Drugs, Health Technologies, Health Systems
Reimbursement Review
Teplizumab (Tzield)
Sponsor: Sanofi-aventis Canada Inc.
Therapeutic area: Delay onset of stage 3 type 1 diabetes
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
ALT
alanine aminotransferase
AUC
area under the concentration-time curve
BSA
body surface area
CDA-AMC
Canada's Drug Agency
CI
confidence interval
CRS
cytokine release syndrome
CSEM
Canadian Society of Endocrinology and Metabolism
DCO
data cut-off
DKA
diabetic ketoacidosis
FAS
full analysis set
GRADE
Grading of Recommendations, Assessment, Development and Evaluations
HR
hazard ratio
HRQoL
health-related quality of life
ITT
intention to treat
OGTT
oral glucose tolerance test
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
T1D
type 1 diabetes
TEAE
treatment-emergent adverse event
ULN
upper limit of normal
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Teplizumab (Tzield), 2 mg/2 mL per vial for IV infusion |
Sponsor | Sanofi-aventis Canada Inc. |
Indication | To delay the onset of stage 3 T1D in adult and pediatric patients 8 years of age and older with stage 2 T1D |
Reimbursement request | As per Health Canada indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | May 5, 2025 |
Recommended dose | Administer teplizumab by IV infusion (over a minimum of 30 minutes), using a body surface area–based dosing, once daily for 14 consecutive days as follows:
|
NOC = Notice of Compliance; T1D = type 1 diabetes.
Introduction
Type 1 diabetes (T1D) is a chronic, progressive autoimmune condition resulting from the destruction of insulin-producing beta cells in the pancreas, culminating in chronic hyperglycemia and reliance on exogenous insulin for survival.1-3 T1D progresses as a continuum across 3 stages: stage 1 T1D is characterized by the presence of at least 2 diabetes-related autoantibodies and normoglycemia; stage 2 is marked by the development of abnormal glucose tolerance in addition to the presence of at least 2 diabetes-related autoantibodies; and stage 3 T1D is characterized by overt hyperglycemia, the presence of 2 or more diabetes-related autoantibodies, and the development of typical clinical symptoms and signs of diabetes requiring the use of life-long insulin replacement therapy.4,5 Patients who advance to stage 2 T1D have a 100% lifetime risk of progressing to stage 3 T1D.5,6 Patients with T1D and their caregivers have compromised health-related quality of life (HRQoL) compared to the general population.7 The diagnosis of T1D is based on the presence of hyperglycemia (such as elevated levels of fasting plasma glucose, 2-hour plasma glucose value during an oral glucose tolerance test [OGTT], or hemoglobin A1C), presence of clinical symptoms, and detection of diabetes-associated autoantibodies.8 In Canada, the incidence rate of T1D among adolescents and young adults (aged 10 years to 24 years) was 31.89 cases per 100,000 population in 2019.9 Moreover, T1D is the most prevalent form of diabetes in children and adolescents, accounting for more than 90% of childhood diabetes in the majority of Western countries.3 The epidemiology of stage 2 T1D is poorly understood and Canadian data on this stage are limited. People with stage 1 or stage 2 T1D often remain undiagnosed until they reach stage 3, by which time there has been a substantial loss in the number of beta cells and endogenous insulin production.1,2 Globally, the mortality of T1D has changed from increasing during the 1990 to 1999 period to decreasing from 2000 to 2019. Major advances in T1D diagnosis, treatment with insulin, and glucose monitoring strategy make possible the near-normal life expectancy in adolescents and young adults with this condition.10 It has been reported that compared to controls, the hazard ratio (HR) for all-cause mortality was 4.11 (95% confidence interval [CI], 3.24 to 5.22) in patients who developed T1D before 10 years of age, and 2.83 (95% CI, 2.38 to 3.37) in those who developed the disease between 26 years to 30 years of age.11 In addition, a younger age at onset of stage 3 T1D has been associated with higher glycated hemoglobin (also known as hemoglobin A1C) levels and impaired kidney function earlier in the disease course, as well as an increased risk of cardiovascular disease.11,12
Currently there are no treatments approved for patients at stage 2 of the disease. There is an unmet need to treat patients for T1D earlier in the continuum of disease and delay the onset of stage 3 disease. Stage 3 T1D is currently managed with insulin replacement therapy.1,13-15 However, even though sufficient glycemic control may be achieved from intensive insulin management balanced with diet and activity, insulin is not a disease-modifying drug and does not delay the continuum of T1D.13-15
Teplizumab is indicated to delay the onset of stage 3 T1D in adult and pediatric patients aged 8 years and older with stage 2 T1D. The sponsor’s reimbursement request aligns with the Health Canada–approved indication. It binds to CD3 (a cell surface antigen present on T lymphocytes). Teplizumab should be administered by IV infusion using body surface area (BSA)–based dosing, once daily for 14 consecutive days.
Testing Procedure Considerations
Testing for diabetes-related autoantibodies and dysglycemia is not part of the current standard care for identifying individuals with early-stage T1D (including stage 2) in Canada. While dysglycemia testing is widely available and publicly funded, the availability, reimbursement status, and access to autoantibody testing varies by jurisdiction. This could be a barrier to implementation, and may result in inequitable access to teplizumab if it were to be funded. Identification of populations eligible for testing remains a key challenge.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to a call for input from Canada’s Drug Agency (CDA-AMC) and from clinical experts consulted for the purpose of this review.
Patient Input
A joint patient group submission was received from Breakthrough T1D Canada and Diabetes Canada. Breakthrough T1D Canada is a national patient advocacy and research funding organization specifically dedicated to people living in Canada with T1D. Diabetes Canada is a national health charity representing Canadians who are affected by diabetes. Breakthrough T1D Canada and Diabetes Canada gathered information through an online survey conducted from January 10 to February 14, 2025. The survey had 463 respondents (258 female, 156 male).
The majority of respondents (n = 351; 83%) living with stage 3 T1D indicated that they are either extremely concerned or very concerned about the progression of T1D, its impact on daily life over time, and the amount of time they have needed off from work to manage their diabetes. According to the patient groups’ input, the only available treatment for patients with T1D is exogenous insulin, which is often accompanied by medical risks, suboptimal clinical outcomes, and a heavy burden on patients.
The patient groups highlighted that most of the respondents (n = 216; 54%) indicated that they feel there are significant gaps in the availability of immunotherapy medications for T1D, such as teplizumab. At the time patient input was collected, teplizumab was not available in Canada. Patients reported that any delay in disease progression would improve their overall well-being and decrease the risk of diabetic complications; and for young children, a delay of 2 to 3 years in progressing to T1D has a significant impact. Eight survey respondents had experience with teplizumab and noted that teplizumab delayed the onset of T1D, helped to maintain independence, and improved their physical and mental health. Despite the limited experience with teplizumab in Canada, the patient groups stated that having access to teplizumab and its potential to delay the onset of stage 3 T1D will have a significant positive impact on the lives of patients with early-stage T1D.
The patient groups clarified that the indication for teplizumab is stage 2 T1D. Autoantibody testing is performed via a blood test and associated assay; however, this is not yet a standard practice in Canada, and the cost of screening to the Canadian health care system is unclear. The majority of respondents (n = 292; 70%) indicated that they would like to participate in screening for T1D-associated autoantibodies if medications to delay the onset of T1D were available.
Clinician Input
Input From Clinical Experts Consulted for This Review
The information in this section is based on input received from a panel of 3 clinical specialists consulted by CDA-AMC for the purpose of this review.
The clinical experts consulted for this review indicated that the most significant unmet need for patients with stage 2 T1D is that currently, there are no treatments targeting this patient population. In addition, no population-based screening program for stage 2 disease is in place in Canada; thus, the clinical experts indicated that the majority of patients are currently unaware that they have stage 2 disease. Because almost all patients in early stages of T1D will progress to stage 3 T1D (according to the literature, patients who advance to stage 2 T1D have a 100% lifetime risk of progressing to stage 3 T1D), the clinical experts noted that the goals of treatment for patients with stage 2 T1D would be to: delay the onset of stage 3 T1D, prevent stage 3 T1D in those identified as being at high risk, prevent serious complications associated with the transition from stage 2 to stage 3 disease (e.g., hyperglycemia, potential diabetic ketoacidosis [DKA]), and alleviate patients’ anxiety and stress.
The clinical experts indicated that teplizumab would be the first and only disease-modifying therapy to delay the onset of stage 3 T1D in this patient population. The experts also noted that teplizumab would be used as first-line treatment and would not be combined with other treatments. Given the lack of alternative therapies, the experts noted that the use of teplizumab would cause a shift in the current treatment paradigm, being a first-in-class medication for stage 2 T1D. However, structured screening programs would need to be put in place to identify the patients who could benefit from this treatment.
The clinical experts noted that patients with stage 2 T1D are best suited for treatment with teplizumab. The experts highlighted the challenges in identifying patients with stage 2 T1D in clinical practice, because T1D at this stage is asymptomatic, and a population-based screening program for T1D has not been implemented in Canada. In the current clinical practice, patients with stage 2 T1D are usually identified in populations at higher risk of developing T1D, such as those with a family member living with T1D; however, the majority of people (approximately 85%) diagnosed with T1D do not have a family history. The clinical experts also raised concerns about the challenges of such a national screening program. Diabetes-related autoantibody testing is needed to identify patients who are suitable for treatment with teplizumab. The challenge is that the current autoantibody screening tests in Canada vary in sensitivity and specificity, as well as availability and accessibility. Also, it is unknown whether this program is cost-effective, or at what ages screening should be performed.
The clinical experts consulted for this review indicated that in general, outcomes used in clinical practice to determine patients’ response to treatment include delay in onset of stage 3 T1D (assessed every 3 months to 6 months); prevention of DKA in those who progress to stage 3 T1D; and patients’ HRQoL, in particular, psychosocial well-being.
The clinical experts consulted for this review noted that initial IV infusions of teplizumab may be associated with immediate adverse events (AEs), although the therapy is generally safe without serious AEs (SAEs) occurring. AEs may result in treatment discontinuation, while discontinuation due to long-term effects of immunosuppression therapies is less of a concern with teplizumab in clinical practice given the short course of treatment and current evidence available.
The clinical experts indicated that a specialist (typically a pediatric or adult endocrinologist, but could also include internists or general pediatricians) would be required to diagnose, treat, and monitor patients with stage 2 T1D who may receive teplizumab. In addition, the experts emphasized the importance of appropriate infrastructure and clinical expertise to provide IV infusions in hospital settings and monitor patient safety during the 14-day infusions.
Clinician Group Input
CDA-AMC received 1 submission from the Canadian Society of Endocrinology and Metabolism (CSEM). CSEM is a professional organization of academic and community-based endocrinologists and researchers that advocates for excellence in endocrinology research, education, and patient care in Canada.
The clinician group agreed with the clinical experts consulted by CDA-AMC that there are no available therapies that modify the disease progression of T1D in Canada and insulin therapy is required for the treatment of T1D when patients are diagnosed at stage 3. The clinician group and clinical experts consulted by CDA-AMC agreed that the major unmet need is lack of treatments to delay the onset of stage 3 T1D. CSEM added that ongoing demands of managing T1D and the associated emotional burden can also impair patients’ quality of life.
The clinician group noted that teplizumab is the first approved disease-modifying therapy in T1D and would be used alone as the first-line treatment to delay the onset of stage 3 T1D in adults and children (aged ≥ 8 years) with stage 2 T1D, and could shift the treatment paradigm from solely managing blood glucose levels to modifying the underlying disease process.
All clinicians noted that a major challenge would be identifying individuals with stage 2 T1D because it is asymptomatic and population screening for T1D has not yet been implemented. The clinical experts consulted by CDA-AMC added that clinicians are most likely to identify stage 2 T1D in people with a family history of T1D, but most people diagnosed with T1D do not have a family history.
The clinician group and the clinical experts consulted by CDA-AMC agreed that the important outcome is a delay in progress from stage 2 to stage 3 T1D, which should be assessed by measuring fasting plasma glucose, OGTT, or hemoglobin A1C every 3 months to 6 months.
CSEM explained that discontinuation of teplizumab therapy should be considered if severe or persistent AEs occur, or with disease progression.
According to CSEM, teplizumab administration requires a multidisciplinary team with expertise in the treatment and monitoring of patients with T1D. Outpatient infusion centres, hospital-based infusion clinics, or specialty pediatric endocrine or diabetes centres are preferred. These locations must have the necessary infrastructure to monitor patients for AEs.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. Please refer to Table 5 for further information. The following were identified as key factors that could potentially impact the implementation of teplizumab:
relevant comparators
considerations for initiation of therapy
considerations for prescribing of therapy
generalizability
care provision issues
system and economic issues.
Clinical Evidence
Systematic Review
Description of Studies
The evidence included in this review consisted of 1 phase II, double-blind, placebo-controlled randomized controlled trial (RCT), the TN-10 study (N = 76). The purpose of this study was to evaluate the efficacy and safety of teplizumab for delaying the onset of stage 3 T1D (also known as clinical T1D) in adults or children aged 8 years or older with a diagnosis of stage 2 disease. These patients were relatives of those with a confirmed diagnosis of stage 3 T1D. Eligible patients were randomly assigned to receive either teplizumab (n = 44) or placebo (n = 32) in a double-blind manner. The primary efficacy end point of this study was time from randomization to stage 3 T1D diagnosis. In addition, changes in levels of C-peptide and hemoglobin A1C, as well as harms were evaluated. This study was projected to last between ██ and ████ years. At baseline, the patient characteristics were generally comparable between the 2 treatment groups. Of the 76 patients, the median age was 14 years in the teplizumab group and 13 years in the placebo group. There were 29 patients (65.9%) aged younger than 18 years in the teplizumab group compared to 26 patients (81.3%) in the placebo group. Before enrolment, all patients were positive for at least 2 autoantibodies, while 73.7% of all patients were positive for 3 or more. The teplizumab and placebo groups were similar in baseline glucose and hemoglobin A1C levels. There were some imbalances in the proportion of patients who were first-degree relatives of siblings with T1D and presence of certain autoantibodies. In this study, patients who were not diagnosed with T1D had OGTTs at 3 months after randomization and then every 6 months thereafter until the study cut-off date or withdrawal. If the patients progressed to stage 3 T1D, they were not followed up further.
At the end of the TN-10 study, patients who had not progressed to stage 3 T1D were continuously followed for up to 80.46 months. Outcomes assessed during this period of time included time from randomization to stage 3 T1D, and changes in levels of C-peptide and hemoglobin A1C. Patients were unblinded to the treatment assignment during the extended follow-up.
Efficacy Results
After a median follow-up of 26.6 months, stage 3 T1D was diagnosed in 20 of 44 participants (45%) in the teplizumab group and 23 of 32 participants (72%) in the placebo group. The median time from randomization to stage 3 T1D diagnosis was 49.5 months (95% CI, 32.2 months to not estimable) in the teplizumab group and 24.9 months (95% CI, 9.5 months to 48.6 months) in the placebo group, with a between-group difference of 24.6 months (95% CI not available). Because the patients who progressed to stage 3 T1D no longer underwent further assessments, the time from randomization to stage 3 T1D was longer than the median follow-up time. The HR obtained from the Cox proportional hazards model was 0.41 (95% CI, 0.22 to 0.78; P = 0.0066). The clinical experts consulted for this review indicated that the approximately 2-year delay in the onset of T1D between teplizumab and placebo is considered clinically meaningful. However, the clinical experts noted that the long-term effects of teplizumab on lowering the risks of macrovascular and microvascular events remain unclear.
Change from baseline in the level of C-peptide reflects beta cell function in patients with T1D. C-peptide levels were collected during OGTT and no longer performed when patients were diagnosed with stage 3 T1D. At 2 years of treatment, results of C-peptide were available in approximately ████% of the study participants (i.e., those who remained in the study because they had not been diagnosed with stage 3 T1D); the 2-hour mean of C-peptide area under the concentration-time curve (AUC) was ████████ (standard deviation [SD] ████████) nmol/L in the teplizumab group and ████████ (SD ████████) nmol/L in the placebo group. The clinical importance of this between-group difference was unclear. In addition, analyses on C-peptide levels were exploratory in the TN-10 study; therefore, the evidence can only be considered supportive. Furthermore, in patients who progressed to stage 3, it is unknown how teplizumab would impact patients’ C-peptide levels once they are diagnosed with T1D.
Change from baseline in the level of hemoglobin A1C was reported in the TN-10 study. At 2 years of treatment, the mean of hemoglobin A1C was ████████% (SD ████████) in the teplizumab group and ████████% (SD ████████) in the placebo group, which are similar to the baseline values. Note that in this study, the values of hemoglobin A1C are considered within the normal range — because patients ceased to be followed after onset of T1D as per the protocol of the TN-10 study, the consistent and normal hemoglobin A1C levels in both treatment groups were an expected result.
HRQoL was considered a clinically important outcome by the patient groups and clinicians. However, HRQoL was not assessed in the current submission; therefore, the effect of teplizumab on patients’ HRQoL, in particular psychosocial well-being, is unknown.
Harms Results
At a median follow-up of 26.6 months, ████████% of patients in the teplizumab group and ████████% in the placebo group experienced at least 1 AE. The most commonly reported AEs in the teplizumab group were lymphopenia (72.7%), leukopenia (20.5%), rash pruritic (████████%), and nasopharyngitis (████████%). Grade 3 treatment-emergent AEs (TEAEs) occurred in ████ (████████%) patients in the teplizumab group and ██ (██████%) patients in the placebo group.
Treatment-emergent SAEs occurred in ██ (████████%) patients in the teplizumab group and ██ (██████%) patients in the placebo group. The SAEs reported in the teplizumab group included ████████████████████ ████████████████████ ██████████ ██████████████████ ██████████ ██████████████████ ██████████████████████████████ ██████████ ██████████ ██████████████████████ ██████████ ████████████████████ ██████ ██████████████████████████████. ██████ case of ██████████████████████████████ ██████████████████████ was reported as SAEs in the placebo group.
██████████ patients discontinued from study treatment because of TEAEs, including ██ ████████ of increased alanine aminotransferase (ALT) (██████%) in the teplizumab group and ██ ██████████ of hyperbilirubinemia (██████%) in the placebo group.
No patient died during the study.
████████ patients (██████%: grade 3 events of cellulitis, gastroenteritis, pneumonia and wound infection) in the teplizumab group had an AE of special interest (AESI), while ████ ██████████████ from the placebo group reported an AESI. There were no grade 3 or higher liver function abnormalities, grade 3 or higher neutropenia, grade 4 or higher cytokine release syndrome (CRS), or lymphocyte count lower than 500 mm3 for 7 days or longer events reported at the data cut-off (DCO) date of November 30, 2018.
The clinical experts consulted for this review noted that most AEs are manageable and there was no unusual safety signals observed.
Critical Appraisal
In the TN-10 study, there were some imbalances between the 2 treatment groups in patients’ baseline characteristics, such as the proportion of patients aged younger than 18 years, proportion of siblings with T1D, and presence of autoantibodies, consistent with the small sample size (N = 76). In general, small studies are at risk of imbalance in prognostic factors, are associated with larger effect sizes, and should be considered in the context of these findings. Teplizumab was developed to delay the onset of stage 3 T1D in patients diagnosed with stage 2 T1D. Time to stage 3 T1D diagnosis was the primary efficacy end point in the TN-10 study. Longer time from randomization to disease progression is associated with delayed treatment with insulin, and related short-term consequences. However, the clinical experts noted that currently it is uncertain whether the delayed onset of stage 3 T1D can be translated to longer-term clinical benefits, such as prolonged survival, and lower risk of macrovascular or microvascular events in patients with stage 3 T1D. It may also have an impact on patients’ HRQoL during the disease-free period, in particular, the psychosocial well-being of the patients and their families; however, this was not examined in this study.
Based on feedback from the clinical experts consulted for this review, the eligibility criteria and baseline characteristics of patients randomized in the TN-10 study are somewhat different than those observed in clinical practice. For example, the proportion of patients aged older than 18 years may be larger in practice than in the TN-10 study. Also, nearly all patients in the study were white, which was inconsistent with those seen in practice. As such, the patients enrolled are unlikely to be representative of the racial or ethnic diversity of those seen in clinical practice in Canada. In addition, the trial used restricted exclusion criteria, while in clinical practice, a broader population may be eligible to receive treatment with teplizumab, such as patients who may have abnormal blood counts or liver function tests. The study findings may not be generalized to the patient population in clinical practice.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations, Assessment, Development and Evaluations (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.16,17
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The threshold for a clinically important effect for time to stage 3 T1D in the study population was not obtained. Therefore, the target of the certainty of evidence assessment was the presence or absence of any non-null effect for this end point. The thresholds for a clinically important effect for the change from baseline in levels of C-peptide and hemoglobin A1C, and change from baseline in the occurrence of harm events in the study population were not obtained either. Therefore, the target of the certainty of evidence assessment was the presence or absence of any non-null effect for these end points.
Table 2 presents the GRADE summary of findings for teplizumab versus placebo.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
time from randomization to stage 3 T1D diagnosis
change from baseline in level of C-peptide
change from baseline in level of hemoglobin A1C
any SAEs
AESIs.
Table 2: Summary of Findings for Teplizumab vs. Placebo for Patients With Stage 2 T1D
Outcome and follow-up | Patients (studies) N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
Placebo | Teplizumab | Difference | ||||||||||
Delay in onset of stage 3 T1D (ITT population) | ||||||||||||
Time from randomization to stage 3 T1D, median months Median follow-up for teplizumab: 27.5 months Median follow-up for placebo: 17.8 months | 76 (1 RCT) | NR | 24.9 months (9.5 months to 48.6 months) | 49.5 months (32.2 months to NE) | 24.6 months (NR) | Moderatea | Teplizumab likely results in an increase in time to onset of stage 3 T1D when compared with placebo. The clinical importance of the delay is uncertain. | |||||
Number of patients diagnosed with stage 3 T1D Median follow-up for teplizumab: 27.5 months Median follow-up for placebo: 17.8 months | 76 (1 RCT) | NR | ██████ per 1,000 (NR) | ██████ per 1,000 (NR) | ██████ less per 1,000 (██████ less to ████ less per 1,000) | Moderateb | Teplizumab likely results in fewer patients progressed to stage 3 T1D when compared with placebo. The clinical importance of the decrease is uncertain. | |||||
Incidence of DKA | ||||||||||||
NRc | NRc | NRc | NRc | NRc | NRc | NRc | NRc | |||||
HRQoL | ||||||||||||
NAd | NAd | NAd | NAd | NAd | NAd | NAd | NAd | |||||
Harms (safety population) | ||||||||||||
SAE Median follow-up for teplizumab: 27.5 months Median follow-up placebo: 17.8 months | 76 (1 RCT) | NR | ██████ per 1,000 (NR) | ██████ per 1,000 (NR) | ██████ more per 1,000 (██ more to ██████ more per 1,000) | Lowe | Teplizumab may result in an increase in the proportion of patients who experience SAEs when compared with placebo. | |||||
AESI Median follow-up for teplizumab: 27.5 months Median follow-up placebo: 17.8 months | 76 (1 RCT) | NR | ██████ | ████ per 1,000 (NR) | ████ more per 1,000 (NE to NE) | Lowf | Teplizumab may result in an increase in the proportion of patients who experience AESIs when compared with placebo. | |||||
AESI = adverse event of special interest; CI = confidence interval; DKA = diabetic ketoacidosis; HRQoL = health-related quality of life; NA = not assessed; NE = not estimable; NR = not reported; RCT = randomized controlled trial; SAE = serious adverse event; T1D = type 1 diabetes; vs. = versus.
Notes: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
No adjustment for multiplicity was made in the analyses in the TN-10 study.
In the TN-10 study, incidence of DKA was assessed as a harm outcome instead of an efficacy outcome. No events of DKA have been reported as of the data cut-off date of November 30, 2018.
aRated down 1 level for serious imprecision. There was no known threshold for a clinically important effect for the time to stage 3 T1D diagnosis. The sample size and/or number of events contributing to the analysis is small.
bRated down 1 level for serious imprecision. There was no known threshold for a clinically important effect for the number of patients who progressed to stage 3 T1D. The sample size and/or number of events contributing to the analysis is small.
cAs this was NR, the evidence is very uncertain about the effect of teplizumab on incidence of DKA compared with any comparator.
dAs this was NA, in the absence of comparative data, the evidence is very uncertain about the effect of teplizumab on HRQoL compared with any comparator.
eRated down 2 levels for very serious imprecision. No threshold of clinical importance could be established; therefore, the null was used. The point estimate suggests harm; however, the 95% CIs were wide and close to null; therefore, the effect of teplizumab on SAE was uncertain.
fRated down 2 levels for very serious imprecision. No threshold of clinical importance could be established; therefore, the null was used. The point estimate suggests harm; however, the 95% CIs were not estimable; therefore, the effect of teplizumab on AESI was uncertain.
Sources: Clinical Study Report for TN-10,18 Sims et al. (2021),19 Lledó-Delgado et al.,20 and additional information provided by the sponsor.21 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Long-Term Extension Studies
Description of Studies
Participants who had not progressed to stage 3 T1D by the end of the TN-10 study in June 2019 were transferred into the TrialNet Pathway to Prevention of T1D (formerly Natural History Study) (TN-01), and continued to be followed up and were included in the extended follow-up analyses of the primary end point, which was conducted after participants had been followed for a median duration up to 80.4 months. Patients were informed of the treatment they received at the end of the TN-10 study and so were aware of treatment assignment in the long-term extension study. The results of median time from randomization to the diagnosis of stage 3 T1D, and metabolic outcomes including measures of C-peptide response and glycemic control as measured by hemoglobin A1C levels were reported.
Efficacy Results
At the 31-month follow-up since initial randomization, the proportion of patients who did not have stage 3 T1D was 50% (22 of 44 patients) in the teplizumab group and 22% (7 of 32 patients) in the placebo group. At the 80-month follow-up, the proportion of patients who did not have stage 3 T1D was 36% (16 of 44 patients) in the teplizumab group and 12% (4 of 32 patients) in the placebo group. Results of these extended follow-up analyses suggested that the treatment effect of teplizumab (delaying the onset of stage 3 T1D) was maintained during the longer follow-up, in patients aged 8 years or older with a diagnosis of stage 2 T1D.
Harms Results
Harm outcomes were not assessed in the long-term extension studies.
Critical Appraisal
Longer-term efficacy and safety data of teplizumab were reported for up to 80.46 months. Missing data handling was not reported during these periods. Time from randomization to stage 3 T1D, and change in the levels of C-peptide and hemoglobin A1C were reported. While these outcomes were objectively measured, the open-label observational design cannot control for the impact of patient behaviours or other treatments received during the extended follow-up period. Insufficient details of the efficacy outcomes were reported (e.g., between-group differences and associated 95% CIs were missing); therefore, a thorough evaluation of the long-term effect of teplizumab in the study population was not feasible. Harm outcomes were not examined in the extended follow-up analyses.
Indirect Comparisons
No indirect comparisons were submitted to this review.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps in the evidence from the systematic review were submitted to this review.
Conclusions
Currently there is a lack of treatment for patients diagnosed with stage 2 T1D. Teplizumab is a first-in-class medication with an indication of delaying the onset of stage 3 T1D in patients with preclinical T1D. One phase II, double-blind, placebo-controlled RCT (the TN-10 study) provided evidence for the efficacy and safety of teplizumab in adults or children aged 8 years or older with stage 2 T1D. The results showed that after a median follow-up of 26.6 months, treatment with teplizumab likely results in delaying the time to progress to stage 3 T1D by approximately 2 years, compared to placebo. However, currently it is uncertain whether this 2-year delay in patients with stage 2 T1D (with or without progression) can be translated to longer-term clinical benefits, such as prolonged survival, and lower risk of macrovascular or microvascular events in patients with stage 3 T1D. In terms of harms, evidence from the TN-10 study indicated that teplizumab may result in an increase in the proportion of patients who experience SAEs or AESIs when compared with placebo. Up to a median follow-up of 80 months since the initial randomization, longer duration to progression to stage 3 T1D was observed in patients in the teplizumab group when compared with those who received placebo. There is uncertainty in long-term safety due to the lack of evidence. In addition, the impact of teplizumab on patients’ HRQoL was unknown, either during the delayed period or after a diagnosis of stage 3 T1D.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of teplizumab (solution of 2 mg/mL teplizumab in single-use vial for IV infusion) to delay the onset of stage 3 T1D in adults and children aged 8 years and older with stage 2 T1D.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
T1D is a chronic, progressive autoimmune condition resulting from the destruction of insulin-producing beta cells in the pancreas, culminating in chronic hyperglycemia and reliance on exogenous insulin for survival.1-3
T1D progresses as a continuum across 3 stages. Stage 1 T1D is characterized by the presence of at least 2 diabetes-related autoantibodies and normoglycemia. Stage 2 is marked by the development of abnormal glucose tolerance in addition to the presence of at least 2 diabetes-related autoantibodies. Stages 1 and 2 are asymptomatic and can start months to years before the onset of stage 3, which is when T1D is clinically diagnosed. Stage 3 T1D is characterized by overt hyperglycemia, presence of 2 or more diabetes-related autoantibodies, and the development of typical clinical symptoms and signs of diabetes requiring the use of life-long exogenous insulin replacement therapy.4,5 Patients who advance to stage 2 T1D have a 60% likelihood of progressing to stage 3 T1D within 2 years, a 75% likelihood within 5 years, and a 100% lifetime risk.5,6 Patients with T1D have compromised HRQoL compared to the general population.7 Caregivers of children with T1D also bear the negative impact of the disease and its management, with parents of children with diabetes reporting lower parenting satisfaction than parents of healthy children.22,23
The diagnosis of T1D is based on the presence of hyperglycemia (such as elevated levels of fasting plasma glucose, 2-hour plasma glucose value during an OGTT, or hemoglobin A1C), presence of clinical symptoms, and detection of diabetes-associated autoantibodies.
Both hypoglycemia and hyperglycemia can escalate to serious, life-threatening complications including altered consciousness and coma if not immediately managed, and therefore often require hospitalization.24 Insulin treatment has been frequently associated with a risk of medication error and injury, and insulin is considered a high-alert medication. Additionally, insulin represented 16% of all medication error events with reported harm in 2008.25
Typical symptoms and signs of diabetes include polyuria, polydipsia, nocturia, enuresis, weight loss, fatigue, polyphagia, blurred vision, and behavioural disturbance.3 DKA is a serious complication of diabetes that is triggered by counter-regulatory metabolic responses to very low circulating insulin levels, and can arise from worsening beta cell function in untreated T1D at diagnosis, or in patients with established T1D due to missed insulin doses or insufficient insulin administration during infection, gastrointestinal illness, and physiological stress.24 It may lead to stupor, coma, and, in the absence of effective treatment, death.3,6 DKA can lead to further long-term complications and is a common cause of diabetes-related mortality in T1D.24,26 The benefits of screening to reduce DKA rate at the time of stage 3 T1D diagnosis have been proven.4 Cerebral edema is a rare but frequently fatal complication of DKA, and it has been estimated to occur in 0.7% to 1.0% of children who develop DKA.27
These autoantibodies are markers of beta cell autoimmunity in T1D: ICA (69% to 90% of patients with T1D), antibodies to glutamic acid decarboxylase 65 (GAD-65) (80% of patients with T1D), IA-2 (54% to 75% of patients with T1D), and IAA (70% in young children with T1D).8 If a patient tests positive for 2 or more diabetes-related autoantibodies, then a positive dysglycemia test (based on the results of fasting plasma glucose level, OGTT, and hemoglobin A1C) is necessary to confirm the diagnosis of stage 2 T1D.5
The global incidence rate of T1D (stages not specified) varies widely. In general, among adolescents and young adults (aged 10 years to 24 years), the incidence increased from 7.78 cases per 100,000 population in 1990 to 11.07 cases per 100,000 population in 2019.9 In Canada, the incidence rate of T1D among adolescents and young adults (aged 10 years to 24 years) was 31.89 cases per 100,000 population in 2019.9 Moreover, T1D is the most prevalent form of diabetes in children and adolescents, accounting for more than 90% of childhood diabetes in the majority of Western countries.3 The epidemiology of stage 2 T1D is poorly understood and Canadian data on this stage are limited. Due to the nature of an asymptomatic condition and because there is no extensive general population early detection testing program available in Canada, there is uncertainty regarding the incidence and prevalence of patients with stage 2 T1D in Canada.28
People with stage 1 or stage 2 T1D often remain undiagnosed until they reach stage 3, by which time there has been a substantial loss in the number of beta cells and endogenous insulin production.1,2 The age at onset of stage 3 T1D may impact mortality. Globally, the mortality of T1D has changed from increasing during the 1990 to 1999 period to decreasing from 2000 to 2019. Major advances in T1D diagnosis, treatment with insulin, and glucose monitoring strategy make possible the near-normal life expectancy in adolescents and young adults with this condition.10 It has been reported that compared to controls, the HR for all-cause mortality was 4.11 (95% CI, 3.24 to 5.22) in patients who developed T1D before 10 years of age, and 2.83 (95% CI, 2.38 to 3.37) in those who developed the disease between 26 years to 30 years of age.11 In addition, a younger age at onset of stage 3 T1D has been associated with higher glycated hemoglobin (also known as hemoglobin A1C) levels and impaired kidney function earlier in the disease course, as well as an increased risk of cardiovascular disease.11,12
Patients with T1D would benefit from early detection of the disease, for example through reduced risk of DKA, delayed disease progression if a disease-modifying therapy is available, lowered incidence of long-term complications of diabetes, and reduced burden from life-long insulin administration. However, diagnosing an asymptomatic rare condition poses significant challenges. According to the clinical experts consulted for this review, a population screening program for T1D has not been implemented across Canada. Many patients are undiagnosed until the development of clinical symptoms and signs. Even though family history is a risk factor for T1D, previous research showed that among newly diagnosed T1D, only up to approximately 15% had a family history of this disease.5
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
According to the clinical experts consulted for this review, there are currently no treatments approved for patients at this stage. The current management for stage 2 T1D is education and glucose monitoring. There is a substantial unmet need to treat patients for T1D earlier in the continuum of disease and delay the onset of stage 3 disease. Delaying the onset of stage 3 T1D for patients with stage 2 T1D would extend the period of life free from the daily burden of diabetes management. This approach would also mitigate the complications associated with diagnosis, insulin use, and the long-term effects of stage 3 T1D.29,30 The clinical experts indicated that the important treatment goals for patients with earlier stages of T1D are delaying the onset of stage 3 T1D, preventing the occurrence of DKA, and reducing patients’ anxiety and stress.
The current standard of care for stage 3 T1D in Canada is limited to managing symptoms and does not combat the pathophysiology of the condition or preserve the body’s own insulin production capacity. There is consensus from Diabetes Canada, the American Diabetes Association, and the European Association for the Study of Diabetes that stage 3 T1D is currently managed with insulin replacement therapy.1,13-15,31 However, even though sufficient glycemic control may be achieved from intensive insulin management balanced with diet and activity, insulin is not a disease-modifying drug and does not delay the continuum of T1D.13-15
Drug Under Review
Key characteristics of teplizumab are summarized in Table 3.
Teplizumab is indicated to delay the onset of stage 3 T1D in adult and pediatric patients aged 8 years and older with stage 2 T1D. The sponsor’s reimbursement request aligns with the approved Health Canada indication.
Teplizumab binds to CD3 (a cell surface antigen present on T lymphocytes). Its mechanism of action may involve partial agonistic signalling and deactivation of pancreatic beta cell autoreactive T lymphocytes. Teplizumab leads to an increase in the proportion of regulatory T cells and of exhausted CD8-positive T cells in peripheral blood.32
Teplizumab should be administered by IV infusion over a minimum of 30 minutes, using BSA-based dosing, once daily for 14 consecutive days as follows:
day 1: 65 mcg/m2
day 2: 125 mcg/m2
day 3: 250 mcg/m2
day 4: 500 mcg/m2
day 5 through day 14: 1,030 mcg/m2.
Teplizumab was approved by Health Canada through an expedited pathway of priority review, and a Notice of Compliance was issued on May 5, 2025.33 The product monograph of teplizumab did not specify the settings in which this drug is to be administered.
Table 3: Key Characteristics of Teplizumab
Characteristic | Teplizumab |
|---|---|
Mechanism of action | Partial agonistic signalling and deactivation of pancreatic beta cell autoreactive T lymphocytes |
Indicationa | To delay the onset of stage 3 T1D in adult and pediatric patients aged ≥ 8 years with stage 2 T1D |
Route of administration | IV |
Recommended dose |
|
Serious adverse effects or safety issues | Lymphopenia, CRS, acute hypersensitivity reactions, serious infections |
Other | The safety of immunization with live-attenuated vaccines in patients treated with teplizumab has not been studied. Additionally, teplizumab may interfere with the immune response to vaccination and decrease vaccine efficacy.
|
CRS = cytokine release syndrome; T1D = type 1 diabetes.
aHealth Canada–approved indication.
Source: Product monograph for teplizumab.32
Testing Procedure Considerations
Detection of 2 or more diabetes-associated autoantibodies, along with evidence of dysglycemia is required to diagnose stage 2 T1D.5 Clinical experts consulted for this review confirmed that testing for diabetes-related autoantibodies and dysglycemia to identify stage 2 T1D is not currently part of the standard care in Canada.
Testing for Diabetes-Related Autoantibodies
In the sponsor-submitted TN-10 trial included in this review,28 the autoantibodies to be confirmed to determine study eligibility were anti-GAD65, IA-2, IAA, anti-ZnT8, and ICA. However, the clinical experts noted that ICA is generally not tested for in Canada. The commonly tested autoantibodies include anti-GAD65, IAA, anti-IA-2, and anti-ZnT8.4,5,34 Among these, anti-GAD65 is the most prevalent in adults with T1D, detected in approximately 80% of cases.35 It is also frequently detected in children with T1D, with prevalence ranging from about 52% to 66%, depending on age at diagnosis.36,37 In Canada, these antibodies are tested by enzyme-linked immunosorbent assay using peripheral blood samples. Testing for these autoantibodies is mostly conducted within research settings. For example, individuals with a family history of T1D (e.g., first-degree relatives), who have a higher risk of developing T1D compared to the general population,38,39 would be referred to the TN-10 trial for autoantibody testing.40 The clinical experts highlighted that this targeted screening is inadequate because approximately 85% of T1D diagnoses occur in individuals without a family history of T1D.41 According to the clinical experts, population-level screening using autoantibody testing could be effective in identifying individuals at risk of developing T1D and has been implemented in several countries.39 For example, Italy has approved and is planning nationwide T1D screening using autoantibody tests in children and adolescents.42,43 In regions of Germany and in some states in the US, diabetes autoantibody screening is available for the pediatric population through primary care provider or at-home tests.39 While Canada currently lacks a systematic, large-scale screening program, family members of people with T1D can be screened through the research consortium offered by the TN-10 study.44 Additionally, a research consortium, the Canadian Population Screening for Risk of Type 1 Diabetes (CanScreen T1D), is exploring the acceptability and feasibility of population-wide T1D screening in Canada.45
According to the clinical experts, a stepwise approach can be used for T1D autoantibody detection, typically beginning with anti-GAD65 and followed by IAA, with anti-IA-2 and anti-ZnT8 assessed if assays are available. Depending on the availability or lack thereof of testing for all 4 antibodies, some individuals with stage 2 T1D may be left unidentified. This could present some inequities in access to treatment with teplizumab, if it were to be funded. The clinical experts also indicated that multiplex autoantibody detection by agglutination polymerase chain reaction panels which simultaneously assess multiple autoantibodies, is also available but its use is limited to certain facilities.46 One of the clinical experts reported that a 4-autoantibody panel including anti-GAD65, IAA, anti-IA-2, and anti-ZnT8 is used by at least 1 hospital in Ontario; however, the samples are referred to a laboratory in the US for the test.
Diabetes-related autoantibody testing for diagnosing stage 2 T1D is currently not part of standard of care, and testing capability varies across the country, which could lead to inconsistent and inequitable access to teplizumab if it were to be funded. The review team considered the potential impacts of diabetes-related autoantibody testing to diagnose stage 2 T1D, including those on health systems, patients (including families and caregivers), and costs. A targeted jurisdictional survey was conducted to gather information about testing availability. Key considerations and relevant information regarding diabetes-related autoantibody testing were sourced from materials submitted by the sponsor, input from the clinical experts including the clinical expert panel consulted by the review team, and sources from the literature. These were validated by the review team when possible and are summarized in Table 4. Additional ethical considerations related to the testing procedure are detailed in the Ethics Review Report.
Testing for Dysglycemia
Dysglycemia can be determined using 1 of 3 tests: hemoglobin A1C, OGTT, or fasting plasma glucose.4 These tests are widely available, publicly funded, and typically performed at community laboratories using blood samples collected in outpatient settings.47 Clinical experts noted that based on clinical guidelines, dysglycemia testing for stage 2 T1D diagnosis is performed once after confirming at least 2 positive diabetes-related autoantibodies and repeated periodically to monitor disease progression following diagnosis.4 An international consensus guideline recommends monitoring metabolic status using hemoglobin A1C every 6 months in adults, and every 3 months in children with stage 2 T1D.4 The clinical experts do not anticipate a significant impact on human and other health care resources from dysglycemia testing if teplizumab were to be funded, as testing would be limited to individuals with 2 or more diabetes-related autoantibodies, representing a relatively small population.
Table 4: Considerations for Diabetes-Related Autoantibody Testing for Diagnosing Stage 2 T1D
Consideration | Criterion | Available Information |
|---|---|---|
Health system related | Number of individuals in Canada expected to require the test (e.g., per year) | The sponsor estimated that approximately ██████████ individuals (i.e., FDR or SDR of patients with T1D) at baseline and over ██████████████ individuals from year 1 onward would undergo testing for diabetes-related autoantibodies.48 However, clinical experts consulted for this review noted that this is likely an underestimate. They indicated that the number of patients tested for these autoantibodies may be doubled if teplizumab were to be funded. They further acknowledged that identifying the eligible population is a key implementation challenge. |
Availability and reimbursement status of the testing procedure in jurisdictions across Canada | Based on responses from a targeted jurisdictional survey and information provided by the clinical experts, the availability and reimbursement status of diabetes-related autoantibody testing is variable across Canada.
No relevant information regarding testing in PEI, NS, NB, or other territories was identified. | |
Testing procedure as part of routine care | Diabetes-related autoantibody testing is not routinely performed for individuals in Canada at risk of having stage 2 T1D. | |
Repeat testing requirements | According to sponsor-submitted materials and the clinical experts, individuals who initially test positive for ≥ 2 diabetes-related autoantibodies should undergo repeat testing to confirm their status. Confirming a positive autoantibody status is important to ensure the persistence of the autoimmune response and the validity of the target antigen.4 Once diagnosed, no further autoantibody testing is required. | |
Impacts on human and other health care resources by provision of the testing procedure | Based on the input from the clinical experts, provision of diabetes autoantibody testing to identify individuals with stage 2 T1D is anticipated to impact human and other health care resources, if teplizumab were to be funded. If teplizumab were to be funded, the number of individuals getting tested would likely increase. Consequentially, the volume of samples requiring out-of-province shipment would also increase, potentially causing delays and backlogs at testing sites. To manage the increased testing volume, investments in infrastructure and equipment along with that in staffing may be needed to establish in-house testing capacity. Upgrading laboratory infrastructure with validated assays for testing these 4 autoantibodies and providing adequate training for laboratory staff may be warranted. In addition, targeted education for health care providers would be necessary to enhance awareness of the autoantibody test. Expanding the screening to a population level would further increase resource requirements. | |
Patient related | Accessibility of the testing procedure in jurisdictions across Canada | Based on responses from the targeted jurisdictional survey and information provided by the clinical experts, testing accessibility is variable across Canada. The clinical experts noted that testing is largely performed in FDRs of patients with T1D, often at the patient’s request. Hence, other populations such as individuals without a family history of T1D, those with unknown family history, including groups such as immigrants, may experience inequitable access to testing. Other possible barriers include low awareness of stage 2 T1D and the role of autoantibody testing among both health care providers and patients, as well as financial barriers (need for out-of-pocket payments).49,50 If teplizumab were to be funded, these factors may be barriers to timely and equitable implementation. |
Expected turnaround times for the testing procedure | According to the clinical experts, the turnaround time for diabetes-related autoantibody testing is approximately 15 days; however, the actual time may vary depending on the testing facility, and delays may occur when the samples are referred out of province (to other provinces or to the US) for testing. In the targeted jurisdictional survey, it was reported that in both SK and MB — where samples are sent out of province — results would be available in approximately 15 days from the date the specimen is received at the testing facility. | |
Burden associated with the testing procedure for patients, families, and caregivers | Input from the patient group for this review indicated that knowing the increased risk of developing T1D may impact the patients and their caregivers’ emotional well-being or mental health. Published studies suggested that T1D screening may lead to psychological stress in parents with positive autoantibody findings, arising from concerns about their child’s risk of developing the chronic disease.51,52,53 A consensus guideline recommends providing psychosocial support for individuals at risk for developing T1D and their families, such as age-specific education.4 | |
Clinical | Clinical utility and validity of the testing procedure | Diabetes-related autoantibodies (anti-GAD65, IAA, anti-IA-2, and anti-ZnT8) are diagnostic markers of presymptomatic stages of T1D.54 According to the clinical experts, although radiobinding assay is considered the gold standard for detecting these autoantibodies, ELISA is more commonly used in Canada. There is evidence showing the clinical utility and validity of diabetes autoantibody testing.54 The sensitivity and specificity of ELISA vary by the specific autoantibody and assay used.55,56,57,58,a One of the clinical experts reported that of the 4 autoantibodies, anti-GAD65 testing is likely the most widely available in Canada. Another clinical expert noted that anti-GAD65 testing generally demonstrates higher sensitivity than the other 3 autoantibodies; however, it should be used in combination with other autoantibody tests to diagnose stage 2 T1D, as recommended in the clinical practice guidelines.4 The clinical experts highlighted that because different autoantibody testing assays can vary in diagnostic accuracy, it is necessary to standardize these assays and cut-offs to improve the sensitivity, specificity, and overall accuracy of testing assays, thereby allowing clinicians to use established diagnostic thresholds. |
Risks of harm associated with the testing procedure | Diabetes-related autoantibody testing is conducted using peripheral blood samples.4 The risk of harm associated with the procedure (e.g., pain from blood collection) is mostly minimal.59 | |
Cost | Projected cost of the testing procedure | According to the sponsor-submitted materials, the cost per test for anti-GAD65 antibody alone is $64.80 using ELISA.60,61 Pricing for the 3-autoantibody panel (IAA, anti-IA-2, and anti-ZnT8) was reported as $288.78,48 and that for the 4-autoantibody panel (anti-GAD65, IAA, anti-IA-2, and anti-ZnT8) as $347.29.62 The clinical experts estimated that diabetes-related autoantibody testing conducted in community laboratories typically costs approximately $150, although this may vary by region, testing method, and assays. Other published sources indicate varying prices for testing.61 |
AB = Alberta; BC = British Columbia; CDA-AMC = Canada's Drug Agency; ELISA = enzyme-linked immunosorbent assay; FDR = first-degree relative; MB = Manitoba; NB = New Brunswick; NL = Newfoundland and Labrador; NS = Nova Scotia; ON = Ontario; PEI = Prince Edward Island; SDR = second-degree relative; SK = Saskatchewan; T1D = type 1 diabetes; YT = Yukon territory.
aCDA-AMC has not evaluated or critically appraised this evidence to determine its validity or reliability.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
A joint patient group submission was received from Breakthrough T1D Canada and Diabetes Canada. Breakthrough T1D Canada is a national patient advocacy and research funding organization specifically dedicated to people in Canada living with T1D. Their mission is to accelerate life-changing breakthroughs to cure, prevent, and treat T1D and its complications, ensuring that people with the disease live healthier lives. Diabetes Canada is a national health charity representing Canadians who are affected by diabetes. Their mission is to prevent diabetes and its complications, help people with diabetes live healthy lives, and work to find a cure. Breakthrough T1D Canada and Diabetes Canada gathered information through an online survey conducted from January 10 to February 14, 2025.
According to the patient groups’ input, the survey had 463 respondents (258 female, 156 male). Of those who responded to the general information section of the survey, 257 identified as living with T1D,182 identified as a caregiver, 20 identified as a person living with T1D and a caregiver, and 6 respondents identified as having no relationship to T1D. Among the respondents to questions about age and time since diagnosis (n = 451), 68% were aged older than 35 years, with the largest number of respondents (n = 83; 18%) in the 25 to 34-year-old category. Up to 43% reported having lived with T1D for more than 20 years. Most of the respondents lived in Ontario (n = 226), British Columbia (n = 74), Alberta (n = 63), Manitoba (n = 24), and Quebec (n = 19). Up to 82% of respondents indicated that they lived in an urban or suburban region (n = 367), with 18% indicating that they lived in a rural or remote area (n = 83). In total, 86% of respondents identified themselves as white Caucasian (n = 385); more than 10% as First Nations, Inuit, and Métis Peoples (n = 3), African, Caribbean, Black (n = 6), Arab (n = 2), Latin American/Hispanic (n = 5), or Chinese (n = 6); and 2% as South Asian (n = 9).
The patient groups explained that because the early symptoms of T1D often present like a virus or flu, these symptoms are likely to be ignored initially, and misdiagnosis is common. In children and adolescents, the progression of T1D is typically faster than in adults and a misdiagnosis of initial symptoms can lead to DKA. Patients with T1D need multiple daily insulin injections via syringe or a continuous infusion of insulin via pump to constantly regulate blood glucose levels in the body to survive. The majority of respondents (n = 351; 83%) living with T1D indicated that they are either extremely concerned or very concerned about the progression of T1D, its impact on daily life over time, and the amount of time they have needed off from work to manage their diabetes. One patient noted that T1D is a daily challenge, both physically (constant attachment to devices, needles, symptoms of lows and highs, and so forth) and mentally (persistent worry about managing blood sugar, constant pharmacy visits and medical appointments, and fear of developing complications such as losing eyesight).
Among the survey respondents, 45% of them experienced hyperglycemia, 40% experienced hypoglycemia (when daily activities are affected, or help is needed) and 21% experienced mental health challenges more than once a week. Most respondents (56%) indicated that they themselves, or the person they care for, had been hospitalized because of T1D. Of those who were hospitalized, 43% had been hospitalized for 1 day or less, 15% for 2 days, 16% for 3 days, and 26% for 4 or more days.
According to the patient groups’ input, the only available treatment for patients with T1D is exogenous insulin, which is often accompanied by medical risks, suboptimal clinical outcomes, and a heavy burden on patients. Too much insulin can lead to severe hypoglycemia, causing confusion, unconsciousness, seizures, or even death. Conversely, insulin deficiency results in hyperglycemia and an increasing risk of long-term complications, such as kidney failure, heart disease, vision loss, and nerve damage. Even with advanced technologies, exogenous insulin delivery is delayed and imprecise, often resulting in excessive or insufficient insulin levels, which has its own risks.
The patient groups noted that based on the survey results, the respondents reported that they use some form of diabetes technology: 85% (n = 350) of respondents reported using a real-time continuous glucose monitor, 10% (n = 42) reported using a flash continuous glucose monitor, 66% (n = 270) reported using an insulin pump, and 38% (n = 154) reported using a hybrid closed-loop system or automatic insulin delivery system. The majority of respondents indicated that their current treatment options and management strategies are very effective (n = 143; 35%) or somewhat effective (n = 253; 61%) in addressing T1D. Only 4% (n = 18) of respondents indicated that their current treatment options and management strategies are not so effective or are limited in addressing T1D. Most of the respondents (n = 264; 63%) indicated that they have experienced financial challenges related to managing their condition such as loss of income, inability to work the hours they would like to, or high out-of-pocket costs.
The patient groups highlighted that most of the respondents (n = 216; 54%) indicated that they feel there are significant gaps in the availability of immunotherapy medications for T1D, such as teplizumab. Due to the unavailability of this drug in Canada and lack of similar or alternative drugs, respondents were asked about their views on how this drug would have improved their quality of life had it been available to them. Patients reported that any delay in disease progression would improve their overall well-being and decrease the risk of diabetic complications; and for young children, a delay of 2 to 3 years in progressing to T1D has significant impact. Children mature significantly over 2 to 3 years, and with maturity, they have a better understanding of why they have to take medicine and follow rules around food and activity.
Eight survey respondents had experience with teplizumab through participation in a clinical trial (n = 6), or paying the full cost out of pocket or through their private medical insurance in the US (n = 2). These patients explained that teplizumab delayed the onset of T1D, helped to maintain independence, and improved their physical and mental health.
The patient groups clarified that the indication for teplizumab is stage 2 T1D, which means that an individual has 2 or more persistent T1D-associated autoantibodies and dysglycemia, but symptoms have not yet been presented to warrant initiation of insulin therapy. Autoantibody testing is performed via a blood test and associated assay; however, this is not yet a standard practice in Canada. Coverage by provincial health programs is limited and many hospitals absorb the costs of these tests internally. Because current autoantibody tests are conducted at a regional or even institutional level, it is unknown what the cost of screening is for the health care system. Based on the results of the survey, most of the respondents indicated that they either strongly agree (n = 103; 25%) or agree (n = 131; 31%) that knowing there is an increased risk of developing T1D if a family member has the condition has negatively impacted their emotional well-being or mental health. With respect to screening for T1D-associated autoantibodies, 28% (n = 118) of respondents have had such screening done, 52% (n = 218) have not had such screening done, and 19% (n = 80) were unsure whether they had such screening done. The majority of respondents (n = 292; 70%) indicated that they would like to participate in screening for T1D-associated autoantibodies if medications to delay the onset of T1D were available.
Many respondents (n = 283; 71%) indicated that public funding should prioritize disease-modifying therapies that can delay the onset of a disease even if they do not provide a cure. Despite the limited experience with teplizumab in Canada, the patient groups stated that having access to teplizumab and its potential to delay the onset of stage 3 T1D will have a significant positive impact on the lives of patients with early-stage diabetes.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the review of teplizumab, a panel of 3 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion follows.
Unmet Needs
The clinical experts consulted for this review indicated that the most significant unmet need for patients with stage 2 T1D is that currently, there are no treatments targeting this patient population. In addition, no population-based screening program for stage 2 disease is in place in Canada; thus, the clinical experts indicated that the majority of patients are currently unaware that they have stage 2 disease. Because almost all patients in early stages of T1D will progress to stage 3 T1D (according to the literature, patients who advance to stage 2 T1D have a 100% lifetime risk of progressing to stage 3 T1D), the clinical experts noted that the goals of treatment for patients with stage 2 T1D would be to delay the onset of stage 3 T1D. An additional unmet need currently is prevention of stage 3 T1D in those identified as being at high risk. Additional goals stemming from delayed onset include the prevention of serious complications associated with the transition from stage 2 to stage 3 disease (e.g., hyperglycemia, potential DKA) and providing patients time to come to terms with life-long treatment needs associated with T1D management, thereby helping to alleviate some anxiety and stress.
Place in Therapy
The clinical experts indicated that currently there is no treatment for stage 2 T1D; therefore, teplizumab would be the first approved disease-modifying therapy to delay the onset of stage 3 T1D in this patient population. The experts also noted that teplizumab would be used as first-line treatment rather than be reserved for a subset of patients. Furthermore, teplizumab will not be combined with other treatments, as there is no other treatment in the target population at this time. Given the lack of alternative therapies, the experts noted that the use of teplizumab would cause a shift in the current treatment paradigm, being a first-in-class medication for stage 2 T1D. However, structured screening programs would need to be put in place to identify the patients who could benefit from this treatment. T1D early detection is a rapidly evolving area, and multiple agents in different drug classes are expected to be available in the future.
Patient Population
The clinical experts noted that patients with stage 2 T1D are best suited for treatment with teplizumab, with the goal of therapy being to delay the onset of stage 3 T1D. A confirmed diagnosis of stage 2 T1D is based on laboratory testing for T1D-associated autoantibodies (≥ 2 being positive) as well as glycemia testing, such as OGTT. The experts highlighted the challenges in identifying patients with stage 2 T1D in clinical practice, because T1D at this stage is asymptomatic, and a population-based screening program for T1D has not been implemented in Canada. In current clinical practice, patients with stage 2 T1D are usually identified in people at higher risk of developing T1D, such as those with a family member living with T1D; however, the majority of people (approximately 85%) diagnosed with T1D do not have a family history. The experts suggested that a process such as that used by the Canadian Population Screening for Risk of Type 1 Diabetes (CanScreen T1D) may help with facilitating early screening, identifying patients with stage 2 disease, and establishing pathways for treatment as has been established in other jurisdictions. However, the clinical experts also raised concerns about the challenges of such a national screening program. Diabetes-related autoantibody testing is needed to identify patients who are suitable for treatment with teplizumab. The challenge is that the current autoantibody screening tests in Canada vary in sensitivity and specificity, as well as in availability and accessibility. Also, it is unknown whether this program is cost-effective, or at what ages screening should be performed.
The experts also noted that in routine clinical practice, it is difficult to determine which patients would be more likely to respond to treatment with teplizumab over others, as compelling clinical evidence is lacking. Clinical trials with longer follow-ups may be helpful for clinicians to further identify subgroups of patients with differential potential for response to treatment.
Assessing the Response Treatment
The clinical experts consulted for this review indicated that in general, outcomes used in clinical practice to determine patients’ response to treatment include delay in onset of stage 3 T1D (defined by testing of fasting glucose, OGTT, and hemoglobin A1C, as well as continuous glucose monitoring; treatment response should be assessed every 3 to 6 months), prevention of DKA in those who progress to stage 3 T1D, and patients’ quality of life, in particular psychosocial well-being.
Discontinuing Treatment
The clinical experts consulted for this review noted that initial IV infusions of teplizumab may be associated with immediate AEs (although the therapy is generally safe without SAEs occurring), and therefore may result in treatment discontinuation. However, the experts noted that discontinuation due to long-term effects of immunosuppression therapies is less of a concern with teplizumab in clinical practice given the short course of treatment (14 days) and current evidence available.
Prescribing Considerations
The clinical experts indicated that a specialist would be required to diagnose, treat, and monitor patients with T1D who may receive teplizumab. A specialist generally refers to a pediatric or adult endocrinologist, but could also include internists or general pediatricians. Along with specialist care, the experts emphasized the importance of appropriate infrastructure and clinical expertise to provide IV infusions in hospital settings and monitor patient safety during the 14-day infusions. Additional clinical considerations post-treatment would include education, psychological support, and metabolic surveillance.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
CDA-AMC received 1 submission from CSEM, with 5 clinicians contributing to the clinician group input. CSEM is a professional organization of academic and community-based endocrinologists and researchers that advocates for excellence in endocrinology research, education, and patient care in Canada.
The clinician group and the clinical experts consulted by CDA-AMC (refer to “Input From Clinical Experts Consulted for This Review”) agreed that there are no available therapies that modify the disease progression of T1D in Canada and insulin therapy is required for the treatment of T1D when patients are diagnosed with stage 3 T1D. CSEM noted that the goal of insulin treatment is to maintain blood glucose levels within a target range to avoid acute complications (e.g., DKA) and chronic complications (e.g., diabetic retinopathy, nephropathy, and neuropathy; cardiovascular disease; stroke; and peripheral artery disease) of diabetes. CSEM added that hypoglycemia is the most common complication of insulin therapy, and it remains the primary limiting factor in achieving optimal glucose control in T1D.
The clinician group and clinical experts consulted by CDA-AMC agreed that the major unmet need is lack of treatments to delay the onset of stage 3 T1D. CSEM added that ongoing demands of managing T1D and the associated emotional burden can also impair patients’ quality of life. Diabetes distress refers to the psychological stress that arises from the relentless self-care requirements, fear of complications, and feelings of frustration, anxiety, and burnout related to diabetes management.
The clinician group agreed with the clinical experts consulted by CDA-AMC that teplizumab is the first approved disease-modifying therapy in T1D and would be used alone as the first-line treatment to delay the onset of stage 3 T1D in adults and children (aged ≥ 8 years) with stage 2 T1D, and could shift the treatment paradigm from solely managing blood glucose levels to modifying the underlying disease process.
All clinicians agreed that patients with stage 2 T1D who are identified through autoantibody screening and glucose tolerance testing are most suitable for teplizumab treatment. CSEM and the clinical experts consulted by CDA-AMC agreed that a major challenge would be identifying individuals with stage 2 T1D because it is asymptomatic and population screening for T1D has not yet been implemented. The clinical experts consulted by CDA-AMC added that clinicians are most likely to identify stage 2 T1D in people with a family history of T1D, but most people diagnosed with T1D do not have a family history.
The clinician group and the clinical experts consulted by CDA-AMC agreed that the important outcome is delay in progress from stage 2 to stage 3 T1D, which should be assessed by measuring fasting plasma glucose, OGTT, or hemoglobin A1C every 3 to 6 months. CSEM added symptom review (common symptoms of T1D such as polyuria, polydipsia, weight loss, and vision changes) to the assessment list.
CSEM explained that discontinuation of teplizumab therapy should be considered under the following circumstances:
severe or persistent AEs, including CRS lasting more than 2 days or requiring hospitalization; persistent lymphopenia, neutropenia, anemia, or thrombocytopenia that does not resolve within 7 days; liver enzyme elevations where ALT or aspartate aminotransferase levels exceed 5 times the upper limit of normal (ULN) or bilirubin levels reach 3 times the ULN; and severe hypersensitivity reactions such as anaphylaxis, angioedema, or serum sickness requiring medical intervention
disease progression, such as the patient progressing to stage 3 T1D during or shortly after treatment.
According to CSEM, teplizumab administration requires a multidisciplinary team with expertise in the treatment and monitoring of patients with T1D, including an endocrinologist, in a controlled health care setting with the capability for IV infusions over 14 consecutive days (with no breaks on weekends or holidays). Outpatient infusion centres, hospital-based infusion clinics, or specialty pediatric endocrine or diabetes centres are preferred. These locations must have the necessary infrastructure to monitor patients for AEs.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
There is no comparator for teplizumab to delay the onset of stage 3 T1D. | This was a comment from the drug programs to inform the CDEC deliberations. |
Considerations for initiation of therapy | |
Stage 2 T1D is diagnosed based on the presence of at least 2 confirmed diabetes-related autoantibodies and dysglycemia (without overt hyperglycemia). However, the autoantibody testing is not readily available in Canada. In clinical practice, what patient population would benefit most from the treatment with teplizumab? For example, those with ≥ 2 diabetes-related autoantibodies (who have access to this test), as well as those with abnormal glucose levels and beta cell loss (how would this be determined in practice)? If a patient starts experiencing clinical symptoms and is diagnosed with stage 3 T1D, will they be excluded from the potential benefit of teplizumab (e.g., preservation of pancreatic beta cells); or by the time they are diagnosed with T1D, are all beta cells destroyed? (in this case, this would be an off-label use for teplizumab). | The clinical experts indicated that the patients who would benefit most from teplizumab are those with at least 2 diabetes-related autoantibodies and with evidence of dysglycemia. These patients need to have the autoantibody testing and glucose assessment (e.g., fasting glucose testing or OGTT). The major issue is the need for a screening program (all screenings are antibody based) to identify such patients. The clinical experts noted that if a patient has progressed to stage 3 T1D, they may still be eligible to receive teplizumab in clinical practice. However, the use of teplizumab should align with Health Canada–approved indication. The treatment with teplizumab in patients who progress to stage 3 disease is off label at present, and there is a lack of clinical evidence to support its use in this patient population. |
Teplizumab is indicated for patients aged ≥ 8 years with stage 2 T1D. Will patients aged < 8 years be eligible for this treatment? Will any patients aged ≥ 8 years possibly be tested or only those with a first-degree or second-degree relative with stage 3 T1D? | The clinical experts indicated that the clinicians would follow the guidance from Health Canada (the product monograph of teplizumab) for the use of teplizumab in patients with stage 2 T1D, including the requirements for patient’s age, given the potential risk of adverse events from the treatment. The clinical experts noted that in general, individuals who are first-degree relatives of those with stage 3 T1D are likely to be screened. However, patients who are not relatives of patients with stage 3 T1D may have a chance to be tested, due to other reasons. |
Teplizumab is a 14-day treatment. Could the treatment course be extended beyond 14 days? Is re-treatment with teplizumab allowed? | The clinical experts stated that the clinicians will follow the guidance from Health Canada. Therefore, it is unlikely for the clinicians to extend the treatment course of teplizumab beyond 14 days. |
Considerations for prescribing of therapy | |
Teplizumab is administered by IV infusion. Please comment on the hospital for infusion vs. home IV program. In some jurisdictions (e.g., PEI), home IV program is not available. | The clinical experts suggested that IV infusion of teplizumab be administered in a hospital or infusion clinic (not necessarily in a hospital but different from a home IV program). The clinical experts noted that a home IV program may not be realistic in clinical practice, because the patients need to have certain laboratory tests (e.g., lymphocyte counts, platelet counts, liver function tests, and so forth) before treatment with teplizumab, and monitor treatment effect and adverse events after teplizumab infusion. |
Generalizability | |
Will patients aged < 8 years be eligible for this treatment? (This question is also asked in “Considerations for initiation of therapy.”) | The clinical experts stated that clinicians will follow the guidance from Health Canada. At present, only children aged ≥ 8 years are eligible for treatment with teplizumab. |
Care provision issues | |
Teplizumab can be administered in outpatient clinic, infusion centre, hospital, or home. Nursing or pharmacy services are required for the preparation of IV infusion. | This was a comment from the drug programs to inform the CDEC deliberations. |
There are costs associated with treatment with teplizumab, such as premedication of antipyretics, antihistamines and/or antiemetics before teplizumab treatment, and monitoring liver enzymes during treatment. | This was a comment from the drug programs to inform the CDEC deliberations. |
Please comment on the issues related to autoantibody testing for patients with preclinical T1D (e.g., accessibility). | Major issues related to the autoantibody testing in patients with stage 2 T1D are as follows.
|
CDEC = Canadian Drug Expert Committee; OGTT = oral glucose tolerance test; PEI = Prince Edward Island; T1D = type 1 diabetes; vs. = versus.
Clinical Evidence
The objective of this Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of teplizumab (2 mg/2 mL per vial for IV infusion) to delay the onset of stage 3 T1D in adult and pediatric patients aged 8 years and older with stage 2 T1D. The focus will be placed on comparing teplizumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of teplizumab is presented in 4 sections with the critical appraisal of the evidence by CDA-AMC included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The assessment by CDA-AMC of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. The third section includes indirect evidence from the sponsor; however, no indirect evidence was submitted by the sponsor. The fourth section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence; however, no studies addressing gaps were submitted by the sponsor.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
1 pivotal study (TN-10) identified in systematic review.18
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
The objective of the TN-10 study was to evaluate the efficacy and safety of teplizumab for prevention of stage 3 T1D (also known as clinical T1D). The TN-10 study was a phase II, double-blind, RCT of teplizumab. Potential patients for the TN-10 study were identified through the TN-01 study; therefore, they were a relative of a patient with confirmed diagnosis of T1D.63 This study planned to enrol approximately 71 patients over approximately 6 years and was projected to last between ██ and ████ years. As the study progressed, projections of the study end were computed and updated based on the rate of enrolment, the observed hazard rate, and the rate of loss to follow-up. The trial was conducted from July 2011 to November 2018, and study participants were enrolled from the US, Canada (1 site), and Germany. The TrialNet Coordinating Center generated the randomization numbers and tables. A total of 76 eligible patients were randomly assigned to receive either teplizumab (n = 44) or placebo (n = 32) in a 1:1 ratio. All patients, clinical investigators, and study personnel were masked to treatment assignment throughout the study. Randomization was stratified according to TrialNet site and age (< 18 years or ≥ 18 years). In this study, T1D was diagnosed using the American Diabetes Association criteria. For example, for individuals who are aged 18 years or older, abnormal glucose tolerance (demonstrated by 2 consecutive OGTTs) and confirmation of 2 or more diabetes-related autoantibodies are required to confirm the diagnosis. Emergency unmasking was allowed upon notification of the TrialNet Central Pharmacy and the TrialNet Coordinating Center. The patients were followed until at least 40 of them reached a diagnosis of T1D.
In the TN-10 study, patients who were diagnosed with T1D ended study participation once diagnosed with T1D or shortly thereafter and no longer underwent further assessments. Patients who were not diagnosed with T1D had OGTTs at 3 months after randomization and then every 6 months thereafter until the study cut-off date or withdrawal. As a result, the number of OGTTs decreased over time and differed among patients.
The DCO date was November 30, 2018.
Characteristics of the included studies are summarized in Table 6.
Table 6: Details of Studies Included in the Systematic Review
Detail | TN-10 |
|---|---|
Designs and populations | |
Study design | A phase II, randomized, placebo-controlled, double-blind trial |
Locations | Participants were enrolled in 3 countries (US, Canada, and Germany) |
Patient enrolment dates | Start date: July 18, 2011 End date: November 30, 2018 |
Randomized (N) | N = 76 (teplizumab group, n = 44; placebo group, n = 32) |
Inclusion criteria | Study participants met the following inclusion criteria:
|
Exclusion criteria | Study participants were excluded for the following reasons:
|
Drugs | |
Intervention | A 14-day course of teplizumab consisting of daily IV doses of 51 mcg/m2, 103 mcg/m2, 207 mcg/m2, and 413 mcg/m2 on days 1 to 4, respectively, and 1 dose of 826 mcg/m2 on each of days 5 to 14 (note that this recommended dosage was indicated in the Clinical Study Report of TN-10) |
Comparators | A 14-day course of IV placebo (saline) only |
Study duration | |
Screening phase | Participants were identified through the ongoing TN-01 study, which included initial confirmation of autoantibody status (within 6 months before randomization), OGTT, and HLA type; screening visit occurred 1 day before treatment |
Treatment phase | Duration of treatment was 14 days; treatment commenced within 7 weeks after confirmatory OGTT and 1 day after screening visit |
Follow-up phase | At the DCO date of the primary analysis (November 30, 2018) the median duration of follow-up was 745 days (26.63 months) |
Outcomes | |
Primary end point |
|
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publication status | |
Publications | Herold et al.64 Sims et al. 202065 Sims et al. 202119 Lledó-Delgado et al.20 |
AESI = adverse event of special interest; ALT = alanine aminotransferase; AST = aspartate aminotransferase; AUC = area under the concentration-time curve; CD3 = cluster of differentiation 3; CMV = cytomegalovirus; DCO = data cut-off; EBV = Epstein-Barr virus; INR = international normalized ratio; ITT = intention to treat; OGTT = oral glucose tolerance test; OKT = Orthoclone-muromonab-CD3; PPD = purified protein derivative test; PMN = polymorphonuclear neutrophil; T1D = type 1 diabetes; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event; ULN = upper limit of normal.
aAbnormal glucose tolerance included: fasting plasma glucose ≥ 6.1 mmol/L and < 7.0 mmol/L; 2-hour plasma glucose ≥ 7.8 mmol/L and < 11.1 mmol/L; or 30, 60, or 90-minute value on OGTT ≥ 11.1 mmol/L.
Sources: Clinical Study Report for TN-10.18 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Populations
Inclusion and Exclusion Criteria
Eligible patients were adult or pediatric patients aged 8 years and older who have a diagnosis of stage 2 T1D (i.e., relatives of people with T1D who do not have clinical diabetes and are high risk for progression to stage 3 clinical T1D).
At randomization, participants aged younger than 18 years must have had a TrialNet-conducted OGTT which demonstrated abnormal glucose tolerance within 7 weeks (52 days) of the baseline visit. Abnormal glucose tolerance was defined as 1 of:
fasting plasma glucose ≥ 6.1 mmol/L and < 7.0 mmol/L
2-hour plasma glucose ≥ 7.8 mmol/L and < 11.1 mmol/L
30, 60, or 90-minute value on OGTT ≥ 11.1 mmol/L.
For participants aged 18 years or older, all must have undergone 2 consecutive TrialNet-conducted OGTTs that demonstrated abnormal glucose tolerance, and the most recent must have been within 7 weeks (52 days) of the baseline visit. They must have had confirmation of 2 or more diabetes-related autoantibodies on 2 occasions. The second occasion must have been within 6 months before study drug administration but did not have to involve the same 2 autoantibodies as those found on the first occasion. The autoantibodies to be confirmed were anti-GAD65, anti-islet cell antigen 512 (ICA512; also known as IA-2), micro-IAA, anti-ZnT8, and/or ICA.
Persons with other clinically relevant medical histories (e.g., type 2 diabetes), abnormal laboratory chemical values, or abnormal blood counts were excluded.
Interventions
Teplizumab or matching placebo (saline) was administered via IV infusion over 14 days. The 14-day course commenced within 7 weeks of the qualifying OGTT. A 14-day course of teplizumab consisted of daily IV doses of 51 mcg/m2 BSA, 103 mcg/m2 BSA, 207 mcg/m2 BSA, and 413 mcg/m2 BSA on days 1 to 4, respectively, and 1 dose of 826 mcg/m2 BSA on each of days 5 to 14. Note that in the product monograph of teplizumab, the 14-day course of teplizumab consisted of daily IV doses of 51 mcg/m2, 103 mcg/m2, 207 mcg/m2, and 413 mcg/m2 on study days 0 to 3, respectively, and 1 dose of 826 mcg/m2 on each of study days 4 to 13. The total dose for a 14-day course is approximately 9,034 mcg/m2.
On day 1, each patient’s BSA was calculated using the Mosteller formula based on their height and weight on that day. This calculation was used for dosing over the entire 14 days. Teplizumab or saline was administered via an IV infusion over a minimum of 30 minutes. This infusion was required to be given at the same time each day ± 4 hours.
Ibuprofen and antihistamine were administered prophylactically before teplizumab or placebo infusion on the first 5 days of treatment. Dosing of ibuprofen, antihistamines, and/or acetaminophen could be used as needed for fever, malaise, headache, arthralgia, or rash.
Patients were instructed not to use prednisone, other immunosuppressive agents, or chronic inhaled or nasal corticosteroids during this trial to reduce the risk of infection and to prevent possible impact on progression to diabetes. However, as an intention-to-treat (ITT) study, no patient was withdrawn from analysis if this occurred. Patients who received teplizumab or placebo were instructed not to receive live vaccinations for 1 year after dosing. In addition, they were required not to receive vaccination with a killed virus vaccine less than 4 weeks after treatment with study drug unless approved by the study chair or a separate study team.
Teplizumab would be withheld during the treatment course if the following occurred: anaphylaxis requiring hemodynamic support or mechanical ventilation, hepatic abnormalities (e.g., total bilirubin > 1.3 mg/dL on day 1, ≥ 2.0 mg/dL on other days; aspartate aminotransferase level > 2 times ULN on day 1; aspartate aminotransferase, ALT, or lactate dehydrogenase ≥ 3 times ULN on other days), thrombocytopenia (a platelet count < 140,000 on day 1 and < 100,000 on other days), grade 3 neutropenia, anemia, coagulopathy, grade 3 fever, other grade 3 or higher AE, or any medically important event, that in the opinion of the investigator, contraindicated continued dosing of teplizumab.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review according to the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, we selected end points that were considered to be most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE.
Table 7: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Outcome type | Time points | ||
|---|---|---|---|---|
TN-1018 | Sims et al. (2021)19 | Lledó-Delgado et al.20 | ||
Time from randomization to stage 3 T1D diagnosis or last contact | Primary | Median follow-up duration: 26.63 months | Median follow-up duration: 31.1 months | Median follow-up duration: 80.46 months |
Percentage of patients diagnosed with stage 3 T1D | Primary | Median follow-up duration: 26.63 months | Median follow-up duration: 31.1 months | Median follow-up duration: 80.46 months |
C-peptide levels | Exploratory | Median follow-up duration: 26.63 months | Median follow-up duration: 31.1 months | NR |
Hemoglobin A1C levels | Exploratory | Median follow-up duration: 26.63 months | Median follow-up duration: 31.1 months | NR |
HRQoLa | Not measured | |||
Occurrence of DKAa | Not measured | |||
Safety | Safety | Median follow-up duration: 26.63 months | NR | NR |
SAE | ||||
AESI | ||||
AESI = adverse event of special interest; DKA = diabetic ketoacidosis; HRQoL = health-related quality of life; NR = not reported; SAE = serious adverse event; T1D = type 1 diabetes.
Note: Multiplicity for all these end points was not adjusted for (e.g., hierarchal testing was not performed).
aHRQoL and the risk of DKA were identified as clinically important outcomes for the study population; however, in the TN-10 study, DKA was assessed as a harm outcome only, while HRQoL was not assessed.
Sources: Clinical Study Report for TN-10.18 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Time From Randomization to Stage 3 T1D
This was the primary end point in the TN-10 study and was defined as the elapsed time from randomization to the clinical diagnosis of diabetes, determined with the use of criteria from the American Diabetes Association. Scheduled OGTTs were performed 3 months and 6 months after the infusions and every 6 months thereafter. Random screening glucose levels were evaluated at 3-month intervals, and an OGTT was performed if the random glucose level was higher than 200 mg/dL (or 11.1 mmol/L) in association with standardized symptoms of diabetes. OGTT results that indicated diabetes were then sequentially confirmed, and the date of diagnosis was identified as the time of the first of the 2 diagnostic tests. The primary end point was censored at the last OGTT laboratory measurement or a visit without OGTT, whichever was later, before the patient ended study participation.
C-Peptide Levels
This outcome is a measure of endogenous insulin production and reflects beta cell function.66,67 While not listed as an FDA-accepted surrogate outcome for measurement in T1D,68 the preservation of C-peptide levels in patients with T1D has been shown to be associated with improved clinical outcomes, such as reduced risk of complications (e.g., severe hypoglycemia, retinopathy, and neuropathy).66,69 Preserved C-peptide levels in patients with recently diagnosed T1D have also been associated with a reduction in the dose of exogenous insulin needed to maintain glycemic control.69 In the TN-10 study, change from baseline in levels of C-peptide was an exploratory end point. Data were collected at each OGTT and the measurements were summarized by treatment groups.
Hemoglobin A1C
Hemoglobin A1C is a marker of the concentration of glucose in the blood over the previous 8 to 12 weeks at measurement.70 As such, hemoglobin A1C levels are indicative of long-term glycemic control.70 Higher levels of hemoglobin A1C have been associated with an increased risk of developing T1D.71 Glycemic control as measured by hemoglobin A1C levels was summarized by treatment groups.
Safety
AEs, TEAEs, AESIs, and treatment-emergent SAEs reported after the first dose of the study treatment were summarized. SAEs and AESIs were selected for GRADE assessment, because they were considered clinically relevant safety outcomes by the clinical experts consulted for this review.
As per the sponsor, AESIs were defined as: grade 3 or higher infections (including all opportunistic infections), acute mononucleosis-like illness, lymphomas or other malignancies, major hypoglycemia, grade 3 or higher liver function abnormalities, grade 3 or higher thrombocytopenia, grade 3 or higher neutropenia, grade 4 or higher allergic or hypersensitivity reactions, grade 3 or higher rash, grade 4 or higher CRS, and lymphocyte count lower than 500 mm3 for 7 days or longer. The clinical experts consulted for this review considered the following as AESIs: acute mononucleosis-like illness, major hypoglycemia, grade 3 or higher liver function abnormalities, grade 3 or higher neutropenia, grade 4 or higher CRS, lymphocyte count lower than 500 mm3 for 7 days or longer, and DKA at time of diagnosis of stage 3 T1D.
Statistical Analysis
Sample Size and Power Calculation
Assuming a HR of 0.4 in the development of stage 3 T1D in the teplizumab group compared to the placebo group and a 5% dropout rate, the study required at least 71 patients who were to be followed until 40 patients had onset of stage 3 T1D to provide 80% power at a 1-sided alpha level of 0.025 to reject a null hypothesis using a Wald test.
Study enrolment was completed with a total of 76 patients being randomized, and patients were followed until at least 40 patients reached T1D diagnosis.
Statistical Test or Model: Primary Analysis
The primary outcome was the time from randomization to the development of stage 3 T1D or time of last contact. In the primary analysis, the effect of teplizumab versus placebo on the cumulative incidence of diabetes onset over time was estimated using the Kaplan-Meier method (proportion surviving diabetes-free as a function of time), in the ITT population. The difference between groups in the cumulative incidence curves, and the associated hazard functions, were tested with a 1-sided Wald test at the 0.025 significance level using the Cox proportional hazards model with discrete time intervals at the 6-month OGTT intervals, stratified by age and the OGTT status (confirmed abnormal or not). In addition, proportion of patients who were diagnosed with stage 3 T1D was summarized by treatment group.
Patients who were lost to follow-up before developing T1D or were ongoing at the study closure were censored at the last OGTT laboratory measurement or a physical examination, whichever was the latest.
Multiple Testing Procedure
No adjustment for multiplicity was made in the analyses.
Data Imputation Methods
In general, missing values were assumed to be missing at random unless empirical evidence to the contrary could be established in the study data. The methodology employed in the time-to-T1DM analysis uses total follow-up recorded for each patient (i.e., maximum use of follow-up time). Presuming no evidence against missing at random, and given the modest size of the trial, no methods were employed to impute additional follow-up of patients who dropped out (i.e., were lost to follow-up). Secondary end points were analyzed using existing data. Multiple imputation was used if missing at random could not be justified and for any sensitivity analyses of secondary end points.
Subgroup Analyses
The effects of teplizumab were compared with placebo in prespecified subgroups based on age at baseline, sex, body mass index at baseline (< median and ≥ median), autoantibodies (anti-GAD65, micro-insulin, anti-IA-2, ICA, anti-ZnT8), HLA type (HLA DR3, HLA DR4), pretreatment C-peptide (< median, ≥ median), and glucose levels (< median, ≥ median) during OGTT. Results were presented in a forest plot as HRs and 95% CIs of T1D onset between teplizumab and placebo for each subgroup.
Sensitivity Analyses
Sensitivity analyses of the primary end point evaluated 3 scenarios:
participants in the placebo group who had onset of stage 3 T1D during the first year (before 12 months) were considered to have onset at 12 months
participants who withdrew consent or were lost to follow-up and thus censored were considered to have onset of stage 3 T1D on their date of withdrawal or the date when lost to follow-up
scenarios 1 and 2 combined.
Other Outcomes of the Studies
The 2-hour C-peptide AUC was calculated using the trapezoidal rule over the 2-hour period (0, 30, 60, 90, and 120 minutes) based on the time points available from the OGTT. Results reported as less than the lower limit of detection were imputed as 0 for those time points of the OGTT. To assess changes over time, C-peptide AUC was compared between groups using a mixed model for repeated measures through 2 years post randomization. The model included treatment, time window, T1D status (diagnosed versus not diagnosed), treatment × time and treatment × T1D status, and baseline C-peptide as covariates. Mean C-peptide concentrations and respective changes from baseline were plotted over time by treatment for all patients and then also plotted for the 4 subgroups (anti-ZnT8 antibody status, HLA types [DR3 and DR4], pre-treatment C-peptide [< median and ≥ median]). In addition, least square means from the mixed model for repeated measures were also plotted.
The number and proportion of patients who had the TEAEs, and the number of events and the proportion of the total number of events, were given by treatment group. Treatment-emergent AESIs were defined retrospectively.
Table 8: Statistical Analysis of Efficacy End Points in the TN-10 Study
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Time from randomization to stage 3 T1D diagnosis or last contact (median follow-up: 26.63 months) | Kaplan-Meier method, Cox proportional hazards model | Age and OGTT status (confirmed abnormal or not) before randomization | No methods were employed to impute additional follow-up of patients who dropped out (i.e., lost to follow-up) | 3 scenarios:
|
OGTT = oral glucose tolerance test; T1D = type 1 diabetes.
Sources: Clinical Study Report for TN-10.18 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Analysis Populations
ITT population: All patients who were randomized. The assigned analysis group was used, regardless of treatment compliance.
Full analysis set (FAS) population: All patients who received any study treatment (including control). The assigned analysis group was used, regardless of treatment compliance.
Safety population: All patients who received any study treatment (including control). Analysis was conducted by actual treatment.
The ITT population was used for the primary, secondary, and other analyses. The safety population was used for all safety analyses.
Table 9: Analysis Populations of the TN-10 Study
Study | Population | Definition | Application |
|---|---|---|---|
TN-10 | ITT population | All subjects who were randomized. The assigned analysis group was used, regardless of treatment compliance. | Used for the primary, secondary, and other analyses. |
FAS | All subjects who received any study treatment (including control). The assigned analysis group was used, regardless of treatment compliance. | NR | |
Safety population | All subjects who received any study treatment (including control). Analysis was conducted by actual treatment. | Used for all safety analyses. |
FAS = full analysis set; ITT = intention to treat; NR = not relevant.
Sources: Clinical Study Report for TN-10.18 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
A total of 146 patients identified through the TN-01 study were assessed for eligibility in the TN-10 study. Among them, 70 patients were not eligible for inclusion (the main reasons for screening failure included normal OGTT result [52.9%], clinical alert OGTT result [28.6%], lost to follow-up [8.6%], withdrew consent before randomization [4.3%], and chronic steroid use [2.9%]). A total of 76 patients were randomly assigned to the teplizumab group (n = 44) or the placebo group (n = 32). ██████████ patients discontinued the 14-day treatment course for protocol-specified reasons (elevated liver function test results), including ██ (██████%) patients in the teplizumab group and ██ (██████%) patients in the placebo group. Six patients discontinued study participation after the infusion was completed, of which 3 (6.8%) were in the teplizumab group and 3 (9.4%) in the placebo group. Among them, 3 completed the study when they were diagnosed with T1D. Of the other 3 patients, 1 was lost to follow-up, and 2 withdrew consent.
By the DCO date of November 30, 2018, the median follow-up time for all 76 patients, including those who completed the study due to T1D onset and those who were censored, was 745 days, or approximately 26.6 months. The median follow-up time was 839 days (approximately 27.5 months) for the teplizumab group and 543 days (approximately 17.8 months) for the placebo group.
All 76 patients received the study treatment and were included in the ITT, FAS, and safety populations (Table 10).
Table 10: Summary of Patient Disposition From Studies Included in the Systematic Review (DCO Date: November 30, 2018)
Patient disposition | TN-10 | |
|---|---|---|
Teplizumab n = 44 | Placebo n = 32 | |
Screened, N | 146 | |
Reason for screening failure, n (%) | 70 (47.9) | |
Normal OGTT result | 37 (52.9) | |
Clinical alert OGTT result | 20 (28.6) | |
Lost to follow-up | 6 (8.6) | |
Withdrew consent before randomization | 3 (4.3) | |
Chronic steroid use | 2 (2.9) | |
Randomized, N (%) | 44 (100) | 32 (100) |
Discontinuation from treatment course, n (%) | ██ (██████) | ██ (██████) |
Protocol-specified drug withholding | ██ (██████) | ██ (██████) |
Discontinuation from study prematurelya, n (%) | 3 (6.8) | 3 (9.4) |
Lost to follow-up | 0 | 1 (3.1) |
Other | 3 (6.8) | 2 (6.3) |
ITT, n (%) | 44 (100) | 32 (100) |
FAS, n (%) | 44 (100) | 32 (100) |
Safety, n (%) | 44 (100) | 32 (100) |
DCO = data cut-off; FAS = full analysis set; ITT = intention to treat; NR = not reported; OGTT = oral glucose tolerance test.
aOf the 6 patients who discontinued from the study, onset of stage 3 T1D occurred in 2 patients in the placebo group and 1 in the teplizumab group (i.e., the primary end point was reached). Therefore, these patients were already included in the primary end point analysis before discontinuing.
Sources: Clinical Study Report for TN-10.18 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
In the TN-10 study, of 76 randomized patients, 44 were assigned to the teplizumab treatment group and 32 were assigned to the placebo group. All 76 patients received the study treatment and were included in the ITT, FAS, and safety populations. The age range among all randomized patients was from 8.5 years to 49.5 years. The median age was 14 years in the teplizumab group and 13 years in the placebo group. There were 29 patients (65.9%) aged younger than 18 years in the teplizumab group compared to 26 patients (81.3%) in the placebo group. Slightly more than half of the patients were male (teplizumab group = 56.8%; placebo group = 53.1%). The median body mass index was also similar between the groups (teplizumab group = 20.0 kg/m2; placebo group = 21.6 kg/m2). Before enrolment, all patients were positive for at least 2 autoantibodies, while 73.7% of all patients were positive for 3 or more. There were some imbalances in the proportion of patients who were first-degree relatives of siblings with T1D, and in the presence of certain autoantibodies. The teplizumab and placebo groups were balanced in baseline glucose and hemoglobin A1C levels. The median baseline glucose level was ██████ (range, ██████ ████ ████████) mmol/L and ██████ (range, ██████ ████ ████████) mmol/L, respectively. The median baseline hemoglobin A1C level was 5.2% (range, 4.6% to 6.1%) and 5.3% (range, 4.3% to 5.6%), respectively.
The baseline demographic and clinical characteristics of the TN-10 study are presented in Table 11.
Table 11: Summary of Baseline Characteristics From Studies Included in the Systematic Review (ITT Population)
Characteristic | TN-10 | |
|---|---|---|
Teplizumab n = 44 | Placebo n = 32 | |
Age (years), median (range) | 14 (8.5 to 49.5) | 13 (8.6 to 45.0) |
Age (< 18 years), n (%) | 29 (65.9) | 26 (81.3) |
Sex, n (%) | ||
Male | 25 (56.8) | 17 (53.1) |
Female | 19 (43.2) | 15 (46.9) |
BMI (kg/m2), median (range) | 20.0 (14.7 to 43.7) | 21.6 (16.0 to 34.6) |
Race, n (%) | ||
Asian | 0 (0.0) | 1 (3.1) |
Ethnicity (non-Hispanic) | 43 (97.7) | 29 (90.6) |
Multiple | 0 (0.0) | 1 (3.1) |
White | 44 (100.0) | 30 (93.8) |
Relationship to person with T1D, n (%) | ||
Siblinga | 30 (68.2) | 19 (59.4) |
Offspring | 7 (15.9) | 6 (18.8) |
Parent | 7 (15.9) | 6 (18.8) |
Sibling and another first-degree relative | 3 (6.8) | 3 (9.4) |
Second-degree relative | 5 (11.4) | 7 (21.9) |
Third-degree relative or further removed | 1 (2.3) | 2 (6.3) |
Presence of autoantibodies,b n (%) | ||
Anti-GAD65 | 40 (90.9) | 28 (87.5) |
mIAA | 19 (43.2) | 11 (34.4) |
Anti-IA-2 | 26 (59.1) | 24 (75.0) |
ICA | 29 (65.9) | 28 (87.5) |
Anti-ZnT8 | 32 (72.7) | 24 (75.0) |
Number of positive autoantibodies,c n (%) | ||
1 | 1d (2.3) | 0 (0.0) |
2 | 12 (27.3) | 7 (21.9) |
3 | 11 (25.0) | 5 (15.6) |
4 | 12 (27.3) | 14 (43.8) |
5 | 8 (18.2) | 6 (18.8) |
Hemoglobin A1C, median (range) | 5.2 (4.6 to 6.1) | 5.3 (4.3 to 5.6) |
C-peptide AUC in OGTT (nmol/L), median (range) | 1.77 (0.6 to 4.4) | 1.73 (0.7 to 3.8) |
HLA risk alleles present, n (%) | ||
Neither DR3 nor DR4 | 5 (11.4) | 3 (9.4) |
DR3 only | 10 (22.7) | 8 (25.0) |
DR4 only | 16 (36.4) | 14 (43.8) |
Both DR3 and DR4 | 11 (25.0) | 7 (21.9) |
Glucosee (mmol/L), median (range) | ████████ | ████████ |
AUC = area under the concentration-time curve; BMI = body mass index; ITT = intention to treat; OGTT = oral glucose tolerance test; T1D = type 1 diabetes.
aParticipants in this category may have had > 1 sibling with stage 3 T1D.
bShown are the autoantibodies for which participants were positive at the time of randomization. All participants were positive for at least 2 autoantibodies before randomization.
cThis was at the time of randomization. All patients were positive for at least 2 autoantibodies before randomization.
dOne patient had a definite autoantibody detected, but the titre for the second autoantibody was borderline between positive and negative. This patient was permitted to enrol in the study at the investigator’s discretion.
eFor patients aged < 18 years, only nonfasting glucose control was performed.
Sources: Clinical Study Report for TN-10.18 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
Study Treatments
In the teplizumab group, 41 (93.2%) patients received all 14 infusions, 2 (4.5%) received 13 infusions, and 1 (2.3%) received 12 infusions. In the placebo group, 28 (87.5%) patients received all 14 infusions, 2 (6.3%) received 13 infusions, 1 (3.1%) received 11 infusions, and 1 (3.1%) received 8 infusions. The total number of patients who completed the 14-day treatment course was 43 (97.7%) in the teplizumab group and 30 (93.8%) in the placebo group. ██████ (██████%) patient in the teplizumab group and ██ (██████%) patients in the placebo group discontinued the 14-day treatment course for protocol-specified reasons (elevated liver function test results).
Efficacy
Time From Randomization to Stage 3 T1D Diagnosis
In the initial analysis, at a DCO date of November 30, 2018, and a median follow-up duration of 26.63 months, T1D was diagnosed in 20 of 44 participants (45%) in the teplizumab group and 23 of 32 participants (72%) in the placebo group (unadjusted HR = 0.13; 95% CI, 0.05 to 0.34). The median time from randomization to stage 3 T1D diagnosis was 49.5 months (95% CI, 32.2 months to not estimable) in the teplizumab group and 24.9 months (95% CI, 9.5 months to 48.6 months) in the placebo group, with a between-group difference of 24.6 months. The HR obtained from the Cox proportional hazards model was 0.41 (95% CI, 0.22 to 0.78; P = 0.0066). Results of the sensitivity analyses were, in general, consistent with the primary analysis and were all statistically significant (results not shown).
Table 12: Summary of Time From Randomization to Stage 3 T1D Diagnosis in the TN-10 Study (DCO Date: November 30, 2018 — ITT Population)
Time from randomization to stage 3 T1D diagnosis | Teplizumab n = 44 | Placebo n = 32 |
|---|---|---|
Follow-up duration (months), median (range) | 26.63 (NR to NR) | |
Number of participants analyzed | 44 | 32 |
Number of censored patients | 24 | 9 |
Number of patients diagnosed with stage 3 T1D, n (%) | 20 (45) | 23 (72) |
Time to diagnosis of stage 3 T1D (months), median (95% CI) | 49.5 (32.2 to NE) | 24.9 (9.5 to 48.6) |
Between-group difference (95% CI) | 24.6 (NR to NR) | |
HR (95% CI) | 0.41 (0.22 to 0.78) | |
P value | 0.0066 | |
CI = confidence interval; DCO = data cut-off; HR = hazard ratio; ITT = intention to treat; NE = not estimable; NR = not reported; OGTT = oral glucose tolerance test; T1D = type 1 diabetes.
Note: Covariates in the model were age and baseline strata (aged ≥ 18 years with confirmed OGTT, < 18 years with confirmed OGTT, and < 18 years without confirmed OGTT).
Sources: Clinical Study Report for TN-10.18 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 1: Kaplan-Meier Curve of Time to Onset of Stage 3 T1D
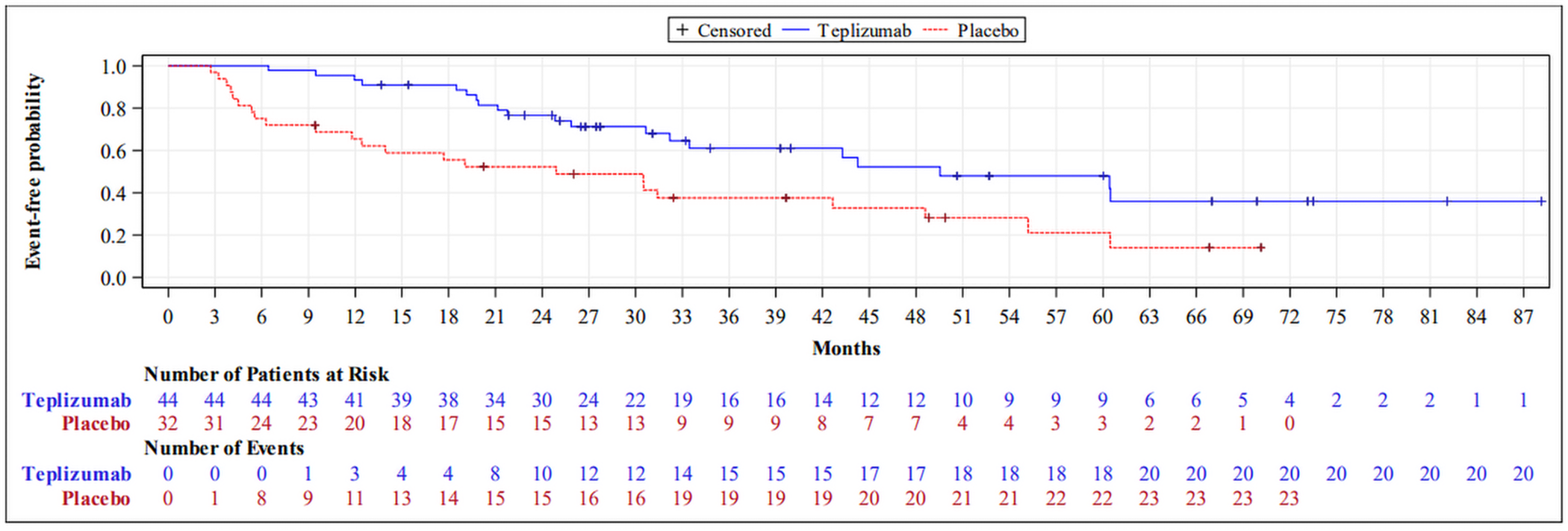
T1D = type 1 diabetes.
Source: Clinical Study Report for TN-10.18
In general, in the preplanned subgroup analyses (Figure 2), the HR for point estimates demonstrated a consistency of effect as in the primary analysis. While there were some differences in certain subgroups (e.g., negative anti-ZnT8 antibodies, HLA DR3 absent, HLA DR4 present, and C-peptide AUC level), the number of patients contributing to each estimate should also be noted.
Figure 2: Subgroup Analyses — HR for Time From Randomization to Diagnosis of Stage 3 T1D
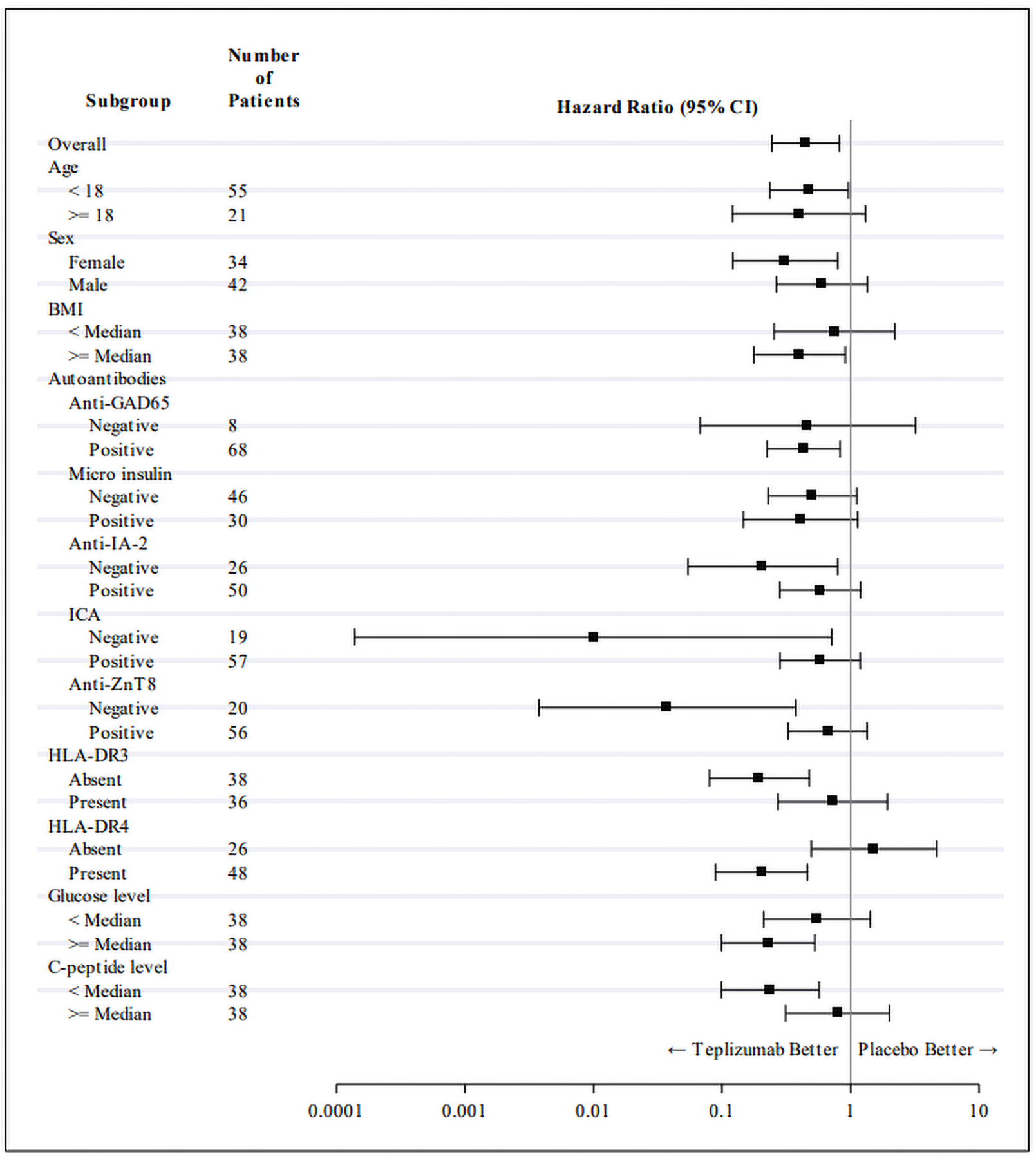
BMI = body mass index; CI = confidence interval; HR = hazard ratio; T1D = type 1 diabetes.
Source: Clinical Study Report for TN-10.18
C-Peptide Levels
At 12 months of treatment, the mean of the C-peptide AUC was ████████ (SD ████████) nmol/L in the teplizumab group and ████████ (SD ████████) nmol/L in the placebo group.
At 24 months of treatment, the mean of the C-peptide AUC was ████████ (SD ████████) nmol/L in the teplizumab group and ████████ (████████) nmol/L in the placebo group.
Details of change in C-peptide levels (AUC) are shown in Table 13.
Table 13: Summary of C-Peptide Levels in the TN-10 Study (ITT Population)
C-Peptide levels | Teplizumab n = 44 | Placebo n = 32 |
|---|---|---|
C-peptide AUC (nmol/L) at baseline, median (range) | 1.77 (0.6 to 4.4) | 1.73 (0.7 to 3.8) |
Number of patients analyzed at 12 months | ████ | ████ |
C-peptide AUC (nmol/L) at 12 months, adjusted mean (SD) | ████████ | ████████ |
Change from baseline at 12 months (nmol/L), mean (SD) | ████████ | ████████ |
Between-group difference (95% CI) | ████ | |
P value | ████ | |
Number of patients analyzed at 24 months | ████ | ████ |
C-peptide AUC (nmol/L) at 24 months, adjusted mean (SD) | ████████ | ████████ |
Change from baseline at 24 months (nmol/L), mean (SD) | ████████ | ████████ |
Between-group difference (95% CI) | ████ | |
P value | ████ | |
AUC = area under the concentration-time curve; CI = confidence interval; ITT = intention to treat; NR = not reported; OGTT = oral glucose tolerance test; SD = standard deviation; T1D = type 1 diabetes.
Note: Patients who were diagnosed with T1D ended study participation once diagnosed with T1D or shortly thereafter and no longer underwent further assessments. Patients who were not diagnosed with T1D had OGTTs at 3 months after randomization and then every 6 months thereafter until the study cut-off date or withdrawal. As a result, the number of OGTTs decreased over time and differed among patients. At 24 months, approximately ████% of the study participants had OGTTs. At 30 months, this declined to ████% of the patients and continued to decline in the remainder of the study. As a result, the sponsor chose to perform the C-peptide analyses up to and including 24 months post randomization in this analysis to avoid comparisons involving too few patients, particularly in the placebo group.
Source: Clinical Study Report for TN-10.18
Hemoglobin A1C Levels
At 12 months of treatment, the mean hemoglobin A1C was ████████% (SD ████████) in the teplizumab group and ████████% (SD ████████) in the placebo group.
At 24 months of treatment, the mean hemoglobin A1C was ████████% (SD ████████) in the teplizumab group and ████████% (SD ████████) in the placebo group (Table 14).
Table 14: Summary of Hemoglobin A1C Levels in the TN-10 Study (ITT Population)
Hemoglobin A1C levels | Teplizumab n = 44 | Placebo n = 32 |
|---|---|---|
Overall population | ||
Number of participants analyzed | 44 | 32 |
Baseline hemoglobin A1C (%), mean (SD) | 5.16 (0.33) | 5.21 (0.26) |
Number of patients contributed to analysis at 12 months | ████ | ████ |
12-month hemoglobin A1C (%) mean (SD) | ████████ | ████████ |
Change from baseline at 12 months (%), mean (SD) | ████ | ████ |
Between-group difference (95% CI) | ████ | |
P value | ████ | |
Number of patients contributed to analysis at 24 months | ████ | ████ |
24-month hemoglobin A1C (%), mean (SD) | ████████ | ████████ |
Change from baseline at 24 months (%), mean (SD) | ████ | ████ |
Between-group difference (95% CI) | ████ | |
P value | ████ | |
CI = confidence interval; ITT = intention to treat; NR = not reported; SD = standard deviation.
Source: Clinical Study Report for TN-10.18
Harms
All patients who received any study treatment were included in the safety population, which was used for all safety analyses. Details of harms outcomes are shown in Table 15.
Adverse Events
As of the DCO date of November 30, 2018, ████████% of patients in the teplizumab group and ████████% in the placebo group experienced at least 1 AE. In the teplizumab group, TEAEs occurred most frequently in the systems organ class of blood and lymphatic system disorders (████████%), infections and infestations (████████%), and skin and subcutaneous disorders (████████%). The most commonly reported AEs in the teplizumab group were lymphopenia (72.7%), leukopenia (20.5%), rash pruritic (████████%), and nasopharyngitis (████████%). Grade 3 TEAEs occurred in ████ (████████%) patients in the teplizumab group and ██ (██████%) patients in the placebo group. No patients had a grade 4 TEAE.
Serious Adverse Events
Treatment-emergent SAEs occurred in ██ (████████%) patients in the teplizumab group and ██ (██████%) patient in the placebo group. The SAEs reported in the teplizumab group included ████████████████████ ████████████████████ ██████████ ██████████████████ ██████████ ██████████████████ ██████████████████████████████ ██████████ ██████████ ██████████████████████ ██████████ ████████████████████ ██████ ██████████████████████████████. ██████ case of ██████████████████████████████ ██████████████████████ was reported as SAE in the placebo group.
Withdrawals Due to AEs
██████████ patients discontinued from study treatment because of TEAEs, including ██ case of increased ALT (██████%) in the teplizumab group and ██ cases of hyperbilirubinemia (██████%) in the placebo group.
Mortality
No patients died in the study.
Notable Harms
████████ patients (██████%: grade 3 events of cellulitis, gastroenteritis, pneumonia, and wound infection) in the teplizumab group had an AESI, while ████ ██████████████ from the placebo group reported AESI. There were no grade 3 or higher liver function abnormalities, grade 3 or higher neutropenia, grade 4 or higher CRS, or lymphocyte count lower than 500 mm3 for 7 days or longer events reported at the DCO date of November 30, 2018. No event of DKA had been reported at the DCO date of November 30, 2018.
Table 15: Summary of Harms Results From the TN-10 Study (DCO Date: November 30, 2018 — Safety Analysis Set)
Harms | Teplizumab n = 44 | Placebo n = 32 | Total |
|---|---|---|---|
AEs occurring in > 5% of patients, n (%) | |||
Patients with ≥ 1 TEAE | ████ (████████) | ████ (████████) | ████ (████████) |
Blood and lymphatic system disorders | ████████ | ████████ | ████████ |
Leukopenia | 9 (20.5) | 0 | 9 (11.8) |
Lymphopenia | 32 (72.7) | 2 (6.3) | 34 (44.7) |
Neutropenia | 3 (6.8) | 1 (3.1) | 4 (5.3) |
Infections and infestations | ████████ | ████████ | ████████ |
Nasopharyngitis | ██ (████████) | ██ (██████) | ██ (████████) |
Pneumonia | 4 (9.1) | 1 (3.1) | 5 (6.6) |
Sinusitis | 4 (9.1) | 1 (3.1) | 5 (6.6) |
Upper respiratory tract infection | 4 (9.1) | 1 (3.1) | 5 (6.6) |
Skin and subcutaneous tissue disorders | ████████ | ████████ | ████████ |
Rash | 6 (13.6) | 0 | 6 (7.9) |
Rash pruritic | ██ (████████) | ██ | ██ (██████) |
Nervous system disorders | 9 (20.5) | 5 (15.6) | 14 (18.4) |
Headache | 5 (11.4) | 3 (9.4) | 8 (10.5) |
Gastrointestinal disorders | 7 (15.9) | 3 (9.4) | 10 (13.2) |
Vomiting | 2 (4.5) | 2 (6.3) | 4 (5.3) |
Respiratory, thoracic, and mediastinal disorders | 7 (15.9) | 1 (3.1) | 8 (10.5) |
Bronchospasm | 3 (6.8) | 0 | 3 (3.9) |
Cough | 3 (6.8) | 0 | 3 (3.9) |
Vascular disorders | 4 (9.1) | 2 (6.3) | 6 (7.9) |
Hypertension | 4 (9.1) | 1 (3.1) | 5 (6.6) |
Hepatobiliary disorders | 0 | 2 (6.3) | 2 (2.6) |
Hyperbilirubinemia | 0 | 2 (6.3) | 2 (2.6) |
SAEs, n (%) | |||
Patients with at least 1 TESAE | ██ (████████) | ██ (██████) | ██ (████████) |
Infections and infestations | ████████ | ██ | ████████ |
Cellulitis | ████████ | ██ | ████████ |
Gastroenteritis | ████████ | ██ | ████████ |
Pneumonia | ████████ | ██ | ████████ |
Wound infection | ████████ | ██ | ████████ |
Immune system disorders | 1 (2.3) | 0 | 1 (1.3) |
Serum sickness | 1 (2.3) | 0 | 1 (1.3) |
Injury, poisoning, and procedural complications | 1 (2.3) | 0 | 1 (1.3) |
Ankle fracture | 1 (2.3) | 0 | 1 (1.3) |
Musculoskeletal and connective tissue disorders | 1 (2.3) | 0 | 1 (1.3) |
Musculoskeletal chest pain | 1 (2.3) | 0 | 1 (1.3) |
Nervous system disorders | 1 (2.3) | 0 | 1 (1.3) |
Dizziness | 1 (2.3) | 0 | 1 (1.3) |
AEs leading to withdrawal, n (%) | |||
Patients with ≥ 1 AE leading to withdrawal | ██ (██████) | ██ (██████) | ██ (██████) |
Hepatobiliary disorders | ██ | ██ (██████) | ██ (██████) |
Hyperbilirubinemia | ██ | ██ (██████) | ██ (██████) |
Investigations | ██ (██████) | ██ | ██ (██████) |
Alanine aminotransferase increase | ██ (██████) | ██ | ██ (██████) |
Skin and subcutaneous tissue disorders | 1 (2.3) | 0 | 1 (1.3) |
Rash pruritic | 1 (2.3) | 0 | 1 (1.3) |
AESIs, n (%) | |||
Patients with at least 1 AESI | ██ (██████) | ██ | ██ (██████) |
Infections and infestations | ██ (██████) | ██ | ██ (██████) |
Cellulitis | ██ (██████) | ██ | ██ (██████) |
Gastroenteritis | ██ (██████) | ██ | ██ (██████) |
Pneumonia | ██ (██████) | ██ | ██ (██████) |
Wound infection | ██ (██████) | ██ | ██ (██████) |
Deaths, n (%) | |||
Number of deaths | 0 | 0 | 0 |
AE = adverse event; AESI = adverse event of special interest; DCO = data cut-off; SAE = serious adverse event; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event.
Sources: Clinical Study Report for TN-10.18 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
In the TN-10 study, appropriate methods of randomization and allocation concealment were employed. The randomization numbers and tables were generated by the TrialNet Coordinating Center. All patients, clinical investigators, and study personnel were masked to treatment assignment throughout the study. There were some imbalances between the 2 treatment groups in patients’ baseline characteristics, such as the proportion of patients aged younger than 18 years, proportion of siblings with T1D, and presence of autoantibodies, consistent with the small sample size.
The HR in the study is imprecise (95% CI, 0.22 to 0.78) and reflects the study’s small size (N = 76); however, a larger study was not practical given the uncertainty regarding the incidence and prevalence of patients with stage 2 T1D. In general, small studies are at risk of imbalance in prognostic factors, are associated with larger effect sizes, and should be considered in the context of these findings.72,73 An example of imbalance in prognostic factors in the TN-10 study is age, which is inversely associated with development of T1D.74 The lower proportion of patients aged younger than 18 years in the teplizumab group could favour teplizumab in the study results; however, the proportional hazards model was adjusted for age greater than and less than 18 years.18 Autoantibody type and distribution between groups might also favour teplizumab;75 the FDA adjusted for autoantibody counts in their review and found the HR was numerically higher (0.44) but still statistically significant after adjustment.76
Teplizumab was developed to delay the onset of stage 3 T1D in patients diagnosed with stage 2 T1D. Time to stage 3 T1D diagnosis was the primary efficacy end point in the TN-10 study. Longer time from randomization to disease progression is associated with delayed treatment with insulin, and related short-term consequences. However, the clinical experts noted that currently it is uncertain whether this delay can be translated to longer-term clinical benefits, such as prolonged survival, and lower risk of macrovascular or microvascular events in patients with stage 3 T1D. It may also have an impact on patients’ HRQoL during the disease-free period, in particular, the psychosocial well-being of the patients and their families; however, this was not examined in this study.
In the TN-10 study, the methodology employed in the time-to-T1D analysis used total follow-up recorded for each patient (i.e., maximum use of follow-up time). Presuming no evidence against missing at random, and given the modest size of the trial, no methods were employed to impute additional follow-up of patients who dropped out (i.e., were lost to follow-up), and there were 3 who discontinued the treatment course: 1 in the teplizumab group and 2 in the placebo group. Predefined sensitivity analyses were conducted to evaluate the robustness of the primary end point using different strategies to handle missing data. Overall, the results of sensitivity analyses aligned with the primary analysis of time from randomization to stage 3 T1D and all reached statistical significance, which supported the robustness of the results.
Prespecified subgroup analyses generally supported consistency of the overall direction of effect of teplizumab across subgroups; some subgroups were small, resulting in wide CIs. Due to the small sample size in the subgroups and the risk of inflated type I error from multiplicity, results should be interpreted with caution, and should be used for hypothesis generation only.
HRQoL and risk of DKA with progression to stage 3 T1D were considered clinically important outcomes by the clinicians and patient groups. No event of DKA was reported in the TN-10 study. Further, the study could not assess whether monitoring and education of people with stage 2 T1D would reduce DKA occurring at diagnosis of stage 3 T1D. Therefore, the effect of teplizumab on occurrence of DKA and patients’ quality of life remained unknown.
C-peptide is a measure that reflects beta cell function, which may support the delay in the onset of clinical T1D and life-long exogenous insulin dependence. While not listed as an FDA-accepted surrogate outcome for measurement in T1D,68 the preservation of C-peptide levels in patients with T1D has been shown to be associated with improved clinical outcomes,66,69 such as a reduced risk of complications (e.g., severe hypoglycemia, retinopathy, and neuropathy).66,69 Preserved C-peptide levels in patients with recently diagnosed T1D have also been associated with a reduction in the dose of exogenous insulin needed to maintain glycemic control.69 In the TN-10 study, change in levels of C-peptide from baseline was an exploratory end point and the data were descriptive. In addition, the results were only available in patients who had not progressed to stage 3 T1D (approximately ████%). Therefore, the effect of the study drug on the level of C-peptide was difficult to interpret. The clinical experts noted that although testing for C-peptide is readily available in Canada, it may not be routinely measured in clinical practice. Similarly, data of change in hemoglobin A1C levels were only collected when patients had not progressed to stage 3 T1D. Follow-ups on the hemoglobin A1C levels stopped after T1D onset.
External Validity
Based on feedback from the clinical experts consulted for this review, the baseline characteristics of patients randomized in the TN-10 study are somewhat different than those observed in clinical practice. For example, the proportion of patients aged older than 18 years may be larger in practice than in the TN-10 study. According to the clinical experts consulted for this review, younger patients are more likely to progress to stage 3 T1D compared to older patients. Also, nearly all patients in the study were white, which was inconsistent with those seen in practice. As such, the patients enrolled are unlikely to be representative of the racial or ethnic diversity of those seen in clinical practice in Canada. In addition, the trial used restricted exclusion criteria, while in clinical practice, a broader population may be eligible to receive treatment with teplizumab, such as patients who may have abnormal blood counts or liver function tests. The clinical experts indicated that, in general, clinicians would follow the recommendations from the product monograph of the study drug, and the study findings may not be generalized to the patient population in clinical practice.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.16,17
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The threshold for a clinically important effect for time to stage 3 T1D in the study population was not obtained. Therefore, the target of the certainty of evidence assessment was the presence or absence of any non-null effect for this end point. The thresholds for a clinically important effect for the change from baseline in levels of C-peptide and hemoglobin A1C, and change from baseline in the occurrence of harm events in the study population were not obtained either. Therefore, the target of the certainty of evidence assessment was the presence or absence of any non-null effect for these end points.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for teplizumab versus placebo.
Teplizumab likely results in an increase in time to onset of stage 3 T1D when compared with placebo. The clinical importance of the delay is uncertain (moderate certainty due to serious imprecision).
Teplizumab likely results in fewer patients progressed to stage 3 T1D when compared with placebo. The clinical importance of the decrease is uncertain (moderate certainty due to serious imprecision).
Teplizumab may result in an increase in the proportion of patients who experience SAEs when compared with placebo (low certainty due to very serious imprecision).
Teplizumab may result in an increase in the proportion of patients who experience AESIs when compared with placebo (low certainty due to very serious imprecision).
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
Participants who had not progressed to stage 3 T1D by the end of the TN-10 study were made aware of their treatment assignment, transferred into the TN-01 study, and continued to be followed up and were included in the extended follow-up analysis of the primary end point, which was conducted after participants had been followed for a median duration of 31.1 months. The original TN-10 study end date was June 2019.
Populations
Patients from the TN-10 study were continuously followed for a median time of 31.1 months (post randomization in the TN-10 study) in the Sims et al. study (2021)19 and 80.46 months (post randomization in the TN-10 study) in the study by Lledó-Delgado and colleagues.20
Interventions
Patients did not receive any treatments during the TN-01 study.
Outcomes
Efficacy analyses of the TN-10 study with an extended follow-up period (median = 31.1 months post randomization; range, 2.4 months to 102.4 months) were published in March 2021 (the Sims et al. study [2021]).19 The publication reported an update on the median time from randomization to the diagnosis of stage 3 T1D and metabolic outcomes, including measures of C-peptide response (which was the focus of this extended follow-up analysis) and glycemic control as measured by hemoglobin A1C levels.19 Furthermore, an efficacy analysis of the TN-10 study with a median follow-up of 80.46 months post randomization (range not reported) was published as part of a mechanistic analyses in August 2024 (the Lledó-Delgado et al. study).20 In the current Clinical Review Report, only results of time to diagnosis of stage 3 T1D are presented.
Statistical Analysis
In the extended follow-up analysis published in 2021 (the Sims et al. study19), analysis of the effect of teplizumab treatment on the incidence of stage 3 T1D was performed using a Cox proportional hazards model adjusted for stratification and age. In the subsequent extended follow-up analysis published in 2024, analysis of the impact of teplizumab on the median time to diagnosis with stage 3 T1D was performed using a log-rank test.20
Details of the statistical methods used in these follow-up analyses are presented in Table 16.
Table 16: Statistical Analysis of Efficacy End Points in the TN-10 Study — Extended Follow-Up
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Sims et al. (2021)19 | ||||
Time from randomization to stage 3 T1D diagnosis or last contact (median follow-up: 31.1 months) | Kaplan-Meier method, Cox proportional hazards model | Age and stratification (“stratification” was not specified in the published article) | NR | NR |
Lledó-Delgado et al.20 | ||||
Time from randomization to stage 3 T1D diagnosis or last contact (median follow-up: 80.46 months) | Kaplan-Meier method, log-rank test | NR | NR | NR |
NR = not reported; T1D = type 1 diabetes.
Source: Sims et al. (2021)19 and Lledó-Delgado et al.20 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Efficacy
Time From Randomization to Stage 3 T1D
In an extended follow-up analysis in the study by Sims and colleagues,19 (median follow-up = 31.1 months since randomization in the TN-10 study; range, 2.4 months to 102.4 months), 22 patients (50%) in the teplizumab group and 25 patients (78%) in the placebo group were diagnosed with stage 3 T1D since randomization. The median time from randomization to stage 3 T1D diagnosis was 59.6 months and 27.1 months for patients treated with teplizumab and placebo, respectively (HR = 0.457; P = 0.01). The between-group difference in median time to T1D diagnosis was 32.5 months.77
In the extended follow-up analysis in the study by Lledó-Delgado and colleagues,20 (median follow-up = 80.46 months since randomization in the TN-10 study; range, NR), 28 patients (64%) in the teplizumab group and 28 patients (88%) in the placebo group were diagnosed with stage 3 T1D. The median time from randomization to stage 3 T1D diagnosis was 52.2 months and 27.3 months for patients treated with teplizumab and placebo, respectively (P = 0.0026, log-rank test).
Table 17: Summary of Time From Randomization to Stage 3 T1D Diagnosis in Extended Follow-Ups (ITT Population)
Time from randomization to stage 3 T1D diagnosis | Sims et al. (2021) | Lledó-Delgado et al. | ||
|---|---|---|---|---|
Teplizumab n = 44 | Placebo n = 32 | Teplizumab n = 44 | Placebo n = 32 | |
Follow-up duration (months), median (range)a | 31.1 (2.4 months to 102.4 months) | 80.46 (NR to NR) | ||
Number of participants analyzed | 44 | 32 | 44 | 32 |
Number of censored patients | NR | NR | ||
Patients diagnosed with stage 3 T1D, n (%) | 22 (50) | 25 (78) | 28 (64) | 28 (88) |
Time to diagnosis of stage 3 T1D (months), median (95% CI)a | 59.6 (NR) | 27.1 (NR) | 52.2 (NR) | 27.3 (NR) |
Between-group difference (95% CI) | NR | NR | ||
HR (95% CI) | 0.457 (NR) | NR | ||
P value | 0.01 | 0.0026 | ||
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; NR = not reported; T1D = type 1 diabetes.
aFollow-up duration since initial randomization in the TN-10 study.
Source: Sims et al. (2021)19 and Lledó-Delgado et al.20 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Harms
Not assessed in the extended follow-up period.
Critical Appraisal
Patients initially enrolled in the TN-10 study and who had not progressed to stage 3 T1D were followed in the extension periods. Their treatment assignment was unblinded at the end of the TN-10 study. Longer-term efficacy of teplizumab was reported for up to 80.46 months. Missing data handling was not reported during these periods. Time from randomization to stage 3 T1D, and change in the levels of C-peptide and hemoglobin A1C were reported. While these outcomes were objectively measured, the open-label observational design cannot control for the impact of patient behaviours or other treatments received. Insufficient details of the efficacy outcomes were reported (e.g., between-group differences and associated 95% CIs were missing); therefore, a thorough evaluation of the long-term effect of teplizumab in the study population was not feasible. Harm outcomes were not examined in the extended follow-up analyses.
Indirect Evidence
No indirect treatment comparison has been submitted to this review.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the systematic review evidence have been submitted to this review.
Discussion
Summary of Available Evidence
The evidence included in this review consisted of 1 phase II, double-blind, placebo-controlled RCT, the TN-10 study (N = 76). The purpose of this study was to evaluate the efficacy and safety of teplizumab for delaying the onset of stage 3 T1D (also known as clinical T1D) in adults or children aged 8 years or older with a diagnosis of stage 2 disease. These patients were relatives of those with confirmed diagnosis of stage 3 T1D. Eligible patients were randomly assigned to receive either teplizumab (n = 44) or placebo (n = 32) in a double-blind manner. The primary efficacy end point of this study was time from randomization to stage 3 T1D diagnosis. In addition, changes in levels of C-peptide and hemoglobin A1C, as well as harms, were evaluated. At baseline, the patient characteristics were generally comparable between the 2 treatment groups. Of the 76 patients, the median age was 14 years in the teplizumab group and 13 years in the placebo group. There were 29 patients (65.9%) aged younger than 18 years in the teplizumab group compared to 26 patients (81.3%) in the placebo group. Before enrolment, all patients were positive for at least 2 autoantibodies, while 73.7% of all patients were positive for 3 or more. The teplizumab and placebo groups were similar in baseline glucose and hemoglobin A1C levels. There were some imbalances in the proportion of patients who were first-degree relatives of siblings with T1D and presence of certain autoantibodies.
At the end of the TN-10 study, patients who had not progressed to stage 3 T1D were continuously followed in the TN-01 study and additional results for up to 80.46 months were reported in 2 publications. Outcomes assessed during this period of time included time from randomization to stage 3 T1D. Patients were unblinded to the treatment assignment during the extended follow-up.
Interpretation of Results
Efficacy
Teplizumab is a first-in-class medication to delay the onset of stage 3 T1D in patients who have a diagnosis of stage 2 T1D. Currently, there is no treatment for patients with stage 2 disease; these patients will eventually progress to stage 3 T1D and require insulin therapy in their lifetime. There is an unmet need for a treatment that prevents or delays progression to stage 3 T1D in patients with stage 2 T1D.
Results of the TN-10 study showed that after a median follow-up of 26.6 months, stage 3 T1D was diagnosed in 20 of 44 participants (45%) in the teplizumab group and 23 of 32 participants (72%) in the placebo group. The median time from randomization to stage 3 T1D diagnosis was 49.5 months (95% CI, 32.2 months to not estimable) in the teplizumab group and 24.9 months (95% CI, 9.5 months to 48.6 months) in the placebo group, with a between-group difference of 24.6 months. The HR obtained from the Cox proportional hazards model was 0.41 (95% CI, 0.22 to 0.78; P = 0.0066). The clinical experts consulted for this review indicated that the approximately 2-year delay in the onset of T1D resulting from treatment with teplizumab (compared to placebo) is considered clinically meaningful. However, the clinical experts noted that the long-term effects of teplizumab on lowering the risks of macrovascular and microvascular events remain unclear, and there are no long-term data for teplizumab in the target population. For pediatric patients, the 2-year delay in disease progression is expected to have a larger impact compared with adults, when children are experiencing rapid development, physically and cognitively. The delay would also enable the children and their family to better prepare for the stage 3 disease that can develop some time in the future.
According to the clinical experts, because there is no cure for T1D, patients with stage 2 T1D could benefit from a delayed onset of stage 3 T1D through improved quality of life, relieved burden of life-long insulin therapy, reduced risk of diabetic complications (e.g., hyperglycemia and potential DKA), more education and monitoring, and increased opportunities to develop better coping strategies. The patient group input echoed that any delay in onset of stage 3 disease would improve their overall well-being and decrease the risk of diabetes complications. The patient group also noted that for young children, a delay of 2 to 3 years for a T1D diagnosis has important and meaningful benefits. However, at present, the evidence supporting the effect of teplizumab on these important outcomes is lacking, and it is unclear if treatment with teplizumab can make a difference for patients with stage 2 disease other than delaying the progression to stage 3 T1D by approximately 2 years.
The clinical experts acknowledged that identifying the eligible population is a key implementation challenge. Currently, stage 2 disease is defined based on the development of dysglycemia in addition to the presence of at least 2 diabetes-related autoantibodies. Because a population-based screening program for autoantibodies is not routinely performed for individuals at risk of having stage 2 T1D in Canada, only a small portion of this population could be tested for autoantibodies. These are first-degree or second-degree relatives of those who have a confirmed diagnosis of stage 3 disease, and testing is often completed at the patient’s request. The majority of the patients with T1D (approximately 85%) are not currently tested with this strategy, and as a result, will not have access to teplizumab. These include other populations who may experience inequitable access to testing (such as individuals without a family history of T1D, those with unknown family history, or groups such as immigrants). The sponsor estimated that approximately ██████████ individuals (i.e., first-degree or second-degree relatives of patients with T1D) at baseline and over ██████████████ individuals from year 1 onward would undergo testing for diabetes-related autoantibodies.48 However, clinical experts consulted for this review noted that this is likely an underestimate. They indicated that the number of patients tested for these autoantibodies may be doubled if teplizumab were to be funded. According to the sponsor-submitted materials and the clinical experts, individuals who initially test positive for 2 or more diabetes-related autoantibodies should undergo repeat testing to confirm their status. Confirming a positive autoantibody status is important to ensure the persistence of the autoimmune response and the validity of the target antigen.4 Once diagnosed, no further autoantibody testing is required. Based on the input from the clinical experts, provision of diabetes autoantibody testing to identify individuals with stage 2 T1D is anticipated to impact human and other health care resources. If teplizumab were to be funded, the number of individuals getting tested would likely increase; consequently, the volume of samples requiring out-of-province shipment would also increase, potentially causing delays and backlogs at testing sites. To manage the increased testing volume, investments in infrastructure and equipment along with that in staffing may be needed to establish in-house testing capacity. Upgrading laboratory infrastructure with validated assays for testing the 4 diabetes-related autoantibodies and providing adequate training for laboratory staff may be warranted. In addition, targeted education for health care providers would be necessary to enhance awareness of the autoantibody test. Expanding the screening to a population level would further increase resource requirements. Even if a population-based screening program can be put into place, other challenges of the implementation include accuracy (sensitivity and specificity) of the autoantibody tests, accessibility, as well as the cost-effectiveness of the screening program. Other possible barriers include low awareness of stage 2 T1D and the role of autoantibody testing among both health care providers and patients, as well as financial barriers (need for out-of-pocket payments).49,50 If teplizumab were to be funded, these factors may be barriers to timely and equitable implementation.
HRQoL was considered a clinically important outcome by the patient groups and clinicians. According to the Ethics Review Report, stage 3 T1D imposes a substantial psychosocial burden on patients and their families, especially for young children and their families. A patient’s daily life with T1D requires constant attention to fluctuating insulin needs, food intake, and stress levels. However, HRQoL was not assessed in the current submission; therefore, the effect of teplizumab on patients’ quality of life, with or without disease progression, in particular psychosocial well-being, is unknown.
Results of the extended follow-up analyses suggested that treatment with teplizumab was associated with a delayed time to stage 3 T1D diagnosis in patients aged 8 years or older who have been previously diagnosed with stage 2 T1D, when compared to placebo.
Harms
At a median follow-up of 26.6 months, ████████% of patients in the teplizumab group and ████████% in the placebo group experienced at least 1 AEs. The most commonly reported AEs in the teplizumab group were lymphopenia (72.7%), leukopenia (20.5%), rash pruritic (████████%), and nasopharyngitis (████████%). Grade 3 TEAEs occurred in ████ (████████%) patients in the teplizumab group and ██ (██████%) patients in the placebo group.
Treatment-emergent SAEs occurred in ██ (████████%) patients in the teplizumab group and ██ (██████%) patient in the placebo group. The SAEs reported in the teplizumab group included ████████████████████ ████████████████████ ██████████ ██████████████████ ██████████ ██████████████████ ██████████████████████████████ ██████████ ██████████ ██████████████████████ ██████████ ████████████████████ ██████ ██████████████████████████████. ██████ case of ██████████████████████████████ ██████████████████████ was reported as SAE in the placebo group.
██████████ patients discontinued from study treatment because of TEAEs, including ██ case of increased ALT (██████%) in the teplizumab group and ██ cases of hyperbilirubinemia (██████%) in the placebo group.
No patients died during the study.
████████ patients (██████%: grade 3 events of cellulitis, gastroenteritis, pneumonia and wound infection) in the teplizumab group had an AESI, while ████ ██████████████ from the placebo group reported AESI. There were no grade 3 or higher liver function abnormalities, grade 3 or higher neutropenia, grade 4 or higher CRS, or lymphocyte count lower than 500 mm3 for 7 days or longer events reported at the DCO date of November 30, 2018.
The clinical experts consulted for this review noted that most AEs are manageable and there were no unusual safety signals observed.
Conclusion
Currently there is a lack of treatment for patients diagnosed with stage 2 T1D. Teplizumab is a first-in-class medication with an indication of delaying the onset of stage 3 T1D in patients with preclinical T1D. One phase II, double-blind, placebo-controlled RCT (TN-10) provided evidence for the efficacy and safety of teplizumab in adults or children aged 8 years or older with stage 2 T1D. The results showed that after a median follow-up of 26.6 months, treatment with teplizumab likely results in delaying the time to progression to stage 3 T1D by approximately 2 years, compared to placebo. However, currently it is uncertain whether this 2-year delay in patients with stage 2 T1D (with or without progression) can be translated to longer-term clinical benefits, such as prolonged survival, and lower risk of macrovascular or microvascular events in patients with stage 3 T1D. In terms of harms, evidence from the TN-10 study indicated that teplizumab may result in an increase in the proportion of patients who experience SAEs or AESIs when compared with placebo. Up to a median follow-up of 80 months since the initial randomization, longer duration to progression to stage 3 T1D was observed in patients in the teplizumab group when compared with those who received placebo. There is uncertainty in long-term safety due to the lack of evidence. In addition, the impact of teplizumab on patients’ HRQoL was unknown, either during the delayed period or after a diagnosis of stage 3 T1D.
References
1.Besser REJ, Bell KJ, Couper JJ, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Stages of type 1 diabetes in children and adolescents. Pediatr Diabetes. 2022;23(8):1175-1187. doi:10.1111/pedi.13410 PubMed
2.ElSayed NA, Aleppo G, Aroda VR, et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S19-S40. doi:10.2337/dc23-S002 PubMed
3.Libman I, Haynes A, Lyons S, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr Diabetes. 2022;23(8):1160-1174. doi:10.1111/pedi.13454 PubMed
4.Phillip M, Achenbach P, Addala A, et al. Consensus Guidance for Monitoring Individuals With Islet Autoantibody–Positive Pre-Stage 3 Type 1 Diabetes. Diabetes Care. 2024;47(8):1276-1298. doi:10.2337/dci24-0042 PubMed
5.Insel RA, Dunne JL, Atkinson MA, et al. Staging Presymptomatic Type 1 Diabetes: A Scientific Statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care. 2015;38(10):1964-1974. doi:10.2337/dc15-1419 PubMed
6.Moore DJ, Leibel NI, Polonsky W, Rodriguez H. Recommendations for Screening and Monitoring the Stages of Type 1 Diabetes in the Immune Therapy Era. Int J Gen Med. 2024;17:3003-3014. doi:10.2147/IJGM.S438009 PubMed
7.Sparring V, Nyström L, Wahlström R, Jonsson PM, Östman J, Burström K. Diabetes duration and health-related quality of life in individuals with onset of diabetes in the age group 15—34 years – a Swedish population-based study using EQ-5D. BMC Public Health. 2013;13:377. doi:10.1186/1471-2458-13-377 PubMed
8.Sarkar S, Donner T. Autoantibodies in Type 1 Diabetes (Johns Hopkins Diabetes Guide). Johns Hopkins Medicine. 2020. Accessed April 28, 2025. https://www.hopkinsguides.com/hopkins/view/Johns_Hopkins_Diabetes_Guide/547013/all/Autoantibodies_in_Type_1_Diabetes
9.Gong B, Yang W, Xing Y, Lai Y, Shan Z. Global, regional, and national burden of type 1 diabetes in adolescents and young adults. Pediatr Res. 2025;97(2):568-576. doi:10.1038/s41390-024-03107-5 PubMed
10.Silfer JL, Tonyushkina KN. Global trends in type 1 diabetes in adolescents and young adults (1990-2019). Pediatr Res. 2025;97(2):459-461. doi:10.1038/s41390-024-03554-0 PubMed
11.Rawshani A, Sattar N, Franzen S, et al. Excess mortality and cardiovascular disease in young adults with type 1 diabetes in relation to age at onset: a nationwide, register-based cohort study. Lancet. 2018;392(10146):477-486. doi:10.1016/S0140-6736(18)31506-X PubMed
12.Edqvist J, Rawshani A, Rawshani A, et al. Trajectories in HbA1c and other risk factors among adults with type 1 diabetes by age at onset. BMJ Open Diabetes Res Care. 2021;9(1):e002187. doi:10.1136/bmjdrc-2021-002187 PubMed
13.Holt RIG, DeVries JH, Hess-Fischl A, et al. The Management of Type 1 Diabetes in Adults. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2021;44(11):2589-2625. doi:10.2337/dci21-0043 PubMed
14.ElSayed NA, Aleppo G, Aroda VR, et al. 14. Children and Adolescents: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S230-S253. doi:10.2337/dc23-S014 PubMed
15.Diabetes Canada Clinical Practice Guidelines Expert Committee. Diabetes Canada 2018 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes. 2018;42(Suppl 1):S1-S325.
16.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
17.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
18.Sanofi. Clinical Study Report: TN-10. Anti-CD3 mab (Teplizumab) for prevention of diabetes in relatives at-risk for type 1 diabetes mellitus [internal sponsor's report]. 2020.
19.Sims EK, Bundy B, Stier K, et al. Teplizumab improves and stabilizes beta cell function in antibody positive high-risk individuals. Sci Transl Med. 2021;13(583):eabc8980. doi:10.1126/scitranslmed.abc8980 PubMed
20.Lledo-Delgado A, Preston-Hurlburt P, Currie S, et al. Teplizumab induces persistent changes in the antigen-specific repertoire in individuals at risk for type 1 diabetes. J Clin Invest. 2024;134(18):e177492. doi:10.1172/JCI177492 PubMed
21.Sanofi. Sanofi-aventis Canada Inc. response to Canada's Drug Agency request for additional information regarding Tzield review on April 11, 2025 [internal additional sponsor's information]. April 17, 2025.
22.Whittemore R, Jaser S, Chao A, Jang M, Grey M. Psychological experience of parents of children with type 1 diabetes: a systematic mixed-studies review. Diabetes Educ. 2012;38(4):562-79. doi:10.1177/0145721712445216 PubMed
23.Rodrigue JR, Geffken GR, Clark JE, Hunt F, Fishel P. Parenting satisfaction and efficacy among caregivers of children with diabetes. Child Health Care. 1994;23(3):181-91. doi:10.1207/s15326888chc2303_3 PubMed
24.Rewers A. Chapter 17: Acute Metabolic Complications in Diabetes [sponsor supplied reference]. In: Cowie CC, Casagrande SS, Menke A, et al, eds. Diabetes in America. 3rd ed. National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018. Accessed August 07, 2024. https://www.ncbi.nlm.nih.gov/books/NBK567993/
25.Institute for Safe Medication Practices (ISMP). ISMP Guidelines for Optimizing Safe Subcutaneous Insulin Use in Adults [sponsor supplied reference]. 2017. Accessed February 10, 2025. https://www.ismp.org/sites/default/files/attachments/2018-09/ISMP138D-Insulin%20Guideline-090718.pdf
26.Lawrence JM, Reynolds K, Saydah SH, et al. Demographic Correlates of Short-Term Mortality Among Youth and Young Adults With Youth-Onset Diabetes Diagnosed From 2002 to 2015: The SEARCH for Diabetes in Youth Study. Diabetes Care. 2021;44(12):2691-2698. doi:10.2337/dc21-0728 PubMed
27.Kitabchi AE, Umpierrez GE, Murphy MB, Kreisberg RA. Hyperglycemic crises in adult patients with diabetes: a consensus statement from the American Diabetes Association. Diabetes Care. 2006;29(12):2739-2748. doi:10.2337/dc06-9916 PubMed
28.Sanofi-aventis Canada Inc. Drug Reimbursement Review sponsor submission: Tzield (teplizumab), 2 mg/2 mL per vial for intravenous infusion [internal sponsor's package]. February 19, 2025.
29.Swediabkids (Swedish Diabetes Registry). Annual Report 2020 [sponsor supplied reference]. Accessed August 06, 2024. https://www.ndr.nu/pdfs/Annual_Report_Swediabkids_2020.pdf
30.Marcovecchio ML, Lucantoni M, Chiarelli F. Role of chronic and acute hyperglycemia in the development of diabetes complications. Diabetes Technol Ther. 2011;13(3):389-394. doi:10.1089/dia.2010.0146 PubMed
31.Haller MJ, Bell KJ, Besser REJ, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Screening, Staging, and Strategies to Preserve Beta-Cell Function in Children and Adolescents with Type 1 Diabetes. Horm Res Paediatr. 2024;97(6):529-545. doi:10.1159/000543035 PubMed
32.Sanofi-aventis Canada Inc. Tzield (teplizumab): 2 mg per 2 mL (1 mg/mL) for intravenous infusion [product monograph]. 2025. Updated May 5, 2025.
33.Health Canada. Notice of compliance (NOC) for Tzield (teplizumab). 2025. Accessed May 20, 2025. https://health-products.canada.ca/noc-ac/nocInfo?no=35295
34.American Diabetes Association Professional Practice Committee. 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes—2025. Diabetes Care. 2024;48(Supplement_1):S27-S49. doi:10.2337/dc25-S002 PubMed
35.Notkins AL, Lernmark A. Autoimmune type 1 diabetes: resolved and unresolved issues. J Clin Invest. 2001;108(9):1247-52. doi:10.1172/jci14257 PubMed
36.Chen BH, Chung SB, Chiang W, Chao MC. GAD65 antibody prevalence and association with thyroid antibodies, HLA-DR in Chinese children with type 1 diabetes mellitus. Diabetes Res Clin Pract. 2001;54(1):27-32. doi:10.1016/s0168-8227(01)00272-8 PubMed
37.Verkauskiene R, Danyte E, Dobrovolskiene R, et al. The course of diabetes in children, adolescents and young adults: does the autoimmunity status matter? BMC Endocr Disord. 2016;16(1):61. doi:10.1186/s12902-016-0145-3 PubMed
38.Parkkola A, Härkönen T, Ryhänen SJ, Ilonen J, Knip M. Extended family history of type 1 diabetes and phenotype and genotype of newly diagnosed children. Diabetes Care. 2013;36(2):348-54. doi:10.2337/dc12-0445 PubMed
39.Sims EK, Besser REJ, Dayan C, et al. Screening for Type 1 Diabetes in the General Population: A Status Report and Perspective. Diabetes. 2022;71(4):610-623. doi:10.2337/dbi20-0054 PubMed
40.Type 1 Diabetes TrialNet. Sign up for T1D Risk Screening. Accessed May 05, 2025. https://www.diabetestrialnet.org/webapp/PreRegTracking/OnlineScreening.aspx
41.Steck AK, Rewers MJ. Genetics of type 1 diabetes. Clin Chem. 2011;57(2):176-85. doi:10.1373/clinchem.2010.148221 PubMed
42.Bosi E, Catassi C. Screening type 1 diabetes and celiac disease by law. Lancet Diabetes Endocrinol. 2024;12(1):12-14. doi:10.1016/s2213-8587(23)00354-6 PubMed
43.Cherubini V, Mozzillo E, Iafusco D, et al. Follow-up and monitoring programme in children identified in early-stage type 1 diabetes during screening in the general population of Italy. Diabetes Obes Metab. 2024;26(10):4197-4202. doi:10.1111/dom.15779 PubMed
44.Type 1 Diabetes TrialNet. Join the TrialNet. Accessed April 24, 2025. https://www.trialnet.org/
45.CanScreen T1D. CanScreen T1D Research Consortium. Accessed April 24, 2025. https://canscreent1d.ca/
46.Lind A, Freyhult E, de Jesus Cortez F, et al. Childhood screening for type 1 diabetes comparing automated multiplex Antibody Detection by Agglutination-PCR (ADAP) with single plex islet autoantibody radiobinding assays. EBioMedicine. 2024;104:105144. doi:10.1016/j.ebiom.2024.105144 PubMed
47.Ontario Ministry of Health. Schedule of Benefits for Laboratory Services: (effective July 24, 2023). 2023. Accessed April 24, 2025. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf
48.Sanofi. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Teplizumab (Tzield), 2 mg per 2 mL (1 mg/mL) for injection. February 19, 2025.
49.Swamy A, Town M, Polonsky WH. Barriers to Screening in Type 1 Diabetes. Children with Diabetes. June 13, 2023. Accessed April 24, 2025. https://childrenwithdiabetes.com/featured/barriers-to-screening-in-type-1-diabetes/
50.Ospelt E, Hardison H, Rioles N, et al. Understanding Providers’ Readiness and Attitudes Toward Autoantibody Screening: A Mixed-Methods Study. Clin Diabetes. 2023;42(1):17-26. doi:10.2337/cd23-0057 PubMed
51.Hummel M, Ziegler AG, Roth R. Psychological impact of childhood islet autoantibody testing in families participating in the BABYDIAB study. Diabet Med. 2004;21(4):324-8. doi:10.1111/j.1464-5491.2004.01142.x PubMed
52.Johnson SB, Lynch KF, Roth R, Schatz D. My Child Is Islet Autoantibody Positive: Impact on Parental Anxiety. Diabetes Care. 2017;40(9):1167-1172. doi:10.2337/dc17-0166 PubMed
53.Weiss A, Zapardiel-Gonzalo J, Voss F, et al. Progression likelihood score identifies substages of presymptomatic type 1 diabetes in childhood public health screening. Diabetologia. 2022;65(12):2121-2131. doi:10.1007/s00125-022-05780-9 PubMed
54.Felton JL, Redondo MJ, Oram RA, et al. Islet autoantibodies as precision diagnostic tools to characterize heterogeneity in type 1 diabetes: a systematic review. Commun Med (Lond). 2024;4(1):66. doi:10.1038/s43856-024-00478-y PubMed
55.Dunseath G, Ananieva-Jordanova R, Coles R, et al. Bridging-type enzyme-linked immunoassay for zinc transporter 8 autoantibody measurements in adult patients with diabetes mellitus. Clin Chim Acta. 2015;447:90-5. doi:10.1016/j.cca.2015.05.010 PubMed
56.Wasserfall C, Montgomery E, Yu L, et al. Validation of a rapid type 1 diabetes autoantibody screening assay for community-based screening of organ donors to identify subjects at increased risk for the disease. Clin Exp Immunol. 2016;185(1):33-41. doi:10.1111/cei.12797 PubMed
57.Lampasona V, Pittman DL, Williams AJ, et al. Islet Autoantibody Standardization Program 2018 Workshop: Interlaboratory Comparison of Glutamic Acid Decarboxylase Autoantibody Assay Performance. Clin Chem. 2019;65(9):1141-1152. doi:10.1373/clinchem.2019.304196 PubMed
58.Marzinotto I, Pittman DL, Williams AJK, et al. Islet Autoantibody Standardization Program: interlaboratory comparison of insulin autoantibody assay performance in 2018 and 2020 workshops. Diabetologia. 2023;66(5):897-912. doi:10.1007/s00125-023-05877-9 PubMed
59.Hoffmann L, Kohls M, Arnolds S, et al. EDENT1FI Master Protocol for screening of presymptomatic early-stage type 1 diabetes in children and adolescents. BMJ Open. 2025;15(1):e088522. doi:10.1136/bmjopen-2024-088522 PubMed
60.Alberta Precision Laboratories. Anti-Glutamic Acid Decarboxylase (Synonym: Anti GAD, Anti-Islet Cell Antibodies, Pancreatic Islet Cell Antibody, GAD65, GAD65 Antibodies, Glutamic Acid Decarboxylase). 2024. Accessed May 09, 2025. https://www.albertahealthservices.ca/webapps/labservices/indexAPL.asp?id=9255&tests=&zoneid=1&details=true
61.BC Diabetes. [Type 1 diabetes auto-antibody testing]. 2023. Accessed May 09, 2025. https://www.bcdiabetes.ca/wp-content/uploads/bcdpdfs/Type-1-diabetes-auto-antibody-testing.pdf
62.Sanofi. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Teplizumab (Tzield), 2 mg per 2 mL (1 mg/mL) for injection. February 19, 2025.
63.Bingley PJ, Wherrett DK, Shultz A, Rafkin LE, Atkinson MA, Greenbaum CJ. Type 1 Diabetes TrialNet: A Multifaceted Approach to Bringing Disease-Modifying Therapy to Clinical Use in Type 1 Diabetes. Diabetes Care. 2018;41(4):653-661. doi:10.2337/dc17-0806 PubMed
64.Herold KC, Bundy BN, Long SA, et al. An Anti-CD3 Antibody, Teplizumab, in Relatives at Risk for Type 1 Diabetes. N Engl J Med. 2019;381(7):603-613. doi:10.1056/NEJMoa1902226 PubMed
65.Sims EK, Bundy BN, Stier K, et al. 277-OR: Teplizumab Reverses the Loss of C-Peptide in Relatives at Risk for Type 1 Diabetes (T1D). Diabetes. 2020;69(Supplement_1):277-OR. doi:10.2337/db20-277-OR
66.Taylor PN, Collins KS, Lam A, et al. C-peptide and metabolic outcomes in trials of disease modifying therapy in new-onset type 1 diabetes: an individual participant meta-analysis. Lancet Diabetes Endocrinol. 2023;11(12):915-925. doi:10.1016/S2213-8587(23)00267-X PubMed
67.Sugahara M, Tanaka T, Nangaku M. Modulating the immune system to delay the clinical onset of type 1 diabetes. Kidney Int. 2020;97(2):248-250. doi:10.1016/j.kint.2019.10.010 PubMed
68.U.S. Food and Drug Administration. Diabetes Mellitus: efficacy endpoints for clinical trials investigating antidiabetic drugs and biological products, guidance for industry. 2023. Accessed April 28, 2025. https://www.fda.gov/media/168475/download
69.Palmer JP, Fleming GA, Greenbaum CJ, et al. C-Peptide Is the Appropriate Outcome Measure for Type 1 Diabetes Clinical Trials to Preserve β-Cell Function: Report of an ADA Workshop, 21–22 October 2001. Diabetes. 2004;53(1):250-264. doi:10.2337/diabetes.53.1.250 PubMed
70.Wang M, Hng T-M. HbA1c: More than just a number. Aust J Gen Pract. 2021;50(9):628-632. doi:10.31128/AJGP-03-21-5866 PubMed
71.Morales JF, Muse R, Podichetty JT, et al. Disease progression joint model predicts time to type 1 diabetes onset: Optimizing future type 1 diabetes prevention studies. CPT Pharmacometrics Syst Pharmacol. 2023;12(7):1016-1028. doi:10.1002/psp4.12973 PubMed
72.Dechartres A, Trinquart L, Boutron I, Ravaud P. Influence of trial sample size on treatment effect estimates: meta-epidemiological study. BMJ. 2013;346:f2304. doi:10.1136/bmj.f2304 PubMed
73.Chu R, Walter SD, Guyatt G, et al. Assessment and implication of prognostic imbalance in randomized controlled trials with a binary outcome--a simulation study. PLoS One. 2012;7(5):e36677. doi:10.1371/journal.pone.0036677 PubMed
74.Leete P, Mallone R, Richardson SJ, Sosenko JM, Redondo MJ, Evans-Molina C. The Effect of Age on the Progression and Severity of Type 1 Diabetes: Potential Effects on Disease Mechanisms. Curr Diab Rep. 2018;18(11):115. doi:10.1007/s11892-018-1083-4 PubMed
75.Jacobsen LM, Bocchino L, Evans-Molina C, et al. The risk of progression to type 1 diabetes is highly variable in individuals with multiple autoantibodies following screening. Diabetologia. 2020;63(3):588-596. doi:10.1007/s00125-019-05047-w PubMed
76.Center for Drug Evaluation Research. Statistical Review(s). In: Tzield (teplizumab). Company: Provention Bio, Inc. Biologic Application No.: 761183 Approval date: 11/17/2022 (FDA drug approval package). U.S. Food and Drug Administration (FDA); 2022. Accessed May 8, 2025. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/761183Orig1s000StatR.pdf
77.Evans-Molina C, Oram RA. Teplizumab approval for type 1 diabetes in the USA. Lancet Diabetes Endocrinol. 2023;11(2):76-77. doi:10.1016/s2213-8587(22)00390-4 PubMed
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
DKA
diabetic ketoacidosis
FPG
fasting plasma glucose
FSDR
first-degree and second-degree relative
HCRU
health care resource use
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
OGTT
oral glucose tolerance test
QALY
quality-adjusted life-year
T1D
type 1 diabetes
Economic Review
The objective of the economic review undertaken by Canada’s Drug Agency (CDA-AMC) is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of teplizumab compared to no intervention to delay the onset of stage 3 type 1 diabetes (T1D) in adult and pediatric patients aged 8 years and older with stage 2 T1D.1 Teplizumab is being reviewed by CDA-AMC through the complex review pathway; as such, CDA-AMC has appraised 2 cost-effectiveness analyses submitted by the sponsor, 1 adopting a publicly funded health care payer perspective and 1 adopting a societal perspective.2
Item | Description |
|---|---|
Drug product | Teplizumab (Tzield), 2 mg/2 mL sterile solution, single-dose vial for IV infusion |
Indication | To delay the onset of Stage 3 T1D in adult and pediatric patients 8 years of age and older with Stage 2 T1D |
Submitted price | $18,410.00 per vial |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | May 5, 2025 |
Reimbursement request | As per Health Canada indication |
Sponsor | Sanofi-aventis Canada Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance; T1D = type 1 diabetes.
Key Messages
Teplizumab is available as a sterile solution for IV infusion (1 mg/mL).1 At the submitted price of $18,410.00 per 2 mL vial, the cost of teplizumab is expected to be $257,740 per patient for a single course of treatment, based on the Health Canada–recommended dosage.1
Clinical efficacy in the economic analysis was derived from the TN-10 trial, which compared teplizumab with placebo in adult and pediatric patients aged 8 years and older with stage 2 T1D (i.e., individuals who have tested positive for ≥ 2 diabetes-related autoantibodies identified by screening and have dysglycemia without overt hyperglycemia).3 Evidence submitted by the sponsor indicated that teplizumab is likely to increase the time to onset of stage 3 T1D (i.e., manifestation of typical clinical symptoms and signs of T1D) compared to placebo among adult and pediatric patients aged 8 years and older with stage 2 T1D. No evidence was provided suggesting that teplizumab is curative (i.e., it will prevent an individual with stage 2 T1D from reaching stage 3 T1D). As noted by the Clinical Review Report, the clinical importance of the delay in onset is highly uncertain.
The results of the CDA-AMC base case suggest that:
Teplizumab will be associated with higher costs to the health care system than no intervention (incremental costs = $221,630), primarily driven by increased costs associated with drug acquisition, partly offset by disease management of stage 3 T1D.
Teplizumab is predicted to be associated with a gain of 0.24 life-years compared to no intervention. When the impact on health-related quality of life (HRQoL) is also considered, teplizumab is predicted to result in a gain of 0.30 quality-adjusted life-years (QALYs) compared to no intervention from the health care payer perspective. When caregiver benefits are considered in the societal perspective, the incremental benefit is increased (incremental benefit = 0.36 QALYs).
The incremental cost-effectiveness ratio (ICER) of teplizumab compared to no intervention was $747,542 per QALY gained in the CDA-AMC base case for the publicly funded health care payer perspective and $608,736 per QALY gained in the societal perspective. The estimated ICER was highly sensitive to the parametric distribution used to estimate the proportion of patients at risk of developing stage 3 T1D. This finding is associated with significant uncertainty because the long-term benefit associated with teplizumab is unknown.
Although the CDA-AMC base case estimated a gain in QALYs with teplizumab compared to no intervention (incremental benefit = 0.30 QALYs), approximately 90% of the incremental benefit was gained in the extrapolated period (i.e., after 26 months of follow-up). In the absence of long-term evidence, the incremental QALYs for teplizumab predicted in the CDA-AMC base case are highly uncertain and may be overestimated. Additionally, health care resource use (HCRU) for stage 3 T1D is associated with significant uncertainty as the mixed regression model used to estimate HCRU costs does not reflect clinical expectations or published literature conducted in Canada. Additional price reductions may therefore be required.
CDA-AMC estimates that the budget impact of reimbursing teplizumab for the indicated population will be approximately $485 million over the first 3 years of reimbursement compared to the amount currently spent on no intervention, which reflects the predicted expenditure over this period. The actual budget impact of reimbursing teplizumab will depend on the number of people eligible and identified for treatment, and the uptake of teplizumab. The economic feasibility of adoption must be addressed, given that the predicted incremental budget impact of reimbursing teplizumab is predicted to be greater than $40 million in year 2 and year 3, and the magnitude of uncertainty in the estimated budget impact.
Screening is a significant factor that was not adequately considered in the economic evaluation or budget impact analysis (BIA). While a targeted screening approach focusing on potential patients with a family history may be most feasible, clinical expert input indicated that this would only identify 15% to 20% of patients with stage 2 T1D who could benefit from teplizumab.4 The potential benefits of a screening program should not be understated, as diabetic ketoacidosis (DKA) often occurs in undiagnosed patients and patient-relevant outcomes may be improved from a screening program itself. The budget impact considers a targeted approach where ██% of first-degree and second-degree relatives (FSDRs) are motivated to receive autoantibody testing; however, this can only capture the 15% of patients with T1D who have a family history.4 Depending on the screening approach, the budget impact may be substantially underestimated. Further information on the implications associated with the testing required to identify individuals with stage 2 T1D can be found in the CDA-AMC Testing Procedure Assessment within the Clinical Review Report.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of teplizumab from the perspective of a public health care payer and from a societal perspective in Canada over a lifetime horizon (100 years).5 The modelled population comprised adult and pediatric patients aged 8 years and older with stage 2 T1D (i.e., those individuals with ≥ 2 diabetes-related autoantibodies and dysglycemia without overt hyperglycemia), which is aligned with the Health Canada–approved indication and was based on the participants in the TN-10 trial.5 The sponsor’s base-case analysis from the health care payer perspective included costs related to drug acquisition (submitted price for teplizumab), administration, stage 2 T1D confirmatory testing, DKA event management, HCRU, and adverse event management.5 The sponsor’s base-case analysis from the societal perspective included additional indirect costs associated with patient and caregiver productivity loss. In the sponsor’s base case, which adopted a health care payer perspective, teplizumab was associated with incremental costs of $179,769 and 0.80 incremental QALYs relative to no intervention. This resulted in an ICER of $224,358 per QALY gained.5 Of the incremental benefit compared to no intervention (0.80 incremental QALYs), approximately 92% of the benefit was predicted to be accrued after the follow-up time of the TN-10 trial (median observation period = 26.62 months). From a societal perspective, the ICER was $176,942 per QALY gained.5 Additional information about the sponsor’s submission is summarized in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 2; full details are provided in Appendix 4). A revised base case was therefore developed.
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The impact of teplizumab on health outcomes is uncertain. | As noted in the clinical review, there is clinical plausibility that teplizumab can delay the onset of stage 3 T1D; however, the long-term impact on health outcomes is unknown. | CDA-AMC was unable to address this issue. | No scenario analysis was conducted due to the lack of plausible alternative evidence. |
Parametric distribution used for risk of progression on teplizumab overestimates the benefit of teplizumab. | Based on the sponsor’s parametric distribution, a proportion of patients at risk for a stage 3 T1D diagnosis would never progress to stage 3 T1D.5 No evidence was provided that teplizumab is curative, and this assumption was considered clinically implausible by clinical expert feedback. | CDA-AMC adopted the gamma distribution for the proportion of patients at risk for stage 3 T1D. | CDA-AMC explored an alternative parametric distribution of the proportion of patients at risk for stage 3 T1D in a scenario analysis due to the uncertainty with the available evidence. |
Disease monitoring of patients with stage 2 T1D was not accounted for. This underestimates the cost of teplizumab. | Patients entering the model were confirmed with stage 2 T1D.5 These patients would be periodically monitored with laboratory glucose tests to determine dysglycemia; yet the sponsor’s base case only considers glucose monitoring strips.6 | CDA-AMC included glucose monitoring strips, OGTT, hemoglobin A1C, and FPG tests7 once per 6-month cycle. | No scenario analysis was conducted because best evidence was used in the CDA-AMC base case. |
DKA events were likely overestimated. This underestimates the cost of teplizumab. | The sponsor applied DKA probabilities upon diagnosis of stage 3 T1D and postdiagnosis.8,9 Clinical experts indicated the clinically unlikelihood of increased postdiagnosis DKA events. Additionally, experts noted that an improved screening program may eliminate DKA events due to dysglycemia monitoring. | CDA-AMC removed the probability of DKA upon diagnosis and adjusted the postdiagnosis DKA probability informed by published literature conducted in Ontario.10 | To explore the uncertainty, CDA-AMC maintained the sponsor’s assumption in a scenario analysis. |
The method to derive utility estimates for stage 3 T1D were inappropriate. This overestimates the benefit for teplizumab. | The sponsor applied 2 stage 3 T1D health state–specific disutilities based on published literature; a flat decrement11 and a linear extrapolation.12 The study cited by the sponsor to support a linear extrapolation is associated with limitations and uncertainty, and does not support the sponsor’s approach. Clinical expert feedback noted patient utility was not expected to decrease over time based solely on diabetes. | CDA-AMC removed the disutility linear extrapolation. | No scenario analysis was conducted because there were no plausible alternative values or approaches. |
Caregiver disutilities were associated with uncertainty. This overestimates the benefit of teplizumab. | The sponsor applied 2 caregiver disutility estimates — 1 due to teplizumab infusion,13 and another applied to caregivers of patients aged < 18 years.14 No adequate evidence was provided to support the caregiver infusion disutility. The caregiver disutility does not apply to the publicly funded health care payer perspective.14 | CDA-AMC removed all caregiver disutilities from the publicly funded health care payer perspective. CDA-AMC removed infusion-related caregiver disutility from the public health care payer and societal perspectives. | No scenario analysis was conducted because there were no plausible alternatives. |
The cost of stage 3 T1D was likely overestimated. This overestimates the cost of no intervention. | Based on the sponsor’s base case, HCRU costs can only increase over time. This did not align with published literature of the cost of diabetes conducted in Canada, nor clinical expert expectations. | CDA-AMC adjusted the starting cost of HCRU based on the average cost of published literature. | No scenario analysis was conducted because there were no plausible alternatives. |
The mortality benefit is associated with uncertainty. This overestimates the benefit of teplizumab. | The sponsor’s model estimates teplizumab is associated with an additional 0.24 life-years compared to no intervention. No evidence was submitted to support this outcome. | CDA-AMC could not address this issue due to limitations with the sponsor’s model structure. | No scenario analysis was conducted. |
The proportion of patients who receive hybrid administration of teplizumab is overestimated. | The sponsor assumed that 45.9% of patients would receive teplizumab at home for days 5 to 14.5 Clinical experts indicated that teplizumab should be administered within a hospital setting. All patients in the trial received teplizumab within hospital. | CDA-AMC adjusted 100% of patients to receive hospital administration. | No scenario analysis was conducted because the input had limited impact on the ICER. |
Indirect costs from productivity loss are likely overestimated. This overestimates the cost to no intervention. | The sponsor elicited clinical expert opinion to estimate time productivity time lost for patients with stage 3 T1D who are employed and caregivers of patients with stage 2 T1D who are aged < 18 years.5 No evidence was submitted to substantiate this assumption from patients or caregivers. | CDA-AMC removed the indirect costs informed by clinical expert opinion. | To explore the uncertainty, CDA-AMC maintained the sponsor’s indirect costs in a scenario analysis. |
CDA-AMC = Canada’s Drug Agency; DKA = diabetic ketoacidosis; FPG = fasting plasma glucose; HCRU = health care resource use; ICER = incremental cost-effectiveness ratio; OGTT = oral glucose tolerance test; T1D = type 1 diabetes.
Note: Full details of the CDA-AMC–identified issues are provided in Appendix 3.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Table 7), in consultation with clinical experts. Detailed information about the base case is provided in Appendix 4.
Impact on Health Care Costs and Societal Costs
From the health care payer perspective, teplizumab is predicted to be associated with additional health care costs compared to no intervention (incremental costs = $221,630). This increase in health care spending primarily results from drug acquisition costs associated with teplizumab, which are partly offset by HCRU costs (refer to Figure 1).
Figure 1: Impact of Teplizumab vs. No Intervention on Health Care Costs
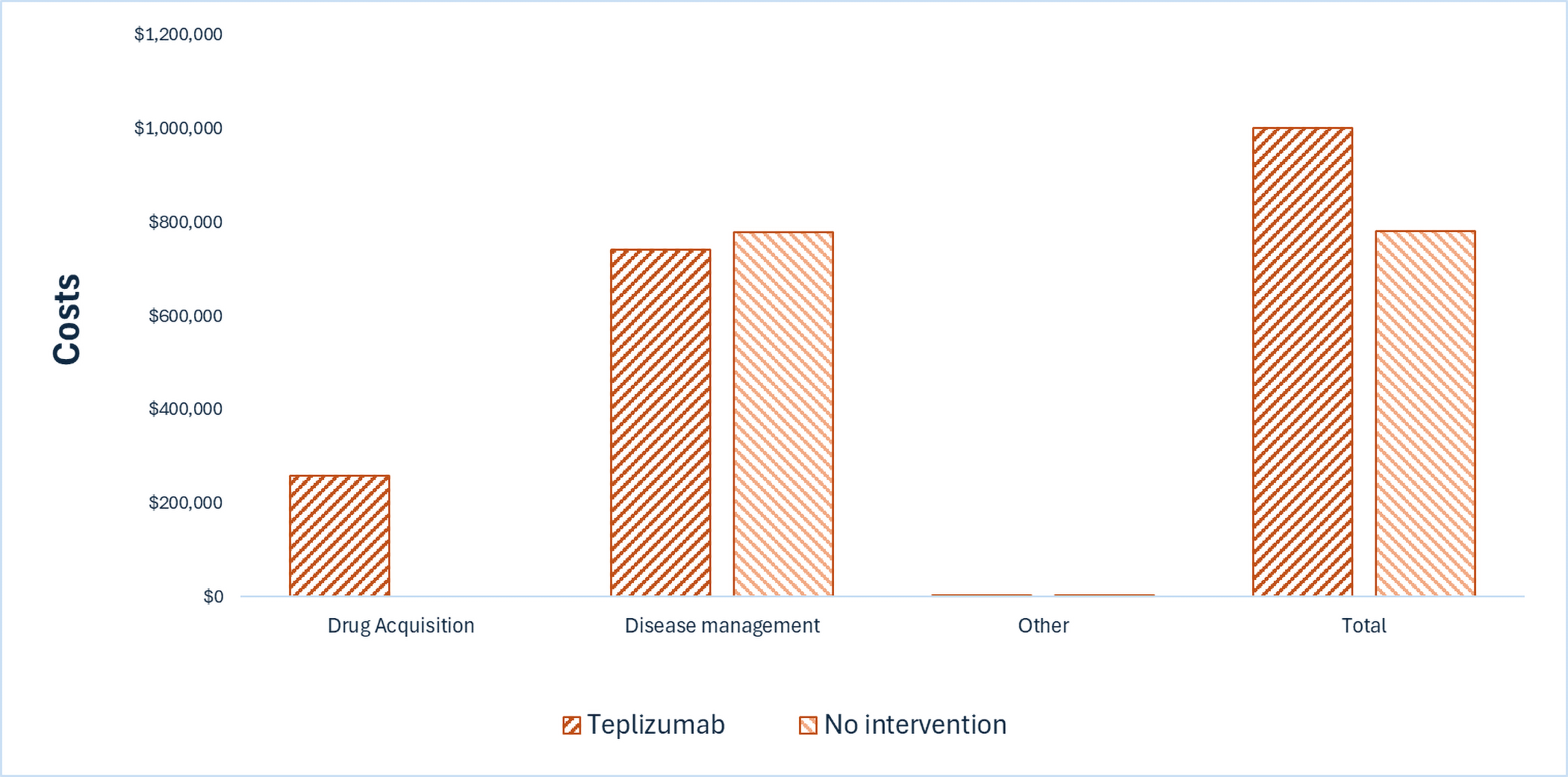
DKA = diabetic ketoacidosis; HCRU = health care resource use; vs. = versus.
Note: Other includes drug administration, adverse event management, treatment-related HCRU, and DKA management.
While teplizumab may result in indirect costs due to productivity loss, the estimates provided to CDA-AMC were not derived from caregivers or patients and so were not included in the base-case societal perspective. A scenario analysis including the sponsor’s clinical expert-derived productivity loss estimates is provided in Appendix 4 (refer to Table 12).
Impact on Health
Relative to no intervention, teplizumab is predicted to increase the amount of time a patient remains in stage 2 T1D by approximately 2 years and to extend life by 0.24 years (refer to Figure 2). Considering the impact of treatment on both quality and length of life, teplizumab is predicted to result in 0.30 additional QALYs per patient compared to no intervention.
Figure 2: Impact of Teplizumab vs. No Intervention on Patient Health
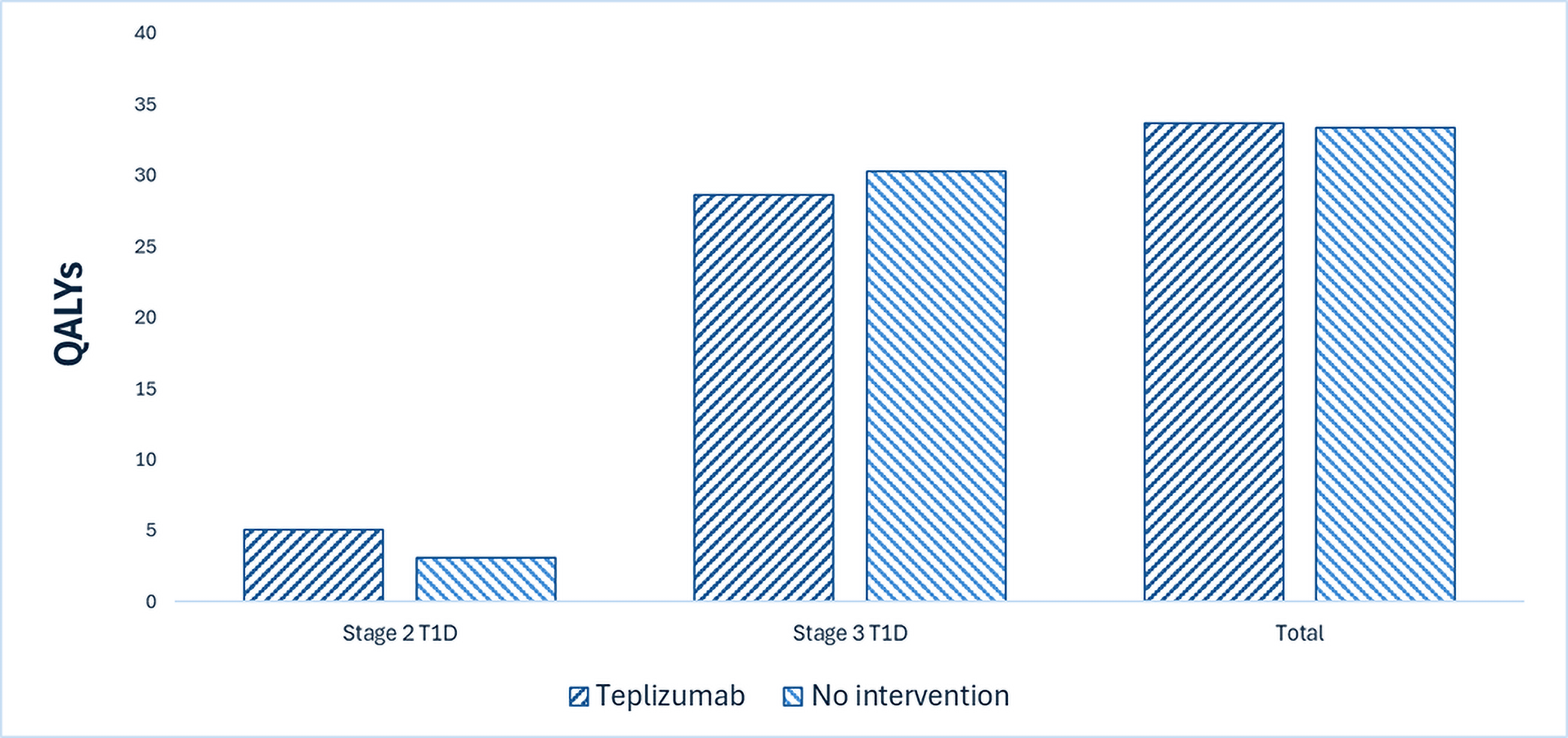
QALY = quality-adjusted life-year; T1D = type 1 diabetes; vs. = versus.
Teplizumab is also anticipated to impact caregiver health. When the impact of teplizumab on caregiver health is additionally considered in a broader perspective, teplizumab is predicted to result in 0.06 additional QALYs per patient compared to no intervention, representing 17% of the incremental benefit of teplizumab (refer to Table 10).
Overall Results
The results of the CDA-AMC base case suggest an ICER of $747,542 per QALY gained for teplizumab compared to no intervention (refer to Table 3). Additional details on the CDA-AMC base case are available in Appendix 4.
When a societal perspective is adopted, the ICER is $608,736 per QALY gained.
Table 3: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | ICER vs. no intervention ($/QALY) |
|---|---|---|---|
Publicly funded health care payer perspective | |||
No intervention | 780,497 | 33.38 | Reference |
Teplizumab | 1,002,127 | 33.68 | 747,542 |
Societal perspectivea | |||
No intervention | 780,659 | 33.33 | Reference |
Teplizumab | 1,000,967 | 33.69 | 608,736 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: The price of teplizumab was based on the sponsor-submitted price.2
aIncludes health impacts to caregivers in addition to all health impacts and costs included in the publicly funded health care payer perspective.
Uncertainty and Sensitivity
Uncertainty was explored in the scenario analyses outlined in Table 2.
Adjusting the parametric fits for the survival curve of the proportion of patients at risk of developing stage 3 T1D over time had the largest impact on cost-effectiveness (refer to Table 12). When adjusting the parametric fit to the Gompertz distribution, the probabilistic ICER decreased significantly. However, the deterministic ICERs were aligned with the analysis using the gamma distribution; as such, the deterministic ICERs were presented. Further information regarding interpretation of these results is provided in Appendix 4.
Screening was noted to be a significant factor that was not captured in its totality and could not be adequately addressed by CDA-AMC.
Summary of the Budget Impact
The sponsor submitted a BIA to estimate the 3-year (2026 to 2028) budget impact of reimbursing teplizumab for use to delay the onset of stage 3 T1D in adult and pediatric patients aged 8 years and older with stage 2 T1D.15 The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach.15 The price of teplizumab was aligned with the price included in the sponsor’s economic evaluation.2 Additional information pertaining to the sponsor’s submission is provided in Appendix 5.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (Appendix 5). CDA-AMC estimated that 4,478 patients would be eligible for treatment with teplizumab over a 3-year period (year 1 = 1,467; year 2 = 1,493; year 3 = 1,519), of whom 1,882 are predicted to receive teplizumab (year 1 = 147; year 2 = 672; year 3 = 1,063). The estimated incremental budget impact of reimbursing teplizumab is predicted to be approximately $485 million over the first 3 years, which also reflects the predicted expenditure as no treatment is currently available. The actual budget impact is dependent on the number of people eligible for treatment and its uptake. The current budget impact estimate from the CDA-AMC base case assumes a screening approach that targets 8 FSDRs per patient with stage 3 T1D, which may not be reflective of a prospective stage 2 T1D screening program; a population-wide screening program may identify more patients who are eligible for teplizumab.
Conclusion
Based on the CDA-AMC base case, teplizumab would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $747,542 or $608,736 for each additional QALY gained from the publicly funded health care payer, or societal perspective, respectively. If the public health care system is not willing to pay either amount, a price reduction should be considered (refer to Figure 3; full details presented in Table 11). The estimated cost-effectiveness of teplizumab compared to no intervention is uncertain because the impact of delaying the onset of stage 3 T1D on long-term benefits is unknown.
The budget impact of reimbursing teplizumab to the public drug plans in the first 3 years is estimated to be approximately $371 million if screening is restricted to FSDRs. The 3-year expenditure on teplizumab (i.e., not accounting for current expenditure on comparators) is estimated to be $485 million. The estimated budget impact is highly uncertain due to model sensitivities to changes to the size of the patient population because there is uncertainty regarding the screening to identify patients who may be eligible for teplizumab. At the sponsor’s submitted price, a price reduction may be required to address concerns of affordability associated with teplizumab.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction

CDA-AMC = Canada's Drug Agency; QALY = quality-adjusted life-year; vs. = versus.
Note: Expenditure includes only the drug cost of teplizumab. The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
References
1.sanofi-aventis Canada Inc. Tzield (Teplizumab): injection, 2 mg per 2 mL (1 mg/mL) [product monograph]. 2025. Updated May 5, 2025.
2.sanofi. Drug Reimbursement Review sponsor submission: Tzield (teplizumab), 2 mg per 2 mL (1 mg/mL) for injection [internal sponsor's package]. February 19, 2025.
3.Provention Bio Inc. Clinical Study Report Addendum for Study TN-10: Anti-CD3 MAB (Teplizumab) for Prevention of Diabetes in Relatives At-Risk for Type 1 Diabetes Mellitus [sponsor supplied reference]. 2020.
4.Insel RA, Dunne JL, Atkinson MA, et al. Staging presymptomatic type 1 diabetes: a scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care. 2015;38(10):1964-74. doi: 10.2337/dc15-1419 PubMed
5.sanofi. Pharmacoeconomic evaluation [internal sponsor's report]. In: Tzield (teplizumab), 2 mg per 2 mL (1 mg/mL) for injection. February 19, 2025.
6.Harris SB, Leiter LA, Yale J-F, Chiasson J-L, Kleinstiver P, Sauriol L. Out-of-pocket Costs of Managing Hyperglycemia and Hypoglycemia in Patients With Type 1 Diabetes and Insulin-treated Type 2 Diabetes. Can J Diabetes. 2007;31(1):25-33. doi: 10.1016/s1499-2671(07)11008-x
7.Ontario Ministry of Health. Schedule of benefits for laboratory services: (effective July 24, 2023). 2023. Accessed May 1, 2025. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf
8.Schneider J, Gemulla G, Kiess W, Berner R, Hommel A. Presymptomatic type 1 diabetes and disease severity at onset. Diabetologia. 2023;66(12):2387-2388. doi: 10.1007/s00125-023-05999-0 PubMed
9.Kao KT, Islam N, Fox DA, Amed S. Incidence Trends of Diabetic Ketoacidosis in Children and Adolescents with Type 1 Diabetes in British Columbia, Canada. J Pediatr. 2020;221:165-173 e2. doi: 10.1016/j.jpeds.2020.02.069 PubMed
10.Weisman A, Booth GL, Everett K, Tomlinson GA. Recent Improvements in Attainment of the Hemoglobin A1c Target of </=7.0% Among Adults with Type 1 Diabetes in Ontario: A Retrospective Cohort Study. Diabetes Technol Ther. 2024;26(9):607-617. doi: 10.1089/dia.2024.0017 PubMed
11.Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making. 2011;31(6):800-4. doi: 10.1177/0272989X11401031 PubMed
12.Sparring V, Nyström L, Wahlström R, Jonsson PM, Östman J, Burström K. Diabetes duration and health-related quality of life in individuals with onset of diabetes in the age group 15—34 years – a Swedish population-based study using EQ-5D. BMC Public Health. 2013;13:377. doi: 10.1186/1471-2458-13-377 PubMed
13.Matza LS, Cong Z, Chung K, et al. Utilities associated with subcutaneous injections and intravenous infusions for treatment of patients with bone metastases. Patient Prefer Adherence. 2013;7:855-65. doi: 10.2147/PPA.S44947 PubMed
14.Lopez-Bastida J, Lopez-Siguero JP, Oliva-Moreno J, et al. Health-related quality of life in type 1 diabetes mellitus pediatric patients and their caregivers in Spain: an observational cross-sectional study. Curr Med Res Opin. 2019;35(9):1589-1595. doi: 10.1080/03007995.2019.1605158 PubMed
15.sanofi. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tzield (teplizumab), 2 mg per 2 mL (1 mg/mL) for injection. February 19, 2025.
16.Government of Canada. Canadian exposure factors used in human health risk assessments. 2025. Accessed May 1, 2025. https://www.canada.ca/en/health-canada/services/chemical-substances/fact-sheets/canadian-exposure-factors-human-health-risk-assessments.html
17.CanScreen T1D Research Consortium. Creating Canada’s First Pilot Type 1 Diabetes Screening Program. 2024. Accessed May 1, 2025. https://canscreent1d.ca/
18.Herold KC, Bundy BN, Long SA, et al. An Anti-CD3 Antibody, Teplizumab, in Relatives at Risk for Type 1 Diabetes. N Engl J Med. 2019;381(7):603-613. doi: 10.1056/NEJMoa1902226 PubMed
19.Statistics Canada. Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island [sponsor supplied reference]. Accessed January 30, 2025. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401
20.Samuelsson J, Bertilsson R, Bulow E, et al. Autoimmune comorbidity in type 1 diabetes and its association with metabolic control and mortality risk in young people: a population-based study. Diabetologia. 2024;67(4):679-689. doi: 10.1007/s00125-024-06086-8 PubMed
21.Herold KC, Gitelman SE, Gottlieb PA, Knecht LA, Raymond R, Ramos EL. Teplizumab: A Disease-Modifying Therapy for Type 1 Diabetes That Preserves beta-Cell Function. Diabetes Care. 2023;46(10):1848-1856. doi: 10.2337/dc23-0675 PubMed
22.Canadian Institute for Health Information. Patient cost estimator [sponsor supplied reference]. 2024. Accessed January 30, 2025. https://www.cihi.ca/en/patient-cost-estimator
23.Guinan K, Mathurin K, Au Y, et al. Venetoclax in Combination with Azacitidine for the Treatment of Newly Diagnosed Acute Myeloid Leukemia: A Canadian Cost-Utility Analysis. Curr Oncol. 2022;29(10):7524-7536. doi: 10.3390/curroncol29100592 PubMed
24.Sanofi Teplizumab PROxy Study - ongoing [sponsor supplied reference]. 2025.
25.Dietitians of Canada. WHO Growth Charts Set 1 [sponsor supplied reference]. Accessed October 2024. https://www.dietitians.ca/Advocacy/Interprofessional-Collaborations-(1)/WHO-Growth-Charts/WHO-Growth-Charts-Set-1
26.Government of Canada Job Bank. Registered Nurse (R.N.) in Canada - Prevailing wages in Canada as updated on December 3, 2024 [sponsor supplied reference]. 2024. Accessed January 13, 2025. https://www.jobbank.gc.ca/explore_career/job_market_report/wage_occupation_report.xhtml
27.Government of Canada Job Bank. Pharmacist in Canada - Prevailing wages in Canada as updated on December 3, 2024 [sponsor supplied reference]. 2024. Accessed January 13, 2025. https://www.jobbank.gc.ca/marketreport/wages-occupation/18196/ca
28.Pettigrew M, Kavan P, Surprenant L, Lim HJ. Comparative net cost impact of the utilization of panitumumab versus cetuximab for the treatment of patients with metastatic colorectal cancer in Canada. J Med Econ. 2016;19(2):135-47. doi: 10.3111/13696998.2015.1105230 PubMed
29.Ontario Ministry of Health. Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)) [sponsor supplied reference]. 2023. Accessed January 30, 2025. https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf
30.Iqvia. DeltaPA [sponsor supplied reference]. 2023. Accessed January 30, 2025. https://www.iqvia.com/
31.British Columbia Ministry of Health. Schedule of Fees For the Laboratory Services Outpatient (2024) [sponsor supplied reference]. 2024. Accessed December 2024. https://www.phsa.ca/plms/Documents/Laboratory%20Services%20Outpatient%20Payment%20Schedule.pdf
32.Manitoba Health. Manitoba Physician's Manual (2024) [sponsor supplied reference]. 2024. Accessed October 2024. https://www.gov.mb.ca/health/documents/physmanual.pdf
33.BC Diabetes. Type 1 diabetes auto-antibody testing, 2023 [sponsor supplied reference]. 2023. Accessed December 2024. https://www.bcdiabetes.ca/wp-content/uploads/bcdpdfs/Type-1-diabetes-auto-antibody-testing.pdf
34.Government of Saskatchewan. Payment Schedule for Insured Services Provided by a Physician (2023) [sponsor supplied reference]. 2023. Accessed October 2024. https://www.phsa.ca/plms/Documents/Laboratory%20Services%20Outpatient%20Payment%20Schedule.pdf
35.Diabetes Canada. Continuous Glucose Monitor (CGM) [sponsor supplied reference]. Accessed October 2024. https://www.diabetes.ca/diabetescanadawebsite/media/managing-my-diabetes/tools%20and%20resources/continuous_glucose_monitoring_advocacy_pkg_4.pdf?ext=.pdf
36.Government of Newfoundland and Labrador. Provincial Laboratory Formulary [sponsor supplied reference]. Accessed October 2024. https://www.gov.nl.ca/labformulary/
37.Alshannaq H, Isitt JJ, Pollock RF, et al. Cost-utility of real-time continuous glucose monitoring versus self-monitoring of blood glucose in people with insulin-treated Type 2 diabetes in Canada. J Comp Eff Res. 2023;12(10):e230075. doi: 10.57264/cer-2023-0075 PubMed
38.Johnson JA, Pohar SL, Majumdar SR. Health care use and costs in the decade after identification of type 1 and type 2 diabetes: a population-based study. Diabetes Care. 2006;29(11):2403-8. doi: 10.2337/dc06-0735 PubMed
39.Ou HT, Yang CY, Wang JD, Hwang JS, Wu JS. Life Expectancy and Lifetime Health Care Expenditures for Type 1 Diabetes: A Nationwide Longitudinal Cohort of Incident Cases Followed for 14 Years. Value Health. 2016;19(8):976-984. doi: 10.1016/j.jval.2016.05.017 PubMed
40.Canadian Expert Opinion [sponsor supplied reference]. 2024.
41.Statistics Canada. Labour Force Survey, April 2024 [sponsor supplied reference]. https://www150.statcan.gc.ca/n1/daily-quotidien/240510/dq240510a-eng.htm
42.Statistics Canada. Retirement age by class of worker, annual [sponsor supplied reference]. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410006001
43.Statistics Canada. Employment, average hourly and weekly earnings (including overtime), and average weekly hours for the industrial aggregate excluding unclassified businesses, monthly, seasonally adjusted [sponsor supplied reference]. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410022201
44.Yeaw J, Lee WC, Wolden ML, Christensen T, Groleau D. Cost of Self-Monitoring of Blood Glucose in Canada among Patients on an Insulin Regimen for Diabetes. Diabetes Ther. 2012;3(1):7. doi: 10.1007/s13300-012-0007-6 PubMed
45.Annemans L, Redekop K, Payne K. Current methodological issues in the economic assessment of personalized medicine. Value Health. 2013;16(6 Suppl):S20-6. doi: 10.1016/j.jval.2013.06.008 PubMed
46.Bank of Canada. Inflation calculator. 2024. Accessed May 1, 2025. https://www.bankofcanada.ca/rates/related/inflation-calculator/
47.CADTH. Guidelines for the economic evaluation of health technologies: Canada. 4th ed. 2017. Accessed May 1, 2025. https://www.cda-amc.ca/guidelines-economic-evaluation-health-technologies-canada-0
48.Draft Product Monograph - Teplizumab [sponsor supplied reference]. 2025.
49.Gong B, Yang W, Xing Y, Lai Y, Shan Z. Global, regional, and national burden of type 1 diabetes in adolescents and young adults. Pediatr Res. 2025;97(2):568-576. doi: 10.1038/s41390-024-03107-5 PubMed
50.Garceau A, Wideroff L, McNeel T, Dunn M, Graubard BI. Population estimates of extended family structure and size. Community Genet. 2008;11(6):331-42. doi: 10.1159/000133305 PubMed
51.Statistics Canada. Population estimates on July 1st, by age and sex [sponsor supplied reference]. Accessed October 2024. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501
52.Statistics Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2022 to 2023 [sponsor supplied reference]. Accessed October 23 2024. https://www.sac-isc.gc.ca/eng/1713194236054/1713194280612
53.Interviews with Canadian Clinical Experts [sponsor supplied reference]. 2024.
54.Sims EK, Geyer S, Johnson SB, et al. Who Is Enrolling? The Path to Monitoring in Type 1 Diabetes TrialNet's Pathway to Prevention. Diabetes Care. 2019;42(12):2228-2236. doi: 10.2337/dc19-0593 PubMed
55.Mahon JL, Sosenko JM, Rafkin-Mervis L, et al. The TrialNet Natural History Study of the Development of Type 1 Diabetes: objectives, design, and initial results. Pediatr Diabetes. 2009;10(2):97-104. doi: 10.1111/j.1399-5448.2008.00464.x PubMed
56.Weiss A, Zapardiel-Gonzalo J, Voss F, et al. Progression likelihood score identifies substages of presymptomatic type 1 diabetes in childhood public health screening. Diabetologia. 2022;65(12):2121-2131. doi: 10.1007/s00125-022-05780-9 PubMed
57.Gagnon-Arpin I, Chen W, Leaver C. Understanding the Gap 2.0: A Pan-Canadian Analysis of Prescription Drug Insurance Coverage [sponsor supplied reference]. The Conference Board of Canada; 2022. https://www.conferenceboard.ca/wp-content/uploads/2022/10/understanding-the-gap-2.0_2022.pdf
58.U.S. Food and Drug Administration. Provention Bio, Inc. TZIELD™ (teplizumab-mzwv). Highlights of Prescribing Information [sponsor supplied reference]. Accessed December 9, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761183s000lbl.pdf
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 4: Cost Comparison for Delay of Stage 3 T1D
Treatment | Strength and/or concentration | Form | Price | Recommended dosage | Daily cost ($)a | Cost per course of treatment ($)a |
|---|---|---|---|---|---|---|
Teplizumab (Tzield) | 2 mg / 2mL (1 mg/mL) | Sterile solution for IV injection | $18,410.0000 per vial | BSA IV infusion once daily for 14 days: Day 1: 65 mcg/m2 Day 2: 125 mcg/m2 Day 3: 250 mcg/m2 Day 4: 500 mcg/m2 Days 5 through 14: 1,030 mcg/m2 | $18,410 | $257,740 |
BSA = body surface area; T1D = type 1 diabetes.
Note: Price of teplizumab was based on the sponsor submitted price.2 Recommended dosing as per respective product monograph.1
aBased on a BSA of 1.72 m2 for people who are 14 to 18 years old and no vial sharing.16 For patients with a BSA less than 1.95 m2, only one vial will be required for each infusion. However, if the patient has a BSA equal to 1.95 m2 and greater, an additional vial will be required for days 5 to 14, resulting in a course cost of $441,840.
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Joint patient input was received from 2 groups: Breakthrough T1D Canada and Diabetes Canada. A total of 463 people (257 patients; 182 caregivers; 20 as both) responded to a 2025 survey conducted by the contributing partners, where 423 indicated that they lived in Canada. Respondents emphasized their concern of T1D disease progression as misdiagnosis of initial symptoms can lead to DKA and its impacts on daily life as mismanagement can result in hyper- or hypoglycemia. Respondents indicated that the only treatment available to patients living with T1D is insulin replacement therapy. 96% of respondents indicated that current treatment options were at least somewhat effective. The majority of respondents (63%) indicated financial hardship related to disease management such as loss of income, inability to work, and out-of-pocket costs. Survey respondents of various ages indicated that patients, caregivers, and families become reliant on private health insurance due to gaps in coverage for insulin and continuous glucose monitoring. Respondents who had experience with teplizumab noted the delay of stage 3 T1D, allowing them to maintain their physical and mental health. The patient group input noted that autoantibody testing is not widely available in Canada.
Clinician group input was received from 1 group: Canadian Society of Endocrinology and Metabolism. Clinician group input indicated that there are no available therapies that modify the disease progression of T1D, case examples provided indicated that patients with family history may be more likely to develop stage 3 T1D compared to the general population. Currently, insulin treatment is utilized to maintain blood glucose to avoid hyperglycemia and to prevent complications such as DKA. Treatment goals include achieving glucose control, reducing the burden of disease management, and improving overall well-being. Clinician group input noted that teplizumab is expected to preserve insulin production, shifting the treatment paradigm by delaying insulin therapy. Clinical group input indicated that the most suitable patients for teplizumab treatment are those identified through autoantibody screening and glucose tolerance testing; potential challenges were noted such as the availability of autoantibody screening to diagnosis stage 2 T1D and broad definitions on dysglycemia, which may lead to underdiagnosis and missed opportunities for early intervention. It was additionally noted that pilot work on a screening program is ongoing (CanScreen T1D).17
Input from CDA-AMC–participating drug plans noted implementation issues as there is no population-wide screening program across Canada. Drug plans also noted that patients may have variable accessibility to at-home programs across Canada. Drug plans highlighted concerns associated with treatment extension, renewal, and potential prescription to patients who are younger than 8 years.
Several of these concerns were addressed in the sponsor’s model:
Patient and caregiver productivity loss from loss of income, and inability to work was captured in the model.
Confirmatory testing for stage 2 T1D was incorporated into the model.
CDA-AMC addressed some of these concerns as follows:
Continued disease monitoring via oral glucose tolerance test (OGTT), hemoglobin A1C, and fasting plasma glucose (FPG) was considered for patients who maintained stage 2 T1D.
CDA-AMC was unable to address the following concerns:
Screening costs for a population-wide program.
Extension or renewal of teplizumab therapy.
Comorbid conditions were not captured in the model.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information in collaboration with clinical experts and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of teplizumab, the sponsor provided a cost-utility analysis and a BIA. The sponsor’s economic submission is summarized in Table 5.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Teplizumab (Tzield), IV solution (2 mg/2mL)1 |
Submitted price of drug under review | $18,410per 2 mL vial2 |
Regimen | BSA IV infusion once daily for 14 days:1 Day 1: 65 mcg/m2 Day 2: 125 mcg/m2 Day 3: 250 mcg/m2 Day 4: 500 mcg/m2 Days 5 through 14: 1,030 mcg/m2 |
Per course cost of drug under review | $257,740 |
Model information | |
Type of economic evaluation | Cost-utility analysis Markov model |
Treatment | Teplizumab (Tzield) |
Included comparator | No intervention |
Perspective | Publicly funded health care payer perspective Societal perspective |
Time horizon | Lifetime (100 years) |
Cycle length | 6 months |
Modelled population | Adults and pediatric patients 8 years of age and older with stage 2 T1D |
Characteristics of modelled population | Derived from TN-10 study18 Starting age: 13.9 years (median age); Female: 44.7%; Baseline BSA: 1.52 m2 |
Model health states |
|
Data sources | |
Comparative efficacy |
|
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities |
|
Costs included in the model |
|
Summary of the submitted results | |
Base-case results |
|
Scenario analysis results | Publicly funded health care payer perspective:
Societal perspective:
|
AE = adverse event; BSA = body surface area; CIHI = Canadian Institute for Health Information; DKA = diabetic ketoacidosis; EQ-5D = European QoL 5 dimensions; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; NICE = National Institute for Health and Care Excellence; NSAID = nonsteroidal anti-inflammatory drugs; QALY = quality-adjusted life-years; T1D = type 1 diabetes; vs. = versus.
aThese scenario analyses included clinical efficacy curve fitting (joint distribution), alternative discount rate, exclusion of caregiver disutility, increasing the age threshold for caregiver disutility and indirect costs, alternative individual curve fits, alternative mortality data, DKA incidence, and alternative cost for health care resource use.
Model Structure
The sponsor submitted a Markov model with 3 health states, representing stage 2 T1D, stage 3 T1D, and death.5 Patients enter the model in the stage 2 T1D health state, where they can maintain their current stage of disease, progress to the stage 3 T1D health state, or die. Patients who progress to stage 3 T1D can remain in the stage 3 T1D health state or die.5
Table 6: Summary of the Sponsor’s Economic Evaluation Results (Probabilistic)
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. ($/QALY) |
|---|---|---|---|---|---|
Publicly Funded Health Care Payer Perspective | |||||
No intervention | 891,261 | Reference | 30.09 | Reference | Reference |
Teplizumab | 1,071,030 | 179,769 | 30.89 | 0.80 | 224,358 |
Societal Perspective | |||||
No intervention | $1,085,281 | Reference | 30.09 | Reference | Reference |
Teplizumab | $1,227,092 | 141,811 | 30.89 | 0.80 | 176,942 |
ICER = incremental cost-effectiveness ratio, QALY = quality-adjusted life-year.
Note: Estimated life-years are 41.46 for teplizumab and 41.22 for no intervention.
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
The CDA-AMC clinical review found that teplizumab may delay disease progression and associated diabetes complications when compared to placebo. Results from TN-10 (phase II, double-blinded, placebo-controlled randomized controlled trial) reported that teplizumab likely results in a clinically important increase (approximately 2 years) in the time to diagnosis of stage 3 T1D after 26 months when compared to placebo. Additionally, teplizumab was reported to be associated with more serious adverse events when compared to placebo. Other outcomes including long-term efficacy and safety were associated with uncertainty, and patient important outcomes such as HRQoL and mortality were not accounted for in the clinical trial design.
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
The long-term benefits associated with teplizumab are associated with significant uncertainty. As noted in the Clinical Review, there is clinical plausibility that teplizumab can delay the onset of stage 3 T1D; however, patients who experienced progression to stage 3 T1D in the TN-10 trial were not followed up. As a result, the long-term impact of teplizumab on health outcomes is unknown. The sponsor’s economic evaluation assumed that patients entering the model have been diagnosed with stage 2 T1D, and estimated the costs and benefits of teplizumab in the aggregate based on published stage 3 T1D costs and outcomes. This approach does not account for potential costs and outcomes related to screening patients for stage 2 T1D; there is significant uncertainty regarding the patient outcomes if a screening program was implemented and the degree of contribution that teplizumab may have on patient outcomes in such a landscape. Multiple published literature sources informing the sponsor’s model were not conducted in an environment with a screening program in place (i.e., HCRU costs, indirect costs, mortality, rate of DKA postdiagnosis), thus it is unclear whether the published evidence used will be generalizable to a setting in which both a standard screening protocol and teplizumab are available for patients with stage 2 T1D. While introduction of teplizumab may result in a paradigm shift in clinical care, the impact that teplizumab has on the lived experience of patients with T1D is uncertain and this economic evaluation is unable to estimate the true cost-effectiveness of teplizumab if a screening program for T1D is implemented.
CDA-AMC is unable to address this limitation as there is a gap in evidence regarding potential costs incurred and patient outcomes if patients were initially screened for T1D.
The parametric distribution of the time to stage 3 T1D diagnosis for the patients treated with teplizumab is associated with uncertainty. The proportion of patients with stage 2 T1D who were treated with teplizumab was derived from a parametric fit of the Kaplan-Meier curves from the TN-10 clinical trial selected by the sponsor. The sponsor selected the log-normal distribution for the teplizumab arm based on statistical fit.5 Based on this parametric distribution, the sponsor estimated that approximately 11% of patients would not progress to stage 3 T1D after 15 years post stage 2 T1D diagnosis when treated with teplizumab; whereas, nearly all patients treated with no intervention developed stage 3 T1D or died (99.2%) by 15 years in the model, suggesting that teplizumab may be considered curative. Clinical expert feedback indicated that all patients with stage 2 T1D will eventually develop stage 3 T1D. The clinical experts noted that while the trial evidence indicates that patients in stage 2 T1D receiving teplizumab may experience a delay in reaching stage 3 T1D, there is currently no evidence that teplizumab will stop patients with stage 2 T1D from developing stage 3 T1D over their lifetime.
In reanalysis, CDA-AMC selected the gamma distribution for the teplizumab survival curve based on fit statistics, visual inspection with the trial period, and clinical expert feedback to ensure convergence with the no intervention survival curve. While the gamma extrapolation appears to visually fit the Kaplan-Meier curve, convergence occurs at approximately 50 years after treatment initiation. To reduce the uncertainty associated with the survival curves, CDA-AMC conducted a scenario analysis selecting the Gompertz distribution for the teplizumab survival curve for which convergence occurs at approximately 19 years post-treatment initiation.
Disease monitoring was not captured: The sponsor’s base case assumes that patients at risk of developing stage 3 T1D are identified by laboratory and autoantibody tests using a one-time cost and the monitoring of patients with stage 2 T1D was captured with glucose monitoring strips; this cost was applied to patients within the stage 2 T1D health state after teplizumab treatment or no intervention.6 Clinical expert feedback obtained by CDA-AMC indicated that monitoring for dysglycemia would involve multiple laboratory tests (i.e., OGTT, hemoglobin A1C, and FPG) on a 3 to 6 month testing schedule, in addition with glucose monitoring strips.
In the submitted pharmacoeconomic model, the sponsor assumed that health care resource cost for patients at risk of developing stage 3 T1D would be monitored using glucose testing strips, corresponding to $42.64 per 6-month cycle, or $85.28 per annum in 2024 Canadian dollars based on published literature.5,6 However, in the cited literature, the average annual cost of monitoring strips for patients with T1D was $360.766 in 2005 Canadian dollars, with a unit cost of $0.785 per strip. According to Diabetes Canada, the average cost of glucose monitoring strips has remained similar to the 2005 estimate from the published literature.44 Therefore, the semiannual cost of glucose monitoring strip is estimated to be $180.38.44
The sponsor assumed that all patients who entered the model tested positive for stage 2 T1D. The sponsor did not consider the accuracy of autoantibody testing to identify patients with stage 2 T1D within the submitted model. As noted in the Clinical Review Report, autoantibody tests for stage 2 T1D can have varying sensitivity and specificity depending on the type of assay conducted. The implications of simplifying screening on economic evaluations have been well documented in literature,45 where the clinical utility of teplizumab is dependent on those who received the treatment and its associated outcomes, and needs to be adequately considered within the economic evaluation.
In reanalysis, CDA-AMC included the cost of laboratory tests (i.e., OGTT, hemoglobin A1C, and FPG) for disease progression of patients with stage 2 T1D once every 6-month cycle.7 Additionally, CDA-AMC revised the cost of monitoring strips to $180.38 per 6-month cycle to reflect the published literature.6,46
CDA-AMC could not address the uncertainty associated with diagnostic test accuracy in the sponsor’s economic evaluation.
The proportion of patients who experience DKA events was likely overestimated. In the sponsor’s submitted model, 2.5%, and 7.41%, of patients, would experience DKA upon diagnosis and postdiagnosis, respectively.8,9 Clinician expert feedback indicated that if patients were screened for stage 2 T1D, DKA would be unlikely to occur, as DKA is usually a symptom for diagnosis of stage 3 T1D, and identification of stage 2 T1D will allow physicians to better manage patients to minimize the risk of DKA. Additionally, clinical expert feedback highlighted the rarity of postdiagnosis DKA events, as DKA occurs when symptoms are mismanaged. Published literature conducted in Ontario noted that approximately 6.2% of patients presented with DKA 1 year after the onset of stage 3 T1D, inclusive of at diagnosis.10 Given the sponsor’s estimate that 2.5% of patients present with DKA upon diagnosis of stage 3 T1D, 3.7% of patients may develop DKA postdiagnosis. There is uncertainty associated with the proportion of patients who present with DKA upon diagnosis if a screening program accompanies the reimbursement of teplizumab.
In reanalysis, CDA-AMC eliminated the risk of DKA upon diagnosis to reduce the uncertainty associated with DKA presentation if a stage 2 T1D screening program was present. Additionally, the proportion of patients who experience postdiagnosis was reduced to 3.7% to reflect published literature conducted in Ontario.8,10 As a scenario analysis, CDA-AMC maintained the sponsor’s original DKA upon diagnosis proportion of 2.5%.8
Disutility estimates for stage 3 T1D were likely overestimated. The sponsor’s model estimates a utility decrement associated with stage 3 T1D via a linear extrapolation informed by a cross-sectional study conducted in Sweden, and a uniform EQ-5D utility decrement based on the National Institute for Health and Care Excellence (NICE) disutility catalogue.11,12 The cross-sectional study suggests that there is a negative relationship between the time since T1D onset and EQ-5D disutility.12 However, the study demonstrates that there was a minimal difference in EQ-5D scores between male patients with diabetes and the general population at 8 and 15 years after the onset of diabetes. Additionally, the study reported that female patients with diabetes had a higher EQ-5D at 24 years postdiagnosis compared to 15 years; albeit a small numerical increase.12 This highlighted the uncertainty that a HRQoL improvement is present for male patients between 8 to 15 years postdiagnosis and an incremental change for female patients between 15 to 24 years. The sponsor’s submitted model continues to extrapolate the disutility decrement until the end of the lifetime of the patient, which did not align with clinical expert opinion obtained for this review. This is associated with significant uncertainty as patients may not experience a continued quality of life impact as HRQoL was not captured in TN-10.18 In addition to the linear extrapolation, a utility decrement was applied based on the National Institute for Health and Care Excellence (NICE) disutility catalogue. This may overestimate the utility decrement associated with diabetes as the linear extrapolation should capture the disutility associated with diabetes.11 The authors of the cross-sectional study did acknowledge that over the years, there have been changes “in the provision of health services such as a shift from hospital inpatient care to daycare and a shift from visits to physicians to visits to diabetes nurses, and in the involvement of patients as part of the expert team around the disease with self-management as an important component. Thus, the patients in this study have received different types of care dependent on the year of diagnosis. These changes in diabetes management likely contribute to reductions or postponements in diabetes-related complications, complications which may have a negative effect on HRQoL for individuals with diabetes.”12 As a result, this also suggests that the utility decrement for those with T1D for longer may be overestimated.
The sponsor also applied a 1-time infusion-related utility decrement for patients who receive teplizumab, where the caregiver of the patient who is receiving teplizumab is assumed to have an identical quality of life decrement to that observed in the patient.13 The published literature examined the utility decrement associated with infusions; however, there was no evidence supporting the assumption that caregivers would experience similar utility decrement as patients who receive an infusion.
Additionally, in the sponsor’s submitted analysis conducted from the perspective of the public health care payer, caregiver utilities were included. As the target population of the economic evaluation was a patient population with stage 2 T1D, the analysis from the perspective of the health care payer should only include the health effects for the target population.47 As such, the inclusion of caregiver utilities in the public health care payer perspective was inappropriate. Given that preferences between caregivers and patients may be conflicting, it is important that a health care payer perspective, that just includes patient impact, is also presented.
In reanalysis, CDA-AMC removed the linear extrapolation utility decrement, and all caregiver disutility estimates in the publicly funded health care payer perspective.
For the societal perspective, CDA-AMC removed the caregiver infusion utility decrement.
Cost of stage 3 T1D HCRU was likely overestimated. In the sponsor’s model, stage 3 T1D HCRU costs were estimated based on published literature and an age-stratified mixed regression model was applied to extrapolate costs throughout the lifetime of the patient. The sponsor-provided literature examined the cost for HCRU in Canada between 1995 to 2005, which found that patients with stage 3 T1D had high initial costs followed by a sharp decrease and a gradual increase over time.38 The regression used to estimate HCRU did not follow the Canadian published literature, rather it estimated that HCRU costs would steadily increase over time.39 The constant gradual increase did not align with clinical expert expectations, which aligned with the Canadian paper.
In reanalysis, CDA-AMC set the intercept of the mixed regression to the annual average of the inflated costs from published literature.
The estimated mortality benefit is associated with uncertainty. The sponsor’s submitted base case estimates that teplizumab is associated with a 0.24 life-year gain when compared to no intervention.5 Mortality was not a key outcome in the TN-10 trial and no deaths were reported in both arms of treatment.18 As noted in the CDA-AMC Clinical Review, while there is plausibility that teplizumab is able to delay the onset of stage 3 T1D, there is significant uncertainty if there are long-term health benefits associated with teplizumab such as improvements in mortality.
CDA-AMC was unable to address this limitation due to a lack of available evidence to address possible long-term benefits of teplizumab treatment.
The proportion of patients who receive hybrid administration of teplizumab is overestimated. Hybrid administration of teplizumab consists of both in-hospital (day 1 to 4) and at-home (day 5 to 14) administration.5 Clinical expert feedback indicated that hybrid administration would not be feasible and only hospital administration would be conducted. Additionally, drug plan input for this review indicated that some provinces do not have at-home programs. Furthermore, the sponsor did not provide any information regarding a patient support program which may assist with in-home infusions.
CDA-AMC set in-hospital administration to 100% based on clinical expert feedback and drug plan input.
Indirect costs from productivity loss are likely overestimated. The sponsor’s submitted model included indirect costs based on the productivity loss from patients aged greater than 18 and caregivers of patients younger than 18, where the number of hours lost to T1D was dependent on the stage of disease, informed by sponsor-elicited clinical experts.40 The productivity loss for patients and caregivers of patients with stage 2 and stage 3 T1D is uncertain, as only clinical expert opinion informed the loss of working hours due to T1D. Clinical expert feedback obtained by CDA-AMC indicated that patients diagnosed with stage 2 T1D are presymptomatic and typically do not require additional care, and noted that as patients become more experienced with metabolic control, T1D may not have an impact on the number of working hours for a patient with stage 3 T1D.
The sponsor’s submitted model did not consider the potential productivity loss and transportation costs due the administration of teplizumab, which the product monograph recommends is infused intravenously over a period of 30 minutes to 4 hours every day for 14 days.48
In reanalysis, CDA-AMC removed all indirect costs informed by clinical expert opinion due to lack of evidence in the number of hours lost for patients or caregivers with diabetes. This reanalysis was conducted due to a lack in evidence; however, CDA-AMC notes that it favours no intervention as patients who spend more time in the stage 3 T1D health state would not incur productivity losses. These indirect costs were included in a scenario analysis, although there is uncertainty with the sponsor’s estimates.
CDA-AMC was unable to address the additional transportation costs and productivity losses due to teplizumab administration.
Additional issues were identified but were not considered to be key issues: Administration costs are likely underestimated, the sponsor only attributed 30 minutes of infusion time for the administration of teplizumab; clinical experts indicated that additional elements such as phlebotomy and preparation for administration were not accounted for.
CDA-AMC Reanalysis of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (refer to Table 7). The impact of these changes, individually and collectively, is presented in Table 8.
Table 7: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Choice of parametric distribution for time to stage 3 T1D | Log-normal | Gamma |
2. Stage 2 monitoring costs | Glucose monitoring strips only. ($42.64 per 6-month cycle) | a. Corrected autoantibody test costs to $353.58 Corrected glucose monitoring strips to $180.38. b. Included OGTT, hemoglobin A1C, and FPG once every 6-month cycle |
3. Linear extrapolation of disutilities | Included | Excluded |
4. DKA rates | Upon diagnosis: 2.5% Postdiagnosis: 7.41% | Upon diagnosis: 0% Postdiagnosis: 3.70% |
5. Health care resource use for stage 3 T1D | Derived by regression: | Average of data: |
Treatment administration setting | In-hospital: 54.1% Hybrid: 45.9% | In-hospital: 100% |
7. Caregiver disutility | Included | a) Caregiver disutility and caregiver disutility due to infusion excluded from the publicly funded health care payer perspective. b) Caregiver disutility due to infusion excluded from the societal perspective. |
8. Indirect costs (societal perspective) | Included | Excluded |
CDA-AMC base case (health care payer perspective) | ― | 1 + 2 + 3 + 4 + 5 + 6 + 7a |
CDA-AMC base case (societal perspective) | ― | 1 + 2 + 3 + 4 + 5 + 6 + 7b + 8 |
CDA-AMC = Canada’s Drug Agency; DKA = diabetic ketoacidosis; FPG = fasting plasma glucose; OGTT = oral glucose tolerance test; T1D = type 1 diabetes.
Note: CDA-AMC was unable to resolve the issues with uncertainty associated with long-term benefits of teplizumab, and the indirect costs of productivity loss.
Table 8: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (Public payer [probabilistic]) | No intervention | 891,261 | 30.09 | Reference |
Teplizumab | 1,071,030 | 30.89 | 224,358 | |
Sponsor’s base case (Societal [probabilistic]) | No intervention | 1,085,281 | 30.09 | Reference |
Teplizumab | 1,227,092 | 30.89 | 176,942 | |
CDA-AMC reanalysis 1 | No intervention | 892,257 | 30.06 | Reference |
Teplizumab | 1,101,289 | 30.66 | 347,262 | |
CDA-AMC reanalysis 2 | No intervention | 899,041 | 30.06 | Reference |
Teplizumab | 1,087,736 | 30.83 | 243,796 | |
CDA-AMC reanalysis 3 | No intervention | 892,257 | 33.26 | Reference |
Teplizumab | 1,074,669 | 33.70 | 419,016 | |
CDA-AMC reanalysis 4 | No intervention | 891,446 | 30.06 | Reference |
Teplizumab | 1,073,902 | 30.83 | 235,736 | |
CDA-AMC reanalysis 5 | No intervention | 775,902 | 30.06 | Reference |
Teplizumab | 968,716 | 30.83 | 249,117 | |
CDA-AMC reanalysis 6 | No intervention | 892,257 | 30.06 | Reference |
Teplizumab | 1,074,677 | 30.83 | 235,689 | |
CDA-AMC reanalysis 7a (Health care payer) | No intervention | 892,257 | 30.18 | Reference |
Teplizumab | 1,074,669 | 30.89 | 255,484 | |
CDA-AMC reanalysis 7b (societal) | No intervention | 1,085,646 | 30.06 | Reference |
Teplizumab | 1,230,758 | 30.83 | 187,274 | |
CDA-AMC reanalysis 8 (societal) | No intervention | 892,257 | 30.06 | Reference |
Teplizumab | 1,074,669 | 30.83 | 235,679 | |
CDA-AMC public payer base case: (1 + 2 + 3 + 4 + 5 + 6 + 7a) (deterministic) | No intervention | 781,875 | 33.38 | Reference |
Teplizumab | 1,002,041 | 33.69 | 710,143 | |
CDA-AMC public payer base case (1 + 2 + 3 + 4 + 5 + 6 + 7a) (probabilistic) | No intervention | 780,497 | 33.38 | Reference |
Teplizumab | 1,002,127 | 33.68 | 747,542 | |
CDA-AMC societal base case: (1 + 2 + 3 + 4 + 5 + 6 + 7b + 8) (deterministic) | No intervention | 781,875 | 33.26 | Reference |
Teplizumab | 1,002,041 | 33.64 | 589,538 | |
CDA-AMC societal base case: (1 + 2 + 3 + 4 + 5 + 6 + 7b + 8) (probabilistic) | No intervention | 780,659 | 33.33 | Reference |
Teplizumab | 1,000,967 | 33.69 | 608,736 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments. Deterministic results are presented, unless otherwise indicated. Estimated life-years are 41.46 for teplizumab and 41.22 for no intervention.
Table 9: Disaggregated Results of the CDA-AMC Base Case — Health Care Payer Perspective
Parameter | Teplizumab | No intervention |
|---|---|---|
Discounted LYs | ||
Total | 41.46 | 41.22 |
Stage 2 T1D | 5.67 | 3.45 |
Stage 3 T1D | 35.79 | 37.77 |
Discounted QALYs | ||
Total | 33.69 | 33.38 |
Stage 2 T1D | 5.03 | 3.05 |
Stage 3 T1D | 28.67 | 30.33 |
Adverse Events | −0.002 | 0.000 |
Discounted costs ($) | ||
Total | 942,896 | 780,935 |
Drug acquisition | 199,472 | 0 |
Administration | 1,066 | 0 |
Adverse event management | 504 | 0 |
Treatment-related HCRU | 1,340 | 367 |
Disease management (stage 2 T1D) | 14,022 | 8,680 |
Disease management (stage 3 T1D) | 726,027 | 771,408 |
DKA management | 463 | 481 |
CDA-AMC = Canada’s Drug Agency; DKA = diabetic ketoacidosis; HCRU = health care resource use; LY = life-year; QALY = quality-adjusted life-year; T1D = type 1 diabetes.
Table 10: Disaggregated Results of the CDA-AMC Base Case — Societal Perspective
Parameter | Teplizumab | No intervention |
|---|---|---|
Discounted LYs | ||
Total | 41.45 | 41.22 |
Stage 2 T1D | 5.70 | 3.52 |
Stage 3 T1D | 35.76 | 37.71 |
Discounted QALYs | ||
Total | 33.69 | 33.33 |
Stage 2 T1D | 5.70 | 3.12 |
Stage 3 T1D | 28.69 | 30.33 |
Caregiver disutility | −0.06 | −0.12 |
Adverse Events | −0.002 | 0.000 |
Discounted costs ($) | ||
Total | 1,000,967 | 780,659 |
Drug acquisition | 257,318 | 0 |
Administration | 1,072 | 0 |
Adverse event management | 501 | 0 |
Treatment-related HCRU | 1,339 | 366 |
Disease management (stage 2 T1D) | 13,993 | 8,716 |
Disease management (stage 3 T1D) | 726,278 | 771,097 |
DKA management | 466 | 480 |
Indirect costs | 0 | 0 |
CDA-AMC = Canada’s Drug Agency; DKA = diabetic ketoacidosis; HCRU = health care resource use; LY = life-year; QALY = quality-adjusted life-year; T1D = type 1 diabetes.
Price Reduction Analysis
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (refer to Table 11).
Table 11: Results of the Price Reduction Analysis
Price reduction | Unit drug cost ($) | One-time cost ($) | ICERs for teplizumab vs. no intervention ($/QALY) | ||
|---|---|---|---|---|---|
Sponsor base case | CDA-AMC public payer base case | CDA-AMC societal base case | |||
No price reduction | 18,410a | 257,740 | 224,358 | 747,542 | 608,736 |
10% | 16,569 | 231,966 | 192,191 | 660,608 | 537,520 |
20% | 14,728 | 206,192 | 160,024 | 573,674 | 466,303 |
30% | 12,887 | 180,418 | 127,857 | 486,740 | 395,087 |
40% | 11,046 | 154,644 | 95,691 | 399,806 | 323,870 |
50% | 9,205 | 128,870 | 63,524 | 312,872 | 252,653 |
60% | 7,364 | 103,096 | 31,357 | 225,938 | 181,437 |
70% | 5,523 | 77,322 | Dominant | 139,004 | 110,220 |
80% | 3,682 | 51,548 | Dominant | 52,070 | 39,004 |
90% | 1,841 | 25,774 | Dominant | Dominant | Dominant |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; vs. = versus.
aSponsor’s submitted price for teplizumab.2
Assessment of Uncertainty
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to address uncertainty within the economic evaluation. The results are provided in Table 12.
Adjusting the survival curve of the proportion of patients at risk of stage 3 T1D using the Gompertz distribution, using the sponsor-provided option to do so, such as that there is convergence of the teplizumab and placebo curves.
Increasing the DKA risk upon diagnosis to 2.5% in line with the sponsor’s base case.
Table 12: Results of CDA-AMC Scenario Analyses
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case (Public payer) | No intervention | 781,875 | 33.38 | Reference |
Teplizumab | 1,002,041 | 33.69 | 710,143 | |
CDA-AMC base case (Societal) | No intervention | 781,875 | 33.26 | Reference |
Teplizumab | 1,002,041 | 33.64 | 589,538 | |
CDA-AMC scenario 1: Gompertz distribution (public payer)b | No intervention | 781,875 | 33.38 | Reference |
Teplizumab | 1,003,229 | 33.69 | 704,672 | |
CDA-AMC scenario 1: Gompertz distribution (societal)b | No intervention | 781,875 | 33.26 | Reference |
Teplizumab | 1,003,229 | 33.63 | 595,317 | |
CDA-AMC scenario 2: DKA upon diagnosis risk (public payer) | No intervention | 782,202 | 33.38 | Reference |
Teplizumab | 1,002,356 | 33.69 | 710,105 | |
CDA-AMC scenario 2: DKA upon diagnosis risk (societal) | No intervention | 782,202 | 33.26 | Reference |
Teplizumab | 1,002,356 | 33.64 | 589,507 | |
CDA-AMC scenario 3: Indirect costs included (societal) | No intervention | 975,265 | 33.26 | Reference |
Teplizumab | 1,161,294 | 33.64 | 498,131 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aDeterministic analyses.
bWhen the probabilistic sensitivity analysis was conducted, results were significantly different than the deterministic analysis (deterministic – Health care payer: $512,582 per QALY; Societal: $433,037). Given the parametric uncertainty that is characterized within the Gompertz distribution for this probabilistic analysis, this can result in long-term extrapolation which does not meet face validity based on the feedback from clinicians consulted by CDA-AMC. This increases the amount of uncertainty associated with the results of the probabilistic analysis.
Issues for Consideration
As noted in the Clinical Review Report, the baseline characteristics of patients in the TN-10 are different compared to patients seen in Canadian clinical practice. (i.e., proportion of patients > 18 years old, racial and ethnic diversity, and parameters associated with blood counts and liver function.)
As noted in the Ethics Review report, the patient group input for this review indicated the substantial emotional impact of T1D on patients and their caregivers and potential benefits of delaying time from stage 2 T1D to stage 3 T1D. However, few patients who received teplizumab treatment had described meaningful emotional relief.
As noted in the Clinical Review Report, testing for stage 2 T1D is not in the current standard of care and accessibility of autoantibody tests are variable across Canada.
As noted in the product monograph, teplizumab requires reconstitution before administration and has specific requirements regarding the viability of the dose. The infusion must be started within 2 hours of preparation, stored at room temperature, and the infusion must be completed within 4 hours of the start of preparation. Any solution not administered within 4 hours of preparation must be discarded.1
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing teplizumab for the treatment to delay the onset of stage 3 T1D in adult and pediatric patients 8 years of age and older with stage 2 T1D.15
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2026 to 2028), with 2025 as the base year.15 The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits Program.15 The sponsor estimated the eligible population using an epidemiological approach.15 Subsequent treatment costs were not included. The sponsor’s base case included drug acquisition costs.2,15 The market uptake for teplizumab was estimated using sponsor assumptions.15 The key inputs to the BIA are documented in Table 13.
The sponsor estimated the 3-year incremental budget impact associated with reimbursing teplizumab for the treatment to delay the onset of stage 3 T1D in adult and pediatric patients 8 years of age and older with stage 2 T1D would be $35,736,291 (year 1 = $1,810,891; year 2 = $11,232,060; year 3 = $22,693,340).15
Table 13: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Total population | 32,953,129 / 33,537,582 / 34,132,623 |
Prevalence of stage 3 T1D | 0.539%49 |
Number of FSDRs per patient with stage 3 T1D | 850 |
Total number of FSDRs of patients with stage 3 T1D | 1,420,939 / 1,446,141 / 1,471,799 |
Proportion of FSDRs who are 8 years and older | |
Proportion of FSDRs who will receive early detection testing | ██%53 |
Proportion of FSDRs that test positive for ≥ 1 autoantibody test | 5.5%54 |
Proportion of FSDRs that test negative for ≥ 1 autoantibody test and are retested | 21.7%54 |
Proportion of FSDRs that retest and test positive for ≥ 1 autoantibody test | 4.5%54 |
Proportion of FSDRs with ≥ 1 positive autoantibody who receive confirmatory autoantibody testing | 87.7%54 |
Proportion of FSDRs that test positive for ≥ 2 autoantibodies on confirmatory testing | 55.4%55 |
Proportion of FSDRs with ≥ 2 positive autoantibodies on confirmatory testing who receive metabolic testing for dysglycemia | 69.4%54 |
Proportion of FDR/SDR with confirmed stage 2 T1D | 8.9%56 |
Proportion of patients eligible for public drug plans in each jurisdiction | 27.8% to 100%a57 |
Proportion of patients eligible for TZIELD treatment | |
Number of patients eligible for drug under review | ███ / ███ / ███ |
Market shares (reference scenario) | |
Teplizumab | 0% / 0% / 0% |
No intervention | 100% / 100% / 100% |
Market shares (new drug scenario) | |
Teplizumab | ███% / ████% / ████% |
No intervention | ████% / ████% / ████% |
Cost of treatment (per patient per course) | |
Teplizumab | $257,740 |
No intervention | $0 |
FSDR = first-degree and second-degree relative; T1D = type 1 diabetes.
aVaries by jurisdiction.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The screening approach undertaken by the sponsor is associated with uncertainty. The sponsor’s submitted BIA assumed that ██% of the FSDRs of patients with stage 3 T1D would be tested for stage 2 T1D.53 Clinical expert feedback discussed different approaches to screening, including focusing on patients with a family history of T1D (FSDRs), or a population-wide approach. The clinical experts consulted indicated that first-degree relatives may be more highly motivated to test for stage 3 T1D and were uncertain that screening second-degree relatives would be widely adopted in a targeted screening program. The sponsor modelled for a targeted screening program assuming only patients with a relative with stage 3 T1D would be identified as having stage 2 T1D and therefore eligible for teplizumab. CDA-AMC cannot comment on the budget impact of a population-wide screening program or the impact of including individuals with stage 2 T1D who do not have a FSDR with stage 3 T1D. Clinical group input for this review noted that a pilot is under way looking at the feasibility of implementing a population-wide screening program in Canada (CanScreen T1D).17 Thus, the market size for teplizumab is highly uncertain.
CDA-AMC was unable to address the limitation regarding a population-wide screening program. However, as approximately 80%4 of patients with stage 3 T1D do not have a family history, a population-wide screening program would be expected to significantly increase the budget impact.
In reanalysis, CDA-AMC increased the proportion of FSDR who received testing to 70% across all 3 years. To reduce the uncertainty of potentially testing unmotivated SDR, CDA-AMC conducted a scenario analysis where only 4 FDR were considered.
Subsequent treatment costs were not considered. Patients who progress to stage 3 T1D are likely to be treated with insulin replacement therapy. As a result, if teplizumab increases the time to progression to stage 3 T1D then there may be cost offsets associated with reduced insulin replacement therapy. It is unclear whether teplizumab would have an impact on long-term use of insulin replacement therapy.
CDA-AMC was unable to address this limitation due to model inflexibility; the time-to-progression parametric distributions would be necessary to stimulate the progression from stage 2 T1D to stage 3 T1D.
The public coverage rate assumed by the sponsor is likely underestimated. The proportion of patients covered by public drug plans were based on eligible population of each province from Understanding the Gap 2.0.57 However, the majority of patients who would be eligible for teplizumab treatment will be likely be under the age of 18 and would be eligible for full coverage. From the baseline characteristics of TN-10, 72.3% of the Intention-to-treat population across the teplizumab and placebo arm were under the age of 18.18 It is likely inappropriate to apply the proportion of eligible patients for drug plans to this patient population.
CDA-AMC modified the proportion of patients who are publicly covered for Ontario, Newfoundland and labrador, Prince Edward Island, and New Brunswick; 72.3% of patients were assumed to be under 18, and therefore, eligible for public coverage, the sponsor’s original public coverage proportion was applied to the remainder. As different jurisdictions have their respective coverage rates for patients aged between 25 and 64, the resulting rates are a function of the proportion of patients who are under 18 and the coverage rate for those over 18.
The market uptake of teplizumab is underestimated: The sponsor’s submitted BIA indicated that teplizumab would result in a market uptake of ███% in Year 1, ████% in Year 2, and ████% in Year 3 based on sponsor assumptions. However, CDA-AMC obtained clinical expert feedback indicating that the market uptake across all 3 years does not align with clinical expectations and indicated the sponsor likely underestimated teplizumab uptake. Currently, patients do not have any treatment in the stage 2 T1D landscape. Therefore, if the patient is eligible to receive treatment, clinical expert feedback indicated that they would likely receive teplizumab. CDA-AMC clinical expert feedback deemed the sponsor’s estimate in Year 1 may be reasonable to account for feasibility, but they indicated that the teplizumab market share would likely grow to 70% by Year 3. Clinical experts discussed the potential variability of market uptake; however, it was noted that there are no alternative treatments available and eligible patients would be considered for teplizumab treatment.
To address this limitation, CDA-AMC undertook a reanalysis by revising the market shares for teplizumab in the new drug scenario to 10%, 45%, and 70% in Year 1, 2, 3, respectively.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, in consultation with clinical experts, as outlined in Table 13.
Table 14: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Proportion of FSDR who receive autoantibody testing | ██% across 3 years | 70% across 3 years |
2. Proportion of patients who are eligible for public coverage | Ontario: 49.4% Newfoundland and labrador: 27.4% Prince Edward Island: 38.9% New Brunswick: 45.0% | Ontario: 86.0% Newfoundland and Labrador: 80.0% Prince Edward Island: 83.1% New Brunswick: 84.8% |
3. Market uptake of teplizumab | Year 1: ███% Year 2: ████% Year 3: ████% | Year 1: 10.0% Year 2: 45.0% Year 3: 70.0% |
CDA-AMC base case | ― | (1 + 2 + 3) |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; FSDR = first- and second-degree relative.
Note: CDA-AMC was unable to resolve the issues with a population-wide screening program.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 15 and a more detailed breakdown is presented in Table 16. In the CDA-AMC base case, the 3-year budget impact of reimbursing teplizumab to delay the onset of stage 3 T1D in adult and pediatric patients 8 years of age and older with stage 2 T1D was $485,007,471 (year 1 = $37,798,412; year 2 = $173,119,238; year 3 = $274,089,821).
Table 15: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 35,736,291 |
CDA-AMC reanalysis 1 | 250,154,039 |
CDA-AMC reanalysis 2 | 45,808,109 |
CDA-AMC reanalysis 3 | 54,051,808 |
CDA-AMC base case: (1 + 2 + 3) | 485,007,471 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to explore uncertainty in the estimated budget impact of reimbursing teplizumab. The results are provided in Table 16.
Considering only first-degree relatives (n = 4) for screening.
Table 16: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference total | $0 | $0 | $0 | $0 | $0 |
Teplizumab | $0 | $0 | $0 | $0 | $0 | |
No intervention | $0 | $0 | $0 | $0 | $0 | |
New drug total | $0 | $1,810,891 | $11,232,060 | $22,693,340 | $35,736,291 | |
Teplizumab | $0 | $1,810,891 | $11,232,060 | $22,693,340 | $35,736,291 | |
No intervention | $0 | $0 | $0 | $0 | $0 | |
Budget Impact | $0 | $1,810,891 | $11,232,060 | $22,693,340 | $35,736,291 | |
CDA-AMC base case | Reference total | $0 | $0 | $0 | $0 | $0 |
Teplizumab | $0 | $0 | $0 | $0 | $0 | |
No intervention | $0 | $0 | $0 | $0 | $0 | |
New drug total | $0 | $37,798,412 | $173,119,238 | $274,089,821 | $485,007,471 | |
Teplizumab | $0 | $37,798,412 | $173,119,238 | $274,089,821 | $485,007,471 | |
No intervention | $0 | $0 | $0 | $0 | $0 | |
Budget Impact | $0 | $37,798,412 | $173,119,238 | $274,089,821 | $485,007,471 | |
CDA-AMC scenario analyses | ||||||
Scenario 1: First-degree relatives only | Reference total | $0 | $0 | $0 | $0 | $0 |
New drug total | $0 | $18,899,206 | $86,559,619 | $137,044,910 | $242,503,735 | |
Budget Impact | $0 | $18,899,206 | $86,559,619 | $137,044,910 | $242,503,735 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
Ethics Review
Abbreviations
CanScreen T1D
Canadian Population Screening for Risk of Type 1 Diabetes
T1D
type 1 diabetes
Ethical Considerations
Type 1 diabetes (T1D) is a chronic, autoimmune condition in which the immune system attacks insulin-producing beta cells in the pancreas, leading to insulin deficiency and eventual dependence on exogenous insulin. Although T1D has historically been considered a childhood-onset disease, current evidence suggests that it is also frequently diagnosed in early adulthood. If left untreated, T1D is life-threatening; even when managed, it carries substantial physical, emotional, and logistical burdens. Stage 2 T1D is a presymptomatic phase defined by the presence of multiple T1D-associated autoantibodies and early signs of dysglycemia.
This report is informed by the sponsor’s submission, patient group, clinician group, and drug plan input received by Canada’s Drug Agency for this review. It has also drawn on direct consultation with 3 clinical experts (2 pediatric endocrinologists and 1 adult endocrinologist) who have experience treating patients with stage 3 T1D and monitoring those with stage 2 T1D. Select published literature was consulted to help clarify points of concern raised by clinical experts or input received for this review.
This report highlights ethical considerations regarding the use of teplizumab to delay the onset of stage 3 T1D in adults and pediatric patients aged 8 years and older with stage 2 T1D. It outlines considerations relevant for decision-making regarding public reimbursement and implementation of teplizumab in Canada. However, it does not present an exhaustive list of all ethical considerations associated with stage 2 T1D and its treatment.
Diagnosis, Treatment, and Experiences of People Living With Stage 2 T1D
An evolving staging model is shaping clinical and policy decision-making: T1D is currently understood as presenting across 3 unique stages with the third representing symptomatic T1D.1-4 Each stage is defined by the presence of at least 2 T1D-associated autoantibodies (commonly glutamic acid decarboxylase 65, islet antigen-2, zinc transporter 8, and insulin autoantibodies), with progression marked by increasing glycemic dysfunction and the onset of clinical symptoms such as polyuria, polydipsia, and unexplained weight loss by stage 3.1 As this staging framework becomes more embedded in clinical and policy decision-making, it raises ethical questions about how risk is modelled, who is diagnosed and when and how, and how access to preventive therapies are offered.
Stage 2 progression is variable and not a uniform risk category: Stage 2 is defined by the presence of at least 2 T1D-associated autoantibodies and the development of abnormal glucose tolerance.1 However, emerging evidence suggests that stage 2 may not be a uniform risk category.5,6 For instance, though the lifetime risk of transitioning from stage 2 to stage 3 approaches 100%, and approximately 75% of individuals progress to stage 3 within 5 years,1 the rate of progression may vary considerably between individuals.2,7 For example, recent evidence has demonstrated that age at stage 2 influences risk of progression, with children progressing faster than adults,5 and that some autoantibody combinations may lead to earlier progression to stage 3.5,8 This lack of consistent progression pattern for all people at stage 2 has direct implications for treatments like teplizumab that may rely on staging to determine eligibility or prioritize access.
Limited access to screening restricts early identification and intervention: Screening for T1D-associated autoantibodies is not routinely available in Canada. Instead, clinical experts indicated that current screening practices are largely limited to research settings and primarily target people with a family history of T1D, who are approximately 15 times more likely to develop T1D than the general population.9 While this targeted approach may be practical in the absence of broader infrastructure, it also raises concerns about fairness and access given that approximately 85% of those who eventually develop T1D have no family history.1 Without a systematic screening strategy, early identification — and therefore access to preventive interventions like teplizumab — is likely to remain limited to a small subset of the stage 2 T1D population. The Canadian Population Screening for Risk of Type 1 Diabetes (CanScreen T1D) initiative is currently exploring the feasibility of building a population-level screening program for T1D, but this is still in preliminary stages. More details regarding current screening practices and the ongoing development of CanScreen T1D are described in the Clinical Review Report.
Stage 3 T1D imposes substantial psychosocial and logistical burdens on patients and their families: Patient group input emphasized the emotional, physical, and logistical burden of managing stage 3 T1D, especially for children and their caregivers. Families described life with T1D as demanding constant attention to fluctuating insulin needs, food intake, and stress levels, creating a daily rhythm of vigilance and adjustment. As most people who develop stage 3 T1D are currently unaware of their stage 2 status, patient group input flagged that this transition can be experienced as abrupt and destabilizing, with little time to prepare for the complex responsibilities of diabetes management. The possibility of even a modest delay in progression from stage 2 to stage 3 was identified as valuable to patients and their caregivers. It was suggested that a delay could offer patients, their families, and their communities (e.g., schools in the case of younger children) time to prepare emotionally, developmentally, and logistically for the responsibilities of chronic disease management. Some participants in the patient group input even hoped that a delay may reduce the risk of common T1D-associated complications (e.g., retinopathy, neuropathy, cardiovascular disease) later in life, improve glycemic outcomes over time, or provide space for emerging therapies to enter standard practice. While clinical experts suggested it is difficult to disentangle which of these desired outcomes might be better addressed through strong screening programs or enhanced diabetes education, they nonetheless illustrate the kinds of value that individuals and families associate with delayed progression, and help clarify the expectations patients and caregivers may place on teplizumab.
Unmet need extends beyond therapy to include identification, education, and planning: The broader context of unmet need in stage 2 is shaped as much by gaps in identification and preparedness as by the absence of therapeutic options. At present, there are no approved interventions for delaying progression from stage 2 to stage 3, and no disease-modifying therapies available for T1D at any stage. While insulin therapy and associated technologies (e.g., insulin pumps and continuous glucose monitors) offer robust support for managing stage 3 disease, access to these tools varies significantly across Canada. As such, patient group input indicated that out-of-pocket costs of the tools used to manage T1D may create barriers to care for some. This is aligned with published literature, which has repeatedly demonstrated that individuals who are racialized or living with lower socioeconomic status often face greater barriers to T1D care and experience poorer outcomes.10-14 However, even before questions of access or treatment arise, most people living with stage 2 T1D remain undiagnosed due to the lack of population-level screening. For children and adolescents, this transition may also carry substantial clinical risk because approximately one-third are diagnosed following an episode of diabetic ketoacidosis, a life-threatening complication that can result in hospitalization, long-term cognitive impacts, or even death.15 Taken together, these observations suggest that unmet need in early T1D is not limited to the absence of treatment options, but extends to broader system gaps in identification, education, and care.
Clinical Evidence Used in the Evaluation of Teplizumab
Trial evidence demonstrated delayed progression to stage 3, but key uncertainties remain: The TN-10 study was a phase II, randomized, double-blind, placebo-controlled trial (N = 76) designed to evaluate the efficacy and safety of teplizumab (delivered via IV infusion over 14 consecutive days) in delaying progression from stage 2 to stage 3 T1D in individuals aged 8 years and older with a known first-degree or second-degree relative diagnosed with stage 3 T1D. The primary outcome was time from randomization to clinical diagnosis of stage 3 T1D. Participants who had not progressed by the end of the trial (n = 20) were followed for up to 80.46 months. Teplizumab was associated with a statistically significant delay in progression, extending time to stage 3 diagnosis by a median of approximately 2 years compared to placebo. While clinical experts considered this delay clinically meaningful, long-term efficacy and safety remain uncertain given limited data, and the trial did not assess outcomes such as glycemic control after diagnosis or impacts on common long-term complications associated with stage 3 T1D.
Several ethical considerations complicate interpretation of the trial evidence:
Limited participant diversity: All participants in the active treatment arm (100%) and nearly all in the placebo arm (94%) were white. Clinical experts suggested that this is more reflective of the demographics seen in opt-in, family-based screening programs rather than the actual T1D population. This raises questions about whether findings can be confidently extended to racialized populations or those less represented in early-stage T1D, particularly in the context of known disparities in T1D diagnosis, management, and outcomes across racial and socioeconomic lines.
Restricted inclusion criteria: Only individuals with a family history of stage 3 T1D were eligible for enrolment. This is particularly problematic given that the majority of people who develop T1D do not have a family history, and that progression rates do not appear to differ based on family history once stage 2 is identified.9 This impacts generalizability of the benefit observed in the trial to the approximately 85% of the patient population who eventually develop T1D where there is no family history, and raises ethical considerations about equitable access to screening, diagnosis, care, and potentially reimbursement, for those patients.
Uncertain value of delay: The primary outcome was time to stage 3 diagnosis, and while the trial demonstrated an average delay in progression of approximately 2 years, the long-term significance of this outcome remains unclear. There is no evidence that delay alters the course of long-term complications, and patient-reported outcomes — such as health-related quality of life — were not assessed. As such, the clinical and experiential value of delayed progression remains difficult to interpret.
Clinical Use of Teplizumab
A first-in-class therapy with potential to shift the T1D treatment paradigm: Teplizumab is positioned as a first-in-class immunotherapy for delaying the onset of symptomatic T1D (stage 3). Clinical experts and patient group input were broadly optimistic about its potential, viewing it as a meaningful step forward in a treatment landscape where no disease-modifying therapies currently exist for T1D at any stage.
Perceived experiential value of delay is not consistently reflected in lived experience: The sponsor’s value proposition rests heavily on the presumed psychosocial benefits of delaying stage 3 disease, but existing evidence complicates this assumption. In a US-based survey of 30 adults and 17 caregivers of children who had all received teplizumab, most respondents expressed general satisfaction with having access to the therapy, but few described meaningful emotional relief.16 Among adult participants, only 20% reported feeling more relaxed posttreatment, and most caregivers continued to express worry about their child’s progression to stage 3. Though caregivers were somewhat more likely to report psychosocial benefit than adult participants, both groups conveyed an enduring sense of vigilance and anticipatory anxiety. These findings suggest that while the concept of delay may be appealing, patients’ experiences may fall short of the emotional or psychosocial reassurance that patients and families hope for.
Safety profile considered manageable, but long-term benefit remains unclear: Teplizumab is an immunosuppressive therapy, and while clinical experts characterized its safety profile as manageable, the long-term consequences of treatment remain unclear. The most common adverse events reported in the trial included lymphopenia, leukopenia, and rash. Although these were generally mild, they must be weighed against the absence of evidence demonstrating psychosocial value of delayed progression or that this delay reduces downstream complications associated with T1D (e.g., retinopathy, neuropathy, cardiovascular disease). This uncertainty is particularly salient given the pediatric indication of teplizumab. Intervening during childhood, in the absence of clear long-term clinical value, raises concerns about benefit-risk proportionality and the potential for unnecessary medicalization. These concerns are compounded by the fact that teplizumab is not curative and progression to stage 3 is simply delayed, making the temporality of benefit difficult to weigh against risk exposure. This uncertainty can make clinical decision-making challenging and will require a robust informed consent process to ensure patients and their caregivers are able to clearly weigh potential harms against potential benefits.
Access and prioritization decisions will be complicated by scientific and structural gaps: If recommended for public reimbursement, designing a fair approach to access teplizumab will be complicated by 2 intersecting considerations: gaps in identifying who is most likely to benefit, and limitations in who is currently identified as living at stage 2 in Canada. While the TN-10 study demonstrated that teplizumab likely delays progression for people at stage 2, variation in short-term progression risk — linked to factors such as age and autoantibody profile1,5,6 — means that all individuals meeting stage 2 criteria may not share the same urgency of need. Yet without validated tools to guide prioritization, clinical experts suggested that any attempt to target those at highest risk remains speculative and risks introducing new forms of inequity. These considerations are compounded by current screening patterns in Canada where individuals identified with stage 2 are primarily those with a family history of T1D.
Structural inequalities may shape who is diagnosed and able to access care: Access to teplizumab will not only depend on clinical eligibility, but on the availability of specialized providers and infusion infrastructure. Clinical experts indicated that diagnosis, prescription, and monitoring would typically require an endocrinologist or pediatrician with experience in T1D as well as access to hospital or community-based IV infusion services. Given that teplizumab is delivered over 14 consecutive days, individuals living in rural or remote areas may face disproportionate barriers to receiving care, where specialist services and infusion infrastructure are less available and travel is often required. Further, clinical experts and published literature highlighted that those who pursue screening and access teplizumab are more likely to be white and relatively affluent.16 Without careful attention to implementation, access to this first-in-class therapy risks reinforcing existing patterns of privilege, offering preventive care not to those most at risk, but to those best positioned to seek it out. This is especially concerning considering persistent racial and socioeconomic disparities in T1D care and outcomes.
Misalignment between approved indication and evolving demand may create pressure for off-label use: The narrow indication for teplizumab, limited to individuals aged 8 years and older with stage 2 T1D, may not align with how demand evolves in practice, raising concerns about off-label use and provider burden. Clinical experts suggested that some families may advocate for access outside of the indicated population, including children under 8 or individuals recently diagnosed with stage 3. While clinical experts indicated that approximately 50% of people with T1D are identified as adults, the peak age of stage 3 onset in children is typically between 10 years and 14 years (and becoming younger in some countries),7 suggesting that stage 2 may begin well before the indicated threshold age of 8 years. Though clinical experts doubted that pediatric endocrinologists would prescribe teplizumab in these situations, they worried that providers may experience moral distress navigating parental pressure or media-influenced expectations, particularly where treatment is viewed as urgent or potentially life-altering if offered earlier in the care pathway. Early trial results on the use of teplizumab for early-stage 3 T1D are also emerging, which may further complicate clinical decision-making. These pressures raise ethical tensions around professional autonomy, responsible prescribing, and balancing patient needs and preferences with limitations in evidence and access, especially in a pediatric setting where beneficence, nonmaleficence, and trust are critical.
Health Systems Impact
Implementation challenges tied to health systems’ readiness and variation: Realizing the potential value of teplizumab will depend not only on clinical outcomes in the real world, but on the health system’s capacity to support equitable and effective implementation. While population-level screening is under exploration in Canada through initiatives such as CanScreen T1D, no such program currently exists, which has limited the identification of stage 2 T1D to those with a family history of T1D. Even if screening were to be expanded, ethical and logistical questions remain around how diagnostic pathways, treatment access, and follow-up care would be structured across jurisdictions. Equitable implementation of teplizumab at scale would require coordination across 3 core areas.
Screening infrastructure to identify individuals in stage 2 through laboratory testing for T1D-associated autoantibodies and early glycemic markers. While glycemic testing is widely available and accessible across Canada, screening for T1D-associated autoantibodies is not routinely offered and may require central coordination and expanded lab capacity in some regions.
Diagnostic and staging protocols to ensure accurate and consistent assessment of risk and eligibility. Introducing teplizumab into the health system would require not only screening infrastructure, but coordinated diagnostic pathways, follow-up care, and specialist oversight to ensure individuals identified in stage 2 receive timely and appropriate support. Managing individuals in a presymptomatic disease stage would also necessitate clearly defined care pathways with involvement of endocrinologists and other specialized health care professionals as well as psychosocial support, raising concerns about provincial variation in readiness and clinical capacity. Without standardized protocols for diagnosis, staging, and follow-up, individuals may face inconsistent care.
Access to infusion services and postinfusion monitoring. Teplizumab requires a 14-day course of IV infusions, typically delivered in hospital-based or outpatient clinics. While some public infrastructure exists, many infusion sites in Canada operate privately and are supported through manufacturer programs or out-of-pocket payment, raising concerns about equitable access, particularly for individuals in rural or underserved areas.17 For children receiving treatment, accessing infusion centres and then undergoing treatment over the course of 14 days may increase caregiver burden related to travel, time off work, and their responsibility in ongoing monitoring. Even after infusion, people may require metabolic surveillance and psychological support during what is still a presymptomatic stage of disease, potentially adding further strain to regions with limited specialist care.
Opportunity costs and alternative funding priorities: In light of ongoing uncertainty regarding the value of delayed progression to stage 3 T1D for health-related quality of life or common long-term T1D complications, some publications have suggested that public funding should also continue to prioritize diabetes education and access to insulin pumps, continuous glucose monitors, or hybrid closed-loop systems — all of which improve health outcomes for individuals already living with T1D.18
References
1.Insel RA, Dunne JL, Atkinson MA, et al. Staging presymptomatic type 1 diabetes: a scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care. 2015;38(10):1964-74. doi:10.2337/dc15-1419 PubMed
2.Beran D, Bandini A, Bosi E, et al. Type 1 diabetes screening: need for ethical, equity, and health systems perspective. Lancet Diabetes Endocrinol. 2025;13(3):175-176. doi:10.1016/S2213-8587(25)00029-4 PubMed
3.Haller MJ, Bell KJ, Besser REJ, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Screening, Staging, and Strategies to Preserve Beta-Cell Function in Children and Adolescents with Type 1 Diabetes. Horm Res Paediatr. 2024;97(6):529-545. doi:10.1159/000543035 PubMed
4.American Diabetes Association Professional Practice Committee. 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes—2025. Diabetes Care. 2024;48(Supplement_1):S27-S49. doi:10.2337/dc25-S002 PubMed
5.Jacobsen LM, Bocchino L, Evans-Molina C, et al. The risk of progression to type 1 diabetes is highly variable in individuals with multiple autoantibodies following screening. Diabetologia. 2020;63(3):588-596. doi:10.1007/s00125-019-05047-w PubMed
6.Felton JL, Redondo MJ, Oram RA, et al. Islet autoantibodies as precision diagnostic tools to characterize heterogeneity in type 1 diabetes: a systematic review. Commun Med (Lond). 2024;4(1):66. doi:10.1038/s43856-024-00478-y PubMed
7.Libman I, Haynes A, Lyons S, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr Diabetes. 2022;23(8):1160-1174. doi:10.1111/pedi.13454 PubMed
8.Jacobsen LM, Atkinson MA, Sosenko JM, Gitelman SE. Time to reframe the disease staging system for type 1 diabetes. Lancet Diabetes Endocrinol. 2024;12(12):924-933. doi:10.1016/S2213-8587(24)00239-0 PubMed
9.Besser REJ, Bell KJ, Couper JJ, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Stages of type 1 diabetes in children and adolescents. Pediatr Diabetes. 2022;23(8):1175-1187. doi:10.1111/pedi.13410 PubMed
10.Ladd JM, Sharma A, Rahme E, et al. Comparison of Socioeconomic Disparities in Pump Uptake Among Children With Type 1 Diabetes in 2 Canadian Provinces With Different Payment Models. JAMA Netw Open. 2022;5(5):e2210464. doi:10.1001/jamanetworkopen.2022.10464 PubMed
11.Tremblay ES, Liu E, Laffel LM. Health Disparities Likely Emerge Early in the Course of Type-1 Diabetes in Youth. J Diabetes Sci Technol. 2022;16(4):929-933. doi:10.1177/19322968221082646 PubMed
12.Agarwal S, Kanapka LG, Raymond JK, et al. Racial-Ethnic Inequity in Young Adults With Type 1 Diabetes. J Clin Endocrinol Metab. 2020;105(8):e2960-9. doi:10.1210/clinem/dgaa236 PubMed
13.Majidi S, Ebekozien O, Noor N, et al. Inequities in Health Outcomes in Children and Adults With Type 1 Diabetes: Data From the T1D Exchange Quality Improvement Collaborative. Clin Diabetes. 2021;39(3):278-283. doi:10.2337/cd21-0028 PubMed
14.Lipman TH, Hawkes CP. Racial and Socioeconomic Disparities in Pediatric Type 1 Diabetes: Time for a Paradigm Shift in Approach. Diabetes Care. 2021;44(1):14-16. doi:10.2337/dci20-0048 PubMed
15.Muñoz C, Floreen A, Garey C, et al. Misdiagnosis and Diabetic Ketoacidosis at Diagnosis of Type 1 Diabetes: Patient and Caregiver Perspectives. Clin Diabetes. 2019;37(3):276-281. doi:10.2337/cd18-0088 PubMed
16.O'Donnell HK, Simmons KM, Gitelman SE, et al. Real-world experiences of adult individuals or caregivers of children who received teplizumab treatment in stage 2 type 1 diabetes. Diabetes Obes Metab. 2025;27(5):2495-2506. doi:10.1111/dom.16246 PubMed
17.Grundy Q, Hart D, Elkhalifa S, et al. Mapping the Landscape of Infusion Care for People Prescribed IV Medicines in Canada. Can J Health Technol. 2025;5(1):1-23. doi:10.51731/cjht.2025.1066
18.Beran D, Abidha C, Adler A, et al. Teplizumab approval for type 1 diabetes in the USA. Lancet Diabetes Endocrinol. 2023;11(2):78-80. doi:10.1016/S2213-8587(22)00384-9 PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.