Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Finerenone (Kerendia)
Indication: As an adjunct to standard of care in adults with heart failure with left ventricular ejection fraction (LVEF) ≥ 40% to reduce the risk of cardiovascular death, hospitalization for heart failure, and urgent heart failure visits.
Sponsor: Bayer Inc.
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Kerendia?
Canada’s Drug Agency (CDA-AMC) recommends that Kerendia be reimbursed by public drug plans as an add-on “to standard of care in adults with heart failure with left ventricular ejection fraction (LVEF) ≥ 40% to reduce the risk of cardiovascular death, hospitalization for heart failure, and urgent heart failure visits,” if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
Evidence from 1 clinical trial showed that adding Kerendia to standard of care (SOC) therapy, improved outcomes, including reduced cardiovascular (CV) deaths, total heart failure (HF) events, and hospitalizations for HF and/or urgent visits, compared to placebo plus SOC therapy in adult patients with HF with LVEF of 40% or more. The Canadian Drug Expert Committee (CDEC) determined that adding Kerendia to SOC therapy provides acceptable clinical value compared with SOC therapy alone for these patients and addresses the needs identified by both patients and clinicians, such as reducing mortality and lowering the risk of initial and recurrent hospitalizations. This determination was enough for CDEC to recommend that Kerendia be reimbursed. Given that Kerendia is expected to be used in addition to SOC therapy, acceptable clinical value refers to added value of Kerendia in combination with SOC therapy versus SOC therapy alone.
Which Patients Are Eligible for Coverage?
Kerendia should only be covered when initiated as an add-on to SOC therapy in adults with HF (New York Heart Association [NYHA] class II to IV) with mildly reduced or preserved ejection fraction (LVEF ≥ 40%). Treatment should not be initiated in patients with serum or plasma potassium levels of greater than 5.0 mmol/L (i.e., severe hyperkalemia) or with an estimated glomerular filtration rate (eGFR) of less than 25 mL/min/1.73 m2.
What Are the Conditions for Reimbursement?
Kerendia should only be reimbursed when prescribed by a clinician who has expertise in managing HF and the cost of Kerendia is reduced. Treatment should be discontinued if the patient develops renal failure or hyperkalemia that cannot be adequately managed. Important budget impact considerations must be addressed for health systems to be able to adopt Kerendia.
Review Background
Disease background: HF is a disorder in which the heart is unable to adequately pump blood through the body to maintain the metabolic needs of tissues and organs. Common symptoms of HF include dyspnea and fatigue, exercise intolerance, and fluid buildup, which in turn may lead to pulmonary congestion and peripheral edema (mainly in the feet, ankles, or legs) that significantly affect quality of life. Patients living with HF often deal with other comorbidities, including diabetes, hypertension, atrial fibrillation, kidney problems, and chronic obstructive pulmonary disease.
In Canada, HF is the third most common reason for hospitalization. It is estimated that more than 750,000 individuals in Canada are living with HF. The crude prevalence of HF among patients aged 40 years or older in Canada has been steadily increasing from 3.62% in 2012 to 4.01% in 2024.
Indication and reimbursement request: Finerenone (Kerendia) has been approved by Health Canada as an adjunct to SOC therapy in adults with HF with LVEF of 40% or more to reduce the risk of CV death, hospitalization for HF, and urgent HF visits. The sponsor is seeking reimbursement for this patient population. This application was submitted by the sponsor before receiving a Notice of Compliance from Health Canada. The CDA-AMC review reflects the sponsor’s originally proposed indication and product monograph, which generally aligned with the final approved indication.
The application was submitted by the sponsor before receiving a Notice of Compliance from Health Canada and the CDA‑AMC review reflects the anticipated indication for finerenone in the sponsor’s submission at the time of the review, where finerenone is “indicated in adults for the treatment of HF with mildly reduced or preserved ejection fraction (LVEF ≥ 40%) to reduce the risk of cardiovascular death, hospitalization for heart failure, and urgent heart failure visits.”
Drug under review: Finerenone is a nonsteroidal mineralocorticoid receptor antagonist. It is available as 10 mg, 20 mg and 40 mg oral tablets. The starting dose of finerenone is 10 mg or 20 mg once daily and is based on eGFR levels. The recommended target dose is 20 mg or 40 mg, depending on eGFR and serum or potassium levels.
Treatment costs: At the submitted price of $3.26 per tablet, the annual cost of finerenone is expected to be $1,189 per patient, based on the Health Canada–recommended dosage.
Highlights of Input From Interested Parties
The following are the patient-identified impacts of HF, unmet needs, and important outcomes as reported in the submission received from a patient group, HeartLife Foundation:
Patients living with HF with mildly reduced or preserved ejection fraction noted swelling in the legs, ankles, and stomach; shortness of breath with light activity; fatigue and low energy; difficulty in sleeping flat and concentrating as some of the burdensome symptoms. In patients with comorbidities such as kidney disease, pulmonary hypertension, chronic obstructive pulmonary disease, or arthritis, identifying the cause of a patient’s symptoms was difficult. Patients could not perform their usual activities such as working, cooking, walking, travelling, or socializing.
Patients living with HF noted that current treatments helped reduce symptoms like swelling or shortness of breath; however, they struggled to keep their condition stable. They highlighted the burden of managing multiple medications, frequent dose adjustments, limited access to specialists, and treatment delays, all of which contribute to emotional distress.
Patients identified outcomes such as fewer hospital stays and emergency visits, reduced risk of death, improved energy and strength for daily activities, and milder side effects with better symptom management and condition stability as important. They also emphasized the importance of affordability and treatments that are easier to incorporate into their daily routines.
Three clinician groups (University of Ottawa and Heart Institute Cardiology and Heart Failure, Regional Wellness Kidney Centre, Graser Health Authority – Cardiology and Nephrology Divisions), a group of clinicians, a cardiologist, and the clinical experts consulted by CDA-AMC noted the following unmet needs regarding HF and the place in therapy for finerenone.
Unmet needs: Patients with HF often lack mortality-reducing therapies, face significant risk of hospitalizations, and have tolerability and safety concerns with current therapies. For example, spironolactone is associated with gynecomastia and sodium-glucose cotransporter-2 (SGLT-2) inhibitors and are associated with genitourinary infections and decreased renal function, and many patients have comorbidities such as advanced kidney disease and type 1 diabetes, for which these treatments are contraindicated.
Anticipated place in therapy: Finerenone would be used as an adjunct to SOC therapy and be considered if a patient had ongoing symptoms, mild renal dysfunction, recurrent risks of hospitalizations, and no contraindications.
The participating public drug programs raised potential implementation issues related to considerations for initiation, renewal, discontinuation, prescribing of therapy, and system and economic issues.
Recommendation
With a vote of 14 in favour to 0 against, CDEC recommends that finerenone be reimbursed “as an adjunct to standard of care in adults with heart failure with left ventricular ejection fraction (LVEF) ≥ 40% to reduce the risk of cardiovascular death, hospitalization for heart failure, and urgent heart failure visits,” only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Treatment with finerenone should be reimbursed when initiated as an adjunct to SOC therapy in adults for the treatment of heart failure (NYHA class II to IV) with mildly reduced or preserved ejection fraction (LVEF ≥ 40%). | Evidence from the FINEARTS-HF trial demonstrated that treatment with finerenone resulted in a clinically meaningful benefit in patients with these characteristics. | According to the clinical experts consulted for this review, the SOC varies across Canada, as there is no universally accepted definition. The experts also noted that finerenone may be used with or without SGLT-2 inhibitors, based on clinical judgment and patient access, because these therapies have distinct mechanisms of action that are expected to provide complementary benefits. CDEC noted that NT-proBNP (or BNP) levels were among the inclusion criteria in the FINEARTS-HF trial. However, the committee agreed with clinical experts that while NT-proBNP may be appropriate for clinical trials, it is not required for diagnosis in practice, may have inconsistent accessibility, and its use could create confusion, potentially excluding patients who might benefit from finerenone. |
2. Treatment with finerenone should not be used in patients with either of the following: 2.1. severe hyperkalemia (serum and/or plasma potassium > 5.0 mmol/L) 2.2. an eGFR < 25 mL/min/1.73 m2. | The FINEARTS-HF trial excluded patients with such characteristics. | — |
Renewal | ||
3. Treatment with finerenone should be continued unless the patient develops renal failure or hyperkalemia that cannot be adequately managed. | The FINEARTS-HF trial excluded patients with renal failure and hyperkalemia. | The clinical experts indicated that there is no objective marker (e.g., biomarker) to determine whether a patient is ready to discontinue treatment. Consequently, patients who tolerate the therapy and remain clinically well would continue receiving the drug. |
Prescribing | ||
4. Finerenone should be prescribed by clinicians with expertise in managing heart failure. | This is meant to ensure that finerenone is prescribed for appropriate patients and that adverse effects are managed in an optimized and timely manner. | — |
Pricing | ||
5. A reduction in price. | Using the CDA-AMC base-case analysis, the ICER for finerenone plus SOC was $77,195 per QALY gained when compared with SOC alone in the indicated population. A band 2a price reduction would be required to achieve cost-effectiveness at a $50,000 per QALY gained threshold. No price reduction would be required to achieve cost-effectiveness at a $100,000 per QALY gained threshold. Price reductions for any given willingness to pay threshold are available in the CDA‑AMC main report and Supplemental Material. | — |
Feasibility of adoption | ||
6. The economic feasibility of adoption of finerenone must be addressed. | At the submitted price, the incremental budget impact of finerenone plus SOC is expected to be greater than $40 million in year 3. | — |
CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; eGFR = estimated glomerular filtration rate, ICER = incremental cost-effectiveness ratio, LVEF = left ventricular ejection fraction, NYHA = New York Heart Association, QALY = quality-adjusted life-year, SGLT-2 = sodium-glucose cotransporter-2; SOC = standard of care.
aRegarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Clinical Value
Based on the totality of the clinical evidence, CDEC concluded that finerenone as an adjunct to SOC therapy demonstrates acceptable clinical value in adult patients with HF, defined as NYHA class II to IV, with mildly reduced or preserved LVEF of 40% or more compared to SOC therapy alone. Given that finerenone is expected to be an additive treatment to SOC therapy, acceptable clinical value refers to added value versus SOC therapy alone.
Evidence from 1 randomized, double-blind, placebo-controlled, multicentre, phase III trial (the FINEARTS-HF trial; N = 6,001) demonstrated that in adult patients with HF (LVEF ≥ 40%), treatment with finerenone plus SOC therapy likely results in added clinical value in the composite outcome of CV death and total HF events (first and recurrent hospitalizations for HF and/or urgent HF visits) compared to placebo plus SOC therapy. After a median follow-up of 32 months, the rate ratio (RR) for the composite outcome was 0.84 (95% confidence interval [CI], 0.74 to 0.95), with a between-group difference of 2.81 (95% CI, █████ ██ █████) in favour of finerenone. Assessment of the individual components of the composite outcome indicated that the between-group difference in incidence rate (per 100 patient years) for CV death was 0.6 (95% CI ████ ██ ███), with a hazard ratio (HR) of 0.93 (95% CI, 0.78 to 1.11). The between-group difference in incidence rate for the total HF events was 2.55 (95% CI, █████ ██ █████), with an RR of 0.82 (95% CI, 0.71 to 0.94), in favour of finerenone versus placebo.
Unmet needs identified by patient groups and clinicians include limited mortality-reducing therapies, a significant risk of hospitalization and repeated hospitalization, and tolerability and safety concerns with current therapies. CDEC acknowledged that HF with mildly reduced to preserved LVEF is a common condition associated with substantial morbidity and mortality, and treatment options are limited. The committee concluded that the results from the FINEARTS-HF trial indicate with moderate to high certainty that finerenone as an adjunct to SOC therapy may address the need for more effective treatments that reduce mortality and the risk of hospitalization.
Further information on the committee’s discussion around clinical value is provided in the Summary of Deliberation section.
Developing the Recommendation
The determination of acceptable clinical value was sufficient for CDEC to recommend reimbursement of finerenone. As part of the deliberation on whether to recommend reimbursement, the committee also considered unmet clinical need, unmet nonclinical need, and health inequity. Information on this discussion is provided in the Unmet Clinical Need and Distinct Social and Ethical Considerations domains in the Summary of Deliberation section.
Because CDEC recommended that finerenone be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations, or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
CDEC considered all domains of value of the deliberative framework before developing its recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Appropriate comparators: CDEC noted that the 4 categories of therapies identified in the 2025 Canadian Cardiovascular Society (CCS) updated guidelines for the pharmacological management of patients with LVEF of 40% or more are appropriate comparators to finerenone. These are SGLT-2 inhibitors, mineralocorticoid receptor antagonists (MRAs) (e.g., spironolactone), angiotensin receptor-neprilysin inhibitors, and evidence-based drugs with glucagon-like peptide-1 receptor agonist activity. CDEC observed that the FINEARTS-HF trial was a placebo-controlled study that did not compare finerenone directly to any active intervention. However, the committee agreed with the clinical experts that at the time of the trial, spironolactone had a weak recommendation with no compelling benefit for use in patients with HF with preserved ejection fraction (HFpEF) and SGLT-2 inhibitors, and the other drugs in the updated CCS guidelines had no official indication for HFpEF, making the placebo-controlled design of the FINEARTS-HF trial acceptable for CDEC to evaluate the effectiveness and safety of finerenone.
Efficacy versus placebo: Evidence from the FINEARTS-HF trial showed an RR of 0.84 (95% CI, 0.74 to 0.95) with a between-group difference of 2.81 (95% CI, █████ ██ █████), in favour of finerenone versus placebo for the primary composite outcome of CV and total HF events after a median follow-up of 32 months. The results indicate that using finerenone as adjunct to SOC therapy provides added value in CV and total HF outcomes compared to SOC therapy alone. The incidence rate (per 100 patient years) for CV death was 3.33 in the finerenone group and 3.59 in the placebo group, with a between-group difference of 0.6 (95% CI, ████ ██ ███) and an HR of 0.93 (95% CI, 0.78 to 1.11). The incidence rate for the total HF events (first and recurrent hospitalizations for HF and/or urgent HF visits) was 11.57 in the finerenone group and 14.12 in the placebo group, with a between-group difference of 2.55 (95% CI, █████ ██ █████), with an RR of 0.82, (95% CI, 0.71 to 0.94). Health-related quality of life (HRQoL) assessed using the Kansas City Cardiomyopathy Questionnaire Total Symptom Score, showed minimal change at 12 months. For the other key secondary end points, including change in NYHA class, composite renal end point, and all-cause mortality, the results demonstrated little to no difference between the finerenone and placebo groups.
Clinical importance of treatment effects: CDEC considered outcomes identified by patients and clinicians, including reductions in hospitalizations for HF, reductions in risk of CV death and/or all-cause mortality, fewer side effects, and improved quality of life. The committee noted that the treatment effect observed at 32 months represents a meaningful benefit for hospitalizations for HF and CV deaths. CDEC discussed the use of finerenone as an adjunct to SGLT-2 inhibitors, noting insufficient evidence to determine the specific incremental value resulting from using them together. However, the committee concluded that there is no mechanistic rationale to expect diminished effectiveness when these therapies are used in combination.
Certainty of the evidence: CDEC discussed the certainty of evidence as assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) method. For the primary composite end point of CV death and total HF events, the certainty was rated as moderate at 32 months, suggesting the reduction was likely clinically important. This reduction was largely driven by the reduction in HF events. For CV death, the certainty of evidence was rated as moderate using GRADE, indicating that treatment with finerenone likely resulted in a reduction of CV deaths compared to placebo. However, conclusions were limited by the imprecision as the 95% CI for the between-group difference spans from potential benefit to potential harm. For total HF events, the GRADE assessment rated the certainty of evidence as high, indicating that treatment with finerenone resulted in a reduction in total HF events compared to placebo. The clinical experts emphasized that total HF events constitute a very important outcome because it impacts patients, treatment outcomes, caregivers, and broader health care systems. For patients’ HRQoL at 12 months, the certainty of evidence was rated as low as the between-group difference was less than the minimal important difference of 5 points between groups suggested by clinical experts consulted by CDA‑AMC. Furthermore, there was uncertainty due to the subjectivity of patient-reported outcome and a risk of attrition bias due to a significant amount of missing data. There was a high certainty of evidence that treatment with finerenone resulted in increased hyperkalemia events and worsening renal function compared to placebo.
Indirect evidence versus SGLT-2 inhibitors (dapagliflozin and empagliflozin): CDEC noted the sponsor-submitted indirect treatment comparison, a network meta-analysis evaluating the efficacy and safety of finerenone versus SGLT‑2 inhibitors with similar indication for patients with HF in Canada (i.e., dapagliflozin and empagliflozin), was insufficient to draw a firm conclusion due to limitations such as significant heterogeneity and sparse network.
Comparative harms: CDEC discussed harm results from the FINEARTS-HF trial, noting that overall treatment-emergent adverse events (TEAEs) and the frequency of serious TEAEs were similar across the finerenone and placebo groups. TEAEs leading to discontinuation were low (3.2% for finerenone versus 2.8% for placebo). The committee observed that treatment-emergent hyperkalemia was higher with finerenone (9.7%) than with placebo (4.2%). However, hyperkalemia leading to hospitalization was rare (0.5% for finerenone and 0.2% for placebo), with most cases being mild or moderate and resolving by the end of the study, and none led to death. CDEC noted that the risk of hyperkalemia is linked to the mechanism of action of MRAs such as finerenone. CDEC also acknowledged the input of clinical experts consulted by CDA-AMC that patients with HF are routinely monitored to address adverse events. CDEC noted that the rate of renal composite end point was higher with finerenone (2.5%) compared to placebo (1.8%) at 3 months but was stable afterwards.
Clinical value: Based on the preceding considerations, CDEC determined that in adult patients with HF (NYHA class II to IV) with mildly reduced or preserved ejection fraction (LVEF ≥ 40%), finerenone as an adjunct to SOC therapy demonstrates acceptable clinical value compared with SOC therapy alone.
Unmet Clinical Need
Input on unmet clinical need: Patients and clinicians emphasized the need for treatments that reduce hospitalizations, lower mortality risk, improve quality of life, and provide better symptom control. They noted that despite the benefits of SGLT‑2 inhibitors, many patients with HFpEF still experience worsening symptoms, high rehospitalization risk, and safety concerns with current therapies. Patients expressed a need for treatments that go beyond symptom control. The committee concluded that the results from the FINEARTS-HF trial indicate with moderate to high certainty that finerenone as an adjunct to SOC therapy may address the need for more effective treatments that reduce mortality and the risk of hospitalization.
Severity of the disease: CDEC acknowledged that HF is a chronic condition leading to frequent hospitalizations, increased mortality, and reduced HRQoL. It is the third most common reason for hospitalizations in Canada and imposes a high disease and economic burden due to intensive resource use. This burden is expected to increase with an aging population and lifestyle factors, contributing to higher prevalence. Worsening HF substantially impacts functional status, the ability to work, and exercise capacity. CDEC noted that HF with mildly reduced to preserved LVEF is a common condition associated with substantial morbidity and mortality, and patients have limited treatment options with proven efficacy and safety.
Availability of treatment options: CDEC noted the 2025 CCS updated guidelines recommends SGLT‑2 inhibitors, MRAs, angiotensin receptor-neprilysin inhibitors, and glucagon-like peptide-1 receptor agonists as pharmacological management of patients with LVEF of 40% or more. Of these, CDEC noted that SGLT-2 inhibitors have the strongest recommendation for use across the ejection fraction spectrum in Canada. However, they are contraindicated in patients with advanced kidney dysfunction and in patients with type 1 diabetes. CDEC discussed that despite the availability of SGLT-2 inhibitors, patients with HF and LVEF of 40% or more continue to face residual risk for mortality, hospitalization for HF, rehospitalizations, and urgent HF visits.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: Patients highlighted the burden of taking multiple medications, frequent dose adjustments, the inability to access specialists, and the treatment delays leading to emotional distress. CDEC acknowledged that managing multiple medications adds to the burden and complexity of treatment to patients, making simplified effective and accessible options highly desirable.
Equity considerations: While CDEC recognized that the risk of HF is disproportionately higher among Indigenous communities, racialized groups, and those of low socioeconomic status, the committee could not find any evidence that finerenone could specifically address this health inequity.
Economic Considerations
Health impacts of finerenone versus relevant comparators: Finerenone plus SOC therapy is predicted to be associated with a gain of 0.02 life-years compared to SOC therapy alone and may result in a gain of 0.03 quality-adjusted life-years compared to SOC therapy alone over a 3-year time horizon.
Cost of finerenone versus relevant comparators: Finerenone plus SOC therapy is predicted to be associated with higher costs to health care systems than SOC therapy alone (incremental costs = $2,538) over a 3-year time horizon, primarily driven by increased costs associated with drug acquisition.
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA‑AMC base-case analysis estimated that the incremental cost-effectiveness ratio for finerenone plus SOC therapy in adults for the treatment of HF with mildly reduced or preserved ejection fraction (LVEF ≥ 40%) was $77,195 per quality-adjusted life-year gained when compared with SOC therapy alone (Figure 1).
Certainty of the evidence: The cost-effectiveness of finerenone using a longer time horizon is highly uncertain due to data limitations. The potential value of finerenone plus SOC therapy is dependent on patients realizing the predicted survival benefit compared to SOC therapy alone, which is uncertain due to limitations with the clinical data and submitted economic model. If these health outcomes are not realized, the incremental cost-effectiveness ratio for finerenone plus SOC therapy compared to SOC therapy alone will be higher than predicted in the CDA-AMC analysis.
Figure 1: Estimate of the ICER Used by CDEC to Inform the Price Condition
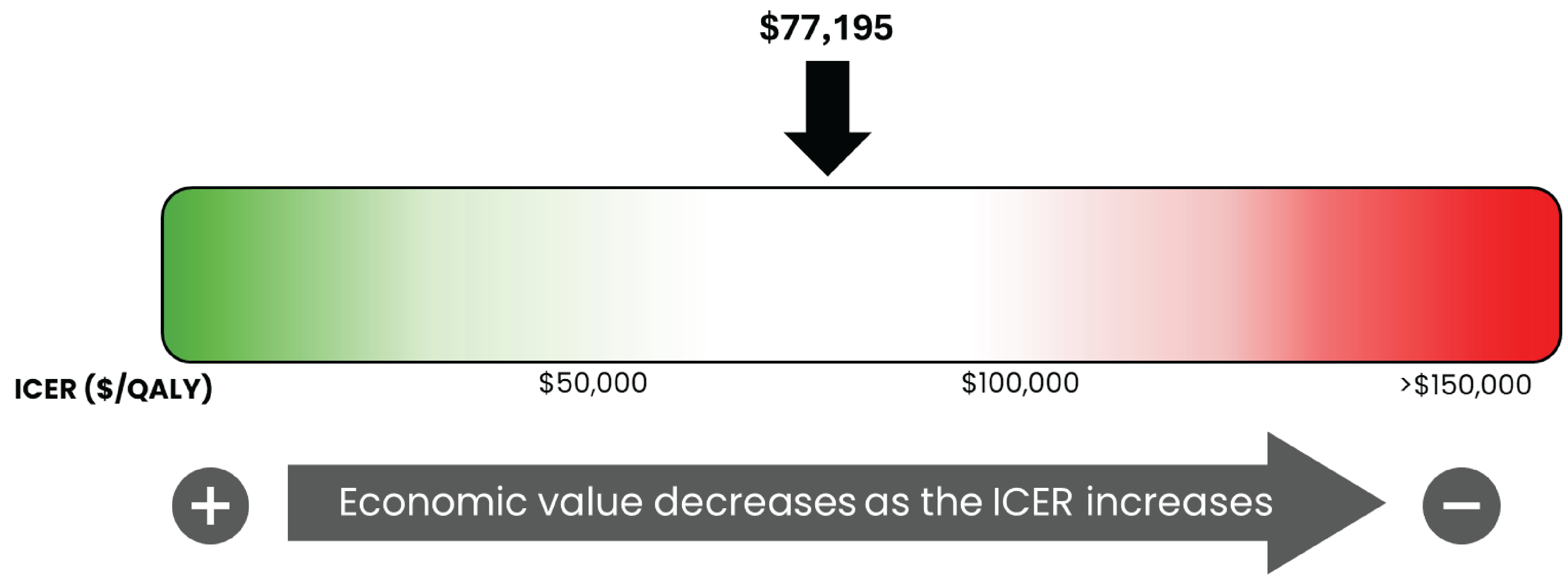
CDEC = Canadian Drug Expert Committee; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year
Impacts on Health Systems
Anticipated budget impact: It is estimated that by year 3 of reimbursement, 358,902 patients would be eligible for treatment with finerenone. Of these patients, 48,868 are expected to receive finerenone. The estimated incremental budget impact of reimbursing finerenone is predicted to be approximately $107 million over the first 3 years. Given finerenone is an add-on to existing care, its estimated expenditure is identical to the budget impact (i.e., $107 million). The actual budget impact of reimbursing finerenone as an adjunct to SOC therapy for adults with HF will depend on the market share of finerenone.
Members of the Committee
Dr. Peter Jamieson (Chair), Dr. Kerry Mansell (Vice-Chair), Sally Bean, Daryl Bell, Dan Dunsky, Dr. Ran Goldman, Dr. Trudy Huyghebaert, Dr. Dennis Ko, Dr. Christine Leong, Dr. Alicia McCallum, Dr. Srinivas Murthy, Dr. Nicholas Myers, Dr. Krishnan Ramanathan, Dr. Marco Solmi, Carla Velastegui, Dr. Edward Xie, and Dr. Peter Zed.
Meeting date: December 18, 2025
Regrets: Two expert committee members did not attend.
Conflicts of interest: None.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.