Drugs, Health Technologies, Health Systems
Reimbursement Review
Nemolizumab (Nemluvio)
Sponsor: Galderma Canada Inc.
Therapeutic area: Atopic dermatitis
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AD
atopic dermatitis
AE
adverse event
AESI
adverse event of special interest
BSA
body surface area
CDA-AMC
Canada’s Drug Agency
CDLQI
Children’s Dermatology Life Quality Index
COPD
chronic obstructive pulmonary disease
CrI
credible interval
CsA
cyclosporine
DAE
discontinuation due to adverse event
DAO
Dermatology Association of Ontario
DLQI
Dermatology Life Quality Index
EASI
Eczema Area and Severity Index
EASI-75
≥ 75% improvement in Eczema Area and Severity Index from baseline
ESC
Eczema Society of Canada
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
IGA
Investigator Global Assessment
IL
interleukin
ITT
intention to treat
LOCF
last observation carried forward
LS
least squares
LTE
long-term extension
MID
minimal important difference
NMA
network meta-analysis
PP-NRS
Peak Pruritus Numeric Rating Scale
RCT
randomized controlled trial
SAE
serious adverse event
SC
subcutaneous
SD
standard deviation
TCI
topical calcineurin inhibitor
TCS
topical corticosteroid
ULN
upper limit of normal
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Nemolizumab powder and solvent for subcutaneous injection, available as:
|
Sponsor | Galderma Canada Inc. |
Indication | For the treatment of patients aged 12 years and older with moderate-to-severe atopic dermatitis (AD) whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable |
Reimbursement request | For the treatment of moderate to severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | December 18, 2025 |
Recommended dose | Adult patients: Initial dose of 60 mg (two 30 mg injections), followed by 30 mg given every 4 weeks; after 16 weeks of treatment, for patients who achieve clinical response, the recommended maintenance dose of nemolizumab is 30 mg every 8 weeks Pediatric patients: No dose adjustment for body weight is recommended for patients aged 12 years or older |
AD = atopic dermatitis; NOC = Notice of Compliance.
Introduction
Atopic dermatitis (AD) is a chronic, relapsing, inflammatory, and noncontagious skin disease that is thought to involve a complex interplay of genetic, immune, and neuroimmune dysregulation, skin barrier dysfunction, microbial imbalance, and environmental factors.1-4 It occurs most frequently in early childhood; it is estimated that the prevalence of eczema in Canada is 15% in children and adolescents (aged 0.5 years to 17 years), and 3.5% in adults.5,6 Acute worsening of AD, commonly referred to as a flare, presents as dry, red, itchy skin that can lead to lesions that blister, ooze, and crust. AD can be mild, moderate, or severe, depending on the extent and the severity of symptoms.7 An intense and debilitating itch and chronically relapsing lesions are the key clinical hallmarks of moderate to severe disease and can result in sleep disturbances, psychosocial distress, and reduced quality of life for patients and caregivers.7
The management of AD involves a multipronged approach including patient education, skin hydration, restoration of the skin, elimination of exacerbating factors, and pharmacologic treatment of skin inflammation.8 The clinical experts consulted for this review noted that the goals of treatment are reduction of signs and symptoms (e.g., red scaly plaques, itch, scratching, lichenification, dyspigmentation, scarring), prevention of secondary infections, improvement of quality of life (e.g., sleep, daily activities, hobbies), maintenance of independence, reduction of caregiver burdens, and enhancement of work and school productivity. Patients with persistent, moderate to severe AD despite optimized topical therapy require systemic treatment to achieve disease control. Topical drugs may be used concurrently with phototherapy or systemic drugs for the maintenance of response, rescue treatment, or control of flares.9 The clinical experts noted that a typical progression would be for patients to trial conventional systemic therapies for a period of 3 months and if well controlled, they would remain on that therapy, but if they do not respond, then they may switch to another conventional systemic therapy or the advanced therapies. They noted a trial of 3 to 6 months is usually used to determine response. If the patient’s skin is not completely clear, they may add a topical therapy. Occasionally, the experts noted that a combination of systemic therapies may be used. Dupilumab, abrocitinib, and upadacitinib are recommended by Canada’s Drug Agency (CDA-AMC) for reimbursement for the treatment of moderate to severe AD. Lebrikizumab and tralokinumab are recommended not to be reimbursed for moderate to severe AD but are approved for use in Canada.
Nemolizumab is a humanized, monoclonal antibody of the IgG2 subclass that inhibits interleukin (IL)-31 signalling by selectively binding to IL-31RA to ameliorate pruritus, inhibit inflammatory responses, and restore barrier integrity in AD. Nemolizumab received a Health Canada indication for the treatment of patients aged 12 years and older with moderate to severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. The sponsor’s reimbursement request is for the treatment of moderate to severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of nemolizumab subcutaneous (SC) (30 mg/0.49 mL in either a single-dose, prefilled dual-chamber pen or prefilled dual-chamber syringe with copackaged needle) for the treatment of moderate to severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to our call for input and from clinical experts consulted by for the purpose of this review.
Patient Input
One patient group submitted input for this review, the Eczema Society of Canada (ESC), a registered charity in Canada aiming to improve the lives of people living in Canada with eczema through support, education, awareness, and research. Information was gathered for this submission through questionnaires, patient interviews, review of published literature, and data from multiple surveys with a combined total of more than 3,000 people living in Canada.
Patients with AD described substantial physical and emotional burdens, including painful, itchy skin lesions that crack, bleed, and lead to scarring, pigment changes, and infection risk. Persistent itching disrupts sleep, school and work, and daily life, with some patients experiencing chronic pain and no relief. Emotionally, patients reported isolation, frustration, anxiety, depression, and difficulties with social and intimate relationships due to low self-esteem and treatment failures. Historically, systemic options were limited to phototherapy, off-label immunosuppressants, and steroids, which many fear using long term. While newer systemic therapies have helped some, access and response remain inconsistent. Patients expressed frustration with the trial-and-error nature of treatment and emphasized that due to the heterogeneous nature of AD, no single therapy works for all.
ESC highlighted the urgency for innovative therapies that can offer long-term relief and improve quality of life. Outcomes of treatment identified as most important to patients with AD include improved disease control, symptom and pain relief (e.g., itch, dryness, inflammation, blistering), convenience, and improved quality of life. ESC described general patient experiences with nemolizumab, although the source of these experiences (e.g., patient interviews, survey responses, general trial observations) was not specified. Patients treated with nemolizumab reported substantial reductions in itch, with noticeable improvements in skin clearance from rashes, lesion, sores, and open wounds, which provided further benefit in improving sleep, productivity, self-esteem, and mental health. ESC noted that many patients who were previously unsuccessful with approved and off-label medications reported success with nemolizumab.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts noted that pruritus (itch) is a very debilitating and unpredictable aspect of AD, and better treatments are needed to target this symptom. In addition, approximately 30% to 40% of patients will either not respond to, or will become refractory to, the currently available nonbiologic treatments (1 expert noted this would be approximately 20% of patients if biologics were also considered); therefore, new treatments are needed. Moderate to severe AD often comes with a high burden of disease, which also impacts patient’s health-related quality of life (HRQoL) and their ability to carry out activities due to symptoms, or due to a feeling of self-consciousness. The currently available treatments (e.g., JAK inhibitors) are not always well tolerated and have contraindications or black box warnings, further reinforcing the need for new treatment options.
The clinical experts noted that nemolizumab is the only treatment with a mechanism of action targeting IL-31, which is involved in the sensation of pruritus. It could be used as monotherapy or in combination with topical therapies, phototherapy, and other conventional immunosuppressing systemic drugs. They noted that nemolizumab should be considered a first-line systemic therapy after topical therapies, and considered alongside the other biologics such as dupilumab, tralokinumab, or lebrikizumab. The clinical experts noted that the reimbursement criteria for dupilumab could also be considered appropriate for nemolizumab (e.g., having been unsuccessful with 1 conventional systemic therapy trial); however, the choice to use a conventional treatment or advanced systemic drug would be partially determined by the drug coverage.
The experts noted that nemolizumab would be suitable for all patients with moderate to severe AD, and 1 expert noted it would also be appropriate for patients who do not tolerate, respond to, or cannot access phototherapy, as well as those who have a relative contraindication to, or have been unsuccessful with, alternate systemic therapies. The experts further noted that patients who are substantially impacted by pruritus, who have substantial flares of AD, whose current therapy has stopped working, or whose AD has a substantial impact on their lives would be those most in need of additional interventions and most likely to benefit. There are no specific criteria or laboratory tests required for diagnosis, as AD is typically diagnosed clinically and is a common disease. The experts noted that there are no biomarkers or tests that would indicate a patient’s likelihood to respond to nemolizumab.
Measures used in the pivotal trials are also used in clinical practice to assess response, including patient global assessment of improvement, Eczema Area and Severity Index (EASI) reduction, numeric rating scale for itch, and Dermatology Life Quality Index (DLQI). The clinical experts also noted that other subjective changes reported by patients in clinical practice may include changes to sleep, daily activities, work productivity, improvement in mental health, and reduction of scratching or itching. They commented that the measures used in clinical practice vary and may be chosen according to the reimbursement criteria set by payers to obtain coverage for a treatment (e.g., change in EASI score at 6 months). Patients are often assessed every 3 months initially and when patients are improved and their condition is considered stable, they are typically assessed every 6 months.
Treatment should be discontinued if there has been no meaningful response after 6 months of therapy, if the patient experiences an allergy or hypersensitivity, or if they experience intolerable adverse events (AEs). The experts noted that definition of a meaningful response could vary and the decision to discontinue is often shared between the clinician and the patient. One expert shared an example that patients with minimal disease response according to a tool such as EASI may still wish to continue treatment if their pruritus is controlled. If there is a partial response, the experts noted that the addition of a new therapy should be considered first, rather than discontinuing the current treatment.
According to the experts, patients should receive a proper diagnosis of AD by a dermatologist before nemolizumab is prescribed. Patients can be managed and monitored by dermatologists in any outpatient clinic (community or hospital). After 6 months of treatment and confirmation of clinical efficacy, primary care providers could also manage the prescribing until reinvolvement of the dermatologist is necessary.
Clinician Group Input
One joint input was submitted for this review by the Dermatology Association of Ontario (DAO) and the Atlantic Dermatology Group. DAO provides broad representation for more than one-half of registered dermatologists in Canada. The Atlantic Dermatology Group is a group of hospital-based and academic-based dermatologists practising in the Atlantic provinces. Information for this submission was gathered through a review of published literature, clinical trial data, and experience with nemolizumab as clinical trialists.
The input from clinician groups was generally consistent with the clinical experts consulted for this review, emphasizing the ongoing unmet need for treatments that provide rapid and sustained relief from pruritus, as well as improvements in sleep and quality of life for patients with moderate to severe AD. Like the experts, the clinician groups highlighted the limitations of current therapies, including slow onset of action with biologics and safety concerns or monitoring requirements with JAK inhibitors. Aligning with expert input, the clinician groups considered nemolizumab a suitable first-line systemic option, to be positioned alongside existing biologics, particularly for patients with an inadequate response to topicals or systemic therapies, or who require more rapid symptom relief. Both also highlighted the novel mechanism and monthly dosing schedule as factors that could improve adherence and convenience. The clinician groups provided additional details on patient selection, noting that nemolizumab may be particularly appropriate for patients with contraindications to JAK inhibitors (e.g., cardiovascular disease, immunosuppression concerns, thromboembolism). They also noted that patients with mild AD that can be managed effectively by topicals alone are less appropriate candidates.
Consistent with expert input, the clinician groups noted a range of clinical and patient-reported tools (e.g., Investigator Global Assessment [IGA], EASI, Peak Pruritus Numeric Rating Scale [PP-NRS], sleep scores) that could be used to assess treatment response, and support reassessment intervals from 4 to 12 months. However, they provided more specific discontinuation criteria, such as the inability to achieve a 4-point or more reduction in PP-NRS or sleep numeric rating scale or less than 50% improvement in EASI by week 16, while the experts emphasized a flexible, shared decision-making approach. Both clinical experts and clinician groups agreed that initiation should be done by dermatologists in an outpatient setting, but the clinician groups added that allergists could also initiate therapy, and that self-injection could be possible after training. The clinician group noted that because misdiagnosis of AD can occur, particularly in adult-onset cases, clinical expertise in differentiating AD from other eczematous conditions (e.g., contact dermatitis, seborrheic dermatitis, cutaneous T-cell lymphoma) is essential to ensure appropriate patient selection.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a recommendation for nemolizumab:
relevant comparators
considerations for initiation of therapy
considerations for continuation or renewal of therapy
considerations for prescribing of therapy
system and economic issues.
The clinical experts provided advice on the potential implementation issues raised by the drug programs. Refer to Table 5 for more details.
Clinical Evidence
Systematic Review
Description of Studies
Three studies were included in the systematic review: ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO.
ARCADIA 1 and ARCADIA 2 Studies
The study designs for the ARCADIA 1 and ARCADIA 2 studies were identical; both were phase III, double-blind, placebo-controlled, multicentre randomized controlled trials (RCTs) evaluating the efficacy and safety of nemolizumab in adults and adolescents (aged ≥ 12 years) with moderate to severe AD. The coprimary end point of the ARCADIA 1 and ARCADIA 2 studies was the proportion of patients with IGA success, and the proportion of patients with a 75% or greater improvement in the EASI score from baseline (EASI-75) at week 16. Key secondary end points also evaluated changes in PP-NRS across the study period. Patients were randomized via interactive response technology 2:1 to receive nemolizumab (ARCADIA 1: n = 620; ARCADIA 2: n = 522) or placebo (ARCADIA 1: n = 321; ARCADIA 2: n = 265) for 16 weeks. After the 16-week initial treatment period, patients in the treatment arm who met the study definition of clinical responders to treatment (i.e., an IGA of 0 [clear] or 1 [almost clear] or EASI-75 at week 16) were rerandomized 1:1:1 to receive either nemolizumab every 4 weeks (n = 169), nemolizumab every 8 weeks (n = 169), or placebo (n = 169) for the maintenance period.
ARCADIA CYCLO Study
The ARCADIA CYCLO study was a phase IIIb, double-blind, placebo-controlled, multicentre RCT evaluating the efficacy and safety of nemolizumab in adult patients aged 18 years or older with chronic AD who had a documented history of inadequate response, intolerance, or unacceptable toxicity to cyclosporine (CsA), or in whom CsA was medically inadvisable. Patients were randomized 1:1 to receive nemolizumab (n = 138) or placebo (n = 138). The primary end point of the ARCADIA CYCLO study was the proportion of patients with EASI-75, and proportion of patients with an improvement in PP-NRS of 4 or more from baseline at week 16.
Efficacy Results
ARCADIA 1 and ARCADIA 2 Studies: Initial Period
Proportion of Patients With IGA Success at Week 16
For patients in the ARCADIA 1 study, at week 16, 35.6% of patients in the nemolizumab arm and 24.6% of patients in the placebo arm attained IGA success (defined as IGA 0 or 1 and a ≥ 2-point reduction from baseline). The strata-adjusted difference between arms was 11.5% (97.5% confidence interval [CI], 4.7% to 18.3%; P = 0.0003). For patients in the ARCADIA 2 study, at week 16, 37.7% of patients in the nemolizumab arm and 26.0% of patients in the placebo arm attained IGA success. The strata-adjusted difference between arms was 12.2% (97.5% CI, 4.6% to 19.8%; P = 0.0006).
Proportion of Patients With EASI-75 at Week 16
For patients in the ARCADIA 1 study, at week 16, 43.5% of patients in the nemolizumab arm and 29.0% of patients in the placebo arm attained EASI-75. The strata-adjusted difference between arms was 14.9% (97.5% CI, 7.8% to 22.0%; P < 0.0001). For patients in the ARCADIA 2 study, at week 16, 42.1% of patients in the nemolizumab arm and 30.2% of patients in the placebo arm attained EASI-75. The strata-adjusted difference between arms was 12.5% (97.5% CI, 4.6% to 20.3%; P = 0.0006).
Change From Baseline to Week 16 in Total EASI Score
For patients in the ARCADIA 1 study, the least squares (LS) mean change from baseline in total EASI score was –12.36 (95% CI, –13.96 to –10.76) in the nemolizumab arm, and –8.68 (95% CI, –10.77 to –6.58) in the placebo arm. The LS mean difference was –3.68 (95% CI, –6.08 to –1.28; P = 0.0026). For patients in the ARCADIA 2 study, the LS mean change from baseline in total EASI score was –13.15 (95% CI, –14.57 to –11.73) in the nemolizumab arm and –9.02 (95% CI, –10.97 to –7.08) in the placebo arm. The LS mean difference between study arms was –4.13 (95% CI, –6.36 to –1.89; P = 0.0003).
Proportion of Patients With an Improvement of PP-NRS of 4 or More at Week 16
For patients in the ARCADIA 1 study, at week 16, 42.7% of patients in the nemolizumab arm and 17.8% of patients in the placebo arm reported a reduction in PP-NRS score of 4 points or greater. The strata-adjusted LS mean difference between arms was 24.9% (97.5% CI, 18.4% to 31.5%; P < 0.0001). For patients in the ARCADIA 2 study, at week 16, 41.0% of patients in the nemolizumab arm and 18.1% of patients in the placebo arm reported a reduction in PP-NRS score of 4 points or greater. The strata-adjusted LS mean difference between arms was 23.2% (97.5% CI, 16.1% to 30.3%; P < 0.0001).
Proportion of Patients With PP-NRS of Less Than 2 Points at Week 16
For patients in the ARCADIA 1 study, at week 16, 30.6% of patients in the nemolizumab arm and 11.2% of patients in the placebo arm reported a PP-NRS score of less than 2 points. The strata-adjusted LS mean difference between arms was –1.84% (97.5% CI, –2.21% to –1.47%; P < 0.0001). For patients in the ARCADIA 2 study, at week 16, 28.4% of patients in the nemolizumab arm and 11.3% of patients in the placebo arm reported a PP-NRS score of less than 2 points. The strata-adjusted LS mean difference between arms was 17.1% (97.5% CI, 10.9% to 23.3%; P < 0.0001).
Change From Baseline to Week 16 in PP-NRS Score
For patients in ARCADIA 1 study, the LS mean change from baseline in PP-NRS score was –3.77 (95% CI, –4.02 to –3.53) in the nemolizumab arm, and –1.94 (95% CI, –2.26 to –1.61) in the placebo arm. The LS mean difference was –1.84 (95% CI, –2.21 to –1.47; P < 0.0001). For patients in the ARCADIA 2 study, the LS mean change from baseline in PP-NRS score was –3.71 (95% CI, –3.94 to –3.47) in the nemolizumab arm and –1.95 (95% CI, –2.27 to –1.63) in the placebo arm. The LS mean difference between study arms was –1.76 (95% CI, –2.13 to –1.39; P < 0.0001).
Change From Baseline to Week 16 in DLQI Total Score
For adult patients in the ARCADIA 1 study, the LS mean change from baseline in DLQI total score was –7.76 (95% CI, –8.49 to –7.03) in the nemolizumab arm, and –5.26 (95% CI, –6.23 to –4.29) in the placebo arm. The LS mean difference was –2.50 (95% CI, –3.63 to –1.37; P < 0.0001). For adult patients in the ARCADIA 2 study, the LS mean change from baseline in DLQI total score was –6.96 (95% CI, –7.67 to –6.25) in the nemolizumab arm and –4.52 (95% CI, –5.48 to –3.56) in the placebo arm. The LS mean difference between study arms was –2.44 (95% CI, –3.58 to –1.30; P < 0.0001).
Change From Baseline to Week 16 in Children’s Dermatology Life Quality Index Total Score
For adolescent patients in the ARCADIA 1 study, the LS mean change from baseline in the Children’s Dermatology Life Quality Index (CDLQI) total score was –6.92 (95% CI, –9.26 to –4.58) in the nemolizumab arm, and –5.10 (95 CI, –7.71 to –2.50) in the placebo arm. The LS mean difference was –1.82 (95% CI, –4.88 to 1.25; P = 0.2454). For adolescent patients in the ARCADIA 2 study, the LS mean change from baseline in CDLQI total score was –7.40 (95% CI, –8.97 to –5.82) in the nemolizumab arm and –5.02 (95% CI, –7.48 to –2.56) in the placebo arm. The LS mean difference between study arms was –2.38 (95% CI, –5.03 to 0.27; P = 0.0788).
Incidence of Rescue Therapy Use
In the ARCADIA 1 study, during the initial period a total of 3.4% of patients in the nemolizumab arm and 4.0% of patients in the placebo arm reported using rescue therapy. In the ARCADIA 2 study, during the initial period a total of 2.1% of patients in the nemolizumab arm and 4.2% of patients in the placebo arm reported using rescue therapy.
ARCADIA 1 and ARCADIA 2 Studies: Pooled Maintenance Period
The ARCADIA 1 and ARCADIA 2 studies were noted by the sponsor to be replicate studies, having identical inclusion and exclusion criteria, study design, and analysis methods. In addition, a similar proportion of patients in each study were considered clinical responders per the study definition and continued on to the maintenance period, and study discontinuations or losses to follow-up were broadly similar. Therefore, the pooled maintenance period results were appraised in the report. Out of the intention-to-treat (ITT) population initially randomized in the initial period, 169 patients were rerandomized to the nemolizumab every 4 weeks arm, 169 to the nemolizumab every 8 weeks arm, and 169 to the placebo arm.
Proportion of Patients Maintaining IGA Success Until Week 48 From the Subset With IGA Success at Week 16
At week 48, 31.7% of patients in the nemolizumab every 4 weeks arm (n = 142), 37.3% of patients in the nemolizumab every 8 weeks arm (n = 142), and 31.3% of patients in the placebo arm (n = 131) reported maintaining IGA success at all study visits until week 48. The strata-adjusted LS mean difference between nemolizumab every 4 weeks and placebo was 0.5% (95% CI, –10.5% to 11.6%). The strata-adjusted LS mean difference between nemolizumab every 8 weeks and placebo was 6.0% (95% CI, –5.2% to 17.1%).
At week 48, 63.4% of patients in the nemolizumab every 4 weeks arm (n = 142), 64.1% of patients in the nemolizumab every 8 weeks arm (n = 142), and 55.0% of patients in the rerandomized placebo arm (n = 131) reported IGA success. The strata-adjusted LS mean difference between nemolizumab every 4 weeks and placebo was 8.5% (95% CI, –3.0% to 20.2%). The strata-adjusted LS mean difference between nemolizumab every 8 weeks and placebo was 9.1% (95% CI, –2.5% to 20.6%).
Proportion of Patients Maintaining EASI-75 Until Week 48 From the Subset With EASI-75 at Week 16
At week 48, 55.8% of patients in the nemolizumab every 4 weeks arm (n = 163), 58.9% of patients in the nemolizumab every 8 weeks arm (n = 163), and 44.6% of patients in the placebo arm (n = 163) reported maintaining EASI-75 at all study visits until week 48. The strata-adjusted LS mean difference between nemolizumab every 4 weeks and placebo was 11.2% (95% CI, 0.3% to 22.1%). The strata-adjusted LS mean difference between nemolizumab every 8 weeks and placebo was 14.1% (95% CI, 3.3% to 24.9%).
At week 48, 76.3% of patients in the nemolizumab every 4 weeks arm (n = 169), 75.7% of patients in the nemolizumab every 8 weeks arm (n = 169), and 63.9% of patients in the rerandomized placebo arm (n = 169) reported attaining EASI-75. The strata-adjusted LS mean difference between nemolizumab every 4 weeks and placebo was 12.4% (95% CI, 2.7% to 22.0%). The strata-adjusted LS mean difference between nemolizumab every 8 weeks and placebo was 11.8% (95% CI, 2.1% to 21.5%).
Change From Week 16 to Week 48 in EASI
The LS mean change from baseline in EASI score was 2.01 (95% CI, –0.16 to 4.19; n = 169) in the nemolizumab every 4 weeks arm; 2.98 (95% CI, 0.80 to 5.17; n = 169) in the nemolizumab every 8 weeks arm, and 6.79 (95% CI, 4.62 to 8.96; n = 169) in the placebo arm. The LS mean difference from placebo was –4.78 (95% CI, –7.85 to –1.70) in the nemolizumab every 4 weeks arm and –3.80 (95% CI, –6.89 to –0.72) in the nemolizumab every 8 weeks arm.
Proportion of Patients With PP-NRS Improvement of 4 or More From Initial Baseline to Week 48 From the Subset With PP-NRS of 4 or More at Week 16
At week 48, of the subset of patients who had a PP-NRS score improvement of 4 points or more at week 16, 46.9% of patients in the nemolizumab every 4 weeks arm (n = 98), 40.4% of patients in the nemolizumab every 8 weeks arm (n = 94), and 31.3% of patients in the placebo arm (n = 83) reported an improvement in PP-NRS of 4 points or more from the initial period baseline. The strata-adjusted proportion difference versus placebo was 15.4% (95% CI, 1.3% to 29.4%) in the nemolizumab every 4 weeks arm and 9.1% (95% CI, –5.0% to 23.2%) in the nemolizumab every 8 weeks arm.
At week 48 of the entire maintenance period population, 36.7% of patients in the nemolizumab every 4 weeks arm (n = 169), 29.0% of patients in the nemolizumab every 8 weeks arm (n = 169), and 21.3% of patients in the placebo arm (n = 169) reported an improvement in PP-NRS of 4 points or more from the initial period baseline. The strata-adjusted proportion difference versus placebo was 15.4% (95% CI, 5.8% to 24.9%) in the nemolizumab every 4 weeks arm and 7.7% (95% CI, –1.5% to 16.9%) in the nemolizumab every 8 weeks arm.
Proportion of Patients With PP-NRS of Less Than 2 at Week 48 From the Subset With PP-NRS of Less Than 2 at Week 16
At week 48, 39.7% of patients in the nemolizumab every 4 weeks arm (n = 169), 43.0% of patients in the nemolizumab every 8 weeks arm (n = 169), and 34.4% of patients in the placebo arm (n = 169) reported a PP-NRS score of less than 2. The strata-adjusted proportion difference versus placebo was 5.9% (95% CI, –10.1% to 21.8%) in the nemolizumab every 4 weeks arm and 8.6% (95% CI, –7.4% to 24.6%) in the nemolizumab every 8 weeks arm.
At week 48, of the entire maintenance period population, 30.2% of patients in the nemolizumab every 4 weeks arm (n = 169), 27.8% of patients in the nemolizumab every 8 weeks arm (n = 169), and 18.9% of patients in the placebo arm (n = 169) reported a PP-NRS score of 2 points or less. The strata-adjusted proportion difference versus placebo was 11.2% (95% CI, 2.1% to 20.3%) in the nemolizumab every 4 weeks arm and 8.9% (95% CI, –0.1% to 17.8%) in the nemolizumab every 8 weeks arm.
Change From Week 16 to Week 48 in PP-NRS
The LS mean change from baseline in PP-NRS score was –0.46 (95% CI, 0.88 to –0.05; n = 143) in the nemolizumab every 4 weeks arm; 0.10 (95% CI, –0.29 to 0.48; n = 155) in the nemolizumab every 8 weeks arm; and 1.35 (95% CI, 0.95 to 1.74; n = 152) in the placebo arm. The LS mean difference from placebo was –1.81 (95% CI, –2.39 to –1.23) in the nemolizumab every 4 weeks arm and –1.25 (95% CI, –1.79 to –0.71) in the nemolizumab every 8 weeks arm.
Change From Week 16 to Week 48 in DLQI Total Score
The LS mean change from baseline in DLQI score was –0.43 (95% CI, –1.11 to 0.24; n = 119) in the nemolizumab every 4 weeks arm, 0.14 (95% CI, –0.50 to 0.79; n = 130) in the nemolizumab every 8 weeks arm, and 0.70 (95% CI, 0.00 to 1.40; n = 110) in the placebo arm. The LS mean difference from placebo was –1.14 (95% CI, –2.11 to –0.16) in the nemolizumab every 4 weeks arm and –0.56 (95% CI, –1.52 to 0.40) in the nemolizumab every 8 weeks arm.
Change From Week 16 to Week 48 in CDLQI Total Score
The LS mean change from baseline in CDLQI score was –0.54 (95% CI, –1.45 to 0.36; n = 29) in the nemolizumab every 4 weeks arm, –1.27 (95% CI, –2.30 to –0.23; n = 22) in the nemolizumab every 8 weeks arm, and 0.34 (95% CI, –0.71 to 1.38; n = 22) in the placebo arm. The LS mean difference from placebo was –0.88 (95% CI, –2.27 to 0.51) in the nemolizumab every 4 weeks arm and –1.60 (95% CI, –3.08 to –0.12) in the nemolizumab every 8 weeks arm.
Incidence of Rescue Therapy Use
In the maintenance period, a total of 1.2% of patients in the nemolizumab every 4 weeks arm, 2.4% in the nemolizumab every 8 weeks arm, and 5.3% of patients in the placebo arm reported using rescue therapy.
ARCADIA CYCLO Study
Proportion of Patients With EASI-75
At week 16 in the ARCADIA CYCLO study, 47.1% of patients in the nemolizumab arm and 34.8% of patients in the placebo arm reported EASI-75. The strata-adjusted difference between the study arms was 12.2% (95% CI, 0.7% to 23.6%; P = 0.040).
Proportion of Patients With Prior CsA Use With EASI-75
██ ████ ███ █████ ██ ████████ ██ ███ ███████████ ███ ██ █ ████ ███ █████ ██ ████████ ██ ███ ███████ ███ ██ █ ████ ████████ ████████ ███ ███████████████ ██████████ ███████ ███ █████ ████ ███ █████ ████ ███ ████ ██ ██████████████.
Percent Change From Baseline in EASI
███ ██ ████ ███████ ██████ ████ ████████ ██ ████ █████ █████ ██ ████ ██ ███ ███████ ████ ███ ███████ ██ ████████ ██ ███ ███████████ ████ ███ ███████ ████ ███ ███████ ██ ████████ ██ ███ ███████ ████ ███ ██ ████ ██████████ ██████ ███████ ███ ██████ ████ ███ ███████ ██ ██████ ████████.
Proportion of Patients With an Improvement of PP-NRS of 4 or More From Baseline to Week 16
At week 16, 39.1% of patients in the nemolizumab arm and 17.4% of patients in the placebo arm reported an improvement in PP-NRS score of 4 points or greater. The strata-adjusted difference versus placebo was 21.7% (95% CI, 11.4% to 32.0%; P < 0.001).
Proportion of Patients With PP-NRS of Less Than 2 at Week 16
██ ████ ███ █████ ██ ████████ ██ ███ ███████████ ███ ███ ████ ██ ████████ ██ ███ ███████ ███ ████████ █ ██████ █████ ██ █ ██████ ██ █████ ███ ██ ████ ██████████ ██████ ███████ ███ █████ ████ ███ ████ ██ █████████████.
Percent Change From Baseline to Week 16 in PP-NRS
███ ██ ████ ███████ ██████ ██ ██████ ████ ████████ ███ ███████ ████ ███ ███████ ██ ████████ ██ ███ ███████████ ███ ███ ███████ ████ ███ ███████ ██ ████████ ██ ███ ███████ ████ ███ ██ ████ ██████████ ██████ ███████ ███ ███████ ████ ███ ███████ ██ ██████████████.
Proportion of Patients With IGA Success
██ ████ ███ █ █████ ██ █████ ██ ████████ ██ ███ ███████████ ███ ███ █████ ██ ████████ ██ ███ ███████ ███ ████████ ███ ███████ ████████ ██ ███ █ ██ █ ███ | | ███████ █████████ ████ ██████████ ███ ██ ████ ██████████ ██████ ███████ ███ ████ ████ ███ █████ ██ ██████ ████████.
Change From Baseline to Week 16 in DLQI Total Score
███ ██ ████ ██████ ████ ████████ ██ ████ █████ █████ ███ █████ ████ ███ █████ ██ ██████ ██ ███ ███████████ ███ ███ █████ ████ ███ █████ ██ ██████ ██ ███ ███████ ████ ███ ██ ████ ██████████ ██████ ███████ ███ █████ ████ ███ █████ ██ ██████ | | ███████.
Incidence of Rescue Treatment Use
██ ██ ████ ███ █ █████ ██ ████ ██ ████████ ██ ███ ███████████ ███ ███ ████ ██ ████████ ██ ███ ███████ ███ ████████ ███ ███ ██ █ ██ ████ ██████ ████████████ ███ ███████████████ ██████████ ██████ ███████ ███ ███ ████ ███ ████ ██ ████ | | ████████.
Harms Results
Adverse Events
ARCADIA 1 Study
During the initial period of the ARCADIA 1 study, 49.7% of patients in the nemolizumab arm and 45.5% of patients in the placebo arm reported at least 1 AE. The most commonly reported AEs during this period were infections and infestations (18.3% in the nemolizumab arm and 20.3% in the placebo arm); skin and SC tissue disorders (18.3% in the nemolizumab arm and 14.0% in the placebo arm); and respiratory, thoracic, or mediastinal disorders (9.4% in the nemolizumab arm and 8.7% in the placebo arm).
During the maintenance period of the ARCADIA 1 study, 58.2% of patients in the nemolizumab every 4 weeks arm, 55.6% in the nemolizumab every 8 weeks arm, 58.2% in the rerandomized placebo arm, and 55.0% in the carryover placebo arm reported AEs. The most common AEs were infections and infestations (34.1% in the nemolizumab every 4 weeks arm, 34.4% in the nemolizumab every 8 weeks arm, 34.1% in the rerandomized placebo arm, and 34.0% in the nonrandomized placebo arm); skin and SC issues (12.1% in the nemolizumab every 4 weeks arm, 11.1% in the nemolizumab every 8 weeks arm, 14.3% in the rerandomized placebo arm, and 14.0% in the nonrandomized placebo arm); and respiratory, thoracic, and mediastinal disorders (12.1% in the nemolizumab every 4 weeks arm, 11.1% in the nemolizumab every 8 weeks arm, 13.2% in the rerandomized placebo arm, and 7.0% in the nonrandomized placebo arm). There was a numerically higher proportion of patients reporting infections and infestations in the maintenance period relative to the initial period, and a numerically higher number of patients in the nemolizumab every 4 weeks arm who reported gastrointestinal disorders (12.1%) relative to the other arms in the maintenance period (ranging from 5.6% to 7.7% of patients).
ARCADIA 2 Study
During the initial period of the ARCADIA 2 study, 41.4% of patients in the nemolizumab arm and 44.5% of patients in the placebo arm reported at least 1 AE. The most commonly reported AEs during this period were infections and infestations (17.0% in the nemolizumab arm and 20.2% in the placebo arm); skin and SC tissue disorders (12.1% in the nemolizumab arm and 9.9% in the placebo arm); and respiratory, thoracic, or mediastinal disorders (5.6% in the nemolizumab arm and 5.3% in the placebo arm).
During the maintenance period of the ARCADIA 1 study, 48.1% of patients in the nemolizumab every 4 weeks arm, 51.9% in the nemolizumab every 8 weeks arm, 58.4% in the rerandomized placebo arm, and 44.0% in the carryover placebo arm reported AEs. The most common AEs were infections and infestations (27.8% in the nemolizumab every 4 weeks arm, 22.1% in the nemolizumab every 8 weeks arm, 31.2% in the rerandomized placebo arm, and 28.6% in the nonrandomized placebo arm); skin and SC issues (13.9% in the nemolizumab every 4 weeks arm, 10.4% in the nemolizumab every 8 weeks arm, 13.0% in the rerandomized placebo arm, and 9.5% in the nonrandomized placebo arm); and respiratory, thoracic, and mediastinal disorders (10.1% in the nemolizumab every 4 weeks arm, 6.5% in the nemolizumab every 8 weeks arm, 11.7% in the rerandomized placebo arm, and 2.4% in the nonrandomized placebo arm). A numerically higher proportion of patients in the rerandomized placebo arm reported COVID-19 infection (16.9%) relative to other study arms (ranging from 3.8% to 7.1%).
ARCADIA CYCLO Study
██ ███████ ██████ █████ ██ ████████ ██ ███ ███████████ ███ ███ █████ ██ ████████ ██ ███ ███████ ███ ████████ ████ ███ ████ ████████ ████████ ███ ████ ██████████ ███ ████████████ ██████ ████████████ █████ █████████ ███ ████ ███ ████████████ █████████ █████ ████████████ █████ █████████ █ ███████████ ██████ ██████████ ██ ████████ ██ ███ ███████████ ███ ████████ ████████████ ████████ ███ ███████████ ███ ██████ ████████ ██ ███ ███████ ███ ███████ ██ ████ ██ ███████████████ ███ ██████████ ██████ █████████ █████ ████████████ ████ █████████.
Serious Adverse Events
ARCADIA 1 Study
During the initial period of the ARCADIA 1 study, 1.0% of patients in the nemolizumab arm and 1.2% of patients in the placebo arm reported any serious AE (SAE). AD SAEs were reported by 2 patients in the nemolizumab arm, and 3 patients in the placebo arm. The remaining SAEs by preferred term were reported in fewer than 2 patients.
During the maintenance phase of the ARCADIA 1 study, 4.4% of patients in the nemolizumab every 4 weeks arm, 3.3% in the nemolizumab every 8 weeks arm, 2.2% in the rerandomized placebo arm, and 1.0% in the nonrandomized placebo arm reported any SAEs. The SAEs by preferred term were reported in fewer than 2 patients.
ARCADIA 2 Study
During the initial period of the ARCADIA 2 study, 2.5% of patients in the nemolizumab arm and 1.1% of patients in the placebo arm reported any SAE. SAEs reported in more than 2 patients in the nemolizumab arm included 3 patients reporting infections and infestations, 3 patients reporting musculoskeletal and connective tissue disorders, 3 patients reporting skin and SC tissue disorders, and 2 patients reporting gastrointestinal disorders.
During the maintenance phase of the ARCADIA 2 study, 7.6% of patients in the nemolizumab every 4 weeks arm, 0% in the nemolizumab every 8 weeks arm, 2.6% in the rerandomized placebo arm, and 1.2% in the nonrandomized placebo arm reported any SAEs. There were no SAEs reported in more than 2 patients.
ARCADIA CYCLO Study
During the ARCADIA CYCLO study, 2.2% of patients in the nemolizumab arm and 1.5% of patients in the placebo arm reported SAEs. In the nemolizumab arm, SAEs were reported in 2 patients in the category of infections and infestations. In the placebo arm, SAEs by preferred term were reported in fewer than 2 patients.
Withdrawals Due to AEs
ARCADIA 1 Study
During the initial period of the ARCADIA 1 study, 1.8% of patients in the nemolizumab arm and 4.0% of patients in the placebo arm discontinued study drug treatment due to AEs. In the maintenance period, 1.1% of patients in the nemolizumab every 4 weeks arm, 3.3% in the nemolizumab every 8 weeks arm, 2.2% in the rerandomized placebo arm, and 2.0% in the carryover placebo arm discontinued due to AEs. In both the initial and maintenance periods, AD was the most common reason for discontinuation (initial period: 1.6% of patients in the nemolizumab arm and 4.0% of patients in the placebo arm; maintenance period: 0% in the nemolizumab every 4 weeks arm, 2.2% in the nemolizumab every 8 weeks arm, 1.1% in the rerandomized placebo arm, and 2.0% in the carryover placebo arm).
ARCADIA 2 Study
During the initial period of the ARCADIA 2 study, 3.5% of patients in the nemolizumab arm and 1.1% of patients in the placebo arm reported discontinuing due to AEs. In the maintenance period, 3.8% of patients in the nemolizumab every 4 weeks arm, 2.6% in the nemolizumab every 8 weeks arm, 3.9% in the rerandomized placebo arm, and 2.4% in the nonrandomized placebo arm withdrew due to AEs. In both the initial and maintenance periods, the most common reason for withdrawal of the study drug was AD (initial period: 1.7% of patients in the nemolizumab arm and 0.8% in the placebo arm; maintenance period: 2.5% in the nemolizumab every 4 weeks arm, 2.6% in the nemolizumab every 8 weeks arm, 2.6% in the rerandomized placebo arm, and 2.4% in the carryover placebo arm).
ARCADIA CYCLO Study
████ ██ ████ ██ ████████ ██ ███ ███████████ ███ ███ ████ ██ ████████ ██ ███ ███████ ███ ███████ ███ █████ █████ ███ ███████ ███ ████████ ██ ███ ███████████ ███ ████ █ ███████ ██████ ████ ██ ██████████ ██████ ████ █████████████████ ███ ███ ███ ███████ ███ ████████ ██ ███ ███████ ███ ████ █ ███████ ██████ ████ ██ ███████████████ █████████ █████████ ███ ███.
Mortality
There were no deaths reported in the ARCADIA 1, ARCADIA 2, or ARCADIA CYCLO studies.
Notable Harms
The AEs of special interest (AESIs) in the ARCADIA 1 and ARCADIA 2 studies identified in the submission were injection site reactions, newly diagnosed or worsening asthma, infections, peripheral edema, and elevated ALT or AST (> 3 × the upper limit of normal [ULN]) in combination with elevated bilirubin (> 2 × ULN). The AESIs identified in the submission for the ARCADIA CYCLO study were injection-related reactions, drug hypersensitivity, infections, COVID-19 infection, asthma, peak expiratory flow rate decrease, and peripheral edema. The submission did not contain details on whether these AESIs were prespecified or identified during the conduct of the studies.
ARCADIA 1 Study
During the initial period, injection-related reactions were reported in 0.2% of patients in the nemolizumab arm and 0 patients in the placebo arm; 0 patients reported injection-related reactions in the maintenance period. Newly diagnosed or worsening asthma was reported in 5.2% of patients in the nemolizumab arm and 3.4% of patients in the placebo arm during the initial period; during the maintenance period, 3.3% of patients in the nemolizumab every 4 weeks arm, 6.7% in the nemolizumab every 8 weeks arm, 2.2% in the rerandomized placebo arm, and 5.0% in the carryover placebo arm reported this AE. Infections were reported in 3.2% of patients in the nemolizumab arm and 3.1% in the placebo arm during the initial period; during the maintenance period, 13.2% of patients in the nemolizumab every 4 weeks arm, 12.2% in the nemolizumab every 8 weeks arm, 13.2% in the rerandomized placebo arm, and 12.0% in the carryover placebo arm reported this AE. Peripheral edema was reported in 1.1% of patients in the nemolizumab arm and 0.3% in the placebo arm during the initial period; in the maintenance period, 1.1% of patients in the nemolizumab every 4 weeks arm, 2.2% in the nemolizumab every 8 weeks arm, 1.1% in the rerandomized placebo arm, and 0 in the carryover placebo arm reported this AE. Elevated ALT or AST in combination with elevated bilirubin was not reported during the trial.
ARCADIA 2 Study
During the initial period and maintenance periods of the ARCADIA 2 study, no injection-related reactions were reported. Newly diagnosed or worsening asthma was reported in 2.9% of patients in the nemolizumab arm and 3.0% of patients in the placebo arm during the initial period; in the maintenance period, 5.1% of patients in the nemolizumab every 4 weeks arm, 0% in the nemolizumab every 8 weeks arm, 2.6% in the rerandomized placebo arm, and 0% in the carryover placebo arm reported this AE. Infections were reported in 3.9% of patients in the nemolizumab arm and 4.6% in the placebo arm during the initial period; in the maintenance period, 5.1% of patients in the nemolizumab every 4 weeks arm, 7.8% in the nemolizumab every 8 weeks arm, 16.9% in the rerandomized placebo arm, and 10.7% in the carryover placebo arm reported this AE. Peripheral edema was reported in 2.3% of patients in the nemolizumab arm and 0.4% in the placebo arm during the initial period; in the maintenance period, 0% of patients in the nemolizumab every 4 weeks arm, 0% in the nemolizumab every 8 weeks arm, 2.6% in the rerandomized placebo arm, and 0% in the carryover placebo arm reported this AE. Elevated ALT or AST in combination with elevated bilirubin was not reported during the trial.
ARCADIA CYCLO Study
███ ████ ████████ ████████ ████ ██ ███████ █████ ████ ████████ ██████████ █████ ██ ████████ ██ ███ ███████████ ████ ████ ██ ████████ ██ ███ ███████ █████ ████████ ██ ██████ █████ ████████████ ████ █████████ ███ ████ ██████████ ████ ████ █████████ █████ ████████████ ████ █████████ ████ ████████████████ ███ ████████ ██ ████ ██ ████████ ██ ███ ███████████ ███ ████ ██ ██ ███████ █████ ███ ███ ███████ ██████ ██ ███ ███████ ███ ████████ ██ █████████████████ ████████ ██ █████████.
Critical Appraisal
Internal Validity
In all ARCADIA studies (ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO), the procedures for randomization, treatment allocation, blinding, and study drug administration were all described and likely at low risk of bias; however, the study design is subject to some limitations. In the ARCADIA 1 and ARCADIA 2 studies, only patients who met the study definition of clinical responder (an IGA score of 0 [clear] or 1 [almost clear] or EASI-75) continued from the initial period on to the maintenance period. This imparts a response bias for the maintenance phase as the patients included in the maintenance phase are an enriched population of patients who have already responded to treatment by 16 weeks. It is not known whether the patients who met the study definition of nonresponder had specific common characteristics which would have impacted their likelihood of responding to treatment. The duration of the initial treatment period, while generally consistent with studies for other treatments reimbursed for moderate to severe AD, may not be long enough to obtain complete treatment response, as the clinical experts consulted for this review noted that a trial of up to 6 months is used in clinical practice, which is a relevant consideration for all ARCADIA trials. There was no run-in period for the ARCADIA CYCLO study, while patients’ background treatment was standardized in the ARCADIA 1 and ARCADIA 2 studies. Because patients in the ARCADIA CYCLO study have more severe disease, this may impact the certainty in the results as patients’ background therapies in the ARCADIA CYCLO study could have differed in efficacy and type of product.
With regards to the statistical analysis across trials, the assessment of outcomes for the coprimary and key secondary outcomes in the initial period is likely at lower risk of bias due to being controlled for multiplicity; however, the order of hypothesis testing for the outcomes is unknown and therefore the alpha spending among the list of outcomes, or when testing might have ended, is also unknown. In the ARCADIA 1 and ARCADIA 2 studies, the results of the sensitivity analyses testing different methods of classifying missing clinical responders and nonresponders were also consistent with the main analysis, which suggests the results are reasonably robust. However the statistical analysis methods are subject to some limitations that impact internal validity, and which increase the uncertainty in the results. In the ARCADIA 1 and ARCADIA 2 studies, there were several protocol amendments, although it is unclear how many patients were impacted by the modification, or what impact this may have had on the results. Per the individual statistical analysis plan for the ARCADIA 1 and ARCADIA 2 studies, no hypothesis testing was conducted on outcomes in the maintenance phase; however, the pooled Clinical Study Report described statistical tests comparing nemolizumab arms to the rerandomized placebo group. In addition, there was no control of multiplicity for the secondary outcomes in the initial period (change from baseline in PP-NRS, EASI, DLQI, and CDLQI) and maintenance period (all outcomes); therefore, there is a risk of increased type I error for these outcomes. The study populations of the ARCADIA 1 and ARCADIA 2 studies appeared broadly similar in terms of disposition, and the studies employed identical designs, inclusion and exclusion criteria, as well as analysis methods. However, the statistical limitations mean that results from the maintenance period should only be considered supportive evidence of the impact of nemolizumab.
External Validity
Patients enrolled in the ARCADIA 1 and ARCADIA 2 studies were required to have an EASI score of 16 or more (≥ 20 in the ARCADIA CYCLO study), and an IGA score of 3 or more in both studies. An EASI score of 7.1 to 21.0 is considered moderate AD, and severe AD ranges from 21.1 to 50.0.9 An IGA score of 3 is considered moderate AD. As such, patients enrolled in the ARCADIA trials may have more severe disease, and therefore the results may not be generalizable to all patients with moderate AD, depending on the disease severity criteria used. However, it is worth noting that an EASI score of 16 and an IGA score of 3 are consistent with other drugs evaluated for moderate to severe AD.
All the ARCADIA studies excluded patients with asthma, chronic obstructive pulmonary disease (COPD), and certain medications which cause sedative effects. Patients who had not improved after 16 weeks of treatment with dupilumab were also excluded from the ARCADIA 1 and ARCADIA 2 trials. The reimbursement request includes patients who are refractory to systemic immunosuppressant therapies, which could include dupilumab; therefore, results from the trials will not be generalizable to patients with a history of dupilumab exposure. The clinical experts consulted for this review noted that these patients could be considered candidates for treatment with nemolizumab in clinical practice. In addition, the fact that only patients who met the study definition of clinical responders were kept in the maintenance phase of the ARCADIA 1 and ARCADIA 2 studies means any results after 16 weeks may not include all the patients represented in the study enrolment criteria.
The ARCADIA trials were all placebo-controlled trials, which allows for adequate evaluation of the treatment effect of nemolizumab; however, it may overestimate the treatment effects. Patients in the ARCADIA 1 and ARCADIA 2 studies had their background therapy stabilized during the run-in period before randomization. There was a high placebo response observed in the ARCADIA trials, although it is unclear whether this is due to the background therapy received by all patients. If so, this also impacts patients receiving nemolizumab. Nemolizumab monotherapy was not evaluated in the evidence submitted, and therefore delineating the true impact of nemolizumab on the disease remains unknown and may overestimate the results of the ARCADIA studies, although, it is worth noting that patients in the real world would continue to receive their background therapies, as was done in the ARCADIA studies. Across all 3 trials, treatment adherence was reported to be high ██ █████; the levels of adherence observed may not be representative of clinical practice settings.
Most patients in the ARCADIA 1 and ARCADIA 2 studies were aged older than 18 years, while only 13.7% to 17.4% of patients were between the ages of 12 and 17 years. Outcomes specific to this population (i.e., the CDLQI) were highly uncertain because they come from a small proportion of patients in the study. Additionally, other results may not be generalized to this population; however, subgroup analyses by age group were generally consistent with the primary analysis.
In addition to the study design, the treatment history described in the inclusion and exclusion criteria does not exactly match the requested reimbursement criteria; the ARCADIA 1 and ARCADIA 2 trials did not require patients to have previous exposure to immunomodulatory therapies, and the ARCADIA CYCLO study only required exposure or inadvisability for CsA. In the ARCADIA 1 and ARCADIA 2 studies, less than 40% of patients had prior exposure to immunomodulatory treatment, less than 15% had exposure to CsA, and approximately 5% had had exposure to dupilumab. Therefore, it is uncertain how applicable the overall results will be to patients with these treatment histories versus patients who are not previously treated with systemic therapies, or who have been treated with other advanced systemic therapies. Subgroup analyses conducted in the ARCADIA 1 and ARCADIA 2 studies on prior use of systemic therapy, biologic therapy, or dupilumab did not show consistent trends between the 2 studies and some subgroups had small sample sizes, thus, firm conclusions could not be drawn. In addition, according to the clinical experts, the criteria for refractoriness to CsA in the ARCADIA CYCLO study were subjective and therefore might be representative of all patients who might not respond to CsA.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for Grading of Recommendations, Assessment, Development and Evaluation (GRADE) assessment was based on the sponsor’s summary of clinical evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members.
ARCADIA 1 and ARCADIA 2 studies:
Proportion of patients with IGA success at week 16
Proportion of patients with EASI-75 at week 16
Proportion of patients with PP-NRS score improvement of 4 or more at week 16
Proportion of patients with PP-NRS score less than 2 at week 16
Change from baseline to week 16 in DLQI
Change from baseline to week 16 in CDLQI
Harms (injection site reactions, newly diagnosed or worsening asthma)
ARCADIA CYCLO study:
Proportion of patients with EASI-75 at week 16
Proportion of patients with PP-NRS score improvement of 4 points or more at week 16
Proportion of patients with PP-NRS score of 2 or more at week 16
Proportion of patients with IGA success at week 16
Change from baseline in DLQI score at week 16
Harms (injection site reactions, newly diagnosed or worsening asthma)
Table 2: Summary of Findings for Nemolizumab vs. Placebo for Patients Aged 12 Years and Older With Moderate to Severe Atopic Dermatitis
Outcome and follow-up | Patients (studies), N | Effect | Certainty | What happens |
|---|---|---|---|---|
Disease activity scores | ||||
Proportion of patients with IGA successa Follow-up: 16 weeks | 1,728 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
| Moderateb | Nemolizumab likely results in an increase in the proportion of patients with IGA success at week 16 when compared with placebo. |
Proportion of patients with EASI-75c Follow-up: 16 weeks | 1,728 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
| Moderateb | Nemolizumab likely results in an increase in the proportion of patients with EASI-75 at week 16 when compared with placebo. |
Proportion of patients with PP-NRS improvement ≥ 4d Follow-up: 16 weeks | 1,728 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
| High | Nemolizumab results in an increase in the proportion of patients with a PP-NRS score improvement of ≥ 4 points at week 16 when compared with placebo. |
Proportion of patients with PP-NRS < 2d Follow-up: 16 weeks | 1,728 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
| High | Nemolizumab results in an increase in the proportion of patients with a PP-NRS score of < 2 at week 16 when compared with placebo. |
HRQoL | ||||
DLQI or CDLQI of 0 (no impact of skin disease on quality of life) to 30 (maximum impact on quality of life) | ||||
LS mean change from baseline in DLQI total scoree Follow-up: 16 weeks | 1,728 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
LS mean difference: –2.44 (95% CI, –3.58 to –1.30) | Moderatef | Nemolizumab may result in a reduction in the change in DLQI total score from baseline to week 16 when compared to placebo. |
LS mean change from baseline in CDLQI total scoree Follow-up: 16 weeks | 266 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
| Moderatef | Nemolizumab may result in a reduction in the change in CDLQI total score from baseline to week 16 when compared to placebo. |
Harms | ||||
Proportion of patients with injection-related reactions Follow-up: 16 weeks | 937 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
| Moderateg | Nemolizumab likely results in little to no difference in the proportion of patients with injection-related reactions when compared to placebo. |
Proportion of patients with newly diagnosed or worsening asthma Follow-up: 16 weeks | 937 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
| Lowg,h | The evidence is very uncertain about the effect of nemolizumab on the proportion of patients with newly diagnosed or worsening asthma when compared to placebo. |
Proportion of patients with 1 or more SAEs, n (%) Follow-up: 16 weeks | 937 (2 RCTs) | ARCADIA 1 study
ARCADIA 2 study
| Lowg,h | The evidence is very uncertain about the effect of nemolizumab on the proportion of patients with ≥ 1 SAEs. |
CDLQI = Children’s Dermatology Life Quality Index; CI = confidence interval; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% in Eczema Area and Severity Index from baseline; HRQoL = health-related quality of life; IGA = Investigator Global Assessment; LS = least squares; NR = not reported; PP-NRS = Peak Pruritus Numeric Rating Scale; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus.
Note: Study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aThe IGA measures the investigator’s global assessment of the patient’s overall severity of atopic dermatitis at that visit, based on a static, numeric 5-point scale ranging from 0 (clear) to 4 (severe). IGA success was defined as an IGA score of 0 or 1 and at least a 2-point reduction from baseline.
bRated down 1 level for serious imprecision. The CI for differences between groups included the potential for little to no difference (based on the threshold for a clinically important between-group difference of 100 per 1,000 provided by the clinical experts consulted for this review).
cThe EASI is a composite index, based on the physician’s assessment of 4 clinical signs of the disease (erythema, infiltration or papulation, excoriation, and lichenification) and the extent of body surface area involved at that visit. It is scored from 0 to 72, with higher scores indicating greater disease severity and/or extent of disease.
dThe PP-NRS is a patient-reported, single-item, daily, 11-point scale. The scale is used by patients to rate their worst itch severity over the previous 24 hours, with 0 indicating no itch and 10 indicating the worst itch imaginable.
eThe DLQI (for patients aged ≥ 16 years) and CDLQI (for those aged < 16 years) are patient-reported, 10-item, HRQoL questionnaires that cover 6 domains (symptoms and feelings, daily activities, leisure, work and school, personal relationships, and treatment) over the previous week. The total score ranges from 0 (no impact of skin disease on quality of life) to 30 (maximum impact on quality of life).
fRated down 1 level for serious imprecision. The CI for differences between groups includes the potential for little to no difference (based on the threshold for clinically important between-group difference of 5 points provided by the clinical experts consulted for this review).
gRated down 1 level for serious imprecision due to the low number of events and lack of 95% CI. The lack of CIs means it cannot be determined whether there is the possibility of benefit, no benefit, or harm in the assessment of this outcome.
hRated down 1 level for very serious indirectness. The duration of follow-up was limited to 16 weeks, which is an insufficient duration of time to detect all occurrences of this harm.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence,10 the ARCADIA 1 Clinical Study Report,11 and the ARCADIA 2 Clinical Study Report.12
Table 3: Summary of Findings for Nemolizumab vs. Placebo for Patients Aged 12 Years and Older With Moderate to Severe Atopic Dermatitis Previously Exposed to Cyclosporine or for Whom Cyclosporine is Medically Inadvisable
Outcome and follow-up | Patients (studies), N | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|
Placebo | Nemolizumab | Difference | ||||
Disease activity measures | ||||||
Proportion of patients with EASI-75a Follow-up: 16 weeks | 276 (1 RCT) | 348 per 1,000 (NR to NR) | 471 per 1,000 (NR to NR) | 122 per 1,000 (NR to NR) (7 to 236 per 1,000) | Moderateb | Nemolizumab likely results in an increase in the proportion of patients with EASI-75 at week 16 when compared with placebo. |
Proportion of patients with PP-NRS improvement ≥ 4c Follow-up: 16 weeks | 276 (1 RCT) | 174 per 1,000 (NR to NR) | 391 per 1,000 (NR to NR) | 217 per 1,000 (NR to NR) (114 to 320 per 1,000) | High | Nemolizumab results in an increase in the proportion of patients with a PP-NRS score improvement of ≥ 4 points at week 16 when compared with placebo. |
Proportion of patients with PP-NRS < 2c Follow-up: 16 weeks | ███ ██ ████ | ██ ███ ████ | ███ ███ ████ | ███ ███ ████ ███ ██ ███ ███ █████ | Moderateb | Nemolizumab likely results in an increase in the proportion of patients with a PP-NRS score < 2 at week 16 when compared with placebo. |
Proportion of patients with IGA successd Follow-up: 16 weeks | ███ ██ ████ | ███ ███ ████ | ███ ███ ████ | ██ ███ ████ █████ ██ ███ ███ █████ | Moderateb | Nemolizumab likely results in little to no difference in the proportion of patients with IGA success at week 16 when compared with placebo. |
HRQoL | ||||||
DLQI or CDLQI of 0 (no impact of skin disease on quality of life) to 30 (maximum impact on quality of life) | ||||||
LS mean change from baseline in DLQI total scoree Follow-up: 16 weeks | ███ ██ ████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | Moderatef | Nemolizumab likely results in a reduction in the change in DLQI total score from baseline to week 16 when compared to placebo. |
Harms | ||||||
Proportion of patients with injection-related reactions Follow-up: 16 weeks | ███ ██ ████ | ██ ████ ████ | ███ ████ ████ | ██ | Moderateg | Nemolizumab likely results in little to no difference in the proportion of patients with injection-related reactions when compared to placebo. |
Proportion of patients with asthma Follow-up: 16 weeks | ███ ██ ████ | ██ ███ ████ ████ | ██ ███ ████ ████ | ██ | Lowg,h | Nemolizumab may result in little to no difference in the proportion of patients with asthma when compared to placebo. |
Proportion of patients with 1 or more SAEs | 274 (1 RCT) | 22 per 1,000 (NR to NR) | 15 per 1,000 (NR to NR) | NR | Lowg,h | Nemolizumab may result in little to no difference in the proportion of patients with ≥ 1 SAEs. |
CDLQI = Children’s Dermatology Life Quality Index; CI = confidence interval; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% improvement in Eczema Area and Severity Index from baseline; HRQoL = health-related quality of life; IGA = Investigator Global Assessment; LS = least squares; NR = not reported; PP-NRS = Peak Pruritus Numeric Rating Scale; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aThe EASI is a composite index, based on the physician’s assessment of 4 clinical signs of the disease (erythema, infiltration or papulation, excoriation, and lichenification) and the extent of body surface area involved at that visit. It is scored from 0 to 72, with higher scores indicating greater disease severity and/or extent of disease.
bRated down 1 level for serious imprecision. The CI for differences between groups included the potential for little to no difference (based on the threshold for a clinically important between-group difference of 100 per 1,000 provided by the clinical experts consulted for this review).
cThe PP-NRS is a patient-reported, single-item, daily, 11-point scale. The scale is used by patients to rate their worst itch severity over the previous 24 hours, with 0 indicating no itch and 10 indicating the worst itch imaginable.
dThe IGA measures the investigator’s global assessment of the patient’s overall severity of atopic dermatitis at that visit, based on a static, numeric 5-point scale ranging from 0 (clear) to 4 (severe). IGA success was defined as an IGA score of 0 or 1 and at least a 2-point reduction from baseline.
eThe DLQI (for patients aged ≥ 16 years) and CDLQI (for those aged < 16 years) are patient-reported, 10-item, HRQoL questionnaires that cover 6 domains (symptoms and feelings, daily activities, leisure, work and school, personal relationships, and treatment) over the previous week. The total score ranges from 0 (no impact of skin disease on quality of life) to 30 (maximum impact on quality of life).
fRated down 1 level for serious imprecision. The CI for differences between groups included the potential for little to no difference (based on the threshold for a clinically important between-group difference of 5 points provided by the clinical experts consulted for this review).
gRated down 1 level for serious imprecision due to the low number of events and lack of 95% CI. The lack of CIs means it cannot be determined whether there is the possibility of benefit, no benefit, or harm in the assessment of this outcome.
hRated down 1 level for serious indirectness. The duration of follow-up was limited to 16 weeks, which is insufficient evidence to detect all occurrences of this harm.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence10 and the ARCADIA CYCLO Clinical Study Report.13
Long-Term Extension Studies
Description of Studies
The ARCADIA long-term extension (LTE) study (NCT03989206; N = 1,751) is an ongoing phase III, single-arm, multicentre, prospective study to evaluate the long-term safety and efficacy of nemolizumab in adult and adolescent patients with moderate to severe AD, when administered with background topical corticosteroid (TCS), with or without topical calcineurin inhibitor (TCI). The ARCADIA LTE study design consisted of a 4-week screening period, a 200-week treatment period, and an 8-week follow-up period. Participants received nemolizumab (30 mg) every 4 weeks via SC injection in the treatment period. Results were from 1 interim analysis (cut-off date of September 30, 2022) up to 56 weeks of treatment, as the sponsor noted that sample sizes beyond this time point were too small to draw meaningful conclusions. The study is estimated to be completed in August 2026.
The primary outcomes in the ARCADIA LTE study were the incidence and severity of AEs throughout the study, the incidence of SAEs throughout the study, and the incidence and severity of AESIs throughout the study. Secondary outcomes aligned with outcomes assessed in the ARCADIA 1 and ARCADIA 2 studies that were identified as important to this review, and included the IGA, EASI, and DLQI and CDLQI.
The study population included patients from prior nemolizumab AD studies, including the ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO studies, and adolescents from selected international sites who had not previously participated in a nemolizumab study. Inclusion criteria for the ARCADIA LTE study were consistent with that of the lead-in studies. Patients were excluded if they had a history of COPD and/or chronic bronchitis, body weight of less than 30 kg, uncontrolled asthma in the preceding 3 months, asthma exacerbation requiring hospitalization in the preceding 12 months, had experienced an AE in a previous nemolizumab study, or had received restricted prior treatments.
Efficacy Results
Proportion of Patients With IGA Success
At LTE study baseline, 23.9% of all patients experienced IGA success (defined as an IGA score between 0 to 1). With treatment before the LTE study, 28.5% of patients previously treated with nemolizumab and 17.7% of patients not previously treated with nemolizumab experienced an IGA score of 0 to 1. At week 20, 42.5% of all patients in the LTE study experienced IGA success. With regards to prior treatment, 45.6% of patients previously treated with nemolizumab and 36.7% of patients not previously treated with nemolizumab experienced an IGA score of 0 to 1. At week 56, 48.9% of all patients in the LTE study experienced IGA success. With prior treatment, 47.1% of patients previously treated with nemolizumab and 49.0% of patients not previously treated with nemolizumab experienced an IGA score of 0 to 1.
Proportion of Patients With EASI-75
At LTE study baseline, 33.7% of all patients achieved EASI-75 improvement from lead-in study baseline. With prior treatment, 38.1% of patients previously treated with nemolizumab and 24.0% of patients not previously treated with nemolizumab achieved EASI-75 improvement from lead-in baseline. At week 20, 66.3% of patients achieved EASI-75 improvement from lead-in baseline and 34% achieved EASI-75 improvement from LTE study baseline. With regards to prior treatment, the proportion of patients achieving EASI-75 from lead-in and LTE study baseline were 69.3% and 32.6% for those previously treated with nemolizumab and 61.5% and 36.2% for patients not previously treated with nemolizumab, respectively. At week 56, 75.6% of patients achieved EASI-75 improvement from lead-in baseline and 57.4% achieved EASI-75 improvement from LTE study baseline. With regards to prior treatment, the proportion of patients achieving EASI-75 from lead-in and LTE study baseline were 73.0% and 52.5% for those previously treated with nemolizumab and 78.7% and 62.3% for patients not previously treated with nemolizumab, respectively.
Change From Baseline in DLQI Total Score
At LTE study baseline, the mean DLQI was 7.6 (standard deviation [SD] = 6.92) across all patients in the LTE study, 6.6 (SD = 6.57) for patients previously treated with nemolizumab, and 9.1 (SD = 7.25) in the group not previously treated with nemolizumab.
At week 20, the mean DLQI score was 4.7 (SD = 5.77) across all patients in the LTE study. Patients previously treated with nemolizumab had a mean DLQI score of 4.6 (SD = 5.84), with a mean change from lead-in baseline and LTE study baseline of −10.4 (SD = 7.52) and −2.0 (SD = 5.54), respectively. Patients not previously treated with nemolizumab had a mean DLQI score of 5.0 (SD = 5.55), with a mean change from lead-in baseline and LTE study baseline of −10.2 (SD = 7.06) and −3.9 (SD = 6.02), respectively.
At week 56, the mean DLQI score was 3.9 (SD = 4.72) across all patients in the LTE study. Patients previously treated with nemolizumab had a mean DLQI score of 4.2 (SD = 4.93), with a mean change from lead-in baseline and LTE study baseline of −11.1 (SD = 7.32) and −3.6 (SD = 6.36), respectively. Patients not previously treated with nemolizumab had a mean DLQI score of 3.7 (SD = 4.58), with a mean change from lead-in baseline and LTE study baseline of −12.2 (SD = 6.92) and −6.4 (SD = 6.71), respectively.
Change From Baseline in CDLQI Total Score
At LTE study baseline, the mean CDLQI score was 6.9 (SD = 6.17) across all patients in the LTE study, 5.3 (SD = 5.83) for patients previously treated with nemolizumab, and 9.1 (SD = 6.00) in the group not previously treated with nemolizumab.
At week 20, the mean CDLQI score was 4.3 (SD = 4.64) across all patients in the LTE study. Patients previously treated with nemolizumab had a mean CDLQI score of 4.1 (SD = 4.62), with a mean change from lead-in baseline and LTE study baseline of −8.3 (SD = 6.15) and −1.9 (SD = 4.41), respectively. Patients not previously treated with nemolizumab had a mean CDLQI score of 4.4 (SD = 4.18), with a mean change from lead-in baseline and LTE study baseline of −8.3 (SD = 6.43) and −5.1 (SD = 5.65), respectively.
At week 56, the mean CDLQI score was 3.4 (SD = 4.48) across all patients in the LTE study. Patients previously treated with nemolizumab had a mean CDLQI score of 2.1 (SD = 2.02), with a mean change from lead-in baseline and LTE study baseline of −9.2 (SD = 6.09) and −4.5 (SD = 5.11), respectively. Patients not previously treated with nemolizumab had a mean CDLQI score of 4.4 (SD = 5.28), with a mean change from lead-in baseline and LTE study baseline of −8.2 (SD = 6.80) and −6.3 (SD = 6.77), respectively.
Harms Results
During the 52-week LTE study treatment period, 63.8% of patients experienced at least 1 AE, most being mild or moderate in severity, and 16.7% experienced a study drug-related AE. A treatment-emergent SAE was experienced by 4.1% of patients. A total of 4.8% of patients experienced a severe AE, with the most common being AD (0.9%), COVID-19 infection (0.3%), increased blood creatine phosphokinase (0.2%), asthma (0.2%), asthenia (0.2%), impetigo (0.2%), and headache (0.2%). A treatment-emergent AESI (by investigator) was experienced by 23.7% of patients, most commonly infections (20.3%) and asthma (newly diagnosed or worsening; 4.3%). Treatment-emergent AEs leading to study drug withdrawal were experienced by 3.3% of patients; 3.1% of patients experienced an AE leading to study discontinuation.
During the LTE study follow-up period, 18.4% of patients experienced at least 1 AE, most being mild or moderate in severity, and 2.7% experienced a study drug-related AE. A treatment-emergent SAE was experienced by 2.7% of patients. A total of 2.0% of patients experienced a severe AE, and the only severe AE occurring in more than 1 patient was AD (0.7%). A treatment-emergent AESI (by investigator) was experienced by 4.8% of patients, most commonly infections (3.1%) and asthma (newly diagnosed or worsening; 1.7%). No treatment-emergent AEs led to study drug withdrawal in the follow-up period; however, 4.4% of patients experienced an AE leading to study discontinuation.
There were no deaths during the treatment or follow-up period of the LTE study.
Critical Appraisal
The ARCADIA LTE study was designed as a single-arm, open-label extension to assess long-term safety and efficacy of nemolizumab in the treatment of adult and adolescent patients with moderate to severe AD. This open-label design could bias the reporting for subjective efficacy outcomes and harms. The direction and magnitude of these potential biases remain unclear. In addition, the absence of statistical hypothesis testing and a control group (i.e., no active comparator or placebo arm) limits the ability to draw definitive conclusions regarding the treatment effect. The study used a dosing regimen of every 4 weeks, which does not align with the dosing schedule of every 8 weeks outlined in the product monograph and may not reflect real-world use.
The extension study partly consisted of patients who took part in the lead-in studies, ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO, and therefore it is reasonable to expect that the same strengths and limitations related to generalizability apply to the extension period. Given that patients needed to complete the lead-in studies before enrolling, the treatment extension population is inherently enriched with patients who met the study definition of clinical responder. Attrition rates were high, particularly for later time points such as week 56, which may limit generalizability and interpretability of long-term outcomes. Although the study follow-up was limited to 56 weeks, the consulted clinical experts indicated that this duration was likely sufficient to assess safety and efficacy. The study is ongoing and is expected to be completed in August 2026.
Indirect Comparisons
One network meta-analysis (NMA) was submitted by the sponsor to fill gaps in the comparative evidence for nemolizumab versus relevant comparators that included abrocitinib, baricitinib, dupilumab, lebrikizumab, tralokinumab, and upadacitinib for the treatment of moderate to severe AD in patients aged 12 years or older who are candidates for systemic therapy. The focus of the NMA was in patients who were experienced with CsA. Because baricitinib, lebrikizumab, and tralokinumab were not relevant to public payers in Canada, they were excluded from this report.
Description of Studies
A feasibility assessment was undertaken to ascertain the extent of clinical heterogeneity across 26 RCTs identified in the systematic literature review. Study design characteristics, baseline characteristics, treatment regimens, outcome definitions, time points, and data availability were considered potential sources of clinical heterogeneity and explored in the feasibility assessment. Of the 26 RCTs, 22 were included in at least 1 network, which included 7 trials of interest (AD Up, ARCADIA 1, ARCADIA 2, ARCADIA CYCLO, JADE DARE, LIBERTY AD CAFÉ, and LIBERTY AD CHRONOS) comparing nemolizumab, dupilumab, abrocitinib, and upadacitinib, connected via placebo comparator arms. The feasibility assessment suggested that the included trials were similar in study design, patient characteristics, treatment regimens, and outcome measures. The authors noted that the main source of heterogeneity was attributed to trial data that included populations experienced with CsA and not experienced with CsA; no other sources of heterogeneity were described. An NMA was considered feasible for patients who were experienced with CsA for the following outcomes of interest at 16 weeks: EASI-75 response, improvement in PP-NRS of 4 points or more (PP-NRS response), IGA score of 0 or 1 (IGA response), DLQI change from baseline, AEs, and discontinuation due to AEs (DAEs). It was assumed that trials with outcome data reported for mixed-age populations, but with a majority (≥ 75%) adult population, could be assessed in adult networks, and that outcome data could be pooled across time points to maintain network integrity. There were no data available for adolescents who were experienced with CsA. Bayesian random-effect NMAs were conducted using generalized linear models to estimate odds ratios and 95% credible intervals (CrIs), except for DLQI change from baseline, which was assessed with mean difference and 95% CrI.
Efficacy and Harm Results
The results for EASI-75 response, PP-NRS response, and IGA response favoured upadacitinib 30 mg versus nemolizumab. The results for IGA response also favoured abrocitinib versus nemolizumab. The results for DLQI mean change from baseline did not favour any treatments. Across all outcomes, there was no difference between dupilumab versus nemolizumab. The results for AEs and DAEs did not favour any treatments.
Critical Appraisal
The protocol of the systematic review and NMA was not a priori registered. The methods used to conduct the systematic literature review used appropriate criteria to search databases, select studies, extract data, and assess risk of bias of the included studies. The NMA included relevant outcomes identified by the CDA-AMC team, which included EASI-75 response, PP-NRS response, IGA response, DLQI change from baseline, AEs, and DAEs. Analysis for all outcomes was performed at 16 weeks and did not include the maintenance treatment phase of 48 weeks for nemolizumab. This was attributed to insufficient data beyond 16 weeks for the comparators of interest, which represents a gap in the available indirect evidence.
The authors noted that the included trials were considered similar in study design, patient eligibility criteria, baseline patient characteristics, and outcome characteristics (i.e., definitions and methods of reporting outcomes). However, there were notable baseline differences with respect to mean body surface area (BSA) (ranging from 42.5% to 59.5% across trials and arms), and proportion of patients with baseline IGA scores of 3 or 4 (IGA = 3 ranging from 46% to 73.9%; IGA = 4 ranging from 26.1% to 54%). The included studies enrolled a combination of patients with inadequate response to, or intolerance to CsA. Efforts were made in the NMA to reduce heterogeneity by stratifying the adult and adolescent patient populations experienced with CsA into subgroups. The results across outcomes showed low heterogeneity via the I2 statistic, which ranged from ██ ██ ██ (indicating low heterogeneity). The results of sensitivity analyses that removed trials with mixed patient populations (with and without experience with CsA), were consistent with the base-case analysis. There were no data available for adolescents who were experienced with CsA, which represents a gap in the available indirect evidence.
Overall, the network was sparse (i.e., many comparisons but few studies). Because most nodes were informed by only 1 trial and had small sample sizes, comparisons were underpowered, which contributed to wide CrIs in the analyses. Most 95% CrIs included both better and worse performance, except for EASI-75, PP-NRS, and IGA response, where upadacitinib 30 mg was favoured over nemolizumab 30 mg (i.e., 95% CrIs did not cross the null). Due to the absence of closed loops in the network, it was not possible to assess for inconsistency across direct and indirect evidence in the NMA.
Conclusions
Results from 2 identical phase III, double-blind, multicentre, placebo-controlled RCTs (ARCADIA 1 and ARCADIA 2) in patients with moderate to severe AD demonstrated that nemolizumab led to statistically significant improvements in markers of disease activity (measured by IGA success and EASI-75) and itch (measured by PP-NRS) at 16 weeks, when compared with placebo. Among the subset of patients who had demonstrated a clinical response by 16 weeks, results suggested that improvements in disease activity and itch were sustained, regardless of whether nemolizumab was given every 4 weeks or every 8 weeks. The clinical experts and patient groups highlighted the debilitating aspect of itch in this population. Results from subgroup analyses at 16 weeks suggested a more pronounced effect on disease activity in patients with severe itch (PP-NRS ≥ 7), although these results were only considered supportive of the overall effect of nemolizumab.
Results from a similar phase IIIb, double-blind, placebo-controlled RCT (ARCADIA CYCLO) in patients refractory to CsA or where CsA was inadvisable, suggested similar trends in EASI-75 and PP-NRS, but not IGA, and the results were more subject to uncertainty due to imprecision. Results from all 3 trials were subject to some uncertainty due to limitations primarily impacting external validity, as patients with certain comorbidities such as uncontrolled or worsening asthma and certain treatment histories were excluded from the ARCADIA 1 and ARCADIA 2 studies; and the ARCADIA CYCLO study enrolled patients with more mixed patient histories. HRQoL results demonstrated a reduction in scores (nominal P value < 0.05 for DLQI) across all trials, although the results were not considered clinically meaningful and did not attain the threshold for a clinically meaningful difference provided by the clinical experts consulted for this review.
In the ARCADIA LTE study, patients previously treated with nemolizumab showed gradual initial improvement in disease activity and symptoms, which appeared to be maintained through the treatment period. Patients who were not previously treated with nemolizumab demonstrated continued improvement throughout the LTE study. However, limitations such as the enriched population and lack of comparator preclude definitive conclusions.
The clinical experts highlighted the safety profile of nemolizumab was considered tolerable and manageable. The long-term safety profile of nemolizumab in the ARCADIA LTE study was consistent with that of the ARCADIA 1 and ARCADIA 2 studies, and no new safety signals were observed.
There was no direct evidence comparing nemolizumab to other systemic therapies used to treat moderate to severe AD in Canada. The results of the sponsor-submitted indirect treatment comparison suggested that upadacitinib 30 mg was favoured over nemolizumab for all efficacy outcomes, and abrocitinib was favoured for IGA response. The results comparing nemolizumab and dupilumab were inconclusive for all outcomes of interest due to the wide 95% CrIs that contained the possibility that either treatment could be favoured or that there could be no difference. The indirect treatment comparison safety results for overall occurrence of any AE and DAE at week 16 did not support a difference between nemolizumab and any relevant comparators. However, the NMA could not support comparisons of specific AEs, which may be of interest to patients and clinicians. Overall, the NMA estimates were subject to uncertainty due to serious imprecision, and a lack of data for adolescents and treatment effect beyond 16 weeks.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of nemolizumab 30 mg/0.49 mL SC injection in the treatment of moderate to severe AD in patients aged 12 years or older who are candidates for systemic therapy.
Disease Background
The contents of this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
AD is a chronic, relapsing, inflammatory, and noncontagious skin disease that is thought to involve a complex interplay of genetic, immune, and neuroimmune dysregulation, skin barrier dysfunction, microbial imbalance, and environmental factors.1-4 AD is a debilitating disease that can negatively impact patients’ quality of life, and has the highest disease burden among skin diseases.14 Patients can experience a range of symptoms; however, the disease is characterized by severe and persistent itch with a chronic duration and a fluctuating course of the eczematous lesions.2 Acute worsening of AD, commonly referred to as a flare, presents as dry, red, itchy skin that can lead to lesions that blister, ooze, and crust. While clinical presentation can vary depending on age, disease stage, geographic location, and race or ethnicity, itch is the leading symptom that characterizes AD.2,4 As the most common and most burdensome symptom of AD, itch has a direct impact on patients’ daily activities and quality of life.15,16 Chronic itch can result in sleep disruption and poor sleep quality, observed in approximately two-thirds of patients with AD.17-21 Sleep disruption can considerably reduce daytime attention levels, in turn negatively impacting school and work performance and relationships. AD is also linked to mental and psychological distress, depression, and a higher risk of suicidal ideation, with itch being a major risk factor and predictor for these psychological comorbidities.22 Patients with AD are also more likely to have or develop other comorbidities, such as allergies or infections.4,23
The prevalence and incidence of AD varies widely between different geographic regions due to genetic, behavioural, cultural, socioeconomic, and climate-related factors.24-26 It is estimated that the prevalence of eczema in Canada is 15% in children and adolescents (aged 0.5 to 17 years) and 3.5% in adults.5,6
The diagnosis of AD and assessment of disease severity is based on clinical judgment and patient-reported history and symptoms.2,7,15,27-30 Diagnostic criteria include the Hanifin-Rajka criteria (with itch and eczema as the essential features), or the UK Working Party diagnostic criteria.3,17 While the Hanifin-Rajka criteria are the gold standard, the UK Working Party criteria are considered easier to employ in clinical practice, although both have been validated and tested in various studies and populations.2,3,17,31 To receive an AD diagnosis, other conditions must be excluded, particularly psoriasis, scabies, contact dermatitis, and seborrheic dermatitis.3,17 Diagnosis of AD is generally more straightforward in infants and young children, as it can be more complicated in more severe cases and adults due to heterogeneous presentation.3,17 Depending on the extent and the severity of symptoms, AD can be classified as mild, moderate, or severe.7 Patients are considered to have moderate to severe disease when they have at least 1 of the following: BSA involvement of 10% or more, moderate to severe lesions, involvement of highly visible areas or those important for function (e.g., neck, face, genitals, palm, and/or soles), or substantially impaired quality of life.7 AD severity can be classified using EASI and intensity of patient burden can be quantified using patient-reported outcomes.9 No biomarkers have been identified for the diagnosis of AD.3,7,15,17,27,29
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
The management of AD involves a multipronged approach including patient education, skin hydration, restoration of the skin, elimination of exacerbating factors, and pharmacologic treatment of skin inflammation.8 The clinical experts consulted for this review noted that the goals of treatment are reduction of signs and symptoms (e.g., red scaly plaques, itch, scratching, lichenification, dyspigmentation, scarring), prevention of secondary infections, improvement of quality of life (e.g., sleep, daily activities, hobbies), maintenance of independence, reduction of caregiver burdens, and enhancement of work and or school productivity.
The typical treatment paradigm for AD is to initiate treatment with a topical drug or combination of drugs, such as a TCS and/or TCI, ruxolitinib, crisaborole, or roflumilast for at least 4 weeks, pending referral to a dermatologist. If this treatment is unsuccessful, patients may be trialled on another topical drug for 4 to 8 weeks. Topical drugs may be used concurrently with narrow band phototherapy (administered in office 2 to 3 times per week) or systemic drugs for the maintenance of response, rescue treatment, or control of flares.32 The clinical experts noted that phototherapy can be limited by factors such as accessibility and convenience.
Patients with persistent, moderate to severe AD despite optimized topical therapy require systemic treatment to achieve disease control, with re-evaluation to rule out concurrent diseases and confirm the diagnosis of AD.8 Dupilumab, tralokinumab, abrocitinib, and upadacitinib are approved in Canada and have recommendations for use in moderate to severe AD. The American Academy of Allergy, Asthma and Immunology and American College of Allergy, Asthma and Immunology Joint Task Force recommends the addition of dupilumab or tralokinumab over continuing standard topical treatment, then switching to a JAK inhibitor if the patient’s disease is not responsive.33 Guidelines on the conventional immunosuppressing systemic therapies is more mixed: some guidelines conditionally suggest the use of methotrexate, mycophenolate mofetil, and CsA with appropriate monitoring,32 while others suggest only CsA (recommending against methotrexate, azathioprine, or mycophenolate mofetil). Systemic corticosteroids are only recommended for acute, severe exacerbations and as a short-term bridge to other therapies.32
The clinical experts noted that a typical progression would be for patients to trial conventional systemic therapies for a period of 3 months and if well controlled, they would remain on that therapy, but if they do not respond, then they may switch to another conventional systemic therapy or the advanced systemic therapies (dupilumab, tralokinumab, abrocitinib, and upadacitinib). They noted a trial of 3 to 6 months is usually used to determine response. If the patient’s skin is not completely clear, they may add a topical therapy. Occasionally, the experts noted that a combination of systemic therapies may be used.
Dupilumab, abrocitinib, and upadacitinib are recommended by CDA-AMC for reimbursement for moderate to severe AD. Lebrikizumab and tralokinumab are approved for use in Canada, but are not recommended to be reimbursed for moderate to severe AD.
Drug Under Review
Key characteristics of nemolizumab and other treatments available for moderate to severe AD are summarized in Table 4.
Nemolizumab is a humanized monoclonal antibody of the IgG2 subclass that inhibits IL-31 signalling by selectively binding to IL-31RA to ameliorate pruritus, inhibit inflammatory responses, and restore barrier integrity in AD.34
Nemolizumab is indicated for the treatment of patients aged 12 years and older with moderate to severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. The reimbursement request is for the treatment of moderate to severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies. Nemolizumab is currently approved for the treatment of AD in the European Union and US.35,36
Nemolizumab is administered as an SC injection and can be used with or without TCSs and TCIs.34 The Health Canada–recommended nemolizumab dose for the treatment of AD is an initial dose of 60 mg (two 30 mg injections), following by 30 mg every 4 weeks.34 After 16 weeks of treatment, the recommended dose for patients who achieve a clinical response is 30 mg every 8 weeks.34
Table 4: Key Characteristics of Treatments for AD
Characteristic | Nemolizumab | Abrocitinib | Dupilumab | Upadacitinib |
|---|---|---|---|---|
Mechanism of action | Humanized monoclonal antibody of the IgG2 subclass that inhibits IL-31 signalling by selectively binding to IL-31 RA to ameliorate pruritus, inhibit inflammatory responses, and restore barrier integrity in AD. | Reversibly and selectively inhibits JAK1 by blocking ATP binding site to prevent STAT phosphorylation and activation, disrupting signalling pathways of proinflammatory cytokines. | Recombinant human IgG4 monoclonal antibody that inhibits IL-4 and IL-13 signalling, key cytokines involved in inflammation associated with atopic disease. | Selective JAK inhibitor that prevents phosphorylation and activation of STATs, disrupting signalling pathways of proinflammatory cytokines. |
Indicationa | For the treatment of patients aged 12 years and older with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. | For the treatment of patients 12 years and older with refractory moderate to severe AD, including the relief of pruritus, who have had an inadequate response to other systemic drugs (e.g., steroid or biologic), or for whom these treatments are not advisable. | For the treatment of patients aged 6 months and older with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. | For the treatment of adults and adolescents 12 years of age and older with refractory moderate to severe AD who are not adequately controlled with a systemic treatment (e.g., steroid or biologic) or when use of those therapies is inadvisable. |
Route of administration | SC | Oral | SC | Oral |
Recommended dose |
|
| For adult patients, initial dose of 600 mg (two 300 mg injections), followed by 300 mg every other week |
|
Serious adverse effects or safety issues | NA | Serious warnings:
|
| Serious warnings:
Other warnings:
|
Other | Completion of all age-appropriate vaccinations should be considered before initiating treatment. Avoid the use of live vaccines. | Completion of all age-appropriate vaccinations should be considered before initiating treatment. Avoid the use of live vaccines. | NA | Completion of all age-appropriate vaccinations should be considered before initiating treatment. Avoid the use of live vaccines. |
AD = atopic dermatitis; ATP = adenosine triphosphate; GI = gastrointestinal; IL = interleukin; MACE = major adverse cardiovascular events; NA = not applicable; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; RA = receptor antagonist; SC = subcutaneous; STAT = signal transducer and activator of transcription.
aHealth Canada–approved indication.
Sources: Nemolizumab product monograph,34 abrocitinib product monograph,37 dupilumab product monograph,38 and upadacitinib product monograph.39
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
One patient group submitted input for this review, the ESC, a registered charity in Canada aiming to improve the lives of people living in Canada with eczema through support, education, awareness, and research. Information was gathered for this submission through questionnaires, patient interviews, review of published literature, and data from multiple surveys with a combined total of more than 3,000 people living in Canada.
When asked about their disease experience, patients with AD highlighted the profound physical and emotional challenges associated with the condition. Physical symptoms include painful and itchy skin lesions that crack, ooze, and bleed; visible skin flares; and persistent itching that disrupts sleep, school and work, and quality of life. Patients reported experiencing skin damage, bleeding, scarring, and pigment changes due to rashes and scratching, with open wounds posing an increased risk of skin infection. Some patients reported living with chronic pain and discomfort due to their AD, never experiencing relief from their symptoms. In addition to physical symptoms, patients also face a substantial emotional toll of AD, including feelings of isolation, hopelessness, frustration, and despair over limited treatment success, as well as anxiety, depression, and low self-esteem. Some patients also have trouble maintaining social and intimate relationships, due to the impact on confidence and comfort. The patient group noted that, until recently, systemic treatments for AD have been limited, including phototherapy, off-label immune-suppressing medication (e.g., CsA, methotrexate), and oral corticosteroids for treatment of flares. However, many patients fear side effects associated with long-term use of treatments such as steroids. Patients have had substantial recent success with new systemic therapies becoming available; however, many are not accessible to all patients, and some patients do not respond. Patients report feeling frustrated over the trial-and-error process of cycling through currently available treatments, and many have exhausted all treatment options. The patient group input noted that because AD is a heterogenous disease, no single treatment option can meet the needs of all patients.
ESC highlighted the urgency for innovative therapies that can offer long-term relief and improve quality of life. Outcomes of treatment identified as most important to patients with AD include improved disease control, symptom and pain relief (e.g., itch, dryness, inflammation, blistering), convenience, and improved quality of life.
ESC described general patient experiences with nemolizumab, although the source of these experiences (e.g., patient interviews, survey responses, general trial observations) was not specified. Patients treated with nemolizumab reported substantial reductions in itch, with noticeable improvements in skin clearance from rashes, lesions, sores, and open wounds, which provided further benefit in improving sleep, productivity, self-esteem, and mental health. ESC noted that many patients who were previously unsuccessful with approved and off-label medications reported success with nemolizumab.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of moderate to severe AD.
Unmet Needs
The clinical experts noted that pruritus (itch) is a very debilitating and unpredictable aspect of AD, and better treatments are needed to target this symptom. In addition, approximately 30% to 40% of patients will either not respond to, or will become refractory to, currently available nonbiologic treatments (1 expert noted this would be approximately 20% if biologics were also considered); therefore, new treatments are needed. Moderate to severe AD often comes with a high burden of disease, which also impacts patients’ HRQoL and their ability to carry out activities due to symptoms, or due to a feeling of self-consciousness. The currently available treatments (e.g., JAK inhibitors) are not always well tolerated and have contraindications or black box warnings, further reinforcing the need for new treatment options.
Place in Therapy
The clinical experts noted that nemolizumab is the only treatment with a mechanism of action targeting IL-31, which is involved in the sensation of pruritus. The experts stated that it could be used as monotherapy or in combination with topical therapies, phototherapy, and other conventional immunosuppressing systemic drugs. They noted that nemolizumab should be considered a first-line systemic therapy after topical therapies, and considered alongside the other biologics such as dupilumab, tralokinumab, or lebrikizumab. The clinical experts noted that the reimbursement criteria for dupilumab could also be considered appropriate for nemolizumab (e.g., having been unsuccessful with 1 conventional systemic therapy trial); however, the choice to use a conventional treatment or advanced systemic drug would be partially determined by the drug coverage.
Patient Population
The experts noted that nemolizumab would be suitable for all patients with moderate to severe AD, and 1 expert noted it would also be appropriate for patients who do not tolerate, respond to, or cannot access phototherapy, as well as those who have a contraindication to alternate systemic therapies. The experts further noted that patients who are substantially impacted by pruritus, who have substantial flares of AD, whose current therapy has stopped working, or whose AD has a substantial impact on their lives would be those most in need of additional interventions and most likely to benefit.
There are no specific criteria or laboratory tests required for diagnosis, as AD is typically diagnosed clinically and is a common disease. The experts noted that there are no biomarkers or tests that would indicate a patient’s likelihood to respond to nemolizumab.
Assessing the Response to Treatment
The clinical experts noted that the measures used in the trial are also used in clinical practice to assess response, including patient global assessment of improvement, EASI reduction, numeric rating scale for itch, and DLQI. The clinical experts also noted that other subjective changes reported by patients in clinical practice may include changes to sleep, daily activities, work productivity, improvement in mental health, and reduction of scratching or itching.
The experts commented that the measures used in clinical practice vary and may be chosen according to the reimbursement criteria set by payers to obtain coverage for a treatment (e.g., change in EASI score at 6 months). Patients are often assessed every 3 months initially and when their condition has improved and stabilized, they are typically assessed every 6 months.
Discontinuing Treatment
The clinical experts stated that treatment should be discontinued if there has been no meaningful response after 6 months of therapy, if the patient experiences an allergy or hypersensitivity, or if they experience intolerable AEs. The definition of a meaningful response could vary and the decision to discontinue is often shared between the clinician and the patient. One expert shared an example that patients with minimal disease response according to a tool such as EASI may still wish to continue treatment if their pruritus is controlled. If there is a partial response, the experts noted that the addition of a new therapy should be considered first, rather than discontinuing the current treatment.
Prescribing Considerations
According to the experts, patients should receive a proper diagnosis of AD by a dermatologist before nemolizumab is prescribed. Patients can be managed and monitored by dermatologists in any outpatient clinic (community or hospital). After 6 months of treatment and confirmation of clinical efficacy, primary care providers could also manage the prescribing until reinvolvement of the dermatologist is necessary.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
One joint input was submitted for this review by DAO and the Atlantic Dermatology Group. DAO provides broad representation for more than one-half of registered dermatologists in Canada. The Atlantic Dermatology Group is a group of hospital-based and academic-based dermatologists practising in the Atlantic provinces. Information for this submission was gathered through a review of published literature, clinical trial data, and experience with nemolizumab as clinical trialists.
The input from clinician groups was generally consistent with the clinical experts consulted for this review, emphasizing the ongoing unmet need for treatments that provide rapid and sustained relief from pruritus, as well as improvements in sleep and quality of life for patients with moderate to severe AD. Like the experts, the clinician groups highlighted the limitations of current therapies, including slow onset of action with biologics and safety concerns or monitoring requirements with JAK inhibitors.
Aligning with expert input, the clinician groups considered nemolizumab a suitable first-line systemic option, to be positioned alongside existing biologics, particularly for patients with an inadequate response to topicals or systemic therapies, or who require more rapid symptom relief. Both also highlighted the novel mechanism and monthly dosing schedule as factors that could improve adherence and convenience. The clinician groups provided additional details on patient selection, noting that nemolizumab may be particularly appropriate for patients with contraindications to JAK inhibitors (e.g., cardiovascular disease, immunosuppression concerns, thromboembolism). They also noted that patients with mild AD that can be managed effectively by topicals alone are less appropriate candidates.
Consistent with expert input, the clinician groups noted a range of clinical and patient-reported tools (e.g., IGA, EASI, PP-NRS, sleep scores) that could be used to assess treatment response, and support reassessment intervals from 4 to 12 months. However, they provided more specific discontinuation criteria, such as not achieving a reduction in PP-NRS or sleep numeric rating scale of 4 points or more or less than 50% improvement in EASI by week 16, while the experts emphasized a flexible, shared decision-making approach. Both clinical experts and clinician groups agreed that initiation should be done by dermatologists in an outpatient setting, but the clinician groups added that allergists could also initiate therapy, and that self-injection could be possible after training. The clinician group noted that because misdiagnosis of AD can occur, particularly in adult-onset cases, clinical expertise in differentiating AD from other eczematous conditions (e.g., contact dermatitis, seborrheic dermatitis, cutaneous T-cell lymphoma) is essential to ensure appropriate patient selection.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
There are comparator treatments funded by jurisdictions, but the studies provided by the sponsor compare nemolizumab to placebo. Would nemolizumab’s anticipated place in therapy be the same as the comparators (i.e., abrocitinib, dupilumab, upadacitinib)? | The experts noted that nemolizumab could be listed alongside the specified comparators. |
Considerations for initiation of therapy | |
The primary and key secondary end points in the ARCADIA 1 and ARCADIA 2 studies were IGA success (defined as a score of 0 [clear skin] or 1 [almost clear skin], representing a ≥ 2-point improvement from baseline) and EASI-75 response (from baseline) at week 16. Past CDEC recommendations have provided a reimbursement condition that both an EASI score and IGA score be provided at initiation; however, only EASI-75 is a required renewal condition. Is there merit to requiring both EASI and IGA scores at baseline, rather than just an EASI score, considering IGA is not required again at renewal for comparator treatments (i.e., are there situations where an individual would not be considered to have moderate to severe AD per their IGA score [score of 3 or 4] but not per EASI [score of ≥ 16])? | The clinical experts noted that there is some ambiguity around the definitions of AD severity when using IGA and EASI scores. An IGA score of 3 is considered moderate AD and 4 is severe. However, an EASI score of 16 would be considered more severe AD and an EASI score as low as 7 would be considered moderate AD. Therefore, a patient with an EASI score of < 16 could also have moderate AD. |
The requested reimbursement criteria are aligned with the key inclusion criteria in the ARCADIA studies (e.g., adult and adolescents aged ≥ 12 years with moderate to severe AD); however, the studies also required individuals to have pruritus associated with their AD (PP-NRS score of ≥ 4). Is the PP-NRS used in clinical practice? If so, should a PP-NRS be obtained at the initiation of therapy? Should patients be required to have a PP-NRS score of ≥ 4 to initiate nemolizumab? | The clinical experts noted that PP-NRS has not been used as a criterion for any other advanced systemics, and its use in clinical practice is likely variable; but may be used in private reimbursement for other disease indications. They noted it should not be mandatory in addition to other reimbursement criteria, but it would have a role as a marker of application and for reimbursement because nemolizumab has a potential mechanism to address pruritus in AD. The clinical experts suggested it could replace either IGA or EASI. |
Reviews by CDEC for comparators (i.e., abrocitinib, dupilumab, and upadacitinib) have resulted in a reimbursement recommendation that therapy be initiated in individuals with refractory disease, who are intolerant to, or are ineligible for:
Although individuals in the ARCADIA 1 and ARCADIA 2 trials were not required to have had a prior trial of phototherapy, should individuals be required to be refractory to maximally tolerated topical therapies with phototherapy (where available) before becoming eligible for nemolizumab? Although individuals in the ARCADIA 1 and ARCADIA 2 trials were not required to have had a prior trial of a systemic immunomodulator, should individuals be required to be refractory to maximally tolerated topical therapies with a systemic immunomodulator before becoming eligible for nemolizumab? | The clinical experts stated that a trial of phototherapy should not be required as only a small proportion of patients can access it. They cited the example of psoriasis, where phototherapy is considered an immunomodulator by some jurisdictions for reimbursement purposes; therefore, patients who are refractory to phototherapy do not have to subsequently trial a systemic immunomodulator before trying advanced systemic drugs. They also noted that ideally, patients should not have had to trial a systemic immunomodulator before becoming eligible for nemolizumab or other advanced systemic drugs for this indication. Several private drug plans do not require this, but they acknowledged that the public plan reimbursement criteria for other advanced systemic drugs currently do. |
Would it be appropriate to initiate nemolizumab in patients whose AD has not responded to previous treatment with a biologic drug or JAK inhibitor? | The clinical experts noted that it is variable whether a patient will respond to 1 class of systemic drug vs. another; therefore, it would be appropriate to initiate nemolizumab in these patients. |
Consider alignment with criteria recommendation for comparators (i.e., abrocitinib, dupilumab, and upadacitinib). | This is a comment from the drug plans intended to inform CDEC deliberations. |
Considerations for continuation or renewal of therapy | |
Considering the key secondary end point related to PP-NRS (described previously), could there be a situation where individuals do not achieve EASI-75 but may continue to benefit from nemolizumab based on improvements in PP-NRS? | The clinical experts noted that given nemolizumab’s potential to address itch, patients who have not yet achieved EASI-75 but have achieved substantial itch reduction may still derive benefit from nemolizumab. |
If consideration for renewal should be given to individuals with improvement in PP-NRS, is there a minimum improvement which should be required? | The clinical experts noted that a change of ≥ 4 points — similar to the pivotal trial — would be reasonable, although they noted that the timing of the assessment would also be important (e.g., 6 months, similar to other assessments). |
Consider alignment with criteria recommendation for comparators (i.e., abrocitinib, dupilumab, and upadacitinib). | This is a comment from the drug plans intended to inform CDEC deliberations. |
Considerations for prescribing of therapy | |
Following the initial 16 weeks of the ARCADIA 1 and ARCADIA 2 studies, patients meeting the study definition of clinical responders to nemolizumab were rerandomized 1:1:1 to nemolizumab 30 mg every 4 weeks, nemolizumab 30 mg every 8 weeks (with placebo every 8 weeks to obtain an every 4 week injection interval), or placebo every 4 weeks. The monograph dosing for nemolizumab is 60 mg initially, followed by 30 mg every 4 weeks. After 16 weeks of treatment, patients who achieve a clinical response are recommended to continue therapy at a maintenance dose of nemolizumab 30 mg every 8 weeks. The rerandomized results showed the percent of individuals maintaining their EASI-75 improvement in the nemolizumab every 4 weeks group, the nemolizumab every 8 weeks group, and the placebo every 4 weeks group, respectively, was:
Should nemolizumab be funded at a maximum of 30 mg every 8 weeks during the maintenance phase (i.e., after 16 weeks of treatment)? Or are there individuals who may benefit from ongoing nemolizumab 30 mg every 4 weeks? | The clinical experts noted that having the option to dose nemolizumab every 8 weeks would be a good option; however, they noted that some patients might achieve more benefit from receiving nemolizumab every 4 weeks, and therefore having the option of every 4 weeks would also be helpful. |
Can nemolizumab be used in combination with other therapies for AD, such as immunosuppressants, phototherapy, biologics, or JAK inhibitors? | The clinical experts noted that nemolizumab could be combined with other therapies for AD. |
System and economic issues | |
The cost of nemolizumab is higher in year 1 than comparators due to loading and the need for an initial 4-week dosing. In subsequent years the cost is lower than dupilumab because individuals who respond to nemolizumab can reduce frequency to every 8 weeks. If individuals may remain on nemolizumab every 4 weeks long term, that could substantially change the annual cost of nemolizumab. A scenario analysis is included to explore the impact of a 4-week dosing interval. | This is a comment from the drug plans intended to inform CDEC deliberations. |
All 3 of the comparators (abrocitinib, dupilumab, and upadacitinib) have confidential pricing in place for AD. | This is a comment from the drug plans intended to inform CDEC deliberations. |
AD = atopic dermatitis; CDEC = Canadian Drug Expert Committee; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% improvement in the Eczema Area and Severity Index from baseline; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; vs. = versus.
Clinical Evidence
The objective of this Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of nemolizumab 30 mg/0.49 mL SC injection in the treatment of moderate to severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, or who are refractory to or ineligible for systemic immunosuppressant therapies. The focus will be placed on comparing nemolizumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of nemolizumab is presented in 3 sections with our critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. Our assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted LTE studies. The third section includes indirect evidence from the sponsor. No studies addressing gaps were included in the review.
Included Studies
Clinical evidence from the following are included in the review and appraised in this document:
3 pivotal studies or RCTs identified in systematic review
1 LTE study
1 indirect treatment comparison consisting of NMAs.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
Three pivotal studies were included in this review (ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO). Characteristics of the included studies are summarized in Table 6.
ARCADIA 1 and ARCADIA 2 Studies
The study designs for the ARCADIA 1 and ARCADIA 2 studies were identical; both were phase III, double-blind, placebo-controlled, multicentre RCTs evaluating the efficacy and safety of nemolizumab in adults and adolescents (aged ≥ 12 years) with moderate to severe AD. The coprimary end point of the ARCADIA 1 and ARCADIA 2 studies was the proportion of patients with IGA success, and the proportion of patients with EASI-75 at week 16. Key secondary end points also evaluated changes in PP-NRS across the study period. Patients were randomized via interactive response technology 2:1 to receive nemolizumab (ARCADIA 1: n = 620; ARCADIA 2: n = 522) or placebo (ARCADIA 1: n = 321; ARCADIA 2: n = 265). Randomization was stratified by disease severity (IGA = 3 or 4), and pruritus severity (PP-NRS < 7 or ≥ 7).
Before randomization for the initial treatment period, there was a 2-week run-in period where patients were started on standardized background topical therapy; background topical therapy included the use of authorized TCS with or without TCI. A medium-potency TCS was to be used on the body, where considered safe (e.g., trunk and extremities). A low-potency TCS or a TCI was to be used in sensitive areas considered unsafe for medium-potency TCSs (e.g., face, neck, intertriginous areas) or where medium-potency TCS was not tolerated. The prescribed background therapy use was within daily limits according to the product labelling. The protocol included guidelines to adjust background therapy use according to disease activity and tolerability.
After the 16-week initial treatment period, patients in the treatment arm who met the study definition of clinical responders (defined as an IGA of 0 [clear] or 1 [almost clear] or EASI-75 at week 16) were rerandomized 1:1:1 via interactive response technology to either continue receiving nemolizumab 30 mg every 4 weeks (n = 169 in both studies), to receive nemolizumab every 8 weeks (n = 169 in both studies), or to receive placebo (n = 169 in both studies). The patients who had been randomized to placebo who met the study definition of clinical responders continued to receive placebo every 4 weeks in the maintenance period (n = 185 in both studies).
Patients who required rescue therapy for clinical worsening of AD before week 16 were considered to be unsuccessful with treatment and may be considered for the LTE study but were required to continue with study visits until the week 16 visit; patients who completed the maintenance period were also eligible to participate in the LTE study. Patients who declined or were not eligible to enter into the LTE study were to complete a follow-up visit 12 weeks after their last study drug injection. The follow-up visit was not required for patients who participated in the LTE study. Patients who discontinued the initial or maintenance periods prematurely were to complete an early termination visit and a follow-up visit 12 weeks after the last study drug injection. Full details of the study design for the ARCADIA 1 and ARCADIA 2 studies are in Figure 1.
ARCADIA CYCLO Study
The ARCADIA CYCLO study was a phase IIIb, double-blind, placebo-controlled, multicentre RCT which included a 16-week treatment period and an 8-week follow-up period for patients who declined or were not eligible to enter the LTE study. There was no run-in period with topical therapy; patients were randomized and began treatment right after the screening period. Patients were randomized 1:1 to receive nemolizumab (n = 138) or placebo (n = 138). Randomization was stratified based on baseline IGA severity (IGA = 3, IGA = 4), and prior CsA exposure (yes, no). The primary end point of the ARCADIA CYCLO study was the proportion of patients with EASI-75, and proportion of patients with an improvement of PP-NRS score of 4 or more from baseline at week 16.
Patients who completed the 16-week treatment period may have been eligible to enrol into the LTE study; the follow-up period, including the follow-up visit, was not required for patients who participated in the LTE study. Patients who declined or were not eligible to enter the LTE study completed a follow-up visit at week 24 (12 weeks after their last study drug injection). Patients who prematurely discontinued the study completed an early termination visit at the time of discontinuation and a follow-up visit 12 weeks after the last study drug injection. Full details of the study design for the ARCADIA CYCLO study are in Figure 2.
Table 6: Details of Studies Included in the Systematic Review
Detail | ARCADIA 1 study | ARCADIA 2 study | ARCADIA CYCLO study |
|---|---|---|---|
Designs and populations | |||
Study design | Phase III, DB, PBO-controlled, MC RCT | Phase III, DB, PBO-controlled, MC RCT | Phase IIIb DB, PBO-controlled, MC RCT |
Locations | 177 centres in 14 countries (Australia, Austria, Canada, Czech Republic, Germany, Korea, Latvia, Lithuania, Netherlands, New Zealand, Poland, Spain, UK, US) | 136 centres in 11 countries (Belgium, Bulgaria, Estonia, France, Georgia, Germany, Hungary, Italy, Poland, Singapore, US) | 50 centres in 6 countries (Czech Republic, Germany, Italy, Latvia, Poland, and Spain ) |
Patient enrolment dates | Start date: August 9, 2019 End date: August 11, 2022 | Start date: August 13, 2019 End date: September 26, 2022 | Start date: February 18, 2022 End date: April 14, 2023 |
Randomized (N) | N = 941 Nemolizumab (n = 620) Placebo (n = 321) | N = 787 Nemolizumab (n = 522) Placebo (n = 265) | N = 276 Nemolizumab (n = 138) Placebo (n = 138) |
Inclusion criteria |
|
| |
Exclusion criteria |
|
| |
Drugs | |||
Intervention | Initial treatment: Nemolizumab 30 mg, with a loading dose of 60 mg at baseline Maintenance period: Nemolizumab 30 mg | ||
Comparator(s) | Placebo | ||
Study duration | |||
Screening phase | Up to 4 weeks | Up to 4 weeks | |
Treatment phase | Initial treatment: 16 weeks Maintenance treatment: 32 weeks | 16 weeks, with last injection at 12 weeks | |
Follow-up phase | 8 weeks | 8 weeks | |
Outcomes | |||
Primary end point |
|
| |
Secondary end points | Key secondary end points:
Other secondary — initial period:
Secondary — maintenance period
|
| |
Publication status | |||
Publications | Silverberg et al. (2024)b EUDRACT No.: 2019-001887-31 NCT Number: NCT03985943 | Silverberg et al. (2024)b EUDRACT No.: 2019-001888-75 NCT Number: NCT03989349 | EUDRACT No.: 2021-002166-40 NCT Number: NCT05056779 |
AAD = American Academy of Dermatology; ACT = Asthma Control Test; AD = atopic dermatitis; AP-NRS = Average Pruritus Numeric Rating Scale; CDLQI = Children’s Dermatology Life Quality Index; COPD = chronic obstructive pulmonary disease; CsA = cyclosporine; DB = double blind; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-50 = ≥ 50% improvement in Eczema Area and Severity Index from baseline; EASI-75 = ≥ 75% improvement in Eczema Area and Severity Index from baseline; EASI-90 = ≥ 90% improvement in Eczema Area and Severity Index from baseline; EUDRACT = European Union Drug Regulating Authorities Clinical Trials Database; HADS = Hospital Anxiety and Depression Scale; HBcAb = hepatitis B core antibody; HBsAg = hepatitis B surface antigen; IGA = Investigator Global Assessment; MC = multicentre; NCT = National Clinical Trial; PBO = placebo; PDE-4 = phosphodiesterase 4; PEF = peak expiratory flow; PGADS = Patient Global Assessment of Disease Status; PGAT = Patient Global Assessment of Treatment effect; POEM = Patient-Oriented Eczema Measure; PP-NRS = Peak Pruritus Numeric Rating Scale; PROMIS = Patient-Reported Outcomes Measurement Information System; RCT = randomized control trial; SCORAD = SCORing Atopic Dermatitis; SD-NRS = Sleep Disturbance Numeric Rating Scale; TCI = topical calcineurin inhibitor; TCS = topical corticosteroid; ULN = upper limit of normal; WASO = wakefulness after sleep onset; WPAI:AD = Work Productivity and Activity Impairment Questionnaire: Atopic Dermatitis.
Note: The language used in the table is as per the sponsor and does not reflect language guidelines used at Canada’s Drug Agency.
aInadequate response was defined as 1 of: failure to achieve or maintain remission or low disease activity (equivalent to IGA ≤ 2) despite treatment with a regimen of a medium-potency, high-potency, or very high-potency TCS (with or without TCI), applied for at least 4 weeks or for the maximum duration per prescribing information; or requirement of a long-term treatment (> 4 weeks) with a high-potency or very high-potency TCS to achieve or maintain remission or low disease activity (equivalent to IGA ≤ 2); or if documentation of inadequate response to topical treatments was not available — patients with a documented recent course of systemic treatment or phototherapy for AD (within 6 months before the visit) were also considered to have had an inadequate response to topical treatments.
bSilverberg JI, Wollenberg A, Reich A, et al. Nemolizumab with concomitant topical therapy in adolescents and adults with moderate-to-severe atopic dermatitis (ARCADIA 1 and ARCADIA 2): results from two replicate, double-blind, randomised controlled phase 3 trials. The Lancet. 2024.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence10 and the ARCADIA 1 Clinical Study Report,11 ARCADIA 2 Clinical Study Report,12 and the ARCADIA CYCLO Clinical Study Report.13
Figure 1: ARCADIA 1 and ARCADIA 2 Study Design
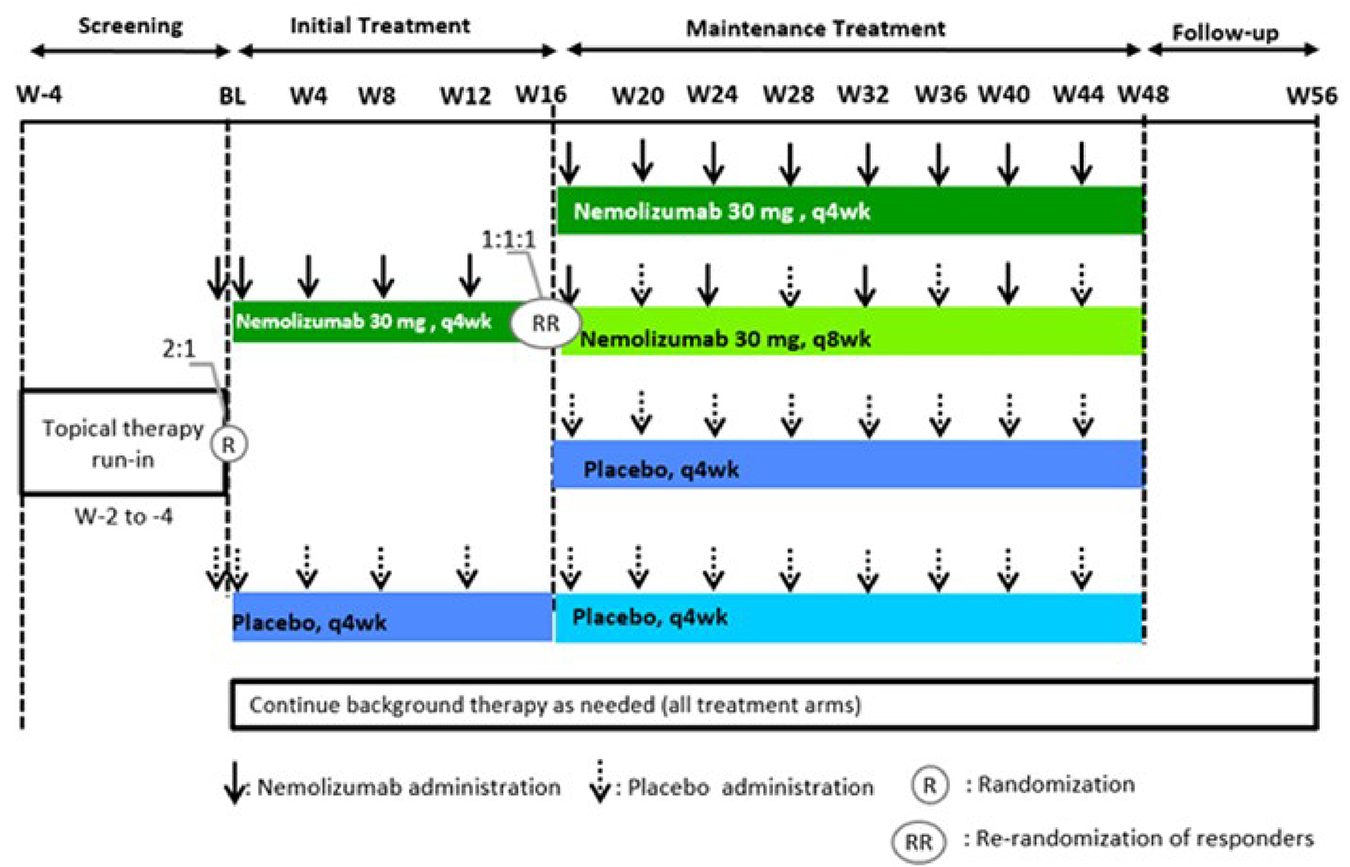
BL = baseline; q4wk = every 4 weeks; q8wk = every 8 weeks; W = week.
Source: Details in the figure are from the sponsor’s ARCADIA 1 Clinical Study Report.11
Figure 2: ARCADIA CYCLO Study Design
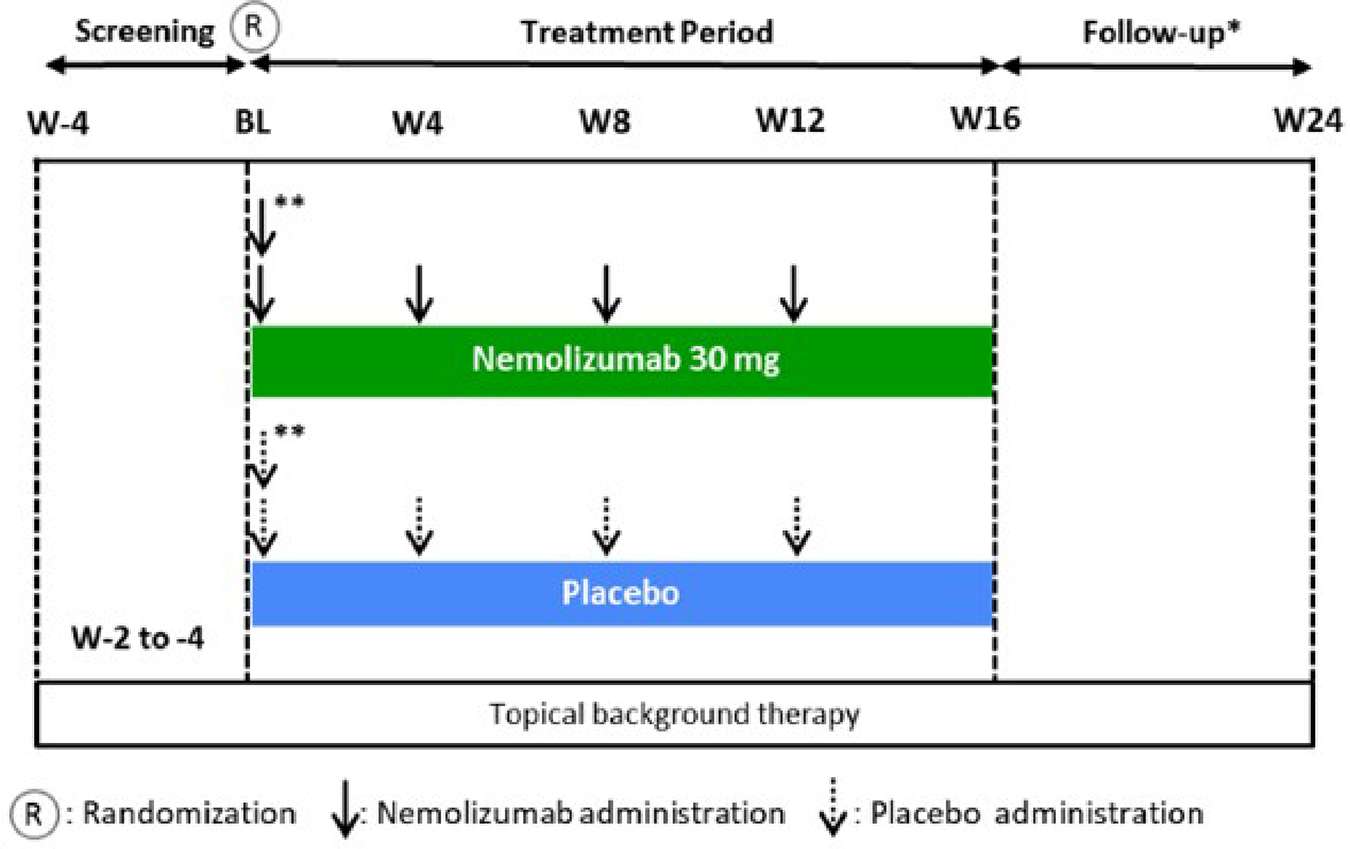
BL = baseline; W = week.
* Applicable for patients who did not participate in the long-term extension study.
Source: Details included in the figure are from the ARCADIA CYCLO Clinical Study Report.13
Populations
Inclusion and Exclusion Criteria: ARCADIA 1 AND ARCADIA 2 Studies
The ARCADIA 1 and ARCADIA 2 studies had the same patient inclusion and exclusion criteria (Table 6). Briefly, patients were required to be aged 12 years or older, meet specific thresholds of IGA (≥ 3), EASI (≥ 16), BSA (≥ 10%), and PP-NRS (≥ 4), and have a minimum disease duration of 2 years. In addition, patients had to have a documented history of inadequate response to topical medications (TCS with or without TCI) within 6 months of study enrolment. Notable exclusion criteria included patients with COPD or chronic bronchitis, uncontrolled asthma, specific medications in the weeks before enrolment, or who either did not improve or worsened after a 16-week trial with dupilumab.
Inclusion and Exclusion Criteria: ARCADIA CYCLO Study
Inclusion and exclusion criteria for the ARCADIA CYCLO study are described in Table 6. Notable inclusion criteria for the ARCADIA CYCLO study were that patients had to be aged 18 years or older, meet specific thresholds of IGA (≥ 3), EASI (≥ 20), BSA (≥ 10%), and PP-NRS (≥ 4), and have a minimum disease duration of 2 years. Of note, patients also had to have a documented history of inadequate response (including at maximum dose per the prescribing information), intolerance or unacceptable toxicity to CsA, or have CsA be medically inadvisable for reasons prespecified in the protocol. Of note, the minimum EASI score required was 20. In addition, patients had to have a documented history of inadequate response to topical medications (TCS with or without TCI) within 6 months of study enrolment. Notable exclusion criteria included patients with COPD or chronic bronchitis or uncontrolled asthma.
Interventions
Interventions and Comparators: ARCADIA 1 and ARCADIA 2 Studies
The interventions were as follows.
Initial treatment phase (week 0 to week 16)
Arm A: 2 injections (2 × nemolizumab 30 mg) SC at baseline, then nemolizumab 30 mg SC every 4 weeks plus topical background therapy
Arm B: 2 injections (2 × placebo) SC at baseline, then placebo SC every 4 weeks plus topical background therapy
Maintenance treatment phase (week 16 to week 48)
Arm A (only patients in the initial phase who met the study definition of clinical responder): nemolizumab 30 mg SC every 4 weeks plus topical background therapy
Arm B (only patients in the initial phase who met the study definition of clinical responder): nemolizumab 30 mg SC every 8 weeks plus topical background therapy
Arm C (only patients in the initial phase who met the study definition of clinical responder): placebo SC every 4 weeks plus topical background therapy
Arm D (placebo arm from the initial phase): continued placebo SC every 4 weeks plus topical background therapy
Dose modification of nemolizumab was not permitted in either study. During the maintenance period, patients who received nemolizumab 30 mg every 8 weeks also had a placebo at weeks 20, 28, 36, and 44 to maintain the blind.
Study drug was prepared by a pharmacist or other qualified study personnel. Members of the study site staff, including those responsible for preparation, did not have access to the randomized treatment assignment. As there may have been detectable differences between active treatment and placebo during the reconstitution process, the treatment was to be delivered for injection after the reconstitution was complete. The pharmacist (or other qualified personnel) preparing study drug was not to be involved with any study assessments and should not have discussed any aspects of study drug reconstitution with the patient or caregiver or study staff involved in patient interviews or study assessments. Injections occurred at the study site and were administered by the investigator or other qualified personnel into the patient’s abdomen or alternative injection location. A different injection location was to be selected for each injection and recorded in the treatment record. For patients willing and able to self-inject or to have a caregiver inject the study drug, study site staff provided training and the patients or caregivers were allowed to inject the medication on subsequent visits under the supervision of the site staff. Patients remained at the study site for at least 30 minutes after the first 2 injections during the study.
Dose modification was not permitted. The dosing frequency was scheduled based on the baseline or day 1 visit date. If a study visit occurred outside the visit window, the study drug could have still been administered, provided there was a minimum 3-week interval between 2 injections. Future visits were to be scheduled within the required windows based on the baseline or day 1 visit date, while maintaining the minimum 3-week interval between 2 injections.
Interventions and Comparators: ARCADIA CYCLO Study
The interventions were as follows.
Arm A: 2 injections (2 × nemolizumab 30 mg) SC at baseline, then nemolizumab 30 mg SC every 4 weeks, plus topical background therapy
Arm B: 2 injections (2 × placebo) SC at baseline, then placebo SC every 4 weeks, plus topical background therapy
Concomitant Therapies: All ARCADIA Trials
Unless specified as prohibited therapies, all therapies were to be authorized, including basic skin care (cleansing and bathing), moisturizers, bleach baths, topical anesthetics, and antihistamines without a sedative effect.
Patients applied a moisturizer at least once daily, and liberally as needed, to dry skin and AD lesions beginning at screening, and throughout the study. The patient’s current moisturizer or a moisturizer recommended by the investigator could be used. Use should not have occurred within 8 hours before each clinic or office visit. Whenever possible, patients were to use the same moisturizer throughout the study.
Patients applied an authorized background topical therapy to all AD lesions beginning within the screening period and at least 14 days before day 1 (i.e., run-in period). A thin layer of treatment was applied at a frequency that was necessary to ensure disease stability and prevent AD flare but that did not exceed the daily frequency recommended in the product labelling — “as needed” treatments were not permitted. Patients applied a medium-potency TCS to areas of the body where use of medium-potency TCS was considered safe (e.g., trunk and extremities). A low-potency TCS or a TCI was to be used in sensitive areas considered unsafe for medium-potency TCS (e.g., face, neck, intertriginous areas) or in cases where medium-potency TCS was not tolerated. The investigator could select either low-potency TCS or TCI for each patient. The patient was allowed to apply only 1 medication to each affected area; concomitant use of low-potency TCS and TCI on the same lesion was not permitted. The investigator adjusted background therapy use during the study according to the disease activity and tolerability, including tapering when signs and symptoms improved, discontinuation when lesions cleared, and restarting if signs and symptoms recurred.
For the ARCADIA 1 and ARCADIA 2 studies only, in transitioning to the maintenance period, patients continued the same background topical therapy used in the initial treatment period leading up to the week 16 visit, including tapering or complete cessation, if applicable. Throughout the maintenance period, adjustments to background topical therapy, as determined by the investigator, were permitted based on clinical response.
Rescue Therapies: All ARCADIA Trials
Rescue therapies included:
higher potency TCS (equivalent to class I to II according to the US classification)
systemic corticosteroids
biologics (including their biosimilars)
systemic nonsteroidal immunosuppressants or immunomodulators
phototherapy.
Whenever possible, investigators were to use topical medication as rescue therapy before escalating to other systemic therapies. If patients received topical treatments or phototherapy as rescue therapy, study drug administration was to continue unless there was a safety concern according to the investigator's judgment. If patients received systemic rescue therapy, study drug administration must have been permanently discontinued. For efficacy analysis, patients receiving any rescue therapies were considered unsuccessful with treatment.
Outcomes
A list of efficacy end points assessed in this Clinical Review report is provided in Table 7 for the ARCADIA 1 and ARCADIA 2 studies, and Table 8 for the ARCADIA CYCLO study. Summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review according to the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, we selected end points that were considered to be most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. The following efficacy outcomes at week 16 (from the initial period) were assessed using GRADE:
proportion of patients with IGA success
proportion of patients with EASI-75
proportion of patients with PP-NRS improvement of 4 or more points
proportion of patients with PP-NRS of less than 2
change from baseline in DLQI or CDLQI.
Select notable harms outcomes considered important for informing expert committee deliberations (injection-related reactions, newly diagnosed or worsening asthma, infections, peripheral edema, elevated AST or ALT plus elevated bilirubin) were also assessed using GRADE. To provide additional context on efficacy, the change from baseline in EASI, change from baseline in PP-NRS, and incidence of topical rescue therapy use was also included in the report but not in the GRADE assessment. The corresponding efficacy outcomes in the maintenance period (from week 16 to week 48) were also included in the report but not in GRADE.
Though not considered to be a critical outcome for this review, the results for the Patient-Oriented Eczema Measure were included at the request of the sponsor to provide additional context on eczema-specific symptoms and quality of life improvements. Results for the Patient-Oriented Eczema Measure can be found in Table 38, Table 39, and Table 40 of Appendix 1.
Table 7: Outcomes Summarized From the ARCADIA 1 and ARCADIA 2 Studies
Outcome measure | Time point | ARCADIA 1 and ARCADIA 2 studies |
|---|---|---|
Initial period | ||
Proportion of patients with IGA success (IGA 0 or 1 and a ≥ 2-point reduction from baseline)a | Week 16 | Primary |
Proportion of patients with EASI-75a | Week 16 | Primary |
Proportion of patients with an improvement of PP-NRS ≥ 4a | Week 16 | Key secondary |
Proportion of patients with PP-NRS < 2a | Week 16 | Key secondary |
Change from baseline in EASI | Week 16 | Secondary |
Change from baseline in PP-NRS | Week 16 | Secondary |
Change from baseline in DLQI or CDLQI total score | Week 16 | Secondary |
Incidence of topical rescue therapy use | Week 16 | Secondary |
Maintenance period | ||
Proportion of patients maintaining IGA success for the subset of patients with IGA success at week 16 | Week 16 to week 48 | Secondary |
Proportion of patients maintaining EASI-75 response for the subset of patients with EASI-75 response at week 16 | Week 16 to week 48 | Secondary |
Proportion of patients with an improvement of PP-NRS ≥ 4 from week 16 up to week 48 and for the subset of patients with such a response at week 16 | Week 16 to week 48 | Secondary |
Proportion of patients with PP-NRS < 2 from week 16 up to week 48 and for the subset of patients with such a response at week 16 | Week 16 to week 48 | Secondary |
Change in PP-NRS | Week 16 to week 48 | Secondary |
Change in EASI | Week 16 to week 48 | Secondary |
Change in DLQI or CDLQI total score | Week 16 to week 48 | Secondary |
Incidence of topical rescue therapy use | Week 16 to week 48 | Secondary |
CDLQI = Children’s Dermatology Life Quality Index; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% improvement in Eczema Area and Severity Index from baseline; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Table 8: Outcomes Summarized From the ARCADIA CYCLO Study
Outcome measure | Time point | ARCADIA CYCLO study |
|---|---|---|
Proportion of patients with EASI-75a | Week 16 | Primary |
Proportion of patients with an improvement of PP-NRS ≥ 4 from baselinea | Week 16 | Primary |
Proportion of patients with PP-NRS < 2 | Week 16 | Secondary |
Proportion of patients with IGA success (IGA 0 or 1 and a ≥ 2-point reduction from baseline) | Week 16 | Secondary |
Proportion of patients with prior CsA use achieving EASI-75 | Week 16 | Secondary |
Change from baseline in DLQI total score at each visit | Week 16 | Secondary |
Percent change from baseline in EASI | Week 16 | Secondary |
Percent change from baseline in PP-NRS | Week 16 | Secondary |
Incidence of rescue therapy use (yes/no) | Week 16 | Secondary |
CsA = cyclosporine; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% improvement in Eczema Area and Severity Index from baseline; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Outcome definitions and details of the measurement properties of the efficacy outcomes are presented in Table 9.
Disease Severity Outcomes
Investigator Global Assessment
IGA is a 5-point scale used by an investigator to evaluate the global severity of AD; scores are associated with specific clinical definitions and range from 0 (clear; defined as minor, residual hypopigmentation or hyperpigmentation, no erythema or induration or papulation, no oozing or crusting) to 4 (severe; deep or bright red erythema with severe induration or papulation with oozing or crusting).40
In all 3 ARCADIA studies, IGA was assessed at every study visit. Change from baseline in IGA score and proportion of patients with IGA success, defined as an IGA score of 0 or 1 and a 2-point or more reduction from baseline, were appraised in the review.
No minimal important difference (MID) for the IGA was identified by the sponsor.
Eczema Area and Severity Index
EASI is a composite score commonly used to assess the severity and extent of AD signs. It ranges from 0 to 72, with higher scores indicating greater severity or extent of AD.41 The severity of erythema, induration or papulation, excoriation, and lichenification was assessed by the investigator or trained designee on a scale of 0 (absent) to 3 (severe) for each of the 4 body areas: head and neck, trunk, upper limbs, and lower limbs, with half points allowed.41 In addition, the extent of AD involvement in each of the 4 body areas was assessed as a percentage by body area of head, trunk, upper limbs, and lower limbs, and converted to a score of 0 to 6.41
In all 3 ARCADIA studies, EASI was assessed at every study visit. Change from baseline in EASI, and the proportion of patients with EASI-75 were appraised in the review.
The sponsor provided a MID of 6.6 points for adult patients, but no MID for adolescent patients was reported.
Peak Pruritus Numerical Rating Scale
The PP-NRS is a scale used by the patients to report the intensity of their pruritus (itch) during the last 24 hours; peak pruritus is an assessment of the maximum itch intensity in that period.42 Patients are asked for maximum itch intensity (PP-NRS): “on a scale of 0 to 10, with 0 being ‘no itch’ and 10 being the ‘worst itch imaginable,’ how would you rate your itch at the worst moment during the previous 24 hours?”
In the initial period of the ARCADIA 1 and ARCADIA 2 studies, as well as for all of the ARCADIA CYCLO study, the PP-NRS was recorded by patients once daily in the evening, beginning after the screening visit. During the maintenance period of the ARCADIA 1 and ARCADIA 2 studies, PP-NRS was assessed for 7 consecutive days before the visits at week 24, 32, 40, and 48.
The sponsor provided a MID of a change from baseline of 2 or more points to 4 points for within-person change; no MID for between study arms or in adolescents was provided.
HRQoL Outcomes
DLQI and CDLQI Questionnaires
The DLQI is a validated 10-item questionnaire for patients aged older than 16 years, covering domains including symptoms or feelings, daily activities, leisure, work or school, personal relationships, and treatment.43 The CDLQI is a comparable validated 10-item questionnaire designed for pediatric patients aged 16 years or younger. Patients rate each question ranging from 0 (not at all) to 3 (very much). The DLQI or CDLQI total score is calculated by summing the individual question scores. The total score ranges from 0 to 30, with higher scores indicating greater quality of life impairment.
In the ARCADIA 1 and ARCADIA 2 studies, the DLQI or CDLQI, as applicable, was assessed at baseline, week 8, and week 16 in the initial period, and week 32 and 48 of the maintenance period. In the ARCADIA CYCLO study, the DLQI was assessed at baseline, week 8, and week 16.
No MID for the DLQI or CDLQI was identified by the sponsor.
Table 9: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Definition | Conclusions about measurement properties | MID |
|---|---|---|---|
IGA | IGA is a 5-point scale used by an investigator to evaluate the global severity of AD. The investigator reviews the patient’s skin and assigns a score of 0 (clear), 1 (almost clear), 2 (mild), 3 (moderate), or 4 (severe).40 IGA success was defined as an IGA score of 0 or 1 and a ≥ 2-point reduction from baseline. | Validity: Moderate to strong correlation with EASI (r = 0.66 to 0.72) in adult patients with AD.40 Reliability: Moderate intrarater (ICC = 0.54; SD = 0.28) and interrater reliability (CV = 33.0; SD = 12.3) in adult patients with AD.40 Responsiveness: No evidence identified. | The sponsor did not identify a MID for the IGA. |
EASI | EASI is a composite score used to assess severity and extent of AD signs, ranging from 0 to 72 with higher scores indicating greater severity or extent of AD.41 The severity of erythema, induration or papulation, excoriation, and lichenification is assessed by the investigator or trained designee on a scale of 0 (absent) to 3 (severe) for each of the 4 body areas: head or neck, trunk, upper limbs, and lower limbs, with half points allowed. In addition, the extent of AD involvement in each of the 4 body areas is assessed as a percentage by body area of head, trunk, upper limbs, and lower limbs, and converted to a score of 0 to 6.41 EASI-50, EASI-75, and EASI-90 is defined as a ≥ 50%, ≥ 75%, ≥ 90% improvement in EASI score from baseline, respectively.41 | Validity: In adult patients with AD, moderate to strong correlation with SCORAD (r = 0.84 to 0.93) was found.9,44,45 In pediatric patients with AD including those aged > 12 years, EASI was correlated strongly with IGA (r > 0.8 at day 43 and 6 months).41 Reliability: The internal consistency of the EASI is adequate in adult patients with AD, with Spearman and Cronbach alpha values of 0.86 and 0.94, respectively.45 Test-retest reliability was also adequate (intrarater and interrater reliability kappa = 0.76)45; whereas, the reliability of each component of the EASI ranged from 0.38 (ICC, lichenification) to 0.75 (ICC, area) indicating poor to good intrarater reliability.40 No evidence of reliability in adolescent patients with AD was identified. Responsiveness: In a study of adult patients with AD (the MAcAD trial), responsiveness to improvement and decline in global severity based on IGA over 24 weeks was demonstrated (AUC = 0.67; 95% CI, 0.60 to 0.76).44 In pediatric patients with AD, sensitivity to change was judged as adequate (P < 0.001; n = 1,068) to detect improvement in disease status from baseline after 8 days of treatment.41 | In adults with AD, the overall MID has been reported to be 6.6 points.44 No MID has been identified specifically for adolescents with AD. |
PP-NRS | Patient-reported worst itch over the past 24 hours using an 11-point NRS, with 0 indicating “no itch” and 10 indicating “worst itch possible.”42 The adolescent version uses the same rating scale as the adult version with wording that is more appropriate for the younger population. | Psychometric assessment was performed in adult patients with moderate to severe AD from clinical trial populations (SOLO 1 and SOLO 2 trials).42 Validity: Content validity was ensured through concept elicitation during development and in-depth, 1 to 1 patient interviews (n = 14). Construct validity with similar constructs (PCS, DLQI itch item, SCORAD itch VAS) was strong (Pearson r = 0.61 to 0.77); whereas, with those with dissimilar constructs (EASI, IGA) was weak to moderate (r = 0.09 to 0.24). Known group validity was established: patients with “absent” or “mild” itch based on PCS, “no impact” on DLQI or “excellent” on PGADS had a significantly lower score on NRS (P < 0.0001).42 Reliability: Test-retest reliability over 1 week was adequate. (ICC = 0.95 to 0.96).42 Responsiveness: Change from baseline at week 16 in NRS was correlated well with those with PCS (Pearson r = 0.71), DLQI itch item (r = 0.66), and SCORAD itch VAS (r = 0.77), less well with EASI (r = 0.50) and IGA (r = 0.50).42 Psychometric assessment in adolescent population with AD has not been identified. | In adults, a change from baseline of ≥ 2 to 4 points has been considered an important within-person change.42,46 Evidence for a MID in adolescents specifically was not identified. |
DLQI or CDLQI | A patient-reported, dermatology-specific HRQoL instrument for use in adults. The DLQI consists of 10 items asking the patient’s perception of the impact of their skin disease on 5 different aspects of quality of life: dermatology-related symptoms and feelings, daily activities and leisure, work and school, personal relationships, and treatment.43,47,48 Over a 1-week recall period, patients rate each question on a 4-point Likert scale ranging from 0 to 3 (0 = not at all; 3 = very much). The DLQI total score is calculated by summing each questionnaire. The total score is the sum of the 10 items (0 to 30), with higher scores indicating greater quality of life impairment.43,47,48 The CDLQI is a comparable validated 10-item questionnaire designed for pediatric patients aged 3 to 16 years. | Validity: DLQI: During the development phase, input from adult patients with AD (n = 9; other eczema, n = 10) ensured content validity.49 Construct validity was demonstrated by a strong correlation with POEM (r = 0.78). CDLQI: Three studies demonstrated concurrent validity; 2 between the CDLQI and Cardiff Acne Disability Index and 1 between the CDLQI and Childhood Atopic Dermatitis Impact Scale.50 Convergent construct validity and divergent construct validity of the CDLQI were demonstrated in 45 and 6 studies, respectively, and a moderate correlation with SCORAD (r = 0.42).50 Reliability: DLQI: In patients with AD that is stabilized, test-retest reliability was adequate (ICC > 0.7). Among adult patients with mixed skin diseases including AD, internal consistency was acceptable (Cronbach alpha = 0.75 to 0.92).51-53 CDLQI: The CDLQI (examined in 6 studies) has good internal consistency, with Cronbach alpha values ranging from 0.82 to 0.92.50,54 Test-retest reliability is adequate, with Spearman rank order correlation coefficient calculated in 4 studies (range, 0.74 to 0.97).5450 One study examined the ICC with finding of 0.86.50 Responsiveness: DLQI: In patients aged > 16 years with a variety of skin conditions including AD (n = 192; patients with eczema = 12.5%), improved DLQI score was observed in those whose disease severity decreased over a 1 to 3 month period (P < 0.0001).48 CDLQI: Examined in 26 studies, which demonstrated responsiveness to change.50 | For DLQI, estimates of the MID have ranged from 2.2 to 6.9, but no information about MID was found specifically for adult patients with AD.43,48 For CDLQI, in adolescent patients with moderate to severe AD, a reduction of 6.0 to 8.0 points has been suggested as the clinically relevant threshold for within-person change corresponding to improvement in anchors.55 |
AD = atopic dermatitis; AUC = area under curve; CDLQI = Children’s Dermatology Life Quality Index; CI = confidence interval; CV = coefficient of variation; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; IGA = Investigator Global Assessment; MID = minimal important difference; NRS = numeric rating scale; PCS = Pruritus Categorical Scale; PGADS = Patient Global Assessment of Disease Status; POEM = Patient-Oriented Eczema Measure; PP-NRS = Peak Pruritus Numeric Rating Scale; SCORAD = SCORing Atopic Dermatitis; SD = standard deviation; VAS = visual analogue scale.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Statistical Analysis
Sample Size and Power Calculations
ARCADIA 1 and ARCADIA 2 Studies
To achieve 90% power for both coprimary end points of the ARCADIA 1 and ARCADIA 2 studies, 270 patients (180 nemolizumab, 90 placebo) were randomized to detect the following differences.
IGA success: To detect a difference of 18%, it was expected that the IGA success at week 16 would be 30% for nemolizumab and 12% for placebo.
EASI-75 response: To detect a difference of 30%, it was expected that the EASI-75 response at week 16 would be 49% for nemolizumab and 19% for placebo.
To ensure sufficient exposure with nemolizumab and sufficient size of the safety database, the sample size was 750 patients in total with a 2:1 randomization ratio. This sample size provided more than 99% power to detect the treatment difference for both coprimary end points at 2.5% significance level.
ARCADIA CYCLO Study
In the ARCADIA CYCLO study, it was estimated that to achieve 90% power for both coprimary end points, 270 patients (135 nemolizumab, 135 placebo) were to be randomized to detect the following differences.
EASI-75 at week 16: To detect a difference of 20%, it was expected that the EASI-75 response at week 16 would be 42% for nemolizumab and 22% for placebo.
PP-NRS at week 16: To detect a difference of 40%, it was expected that the PP-NRS response at week 16 would be 60% for nemolizumab and 20% for placebo.
An attrition rate of 15% was assumed.
Statistical and Analytical Plans
ARCADIA 1 and ARCADIA 2 Studies
Initial Period Analyses
Primary analyses were performed in the ITT population and compared nemolizumab 30 mg every 4 weeks to placebo every 4 weeks. In the initial period of the ARCADIA 1 and ARCADIA 2 studies, the coprimary end points and key secondary end points were analyzed using a Cochran-Mantel-Haenszel test adjusted for the randomized stratification variables (IGA severity [3 = moderate, 4 = severe] and PP-NRS [≥ 7, < 7] for the full population; IGA severity only for the baseline PP-NRS ≥ 7 population), at a 2-sided significance level of 2.5%. The estimate of treatment unadjusted difference with the corresponding 2-sided 95% CIs, as well as the strata-adjusted differences with corresponding 97.5% CIs, were presented.
Binary secondary end points in the initial period were also analyzed using a Cochran-Mantel-Haenszel test, adjusted for randomized stratification variables (IGA severity and PP-NRS for full population; IGA severity only for baseline PP-NRS ≥ 7 population). Analyses were performed for observed cases. In addition, for binary end points of EASI (global score), IGA, and PP-NRS, supplemental analyses, where data collected after rescue and missing data were considered nonresponders, were performed. Continuous secondary end points in the initial period were analyzed using analysis of covariance adjusted for treatment group, the randomized stratification variables, and appropriate baseline values. The missing information under the missing at random assumption approach and the mixed model for repeated measures approach were used to handle the missing data of continuous variables. Missing HRQoL data were imputed using last observation carried forward (LOCF), where applicable.
Maintenance Period Pooled Analysis
Given the similarities in design and conduct of the ARCADIA 1 and ARCADIA 2 studies, a pooled analysis of the maintenance phase results had been conducted. The submission did not provide a detailed rationale for pooling the studies and did not specify whether the decision to pool was preplanned.
In the maintenance period, statistical tests compared the nemolizumab 30 mg every 4 weeks to every 4 weeks and nemolizumab 30 mg every 4 weeks to every 8 weeks treatment groups with the nemolizumab 30 mg every 4 weeks to placebo treatment group. Patients randomized to placebo in the initial treatment period and reassigned to placebo in the maintenance period were not included in the pooled analysis. Week 16 measurements served as baseline measurements (i.e., maintenance baseline). If week 16 measurements were missing for rerandomized participants, the last valid nonmissing measurement in the initial treatment period (i.e., before dosing for the maintenance period at week 16 visit) was taken as the maintenance baseline measurement for the maintenance period.
For the analysis of change in EASI from week 16 up to week 48 and change in PP-NRS from week 16 up to week 48, data collected after the use of rescue medication were imputed to worst possible value and missing values were imputed using a missing information, missing at random assumption. Continuous end points (change from maintenance baseline to each visit in EASI and PP-NRS) and HRQoL (change from maintenance baseline to each visit in CDLQI or DLQI) were analyzed using an analysis of covariance including treatment group and stratification variables study as factors and appropriate maintenance baseline values as covariates, if applicable; the submission did not specify which baseline variables were included in the analyses. The LS mean, estimated standard error, and 95% CIs for each end point were presented for each treatment group and analysis visit. The estimated treatment difference for each end point at each analysis visit was summarized by presenting the difference in LS mean between treatment groups, the 2-sided 95% CIs, and P value.
ARCADIA CYCLO Study
In the ARCADIA CYCLO study, the coprimary end points and binary secondary end points were analyzed using the Cochran-Mantel-Haenszel test, adjusting for the randomized stratification variables (baseline IGA severity [3 = moderate, 4 = severe] and prior CsA exposure). The estimate of treatment difference, the corresponding 2-sided 95% CI, and P values were presented. Missing data were not imputed in this trial; however, for the coprimary end points, a tipping point analysis and analysis based on MI were conducted to assess the robustness of the analyses. Analysis of primary end points was repeated on the per-protocol population. Secondary continuous end points were analyzed using both analysis of covariance adjusted for treatment group, baseline IGA severity, CsA exposure, and appropriate baseline values, and a mixed model for repeated measures adjusting for treatment group, baseline IGA severity, prior CsA exposure, visit, an interaction term between treatment and visit, and appropriate baseline values. The submission did not specify which baseline variables were included in the analyses.
Details of the statistical analysis, adjustments, and handling of missing data, by outcome, are presented for the ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO studies in Table 10.
Table 10: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
ARCADIA 1 and ARCADIA 2 initial phase | ||||
Proportion of patients with IGA success (IGA 0 or 1 and a ≥ 2-point reduction from baseline) | Cochran-Mantel-Haenszel |
| All missing values were treated as a nonresponder for the binary end points for primary, key secondary, and secondary end points during the initial period. |
|
The proportion of patients with EASI-75 | Cochran-Mantel-Haenszel |
| All missing values were treated as a nonresponder for the binary end points for primary, key secondary, and secondary end points during the initial period. |
|
Proportion of patients with an improvement of PP-NRS ≥ 4 | Cochran-Mantel-Haenszel |
| All missing values were treated as a nonresponder for the binary end points for primary, key secondary, and secondary end points during the initial period. |
|
Proportion of patients with PP-NRS < 2 | Cochran-Mantel-Haenszel |
| All missing values were treated as a nonresponder for the binary end points for primary, key secondary, and secondary end points during the initial period. |
|
Change from baseline in EASI | ANCOVA using MI-MAR, MMRM | Adjusted for treatment group and the randomized stratification variables (IGA severity [3 = moderate, 4 = severe] and PP-NRS [≥ 7, < 7]), appropriate baseline values, visit, and interactions between baseline score with visit |
| NA |
Change from baseline in PP-NRS | ANCOVA using MI-MAR, MMRM | Adjusted for treatment group and the randomized stratification variables (IGA severity [3 = moderate, 4 = severe] and PP-NRS [≥ 7, < 7]), appropriate baseline values, visit, and interactions between baseline score with visit |
| NA |
Change from baseline in DLQI or CDLQI total score | ANCOVA using MI-MAR | Adjusted for treatment group and the randomized stratification variables (IGA severity [3 = moderate, 4 = severe] and PP-NRS [≥ 7, < 7]), appropriate baseline values, visit, and interactions between baseline score with visit |
| NA |
Incidence of topical rescue therapy use | Descriptive analysis | NR | NR | NA |
ARCADIA 1 and ARCADIA 2 maintenance phase: pooled analysis | ||||
Proportion of patients maintaining IGA success for the subset of patients with IGA success at week 16 | Cochran-Mantel-Haenszel | Stratification variables | OC (no imputation for missing and/or for assessments after use of rescue medication) | NA |
Proportion of patients maintaining EASI-75 response for the subset of patients with EASI-75 response at week 16 | Cochran-Mantel-Haenszel | Stratification variables | OC (no imputation for missing and/or for assessments after use of rescue medication) | NA |
Proportion of patients with an improvement of PP-NRS ≥ 4 from week 16 up to week 48 and for the subset of patients with such a response at week 16 | Cochran-Mantel-Haenszel | Stratification variables | OC (no imputation for missing and/or for assessments after use of rescue medication) | NA |
Proportion of patients with PP-NRS < 2 from week 16 up to week 48 and for the subset of patients with such a response at week 16 | Cochran-Mantel-Haenszel | Stratification variables | OC (no imputation for missing and/or for assessments after use of rescue medication) | NA |
Change in PP-NRS | ANCOVA using OC | Treatment group, study, and appropriate baseline values (not specified in submission) | OC (no imputation for missing and/or for assessments after use of rescue medication) | NR |
Change in EASI | ANCOVA using OC | Treatment group, study, and appropriate baseline values (not specified in submission) | OC (no imputation for missing and/or for assessments after use of rescue medication) | NR |
Change in DLQI or CDLQI total score | ANCOVA using OC | Treatment group, study, and appropriate baseline values (not specified in submission) | OC (no imputation for missing and/or for assessments after use of rescue medication) | NR |
Incidence of topical rescue therapy use | Descriptive Summary | NR | OC (no imputation for missing and/or for assessments after use of rescue medication) | NA |
ARCADIA CYCLO study | ||||
Proportion of patients with EASI-75 | Cochran-Mantel-Haenszel | Randomized stratification variables (baseline IGA severity [3 = moderate, 4 = severe] and prior CsA exposure) | All missing values for binary outcomes were treated as nonresponder and data for continuous outcomes were not imputed. | Same analysis on PP population Tipping point analysis and analysis based on multiple imputation was conducted to assess the robustness of the analyses |
Proportion of patients with an improvement of PP-NRS ≥ 4 from baseline | Cochran-Mantel-Haenszel | Randomized stratification variables (baseline IGA severity [3 = moderate, 4 = severe] and prior CsA exposure) | All missing values for binary outcomes were treated as nonresponder and data for continuous outcomes were not imputed. | Same analysis on PP population Tipping point analysis and analysis based on multiple imputation was conducted to assess the robustness of the analyses |
Proportion of patients with PP-NRS < 2 | Cochran-Mantel-Haenszel | Randomized stratification variables (baseline IGA severity [3 = moderate, 4 = severe] and prior CsA exposure) | All missing values for binary outcomes were treated as nonresponder and data for continuous outcomes were not imputed. | NA |
Proportion of patients with IGA success (IGA 0 or 1 and a ≥ 2-point reduction from baseline) | Cochran-Mantel-Haenszel | Randomized stratification variables (baseline IGA severity [3 = moderate, 4 = severe] and prior CsA exposure) | All missing values for binary outcomes were treated as nonresponder and data for continuous outcomes were not imputed. | NA |
Proportion of patients with prior CsA use achieving EASI-75 | Cochran-Mantel-Haenszel | Randomized stratification variables (baseline IGA severity [3 = moderate, 4 = severe] and prior CsA exposure) | All missing values for binary outcomes were treated as nonresponder and data for continuous outcomes were not imputed. | NA |
Change from baseline in DLQI total score at each visit | ANCOVA MMRM | For ANCOVA: Treatment group, baseline IGA severity (3 = moderate, 4 = severe), and CsA exposure as factors, and appropriate baseline values For MMRM: Treatment group, baseline IGA severity (3 = moderate, 4 = severe), prior CsA exposure, visit, interaction term between treatment and visit, and appropriate baseline value | All missing values for binary outcomes were treated as nonresponder and data for continuous outcomes were not imputed. | NA |
Incidence of rescue therapy use (yes or no) | Cochran-Mantel-Haenszel | Randomized stratification variables (baseline IGA severity [3 = moderate, 4 = severe] and prior CsA exposure) | All missing values for binary outcomes were treated as nonresponder and data for continuous outcomes were not imputed. | NA |
ANCOVA = analysis of covariance; CDLQI = Children’s Dermatology Life Quality Index; CsA = cyclosporine; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% improvement in Eczema Area and Severity Index from baseline; IGA = Investigator Global Assessment; LOCF = last observation carried forward; MAR = missing at random; MI = multiple imputation; MMRM = mixed effects model for repeated measures; NA = not applicable; NR = not reported; OC = observation case; PP = per protocol; PP-NRS = Peak Pruritus Numeric Rating Scale; QoL = quality of life.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Subgroup Analyses
In the ARCADIA 1 and ARCADIA 2 studies, subgroup analyses were performed on the ITT population (full population; baseline PP-NRS ≥ 7) for primary and key secondary end points. The following subgroups were descriptively evaluated in the ARCADIA 1 and ARCADIA 2 studies:
region (Europe, North America, Asia Pacific)
age groups (12 to 17 years, 18 to 65 years, and > 65 years)
sex
race
baseline IGA (3 or 4)
baseline PP-NRS (≥ 7 and < 7)
previous use of any systemic therapy for AD (yes, no)
previous use of any biologic therapy for AD (yes, no)
previous use of any immunosuppressive or immunomodulatory drugs for AD (yes, no)
previous use of dupilumab for AD (yes, no)
previous use of CsA for AD (yes, no)
country.
Subgroup results by age group, sex, baseline IGA score, baseline PP-NRS, previous use of any systemic therapy for AD, previous use of any biologic therapy for AD, previous use of any immunosuppressive or immunomodulatory drugs for AD, previous use of dupilumab for AD, and previous use of CsA for AD were of interest to this review.
There were no subgroup analyses in the ARCADIA CYCLO study.
Multiple Testing Procedure
ARCADIA 1 and ARCADIA 2 Studies
Multiplicity control was applied to the coprimary and key secondary end points. To control the type I error at 5%, a serial gatekeeping approach was implemented. The coprimary end points were tested at 2.5% significance level for each population. If both coprimary end points were statistically significant at a 2.5% significance level, the key secondary end points were tested sequentially following a hierarchical testing procedure using the prespecified order of end points for each population; the submission did not list the end points but noted that they were tested in a prespecified order. The comparisons for key secondary end points were made sequentially, and the subsequent testing was stopped when no statistical difference was found. Secondary end points were not controlled for multiplicity.
In the pooled analysis of the maintenance period of the ARCADIA 1 and ARCADIA 2 studies, none of the efficacy analyses were adjusted for multiplicity and they were tested at a 5% significance level.
ARCADIA CYCLO Study
To control the type I error at a 5% significance level, the primary end points were tested sequentially following a hierarchical testing procedure. The proportion of patients with EASI-75 at week 16 was tested first at the 2-sided 0.05 significant level. To preserve the overall alpha level at 0.05 across the 2 primary end points, formal statistical inference for the proportion of patients with an improvement of PP-NRS of 4 or more at week 16 could only be made if superiority of nemolizumab was demonstrated for the first primary efficacy end point, at the 2-sided 0.05 significance level. Apart from the primary end points, no other adjustments for multiplicity were made.
Analysis Populations
The analysis populations used in the ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO studies are provided in Table 11.
Table 11: Analysis Populations of the ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO Studies
Study | Population | Definition | Application |
|---|---|---|---|
ARCADIA 1 and ARCADIA 2 studies | ITT | All patients who were randomized. For the maintenance period, the ITT population included only patients who were rerandomized after the initial treatment period. | All primary and secondary efficacy end points were analyzed based on the ITT population. The ITT population was the primary population for all efficacy analyses. |
Safety | All patients in the ITT population who received at least 1 dose of study drug. For the maintenance period, only patients in the ITT population who received at least 1 dose of any drug in the maintenance period were included in the population. | All safety data were summarized based on the safety population under the treatment group “as treated.” | |
PP | All patients in the ITT population who had no major protocol deviations that would have had a substantial effect on the efficacy of the study drug. | Only primary and key secondary end points were analyzed using the PP population under the treatment group as randomized. | |
ARCADIA CYCLO study | ITT | All patients who were randomized. | All primary and secondary efficacy end points were analyzed based on the ITT population under the treatment group “as randomized.” As the ITT set and enrolled set are equivalent, only the ITT set will be used for the analyses. |
Safety | All patients in the ITT population who received at least 1 dose of study drug. | All safety data were summarized based on the safety population under the treatment group “as treated.” | |
PP | All patients in the ITT population who had no major protocol deviations that would have had a substantial effect on the efficacy of the study drug. | Only primary and selected secondary end points were analyzed using the PP population. |
ITT = intention to treat; PP = per protocol.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Protocol Amendments and Deviations
The original protocol for the ARCADIA 1 study (dated January 17, 2019) and the ARCADIA 2 study (dated January 29, 2019) were amended 7 times each. Notable amendments for the ARCADIA 1 and ARCADIA 2 studies included allowing the investigator to prescribe background topical therapy and adding the incidence of rescue therapy use as an outcome, correcting and clarifying randomization methods (not specified how), updating statistical analysis and analysis populations (October 2019), clarifying the exclusion criteria around asthma, updating exclusion criteria (not specified how), and updating statistical methodology (not specified how) (June 2020). The first patient was randomized on August 9, 2019, in the ARCADIA 1 study and August 13, 2019, in the ARCADIA 2 study. It is unknown how many patients were impacted by changes to the protocol after enrolment. There was 1 country-specific amendment made to the original protocol of the ARCADIA CYCLO study (dated August 9, 2021), although it was not considered to impact study conduct.
In the ARCADIA 1 study, a total of 172 patients (27.7%) in the nemolizumab arm and 87 patients (27.1%) in the placebo arm had major protocol deviations during the initial treatment period. In the ARCADIA 2 study, a total of 139 patients (26.6%) in the nemolizumab arm and 63 patients (23.8%) in the placebo arm had major protocol deviations during the initial treatment period. In both studies, the most common major protocol deviations pertained to enrolment criteria (ARCADIA 1: 10.8% nemolizumab, 7.8% placebo; ARCADIA 2: 10.0% nemolizumab, 9.4% placebo) and other (ARCADIA 1: 12.3% nemolizumab, 13.1% placebo; ARCADIA 2: 9.0% nemolizumab, 8.7% placebo).
In the maintenance period of the ARCADIA 1 study, 6.7%, 12.1%, and 4.4% of patients in the nemolizumab every 4 weeks to every 4 weeks, nemolizumab every 4 weeks to every 8 weeks, and nemolizumab every 4 weeks to placebo groups had major protocol deviations, respectively. In the maintenance period of the ARCADIA 2 study, 12.7%, 10.3%, and 19.2% of patients in the nemolizumab every 4 weeks to every 4 weeks, nemolizumab every 4 weeks to every 8 weeks, and nemolizumab every 4 weeks to placebo groups had major protocol deviations, respectively.
██ ███████ ██████ █ █████ ██ ██ ███████ ████████ ██ ███ ███████████ ███ ███ ██ ███████ ████████ ██ ███ ███████ ███ ███ █████ ████████ ███████████ ████ ████████ ███ ██ ███████ ████████ ███████████ █████ ████████████ █████ ████████ ███ █████ ██████████████████████ █████ ████████████ ████ █████████.
Results
Patient Disposition
ARCADIA 1 and ARCADIA 2 Studies
Details of the patient disposition for the initial treatment period in the ARCADIA 1 and ARCADIA 2 studies are in Table 12. The submission did not report reasons for unsuccessful screening but reported that 29.4% of patients did not meet screening criteria in the ARCADIA 1 study and 26.5% did not meet screening criteria in the ARCADIA 2 study. A total of 10% or fewer of patients discontinued from the ARCADIA 1 or ARCADIA 2 studies, across treatment arms during the initial treatment period. The reasons for study discontinuation and the proportion of patients who discontinued the study were broadly similar between the nemolizumab and placebo arms of the ARCADIA 1 and ARCADIA 2 studies, with the exception that a numerically higher proportion of patients (3.4%) in the nemolizumab arm discontinued due to AEs than in the placebo arm (1.5%) in the ARCADIA 2 study. A total of 272 patients met the study definition for clinical responders after the initial period of the ARCADIA 1 and ARCADIA 2 studies were rerandomized for follow-up in the maintenance period.
Table 12: Summary of Patient Disposition From the ARCADIA 1 and ARCADIA 2 Studies — Initial Period
Patient disposition | ARCADIA 1 study | ARCADIA 2 study | ||
|---|---|---|---|---|
Nemolizumab n = 620 | Placebo n = 321 | Nemolizumab n = 522 | Placebo n = 265 | |
Screened, N | 1,333 | 1,071 | ||
Unsuccessful screening, n (%)a | 392 (29.4) | 284 (26.5) | ||
Randomized, n (%) | 620 (100) | 321 (100) | 522 (100) | 265 (100) |
Randomized but not treated, n (%) | 4 (0.6) | 0 (0.0) | 3 (0.6) | 2 (0.8) |
Initial treatment period | ||||
Completed treatment | 560 (90.3) | 296 (92.2) | 470 (90.0) | 241 (90.9) |
Discontinued from study during initial treatment period, n (%) | 56 (9.0) | 25 (7.8) | 49 (9.4) | 22 (8.3) |
Reason for discontinuation, n (%) | ||||
Pregnancy | 2 (0.3) | 0 | 0 | 0 |
Lack of efficacy | 4 (0.6) | 2 (0.6) | 3 (0.6) | 0 |
Adverse event | 8 (1.3) | 5 (1.6) | 18 (3.4) | 4 (1.5) |
Patient’s request | 25 (4.0) | 12 (3.7) | 25 (4.8) | 15 (5.7) |
Lost to follow-up | 10 (1.6) | 0 | 1 (0.2) | 1 (0.4) |
Protocol deviation | 8 (1.3) | 3 (0.9) | 4 (0.8) | 3 (1.1) |
Other | 2 (0.3) | 0 | 2 (0.4) | 1 (0.4) |
Completed or exited the study after the initial treatment period, n (%) | 289 (46.6) | 199 (62.0) | 234 (44.8) | 156 (58.9) |
Analysis populations | ||||
ITT, n | 620 | 321 | 522 | 265 |
PP, n (%) | 501 (80.8) | 256 (79.8) | 454 (87.0) | 227 (85.7) |
Safety, n | 616 | 321 | 519 | 263 |
ITT = intention to treat; PP = per protocol.
aUnsuccessful screening percentages were out of the total number screened; the remaining percentages are out of the number of patients randomized.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Details of the patient disposition during the maintenance phase for the ARCADIA 1 and ARCADIA 2 studies are presented in Table 13. In the ARCADIA 1 study, of the 620 patients initially randomized to nemolizumab, a total of 272 patients (43.9%) were rerandomized, and a total of 100 patients (31.2%) initially randomized to placebo were eligible to continue in the maintenance period. A numerically higher proportion of patients in the rerandomized placebo arm discontinued the maintenance treatment in general (24.2% of patients) relative to the other study arms (15.6% nemolizumab every 4 weeks, 13.2% nemolizumab every 8 weeks, and 18.0% placebo). A numerically higher proportion of patients who were rerandomized to placebo discontinued the treatment due to lack of efficacy (13.2% of patients) than in the ARCADIA 2 study (3.8% of patients). Otherwise, the patient disposition was broadly balanced between the study arms in the ARCADIA 1 study.
In the ARCADIA 2 study, of the 522 patients initially rerandomized to nemolizumab, 235 patients (45.0%) were rerandomized, and 85 patients (32.0%) of the original 265 randomized to the placebo arm were eligible to continue in the maintenance period. The proportions of patients discontinuing maintenance treatment and the reasons for discontinuation were broadly similar across treatment arms. With the exception of the proportion of patients in the rerandomized placebo arm discontinuing maintenance treatment (described previously), the proportions of patients discontinuing treatment in the other study arms was generally consistent with the ARCADIA 2 study.
Table 13: Summary of Patient Disposition From the ARCADIA 1 and ARCADIA 2 Studies — Maintenance Period
Patient disposition | ARCADIA 1 study | ARCADIA 2 study | ||||||
|---|---|---|---|---|---|---|---|---|
Nemo q.4.w. to nemo q.4.w. n = 90 | Nemo q.4.w. to nemo q.8.w. n = 91 | Nemo q.4.w. to PBO n = 91 | Reassigned to PBO n = 100 | Nemo q.4.w. to nemo q.4.w. n = 79 | Nemo q.4.w. to nemo q.8.w. n = 78 | Nemo q.4.w. to PNO n = 78 | Reassigned to PBO n = 85 | |
Rerandomized, N | 90 | 91 | 91 | 100 | 79 | 78 | 78 | 85 |
Assigned but not treated, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (1.3) | 0 (0.0) | 1 (1.3) | 1 (1.2) |
Treated, n (%) | 90 (100.0) | 91 (100.0) | 91 (100.0) | 100 (100.0) | 78 (98.7) | 78 (100.0) | 77 (8.7) | 84 (98.8) |
Completed maintenance period treatment, n (%) | 76 (84.4) | 79 (86.8) | 69 (75.8) | 82 (82.0) | 65 (82.3) | 68 (87.2) | 65 (83.3) | 74 (87.1) |
Discontinued maintenance period treatment, n (%) | 14 (15.6) | 12 (13.2) | 22 (24.2) | 18 (18.0) | 13 (16.5) | 10 (12.8) | 12 (15.4) | 10 (11.8) |
Reason for discontinuation, n (%) | ||||||||
Pregnancy | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Lack of efficacy | 4 (4.4) | 3 (3.3) | 12 (13.2) | 4 (4.0) | 2 (2.5) | 2 (2.6) | 3 (3.8) | 3 (3.5) |
Adverse event | 1 (1.1) | 3 (3.3) | 1 (1.1) | 1 (1.0) | 3 (3.8) | 2 (2.6) | 3 (3.8) | 2 (2.4) |
Patient’s request | 6 (6.7) | 4 (4.4) | 5 (5.5) | 9 (9.0) | 2 (2.5) | 3 (3.8) | 1 (1.3) | 4 (4.7) |
Lost to follow-up | 0 (0.0) | 1 (1.1) | 1 (1.1) | 1 (1.0) | 1 (1.3) | 0 (0.0) | 3 (3.8) | 0 (0.0) |
Physician decision | NR | NR | NR | NR | 1 (1.3) | 1 (1.3) | 0 (0.0) | 1 (1.2) |
Protocol deviation | 1 (1.1) | 0 (0.0) | 1 (1.1) | 0 (0.0) | 2 (2.2) | 1 (1.1) | 1 (1.1) | 2 (2.0) |
Other | 0 (0.0) | 0 (0.0) | 1 (1.1) | 1 (1.0) | 4 (5.1) | 2 (2.6) | 2 (2.6) | 0 (0.0) |
Completed or exited the study after the maintenance treatment period, n (%) | 77 (85.6) | 79 (86.8) | 70 (76.9) | 82 (82.0) | 65 (82.3) | 68 (87.2) | 63 (80.8) | 74 (87.1) |
Entered LTE after maintenance period treatment, n (%) | 79 (87.8) | 83 (91.2) | 73 (80.2) | 78 (78.0) | 66 (83.5) | 69 (88.5) | 63 (80.8) | 77 (90.6) |
LTE = long-term extension; Nemo = nemolizumab; NR = not reported; PBO = placebo; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks.
Sources: Details included in the table are from the sponsor’s ARCADIA 1 Clinical Study Report11 and ARCADIA 2 Clinical Study Report.12
ARCADIA CYCLO Study
Details of the patient disposition for the ARCADIA CYCLO study are in Table 14. ███ ██████████ ███ ███ ██████ ███████ ███ █████████ ███████ ███ █████ ████ █████ ██ ████████ ██████ ██████████ █ █████ ██ ████ ██ ████████ ████████████ ████ ███ █████ ██ ███ ███████ ████ ███ ████ ████████████ ████ ███ ███████████ ████ ███ ████ ██████ ██████ ███ █████████████ ██ ███ ███████ ███ ███ ███████ ███████ ██████ ███ ██ ███ ███████████ ███ ██ ███ ████ ███████ ███████ ██████ ███ ████ ██ █████████ ███████.
Table 14: Summary of Patient Disposition From the ARCADIA CYCLO Study
Patient disposition | ARCADIA CYCLO study | |
|---|---|---|
Nemolizumab n = 138 | Placebo n = 138 | |
Screened, N | 326 | |
Unsuccessful screening, n (%)a | ██ ██████ | |
Randomized, n (%) | 138 (100) | 138 (100) |
Randomized but not treated, n (%) | ███████ | ██████ |
Completed the study, n (%) | ███ ██████ | ███ ██████ |
Discontinued from study, n (%) | ██████ | ██████ |
Reason for discontinuation, n (%) | ||
Adverse event | ██████ | ██████ |
Patient’s request | ██████ | ██████ |
Lost to follow-up | ██████ | || |
Protocol deviation | ██████ | || |
Continued to LTE, n (%) | ███ ██████ | ███ ██████ |
Analysis populations | ||
ITT, n | ███ █████ | ███ █████ |
PP, n (%) | ███ ██████ | ███ ██████ |
Safety, n | ███ ██████ | ███ ██████ |
ITT = intention to treat; LTE = long-term extension; PP = per protocol.
aUnsuccessful screening percentages were out of the total number screened; the remaining percentages are out of the number of patients randomized.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Baseline Characteristics
ARCADIA 1 and ARCADIA 2 Studies
The mean age, proportion of female patients, height, weight, and smoking status were similar between the ARCADIA 1 and ARCADIA 2 studies and were also generally balanced between the 2 arms within each study. The mean age in the ARCADIA 1 study was approximately 33 years in both study arms and was 35 years in the ARCADIA 2 study, in both study arms. Of note, the ARCADIA 1 study enrolled a higher proportion of patients who self-identified as Asian (15.8% in the nemolizumab arm, 16.2% in the placebo arm) than the ARCADIA 2 study (1.9% in the nemolizumab arm, 1.5% in the placebo arm), and a lower proportion of white patients (72.7% in the nemolizumab arm, 76.0% in the placebo arm), than the ARCADIA 2 study (87.7% in the nemolizumab arm, 85.7% in the placebo arm).
In terms of AD and prior treatment characteristics, the 2 studies were broadly similar and within each study, and the 2 treatment arms were generally balanced. The mean EASI score was approximately 27 in both treatment arms in both studies, and the majority of patients reported a mean IGA score of 3 (ARCADIA 1: 70.6% in the nemolizumab arm, 73.5% in the placebo arm; ARCADIA 2: 67.4% in the nemolizumab arm, 69.8% in the placebo arm). The weekly average PP-NRS score was approximately 7 in both treatment arms in both studies. The average BSA involvement was also consistent across treatment arms within the studies (ARCADIA 1: 44.9% in the nemolizumab arm, 43.8% in the placebo arm; ARCADIA 2: 44.6% in the nemolizumab arm, 45.0% in the placebo arm). The total mean DLQI score was approximately 15 in the ARCADIA 1 study and 14 in the ARCADIA 2 study; the mean total CDLQI score was approximately 12 in the ARCADIA 1 and ARCADIA 2 studies, in all study arms. Prior treatment characteristics were reasonably balanced across treatment arms; the majority of patients (> 97% in all arms in the ARCADIA 1 and ARCADIA 2 studies) reported the use of moderately potent corticosteroids before enrolment, and approximately one-half (48% to 55% across all arms in the ARCADIA 1 and ARCADIA 2 studies) reported the use of other drugs. Immunomodulating drugs were the most commonly reported systemic drug in both trials (ARCADIA 1: 38.1% in the nemolizumab arm, 36.4% in the placebo arm; ARCADIA 2: 29.1% in the nemolizumab arm, 31.7% in the placebo arm); less than 15% of patients in both arms of both trials reported the use of CsA, and less than 8% reported the use of biologics.
Details of the baseline characteristics from ARCADIA 1 and ARCADIA 2 studies are outlined in Table 15; these limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
Table 15: Summary of Baseline Characteristics From the ARCADIA 1 and ARCADIA 2 Studies (ITT) — Initial Treatment Period
Characteristic | ARCADIA 1 study | ARCADIA 2 study | ||
|---|---|---|---|---|
Nemolizumab n = 620 | Placebo n = 321 | Nemolizumab n = 522 | Placebo n = 265 | |
Demographic characteristics | ||||
Age (years) | ||||
Mean (SD) | 33.5 (15.9) | 33.3 (15.6) | 34.9 (17.7) | 35.2 (17.0) |
Median (range) | 29.0 (12 to 82) | 29.0 (12 to 81) | 30.0 (12 to 84) | 32.0 (12 to 85) |
12 to 17 years, n (%) | 85 (13.7) | 49 (15.3) | 91 (17.4) | 41 (15.5) |
18 to 65 years, n (%) | 505 (81.5) | 263 (81.9) | 394 (75.5) | 209 (78.9) |
> 65 years, n (%) | 30 (4.8) | 9 (2.8) | 37 (7.1) | 15 (5.7) |
Sex, n (%) | ||||
Female | 297 (47.9) | 144 (44.9) | 270 (51.7) | 136 (51.3) |
Male | 323 (52.1) | 177 (55.1) | 252 (48.3) | 129 (48.7) |
Race, n (%) | ||||
American Indian or Alaska Native | 2 (0.3) | 3 (0.9) | 1 (0.2) | 0 (0.0) |
Asian | 117 (18.9) | 51 (15.9) | 35 (6.7) | 18 (6.8) |
Black or African American | 36 (5.8) | 18 (5.6) | 25 (4.8) | 20 (7.5) |
Native Hawaiian or other Pacific Islander | 1 (0.2) | 0 (0.0) | 1 (0.2) | 0 (0.0) |
White | 451 (72.7) | 244 (76.0) | 458 (87.7) | 227 (85.7) |
Other or multiple | 3 (0.5) | 1 (0.3) | 2 (0.4) | 0 (0.0) |
Body mass index (kg/m2), mean (SD) | 26.01 (5.73) | 26.53 (5.77) | 25.90 (5.23) | 25.60 (6.34) |
AD disease characteristics | ||||
EASI score | ||||
Mean (SD) | 27.77 (10.64) | 27.06 (9.37) | 27.43 (10.81) | 27.58 (10.88) |
Median (range) | 24.4 (16.0 to 70.8) | 24.8 (16.0 to 61.7) | 24.3 (13.4 to 72.0) | 24.4 (16.0 to 66.0) |
IGA score, n (%) | ||||
3 (moderate) | 438 (70.6) | 236 (73.5) | 352 (67.4) | 185 (69.8) |
4 (severe) | 182 (29.4) | 85 (26.5) | 170 (32.6) | 80 (30.2) |
Weekly average PP-NRS, mean (SD) | 7.17 (1.40) | 7.15 (1.44) | 7.04 (1.53) | 7.16 (1.51) |
Weekly average AP-NRS, mean (SD) | 6.46 (1.57) | 6.47 (1.60) | 6.47 (1.68) | 6.50 (1.68) |
Weekly average SD-NRS, mean (SD) | 5.94 (2.14) | 5.74 (2.26) | 5.76 (2.30) | 5.72 (2.36) |
BSA (%) of AD involvement, mean (SD) | 44.85 (19.89) | 43.81 (18.65) | 44.61 (19.42) | 44.95 (19.28) |
SCORAD, mean (SD) | 64.09 (11.65) | 63.32 (11.28) | 64.87 (11.98) | 64.93 (13.32) |
Pain frequency, n (%) | ||||
Never | 28 (4.5) | 14 (4.4) | 23 (4.4) | 14 (5.3) |
Less than once a week | 50 (8.1) | 22 (6.9) | 46 (8.8) | 28 (10.6) |
1 to 2 days a week | 84 (13.5) | 51 (15.9) | 79 (15.1) | 42 (15.8) |
3 to 4 days a week | 140 (22.6) | 75 (23.4) | 133 (25.5) | 54 (20.4) |
5 to 6 days a week | 116 (18.7) | 46 (14.3) | 69 (13.2) | 47 (17.7) |
Every day | 193 (31.1) | 108 (33.6) | 165 (31.6) | 74 (27.9) |
Not reported | 9 (1.5) | 5 (1.6) | 7 (1.3) | 6 (2.3) |
Pain intensity, n (%) | ||||
0 | 23 (3.7) | 12 (3.7) | 26 (5.0) | 12 (4.5) |
1 | 16 (2.6) | 6 (1.9) | 14 (2.7) | 8 (3.0) |
2 | 24 (3.9) | 11 (3.4) | 31 (5.9) | 10 (3.8) |
3 | 31 (5.0) | 18 (5.6) | 29 (5.6) | 16 (6.0) |
4 | 40 (6.5) | 20 (6.2) | 43 (8.2) | 27 (10.2) |
5 | 65 (10.5) | 36 (11.2) | 49 (9.4) | 23 (8.7) |
6 | 79 (12.7) | 50 (15.6) | 62 (11.9) | 32 (12.1) |
7 | 129 (20.8) | 53 (16.5) | 91 (17.4) | 36 (13.6) |
8 | 94 (15.2) | 66 (20.6) | 94 (18.0) | 53 (20.0) |
9 | 77 (12.4) | 32 (10.0) | 43 (8.2) | 31 (11.7) |
10 | 33 (5.3) | 12 (3.7) | 33 (6.3) | 11 (4.2) |
Not reported | 9 (1.5) | 5 (1.6) | 7 (1.3) | 6 (2.3) |
DLQI, n | 540 | 279 | 440 | 228 |
Mean (SD) | 15.4 (6.60) | 15.5 (6.75) | 14.5 (6.85) | 14.2 (6.98) |
Median (range) | 15.0 (1.0 to 30.0) | 15.0 (1.0 to 30.0) | 14.0 (1.0 to 30.0) | 14.0 (1.0 to 30.0) |
CDLQI, n | 71 | 37 | 75 | 30 |
Mean (SD) | 12.7 (6.70) | 12.5 (5.83) | 12.2 (5.98) | 12.4 (5.40) |
Median (range) | 12.0 (1.0 to 30.0) | 13.0 (1.0 to 23.0) | 11.0 (1.0 to 26.0) | 14.0 (2.0 to 21.0) |
Prior topical therapy, n (%) | ||||
At least 1 background topical therapy | 618 (99.7) | 319 (99.4) | 512 (98.1) | 261 (98.5) |
Corticosteroids, very potent | 8 (1.3) | 10 (3.1) | 9 (1.7) | 7 (2.6) |
Corticosteroids, potent | 422 (68.1) | 226 (70.4) | 395 (75.7) | 208 (78.5) |
Corticosteroids, moderately potent | 613 (98.9) | 313 (97.5) | 508 (97.3) | 259 (97.7) |
Corticosteroids, weak | 173 (27.9) | 89 (27.7) | 119 (22.8) | 51 (19.2) |
Drugs for dermatitis, excluding corticosteroids | 345 (55.6) | 180 (56.1) | 256 (49.0) | 128 (48.3) |
Prior AD medications, n (%) | ||||
Biologics | 38 (6.1) | 24 (7.5) | 28 (5.4) | 19 (7.2) |
Immunosuppressive or immunomodulatory drugs | 236 (38.1) | 117 (36.4) | 152 (29.1) | 84 (31.7) |
Dupilumab | 36 (5.8) | 19 (5.9) | 27 (5.2) | 17 (6.4) |
Cyclosporine | 92 (14.8) | 41 (12.8) | 70 (13.4) | 39 (14.7) |
AD = atopic dermatitis; AP-NRS = Average Pruritus Numeric Rating Scale; BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; IGA = Investigator Global Assessment; ITT = intention to treat; PP-NRS = Peak Pruritus Numeric Rating Scale; SCORAD = SCORing Atopic Dermatitis; SD = standard deviation; SD-NRS = Sleep Disturbance Numeric Rating Scale.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
In the maintenance period of the ARCADIA 1 study, 90 patients were rerandomized from nemolizumab every 4 weeks to every 4 weeks, 91 patients were rerandomized from nemolizumab every 4 weeks to every 8 weeks, 91 patients were rerandomized from nemolizumab every 4 weeks to placebo, and 100 patients from the initial placebo group were reassigned to placebo. Across treatment arms, the demographic and AD characteristics postrandomization in the maintenance population from the ARCADIA 1 study were broadly balanced. Relative to the patients who responded to placebo, those who responded to treatment in the intervention arm had a numerically higher proportion of female patients (58.9% to 61.5% in the nemolizumab arms, 47.0% in the placebo arm). The majority of the maintenance population was white (77.8% to 86.0% across all 4 treatment arms), with an EASI score ranging from 2.74 to 3.1 across study arms, and a PP-NRS score ranging from 2.13 to 3.34 across study arms. Detailed baseline characteristics of the maintenance population are in Table 16.
Table 16: Summary of Baseline Characteristics From the ARCADIA 1 Study (ITT) — Maintenance Treatment Period
Characteristic | Patients who responded to the ARCADIA 1 study | Patients who responded to placebo to placebo n = 100 | ||
|---|---|---|---|---|
Nemolizumab q.4.w. to nemolizumab q.4.w. n = 90 | Nemolizumab q.4.w. to nemolizumab q.8.w. n = 91 | Nemolizumab q.4.w. to placebo n = 91 | ||
Demographic characteristics | ||||
Age (years) | ||||
Mean (SD) | 30.7 (15.35) | 32.2 (15.43) | 33.4 (18.55) | 33.3 (17.15) |
Median (range) | 25.5 (12.0 to 74.0) | 27.0 (12.0 to 75.0) | 28.0 (12.0 to 82.0) | 30.0 (12.0 to 81.0) |
12 to 17 years, n (%) | 16 (17.8) | 16 (17.6) | 18 (19.8) | 23 (23.0) |
18 to 65 years, n (%) | 71 (78.9) | 72 (79.1) | 64 (70.3) | 71 (71.0) |
> 65 years, n (%) | 3 (3.3) | 3 (3.3) | 9 (9.9) | 6 (6.0) |
Sex, n (%) | ||||
Female | 53 (58.9) | 56 (61.5) | 55 (60.4) | 47 (47.0) |
Male | 37 (41.1) | 35 (38.5) | 36 (39.6) | 53 (53.0) |
Race, n (%) | ||||
American Indian or Alaska Native | 13 (14.4) | 12 (13.2) | 10 (11.0) | 6 (6.0) |
Asian | 6 (6.7) | 4 (4.4) | 3 (3.3) | 6 (6.0) |
Black or African American | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Native Hawaiian or other Pacific Islander | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
White | 70 (77.8) | 75 (82.4) | 76 (83.5) | 86 (86.0) |
Other or multiple | 1 (1.1) | 0 (0.0) | 2 (2.2) | 2 (2.0) |
Body mass index (kg/m2), mean (SD) | 24.84 (5.35) | 26.19 (6.03) | 25.31 (5.75) | 26.29 (5.75) |
AD disease characteristics | ||||
EASI score | ||||
Mean (SD) | 3.10 (3.18) | 2.82 (3.09) | 2.74 (2.40) | 2.91 (2.38) |
Median (range) | 2.25 (0.0 to 21.6) | 2.00 (0.0 to 22.0) | 2.20 (0.0 to 9.5) | 2.40 (1.00 to 4.40) |
IGA score, n (%) | ||||
0 (clear) | 11 (2.2) | 9 (9.9) | 6 (6.6) | 4 (4.0) |
1 (almost clear) | 66 (73.3) | 64 (70.3) | 62 (68.1) | 73 (73.0) |
2 (mild) | 10 (11.1) | 18 (19.8) | 21 (23.1) | 18 (18.0) |
3 (moderate) | 3 (3.3) | 0 (0.0) | 2 (2.2) | 5 (5.0) |
4 (severe) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Weekly average PP-NRS, n | 77 | 83 | 81 | 89 |
Mean (SD) | 2.13 (2.20) | 2.20 (2.04) | 2.68 (2.21) | 3.34 (2.13) |
Weekly average AP-NRS, n | 77 | 83 | 81 | 89 |
Mean (SD) | 1.64 (1.89) | 1.84 (1.84) | 2.38 (2.21) | 2.79 (2.00) |
Weekly average SD-NRS, n | 72 | 82 | 80 | 89 |
Mean (SD) | 1.17 (1.59) | 1.61 (1.93) | 1.98 (2.07) | 1.95 (1.99) |
BSA (%) of AD involvement, mean (SD) | 8.91 (9.58) | 8.80 (11.60) | 9.12 (8.79) | 7.78 (7.65) |
SCORAD, mean (SD) | 19.35 (11.54) | 19.08 (9.69) | 19.10 (9.34) | 21.61 (9.45) |
Pain frequency, n (%) | ||||
Never | 49 (54.4) | 43 (47.3) | 41 (45.1) | 31 (31.0) |
Less than once a week | 29 (32.2) | 30 (33.0) | 24 (26.4) | 35 (35.0) |
1 to 2 days a week | 8 (8.9) | 9 (9.9) | 14 (15.4) | 24 (24.0) |
3 to 4 days a week | 2 (2.2) | 6 (6.6) | 6 (6.6) | 5 (5.0) |
5 to 6 days a week | 2 (2.2) | 3 (3.3) | 1 (1.1) | 2 (2.0) |
Every day | 0 (0.0) | 0 (0.0) | 5 (5.5) | 3 (3.0) |
Not reported | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Pain intensity, n (%) | ||||
0 | 51 (56.7) | 44 (48.4) | 41 (45.1) | 24 (24.0) |
1 | 14 (15.6) | 17 (18.7) | 14 (15.4) | 20 (20.0) |
2 | 9 (10.0) | 10 (11.0) | 9 (9.9) | 18 (18.0) |
3 | 5 (5.6) | 5 (5.5) | 11 (12.1) | 8 (8.0) |
4 | 7 (7.8) | 3 (3.3) | 2 (2.2) | 11 (11.0) |
5 | 1 (1.1) | 4 (4.4) | 4 (4.4) | 7 (7.0) |
6 | 0 (0.0) | 3 (3.3) | 7 (7.7) | 5 (5.0) |
7 | 2 (2.2) | 1 (1.1) | 2 (2.2) | 3 (3.0) |
8 | 0 (0.0) | 4 (4.4) | 1 (1.1) | 3 (3.0) |
9 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (1.0) |
10 | 1 (1.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Not reported | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
DLQI, n | 75 | 82 | 75 | 81 |
Mean (SD) | 3.00 (3.81) | 3.10 (3.33) | 4.10 (4.79) | 3.70 (3.72) |
Median (range) | 2.0 (0 to 19) | 2.0 (0 to 13) | 2.0 (0 to 21) | 2.0 (0 to 19) |
CDLQI, n | 15 | 9 | 16 | 19 |
Mean (SD) | 1.90 (2.05) | 4.10 (4.51) | 4.30 (4.68) | 3.70 (3.62) |
Median (range) | 2.0 (0 to 6) | 1.0 (0 to 10) | 2.5 (0 to 15) | 3.0 (0 to 12) |
AD = atopic dermatitis; AP-NRS = Average Pruritus Numeric Rating Scale; BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; IGA = Investigator Global Assessment; ITT = intention to treat; PP-NRS = Peak Pruritus Numeric Rating Scale; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SCORAD = SCORing Atopic Dermatitis; SD = standard deviation; SD-NRS = Sleep Disturbance Numeric Rating Scale.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Source: Details included in the table are from the sponsor’s ARCADIA 1 Clinical Study Report.11
In the maintenance phase of the ARCADIA 2 study, 79 patients were rerandomized from nemolizumab every 4 weeks to every 4 weeks, 78 patients were rerandomized from nemolizumab every 4 weeks to every 8 weeks, 78 patients were rerandomized from nemolizumab every 4 weeks to placebo, and 85 patients from the initial placebo group were reassigned to placebo. The maintenance population had mean EASI and PP-NRS scores similar to the maintenance population of the ARCADIA 1 study (EASI ranged from 1.85 to 3.39 across all 4 study arms; PP-NRS ranged from 2.03 to 3.60 across all 4 study arms). Of note, there were some numeric imbalances between the rerandomized study arms in the ARCADIA 2 study. A total of 11.5% of patients in the nemolizumab every 4 weeks to every 8 weeks arm reported an IGA score of 2, relative to 19.2% in the nemolizumab every 4 weeks to placebo arm; 33.3% of patients in the nemolizumab every 4 weeks to placebo arm were male, relative to 47.4% in the nemolizumab every 4 weeks to every 8 weeks arm; and patients in the nemolizumab every 4 weeks to every 8 weeks arm had 5.9% mean BSA involvement, relative to nemolizumab every 4 weeks to placebo with 11.5% mean BSA involvement. Detailed baseline characteristics for the ARCADIA 2 study maintenance period are in Table 17.
Table 17: Summary of Baseline Characteristics From the ARCADIA 2 Study (ITT) — Maintenance Treatment Period
Characteristic | Patients who responded to the ARCADIA 2 study | Patients who responded to placebo to placebo n = 85 | ||
|---|---|---|---|---|
Nemolizumab q.4.w. to nemolizumab q.4.w. n = 79 | Nemolizumab q.4.w. to nemolizumab q.8.w. n = 78 | Nemolizumab q.4.w. to placebo n = 78 | ||
Demographic characteristics | ||||
Age (years) | ||||
Mean (SD) | 32.5 (16.94) | 34.2 (17.25) | 37.3 (20.10) | 34.7 (19.26) |
Median (range) | 29.0 (12.0 to 77.0) | 31.5 (12.0 to 72.0) | 32.0 (12.0 to 84.0) | 30.0 (12.0 to 85.0) |
12 to 17 years, n (%) | 18 (22.8) | 17 (21.8) | 13 (16.7) | 19 (22.4) |
18 to 65 years, n (%) | 57 (72.2) | 57 (73.1) | 55 (70.5) | 59 (69.4) |
> 65 years, n (%) | 4 (5.1) | 4 (5.1) | 10 (12.8) | 7 (8.2) |
Sex, n (%) | ||||
Female | 47 (59.5) | 41 (52.6) | 52 (66.7) | 47 (55.3) |
Male | 32 (40.5) | 37 (47.4) | 26 (33.3) | 38 (44.7) |
Race, n (%) | ||||
American Indian or Alaska Native | 0 (0.0) | 0 (0.0) | 1 (1.3) | 0 (0.0) |
Asian | 2 (2.5) | 7 (9.0) | 1 (1.3) | 4 (4.7) |
Black or African American | 2 (2.5) | 2 (2.6) | 5 (6.4) | 2 (2.4) |
Native Hawaiian or other Pacific Islander | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
White | 75 (94.9) | 68 (87.2) | 71 (91.0) | 79 (92.9) |
Other | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) |
Body mass index (kg/m2), mean (SD) | 25.52 (4.90) | 25.09 (4.55) | 26.72 (6.27) | 24.70 (5.05) |
AD disease characteristics | ||||
EASI score | ||||
Mean (SD) | 2.69 (3.15) | 1.85 (2.10) | 3.39 (3.83) | 2.09 (2.03) |
Median (range) | 1.80 (0.0 to 20.1) | 1.20 (0.0 to 8.5) | 2.65 (0.0 to 22.4) | 1.60 (0.0 to 7.6) |
IGA score, n (%) | ||||
0 (clear) | 13 (16.5) | 15 (19.2) | 10 (12.8) | 15 (17.6) |
1 (almost clear) | 52 (65.8) | 54 (69.2) | 53 (67.9) | 53 (62.4) |
2 (mild) | 14 (17.7) | 9 (11.5) | 15 (19.2) | 17 (20.0) |
3 (moderate) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
4 (severe) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Weekly average PP-NRS, n | 66 | 72 | 71 | 76 |
Mean (SD) | 2.03 (1.79) | 2.20 (2.15) | 2.70 (2.35) | 3.60 (2.09) |
Weekly average AP-NRS, n | 66 | 72 | 71 | 76 |
Mean (SD) | 1.76 (1.63) | 1.91 (2.09) | 2.43 (2.33) | 3.12 (2.05) |
Weekly average SD-NRS, n | 71 | 72 | 72 | 75 |
Mean (SD) | 1.50 (1.71) | 1.69 (2.02) | 2.04 (2.19) | 2.60 (2.29) |
BSA (%) of AD involvement, mean (SD) | 9.59 (11.91) | 5.88 (7.01) | 11.29 (14.12) | 6.42 (6.11) |
SCORAD, mean (SD) | 17.48 (10.06) | 15.20 (8.95) | 20.87 (12.52) | 19.33 (11.42) |
Pain frequency, n (%) | ||||
Never | 40 (50.6) | 37 (47.4) | 38 (48.7) | 31 (36.5) |
Less than once a week | 21 (26.6) | 22 (28.2) | 18 (23.1) | 28 (32.9) |
1 to 2 days a week | 12 (15.2) | 14 (17.9) | 11 (14.1) | 16 (18.8) |
3 to 4 days a week | 4 (5.1) | 2 (2.6) | 8 (10.3) | 5 (5.9) |
5 to 6 days a week | 0 (0.0) | 2 (2.6) | 2 (2.6) | 1 (1.2) |
Every day | 2 (2.5) | 1 (1.3) | 1 (1.3) | 4 (4.7) |
Not reported | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Pain intensity, n (%) | ||||
0 | 40 (50.6) | 38 (48.7) | 36 (46.2) | 30 (35.3) |
1 | 11 (13.9) | 13 (16.7) | 10 (12.8) | 11 (12.9) |
2 | 15 (19.0) | 9 (11.5) | 10 (12.8) | 19 (22.4) |
3 | 6 (7.6) | 8 (10.3) | 7 (9.0) | 5 (5.9) |
4 | 0 (0.0) | 4 (5.1) | 5 (6.4) | 6 (7.1) |
5 | 1 (1.3) | 4 (5.1) | 1 (1.3) | 5 (5.9) |
6 | 3 (3.8) | 0 (0.0) | 5 (6.4) | 5 (5.9) |
7 | 1 (1.3) | 0 (0.0) | 1 (1.3) | 3 (3.5) |
8 | 2 (2.5) | 2 (2.6) | 3 (3.8) | 1 (1.2) |
DLQI, n | 64 | 64 | 68 | 70 |
Mean (SD) | 3.2 (3.70) | 2.8 (3.33) | 3.1 (3.67) 3 | 0.9 (3.73) |
Median (range) | 2.0 (0.5, 4.5) | 2.0 (0.0, 13.0) | 2.0 (0.0, 15.0) | 3.0 (0.0, 16.0) |
CDLQI, n | 15 | 14 | 10 | 15 |
Mean (SD) | 2.30 (3.50) | 3.40 (2.31) | 1.70 (2.36) | 4.10 (2.85) |
Median (range) | 1.0 (0.0 to 10.0) | 3.0 (0.0 to 8.0) | 1.0 (0.0 to 6.0) | 4.0 (0.0 to 9.0) |
AD = atopic dermatitis; AP-NRS = Average Pruritus Numeric Rating Scale; BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; IGA = Investigator Global Assessment; ITT = intention to treat; PP-NRS = Peak Pruritus Numeric Rating Scale; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SCORAD = SCORing Atopic Dermatitis; SD = standard deviation; SD-NRS = Sleep Disturbance Numeric Rating Scale.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Source: Details included in the table are from the sponsor’s ARCADIA 2 Clinical Study Report.12
ARCADIA CYCLO Study
Details of the baseline characteristics from the ARCADIA CYCLO study are outlined in Table 18. ███████ ███ ████████ ███████████ ████████████████ ██ ███████ ████████████████ ███ █████ █████████ ███████████████ ████ ███████ ████████ ███████ █████ █████ ███ ████ ███ ██ ████████ ███ ████ ██ ███ ███████████ ████ ████ ██ ███ ███████ ████ ███ ███ ████████ ██ ████████ ██ ████ █████████ ████ ████ █████ ██████ ███████████ ████ █████ ███████ █████ ███ ███████ ████ █████ ███ █████ ██ ███ ███████████ ████ █████ ██ ███ ███████ ████ ███ ███ ████████ ██ ████████ ██ ████ ████ ████████ ██ ███ █████ ██ █ ██████████████ ██ ██ ████ ██████ ███ ████ ██████ ██████ █████ ███ █████████████ ███ ██ ████ █████ ███ ███ ████ ███ ███ █████████████ ███ ██ ████ █████ ███ ████████ ██ ████████ ██████ ██ ████ █████ █████ ████████ ████████ █████████████████ ████ ████ ███ ████ ██████ █████ ████████ ██████████████████ ██████ ███████████ ████ █████ ███████ ████ ███ ████████ ███████████████ ██████ ███████████ ████ █████ ███████ █████ █ █████ ██ █████ ██ ████████ ██ ███ ███████████ ███ ███ █████ ██ ████████ ██ ███ ███████ ███ ████████ ████████ ███ █████████ ███ ████ ████████ ████████ ██████ ███ ████████ ███ ████ ██████ █████ ███ ███ ███ ███████████ ██████ ████████ ████ ████████ ██████ ██ ████████ ██ ███ ███████████ ████ █████ ██ ████████ ██ ███ ███████ █████.
Table 18: Summary of Baseline Characteristics From the ARCADIA CYCLO Study (ITT)
Characteristic | ARCADIA CYCLO study | |
|---|---|---|
Nemolizumab n = 138 | Placebo n = 138 | |
Demographic characteristics | ||
Age (years) | ||
Mean (SD) | 38.3 (13.15) | 36.1 (12.21) |
Median (range) | ███ █████ ████ | ███ █████ ████ |
Sex, n (%) | ||
Female | 66 (47.8) | 66 (47.8) |
Male | 72 (52.2) | 72 (52.2) |
Race, n (%) | ||
Asian | | █████ | | █████ |
White | ███ ██████ | ███ ██████ |
Other | || | | █████ |
Body mass index (kg/m2), mean (SD) | █████ ██████ | █████ ██████ |
AD disease characteristics | ||
EASI score | ||
Mean (SD) | 29.54 (8.50) | 31.33 (9.67) |
Median (range) | █████ ███████ ██████ | █████ ███████ ██████ |
IGA score, n (%) | ||
3 (moderate) | ███ ██████ | ███ ██████ |
4 (severe) | ██ ██████ | ██ ██████ |
Weekly average PP-NRS, mean (SD) | 7.41 (1.38) | 7.46 (1.46) |
Weekly average AP-NRS, mean (SD) | ████ ██████ | ████ ██████ |
Weekly average SD-NRS, mean (SD) | █████ ███████ | █████ ███████ |
BSA (%) of AD involvement, mean (SD) | █████ ███████ | █████ ███████ |
SCORAD, mean (SD) | █████ ███████ | █████ ███████ |
Pain frequency, n (%) | ||
Never | ██ █████ | ██████ |
Less than once a week | ██████ | ██ ██████ |
1 to 2 days a week | ██ ██████ | ██ ██████ |
3 to 4 days a week | ██ ██████ | ██ ██████ |
5 to 6 days a week | ██ ██████ | ██ ██████ |
Every day | ██ ██████ | ██ ██████ |
Not reported | ██████ | || |
AD-associated pain intensity, mean (SD) | ███ ██████ | ███ ██████ |
DLQI | ||
Mean (SD) | ████ ██████ | ████ ██████ |
Median (range) | ███ ████ ████ | ███ ████ ████ |
Prior therapy, n (%) | ||
At least 1 background topical therapy | ███ ██████ | ███ ██████ |
Corticosteroids | ███ ██████ | ██ ██████ |
Corticosteroids, very potent | ██ ██████ | ██ ██████ |
Corticosteroids, potent | ██ ██████ | ██ ██████ |
Corticosteroids, moderately potent | ██ ██████ | ██ ██████ |
Corticosteroids, weak | ██ ██████ | ██ ██████ |
Drugs for dermatitis, excluding corticosteroids | ██ ██████ | ██ ██████ |
Any previous immunosuppressant use | ███ ██████ | ███ ██████ |
Systemic corticosteroids or systemic immunosuppressants | ███ ██████ | ███ ██████ |
Systemic corticosteroids | ██ ██████ | ██ ██████ |
Methotrexate | ██████ | ██████ |
Azathioprine | ██████ | ██████ |
Dupilumab for AD | ██████ | ██████ |
JAK inhibitors | ██ █████ | ██████ |
Systemic immunosuppressants | ██ ██████ | ██ ██████ |
Omalizumab | ██████ | ██████ |
Previous CsA exposure | ███ ██████ | ███ ██████ |
Reasons for stopping the most recent CsA treatment | ||
Flare while CsA tapering from maximum of 6 weeks of high dose to maintenance dose | ██████ | ██████ |
Flare after a minimum of 3 months on maintenance dose | ██ ██████ | ██ ██████ |
Previous CsA at dose > 5 mg/kg/day | ██████ | ██████ |
Duration beyond prescribing advice > 1 year | ██ ██████ | ██ ██████ |
Intolerance or toxicity with exposure | ██ ██████ | ██ ██████ |
Other | ██ ██████ | ██ █████ |
AD = atopic dermatitis; AP-NRS = Average Pruritus Numeric Rating Scale; BSA = body surface area; CsA = cyclosporine; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; IGA = Investigator Global Assessment; ITT = intention to treat; PP-NRS = Peak Pruritus Numeric Rating Scale; SCORAD = SCORing Atopic Dermatitis; SD = standard deviation; SD-NRS = Sleep Disturbance Numeric Rating Scale.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence10 and ARCADIA CYCLO Clinical Study Report.13
Exposure to Study Treatments
Details of the adherence and exposure to study treatments are in Table 19 (the initial period of the ARCADIA 1 and ARCADIA 2 studies), Table 20 (the maintenance period of the ARCADIA 1 and ARCADIA 2 studies), and Table 21 (the ARCADIA CYCLO study). Briefly, patient adherence was greater than ███ in the initial period of the ARCADIA 1 and ARCADIA 2 studies, greater than ███ in the maintenance period of the ARCADIA 1 and ARCADIA 2 studies, and greater than ███ in the ARCADIA CYCLO studies. Treatment duration during the initial 16 weeks was consistent between the ARCADIA studies, ranging from 79.9 days to 83.4 days, and was consistent across the ARCADIA 1 and ARCADIA 2 studies during the maintenance phase.
Table 19: Summary of Patient Adherence From the ARCADIA 1 and ARCADIA 2 Studies (SAS) — Initial Period
Exposure | ARCADIA 1 study | ARCADIA 2 study | ||
|---|---|---|---|---|
Nemolizumab n = 616 | Placebo n = 321 | Nemolizumab n = 519 | Placebo n = 263 | |
Adherence (%) | ||||
Mean (SD) | 95.98 (12.54) | 96.14 (11.59) | 96.54 (11.83) | 96.45 (12.08) |
Minimum, maximum | 40.00, 100.00 | 40.00, 100.00 | 40.00, 100.00 | 40.00, 100.00 |
Total number of doses administered | ||||
Mean (SD) | 4.8 (0.67) | 4.8 (0.62) | 4.8 (0.64) | 4.8 (0.63) |
Median (minimum, maximum) | 5 (2, 5) | 5 (2, 5) | 5 (2, 5) | 5 (2, 5) |
Patients who missed at least 1 dose, n (%) | 68 (11.0) | 38 (11.8) | 49 (9.4) | 26 (9.9) |
Treatment duration (days) | ||||
Mean (SD) | 79.9 (18.99) | 80.3 (17.51) | 80.3 (18.27) | 81.0 (17.85) |
Median (minimum, maximum) | 85 (1, 118) | 85 (1, 102) | 85 (1, 114) | 85 (1, 104) |
SAS = safety analysis set; SD = standard deviation.
Sources: Details included in the table are from the sponsor’s ARCADIA 1 Clinical Study Report11 and ARCADIA 2 Clinical Study Report.12
Table 20: Summary of Patient Adherence From the ARCADIA 1 and ARCADIA 2 Studies (SAS) — Maintenance Period
Exposure | Nemo q.4.w. to Nemo q.4.w. | Nemo q.4.w. to Nemo q.8.w. | Nemo q.4.w. to PBO | Patients who responded to PBO to PBO |
|---|---|---|---|---|
ARCADIA 1 study | ||||
N | 90 | 91 | 91 | 100 |
Adherence (%) | ||||
Mean (SD) | 93.96 (14.95) | 95.19 (12.93) | 91.99 (15.50) | 91.03 (20.06) |
Minimum, maximum | 25.00, 100.00 | 20.00, 100.00 | 25.00, 100.00 | 12.50, 100.00 |
Total number of doses administered | ||||
Mean (SD) | 7.5 (1.34) | 7.4 (1.49) | 6.9 (1.72) | 7.1 (1.87) |
Median (minimum, maximum) | 8 (1, 8) | 8 (1, 8) | 8 (1, 8) | 8 (1, 8) |
Patients who missed at least 1 dose, n (%) | 18 (19.8) | 17 (18.9) | 25 (27.5) | 24 (24.0) |
Treatment duration (days) | ||||
Mean (SD) | 183.1 (36.27) | 182.0 (41.67) | 169.8 (48.36) | 174.7 (51.98) |
Median (minimum, maximum) | 196.0 (1, 212) | 197.0 (1, 214) | 195.0 (1, 217) | 197.0 (1, 218) |
ARCADIA 2 study | ||||
N | 78 | 79 | 79 | 85 |
Adherence (%) | ||||
Mean (SD) | 93.00 (17.91) | 93.72 (15.74) | 91.48 (16.82) | 93.80 (14.61) |
Minimum, maximum | 16.70, 100.00 | 25.00, 100.00 | 37.50, 100.00 | 37.50, 100.00 |
Total number of doses administered | ||||
Mean (SD) | 7.2 (1.69) | 7.4 (1.43) | 7.2 (1.49) | 7.4 (1.32) |
Median (minimum, maximum) | 8 (1, 8) | 8 (2, 8) | 8 (3, 8) | 8 (3, 8) |
Patients who missed at least 1 dose, n (%) | 17 (21.5) | 14 (18.2) | 21 (27.3) | 18 (21.4) |
Treatment duration (days) | ||||
Mean (SD) | 178.5 (47.68) | 180.7 (39.57) | 178.9 (41.13) | 182.5 (34.90) |
Median (minimum, maximum) | 196.0 (1, 222) | 197.0 (28, 209) | 196.0 (57, 218) | 196.0 (71, 220) |
Nemo = nemolizumab; PBO = placebo; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SAS = safety analysis set; SD = standard deviation.
Sources: Details included in the table are from the sponsor’s ARCADIA 1 Clinical Study Report11 and ARCADIA 2 Clinical Study Report.12
Table 21: Summary of Patient Adherence From the ARCADIA CYCLO Study
Exposure | ARCADIA CYCLO study | |
|---|---|---|
Nemolizumab n = 137 | Placebo n = 137 | |
Adherence (%) | ||
Mean (SD) | █████ ██████ | █████ ███████ |
Minimum, maximum | ██████ ██████ | ██████ ██████ |
Total dose administered (mg) | ||
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum, maximum) | ███ ████ ████ | ███ ████ ████ |
Treatment duration (days) | ||
Mean (SD) | ████ ███████ | ████ ███████ |
Median (minimum, maximum) | ██ ███ ████ | ██ ███ ███ |
SD = standard deviation.
Source: Details included in the table are from the sponsor’s ARCADIA CYCLO Clinical Study Report.13
Concomitant Medications
Details of the most common (i.e., ≥ 10% of patients) concomitant medications for the initial period of the ARCADIA 1 and ARCADIA 2 studies are in Table 22. Briefly, all patients in the ARCADIA 1 and ARCADIA 2 studies reported concomitant medication use. The most commonly reported type of concomitant medication in both the ARCADIA 1 and ARCADIA 2 studies was emollients and protectives (ARCADIA 1: 69.8% of patients in the nemolizumab arm, 70.4% of patients in the placebo arm; ARCADIA 2: 76.8% of patients in the nemolizumab arm, 74.7% of patients in the placebo arm), as well as group II (potent) corticosteroids (ARCADIA 1: 68.1% of patients in the nemolizumab arm, 70.4% of patients in the placebo arm; ARCADIA 2: 75.4% of patients in the nemolizumab arm, 78.5% of patients in the placebo arm). The use of concomitant medications was broadly balanced between study arms within each study, and also between the ARCADIA 1 and ARCADIA 2 studies. The submission did not specify whether the corticosteroids were used as authorized background therapy.
Table 22: Summary of Most Common (10% or More of Patients) Concomitant Medications in the ARCADIA 1 and ARCADIA 2 Studies (ITT) — Initial Period
ATC level 4 preferred term | ARCADIA 1 study | ARCADIA 2 study | ||
|---|---|---|---|---|
Nemolizumab n = 620 | Placebo n = 321 | Nemolizumab n = 522 | Placebo n = 265 | |
Patients with at least 1 concomitant medication | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
Other antihistamines for systemic use | ██ ██████ | ██ ██████ | ███ █████ | ██ ██████ |
Piperazine derivatives | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Corticosteroids, moderately potent (group II) | ██ ██████ | ███ █████ | ███ █████ | ██ ██████ |
Hydrocortisone butyrate | || | || | ██ █████ | ██ ██████ |
Corticosteroids, potent (group III) | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
Mometasone furoate | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
Corticosteroids, weak (group I) | ███ █████ | ██ ██████ | ███ █████ | ██ ██████ |
Hydrocortisone | ███ █████ | ██ ██████ | ██ ██████ | ██ █████ |
Hydrocortisone acetate | || | || | ██ ██████ | ██ ██████ |
Adrenergics in combination with corticosteroids or other drugs, excluding anticholinergics | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Selective beta 2–adrenoreceptor agonists | ███ █████ | ██ ██████ | ██ ██████ | ██ ██████ |
Salbutamol | ██ ██████ | ██ ██████ | ██ █████ | ██ ██████ |
Other emollients and protectives | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
Other emollients and protectives | ███ █████ | ███ █████ | ███ █████ | ██ ██████ |
Butyl hydroxybenzoate, cetyl alcohol, propylene glycol, sodium lauryl sulphate, stearyl alcohol, water purified | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Glycerol; paraffin, liquid; white soft paraffin | ██ ██████ | ██ ██████ | ██ █████ | ██ █████ |
Dimethicone, propylene glycol | || | || | ██ █████ | ██ ██████ |
Soft paraffin and fat products | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Drugs for dermatitis, excluding corticosteroids | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
Tacrolimus monohydrate | ███ █████ | ██ ██████ | ███ █████ | ██ ██████ |
Pimecrolimus | ███ █████ | ██ ██████ | ██ ██████ | ██ ██████ |
Tacrolimus | ██ ██████ | ██ ██████ | ██ ██████ | ██ █████ |
Other viral vaccines | ███ █████ | ██ ██████ | ██ ██████ | ██ ██████ |
Tozinameran | ██ ██████ | ██ ██████ | ██ █████ | ██ █████ |
ATC = anatomic therapeutic class; ITT = intention to treat.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Details of the concomitant medications for the ARCADIA CYCLO study are in Table 23. All patients, except for 1 patient in both arms, reported concomitant medication use. Similar to the ARCADIA 1 and ARCADIA 2 studies, the most commonly reported medication class was potent corticosteroids (█████ ████████████ █████ ███████). The second most commonly reported type of medication was emollients and protectives (█████ ███████████ █████████ █████ ███████ patients) potent corticosteroids (█████ nemolizumab, █████ placebo).
Table 23: Summary of Most Common (10% or More of Patients) Concomitant Medications in the ARCADIA CYCLO Study (ITT)
ATC level 4 preferred term | ARCADIA CYCLO study | |
|---|---|---|
Nemolizumab n = 138 | Placebo n = 138 | |
Patients with at least 1 concomitant medication | ███ ██████ | ███ ██████ |
Other antihistamines for systemic use | ██ ██████ | ██ ██████ |
Bilastine | ██ ██████ | ██ ██████ |
Piperazine derivatives | ██ ██████ | ██ ██████ |
Cetirizine hydrochloride | ██ █████ | ██ ██████ |
Propionic acid derivatives | ██ ██████ | ██ ██████ |
Ibuprofen | ██ ██████ | ██ █████ |
Corticosteroids, potent (group III) | ███ ██████ | ███ ██████ |
Mometasone furoate | ██ ██████ | ██ ██████ |
Mometasone | ██ ██████ | ██ ██████ |
Corticosteroids, weak (group I) | ██ ██████ | ██ ██████ |
Hydrocortisone | ██ ██████ | ██ ██████ |
Adrenergics in combination with corticosteroids or other drugs, excluding anticholinergics | ██ ██████ | ██ ██████ |
Selective beta 2–adrenoreceptor agonists | ██ ██████ | ██ ██████ |
Salbutamol | ██ █████ | ██ ██████ |
Emollients and protectives | ███ ██████ | ███ ██████ |
Other emollients and protectives | ██ ██████ | ███ ██████ |
Aquaphilus dolomiae; elaeis guineensis oil; glycerol; oenothera biennis oil; paraffin, liquid; tocopherol | ██ ██████ | ██ ██████ |
Glycerol; paraffin, liquid; white soft paraffin | ██ ██████ | ██ ██████ |
Dimethicone; propylene glycol | ██ ██████ | ██████ |
Soft paraffin and fat products | ██ ██████ | ██ ██████ |
Aloin; beeswax; glycerol; levomenol; palmitic acid | ██ ██████ | ██ ██████ |
Drugs for dermatitis, excluding corticosteroids | ██ ██████ | ██ ██████ |
Tacrolimus monohydrate | ██ ██████ | ██ ██████ |
Pimecrolimus | ██ ██████ | ██ ██████ |
Sex hormones and modulators of the genital system | ██ ██████ | ██ ██████ |
Progestogens and estrogens, fixed combinations | ██ ██████ | ██ ██████ |
Drugs acting on the renin-angiotensin system | ██ ██████ | ██ ██████ |
Antibacterials for systemic use | ██ ██████ | ██ ██████ |
ATC = anatomic therapeutic category; ITT = intention to treat.
Source: Details included in the table are from the sponsor’s ARCADIA CYCLO Clinical Study Report.
Efficacy
ARCADIA 1 and ARCADIA 2 Studies: Initial Period Results
Detailed results from the initial period in the ARCADIA 1 and ARCADIA 2 studies are presented in Table 24.
Proportion of Patients With IGA Success at Week 16
For patients in the ARCADIA 1 study, at week 16, 35.6% of patients in the nemolizumab arm and 24.6% of patients in the placebo arm attained IGA success (defined as IGA of 0 or 1 and a ≥ 2-point reduction from baseline). The strata-adjusted difference between arms was 11.5% (97.5% CI, 4.7% to 18.3%; P = 0.0003). For patients in the ARCADIA 2 study, at week 16, 37.7% of patients in the nemolizumab arm and 26.0% of patients in the placebo arm attained IGA success. The strata-adjusted difference between arms was 12.2% (97.5% CI, 4.6% to 19.8%; P = 0.0006).
Subgroup analyses for the proportion of patients with IGA success at week 16 in the ARCADIA 1 and ARCADIA 2 studies are summarized in Figure 10, Figure 11, Figure 12, Figure 13, Figure 14, Figure 15, Figure 16, and Figure 17, with pooled results summarized in Figure 18, Figure 19, Figure 20, and Figure 21.
Proportion of Patients With EASI-75 at Week 16
For patients in the ARCADIA 1 study, at week 16, 43.5% of patients in the nemolizumab arm and 29.0% of patients in the placebo arm attained EASI-75. The strata-adjusted difference between arms was 14.9% (97.5% CI, 7.8% to 22.0%; P < 0.0001). For patients in the ARCADIA 2 study, at week 16, 42.1% of patients in the nemolizumab arm and 30.2% of patients in the placebo arm attained EASI-75. The strata-adjusted difference between arms was 12.5% (97.5% CI, 4.6% to 20.3%; P = 0.0006).
Subgroup analyses for the proportion of patients with EASI-75 at week 16 in the ARCADIA 1 and ARCADIA 2 studies are summarized in Figure 10, Figure 11, Figure 12, Figure 13, Figure 14, Figure 15, Figure 16, and Figure 17, with pooled results summarized in Figure 18, Figure 19, Figure 20, and Figure 21.
Change From Baseline to Week 16 in Total EASI Score
For patients in the ARCADIA 1 study, the LS mean change from baseline in total EASI score was –12.36 (95% CI, –13.96 to –10.76) in the nemolizumab arm, and –8.68 (95% CI, –10.77 to –6.58) in the placebo arm. The LS mean difference was –3.68 (95% CI, –6.08 to –1.28; P = 0.0026). For patients in the ARCADIA 2 study, the LS mean change from baseline in total EASI score was –13.15 (95% CI, –14.57 to –11.73) in the nemolizumab arm and –9.02 (95% CI, –10.97 to –7.08) in the placebo arm. The LS mean difference between study arms was –4.13 (95% CI, –6.36 to –1.89; P = 0.0003).
Proportion of Patients With an Improvement of 4 or More in PP-NRS at Week 16
For patients in the ARCADIA 1 study, at week 16, 42.7% of patients in the nemolizumab arm and 17.8% of patients in the placebo arm reported a reduction in PP-NRS score of 4 points or greater. The strata-adjusted LS mean difference between arms was 24.9% (97.5% CI, 18.4% to 31.5%; P < 0.0001). For patients in the ARCADIA 2 study, at week 16, 41.0% of patients in the nemolizumab arm and 18.1% of patients in the placebo arm reported a reduction in PP-NRS score of 4 points or greater. The strata-adjusted LS mean difference between arms was 23.2% (97.5% CI, 16.1% to 30.3%; P < 0.0001).
Subgroup analyses for the proportion of patients with PP-NRS scores of 4 or more at week 16 in the ARCADIA 1 and ARCADIA 2 studies are summarized in Figure 10, Figure 11, Figure 12, Figure 13, Figure 14, Figure 15, Figure 16, and Figure 17, with pooled results summarized in Figure 18, Figure 19, Figure 20, and Figure 21.
Proportion of Patients With PP-NRS Less Than2 at Week 16
For patients in the ARCADIA 1 study, at week 16, 30.6% of patients in the nemolizumab arm and 11.2% of patients in the placebo arm reported a PP-NRS score of less than 2 points. The strata-adjusted LS mean difference between arms was 19.5% (97.5% CI, 13.7% to 25.2%; P < 0.0001). For patients in the ARCADIA 2 study, at week 16, 28.4% of patients in the nemolizumab arm and 11.3% of patients in the placebo arm reported a PP-NRS score of less than 2 points. The strata-adjusted LS mean difference between arms was 17.1% (97.5% CI, 10.9% to 23.3%; P < 0.0001).
Subgroup analyses for the proportion of patients with PP-NRS scores of 2 or less at week 16 in the ARCADIA 1 and ARCADIA 2 studies are summarized in Figure 10, Figure 11, Figure 12, Figure 13, Figure 14, Figure 15, Figure 16, and Figure 17, with pooled results summarized in Figure 18, Figure 19, Figure 20, and Figure 21.
Change From Baseline to Week 16 in PP-NRS Score
For patients in the ARCADIA 1 study, the LS mean change from baseline in PP-NRS score was –3.77 (95% CI, –4.02 to –3.53) in the nemolizumab arm, and –1.94 (95% CI, –2.26 to –1.61) in the placebo arm. The LS mean difference was –1.84 (95% CI, –2.21 to –1.47; P < 0.0001). For patients in the ARCADIA 2 study, the LS mean change from baseline in PP-NRS score was –3.71 (95% CI, –3.94 to –3.47) in the nemolizumab arm and –1.95 (95% CI, –2.27 to –1.63) in the placebo arm. The LS mean difference between study arms was –1.76 (95% CI, –2.13 to –1.39; P < 0.0001).
Change From Baseline to Week 16 in DLQI Total Score
For adult patients in the ARCADIA 1 study, the LS mean change from baseline in DLQI total score was –7.76 (95% CI, –8.49 to –7.03) in the nemolizumab arm, and –5.26 (95% CI, –6.23 to –4.29) in the placebo arm. The LS mean difference was –2.50 (95% CI, –3.63 to –1.37; P < 0.0001). For adult patients in the ARCADIA 2 study, the LS mean change from baseline in DLQI total score was –6.96 (95% CI, –7.67 to –6.25) in the nemolizumab arm and –4.52 (95% CI, –5.48 to –3.56) in the placebo arm. The LS mean difference between study arms was –2.44 (95% CI, –3.58 to –1.30; P < 0.0001).
Change From Baseline to Week 16 in CDLQI Total Score
For adolescent patients in the ARCADIA 1 study, the LS mean change from baseline in DLQI total score was –6.92 (95% CI, –9.26 to –4.58) in the nemolizumab arm, and –5.10 (95 CI, –7.71 to –2.50) in the placebo arm. The LS mean difference was –1.82 (95% CI, –4.88 to 1.25; P = 0.2454). For adolescent patients in the ARCADIA 2 study, the LS mean change from baseline in DLQI total score was –7.40 (95% CI, –8.97 to –5.82) in the nemolizumab arm and –5.02 (95% CI, –7.48 to –2.56) in the placebo arm. The LS mean difference between study arms was –2.38 (95% CI, –5.03 to 0.27; P = 0.0788).
Incidence of Rescue Therapy Use
In the ARCADIA 1 study, during the initial period, a total of 3.4% of patients in the nemolizumab arm and 4.0% of patients in the placebo arm reported using rescue therapy. In the ARCADIA 2 study, during the initial period, a total of 2.1% of patients in the nemolizumab arm and 4.2% of patients in the placebo arm reported using rescue therapy.
Table 24: Summary of Key Efficacy Results From the ARCADIA 1 and ARCADIA 2 Studies (ITT) — Initial Period
Variable | ARCADIA 1 study | ARCADIA 2 study | ||
|---|---|---|---|---|
Nemolizumab n = 620 | Placebo n = 321 | Nemolizumab n = 522 | Placebo n = 265 | |
Proportion of patients with IGA successa at week 16: coprimary outcome | ||||
Number of patients contributing to the analysis, n | 620 | 321 | 522 | 265 |
Proportion with IGA success, n (%) | 221 (35.6) | 79 (24.6) | 197 (37.7) | 69 (26.0) |
Strata-adjusted difference, % (97.5% CI) | 11.5 (4.7 to 18.3) | 12.2 (4.6 to 19.8) | ||
Strata-adjusted P valueb | 0.0003 | 0.0006 | ||
Proportion of patients with EASI-75 at week 16: coprimary outcome | ||||
Number of patients contributing to the analysis, n | 620 | 321 | 522 | 365 |
Proportion with EASI-75, n (%) | 270 (43.5) | 93 (29.0) | 220 (42.1) | 80 (30.2) |
Strata-adjusted difference, % (97.5% CI) | 14.9 (7.8 to 22.0) | 12.5 (4.6 to 20.3) | ||
Strata-adjusted P valueb | < 0.0001 | 0.0006 | ||
Change from baseline to week 16 in EASI: secondary outcome | ||||
Number of patients contributing to the analysis, n (%) | 620 | 321 | 522 | 265 |
Baseline, mean (SD) | 27.77 (10.64) | 27.06 (9.37) | 27.43 (10.81) | 27.58 (10.87) |
LS mean change from baseline (95% CI) | –12.36 (–13.96 to –10.76) | –8.68 (–10.77 to –6.58) | –13.15 (–14.57 to –11.73) | –9.02 (–10.97 to –7.08) |
LS mean difference vs. placebo (95% CI) | –3.68 (–6.08 to –1.28) | –4.13 (–6.36 to –1.89) | ||
P value | 0.0026 | 0.0003 | ||
Proportion of patients with an improvement of PP-NRS ≥ 4 at week 16: key secondary outcome | ||||
Number of patients contributing to the analysis, n | 620 | 321 | 522 | 265 |
Proportion with PP-NRS improvement ≥ 4 points, n (%) | 265 (42.7) | 57 (17.8) | 214 (41.0) | 48 (18.1) |
Strata-adjusted difference, % (97.5% CI) | 24.9 (18.4 to 31.5) | 23.2 (16.1 to 30.3) | ||
P valueb | < 0.0001 | < 0.0001 | ||
Proportion of patients with PP-NRS < 2 at week 16: key secondary outcome | ||||
Number of patients contributing to the analysis, n | 620 | 321 | 522 | 265 |
Proportion with PP-NRS < 2, n (%) | 190 (30.6) | 36 (11.2) | 148 (28.4) | 30 (11.3) |
Strata-adjusted difference, % (97.5% CI) | 19.5 (13.7 to 25.2) | 17.1 (10.9 to 23.3) | ||
P valueb | < 0.0001 | < 0.0001 | ||
Change from baseline to week 16 in PP-NRS: secondary outcome | ||||
Number of patients contributing to the analysis, n (%) | 618 | 320 | 521 | 264 |
Baseline, mean (SD) | 7.17 (1.40) | 7.15 (1.44) | 7.04 (1.53) | 7.16 (1.51) |
LS mean change from baseline (95% CI) | –3.77 (–4.02 to –3.53) | –1.94 (–2.26 to –1.61) | –3.71 (–3.94 to –3.47) | –1.95 (–2.27 to –1.63) |
LS mean difference vs. placebo (95% CI) | –1.84 (–2.21 to –1.47) | –1.76 (–2.13 to –1.39) | ||
P value | < 0.0001 | < 0.0001 | ||
Change from baseline to week 16 in DLQI total score: secondary outcome | ||||
Number of patients contributing to the analysis, n (%) | 540 | 279 | 440 | 228 |
Baseline, mean (SD) | 15.40 (6.60) | 15.50 (6.75) | 14.50 (6.85) | 14.20 (6.98) |
LS mean change from baseline (95% CI) | –7.76 (–8.49 to –7.03) | –5.26 (–6.23 to –4.29) | –6.96 (–7.67 to –6.25) | –4.52 (–5.48 to –3.56) |
LS mean difference vs. placebo (95% CI) | –2.50 (–3.63 to –1.37) | –2.44 (–3.58 to –1.30) | ||
P value | < 0.0001 | < 0.0001 | ||
Change from baseline to week 16 in CDLQI total score: secondary outcome | ||||
Number of patients contributing to the analysis, n (%) | 71 | 37 | 75 | 30 |
Baseline, mean (SD) | 12.70 (6.70) | 12.50 (5.83) | 12.2 (5.98) | 12.4 (5.40) |
LS mean change from baseline (95% CI) | –6.92 (–9.26 to –4.58) | –5.10 (–7.71 to –2.50) | –7.40 (–8.97 to –5.82) | –5.02 (–7.48 to –2.56) |
LS mean difference vs. placebo (95% CI) | –1.82 (–4.88 to 1.25) | –2.38 (–5.03 to 0.27) | ||
P value | 0.2454 | 0.0788 | ||
Incidence of rescue treatment use from baseline to week 16: secondary outcome | ||||
Number of patients contributing to the analysis, n | 620 | 321 | 522 | 265 |
Proportion of patients with any topical therapy, n (%) | 21 (3.4) | 13 (4.0) | 11 (2.1) | 11 (4.2) |
CDLQI = Children’s Dermatology Life Quality Index; CI = confidence interval; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% improvement in the Eczema Area and Severity Index; IGA = Investigator Global Assessment; ITT = intention to treat; LS = least squares; PP-NRS = Peak Pruritus Numeric Rating Scale; SD = standard deviation; vs. = versus.
aIGA success was defined as IGA of 0 or 1 and a ≥ 2-point reduction from baseline.
bStatistical analysis was adjusted for multiple comparisons.
Sources: Details included in the table are from the sponsor’s ARCADIA 1 Clinical Study Report11 and ARCADIA 2 Clinical Study Report.12
ARCADIA 1 and ARCADIA 2 Studies: Pooled Maintenance Period Results
The ARCADIA 1 and ARCADIA 2 studies were noted by the sponsor to be replicate studies, having identical inclusion and exclusion criteria, study design, and analysis methods. In addition, a similar proportion of patients in each study met the study definition of clinical responders and continued on to the maintenance period, and study discontinuations or losses to follow-up were broadly similar. Therefore, the pooled maintenance period results were appraised in the report. Out of the ITT population initially randomized in the initial period, 169 patients were rerandomized to the nemolizumab every 4 weeks arm, 169 to the nemolizumab every 8 weeks arm, and 169 to the placebo arm. Detailed results from the pooled results from the maintenance period of the ARCADIA 1 and ARCADIA 2 studies are presented in Table 25.
Proportion of Patients Maintaining IGA Success Until Week 48 From the Subset With IGA Success at Week 16
At week 48, 31.7% of patients in the nemolizumab every 4 weeks arm (n = 142), 37.3% of patients in the nemolizumab every 8 weeks arm (n = 142), and 31.3% of patients in the placebo arm (n = 131) reported maintaining IGA success at all study visits until week 48. The strata-adjusted LS mean difference between nemolizumab every 4 weeks and placebo was ████ ████ ███ ██████ ██ ███████ ███ ███████████████ ██ ████ ██████████ ███████ ███████████ ███ ███ ███████ ███ ████ ████ ███ █████ ██ ███████.
At week 48, 63.4% of patients in the nemolizumab every 4 weeks arm (n = 142), 64.1% of patients in the nemolizumab every 8 weeks arm (n = 142), and 55.0% of patients in the rerandomized placebo arm (n = 131) reported IGA success. The strata-adjusted LS mean difference between nemolizumab every 4 weeks and placebo was 8.5% (95% CI, –3.0% to 20.2%). The strata-adjusted LS mean difference between nemolizumab every 8 weeks and placebo was 9.1% (95% CI, –2.5% to 20.6%).
Proportion of Patients Maintaining EASI-75 Until Week 48 From the Subset With EASI-75 at Week 16
At week 48, 55.8% of patients in the nemolizumab every 4 weeks arm (n = 163), 58.9% of patients in the nemolizumab every 8 weeks arm (n = 163), and 44.6% of patients in the placebo arm (n = 163) reported maintaining EASI-75 at all study visits until week 48. The strata-adjusted LS mean difference between nemolizumab every 4 weeks and placebo was 11.2 ████ ███ ████ ██ ███████ ███ ███████████████ ██ ████ ██████████ ███████ ███████████ ███ ███ ███████ ███ █████ ████ ███ ████ ██ ███████.
At week 48, 76.3% of patients in the nemolizumab every 4 weeks arm (n = 169), 75.7% of patients in the nemolizumab every 8 weeks arm (n = 169), and 63.9% of patients in the rerandomized placebo arm (n = 169) reported attaining EASI-75. The strata-adjusted LS mean difference between nemolizumab every 4 weeks and placebo was 12.4% (95% CI, 2.7% to 22.0%). The strata-adjusted LS mean difference between nemolizumab every 8 weeks and placebo was 11.8% (95% CI, 2.1% to 21.5%).
Change From Week 16 to Week 48 in EASI
The LS mean change from baseline in EASI score was 2.01 (95% CI, █████ ██ █████ ████ ██ ███ ███████████ ███ ████ ████ ████ ███ ████ ██ █████ ████ ██ ███ ███████████ ███ ████ ███ ████ ████ ███ ████ ██ █████████ ██ ███ ███████ ████ ███ ██ ████ ██████████ ████ ███████ ███ █████ ████ ███ █████ ██ ██████ ██ ███ ███████████ ███ ███ ███ █████ ████ ███ █████ ██ ██████ ██ ███ ███████████ ███ ████.
Proportion of Patients With PP-NRS Improvement of 4 or More From Initial Baseline to Week 48 From the Subset With PP-NRS of 4 or More at Week 16
At week 48, out of the subset of patients who had a PP-NRS score improvement of 4 points or more at week 16, a total of 46.9% of patients in the nemolizumab every 4 weeks arm (n = 98), 40.4% of patients in the nemolizumab every 8 weeks arm (n = 94), and 31.3% of patients in the placebo arm (n = 83) reported an improvement in PP-NRS of 4 points or more from the initial period baseline. The strata-adjusted proportion difference versus placebo was █████ ████ ███ ████ ██ ██████ ██ ███ ███████████ ███ ███ ███ ████ ████ ███ █████ ██ ██████ ██ ███ ███████████ ███ ████.
At week 48, out of the entire maintenance period population, ████ ██ █████ ██ ████████ ██ ███ ███████████ ███ ███ ██ █ █████ █████ ██ ████████ ██ ███ ███████████ ███ ███ ██ █ ████ ███ █████ ██ ████████ ██ ███ ███████ ███ ██ █ ████ ████████ ██ ███████████ ██ ██████ ██ █ ██████ ██ ████ ████ ███ ███████ ██████ █████████ ███ ███████████████ ██████████ ██████████ ██████ ███████ ███ 15.4% (95% CI, 5.8% to 24.9%) in the nemolizumab every 4 weeks arm and 7.7% (95% CI, –1.5% to 16.9%) in the nemolizumab every 8 weeks arm.
Proportion of Patients With PP-NRS Less Than 2 at Week 48 From the Subset With PP-NRS Less Than 2at Week 16
At week 48, a total of 39.7% of patients in the nemolizumab every 4 weeks arm (n = 169), 43.0% of patients in the nemolizumab every 8 weeks arm (n = 169), and 34.4% of patients in the placebo arm (n = 169) reported a PP-NRS score of 2 or less. The strata-adjusted proportion difference versus placebo was 5.9% (95% CI, –10.1% to 21.8%) in the nemolizumab every 4 weeks arm and 8.6% (95% CI, –7.4% to 24.6%) in the nemolizumab every 8 weeks arm.
At week 48, out of the entire maintenance period population, a total of 30.2% of patients in the nemolizumab every 4 weeks arm (N = 169), 27.8% of patients in the nemolizumab every 8 weeks arm (n = 169) and 18.9% of patients in the placebo arm (n = 169) reported a PP-NRS score of 2 points or less. The strata-adjusted proportion difference versus placebo was 11.2% (95% CI, 2.1% to 20.3%) in the nemolizumab every 4 weeks arm and 8.9% (95% CI, –0.1% to 17.8%) in the nemolizumab every 8 weeks arm.
Change From Week 16 to Week 48 in PP-NRS
The LS mean change from baseline in PP-NRS score was –0.46 (95% CI, 0.88 to –0.05; n = 143) in the nemolizumab every 4 weeks arm, 0.10 (95% CI, –0.29 to 0.48; n = 155) in the nemolizumab every 8 weeks arm, and 1.35 (95% CI, 0.95 to 1.74; n = 152) in the placebo arm. The LS mean difference from placebo was –1.81 (95% CI, –2.39 to –1.23) in the nemolizumab every 4 weeks arm and –1.25 (95% CI, –1.79 to –0.71) in the nemolizumab every 8 weeks arm.
Change From Week 16 to Week 48 in DLQI Total Score
The LS mean change from baseline in DLQI score was –0.43 (95% CI, –1.11 to 0.24; n = 119) in the nemolizumab every 4 weeks arm, 0.14 (95% CI, –0.50 to 0.79; n = 130) in the nemolizumab every 8 weeks arm, and 0.70 (95% CI, 0.00 to 1.40; n = 110) in the placebo arm. The LS mean difference from placebo was –1.14 (95% CI, –2.11 to –0.16) in the nemolizumab every 4 weeks arm and –0.56 (95% CI, –1.52 to 0.40) in the nemolizumab every 8 weeks arm.
Change From Week 16 to Week 48 in CDLQI Total Score
The LS mean change from baseline in CDLQI score was –0.54 (95% CI, –1.45 to 0.36; n = 29) in the nemolizumab every 4 weeks arm, –1.27 (95% CI, –2.30 to –0.23; n = 22) in the nemolizumab every 8 weeks arm, and 0.34 (95% CI, –0.71 to 1.38; n = 22) in the placebo arm. The LS mean difference from placebo was –0.88 (95% CI, –2.27 to 0.51) in the nemolizumab every 4 weeks arm and –1.60 (95% CI, –3.08 to –0.12) in the nemolizumab every 8 weeks arm.
Incidence of Rescue Therapy Use
In the maintenance period, a total of 1.2% of patients in the nemolizumab every 4 weeks arm, 2.4% in the nemolizumab every 8 weeks arm, and 5.3% of patients in the placebo arm reported using rescue therapy.
Table 25: Summary of Key Efficacy Results From the ARCADIA 1 and ARCADIA 2 Pooled Analysis (ITT) — Maintenance Period
Variable | Patients meeting the definition of clinical responder in the ARCADIA 1 and ARCADIA 2 studies (rerandomized) | ||
|---|---|---|---|
Nemolizumab q.4.w. to nemolizumab q.4.w. n = 169 | Nemolizumab q.4.w. to nemolizumab q.8.w. n = 169 | Nemolizumab q.4.w. to placebo n = 169 | |
Proportion of patients maintaining IGA success at all visits until week 48a (subset with IGA success at week 16) | |||
Number of patients contributing to the analysis, n | 142 | 142 | 131 |
Proportion with IGA success, n (%) | 45 (31.7) | 53 (37.3) | 41 (31.3) |
Strata-adjusted difference vs. placebo (95% CI) | 0.5 (–10.5 to 11.6) | 6.0 (–5.2 to 17.1) | NA |
P value | 0.9268 | 0.2972 | NA |
Proportion of patients maintaining EASI-75 until week 48a (subset with EASI-75 at week 16) | |||
Number of patients contributing to the analysis, n | 163 | 163 | 157 |
Proportion with EASI-75, n (%) | 91 (55.8) | 96 (58.9) | 70 (44.6) |
Strata-adjusted difference vs. placebo (95% CI) | 11.2 (0.3 to 22.1) | 14.1 (3.3 to 24.9) | NA |
P value | 0.0459 | 0.0114 | NA |
Change from week 16 to week 48 in EASI | |||
Number of patients contributing to the analysis, n | 169 | 169 | 169 |
Week 16 maintenance baseline, mean (SD) | 2.91 (3.16) | 2.37 (2.72) | 3.04 (3.15) |
LS mean change from baseline (95% CI) | 2.01 (–0.16 to 4.19) | 2.98 (0.80 to 5.17) | 6.79 (4.62 to 8.96) |
LS mean difference vs. placebo (95% CI) | –4.78 (–7.85 to –1.70) | –3.80 (–6.89 to –0.72) | NA |
P value | 0.0023 | 0.0157 | NA |
Proportion with PP-NRS improvement ≥ 4 from initial baseline to week 48 (subset with PP-NRS improvement ≥ 4 at week 16) | |||
Number of patients contributing to the analysis, n | 98 | 94 | 83 |
Improvement of ≥ 4 from initial period baseline, n (%) | 46 (46.9) | 38 (40.4) | 26 (31.3) |
Strata-adjusted proportion difference vs. placebo (95% CI) | 15.4 (1.3 to 29.4) | 9.1 (–5.0 to 23.2) | NA |
P value | 0.0358 | 0.2124 | NA |
Proportion of patients with PP-NRS < 2 at week 48 (subset with PP-NRS < 2 at week 16) | |||
Number of patients contributing to the analysis, n | 73 | 79 | 64 |
Proportion with PP-NRS < 2 | 29 (39.7) | 34 (43.0) | 22 (34.4) |
Strata-adjusted proportion difference vs. placebo (95% CI) | 5.9 (–10.1 to 21.8) | 8.6 (–7.4 to 24.6) | NA |
P value | 0.4733 | 0.2969 | NA |
Change from week 16 to week 48 in PP-NRS | |||
Number of patients contributing to the analysis, n | 143 | 155 | 152 |
Week 16 maintenance baseline, mean (SD) | 2.08 (2.01) | 2.20 (2.08) | 2.69 (2.27) |
LS mean change from baseline (95% CI) | –0.46 (0.88 to –0.05) | 0.10 (–0.29 to 0.48) | 1.35 (0.95 to 1.74) |
LS mean difference vs. placebo (95% CI) | –1.81 (–2.39 to –1.23) | –1.25 (–1.79 to –0.71) | NA |
P value | < 0.0001 | < 0.0001 | NA |
Change from week 16 to week 48 in DLQI total score | |||
Number of patients contributing to the analysis, n | 119 | 130 | 110 |
Week 16 maintenance baseline, mean (SD) | 3.10 (3.74) | 3.00 (3.32) | 3.70 (4.31) |
LS mean change from baseline (95% CI) | –0.43 (–1.11 to 0.24) | 0.14 (–0.50 to 0.79) | 0.70 (0.00 to 1.40) |
LS mean difference vs. placebo (95% CI) | –1.14 (–2.11 to –0.16) | –0.56 (–1.52 to 0.40) | NA |
P value | 0.0222 | 0.2498 | NA |
Change from week 16 to week 48 in CDLQI total score | |||
Number of patients contributing to the analysis, n | 29 | 22 | 22 |
Week 16 maintenance baseline, mean (SD) | 2.10 (2.83) | 3.70 (3.27) | 3.30 (4.09) |
LS mean change from baseline (95% CI) | –0.54 (–1.45 to 0.36) | –1.27 (–2.30 to –0.23) | 0.34 (–0.71 to 1.38) |
LS mean difference vs. placebo (95% CI) | –0.88 (–2.27 to 0.51) | –1.60 (–3.08 to –0.12) | NA |
P value | 0.2098 | 0.0343 | NA |
Incidence of rescue treatment use from week 16 to week 48 | |||
Number of patients contributing to the analysis, n | 169 | 169 | 169 |
Proportion of patients with any topical therapy, n (%) | 2 (1.2) | 4 (2.4) | 9 (5.3) |
CDLQI = Children’s Dermatology Life Quality Index; CI = confidence interval; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% improvement in the Eczema Area and Severity Index; IGA = Investigator Global Assessment; ITT = intention to treat; LS = least squares; NA = not applicable; PP-NRS = Peak Pruritus Numeric Rating Scale; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SD = standard deviation; vs. = versus.
aMaintaining IGA success and EASI-75 was defined for participants achieving IGA success (or EASI-75, as applicable) at week 16 and achieving that outcome at every analysis visit until the analysis visit was summarized.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence10 and the ARCADIA 1 and ARCADIA 2 pooled analysis Clinical Study Reports.56
ARCADIA CYCLO Study
Detailed results from the final analysis of the ARCADIA CYCLO study are presented in Table 26.
Proportion of Patients With EASI-75
At week 16, 47.1% of patients in the nemolizumab arm and 34.8% of patients in the placebo arm reported EASI-75. The strata-adjusted difference between the study arms was 12.2% (95% CI, 0.7% to 23.6%; P = 0.040).
Proportion of Patients With Prior CsA Use With EASI-75
██ ████ ███ █████ ██ ████████ ██ ███ ███████████ ███ ██ █ ████ ███ █████ ██ ████████ ██ ███ ███████ ███ ██ █ ████ ████████ ████████ ███ ███████████████ ██████████ ███████ ███ █████ ████ ███ █████ ████ ███ ████ ██ ██████████████.
Percent Change From Baseline in EASI
███ ██ ████ ███████ ██████ ████ ████████ ██ ████ █████ █████ ██ ████ ██ ███ ███████ ████ ███ ███████ ██ ████████ ██ ███ ███████████ ████ ███ ███████ ████ ███ ███████ ██ ████████ ██ ███ ███████ ████ ███ ██ ████ ██████████ ██████ ███████ ███ ██████ ████ ███ ███████ ██ ██████ ████████.
Proportion of Patients With an Improvement of PP-NRS of 4 or More From Baseline to Week 16
At week 16, 39.1% of patients in the nemolizumab arm and 17.4% of patients in the placebo arm reported an improvement in PP-NRS score of 4 points or greater. The strata-adjusted difference versus placebo was 21.7% (95% CI, 11.4% to 32.0%; P < 0.0010).
Proportion of Patients With PP-NRS of Less Than 2 at Week 16
██ ████ ███ █████ ██ ████████ ██ ███ ███████████ ███ ███ ████ ██ ████████ ██ ███ ███████ ███ ████████ █ ██████ █████ ██ █ ██████ ██ █████ ███ ██ ████ ██████████ ██████ ███████ ███ █████ ████ ███ ████ ██ ██████ | | | ████████.
Percent Change From Baseline to Week 16 in PP-NRS
███ ██ ████ ███████ ██████ ██ ██████ ████ ████████ ███ ███████ ████ ███ ███████ ██ ████████ ██ ███ ███████████ ███ ███ ███████ ████ ███ ███████ ██ ████████ ██ ███ ███████ ████ ███ ██ ████ ██████████ ██████ ███████ ███ ███████ ████ ███ ███████ ██ ███████ | | | ████████.
Proportion of Patients With IGA Success
██ ████ ███ █ █████ ██ █████ ██ ████████ ██ ███ ███████████ ███ ███ █████ ██ ████████ ██ ███ ███████ ███ ████████ ███ ███████ ████████ ██ ███ █ ██ █ ███ | | ███████ █████████ ████ ██████████ ███ ██ ████ ██████████ ██████ ███████ ███ ████ ████ ███ █████ ██ ██████ ████████.
Change From Baseline to Week 16 in DLQI Total Score
███ ██ ████ ██████ ████ ████████ ██ ████ █████ █████ ███ █████ ████ ███ █████ ██ ██████ ██ ███ ███████████ ███ ███ █████ ████ ███ █████ ██ ██████ ██ ███ ███████ ████ ███ ██ ████ ██████████ ██████ ███████ ███ █████ ████ ███ █████ ██ ██████ | | ████████.
Incidence of Rescue Treatment Use
██ ██ ████ ███ █ █████ ██ ████ ██ ████████ ██ ███ ███████████ ███ ███ ████ ██ ████████ ██ ███ ███████ ███ ████████ ███ ███ ██ █ ██ ████ ██████ ████████████ ███ ███████████████ ██████████ ██████ ███████ ███ ███ ████ ███ ████ ██ ████ | | ████████.
Table 26: Summary of Key Efficacy Results From the ARCADIA CYCLO Study (ITT)
Variable | ARCADIA CYCLO study | |
|---|---|---|
Nemolizumab n = 138 | Placebo n = 138 | |
Proportion of patients with EASI-75: primary outcome | ||
Number of patients contributing to the analysis, n | 138 | 138 |
Proportion with EASI-75, n (%) | ██ (47.1) | ██ (34.8) |
Strata-adjusted difference vs. placebo (95% CI) | 12.2 (0.7 to 23.6) | |
P value | 0.040 | |
Proportion of patients with prior CsA use with EASI-75: secondary outcome | ||
Number of patients contributing to the analysis, n | ███ | ███ |
Proportion with EASI-75, n (%) | ██ ██████ | ██ ██████ |
Strata-adjusted difference vs. placebo (95% CI) | ████ █████ █████ | |
P value | ██████ | |
Percent change from baseline to week 16 in EASI: secondary outcome | ||
Number of patients contributing to the analysis, n | ███ | ███ |
Baseline, mean (SD) | █████ ██████ | █████ ██████ |
LS mean % change from baseline (95% CI) | ████ ██████ █████ | ████ ██████ █████ |
LS mean difference vs. placebo (95% CI) | █████ ████████ █████ | |
P value | ██████ | |
Proportion of patients with an improvement of PP-NRS ≥ 4 from baseline to week 16: primary outcome | ||
Number of patients contributing to the analysis, n | 138 | 138 |
Proportion with PP-NRS ≥ 4 at week 16, n (%) | ██ (39.1) | ██ (17.4) |
Strata-adjusted difference vs. placebo (95% CI) | 21.7 (11.4 to 32.0) | |
P value | < 0.0010 | |
Proportion of patients with PP-NRS < 2 at week 16: secondary outcome | ||
Number of patients contributing to the analysis, n | ███ | ███ |
Proportion with PP-NRS < 2 at week 16, n (%) | ██ ██████ | ██ █████ |
Strata-adjusted difference vs. placebo (95% CI) | ████ █████ █████ | |
P value | ██████ | |
Percent change from baseline to week 16 in PP-NRS: secondary outcome | ||
Number of patients contributing to the analysis, n | ███ | ███ |
Baseline, mean (SD) | ████ ██████ | ████ ██████ |
LS mean % change from baseline (95% CI) | ████ ██████ █████ | ████ ██████ █████ |
LS mean difference vs. placebo (95% CI) | ██████ ████████ ██████ | |
P value | ██████ | |
Proportion of patients with IGA successa at week 16: secondary outcome | ||
Number of patients contributing to the analysis, n | ███ | ███ |
Proportion with IGA success at week 16, n (%) | ██ ██████ | ██ ██████ |
Strata-adjusted difference vs. placebo (95% CI) | ███ ██████ █████ | |
P value | ██████ | |
Change from baseline to week 16 in DLQI total score: secondary outcome | ||
Number of patients contributing to the analysis, n | ███ | ███ |
Baseline, mean (SD) | █████ ██████ | █████ ██████ |
LS mean change from baseline (95% CI) | ████ ██████ █████ | ████ ██████ █████ |
LS mean difference vs. placebo (95% CI) | █████ ███████ ██████ | |
P value | ██████ | |
Incidence of rescue treatment use through week 16: secondary outcome | ||
Number of patients contributing to the analysis, n | ███ | ███ |
Patients with ≥ 1 rescue medication, n (%) | ██████ | ██████ |
Strata-adjusted difference (95% CI) | ███ ██████ ████ | |
P value | ██████ | |
CI = confidence interval; CsA = cyclosporine; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; EASI-75 = ≥ 75% improvement in the Eczema Area and Severity Index from baseline; IGA = Investigator Global Assessment; ITT = intention to treat; LS = least squares; PP-NRS = Peak Pruritus Numeric Rating Scale; SD = standard deviation; vs. = versus.
aIGA success was defined as IGA 0 or 1 and a ≥ 2-point reduction from baseline.
Source: Details included in the table are from the sponsor’s ARCADIA CYCLO Clinical Study Report.10
Harms
Refer to Table 27 for harms data from the ARCADIA 1 study, Table 28 for harms data from the ARCADIA 2 study, and Table 29 for harms data from the ARCADIA CYCLO study.
Adverse Events
ARCADIA 1 Study
During the initial period of the ARCADIA 1 study, 49.7% of patients in the nemolizumab arm and 45.5% of patients in the placebo arm reported at least 1 AE. The most commonly reported AEs during this period were infections and infestations (18.3% in the nemolizumab arm, 20.3% in the placebo arm); skin and SC tissue disorders (18.3% in the nemolizumab arm, 14.0% in the placebo arm); and respiratory, thoracic, or mediastinal disorders (9.4% in the nemolizumab arm, 8.7% in the placebo arm). The proportion of patients reporting AEs was generally balanced between the nemolizumab and placebo arms.
During the maintenance period of the ARCADIA 1 study, 58.2% of patients in the nemolizumab every 4 weeks arm, 55.6% in the nemolizumab every 8 weeks arm, 58.2% in the rerandomized placebo arm, and 55.0% in the carryover placebo arm reported AEs. The most common AEs were infections and infestations (34.1% in the nemolizumab every 4 weeks arm, 34.4% in the nemolizumab every 8 weeks arm, 34.1% in the rerandomized placebo arm, and 34.0% in the nonrandomized placebo arm); skin and SC issues (12.1% in the nemolizumab every 4 weeks arm, 11.1% in the nemolizumab every 8 weeks arm, 14.3% in the rerandomized placebo arm, and 14.0% in the nonrandomized placebo arm); and respiratory, thoracic, and mediastinal disorders (12.1% in the nemolizumab every 4 weeks arm, 11.1% in the nemolizumab every 8 weeks arm, 13.2% in the rerandomized placebo arm, and 7.0% in the nonrandomized placebo arm). There was a numerically higher proportion of patients reporting infections and infestations in the maintenance period relative to the initial period, and a numerically higher number of patients in the nemolizumab every 4 weeks arm reported gastrointestinal disorders (12.1%) relative to the other arms in the maintenance period (ranging from 5.6% to 7.7% of patients).
ARCADIA 2 Study
During the initial period of the ARCADIA 2 study, 41.4% of patients in the nemolizumab arm and 44.5% of patients in the placebo arm reported at least 1 AE. The most commonly reported AEs during this period were infections and infestations (17.0% in the nemolizumab arm, 20.2% in the placebo arm); skin and SC tissue disorders (12.1% in the nemolizumab arm, 9.9% in the placebo arm); and respiratory, thoracic, or mediastinal disorders (5.6% in the nemolizumab arm, 5.3% in the placebo arm). The proportion of patients reporting AEs was generally balanced between the nemolizumab and placebo arms.
During the maintenance period of the ARCADIA 1 study, 48.1% of patients in the nemolizumab every 4 weeks arm, 51.9% in the nemolizumab every 8 weeks arm, 58.4% in the rerandomized placebo arm, and 44.0% in the carryover placebo arm reported AEs. The most common AEs were infections and infestations (27.8% in the nemolizumab every 4 weeks arm, 22.1% in the nemolizumab every 8 weeks arm, 31.2% in the rerandomized placebo arm, and 28.6% in the nonrandomized placebo arm); skin and SC issues (13.9% in the nemolizumab every 4 weeks arm, 10.4% in the nemolizumab every 8 weeks arm, 13.0% in the rerandomized placebo arm, and 9.5% in the nonrandomized placebo arm); and respiratory, thoracic, and mediastinal disorders (10.1% in the nemolizumab every 4 weeks arm, 6.5% in the nemolizumab every 8 weeks arm, 11.7% in the rerandomized placebo arm, and 2.4% in the nonrandomized placebo arm). A numerically higher proportion of patients in the rerandomized placebo arm reported COVID-19 infection (16.9%) relative to other study arms (ranging from 3.8% to 7.1%).
ARCADIA CYCLO Study
██████ ███████ ██████ █████ ██ ████████ ██ ███ ███████████ ███ ███ █████ ██ ████████ ██ ███ ███████ ███ ████████ ████ ███ ████ ████████ ████████ ███ ████ ██████████ ███ ████████████ ██████ ████████████ █████ █████████ ███ ████ ███ ████████████ █████████ █████ ████████████ █████ █████████ █ ███████████ ██████ ██████████ ██ ████████ ██ ███ ███████████ ███ ████████ ████████████ ████████ ███ ███████████ ███ ██████ ████████ ██ ███ ███████ ███ ███████ ██ ████ ██ ███████████████ ███ ██████████ ██████ █████████ █████ ████████████ ████ █████████.
Serious Adverse Events
ARCADIA 1 Study
During the initial period of the ARCADIA 1 study, 1.0% of patients in the nemolizumab arm and 1.2% of patients in the placebo arm reported any SAE. The following SAEs were reported in 2 or more patients: AD was reported by 2 patients in the nemolizumab arm and 3 patients in the placebo arm. The remaining SAEs by preferred term were reported in fewer than 2 patients.
During the maintenance phase of the ARCADIA 1 study, 4.4% of patients in the nemolizumab every 4 weeks arm, 3.3% in the nemolizumab every 8 weeks arm, 2.2% in the rerandomized placebo arm, and 1.0% in the nonrandomized placebo arm reported any SAEs. The SAEs by preferred term were reported in fewer than 2 patients.
ARCADIA 2 Study
During the initial period of the ARCADIA 2 study, 2.5% of patients in the nemolizumab arm and 1.1% of patients in the placebo arm reported any SAE. SAEs reported in more than 2 patients in the nemolizumab arm included 3 patients reporting infections and infestations, 3 patients reporting musculoskeletal and connective tissue disorders, 3 patients reporting skin and SC tissue disorders, and 2 patients reporting gastrointestinal disorders.
During the maintenance phase of the ARCADIA 2 study, 7.6% of patients in the nemolizumab every 4 weeks arm, 0 in the nemolizumab every 8 weeks arm, 2.6% in the rerandomized placebo arm, and 1.2% in the nonrandomized placebo arm reported any SAEs. There were no SAEs reported in more than 2 patients.
ARCADIA CYCLO Study
During the ARCADIA CYCLO study, 2.2% of patients in the nemolizumab arm and 1.5% of patients in the placebo arm reported SAEs. In the nemolizumab arm, SAEs were reported in 2 patients in the category of infections and infestations. In the placebo arm, SAEs by preferred term were reported in fewer than 2 patients.
Withdrawals Due to AEs
ARCADIA 1 Study
During the initial period of the ARCADIA 1 study, 1.8% of patients in the nemolizumab arm and 4.0% of patients in the placebo arm discontinued study drug treatment due to AEs. In the maintenance period, 1.1% of patients in the nemolizumab every 4 weeks arm, 3.3% in the nemolizumab every 8 weeks arm, 2.2% in the rerandomized placebo arm, and 2.0% in the carryover placebo arm discontinued due to AEs. In both the initial and maintenance periods, AD was the most common reason for discontinuation (initial period: 1.6% of patients in the nemolizumab arm, 4.0% of patients in the placebo arm; maintenance period: 0% in the nemolizumab every 4 weeks arm, 2.2% in the nemolizumab every 8 weeks arm, 1.1% in the rerandomized placebo arm, and 2.0% in the carryover placebo arm).
ARCADIA 2 Study
During the initial period of the ARCADIA 2 study, 3.5% of patients in the nemolizumab arm and 1.1% of patients in the placebo arm reported discontinuing due to AEs. In the maintenance period, 3.8% of patients in the nemolizumab every 4 weeks arm, 2.6% in the nemolizumab every 8 weeks arm, 3.9% in the rerandomized placebo arm, and 2.4% in the nonrandomized placebo arm withdrew due to AEs. In both the initial and maintenance periods, the most common reason for withdrawal of the study drug was AD (initial period: 1.7% of patients in the nemolizumab arm, 0.8% in the placebo arm; maintenance period: 2.5% in the nemolizumab every 4 weeks arm, 2.6% in the nemolizumab every 8 weeks arm, 2.6% in the rerandomized placebo arm, and 2.4% in the carryover placebo arm).
ARCADIA CYCLO Study
████ ██ ████ ██ ████████ ██ ███ ███████████ ███ ███ ████ ██ ████████ ██ ███ ███████ ███ ███████ ███ █████ █████ ███ ███████ ███ ████████ ██ ███ ███████████ ███ ████ █ ███████ ██████ ████ ██ ██████████ ██████ ████ █████████████████ ███ ██████ ███████████ ███ ███████ ███ ████████ ██ ███ ███████ ███ ████ █ ███████ ██████ ████ ██ ███████████████ █████████ █████████ ███ ██████ ███████████.
Mortality
There were no deaths reported in the ARCADIA 1, ARCADIA 2, or ARCADIA CYCLO studies.
Notable Harms
The AESIs identified in the submission for the ARCADIA 1 and ARCADIA 2 studies were injection site reactions, newly diagnosed, or worsening asthma, infections, peripheral edema, and elevated ALT or AST (> 3 × ULN) in combination with elevated bilirubin (> 2 × ULN). The AESIs identified in the submission for the ARCADIA CYCLO studies were injection-related reactions, drug hypersensitivity, infections, COVID-19 infection, asthma, peak expiratory flow rate decrease, and peripheral edema. The submission did not contain details on whether these AESIs were prespecified or identified during the conduct of the studies.
ARCADIA 1 Study
During the initial period of the ARCADIA 1 study, injection-related reactions were reported in 0.2% of patients in the nemolizumab arm, and 0 patients in the placebo arm; 0 patients reported injection-related reactions in the maintenance period. Newly diagnosed or worsening asthma was reported in 5.2% of patients in the nemolizumab arm and 3.4% of patients in the placebo arm during the initial period; and in the maintenance period, 3.3% in the nemolizumab every 4 weeks arm, 6.7% in the nemolizumab every 8 weeks arm, 2.2% in the rerandomized placebo arm, and 5.0% in the carryover placebo arm reported this AE. Infections were reported in 3.2% of patients in the nemolizumab arm and 3.1% in the placebo arm during the initial period; and in the maintenance period, 13.2% in the nemolizumab every 4 weeks arm, 12.2% in the nemolizumab every 8 weeks arm, 13.2% in the rerandomized placebo arm, and 12.0% in the carryover placebo arm reported this AE. Peripheral edema was reported in 1.1% of patients in the nemolizumab arm and 0.3% in the placebo arm during the initial period; and in the maintenance period, 1.1% in the nemolizumab every 4 weeks arm, 2.2% in the nemolizumab every 8 weeks arm, 1.1% in the rerandomized placebo arm, and 0 in the carryover placebo arm reported this AE. Elevated ALT or AST in combination with elevated bilirubin was not reported during the trial.
ARCADIA 2 Study
During the initial period and maintenance periods in the ARCADIA 2 study, no injection-related reactions were reported. Newly diagnosed or worsening asthma was reported in 2.9% of patients in the nemolizumab arm and 3.0% of patients in the placebo arm during the initial period; and in the maintenance period, 5.1% in the nemolizumab every 4 weeks arm, 0% in the nemolizumab every 8 weeks arm, 2.6% in the rerandomized placebo arm, and 0% carryover placebo arm reported this AE. Infections were reported in 3.9% of patients in the nemolizumab arm and 4.6% in the placebo arm during the initial period; and in the maintenance period, 5.1% in the nemolizumab every 4 weeks arm, 7.8% in the nemolizumab every 8 weeks arm, 16.9% in the rerandomized placebo arm, and in the 10.7% carryover placebo arm reported this AE. Peripheral edema was reported in 2.3% of patients in the nemolizumab arm and 0.4% in the placebo arm during the initial period; and in the maintenance period, 0% in the nemolizumab every 4 weeks arm, 0% in the nemolizumab every 8 weeks arm, 2.6% in the rerandomized placebo arm, and 0% in the carryover placebo arm reported this AE. Elevated ALT or AST in combination with elevated bilirubin was not reported during the trial.
ARCADIA CYCLO Study
███ ████ ████████ ████████ ████ ██ ███████ █████ ████ ████████ ██████████ █████ ██ ████████ ██ ███ ███████████ ████ ████ ██ ████████ ██ ███ ███████ █████ ████████ ██ ██████ █████ ████████████ ████ █████████ ███ ████ ██████████ ████ ████ █████████ █████ ████████████ ████ █████████ ████ ████████████████ ███ ████████ ██ ████ ██ ████████ ██ ███ ███████████ ███ ████ ██ ██ ███████ █████ ███ ███ ███████ ██████ ██ ███ ███████ ███ ████████ ██ █████████████████ ████████ ██ ██████████.
Table 27: Summary of Harms Results From the ARCADIA 1 Study (SAS)
AEs | Initial period | Maintenance period | ||||
|---|---|---|---|---|---|---|
Nemolizumab n = 616 | Placebo n = 321 | Nemolizumab q.4.w. to nemolizumab q.4.w. n = 91 | Nemolizumab q.4.w. to nemolizumab q.8.w. n = 90 | Nemolizumab q.4.w. to placebo n = 91 | Placebo to placebo n = 100 | |
Most common (≥ 5% of patients) AEs, n (%) | ||||||
≥ 1 AE | 306 (49.7) | 146 (45.5) | 53 (58.2) | 50 (55.6) | 53 (58.2) | 55 (55.0) |
Infections and infestations | 113 (18.3) | 67 (20.9) | 31 (34.1) | 31 (34.4) | 31 (34.1) | 34 (34.0) |
COVID-19 infection | 10 (1.6) | 6 (1.9) | 10 (11.0) | 9 (10.0) | 6 (6.6) | 10 (10.0) |
Nasopharyngitis | 9 (1.5) | 8 (2.5) | 7 (7.7) | 5 (5.6) | 7 (7.7) | 6 (6.0) |
Upper respiratory tract infection | 9 (1.5) | 14 (4.4) | 3 (3.3) | 3 (3.3) | 5 (5.5) | 9 (9.0) |
Skin and subcutaneous tissue disorders | 113 (18.3) | 45 (14.0) | 11 (12.1) | 10 (11.1) | 13 (14.3) | 14 (14.0) |
Dermatitis atopic | 75 (12.2) | 34 (10.6) | 7 (7.7) | 8 (8.9) | 12 (13.2) | 10 (10.0) |
Respiratory, thoracic, and mediastinal disorders | 58 (9.4) | 28 (8.7) | 11 (12.1) | 10 (11.1) | 12 (13.2) | 7 (7.0) |
Asthma | 33 (5.4) | 13 (4.0) | 3 (3.3) | 6 (6.7) | 5 (5.5) | 5 (5.0) |
Nervous system disorders | 41 (6.7) | 15 (4.7) | 5 (5.5) | 8 (8.9) | 3 (3.3) | 3 (3.0) |
Headache | 28 (4.5) | 11 (3.4) | 5 (5.5) | 5 (5.6) | 3 (3.3) | 1 (1.0) |
Gastrointestinal disorders | 35 (5.7) | 15 (4.7) | 11 (12.1) | 5 (5.6) | 7 (7.7) | 6 (6.0) |
General disorders and administration site conditions | 33 (5.4) | 15 (4.7) | 4 (4.4) | 5 (5.6) | 4 (4.4) | 4 (4.0) |
Musculoskeletal and connective tissue disorders | 33 (5.4) | 12 (3.7) | 5 (5.5) | 4 (4.4) | 4 (4.4) | 4 (4.0) |
Investigations | 18 (2.9) | 11 (3.4) | 2 (2.2) | 5 (5.6) | 2 (2.2) | 4 (4.0) |
SAEs, n (%) | ||||||
Patients with ≥ 1 SAE | 6 (1.0) | 4 (1.2) | 4 (4.4) | 3 (3.3) | 2 (2.2) | 1 (1.0) |
Infections and infestations | 0 | 1 (0.3) | 2 (2.2) | 1 (1.1) | 1 (1.1) | 0 |
Musculoskeletal and connective tissue disorders | 0 | 0 | 2 (2.2) | 0 | 0 | 0 |
Neoplasms benign, malignant, and unspecified | 2 (0.3) | 0 | 0 | 0 | 1 (1.1) | 0 |
Skin and subcutaneous tissue disorders | 2 (0.3) | 3 (0.9) | 0 | 0 | 0 | 0 |
Dermatitis atopic | 2 (0.3) | 3 (0.9) | 0 | 0 | 0 | 0 |
Patients who stopped treatment due to AEs, n (%) | ||||||
Patients who stopped study drug treatment | 11 (1.8) | 13 (4.0) | 1 (1.1) | 3 (3.3) | 2 (2.2) | 2 (2.0) |
Infections and infestations | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Neoplasms benign, malignant, and unspecified | 1 (0.2) | 0 | 0 | 0 | 1 (1.1) | 0 |
Respiratory, thoracic, and mediastinal disorders | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Skin and subcutaneous tissue disorders | 10 (1.6) | 13 (4.0) | 0 | 2 (2.2) | 1 (1.1) | 2 (2.0) |
Dermatitis atopic | 10 (1.6) | 13 (4.0) | 0 | 2 (2.2) | 1 (1.1) | 2 (2.0) |
Patients who discontinued study | 9 (1.5) | 3 (0.9) | 0 | 3 (3.3) | 1 (1.1) | 1 (1.0) |
AESIs, n (%) | ||||||
Injection-related reactions | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
Newly diagnosed asthma or worsening of asthma | 32 (5.2) | 11 (3.4) | 3 (3.3) | 6 (6.7) | 2 (2.2) | 5 (5.0) |
Infections | 20 (3.2) | 10 (3.1) | 12 (13.2) | 11 (12.2) | 12 (13.2) | 12 (12.0) |
Peripheral edema: limbs, bilateral; facial edema | 7 (1.1) | 1 (0.3) | 1 (1.1) | 2 (2.2) | 1 (1.1) | 0 |
Elevated ALT or AST (> 3 × ULN) in combination with elevated bilirubin (> 2 × ULN) | 0 | 0 | 0 | 0 | 0 | 0 |
AE = adverse event; AESI = adverse event of special interest; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SAE = serious adverse event; SAS = safety analysis set; ULN = upper limit of normal.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Table 28: Summary of Harms Results From the ARCADIA 2 Study (SAS)
AEs | Initial period | Maintenance period | ||||
|---|---|---|---|---|---|---|
Nemolizumab n = 616 | Placebo n = 321 | Nemolizumab q.4.w. to nemolizumab q.4.w. n = 91 | Nemolizumab q.4.w. to nemolizumab q.8.w. n = 90 | Nemolizumab q.4.w. to placebo n = 91 | Placebo to placebo n = 100 | |
Most common (≥ 5% of patients) AEs, n (%) | ||||||
≥ 1 AE | 215 (41.4) | 117 (44.5) | 38 (48.1) | 40 (51.9) | 45 (58.4) | 37 (44.0) |
Infections and infestations | 88 (17.0) | 53 (20.2) | 22 (27.8) | 17 (22.1) | 24 (31.2) | 24 (28.6) |
COVID-19 infection | 14 (2.7) | 8 (3.0) | 3 (3.8) | 4 (5.2) | 13 (16.9) | 6 (7.1) |
Nasopharyngitis | 19 (3.7) | 12 (4.6) | 7 (8.9) | 3 (3.9) | 5 (6.5) | 6 (7.1) |
Upper respiratory tract infection | 6 (1.2) | 5 (1.9) | 1 (1.3) | 2 (2.6) | 5 (6.5) | 2 (2.4) |
Skin and subcutaneous tissue disorders | 63 (12.1) | 26 (9.9) | 11 (13.9) | 8 (10.4) | 10 (13.0) | 8 (9.5) |
Dermatitis atopic | 37 (7.1) | 15 (5.7) | 6 (7.6) | 3 (3.9) | 6 (7.8) | 5 (6.0) |
Respiratory, thoracic, and mediastinal disorders | 29 (5.6) | 14 (5.3) | 8 (10.1) | 5 (6.5) | 9 (11.7) | 2 (2.4) |
Musculoskeletal and connective tissue disorders | 27 (5.2) | 9 (3.4) | 6 (7.6) | 5 (6.5) | 7 (9.1) | 2 (2.4) |
Nervous system disorders | 25 (4.8) | 14 (5.3) | 4 (5.1) | 3 (3.9) | 3 (3.9) | 4 (4.8) |
Gastrointestinal disorders | 22 (4.2) | 16 (6.1) | 7 (8.9) | 4 (5.2) | 5 (6.5) | 1 (1.2) |
Investigations | 13 (2.5) | 10 (3.8) | 4 (5.1) | 3 (3.9) | 3 (3.9) | 2 (2.4) |
Injury, poisoning, and procedural complications | 0 | 0 | 2 (2.5) | 5 (6.5) | 1 (1.3) | 1 (1.2) |
SAEs, n (%) | ||||||
Patients with ≥ 1 SAE | 13 (2.5) | 3 (1.1) | 6 (7.6) | 0 (0.0) | 2 (2.6) | 1 (1.2) |
Gastrointestinal disorders | 2 (0.4) | 1 (0.4) | 1 (1.3) | 0 | 0 | 0 |
Infections and infestations | 3 (0.6) | 2 (0.8) | 1 (1.3) | 0 | 0 | 0 |
Musculoskeletal and connective tissue disorders | 3 (0.6) | 0 | 1 (1.3) | 0 | 0 | 0 |
Intervertebral disc protrusion | 2 (0.4) | 0 | 1 (1.3) | 0 | 0 | 0 |
Skin and subcutaneous tissue disorders | 3 (0.6) | 0 | 0 | 0 | 0 | 0 |
Dermatitis atopic | 3 (0.6) | 0 | 0 | 0 | 0 | 0 |
Patients who stopped treatment due to AEs, n (%) | ||||||
Patients who stopped study drug treatment | 18 (3.5) | 3 (1.1) | 3 (3.8) | 2 (2.6) | 3 (3.9) | 2 (2.4) |
Blood and lymphatic system disorders | 2 (0.4) | 0 | 0 | 0 | 0 | 0 |
Lymphadenopathy | 2 (0.4) | 0 | 0 | 0 | 0 | 0 |
General disorders and administration site conditions | 2 (0.4) | 0 | 0 | 0 | 0 | 0 |
Edema peripheral | 2 (0.4) | 0 | 0 | 0 | 0 | 0 |
Psychiatric disorders | 2 (0.4) | 0 | 0 | 0 | 0 | 0 |
Respiratory, thoracic, and mediastinal disorders | 2 (0.4) | 0 | 0 | 0 | 1 (1.3) | 0 |
Skin and subcutaneous tissue disorders | 10 (1.9) | 3 (1.1) | 2 (2.5) | 2 (2.6) | 2 (2.6) | 2 (2.4) |
Dermatitis atopic | 9 (1.7) | 2 (0.8) | 2 (2.5) | 2 (2.6) | 2 (2.6) | 2 (2.4) |
Patients who discontinued study | 15 (2.9) | 3 (1.1) | 3 (3.8) | 2 (2.6) | 3 (3.9) | 1 (1.2) |
AESIs, n (%) | ||||||
Injection-related reactions | 0 | 0 | 0 | 0 | 0 | 0 |
Newly diagnosed asthma or worsening of asthma | 15 (2.9) | 8 (3.0) | 4 (5.1) | 0 | 2 (2.6) | 0 |
Infections | 20 (3.9) | 12 (4.6) | 4 (5.1) | 6 (7.8) | 13 (16.9) | 9 (10.7) |
Peripheral edema: limbs, bilateral; facial edema | 12 (2.3) | 1 (0.4) | 0 | 0 | 2 (2.6) | 0 |
Elevated ALT or AST (> 3 × ULN) in combination with elevated bilirubin (> 2 × ULN) | 0 | 0 | 0 | 0 | 0 | 0 |
AE = adverse event; AESI = adverse event of special interest; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SAE = serious adverse event; SAS = safety analysis set; ULN = upper limit of normal.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Table 29: Summary of Harms Results From the ARCADIA CYCLO Study (SAS)
AEs | ARCADIA CYCLO study | |
|---|---|---|
Nemolizumab n = 137 | Placebo n = 137 | |
Most common (≥ 5% of patients) AEs, n (%) | ||
≥ 1 AE | ██ ██████ | ██ ██████ |
Infections and infestations | ██ ██████ | ██ ██████ |
COVID-19 infection | ██████ | | █████ |
Investigations | ██████ | ██████ |
Musculoskeletal and connective tissue disorders | ██ █████ | ██████ |
Respiratory, thoracic, and mediastinal disorders | ██ █████ | ██████ |
Skin and subcutaneous tissue disorders | ██ █████ | ██ ██████ |
Dermatitis atopic | ██ █████ | ██████ |
SAEs, n (%) | ||
Patients with ≥ 1 SAE | 3 (2.2) | 2 (1.5) |
Infections and infestations | ██████ | █ |
Patients who stopped treatment due to AEs, n (%) | ||
Patients who stopped taking the study drug | ██████ | ██████ |
Blood and lymphatic system disorders | █ | ██████ |
Thrombocytosis | █ | ██████ |
General disorders and administration site conditions | ██████ | █ |
Edema peripheral | ██████ | █ |
Immune system disorders | ██████ | █ |
Drug hypersensitivity | ██████ | █ |
Psychiatric disorders | █ | ██████ |
Psychotic symptom | █ | ██████ |
Skin and subcutaneous tissue disorders | ██████ | ██████ |
Dermatitis atopic | ██████ | ██████ |
Patients who discontinued study | ██████ | ██████ |
AESIs, n (%) | ||
Injection-related reaction (urticaria) | █ | ██████ |
Drug hypersensitivity | ██████ | █ |
Infections | ██████ | ██████ |
COVID-19 infection | ██████ | ██████ |
Asthma | ██████ | ██████ |
Peak expiratory flow rate decreased | ██████ | ██████ |
Peripheral edema: limbs, bilateral; facial edema | ██████ | █ |
AE = adverse event; AESI = adverse event of special interest; SAE = serious adverse event; SAS = safety analysis set.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.10
Critical Appraisal
Internal Validity
In all of the ARCADIA studies (ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO), the procedures for randomization, treatment allocation, blinding, and study drug administration were all described and likely at low risk of bias; however, the study design is subject to some limitations. In the ARCADIA 1 and ARCADIA 2 studies, only patients meeting the definition of clinical responder in the studies (with an IGA score of 0 [clear] or 1 [almost clear] or EASI-75) continued from the initial period onto the maintenance period. This imparts a response bias for the maintenance phase as the patients included in the maintenance phase are an enriched population of patients who have already responded to treatment by 16 weeks. It is not known whether patients who did not have a favourable outcome to treatment had specific common characteristics that would have impacted their likelihood of responding to treatment. The duration of initial treatment period, while generally consistent with studies for other treatments reimbursed for moderate to severe AD, may not be long enough to obtain complete treatment response, as the clinical experts consulted for this review noted that a trial of up to 6 months is used in clinical practice, which is a relevant consideration for all ARCADIA trials. There was no run-in period for the ARCADIA CYCLO study, while patients’ background treatment was standardized in the ARCADIA 1 and ARCADIA 2 studies. As patients in the ARCADIA CYCLO study have more severe disease, this may impact the certainty in the results as patients’ background therapies in the ARCADIA CYCLO study could have differed in efficacy and type of product.
With regards to the statistical analysis across trials, the assessment of outcomes for the coprimary and key secondary outcomes in the initial period is likely at lower risk of bias due to being controlled for multiplicity; however, the order of hypothesis testing for the outcomes is unknown and therefore the alpha spending among the list of outcomes, or when testing might have ended, is also unknown. In the ARCADIA 1 and ARCADIA 2 studies, the results of the sensitivity analyses testing different methods of classifying missing clinical responders and clinical nonresponders were also consistent with the main analysis, which suggests the results are reasonably robust. However the statistical analysis methods are subject to some limitations that impact internal validity, and which increase the uncertainty in the results. In the ARCADIA 1 and ARCADIA 2 studies, there were several protocol amendments, although it is unclear how many patients were impacted by the modification, or what impact this may have had on the results. Per the individual statistical analysis plan for the ARCADIA 1 and ARCADIA 2 studies, no hypothesis testing was conducted on outcomes in the maintenance phase’ however, the pooled Clinical Study Report described statistical tests comparing the nemolizumab arms to the rerandomized placebo group. In addition, there was no control of multiplicity for the secondary outcomes in the initial period (change from baseline in PP-NRS, EASI, DLQI, and CDLQI) and maintenance period (all outcomes); therefore, there is a risk of increased type I error for these outcomes. The study populations of the ARCADIA 1 and ARCADIA 2 studies appeared broadly similar in terms of disposition because the studies employed identical designs, inclusion and exclusion criteria, as well as analysis methods. However, these statistical limitations mean that results from the maintenance period should only be considered supportive evidence of the impact of nemolizumab.
External Validity
Patients enrolled in the ARCADIA 1 and ARCADIA 2 studies were required to have an EASI score of 16 or more (≥ 20 in the ARCADIA CYCLO study), and IGA score of 3 or more in both studies. An EASI score of 7.1 to 21.0 is considered moderate AD, and severe AD ranges from 21.1 to 50.0.9 An IGA score of 3 is considered moderate AD. As such, patients enrolled in the ARCADIA trials may have more severe disease, and therefore the results may not be generalizable to all patients with moderate AD, depending on the disease severity criteria used. However, it is worth noting that EASI of 16 and IGA of 3 are consistent with other drugs evaluated for moderate to severe AD.
All the ARCADIA studies excluded patients with asthma, COPD, and certain medications which cause sedative effects; the results would therefore not be generalizable to patients with these conditions and taking these medications. Patients who had not improved after 16 weeks of treatment with dupilumab were also excluded from the ARCADIA 1 and ARCADIA 2 trials. The reimbursement request includes patients who are refractory to systemic immunosuppressant therapies, which could include dupilumab; therefore, results from the trials will not be generalizable to patients with a history of dupilumab exposure. The clinical experts consulted for this review noted that these patients could be considered candidates for treatment with nemolizumab in clinical practice. Subgroup analyses conducted in the ARCADIA 1 and ARCADIA 2 studies on prior use of systemic therapy, biologic therapy, or dupilumab did not show consistent trends between the 2 studies and some subgroups had small sample sizes; thus, firm conclusions could not be drawn. In addition, the fact that only patients meeting the study definition of clinical responder were kept in the maintenance phase of the ARCADIA 1 and ARCADIA 2 studies means any results after 16 weeks may not include all the patients represented in the study enrolment criteria.
The ARCADIA trials were all placebo-controlled trials, which allows for adequate evaluation of the treatment effect of nemolizumab; however, it may overestimate the treatment effects. Patients in the ARCADIA 1 and ARCADIA 2 studies had their background therapy stabilized during the run-in period before randomization. There was a high placebo response observed in the ARCADIA trials. It is unclear whether this is due to the background therapy received by all patients, although this also impacts patients receiving nemolizumab. Nemolizumab monotherapy was not evaluated in the evidence submitted, and therefore delineating the true impact of nemolizumab on the disease remains unknown and may overestimate the results of the ARCADIA studies. It is worth noting that patients in the real world would continue to receive their background therapies, as was done in the ARCADIA studies. Across all 3 trials, treatment adherence was reported to be high ██ █████ the levels of adherence observed may not be representative of clinical practice settings.
Most patients in the ARCADIA 1 and ARCADIA 2 studies were aged older than 18 years, while only 13.7% to 17.4% of patients were between the ages of 12 and 17 years. Outcomes specific to this population (i.e., the CDLQI) were highly uncertain because they come from a small proportion of patients in the study. Additionally, other results may not be generalized to this population; however, subgroup analyses by age group were generally consistent with the primary analysis.
In addition to the study design, the treatment history described in the inclusion and exclusion criteria does not exactly match the requested reimbursement criteria; the ARCADIA 1 and ARCADIA 2 trials did not require patients to have previous exposure to immunomodulatory therapies, and the ARCADIA CYCLO study only required exposure or inadvisability for CsA. In the ARCADIA 1 and ARCADIA 2 studies, less than 40% of patients had prior exposure to immunomodulatory treatment, less than 15% had exposure to CsA, and approximately 5% had had exposure to dupilumab. Therefore, it is uncertain how applicable the overall results will be to patients with these treatment histories versus patients who have not previously received treatment with systemic therapies, or who have been treated with other advanced systemic therapies. However, subgroup analyses by treatment history conducted in the ARCADIA 1 and ARCADIA 2 studies, while including small sample sizes and not perfectly consistent between the 2 studies, provide some supportive evidence of benefit for nemolizumab relative to placebo for IGA success, EASI-75, PP-NRS improvement of 4 points or more, and PP-NRS less than 2. In addition, according to the clinical experts, the criteria for refractoriness to CsA in the ARCADIA CYCLO study were subjective and therefore might not be representative of all patients who might be unsuccessful with CsA.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.57,58
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. For the proportion of patients with IGA success at week 16, proportion of patients with EASI-75 at week 16, and both outcomes relating to PP-NRS (proportion of patients with improvement of ≥ 4 points and proportion of patients with PP-NRS < 2 at week 16), the presence or absence of an important effect was based on thresholds informed by the clinical experts consulted for this review. For the change from baseline in CDLQI and DLQI, the presence or absence of an important effect was based on a threshold provided by the sponsor.
For the GRADE assessments, findings from the ARCADIA 1 and ARCADIA 2 studies were considered together and summarized narratively per outcome because these studies were nearly identical in population, interventions, design, and outcome measures. Findings from ARCADIA CYCLO study were summarized individually as the study population and outcome measures were different.
Results of GRADE Assessments
Nemolizumab Versus Placebo
Table 2 presents the GRADE summary of findings for nemolizumab versus placebo in patients with moderate to severe AD. Table 3 presents the GRADE summary of findings for nemolizumab versus placebo in patients with moderate to severe AD who have either had an inadequate response to CsA or for whom CsA is not advisable.
LTE Studies
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
The ARCADIA LTE study (NCT03989206) is an ongoing phase III, single-arm, multicentre, prospective study to evaluate the long-term safety and efficacy of SC nemolizumab 30 mg every 4 weeks in adult and adolescent patients with moderate to severe AD, when administered with background TCS, with or without TCI, over a 4-year (200 week) treatment period.
Results were from 1 interim analysis (data cut-off date of September 30, 2022) up to 56 weeks of treatment, as the sponsor noted that sample sizes beyond this time point were too small to draw meaningful conclusions. Preliminary data from the second interim analysis (data cut-off date of July 21, 2024) were submitted up to 104 weeks of follow-up, but this analysis was not yet complete and full results were not available at the time of submission. The study is estimated to be completed in August 2026.
Populations
A total of 1,751 patients were enrolled in the study, including 89 patients from Canada. The study population included patients from prior nemolizumab AD studies, including a phase IIb, 24-week dose-ranging study59; a phase II, 16-week adolescent pharmacokinetics and safety study60; a phase II, 16-week vaccination safety study61; a phase II, 24-week drug-drug interaction study62; a phase IIIb, 16-week study ARCADIA CYCLO trial13; and the 2 phase III pivotal ARCADIA 1 and ARCADIA 2 trials.11,12 Adolescents from selected sites in Australia, Austria, Canada, and the US, who had not previously participated in a nemolizumab study (hereafter referred to as “new adolescent patients”) were also eligible.
Inclusion criteria for the ARCADIA LTE study were consistent with that of the lead-in studies. For new adolescents entering the LTE study, key inclusion criteria included the presence of chronic AD for at least 2 years involving at least 10% BSA involvement, EASI score of 16 or more, IGA score of 3 or more, SCORing Atopic Dermatitis visual analogue scale of 4 or more, and an inadequate response to TCS treatments (with or without TCI). Patients were excluded from the ARCADIA LTE study if they had a history of COPD and/or chronic bronchitis, body weight of less than 30 kg, uncontrolled asthma in the preceding 3 months, asthma exacerbation requiring hospitalization in the preceding 12 months, had experienced an AE in previous nemolizumab study, or had received restricted prior treatments.
To maintain the blind of ongoing lead-in studies (RD.06.SPR.118161, RD.06.SPR.118169, RD.06.SPR.118380, RD.06.SPR.201591), enrolment into the LTE study was not restricted by prior blinded treatment assignment.
Baseline Characteristics
Refer to Table 30 for a summary of baseline characteristics of patients in the first interim analysis of the ARCADIA LTE study. The mean age of patients in the ARCADIA LTE study was 33.7 years (SD = 15.8 years). Of all patients, 49.1% were female, and the proportion of female patients was higher in patients who were retreated (62.9%) compared to other groups (ranging from 46.6% to 52.9%). Most patients in the LTE study were aged between 18 to 65 years (80.9%), with 14.6% being adolescents (aged 12 to 17 years), and 4.5% aged older than 65 years. Mean weight at baseline was 75.7 kg overall, and similar in patients aged 18 to 65 years (77.8 kg) compared to those aged older than 65 years (79.8 kg). Disease severity, as measured by EASI and IGA, was lower in patients who were retreated with nemolizumab compared to patients who have not previously received treatment and those who enrolled in a blinded lead-in study. Mean DLQI and CDLQI score at baseline was lower in those retreated (5.5; SD = 5.91 and 5.0; SD = 5.15, respectively) compared to those who have not previously received treatment (9.1; SD = 7.25 and 9.1; SD = 6.00).
Table 30: Summary of Baseline Characteristics in the ARCADIA LTE Study — First Interim Analysis
Characteristic | Nemolizumab 30 mg q.4.w. | By treatment before the LTE | ||||
|---|---|---|---|---|---|---|
Previously treated with nemolizumab | Patients who have not previously received treatment with nemolizumab | Blinded lead-in study | ||||
All | Continuous nemolizumab | Re-treatment | ||||
n = 1,740 | n = 962 | n = 792 | n = 170 | n = 536 | n = 242 | |
Demographic characteristics | ||||||
Age (years), mean (SD) | 33.7 (15.8) | 33.8 (16.4) | 33.7 (15.9) | 34.4 (18.9) | 32.6 (15.9) | 35.6 (12.3) |
Age group, n (%) | ||||||
12 to 17 years | 254 (14.6) | 141 (14.7) | 110 (13.9) | 31 (18.2) | 107 (20.0) | 6 (2.5) |
18 to 65 years | 1408 (80.9) | 765 (79.5) | 642 (81.1) | 123 (72.4) | 410 (76.5) | 233 (96.3) |
> 65 years | 78 (4.5) | 56 (5.8) | 40 (5.1) | 16 (9.4) | 19 (3.5) | 3 (1.2) |
Female sex, n (%) | 855 (49.1) | 476 (49.5) | 369 (46.6) | 107 (62.9) | 251 (46.8) | 128 (52.9) |
Region, n (%) | ||||||
Asia Pacific | 145 (8.3) | 87 (9.0) | 81 (10.2) | 6 (3.5) | 58 (10.8) | 0 |
Europe | 1,041 (59.8) | 609 (63.3) | 505 (63.8) | 104 (61.2) | 323 (60.3) | 109 (45.0) |
North America | 554 (31.8) | 266 (27.7) | 206 (26.0) | 60 (35.3) | 155 (28.9) | 133 (55.0) |
Race, n (%) | ||||||
American Indian or Alaska Native | 3 (0.2) | 1 (0.1) | 1 (0.1) | 0 | 1 (0.2) | 1 (0.4) |
Asian | 225 (12.9) | 134 (13.9) | 120 (15.2) | 14 (8.2) | 73 (13.6) | 18 (7.4) |
Black or African American | 114 (6.6) | 46 (4.8) | 32 (4.0) | 14 (8.2) | 32 (6.0) | 36 (14.9) |
Native Hawaiian or other Pacific Islander | 2 (0.1) | 2 (0.2) | 2 (0.3) | 0 | 0 | 0 |
White | 1,370 (78.7) | 768 (79.8) | 628 (79.3) | 140 (82.4) | 418 (78.0) | 184 (76.0) |
Other or multiple | 26 (1.5) | 11 (1.1) | 9 (1.1) | 1(0.6) | 12 (2.2) | 3 (1.2) |
Disease characteristics | ||||||
EASI score, mean (SD) | 13.34 (12.3) | 12.03 (11.9) | 13.08 (12.2) | 7.11 (8.8) | 16.24 (12.9) | 12.17 (11.0) |
IGA score, n (%) | ||||||
Clear | 158 (9.1) | 106 (11.0) | 76 (9.6) | 30 (17.6) | 41 (7.6) | 11 (4.5) |
Almost clear | 257 (14.8) | 168 (17.5) | 120 (15.2) | 48 (28.2) | 54 (10.1) | 35 (14.5) |
Mild | 478 (27.5) | 267 (27.8) | 222 (28.0) | 45 (26.5) | 131 (24.4) | 80 (33.1) |
Moderate | 687 (39.5) | 346 (36.0) | 304 (38.4) | 42 (24.7) | 241 (45.0) | 100 (41.3) |
Severe | 158 (9.1) | 74 (7.7) | 69 (8.7) | 5 (2.9) | 69 (12.9) | 15 (6.2) |
Not reported | 2 (0.1) | 1 (0.1) | 1 (0.1) | 0 | 0 | 1 (0.4) |
DLQI, mean (SD) | 7.6 (6.92) | 6.6 (6.57) | 6.8 (6.67) | 5.5 (5.91) | 9.1 (7.25) | 8.1 (6.96) |
CDLQI, mean (SD) | 6.9 (6.17) | 5.3 (5.83) | 5.4 (6.06) | 5.0 (5.15) | 9.1 (6.00) | 10.0 (7.07) |
CDLQI = Children’s Dermatology Life Quality Index; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; IGA = Investigator Global Assessment; LTE = long-term extension; q.4.w. = every 4 weeks; SD = standard deviation.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Source: ARCADIA LTE Interim Clinical Study Report.63
Interventions
The ARCADIA LTE study design consists of a 4-week screening period, a 200-week treatment period, and an 8-week follow-up period. Participants received nemolizumab (30 mg) every 4 weeks via SC injection in the treatment period. The same dose (30 mg with a 60 mg loading dose) was administered to adolescents aged 12 to 17 years and adults in this study. Participants were able to continue to use background TCS and/or TCI.
Participants from the ARCADIA 1 and ARCADIA 2 studies who received nemolizumab every 8 weeks in the maintenance period switched to every 4 weeks for the LTE study. It was noted by the sponsor that when the LTE study was designed, the data from every 8 weeks dosing in the pivotal trials were not yet available and all patients were assigned to receive dosing every 4 weeks from baseline.
Outcomes
The primary outcomes in the ARCADIA LTE study were the incidence and severity of AEs throughout the study, the incidence of SAEs throughout the study, and the incidence and severity of AESIs throughout the study. Secondary outcomes aligned with outcomes assessed in the ARCADIA 1 and ARCADIA 2 studies that were identified as important to this review, and included the IGA, EASI, and DLQI or CDLQI. Assessment time points in year 1 of the ARCADIA LTE study are provided in Table 31.
Table 31: Outcomes Assessment Time Points in Year 1 of the ARCADIA LTE Study
Outcomes | Assessment time points |
|---|---|
Safety assessments and AEs | Baseline and q.4.w. to week 208 |
Efficacy assessments | |
IGA, EASI | Baseline, week 4, week 8, week 20, week 32, week 44, week 56, week 80, week 104, week 128, week 152, week 176, and week 200 |
PRO assessments | |
DLQI or CDLQI | Baseline, week 20, week 56, week 80, week 104, week 128, week 152, week 176, and week 200 |
AE = adverse event; CDLQI = Children’s Dermatology Life Quality Index; DLQI = Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; IGA = Investigator Global Assessment; LTE = long-term extension; PRO = patient-reported outcome; q.4.w. = every 4 weeks.
Source: ARCADIA LTE Interim Clinical Study Report.63
Statistical Analysis
Sample Size Calculation
No formal sample size calculations were performed for this LTE study. A sample size of approximately 1,700 patients, including adult and adolescent patients (aged 12 to 17 years), was projected to support long-term safety and efficacy evaluation of nemolizumab.
Method of Analysis
No formal hypothesis testing was performed in the ARCADIA LTE study. All efficacy assessments were summarized by visit and safety data, based on the safety population, was summarized by study period (treatment period and follow-up period). Screened patients were defined as patients who signed the informed consent form. The safety population was defined as all patients who received at least 1 dose of the study drug.
Baseline Assessment
Two different baselines were used. The LTE baseline was defined as the last nonmissing value before the date of first treatment in the LTE study, while the lead-in study baseline was defined as the last nonmissing value before the first dose of the study drug of the lead-in studies. This definition applied only to patients who rolled over to the LTE study within 6 months of the completion of the lead-in study (i.e., patients whose interval between the LTE baseline and the date of last study drug administration in the lead-in study was ≤ 6 months). For patients who enrolled directly into the LTE study or who enrolled in the LTE study more than 6 months after the last lead-in study dose, the lead-in study baseline was not applicable.
Handling of Missing Values
For AEs and concomitant medications and procedures, any missing assessment times had imputed times for the purposes of assessing treatment emergence for AEs or classifying medications into prior or concomitant. If an AE had the start date completely missing and the stop date on or after the first dose date of the study drug, the AE was considered as a treatment-emergent AE. If a medication had the stop date completely missing, the medication was considered as ongoing and concomitant. If the start date of a medication was completely missing and impossible to identify differently by the stop date, this medication was considered as concomitant.
Results
Patient Disposition
Information pertaining to patient disposition was available for the first interim analysis only (data cut-off date September 30, 2022). A total of 1,776 patients were screened, and 1,751 patients were enrolled. Of all the patients enrolled, 0.6% did not receive the study drug and were excluded from the safety population, and 24.1% discontinued treatment. Overall, the most common reasons for treatment discontinuation were patient request (13.3%) and AEs (3.8%). The reasons for discontinuation were similar between patients who received continuous nemolizumab, those who were retreated, those who had not previously received treatment with nemolizumab, and those who enrolled from a lead-in study.
Table 32: Patient Disposition in the ARCADIA LTE Study — First Interim Analysis
Patient disposition | Nemolizumab 30 mg q.4.w. |
|---|---|
Patients screened, N | 1,776 |
Patients enrolled, n | 1,751 |
Treated, n (%) | 1,740 (99.4) |
Completed treatment, n (%) | 0 |
Discontinued treatment, n (%) | 422 (24.1) |
Primary reasons for study discontinuation of treatment (≥ 2%), n (%) | |
Pregnancy | 2 (0.1) |
Lack of efficacy | 45 (2.6) |
Adverse event | 67 (3.8) |
Lost to follow-up | 48 (2.7) |
Patient’s request | 233 (13.3) |
Patients entered into the follow-up period | 293 (16.7) |
Patients completed the study | 0 |
Patients discontinued from the study | 392 (22.4) |
Primary reason for discontinuation from the study (≥ 2%), n (%) | |
Lack of efficacy | 42 (2.4) |
Adverse event | 59 (3.4) |
Lost to follow-up | 45 (2.6) |
Patient’s request | 220 (12.6) |
Patients completed follow-up | 163 (9.3) |
LTE = long-term extension; q.4.w. = every 4 weeks.
Source: ARCADIA LTE Interim Clinical Study Report.63
Exposure to Study Treatments
In the first interim analysis, patients had a mean of 13.7 planned total doses and received a mean of 13.2 total doses, and 31.3% missed at least 1 dose of the study drug. The mean and median treatment durations were 322.2 days and 312.5 days, respectively. Most patients (58.0%) had received between 6 to 18 months of treatment at the time of data cut-off. Of the 1,740 patients who received at least 1 dose of nemolizumab, the percentage of patients with 365 days or more overall treatment exposure were as follows: 7.8% of adolescent patients (aged 12 to 17 years), 50.2% of patients aged 18 to 65 years, and 2.3% of patients aged older than 65 years. Mean treatment compliance was 95.1% overall and 95.5% in the first year of the LTE study.
Results on the exposure to study medication and the duration of treatment from the second interim analysis were not yet available.
Concomitant and Rescue Medications
Almost all patients (99.9%) received at least 1 concomitant medication; the most common concomitant medications were mometasone furoate (47.2%), other emollients and protectives (27.1%), tacrolimus monohydrate (25.1%), and tozinameran (23.1%). Of note, mometasone furoate and tacrolimus monohydrate were considered background therapies.
The use of very high-potency TCS (group IV) was prohibited during the study and was to be reported as a protocol deviation unless used as a rescue medication. Among the 70 patients who received a very potent TCS (group IV), 43 used it as a rescue medication. The percentage of patients with at least 1 background topical therapy during the treatment period was 89.1%. The most frequently reported background topical therapy was mometasone furoate (47.2%).
Results on concomitant medications and topical background therapy from the second interim analysis were not yet available.
Efficacy
Refer to Table 33 for a summary of efficacy results from the ARCADIA LTE study (first interim analysis).
Proportion of Patients With IGA Success
At LTE baseline, 23.9% of all patients experienced IGA success (defined as an IGA score between 0 to 1). In terms of treatment before the LTE study, 28.5% of patients previously treated with nemolizumab and 17.7% of patients who have not previously received treatment with nemolizumab experienced an IGA score of 0 to 1.
At week 20, 42.5% of all patients in the LTE study experienced IGA success. By prior treatment, 45.6% of patients previously treated with nemolizumab and 36.7% of patients who have not previously received treatment with nemolizumab experienced an IGA score of 0 to 1.
At week 56, 48.9% of all patients in the LTE study experienced IGA success. By prior treatment, 47.1% of patients previously treated with nemolizumab and 49.0% of patients who have not previously received treatment with nemolizumab experienced an IGA score of 0 to 1.
Proportion of Patients With EASI-75
EASI-75 was defined as a 75% or higher improvement in EASI from baseline.
At LTE baseline, 33.7% of all patients achieved EASI-75 improvement from lead-in study baseline. By prior treatment, 38.1% of patients previously treated with nemolizumab and 24.0% of patients who have not previously received treatment with nemolizumab achieved EASI-75 improvement from lead-in baseline.
At week 20, 66.3% of patients achieved EASI-75 improvement from lead-in baseline and 34% achieved EASI-75 improvement from LTE baseline. By prior treatment, the proportion of patients achieving EASI-75 from lead-in and LTE baseline were 69.3% and 32.6% for those previously treated with nemolizumab and 61.5% and 36.2% for patients who have not previously received treatment with nemolizumab, respectively.
At week 56, 75.6% of patients achieved EASI-75 improvement from lead-in baseline and 57.4% achieved EASI-75 improvement from LTE baseline. By prior treatment, the proportion of patients achieving EASI-75 from lead-in and LTE baseline were 73.0% and 52.5% for those previously treated with nemolizumab and 78.7% and 62.3% for patients who have not previously received treatment with nemolizumab, respectively.
Change From Baseline in DLQI Total Score
At LTE baseline, the mean DLQI was 7.6 (SD = 6.92) across all patients in the LTE study, 6.6 (SD = 6.57) for patients previously treated with nemolizumab, and 9.1 (7.25) in the group who have not previously received treatment with nemolizumab.
At week 20, the mean DLQI score was 4.7 (SD = 5.77) across all patients in the LTE study. Patients previously treated with nemolizumab had a mean DLQI score of 4.6 (SD = 5.84), with a mean change from lead-in baseline and LTE baseline of −10.4 (SD = 7.52) and −2.0 (SD = 5.54), respectively. Patients who have not previously received treatment with nemolizumab had a mean DLQI score of 5.0 (SD = 5.55), with a mean change from lead-in baseline and LTE baseline of −10.2 (SD = 7.06) and −3.9 (SD = 6.02), respectively.
At week 56, the mean DLQI score was 3.9 (SD = 4.72) across all patients in the LTE study. Patients previously treated with nemolizumab had a mean DLQI score of 4.2 (SD = 4.93), with a mean change from lead-in baseline and LTE baseline of −11.1 (SD = 7.32) and −3.6 (SD = 6.36), respectively. Patients who have not previously received treatment with nemolizumab had a mean DLQI score of 3.7 (SD = 4.58), with a mean change from lead-in baseline and LTE baseline of −12.2 (SD = 6.92) and −6.4 (SD = 6.71), respectively.
Change From Baseline in CDLQI Total Score
At LTE baseline, the mean CDLQI score was 6.9 (SD = 6.17) across all patients in the LTE study, 5.3 (SD = 5.83) for patients previously treated with nemolizumab and 9.1 (SD = 6.00) in the group who have not previously received treatment with nemolizumab.
At week 20, the mean CDLQI score was 4.3 (SD = 4.64) across all patients in the LTE study. Patients previously treated with nemolizumab had a mean CDLQI score of 4.1 (SD = 4.62), with a mean change from lead-in baseline and LTE baseline of −8.3 (SD = 6.15) and −1.9 (SD = 4.41), respectively. Patients who have not previously received treatment with nemolizumab had a mean CDLQI score of 4.4 (SD = 4.18), with a mean change from lead-in baseline and LTE baseline of −8.3 (SD = 6.43) and −5.1 (SD = 5.65), respectively.
At week 56, the mean CDLQI score was 3.4 (SD = 4.48) across all patients in the LTE study. Patients previously treated with nemolizumab had a mean CDLQI score of 2.1 (SD = 2.02), with a mean change from lead-in baseline and LTE baseline of −9.2 (SD = 6.09) and −4.5 (SD = 5.11), respectively. Patients who have not previously received treatment with nemolizumab had a mean CDLQI score of 4.4 (SD = 5.28), with a mean change from lead-in baseline and LTE baseline of -–8.2 (SD = 6.80) and −6.3 (SD = 6.77), respectively.
Table 33: Summary of Efficacy Results From the ARCADIA LTE Study — First Interim Analysis
Characteristic | Nemolizumab 30 mg q.4.w. | By treatment before the LTE | ||||
|---|---|---|---|---|---|---|
Previously treated with nemolizumab | Patients who have not previously received treatment with nemolizumab | Blinded lead-in study | ||||
All | Continuously received nemolizumab | Re-treatment | ||||
n = 1,740 | n = 962 | n = 792 | n = 170 | n = 536 | n = 242 | |
Proportion of patients with IGA success | ||||||
LTE baseline, n | 1,738 | 961 | 791 | 170 | 536 | 241 |
IGA score 0 to 1, n (%) | 415 (23.9) | 274 (28.5%) | 196 (24.8) | 78 (45.9) | 95 (17.7) | 46 (19.1) |
Week 20, n | 1,427 | 859 | 711 | 148 | 471 | 97 |
IGA score 0 to 1, n (%) | 607 (42.5) | 392 (45.6) | 296 (41.6) | 96 (64.9) | 173 (36.7) | 42 (43.3) |
Week 56, n | 741 | 433 | 389 | 44 | 253 | 55 |
IGA score 0 to 1, n (%) | 362 (48.9) | 204 (47.1) | 175 (45.0) | 29 (65.9) | 124 (49.0) | 34 (61.8) |
Proportion of patients with EASI-75 | ||||||
LTE baseline, n | 1,672 | 938 | 790 | 148 | 495 | 239 |
EASI-75 (lead-in), n (%) | 563 (33.7) | 357 (38.1) | 253 (32.0) | 104 (70.3) | 119 (24.0) | 87 (36.4) |
Week 20 | ||||||
n (lead-in/LTE) | 1,368/1,301 | 838/772 | 711/647 | 127/125 | 434/437 | 96/92 |
EASI-75 (lead-in), n (%) | 907 (66.3) | 581 (69.3) | 468 (65.8) | 113 (89.0) | 267 (61.5) | 59 (61.5) |
EASI-75 (LTE), n (%) | 442 (34.0) | 252 (32.6) | 197 (30.4) | 55 (44.0) | 158 (36.2) | 32 (34.8) |
Week 56 | ||||||
n (lead-in/LTE) | 709/711 | 415/413 | 389/376 | 26/37 | 239/247 | 55/51 |
EASI-75 (lead-in), n (%) | 536 (75.6) | 303 (73.0) | 282 (72.5) | 21 (80.8) | 188 (78.7) | 45 (81.8) |
EASI-75 (LTE), n (%) | 408 (57.4) | 217 (52.5) | 193 (51.3) | 24 (64.9) | 154 (62.3) | 37 (72.5) |
Change from baseline in DLQI total score | ||||||
LTE baseline, n | 1,411 | 805 | 674 | 131 | 426 | 180 |
Mean (SD) | 7.6 (6.92) | 6.6 (6.57) | 6.8 (6.67) | 5.5 (5.91) | 9.1 (7.25) | 8.1 (6.96) |
Week 20 | ||||||
Patients with nonmissing data, n | 1,286 | 783 | 655 | 128 | 410 | 93 |
Mean (SD) | 4.7 (5.77) | 4.6 (5.84) | 4.8 (5.95) | 3.4 (5.08) | 5.0 (5.55) | 4.3 (6.13) |
Change from lead-in baseline, n | 1,135 | 747 | 637 | 110 | 388 | 0 |
Mean (SD) | −10.3 (7.36) | −10.4 (7.52) | −10.3 (7.59) | −10.9 (7.13) | −10.2 (7.06) | NA |
Change from LTE baseline, n | 1,204 | 754 | 630 | 124 | 390 | 60 |
Mean (SD) | −2.6 (5.84) | −2.0 (5.54) | −2.0 (5.45) | −2.0 (6.04) | −3.9 (6.02) | −2.4 (6.94) |
Week 56 | ||||||
Patients with nonmissing data, n | 674 | 397 | 360 | 37 | 228 | 49 |
Mean (SD) | 3.9 (4.72) | 4.2 (4.93) | 4.4 (4.96) | 2.9 (4.53) | 3.7 (4.58) | 2.1 (2.87) |
Change from lead-in baseline, n | 600 | 378 | 355 | 23 | 222 | 0 |
Mean (SD) | −11.5 (7.19) | −11.1 (7.32) | −11.1 (7.34) | −11.3 (7.18) | −12.2 (6.92) | NA |
Change from LTE baseline, n | 629 | 379 | 343 | 36 | 217 | 33 |
Mean (SD) | −4.7 (6.64) | −3.6 (6.36) | −3.6 (6.40) | −3.8 (6.05) | −6.4 (6.71) | −5.2 (6.91) |
Change from baseline in CDLQI total score | ||||||
LTE baseline, n | 198 | 115 | 87 | 28 | 81 | 2 |
Mean (SD) | 6.9 (6.17) | 5.3 (5.83) | 5.4 (6.06) | 5.0 (5.15) | 9.1 (6.00) | 10.0 (7.07) |
Week 20 | ||||||
Patients with nonmissing data, n | 166 | 92 | 73 | 19 | 72 | 2 |
Mean (SD) | 4.3 (4.64) | 4.1 (4.62) | 4.3 (4.95) | 3.5 (3.10) | 4.4 (4.18) | 11.5 (16.26) |
Change from lead-in baseline, n | 132 | 89 | 73 | 16 | 43 | 0 |
Mean (SD) | −8.3 (6.22) | −8.3 (6.15) | −8.1 (6.12) | −8.9 (6.41) | −8.3 (6.43) | NA |
Change from LTE baseline, n | 163 | 90 | 71 | 19 | 72 | 1 |
Mean (SD) | −3.4 (5.30) | −1.9 (4.41) | −1.8 (4.48) | −2.2 (4.22) | −5.1 (5.65) | −15.0 (NA) |
Week 56 | ||||||
Patients with nonmissing data, n | 64 | 32 | 27 | 5 | 30 | 2 |
Mean (SD) | 3.4 (4.48) | 2.1 (2.02) | 2.0 (2.04) | 2.4 (2.07) | 4.4 (5.28) | 10.5 (12.02) |
Change from lead-in baseline, n | 48 | 29 | 27 | 2 | 19 | 0 |
Mean (SD) | −8.8 (6.33) | −9.2 (6.09) | −9.4 (6.25) | −6.5 (2.12) | −8.2 (6.80) | NA |
Change from LTE baseline, n | 62 | 31 | 26 | 5 | 30 | 1 |
Mean (SD) | −5.5 (6.04) | −4.5 (5.11) | −4.0 (5.20) | −7.0 (4.12) | −6.3 (6.77) | −13.0 (NA) |
CDLQI = Children’s Dermatology Life Quality Index; DLQI = Dermatology Life Quality Index; EASI-75 = ≥ 75% improvement in the Eczema Area and Severity Index from baseline; IGA = Investigator Global Assessment; LTE = long-term extension; NA = not applicable; q.4.w. = every 4 weeks; SD = standard deviation.
Note: Lead-in study baseline was defined as the last nonmissing value before the first dose of study drug of the lead-in studies. LTE baseline was the last available measurement before the first treatment in this study. DLQI and CDLQI index score ranges from 0 to 30. The higher the score, the more quality of life is impaired. Only participants previously included in studies SPR.116912, SPR.118161, SPR.118169, and SPR.201591, who rolled over to the LTE study within 6 months of the last dose in the lead-in study contributed to the change from lead-in study baseline analyses. All treated by nemolizumab included participants who had been treated by nemolizumab at least once before the LTE study. Continuous nemolizumab included participants with < 12 weeks interval between lead-in last dose of nemolizumab and the first dose in the LTE study. Re-treatment included participants with ≥ 12 weeks interval between lead-in last dose of nemolizumab and the first dose in the LTE study. Participants who have not previously received treatment with nemolizumab included those never exposed to nemolizumab before the LTE study. Blinded lead-in study included participants who rolled over from the ongoing blinded study.
Source: ARCADIA LTE Interim Clinical Study Report.63
Harms
Refer to Table 34 for harms data. During the 52-week LTE treatment period, 63.8% of patients experienced at least 1 AE, most being mild or moderate in severity, and 16.7% experienced a study drug-related AE. A treatment-emergent SAE was experienced by 4.1% of patients. A total of 4.8% of patients experienced a severe AE, with the most common being AD (0.9%), COVID-19 infection (0.3%), increased blood creatine phosphokinase (0.2%), asthma (0.2%), asthenia (0.2%), impetigo (0.2%), and headache (0.2%). A treatment-emergent AESI (by investigator) was experienced by 23.7% of patients, most commonly infections (20.3%) and asthma (newly diagnosed or worsening; 4.3%). Treatment-emergent AEs leading to study drug withdrawal were experienced by 3.3% of patients; 3.1% of patients experienced an AE leading to study discontinuation.
During the LTE follow-up period, 18.4% of patients experienced at least 1 AE, most being mild or moderate in severity, and 2.7% experienced a study drug-related AE. A treatment-emergent SAE was experienced by 2.7% of patients. A total of 2.0% of patients experienced a severe AE, and the only severe AE occurring in more than 1 patient was AD (0.7%). A treatment-emergent AESI (by investigator) was experienced by 4.8% of patients, most commonly infections (3.1%) and asthma (newly diagnosed or worsening; 1.7%). No treatment-emergent AEs led to study drug withdrawal in the follow-up period; however, 4.4% of patients experienced an AE leading to study discontinuation.
There were no patient deaths during the treatment or follow-up period of the LTE study.
Table 34: Summary of Harms in the ARCADIA LTE Study — First Interim Analysis
Summary of treatment-emergent AEs | Treatment period n = 1,740 | Follow-up period n = 293 |
|---|---|---|
Patients with at least 1 AE, n (%) | 1,110 (63.8) | 54 (18.4) |
AEs occurring in ≥ 2% of patients, n (%) | ||
Any AE | 1,110 (63.8) | 54 (18.4) |
Blood and lymphatic system disorders | 47 (2.7) | 2 (18.4) |
Eye disorders | 49 (2.8) | 1 (0.3) |
Gastrointestinal disorders | 135 (7.8) | 2 (0.7) |
Diarrhea | 40 (2.3) | 0 |
General disorders and administration site conditions | 101 (5.8) 156 | 2 (0.7) |
Infections and infestations | 721 (41.4) | 24 (8.2) |
COVID-19 infection | 281 (16.1) | 5 (1.7) |
Nasopharyngitis | 166 (9.5) | 0 |
Upper respiratory tract infection | 97 (5.6) | 1 (0.3) |
Urinary tract infection | 44 (2.5) | 0 |
Asymptomatic COVID-19 infection | 38 (2.2) | 1 (0.3) |
Injury, poisoning, and procedural complications | 127 (7.3) | 0 |
Investigations | 105 (6.0) | 6 (2.0) |
Blood creatine phosphokinase increased | 44 (2.5) | 3 (1.0) |
Metabolism and nutrition disorders | 51 (2.9) | 1 (0.3) |
Musculoskeletal and connective tissue disorders | 149 (8.6) | 4 (1.4) |
Back pain | 36 (2.1) | 2 (0.7) |
Nervous system disorders | 124 (7.1) | 4 (1.4) |
Headache | 79 (4.5) | 1 (0.3) |
Psychiatric disorders | 51 (2.9) | 0 |
Respiratory, thoracic, and mediastinal disorders | 188 (10.8) | 5 (1.7) |
Asthma | 69 (4.0) | 2 (0.7) |
Cough | 38 (2.2) | 0 |
Skin and subcutaneous tissue disorders | 348 (20.0) | 17 (5.8) |
Dermatitis atopic | 227 (13.0) | 13 (4.4) |
Vascular disorders | 38 (2.2) | 2 (0.7) |
AE by maximum severity, n (%) | ||
Mild | 529 (30.4) | 27 (9.2) |
Moderate | 498 (28.6) | 21 (7.2) |
Severe | 83 (4.8) | 6 (2.0) |
Study drug-related AE, n (%) | 291 (16.7) | 8 (2.7) |
Study drug-related AE by maximum severity, n (%) | ||
Mild | 128 (7.4) | 3 (1.0) |
Moderate | 141 (8.1) | 4 (1.4) |
Severe | 22 (1.3) | 1 (0.3) |
AE related to protocol procedure, n (%) | 78 (4.5) | 2 (0.7) |
Severe AE, n (%) | 83 (4.8) | 6 (2.0) |
SAEs (occurring in ≥ 1% of patients), n (%) | ||
Patients with ≥ 1 SAE | 72 (4.1) | 8 (2.7) |
Infections and infestations | 20 (1.1) | 1 (0.3) |
Skin and subcutaneous tissue disorders | 8 (0.5) | 4 (1.4) |
SAE related to study drug, n (%) | 8 (0.5) | 2 (0.7) |
AE leading to study drug interruption, n (%) | 170 (9.8) | 0 |
AE leading to study discontinuation, n (%) | 54 (3.1) | 13 (4.4) |
Any AE leading to permanent discontinuation of study drug, n (%) | 57 (3.3) | 0 |
Skin and subcutaneous tissue disorders | 38 (2.2) | 0 |
Deaths, n | ||
AE leading to death | 0 | 0 |
AE related to study drug leading to death | 0 | 0 |
Treatment-emergent AESI, n (%) | ||
AESI by categories (by investigator; occurring in ≥ 1% of patients) | 413 (23.7) | 14 (4.8) |
Newly diagnosed asthma or worsening of asthma | 75 (4.3) | 5 (1.7) |
Infections | 353 (20.3) | 9 (3.1) |
AESI by categories (MedDRA search; occurring in ≥ 1% of patients) | 892 (51.3) | 43 (14.7) |
Injection-related reactions | 414 (23.8) | 18 (6.1) |
Newly diagnosed asthma or worsening of asthma | 94 (5.4) | 7 (2.4) |
Infections | 723 (41.6) | 24 (8.2) |
Peripheral edema: limbs, bilateral; facial edema | 21 (1.2) | 0 |
AE = adverse event; AESI = adverse event of special interest; LTE = long-term extension; MedDRA = Medical Dictionary for Regulatory Activities; SAE = serious adverse event.
Source: ARCADIA LTE Interim Clinical Study Report.63
Critical Appraisal
The ARCADIA LTE study was designed as a single-arm, open-label extension to assess long-term safety and efficacy of nemolizumab in the treatment of adult and adolescent patients with moderate to severe AD. This open-label design could bias the reporting for subjective efficacy outcomes and harms. The direction and magnitude of these potential biases remains unclear. In addition, the absence of statistical hypothesis testing and a control group (i.e., no active comparator or placebo arm) limits the ability to draw definitive conclusions regarding the treatment effect. The study used a dosing regimen of every 4 weeks, which does not align with the every 8 weeks dosing schedule outlined in the product monograph and may not reflect real-world use.
The extension study partly consisted of patients who took part in the lead-in studies, the ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO studies, and therefore it is reasonable to expect that the same strengths and limitations related to generalizability apply to the extension period. Given that patients needed to complete the lead-in studies before enrolling, the treatment extension population is inherently enriched with patients meeting the study definition of clinical responders. Attrition rates were high, particularly for later time points such as week 56, which may limit generalizability and interpretability of long-term outcomes. Although study follow-up was limited to 56 weeks, the consulted clinical experts indicated that this duration was likely sufficient to assess safety and efficacy. The study is ongoing and is expected to be completed in August 2026.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
The aim of this section is to summarize and critically appraise 1 sponsor-submitted NMA to fill gaps in the comparative evidence for nemolizumab versus other treatments of interest for patients aged 12 years and older with moderate to severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable and who are refractory to or ineligible for systemic immunosuppressant therapies.
Description of Indirect Comparisons
The systematic literature search and study selection criteria for the NMA are summarized in Table 35.
Table 35: Study Selection Criteria and Methods for the NMA Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Patients with moderate to severe AD and CsA experience |
Intervention | Nemolizumab 40 mg q.4.w. |
Comparator |
|
Outcome |
Assessment time point: 16 weeks for all outcomes |
Study designs | Randomized double-blind control trials |
Publication characteristics | Published and nonpublished studies |
Exclusion criteria | Trials that did not report findings for patients with CsA experience, including comparators and outcomes of interest |
Databases searched | Refer to details of literature search strategy in Literature Search Methodology in Section 2 of this report |
Selection process | Titles, abstracts, and full-text articles were screened independently by 2 reviewers Disagreements were resolved by a third reviewer |
Data extraction process | Data from the included studies were extracted into data extraction templates designed in Microsoft Excel; the data were extracted by 1 reviewer and as a validation step, a second reviewer assessed the entries to ensure consistency and accuracy against the source article; a third reviewer was consulted to resolve disagreements |
Quality assessment | The Cochrane RoB 2.0 was used for quality assessment. |
AD = atopic dermatitis; AE = adverse event; CsA = cyclosporine; DAE = discontinuation due to adverse event; DLQI = Dermatology Life Quality Index; EASI-50 = ≥ 50% improvement in Eczema Area and Severity Index from baseline; EASI-75 = ≥ 75% improvement in Eczema Area and Severity Index from baseline; EASI-90 = ≥ 90% improvement in Eczema Area and Severity Index from baseline; IGA = Investigator Global Assessment; NMA = network meta-analysis; PP-NRS = Peak Pruritus Numeric Rating Scale; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.d. = every day; RoB = risk of bias.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence10 and the NMA Technical Report.64
NMA Design
Objectives
The objective of the sponsor-submitted NMA64 was to compare the treatment effects of nemolizumab versus relevant comparators that included abrocitinib, baricitinib, dupilumab, lebrikizumab, tralokinumab, and upadacitinib for the treatment of moderate to severe AD in patients aged 12 years who are candidates for systemic therapy. The focus of the NMA was in patients with CsA experience. Because baricitinib, lebrikizumab, and tralokinumab were not relevant to public payers in Canada, they were excluded from this report.
Study Selection Methods
The systematic literature search criteria for the NMA are described in Table 35, and are the same criteria used in the first section of this report (i.e., pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol), albeit more focused criteria were used to identify relevant trials and outcomes. The NMA included trials investigating treatments in patients aged 12 years and older with moderate to severe AD who had been previously treated with CsA (i.e., experience with CsA). Identified trials were assessed for eligibility against predefined inclusion and exclusion criteria. Two reviewers independently screened titles and abstracts and relevant full-text citations for inclusion. Discrepancies were resolved through consensus or by a third reviewer. Data extraction and quality assessment of included studies were performed by 1 reviewer and validated by a second reviewer, and discrepancies were resolved through by a third reviewer. Risk of bias assessment of included studies was performed using the Cochrane Collaboration’s Risk of Bias tool (Version 2) at the study level.
NMA Analysis Methods
Details of the NMA analysis methods are summarized in Table 36. A feasibility assessment was undertaken before the NMA to assess the heterogeneity of the included trials, including study characteristics, baseline characteristics, treatment regimens, outcome definitions, time points, and data availability. NMAs were performed using a Bayesian framework, whereby posterior distributions for treatment effects were estimated using a generalized linear model framework to synthesize data from the included trials and outcomes reported from the nemolizumab ARCADIA trials. Both fixed-effects and random-effects models with vague and informative priors were run and model fit was compared for each analysis. Absolute model fit was assessed by the total residual deviance. The deviance information criterion was used to compare the fit of the different models. Lower values of the deviance information criterion suggest a more parsimonious model, which informed which models were given most weight when interpreting the results. A deviance information criterion between 3 and 5 was considered a meaningful difference in models.172 Model choice was also determined by the presence of heterogeneity of the treatment effect via the I2 statistic and model convergence. Where networks contained closed loops, consistency was assessed using node splitting. Odds (risk) ratios and 95% CrIs were constructed for all outcomes except DLQI change from baseline at 16 weeks, which was assessed with mean difference and 95% CrI.
Posterior densities were estimated for treatment effects for all treatment comparisons in the networks using Markov Chain Monte Carlo simulation. Each analysis consisted of multiple Markov Chain Monte Carlo chains, with each chain simulated from different sets of starting values. Convergence was evaluated by the visual assessment of the overlapping history plots of the chains. Inferences were made from the posterior distributions of the treatment effects between treatments for outcomes of interest, derived from more than at least 50,000 iterations following burn-in and the iterations were discarded once the chains converged. The number of iterations for burn-in was 50,000, and no additional iterations were required to ensure convergence. Reference treatments for analyzed networks were chosen as the treatment to which most other treatments were directly connected (i.e., the centre of the network).
The following sensitivity analyses were conducted, with the random Turner model applied to assess consistency.
Because the ARCADIA 1 and ARCADIA 2 studies enrolled patients who were experienced with CsA and those who had no previous experience with CsA, exclusion of either population was performed to allow for comparison of these trials. To explore the impact of these exclusions, a sensitivity analysis was performed using only the ARCADIA CYCLO trial, which only included patients with CsA experience.
For patients defined as EASI-75 responders at 16 weeks, heterogenous data were removed for abrocitinib from the JADE DARE trial, which had mixed patient populations with CsA experience and those without CsA experience. The analysis was repeated with the heterogeneous trial removed.
Placebo regression adjustment was performed by including the nemolizumab phase IIb trial.
Table 36: NMA Analysis Methods
Methods | Description |
|---|---|
Analysis methods | NMAs were conducted using a generalized linear model framework using Bayesian MCMC simulations. Data inputs were counts or mean change from baseline. |
Priors | Vague prior distributions were used throughout the analysis for baseline and nuisance parameters, as well as the between-trial variance in the first instance. Random-effects informed priors, as recommended by NICE,65 were also used. Sensitivity analyses were performed comparing informed vs. vague priors. |
Assessment of model fit | Model fit was assessed by comparing the total residual deviance with the number of unconstrained data points, and minimizing the DIC, and between-study variance (i.e., I2 statistic). |
Assessment of consistency | Where networks contained closed loops, consistency was assessed using node splitting. |
Assessment of convergence | Convergence was evaluated via the visual assessment of the overlapping history plots of the chains. Inferences were made from the posterior distributions of the treatment effects between treatments for outcomes of interest, derived over at least 50,000 iterations following burn-in. The iterations were discarded once the chains converged. |
Outcomes | Odds (risk) ratios and 95% credible intervals were constructed for all outcomes except DLQI change from baseline at 16 weeks, which was assessed with mean difference and 95% credible interval. |
Follow-up time points | 16 weeks. |
Construction of nodes | Nodes were constructed according to individual treatments, their dosages, and the frequency of treatment. |
Sensitivity analyses | Inclusion of the ARCADIA CYCLO study; removal of heterogenous trials; and placebo adjustment. |
Subgroup analysis | NA |
Methods for pairwise meta-analysis | NA |
DIC = deviance information criterion; DLQI = Dermatology Life Quality Index; MCMC = Markov Chain Monte Carlo; NA = not applicable; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; vs. = versus.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence10 and the NMA Technical Report.64
Results of the NMA
Summary of Included Studies
The search identified 26 RCTs that underwent feasibility assessment. The feasibility of conducting an NMA was assessed for adults and adolescents with CsA experience, and for a mixed population of adults and adolescents with and without CsA experience. The feasibility assessment for the population with treatment experience was sparse. One trial was excluded because it did not include a relevant comparator, and 3 trials were excluded because they did not report on relevant outcomes. The remaining 22 trials were included in at least 1 network, which included 7 trials of interest (AD Up,66 ARCADIA 1,11 ARCADIA 2,12 ARCADIA CYCLO,13 JADE DARE,67 LIBERTY AD CAFÉ,68 and LIBERTY AD CHRONOS69) comparing nemolizumab, dupilumab, abrocitinib, and upadacitinib connected via placebo (Figure 3). The feasibility assessment suggested that the included trials were similar in study design, patient characteristics, treatment regimens, and outcome measures. The authors noted that the main source of heterogeneity was attributed to trial data that included the population with CsA experience as well as those without CsA experience; no other sources of heterogeneity were described. The proportion of patients with CsA experience in each relevant treatment group was 10.8% and 13.7% for the JADE DARE trial (abrocitinib 200 mg once daily and dupilumab 300 mg every 2 weeks, respectively), and 62.7% and 64.5% for the LIBERTY AD CAFÉ study (dupilumab 300 mg every week and 300 mg every 2 weeks, respectively). An NMA was considered feasible for patients with CsA experience for the following outcomes of interest at 16 weeks: EASI-75 response, improvement in PP-NRS of 4-points or more (PP-NRS response), IGA score of 0 (completely clear) or 1 (almost clear), DLQI change from baseline, AEs, and DAEs. It was assumed that trials with outcome data reported for mixed-age populations, but with a majority (≥ 75%) adult population, could be assessed in adult networks, and that outcome data could be pooled across time points to maintain network integrity.
Key characteristics of the included relevant trials are summarized in Table 37. Across the trials, most patients were male, and the mean age of patients ranged from 32.5 to 39.6 years. The authors noted that patients were comparable across studies with respect to BSA affected, and baseline EASI, DLQI, IGA, and PP-NRS scores. The proportion of adult patients in the trials which included a mix of patients with or without CsA experience ranged from 10.8% (JADE DARE trial) to 66.7% (LIBERTY AD CAFÉ trial); these data were not reported in the LIBERTY AD CHRONOS trial.
Figure 3: Network Diagram of All Treatments for Patients With CsA Experience and Mixed Populations
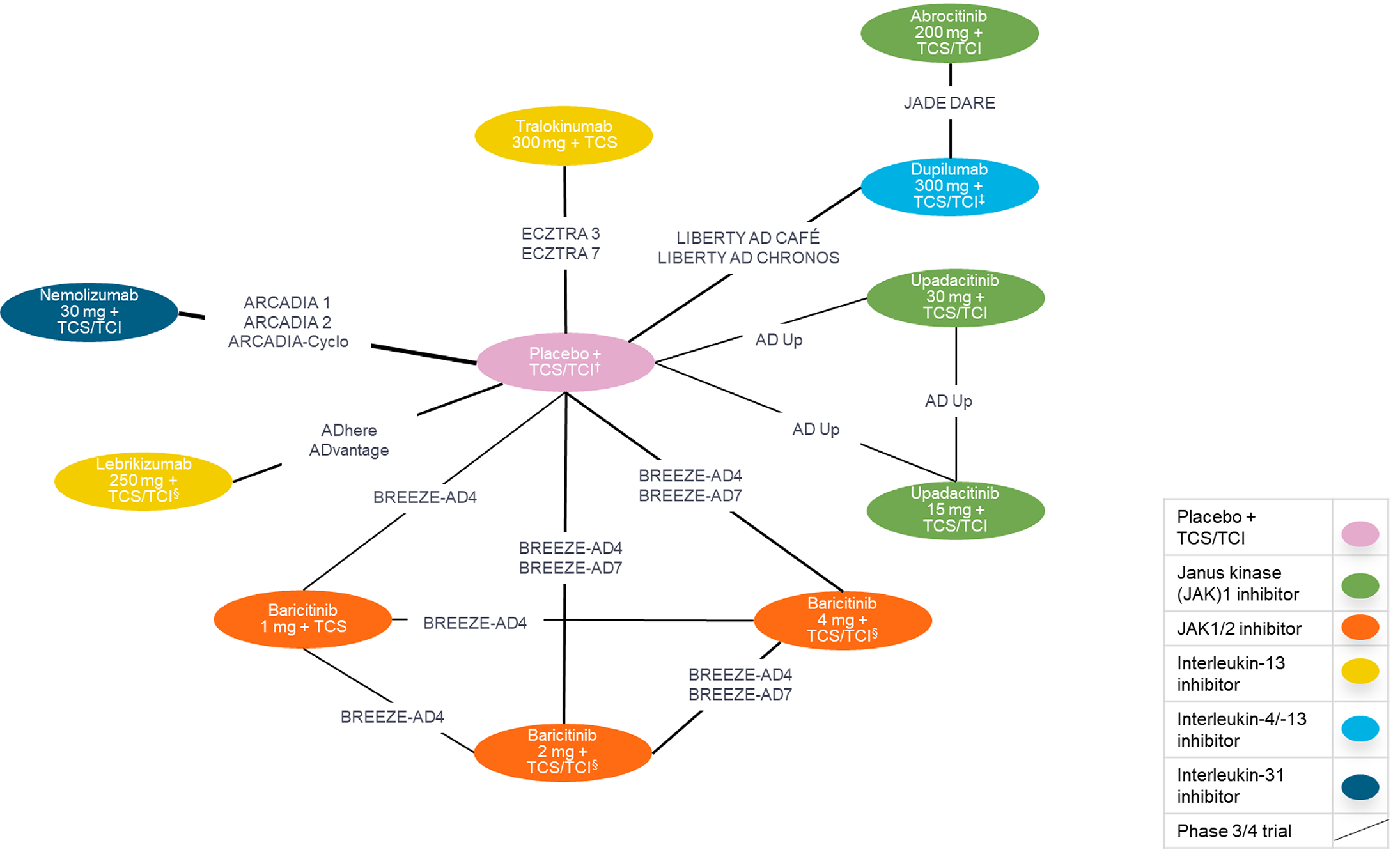
q.d. = every day; q.w. = once weekly; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; RCT = randomized controlled trial; TCI = topical calcineurin inhibitor; TCS = topical corticosteroid.
Notes: Thickness of connecting lines denotes the number of RCTs available for comparison. The symbol † refers to q.d., q.w., q.2.w., or q.4.w. administered orally or subcutaneously. The symbol ‡ refers to q.w. or q.2.w.
Sources: Network Meta-Analysis Technical Report.64 Details included in the table are from the sponsor’s summary of clinical evidence.
Table 37: Key Characteristics of Included Studies in the NMA
Trial name | Study design and population | Study duration | Intervention | Sample size | Age mean (SD) | Males % | BL BSA % mean (SD) | BL EASI mean score (SD) | BL DLQI mean score (SD) | BL IGA score, n (%) | BL PP-NRS mean score (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|
AD Up | Phase III, double-blind RCT Adults and adolescents aged 12 to 75 years | 16 weeks; subsequent 120-week blinded extension period | Placebo + TCS | 304 | 34.3 (NR) | 59 | 48.6 (23.1) | 30.3 (13) | 16.3 (7) | 4, 163 (54) 3, 141 (46) | 7.1 (1.6) |
Upadacitinib, 15 mg q.d. + TCS | 300 | 32.5 (NR) | 60 | 46.7 (21.6) | 29.2 (11.8) | 16.4 (7.2) | 4, 157 (52) 3, 143 (48) | 7.1 (1.8) | |||
Upadacitinib, 30 mg q.d. + TCS | 297 | 35.5 (NR) | 64 | 48.5 (23.1) | 29.7 (11.8) | 17.1 (7) | 4, 157 (53) 3, 140 (47) | 7.4 (1.6) | |||
ARCADIA 1 | Phase III, double-blind RCT Adults and adolescents aged 12 to 75 years | 16 weeks | Nemolizumab + TCS-TCIs | 620 | 33.5 (15.92) | 52.1 | 44.9 (19.9) | 27.77 (10.64) | 15.4 (6.6) | 4, 182 (29.4) 3, 438 (70.6) | 7.2 (1.4) |
Placebo + TCS/TCIs | 321 | 33.3 (15.61) | 55.1 | 43.8 (18.7) | 27.06 (9.37) | 15.5 (6.75) | 4, 85 (26.5) 3, 236 (73.5) | 7.2 (1.4) | |||
ARCADIA 2 | Phase III, double-blind RCT Adults and adolescents aged 12 to 75 years | 16 weeks | Placebo + TCS/TCIs | 265 | 35.2 (16.98) | 48.3 | 44.61 (19.42) | 27.43 (10.81) | 14.5 (6.85) | 4, 170 (32.6) 3, 352 (67.4) | 7.038 (1.5) |
Nemolizumab + TCS-TCIs | 522 | 34.9 (17.66) | 48.7 | 44.95 (19.28) | 27.58 (10.88) | 14.2 (6.98) | 4, 80 (30.2) 3, 185 (69.8) | 7.164 (1.5) | |||
ARCADIA CYCLO | Phase III, double-blind RCT Adults aged ≥ 18 years | 16 weeks | Nemolizumab 30 mg + TCS | 138 | 38.3 (13.15) | 52.2 | 44.61 (17.53) | 29.54 (8.5) | 14.8 (6.3) | 4, 36 (26.1) 3, 102 (73.9) | 7.405 (1.4) |
Placebo + TCS | 138 | 36.1 (12.21) | 52.2 | 46.09 (17.97) | 31.33 (9.67) | 16.3 (7.02) | 4, 37 (26.8) 3, 101 (73.2) | 7.475 (1.5) | |||
JADE DARE | Phase III, double-blind RCT Adults aged ≥ 18 years | 26 weeks | Abrocitinib + TCS | 362 | 36.6 (14.6) | 53 | 42.5 (19.9) | 28.1 (11.5) | 14 (6.8) | 4, 146 (40) 3, 216 (60) | 7.4 (1.6) |
Dupilumab + TCS | 365 | 35.5 (13.3) | 56 | 42.6 (21.3) | 28.1 (11.9) | 14.2 (6.3) | 4, 145 (40) 3, 220 (60) | 7.4 (1.6) | |||
LIBERTY AD CAFÉ | Phase III, double-blind RCT Adults aged ≥ 18 years | 16 weeks | Placebo + TCS | 108 | 38.9 (13.4) | 63 | 53 (38.3, 69.3)a | 31.7 (24.2, 40.7)a | 13 (6.8) | 4, 52 (48.1) | 6.9 (NR)a |
Dupilumab, 300 mg q.2.w. + TCS | 107 | 37.5 (12.9) | 60.7 | 55 (44, 66)a | 31.6 (25.2, 39.2)a | 13.3 (7.8) | 4, 50 (46.7) | 7 (NR)a | |||
Dupilumab, 300 mg q.w. + TCS | 110 | 38 (29, 48)a | 60 | 55.8 (41.5, 68)a | 31.1 (24.5, 39.0)a | 13 (7, 21)a | 4, 52 (47.3) | 6.4 (NR)a | |||
LIBERTY AD CHRONOS | Phase III, double-blind RCT Adults aged ≥ 18 years | 52 weeks | Dupilumab, 300 mg q.2.w. + TCS | 106 | 39.6 (13.98) | 58.5 | 59.5 (20.84) | 33.6 (13.3) | 14.5 (7.31) | 4, 53 (50) 3, 53 (50) | 7.4 (1.7) |
Dupilumab, 300 mg q.w. + TCS | 319 | 36.9 (13.67) | 60 | 54.1 (21.76) | 32.1 (12.76) | 14.4 (7.17) | 4, 147 (46) 3, 172 (54) | 7.1 (1.9) | |||
Placebo + TCS | 315 | 36.6 (13.01) | 61.3 | 56.9 (21.69) | 32.6 (12.93) | 14.7 (7.37) | 4, 147 (47) 3, 168 (53) | 7.3 (1.8) |
BL = baseline; BSA = body surface area; EASI = Eczema Area and Severity Index; DLQI = Dermatology Life Quality Index; IGA = Investigator Global Assessment; NMA = network meta-analysis; NR = not reported; PP-NRS = Peak Pruritus Numeric Rating Scale; q.2.w. = once every 2 weeks; q.d. = once daily; q.w. = once weekly; RCT = randomized controlled trial; SD = standard deviation; TCI = topical calcineurin inhibitors; TCS = topical corticosteroids.
aMedian (interquartile range).
Sources: Details included in the table are from the sponsor’s summary of clinical evidence10 and the NMA Technical Report.64
Results
For all outcomes of interest, both fixed and random-effects models showed similar deviance information criterion within a range of 3, with no model showing substantially lower deviance information criterion. As such, the authors selected the random-effects model with informed priors for all outcome analyses; the results of the sensitivity analysis comparing informed versus vague priors were similar for each outcome. Across analyses, the I2 statistic showed low heterogeneity that ranged from ██ ██ ██. The authors noted that the risk of bias assessment for all included trials showed low risk of bias, although their results were not considered in the NMA. Sensitivity analyses (data not shown) that removed the heterogenous trial with mixed patient populations had similar results compared to the base case for the remaining comparators, where trials remained. Sensitivity analyses (data not shown) that removed the ARCADIA 1 and ARCADIA 2 studies and included only the ARCADIA CYCLO study data were less favourable for nemolizumab but were generally consistent with the base-case analysis; the authors noted that this finding would be expected due to the reduced sample size. Sensitivity analyses that included a placebo adjustment were generally consistent with the base-case analysis (data not shown).
EASI-75 Response
For EASI-75 response at week 16, the network was informed by 6 trials, excluding the LIBERTY AD CHRONOS trial. The results (i.e., the odds of response) favoured upadacitinib 30 mg versus nemolizumab 30 mg (Figure 4). For all other relevant comparisons, there was insufficient evidence to detect a difference between point estimates and the 95% CrIs crossed the null.
Figure 4: Forest Plot of EASI-75 Response at Week 16 — Random-Effects NMA, Population With CsA Experience [Redacted]

CsA = cyclosporine; EASI-75 = ≥ 75% improvement in Eczema Area and Severity Index from baseline; NMA = network meta-analysis.
███ █ ████████ █████████ ██ █ ███████████ ██ █ ████ ██████ ██ █ ████ ██████ ███ █ ████ █████ █ ██████
████████ ███ █████████ ███████64███████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ █████████
PP-NRS Response (Improvement of 4 Points or More)
For PP-NRS response (≥ 4-point improvement) at week 16, the network was informed by all 7 trials. The results (i.e., the odds of response) favoured upadacitinib 30 mg versus nemolizumab 30 mg (Figure 6). For all other relevant comparisons, there was insufficient evidence to detect a difference between results and the 95% CrIs crossed the null.
Figure 5: Forest Plot of PP-NRS Response at Week 16 — Random-Effects NMA, Population With CsA Experience [Redacted]

CsA = cyclosporine; NMA = network meta-analysis; PP-NRS = Peak Pruritus Numeric Rating Scale.
███ █ ████████ █████████ ██ █ ███████████ ██ █ ████ ██████ ██ █ ████ ██████ ███ █ ████ █████ █ ██████
████████ ███ █████████ ███████64███████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ █████████
IGA Response (Score of 0 or 1)
For IGA response (score of 0 or 1) at week 16, the network was informed by all 7 trials. The results (i.e., the odds of response) favoured upadacitinib 30 mg and abrocitinib 200 mg versus nemolizumab 30 mg (Figure 6). For all other relevant comparisons, there was insufficient evidence to detect a difference as the 95% CrIs crossed the null.
Figure 6: Forest Plot of IGA Response at Week 16 — Random-Effects NMA, Population With CsA Experience [Redacted]

CsA = cyclosporine; IGA = Investigator Global Assessment; NMA = network meta-analysis.
███ █ ████████ █████████ ██ █ ███████████ ██ █ ████ ██████ ██ █ ████ ██████ ███ █ ████ █████ █ ██████
████████ ███ █████████ ███████64███████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ █████████
Dermatology Life Quality Index
For DLQI mean change from baseline at week 16, the network was informed by 6 trials, excluding the AD Up trial. There was insufficient evidence to detect a difference between nemolizumab 30 mg and any relevant comparator (Figure 7).
Figure 7: Forest Plot of DLQI Mean Change at Week 16 — Random-Effects NMA, Population With CsA Experience [Redacted]

CsA = cyclosporine; DLQI = Dermatology Life Quality Index; NMA = network meta-analysis.
███ █ ████████ █████████ ██ █ ███████████ ██ █ ████ ██████ ███ █ ████ █████ █ ██████
████████ ███ █████████ ███████64███████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ █████████
Adverse Events
For AEs at week 16, the network was informed by 6 trials, excluding the JADE DARE trial. There was insufficient evidence to detect a difference between nemolizumab 30 mg or any relevant comparator in odds of AEs (i.e., 95% CrIs crossed the null; Figure 8).
Figure 8: Forest Plot of AEs at Week 16 — Random-Effects NMA, Population With CsA Experience [Redacted]

AE = adverse event; CsA = cyclosporine; NMA = network meta-analysis.
███ █ ████████ █████████ ██ █ ███████████ ██ █ ████ ██████ ██ █ ████ ██████ ███ █ ████ █████ █ ██████
████████ ███ █████████ ███████ ███████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ █████████
Discontinuation Due to AEs
For DAEs at week 16, the network was informed by 6 trials, excluding the JADE DARE trial. There was insufficient evidence to detect a difference in the odds of DAEs between nemolizumab 30 mg and any relevant comparator (i.e., 95% CrIs crossed the null; Figure 9).
Figure 9: Forest Plot of DAEs at Week 16 — Random-Effects NMA, Population With CsA Experience [Redacted]

CsA = cyclosporine; DAE = discontinuation due to adverse event; NMA = network meta-analysis.
███ █ ████████ █████████ ██ █ ███████████ ██ █ ████ ██████ ██ █ ████ ██████ ███ █ ████ █████ █ ██████
████████ ███ █████████ ███████ ███████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ █████████
Critical Appraisal of NMA
The protocol of the systematic review and NMA was not a priori registered. The methods used to conduct the systematic literature review used appropriate criteria to search databases, select studies, extract data, and assess risk of bias of the included studies. Selection bias is expected to be low given the comprehensiveness of the searches and methods for study selection. The risk of bias assessment at the outcome level and their potential impact on the NMA effect estimates were not explicitly assessed or discussed, although the authors of the NMA stated that in general, trials were found to have low risk of bias.
The NMA included relevant outcomes identified by the CDA-AMC team, which included EASI-75, improvement in PP-NRS of 4-points or more, IGA score of 0 or 1, DLQI, AEs, and DAEs. Analysis for all outcomes was performed at 16 weeks and did not include the maintenance treatment phase of 48 weeks for nemolizumab. This was attributed to insufficient data beyond 16 weeks for the comparators of interest, which represents a gap in the available indirect evidence.
The authors noted that the included trials were considered similar in study design, patient eligibility criteria, baseline patient characteristics, and outcome characteristics (i.e., definitions and methods of reporting outcomes). However, there were notable baseline differences with respect to mean BSA involvement (ranging from 42.5% to 59.5% across trials and arms), and proportion of patients with baseline IGA scores of 3 or 4 (IGA = 3 ranging from 46% to 73.9%; IGA = 4 ranging from 26.1% to 54%). The included studies enrolled a combination of patients with inadequate response to, or intolerance to CsA. Efforts were made in the NMA to reduce heterogeneity by stratifying the adult and adolescent patient populations into subgroups with CsA experience. The results across outcomes showed low heterogeneity via the I2 statistic, which ranged from 0% to 6% (indicating low heterogeneity), and the results of sensitivity analyses that removed trials with mixed patient populations (those with CsA experience and those without CsA experience), were consistent with the base-case analysis. There were no data available for adolescents with CsA experience, which represents a gap in the available indirect evidence.
Overall, the network was sparse (i.e., many comparisons but few studies). Because most nodes were informed by only 1 trial and had small sample sizes, comparisons were underpowered, which contributed to wide CrIs in the analyses. Most 95% CrIs included both better and worse performance, except for EASI-75, PP-NRS, and IGA response, where upadacitinib 30 mg was favoured over nemolizumab 30 mg (i.e., 95% CrIs did not cross the null). It was not possible to assess for inconsistency across direct and indirect evidence in the NMA outcomes, due to the absence of closed loops in the network.
Discussion
Summary of Available Evidence
The evidence included in this review consisted of 2 pivotal studies (ARCADIA 1 and ARCADIA 2), and 1 additional study in the systematic literature review (ARCADIA CYCLO). Additional evidence included 1 LTE study (ARCADIA LTE), and an NMA. No studies addressing gaps were included.
The submission contained results from the initial (16 weeks) and maintenance period (additional 32 weeks) of the ARCADIA 1 study (initial period: n = 971) and the ARCADIA 2 study (initial period: n = 787) which were 2 randomized, placebo-controlled, double-blind, multicentre trials enrolling patients with moderate to severe AD (based on EASI score of ≥ 16, IGA score ≥ 3, and AD involvement ≥ 10% of BSA); in addition, patients were required to meet specific thresholds for itch (PP-NRS score ≥ 4) and report recent inadequate response to topical therapies. Patients who met the study definition of clinical responder (IGA of 0 [clear] or 1 [almost clear] or EASI-75 at week 16) were rerandomized to the maintenance phase which consisted of 3 treatment arms (nemolizumab every 4 weeks [n = 169], every 8 weeks [n = 169], or placebo [n = 169]) and followed for up to 48 weeks total alongside the patients who met the study definition of clinical responder from the placebo arms of both trials (n = 185). The ARCADIA CYCLO study (n = 276) was a 16-week randomized, placebo-controlled, double-blind, multicentre trial enrolling patients with moderate to severe AD but at higher EASI threshold than the ARCADIA 1 and ARCADIA 2 studies (EASI score ≥ 20); IGA score, PP-NRS score, BSA requirement, and the requirement to have inadequate response to topical therapy was the same. The ARCADIA CYCLO study additionally required patients to either be refractory to CsA or have CsA be medically inadvisable. Patients who completed the ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO study were eligible to enrol in the ARCADIA LTE study (n = 1,740); an ongoing, phase III, multicentre, single-arm, open-label extension study to assess the long-term safety and efficacy of SC nemolizumab 30 mg every 4 weeks in adolescent and adult patients with moderate to severe AD. Patients who participated in other nemolizumab AD studies, and adolescents from selected international sites who had not previously participated in a nemolizumab AD study, were also eligible. Results were from 1 interim analysis (data cut-off date of September 30, 2022) up to 56 weeks of treatment.
In the absence of direct comparative evidence of nemolizumab versus relevant comparators of interest, an NMA was conducted by the sponsor. The NMA assessed the treatment effects of nemolizumab versus abrocitinib, dupilumab, and upadacitinib for the treatment of moderate to severe AD in patients aged 12 years or older who are candidates for systemic therapy. Some comparators included in the NMA (i.e., baricitinib, lebrikizumab, and tralokinumab) were not relevant to public payers in Canada and were therefore excluded from this report. The focus of the NMA was in patients with CsA experience, and the trials included patients who were intolerant to, or ineligible for CsA. Outcomes of interest were assessed at 16 weeks, which included EASI-75 response, PP-NRS response, IGA response, DLQI change from baseline, AEs, and DAEs. Bayesian random-effect NMAs were conducted using generalized linear models to estimate odds ratios and 95% CrIs, except for DLQI change from baseline, which was assessed with mean difference and 95% CrI.
Interpretation of Results
Efficacy
The sponsor is seeking reimbursement criteria that mimics dupilumab for patients with moderate to severe AD. In general, the patient populations in all 3 trials do not fully match the proposed reimbursement criteria requested by the sponsor as patients in the ARCADIA 1 and ARCADIA 2 studies were not required to have been unsuccessful with a previous systemic therapy, and 33.5% and 40.6% of patients in the ARCADIA 1 and ARCADIA 2 studies had no prior systemic therapy. As previously noted, an EASI score of 7.1 to 21.0 may be considered moderate, and scores ranging from 21.1 to 50.0 represent severe AD. Additionally, IGA scores of 3 are indicative of moderate AD. Patients in the ARCADIA 1 and ARCADIA 2 studies had mean EASI scores at baseline of approximately 27, with EASI scores greater than ██ in the ARCADIA CYCLO study, suggesting that most patients had severe disease per the EASI. Most patients had IGA scores of 3 at baseline in all ARCADIA studies, which was suggestive of moderate disease. All 3 trials had a baseline PP-NRS score which the experts noted would correspond to a severe itch (mean score ranged from 7.04 to 7.46), where 65.5% and 61.0% of patients in the ARCADIA 1 and ARCADIA 2 studies had PP-NRS scores of 7 or more at baseline. The patient population enrolled in the ARCADIA 1 and ARCADIA 2 studies was not required to be refractory to systemic therapy or have it be medically inadvisable, and approximately 38% of patients enrolled in these trials reported a prior history of immunomodulating drugs (including 12% to 15% with prior CsA exposure across treatment arms in the ARCADIA 1 and ARCADIA 2 studies). The ARCADIA CYCLO study enrolled a mixed population where most patients had CsA experience, and some were experienced with other systemic drugs. Patients in the ARCADIA 1 and ARCADIA 2 studies were on optimized background topical treatment initiated during a 2-week run-in period. Patients in the ARCADIA CYCLO study did not have this run-in but were required to follow authorized background topical therapy. This likely contributed to the numerically high placebo response observed in these trials. Therefore, treatment history and adherence to pre-existing topical therapy will be an important consideration when determining the place in therapy.
Patient groups emphasized the need for improved disease control as well as symptom and pain relief (e.g., itch, dryness, inflammation, blistering), convenience, and improved quality of life. The results from the body of evidence comprising the ARCADIA and ARCADIA 2 studies’ initial 16-week periods, and the 16-week ARCADIA CYCLO trial demonstrated that nemolizumab had a meaningful impact relative to placebo on disease activity and symptoms, particularly itch, which patients and clinicians noted is a key concern for this population. Treatment with nemolizumab likely led to an increased proportion of patients with treatment success (per IGA) and EASI-75 relative to placebo, and there was a greater magnitude of EASI score reduction in the nemolizumab arm relative to the placebo arm in all 3 trials over 16 weeks. However, based on the between-group MID of 10% provided by the clinical experts, results for the proportion of patients achieving treatment success and proportion of patients achieving EASI-75 may not be clinically meaningful as the 95% CIs included the possibility of no clinically meaningful benefit. In the ARCADIA 1 and ARCADIA 2 studies, treatment with nemolizumab led to a greater proportion of patients with a PP-NRS score improvement of 4 or greater which was considered clinically meaningful based on the MID of 10% suggested by the clinical experts. Additionally, there was a greater proportion of patients with PP-NRS less than 2 at 16 weeks, relative to placebo, with up to 30% of patients receiving nemolizumab across ARCADIA trials reporting PP-NRS scores less than 2 (where scores of 0 equal no itch) at week 16 compared to approximately 10% of patients receiving placebo. In both trials, a greater proportion of patients treated with nemolizumab in the subgroup with PP-NRS less than 7 at baseline was able to achieve this outcome (ARCADIA 1: 36.0% versus 18.0%; strata-adjusted difference versus placebo = 17.9%; 95% CI, 8.3% to 27.5% and ARCADIA 2: 30.6% versus 15.8%; strata-adjusted difference versus placebo = 15.0%; 95% CI, 5.5% to 24.5%) compared to patients with PP-NRS scores of 7 or more at baseline (ARCADIA 1: 27.8% versus 7.6%; strata-adjusted difference versus placebo = 20.5%; 95% CI, 14.6% to 25.9% and ARCADIA 2: 26.9% versus 8.5%; strata-adjusted difference versus placebo = 18.4%; 95% CI, 11.9% to 24.9%). This overall finding was supported by net reductions in PP-NRS scores from baseline in all treatment arms in all studies.
Several subgroup analyses were included in the submission for primary and secondary outcomes. Subgroup analyses were generally consistent with the primary analyses, although many were affected by small sample sizes. Subgroup analyses by prior therapy (systemic, biologic, immunosuppressive, dupilumab, or CsA) did not show consistent trends across the ARCADIA 1 and ARCADIA 2 studies, with patients with prior use of these treatments in the ARCADIA 2 study often demonstrating no benefit over placebo across outcomes of interest, challenging the interpretation of the subgroup results. Subgroup analyses by PP-NRS at baseline were generally suggestive that patients with more severe itch (PP-NRS > 7) experienced greater improvement in IGA success and EASI-75, as the 95% CI for the subgroup of patients with PP-NRS scores less than 7 at baseline crossed the null threshold and included the possibility of no benefit.
Results for the ARCADIA CYCLO study were broadly consistent with the ARCADIA 1 and ARCADIA 2 studies for EASI and PP-NRS outcomes, although more impacted by imprecision. As previously noted, the ARCADIA CYCLO study required patients to have higher EASI scores (minimum 20) to be enrolled in the trial, as well as experience with CsA, compared to the ARCADIA 1 and ARCADIA 2 studies, and therefore patients in the ARCADIA CYCLO study were considered to have more severe disease. Results for EASI-75 were not considered clinically meaningful based on the 10% threshold identified by the experts, but PP-NRS results were clinically meaningful, in line with the ARCADIA 1 and ARCADIA 2 studies. However, the proportion of patients achieving IGA success in the ARCADIA CYCLO study (█████ ███ █████) was lower than in the ARCADIA 1 and ARCADIA 2 studies (35.6% versus 24.6% and 37.7% versus 26.0%, respectively) and the between-group difference results were affected by imprecision based on the wide CIs, which also allowed for the possibility of worsening in the outcome (███ ███████ ███ ███ ████ ██ ████).
With regards to HRQoL, the DLQI and CDLQI results for the initial period of the ARCADIA 1 and ARCADIA 2 studies, and the ███████ ████████ of the ARCADIA CYCLO studies demonstrated a reduction (improvement) in scores from baseline; however, the between-group results did not attain the MID of 5 points provided by the experts and were not considered clinically meaningful relative to placebo.
The initial period of the ARCADIA 1 and ARCADIA 2 studies and the full duration of the ARCADIA CYCLO study were 16 weeks which the clinical experts noted might not be sufficient to ascertain complete response. The ARCADIA 1 and ARCADIA 2 trials included a maintenance period which rerandomized patients who met the study definition of clinical responder to treatment with nemolizumab either every 4 weeks, every 8 weeks, or to placebo. The results from the maintenance phase represent a selected subgroup of patients who were considered responders to treatment in the initial period. While this provides results from a longer duration of follow-up, it does not provide information on which of the patients in the initial period were more or less likely to respond to treatment in the time frame; it is also unknown whether patients who initially had not responded to treatment in the initial period would have responded if treated for a longer period, as the clinical experts consulted for this review noted that patients may be evaluated for response over a period of 6 months.
Overall, the results from the pooled maintenance period of the ARCADIA 1 and ARCADIA 2 trials suggested that the treatment effects observed among patients who had responded by week 16 in the initial period were maintained across the 48-week maintenance period, and at the end of the 48-week maintenance period. In the group of patients that were rerandomized to placebo, the proportion of patients with each outcome was similar to patients rerandomized to nemolizumab every 4 weeks or every 8 weeks, albeit slightly lower (proportion of patients with IGA success: 63.4% and 64.1% versus 55.0%; EASI-75 at week 48: 76.3% and 75.7% versus 63.9%; proportion of patients with PP-NRS improvement of 4 or more: 36.7% and 29.0% versus 21.3%). It remains unclear whether the high placebo response was due to continued effects of nemolizumab, or background therapy. No information was provided on the duration of this apparent sustained response after stopping nemolizumab. Despite the observed maintained effects, the maintenance phase was at a higher risk of bias due to only enrolling patients who demonstrated a response to treatment at week 16 using the IGA or EASI-75, and there was no formal statistical analysis or control for multiplicity for secondary outcomes. Although achievement of EASI-75 is a common response criterion for renewal in other CDA-AMC recommendations for AD, response using IGA is not considered during renewal. It is unclear how many patients in the ARCADIA trials who achieved IGA success also achieved EASI-75 response. It is also unclear if there would be substantial differences across these patient groups; thus, this population may not be comparable to patients who would receive long-term nemolizumab in clinical practice.
From the ARCADIA LTE study baseline, the proportion of patients achieving IGA success, EASI-75, and DLQI improvements from baseline showed continued improvement in groups with prior treatment with nemolizumab and those without prior treatment with nemolizumab. Across these outcomes, the group with prior treatment with nemolizumab demonstrated gradual early improvements that were maintained to week 56, while the group with no prior treatment with nemolizumab continued to increase over the LTE treatment period. By week 56, there were a similar proportion of patients achieving IGA success and EASI-75 between groups, and mean DLQI total scores were similar. No meaningful conclusion could be made for the mean change from lead-in or LTE baseline in CDLQI by previous treatment at week 20 and week 56 due to the small sample sizes.
Given the lack of direct comparative evidence for nemolizumab and relevant comparators in the context in Canada, the sponsor submitted an NMA comparing nemolizumab to other advanced systemic therapies in patients who were refractory to, or ineligible for CsA. In general, the trials included in the NMA were considered similar in study design, patient eligibility criteria, baseline patient characteristics (except for percent BSA affected and IGA score), and outcome characteristics. The results across outcomes showed low heterogeneity via the I2 statistic, which ranged from ██ ██ ██ (indicating low heterogeneity); however, 95% CrIs were wide and imprecise suggesting considerable heterogeneity in the results. Overall, the network was sparse (i.e., many comparisons but few studies). Because most nodes were informed by only 1 trial and had small sample sizes, comparisons were underpowered, which also contributed to wide CrIs in the analyses. █████ ██ ███ █████████████████ ████ ███ ███████ ███ ███████ █████████ ██████ ████████ ███ ███ ████████ ████████ ████████████ ██ ██ ██████ ████████████ ███ ███████ ███ ███ ████████ ████ ████████ ███████████ ██████ ████████████ ███ ███████ ███ ████ ████ ██████ ████ ████████ ███ ███ ██████ ███ ███████████ ██████ ███ █████████ █████ ███ ██ ██████████ ████████ ███████ █████████ ██████ ████████████ ████ ███ ████ ████████ ████ ██████ ███ █████ ████████████ ██████ ███ ████████ ██████ ███ ███ █████████ █████ ████████████ ██ ██ ███ ████████ ████ ███████████ ██████ ███ ████ ███ ███ █████ ███ ██████. Due to insufficient data beyond 16 weeks for the comparators of interest, analyses for all outcomes were performed at 16 weeks, and did not include the maintenance treatment phase of 48 weeks for nemolizumab. The results of sensitivity analyses that removed trials with mixed patient populations (those with CsA experience and those without CsA experience), were consistent with the base-case analysis. There were no data available for adolescents with CsA experience, which represents a gap in the available indirect evidence.
Harms
The most commonly reported AEs in all ARCADIA trials during the first 16 weeks were infections and infestations; skin and SC tissue disorders; and respiratory, thoracic, or mediastinal disorders. However, the overall occurrences of AEs during the initial 16-week trial period of the ARCADIA studies were low (< 52%), and there were no meaningful differences across nemolizumab and placebo groups. In general, in the ARCADIA 1 and ARCADIA 2 studies, AEs in the maintenance period were consistent with those in the initial treatment period in terms of type and frequency. Notably, in the ARCADIA 1 and ARCADIA 2 studies, patients in the maintenance phase who were rerandomized from nemolizumab to placebo did not experience a reduction in AEs relative to the initial phase or compared to the other rerandomized groups. Infections were generally higher in the maintenance phase in all groups, which was most likely driven by the COVID-19 pandemic, and is not necessarily related to treatment with nemolizumab. No deaths were reported in the studies arms and a numerically small proportion of patients reported SAEs during the conduct of all 3 studies (< 5% across study arms in all 3 trials). In addition, withdrawals were balanced between patients receiving nemolizumab and patients in the placebo arms.
The clinical experts noted that the tolerability profile of nemolizumab was consistent with those expected of biologics used in the treatment of AD and there was fewer safety concerns compared to JAK inhibitors. The exclusion of patients with uncontrolled asthma limits the generalizability of the results as it is not known whether these patients would be at risk for additional harm. However, while this may be a signal of interest in the ARCADIA trials, a numerically low proportion of patients reported these AESIs.
The safety profile of nemolizumab in the ARCADIA LTE study was consistent with that of the ARCADIA 1 and ARCADIA 2 studies, and no new safety signals were observed. █████ ██ ███ █████████████████ ████ █████ ███ ██ ██████████ ████████ ███████ ███████████ ███ ███ █████ ██████████ ███ ███ ███ ████.
Conclusion
Results from 2 identical phase III, double-blind, multicentre, placebo-controlled RCTs (ARCADIA 1 and ARCADIA 2) in patients with moderate to severe AD demonstrated that nemolizumab led to statistically significant improvements in markers of disease activity (measured by IGA success and EASI-75) and itch (measured by PP-NRS) at 16 weeks, when compared with placebo. Among the subset of patients who had demonstrated a clinical response by 16 weeks, results suggested that improvements in disease activity and itch were sustained, regardless of whether nemolizumab was given every 4 weeks or every 8 weeks. The clinical experts and patient groups highlighted the debilitating aspect of itch in this population. Results from subgroup analyses at 16 weeks suggested a more pronounced effect on disease activity in patients with severe itch (PP-NRS ≥ 7), although these results were only considered supportive of the overall effect of nemolizumab.
Results from a similar phase IIIb, double-blind, placebo-controlled RCT (ARCADIA CYCLO) in patients refractory to CsA or where CsA was inadvisable, suggested similar trends in EASI-75 and PP-NRS, but not IGA, and the results were more subject to uncertainty due to imprecision. Results from all 3 trials were subject to some uncertainty due to limitations primarily impacting external validity, as patients with certain comorbidities such as uncontrolled or worsening asthma and certain treatment histories were excluded from the ARCADIA 1 and ARCADIA 2 studies, and the ARCADIA CYCLO study enrolled patients with more mixed patient history. HRQoL results demonstrated a reduction in scores (nominal P value < 0.05 for DLQI) across all trials, although the results were not considered clinically meaningful and did not attain the threshold for a clinically meaningful difference provided by the clinical experts consulted for this review.
In the ARCADIA LTE study, patients previously treated with nemolizumab showed gradual initial improvement in disease activity and symptoms, which appeared to be maintained through the treatment period. Patients who had not previously received treatment with nemolizumab demonstrated continued improvement throughout the LTE study. However, limitations such as the enriched population and lack of comparator preclude definitive conclusions.
The clinical experts highlighted the safety profile of nemolizumab was considered tolerable and manageable. The long-term safety profile of nemolizumab in the ARCADIA LTE study was consistent with that of the ARCADIA 1 and ARCADIA 2 studies, and no new safety signals were observed.
There was no direct evidence comparing nemolizumab to other systemic therapies used to treat moderate to severe AD in Canada. The results of the sponsor-submitted indirect treatment comparison suggested that upadacitinib 30 mg was favoured over nemolizumab for all efficacy outcomes, and abrocitinib was favoured for IGA response. The results comparing nemolizumab and dupilumab were inconclusive for all outcomes of interest due to the wide 95% CrIs that contained the possibility that either treatment could be favoured or that there could be no difference. The indirect treatment comparison safety results for overall occurrence of any AEs and DAEs at week 16 did not support a difference between nemolizumab and any relevant comparators. However, the NMA could not support comparisons of specific AEs, which may be of interest to patients and clinicians. Overall, the NMA estimates were subject to uncertainty due to serious imprecision, and a lack of data for adolescents, as well as lack of comparative evidence of treatment effect beyond 16 weeks.
References
1.Datsi A, Steinhoff M, Ahmad F, Alam M, Buddenkotte J. Interleukin-31: The “itchy” cytokine in inflammation and therapy. Allergy. 2021;76(10):2982-2997. doi:10.1111/all.14791 PubMed
2.Ständer S. Atopic Dermatitis. N Engl J Med. 2021;384(12):1136-1143. doi:10.1056/NEJMra2023911 PubMed
3.Fishbein AB, Silverberg JI, Wilson EJ, Ong PY. Update on Atopic Dermatitis: Diagnosis, Severity Assessment, and Treatment Selection. J Allergy Clin Immunol Pract. 2020;8(1):91-101. doi:10.1016/j.jaip.2019.06.044 PubMed
4.Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet. 2020;396(10247):345-360. doi:10.1016/s0140-6736(20)31286-1 PubMed
5.Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy. 2018;73(6):1284-1293. doi:10.1111/all.13401 PubMed
6.Silverberg JI, Barbarot S, Gadkari A, et al. Atopic dermatitis in the pediatric population: A cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol. 2021;126(4):417-428.e2. doi:10.1016/j.anai.2020.12.020 PubMed
7.Boguniewicz M, Alexis AF, Beck LA, et al. Expert Perspectives on Management of Moderate-to-Severe Atopic Dermatitis: A Multidisciplinary Consensus Addressing Current and Emerging Therapies. J Allergy Clin Immunol Pract. 2017;5(6):1519-1531. doi:10.1016/j.jaip.2017.08.005 PubMed
8.Paller AS, Butala S, Howe W. Treatment for atopic dermatitis (eczema). UpToDate; 2025. February 21, 2025.
9.Hanifin JM, Baghoomian W, Grinich E, Leshem YA, Jacobson M, Simpson EL. The Eczema Area and Severity Index-A Practical Guide. Dermatitis. 2022;33(3):187-192. doi:10.1097/der.0000000000000895 PubMed
10.Galderma Canada I. CDA Reimbursement Review Sponsor summary of clinical evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Nemolizumab 30mg/0.49mL. 2025.
11.Galderma. ARCADIA 1 - Clinical Study Report – RD.06.SRE.118161. 2023.
12.Galderma. ARCADIA 2 - Clinical Study Report – RD.06.SRE.118169. 2023.
13.Galderma. ARCADIA Cyclo Topline - Clinical Study Report - RD.06.SPR.201591. 2024.
14.Laughter MR, Maymone MBC, Mashayekhi S, et al. The global burden of atopic dermatitis: lessons from the Global Burden of Disease Study 1990-2017. Br J Dermatol. 2021;184(2):304-309. doi:10.1111/bjd.19580 PubMed
15.Legat FJ. Itch in Atopic Dermatitis - What Is New? Front Med (Lausanne). 2021;8:644760. doi:10.3389/fmed.2021.644760 PubMed
16.Augustin M, Langenbruch A, Blome C, et al. Characterizing treatment-related patient needs in atopic eczema: insights for personalized goal orientation. J Eur Acad Dermatol Venereol. 2020;34(1):142-152. doi:10.1111/jdv.15919 PubMed
17.Avena-Woods C. Overview of atopic dermatitis. Am J Manag Care. 2017;23(8 Suppl):S115-s123. PubMed
18.Jeon C, Yan D, Nakamura M, et al. Frequency and Management of Sleep Disturbance in Adults with Atopic Dermatitis: A Systematic Review. Dermatol Ther (Heidelb). 2017;7(3):349-364. doi:10.1007/s13555-017-0192-3 PubMed
19.Bruin-Weller M, Pink AE, Patrizi A, et al. Disease burden and treatment history among adults with atopic dermatitis receiving systemic therapy: baseline characteristics of participants on the EUROSTAD prospective observational study. J Dermatolog Treat. 2021;32(2):164-173. doi:10.1080/09546634.2020.1866741 PubMed
20.Gilhooley E, O'Grady C, Roche D, et al. High Levels of Psychological Distress, Sleep Disturbance, and Alcohol Use Disorder in Adults With Atopic Dermatitis. Dermatitis. 2021;32(1s):S33-s38. doi:10.1097/der.0000000000000687 PubMed
21.Kwatra SG, Gruben D, Fung S, DiBonaventura M. Psychosocial Comorbidities and Health Status Among Adults with Moderate-to-Severe Atopic Dermatitis: A 2017 US National Health and Wellness Survey Analysis. Adv Ther. 2021;38(3):1627-1637. doi:10.1007/s12325-021-01630-z PubMed
22.Halvorsen JA, Lien L, Dalgard F, Bjertness E, Stern RS. Suicidal ideation, mental health problems, and social function in adolescents with eczema: a population-based study. J Invest Dermatol. 2014;134(7):1847-1854. doi:10.1038/jid.2014.70 PubMed
23.Roh YS, Huang AH, Sutaria N, et al. Real-world comorbidities of atopic dermatitis in the US adult ambulatory population. J Am Acad Dermatol. 2022;86(4):835-845. doi:10.1016/j.jaad.2021.11.014 PubMed
24.Maspero J, Rubini NDPM, Zhang J, et al. Epidemiology of adult patients with atopic dermatitis in AWARE 1: A second international survey. World Allergy Organization Journal. 2023;16(3):100724. PubMed
25.Raimondo A, Lembo S. Atopic Dermatitis: Epidemiology and Clinical Phenotypes. Dermatol Pract Concept. 2021;11(4):e2021146. doi:10.5826/dpc.1104a146 PubMed
26.Yew YW, Thyssen JP, Silverberg JI. A systematic review and meta-analysis of the regional and age-related differences in atopic dermatitis clinical characteristics. J Am Acad Dermatol. 2019;80(2):390-401. doi:10.1016/j.jaad.2018.09.035 PubMed
27.Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338-51. doi:10.1016/j.jaad.2013.10.010 PubMed
28.Hill MK, Kheirandish Pishkenari A, Braunberger TL, Armstrong AW, Dunnick CA. Recent trends in disease severity and quality of life instruments for patients with atopic dermatitis: A systematic review. J Am Acad Dermatol. 2016;75(5):906-917. doi:10.1016/j.jaad.2016.07.002 PubMed
29.Reynolds M, Gorelick J, Bruno M. Atopic Dermatitis: A Review of Current Diagnostic Criteria and a Proposed Update to Management. J Drugs Dermatol. 2020;19(3):244-248. PubMed
30.Silverberg JI. Public Health Burden and Epidemiology of Atopic Dermatitis. Dermatol Clin. 2017;35(3):283-289. doi:10.1016/j.det.2017.02.002 PubMed
31.Kim J, Kim BE, Leung DYM. Pathophysiology of atopic dermatitis: Clinical implications. Allergy Asthma Proc. 2019;40(2):84-92. doi:10.2500/aap.2019.40.4202 PubMed
32.Davis DM, Drucker AM, Alikhan A, et al. Guidelines of care for the management of atopic dermatitis in adults with phototherapy and systemic therapies. J Am Acad Dermatol. 2023;90(2):e43-e56. PubMed
33.Chu DK, Schneider L, Asiniwasis RN, et al. Atopic dermatitis (eczema) guidelines: 2023 American Academy of Allergy, Asthma and Immunology/American College of Allergy, Asthma and Immunology Joint Task Force on Practice Parameters GRADE– and Institute of Medicine–based recommendations. Ann Allergy Asthma Immunol. 2024;132(3):274-312. doi:10.1016/j.anai.2023.11.009 PubMed
34.Galderma Canada I. NEMLUVIOTM Product Monograph (Draft dated February 12, 2024). 2024.
35.Agency EM. Nemluvio (Nemolizumab). 2025. Accessed June 2, 2025. https://www.ema.europa.eu/en/medicines/human/EPAR/nemluvio
36.Administration USFaD. Nemluvio (Nemolizumab): for injection, for subcutaneous use [Prescribing Information]. 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/761391s000lbl.pdf
37.Pfizer C. CIBINQO (abrocitinib) product monograph [Internet]. 2022. https://pdf.hres.ca/dpd_pm/00066473.PDF
38.Inc. S-aC. Dupilumab (Dupixent): solution for subcutaneous injection [Product Monograph]. 2024. https://pdf.hres.ca/dpd_pm/00077903.PDF
39.AbbVie C. RINVOQ (upadacitinib) product monograph [Internet]. 2022. https://pdf.hres.ca/dpd_pm/00068075.PDF
40.Bożek A, Reich A. Assessment of Intra- and Inter-Rater Reliability of Three Methods for Measuring Atopic Dermatitis Severity: EASI, Objective SCORAD, and IGA. Dermatology. 2017;233(1):16-22. doi:10.1159/000472711 PubMed
41.Barbier N, Paul C, Luger T, et al. Validation of the Eczema Area and Severity Index for atopic dermatitis in a cohort of 1550 patients from the pimecrolimus cream 1% randomized controlled clinical trials programme. Br J Dermatol. 2004;150(1):96-102. doi:10.1111/j.1365-2133.2004.05696.x PubMed
42.Yosipovitch G, Reaney M, Mastey V, et al. Peak Pruritus Numerical Rating Scale: psychometric validation and responder definition for assessing itch in moderate-to-severe atopic dermatitis. Br J Dermatol. 2019;181(4):761-769. doi:10.1111/bjd.17744 PubMed
43.Shikiar R, Harding G, Leahy M, Lennox RD. Minimal important difference (MID) of the Dermatology Life Quality Index (DLQI): results from patients with chronic idiopathic urticaria. Health Qual Life Outcomes. 2005;3:36. doi:10.1186/1477-7525-3-36 PubMed
44.Schram ME, Spuls PI, Leeflang MM, Lindeboom R, Bos JD, Schmitt J. EASI, (objective) SCORAD and POEM for atopic eczema: responsiveness and minimal clinically important difference. Allergy. 2012;67(1):99-106. doi:10.1111/j.1398-9995.2011.02719.x PubMed
45.Schmitt J, Langan S, Deckert S, et al. Assessment of clinical signs of atopic dermatitis: a systematic review and recommendation. J Allergy Clin Immunol. 2013;132(6):1337-47. doi:10.1016/j.jaci.2013.07.008 PubMed
46.Simpson El BLAGAELRM. Defining a responder on the Peak Pruritus Numerical Rating Scale (NRS) in patients with moderate-to-severe atopic dermatitis: detailed analysis from randomized trials of dupilumab [abstract]. JAAD. 2017;76(6)(1):AB93.
47.Howells L, Ratib S, Chalmers JR, Bradshaw L, Thomas KS. How should minimally important change scores for the Patient-Oriented Eczema Measure be interpreted? A validation using varied methods. Br J Dermatol. 2018;178(5):1135-1142. doi:10.1111/bjd.16367 PubMed
48.Basra MK, Salek MS, Camilleri L, Sturkey R, Finlay AY. Determining the minimal clinically important difference and responsiveness of the Dermatology Life Quality Index (DLQI): further data. Dermatology. 2015;230(1):27-33. doi:10.1159/000365390 PubMed
49.Barrett A, Hahn-Pedersen J, Kragh N, Evans E, Gnanasakthy A. Patient-Reported Outcome Measures in Atopic Dermatitis and Chronic Hand Eczema in Adults. Patient. 2019;12(5):445-459. doi:10.1007/s40271-019-00373-y PubMed
50.Salek MS, Jung S, Brincat-Ruffini LA, et al. Clinical experience and psychometric properties of the Children's Dermatology Life Quality Index (CDLQI), 1995-2012. Br J Dermatol. 2013;169(4):734-59. doi:10.1111/bjd.12437 PubMed
51.Basra MK, Fenech R, Gatt RM, Salek MS, Finlay AY. The Dermatology Life Quality Index 1994-2007: a comprehensive review of validation data and clinical results. Br J Dermatol. 2008;159(5):997-1035. doi:10.1111/j.1365-2133.2008.08832.x PubMed
52.Lewis V, Finlay AY. 10 years experience of the Dermatology Life Quality Index (DLQI). J Investig Dermatol Symp Proc. 2004;9(2):169-80. doi:10.1111/j.1087-0024.2004.09113.x PubMed
53.Badia X, Mascaró JM, Lozano R. Measuring health-related quality of life in patients with mild to moderate eczema and psoriasis: clinical validity, reliability and sensitivity to change of the DLQI. The Cavide Research Group. Br J Dermatol. 1999;141(4):698-702. doi:10.1046/j.1365-2133.1999.03112.x PubMed
54.Lewis-Jones MS, Finlay AY. The Children's Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol. 1995;132(6):942-9. doi:10.1111/j.1365-2133.1995.tb16953.x PubMed
55.Simpson EL, de Bruin-Weller M, Eckert L, et al. Responder Threshold for Patient-Oriented Eczema Measure (POEM) and Children's Dermatology Life Quality Index (CDLQI) in Adolescents with Atopic Dermatitis. Dermatol Ther (Heidelb). 2019;9(4):799-805. doi:10.1007/s13555-019-00333-2 PubMed
56.Galderma. Pooled Analysis of ARCADIA1 and ARCADIA 2 - Clinical Study Report - RD.06.SRE.118161 and RD.06.SRE.118169 POOL. 2023.
57.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
58.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
59.Silverberg JI, Pinter A, Pulka G, et al. Phase 2B randomized study of nemolizumab in adults with moderate-to-severe atopic dermatitis and severe pruritus. J Allergy Clin Immunol. 2020;145(1):173-182. doi:10.1016/j.jaci.2019.08.013 PubMed
60.Sidbury R, Alpizar S, Laquer V, et al. Pharmacokinetics, Safety, Efficacy, and Biomarker Profiles During Nemolizumab Treatment of Atopic Dermatitis in Adolescents. Dermatol Ther (Heidelb). 2022;12(3):631-642. doi:10.1007/s13555-021-00678-7 PubMed
61.NCT04365387. A Study to Assess Immunization Responses in Adult and Adolescent Participants With Moderate-to-Severe Atopic Dermatitis Treated With Nemolizumab. https://clinicaltrials.gov/ct2/show/NCT04365387
62.NCT04562116. A Study to Assess the Effects of Nemolizumab on Cytochrome P450 Substrates in Participants With Moderate-to-Severe Atopic Dermatitis. https://clinicaltrials.gov/ct2/show/NCT04562116?term=nemolizumab&cond=Atopic+Dermatitis&draw=2&rank=1
63.Galderma. ARCADIA LTE - Interim Clinical Study Report - RD.06.SIR.118163. 2023.
64.Inc. GC. Nemolizumab for treatment of atopic dermatitis: network meta-analysis report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Nemolizumab (Nemluvio); 30 mg subcutaneous injection. 2024.
65.National Institute for Health and Care. Upadacitinib, abrocitinib and tralokinumab or for treating dermatitis. ID3960 Committee papers. 2022. Accessed 12/04/2024. https://www.nice.org.uk/guidance/ta814
66.Reich K, Teixeira HD, de Bruin-Weller M, et al. Safety and efficacy of upadacitinib in combination with topical corticosteroids in adolescents and adults with moderate-to-severe atopic dermatitis (AD Up): results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2021;397(10290):2169-2181. doi:10.1016/s0140-6736(21)00589-4 PubMed
67.Reich K, Thyssen JP, Blauvelt A, et al. Efficacy and safety of abrocitinib versus dupilumab in adults with moderate-to-severe atopic dermatitis: a randomised, double-blind, multicentre phase 3 trial. Lancet. 2022;400(10348):273-282. doi:10.1016/S0140-6736(22)01199-0 PubMed
68.de Bruin-Weller M, Thaçi D, Smith CH, et al. Dupilumab with concomitant topical corticosteroid treatment in adults with atopic dermatitis with an inadequate response or intolerance to ciclosporin A or when this treatment is medically inadvisable: a placebo-controlled, randomized phase III clinical trial (LIBERTY AD CAFÉ). Br J Dermatol. 2018;178(5):1083-1101. doi:10.1111/bjd.16156 PubMed
69.Blauvelt A, de Bruin-Weller M, Gooderham M, et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet. 2017;389(10086):2287-2303. doi:10.1016/s0140-6736(17)31191-1 PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Figure 10: Subgroup Results for the Proportion of Patients With IGA Success at Week 16 — The ARCADIA 1 Study Initial Period
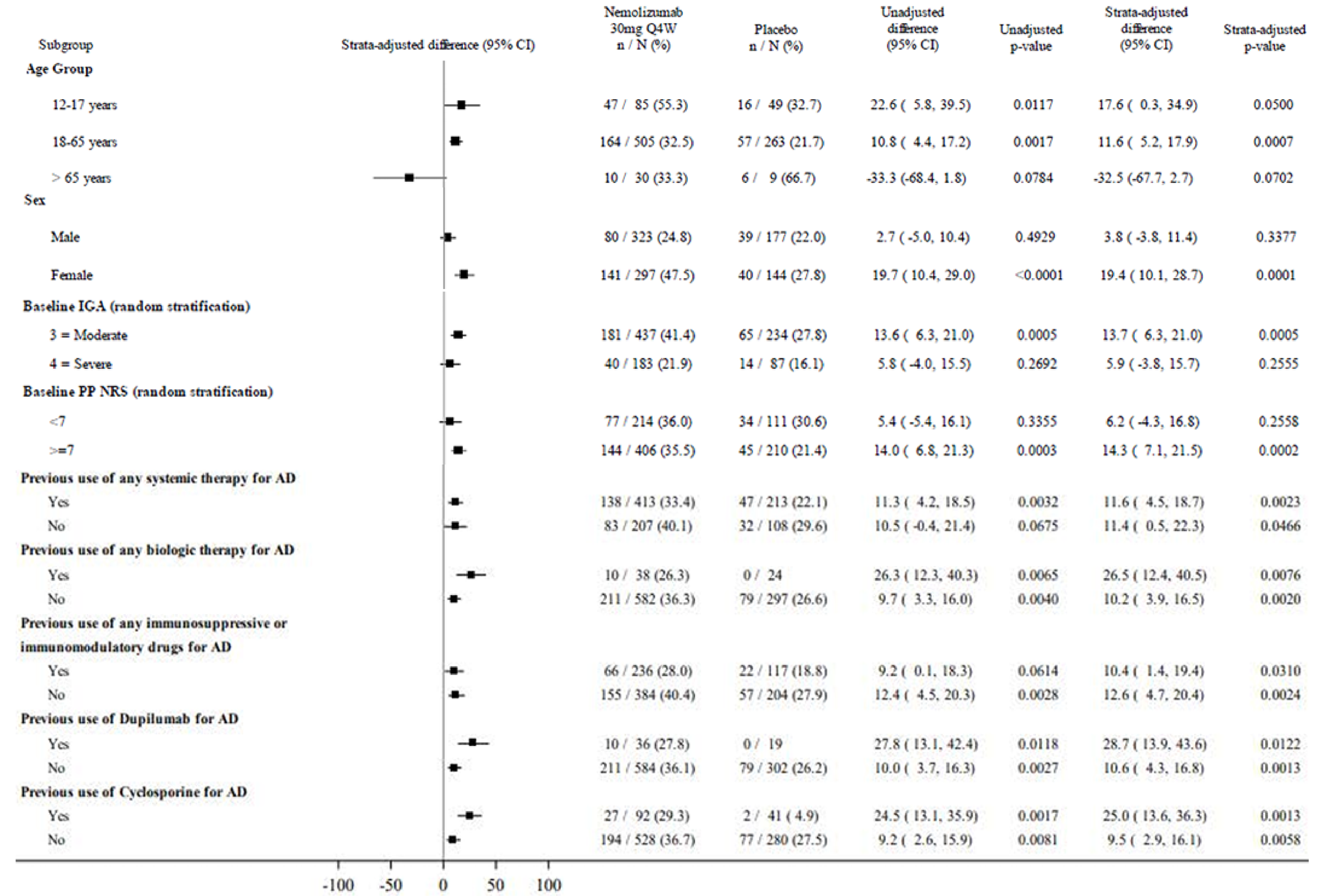
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; Q4W = every 4 weeks.
Source: Details included in the figure are from the sponsor’s ARCADIA 1 Clinical Study Report.11
Figure 11: Subgroup Results for the Proportion of Patients With EASI-75 at Week 16 by Relevant Subgroup — The ARCADIA 1 Study Initial Period
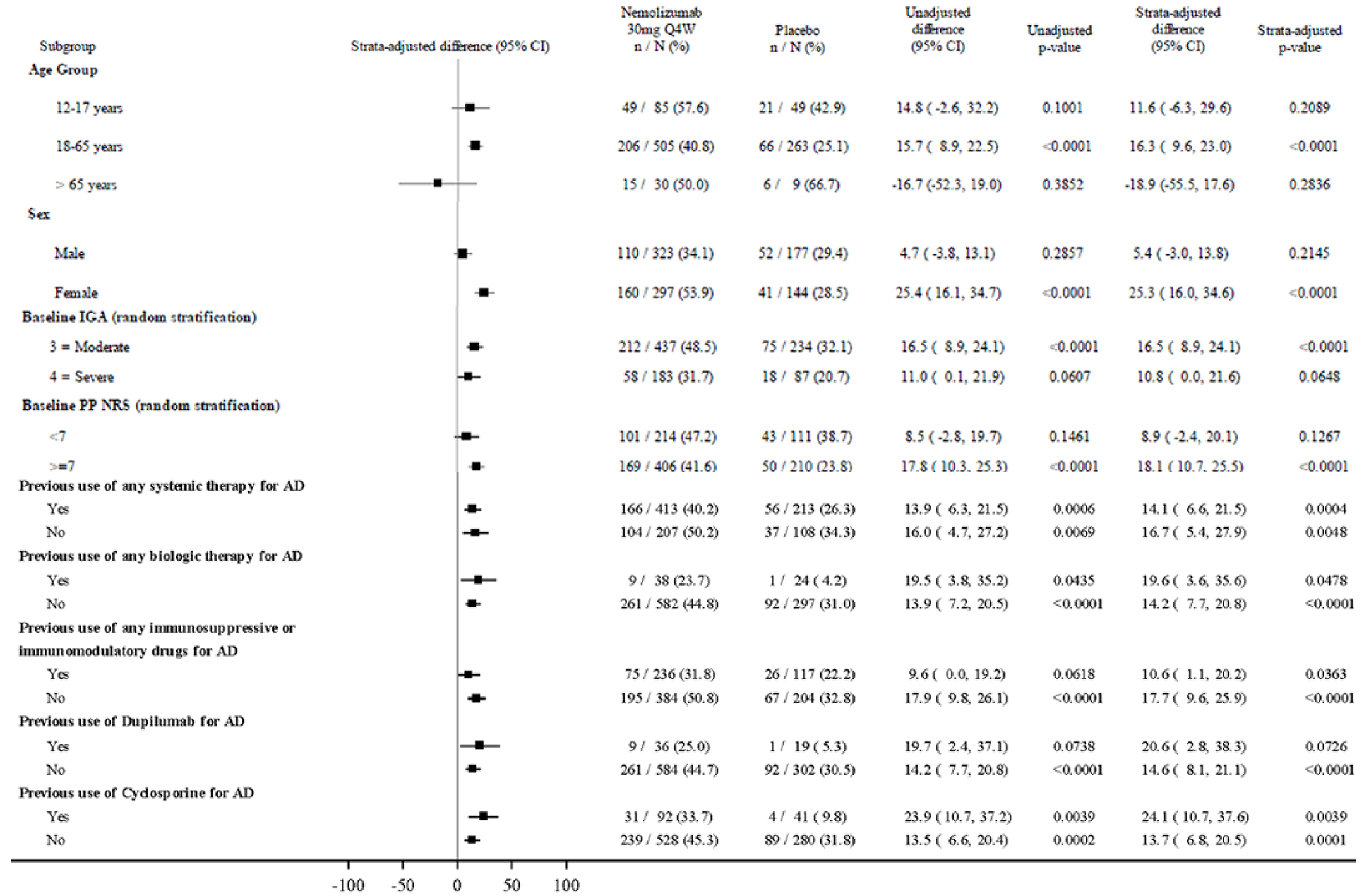
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; Q4W = every 4 weeks.
Source: Details included in the figure are from the sponsor’s ARCADIA 1 Clinical Study Report.11
Figure 12: Subgroup Results for the Proportion of Patients With PP-NRS Score Improvement of 4 Points or More at Week 16 by Relevant Subgroup — The ARCADIA 1 Study Initial Period
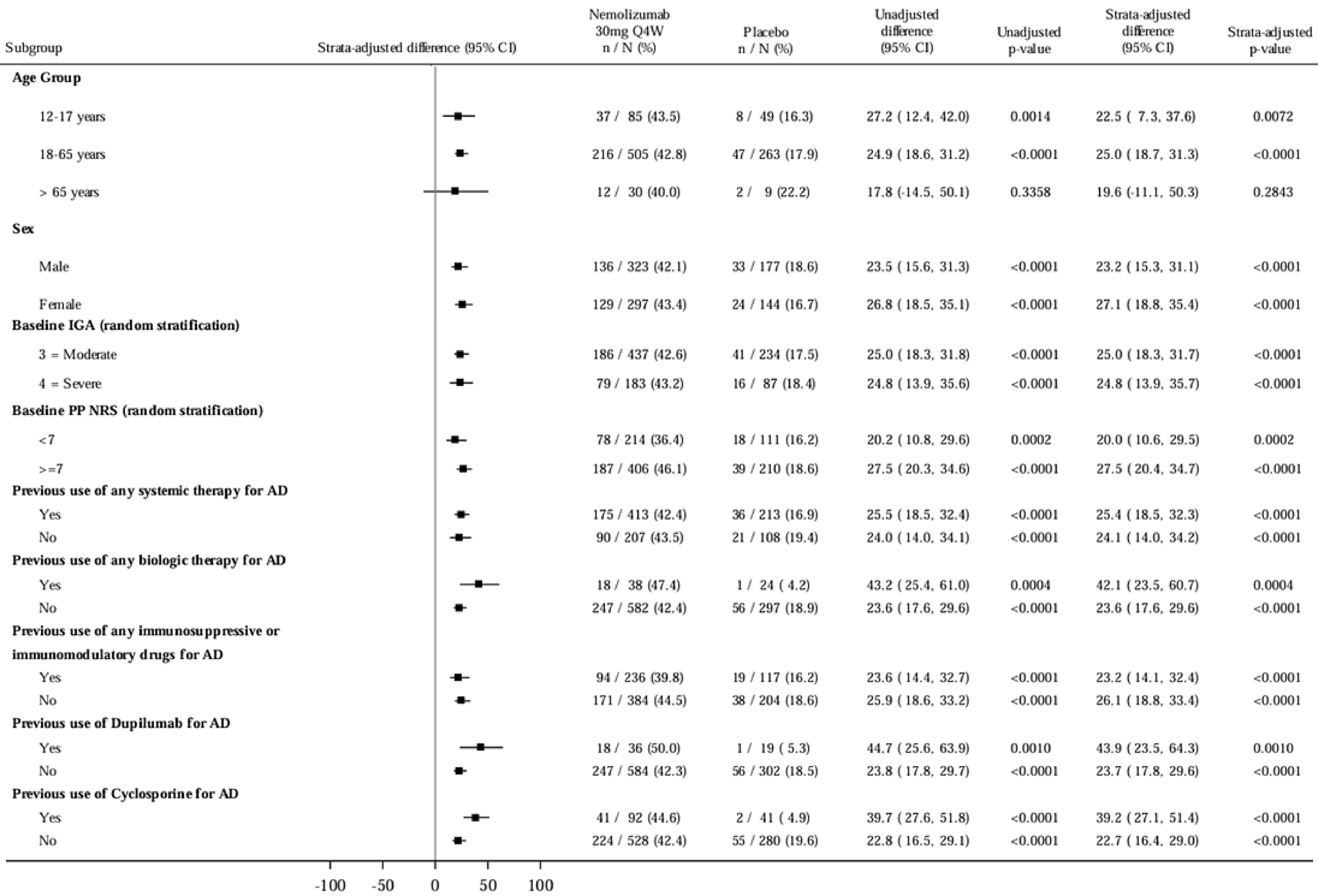
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; Q4W = every 4 weeks.
Source: Details included in the figure are from the sponsor’s ARCADIA 1 Clinical Study Report.11
Figure 13: Subgroup Results for the Proportion of Patients With PP-NRS Score of Less Than 2 at Week 16 by Relevant Subgroup — The ARCADIA 1 Study Initial Period
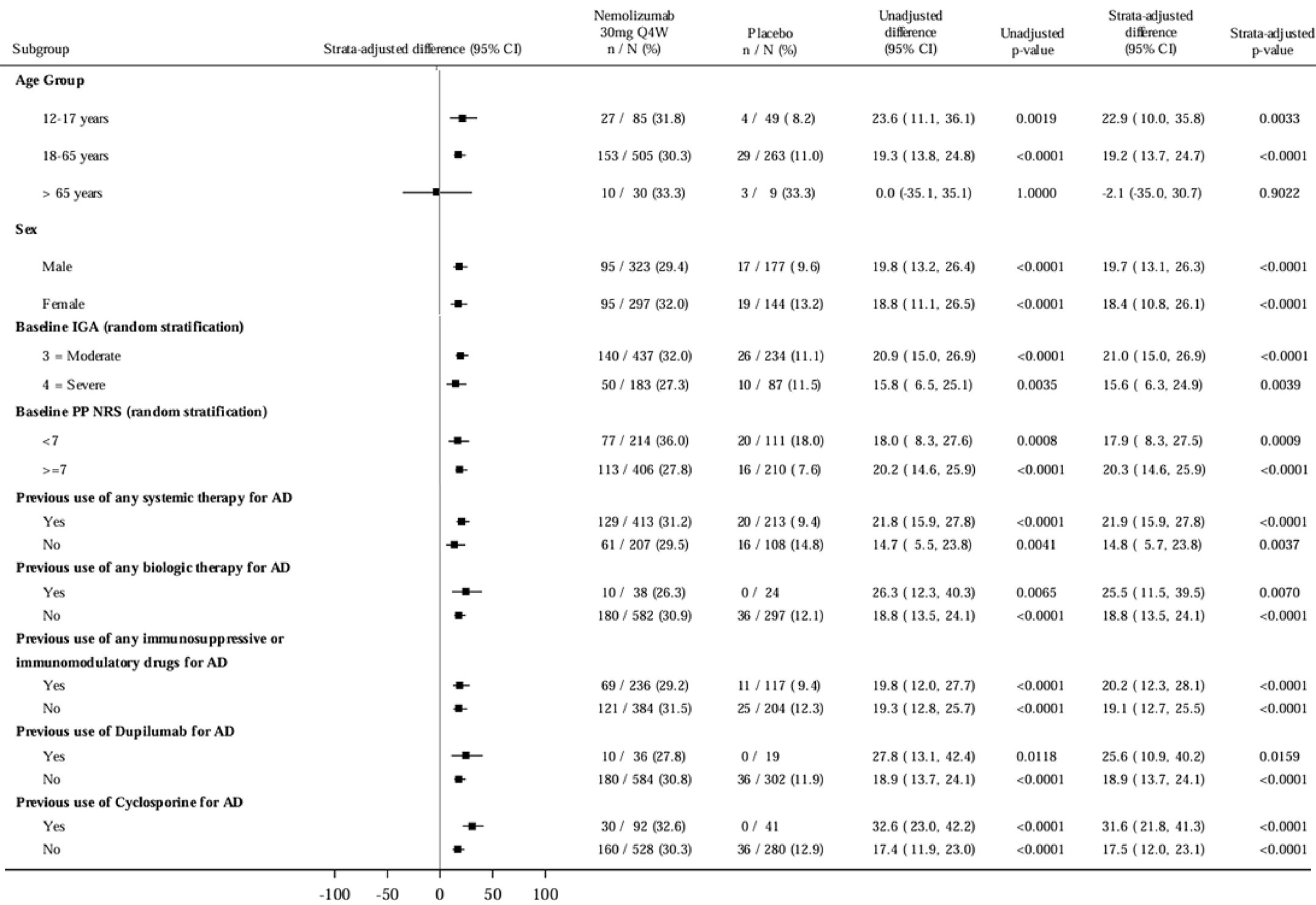
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; Q4W = every 4 weeks.
Source: Details included in the figure are from the sponsor’s ARCADIA 1 Clinical Study Report.11
Figure 14: Subgroup Results for the Proportion of Patients With IGA Success at Week 16 — The ARCADIA 2 Study Initial Period
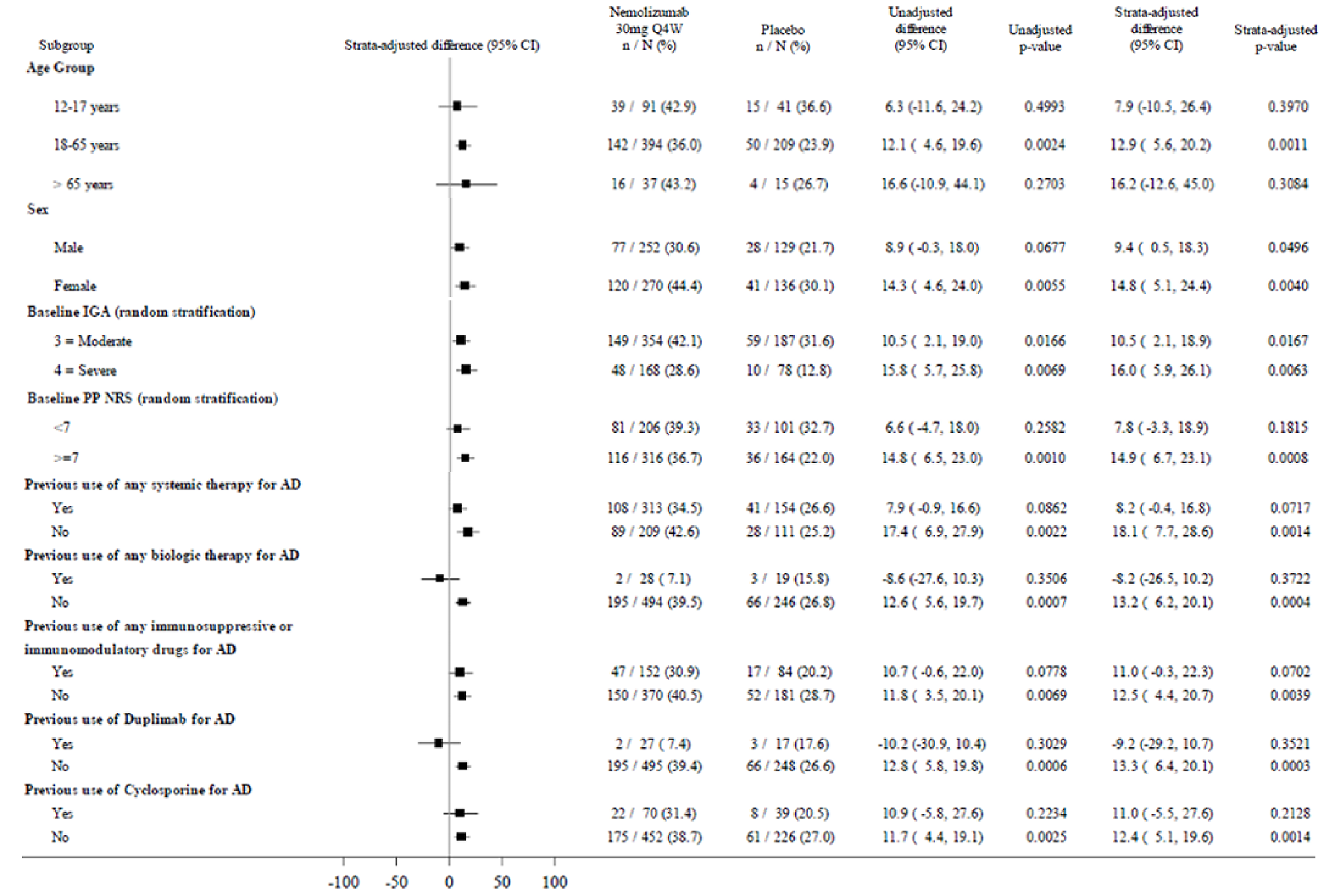
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; Q4W = every 4 weeks.
Source: Details included in the figure are from the sponsor’s ARCADIA 2 Clinical Study Report.12
Figure 15: Subgroup Results for the Proportion of Patients With EASI-75 at Week 16 — The ARCADIA 2 Study Initial Period
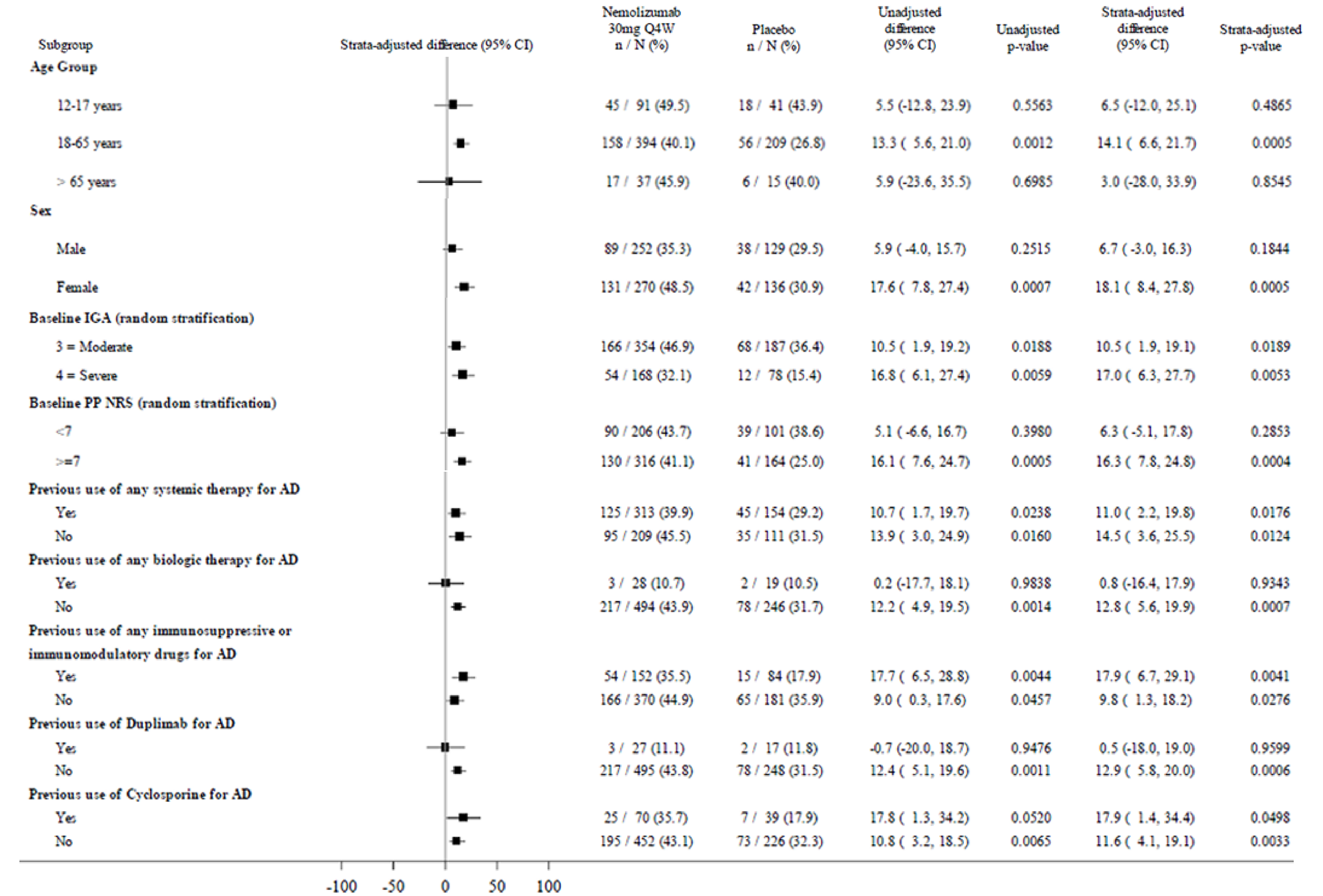
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; Q4W = every 4 weeks.
Source: Details included in the figure are from the sponsor’s ARCADIA 2 Clinical Study Report.12
Figure 16: Subgroup Results for the Proportion of Patients With PP-NRS Score Improvement of 4 Points or More at Week 16 — The ARCADIA 2 Study Initial Period
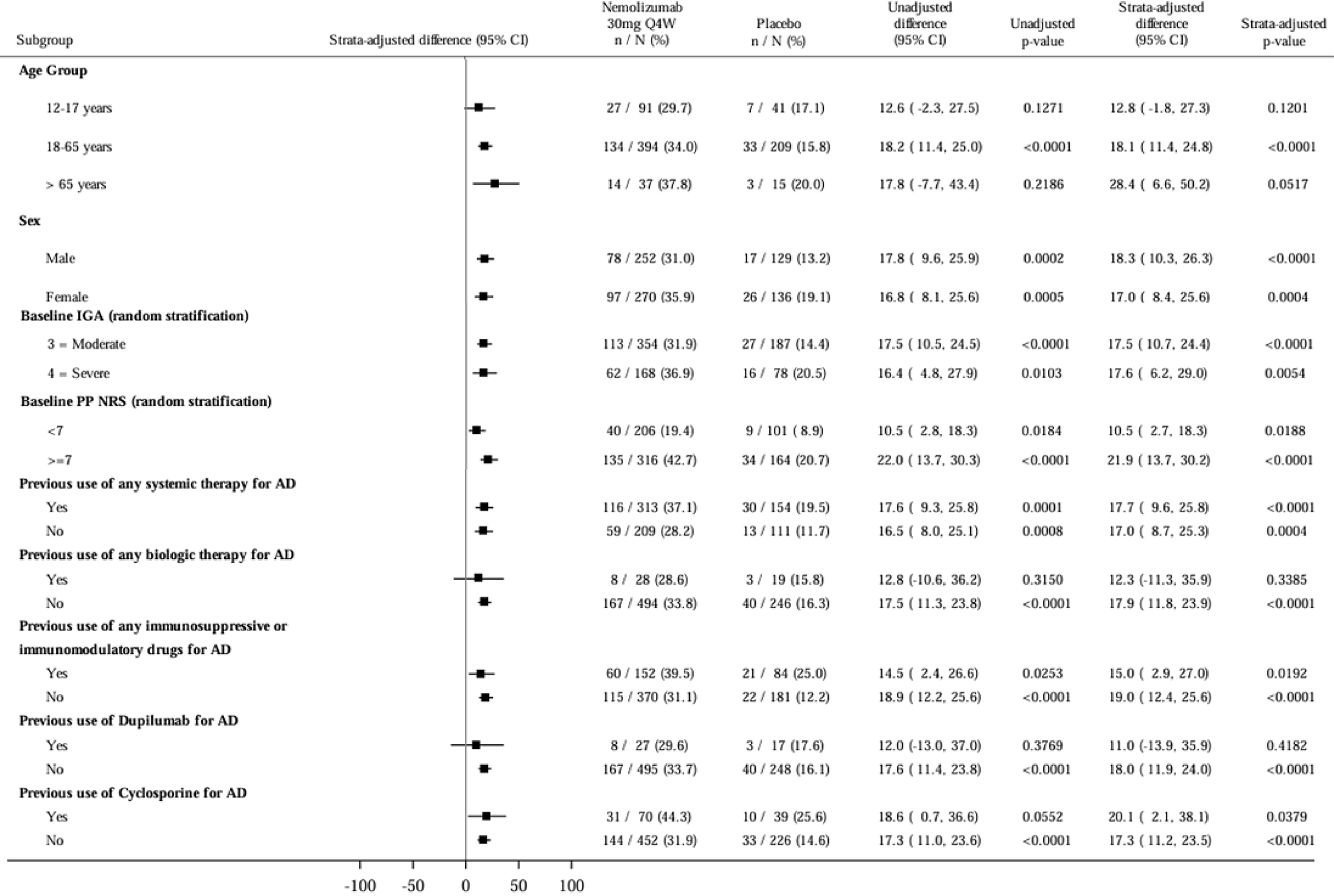
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; Q4W = every 4 weeks.
Source: Details included in the figure are from the sponsor’s ARCADIA 2 Clinical Study Report.12
Figure 17: Subgroup Results for the Proportion of Patients With PP-NRS Score of Less Than 2 at Week 16 — The ARCADIA 2 Study Initial Period
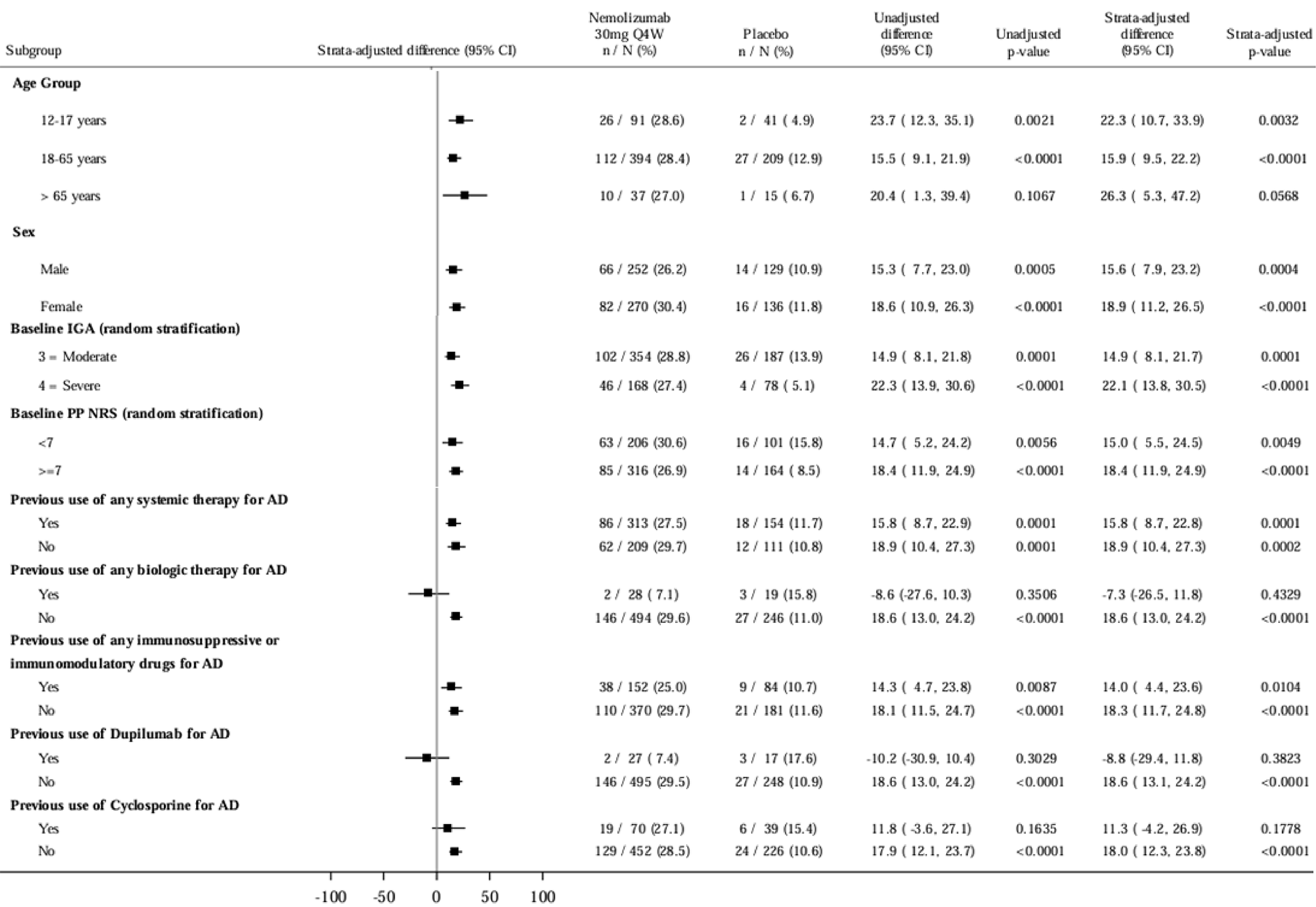
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale; Q4W = every 4 weeks.
Source: Details included in the figure are from the sponsor’s ARCADIA 2 Clinical Study Report.12
Figure 18: Subgroup Results for the Proportion of Patients With IGA Success at Week 16 — The ARCADIA 1 and ARCADIA 2 Studies Initial Period Pooled Analyses
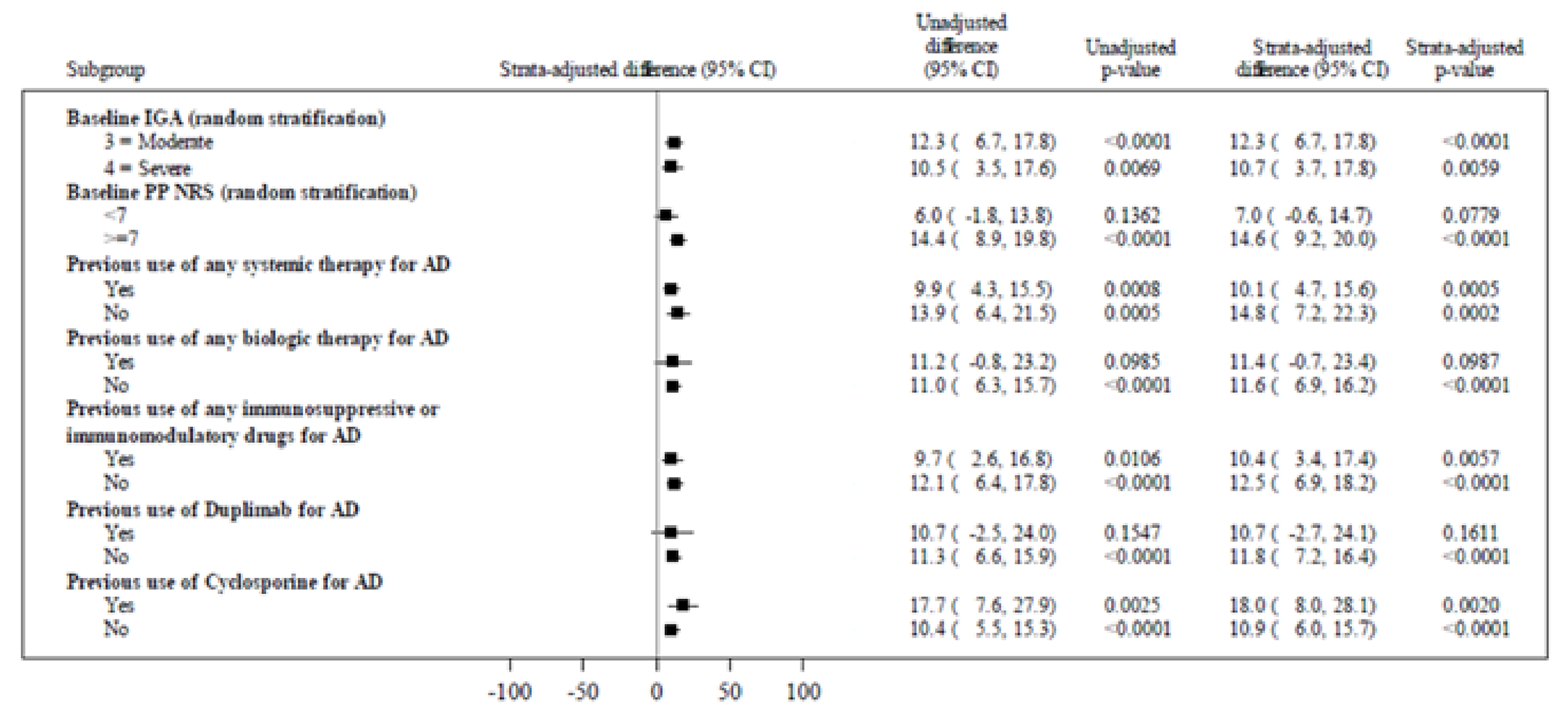
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale.
Source: Details are from the sponsor’s summary of clinical evidence.10
Figure 19: Subgroup Results for the Proportion of Patients With EASI-75 at Week 16 — The ARCADIA 1 and ARCADIA 2 Studies Initial Period Pooled Analyses
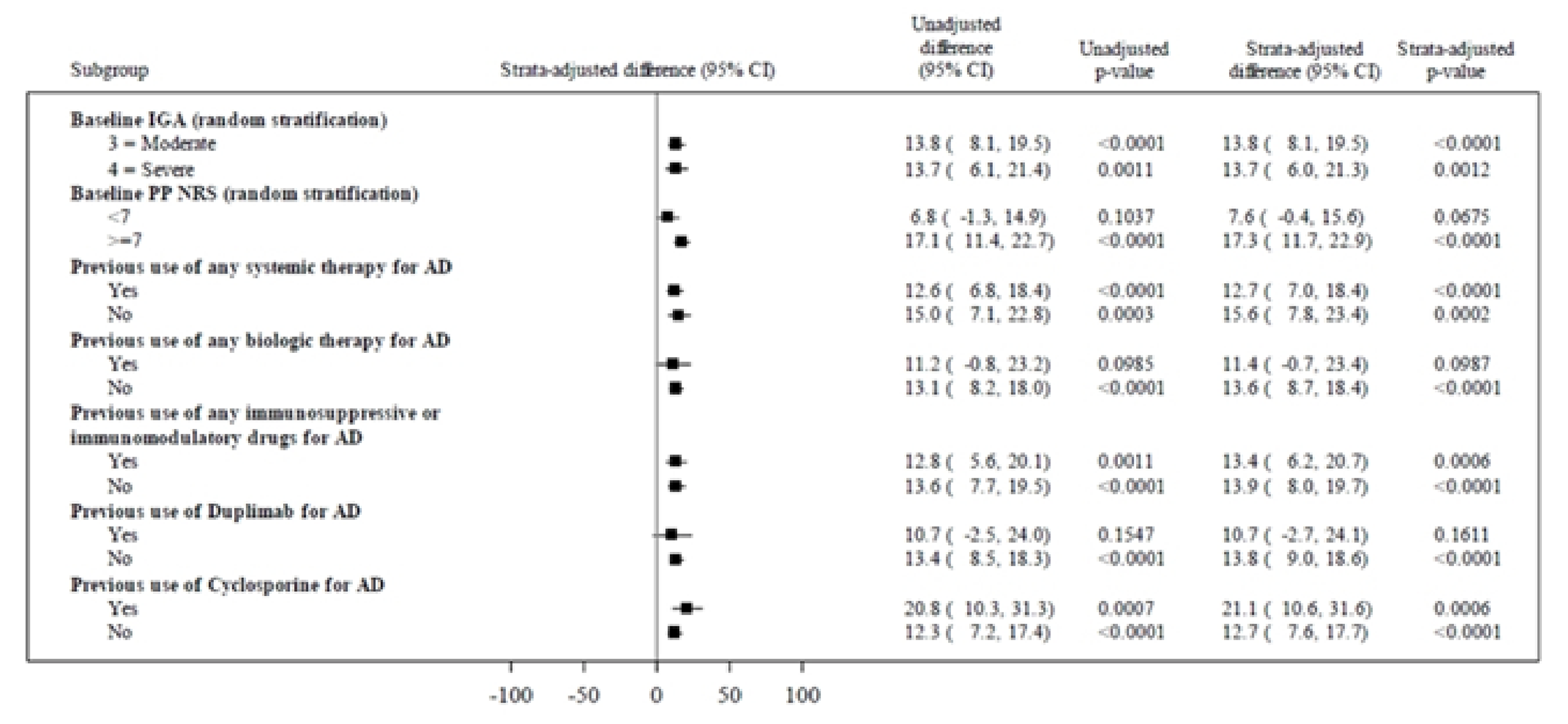
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale.
Source: Details are from the sponsor’s summary of clinical evidence.10
Figure 20: Subgroup Results for the Proportion of Patients With PP-NRS Score Improvement of 4 Points or More at Week 16 — The ARCADIA 1 and ARCADIA 2 Studies Initial Period Pooled Analyses
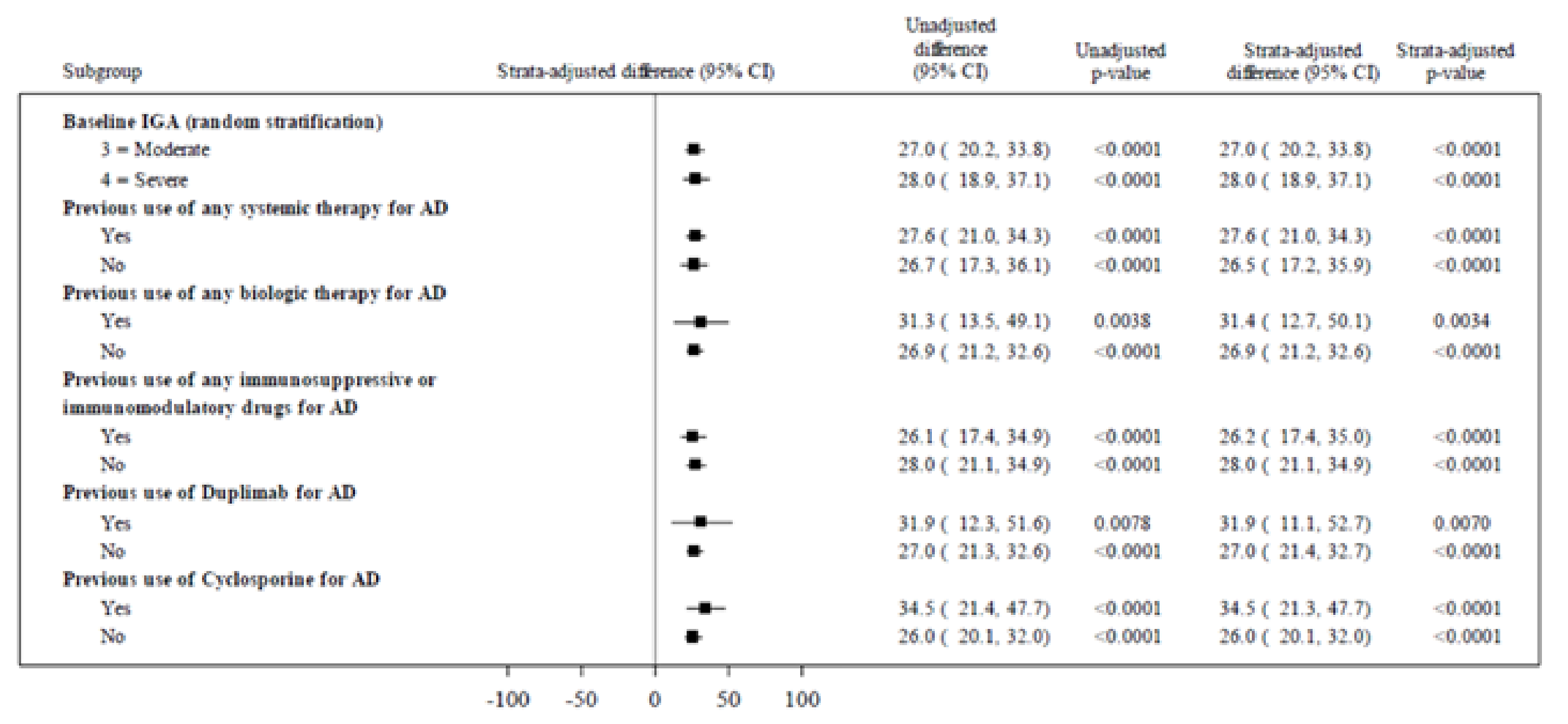
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale.
Source: Details are from the sponsor’s summary of clinical evidence.10
Figure 21: Subgroup Results for the Proportion of Patients With PP-NRS Score of Less Than 2 at Week 16 — The ARCADIA 1 and ARCADIA 2 Studies Initial Period Pooled Analyses
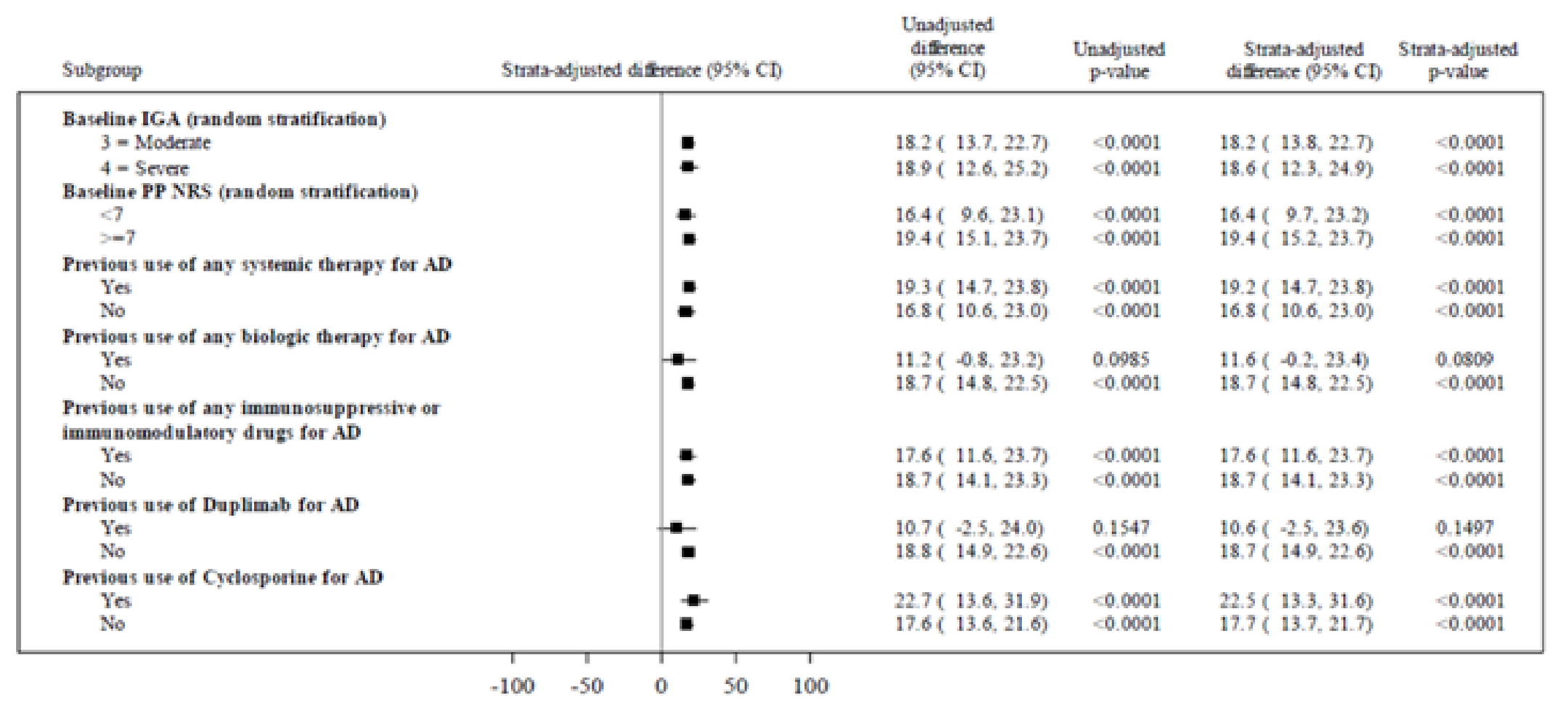
AD = atopic dermatitis; CI = confidence interval; IGA = Investigator Global Assessment; PP-NRS = Peak Pruritus Numeric Rating Scale.
Source: Details are from the sponsor’s summary of clinical evidence.10
Table 38: Summary of POEM Scores for the ARCADIA 1 and ARCADIA 2 Studies (ITT) — Initial Period
Variable | ARCADIA 1 study | ARCADIA 2 study | ||
|---|---|---|---|---|
Nemolizumab N = 620 | Placebo N = 321 | Nemolizumab N = 522 | Placebo N = 265 | |
Number of patients contributing to the analysis, n (%) | 620 | 321 | 515 | 265 |
Baseline, mean (SD) | 20.30 (5.52) | 19.90 (5.81) | 19.90 (5.20) | 19.80 (5.59) |
LS mean change from baseline (95% CI) | –9.04 (–9.72, –8.35) | –5.00 (–5.91, –4.09) | –8.87 (–9.59, –8.26) | –4.95 (–5.93, –3.96) |
LS mean difference vs. placebo (95% CI) | –4.04 (–5.09, –2.99) | –3.93 (–5.07, –2.78) | ||
P value | < 0.0001 | < 0.0001 | ||
CI = confidence interval; ITT = intention to treat; LS = least square; POEM = patient-oriented eczema measure; SD = standard deviation
Sources: Details included in the table are from the sponsor’s ARCADIA 111 and ARCADIA 2 Clinical Study Report.12
Table 39: Summary of POEM Scores for the ARCADIA 1 and ARCADIA 2 Studies (ITT) — Maintenance Period
Variable | ARCADIA 1 and ARCADIA 2 studies | ||
|---|---|---|---|
Nemolizumab q.4.w. to nemolizumab q.4.w. (N = 169) | Nemolizumab q.4.w. to nemolizumab q.8.w. (N = 169) | Nemolizumab q.4.w. to placebo (N = 169) | |
Number of patients contributing to the analysis, n (%) | 148 | 152 | 133 |
Baseline, mean (SD) | 5.70 (5.30) | 6.30 (5.41) | 6.80 (5.87) |
LS mean change from baseline (95% CI) | –0.76 (–1.62, 0.11) | 0.26 (–0.60, 1.11) | 1.65 (0.73, 2.56) |
LS mean difference vs. placebo (95% CI) | –2.40 (–3.66, –1.14) | –1.39 (–2.64, –0.13) | NA |
P value | 0.0002 | 0.0300 | NA |
CI = confidence interval; ITT = intention to treat; LS = least square; NA = not applicable; POEM = patient-oriented eczema measure; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SD = standard deviation.
Sources: Details included in the study are from the sponsor’s ARCADIA 1 and ARCADIA 2 Pooled Maintenance Clinical Study Report.
Table 40: Summary of POEM Scores for the ARCADIA CYCLO Study (ITT) — Initial Period
Variable | ARCADIA CYCLO study | |
|---|---|---|
Nemolizumab N = 138 | Placebo N = 138 | |
Number of patients contributing to the analysis, n (%) | ███ | ███ |
Baseline, mean (SD) | █████ ██████ | █████ ██████ |
LS mean change from baseline (95% CI) | ███ █████ ████ | ███ ████ █████ |
LS mean difference vs. placebo (95% CI) | █████ ███████ ██████ | |
P value | ███████ | |
CI = confidence interval; ITT = intention to treat; LS = least square; POEM = patient-oriented eczema measure; SD = standard deviation.
Source: Details included in the table are from the sponsor’s ARCADIA CYCLO Clinical Study Report.13
Pharmacoeconomic Review
Abbreviations
AD
atopic dermatitis
BIA
budget impact analysis
BSC
best supportive care
CDA-AMC
Canada’s Drug Agency
CMA
cost-minimization analysis
EASI-75
≥ 75% improvement in Eczema Area and Severity Index from baseline
IGA
Investigator Global Assessment
NIHB
Non-Insured Health Benefits
NMA
network meta-analysis
NOC
Notice of Compliance
ODB
Ontario Drug Benefit
Economic Review
The objective of the economic review is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor on the cost and budget impact of nemolizumab compared to dupilumab, upadacitinib, and abrocitinib for the requested reimbursement population (i.e., treatment of moderate to severe atopic dermatitis [AD] in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies). The sponsor’s reimbursement request also included the text “The sponsor is seeking reimbursement criteria that mimics the CDA-AMC recommendation and CDA-AMC-participating jurisdiction implementation for dupilumab for patients with moderate-to-severe AD.” The reimbursement population is narrower than the Health Canada–approved indication. Additional information about the sponsor’s submission is summarized in Appendix 2.
The sponsor’s application was filed on a pre-Notice of Compliance (NOC) basis and the pharmacoeconomic submission and budget impact analysis (BIA) are reflective of the indication that was initially submitted to Health Canada and Canada’s Drug Agency (CDA-AMC). The CDA-AMC appraisal was undertaken based on the submitted information, and the appraisal was not revised after the NOC was received. The updated indication is not expected to materially impact conclusions on cost-effectiveness. Note that the Health Canada–indicated population submitted for the BIA was for the treatment of patients aged 12 years and older with moderate to severe AD who are candidates for systemic therapy, rather than the final approved indication.
Item | Description |
|---|---|
Drug product | Nemolizumab (Nemluvio), 30 mg/0.49 mL powder and solvent solution for subcutaneous injection |
Indication | For the treatment of patients aged 12 years and older with moderate-to-severe atopic dermatitis (AD) whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable |
Submitted price | $2,995.00 per 30 mg prefilled pen |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | December 18, 2025 |
Reimbursement request | For the treatment of moderate to severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies |
Sponsor | Galderma Canada Inc. |
Submission history | Previously reviewed: Yes Indication: For the treatment of moderate to severe prurigo nodularis Recommendation date: Currently under review Recommendation: To be determined |
AD = atopic dermatitis; NOC = Notice of Compliance.
Key Messages
Nemolizumab is available as a prefilled pen for subcutaneous injection (30 mg/0.49 mL). At the submitted price of $2,995.00 per 30 mg prefilled pen, the annual cost of nemolizumab is expected to be $28,519 per patient in the first year of treatment and $19,534 in subsequent years, based on the Health Canada–recommended dosage.
Based on the results of the sponsor’s cost comparison, nemolizumab is expected to be associated with higher drug costs compared to dupilumab, abrocitinib, and upadacitinib in the first year of treatment (incremental costs = $3,357 to $13,683 per patient). In subsequent years, costs to the health system are expected to be lower than those of dupilumab and upadacitinib 30 mg (incremental savings = $5,381 to $8,623 per patient per year), but higher than those of both doses of abrocitinib and upadacitinib 15 mg (incremental costs = $604 to $1,703 per patient per year).
CDA-AMC estimates that the budget impact of reimbursing nemolizumab for the treatment of moderate to severe AD in the reimbursement-requested population will be approximately $45 million over the first 3 years of reimbursement compared to the amount currently spent on dupilumab, abrocitinib, and upadacitinib, with an estimated expenditure of $392 million on nemolizumab over this period. The actual budget impact of reimbursing nemolizumab is uncertain and will depend on the proportion of patients treated at each line of therapy, the proportion who are refractory to or ineligible for each line of therapy, and the proportion who will be publicly funded.
The budget impact of reimbursing nemolizumab for the full Health Canada–indicated population is unknown but would be substantially higher than estimations for the reimbursement-requested population.
Summary of the Submitted Economic Evaluation
The sponsor-submitted cost comparisons for the first year and the average annual cost of subsequent years of treatment including only drug acquisition costs. For adult patients, nemolizumab was more costly than all comparators in year 1 (incremental costs = $3,357 to $13,683 per patient), while in subsequent years nemolizumab was more costly than upadacitinib 15 mg and both doses of abrocitinib (incremental costs = $604 to $1,703 per patient per year), but less costly than dupilumab and upadacitinib 30 mg (incremental savings = $5,979 to $8,623 per patient per year). For adolescent patients, nemolizumab was more costly than all comparators in year 1 (incremental costs = $4,924 to $13,683 per patient), while in subsequent years it was more costly than upadacitinib 15 mg and both doses of abrocitinib (incremental costs = $604 to $1,703 per patient per year), but less expensive than dupilumab (incremental savings = $5,381 per patient per year).
The sponsor also submitted 2 long-term cost-minimization analyses (CMAs) comparing nemolizumab plus best supportive care (BSC) to dupilumab plus BSC, upadacitinib plus BSC, abrocitinib plus BSC, and BSC alone (i.e., placebo) from the perspective of a public drug plan payer in Canada over a lifetime horizon (60 years). The modelled populations comprised adults (aged ≥ 18 years) or adolescents (aged ≥ 12 to < 18 years) with moderate to severe AD after failure of topical therapies and at least 1 systemic immunosuppressant or for whom these are not suitable, which is narrower than the Health Canada–indicated population. Baseline characteristics were informed by a multiple technology appraisal report by the National Institute for Health and Care Excellence.1 The sponsor’s base-case analysis included costs related to drug acquisition, including BSC, administration, disease monitoring, and adverse events. Based on the sponsor’s assumption of clinical similarity, all costs aside from drug acquisition costs were assumed to be equal across all comparators.
For adult patients, in the sponsor’s CMA and against active comparators, nemolizumab plus BSC was associated with a difference in costs ranging from a savings of $74,413 relative to upadacitinib 30 mg daily to an incremental cost of $37,054 relative to abrocitinib 100 mg or 200 mg daily. For adolescent patients, differential costs associated with nemolizumab plus BSC ranged from a savings of $49,915 relative to dupilumab to additional costs of $37,625 relative to abrocitinib 100 mg or 200 mg daily. Relative to placebo, the incremental cost of nemolizumab was $228,821 for adult patients and $233,628 for adolescent patients. All differences in costs were based on differences in drug acquisition costs. Additional information about the sponsor’s submission is summarized in Appendix 2.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 2; full details are provided in Appendix 3). As the sponsor had also submitted a short-term cost comparison, CDA-AMC did not conduct reanalyses on the CMAs.
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The clinical similarity of nemolizumab to relevant comparators is uncertain. | There have been no head-to-head trials comparing nemolizumab to relevant comparators. The conclusion that nemolizumab is clinically similar to its comparators is uncertain based on NMA evidence demonstrating that some comparators were favoured over nemolizumab. For other comparisons, the NMA reported wide credible intervals where either nemolizumab or its comparators could be favoured. Additionally, the NMA’s results were uncertain due to a spare network and because the timing of response assessment in the NMA was not aligned with clinical practice, increasing uncertainty in the clinical similarity of nemolizumab to its comparators over a relevant time period. Finally, there was a lack of data supporting the claim of clinical similarity in adolescents with systemic therapy experience. | CDA-AMC could not address uncertainty in the comparative clinical evidence. | No scenario analysis was conducted because of a lack of robust clinical data. |
The inputs informing the long-term CMA were inappropriate. | The sponsor assumed that 100% of patients would initially respond to all comparators and that, upon losing response, they would discontinue to a basket of therapies that included therapies patients already received as well as those not funded in Canada. This resulted in the submitted CMA not adequately representing the costs that would be incurred by the public health care system for each comparator, or their relative costs. | CDA-AMC could not address this limitation in reanalysis, but instead accepted the sponsor’s submitted short-term cost comparison. | No scenario analyses were conducted. |
Poor modelling practices were employed. | The submitted CMA was overly complex considering the assumptions of clinical similarity, and contained numerous IFERROR statements, limiting the ability of the CDA-AMC to fully validate the analysis. | CDA-AMC could not address this limitation, but instead accepted the sponsor’s submitted short-term cost comparison. | No scenario analyses were conducted. |
The sponsor’s analyses rely on publicly accessible list prices and do not reflect existing confidential prices negotiated by public plans. | Dupilumab, abrocitinib, and upadacitinib have successfully undergone price negotiations for the treatment of atopic dermatitis, and it is likely that the current unit costs paid by public drug plans for these treatments are lower than the submitted prices. | CDA-AMC was unable to incorporate the presence of confidential negotiated prices in the reanalysis. | No scenario analyses were conducted. |
CDA-AMC = Canada’s Drug Agency; CMA = cost-minimization analysis, NMA = network meta-analysis.
Note: Full details of the issues identified by CDA-AMC are provided in Appendix 3.
CDA-AMC Assessment of Cost
CDA-AMC did not conduct a reanalysis of the CMA due to limitations in the submitted analysis. CDA-AMC focused on results from the short-term cost comparison.
Summary of the Budget Impact
The sponsor submitted a BIA to estimate the 3-year (2027 to 2029) budget impact of reimbursing nemolizumab for use in the reimbursement-requested population. The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach. The price of nemolizumab was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in Appendix 4.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (Appendix 4). CDA-AMC estimated that approximately 28,000 patients per year would be eligible for treatment with nemolizumab over a 3-year period, of whom approximately 8,000 are expected to receive nemolizumab by year 3 of the analysis. The estimated incremental budget impact of reimbursing nemolizumab is expected to be approximately $45 million over the first 3 years, with an expected expenditure of $392 million on nemolizumab. The actual budget impact of reimbursing nemolizumab is uncertain and will depend on the proportion of patients treated at each line of therapy, the proportion who are refractory to or ineligible for each line of therapy, the proportion who will be publicly funded, and the actual prices for comparators paid by public plans.
The budget impact of reimbursing nemolizumab for its indicated population is unknown but would be substantially higher than funding it for the reimbursement-requested population.
Conclusions
At the submitted price for nemolizumab, and using publicly available list prices for comparators, nemolizumab is expected to be more costly than dupilumab, abrocitinib, and upadacitinib in the first year of treatment in adults and adolescents with moderate to severe AD. In subsequent years, nemolizumab is expected to be more costly than both doses of abrocitinib and upadacitinib 15 mg but less costly than dupilumab and upadacitinib 30 mg. To ensure cost-effectiveness, nemolizumab should be priced to ensure no additional costs to the health system relative to the lowest-cost alternative for treating patients with moderate to severe AD.
The budget impact of reimbursing nemolizumab to the public drug plans in the first 3 years is estimated to be approximately $45 million, if funded for the reimbursement-requested population. The 3-year expenditure on nemolizumab is estimated to be $392 million. The budget impact of funding nemolizumab for its full indicated population is unknown but is expected to be substantially higher. The actual budget impact of reimbursing nemolizumab is uncertain and will depend on the proportion of patients treated at each line of therapy, the proportion who are refractory to or ineligible for each line of therapy, the proportion who will be publicly funded, and any confidential pricing that may exist for the comparators.
Economic Review Appendices
The sponsor’s application was filed on a pre-NOC basis and the pharmacoeconomic submission is reflective of the indication and product monograph that were initially submitted to Health Canada and CDA-AMC. There were no changes to the dosing regimen, but the sponsor’s submission was not specific to those whose disease was not adequately controlled with topical prescription therapies or when those therapies were not advisable. The CDA-AMC appraisal was undertaken based on the submitted information, and the appraisal was not revised after the NOC was received.
References
1.National Institute of H, Care E. Abrocitinib, tralokinumab or upadacitinib for treating moderate to severe atopic dermatitis [TA814][sponsor supplied reference]. 2022. Accessed 20/02/2023. https://www.nice.org.uk/guidance/ta814
2.Galderma Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Nemluvio (nemolizumab), 30 mg/0.49 mL lyophilized powder and solvent solution for subcutaneous injection. February 27, 2025.
3.Ontario Ministry of Health. Exceptional Access Program (EAP). Accessed March 28, 2025. http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx
4.Government of Saskatchewan. Saskatchewan Drug Plan: search formulary. 2024. Accessed March 28, 2025. http://formulary.drugplan.ehealthsask.ca/SearchFormulary
5.Ontario Ministry of Health. Ontario drug benefit formulary/comparative drug index. Accessed March 28, 2025. https://www.formulary.health.gov.on.ca/formulary/
6.Sidbury R, Davis DM, Cohen DE, et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. J Am Acad Dermatol. 2014;71(2):327-49. doi:10.1016/j.jaad.2014.03.030 PubMed
7.Davis DMR, Drucker AM, Alikhan A, et al. Guidelines of care for the management of atopic dermatitis in adults with phototherapy and systemic therapies. J Am Acad Dermatol. 2024;90(2):e43-e56. doi:10.1016/j.jaad.2023.08.102 PubMed
8.Galderma Canada Inc. Nemolizumab for treatment of atopic dermatitis: network meta-analysis report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Nemolizumab (Nemluvio); 30 mg subcutaneous injection. 2024.
9.Galderma Data on F. ARCADIA 1 Clinical Study Report [sponsor supplied reference]. 2023;
10.Galderma Data on F. ARCADIA 2 Clinical Study Report [sponsor supplied reference]. 2023;
11.Galderma Data on F. ARCADIA-CYCLO Clinical Study Report [sponsor supplied reference]. 2023;
12.Ministry of Health O. Schedule of Benefits, Physician Services Under the Health Insurance Act (June 29, 2023 (effective July 24, 2023)) [sponsor supplied reference]. 2023. Accessed 12/12/23. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-2024-01-24.pdf
13.National Institute of H, Care E. Dupilumab for treating moderate to severe atopic dermatitis [TA534] [sponsor supplied reference]. 2018. Accessed 20/02/2023. https://www.nice.org.uk/guidance/ta534
14.Galderma Canada Inc. Drug Reimbursement Review sponsor submission: Nemluvio (nemolizumab), 30 mg/0.49 mL, lyophilized powder and solvent solution for subcutaneous injection [internal sponsor's package]. February 27, 2025.
15.pan-Canadian Pharmaceutical Alliance. Dupixent (dupilumab) for atopic dermatitis. 2023. Accessed 2025 May 19. https://www.pcpacanada.ca/negotiation/22214
16.pan-Canadian Pharmaceutical Alliance. Dupixent (dupilumab) for atopic dermatitis, pediatrics. 2024. Accessed 2025 May 19. https://www.pcpacanada.ca/negotiation/22496
17.pan-Canadian Pharmaceutical Alliance. Cibinqo (abrocitinib) for atopic dermatitis, moderate to severe. 2023. Accessed 2025 May 19. https://www.pcpacanada.ca/negotiation/21987
18.pan-Canadian Pharmaceutical Alliance. Rinvoq (upadacitinib) for atopic dermatitis. 2023. Accessed 2025 May 19. https://www.pcpacanada.ca/negotiation/21907
19.Galderma Canada Inc. Nemluvio (nemolizumab): 30 mg powder and solvent solution for subcutaneous injection [DRAFT product monograph]. February 12th, 2024. Updated January 1, 1800.
20.Sanofi-aventis Canada Inc. Dupixent (dupiluamb): 300 mg single-use syringe (300 mg/2 mL), 300 mg single-use pen (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL), 200 mg single-use pen (200 mg/1.14 mL), solution for subcutaneous injection [product monograph]. 2017. Accessed May 17, 2025. https://pdf.hres.ca/dpd_pm/00077903.PDF
21.Eli Lilly Canada Inc. Ebglyss (lebrikizumab injection) solution for subcutaneous injection [product monograph]. Eli Lilly Canada, Inc.; 2024. Accessed May 30, 2025. https://pdf.hres.ca/dpd_pm/00076063.PDF
22.LEO Pharma Inc. Adtralza (tralokinumab injection) solution for subcutaneous injection [product monograph]. LEO Pharma Inc.; 2021. Accessed May 30, 2025. https://pdf.hres.ca/dpd_pm/00071936.PDF
23.Canada's Drug A. Reimbursement recommendation: lebrikizumab (Ebglyss). Can J Health Technol. 2024;vol 4(iss 11)doi:DOI.
24.Canada's Drug A. Reimbursement recommendation: tralokinumab (Adtralza). Can J Health Technol. 2024;vol 4(iss 5)doi:DOI.
25.Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy. 2018;73(6):1284-1293. doi:10.1111/all.13401 PubMed
26.Silverberg JI, Barbarot S, Gadkari A, et al. Atopic dermatitis in the pediatric population: A cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol. 2021;126(4):417-428.e2. doi:10.1016/j.anai.2020.12.020 PubMed
27.Galderma. ClearView Analysis [sponsor supplied reference]. 2024.
28.Canada's Drug Agency. Pharmacoeconomic Review Report for Upadacitinib (RINVOQ) [sponsor supplied reference]. 2022.
29.Galderma Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Nemluvio (nemolizumab), 30 mg/0.49 mL lyophilized powder and solvent solution for subcutaneous injection. March, 2025.
30.Galderma. Galderma response to Canada's Drug Agency request for additional information regarding nemolizumab review on April 11, 2025: Sections of the ClearView Analysis 2024 [internal additional sponsor's information]. 2025.
31.Canada's Drug A. Reimbursement Review: upadacitinib (Rinvoq). Can J Health Technol. 2022;vol 2(iss 10)doi:DOI.
32.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada; 2017. Accessed May 21, 2025. https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326
33.Gagnon-Arpin I, Chen, W. and Leaver, C. Understanding the Gap 2.0: A Pan-Canadian Analysis of Prescription Drug Insurance Coverage. The Conference Board of Canada; 2022. Accessed 2025 May 21. https://www.conferenceboard.ca/product/understanding-the-gap-2-0-a-pan-canadian-analysis-of-prescription-drug-insurance-coverage-2/
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 3: CDA-AMC Cost Comparison Table for Treatment of Moderate to Severe Atopic Dermatitis
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Nemolizumab (Nemluvio) | 30 mg / 0.49 mL | Prefilled syringe or prefilled pen | 2,995.0000a | 60 mg initially, followed by 30 mg every 4 weeks; after 16 weeks, the recommended maintenance dose for patients who achieve a clinical response is 30 mg every 8 weeks | Year 1: 78.08 Year 2: 53.48 | Year 1: 28,519 Year 2+: 19,534 |
Systemic therapies | ||||||
Abrocitinib (Cibinqo) | 50 mg 100 mg 200 mg | Tablet | 48.6667b 48.6667b 54.4667b | 100 mg or 200 mg once daily | 48.67 or 54.47 | 17,776 or 19,894 |
Dupilumab (Dupixent) | 200 mg / 1.14 mL 300 mg / 2 mL | Prefilled syringe or prefilled pen | 978.7000b | Adolescents 30 kg to < 60 kg: 400 mg as an initial dose, followed by 200 mg every 2 weeks Adolescents ≥ 60 kg and adults: 600 mg as an initial dose, followed by 300 mg every 2 weeks | Year 1: 72.59 Year 2+: 69.91 | Year 1: 26,512 Year 2+: 25,534 |
Upadacitinib (Rinvoq) | 15 mg 30 mg | Extended-release tablet | 51.6810c 76.9600c | Adolescents (12 to 17 years) > 40 kg: 15 mg once daily Adults: 15 mg or 30 mg once daily depending on individual patient presentation | Adolescents: 51.68 Adults: 51.68 to 76.96 | Adolescents: 18,876 Adults: 18,876 to 28,110 |
Note: Assumes a 365.25 day (52.18 week) year.
aSponsor-submitted price.2
bOntario Drug Benefit Exceptional Access Program list price (accessed March 2025).3
cSaskatchewan Formulary (accessed March 2025).4
Table 4: Cost Comparison for Treatment of Moderate to Severe Atopic Dermatitis (Off-Label)
Drug/ comparator | Strength / concentration | Dosage form | Price ($) | Recommended dosage | Daily cost ($)a | Annual ($)a |
|---|---|---|---|---|---|---|
Immunosuppressants | ||||||
Azathioprine (generic) | 50 mg | Tablet | 0.2405 | Adolescents: 1.0 to 4.0 mg/kg per day Adults: 2.5 to 5 mg/kg per day | Adolescent: 0.24 to 0.96 Adult: 0.96 to 1.92 | Adolescent: 88 to 351 Adult: 176 to 439 |
Cyclosporine (generic) | 10 mg 25 mg 50 mg 100 mg | Capsule | 0.7526 0.8657 1.6885 3.3792 | Adolescent: 3.0 to 6.0 mg/kg per day Adult: 3 to 5 mg/kg per day | Adolescent: 5.07 to 10.14 Adult: 8.49 to 13.52 | Adolescent: 1,851 to 3,703 Adult: 3,101 to 4,937 |
Methotrexate (generic) | 2.5 mg | Tablet | 0.2513 | Adolescent: 0.2 to 0.7 mg/kg per week Adult: 10 to 25 mg per week | Adolescent: 0.14 to 0.36b Adult: 0.14 to 0.36 | Adolescent: 52 to 131b Adult: 52 to 131 |
Mycophenolate mofetil | 250 mg 500 mg | Capsule | 0.3712 0.7423 | Adolescent: 30 to 50 mg/kg per day Adult: Up to 3,000 mg per day, in 2 doses | Adolescent: 2.23 to 3.71 Adult: Up to 4.45 | Adolescent: 813 to 1,355 Adult: Up to 1,627 |
Note: Unit prices of medications are taken from the Ontario Drug Benefit Formulary (accessed March 2025),5 unless otherwise indicated, and do not include dispensing fees. Recommended dosage is based on the American Academy of Dermatology Guidelines from 2014 for adolescents6 and 2024 for adults.7 Annual costs assumes 365.25 days for all comparators.
aAssumes a mean adult weight of 80 kg and a mean adolescent weight of 50 kg.
bAssumes adolescent dose will be capped at upper end of adult range.
Appendix 2: Additional Details of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Nemolizumab (Nemluvio), 30 mg/0.49 mL powder and solvent solution for subcutaneous injection |
Submitted price of drug under review | $2,995.00 per 30 mg prefilled pen |
Regimen | Nemolizumab: 60 mg loading dose, followed by 30 mg every 4 weeks until week 24, then 30 mg every 8 weeks plus SOC.a |
Annual cost | Year 1: $31,448 per patient. Subsequent years: $19,468 per patient per year. |
Model information | |
Type of economic evaluation | Short-term cost comparison, long-term CMA |
Treatment | Nemolizumab plus SOC |
Included comparators | Adults: Abrocitinib 100 mg or 200 mg daily plus SOC, dupilumab 300 mg every 2 weeks (after 600 mg loading dose) plus SOC, upadacitinib 15 mg or 30 mg daily plus SOC, SOC alonea Adolescents: Abrocitinib 100 mg or 200 mg daily plus SOC, dupilumab 200 mg every 2 weeks (after 400 mg loading dose) plus SOC, upadacitinib 15 mg daily plus SOC, SOC alonea |
Perspective | Publicly funded health care payer |
Time horizon | Cost comparison: 2 years (year 1 and year 2 costs separately) CMA: Lifetime (60 years) |
Modelled populations | Adults (≥ 18 years) with moderate to severe AD after failure of topical therapies and at least 1 systematic immunosuppressant or for whom these are not suitable (mean age = 34.6 years; mean weight = 76 kg; 32.6% female, 67.4% male). Adolescents (≥ 12 to < 18 years) with moderate to severe AD after failure of topical therapies and at least 1 systematic immunosuppressant or for whom these are not suitable (adolescent mean age = 15.5 years; adolescent mean weight 63 kg; 50% female, 50% male.) Baseline characteristics were based on a NICE Multiple Technology Appraisal, which reported evidence from the Measure UP 1, Measure UP 2, and AD UP upadacitinib trials.1 |
Model health states | Maintenance (patients receive an initial therapy plus a basket of creams), SOC (patients have discontinued initial therapy and receive a basket of creams, biologics, and JAK inhibitors), and deatha |
Data sources | |
Comparative efficacy | The assumption of clinical efficacy was based on the sponsor-submitted NMA,8 allowing the comparison of nemolizumab, as studied in the ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO trials,9-11 with dupilumab, abrocitinib, and upadacitinib. |
Resource use and costs |
|
Summary of the submitted results | |
Short-term cost comparison results |
|
Long-term cost-minimization analysis results |
|
AD = atopic dermatitis; CMA = cost-minimization analysis; SC = subcutaneous; SOC = standard of care; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis.
aSOC was composed of a basket of topical calcineurin inhibitors, topical corticosteroids, and emollients during treatment with the initial therapy. After discontinuation of the initial therapy, the casket was composed of topical calcineurin inhibitors, topical corticosteroids, emollients, biologics, and JAK inhibitors.
Appendix 3: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
Assuming similar clinical efficacy and safety for nemolizumab compared to dupilumab, abrocitinib, and upadacitinib, the sponsor submitted a cost comparison and a CMA. The cost comparisons compared drug acquisition costs, while the CMA compared drug acquisition, administration, and health care resource use for the treatment of moderate to severe AD in patients aged 12 to 17 years (adolescent population) and 18 years and older (adult population) whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies. Based on the CDA-AMC Clinical Review of the sponsor-submitted network meta-analysis (NMA), the assumption that nemolizumab has comparable clinical efficacy to its comparators, which is required to support a CMA, is uncertain due to the results suggesting a more favourable efficacy profile for upadacitinib 30 mg across all outcomes and to a lesser extent abrocitinib (which was favoured over nemolizumab for Investigator Global Assessment [IGA] response), with no difference observed for dupilumab compared to nemolizumab. When considering safety, results of the NMA did not support a difference between nemolizumab and its comparators. Overall, the CDA-AMC Clinical Review concluded that evidence from the NMA was subject to uncertainty due to imprecision, a lack of comparative data beyond 16 weeks, and a lack of data in adolescents who are refractory or ineligible for systemic immunosuppressant therapies.
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
The clinical similarity of nemolizumab to relevant comparators is uncertain: The sponsor submitted a CMA assuming clinical similarity between nemolizumab and comparators. In the absence of direct evidence comparing nemolizumab to dupilumab, abrocitinib, or upadacitinib, the sponsor submitted an NMA using data from the ARCADIA 1, ARCADIA 2, and ARCADIA CYCLO trials. For adults with systemic therapy experience, NMA results for an improvement of 75% or more in the Eczema Area and Severity Index from baseline (EASI-75), Peak Pruritus Numeric Rating Scale, and IGA response at week 16 favoured upadacitinib 30 mg over nemolizumab. Results for IGA response also favoured abrocitinib over nemolizumab. No data were available for adolescents with systemic therapy experience. There was no difference between nemolizumab and dupilumab for any outcomes of interest in the NMAs. As well, safety results from the NMA did not detect a difference between nemolizumab and any relevant comparators. Overall, the network was sparse, and the results were subject to uncertainty due to imprecision. Taken together, it is uncertain whether nemolizumab is clinically similar to other advanced therapies. If differences between nemolizumab and comparators exist, a CMA would be insufficient to assess cost-effectiveness.
Additionally, outcomes in the NMA were assessed at 16 weeks, which is inconsistent with current reimbursement renewal criteria for dupilumab, upadacitinib, and abrocitinib, where response is defined as achieving an EASI-75 response within 6 months for dupilumab, or within 20 weeks for the JAK inhibitors.3,4 As the sponsor has requested reimbursement implementation similar to that of dupilumab,14 response to nemolizumab is presumably also intended to be assessed at 6 months. The efficacy and safety of nemolizumab relative to its comparators at 6 months is unknown.
Due to limitations of the model and a lack of clinical data, CDA-AMC was unable to adjust the time point of response to 6 months to better reflect current funding criteria and renewal in Canada, nor to account for a lack of response data for adolescent patients who are refractory to or ineligible for systemic immunotherapies.
The inputs informing the long-term CMA were inappropriate: In the submitted CMA, the sponsor assumed that all comparators, including placebo (representing standard of care alone), were associated with a 100% EASI-75 response rate. All patients therefore continued their initially assigned treatment throughout the first year, after which the sponsor assumed patients would begin to discontinue due to treatment waning. In contrast, 43.5% of patients in the nemolizumab group of the ARCADIA 1 trial attained an EASI-75 response, while 42.1% did so in the ARCADIA 2 trial by week 16.9,10 While it was appropriate to assume equal response rates between active comparators due to the underlying assumption of clinical equivalence necessary for a CMA, the assumption that all patients initially respond to therapy inappropriately inflates costs for all comparators. Additionally, after discontinuation due to treatment waning, patients were assumed to take a standard of care basket of treatments that included topical treatments (e.g., emollients, calcineurin inhibitors, and corticosteroids) as well as systemic biologics (dupilumab and tralokinumab) and JAK inhibitors (upadacitinib, abrocitinib, and baricitinib). As such, patients discontinuing their initially modelled therapy were often assumed to be switched to a therapy they may have just discontinued (abrocitinib, upadacitinib, or dupilumab) or 1 which is not publicly funded in Canada (tralokinumab or baricitinib). Patients who were initially assigned to standard of care alone (i.e., placebo), also gained access to this expanded basket of therapies (i.e., topicals, biologics, and JAK inhibitors) once their initially assumed response waned. Additionally, baseline patient characteristics were ultimately derived from the upadacitinib trials rather than the nemolizumab trials,1 and, when considering the adolescent population, the sponsor assumed costs for adverse events for patients receiving nemolizumab but not for the other comparators. Finally, the sponsor’s long-term CMA included BSC as a comparator which is uncertain because clinical expert feedback obtained by CDA-AMC indicated that nemolizumab reimbursement is not expected to expand the number of patients who will receive advanced therapies beyond those who would otherwise already receive 1 of the available biologics (i.e., dupilumab) or JAK inhibitors (i.e., upadacitinib, abrocitinib) funded for the treatment of moderate to severe AD. As such, it is unlikely that BSC would be considered to be a relevant comparator. The sponsor’s long-term CMA therefore does not adequately represent costs to the public health care system that would result from the use of each included comparator and thus does not adequately reflect relative costs between comparators.
Given the lack of clinical evidence supporting a price premium for nemolizumab, and as a relevant cost comparison was also presented, CDA-AMC did not conduct reanalyses on the long-term CMA and instead focused on the cost comparison.
Poor modelling practices were employed: The sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical. It remains unclear whether the model is running inappropriately by overriding errors. Additionally, given the assumption of clinical similarity and thus the assumption of equivalent costs for adverse events, health states, and so forth, the sponsor’s submitted CMA was overly complex, increasing the time required to validate the model.
CDA-AMC was unable to address this limitation.
Confidential pricing agreements: The sponsor’s analysis appropriately incorporated pricing available from the Ontario Drug Benefit (ODB) Formulary5 and Exceptional Access Program.3 However confidential pricing agreements exist for dupilumab,15,16 abrocitinib,17 and upadacitinib18 for AD. Therefore, the submitted price of nemolizumab may require a further price reduction to avoid incurring additional costs relative to its comparators.
CDA-AMC was unable to address this limitation as the negotiated prices of the comparators are unknown.
CDA-AMC Cost Analysis
Due to limitations in clinical data and methods, CDA-AMC was unable to address key issues in the sponsor’s submitted long-term CMA, including uncertainty in the assumption of clinical similarity as well as the inappropriate modelling of long-term costs. As such, CDA-AMC did not conduct reanalyses on the sponsor’s long-term CMA, but instead accepted the short-term cost comparison, which compared drug acquisition costs between comparators in year 1 and in subsequent years of therapy.
Issues for Consideration
Nemolizumab is associated with less frequent dosing than dupilumab: The recommended dosing schedule for nemolizumab is once every 4 weeks during the induction period, and once every 8 weeks thereafter,19 whereas that of dupilumab is once every 2 weeks.20 This less frequent dosing schedule may be preferable for some patients, such as those who travel frequently due to the lower likelihood of needing to bring their injectable therapy with them, or those with an aversion to injections.
Other advanced therapies are indicated for moderate to severe AD but not publicly funded: Lebrikizumab (Ebglyss)21 and tralokinumab (Adtralza)22 are indicated for the treatment of moderate to severe AD in adults and adolescents aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. However, neither product was recommended for reimbursement by CDA-AMC23,24 and thus they are not currently reimbursed by public drug plans in Canada.
Appendix 4: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing nemolizumab for the treatment of moderate to severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies. This population is aligned with the sponsor’s accepted deviation request and is narrower than the Health Canada–approved indication.
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2027 to 2029), with 2026 as the base year. The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits (NIHB) Program. The sponsor estimated the eligible population using an epidemiological approach. The sponsor’s base case included drug acquisition costs. The market share of comparators in the reference scenario and the uptake for nemolizumab in the new drug scenario were estimated using the sponsor’s internal market research. The key inputs to the BIA are documented in Table 6.
The sponsor estimated that the 3-year incremental budget impact associated with reimbursing nemolizumab for the reimbursement-requested population of patients aged 12 years and older with moderate to severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies would be $35,369,152 (year 1 = $22,371,289; year 2 = $15,770,604; year 3 = –$2,772,238). When considering the reimbursement of nemolizumab for the proposed Health Canada–indicated population of patients aged 12 years and older with moderate to severe AD who are candidates for systemic therapy, the sponsor’s model reported an incremental 3-year budgetary impact of $78,598,115 (year 1 = $49,713,970; year 2 = $35,045,786; year 3 = –$6,161,641). Note that this result for the indicated population is as programmed into the BIA model file, which is inconsistent with the sponsor’s submitted BIA report, which indicated that the budget impact of reimbursing nemolizumab for the entire Health Canada indication would be identical to the budget impact of reimbursement in the sponsor’s reimbursement request.
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) | |
|---|---|---|
Adults (≥ 18 years) | Adolescents (≥ 12 to < 18 years) | |
Target population | ||
Starting number of people | 25,916,220 | 2,130,132 |
Prevalence of AD, diagnosed | 3.5%25 | 15.8%26 |
Proportion diagnosed who are treated | 74%25 | 74%25 |
Proportion diagnosed and treated who have moderate to severe AD | 52%25 | 40%26 |
Proportion treated with topical therapies | ██%27 | ██%27 |
Proportion who are intolerant to, ineligible for, or whose topical and phototherapy treatment was unsuccessful | ██%27 | ██%27 |
Patients that progress to systemic therapy | 40%28 | 40%28 |
Proportion who are intolerant to, ineligible for, or whose systemic therapy was unsuccessful | 45%27 | 45%27 |
Percentage of patients covered by public drug plan | 47%a | 34%a |
Number of patients eligible for drug under review | 15,361 / 15,531 / 15,699 | 3,390 / 3,428 / 3,466 |
Market shares (reference scenario)b | ||
Nemolizumab plus SOC | 0% / 0% / 0% | 0% / 0% / 0% |
Dupilumab plus SOC | ██% / ██% / ██% | ██% / ██% / ██% |
Abrocitinib plus SOC | ||% / ||% / ||% | ||% / ||% / ||% |
Upadacitinib plus SOC | ██% / ██% / ██% | ||% / ||% / ||% |
SOC alone | ||% / ||% / ||% | ||% / ||% / ||% |
Market shares (new drug scenario)b | ||
Nemolizumab plus SOC | ██ % / ██ % / ██ % | ██ % / ██ % / ██ % |
Dupilumab plus SOC | ██ % / ██ % / ██ % | ██ % / ██ % / ██ % |
Abrocitinib plus SOC | || % / || % / || % | || % / || % / || % |
Upadacitinib plus SOC | ██ % / ██ % / ██ % | || % / || % / || % |
SOC alone | || % / || % / || % | || % / || % / || % |
Cost of treatment (year 1/ year 2+, per patient per year) | ||
Nemolizumab plus SOC | $28,902 / $17,521 | $28,902 / $17,521 |
Dupilumab plus SOC | $23,978 / $22,902 | $23,978 / $22,902 |
Abrocitinib plus SOC | $12,435 / $12,435 | $12,435 / $12,435 |
Upadacitinib plus SOC | $20,709 / $20,709 | $13,205 / $13,205 |
SOC alone | $0 / $0 | $0 / $0 |
AD = atopic dermatitis; SOC = standard of care.
aCited as “PDCI Market Access CHRIS Model, 2024,”29 later clarified to be PDCI’s Canadian Health & Reimbursement Insurance Simulation, a model projecting patient access to private and public insurance for pharmaceutical products in Canada.30
bCited as based on internal market research.29
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The full Health Canada indication population scenario was underestimated and inconsistently conducted: In the scenario estimating the budgetary impact of reimbursing nemolizumab for its full proposed indication (i.e., for the treatment of moderate to severe AD in patients aged 12 years and older who are candidates for systemic therapy), the sponsor appropriately removed the requirement for patients to have been intolerant, ineligible, or were previously unsuccessful with systemic therapy. However, in the submitted BIA Excel file, the BSC market share was still assumed to be 0% in the full Health Canada indication scenario, and nemolizumab was assumed to capture the same proportions of the comparators as in the base case, resulting in an estimated budget impact of $78.6 million over 3 years. In contrast, in the submitted BIA report, the sponsor assumed that, if nemolizumab was reimbursed for the entire Health Canada indication, BSC would have 55% of the reference scenario market share and that nemolizumab would capture only 45% of the share it would in the base case, all of which was assumed to come from the other advanced comparators, such that the resulting estimated budget impact was the same as the base case, $35.4 million over 3 years. Within the review period, the sponsor clarified that the information in the report was the intended analysis for the Health Canada indication scenario. Both methods are inappropriate and underestimate the expected budget impact of reimbursing nemolizumab for its full indication. Based on clinical expert feedback received for this review, if nemolizumab was reimbursed without requiring prior failure of, or intolerability or ineligibility to, conventional systemic therapies (i.e., azathioprine, cyclosporine, methotrexate, mycophenolate mofetil, oral corticosteroids), nemolizumab would be expected to displace those therapies. When queried as to what proportion of patients with moderate to severe AD who would otherwise receive conventional systemic therapies would instead be given nemolizumab if funded at the same line of therapy, clinical expert opinion obtained by CDA-AMC noted “virtually all of them.” Given the much lower cost of conventional systemic therapies (refer to Table 4) compared to advanced therapies (refer to Table 3), funding nemolizumab for its full proposed Health Canada indication would lead to a much larger budgetary impact than either estimate submitted by the sponsor.
Due to hard coding within the submitted BIA file, and to limitations noted in the following, CDA-AMC was unable to estimate the budgetary impact of reimbursing nemolizumab for its full proposed Health Canada–indicated population. The budgetary impact of reimbursing nemolizumab for its full proposed indication is expected to be substantially larger than estimated by the sponsor.
The number of patients eligible for nemolizumab is uncertain: In determining the number of patients who will be eligible for nemolizumab and the other advanced therapies, the sponsor inappropriately assumed that all epidemiology inputs are independent of each other. For example, the sponsor’s analysis assumed that if 74% of adult patients diagnosed with AD are treated, and if 52% of adult patients diagnosed with AD have moderate to severe disease, then 74% of adult patients with moderate to severe AD are treated.29 However, these variables are unlikely to be independent of each other as patients with more severe forms of AD are expected to receive treatment in greater proportions than the overall population of patients with that condition. The sponsor provided selected figures from an internal report cited as the ClearView Analysis reporting that ██% of patients with moderate to severe AD █████████████████████████ have received a topical therapy, rather than 74% of ██% as estimated by the sponsor, with a further ||% not being candidates for topicals.27,30 As the sponsor’s requested reimbursement population specifies “those whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable,” when using this data, the ||% of patients with moderate to severe AD who were not candidates for topical therapies should also have been considered part of the population who would move on to systemic therapy rather than being excluded. This is consistent with clinical expert input obtained by CDA-AMC that indicated the assumption that ██% of the population considered moderate to severe would either receive or be ineligible for topical therapy was an underestimate, as many of those who are ineligible for topicals are because too great a percentage of their body surface area was affected.
The sponsor also estimated that 40% of patients for whom topical therapies are insufficient move on to a conventional systemic therapy, consistent with previous reviews submitted to CDA-AMC,23,24,31 and that of these, 45% are unable to tolerate their systemic therapy.29 In contrast, the sponsor-provided data extracted from the analysis of patients with moderate to severe AD ██ ███████████████████████ indicated that approximately 20% of patients who were inadequately controlled on topical treatments were receiving a systemic immunosuppressant in 2024, and that a further 40% to 50% were receiving an advanced therapy.30 This would more closely correspond to an estimated 65% of patients for whom topical therapy was inadequate moving on to a systemic treatment, with approximately 70% of those (45% of 65%), using an advanced therapy rather than conventional systemic therapy. Clinical expert input obtained by CDA-AMC also noted that conventional systemic therapy is often inadequate, estimating that two-thirds of patients would have an inadequate response.
However, it was unclear whether the proportions of patients receiving conventional and advanced therapies after the failure of topical treatments that were provided for ███████ ████████ ███ ███ ██ ████████ reflect proportions seen in clinical practice when considering patients who are publicly funded in Canada alone.
In reanalysis, CDA-AMC assumed that 85% of patients with moderate to severe AD would receive some form of topical therapy, and of these, 64% would have an inadequate response. A further 7% of patients with moderate to severe AD would be ineligible for topical therapy, all of whom would be considered to have an inadequate response due to not receiving the topical therapy. A scenario analysis was conducted assuming that of patients accessing conventional therapies, 67% would have an inadequate response or be ineligible and move on to advanced therapies.
Market share estimates are uncertain: The sponsor estimated market shares for the comparator products, as well as the uptake of nemolizumab, using internal, unspecified, market research. Clinical expert feedback obtained by CDA-AMC indicated that the sponsor’s market share assumptions, particularly in the adolescent population, did not align with clinical practice in Canada. Estimates informed by clinical expert opinion were relatively similar to those used by the sponsor in the adult population, with the market share for upadacitinib being slightly lower than expected, as well as the proportion of nemolizumab’s market capture coming from the JAK inhibitors. In contrast, clinical expert feedback obtained by CDA-AMC indicated that a greater proportion of the adolescent population are expected to use oral JAK inhibitors than estimated by the sponsor due to ease of use and transportability relative to prefilled pens or syringes. Expert feedback estimated that JAK inhibitors likely make up 25% to 33% of the adolescent market, with 80% of that being upadacitinib. This expert input also believed that uptake of nemolizumab was likely overestimated, particularly in the adolescent population, where most capture would be due to displacing dupilumab.
In the adolescent population, CDA-AMC assumed that 20% of the reference scenario market would be upadacitinib, 5% would be abrocitinib, and 75% would be dupilumab. The market uptake of nemolizumab in the adolescent population was reduced by one-half in this population and assumed to exclusively come from dupilumab.
The price of drugs paid by public plans is uncertain: The sponsor’s analysis appropriately incorporated pricing available from the ODB Formulary5 and Exceptional Access Program.3 However confidential pricing agreements likely exist for dupilumab,15,16 abrocitinib,17 and upadacitinib18 for AD. As such, the price paid by public plans for the comparators is likely lower than incorporated into the sponsor’s analysis.
CDA-AMC was unable to address this limitation as the negotiated prices of the comparators are unknown. The budgetary impact of reimbursing nemolizumab at its submitted price is likely underestimated.
The proportion of patients funded by public drug plans is uncertain: The sponsor’s BIA estimates the proportion of patients who will receive publicly funded advanced therapies for AD using the PDCI Canadian Health & Reimbursement Insurance Simulation model. The methods used within the Canadian Health & Reimbursement Insurance Simulation model to estimate the proportion of patients with moderate to severe AD who will be eligible for public drug funding were not provided and differ from proportions listed in the Understanding the Gap 2.032,33 report for either the enrolled or eligible population for each jurisdiction. The proportions of patients eligible assumed by the sponsor are generally higher than the proportion of patients enrolled in each jurisdiction, and generally lower than the proportion eligible within each jurisdiction. Given the annual cost of advanced therapies for AD, it would be expected that patients with moderate to severe AD would be more likely to enrol in public drug plans than the general population, specifically to access their advanced therapies. However, given the relatively young age of the population affected, it would also be expected that many would have private drug coverage through their employers or their parents’ employers.
CDA-AMC did not adjust for this limitation, as it is likely that the proportion of patients who will be funded for nemolizumab is greater than the proportion of the general population who are enrolled in public plans, but less than the proportion who would be eligible to enrol. However, uncertainty remains in the proportion of eligible patients who will be publicly funded.
The NIHB population was inappropriately calculated: Clients of the NIHB Program residing within Ontario who are aged younger than 25 years or 65 years and older are eligible for reimbursement by ODB and thus should be counted as clients of the ODB and included in the Ontario population estimates rather than as clients of the NIHB clients for the purposes of modelling the budget impact of reimbursing nemolizumab for the treatment of moderate to severe AD.
CDA-AMC did not adjust for this limitation in reanalysis. The impact of this limitation on the pan-Canadian model results is expected to be minimal.
Additional limitations were identified but were not considered to be key limitations: The sponsor’s BIA employed poor modelling practices, with many inputs hard coded and not easy to change for all jurisdictions. A full summary of the pan-Canadian analysis was not provided and needed to be calculated by CDA-AMC.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, in consultation with clinical experts, as outlined in Table 7.
Table 7: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Eligible population | Proportion of patients with moderate to severe AD treated with topicals: 74%*██% = ██% Proportion of patients with an inadequate response to topicals = ██% Proportion of patients ineligible for topicals = excluded | Proportion of patients with moderate to severe AD treated with topicals = 85% Proportion of patients with an inadequate response to topicals = 64% Proportion of patients ineligible for topicals = 7% of those with moderate to severe AD |
2. Reference scenario market shares, adolescent | Dupilumab = ██% Upadacitinib = ||% Abrocitinib = ||% | Dupilumab = 75% Upadacitinib = 20% Abrocitinib = 5% |
3. Nemolizumab uptake, adolescent (year 1/year 2/year 3) | ██% / ██% / ██% Uptake is ██% from dupilumab, ██% from ██████ abrocitinib and upadacitinib | 9% / 14% / 20% Uptake is 100% from dupilumab |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 |
AD = atopic dermatitis; BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 8 and a more detailed breakdown is presented in Table 9. In the CDA-AMC base case, the 3-year budget impact of reimbursing nemolizumab for treatment of moderate to severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and who are refractory to or ineligible for systemic immunosuppressant therapies was $44,898,762 (year 1 = $29,713,106; year 2 = $21,980,270; year 3 = –$6,794,614). Note that the budgetary impact of reimbursing nemolizumab becomes negative in year 3 due to a greater proportion of market uptake coming from dupilumab at that time point, and because nemolizumab is most expensive in its first year of therapy compared to subsequent years, whereas the cost of the comparators is similar between the first year of therapy and subsequent years.
Table 8: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 35,369,152 |
CDA-AMC reanalysis 1 | 53,946,391 |
CDA-AMC reanalysis 2 | 54,686,172 |
CDA-AMC reanalysis 3 | 30,287,949 |
CDA-AMC base case: Reanalyses 1 + 2 + 3 | 44,898,762 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments
CDA-AMC conducted the following scenario analysis (Table 9) to highlight uncertainty associated with the potential budget impact:
Increasing the proportion of patients who have an inadequate response or are ineligible to conventional systemic therapy from 45% to 67%.
Table 9: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base casea | Reference total | $395,623,797 | $393,025,450 | $391,440,401 | $392,740,602 | $1,177,206,453 |
Nemolizumab | $0 | $0 | $0 | $0 | $0 | |
All other comparators | $395,623,797 | $393,025,450 | $391,440,401 | $392,740,602 | $1,177,206,453 | |
New drug total | $395,623,797 | $415,396,737 | $407,211,005 | $389,967,863 | $1,212,575,605 | |
Nemolizumab | $0 | $65,505,460 | $104,196,139 | $120,466,859 | $290,168,458 | |
All other comparators | $395,623,797 | $349,891,277 | $303,014,865 | $269,501,005 | $922,407,147 | |
Budget Impact | $0 | $22,371,286 | $15,770,604 | -$2,772,738 | $35,369,152 | |
CDA-AMC base case | Reference total | $593,823,329 | $591,923,760 | $589,424,064 | $591,324,167 | $1,772,671,991 |
Nemolizumab | $0 | $0 | $0 | $0 | $0 | |
All other comparators | $593,823,329 | $591,923,760 | $589,424,064 | $591,324,167 | $1,772,671,991 | |
New drug total | $593,823,329 | $621,636,867 | $611,404,334 | $584,529,553 | $1,817,570,754 | |
Nemolizumab | $0 | $87,203,169 | $143,524,516 | $161,218,074 | $391,945,759 | |
All other comparators | $593,823,329 | $534,433,698 | $467,879,818 | $423,311,479 | $1,425,624,995 | |
Budget Impact | $0 | $29,713,106 | $21,980,270 | -$6,794,614 | $44,898,762 | |
CDA-AMC scenario 1: Higher proportion inadequately respond to conventional systemics | Reference total | $879,738,265 | $876,924,090 | $873,220,835 | $876,035,803 | $2,626,180,728 |
Nemolizumab | $0 | $0 | $0 | $0 | $0 | |
All other comparators | $879,738,265 | $876,924,090 | $873,220,835 | $876,035,803 | $2,626,180,728 | |
New drug total | $879,738,265 | $920,943,507 | $905,784,198 | $865,969,708 | $2,692,697,413 | |
Nemolizumab | $0 | $129,189,879 | $212,628,913 | $238,841,591 | $580,660,383 | |
All other comparators | $879,738,265 | $791,753,627 | $693,155,285 | $627,128,117 | $2,112,037,030 | |
Budget Impact | $0 | $44,019,417 | $32,563,363 | -$10,066,094 | $66,516,685 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
aThe sponsor’s model did not report the reference and new drug scenarios for the pan-Canadian analysis as submitted. CDA-AMC calculated full pan-Canadian results from the individual jurisdictional results.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.