Drugs, Health Technologies, Health Systems
Reimbursement Review
Ravulizumab (Ultomiris)
Sponsor: Alexion Pharma GmbH
Therapeutic area: Generalized myasthenia gravis
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AChE
acetylcholinesterase
AChR
acetylcholine receptor
AE
adverse event
AESI
adverse event of special interest
Anti-AChR
anti–acetylcholine receptor
Anti-MuSK
anti–muscle-specific kinase
CDA-AMC
Canada’s Drug Agency
CDEC
Canadian Drug Expert Committee
CI
confidence interval
CrI
credible interval
DIC
deviance information criterion
FAS
full analysis set
FE
fixed-effect
gMG
generalized myasthenia gravis
HRQoL
health-related quality of life
IPD
individual patient data
IST
immunosuppressive therapy
ITC
indirect treatment comparison
IVIg
IV immunoglobulin
LSM
least squares mean
MAIC
matching-adjusted indirect comparison
MCID
minimal clinically important difference
MCMC
Markov Chain Monte Carlo
MDC
Muscular Dystrophy Canada
MG
myasthenia gravis
MG-ADL
Myasthenia Gravis Activities of Daily Living
MG-QoL15r
Myasthenia Gravis Quality of Life 15-item Scale - Revised
MGFA
Myasthenia Gravis Foundation of America
MID
minimal important difference
MMRM
mixed model of repeated measures
MuSK
muscle-specific kinase
Neuro-QoL
Quality of Life in Neurological Disorders
NMA
network meta-analysis
NMD4C
Neuromuscular Disease Network for Canada
NSIST
nonsteroidal immunosuppressive therapy
OLE
open-label extension
OR
odds ratio
PICOS
Population, Intervention, Comparison, Outcomes, and Study
PLEX
plasma exchange or plasmapheresis
QMG
Quantitative Myasthenia Gravis
RCP
randomized controlled period
RCT
randomized controlled trial
RE
random-effect
RTS
ravulizumab-treated set
SAE
serious adverse event
SEM
standard error of the mean
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Ravulizumab (Ultomiris) for IV infusion, 10 mg/mL and 100 mg/mL concentrate for solution for IV infusion |
Sponsor | Alexion Pharma GmbH |
Indication | For the treatment of adult patients with anti–AChR antibody–positive gMG |
Reimbursement request | As add-on therapy for adult patients with anti–AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChEIs, corticosteroids, and/or NSISTs |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | January 6, 2023 |
Recommended dosage | Loading dose on day 1, and maintenance dose on day 15 and q.8.w. thereafter by IV infusion:
|
AChEI = acetylcholinesterase inhibitor; AChR = acetylcholine receptor; gMG = generalized myasthenia gravis; NOC = Notice of Compliance; NSIST = nonsteroidal immunosuppressive therapy; q.8.w. = every 8 weeks.
Introduction
Myasthenia gravis (MG) is a chronic autoimmune disease in which antibodies against acetylcholine receptors (AChRs) or functionally associated molecules in the neuromuscular junction disrupt nerve impulse conduction, resulting in localized or generalized skeletal muscle weakness.1-4 In 10% to 15% of all patients with MG, weakness remains restricted exclusively to the eyes (ocular MG).1,3,5,6 The remainder of patients either are diagnosed with or progress within a few years to generalized myasthenia gravis (gMG), and their symptoms include eyelid drooping and double vision, altered facial expression, difficulty chewing and swallowing food, difficulty speaking, and in patients with more severe disease, problems with limb movement and breathing.3,6 Collectively, symptoms of MG negatively impact patients’ health-related quality of life (HRQoL).3 Globally, the prevalence rates of MG range from 150 cases to 200 cases per 1 million population, and the incidence rates range from 4 cases to 30 cases per million person-years.3,7 In Canada, the prevalence of MG is approximately 263 cases to 320 cases per 1 million population and its incidence is approximately 23 cases per 1 million population annually.8 Autoantibodies against AChR can be detected in approximately 80% of patients with gMG.3 According to the clinical expert consulted by Canada’s Drug Agency (CDA-AMC) for this review, 15% to 20% of patients with gMG have refractory disease. The prognosis of MG varies by symptom severity and response to treatment. Patients with severe or refractory symptoms are at higher risk for complications compared with those with mild or nonbulbar symptoms. MG may be associated with increased mortality.9
According to the clinician expert, the goal of treatment in most patients with gMG is to reduce disease symptoms (ideally aiming for minimal disease manifestation) as well as adverse effects of MG therapy and to allow the patient to function and work normally with good HRQoL. Other goals of treatment include avoiding MG exacerbations and myasthenic crisis, minimizing hospitalizations and intensive care unit admissions, and reducing the numbers and doses of therapies required for symptom control.
The initial symptomatic treatment for most patients with gMG is an acetylcholinesterase (AChE) inhibitor such as pyridostigmine. According to the expert, peripherally acting AChE inhibitors are used as symptomatic treatments for temporarily alleviating muscle weakness in these patients. A minority of patients with MG have a spontaneous remission or respond to AChE inhibitors; however, most patients need treatment with corticosteroids and/or steroid-sparing drugs when they do not reach their treatment goals with AChE inhibitors.
Corticosteroids are the first-line immunosuppressive therapy (IST) for patients with MG who remain symptomatic while on AChE inhibitors or those who desire better symptom control. Early use of oral steroids in patients with pure ocular symptoms may delay or reduce the risk of generalization and worsening of the underlying symptoms.10,11 Patients who do not respond to corticosteroids or who have comorbidities that are not suitable for treatment with corticosteroids may initiate treatment with nonsteroidal immunosuppressive therapies (NSISTs).12 The use of conventional therapy (AChE inhibitors, corticosteroids, and/or NSISTs) is associated with the slow onset of benefit, incomplete efficacy in eliminating MG symptoms, and significant toxicities.13-15 Other treatment options, such as immunomodulating therapies like plasma exchange or plasmapheresis (PLEX) and IV immunoglobulin (IVIg), are usually reserved for use on a short-term basis for life-threatening situations or crises, for use in some patients before surgery or corticosteroid treatment, to obtain a rapid treatment response, or for when treatments have been ineffective.10 Novel biologic treatments include efgartigimod alfa, eculizumab, and rituximab.12,16-21 Surgery (thymectomy) is a treatment option in select circumstances.20 Thymectomy is recommended in nonthymomatous, anti–AChR antibody–positive adult patients with gMG aged 50 years or younger if they are stable (as an early treatment option), as well as in patients with or without AChR antibodies if ISTs (which include both corticosteroids and NSISTs) elicit an insufficient response or are intolerable due to side effects.12
Ravulizumab is a terminal complement inhibitor that specifically binds to the complement protein C5 with high affinity, thereby inhibiting its cleavage to C5a and C5b and preventing the generation of membrane attack complex.22 In January 2023, ravulizumab was approved by Health Canada for the treatment of adult patients with anti–AChR antibody–positive gMG.22 It is supplied as a 10 mg/mL or 100 mg/mL concentrate for IV infusion. The recommended ravulizumab maintenance dosing in adult patients with gMG (aged 18 years or older) with a body weight greater than or equal to 40 kg is based on the patient’s body weight with maintenance doses administered every 8 weeks, starting 2 weeks after the loading dose. Patients must be vaccinated against meningococcal infections before, or at the time of, initiating ravulizumab unless the risks of delaying ravulizumab therapy outweigh the risks of developing a meningococcal infection.22 Ravulizumab was initially reviewed by CDA-AMC for the treatment of adults with anti–AChR antibody–positive gMG and received a negative funding recommendation from the Canadian Drug Expert Committee (CDEC) on August 24, 2023.23 The drug was resubmitted for review by the sponsor on the basis of the availability of new evidence from the pivotal CHAMPION-MG trial: the efficacy and harms of ravulizumab in 2 post hoc subgroups, the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort; additional open-label extension (OLE) follow-up data (with the final analysis representing up to 3.5 years of follow-up duration); and a new indirect treatment comparison (ITC). In this resubmission, the sponsor’s reimbursement request is as add-on therapy for adult patients with anti–AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChE inhibitors, corticosteroids, and/or NSISTs.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the call for input by CDA-AMC and from clinical experts consulted by CDA-AMC for the purpose of this review. The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Input
CDA-AMC received 1 patient group submission from Muscular Dystrophy Canada (MDC). MDC is a health charity that supports people affected by muscular dystrophies and related muscle diseases in Canada. MDC collected information from 215 patients impacted by MG through a health care experience survey and semistructured phone or virtual interviews. These patients consisted of 83 males and 132 females aged between 22 years and 78 years from all provinces in Canada. MDC also conducted an MG Canadian journey mapping project among patients living with MG via the completion of virtual interviews, round table sessions, surveys, and HRQoL measures. Respondents indicated that MG has a significant impact on productivity; fatigue, energy levels, and quality of sleep; respiratory health; mobility and strength; independence; relationships and social participation; eyes, vision, speech, and swallowing; mental health; quality of life; and the well-being of respondents’ families. MDC added that according to the respondents, while supportive treatments have had positive health outcomes, there are concerns about the long-term and sustained benefits of these treatments.
MDC noted that patients with gMG seek better control over their condition to minimize the impact of symptoms, side effects, and disease exacerbations on their lives, allowing them to maintain their independence and avoid serious hospital admissions. MDC added that patients stated that they would be willing to deal with the side effects of medications if these aspects of MG were better controlled. According to MDC, respondents indicated that currently available therapies may decrease MG exacerbations but do not improve their overall HRQoL.
Based on the patient group input, the factors that are important in evaluating different treatments include treatment administration, potential side effects, the duration and frequency of treatments, convenience (e.g., travel time and parking for clinic visits), and financial impact (costs).
MDC explained that patients value new treatments that offer improved disease control and symptom relief, and extend dosing intervals.
In terms of diagnostic testing, MDC stated that 85% of respondents reported significant difficulty in getting diagnosed. The vast majority of patients found the test to be cost-effective but noted the overall lengthy process with many missed opportunities (e.g., delays, misdiagnoses, costs incurred). A diagnosis received as part of hospitalization was reported as a seamless experience.
MDC believed that there is a pressing need for improved treatment options to address the ongoing challenges faced by patients with MG and ravulizumab provides a new treatment option for patients with MG that has demonstrated efficacy, safety, and improved dosing convenience compared to other treatment options.
Clinician Input
Input From Clinical Experts Consulted by the Review Team for This Resubmission
The clinical expert consulted for this review identified unmet needs associated with currently available treatments for patients with gMG whose symptoms persist even if they have been treated with conventional medications for this disease (such as AChE inhibitors, corticosteroids, and/or NSISTs). The unmet needs are as follows: although multiple treatment options are available to patients with gMG, some patients do not have adequate response to the existing treatments and 15% to 20% of patients have refractory disease and require alternative therapeutic options; patients may become intolerant of ISTs; and some exiting treatments are only suitable for select patients. Because of its unique mechanism of action, ravulizumab — a complement C5 inhibitor — could be another treatment option for patients living in Canada with gMG whose disease had an inadequate response to or did not respond to or who cannot tolerate conventional ISTs.
The clinical expert indicated that patients in Canada with significant symptoms of gMG whose disease has not responded to or who cannot tolerate conventional immunosuppressants would be eligible to receive treatment with ravulizumab. The initiation of ravulizumab therapy could be considered when patients are experiencing significant symptoms of gMG; are resistant to conventional therapies, requiring multiple concomitant ISTs (which include corticosteroids and NSISTs); or are patients who cannot tolerate the significant side effects of conventional immunosuppressants.
The expert noted that in clinical practice, regular follow-up visits with a neuromuscular specialist or a neurologist are required to monitor the patient’s response to treatment, using certain MG-specific scales (e.g., the Myasthenia Gravis Activities of Daily Living [MG-ADL]) tool as well as the treating physician’s clinical examination.
The expert also noted that treatment with ravulizumab should be discontinued when a patient does not respond well to the treatment or experiences significant side effects of the treatment such as meningococcal infections, or when a patient prefers to discontinue treatment. In addition, if the patient shows long-term stability of neurologic status and is perceived to have achieved remission, the clinician may suggest holding the treatment under observation.
The expert indicated that the initiation of treatment with ravulizumab and the follow-up assessments could be provided by a neurologist with expertise in MG management.
Clinician Group Input
One input was received from the Neuromuscular Disease Network for Canada (NMD4C), a new pan-Canadian network that brings together clinical, scientific, technical, and patient expertise to improve care, research, and collaboration in neuromuscular disease. The mission of NMD4C is to improve the care, research, and treatment of neuromuscular diseases for all people living in Canada. The information presented in this submission was gathered from 8 clinicians with experience in treating gMG.
NMD4C noted that the goals of therapy are to minimize morbidity and mortality from MG, keep patients out of hospital, improve quality of life, prevent repeated attacks, and prevent prolonged, untreated, or partially treated MG. According to the clinician input, the current mainstay of therapies for MG includes supportive therapies, symptomatic treatments, and disease-modifying strategies. NMD4C provided opinions consistent with the clinical expert consulted for this review regarding the unmet needs with currently available treatments: limited available options for active and refractory disease, limited response to the traditional immunotherapies, the slow onset of treatment action, and serious side effects.
NMD4C believes ravulizumab inhibits immune-mediated damage to the neuromuscular junction rather than being a symptomatic treatment. The place in therapy for ravulizumab would likely be in patients with inadequate MG response: after treatment with pyridostigmine, and after treatment with either steroids and/or other ISTs, including steroid-sparing immunosuppressive drugs. Ravulizumab is likely to affect the treatment paradigm of patients with refractory and nonrefractory MG who are not responsive to first-line and second-line therapies or require chronic IVIg infusions or PLEX. It may also be considered in patients who are intolerant of other immunomodulatory treatments.
NMD4C stated that patients with MG should try other treatments before initiating ravulizumab, which requires periodic IV infusions over an extended period, is unlikely to induce long-term disease remission, is likely to be expensive, will likely not be available in smaller cities or nonspecialized centres, and requires extensive expertise.
Based on the clinician group input, adult patients who are seropositive for anti–AChR antibodies and have gMG would be best suited for treatment with ravulizumab; there are no data on the efficacy of ravulizumab for a minority population of patients with MG — including those aged younger than 18 years, those who had thymectomy within the past year, those with thymic carcinoma or who are pregnant or breastfeeding, those with anti–muscle-specific kinase (anti–MuSK) or anti–LRP4 antibodies, or seronegative patients. Patients with MG who are anti–AChR antibody–positive who have not responded to pyridostigmine and to steroids and/or oral ISTs or are additionally dependent on periodic PLEX or chronic IVIg therapy are most in need.
NMD4C noted that the diagnosis must have been confirmed clinically and supported by confirmatory laboratory tests before treatment with ravulizumab.
NMD4C explained that the outcomes that are used to determine whether a patient is responding to treatment in clinical practice include increased survival, the avoidance of emergency department visits or hospital admissions (including intensive care unit admissions), the avoidance of the need for rescue therapy as well as maintenance therapy with IVIg and plasmapheresis, a reduction in the dose and/or duration of concomitant steroids, a reduction in the level of fatigable weakness, and an improvement in activities of daily living and quality of life.
Based on the NMD4C input, the factors that should be considered when deciding to discontinue treatment include the amount of clinical improvement or response, the duration of time spent in a clinically stable state, adverse events (AEs) associated with the treatments, and inconvenience associated with the therapy.
NMD4C added that an appropriate setting for treatment includes a clinical team with general knowledge of MG, as well as appropriate nursing experience in venous access issues, managing IV medications, and managing potential adverse effects. It is recommended that ravulizumab be prescribed by neurology specialists with expertise in MG diagnosis, assessment, monitoring, and the management of patients with MG.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. Please refer to Table 5 for further information. The following were identified as key factors that could potentially impact the implementation of the CDA-AMC recommendation for ravulizumab:
relevant comparators
considerations for the initiation of therapy
considerations for the continuation or renewal of therapy
considerations for the discontinuation of therapy
considerations for the prescribing of therapy
generalizability
care provision issues
system and economic issues.
Clinical Evidence
Systematic Review
Description of Studies
The CHAMPION-MG trial (N = 175)24 was a phase III, double-blind, multicentre, placebo-controlled randomized controlled trial (RCT) with an OLE period of up to 4 years. The primary objective of the CHAMPION-MG trial was to evaluate the safety and efficacy of ravulizumab compared with placebo in complement inhibitor–naive adult patients with gMG. The randomized controlled period (RCP) portion of the trial is complete (the data cut-off date was May 11, 2021; the database was locked on June 30, 2021) and the OLE concluded on May 25, 2023 (the last patient’s last visit).
In this resubmission, the sponsor provided new clinical evidence to support its revised reimbursement request: ravulizumab as add-on therapy for adult patients with anti–AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChE inhibitors, corticosteroids, and/or NSISTs. Post hoc analyses were performed in 2 cohorts, the concomitant IST optimized cohort (N = ███, █████ and the refractory concomitant IST optimized cohort (N = █████████); these cohorts were the focus of this Clinical Review Report. The purpose of the post hoc analyses was to evaluate the efficacy and safety of 26-week treatment with ravulizumab or placebo in patients with anti–AChR antibody–positive gMG. Therefore, the inclusion criteria of the previous Study ADAPT (efgartigimod alfa versus placebo) and Study REGAIN (eculizumab versus placebo) were adopted to select patients who would be considered to have either IST optimization, or IST optimization with refractory disease (patients who do not achieve symptom control after 12 months of treatment with 2 or more ISTs, or 1 or more IST and chronic IVIg or PLEX treatment based on the criteria for eculizumab in the pivotal Study REGAIN) at the time of study enrolment from the CHAMPION-MG trial, respectively. The primary efficacy end point (change from baseline in the MG-ADL score at week 26) was the same as that in the primary analysis in the full population. Other outcomes in these analyses included change from baseline in the Quantitative Myasthenia Gravis (QMG) total score, improvement of at least 5 points in the QMG total score from baseline, change from baseline in the Myasthenia Gravis Quality of Life 15-item Scale - Revised (MG-QoL15r) score, change from baseline in the Quality of Life in Neurological Disorders (Neuro-QoL) fatigue score, improvement of at least 3 points in the MG-ADL total score from baseline, the incidence of clinical deterioration and/or an MG crisis, and safety. In the subgroup population of patients who received optimized IST or patients who were refractory despite having received optimized IST, all outcomes analyzed were exploratory. Baseline demographic and disease characteristics of the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort were consistent with the full CHAMPION-MG trial population in terms of the distribution of the Myasthenia Gravis Foundation of America (MGFA) classification, the baseline MG-ADL score (approximately 9 points across the 3 groups), the baseline QMG score (ranging from 14 points to 15 points across the 3 groups), and age at diagnosis.
Efficacy Results
The evidence examined in this review was informed by 2 post hoc cohorts: the concomitant IST optimized cohort (patients receiving concomitant optimized IST, with or without refractory disease), and the refractory concomitant IST optimized cohort (patients receiving concomitant optimized IST, with refractory disease).
MG-ADL Total Score
The MG-ADL total score ranges from 0 to 24; higher scores indicate a greater severity of symptoms and a more significant impact on a patient’s daily activities. Although no minimal important difference (MID) has been estimated, an improvement of approximately 2 points in the MG-ADL total score represents the minimal clinically important difference (MCID) and is a recommended response threshold in patients with MG.25 This MID was estimated to interpret the change from baseline in an individual patient; an MID for between-group effects has not been estimated. In the concomitant IST optimized cohort, during the RCP, the least squares mean (LSM) (95% confidence interval [CI]) change from baseline to week 26 in the MG-ADL total score was █████████████████ in the ravulizumab group compared to █████████████████ in the placebo group. The LSM treatment difference was ███████████████████████). In the refractory concomitant IST optimized cohort, the LSM (95% CI) change from baseline to week 26 in the MG-ADL total score was ████████████████) in the ravulizumab group compared to ████████████████) in the placebo group. The LSM treatment difference was ███████████████████████). ███████████████████████████████████████████████████████████
QMG Total Score
The QMG total score ranges from 0 to 39, where higher scores indicate greater disease severity. A definite MID for the QMG scale has not been established, although a threshold ranging between 2 points and 3 points depending on disease severity has been suggested for patients with MG,26,27 which represents the MCID for the QMG scale. This MID was estimated to interpret the change from baseline in an individual patient; an MID for between-group effects has not been estimated. In the concomitant IST optimized cohort, the LSM (standard error of the mean [SEM]) change from baseline to week 26 in the QMG total score was ████ (████) in the ravulizumab group and ████████) in the placebo group. The LSM treatment difference was ████ (████████████████████). In the refractory concomitant IST optimized cohort, the LSM (SEM) change from baseline to week 26 in the QMG total score was ████ (████) in the ravulizumab group and ████ (████) in the placebo group during the RCP. The LSM treatment difference was ███████████████████████). ███████████████████████████████████████████████████████████████████
QMG 5-Point or Greater Response
A clinical responder was defined as a patient who achieved a 5-point or greater improvement in the QMG total score. A 5-point or greater improvement in the QMG total score represents a higher threshold and exceeds the established MCID of 2 points or 3 points for the QMG total score scale. In the concomitant IST optimized cohort, █████ of patients in the ravulizumab group compared to ████ in the placebo group achieved at least a 5-point improvement. The between-group difference was ███████████████████ and the OR was █████ (██████████████████████). In the refractory concomitant IST optimized cohort, the proportion of patients meeting the clinical responder definition for QMG improvement was █████ in the ravulizumab group versus ████ in the placebo group, with a between-group difference of █████ (█████████████) and an OR of █████ (95% █████████████; | | ██████). ████████████████████████████████████████████████████████.
MG-ADL 3-Point or Greater Response
Patients who achieved at least a 3-point improvement in the MG-ADL total score were considered responders. A 3-point or greater improvement in MG-ADL total score represents a higher threshold and exceeds the established MCID of 2 points for the MG-ADL total score scale. In the full analysis set (FAS) of the CHAMPION-MG trial, this outcome was tested after a prior nonsignificant result of the hierarchical testing procedure and therefore is at an increased risk of type I error (falsely rejecting the null hypothesis). In the concomitant IST optimized cohort, the proportion of patients who met the clinical responder definition for MG-ADL improvement of at least 3 points was ████% (███████████) in the ravulizumab group compared to ████% █████████████) in the placebo group, with a between-group difference of ███████████████████ and an OR of █████ (██████████). In the refractory concomitant IST optimized cohort, the proportion of patients meeting the clinical responder definition for MG-ADL improvement was █████ (███████████) in the ravulizumab group compared to ████% (███████████) in the placebo group, with a between-group difference of ███████████████████ and an OR of █████ (██████████). ██████████████████████████████████████████████████
MG-QoL15r Total Score and Neuro-QoL Fatigue Score
HRQoL and fatigue were assessed based on LSM change from baseline in the MG-QoL15r total score and Neuro-QoL fatigue score. An MID for MG-QoL15r or Neuro-QoL fatigue in patients with MG has not been estimated. Since the MG-QoL15r outcome did not reach statistical significance in the overall trial population, the P values for the subsequent secondary end points included in the prespecified hierarchical testing order including the Neuro-QoL fatigue score were considered nominal. The between-group differences in these outcomes for both the primary analysis and the 2 cohorts were consistent. In the concomitant IST optimized cohort, the LSM change from baseline to week 26 in the MG-QoL15r total score was ████ (███████████) in the ravulizumab group and ████ (███████████) in the placebo group during the RCP. The LSM treatment difference was ████ (███████████████████). In the refractory concomitant IST optimized cohort, the LSM change from baseline to week 26 in the MG-QoL15r total score was ████████████████ in the ravulizumab group and ████ (███████████) in the placebo group during the RCP. The LSM treatment difference was ████ (███████████████████). In the concomitant IST optimized cohort, the LSM change from baseline to week 26 in the Neuro-QoL fatigue score was ████ (█████████████) in the ravulizumab group and ████ (███████████) in the placebo group during the RCP. The LSM treatment difference was ████ (███████████████████). In the refractory concomitant IST optimized cohort, the LSM change from baseline to week 26 in the Neuro-QoL fatigue score was -███ (████████████) in the ravulizumab group and ████ (████████████) in the placebo group during the RCP. The LSM treatment difference was ████ (███████████████████). █████████████████████████████████████████████████████████
Incidence of Clinical Deterioration and MG Crisis
During the RCP, in the concomitant IST optimized cohort, █████████████ in the ravulizumab group and ███████████████ in the placebo group reported clinical deterioration. In the refractory concomitant IST optimized cohort, ████████ (██████ in the ravulizumab group and ██████████████ in the placebo group reported clinical deterioration. In each cohort, an MG crisis was reported by || patient from the placebo group. No patients from the ravulizumab group reported an MG crisis.
Harms Results
███████████████████████████████████████████████████████████████████████████
The percentage of patients with any AEs was █████ (██ patients) of placebo-treated patients and █████ (██ patients) of ravulizumab-treated patients in the concomitant IST optimized cohort and █████ (██ patients) of placebo-treated patients and █████ (██ patients) of ravulizumab-treated patients in the refractory concomitant IST optimized cohort. The most commonly reported AEs in these 2 cohorts included diarrhea (concomitant IST optimized cohort = █████ in the ravulizumab group versus █████ in the placebo group; refractory concomitant IST optimized cohort = █████ in the ravulizumab group versus █████ in the placebo group) and headache (concomitant IST optimized cohort = █████ in the ravulizumab group versus █████ in the placebo group; refractory concomitant IST optimized cohort = █████ in the ravulizumab group versus █████ in the placebo group). Most AEs were grade 1 and grade 2 in severity.
In the concomitant IST optimized cohort, the percentage of patients with serious adverse events (SAEs) was higher in the ravulizumab group (█████) compared to the placebo group (█████). In the refractory concomitant IST optimized cohort, █████ of ravulizumab-treated patients and █████ of patients in the placebo group experienced at least 1 SAE. Commonly reported SAEs were not reported for these 2 cohorts.
In both cohorts, there was ████████ treated with ravulizumab who discontinued the study drug due to an AE. In both cohorts, there were █████████ treated with ravulizumab who died, and ██ death was reported for the placebo group. Meningococcal infection was considered a notable harm for treatment with ravulizumab. No events of meningococcal infection were reported during the RCP in the entire study population.
Table 2: Summary of Key Results From the Randomized Controlled Period of CHAMPION-MG Trial, Cohort Analyses
Outcome | Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort | Full population | |||
|---|---|---|---|---|---|---|
Placebo ████ | Ravulizumab ████ | Placebo ████ | Ravulizumab ████ | Placebo N = 89 | Ravulizumab N = 86 | |
Change from baseline in total MG-ADL score at week 26 (FAS)a | ||||||
Baseline MG-ADL score, mean (SD) | ███████ | ███████ | ███████ | ███████ | 8.9 (2.30) | 9.1 (2.62) |
LSM (SEM or 95% CI) | █████████ | █████████ | █████████ | █████████ | −1.4 (−2.1 to −0.7) | −3.1 (−3.8 to −2.3) |
LSM treatment group difference vs. control (95% CI) | ████████████████ | ████████████████ | −1.6 (−2.6 to −0.7) | |||
P value | ██████ | ██████ | 0.0009 | |||
Change from baseline in total QMG score at week 26 (FAS)a | ||||||
Baseline QMG score, mean (SD) | █████████ | █████████ | █████████ | █████████ | 14.5 (5.26) | 14.8 (5.21) |
LSM (SEM or 95% CI) | █████████ | █████████ | █████████ | █████████ | −0.8 (−1.7 to 0.1) | −2.8 (−3.7 to −1.9) |
LSM treatment group difference vs. control (95% CI) | ████████████████ | ███████████████ | −2.0 (−3.2 to −0.8) | |||
P value | ██████ | ██████ | 0.0009 | |||
Proportion of patients with improvements of at least 5 points in QMG score at week 26 (FAS)a | ||||||
Adjusted percentage (95% CI) | ████████████ | ██████████████ | ████████████ | ██████████████ | 11.3 (5.6 to 21.5) | 30.0 (19.2 to 43.5) |
OR (95% CI) | ████████████████ | ████████████████ | 3.350 (1.443 to 7.777) | |||
P value | ██████ | ██████ | 0.0052 | |||
Proportion of patients with improvements of at least 3 points in MG-ADL score at week 26 (FAS)a | ||||||
Adjusted percentage (95% CI) | ██████████████ | ██████████████ | ██████████████ | ██████████████ | 34.1 (23.8 to 46.1) | 56.7 (44.3 to 68.3) |
OR (95% CI) | ███████████████ | ███████████████ | 2.5 (1.33 to 4.80) | |||
P value | ██████ | ██████ | 0.0049 | |||
Change from baseline in MG-QoL15r score at week 26 (FAS)a | ||||||
LSM (SEM) | █████████ | █████████ | █████████ | █████████ | −1.6 (0.70) | −3.3 (0.71) |
Ravulizumab difference vs. placebo (95% CI) | ██████████████ | ██████████████ | −1.7 (−3.4 to 0.1) | |||
P value | ██████ | ██████ | 0.0636 | |||
Change from baseline in Neuro-QoL fatigue score at week 26 (FAS)a | ||||||
LSM (SEM) | █████████ | █████████ | █████████ | █████████ | −4.8 (1.87) | −7.0 (−1.92) |
Ravulizumab difference vs. placebo (95% CI) | ███████████████ | ███████████████ | −2.2 (−6.9 to 2.6) | |||
P value | ██████ | ██████ | 0.3734 | |||
Harms, n (%) (safety population) | ||||||
AEs | ███████ | ███████ | ███████ | ███████ | 77 (86.5) | 78 (90.7) |
SAEs | ███████ | ███████ | ██████ | ███████ | 14 (15.7) | 20 (23.3) |
WDAEs | || | ██████ | || | █████ | 3 (3.4) | 2 (2.3) |
Deaths | 0 | ██████ | 0 | █████ | 0 | 2 (2.3) |
Notable harms, n (%) (safety population) | ||||||
Meningococcal infection | 0 | 0 | 0 | 0 | 0 | 0 |
AE = adverse event; CI = confidence interval; FAS = full analysis set; IST = immunosuppressive therapy; LSM = least squares mean; MG-ADL = Myasthenia Gravis Activities of Daily Living; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item Scale - Revised; MMRM = mixed model of repeated measures; Neuro-QoL = Quality of Life in Neurological Disorders; OR = odds ratio; QMG = Quantitative Myasthenia Gravis; SAE = serious adverse event; SD = standard deviation; SEM = standard error of the mean; vs. = versus; WDAE = withdrawal due to adverse event.
aAll efficacy outcomes in Table 2 analyzed in the full population were multiplicity-adjusted using a hierarchical testing strategy. However, none of the P values in the cohort analyses were multiplicity-adjusted.
Sources: Clinical Study Report for the CHAMPION-MG trial,24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
This is a resubmission of the initial ravulizumab review. In the previous review on ravulizumab, CDEC issued a negative reimbursement recommendation in 2023 based on the evidence submitted to CDA-AMC. The current review focuses on 2 post hoc cohorts that were identified from the FAS in the CHAMPION-MG trial: a concomitant IST optimized cohort and a refractory concomitant IST optimized cohort. The criteria and definitions used for patient selection for these 2 cohorts were considered reasonable and acceptable in clinical practice, according to the clinical expert consulted for this review. Based on the patient characteristics at baseline (which were similar to those reported in the full population) and the patients’ previous IST treatment history, the selected cohorts of patients represented a heavily pretreated patient population that, despite a lengthy duration of IST treatment, continued to experience significant gMG symptoms. Theoretically, post hoc analyses that are not prespecified in a trial’s analysis plan can be at risk of bias due to selective reporting. However, the sponsor provided clear justification for the selected subpopulations using criteria informed by the other gMG trials to provide directly relevant information related to a previous negative reimbursement recommendation. Additionally, the same prespecified analysis methods of the CHAMPION-MG trial were used to analyze the subgroup data, and results for all relevant end points were presented. As a result, any concern for selective reporting is minimized. In these 2 subgroups, patients’ baseline demographic and disease characteristics were generally well balanced between treatment groups and were similar to the FAS population. Also similar to the FAS, minor imbalances were observed for ████████████████████ (██████████████████████████████████████████████████████████████████████████████████████████████████) and ████████████████████████. The imbalances in the FAS could be due to the small sample size, which would have been exacerbated in the smaller subgroups. The clinical expert consulted by the review team noted that these may not have a significant impact on result interpretation. Tests for subgroup differences between the subgroup populations and the rest of the FAS were performed for the MG-ADL score and QMG score. However, these analyses were post hoc and the CHAMPION-MG trial was not powered to find a difference between the groups. Otherwise, results from these post hoc subgroups can be interpreted as having consistency with the main analyses of the CHAMPION-MG study and sharing the same limitations of those analyses. In addition, it should be considered that the small sample size in these 2 subgroups (the concomitant IST optimized cohort accounted for ███ of the full population and the refractory concomitant IST optimized cohort was ████ of the full population) could have resulted in insufficient power to detect true between-group differences, and multiplicity was not controlled using hierarchical testing. Therefore, there was an increasing risk of type I error (i.e., falsely rejecting the null hypothesis) rate for the investigated outcomes that achieved statistical significance at a conventional alpha of 0.05.
The reimbursement request also includes patients who have had an adequate trial of AChE inhibitors and no ISTs; these patients are not included in the 2 post hoc cohorts but were studied in the FAS in the CHAMPION-MG trial. A similar proportion of patients who received AChE inhibitors but no ISTs were enrolled in the CHAMPION-MG and ADAPT trials (i.e., approximately 10% of the overall trial populations). The NMD4C clinician group and the clinical expert consulted for this review agreed that while the place in therapy for ravulizumab would also include patients who had received AChE inhibitors but not ISTs, it would be reasonable for patients with gMG to try other treatments before initiating ravulizumab, which requires periodic IV infusions over an extended period, is likely to be expensive, may not be available in smaller cities or nonspecialized centres, and requires extensive expertise.
Patient selection for these 2 subgroups was based on the inclusion criteria from other RCTs: Study ADAPT and Study REGAIN. According to the clinical expert consulted for this review, the definitions used to identify patients are reasonable and adequately reflect the patients who experience unmet needs in the treatment of gMG in clinical settings in Canada (i.e., patients with refractory gMG as well as those whose disease showed response to a prior gMG treatment but responded inadequately to existing standards of gMG therapy). Furthermore, based on the duration of prior ISTs and concomitant ISTs used in the 2 subgroups before enrolment in the CHAMPION-MG trial, the clinical expert consulted for this review considered patients in these subgroups to have entered the CHAMPION-MG trial on optimized ISTs.
Because the concomitant conventional therapy was required to remain stable during the RCP, except in the case of rescue therapy, ravulizumab was not compared to any individual or combination conventional therapy as it would typically be used in clinical practice (i.e., altering doses or adding additional medications to suit patients’ current symptoms or other needs). Similar protocol requirements for concomitant ISTs are common across trials in patients with gMG to ensure consistency and to prevent the confounding of trial results. Notably in Study ADAPT (efgartigimod alfa versus placebo) and Study REGAIN (eculizumab versus placebo), a change in the type or dose of concomitant conventional care was not allowed unless deemed medically necessary.
The RCP of the CHAMPION-MG trial was 26 weeks. The longer-term treatment effect of ravulizumab can only be assessed in the OLE period of this study. Moreover, the CHAMPION-MG trial did not provide evidence for the comparisons between ravulizumab and other currently available active treatments for gMG.
Long-Term Extension Studies
Description of Studies
One long-term extension study is summarized here to provide evidence regarding the long-term efficacy and safety of ravulizumab in patients with gMG. In the current resubmission, OLE data from the pivotal study of up to 3.5 years is available. At the end of the 26-week RCP, all patients were eligible to enter the OLE and receive open-label ravulizumab. Following the 26-week RCP, patients in the placebo group received a blinded loading dose of ravulizumab and patients in the ravulizumab group received a blinded ravulizumab dose of 900 mg. Starting week 28, all patients began open-label ravulizumab maintenance doses every 8 weeks.
Efficacy Results
In the OLE set in the ravulizumab-ravulizumab group, the LSM change from RCP baseline in the MG-ADL total score was −4.0 (95% CI, −5.3 to −2.8) at week 164 during the OLE period. In the placebo-ravulizumab group, the LSM change from RCP baseline was −3.6 (95% CI, −4.8 to −2.3) at week 164. In the ravulizumab-ravulizumab concomitant IST optimized cohort, the LSM change from OLE baseline in the MG-ADL total score was ███████████████ at week 28 and ████████████████ at week 164. In the placebo-ravulizumab concomitant IST optimized cohort, the LSM change from OLE baseline was █████████████████ at week 28 and █████████████████ at week 148. In the ravulizumab-ravulizumab refractory concomitant IST optimized cohort, the LSM change from OLE baseline in the MG-ADL total score was ███████████████ at week 28 and ████████████████ at week 148. In the placebo-ravulizumab refractory concomitant IST optimized cohort group, the LSM change in the MG-ADL total score from OLE baseline was █████████████████ at week 28 and █████████████████ at week 148. In the OLE set, in the ravulizumab-ravulizumab and placebo-ravulizumab groups, the LSM change from RCP baseline in the QMG total score was █████████████████ and █████████████████ at week 164, respectively. In the ravulizumab-ravulizumab and placebo-ravulizumab groups of the concomitant IST optimized cohort, the LSM change from OLE baseline in the QMG total score was ████████████████ at week 164 and █████████████████ at week 148, respectively.
In the ravulizumab-ravulizumab and placebo-ravulizumab groups of the refractory concomitant IST optimized cohort, the LSM change from OLE baseline in the QMG total score was ███████████████ and █████████████████ at week 148, respectively. In the OLE set, based on a 5-point or greater improvement in the QMG total score from the RCP baseline, the proportion of clinical responders in the ravulizumab-ravulizumab group and placebo-ravulizumab group was ██████████████████ and █████████████████ at week 164, respectively.
In the ravulizumab-ravulizumab and placebo-ravulizumab groups of the concomitant IST optimized cohort, the proportion of patients with a 5-point or greater improvement in the QMG total score from the RCP baseline was ██████████████████ and █████████████████) at week 164, respectively.
In the ravulizumab-ravulizumab and placebo-ravulizumab groups of the refractory concomitant IST optimized cohort, the proportion of patients with a 5-point or greater improvement in their QMG total score from the RCP baseline was ██████████████████ and ██████████████████ at week 164, respectively.
In the OLE set, in the ravulizumab-ravulizumab and placebo-ravulizumab groups, the LSM change from RCP baseline in the MG-QoL15r total score was ████████████████ and █████████████████ at week 164, respectively.
In the OLE set, in the ravulizumab-ravulizumab and placebo-ravulizumab groups, the LSM change from RCP baseline in the Neuro-QoL fatigue score was ███████████████████ and ███████████████████ at week 164, respectively.
In the OLE set, based on a 3-point or greater improvement in the MG-ADL total score from RCP baseline, the proportion of clinical responders in the ravulizumab-ravulizumab and placebo-ravulizumab groups was ██████████████████ and ██████████████████ at week 164, respectively.
Harms Results
During ravulizumab treatment, 96.4% of patients experienced at least 1 AE. The most commonly reported AEs (≥ 10% of total patients) in the ravulizumab-treated set (RTS) were COVID-19 (36.1%), headache (23.1%), diarrhea (17.2%), arthralgia (13.6%), back pain (13%), nausea (13%), urinary tract infection (12.4%), nasopharyngitis (11.8%), fatigue (10.7%), and dizziness (10.1%). The total number of patients with ravulizumab infusion interruption due to AEs was 8 (4.7%) patients and 74 (43.8%) patients who reported potential infusion reactions during ravulizumab treatment. SAEs reported by 1 patient or more included COVID-19 (6 patients), MG (5 patients), COVID-19 pneumonia (4 patients), cellulitis and pneumonia (3 patients each), and erysipelas, urinary tract infection, spinal compression fracture, intervertebral disc protrusion, transient ischemic attack, congestive cardiac failure, pyrexia, dyspnea, dysphagia, dehydration, and nephrolithiasis (2 patients each).
In the RTS, there were 8 deaths throughout the entirety of the study period. Two deaths occurred during the RCP (due to COVID-19 pneumonia and cerebral hemorrhage) and 6 deaths occurred during the OLE period due to the following reasons: COVID-19 (3 patients), toxicity due to various drugs (1 patient), dehydration (1 patient), and an unknown reason (1 patient).
████ patients had AEs that were unrelated to the study drug and led to discontinuation. No meningococcal infections were reported during the study.
Critical Appraisal
The lack of control group precludes causal statements about benefit and harm compared with any comparator. The open-label nature of the study may increase the risk of bias in determining the magnitude of the safety outcomes and efficacy end points that include more subjective assessments because the lack of blinding may affect patients’ expectations of treatment. The direction and magnitude of these potential biases remain unclear. Patients of the OLE were patients who did not drop out of the placebo-controlled study (92%), which puts the results at some risk of selection bias that is likely to be favouring ravulizumab. Of the patients who started the placebo-controlled phase, 123 patients completed the OLE. There is therefore a risk of bias due to missing outcome data in both the placebo-ravulizumab and ravulizumab-ravulizumab arms, with the impact on the direction of treatment effect over time not clear. The limitations of the post hoc analyses of the subgroups mirror those discussed in the systematic review section; however, these concerns are minimized as the findings for these groups were generally consistent with the overall population.
Indirect Comparisons
Description of Studies
One sponsor-submitted network meta-analysis (NMA) report compared the efficacy and harms of ravulizumab relative to currently available active treatments (efgartigimod alfa, eculizumab, IVIg, and rituximab) for the treatment of adult patients with anti–AChR antibody–positive gMG in the concomitant IST optimized cohort as well as the refractory concomitant IST optimized cohort.29 In total, 7 RCTs were included in the ITC. The sponsor also submitted a matching-adjusted indirect comparison (MAIC) report comparing ravulizumab relative to efgartigimod alfa at various time points, although this was for the overall trial populations rather than for specific subgroups.30
Efficacy Results
Comparative evidence of ravulizumab to other active treatments for gMG in the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort was available through sponsor-submitted NMA. Based on the results of the NMA, the evidence is insufficient to conclude whether ravulizumab differs from efgartigimod alfa, rituximab, or IVIg in terms of change from baseline in the MG-ADL total score or QMG total score in the concomitant IST optimized cohort, or whether ravulizumab differs from eculizumab in terms of change in the MG-ADL total score or QMG total score in the refractory concomitant IST optimized cohort.
Evidence from the MAIC report is insufficient to conclude whether ravulizumab differs from efgartigimod alfa in improvement in the MG-ADL total score in patients with gMG who received a previous stable dose of IST.
Harms Results
The evidence from the NMA was not sufficient to conclude whether ravulizumab differs from the other active treatments in the risk of discontinuation of the study drug due to AEs in the overall patient population with gMG.
Critical Appraisal
A priori protocols for the sponsor-submitted NMA or MAIC were not available; therefore, it cannot be known whether the analyses presented were selected from multiple analyses of the data.
One of the major concerns for NMA is that the included trials could be highly heterogeneous in terms of study design and patient characteristics at baseline. Seven RCTs were included in the NMA: 6 for the analyses in the concomitant IST optimized cohort and 2 for the analyses in the refractory concomitant IST optimized cohort. Heterogeneities were identified in the analysis populations, which included study design (phase of study, study time points, and outcome measures in different ways) and patient characteristics at baseline (age, gender, and baseline MG-ADL scores).
These differences would undermine the validity of the NMA, which relies on the transitivity assumption being upheld (i.e., that the trials are similar on all important effect modifiers). The limited number of included studies did not allow for metaregression or other techniques to adjust for differences in effect modifiers across studies within the NMA. The rarity of the population of interest limits the size and number of clinical studies completed with potential comparators and adds to the practical challenges when indirectly comparing treatment options.
Usually, including post hoc subgroups in the analyses may raise concerns since these analyses are not prespecified and can be at risk of bias due to selective reporting (e.g., there is a risk that the presented results are selected from multiple analyses of the data based on their direction, magnitude, or statistical significance). However, the sponsor provided clear justification for the selected subpopulations using criteria informed by other MG trials. Additionally, various sensitivity analyses were conducted to examine the robustness of the results from base-case analysis, and results of the sensitivity analyses were consistent with the base-case analysis. As a result, any concern for selective reporting was minimized.
In the NMA, given the lack of closed loops in the networks, consistency in the ITC analyses could not be tested. All comparisons were therefore informed only by indirect evidence, which increases the level of uncertainty. Efficacy data were sparse in the NMA for the comparison of ravulizumab versus other active treatments. Overall, the 95% credible intervals (CrIs) for the point estimates were wide for the efficacy and harms outcomes and spanned the null when compared with other regimens; therefore, confidence in the effect estimates for efficacy of the study drugs was limited due to imprecision indicated by the wide CrIs for these outcomes and precluded any conclusions as to which treatment may be favoured.
In this NMA, 2 efficacy outcomes were analyzed (the MG-ADL score and the QMG score). Therefore, the relative treatment effect of ravulizumab versus relevant comparators on other important clinical outcomes such as patients’ survival or HRQoL remains unknown. Harms were only assessed in a full population instead of the IST optimized cohorts, which were the focus of this current review.
In the MAIC analysis, various patient characteristics at baseline were considered for involvement in the adjusted analyses, including age, sex, MGFA class, disease duration, MG-ADL score, steroid use at study entry, and NSIST use at study entry. It was not clear whether other potential effect modifiers were missing. Therefore, there remains a risk that the results are biased due to residual confounding. In this analysis, the effect sample size in the CHAMPION-MG trial after matching was substantially reduced by ███ for patients treated with ravulizumab, and ███ for those treated with placebo, suggesting that results were heavily influenced by a subset of the sample in the trial that may not be representative of the full sample, nor generalizable to the original population represented by the CHAMPION-MG trial. In general, the 95% CIs for the point estimates often crossed the null (except for at 4 weeks) and precluded definitive conclusions as to which treatment may be favoured. In this MAIC analysis, change in the MG-ADL score was the only assessed outcome; therefore, other relevant outcomes were not assessed, such as HRQoL, symptom relief, or safety.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps were submitted by the sponsor.
Conclusions
Evidence from 1 phase III, multicentre, double-blind, randomized, placebo-controlled trial (the CHAMPION-MG study) suggested that administration of ravulizumab in adult patients with anti–AChR antibody–positive gMG resulted in statistically significant improvements compared with placebo in activities of daily living (change from baseline in the MG-ADL total score) and gMG disease severity (change from baseline in the QMG total score and the proportion of patients with a QMG 5-point response) after 26 weeks of treatment. Two post hoc cohorts of the CHAMPION-MG trial aligned with the reimbursement request under review: the concomitant IST optimized cohort (████████) and the refractory concomitant IST optimized cohort (█████████), which were the focus of this resubmission. The clinical benefit observed in the 2 cohorts was consistent with the results shown in the overall trial population. Evidence from the 2 post hoc cohorts suggested that in adult patients with anti–AChR antibody–positive gMG, ravulizumab likely results in clinically meaningful improvements in activities of daily living (the MG-ADL total score) compared with placebo. Results for other outcomes related to relief in MG disease severity (change from baseline in the QMG total score, at least a 5-point improvement in the QMG total score, and at least a 3-point improvement in the MG-ADL total score) were supportive of the analyses of changes in the MG-ADL total score. Note that confidence in the between-group differences for efficacy in the 2 cohorts were limited due to imprecision, which was indicated by the associated CIs that included small effects close to the null or that crossed the null (the CI crossed the null for the QMG total score in the refractory concomitant IST optimized cohort). The treatment effect of ravulizumab on HRQoL (the MG-QoL15r score and the Neuro-QoL fatigue score) remains uncertain. Results of post hoc cohort analyses were subject to limitations such as the potential for randomization to not be upheld, a reduced sample size, and a lack of formal statistical approaches to control for inflated type I error rate in multiple comparisons. However, in all cases, the findings of the subgroup analyses were consistent with the analyses of the full trial population. Results of an OLE study (with up to 3.5 years of follow-up) suggested that improvement in daily living activities and disease severity was sustained during the long-term follow-up and that patients who switched from placebo to ravulizumab continuously reported improvements in their MG-ADL total score. The safety profile of ravulizumab in the 2 subgroups was consistent with that reported in the full population with no unexpected safety signals and was considered manageable by the clinical expert consulted for this review.
Evidence from sponsor-submitted ITCs (an NMA and an MAIC) comparing ravulizumab to other active treatments was insufficient to make conclusions on the relative efficacy of ravulizumab to these active treatments (i.e., the NMA examined ravulizumab versus efgartigimod alfa, IVIg, and rituximab in the concomitant IST optimized cohort, and ravulizumab versus eculizumab in the refractory concomitant IST cohort; the MAIC examined ravulizumab versus efgartigimod alfa in the overall population of the CHAMPION-MG trial). Limitations identified in these ITCs included a limited number of included studies, heterogeneity in trial characteristics and patient characteristics across these trials, and CrIs or CIs that crossed the null.
Introduction
The objective of this report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of ravulizumab (10 mg/mL and 100 mg/mL for IV infusion) in the treatment of adult patients with gMG. This is a resubmission and the focus of this report has been placed on comparing ravulizumab to relevant comparators (in particular, subsets of patients with gMG) and identifying gaps in the current evidence.
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
MG is a chronic autoimmune disease in which antibodies against AChRs or functionally associated molecules in the neuromuscular junction disrupt nerve impulse conduction, resulting in localized or generalized skeletal muscle weakness.1-4 In approximately two-thirds of patients with MG, the disease initially affects the extraocular muscles. These patients present with isolated ptosis, diplopia, or both, and no signs or symptoms of muscle weakness elsewhere.5 In 10% to 15% of all patients with MG, weakness remains restricted exclusively to the eyes (ocular MG).1,3,5,6 The remainder of patients either are diagnosed with or progress within a few years to gMG, where symptoms affect muscle groups in the head, neck, trunk, and/or limbs and are not limited to only eye muscles.31-35 Symptoms of gMG include eyelid drooping and double vision, altered facial expression, difficulty chewing and swallowing food, difficulty speaking, and in patients with more severe disease, problems with limb movement and breathing.3,6 Collectively, symptoms of MG negatively impact patients’ HRQoL.3 The disease has a fluctuating natural history: MG exacerbation (an increase in symptoms in patients who were previously asymptomatic or minimally symptomatic) and myasthenic crisis (muscle weakness causing life-threatening difficulties with breathing and swallowing and requiring ventilator support) can occur gradually or without warning.36 A widely used classification system from a task force of the MGFA stratifies patients by the extent and severity of muscle weakness, where class I equals isolated ocular muscle weakness, class II equals mild generalized weakness involving nonocular muscles, class III equals moderate generalized weakness involving nonocular muscles, class IV equals severe generalized weakness involving nonocular muscles, and class V equals intubation due to respiratory muscle weakness.37 For MG symptoms that fluctuate, the patient’s most severe weakness was used to assess the MGFA clinical class.2
Globally, the prevalence rates of MG range from 150 cases to 200 cases per 1 million population, and they have steadily increased over the past 50 years, at least partly due to improvements in recognition, diagnosis, treatment, and an overall increase in life expectancy. More recent studies addressing incidence rates show a wide range from 4 cases to 30 cases per million person-years.3,7 In Canada, the prevalence of MG is approximately 263 cases to 320 cases per 1 million population and its incidence is approximately 23 cases per 1 million population annually, based on the data in Ontario from 1996 to 2013.8 Autoantibodies against AChR, muscle-specific kinase (MuSK), and LRP4 can be detected in approximately 80%, 1% to 10%, and 1% to 3% of patients with gMG, respectively.3 Ten percent of patients with MG have a thymoma, and the prevalence of thymoma increases with increasing age and is associated with more severe disease.3,38 According to the clinical expert consulted by this review, 15% to 20% of patients with gMG have refractory disease, which may be defined by not achieving symptom control even though sufficient or multiple conventional therapies have been given, although a commonly accepted definition of refractory disease is unavailable. A web-based observational disease and outcomes registry also estimated that approximately 15% of patients with MG is considered medically refractory to conventional treatment strategies.31 Diagnosis of MG and gMG is made based on the combination of relevant symptoms and signs, a positive test for specific autoantibodies (e.g., AChR, MuSK, and LRP4 autoantibodies), and neurophysiological testing. Thymic status should be determined by means of mediastinal imaging.3 In patients with mild symptoms, the disease may be underdiagnosed.
The prognosis of MG varies by symptom severity and response to treatment. Patients with severe or refractory symptoms, including those hospitalized for myasthenic crisis, are at higher risk for complications compared with those with mild or nonbulbar symptoms. MG may be associated with increased mortality. In a population-based study from Denmark, overall mortality was significantly increased for patients with anti–AChR antibody–positive MG compared with matched controls from the general population (mortality rate ratio = 1.41 [95% CI, 1.24 to 1.60]).9 However, other contemporary studies have not found an increased mortality rate, perhaps due to better disease management with the increasing availability of effective immunotherapies.2
Standards of Therapy
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
According to the clinician expert consulted for this review, the goal of treatment in most patients with gMG is to reduce disease symptoms (ideally aiming for minimal disease manifestation) as well as adverse effects of MG therapy and to allow the patient to function and work normally with good HRQoL. Other goals of treatment include avoiding MG exacerbations and myasthenic crisis, minimizing hospitalizations (including intensive care unit admissions), and reducing the numbers and doses of therapies required for symptom control.
The initial symptomatic treatment for most patients with gMG is an AChE inhibitor such as pyridostigmine. According to the clinical expert consulted for this review, peripherally acting AChE inhibitors are used as symptomatic treatments for temporarily alleviating muscle weakness in these patients. A minority of patients with MG have a spontaneous remission or respond to AChE inhibitors; however, most patients need treatment with corticosteroids and/or steroid-sparing drugs when they do not reach their treatment goals with AChE inhibitors.
Corticosteroids are the first-line immunosuppressive therapy for patients with MG who remain symptomatic while on AChE inhibitors or who desire better symptom control. Early use of oral steroids in patients with pure ocular symptoms may delay or reduce the risk of generalization and the worsening of underlying symptoms.10,11 Patients who do not respond to corticosteroids or who have comorbidities that are not suitable for treatment with corticosteroids may initiate treatment with NSISTs.12 Among the NSISTs, azathioprine and mycophenolate mofetil are commonly used in gMG. The use of conventional therapy (AChE inhibitors, corticosteroids, and/or NSISTs) is associated with the slow onset of benefit, and incomplete efficacy in eliminating MG symptoms and significant toxicities. Corticosteroids, particularly if used at high doses or over prolonged periods, are associated with cataracts, cushingoid appearance, osteoporosis and fractures, glucose intolerance and diabetes, hypertension, infections, mood disturbances, and weight gain.13-15
Other treatment options, such as immunomodulating therapies like PLEX and IVIg, are usually reserved for use on a short-term basis for life-threatening situations or crises, for use in some patients before surgery or corticosteroid treatment, to obtain a rapid treatment response, or for when treatments have been ineffective.10 The choice of whether to use IVIg or PLEX depends on patient comorbidities such as sepsis (PLEX-contraindicated) or renal failure (IVIg-contraindicated) and on treatment availability due to blood supply shortages.10 Importantly, PLEX or IVIg have no long-term impact on the disease course in gMG.20 Significant limitations of IVIg or PLEX39 have been noted by clinicians in Canada: venous access issues, potentially serious cardiovascular and systemic adverse effects or contraindications to these therapies, waning efficacy in spite of an initial response to IVIg or PLEX, considerable infusion or transfusion requirements that make these efforts unsustainable, a lack of supply of product (IVIg or subcutaneous immunoglobulin) that threatens to interrupt therapy abruptly to the detriment of patients, and finally, that PLEX is available in very few large centres in each province and IVIg can only be infused in hospital infusion rooms across the country, which contributes to considerable delay in instituting this therapy.
Novel biologic treatments such as efgartigimod alfa and eculizumab have emerged. Efgartigimod alfa is an FcRn inhibitor, and was approved by Health Canada in 2023 for the treatment of adult patients with gMG who are anti–AChR antibody–positive.16 This therapy also received a positive reimbursement recommendation with conditions from CDA-AMC as an add-on therapy for adult patients with anti–AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChE inhibitors, corticosteroids, and/or NSISTs.17 Efgartigimod alfa is currently undergoing negotiations for product listing agreements. Eculizumab, a monoclonal antibody that specifically binds to the complement protein C5 with high affinity, was approved for use in adult patients with gMG by Health Canada in 2018.18 Although eculizumab is indicated for use in all adult patients with gMG, CDEC recommended that it be reimbursed in patients with refractory gMG who are anti–AChR antibody–positive and have inadequate symptom control after undergoing at least 2 ISTs in the previous 12 months, or at least 1 IST and chronic IVIg or PLEX in the previous 12 months, along with other conditions.19,20 A successful product listing agreement for eculizumab was not reached between the drug plans and the sponsor, and therefore is not listed in any jurisdictions in Canada. The international consensus guidance from 2021 states that rituximab (an immunomodulatory drug) is generally recommended only for patients with anti–MuSK antibody–positive MG considering the great uncertainty of its efficacy in anti–AChR antibody–positive MG.12 The 2021 CDA-AMC technology review of rituximab concluded that rituximab may be associated with improvements in clinical status, the use of concurrent immunomodulatory therapies, quality of life, and various laboratory parameters in patients with MG compared to their previous treatments; however, the use of these findings in informing clinical and policy decisions was limited due to the substantial methodological limitations of the included literature in this report.21 Challenges with rituximab include the slow onset of action (a minimum of 3 months), a lack of efficacy in the anti–AChR antibody–positive gMG population, and significant side effects owing to its broad immunosuppressive mechanism — including life-threatening infections, hepatitis B reactivation, severe mucocutaneous reactions, and progressive multifocal leukoencephalopathy.40-43 In many jurisdictions in Canada, rituximab is listed with relatively accessible criteria, although it remains challenging to access in certain provinces.
Lastly, surgery (thymectomy) is a treatment option in select circumstances.20 Thymectomy is recommended in nonthymomatous adult patients with anti–AChR antibody–positive gMG aged 50 years or younger if they are stable (as an early treatment option), as well as in patients with or without AChR antibodies if ISTs elicit an insufficient response or are intolerable due to side effects.12
According to the clinician expert input received for the original submission for ravulizumab, as MG symptoms improve, doses of AChE inhibitors, corticosteroids, and then other ISTs are reduced and the frequency of IVIg or PLEX is reduced until the minimal maintenance therapy required for remission is identified. Patients whose symptoms persist despite treatment with adequate doses of corticosteroids, ISTs, and/or chronic IVIg or PLEX, or patients for whom the doses or frequencies of these therapies cannot be reduced, are considered to have refractory gMG, which accounts for approximately 10% to 15% of patients with gMG.
Drug Under Review
Ravulizumab is a terminal complement inhibitor that specifically binds to the complement protein C5 with high affinity, thereby inhibiting its cleavage to C5a and C5b and preventing the generation of membrane attack complex.22 The precise mechanism by which ravulizumab exerts its therapeutic effect in patients with gMG is unknown but is presumed to involve the reduction of terminal complement complex C5b-9 deposition at the neuromuscular junction.
In January 2023, ravulizumab was approved by Health Canada for the treatment of adult patients with anti-AChR antibody–positive gMG. It is supplied as a 10 mg/mL or 100 mg/mL concentrate for IV infusion. The recommended ravulizumab maintenance dosing in adult patients (aged 18 years or older) with gMG with a body weight greater than or equal to 40 kg is based on the patient’s body weight, with maintenance doses administered every 8 weeks, starting 2 weeks after the loading dose (Table 3). Patients must be vaccinated against meningococcal infections before, or at the time of, initiating ravulizumab, unless the risks of delaying ravulizumab therapy outweigh the risks of developing a meningococcal infection.22
Table 3: Ravulizumab Weight-Based Dosing Regimen
Weight-based dosing regimen, indication | Body weight range (kg) | Loading dose (mg) | Maintenance dose (mg) | Dosing interval |
|---|---|---|---|---|
gMG | ≥ 40 to < 60 | 2,400 | 3,000 | Every 8 weeks |
≥ 60 to < 100 | 2,700 | 3,300 | Every 8 weeks | |
≥ 100 | 3,000 | 3,600 | Every 8 weeks |
gMG = generalized myasthenia gravis.
Source: Product monograph for ravulizumab.22
In this resubmission, the sponsor’s current reimbursement request is as add-on therapy for adult patients with anti–AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChE inhibitors, corticosteroids, and/or NSISTs.
Key characteristics of ravulizumab are summarized in Table 4 with other treatments available for gMG.
Table 4: Key Characteristics of Ravulizumab and Other Drugs Used for the Treatment of gMG
Characteristic | Ravulizumab | Efgartigimod alfa | Eculizumab | AChEI (e.g., pyridostigmine) | IST (e.g., corticosteroids, steroid-sparing drugs, rituximab) | Rituximab | IVIg | PLEX |
|---|---|---|---|---|---|---|---|---|
Mechanism of action | Terminal complement inhibitor | Human IgG1 antibody fragment engineered for increased affinity to FcRn | Terminal complement inhibitor | Cholinesterase inhibitor | Suppression of production of AChR antibodies | Binds to antigen CD20. CD20 regulates an early step(s) in the activation process for cell cycle initiation and differentiation, and possibly functions as a calcium ion channel. | Unknown | Removal of AChR antibodies |
Relevant indicationa | For the treatment of adult patients with anti–AChR antibody–positive gMG | For the treatment of adult patients with anti–AChR antibody–positive gMG | Adult patients with gMG | For the symptomatic treatment of myasthenia gravis | NA | Off-label use | NA | NA |
Route of administration | IV | IV | IV | PO | PO or IV | IV | IV | IV |
Recommended dosage | 2,400 mg to 3,000 mg (loading) 3,000 mg to 3,600 mg every 8 weeks starting 2 weeks after loading dose (maintenance)b | The recommended dosage of efgartigimod alfa is 10 mg/kg administered as an IV infusion over 1 hour once weekly for 4 weeks. In patients weighing 120 kg or more, the recommended dose of efgartigimod alfa is 1,200 mg (3 vials) per infusion. Administer subsequent treatment cycles based on clinical evaluation. The frequency of efgartigimod alfa treatment cycles may vary by patient. | 900 mg weekly for 4 weeks followed by 1,200 mg 1 week later (loading) 1,200 mg every 2 weeks (maintenance)c | 60 mg to 1,500 mg per day | Various | Off-label use. There was no recommended dosage. | 1 g/kg to 2 g/kg administered over 2 days to 5 days | 1 plasma volume to 1.5 plasma volumes daily, usually 5 to 6 exchanges |
Serious adverse effects or safety issues | Infections, including serious meningococcal infections | Infections. As efgartigimod alfa causes transient reduction in IgG levels, the risk of infections may increase. The most common infections observed in clinical trials were upper respiratory tract infections. | Infections, including serious meningococcal infections | Increased salivation and fasciculation, diarrhea, nausea, vomiting | Infections, infusion reactions | Infusion reactions, PML, TSL, hepatitis B reactivation, mucocutaneous reactions, infections, and serious cardiovascular events | Infusion reactions | Infections, bleeding, thrombosis, transfusion reactions |
AChEI = acetylcholinesterase inhibitor; AChR = acetylcholine receptor; gMG = generalized myasthenia gravis; IgG = immunoglobulin G; IgG1 = immunoglobulin G1; IST = immunosuppressive therapy; IVIg = IV immunoglobulin; NA = not applicable; PLEX = plasma exchange or plasmapheresis; PML = progressive multifocal leukoencephalopathy; PO = orally; TSL = tumour lysis syndrome.
aRelevant Health Canada–approved indications.
bSupplemental ravulizumab doses of 1,200 mg to 1,800 mg are given following PLEX and supplemental doses of 600 mg are given following IVIg.
cSupplemental eculizumab doses of 300 mg to 600 mg are given following PLEX.
Sources: Product monographs for ravulizumab,22 efgartigimod alfa,16 eculizumab,19 pyridostigmine,44 and rituximab.45
Submission History
Ravulizumab was initially reviewed by CDA-AMC for the treatment of adults with anti-AChR antibody–positive gMG and received a negative funding recommendation from CDEC on August 24, 2023.23 The recommendation was based on evidence assessed in the CDA-AMC Clinical Review Report for the initial submission of ravulizumab.46 Key reasons for the negative recommendation included the following.
There was a lack of IST dosing information to conclude whether IST was optimized for patients at the time of study enrolment. Without IST dosing information at study entry, the committee was uncertain if the dose and durations of corticosteroid and NSIST therapies at study enrolment were sufficient to achieve maximal responses. During the RCP, dosage changes in concomitant ISTs were discouraged; however, rescue therapy was allowed upon patients’ clinical deterioration and dosage changes were permitted if deemed medically necessary by the investigator. The committee noted that changes in concomitant MG therapies were not generalizable to clinical practice since changes to these medications were discouraged by the study protocol. Therefore, there was insufficient evidence on the treatment effect of ravulizumab compared to conventional therapies such as those used in clinical practice.
There was insufficient evidence on the treatment effect of ravulizumab in patients who remained symptomatic and were not necessarily considered refractory. While subgroup analyses conducted among patients who had been exposed to at least 2 ISTs were consistent with the main analyses, these results were limited by smaller numbers of patients and the lack of formal statistical testing with adjustment for multiple testing (an increased risk of type I error). Given the lack of IST dosing information, it was unclear whether IST dosing was optimized at study entry in this subgroup.
There was insufficient evidence on the treatment effect of ravulizumab in patients with refractory gMG. Patients enrolled in the CHAMPION-MG trial were not required to be refractory and therefore it was unknown how many patients were refractory and whether the results observed in the overall patient population would be the same in these patients.
There was a lack of evidence on the relative efficacy and harms of ravulizumab compared to relevant comparators (e.g., rituximab, IVIg, PLEX). Evidence from sponsor-submitted ITCs and an observational study comparing ravulizumab to eculizumab suggested uncertainty in the relative efficacy of these drugs. In addition, the ITCs were limited by differences in the study populations, a small effective sample size, selection criteria, and demographic differences between included studies and the absence of adjustment for potentially important clinical covariates.
In response to the draft CDEC recommendation, the sponsor submitted a request for reconsideration in which the sponsor requested that CDEC reconsider the following.
The study design of the CHAMPION-MG trial allowed for the robust comparison of ravulizumab with relevant standard of care treatments in gMG. The sponsor noted that the CHAMPION-MG trial enrolled patients on stable and optimized doses of ISTs with mean treatment durations well above the minimum treatment length requirement in both treatment arms. According to the sponsor, the CHAMPION-MG trial compared ravulizumab to current standard of care therapies at optimized doses.
The sponsor noted that rituximab and IVIg or PLEX are not considered relevant comparators for ravulizumab in the treatment of anti–AChR antibody–positive gMG largely due to their limited accessibility and limited evidence to support their efficacy.
There are significant unmet needs in patients with gMG who are symptomatic despite treatment due to the limitations of current standard of care. The sponsor noted that ravulizumab selectively targets the underlying disease pathogenesis and has a rapid onset of action, sustained clinical benefit, and a well-tolerated safety profile that fulfills the current gaps in the management of patients with gMG.
The sponsor proposed that the reimbursement criteria for ravulizumab align with the unmet needs of patients, the studied population most represented by the pivotal CHAMPION-MG trial — specifically, patients with gMG who remain symptomatic (the MG-ADL score of ≥ 6 and the MGFA classification of class II to class IV) despite 2 or more prior ISTs. According to the sponsor, the results of the prespecified subgroup analyses in patients with more than 2 prior ISTs are consistent with the results of the primary analysis and demonstrated statistically significant MG-ADL improvements from baseline to week 26 in the ravulizumab group compared to placebo.
However, CDEC maintained its initial position that there was insufficient information on IST dosing to conclude whether patients in the CHAMPION-MG trial were on optimized IST dosages at study entry, that rituximab and IVIg or PLEX were relevant comparators, that it remained unclear from the evidence in the CHAMPION-MG trial whether ravulizumab could be more effective and safer than currently available treatments in patients with symptomatic but nonrefractory gMG, and that the proportion of patients with refractory gMG who received an adequate trial of IST could not be determined in the CHAMPION-MG trial.
The drug was resubmitted for review by the sponsor on June 4, 2024, on the basis of the availability of new evidence and a revised reimbursement request for ravulizumab as an add-on therapy for adult patients with anti–AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChE inhibitors, corticosteroids, and/or NSISTs. The new evidence included the following.
The efficacy and harms of ravulizumab in 2 post hoc subgroups in the CHAMPION-MG trial: These subgroups were the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort.28 The sponsor noted that there is no universally accepted definition of IST “optimization” in clinical practice due to variability in the disease symptoms, adverse effects of the current therapies, and individual patient characteristics. Therefore, the inclusion criteria of Study ADAPT (efgartigimod alfa versus placebo) and Study REGAIN (eculizumab versus placebo) were adopted to select patients who would be considered to have IST optimization, or were IST optimized but still with refractory disease at the time of study enrolment in the CHAMPION-MG trial, respectively. These criteria were based on total treatment duration and stable dose duration.
NMA:30 The relative efficacy of ravulizumab was assessed against efgartigimod alfa, rituximab, IVIg, and eculizumab in the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort. In addition, the sponsor submitted an MAIC report comparing the efficacy of ravulizumab relative to efgartigimod alfa in the overall trial populations.30
OLE data47 in the CHAMPION-MG trial: In the end-of-study analysis (the last patient’s last visit on May 25, 2023), a total of 161 patients had entered the OLE period. The efficacy and safety of ravulizumab were assessed in the 2 cohorts during the OLE phase.
The sponsor noted that the new evidence addressed concerns raised by CDEC during the initial submission; these concerns were related to IST optimization during the CHAMPION-MG trial, the treatment effect of ravulizumab in patients with refractory disease, comparative evidence of ravulizumab versus relevant comparators, and the long-term efficacy and harms of ravulizumab.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
CDA-AMC received 1 patient group submission from MDC. MDC is a health charity that supports people affected by muscular dystrophies and related muscle diseases in Canada. MDC’s mission is to enhance the lives of those impacted by neuromuscular disorders by continually working to provide ongoing support and resources while relentlessly searching for a cure through well-funded research.
MDC identified and contacted adults living with MG to participate in a survey and in semistructured interviews. Surveys were shared with members via e-blasts, personalized invites, and online patient groups. MDC also conducted an MG Canadian journey mapping project among adults living with MG via virtual interviews, round table sessions, surveys, and HRQoL measures (EQ visual analogue scale, EQ-5D, MG-ADL, and MG-QoL). MDC collected information from 215 patients impacted by MG through a health care experience survey and semistructured phone or virtual interviews. These patients consisted of 83 males and 132 females aged between 22 years and 78 years from all provinces in Canada.
In addition, MDC sought patients’ opinions on the value of having ravulizumab approved for use in Canada from those affected by gMG. In total, 14 patients (11 females and 3 males) aged 32 years to 69 years (mean age of 53 years) provided input on their experience with MG and their knowledge of ravulizumab. These patients were recruited from all regions across Canada (the Atlantic, Central, and Prairies regions) except for the North (Nunavut, the Northwest Territories, and Yukon).
Respondents indicated that MG has a significant impact on productivity; fatigue, energy levels, and quality of sleep; respiratory health; mobility and strength; independence; relationships and social participation; eyes, vision, speech, and swallowing; mental health; quality of life; and the well-being of their families.
With respect to the currently available treatments, MDC noted that patients reported negative experiences with steroids and prednisone, the slow onset of medication effects, and a feeling of trial and error with medications, but a positive experience with IVIg. MDC added that, while according to the respondents, supportive treatments have had positive health outcomes, there are concerns about the long-term and sustained benefits of these treatments.
MDC noted that patients with gMG seek better control over their condition to minimize the impact of symptoms, side effects, and disease exacerbations on their lives, allowing them to maintain their independence and avoid serious hospital admissions. MDC added that patients stated that they would be willing to deal with the side effects of medications if these aspects of MG were better controlled. According to MDC, respondents indicated that currently available therapies may decrease MG exacerbations but do not improve their overall HRQoL.
Based on the patient group input, the important factors in evaluating different treatments include treatment administration, potential side effects, the duration and frequency of treatments, convenience (e.g., travel time and parking for clinic visits), and financial impact (costs).
MDC explained that according to the recent round table of patients with gMG in Canada, patients value new treatments that offer improved disease control and disease symptoms and extend dosing intervals.
In terms of diagnostic testing, MDC stated that 85% of respondents reported significant difficulty in getting diagnosed. The vast majority of patients found the test to be cost-effective but noted the overall lengthy process with many missed opportunities for improvement (e.g., delays, misdiagnoses, costs incurred). A diagnosis received as part of hospitalization was reported as a seamless experience.
MDC believed that there is a pressing need for improved treatment options to address the ongoing challenges faced by patients with MG and that ravulizumab provides a new treatment option for patients with MG that has demonstrated efficacy, safety, and improved dosing convenience compared to other treatment options.
Clinician Input
Input From Clinical Experts Consulted by the Review Team
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of gMG.
Unmet Needs
The clinical expert consulted for this review identified unmet needs associated with currently available treatments for patients with gMG whose symptoms persist even if they have been treated with conventional medications for this disease (such as AChE inhibitors, corticosteroids, and/or NSISTs). The unmet needs are as follows: although multiple treatment options are available to patients with gMG, some patients do not have an adequate response to the existing treatments, and 15% to 20% of patients have refractory disease and require alternative therapeutic options; patients may become intolerant of ISTs (e.g., from treatment with corticosteroids); and some exiting treatments are only suitable for select patients. Treatments with a more rapid onset of action, longer-lasting benefits, improved efficacy in patients with refractory gMG, and fewer side effects are needed.
Place in Therapy
The clinical expert consulted for this review noted that treatment with traditional immunosuppressants sometimes is not satisfactory (e.g., prednisone is associated with a wide spectrum of side effects, especially in the chronic use; azathioprine may not be effective and may require 9 months to 12 months to reach its maximum effect; mycophenolate mofetil may not be effective either and poses a risk of teratogenicity). In addition, there were no good-quality RCTs supporting the use of these drugs, even though they are widely accepted and routinely used in clinical practice. The expert stated that because of its unique mechanism of action (a complement C5 inhibitor), ravulizumab could be another treatment option for patients living in Canada with gMG whose disease has had an inadequate response to or has not responded to conventional ISTs or those who cannot tolerate traditional ISTs.
Patient Population
According to the clinical expert consulted for this review, patients with significant symptoms of gMG and resistance to conventional therapies, patients who require multiple concomitant ISTs, or patients who may experience significant side effects or intolerance of standard immunosuppressants may benefit from treatment with ravulizumab.
The expert also noted that candidates for ravulizumab therapy (primarily patients with refractory gMG and those with severe but nonrefractory gMG) would be identified through the judgment of an expert neurologist based on clinical evaluation following serologic testing for AChR antibodies and, potentially, following a chest CT scan to rule out thymoma and thymic carcinoma. The expert also noted that although patients with thymoma were excluded from the clinical trials of complement inhibitors, there is no reason to expect that these patients would not benefit from these drugs. These new treatments are likely to reduce the chronic use of corticosteroids, diminish side effects of immunosuppressants, and decrease the number of patients with refractory disease.
Assessing Response to Treatment
The clinical expert stated that a patient’s response to treatment with ravulizumab would be assessed by certain MG scales (e.g., a decrease of approximately 2 points in the MG-ADL total score and/or a decrease of approximately 3 points in the QMG score, every 1 month to 3 months), by a physician’s clinical examination of MG symptoms and signs, and via the reduction of other MG therapies, such as corticosteroid use, chronic IVIg or PLEX, and the number of emergency department visits and hospitalizations.
Patients need regular follow-up visits with a neuromuscular specialist or neurologist to monitor the degree of response to treatment. Depending on the severity of the patients’ symptoms, the follow-up visits can range from every 1 month to 3 months when ravulizumab is initiated, and every 3 months thereafter if the patients have a stable neurologic status.
Discontinuing Treatment
The clinical expert consulted for this review stated that ravulizumab would be discontinued in patients who do not respond favourably to treatment with ravulizumab (e.g., less than 2-point improvement of MG-ADL total score), continue to require therapy with multiple concomitant ISTs, or exhibit recurrent MG crises or exacerbations of symptoms requiring rescue therapies with IVIg or PLEX. Ravulizumab would also be discontinued in patients who experience serious side effects or secondary infection such as meningococcal meningitis, or in patients who prefer to discontinue. At present, there is no available data or anecdotal experience to inform decision-makers and clinicians on whether it may be plausible to hold the treatment once the patient achieves sustained stable neurologic status or whether in some patients, lifelong treatment with complement inhibitors — including ravulizumab — would be required to maintain the achieved clinical benefit.
Prescribing Conditions
The clinical expert consulted for this review stated that the initiation of ravulizumab would be supervised by a neurologist with expertise in managing patients with MG (a neuromuscular expert). Given the small group of neuromuscular experts in Canada and the high demand on their time, it may not be realistic to restrict the use of ravulizumab to academic expert settings only. Therefore, a trained neurologist may be starting the therapy and providing the follow-up assessments.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
One input was received from NMD4C, a new pan-Canadian network that brings together clinical, scientific, technical, and patient expertise to improve care, research, and collaboration in neuromuscular disease. The mission of NMD4C is to improve the care, research, and treatment of neuromuscular diseases for all people living in Canada. The information presented in this submission was gathered from 8 clinicians with experience in treating gMG.
According to the clinician input, the current mainstay of therapies for MG includes supportive therapies, symptomatic treatments, and disease-modifying strategies. NMD4C added that outside the setting of crisis or imminent crisis, the effects of disease-modifying therapy are usually transient, lasting a few weeks, and additional ongoing immunotherapy is often needed.
NMD4C noted that the goals of therapy are to minimize morbidity and mortality from MG, keep patients out of hospital, improve quality of life, prevent repeated attacks, and prevent prolonged, untreated, or partially treated MG.
NMD4C stated that some of the treatment gaps include limited therapy options for active and refractory disease, inadequate response to the traditional immunotherapies, the slow onset of treatment action, side effects, a lack of response, and treatments for pediatric patients.
In terms of place in therapy, NMD4C believes ravulizumab addresses the underlying disease process by inhibiting the immune-mediated damage to the neuromuscular junction rather than being a symptomatic treatment. Ravulizumab will complement other treatments that act upstream in the immune-mediated damage. Conversely, the concomitant use of PLEX or IVIg may reduce the efficacy of ravulizumab by reducing its concentrations. The place in therapy for ravulizumab would likely be after treatment with pyridostigmine, and after treatment with either steroids and/or other ISTs, including steroid-sparing immunosuppressive drugs. Ravulizumab is likely to affect the treatment paradigm of patients with refractory and nonrefractory MG who are not responsive to first-line and second-line therapies or require chronic IVIg infusions or PLEX. It may also be considered in patients who are intolerant of other immunomodulatory treatments.
NMD4C stated that it would be appropriate to recommend that patients with gMG try other treatments before initiating ravulizumab, which requires periodic IV infusions over an extended period, is unlikely to induce long-term disease remission, is likely to be expensive, may not be available in smaller cities or nonspecialized centres, and requires extensive expertise. Ravulizumab will be contraindicated in patients who have had previous infection with Neisseria meningitidis; vaccination for this pathogen is required before consideration of treatment with ravulizumab.
Based on the clinician group input, adult patients who are seropositive for AChR antibodies and have gMG would be best suited for treatment with ravulizumab; there are no data on the efficacy of ravulizumab for a minority population of patients with MG — including those aged younger than 18 years, those who had thymectomy within the past year, those with thymic carcinoma, those who are pregnant or breastfeeding, patients with anti–MuSK or anti–LRP4 antibodies, or seronegative patients. Patients with MG who are seropositive for AChR antibodies who have not responded to pyridostigmine and to steroids and/or oral ISTs or are additionally dependent on periodic PLEX or chronic IVIg therapy are most in need.
NMD4C noted that the diagnosis must have been confirmed clinically and supported by confirmatory laboratory tests before treatment with ravulizumab.
NMD4C explained that the outcomes that are used to determine whether a patient is responding to treatment in clinical practice include increased survival, the avoidance of emergency department visits or hospital admissions (including admissions to the intensive care unit), the avoidance of the need for rescue as well as maintenance therapy with IVIg and plasmapheresis, a reduction in the dose and/or duration of concomitant steroids, a reduction in the level of fatigable weakness, and an improvement in activities of daily living and quality of life.
Based on the NMD4C input, the factors that should be considered when deciding to discontinue treatment include the amount of clinical improvement or response, the duration of time spent in a clinically stable state, the AEs associated with the treatments, and the inconvenience associated with the therapy.
NMD4C added that an appropriate setting for treatment includes a clinical team with general knowledge of MG, appropriate nursing experience in managing IV medications, and familiarity with venous access issues and managing potential adverse effects. It is recommended that ravulizumab be prescribed by neurology specialists with expertise in MG diagnosis, assessment, monitoring, and management of patients with MG.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation question | Clinical expert response |
|---|---|
Relevant comparators | |
The efficacy and safety of ravulizumab for gMG was previously reviewed by CDA-AMC, based on the evidence from a phase III, multicentre, double-blind, placebo-controlled RCT (the CHAMPION-MG trial). This drug received a CDEC recommendation of “do not reimburse.” In this resubmission, the sponsor is requesting different reimbursement criteria and provided new clinical evidence, including post hoc analyses in the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort, new open-label extension study data on up to 3.5 years of treatment with ravulizumab, and a new ITC, in which the relative efficacy of ravulizumab vs. efgartigimod alfa, rituximab, IVIg, and eculizumab were evaluated in the concomitant IST optimized cohort. The sponsor noted that based on the results of the ITC, ravulizumab was, at minimum, comparable to other active treatments at the time points considered. Is this indirect comparison analysis sufficient to demonstrate that ravulizumab is comparable to other active treatments in patients with gMG whose symptoms persist despite adequate treatment with AChEIs, corticosteroids, and/or NSISTs? | The clinical expert noted that there is currently no robust direct or indirect evidence of ravulizumab compared to other active treatments in patients with gMG whose symptoms persist despite adequate treatment with AChEIs, corticosteroids, and/or NSISTs. Based on expert opinion, the clinical expert anticipated that ravulizumab and efgartigimod alfa would have similar efficacy. |
In many jurisdictions, rituximab is listed with relatively accessible criteria although it is used off-label for patients with gMG, and it has not been reviewed by CDEC. Eculizumab (Soliris) has received a positive recommendation for patients with gMG from CDEC; however, a successful PLA was not reached for it between the drug plans and the sponsor, and therefore it was not listed in any jurisdictions in Canada. Efgartigimod alfa has recently received a positive recommendation from CDEC for patients with gMG who are anti–AChR antibody–positive. It is currently undergoing PLA negotiations. | Comment from the drug programs to inform CDEC deliberations. |
Considerations for initiation of therapy | |
In accordance with the requested reimbursement criteria, how are patients identified as having persistent symptoms despite adequate treatment? Do all standard or conventional therapies need to be maximized first? How should an adequate trial on these drugs be defined? The sponsor has noted that ravulizumab would be used as an add-on therapy in patients who continue to experience debilitating symptoms despite adequate conventional therapies. This is different from the eculizumab review, where eculizumab was used in patients with refractory disease. Is there a clear definition of “refractory disease” for the population with gMG? Can ravulizumab be used for patients with refractory disease as well? | The expert suggested that patients’ MG symptoms can be identified using MG-related scales (e.g., MG-ADL). The number of symptoms that the patient experienced will be recorded — the higher the number, the more symptomatic the patient is. The expert indicated that in clinical practice, it is not realistic for patients to maximize all standard or conventional therapies before receiving ravulizumab since not every patient is a good candidate for all standard or conventional treatments; in addition, it also depends on how conservative the treatment plan would be. However, the expert anticipated that most clinicians would likely attempt to maximize at least 1 IST before ravulizumab. The expert also noted that different drugs have different requirements for being considered maximized. For example, patients who receive steroids, IVIg, or other therapies need to be kept on these treatments for approximately 6 months to 9 months before they can be considered to have been used for a sufficient length of time and whether they are effective for the patients or not. In clinical trials of MG, treatment effects of the investigated medications can be determined using certain scales — for example, the MG-ADL scale to capture the changes in symptoms. In this scale, higher scores indicate more severely impacted daily activities for the patients. The expert noted that in practice, there is no standard definition for patients with refractory disease. Usually, if the patients have persistent symptoms despite adequate conventional therapies and the scores of certain scales (e.g., MG-ADL) are higher than predefined values, the patients are considered as having refractory disease. Other approaches for defining refractory disease include the history of treatments for MG. For example, if patients do not respond well to multiple ISTs, or require chronic IVIg therapy or PLEX, they are considered as having refractory disease. The expert noted that ravulizumab can be used in patients with refractory MG. |
Should patients who have experienced other drug treatments in this area (eculizumab, efgartigimod alfa, or rituximab) be eligible for the treatment with ravulizumab? | The expert agreed that patients are still eligible for treatment with ravulizumab if they received previous gMG medications, such as eculizumab, efgartigimod alfa, or rituximab. |
FWG noted that consistency with initiation criteria associated with other drugs in the same therapeutic space, specifically efgartigimod alfa, should be considered. This drug has been reviewed by CDA-AMC in the same population and a positive CDEC recommendation was issued in December 2023. Is there a specific place in therapy before or after efgartigimod alfa and eculizumab that will be considered for ravulizumab? | The expert indicated that ravulizumab should be included as a treatment option for patients with gMG, as efgartigimod alfa and eculizumab are. Even though these patients may have received multiple therapies for MG, they may still experience significant symptoms. |
Considerations for continuation or renewal of therapy | |
FWG noted that consistency with continuation or renewal criteria associated with other drugs in the same therapeutic space, specifically efgartigimod alfa, should be considered. This drug has been reviewed by CDA-AMC in the same population and a positive CDEC recommendation was issued in December 2023. | This is a comment from the drug programs to inform CDEC deliberations. |
Considerations for discontinuation of therapy | |
What are the differences between “refractory disease” and “inadequate response to conventional therapy”? Can these 2 terms be clearly defined? | The expert indicated that these 2 terms overlap significantly, although there are no accepted definitions available for them. Based on the expert’s opinion, “refractory disease” implies a poorer response to treatment and being harder to treat when compared to “inadequate response to conventional therapy.” Patients with refractory disease can be identified if they have persistent symptoms despite adequate conventional therapies, which imply inadequate response to those treatments. Patients’ responses can be measured using scales specific for MG. For example, in MG-ADL, higher scores indicate a greater severity of symptoms. Other approaches for defining refractory disease include the history of treatments for MG. |
Are there guidelines for switching from eculizumab or efgartigimod alfa to ravulizumab and vice versa? | The expert noted that currently, there are no guidelines for switching from eculizumab or efgartigimod alfa to ravulizumab and vice versa. |
FWG noted that consistency with continuation or renewal criteria associated with other drugs in the same therapeutic space, specifically efgartigimod alfa, should be considered. | This is a comment from the drug programs to inform CDEC deliberations. |
Considerations for prescribing of therapy | |
Life-threatening meningococcal infections and sepsis have been reported in patients treated with ravulizumab. Therefore, patients are required to be vaccinated against meningococcal infections before or at the time of initiating ravulizumab, and to be monitored for early signs of meningococcal infections and be treated immediately if infection is suspected. | This is a comment from the drug programs to inform CDEC deliberations. |
Please indicate if there are any concerns with adding ravulizumab to a regimen already containing 1 of the other recommended drugs (e.g., eculizumab, efgartigimod alfa) for patients with gMG. | The expert indicated that when combining multiple ISTs in patients with MG, there is always a risk of potential superimposed infections due to a patient’s compromised immune system. This is not unique to ravulizumab but applies to all ISTs. Since meningococcal vaccination is mandatory before initiating treatment with ravulizumab, the expert had no additional concerns for this type of infection. |
FWG noted that consistency with prescribing criteria associated with other drugs in the same therapeutic space, specifically efgartigimod alfa, should be considered. | This is a comment from the drug programs to inform CDEC deliberations. |
Generalizability | |
Patients who are currently receiving an active comparator treatment to ravulizumab may have a time-limited opportunity to switch to ravulizumab, if ravulizumab is a preferred treatment option. Would there be any concerns with this approach? | The expert did not have concerns regarding the time-limited opportunity to switch to ravulizumab if patients are currently receiving another active comparator treatment, such as eculizumab, efgartigimod alfa, or rituximab. |
Care provision issues | |
FWG noted that meningococcal vaccination is required before treatment with ravulizumab, and patients receiving ravulizumab should be monitored for early signs of meningococcal infections. | This is a comment from the drug programs to inform CDEC deliberations. |
System and economic issues | |
FWG noted that the provision of ravulizumab may have a substantial budget impact due to an easier dosing regimen of this drug. | This is a comment from the drug programs to inform CDEC deliberations. |
Efgartigimod alfa, 1 of the comparators for ravulizumab, is currently undergoing price negotiations for the same indication. | This is a comment from the drug programs to inform CDEC deliberations. |
AChEI = acetylcholinesterase inhibitor; AChR = acetylcholine receptor; CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; FWG = Formulary Working Group; gMG = generalized myasthenia gravis; IST = immunosuppressive therapy; ITC = indirect treatment comparison; IVIg = IV immunoglobulin; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; NSIST = nonsteroidal immunosuppressive therapy; PLA = product listing agreement; PLEX = plasma exchange or plasmapheresis; RCT = randomized controlled trial; vs. = versus.
Clinical Evidence
The objective of this Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of ravulizumab (10 mg/mL and 100 mg/mL for IV infusion) in the treatment of gMG. The focus will be placed on comparing ravulizumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of ravulizumab is presented in 3 sections with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second section includes sponsor-submitted long-term extension studies. The third section includes indirect evidence from the sponsor. There can also be a fourth section in such reviews that includes additional studies considered by the sponsor to address important gaps in the systematic review evidence. However, no studies addressing gaps were submitted by the sponsor in the review of ravulizumab.
Included Studies
Clinical evidence from the following are included in the review and appraised in this document:
1 pivotal study (the CHAMPION-MG trial)24 identified in the systematic review, including data from 2 post hoc cohorts28 submitted for this resubmission
1 long-term extension study47
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
Characteristics of the included study are summarized in Table 6.
Table 6: Details of CHAMPION-MG Study
Characteristic | CHAMPION-MG study |
|---|---|
Designs and populations | |
Study design | Phase III, randomized, double-blind, placebo-controlled, multicentre RCT Post hoc analyses were conducted in 2 specific cohorts:
|
Locations | 85 sites in 13 countries (Canada, Czech Republic, Denmark, France, Germany, Israel, Italy, Japan, the Netherlands, South Korea, Spain, Switzerland, and the US) |
Key dates | Study initiation date: March 26, 2019 (first patient randomized) Primary analysis data cut-off date: May 11, 2021 (last RCP visit) End-of-study data cut-off date: May 25, 2023 (last participant’s last visit) |
Randomized (N) | 175 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Ravulizumab (loading dose on day 1, and maintenance dose on day 15 and q.8.w. thereafter) by IV infusion over approximately 2 hours:
|
Comparator(s) | Matching placebo solution, administered by IV infusion, as a loading dose on day 1 and maintenance doses on day 15 and q.8.w. thereafter |
Study duration | |
Screening phase | Up to 4 weeks |
RCP phase | 26 weeks |
OLE phase | Up to 4 years |
Outcomes | |
Primary end point | Change from baseline in MG-ADL total score at week 26 of the RCP |
Secondary and exploratory end points | Secondary end points
Exploratory end points
|
Publication status | |
Publications | Vu T, Meisel A, Mantegazza R, et al. Terminal Complement Inhibitor Ravulizumab in Generalized Myasthenia Gravis. NEJM Evid, 2022; 1(5). DOI: 10.1056/EVIDoa2100066 Meisel A, Annane D, Vu T et al. Long-term efficacy and safety of ravulizumab in adults with anti-acetylcholine receptor antibody-positive generalized myasthenia gravis: results from the phase 3 CHAMPION MG open-label extension. J Neurol. 2023 Aug;270(8):3862 to 3875. DOI: 10.1007/s00415-023-11699-x. NCT03920293: https://classic.clinicaltrials.gov/ct2/show/NCT03920293 |
AChR = acetylcholine receptor; gMG = generalized myasthenia gravis; IST = immunosuppressive therapy; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item Scale - Revised; MGC = Myasthenia Gravis Composite; MGFA = Myasthenia Gravis Foundation of America; MGFA-PIS = Myasthenia Gravis Foundation of America Post-intervention Status; Neuro-QoL = Quality of Life in Neurological Disorders; OLE = open-label extension; q.8.w. = every 8 weeks; QMG = Quantitative Myasthenia Gravis; RCP = randomized controlled period; RCT = randomized controlled trial.
Sources: Clinical Study Report for the CHAMPION-MG trial,24 and addendum of the CHAMPION-MG trial.28,47 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The CHAMPION-MG trial (N = 175)24 was a phase III, double-blind, multicentre, placebo-controlled RCT with an OLE period of up to 4 years. The primary objective of the CHAMPION-MG trial was to evaluate the safety and efficacy of ravulizumab compared with placebo in complement inhibitor–naive adult patients with gMG.
The study design consisted of 3 periods: a screening period of up to 4 weeks, a 26-week double-blind RCP, and an OLE period of up to 4 years (or until the product is registered or approved and available by prescription [in accordance with country-specific regulations], or until the study drug can be provided via an Alexion post-trial access program, whichever occurs first). After screening, if all of the inclusion criteria and none of the exclusion criteria were met, patients were vaccinated against N. meningitidis, if not already vaccinated within the 3 years before their enrolment in the study.48 Following screening, adult patients with anti–AChR antibody–positive gMG were enrolled at 85 centres in 13 countries (primarily North America and Europe; 5 sites in Canada) and randomized 1:1 to receive either a weight-based dose of ravulizumab or a matching placebo for 26 weeks. Randomization was stratified by region (North America, Europe, Asia-Pacific, and Japan). The matching placebo, consisting of a sterile clear solution in an identically packaged 30-mL vial, was administered on the same schedule. All investigative site personnel, sponsor staff and designees, staff directly associated with the conduct of the study, and patients were blinded to treatment assignment.
The RCP portion of the trial is complete (the data cut-off date was May 11, 2021; the database was locked on June 30, 2021) and the OLE concluded on May 25, 2023 (the date of the last patient’s last visit). Patients receiving an IST at screening could continue taking their baseline ISTs throughout the RCP and OLE portions.
Populations
Inclusion and Exclusion Criteria
Patients enrolled in the CHAMPION-MG study were male and female adults diagnosed with anti-AChR antibody–positive gMG at least 6 months before the screening visit. Patients had MGFA clinical classification of class II to class IV at screening and their MG-ADL profile score must have been 6 or greater at both screening and randomization. Patients who were currently receiving treatment with AChE inhibitors and/or ISTs (i.e., oral corticosteroids, azathioprine, mycophenolate mofetil, methotrexate, cyclosporine, tacrolimus, or cyclophosphamide) must have been receiving treatment and must have been on a stable dose for protocol-specified time periods. Patients were excluded from the study if they had any active or untreated thymoma, or a history of thymic carcinoma or thymic malignancy. Patients with a history of thymectomy, thymomectomy, or any thymic surgery within the 12 months before screening were also excluded. Additionally, if patients presented with clinical features that were consistent with an MG crisis or exacerbation or with clinical deterioration at the time of the screening visit, or before randomization, they were ineligible for study participation. Finally, patients did not advance past screening if they had received previous treatment with complement inhibitors. In total, 175 patients (86 patients in the ravulizumab group and 89 patients in the placebo group) from 13 countries were enrolled; of those, 6 patients were enrolled from sites in Canada.
In this resubmission, the sponsor provided new clinical evidence to support its revised reimbursement request: ravulizumab as add-on therapy for adult patients with anti-AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChE inhibitors, corticosteroids, and/or NSISTs. Post hoc analyses were performed in a concomitant IST optimized cohort and a refractory concomitant IST optimized cohort.
The sponsor noted that there is no universally accepted definition of IST “optimization” in clinical practice. Therefore, the inclusion criteria of the previous Study ADAPT (efgartigimod alfa versus placebo) and Study REGAIN (eculizumab versus placebo) were adopted to select patients who would be considered to have IST optimization and IST optimization with refractory disease at the time of study enrolment from the CHAMPION-MG trial, respectively. These criteria were based on “total treatment duration” and “stable dose duration” before screening. Therefore, the definitions of the 2 cohorts were as follows.
Concomitant IST optimized cohort: This was a subset of the full population in the CHAMPION-MG trial (n = ███ of 175 patients in the full population, █████ included patients who were on at least 1 concomitant IST at screening and met the following:
if on a concomitant corticosteroid, the patient had been treated with that steroid for 3 or more months before screening and had been on a stable dose for 1 or more month
if on a concomitant NSIST (e.g., azathioprine), the patient had been treated with that NSIST for 6 or more months before screening and had been on a stable dose of that NSIST for 3 or more months.
Refractory concomitant IST optimized cohort: This was a subset of the full population in the CHAMPION-MG trial ██ ██ of 175 patients in the full population █████████████ patients in the concomitant IST optimized cohort, █████). Patients in this refractory cohort met both the concomitant IST optimized cohort criteria as well as the definition of refractory disease per the inclusion criteria of Study REGAIN. Specifically, patients in this cohort of the CHAMPION-MG trial were defined as not achieving symptom control after 12 months of treatment with either of the following:
2 or more ISTs
1 or more IST and chronic IVIg or PLEX.
Interventions
During the randomization period, patients received a weight-based loading dose of ravulizumab or placebo on day 1, followed by maintenance doses of ravulizumab or placebo on day 15 and every 8 weeks thereafter until week 26. Both ravulizumab and placebo were administered by IV infusion. Following week 26, all patients could transition into the OLE phase, which continued for up to 4 years.
Patients received a body weight–based loading dose of ravulizumab (10 mg/mL concentrate) on day 1 as follows:
a body weight of 40 kg or greater but less than 60 kg meant a loading dose of 2,400 mg
a body weight of 60 kg or greater but less than 100 kg meant a loading dose of 2,700 mg
a body weight of 100 kg or greater meant a loading dose of 3,000 mg.
Subsequently, patients received body weight–based maintenance doses of ravulizumab on day 15 and every 8 weeks (± 2 weeks) thereafter during the RCP (week 10 and week 18) as follows:
a body weight of 40 kg or greater but less than 60 kg meant a maintenance dose of 3,000 mg
a body weight of 60 kg or greater but less than 100 kg meant a maintenance dose of 3,300 mg
a body weight of 100 kg or greater meant a maintenance dose of 3,600 mg.
Supplemental doses of ravulizumab were administered if IVIg or PLEX rescue therapy was provided on nondosing days (no supplemental drug was given if rescue therapy was provided before study drug administration on a dosing day). Supplemental ravulizumab was administered within 4 hours of each PLEX session or within 4 hours of the completion of each IVIg cycle. This is consistent with the recommendation in the product monograph.22 A fixed dose of 600 mg of ravulizumab was administered following IVIg (with a minimum infusion time of 0.4 hours to 0.5 hours). Patients received a body weight–based supplemental dose of ravulizumab following PLEX as follows:
a body weight of 40 kg or greater but less than 60 kg meant if the most recent dose was 2,400 mg, the supplemental dose was 1,200 mg and the minimum infusion time was 1.0 hour; if the most recent dose was 3,000 mg, the supplemental dose was 1,500 mg and the minimum infusion time was 1.2 hours
a body weight of 60 kg or greater but less than 100 kg meant if the most recent dose was 2,700 mg, the supplemental dose was 1,500 mg and the minimum infusion time was 1.0 hour; if the most recent dose was 3,300 mg, the supplemental dose was 1,800 mg and the minimum infusion time was 1.1 hours
a body weight of 100 kg or greater meant if the most recent dose was 3,000 mg, the supplemental dose was 1,500 mg and the minimum infusion time was 1.0 hour; if the most recent dose was 3,600 mg, the supplemental dose was 1,800 mg and the minimum infusion time was 1.1 hours.
Allowed concomitant medications included AChE inhibitors, immunosuppressive drugs (corticosteroids, azathioprine, mycophenolate, methotrexate, tacrolimus, cyclosporine, and cyclophosphamide), and rescue therapy with IVIg or PLEX. Patients who entered the study receiving AChE inhibitors were to maintain the dose and schedule unless there was a compelling medical need and the sponsor approval had to be obtained before the change in order for the patient to remain on the study. AChE inhibitors were withheld for at least 10 hours before QMG and Myasthenia Gravis Composite assessments. Patients who entered the study receiving corticosteroids or IST were to maintain their dose and schedule; dose changes needed to be authorized by the sponsor and corticosteroid dose increases could not exceed the dose at baseline. Disallowed concurrent medications included rituximab and eculizumab (or other complement inhibitors).
Rescue therapy with IVIg or PLEX could be administered for clinical deterioration, defined per protocol as 1 of the following:
there was an MG crisis (respiratory muscle weakness severe enough to necessitate intubation or to delay extubation following surgery, often accompanied by severe bulbar muscle weakness)
there was a significant symptomatic worsening to a score of 3 points or a 2-point worsening from baseline on any 1 of the individual MG-ADL items other than double vision or eyelid droop
patient health would be in jeopardy if rescue therapy was not given, in the opinion of the investigator or investigator-designated physician.
Outcomes
A list of efficacy and harms outcomes assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence72 as well as any outcomes identified as important to this review according to the clinical expert consulted by the review team and input from patient and clinician groups and public drug plans. Using the same considerations, the review team selected end points that were considered to be most relevant to inform expert committee deliberations. Note that these outcomes were selected for the analyses of the full population in the CHAMPION-MG trial. However, all the new analyses in the 2 subgroups are post hoc and unadjusted for multiplicity.
Table 7: Main Outcomes Summarized From CHAMPION-MG Study
Outcome measure | Time point | CHAMPION-MG study |
|---|---|---|
Change from baseline in the MG-ADL total score | At week 26 | Primary |
Change from baseline in QMG total score | At week 26 | Key secondary #1a |
Improvement of at least 5 points in the QMG total score from baseline | At week 26 | Key secondary #2a |
Change from baseline in the MG-QoL15r score | At week 26 | Key secondary #3a |
Change from baseline in the Neuro-QoL fatigue score | At week 26 | Key secondary #4a |
Improvement of at least 3 points in the MG-ADL total score from baseline | At week 26 | Key secondary #5a |
Incidence of clinical deterioration or an MG crisis | At week 26 | Exploratory |
Incidence of AEs and SAEs | At week 26 | Safety |
AE = adverse event; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item Scale - Revised; Neuro-QoL = Quality of Life in Neurological Disorders; QMG = Quantitative Myasthenia Gravis; SAE = serious adverse event.
aStatistical testing for these end points was adjusted for multiple comparisons in the primary analyses (e.g., hierarchical testing) in the full population in the CHAMPION-MG trial, using a closed testing procedure. If an end point did not achieve statistical significance (P value > 0.05), then subsequent end points in the prespecified order were considered to be not statistically significant and reported P values were considered nominal. Numbers included in parentheses denote testing order. No end points were adjusted for multiple comparisons in the post hoc analyses in the 2 cohorts.
Sources: Clinical Study Report for the CHAMPION-MG trial.24 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Primary Outcome
The primary efficacy outcome was the change from baseline in the MG-ADL total score at week 26. The MG-ADL is an 8-item survey to measure the severity of patient-reported MG symptoms and their impact on patients’ daily activities, with each response rated from 0 (normal) to 3 (most severe); the total MG-ADL score is the sum of the scores of the 8 items and ranges from 0 to 24.49,50 A reduction in score indicates improvement and the MCID on the MG-ADL scale is estimated to be 2 points based on the change within an individual patient.25 The MG-ADL assessment was performed by a properly trained clinical evaluator, delegated by the investigator. The MG-ADL is a commonly used assessment tool in clinical practice as no objective tests (e.g., blood or other laboratory test) are available for monitoring efficacy in patients with gMG.
Secondary Outcomes
The secondary efficacy outcomes (all measured at week 26) were as follows:
change from baseline in QMG total score
improvement from baseline of 5 or more points in the QMG total score
change from baseline in MG-QoL15r score
change from baseline in Neuro-QoL fatigue score
improvement from baseline of 3 or more points in the MG-ADL total score.
The QMG is a 13-item clinician-determined assessment of MG disease status, with each item graded for severity from 0 (normal function) to 3 (loss of ability to perform that function); the total score of QMG is the sum of the scores of the 13 items and ranges from 0 to 39.51 A higher score is indicative of more severe disease. A definite MID for the QMG scale has not been established, although a threshold ranging between 2 points and 3 points depending on disease severity has been suggested in previous studies enrolling patients with MG.26,27 The MCID for QMG is estimated to be 3 points for patients with higher baseline QMG scores (> 16) within an individual patient.27 A 5-point or greater improvement in the QMG total score from baseline at week 26 was selected as a robust clinical significance threshold for the second hierarchical secondary end point. The QMG assessment was performed by a properly trained clinical evaluator, delegated by the investigator.
The MG-QoL15r questionnaire (a revised version of the Myasthenia Gravis Quality of Life 15-item Scale) is a 15-item patient-reported HRQoL instrument for MG, with each item having 3 response options: 0 (not at all), 1 (somewhat), and 2 (very much); total scores range from 0 to 30, with higher scores indicating a greater extent of dissatisfaction with MG-related dysfunction.52 MCIDs have yet to be established for the MG-QoL15r questionnaire.
The Neuro-QoL fatigue subscale is an instrument evaluating the effect of fatigue on the quality of life of patients with neurologic disorders.53 It comprises 19 patient-reported items assessing the frequency of different aspects of fatigue over the previous 7 days, answered using a 5-point scale ranging from 1 (never) to 5 (always); total scores range from 19 to 95. Higher scores indicate greater fatigue and a greater impact of MG on activities. MCIDs have yet to be established for the Neuro-QoL fatigue subscale.
The proportion of patients who experienced a 3-point or greater improvement in MG-ADL total score at week 26 was another secondary end point. The 3-point reduction threshold was selected to exceed the estimated MCID of 2 points for the MG-ADL scale.25
Exploratory Outcomes
The incidence of clinical deterioration was 1 of the exploratory outcomes in the CHAMPION-MG trial. Clinical deterioration was defined as 1 of the following: an MG crisis (respiratory muscle weakness severe enough to necessitate intubation or delay extubation following surgery, often accompanied by severe bulbar muscle weakness); significant symptomatic worsening to a score of 3 points or a 2-point worsening from baseline on any 1 of the individual MG-ADL items other than double vision or eyelid droop; or the fact that patient health would be in jeopardy if rescue therapy were not given, in the opinion of the investigator or investigator-designated physician.
The incidence of an MG crisis was another exploratory outcome.
Harms Outcomes
Safety and tolerability of ravulizumab was evaluated by the incidence of patients with at least 1 AE, SAE, and adverse events of special interest (AESIs) over time. Meningococcal infections were collected as the AESI for this study. All AEs were treatment-emergent (unless otherwise specified) and were summarized according to the number and percentage of patients with events.
AEs were defined as:
any abnormal laboratory result or other safety assessment
the exacerbation of a chronic or intermittent pre-existing condition
new conditions detected or diagnosed after study drug administration
signs, symptoms, or the clinical sequelae of a suspected drug-drug interaction.
An SAE was defined as an AE at any dose that:
resulted in death
was life-threatening
required hospitalization
resulted in persistent disability or incapacity.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
MG-ADL questionnaire | An 8-item patient-reported outcome measure assessing MG symptoms and functional activities related to patients’ daily life and producing a total score ranging from 0 to 24, where higher scores indicate greater severity of symptoms. The MG-ADL is composed of items related to patients’ assessment of functional disability secondary to ocular (2 items), bulbar (3 items), respiratory (1 item), and gross motor or limb (2 items) impairment.49 | Validity The MG-ADL highly correlated with the MGC (r = 0.85; P < 0.0001) and MG-QoL15 (r = 0.76; P < 0.0001) (n = 87). Correlation of the MG-ADL score and physician impression of change between the visits was strong (r = 0.70; P < 0.0001) (n = 76).54 Reliability Test-retest reliability coefficient of 93.7% among 20 patients, with lower bound of the 95% CI at 87.3%, tested twice within 1 week54 Responsiveness The MG-ADL was assessed at 2 visits, where the mean improvement in score in patients who improved, based on the gold standard, was 3.88 (SD = 2.72) (n = 76).54 Note: The measurement properties of the subcomponents of the scale have not been investigated. | An MID in patients with MG has not been estimated. A 2-point improvement in MG-ADL score was a threshold that provided the best balance of sensitivity (n = 26) and specificity (n = 50) when referenced to MG-QoL15 and physician impression of change for predicting clinical improvement at the level of the individual for patients with MG.25 |
QMG scale | A 13-item direct physician assessment scoring system that quantifies disease severity, based on impairments of body functions and structures. The total QMG score ranges from 0 to 39, where higher scores indicated greater disease severity. The QMG score is composed of the following items: ocular (2 items), facial (1 item), bulbar (2 items), gross motor | Validity Construct validity was assessed through correlations with MMT (r = 0.69 in 303 patients35 and r = 0.73 in 53 patients55). Reliability Internal consistency assessed via a Cronbach alpha value was 0.74 for the QMG, demonstrating an acceptable threshold (n = 251).56,57 Test-retest reliability was studied in 209 stable patients assessed 2 weeks apart. The intraclass correlation coefficient for the total scores was 0.88 (95% CI, 0.85 to 0.91).56,57 Responsiveness The index of responsiveness (signal-to-noise ratio) was 1.45 (n = 53).55 Note that the measurement properties of the subcomponents of the scale have not been investigated. | Based on results from 5 patients with MG and 4 healthy individuals and an interrater reliability of 1.342 SD, any change in the QMG score of up to 2.6 points was expected to occur due to the variability of repeated observations; therefore, a change of 2.6 points was estimated to be the threshold of clinical significance in patients with MG.51 Using the anchor-based method with the patients’ perception of overall improvement as assessed by a VAS, there was some evidence that the MID should be higher in patients with higher baseline QMG scores, where the MID with mild to moderate MG (QMG ≤ 16) was estimated to be 2 points (n = 38), compared to patients with higher baseline values (QMG > 16) for whom the estimated MID was 3 points (n = 12).26,27 |
MG-QoL15r scale | The MG-QoL15 is a patient-reported 15-item questionnaire that allows clinicians to estimate a patient’s quality of life relevant to MG. Items on the MG-QoL15 relate to physical, social, and psychological components and are scored from 0 (not at all) to 4 (quite a bit). The cumulative scores range from 0 to 60, with higher scores representing a worse quality of life.52 The MG-QoL15r is a revised version of the MG-QoL15 questionnaire. Items on the MG-QoL15r relate to physical, social, and psychological components and are scored on a 3-response option scale (0 = not at all; 1 = somewhat; 2 = very much), with higher scores indicating worse quality of life over the past few weeks.52 | The psychometric properties of MG-QoL15r, QMG, MG-ADL, and MGC were evaluated and compared to response to disease change in patients with autoimmune MG (N = 872).58 Validity Construct validity was demonstrated for MG-QoL15r with QMG (r = 0.550), MG-ADL (r = 0.701), and MGC (r = 0.635). For discriminant validity, the MG-QoL15r scores differed between patients based on their MGFA classification and MGC scores.58 Reliability Internal consistency reliability was demonstrated by the Cronbach alpha of 0.93 for MG-QoL15r.58 Responsiveness For responsiveness to change, the Pearson correlation coefficients between changes in the 4 scales after treatment ranged from 0.423 (MG-QoL15r and QMG) to 0.849 (MGC and QMG).58 | An MID for patients with MG was not estimated. |
Neuro-QoL fatigue scale | The Neuro-QoL fatigue scale is a generic 19-item patient-reported survey of fatigue. Items are scored from 1 (never) to 5 (sometimes). Total scores range from 19 to 95, where higher scores indicate greater fatigue and greater impact of MG on activities.24,53 | Validity Based on data from 125 patients with refractory gMG, the correlations of the Neuro-QoL fatigue scale with the MG-QoL15 were identified for patients treated with eculizumab (r = 0.74 [95% CI, 0.59 to 0.84; P = 0.0002]) and placebo (r = 0.65 [95% CI, 0.47 to 0.78; P = 0.01]).59 Reliability No information Responsiveness No information | An MID for patients with MG has not been estimated. |
CI = confidence interval; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MG-QoL15 = Myasthenia Gravis Quality of Life 15-item Scale; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item Scale - Revised; MGC = Myasthenia Gravis Composite; MGFA = Myasthenia Gravis Foundation of America; MID = minimal important difference; MMT = manual muscle testing; Neuro-QoL = Quality of Life in Neurological Disorders; QMG = Quantitative Myasthenia Gravis; r = correlation coefficient; SD = standard deviation; VAS = visual analogue scale.
Statistical Analysis
Statistical analyses of efficacy and harms outcomes in the full population in the CHAMPION-MG trial have been described in detail in the Clinical Review Report of the previous ravulizumab submission.
In the primary analysis of the full population, a sample size of approximately 160 patients was planned to ensure at least 90% nominal power to reject the null hypotheses of no treatment difference for the primary and secondary end points at a 2-sided alpha level of 0.05 and based on a t statistic for 2 independent samples. Sample size calculation in the CHAMPION-MG trial was not based on the concomitant IST optimized cohort or the refractory concomitant IST optimized cohort, which are the focus of this report.
In the full population, type I error was controlled using a closed-loop hierarchical testing strategy to limit the overall 2-sided type I error rate to alpha equalling 0.05. Between the primary and secondary efficacy outcomes, and within the secondary outcomes, a sequential hypothesis testing procedure was used for multiplicity adjustment. The primary outcome (change in the MG-ADL total score from baseline to week 26) was tested first, followed by 5 secondary outcomes (refer to Table 6 for the order of testing). All null hypotheses were tested at alpha equalling 0.05. If statistical significance was not achieved for an end point within the hierarchy, subsequent end points in the prespecified order were not to be considered statistically significant and all P values were considered nominal. Exploratory efficacy outcomes were not included in the hierarchical testing strategy and statistical tests of these outcomes were not adjusted for multiplicity. There was no hierarchical testing procedure used to control the overall type I error to control for multiple comparisons in the 2 post hoc cohorts.
Sensitivity analyses of the primary outcome included a placebo-based analysis (i.e., considering a potential missing not at random mechanism for the missing data) and a tipping point analysis. Sensitivity analyses of both the primary and secondary outcomes included identical mixed model of repeated measures (MMRM) analyses conducted in the per-protocol set and the modified FAS as well as an MMRM excluding randomization stratification region and an MMRM including rescue therapy received in the model.
In the primary analysis, subgroup analyses were performed for all secondary outcomes as per the primary analysis using an MMRM except with an additional subgroup covariate — by treatment interaction. The following prespecified subgroup analyses were performed based on geographic region, sex, race, age at first study drug infusion, IST use at baseline, years from diagnosis to informed consent, baseline MGFA classification, and baseline body weight. The study was not specifically powered to evaluate differences in outcomes among the individual strata.
Post Hoc Analyses in the Concomitant IST Optimized Cohort and Refractory Concomitant IST Optimized Cohort
The statistical analyses used were consistent with the statistical methods used for the primary analysis and followed the methods in the CHAMPION-MG trial’s statistical analysis plan (Table 9). All demographic, baseline, and disease characteristics were summarized by treatment group. The number of patients who received a stable dose of NSIST, corticosteroid, or both per inclusion triggers was summarized by treatment group. Descriptive statistics on the duration of use were provided, concomitant ISTs were used during the RCP, and changes in concomitant MG medication therapies used were summarized.
For primary and secondary continuous end points, changes from baseline at week 26 were analyzed using an MMRM model. The model included the change from baseline score as the response variable, fixed categorical effects of treatment, study visit and treatment-by-study-visit interaction, the randomization stratification variable geographic region, and a fixed covariate of baseline score. A difference in treatment effect between the ravulizumab and placebo treatment groups along with a 2-sided 95% CI and P value were calculated. Missing data were not imputed. In addition to these analyses, differences in treatment effect for the concomitant IST optimized cohort versus the remainder of the FAS for both change from baseline to week 26 in MG-ADL (and QMG) were assessed using an MMRM as specified for the primary end point with the inclusion of cohort status, treatment by cohort status interaction, and treatment by cohort-status-by-visit interaction. For the primary efficacy end point (change in the MG-ADL total score) and key secondary efficacy end points, sensitivity analyses were conducted in the concomitant IST optimized cohort by excluding patients with any increases in IST dosing during the RCP.
The secondary end points of at least a 5-point improvement in QMG total score from baseline to week 26 (and at least a 3-point improvement in MG-ADL) were analyzed using a generalized linear mixed model including the same explanatory covariates as for the continuous end points. Odds ratios (ORs) of the treatment effect (ravulizumab group compared to placebo) along with 2-sided 95% CIs and P values were calculated. An estimate of an OR greater than 1 indicated a beneficial treatment effect.
For the exploratory outcomes of incidence of clinical deterioration and MG crisis, the number of patients who experienced these events was summarized by treatment group.
Table 9: Statistical Analysis of Efficacy End Points in the Cohorts and Full Population in CHAMPION-MG Study
End point: analysis sets | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses | |
|---|---|---|---|---|---|
Statistical analysis methods (model, adjustment factors, and missing data handling) were the same in full population, concomitant IST optimized cohort, and refractory concomitant IST optimized cohort | Cohorts | Full population | |||
Primary end point: Change from baseline in MG-ADL total score at week 26 | MMRM | Fixed categorical effects of treatment, study visit and treatment-by-study-visit interaction, and region; fixed covariate of baseline MG-ADL total score | No imputation MAR assumption | Conducted in the concomitant IST optimized cohort by excluding patients with any increases in IST dosing during the RCP |
|
Secondary end point #1: Change from baseline in QMG total score | MMRM | As per primary analysis (using baseline QMG total score) | No imputation | Conducted in the concomitant IST optimized cohort by excluding patients with any increases in IST dosing during the RCP |
|
Secondary end point #2: Improvement of at least 5 points in the QMG total score from baseline | GLMM | Fixed categorical effects of treatment, study visit and treatment-by-study-visit interaction, and region; fixed covariate of baseline QMG total score | No imputation MAR assumption | Conducted in the concomitant IST optimized cohort by excluding patients with any increases in IST dosing during the RCP |
|
Secondary end point #3: Change from baseline in the MG-QoL15r score | MMRM | As per primary analysis (using baseline MG-QoL15r score) | No imputation MAR assumption | Conducted in the concomitant IST optimized cohort by excluding patients with any increases in IST dosing during the RCP |
|
Secondary end point #4: Change from baseline in Neuro-QoL fatigue score | MMRM | As per primary analysis (using baseline Neuro-QoL fatigue score) | No imputation MAR assumption | Conducted in the concomitant IST optimized cohort by excluding patients with any increases in IST dosing during the RCP |
|
Secondary end point #5: Improvement of at least 3 points in the MG-ADL total score from baseline | GLMM | Fixed categorical effects of treatment, study visit and treatment-by-study-visit interaction, and region; fixed covariate of baseline MG-ADL total score | No imputation | Conducted in the concomitant IST optimized cohort by excluding patients with any increases in IST dosing during the RCP |
|
FAS = full analysis set; GLMM = generalized linear mixed model; IST = immunosuppressive therapy; MAR = missing at random; mFAS = modified full analysis set; MG-ADL = Myasthenia Gravis Activities of Daily Living; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item Scale - Revised; MMRM = mixed model of repeated measures; MNAR = missing not at random; OR = odds ratio; PPS = per-protocol set; QMG = Quantitative Myasthenia Gravis; RCP = randomized controlled period.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Analysis Populations
In the CHAMPION-MG study, the FAS included all patients who had received at least 1 dose of the study drug; patients were analyzed according to the treatment they were randomized to receive, regardless of the treatment received. The per-protocol set included all patients in the FAS without any major protocol deviations during the RCP. The overall safety analysis set in the CHAMPION-MG study included all patients who had received at least 1 dose of the study drug; patients were analyzed according to the treatment they actually received, and must have received that treatment for the entire duration of the RCP. The safety set in the 2 post hoc subgroups was a subset of the overall safety analysis set.
The populations used in the cohort analyses in this study are described in Table 10.
Table 10: Populations in Cohort Analyses in the CHAMPION-MG Study During Randomization Controlled Period
Cohort | Population | Definition | Application |
|---|---|---|---|
Cohort 1 | FAS concomitant IST optimized cohort | Subset of the FAS, including participants who were on ≥ 1 concomitant IST at screening and met the following criteria:
| Efficacy analyses |
Cohort 2 | FAS refractory concomitant IST optimized cohort | Subset of FAS concomitant IST optimized cohort excluding nonrefractory participants defined as participants treated with only 1 IST and who had not received chronic IVIg or PLEX at least every 3 months, or no IST within the last 12 months before the screening visit | Efficacy analyses |
Safety set | A subset of the overall safety analysis set | Included all patients who received at least 1 dose of the study drug; patients were analyzed according to the treatment they actually received, and must have received that treatment for the entire duration of the randomized controlled period | Safety analyses |
CS = corticosteroid; FAS = full analysis set; IST = immunosuppressive therapy; IVIg = IV immunoglobulin; NSIST = nonsteroidal immunosuppressive therapy; PLEX = plasma exchange or plasmapheresis.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
Patient disposition in the full population and 2 post hoc subgroups of the CHAMPION-MG trial is summarized in Table 11. In the full population, among 242 patients screened, 175 (72.3%) patients were randomized and 67 (27.7%) patients did not advance past screening. The most common reasons for not advancing past screening were not having a positive serologic test for anti-AChR antibodies (25 [10.3%] patients) and an MG-ADL score of 6 or less (16 [6.6%] patients). All 175 of the randomized patients were treated with the study drug.
Thirteen of the 175 (7.4%) randomized patients withdrew from the study before completing the RCP (6 patients in the placebo group and 7 patients in the ravulizumab group). The most common reasons for discontinuation were patient decision (3 patients), physician decision (3 patients), death (2 patients), and AEs (2 patients). Overall, 161 (92%) patients entered the OLE period.
In the concomitant IST optimized cohort █| patients (████) in the ravulizumab group and || (████) in the placebo group withdrew from the study before completing the 26-week treatment. In the refractory concomitant IST optimized cohort, || patients (█████) in the ravulizumab group and || (████) in the placebo group withdrew before completing the 26-week treatment. The reasons for early discontinuation in these 2 cohorts were similar to those in the full population.
Table 11: Patient Disposition in CHAMPION-MG Study
Patient disposition | CHAMPION-MG study Full population | Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort | |||
|---|---|---|---|---|---|---|
Placebo | Ravulizumab | Placebo | Ravulizumab | Placebo | Ravulizumab | |
Screened, N | 242 | NA | NA | |||
Randomized, N (%) | 89 (100.0) | 86 (100.0) | ██████ | ██████ | ██████ | ██████ |
Treated, n (%) | 89 (100.0) | 86 (100.0) | ██████ | ██████ | ██████ | ██████ |
Discontinued from study, n (%) | 6 (6.7) | 7 (8.1) | ██████ | ██████ | ██████ | ███████ |
Reason for discontinuation, n (%) | ||||||
Death | 0 | 2 (2.3) | 0 | ██████ | 0 | ██████ |
Patient decision | 1 (1.1) | 2 (2.3) | || | ██████ | || | ██████ |
Noncompliance | 0 | 1 (1.2) | 0 | ██████ | 0 | ██████ |
Physician decision | 2 (2.2) | 1 (1.2) | || | || | || | || |
AE | 2 (2.2) | 0 | || | 0 | || | 0 |
Protocol violation | 0 | 1 (1.2) | 0 | ██████ | 0 | █████ |
Other | 1 (1.1) | 0 | ██████ | 0 | ██████ | 0 |
Entered OL extension period, n (%) | 81 (91.0) | 77 (89.5) | ██████ | ███████ | ██████ | ██████ |
FAS, N (%) | 89 (100.0) | 86 (100.0) | ██████ | ██████ | ██████ | ██████ |
PPS, N (%) | 79 (88.8) | 76 (88.4) | ██ | ██ | ||
Safety set, N (%) | 89 (100.0) | 86 (100.0) | ██████ | ███████ | ██████ | ██████ |
AE = adverse event; FAS = full analysis set; IST = immunosuppressive therapy; mFAS = modified full analysis set; NA = not applicable; NR = not reported; OL = open-label; PPS = per-protocol set.
Note: Patient disposition information in Table 11 was collected through the end of the week 26 randomized controlled period for all patients. Results were presented for patients who received 1 or more doses of ravulizumab in the OLE period and who completed (or would have completed but discontinued) a total of 52 weeks of treatment as of the data cut-off date of May 11, 2021.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
Of the full CHAMPION-MG trial population (n = 175), ██████████████ (███/175 patients = █████) were receiving concomitant IST at baseline and met the dose optimization criteria used in Study ADAPT. In Study ADAPT, patients were required to be on a stable dose of at least 1 treatment for gMG (e.g., AChE inhibitors, corticosteroids, NSISTs) before screening and throughout the trial. These patients formed the concomitant IST optimized cohort; a ███████ number of patients were included in the ravulizumab arm (n ███) and the placebo arm (n = ██). The refractory concomitant IST optimized cohort included ██ patients (█████ of the FAS population) with refractory disease despite concomitant optimized ISTs.
Baseline demographic and disease characteristics of the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort were ██████████ with the full CHAMPION-MG study population in terms of distribution of ███████████████████████████████████████████████ ████████ ████████████████████████████████████████ ██████████████████████████████████████, as shown in Table 12.
The baseline characteristics outlined in Table 12 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
Table 12: Baseline Characteristics in CHAMPION-MG Study — Concomitant IST Optimized Cohort Versus Refractory Concomitant IST Optimized Cohort Versus FAS Population
Characteristic | Placebo | Ravulizumab | ||||
|---|---|---|---|---|---|---|
Concomitant IST optimized cohort (N = 69) | Refractory concomitant IST optimized cohort (████) | FAS (N = 89) | Concomitant IST optimized cohort (N = 63) | Refractory concomitant IST optimized cohort (████) | FAS (N = 86) | |
Age at MG diagnosis (years) | ||||||
Mean (SD) | ██████████ | ██████████ | 43.7 (19.04) | ██████████ | ██████████ | 48.6 (18.54) |
Median (range) | ███████████ | ███████████ | 44.8 (12 to 81) | █████████ | ██████████ | 50.4 (12 to 77) |
Time since MG diagnosis (years) | ||||||
Mean (SD) | █████████ | ███████ | 10.0 (8.90) | ███████ | ███████ | 9.8 (9.68) |
Median (range) | ███████████ | ███████████ | 7.6 (0.5 to 36.1) | ███████████ | ███████████ | 5.7 (0.5 to 39.5) |
Sex | ||||||
Male | ███████ | ███████ | 44 (49.4) | █████ | █████ | 42 (48.8) |
Female | ███████ | ███████ | 45 (50.6) | █████ | ███████ | 44 (51.2) |
Type of first MG clinical presentation, n (%) | ||||||
Ocular MG | ███████ | ███████ | 29 (32.6) | ███████ | ███████ | 21 (24.4) |
Generalized MG | ███████ | ███████ | 60 (67.4) | ███████ | ███████ | 65 (75.6) |
Baseline MGFA clinical classification, n (%) | ||||||
Class IIa | ███████ | ███████ | 24 (27.0) | ███████ | ███████ | 22 (25.6) |
Class IIb | ███████ | ███████ | 15 (16.9) | ███████ | ██████ | 17 (19.8) |
Class IIIa | ███████ | ███████ | 34 (38.2) | ███████ | ███████ | 22 (25.6) |
Class IIIb | ███████ | ███████ | 11 (12.4) | ███████ | ███████ | 19 (22.1) |
Class IVa | ██████ | ██████ | 4 (4.5) | ██████ | ██████ | 2 (2.3) |
Class IVb | ██████ | ██████ | 1 (1.1) | ██████ | ██████ | 4 (4.7) |
Baseline MG-ADL total score | ||||||
Mean (SD) | ██████ | ██████ | 8.9 (2.30) | ██████ | ██████ | 9.1 (2.62) |
Median (range) | ███████████ | ███████ | 9.0 (6.0 to 15.0) | ███████████ | █████████ | 9.0 (6.0 to 24.0) |
Baseline QMG total score | ||||||
Mean (SD) | █████████ | █████████ | 14.5 (5.26) | █████████ | █████████ | 14.8 (5.21) |
Median (range) | ██████████ | ████████ | 14.0 (2.0 to 27.0) | ████████ | ████████ | 15.0 (6.0 to 39.0) |
FAS = full analysis population; IST = immunosuppressive therapy; IVIg = IV immunoglobulin; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; NSIST = nonsteroidal immunosuppressive therapy; PLEX = plasma exchange or plasmapheresis; QMG = Quantitative Myasthenia Gravis; SD = standard deviation.
Notes: The IST optimized cohort included patients on 1 or more concomitant IST at screening and who met the following criteria: if on a concomitant steroid, the patient had been treated with that steroid for the 3 or more months before screening and had been on a stable dose for 1 or more month; if on a concomitant NSIST, the patient had been treated with that NSIST for the 6 or more months before screening and had been on a stable dose of that NSIST for 3 or more months.
Patients in the refractory concomitant IST optimized cohort met both the concomitant IST optimized cohort criteria as well as the definition of refractory disease, which was defined as not achieving symptom control after 12 months of treatment with either 2 or more ISTs, or with 1 or more IST and chronic IVIg or PLEX.
Exposure to Study Treatments
During the RCP, treatment compliance was 94.4% in the placebo group and 96.5% in the ravulizumab group in the full population. Reasons for missed infusions were documented as either COVID-19–related or “other” reasons (due to AEs and unknown). Per the protocol, 12 (13.5%) patients in the placebo group and 7 (8.1%) patients in the ravulizumab group were administered supplemental study drug doses when PLEX or IVIg rescue therapy was administered.
In the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort, the results of study duration and treatment duration were similar to those observed in the full population (Table 13). The mean study duration in the ravulizumab group was 202.5 days, █████ days, and █████ days in the FAS, the concomitant IST optimized cohort, and the refractory concomitant IST optimized cohort, respectively. The mean study duration in the placebo group was 198.9 days, █████ days, and █████ days in the FAS, the concomitant IST optimized cohort, and the refractory concomitant IST optimized cohort, respectively. The mean treatment duration in the ravulizumab group was 179.6 days, █████ days, and █████ days in the FAS, the concomitant IST optimized cohort, and the refractory concomitant IST optimized cohort, respectively. The mean treatment duration in the placebo group was 176.5 days, █████ days, and █████ days in the FAS, the concomitant IST optimized cohort, and the refractory concomitant IST optimized cohort, respectively.
Table 13: Patient Exposure During Randomized Controlled Period of the CHAMPION-MG Study (FAS Population and Post Hoc Cohorts)
Exposure | Placebo | Ravulizumab |
|---|---|---|
Full population, n | 89 | 86 |
Study duration from informed consent (days) | ||
Mean (SD) | 198.9 (27.40) | 202.5 (22.61) |
Median (range) | 205.0 (60.0 to 218.0) | 205.0 (40.0 to 240.0) |
Treatment duration (days), n | ||
Mean (SD) | 176.5 (27.20) | 179.6 (22.39) |
Median (range) | 183.0 (46.0 to 201.0) | 183.0 (14.0 to 222.0) |
Compliance, % | 94.4 | 96.5 |
Reasons for missed infusions, n (%) | ||
COVID-19–related | 3 (3.4) | 2 (2.3) |
Other | 2 (2.2) | 2 (2.3) |
Concomitant IST optimized cohort, n | ██ | ██ |
Study duration from informed consent (days), n | ||
Mean (SD) | ███████████ | ███████████ |
Median (range) | ████████████████ | ████████████████ |
Treatment duration (days), n | ||
Mean (SD) | ███████████ | ███████████ |
Median (range) | ████████████████ | ████████████████ |
Refractory concomitant IST optimized cohort, n | ██ | ██ |
Study duration from informed consent (days), n | ||
Mean (SD) | ███████████ | ███████████ |
Median (range) | ████████████████ | ████████████████ |
Treatment duration (days), n | ||
Mean (SD) | ███████████ | ███████████ |
Median (range) | ████████████████ | ████████████████ |
FAS = full analysis set; IST = immunosuppressive therapy; SD = standard deviation.
Sources: Clinical Study Report for the CHAMPION-MG trial,24 cohort analyses of the CHAMPION-MG trial,28 and the sponsor’s Summary of Clinical Evidence.
Table 14 provides details on the median doses of the concomitant IST for the concomitant IST optimized cohort (n = ███) and the refractory concomitant IST optimized cohort (n = ██) at study enrolment. Doses are broken down into 3 categories based on the IST(s) received at the time of study enrolment: NSIST only, corticosteroid only, or corticosteroid in combination with NSIST. Note that the following drugs are considered usual care in the CHAMPION-MG trial: pyridostigmine, prednisone, azathioprine, cyclosporine, mycophenolate mofetil, and tacrolimus. Table 38 in Appendix 1 summarizes the types and frequencies of patients’ use of ISTs at baseline in the CHAMPION-MG study’s FAS population.
Table 14: Median Stable Doses of IST Treatments in Concomitant IST Optimized Cohort and Refractory Concomitant IST Optimized Cohort in the CHAMPION-MG Study at Time of Study Enrolment
IST treatment | Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort | ||||||
|---|---|---|---|---|---|---|---|---|
Ravulizumab (n = ██) | Placebo (n = ██) | Ravulizumab (n = ██) | Placebo (n = ██) | |||||
█████████ ███ | █████████ ██ | |||||||
███ | || | ██████ | || | █████ | || | █████ | || | █████ |
AZA (mg) | || | ███ | || | ███ | || | ███ | || | ███ |
AZA (mg/kg) | || | ███ | || | ███ | || | ███ | || | ███ |
MMF (mg) | || | ████ | || | ████ | || | ████ | || | ████ |
TAC (mg) | || | ███ | || | ███ | || | ██ | || | ██ |
CyS (mg) | || | ███ | || | ███ | || | ██ | || | ██ |
CyS (mg/kg) | || | ███ | || | ███ | || | ██ | || | ██ |
MTX (mg) | || | ██ | || | ██ | || | ██ | || | ██ |
██████ ███ | ██████ ███ | |||||||
███ | || | █████ | || | █████ | || | █████ | || | █████ |
CS (mg) | ██ | ██ | ██ | ██ | || | ██ | || | ████ |
CS (mg/kg) | ██ | ███ | ██ | ███ | || | ███ | || | ███ |
█████████ ███ | █████████ ███ | |||||||
███ | || | ██████ | || | █████ | || | █████ | || | █████ |
CS (mg) | ██ | ████ | ██ | ██ | ██ | ████ | ██ | ██ |
CS (mg/kg) | ██ | ███ | ██ | ███ | ██ | ███ | ██ | ███ |
AZA (mg) | ██ | ███ | ██ | ███ | ██ | ███ | ██ | ███ |
AZA (mg/kg) | ██ | ███ | ██ | ███ | ██ | ███ | ██ | ███ |
MMF (mg) | ██ | ████ | ██ | ████ | ██ | ████ | ██ | ████ |
TAC (mg) | || | ███ | || | ███ | || | ███ | || | ███ |
CyS (mg) | || | ███ | || | ███ | || | ███ | || | ███ |
CyS (mg/kg) | || | ███ | || | ███ | || | ███ | || | ███ |
MTX (mg) | || | ██ | || | ███ | || | ██ | || | ███ |
AZA = azathioprine; CS = corticosteroid; CyS = cyclosporine; IST = immunosuppressive therapy; MMF = mycophenolate mofetil; MTX = methotrexate; NA = not applicable; NSIST = nonsteroidal immunosuppressive therapy; TAC = tacrolimus.
Note: The mg/kg doses were reported for select ISTs, which were dosed based on body weight.
Sources: Cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The median durations of IST treatment at baseline in the cohort populations were longer than the minimum inclusion requirements based on Study ADAPT (Table 15).60 In the concomitant IST optimized cohort, patients receiving corticosteroids had a median treatment duration of █████████████████ in the placebo group and ███████████████████ in the ravulizumab group. Similar results were observed in the refractory concomitant IST optimized cohort (the median duration was ███████████████ in the placebo and ravulizumab groups, respectively), reflecting a far longer duration than the minimum requirement of 3 months in the cohort inclusion criteria. Similarly, the median duration of azathioprine treatment surpassed the minimum criteria of 6 months by a wide margin; the median duration of azathioprine was over █████████████) and over ██████████████) in the placebo group and ravulizumab group, respectively. This was also observed in the refractory concomitant IST optimized cohort, with a median treatment duration of █████ days and ████ days in the placebo and ravulizumab groups, respectively. Mycophenolate mofetil was the most commonly used NSIST apart from azathioprine in both cohorts. The median duration of mycophenolate mofetil was over █████████████) in the placebo group and over ███████████████) in the ravulizumab group in the concomitant IST optimized cohort, whereas in the refractory concomitant IST optimized cohort, the median duration was ███ days and █████ days in the placebo and ravulizumab groups, respectively. In addition to exceeding the minimum criteria for inclusion in the concomitant IST optimized cohort, the median durations of corticosteroid and NSIST use also exceeded the typical IST treatment duration for maximal responses of 2 months to 6 months for corticosteroids, and 9 months to 18 months for NSISTs as outlined in the clinician input received by CDA-AMC.17,61
Table 40 and Table 41 in Appendix 1 summarize mean, median, range, and at least 6 months’ and at least 12 months’ duration of treatment for ISTs before the first dose of the study drug in the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort.
Table 15: Median Duration of IST Treatment in Concomitant IST Optimized Cohort and Refractory Concomitant IST Optimized Cohort at Time of Study Enrolment
Treatment | Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort | |||
|---|---|---|---|---|---|
Placebo (N = ██) | Ravulizumab (N = ██) | Placebo (N = ██) | Ravulizumab (N = ██) | ||
CS | n | ██ | ██ | ██ | ██ |
Median (days) | █████ | █████ | █████ | █████ | |
AZA | n | ██ | ██ | ██ | ██ |
Median (days) | █████ | ██████ | █████ | ██████ | |
MMF | n | ██ | ██ | ██ | ██ |
Median (days) | █████ | █████ | █████ | █████ | |
CyS | n | || | || | || | || |
Median (days) | ██████ | █████ | ██████ | ██████ | |
TAC | n | || | || | || | || |
Median (days) | █████ | ██████ | █████ | ██████ | |
MTX | n | || | || | || | || |
Median (days) | █████ | ██ | █████ | ██ | |
AZA = azathioprine; CS = corticosteroid; CyS = cyclosporine; FAS = full analysis set; IST = immunosuppressive therapy; MMF = mycophenolate mofetil; MTX = methotrexate; NA = not applicable; TAC = tacrolimus.
Sources: Cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 39 in Appendix 1 summarizes the changes (replacement, addition or removal, or dose and/or frequency adjustment) in concomitant ISTs in the safety analysis set in the CHAMPION-MG trial.
Efficacy
MG-ADL Total Score
The MG-ADL total score ranges from 0 to 24, and higher scores indicate a greater severity of symptoms and a more significant impact on a patient’s daily activities. Although no MID has been estimated, an improvement of approximately 2 points in the total MG-ADL score is a recommended response threshold that indicates clinical improvement at the level of individual patients with MG.25
In the concomitant IST optimized cohort, during the RCP, the LSM (95% CI) change from baseline to week 26 in the MG-ADL total score was █████████████████ in the ravulizumab group compared to █████████████████ in the placebo group, as summarized in Table 16. The LSM treatment difference was -████████████████ |███████. Differences in treatment effect for the concomitant IST optimized cohort versus the remainder of the FAS for change from baseline to week 26 in the MG-ADL total score were assessed using an MMRM. The results showed that there was █████████████████████ between the cohort and the remainder of the FAS (the LSM treatment difference was █████████████████, supporting the ██████████████████████████████████ determined by visual inspection.
In the refractory concomitant IST optimized cohort, the LSM (95% CI) change from baseline to week 26 in the MG-ADL total score was █████████████████ in the ravulizumab group compared to █████████████████ in the placebo group. The LSM treatment difference was █████████████████████████. Differences in treatment effect for the refractory concomitant IST optimized cohort versus the remainder of the FAS for change from baseline to week 26 in the MG-ADL total score were assessed using an MMRM. The results showed that there was █████████████████████ between the cohort and the remainder of the FAS (the LSM treatment difference was █████████████████, supporting the ██████████████████████████████████ determined by visual inspection.
The treatment effect of ravulizumab over placebo observed in the 2 cohorts is consistent with results from the primary analysis population in the CHAMPION-MG trial. Sensitivity analyses for the MG-ADL total score from baseline to week 26 were performed in the FAS, and the results were consistent with those from the primary analysis. Sensitivity analyses were performed in the concomitant IST optimized cohort by removing patients with increases in IST dosing during the RCP. Results of the sensitivity analysis were aligned with those in the primary analysis. Please refer to Table 39 (Appendix 1) for changes in IST dosing during the RCP in the safety analysis set in the CHAMPION-MG trial.
Table 16: Change From Baseline to Week 26 in MG-ADL Total Score in 2 Cohorts and FAS
Change from baseline in MG-ADL score | Concomitant IST optimized cohorta | Refractory concomitant IST optimized cohorta | FASb | |||
|---|---|---|---|---|---|---|
Placebo N = ██ | Ravulizumab N = ██ | Placebo N = ██ | Ravulizumab N = ██ | Placebo N = 89 | Ravulizumab N = 86 | |
Number of patients contributing to the analysis, n | ██ | ██ | ██ | ██ | 82 | 78 |
Baseline MG-ADL score, mean (SD) | ████████ | ████████ | ████████ | ████████ | 8.9 (2.30) | 9.1 (2.62) |
LSM change from baseline (SEM or 95% CI) | █████████ | ████████ | █████████ | ████████ | −1.4 (−2.1 to −0.7) | −3.1 (−3.8 to −2.3) |
LSM difference in change from baseline (95% CI) | █████████████ | █████████████ | −1.6 (−2.6 to −0.7) | |||
P value | ██████ | ██████ | 0.0009 | |||
CI = confidence interval; FAS = full analysis set; IST = immunosuppressive therapy; LSM = least squares mean; MG-ADL = Myasthenia Gravis Activities of Daily Living; MMRM = mixed model of repeated measures; SD = standard deviation; SEM = standard error of the mean.
aEstimates were based on an MMRM that included treatment group, stratification factor region, and MG-ADL total score at baseline, study visit and study-visit-by-treatment-group interaction. The P value was from a restricted maximum likelihood–based MMRM that tested whether the LSMs for the 2 treatments were equal. An unstructured covariance structure was used. P values were unadjusted for multiplicity; as a result, there was an increased risk of type I error (i.e., falsely rejecting the null hypothesis).
bThe P value was from an MMRM that included change from baseline at postdosing visits as the response variable; fixed categorical effects of treatment, study visit and treatment-by-study-visit interaction; the randomization stratification variable geographic region; and the fixed covariate of baseline score.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
QMG Total Score
The total QMG score ranges from 0 to 39, where higher scores indicate greater disease severity. A definite MID for the QMG scale has not been established, although a threshold ranging between 2 points and 3 points depending on disease severity was suggested for patients with MG.26,27
In the concomitant IST optimized cohort, the LSM (SEM) change from baseline to week 26 in the QMG total score was █████████ in the ravulizumab group and █████████ in the placebo group (Table 17). The LSM treatment difference was █████████████████████████. Differences in treatment effect for the concomitant IST optimized cohort versus the remainder of the FAS for change from baseline to week 26 in the QMG score were assessed using an MMRM. The results showed that there ███████████████████████ between the cohort and the remainder of the FAS (the LSM treatment difference was █████████████████, supporting the ██████████████████████████████████ determined by visual inspection.
In the refractory concomitant IST optimized cohort, the LSM (SEM) change from baseline to week 26 in the QMG total score was █████████ in the ravulizumab group and -████████ in the placebo group. The LSM treatment difference was ████████████████████████. Differences in treatment effect for the refractory concomitant IST optimized cohort versus the remainder of the FAS for change from baseline to week 26 in the QMG score were assessed using an MMRM. The results showed that there was █████████████████████ between the cohort and the remainder of the FAS (the LSM treatment difference was ████████████████, supporting ████████████████████████████████████ determined by visual inspection.
Results of the 2 cohorts were consistent with those in the primary analysis conducted in the FAS of the CHAMPION-MG trial. A sensitivity analysis was performed in the concomitant IST optimized cohort by removing patients with increases in IST dosing during the RCP. Results of the sensitivity analysis were aligned with those in the primary analysis.
Table 17: Change From Baseline to Week 26 in QMG Total Score in 2 Cohorts and FAS
Change from baseline in QMG total score | Concomitant IST optimized cohorta | Refractory concomitant IST optimized cohorta | FASb | |||
|---|---|---|---|---|---|---|
Placebo N = ██ | Ravulizumab N = ██ | Placebo N = ██ | Ravulizumab N = ██ | Placebo N = 89 | Ravulizumab N = 86 | |
Number of patients contributing to the analysis, n | ██ | ██ | ██ | ██ | 78 | 76 |
Baseline QMG score, mean (SD) | ████████ | █████████ | █████████ | █████████ | 14.5 (5.26) | 14.8 (5.21) |
LSM change from baseline (SEM or 95% CI) | ████████ | █████████ | █████████ | █████████ | −0.8 (−1.7 to 0.1) | −2.8 (−3.7 to −1.9) |
LSM difference in change from baseline (95% CI) | ████████████████ | ████████████ | −2.0 (−3.2 to −0.8) | |||
P value | ██████ | ██████ | 0.0009 | |||
CI = confidence interval; FAS = full analysis set; IST = immunosuppressive therapy; LSM = least squares mean; MMRM = mixed model of repeated measures; QMG = Quantitative Myasthenia Gravis; SD = standard deviation; SEM = standard error of the mean.
aEstimates were based on an MMRM that included treatment group, stratification factor region, and QMG total score at baseline, study visit and study-visit-by-treatment-group interaction. The P value was from a restricted maximum likelihood–based MMRM that tested whether the LSMs for the 2 treatments were equal. An unstructured covariance structure was used. P values were unadjusted for multiplicity; as a result, there was an increased risk of type I error (i.e., falsely rejecting the null hypothesis).
bThe P value was from an MMRM that included change from baseline at postdosing visits as the response variable; fixed categorical effects of treatment, and study visit and treatment-by-study visit interaction; the randomization stratification variable geographic region; and the fixed covariate of baseline score.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
QMG 5-Point Response
Clinical responder was defined as patients who achieved a greater than 5-point improvement in the QMG total score; this is larger than the proposed MID of 2 points to 3 points.26,27
In the concomitant IST optimized cohort, █████ of patients in the ravulizumab group compared to ████ in the placebo group achieved at least a 5-point improvement. The between-group difference was ███████████████████ and the OR was ████████████████████████████████████████ ███████ (Table 18).
In the refractory concomitant IST optimized cohort, the proportion of patients meeting the clinical responder definition for QMG improvement was █████ in the ravulizumab group versus ████ in the placebo group, with a between-group difference of ███████████████████ and an OR of ███████████████████████████████████████████████.
Results in the 2 cohorts aligned with those in the primary analysis: the QMG improvement was █████ in the ravulizumab group versus █████ in the placebo group (██████████████████████████████████████ █| █████████████████████████.
Table 18: Improvement of 5 or More Points in the QMG Score From Baseline to Week 26 in 2 Cohorts and FAS
Improvement of ≥ 5 points in the QMG score from baseline | Concomitant IST optimized cohorta | Refractory concomitant IST optimized cohorta | FASb | |||
|---|---|---|---|---|---|---|
Placebo ████ | Ravulizumab ████ | Placebo ████ | Ravulizumab ████ | Placebo N = 89 | Ravulizumab N = 86 | |
Adjusted percentage (95% CI) | ███████████ | ███████████ | ███████████ | ██████████ | 11.3 (5.6 to 21.5) | 30.0 (19.2 to 43.5) |
Absolute between-group difference (95% CI) | ██ | ██ | NR | |||
OR (95% CI) | ████████████████ | █████████████████ | 3.350 (1.443 to 7.777) | |||
P value | ██████ | ██████ | 0.0052 | |||
CI = confidence interval; FAS = full analysis set; IST = immunosuppressive therapy; NR = not reported; OR = odds ratio; QMG = Quantitative Myasthenia Gravis.
aBaseline was defined as the last available assessment value before the first study drug infusion. In the event that a cholinesterase inhibitor was not withheld for at least 10 hours before administration of the QMG assessment, the screening visit assessment was to be used as baseline. Estimates were based on a generalized linear mixed model that included treatment group, stratification factor region and QMG total score at baseline, study visit and study-visit-by-treatment-group interaction. An autoregressive covariance structure was used. P values were unadjusted for multiplicity; as a result, there was an increased risk of type I error (falsely rejecting the null hypothesis).
bBaseline was defined as the last available assessment value before the first study drug infusion. In the event that a cholinesterase inhibitor was not withheld for at least 10 hours before administration of the QMG assessment, the screening visit assessment was to be used as baseline. Estimates were based on a generalized linear mixed model that included treatment group, stratification factor region and QMG total score at baseline, study visit and study-visit-by-treatment-group interaction. An unstructured covariance structure was used.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
MG-QoL15r Total Score
MG-QoL15r is used to measure a patient’s MG-specific HRQoL. The cumulative scores in the MG-QoL15r tool range from 0 to 60, with higher scores representing a worse quality of life.52 An MID for patients with MG has not been estimated.
This outcome did not reach statistical significance in the FAS population and therefore the P values for the subsequent secondary end points included in the prespecified hierarchical testing order (i.e., change from baseline in Neuro-QoL fatigue score at week 26 and an MG-ADL 3-point response at week 26) were considered nominal. In the concomitant IST optimized cohort, the LSM change from baseline to week 26 in the MG-QoL15r total score was ████████████████ in the ravulizumab group and ████████████████ in the placebo group during the RCP. The LSM treatment difference was ███████████████████████.
In the refractory concomitant IST optimized cohort, the LSM change from baseline to week 26 in the MG-QoL15r total score was ████████████████ in the ravulizumab group and ████████████████ in the placebo group during the RCP. The LSM treatment difference was ████████████████████████.
The results of the 2 cohorts are aligned with the primary analysis in the FAS (Table 19).
Table 19: Change From Baseline in MG-QoL15r Total Score at Week 26 in 2 Cohorts and FAS
Change from baseline in MG-QoL15r total score | Concomitant IST optimized cohorta | Refractory concomitant IST optimized cohorta | FAS | |||
|---|---|---|---|---|---|---|
Placebo N = ██ | Ravulizumab N = ██ | Placebo N = ██ | Ravulizumab N = ██ | Placebo N = 89 | Ravulizumab N = 86 | |
Number of patients contributing to the analysis, n | ██ | ██ | ██ | ██ | 82 | 78 |
Baseline MG-QoL15r total score, mean (SD) | ██ | ██ | NR | |||
LSM change from baseline (SEM) | ████████ | █████████ | █████████ | █████████ | −1.6 (0.70) | −3.3 (0.71) |
LSM difference in change from baseline (95% CI) | ████████████ | ████████████ | −1.7 (−3.4 to 0.1) | |||
P value | ██████ | ██████ | 0.0636 | |||
CI = confidence interval; FAS = full analysis set; IST = immunosuppressive therapy; LSM = least squares mean; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item Scale - Revised; MMRM = mixed model of repeated measures; NR = not reported; SD = standard deviation; SEM = standard error of the mean.
aEstimates were based on an MMRM that included treatment group, stratification factor region and MG-QoL15r score at baseline, study visit and study-visit-by-treatment-group interaction. The P value was from a restricted maximum likelihood–based MMRM that tested whether the LSMs for the 2 treatments were equal. An unstructured covariance structure was used.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Neuro-QoL Fatigue Score
The Neuro-QoL fatigue scale is a generic 19-item patient-reported survey of fatigue with a score that ranges from 19 to 95. Higher scores represent greater fatigue and a greater impact of MG on a patient’s activities.24,53 An MID of Neuro-QoL fatigue score has not been established in patients with MG. This outcome was tested after a prior nonsignificant result of the hierarchical testing procedure and therefore P values were considered nominal in the FAS population.
In the concomitant IST optimized cohort, the LSM change from baseline to week 26 in the Neuro-QoL fatigue score was ██████████████████ in the ravulizumab group and ████████████████ in the placebo group during the RCP. The LSM treatment difference was ████████████████████████.
In the refractory concomitant IST optimized cohort, the LSM change from baseline to week 26 in the Neuro-QoL fatigue score was █████████████████ in the ravulizumab group and █████████████████ in the placebo group during the RCP. The LSM treatment difference was ████████████████████████.
The results of the ██████████████████████████████████████████████████████████████████████████████████████████ (Table 20).
Table 20: Change From Baseline in Neuro-QoL Fatigue Score at Week 26 in 2 Cohorts and FAS
Change from baseline in Neuro-QoL fatigue score | Concomitant IST optimized cohorta | Refractory concomitant IST optimized cohorta | FAS | |||
|---|---|---|---|---|---|---|
Placebo N = ██ | Ravulizumab N = ██ | Placebo N = ██ | Ravulizumab N = ██ | Placebo N = 89 | Ravulizumab N = 86 | |
Number of patients contributing to the analysis, n | ██ | ██ | ██ | ██ | 82 | 77 |
LSM (SEM) | ████████ | █████████ | █████████ | █████████ | −4.8 (1.87) | −7.0 (−1.92) |
Ravulizumab difference vs. placebo (95% CI) | ████████████ | ████████████ | −2.2 (−6.9 to 2.6) | |||
P value | ██████ | ██████ | 0.3734 | |||
CI = confidence interval; FAS = full analysis set; IST = immunosuppressive therapy; LSM = least squares mean; MMRM = mixed model of repeated measures; Neuro-QoL = Quality of Life in Neurological Disorders; NR = not reported; SEM = standard error of the mean; vs. = versus.
aEstimates were based on an MMRM that included treatment group, stratification factor region and Neuro-QoL fatigue score at baseline, and study visit and study-visit-by-treatment-group interaction. The P value was from a restricted maximum likelihood–based MMRM that tested whether the LSMs for the 2 treatments were equal. An unstructured covariance structure was used.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
MG-ADL 3-Point or Greater Response
Patients who achieved at least a 3-point improvement in their MG-ADL total score were considered responders; this exceeds the estimated MID of 2 points.25,54 This outcome was tested after a prior nonsignificant result of the hierarchical testing procedure and therefore is at an increased risk of type I error (falsely rejecting the null hypothesis).
In the concomitant IST optimized cohort, the proportion of patients who met the clinical responder definition for MG-ADL improvement of at least 3 points was █████████████████ in the ravulizumab group compared to ██████████████████ in the placebo group, with a between-group difference of ███████████████████ and an OR of ███████████████████████████████████ ███████.
In the refractory concomitant IST optimized cohort, the proportion of patients meeting the clinical responder definition for MG-ADL improvement was █████████████████ in the ravulizumab group compared to █████████████████ in the placebo group, with a between-group difference of ███████████████████ and an OR of ████████████████, ███████████████████ (Table 21).
The results in the 2 cohorts were aligned with the primary analysis in the FAS.
Table 21: Improvement of 3 or More Points in the MG-ADL Total Score From Baseline at Week 26 in 2 Cohorts and FAS
Improvement of total score ≥ 3 points in the MG-ADL total score | Concomitant IST optimized cohorta | Refractory concomitant IST optimized cohortb | FASc | |||
|---|---|---|---|---|---|---|
Placebo N ███ | Ravulizumab N = ██ | Placebo N = ██ | Ravulizumab N = ██ | Placebo N = 89 | Ravulizumab N = 86 | |
Adjusted percentage (95% CI) | ████████████ | ██████████████ | ██████████████ | ██████████████ | 34.1 (23.8 to 46.1) | 56.7 (44.3 to 68.3) |
OR (95% CI) | ████████████████ | ████████████████ | 2.526 (1.330 to 4.799) | |||
P value | ██████ | ██████ | 0.0049 | |||
CI = confidence interval; FAS = full analysis set; IST = immunosuppressive therapy; MG-ADL = Myasthenia Gravis Activities of Daily Living; OR = odds ratio.
aEstimates were based on a generalized linear mixed model that included treatment group, stratification factor region and MG-ADL total score at baseline, study visit and study-visit-by-treatment-group interaction. An unstructured covariance structure was used. This analysis was unadjusted for multiplicity; as a result, there was an increased risk of type I error (falsely rejecting the null hypothesis).
bEstimates were based on a generalized linear mixed model that included treatment group, stratification factor region and MG-ADL total score at baseline, study visit and study-visit-by-treatment-group interaction. A Toeplitz covariance structure was used.
cThis analysis occurred after a failure of the testing hierarchy. There was an increased risk of type I error (falsely rejecting the null hypothesis).
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Incidence of Clinical Deterioration and MG Crisis
During the RCP, in the concomitant IST optimized cohort, || patients (████) in the ravulizumab group and ██ patients (█████) in the placebo group reported clinical deterioration. In the refractory concomitant IST optimized cohort, || patients (█████) in the ravulizumab group and || patients (█████) in the placebo group reported clinical deterioration.
In each cohort, an MG crisis was reported by || patient from the placebo group. No patients from the ravulizumab group reported an MG crisis (Table 22).
Table 22: Incidence of Clinical Deterioration and MG Crisis During RCP in 2 Cohorts and FAS
Clinical deterioration or MG crisis | Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort | FAS | |||
|---|---|---|---|---|---|---|
Placebo N = ██ | Ravulizumab N = ██ | Placebo N = ██ | Ravulizumab N = ██ | Placebo N = 89 | Ravulizumab N = 86 | |
Incidence of clinical deterioration, n (%) | ██████ | ██████ | ███████ | ███████ | 15 (16.9) | 8 (9.3) |
Incidence of an MG crisis, n (%) | ██████ | 0 | ██████ | 0 | 1 (1.1) | 0 |
FAS = full analysis set; IST = immunosuppressive therapy; MG = myasthenia gravis; RCP = randomized controlled period.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Harms
Results for the safety end points in the 2 cohorts are presented in Table 23. The incidence of treatment-emergent AEs and SAEs during the RCP in the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort were ██████████ with the harm results from the primary analysis.
Adverse Events
The percentage of patients with AEs was similar between the treatment groups (████████ of placebo-treated patients and ████████ of ravulizumab-treated patients in the concomitant IST optimized cohort and ████████ of placebo-treated patients and ████████ of ravulizumab-treated patients in the refractory concomitant IST optimized cohort). The most commonly reported AEs in these 2 cohorts included ████████ (concomitant IST optimized cohort = █████ in the ravulizumab group versus █████ in the placebo group; refractory concomitant IST optimized cohort = █████ in the ravulizumab group versus █████ in the placebo group) and ████████ (concomitant IST optimized cohort = █████ in the ravulizumab group versus █████ in the placebo group; refractory concomitant IST optimized cohort = █████ in the ravulizumab group versus █████ in the placebo group). Most AEs were █████ ███ █████████.
In the safety set of the CHAMPION-MG trial, during the RCP, most patients (90.7% of ravulizumab-treated patients and 86.5% of placebo-treated patients) experienced AEs. The most common AEs were headache (25.8% of patients in the ravulizumab group and 18.6% of patients in the placebo group), diarrhea (12.4% of patients in the ravulizumab group and 15.1% of patients in the placebo group) and nausea (10.1% of patients in the ravulizumab group and 10.5% of patients in the placebo group).
Serious Adverse Events
The percentage of patients with SAEs was higher in the ravulizumab group compared to the placebo group. In the concomitant IST optimized cohort, █████ of ravulizumab-treated patients and █████ of placebo-treated patients experienced at least 1 SAE. In the refractory concomitant IST optimized cohort, █████ of ravulizumab-treated patients and █████ of patients in the placebo group experienced at least 1 SAE. Commonly reported SAEs were not reported for these 2 cohorts.
Withdrawals Due to Adverse Events
In both cohorts, there was || patient treated with ravulizumab who discontinued the study drug due to an AE.
Mortality
In both cohorts, there were || patients treated with ravulizumab who died, and ██ death was reported for the placebo group.
Notable Harms
Meningococcal infection was considered a notable harm for treatment with ravulizumab. No events were reported during the RCP in the entire study population.
Table 23: Overview of All Treatment-Emergent Adverse Events and Serious Adverse Events During the Randomized Controlled Period in the Concomitant IST Optimized, Refractory Concomitant IST Optimized Cohorts and Full Safety Set
AE, n (%) | Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort | Full safety set | |||
|---|---|---|---|---|---|---|
Placebo (N = ██) | Ravulizumab (N = ██) | Placebo (N = ██) | Ravulizumab (N = ██) | Placebo (N = 89) | Ravulizumab (N = 86) | |
Any AEs | ███████ | ███████ | ███████ | ███████ | 77 (86.5) | 78 (90.7) |
Commonly reported AEs (frequency ≥ 10%) | ||||||
Diarrhea | ███████ | ███████ | ███████ | ███████ | 11 (12.4) | 13 (15.1) |
Headache | ███████ | ███████ | ███████ | ███████ | 23 (25.8) | 16 (18.6) |
Nausea | ██████ | ███████ | ██████ | ███████ | 13 (10.2) (ravulizumab-treated set) | |
≥ grade 3 AEs | ███████ | ███████ | ██████ | ███████ | 15 (16.8) | 25 (29.1) |
Any SAEs | ███████ | ███████ | ███████ | ███████ | 14 (15.7) | 20 (23.3) |
Death | || | ██████ | || | ██████ | 0 | 2 (2.3) |
WDAEs | || | ██████ | || | ██████ | 3 (3.4) | 2 (2.3) |
Notable harm | ||||||
Meningococcal infection | 0 | 0 | 0 | 0 | 0 | 0 |
AE = adverse event; IST = immunosuppressive therapy; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Sources: Clinical Study Report for the CHAMPION-MG trial24 and cohort analyses of the CHAMPION-MG trial.28 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
This is a resubmission of the initial ravulizumab review. The CHAMPION-MG trial (N = 175) was the pivotal study. This was a phase III, double-blind, multicentre, placebo-controlled RCT with an OLE period of up to 4 years. The primary objective of the CHAMPION-MG trial was to evaluate the safety and efficacy of ravulizumab compared with placebo in complement inhibitor–naive adult patients with anti-AChR antibody–positive gMG. CDEC issued a negative reimbursement recommendation in 2023 (refer to the Submission History section in this report for details). The current review focuses on 2 post hoc subgroups that were identified from the FAS in the CHAMPION-MG trial: the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort.
According to the critical appraisal of the CHAMPION-MG trial in the initial ravulizumab submission, there were no major validity concerns regarding this trial. █████ baseline imbalances between study arms were viewed as unlikely to be prognostic or to significantly affect the study results. Study discontinuations before completing the RCP were relatively ██████████ (████ of patients) and missing data for reasons other than discontinuation were █████████████ (███ ████████ in each arm, depending on outcome). During the study, concomitant MG therapy was generally ███████ in both study arms, apart from ███████████████ █████████████████████████████ █████████████. Important protocol deviations occurred █████████ in both arms and were not viewed as likely to impact the study results. The instruments used to evaluate the primary and secondary efficacy outcomes (MG-ADL, QMG, MG-QoL15r, and Neuro-QoL fatigue) were appropriate and their psychometric properties have been investigated in patients with MG, although no MIDs have been estimated for the MG-QoL15r and Neuro-QoL fatigue scores. Statistical tests were appropriate overall, power was adequate for the primary analysis, and multiplicity was controlled using a hierarchical testing strategy. Statistical testing for a 3-point or greater improvement in the MG-ADL score and changes from baseline in the Neuro-QoL fatigue score at 26 weeks occurred after a prior nonsignificant result (MG-QoL15r total scores) in the statistical hierarchy, so there is an increased risk of type I error. Subgroup analyses identified were not adjusted for multiplicity nor were they specifically powered to detect differences among strata. In addition, an MID for MG-QoL15r or Neuro-QoL fatigue in patients with MG has not been estimated. Definite conclusions regarding the effect of the study drug on HRQoL cannot be drawn, due to the small sample size in the cohorts (HRQoL results were not available in 11% to 15% of patients treated with ravulizumab), and 95% CIs that were wide and crossed the null.
Post hoc analyses that are not prespecified in a trial’s analysis plan can be at risk of bias due to selective reporting (i.e., there is a risk that the presented results are selected from multiple analyses of the data based on their direction, magnitude, or statistical significance). However, the sponsor furnished clear justification for the selected subpopulations using criteria informed by Study ADAPT and Study REGAIN to provide directly relevant information related to a previous negative reimbursement recommendation. Additionally, the same prespecified analysis methods of the CHAMPION-MG trial were used to analyze the subgroup data and results for all relevant end points were presented. As a result, any concern for selective reporting was minimized.
Whether patients had received an optimized IST was not a stratification factor in the randomization of the CHAMPION-MG trial; therefore, there is a risk that the randomization was not fully upheld in the subgroups. Nevertheless, in these 2 subgroups, patients’ baseline demographic and disease characteristics were generally ███████████ between treatment groups and were similar to the FAS population. Also ███████ to the FAS, ██████████████ were observed for ████ ███████ █████████████████ ███████████████████████████████████████████ █████████████████████████ ██████████████████████) and ████████████████████████. The imbalances in the FAS could be due to the small sample size, which would have been ███████████ in the smaller subgroups. The clinical expert consulted by the review team noted that these may not have a significant impact on result interpretation.
Tests for subgroup differences between the subgroup populations and the rest of the FAS were performed for the MG-ADL score and QMG score. However, these analyses were post hoc and the CHAMPION-MG trial was not powered to find a difference between the groups. Otherwise, results from these post hoc subgroups can be interpreted for consistency with the main analyses of the CHAMPION-MG trial as they share the same limitations of those analyses. In addition, it should be considered that the small sample size in these 2 subgroups (the concomitant IST optimized cohort accounted for ███ of the full population and the refractory concomitant IST optimized cohort was ████ of the full population) could have resulted in insufficient power to detect true between-group differences, and multiplicity was not controlled using hierarchical testing. Therefore, there was an increasing risk of type I error (i.e., falsely rejecting the null hypothesis) rate for the investigated outcomes that achieved statistical significance at a conventional alpha of 0.05.
Efficacy data during the OLE period for the 2 cohorts were ██████████ with those from the RCP for the 2 cohorts and the FAS. Patients who switched from placebo to ravulizumab showed █████████ improvements in daily activities and other efficacy outcomes at week 164. However, further interpretation of these data was limited by the open-label and descriptive nature of the extension study. Attrition bias is also a concern in OLE studies; it increases the uncertainty in the study results.
External Validity
The drug was resubmitted for review by the sponsor on the basis of the availability of new evidence and a revised reimbursement request for ravulizumab as an add-on therapy for adult patients with anti–AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChE inhibitors, corticosteroids, and/or NSISTs. The new evidence provided by the sponsor consisted of 2 post hoc subgroups in the CHAMPION-MG trial: the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort. These cohorts aligned with the reimbursement request in that patients in these cohorts had anti-AChR antibody–positive gMG and were symptomatic despite having had “adequate” ISTs (i.e., corticosteroids and/or NSISTs). However, the reimbursement request also includes patients who have had an adequate trial of AChE inhibitors and no ISTs; these patients were not included in the 2 post hoc cohorts but were studied in the FAS in the CHAMPION-MG trial. A similar proportion of patients who received AChE inhibitors but no ISTs were enrolled in the CHAMPION-MG trial and Study ADAPT (i.e., approximately 10% of the overall trial populations). The review team noted that the conditions for reimbursement for efgartigimod alfa align with the sponsor’s reimbursement request for this resubmission. CDEC noted in the final CDA-AMC recommendation for efgartigimod alfa that it would be reasonable to consider efgartigimod alfa after a trial of at least 1 of AChE inhibitors, corticosteroids, and/or NSISTs in the previous 12 months. The NMD4C clinician group, which provided input to this resubmission for ravulizumab, agreed that the place in therapy for ravulizumab would also include patients who had received AChE inhibitors but not ISTs. However, both the clinician group and the clinical expert consulted for this review noted that it would be reasonable for patients with gMG to try other treatments before initiating ravulizumab, which requires periodic IV infusions over an extended period, is likely to be expensive, may not be available in smaller cities or nonspecialized centres, and requires extensive expertise. The clinical expert consulted for this review noted that most clinicians would likely continue offering AChE inhibitors and ISTs before ravulizumab.
Patient selection for the 2 post hoc cohorts was based on the inclusion criteria from other RCTs: Study ADAPT and Study REGAIN. According to the clinical expert consulted for this review, the definitions used to identify patients are reasonable and acceptable in clinical practice. These 2 subgroups reflect patients who did not experience improvement on a prior gMG treatment (known as patients with refractory gMG) and patients whose disease responded on a prior gMG treatment but had responded inadequately to existing standards of gMG therapy. According to the clinical expert consulted for this review, the population included in the 2 cohorts is adequately reflective of the patients who experience unmet needs in the treatment of gMG in clinical settings in Canada.
According to Table 14 and Table 15 in this report, the median duration of prior corticosteroid and NSIST use exceeded the typical IST treatment duration for maximal responses (2 months to 6 months for corticosteroids, and 9 months to 18 months for NSISTs) as outlined in the clinician input received for the initial ravulizumab submission. In addition, the median treatment durations for IST treatment surpassed the minimum criteria for inclusion in the concomitant IST optimized cohort. The clinical expert consulted for this review had no concerns about suboptimal management with IST treatment (i.e., inadequate dosing or duration of therapy) in patients at the time of enrolment in the CHAMPION-MG trial. The clinical expert agreed that median durations of corticosteroid and NSIST treatment appeared adequate and allowed sufficient time to achieve maximal responses with IST. Therefore, the patient population in the 2 cohorts aligned with the reimbursement request in that patients with anti-AChR antibody–positive gMG were symptomatic despite “adequate” ISTs (i.e., corticosteroids and/or NSISTs).
Concomitant conventional therapy such as AChE inhibitors and ISTs (e.g., corticosteroids, azathioprine, mycophenolate mofetil, tacrolimus) were allowed during the CHAMPION-MG trial. As per the protocol of the CHAMPION-MG study, the dosage of these drugs was not allowed to be changed and no new ISTs were allowed to be added throughout the RCP, unless deemed medically necessary. Rescue therapy (e.g., a high-dose corticosteroid, PLEX, IVIg) was allowed if a patient experienced protocol-defined clinical deterioration. Similar protocol requirements for concomitant ISTs are common across trials in patients with gMG to ensure consistency and to prevent the confounding of trial results. Notably in Study ADAPT (efgartigimod alfa versus placebo) and Study REGAIN (eculizumab versus placebo), a change in the type or dose and/or regimen of standard of care (replacing, adding, or removing standard of care, or adjusting the standard of care dose and/or frequency) was not allowed unless deemed medically necessary (standard of care referred to NSISTs, steroids, and AChE inhibitors). Because the concomitant conventional therapy was required to remain stable except in the case of rescue therapy, ravulizumab was not compared to any individual or combination conventional therapy as it would typically be used in clinical practice (i.e., altering doses or adding additional medications to suit patients’ current symptoms or other needs). According to the sponsor for the present submission, a change of ISTs (their introduction or discontinuation, or an increased or decreased dosage) occurred in 17% of patients overall (12% in the placebo group and 20% in the ravulizumab group) during the RCP of the CHAMPION-MG trial. The clinical expert consulted for this review was not concerned about discouraging dose changes in concomitant medications over the course of the 26 weeks in the RCP. The clinical experts noted that patients were on optimized and stable concomitant therapy entering the trial and were allowed to continue those therapies. Rescue therapy, including high-dose corticosteroids, PLEX, or IVIg, was permitted throughout the study for patients experiencing clinical deterioration, which was considered appropriate by the clinical expert consulted for this review. During the OLE (OLE data were available for up to 3.5 years of follow-up), physicians could adjust ISTs and changes to MG medication occurred in the majority of patients (68.3%). The most common reason for change was due to improvements in MG symptoms (43.5% of patients). By the end of the study, 30.1% (34 of 113) of patients had decreased their daily dose of corticosteroid therapy and 12.4% (14 of 113) of patients had stopped corticosteroid therapy.
According to the clinical expert consulted for this review, the eligibility criteria for patients of an MGFA class II to class IV and an MG-ADL total score of 6 or more would select patients with symptomatic gMG most in need of intervention. Patients with MGFA class I and class V were excluded. Very few patients with class IV gMG were included in the CHAMPION-MG trial (11 patients in the FAS). Whether the findings of the CHAMPION-MG trial can be generalized to patients with MGFA class I or MGFA class V is uncertain. The clinical expert consulted for this review indicated that a subset of patients with an MGFA class I (ocular MG) or class V and MG-ADL scores of less than 6, who were excluded from the trial, would be suitable for treatment. Specifically, the clinical expert indicated that patients with ocular MG or mild symptoms can still be refractory to other therapies, and patients with MGFA class V (on a ventilator) who have no contraindications would potentially benefit from ravulizumab. However, the results of the trial cannot be directly generalized to these groups of patients.
The median baseline MG-ADL score was approximately 9 points and the median QMG score of 14 points to 15 points across study groups in the FAS and the 2 post hoc cohorts. In addition, the IST treatment history of the cohort populations (Table 15 of this report) reflected a heavily pretreated patient population that, despite a lengthy duration of IST treatment, continued to experience significant gMG symptoms. The MG-ADL total score cut-off value was 6 or more points as an inclusion criterion in the CHAMPION-MG trial and in previous gMG clinical trials (i.e., in Study REGAIN). However, the review team noticed that the inclusion criteria for recruiting patients in Study ADAPT was 5 or more points on the MG-ADL total score. Patients in Study ADAPT who had 5 points on the MG-ADL total score at baseline were relatively few. The clinical expert consulted for this review indicated that severity status based on the MG-ADL was subjective; a difference of 1 point may not be clinically important in terms of disease severity and is unlikely to have a meaningful impact on the patient’s response to the treatment. Whether the results of the CHAMPION-MG trial can be generalized to patients who have an MG-ADL total score of less than 6 despite a stable dose of conventional therapies remains uncertain.
The RCP of the CHAMPION-MG trial was 26 weeks. The longer-term treatment effect of ravulizumab can only be assessed in the OLE period of this study. Moreover, the CHAMPION-MG trial did not provide evidence for comparisons between ravulizumab and other currently available active treatments for gMG.
Long-Term Extension Studies
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
The CHAMPION-MG OLE, with the last patient’s last visit being on May 25, 2023, represents up to 3.5 years of ravulizumab treatment exposure. At the end of the 26-week RCP, all patients were eligible to enter the OLE and receive open-label ravulizumab. Following the 26-week RCP, patients in the placebo group received a blinded loading dose of ravulizumab and patients in the ravulizumab group received a blinded ravulizumab dose of 900 mg. Starting week 28, all patients began open-label ravulizumab maintenance doses every 8 weeks. The OLE period for each patient started when the patient received their dose of ravulizumab on week 26 (day 183) and was intended to continue for up to 4 years or until the product is registered or approved and available by prescription.
Populations
There were no additional criteria to continue from the CHAMPION-MG study to the extension study (refer to section 2 eligibility criteria). All patients were eligible to receive open-label ravulizumab during the OLE period.
Interventions
During the OLE period, patients were given a blinded dose of ravulizumab at week 26 (day 183). As of 2 weeks following the blinded dose (week 28), all patients began receiving open-label ravulizumab maintenance doses every 8 weeks. Supplemental ravulizumab (or placebo) dosing was required following PLEX or IVIg rescue treatment on nondosing days. While all patients who entered the OLE period received ravulizumab, patients randomized to the ravulizumab group had previously received 26 weeks of ravulizumab treatment during the RCP (the ravulizumab-ravulizumab treatment group). Patients randomized to receive placebo during the RCP had their first dose of ravulizumab at the start of the OLE period (the day 183 visit in the placebo-ravulizumab treatment group).
Outcomes
The efficacy and safety outcomes assessed in the OLE were the same as the outcomes assessed during the RCP.
The primary efficacy end point was the MG-ADL total score. The key secondary end points were the QMG total score, a QMG 5-point or greater improvement, the MG-QoL15r total score, the Neuro-QoL fatigue score, and an MG-ADL 3-point or greater improvement. Data on clinical deterioration and MG crisis were not available.
Safety outcomes included infusion interruptions, SAEs, treatment-emergent AEs, common AEs, withdrawals due to adverse events (WDAEs), deaths, and AESIs.
Statistical Analysis
For continuous variables, the change from baseline, defined as the last available assessment value before the first study drug infusion during the RCP, was analyzed using an MMRM. The RCP estimates were based on an MMRM that included treatment group, stratification factor region, baseline score, and study visit and study-visit-by-treatment-group interaction. Visits up to week 26 were included in the model. The OLE estimates were based on an MMRM that included stratification factor region, baseline score, and study visit. A model was fit for the ravulizumab and placebo arm of the OLE set separately.
Summary statistics included the number of observations (n), the mean, the standard deviation, and median, minimum, and maximum values. Frequencies and percentages were calculated for categorical variables.
Long-term analyses of change from the OLE baseline in the MG-ADL and QMG total scores through to the end of the OLE period were performed post hoc for both the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort, and were analyzed using an MMRM. Visits with assessments performed on at least 10 patients were used. Missing data were not imputed. A 2-sided 95% CI at each visit for each treatment sequence was calculated.
Of the 175 patients randomized in the RCP, 161 were included in the OLE set (patients who had received 1 dose or more of ravulizumab in the OLE period) and 169 were included in the RTS (all patients who received ≥ 1 dose of ravulizumab either in the RCP or the OLE period; the primary population for assessment of safety during ravulizumab treatment was this patient set). Additional cohort analyses were performed using a subset of the FAS concomitant IST optimized cohort (the OLE set concomitant IST optimized cohort). These patients received 1 dose or more of ravulizumab beginning from week 26 onward and were included in all efficacy analyses during the OLE period.
Results
Patient Disposition
Of the 175 patients randomized in the CHAMPION-MG trial, a total of 161 (92%) patients from the RCP entered the OLE study and received open-label treatment. Of these patients, 123 completed the study, with 38 patients discontinuing. Reasons for discontinuation were withdrawal by patient (9.9%), physician decision (5.0%), death (3.7%), and “other” (5.0%). Of the 6 deaths, 3 patient deaths were assessed as COVID-19–related. All 8 patients designated as “other” were patients in South Korea who transitioned to alternative treatment by the investigator when the study finished. Patient disposition for all study phases was previously illustrated in Figure 4.
Details of patient disposition are provided in Table 24.
Table 24: Patient Disposition During the OLE Period
Patient disposition | Placebo-ravulizumab | Ravulizumab-ravulizumab | ||||
|---|---|---|---|---|---|---|
Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort | Open-label extension set | Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort | Open-label extension set | |
Entered into open-label extension period, n (%) | ██████ | ██████ | 83 (100) | ██████ | ██████ | 78 (100) |
Treated, n (%) | ██████ | ██████ | 83 (100) | ██████ | ██████ | 78 (100) |
Completed, n (%) | ███████ | ███████ | 63 (75.9) | ███████ | ███████ | 60 (76.9) |
Discontinued, n (%) | ███████ | ███████ | 20 (24.1) | ███████ | ███████ | 18 (23.1) |
Physician decision | ██████ | ██████ | 3 (3.6) | ██████ | ███████ | 5 (6.4) |
Death | ██████ | ██████ | 3 (3.6) | ██████ | ██████ | 3 (3.8) |
Withdrawal by patient | ███████ | ██████ | 9 (10.8) | ██████ | ██████ | 7 (9.0) |
Adverse event | || | || | 0 | || | || | 0 |
Lost to follow-up | || | || | 0 | || | || | 0 |
Noncompliance with study drug | || | || | 0 | || | || | 0 |
Pregnancy | || | || | 0 | || | || | 0 |
Protocol violation | || | || | 0 | || | || | 0 |
Study terminated by sponsor | || | || | 0 | || | || | 0 |
Other | ██████ | ██████ | 5 (6.0) | ██████ | ██████ | 3 (3.8) |
IST = immunosuppressive therapy; PBO = placebo; RAV = ravulizumab.
Sources: Additional information provided by the sponsor: Response to CDA request on August 6, 2024 (concomitant IST optimized cohort),73 Response to CDA request on August 6, 2024 (refractory concomitant IST optimized cohort),74 and Study 306 End of Study Tables and Figures.75
Baseline Characteristics
The baseline characteristics are summarized in Table 25. Baseline was defined as the last available assessment value before the first study drug infusion.
Table 25: Demographics and Baseline Characteristics (Open-Label Extension Set)
Baseline characteristic | Placebo-ravulizumab | Ravulizumab-ravulizumab | ||||
|---|---|---|---|---|---|---|
Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort N = 47 | Open-label extension set | Concomitant IST optimized cohort | Refractory concomitant IST optimized cohort N = 35 | Open-label extension set | |
Sex, n (%) | ||||||
Male | ███████ | ███████ | 41 (49.4) | ██████ | ███████ | 38 (48.7) |
Female | ███████ | ███████ | 42 (50.6) | ██████ | ███████ | 40 (51.3) |
Ethnicity, n (%) | ||||||
Not Hispanic or Latino | ███████ | ███████ | 72 (86.7) | ██████ | █████ | 71 (91.0) |
Hispanic or Latino | ██████ | ██████ | 5 (6.0) | ██████ | ██████ | 2 (2.6) |
Race, n (%) | ||||||
Asian | ███████ | ███████ | 14 (16.9) | ███████ | ███████ | 13 (16.7) |
Black or African American | ██████ | ██████ | 4 (4.5) | ██████ | ██████ | 2 (2.6) |
White | ███████ | ███████ | 57 (68.7) | ██████ | ███████ | 61 (78.2) |
Not reported | ██████ | ██████ | 5 (6.0) | || | || | 2 (2.6) |
Age at first infusion (years) | ||||||
Mean (SD) | ██████████ | ██████████ | 53.6 (16.42) | ██████ | ██████████ | 58.2 (13.56) |
18 years to 65 years, n (%) | ███████ | ███████ | 59 (71.1) | ██████ | ███████ | 51 (65.4) |
> 65 years | ███████ | ███████ | 24 (28.9) | ██████ | ███████ | 27 (34.6) |
Baseline weight (kg) | ||||||
Mean (SD) | ██████████ | ██████████ | 90.5 (29.62) | ██████ | ██████████ | 91.7 (23.27) |
≥ 40 kg to < 60 kg, n (%) | ███████ | ██████ | 10 (12.0) | ██████ | ██████ | 5 (6.4) |
≥ 60 kg to < 100 kg, n (%) | ███████ | ███████ | 45 (54.2) | ██████ | ███████ | 44 (56.4) |
≥ 100 kg, n (%) | ███████ | ███████ | 28 (33.7) | ██████ | ███████ | 29 (37.2) |
Randomization stratification region, n (%) | ||||||
North America | ███████ | ███████ | 38 (45.8) | ██████ | ███████ | 37 (47.4) |
Europe | ███████ | ███████ | 31 (37.3) | ██████ | ███████ | 28 (35.9) |
Asia-Pacific | ███████ | ███████ | 9 (10.8) | ██████ | ███████ | 8 (10.3) |
Japan | ██████ | ██████ | 5 (6.0) | ██████ | ██████ | 5 (6.4) |
Baseline MGFA clinical classification, n (%) | ||||||
Class IIa | ███████ | ███████ | 21 (25.3) | ██████ | ███████ | 21 (26.9) |
Class IIb | ███████ | ███████ | 14 (16.9) | ███████ | ██████ | 15 (19.2) |
Class IIIa | ███████ | ███████ | 33 (39.8) | ██████ | ███████ | 20 (25.6) |
Class IIIb | ███████ | ███████ | 10 (12.0) | ██████ | ███████ | 17 (21.8) |
Class IVa | ██████ | ██████ | 4 (4.8) | ██████ | ██████ | 2 (2.6) |
Class IVb | ██████ | ██████ | 1 (1.2) | ██████ | ██████ | 3 (3.8) |
IST = immunosuppressive therapy; MGFA = Myasthenia Gravis Foundation of America; PBO = placebo; RAV = ravulizumab; SD = standard deviation.
Sources: Clinical Study Report Addendum (End of Study),47 and additional information from the sponsor (Response to CDA request on August 15, 2024 (refractory concomitant IST optimized cohort),76 and Response to CDA request on August 15, 2024 (concomitant IST optimized cohort). 77
Exposure to Study Treatments
The ravulizumab-ravulizumab treatment group had a longer mean exposure to ravulizumab due to the prior 26 weeks of exposure in the RCP. In total, the exposure to ravulizumab at the end of the study was ███ patient-years included █████ patient-years in the placebo-ravulizumab group and █████ patient-years in the ravulizumab-ravulizumab group. The mean duration of ravulizumab treatment by the end of the study (during the RCP and the OLE period) was █████ days and the maximum exposure was ██████ days. From the first dose of ravulizumab through to the end of the study, █████ of patients had 100% compliance. Overall, ████████ patients missed 1 or more scheduled infusion during the ravulizumab treatment period and 19 (11.2%) patients had infusion interruptions.
During the long-term extension period in the concomitant IST optimized cohort, the mean treatment duration (SD) was ████████████ in the ravulizumab-ravulizumab group and ████████████ in the placebo-ravulizumab group. In the refractory concomitant IST optimized cohort, the mean treatment duration (SD) was ████████████ in the ravulizumab-ravulizumab group and ████████████ in the placebo-ravulizumab group. The drug compliance in the 2 cohorts has not been provided.
The patient-years of OLE exposure to ravulizumab in the concomitant IST optimized cohort was ████ in the ravulizumab-ravulizumab group and ████ in the placebo-ravulizumab group. In the refractory concomitant IST optimized cohort, patient-years of OLE exposure to ravulizumab was █████ in the ravulizumab-ravulizumab group and █████ in the placebo-ravulizumab group.
Table 26: Exposure to Treatments (Ravulizumab-Treated Set)
Exposure | Placebo-ravulizumab (N = 83) | Ravulizumab-ravulizumab (N = 86) |
|---|---|---|
Study duration from informed consent (days), mean (SD) | ████████████ | ███████████ |
Ravulizumab treatment duration (days), mean (SD) | ████████████ | ███████████ |
Maximum exposure (days) | ██████ | ██████ |
Patient-years of exposure | █████ | █████ |
100% drug compliance, n (%) | ███████ | ███████ |
Patients with infusion interruption, n (%) | ██████ | ███████ |
PBO = placebo; RAV = ravulizumab; SD = standard deviation.
Note: Percentages were based on the total number of patients in each group. Study duration equalled the date of study completion or discontinuation minus (the date of informed consent + 1). Treatment duration equalled the date of study completion or discontinuation minus (the first ravulizumab infusion date + 1). Percentage compliance equalled 100% minus (total percentage of time participants were noncompliant with scheduled ravulizumab doses in the ravulizumab treatment period).
Source: Clinical Study Report Addendum (End of Study).47
Concomitant Medications and Cointerventions
All patients in the RTS used concomitant MG medications during the ravulizumab treatment period (i.e., concomitant MG medications were those received by the patients on or after the first ravulizumab infusion in the RCP or the OLE period). Overall, concomitant MG medications (other than IVIg) used by more than 25% of patients in the RTS were pyridostigmine bromide (███████ prednisone (███████ and mycophenolate mofetil (███████ The most commonly used IST in the RTS was corticosteroids (███████ In the RTS, █████ of patients used IVIg and ████ of participants used any PLEX.
In the OLE period, physicians had the option to adjust IST therapies. A ███████████████████ of patients had a change in concomitant MG medication (i.e., concomitant MG medications received by the patients on or after the first study drug infusion in the OLE period) during the OLE period. The most common reason for change in corticosteroid therapies was improvement in MG symptoms in █████ of patients. At the end of the OLE period, ███████████ of patients decreased their daily dose of corticosteroid therapy and ███████████ of patients stopped corticosteroid therapy. Similar data were not provided for the cohorts separately.
Efficacy
MG-ADL Total Score
The MG-ADL is an 8-item survey of patient-reported MG symptom severity and the symptoms’ functional impact on the patient, with each response graded from 0 (normal) to 3 (most severe); the total MG-ADL score ranges from 0 to 24.49 A reduction in score indicates improvement and the MCID on the MG-ADL scale is estimated to be 2 points based on the change within an individual patient.25
Primary Analysis
In the OLE set, in the ravulizumab-ravulizumab group, the LSM change from RCP baseline in the MG-ADL total score was −4.0 (95% CI, −5.3 to −2.8) at week 164. In the placebo-ravulizumab group, the LSM change from RCP baseline was −3.3 (95% CI, −4.2 to −2.4) at week 28 and −3.6 (95% CI, −4.8 to −2.3) at week 164.
OLE Set Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab concomitant IST optimized cohort, the LSM change from the OLE baseline (OLE period baseline is defined as the last available assessment before administration of the first study drug in the OLE period) in the MG-ADL total score was ██████████████) at week 28 and ███████████████) at week 164.
In the placebo-ravulizumab concomitant IST optimized cohort, the LSM change from the OLE baseline in the MG-ADL total score was ████ (95% ██████████) at week 28 and ████████████████) at week 148.
OLE Set Refractory Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab refractory concomitant IST optimized cohort, the LSM change from the OLE baseline in the MG-ADL total score was ██████████████) at week 28 and ███████████████) at week 164.
In the placebo-ravulizumab refractory concomitant IST optimized cohort, the LSM change from the OLE baseline in the MG-ADL total score was ████████████████) at week 28 and ████████████████) at week 148.
QMG Total Score
The QMG is a 13-item clinician-determined assessment of MG disease status, with each item graded for severity from 0 (none) to 3 (severe); total scores range from 0 to 39.51 A higher score is indicative of more severe disease. A definite MID for the QMG scale has not been established, although a threshold ranging between 2 points and 3 points depending on disease severity has been suggested in previous studies enrolling patients with MG.26,27
Primary Analysis
In the OLE set in the ravulizumab-ravulizumab group, the LSM change from the RCP baseline in the QMG total score was −2.9 (95% CI, −4.1 to −1.8) at week 28 and −4.3 (95% CI, −6.0 to −2.7) at week 164.
In the placebo-ravulizumab group, the LSM change from the RCP baseline was −3.0 (95% CI, −4.3 to −1.7) at week 28 and −3.7 (95% CI, −5.5 to −1.9) at week 164.
OLE Set Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab concomitant IST optimized cohort, the LSM change from the OLE baseline in the QMG total score was ██████████████) at week 28 and ███████████████) at week 164.
In the placebo-ravulizumab concomitant IST optimized cohort, the LSM change from the OLE baseline in the QMG total score was ████████████████) at week 28 and ████████████████) at week 148.
OLE Set Refractory Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab refractory concomitant IST optimized cohort, the LSM change from the OLE baseline in the QMG total score was ███ (███████████) at week 28 and ██████████████) at week 148.
In the placebo-ravulizumab refractory concomitant IST optimized cohort, the LSM change from the OLE baseline in the QMG total score was █████████████████ at week 28 and ████████████████) at week 148.
QMG 5-Point or Greater Response
Based on a 5-point or greater improvement in the QMG total score from the RCP baseline, the proportion of clinical responders in the ravulizumab-ravulizumab group was 38.0% (95% CI, 26.8% to 50.3%) at week 28 and 61.5% (95% CI, 31.6% to 86.1%) at week 164.
The proportion of clinical responders in the placebo-ravulizumab group was 31.9% (95% CI, 21.2% to 44.2%) at week 28 and 58.3% (95% CI, 27.7% to 84.8%) at week 164.
Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab group, the proportion of patients with a 5-point or greater improvement in the QMG total score from the RCP baseline was █████████████████) at week 28 and █████████████████) at week 164.
In the placebo-ravulizumab group, the proportion of patients with a 5-point or greater improvement in the QMG total score from the RCP baseline was █████████████████) at week 28 and █████████████████) at week 164.
OLE Set Refractory Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab group, the proportion of patients with a 5-point or greater improvement in the QMG total score from the RCP baseline was █████████████████) at week 28 and █████████████████) at week 164.
In the placebo-ravulizumab group, the proportion of patients with a 5-point or greater improvement in the QMG total score from the RCP baseline was █████████████████) at week 28 and █████████████████) at week 164.
MG-QoL15r Total Score
The MG-QoL15r questionnaire (a revised version of the Myasthenia Gravis Quality of Life 15-item Scale tool) is a 15-item HRQoL instrument for MG, with each item having 3 response options that include 0 (not at all), 1 (somewhat), and 2 (very much); total scores range from 0 to 30, with higher scores indicating a greater extent of dissatisfaction with MG-related dysfunction.52 An MID has not been estimated for patients with MG.
In the OLE set, in the ravulizumab-ravulizumab group, the LSM change from the RCP baseline in the MG-QoL15r total score was −3.7 (95% CI, −5.4 to −2.0) at week 26 and −5.2 (95% CI, −7.3 to −3.1) at week 164.
In the placebo-ravulizumab group, the LSM change from the RCP baseline was −5.9 (95% CI, −8.0 to −3.7) at week 30 and −5.4 (95% CI, −7.8 to −3.0) at week 164.
OLE Set Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab group, the LSM change from the OLE baseline in the MG-QoL15r total score was ████████████████) at week 30 and ████████████████) at week 164.
In the placebo-ravulizumab group, the LSM change from the OLE baseline in the MG-QoL15r total score was ████████████████) at week 30 and ████████████████) at week 164.
OLE Set Refractory Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab group, the LSM change from the OLE baseline in the MG-QoL15r total score was ███████████████) at week 30 and ██████████████) at week 132.
In the placebo-ravulizumab group, the LSM change from the OLE baseline in the MG-QoL15r total score was ████████████████) at week 30 and ████████████████) at week 164.
Neuro-QoL Fatigue Score
The Neuro-QoL fatigue subscale is an instrument evaluating the effect of fatigue on the quality of life of patients with neurologic disorders.53 It comprises 19 patient-reported items assessing the frequency of different aspects of fatigue over the previous 7 days, answered using a 5-point scale ranging from 1 (never) to 5 (always); total scores range from 19 to 95. Higher scores indicate greater fatigue and a greater impact of MG on activities. An MID has not been estimated for patients with MG.
In the ravulizumab-ravulizumab group, the LSM change from the RCP baseline in the Neuro-QoL fatigue score was −7.7 (95% CI, −12.2 to −3.2) at week 26 and −10.4 (95% CI, −16.4 to −4.7) at week 164.
In the placebo-ravulizumab group, the LSM change from the RCP baseline was −16.9 (95% CI, −21.4 to −12.5) at week 30 and −14.7 (95% CI, −20.1 to −9.3) at week 164.
OLE Set Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab group, the LSM change from the OLE baseline in the Neuro-QoL fatigue score was ███████████████) at week 30 and ███████████████) at week 164.
In the placebo-ravulizumab group, the LSM change from the OLE baseline was ██████████████████) at week 30 and █████████████████) at week 164.
OLE Set Refractory Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab group, the LSM change from the OLE baseline in the Neuro-QoL fatigue score was █████████████████) at week 30 and ████████████████) at week 132.
In the placebo-ravulizumab group, the LSM change from the OLE baseline was ███████████████████ at week 30 and █████████████████) at week 164.
MG-ADL 3-Point or Greater Response
Based on a 3-point or greater improvement in the MG-ADL total score from the RCP baseline, the proportion of clinical responders in the ravulizumab-ravulizumab group was 64.0% (95% CI, 52.1% to 74.8%) at week 28 and 71.4% (95% CI, 41.9% to 91.6%) at week 164.
The proportion of clinical responders in the placebo-ravulizumab group in the MG-ADL total score from the RCP baseline was 62.5% (95% CI, 51.0% to 73.1%) at week 28 and 75.0% (95% CI, 42.8% to 94.5%) at week 164.
OLE Set Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab group, the proportion of patients with a 3-point or greater improvement in the MG-ADL total score from the RCP baseline was ████ █████████████) at week 28 and ██████████████████ at week 164.
In the placebo-ravulizumab group, the proportion of patients with a 3-point or greater improvement in the MG-ADL total score from the RCP baseline was █████████████████) at week 28 and ██████████████████ at week 164.
OLE Set Refractory Concomitant IST Optimized Cohort Analysis
In the ravulizumab-ravulizumab group, the proportion of patients with a 3-point or greater improvement in the MG-ADL total score from the RCP baseline was █████████████████) at week 28 and ████████████████ at week 164.
In the placebo-ravulizumab group, the proportion of patients with a 3-point or greater improvement in the MG-ADL total score from the RCP baseline was █████████████████) at week 28 and ██████████████████ at week 164.
Harms
Results for the safety end points in this section are presented for the 169 patients in the RTS — all 86 patients in the ravulizumab-ravulizumab group and 83 patients in the placebo-ravulizumab group. A summary of harms is reported from the first ravulizumab treatment exposure during the RCP through to the end of the OLE period in the OLE set and in both cohorts. In all cases of AEs, SAEs, and death, the results for the 2 cohorts were similar to the OLE set. WDAEs were rare in the full population and only 1 case was reported in the ravulizumab-ravulizumab concomitant IST optimized cohort.
Adverse Events
During ravulizumab treatment, 96.4% of patients experienced at least 1 AE. The most commonly reported AEs (≥ 10% of total patients) in the RTS were COVID-19 (36.1%), headache (23.1%), diarrhea (17.2%), arthralgia (13.6%), back pain (13%), nausea (13%), urinary tract infection (12.4%), nasopharyngitis (11.8%), fatigue (10.7%), and dizziness (10.1%).
Serious Adverse Events
SAEs reported by 1 patient or more included COVID-19 (6 patients), MG (5 patients), COVID-19 pneumonia (4 patients); SAEs reported by 3 patients each included cellulitis and pneumonia; and SAEs reported by 2 patients each included erysipelas, urinary tract infection, spinal compression fracture, intervertebral disc protrusion, transient ischemic attack, congestive cardiac failure, pyrexia, dyspnea, dysphagia, dehydration, and nephrolithiasis.
There were 8 patient deaths throughout the entirety of the study period. There were 2 patient deaths in the RCP (due to COVID-19 pneumonia and cerebral hemorrhage). Six patients died in the OLE period due to the following reasons: COVID-19 (3 patients), toxicity due to various drugs (1 patient), dehydration (1 patient), and an unknown reason (1 patient).
Withdrawals Due to Adverse Events
Four patients had AEs that led to WDAEs. Two AEs occurred during the RCP (infected skin ulcer and COVID-19 pneumonia) and 2 AEs occurred during the OLE period (COVID-19 and MG). All 4 AEs occurred in the ravulizumab-ravulizumab treatment group. No patients in the placebo-ravulizumab group discontinued the study drug. The total number of patients with ravulizumab infusion interruption due to an AE was 8 (4.7%) patients and 74 (43.8%) patients reported potential infusion reactions during ravulizumab treatment.
Adverse Events of Special Interest
There were no meningococcal infections reported during the study, although there was 1 event of meningitis of unknown etiology reported in the OLE period in the placebo-ravulizumab group (Table 27 and Table 28).
Table 27: Summary of Harms Results From Long-Term Extension Phase of CHAMPION-MG Study
AE | Placebo-ravulizumab | Ravulizumab-ravulizumab | ||||
|---|---|---|---|---|---|---|
Concomitant IST optimized cohort N (%) | Refractory concomitant IST optimized cohort N (%) | Open-label extension set N (%) | Concomitant IST optimized cohort N (%) | Refractory concomitant IST optimized cohort N (%) | Open-label extension set N (%) | |
Any AE | ███████ | ███████ | 80 (96.4) | ███████ | ███████ | 83 (96.5) |
Any SAE | ███████ | ███████ | 32 (38.6) | ███████ | ███████ | 34 (39.5) |
Death | █████ | █████ | 3 (3.6) | █████ | █████ | 5 (5.8) |
AE leading to withdrawal of study drug | || | || | 0 | ██████ | || | 4 (4.7) |
AE by toxicity | ||||||
Grade 1 | ███████ | ███████ | 68 (81.9) | ███████ | ███████ | 79 (91.9) |
Grade 2 | ███████ | ██████ | 51 (61.4) | ███████ | ███████ | 61 (70.9) |
Grade 3 | ███████ | ███████ | 31 (37.3) | ███████ | ███████ | 36 (41.9) |
Grade 4 | ██████ | ██████ | 5 (6.0) | ██████ | ██████ | 7 (8.1) |
Grade 5 | ██████ | ██████ | 3 (3.6) | ██████ | ██████ | 5 (5.8) |
Toxicity grade ≥ 3 | ███████ | ███████ | NR | ███████ | ███████ | NR |
Notable harm | ||||||
AE of meningococcal infection | 0 | 0 | — | 0 | 0 | — |
AE = adverse event; IST = immunosuppressive therapy; NR = not reported; PBO = placebo; RAV = ravulizumab; SAE = serious adverse event; SD = standard deviation.
Sources: Additional information provided by sponsor: Response to CDA request on August 6, 2024 (concomitant IST optimized cohort) 73, and Response to CDA request on August 6, 2024 (refractory concomitant IST optimized cohort).74
Table 28: All Treatment-Emergent Adverse Events and Serious Adverse Events During Ravulizumab Treatment Period in Ravulizumab-Treated Set
AE | Total (N = 169) |
|---|---|
Most common AEs (≥ 5% of patients), n (%) | |
≥ 1 AE | 163 (96.4) |
COVID-19 | 61 (36.1) |
Headache | 39 (23.1) |
Diarrhea | 29 (17.2) |
Arthralgia | 23 (13.6) |
Back pain | 22 (13.0) |
Nausea | 22 (13.0) |
Urinary tract infection | 21 (12.4) |
Nasopharyngitis | 20 (11.8) |
Fatigue | 18 (10.7) |
Dizziness | 17 (10.1) |
SAEs in ≥ 2 patients, n (%) | |
Patients with ≥ 1 SAE | 66 (39.1) |
COVID-19 | 6 (6.3) |
Myasthenia gravis | 5 (3.0) |
COVID-19 pneumonia | 4 (2.4) |
Cellulitis | 3 (1.8) |
Pneumonia | 3 (1.8) |
Erysipelas | 2 (1.2) |
Urinary tract infection | 2 (1.2) |
Spinal compression fracture | 2 (1.2) |
Intervertebral disc protrusion | 2 (1.2) |
Transient ischemic attack | 2 (1.2) |
Cardiac failure, congestive | 2 (1.2) |
Pyrexia | 2 (1.2) |
Dyspnea | 2 (1.2) |
Dysphagia | 2 (1.2) |
Dehydration | 2 (1.2) |
Nephrolithiasis | 2 (1.2) |
Patients who stopped treatment due to AEs, n (%) | |
AE leading to withdrawal | 4 (2.4) |
SAE leading to withdrawal | 3 (1.8) |
Deaths, n (%) | |
Patients who died | 8 (4.7) |
AEs of special interest, n (%) | |
Meningococcal infections (%) | 0 |
AE = adverse event; SAE = serious adverse event.
Source: The sponsor’s Summary of Clinical Evidence.72
Critical Appraisal
Internal Validity
The lack of a control group precludes causal statements about benefit and harm compared with any comparator. The open-label nature of the study may increase the risk of bias in determining the magnitude of the safety outcomes and the efficacy end points that include more subjective assessments, because the lack of blinding may affect patients’ expectations of treatment. The direction and magnitude of this potential bias remains unclear. Patients of the OLE were patients who did not drop out of the placebo-controlled study (92%), which puts the results at some risk of selection bias, likely to be favouring ravulizumab. Of the 175 patients randomized in the CHAMPION-MG trial, 123 patients completed the OLE. There is therefore a risk of bias due to missing outcome data in both the placebo-ravulizumab and the ravulizumab-ravulizumab arms, with the impact on the direction of treatment effect over time not clear. The limitations of the post hoc analyses of the subgroups mirror those discussed in the systematic review section; however, these concerns have been minimized as the findings for these groups were generally consistent with the overall population.
External Validity
The appraisal of the external validity of the RCP, presented in the Critical Appraisal subsection regarding the CHAMPION-MG study in the Clinical Evidence section, is also applicable to the OLE period.
Indirect Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
The objective of this section is to summarize and appraise the ITCs that provide evidence for the relative efficacy and safety of ravulizumab versus relevant comparators for the treatment of adult patients with anti–AChR antibody–positive gMG in the concomitant IST optimized cohort as well as the refractory concomitant IST optimized cohort in an NMA analysis, and for the treatment of patients with gMG, although not for a specific subgroup, in an MAIC analysis.
Description of Indirect Comparison
Study Selection Methods
To inform the NMA, a systematic literature review was performed in February 2022 and updated in January of 2024 to identify literature published from 2000 to 2024. Published literature was identified by searching the following databases: MEDLINE All (1946–), Embase (1974–), and Evidence-Based Medicine Reviews. The search strategies used medical subject headings and keywords related to the study population of interest. Study design filters for clinical trials were also used. Comparators and outcomes were not prespecified in the search strategy. Instead, these characteristics were screened for in the abstract and full-text review steps to ensure that all potentially relevant studies were identified.
Study selection was conducted by 2 independent reviewers. All abstracts identified by the search strategy were reviewed and compared against the predetermined Population, Intervention, Comparison, Outcomes, and Study (PICOS) tool. If any discrepancies occurred between the studies selected for inclusion by the 2 reviewers, a third reviewer provided arbitration. Following abstract screening, the full texts of included citations were accessed. Similar to the abstract screening process, full-text review was conducted by 2 reviewers independently and decisions were made to include or exclude full-text articles depending on whether the PICOS criteria were met. It is important to note that studies describing patient populations comprising both anti–AChR antibody–positive MG and anti-MuSK antibody–positive MG were considered for inclusion. In general, 80% to 85% of patients with gMG have AChR, nearly 15% of patients are anti-AChR antibody–negative, and approximately 1% to 10% of patients have MuSK or LRP4.3 Further details regarding PICOS, data extraction, and the assessment of study quality are described in Table 29.
Table 29: Study Selection Criteria and Methods for Network Meta-Analyses
Characteristic | Indirect comparison |
|---|---|
Population | Patients with anti–AChR antibody–positive gMG |
Intervention |
|
Comparator |
|
Outcome | Efficacy:
Safety:
|
Study designs |
|
Publication characteristics | Published studies, with results presented in articles, conference proceedings, or abstracts, or posted on clinical trial registries For ravulizumab, clinical study reports were also used. |
Exclusion criteria |
|
Databases searched | MEDLINE Embase EBM Reviews |
Selection process | The selection process was conducted in 2 steps. At the first pass, all titles and abstracts were reviewed for inclusion, and at the second pass, all full-text articles deemed relevant were screened for final inclusion. Disagreements between reviewers were resolved with a third researcher who provided arbitration. |
Data extraction process | One reviewer extracted data and a second reviewer independently checked for errors against the original study report. Multiple publications of the same study were linked together and extracted as a single reference. |
Quality assessment | The risk of bias of the studies to be included in the analyses was assessed at the study level using the Cochrane risk-of-bias tool for RCTs.62 The Cochrane risk-of-bias tool addresses the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. For each domain, the risk of bias is graded as “low,” “high,” or “unclear” (if study information is insufficient to conclude). In addition, based on the risk of bias of the studies included in the analyses, a sensitivity analysis was planned to exclude studies with a high risk of bias in at least 1 domain. Note that this is an older version of the quality assessment tool. |
AChR = acetylcholine receptor; AE = adverse event; EBM = Evidence-Based Medicine; gMG = generalized myasthenia gravis; IVIg = IV immunoglobulin; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MGFA-PIS = Myasthenia Gravis Foundation of America Post-intervention Status; MMS = minimal manifestation status; MSE = minimal symptom expression; PLEX = plasma exchange or plasmapheresis; QMG = Quantitative Myasthenia Gravis; RCT = randomized controlled trial; SAE = serious adverse event.
Sources: Sponsor-submitted network meta-analysis report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The sponsor also submitted an MAIC to assess the relative efficacy of ravulizumab compared to efgartigimod alfa for the management of patients with gMG and anti–AChR antibody–positive. In this MAIC, change in the MG-ADL total score at select follow-up time points (week 4, week 8, week 10, and week 26) was the only outcome that was examined. There was no description of study selection, data extraction, or assessment on the risk of bias of the included studies.
ITC Analysis Methods
Network Meta-Analyses
An NMA was performed for the concomitant IST optimized population. Given the limited data available for the refractory concomitant IST optimized population, comprising only 2 studies and 2 treatments, an ITC was conducted using placebo as the common comparator. To integrate the convergence diagnosis and output analysis into the economic model, the ITC was performed with a Bayesian approach. Supplementary analyses were performed using the frequentist method (i.e., Bucher).
Description of Model
The NMA was performed using a Bayesian framework. The results were calculated with Markov Chain Monte Carlo (MCMC) simulations, which allow reproducing the model several times until convergence.63 Using the software gemtc (version 1.0 to 2) package of the R, a fixed-effect (FE) model and a random-effect (RE) model with a normal likelihood and an identity link function were performed for the continuous outcomes, and with a binomial likelihood and a log link function were performed for the binary outcomes.64
The FE model assumes homogeneity between studies while the RE approach assumes that the studies were drawn from different populations, which could impact the estimated treatment effect. With the RE approach, between-study heterogeneity (tau-squared) is considered.65 Due to the limited number of studies (n = 7) and in accordance with the Cochrane Scientific Committee (2018) — recommendations for meta-analyses that included fewer than 10 studies — informative priors for the tau-squared were used in the RE model.66 The choice between the FE model and the RE model was based on the lowest deviance information criterion (DIC) score.67 However, with similar DICs (i.e., a difference of less than 2), the FE model was preferred and selected.68 As a result, the RE model was provided as supplementary analysis.
Vague priors (noninformative priors [uniform distribution]) were assigned to the parameters mu (mean effect) and d (treatment effect). The RE model was fitted with informative priors for the heterogeneity parameter (i.e., log-normal ([mean = −3.02, standard deviation = 1.85]2 for semiobjective outcomes). The sponsor noted that due to the limited number of studies (n = 7) and in accordance with the Cochrane Scientific Committee (2018) recommendations for meta-analyses that included fewer than 10 studies, informative priors for the tau-squared were used in the RE model.66 A sensitivity analysis was performed using vague priors (i.e., noninformative).
MCMC sampling was done with 4 chains, with an initial number of iterations discarded as the “burn-in” period. The burn-in was initially 20,000 samples, but this was increased if there was evidence that the MCMC did not converge. Once convergence was achieved, another minimum of 20,000 samples was generated from the posterior distribution to estimate treatment effects and the 95% Crls. The Potential Scale Reduction Factor was verified to be under a threshold of 1.05 and the convergence was assessed with the Brooks-Gelman-Rubin method using the same package. Specifically, Gelman and Rubin (1992) proposed a general approach to monitor the convergence of MCMC outputs in which 2 or more parallel chains are run with starting values that are overdispersed relative to the posterior distribution. The convergence is assessed by comparing the estimated between-chain and within-chain variances for each model parameter. Large differences between these variances indicate nonconvergence.
The model provided the mean difference for the efficacy outcomes or the risk ratio for the safety outcome for each comparison of treatments. Results of pairwise treatment comparisons were considered statistically significant when the 95% CrI did not cross the line of equality (mean difference = 0 or risk ratio = 1).
Heterogeneity Assessment
Because of the multiple comparisons involved in the NMA, which may generate inconsistency or incoherence in the model, these 3 assumptions were made: similarity, homogeneity, and consistency.63
Heterogeneity between baseline characteristics and between study characteristics among trials were evaluated by conducting subgroups analyses, when relevant and possible. The statistical assessment of heterogeneity was based on the I2 statistic, derived from a direct head-to-head meta-analysis of the treatment comparisons in each network that were evaluated in more than 1 study.69 All comparisons with I2 higher than 50% (indicating substantial or considerable heterogeneity) were investigated. The studies included in these treatment nodes were examined to determine the cause of the observed heterogeneity. If needed, sensitivity analyses without the studies at the origin of the observed heterogeneity were performed.
To verify the consistency of the direct and indirect comparisons, a node-splitting approach was considered. With this approach, the direct evidence for a specific treatment comparison is contrasted with the indirect evidence coming from the rest of the network. When direct and indirect evidence differed substantially, that indicated that inconsistency was present. However, due to the limited number of studies, the node-split analysis was not feasible for any outcomes.
Since outcomes were not prespecified, no preplanned analyses were excluded. An NMA was conducted at the end of the study (the longest follow-up time point) for the 2 efficacy outcomes (i.e., the mean change from baseline in the MG-ADL and QMG total scores). Additionally, a sensitivity analysis was performed at 8 weeks plus or minus 2 weeks (range, 6 weeks to 10 weeks) to ensure a maximum inclusion of studies at a similar time point. An NMA for WDAEs was also completed.
Table 30: Analysis Methods Used in Sponsor-Submitted NMA
Method | Description |
|---|---|
Analysis methods | NMA using an FE or RE Bayesian model |
Priors | Vague priors (noninformative [uniform distribution]) were assigned to the parameters mu (mean effect) and d (treatment effect), and informative priors for the between-study heterogeneity were assigned to the RE model (log-normal [mean = −3.02; standard deviation = 1.85]2). |
Assessment of model fit | Deviance information criterion |
Assessment of consistency | I2 statistic (heterogeneity assessment). A node-splitting approach (consistency assessment) was planned but not completed due to too few studies. |
Assessment of convergence | Brooks-Gelman-Rubin method |
Outcomes | Efficacy:
Safety:
|
Follow-up time points | Outcomes were reported using end-of-study time points, which varied between studies |
Construction of nodes | Phase II or III clinical studies of relevant comparators in the population of interest (patients with anti–AChR antibody–positive gMG) |
Sensitivity analyses | Wolfe et al. (2002)78 was excluded due to the high risk of bias in at least 1 domain. The CHAMPION-MG trial’s concomitant IST optimized cohort was replaced with the CHAMPION-MG trial’s FAS. The time point analysis was at 8 weeks ± 2 weeks. |
Subgroup analysis | None |
Methods for pairwise meta-analysis | Direct head-to-head meta-analysis of the treatment comparisons in each network that were evaluated in more than 1 study (i.e., 2 studies) was performed with both the FE and RE models. |
AChR = acetylcholine receptor; CFB = change from baseline; FAS = full analysis set; FE = fixed-effect; gMG = generalize myasthenia gravis; IST = immunosuppressive therapy; MG-ADL = Myasthenia Gravis Activities of Daily Living; NMA = network meta-analysis; QMG = Quantitative Myasthenia Gravis; RE = random-effect; WDAE = withdrawal due to adverse event.
Sources: Sponsor-submitted network meta-analysis report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Matching-Adjusted Indirect Comparison
The MAIC was conducted following the recommendations of the National Institute for Health and Care Excellence Decision Support Unit Technical Support Document67 on population-adjusted indirect comparisons. Baseline characteristics of the study populations were compared before undertaking the MAIC. Imbalances across those baseline characteristics were identified, as were prognostic factors or treatment-effect modifiers. The subset of baseline characteristics available in both studies that were identified as potentially being prognostic or a treatment-effect modifier were selected for adjustment.
Mean changes from baseline in the MG-ADL score were compared at the following time points: week 4, week 10, and time of best response (week 26 for ravulizumab versus week 4 for efgartigimod alfa).
The MAIC was based on 2 data sources:
Ravulizumab data were drawn from individual patient data (IPD) from the CHAMPION-MG trial (n = 86 for the ravulizumab group; n = 89 for the placebo group). These were adults diagnosed with MG, anti-AChR antibody–positive, and an MG-ADL score at baseline of 6 or more. They had no requirement for prior treatment failure but stable standard of care was allowed.
Efgartigimod alfa data were drawn from aggregate data reported for the anti-AChR antibody–positive subgroup of Study ADAPT (n = 65 for the efgartigimod alfa group; n = 64 for the placebo group). These were adults diagnosed with MG and an MG-ADL score of 5 or more. Patients were also required to be on a stable dose of at least 1 treatment for gMG (e.g., AChE inhibitors, corticosteroids, NSISTs) before screening and throughout the trial
The analyses were anchored on the placebo groups of Study ADAPT and the CHAMPION-MG trial. The MAIC was conducted by matching the IPD from the CHAMPION-MG trial to baseline summary characteristics from Study ADAPT; this was performed at the arm-level (active arm to active arm, placebo arm to placebo arm) to account for differences between the treatment groups of Study ADAPT in characteristics such as mean age and mean time since diagnosis. Adjustment for differences in selected baseline characteristics was achieved by reweighting the influence of patients in each CHAMPION-MG trial arm’s IPD such that the weighted average of the characteristics matched the profile of the cohort reported by the respective arm in Study ADAPT.
Results of ITCs
Summary of Included Studies
Network Meta-Analyses
In total, 7 studies were included in the NMA, as summarized in Table 31.
Table 31: Studies Included in NMA Analyses
Trial | Publication year | Trial start year | Design | Intervention | End of study |
|---|---|---|---|---|---|
CHAMPION-MG study | 2022 | 2019 | Phase III RCT | Ravulizumab Placebo | 26 weeks |
Study ADAPT | 2021 | 2018 | Phase III RCT | Efgartigimod alfa Placebo | 10 weeks |
Howard et al. study 79 | 2019 | 2016 | Phase II RCT | Efgartigimod alfa Placebo | 77 days (11 weeks) |
Study REGAIN | 2017 | 2013 | Phase III RCT | Eculizumab Placebo | 26 weeks |
Wolfe et al. study78 | 2002 | NR | Phase NR RCT | IVIg Placebo | 42 days (6 weeks) |
NCT02473952 study (this study is unpublished) | 2019 | 2015 | Phase II RCT | IGIV-C Placebo | 24 weeks |
Study BeatMG | 2022 | 2014 | Phase II RCT | Rituximab Placebo | 52 weeks |
IVIg = IV immunoglobulin; IGIV-C = IV immunoglobulin-10% caprylate/chromatography purified; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial.
Sources: Sponsor-submitted network meta-analysis report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Between-Study Heterogeneity
In terms of trial characteristics, eligibility criteria and study designs were similar between studies. The time period during which the trials were conducted varied. Patients were enrolled from 2013 (Study REGAIN70) to 2019 (the CHAMPION-MG trial71), except for the Wolfe et al. study, which was published in 2002. Also, Wolfe et al. (2002) did not specify the study phase whereas the identified trials were classified as phase III (i.e., the CHAMPION-MG, ADAPT, and REGAIN studies) and the remaining studies were phase II.
In terms of treatment characteristics, all of the trials were placebo-controlled. There were various study populations depending on treatment history such as being stable on ISTs, IST optimized, and IST optimized and refractory populations. Since treatment may be a potential effect modifier, 2 separate NMAs were conducted based on population type; this was adult patients with anti–AChR antibody–positive gMG with a concomitant IST optimized population and with concomitant IST optimized and refractory population (i.e., inadequate symptom control after 2 or more ISTs in the previous 12 months, or 1 or more IST and chronic IVIg or PLEX in the previous 12 months).
While it was not possible to determine whether patients included in the IVIg trials were IST optimized or not, these trials were also added in the concomitant IST optimized NMA, given that IVIg should be used as the last resort.10 Therefore, it was assumed that patients on IVIg would have been optimized on IST before the initiation of IVIg therapy. The 2 networks included the following studies:
the concomitant IST optimized network, excluding concomitant IST optimized and refractory exclusively, had 6 studies in the network —
the CHAMPION-MG trial (concomitant IST optimized subgroup)
Study ADAPT
Study BeatMG
Howard et al. (2019)
Wolfe et al. (2002)
NCT02473952 study (this study is unpublished)
the concomitant IST optimized and refractory network included 2 studies in the network —
the CHAMPION-MG trial (concomitant IST optimized and refractory subgroup)
Study REGAIN.
With regard to baseline patient characteristics, the mean age was consistent between the studies (range, 44.7 years to 58.5 years), although the proportion of male patients varied from 29% (Study ADAPT) to 53.3% (the NCT02473952 trial; this study is unpublished). The distribution of disease severity was similar between trials, with most trials reporting a similar proportion of MGFA class II to class IV patients and few patients in class V, and excluding class I patients altogether. The baseline clinical scores, specifically the mean MG-ADL total score at baseline, was lower in Study BeatMG and Wolfe et al. (2022) (5.8 points and 5.3 points, respectively) compared to the other trials, indicating a population with less severe disease. The mean baseline MG-ADL score was higher in Study REGAIN (10.5 points) as this study was conducted in a refractory population, thus indicating more severe disease. Similarly, the mean QMG score at baseline was lower in the Wolfe et al. (2022) study (8.5 points) and higher in Study REGAIN (17.3 points) compared to the other trials.
Since the primary end point of the CHAMPION-MG trial was the mean change from baseline in the MG-ADL total score, the key secondary end point was the mean change from baseline in the QMG total score; as both outcomes were reported in all included studies, these end points were considered the outcomes of interest in the NMA. However, the primary end point differed between the other studies and was reported as the proportion of MG-ADL responders in Study ADAPT. An analysis based on the percentage of responders that was centred on the MG-ADL score was not deemed appropriate due to variable reporting of this outcome (i.e., ≥ 2-point improvement sustained ≥ 4 weeks in Study ADAPT) and was not reported in 3 of the 7 studies. The same rationale was applied for the proportion of QMG responders. Two different definitions were reported for WDAE: AEs leading to the discontinuation of the study and AEs leading to the discontinuation of the study drug. As a conservative approach, WDAE relating to the study drug was preferred over WDAE relating to the study. Due to 0 WDAEs, Howard et al. (2019) was excluded from the WDAE analyses.
Study time points for each end point varied from 1 week to 52 weeks. Since the outcomes of interest were change from baseline, the time at which the outcomes were assessed was considered a potential effect modifier. Based on time point availability, the base-case analysis was at the end of the study (from 6 weeks to 52 weeks). A sensitivity analysis was performed at the time point of 8 weeks plus or minus 2 weeks, which permitted the comparison of treatments using a similar time point according to the opinion of a clinical expert consulted by the sponsor. The time point of 8 weeks plus or minus 2 weeks was chosen given that 6 weeks was the shortest trial duration reported in relevant clinical trials (Wolfe et al. [2002]), that data within the time range of 8 weeks plus or minus 2 weeks was reported for most trials of interest, and that treatments would have at least 1 maintenance dose before the time point. Since Study BeatMG only reported data at the end of study, rituximab was excluded from this analysis. No sensitivity analysis was performed for the concomitant IST optimized and refractory network given that both the CHAMPION-MG trial (ravulizumab) and Study REGAIN (eculizumab) have a 26-week trial duration.
With respect to comparator dosing, all studies employed a dosing schedule involving infusions at a specific time. The formulation of efgartigimod alfa remained consistent across Study ADAPT and Howard et al. (2019); thus, no distinction was required. IVIg and IV immunoglobulin-10% caprylate/chromatography purified were combined into the IVIg group, since no difference in efficacy was expected. In terms of frequency of treatment, ravulizumab was administered less frequently than the other treatments (every 8 weeks) whereas eculizumab was administered most frequently (every 2 weeks). Table 32 shows the assessment of homogeneity for the gMG trials.
Overall, the risk of bias of the studies was assessed using the Cochrane risk-of-bias RCTs tool. This assessment was made using only publicly available reports in order to not favour ravulizumab. Overall bias was judged as low for 5 of the 7 studies, as high risk for Wolfe et al. (2002), and as uncertain for the NCT02473952 trial (this study is unpublished). Therefore, a sensitivity analysis excluding Wolfe et al. (2022) was performed in the NMA. Note that the risk of bias was likely assessed using an older version of the tool and this assessment was done at the study level instead of at the outcome level.
Table 32: Assessment of Homogeneity for gMG Trials
Characteristic | Description and handling of potential effect modifier |
|---|---|
Disease severity | Patients with MGFA class I were excluded from all studies. When looking at MGFA class II to class IV patients, the distribution was similar across studies. |
Clinical score | The mean MG-ADL total scores at baseline were lower in the BeatMG and Wolfe et al. 2022 studies, indicating a less severe population. The MG-ADL score was higher in Study REGAIN, as this study was conducted in a refractory population; thus, the score was more severe. Consistently, the mean QMG score at baseline was lower in the Wolfe et al. 2022 study but higher in Study REGAIN. |
Treatment history | There were various study populations, depending on treatment history such as stable on IST, IST optimized, and IST optimized and refractory. As treatment history may be a potential effect modifier, it was decided to conduct 2 separate NMAs based on population type, which was adult patients with anti-AChR antibody-positive gMG with concomitant IST optimized, and with refractory concomitant IST optimized. |
Trial eligibility criteria | Inclusion and exclusion criteria were similar across studies. |
Dosing of comparators | All studies employed a dosing schedule involving infusions at a specific time. |
Placebo response | Placebo response was generally comparable between studies. |
Definitions of end points | The primary end point of the CHAMPION-MG study was the mean CFB in the MG-ADL total score; it was reported in all included studies and was chosen as the primary efficacy outcome for the NMA. However, the primary end point differed between studies and was the proportion of MG-ADL responders in Study ADAPT. Since the definition of responders was inconsistent between the trials and was not reported in 3 of the 7 studies, it was decided to not use this outcome in the NMA. The same rationale was applied for the QMG total score. |
Timing of end point evaluation | Different time points were available for the CFB in the MG-ADL total score and the CFB in the QMG score from 1 week to 52 weeks. Since the outcomes of interest were CFB, the timing of outcome assessment was considered as a potential effect modifier and was thus further explored during this feasibility assessment. Based on the availability of the different time points, 2 analyses were performed.
|
Withdrawal frequency | Definitions were reported as:
To be conservative, discontinuation of the study drug was preferred when both were available. |
Study design | All studies were RCTs compared with placebo. Three studies were phase III, 2 studies were phase II, and 1 study phase was NR. |
AChR = acetylcholine receptor; AE = adverse event; CFB = change from baseline; gMG = generalized myasthenia gravis; IST = immunosuppressive therapy; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; NMA = network meta-analysis; NR = not reported; QMG = Quantitative Myasthenia Gravis; RCT = randomized controlled trial.
Sources: Sponsor-submitted network meta-analysis report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Matching-Adjusted Indirect Comparison
The baseline patient characteristics in the CHAMPION-MG trial before and after reweighting are presented in Table 33, along with those reported in Study ADAPT. Discrepancies in age, sex, MGFA classification, and prior IST use between the 2 trials were observed. After matching, the effective sample sizes were 34.5 for the ravulizumab group (40.1% of the original size) and 65.1 for the placebo group (73.1% of the original size).
Table 33: Baseline Patient Characteristics From CHAMPION-MG Trial and Study ADAPT Before and After Matching
Baseline characteristic used for matching | CHAMPION-MG trial Ravulizumab (n = 86) | Study ADAPT Efgartigimod alfa (n = 65) | CHAMPION-MG trial Placebo (n = 89) | Study ADAPT Placebo (n = 64) | ||
|---|---|---|---|---|---|---|
Before matching | After matchinga | Before matching | After matchinga | |||
Mean age, years | 58.0 | 44.7 | 44.7 | 53.3 | 49.2 | 49.2 |
Female, n (%) | 44 (51.2) | 61 (70.8) | 46 (70.8) | 45 (50.6) | 56 (62.5) | 40 (62.5) |
MGFA class, n (%) | ||||||
MGFA class II | 39 (45.3) | 37 (43.1) | 28 (43.1) | 39 (43.8) | 35 (39.1) | 25 (39.1) |
MGFA class III | 41 (47.7) | 46 (53.8) | 35 (53.8) | 45 (50.6) | 50 (56.3) | 36 (56.3) |
MGFA class IV | 6 (7.0) | 3 (3.1) | 2 (3.1) | 5 (5.6) | 4 (4.7) | 3 (4.7) |
Mean years since diagnosis | 9.8 | 9.7 | 9.7 | 10.0 | 8.9 | 8.9 |
Mean MG-ADL score | 9.1 | 9.0 | 9.0 | 8.9 | 8.6 | 8.6 |
Steroid use at study entry, n (%) | 56 (65.1) | 61 (70.8) | 46 (70.8) | 65 (73.0) | 71 (79.7) | 51 (79.7) |
NSIST use at study entry, n (%) | 56 (65.1) | 53 (61.5) | 40 (61.5) | 63 (70.8) | 51 (57.8) | 37 (57.8) |
MAIC = matching-adjusted indirect comparison; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; NSIST = nonsteroidal immunosuppressive therapy.
aPercentages in the “after matching” columns may show small discrepancies versus n/N, as the n’s are computed as the sum of MAIC weights and are not complete integers.
Source: Sponsor-submitted matching-adjusted indirect comparison.30
Results
Network Meta-Analyses
Evidence Networks
Concomitant IST Optimized Population
For the mean change from baseline in the MG-ADL total score end point, the NMA network comprised 6 trials and 405 patients in total.
For the mean change from baseline in the QMG total score end point, the NMA network comprised 6 trials and 400 patients in total.
The network diagram for both the mean change from baseline in the MG-ADL total score and the QMG total score is presented in Figure 1.
Figure 1: Network Diagram for the Mean Change From Baseline in MG-ADL Total Score and Change From Baseline in QMG Total Score (Concomitant IST Optimized Population)
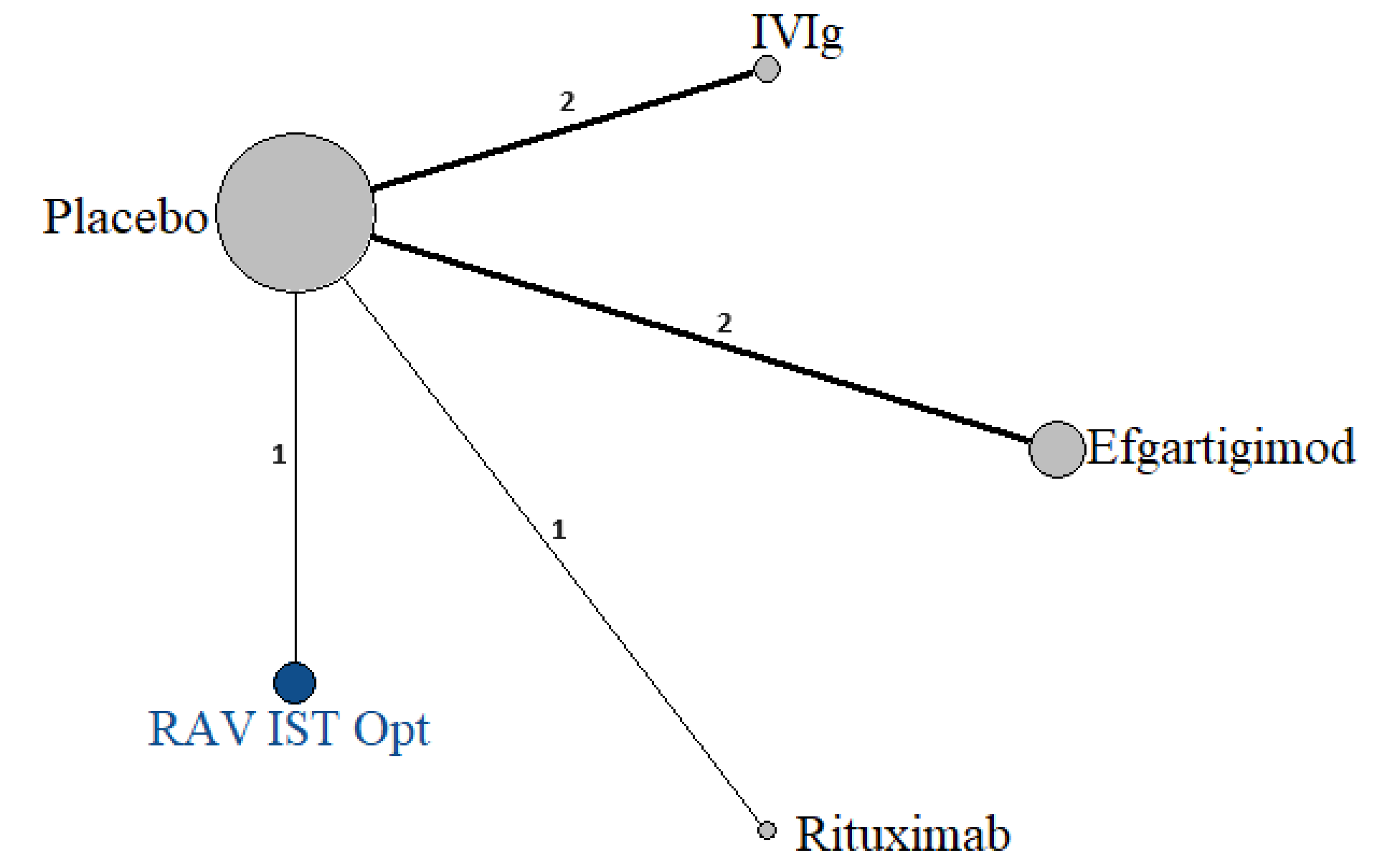
IST = immunosuppressive therapy; IVIg = IV immunoglobulin; MG-ADL = syasthenia gravis activities of daily living; QMG = Quantitative Myasthenia Gravis; RAV IST Opt = ravulizumab concomitant immunosuppressive therapy optimized subgroup.
Note: The nodes are weighted according to the number of participants. The edges are weighted according to the number of studies with a direct comparison between drugs.
Source: Sponsor-submitted network meta-analysis report.29
Refractory Concomitant IST Optimized Population
For both the mean change from baseline in the MG-ADL total score end point and the mean change from baseline in the QMG total score end point, the NMA network comprised 2 trials and a total of 205 and 204 patients, respectively.
Figure 2: Network Diagram for the Mean Change From Baseline in MG-ADL Total Score and Change From Baseline in QMG Total Score (Concomitant IST Optimized and Refractory Population)
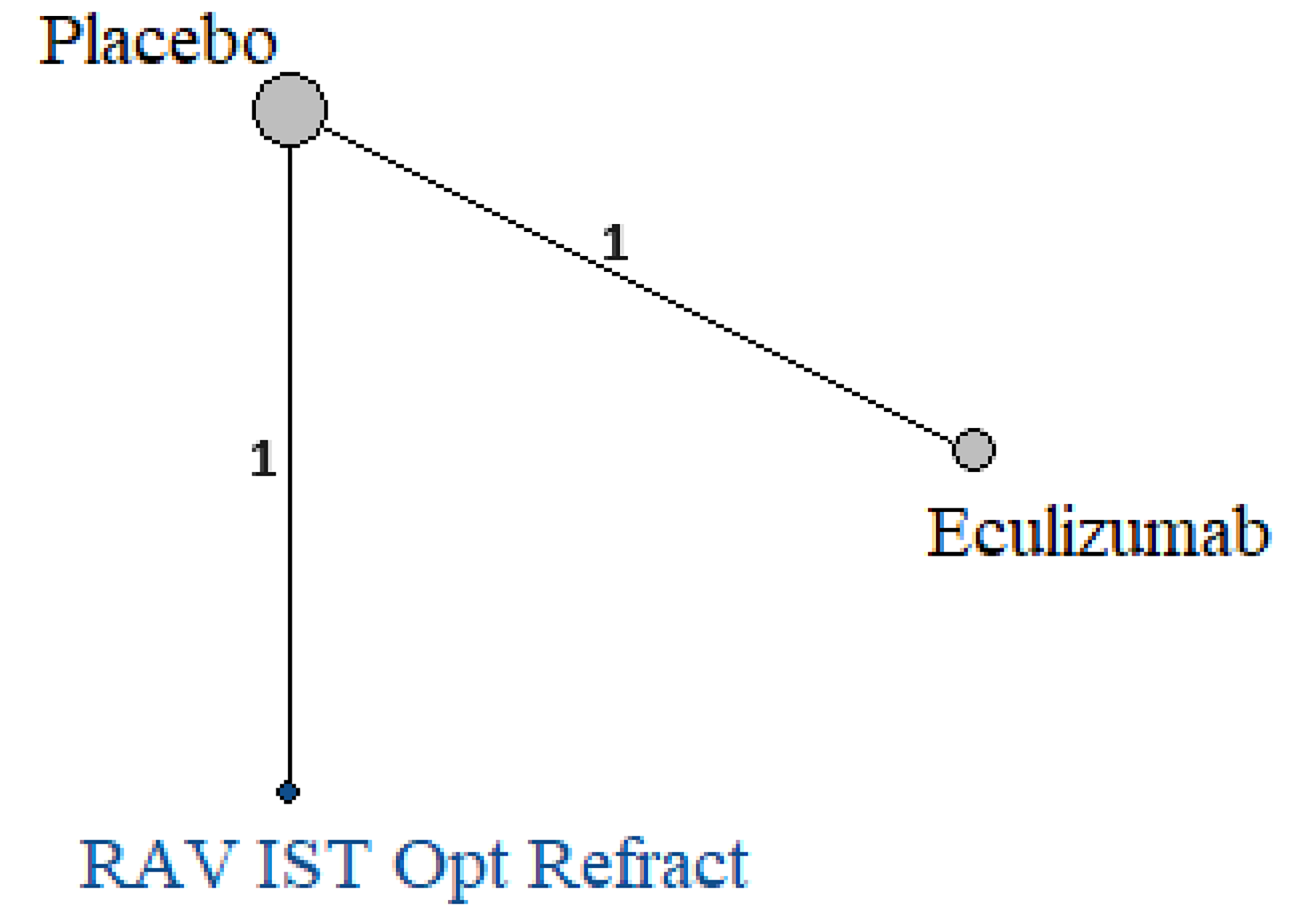
MG-ADL = Myasthenia Gravis Activities of Daily Living; IST = immunosuppressive therapy; QMG = Quantitative Myasthenia Gravis; RAV IST Opt Refract = ravulizumab concomitant immunosuppressive therapy optimized and refractory subgroup.
Note: The nodes are weighted according to the number of participants.
Source: Sponsor-submitted network meta-analysis report.29
Withdrawal Due to Adverse Events
The ITC report indicated that since no distinction regarding the population was made given the nature of the WDAE safety outcome, the full population of the CHAMPION-MG trial was included and the analysis was performed across all trials. When both definitions were available, the WDAE relating to the study drug was preferred over the WDAE relating to the study as a conservative approach (the WDAE rate of the study drugs is always at least equal to that of the study itself).
The analysis included 6 trials (Howard et al. [2019] was excluded from the analysis due to 0 events in both groups [i.e., the placebo group and the efgartigimod alfa group]).
Figure 3: Network Diagram for WDAE
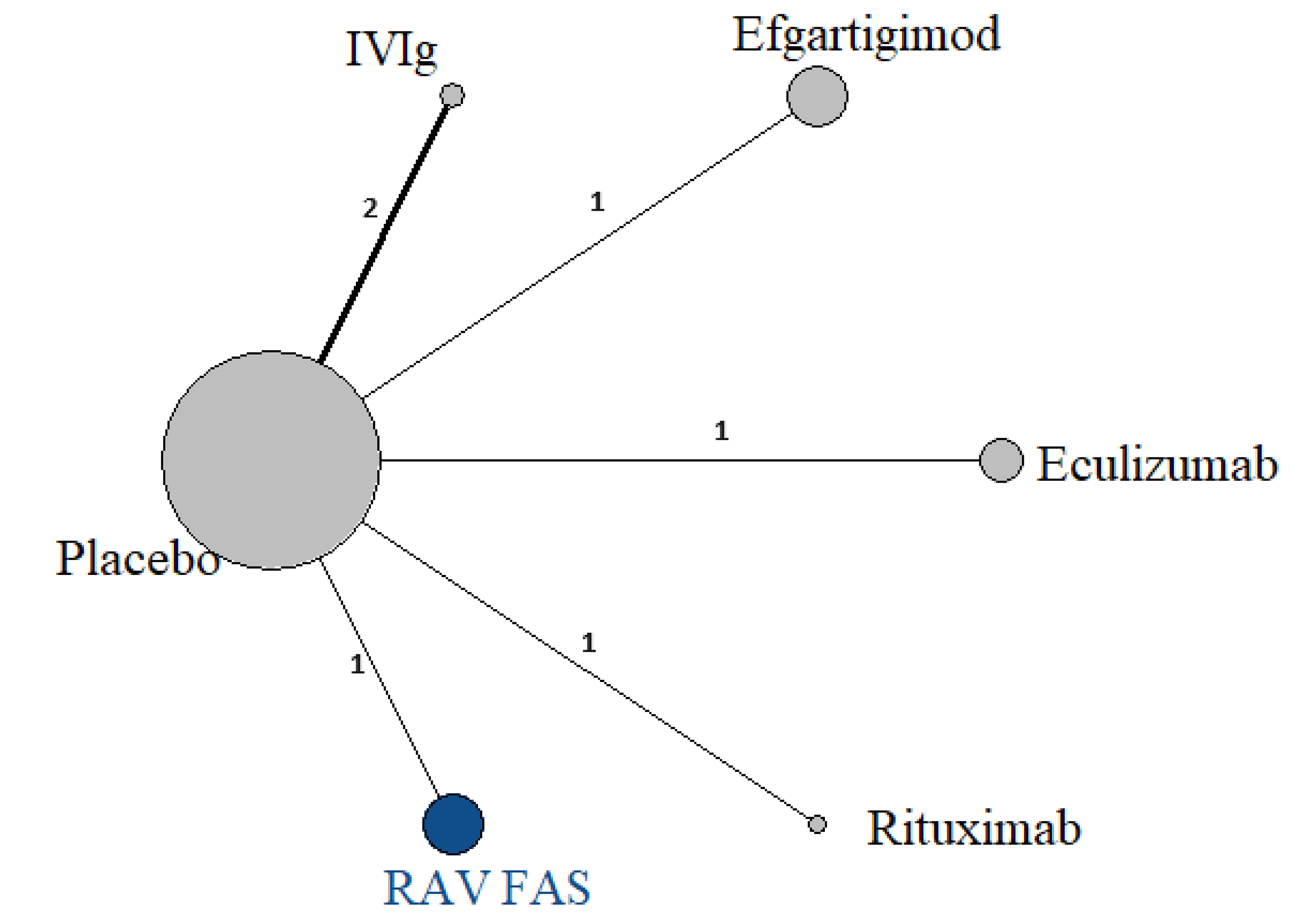
IVIg = IV immunoglobulin; RAV FAS = ravulizumab full analysis set; WDAE = withdrawal due to adverse event.
Note: The nodes are weighted according to the number of participants. The edges are weighted according to the number of studies with a direct comparison between drugs.
Source: Sponsor-submitted network meta-analysis report.29
Efficacy
Efficacy outcomes were assessed using 2 separate populations: the concomitant IST optimized population and the refractory concomitant IST optimized population.
Concomitant IST Optimized Population
Study REGAIN was excluded from the concomitant IST optimized population analysis due to the enrolment of patients who were refractory.
Mean Change From Baseline in MG-ADL Total Score
An FE model was used in the base-case analysis. ███████████████████████ █████ ████████████████ ████ ████████ █████████████████ █████████████ ███████████████████ █████████████████████ █████ █████████████████ ███████████ ████████ ██████████████████ ████ ██████████████████ In the sensitivity analysis including the CHAMPION-MG trial’s FAS rather than its concomitant IST optimized subgroup, ███████████████████████ ████████████████████████████ █████████████ █████ ████████████████████ ██████████████████████████ ███████████████████ ███████████ ███████████████████ ████████████████████ ████████████ █████████████████████████ █████████████ ███████████████████████ ███████ ████████████████████████ ██████████ ████████████████ ████████ ██████████████████████████ ████████████████████████████ ███████████ ███ █████████████ █████████████████ ███████████ ████ ████████████████████ ██████ ████████████████ ████████████████████████ ██████████████████████████████ ████████ ████ ████████████████████████
Mean Change From Baseline in QMG Total Score
An FE model was used as the base-case analysis. ███████████ █████████████████ ██████████████████████ ███████████████████████ █████████████████████████ ████ █████████ (Table 34).
In the sensitivity analysis including the CHAMPION-MG trial’s FAS rather than its concomitant IST optimized subgroup, ███████████████████ █████████████ ██████████████████████ ████████████████████████████ ████ ███████ ██████ ████████████ █████ ███████ ████████████ ██████ ████████████████████ ████████████████████████ ███████████████████████ ██████████ █████████████████████████████████ ███████ ████████████ ██████████ █████████ ████████ █████████████ ███████████ █████████████████████████████ ████████████████ ███████ ████████████ ████ ███████ █████████████████ ███████████████████████ ████
Table 34: Summary of Efficacy Outcome Measures in the Sponsor-Submitted ITC at the End of the Study Time Point (Concomitant IST Optimized Cohort)
Ravulizumab vs. | Mean change from baseline in MG-ADL total score MD (95% CrI) from FE model | Mean change from baseline in QMG total score MD (95% CrI) from FE model |
|---|---|---|
Efgartigimod alfa | ███████████████ | ███████████████ |
Rituximab | ███████████████ | ███████████████ |
IVIg | ████████████████ | ███████████████ |
Placebo | ████████████████ | ████████████████ |
CrI = credible interval; FE = fixed-effect; IST = immunosuppressive therapy; ITC = indirect treatment comparison; IVIg = IV immunoglobulin; MD = mean difference; MG-ADL = Myasthenia Gravis Activities of Daily Living; QMG = Quantitative Myasthenia Gravis; vs. = versus.
Note: Results in bold are significant; an MD of less than 0 favours the drug in the column (a result of a greater reduction in the MG-ADL score or the QMG score from baseline).
Source: Sponsor-submitted network meta-analysis report.29
The forest plots of all treatments compared to ravulizumab for the assessment of change from baseline in the MG-ADL score and the QMG score to the end-of-study time point in the concomitant IST optimized population are presented in Figure 4 to Figure 5.
Figure 4: Forest Plot, All Treatments Compared With Ravulizumab (MD With 95% CrI) for Mean Change From Baseline in MG-ADL Total Score at the End of the Study Time Point (Concomitant IST Optimized Population) [Redacted]

Source: Sponsor-submitted network meta-analysis report.29
Figure 5: Forest Plot, All Treatments Compared With Ravulizumab (MD With 95% Crl) for Mean Change From Baseline in QMG Total Score at the End-of-Study Time Point (Concomitant IST Optimized Population) [Redacted]

Source: Sponsor-submitted network meta-analysis report.29
Concomitant IST Optimized and Refractory Population
Study REGAIN was the only comparator study included in the concomitant IST optimized and refractory population analysis due to the enrolment of patients who were refractory. The ravulizumab concomitant IST optimized and refractory cohort was the only ravulizumab group in this analysis. Since the analysis included 2 studies, an ITC was conducted using placebo as the common comparator. The end of study for both trials was 26 weeks; therefore, no other time points were evaluated. A sensitivity analysis was not performed in this subgroup.
Mean Change From Baseline in MG-ADL Total Score
The ITC comprised a total of 205 patients.
The CrI for the mean change from baseline in the MG-ADL total score between the ravulizumab and eculizumab groups included the null (Table 33, Table 35, and Figure 6).
Mean Change From Baseline in QMG Total Score
The ITC comprised a total of 204 patients in total.
The CrI for the mean change from baseline in the QMG total score between the ravulizumab and eculizumab groups included the null (Table 35 and Figure 7).
Table 35: Summary of Efficacy Outcome Measures in the Sponsor-Submitted ITC at Week 26 (Concomitant IST Optimized and Refractory Population)
Ravulizumab vs. | Mean change from baseline in MG-ADL total score MD (95% CrI) | Mean change from baseline in QMG total score MD (95% CrI) |
|---|---|---|
Eculizumab | ███████████████ | ██████████████ |
Placebo | ████████████████ | ████████████████ |
CrI = credible interval; IST = immunosuppressive therapy; ITC = indirect treatment comparison; MD = mean difference; MG-ADL = Myasthenia Gravis Activities of Daily Living; QMG = Quantitative Myasthenia Gravis; vs. = versus.
Note: Results in bold are significant; an MD of less than 0 favours the drug in the column (a result of a greater reduction in the MG-ADL score or the QMG score from baseline).
Source: Sponsor-submitted network meta-analysis report.29
Forest plots of eculizumab compared to ravulizumab are presented in Figure 6 and Figure 7.
Figure 6: Forest Plot of the Indirect Comparison of Eculizumab and Ravulizumab (MD With 95% Crl) for Mean Change From Baseline in MG-ADL Total Score at the End-of-Study Time Point (Concomitant IST Optimized and Refractory Population) [Redacted]

Source: Sponsor-submitted network meta-analysis report.29
Figure 7: Forest Plot of the Indirect Comparison of Eculizumab and Ravulizumab (MD With 95% Crl) for Mean Change From Baseline in QMG Total Score at the End-of-Study Time Point (Concomitant IST Optimized and Refractory Population) [Redacted]

Source: Sponsor-submitted network meta-analysis report.29
Harms
WDAEs (Full Population)
For indirect evidence, relative effects are presented in Table 36 and the forest plot of all treatments compared to ravulizumab is presented in Figure 8. Based on the model fits for this outcome, the FE model was used as the base-case analysis. Although DIC values were similar for the FE model (DIC = 24.6) and the RE model (DIC = 23.4), the FE model was preferred.
Due to the limited number of studies and treatments with no events (0 events for the placebo group in Study REGAIN and Wolfe et al. [2002]), this outcome encountered difficulty in converging, particularly with eculizumab, where the comparison with placebo tends toward infinity (placebo is infinitely better). This resulted in all treatments being significantly better than eculizumab. However, this result should be interpreted with caution. Other results had wide CrIs including the null.
Table 36: Relative Effect From NMA Results (RR With 95% CrI) for WDAE
Ravulizumab FAS vs. | Safety outcome: relative effect in WDAE RR (95% CrI) from FE model |
|---|---|
Efgartigimod alfa | █████████████ |
Eculizumab | █████████████ |
Rituximab | █████████████ |
IVIg | █████████████ |
Placebo | █████████████ |
CrI = credible interval; FAS = full analysis set; FE = fixed-effect; Inf = tends to infinity (i.e., > 1,000); IVIg = IV immunoglobulin; NMA = network meta-analysis; RR = risk ratio; vs. = versus; WDAE = withdrawal due to adverse event.
Note: Results in bold are significant; an RR of less than 1 favours ravulizumab (as a result, there is a lower risk of WDAE).
Source: Sponsor-submitted network meta-analysis report.29
Figure 8: Forest Plot of All Treatments Compared With Ravulizumab (RR With 95% CrI) for DAE [Redacted]

Source: Sponsor-submitted network meta-analysis report.29
Matching-Adjusted Indirect Comparison
The mean change from baseline in the MG-ADL total scores at various time points in the CHAMPION-MG trial and Study ADAPT from the MAIC are shown in Table 37. Overall, the between-group difference in the MG-ADL score had CIs that crossed the null for all comparisons, except for week 4 (wide CIs were observed for this time point even though the 95% CIs did not cross 0, and the result favoured efgartigimod alfa).
Table 37: Mean (95% CI) Change From Baseline in MG-ADL Total Score at Various Time Points (MAIC Analysis)
Time point | CHAMPION-MG trial | Study ADAPT | MAIC Difference: Ravulizumab vs. efgartigimod alfa |
|---|---|---|---|
Ravulizumab vs. placebo | Efgartigimod alfa vs. placebo | ||
Week 4 | ███████████████ | ███████████████ | ██████████████ |
Week 10 | ███████████████ | ██████████████ | ██████████████ |
Time of best response: Week 26 (ravulizumab) vs. week 4 (efgartigimod alfa) | ███████████████ | ███████████████ | ██████████████ |
Week 26 (ravulizumab) vs. week 8 (efgartigimod alfa) | ███████████████ | ███████████████ | ██████████████ |
CI = confidence interval; MAIC = matching-adjusted indirect comparison; MG-ADL = Myasthenia Gravis Activities of Daily Living; vs. = versus.
Note: Negative values indicate a favourable relative effect for ravulizumab. The difference is statistically significant if its CIs do not cross 0.
Source: Sponsor-submitted matching-adjusted indirect comparison.30
Critical Appraisal of ITC
A priori protocols for the sponsor-submitted NMA or MAIC were not available; therefore, it cannot be known whether the analyses presented were selected from multiple analyses of the data.
For the NMA, studies were identified by searching multiple databases based on prespecified inclusion and exclusion criteria. Studies were selected by 2 independent reviewers; thus, the error and bias in the study selection process were minimized. Appropriate methods were used to reduce the risk of bias and error in data extraction. It was unknown if the risk of bias of the included trials was assessed by 2 independent reviewers. In addition, risk of bias was assessed at the level of the trial, rather than at the level of the reported results (i.e., per outcome), which ignores that risk of bias can vary by reported result within a trial. Some of the studies included within the NMA had some concerns for risk of bias.
One of the major concerns for NMA is that the included trials could be highly heterogeneous in terms of study design and patient characteristics at baseline. Seven RCTs were included in the NMA: 6 for the analyses in the concomitant IST optimized cohort and 2 for the analyses in the refractory concomitant IST optimized cohort (the CHAMPION-MG trial was included in both analyses). Heterogeneities were identified in the analysis populations, which included study design (phase of study, study time points, and outcomes measured in different ways) and patient characteristics at baseline (age, gender, or baseline MG-ADL scores). In the NMA, a sensitivity analysis using the time point of 8 weeks plus or minus 2 weeks was conducted. The results were similar to the base-case analysis; therefore, the results were supportive of the treatment effect of the study drugs, which was evaluated at the end of the study (the time point ranged from 6 weeks to 1 year across the included RCTs). However, this is still limited because week 8 is considered a short-term effect only. When the outcomes were measured in different ways, they imply that the comparisons to some relevant drugs were not feasible (e.g., rituximab was not able to be assessed in this sensitivity analysis since its efficacy was assessed at week 52 in Study BeatMG).
These differences would undermine the validity of the NMA, which relies on the transitivity assumption being upheld (i.e., that the trials are similar regarding all important effect modifiers). The use of FE models was chosen based on the DIC. However, the use of FE models (assuming no between-study heterogeneity) rather than RE models means that the CrIs are unlikely to adequately express the uncertainty arising from the heterogeneity. The limited number of included studies did not allow for metaregression or other techniques to adjust for differences in effect modifiers across studies within the NMA. The rarity of the population of interest limits the size and number of clinical studies completed with potential comparators and adds to the practical challenges when indirectly comparing treatment options.
Usually, including post hoc subgroups in the analyses may raise concerns since these analyses are not prespecified and can be at risk of bias due to selective reporting (e.g., there is a risk that the presented results are selected from multiple analyses of the data based on their direction, magnitude, or statistical significance). However, the sponsor provided clear justification for the selected subpopulations using criteria informed by other MG trials. Additionally, various sensitivity analyses were conducted to examine the robustness of the results from the base-case analysis, and results of the sensitivity analyses were consistent with the base-case analysis. As a result, any concern for selective reporting is minimized.
In the NMA, given the lack of closed loops in the networks, consistency in the NMA analyses could not be tested. All comparisons were therefore informed only by indirect evidence, which increases the level of uncertainty. Efficacy data were sparse in this NMA for the comparison of ravulizumab versus other active treatments. Overall, the 95% CrIs for the point estimates were wide for the efficacy and harms outcomes and spanned the null when compared with other regimens; therefore, confidence in the effect estimates for efficacy of the study drugs was limited due to imprecision indicated by the wide CrIs for these outcomes and precluded definitive conclusions as to which treatment may be favoured.
The study population for this review is patients with anti-AChR antibody–positive MG. However, some of the selected trials also included patients with MuSK antibody–positive MG. According to the clinical expert consulted for this review, MuSK antibody–positive MG accounts for a small portion of all types of MG (1% to 10%); the results in the mixed patient population may be generalized to patients with anti-AChR antibody–positive MG.
In the NMA, 2 efficacy outcomes were analyzed (the MG-ADL score and the QMG score). Therefore, the relative treatment effect of ravulizumab versus relevant comparators on other important clinical outcomes such as patients’ survival or HRQoL remains unknown. Harms were only assessed in a full population instead of the IST optimized cohorts, which were the focus of this current review.
In the sponsor-provided MAIC analyses, the CHAMPION-MG trial (ravulizumab versus placebo) and Study ADAPT (efgartigimod alfa versus placebo) were included. In Study ADAPT, 14.7% of the anti-AChR antibody–positive population (13 [20%] patients in the efgartigimod alfa group and 6 [9%] patients in the placebo group) did not receive prior corticosteroids or NSISTs at baseline, which means these patients received AChE inhibitors only and were not IST optimized. Even though patients in this trial were required to be on a stable dose of at least 1 treatment for gMG (i.e., AChE inhibitors, corticosteroids, or NSISTs) before screening and throughout the trial, detailed information regarding the duration of the stable dose or the mean or median dose of ISTs was not provided. Previous steroid and/or IST use were somewhat different between the CHAMPION-MG trial and Study ADAPT before matching (Table 33). Various patient characteristics at baseline were considered for inclusion in the adjusted analyses, including age, sex, MGFA class, disease duration, MG-ADL score, steroid use at study entry, and NSIST use at study entry. A rationale for how these factors were identified was not provided and was limited to factors that were available from both trials. It was not clear whether other potential effect modifiers were missing. The validity of the MAIC result requires that all sources of heterogeneity that exist between the index trial and the comparator trial are identified and adjusted for. Since it is not clear that this was achieved, there remains a risk that the results are biased due to residual confounding. Before adjustment, the mean age, proportion of female patients, steroid use, and NSIST use at study entry were somewhat different, suggesting reduced comparability of the populations. Patients in the CHAMPION-MG trial were older, fewer patients were female, and patients received fewer steroid but more IST treatments. In terms of effect sample size, the effect sample size was substantially reduced by ███ for patients treated with ravulizumab, █████ for those treated with placebo, suggesting that results are heavily influenced by a subset of the sample in the trial who may not be representative of the full sample, nor generalizable to the original population represented by the CHAMPION-MG study. In general, the 95% CIs for the point estimates often (except for at 4 weeks) ████████████, and precluded definitive conclusions as to which treatment may be favoured. In this MAIC analysis, change in the MG-ADL score was the only assessed outcome; therefore, other relevant outcomes were not assessed, such as HRQoL, symptom relief, or safety. In this analysis, the treatment effect of ravulizumab was assessed up to week 26, and longer-term benefits or harms of the study drug could not be examined.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the systematic review evidence were submitted.
Discussion
Summary of Available Evidence
The evidence included in this review consisted of 1 pivotal phase III, double-blind RCT. The CHAMPION-MG trial (N = 175) met the inclusion criteria for the systematic review conducted by the sponsor, and 2 post hoc subgroups of patients — the concomitant IST optimized cohort (████████) and the refractory concomitant IST optimized cohort (█████████) — were the focus of this Clinical Review Report. The purpose of the post hoc analyses was to evaluate the efficacy and safety of 26-week treatment with ravulizumab or placebo in patients with anti-AChR antibody–positive gMG in these 2 specific subgroups. The primary efficacy end point (change from baseline in MG-ADL at week 26) was the same as that in the primary analysis in the full population. Other outcomes in these analyses included change from baseline in the QMG total score and other HRQoL questionnaires, or the proportion of responders to QMG or MG-ADL, and safety. In the subgroup population of patients who received optimized IST or patients who were refractory despite having received optimized IST, all outcomes analyzed were exploratory. Baseline demographic and disease characteristics of the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort were consistent with the full CHAMPION-MG trial’s population in terms of the distribution of MGFA classifications, the baseline MG-ADL score (approximately 9 points across the 3 groups), the baseline QMG score (it ranged from 14 points to 15 points across the 3 groups), and age at diagnosis.
At the end of the RCP, all patients were eligible to enter the OLE phase and receive open-label ravulizumab therapy. A total of 161 (92%) patients from the RCP entered the OLE and received open-label treatment. In the current resubmission, OLE data from the pivotal study were available for up to 3.5 years of follow-up.
One sponsor-submitted NMA report compared the efficacy and harms of ravulizumab relative to currently available active treatments (efgartigimod alfa, eculizumab, IVIg, and rituximab) for the treatment of adult patients with anti-AChR antibody–positive gMG in the concomitant IST optimized cohort as well as the refractory concomitant IST optimized cohort. In total, 7 RCTs were included in the ITC. A sponsor-submitted MAIC compared MG-ADL scores between ravulizumab and efgartigimod alfa at various time points using the full trial populations; eligible patients in this study were required to be on a stable dose of at least 1 treatment for gMG (such as AChE inhibitors, corticosteroids, or NSISTs). Data of the baseline patient characteristics showed that 86% of this population (anti-AChR antibody–positive patients) had received at least 1 previous NSIST. Although Study ADAPT was not exclusively designed for patients who had received optimized IST, the majority of the study participants had received a stable dose of AChE inhibitors, corticosteroids, or NSISTs, and it is unlikely that generalizing the study results to patients who had received concomitant optimized IST is a major issue.
Interpretation of Results
Efficacy
The final CDEC recommendation for the initial submission of ravulizumab identified the following areas as having insufficient evidence regarding the efficacy and safety of ravulizumab: insufficient IST dosing information to conclude whether IST was optimized for patients at the time of study enrolment, insufficient evidence on the treatment effect of ravulizumab compared to conventional therapy as used in clinical practice, insufficient evidence on the treatment effect of ravulizumab in patients with refractory and nonrefractory disease, and a lack of evidence on the relative efficacy and harms of ravulizumab compared to relevant comparators (e.g., rituximab, IVIg, PLEX).
The interpretation of efficacy results in the following is organized for each of these points separately.
1. Lack of IST dosing information to conclude whether IST was optimized for patients at the time of study enrolment
In total, ██████████ (███ of the full population in the CHAMPION-MG trial) were included in the concomitant IST optimized cohort. These participants were defined as patients who were on at least 1 concomitant IST at screening and met 1 of the following criteria: if on a concomitant corticosteroid, the patient had been treated with that steroid for the 3 months or more before screening and had been on a stable dose for 1 month or more; if on a concomitant NSIST (e.g., azathioprine), the patient had been treated with that NSIST for the 6 months or more before screening and had been on a stable dose of that NSIST for 3 months or more. These patients met the inclusion criteria of Study ADAPT and were symptomatic but not considered refractory to IST treatment.
In the CHAMPION-MG trial, there were █████████ (███ of the full population in the CHAMPION-MG trial) included in the refractory concomitant IST optimized cohort. These patients met both the concomitant IST optimized cohort criteria as well as the definition of refractory disease per the inclusion criteria of the REGAIN trial. Specifically, patients in this cohort of the CHAMPION-MG trial were defined as not having achieved symptom control after 12 months of treatment with either at least 2 ISTs, or at least 1 IST plus chronic IVIg or PLEX.
According to Table 14 and Table 15, the concomitant treatments that patients in the 2 post hoc cohorts received before randomization were consistent with the dosing and management of patients with currently available therapies, according to the clinical expert consulted for this review. The median duration of prior corticosteroid and NSIST use in both cohorts exceeded the typical IST treatment duration for maximal responses (2 months to 6 months for corticosteroids, and 9 months to 18 months for NSISTs) as per the clinician expert opinion consulted for this review. In addition, the median treatment durations for IST treatment surpassed the minimum criteria for inclusion in the concomitant IST optimized cohort. The clinical expert consulted for this review had no concerns about suboptimal management with IST treatment (i.e., inadequate dosing or duration of therapy) in patients at the time of enrolment in the CHAMPION-MG trial. The clinical expert agreed that the dosages as well as median durations of corticosteroid and NSIST treatment appeared adequate and allowed sufficient time to achieve maximal responses with IST. Therefore, the patient population in the 2 cohorts aligned with the reimbursement request in that patients with anti-AChR antibody–positive gMG were symptomatic despite “adequate” ISTs (i.e., corticosteroids and/or NSISTs).
2. Insufficient evidence on the treatment effect of ravulizumab compared to conventional therapy as used in clinical practice
Concomitant conventional therapy such as AChE inhibitors and ISTs (e.g., corticosteroids, azathioprine, mycophenolate mofetil, tacrolimus) were allowed during the CHAMPION-MG trial. As per the protocol of the CHAMPION-MG trial, the dosage of these drugs was not allowed to be changed and no new ISTs were allowed to be added throughout the RCP, unless deemed medically necessary. Rescue therapy was allowed if a patient experienced protocol-defined clinical deterioration. Similar protocol requirements for concomitant ISTs are common across trials in patients with gMG (e.g., Study ADAPT [efgartigimod alfa versus placebo], Study REGAIN [eculizumab versus placebo]) to ensure consistency and to prevent the confounding of trial results. Because the concomitant conventional therapy was required to remain stable except in the case of rescue therapy, ravulizumab was not compared to any individual or combination conventional therapy as it would typically be used in clinical practice (i.e., altering doses or adding additional medications to suit patients’ current symptoms or other needs). The clinical expert consulted for this review was not concerned about discouraging dose changes in concomitant medications over the course of the 26 weeks in the RCP. The clinical experts noted that patients were on optimized and stable concomitant therapy entering the trial and were allowed to continue those therapies. Rescue therapy, including high-dose corticosteroids, PLEX, or IVIg, was permitted throughout the study for patients experiencing clinical deterioration, which was considered appropriate by the clinical expert consulted for this review.
3. Insufficient evidence on the treatment effect of ravulizumab in patients with refractory gMG, and in patients who were symptomatic but not considered refractory to IST
Patient selection for these 2 subgroups was based on the inclusion criteria from other RCTs: Study ADAPT and Study REGAIN. According to the clinical expert consulted for this review, the definitions used to identify patients are reasonable and acceptable in clinical practice. The population included in the 2 cohorts is adequately reflective of the patients who experience unmet needs in the treatment of gMG in clinical settings in Canada; this includes patients with refractory gMG as well as those whose disease had responded to prior gMG treatment but had responded inadequately to the existing standard of gMG therapy.
In the concomitant IST optimized cohort, during the RCP, the LSM treatment difference in the change from baseline for the MG-ADL total score was ████████████████████████). In the refractory concomitant IST optimized cohort, the LSM treatment difference in the MG-ADL total score was ████████████████████████). The treatment effect of ravulizumab over placebo observed in the 2 cohorts is consistent with the statistically significant results from the FAS population in the CHAMPION-MG trial. Results in both subgroups suggested an improvement in disease severity and its impact on a patient’s daily activities, and favoured ravulizumab. The between-group difference was close to the MID for the MG-ADL total score (a change of approximately 2 points). The clinical expert noted that this difference can be considered clinically important. However, it should be noted that there is some uncertainty about the clinical importance of the benefit due to imprecision; the upper bound of the CIs include effects that are small (close to the null).
Results of the change in the QMG total score at week 26 in both subgroups suggested improvement in disease severity after the 26-week treatment and favoured ravulizumab, which is consistent with the statistically significant results from the FAS population in the CHAMPION-MG trial. The clinical expert consulted for this review noted that the results appeared clinically important; patients with refractory disease appeared to do slightly less well. The expert noted that in clinical practice, patients with refractory disease would be expected to have lower response rates than patients with nonrefractory disease. In the concomitant IST optimized cohort, the LSM treatment difference was ████████████████████████), and in the refractory concomitant IST optimized cohort, the LSM treatment difference was ███████████████████████). A definite MID for the QMG scale has not been established, although a threshold ranging between 2 points and 3 points depending on disease severity has been suggested in previous studies enrolling patients with MG (refer to Table 8). There is some uncertainty about the clinical importance of the benefit gained from treatment with ravulizumab because of imprecision. The upper bounds of the 95% CIs included effects that are small (< 2 in the concomitant IST optimized cohort) and that crossed the null in the refractory concomitant IST optimized cohort.
In both cohorts, there was a larger proportion of clinical responders in the ravulizumab group than in the placebo group based on a 5-point or greater reduction in the QMG total score and a 3-point or greater reduction in the MG-ADL total score from baseline to week 26, although the clinical expert indicated that in practice, clinicians may use different thresholds in decision-making. Results in the 2 cohorts for the proportion of responders after the treatment (a QMG 5-point response or an MG-ADL 3-point response) were consistent with the primary analysis in the full population (a QMG 5-point response reached a statistically significant level in the FAS population, while the MG-ADL 3-point response was tested after a prior nonsignificant result of the hierarchical testing procedure and, therefore, P values were considered nominal).
HRQoL and fatigue were assessed based on LSM change from baseline in the MG-QoL15r total score and the Neuro-QoL fatigue score. An MID for MG-QoL15r or Neuro-QoL fatigue in patients with MG has not been estimated. Definite conclusions regarding the effect of the study drug on HRQoL cannot be drawn, due to the small sample size in the cohorts (HRQoL results were not available in 11% to 15% of patients treated with ravulizumab), and 95% CIs that were wide and crossed the null. The clinical expert consulted for this review noted that it was not surprising to see insignificant between-group differences for HRQoL measurements in this trial, given the chronicity of the condition, patients’ other comorbidities, and the potential for a placebo effect, which may also contribute to the insignificant between-group differences for this outcome. Results in the 2 subgroups were consistent with those in the primary analysis in the full population of the CHAMPION-MG trial.
The incidence of clinical deterioration and the incidence of an MG crisis were exploratory outcomes in the CHAMPION-MG trial. Patients treated with ravulizumab had a numerically lower incidence of clinical deterioration compared to those treated with placebo. An MG crisis was rare in the 2 cohorts; only 1 patient from the placebo group in each cohort reported an MG crisis. The effect of ravulizumab in lowering the risk of clinical deterioration or an MG crisis remains uncertain due to the low number of events and lack of formal analysis.
Efficacy data from the OLE period for the 2 cohorts were consistent with those from the RCP for the 2 cohorts and the FAS. Patients who switched from placebo to ravulizumab experienced numeric improvements in the LSM change from baseline in the MG-ADL total score at week 164. Improvements in other efficacy outcomes were also sustained over the observation period in both cohorts. However, further interpretation of these data was limited by the open-label and descriptive nature of the extension study. Attrition bias is also a concern in the OLE studies; this increases the uncertainty in the study results.
4. Lack of evidence on the relative efficacy and harms of ravulizumab compared to relevant comparators (e.g., rituximab, immunomodulating therapies such as IVIg and PLEX)
Comparative evidence of ravulizumab to other active treatments for gMG in the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort was available through a sponsor-submitted NMA. The rarity of the population of interest limits the size and number of clinical studies completed with potential comparators and adds to the practical challenges when indirectly comparing treatment options. Based on the results of the NMA, the evidence is insufficient to conclude which treatment may be favoured when comparing ravulizumab to efgartigimod alfa, IVIg, or rituximab in terms of change from baseline in the MG-ADL total score or the QMG total score in the concomitant IST optimized cohort, or whether ravulizumab or eculizumab may be superior in terms of the MG-ADL total score or the QMG total score in the refractory concomitant IST optimized cohort. The uncertainty in the study results from the NMA mainly resulted from the heterogeneity in the patient population and trial design across the included RCTs, from the fact that all included evidence was indirect, and from CrIs crossing the null (and wide CrIs were observed in many cases).
Evidence from an MAIC analysis provided by the sponsor examined the change in the MG-ADL total score of ravulizumab (evidence from the CHAMPION-MG trial) relative to efgartigimod alfa (evidence from Study ADAPT). Evidence from this MAIC analysis was insufficient to conclude whether ravulizumab differs from efgartigimod alfa in improvement in the MG-ADL total score at different time points in patients with gMG who received a previous stable dose of IST. This analysis was limited by a likelihood of residual confounding and a large reduction in effective sample size, suggesting that the findings are being driven by a small subset of the population in the CHAMPION-MG trial.
Harms
Limited results were reported for harms in the subgroup of interest. The incidence of treatment-emergent AEs and SAEs during the RCP in the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort were consistent with the harms results from the primary analysis in the full population of the CHAMPION-MG trial.
The percentage of patients with AEs was similar between the treatment groups (████████ of placebo-treated patients and ████████ of ravulizumab-treated patients in the concomitant IST optimized cohort and ████████ of placebo-treated patients ██████████ of ravulizumab-treated patients in the refractory concomitant IST optimized cohort). The most commonly reported AEs in these 2 cohorts included diarrhea and headache. Most AEs were grade 1 and grade 2 in severity.
The percentage of patients with SAEs was higher in the ravulizumab group compared to the placebo group. In the concomitant IST optimized cohort, █████ of ravulizumab-treated patients and █████ of placebo-treated patients experienced at least 1 SAE. In the refractory concomitant IST optimized cohort, █████ of ravulizumab-treated patients and █████ of patients in the placebo group experienced at least 1 SAE.
In both cohorts, there was 1 patient treated with ravulizumab who discontinued the study drug due to an AE. In both cohorts, there were |█patients treated with ravulizumab who died, and ██ death was reported for the placebo group. Deaths were deemed not related to the study drug by the investigator. Meningococcal infection was considered a notable harm for treatment with ravulizumab. No events were reported during the RCP in the entire study population.
During the OLE period, 96.4% of patients experienced at least 1 AE. Commonly reported AEs included COVID-19 infection (36.1%), headache (23.1%), and diarrhea (17.2%). Six patients died in the OLE period due to the following reasons: COVID-19 (3 patients), toxicity due to various drugs (1 patient), dehydration (1 patient), and an unknown reason (1 patient). There were no meningococcal infections reported during the OLE period.
The evidence from the ITC was not sufficient to conclude whether ravulizumab differs from the other active treatment in the risk of discontinuation of the study drug due to AEs in the overall patient population with gMG. Due to very few events across trials, the CrIs were wide.
Overall, the clinical expert considered the harms related to the treatment of ravulizumab manageable, and no unexpected safety signal was observed.
Conclusion
Evidence from 1 phase III, multicentre, double-blind, randomized, placebo-controlled trial (the CHAMPION-MG study) suggested that the administration of ravulizumab in adult patients with anti-AChR antibody–positive gMG resulted in statistically significant improvements compared with placebo in activities of daily living (change from baseline in the MG-ADL total score) and gMG disease severity (change from baseline in the QMG total score and the proportion of patients with a QMG 5-point response) after 26 weeks of treatment. Two post hoc cohorts of the CHAMPION-MG trial aligned with the reimbursement request under review — a concomitant IST optimized cohort (█|██████) and a refractory concomitant IST optimized cohort (█████████); these were the focus of this resubmission. The clinical benefit observed in the 2 cohorts was consistent with the results shown in the overall trial population. Evidence from the 2 post hoc cohorts suggested that in adult patients with anti-AChR antibody–positive gMG, ravulizumab likely results in clinically meaningful improvements in activities of daily living (the MG-ADL total score) compared with placebo. Results for other outcomes related to relief in MG disease severity (change from baseline in the QMG total score, at least a 5-point improvement in the QMG total score, and at least a 3-point improvement in the MG-ADL total score) were supportive of the analyses of changes in the MG-ADL total score. Note that confidence in the between-group differences for efficacy in the 2 cohorts was limited due to imprecision, which was indicated by the associated CIs that included small effects close to the null or that crossed the null (the CI crossed the null for the QMG total score in the refractory concomitant IST optimized cohort). The treatment effect of ravulizumab on HRQoL (the MG-QoL15r score and the Neuro-QoL fatigue score) remains uncertain. Results of post hoc cohort analyses are subject to limitations such as the potential for randomization to not be upheld, a reduced sample size, and a lack of formal statistical approaches to control for inflated type I error rate in multiple comparisons. However, in all cases, the findings of the subgroup analyses were consistent with the analyses of the full trial population. Results of an OLE study (based on up to 3.5 years of follow-up) suggested that improvement in daily living activities and disease severity was sustained during the long-term follow-up and that patients who switched from placebo to ravulizumab continuously reported improvements in their MG-ADL total score. The safety profile of ravulizumab in the 2 subgroups was consistent with that reported in the full population with no unexpected safety signals and was considered manageable by the clinical expert consulted for this review.
Evidence from sponsor-submitted ITCs (an NMA and an MAIC) comparing ravulizumab to other active treatments was insufficient to make conclusions on the relative efficacy of ravulizumab to these active treatments (i.e., the NMA examined ravulizumab versus efgartigimod alfa, IVIg, and rituximab in the concomitant IST optimized cohort, and ravulizumab versus eculizumab in the refractory concomitant IST cohort; the MAIC examined ravulizumab versus efgartigimod alfa in the overall population of the CHAMPION-MG trial). Limitations identified in these ITCs included a limited number of included studies, heterogeneity in trial characteristics and patient characteristics across these trials, and CrIs or CIs that crossed the null.
References
1.Conti-Fine BM, Milani M, Kaminski HJ. Myasthenia gravis: Past, present, and future. J Clin Invest. 2006;116(11):2843-2854. PubMed
2.Bird SJ. Clinical manifestations of myasthenia gravis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com. Accessed 2024 Jun 4.
3.Gilhus NE. Myasthenia gravis. N Engl J Med. 2016;375(26):2570-2581. PubMed
4.Meriggioli MN, Sanders DB. Autoimmune myasthenia gravis: Emerging clinical and biological heterogeneity. Lancet Neurol. 2009;8(5):475-490. PubMed
5.Pelak VS, Quan D. Ocular myasthenia gravis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com. Accessed 2024 Jun 4.
6.Jayam Trouth A, Dabi A, Solieman N, Kurukumbi M, Kalyanam J. Myasthenia gravis: A review. Autoimmune Dis. 2012;2012:874680. PubMed
7.Dresser L, Wlodarski R, Rezania K, Soliven B. Myasthenia gravis: Epidemiology, pathophysiology and clinical manifestations. J Clin Med. 2021;10(11). PubMed
8.Breiner A, Widdifield J, Katzberg HD, Barnett C, Bril V, Tu K. Epidemiology of myasthenia gravis in Ontario, Canada. Neuromuscul Disord. 2016;26(1):41-46. PubMed
9.Hansen JS, Danielsen DH, Somnier FE, et al. Mortality in myasthenia gravis: A nationwide population-based follow-up study in Denmark. Muscle Nerve. 2016;53(1):73-77. PubMed
10.Sanders DB, Wolfe GI, Benatar M, et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology. 2016;87(4):419-425. PubMed
11.Schneider-Gold C, Gajdos P, Toyka KV, Hohlfeld RR. Corticosteroids for myasthenia gravis. Cochrane Database Syst Rev. 2005;2005(2):CD002828. PubMed
12.Narayanaswami P, Sanders DB, Wolfe G, et al. International consensus guidance for management of myasthenia gravis: 2020 Update. Neurology. 2021;96(3):114-122. PubMed
13.Gilhus NE, Nacu A, Andersen JB, Owe JF. Myasthenia gravis and risks for comorbidity. Eur J Neurol. 2015;22(1):17-23. PubMed
14.Pascuzzi RM, Coslett HB, Johns TR. Long-term corticosteroid treatment of myasthenia gravis: report of 116 patients. Ann Neurol. 1984;15(3):291-298. PubMed
15.Schneider-Gold C, Hagenacker T, Melzer N, Ruck T. Understanding the burden of refractory myasthenia gravis. Ther Adv Neurol Disord. 2019;12:1756286419832242. PubMed
16.Argenx BV. Product Monograph: Vyvgart (efgartigimod alfa) [sponsor provided reference]. 2023.
17.CADTH Reimbursement Recommendation: Efgartigimod Alfa (Vyvgart) [accessed by sponsor]. Can J Health Technol. 2024;4(1).
18.Government of Canada. Notice of Compliance Information. Soliris (eculizumab) Supplement to a New Drug Submission. New Indication: Myasthenia Gravis [sponsor provided reference]. 2018.
19.Alexion Pharma GmbH. Product Monograph: Soliris (eculizumab) [sponsor provided reference]. 2021.
20.CADTH Common Drug Review Clinical Review Report: Eculizumab (Soliris) [accessed by sponsor]. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/clinical/sr0605-soliris-mg-clinical-review-report.pdf.
21.CADTH Health Technology Review. Rituximab for the treatment of myasthenia gravis: A 2021 update [accessed by sponsor]. Can J Health Technol. 2021;1(14).
22.Alexion Pharma GmbH. Product Monograph: Ultomiris (ravulizumab) [sponsor provided reference]. 2023.
23.CADTH Drug Reimbursement Expert Review Committee final recommendation: Ravulizumab (Ultomiris - Alexion Pharma GmBH). Can J Health Technol. 2023;3(8). https://www.cda-amc.ca/sites/default/files/DRR/2023/SR0765Ultomiris%20-%20Confidential%20Final%20CADTH%20Recommendation%20August%2024,%202023%20revised.pdf. Accessed 2024 Aug 18.
24.Clinical Study Report: ALXN1210-MG-306. A phase 3, randomized, double-blind, placebo-controlled, multicenter study to evaluate the safety and efficacy of ravulizumab in complement-inhibitor-naive adult patients with generalized myasthenia gravis [internal sponsor's report]. Boston (MA): Alexion Pharmaceuticals, Inc; 2021 Oct 5.
25.Muppidi S. The myasthenia gravis--specific activities of daily living profile. Ann N Y Acad Sci. 2012;1274:114-119. PubMed
26.Barnett C, Herbelin L, Dimachkie MM, Barohn RJ. Measuring clinical treatment response in myasthenia gravis. Neurol Clin. 2018;36(2):339-353. PubMed
27.Katzberg HD, Barnett C, Merkies IS, Bril V. Minimal clinically important difference in myasthenia gravis: Outcomes from a randomized trial. Muscle Nerve. 2014;49(5):661-665. PubMed
28.Alexion Pharmaceuticals Inc. CHAMPION-MG: Cohort Analyses 2024 [sponsor provided reference]. 2024.
29.Ultomiris (ravulizumab) for the treatment of generalized Myasthenia Gravis: Systematic literature review and network meta-analyses [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ravulizumab, 10 mg/mL & 100 mg/mL for intravenous infusion. Montreal (QC): PeriPharm Inc. for Alexion Pharmaceuticals Inc; 2024 May.
30.Efficacy of ravulizumab vs efgartigimod for the treatment of generalized myasthenia gravis: Indirect treatment comparison technical report [internal sponsor's report]. Alexion; 2023 Aug 15.
31.Anil R, Kumar A, Alaparthi S, et al. Exploring outcomes and characteristics of myasthenia gravis: Rationale, aims and design of registry - The EXPLORE-MG registry. J Neurol Sci. 2020;414:116830. PubMed
32.Oh SJ, Morgan MB, Lu L, et al. Racial differences in myasthenia gravis in Alabama. Muscle Nerve. 2009;39(3):328-332. PubMed
33.Pallaver F, Riviera AP, Piffer S, et al. Change in myasthenia gravis epidemiology in Trento, Italy, after twenty years. Neuroepidemiology. 2011;36(4):282-287. PubMed
34.Santos E, Coutinho E, Moreira I, et al. Epidemiology of myasthenia gravis in Northern Portugal: Frequency estimates and clinical epidemiological distribution of cases. Muscle Nerve. 2016;54(3):413-421. PubMed
35.Sanders DB, Raja SM, Guptill JT, Hobson-Webb LD, Juel VC, Massey JM. The Duke myasthenia gravis clinic registry: I. Description and demographics. Muscle Nerve. 2021;63(2):209-216. PubMed
36.Wendell LC, Levine JM. Myasthenic crisis. Neurohospitalist. 2011;1(1):16-22. PubMed
37.Jaretzki A, 3rd, Barohn RJ, Ernstoff RM, et al. Myasthenia gravis: Recommendations for clinical research standards. Task Force of the Medical Scientific Advisory Board of the Myasthenia Gravis Foundation of America. Neurology. 2000;55(1):16-23. PubMed
38.Romi F. Thymoma in myasthenia gravis: From diagnosis to treatment. Autoimmune Dis. 2011;2011:474512. PubMed
39.CADTH Reimbursement Review: Stakeholder feedback on draft recommendation: Ravulizumab (Ultomiris) [accessed by sponsor]. Ottawa (ON): CADTH; 2023: https://www.cda-amc.ca/sites/default/files/DRR/2023/SR0765_Ultomiris_Stakeholder_Feedback.pdf.
40.Araujo-Neto JM, Guimaraes GS, Fernandes FF, Soares MA. Hepatitis B surface antibody (Anti-HBs) kinetics during rituximab chemotherapy and performance of hepatitis B vaccine before immunosuppression: Two prospective studies. Viruses. 2022;14(8). PubMed
41.Carson KR, Evens AM, Richey EA, et al. Progressive multifocal leukoencephalopathy after rituximab therapy in HIV-negative patients: A report of 57 cases from the Research on Adverse Drug Events and Reports project. Blood. 2009;113(20):4834-4840. PubMed
42.Gkrania-Klotsas E, Kumararatne DS. Serious infectious complications after rituximab therapy in patients with autoimmunity: Is this the final word? Clin Infect Dis. 2021;72(5):738-742. PubMed
43.Fouda GE, Bavbek S. Rituximab hypersensitivity: From clinical presentation to management. Front Pharmacol. 2020;11:572863. PubMed
44.Valeant Canada LP. Product Monograph: Pyridostigmine Bromide [sponsor provided reference]. 2014.
45.Rituxan (rituximab): 10 mg/mL for intravenous Infusion [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; 2023 Jun 2: https://assets.roche.com/f/173850/x/5af6aeabe9/rituxaniv_pm_e.pdf.
46.CADTH Drug Reimbursement Review: Ravulizumab (Ultomiris) [accessed by sponsor]. Ottawa (ON): CADTH; 2023.
47.Clinical Study Report: ALXN1210-MG-306 (addendum). Phase 3, randomized, double-blind, placebo-controlled, multicenter study to evaluate the safety and efficacy of ravulizumab in complement-inhibitor naive adult patients with generalized myasthenia gravis [internal sponsor's report]. Boston (MA): Alexion Pharmaceuticals, Inc; 2023 Dec 8.
48.Clinical Study Report: ALXN1210-MG-306 Protocol or Amendment. New Haven (CT): Alexion Pharma Corporation; 2018 Nov 16.
49.Wolfe GI, Herbelin L, Nations SP, Foster B, Bryan WW, Barohn RJ. Myasthenia gravis activities of daily living profile. Neurology. 1999;52(7):1487-1489. PubMed
50.Muppidi S, Silvestri NJ, Tan R, Riggs K, Leighton T, Phillips GA. Utilization of MG-ADL in myasthenia gravis clinical research and care. Muscle Nerve. 2022;65(6):630-639. PubMed
51.Barohn RJ, McIntire D, Herbelin L, Wolfe GI, Nations S, Bryan WW. Reliability testing of the quantitative myasthenia gravis score. Ann N Y Acad Sci. 1998;841:769-772. PubMed
52.Burns TM, Grouse CK, Conaway MR, Sanders DB, MG Composite, MG-QOL15 Study Group. Construct and concurrent validation of the MG-QOL15 in the practice setting. Muscle Nerve. 2010;41(2):219-226. PubMed
53.Gershon RC, Lai JS, Bode R, et al. Neuro-QOL: Quality of life item banks for adults with neurological disorders: item development and calibrations based upon clinical and general population testing. Qual Life Res. 2012;21(3):475-486. PubMed
54.Muppidi S, Wolfe GI, Conaway M, Burns TM, Mg C, Mg-Qol15 Study G. MG-ADL: Still a relevant outcome measure. Muscle Nerve. 2011;44(5):727-731. PubMed
55.Bedlack RS, Simel DL, Bosworth H, Samsa G, Tucker-Lipscomb B, Sanders DB. Quantitative myasthenia gravis score: Assessment of responsiveness and longitudinal validity. Neurology. 2005;64(11):1968-1970. PubMed
56.Barnett C, Merkies IS, Katzberg H, Bril V. Psychometric properties of the Quantitative Myasthenia Gravis Score and the Myasthenia Gravis Composite Scale. J Neuromuscul Dis. 2015;2(3):301-311. PubMed
57.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
58.Luo Y, Dong X, Peng Y, et al. Evaluation of outcome measures for myasthenia gravis subgroups. J Clin Neurosci. 2021;91:270-275. PubMed
59.Andersen H, Mantegazza R, Wang JJ, et al. Eculizumab improves fatigue in refractory generalized myasthenia gravis. Qual Life Res. 2019;28(8):2247-2254. PubMed
60.Howard JF, Jr., Bril V, Vu T, et al. Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): A multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021;20(7):526-536. PubMed
61.Drug Reimbursement Review: Efgartigimod Alfa (Vyvgart) for the treatment of generalized myasthenia gravis (gMG) [accessed by sponsor]. Ottawa (ON): CADTH; 2024: https://www.cda-amc.ca/efgartigimod-alfa.
62.Quality assessment tools project report. Ottawa (ON): CADTH; 2012: https://www.cda-amc.ca/sites/default/files/pdf/QAT_final.pdf. Accessed 2024 Aug 21.
63.Tonin FS, Rotta I, Mendes AM, Pontarolo R. Network meta-analysis: A technique to gather evidence from direct and indirect comparisons. Pharm Pract (Granada). 2017;15(1):943. PubMed
64.Van Valkenhoef G, Kuiper J. Package “gemtc”- Network Meta-Analysis Using Bayesian Methods, Version 1.0-2 [sponsor provided reference]. 2023.
65.Borenstein M, Hedges L, Rothstein H. Meta-Analysis Fixed effect vs. random effects [sponsor provided reference]. 2017.
66.Cochrane Scientific Committee. Cochrane Scientific Committee Agenda Meeting 8th November 2018 [accessed by sponsor]. 2018; https://methods.cochrane.org/sites/default/files/public/uploads/2018_8th_november_agenda_and_papers_final.pdf. Accessed 2024 May 26.
67.Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU Technical Support Document 2: A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials [sponsor provided reference]. 2014.
68.Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: A generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making. 2013;33(5):607-617. PubMed
69.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539-1558. PubMed
70.Howard JF, Jr., Utsugisawa K, Benatar M, et al. Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): A phase 3, randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol. 2017;16(12):976-986. PubMed
71.Vu T, Meisel A, Mantegazza R, et al. Terminal complement inhibitor ravulizumab in generalized myasthenia gravis. NEJM Evid. 2022;1(5):EVIDoa2100066.
72.ULTOMIRIS® (ravulizumab) for the treatment of adult patients with anti-acetylcholine receptor (AChR) antibody-positive generalized Myasthenia Gravis (gMG) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ravulizumab, 10 mg/mL and 100 mg/mL for intravenous infusion. Mississauga (ON): Alexion Pharma GmbH; 2024.
73.Alexion Pharma GmbBH. Alexion Pharma GmbBH response to Aug 6, 2024 CDA-AMC request for additional information regarding Ultomiris. Information on the Concomitant IST Optimized Cohort and Refractory Concomitant IST Optimized Cohort [internal sponsor report]. Mississaugua (ON): Alexion Pharma GmbBH; 2024.
74.Alexion Pharma GmbBH. Alexion Pharma GmbBH response to Aug 6, 2024 CDA-AMC request for additional information regarding Ultomiris. Information in the Concomitant IST Optimized Cohort and Refractory Concomitant IST Optimized Cohort - Refractory [internal sponsor report]. Mississaugua (ON): Alexion Pharma GmbBH; 2024.
75.Clinical Study Report: ALXN1210-MG-306 (figures). Phase 3, randomized, double-blind, placebo-controlled, multicenter study to evaluate the safety and efficacy of ravulizumab in complement-inhibitor naive adult patients with generalized myasthenia gravis [internal sponsor's report]. Boston (MA): Alexion Pharmaceuticals, Inc; 2023.
76.Alexion Pharma GmbBH. Alexion Pharma GmbBH response to Aug 6, 2024 CDA-AMC request for additional information regarding Ultomiris. Information in the Concomitant IST Optimized Cohort and Refractory Concomitant IST Optimized Cohort for the open-label extension period - Refractory Concomitant IST Optimized Cohort [internal sponsor report]. Mississauga (ON): Alexion Pharma GmbBH; 2024.
77.Alexion Pharma GmbBH. Alexion Pharma GmbBH response to Aug 15, 2024 CDA-AMC request for additional information regarding Ultomiris. Information in the Concomitant IST Optimized Cohort and Refractory Concomitant IST Optimized Cohort for the open-label extension period [internal sponsor report]. Mississaugua (ON): Alexion Pharma GmbBH; 2024.
78.Wolfe GI, Barohn RJ, Foster BM, et al. Randomized, controlled trial of intravenous immunoglobulin in myasthenia gravis. Muscle Nerve. 2002;26(4):549-552.
79.Howard JF, Jr., Bril V, Burns TM, et al. Randomized phase 2 study of FcRn antagonist efgartigimod in generalized myasthenia gravis. Neurology. 2019;92(23):e2661-e2673.
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 38: Summary of Patients’ Use of Immunosuppressive Therapies for MG at Baseline in CHAMPION-MG Study (FAS)
IST use, n (%) | Placebo (N = 89) | Ravulizumab (N = 86) | All patients (N = 175) |
|---|---|---|---|
Patients with no IST use | 8 (9) | 10 (12) | 18 (10) |
Patients with any IST use | 81 (91) | 76 (88) | 157 (90) |
Glucocorticoids | 65 (73) | 56 (65) | 121 (69) |
Azathioprine | 22 (25) | 18 (21) | 40 (23) |
Mycophenolate mofetil | 24 (27) | 24 (28) | 48 (27) |
Cyclosporine | 4 (4) | 6 (7) | 10 (6) |
Tacrolimus | 12 (13) | 8 (9) | 20 (11) |
Methotrexate | 1 (1) | 0 (0) | 1 (1) |
Patients using 1 IST | 34 (38) | 40 (47) | 74 (42) |
Glucocorticoids | 18 (20) | 20 (23) | 38 (22) |
Other IST | 16 (18) | 20 (23) | 36 (21) |
Patients using 2 IST | 47 (53) | 36 (42) | 83 (47) |
Glucocorticoids and azathioprine | 13 (15) | 12 (14) | 25 (14) |
Glucocorticoids and mycophenolate mofetil | 20 (22) | 12 (14) | 32 (18) |
Glucocorticoids and cyclosporine | 3 (3) | 5 (6) | 8 (5) |
Glucocorticoids and tacrolimus | 10 (11) | 7 (8) | 17 (10) |
Glucocorticoids and methotrexate | 1 (1) | 0 (0) | 1 (1) |
FAS = full analysis set; IST = Immunosuppressive therapy; MG = myasthenia gravis.
Source: Clinical Study Report for the CHAMPION-MG trial.24
Table 39: Change in Concomitant IST Used During RCP in CHAMPION-MG Study (SAS)
IST use | FAS | |
|---|---|---|
Placebo (N = 89) n (%) | Ravulizumab (N = 86) n (%) | |
Corticosteroids | ||
New | 1 (1) | 2 (2) |
Discontinued | 0 | 2 (2) |
Increased | 3 (3) | 3 (3) |
Decreased | 5 (6) | 4 (5) |
Immunosuppressants | ||
New | 0 | 0 |
Discontinued | 0 | (1) |
Increased | 1 (1) | 2 (2) |
Decreased | 1 (1) | 3 (3) |
IST = immunosuppressive therapy; MG = myasthenia gravis; RCP = randomized controlled period; SAS = safety analysis set.
Source: Clinical Study Report for the CHAMPION-MG trial.24
Table 40: Duration of Corticosteroid and Nonsteroidal Immunosuppressive Therapies Before First Dose of Study Drug (Concomitant IST Optimized Cohort in CHAMPION-MG Study)
Variable | Statistic | ██████████ ███ | ███████ ███ |
|---|---|---|---|
Duration of corticosteroids (days) | n | ██ | ██ |
Mean (SD) | █████████████ | ████████████ | |
Median | █████ | █████ | |
Minimum to maximum | ████████ | ███████ | |
At least 6 months, n (%) | ███████ | ███████ | |
At least 12 months, n (%) | ███████ | ███████ | |
Duration of azathioprine (days) | n | ██ | ██ |
Mean (SD) | █████████████ | ████████████ | |
Median | ██████ | █████ | |
Minimum to maximum | ███████ | ████████ | |
At least 6 months, n (%) | ██████ | ███████ | |
At least 12 months, n (%) | ███████ | ████████ | |
Duration of mycophenolate mofetil (days) | n | ██ | ██ |
Mean (SD) | ████████████ | █████████████ | |
Median | █████ | █████ | |
Minimum to maximum | ████████ | ███████ | |
At least 6 months, n (%) | ███████ | ███████ | |
At least 12 months, n (%) | ████████ | ████████ | |
Duration of cyclosporine (days) | n | || | || |
Mean (SD) | ██████████████ | ████████████ | |
Median | █████ | ██████ | |
Minimum to maximum | ███████ | ███████ | |
At least 6 months, n (%) | ██████ | ██████ | |
At least 12 months, n (%) | ██████ | ███████ | |
Duration of tacrolimus (days) | n | || | || |
Mean (SD) | █████████████ | ██████████████ | |
Median | ██████ | █████ | |
Minimum to maximum | ███████ | ███████ | |
At least 6 months, n (%) | ██████ | ██████ | |
At least 12 months, n (%) | ███████ | ██████ | |
Duration of methotrexate (days) | n | || | || |
Mean (SD) | ██ | ████████ | |
Median | ██ | █████ | |
Minimum to maximum | ██ | ██████ | |
At least 6 months, n (%) | || | ██████ | |
At least 12 months, n (%) | || | ██████ |
CS = corticosteroid; NA = not applicable; NSIST = nonsteroidal immunosuppressive therapy.
Notes: Duration of IST use for inclusion was calculated for the continuous IST use regardless of dose that triggered the cohort inclusion. If the end date is after the first dose of study drug, the date of the first dose of study drug was used for calculation. Per protocol, no ISTs were discontinued between screening date and the first dose of study drug date.
The concomitant IST optimized cohort included patients on 1 or more concomitant IST at screening and who met the following: if on a concomitant steroid, the patient had been treated with that steroid for the 3 or more months before screening and had been on a stable dose for 1 or more month; and if on a concomitant NSIST, the patient had been treated with that NSIST for the 6 or more months before screening and had been on a stable dose of that NSIST for 3 or more months.
Source: Cohort analyses of CHAMPION-MG trial.28
Table 41: Duration of Corticosteroid and Nonsteroidal Immunosuppressive Therapies Before First Dose of Study Drug (Refractory Concomitant IST Optimized Cohort in CHAMPION-MG Study)
Variable | Statistic | Ravulizumab (████) | Placebo (████) |
|---|---|---|---|
Duration of corticosteroids (days) | n | ██ | ██ |
Mean (SD) | █████████████ | ████████████ | |
Median | █████ | █████ | |
Minimum to maximum | ████████ | ███████ | |
At least 6 months, n (%) | ███████ | ███████ | |
At least 12 months, n (%) | ███████ | ███████ | |
Duration of azathioprine (days) | n | ██ | ██ |
Mean (SD) | █████████████ | ████████████ | |
Median | ██████ | █████ | |
Minimum to maximum | ███████ | ████████ | |
At least 6 months, n (%) | ██████ | ██████ | |
At least 12 months, n (%) | ███████ | ███████ | |
Duration of mycophenolate mofetil (days) | n | ██ | ██ |
Mean (SD) | ████████████ | ███████████ | |
Median | █████ | █████ | |
Minimum to maximum | ███████ | ███████ | |
At least 6 months, n (%) | ██████ | ██████ | |
At least 12 months, n (%) | ███████ | ███████ | |
Duration of cyclosporine (days) | n | █████ | ██ |
Mean (SD) | ██████████████ | ████████████ | |
Median | ██████ | ██████ | |
Minimum to maximum | ███████ | ███████ | |
At least 6 months, n (%) | █████ | █████ | |
At least 12 months, n (%) | █████ | ██████ | |
Duration of tacrolimus (days) | n | █████ | █████ |
Mean (SD) | █████████████ | ████████████ | |
Median | ██████ | █████ | |
Minimum to maximum | █████████ | ████████ | |
At least 6 months, n (%) | █████ | █████ | |
At least 12 months, n (%) | █████ | █████ | |
Duration of methotrexate (days) | n | █████ | █████ |
Mean (SD) | ██ | █████████ | |
Median | ██ | █████ | |
Minimum to maximum | ██ | ███████ | |
At least 6 months, n (%) | █████ | █████ | |
At least 12 months, n (%) | █████ | █████ |
CS = corticosteroid; NA = not applicable; NSIST = nonsteroidal immunosuppressive therapy.
Notes: The duration of IST use for inclusion was calculated for the continuous IST use regardless of dose that triggered the cohort inclusion. If the end date is after the first dose of study drug, the date of the first dose of study drug was used for calculation. Per protocol, no ISTs were discontinued between screening date and the first dose of study drug date.
The refractory concomitant IST optimized cohort includes patients of concomitant IST optimized cohort excluding the patients who were nonrefractory defined as patients treated with only 1 IST and who had not received chronic IVIg or PLEX at least every 3 months, or no IST within the last 12 months before the screening visit.
Source: Cohort analyses of the CHAMPION-MG trial.28
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AChEI
acetylcholinesterase inhibitor
AChR
acetylcholine receptor
Anti-AChR
anti–acetylcholine receptor
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
gMG
generalized myasthenia gravis
ICER
incremental cost-effectiveness ratio
IST
immunosuppressive therapy
IVIg
IV immunoglobulin
LY
life-year
MAIC
matching-adjusted indirect comparison
MG
myasthenia gravis
MG-ADL
myasthenia gravis activities of daily living
MGFA
Myasthenia Gravis Foundation of America
NMA
network meta-analysis
NSIST
nonsteroidal immunosuppressive therapy
pCPA
pan-Canadian Pharmaceutical Alliance
PLEX
plasma exchange or plasmapheresis
QALY
quality-adjusted life-year
QMG
Quantitative Myasthenia Gravis
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Ravulizumab (Ultomiris), 10 mg/mL and 100 mg/mL concentrate for solution for IV infusion |
Indication | For the treatment of adult patients with anti-AChR antibody–positive gMG |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | January 6, 2023 |
Reimbursement request | Add-on therapy for adult patients with anti-AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChEIs, corticosteroids, and/or NSISTs |
Sponsor | Alexion Pharma GmbH |
Submission history | Previously reviewed: Yes Indication: Neuromyelitis optica spectrum disorder Recommendation date: March 13, 2024 Recommendation: Reimburse with clinical criteria and/or conditions Previously reviewed: Yes Indication: anti-AChR antibody–positive gMG Recommendation date: August 8, 2023 Recommendation: Do not reimburse Previously reviewed: Yes Indication: Atypical hemolytic uremic syndrome Recommendation date: February 27, 2023 Recommendation: Reimburse with clinical criteria and/or conditions Previously reviewed: Yes Indication: Paroxysmal nocturnal hemoglobinuria Recommendation date: February 11, 2022 Recommendation: Reimburse with clinical criteria and/or conditions |
AChEI = acetylcholinesterase inhibitor; AChR = acetylcholine receptor; gMG = generalized myasthenia gravis; NOC = Notice of Compliance; NSIST = nonsteroidal immunosuppressive therapy.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adults with anti-AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChEIs, corticosteroids, and/or NSISTs |
Treatment | Ravulizumab plus usual care |
Dose regimen | A single loading dose (2,400 mg, 2,700 mg, and 3,000 mg for body weights of ≥ 40 kg to < 60 kg, ≥ 60 kg to < 100 kg, and ≥ 100 kg, respectively), followed by maintenance dosing (3,000 mg, 3,300 mg, and 3,600 mg for body weights of ≥ 40 kg to < 60 kg, ≥ 60 kg to < 100 kg, and ≥ 100 kg, respectively) |
Submitted price | Ravulizumab, 300 mg vial (as a 30 mL vial, 10 mg/mL, or as a 3 mL vial, 100 mg/mL) = $7,282.15 Ravulizumab, 1,100 mg vial (as an 11 mL vial, 100 mg/mL) = $26,701.20 |
Submitted treatment cost |
|
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (44 years) |
Key data source | CHAMPION-MG trial, a multicentre, double-blind, randomized, placebo-controlled trial (full analysis set and concomitant IST optimized cohort) and a sponsor-conducted NMA that assessed the relative efficacy of ravulizumab vs. usual care, efgartigimod, IVIg, and rituximab |
Submitted results | ICER vs. rituximab = $2,102,671 per QALY gained (incremental QALYs = 0.93; incremental costs = $1,954,093) |
Key limitations |
|
CDA-AMC reanalysis results |
|
AChEI = acetylcholinesterase inhibitor; AChR = acetylcholine receptor; CDA-AMC = Canada’s Drug Agency; gMG = generalized myasthenia gravis; ICER = incremental cost-effectiveness ratio; IST = immunosuppressive therapy; IVIg = IV immunoglobin; LY = life-year; MAIC = matching-adjusted indirect comparison; MG-ADL = myasthenia gravis activities of daily living; NMA = network meta-analysis; NSIST = nonsteroidal immunosuppressive therapy; QALY = quality-adjusted life-year; QMG = Quantitative Myasthenia Gravis; vs. = versus; WTP = willingness to pay.
Conclusions
The clinical review by Canada’s Drug Agency (CDA-AMC) concluded that evidence from the concomitant immunosuppressive therapy (IST) optimized cohort and the refractory concomitant IST optimized cohort of the CHAMPION-MG trial suggested that in adult patients with anti–acetylcholine receptor (anti-AChR) antibody–positive generalized myasthenia gravis (gMG) with a classification of Myasthenia Gravis Foundation of America (MGFA) class II to class IV at screening, and with a myasthenia gravis activities of daily living (MG-ADL) total score of 6 points or more, ravulizumab likely results in clinically meaningful improvement in MG-ADL total score compared with placebo. Results for other outcomes related to relief in myasthenia gravis (MG) disease severity (change from baseline in the Quantitative Myasthenia Gravis [QMG] total score, at least a 5-point improvement in the QMG total score, and at least a 3-point improvement in the MG-ADL total score) were supportive of the analyses of changes in the MG-ADL total score. The CDA-AMC clinical review also concluded that based on indirect evidence submitted by the sponsor, there remains uncertainty with respect to the relative efficacy and safety of ravulizumab compared to active treatments (i.e., efgartigimod, rituximab, and IV immunoglobulin [IVIg]) due to limitations in the network meta-analysis (NMA) and matching-adjusted indirect comparison (MAIC) such as a limited number of included studies, significant heterogeneity across the included trials, and wide credible intervals that crossed the null. As such, the clinical review noted that there is insufficient evidence to conclude whether ravulizumab differs from efgartigimod, IVIg, or rituximab in terms of change from baseline in the MG-ADL total score or the QMG total score in the concomitant IST optimized cohort, or whether ravulizumab differs from eculizumab in terms of the MG-ADL total score or the QMG total score in the refractory concomitant IST optimized cohort.
CDA-AMC undertook reanalyses to address limitations in the sponsor’s pharmacoeconomic evaluation by assuming no annual increase in the MG-ADL score for patients receiving usual care. However, as several key limitations remained unresolved, the reanalysis performed by CDA-AMC is associated with uncertainty. In the CDA-AMC base case, the incremental cost-effectiveness ratio (ICER) for ravulizumab plus usual care is $2,996,852 per quality-adjusted life-year (QALY) gained, compared with rituximab plus usual care. The CDA-AMC base case is aligned with the sponsor’s results; that is, there was a 0% probability of ravulizumab plus usual care being cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained. A price reduction of at least 97% would be required for ravulizumab to be considered cost-effective at this threshold, reducing the unit price of ravulizumab for a 300 mg vial from $7,282 to $218 or annual per patient costs from $533,224 to $15,997 in subsequent years of treatment.
To address the clinical review’s conclusion that there is insufficient evidence to conclude whether ravulizumab differs from efgartigimod, IVIg, or rituximab, CDA-AMC conducted a scenario analysis in which all active treatments were assumed to be equally efficacious. In this scenario, ravulizumab was associated with the same QALYs as rituximab and efgartigimod; however, ravulizumab was more costly than rituximab and efgartigimod. Based on the conclusions of the clinical review, there is no evidence provided to support a price premium for ravulizumab over efgartigimod, IVIg, or rituximab.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Muscular Dystrophy Canada, which collected patient perspectives from patients living with MG through online surveys and interviews in Canada. All patients had a confirmed diagnosis of gMG through clinical reports. Patients with MG reported negative impacts of the disease on their quality of life and symptoms including fatigue, low energy levels, impacts on respiratory health, impacts on mobility and strength, difficulty completing daily life activities, loss of independence, double vision, and difficulty swallowing and speaking. Current treatments being used by patients included prednisone, mycophenolate mofetil, pyridostigmine, thymectomy, azathioprine, and IVIg. Side effects reported by patients associated with current treatments included depression, weight gain, unstable sugar levels, diarrhea, and nausea. Patient-reported shortcomings of current treatments included the slow onset of medication effects and the need for trial and error with medications. Treatment goals were identified as decreased intensity and severity of exacerbations, reduced side effects, maintenance of independence in conducting daily activities, and fewer hospitalizations. Patients expressed a preference for an extended dosing interval of 8 weeks for ravulizumab compared to other treatments such as IVIg, which needs to be administered more frequently. Caregivers and patients with MG also valued treatments that were noninvasive and less costly.
Clinician input was received from the Neuromuscular Disease Network for Canada with the participation of a group of experts in the disease area, MG. The clinician input noted that current treatments for patients with MG included pyridostigmine, thymectomy, immunotherapy (including prednisone, azathioprine, mycophenolate mofetil, methotrexate, cyclophosphamide, or cyclosporine), IVIg, plasmapheresis, eculizumab, and rituximab. The clinicians noted that clinically meaningful treatment goals included safe and effective treatment for patients with refractory and nonrefractory MG and an improved side effects profile. Clinically meaningful treatment response was described as increased survival, fewer hospital admissions (including emergency department visits, hospital admissions, and intensive care unit stays), decreased needs for rescue treatment, and reductions in concomitant steroids. The input noted that ravulizumab is likely to be used after treatment with pyridostigmine, and after treatment with either steroids or other immunosuppressants. Ravulizumab may shift the treatment paradigm for patients with severe and refractory disease who currently require chronic IVIg and plasma exchange.
The drug plans noted considerations of using ravulizumab after experience with other active treatments (e.g., eculizumab, efgartigimod, rituximab), as well as switching from an active treatment to ravulizumab. Further, the plans indicated that meningococcal vaccination and monitoring for meningococcal infections is required.
Several of these concerns were addressed in the sponsor’s model:
Model health states were based on the MG-ADL scale, which considers symptoms of MG, including double vision and difficulty swallowing and speaking.
The cost of meningococcal vaccination was included in the sponsor’s pharmacoeconomic analyses and budget impact analysis (BIA).
CDA-AMC was unable to address the following concerns raised from the input relevant to the economic review:
The sponsor’s model did not consider the use of ravulizumab after trialling eculizumab, efgartigimod, and rituximab or switching from eculizumab, efgartigimod, and rituximab to ravulizumab.
Economic Review
The current review is for ravulizumab (Ultomiris) for the treatment of adults with anti-acetylcholine receptor (AChR) antibody–positive gMG whose symptoms persist despite adequate treatment with acetylcholinesterase inhibitors (AChEIs), corticosteroids, and/or nonsteroidal immunosuppressive therapies (NSISTs).
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Ravulizumab was previously reviewed by CDA-AMC for the treatment of adult patients with anti-AChR antibody–positive gMG and received a do not reimburse recommendation.1 For this resubmission, the sponsor submitted a deviation request to consider ravulizumab as an add-on therapy for adults whose symptoms persist despite adequate treatment with AChEIs, corticosteroids, and/or NSISTs, which was accepted by CDA-AMC. For this resubmission, the sponsor submitted new evidence from the pivotal CHAMPION-MG trial and new indirect treatment comparison studies that focused on the efficacy of ravulizumab in 2 post hoc subgroups: a concomitant IST optimized cohort (aligned with the reimbursement request, according to the CDA-AMC clinical review) and a refractory concomitant IST optimized cohort. However, as noted in the CDA-AMC clinical review, the reimbursement request also includes patients who have had an adequate trial of AChEIs and no ISTs; these patients were not included in the 2 post hoc cohorts. As such, the base-case model population was aligned with the reimbursement request population, apart from the exclusion of patients who had had an adequate trial of AChEIs and no ISTs. The sponsor submitted a cost-utility analysis assessing ravulizumab plus usual care compared with efgartigimod plus usual care, rituximab plus usual care, blood products (i.e., IVIg) plus usual care, and usual care alone in adult patients with anti-AChR antibody–positive gMG.2 Usual care alone consisted of AChEIs (pyridostigmine) and ISTs (i.e., azathioprine, mycophenolate mofetil, cyclosporine, tacrolimus, methotrexate, cyclophosphamide, and prednisone).
Ravulizumab is available as a solution for IV infusion (300 mg per 30 mL, 300 mg per 3 mL, and 1,100 mg per 11 mL, single-use vials).3 The recommended dose for ravulizumab is weight-based and consists of a single loading dose (2,400 mg, 2,700 mg, and 3,000 mg for body weights of ≥ 40 kg to < 60 kg, ≥ 60 kg to < 100 kg, and ≥ 100 kg, respectively) followed by maintenance dosing (3,000 mg, 3,300 mg, and 3,600 mg for body weights of ≥ 40 kg to < 60 kg, ≥ 60 kg to < 100 kg, and ≥ 100 kg, respectively).3 Maintenance doses are initiated 2 weeks after the loading dose and then administered every 8 weeks thereafter. At the submitted price of $7,282.1500 per 300 mg vial, the cost per maintenance dose is $72,822, $80,104, and $87,386 for body weights of at least 40 kg to less than 60 kg, at least 60 kg to less than 100 kg, and 100 kg or more, respectively.2 Assuming patients receive 6.5 administrations annually beyond the first year, the estimated annual costs of maintenance treatment ranged between $473,340 and $568,008 depending on patient weight (Table 8). In the model, ravulizumab treatment costs were based on the weight distribution observed in the concomitant IST optimized cohort of the CHAMPION-MG trial (████% of individuals ≥ 40 kg to < 60 kg, █████% of individuals between ≥ 60 kg to < 100 kg, and █████% of individuals ≥ 100 kg), resulting in an annual treatment cost of $631,458 per patient in the first year and $533,224 per patient in subsequent years.4 The annual costs of comparators included in the sponsor’s model were $395,479 for efgartigimod, $26,136 for rituximab, and $132,563 for the first year of IVIg use, followed by $79,710 in subsequent years. Ravulizumab, efgartigimod, and rituximab were add-on treatment to usual care. The treatment costs contributing to usual care in the model consisted of background therapy drugs used in the CHAMPION-MG trial and was associated with an annual cost of $1,667 per patient.2
The clinical outcomes of interest were QALYs and life-years (LYs). The economic analysis was undertaken over a lifetime time horizon (44 years) from the perspective of the Canadian public health care payer. Both costs and health outcomes were discounted at an annual rate of 1.5%.
Model Structure
A Markov model with 9 health states and 3-month cycle lengths was submitted by the sponsor. Patients entered the model distributed across health states characterized by the extent of their MG-ADL score improvement at 26 weeks (refer to Figure 1) based on efficacy data in the CHAMPION-MG trial for usual care and a sponsor-submitted NMA for ravulizumab, efgartigimod, rituximab, and IVIg.4 The sponsor defined health states based on the extent of MG-ADL score improvement compared with baseline data (i.e., people in the 3-point to 4-point MG-ADL score change category health state had to have had a score decrease of 3 points in the CHAMPION-MG trial). In the first cycle, all patients started with a total MG-ADL score of 9.0 points, based on the mean baseline MG-ADL score of patients in the IST optimized cohort of the CHAMPION-MG trial. In the next cycle, a patient’s MG-ADL score in each health state decreased based on their score change category (refer to Table 12 for MG-ADL total score change by category). These scores were then maintained for the following 3 cycles, after which a percentage of patients on treatment could discontinue. Upon discontinuation, a patient’s MG-ADL scores increased at a rate of 0.5 points annually. Patients in the model did not transition between MG-ADL score change health states. Instead, during a given cycle, patients could experience myasthenic exacerbations or crises based on their MG-ADL score. Those who experienced an exacerbation remained in the given health state but a crisis could result in death.
Model Inputs
The base-case pharmacoeconomic model was primarily informed by inputs from the concomitant IST optimized gMG population of the CHAMPION-MG trial, a multicentre, double-blind, randomized, placebo-controlled trial.4 The model’s baseline population characteristics were derived from the IST optimized cohort of the CHAMPION-MG trial (mean age ████ years; ████% of patients female; mean MG-ADL total score ███).
Efficacy data were characterized by the proportion of patients distributed across MG-ADL score change categories and the MG-ADL total score change by category at 26 weeks (Table 11). For usual care, efficacy inputs were based on patient-level data obtained from the placebo arm of the IST optimized cohort of the CHAMPION-MG trial.4 For ravulizumab, efgartigimod, rituximab, and IVIg, efficacy was informed by applying mean reductions in MG-ADL scores from the sponsor-submitted NMA to the patient-level data from the placebo arm of the IST optimized cohort of the sponsor-submitted NMA to determine the distribution of patients across MG-ADL score change categories at 26 weeks.5 As the sponsor’s model structure was based on MG-ADL score change categories, a change of 1 full point was required to move a score change category, meaning that only treatments from the sponsor’s NMA that resulted in a greater than 1-point mean change from baseline in MG-ADL total score at the end of the study resulted in a change in distribution of patients across score change categories (Table 11).5 Once people were distributed across score change categories, their baseline MG-ADL score was reduced by the amount of the score change category they occupied (e.g., those in the 3-point to 4-point score change category had a reduction in their MG-ADL score of 3 points) (Table 12). The mean change in scores for score change categories that represented more than 1 score change (i.e., the score change category of less than 2 points and greater than 8 points) was derived from the patient-level data from the placebo arm of the concomitant IST optimized cohort after the mean reduction in MG-ADL score was applied. For example, in the less than 2-point score change category, which could include a 1-point reduction, or for those MG-ADL scores staying constant or increasing, ravulizumab was associated with an average change of −0.53 points whereas all other treatments were associated with a score increase (Table 12).
Treatment response for those on active treatments (i.e., ravulizumab, efgartigimod, rituximab, and IVIg) was defined as a decrease of 3 or more points in their total MG-ADL score.4 Patients who reached this response threshold within 6 months were considered responders and continued to receive active treatment. Patients who did not meet this threshold were considered nonresponders and were assumed to discontinue active treatment and receive usual care only thereafter. A proportion of the initial responders could also discontinue active treatment at an annual rate of 8.8% based on a retrospective chart review of eculizumab patients in the US.2 Nonresponders, patients who discontinued active treatment, and all patients on usual care were assumed to experience a worsening disease trajectory, modelled by an annual increase in their total MG-ADL score of 0.5 points (informed by the sponsor’s assumption); this was assumed to begin 1 year after discontinuation or nonresponse.
In each cycle, patients could experience clinical events (i.e., myasthenic exacerbations or myasthenic crises). The annual rate of patients experiencing these clinical events was determined by their total MG-ADL score, and this relationship was estimated based on data from the CHAMPION-MG trial. As event rates were linked to MG-ADL scores, there was no difference in MG-ADL score-specific event rates between treatments. The sponsor estimated that of all clinical events, 97.2% were myasthenic exacerbations while the remaining 2.9% were myasthenic crises based on the full analysis of the CHAMPION-MG trial.6
Patients experiencing a myasthenic crisis had an increased risk of death, with 4.47% of crises resulting in death, based on an analysis of a US sample of hospitalized patients with MG.7 Apart from myasthenic crises, patients were assumed to have the same mortality as their age- and gender-matched general population.8 Adverse events (AEs) occurring in 10% or more of patients in the CHAMPION-MG trial for ravulizumab and usual care were included in the model.6 The rates of AEs were obtained from the ADAPT, BeatMG, and NCT02473965 trial for efgartigimod, rituximab, and IVIg, respectively.9-11 AEs were assumed to only occur in the first 3 months of the model.
Utility values were derived by conducting post hoc analyses on the CHAMPION-MG (full analysis set) trial data to determine EQ-5D utility scores using MG-ADL scores and disease duration as a predictor.6 The sponsor used a regression equation to predict change in utility from the baseline EQ-5D score based on the baseline MG-ADL score, the MG-ADL score over time, and disease duration. In the sponsor’s approach, patients had an EQ-5D score of 0.5927 at baseline (in the full population) and the health utility was adjusted for the baseline MG-ADL score by using a coefficient of 0.0280. The model predicted a decrease in the health utility with an increase in the MG-ADL score (using a coefficient of −0.0278) and disease duration (using a coefficient of −0.0030). As the health utility was predicted by the MG-ADL score and the MG-ADL score in a health state changed over time, the utility values were not specific to a health state. Myasthenic exacerbations and myasthenic crises were associated with disutilities in the model, derived from patient-level data in the CHAMPION-MG trial (exacerbation disutility = −0.0615 lasting for 11.8 days; crisis disutility = −0.3863 lasting for 31.1 days).6 Utilities for AEs were obtained from published literature and were assumed to occur for 2 to 14 days.12-15
Costs in the model included drug acquisition, treatment administration, vaccination, routine care, and management of clinical events and AEs. Information on the dosing of efgartigimod was obtained from its product monograph and the price was obtained from the CDA-AMC review of efgartigimod.16,17 Rituximab dosing was adopted as per BeatMG trial and price was obtained from the Ontario Drug Benefit Formulary.10,18 The dosage of IVIg was informed by published literature and sponsor-sought expert opinion.17,19-26 IVIg costs were from a report published by the Ontario Ministry of Health and Long-Term Care.27,28 IST dosing was obtained from the CHAMPION-MG trial and published literature and costs were sourced from the Ontario Drug Benefit Formulary.4,18 The proportion of patients on each drug in usual care was based on data from the CHAMPION-MG trial.4 Treatment administration costs included the cost of nursing time and transportation, supplies, and physician supervision.18,29-31 The sponsor assumed that 50% of patients incurred routine care costs, which included 1 family physician and neurologist visit every 28 days.22 Myasthenic exacerbation and crisis management costs were broken into initial acute care and postacute care costs. Initial acute care costs included outpatient care, hospital stay, stay in an intensive care unit and rescue treatment with plasma exchange (PLEX) or IVIg with costs sourced from Ontario Case Costing Initiative Analysis Tool, Canadian Institute for Health Information, and published literature.32-35 The postacute care phase consisted of outpatient care, short-term nursing care, and PLEX or IVIg. The proportion of patients receiving each component of initial and postacute care were based on the sponsor’s assumption, the expert opinion sought by the sponsor, and published literature.7,34 It was assumed that 100% of patients would require IVIg or PLEX in the initial acute care phase. AE management costs were based on ambulatory care codes from the Alberta Interactive Health Data Application.36
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations), with the deterministic and probabilistic results being similar. The probabilistic findings are presented as follows.
Base-Case Results
In the base case, the sponsor reported that ravulizumab plus usual care was associated with an additional cost of $1,954,093 and 0.93 QALYs compared with rituximab, leading to an ICER of $2,102,671 per QALY gained (Table 3). Ravulizumab plus usual care was not associated with any additional LYs compared to comparators (Table 13). At a WTP threshold of $50,000 per QALY gained, there was a 0% probability of ravulizumab being cost-effective. Approximately 97% of patients in each arm were alive at the end of the time horizon. Of the 0.93 incremental QALYs predicted by the sponsor’s model to be gained for ravulizumab plus usual care compared to rituximab plus usual care, only 0.01 (1%) QALYs were accrued during the trial period. The remaining 99% of QALYs were accrued during the extrapolated period. Drug acquisition costs accounted for the majority of incremental costs for ravulizumab ($2,059,825, 105%); this was partly offset by reduced costs of treating myasthenic exacerbations and myasthenic crises for patients using ravulizumab compared with rituximab (incremental savings = $98,638) (Table 13).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Usual care | 866,247 | 9.33 | Reference |
Rituximab | 1,095,394 | 10.28 | 241,628 vs. usual care |
Ravulizumab | 3,049,488 | 11.21 | 2,102,671 vs. rituximab |
Dominated treatments | |||
Blood products (IVIg) | 1,025,077 | 9.66 | Extendedly dominated by rituximab |
Efgartigimod | 1,968,733 | 10.29 | Extendedly dominated by rituximab and ravulizumab |
ICER = incremental cost-effectiveness ratio; IVIg = IV immunoglobulin; QALY = quality-adjusted life-year; vs. = versus.
Note: Probabilistic results are presented.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor conducted a variety of deterministic sensitivity and scenario analyses to test the influence that changes in model parameters had on the cost-effectiveness of ravulizumab. Cost-effectiveness results were robust to changes in most parameters and sponsor’s assumptions. The scenarios with the greatest impact on the ICER assumed alternative estimates for change in the MG-ADL score for patients on usual care, with the ICER increasing to $2,413,302 per QALY gained versus rituximab when assuming an annual MG-ADL score increase of 0.25 points. Results were also sensitive to the MG-ADL response threshold, changing to $2,815,883 and $1,637,217 per QALY gained versus rituximab when the threshold was changed to 2 points and 4 points, respectively. The model was also sensitive to discount rates and the use of a shorter time horizon (20 years).
The sponsor conducted a scenario analysis from a societal perspective; this analysis included additional costs associated with the loss of productivity (calculated based on hourly wage and the number of work hours lost with exacerbation and crisis across the MG-ADL score categories) and caregiver lost income. In this analysis, relative to rituximab, the ICER was $2,122,851 per QALY gained. This was similar to the sponsor’s base-case analysis using a health care payer perspective.
The sponsor also submitted a scenario analysis assessing the cost-effectiveness of ravulizumab plus usual care compared with eculizumab plus usual care and usual care alone in the refractory concomitant IST optimized patient population pooled from the CHAMPION-MG trial and REGAIN trials. As there was no direct evidence regarding the relative efficacy of ravulizumab compared with eculizumab, efficacy for the pooled population was informed by a sponsor-commissioned NMA, which was conducted using patient-level data from the IST optimized and refractory cohort of the CHAMPION-MG trial (ravulizumab) and REGAIN (eculizumab) trials. Ravulizumab plus usual care was associated with an ICER of $1,083,808 per QALY gained versus usual care alone in this population (eculizumab was dominated by ravulizumab).
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The comparative efficacy and safety of ravulizumab is uncertain. The IST optimized cohort of the CHAMPION-MG trial compared ravulizumab with placebo, which was assumed to be representative of usual care in the sponsor’s economic evaluation due to the use of concomitant AChEIs, corticosteroids, and/or NSISTs.2 There have been no head-to-head trials of ravulizumab versus other active treatments (i.e., efgartigimod, rituximab, and IVIg). The sponsor therefore submitted an NMA and MAIC analysis to inform the comparative efficacy of ravulizumab versus other active treatments and placebo. The clinical review report identified several limitations with the sponsor-submitted indirect treatment comparisons,5 including significant heterogeneity in study design and patient characteristics at baseline, and a limited number of studies, which undermined the internal validity of the sponsor’s analyses. Further, the confidence in the effect estimates for efficacy was also limited due to imprecision indicated by the wide credible intervals and precluded any firm conclusions on comparative efficacy. Overall, according to the Clinical Review Report, based on the results of the NMA, the evidence is insufficient to conclude whether ravulizumab differs from efgartigimod, IVIg, or rituximab in terms of change from the baseline MG-ADL total score or QMG total score in the concomitant IST optimized cohort. Furthermore, evidence from a sponsor-submitted MAIC that compared ravulizumab with efgartigimod was insufficient to determine which treatment may be favoured in terms of MG-ADL score.
The mean reduction in the MG-ADL score from the sponsor’s NMA was applied directly to patient-level data from the placebo arm of the IST optimized cohort of the CHAMPION-MG trial to inform the relative MG-ADL improvement category at 26 weeks for the active treatments.4,5 As the sponsor’s model was based on MG-ADL score change categories that were defined by 1-point increments, the sponsor’s approach to modelling gMG assumed that a full 1-point increment was needed to move patients into a new MG-ADL score change category. If the change in the mean change from baseline in the MG-ADL total score was less than a full 1-point increment, the sponsor’s chosen modelling approach meant that there was no change in the proportion of patients across MG-ADL score change categories. As both efgartigimod and rituximab had a mean change in the baseline MG-ADL score of less than 1 point, this meant that the sponsor assumed that these treatments have no impact on the distribution of patients across MG-ADL score change categories compared with usual care (refer to Table 11). Further, because results of the sponsor’s NMA for IVIg predicted an increase in the MG-ADL score, patients who received IVIg were assigned to poorer score change categories than usual care at week 26, meaning the use of IVIg made a patient’s disease worse compared with the use of usual care alone.
Based on the results of the NMA, the sponsor also estimated that in patients who have a less than 2-point change in MG-ADL scores, only patients receiving ravulizumab will experience improvement in the disease (i.e., a decrease in MG-ADL scores) and patients on all other treatments will experience a worsening of the disease (i.e., an increase in MG-ADL scores) and that, among those in the score change category of equal to or greater than 8 points, ravulizumab will have the greatest change in total MG-ADL score (Table 12). Both of these assumptions are uncertain due to the limitations of the sponsor-conducted NMA and potentially bias the results in favour of ravulizumab. Furthermore, according to clinical expert feedback received by CDA-AMC, the parameterization of gMG treatment efficacy such that efgartigimod and rituximab result in a minimal improvement compared with usual care alone did not meet face validity. To elaborate, efgartigimod and rituximab both resulted in a 0.4-point score improvement compared with the use of usual care alone in cycle 2. Finally, the finding that IVIg would result in a worsening of the MG-ADL score compared to usual care alone did not meet face validity according to clinical expert feedback received by CDA-AMC for this review.
Regarding AEs, the comparative safety of the active treatments was also not assessed in the IST optimized cohorts and therefore is unknown. The sponsor’s approach to adopting AE rates from respective trials to populate safety in the economic model is prone to confounding.
CDA-AMC was unable to address this limitation in reanalyses. Due to the lack of direct evidence and limitations with the indirect comparative evidence used by the sponsor in the pharmacoeconomic analysis, the cost-effectiveness of ravulizumab compared to efgartigimod, rituximab, and IVIg is highly uncertain. As the clinical review noted that the evidence is insufficient to conclude whether ravulizumab differs from efgartigimod, IVIg, or rituximab in terms of change in the baseline MG-ADL total score, CDA-AMC explored a scenario analysis where all of the active treatments were assumed to be equally efficacious.
The model structure does not adequately reflect gMG in clinical practice. The sponsor submitted a Markov model with health states defined by MG-ADL score change categories.2 The sponsor-submitted model structure includes the following MG-ADL score categories: less than 2 points, 2 or more points, 3 or more points, 4 or more points, 5 or more points, 6 or more points, 7 or more points, and 8 or more points, and defined treatment response as a decrease of 3 or more points in the total MG-ADL score.2 Occupancy in a health state in the second cycle and beyond in the model was determined by the change in a patient’s total MG-ADL score at 26 weeks compared with baseline in the placebo arm of the IST optimized cohort of the CHAMPION-MG trial.4 For example, patients with an MG-ADL total score change of 4 points were assigned to the 4 points to 5 points health state, and those with a score change of 5 points were assigned to the 5 points to 6 points health state. The distribution of patients across MG-ADL score change category health states (Table 11) was used to determine their total MG-ADL score in the model’s second cycle, as a patient’s total baseline MG-ADL score was decreased by the number of points associated with their score change category (Table 12). This modelling approach is uncertain for several reasons. It is uncertain whether the MG-ADL score change categories defined by the sponsor were clinically meaningfully different from one another. For example, according to clinical expert feedback obtained by CDA-AMC for this review, it was noted that a 3-point change in the MG-ADL score may not be clinically meaningfully different from a 4-point change. No justification was provided for the sponsor’s cut-offs that were used to define health states. Additionally, despite treatment response being defined as a decrease of 3 or more points, the sponsor’s model included a less than 2 points health state, meaning that it was expected that nonresponders across different treatments would have different changes in MG-ADL scores. This modelling approach to modelling nonresponse is uncertain and biased results in favour of ravulizumab (refer to the previous limitation).
Additionally, because the MG-ADL score is a summary score, 2 patients in the same MG-ADL score change category could have markedly different clinical statuses. To elaborate, the MG-ADL assesses the functional ability of 8 signs or symptoms such as the ability to speak, chew, swallow, breathe, perform self-care activities, and perform physical activities, and vision-related parameters (2 items).37 A change in the MG-ADL total score does not clarify which element of functional ability has changed and therefore, 2 people with the same score change could have experienced very different changes in symptoms. CDA-AMC additionally notes that an MG-ADL score change category is not a distinct health state (i.e., it is not possible to describe the clinical picture of a patient in a given MG-ADL change category). Given this, CDA-AMC was unable to validate health state utility values or clinical event rates (i.e., crises and exacerbations) by score change category. Furthermore, even though the score change category is translated to a total MG-ADL score, as the MG-ADL score is a summary score, the components of the MG-ADL scale resulting in the total MG-ADL score could be very different for patients with the same total MG-ADL score. Therefore, the use of MG-ADL scores to define health states is problematic because patients within the same MG-ADL score change category and with the same total MG-ADL score can have very different symptoms. From a methodological perspective, a health state in an economic model should represent a homogenous group of patients who have similar expected costs and quality-of-life considerations. The implications of heterogeneity in health states have been well documented in the literature.38
As noted in the CADTH guidelines for economic evaluation, model health states should be based on the clinical or care pathway for the condition of interest.39 No health state transitions occurred in the model and patients did not move between sponsor-defined MG-ADL score categories. Clinical expert feedback received for this review noted that the sponsor’s assumption that patients remain in the initial MG-ADL score change categories lacks face validity because it is not reasonable to predict that there would be no change in MG-ADL total score change over the time horizon and because initial change in the MG-ADL score at week 26 was not deemed to be a clinically appropriate way to predict disease progression. A valid Markov model structure should allow patients to move between mutually exclusive health states and movement between health states should represent patients’ progression through the disease course, both of which were not captured appropriately in the sponsor’s model.39 This has implications for appropriately capturing differences in costs and health outcomes.39
CDA-AMC was unable to address limitations related to the model structure, and the direction and magnitude of the impact of these model structure limitations are unknown.
Natural history and long-term efficacy assumptions lack face validity. The sponsor applied natural history assumptions after the second model cycle to model gMG disease trajectory and long-term disease outcomes for the remainder of the model time horizon. The sponsor assumed that all patients receiving usual care (i.e., patients who started treatment on usual care and patients who discontinued active treatment due to nonresponse [with an MG-ADL score change of < 3 points] or patients who initially responded but discontinued throughout the model time horizon) would experience a deteriorating disease course by modelling an increase in a patient’s MG-ADL score by 0.5 points each year.2 This value was informed by the opinion of the sponsor’s clinical expert and was not based on the literature or trial findings (i.e., there was no comparative evidence to support the assumption).2 According to clinical expert feedback, the sponsor’s assumption that the MG-ADL score would increase over time for all patients treated with usual care lacks face validity; rather, the natural history of gMG is expected to fluctuate instead of progressively deteriorating. Further, a published study describing the natural history of gMG found that the majority of patients demonstrated improvement after 2 years of illness.40 Finally, only 14.5% of patients receiving placebo in the concomitant IST optimized cohort of the CHAMPION-MG trial experienced clinical deterioration, indicating that not all patients on usual care would be expected to experience a worsening disease course. Therefore, the assumption of a worsening disease course for all patients receiving usual care was deemed to be inappropriate. Assuming a progressively higher total MG-ADL score for usual care patients directly impacts health utility and clinical event rates because utility and event rates are determined by total MG-ADL scores and bias the results in favour of active treatments, including ravulizumab.
Finally, the effectiveness of active treatments from the CHAMPION-MG trial and sponsor-conducted NMA was captured in the sponsor’s modelling approach using the change in the MG-ADL score in cycle 1 and cycle 2. The remainder of the efficacy parameters informing the MG-ADL total score were based on the sponsor’s assumptions on long-term treatment effectiveness, such as a sustained change in the MG-ADL score or a progressively worsening disease course. As such, the majority of the total incremental QALYs for ravulizumab (99%) accrued after cycle 2 were based on extrapolation assumptions, which are highly uncertain.
In CDA-AMC reanalyses, a stable disease course (i.e., no deterioration or improvement) was assumed for patients receiving usual care. The model was not sufficiently flexible to allow for changes that accurately reflected a fluctuating disease progression (i.e., MG-ADL scores increasing after a clinical event, patient improvement, or patient stabilization).
Additional limitations were identified but were not considered to be key limitations. These limitations are outlined subsequently.
Utility values were not specific to health states and lacked face validity. Changes in utility values from baseline were derived from a mixed-effects model using a US index to derive a regression equation.2 In the sponsor’s modelling approach, the baseline MG-ADL score, the MG-ADL score over time, and disease duration predicted the change in utility from the baseline EQ-5D score. As the health utility was predicted by the MG-ADL score and the MG-ADL score in a health state changed over time, the utility values were not specific to a health state. Utility values should be specific to a clinically homogeneous group of patients.39 Further, given the limitations with the sponsor’s approach to modelling disease progression based on MG-ADL scores described earlier, the sponsor’s approach to linking health utilities with MG-ADL scores inappropriately estimated QALYs.
CDA-AMC could not address this limitation.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, which led to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical and it remains unclear whether the model is running inappropriately by overriding errors.
CDA-AMC could not address this limitation and notes that a thorough validation of the sponsor’s model was not possible.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Usual care was assumed to be equal to the placebo arm of the IST optimized cohort of the CHAMPION-MG trial. | According to the CDA-AMC Clinical Review Report, because the concomitant conventional therapy was required to remain stable except in the case of rescue therapy, ravulizumab was not compared to any individual or combination conventional therapy as it would typically be used in clinical practice (i.e., altering doses or adding additional medications to suit patients’ current symptoms or other needs). |
The sponsor-submitted model structure includes the following MG-ADL score categories of points: < 2, ≥ 2, ≥ 3, ≥ 4, ≥ 5, ≥ 6, ≥ 7, and ≥ 8. However, it defined treatment response as a decrease of 3 or more points in the total MG-ADL score. | It is uncertain if patients in the MG-ADL score category had a decrease of 3 or more points in the total MG-ADL score. |
Discontinuation among initial responders was assumed to be equal among those receiving active treatments. | This is likely appropriate according to clinical expert opinion received as part of this review. Additionally, while no evidence was available in the IST optimized population, evidence from the sponsor’s submitted ITC in the overall patient population with gMG was not sufficient to conclude whether ravulizumab differs from other active treatment in the risk of discontinuation of the study drug due to AEs. |
The sponsor assumed that patients who discontinued active treatment experienced disease progression (noted by an increase in MG-ADL score) 1 year after discontinuation. | There was no evidence to support a delay in disease progression. As such, the modelling approach is uncertain but unlikely to influence the results. |
The sponsor assumed the rate of myasthenic exacerbations would increase with an increase in MG-ADL score. | As the sponsor-modelled rate of myasthenic exacerbations and crises was based on MG-ADL scores and because ravulizumab was associated with the greatest change in MG-ADL score in the sponsor’s model based on their NMA, ravulizumab treatment was associated with the fewest clinical events in the sponsor’s model. However, there is insufficient clinical evidence to show the relative effect of different treatments on the number of exacerbations and crises. The CHAMPION-MG trial included the exploratory outcomes of incidence of clinical deterioration and crisis; however, the effect of ravulizumab in lowering the risk of clinical deterioration and crisis was uncertain due to the lower number of events and lack of formal analysis. Additionally, comparative evidence regarding myasthenic exacerbations and crises was not available for ravulizumab vs. active comparators. CDA-AMC explored the impact of excluding the modelled relationship between MG-ADL score and all clinical events (both exacerbations and crises) and found the sponsor’s assumption had minimal impact on the results. |
The sponsor assumed that AEs could occur only once during treatment. | This assumption is likely inappropriate but likely has minimal impact on the cost-effectiveness of ravulizumab. |
The sponsor used the results of a regression equation to predict change in utility from the baseline EQ-5D score based on the baseline MG-ADL score, the MG-ADL score over time, and disease duration. | Uncertain. CDA-AMC tested the impact of varying the coefficients of a regression equation for baseline MG-ADL score, MG-ADL score over time, and disease duration, and observed that it had an impact on total QALYs and minimal impact on the incremental changes. This finding suggests that while the total QALYs may be susceptible to fluctuations in the coefficients, the incremental differences are relatively stable. |
Supplemental dosing of ravulizumab following administration of PLEX or IVIg was not incorporated. | Inappropriate. The product monograph for ravulizumab indicates that supplemental dosing of a complement inhibitor is required with PLEX or IVIg to maintain the serum concentration of the complement inhibitor. As per the product monograph, the supplemental dose of ravulizumab required is approximately half of the “most recent” ravulizumab dose. The sponsor assumed no supplemental doses for patients on ravulizumab who received PLEX or IVIg. As such, treatment acquisition costs for ravulizumab are likely underestimated, biasing the results in favour of ravulizumab. |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; gMG = generalized myasthenia gravis; IST = immunosuppressive therapy; ITC = indirect treatment comparison; IVIg = IV immunoglobulin; MG-ADL = myasthenia gravis activities of daily living; NMA = network meta-analysis; PLEX = plasma exchange or plasmapheresis; QALY = quality-adjusted life-year; vs. = versus.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
CDA-AMC undertook reanalyses that addressed limitations within the model, as summarized in Table 5. The CDA-AMC base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts. All CDA-AMC probabilistic reanalyses were based on 3,000 iterations.
CDA-AMC was unable to address other key limitations of the model (as previously described), including uncertainty in the comparative efficacy of ravulizumab versus active treatment comparators, structural concerns with the submitted model that introduced significant uncertainty to the analysis, and natural history assumptions that did not accurately reflect disease progression. Due to these key limitations, it is uncertain that costs and health outcomes have been appropriately captured.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | ― | ― |
Changes to derive the CDA-AMC base case | ||
1. Annual MG-ADL score increase for usual care | 0.5 | 0 |
CDA-AMC base case | ― | Reanalysis 1 |
CDA-AMC = Canada’s Drug Agency; MG-ADL = myasthenia gravis activities of daily living.
CDA-AMC undertook a stepped analysis, incorporating each change proposed in Table 5 into the sponsor’s base case to highlight the impact of each change (Table 14). In the CDA-AMC base case, ravulizumab plus usual care was associated with higher costs (incremental costs = $2,020,771) and higher QALYs (incremental QALYs = 0.67) compared with rituximab plus usual care over a 44-year horizon, resulting in an ICER of $2,996,852 per QALY gained (Table 6). Ravulizumab plus usual care was not associated with any additional LYs compared to the comparators. Similar to the sponsor’s base case, there is a 0% probability that ravulizumab plus usual care is cost-effective at a WTP threshold of $50,000 per QALY gained. Of the 0.67 incremental QALYs gained for ravulizumab plus usual care, 0.01 (1%) QALYs were accrued during the trial period.
Disaggregated results can be found in Table 15. Drug acquisition costs accounted for nearly all of the incremental costs for ravulizumab versus comparators. Drug acquisition costs were partially offset by the costs of managing myasthenic crises and exacerbations. Incremental QALYs for ravulizumab were derived from patients spending more time in higher score change categories compared with other comparators, which resulted in ravulizumab patients achieving a lower MG-ADL score versus comparators. Note that despite efgartigimod and IVIg resulting in no change in the distribution of people across health states, they still resulted in incremental QALYs compared with usual care arising from having a better MG-ADL total score change in the less than 2 points and greater than or equal to 8 points score change category states (refer to Table 12).
Table 6: Summary of the CDA-AMC Reanalysis Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor base case (probabilistic) | |||
Usual carea | 866,247 | 9.33 | Reference |
Rituximab | 1,095,394 | 10.28 | 241,628 vs. usual care |
Ravulizumab | 3,049,488 | 11.21 | 2,102,671 vs. rituximab |
Dominated treatments | |||
Blood products (IVIg) | 1,025,077 | 9.66 | Extendedly dominated by rituximab |
Efgartigimod | 1,968,733 | 10.29 | Extendedly dominated by rituximab and ravulizumab |
CDA-AMC base case (probabilistic) | |||
Usual carea | 426,145 | 12.99 | Reference |
Rituximab | 756,446 | 13.28 | 1,138,505 vs. usual care |
Ravulizumab | 2,777,217 | 13.96 | 2,996,852 vs. rituximab |
Dominated treatments | |||
Blood products (IVIg) | 632,095 | 12.84 | Dominated by usual care |
Efgartigimod | 1,625,950 | 13.28 | Dominated by rituximab |
AChEI = acetylcholinesterase inhibitor; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; IST = immunosuppressive therapy; IVIg = IV immunoglobulin; QALY = quality-adjusted life-year; vs. = versus.
aUsual care consisted of AChEIs (pyridostigmine) and ISTs (azathioprine, mycophenolate mofetil, cyclosporine, tacrolimus, methotrexate, cyclophosphamide, and prednisone).
Source: Sponsor’s pharmacoeconomic submission.2
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s base case and the CDA-AMC base case. In the CDA-AMC base case, a price reduction of at least 97% is required for ravulizumab plus usual care to be considered cost-effective at a WTP threshold of $50,000 per QALY gained (Table 7). At a price reduction of approximately 60%, ravulizumab becomes less costly than rituximab, and only ravulizumab and usual care remain on the cost-effectiveness frontier.
Table 7: CDA-AMC Price Reduction Analyses
Analysis: price reduction | Unit drug cost ($) | Sequential ICERs for ravulizumab plus usual care ($/QALY) | |
|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | ||
No price reduction | 7,282 | 2,102,671 vs. rituximab | 2,996,852 vs. rituximab |
10% | 6,554 | 1,846,556 vs. rituximab | 2,643,873 vs. rituximab |
20% | 5,826 | 1,590,442 vs. rituximab | 2,290,894 vs. rituximab |
30% | 5,098 | 1,334,327 vs. rituximab | 1,937,915 vs. rituximab |
40% | 4,369 | 1,078,212 vs. rituximab | 1,584,936 vs. rituximab |
50% | 3,641 | 822,097 vs. rituximab | 1,231,957 vs. rituximab |
60% | 2,913 | 565,983 vs. rituximab | 957,049 vs. usual care |
70% | 2,185 | 309,868 vs. rituximab | 710,255 vs. usual care |
80% | 1,456 | 148,642 vs. usual care | 463,460 vs. usual care |
90% | 728 | 21,881 vs. usual care | 216,665 vs. usual care |
100% | 0 | Dominant | Dominant |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
CDA-AMC also explored several scenario analyses, including assuming equal efficacy for active treatments and excluding rituximab as a comparator.
Ravulizumab plus usual care was dominated by efgartigimod and rituximab in the scenario assuming equal efficacy of active treatments (ravulizumab, rituximab, efgartigimod, and IVIg). When rituximab plus usual care was excluded as a comparator, the ICER for ravulizumab plus usual care compared with usual care alone was $2,584,140 per QALY gained (Appendix 4, Table 16). As in the CDA-AMC base case, in this scenario, a 97% price reduction is required for ravulizumab to be considered cost-effective at a $50,000 per QALY WTP threshold.
Issues for Consideration
Modelled population is narrower than that of the Health Canada indication: Although the Health Canada indication does not specify MGFA classification and MG-ADL score, the product monograph notes that ravulizumab was studied in adult patients with gMG with an MGFA clinical classification of class II to class IV and with an MG-ADL score of 6 or more points.4 The sponsor’s analyses reflect the cost-effectiveness of ravulizumab plus usual care in only a subset of the Health Canada indicated population.31
Exclusion of patients with thymoma from the CHAMPION-MG trial: The CHAMPION-MG trial excluded patients with thymoma but the Health Canada indication covers this patient subpopulation.4,31 According to the clinical expert feedback received for this review, patients with thymoma may benefit from treatment with ravulizumab. However, the cost-effectiveness of ravulizumab in patients with thymoma is unknown due to the fact there is no efficacy data for ravulizumab in this population.
Anticipated patent expiration of eculizumab: Pan-Canadian Pharmaceutical Alliance (pCPA) negotiations for eculizumab for gMG concluded without an agreement.41 The patent for eculizumab is expected to expire on March 15, 2027.42 If eculizumab biosimilars become available and are considered clinically equivalent to eculizumab, ravulizumab is unlikely to remain less costly than eculizumab biosimilars (Table 8).
Previous submission history of ravulizumab: Ravulizumab has been previously reviewed by CDA-AMC for anti-AChR antibody–positive gMG and received a do not reimburse recommendation.43 Previously, the committee was concerned about the population being a mix of those who were exposed to IST and those who were refractory to IST, creating uncertainty about the effectiveness of ravulizumab in the population in which ravulizumab is expected to be used. The sponsor acknowledged this concern by performing the analyses in the IST optimized cohort of the CHAMPION-MG trial and the clinical expert feedback obtained for this review found the sponsor’s definition of IST optimization acceptable.
Alternative dosage form of ravulizumab: Ravulizumab is also available in an 1,100 mg/11 mL vial but the sponsor estimated the treatment cost of ravulizumab in this review based on the 300 mg/30 mL vial.31 As the cost per mg of ravulizumab is the same across dosage forms, the impact of this on the cost-effectiveness results is expected to be minimal.
Concerns about relevant comparators: Based on drug plan feedback received, rituximab may not be readily available in some jurisdictions. The sponsor also excluded chronic PLEX as a relevant comparator; however, it was identified as a relevant treatment option for the refractory population based on clinical expert feedback received for this review. As PLEX was not included in the analysis, the cost-effectiveness compared with ravulizumab is unknown.
Availability of efgartigimod for gMG is uncertain: Efgartigimod for the treatment of adult patients with gMG who are anti-AChR antibody–positive received a positive reimbursement recommendation and is currently in active pCPA negotiations.44,45 As such, whether efgartigimod will be reimbursed by jurisdictions for gMG is uncertain.
Overall Conclusions
The CDA-AMC clinical review concluded that evidence from the concomitant IST optimized cohort and the refractory concomitant IST optimized cohort of the CHAMPION-MG trial suggested that in adult patients with anti-AChR antibody–positive gMG with an MGFA classification of class II to class IV at screening, and with an MG-ADL total score of 6 or more points, ravulizumab likely results in clinically meaningful improvement in MG-ADL total score compared with placebo. Results for other outcomes related to relief in MG disease severity (change from baseline in the QMG total score, at least a 5-point improvement in the QMG total score, and at least a 3-point improvement in the MG-ADL total score) were supportive of the analyses of changes in the MG-ADL total score. The CDA-AMC clinical review also concluded that based on indirect evidence submitted by the sponsor, there remains uncertainty with respect to the relative efficacy and safety of ravulizumab relative to active treatments (i.e., efgartigimod, rituximab, and IVIg due to limitations in the NMA and MAIC such as a limited number of included studies, significant heterogeneity across the included trials, and wide credible intervals that crossed the null. As such, the clinical review noted that there is insufficient evidence to conclude whether ravulizumab differs from efgartigimod, IVIg, or rituximab in terms of change from baseline in the MG-ADL total score or the QMG total score in the concomitant IST optimized cohort, or whether ravulizumab differs from eculizumab in terms of the MG-ADL total score or the QMG total score in the refractory concomitant IST optimized cohort.
CDA-AMC undertook reanalyses to address limitations in the sponsor’s pharmacoeconomic evaluation by assuming no annual increase in the MG-ADL score for patients receiving usual care. However, as several key limitations remained unresolved, the reanalysis performed by CDA-AMC is associated with uncertainty. In the CDA-AMC base case, the ICER for ravulizumab plus usual care is $2,996,852 per QALY gained compared with rituximab plus usual care. The CDA-AMC base case is aligned with the sponsor’s results; that is, there was a 0% probability of ravulizumab plus usual care being cost-effective at a WTP threshold of $50,000 per QALY gained. A price reduction of at least 97% would be required for ravulizumab to be considered cost-effective at this threshold, reducing the unit price of ravulizumab for a 300 mg vial from $7,282 to $218 or annual per patient costs from $533,224 to $15,997 in subsequent years of treatment.
To address the clinical review’s conclusion that there is insufficient evidence to conclude whether ravulizumab differs from efgartigimod, IVIg, or rituximab, CDA-AMC conducted a scenario analysis in which all active treatments were assumed to be equally efficacious. In this scenario, ravulizumab was associated with the same QALYs as rituximab and efgartigimod; however, it was more costly than rituximab and efgartigimod. Based on the conclusions of the clinical review, there is no evidence provided to support a price premium for ravulizumab over efgartigimod, IVIg, or rituximab.
References
1.CADTH Reimbursement Recommendation: Ravulizumab (Ultomiris). Can J Health Technol. 2023;3(8). https://www.cda-amc.ca/sites/default/files/DRR/2023/SR0765Ultomiris%20-%20Confidential%20Final%20CADTH%20Recommendation%20August%2024,%202023%20revised.pdf. Accessed 2024 Aug 27.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab), 10 mg/mL & 100 mg/mL, concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma GmbH; 2024 Jun 4.
3.Ultomiris (ravulizumab): 10 mg/mL & 100 mg/mL, concentrate for solution for intravenous infusion [product monograph]. Mississauga (ON): Alexion Pharma Canada Corp; 2023.
4.Alexion Pharma Corporation. [CONFIDENTIAL] Clinical Study Report for ALXN1210-MG-306. A phase 3, randomized, double-blind, placebo-controlled, multicenter study to evaluate the safety and efficacy of ravulizumab in complement-inhibitor-naive adult patients with generalized Myasthenia Gravis. Primary Analysis Data Cut-off 11 May 2021. Date of Report: 05 October 2021 [sponsor supplied reference].
5.PeriPharm Inc. ULTOMIRIS® (ravulizumab) for the Treatment of Generalized Myasthenia Gravis: Systematic Literature Review and Network Meta-Analyses (Data on file) [sponsor supplied reference]. 2024.
6.Alexion Pharma Corporation. [CONFIDENTIAL] 60-Week Clinical Study Report Addendum for ALXN1210-MG-306. A phase 3, randomized, double-blind, placebo-controlled, multicenter study to evaluate the safety and efficacy of ravulizumab in complement-inhibitor-naive adult patients with generalized Myasthenia Gravis. Data Cut-off 9 November 2021. Date of Report: 23 March 2022 [sponsor supplied reference].
7.Alshekhlee A, Miles JD, Katirji B, Preston DC, Kaminski HJ. Incidence and mortality rates of myasthenia gravis and myasthenic crisis in US hospitals. Neurology. 2009;72(18):1548-1554. PubMed
8.Statistics Canada. Table 13-10-0114-01, based on data for the years 2018-2020. Available at: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401 [sponsor supplied reference]. 2022.
9.Howard JF, Jr., Bril V, Vu T, et al. Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): a multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021;20(7):526-536. PubMed
10.Nowak RJ, Coffey CS, Goldstein JM, et al. Phase 2 Trial of Rituximab in Acetylcholine Receptor Antibody-Positive Generalized Myasthenia Gravis: The BeatMG Study. Neurology. 2022;98(4):e376-e389. PubMed
11.Grifols Therapeutics LLCCG. NCT02473952 - A Study to Evaluate the Efficacy and Safety of IGIV-C in Symptomatic Subjects With Generalized Myasthenia Gravis [sponsor supplied reference]. 2019.
12.Chirikov V, Ma I, Joshi N, et al. Cost-Effectiveness of Alemtuzumab in the Treatment of Relapsing Forms of Multiple Sclerosis in the United States. Value Health. 2019;22(2):168-176. PubMed
13.Jit M, Cromer D, Baguelin M, Stowe J, Andrews N, Miller E. The cost-effectiveness of vaccinating pregnant women against seasonal influenza in England and Wales. Vaccine. 2010;29(1):115-122. PubMed
14.Little P, Williamson I, Warner G, Gould C, Gantley M, Kinmonth AL. Open randomised trial of prescribing strategies in managing sore throat. BMJ (Clinical research ed). 1997;314(7082):722-727. PubMed
15.Matza LS, Boye KS, Yurgin N, et al. Utilities and disutilities for type 2 diabetes treatment-related attributes. Qual Life Res. 2007;16(7):1251-1265. PubMed
16.Argenx BV. VYVGART (efgartigimod alfa) [monograph] [sponsor supplied reference]. 2023.
17.Health CAfDaTi. CADTH Reimbursement Review: Efgartigimod Alfa (Vyvgart) [sponsor supplied reference]. 2024.
18.Ontario Ministry of Health and Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2024; https://www.formulary.health.gov.on.ca/formulary/. Accessed by sponsor 2024 Apr 30; by CDA-AMC 2024 Aug 1.
19.Bril V, Szczudlik A, Vaitkus A, et al. Randomized Double-Blind Placebo-Controlled Trial of the Corticosteroid-Sparing Effects of Immunoglobulin in Myasthenia Gravis. Neurology. 2023;100(7):e671-e682. PubMed
20.Blackhouse G, Gaebel K, Xie F, et al. Cost-utility of Intravenous Immunoglobulin (IVIG) compared with corticosteroids for the treatment of Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) in Canada. Cost Effectiveness and Resource Allocation. 2010;8(1):1-9. PubMed
21.Alhaidar MK, Abumurad S, Soliven B, Rezania K. Current Treatment of Myasthenia Gravis. J Clin Med. 2022;11(6). PubMed
22.Ministry of Health of Ontario. Schedule of Benefits. Physician Services Under the Health Insurance Act. Available from: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf [sponsor supplied reference]. 2024.
23.LifeSupply. SKU: B.Braun V1415-15-x. Available [Last accessed: April 2024]. Available from: https://www.lifesupply.ca/search.php?search_query=B.Braun%20V1415-15-x.§ion=product [sponsor supplied reference].
24.LifeSupply. Covidien 8881540111 Monoject SMARTIP NEEDLESS VIAL ACCESS CANNULA BX/100 (CS/10). [Last accessed: April 2024]. Available from: https://www.lifesupply.ca/monoject-smartip-needless-vial-access-cannula-bx-100-cs-10-mdt-8881540111 [sponsor supplied reference].
25.LifeSupply. Dressing IV Transparent 3M TEGADERM HP 6 Cm X 7cm BX/100 (3M-9534HP). [Last accessed: April 2024]. Available from: https://www.lifesupply.ca/dressing-iv-transparent-3m-tegaderm-hp-6-cm-x-7cm-bx-100-3m-9534hp [sponsor supplied reference].
26.Health Quality O. Home-Based Subcutaneous Infusion of Immunoglobulin for Primary and Secondary Immunodeficiencies: A Health Technology Assessment. Ontario health technology assessment series, 17(16). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6548531/pdf/ohtas-17-1.pdf [sponsor supplied reference]. 2017.
27.Statistics Canada. Table: 18-10-0004-13. Consumer Price Index, monthly, percentage change, not seasonally adjusted, Canada, provinces, Whitehorse and Yellowknife [sponsor supplied reference]. 2024.
28.Ontario Reginal Blood Coordination Network. Ontario Immune Globulin (IG) Utilization Management Guidelines [sponsor supplied reference]. https://transfusionontario.org/en/ontario-ig-utilization-management-guidelines/. Accessed 30 April 2024.
29.Statistics Canada. Job Bank Canada, Wage Report. NOC 3012. [Last Accessed: April 2024]. Available from: https://www.jobbank.gc.ca/marketreport/wages-occupation/696/ca [sponsor supplied reference]. 2024.
30.Alexion Pharma GmbH. SOLIRIS (eculizumab for injection) 10 mg/mL parenteral solution [Monograph] [sponsor supplied reference]. 2021.
31.Alexion Pharma GmbH. ULTOMIRIS (ravulizumab) [Monograph] [sponsor supplied reference]. 2023; https://alexion.com/documents/ultomiris_product_monograph_approved_english.
32.Canadian Institute for Health Information (2016). Care in Canadian ICUs. CIHI. Ottawa, ON [sponsor supplied reference].
33.Ontario Case Costing Analysis Tool. [Last accessed: 24 Sep 2019]. Available from: https://www.ontario.ca/data/ontario-case-costing-initiative-occi [sponsor supplied reference].
34.Neumann B, Angstwurm K, Mergenthaler P, et al. Myasthenic crisis demanding mechanical ventilation: a multicenter analysis of 250 cases. Neurology. 2020;94(3):e299-e313. PubMed
35.Furlan JC, Barth D, Barnett C, Bril V. Cost-minimization analysis comparing intravenous immunoglobulin with plasma exchange in the management of patients with myasthenia gravis. Muscle Nerve. 2016;53(6):872-876. PubMed
36.Alberta Health Interactive Health Data Team. Hospital Inpatient Care Case Costs - CMG/Plex. 2015; https://open.alberta.ca/opendata/hospital-inpatient-care-case-costs-cmgplex. Accessed 2024 Apr 1.
37.Wolfe GI HL, Nations SP, Foster B, Bryan WW, Barohn RJ. Myasthenia gravis activities of daily living profile. Neurology. 1999;52(7):1487-1489. PubMed
38.GS Z. The impact of ignoring population heterogeneity when Markov models are used in cost-effectiveness analysis. Med Decis Making. 2003;23(5):379-396. PubMed
39.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2024 Aug 26.
40.Grob D, Brunner N, Namba T, Pagala M. Lifetime course of myasthenia gravis. Muscle Nerve. 2008;37(2):141-149. PubMed
41.pan-Canadian Pharmaceutical Alliance. Soliris (eculizumab) [sponsor supplied reference]. 2024; https://www.pcpacanada.ca/negotiation/21306.
42.Health Canada. Patient register. Ottawa (ON): Government of Canada; 2022: https://pr-rdb.hc-sc.gc.ca/pr-rdb/start-debuter.do?access=external&lang=en. Accessed 2023 Jan 23.
43.Canadian Agency for Drugs and Technologies in Health. CADTH Reimbursement Review: Ravulizumab (Ultomiris) [sponsor supplied reference]. 2023.
44.pan-Canadian Pharmaceutical Alliance. Vyvgart (efgartigimod alfa) [sponsor supplied reference]. 2024; https://www.pcpacanada.ca/negotiation/22530.
45.CADTH Reimbursement Recommendation: Efgartigimod Alfa (Vyvgart). CanJ Health Technol. 2024;4(1). https://www.cda-amc.ca/sites/default/files/DRR/2024/SR0782REC-Vyvgart-meta.pdf. Accessed 2024 Aug 27.
46.Cadth. CADTH Reimbursement Review Reports: Efgartigimod Alfa (Vyvgart) [sponsor supplied reference]. 2024.
47.Government of Alberta. Interactive drug benefit list. 2024; https://idbl.ab.bluecross.ca/idbl/load.do. Accessed 2024 Aug 1.
48.Farmakidis C PM, Dimachkie MM, Barohn RJ. Treatment of myasthenia gravis. Neurol Clin. 2018;36(2). PubMed
49.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2024: http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2024 Aug 1.
50.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 Aug 1.
51.Saskatchewan Drug Plan: search formulary. 2024; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2024 Aug 13.
52.Heckmann JM RA, Bateman K, Renison R, Badri M. A single-blinded trial of methotrexate versus azathioprine as steroid-sparing agents in generalized myasthenia gravis. BMC Neurol. 2011:11:97. PubMed
53.PrMestinon® and PrMestinon®-SR (pyridostigmine bromide): 60 mg tablets and 180 mg slow-release tablets [product monograph]. Laval (QC): Bausch Health; 2019: https://pdf.hres.ca/dpd_pm/00052033.PDF. Accessed August 20, 2024.
54.Melzer N RT, Fuhr P, et al. Clinical features, pathogenesis, and treatment of myasthenia gravis: a supplement to the Guidelines of the German Neurological Society. J Neurol. 2016;263(8):1473-1494. PubMed
55.Inflation Calculator. Ottawa (ON): Bank of Canada: https://www.bankofcanada.ca/rates/related/inflation-calculator/. Accessed 2024 Aug 20.
56.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab), 10 mg/mL & 100 mg/mL, concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma GmbH; 2024 Jun 4.
57.Westerberg E PA. Epidemiology of Myasthenia Gravis in Sweden 2006-2016. Brain Behav. 2020;10(11):e01819. PubMed
58.Anil R, Kimar A, Aaprthi S, et al. Exploring outcomes and characteristics of myasthenia gravis: Rationale, aims and design of registry - The EXPLORE-MG registry. Journal of Neurological Sciences. 2020;414:116830. PubMed
59.Hendricks TM, Bhatti MT, Hodge DO, Chen JJ. Incidence, Epidemiology, and Transformation of Ocular Myasthenia Gravis: A Population-Based Study. Am J Ophthalmol. 2019;205:99-105. PubMed
60.Petersson M, Feresiadou A, Jons D, et al. Patient-Reported Symptom Severity in a Nationwide Myasthenia Gravis Cohort: Cross-sectional Analysis of the Swedish GEMG Study. Neurology. 2021;97(14):e1382-e1391. PubMed
61.Oh SJ. Muscle-specific receptor tyrosine kinase antibody positive myasthenia gravis current status. J Clin Neurol. 2009;5(2):53-64. PubMed
62.Pallaver F RA, Piffer S, et al. Change in myasthenia gravis epidemiology in Trento, Italy, after twenty years. . Neuroepidemiology. 2011;36(4):282-287. PubMed
63.Sanders DB RS, Guptill JT, Hobson-Webb LD, Juel VC, Massey JM. The Duke myasthenia gravis clinic registry: I. Description and demographics. Muscle Nerve. 2021;63(2):209-216. PubMed
64.Santos E CE, Moreira I, et al. Epidemiology of myasthenia gravis in Northern Portugal: frequency estimates and clinical epidemiological distribution of cases. Muscle Nerve. 2016;54(3):413-421. PubMed
65.Association québécoise des pharmaciens p. AQPP Drug Price List. April 2024.
66.O'Reilly DJ, Blackhouse G, Burns S, et al. Economic analysis of pharmacist-administered influenza vaccines in Ontario, Canada. Clinicoecon Outcomes Res. 2018;10:655-663. PubMed
67.Procedures for CADTH reimbursement reviews. Ottawa (ON): Canada's Drug Agency; 2024: https://www.cadth.ca/sites/default/files/Drug_Review_Process/CADTH%20Drug%20Reimbursement%20Review%20Procedures.pdf. Accessed 2024 Aug 28.
68.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2024 Aug 26.
69.Pan-Canadian Prescription Drug Data Landscape. Ottawa (ON): Canadian Institute for Health Information; 2024: https://www.cihi.ca/sites/default/files/document/pan-canadian-prescription-drug-data-landscape-report-en.pdf. Accessed 20224 Aug 8.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Complement Inhibitors Indicated for the Treatment of Generalized Myasthenia Gravis
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Ravulizumab (Ultomiris) | 300 mg/3 mL 300 mg/30 mL 1,100 mg/11 mL | Single-use vial for IV infusion | 7,282.1500a 7,282.1500a 26,701.2000a | Loading dose, with maintenance doses given starting 2 weeks after, then administered every 8 weeks thereafter based on weight as follows:b ≥ 40 kg to < 60 kg Loading: 2,400 mg Maintenance: 3,000 mg ≥ 60 kg to < 100 kg Loading: 2,700 mg Maintenance: 3,300 mg ≥ 100 kg Loading: 3,000 mg Maintenance: 3,600 mg | ≥ 40 kg to < 60 kg Year 1c: 1,406.55 Subsequent yearsd: 1,296.82 ≥ 60 kg to < 100 kg: Year 1c: 1,551.20 Subsequent yearsd: 1,426.50 ≥ 100 kg Year 1c: 1,695.84 Subsequent yearsd: 1,556.19 | ≥ 40 kg to < 60 kg: Year 1c: 513,392 Subsequent yearsd: 473,340 ≥ 60 kg to < 100 kg: Year 1c: 566,187 Subsequent yearsd: 520,674 ≥ 100 kg: Year 1c: 618,983 Subsequent yearsd: 568,008 |
Efgartigimod alfa (Vyvgart) | 20 mg/mL | 400 mg single-use vial for IV infusion | 7,900.0000e | Loading dose: 10 mg/kg (max 1,200 mg) weekly for 4 weeks. Subsequent treatment cycles are based on clinical evaluation and may vary by patient. | Patient weight 41 to 80 kg: 408.41 to 817.27f Patient weight above 80 kg: 1,225.91f | Patient weight 41 to 80 kg: 298,304f Patient weight above 80 kg: 447,456f |
Eculizumab (Soliris) | 10 mg/mL | 300 mg single-use vial for IV infusion | 6,675.3000g | Loading: 900 mg weekly for 4 weeks, then 1,200 mg for the fifth dose 1 week later Maintenance: 1,200 mg every 2 weeks thereafter | First year:h 1,975.16 Subsequent years:i 1,902.00 | First year:h 720,932 Subsequent years:i 694,231 |
CDA-AMC = Canada’s Drug Agency.
Note: A year is 365 days.
aSponsor-submitted price.2
bFor patients switching from eculizumab, the loading dose of ravulizumab is given 2 weeks after the last eculizumab infusion. Maintenance doses are then given every 8 weeks, starting 2 weeks after the loading dose.30
cYear 1 costs assume 1 loading dose and 6.25 maintenance doses.
dSubsequent year dosing are based on an average of 6.5 (52/8) administrations per year.
ePrice obtained from CDA-AMC review of Efgartigimod alfa.46
fAssumes an average of 4.72 4-week courses per year, as reportedly administered to patients with anti-AChR antibody–positive gMG in pooled ADAPT and ADAPT+ data. Cost per 4-week course is $63,200 for patients weighing 41 kg to 80 kg and $94,800 for patients weighing more than 80 kg.9
gAlberta formulary, accessed August 1, 2024.47
hYear 1 costs assume four 900 mg doses and 24 1,200 mg doses.
iSubsequent year costs assume 26 administrations per year.
Table 9: CDA-AMC Cost Comparison Table for Generalized Myasthenia Gravis (Off-Label Treatments)
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Other Biologics | ||||||
Rituximab (biosimilars) | 10 mg/mL | 10 mL 50 mL Vial for IV infusion | 297.0000 1,485.0000 | 375 mg/m2 weekly for 4 doses Alternate dosing: 1 g, followed by 1 g 2 weeks later, and then every 6 months | NA | Cost per course: 8,316 Alternate dosing in year 1: 11,652 |
Glucocorticoids | ||||||
Prednisone (Winpred, generics) | 1 mg 5 mg 50 mg | Tablet | 0.1276 0.0220 0.1735 | Initiate at 10 to 20 mg/day, increase by 5 mg/day per week until stable remission (target 1 mg/kg/day) | 0.04 to 0.11 | 16 to 40 |
Alternate dosing: Initiate at 60 to 80 mg/day, then taper after improvement | 0.26 to 0.35 | 96 to 127 | ||||
Immunosuppressive drugs | ||||||
Azathioprine | 50 mg | Tablet | 0.5185 | Initiate at 50 mg/day for 5 days, and then, escalate to 2.5 to 3 mg/kg/dayd | First year: 2.05 Subsequent years: 2.07 | First year: 749 Subsequent years: 757 |
Cyclophosphamide (Procytox, generics) | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 500 mg/m2 to 1,000 mg/m2 every month for 6 months | NA | Cost per course: 52 to 103 |
200 mg 500 mg 1,000 mg 2,000 mg | IV vial, powder for injection | Not available 107.8100b 195.4200b 359.4000b | NA | Cost per course: 1,173 to 2,156 | ||
Cyclosporine (Neoral, generic) | 10 mg 25 mg 50 mg 100 mg | Capsule | 0.7526 0.7870 1.5350 3.0720 | Starting dose: 100 mg twice daily Target dose: 5 to 6 mg/kg/day in 2 divided doses, adjust for serum trough level of 75 to 150 ng/mL | First year: 20.45 to 24.63 Subsequent years: 20.46 to 24.56 | First year: 7,463 to 8,989 Subsequent years: 7,469 to 8,964 |
Methotrexate (generic, Metoject Subcutaneous) | 2.5 mg 10 mg | Tablet | 0.2513 2.7983c | 10 mg to 20 mg per week, orally or SC | 1.01 to 2.01 | 52 to 105 |
10 mg/mL 25 mg/mL 15 mg/0.3 mL 17.5mg/0.35 20mg/0.4mL 22.5mg/0.45mL 25mg/0.5mL 10mg/0.2mL 12.5mg/0.25mL | Prefilled syringe for SC use | 12.5000 8.9200 16.3800 16.0000 17.5000 17.5000 19.5000 22.2300 23.4000 | 12.50 to 17.50 | 650 to 910 | ||
Mycophenolate mofetil (Cellcept, generics) | 250 mg | Capsule | 0.3712 | 1,000 mg twice daily | 2.97 | 1,084 |
500 mg | Tablet | 0.7423 | 2.97 | 1,084 | ||
Mycophenolate Sodium (Myfortic, generics) | 180 mg 360 mg | Enteric Tablet | 0.9989 1.9977 | 720 mg twice dailye | 7.99 | 2,917 |
Tacrolimus (generics) | 0.5 mg 1 mg 5 mg | Capsule | 1.0146 1.2978 6.4993 | 3 mg to 5 mg per dayf | 3.90 to 6.51 | 1,425 to 2,375 |
Cholinesterase inhibitors | ||||||
Pyridostigmine (Mestinon) | 60 mg | Tablet | 0.2673 | 60 mg to 120 mg every 3 to 8 hours while awake | 0.80 to 1.60 | 293 to 585 |
180 mg | SR tablet | 1.3919 | 4.19 to 8.37 | 1,528 to 3,066 | ||
Blood products | ||||||
IV immunoglobulin | 10,611 per exacerbationg | |||||
Plasma Exchange | 7,800 per exacerbationg | |||||
CDA-AMC = Canada’s Drug Agency.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed August 1, 2024),18 unless otherwise indicated, and do not include dispensing fees. All cost calculations for drugs with weight or body surface area-based dosing was calculated using the mean body surface area of 1.8 m2 and mass of 65 kg. Drug wastage was included. Dosing is from a study by Farmakidis et al., unless otherwise indicated.48
aOntario Drug Benefit Formulary Exceptional Access Program (accessed August 1, 2024).49
bDeltaPA database wholesale prices (accessed August 13, 2024).50
cSaskatchewan Drug Plan formulary (accessed August 13, 2024).51
dAzathioprine dosing was obtained from published literature.52
eMyfortic product monograph, dose indicated for the prophylaxis of organ rejection in patients receiving allogeneic renal transplants, confirmed with clinical expert opinion as also use for generalized myasthenia gravis.53
fTacrolimus dose reported for patients with therapy-refractory myasthenia gravis in Clinical features, pathogenesis, and treatment of myasthenia gravis: a supplement to the Guidelines of the German Neurologic Society.54
gThe cost of IV immunoglobulin and plasma exchange, totalling $8,277 and $6,084, respectively, in 2014 dollars,35 was for rescue therapy and included cost of blood products and hospital costs and was inflated to 2024 dollars by CDA-AMC.55 Due to confidential prices of IV immunoglobulin products and plasma exchange, chronic treatment cost is unknown.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comment |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | Refer to limitation “Poor modelling practices were employed” and “The model structure does not adequately reflect generalized myasthenia gravis in clinical practice.” |
Model structure is adequate for decision problem | No | Refer to limitation “The model structure does not adequately reflect generalized myasthenia gravis in clinical practice.” |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Explanation of model structure was inadequate. For example, it was difficult to understand the movement of individuals through health states. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
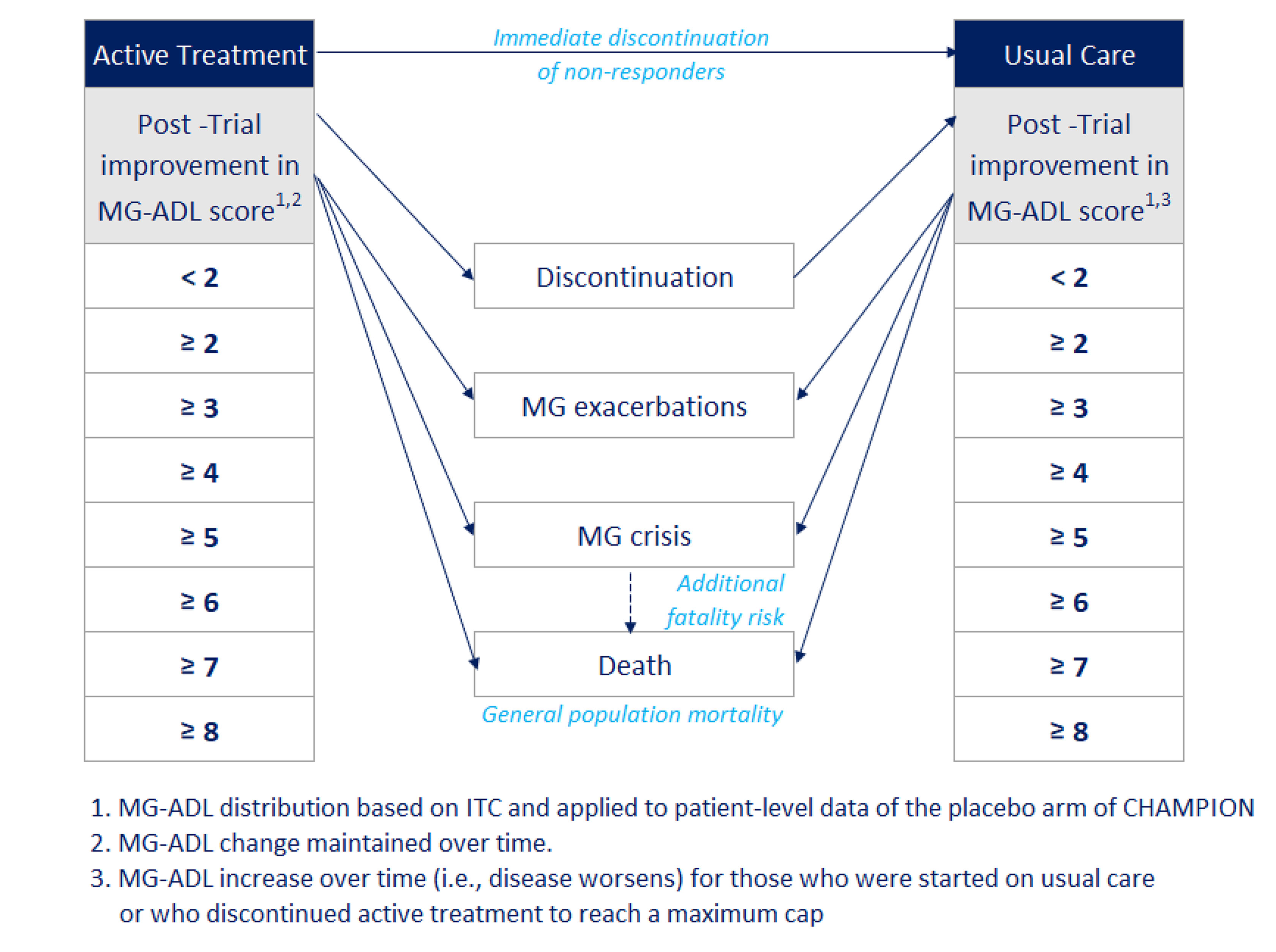
ITC = indirect treatment comparison; MG = myasthenia gravis; MG-ADL = myasthenia gravis activities of daily living.
Source: Sponsor’s pharmacoeconomic submission.2
Table 11: Proportion of Patients in Each MG-ADL Score Change Category at Month 6
MG-ADL total score change category | Proportion of patients in each category | ||||
|---|---|---|---|---|---|
Ravulizumab | Usual care | Efgartigimod | Rituximab | IVIg | |
< 2 | 39.71% | 51.47% | 51.47% | 51.47% | 66.18% |
≥ 2 | 60.29% | 48.53% | 48.53% | 48.53% | 33.82% |
≥ 3 | 48.53% | 33.82% | 33.82% | 33.82% | 23.53% |
≥ 4 | 33.82% | 23.53% | 23.53% | 23.53% | 13.24% |
≥ 5 | 23.53% | 13.24% | 13.24% | 13.24% | 8.82% |
≥ 6 | 13.24% | 8.82% | 8.82% | 8.82% | 2.94% |
≥ 7 | 8.82% | 2.94% | 2.94% | 2.94% | 1.47% |
≥ 8 | 2.94% | 1.47% | 1.47% | 1.47% | 0.00% |
IVIg = IV immunoglobulin; MG-ADL = myasthenia gravis activities of daily living.
Source: Sponsor’s pharmacoeconomic submission.2
Table 12: Mean Change in MG-ADL Score Within Each Category
MG-ADL change category | Proportion of patients in each category | ||||
|---|---|---|---|---|---|
Ravulizumab | Usual care | Efgartigimod | Rituximab | IVIg | |
< 2 | −0.53 | 0.89 | 0.15 | 0.18 | 0.30 |
2 to 3 | −2.00 | −2.00 | −2.00 | −2.00 | −2.00 |
3 to 4 | −3.00 | −3.00 | −3.00 | −3.00 | −3.00 |
4 to 5 | −4.00 | −4.00 | −4.00 | −4.00 | −4.00 |
5 to 6 | −5.00 | −5.00 | −5.00 | −5.00 | −5.00 |
6 to 7 | −6.00 | −6.00 | −6.00 | −6.00 | −6.00 |
7 to 8 | −7.00 | −7.00 | −7.00 | −7.00 | −7.00 |
≥ 8 | −9.48 | −8.00 | −8.74 | −8.70 | −8.00 |
IVIg = IV immunoglobulin; MG-ADL = myasthenia gravis activities of daily living.
Source: Sponsor’s pharmacoeconomic submission.2
Detailed Results of the Sponsor’s Base Case
Table 13: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Ravulizumab | Usual care | Efgartigimod | Rituximab | IVIg |
|---|---|---|---|---|---|
Discounted LYs | |||||
Total | 22.79 | 22.78 | 22.79 | 22.79 | 22.78 |
Discounted QALYs | |||||
Total | 11.21 | 9.33 | 10.29 | 10.28 | 9.66 |
QALYs by health states (MG-ADL total score change) | |||||
Score change < 2 | 2.72 | 4.20 | 4.13 | 4.11 | 4.93 |
Score change < 3 | 1.39 | 1.41 | 1.29 | 1.26 | 1.17 |
Score change 3 to 4 | 1.60 | 1.05 | 1.40 | 1.39 | 1.19 |
Score change 4 to 5 | 1.54 | 1.10 | 1.23 | 1.18 | 0.90 |
Score change 5 to 6 | 1.34 | 0.50 | 0.85 | 0.90 | 0.67 |
Score change 6 to 7 | 0.99 | 0.70 | 0.69 | 0.67 | 0.47 |
Score change 7 to 8 | 0.74 | 0.18 | 0.41 | 0.43 | 0.22 |
Score change ≥ 8 | 0.89 | 0.19 | 0.29 | 0.34 | 0.11 |
Discounted costs ($) | |||||
Total | 3,049,488 | 866,247 | 1,968,733 | 1,095,394 | 1,025,077 |
Drug acquisition | 2,380,173 | 0 | 1,207,181 | 320,348 | 171,597 |
Drug infusion | 10,181 | 0 | 5,706 | 17,333 | 26,956 |
Meningococcal vaccination | 333 | 0 | 0 | 0 | 0 |
Standard of care | 37,939 | 37,936 | 37,938 | 37,938 | 37,937 |
Routine care | 40,455 | 40,451 | 40,453 | 40,453 | 40,452 |
Clinical event management | 580,121 | 787,554 | 677,110 | 678,759 | 747,756 |
Adverse event management | 286 | 305 | 344 | 563 | 380 |
Productivity loss | 0 | 0 | 0 | 0 | 0 |
IVIg = IV immunoglobulin; MG-ADL = myasthenia gravis activities of daily living; QALY = quality-adjusted life-year; LY = life-year.
Source: Sponsor’s pharmacoeconomic submission.2
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 14: Summary of the Stepped Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case, probabilistic | Usual carea | 866,247 | 9.33 | Reference |
Rituximab | 1,095,394 | 10.28 | 241,628 vs. usual care | |
Ravulizumab | 3,049,488 | 11.21 | 2,102,671 vs. rituximab | |
Dominated treatments | ||||
Blood products (IVIg) | 1,025,077 | 9.66 | Extendedly dominated by rituximab | |
Efgartigimod | 1,968,733 | 10.29 | Extendedly dominated by rituximab and ravulizumab | |
Sponsor’s base case, deterministic | Usual carea | 812,522 | 9.35 | Reference |
Rituximab | 1,030,722 | 10.15 | 270,839 vs. usual care | |
Ravulizumab | 2,794,060 | 10.97 | 2,149,700 vs. rituximab | |
Dominated treatments | ||||
Blood products (IVIg) | 957,339 | 9.51 | Extendedly dominated by rituximab | |
Efgartigimod | 1,813,402 | 10.16 | Extendedly dominated by rituximab and ravulizumab | |
CDA-AMC base case, deterministic | Usual carea | 419,059 | 12.99 | Reference |
Rituximab | 721,642 | 13.21 | 1,397,664 vs. usual care | |
Ravulizumab | 2,535,147 | 13.81 | 3,010,550 vs. rituximab | |
Dominated treatments | ||||
Blood products (IVIg) | 600,938 | 12.77 | Dominated by usual care | |
Efgartigimod | 1,504,367 | 13.22 | Extendedly dominated by rituximab and ravulizumab | |
CDA-AMC base case, probabilistic | Usual carea | 426,145 | 12.99 | Reference |
Rituximab | 756,446 | 13.28 | 1,138,505 vs. usual care | |
Ravulizumab | 2,777,217 | 13.96 | 2,996,852 vs. rituximab | |
Dominated treatments | ||||
Blood products (IVIg) | 632,095 | 12.84 | Dominated by usual care | |
Efgartigimod | 1,625,950 | 13.28 | Dominated by rituximab | |
ICER = incremental cost-effectiveness ratio; IVIg = IV immunoglobulin; QALY = quality-adjusted life-year.
aUsual care consisted of AChEIs (pyridostigmine) and ISTs (azathioprine, mycophenolate mofetil, cyclosporine, tacrolimus, methotrexate, cyclophosphamide, and prednisone).
Table 15: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Ravulizumab | Usual care | Efgartigimod | Rituximab | IVIg |
|---|---|---|---|---|---|
Discounted LYs | |||||
Total | 22.79 | 22.79 | 22.79 | 22.79 | 22.79 |
Discounted QALYs | |||||
Total | 13.96 | 12.99 | 13.28 | 13.28 | 12.84 |
QALYs by health states (MG-ADL total score change) | |||||
Score change < 2 | 3.86 | 6.01 | 5.89 | 5.85 | 7.06 |
Score change < 3 | 1.93 | 1.97 | 1.79 | 1.74 | 1.63 |
Score change 3 to 4 | 1.86 | 1.44 | 1.63 | 1.63 | 1.40 |
Score change 4 to 5 | 1.78 | 1.50 | 1.42 | 1.37 | 1.05 |
Score change 5 to 6 | 1.54 | 0.67 | 0.97 | 1.05 | 0.78 |
Score change 6 to 7 | 1.14 | 0.92 | 0.79 | 0.76 | 0.54 |
Score change 7 to 8 | 0.85 | 0.24 | 0.47 | 0.50 | 0.26 |
Score change ≥ 8 | 1.00 | 0.25 | 0.32 | 0.38 | 0.13 |
Discounted costs ($) | |||||
Total | 2,777,217 | 426,145 | 1,625,950 | 756,446 | 632,095 |
Drug acquisition | 2,380,130 | 0 | 1,202,913 | 322,490 | 171,023 |
Drug infusion | 10,180 | 0 | 5,706 | 17,332 | 26,992 |
Meningococcal vaccination | 333 | 0 | 0 | 0 | 0 |
Standard of care | 37,990 | 37,990 | 37,990 | 37,990 | 37,989 |
Routine care | 40,459 | 40,458 | 40,459 | 40,459 | 40,458 |
Clinical event management | 307,838 | 347,392 | 338,538 | 337,616 | 355,251 |
Adverse event management | 286 | 304 | 345 | 559 | 382 |
Productivity loss | 0 | 0 | 0 | 0 | 0 |
IVIg = IV immunoglobulin; MG-ADL = myasthenia gravis activities of daily living; QALY = quality-adjusted life-year; LY = life-year.
Scenario Analyses
Table 16: Summary of the Scenario Analyses of the CDA-AMC Base-Case Results, Deterministic
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case | Usual care | 419,059 | 12.99 | Reference |
Rituximab | 721,642 | 13.21 | 1,397,664 vs. usual care | |
Ravulizumab | 2,535,147 | 13.81 | 3,010,550 vs. rituximab | |
Dominated treatments | ||||
Blood products (IVIg) | 600,938 | 12.77 | Dominated by usual care | |
Efgartigimod | 1,504,367 | 13.22 | Extendedly dominated by rituximab and ravulizumab | |
CDA-AMC scenario analysis – equal efficacy of rituximab, efgartigimod, and ravulizumab | Usual care | 419,059 | 12.99 | Reference |
Rituximab | 814,781 | 13.81 | 483,437 | |
Dominated treatments | ||||
Blood products (IVIg) | 600,938 | 12.77 | Dominated by usual care | |
Efgartigimod | 1,942,981 | 13.81 | Dominated by rituximab | |
Ravulizumab | 2,535,147 | 13.81 | Dominated by efgartigimod and rituximab | |
CDA-AMC scenario analysis – rituximab is excluded as a comparator | Usual care | 419,059 | 12.99 | Reference |
Ravulizumab | 2,535,147 | 13.81 | 2,584,140 | |
Dominated treatments | ||||
Blood products (IVIg) | 600,938 | 12.77 | Dominated by usual care | |
Efgartigimod | 1,504,367 | 13.22 | Extendedly dominated by ravulizumab | |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; IVIg = IV immunoglobulin; QALY = quality-adjusted life-year.
Appendix 5: Submitted BIA and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 17: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
CDA-AMC = Canada’s Drug Agency.
Summary of Sponsor’s BIA
The sponsor submitted a BIA estimating the incremental budget impact of reimbursing ravulizumab for patients aged 18 years and older with anti-AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChEIs, corticosteroids, and/or NSIST.56 The BIA was undertaken over a 3-year time horizon (2025 to 2027), and the sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec). Key inputs to the BIA are documented in Table 18.
The sponsor estimated the number of eligible patients for ravulizumab treatment using an epidemiologic approach with data obtained from published sources and sponsor’s-consulted clinical experts.43,57-64 Comparators included efgartigimod, rituximab, IVIg, eculizumab, and usual care. Usual care comprised a basket of cholinesterase inhibitors (pyridostigmine) and immunosuppressive therapies (azathioprine, mycophenolate mofetil, cyclosporine, tacrolimus, methotrexate, cyclophosphamide, and prednisone). Doses for usual care drugs and the proportion of patients on each drug were derived using data on IST optimized cohort of the CHAMPION-MG trial.4 Drug dosages for ravulizumab, efgartigimod and eculizumab were obtained from respective product monographs and doses for rituximab and IVIg were obtained from previous CDA-AMC review.17 Ravulizumab, efgartigimod, and eculizumab costs were estimated by calculating a weighed annual cost using the weight distribution from the concomitant IST optimized cohort of the CHAMPION-MG trial and were incorporated as first year costs (which included loading doses and vaccination costs) and subsequent year costs (which included maintenance dose).
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3 if appropriate) |
|---|---|
Target population | |
MG prevalence | 361 in 1,000,00057 |
Proportion of adult patients with MG | 97.0%57 |
Proportion of gMG (MGFA class II to class IV) in MG | |
Proportion of anti-AChR antibody–positive gMG | |
Proportion of with MG-ADL score of > 6 | 17.0%60 |
Proportion of treated population | 100.0%a |
Proportion of patients with gMG with an MGFA class II to class IV and an MG-ADL total score ≥ 6 who require treatment | 80.0%a |
Proportion of patients covered by public drug programs | 80%43 |
Number of patients eligible for drug under review | 779 / 788 / 798 |
Market uptake (3 years) | |
Uptake (reference scenario) Eculizumab plus usual care Efgartigimod plus usual care Rituximab plus usual care IVIg plus usual care Usual care | 0% / 0% / 0% 27% / 34% / 39% 3% / 1% / 1% 20% / 15% / 10% 50% / 50% / 50% |
Uptake (new drug scenario) Ravulizumab plus usual care Eculizumab plus usual care Efgartigimod plus usual care Rituximab plus usual care IVIg plus usual care Usual care | 15% / 19% / 22% 0% / 0% / 0% 17% / 20% / 22% 3% / 1% / 1% 15% / 10% / 5% 50% / 50% / 50% |
Cost of treatment (per patient) | |
Cost of treatment over year Ravulizumab – new patientsb, c Ravulizumab – existing patientsb, c Efgartigimodd Rituximabe IVIg – new patientsf IVIg – existing patientsf Usual care Eculizumab – new patientsg Eculizumab – existing patientsg | $581,653 $534,692 $395,477 $25,750 $92,034 $78,887 $1,683 $736,190 $696,138 |
Cost of vaccination (per patient) | |
Meningococcal vaccinationh | $333 |
AChR = acetylcholine receptor; MG-ADL = Myasthenia gravis activities of daily living; MGFA = Myasthenia Gravis Foundation of America; gMG = generalized myasthenia gravis; MG = myasthenia gravis.
aSponsor’s assumption.
bThe weighted cost of ravulizumab treatment costs was estimated using the weight distribution observed in the IST optimized cohort of the CHAMPION-MG trial (████% of individuals between 40 and 60 kg, █████% of individuals between 60 and 100 kg and █████% of individuals equal or greater than 100 kg).
cThe treatment cost of new patients included cost of a loading dose and 6.3 maintenance doses, while the treatment cost of existing patients included the cost of 6.5 maintenance doses.
dThe weighted cost of efgartigimod was estimated using the weight distribution observed in the IST optimized cohort of the CHAMPION-MG trial (34.85% of individuals weighing less than 80 kg and receiving the dose of 800 mg, while the remaining 65.15% of patients weighing greater than or equal to 80 kg and receiving 1,200 mg).
eAll patients were receiving 375 mg/m2 weekly for 4 doses, repeated every 6 months.
fThe treatment cost of new patients included a loading dose and 12 maintenance doses, while the treatment cost of existing patients included the cost of 12 maintenance doses.
gThe treatment cost of new patients included cost of a loading dose of 900 mg in Week 1 to 4, a loading dose of 1,200 mg in Week 5 and 24 maintenance doses, while the treatment cost of existing patients included the cost of 26 maintenance doses.
hThe vaccination cost consisted of 2 doses of Bexsero (multicomponent Meningococcal B vaccine), and 1 dose of Nimenrix (meningococcal polysaccharide groups A, C, Y, and W-135 conjugate vaccine), as well as a vaccination administration cost per dose. The costs of vaccines were retrieved from the Association québécoise des pharmaciens propriétaires Drug List.65 The administration cost was obtained from the Ontario Schedule of Benefits for Physician Services and published literature.66
Summary of the Sponsor’s BIA Results
The sponsor estimated the net 3-year budget impact of introducing ravulizumab for treatment of patients aged 18 years and older with anti-AChR antibody–positive gMG to be $101,061,496 (Year 1: $29,138,279; Year 2: $34,034,934; Year 3: $37,888,283).
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The distribution of patients across current treatments does not represent clinical practice. The sponsor estimated that approximately 20% of eligible patients will be receiving efgartigimod plus usual care over the modelled time horizon in the reference scenario. CDA-AMC notes that pCPA negotiations for efgartigimod for gMG are ongoing and the outcome and the timeline of these negotiations is uncertain.44 Consequently, the uptake of efgartigimod should it receive a letter of intent is currently unknown.
According to the clinical expert feedback received for this review, the market share allocated to usual care was also deemed to be an overestimate.
CDA-AMC could not address these limitations. As such, there is uncertainty in the market share estimates in the reference scenario.
Market uptake of ravulizumab is uncertain. CDA-AMC obtained clinical expert feedback that the uptake of ravulizumab and efgartigimod is uncertain and could possibly be lower than estimated by the sponsor as changes in prescribing behaviour of physicians may be gradual. Additionally, according to the clinical expert feedback obtained for this review, the sponsor’s assumption that there is no market capture of ravulizumab or efgartigimod from usual care alone was not deemed to be reasonable. As all market capture for ravulizumab comes from efgartigimod and IVIg, which are more costly than usual care, this assumption likely underestimates the budget impact of reimbursing ravulizumab.
CDA-AMC could not address these limitations. It should be noted that the market share estimates for ravulizumab plus usual care and comparators is highly uncertain due to ongoing negotiations and reviews of treatments for gMG.
Drug plan payer perspective: According to the CDA-AMC Procedures for Reimbursement Reviews,67 the BIA base case should be undertaken from the perspective of a pan-Canadian drug plan program. As such, costs relating to the use of blood products (i.e., IVIg) and administration costs of drugs and vaccinations are not funded by jurisdictional drug plan budgets and should, thus, be excluded from the drug plan perspective.
In reanalysis, costs associated with the use of blood products and vaccination administration were excluded from the drug plan perspective. The costs of vaccinations were not excluded. Blood product costs and administration costs were included within a health care system perspective.
Public coverage rate is uncertain. The sponsor assumed a public coverage rate of 80%, referencing the clinical expert feedback obtained in the CDA-AMC review of ravulizumab for gMG.43 Approximately ██% of patients in the concomitant IST optimized cohort were 65 years or older.6 According to the Understanding the Gap report by Sutherland et al., 100% of individuals aged 65 years and older are eligible for public coverage through formularies in many jurisdictions.68 Many jurisdictions also have support programs available to help cover the cost of expensive drugs for rare disease.69 The results of the BIA are sensitive to the proportion of patients covered by public drug programs.
In reanalysis, CDA-AMC adopted a conservative estimate of 100% coverage rate, consistent with the original BIA submission for ravulizumab for gMG. In scenario analyses, CDA-AMC explored the impact of assuming a public coverage rate of 80%.
The ravulizumab may be used in a broader population than modelled. The sponsor submitted analyses reflected the budget impact of reimbursing ravulizumab plus usual care among treated adult patients with anti-AChR antibody–positive gMG in MGFA class II to class IV and an MG-ADL total score of greater than or equal to 6, aligned with the CHAMPION-MG trial inclusion criteria and assumed to be aligned with the sponsor’s submitted reimbursement request (i.e., ravulizumab as an add-on therapy for adult patients with anti-AChR antibody–positive gMG whose symptoms persist despite adequate treatment with AChEIs, corticosteroids, and/or NSISTs).4 The CHAMPION-MG trial excluded patients with MGFA class I and V as well as patients with an MG-ADL total score of 5 or less.4 The Health Canada indication is agnostic to MGFA class and MG-ADL score, meaning that the CHAMPION-MG trial was narrower than the indicated population. Clinical expert feedback received by CDA-AMC noted that while class I patients are not severe, they can be refractory and that ravulizumab would ideally be considered for use in this group. Further, regarding use in class V patients, experts noted that ravulizumab could be useful especially in severe cases.
As a scenario analysis, CDA-AMC explored the budget impact of reimbursing ravulizumab in the Health Canada population, which is not restricted by MGFA class and MG-ADL score.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s base case by adopting a public coverage rate of 100% and removing the cost of blood products (IVIg) and vaccination administration costs, which are not relevant to the public drug payer perspective. CDA-AMC also conducted a health care system perspective in which the administration and blood product costs were included. The changes applied to derive the CDA-AMC base case from both perspectives are described in Table 19.
Table 19: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CDA-AMC base case | ||
1. Coverage rate | 80% | 100% |
2a. Blood product and vaccination administration costs (drug plan perspective) | Included | Set to $0 |
2b. Drug administration costs (health care system perspective) | Drug administration costs excluded | Drug administration costs included |
CDA-AMC base case (drug plan perspective) | Reanalysis 1 + 2a | |
CDA-AMC base case (health care system perspective) | Reanalysis 1 + 2b | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21. For the reimbursement requested population (i.e., adult patients with symptomatic anti-AChR antibody–positive gMG characterized with MGFA class II to class IV and an MG-ADL score of > 6), CDA-AMC reanalyses suggest that the 3-year budget impact of reimbursing ravulizumab plus usual care from the public drug plan perspective increased to $138,415,412 (Year 1: $40,405,866; Year 2: $46,573,094; Year 3: $51,436,451). However, the estimated budget impact is highly uncertain due to uncertainty associated with sponsor’s market share assumptions.
Table 20: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | 3-year total ($) |
|---|---|
Submitted base case | 101,061,496 |
CDA-AMC reanalysis 1 | 126,326,870 |
CDA-AMC reanalysis 2a – no blood product and vaccination administration costs | 110,732,330 |
CDA-AMC reanalysis 2b – drug administration costs | 100,864,775 |
CDA-AMC base case, drug plan perspective | 138,415,412 |
CDA-AMC base case, health care system perspective | 126,080,969 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
CDA-AMC conducted scenario analyses to address uncertainty in the population treated with ravulizumab plus, using the CDA-AMC base case from the health care payer perspective (results are provided in Table 21). The use of ravulizumab in all adult patients with anti-AChR antibody–positive gMG (regardless of MGFA class and MG-ADL score) increased the 3-year budget impact to $1,071,326,718.
Table 21: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | 3-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 78,608,219 | 97,600,287 | 117,023,098 | 130,978,108 | 345,601,493 |
New drug | 78,608,219 | 126,738,566 | 151,058,032 | 168,866,392 | 446,662,989 | |
Budget impact | 0 | 29,138,279 | 34,034,934 | 37,888,283 | 101,061,496 | |
CDA-AMC base case, drug plan perspective | Reference | 78,562,128 | 106,051,461 | 134,174,413 | 155,557,805 | 395,783,680 |
New drug | 78,562,128 | 146,457,327 | 180,747,508 | 206,994,257 | 534,199,092 | |
Budget impact | 0 | 40,405,866 | 46,573,094 | 51,436,451 | 138,415,412 | |
CDA-AMC base case, health care system perspective | Reference | 99,685,548 | 123,418,366 | 147,689,029 | 165,111,654 | 436,219,049 |
New drug | 99,685,548 | 159,768,932 | 190,149,999 | 212,381,087 | 562,300,018 | |
Budget impact | 0 | 36,350,565 | 42,460,970 | 47,269,434 | 126,080,969 | |
CDA-AMC scenario analysis, drug plan perspective 1: all adult patients with anti-AChR antibody–positive gMG | Reference | 608,066,010 | 820,831,742 | 1,038,501,652 | 1,204,007,781 | 3,063,341,175 |
New drug | 608,066,010 | 1,133,570,646 | 1,398,974,518 | 1,602,122,729 | 4,134,667,892 | |
Budget impact | 0 | 312,738,904 | 360,472,866 | 398,114,948 | 1,071,326,718 | |
CDA-AMC scenario analysis, drug plan perspective 2: 80% coverage rate | Reference | 62,849,703 | 84,841,169 | 107,339,531 | 124,446,244 | 316,626,944 |
New drug | 62,849,703 | 117,165,862 | 144,598,006 | 165,595,405 | 427,359,273 | |
Budget impact | 0 | 32,324,693 | 37,258,475 | 41,149,161 | 110,732,330 |
anti-AChR = anti–acetylcholine receptor; BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; gMG = generalized myasthenia gravis.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.