of Lemborexant
Item | Description |
|---|---|
Drug product | Lemborexant (Dayvigo), 5 mg per tablet and 10 mg per tablet, oral |
Indication | For the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 4, 2020 |
Sponsor | Eisai Limited |
NOC = Notice of Compliance.
Source: Sponsor’s submission package for review of lemborexant.49
Introduction
Insomnia disorder is the most common sleep disorder and, according to the DSM-5, is described as being dissatisfied with the quality or quantity of sleep, difficulty initiating and/or maintaining sleep, and is associated with daytime impairment.50,51 The DSM-5 criteria include sleep disturbances occurring at least 3 nights per week for at least 3 months.2,51 In Canada, the prevalence is estimated to be between 12% and 24%52,53 and the incidence is estimated to be between 3.8% and 7.3% per year.54,55 Older age, female sex, comorbid medical or psychiatric conditions, and social and environmental factors have been identified as common risk factors for insomnia.50,51 Insomnia can be diagnosed as a disorder on its own or as a symptom associated with many other medical conditions and has been closely linked to reduced life expectancy and increased economic costs through lost productivity, workplace and motor vehicle accidents (MVAs), and greater health care utilization.10,50,51,54-56
Per the Alberta Medical Association’s Clinical Practice Guidelines, insomnia can be treated and managed in a primary care setting or by a specialist when the problem cannot be diagnosed or if the insomnia is resistant to treatment.51 Non-pharmacological treatment options such as CBT-I are recommended as an initial treatment.10,51,57 Pharmacological treatments include BZRA (including benzodiazepines and Z-drugs), DORA, histamine receptor antagonists, and melatonin receptor agonists.58 Off-label medications that have sedating effects (e.g., antidepressants, antihistamines, anticonvulsants, and antipsychotics) may be used in specific situations but are generally not recommended as a first-line treatment due to the lack of efficacy and safety evidence in this population.51,58 Long-term use of hypnotics is discouraged as the studies supporting their approval were based on short-term use50 and are not recommended as a first-line treatment option.51,58
Lemborexant is a DORA indicated for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.49 The recommended dose is 5 mg once per night and may be increased to the maximum recommended dose of 10 mg based on clinical response and tolerability.59 Lemborexant is taken orally once per night within a few minutes before going to bed with at least 7 hours before planned awakening time.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of lemborexant 5 mg (LEM5) or 10 mg (LEM10) tablets taken orally once daily at bedtime for the treatment of patients with insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.
Following the issuance of the draft CADTH Canadian Drug Expert Committee (CDEC) recommendation for lemborexant in August 2022, the following additional information was provided to CADTH:
One unpublished manuscript by Drake et al. (2021)60 that provided evidence for lemborexant’s efficacy as measured by the Patient Global Impression – Insomnia (PGI-Insomnia) in SUNRISE 2;
A periodic safety update report61 that included aggregate data from approximately 4,024 adult patients with insomnia disorder, Irregular Sleep-Wake Rhythm Disorder, or healthy volunteers who were enrolled in the lemborexant clinical development program; and
A published network meta-analysis (NMA) by De Crescenzo et al. (2022)62 comparing lemborexant to other pharmacological treatments for the acute and long-term treatment of adults with insomnia.
These data were not included in the submission to CADTH and provided more information on the clinical meaningfulness of the subjective PGI-Insomnia instrument, safety, and comparison to other drugs for the treatment of insomnia. The information has been summarized and critically appraised as an addendum to the CADTH report in Appendix 6.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input, clinician input, and from a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
CADTH received input from 3 patient groups: the MDSC, Migraine Canada, and Menopause Chicks. The 3 groups conducted surveys and interviews with patients and caregivers to inform their input. Respondents from all 3 patient groups indicated that sleep problems significantly impacted their quality of life, energy level, cognitive function, mood the next day, and daytime activities. Most respondents reported having tried various treatments (e.g., benzodiazepines, Z-drugs) for sleep problems. Many reported being dissatisfied and discontinued treatment due to side effects such as next day sedation and cognitive impairment, and fear of developing a substance use disorder. The groups indicated the following as key outcomes for patients and caregivers: uninterrupted and restorative sleep, greater access to treatment, more effective treatment options, long-term effectiveness, fewer side effects, less stress and anxiety, improved productivity, and improved relationships. The MDSC input included 3 respondents who had experience with lemborexant and accessed the drug through private health insurance. They described being able to manage their sleep problems without becoming dependent on the medication or experiencing serious side effects, and without feeling lethargic and sleepy the next morning.
Clinician Input
Input From the Clinical Expert Consulted by CADTH
The clinical expert consulted for this review stated that the current goals of treatment are to improve sleep initiation, maintenance, and terminal insomnia leading to restorative sleep. According to the clinical expert, CBT-I is the first-line treatment for insomnia, but many patients have limited access to and/or success with this option, thus pharmacotherapy is often used in addition to or in place of CBT-I. Per the expert, when a medication is used for extended periods of time, a patient may have a waning response or no response. At this point it can be difficult to withdraw the therapy if the patient has developed tolerance to the drug and the patient may experience rebound insomnia. Another concern raised by the clinical expert was the risk of cognitive and behavioural changes the next morning that can lead to falls and other dangers, particularly for older adult patients.
The clinical expert suggested that lemborexant may be a first-line pharmacological treatment for insomnia and noted that it would be necessary to determine how to optimally transition from other currently available medications (e.g., Z-drugs) to lemborexant. The expert indicated that most patients with insomnia may be candidates for treatment with lemborexant except for those who are pregnant, nursing, or have narcolepsy. According to the clinical expert, patients are asked general questions about their sleep rather than taking measurements in clinics which the expert thought does not tend to vary among physicians. The clinical expert indicated that few clinics are performing sleep studies for insomnia (except where another sleep disorder is suspected) because access is limited across Canada.
The expert noted that chronic insomnia generally does not go away and tends to worsen with age, menopause, or as a result of other major negative life events. The expert suggested that a patient may wish to trial being off medication and can be supported by additional sleep management tools such as CBT-I. When deprescribing a medication, the clinical expert would observe for a return of symptoms or rebound insomnia. Per the clinical expert, insomnia is typically treated by family physicians or psychiatrists.
Clinician Group Input
CADTH received input from 2 clinician groups: the Canadian Consortium of Sleep and Sleep Interested Physicians (CCSSP) and the National Advisory Board. The clinician group input was aligned with that given by the clinical expert consulted by CADTH.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. Key issues raised by the drug plans included concerns over the most appropriate comparator to lemborexant, the necessity for patients to fail a treatment for insomnia before accessing lemborexant, exclusion of comorbid conditions, and the use of polysomnography for measuring efficacy. The clinical expert indicated uncertainty of zolpidem being the most appropriate comparator and how it compared to zopiclone, the latter of which was noted as being more commonly used in Canadian practice. The expert also stated that it would not be reasonable for patients to have to fail a less expensive drug with greater risk of harms before accessing safer alternatives if the 2 had similar efficacy. Further, the clinical expert noted that there is currently a lack of evidence supporting the use of lemborexant in patients with comorbid conditions that were excluded from SUNRISE 1 and SUNRISE 2 (based on Beck Depression Inventory–II [BDI-II], Beck Anxiety Inventory [BAI], and Apnea-Hypopnea Index [AHI] scores), but given that insomnia is closely linked to anxiety and depression, it would be very difficult to exclude these comorbidities until trials could be performed. Lastly, the expert stated that polysomnography results should not be used as a marker for efficacy or a necessary criterion for accessing lemborexant.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
Two double-blind (DB), phase III, RCTs (SUNRISE 1 and SUNRISE 2) were included in the systematic review of lemborexant.
SUNRISE 1 (N = 1,006) was designed to assess the safety and efficacy of LEM5 and LEM10 for 30 days in females who were 55 years or older and males who were 65 years or older, all of whom had insomnia disorder according to the DSM-5. Comparators included zolpidem tartrate extended-release 6.25 mg and appearance-matched placebos (PBOs) for both active compounds. The primary outcome was latency to persistent sleep (LPS) and key secondary outcomes were WASO, wake after sleep onset in the second half of the night (WASO2H), and sleep efficiency as measured by polysomnography. Other secondary and exploratory outcomes important to the CADTH review included patient-reported outcomes such as the European quality of life-5 dimensions-3 levels (EQ-5D-3L), ISI, Fatigue Severity Scale (FSS), PGI-Insomnia, and quality of sleep questionnaires. Patients had a mean age of 63.9 years (SD = 6.81 years) and 86.4% were female. At baseline, mean LPS was approximately 45 minutes, mean WASO was around 114 minutes, mean WASO2H was 77 minutes, and mean sleep efficiency was 68%.
SUNRISE 2 (N = 971) was designed to assess the long-term safety and efficacy of LEM5 and LEM10 for up to 12 months in adults 18 years or older who had insomnia disorder according to the DSM-5. The first 6 months of SUNRISE 2 consisted of 3 treatment groups: LEM5, LEM10, and PBO. For the next 6 months of the trial, patients who were randomized to PBO were rerandomized to active treatment (i.e., LEM5 or LEM10) for the remainder of the trial. The primary outcome was subjective sleep onset latency (sSOL) and key secondary outcomes were subjective WASO (sWASO) and subjective sleep efficiency as recorded in the sleep diary. Other secondary and exploratory outcomes important to the CADTH review were the same as the patient-reported outcomes listed for SUNRISE 1. Patients had a mean age of 54.5 years (SD = 13.80 years) and 68.2% were female. At baseline, mean sSOL was approximately 64 minutes, sWASO was 134 minutes, and subjective sleep efficiency was 62%.
Efficacy Results
Statistical testing was conducted based on a gate-keeping procedure for both studies. In SUNRISE 1, the following outcomes were controlled for multiplicity: LPS, sleep efficiency, WASO, and WASO2H. In SUNRISE 2, the following outcomes were controlled for multiplicity: sSOL, subjective sleep efficiency, and sWASO. Efficacy data have been summarized in Table 12 for SUNRISE 1 and Table 13 for SUNRISE 2.
Health-Related Quality of Life and Severity of Symptoms
The clinical expert emphasized the importance of patient-reported outcomes such as the EQ-5D-3L, ISI, FSS, PGI-Insomnia, and quality of sleep questionnaires. For the EQ-5D-3L visual analogue scale in SUNRISE 1, the least squares mean (LSM) treatment difference for LEM10 versus PBO was 2.53 (95% CI, 0.69 to 4.38) and for LEM5 versus PBO was 0.52 (95% CI, –1.32 to 2.37). In SUNRISE 2, the LSM treatment difference for LEM10 versus PBO was 1.04 (95% CI, –1.36 to 3.43) and for LEM5 versus PBO was –0.96 (95% CI, –3.31 to 1.39). All patient-reported outcome questionnaires were other secondary or exploratory outcomes and were not adjusted for multiplicity, therefore definitive conclusions could not be made from the results.
Sleep Latency (Sleep Onset): LPS, sSOL
In SUNRISE 1, the least squares geometric mean (LSGM) treatment ratio for LPS for LEM10/PBO was 0.72 (95% CI, 0.63 to 0.83; P < 0.0001) and for LEM5/PBO was 0.77 (95% CI, 0.67 to 0.89; P = 0.0003).
In SUNRISE 2, the LSGM treatment ratio for LPS for LEM10/PBO was 0.70 (95% CI, 0.61 to 0.81; P < 0.0001) and for LEM5/PBO was 0.73 (95% CI, 0.64 to 0.84; P < 0.0001).
Waking After Sleep Onset (Sleep Maintenance): WASO, WASO2H, sWASO
In SUNRISE 1, the LSM treatment differences for WASO for LEM10 versus PBO was –25.35 minutes (95% CI, –31.36 to –19.34 minutes; P < 0.0001) and for LEM5 versus PBO was –23.96 minutes (95% CI, –29.98 to –17.95 minutes; P < 0.0001). The LSM treatment differences for WASO2H for LEM10 versus zolpidem was –8.00 minutes (95% CI, –12.53 to –3.47 minutes; P = 0.0005) and for WASO2H for LEM5 versus zolpidem was –6.65 minutes (95% CI, –11.15 to –2.15 minutes; P = 0.0038).
In SUNRISE 2, the LSM treatment differences for LEM10 versus PBO was –12.67 minutes (95% CI, –22.38 to –2.96 minutes; P = 0.0105) and for LEM5 versus PBO was –17.47 minutes (95% CI, –27.31 to –7.64 minutes; P = 0.0005).
Sleep Efficiency: Sleep Efficiency and Subjective Sleep Efficiency
In SUNRISE 1, the LSM treatment differences for LEM10 versus PBO was 8.03% (95% CI, 6.57 to 9.49%; P < 0.0001) and for LEM5 versus PBO was 7.07% (95% CI, 5.61 to 8.54%; P < 0.0001).
In SUNRISE 2, the LSM treatment differences for LEM10 versus PBO was 4.67% (95% CI, 2.37 to 6.96%; P < 0.0001) and for LEM5 versus PBO was 4.55% (95% CI, 2.24 to 6.86%; P = 0.0001).
Harms Results
Harms data have been summarized in Table 12 for SUNRISE 1 and Table 13 for SUNRISE 2.
Adverse Events
In SUNRISE 1, approximately one-third of patients experienced a treatment-emergent adverse event (TEAE), and rates were relatively similar among all groups: 82 (30.6%), 74 (27.8%), 93 (35.4%), and 53 (25.4%) patients in LEM10, LEM5, zolpidem, and PBO groups, respectively. In SUNRISE 2, more than half of the patients experienced a TEAE and rates were similar among all groups: 187 (59.6%), 192 (61.1%), and 200 (62.7%) of patients in LEM10, LEM5, and PBO groups, respectively. The most common events in both studies were headache, somnolence, and nasopharyngitis.
Serious AEs
Serious adverse events (SAEs) were rare in both studies. In SUNRISE 1, 2 (0.8%) and 4 (1.5%) patients in LEM5 and zolpidem groups, respectively, experienced at least 1 SAE. No patients in LEM10 or PBO groups reported a SAE. In SUNRISE 2, 9 (2.9%), 7 (2.2%), and 5 (1.6%) patients in LEM10, LEM5, and PBO groups, respectively, experienced at least 1 SAE. No SAE occurred in more than 1 patient per treatment group.
Withdrawals Due to AEs
In general, there were few withdrawals from treatment due to AEs in both studies. In SUNRISE 1, 3 (1.1%), 2 (0.8%), 7 (2.7%), and 2 (1.0%) patients in LEM10, LEM5, zolpidem, and PBO groups, respectively, stopped treatment due to an AE. No events occurred in more than 1 patient in any treatment group. In SUNRISE 2, 26 (8.3%), 13 (4.1%), and 12 (3.8%) patients in LEM10, LEM5, and PBO groups, respectively, stopped treatment due to an AE. The following events occurred in more than 1 patient in any group: headache, somnolence, nightmare, and palpitations.
Mortality
No deaths were reported in either SUNRISE 1 or SUNRISE 2 trials.
Notable Harms
In both studies, rates of somnolence were numerically higher among patients who received LEM10 compared to LEM5 (7.1% versus 4.1% in SUNRISE 1 and 13.1% versus 8.6% in SUNRISE 2) and were greater than either zolpidem (1.5%) or PBO (1.9%) in SUNRISE 1 or PBO (1.6%) in SUNRISE 2.
Falls were rare in SUNRISE 1 (1.5% in the LEM5 group and 0% for all other groups) and SUNRISE 2 (1.6% in each of the LEM10 and LEM5 groups and 3.1% for PBO).
A road traffic accident (MVA for the CADTH systematic review protocol) was described for 1 patient who received zolpidem in SUNRISE 1 and no other treatment groups reported a MVA. In SUNRISE 2, 1 patient each in LEM10 and PBO groups reported a MVA and no MVAs were reported in the LEM5 group.
Reports of hallucinations were rare in both studies. In SUNRISE 1, tactile hallucination was reported for 1 patient who received LEM10 (0 patients for all other treatments). In SUNRISE 2, hypnagogic hallucination was reported for 3 patients (2 patients who received LEM10 and 1 patient who received LEM5) while hypnopompic hallucination was reported for 1 patient who received LEM10. The PBO group did not have any reports of hallucinations.
No intentional overdoses were reported in SUNRISE 1. Intentional overdoses were reported for 2 patients who received LEM5, 1 patient who received PBO, and 0 patients who received LEM10 in SUNRISE 2.
Impaired driving and workplace accidents were not reported in either trial.
Postural instability was assessed in SUNRISE 1. On Days 2/3, the LSM treatment difference between LEM10 and PBO was 2.91 units (95% CI, –0.28 to 6.10 units) and between LEM5 and PBO was 2.49 units (95% CI, –0.70 to 5.67 units). The LSM treatment difference between LEM10 and zolpidem was –4.29 units (95% CI, –7.32 to –1.26 units) and between LEM5 and zolpidem was –4.71 units (95% CI, –7.73 to –1.70 units). On Days 30/31, the LSM treatment difference between LEM10 and PBO was –0.58 units (95% CI, –3.68 to 2.53 units) and between LEM5 and PBO was –0.71 units (95% CI, –3.80 to 2.38 units). The LSM treatment difference between LEM10 and zolpidem was –2.57 units (95% CI, –5.53 to 0.39 units) and between LEM5 and zolpidem was –2.70 units (95% CI, –5.64 to 0.23 units). Since there was no adjustment for multiplicity, the results are uncertain.
Impaired attention was assessed in SUNRISE 1 using 2 components of the Cognitive Performance Assessment Battery: power of attention and continuity of attention. On both Days 2/3 and Days 30/31, the mean change from baseline for power of attention decreased for PBO group and increased for LEM10, LEM5, and zolpidem groups. On Days 2/3, the mean change from baseline for continuity of attention increased for LEM5 group and decreased for LEM10, PBO, and zolpidem groups. On Days 30/31, the mean change from baseline for continuity of attention decreased for all groups. Since there was no adjustment for multiplicity for this outcome, conclusions based on the results cannot be drawn with certainty.
In SUNRISE 1, differences in reports of rebound insomnia during the follow-up period between the treatment groups were not tested statistically. The frequency of rebound insomnia appeared similar between LEM10 and LEM5 groups based on sSOL measures (17% to 21% for the first 7 nights of follow-up and 22% to 24% for the last 7 nights of follow-up) and proportions were numerically higher for zolpidem and PBO groups (23% to 27% for the first 7 nights and 23% to 27% for the last 7 nights). The results using sWASO measures were similar for LEM10 and LEM5 groups (16% to 19% for the first 7 nights and 18% to 19% for the last 7 nights) as well as zolpidem and PBO groups (15% to 22% for the first 7 nights and 18% for the last 7 nights). Rates of rebound insomnia were generally lower in SUNRISE 2 and similar between LEM10 and LEM5 groups based on sSOL measures (11% to 12% for the first 7 nights and 9% to 12% for the last 7 nights) and sWASO measures (12% to 14% for both the first and last 7 nights).
Rates of withdrawal symptoms were similar among LEM10, LEM5, zolpidem, and PBO groups in SUNRISE 1 (10.0%, 11.6%, 14.7%, and 14.1%, respectively) and for LEM10 and LEM5 groups in SUNRISE 2 (16.8% and 20.7%, respectively).
In both SUNRISE 1 and SUNRISE 2, suicidal ideation was reported in no more than 3 patients in any treatment group at any post-baseline time point.
Table 12: Summary of Key Results From SUNRISE 1
Results | SUNRISE 1 | |||
|---|---|---|---|---|
PBO (N = 208) | Zolpidem (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) | |
Key efficacy results – FAS | ||||
LPS | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Geometric mean (SD), minutes | 33.61 (NR) | 30.96 (NR) | 32.98 (NR) | 33.31 (NR) |
Median (Q1, Q3), minutes | 33.63 (20.75, 59.50) | 31.50 (17.50, 61.25) | 33.13 (20.25, 62.25) | 38.50 (17.75, 62.00) |
Days 29/30, na | 200 | 250 | 260 | 260 |
Geometric mean (SD), minutes | 24.88 (NR) | 27.88 (NR) | 18.87 (NR) | 17.49 (NR) |
Median (Q1, Q3), minutes | 27.25 (15.25, 45.63) | 27.00 (15.00, 41.00) | 21.63 (14.50, 33.00) | 21.75 (13.25, 33.00) |
Change from baseline, median (Q1, Q3), minutes | –6.63 (–20.75, 6.88) | –2.88 (–23.75, 12.50) | –12.00 (–32.25, –0.25) | –16.25 (–37.50, –1.88) |
LSGM treatment ratio active/PBO (95% CI)b,c | Reference | 1.22 (1.06, 1.40) | 0.77 (0.67, 0.89) | 0.72 (0.63, 0.83) |
P valueb,d | Reference | 0.0063 | 0.0003 | < 0.0001 |
WASO | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 111.75 (37.18) | 114.31 (39.92) | 113.44 (38.95) | 114.83 (40.00) |
Days 29/30, na | 200 | 250 | 260 | 260 |
Mean (SD), minutes | 92.09 (40.97) | 77.71 (39.93) | 69.10 (34.53) | 68.60 (35.20) |
Change from baseline, mean (SD), minutes | –18.58 (41.93) | –36.50 (43.41) | –43.89 (39.26) | –46.43 (39.60) |
LSM visit estimate (SE),e minutes | –21.43 (2.46) | –37.68 (2.22) | –45.40 (2.19) | –46.78 (2.19) |
LSM treatment difference (active – PBO) (95% CI)c,e | Reference | –16.25 (–22.31, –10.18) | –23.96 (–29.98, –17.95) | –25.35 (–31.36, –19.34) |
P valued,e | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
WASO2H | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 74.44 (30.11) | 78.04 (33.85) | 76.60 (32.90) | 76.88 (32.13) |
Days 29/30, na | 200 | 250 | 260 | 260 |
Mean (SD), minutes | 64.37 (32.45) | 56.74 (31.11) | 49.11 (28.18) | 48.15 (27.84) |
Change from baseline, mean (SD), minutes | –8.92 (31.91) | –21.42 (36.26) | –27.19 (33.05) | –28.84 (33.14) |
LSM visit estimate (SE),f minutes | –10.98 (1.97) | –20.74 (1.78) | –27.39 (1.75) | –28.74 (1.76) |
LSM treatment difference (active – zolpidem) (95% CI)f,g | NA | Reference | –6.65 (–11.15, –2.15) | –8.00 (–12.53, –3.47) |
P valued,f | NA | Reference | 0.0038 | 0.0005 |
Sleep efficiency | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), % | 68.89 (9.64) | 68.13 (11.42) | 68.36 (11.27) | 67.85 (10.85) |
Days 29 /30, na | 200 | 250 | 260 | 260 |
Mean (SD), % | 74.49 (9.85) | 77.17 (10.19) | 81.29 (8.80) | 81.99 (8.80) |
Change from baseline, mean (SD), % | 5.35 (9.90) | 9.06 (11.23) | 12.93 (9.74) | 14.09 (10.51) |
LSM visit estimate (SE),h % | 6.34 (0.60) | 9.50 (0.55) | 13.42 (0.53) | 14.37 (0.54) |
LSM treatment difference (active – PBO) (95% CI)c,h | Reference | 3.15 (1.67, 4.63) | 7.07 (5.61, 8.54) | 8.03 (6.57, 9.49) |
P valued, h | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
Harms | ||||
Safety population, N | 209 | 263 | 266 | 268 |
TEAEs, n (%) | 53 (25.4) | 93 (35.4) | 74 (27.8) | 82 (30.6) |
SAEs, n (%) | 0 | 4 (1.5) | 2 (0.8) | 0 |
WDAE from study treatment, n (%) | 2 (1.0) | 7 (2.7) | 2 (0.8) | 3 (1.1) |
Deaths, n (%) | 0 | 0 | 0 | 0 |
Notable harms | ||||
Somnolence, n (%) | 4 (1.9) | 4 (1.5) | 11 (4.1) | 19 (7.1) |
Impaired driving performance, n (%) | NR | NR | NR | NR |
Falls, n (%) | 0 | 0 | 4 (1.5) | 0 |
MVA (road traffic accident), n (%) | 0 | 1 (0.4) | 0 | 0 |
Workplace accidents, n (%) | NR | NR | NR | NR |
Hallucination – tactile, n (%) | 0 | 0 | 0 | 1 (0.4) |
Drug misuse (intentional overdose), n (%) | 0 | 0 | 0 | 0 |
Postural instabilityi | NA | NA | NA | NA |
Baseline mean (SD) | 23.08 (17.51) | 26.01 (22.13) | 26.40 (20.78) | 23.69 (19.52) |
Days 2/3 change from baseline, mean (SD) | –2.02 (13.66) | 4.07 (18.92) | –0.82 (20.38) | 0.56 (17.08) |
Days 30/31 change from baseline, mean (SD) | 1.68 (16.58) | 2.12 (18.36) | –0.85 (16.20) | 0.48 (14.85) |
Impaired attention – power of attentioni | NA | NA | NA | NA |
Baseline mean (SD), msec | 1,421.0 (210.27) | 1,418.7 (195.95) | 1,452.9 (263.04) | 1,399.2 (192.47) |
Days 2/3 change from baseline, LSM (SE), msec | –22.53 (10.48) | 27.46 (9.57) | 8.24 (9.47) | 17.14 (9.59) |
Days 30/31 change from baseline, LSM (SE), msec | –5.97 (13.23) | 37.76 (12.02) | 37.29 (11.77) | 31.22 (11.89) |
Impaired attention – continuity of attentioni | NA | NA | NA | NA |
Baseline mean (SD), units | 90.7 (4.77) | 90.6 (6.04) | 91.0 (5.15) | 91.3 (4.15) |
Days 2/3 change from baseline, LSM (SE), units | –0.09 (0.32) | –1.12 (0.30) | 0.26 (0.29) | –0.53 (0.30) |
Days 30/31 change from baseline, LSM (SE), units | –0.25 (0.37) | –0.32 (0.33) | –0.14 (0.32) | –0.57 (0.33) |
Rebound insomniai | NA | NA | NA | NA |
sSOL average first 7 nights, n (%) | 45 (23.3) | 66 (27.4) | 52 (20.7) | 44 (17.3) |
sSOL average last 7 nights, n (%) | 44 (23.3) | 63 (26.9) | 53 (21.8) | 60 (24.4) |
sWASO average first 7 nights, n (%) | 29 (14.9) | 52 (21.6) | 48 (19.4) | 41 (16.3) |
sWASO average last 7 nights, n (%) | 33 (17.5) | 41 (17.5) | 46 (19.1) | 43 (17.7) |
Withdrawal symptoms, n (%) | 28 (14.1) | 37 (14.7) | 30 (11.6) | 26 (10.0) |
C-SSR – suicidal ideation at end of study, n (%) | 0 | 2 (0.8) | 0 | 0 |
AE = adverse event; C-SSRS = Columbia-Suicide Severity Rating Scale; CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; LSGM = least squares geometric mean; LSM = least squares mean; MMRM = mixed effect model repeated measurement; MVA = motor vehicle accident; NA = not applicable; NR = not reported; PBO = placebo; Q1 = first quartile; Q3 = third quartile; SAE = serious adverse event; SD = standard deviation; SE = standard error; sSOL = subjective sleep onset latency; sWASO = subjective wake after sleep onset; TEAE = treatment-emergent adverse event; WASO = wake after sleep onset; WASO2H = wake after sleep onset in the second half of the night; WDAE = withdrawal due to adverse event.
aThe number of patients analyzed for the change from baseline at this time point (not the number who provided data at this time point).
bBased on MMRM model with log transformation of LPS and factors for age group, region, treatment, visit (Days 1/2, and Days 29/30), and treatment-by-visit interaction as fixed effects, and the baseline LPS as a covariate. Missing values are imputed using multiple imputation and assumed to be missing not at random.
c“active/PBO” or “active – PBO” means LEM10, LEM5, or zolpidem compared to PBO.
dP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
eBased on MMRM model with factors of age group, region, treatment, visit (Days 1/2, and Days 29/30), and treatment-by-visit interaction as fixed effect, and the baseline WASO as a covariate. Missing values are imputed using multiple imputation and assumed to be missing not at random.
fBased on MMRM model with factors of age group, region, treatment, visit (Days 1/2, and Days 29/30), and treatment-by-visit interaction as fixed effect, and the baseline WASO2H as a covariate. Missing values are imputed using multiple imputation and assumed to be missing not at random.
g“active – zolpidem” means LEM10 or LEM5 minus zolpidem.
hBased on MMRM model with factors of age group, region, treatment, visit (Days 1/2, and Days 29/30), and treatment-by-visit interaction as fixed effect, and the baseline SE as a covariate. Missing values are imputed using multiple imputation and assumed to be missing not at random.
iSafety results based on the FAS population.
Source: SUNRISE 1 Clinical Study Report.63
Table 13: Summary of Key Results From SUNRISE 2
Outcome | SUNRISE 2 | ||
|---|---|---|---|
PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) | |
Key efficacy results – FAS | |||
sSOL | |||
Baseline, n | 316 | 314 | 312 |
Geometric mean (SD), minutes | 44.99 (NR) | 42.97 (NR) | 45.05 (NR) |
Median (Q1, Q3), minutes | 55.86 (34.14, 78.93) | 53.57 (32.86, 75.71) | 55.71 (33.57, 85.07) |
Month 6, na | 249 | 245 | 229 |
Geometric mean (SD), minutes | 27.42 (NR) | 18.62 (NR) | 19.35 (NR) |
Median (Q1, Q3), minutes | 50.71 (29.29, 75.71) | 36.58 (21.50, 57.36) | 35.71 (21.67, 60.00) |
Change from study baseline, median (Q1, Q3), minutes | –11.43 (–33.57, 0.00) | –21.81 (–44.29, –11.14) | –28.21 (–54.43, –9.29) |
LSGM treatment ratio active/PBO (95% CI)a | Reference | 0.732 (0.64, 0.84) | 0.701 (0.61, 0.81) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
sWASO | |||
Baseline, n | 314 | 313 | 311 |
Mean (SD), minutes | 132.49 (80.20) | 132.77 (82.52) | 136.83 (87.39) |
Month 6, na | 248 | 244 | 227 |
Mean (SD), minutes | 103.15 (82.29) | 81.79 (76.80) | 86.38 (77.79) |
Change from study baseline, mean (SD), minutes | –32.14 (55.28) | –51.45 (67.30) | –48.12 (68.55) |
LSM visit estimate (95% CI),d minutes | –29.28 (–36.34, –22.21) | –46.75 (–53.92, –39.58) | –41.95 (–49.19, –34.70) |
LSM treatment difference (active – PBO) (95% CI),d minutes | Reference | –17.47 (–27.31, –7.64) | –12.67 (–22.38, –2.96) |
P valuec,d | Reference | 0.0005 | 0.0105 |
Subjective sleep efficiency | |||
Baseline, n | 307 | 302 | 299 |
Mean (SD), % | 61.34 (17.84) | 63.14 (18.23) | 62.03 (17.25) |
Month 6, na | 242 | 235 | 220 |
Mean (SD), % | 71.40 (18.31) | 78.55 (16.24) | 76.53 (17.99) |
Change from study baseline, mean (SD), % | 10.36 (13.80) | 15.34 (14.61) | 15.55 (15.62) |
LSM visit estimate (95% CI),e % | 9.64 (7.99, 11.30) | 14.19 (12.50, 15.88) | 14.31 (12.60, 16.02) |
LSM treatment difference (active – PBO) (95% CI),e % | Reference | 4.55 (2.24, 6.86) | 4.67 (2.37, 6.96) |
P valuec,e | Reference | 0.0001 | < 0.0001 |
Harms – Safety population | |||
Safety population, N | 319 | 314 | 314 |
AEs, n (%) | 200 (62.7) | 192 (61.1) | 187 (59.6) |
SAEs, n (%) | 5 (1.6) | 7 (2.2) | 9 (2.9) |
WDAE from study treatment, n (%) | 12 (3.8) | 13 (4.1) | 26 (8.3) |
Deaths, n (%) | 0 | 0 | 0 |
Notable harms | |||
Somnolence, n (%) | 5 (1.6) | 27 (8.6) | 41 (13.1) |
Impaired driving performance, n (%) | NR | NR | NR |
Falls, n (%) | 10 (3.1) | 5 (1.6) | 5 (1.6) |
MVA (road traffic accident), n (%) | 1 (0.3) | 0 | 1 (0.3) |
Workplace accidents, n (%) | NR | NR | NR |
Hallucination – hypnagogic, n (%) | 0 | 1 (0.3) | 2 (0.6) |
Hallucination – hypnopompic, n (%) | 0 | 0 | 1 (0.3) |
Drug misuse (intentional overdose), n (%) | 1 (0.3) | 2 (0.6) | 0 |
On-treatment FAS, N | NA | 444 | 437 |
Rebound insomnia | NA | NA | NA |
sSOL average first 7 nights, n (%) | NA | 53 (11.94) | 46 (10.53) |
sSOL average last 7 nights, n (%) | NA | 52 (11.71) | 41 (9.38) |
sWASO average first 7 nights, n (%) | NA | 55 (12.39) | 62 (14.19) |
sWASO average last 7 nights, n (%) | NA | 60 (13.51) | 52 (11.90) |
On-treatment safety analysis set, N | NA | 447 | 437 |
Withdrawal symptoms, n (%) | NA | 84 (20.7) | 65 (16.8) |
C-SSR – suicidal ideation at 12 months, n (%) | NA | 1 (0.5) | 1 (0.5) |
AE = adverse event; C-SSR = Columbia-Suicide Severity Rating Scale; CCMV = complete case missing value; CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSGM = least squares geometric mean; LSM = least squares mean; MMRM = mixed effect model repeated measurement; MNAR = missing not at random; MVA = motor vehicle accident; NA = not applicable; NR = not reported; PBO = placebo; Q1 = first quartile; Q3 = third quartile; SAE = serious adverse event; SD = standard deviation; sSOL = subjective sleep onset latency; sWASO = subjective wake after sleep onset; TEAE = treatment-emergent adverse event; WDAE = withdrawal due to adverse event.
aThe number of patients analyzed for the change from baseline at this time point (not the number who provided data at this time point).
bBased on MMRM model with log transformation of sSOL and factors for age group, region, treatment, visit (First 7 nights, Month 1, Month 3, and Month 6), and treatment-by-visit interaction as fixed effects, and the Study Baseline sSOL as a covariate. Missing values are imputed using multiple imputation and assumed to be missing not at random (MNAR/CCMV).
cP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
dBased on MMRM model with factors of age group, region, treatment, visit (First 7 nights, Month 1, Month 3, and Month 6), and treatment-by-visit interaction as fixed effect, and the Study Baseline sWASO as a covariate. Missing values are imputed using multiple imputations and assumed to be missing not at random (MNAR/CCMV).
eBased on MMRM model with factors of age group, region, treatment, visit (First 7 nights, Month 1, Month 3, and Month 6), and treatment-by-visit interaction as fixed effect, and the Study Baseline subjective sleep efficiency as a covariate. Missing values are imputed using multiple imputation and assumed to be missing not at random (MNAR/CCMV).
Source: SUNRISE 2 Clinical Study Report.64
Critical Appraisal
Both SUNRISE 1 and SUNRISE 2 appeared to have appropriate methods for blinding to the assigned treatment, randomization with stratification, and adequate power for the primary and secondary outcomes. Adjustments for multiplicity were made for all primary and key secondary outcomes and the type I error was controlled for in both studies. All primary and key secondary outcomes were objective polysomnography measures (SUNRISE 1), or subjective measures based on sleep diary responses (SUNRISE 2). The sponsor noted the importance of having objective outcomes to assess the physiological effect of the medication along with subjective outcomes to measure the patient’s perception of the medication’s effect. According to the clinical expert, polysomnography results may not always be interpreted meaningfully or consistently when compared side-by-side with subjective or patient-reported outcomes and consequently, may not be the most meaningful marker of efficacy. The expert further emphasized that insomnia is a subjective issue, therefore patient-reported outcomes and perceptions of sleep changes may be more appropriate for assessing treatment effect. With all subjective measures, there is risk of bias which cannot be measured and leads to uncertainty of how meaningful the results are. The direction of the treatment effect for objective and subjective measures aligned in SUNRISE 1 which contributes to the certainty of the results. The numerically higher rates of discontinuations in the LEM10 group compared to the LEM5 group may bias the results though the magnitude and direction of bias is unknown. There was some amount of missing data at post-baseline visits for all outcomes in either trial, particularly for long-term end points in SUNRISE 2, which prevent strong conclusions from being made. Pre-specified subgroup analyses by age were considered exploratory, may not have been powered to detect a treatment difference, were not adjusted for multiplicity, and there was variability in the change from baseline results (noted by large SDs and interquartile ranges [IQRs]). For responder analyses, SUNRISE 1 was not powered to detect a treatment difference and neither trial adjusted for multiplicity. As a result of these limitations, conclusions could not be drawn from the either subgroup or responder analysis results.
In general, the clinical expert consulted for this review confirmed that the populations of SUNRISE 1 and SUNRISE 2 were similar to patients seen in Canadian clinics and the trial results would be generalizable with some limitations. There was a large proportion of individuals screened out before randomization, thus producing a study population that may not adequately represent the broader Canadian population with insomnia who would otherwise be eligible for treatment with lemborexant. Eligibility for SUNRISE 1 was restricted to females 55 years or older and males 65 years or older and the clinical expert stated that the generalizability of the results would be limited to patients matching these demographics. Further, both SUNRISE 1 and SUNRISE 2 excluded a number of comorbid conditions (e.g., based on BDI–II and BAI scores) and had AHI cut-offs that the clinical expert suggested may have captured individuals with insomnia related to mild sleep apnea rather than psychophysiological insomnia. It is uncertain how applicable the trial results would be to patients with the excluded comorbidities or different AHI scores. No dose changes were allowed during the study and it is noted in the Health Canada product monograph that the recommended nightly dose for lemborexant is 5 mg which may be increased to 10 mg based on clinical response and tolerability.65 Zolpidem was the active comparator in SUNRISE 1 and discussions with the clinical expert and a representative from the Canadian public drug plans indicated that zolpidem is not publicly funded by all drug plans in Canada and is less commonly used for the treatment of insomnia, therefore it is uncertain if it is the most appropriate comparator for a Canadian setting. Patients were required to maintain a sleep diary throughout the course of both studies, and the clinical expert stated a sleep diary may not be required in clinical practice. Thus, screening out patients who could not comply with completing a daily sleep diary excluded patients who could be candidates for lemborexant. Most outcomes identified in the input received by CADTH from patient groups aligned with efficacy and harms outcomes in the studies though there are still gaps in the evidence for the use of lemborexant in patients with comorbid conditions and alongside other medications.
Indirect Comparisons
Description of Studies
One sponsor-submitted indirect treatment comparison (ITC) and a published NMA were included. The first is a systematic review and NMA, with 11 studies, evaluated the efficacy and safety of lemborexant in patients with insomnia by comparing it to relevant drugs in Canadian public formularies (e.g., zopiclone, temazepam, triazolam, flurazepam, and nitrazepam) with respect to clinical end points evaluated objectively (by polysomnography) or subjectively (patient reported). The clinical end points included LPS, WASO, sleep efficiency, and total sleep time (TST) with subjective assessment in these same end points. Harms related to the use of lemborexant were also evaluated in an ITC analysis, including treatment discontinuations, somnolence, dizziness, headache, and in a post hoc analysis, risk of falls. The second NMA is a published comparative efficacy analysis aimed at evaluating the efficacy and safety of lemborexant against other insomnia treatments through a systematic literature review and network meta-analysis.66 The ITC search strategy included RCTs of drugs used in adults with primary insomnia (not all reimbursed in Canada). The drugs of interest in McElroy et al.’s NMA were lemborexant, suvorexant, benzodiazepines, Z-drugs (zolpidem, eszopiclone, zaleplon, zopiclone), trazodone, and ramelteon. Of these, only zolpidem, zopiclone, eszopiclone, trazodone, triazolam, and temazepam were available in the body of evidence from the NMA and of interest to this CADTH reimbursement review.
Efficacy Results
Indirect evidence from the NMAs suggest that for the end point of LPS, LEM5 is superior to triazolam and PBO but no evidence of a difference between LEM5 and LEM10 was observed. With LEM5 as reference, LPS was longer in the PBO group (mean difference of –19.1 minutes; 95% CI, –3.20 to –35.0 minutes, in which a negative value in the mean difference implies improvement in favour of LEM5). Patients treated with LEM5 had a reduction of in LPS when compared to triazolam 0.5 mg (mean difference –34.1 minutes; 95% CI, –5.47 to –62.8 minutes). The results for LEM10 were consistent with LEM5. In the second NMA, lemborexant showed a reduction in LPS when compared to placebo (–18.6 minutes; 95% credible interval [CrI], –29.0 to –10.9), zolpidem-ER (–13.4 minutes; 95% CrI, –24.4 to –4.9), and triazolam (–23.2 minutes; 95% CrI, –38.8 to –9.6).
For the end point of WASO, the evidence suggests LEM5 and LEM10 were superior to PBO, but the evidence against triazolam was very imprecise to detect a difference in polysomnography assessed WASO between LEM5, LEM10, and triazolam 0.5 mg. In the second NMA, for WASO, lemborexant was superior to placebo and zolpidem-IR, with an average reduction of 21.3 (95% CrI, −29.6 to −10.1) minutes and 19.6 (−31.9 to −0.3) minutes, respectively.
For the evaluation of objectively measured sleep efficiency, LEM5, LEM10, flurazepam 30 mg, and triazolam 0.5 mg could be compared in the NMA. The mean differences in sleep efficiency for LEM5 and LEM10 compared with PBO were 7.62% (95% CI, 5.93 to 9.31%) and 8.80% (95% CI, 10.5 to 7.06%), respectively (where higher values mean improvement in favour of lemborexant). The mean differences in sleep efficiency for LEM5 and LEM10 compared with triazolam were 9.62% (95% CI, 14.3 to 4.92%) and 10.8% (95% CI, 15.5 to 6.09%), respectively. Effect estimates for the comparisons between LEM5 and LEM10 and flurazepam were too imprecise to draw a conclusion.
Total sleep time data were only available for LEM5 and LEM10 against PBO. The NMA showed that effect estimates were imprecise to detect a difference between LEM5 and LEM10 (–4.65 minutes; 95% CI, –2.45 to 11.8 minutes). Although relative to PBO, LEM5 and LEM10 were associated with an improvement of 34.8 minutes (95% CI, 27.4 to 42.4 minutes) and 39.5 minutes (95% CI, 32.1 to 46.9 minutes), respectively.
In the second NMA, for the subjective outcomes, lemborexant was superior to placebo in all end points evaluated but not against eszopiclone for the subjective quality of sleep (sQUAL) end point (mean difference of −0.6; 95% CrI, −0.9 to −0.2). For the rest of comparisons, no evidence of effect was observed.
Harms Results
The evidence from the ITC suggested that LEM10 had an increased risk of drug discontinuation when compared to LEM5 (OR = 1.99 [95% CI, 1.06 to 3.74]) and PBO, but not against the other comparators. The odds of discontinuations were less for PBO compared with LEM10 (OR, 0.48 [95% CI, 0.25 to 0.91]). The effect estimates for all other comparisons with LEM10 were too imprecise to draw a conclusion.
For the end point of somnolence, when compared with LEM 5, PBO had reduced odds of somnolence (OR, 0.25; 95% CI, 0.12 to 0.52), similarly the odds were reduced in triazolam 0.25 mg (OR, 0.31; 95% CI, 0.14 to 0.69), and zopiclone arms. Increased odds of somnolence for LEM10 were observed against PBO, triazolam 0.25 mg, and zopiclone 7.5 mg. For other comparisons (i.e., LEM5 and LEM10 versus flurazepam, temazepam, and triazolam 0.125 mg), the effect estimates were too imprecise to detect a difference.
For the end point of dizziness, the effect estimates were too imprecise to draw conclusions about the effect of LEM5 or LEM10 compared with PBO, flurazepam, triazolam, or zopiclone.
For the end point of headache, the results were also too imprecise to detect a difference in the odds of headache between LEM5 and each of alternatives. This situation also occurred in the comparison of LEM10 to the other comparators.
In an additional post hoc analysis (Bucher ITCs) of studies reporting falls, using LEM5 as the reference, no evidence of any difference could be detected when comparing to patients receiving triazolam, flurazepam, lorazepam, trazodone, benzodiazepines, and Z-drugs due to the high imprecision of the results. When LEM10 was used as the reference, the odds of falls were higher with triazolam, flurazepam, and lorazepam when compared to LEM10. When the entire class of benzodiazepines and trazodone were compared to LEM10, the odds of falls were also higher with the former drugs. Even though these findings suggested that LEM10 is associated with a reduction in the odds of falls when compared to other drugs, the results are very imprecise with wide CIs to draw conclusions.
In the second NMA evaluated in this CADTH report, there was no evidence of increased or decreased odds for presenting SAEs for patients receiving lemborexant when compared to relevant comparators, mainly due to wide CrIs. Similarly, no difference was observed in the odds of withdrawals due to AEs or in the odds of falls. Lemborexant was associated with lower odds of dizziness compared with zolpidem-IR, zolpidem-ER, and eszopiclone. Lemborexant, however, increased the odds of somnolence when compared to placebo, zolpidem, and eszopiclone.
Critical Appraisal
The results from both NMAs have uncertainty due to risk of bias in the individual studies (i.e., unclear randomization, allocation concealment, baseline imbalances), heterogeneity in the pairwise comparisons, and suspected publication bias. Furthermore, the evidence is imprecise in most of the effect estimates from both NMAs, with wide confidence intervals that could include an appreciable threshold of benefit or harm. In the NMAs there were concerns of incomplete information and discrepancies in the included studies that could affect the plausibility of the transitivity assumption. Overall, the populations included in the individual studies of the network are generalizable to the Canadian population without comorbid conditions.
Other Relevant Evidence
Description of Studies
Study 312 was an open-label, phase IIIb, pilot, multi-centre trial (N = 53) investigating next-dose transition from zolpidem to lemborexant for the treatment of insomnia. The trial included adult patients with insomnia who were receiving zolpidem as monotherapy, and who agreed to substitute it with lemborexant.
Efficacy Results
Overall, 81.1% of patients successfully transitioned to lemborexant at the end of the 2-week titration period and entered the extension phase. A total of 15 (48.4%) patients had a lemborexant dose increase from 5 mg to 10 mg while 5 (22.7%) patients had a lemborexant dose decrease from 10 mg to 5 mg at the end of the 2-week titration period.
At the end of the titration period, patients in both LEM5 and LEM10 groups indicated that lemborexant had a positive effect on sleep, time to fall asleep, and TST. A large proportion of patients felt that the medication was “too weak.” In the overall trial population, the mean change in ISI total score was –4.6 (SD = 6.26) and the mean change in quality of sleep score was –0.19 (SD = 0.92) at the end of the titration period.
In the overall trial population, at baseline and at the end of the titration period, the mean sleep efficiency scores were 79.03% (SD = 85.4%) and 80.17% (SD = 8.49%), respectively; the mean WASO scores were 80.90 minutes (SD = 33.23 minutes) and 83.92 minutes (SD = 35.44 minutes), respectively; and the mean TST scores were 403.44 minutes (SD = 62.07 minutes) and 412.11 minutes (SD = 60.17 minutes), respectively.
Harms Results
Of the 53 patients enrolled in the core study, 20 (37.7%) experienced at least 1 TEAE (5 patients from the LEM5 group and 15 patients from the LEM10 group). The most common TEAEs were abnormal dreams (7.5%) and somnolence (7.5%). In the overall trial population, 13% of patients withdrew from treatment due to an AE. No deaths or SAEs leading to study drug discontinuation were reported in the study.
Critical Appraisal
Study 312 had an open-label design, small sample size, short study duration, no formal statistical testing, subjective secondary end points, 50% screening failures, and chose zolpidem as the previous treatment to transition from (rather than other treatments that may have been more relevant to Canadian clinical practice), which prevent conclusions from being drawn and limits generalizability to the Canadian population with insomnia.
Conclusions
Both LEM10 and LEM5 demonstrated statistically significant improvements in sleep onset, sleep maintenance, and sleep efficiency among adults with insomnia relative to PBO in the SUNRISE 1 and SUNRISE 2 trials. In SUNRISE 1, all primary and key secondary outcomes were for objective polysomnography measures and were clinically meaningful based on suggested thresholds for a clinically important effect identified from the literature, except for WASO2H which did not have a MID, or threshold identified. In SUNRISE 2, all primary and key secondary outcomes were for subjective sleep diary measures, and none reached the suggested thresholds for a clinically important effect identified from the literature. Numerical differences in the ISI items 4 to 7 and FSS indicated a benefit from treatment with lemborexant over PBO, but due to the lack of adjustment for multiple comparisons and no established MID for the ISI items 4 to 7 and FSS, conclusions could not be drawn from these outcomes. Other patient-reported outcomes such as the EQ-5D-3L, PGI-Insomnia, and quality of sleep scale were exploratory, not controlled for multiplicity, and did not have MIDs for populations with insomnia, therefore no conclusions could be drawn regarding whether treatment with lemborexant confers a benefit for these outcomes. The clinical expert consulted for this review emphasized the importance of subjective outcomes and how patients perceive changes in their sleep, and sponsor-submitted post-hoc analyses of SUNRISE 2 data lend support to the meaningfulness of the PGI-Insomnia and ISI subjective outcomes. However, the sleep improvements based on polysomnography and sleep diary outcomes observed in the studies did not appear to be reflected in the results from the patient-reported questionnaires (i.e., ISI, FSS, and perceived sleep quality). It is uncertain if the differences in treatment effect observed in SUNRISE 1 and SUNRISE 2 would be experienced by and be meaningful to all patients who could be treated with lemborexant. There did not appear to be a clear difference in efficacy between LEM10 and LEM5, although differences in efficacy between the 2 doses was not tested statistically in the trials. The product monograph’s recommendation to start with LEM5 and the higher rates of somnolence and treatment discontinuations for LEM10 would be considerations when prescribing or increasing a patient’s dose. Overall, the clinical expert indicated that lemborexant demonstrated a minor harms profile with few SAEs, low rates of withdrawals from treatment due to AEs, and no deaths. Patients with specific comorbid conditions such as sleep apnea, anxiety, and depression were excluded from the studies based on the exclusion criteria for AHI, BAI, and BDI–II scores, and further research showing adequate efficacy and safety is needed to inform broader treatment with lemborexant. Indirect evidence suggested lemborexant is superior to triazolam 0.5 mg for LPS and sleep efficiency, to zolpidem for WASO and LPS, and inferior to eszopiclone in sleep quality; however, there is uncertainty in this conclusion due to limitations of the NMAs and differences in conclusions for some outcome comparisons across NMAs. Evidence was very uncertain or absent for the other comparisons and end points due to imprecision, risk of bias, and heterogeneity in the pairwise comparisons. Additionally, evidence for transitioning from zolpidem to lemborexant from the pilot study 312 was limited by the study design, small sample size, and large proportion of screening failures preventing conclusions from being drawn. Overall, lemborexant appears to be effective relative to PBO for important sleep-related outcomes, and long-term results from SUNRISE 2 supported those observed during the first 6 months of treatment. There were no serious safety concerns, but efficacy for HRQoL and subjective appraisals of symptoms and sleep quality are less certain due to limitations of the trials. Zolpidem may not have been the most relevant comparator in Canadian practice, and comparisons with zolpidem in the trial (except for WASO2H) were not controlled for multiplicity, therefore, there is uncertainty in the conclusions about the comparative efficacy. Lemborexant appeared to be more effective than zolpidem for the outcome of WASO2H, which was noted as being important for sleep maintenance, though there was no MID identified and there is uncertainty if the change observed in SUNRISE 1 was clinically meaningful. Moreover, there is no direct evidence for efficacy or harms relative to other relevant comparators that may be used in Canadian clinical practice, and the indirect evidence is uncertain. Owing to its superiority over PBO, lemborexant may be another treatment option for patients with insomnia.
Appendix 2: Details on Excluded Studies
Please note that this appendix has not been copy-edited.
Table 14: Details on Studies Excluded by CDA-AMC
Author (year) | Details | Rationale for exclusion |
|---|---|---|
Henmi et al. (2024)67 | Funding source: Not reported Location or setting: A hospital in Japan Study design: Retrospective cohort study Population: Patients who were admitted to a general hospital, treated for general medical-surgical settings for nonpsychiatric conditions, and underwent consultation-liaison psychiatry consult. Number of patients or patient record: 1,886 Intervention or exposure: Fourteen factors that have been reported to be associated with the occurrence of delirium in the literature. Out of these 14 factors, 11 were reported to increase the risk of delirium, including age, sex, previous cerebral hemorrhage-infarction, major neurocognitive disorder, electrolyte imbalance (sodium, potassium, chlorine, or calcium), habitual use of alcohol, history of delirium, after surgery (under general anesthesia), use of potentially deliriogenic medication (e.g., antiparkinsonian drugs, H2 receptor antagonists, and corticosteroids), benzodiazepines, and Z-drugs. Three factors were reported to decrease the risk of delirium, i.e., ramelteon, suvorexant, and lemborexant. The 14 factors were retrospectively examined from medical records. Main outcomes: Incidence of delirium during hospitalization in patients with insomnia. | The study investigated the relationship among sleep-inducing drugs (ramelteon, suvorexant, lemborexant, benzodiazepines, and Z-drugs) and the prevention of delirium in patients who were hospitalized. Delirium was not identified as an important outcome for patients and clinicians, was not included in the initial review’s protocol, and does not frequently occur in the outpatient setting according to clinical experts. |
Horikoshi et al. (2023)68 | Funding source: Not reported Location or setting: A psychosomatic clinic in Japan Study design: Analysis of medical records Population: Patients with mental health disorders who underwent treatment with lemborexant Number of patients-patient record: 61 Intervention or exposure: Lemborexant Main outcomes: The Athens Insomnia Scale (AIS), Epworth Sleepiness Scale (ESS), Perceived Deficits Questionnaire-5 (PDQ-5). | The study investigated the efficacy and safety of switching from benzodiazepines, Z-drugs, suvorexant, ramelteon, mirtazapine, trazodone, and antipsychotics to lemborexant. How to switch to lemborexant was not a gap identified by CDEC. |
Kamboj et al. (2024) | Funding source: Eisai Co., Ltd., Canada Location or setting: Administrative databases Study design: Retrospective observational study Population: Patients with any claims for medications approved for insomnia in Canada Number of patients-patient record: 597,222 (2019) Intervention or exposure: Interventions for insomnia Main outcomes: Patient characteristics, insomnia medication use and costs, inappropriate medication usage | This study focused on real-world prescribing practices, medication utilization, costs, and lines of treatment among patients with insomnia in Canada. This information was not considered a gap by CDEC. |
Katsuta et al. (2023)69 | Funding source: the Juntendo Mental Health Institute Location or setting: A mental health clinic in Japan Study design: A retrospective cohort study Population: Patients who were diagnosed with an axis I mental disorder and prescribed lemborexant during the target period Number of patients-patient record: 649 Intervention or exposure: Lemborexant Main outcomes: The Clinical Global Impression improvement | This noncomparative study does not support causal interpretations, therefore did not address a gap related to lack of efficacy or safety data relative to other treatments used in Canada. |
Mishima et al. (2024)70 | Funding source: Eisai Co., Ltd., Japan Location or setting: A medical institution in Japan Study design: Prospective observational study Population: Patients who received lemborexant for the first time Number of patients-patient record: 550 Intervention or exposure: Lemborexant Main outcomes: Discontinuation, safety, improvement | This noncomparative study does not support causal interpretations, therefore did not address a gap related to lack of efficacy or safety data relative to other treatments used in Canada. |
Miyata et al. (2024)71 | Funding source: Eisai Co., Ltd. Location or setting: A hospital in Japan Study design: Single-arm trial Population: Patients with insomnia disorder Number of patients-patient record: 31 Intervention or exposure: Lemborexant Main outcomes: Latency to persistent sleep, wake after sleep onset, total sleep time, and sleep efficacy | This noncomparative study does not support causal interpretations, therefore did not address a gap related to lack of efficacy or safety data relative to other treatments used in Canada. |
Moline et al. (2023)72 (conference abstract) | Funding source: Eisai Inc. Location or setting: US Study design: A retrospective study Population: Four databases where adverse events were reported Number of patients-patient record: 64,213 Intervention or exposure: DORAs, benzodiazepines, Z-drugs, approved nonscheduled hypnotics, trazodone, diphenhydramine Main outcomes: Adverse events | This study provided descriptive statistics on DORAs as a category (no data on lemborexant alone) and thus did not address a gap related to lack of efficacy or safety data relative to other treatments used in Canada. |
Ozone et al. (2024)73 | Funding source: Eisai Co., Ltd. Location or setting: Multiple centres in Japan Study design: Prospective, nonrandomized, open-label study Population: Patients transitioning to lemborexant Number of patients-patient record: 97 Intervention or exposure: Lemborexant Main outcomes: Proportion of successful cases of continuous transition to lemborexant | The study investigated the transition to lemborexant from other drugs. How to switch to lemborexant was not a gap identified by CDEC. |
Tanaka-Mizuno et al. (2024)74 | Funding source: Eisai Co., Ltd. and Kyoto University Location or setting: Japan Study design: Retrospective cohort study Population: Patients with at least 1 prescription for lemborexant Number of patients-patient record: 38,022 Intervention or exposure: Lemborexant Main outcomes: The proportion of patients who successfully switched to lemborexant. | The study investigated the transition to lemborexant from other drugs. How to switch to lemborexant was not a gap identified by CDEC. |
AIS = Athens Insomnia Scale; CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; DORA = dual orexin receptor antagonist; ESS = Epworth Sleepiness Scale; PDQ-5 = Perceived Deficits Questionnaire-5.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CBT-I
cognitive behavioural therapy for insomnia
CDA-AMC
Canada’s Drug Agency
CID
chronic insomnia disorder
DSM
Diagnostic and Statistical Manual of Mental Disorders
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
MVA
motor vehicle accident
QALY
quality-adjusted life-year
sSOL
subjective sleep onset latency
WPA
workplace accident
Economic Review
The objective of the economic review is to review and critically appraise the submitted pharmacoeconomic evidence, which included an economic evaluation comparing the cost-effectiveness of lemborexant to benzodiazepines (flurazepam, nitrazepam, triazolam, temazepam, lorazepam), Z-drugs (zopiclone), antidepressants (trazodone), and antipsychotics (quetiapine) for the requested reimbursement population. The requested reimbursement population is for the treatment of insomnia in adults diagnosed according to the most recent version of the Diagnostic and Statistical Manual of Mental Disorders (DSM) referring to chronic insomnia disorder (CID), which is narrower than the Health Canada indication. The sponsor additionally submitted a budget impact analysis (BIA) assessing the budgetary impact of reimbursing lemborexant for the requested reimbursement population as well as for the full Health Canada indication (i.e., the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance).
Item | Description |
|---|---|
Drug product | Lemborexant (Dayvigo), 5 mg film-coated tablet and 10 mg film-coated tablet, oral |
Indication | The treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance. |
Submitted price | $1.76 per 5 mg or 10 mg tablet |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 4, 2020 |
Reimbursement request | For the treatment of insomnia in adults diagnosed according to the most recent version of the Diagnostic and Statistical Manual of Mental Disorders (DSM) referring to chronic insomnia disorder. |
Sponsor | Eisai Limited |
Submission history | Previously reviewed: Yes Indication: The treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance Recommendation date: January 26, 2023 Recommendation: Do not reimburse |
DSM = Diagnostic and Statistical Manual of Mental Disorders; NOC = Notice of Compliance.
Summary
Lemborexant is available as 5 mg and 10 mg oral tablets. At the submitted price of $1.76 per 5 mg or 10 mg tablet,1 the annual cost of lemborexant is expected to be $641 per patient, based on the Health Canada–recommended dosage.2
The economic analysis was informed by clinical evidence previously submitted to Canada’s Drug Agency (CDA-AMC). Evidence generated from the randomized clinical trials and an indirect treatment comparison (ITC) remains unchanged from the initial submission.3 The clinical efficacy of lemborexant was informed by the SUNRISE-1 and SUNRISE-2 clinical trials.4-6 The efficacy of the modelled treatments was derived from a sponsor-submitted ITC that compared the efficacy and safety of lemborexant to placebo, triazolam, and temazepam.7 The indirect evidence submitted by the sponsor suggests that lemborexant may improve subjective sleep onset latency (sSOL) compared to triazolam. However, substantial imprecision, unresolved heterogeneity, and uncertainty in the plausibility of the transitivity assumption was identified by CDA-AMC, which precludes the use of the ITC to inform decision-making.3
The results of the CDA-AMC base case suggest that over 180 days:
Lemborexant is predicted to be associated with higher costs to health care systems than lorazepam, quetiapine, flurazepam, temazepam, trazodone, triazolam, zopiclone, nitrazepam, or no treatment (incremental costs = $276 to $321), primarily driven by increased costs associated with drug acquisition.
Lemborexant is not predicted to extend life compared to all modelled treatments but may slightly improve quality of life due to increasing the likelihood that a patient becomes a good sleeper. This results in a gain of 0.003 quality-adjusted life-years (QALYs) compared to quetiapine.
The incremental cost-effectiveness ratio (ICER) of lemborexant compared to quetiapine was $103,511 per QALY gained in the CDA-AMC base case. The estimated ICER was sensitive to efficacy parameters (i.e., sSOL) and to the relative risk of falls, motor vehicle accidents (MVAs), and workplace accidents(WPAs). Because no comparative evidence was presented for lorazepam, quetiapine, flurazepam, zopiclone, or nitrazepam, there is uncertainty associated with the cost-effectiveness of lemborexant compared to these treatments. Given the level of clinical uncertainty in the submitted ITC, it is unclear whether lemborexant provides incremental benefit relative to currently reimbursed treatments.
CDA-AMC estimates that the budget impact of reimbursing for the treatment of CID (i.e., the population in the reimbursement request) will be approximately $165 million over the first 3 years of reimbursement, compared to the amount currently spent on comparators, with an estimated expenditure of $189 million on lemborexant over this period. When considering the Health Canada indication (i.e., acute and chronic insomnia), the budget impact is estimated to be $257 million for the first 3 years of reimbursement. The actual budget impact of reimbursing lemborexant will depend on the market uptake of lemborexant and the number of people eligible for treatment. At the submitted price, the incremental budget impact of lemborexant is predicted to be greater than $40 million in year 2 and year 3 of reimbursement, and the economic feasibility of adoption must be addressed. Additionally, the magnitude of uncertainty in the budget impact must be addressed to ensure the feasibility of adoption, given the difference between the sponsor’s estimate and the CDA-AMC estimate.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of lemborexant from the perspective of a public health care payer in Canada over a 6-month time horizon.8 The modelled population comprised adults with insomnia diagnosed according to the most recent DSM referring to CID, which is aligned with the reimbursement request, and was based on the participants in the SUNRISE-2 trial; however, the modelled population is narrower than the Health Canada–indicated population.8 The sponsor’s base-case analysis included costs related to drug acquisition, medical resource use (physician visits, cognitive behavioural therapy for insomnia [CBT-I]), and the treatment of falls, WPAs, and MVAs.8
In the sponsor’s base case, lemborexant was associated with lower costs and greater QALYs than all other treatments (i.e., it was dominant).8 Additional information about the sponsor’s submission is summarized in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 2; full details are provided in Appendix 4).
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
Relevant comparators were omitted from the analysis. | The clinical experts noted that doxepin and mirtazapine are commonly prescribed medications in clinical practice and are reimbursed. Thus, these treatments should have been considered in the economic analysis. | CDA-AMC could not address this issue in the base case due to a lack of comparative evidence of lemborexant vs. doxepin and mirtazapine. | No scenario analysis was conducted due to a lack of evidence. |
The response rate with lemborexant relative to active comparators is highly uncertain. This may overestimate the relative benefit of lemborexant. | The economic analysis was based on the sponsor’s submitted ITC; however, comparative efficacy was only available for triazolam and for temazepam.7 The other comparators were assumed to have equal efficacy to triazolam or temazepam.8 Additionally, the Clinical Review of the sponsor’s ITC identified several limitations that may confound results.3 | CDA-AMC could not address this issue in the base case due to the lack of alternative efficacy estimates. | To explore the uncertainty of the comparative efficacy of active comparators, CDA-AMC conducted a scenario analysis in which “no differences in sSOL” was assumed for lemborexant and active comparators (refer to Table 11). |
The submitted evidence on the impact of insomnia treatment on MVAs and WPAs was insufficient and lacked validity. This may overestimate the benefit for lemborexant. | The sponsor used a threshold value to determine driving impairment for a BAC of 0.05%9 to estimate the risk of an MVA for lemborexant and zopiclone; other comparators were assumed to be equal to zopiclone. Additionally, the study comparing driving impairment while taking lemborexant or zopiclone was conducted on healthy [wording from original source] volunteers, limiting the external validity.10 WPAs were assumed to have an equivalent relative risk to MVAs.8 | CDA-AMC assumed there is no difference in the risk of MVAs and WPAs between lemborexant and all relevant comparators. | No scenario analysis was conducted due to a lack of evidence. |
The impact of insomnia treatment on the risk of falls is highly uncertain. This may overestimate the benefit for lemborexant. | The pooled clinical trial estimates for falls had wide overlapping confidence intervals, resulting in imprecision.11,12 The published literature cited may not be generalizable to the overall population of patients with insomnia because the studies may have included patients with other conditions and did not match for age or sex.13,14Additionally, the patients taking an active comparator appeared to be experiencing more illnesses than the control arm, biasing the results against the active comparators.13,14 | CDA-AMC assumed there is no difference in the relative risk of falls between lemborexant and all relevant comparators. | CDA-AMC conducted a scenario analysis maintaining the sponsor’s relative risk estimate for benzodiazepines only. |
The number of additional primary care visits and CBT-I sessions was overestimated. This may overestimate the cost for relevant comparators. | The clinical experts noted that the modelled differences in primary care and CBT-I sessions did not meet face validity, and they expect no meaningful differences between treatments over the 6-month time horizon. | CDA-AMC assumed there is no difference in the number of primary care visits or CBT-I sessions for all relevant comparators. | No scenario analysis was conducted due to a lack of evidence. |
The model does not fully capture the natural history of the disease. | The submitted model did not capture mood disorders that often accompany insomnia or the often cyclic nature of insomnia (including rebound insomnia) and the potential costs and impact on quality of life these may have. | CDA-AMC was unable to address this limitation due to the model structure. | No scenario analysis was conducted due to the submitted model structure. |
BAC = blood alcohol concentration; CBT-I = cognitive behavioural therapy for insomnia; CDA-AMC = Canada’s Drug Agency; ITC = indirect treatment comparison; MVA = motor vehicle accident; sSOL = subjective sleep onset latency; vs. = versus; WPA = workplace accident.
Note: Full details of the issues identified by CDA-AMC are provided in Appendix 3.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Table 7) in consultation with clinical experts. Detailed information about the CDA-AMC base case is provided in Appendix 4. Comparators on the cost-effectiveness frontier include no treatment, lorazepam, quetiapine, and lemborexant.
Impact on Health Care Costs
Lemborexant is predicted to be associated with additional health care costs compared to quetiapine (incremental costs = $304). This increase in health care spending results from the drug acquisition costs associated with lemborexant (refer to Figure 1).
Figure 1: Impact of Lemborexant Versus Comparators on Health Care Costs
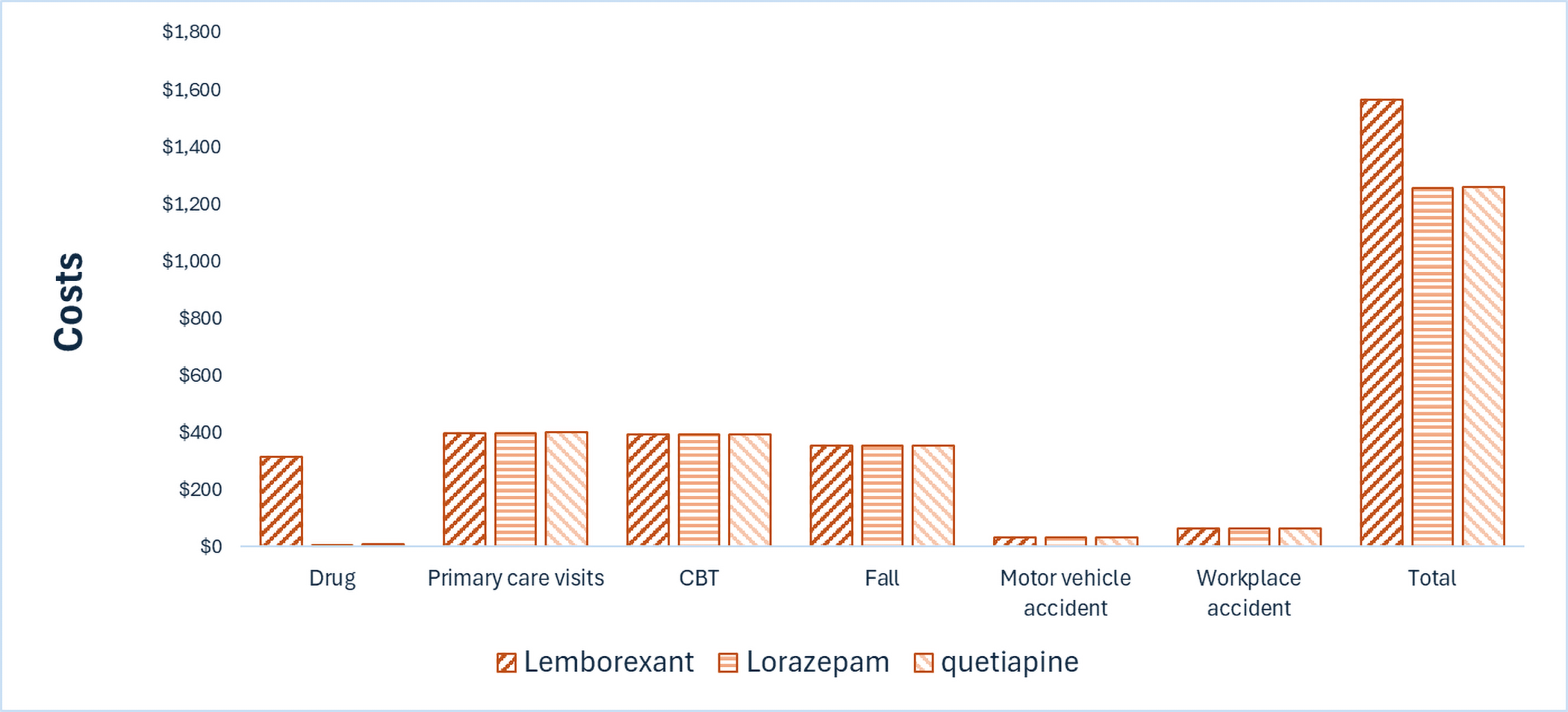
CBT = cognitive behavioural therapy.
Note: Results for other comparators are not presented in this figure. Refer to Appendix 4 for full results.
Impact on Health
Relative to quetiapine, lemborexant is not anticipated to impact the number of patient falls, MVAs, WPAs, or premature deaths. Based on results from the ITC, lemborexant may increase the proportion of patients who become good sleepers relative to quetiapine from 19.8% to 26.5%. The utility gain associated with this improvement results in 0.003 additional QALYs per patient over a 6-month time horizon (refer to Table 9). There is no evidence to inform relative differences in quality of life associated with treatment side effects.
Overall Results
Based on the CDA-AMC analysis, the following treatments are on the cost-effectiveness frontier (i.e., they are not dominated by other treatments): no treatment, lorazepam, quetiapine, and lemborexant. Compared with the next drug on the frontier (i.e., quetiapine), the ICER for lemborexant is $103,511 per QALY gained.
Table 3: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Untreated | 1,243 | 0.316 | Reference |
Lorazepam | 1,257 | 0.317 | 9,436 vs. untreated |
Quetiapine | 1,260 | 0.318 | 4,255 vs. lorazepam |
Lemborexant | 1,564 | 0.321 | 103,511 vs. quetiapine |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators. All other treatments were dominated or extendedly dominated.
Uncertainty and Sensitivity
CDA-AMC explored the uncertainty associated with the cost-utility analysis through 2 scenario analyses (outlined in Table 2). Given the uncertainty in the comparative efficacy of lemborexant versus other comparators with regard to risk of falls, CDA-AMC considered a scenario in which lemborexant reduced the risk of falls compared to benzodiazepine comparators. The results were similar to the CDA-AMC base case: lemborexant was associated with an ICER of $103,425 versus quetiapine (Table 11). In the CDA-AMC scenario analysis assuming equivalent efficacy, the total QALYs for all comparators except for no treatment were equivalent, and lorazepam was associated with the lowest total cost, which was $308 less than the total cost associated with lemborexant over the 6-month time horizon.
Summary of the Budget Impact
The sponsor submitted a BIA to estimate the 3-year (July 2026 to June 2029) budget impact of reimbursing lemborexant for use in the Health Canada–indicated population.15 The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach.15 The price of lemborexant was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices.1 Additional information pertaining to the sponsor’s submission is provided in Appendix 5.
CDA-AMC identified several issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (Appendix 5). CDA-AMC estimated that 795,967 patients would be eligible for treatment with lemborexant over a 3-year period (year 1 = 257,520; year 2 = 265,245; year 3 = 273,203), of whom 294,203 are expected to receive lemborexant (year 1 = 51,504; year 2 = 106,098; year 3 = 136,601). The estimated incremental budget impact of reimbursing lemborexant is predicted to be approximately $165 million over the first 3 years, with an expected expenditure of $189 million on lemborexant. The actual budget impact will depend on the market uptake of lemborexant.
Conclusion
Based on the CDA-AMC base case, lemborexant would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $103,511 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (refer to Figure 2; full details of the impact of price reductions on cost-effectiveness are presented in Table 10). However, the estimated cost-effectiveness of lemborexant compared to all relevant comparators is highly uncertain due to the limitations associated with the indirect evidence. If lemborexant is anticipated to produce similar health outcomes to currently available treatments, then it should be priced no more than the lowest cost comparator.
The budget impact of reimbursing lemborexant to the public drug plans in the first 3 years is estimated to be approximately $165 million. The 3-year expenditure on lemborexant (i.e., not accounting for current expenditure on comparators) is estimated to be $189 million. The estimated budget impact is uncertain due to uncertainty about the market uptake of lemborexant and the number of patients with chronic insomnia.
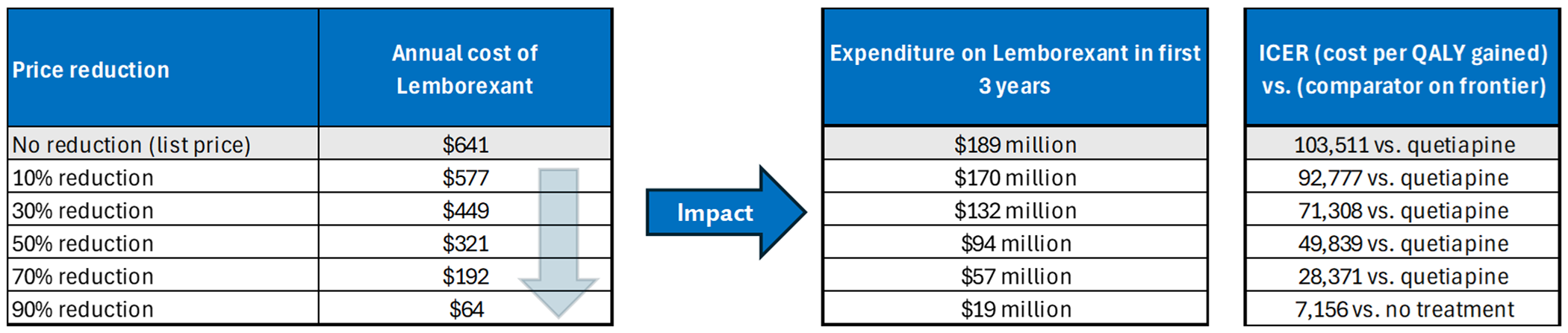
References
1.Eisai Limited. Drug Reimbursement Review sponsor submission: DAYVIGO (lemborexant) tablet for oral use, 5 mg, 10 mg [internal sponsor's package]. April 10, 2025.
2.Eisai Limited. DAYVIGO (lemborexant): Tablet for oral use, 5 mg, 10 mg [product monograph]. January 30, 2025.
3.CADTH Reimbursement Review: Lemborexant (Dayvigo). Can J Health Technol. 2023;3(4). doi:10.51731/cjht.2023.624
4.Eisai Inc. Clinical Study Report: E2006-G000-303. A Long-Term Multicenter, Randomized, Double-Blind, Controlled, Parallel-Group Study of the Safety and Efficacy of Lemborexant in Subjects With Insomnia Disorder [internal sponsor's report]. March 25, 2019.
5.Eisai Inc. Clinical Study Report: E2006-G000-304. A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Active Comparator, Parallel-Group Study of the Efficacy and Safety of Lemborexant in Subjects 55 Years and Older with Insomnia Disorder [internal sponsor's report]. November 29, 2018.
6.Eisai Inc. Core Clinical Study Report: E2006-G000-303. A Long-Term Multicenter, Randomized, Double-Blind, Controlled, Parallel-Group Study of the Safety and Efficacy of Lemborexant in Subjects With Insomnia Disorder [internal sponsor's report]. December 4, 2018.
7.Eisai Limited. Lemborexant (DAYVIGO) for the Treatment of Adults with Insomnia Disorder: A Systematic Review and Network Meta-Analysis to Indirectly Compare Safety and Efficacy to Agents Available on Canadian Public Drug Plans [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: DAYVIGO (lemborexant) tablet for oral use, 5 mg, 10 mg April 10, 2025.
8.Eisai Limited. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: DAYVIGO (lemborexant) tablet for oral use, 5 mg, 10 mg. April 10, 2025.
9.Taylor B, Rehm J. The relationship between alcohol consumption and fatal motor vehicle injury: high risk at low alcohol levels. Alcohol Clin Exp Res. 2012;36:1827-34. PubMed
10.Vermeeren A, Jongen S, Murphy P, et al. On-the-road driving performance the morning after bedtime administration of lemborexant in healthy adult and elderly volunteers. Sleep. 2019;42(4). doi: 10.1093/sleep/zsy260 PubMed
11.Karppa M, Yardley J, Pinner K, et al. Long-term efficacy and tolerability of lemborexant compared with placebo in adults with insomnia disorder: results from the phase 3 randomized clinical trial SUNRISE 2. Sleep. 2020;43(9). doi: 10.1093/sleep/zsaa123 PubMed
12.Rosenberg R, Zammit G, Yardley J, et al. 164 Pooled Analyses of Patient-Reported Sleep Onset and Maintenance from Two Phase 3 Studies of Lemborexant. CNS spectrums. 2020;25(2):304-305. doi: 10.1017/s1092852920000802
13.Amari D FF JT, Wang W, Gor D, Wickwire E. Risk of Falls Among Adult Patients on Commonly Used Insomnia Medications in the United States. presented at: Academy of Managed Care Pharmacy (AMCP) Managed Care & Specialty Pharmacy Nexus 2020; 2020; Alexandria (VA).
14.Neutel CI, Hirdes JP, Maxwell CJ, Patten SB. New evidence on benzodiazepine use and falls: the time factor. Age Ageing. 1996;25(4):273-8. doi: 10.1093/ageing/25.4.273 PubMed
15.Eisai Limited. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: DAYVIGO (lemborexant) tablet for oral use, 5 mg, 10 mg. April 10, 2025.
16.Government of Alberta. Interactive drug benefit list. Accessed May 1, 2025. https://idbl.ab.bluecross.ca/idbl/load.do
17.BC Government. BC PharmaCare formulary search. Accessed May 1, 2025. https://pharmacareformularysearch.gov.bc.ca
18.Ontario Ministry of Health. Ontario drug benefit formulary/comparative drug index. Accessed May 1, 2025. https://www.formulary.health.gov.on.ca/formulary/
19.Manis DR, Caitlin M, Costa AP. Associations with rates of falls among home care clients in Ontario, Canada: a population-based, cross-sectional study. BMC Geriatr. 2020;20. PubMed
20.Zecevic AA, Chesworth BM, Zaric GS, et al. Estimating the cost of serious injurious falls in a Canadian acute care hospital. Can J Aging. 2012;31(2):139-47. doi: 10.1017/S0714980812000037 PubMed
21.Australian Institute of Health and Welfare. Hip Fracture incidence and hospitalisation in Australia 2015–16 Data tables. Table S3.1: Hospitalisation for new hip fracture, by age and sex, 2015–16 [sponsor supplied reference]. 2017. Accessed May 2019. https://www.aihw.gov.au/getmedia/d4236d00-0277-48a6-bb6d-b7c911ed7207/aihw-phe-226-data-tables.xlsx.aspx
22.Blincoe LJ, Miller TR, Zaloshnja E, Lawrence BA. The economic and societal impact of motor vehicle crashes, 2010. (Revised) (Report No. DOT HS 812 013). Washington, DC: National Highway Traffic Safety Administration [sponsor supplied reference]. 2015. Accessed March 2019. https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812013.
23.Tefft BC, AAA Foundation for Traffic Safety. Motor Vehicle Crashes, Injuries, and Deaths in Relation to Driver Age: United States, 1995 – 2010. AAA Foundation for Traffic Safety [sponsor supplied reference]. 2012. https://aaafoundation.org/motor-vehicle-crashes-injuries-deaths-relation-driver-age-united-states-1995-2010/
24.Gustavsen I, Bramness JG, Skurtveit S, Engeland A, Neutel I, Morland J. Road traffic accident risk related to prescriptions of the hypnotics zopiclone, zolpidem, flunitrazepam and nitrazepam. Sleep Med. 2008;9(8):818-22. doi: 10.1016/j.sleep.2007.11.011 PubMed
25.U.S. Bureau of Labor Statistics. Labor Force Statistics from the Current Population Survey, Occupation: Employed persons by detailed occupation and age, including median age. 2018. Accessed May 2019. https://www.bls.gov/cps/demographics.htm#age
26.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-18. doi: 10.1111/j.1524-4733.2010.00700.x PubMed
27.Olfson M, Wall M, Liu SM, Morin CM, Blanco C. Insomnia and Impaired Quality of Life in the United States. J Clin Psychiatry. 2018;79(5). doi: 10.4088/JCP.17m12020 PubMed
28.Tannenbaum C, Diaby V, Singh D, Perreault S, Luc M, Vasiliadis HM. Sedative-hypnotic medicines and falls in community-dwelling older adults: a cost-effectiveness (decision-tree) analysis from a US Medicare perspective. Drugs Aging. 2015;32(4):305-14. doi: 10.1007/s40266-015-0251-3 PubMed
29.Spicer RS, Miller TR, Hendrie D, Blincoe LJ. Quality-adjusted life years lost to road crash injury: updating the injury impairment index. Ann Adv Automot Med. 2011;55:365-77. PubMed
30.Government of Newfoundland and Labrador. Newfoundland and Labrador interchangeable drug products formulary [sponsor supplied reference].
31.IQVIA. PharmaStat [sponsor supplied reference]. 2023. https://www.iqvia.com/
32.Ontario Ministry of Health. Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)). 2023. Accessed May 1, 2025. https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf
33.Canadian Institute for Health Information. Patient cost estimator [sponsor supplied reference]. 2024. https://www.cihi.ca/en/patient-cost-estimator
34.Pincus D, Wasserstein D, Nathens AB, Bai YQ, Redelmeier DA, Wodchis WP. Direct medical costs of motorcycle crashes in Ontario. CMAJ. 2017;189(46):E1410-E1415. doi: 10.1503/cmaj.170337 PubMed
35.Government of Saskatchewan. Saskatchewan Drug Plan: search formulary. 2024. Accessed June 30, 2025. http://formulary.drugplan.ehealthsask.ca/SearchFormulary
36.Morin CM, Vezina-Im LA, Chen SJ, et al. Prevalence of insomnia and use of sleep aids among adults in Canada. Sleep Med. 2024;124:338-345. doi: 10.1016/j.sleep.2024.09.044 PubMed
37.Chaput JP, Janssen I, Sampasa-Kanyinga H, et al. Economic burden of insomnia symptoms in Canada. Sleep Health. 2023;9(2):185-189. doi: 10.1016/j.sleh.2022.09.010 PubMed
38.eHealth Saskatchewan. Saskatchewan Covered Population Reports [sponsor supplied reference]. 2015. https://opendata.ehealthsask.ca/MicroStrategyPublic/asp/Main.aspx
39.Government of Alberta. Alberta Health Care Insurance Plan statistical supplement [sponsor supplied reference]. 2021. Accessed June 15, 2022. https://open.alberta.ca/publications/0845-4775
40.Government of Canada. Non-Insured Health Benefits Program - First Nations and Inuit Health Branch: Annual Reports [sponsor supplied reference]. 2023. https://www.sac-isc.gc.ca/eng/1713194236054/1713194280612
41.Government of Manitoba. Manitoba Health Population Reports [sponsor supplied reference]. 2020. https://www.gov.mb.ca/health/population/index.html
42.Government of Newfoundland and Labrador. Newfoundland and Labrador Prescription Drug Program [accessed by sponsor]. 2025. Accessed March 21, 2025. https://www.health.gov.nl.ca/health/prescription/newformulary.asp
43.Government of New Brunswick. New Brunswick Prescription Monitoring Program and Drug Information System [sponsor supplied reference]. Accessed April 3, 2025. https://www2.gnb.ca/content/gnb/en/departments/health/DrugPlans/prescription-monitoring-program.html
44.Government of Prince Edward Island. Prince Edward Island Prescription Monitoring Report Narcotics (Opioids & Monitored Drugs) [sponsor supplied reference]. 2017. Accessed April 3, 2025.
45.Nova Scotia Prescription Monitoring Program. Drugs Monitored by the Nova Scotia Prescription Monitoring Program [sponsor supplied reference]. 2022. Accessed April 3, 2025. https://nspmp.s3.ca-central-1.amazonaws.com/pdfs/NSPMP-Drug-List_April-5-2022_2023.pdf
46.Ontario Public Drug Programs. Direct data request of elgible beneficiaries by age group (2007-2014) [sponsor supplied reference]. 2014.
47.BC Pharmacare. BC PharmaCare Annual Performance Reports and BC PharmaCare Trends [sponsor supplied reference]. 2022. Accessed April 3, 2025. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/pharmacare/pharmacare-publications
48.Statistics Canada. Table: 17-10-0057-01. Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Accessed July 3, 2025. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701
49.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada; 2017. Accessed July 3, 2025. https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326
50.Government of Canada. Annual Demographic Estimates: Canada, Provinces and Territories, 2024. Statistics Canada. 2024. Accessed June 30, 2025.
51.Weir DL, Samanani S, Gilani F, Jess E, Eurich DT. Benzodiazepine receptor agonist dispensations in Alberta: a population-based descriptive study. CMAJ Open. 2018;6(4):E678-E684. doi: 10.9778/cmajo.20180121 PubMed
52.Morin CM, Khullar A, Robillard R, et al. Delphi consensus recommendations for the management of chronic insomnia in Canada. Sleep Med. 2024;124:598-605. doi: 10.1016/j.sleep.2024.09.038 PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans
Table 4: Cost Comparison for Chronic Insomnia Disorder
Treatment | Strength and/or concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($)a |
|---|---|---|---|---|---|---|
Lemborexant | 5 mg 10 mg | Oral tablet | 1.75591 | 5 mg or 10 mg nightly. | 1.76 | 641 |
aAnnual cost based on 365.25 days per year.
Table 5: Cost Comparison for Chronic Insomnia Disorder (Off-Label Treatment)
Treatment | Strength and/or concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($)a |
|---|---|---|---|---|---|---|
Benzodiazepines | ||||||
Clonazepam | 0.25 mg 0.5 mg 1 mg 2 mg | Oral tablet | 0.0850b 0.0418 0.1721b 0.0721 | 0.25 mg to 2 mg nightly | 0.04 to 0.17 | 63 |
Flurazepam | 15 mg 30 mg | Oral tablet | 0.1166 0.1364 | 15 to 30 mg nightly | 0.12 to 0.14 | 43 to 50 |
Lorazepam | 0.5 mg 1 mg 2 mg | Oral tablet | 0.0359 0.0447 0.0699 | 0.5 mg to 2 mg nightly | 0.04 to 0.07 | 13 to 26 |
Temazepam | 15 mg 30 mg | Oral tablet | 0.1431 0.0877 | 30 mg nightly | 0.09 | 32 |
Triazolam | 0.125 mg 0.25 mg | Oral tablet | 0.1496 0.2551 | 0.125 mg to 0.25 mg nightly | 0.15 to 0.26 | 55 to 93 |
Z-drugs | ||||||
Zopiclone | 3.75 mg 5 mg 7.5 mg | Oral tablet | 0.0675c 0.1069c 0.1350c | 3.75 to 7.5 mg nightly | 0.07 to 0.14 | 26 to 81 |
Zolpidem tartrate | 5 mg 10 mg | Oral tablet | 1.1825c 1.1883c | 5 to 10 mg nightly | 1.18 to 1.19 | 432 to 434 |
Antidepressants | ||||||
Amitriptyline | 10 mg 25 mg 50 mg 75 mg 100 mg | Tablet | 0.0305 0.0829 0.1540 0.2544b 0.2993c | 10 mg to 100 mg nightly | 0.03 to 0.30 | 11 to 109 |
Doxepin | 10 mg 25 mg 50 mg 75 mg 100 mg | Tablet | 0.4075 0.5000 0.9274 0.8711c 1.7388c | 10 mg to 100 mg nightly | 0.41 to 1.74 | 149 to 635 |
Mirtazapine | 15 mg 30 mg 45 mg | Tablet | 0.3750 0.3100 1.1250 | 15 mg to 45 mg nightly | 0.31 to 1.13 | 113 to 411 |
Trazodone | 50 mg 75 mg 100 mg 150 mg | Tablet | 0.0554 0.4422b 0.0989 0.1453 | 50 mg to 150 mg nightly | $0.06 to $0.44 | 20 to 162 |
Antipsychotics | ||||||
Quetiapine | 25 mg 100 mg 200 mg 300 mg | Immediate release tablet | 0.0494 0.1318 0.2647 0.3863 | 25 mg to 300 mg nightly | 0.05 to 0.39 | 18 to 141 |
50 mg 150 mg 200 mg 300 mg 400 mg | Extended-release tablet | 0.2501 0.4926 0.6661 0.9976 $1.3270 | 50 mg to 400 mg nightly | 0.25 to 1.33 | 91 to 485 | |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed May 2025), unless otherwise indicated, and do not include dispensing fees.18
aAnnual cost based on 365.25 days per year.
bDrug cost sourced from the Alberta Health Interactive Drug Formulary.16
cDrug cost sourced from the British Columbia Pharmacare Formulary.17
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Alzheimer Society of Ontario, Migraine Canada, and Mood Disorders Society of Canada. Survey and interviews with people with lived experience and health care professionals indicated that chronic insomnia is a debilitating condition which significantly impacts daily living resulting in physical, mental, emotional, and social anguish. In addition, patients often experience comorbid conditions such as cardiovascular disease, diabetes, obesity, cancer, and gastrointestinal diseases and disorders. Patient groups indicated multiple different treatment options with varying levels of success including cognitive behavioural therapy, life-style adjustments and off-label medication such as over-the-counter medication or supplements, benzodiazepines, Z-drugs, antidepressants, antipsychotics and, in extreme circumstances, alcohol and recreational drug use. Patient groups indicated that current treatments are for short-term use only yet are still prescribed for chronic insomnia; these off-label treatments can carry risks for dependency, abuse, misuse, withdrawal, next-day sedation, and other side effects. Patient input indicated that the most important outcomes were the alleviation of symptoms (daytime functioning) and improvement of well-being while minimizing side effects. Among patients who provided input, 20 had experience with lemborexant, of which, 60% indicated some to significant improvement in their condition with 50% reporting no side effects.
Clinician group input was received from Gastrointestinal Society, Primary Care Clinician Group, Aging Patients Clinician Group, Chronic Insomnia Clinician Group, Addiction Medicine Specialists, Alberta Psychiatrists, Cardiometabolic Patient Clinician Group, Depression and Anxiety Clinician Group, and Women’s Health Clinician Group. Clinician group input indicated that the current pathway of care includes nonpharmacological (i.e., CBT-I, and sleep hygiene) and pharmacological options (i.e., short-term insomnia: benzodiazepines and Z-drugs; off-label: antidepressants and antipsychotics). All clinician groups indicated that CBT-I is preferred over all other treatment options; however, patients often do not have access. Conversely, pharmacological medications have cognitive side effects, result in dependency, become refractory due to tolerance, and are not appropriate for long-term use. Clinician groups indicated that treatment goals are to improve sleep quality, sleep architecture, and enhance daytime functioning without additional side effects. Clinician groups indicated that lemborexant would be most suitable for patients after CBT-I and is preferred over all currently available pharmacological treatments.
Input from CDA-AMC–participating drug plans questioned if inclusion or exclusion criteria based on the clinical trials is appropriate for initiation of lemborexant treatment. The plans also sought to understand how disease progression is measured in clinical practice, along with renewal conditions based on disease progression.
The following concern was addressed in the sponsor’s model: CBT-I was included in the economic analysis.
CDA-AMC was unable to address the following concerns:
Comorbidities such as cardiovascular disease, diabetes, obesity, cancer, and gastrointestinal diseases and disorders were not captured in the submitted model.
Over-the-counter medications or supplements were not considered in the economic analysis.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information in collaboration with clinical experts and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of lemborexant, the sponsor provided a cost-utility analysis and a BIA.1 The sponsor’s economic submission is summarized in Table 6.
Table 6: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Lemborexant (Dayvigo), 5 mg and 10 mg tablets |
Submitted price of drug under review | $1.76 per 5 mg or 10 mg tablet1 |
Regimen | 5 mg nightly or 10 mg nightly2 |
Annual cost of drug under review | $641 per patient1 |
Model information | |
Type of economic evaluation | Cost-utility analysis Decision tree |
Treatment | Lemborexant |
Included comparators |
|
Perspective | Publicly funded health care payer perspective |
Time horizon | 6 months |
Cycle length | Not applicable |
Modelled population | Patients aged 18 years and older with insomnia diagnosed according to the most recent DSM referring to chronic insomnia disorder, characterized by difficulties with sleep onset and/or maintenance lasting for 3 nights or more per week for at least 3 months8 |
Characteristics of modelled population | Derived from the SUNRISE-2 trial (patients aged 18 to 64 years: 72.4%, mean age: 55 years; patients aged 65 years and older: 27.6%, mean age: 70 years; female: 68.2%; male: 31.8%)8 |
Model health states |
For additional information, refer to Model Structure |
Data sources | |
Comparative efficacy | The rate of treatment response based on the relative standardized mean differences in sSOL for comparators were obtained from the sponsor-submitted NMA, which included the SUNRISE-2 trial for lemborexant.8 |
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities | |
Costs |
|
Summary of the submitted results | |
Base-case results | Lemborexant was dominant vs. all comparators (i.e., less costly and more effective). |
Scenario analysis results |
|
CBT-I = cognitive behavioural therapy for insomnia; CID = chronic insomnia disorder; CIHI = Canadian Institute for Health Information; DSM = Diagnostic and Statistical Manual of Mental Disorders; ICER = incremental cost-effectiveness ratio; MVA = motor vehicle accident; NMA = network meta-analysis; sSOL = subjective sleep onset latency; QALY = quality-adjusted life-years; vs. = versus; WASO = wake after sleep onset; WPA = workplace accident.
Model Structure
The sponsor submitted a decision tree to compare the efficacy, safety, and mortality impacts of chronic insomnia treatments (Figure 3).8 Patients entered the model and received treatment, and could then transition to ‘Response’ or ‘No Response,’ resulting in the presence or absence of disease response.8 From here, patients would experience an event (i.e., falls, MVAs, workplace accidents).8 At the end of the decision tree, patients remain alive or die.8 Patients were assigned lemborexant, 1 of the comparators, or no treatment and were assumed to receive the same treatment until the end of the modelled time horizon.8
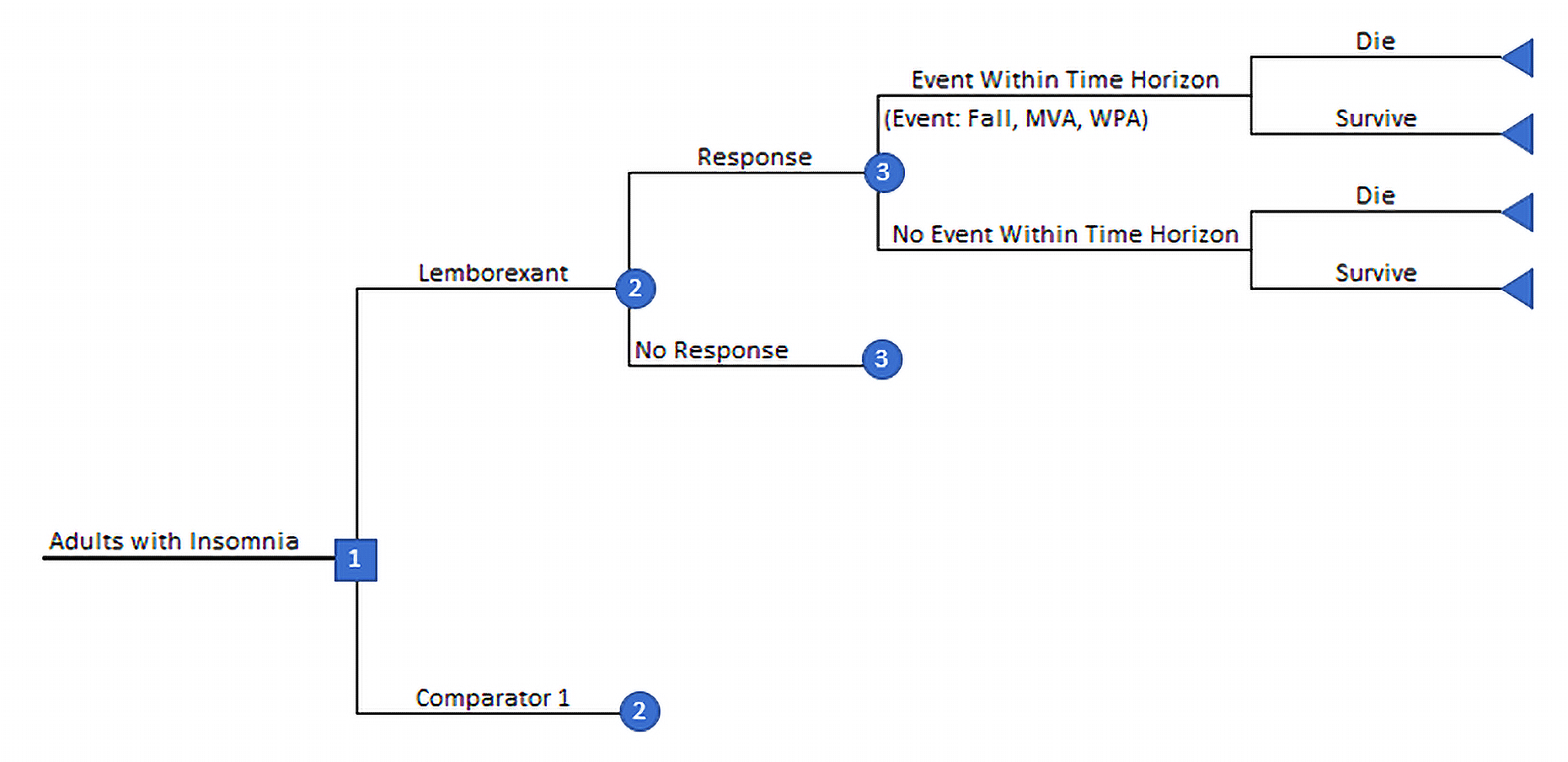
MVA = motor vehicle accident; WPA = workplace accident.
Source: Sponsor’s pharmacoeconomic submission8
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
Clinical evidence informing the economic model was previously submitted and appraised by CDA-AMC.3 While there was no submitted direct evidence comparing lemborexant against any comparators used in the cost-utility analysis, the sponsor conducted an ITC, which suggested that lemborexant may improve sSOL compared to triazolam; however, the CDA-AMC Clinical Review concluded that results of the ITC were uncertain due to substantial imprecision, unresolved heterogeneity, and implausibility in the transitivity assumption.3
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
Relevant comparators omitted from the analysis: The clinical expert consulted for this review noted that some pharmacological treatments for insomnia were not included in the analysis. Doxepin and mirtazapine are commonly prescribed medications in clinical practice in Canada that are reimbursed by several of the public formularies.16-18,30,35 As these comparators were not included in the analysis, their cost-effectiveness compared to lemborexant is unknown; however, notably, their list price on the Ontario Drug Benefit Formulary is less costly than lemborexant (Appendix 1).18
CDA-AMC could not address this limitation.
The response rate with lemborexant use relative to active comparators is highly uncertain: The sponsor modelled a higher response rate on lemborexant relative to active comparators.8 The sponsor submitted an ITC of treatment response measured using sSOL; however, the comparative clinical evidence is only available for triazolam 0.125 mg and temazepam 15 mg.7 There is no comparative evidence available for the sponsor’s other active comparators: flurazepam, lorazepam, nitrazepam, zopiclone, trazodone and quetiapine.7 Further, the ITC suggested lemborexant is superior to triazolam 0.125 mg; however, the effect estimates are imprecise, which make it difficult to ascertain the magnitude and direction of comparative treatment response.3 Additional limitations of the network meta-analysis were also identified, and include risk of bias, heterogeneity in the pairwise comparisons, and uncertainty in the plausibility of the transitivity assumption.3 As such, no firm conclusions about the comparative efficacy of lemborexant can be drawn relative to active comparators that may be used in clinical practice in Canada.
In a scenario analysis, CDA-AMC explored the uncertainty in comparative treatment response based on sSOL by assuming no differences in the response rates between lemborexant and active comparators.
There was insufficient evidence for the impact insomnia treatment on the risk of MVAs or WPAs: In the sponsor’s submission, the impact of insomnia treatment on the risk of MVAs, was based on the standard deviation of lateral position on a standardized on the road driving test (a measure of lane swerving). Specifically, the cut-off of those at increased risk of an MVA was assumed to be at least 2.4 cm, a value demonstrated in a systematic review to be equivalent to a person driving with a blood alcohol concentration of 0.05%.9 Using that threshold, the sponsor applied the standard deviation of lateral position cut-off to a study by Vermeeren et al., (2019) that aimed to evaluate the effect of lemborexant compared to zopiclone on driving performance in 48 healthy [wording from original source] volunteers.10 Based on those findings, the sponsor assumed lemborexant would not have an increased risk of a MVA, while zopiclone and all other relevant comparators in the model would have a risk of an MVA equivalent to those driving with a blood alcohol concentration of 0.05%. There were important limitations to this approach, where primarily the assumption to naively use the standard deviation of lateral position cut-off for blood alcohol concentrations to estimate the odds of an MVA after taking zopiclone or lemborexant is unlikely to be valid. There are likely differences in the relationship between alcohol and MVAs, and medications used to treat insomnia (e.g., lemborexant and zopiclone) and MVAs, that would impact the odds of MVAs. Therefore, both the direction and magnitude of difference between these relationships cannot be inferred and are likely different from that used by the sponsor. According to the clinical expert consulted for this review by CDA-AMC, the evidence linking insomnia treatments to MVAs is uncertain, and in clinical practice they typically see MVAs in disorders of hypersomnolence such as sleep apnea and narcolepsy rather than chronic insomnia.
The sponsor-submitted report on MVAs also lacks external validity. The study by Vermeeren et al., included only healthy [wording from original source] volunteers (who explicitly had no sleep disorders and were described as “good sleepers”), which limits generalizability of the trial results to patients with insomnia.10 The small sample size further limits generalizability of this study to the population in Canada.
The clinical expert for this review also noted that any evidence of MVA in patients with severe sleep apnea is not directly transferable to a patient population with insomnia.
The effect of insomnia treatments on WPAs was assumed to be the same as MVAs. As the evidence on MVAs is insufficient, and no causal evidence was provided between WPAs and insomnia treatments, the sponsor biased the results of their cost-effectiveness analysis in favour of lemborexant by assuming a difference in MVA and WPA risk for lemborexant versus relevant comparators.
CDA-AMC assumed there would be no difference in the risk of MVAs and WPAs between lemborexant and all relevant comparators.
The impact of insomnia treatments on the risk falls is highly uncertain: The sponsor assumed lemborexant use is associated with an increased risk of falls compared to placebo, but at a reduced risk compared to other active comparators. However, the impact of insomnia treatments on the risk of falls is highly uncertain. The sponsor estimated the risk of falls with lemborexant use by pooling results from the SUNRISE 1 and 2 trials (lemborexant 5 mg: odds ratio = 1.32; 95% confidence interval, 0.11 to 16.31; lemborexant 10 mg: odds ratio = 0.52; 95% confidence interval, 0.18 to 1.47).11,12 As exhibited by the wide overlapping 95% confidence intervals, no firm conclusions can be drawn due to serious imprecision.
The sponsor derived the risk of falls compared to other active comparators from the literature.13,14 The study they used by Neutel et al. was conducted more than 25 years ago, and it is unclear whether all participants in the study were diagnosed with insomnia because the study selected a population based on claims data which did not provide the health indication for which treatment is prescribed.14 The odds of falls after benzodiazepine use in patients with insomnia may be different than in a population with conditions other than insomnia, which limits the applicability of the results of this study to the indicated population considered in this review. Further, the study by Amari et al. compared the risk of falls among adult patients with insomnia treated with commonly used prescription medications relative to a matched control cohort without sleep disorders.13 The results of Amari et al. are prone to confounding, the comparator and control arm were only matched on age and sex, and not on the presence of disease.13 The risk of falls associated with insomnia treatment may have also been overestimated by having a control group that is healthier [wording from original source] than the intervention group. The study notes a higher Charlson Comorbidity Index score for the intervention group, indicating the patients receiving insomnia treatment were experiencing more illnesses than the control arm, which may have biased the results against the active comparators.
The sponsor-submitted supplementary ITC of lemborexant to active insomnia treatments produced estimates with wide 95% confidence intervals that included the null value. The sponsor biased the results of their cost-effectiveness analysis in favour of lemborexant by modelling a reduced risk of falls for lemborexant compared to other active comparators. As a part of their resubmission, CDA-AMC appraised additional evidence on risk of falls from Juday et al., and Hirata et al., as noted in the Clinical Review report, both studies were limited by internal and external validity and significant imprecision. As such, it was determined that falls risk was unable to be attributable to specific treatments, and any conclusions regarding the relative risk of falls with lemborexant use compared to other active insomnia treatments is highly uncertain due to the lack of direct evidence and imprecision in the indirect estimates.
CDA-AMC assumed there would be no difference in the risk of falls between lemborexant and all relevant comparators.
CDA-AMC explored the impact of an increased risk of falls associated with benzodiazepines in a scenario analysis.
The number of additional primary care visits for patients with no treatment was overestimated: The sponsor assumed patients who were not treated seek primary care 4 times more than patients taking lemborexant. The clinical expert consulted for this review noted the sponsor overestimated the number of additional primary care visits sought for insomnia by patients who were not treated over the 6-month time horizon. The clinical expert also noted the modelled differences in primary care visits between active comparators was not meaningful.
CDA-AMC assumed that there is no difference in the number of additional primary care visits or cognitive behavioural therapy visits for all relevant comparators.
The submitted model does not capture key aspects of the treatment paradigm: The sponsor’s submitted decision tree model was based primarily on patient response and nonresponse captured by the sSOL scale. According to the clinical expert consulted by CDA-AMC for this review, sleep treatment is often associated with depression or anxiety; however, mood disorders accompanying insomnia have not been considered in this analysis. Further, insomnia is often cyclic in nature where some patients continue their medication and obtain some benefit, while others discontinue and have rebound insomnia. The decision tree framework and chosen time horizon do not capture all these possibilities, and their associated costs and the impact on quality of life.
CDA-AMC could not address this limitation.
CDA-AMC Reanalysis of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (refer to Table 7). The impact of these changes, individually and collectively, is presented in Table 8.
Table 7: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. MVAs and WPAs | The sponsor assumed an increased risk of having an MVA and WPA (RR = 2.18) while patients were treated with flurazepam, nitrazepam, zopiclone, triazolam, temazepam, quetiapine, trazodone or lorazepam compared with placebo | CDA-AMC assumed no difference in the relative risk of MVAs and WPAs (RR = 1). |
2. Falls | The sponsor assumed an increased risk of falls while patients were treated with lemborexant (RR = 1.18), flurazepam (RR = 3.05), nitrazepam (RR = 2.16), zopiclone (RR = 2.16), triazolam (RR = 2.50), temazepam (RR = 2.16), quetiapine (RR = 2.63), trazodone (RR = 2.63) or lorazepam (RR = 1.91), compared with placebo. | CDA-AMC assumed no difference in the relative risk of falls (RR = 1). |
3. Additional primary care and CBT-I visits | Primary care visits: Lemborexant: 0.5 visits per 30 days Benzodiazepines: 0.667 visits per 30 days Quetiapine and trazodone: 0.5 visits per 30 days Untreated: 2 visits per 30 days CBT-I sessions: Patients who were treated: 6 sessions of CBT-I Patients who were not treated: 12 sessions of CBT-I | Assumed no difference in the number of primary care and CBT-I visits between lemborexant and all comparators |
CDA-AMC base case (health care payer perspective) | ― | Reanalysis 1 + 2 + 3 |
CBT-I = cognitive behavioural therapy for insomnia; CDA-AMC = Canada’s Drug Agency; MVA = motor vehicle accident; RR = relative risk; WPA = workplace accident.
Note: CDA-AMC was unable to resolve the issues with the excluded comparators and could not address aspects of the treatment paradigm.
Table 8: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | Lemborexant | 1,749 | 0.313 | Reference |
Quetiapine | 1,865 | 0.267 | Dominated by lemborexant | |
Trazodone | 1,866 | 0.267 | Dominated by lemborexant and quetiapine | |
Lorazepam | 1,895 | 0.282 | Dominated by lemborexant | |
Temazepam | 1,947 | 0.275 | Dominated by lorazepam and lemborexant | |
Zopiclone | 1,955 | 0.275 | Dominated by temazepam, lorazepam and lemborexant | |
Nitrazepam | 1,964 | 0.275 | Dominated by zopiclone, temazepam, and lemborexant | |
Triazolam | 2,003 | 0.269 | Dominated by nitrazepam, zopiclone, temazepam, lorazepam and lemborexant | |
Flurazepam | 2,056 | 0.260 | Dominated by triazolam, nitrazepam, zopiclone, temazepam, lorazepam, trazodone, quetiapine and lemborexant | |
Untreated | 3,139 | 0.313 | Dominated by lemborexant | |
CDA-AMC reanalysis 1 | Lemborexant | 1,749 | 0.313 | Reference |
Quetiapine | 1,753 | 0.270 | Dominated by lemborexant | |
Trazodone | 1,754 | 0.270 | Dominated by quetiapine and lemborexant | |
Lorazepam | 1,784 | 0.284 | Dominated by lemborexant | |
Temazepam | 1,835 | 0.278 | Dominated by lorazepam and lemborexant | |
Zopiclone | 1,843 | 0.278 | Dominated by temazepam, lorazepam and lemborexant | |
Nitrazepam | 1,852 | 0.278 | Dominated by zopiclone, temazepam, lorazepam and lemborexant | |
Triazolam | 1,891 | 0.271 | Dominated by lemborexant | |
Flurazepam | 1,945 | 0.263 | Dominated by triazolam, nitrazepam, zopiclone, temazepam, lorazepam, trazodone, quetiapine and lemborexant | |
Untreated | 3,027 | 0.316 | 454,736 vs. lemborexant | |
CDA-AMC reanalysis 2 | Quetiapine | 1,534 | 0.315 | Reference |
Trazodone | 1,535 | 0.315 | Dominated by quetiapine | |
Lorazepam | 1,668 | 0.314 | Dominated by quetiapine and trazodone | |
Temazepam | 1,676 | 0.314 | Dominated by quetiapine, trazodone, and lorazepam | |
Zopiclone | 1,684 | 0.314 | Dominated by quetiapine, trazodone, lorazepam, and temazepam | |
Flurazepam | 1,685 | 0.314 | Dominated by quetiapine, trazodone, lorazepam, temazepam, and zopiclone | |
Triazolam | 1,687 | 0.314 | Dominated by quetiapine, trazodone, lorazepam, temazepam, zopiclone, and flurazepam | |
Nitrazepam | 1,693 | 0.314 | Dominated by quetiapine, trazodone, lorazepam, temazepam, zopiclone, flurazepam, and nitrazepam | |
Lemborexant | 1,693 | 0.321 | 27,343 vs. quetiapine | |
Untreated | 3,139 | 0.313 | Dominated by quetiapine, trazodone, lorazepam, temazepam, zopiclone, flurazepam, triazolam, nitrazepam, and lemborexant | |
CDA-AMC reanalysis 3 | Lorazepam | 1,725 | 0.281 | Reference |
Lemborexant | 1,749 | 0.313 | 787 vs. lorazepam | |
Temazepam | 1,776 | 0.275 | Dominated by lorazepam and lemborexant | |
Zopiclone | 1,784 | 0.275 | Dominated by lorazepam, lemborexant, and temazepam | |
Nitrazepam | 1,793 | 0.275 | Dominated by lorazepam, lemborexant, temazepam, and zopiclone | |
Quetiapine | 1,829 | 0.267 | Dominated by lorazepam, lemborexant, temazepam, zopiclone, and nitrazepam | |
Trazodone | 1,830 | 0.267 | Dominated by lorazepam, lemborexant, temazepam, zopiclone, nitrazepam, and quetiapine | |
Triazolam | 1,832 | 0.268 | Dominated by lorazepam, lemborexant, temazepam, zopiclone, and nitrazepam | |
Untreated | 1,884 | 0.313 | Dominated by lemborexant | |
Flurazepam | 1,885 | 0.260 | Dominated by lorazepam, lemborexant, zopiclone, nitrazepam, quetiapine, trazodone, triazolam, and untreated | |
CDA-AMC base case Reanalysis 1 + 2 + 3 (deterministic) | Untreated | 1,377 | 0.316 | Reference |
Lorazepam | 1,385 | 0.317 | 5,334 vs. untreated | |
Quetiapine | 1,386 | 0.318 | 1,670 vs. lorazepam | |
Trazodone | 1,387 | 0.318 | Dominated by quetiapine | |
Temazepam | 1,393 | 0.317 | Dominated by lorazepam, quetiapine and trazodone | |
Zopiclone | 1,402 | 0.317 | Dominated by lorazepam, quetiapine, trazodone, and temazepam | |
Flurazepam | 1,402 | 0.317 | Dominated by lorazepam, quetiapine, trazodone, temazepam, and zopiclone | |
Triazolam | 1,404 | 0.317 | Dominated by lorazepam, quetiapine, trazodone, temazepam, zopiclone, and flurazepam | |
Nitrazepam | 1,410 | 0.317 | Dominated by lorazepam, quetiapine, trazodone, temazepam, zopiclone, flurazepam, and nitrazepam | |
Lemborexant | 1,693 | 0.321 | 103,425 vs. quetiapine | |
CDA-AMC base case Reanalysis 1 + 2 + 3 (probabilistic) | Untreated | 1,243 | 0.316 | Reference |
Lorazepam | 1,257 | 0.317 | 9,436 vs. untreated | |
Quetiapine | 1,260 | 0.318 | 4,255 vs. lorazepam | |
Flurazepam | 1,265 | 0.317 | Dominated by quetiapine and lorazepam | |
Temazepam | 1,265 | 0.317 | Dominated by flurazepam, quetiapine and lorazepam | |
Trazodone | 1,270 | 0.318 | Dominated by quetiapine | |
Triazolam | 1,273 | 0.317 | Dominated by trazodone, temazepam, flurazepam, quetiapine and lorazepam | |
Zopiclone | 1,281 | 0.317 | Dominated by triazolam, trazodone, temazepam, flurazepam, quetiapine and lorazepam | |
Nitrazepam | 1,289 | 0.317 | Dominated by zopiclone, triazolam, trazodone, temazepam, flurazepam, quetiapine and lorazepam | |
Lemborexant | 1,564 | 0.321 | 103,511 vs. quetiapine |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years; vs. = versus.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
Table 9: Disaggregated Results of the CDA-AMC Base Case (Probabilistic)
Parameter | Lemborexant | Flurazepam | Nitrazepam | Zopiclone | Triazolam | Temazepam | Quetiapine | Trazodone | Lorazepam | Untreated |
|---|---|---|---|---|---|---|---|---|---|---|
Discounted LYs | ||||||||||
Total | 0.492 | 0.492 | 0.492 | 0.492 | 0.492 | 0.492 | 0.492 | 0.492 | 0.492 | 0.492 |
Discounted QALYs | ||||||||||
Total | 0.321 | 0.317 | 0.317 | 0.317 | 0.317 | 0.317 | 0.318 | 0.318 | 0.317 | 0.316 |
Treatment | 0.373 | 0.369 | 0.369 | 0.369 | 0.369 | 0.369 | 0.370 | 0.370 | 0.369 | 0.368 |
Falls | −0.014 | −0.014 | −0.014 | −0.014 | −0.014 | −0.014 | −0.014 | −0.014 | −0.014 | −0.014 |
MVAs | −0.0003 | −0.0003 | −0.0003 | −0.0003 | −0.0003 | −0.0003 | −0.0003 | −0.0003 | −0.0003 | −0.0003 |
WPAs | −0.001 | −0.001 | −0.001 | −0.001 | −0.001 | −0.001 | −0.001 | −0.001 | −0.001 | −0.001 |
Premature death | −0.037 | −0.037 | −0.037 | −0.037 | −0.037 | −0.037 | −0.037 | −0.037 | −0.037 | −0.037 |
Discounted costs ($) | ||||||||||
Total | 1,564 | 1,265 | 1,289 | 1,281 | 1,273 | 1,265 | 1,260 | 1,270 | 1,257 | 1,243 |
Drug | 316 | 25 | 33 | 24 | 27 | 16 | 9 | 10 | 8 | 0 |
Primary care visits | 399 | 390 | 406 | 407 | 396 | 400 | 401 | 410 | 399 | 393 |
CBT | 395 | 395 | 395 | 395 | 395 | 395 | 395 | 395 | 395 | 395 |
Falls | 355 | 355 | 355 | 355 | 355 | 355 | 355 | 355 | 355 | 355 |
MVA | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 |
WPA | 66 | 66 | 66 | 66 | 66 | 66 | 66 | 66 | 66 | 66 |
CBT = cognitive behavioural therapy; CDA-AMC = Canada’s Drug Agency; LY = life-year; MVA = motor vehicle accident; QALY = quality-adjusted life-year; WPA = workplace accident.
Price Reduction Analysis
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (refer to Table 10).
Table 10: Results of the Price Reduction Analysis
Price reduction | Unit drug cost ($) | Annual cost ($) | ICERs for lemborexant vs. comparators ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC base case | |||
No price reduction | 1.76 | 641 | Dominant | 103,511 vs. quetiapine |
10% | 1.58 | 577 | Dominant | 92,777 vs. quetiapine |
20% | 1.40 | 513 | Dominant | 82,042 vs. quetiapine |
30% | 1.23 | 449 | Dominant | 71,308 vs. quetiapine |
40% | 1.05 | 385 | Dominant | 60,574 vs. quetiapine |
50% | 0.88 | 320 | Dominant | 49,839 vs. quetiapine |
60% | 0.70 | 256 | Dominant | 39,105 vs. quetiapine |
70% | 0.53 | 192 | Dominant | 28,371 vs. quetiapine |
80% | 0.35 | 128 | Dominant | 17,637 vs. quetiapine |
90% | 0.18 | 64 | Dominant | 7,156 vs. no treatment |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
aSponsor’s submitted price for lemborexant.1
Assessment of Uncertainty
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to address uncertainty within the economic evaluation. The results are provided in Table 11.
Assuming no differences in sSOL between lemborexant and all comparators.
Retaining the sponsor-provided risk of falls associated with benzodiazepines.
In the first CDA-AMC scenario analysis (results not shown in table), the total QALYs for all comparators except for no treatment were equivalent, and lorazepam was associated with the lowest total cost, which was $308 less than the total cost associated with lemborexant over the 6-month time horizon.
Table 11: Results of CDA-AMC Scenario Analyses
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case | Untreated | 1,377 | 0.316 | Reference |
Lorazepam | 1,385 | 0.317 | 5,334 vs. untreated | |
Quetiapine | 1,386 | 0.318 | 1,670 vs. lorazepam | |
Lemborexant | 1,693 | 0.321 | 103,425 vs. quetiapine | |
CDA-AMC scenario 2: increased risk of falls for benzodiazepines | Quetiapine | 1,386 | 0.318 | Reference |
Lemborexant | 1,693 | 0.321 | 103,425 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
aDeterministic analysis: Treatments that were not on the cost-effectiveness frontier (i.e., are dominated by 1 or more other treatments) are not reported.
Issues for Consideration
Lemborexant was previously reviewed by CDA-AMC for insomnia, which a recommendation to not reimburse was issued. The submitted economic model updated the cost of lemborexant and other comparators and retained the original model structure from the previous submission.
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing lemborexant for the treatment of insomnia in adults diagnosed according to the most recent version of the DSM referring to CID and the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.1
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2026 to 2028), with 2025 as the base year.15 The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits Program.15 The sponsor estimated the eligible population using an epidemiological approach starting from the number of public drug plan beneficiaries.15,36,37 The sponsor’s base case included drug acquisition costs.15 The market uptake for lemborexant was estimated using the sponsor’s market forecast.15 The key inputs to the BIA are documented in Table 12.
The sponsor estimated the 3-year incremental budget impact associated with reimbursing lemborexant would be $99,482,389 (year 1 = $21,152,890: year 2 = $32,877,469; year 3 = $45,452,030) for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.15 In the reimbursement request population (i.e., only those with CID), the sponsor estimated the 3-year incremental budget impact associated with reimbursing lemborexant would be $64,093,397 (year 1 = $13,628,146: year 2 = $21,181,927; year 3 = $29,283,324).15
Table 12: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) | |
|---|---|---|
Target population | ||
Number of public drug plan beneficiaries, 18 years and older | ||
Growth ratea | 3.69% / 3.75% / 3.81%15 | |
Prevalence of insomniab | 25.3%37 | |
Proportion of patients receiving prescription treatment | 14.7%36 | |
Number of patients eligible for drug under review | 372,762 / 386,730 / 401,456 | |
Market shares (reference scenario) | ||
Lemborexant | 0% / 0% / 0% | |
Antidepressants | 50.1% / 51.6% / 53.0% | |
Antipsychotics | 2.2% / 2.3% / 2.3% | |
Benzodiazepines | 33.2% / 31.8% / 30.4% | |
Z-drugs | 14.5% / 14.4% / 14.2% | |
Market shares (new drug scenario) | ||
Lemborexant | 10.0% / 15.0% / 20.0% | |
Antidepressants | 45.1% / 43.8% / 42.4% | |
Antipsychotics | 2.0% / 1.9% / 1.9% | |
Benzodiazepines | 29.8% / 27.0% / 24.4% | |
Z-drugs | 13.1% / 12.2% / 11.4% | |
Cost of treatment (per patient per dayc) | ||
Lemborexant | $1.761 | |
Antidepressants | ||
Antipsychotics | ||
Benzodiazepines | ||
Z-drugs | ||
aGrowth rates were calculated as an aggregate of the growth in beneficiaries based on population growth rates.
bWhen adjusting for the reimbursement request population, the prevalence of chronic insomnia was 16.3%.
cDaily costs were calculated based on a weighted average of dosages.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The starting population is associated with uncertainty. The sponsor’s model began their market size narrowing with the number of public drug plan beneficiaries. Subsequently, the sponsor applied a stepwise narrowing approach using published literature.36-47 Starting with the number of people in the public drug plan beneficiaries may be inappropriate because there may be a difference in baseline characteristics and demographics when compared to the general population. The sponsor’s subsequent narrowing steps were based published literature examining the prevalence of insomnia in the general population of Canada and may not be applicable to people within the drug plan beneficiaries.
In reanalysis, CDA-AMC adjusted the starting population to be the general population of Canada, stratified into 2 age groups: 18 to 64 years, and 65 years and older. A narrowing step was applied to reduce the patient population to reflect patients enrolled in the public drug plans based on Understanding the Gap 2.0, and the average population growth rate in Canada was considered.48-50
The market size for patients with chronic insomnia may be underestimated. The sponsor based the proportion of patients with insomnia who would receive pharmacologic treatment (14.7%) on a phone interview study conducted in Canada in their analysis of all patients with insomnia symptoms or insomnia disorder.36 However, in the subgroup of patients classified as having insomnia disorder (based on DSM, Fifth Edition, diagnostic criteria for insomnia) 36.9% reported using prescribed sleep medication.36 According to clinical expert feedback, patients with chronic insomnia would be more likely to be prescribed pharmacological treatment, which aligns with the subgroup analysis in the sponsor-cited study for patients classified as having insomnia disorder.
CDA-AMC conducted a scenario analysis where the proportion of patients who receive prescription treatment was increased to 36.9%.36
The market shares of comparator treatments are associated with uncertainty. The sponsor calculated the market shares of comparator treatments based on the historical claims from the IQVIA private drug plan database for each treatment, while assuming a proportion of those claims were prescribed for insomnia.15,31 This approach introduces significant uncertainty as drug claims do not represent utilization per indication, and therefore, some included comparators may not be used for insomnia or CID treatment. Additionally, clinical experts indicated that doxepin and zolpidem were not included as relevant comparators; however, are commonly used in clinical practice to treat insomnia.
In reanalysis, CDA-AMC included the missing comparators. As a result, market shares and drug costs were revised in line with the clinical expert feedback obtained by CDA-AMC. Clinical expert feedback indicated that the sponsor’s reference scenario market shares were somewhat aligned with clinical practice as trazodone and zopiclone capture the majority of the market share.
The duration of treatment is associated with uncertainty. In the submitted analysis, the sponsor assumed that all treatments would be taken daily for 1 year. In the sponsor’s BIA report, it was noted that the duration of treatment of relevant comparators is associated with uncertainty as prescribing behaviours may vary across jurisdictions.15 Clinical experts consulted for this review indicated that benzodiazepines and Z-drugs are most typically prescribed with interval dosing and patients would not be expected to on benzodiazepine or Z-drug treatment for 365 days of a year.
In reanalysis, CDA-AMC selected to change the number of days on benzodiazepines and Z-drugs to 137 days based on the published literature.51
The market uptake of lemborexant is likely underestimated. The sponsor based their market uptake of lemborexant on internal market forecasting. Multiple clinical guidelines recommend against the routine use of benzodiazepines, Z-drugs, antipsychotics, or antidepressants to treat insomnia.52 Additionally, the 2024 Delphi consensus recommendations concluded that dual orexin receptor antagonists have a more favourable side effect profile when compared to other treatments.52 Given the consensus guidelines and discussions with clinical experts consulted for this review, a market uptake of 10%, 15%, and 20% in years 1 to 3, respectively, may be underestimated.
In reanalysis, CDA-AMC adjusted the market uptake of lemborexant to 20%, 40%, and 50% for years 1, 2, and 3 to reflect clinical guidelines and expectations of use in clinical practice in Canada if lemborexant was publicly funded.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, in consultation with clinical experts, as outlined in Table 13.
Table 13: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Starting population | Started with drug plan beneficiaries | Started with the population aged 18 years and older in Canada and applied a narrowing step to obtain the people eligible for a public drug plan. |
2. Reference scenario market shares | Zolpidem and doxepin were excluded. Alprazolam, bromazepam, diazepam, flurazepam, nitrazepam, oxazepam, triazolam, chlordiazepoxide, and clobazam: included | Zolpidem and doxepin were included. Alprazolam, bromazepam, diazepam, flurazepam, nitrazepam, oxazepam, triazolam, chlordiazepoxide, and clobazam: excluded. Refer to Table 14 |
3. Duration of treatment for benzodiazepines and Z-drugs | 365 days | 137 days |
4. Market uptake of lemborexant | Year 1: 10% Year 2: 15% Year 3: 20% | Year 1: 20% Year 2: 40% Year 3: 50% |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 + 4 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 15 and a more detailed breakdown is presented in Table 16. In the CDA-AMC base case, the 3-year budget impact of reimbursing lemborexant for the treatment of insomnia in adults diagnosed according to the most recent version of the DSM referring to CID was $165,454,416 (year 1 = $28,964,842; year 2 = $59,667,574; year 3 = $76,822,001).
Table 14: Market Shares for the CDA-AMC Base Case
Pharmacological treatment | Drugs | Market shares years 1 to 3 |
|---|---|---|
Antidepressants (54%) | Amitriptyline | 4% |
Doxepin | 3% | |
Mirtazapine | 5% | |
Trazodone | 42% | |
Antipsychotics (7%) | Quetiapine | 7% |
Benzodiazepines (13%) | Clonazepam | 7% |
Lorazepam | 5% | |
Temazepam | 1% | |
Z-drugs (26%) | Zopiclone | 21% |
Zolpidem | 5% |
CDA-AMC = Canada’s Drug Agency.
Table 15: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 64,093,397 |
CDA-AMC reanalysis 1 | 68,094,309 |
CDA-AMC reanalysis 2 | 44,825,858 |
CDA-AMC reanalysis 3 | 65,920,545 |
CDA-AMC reanalysis 4 | 156,327,722 |
CDA-AMC base case: Reanalysis 1 + 2 + 3 + 4 | 165,454,416 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to explore uncertainty in the estimated budget impact of reimbursing lemborexant (results are provided in Table 16):
Adjusting the patient population to include the Health Canada indication.
Increasing the proportion of patients who receive prescribed treatment to 36.9%.
Table 16: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference total | 16,843,429 | 17,637,083 | 18,473,613 | 19,350,097 | 55,460,794 |
Lemborexant | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 16,843,429 | 17,637,083 | 18,473,613 | 19,350,097 | 55,460,794 | |
New drug total | 16,843,429 | 31,265,230 | 39,655,540 | 48,633,421 | 119,554,191 | |
Lemborexant | 0 | 15,391,855 | 23,952,969 | 33,153,343 | 72,498,167 | |
All other comparators | 16,843,429 | 15,873,375 | 15,702,571 | 15,480,078 | 47,056,024 | |
Budget Impact | 0 | 13,628,146 | 21,181,927 | 29,283,324 | 64,093,397 | |
CDA-AMC base case | Reference total | 19,632,048 | 20,221,009 | 20,827,639 | 21,452,468 | 62,501,117 |
Lemborexant | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 19,632,048 | 20,221,009 | 20,827,639 | 21,452,468 | 62,501,117 | |
New drug total | 19,632,048 | 49,185,851 | 80,495,213 | 98,274,469 | 227,955,533 | |
Lemborexant | 0 | 33,009,043 | 67,998,629 | 87,548,235 | 188,555,908 | |
All other comparators | 19,632,048 | 16,176,807 | 12,496,584 | 10,726,234 | 39,399,625 | |
Budget Impact | 0 | 28,964,842 | 59,667,574 | 76,822,001 | 165,454,416 | |
CDA-AMC scenario analyses | ||||||
Scenario 1: Health Canada indication | Reference total | 30,471,828 | 31,385,983 | 32,327,563 | 33,297,390 | 97,010,935 |
New drug total | 30,471,828 | 76,343,682 | 124,940,422 | 152,536,446 | 353,820,551 | |
Budget Impact | 0 | 44,957,699 | 92,612,860 | 119,239,057 | 256,809,616 | |
Scenario 2: Increased proportion receiving prescribed treatment | Reference total | 49,280,446 | 50,758,859 | 52,281,625 | 53,850,074 | 156,890,558 |
New drug total | 49,280,446 | 123,466,523 | 202,059,412 | 246,688,974 | 572,214,909 | |
Budget Impact | 0 | 72,707,664 | 149,777,787 | 192,838,901 | 415,324,351 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.