Drugs, Health Technologies, Health Systems
Reimbursement Review
Dupilumab (Dupixent)
Sponsor: Sanofi-Aventis Canada Inc.
Therapeutic area: Chronic rhinosinusitis with nasal polyps
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AC
Asthma Canada
AE
adverse event
AESI
adverse event of special interest
ANCOVA
analysis of covariance
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CRS
chronic rhinosinusitis
CRSsNP
chronic rhinosinusitis without nasal polyps
CRSwNP
chronic rhinosinusitis with nasal polyps
EPOS
European position paper on rhinosinusitis and nasal polyps
EUFOREA
European Forum for Research and Education in Allergy and Airway Diseases
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
IgE
immunoglobulin E
IgG4
immunoglobulin G4
IL-4
interleukin 4
IL-13
interleukin 13
INCS
intranasal corticosteroid
ITC
indirect treatment comparison
ITT
intention-to-treat
LS
least squares
MAIC
matching-adjusted indirect comparison
MeD
median difference
MID
minimal important difference
MD
mean difference
MFNS
mometasone furoate nasal spray
MI
multiple imputation
MMRM
mixed-effects model with repeated measures
NC
nasal congestion and obstruction
NPS
nasal polyp score
NSAID
nonsteroidal anti-inflammatory drug
NSAID-ERD
nonsteroidal anti-inflammatory drug–exacerbated respiratory disease
OR
odds ratio
RCT
randomized controlled trial
SAE
serious adverse event
SC
subcutaneous
SCS
systemic corticosteroid
SD
standard deviation
SLR
systematic literature review
SMD
standardized mean difference
SNOT-22
22-item Sino-Nasal Outcome Test
TEAE
treatment-emergent adverse event
TSS
total symptom score
UPSIT
University of Pennsylvania Smell Identification Test
VAS
visual analogue scale
WOCF
worst observation carried forward
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Dupilumab (Dupixent), 300 mg single-use prefilled syringe or pen administered by subcutaneous injection |
Sponsor | Sanofi-Aventis Canada Inc. (Sanofi) |
Indication | As an add-on maintenance treatment with intranasal corticosteroids in adult patients with severe chronic rhinosinusitis with nasal polyposis (CRSwNP) inadequately controlled by systemic corticosteroids and/or surgery |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | August 12, 2020 |
Recommended dose | 300 mg q.2.w. |
CRSwNP = chronic rhinosinusitis with nasal polyposis; NOC = Notice of Compliance; q.2.w. = every 2 weeks.
Introduction
Chronic rhinosinusitis (CRS) is a heterogeneous disease characterized by inflammation of the nose and paranasal sinuses, tissue edema, nasal obstruction, and increased mucus production. CRS presents with symptoms such as nasal congestion and/or obstruction (NC) and rhinorrhea that persist for at least 12 weeks.1 Current medical consensus categorizes CRS into 2 major phenotypes based on the presence or absence of nasal polyps. These 2 categories are CRS with nasal polyposis (CRSwNP) and CRS without nasal polyposis (CRSsNP).2-4 Nasal polyps in CRSwNP occur bilaterally and are noncancerous, edematous, inflammatory lesions that usually originate from the mucosa of the ethmoid, maxillary, and sphenoidal sinuses.5 A retrospective study in Alberta (2004 to 2014) estimated the prevalence of CRS to range from 18.8 to 23.3 per 1,000 population.6 Among all patients with CRS, between 25% and 30% have CRSwNP.7 The peak incidence of CRSwNP generally occurs in working adults between the ages of 45 to 60 years.2,8 Patients with CRSwNP suffer with a high symptom burden, including NC, loss of sense of smell, facial pain or pressure, discoloured sinonasal discharge, breathing impairment, sleep disorders, fatigue, and increased risk of infection.3,8,9 Among these, the symptoms with the greatest impact on patients’ health-related quality of life (HRQoL) are sinonasal congestion, loss of sense of smell, and sleep impairment.10 CRSwNP is diagnosed based on the presence of 2 or more symptoms of rhinosinusitis (NC, rhinorrhea, loss of sense of smell, facial pain and/or headache), presence of polyps in nasal endoscopy, and evidence of sinus inflammation on CT scan.11 In addition, the assessment of CRSwNP also takes into consideration the severity of the disease, often categorized using a visual analogue scale (VAS), and the duration of symptoms.12,13
International guidelines recommend a stepwise treatment approach based on disease severity for the treatment and management of CRSwNP. In this context, CRSwNP treatment is limited to the chronic use of intranasal corticosteroids (INCSs), short courses of systemic corticosteroids (SCSs) when symptoms worsen, and sinonasal surgery when medical therapy fails. In clinical settings in Canada, the use of INCSs for initial treatment for CRSwNP includes mometasone furoate nasal spray (MFNS).14 SCSs are typically more effective than INCSs in reducing polyp size and nasal symptoms.2 However, long-term SCS use for severe CRSwNP has been associated with increased adverse events (AEs), including infections, gastrointestinal events, pneumonia, and retinopathy, as well as long-term diseases such as diabetes, hypertension, kidney disease, peptic ulcer disease, and osteoporosis or osteopenia.15 In patients who do not respond to medical therapy, surgical management may be required to provide symptom relief and to remove inflammatory tissue. However, the recurrence of CRSwNP symptoms after surgery is common,16 and multiple surgeries may be needed to address recurrent symptoms.8,17,18 The current stepwise approach to CRSwNP treatment does not address the underlying chronic type 2 inflammation pathology and leads to a cycle of high morbidity, poor symptom control, loss of smell and/or taste, and poor HRQoL. The Canadian Rhinology Working Group recommends the use of biologic therapies for patients with CRSwNP to address the gaps in treatment.19,20 Biologic therapies that are currently available in Canada include dupilumab, omalizumab, and mepolizumab. Although omalizumab is approved by Health Canada for use in CRSwNP, it is not publicly reimbursed in Canada. Not all patients respond to mepolizumab.21
Dupilumab is a human immunoglobulin G4 (IgG4) monoclonal antibody that inhibits interleukin-4 (IL-4) and interleukin-13 (IL-13) signalling by binding to the IL-4 receptor alpha subunit shared by the IL-4 and IL-13 receptor complexes.22 IL-4 and IL-13 are key type 2 cytokines (including T-helper 2 cells) involved in atopic disease and type 2 inflammation, which are important components in the pathogenesis of CRSwNP.22 The recommended dose of dupilumab is 300 mg single-use prefilled syringe or pen administered by subcutaneous (SC) injection. Dupilumab was approved by Health Canada in 2020 as an add-on maintenance treatment with INCSs in adult patients with severe CRSwNP inadequately controlled by SCSs and/or surgery. The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of dupilumab for the treatment of adult patients with severe CRSwNP inadequately controlled by SCSs and/or surgery.
Dupilumab has been previously reviewed by Canada’s Drug Agency (CDA-AMC) for other indications (atopic dermatitis and asthma). At the time of this review, dupilumab was also being actively reviewed for chronic obstructive pulmonary disease and prurigo nodularis.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to our call for input and from clinical experts consulted by CDA-AMC for the purpose of this review.
Patient Input
One patient group input submission from Asthma Canada (AC) was received for this review. AC is a national charitable patient-driven organization that advocates for improved health and quality of life for people living with asthma and respiratory allergies through effective collaboration with policy-makers, researchers, and health care providers. AC gathered information for this submission through an online survey involving Canadians living with or caring for patients with nasal polyps between October 30, 2024, to November 28, 2024. The survey received 8 responses from adults living with nasal polyps, including 3 people in British Columbia, 1 in Manitoba, and 4 in Ontario. Of the 8 respondents, 1 was chosen at random for a 1-to-1 interview to gain an in-depth knowledge of the impacts of nasal polyps on the quality of life of people living with the condition.
When asked about their disease experience, respondents indicated that NC, trouble breathing, frequent sneezing, and loss of sense of smell and taste are the most common symptoms associated with nasal polyps. Overall, respondents highlighted that the most challenging aspects of living with nasal polyps include breathing difficulties, persistent NC, navigating the health care system, the possibility of surgery, and associated pain. These physical discomforts interfere with daily activities, sleep, and overall well-being. According to respondents, frequent medical appointments, financial difficulty, and an increase in missed days from work or school are among the several challenges that family and caregivers face while caring for an individual with nasal polyps.
The respondents indicated that currently available treatment options for nasal polyps include INCS sprays, over-the-counter nasal sprays, nasal irrigation or saline rinse, and biologics such as mepolizumab and omalizumab. In regard to these treatments, 4 respondents noted that their current treatments are largely ineffective and provide poor symptom control. Six respondents expressed concerns about side effects of available medications, especially oral corticosteroids, such as frequent sinus infections, allergic reactions, and headaches or dizziness. The patient who participated in the 1-to-1 interview indicated that they struggled to find effective treatment, having undergone 2 surgeries and a short trial of omalizumab, which eventually became ineffective.
Overall, respondents expressed a need for new, more effective relief for day-to-day symptoms, emphasizing the need for new therapies that can provide longer-lasting benefits and reduce recurrence, the need for surgery, and reliance on oral corticosteroids. These preferences underline the desire for treatments that not only alleviate immediate symptoms but also provide sustainable relief and minimize the physical and emotional burdens associated with managing the condition. Although none of the respondents had direct experience with dupilumab, 4 respondents indicated that the advantages of dupilumab, including easier management of disease symptoms and better long-term results, would outweigh the potential side effects of other treatment options.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts consulted for this review indicated that the most important treatment goals for patients with CRSwNP include reducing symptom severity, preventing disease progression, minimizing complications, improving HRQoL, and reducing the need for surgery. The clinical experts noted that the current standard of care for patients with CRSwNP in Canada is to start treatment with INCSs in a standard or high dose, as tolerated. If INCSs fails to control disease severity, which is often the case, oral steroids and surgical options are pursued. Oral corticosteroids provide only temporary improvement in severe symptoms and have significant side effects when used frequently. Although surgical intervention leads to symptom relief, nasal polyps often recur, requiring repeat procedures. The clinical experts indicated that patients often become refractory to current treatment options, particularly INCSs and even surgery, and available treatment cannot reverse the course of the disease or modify the underlying pathophysiology of CRSwNP. Therefore, new therapies that are better tolerated, are more effective, and can improve HRQoL relative to current standard of care are needed.
The clinical experts noted that dupilumab has a unique mechanism of action that is more targeted to the underlying inflammation driving CRSwNP. The clinical experts indicated that, based on their clinical experience, dupilumab is more effective than INCSs, oral corticosteroids, and surgery, because it particularly targets the underlying type 2 inflammation in the pathogenesis of CRSwNP. This is because dupilumab’s mechanism of action makes it a disease-modifying treatment, distinguishing it from traditional therapies that only manage symptoms without altering the disease process. Compared to available treatment options in the current landscape in Canada, the clinical experts noted that dupilumab will not be a first-line therapy but rather a second-line therapy after INCSs and/or surgery have failed. The experts also noted that it would be appropriate to consider use in combination with other treatments, such as INCSs or surgery.
According to the clinical experts, patients best suited for dupilumab include those with severe, uncontrolled symptoms, particularly those whose CRSwNP has not responded to traditional therapies such as INCSs, oral corticosteroids, and/or surgery or those who are intolerant to other therapies. Based on the experience of the clinical experts consulted for this review, they suggested that patients with eosinophilic-driven inflammation and significant nasal polyp burden may be best suited for dupilumab, whereas patients with mild disease or those with noneosinophilic CRSwNP may be least suited for dupilumab. The clinical experts indicated that there are no issues related to CRSwNP diagnosis, and no companion diagnostic test is needed.
The clinical experts noted that response to dupilumab should be assessed based on clinical symptoms (e.g., nasal obstruction, loss of sense of smell), change in scores on the 22-item Sino-Nasal Outcome Test (SNOT-22), anterior rhinoscopy, and, when available, in-office nasal endoscopy, which is commonly performed to objectively assess nasal polyp size and severity. According to the clinical experts, treatment response to dupilumab should be assessed at 6 months and 1 year after treatment initiation. According to the clinical experts, outcomes used in clinical practice align closely with those in clinical trials.
According to the clinical experts, dupilumab should be discontinued if patients do not respond to treatment by 1 year or develop AEs (such as eosinophilia) that are clinically significant, blepharitis/conjunctivitis that cannot be managed, or myalgias that are intolerable to the patient. The need for discontinuation should be determined based on persistence and severity of symptoms and, when relevant, imaging.
The clinical experts indicated that dupilumab is typically prescribed in specialty settings, such as outpatient clinics or specialty clinics with access to comprehensive diagnostic and monitoring tools. In addition, dupilumab should be prescribed only by a specialist (allergist, respirologist, or ear, nose, and throat specialist).
Clinician Group Input
No clinician group input was received for this submission.
Drug Program Input
Input was obtained from the drug programs that participate in our Reimbursement Review process. Please refer to Table 4 for further information. The following were identified as key factors that could potentially impact the implementation of dupilumab:
considerations for initiation of therapy
considerations for continuation or renewal of therapy
considerations for prescribing of therapy
generalizability
system and economic issues.
Clinical Evidence
Systematic Review
Description of Studies
Two studies met the inclusion criteria of the sponsor-submitted systematic literature review (SLR): LIBERTY-NP SINUS-24 (NCT0291246823) and LIBERTY-NP SINUS-52 (NCT0289845424), herein referred to as SINUS-24 and SINUS-52 respectively.
The SINUS-24 and SINUS-52 trials were multinational, multicentre, randomized, double-blind, placebo-controlled, parallel-group studies that assessed the efficacy and safety of dupilumab in adult patients with severe CRSwNP. The SINUS-24 trial was conducted in 67 centres in 13 countries, while the SINUS-52 trial was conducted in 117 centres in 14 countries. There were no Canadian sites in the SINUS-24 trial; however, there were 8 Canadian sites in the SINUS-52 trial. Both trials are completed, and the data presented in this report correspond with a data cut-off date of July 5, 2018, for the SINUS-24 trial, and August 29, 2018, for the SINUS-52 trial.
In the SINUS-24 trial, 276 patients were randomized 1:1 to receive dupilumab 300 mg (N = 133) or a matching placebo (N = 143) every 2 weeks for 24 weeks. In the SINUS-52 trial, 448 patients were randomly assigned (1:1:1) to dupilumab 300 mg every 2 weeks for 52 weeks (arm A) (N = 150), the same schedule for the first 24 weeks followed by dupilumab 300 mg every 4 weeks for additional 28 weeks (arm B) (N = 145), or placebo (arm C) (N = 153). Randomization was stratified by the presence of comorbid asthma and/or nonsteroidal anti-inflammatory drug–exacerbated respiratory disease (NSAID-ERD), prior surgery for nasal polyps (yes or no), and country.
In both trials, patients were included if they were diagnosed with CRSwNP and had bilateral sinonasal polyposis, chronic symptoms of NC, and another symptom, such as loss of sense of smell or rhinorrhea, despite background treatment with INCSs and maximum standard of care therapy, including SCSs and/or surgery for nasal polyps, in the past and had signed a written informed consent. Patients with persistent signs and symptoms or disease relapse after short courses of SCSs or after surgery were permitted in the trials. Key exclusion criteria included patients with systemic immunosuppressant to treat inflammatory disease or autoimmune disease, patients on anti-IgE therapy (e.g., omalizumab) up to 130 days before baseline, patients who had undergone intranasal and/or sinonasal surgery (including polypectomy) up to 6 months before baseline, or patients who had undergone sinonasal surgery changing the lateral wall structure of the nose, making the evaluation of nasal polyps impossible.
The coprimary objectives of both the SINUS-24 and SINUS-52 trials were to evaluate the efficacy of dupilumab compared to placebo based on the change from baseline in NC score and nasal polyp score (NPS) at week 24 in both trials. In the SINUS-52 trial, outcomes were also assessed at week 52. Key secondary objectives of both trials were to evaluate the efficacy and safety of dupilumab in improving total symptom score (TSS), HRQoL (SNOT-22), and sense of smell, as well as the proportion of patients who received SCSs or planned to undergo sinonasal surgery. A prespecified hierarchical testing procedure was used to control the overall type I error rate for both NPS and NC as well as selected secondary end points, including SNOT-22, TSS, and decreased or loss of sense of smell. Safety outcomes included AEs, serious adverse events (SAEs), AEs of special interest (AESIs), deaths, and notable harms, including myalgia, eosinophilia, nasopharyngitis, and headaches.
In the SINUS-24 trial, the median age of patients was 51 years (range, ███) and most were male (N = 158; 57.2%), whereas in the SINUS-52 trial, the median age of patients was 52 years (range, █████████). The number of patients with any medical history of type 2 inflammation, including asthma and/or NSAID-ERD, was 75.4% and 82.4% in the SINUS-24 and SINUS-52 trials, respectively. In the SINUS-24 trial, 71.7% of patients had prior nasal polyp surgery, while 58.2% of patients included the SINUS-52 trial had prior nasal polyp surgery. The mean time since first diagnosis of CRSwNP in the overall study population of the SINUS-24 trial was 11.11 years (range, 0.2 to 42.5) and 10.94 years (range, 0.1 to 61.3) in the SINUS-52 trial. In both trials, nearly all patients had chronic symptoms of nasal polyposis (i.e., NC, rhinorrhea, or loss of sense of smell) and the majority of patients presented with at least 2 symptoms 8 weeks before screening. The mean time since asthma onset was 15.51 years (range, █████████) in the SINUS-24 trial and 17.72 years (range, ██████) in the SINUS-52 trial. There were 208 (75.4%) patients in the SINUS-24 trial and 369 (82.4%) in the SINUS-52 trial who had a medical history of at least 1 type 2 inflammation–mediated condition.
Efficacy Results
In the SINUS-52 trial, results for dupilumab 300 mg every 2 weeks and placebo groups are reported. Results for the dupilumab 300 mg every 2 weeks followed by every 4 weeks group are not reported because they do not match the indication for this review. For week 24 results, the 2 dupilumab arms were pooled, so results are for N = 295 and comparisons are for the pooled dupilumab arms versus placebo.
Severity of Nasal Polyps and Nasal Obstruction
NPS: NPS was a coprimary outcome and was assessed based on centrally read video recordings of nasal endoscopy by 2 physicians. In the SINUS-24 trial, the least squares (LS) mean change from baseline in NPS at week 24 was –1.89 for the dupilumab 300 mg every 2 weeks group and 0.17 for the placebo group, with mean difference versus placebo of –2.06 (95% confidence interval [CI], –2.43 to –1.69; P < 0.0001). In the SINUS-52 trial, the LS mean change in NPS score at week 24 in the dupilumab group was lower (–1.72; standard deviation [SD] 1.77) compared to the placebo (0.12; SD 0.95). The LS mean difference at week 24 was –1.80 (95% CI, –2.10 to –1.51; P < 0.0001) in favour of dupilumab treatment group. At week 52, the LS mean difference between the dupilumab and placebo group was –2.40 (95% CI, –2.77 to –2.02; P < 0.0001).
In both trials, responder analysis of the change from baseline in NPS at week 24 was conducted as supportive analysis to determine the proportion of patients with improvement of at least 1 point in NPS based on the minimal important difference (MID) identified in the literature. In the SINUS-52 trial, a responder analysis was also conducted for the change from baseline to week 52. In the SINUS-24 trial, the proportion of patients with an improvement of at least 1 point decrease in NPS was 65.0% in the dupilumab group compared to 17.3% in the placebo group. In the SINUS-52 trial, the proportion of patients with at least 1 point decrease in NPS in the dupilumab group compared to placebo group at weeks 24 and 52 was 62.0% and ██ versus 10.5% and ██ respectively.
NC score: The change from baseline in NC was a coprimary outcome in both trials. NC was a patient-reported outcome that assessed the severity of NC on a daily basis. Scores were calculated based on a weekly average of the daily scores. In the SINUS-24 trial, the LS mean change from baseline in NC scores at week 24 was –1.34 for the dupilumab every 2 weeks group and –0.45 for placebo. The LS mean difference in change from baseline in NC scores at week 24 between dupilumab and placebo was –0.89 (95% CI, –1.07 to –0.71; P < 0.0001) in favour of dupilumab group. In the SINUS-52 trial, the LS mean change in NC scores from baseline to week 24 was –1.25 for the dupilumab group and –0.38 for the placebo group, with a mean difference of –0.87 (95% CI, –1.03 to –0.71; P < 0.0001) in favour of placebo. At week 52, the LS mean difference in change from baseline in NC was –0.98 (95% CI, –1.17 to –0.79; P < 0.0001).
A responder analysis was conducted in both trials as supportive evidence. ████ ███ ███ ███ ███ ████ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ████ ███ ███ ███ ██ █.
Health-Related Quality of Life
SNOT-22: SNOT-22 was a patient-reported outcome used to assess the impact of CRSwNP on HRQoL in the preceding 2 weeks. SNOT-22 is a 22-item validated questionnaire, in which each item is scored on a scale from 0 (no impact of CRSwNP on HRQoL) to 5 (impact of CRSwNP on HRQoL). The sum of the response to each of the 22 questions informed the global score. The change from baseline in SNOT-22 was included as a key secondary outcome. In the SINUS-24 trial, the LS mean change from baseline to week 24 was –30.43 (SD 1.54) for the dupilumab group and –9.31 (SD 1.62) for the placebo group. The LS mean difference in change from baseline in SNOT-22 scores was –21.12 (95% CI, –25.17 to –17.06; P < 0.0001) in favour of dupilumab. In the SINUS-52 trial, the LS mean difference in change from baseline in SNOT-22 scores at both week 24 and week 52 were –17.36 (95% CI, –20.87 to –13.85; P < 0.0001) and –20.96 (95% CI, –25.03 to –16.89; P < 0.0001).
A responder analysis of the proportion of patients with at least 8.9-point decrease in SNOT-22, based on the MID identified in the literature, was conducted as supportive evidence in both trials. ████ ███ ███ ███ ███ ████ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ███ ████ ███ ███ ███ ██ █.
Disease Symptoms and Severity
TSS: The TSS was assessed as a composite score (ranging between 0 and 9) based on the sum of the following symptoms: NC, decreased or loss of sense of smell, rhinorrhea (average of anterior and posterior nasal discharge). The symptom scores were calculated using the same approach as for NC (a weekly average based on daily scores). The change from baseline in TSS score was included as a key secondary outcome in both trials. In the SINUS-24 trial, the LS mean change from baseline in TSS scores at week 24 to 3.69 (SD 2.04) for the dupilumab group and –1.26 (SD 1.71) for the placebo group. The LS mean difference in change from baseline to TSS score between dupilumab and placebo groups was –2.61 (95% CI, –3.04 to –2.17; P < 0.0001). In the SINUS-52 trial, the LS change from baseline in TSS scores at week 24 was –3.54 (SD 2.47) for the dupilumab group every 2 weeks and –1.03 (SD 1.66) for the placebo group. The LS mean difference in the change from baseline in TSS between dupilumab and placebo groups was –2.44 (95% CI, –2.87 to –2.02; P < 0.0001). At week 52, the LS mean difference in the change from baseline TSS was ████ ███ █████ ███ █ also in favour of the dupilumab group.
Decreased or loss of sense of smell: The decreased or loss of sense of smell was a patient-reported outcome that assessed the severity of CRSwNP symptoms daily during the trials. Scores were calculated using a 0 to 3 categorical scale (where 0 = no symptoms, 1 = mild symptoms, 2 = moderate symptoms, and 3 = severe symptoms). The symptom scores were calculated using the same approach as for NC, where a weekly average of daily scores was calculated. The change from baseline in decreased or loss of sense of smell was included as a key secondary outcome. In the SINUS-24 trial, the LS mean difference in the change from baseline in decreased or loss of sense of smell at week 24 was –1.12 (95% CI, –1.31 to –0.93) in favour of the dupilumab treatment group. In the SINUS-52 trial, the LS mean difference in the change from baseline in decreased or loss of sense of smell at week 24 and week 52 was –0.98 (95% CI, –1.15 to –0.81; P < 0.0001) and ████ ███ █████ respectively.
Rescue Therapy
Proportion of patients who received SCS rescue therapy or surgery for nasal polyps (actual or planned): SCS or sinonasal surgery (actual or planned) was considered rescue therapy for CRSwNP in both trials. The proportion of patients who received SCS or planned surgery for nasal polyps was included as a secondary outcome. In the SINUS-24 trial, the number of patients who received SCS as rescue therapy in the dupilumab group was 6.3% compared to 18.8% in the placebo group. Nine (6.8%) patients in the placebo group and 3 (2.1%) in the dupilumab group had surgery for nasal polyps (actual or planned). Compared to the placebo group, the proportion of patients who received SCS as rescue therapy during the treatment period in the SINUS-52 trial was lower in the dupilumab group (14.7%; N = 22) compared to the placebo group (41.2%; N = 63). Additionally, 13 (8.5%) patients in the placebo and 2 (1.3%) patients in the dupilumab group had surgery for nasal polyps (actual or planned).
Harms Results
Adverse Events
In the SINUS-24 trial, 65.0% of patients in the dupilumab group experienced treatment-emergent AEs (TEAEs) during the entire treatment period, compared to 70.5% of patients in the placebo group. In the SINUS-52 trial, the proportion of patients with at least 1 TEAE during the entire treatment period was lower in dupilumab treatment group (83.2%) compared with the placebo group (90.7%).
Serious Adverse Events
In the SINUS-24 trial, the incidence of treatment-emergent SAEs was lower in the dupilumab group, with 4.2% in the dupilumab group versus 14.4% in the placebo group experiencing an SAE. In the SINUS-52 trial, a total of 15 (10.0%) patients in the placebo group compared to 8 (5.4%) patients in the dupilumab group 300 mg every 2 weeks treatment group experienced a treatment-emergent SAE.
Withdrawals Due to Adverse Events
The discontinuation rate due to TEAEs in the SINUS-24 trial was 3.5% in the dupilumab group compared to 2.3% in the placebo group. The most frequently reported TEAE that led to permanent treatment discontinuation was nasal polyps, and this occurred in 2 (1.4%) patients in the dupilumab group and 1 (0.8%) patient in the placebo group. In the SINUS-52 trial, 11.3% of patients in the placebo group and 4.0% in the dupilumab group discontinued treatment due to TEAE.
Mortality
In the SINUS-24 trial, 1 patient in the placebo group died during the posttreatment period due to myocardial infarction, which was assessed as unrelated to the study drug. In the SINUS-52 trial, 1 patient died during the follow-up period due to a traumatic intracranial hemorrhage arising from an accidental fall from a bicycle, assessed as unrelated to the study drug by the investigator.
Notable Harms
Notable harms included in this review were the proportion of patients who had myalgia, eosinophilia, nasopharyngitis, and headaches during the treatment period. In the SINUS-24 trial, ████ ███ █████ ███ █████ ██████ ███ █████ ███ ██ █, and headache (4.9% versus 8.3%) compared to the placebo group, while the incidence of nasopharyngitis (13.3% versus 15.2%) was lower in the dupilumab group. There were 9 (6.8%) patients in the placebo group and 6 (4.2%) patients in the dupilumab group who experienced an AESI. In the SINUS-52 trial, ████ ███ █████ ███ █████ ███ █████, nasopharyngitis (20.1% versus 24.0%) and headache (10.8% versus 12.0%) compared to the placebo group. ████ ███ █████ ██████ ███ █████ ███ ██ █. There were 13 (8.7%) patients in the placebo group and 8 (5.4%) patients in the dupilumab group who experienced AESI.
Critical Appraisal
The SINUS-24 and SINUS-52 trials were randomized, double-blind, and placebo-controlled. Both trials employed appropriate methods for blinding and treatment allocation, and randomization was stratified based on presence of comorbid asthma and/or NSAID-ERD, prior nasal polyp surgery, and country. Although the trials were powered to detect differences in the coprimary outcomes, they were not powered to detect differences in subgroups of patients with or without prior nasal polyp surgery. However, a prespecified subgroup analysis demonstrated consistent treatment effect of dupilumab in patients with and without prior nasal polyp surgery. CDA-AMC notes that there were differences in concomitant medication use between treatment groups in both trials, which could signal differences in underlying morbidity. However, it is unclear whether this would result in an increased risk of bias in the results. Missing data ranged from ████ per treatment group for outcomes including NPS, NC, and SNOT-22 in both trials. Worst observation carried forward (WOCF) and multiple imputation (MI) methods were used to handle missing values. MI methods can introduce bias because they depend on the assumption that data are missing at random, which is often not realistic. However, sensitivity analyses for approaches to missing data demonstrated similar results as the main analysis. The relatively short follow-up duration (24 to 52 weeks) and absence of long-term extension studies limit the assessment of sustained efficacy and long-term safety, which is particularly important for CRSwNP.
The study population was generally representative of patients with severe CRSwNP. However, the exclusion of patients with mild to moderate forms of CRSwNP, systemic immunosuppressant use, autoimmune diseases, or recent sinonasal surgery limits generalizability of the findings to these populations. The lack of Canadian sites in the SINUS-24 trial and the inclusion of few patients (nearly all white) from Canada in the SINUS-52 trial raise concerns about the generalizability to the Canadian practice landscape, given the ethnic diversity of patients seen in clinical practice in Canada. However, the clinical experts consulted for the review indicated that they do not expect different results in populations in Canada. Both trials included NPS and NC as coprimary outcomes, which were also identified as important outcomes, based on the inputs from patient groups and clinical experts consulted for this review. Notably, SNOT-22, which measures the impact of CRSwNP on HRQoL, was a key secondary outcome and was controlled for multiplicity. Of note, the pivotal trials were placebo-controlled, and no studies were submitted that evaluated a direct comparison to other biologics such as mepolizumab.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.25,26
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect. If this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The target of the certainty-of-evidence assessment for the change from baseline in NPS and NC was informed by the literature and expert opinion (an MID of a decrease in score greater than or equal to 1).27 The target of the certainty-of-evidence assessment for the change from baseline in SNOT-22 was also informed by the literature and expert opinion (an MID of a decrease in score greater than or equal to 8.9).28
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The target of the certainty-of-evidence assessment for all other outcomes assessed by GRADE were informed by the clinical experts consulted for this review. The following list of outcomes was finalized in consultation with expert committee members:
severity of nasal polyp (change from baseline in NPS)
severity of NC (change from baseline in NC)
HRQoL (change from baseline in SNOT-22)
notable harms (myalgia, eosinophilia, nasopharyngitis, headaches).
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for dupilumab as an add-on maintenance treatment with INCSs in adult patients with severe CRSwNP inadequately controlled by SCSs and/or surgery.
Dupilumab results in a reduction in NPS at 24 and 52 weeks of follow-up when compared with placebo.
Dupilumab likely results in a reduction in NC at 24 and 52 weeks of follow-up when compared with placebo (moderate certainty due to serious imprecision).
Dupilumab results in a reduction in SNOT-22 score at 24 and 52 weeks of follow-up when compared with placebo.
Dupilumab may result in little to no difference in myalgia at 52 weeks of follow-up when compared with placebo (low certainty due to very serious imprecision).
Dupilumab may result in little to no difference in eosinophilia at 52 weeks of follow-up when compared with placebo (low certainty due to very serious imprecision).
Dupilumab likely results in little to no difference in nasopharyngitis at 52 weeks of follow-up when compared with placebo (moderate certainty due to serious imprecision).
Dupilumab likely results in little to no difference in headaches at 52 weeks of follow-up when compared with placebo. (moderate certainty due to serious imprecision).
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
Description of Studies
In the absence of direct head-to-head evidence, the sponsor conducted indirect treatment comparisons (ITCs) to evaluate dupilumab versus mepolizumab for adults with uncontrolled CRSwNP. A Bucher method ITC was performed using placebo as the common comparator, and a matching-adjusted indirect comparison (MAIC) served as a supporting analysis to account for baseline differences across trials.
The ITCs drew results from 3 key RCTs: SINUS-24, SINUS-52, and SYNAPSE. In the SINUS-24 and SINUS-52 trials, dupilumab was examined over 24 and 52 weeks, respectively, in patients with severe CRSwNP who had a history of nasal polyp surgery or SCS use. The SYNAPSE trial, by contrast, evaluated mepolizumab but required at least 1 nasal surgery in the past 10 years and a higher threshold for symptom severity on a VAS.
To address the substantial differences in eligibility criteria between the SINUS and SYNAPSE trials, the ITC restricted its comparative analyses to a “SYNAPSE-like” subgroup from the SINUS studies. This subgroup included only patients who met the more stringent criteria in the SYNAPSE study, thereby helping to control for clinical heterogeneity and enabling a more consistent basis for indirect comparison. As a result, the final analyses of dupilumab versus mepolizumab reflect outcomes solely in this matched population.
Efficacy Results
Across both the Bucher ITC and the MAIC analyses, dupilumab demonstrated greater improvements than mepolizumab in key clinical outcomes — such as NPS, NC, and smell function — at 24 and 52 weeks. Dupilumab was also associated with numerically lower rates of nasal polyp surgery and reduced need for SCS compared to mepolizumab. While point estimates favoured dupilumab in most comparisons, the CI for the mean change in the SNOT-22 score crossed the null in continuous analyses. However, other patient-reported outcomes presented in the ITC, such as the loss of sense of smell score, VAS, and the SNOT-22 responder analysis, showed improvements favouring dupilumab that excluded the null, despite some analyses having wider CIs, potentially reflecting variations such as scale conversions or smaller effective sample sizes.
Table 2: Summary of Findings for the Efficacy and Safety of Dupilumab Versus Placebo in Adult Patients With Severe CRSwNP Inadequately Controlled by Systemic Corticosteroids and/or Surgery
Outcome and follow-up | Patients (studies), N | Effect | Certainty | What happens |
|---|---|---|---|---|
Severity of nasal polyps | ||||
Change from baseline in NPS (0 [no polyps] to 8 [large polyps causing complete obstruction]),a LS mean change from baseline, score (95% CI) Follow-up: week 24 | 724 (2 RCT) | SINUS-24 Dupilumab: –1.89 (██ █))) Placebo: 0.17 (██ █))) Difference: –2.06 (–2.43 to –1.69) SINUS-52 Dupilumab: –1.71 (██ █))) Placebo: 0.10 (██ █))) Difference: –1.80 (–2.10 to –1.51) | Highb | Dupilumab results in a reduction in nasal polyp score when compared with the placebo. |
Change from baseline in NPS (0 [no polyps] to 8 [large polyps causing complete obstruction]),c LS mean change from baseline, score (95% CI) Follow-up: week 52 | 448 (1 RCT) | SINUS-52 Dupilumab: –2.24 (██ █))) Placebo: 0.15 (██ █))) Difference: –2.40 (–2.77 to –2.02) | Highb | Dupilumab results in a reduction in nasal polyp score when compared with the placebo. |
Severity of NC | ||||
Change from baseline in NC (0 [no symptoms] to 6 [severe symptoms]),a LS mean change from baseline, score (95% CI) Follow-up: week 24 | 724 (2 RCT) | SINUS-24 Dupilumab: –1.34 (██ █))) Placebo: –0.45 (██ █))) Difference: –0.89 (–1.07 to –0.71) SINUS-52 Dupilumab: –1.25 (██ █))) Placebo: –0.38 (██ █))) Difference: –0.87 (–1.03 to –0.71) | Moderated | Dupilumab likely results in a reduction in NC score when compared with the placebo. |
Change from baseline in NC (0 [no symptoms] to 6 [severe symptoms]),c LS mean change from baseline, score (95% CI) Follow-up: week 52 | 448 (1 RCT) | SINUS-52 Dupilumab: –1.35 (██ █))) Placebo: –0.37 (██ █))) Difference: –0.98 (–1.17 to –0.79) | Moderated | Dupilumab likely results in a reduction in NC score when compared with the placebo. |
HRQoL | ||||
Change from baseline in SNOT-22 (0 [less impact of CRSwNP on HRQoL] to 110 [most impact of CRSwNP on HRQoL]), LS mean change from baseline, score (95% CI) Follow-up: week 24 | 724 (2 RCT) | SINUS-24 Dupilumab: –30.43 (██ █))) Placebo: –9.31 (██ █))) Difference: –21.12 (–25.17 to –17.06) SINUS-52 Dupilumab: –27.77 (██ █))) Placebo: –10.40 (██ █))) Difference: –17.36 (–20.87 to –13.85) | Highe | Dupilumab results in a reduction in SNOT-22 score when compared with the placebo. |
Change from baseline in SNOT-22 (0 [less impact] to 110 [most impact]), LS mean change from baseline, score (95% CI) Follow-up: week 52 | 448 (1 RCT) | SINUS-52 Dupilumab: –29.84 (██ █))) Placebo: –8.88 (██ █))) Difference: –20.96 (–25.03 to –16.89) | Highe | Dupilumab results in a reduction in SNOT-22 score when compared with the placebo. |
Harms | ||||
Patients with myalgia, n (95% CI) Follow-up: week 52 | 448 (1 RCT) | SINUS-52 Dupilumab: ████ ███ █ Placebo: ████ ███ █ Difference: ████ ███ █ | Lowf | Dupilumab may result in little to no difference in myalgia when compared with the placebo. |
Patients with eosinophilia, n (95% CI) Follow-up: week 52 | 448 (1 RCT) | SINUS-52 Dupilumab: ████ ███ █ Placebo: ████ ███ █ Difference: ████ ███ █ | Lowg | Dupilumab may result in little to no difference in eosinophilia when compared with the placebo. |
Patients with nasopharyngitis, n (95% CI) Follow-up: week 52 | 448 (1 RCT) | SINUS-52 Dupilumab: 201 per 1,000 (██))) Placebo: 240 per 1,000 (█ █) Difference: 39 less per 1,000 (█ █) | Moderateh | Dupilumab likely results in little to no difference in nasopharyngitis when compared with the placebo. |
Patients with headaches, n (95% CI) Follow-up: week 52 | 448 (1 RCT) | SINUS-52 Dupilumab: 94 per 1,000 (██ █))) Placebo: 120 per 1,000 (██ █))) Difference: 26 less per 1,000 (█))) | Moderatei | Dupilumab likely results in little to no difference in headaches when compared with the placebo. |
CI = confidence interval; CRSwNP = chronic rhinosinusitis with nasal polyps; HRQoL = health-related quality of life; LS = least squares; NC = nasal congestion and/or obstruction; NPS = nasal polyp score; RCT = randomized controlled trial; SNOT-22 = 22-item Sino-Nasal Outcome Test.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aThe score of NPS is 0 to 4 per each nostril; the overall score is a sum of the right and left nostril scores (range from 0 to 8).
bBased on a literature-based MID of 1 estimated for within-group effects; input from the clinical expert consulted by the review team considered that a between-group difference smaller than 1 point was not likely to be clinically important. A reduction in the NPS corresponds to a reduction in the size of nasal polyp.
cThe score of NC is 0 to 3 per each nostril; the overall score is a sum of the right and left nostril scores (range from 0 to 6).
dRated down 1 level for serious imprecision. A literature-based MID of 1 estimated for within-group effects was also considered clinically relevant for a between-group difference (i.e., a between-group difference smaller than 1 point was not likely to be clinically important) based on input from the clinical expert consulted by the review team. 95% CIs for difference between groups includes the possibility of no difference.
eBased on MID of 8.9 from the literature for within-group effects; input from the clinical expert consulted by the review team considered that a between-group difference smaller than 8.9 points was not likely to be clinically important.
fThreshold for a clinically important difference was 10% or more (100 per 1,000), as informed by clinical expert consulted for the review. Rated down 2 levels for very serious imprecision; the between-group effect was based on a very low number of events.
gThreshold for a clinically important difference was 3% or more (100 per 1,000), as informed by clinical expert consulted for the review. Rated down 2 levels for very serious imprecision; the between-group effect was based on a very low number of events.
hThreshold for a clinically important difference was 20% or more (100 per 1,000), as informed by clinical experts consulted for the review. Rated down 1 level for serious imprecision; the between-group effect was based on a low number of events.
IRated down 1 level for serious imprecision. Lower bound of CI shows potential for reduction in harm based on a threshold of 5% or more (100 per 1,000), as informed by the clinical experts consulted for the review.
Source: SINUS-24 Clinical Study Report;29 SINUS-52 Clinical Study Report.30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Harms Results
The submitted indirect comparisons did not assess harms.
Critical Appraisal
The ITCs offer useful insights into comparative efficacy where direct evidence is lacking. However, methodological constraints introduce limitations to the level of certainty and generalizability of the results. The reliance on fixed-effects models (potentially overstating precision for results close to the null, such as the NC score), the use of less than half the sample of the SINUS trials in the clinically similar analysis of SYNAPSE-like population, the necessity to “downscale” outcome measures (e.g., NC) between trials, and the reduced effective sample sizes following MAIC reweighting introduce uncertainty. Notably, the comparison for NC score is subject to compounded uncertainty, and the SNOT-22 mean difference did not show a statistically significant advantage for dupilumab. Moreover, the SYNAPSE-like results limit generalizability beyond the most severe CRSwNP patient profile, i.e., those who have had prior surgery. Taken together, the consistent direction of effect favouring dupilumab is notable, and dupilumab is likely as effective as and might be more effective than mepolizumab in patients who have had prior nasal polyp surgery, but residual heterogeneity and gaps in external validity are considered limitations in the analysis. There is no comparative evidence for patients with CRSwNP who did not have prior surgery. A head-to-head study of dupilumab and mepolizumab is expected to be completed in 2026 and has also limited its enrolment to patients with prior nasal polyp surgery.
Studies Addressing Gaps in the Evidence From the Systematic Review
One real-world, observational cohort study31 conducted in a single tertiary referral centre was submitted by the sponsor to address the gaps in long-term efficacy and safety evidence from the systematic review. However, in the observational study, patients increased the dosage interval over time, which was not consistent with the approved Health Canada indication and recommended dosage21 under review. At 48 weeks, 80% of patients were taking dupilumab 300 mg at an interval of every 4 or every 6 weeks. Therefore, the efficacy and safety findings of this study were not considered relevant to this review.
Conclusions
The SINUS-24 and SINUS-52 trials demonstrated that dupilumab as an add-on to INCSs results in a clinically meaningful reduction in the severity of nasal polyps, based on the NPS, and an improvement in HRQoL, based on the SNOT-22, for adult patients with severe chronic CRSwNP inadequately controlled by SCSs and/or surgery when compared to placebo. Dupilumab also likely results in a clinically meaningful improvement in NC when compared to placebo. Additionally, evidence from both trials suggests that treatment with dupilumab is associated with improvements in severity of symptoms, based on the change from baseline in TSS, as well as improved sense of smell, based on the change from baseline in decreased or loss of sense of smell, which aligned with the results for NPS, NC, and SNOT-22. Dupilumab was well tolerated, and the reported AEs were generally consistent with what is anticipated in adult patients with severe CRSwNP. In the 24-week safety population, SAEs were more common in the placebo group than in the dupilumab group. Notable harms — including myalgia, eosinophilia, nasopharyngitis, and headache — were assessed to range from low to moderate certainty, suggesting that there was little to no difference in notable harms in the dupilumab group compared to the placebo group. However, long-term safety data remain limited due to the absence of long-term extension studies, and the absence of direct comparisons with other biologics (e.g., mepolizumab) limits conclusions about the safety profile of dupilumab relative to mepolizumab.
Results from the ITC suggest that dupilumab is likely as effective as and might be more effective than mepolizumab when assessed using end points of NPS, NC, and smell function among patients with severe CRSwNP who had prior surgery. However, there is increased uncertainty related to superiority due to methodological limitations and population differences across the included studies. There is no comparative evidence, direct or indirect, for patients with CRSwNP without prior surgery.
Based on the evidence available for this review, dupilumab represents an additional treatment option for patients with severe CRSwNP that is inadequately controlled by SCSs and/or nasal polyp surgery.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of dupilumab 300 mg (SC injection) in adult patients with severe CRSwNP that is inadequately controlled by SCSs and/or surgery.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
Rhinosinusitis occurs when the lining of the sinuses becomes infected, irritated, and swollen, and it causes symptoms such as extra mucus due to congestion, mucus discharge from the nose (or mucus that drips down the back of the throat), or a decreased sense of smell. CRS is a heterogeneous disease characterized by inflammation of the nose and paranasal sinuses, tissue edema, nasal obstruction, and increased mucus production, causing symptoms (including NC and rhinorrhea) that persist for at least 12 weeks.1 Current medical consensus categorizes CRS into 2 major phenotypes based on the presence (CRSwNP) or absence (CRSsNP) of nasal polyps.2-4
CRSwNP is a distinct subtype of CRS due to the presence of nasal polyps in the upper airway. These polyps are noncancerous, edematous, inflammatory lesions that usually originate from the mucosa of the ethmoid, maxillary, and sphenoidal sinuses and occur bilaterally.5 As the polyps grow, they protrude into the nasal cavities and obstruct nasal passages, further increasing the disease burden of CRSwNP. The pathophysiology of CRSwNP involves a complex interaction between impaired epithelial barrier function and mucociliary dysfunction, imbalance of the sinonasal microbiome, and immune dysfunction that leads to the pathologic features of inflammation. The estimated prevalence of CRSwNP in the US and Europe is 4.2% and 4.3%, respectively.32 Although data in Canada are scarce, cross-sectional data from the 1996 to 1997 National Population Health Survey (N = 73,364) reported that the prevalence of CRS among Canadians aged 12 years and older was 5.7% in females and 3.4% in males.33 One retrospective study in Alberta (2004 to 2014) involving 2,925,930 adults aged 18 years or older reported the estimated prevalence of CRS to range from 18.8 to 23.3 per 1,000 population.6 Among all patients with CRS, it is estimated that between 25% and 30% have CRSwNP.7 The peak incidence of CRSwNP generally occurs in working adults between the ages of 45 to 60 years.2,8 Established risk factors for CRSwNP include asthma, allergic conditions affecting the sinuses, sinonasal passage abnormality, immune system disorder, obesity, regular exposure to pollutants, familial history of nasal polyps, male gender, and older age.2,12,34-37
Patients with CRSwNP suffer from a high symptom burden, including sinonasal congestion and/or obstruction, loss of sense of smell, facial pain or pressure, discoloured sinonasal discharge, breathing impairment, sleep disorders, fatigue, and increased risk of infection.3,8,9 However, the symptoms with the greatest impact on patients’ HRQoL are sinonasal congestion and/or obstruction, loss of sense of smell, and sleep impairment.10 Patients with CRSwNP tend to have a longer duration of disease and are more resistant to therapy than patients with CRSsNP. This is primarily because conventional medical therapies, including INCSs, tend to fail in patients with CRSwNP.8
The International Consensus Statement on Allergy and Rhinology for Rhinosinusitis and International Consensus Statement on Allergy and Rhinology recommend the diagnosis of CRSwNP based on the presence of 2 or more symptoms of rhinosinusitis (NC, rhinorrhea, loss of sense of smell, facial pain or headache), presence of nasal polyps on nasal endoscopy, or evidence of sinus inflammation on CT scan.11 This is consistent with the diagnostic criteria in current Canadian guidelines, which include a clinical observation of at least 2 disease symptoms plus the presence of bilateral polyps in the middle meatus on endoscopy or bilateral mucosal disease on CT scan.38 In addition, the assessment of CRSwNP also takes into consideration the severity of the disease, often categorized using a VAS, and the duration of symptoms.12,13 Severe CRSwNP is the most bothersome phenotype of CRS and is often characterized by the need for long-term treatment. It has a high risk of recurrence even after surgery. Severity of CRSwNP is categorized using the VAS score, as follows: mild (0 to 3), moderate (> 3 to 7), and severe (> 7 to 10).12,13 The higher the VAS score (> 5), the lower the patient’s quality of life.
The diagnosis and management of CRSwNP are performed by specialist physicians, including otolaryngologists, allergists, or respirologists.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
The overall goal for the management of severe CRSwNP includes reduction in sinus and nasal inflammation and the size of polyps to establish patency of upper airways and restore nasal breathing and sense of smell.12,38,39 Timely management of CRSwNP is important, not only to alleviate the disease and treatment-related burden, but also to prevent further disease development and to enhance long-term clinical outcomes.40 The clinical experts consulted for this review indicated that the management of CRSwNP typically involves the use of nondrug-based and drug-based approaches. Overall, international guidelines recommend a stepwise treatment approach based on disease severity that includes nasal saline irrigation and topical nasal steroids for all severity levels, short courses of oral corticosteroids for moderate and/or severe disease, and surgical intervention if medical management is unsuccessful.12
Treatment of CRSwNP is limited to the chronic use of INCSs, short courses of SCS when symptoms worsen, and sinonasal surgery when medical therapy fails. While antibiotics may be useful in treating infectious exacerbations of CRSwNP, they provide minimal to no effect in reducing polyp size in randomized trials.41 In clinical settings in Canada, the use of INCSs for initial treatment for CRSwNP includes MFNS (two 50 mcg sprays in each nostril twice daily or equivalent).14 Although use of INCSs does lead to improvement in nasal symptoms, these drugs fail to treat many components of the underlying disease. Topical INCSs do not improve the sense of smell, and they may be associated with loss of smell and taste.42 INCSs have limited effects on improving sinus disease, as measured by CT scan, likely because only a small portion of the administered dose reaches the middle meatus and sinuses, where nasal polyps originate.43 Most topical INCSs are generally associated with mild AEs, which include epistaxis, dry nose, nasal irritation, headache, and cough.42 SCSs are typically more effective than INCSs in reducing polyp size and nasal symptoms.2 The maximal treatment effects with SCSs are usually noted after 2 weeks of treatment, but the duration of these effects is limited after completing a treatment course. Long-term SCSs use for severe CRSwNP has been associated with increased AEs, including infections, gastrointestinal events, pneumonia, and retinopathy, as well as long-term diseases such as diabetes, hypertension, kidney disease, peptic ulcer disease, and osteoporosis or osteopenia.15 According to the clinical experts consulted for this review, contraindications to SCS use include poorly controlled diabetes, hypertension, kidney disease, peptic ulcer disease, retinopathy, cataracts, glaucoma, active infections, latent infections (e.g., untreated tuberculosis), history of upper gastrointestinal bleed, osteoporosis or osteopenia, and first trimester of pregnancy.
In patients who do not respond to medical therapy, the clinical experts consulted for the review noted that surgical management may be required to provide symptom relief and to remove inflammatory tissue. The goals of sinonasal surgery for CRSwNP are to reduce sinus outflow obstruction by establishing a nasal airway, reduce the number of proinflammatory cells and tissue parts (inflammatory load), and open the sinuses for postoperative topical drug delivery (e.g., INCSs).11,44 The gold standard surgical procedure for CRSwNP is endoscopic sinus surgery.44 Even if surgery is successful, the recurrence of CRSwNP symptoms and nasal polyps is common.16 Often patients will achieve only temporary and/or partial symptom relief, with nasal polyp recurrence reported in 35% of patients after 6 months, 38% after 12 months, and 40% after 18 months postsurgery.45 Further, multiple surgeries may be needed to address recurrent symptoms.8,17,18
According to the clinical experts consulted for this review, the current stepwise approach to CRSwNP treatment (i.e., chronic INCSs, intermittent SCSs, and surgery) does not address the underlying chronic type 2 inflammation pathology and leads to a cycle of high morbidity, poor symptom control, loss of smell and/or taste, poor HRQoL (including sleep quality), and diminished productivity in patients. As a result, the Canadian Rhinology Working Group recommends the use of biologic therapies for patients with CRSwNP to address the gaps in treatment.19,20 The clinical experts consulted for this review indicated that biologic therapies that are currently available in Canada for add-on maintenance treatment of CRSwNP include dupilumab, omalizumab, and mepolizumab. Although omalizumab is approved by Health Canada for use in CRSwNP, it is not publicly reimbursed in Canada. Mepolizumab is a targeted anti-interleukin-5 (IL-5) IgG1 kappa monoclonal antibody, indicated as add-on maintenance treatment with INCSs in adult patients with severe CRSwNP inadequately controlled by INCSs alone.21 According to the clinical experts consulted for this review, mepolizumab is the relevant comparator for the drug under review. Omalizumab is not publicly reimbursed in Canada and was not considered as a comparator for the drug under review by the clinical experts.
Drug Under Review
Key characteristics of dupilumab are summarized in Table 3 with other treatments available for CRSwNP.
Table 3: Key Characteristics of Dupilumab and Relevant Comparators for the Treatment of CRSwNP
Characteristic | Dupilumab | Mepolizumab |
|---|---|---|
Mechanism of action | Inhibits IL-4 signalling via the type I receptor (IL-4 receptor alpha/γc), and both IL-4 and IL-13 signalling through the type II receptor (IL-4 receptor alpha or IL-13 receptor alpha). | Binds to soluble IL-5 with high affinity, preventing IL-5 from binding to the alpha chain of the IL-5 receptor complex expressed on the eosinophil cell surface. |
Indicationa | As an add-on maintenance treatment with INCSs in adult patients with severe chronic rhinosinusitis with nasal polyposis (CRSwNP) inadequately controlled by SCSs and/or surgery | As an add-on maintenance treatment with INCSs in adult patients with severe CRSwNP inadequately controlled by INCSs alone |
Route of administration | SC | SC |
Recommended dose | 300 mg q.2.w. | 100 mg q.4.w. |
Serious adverse effects or safety issues |
|
|
CRSwNP = chronic rhinosinusitis with nasal polyps; IL-4 = interleukin-4; IL-13 = interleukin-13; INCS = intranasal corticosteroid; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SC = subcutaneous; SCS = systemic corticosteroid.
aSCSs are a component of standard medical therapy in the case of worsening signs and/or symptoms of CRSwNP requiring medical intervention and are used for short or intermittent courses only.
Source: Dupixent Product Monograph;22 Nucala Product Monograph.21
Dupilumab is indicated add-on maintenance treatment with INCSs in adult patients with severe CRSwNP inadequately controlled by SCSs and/or surgery.22 The recommended dosage of dupilumab for CRSwNP is 300 mg single-use prefilled syringe or pen administered by SC injection every other week. Dupilumab is also approved for the treatment of atopic dermatitis, asthma, eosinophilic esophagitis, and prurigo nodularis.
Dupilumab is a human IgG4 monoclonal antibody that inhibits IL-4 and IL-13 signalling by binding to the IL-4 receptor alpha subunit shared by the IL-4 and IL-13 receptor complexes.22 Dupilumab inhibits IL-4 signalling via the type I receptor (IL-4 receptor alpha/γc) and both IL-4 and IL-13 signalling through the type II receptor (IL-4 receptor alpha or IL-13 receptor alpha).22 IL-4 and IL-13 are key type 2 cytokines (including T-helper 2 cells) involved in atopic disease and type 2 inflammation, which is an important component in the pathogenesis of CRSwNP.22 Multiple cell types that express IL-4 receptor alpha (e.g., mast cells, eosinophils, macrophages, lymphocytes, epithelial cells, goblet cells) and inflammatory mediators (e.g., histamine, eicosanoids, leukotrienes, cytokines, chemokines) are involved in inflammation.22 Blocking IL-4 receptor alpha with dupilumab inhibits IL-4 and IL-13 cytokine-induced inflammatory responses, including the release of proinflammatory cytokines, chemokines, nitric oxide, and IgE.22 The reimbursement request by the sponsor is consistent with the approved Health Canada indication for dupilumab. Of note, dupilumab has been previously reviewed by CDA-AMC for other indications (atopic dermatitis and asthma). At the time of this review, dupilumab was also being actively reviewed for chronic obstructive pulmonary disease and prurigo nodularis.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
One patient group input submission from AC was received for this review. AC is a national charitable patient-driven organization that advocates improved health and quality of life for people living with asthma and respiratory allergies. The goal of AC is to help people living with asthma and respiratory allergies to live a symptom-free life by providing credible information, guidance, and education to patients through effective collaboration with policy-makers, researchers, and health care providers. AC gathered information for this submission through an online survey involving Canadians living with or caring for patients with nasal polyps from October 30, 2024, to November 28, 2024. The survey received 8 responses from adults living with nasal polyps, including 3 people in British Columbia, 1 in Manitoba, and 4 in Ontario. Of the 8 respondents, 1 was chosen at random for a 1-to-1 interview to gain an in-depth knowledge of the impacts of nasal polyps on the quality of life of people living with the condition.
Regarding disease experience, respondents indicated NC, trouble breathing, frequent sneezing, and loss of sense of smell and taste as the most common symptoms associated with nasal polyps. Overall, respondents indicated that difficulty in breathing, NC, daily struggle with the health care system, and the risk of surgeries and pain are the most difficult discomforts for patients living with nasal polyps. The physical discomforts interfere with daily activities, sleep, and overall well-being. Four respondents indicated that nasal polyps aggravate their asthma symptoms, 5 indicated that nasal polyps require additional medications for management, and 2 respondents said that nasal polyps lead to more frequent asthma flare-ups. Respondents indicated that frequent medical appointments, financial difficulty, poor quality of life, and an increase in missed days from work or school are among the several challenges that family and/or caregivers face while caring for individuals with nasal polyps.
The survey participants indicated that currently available treatment options for nasal polyps include INCS sprays, over-the-counter nasal sprays, nasal irrigation or saline rinse, and biologics such as mepolizumab and omalizumab. In regard to these treatment options, 4 respondents noted that their current treatments are largely ineffective and provide poor symptom control. None of the respondents had direct experience with dupilumab. Six respondents expressed concerns such as frequent sinus infection, allergic reactions, and headaches or dizziness as side effects of available medications, especially oral corticosteroids. Another major concern for respondents was that drugs are costly. While some patients do have insurance coverage, insurance does not cover the entire cost of medication. The patient who participated in the 1-to-1 interview indicated that they struggled to find effective treatment (currently using mepolizumab), having undergone 2 surgeries and a short trial with omalizumab, which eventually became ineffective.
The respondents expressed a need for new, more effective symptom relief for day-to-day symptoms, emphasizing the desire for new therapies that can provide longer-lasting benefits and reduce recurrence of polyps, the need for surgery, and reliance on oral corticosteroids. These preferences underline the desire for treatments that not only alleviate immediate symptoms but also provide sustainable relief and minimize the physical and emotional burdens associated with managing the condition. Of the 8 respondents who participated in the survey, 4 believed that the advantages of dupilumab, which include easier management of disease symptoms and better long-term results, would outweigh the potential side effects.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of CRSwNP.
Unmet Needs
The clinical experts consulted for this review indicated that the most important treatment goals for patients with CRSwNP include controlling symptoms (reducing severity), reducing inflammation, preventing disease progression, minimizing complications, improving HRQoL, and reducing the risk of surgery. The clinical experts noted that the current standard of care for patients with CRSwNP in Canada starts with INCSs at a standard or high dose, as tolerated. When this fails to control disease severity, which is often the case, oral steroids and surgical options are pursued. Oral corticosteroids provide only temporary improvement of severe symptoms and have significant side effects when used frequently. Although surgical intervention leads to symptom relief, nasal polyps often recur, requiring repeat procedures. The clinical experts indicated that the disease often becomes refractory to current treatment options, particularly INCSs and even surgery, and available treatment cannot reverse the course of the disease or modify the underlying pathophysiology of CRSwNP. Although mepolizumab, a biologic therapy, recently received a positive reimbursement recommendation from CDA-AMC, not all patients respond to treatment. The long-term follow-up for treating CRSwNP can be challenging for patients who have difficulty accessing health care, particularly those in underserved areas. Therefore, new therapies that are better tolerated, are more effective, and can improve HRQoL relative to current standard of care are needed.
Place in Therapy
The clinical experts noted that dupilumab has a unique mechanism of action that is more targeted to the underlying inflammation driving CRSwNP. The clinical experts indicated that, based on their clinical experience, dupilumab is more effective than INCSs, oral corticosteroids, or surgery, because dupilumab particularly targets the underlying type 2 inflammation in the pathogenesis of CRSwNP. Dupilumab’s mechanism of action makes it a disease-modifying treatment, distinguishing it from traditional therapies that manage symptoms without altering the disease process. Compared to available treatment options in the current landscape in Canada, the clinical experts noted that dupilumab would not be a first-line therapy but, rather, a second-line therapy after failure of INCSs and/or surgery. The experts also noted that it would be appropriate to consider use in combination with INCSs or surgery.
Patient Population
The clinical experts noted that patients best suited for dupilumab should be identified through assessment of clinical symptoms, including persistent nasal obstruction, loss of sense of smell, blood eosinophil count (for some patients), and endoscopic or imaging findings of polyposis. According to the clinical experts, patients best suited for dupilumab include those with severe, uncontrolled symptoms, particularly those who have not responded or are intolerant to traditional therapies such as INCSs, surgery, and oral steroids. Based on the experience of the clinical experts consulted for the review, they suggested that patients with type 2 and/or eosinophilic-driven inflammation and significant nasal polyp burden may be best suited for dupilumab treatment. The clinical experts indicated that patients with mild disease, or those with noneosinophilic CRSwNP, may be least suited for dupilumab. The clinical experts indicated that there are no issues related to CRSwNP diagnosis, and no companion diagnostic test is needed. However, underdiagnosis is a possibility at primary care centres, where patients with milder or atypical presentations may be overlooked.
Assessing the Response Treatment
The clinical experts noted that response to dupilumab should be assessed based on clinical symptoms (e.g., nasal obstruction, loss of smell), change in SNOT-22 scores, anterior rhinoscopy, and in-office nasal endoscopy, which is commonly performed to objectively assess nasal polyp size and severity. Also, an improvement in sense of smell is a clinically relevant indicator of treatment response, as it is associated with an improvement in patient quality of life. In addition, although NPS and NC scores are not routinely used in clinical practice, they are increasingly used for identifying candidates for biologic therapies. According to the clinical experts, treatment response to dupilumab should be assessed at 6 months and 1 year after treatment initiation. According to the clinical experts, outcomes used in clinical practice align closely with those in clinical trials, although clinical trials may more rigorously quantify improvements (e.g., using precise polyp scores).
Discontinuing Treatment
According to the clinical experts, dupilumab should be discontinued if patients do not respond to treatment by 1 year. This should be determined based on persistence and severity of symptoms and imaging. In addition, the clinical experts noted that dupilumab should be discontinued if patients develop AEs such as clinically significant eosinophilia, blepharitis or conjunctivitis that cannot be managed, or myalgias that are intolerable to the patient.
Prescribing Considerations
The clinical experts indicated that dupilumab is typically prescribed in specialty settings, such as outpatient clinics or specialty clinics with access to comprehensive diagnostic and monitoring tools. However, it can be safely administered at home after at least 1 supervised injection in an approved training centre or location. In addition, dupilumab should only be prescribed by a specialist (allergist; ear, nose and throat specialist; respirologist; and subspecialist and generalist physicians with airway-focused practices). However, allergists who do not perform endoscopy can prescribe dupilumab, as nasal polyps can be determined with a combination of anterior rhinoscopy and CT assessment.
Clinician Group Input
No clinician group input was received for this submission.
Drug Program Input
The drug programs provide input on each drug being reviewed through the Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC for this review are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
Should severe CRSwNP be defined and, if so, what criteria are used to diagnose severe CRSwNP? | According to the clinical experts, criteria for diagnosing severe CRSwNP include patients with disease refractory to high-dose intranasal corticosteroid sprays, and those who have required SCSs or surgery to manage their condition (or have contraindications to SCSs or surgery). Patients who have CRSwNP that has had a significant impact on their HRQoL fall under the criteria for severe CRSwNP. In addition, Health Canada definitions for severe CRSwNP are referenced in practice. |
Dupilumab is used in pediatric populations for other indications. Is there a place in therapy for dupilumab in children with CRSwNP? | The 2 clinical experts noted that CRSwNP is very uncommon in individuals younger than age 18 and rare in adolescents. The experts also indicated that safety of dupilumab for indications other than CRSwNP in pediatric populations has been shown. |
What dose, duration, and timeline of therapy for SCSs would be considered for the criterion of “previous use”? What would constitute a “medical contraindication” to SCS use? If SCS use is for temporary symptom relief, and not a long-term treatment, should its use be required at all? | The clinical experts indicated that any requirement for SCS use, such as history of 1 course of prednisone in the past, is sufficient for the previous-use criterion. According to the clinical experts, contraindications to SCS use include poorly controlled diabetes, hypertension, or kidney disease, or peptic ulcer disease, retinopathy, cataracts, glaucoma, active infections, latent infections (e.g., untreated tuberculosis), peptic ulcer disease, history of upper gastrointestinal bleed, osteoporosis or osteopenia, and first trimester of pregnancy. The 2 clinical experts suggested that experience with the use of SCSs should not be a requirement for treatment with dupilumab, as the need for SCSs is more of a criterion for defining severe disease. |
Referring to the indication, should the type of surgery required be specified, or is any reference to surgery within the past 10 years sufficient? | According to the clinical experts, the type of surgery should be sinus surgery. However, previous surgery should not be a barrier to accessing dupilumab. The experts indicated that disease severity should be considered more important than prior surgery when determining a patient’s eligibility for dupilumab. The experts also noted that wait times for an appointment with an ear, nose, and throat specialist followed by wait times for surgery can delay access to effective treatment for CRSwNP when prior surgery is an eligibility criterion for treatments like dupilumab. |
Are there scenarios where a patient eligible for surgery would replace surgery with SCS use? If a patient is ineligible for surgery, should they be required to use SCSs? Are there scenarios where the patient is ineligible for both surgery and SCSs? | The 2 clinical experts noted that SCS should not be used to replace surgery; however, patients who are on a waitlist for surgery should be eligible for SCSs. The clinical experts noted that this will depend on the observation of an ear, nose, and throat specialist. Patients ineligible for surgery can use SCSs if there is no contraindication. According to the clinical experts, patients are ineligible for surgery if they have uncontrolled medical conditions, such as poorly managed diabetes or hypertension, infections including active sinus or systemic infections, bleeding disorders including hemophilia or use of anticoagulants, or untreated dental issues or periodontal disease. Other concerns may be indicated by the ear, nose, and throat specialist caring for the patient. |
Considerations for continuation or renewal of therapy | |
If a patient does not meet the criterion for “clinically meaningful response” and is denied renewal, should they be eligible for re-treatment in the future? Are there any scenarios to consider as “extenuating circumstances” for renewal consideration for a patient not reaching the required clinically meaningful response beyond 52 weeks? | The clinical experts indicated that they had no experience with patients who did not respond to dupilumab yet. However, they noted that a previous denial of renewal should not impact eligibility for re-treatment in the future. The clinical experts indicated that unexpected treatment interruptions such as pregnancy or other reasons beyond the control of patients are some of the scenarios to consider as “extenuating circumstances” for renewal consideration. |
Considerations for prescribing of therapy | |
Is there potential for dose escalation for this indication? | The clinical experts indicated that, based on their clinical experience, there is no need for potential dose escalation for this indication. |
Should tapering be considered after 24 weeks, 52 weeks, or specific to clinical needs for this indication? | The clinical experts indicated that off-label use should not be considered. The currently approved Health Canada dosage recommendations for dupilumab for CRSwNP do not include tapering. |
Generalizability | |
It is appropriate to consider switching a patient to dupilumab from another product, such as mepolizumab? If so, should different initiation criteria be used for patients who would like to switch between products? And would achieving a clinically meaningful response be a factor when switching? Can baseline values before comparator therapy be used for initial assessment? | According to the clinical experts, given the different mechanism of action of dupilumab, switching patients from another biologic (e.g., mepolizumab) to dupilumab should be considered. The clinical experts indicated that patients who are eligible for mepolizumab should be eligible for dupilumab. The experts noted that initiation criteria for switching product should include evidence of minimal improvement in symptoms despite 4 to 6 months of treatment. According to the clinical experts, baseline values should be considered for initial assessment before comparator therapy. |
System and economic issues | |
Should reimbursement of multiple biologics be considered for differing indications? | The clinical experts indicated that reimbursement of multiple biologics can be considered for different indications but not for the same indication. They also indicated that multiple biologics should not be used concurrently for the same indication. The CDA-AMC review team notes that there is no evidence to support the use of dupilumab for the treatment of CRSwNP in combination with other biologics. |
Should patients be eligible for both mepolizumab and dupilumab at the same time for treatment of CRSwNP, considering they have different mechanisms of action? | The 2 clinical experts indicated that dupilumab and mepolizumab should not be used concurrently. |
CDA-AMC = Canada’s Drug Agency; CRSwNP = chronic rhinosinusitis with nasal polyposis; HRQoL = health-related quality of life; SCS = systemic corticosteroid.
Clinical Evidence
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of dupilumab 300 mg every 2 weeks administered by SC injection as an add-on maintenance treatment with INCSs in adult patients with severe CRSwNP that is inadequately controlled by SCSs and/or surgery. The focus will be placed on comparing dupilumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of dupilumab is presented in 4 sections with the CDA-AMC critical appraisal of the evidence at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor. The third section includes additional studies that were considered by the sponsor to address the lack of long-term extension studies of the pivotal trials.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
2 pivotal studies (SINUS-24 and SINUS-52) identified in systematic review
1 ITC
1 observational study to address lack of long-term evidence of efficacy and safety.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
Two studies — SINUS-24 (NCT0291246823) and SINUS-52 (NCT0289845424) — met the inclusion criteria of the sponsor-submitted SLR. The SINUS-24 and SINUS-52 trials were multinational, multicentre, randomized, double-blind, placebo-controlled, parallel-group studies that assessed the efficacy and safety of dupilumab in adult patients with severe uncontrolled CRSwNP. The SINUS-24 trial was conducted in 67 centres in 13 countries, while the SINUS-52 trial was conducted in 117 centres in 14 countries. There were no Canadian sites in the SINUS-24 trial; however, there were 8 Canadian sites in the SINUS-52 trial. Both trials are completed, and the data presented in this report correspond to a data cut-off of July 5, 2018, for the SINUS-24 trial, and of August 29, 2018, for the SINUS-52 trial. Unless otherwise specified, all reported data are from the corresponding clinical study reports for these data cut-offs.
In the SINUS-24 trial, 276 patients were randomized 1:1 to receive dupilumab 300 mg (N = 133) or a matching placebo (N = 133) every 2 weeks until week 24. In the SINUS-52 trial, 448 patients were randomly assigned (1:1:1) to dupilumab 300 mg every 2 weeks for 52 weeks (arm A) (N = 150), the same schedule for the first 24 weeks followed by dupilumab 300 mg every 4 weeks for additional 28 weeks (arm B) (N = 145), or placebo (arm C) (N = 153). The trials included a 4-week run-in period (plus or minus 3 days), a randomized double-blind 24-week (SINUS-24) or 52-week (SINUS-52) treatment period (plus or minus 3 days), and a 24-week (SINUS-24) or 12-week (SINUS-52) posttreatment follow-up period (plus or minus 3 days). The purpose of the run-in period was to determine a patient’s eligibility for inclusion and for run-in or standardization of background INCSs before randomization. Patients received MFNS, 2 actuations (50 mcg per actuation) in each nostril twice daily, for a total daily dose of 400 mcg. If patients were unable to tolerate this dose or when a specific regulatory requirement prevented its use, patients were permitted to stay on a lower-dose regimen (200 mcg MFNS). Patients were randomly assigned centrally with a permuted block randomization schedule by Interactive Voice Response System or Interactive Web Response System. The randomization block size was 4 for the SINUS-24 trial and 6 for the SINUS-52 trial. Randomization was stratified by the presence of comorbid asthma and/or NSAID-ERD, prior nasal polyp surgery (yes or no), and country. Both patients and investigators were masked to either treatment group.
The primary objective of both the SINUS-24 and SINUS-52 trials was to evaluate the efficacy of dupilumab compared to placebo in reducing NC severity and nasal polyp size in adult patients with bilateral nasal polyps and persistent CRSwNP that had failed to respond to currently available therapies. Key secondary objectives of both trials were to evaluate the efficacy of dupilumab in improving TSS and sense of smell, and the proportion of patients who require treatment with SCSs or surgery for nasal polyps. The study designs of the SINUS-24 and SINUS-52 trials are illustrated in Figure 1 and Figure 2, respectively.
Figure 1: Study Design for the SINUS-24 Trial
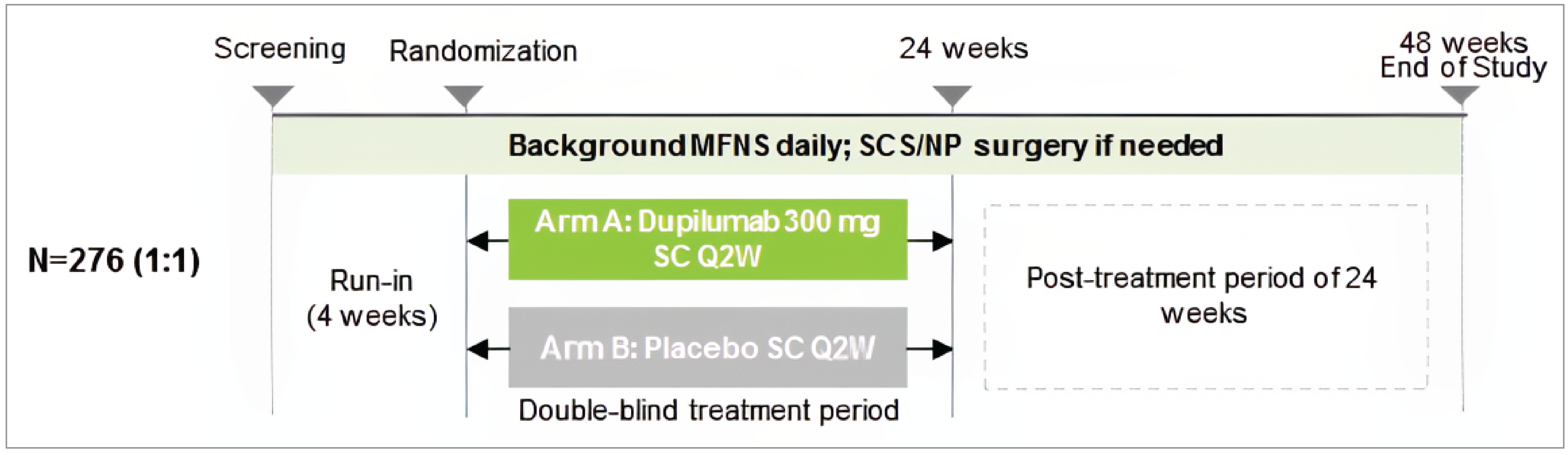
MFNS = mometasone furoate nasal spray; NP = nasal polyp; Q2W = every 2 weeks; SC = subcutaneous; SCS = systemic corticosteroid.
Source: SINUS-24 Clinical Study Report.29
Figure 2: Study Design for the SINUS-52 Trial
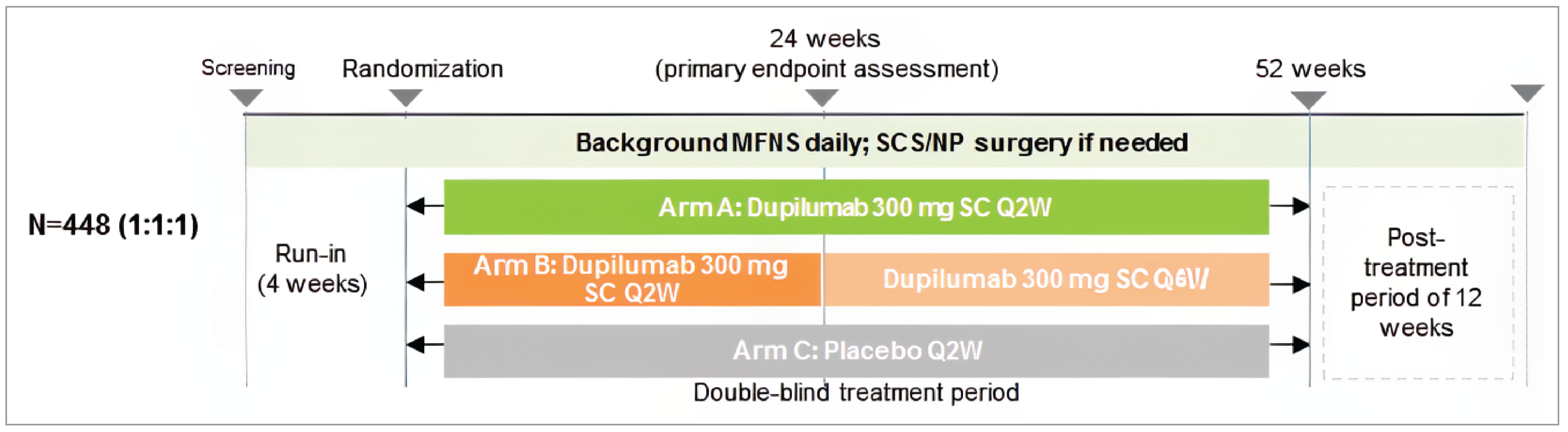
MFNS = mometasone furoate nasal spray; NP = nasal polyp; Q2W = every 2 weeks; Q4W = every 4 weeks; SC = subcutaneous; SCS = systemic corticosteroid.
Source: SINUS-52 Clinical Study Report.30
Characteristics of the included studies are summarized in Table 5.
Table 5: Details of Studies Included in the Systematic Review
Detail | SINUS-24 | SINUS-52 |
|---|---|---|
Designs and populations | ||
Study design | Phase III, double-blind, multicentre, placebo-controlled, parallel-group RCT | |
Locations | 67 centres in 13 countries (Bulgaria, Czechia, France, Germany, Hungary, Italy, Netherlands, Poland, Romania, Russia, Ukraine, the UK, and the US) | 117 centres in 14 countries (Argentina, Australia, Belgium, Canada, Chile, Israel, Mexico, Portugal, Russia, Spain, Sweden, Turkey, Japan, and the US) |
Patient enrolment dates | Start date: December 5, 2016 End date: July 5, 2018 | Start date: November 28, 2016 End date: August 29, 2018 |
Randomized (N) | Total N = 276 Dupilumab 300 mg q.2.w. N = 133 Placebo N = 143 | Total N = 448 Dupilumab 300 mg q.2.w. N = 150 Dupilumab 300 mg q.2.w.–q.4.w. N = 145 Placebo N = 153 |
Inclusion criteria | Patients (18 years or older) with bilateral sinonasal polyposis that persisted despite prior treatment with SCSs any time within the past 2 years, and/or had a medical contraindication to SCSs, and/or had prior sinonasal surgery for nasal polyps, and had:
| |
Exclusion criteria |
| |
Drugs | ||
Intervention | Dupilumab 300 mg SC q.2.w. | Dupilumab 300 mg q.2.w. to week 52 (arm A) Dupilumab 300 mg q.2.w. to week 24–300 mg q.4.w. to week 52 (arm B) |
Comparator(s) | Placebo | Placebo |
Study duration | ||
Run-in phase | 4 weeks (± 3 days) | 4 weeks (± 3 days) |
Treatment phase | 24 weeks (± 3 days) | 52 weeks (± 3 days) |
Follow-up phase | 24 weeks (± 3 days) | 12 weeks (± 3 days) |
Outcomes | ||
Coprimary end points |
| |
Key secondary end points | Change from baseline to week 24 in:
| Change from baseline to week 24 in:
Change from baseline to week 52 in:
|
Other secondary end points | Other secondaryc:
| |
Publication status | ||
Publications | ||
ACQ-6 = 6-question Asthma Control Questionnaire; FEV1 = forced expiratory volume in 1 second; IBD = inflammatory bowel disease; IgE = immunoglobulin E; LMK-CT = Lund-Mackay CT; LTRA = leukotriene receptor antagonist; mAb = monoclonal antibody; MS = multiple sclerosis; NC = nasal congestion and/or obstruction; NPIF = nasal peak inspiratory flow; NPS = nasal polyps score; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; RA = rheumatoid arthritis; RCT = randomized controlled trial; SC = subcutaneous; SCS = systemic corticosteroid; SLE = systemic lupus erythematosus; SNOT-22 = 22-item Sino-Nasal Outcome Test; TSS = total symptom score; UPSIT = University of Pennsylvania Smell Identification Test; VAS = visual analogue scale.
aEight weeks or more before screening followed by 4 weeks before randomization (total 12 weeks of symptoms).
bTwo prespecified analyses were included in the statistical hierarchy based on a prespecified pooled analysis of the 2 trials.
cNot included in the statistical hierarchy.
Source: SINUS-24 Clinical Study Report;29 SINUS-52 Clinical Study Report;30 Bachert et al., 2019.32
Populations
Inclusion and Exclusion Criteria
Eligibility criteria were identical for both trials. Detailed inclusion and exclusion criteria are provided in Table 5. Patients were included if they were diagnosed with CRSwNP and had bilateral sinonasal polyposis (NPS by endoscopy, described in the next section), chronic symptoms of NC, and another symptom, such as loss of smell or rhinorrhea, despite background treatment with INCSs and maximum standard of care therapy, including SCSs and/or surgery for nasal polyps in the past, and if they had signed a written informed consent. Patients with persistent signs and symptoms or disease relapse after short courses of SCSs or after surgery were permitted in the trials. Additionally, patients with comorbid asthma and/or NSAID-ERD were also eligible and were stratified at randomization by the presence of these conditions. Analyses were prespecified to assess efficacy in these subgroups. Key exclusion criteria included patients with systemic immunosuppressant to treat inflammatory disease or autoimmune disease, patients on anti-IgE therapy (e.g., omalizumab) 130 days or less before baseline, patients who had intranasal and/or sinonasal surgery (including polypectomy) 6 months or less before baseline or sinonasal surgery changing the lateral wall structure of the nose, making the evaluation of NPS impossible.
Interventions
The study intervention was dupilumab 300 mg every 2 weeks (or 300 mg every 4 weeks after 24 weeks in the SINUS-52 trial) by SC injection, provided as 150 mg/mL in a prefilled syringe to deliver 300 mg in 2 mL volume. The comparator was matched placebo administered in the same manner as the intervention and supplied in an identically matched prefilled syringe to deliver 2 mL volume.
In the SINUS-24 trial, patients were randomized to 1 of the following treatment groups: dupilumab 300 mg SC every 2 weeks (2 mL) or placebo matched to dupilumab 300 mg (2 mL) for 24 weeks. All randomized patients received every 2 weeks SC administrations of either dupilumab or placebo on day 1. Every other week, the administrations of dupilumab or matched placebo were separated by at least 11 days. In the SINUS-52 trial, patients were randomized to 1 of the following treatment groups: arm A: dupilumab 300 mg every 2 weeks SC until week 52; arm B: dupilumab 300 mg every 2 weeks SC until week 24 then 300 mg every 4 weeks until week 52; and arm C: placebo matching dupilumab every 2 weeks SC until week 52. For arm B, after week 24, dupilumab administration was alternated with a matched placebo injection every other week up to week 50 (last administration).
In both trials, the investigator performed the injection of dupilumab or matched placebo on day 1. After day 1, every other week administration of dupilumab or matched placebo was performed at the investigational site up to at least week 8. Dupilumab or matched placebo was administered following clinic procedures and blood collection. Patients were monitored at the study site for at least 30 minutes or the minimum time required by the local regulator after injections for signs of hypersensitivity reaction. Starting at week 10, administration of dupilumab or matched placebo by patient or caregiver was allowed if the patient or caregiver had been trained for 4 injections. SC injection sites were alternated among the 4 quadrants of the abdomen (avoiding navel and waist areas), the upper thighs, or the upper arms so that the same site was not injected twice consecutively. During the 4-week run-in period and throughout the trials, patients received MFNS 50 mcg per actuation as background therapy. Patients administered 2 actuations (100 mcg) of MFNS in each nostril twice daily (total daily dose of 400 mcg) unless they were intolerant to the twice-daily regimen or if the dose was not approved in specific countries, in which case, they followed a once-daily regimen.
During the study treatment period and off-treatment follow-up, the following rescue medications were used if needed: nasal lavage with saline and/or systemic antibiotics (up to 2 weeks in case of acute infection); short course SCSs (prednisone or prednisolone up to 2 weeks), or sinonasal surgery for nasal polyps (8 weeks of treatment was recommended before surgery to allow for onset of treatment effect). Permitted concomitant medications included short-term antibiotics (less than 2 weeks), short and long-acting beta agonists, long-acting muscarinic antagonists, methylxanthines, inhaled corticosteroids, and systemic antihistamines. In addition, leukotriene antagonists or modifiers and allergen immunotherapy were permitted if patients were already on treatment before screening. Cytochrome P450 substrates were not prohibited; however, investigators were advised to use caution and closely monitor patients receiving them.
Outcomes
A list of efficacy end points assessed in this clinical review report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review according to the clinical expert(s) consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, we selected end points that were considered most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Selected notable harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE.
Table 6: Outcomes Summarized From the SINUS-24 and SINUS-52 Trial
Outcome measure | Time point | SINUS-24 | SINUS-52 |
|---|---|---|---|
Severity of nasal polyps and nasal obstruction | |||
Change from baseline in endoscopic NPS | Baseline, week 24 and 52 | Coprimary | Coprimary |
Change from baseline in NC score | Baseline, week 24 and 52 | Coprimary | Coprimary |
HRQoL | |||
Change from baseline in SNOT-22 | Baseline, week 24 and 52 | Key secondary | Key secondary |
Disease symptoms | |||
Change from baseline in TSS | Baseline, week 24 | Key secondary | Key secondary |
Change from baseline in daily symptoms of decreased or loss of sense of smell | Baseline, week 24 | Key secondary | Key secondary |
Rescue therapy | |||
The proportion of patients who received SCSs | Baseline, week 24 | Key secondary | Key secondary |
Proportion of patients who planned to undergo sinonasal surgery | Baseline, week 24 | Key secondary | Key secondary |
Harms | |||
Number (%) of patients with AEs, SAEs, AESI, mortality | Baseline, week 24 and 52 | Key secondary | Key secondary |
AE = adverse event; AESI = adverse event of special interest; HRQoL = health-related quality of life; NC = nasal congestion and/or obstruction; NPS = nasal polyp score; SAE = serious adverse event; SCS = systemic corticosteroid; SNOT-22 = 22-item Sino-Nasal Outcome Test; TSS = total symptom score; UPSIT = University of Pennsylvania Smell Identification Test.
Note: Statistical testing for these end points was adjusted for multiple comparisons and tested according to a prespecified statistical hierarchy.
Source: SINUS 24 Clinical Study Report;29 SINUS-52 Clinical Study Report.30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Severity of Nasal Polyps and Nasal Obstruction
NPS: The NPS assesses the severity of nasal polyps in patients with CRSwNP. The change in NPS from baseline was a coprimary efficacy end point in both trials. NPS was assessed by at least 2 physicians based on centrally read video recordings of nasal endoscopy. The total score of NPS was calculated as the sum scores of the right and left nostril scores (range 0 to 4 points on each nostril), as evaluated by nasal endoscopy. The NPS was graded based on polyp size in each nostril (Table 7) where higher scores correspond to larger nasal polyp. If the NPS total scores assigned by the 2 independent readers differed by at least 1 point, the assigned NPS total score was the average of the 2 readings. A prespecified adjudication process was in place in case of disagreements between the 2 readings by more than 1 point. In such instances, the NPS total score was taken to be the average of the adjudicator’s score and the score of the reader whose NPS total score was closer to the adjudicator’s reading. If the 2 readers’ NPS scores were equidistant from that of the adjudicator, the higher score was used in the calculation. The NPS has shown high intrarater reliability (interclass correlation coefficient = 0.88) and demonstrated moderate correlation between change in rhinologic symptoms and the change in the total NPS (r = 0.51), reflecting responsiveness of the NPS to nasal symptoms of CRS (Table 8).27 An MID for the NPS is a decrease in score from baseline of 1 point or greater in adult patients with CRSwNP who were medically managed.46
Table 7: Scoring of Nasal Polyp Score and Nasal Congestion/Obstruction Scale
NPS | NC scale | ||
|---|---|---|---|
Polyp score | Polyp size | Scale | Symptoms |
0 | No polyps | 0 | No symptoms |
1 | Small polyps in the middle meatus not reaching below the interior border of the middle turbinate | 1 | Mild symptoms (symptoms clearly present, but minimal awareness and easily tolerated) |
2 | Polyps reaching below the lower border of the middle turbinate | 2 | Moderate symptoms (definite awareness of symptoms that are bothersome but tolerable) |
3 | Large polyps reaching the lower border of the inferior turbinate or polyps medial to the middle turbinate | 3 | Severe symptoms (symptoms that are hard to tolerate or cause interference with activities or daily living) |
4 | Large polyps causing complete obstruction of the inferior nasal cavity | ||
NC = nasal congestion and/or obstruction; NPS = nasal polyps score.
Source: SINUS-24 Clinical Study Report.29
NC score: NC is a patient-reported outcome that assesses the severity of nasal symptoms of CRSwNP. The change in NC from baseline to week 24 was a coprimary outcome in both trials. The SINUS-52 trial also reported NC at 52 weeks. NC was scored by the patient as a reflective score, evaluating symptom severity over the past 24 hours. The NC score is based on a 0 to 3 categorical scale for each nostril, where 0 = no symptoms, 1 = mild symptoms, 2 = moderate symptoms, and 3 = severe symptoms. In the SINUS trials, the NC score was recorded by the patient every morning in an e-diary, starting at screening and throughout the study, using the scale presented in Table 7. Daily scores were averaged to generate a weekly score. If 4 or more measurements collected within 7 days before randomization were available, the baseline was the average of these measurements. If fewer than 4 measurements were collected within 7 days before randomization, the baseline was the average of the most recent 4 measurements before randomization. For the baseline to end-of-treatment analysis, 4 weeks’ average of the symptom scores was used. NC has demonstrated reasonable validity (Cronbach alpha > 0.7) between individual nasal symptom (nasal obstruction, nasal discharge, mucus in the throat, loss of sense of smell) in patients with CRSwNP.47 NC is also moderately correlated with SNOT-22 total (interclass correlation coefficient = 0.354), supporting its validity as a measure of nasal symptom severity.47 An MID for NC is a decrease in score from baseline of 1 point or greater in adult patients with CRSwNP who were medically managed.46
Health-Related Quality of Life
SNOT-22: The change from baseline in SNOT-22 was a key secondary outcome in both trials. The SNOT-22 is a validated questionnaire that was used to assess the impact of CRSwNP on HRQoL in the preceding 2 weeks. The SNOT-22 has 22 items on a 5-category scale applicable to sinonasal conditions and surgical treatments. Each item is scored on a scale from 0 (no problem) to 5 (problem is as bad as it can be). The range of the global score is 0 to 110, based on the sum of response to each of the 22 questions. The SNOT-22 has been shown to have excellent construct validity and a high degree of internal consistency (Cronbach alpha > 0.9) as well as test-retest reliability (correlation coefficient > 0.9).28 SNOT-22 has been shown to discriminate between patients with and without CRS (Table 8).28 On the 110-point scale of the SNOT-22, a change or difference in score of 8.9 is the smallest change that was considered clinically important (MID) for patients in whom CRSwNP is managed surgically, whereas an MID of 12 is considered clinically meaningful in patients in whom CRSwNP is managed medically.46 Other studies have reported the MID for the SNOT-22 to range from 8 to 12 points.48-51
Disease Symptoms
TSS: The change from baseline in TSS at week 24 or week 52 was a key secondary efficacy end point. TSS was assessed by the patient to determine symptom severity. Patients used an e-diary to respond to questions regarding individual rhinosinusitis symptoms every morning using a 0 to 3 categorical scale, where 0 = no symptoms, 1 = mild symptoms, 2 = moderate symptoms, and 3 = severe symptoms. The TSS is a composite score (ranging between 0 and 9) consisting of the sum of the following symptoms assessed daily in the morning: NC, loss of sense of smell, and rhinorrhea (average of anterior/posterior nasal discharge). The symptom scores at baseline and from baseline to end-of-treatment analysis were calculated using the same approach as for NC based on 4 weeks’ average of the symptom scores at each visit. The MID for the within-patient change in the TSS score is reported to be 3 points.27
Decreased or loss of sense of smell: Decreased or loss of sense of smell is a patient-reported outcome that assesses the severity of loss of sense of smell. A change from baseline in decreased or loss of sense of smell was a key secondary outcome in both trials. The severity of the decreased or loss of sense of smell was scored by the patient as a reflective score, evaluating the symptom severity every morning throughout the study, using a 0 to 3 categorical scale (where 0 = no symptoms, 1 = mild symptoms, 2 = moderate symptoms, and 3 = severe symptoms). The symptom scores at baseline and from baseline to end-of-treatment analysis were calculated using the same approach as for NC, using 4 weeks’ average of the symptom scores at each visit. The MID for the decreased or loss of sense of smell is a decrease in score from baseline of 1 point.46
Rescue Therapy
Proportion of patients who received SCS rescue therapy or surgery for nasal polyps (actual or planned): The proportion of patients who received SCSs or surgery for NP (actual or planned) was a secondary outcome in both pivotal trials. The prescribing of SCSs as rescue treatment for CRSwNP or for another reason by the investigator was dependent on local treatment guidelines. The investigator recorded the date and dosing information (e.g., daily dose, duration, indication) on the appropriate page(s) of the electronic case report form. The indication for SCS use was also captured by selecting 1 or more of the following categories: nasal polyposis; asthma; other respiratory disease; other ear, nose, or throat disease; or other reasons. For patients who had sinonasal surgery (actual or planned) for nasal polyps, the reason (e.g., worsening signs and/or symptoms during the study), the expected or actual surgery date, and the type and outcome of surgery were recorded. For patients who had had surgery or had a scheduled date for sinonasal surgery for nasal polyps, the reason (worsening signs and/or symptoms during the study), the expected or actual surgery date, the type and outcome of surgery were recorded.
Harms
The number and percentage of patients with AEs, SAEs, and AESIs, as well as those who died, were assessed for each trial. TEAEs, including SAEs and AESIs, were collected at every study visit. The AESIs included anaphylactic reactions or systemic allergic reactions related to the study drug and requiring treatment; severe injection-site reactions lasting more than 24 hours; any infection that qualified as an SAE, required parenteral antimicrobial therapy, required oral antimicrobial therapy for more than 2 weeks, or was a parasitic or opportunistic infection; and symptomatic overdose (serious or nonserious) with study drug.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
NPS | The NPS is the sum of the right and left nostril scores, as assessed by central video recordings of nasal endoscopy. The nasal polyps are graded using scoring systems that use the lower edges of the middle and inferior turbinates as vertical landmarks. The NPS has a possible score ranging from 0 to 8, based on polyp size on each side of the nostril, with 0 indication no polyps and 4 indicating large polyps causing complete obstruction of the inferior nasal cavity. | NPS is used as a coprimary end point in several trials assessing the effectiveness of biologics in patients with CRSwNP. It is currently the most used scoring system for nasal polyp size. Validity: A recent study showed a moderate correlation between change in rhinologic symptoms and the change in the total NPS (r = 0.51), reflecting responsiveness of the NPS to nasal symptoms of CRS.27 Reliability: The NPS has shown high intrarater reliability (interclass correlation coefficient = 0.88) and moderate to substantial interrater reliability in previous trials.52 | The MID for within-patient change in NPS is reported to be ≥ 1 point.27 |
NC | The NC score is a patient reflective score of the severity of NC. It is based on symptom severity over the past 24 hours and recorded by the patient every morning in an e-diary. The NC score consists of a 0 to 3 categorical scale (where 0 = no symptoms, 1 = mild symptoms, 2 = moderate symptoms, and 3 = severe symptoms). | The NC score is a particularly important individual symptom severity score and is often used as a coprimary end point in CRSwNP trials. Validity: Strong correlations (Cronbach alpha > 0.7) between individual nasal symptom (nasal obstruction, nasal discharge, mucus in the throat, loss of sense of smell) and their corresponding SNOT-22 items.47 In patients with severe CRSwNP, NC is moderately correlated with SNOT-22 total (interclass correlation coefficient = 0.354), supporting its validity as a measure of nasal symptom severity.47 | The MID for the within-patient change in the NC score is reported to be ≥ 1 point.27 |
SNOT-22 | A validated questionnaire that assesses the burden of CRS, with a recall period of 2 weeks. The SNOT-22 has 22 items on a 5-category scale applicable to sinonasal conditions and surgical treatments. The burden of each of the 22 items on the SNOT-22 is scored with a 6-item Likert scale corresponding to numerical scores ranging from 0 to 5, respectively. The SNOT-22 total score ranges from 0 to 110. There are 5 domains that can be described within SNOT-22, including nasal, ear, sleep, general and practical, and emotional. A classification of CRS severity based on the SNOT-22 score is as follows: mild (8 to 20), moderate (> 20 to 50), and severe (> 50).46 The SNOT-22 is validated for CRS and allergic rhinitis. | The SNOT-22 score has been used in a multitude of studies and has been recommended to be a standard patient-reported outcome measure used to assess CRS outcomes.28,46 Validity: The SNOT-22 has been shown to have excellent construct validity, with previous studies showing strong correlation of SNOT-22 with measures of general HRQoL as well as the ability of the SNOT-22 to discriminate between patients with and without CRS.28 Reliability: The SNOT-22 has a high degree of internal consistency (Cronbach alpha > 0.9) as well as test-retest reliability (correlation coefficient > 0.9).28 The SNOT-22 has demonstrated excellent responsiveness with large effect size (d = 0.81 for all CRS, d = 0.90 for CRSwNP, d = 0.63 for CRSsNP) after treatment of CRS. | In a population of patients with chronic rhinosinusitis that is medically managed, the mean change from baseline that is interpreted as MID is 8.9. In a population of patients with chronic rhinosinusitis that is surgically managed, the mean change from baseline that is interpreted as MID is 12. |
CRS = chronic rhinosinusitis; CRSsNP = chronic rhinosinusitis without nasal polyposis; CRSwNP = chronic rhinosinusitis with nasal polyposis; HRQoL = health-related quality of life; MID = minimal important difference; NC = nasal congestion and/or obstruction; NPS = nasal polyp score; SNOT-22 = 22-Item Sino-Nasal Outcome Test.
Statistical Analysis
Sample Size and Power Calculation
For the SINUS-24 trial, based on a previous phase II study,53 it was estimated that a sample size of approximately 120 patients per treatment group would provide 98% power (2-tailed test at an alpha level of 0.05) to detect an effect size of 0.588 in NPS (on the basis of assumed mean difference of 1.24 and common SD of 2.11). The sample size would also provide 95% power to detect an effect size of 0.534 in NC score (on the basis of assumed mean difference of 0.55 and common SD of 1.03) at week 24 in the dupilumab group. The combined power for both outcomes would be 93%, assuming no negative correlation between outcomes.32 The study was not powered to detect differences in subgroups.
For the SINUS-52 trial, in which 3 groups were randomized 1:1:1, the pooling of arms A and B for the primary analyses resulted in the use of an allocation ratio of 2:1 to assess the sample size.32 The pooling of arms A and B at week 24 (approximately 240 patients) provided 99% power to detect the same effect size as previously described for NPS and NC in patients treated with dupilumab, with 98% combined power.32 The study was not powered to detect differences in subgroups.
Statistical Testing
Table 9 summarizes the statistical test or model used for the coprimary and key secondary efficacy outcomes, along with covariates and/or baseline values that were included in the statistical models. The analysis presented in this report is the final analysis for both the SINUS-24 and SINUS-52 trials, as both trials are now completed.
Coprimary outcomes: Each of the coprimary efficacy outcomes was analyzed as a change from baseline to end point (either 24 week or 52 weeks, depending on the study) using a hybrid method of the WOCF and MI methods. Data collected after treatment discontinuation was included in the analysis. The imputed completed data were analyzed by fitting an analysis of covariance (ANCOVA) model with the baseline value of the corresponding coprimary outcome, treatment group, asthma or NSAID-ERD status, prior surgery history, and regions as covariates. Statistical inference obtained from all imputed data was combined using Rubin’s rule.
Secondary outcomes: Analyses of the key secondary outcomes were conducted using the hybrid method of the WOCF and MI in the same way as the primary analysis of the coprimary outcomes, as described previously. Prespecified pooled analyses of results from SINUS 24 and SINUS 52 for the proportion and time to event of patients requiring rescue therapy (SCSs or nasal polyp surgery [actual or planned]) were derived and analyzed using the Cox proportional hazards model. For the responder analyses, treatment groups were compared using the Cochran-Mantel-Haenszel test stratified by the randomization stratification factors.
Multiplicity Adjustment
A prespecified hierarchical testing procedure was used to control the overall type I error rate for testing the coprimary and selected secondary end points. The overall alpha was 0.05. The comparisons with placebo were tested based on the hierarchical order in Figure 3 at a 2-sided alpha of 0.05. Each trial was considered positive when both coprimary outcomes achieved statistical significance at week 24.
Figure 3: Hierarchical Statistical Testing Order for Coprimary and Selected Secondary Outcomes
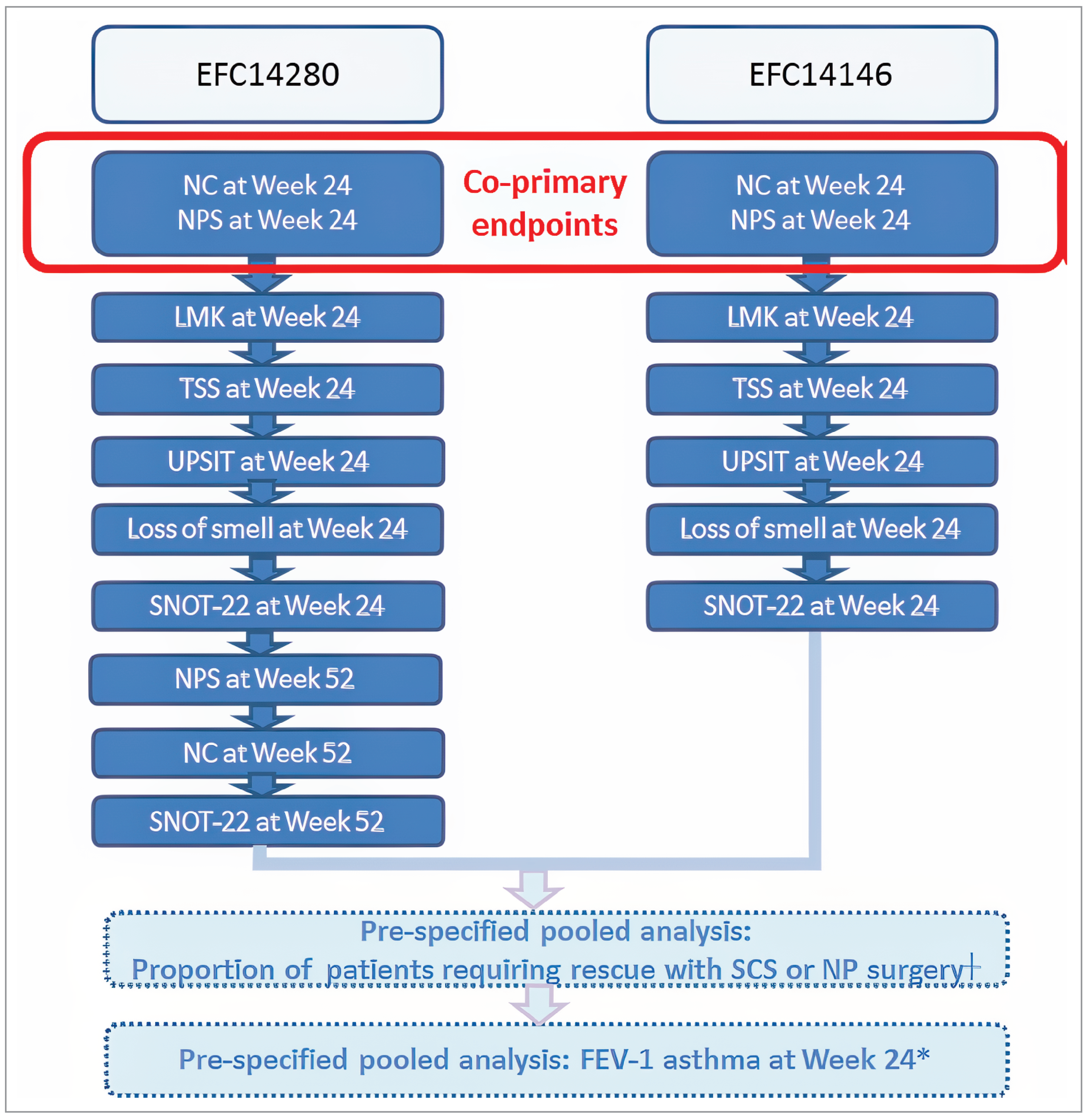
FEV-1 = forced expiratory volume in 1 second; LMK = Lund-Mackay score; NC = nasal congestion and/or obstruction; NP = nasal polyp; NPS = nasal polyp score; SCS = systemic corticosteroid; SNOT-22 = 22-item Sino-Nasal Outcome Test; TSS = total symptom score; UPSIT = University of Pennsylvania Smell Identification Test.
Note: EFC14280 = LIBERTY SINUS-52 trial and EFC14146 = LIBERTY SINUS-24 trial.
┼In both studies, the pooled analysis for this end point (proportion of patients requiring rescue treatment of SCS or nasal polyp surgery) was tested in the hierarchy only when, all previous end points reached statistical significance with a P value ≤ 0.05.
*The pooled analysis for this end point (change from baseline in FEV1 at week 24) was tested in the hierarchy only when the previous end point (the pooled analysis for the proportion of patients requiring rescue treatment of SCS or nasal polyp surgery) achieved statistical significance.
Source: LIBERTY SINUS-24 Clinical Study Report (statistical analysis plan).29
Prespecified Pooled Data Analyses
Preplanned pooled analyses of data from the SINUS-24 and SINUS-52 trials were conducted for the proportion of patients requiring rescue treatment (i.e., SCS or nasal polyp surgery [actual or planned]). Although the subgroup of patients with prior nasal polyp surgery (yes, no) was a prespecified subgroup in both trials, the subgroup analyses were not adjusted for multiplicity or included in the statistical hierarchical testing. The proportion of patients requiring rescue treatment was analyzed using the Cox proportional hazards model and the Kaplan-Meier method. The Cox model used the event as the dependent variable and the study indicator, treatment group, asthma or NSAID-ERD strata, previous surgery strata, and study region as covariates.
Subgroup Analyses
Prespecified subgroup analyses of the coprimary outcomes at week 24 were conducted regarding age, gender, baseline weight, baseline body mass index, region, territory, prior nasal polyp surgery, race, ethnicity, asthma comorbidity, asthma and/or NSAID-ERD, NSAID-ERD, allergic rhinitis at baseline, and SCS use in the prior 2 years. The analysis was performed based on the imputed datasets from the primary analysis. The subgroup analyses were not adjusted for multiplicity or included in the statistical hierarchical testing procedure.
Sensitivity Analyses
Sensitivity analyses (e.g., mixed-effects model with repeated measures [MMRM], pattern mixture model with copy increment from placebo, tipping point analysis, as-observed analysis, MMRM approach for NC as binary response data) were conducted on the coprimary outcomes (Table 9). For all sensitivity analysis (except for the “as-observed” analysis), data collected postsurgery or post-SCSs were set to missing for patients who underwent surgery for nasal polyps or received SCSs for any reason.
Table 9: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing dataa | Supportive and sensitivity analyses |
|---|---|---|---|---|
SINUS-24 and SINUS-52 | ||||
Change from baseline in NPS score Change from baseline in NC score | ANCOVA | Baseline value of corresponding coprimary outcome, treatment group, asthma or NSAID-ERD status, prior surgery history, and regions as covariates |
|
|
Change from baseline in LMK-CT score Change from baseline in TSS Change from baseline in UPSIT Change from baseline in daily loss of smell Change from baseline in SNOT-22 | ANCOVA | Baseline value of corresponding coprimary outcome, treatment group, asthma or NSAID-ERD status, prior surgery history, and regions as covariates |
| NR |
Proportion and time to event of patients requiring rescue treatment (SCS or nasal polyp surgery)b (prespecified pooled analysis) | Cox proportional hazards model Kaplan-Meier method | Cox model includes events as the dependent variable and study indicator, treatment group, asthma or NSAID-ERD strata, prior surgery strata, and region (pooled countries) as covariates | If the decision date of nasal polyp surgery was missing, the planned surgery date was used or, if missing, the actual surgery date was used | NR |
Responder analysesc | Cochran-Mantel-Haenszel test | Stratified by asthma or NSAID-ERD status, prior surgery history, and region | Missing data considered as nonresponders | NR |
ANCOVA = analysis of covariance; LMK-CT score = Lund-Mackay CT score; MI = multiple imputation; MMRM = mixed-effects model with repeated measures; NC = nasal congestion and/or obstruction; NPS = nasal polyps score; NR = not reported; NSAID-ERD = nonsteroidal anti-inflammatory drug–exacerbated respiratory disease; SCS = systemic corticosteroid; SNOT-22 = 22-item Sino-Nasal Outcome Test; TSS = total symptom score; UPSIT = University of Pennsylvania Smell Identification Test; WOCF = worst observation carried forward.
aFor patients who received SCS or underwent nasal polyp surgery for any reason, data collected postsurgery (actual date) or post-SCS treatment were set to missing in the WOCF-MI approach. The worst baseline value on or before the time of surgery or SCS treatment was used to impute missing week 24 or 52 values (depending on the study; baseline values were used for patients whose postbaseline values were all missing). For patients who discontinued treatment without rescue by nasal polyp surgery or SCSs, an MI approach to impute missing data was used, using all patients who had not been rescued by surgery or were not receiving SCSs.
bDue to the potential low number of events in each single study, the proportion of patients requiring rescue treatment (SCS or nasal polyp surgery [actual or planned]) during the treatment period was analyzed by pooling results from SINUS-24 and SINUS-52.
cResponder analyses at week 24 defined responders as the proportion of patients with improvement by 1 point in NPS,3 2 points in NPS,3 1 point in NPS and 0.5 reductions in NC,3 8.9 MCID for SNOT-22, and VAS ≤ 7. All P values reported for the responder analyses are nominal.
Source: SINUS-24 Clinical Study Report;29 SINUS-52 Clinical Study Report;30 Bachert et al., 2019.32
Analysis Populations
The analysis populations are defined in Table 10 and are summarized as follows:
Table 10: Analysis Populations of the SINUS-24 and SINUS-52 Trials
Study | Population | Definition | Application |
|---|---|---|---|
SINUS-24 and SINUS-52 | Efficacy population | ITT population defined as the randomized population analyzed according to the treatment group allocated by randomization, regardless of whether the treatment kit was used. | Primary efficacy population for all efficacy analyses |
Safety population | All patients who received at least 1 dose or part of a dose of study drug, analyzed according to the treatment actually received. Patients who were treated without randomization were also included in the safety population. | Primary safety population for all safety analyses |
ITT = intention-to treat.
Source: LIBERTY SINUS-24 Clinical Study Report;29 LIBERTY SINUS-52 Clinical Study Report.30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
A summary of patient disposition of the SINUS-24 and SINUS-52 trials is presented in Table 11.
A total of 276 patients were enrolled in the SINUS-24 trial, and 448 patients were enrolled in the SINUS-52 trial. The most common reason patients were not eligible for randomization in both studies was that they did not meet the inclusion criteria of a minimum score of 5 points on the bilateral NPS. The proportion of patients who completed the 24-week study period was high (at least 97% in all treatment groups) in both trials. Similarly, the proportion of patients who completed the 48-week (SINUS-24) and 52-week (SINUS-52) study period was at least 92% in all treatment groups in both trials.
Table 11: Summary of Patient Disposition in the SINUS-24 and SINUS-52 Trials (ITT Population)
Patient disposition | SINUS-24 | SINUS-52 | |||
|---|---|---|---|---|---|
Dupilumab 300 mg q.2.w. (N = 143) | Placebo (N = 133) | Dupilumab 300 mg q.2.w. (N = 150) | Dupilumab 300 mg q.2.w.–q.4.w. (N = 145) | Placebo (N = 153) | |
Screened, N | 506 | 806 | |||
Main reasons for screening failure, N (%) | 230 (45.5) | 358 (44.4) | |||
██ █))██ █))██ █)) | █))██ █)) | █))██ █)) | |||
██ █))██ █))██ █)) | █))██ █)) | █))██ █)) | |||
██ █))██ █))██ █)) | █))██ █)) | █))██ █)) | |||
Randomized, N (%) | 143 (100.0) | 133 (100.0) | 150 (100.0) | 145 (100.0) | 153 (100.0) |
Randomized and treated, N (%) | █))██ █)) | █))██ █)) | █))██ █)) | █))██ █)) | █))██ █)) |
Completed 24-week study period, N (%) | 141 (98.6) | 130 (97.7) | 147 (98.0) | 144 (99.3) | 148 (96.7) |
Discontinued study before week 48 (SINUS-24) or week 52 (SINUS-52), N (%) | 4 (3.0) | 9 (6.7) | 13 (8.7) | 5 (3.4) | 31 (20.3) |
Reason for discontinuation before week 48 (SINUS-24) or week 52 (SINUS-52), N (%) | |||||
Adverse events | 2 (1.4) | 3 (2.3) | 6 (4.0) | 1 (0.7) | 16 (10.5) |
No treatment efficacy | 0 (0) | 0 (0) | 1 (0.7) | 2 (1.4) | 8 (5.2) |
Poor compliance | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.7) |
Other reasons | 2 (1.4) | 6 (4.5) | 6 (4.0) | 2 (1.4) | 6 (3.9) |
Completed study period (48-week for SINUS-24 and 52-week for SINUS-52), N (%) |
| 124 (93.2) | 146 (97.3) | 142 (97.9) | 140 (91.5) |
Analysis set | |||||
ITT, N | 143 | 133 | 150 | 145 | 153 |
Safety, N | 143 | 132 | 149 | 148 | 150 |
ITT = intention-to-treat; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks.
Source: LIBERTY SINUS-24 Clinical Study Report;29 LIBERTY SINUS-52 Clinical Study Report.30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
The baseline characteristics of patients in the SINUS-24 and SINUS-52 trials are summarized in Table 12. The baseline demographic and disease characteristics were similar in both treatment arms of both trials. In the SINUS-24 trial, the median age of patients was 51 years (range: █))██) and most were male (N = 158; 57.2%), whereas in the SINUS-52 trial, the median age of patients was 52 years (range: █))██). The number of patients with any medical history of type 2 inflammation, including asthma and/or NSAID-ERD, was 75.4% and 82.4% in the SINUS-24 trial and the SINUS-52 trial, respectively. In the SINUS-24 trial, 71.7% of patients had prior nasal polyp surgery, whereas 58.2% of patients included in the SINUS-52 trial had prior nasal polyp surgery. The mean time since first diagnosis of CRSwNP in the overall study population of the SINUS-24 trial was 11.11 years (range, 0.2 to 42.5) and 10.94 years (range, 0.1 to 61.3) in the SINUS-52 trial. Further, 198 (71.7%) of patients in the SINUS-24 trial had previous surgery for nasal polyps and 58.3% of patients in the SINUS-52 trial had previous nasal polyp surgery. In both trials, nearly all patients had chronic symptoms, with nasal polyposis (i.e., NC, rhinorrhea, or loss of sense of smell) and the majority of patients presented at least 2 symptoms 8 weeks before screening. CRSwNP symptoms, as assessed by NC score, loss of sense of smell, rhinorrhea symptom scores, and TSS at both 8 and 4 weeks before screening, were severe and comparable among groups.
Table 12: Summary of Baseline Characteristics of Patients in the SINUS-24 and SINUS-52 Trials (ITT Population)
Characteristic | SINUS-24 | SINUS-52 | |||
|---|---|---|---|---|---|
Dupilumab 300 mg q.2.w. (N = 143) | Placebo (N = 133) | Dupilumab 300 mg q.2.w. (N = 150) | Dupilumab 300 mg q.2.w.–q.4.w. (N = 145) | Placebo (N = 153) | |
Age | |||||
Mean (SD) | 50.17 (13.59) | 50.83 (13.21) | 51.91 (11.88) | 52.28 (12.87) | 51.67 (12.66) |
Median (range) | 52.0 (█))██) | 50.0 (█))██) | 51.0 (█))██) | 53.0 (█))██) | 53.0 (█))██) |
Sex, n (%) | |||||
Female | 55 (38.5) | 63(47.4) | 53(35.3) | 58(40.0) | 58(37.9) |
Male | 88 (61.5) | 70 (52.6) | 97 (64.7) | 87 (60.0) | 95 (62.1) |
Race, n (%) | |||||
American Indian or Alaska Native | 1 (0.7) | 1 (0.4) | 7 (4.7) | 2 (1.4) | 3 (2.0) |
Asian or Orientala | 1 (0.7) | — | 17 (11.3) | 19 (13.1) | 18 (11.8) |
Japanese | 0 | 0 | 16 (10.7) | 17 (11.7) | 17 (11.1) |
Black or of African descent | 2 (1.4) | 7 (5.3) | 2 (1.3) | 2 (1.4) | 3 (2.0) |
Caucasiana/white | 138 (96.5) | 126 (94.7) | 124 (82.7) | 120 (82.8) | 128 (83.7) |
Multiple | — | — | — | 1 (0.7) | 1 (0.7) |
Native Hawaiian or other Pacific Islander | — | — | — | 1 (0.7) | — |
Unknown | 1 (0.7) | — | — | — | — |
BMI | |||||
Mean (SD) | 27.49 (5.11) | 28.36 (5.76) | 27.96 (5.53) | 27.96 (5.51) | 27.91 (5.50) |
Median (range) | 26.84 (16.4 to 41.7) | 26.87 (18.4 to 45.0) | 27.06 (18.0 to 59.9) | 27.44 (16.4 to 52.3) | 27.48 (17.5 to 45.8) |
Smoking history, n (%) | |||||
Former | 38 (26.6) | 33 (24.8) | 40 (26.7) | 43 (29.7) | 49 (32.0) |
Current | 14 (9.8) | 14 (10.5) | 14 (9.3) | 11 (7.6) | 17 (11.1) |
Never | 91 (63.6) | 86 (64.7) | 96 (64.0) | 91 (62.8) | 87 (56.9) |
Time since first diagnosis of nasal polyp, years | |||||
Mean (SD) | 11.42 (9.69) | 10.77 (8.57) | 11.28 (10.38) | 10.67 (9.12) | 10.88 (9.40) |
Median (range) | 9.68 (0.3 to 42.5) | 9.49 (0.2 to 37.5) | 9.05 (0.1 to 61.3) | 7.71 (0.2 to 55.1) | 7.52 (0.2 to 42.3) |
No. of patients with prior nasal polyp surgery, n (%) | 99 (69.2) | 99 (74.4) | 88 (58.7) | 85 (58.6) | 88 (57.5) |
No. of previous surgeries for nasal polyp | |||||
Mean (SD) | 2.34 (1.93) | 2.13 (1.50) | 1.93 (1.57) | 1.54 (1.17) | 1.76 (1.37) |
Median (range) | 2.0 (1.0 to 11.0) | 2.0 (1.0 to 8.0) | 1.0 (1.0 to 11.0) | 1.0 (1.0 to 8.0) | 1.00 (1.0 to 8.0) |
1 previous surgery, n (%) | 45 (45.5) | 45 (45.5) | 49 (55.7) | 59 (69.4) | 56 (63.6) |
2 previous surgeries, n (%) | 21 (21.2) | 25 (25.3) | 17 (19.3) | 17 (20.0) | 14 (15.9) |
≥ 3 surgeries, n (%) | 33 (33.3) | 29 (29.3) | 22 (25.0) | 9 (10.6) | 18 (20.5) |
No. of patients with SCS use during past 2 years, n (%) | 92 (64.3) | 87 (65.4) | 121 (80.7) | 116 (80.0) | 122 (79.7) |
No. of courses of SCS use during past 2 years | |||||
Mean (SD) | 1.43 (0.83) | 1.45 (0.85) | 1.61 (1.37) | 1.72 (1.60) | 1.49 (0.95) |
Median (range) | 1.0 (1.0 to 6.0) | 1.0 (1.0 to 5.0) | 1.0 (1.0 to 11.0) | 1.0 (1.0 to 12.0) | 1.0 (1.0 to 7.0) |
Patients with medical history of asthma, n (%) | 82 (57.3) | 79 (59.4) | 85 (56.7) | 91 (62.8) | 91 (59.5) |
Patients with NSAID-ERD, n (%) | 46 (32.2) | 38 (28.6) | 35 (23.3) | 41 (28.3) | 44 (28.8) |
Patients with comorbid type 2 inflammatory medical history including asthma or NSAID-ERD, n (%) | 109 (76.2) | 99 (74.4) | 122 (81.3) | 120 (82.8) | 127 (83.0) |
Patients with comorbid type 2 inflammatory medical history excluding asthma or NSAID-ERD, n (%) | 81 (56.6) | 75 (56.4) | 96 (64.0) | 99 (68.3) | 98 (64.1) |
BMI = body mass index; ITT = intention-to-treat; NSAID-ERD = nonsteroidal anti-inflammatory–exacerbated respiratory disease; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SCS = systemic corticosteroid; SD = standard deviation.
aWording from original source.
Source: SINUS-24 Clinical Study Report;29 SINUS-52 Clinical Study Report.30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
█))██))███))███))███))███))███))████))██))███))███))███))███))███))███))██))███))███))███))███))███))████))██))███))███))███))███))███))██))██))███))███))███))███))███))████))██))███))███))███))█████.
█))██))███))███))███))███))███))████))██))███))███))███))███))███))███))██))███))███))███))███))███))████))██))███))███))███))███))███))██))██))███))███))███))███))███))████))██))██. Table 13 is a summary of the patient exposure to treatment in both trials.
Table 13: Patient Exposure in the SINUS-24 and SINUS-52 Trials (Safety Population)
Exposure | SINUS-24 | SINUS-52 | |||
|---|---|---|---|---|---|
Dupilumab 300 mg q.2.w. (N = 143) | Placebo (N = 132) | Dupilumab 300 mg q.2.w. (N = 149) | Dupilumab 300 mg q.2.w.–q.4.w. (N = 148) | Placebo (N = 150) | |
Cumulative exposure to treatment, patient-years | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Duration, days | |||||
Mean (SD) | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Median (range) | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SD = standard deviation.
Source: SINUS-24 Clinical Study Report;29 SINUS-52 Clinical Study Report.30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Concomitant Medications
█))██))███))███))███))███))███))████))██))███))███))███))███))███))███))██))███))███))███))███))███))████))██))███))███))███))███))███))██))██))███))███))███))███))███))████))██))██. Table 14 provides a detailed summary of the concomitant medications (other than MFNS) taken by the highest proportion of patients between the treatment groups in both trials.
Table 14: Summary of Concomitant Medication Use by Anatomic Class in the SINUS-24 and SINUS-52 Trials During the Treatment Period (Randomized Population)
Concomitant medication, n (%) | SINUS-24 | SINUS-52 | |||
|---|---|---|---|---|---|
Dupilumab 300 mg q.2.w. (N = 143) | Placebo (N = 133) | Dupilumab 300 mg q.2.w. (N = 150) | Dupilumab 300 mg q.2.w.–q.4.w. (N = 145) | Placebo (N = 153) | |
Any concomitant medication | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Dermatologicals | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Respiratory system | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Sensory organs | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Cardiovascular system | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Alimentary tract and metabolism | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Nervous system | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Genitourinary system and sex hormones | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Systemic hormonal preparations excluding sex hormones and insulins | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Blood and blood-forming organs | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Various | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Musculoskeletal system | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Anti-infectives for systemic use | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Antiparasitic products, insecticides, and repellants | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
Antineoplastic and immunomodulating agents | )██))██ | )██))██ | )██))██ | )██))██ | )██))██ |
q.2.w. = every 2 weeks; q.4.w. = every 4 weeks.
Source: SINUS-24 Clinical Study Report;29 SINUS-52 Clinical Study Report.30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Efficacy
A summary of the key efficacy outcomes of the SINUS-24 and SINUS-52 trials are presented in Table 15. This summary focused on reporting the results in both arms (dupilumab 300 mg every 2 weeks and placebo groups) of the SINUS-24 trial. In the SINUS-52 trial, we reported results for dupilumab 300 mg every 2 weeks and placebo groups. The week 24 results for the dupilumab treatment group were based on a pooled group of all patients who were treated with dupilumab every 2 weeks, i.e., a pooled group of patients from the dupilumab 300 mg every 2 weeks group and dupilumab 300 mg every 2 weeks–every 4 weeks group (N = 295). Comparisons are for the pooled dupilumab arms versus placebo. Results of the dupilumab 300 mg every 2 weeks–every 4 weeks group are not reported because they do not match the indication for this review.
Severity of Nasal Polyps and Nasal Obstruction
NPS: The baseline NPS scores were comparable between the treatment groups in both trials. In the SINUS-24 trial, the LS mean change from baseline in NPS to week 24 was –1.89 for the dupilumab 300 mg every 2 weeks group and 0.17 for the placebo group. The LS mean difference in the change from baseline in NPS between dupilumab treatment group and placebo was –2.06 (95% CI, –2.43 to –1.69; P < 0.0001). The LS change from baseline in NPS to week 24 in the SINUS-52 trial was lower (–1.72 [SD = 1.77]) compared to the placebo (0.12 [SD = 0.95]) with an LS mean difference of –1.80 (95% CI, –2.10 to –1.51; P < 0.0001) in favour of the dupilumab treatment group. At week 52, the LS mean difference in change from baseline was –2.40 (95% CI, –2.77 to –2.02; P < 0.0001), also in favour of the dupilumab treatment group. Sensitivity analysis of the change from baseline in NPS using the MMRM approach showed similar results to the primary analyses in both trials.
A responder analysis of the change from baseline in NPS at week 24 and week 52 (SINUS-52) was conducted as a supportive analysis to determine the proportion of patients with a decrease of at least 1 point in NPS, for both trials. In the SINUS-24 trial, the proportion of patients with an improvement (decrease) of at least 1 point in NPS at week 24 was 65.0% in the dupilumab treatment group compared to 17.3% in the placebo group. In the SINUS-52 trial, the proportion of patients with a decrease of at least 1 point in NPS at weeks 24 and 52 was higher in the dupilumab treatment group compared to the placebo group: 62.0% versus 10.5% at week 24 and )██ versus )██ at week 52.
NC: In the SINUS-24 trial, the LS mean change from baseline in NC scores to week 24 was –1.34 for the dupilumab group and –0.45 for placebo group. The LS mean difference in change from baseline in NC scores between dupilumab and placebo was –0.89 (95% CI, –1.07 to –0.71; P < 0.0001) in favour of the dupilumab treatment group. In the SINUS-52 trial, the LS mean difference in the change from baseline in NC scores to week 24 was –0.87 (95% CI, –1.03 to –0.71; P < 0.0001) in favour of the dupilumab treatment group. The results at week 52 were also in favour of the dupilumab treatment group (LS mean difference in change from baseline –0.98; 95% CI, –1.17 to –0.79; P < 0.0001). Sensitivity analysis of the change from baseline in NC score in both trials using MMRM approach was consistent with the primary analysis.
A responder analysis was performed as supportive evidence in both trials. ██))████))███))███))███))████))██))███))███))███))███))████))██))██))███))███))███))████))██))███))███)██))███))███))███))████))██))███))███))███))███))████))██))███))██))██.
Health-Related Quality of Life
SNOT-22: SNOT-22 total scores at baseline were comparable between treatment groups in both trials. The LS mean change from baseline in SNOT-22 to week 24 was –30.43 (SD =.54) for the dupilumab group and –9.31 (SD = 1.62) for the placebo group in the SINUS-24 trial. The LS mean difference was –21.12 (95% CI, –25.17 to –17.06; P < 0.0001) in favour of the dupilumab treatment group. Similarly, results in the SINUS-52 trial favoured the dupilumab treatment group. The LS mean difference in change from baseline in SNOT-22 to week 24 was –17.36 (95% CI, –20.87 to –13.85; P < 0.0001) and to week 52 was –20.96 (95% CI, –25.03 to –16.89; P < 0.0001).
In a responder analysis performed as supportive evidence, ██))███))███))███))████))██))███))███))███))███))████))██))███))███))███))███))████))██))███))███))███))███))████))██))███))███))███))███))████))██))█.
Disease Symptoms and Severity
TSS: In the SINUS-24 trial, the LS mean change from baseline in TSS scores to week 24 was –3.69 (SD = 2.04) for the dupilumab and –1.26 (SD = 1.71) for the placebo group. The LS mean difference in change from baseline in TSS score at week 24 was –2.61 (95% CI, –3.04 to –2.17; P < 0.0001) in favour of dupilumab. In the SINUS-52 trial, the LS mean change from baseline in TSS scores was –3.54 (SD = 2.47) for the dupilumab treatment group and –1.03 (SD = 1.66) for the placebo group. The LS mean difference in the change from baseline in TSS to week 24 was –2.44 (95% CI, –2.87 to –2.02; P < 0.0001), and, at week 52, the LS mean difference was ██))██))███))███))███)) both favour of the dupilumab treatment group.
Decreased or loss of sense of smell: In the SINUS-24 trial, the LS mean difference in the change from baseline in decreased or loss of sense of smell to week 24 was –1.12 (95% CI, –1.31 to –0.93) in favour of the dupilumab treatment group. These results were similar in the SINUS-52 trial, where the LS mean difference in the change from baseline to week 24 and week 52 were –0.98 (95% CI, –1.15 to –0.81; P < 0.0001) and ██))██))███))███))███) respectively, both in favour of the dupilumab treatment group.
Rescue Therapy
Proportion of patients who received SCS rescue or surgery for nasal polyps (actual or planned): The proportion of patients who received SCSs or NP surgery during the treatment period in the SINUS-24 trial was lower in the dupilumab treatment group compared to the placebo group (██))██))███))██). Compared to the placebo group, the number of patients with SCS use was lower (6.3% [N = 9] versus 18.8% [N = 25]). The most common reason for SCS rescue treatment was for nasal polyps, and SCS rescue treatment was lower in the dupilumab group (██))██))█ compared with the placebo group ██))██))█ During the study, 9 (6.8%) patients in the placebo group and 3 (2.1%) in the dupilumab group had surgery for nasal polyps (actual or planned).
Table 15: Key Efficacy Outcomes in the SINUS-24 and SINUS-52 Trials (ITT Population)
Outcome | SINUS-24 | SINUS-52 | ||
|---|---|---|---|---|
Dupilumab 300 mg q.2.w. (N = 143) | Placebo (N = 133) | Dupilumab 300 mg q.2.w. (N = 295) | Placebo (N = 153) | |
Severity of nasal polyps and nasal obstruction | ||||
Change in NPS from baseline to week 24 | ||||
N | 137 | 128 | 283 | 145 |
Baseline, mean (SD) | 5.64 (1.23) | 5.86 (1.31) | 6.18 (1.21)a | 5.96 (1.21) |
Week 24, mean (SD) | 3.75 (1.98) | 5.94 (1.44) | 4.46 (1.89)a | 6.09 (1.19) |
Change from baseline | ||||
LS mean (SE) | −1.89 (0.14) | 0.17 (0.15) | −1.71 (0.11)a | 0.10 (0.14) |
LS mean difference versus placebo (95% CI)b | −2.06 (−2.43 to −1.69) | −1.80 (−2.10 to −1.51) | ||
P value | < 0.0001 | < 0.0001 | ||
Change in NPS from baseline to week 52 | ||||
N | — | — | 141 | 142 |
Baseline, mean (SD) | — | — | 6.07 (1.22) | 5.96 (1.21) |
Week 52, mean (SD) | — | — | 3.76 (2.20) | 6.10 (1.52) |
Change from baseline | — | — | ||
LS mean (SE) | — | — | −2.24 (0.15) | 0.15 (0.15) |
LS mean difference versus placebo (95% CI)b | — | — | −2.40 (−2.77 to −2.02) | |
P value | — | — | < 0.0001 | |
Change in NC from baseline to week 24 | ||||
N | 141 | 130 | 289 | 147 |
Baseline, mean (SD) | 2.26 (0.57) | 2.45 (0.55) | 2.46 (0.61)a | 2.38 (0.54) |
Week 24, mean (SD) | 0.94 (0.75) | 1.90 (0.85) | 1.19 (0.90)a | 2.02 (0.77) |
Change from baseline | ||||
LS mean (SE)b | −1.34 (0.07) | −0.45 (0.07) | −1.25 (0.06)a | −0.38 (0.07) |
LS mean difference versus placebo (95% CI)b | −0.89 (−1.07 to −0.71) | −0.87 (−1.03 to −0.71) | ||
P value | < 0.0001 | < 0.0001 | ||
Change in NC from baseline to week 52 | ||||
N | — | — | 145 | 144 |
Baseline, mean (SD) | — | — | 2.48 (0.62) | 2.38 (0.54) |
Week 52, mean (SD) | — | — | 1.10 (0.92) | 2.04 (0.78) |
Change from baseline | — | — | ||
LS mean (SE) | — | — | −1.35 (0.07) | −0.37 (0.08) |
LS mean difference versus placebo (95% CI)b | — | — | −0.98 (−1.17 to −0.79) | |
P value | — | — | < 0.0001 | |
HRQoL | ||||
Change from baseline to week 24 in SNOT-22 | ||||
N | 135 | 128 | 282 | 145 |
Baseline, mean (SD) | 48.00 (20.16) | 50.87 (20.22) | 51.02 (20.37)a | 53.48 (21.85) |
Week 24, mean (SD) | 18.58 (14.92) | 40.49 (23.06) | 23.89 (18.77)a | 42.16 (23.26) |
Change from baseline | ||||
LS mean (SE)b | −30.43 (1.54) | −9.31 (1.62) | −27.77 (1.26)a | −10.40 (1.61) |
LS mean difference versus placebo (95% CI) | −21.12 (−25.17 to −17.06) | −17.36 (−20.87 to −13.85) | ||
P value | < 0.0001 | < 0.0001 | ||
Change from baseline to week 52 in SNOT-22 | ||||
N | — | 143 | 143 | |
Baseline, mean (SD) | — | — | 50.16 (19.72) | 53.48 (21.85) |
Week 52, mean (SD) | — | — | 21.67 (19.16) | 44.05 (22.66) |
Change from baseline | — | — | ||
LS mean (SE) | — | — | −29.84 (1.63) | −8.88 (1.61) |
LS mean difference versus placebo (95% CI)b | — | — | −20.96 (−25.03 to −16.89) | |
P value | — | — | < 0.0001 | |
Disease symptoms | ||||
Change from baseline to week 24 in TSS | ||||
N | 141 | 129 | 289 | 145 |
Baseline, mean (SD) | ██))██) | ██))██) | ██))██) | ██))██) |
Week 24, mean (SD) | 3.16 (1.93) | 6.02 (2.02) | 3.77 (2.44)a | 6.08 (1.97) |
Change from baseline | ||||
LS mean (SE)b | −3.77 (0.16) | −1.17 (0.17) | −3.45 (0.15)a | −1.00 (0.20) |
LS mean difference versus placebo (95% CI) | −2.61 (−3.04 to −2.17) | −2.44 (−2.87 to −2.02) | ||
P value | < 0.0001 | < 0.0001 | ||
Change from baseline to week 52 in TSS | ||||
N | ██))██) | ██))██) | ██))██) | ██))██) |
Baseline, mean (SD) | ██))██) | ██))██) | ██))██) | ██))██) |
Week 52, mean (SD) | ██))██) | ██))██) | ██))██) | ██))██) |
Change from baseline | ██))██) | ██))██) | ██))██) | ██))██) |
LS mean (SE)b | ██))██) | ██))██) | ██))██) | ██))██) |
LS mean difference versus placebo (95% CI) | ██))██) | ██))██) | ||
P value | ██))██) | ██))██) | ||
Change from baseline to week 24 in decreased or loss of sense of smell | ||||
N | 141 | 130 | 289 | 147 |
Baseline, mean (SD) | 2.70 (0.57) | 2.73 (0.51) | 2.77 (0.53)a | 2.72 (0.52) |
Week 24, mean (SD) | 1.35 (0.99) | 2.50 (0.77) | 1.55 (1.02)a | 2.49 (0.79) |
Change from baseline | ||||
LS mean (SE)b | −1.41 (0.07) | −0.29 (0.07) | −1.21 (0.06)a | −0.23 (0.08) |
LS mean difference versus placebo (95% CI) | −1.12 (−1.31 to −0.93) | −0.98 (−1.15 to −0.81) | ||
P value | < 0.0001 | < 0.0001 | ||
Change from baseline to week 52 in decreased or loss of sense of smell | ||||
N | ██))██) | ██))██) | ██))██) | ██))██) |
Baseline, mean (SD) | ██))██) | ██))██) | ██))██) | ██))██) |
Week 52, mean (SD) | ██))██) | ██))██) | ██))██) | ██))██) |
Change from baseline | ██))██) | ██))██) | ██))██) | ██))██) |
LS mean (SE)b | ██))██) | ██))██) | ██))██) | ██))██) |
LS mean difference versus placebo (95% CI) | ██))██) | ██))██) | ||
P value | ██))██) | ██))██) | ||
Rescue therapyc | ||||
Summary of rescue therapy (SCS or nasal polyp surgery) by reason, n (%) | ||||
Patients with SCS use | 9 (6.3) | 25 (18.8) | 22 (14.7) | 63 (41.2) |
For nasal polyps | ██))██) | ██))██) | ██))██) | ██))██) |
For asthma | ██))██) | ██))██) | ██))██) | ██))██) |
For other respiratory disease | ██))██) | ██))██) | ██))██) | ██))██) |
Other ear, nose, or throat disease | ██))██) | ██))██) | ██))██) | ██))██) |
For other reason | ██))██) | ██))██) | ██))██) | ██))██) |
Patients with nasal polyp surgery | 3 (2.1) | 9 (6.8) | 2 (1.3) | 13 (8.5) |
Patients with SCS use and/or nasal polyp surgery | ██))██) | ██))██) | ██))██) | ██))██) |
CI = confidence interval; HRQoL = health-related quality of life; ITT = intention-to-treat; LS = least squares; NC = nasal congestion and/or obstruction; NPS = nasal polyp score; q.2.w. = every 2 weeks; SCS = systemic corticosteroid; SD = standard deviation; SE = standard error; SNOT-22 = 22-item Sino-Nasal Outcome Test; TSS = total symptom score.
aFor the week 24 results, the 2 dupilumab 300 mg every 2 weeks arms were combined, so results are for N = 295 and comparisons are for the pooled dupilumab arms versus the placebo arm.
bData analyzed by fitting an ANCOVA model with the corresponding baseline value, treatment group, asthma or NSAID-ERD status, prior surgery history, and region as covariates. Data collected after treatment discontinuation were included. Data post-SCS or nasal polyp surgery were set to missing and imputed by WOCF; other missing data were imputed by MI. Descriptive statistics at week 24 included patients after WOCF at week 24, and patients whose week 24 values were imputed by MI were excluded from the descriptive analysis.
cData reported for the treatment period; the total number of patients in the dupilumab 300 mg every 2 weeks group for this outcome is 150 patients.
Source: SINUS-24 Clinical Study Report;29 SINUS-52 Clinical Study Report30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
In the SINUS-52 trial, the proportion of patients who required treatment with SCS or nasal polyp surgery during the treatment period was lower in the dupilumab group compared to the placebo group (██))██))█). Similarly, the number of patients with rescue SCS use was lower in the dupilumab group (14.7% [N = 22]) compared to the placebo group (41.2%). The most common reason for SCS rescue treatment was for nasal polyps, and SCS rescue treatment was lower in the dupilumab group (██)) compared with the placebo group (██))). During the study, 13 (8.5%) patients in the placebo group and 2 (1.3%) patients in the dupilumab group had surgery for nasal polyps (actual or planned).
Prespecified Pooled Analyses
Prespecified pooled analyses of data from the SINUS-24 and SINUS-52 trials were conducted (Table 16) for the proportion of patients requiring rescue treatment (i.e., SCSs or nasal polyp surgery; actual or planned) in the pooled intention-to-treat (ITT) population.
Proportion of Patients Requiring Rescue Treatment (SCS and/or Nasal Polyp Surgery)
The probability of patients who required treatment with SCS or sinus surgery during the treatment period was lower in the pooled dupilumab 300 mg every 2 weeks group (n = 42 [9.6%]) compared with the pooled placebo group (n = 97 [33.9%]). The corresponding hazard ratio = 0.243 (95% CI, 0.169 to 0.351). The Kaplan-Meier curve for time to first SCS use and/or nasal polyp surgery is depicted in Figure 4.
Figure 4: The SINUS-24 and SINUS-52 Trials — Kaplan-Meier Curve for Time to First SCS Use and/or Surgery (Actual or Planned) During the Treatment Period (Pooled ITT Population)
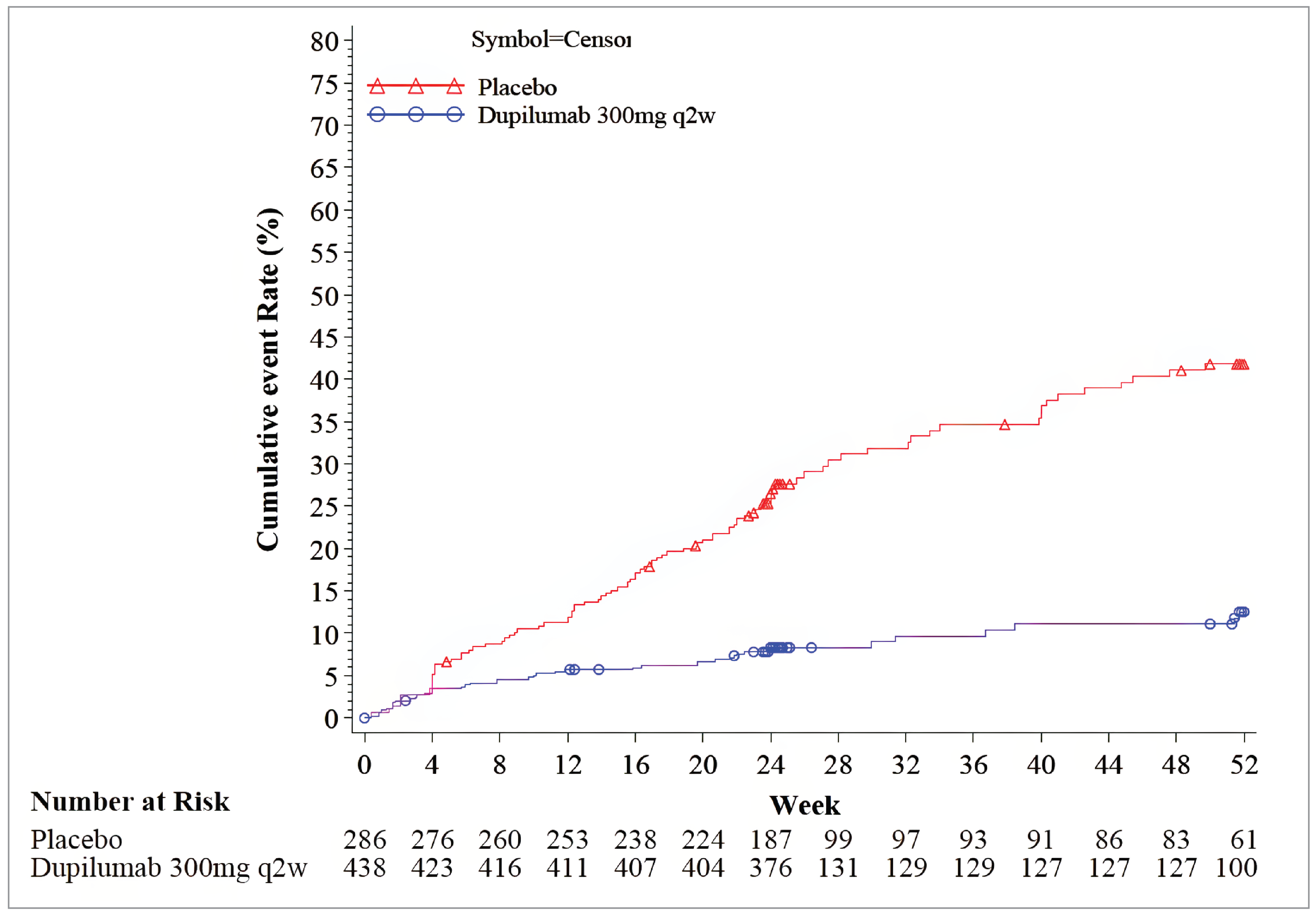
ITT = intention-to-treat; q2w = every 2 weeks; SCS = systemic corticosteroids.
Source: Common Technical Document 2.7.3: Summary of Clinical Efficacy.54
Table 16: The SINUS-24 and SINUS-52 Trials — Patients With SCS and/or Nasal Polyp Surgery (Actual or Planned) During the Treatment Period (Pooled ITT Population)
Outcome | Dupilumab 300 mg q.2.w. (N = 438) | Placebo (N = 286) |
|---|---|---|
Patients with SCS use and/or nasal polyp surgery | ||
n (%) | 42 (9.6) | 97 (33.9) |
Kaplan-Meier estimates for probability of patient with 1 event (95% CI) up to: | ||
16 weeks | ██))██) | ██))██) |
24 weeks | ██))██) | ██))██) |
40 weeks | ██))██) | ██))██) |
52 weeks | ██))██) | ██))██) |
HR (95% CI)a | 0.243 (0.169 to 0.351) | |
P value versus placeboa | < 0.0001 | |
CI = confidence interval; HR = hazard ratio; ITT = intention-to-treat; q.2.w. = every 2 weeks; SCS = systemic corticosteroids.
aHazard ratio was derived from the Cox proportional hazards model, with the event of first SCS use and/or nasal polyp surgery (actual or planned; whichever is earlier) as the response variable, and treatment, asthma or NSAID-ERD status, prior surgery history, region (pooled country), and study indicator as covariates.
Source: Common Technical Document 2.7.3: Summary of Clinical Efficacy.54
Subgroup Analyses
In both trials, a prespecified subgroup analysis of the coprimary outcomes at week 24 was conducted to assess efficacy in subgroups of patients with and without prior nasal polyp surgery. In the SINUS-24 trial, the change from baseline in NPS at week 24 in patients with and without a history of nasal polyp surgery was –2.00 (95% CI, –2.45 to –1.54) and –2.26 (95% CI, –2.87 to –1.66), respectively, both in favour of the dupilumab treatment group. Similarly, the change from baseline in NC score at week 24 in patients with (–0.89; 95% CI, –1.11 to –0.67) and without prior NPS surgery (–0.89; 95% CI, –1.19 to –0.59) was also in favour of the dupilumab treatment group. In the SINUS-52 trial, the LS mean change from baseline in NPS at week 24 in patients with (–1.95; 95% CI, –2.36 to –1.54) and without prior nasal polyp surgery (–1.55; 95% CI, –1.97 to –1.13) was in favour of the dupilumab treatment group. Additionally, the LS mean change from baseline in NC score in patients with prior nasal polyp surgery was –1.03 (95% CI, –1.24 to –0.82) and without prior nasal polyp surgery was –0.64 (95% CI, –0.89 to –0.39).
Harms
Adverse Events
Harms data for the SINUS-24 and SINUS-52 trials are summarized in Table 17. In the SINUS-24 trial, 65.0% (N = 93) of patients in the dupilumab group experienced TEAEs during the entire treatment period compared to 70.5% (N = 93) in the placebo group. The most frequent TEAEs were nasopharyngitis, nasal polyps, epistaxis, injection-site erythema, headache, cough, asthma, and bronchitis. Of these, the only TEAE that occurred more frequently in the dupilumab group compared to the placebo group was epistaxis (n = 11 [7.7%] versus n = 4 [3.0%], respectively). In the SINUS-52 trial, the proportion of patients with at least 1 TEAE during the entire treatment period was lower in the dupilumab group (83.2%) compared with the placebo group (90.7%). Compared to the placebo group, arthralgia and injection-site reactions were more frequently reported in the dupilumab group.
Serious Adverse Events
The incidence of treatment-emergent SAEs was lower in the dupilumab group (4.2%) compared to the placebo group (14.4%) in the SINUS-24 trial. Compared to the placebo group, SAEs that occurred in at least 2 patients in either treatment group were ██))██)████))██)██))██)██))██)██))██)██))██)██))██)))██)██))██). In the SINUS-52 trial, 10.0% of patients in the placebo group compared to 5.4% patients in the dupilumab group experienced treatment-emergent SAEs. Of these, the SAEs that occurred in at least 2 patients in any treatment group were ██))██)████))██)██))██)██))██)██))██)██)██)██))██)))██)██))███))██)████))██)██))██)██))██)██))██)██))██)██))██)))██)██))██).
Withdrawals Due to Adverse Events
The discontinuation rate due to TEAEs in the SINUS-24 trial was 3.5% in the dupilumab group compared to 2.3% in the placebo group, while in the SINUS-52 trial, the proportion of patients who discontinued treatment due to a TEAE was lower in the dupilumab group (4.0%) compared to the placebo group (11.3%). The most frequently reported TEAE that led to permanent treatment discontinuation was nasal polyps in both trials, occurring in 2 (1.4%) patients in the dupilumab and 1 (0.8%) patient in the placebo in the SINUS-24 trial. In the SINUS-52 trial, 6 patients in the placebo group and no patient in the dupilumab group discontinued treatment due to nasal polyps.
Mortality
In both trials, there were no reports of deaths due to AEs during the treatment period. In the SINUS-24 trial, 1 patient in the placebo group died during the posttreatment period due to myocardial infarction, which was assessed as unrelated to the study drug. In the SINUS-52 trial, 1 patient experienced a TEAE leading to death in the follow-up period, involving a traumatic intracranial hemorrhage arising from an accidental fall from a bicycle, which was assessed as unrelated to the study drug.
Notable Harms
Notable harms included in this review were the proportion of patients who had myalgia, eosinophilia, nasopharyngitis, and headaches during the treatment period. In the SINUS-24 trial, ██))██)████))██)██))██)██))██)██))██)██))██)██))██)))██)██))███))██)████))██)██))██)██))██)██))██)██))██)██))██)))██)██))██). and headache (4.9% versus 8.3%) compared to the placebo group, while the incidence of nasopharyngitis (13.3% versus 15.2%) was lower in the dupilumab ██))██)████))██)██))██)██))██)███))██)████))██)██))██)██))██)███))██)████))██)██))██)██))██)█ nasopharyngitis (20.1% versus 24.0%) and headache (10.8% versus 12.0%) compared to the placebo group. ██))██)████))██)██))██)██))██)███))██)████))██)██))██)██))██)███))██)████))██)██))██)██))██)█.
There were ██))██ patients in the placebo group and ██))██ patients in the dupilumab group in the SINUS-24 trial who experienced AESIs, and the most frequently reported AESI was ██))██)████))██)██))██)██))██)███))██)████))██)██))██)██))██)█. There were more cases of ██))██)████))██)██))██)██))██)███))██)████))██)██))██)██))██)█. Similarly ██))██)████ patients in the placebo group, and ██))██) patients in the dupilumab treatment group in the SINUS-52 trial experienced AESIs, and the most frequently reported AESIs were ██))██)████))██)██))██)██))██)███))██)████))██)██))██)██))██)███))██)████.
Table 17: Summary of Harms Results From Studies Included in the Systematic Review
Characteristic | SINUS-24 | SINUS-52 | ||
|---|---|---|---|---|
Dupilumab 300 mg q.2.w. (N = 143) | Placebo (N = 132) | Dupilumab 300 mg q.2.w. (N = 148) | Placebo (N = 150) | |
Most common adverse events, n (%)a | ||||
Patients with ≥ 1 TEAE | 93 (65.0) | 93 (70.5) | 132 (89.2) | 136 (90.7) |
Nasopharyngitis | 19 (13.3) | 20 (15.2) | 30 (20.1) | 36 (24.0) |
Nasal polyps | 17 (11.9) | 24 (18.2) | 15 (10.1) | 25 (16.7) |
Epistaxis | 11 (7.7) | 4 (3.0) | 7 (4.7) | 20 (13.3) |
Injection-site erythema | 8 (5.6) | 12 (9.1) | 10 (6.8) | 11 (7.3) |
Headache | 7 (4.9) | 11 (8.3) | 16 (10.8) | 18 (12.0) |
Cough | 4 (2.8) | 7 (5.3) | 9 (6.1) | 8 (5.3) |
Asthma | 3 (2.1) | 10 (7.6) | 13 (8.8) | 19 (12.7) |
Bronchitis | 0 (0) | 8 (6.1) | 9 (6.1) | 8 (5.3) |
URTI | — | — | 8 (5.4) | 19 (12.7) |
Sinusitis | — | — | 13 (8.8) | 17 (11.3) |
Acute sinusitis | — | — | 5 (3.4) | 16 (10.7) |
Back pain | — | — | 6 (4.1) | 9 (6.0) |
Arthralgia | — | — | 11 (7.4) | 2 (1.3) |
Injection-site reaction | — | — | 8 (5.4) | 3 (2.0) |
Accidental overdose | — | — | 12 (8.1) | 11 (7.3) |
Eosinophilia | 2 (1.4) | 1 (0.8) | 2 (1.3) | 1 (0.7) |
Myalgia | 0 (0) | 1 (0.8) | 2 (1.3) | 5 (3.3) |
Serious adverse events, n (%)b | ||||
Patients with ≥ 1 SAE | 6 (4.2) | 19 (14.4) | 10 (6.8) | 15 (10.0) |
██))██ | ██))██ | ██))██ | ██))██ | ██))██ |
██))██ | ██))██ | ██))██ | ██))██ | ██))██ |
██))██ | — | — | ██))██ | ██))██ |
Discontinuation due to adverse events, n (%)b | ||||
Patients with any TEAE leading to permanent treatment discontinuation | 5 (3.5) | 3 (2.3) | 2 (1.4) | 17 (11.3) |
Nasal polyps | 2 (1.4) | 1 (0.8) | 0 (0) | 6 (4.0) |
Deaths, n (%) | ||||
Death related to any TEAE | 0 (0) | 0 (0) | 1 (0.7) | 0 (0) |
Adverse events of special interest, n (%) | ||||
Any treatment-emergent AESI | 5 (4.2) | 9 (6.8) | 7 (4.7) | 13 (8.7) |
Anaphylactic reaction | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Hypersensitivity (medically reviewed) | 3 (2.1) | 4 (3.0) | 2 (1.4) | 8 (5.3) |
Serious injection-site reactions or severe injection-site reactions lasting > 24 hours | 0 (0) | 0 (0) | 1 (0.7) | 0 (0) |
Severe or serious infections | 2 (1.4) | 5 (3.8) | 3 (2.0) | 5 (3.3) |
Parasitic infections | 0 (0) | 1 (0.8) | 0 (0) | 0 (0) |
Opportunistic infections | 0 (0) | 1 (0.8) | 0 (0) | 0 (0) |
Potential drug-related hepatic Disorders | 1 (0.7) | 0 (0) | 1 (0.7) | 1 (0.7) |
Pregnancy | 0 (0) | 0 (0) | 0 (0) | 1 (0.7) |
Symptomatic overdose | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
AESI = adverse event of special interest; q.2.w. = every 2 weeks; SAE = serious adverse event; TEAE = treatment-emergent adverse event; URTI = upper respiratory tract infection.
aMost common TEAEs occurring in 5% patients in either treatment group.
bMost common occurring in 2 patients in either treatment group.
Source: SINUS-24 Clinical Study Report29 and SINUS-52 Clinical Study Report.30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
The 2 pivotal trials (SINUS-24 and SINUS-52) were both randomized, double-blind, placebo-controlled studies. Both trials employed appropriate methods for blinding, treatment allocation, and randomization. The trials stratified randomization by the presence of comorbid asthma, NSAID-ERD, prior nasal polyp surgery, and country. Regarding baseline demographic characteristics of patients, there were some minor demographic differences between groups at baseline, but the clinical experts consulted by CDA-AMC agreed that any baseline discrepancies were unlikely to bias the findings. CDA-AMC noted that concomitant medication use for many categories was higher in the placebo groups, but it is unclear whether this reflects baseline imbalance or whether differences would bias the findings.
In the SINUS-52 trial, results for efficacy end points at week 24 were pooled, i.e., data from the 2 dupilumab groups (every 2 weeks and every 2 weeks–every 4 weeks) were combined for the comparison with the placebo group. CDA-AMC notes that the pooling of the 2 dupilumab groups is appropriate because both groups received the same every 2 weeks dosage up to week 24 and, thus, the assumption of similar treatment effects during this period is reasonable. The statistical methods used for pooling, including an ITT analysis, ensured that all randomized patients were included in the analysis. Additionally, pooling of the 2 dupilumab groups in the SINUS-52 trial at week 24 provided enough power to detect differences in primary outcomes with similar effect sizes observed in the SINUS-24 trial.
The outcomes assessed in both trials are common to CRSwNP trials. The coprimary outcomes in both trials were change from baseline in the NPS and NC. The NPS, determined by independent physician assessments of centrally recorded nasal endoscopy, provides an objective measure of the size and burden of nasal polyps. In contrast, the NC score, which relies on patient-reported data, reflects the severity of NC. According to the clinical experts consulted for this review, both outcomes are clinically relevant, as they directly address the core pathophysiological features of CRSwNP, i.e., the presence of polyps and the resultant symptom burden. Based on the inputs from patient groups and the clinical experts consulted for this review, 1 key outcome was improvement in HRQoL, as measured by SNOT-22 and decreased or loss of sense of smell, which were included as key secondary end point in both trials. Outcomes such as NC and SNOT-22, although validated, are subjective to recall bias, particularly when participants perceive improvement due to expectations rather than actual treatment effect. However, this is not expected to bias results, since patients and clinicians were blinded to treatment assignment. CDA-AMC acknowledges the benefits of using the University of Pennsylvania Smell Identification Test (UPSIT) score as a measure of sense of smell in the clinical trial setting. However, this outcome was not considered as a clinically relevant outcome for this review because it is not routinely used in clinical practice in Canada due to the cost and time required to administer the test, based on inputs from clinical experts consulted for the review. To assess sense of smell, change from baseline in TSS and decreased or loss of sense of smell were summarized for this review.
The 2 trials were powered to detect differences in coprimary outcomes but not to detect differences in subgroups. However, a prespecified subgroup analysis demonstrated consistent treatment effect of dupilumab in patients with and without prior nasal polyp surgery. All analyses were performed using the ITT method, ensuring randomization was maintained. Patients who discontinued or deviated from the interventions were accounted for in the ITT approach. Regarding multiplicity, a prespecified hierarchical testing procedure was performed to control for type I error rates in the coprimary outcomes (NPS and NC) and key secondary outcomes, including SNOT-22. The hierarchical testing strategy required the 2 coprimary outcomes (change from baseline in NPS and NC) to first meet the threshold for statistical significance. Once the coprimary outcomes met this threshold (P < 0.0001), the hierarchy testing moved on to the key secondary end points, notably the SNOT-22, which assesses HRQoL, along with other secondary measures, such as the change from baseline in TSS or decreased or loss of sense of smell. CDA-AMC notes that this hierarchical approach minimizes the risk of false-positive findings that can occur when several end points are analyzed simultaneously.
WOCF and MI methods were used to impute missing values in the main analyses. MI methods can introduce bias because they depend on the often-unrealistic assumption that data are missing at random, and single imputation methods such as WOCF can bias results and may artificially improve precision in the CI. Sensitivity analyses were performed to assess the robustness of the approach to missing data. MMRM, pattern mixture model with copy increments from placebo, tipping point analysis, and as-observed analysis, were performed in both trials, and their results were consistent with the primary analysis. Additionally, discontinuations due to AEs were reportedly low in both trials. Notably, discontinuation due to TEAEs occurred in 3.5% of patients in the dupilumab group compared to 2.3% in the placebo group in the SINUS-24 trial, while in the SINUS-52 trial, it occurred in 4.0% of patients in the dupilumab group compared to 11.3% in the placebo group.
Both trials had a relatively short duration, at 24 (SINUS-24) and 52 weeks (SINUS-52). The clinical experts consulted for this review noted that, based on their clinical experience, nearly all patients demonstrate a treatment response within 1 year and some even within 6 months. Thus, they considered the duration of the trials sufficient. However, CDA-AMC notes that, although data from the SINUS-52 trial include improvement in NPS, NC, and HRQoL (via SNOT-22) up to 1 year, it remains uncertain whether 52 weeks is sufficient to assess longer-term safety and efficacy outcomes for a chronic condition.
External Validity
The demographic characteristics of the study population in both trials were considered by the clinical expert consulted for the review to be generally reflective of the population of patients with severe CRSwNP in Canada. Both trials included adult patients with severe CRSwNP previously treated with SCSs or nasal polyp surgery, making the results primarily generalizable to patients with severe CRSwNP. CDA-AMC notes that the exclusion of patients with mild to moderate forms of the disease, systemic immunosuppressant use, autoimmune diseases, or recent sinonasal surgery raises concerns about the generalizability of the results to the broader population of patients with CRSwNP, particularly those with complex medical histories or multiple comorbidities.
In both trials, placebo was the comparator in evaluating the efficacy of dupilumab in adult patients with CRSwNP. The absence of a biologic comparator, such as mepolizumab, limits the interpretation of the efficacy of dupilumab relative to other biologics.
The SINUS-24 trial did not include any sites in Canada, while the SINUS-52 trial included only 8 Canadian centres. Given that the prevalence and management approaches for CRSwNP may vary by country, the limited inclusion of patients in Canada may reduce the generalizability of the findings to the Canadian context. There was a high degree of overlap between the trial populations and patients in Canada with severe CRSwNP in terms of disease characteristics and comorbidities. Although these patients may not generally reflect the broader population of patients with CRSwNP, the 2 clinical experts indicated that the results were generalizable to the practice setting in Canada.
Endoscopic NPS and NC were the coprimary end points the SINUS trials. These coprimary outcomes were considered clinically relevant, as they measure relevant symptoms of CRSwNP. In the clinical practice setting, the applicability of the NC score and NPS to determine the course of treatment is limited. Although nasal endoscopy was performed at each scheduled visits in the trials, this is not the case in the clinical setting due to the longer wait times for endoscopy and its availability, as noted by the clinical experts consulted for the review. As a result, SNOT-22 is usually preferred and used to determine response to treatment, as it assesses impact of CRSwNP on patients’ HRQoL. Additionally, SNOT-22 is used by ear, nose, and throat specialists to decide when a patient needs sinonasal surgery. Both clinical experts noted that, if a reduction in NPS or NC is not accompanied by improved symptoms, patients are unlikely to continue with treatment. In Canada, response to biologics in the treatment of CRSwNP is based on both subjective and objective improvement in patients’ symptoms as well as endoscopy results, according to the input received from the clinical experts consulted for this review.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined, as outlined by the GRADE Working Group.25,26
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — that is, the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — that is, the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — that is, the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty-of-evidence assessment was the presence or absence of an important improvement in NPS, NC, and SNOT-22, which were considered the most important outcomes for treatment by clinical experts consulted for this review. For the coprimary outcomes of change from baseline in NPS and NS at week 24 or 52, an MID of a decrease in score greater than or equal to 1 was the threshold. For the key secondary outcome, the change from baseline in SNOT-22, an MID of a decrease in score between 8 and 12 was the threshold.
For the GRADE assessments, findings from SINUS 24 and SINUS 52 were considered together for week 24 follow-up because these studies were similar in population, interventions, design, and outcome measures. Outcomes at week 52 were assessed only for the SINUS-52 trial because the SINUS-24 trial did not include follow-up at week 24.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for dupilumab as an add-on maintenance treatment with INCSs in adult patients with severe CRSwNP inadequately controlled by SCSs and/or surgery.
Dupilumab results in a reduction in NPS at 24 and 52 weeks of follow-up when compared with the placebo.
Dupilumab likely results in a reduction in NC at 24 and 52 weeks of follow-up when compared with the placebo (moderate certainty due to serious imprecision).
Dupilumab results in a reduction in SNOT-22 score at 24 and 52 weeks of follow-up when compared with the placebo.
Dupilumab may result in little to no difference in myalgia at 52 weeks of follow-up when compared with the placebo (low certainty due to very serious imprecision).
Dupilumab may result in little to no difference in eosinophilia at 52 weeks of follow-up when compared with the placebo (low certainty due to very serious imprecision).
Dupilumab likely results in little to no difference in nasopharyngitis at 52 weeks of follow-up when compared with the placebo (moderate certainty due to serious imprecision).
Dupilumab likely results in little to no difference in headaches at 52 weeks of follow-up when compared with the placebo. (moderate certainty due to serious imprecision).
Long-Term Extension Studies
There were no relevant long-term extension studies submitted for this review.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
As the SINUS-24 and SINUS-52 trials investigated the use of dupilumab versus placebo, indirect evidence was needed to evaluate comparative effectiveness of dupilumab versus relevant comparators. Mepolizumab was determined to be the relevant comparator for dupilumab for CRSwNP. The aim of this ITC was to evaluate and synthesize the empirical evidence on the clinical efficacy of dupilumab compared with mepolizumab for the treatment of adults with uncontrolled CRSwNP.
Description of Indirect Comparison(s)
One ITC was submitted by the sponsor to evaluate and synthesize empirical evidence on the clinical efficacy of dupilumab compared to mepolizumab for the treatment of adults with uncontrolled CRSwNP.
Table 18: Study Selection Criteria and Methods for ITC Submitted by the Sponsor
Characteristics | Inclusion criteria | Exclusion criteria |
|---|---|---|
Population | Adults ≥ 18 years of age with severe CRSwNP; for studies assessing biologics, patients with nonsevere CRSwNP will also be included | Children < 18 years of age |
Intervention |
|
|
Comparator |
|
|
Outcome | Efficacy outcomes:
Patient-reported outcomes:
Safety and tolerability:
| Relevant outcomes unreported |
Study designs | RCTs (phase II, III) including follow-up or extensions, subgroup analysis, and post hoc analysis |
|
Publication characteristics |
| • -Not published in English |
Selection process | Studies were screened and selected for inclusion based on the population, intervention, comparator, outcomes, and study design (PICOS) time frame criteria. Screening questions were developed based on these criteria. Before the formal screening process, the researchers tested the questions via pilot screening and refined them to ensure appropriateness for use. The screening process involved the following stages: dual screening conducted by 2 independent researchers with any discrepancies resolved by a third researcher. | |
Data extraction process | Data extraction of the included studies was performed in a data extraction template (DET) and developed in Microsoft Excel specifically for this SLR. All data were extracted by 1 researcher and quality-checked by an independent reviewer. When data from a single study were reported in multiple sources (e.g., a poster and a published report) or when trials were linked (e.g., an open-label extension to an RCT), this was captured as a link between the primary and secondary publications. | |
Study limits |
| Journal articles and conference abstracts not available in English |
Quality assessment | The quality assessment of the identified RCT included in the SLR was conducted using the Cochrane Risk-of-Bias Tool.55 | |
CRSwNP = chronic rhinosinusitis; DET = data extraction template; ITC = indirect treatment comparison; LOS = loss of smell; NC = nasal congestion and/or obstruction; NPS = nasal polyp score; PICOS = population, intervention, comparator, outcomes, and study design; QoL = quality of life; RCT = randomized controlled trial; SCS = systemic corticosteroid; SLR = systematic literature review; SNOT = Sino-Nasal Outcome Test; UPSIT = University of Pennsylvania Smell Identification Test; VAS = visual analogue scale.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
ITC Design
Objectives
The ITC was to evaluate the comparative clinical efficacy of dupilumab versus mepolizumab in adult patients with uncontrolled CRSwNP. This ITC aimed to synthesize available RCT evidence in the absence of direct head-to-head trials, facilitating an evidence-based assessment of relative treatment effects.
Study Selection Methods
An SLR was conducted to identify relevant RCT evidence on the clinical efficacy and safety of dupilumab compared with other biologics, including mepolizumab, in adult patients with uncontrolled CRSwNP. The SLR was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.56 Searches were performed in Embase (via OvidSP), MEDLINE (via OvidSP), the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews (via Ovid) to identify articles published in English between January 1980 and May 18, 2020. Phase IV studies were excluded from the search strategy. Following the completion of the SLR, additional publications related to previously included or relevant trials were identified via handsearching to ensure all relevant publications would be captured before conducting the ITC. The strategies for each electronic literature database included a combination of free text and medical subject headings, grouped into the following categories: population, interventions, study design, and limits. The bibliographies of relevant SLRs identified across the electronic database searches were screened to check for any additional relevant references. After the systematic searches and removal of duplicates, title, abstracts, and full-text screening for study selection was based on the predefined patient, intervention, comparator, outcome, and study design criteria (Table 18). The SLR was completed before the primary publication reporting results from the SYNAPSE trial were published. Therefore, this publication was subsequently identified by a handsearch.
Study selection involved a dual-review process, with 2 independent reviewers screening titles, abstracts, and full-text articles to ensure eligibility. Any discrepancies were resolved by a third independent reviewer. Data extraction followed a structured process, where 1 researcher extracted data into a standardized data extraction template, and a second researcher conducted a quality check for accuracy. For quality assessment, the Cochrane Risk-of-Bias Tool was used to evaluate the methodological rigour of included studies, assessing key domains such as selection bias, performance bias, detection bias, attrition bias, and reporting bias. Studies deemed to have a high risk of bias were excluded from the primary ITC analysis.
The primary time points for analysis were 24 and 52 weeks. At 24 weeks, outcomes included changes in NPS, NC, and SNOT-22, along with the proportion of patients achieving 1-point or higher or 2-point or higher improvement in NPS. At 52 weeks, additional assessments included UPSIT scores, SCS use, nasal polyp surgery rates, and responder outcomes for SNOT-22 improvement (≥ 8.9 points). Safety outcomes included the incidence of AEs, SAEs, and treatment discontinuations.
A feasibility assessment was conducted that considered all available studies of patients with CRSwNP that were identified from the SLR and retrieved by hand searches. Three RCTs were considered suitable for inclusion in the ITC to compare dupilumab with mepolizumab, including the SINUS-24 trial, assessing dupilumab up to 24 weeks; the SINUS-52 trial, assessing dupilumab up to 52 weeks; and the SYNAPSE trial, assessing mepolizumab up to 52 weeks.22,57 A key difference in the eligibility criteria of the included trials was that patients were required to have prior surgical treatment in the SYNAPSE trial and but not in the SINUS trials. In the SINUS-24 trial, all patients in the dupilumab every 2 weeks arm received dupilumab in line with the FDA recommendation and data from these patients were used in the 24-week outcomes analysis. In the SINUS-52 trial, patients in the dupilumab every 2 weeks–every 4 weeks arm of the trial received dupilumab every 2 weeks for the first 24 weeks of the study, and data from these patients for the first 24 weeks contributed to the 24-week outcomes analysis. Further, in the SINUS-52 trial, patients in the dupilumab every 2 weeks arm who received dupilumab every 2 weeks throughout the 52-week duration of the trial were included in both the 24-week and the 52-week outcome analyses.
ITC Analysis Methods
The Bucher method was used to conduct ITCs, with placebo as a common comparator.58
For all binary outcomes, the raw number of responders or events and corresponding number evaluated (arm-based data) were used as input data to compute an unadjusted estimate of an odds ratio (OR) in an individual or pooled study for each responder outcome; log-ORs were used in meta-analyses, if appliable, and indirect comparison (which were back-transformed to ORs for final reporting).
Given the differences in study inclusion criteria between the studies, all patients in the SYNAPSE trial would have been eligible for inclusion in SINUS trials, but not all patients in the SINUS trials would have been eligible for inclusion in the SYNAPSE trial. Thus, an analysis of patients in the SINUS trials who were similar to the SYNAPSE trial population (“SYNAPSE-like” population) was reported. This subgroup of patients from the SINUS trials had at least 1 prior surgery, were nonsmokers or former smokers for at least 6 months, and had a VAS symptom score of more than 7. Using the pairwise Bucher ITC approach,58 data from the SYNAPSE-like subgroup from the SINUS trials were compared with those from the ITT population from the SYNAPSE trial. For 24-week outcomes, data from the SYNAPSE-like subgroup patients from the dupilumab every 2 weeks arms of the SINUS-24 and SINUS-52 trials were pooled to give a SYNAPSE-like SINUS subgroup, before comparing with the SYNAPSE trial mepolizumab every 4 weeks arm. For 52-week outcomes, data from only the SYNAPSE-like SINUS-52 trial dupilumab every 2 weeks subgroup were used. Table 19 presents the indirect comparison analysis methods.
A frequentist approach was used in the ITC. Because only 1 dataset was available per treatment arm in each trial, no additional meta-analytical pooling was required. The sponsor applied a fixed-effects model approach.
The main outcomes assessed at 24 and 52 weeks included change from baseline in NPS, NC, UPSIT, SNOT-22, and loss of smell scores, as well as the proportion of patients requiring SCSs or surgery. For binary outcomes, ORs were calculated, while for continuous outcomes, mean differences (MDs) and standardized mean differences (SMDs) were used, depending on the scale of measurement.
Consistency between direct (A versus B) and indirect comparisons (A versus C via B) could not be formally assessed, as there were no direct head-to-head trials of dupilumab and mepolizumab. However, descriptive comparisons of baseline characteristics and placebo arm responses were conducted to check for any major inconsistencies. Heterogeneity within the placebo arms of the SYNAPSE and SINUS trials was evaluated, and any observed differences in placebo response were taken into account during sensitivity analyses.
For trials that used different outcome scales, SMDs were calculated, and when necessary, scales were rescaled to a common range (e.g., NC score and loss of smell scores were converted from a 0 to 10 scale in SYNAPSE to a 0 to 3 scale in SINUS trials). This ensured that results remained comparable across studies.
In addition to the pairwise Bucher ITC, an MAIC of dupilumab versus mepolizumab based on balanced covariates has been conducted as a supporting analysis. The MAIC analyses were conducted on a subset of key outcomes.
For the MAIC analysis, adjustments were made for key covariates, including time since last nasal polyp surgery, baseline NC score, baseline SNOT-22 score, baseline eosinophil count (≥ 300 cells/μL), asthma history, NPS, loss of smell score, and SCS use in the previous year. These characteristics were identified as known effect modifiers by the sponsor. The sponsor justified this selection on prior clinical evidence and expert input.
The weighting of individual patient data for the MAIC was performed using a logistic regression model to estimate the probability of trial enrolment, and the method of moments was applied to reweight the individual patient data from the SINUS trials to align with the population in the SYNAPSE trial. The effective sample size was reported to assess the impact of reweighting, and baseline demographics were compared before and after weighting to assess for successful adjustment on characteristics presented.
Table 19: ITC Analysis Methods
Methods | Description |
|---|---|
Analysis methods | Pairwise Bucher ITC |
Outcomes | Pairwise ITCs were conducted at 52 weeks for CFB NC score, NPS, UPSIT, LOS, SNOT-22, and VAS, as well as binary responder outcomes of NPS improvement ≥ 1, NPS improvement ≥ 2, and SNOT-22 improvement ≥ 8.9 points from baseline outcomes. |
Follow-up time points | Primary outcome assessment conducted at week 52 |
Construction of nodes | Not relevant to a pairwise Bucher ITC |
Sensitivity analyses | Sensitivity analyses based on balanced covariates were conducted using an MAIC that adjusted for time since last nasal polyp surgery, baseline NC, baseline SNOT-22 score, baseline EOSs ≥ 300 cells/L, asthma history, NERD history, baseline age, baseline NPS, baseline LOS score, and SCS use in the year prior. |
Methods for pairwise meta-analysis | Bucher method58 |
CFB = change from baseline; EOS = eosinophil; ITC = indirect treatment comparison; LOS = loss of smell; MAIC = matching-adjusted indirect comparison; NC = nasal congestion and/or obstruction; NERD = nonsteroidal anti-inflammatory drug–exacerbated respiratory tract disease; NPS = nasal polyposis score; SCS = systemic corticosteroid; SNOT-22 = 22-item Sino-Nasal Outcome Test; UPSIT = University of Pennsylvania Smell Identification Test; VAS = visual analogue score.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results of ITC
Summary of Included Studies
Three trials were included in the analysis: SINUS-24, SINUS-52, and SYNAPSE. The SYNAPSE trial required participants to have at least 1 surgery in the previous 10 years for the removal of nasal polyps versus the SINUS-52 trial, which included patients with SCS within the past 2 years, and/or those with a medical contraindication or intolerance to SCS, and/or those with prior surgery for nasal polyps at the screening visit. The SYNAPSE trial also required included patients to be nonsmokers or former smokers (i.e., had quit smoking for > 6 months) and have an overall VAS rhinosinusitis symptom score greater than 7, requirements that were not included in the SINUS trials. Also, most patients in the SYNAPSE trial had baseline eosinophil levels of 150 cells/µL or higher. To account for some differences in the eligibility criteria, pairwise ITCs in matched subgroups (at least 1 prior surgery, nonsmokers or former smokers > 6 months, and VAS > 7 among ITT population of SINUS trials) were performed and reported as a key analysis, referred to as the “SYNAPSE-like” subgroup. Thus, the pairwise ITC of dupilumab versus mepolizumab was conducted in the SYNAPSE-like subgroup of the SINUS trials versus the ITT population of the SYNAPSE trial. To increase the likelihood of maintaining the assumption of homogeneity among included studies in the ITC, the rest of the ITC section will focus on the results from the SYNAPSE-like subgroup analysis.
In the SYNAPSE-like subgroup from the SINUS trials, patients generally presented with lower baseline SNOT-22 total scores (about 55 to 56) than the ITT population in the SYNAPSE trial (64.1), suggesting slightly less severe nasal symptoms. While their NPS was marginally higher (6.0) compared with that in the SYNAPSE trial (5.5), they also had higher rates of prior SCS use within the last year (57% to 63% versus 49%). Comorbid asthma was observed at a similar frequency (67% to 69% versus 71%), but the SYNAPSE population had worse baseline asthma control, as shown by higher 5-question Asthma Control Questionnaire (ACQ-5) scores (2.3 versus 1.6 to 1.7 in the SINUS subgroups). Both groups were comparable in age (roughly 50 to 51 versus 48.8), sex distribution, and blood eosinophil counts.
Table 20: Baseline Characteristics of the SYNAPSE-Like SINUS Subgroups and the SYNAPSE ITT Population
Parameter | SYNAPSE-like SINUS 24 and 52 subgroup used for 24-week outcomesa,b,c (N = 298) | SYNAPSE-like SINUS-52 subgroup used for 52-week outcomesa,b,c (N = 127) | SYNAPSEa,c (N = 407) |
|---|---|---|---|
Mean age, years | 50.6 | 50.7 | 48.8 |
Male, % | 59 | 66 | 65 |
Prior surgery, % | 100 | 100 | 100 |
Prior SCS within 1 year, % | 57 | 63 | 49 |
Mean NPS, 0 to 8 | 6.0 | 6.0 | 5.5 |
Mean NC | 2.6 (scale: 0 to 3) | 2.5 (scale: 0 to 3) | 9.0 (scale: 0 to 10) |
Mean SNOT-22 total score, 0 to 110 | 55.5 | 54.8 | 64.1 |
Mean LOS score | 2.8 (scale: 0 to 3) | 2.8 (scale: 0 to 3) | 9.0 (scale: 0 to 10) |
Mean overall VAS scored | 8.9 | 9.0 | 9.0 |
Mean comorbid asthma, % | 69 | 67 | 71 |
Mean ACQ-5e, 0 to 6 | 1.7 (n = 205) | 1.6 (n = 85) | 2.3 (n = 289) |
Geometric mean blood eosinophil count, cells/L | 0.38 | 0.41 | 0.39 |
ACQ-5 = 5-item Asthma Control Questionnaire; ITT = intention-to-treat; LOS = loss of smell; NC = nasal congestion and/or obstruction; NPS = nasal polyp score; SCS = systemic corticosteroid; SNOT-22 = 22-item Sino-Nasal Outcome Test; VAS = visual analogue score.
aSINUS-24: NCT02912468; SINUS-52: NCT02898454; SYNAPSE: NCT03085797.
bSYNAPSE trial inclusion criteria (≥ 1 prior surgery; nonsmokers or former smokers for ≥ 6 months; VAS ≥ 7) were used to identify a SYNAPSE trial population-like (“SYNAPSE-like”) subgroup of patients from the SINUS trials.
cWeighted mean of all randomized patients from mean reported by treatment arms. (For SYNAPSE, 414 patients were randomized, but the baseline characteristics are available among only 407 patients.)
dSINUS-24 and SINUS-52 assessed VAS rhinosinusitis score only.
eAmong those with comorbid asthma.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 21: Baseline Characteristics of the SYNAPSE-Like Subgroups in the SINUS Trials (Unweighted and Weighted) and the ITT Population in the SYNAPSE Trial (Unweighted only) Identified as Effect Modifiers for Use in MAIC Analysis
Parameter | Unweighted | Weighted | |||||
|---|---|---|---|---|---|---|---|
SYNAPSE (N = 407) | SYNAPSE-like SINUS-52 subgroup used for 52-week outcomes (N = 126a) | SYNAPSE-like SINUS-24 and -52 subgroup used for 24-week outcomes (N = 295a) | SYNAPSE-like SINUS-52 subgroup base caseb (ESS = 58.7) | SYNAPSE-like SINUS-52 subgroup sensitivity analysisc (ESS = 40.2) | SYNAPSE-like SINUS-24 and 52 subgroup base caseb (ESS = 174.1) | SYNAPSE-like SINUS-24 and 52 subgroup sensitivity analysisc (ESS = 150.5) | |
Mean age, years | 48.8 | 50.7 | 50.6 | 48.9 | 48.7 | 48.4 | 48.7 |
Time since last nasal polyp surgery, year | 4.0 | 8.3 | 7.3 | 4.0 | 4.0 | 4.0 | 4.0 |
Prior SCS within 1 year, % | 48 | 63 | 57 | 70 | 50 | 61 | 48 |
Mean NPS, 0 to 8 | 5.5 | 6.0 | 6.0 | 6.1 | 5.5 | 5.8 | 5.5 |
Mean NC | 2.7d | 2.5 | 2.6 | 2.7 | 2.7 | 2.7 | 2.7 |
Mean SNOT-22 total score, 0 to 110 | 64.1 | 54.8 | 55.5 | 64.0 | 64.0 | 64.0 | 64.0 |
Mean LOS score | 2.9d | 2.8 | 2.8 | 2.9 | 2.9 | 2.9 | 2.9 |
Comorbid asthma, % | 71 | 67 | 69 | 71 | 71 | 71 | 71 |
NERD history, % | 26 | 33 | 35 | 27 | 27 | 26 | 26 |
Blood eosinophil count ≥ 300 cells/L, % | 68 | 70 | 67 | 68 | 68 | 68 | 68 |
ESS = effective sample size; ITT = intention-to-treat; LOS = loss of smell; MAIC = matching-adjusted indirect comparison; NC = nasal congestion and/or obstruction; NERD = nonsteroidal anti-inflammatory drug–exacerbated respiratory tract disease; NPS = nasal polyp score; SCS = systemic corticosteroid; SNOT-22 = 22-item Sino-Nasal Outcome Test.
aBaseline data presented here were for the patients with nonmissing baseline data in the covariates adjusted in the MAIC analysis.
bThe base case adjusted for 6 variables (time since last nasal polyp surgery, baseline NC, baseline SNOT-22 score, baseline blood eosinophil count ≥ 300 cells/L, asthma history, and nonsteroidal anti-inflammatory drug–exacerbated respiratory tract disease history).
cThe sensitivity analysis adjusted for 10 variables (all 6 base case variables as well as baseline age, baseline NPS, baseline LOS score, and SCS use in the year prior).
dScoring for NC and LOS ranged from 0 to 3 (0 = no symptoms to 3 = severe symptoms) in the SINUS trials and from 0 to 10 (0 = not troublesome to 10 = worst thinkable, troublesome) in the SYNAPSE trial. As the scale was smaller in SINUS, it was not appropriate to “upscale” the scale (0 to 3) in the SINUS trials to match the scale (0 to 10) in the SYNAPSE trial; instead, the scale in the SYNAPSE trial was “downscaled” to that in the SINUS trials.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 22: Description of Important Differences Across Trials for Key Characteristics
Characteristics | SINUS-24 and SINUS-52 | SYNAPSE | Description and handling of potential effect modifiers |
|---|---|---|---|
Disease severity | Patients must be experiencing severe disease. At screening, patients were required to have a bilateral endoscopic nasal polyp score of at least 5 (maximum 8), with a minimum score of 2 for each nostril, and exhibit at least 2 of the following symptoms: nasal congestion or obstruction (patient-assessed symptom severity score of at least 2 of 3, and a weekly average score of at least 1 at randomization; 0 = no symptoms, 1 = mild, 2 = moderate, and 3 = severe) and either loss of smell or nasal discharge (anterior or posterior). These criteria resulted in a study population with severe disease. | Patients must be experiencing severe disease, defined as recurrent, refractory, severe, bilateral nasal polyp symptoms (nasal obstruction symptom visual analogue scale [VAS] score of > 5 [maximum 10]) and eligibility for repeat nasal surgery (overall symptoms VAS score > 7 and endoscopic nasal polyps score of ≥ 5 [maximum 8], with a minimum score of 2 in each nasal cavity), despite standard of care treatment. | Key scenario analysis was conducted and reported, consisting of a SYNAPSE-like subgroup population of the SYNAPSE trial population to address difference in trial populations. The MAIC analyses adjusted for 6 variables (time since last nasal polyp surgery, baseline NC score, baseline SNOT-22 score, baseline EOS ≥ 300 cells/L, asthma history, and NERD history) and a sensitivity analysis adjusted for 10 variables (all 6 base case variables as well as baseline age, baseline NPS, baseline LOS score, and SCS use in the year prior). In addition, an MAIC of dupilumab versus mepolizumab based on balanced covariates was conducted as a scenario analysis. |
Treatment history | Patients were required to have had intranasal corticosteroid therapy before randomization and had received SCSs in the preceding 2 years (or had a medical contraindication or intolerance to SCSs) or previous sinonasal surgery. | Patients had to have at least 1 nasal surgery (defined as any incision [cutting open] of the paranasal sinuses and removal of polyp tissue from the nasal cavity [polypectomy] and the sinuses) in the past 10 years and be on maintenance therapy. | |
Trial eligibility criteria | Eligible patients were aged 18 years or older with bilateral nasal polyps and symptoms of chronic rhinosinusitis despite intranasal corticosteroid therapy before randomization and had received SCSs in the preceding 2 years (or had a medical contraindication or intolerance to SCSs) or previous sinonasal surgery. | Eligible patients were aged 18 years or older with recurrent, refractory, severe, bilateral nasal polyp symptoms (nasal obstruction symptom visual analogue scale [VAS] score of > 5 [maximum 10]) and were eligible for repeat nasal surgery (overall symptoms VAS score > 7 and endoscopic nasal polyps score of ≥ 5 [maximum 8], with a minimum score of 2 in each nasal cavity), despite standard of care treatment. | Given the differences in study inclusion criteria, all patients in the SYNAPSE trial would have been eligible for inclusion in the SINUS-24 and SINUS-52 trials, but not all patients in the SINUS-24 and SINUS-52 trials would have been eligible for inclusion in the SYNAPSE trial. Thus, inclusion criteria in the SYNAPSE trial were used to identify a SYNAPSE trial population-like (“SYNAPSE-like”) subgroup of patients from the SINUS trials, which included patients who had at least 1 prior surgery, were nonsmokers or former smokers for at least 6 months, and had a VAS of more than 7. |
Dosing | In the SINUS-24 trial, patients were randomly assigned (1:1) to dupilumab 300 mg every 2 weeks or to matching placebo. In the SINUS-52 trial, patients were randomly assigned (1:1:1) to dupilumab 300 mg every 2 weeks for 52 weeks (group A), the same schedule for the first 24 weeks, followed by dupilumab 300 mg every 4 weeks (group B), or placebo (group C). In both trials, adjunct noninvestigational medicinal products were available to patients, including twice daily mometasone furoate nasal spray (50 mcg/actuation). Rescue medication available included nasal or systemic antibiotics (maximum 2 weeks), short course prednisone or prednisolone, and sinonasal surgery. | Following a 4-week run-in period, patients received mepolizumab at 100 mg subcutaneously or placebo once every 4 weeks (using a safety syringe), in addition to standard of care (mometasone furoate intranasal spray for at least 8 weeks before screening and during the study, saline nasal irrigations, SCSs or antibiotics, or both), as required, for 52 weeks. The SYNAPSE trial also allowed for rescue therapy with sinonasal surgery or oral corticosteroids, as needed. | For the placebo arms, the SYNAPSE and SINUS-52 trials showed some variation in the observed CFB at week 52 for SNOT-22 total score in the placebo arms, with a greater change observed in SYNAPSE (–15.7 versus −13.3), which also had a higher baseline score in the placebo arm (mean 64.4) compared with the SINUS-52 trial (mean 53.5). Differences were also observed across the placebo arms of the SYNAPSE trial and the SINUS-52 trial in the proportion of patients with improvement in NPS ≥ 1 point (28% versus 21.6%, respectively) and in NPS ≥ 2 points (26% versus 11.8%, respectively). Dosing was not identified as a significant treatment modifier. |
Definitions of end points | The coprimary end points in both studies were change from baseline in both endoscopic NPS and nasal congestion severity (based on monthly average of daily score recorded by patients) at week 24. Key secondary end points were change from baseline at week 24 in sinus opacification, assessed by Lund-Mackay CT score (third coprimary end point in Japan); patient-reported total symptom score (a composite severity score consisting of the sum of daily symptoms of nasal congestion, loss of smell, and anterior or posterior rhinorrhea); daily loss of smell or smell impairment; SNOT-22 score; and UPSIT smell test. Multiplicity-tested key secondary end points for the SINUS-52 trial were change from baseline at week 52 in NPS, nasal congestion, and SNOT-22 score (group A alone). NPS and Lund-Mackay CT scan scoring was done centrally by masked review of the video recordings of standardized endoscopies (for NPS) and sinus images (for Lund-Mackay CT). | The coprimary end points were change from baseline in total endoscopic nasal polyp score at week 52 and in mean nasal obstruction VAS score during weeks 49 to 52. Total endoscopic nasal polyp score was the sum of left and right nostril scores ranging from 0 (no polyps) to 4 (large polyps causing complete obstruction of the inferior meatus) for each nostril, giving a total score of up to 8. The VAS score could range from 0 to 10, as used in previous studies of nasal polyps. The key secondary end point was time to first nasal surgery until week 52. Other secondary end points were the proportion of patients requiring SCS for nasal polyps until week 52 and change from baseline in: mean overall VAS symptom score during weeks 49 to 52, SNOT-22 total score at week 52, mean composite VAS score (combining scores for nasal obstruction, nasal discharge, throat mucus, and loss of smell) during weeks 49 to 52, and mean VAS score for loss of smell during weeks 49 to 52. | Outcomes were assessed using different scales in the SYNAPSE trial and the SINUS trials and were therefore compared by converting to standardized mean differences in the analysis. The MAIC analyses were conducted on a subset of key outcomes (NPS at week 24, and NPS, NC score, and SNOT-22 at week 52) and also compared the SYNAPSE-like subgroup from the SINUS studies with the ITT population from the SYNAPSE trial. |
Clinical trial setting and study design | Trials were multinational, multicentre, randomized, double-blind, placebo-controlled, parallel-group studies. The SINUS-24 trial was conducted in 67 hospitals or clinical centres in 13 countries (Bulgaria, Czechia, France, Germany, Hungary, Italy, the Netherlands, Poland, Romania, Ukraine, Russia, the UK, and the US). The SINUS-52 trial was conducted in 117 hospitals or clinical centres in 14 countries (Argentina, Australia, Belgium, Canada, Chile, Israel, Mexico, Portugal, Russia, Spain, Sweden, Turkey, Japan, and the US). | This trial was a randomized, double-blind, placebo-controlled, parallel-group, phase III trial done at 93 centres, mainly hospitals, in 11 countries (Argentina, Australia, Canada, Germany, the Netherlands, South Korea, Romania, Russia, Sweden, the UK, and the US). | NA |
CFB = change from baseline; EOS = eosinophil; ITT = intention-to-treat; LOS = loss of smell; MAIC = matching-adjusted indirect comparison; NA = not applicable; NC = nasal congestion and/or obstruction; NERD = nonsteroidal anti-inflammatory drug–exacerbated respiratory tract disease; NPS = nasal polyp score; SCS = systemic corticosteroid; SNOT-22 = 22-item Sino-Nasal Outcome Test; VAS = visual analogue scale.
Source: Bachert et al. (2019) for the SINUS-24 and SINUS-52 trials,32 Han et al. (2021) for the SYNAPSE trial.59 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Efficacy
Given the differences in the populations in the SINUS trials and the SYNAPSE trial, we present the analysis of interest, which was conducted using SYNAPSE-like subgroup data (N = 298 for analyses at 24 weeks and N = 127 for analysis at 52 weeks) from the SINUS-52 trial. The subgroup included patients with at least 1 prior surgery, nonsmokers or former smokers for more than 6 months, and VAS greater than 7 among ITT population that aligned with the ITT population in the SYNAPSE trial at 52 weeks as base case for SNOT-22 improvement ≥ 8.9 points and NPS improvement ≥ 1-point. Of note, this SYNAPSE-like subgroup of the SINUS-52 trial had lower baseline mean SNOT-22 scores than in the ITT population in the SYNAPSE trial (55.1 versus 64.1).32
Included in the following paragraphs are the results of the analysis (ITC based on the comparison of the SYNAPSE-like subgroup in the SINUS trials) from the SINUS-24 and SINUS-52 trials (n = 298) and from the SINUS-52 trial (n = 127), in which the inclusion criteria from the SYNAPSE trial were applied.
Nasal Polyps Score
In the SYNAPSE-like subgroup, multiple analyses for NPS favour dupilumab over mepolizumab. In the Bucher ITC at 52 weeks, the continuous outcome showed an MD of –1.35 (95% CI, –2.14 to –0.56) and a median difference (MeD) of ██))████))████))██ versus mepolizumab. The corresponding responder analysis at 52 weeks indicated that the OR for achieving a 1-point or greater improvement was 4.36 (95% CI, 1.71 to 11.13) and for a 2-point or greater improvement was 2.85 (95% CI, 1.06 to 7.66). The MAIC analysis within the SYNAPSE-like subgroup provided a continuous outcome at 24 weeks with a base case MD of –1.93 (95% CI, –2.48 to –1.38) and a sensitivity analysis MD of –1.90 (95% CI, –2.51 to –1.29) versus mepolizumab; at 52 weeks, the MAIC sensitivity analysis reported an MD of –1.82 (95% CI, –3.46 to –0.17).
Nasal Congestion and/or Obstruction
In the SYNAPSE-like subgroup, the Bucher ITC analysis of NC at 52 weeks indicated that the continuous outcome favoured dupilumab over mepolizumab, with an adjusted MD of –0.39 (95% CI, –0.77 to –0.01). In addition, when expressed as a standardized MD, the estimate was –0.48 (95% CI, –0.90 to –0.06). MAIC analyses for NC at 52 weeks were also reported within the SYNAPSE-like subgroup comparison; the base case yielded an MD of –0.54 (95% CI, –1.01 to –0.07) versus mepolizumab, and the sensitivity analysis reported an MD of –0.48 (95% CI, –1.19 to 0.23).
22-Item Sino-Nasal Outcome Test
For the SNOT-22 outcome assessing HRQoL, the Bucher ITC analysis in the SYNAPSE-like subgroup at 52 weeks produced an unadjusted MD of –4.13 (95% CI, –12.24 to 3.98). Additional analyses using MeD at 52 weeks were also reported (Table 24). The MeD for the SYNAPSE-like subgroup comparison was ██))████))████))██.
Table 23: Bucher ITC Estimates for Dupilumab Versus Mepolizumab on CFB in Continuous Outcomes at 52 Weeks
Outcome | Covariate adjustment | Effect measure | SYNAPSE-like subgroup |
|---|---|---|---|
NPS | Adjusted | MD (95% CI) | −1.35 (−2.14 to −0.56) |
NC | Adjusted | SMD (95% CI) | −0.48 (−0.90 to −0.06) |
NC | Adjusted | MDa (95% CI) | −0.39 (−0.77 to −0.01) |
LOS | Unadjusted | SMD (95% CI) | −0.76 (−1.19 to −0.33) |
SNOT-22 | Unadjusted | MD (95% CI) | −4.13 (−12.24 to 3.98) |
CFB = change from baseline; CI = confidence interval; ITC = indirect treatment comparison; LOS = loss of sense of smell; MD = mean difference; NC = nasal congestion and/or obstruction; NPS = nasal polyp score; SMD = standardized mean difference; SNOT-22 = 22-item Sino-Nasal Outcome Test.
aThe estimate of MD in a 0 to 10 scale from the SYNAPSE trial was converted to 0 to 3 range (same as in the SINUS-52 trial) by dividing by 3.33 before performing ITC.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Loss of Sense of Smell Score
The Bucher ITC analysis for the loss of sense of smell score at 52 weeks demonstrated an unadjusted standardized mean difference of –0.76 (95% CI, –1.19 to –0.33), favouring dupilumab over mepolizumab. No additional MAIC or responder analyses for loss of smell score were reported, yet the available continuous outcome data robustly support the enhanced efficacy of dupilumab in restoring the sense of smell (Table 24 and Table 25).
Table 24: Bucher ITC Estimates for Dupilumab Versus Mepolizumab on CFB in Continuous Outcomes at 52 Weeks
Outcomea | Effect measureb | SYNAPSE-like subgroup | ITT population |
|---|---|---|---|
NPS | ██))██ | ██))██ | ██))██ |
NC | ██))██ | ██))██ | ██))██ |
NC | ██))██ | ██))██ | ██))██ |
VAS | ██))██ | ██))██ | ██))██ |
SNOT-22 | ██))██ | ██))██ | ██))██ |
CFB = change from baseline; CI = confidence interval; ITC = indirect treatment comparison; ITT = intention-to-treat; MeD = median difference; NC = nasal congestion and/or obstruction; NPS = nasal polyp score; SMeD = standardized median difference; SNOT-22 = 22-item Sino-Nasal Outcome Test; VAS = visual analogue scale.
aAll data were measured at 52 weeks.
bAdjusted MeDs from both the SINUS-52 and SYNAPSE trials were used, where the normality of MeDs was assumed (i.e., MeDs were treated as if they were MDs so that the standard errors of the MeDs were computed using the 95% CI of MeDs).
cThe estimate of MeD in a 0 to 10 scale from the SYNAPSE trial was converted to 0 to 3 range (same as in the SINUS-52 trial) by dividing by 3.33 before performing ITC.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 25: Bucher ITC Estimates for Dupilumab Versus Mepolizumab on Binary Outcomes at 52 Weeks
Outcome | SYNAPSE-like subgroup, OR (95% CI) |
|---|---|
NPS improvement ≥ 1 | 4.36 (1.71 to 11.13) |
SNOT-22 improvement ≥ 8.9 | 3.37 (1.10 to 10.32) |
SCS use for nasal polyps | 0.32 (0.10 to 0.99) |
Surgery for nasal polyps | 0.50 (0.05 to 4.63) |
CI = confidence interval; ITC = indirect treatment comparison; NPS = nasal polyp score; OR = odds ratio; SCS = systemic corticosteroid; SNOT-22 = 22-item Sino-Nasal Outcome Test.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 26: Estimates of Mean Differences of Dupilumab Versus Mepolizumab in the MAIC and the SYNAPSE-Like Subgroup Comparison
Outcome | SYNAPSE-like subgroup comparison, MD (95% CI) (pairwise Bucher ITC) | MAIC, MD (95% CI) | |
|---|---|---|---|
Base casea | Sensitivity analysisb | ||
ESS, 24 weeks | NA | 174 | 151 |
ESS, 52 weeks | NA | 59 | 40 |
NPS at 24 weeks | −1.38 (−1.86 to −0.90) | –1.93 (–2.48 to –1.38) | –1.90 (–2.51 to –1.29) |
NPS at 52 weeks | −1.35 (−2.14 to −0.56) | −2.31 (−3.41, −1.21) | –1.82 (–3.46 to –0.17) |
NC score at 52 weeksc | –0.39 (0.77 to –0.01) | –0.54 (–1.01 to –0.07) | –0.48 (–1.19 to 0.23) |
SNOT-22 at 52 weeks | –4.13 (–12.24 to 3.98) | –4.33 (–15.31 to 6.66) | –5.28 (–22.97 to 12.42) |
CI = confidence interval; ESS = effective sample size; MAIC = matching-adjusted indirect comparison; MD = mean difference; NA = not applicable; NC = nasal congestion/obstruction; NPS = nasal polyp score; SNOT-22 = 22-item Sino-Nasal Outcome Test.
aThe base case adjusted for 6 variables (time since last NP nasal polyp surgery, baseline NC, baseline SNOT-22 score, baseline eosinophils ≥ 300 cells/L, asthma history, and nonsteroidal anti-inflammatory drug–exacerbated respiratory tract disease history).
bThe sensitivity analysis adjusted for 10 variables (all 6 base case variables as well as baseline age, baseline NPS, baseline loss of smell score, and SCS use in the year prior).
cScoring for NC ranged from 0 to 3 (0 = no symptoms to 3 = severe symptoms) in the SINUS trials and from 0 to 10 (0 = not troublesome to 10 = worst thinkable, troublesome) in the SYNAPSE trial. As the scale was smaller in the SINUS trials, it was not appropriate to “upscale” the SINUS trials scale (0 to 3) to match the SYNAPSE trial scale (0 to 10); instead, the scale in the SYNAPSE was “downscaled” to that in the SINUS trials.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Harms
Harms data were not captured as part of the ITC that informed efficacy in the pharmacoeconomic model.
Critical Appraisal of ITC
The sponsor conducted an SLR to identify relevant studies comparing dupilumab and mepolizumab for the treatment of adults with uncontrolled CRSwNP. While the search encompassed articles up to May 18, 2020, and additional handsearching was done to capture missed evidence, it remains unclear whether any key studies published after May 2020 were missing. The search and selection strategy excluded phase IV studies, despite the sponsor’s drug being commercially available and with the indication under review approved for several years (since 2020). Therefore, there is a risk of bias due to missing evidence in the synthesis. The data extraction involved a single reviewer with subsequent quality checks rather than the dual extraction typical of best-practice guidelines, potentially increasing the risk of missing or misinterpreting data. Moreover, the risk-of-bias assessment was applied at the study level and did not clarify how studies with a high risk of bias would be handled in subsequent analyses.
The ITC relied on the Bucher method with placebo as the common comparator. While this approach is well established, it employs fixed-effects models, which assume minimal heterogeneity between studies (an assumption that may not hold, given notable differences in patient populations) and can result in narrower CIs than would occur using methods allowing for more heterogeneity. Therefore, the Bucher analysis might exclude the null (i.e., show a significant difference between treatments), whereas a method that allowed for more heterogeneity might not. This potential overestimation of precision is particularly relevant for outcomes where the confidence interval under the fixed-effects model is close to the null value, such as the NC score in this analysis (e.g., 95% CI for adjusted MD, –0.77 to –0.01), where a random-effects model incorporating potential heterogeneity might yield a nonsignificant result. Further, the point estimates for differences in the NC score and SNOT-22, 2 of the outcomes of interest in the clinical review, were not as large as established MIDs.46
The sponsor attempted to address differences in study populations among the SINUS and SYNAPSE trials by focusing on a SYNAPSE-like subgroup within the SINUS trials (patients with at least 1 prior surgery, nonsmokers or former smokers, and VAS symptom score > 7), which is a methodological strength that reduces clinical heterogeneity in the analysis. However, restricting the population in this way meant that less than half of the SINUS trial population met these tighter criteria, leaving an evidence gap regarding patients who would not have been eligible for the SYNAPSE trial. Therefore, the available comparative evidence is limited to those with prior surgery, nonsmokers or former smokers, and VAS symptom scores greater than 7.
Furthermore, the sponsor performed an MAIC as a sensitivity analysis, adjusting for key baseline covariates (e.g., time since last nasal polyp surgery, baseline NC score, baseline SNOT-22 score, asthma history) to reduce imbalance between trials. The results of the MAIC sensitivity analyses were in line with the SYNAPSE-like subgroup analysis. Typical limitations of MAICs apply to the sensitivity analysis: the effective sample size was reduced, increasing uncertainty and limiting power. Additionally, the baseline differences (e.g., in SNOT-22 scores) were not fully eradicated even after reweighting, and the lack of a formal meta-regression analysis leaves open the possibility of residual confounding. However, the MAICs analyses were generally in line with the SYNPSE-like results.
A practical challenge arose from the distinct measurement scales used in the SINUS versus SYNAPSE trials for key outcomes such as NC (0 to 3 in the SINUS trials; 0 to 10 in the SYNAPSE trials); the sponsor “downscaled” scores from the SYNAPSE trial by dividing by 3.33. While this is a common strategy, it assumes a linear relationship across 2 inherently different scales, which may not perfectly reflect clinical reality. Finally, the sponsor’s ITC focused on clinical efficacy outcomes, with no discussion of safety data; this omission is notable given the importance of such outcomes in decision-making.
Despite these limitations, the direction of effect across the Bucher ITC, SYNAPSE-like subgroup analyses, and MAIC favoured dupilumab over mepolizumab at both 24 and 52 weeks for key efficacy outcomes such as NPS and NC score. However, the finding for NC carries substantial uncertainty, given that its statistical significance might be dependent on the fixed-effects model assumption and the comparison itself relies on potentially problematic scale conversion. Furthermore, wide CIs (observed particularly for the SNOT-22 mean difference and several responder outcomes such as NPS improvement ≥ 2 points or need for surgery or SCSs), the potential differences that remained between the SYNAPSE-like subgroup of the SINUS trials and the population in the SYNAPSE trial, and the assumptions involved in the fixed-effects models, downscaling, and MAIC inevitably introduce residual uncertainty. Collectively, these issues highlight a reasonable but imperfect comparison, with consistency of directionality supporting a dupilumab advantage but with limitations that should be considered when interpreting the results and generalizing them to the wider CRSwNP population.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
The sponsor submitted 5 studies31,60-63 to address the gap in evidence identified in the pivotal trial. Specifically, 231,63 of the 5 studies were submitted to address the gap in long-term efficacy of dupilumab. Of these studies, CDA-AMC included only the study by van der Lans et al.31 as evidence that may address a gap in the pivotal evidence reported in Section 2. The gap identified by the sponsor was a lack of long-term data, with the study providing evidence of patients with CRSwNP treated with add-on dupilumab for up to 96 weeks.
Description of Studies
The study by van der Lans et al. was described as a real-life, prospective, observational cohort study conducted in a single tertiary referral centre (i.e., Department of Otorhinolaryngology and Head and Neck Surgery, University of Amsterdam) and was submitted to demonstrate the long-term efficacy and safety of dupilumab as treatment for CRSwNP in an adult population. Upon further review by the CDA-AMC review team, it was determined that this study31 reports on data from a registry and is more accurately described as an observational retrospective study.
Populations
A total of 228 patients were included. Included patients were adults (at least 18 years of age) with severe CRSwNP with an indication for biologic treatment as per the 2020 European position paper on rhinosinusitis and nasal polyps (EPOS) criteria2 who started dupilumab as their primary biologic add-on treatment in a tertiary referral centre. They were included if they had at least 48 weeks of follow-up data in the registry as of December 2022. No exclusion criteria were reported in the study publication.
Interventions
Patients self-administered dupilumab initially at a dosage of 300 mg every 2 weeks. The frequency of dosing was tapered based on therapeutic effect, prolonging the time between doses beyond 2 weeks over time. More specifically, the publication described this as follows: “stepwise tapering by interdose interval prolongation of 2 weeks conditional to therapeutic effect was undertaken in patients with moderate-to-excellent response as per EPOS 2020 criteria,2 with minimal 24-week interim periods.” No further description of dose reduction was provided by the sponsor. Of note, by week 48, less than 20% of patients were treated with dupilumab at the recommended dosage approved by Health Canada of 300 mg every 2 weeks.22,31
Outcomes
The coprimary outcomes were NPS, SNOT-22, and Sniffin Sticks 12 smell identification test, and asthma control test. Other outcomes were modified Lund-Kennedy score, peak nasal inspiratory flow, EPOS 2020 CRS control, European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) 2023 biological response, and information on tapering of the dupilumab dose interval. Outcomes identified as clinically relevant for this review include NPS and SNOT-22 and are thus reported in this summary.
Statistical Analysis
One-way repeated measures analysis of variance (ANOVA) of coprimary outcome mean scores was performed to determine the differences across observation time points. Post hoc analysis with multiple pairwise t tests between observations was performed, with P values adjusted using the Bonferroni multiple testing correction method. Statistical significance was assumed for P values of 0.05 or less.
Results
Patient Disposition
Limited patient disposition data were reported in the study publication. Treatment discontinuation occurred in 31 (13.3%) of patients; discontinuation was temporary in 7 patients, definite in 17 patients, and unknown in 7 patients. Overall, 11 (4.8%) patients discontinued therapy due to insufficient response and 6 (2.6%) patients discontinued treatment due to AEs. Follow-up until 48 weeks was available for n = 214 patients and for up to 96 weeks for n = 99 patients.
Baseline Characteristics
Patients were predominantly male (63.7%) with a mean age of 51 years (range, 18 to 90). All patients had undergone prior sinonasal surgery (except 1 patient who was unfit for surgery), with 117 (51.3%) and 39 (17.1%) patients having at least 3 and 5 surgeries, respectively. At baseline, 205 (89.9%) patients were anosmic, 184 (80.7%) reported comorbid asthma, and 85 (40.6%) reported NSAID-ERD. EPOS 2020 CRS control was insufficient in 144 (69.2%) patients.
Exposure to Study Treatments
The proportion of participants receiving dupilumab at a dosage interval greater than that consistent with the indication increased over time. At week 24, more than 75% of patients were taking dupilumab 300 mg every 4 weeks. At 48 weeks, more than 80% were taking dupilumab 300 mg at an interval of every 4 or every 6 weeks. At 96 weeks, 50% of participants were receiving dupilumab at an interval of every 8 or 12 weeks. No information on concomitant medication use, cointerventions, or confounding treatments was included in the study publication.
Efficacy
A summary of key efficacy outcomes is provided in Table 27.
Harms
There were 6 (2.6%) patients who discontinued treatment due to AEs, of whom 4 definitely discontinued and 2 discontinued temporarily. Persistent hypereosinophilia occurred in 3 of the 6 patients, without signs or symptoms of hypereosinophilic syndrome. All 3 patients switched to another biologic therapy. One of the 6 patients developed pericarditis, and 2 patients experienced arthralgia and myalgia. Of these, 2 patients reinitiated dupilumab.
Table 27: Summary of Efficacy Outcomes
Outcome | Baseline (0 weeks) N = 228 | 48 weeksa N = 214 | 96 weeksb N = 99 |
|---|---|---|---|
NPS (range, 0 to 8), mean (SD) | 5.3 (1.9) | 1.4 (1.8) | 1.3 (1.7) |
0, n (%) | 12 (5.3) | 112 (52.2) | 48 (48.4) |
1, n (%) | 3 (1.3) | 26 (12.1) | 16 (15.8) |
2, n (%) | 8 (3.5) | 30 (14.0) | 18 (18.6) |
3 to 4, n (%) | 35 (15.4) | 31 (14.5) | 8 (8.4) |
5 to 6, n (%) | 130 (57.0) | 15 (6.8) | 8 (8.4) |
7 to 8, n (%) | 40 (17.5) | 1 (0.5) | 0 (0) |
1-point change from baseline, n (%) | — | 191 (89.4) | 86 (87.0) |
2-point change from baseline, n (%) | — | 189 (88.4) | 82 (83.2) |
SNOT-22 (range, 0 to 110), mean SD) | 53.6 (19.6) | 20.2 (15.4) | 21.2 (15.6) |
NPS = nasal polyp score; SD = standard deviation; SNOT-22 = 22-item Sino-Nasal Outcome Test.
aAt 48 weeks, more than 80% were taking dupilumab 300 mg at an interval of every 4 or every 6 weeks.
bAt 96 weeks, 50% of participants were receiving dupilumab at an interval of every 8 or 12 weeks.
Source: van der Lans et al.31
Harms
There were 6 (2.6%) patients who discontinued treatment due to AEs, of whom 4 definitely discontinued and 2 discontinued temporarily. Persistent hypereosinophilia occurred in 3 of the 6 patients, without signs or symptoms of hypereosinophilic syndrome. All 3 patients switched to another biologic therapy. One of the 6 patients developed pericarditis, and 2 patients experienced arthralgia and myalgia. Of these, 2 patients reinitiated dupilumab.
Critical Appraisal
The study was an observational, retrospective, noncomparative study of adults with severe CRSwNP. Almost all patients had prior sinosinal surgery. The study was designed to increase the dosage interval (i.e., change from every 2 weeks to every 4 weeks, up to every 12 weeks over the duration of the data available), which is inconsistent with the indication and recommended dosage for dupilumab for CRSwNP under review. Therefore, results from this study do not address the gap in evidence identified by the sponsor, as the study does not provide evidence for long-term effectiveness or safety questions about dupilumab for the indication under review, i.e., dupilumab 300 mg every 2 weeks. Safety findings are overly optimistic, given that the drug exposure was lower than the recommended dosage. Efficacy findings are not relevant to this review because they are inconsistent with the indication. Further, the findings may also be overly optimistic given that patients successfully maintained treatment for at least 48 weeks to be included in the study. Additionally, results may be overly optimistic because patients and physicians had knowledge of treatment assignments and several outcomes were self-assessed. The lack of a control group also limits causal inference.
Discussion
Summary of Available Evidence
The SINUS-24 trial (N = 276) and the SINUS-52 trial (N = 448) were randomized, double-blind, multicentre, placebo-controlled, phase III trials and were included in the sponsor’s SLR. Both trials evaluated the efficacy and safety of dupilumab 300 mg every 2 weeks as an add-on maintenance treatment with INCSs in adult patients with severe CRSwNP inadequately controlled by SCS and/or surgery. Patients were randomized at 1:1 (or 1:1:1 in the SINUS-52 trial) to dupilumab or placebo, and randomization was stratified by the presence of comorbid asthma and/or NSAID-ERD, prior sinonasal surgery for nasal polyps, and country.
The coprimary outcomes in both trials were the change from baseline to week 24 in NPS and the NC score. Other efficacy outcomes were the change from baseline in TSS, daily symptoms of decreased or loss of sense of smell, change from baseline in SNOT-22 score, and change from baseline in the proportion of patients who received either SCS or sinonasal surgery as rescue therapy. The SINUS-52 trial also included assessments at week 52. A prespecified hierarchical testing procedure was used to control the overall type I error rate for testing the coprimary outcomes and selected secondary end points, including SNOT-22 score and decreased or loss of sense of smell. In the SINUS-24 trial, the mean age of patients was 50 ██))████))████))██, the mean time since first diagnosis of CRSwNP was 11 years ██))████))██ and 198 (71.7%) patients had previous nasal polyp surgery. These baseline characteristics were similar for the SINUS-52 trial, where the mean age of patients was 51.6 ██))████))████))██ and the mean time since first diagnosis of CRSwNP was 10.9 ██))████). Fewer patients (58.3%) had previous nasal polyp surgery in the SINUS-52 trial.
The key limitations of the body of evidence were a lack of head-to-head evidence of dupilumab versus other biologics such as mepolizumab and a lack of safety and efficacy data beyond 52 weeks.
A sponsor-submitted ITC estimated the comparative effectiveness of dupilumab and mepolizumab for the indication under review. Of note, the ITC was focused on a subgroup of patients from the SINUS trials with prior nasal polyp surgery. As a consequence, there is no comparative evidence for patients with CRSwNP without prior nasal polyp surgery.
There was no evidence of efficacy and safety of dupilumab beyond 52 weeks in the submission based on the pivotal trials. The sponsor submitted a single-centre observational cohort study (van der Lans et al.)31 with data up to 96 weeks to address the lack of long-term efficacy and safety based on the evidence from the systematic review. The study was not considered relevant to the review because the majority of patients were receiving dupilumab at intervals greater than 2 weeks at 48 weeks and beyond.
Interpretation of Results
Efficacy
Input from patients and clinicians indicated that the most important treatment goals for patients with severe CRSwNP are to prevent disease progression, reduce severity of symptoms, improve HRQoL, and reduce the need for surgery. Input from both patients and clinical experts indicated that the disease often becomes refractory to current treatment options, particularly INCSs and surgery, and available treatment cannot reverse the course of the disease or modify the underlying pathophysiology of CRSwNP. Consistent with the clinical expert input, the patient group agreed that new therapies that are better tolerated and more effective, and that can improve HRQoL more than the current standard of care, are needed.
The efficacy of dupilumab as an add-on maintenance treatment with INCSs in adult patients with severe CRSwNP inadequately controlled by SCSs and/or surgery was assessed in 2 pivotal trials, SINUS-24 and SINUS-52. The severity of nasal polyps and of NC were identified as clinically relevant outcomes of importance for this review. In both trials, treatment with dupilumab 300 mg every 2 weeks for 24 weeks resulted in a reduction in NPS compared to the placebo, as measured by the change from baseline in NPS. In the SINUS-52 trial, treatment with dupilumab for 52 weeks resulted in sustained reduction in NPS compared to placebo. In the SINUS-24 trial, dupilumab treatment led to a higher proportion of patients who had at least 1 point or 2 points improvement in NPS at week 24. Compared to the SINUS-24 trial, a higher proportion of patients had at least 1 point and 2 points reduction in NPS at week 52 in the SINUS-52 trial. The results were considered robust, given the consistency of the primary results with various sensitivity analyses. The reduction in NPS was reflected in the CDA-AMC GRADE assessment as high-level certainty, based on the within-group MID identified in the literature.27 CDA-AMC notes that, although the MID was drawn from within-group change of at least 1 point difference in NPS, the clinical experts agreed that a 1-point between-group difference in NPS was clinically relevant.
Regarding NC, dupilumab treatment for 24 weeks likely resulted in a reduction in NC score when compared with placebo. In the SINUS-52 trial, patients treated with dupilumab over 52 weeks maintained meaningful improvements in NC compared to those receiving placebo. Compared to the SINUS-24 trial, the proportion of patients with improvement in NC score was higher (58.7% in the SINUS-52 trial versus 56.6% in the SINUS-24 trial). Although the overall pattern of benefit was similar to that observed for NPS, the evidence of the reduction in NC was assessed as of moderate certainty based on GRADE. The rationale for the moderate certainty assessment was that the point estimate and 95% CIs for change from baseline in NC between groups included the possibility of no MID. The MID for NC is drawn from within-group change of at least 1 point27 estimated in the literature; the clinical experts agreed that a 1-point between-group difference is clinically relevant.
The input received from the patient group indicated that patients experience breathing problems, involving physical discomfort that interferes with daily activities, including sleep, overall well-being, and HRQoL. The clinical experts indicated that SNOT-22 is preferred and used to assess response to treatment in clinical practice and is also used by specialists treating CRSwNP to decide when a patient needs sinonasal surgery. In both trials, the change from baseline in SNOT-22 was a key secondary outcome. Evidence from both trials showed that treatment with dupilumab for 24 weeks resulted in a reduction in SNOT-22 scores compared to placebo. In the SINUS-52 trial, the improvement in SNOT-22 at week 24 was maintained at 52 weeks. Further, a responder analysis performed in both trials showed that the proportion of patients with at least an 8.9-point improvement in SNOT-22 was greater in the dupilumab group compared to the placebo group. CDA-AMC notes that the improvement in SNOT-22 at week 24 or 52 was clinically meaningful. This improvement was assessed to be of high certainty in the GRADE assessment, based on a within-group MID of 8.9 identified in the literature,28 which was considered to be similar to a between-group difference by the clinical experts consulted for this review.
Consistent with the patient group input, the clinical experts noted that response to dupilumab is assessed in clinical practice based on symptom severity and sense of smell, usually assessed by TSS and/or decreased or loss of sense of smell. TSS is a composite score of NC, loss of sense of smell, and rhinorrhea, while decreased or loss of sense of smell assesses the severity of daily symptoms of CRSwNP. As measured by the change from baseline to week 24 in TSS, treatment with dupilumab in both trials resulted in a greater improvement in symptoms of CRSwNP compared to placebo that was both statistically significant and clinically meaningful. Similarly, dupilumab resulted in an improvement in severity of CRSwNP compared to placebo, as measured by change from baseline to week 24 in decreased or loss of sense of smell in both trials. CDA-AMC notes that the improvement in TSS and decreased or loss of sense of smell was clinically relevant, based on the within-group MIDs of 3 points27 and 1 point,46 respectively, identified in the literature and consistent with the opinion of the clinical experts consulted for the review. The change from baseline in TSS was not included in CDA-AMC GRADE certainty assessment because TSS was not considered a priority outcome for clinical decision-making by the clinical experts consulted for this review. Although TSS captures a broad range of CRSwNP symptoms, it overlaps with outcomes such as NC and SNOT-22, which were both assessed using GRADE. Similarly, decreased or loss of sense of smell was not included because it is a key item in the SNOT-22 measure.
The clinical experts consulted for this review considered the duration of the trials to be sufficient, based on their clinical experience. Nearly all patients demonstrated a treatment response to dupilumab within 1 year, and some within 6 months. CDA-AMC notes that CRSwNP is a chronic condition in which patients are expected to be on long-term treatment. Therefore, 52 weeks may not be sufficient to evaluate the sustained improvement in these outcomes. Long-term results are needed for an adequate efficacy and safety assessment. As a result, the lack of long-term extension studies of the pivotal trials is a limitation. To address this gap, the sponsor submitted an observational single-centre study, but it was not relevant to this review. Of note, the pivotal trials were placebo-controlled, and no studies were submitted that evaluated a direct comparison to other biologics such as mepolizumab.
In the absence of direct head-to-head evidence, a Bucher ITC and a supporting MAIC were conducted using data from the SINUS and SYNAPSE trials. Across both the main Bucher ITC and the MAIC, dupilumab is likely as effective as mepolizumab in key end points for CRSwNP in patients with prior nasal polyp surgery, such as NC and smell function. It might be more effective than mepolizumab based on the NPS at both 24 and 52 weeks. Despite the consistent direction of effect, there are noteworthy methodological limitations that may introduce a level of uncertainty in the estimates. The reliance on fixed-effects ITCs, baseline population differences between the SINUS trials and the SYNAPSE trial (necessitating the SYNAPSE-like subgroup and the MAIC reweighting), and the downscaling of certain outcome measures (e.g., NC) introduce uncertainties. Further, the SYNAPSE-like subset represented only a fraction of the broader SINUS population, limiting the generalizability of these findings beyond those with prior nasal polyp surgery. Taken together, the body of indirect evidence suggests dupilumab is as effective as, and might be more effective than, mepolizumab. Unaccounted heterogeneity, evidence gaps in patients outside the eligibility criteria for the SYNAPSE trial, smaller effective sample sizes, and certain methodological limitations introduce uncertainty in the results indicating superiority. While such uncertainty exists, the magnitude of effect and consistent direction is still supportive of the effectiveness of dupilumab. The comparative effectiveness of dupilumab and mepolizumab is currently being assessed in an ongoing RCT in Denmark of dupilumab versus mepolizumab in 220 patients with CRSwNP with prior surgery. The RCT is anticipated to finish in March 2026.64 The primary objective is to establish noninferiority of dupilumab versus mepolizumab and, if that is achieved, to test for possible superiority of dupilumab over mepolizumab. There is no comparative evidence for patients with CRSwNP who have not had surgery. According to the clinical experts consulted for this review, patients are required to have prior sinus surgery before accessing mepolizumab. However, delays in access to endoscopic sinus surgery due to long specialist wait times can disproportionately affect patients who are otherwise eligible for biologic therapy but cannot meet the surgical requirement in a timely manner. In contrast, the SINUS-24 and SINUS-52 trials included patients without prior sinus surgery and still demonstrated clinically meaningful benefits, suggesting that disease severity should be considered more important than prior surgery when determining a patient’s eligibility for biologic therapy.
Harms
In the SINUS-24 and SINUS-52 trials, safety analyses were conducted for all patients who received at least 1 dose of dupilumab. Overall, dupilumab was well tolerated and, according to the clinical experts consulted for this review, the reported AEs were generally consistent with what they would anticipate in patients with severe CRSwNP. The AEs reported in both trials were consistent with the known and acceptable safety profile of dupilumab in adults with severe CRSwNP. Dupilumab was associated with higher rates of injection-site reactions, nasopharyngitis, and conjunctivitis compared to placebo in both the SINUS-24 and SINUS-52 trials. While the overall rate of TEAEs was similar or lower in the dupilumab groups, events such as eosinophilia were more frequently reported. Most AEs were mild to moderate severity. SAEs occurred less frequently in the dupilumab groups, and no new safety signals were identified during the study periods in both the SINUS-24 and SINUS-52 trials. Discontinuation due to AEs was low: 3.5% in the dupilumab group versus 2.3% in the placebo group in the SINUS-24 trial, and 1.4% versus 11.3%, respectively, in the SINUS-52 trial. No deaths were attributed to dupilumab in both trials. █))████))████))████))████))████))██.
While the duration of the SINUS-52 trial was 52 weeks, the SINUS-24 trial lasted for 24 weeks. No long-term extension studies of the pivotal trials was submitted by the sponsor, making it impossible to assess the safety of dupilumab beyond 52 weeks or whether long-term use presents additional safety concerns based on the available evidence. CDA-AMC notes that the lack of long-term data is an important concern, given that CRSwNP is a chronic condition requiring sustained long-term management. Despite these, the clinical experts consulted for this review indicated that the harms data at week 52 are consistent with clinical practice. An assessment of harms data was not conducted in the ITCs submitted by the sponsor. The absence of head-to-head comparisons makes it unclear whether dupilumab offers a clinically meaningful safety advantage over other biologics.
Conclusion
The SINUS-24 and SINUS-52 trials demonstrated that dupilumab, as an add-on to INCSs, results in a clinically meaningful reduction in the severity of nasal polyps, based on the NPS, as well as an improvement in HRQoL, based on the SNOT-22, for adult patients with severe chronic CRSwNP inadequately controlled by SCSs and/or surgery when compared to placebo. Dupilumab also likely results in a clinically meaningful improvement in NC when compared to placebo. Additionally, evidence from both trials suggests that treatment with dupilumab is associated with improvements in severity of symptoms, based on the change from baseline in TSS, as well as improved sense of smell, based on the change from baseline in decreased or loss of sense of smell, which aligned with the results for NPS, NC, and SNOT-22. Dupilumab was well tolerated, and the reported AEs were generally consistent with those anticipated in adult patients with severe CRSwNP. In the 24-week safety population, SAEs were more common in the placebo group than in the dupilumab group. Notable harms, including myalgia, eosinophilia, nasopharyngitis, and headache, were assessed to range from low to moderate certainty, suggesting that there was little to no difference in notable harms between the dupilumab group and the placebo group. However, long-term safety data remain limited due to the absence of long-term extension studies. The absence of direct comparisons with other biologics (e.g., mepolizumab) limits conclusions about the safety profile of dupilumab relative to mepolizumab.
Results from the ITC suggest that dupilumab is likely as effective as, and might be more effective than, mepolizumab when assessed using end points of NPS, NC, and smell function among patients with severe CRSwNP who had prior surgery. However, there is increased uncertainty related to superiority due to methodological limitations and population differences across the included studies. There is no comparative evidence, direct or indirect, for patients with CRSwNP without prior surgery.
Based on the evidence available for this review, dupilumab represents an additional treatment option for patients with severe CRSwNP that is inadequately controlled by SCSs and/or nasal polyp surgery.
References
1.Kato A. Immunopathology of chronic rhinosinusitis. Allergol Int. 2015;64(2):121-30. doi:10.1016/j.alit.2014.12.006. PubMed
2.Fokkens WJ, Lund VJ, Hopkins C, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58(Suppl S29):1-464. doi:10.4193/Rhin20.600 PubMed
3.Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 Suppl):S1-S39. doi:10.1177/0194599815572097 PubMed
4.Dass K, Peters AT. Diagnosis and management of rhinosinusitis: highlights from the 2015 practice parameter. Curr Allergy Asthma Rep. 2016;16(4):29. doi:10.1007/s11882-016-0607-8 PubMed
5.Dalziel K, Stein K, Round A, et al. Systematic review of endoscopic sinus surgery for nasal polyps. Health Technol Assess. 2003;7(17):iii, 1-159. doi:10.3310/hta7170 PubMed
6.Xu Y, Quan H, Faris P, et al. Prevalence and incidence of diagnosed chronic rhinosinusitis in Alberta, Canada. JAMA Otolaryngol Head Neck Surg. 2016;142(11):1063-1069. doi:10.1001/jamaoto.2016.2227 PubMed
7.Stevens WW, Schleimer RP, Kern RC. Chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol Pract. 2016;4(4):565-72. doi:10.1016/j.jaip.2016.04.012 PubMed
8.Hulse KE, Stevens WW, Tan BK, et al. Pathogenesis of nasal polyposis. Clin Exp Allergy. 2015;45(2):328-46. doi:10.1111/cea.12472 PubMed
9.Hopkins C. Chronic rhinosinusitis with nasal polyps. N Engl J Med. 2019;381(1):55-63. doi:10.1056/NEJMcp1800215 PubMed
10.Orlandi RR, Kingdom TT, Hwang PH, et al. International consensus statement on allergy and rhinology: rhinosinusitis. Int Forum Allergy Rhinol. 2016;6 Suppl 1:S22-209. doi:10.1002/alr.21695 PubMed
11.Orlandi RR, Kingdom TT, Smith TL, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol. 2021;11(3):213-739. doi:10.1002/alr.22741 PubMed
12.Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50(1):1-12. doi:10.4193/Rhino12.000 PubMed
13.Doulaptsi M, Prokopakis E, Seys S, et al. Visual analogue scale for sino-nasal symptoms severity correlates with sino-nasal outcome test 22: paving the way for a simple outcome tool of CRS burden. Clin Transl Allergy. 2018;8:32. doi:10.1186/s13601-018-0219-6 PubMed
14.Canada’s Drug Agency. Reimbursement Review: mepolizumab (Nucala). Can J Health Technol. 2023;3(2). doi:10.51731/cjht.2023.588 Accessed July 31, 2024. https://www.cadth.ca/sites/default/files/DRR/2023/SR0735-Nucala_combined.pdf
15.Price DB, Trudo F, Voorham J, et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy. 2018;11:193-204. doi:10.2147/jaa.S176026 PubMed
16.Dessouky O, Hopkins C. Surgical versus medical interventions in CRS and nasal polyps: comparative evidence between medical and surgical efficacy. Curr Allergy Asthma Rep. 2015;15(11):66. doi:10.1007/s11882-015-0566-5 PubMed
17.Philpott C, Hopkins C, Erskine S, et al. The burden of revision sinonasal surgery in the UK-data from the Chronic Rhinosinusitis Epidemiology Study (CRES): a cross-sectional study. BMJ Open. 2015;5(4):e006680. doi:10.1136/bmjopen-2014-006680 PubMed
18.Van Zele T, Holtappels G, Gevaert P, et al. Differences in initial immunoprofiles between recurrent and nonrecurrent chronic rhinosinusitis with nasal polyps. Am J Rhinol Allergy. 2014;28(3):192-8. doi:10.2500/ajra.2014.28.4033 PubMed
19.Thamboo AV, Lee M, Bhutani M, et al. Canadian multidisciplinary expert consensus on the use of biologics in upper airways: a Delphi study. J Otolaryngol Head Neck Surg. 2023;52(1):30. doi:10.1186/s40463-023-00626-9 PubMed
20.Thamboo A, Kilty S, Witterick I, et al. Canadian Rhinology Working Group consensus statement: biologic therapies for chronic rhinosinusitis. J Otolaryngol Head Neck Surg. 2021;50(1):15. doi:10.1186/s40463-021-00493-2 PubMed
21.GlaxoSmithKline Inc. Nucala (mepolizumab for injection): 100 mg/mL lyophilized powder, 100 mg/mL solution, 40 mg/0.4 mL solution for subcutaneous injection [product monograph]. September 15, 2022.
22.Sanofi-Aventis Canada Inc. Dupixent (dupilumab for injection): 300 mg single-use syringe (300 mg/2 mL), 300 mg single-use pen (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL), 200 mg single-use pen (200 mg/1.14 mL) solution for subcutaneous injection [product monograph]. November 18, 2024.
23.Sanofi. NCT02912468. A controlled clinical study of dupilumab in patients with bilateral nasal polyps (SINUS-24). ClinicalTrials.gov. Accessed July 31, 2024. https://clinicaltrials.gov/study/NCT02912468?term=nct02912468&rank=1
24.Sanofi. NCT02898454. A controlled clinical study of dupilumab in patients with nasal polyps (SINUS-52). ClinicalTrials.gov. Accessed July 31, 2024. https://clinicaltrials.gov/study/NCT02898454?term=nct02898454&rank=1
25.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
26.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
27.Han JK, Bachert C, Lee SE, et al. Estimating clinically meaningful change of efficacy outcomes in inadequately controlled chronic rhinosinusitis with nasal polyposis. Laryngoscope. 2022;132(2):265-271. doi:10.1002/lary.29888 PubMed
28.Hopkins C, Gillett S, Slack R, et al. Psychometric validity of the 22-item Sinonasal Outcome Test. Clin Otolaryngol. 2009;34(5):447-54. doi:10.1111/j.1749-4486.2009.01995.x PubMed
29.Sanofi. Clinical Study Report: EFC14146 (SINUS-24). A randomized, 24-week treatment, double-blind, placebo-controlled efficacy and safety study of dupilumab 300 mg every other week, in patients with bilateral nasal polyposis on a background therapy with intranasal corticosteroids [internal sponsor's report]. December 11, 2018.
30.Sanofi. Clinical Study Report: EFC14280 (SINUS-52). A randomized, double-blind, 52-week, placebo-controlled effiacy and safety study of dupilumab in patients with bilateral nasal polyposis on a background therapy with intranasal corticosteroids [internal sponsor's report] January 29, 2019.
31.van der Lans RJL, Otten JJ, Adriaensen G, et al. Two-year results of tapered dupilumab for CRSwNP demonstrates enduring efficacy established in the first 6 months. Allergy. 2023;78(10):2684-2697. doi:10.1111/all.15796 PubMed
32.Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet. 2019;394(10209):1638-1650. doi:10.1016/S0140-6736%2819%2931881-1 PubMed
33.Chen Y, Dales R, Lin M. The epidemiology of chronic rhinosinusitis in Canadians. Laryngoscope. 2003;113(7):1199-205. doi:10.1097/00005537-200307000-00016 PubMed
34.Mayo Clinic. Chronic sinusitis: risk factors. September 19, 2023. Accessed July 31, 2024. https://www.mayoclinic.org/diseases-conditions/chronic-sinusitis/symptoms-causes/syc-20351661
35.Ahn JC, Kim JW, Lee CH, et al. Prevalence and risk factors of chronic rhinosinusitus, allergic rhinitis, and nasal septal deviation: results of the Korean national health and nutrition survey 2008-2012. JAMA Otolaryngol Head Neck Surg. 2016;142(2):162-7. doi:10.1001/jamaoto.2015.3142 PubMed
36.Bohman A, Oscarsson M, Holmberg K, et al. Heredity of nasal polyps. Rhinology. 2015;53(1):25-8. doi:10.4193/Rhino14.032 PubMed
37.Alexiou A, Sourtzi P, Dimakopoulou K, et al. Nasal polyps: heredity, allergies, and environmental and occupational exposure. J Otolaryngol Head Neck Surg. 2011;40(1):58-63. PubMed
38.Kaplan A. Canadian guidelines for chronic rhinosinusitis: clinical summary. Can Fam Physician. 2013;59(12):1275-81, e528-34.
39.Fokkens WJ, Viskens AS, Backer V, et al. EPOS/EUFOREA update on indication and evaluation of biologics in chronic rhinosinusitis with nasal polyps 2023. Rhinology. 2023;61(3):194-202. doi:10.4193/Rhin22.489 PubMed
40.Fokkens WJ, Lund V, Bachert C, et al. EUFOREA consensus on biologics for CRSwNP with or without asthma. Allergy. 2019;74(12):2312-2319. doi:10.1111/all.13875 PubMed
41.Van Zele T, Gevaert P, Holtappels G, et al. Oral steroids and doxycycline: two different approaches to treat nasal polyps. J Allergy Clin Immunol. 2010;125(5):1069-1076.e4. doi:10.1016/j.jaci.2010.02.020 PubMed
42.Teva Canada Limited. Teva-Mometasone (mometasone furoate aqueous nasal spray): 50 mcg per metered spray [product monograph]. November 2, 2022.
43.Aukema AA, Mulder PG, Fokkens WJ. Treatment of nasal polyposis and chronic rhinosinusitis with fluticasone propionate nasal drops reduces need for sinus surgery. J Allergy Clin Immunol. 2005;115(5):1017-23. doi:10.1016/j.jaci.2004.12.1144 PubMed
44.Weber RK, Hosemann W. Comprehensive review on endonasal endoscopic sinus surgery. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2015;14:Doc08. doi:10.3205/cto000123 PubMed
45.DeConde AS, Mace JC, Levy JM, et al. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope. 2017;127(3):550-555. doi:10.1002/lary.26391 PubMed
46.Sedaghat AR, Campbell RG, Douglas RG, et al. Outcome measures for chronic rhinosinusitis with nasal polyps. Rhinology. 2024;62(34):1-37. doi:10.4193/Rhin24.090. PubMed
47.Shih VH, Slagle AF, Ivanescu C, et al. Psychometric validation and meaningful change thresholds of the new nasal polyposis symptom diary. Ann Otol Rhinol Laryngol 2023;132(12):1638-1648. doi:10.1177/00034894231177769 PubMed
48.Chowdhury NI, Mace JC, Bodner TE, et al. Investigating the minimal clinically important difference for SNOT-22 symptom domains in surgically managed chronic rhinosinusitis. Int Forum Allergy Rhinol. 2017;7(12):1149-1155. doi:10.1002/alr.22028 PubMed
49.Phillips KM, Hoehle LP, Caradonna DS, et al. Minimal clinically important difference for the 22-item Sinonasal Outcome Test in medically managed patients with chronic rhinosinusitis. Clin Otolaryngol. 2018;43(5):1328-1334. doi:10.1111/coa.13177 PubMed
50.Phillips KM, Houssein FA, Boeckermann LM, et al. Multi-institutional minimal clinically important difference of the 22-item Sinonasal Outcome Test in medically managed chronic rhinosinusitis. Rhinology. 2021;59(6):552-559. doi:10.4193/Rhin21.253 PubMed
51.Chowdhury NI, Mace JC, Bodner TE, et al. Does medical therapy improve SinoNasal Outcomes Test-22 Domain Scores? An analysis of clinically important differences. Laryngoscope. 2019;129(1):31-36. doi:10.1002/lary.27470 PubMed
52.Hellings PW, Verhoeven E, Fokkens WJ. State-of-the-art overview on biological treatment for CRSwNP. Rhinology. 2021;59(2):151-163. doi:10.4193/Rhin20.570 PubMed
53.Bachert C, Mannent L, Naclerio RM, et al. Effect of subcutaneous dupilumab on nasal polyp burden in patients with chronic sinusitis and nasal polyposis: a randomized clinical trial. JAMA. 2016;315(5):469-79. doi:10.1001/jama.2015.19330 PubMed
54.Sanofi-aventis Canada Inc. Common technical document. 2.7.3 summary of clinical efficacy (chronic rhinosinusitis with nasal polyposis) In: Drug Reimbursement Review sponsor submission: Dupixent (dupilumab for injection), 300 mg subcutaneous injectionDrug Reimbursement Review sponsor submission: Dupixent (dupilumab for injection), 300 mg subcutaneous injection. December 14, 2018.
55.Cochrane Methods Bias. Assessing risk of bias in included studies [sponsor submitted reference]. Accessed December 13, 2024. https://methods.cochrane.org/bias/assessing-risk-bias-included-studies
56.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097 PubMed
57.US Food and Drug Administration (FDA). Highlights of prescribing information for Dupixent. 2017. Accessed December 13, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761055lbl.pdf
58.Bucher HC, Guyatt GH, Griffith LE, et al. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol. 1997;50(6):683-91. doi:10.1016/s0895-4356(97)00049-8 PubMed
59.Han JK, Bachert C, Fokkens W, et al. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. 2021;9(10):1141-1153. doi:10.1016/s2213-2600(21)00097-7 PubMed
60.Albrecht T, Sailer MM, Capitani F, et al. Real-world evidence for the effectiveness and safety of dupilumab in patients with CRSwNP after 1 year of therapy. World Allergy Organ J. 2023;16(5):100780. doi:10.1016/j.waojou.2023.100780 PubMed
61.De Corso E, Pasquini E, Trimarchi M, et al. Dupilumab in the treatment of severe uncontrolled chronic rhinosinusitis with nasal polyps (CRSwNP): a multicentric observational phase IV real-life study (DUPIREAL). Allergy. 2023;78(10):2669-2683. doi:10.1111/all.15772 PubMed
62.Grose E, Li AY, Lee JM. Clinical outcomes of dupilumab therapy in chronic rhinosinusitis with nasal polyps in a Canadian tertiary care rhinology practice. Allergy Asthma Clin Immunol. 2023;19(1):26. doi:10.1186/s13223-023-00782-7 PubMed
63.Kilty SJ, Lasso A. Canadian Real-World Study Long-Term Clinical Results Using Dupilumab for Chronic Rhinosinusitis With Polyps. J Otolaryngol Head Neck Surg. 2024;53:19160216241278659. doi:10.1177/19160216241278659 PubMed
64.Rigshospitalet Denmark. NCT05942222: Treatment of rhinosinusitis with nasal polyposis with dupilumab and mepolizumab: A randomized, multi-centre, head-to-head comparison in real-world Danish patients. ClinicalTrials.gov; 2023. Accessed July 31, 2024. https://clinicaltrials.gov/study/NCT05942222
Appendix 1: The SINUS-24 Trial — LS Mean Change From Baseline to Week 24 in Bilateral NPS Score (ITT Population)
Please note that this appendix has not been copy-edited.
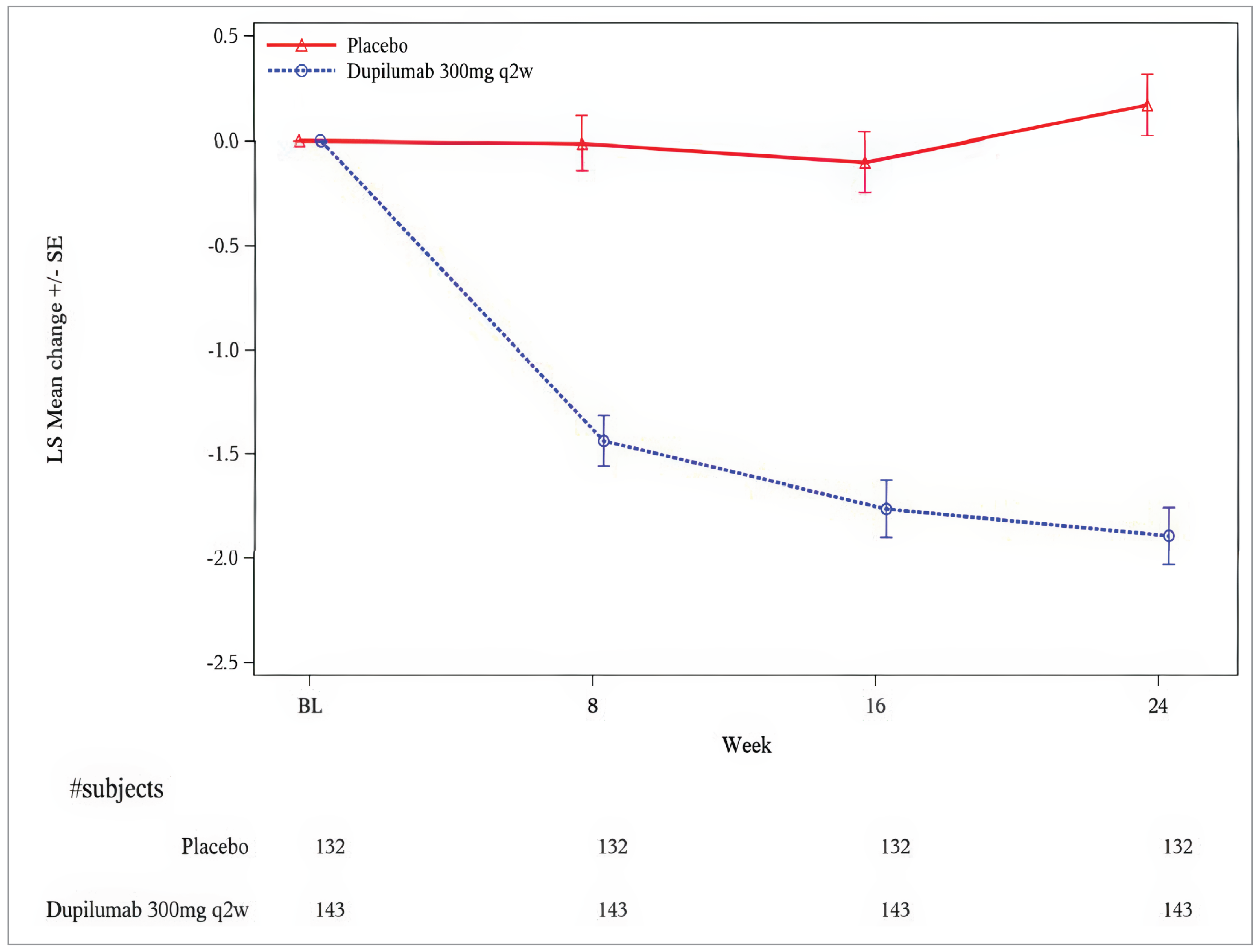
Appendix 2: The SINUS-52 Trial — LS Mean Change From Baseline to Week 52 in NPS Score (ITT Population)
Please note that this appendix has not been copy-edited.
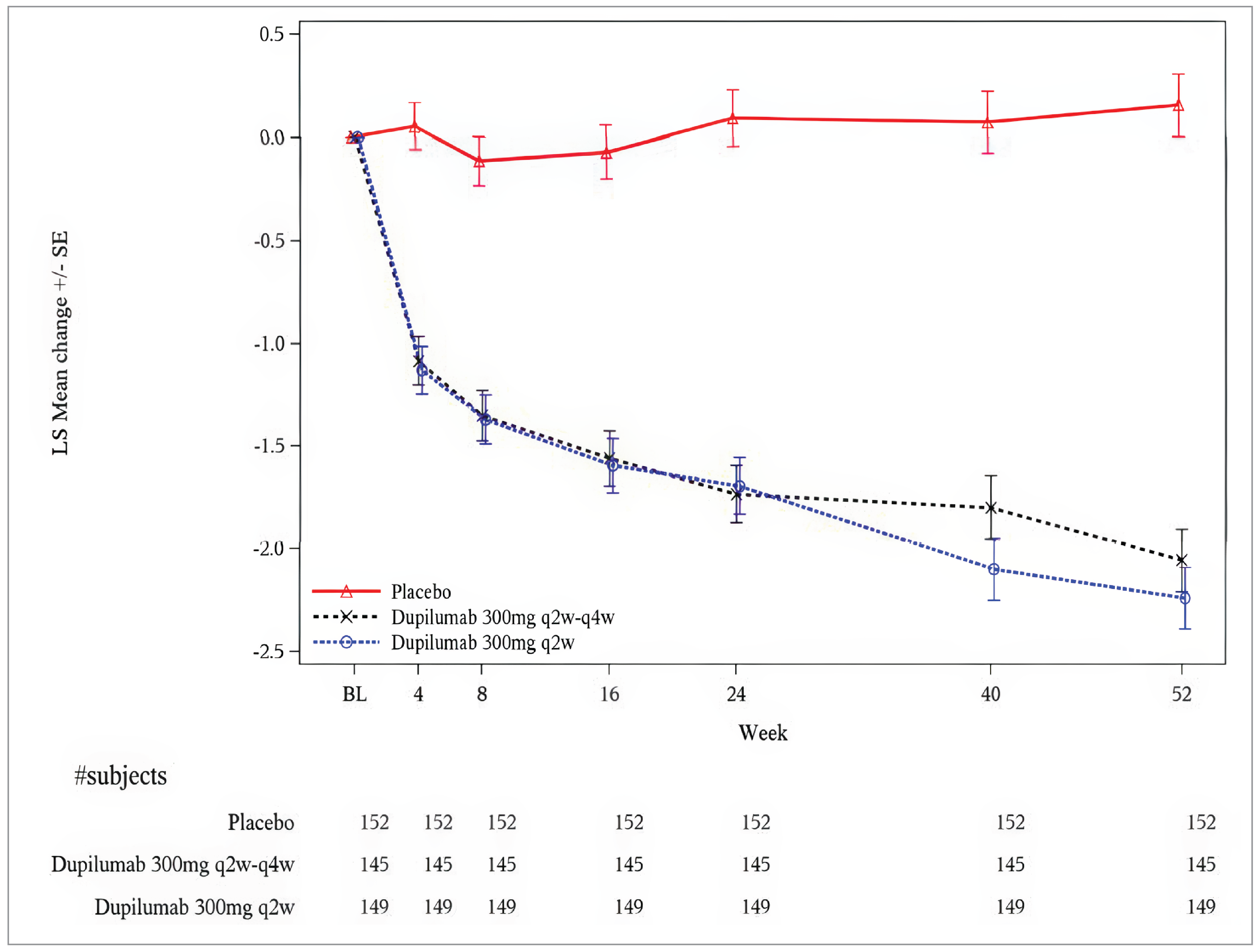
Appendix 3: The SINUS-24 Trial — LS Mean Change From Baseline to Week 24 in NC Score (ITT Population)
Please note that this appendix has not been copy-edited.
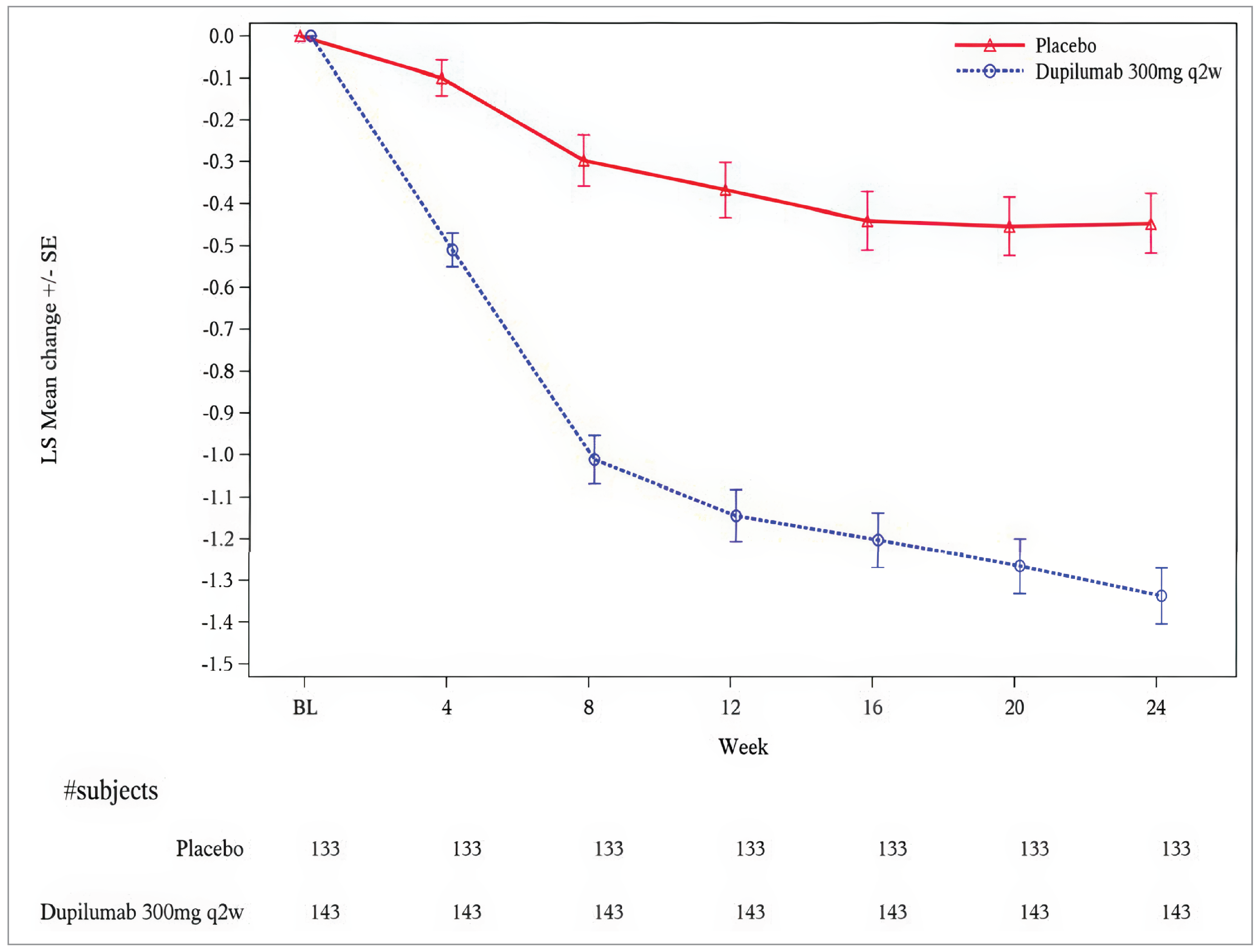
Appendix 4: The SINUS-52 Trial — LS Mean Change From Baseline to Week 52 in NC Score (ITT Population)
Please note that this appendix has not been copy-edited.
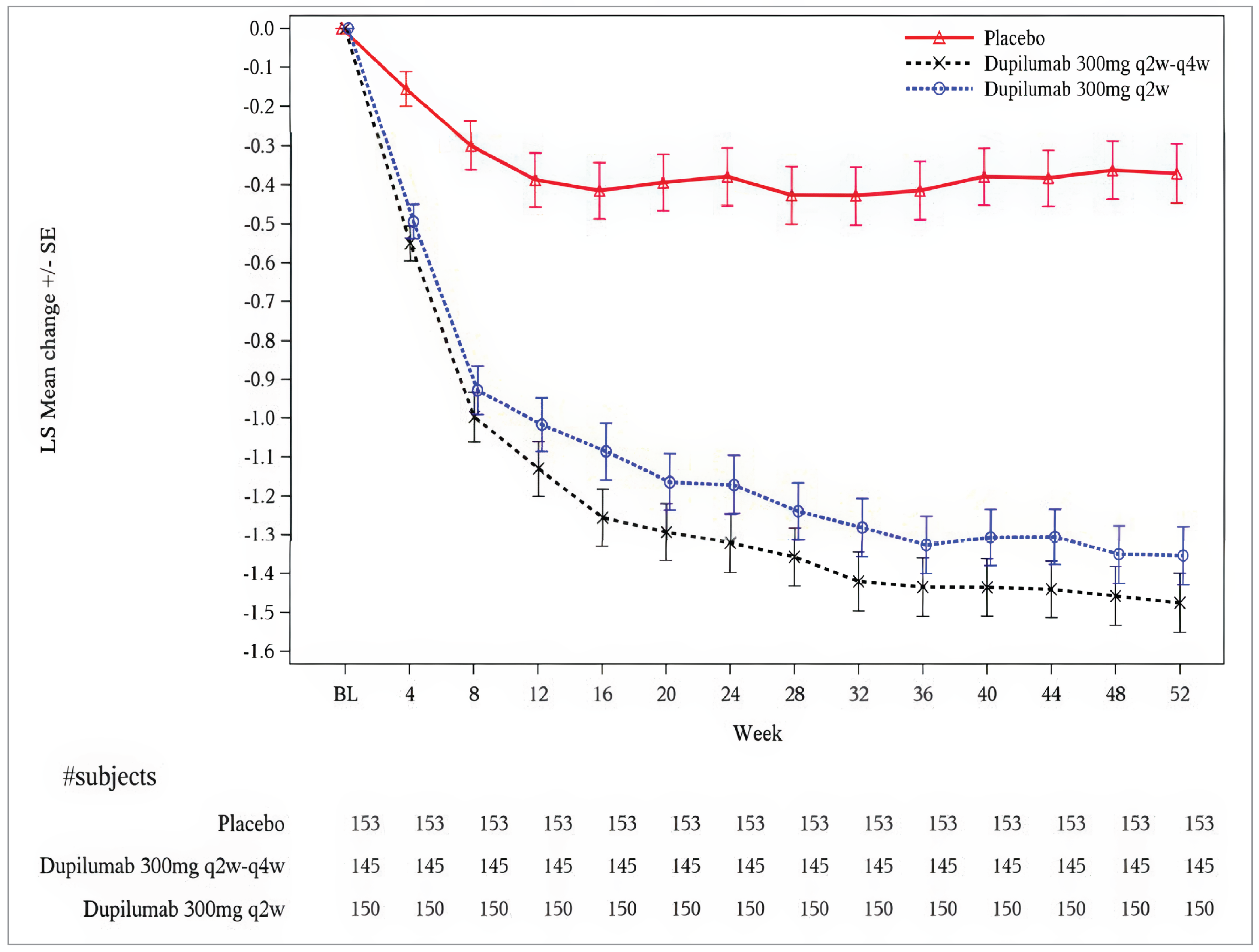
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
BSC
best supportive care
CDA-AMC
Canada’s Drug Agency
CRS
chronic rhinosinusitis
CRSwNP
chronic rhinosinusitis with nasal polyposis
ED
emergency department
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
ITT
intention-to-treat
LY
life-year
NPS
nasal polyp score
OR
odds ratio
QALY
quality-adjusted life-year
SNOT-22
22-item Sino-Nasal Outcome Test
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Dupilumab (Dupixent) 300 mg/2 mL single-use syringe or pen for subcutaneous injectiona |
Indication | As add-on maintenance treatment with intranasal corticosteroids in adult patients with severe CRSwNP inadequately controlled by systemic corticosteroids and/or surgery |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | August 12, 2020 |
Reimbursement request | As per indication |
Sponsor | Sanofi-Aventis Canada Inc. |
Submission history | Yesb Indication: As an add-on maintenance treatment in patients aged 12 years and older with severe asthma with a type 2 eosinophilic phenotype or oral corticosteroid–dependent asthma Recommendation date: June 8, 2021 Recommendation: Reimburse with clinical criteria and/or condition Indication: As an add-on maintenance treatment in patients aged 6 years and older with severe asthma with a type 2 eosinophilic phenotype or oral corticosteroid–dependent asthma Recommendation date: January 20, 2023 Recommendation: Reimburse with clinical criteria and/or condition Indication: As an add-on maintenance treatment in adult patients with uncontrolled COPD associated with type 2 inflammation Recommendation date: TBD (currently an active review) Recommendation: TBD |
COPD = chronic obstructive pulmonary disease; CRSwNP = chronic rhinosinusitis with nasal polyposis; NOC = Notice of Compliance; TBD = to be determined.
aDupilumab is also available in 200 mg/1.14 mL prefilled pens and syringes.1 However, this size is not relevant to the recommended dose for severe chronic rhinosinusitis (CRS).
bDupilumab had also been reviewed by CADTH for atopic dermatitis and is currently under review for prurigo nodularis.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision tree followed by Markov model |
Target population | Adult patients with severe CRSwNP inadequately controlled by systemic corticosteroids and/or surgery |
Treatment | Dupilumab as an add-on to BSC BSC consists of daily intranasal corticosteroids, occasional short courses of systemic steroids in case of worsening signs and/or symptoms requiring medical intervention, and/or systemic antibiotics in case of acute infection. |
Dose regimen | 300 mg given every 2 weeks |
Submitted price | Dupilumab: $978.70 per 300 mg single-use syringe or pen |
Submitted treatment cost | $25,534 per year, not including BSC |
Comparators |
|
Perspective | Publicly funded health care payer in Canada |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (50 years) |
Key data sources | Pooled data from the LIBERTY NP SINUS-24 (SINUS-24) and LIBERTY NP SINUS-52 (SINUS-52) trials, as well as a sponsor-conducted ITC |
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; CRSwNP = chronic rhinosinusitis with nasal polyposis; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; LY = life-year; NPS = nasal polyp score; QALY = quality-adjusted life-year; SNOT-22 = 22-item Sino-Nasal Outcome Test.
Conclusions
Based on data from the SINUS-24 and SINUS-52 trials, the Canada’s Drug Agency (CDA-AMC) clinical review concluded that dupilumab as an add-on treatment to best supportive care (BSC) for adult patients with severe chronic rhinosinusitis (CRS) with nasal polyposis (CRSwNP) inadequately controlled by systemic corticosteroid and/or surgery resulted in improvements in nasal polyp score (NPS), nasal congestion and/or obstruction score, and 22-item Sino-Nasal Outcome Test (SNOT-22) score compared to BSC alone. The CDA-AMC clinical review also reported that dupilumab plus BSC resulted in improvements in the probability of response compared to placebo plus BSC, while being well tolerated. Results from the sponsor’s submitted indirect treatment comparison (ITC) suggest that dupilumab plus BSC is likely as effective, and might be more effective, than mepolizumab, as measured by NPS, nasal congestion, and smell function, in patients with severe CRSwNP who had prior surgery. The sponsor’s ITC was associated with limitations, including differences between trial eligibility criteria, which led to a subgroup representing patients meeting the eligibility criteria of the pivotal trial for mepolizumab (SYNAPSE trial) used as the main analysis, limiting generalizability to the full population included in the Health Canada indication for dupilumab.
The sponsor submitted an economic analysis comparing the cost-effectiveness of dupilumab plus BSC with mepolizumab plus BSC and BSC alone, based on pooled data from the SINUS-24 and SINUS-52 trials and an exploratory analysis in the submitted ITC, which included the intention-to-treat (ITT) population of both the SINUS and SYNAPSE trials. CDA-AMC undertook reanalyses to address several limitations in the sponsor’s analysis, including assuming relative efficacy based on the main SYNAPSE-like population analysis from the submitted ITC, using the Saskatchewan public list price for mepolizumab, modelling clinical response as an improvement in SNOT-22 score, adjusting the utility gain and the probability of recurrence after surgery, assuming the proportion of patients experiencing disutility due to asthma can only impact patients with asthma, and adjusting health care resource use in uncontrolled health states. Similar to the sponsor’s results, in the CDA-AMC base case, dupilumab plus BSC is associated with higher costs (incremental costs: $446,568) and higher quality-adjusted life-years (QALYs) (incremental QALYs: 4.17) when compared to BSC alone, resulting in an incremental cost-effectiveness ratio (ICER) of $106,988 per QALY gained. Mepolizumab plus BSC was extendedly dominated (more expensive, less effective) than if the population used a mix of dupilumab plus BSC and BSC alone, similar to the sponsor’s results. A price reduction of approximately 50% would be required for dupilumab to be considered cost-effective relative to BSC at a willingness-to-pay threshold of $50,000 per QALY gained, reflecting a cost of $489 per 300 mg/2 mL prefilled syringe or pen. When considering public list prices, the annual drug acquisition cost of dupilumab is less expensive than that of mepolizumab, where funded.
Results of the CDA-AMC analyses are dependent upon the estimated life extension for dupilumab plus BSC compared to BSC alone (incremental life-years [LYs]: 1.33) being realized. Apart from a small mortality benefit associated with avoiding surgery, the mortality benefit was largely based on uncertain assumptions about the impact of severe asthma on patients with CRSwNP. These assumptions included the proportion of patients with severe asthma and the relative risk of mortality for severe asthma compared to the general population, both of which were likely overestimated. In the absence of alternative data, CDA-AMC was unable to fully resolve this uncertainty in reanalysis. Additionally, CDA-AMC was unable to adjust the analysis to reflect the time point of response assessment used in clinical practice. Given the outstanding clinical uncertainty, higher price reductions may be warranted.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Asthma Canada, which conducted a survey and received 8 responses, 7 of which were completed by adults living with nasal polyps in Canada (3 in Ontario, 1 in Manitoba, and 3 in British Columbia). One of the 7 respondents was randomly selected and interviewed to gain in-depth knowledge on the impacts of nasal polyps on quality of life. Asthma Canada noted that about 50% of patients with CRSwNP eventually develop asthma and noted the following symptoms of CRSwNP: nasal congestion, trouble breathing, frequent sneezing, postnasal drip, runny nose, impaired sense of smell, and loss of sense of taste. Respondents also noted sleep deprivation, nausea and vomiting due to phlegm, impacts on family due to frequent medical appointments, financial difficulty due to treatment cost, increased missed work or school days, and impacts on sleep. Respondents reported experience with intranasal sprays, both over the counter (fluticasone propionate and triamcinolone acetonide) and prescription options (beclomethasone, budesonide, ciclesonide, fluticasone furoate, and mometasone), as well as nasal irrigation or saline rinse, oral corticosteroids, biologics, and surgery. Patients noted that their current treatments are largely ineffective, expensive, provide poor symptom control, and are associated with side effects, such as increased risk of sinus infection, allergic reactions, and headaches and dizziness. Six out of 7 respondents expressed concern about the adverse effects of oral corticosteroids. The interviewed patient reported good results with mepolizumab in managing both nasal polyps and asthma after 2 surgeries, as well as treatment with omalizumab, which stopped working, but noted concerns about continued access to mepolizumab due to funding availability. When asked what aspects of a new treatment were most important, respondents chose easier management of symptoms, better long-term results, reduced need for surgery, reduced reliance on oral corticosteroids, and less anxiety about their nasal polyps. The interviewed patient did not have experience with dupilumab. While it was unclear whether any of the survey respondents did, 4 of 7 reported believing the advantages of dupilumab treatment outweigh the potential side effects in improving management of nasal polyps.
No clinician group input was received for this review.
The drug plans noted that the SINUS trials included a group that extended the treatment interval to every 4 weeks after 24 weeks of treatment. However, the Health Canada recommended dosage is 300 mg every 2 weeks. The plans also noted that mepolizumab is not yet funded for CRSwNP in all jurisdictions.
Several of these concerns were addressed in the sponsor’s model:
Model health states were based on SNOT-22 scores in the SINUS trials, a questionnaire that considers many of the symptoms mentioned by patients.
59% of modelled patients with severe CRSwNP were assumed to have comorbid asthma, affecting quality and length of life.
In addition, CDA-AMC addressed some of these concerns, as follows:
Use of the SNOT-22 score to assess probability of response incorporates many of the symptoms described by patients as important.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Dupilumab (Dupixent) is indicated as an add-on maintenance treatment with intranasal corticosteroids in adult patients with severe CRSwNP inadequately controlled by systemic corticosteroids and/or surgery.1 The sponsor submitted a cost-utility analysis2 of dupilumab plus BSC compared with mepolizumab plus BSC, and with BSC alone. BSC was defined as standardized background treatment of daily intranasal corticosteroids (i.e., mometasone furoate), short courses of systemic corticosteroids in case of worsening signs and/or symptoms requiring medical intervention, and/or systemic antibiotics in case of acute infection. The modelled population, as well as the sponsor’s reimbursement request, are aligned with the Health Canada indication.
Dupilumab is available in 300 mg/2 mL single-use syringes and pens, as well as 200 mg/1.14 mL single-use syringes and pens.1 As the recommended dose for CRSwNP is 300 mg every 2 weeks, only the 300 mg/2 mL products are relevant to this review. At the submitted price of $978.70 per 300 mg syringe or pen, the annual cost of therapy with dupilumab is $25,534 per patient. The annual cost of mepolizumab, as reported by the sponsor, was $30,239 per patient. The modelled cost of BSC, including daily mometasone furoate nasal spray, occasional prednisone, and occasional amoxicillin plus clavulanic acid, was $455 to $461 per patient per year, depending on the health state.
The clinical outcomes of interest were LYs and QALYs. The sponsor adopted a lifetime time horizon (50 years), with the analysis conducted from the perspective of a publicly funded health care payer. Future costs and benefits were discounted at a rate of 1.5% per year. The decision tree portion of the model was 1 year long, and the subsequent Markov model cycles also had a length of 1 year. Half-cycle corrections were applied.
Model Structure
The sponsor submitted a 1-year decision tree (Figure 1) to represent short-term response, followed by a Markov model representing long-term response, the potential for nasal polyp surgery, and long-term outcomes (Figure 2). Patients entering the decision tree can be treated either with a biologic (dupilumab or mepolizumab) in addition to BSC, or BSC alone. At the first assessment time point (24 weeks), when response was defined as a change from baseline of at least 1 on the endoscopic NPS, responding patients continued on their assigned therapy with the decision tree, while nonresponders discontinued their add-on biologic, if applicable, and entered the Markov model in the inadequately controlled disease or postoperative controlled health states. At week 52, response was assessed once again, and those who continued to respond entered the Markov model in the controlled disease state, while those whose disease was no longer responding discontinued their add-on biologic, if applicable, and entered the Markov model in the inadequately controlled disease or postoperative controlled health states.
The Markov model consisted of 4 health states (controlled disease, inadequately controlled disease, postoperative controlled, and uncontrolled) with an additional state of death (not pictured in Figure 2). As described, patients could enter the Markov process from the decision tree in the controlled disease, inadequately controlled disease, or postoperative controlled health states. Patients in the controlled state could remain in that state every cycle or move to the inadequately controlled state. The inadequately controlled state functioned as a tunnel state, with patients either having surgery within the year and entering the postoperative controlled state, or not having surgery and entering the uncontrolled state. Patients in the uncontrolled state could remain in that state or have surgery and enter the postoperative controlled state. Those in the postoperative controlled state could remain in that state or move to the uncontrolled state. The model also included a death state based on general population mortality, with additional risks for uncontrolled asthma and surgery.
Model Inputs
The baseline population characteristics used to inform the model were based on pooled patient characteristics from the SINUS-243 and SINUS-52 trials,4 double-blind, placebo-controlled, multicentre randomized trials in patients aged 18 years or older (mean 51.39) with severe CRSwNP who had an NPS of 5 or greater (mean 5.97) and ongoing moderate to severe symptoms despite prior treatment with currently available therapies such as systemic corticosteroids and surgery. Patients in the pooled SINUS-24 and SINUS-52 data were 39.6% female and 60.4% male.
The primary measure of efficacy in the model was the probability of treatment response at 24 weeks, followed by the probability of maintaining that response at 52 weeks. Response rates at 24 and 52 weeks, defined as an improvement in NPS score of 1 or higher, were informed by pooled data from the SINUS-24 and SINUS-52 trials for dupilumab plus BSC (63.0% at week 24; of these, 95.4% patients maintained response at week 52) and BSC alone (13.6% at week 24; of these, 43.8% patients maintained response at week 52), with BSC assumed equivalent to placebo.3,4 Response rates for mepolizumab plus BSC were informed by the sponsor’s ITC5 comparing dupilumab to mepolizumab (odds ratio [OR] for NPS improvement ≥ 1 response at 24 weeks = 4.60, and at 52 weeks = 4.64) leading to estimated response rates for mepolizumab plus BSC of 27.0% at week 24, with 90.7% of responding patients still responding at week 52.
Patients who did not respond at 24 weeks or who lost response by 52 weeks discontinued their add-on biologic, if applicable. Within the decision tree, ███% of patients receiving dupilumab plus BSC and receiving mepolizumab plus BSC were assumed to receive surgery for nasal polyps during weeks 0 to 24, all of them nonresponders, while ███% of patients receiving BSC did, with a further ███% of patients receiving BSC receiving surgery during weeks 25 to 52 (████% for dupilumab plus BSC and mepolizumab plus BSC). Patients then entered the Markov model in the controlled state if they were still responding, in the inadequately controlled tunnel state if they were not, and in the postoperative controlled state if they had received surgery. Patients in the controlled state had a 0% annual probability of moving to the inadequately controlled state if they were receiving add-on dupilumab or mepolizumab, based on expert opinion obtained by the sponsor, and a ████% annual probability of losing response if they were receiving BSC alone, based on the proportion of patients in the BSC group who responded at week 24 and who were still responding at week 52.2 Patients in the inadequately controlled tunnel state or the uncontrolled state had an 11.4% annual probability of receiving surgery and entering the postoperative controlled state the following cycle, with the rest entering or remaining in the uncontrolled state.6,7 Patients in the postoperative controlled state had a 38.4% annual probability of losing response to surgery and entering the uncontrolled state, after which they were eligible to receive another surgery.6,7
Based on pooled data from the SINUS trials,3,4 59.1% of patients were assumed to have comorbid asthma, with 71.8% of patients receiving dupilumab plus BSC and 23.1% of patients receiving BSC having controlled asthma; mepolizumab plus BSC was assumed to have the same impact on controlled asthma rates as dupilumab plus BSC. At any time in the model, patients with controlled asthma had an underlying risk of mortality consistent with that of the age-specific general population,8 weighted by gender, while those with uncontrolled asthma had a relative risk of death of 2.1 compared to the general population.9 Additionally, modelled patients were assumed to have a 0.01% risk of death from surgery.6,10
Utility values were derived by mapping SNOT-22 scores from pooled data from the SINUS trials3,4 to the EQ-5D using a published mapping algorithm, the Crump method.11 At model entry, patients were assumed to have a utility of █████, derived from patients’ baseline SNOT-22 scores from the SINUS trials, across treatment arms. In weeks 25 to 52 of the decision tree, responding patients were assigned a utility of █████, calculated from pooled week 24 data from responders in the SINUS trial, while those not responding were assigned a utility derived from patients who were not responders to BSC (█████). In weeks 13 to 24, patients were assigned the average utility between baseline and week 24, across treatment arms (█████). Once in the Markov model, patients in the controlled state were assigned a utility of █████, derived from week 52 pooled SINUS data for responders. Patients in the uncontrolled or inadequately controlled states were assigned the baseline utility score (█████). Patients in the postoperative controlled state were assigned a utility gain from surgery of 0.051, added to the utility of the state from which they came, based on a subgroup of patients with nasal polyposis in a US cohort study of endoscopic sinus surgery,12 along with a temporary disutility of −0.200 applied for 10 days due to having surgery, based on assumption and clinical expert opinion obtained by the sponsor.2 Finally, disutilities were applied for nasopharyngitis (−0.010, chronic), asthma (−0.025, chronic), and injection-site reactions (−0.030, 7 days).
Costs in the model included drug acquisition, administration, surgical, health care resource use (routine and emergency), asthma, and adverse event costs. All patients were assumed to receive BSC, with 100% of patients assumed to use mometasone nasal spray, while the use of prednisone and amoxicillin plus clavulanic acid varied by health state. Drug acquisition costs were from the Ontario Drug Benefit Formulary and its Exceptional Access Program.13,14 Dupilumab and mepolizumab were associated with a 1-time administration cost based on the median hourly wage of nurses in Canada,15 with patients assumed to self-administer thereafter. Costs of using health care resources included general practitioner (GP), specialist, emergency department (ED), and nurse visits, as well as hospitalization, CT scans, and rhinoscopies, based on frequencies derived from clinical expert input received by the sponsor, which varied by health state, and Canadian cost sources.15-18 Annual costs of resource use, excluding asthma and surgery, totalled $161 per year for patients with controlled disease, and $1,900 per year for those with uncontrolled disease. Patients with controlled and uncontrolled asthma were assigned additional costs of $4,109 and $6,214 per year, respectively, based on asthma-related costs reported in a cohort study of patients with severe eosinophilic asthma before and after receiving treatment with mepolizumab, also respectively.19 A cost of $4,990 per sinonasal surgery was applied,20 and a cost of $77, representing an extra GP visit, was applied per nasopharyngitis, headache, or epistaxis event.16
Summary of Sponsor’s Economic Evaluation Results
The sponsor’s base-case analysis was run probabilistically (500 iterations), while scenario analyses were conducted deterministically. Deterministic and probabilistic results for the base case were similar. The probabilistic findings are presented in the following paragraphs, where possible.
Base-Case Results
In sequential analysis, the sponsor’s probabilistic base case reported that dupilumab plus BSC was associated with an ICER of $74,785 per QALY gained (incremental cost: $305,969, incremental QALYs: 4.09) compared to BSC alone (Table 3), with mepolizumab plus BSC being extendedly dominated (more costly and less effective) than if the population used a mix of the other 2 comparators. At a willingness-to-pay threshold of $50,000 per QALY gained, dupilumab had a 0% probability of being cost-effective relative to BSC alone or mepolizumab plus BSC in pairwise comparisons. Compared to BSC, both dupilumab plus BSC and mepolizumab plus BSC were associated with gain of 1.4 LYs per patient. At the end of the 50-year time horizon, 1.7% of patients receiving dupilumab plus BSC were still alive.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
BSC | 135,622 | 12.34 | Reference |
Dupilumab plus BSC | 441,591 | 16.44 | 74,785 |
Dominated treatments | |||
Mepolizumab plus BSC | 297,551 | 14.44 | Extendedly dominated by mix of BSC and dupilumab plus BSC |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor presented deterministic sensitivity analyses for dupilumab plus BSC compared to BSC alone considering alternate inputs for the discount rate, the proportion of patients with asthma who have uncontrolled asthma when receiving dupilumab or mepolizumab, the proportion of patients with asthma who have uncontrolled asthma when receiving BSC alone, the utility weight for patients in the uncontrolled state, the baseline utility weight, the utility weight for patients receiving dupilumab plus BSC during the first 12 weeks of the decision tree, the transition probability of patients with inadequately controlled disease to postoperative controlled, and the annual cost of uncontrolled asthma. Of these, the sponsor reported that only varying the discount rate of outcomes and costs from 1.5% to 0% or 3% had substantial effects on the reported ICER. The sponsor also conducted a variety of scenario analyses, including limiting the patient population to be similar to that of the mepolizumab pivotal trial; limiting to patients who had previously had surgery; limiting to patients with a baseline visual analogue scale (VAS) score of 7 or greater; limiting to patients with medical history of type 2 inflammation, including asthma, or nonsteroidal anti-inflammatory drug–exacerbated respiratory disease as well as to those who had also had surgery; limiting to patients not eligible for surgery; changing the response definition to an improvement from baseline of 8.9 or higher on the SNOT-22 scale; and reducing the frequency of dupilumab doses to every 4 weeks after 24 weeks. Of these scenarios, only reducing the dose frequency of dupilumab had a substantial impact on results.
The sponsor also conducted a scenario analysis from a societal perspective. This deterministic analysis included additional costs associated with productivity loss due to absenteeism (missing work) and presenteeism (coming to work while ill). In this analysis, relative to BSC, the ICER was $54,994 per QALY gained. This was lower than the sponsor’s base-case analysis using a health care payer perspective.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The relative clinical efficacy of dupilumab is uncertain. In the absence of direct evidence comparing dupilumab plus BSC to mepolizumab plus BSC, the sponsor submitted a Bucher ITC using data from the SINUS and SYNAPSE trials, including an exploratory analysis including the ITT populations of the SINUS and SYNAPSE trials.5 In these indirect comparisons, dupilumab plus BSC consistently demonstrated greater improvements in outcomes such as change in NPS, proportion of responders (NPS improvement ≥ 1, SNOT-22 improvement ≥ 8.9), nasal congestion, loss of smell score, and overall VAS. However, not all patients in the SINUS trials would have been eligible for the SYNAPSE trial, leading to differences in underlying condition severity and treatment history between the trials. Thus, there is uncertainty that the relative efficacy derived from the ITC’s exploratory ITT analysis represents actual differences between dupilumab and mepolizumab, rather than reflecting differences in the underlying populations. The sponsor’s main ITC analysis considered a “SYNAPSE-like” subgroup, which included only patients from the SINUS trials who were similar to the population included in SYNAPSE (i.e., they had had at least 1 prior sinus surgery, were nonsmokers or former smokers, and had a VAS symptom score of more than 7). However, the sponsor’s base-case economic analysis incorporated ITC results from the overall ITT population analysis, which likely overestimates the relative efficacy of dupilumab plus BSC compared to mepolizumab plus BSC. Of note, the comparative efficacy of dupilumab compared to mepolizumab in patients who have not previously had sinus surgery is unknown.
The CDA-AMC reanalysis incorporated the model’s option to base efficacy inputs on the sponsor’s main SYNAPSE-like population analysis from the submitted ITC. A scenario was conducted on the CDA-AMC base case, reverting these inputs to represent the ITT population of the ITC.
Response assessment may not represent clinical practice. The sponsor’s model assumed that response to treatment would be assessed at 6 months, with patients who have not responded to dupilumab or mepolizumab discontinuing treatment at that time point, and those who do not sustain that response through to 1 year also discontinuing. However, when used to treat CRSwNP, mepolizumab is typically funded for 1 year,21,22 with additional renewals occurring annually thereafter. Clinical expert feedback obtained by CDA-AMC indicated that, while many patients receiving mepolizumab would have started to respond by 6 months, some require up to 1 year to fully realize a response. Additionally, this feedback suggested that, while most patients responding to dupilumab do so within 6 months, some also require longer to reach the response definition threshold (i.e., NPS improvement ≥ 1 or SNOT-22 improvement ≥ 8.9). By discontinuing all patients who have not reached the response definition threshold at 6 months, the sponsor’s model does not represent current clinical and funding practice in Canada.
According to clinical expert feedback obtained by CDA-AMC, while NPS is an objective measure useful in clinical trials, it is not typically used to assess response in clinical practice. Instead, clinicians reportedly use either the SNOT-22 scale or a VAS to determine symptom status and perceived improvement with treatment. Hence, use of the SNOT-22 response threshold (improvement ≥ 8.9 points) is likely more representative of how response will be assessed in clinical practice than using a threshold based on NPS.
Due to the structure of the model, CDA-AMC was unable to adjust for this limitation regarding time point of assessment. CDA-AMC reanalyses did incorporate the model’s option for response determination based on the SNOT-22 scale rather than NPS, although a scenario analysis was also conducted reverting response determination to NPS improvement.
The cost of mepolizumab may be overestimated. When estimating the cost of mepolizumab, the sponsor used the Ontario Drug Benefit Exceptional Access Program list price of $2,318 per 100 mg dose.13 However, CDA-AMC notes that the list price of mepolizumab on the Saskatchewan formulary is $21.37 per mg or $2,137 per 100 mg dose.22 As mepolizumab was funded following a positive recommendation from CDA-AMC,23 which included a substantial price reduction recommendation, and successful negotiations with the pan-Canadian Pharmaceutical Alliance,24 it is likely that confidential pricing exists for mepolizumab. Thus, it is likely that Saskatchewan’s lower list price is a closer approximation of this confidential price.
In reanalysis, CDA-AMC used a price of $2,137.15 per 100 mg dose of mepolizumab.
The benefits of nasal surgery are likely underestimated. The sponsor’s model assumed that patients undergoing nasal surgery due to uncontrolled CRSwNP would experience a utility gain of 0.051, based on a 2011 utility study of patients with CRS undergoing endoscopic sinus surgery by Soler et al. (nasal polyposis subgroup).12 However, this study derived utility scores using the Short Form-6D Health Questionnaire (SF-6D) which, as described in the sponsor’s submission, is less sensitive to CRSwNP-related symptoms than the SNOT-22 scale on which the model’s other health state utility values are based.2 A 2006 study by Hopkins et al. found that sinonasal surgery was associated with a mean SNOT-22 improvement from baseline of 17.9 points at 3 months for patients with nasal polyps and 15.4 points at 36 months (at which point 11% of patients had received surgery),25 compared to a mean improvement from baseline of 27.7 to 30 points at 24 weeks for dupilumab in the SINUS-24 and SINUS-52 trials (refer to CDA-AMC Clinical Report). Given that response to dupilumab was associated with a utility gain of ████ compared to baseline (an increase to ████ from ████) in the model, a utility gain of only 0.051 likely underestimates the quality-of-life improvement associated with sinonasal surgery in patients with severe CRSwNP. Additionally, patients who underwent surgery were assumed to have a 38% chance of losing their response to surgery (i.e., having a recurrence of nasal polyps) each year, based on a prospective cohort study of adult patients undergoing endoscopic sinus surgery for treatment-resistant CRSwNP.7 However, the proportion of patients who had a recurrence of nasal polyposis in this study was 35% at 6 months, 38% at 12 months, and 40% at 18 months, indicating that the risk of recurrence is not linear over time. Thus, the assumption that 38% of postsurgical patients will have a recurrence every year after surgery overestimates the rate of recurrence. According to clinical expert input obtained by CDA-AMC, patients typically maintain improvements gained through surgery for several years, which is consistent with the maintained SNOT-22 improvement reported at 36 months by Hopkins et al.25
In reanalysis, CDA-AMC assumed that nasal surgery would be associated with a utility gain of 0.125 (i.e., ████ ███ ████ experienced by patients responding to dupilumab plus BSC, mepolizumab plus BSC, or BSC alone) and that, conservatively, 29.3% of patients would have a polyp recurrence each year postsurgery, corresponding to an assumption that 50% of patients would have a recurrence within 2 years, rather than 62% as assumed by the sponsor (i.e., assuming 38% per year).
Resource use in uncontrolled CRSwNP and asthma is likely overestimated. The sponsor’s model assumed that, excluding resource use associated with asthma, patients in the response and controlled health states would require 1 GP and 1 specialist visit per year, while those in the nonresponse, inadequately controlled, and uncontrolled health states would require 5 GP visits, 6 specialist visits, 2 ED visits, a CT scan, and 6 rhinoscopies per year, based on clinical expert input obtained by the sponsor.2 In contrast, clinical expert input obtained by CDA-AMC considered the resource use assumptions for patients whose severe CRSwNP was not controlled to be too high, estimating instead that patients in these health states would visit a GP 5 times per year, a specialist 3 to 5 times per year, and an ED 1 to 2 times per year, as well as having a CT scan every 2 to 3 years and 2 rhinoscopies per year. The sponsor’s model then added additional resource use for patients with comorbid asthma, based on an observational study of patients with severe eosinophilic asthma before and after receiving mepolizumab,19 which was used to represent modelled patients with uncontrolled and controlled asthma, respectively. Exact resource use included in the observational study’s overall cost estimates is unclear due to multiple datasets in the article and supplementary material. However, resource use appears to include approximately 2 more GP visits, 3.5 more specialist visits, and 0.5 more ED visits for patients with controlled asthma (represented by the overall population that had received mepolizumab in the observational study), and 3.5 additional GP visits, 5.0 additional specialist visits, and 1 additional ED visits for patients with uncontrolled asthma (based on the population that had not yet received mepolizumab in the observational study). Clinical expert input obtained by CDA-AMC did not consider resource use before and after receiving mepolizumab for severe eosinophilic asthma to be a good proxy for asthma-related resource use associated with severe CRSwNP, indicating that resource use for asthma in those with severe eosinophilic asthma is likely higher than for those with severe CRSwNP and uncontrolled asthma. It is therefore likely that both the magnitude of resource use for asthma as well as differences in resource use costs for patients with differing extents of asthma (i.e., controlled, uncontrolled, and without asthma) are also overestimated.
CDA-AMC assumed that patients with uncontrolled severe CRSwNP would have 4 specialist visits, 1.5 ED visits, 0.5 CT scans, and 2 rhinoscopies per year. CDA-AMC was unable to adjust for limitations to the additional costs associated with uncontrolled and controlled asthma.
Asthma-related impacts are likely overestimated. The sponsor’s model assumed that 59.1% of patients have comorbid asthma, and that, of these, 28.2% of those receiving dupilumab or mepolizumab have uncontrolled asthma, while 76.9% of those receiving BSC alone do so, based on pooled data from the SINUS trials.2 CDA-AMC notes that patients with severe eosinophilic asthma already have access to dupilumab and mepolizumab in most jurisdictions, as assumed within the sponsor’s budget impact analysis (BIA).26 According to clinical expert input obtained by CDA-AMC, when a patient has both CRSwNP and asthma, clinicians generally treat the asthma first. As a result, it is likely that, in clinical practice, many patients with asthma severe enough to substantially impact their quality of life (i.e., to be assumed to have an asthma-related disutility) and to increase their health care resource use, and whose asthma would be improved by the use of dupilumab or mepolizumab (i.e., type 2 asthma), would already have access to these therapies and not be additionally seeking them for CRSwNP. Thus, the proportion of patients seeking reimbursement for dupilumab for CRSwNP who have uncontrolled asthma is likely lower than the proportion reported in the SINUS trials. The difference in rates of uncontrolled asthma between treatment groups would therefore be smaller than estimated within the model.
The sponsor also assumed that patients with uncontrolled asthma have 2.1 times the mortality of the general population of the same age and gender, based on a Danish case-control study of patients enrolled at an allergy clinic between 1974 and 1990 and followed up to 2011.9 Clinical expert opinion obtained by CDA-AMC indicated that, while asthma is associated with an increased risk of mortality, it is unlikely to carry double the risk in current clinical practice in Canada. While a 2017 study conducted in Utah reported that patients with CRSwNP had higher mortality than CRS patients without nasal polyps, the extent to which this higher mortality rate was related to asthma was unclear. Patients in this study with both asthma and CRS (mainly CRS without nasal polyps) had a lower risk of mortality than those with asthma alone, suggesting that overall asthma mortality rates may not be fully generalizable to the CRS population.27 As a result, the increased risk of mortality associated with uncontrolled asthma in the model may be overestimated.
The sponsor also assigned a disutility for having asthma to 28.2% of patients receiving dupilumab plus BSC or mepolizumab plus BSC, and to 76.9% of patients receiving BSC alone. These proportions are consistent with the proportion of patients with asthma in each treatment group who have uncontrolled asthma. However, for the disutility calculation, the model does not appropriately consider that only 59.1% of modelled patients have asthma.
In its base-case reanalysis, CDA-AMC altered the disutility associated with having uncontrolled asthma to apply to 28% of the 59% of patients with asthma receiving dupilumab or mepolizumab, and to 77% of the 59% of patients with asthma receiving BSC alone. A scenario analysis was conducted removing the additional costs, mortality, and disutility associated with asthma. The true effect of improvements in asthma control on the ICER likely lies between the CDA-AMC base-case analysis and this scenario.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical. It remains unclear whether the model is running inappropriately by overriding errors.
Additionally, the model did not adequately represent uncertainty in clinical parameters. When considering the binary outcome of NPS improvement of 1 or higher for the ITT population comparison of dupilumab plus BSC compared to mepolizumab plus BSC, the sponsor’s ITC reported an OR 4.60 (95% CI, 2.65 to 7.99, refer to the CDA-AMC Clinical Report). However, with the submitted model, variation in response for each comparator is based solely on an OR of 4.60, with calculated beta distributions based on the resulting response rates for each comparator, without accounting for variation in the OR rate itself. For example, the modelled beta distribution for response rate for mepolizumab plus BSC at 24 weeks (mean 27%) is based on the response rate at 24 weeks for dupilumab plus BSC (mean 63%) and has upper and lower bounds of 23% and 31%, respectively. However, if the extremes of the 95% confidence interval around the ITC’s reported OR are used (i.e., 2.65 and 7.99), this range should encompass values from at least 18% to 39% (14% to 44% when beta distributions are constructed around each mean result). Therefore, uncertainty in differences in response rates between dupilumab plus BSC and mepolizumab plus BSC have not been adequately captured, underestimating the uncertainty in the model’s predicted ICERs.
CDA-AMC was unable to address this limitation. The use of IFERROR statements precludes a thorough validation of the sponsor’s model. Limitations around insufficient representation of clinical uncertainty are not expected to have a substantial impact on mean model results (i.e., the ICER), but lead to an overestimation of certainty in, and thus stability of, modelled results.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
An increased relative risk of mortality can be directly applied to annual probabilities of death. | Inappropriate. The sponsor directly multiplied the annual probability of death for patients of any given age8 by the assumed increased relative risk of death for uncontrolled asthma (2.1). However, when mortality multiplies are applied to annual probabilities of death, the probabilities should first be converted to instantaneous rates, then multiplied by the appropriate relative risk, and then converted back to annual probabilities. Correcting this error had minimal impact on model results for this review. |
Mepolizumab injection-site reactions have the same incidence as dupilumab injection-site reactions. | Uncertain. The recommended schedule for dupilumab is every 2 weeks, compared to every 4 weeks for mepolizumab. It is likely that patients who experience injection-site reactions would have fewer with mepolizumab than dupilumab due to receiving fewer injections. However, halving the incidence of injection-site reactions for mepolizumab has minimal impact on model results. |
Modelled patients do not discontinue add-on biologic therapy after 1 year. | Uncertain. The sponsor’s model assumed that 100% of patients receiving dupilumab or mepolizumab who entered the controlled health state of the Markov portion of the model remained on their add-on biologic therapy, maintaining response until death or the end of the time horizon. Clinical expert input obtained by CDA-AMC indicated there are insufficient long-term data to support such an assumption, noting that most patients are likely to maintain a durable response based on experience with older biologics such as omalizumab, but some may experience disease progression and require dose adjustment, adjunctive treatment, or alternate therapy. The model also does not consider any other reason for discontinuation, such as side effects, pregnancy planning, injection burden, perceived lack of necessity, patient preference, or comorbidities that change treatment needs (e.g., development of a malignancy requiring immunosuppressive therapy). |
CDA-AMC = Canada’s Drug Agency.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base-case analysis was derived by making changes to model parameters and assumptions, in consultation with clinical experts, as summarized in Table 5. These changes included assuming relative efficacy based on the SYNAPSE-like subgroup analysis from the submitted ITC, using the Saskatchewan public list price for mepolizumab, altering the definition of clinical response to be an improvement in SNOT-22 score of 8.9 points or higher, adjusting the utility gain associated with surgery and the probability of recurrence after surgery, assuming the proportion of patients experiencing disutility due to uncontrolled asthma can impact only patients with asthma, and adjusting health care resource use in uncontrolled health states.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. ITC analysis population | Intention-to-treat population | “SYNAPSE-like” subgroup |
2. Unit price of mepolizumab 100 mg | Ontario list price: $2,318.13 | Saskatchewan list price: $2,137.15 |
3. Definition of response | NPS improvement ≥ 1 | SNOT-22 improvement ≥ 8.9 |
4. Surgery parameters | Utility gain after surgery: 0.051 Postoperative annual recurrence: 38.4% | Utility gain after surgery: 0.125 Postoperative annual recurrence: 29.3% |
5. Proportion of patients with asthma disutility | Dupilumab/mepolizumab: 28.2% BSC: 76.9% | Dupilumab/mepolizumab: 16.7% BSC: 45.5% |
6. Resource use in uncontrolled states (annual) | Specialist visits: 6.0 Emergency department: 2.0 CT scans: 1.0 Rhinoscopy: 6.0 | Specialist visits: 4.0 Emergency department: 1.5 CT scans: 0.5 Rhinoscopy: 2.0 |
CDA-AMC base case | ― | Reanalyses 1 through 6 |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ITC = indirect treatment comparison; NPS = nasal polyp score; SNOT-22 = 22-item Sino-Nasal Outcome Test.
CDA-AMC undertook a stepped analysis, incorporating each change proposed in Table 5 to the sponsor’s base case. Results for these stepwise analyses are reported in Table 10. Results of the CDA-AMC probabilistic base case are reported in Table 6, with disaggregated results reported in Table 11. All CDA-AMC probabilistic analyses were run for 500 iterations.
Results from the CDA-AMC base case suggest that dupilumab plus BSC is associated with higher costs (incremental costs: $446,568) and higher QALYs (incremental QALYs: 4.17) when compared to BSC alone, resulting in an ICER of $106,988 per QALY gained. Mepolizumab plus BSC was extendedly dominated (i.e., more costly and less effective) than if the population used a mix of dupilumab plus BSC and BSC alone. At a willingness to pay of $50,000 per QALY gained, dupilumab had a 0% probability of being cost-effective compared to BSC alone in pairwise analysis and a 4% probability of being cost-effective compared to mepolizumab plus BSC.
Table 6: Summary of the CDA-AMC Reanalysis Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor base case (probabilistic) | |||
BSC | 135,622 | 12.34 | Reference |
Dupilumab plus BSC | 441,591 | 16.44 | 74,785 |
Dominated treatments | |||
Mepolizumab plus BSC | 297,551 | 14.44 | Extendedly dominated by mix of BSC and dupilumab plus BSC |
CDA-AMC base case (probabilistic) | |||
BSC | 121,016 | 12.59 | Reference |
Dupilumab plus BSC | 567,584 | 16.76 | 106,988 |
Dominated treatments | |||
Mepolizumab plus BSC | 489,119 | 15.76 | Extendedly dominated by mix of BSC and dupilumab plus BSC |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s results and the CDA-AMC base case. The CDA-AMC base case suggests that a price reduction of approximately 50% would be required for dupilumab plus BSC to be considered cost-effective at a willingness to pay of $50,000 per QALY gained relative to BSC alone, or $489 per 300 mg/2 mL prefilled syringe or pen.
Table 7: CDA-AMC Price Reduction Analyses
Price reduction | Unit drug cost ($) | ICERs for dupilumab + BSC versus BSCa ($/QALY) | |
|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | ||
No price reduction | 979 | 74,785 | 106,988 |
10% | 880 | 66,024 | 95,531 |
20% | 783 | 57,263 | 84,074 |
30% | 685 | 48,502 | 72,617 |
40% | 587 | 39,741 | 61,161 |
50% | 489 | 30,980 | 49,704 |
60% | 391 | 22,219 | 38,247 |
70% | 294 | 13,458 | 26,790 |
80% | 196 | 4,697 | 15,333 |
90% | 98 | Dominant | 3,876 |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aAs mepolizumab is extendedly dominated in both the sponsor’s and the CDA-AMC base cases, it remains either extendedly or simply dominated for all dupilumab price reductions.
CDA-AMC also conducted scenario analyses to explore remaining uncertainty in the economic analysis:
Removal of the additional resource use for patients with controlled and uncontrolled asthma, the disutility associated with uncontrolled asthma, and the increased mortality associated with uncontrolled asthma.
Reverting the proportion of responders for each comparator to represent the results of the overall ITT population of the submitted ITC.
Reverting response determination to be based on achieving an NPS improvement of 1 or higher.
The scenario removing asthma-based differences between groups resulted in dupilumab plus BSC being associated with an ICER of $130,377 per QALY gained compared to BSC alone (incremental costs: $470,128; incremental QALYs: 3.61), with mepolizumab plus BSC still extendedly dominated by a mix of the other 2 comparators (Table 12). The actual impact of asthma-related costs and quality of life effects on the ICER associated with dupilumab plus BSC relative to BSC alone would lie between the CDA-AMC base-case estimate and this scenario. When considering clinical efficacy informed by the overall ITT analysis of the submitted ITC, dupilumab plus BSC was associated with an ICER of $88,891 per QALY gained compared to BSC alone (incremental costs: $377,774, incremental QALYs: 4.25). Finally, when considering clinical efficacy. when response was defined as an improvement in NPS of 1 or higher, dupilumab plus BSC was associated with an ICER of $85,467 per QALY gained compared to mepolizumab plus BSC (incremental costs: $78,466, incremental QALYs: 1.00).
Issues for Consideration
Dupilumab is currently being reviewed by CDA-AMC for 2 other distinct indications: for the treatment of adult patients with moderate to severe prurigo nodularis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable,28 and as add-on maintenance treatment in adult patients with uncontrolled chronic obstructive pulmonary disease associated with type 2 inflammation.29
CDA-AMC notes that the pan-Canadian Pharmaceutical Alliance concluded negotiations with a letter of intent for dupilumab for the treatment of asthma and atopic dermatitis.30,31 Hence, dupilumab has a confidential negotiated price. Additionally, the pan-Canadia Pharmaceutical Alliance has concluded negotiations with a letter of intent for mepolizumab for the treatment of severe CRSwNP and severe eosinophilic asthma.32-34 The CDA-AMC reanalyses are based on the publicly available price of mepolizumab and dupilumab, which may be different from the confidential prices and may influence the results of the cost-effectiveness and BIAs.
Overall Conclusions
Based on data from the SINUS-24 and SINUS-52 trials, the CDA-AMC clinical review concluded that dupilumab as an add-on treatment to BSC for adult patients with severe CRSwNP inadequately controlled by systemic corticosteroid and/or surgery resulted in improvements in NPS, nasal congestion/obstruction score, and SNOT-22 score compared to BSC alone. The CDA-AMC clinical review also reported that dupilumab plus BSC resulted in improvements in the probability of response compared to placebo plus BSC, while being well tolerated. Results from the sponsor’s submitted ITC suggest that dupilumab plus BSC is likely as effective, and might be more effective, than mepolizumab, as measured by NPS, nasal congestion, and smell function, in patients with severe CRSwNP who had prior surgery. The sponsor’s ITC was associated with limitations, including differences between trial eligibility criteria which led to a subgroup representing patients meeting the eligibility criteria of the pivotal trial for mepolizumab (SYNAPSE trial) being used as the main analysis, limiting generalizability to the full population included in the Health Canada indication for dupilumab.
The sponsor submitted an economic analysis comparing the cost-effectiveness of dupilumab plus BSC with mepolizumab plus BSC and BSC alone based on pooled data from the SINUS-24 and SINUS-52 trials and an exploratory analysis in the submitted ITC, which included the ITT population of both the SINUS and SYNAPSE trials. CDA-AMC identified several limitations with the sponsor’s submitted analysis, including uncertainty in the relative clinical efficacy of dupilumab compared to mepolizumab when based on an exploratory ITC analysis, timing of modelled response assessment relative to current clinical practice in Canada and funding criteria, overestimation of the cost of mepolizumab, likely underestimation of the benefits of surgery, overestimation of the resource use associated with having uncontrolled CRSwNP, overestimation of the impact dupilumab is likely to have on asthma-related parameters, and poor modelling practices.
CDA-AMC undertook reanalyses to address several limitations in the sponsor’s analysis, including assuming relative efficacy based on the main SYNAPSE-like population analysis from the submitted ITC, using the Saskatchewan public list price for mepolizumab, modelling clinical response as an improvement in SNOT-22 score, adjusting the utility gain and the probability of recurrence after surgery, assuming the proportion of patients experiencing disutility due to asthma can impact only patients with asthma, and adjusting health care resource use in uncontrolled health states. Similar to the sponsor’s results, in the CDA-AMC base case, dupilumab plus BSC is associated with higher costs (incremental costs: $446,568) and higher QALYs (incremental QALYs: 4.17) when compared to BSC alone, resulting in an ICER of $106,988 per QALY gained. Mepolizumab plus BSC was extendedly dominated (more expensive, less effective) than if the population used a mix of dupilumab plus BSC and BSC alone, similar to the sponsor’s results. A price reduction of approximately 50% would be required for dupilumab to be considered cost-effective relative to BSC at a willingness-to-pay threshold of $50,000 per QALY gained, reflecting a cost of $489 per 300 mg/2 mL prefilled syringe or pen. When considering public list prices, the annual drug acquisition cost of dupilumab is less expensive than that of mepolizumab, where funded.
Results of the CDA-AMC analyses are dependent upon the estimated life extension for dupilumab plus BSC compared to BSC alone (incremental LYs: 1.33) being realized. Apart from a small mortality benefit associated with avoiding surgery, the mortality benefit was largely based on uncertain assumptions about the impact of severe asthma on patients with CRSwNP. These assumptions included the proportion of patients with severe asthma and the relative risk of mortality for severe asthma compared to the general population, both of which were likely overestimated. In the absence of alternative data, CDA-AMC was unable to fully resolve this uncertainty in its reanalysis. Additionally, CDA-AMC was unable to adjust the analysis to reflect the time point of response assessment used in clinical practice. Given the outstanding clinical uncertainty, higher price reductions may be warranted.
References
1.Sanofi-aventis Canada Inc. Dupixent (dupilumab for injection): 300 mg single-use syringe (300 mg/2 mL), 300 mg single-use pen (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL), 200 mg single-use pen (200 mg/1.14 mL) solution for subcutaneous injection [product monograph]. November 18, 2024.
2.Sanofi-aventis Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dupixent (dupilumab for injection), 300 mg subcutaneous injection. December 18, 2024.
3.Sanofi. Clinical Study Report: EFC14146 (SINUS-24). A randomized, 24-week treatment, double-blind, placebo-controlled efficacy and safety study of dupilumab 300 mg every other week, in patients with bilateral nasal polyposis on a background therapy with intranasal corticosteroids [internal sponsor's report]. December 11, 2018.
4.Sanofi. Clinical Study Report: EFC14280 (SINUS-52). A randomized, double-blind, 52-week, placebo-controlled efficacy and safety study of dupilumab in patients with bilateral nasal polyposis on a background therapy with intranasal corticosteroids [internal sponsor's report] January 29, 2019.
5.Sanofi. Indirect treatment comparison of dupilumab vs. biologic therapies for severe chronic rhinosinusitis with nasal polyps executive summary report [internal sponsor’s report] In: Drug Reimbursement Review sponsor submission: Dupixent (dupilumab for injection), 300 mg subcutaneous injection. February 18, 2022.
6.Canada’s Drug Agency. Reimbursement Review: Mepolizumab (Nucala). Can J Health Technol. 2023;3(2). doi:10.51731/cjht.2023.588 Accessed July 31, 2024. https://www.cadth.ca/sites/default/files/DRR/2023/SR0735-Nucala_combined.pdf
7.DeConde AS, Mace JC, Levy JM, et al. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope. 2017;127(3):550-555. doi:10.1002/lary.26391 PubMed
8.Statistics Canada. Table: 84-537-X. Life expectancy and other elements of the complete life table, three-year estimates, Canada, all provinces except Prince Edward Island. 2020-2022. 2024. Accessed by sponsor, no date provided. https://www150.statcan.gc.ca/n1/en/catalogue/84-537-X
9.Ali Z, Dirks CG, Ulrik CS. Long-term mortality among adults with asthma: a 25-year follow-up of 1,075 outpatients with asthma. Chest. 2013;143(6):1649-1655. doi:10.1378/chest.12-2289 PubMed
10.Scangas GA, Wu AW, Ting JY, et al. Cost utility analysis of dupilumab versus endoscopic sinus surgery for chronic rhinosinusitis with nasal polyps. Laryngoscope. 2021;131(1):E26-E33. doi:10.1002/lary.28648 PubMed
11.Crump LJS. Establishing utility values for the 22-item Sino-Nasal Outcome Test (SNOT-22) using a crosswalk to the EuroQol–five-dimensional questionnaire–three-level version (EQ-5D-3L). 2017;doi:10.1002/alr.21917
12.Soler ZM, Wittenberg E, Schlosser RJ, et al. Health state utility values in patients undergoing endoscopic sinus surgery. Laryngoscope. 2011;121(12):2672-2678. doi:10.1002/lary.21847 PubMed
13.Ontario Ministry of Health. Exceptional Access Program product prices. 2024. Accessed by sponsor, no date provided. https://www.ontario.ca/page/exceptional-access-program-product-prices
14.Ontario Ministry of Health. Ontario drug benefit formulary/comparative drug index. 2024. Accessed by sponsor, no date provided. https://www.formulary.health.gov.on.ca/formulary/
15.Government of Canada. Wages. Registered Nurse (R.N.) in Canada. 2023. Accessed by sponsor, no date provided. https://www.jobbank.gc.ca/marketreport/wages-occupation/993/ca
16.Ontario Ministry of Health. Schedule of benefits and fees [sponsor submitted reference]. 2024. Accessed by sponsor, no date provided. https://www.health.gov.on.ca/en/pro/programs/ohip/sob/
17.Canadian Institute of Health Information. Cost of a standard hospital stay. 2022. Accessed by sponsor, no date provided. https://yourhealthsystem.cihi.ca/hsp/inbrief?lang=en#!/indicators/015/cost-of-a-standard-hospital-stay-cshs/;mapC1;mapLevel2;provinceC9001;/
18.CADTH. Canadian Medical Imaging Inventory. Private imaging facilities in Canada: MRI and CT. 2022. Accessed by sponsor, no date provided. https://www.cda-amc.ca/sites/default/files/attachments/2022-06/CMII-MRI-CT-Final_3.pdf
19.Chapman KR, Cogger K, Arthurs E, et al. Real-world outcomes of mepolizumab for the treatment of severe eosinophilic asthma in Canada: an observational study. Allergy Asthma Clin Immunol. 2024;20(1):11. doi:10.1186/s13223-023-00863-7 PubMed
20.Au J, Rudmik L. Cost of outpatient endoscopic sinus surgery from the perspective of the Canadian government: a time-driven activity-based costing approach. Int Forum Allergy Rhinol. 2013;3(9):748-754. doi:10.1002/alr.21181 PubMed
21.Ontario Ministry of Health. Exceptional Access Program reimbursement criteria for frequently requested drugs. 2025. Accessed January 30, 2025. https://www.ontario.ca/files/moh-frequently-requested-drugs.pdf
22.Government of Saskatchewan. Saskatchewan Drug Plan: search formulary. 2024. Accessed January 30, 2025. https://formulary.drugplan.ehealthsask.ca/SearchFormulary
23.Canada’s Drug Agency. Reimbursement Recommendation: Mepolizumab (Nucala). Can J Health Technol.2(12). doi:10.51731/cjht.2022.515 Accessed July 31, 2024. https://www.cadth.ca/sites/default/files/DRR/2022/SR0735%20Nucala%20-%20CADTH%20Final%20Recommendation%20(with%20corrections)_Final.pdf
24.pan-Canadian Pharmaceutical Alliance. Nucala (mepolizumab): severe chronic rhinosinusitis with nasal polyps [sponsor submitted reference]. 2024. Accessed July 31, 2024. https://www.pcpacanada.ca/negotiation/22092
25.Hopkins C, Browne JP, Slack R, et al. The national comparative audit of surgery for nasal polyposis and chronic rhinosinusitis. Clin Otolaryngol. 2006;31(5):390-398. doi:10.1111/j.1749-4486.2006.01275.x PubMed
26.Sanofi-aventis Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dupixent (dupilumab for injection), 300 mg subcutaneous injection December 18, 2024.
27.Alt JA, Thomas AJ, Curtin K, et al. Mortality risk in patients with chronic rhinosinusitis and its association to asthma. Int Forum Allergy Rhinol. 2017;7(6):591-599. doi:10.1002/alr.21931 PubMed
28.Canada's Drug Agency. Reimbursement Review: Dupilumab for prurigo nodularis. 2025. Accessed March 7, 2025. https://www.cda-amc.ca/dupilumab-8
29.Canada's Drug Agency. Reimbursement Review: Dupilumab for chronic obstructive pulmonary disease. 2025. Accessed March 7, 2025. https://www.cda-amc.ca/dupilumab-6
30.pan-Canadian Pharmaceutical Alliance. Dupixent (dupilumab): asthma. 2023. Accessed March 17, 2025. https://www.pcpacanada.ca/negotiation/22270
31.pan-Canadian Pharmaceutical Alliance. Dupixent (dupilumab): atopic dermatitis. 2023. Accessed March 17, 2025. https://www.pcpacanada.ca/negotiation/22214
32.pan-Canadian Pharmaceutical Alliance. Nucala (mepolizumab): severe eosinophilic asthma. 2017. Accessed March 17, 2025. https://www.pcpacanada.ca/negotiation/20946
33.pan-Canadian Pharmaceutical Alliance. Nucala (mepolizumab): severe eosinophilic asthma, add-on maintenance treatment of in children (aged 6 years and older). 2024. Accessed March 17, 2025. https://www.pcpacanada.ca/negotiation/22535
34.pan-Canadian Pharmaceutical Alliance. Nucala (mepolizumab): severe chronic rhinosinusitis with nasal polyps. 2024. Accessed March 17, 2025. https://www.pcpacanada.ca/negotiation/22092
35.GlaxoSmithKline Inc. Nucala (mepolizumab for injection): 100 mg/mL lyophilized powder, 100 mg/mL solution, 40 mg/0.4 mL solution for subcutaneous injection [product monograph]. November 28, 2023. Accessed January 30, 2025. https://pdf.hres.ca/dpd_pm/00073581.PDF
36.INESSS. Extract Notice to Minister. Nucala (Polypes) Accessed by sponsor, no date provided. https://www.inesss.qc.ca/en/themes/medicaments/drug-products-undergoing-evaluation-and-evaluated/extract-notice-to-the-minister/nucala-polypes-6879.html
37.Statistics Canada. Table: 17-10-0005-01. Population estimates on July 1, by age and gender. 2024. Accessed February 7, 2025. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501
38.Indigenous Services Canada. Non-insured health benefits program: First Nations and Inuit Health Branch: annual report 2022 to 2023. 2024. Accessed February 7, 2025. https://www.sac-isc.gc.ca/eng/1713194236054/1713194280612#sec2
39.Chen Y, Dales R, Lin M. The epidemiology of chronic rhinosinusitis in Canadians. Laryngoscope. 2003;113(7):1199-205. doi:10.1097/00005537-200307000-00016 PubMed
40.Khan A, et al. The Global Allergy and Asthma European Network (GALEN rhinosinusitis cohort: a large European cross-sectional study of chronic rhinosinusitis patients with and without nasal polyps. Rhinology. 2019;57(1):32-42. doi:10.4193/Rhin17.255 PubMed
41.Alsharif S, Jonstam K, van Zele T, et al. Endoscopic sinus surgery for type-2 CRS wNP: an endotype-based retrospective study. Laryngoscope. 2019;129(6):1286-92. doi:10.1002/lary.27815 PubMed
42.Mascarenhas JG, da Fonseca VMG, Chen VG, et al. Long-term outcomes of endoscopic sinus surgery for chronic rhinosinusitis with and without nasal polyps. Braz J Otorhinolaryngol. 2013;79(3):306-11. doi:10.5935/1808-8694.20130055 PubMed
43.Veloso-Teles R, Cerejeira R, et al. Endoscopic sinus surgery for chronic rhinosinusitis with nasal polyps: clinical outcome and predictive factors of recurrence. Am J Rhinol Allergy. 2017;31(1):56-62. doi:10.2500/ajra.2017.31.4402 PubMed
44.Min HK, Lee S, Kim S, et al. Global incidence and prevalence of chronic rhinosinusitis: a systematic review. Clin Exp Allergy. 2025;55(1):52-66. doi:10.1111/cea.14592 PubMed
45.Bachert C, Bhattacharyya N, Desrosiers M, et al. Burden of disease in chronic rhinosinusitis with nasal polyps. J Asthma Allergy. 2021;14:127-134. doi:10.2147/JAA.S290424 PubMed
46.Toppila-Salmi S, Hallfors J, Aakko J, et al. The burden of chronic rhinosinusitis with nasal polyps and its relation to asthma in Finland. Clin Transl Allergy. 2022;12(10):e12200. doi:10.1002/clt2.12200 PubMed
47.Sutherland G, Thy D. Understanding the gap. A pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada; 2017.
48.Lau SWJ, Huang Y, Hsieh J, et al. Participation of older adults in clinical trials for new drug applications and biologics license applications from 2010 through 2019. JAMA Netw Open. 2022;5(10):e2236149. doi:10.1001/jamanetworkopen.2022.36149 PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Severe Chronic Rhinosinusitis With Nasal Polyposis
Treatment | Strength/concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Dupilumab (Dupixent) | 300 mg/2 mL | Single-use syringe | 978.7000a | 300 mg every other week1 | 69.91 | 25,534 |
Single-use pen | 978.7000a | |||||
Mepolizumab (Nucala) | 100 mg/1 mL | Powder for injection | 2,058.6400 | 100 mg every 4 weeks35 | 73.52 | 26,854 |
Prefilled autoinjector | 2,137.1500 | 76.33 | 27,878 | |||
Prefilled syringe | 2,137.1500 | 76.33 | 27,878 |
CDA-AMC = Canada’s Drug Agency.
Note: All prices are from the Saskatchewan Drug Plan Formulary (accessed January 2025),22 unless otherwise indicated, and do not include dispensing fees. A year is assumed to be 365.25 days.
aSponsor’s submitted price.2 Dupilumab is also available in 200 mg/1.14 mL prefilled pens and syringes at a list price of $978.7000;22 however, this size is not relevant to the recommended dose for severe CRS.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | The model includes numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. |
Model structure is adequate for decision problem | No | The model’s response assessment time point was not consistent with current clinical practice or funding criteria and could not be changed. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Uncertainty in the odds of responding to mepolizumab relative to dupilumab was not fully implemented, nor was uncertainty in the probability of having asthma or uncontrolled asthma incorporated. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough detail) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
Figure 1: Decision Tree Model Structure
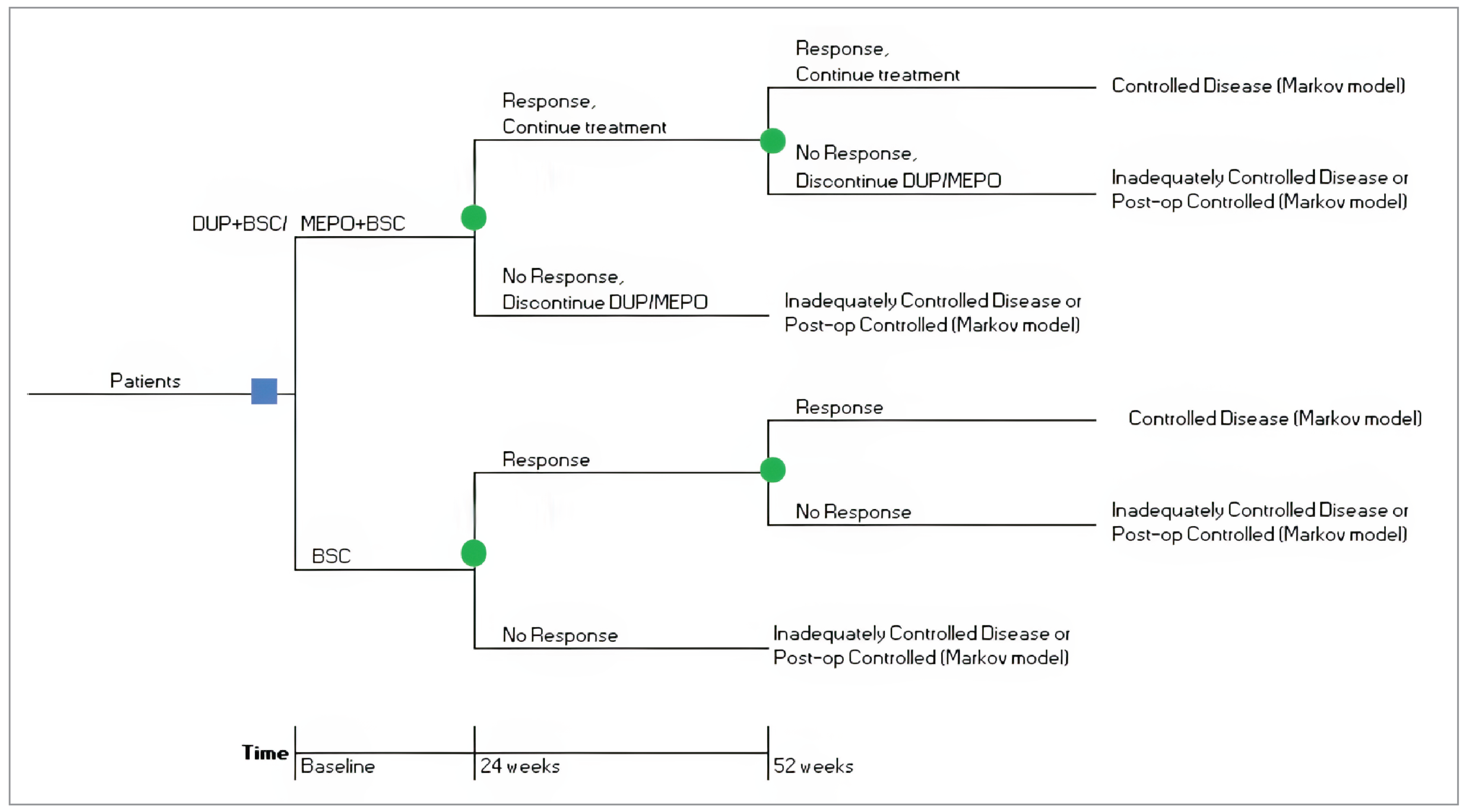
BSC = best supportive care; CRSwNP = chronic rhinosinusitis with nasal polyposis; DUP = dupilumab; MEPO = mepolizumab.
Source: Sponsor’s pharmacoeconomic submission.2
Figure 2: Markov Model Structure
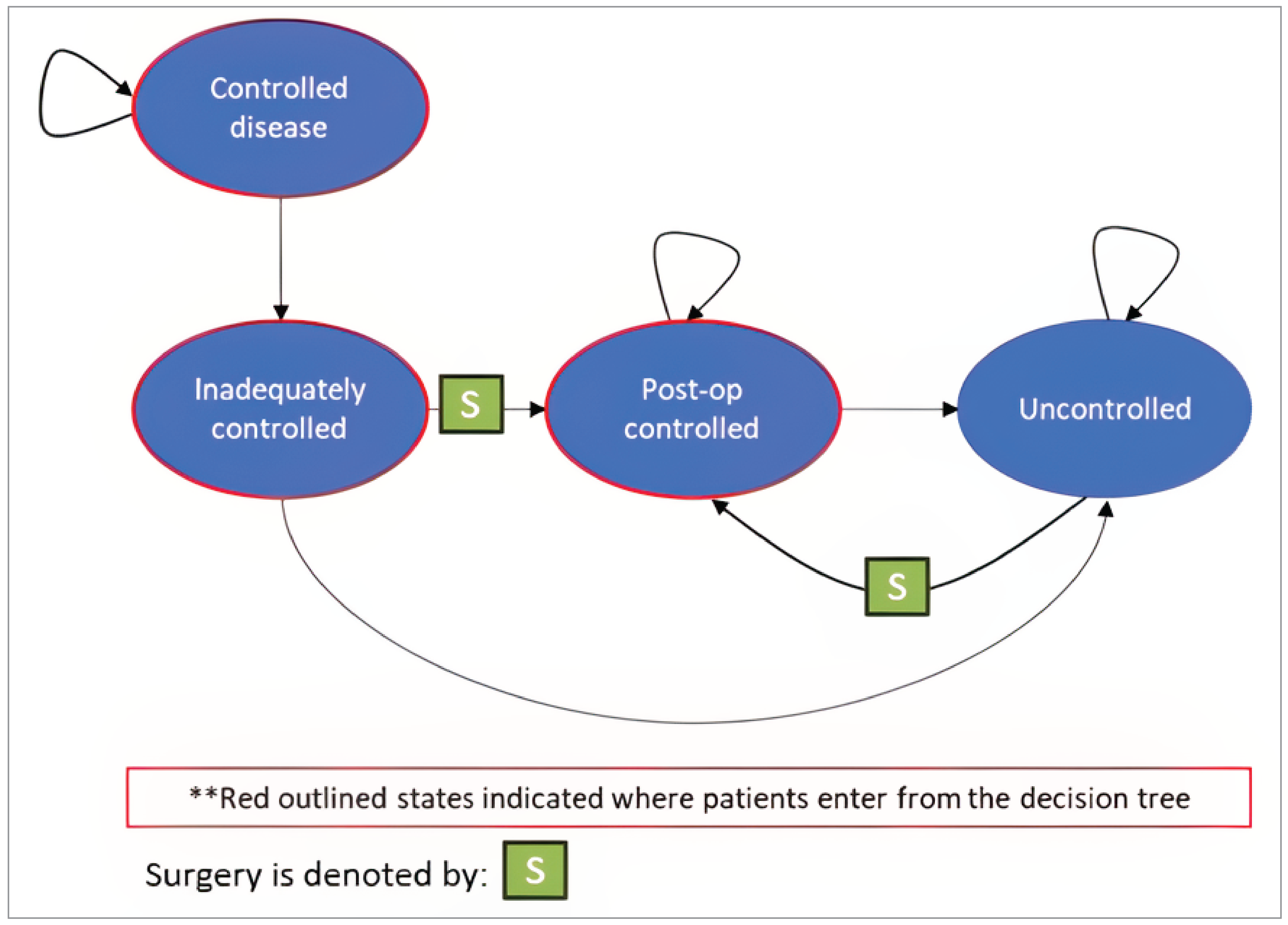
Post-op = postoperative.
Source: Sponsor’s pharmacoeconomic submission.2
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of the CDA-AMC Base Case
Table 10: Summary of the Stepped Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case (probabilistic) | BSC | 135,622 | 12.34 | Reference |
Dupilumab plus BSC | 441,591 | 16.44 | 74,785 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 297,551 | 14.44 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
Sponsor base case (deterministic) | BSC | 135,144 | 11.93 | Reference |
Dupilumab plus BSC | 443,473 | 16.16 | 72,878 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 229,359 | 14.05 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC reanalysis 1: SYNAPSE-like population (deterministic) | BSC | 136,328 | 11.93 | Reference |
Dupilumab plus BSC | 501,215 | 16.68 | 76,896 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 339,474 | 14.36 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC reanalysis 2: Saskatchewan price for mepolizumab (deterministic) | BSC | 135,144 | 11.93 | Reference |
Mepolizumab plus BSC | 285,982 | 14.05 | 71,120 | |
Dupilumab plus BSC | 443,473 | 16.16 | 74,645 vs. mepolizumab plus BSC | |
CDA-AMC reanalysis 3: Response based on SNOT-22 (deterministic) | BSC | 134,417 | 11.99 | Reference |
Dupilumab plus BSC | 505,136 | 16.73 | 78,292 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 476,730 | 15.70 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC reanalysis 4: Greater impact of surgery (deterministic) | BSC | 132,915 | 12.42 | Reference |
Dupilumab plus BSC | 442,544 | 16.36 | 78,525 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 297,612 | 14.43 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC reanalysis 5: Disutility for uncontrolled asthma (deterministic) | BSC | 135,144 | 12.11 | Reference |
Dupilumab plus BSC | 443,473 | 16.28 | 73,985 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 299,359 | 14.21 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC reanalysis 6: Resource use in uncontrolled states (deterministic) | BSC | 123,260 | 11.93 | Reference |
Dupilumab plus BSC | 438,390 | 16.16 | 74,485 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 289,717 | 14.05 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC base case (deterministic) Reanalysis 1 through 6 | BSC | 130,821 | 11.96 | Reference |
Dupilumab plus BSC | 569,259 | 16.27 | 101,796 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 492,933 | 15.25 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC base case (probabilistic) Reanalysis 1 through 6 | BSC | 121,016 | 12.59 | Reference |
Dupilumab plus BSC | 567,584 | 16.76 | 106,988 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 489,119 | 15.76 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically.
Table 11: Disaggregated Summary of CDA-AMC Economic Evaluation Results
Parameter | Dupilumab + BSC | Mepolizumab + BSC | BSC |
|---|---|---|---|
Discounted LYs | |||
Total LYs | 26.61 | 26.62 | 25.28 |
Response | 2.55 | 1.88 | 1.62 |
No response | 0.28 | 0.73 | 0.80 |
Controlled disease | 20.11 | 14.82 | 1.43 |
Inadequately controlled disease | 0.20 | 0.53 | 1.00 |
Postoperative controlled disease | 0.85 | 2.02 | 5.13 |
Uncontrolled disease | 2.63 | 6.64 | 15.30 |
Discounted QALYs | |||
Total QALYs | 16.76 | 15.76 | 12.59 |
Response | 0.57 | 0.42 | 0.32 |
No response | 0.04 | 0.10 | 0.11 |
Controlled disease | 14.26 | 10.51 | 1.01 |
Inadequately controlled disease | 0.07 | 0.19 | 0.44 |
Postoperative controlled disease | 0.52 | 1.25 | 3.11 |
Uncontrolled disease | 1.31 | 3.30 | 7.61 |
Short-term disutility due to surgery | 0.00 | 0.00 | 0.01 |
Discounted costs ($) | |||
Total | 567,584 | 489,119 | 121,016 |
Drug acquisition (add-on) | 476,350 | 387,766 | 0 |
BSC costs | 11,291 | 11,427 | 10,847 |
Health state costs | 7,024 | 11,689 | 21,338 |
Surgery costs | 1,366 | 3,230 | 8,341 |
Adverse event costs | 952 | 1,093 | 1,578 |
Asthma-related costs | 70,603 | 73,914 | 78,912 |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 12: Scenario Analyses Conducted on the CDA-AMC Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case (probabilistic) Reanalysis 1 through 6 | BSC | 121,016 | 12.59 | Reference |
Dupilumab plus BSC | 567,584 | 16.76 | 106,988 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 489,119 | 15.76 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC Scenario 1: Asthma-related impacts removeda | BSC | 46,363 | 13.81 | Reference |
Dupilumab plus BSC | 516,491 | 17.42 | 130,377 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 430,188 | 16.37 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC Scenario 2: Efficacy informed by ITT analysis of submitted ITC | BSC | 119,686 | 12.77 | Reference |
Dupilumab plus BSC | 497,460 | 17.02 | 88,891 | |
Dominated treatments | ||||
Mepolizumab plus BSC | 436,921 | 16.12 | Extendedly dominated by mix of BSC and dupilumab plus BSC | |
CDA-AMC Scenario 3: Response based on NPS | BSC | 122,846 | 12.35 | Reference |
Mepolizumab plus BSC | 312,761 | 14.66 | 82,279 | |
Dupilumab plus BSC | 499,230 | 16.84 | 85,467 | |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; ITT = intention-to-treat; NPS = Nasal Polyp Score; QALY = quality-adjusted life-year.
aThe magnitude of the impacts of asthma on health care costs, mortality, and quality of life is uncertain. The true effect of improvements in asthma control on the ICER likely lies between the CDA-AMC base-case analysis and this scenario.
Appendix 5: Submitted BIA and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key Take-aways of the BIA |
|---|
|
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CRS = chronic rhinosinusitis; CRSwNP = chronic rhinosinusitis with nasal polyposis; NIHB = Non-Insured Health Benefits.
Summary of Sponsor’s BIA
The sponsor submitted a BIA estimating the expected incremental budget impact of reimbursing dupilumab as an add-on maintenance treatment with intranasal corticosteroids in adult patients with severe CRSwNP inadequately controlled by systemic corticosteroids and/or surgery.26 The BIA was conducted from the perspective of public health care payers in Canada over a 3-year time horizon (2026 through 2028, with 2025 as the base year). The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets, excluding Quebec, as well as the Non-Insured Health Benefits (NIHB) program. The sponsor’s base case included drug acquisition costs only, and the cost of BSC was assumed to be equal for all patients and thus was assumed to be $0 within the analysis. Market shares in the reference scenario were based on sponsor-obtained clinical expert opinion and a reanalysis conducted by the Institut national d’excellence en santé et en services sociaux (INESSS) during its review of mepolizumab for CRSwNP.36 Market uptake of dupilumab was estimated based on internal sponsor estimates. Dupilumab was expected to capture 90% of its market share from mepolizumab. Key inputs to the BIA are documented in Table 14.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3 if appropriate) |
|---|---|
Target population | |
Pan-Canadian population (year before base year) | |
Adult population (varies by jurisdiction) | 81.32%37 |
Prevalence of CRS | 5.0%39 |
Proportion of CRS who have CRSwNP | |
Proportion treated with intranasal corticosteroids | 90.4%40 |
Proportion without severe eosinophilic asthma | 87.6%25 |
Proportion previously treated with oral corticosteroids and/or surgery | 47.0%a |
Proportion with uncontrolled symptoms | 40.0%b |
Proportion eligible for public drugs | 48.42%c |
Average annual population growth (varies by jurisdiction) | 0.967% |
Number of patients eligible for drug under review | 5,836 / 5,894 / 5,953 |
Market shares (reference scenario, 3 years) | |
Dupilumab plus BSC | 0% / 0% / 0% |
Mepolizumab plus BSC | ████% / ████% / ████% |
BSC alone | ████% / ████% / ████% |
Market shares (new drug scenario, 3 years) | |
Dupilumab plus BSC | ████% / ████% / ████% |
Mepolizumab plus BSC | ████% / ████% / ████% |
BSC alone | ████% / ████% / ████% |
Cost of treatment (per patient, per year) | |
Dupilumab (adherence: ████%)d | $22,582 |
Mepolizumab (adherence: ████%)d | $26,743 |
BSC alone (adherence: ███%) | $0 |
BSC = best supportive care; CRS = chronic rhinosinusitis; CRSwNP = chronic rhinosinusitis with nasal polyposis.
aCited as based on a US database of employer claims based on more than 39.7 million patients, which found that 47% of patients with CRSwNP had been previously treated with systemic corticosteroids or surgery.26
bBased on the range of values reported across multiple population studies.7,40-43
cBased on 82.9% of patients within the SINUS-24 and SUNIS-52 trials being less than 65 years of age. Patients older than 65 years were assumed to have 100% eligibility for public funding, while those younger than 65 years were assumed to be publicly funded in proportions consistent a mix of enrolled and eligible patients within each jurisdiction as reported by the Conference Board of Canada.26
dAdherence was based on that reported in the SINUS-52 clinical trial of dupilumab, with mepolizumab assumed to be the same.26
Summary of the Sponsor’s BIA Results
The results for the sponsor’s analysis suggested that the reimbursement of dupilumab for the add-on treatment of adults with severe CRSwNP inadequately controlled by systemic corticosteroids and/or surgery would be associated with an incremental savings of $1,475,592 in year 1, $2,805,187 in year 2, and $3,806,943 in year 3, for a 3-year incremental savings of $8,087,722.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The prevalence of CRSwNP may be underestimated. The sponsor estimated that 5% of adults in Canada have CRS, based on a population health survey conducted from 1996 to 1997.39 The sponsor also assumed that 6.1% of patients with CRS have CRSwNP, based on a Utah database study of mortality with CRS and asthma.27 These figures have previously been used in a CDA-AMC review for CRSwNP, however, were noted to be uncertain at the time.6 According to clinical expert input obtained by CDA-AMC, the prevalence of CRS has been rising due to increased awareness and diagnosis, while a recent systematic review hypothesized that increasing global incidence may stem from a variety of factors, including a general trend in increasing prevalence of allergic diseases.44 Clinical expert input obtained by CDA-AMC indicated that estimates between 8 to 12% may be more reflective of the current prevalence of CRS in Canada, consistent with the pooled prevalence of CRS of 8% for North America reported in the global systematic review.44 Clinical expert input obtained by CDA-AMC also indicated that the assumed proportion of patients with CRS who have nasal polyps (6.1%) may also be underestimated, with sources in the literature estimating rates of nasal polyps in CRS as high as 20 to 30%.45,46
In reanalysis, CDA-AMC assumed the prevalence of CRS to be 8% of the adult population. In a scenario analysis, CDA-AMC also assumed that 20% of patients with CRS have NP.
The cost of mepolizumab may be overestimated. When estimating the cost of mepolizumab, the sponsor used the Ontario Drug Benefit Exceptional Access Program list price of $2,318 per 100 mg dose.13 However, CDA-AMC notes that the list price of mepolizumab on the Saskatchewan formulary is $21.37 per mg, or $2,137 per 100 mg dose22 As mepolizumab was funded following a positive recommendation from CDA-AMC,23 which included a substantial price reduction recommendation, and successful negotiations with the pan-Canadian Pharmaceutical Alliance,24 it is likely that confidential pricing exists for mepolizumab. As such, it is likely that Saskatchewan’s lower list price is a closer approximation of this confidential price.
In reanalysis, CDA-AMC used a price of $2,137.15 per 100 mg dose of mepolizumab.
The proportion of patients eligible for funding is uncertain. The sponsor assumed that 48.4% of patients meeting the criteria for dupilumab would be publicly funded, which was based on the assumption that 82.9% of otherwise eligible patients are younger than 65 years, consistent with the population of the SINUS trials. The sponsor then assumed that 100% of patients aged 65 years or older would receiving public funding, whereas younger than 65 years would be funded at rates consistent with the proportion enrolled in public drug plans in each jurisdiction as reported by the Conference Board of Canada.47 While the SINUS trials did not limit patient enrolment by an upper age criterion, it is possible that older adults are underrepresented in the SINUS populations, as they often are in clinical trials.48 CDA-AMC notes that in the recent global prevalence of CRS systematic review, prevalence rates reported for adults younger than age 65 and those 65 years of age and older were almost identical (7.4% and 7.5%, respectively), which would indicate that the age distribution of the CRS population may be more closely aligned with that of the overall adult population than estimated. CDA-AMC notes that for mepolizumab, currently funded for severe eosinophilic asthma and severe CRSwNP in patients who have had nasal surgery, approximately ████% of all 2024 claims within the IQVIA Pharmastat database, excluding Quebec, were publicly funded. Clinical expert input obtained by CDA-AMC indicated that patients with severe CRSwNP may experience underemployment due to absenteeism, decreased productivity, and disability as a result of their condition, in which case their access to private drug insurance may be somewhat lower than average, increasing the proportion who may seek public funding relative to the overall population. As such, it is likely that the assumption that 48.4% of patients within the BIA would receive public funding is an underestimate.
CDA-AMC did not adjust for this limitation in its base case as the proportion of patients with CRSwNP who are older than 65 years is uncertain, as is the proportion or patients with severe CRSwNP who are enrolled in public plans and the proportion who would newly enrol in public plans to access dupilumab. The base case estimated budgetary impact of reimbursing dupilumab is likely underestimated. CDA-AMC conducted a scenario analysis assuming 60% of the pan-Canadian patient population would be eligible for public funding, consistent with the approximate proportion assumed in its review of mepolizumab for CRSwNP.6
The proportion of dupilumab uptake coming from mepolizumab is overestimated. The sponsor’s BIA assumed that ██% of the uptake of dupilumab would be due to the displacement of mepolizumab, while only ██% would be from patients who would otherwise be on BSC alone. However, the requested reimbursement for dupilumab is for adult patients with severe CRSwNP inadequately controlled by systemic corticosteroids and/or surgery, while current funding criteria for mepolizumab is for adult patients with severe CRSwNP who have undergone at least 1 prior surgical intervention or who have a contraindication to surgery. As such, the population of patients who would be eligible for dupilumab if funded as requested is broader than those who can currently access mepolizumab. The sponsor’s BIA has an option to restrict the eligible patient population to those who have previously had surgery, which estimates that ████% of patients have previously had a nasal surgery, compared to the estimated ████% of patients who were estimated to have been treated with oral corticosteroids and/or surgery. This therefore assumes that ██% of patients (██████%) have had oral corticosteroids but not surgery, and thus most of that ██% who could be eligible for dupilumab could not be eligible for mepolizumab under current funding criteria (some would still be eligible due to having a contraindication for surgery).
In reanalysis, CDA-AMC assumed that 70% of the market uptake of dupilumab would come from patients who would otherwise receive mepolizumab, due to the broader population who would be eligible for dupilumab compared to mepolizumab. The remaining 30% would come from patients who would otherwise receive BSC due to not being eligible for mepolizumab, or who would choose not to receive mepolizumab but would receive dupilumab.
The NIHB population was inappropriately calculated. The sponsor calculated the total population of CDA-AMC-participating drug plans by adding the population of the provinces, excluding Quebec, to the population of NIHB clients. NIHB clients living within the borders of a province are counted within provincial population data as reported by Statistics Canada, thus the NIHB population was double counted in the sponsor’s analysis. Additionally, NIHB clients residing within Ontario who are aged < 25 years or ≥ 65 years are eligible for reimbursement by the Ontario Drug Benefit (ODB) and thus should be counted as ODB clients (and included in the Ontario population estimates) rather than NIHB clients for the purposes of modelling the budget impact of reimbursing dupilumab. Finally, in determining the proportion of the NIHB client population who are adults, the sponsor summed the number of adults in each of the 3 territories (i.e., Northwest Territory, Yukon, and Nunavut) and divided it by the sum of the total population of the 3 territories. As less than 10% of the NIHB’s client population reside in the territories, and the NIHB’s annual reports include a breakdown of their client population by jurisdiction and age, it is more appropriate to estimate the proportion of the NIHB client population that are adults using the NIHB annual reports.
CDA-AMC did not adjust for this limitation in reanalysis. The impact on pan-Canadian model results is expected to be minimal, however the impact on the jurisdictional results, particularly those of the NIHB, is expected to be more substantial.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by increasing the prevalence of CRS, reducing the unit cost of mepolizumab, and decreasing the proportion of dupilumab market uptake that is displacing mepolizumab. The changes made to derive the CDA-AMC base case are described in Table 15.
Table 15: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Prevalence of CRS | 5.0% | 8.0% |
2. Unit cost of mepolizumab | $2,318 | $2,137 |
3. Proportion of dupilumab share that is displacing mepolizumab | ███████% | 70% |
CDA-AMC base-case | Reanalysis 1 through 3 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CRS = chronic rhinosinusitis.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17. In the CDA-AMC base case, the 3-year budget impact of reimbursing dupilumab as an add-on maintenance treatment with intranasal corticosteroids in adult patients with severe CRSwNP inadequately controlled by systemic corticosteroids and/or surgery is expected to be $46,313,639 (year 1: $8,449,849, year 2: $16,063,660, year 3: $21,800,130).
Table 16: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | −8,087,722 |
CDA-AMC reanalysis 1: Prevalence of CRS | −12,940,356 |
CDA-AMC reanalysis 2: Unit cost of mepolizumab | 2,130,824 |
CDA-AMC reanalysis 3: 70% of dupilumab uptake is from mepolizumab | 20,998,266 |
CDA-AMC base case (reanalysis 1 through 3) | 46,313,639 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CRS = chronic rhinosinusitis.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 17):
Assuming that of patients with CRS, 20% have nasal polyps.
Assuming that 60% of the pan-Canadian patient population will be publicly funded.
Table 17: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 54,090,390 | 62,431,668 | 70,933,593 | 79,598,624 | 212,963,885 |
New drug | 54,090,390 | 60,956,076 | 68,128,406 | 75,791,681 | 204,876,162 | |
Budget impact | 0 | −1,475,592 | −2,805,187 | −3,806,943 | −8,087,722 | |
CDA-AMC base case | Reference | 79,787,951 | 92,092,049 | 104,633,116 | 117,414,778 | 393,927,894 |
New drug | 79,787,951 | 100,541,898 | 120,696,776 | 139,214,909 | 440,241,533 | |
Budget impact | 0 | 8,449,849 | 16,063,660 | 21,800,130 | 46,313,639 | |
CDA-AMC scenario analysis 1: 20% of patients with CRS have NPs | Reference | 261,599,838 | 301,941,145 | 343,059,395 | 384,966,486 | 1,291,566,865 |
New drug | 261,599,838 | 329,645,567 | 395,727,133 | 456,442,324 | 1,443,414,863 | |
Budget impact | 0 | 27,704,423 | 52,667,737 | 71,475,838 | 151,847,998 | |
CDA-AMC scenario analysis 2: 60% of patients are eligible for public funding | Reference | 98,717,903 | 113,925,702 | 129,422,508 | 145,212,703 | 487,278,816 |
New drug | 98,717,903 | 124,378,884 | 149,291,927 | 172,174,010 | 544,562,723 | |
Budget impact | 0 | 10,453,182 | 19,869,418 | 26,961,307 | 57,283,908 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CRS = chronic rhinosinusitis; NP = nasal polyp.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.