Drugs, Health Technologies, Health Systems
Reimbursement Review
Baricitinib (Olumiant)
Sponsor: Eli Lilly Canada Inc.
Therapeutic area: Alopecia areata, severe
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AA
alopecia areata
AE
adverse event
CANAAF
Canadian Alopecia Areata Foundation
CDA-AMC
Canada's Drug Agency
CI
confidence interval
ClinRO
clinician-reported outcome
EB
eyebrow
EL
eyelash
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HADS
Hospital Anxiety and Depression Scale
HRQoL
health-related quality of life
IP
immune privilege
IR
incidence rate
JAK
Janus kinase
LOCF
last observation carried forward
MACE
major adverse cardiac event
MID
minimal important difference
mLOCF
modified last observation carried forward
NRI
nonresponder imputation
PRO
patient-reported outcome
RCT
randomized controlled trial
SAE
serious adverse event
SALT
Severity of Alopecia Tool
SALT50
at least a 50% reduction in the Severity of Alopecia Tool score from baseline
SALT75
at least a 75% reduction in the Severity of Alopecia Tool score from baseline
SD
standard deviation
SF-36
Short Form (36) Health Survey
Skindex-16 for AA
Skindex-16 for Alopecia Areata
TEAE
treatment-emergent adverse event
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Baricitinib (Olumiant), 2 mg and 4 mg oral tablets |
Sponsor | Eli Lilly Canada Inc. |
Indication | Baricitinib is indicated for the treatment of adult patients with severe alopecia areata. |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | January 26, 2024 |
Recommended dose |
|
NOC = Notice of Compliance.
Introduction
Alopecia areata (AA) is a chronic autoimmune disease characterized by nonscarring hair loss at the scalp as well as the loss of eyebrow (EB), eyelash (EL), beard, pubic, or axillary hair. The onset of hair loss in AA is typically rapid and the progression is unpredictable, with the majority of patients experiencing disease onset by aged 40 years.1 AA is associated with psychological impacts and impairment in health-related quality of life (HRQoL). It is estimated that the prevalence of AA in Canada is between 0.1% and 0.58%.2-5 Canadian clinical practice guidelines for AA are not available to date. As per input from the clinical experts consulted by Canada’s Drug Agency (CDA-AMC), clinicians in Canada consider systemic drugs for the treatment of adults with severe AA, including off-label conventional immunosuppressants (cyclosporine, methotrexate, azathioprine, and mycophenolate mofetil) and Janus kinase (JAK) inhibitors (i.e., ritlecitinib, which has been recently approved by Health Canada for the treatment of adults and adolescents aged 12 years and older with severe AA, as well as tofacitinib, upadacitinib, and abrocitinib, which are off-label treatments for severe AA). Conventional immunosuppressants are currently reimbursed by the public drug plans in Canada. The clinical experts noted that conventional immunosuppressants are associated with poor efficacy, a risk of relapse with dose reduction and/or discontinuation, as well as potential serious adverse events (SAEs) when used long-term.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of baricitinib 2 mg and baricitinib 4 mg oral tablets in the treatment of adult patients with severe AA.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the call for input by CDA-AMC and from clinical experts we consulted for the purpose of this review.
Patient Input
CDA-AMC received 1 patient group submission from the Canadian Alopecia Areata Foundation (CANAAF). CANAAF was registered as a charitable organization in 2010 and is described as the voice for all patients and families affected by AA living in Canada. CANAAF collected data on the psychosocial and emotional impact of AA from peer-reviewed literature, as well as patient perspectives on AA from patient reports and support sessions.
CANAAF commented that AA is incredibly burdensome on a patient’s mental health and quality of life, and the disease causes disfiguring hair loss that occurs unexpectedly and can progress rapidly. Based on a patient report, CANAAF further stated that the anxiety, depression, and other resultant psychological conditions are not minor in nature; therefore, the loss of hair can create layers of stigma and misunderstandings. Short hair or baldness may be associated with a preference for an “edgy” look or having a certain sexuality, which may not be accurate. Those with this disease may feel less feminine or less masculine without hair. Children and teenagers may experience bullying. In addition, CANAAF revealed that there is also a significant financial burden associated with AA; this was supported by the findings of a CANAAF community alopecia patient focus group conducted in 2023. The most significant cost item was a wig purchase and maintenance, which can cost more than $2,500 a year. Some patients experienced significant impacts on their ability to work.
Based on the literature, CANAAF identified limitations of the currently available treatments for AA, including topical corticosteroids (limited effectiveness, effective only for patients with very limited AA, difficult product application, and scalp irritation), intralesional corticosteroids (painful injections and limited drug coverage by drug plans), oral corticosteroids (variable success rates, a high relapse rate, limited drug coverage, and unfavourable side effects), topical minoxidil (nondurable benefits for very mild AA, and adverse events [AEs] such as excessive hair growth on body parts other than the site of application, irritation, and allergic contact dermatitis), oral minoxidil (systemic AEs relating to its antihypertensive property and limited drug coverage), and systemic immunosuppressants (variable effectiveness; a risk of organ toxicity, infection, and malignancy; concomitant administration of oral corticosteroids required for some drugs; and limited drug coverage).
CANAAF identified a need for an effective treatment option that could result in full and sustained hair growth and alleviate anxiety and depression associated with AA. CANAAF believed that baricitinib may fulfill this need by serving as an effective treatment that has a favourable side effect profile and is easy to administer. The group noted that most patients regrew all their hair with baricitinib treatment. CANAAF also noted that the side effect profile of baricitinib is much more favourable compared to existing treatments. Baricitinib is also a much easier treatment option for patients as it only requires that they take 1 pill, once a day. This is in comparison to other treatments that must be applied topically, injected (often by a health care professional), or taken orally more than once a day.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
The clinical experts we consulted noted that currently reimbursed off-label systemic treatments for severe AA are associated with poor efficacy, a risk of relapse with dose reduction and/or discontinuation, and potential SAEs when used long-term (especially with conventional immunosuppressants). Also, access to emerging therapies, such as ritlecitinib, is currently limited as per clinical expert input. The clinical experts noted that, because of the limited efficacy of the conventional systemic immunomodulators, it is rational to use baricitinib (and JAK inhibitors in general) as a first-line systemic therapy in severe AA rather than as the last line of treatment after the failure of conventional systemic immunomodulators. The clinical experts noted that it would be appropriate to use baricitinib in combination with topical treatments and/or intralesional corticosteroids but not in combination with other immunomodulators, except for prednisone where concomitant use with baricitinib may be appropriate.
In the clinical experts’ opinion, patients who have severe AA with scalp involvement as reflected by a Severity of Alopecia Tool (SALT) score of 50 or more and have a current episode of AA of a duration greater than 1 year but less than 10 years are potential candidates for baricitinib treatment, though the clinical experts noted that adhering to the inclusion criterion on the duration of a current episode used in the pivotal trials (i.e., more than 6 months and less than 8 years in duration) would also be reasonable. One clinical expert considered the use of baricitinib in older adults (i.e., older than 60 years for males or older than 70 years for females, which were categories of patients excluded from the pivotal trials) to be reasonable, while the other clinical expert suggested restricting the use of baricitinib as per the age restriction in the pivotal trials because of a lack of clinical trial data and unknown clinical treatment benefits.
The clinical experts felt that it is reasonable to define meaningful response to treatment as the attainment of a SALT score of 20 or less after 36 weeks of baricitinib treatment, consistent with the pivotal trials. The clinical experts noted that it would be reasonable to consider the discontinuation of baricitinib treatment in patients who do not attain cosmetically acceptable hair regrowth at 36 weeks, who have further loss of hair at 36 weeks, who experience severe AEs deemed to be related to the use of a JAK inhibitor, or who develop intercurrent conditions, making the discontinuation of a JAK inhibitor advisable (e.g., malignancy). In the clinical expert’s opinion, baricitinib treatment should be prescribed by dermatologists with experience in diagnosing, treating, and monitoring patients with severe AA.
Clinician Group Input
We received no clinician group input for the drug under review.
Drug Program Input
Input was obtained from the drug programs that participate in our reimbursement review process. The following were identified as key factors that could potentially affect the implementation of a CDA-AMC recommendation for baricitinib:
relevant comparators
considerations for the initiation of therapy
considerations for the continuation or renewal of therapy
considerations for the discontinuation of therapy
considerations for the prescribing of therapy
generalizability
care provision issues
system and economic issues.
The clinical experts we consulted provided advice on the potential implementation issues raised by the drug programs. Refer to Table 5 for more details.
Clinical Evidence
Systematic Review
Description of Studies
The sponsor-conducted systematic literature review identified 2 pivotal double-blind, randomized, placebo-controlled trials (Study BRAVE-AA1, N = 654; Study BRAVE-AA2, N = 546)6 that assessed the efficacy and safety of baricitinib relative to placebo in adult patients who had severe or very severe AA with at least 50% scalp involvement (i.e., a SALT score of at least 50) and had a current AA episode lasting more than 6 months and less than 8 years. In the double-blind, placebo-controlled treatment period, patients were randomized in a 2:2:3 ratio to receive placebo, baricitinib 2 mg, and baricitinib 4 mg once daily for 36 weeks, at which time the primary analysis of efficacy and safety was conducted. In the 68-week long-term extension period, patients continued the existing intervention or were reassigned a new intervention (placebo, baricitinib 2 mg, or baricitinib 4 mg), depending on response to treatment at week 36 (for patients initially assigned to placebo) or week 52 (for patients initially assigned to baricitinib 2 mg or baricitinib 4 mg) as per-protocol-defined criteria. This was followed by a 96-week bridging extension where patients continued to receive the same intervention until the end of the study. The long-term extension period is ongoing in both trials.
Efficacy end points of interest to this review included the proportion of patients attaining a SALT score of 20 or less (the primary end point), a response of at least a 50% reduction in the Severity of Alopecia Tool score from baseline (SALT50), clinician-reported outcome (ClinRO) measures for EB and EL hair loss scores of 0 or 1 with at least a 2-point reduction from baseline (key secondary end points), change from baseline in Hospital Anxiety and Depression Scale (HADS) anxiety and depression domain scores, and Skindex-16 for Alopecia Areata (Skindex-16 for AA) symptoms, emotions, and functioning domain scores (secondary or exploratory outcomes). All of these were assessed at week 36.
In both trials, at baseline, there was about an equal proportion of patients with severe AA and very severe AA. The mean duration of the current AA episode was 3.6 (standard deviation [SD] = 3.9) years and 4.3 (SD = 4.9) years in Study BRAVE-AA1 and Study BRAVE-AA2, respectively. Approximately 90% of patients had received prior AA treatment, with the most common ones (reported in at least 40% of patients) being topical therapies, intralesional therapy, and systemic immunosuppressants and immunomodulators.
Efficacy Results
Proportion of Patients Attaining SALT Score of 20 or Less
The proportion of patients attaining a SALT score of 20 or less at week 36 was the primary end point in both trials. At week 36, the between-group difference comparing baricitinib 2 mg versus placebo was 16.4% (95% confidence interval [CI], 9.7% to 23.4%; P < 0.001) in Study BRAVE-AA1 and 14.7% (95% CI, 8.3% to 21.6%; P < 0.001) in Study BRAVE-AA2. The between-group difference comparing baricitinib 4 mg and placebo was 29.9% (95% CI, 23.2% to 36.2%; P < 0.001) in Study BRAVE-AA1 and 29.9% (95% CI, 23.1% to 36.3%; P < 0.001) in Study BRAVE-AA2. Results were in favour of both regimens of baricitinib treatment. In both trials, subgroup analyses by baseline disease severity and duration of the current episode of AA were consistent with the primary analysis.
The percentage change from baseline in the SALT score was assessed at week 36 in both trials (a key secondary end point). In both trials, the between-group difference comparing baricitinib and placebo was in favour of baricitinib for both the 2 mg regimen (–23.1% [95% CI, –30.6% to –15.6%; P < 0.001] in Study BRAVE-AA1 and –25.3% [95% CI, –32.8% to –17.7%] in Study BRAVE-AA2) and the 4 mg regimen (–37.7% [95% CI, –44.4% to –30.9%; P < 0.001] in Study BRAVE-AA1 and 44.5% [95% CI, –51.3% to –37.7%; P < 0.001] in Study BRAVE-AA2).
Proportion of Patients Attaining SALT50 Response
The between-group difference in the proportion of patients attaining a SALT50 response at week 36 (a secondary end point) comparing baricitinib 2 mg versus placebo was 17.7% (95% CI, 9.5% to 25.8%; P < 0.001) in Study BRAVE-AA1 and 23.1% (95% CI, 15.1% to 31.0%; P < 0.001) in Study BRAVE-AA2. The between-group difference comparing baricitinib 4 mg with placebo was 33.6% (95% CI, 25.6% to 40.7%; P < 0.001) in Study BRAVE-AA1 and 41.9% (95% CI, 34.0% to 48.7%; P < 0.001) in Study BRAVE-AA2. Results of the responder analysis for at least a 75% reduction in the Severity of Alopecia Tool score from baseline (SALT75) were consistent with the SALT50 responder analysis. Neither end point was adjusted for multiplicity in the trials.
Proportion of Patients Attaining ClinRO Measure for EB Hair Loss Score of 0 or 1 With an Improvement of 2 Points or More From Baseline Among Patients With ClinRO Measure for EB Hair Loss Score of 2 or More at Baseline
Between 66.3% and 73.9% of all randomized patients had a ClinRO measure for EB hair loss score of at least 2 at baseline in the trials and contributed to the analysis of the proportion of patients with a ClinRO measure for EB hair loss score of 0 or 1 with at least a 2-point improvement from baseline at week 36 (a key secondary end point).
The between-group difference comparing baricitinib 2 mg versus placebo was 15.9% (95% CI, 8.4% to 23.6%; P < 0.001) in favour of baricitinib 2 mg in Study BRAVE-AA1 and 7.1% (95% CI, –0.3% to 15.0%; P = 0.08) in Study BRAVE-AA2. In Study BRAVE-AA2, no formal testing was conducted for subsequent end points in the statistical hierarchy because of the failure of this end point in the study. The between-group difference was in favour of baricitinib 4 mg over placebo in both trials (28.2% [95% CI, 20.3% to 35.4%; P < 0.001] in Study BRAVE-AA1 and 30.3% [95% CI, 21.4% to 38.4%; P < 0.001] in Study BRAVE-AA2). Results based on the patient-reported outcome (PRO) measure showed consistent results.
Proportion of Patients Attaining ClinRO Measure for EL Hair Loss Score of 0 or 1 With an Improvement of 2 Points or More From Baseline Among Patients With ClinRO Measure for EL Hair Loss Score of 2 or More at Baseline
Between 51.3% and 60.3% of all randomized patients had a ClinRO measure for EL hair loss score of at least 2 at baseline in the trials and contributed to the analysis of the proportion of patients who had a ClinRO measure for EL hair loss score of 0 or 1 with at least a 2-point improvement from baseline at week 36 (a key secondary end point).
The between-group difference comparing baricitinib 2 mg and placebo was 10.4% (95% CI, 2.7% to 18.3%) in Study BRAVE-AA1 and 4.6% (95% CI, –3.7% to 13.2%) in Study BRAVE-AA2; neither difference was formally tested for statistical significance because of the prior failure of an outcome in the statistical hierarchy. The between-group difference favoured baricitinib 4 mg treatment over placebo in both trials (30.4% [95% CI, 21.6% to 38.1%; P < 0.001] in Study BRAVE-AA1 and 28.7% [95% CI, 18.7% to 37.5%; P < 0.001] in Study BRAVE-AA2). Results based on the PRO measure showed consistent results.
Change From Baseline in HADS Anxiety Domain Score
The between-group difference comparing baricitinib 2 mg and placebo with respect to change from baseline in the HADS anxiety domain score at week 36 (a secondary end point) favoured baricitinib 2 mg in Study BRAVE-AA1 at –0.8 (95% CI, –1.4 to –0.3; P ≤ 0.01) and at 0.2 (95% CI, –0.8 to 0.4; P = 0.5) in Study BRAVE-AA2. The between-group difference comparing baricitinib 4 mg and placebo favoured baricitinib 4 mg in both trials (–0.5 [95% CI, –1.1 to 0.0; P = 0.04] in Study BRAVE-AA1 and –0.7 [95% CI, –1.3 to –0.2; P = 0.01] in Study BRAVE-AA2). This end point was not adjusted for multiplicity.
Change From Baseline in HADS Depression Domain Score
The between-group difference comparing baricitinib 2 mg and placebo with respect to change from baseline in the HADS depression domain score at week 36 (a secondary end point) was –0.42 (95% CI, –0.93 to 0.109; P = 0.107) in Study BRAVE-AA1 and 0.51 (95% CI, –1.108 to 0.107; P = 0.083) in Study BRAVE-AA2. The between-group difference comparing baricitinib 4 mg and placebo favoured baricitinib 4 mg in Study BRAVE-AA2 at –0.768 (95% CI, –1.20 to –0.216; P = 0.010) and at –0.32 (95% CI, –0.78 to 0.14; P = 0.174) in Study BRAVE-AA1. This end point was not adjusted for multiplicity.
Change From Baseline in Skindex-16 for AA Symptoms Domain Score
The difference between baricitinib 2 mg and placebo with respect to change from baseline in the Skindex-16 AA symptoms domain score at week 36 favoured baricitinib 2 mg in Study BRAVE-AA1 at –4.76 (95% CI, –9.13 to –0.40; P = 0.033) and at –3.02 (95% CI, –6.91 to 0.88; P = 0.129) in Study BRAVE-AA2. The difference between baricitinib 4 mg and placebo favoured baricitinib 4 mg in Study BRAVE-AA2 at –4.21 (95% CI, –7.75 to –0.68; P = 0.020) and at –2.75 (95% CI, –6.67 to 1.17; P = 0.168) in Study BRAVE-AA1. This was an exploratory end point in Study BRAVE-AA1 and a secondary end point in Study BRAVE-AA2. It was not adjusted for multiplicity.
Change From Baseline in Skindex-16 for AA Emotions Domain Score
The between-group difference with respect to change from baseline in the Skindex-16 for AA emotions domain score at week 36 was in favour of baricitinib over placebo in both trials for both the baricitinib 2 mg regimen (–11.50 [95% CI, –17.71 to –5.30; P < 0.001] in Study BRAVE-AA1 and –6.75 [95% CI, –12.68 to –0.82; P = 0.026] in Study BRAVE-AA2) and the baricitinib 4 mg regimen (–11.01 [95% CI, –16.57 to –5.45; P < 0.001] in Study BRAVE-AA1 and –13.42 [95% CI, –18.80 to –0.84; P < 0.001] in Study BRAVE-AA2). This was an exploratory end point in Study BRAVE-AA1 and a secondary end point in Study BRAVE-AA2. It was not adjusted for multiplicity.
Change From Baseline in Skindex-16 for AA Functioning Domain Score
The difference between baricitinib 2 mg and placebo with respect to change from baseline in the Skindex-16 for AA functioning domain score at week 36 was –5.07 (95% CI, –10.94 to 0.80; P = 0.090) in Study BRAVE-AA1 and –4.38 (95% CI, –9.65 to 0.88; P = 0.103) in Study BRAVE-AA2. The difference between baricitinib 4 mg and placebo favoured baricitinib 4 mg in both trials (–7.04 [95% CI, –12.31 to –1.77; P = 0.009] in Study BRAVE-AA1 and –8.33 [95% CI, –13.10 to –3.56; P < 0.001] in Study BRAVE-AA2). This was an exploratory end point in Study BRAVE-AA1 and a secondary end point in Study BRAVE-AA2. It was not adjusted for multiplicity.
Harms Results
Treatment-Emergent Adverse Events, SAEs, Withdrawal Due to Adverse Events, and Mortality
Treatment-emergent adverse events (TEAEs) were reported in 50.8% to 68.4% of patients across the trials and occurred in similar proportions of patients across treatment groups. The most common TEAEs of baricitinib (reported in at least 5% of patients in either baricitinib group) were upper respiratory tract infection, headache, urinary tract infection, nasopharyngitis, acne, and increased blood creatine phosphokinase. SAEs (1.6% to 3.4%) and withdrawal due to adverse events (WDAEs) (1.1% to 2.6%) were uncommon in the studies. No deaths were reported in the trials.
Notable Harms (Infections, Cardiovascular and Thromboembolic Events, Gastrointestinal Perforations, Malignancies)
Treatment-emergent infections were reported in 25.1% to 37.4% of patients across treatment groups in the trials. In Study BRAVE-AA2, the frequency of infection was higher in the baricitinib 2 mg group (37.4% of patients) compared with the placebo group (29.2% of patients), but this was not observed in Study BRAVE-AA1. In Study BRAVE-AA1, none of the infections was reported to be serious or leading to treatment discontinuation. In Study BRAVE-AA2, serious infection was reported in 2 (1.3%) patients and 1 (0.4%) patient in the baricitinib 2 mg and baricitinib 4 mg groups, respectively, and infection leading to treatment discontinuation was reported in 1 (0.6%) patient in the baricitinib 2 mg group. Infection leading to treatment interruption was reported in 1.1% to 5.2% of patients across the trials.
In Study BRAVE-AA1, myocardial infarction and coronary revascularization was reported in 1 (0.5%) patient in the baricitinib 2 mg group. Serious arrhythmia was reported in 1 (0.5%) patient in the baricitinib 4 mg group. There was no report of cardiovascular events in Study BRAVE-AA2. There were no reports of venous or pulmonary thromboembolic events, gastrointestinal perforations, or nonmelanoma skin cancers in either trial. One patient in each of the placebo group (0.6% of patients) and the baricitinib 4 mg group (0.4% of patients) reported other forms of malignancies.
Critical Appraisal
The trials used adequate methods of randomization and allocation concealment. There were a few small baseline imbalances in patient characteristics that may be compatible with chance and were not believed to have a substantial impact on study results. The trials were adequately blinded; however, there was a potential for bias in the measurement of subjective outcomes (i.e., ClinRO measures, HADS, and Skindex-16 for AA). This could have led to the inflated efficacy of baricitinib based on the inferred judgment by patients and investigators regarding treatment assignment premised on response to treatment, without being unblinded. SALT50 responder analysis, HADS, and Skindex-16 for AA outcomes were not adjusted for multiplicity, so statistically significant results were at an increased risk of type I error (false-positive results). Between 31% and 42% of patients were excluded from ClinRO measures–based outcomes because of not having the specified baseline score, which could have impacted randomization, although the extent and direction of the resulting bias was unclear. There was a risk of attrition bias in favour of baricitinib with respect to change from baseline in HADS and Skindex-16 for AA domain scores, given the differential discontinuation rate between the baricitinib and placebo groups (there was a higher proportion of dropouts in the placebo group) and the use of last observation carried forward (LOCF) or modified last observation carried forward (mLOCF) as the data imputation method. There was a lack of sample size consideration and control for multiplicity for subgroup analyses, which precluded definitive conclusions on subgroup effects. Evidence for the validity and minimal important difference (MID) estimate of HADS and Skindex-16 for AA outcomes in patients with AA was not identified by the sponsor.
The clinical experts we consulted noted that the inclusion and exclusion criteria of the trials in general were reflective of the patient population eligible for baricitinib treatment in Canada, although patients with a primarily diffuse type of AA would not necessarily be excluded from treatment in clinical practice. As well, older adults (i.e., males older than 60 years and females older than 70 years) were excluded from the trials. There are differing opinions from the clinical experts suggesting that older adults may or may not be eligible for baricitinib treatment in clinical practice. In addition, the clinical experts noted that compared to clinical practice, the trials appeared to have enrolled a higher proportion of patients with very severe AA. As well, the trial populations had a lower degree of anxiety and depression at baseline as per clinical expert input, which could have impacted the generalizability of HADS outcomes. The clinical experts noted that a longer duration of follow-up beyond 36 weeks is required to adequately capture the long-term safety of baricitinib, including potential rare AEs, since baricitinib is expected to be a lifelong treatment for many patients. No head-to-head evidence comparing baricitinib with systemic treatments for severe AA that are currently reimbursed by the public drug plans (conventional immunosuppressants) was submitted. As well, the absence of evidence for baricitinib in older adults (males older than 60 years and females older than 70 years — categories that were excluded from the trials), represents another gap in evidence.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool was used to assess the certainty of the evidence for outcomes considered most relevant to inform our expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group. Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias.
The selection of outcomes for the GRADE assessment was based on the sponsor’s Summary of Clinical Evidence,9 consultation with clinical experts, and input received from a patient group and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
scalp hair regrowth (the proportion of patients with a SALT score of 20 or less and a SALT50 response)
EB and EL hair regrowth (the proportion of patients attaining an EB [or EL] score of 0 or 1 with ≥ 2-point improvement from baseline, among patients with a baseline score of ≥ 2)
anxiety and depression (the change from baseline in HADS anxiety and depression domain scores)
HRQoL (the change from baseline in Skindex-16 for AA symptoms, emotions, and functioning domain scores)
harms (SAEs).
The GRADE summary of findings for baricitinib versus placebo for the treatment of adults with severe or very severe AA is presented in Table 2 (baricitinib 2 mg versus placebo) and Table 3 (baricitinib 4 mg versus placebo).
Table 2: Summary of Findings for Baricitinib 2 mg Versus Placebo for Adults With Severe or Very Severe AA
Outcome and follow-up | Patients (studies), N | Effect | Certainty | What happens |
|---|---|---|---|---|
Scalp hair regrowth | ||||
SALT score (0 [no scalp hair loss] to 100 [complete scalp hair loss]), proportion of patients attaining a SALT score ≤ 20 (95% CI) Follow-up: 36 weeks | 685 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Moderatea | Baricitinib 2 mg likely results in a clinically important increase in the proportion of patients attaining SALT ≤ 20 when compared with placebo. |
Proportion of patients attaining a SALT50 response (i.e., at least a 50% reduction in score from baseline) (95% CI) Follow-up: 36 weeks | 685 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Highc | Baricitinib 2 mg results in a clinically important increase in a SALT50 response when compared with placebo. |
EB hair regrowth | ||||
ClinRO measure for EB hair loss (0 [full coverage and no areas of hair loss] to 3 [no notable EB hair]), proportion of patients attaining a score of 0 (full coverage and no areas of hair loss) or 1 (minimal gaps in EB hair and even distribution) with ≥ 2-point improvement from baseline, among patients with a baseline score of ≥ 2 (95% CI) Follow-up: 36 weeks | 476 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowd, e | Baricitinib 2 mg may result in a clinically important increase in EB hair regrowth when compared with placebo. |
EL hair regrowth | ||||
ClinRO measure for EL hair loss (0 [continuous line of ELs along the rim of eyelids] to 3 [no notable ELs]), proportion of patients attaining a score of 0 (continuous line of ELs along the rim of eyelids) or 1 (minimal gaps in EL hair and even distribution) with ≥ 2-point improvement from baseline, among patients with a baseline score of ≥ 2 (95% CI) Follow-up: 36 weeks | 386 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowd, e | Baricitinib 2 mg may result in little to no clinically important difference in EL hair regrowth when compared with placebo. |
Anxiety and depression | ||||
HADS anxiety domain score (0 [least anxiety] to 21 [greatest anxiety]), change from baseline in score (95% CI) Follow-up: 36 weeks | 580 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Very lowg, h | The evidence is very uncertain about the effect of baricitinib 2 mg on anxiety when compared with placebo. |
HADS depression domain score (0 [least depression] to 21 [greatest depression]), change from baseline in score (95% CI) Follow-up: 36 weeks | 580 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Very lowg, h | The evidence is very uncertain about the effect of baricitinib 2 mg on depression when compared with placebo. |
HRQoL | ||||
Skindex-16 for AA symptoms score (0 [no effect] to 100 [effect experienced all the time]), change from baseline in score (95% CI) Follow-up: 36 weeks | 449 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowg, i | Baricitinib 2 mg may result in an improvement in symptoms when compared with placebo. The clinical importance of the improvement is unclear. |
Skindex-16 for AA emotions score (0 [no effect] to 100 [effect experienced all the time]), change from baseline in score (95% CI) Follow-up: 36 weeks | 449 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowg | Baricitinib 2 mg may result in an improvement in emotions when compared with placebo. The clinical importance of the improvement is unclear. |
Skindex-16 for AA functioning score (0 [no effect] to 100 [effect experienced all the time]), change from baseline in score (95% CI) Follow-up: 36 weeks | 449 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowg, j | Baricitinib 2 mg may result in an improvement in functioning when compared with placebo. The clinical importance of the improvement is unclear. |
Harms | ||||
Serious adverse event Follow-up: 36 weeks | 681 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowk | Baricitinib 2 mg may result in little to no difference in serious adverse events compared with placebo. |
AA = alopecia areata; CDA-AMC = Canada’s Drug Agency; CI = confidence interval; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; HADS = Hospital Anxiety and Depression Scale; HRQoL = health-related quality of life; NR = not reported; RCT = randomized controlled trial; SALT = Severity of Alopecia Tool; SALT50 = at least a 50% improvement from baseline in the Severity of Alopecia Tool score; SE = standard error; Skindex-16 for AA = Skindex-16 for Alopecia Areata.
Notes: Details included in Table 2 are from the sponsor’s Summary of Clinical Evidence.9
Study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 1 level for serious imprecision. The clinical experts consulted by CDA-AMC indicated that a difference of 100 patients per 1,000 patients could be considered clinically important. The 95% CI included the possibility of benefit and no difference in both trials.
bStatistical testing for this outcome was not adjusted for multiplicity. The results are considered as supportive evidence.
cDid not rate down for imprecision. Although the lower boundary of the 95% CI in Study BRAVE-AA1 was 95 more patients per 1,000 patients, this was not considered to be a source of serious imprecision because of the lower boundary’s proximity to the threshold of 100 more patients per 1,000 patients as per clinical expert input.
dRated down 1 level for serious study limitations. Randomization could potentially be impacted because of the exclusion of patients whose baseline score did not meet the specified value of at least 2, from each treatment group. The extent and direction of the resulting bias was unclear.
eRated down 1 level for serious imprecision. The clinical experts we consulted indicated that a difference of 100 patients per 1,000 patients could be considered clinically important. In both trials, the 95% CI included the possibility of benefit and little to no difference. This was not rated down for inconsistency, though the point estimates from the trials were in different directions based on the threshold of 100 patients per 1,000 patients as per clinical expert input. This is because of overlap in the 95% CIs in the trials, including the possibility of benefit and little to no difference for both.
fNo formal statistical testing was conducted because of a prior failure of an outcome in the statistical hierarchy. The results are considered as supportive evidence.
gRated down 2 levels for very serious study limitations. Study treatment discontinuation was notably higher in the placebo group compared with the baricitinib 2 mg group in both trials. The differential discontinuation rate, along with the use of modified LOCF or LOCF as the data imputation method, could potentially lead to attrition bias in favour of the baricitinib 2 mg group. In addition, evidence for the validity of this outcome measure in the patient population under review (i.e., patients with AA) were not identified by the sponsor.
hRated down 1 level for serious indirectness. The trial population had a higher mean baseline score (less severe anxiety or depression) than patients in clinical practice as per clinical expert input.
iDid not rate down for imprecision using null as a threshold. Although the upper boundary of the 95% CI in Study BRAVE-AA2 was 0.88, this was not considered to be a source of serious imprecision because of the upper boundary’s proximity to the null.
jThere were no concerns with imprecision using the null as a threshold. Although the upper boundary of the 95% CI was 0.80 and 0.88 in Study BRAVE-AA1 and Study BRAVE-AA2, respectively, this was not considered to be a source of serious imprecision because of the upper boundary’s proximity to the null.
kRated down 1 level for serious indirectness. The duration of follow-up of 36 weeks is inadequate for capturing potential rare serious adverse events of baricitinib as per clinical expert input. We were also rated this down 1 level for serious imprecision since the results were based on a small number of events across the trials.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Reports.7,8
Table 3: Summary of Findings for Baricitinib 4 mg Versus Placebo for Adults With Severe or Very Severe AA
Outcome and follow-up | Patients (studies), N | Effect | Certainty | What happens |
|---|---|---|---|---|
Scalp hair regrowth | ||||
SALT score (0 [no scalp hair loss] to 100 [complete scalp hair loss]), proportion of patients attaining a SALT score of ≤ 20 (95% CI) Follow-up: 36 weeks | 860 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| High | Baricitinib 4 mg results in a clinically important increase in the proportion of patients attaining a SALT score of ≤ 20 when compared with placebo. |
Proportion of patients attaining a SALT50 response (i.e., at least a 50% reduction in score from baseline) (95% CI) Follow-up: 36 weeks | 860 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| High | Baricitinib 4 mg results in a clinically important increase in SALT50 response when compared with placebo. |
EB hair regrowth | ||||
ClinRO measure for EB hair loss (0 [full coverage and no areas of hair loss] to 3 [no notable EB hair]), proportion of patients attaining a score of 0 (full coverage and no areas of hair loss) or 1 (minimal gaps in EB hair and even distribution) with ≥ 2-point improvement from baseline, among patients with a baseline score of ≥ 2 (95% CI) Follow-up: 36 weeks | 585 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Moderateb | Baricitinib 4 mg likely results in a clinically important increase in EB hair regrowth when compared with placebo. |
EL hair regrowth | ||||
ClinRO measure for EL hair loss (0 [continuous line of ELs along the rim of eyelids] to 3 [no notable ELs]), proportion of patients attaining a score of 0 (continuous line of ELs along the rim of eyelids) or 1 (minimal gaps in EL hair and even distribution) with ≥ 2-point improvement from baseline, among patients with a baseline score of ≥ 2 (95% CI) Follow-up: 36 weeks | 493 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Moderateb | Baricitinib 4 mg likely results in a clinically important increase in EL hair regrowth when compared with placebo. |
Anxiety and depression | ||||
HADS anxiety domain score (0 [least anxiety] to 21 [greatest anxiety]), change from baseline in score (95% CI) Follow-up: 36 weeks | 740 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Very lowc, d | The evidence is very uncertain about the effect of baricitinib 4 mg on anxiety when compared with placebo. |
HADS depression domain score (0 [least depression] to 21 [greatest depression]), change from baseline in score (95% CI) Follow-up: 36 weeks | 740 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Very lowc, d | The evidence is very uncertain about the effect of baricitinib 4 mg on depression when compared with placebo. |
HRQoL | ||||
Skindex-16 for AA symptoms score (0 [no effect] to 100 [effect experienced all the time]), change from baseline in score (95% CI) Follow-up: 36 weeks | 579 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowc | Baricitinib 4 mg may result in an improvement in symptoms when compared with placebo. The clinical importance of the improvement is unclear. |
Skindex-16 for AA emotions score (0 [no effect] to 100 [effect experienced all the time]), change from baseline in score (95% CI) Follow-up: 36 weeks | 579 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowc | Baricitinib 4 mg may result in an improvement in emotions when compared with placebo. The clinical importance of the improvement is unclear. |
Skindex-16 for AA functioning score (0 [no effect] to 100 [effect experienced all the time]), change from baseline in score (95% CI) Follow-up: 36 weeks | 579 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowc | Baricitinib 4 mg may result in an improvement in functioning when compared with placebo. The clinical importance of the improvement is unclear. |
Harms | ||||
Serious adverse event (95% CI) Follow-up: 36 weeks | 856 (2 RCTs) | Study BRAVE-AA1
Study BRAVE-AA2
| Lowe | Baricitinib 4 mg may result in little to no difference in serious adverse events compared with placebo. |
AA = alopecia areata; CI = confidence interval; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; HADS = Hospital Anxiety and Depression Scale; HRQoL = health-related quality of life; NR = not reported; RCT = randomized controlled trial; SALT = Severity of Alopecia Tool; SALT50 = at least a 50% improvement from baseline in the Severity of Alopecia Tool score; SE = standard error; Skindex-16 for AA = Skindex-16 for Alopecia Areata.
Notes: Details included in Table 3 are from the sponsor’s Summary of Clinical Evidence.9
Study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aStatistical testing for this outcome was not adjusted for multiplicity. The results are considered as supportive evidence.
bRated down 1 level for serious study limitations. Randomization could potentially be impacted because of the exclusion of a large proportion of patients from each treatment group whose baseline score did not meet the specified value of at least 2. The extent and direction of the resulting bias was unclear.
cRated down 2 levels for serious study limitations. Study treatment discontinuation was notably higher in the placebo group compared with the baricitinib 4 mg group in both trials. The differential discontinuation rate, along with the use of modified LOCF or LOCF as the data imputation method, could potentially lead to attrition bias in favour of the baricitinib 4 mg group. In addition, evidence for the validity of this outcome measure in the patient population under review (i.e., patients with AA) were not identified by the sponsor.
dRated down 1 level for serious indirectness. The trial population had a higher mean baseline score (less severe anxiety or depression) than patients in clinical practice as per clinical expert input.
eRated down 1 level for serious indirectness. The duration of follow-up of 36 weeks is inadequate for capturing potential rare serious adverse events of baricitinib as per clinical expert input. We also rated this down 1 level for serious imprecision since the results were based on a small number of events across the trials.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Long-Term Extension Studies
Description of Studies
Study BRAVE-AA1
This is a long-term extension study (week 36 onward) of Study BRAVE-AA1.10 The purpose of this study is to provide the safety and efficacy analyses through week 104 to support dosing recommendations in the product labelling of baricitinib.
At week 52, patients initially randomized to baricitinib who were responders (with a SALT score of 20 or less) were rerandomized at a 3:1 ratio to stay on their current dose of baricitinib or to transition to placebo (randomized withdrawal). Responders who had been rerandomized to placebo and had experienced a loss of treatment benefit at any time after week 52 (more than a 20-point worsening in the SALT score from week 52) were re-treated with their original baricitinib dose and the efficacy of re-treatment was analyzed as part of the other secondary end points of Study BRAVE-AA1.
This extension study included week 0 to week 52 and week 52 to week 76 efficacy and safety data for patients who up-titrated at week 52. The up-titration cohort included ███ patients randomized to baricitinib 2 mg at week 0 who did not attain a SALT score of 20 or less at week 52. All ███ patients were titrated up to baricitinib 4 mg.
Study BRAVE-AA2
This is a long-term extension study (week 36 onward) of Study BRAVE-AA2.11 The purpose of this study is to provide efficacy and safety analyses to support dosing recommendations in product labelling.
At week 52, patients were divided into 2 cohorts. The randomized down-titration cohort included 82 patients who were randomized at week 0 to baricitinib 4 mg, having attained a SALT score of 20 or less at week 52. Of these patients, 42 were randomly assigned to remain on baricitinib 4 mg and 40 patients were randomly assigned to down-titrate to baricitinib 2 mg. The up-titration cohort included ██ patients randomized to baricitinib 2 mg at week 0 who did not attain a SALT score of 20 or less at week 52. All ██ patients were titrated up to baricitinib 4 mg.
Efficacy Results
Proportion of Patients Attaining SALT Score of 20 or Less
In both trials, the proportion of patients attaining a SALT score of 20 or less continuously increased over the treatment period beyond 36 weeks for the baricitinib 4 mg cohort. At week 52, 40.9% and 21.2% of patients receiving baricitinib 4 mg and baricitinib 2 mg, respectively, attained a SALT score of 20 or less in Study BRAVE-AA1. Similarly, 36.8% and 24.4% of patients receiving baricitinib 4 mg and baricitinib 2 mg, respectively, attained a SALT score of 20 or less at week 52 in Study BRAVE-AA2.
Study BRAVE-AA1: Up-Titration Cohort
At week 52, ███ patients who were originally randomized to the baricitinib 2 mg group were considered nonresponders and were eligible for inclusion in the up-titration cohort titrated up to baricitinib 4 mg. At week 76, following 24 weeks of treatment on baricitinib 4 mg, ██ of ███ patients (████ ███ ███ █████ ██ █████) in the up-titration cohort attained a SALT score of 20 or less.
Study BRAVE-AA2: Randomized Down-Titration Cohort
At week 52, 82 patients who were originally randomized to the baricitinib 4 mg group were eligible for randomized down-titration to baricitinib 2 mg. At week 52, █████ ███ ██ ███ ███ ███ █████ ██████ of patients attained a SALT score of 20 or less. ███ ███████ ███ █ ███████ █████ ██ ████ ███ ███ ████████ ████ █████████ █████ ████ ██████ ███ █████████ ████ ███ ████████ ████ ██ ████ ██ ██ ███ █████
Among patients receiving baricitinib 4 mg who attained a SALT score of 20 or less at week 52, this response was retained up to week 76 in 75% (30 of 40, ███ ███ █████ ██ █████) of patients who were down-titrated to baricitinib 2 mg, and 98% (41 of 42, ███ ███ █████ ██ █████) of patients who remained on baricitinib 4 mg.
Study BRAVE-AA2: Up-Titration Cohort
At week 52, ██ patients who were originally randomized to the baricitinib 2 mg group were considered nonresponders and were eligible for inclusion in the up-titration cohort that was titrated up to baricitinib 4 mg. At week 76, after 24 weeks of titration up treatment on baricitinib 4 mg, ██ of ██ patients (██████ ███ ██ █████ ██ █████) attained a SALT score of 20 or less.
ClinRO Measures for EB and EL Hair Loss
At week 52, 39.4% and 27.9% of patients receiving baricitinib 4 mg and baricitinib 2 mg, respectively, attained a ClinRO measure for EB hair loss (0 or 1) (with ≥ 2-point improvement from baseline through week 52 among patients with a score of ≥ 2 at baseline) in Study BRAVE-AA1. Similarly, 49.7% and 16.3% of patients receiving baricitinib 4 mg and baricitinib 2 mg, respectively, attained a ClinRO measure for EB hair loss (0 or 1) (with ≥ 2-point improvement from baseline through week 52 among patients with a score of ≥ 2 at baseline) at week 52 in Study BRAVE-AA2.
At week 52, 40.7% and 21.6% of patients receiving baricitinib 4 mg and baricitinib 2 mg, respectively, attained a ClinRO measure for EL hair loss (0 or 1) (with ≥ 2-point improvement from baseline through week 52 among patients with a score of ≥ 2 at baseline) in Study BRAVE-AA1. Similarly, 50.7% and 30.3% of patients receiving baricitinib 4 mg and baricitinib 2 mg, respectively, attained a ClinRO measure for EL hair loss (0 or 1) (with ≥ 2-point improvement from baseline through week 52 among patients with a score of ≥ 2 at baseline) at week 52 in Study BRAVE-AA2.
Harms Results
Study BRAVE-AA1: Up-Titration Cohort
TEAEs were reported for ████ █ ███ ██ ████ of patients who up-titrated to baricitinib 4 mg up to week 76. Most events were mild in severity. █████ ████ █ ████████ ███ ████████ ████ ████ ████ ██████ ██████ ███ ███████ discontinued the study drug and study because of ██████ ████. There were no deaths in the up-titration cohort.
Study BRAVE-AA2: Randomized Down-Titration Cohort
For both treatment groups, most events were mild or moderate in severity. Up to week 76, of the patients who remained on baricitinib 4 mg, | ████████ ████████ ████ ███ ███ █ ███████ ████ █████ ███ █ ██████ ████. ██ ███████ ██████ ███ ████ ████████ for patients who down-titrated to baricitinib 2 mg. ██████████ ████████████ █████ ████ ██ ███ █████ ███ ██ ███ ██ ███ ████ ██████ There were no deaths in the randomized down-titration cohort.
Study BRAVE-AA2: Up-Titration Cohort
TEAEs were reported for █████ ███ ██ ███ of patients who titrated up to baricitinib 4 mg up to week 76. Most events were mild or moderate in severity; | ███████ ████████ █ ██████ █████ ██ ████████ ████████ ████ ██ ████████████ █████ ████ ██ ███ █████ ███ ██ ████ There were no deaths in the up-titration cohort.
Critical Appraisal
Both the BRAVE-AA1 and BRAVE-AA2 extension studies were limited by their noncomparative design. At time points after 36 weeks, there remained no randomized comparison to placebo, challenging causal interpretations. Although the patients and investigators remained blinded to the assigned interventions, there is still the possibility that patients may be able to infer treatment assignment because of differences in efficacy (relative to placebo during the double-blind treatment phase). As such, there may be a risk of bias in the reporting of efficacy outcomes that required some level of subjective judgment by the evaluators (e.g., ClinRO) and harms outcomes, although the extent and direction of bias cannot be predicted. It is unlikely that bias would be introduced for the SALT response, since it is measured objectively. Finally, missing information such as pooling strategies constrained a robust critical appraisal; hence, a firm conclusion cannot be drawn on the long-term efficacy and safety. Since both Study BRAVE-AA1 and Study BRAVE-AA2 included rollover patients consistent with their characteristics at entry in the core study, it is reasonable to expect similar limitations to the generalizability of study results are relevant to the long-term extension phase. Further, some outcomes that are important to patients (e.g., HRQoL, anxiety, depression) could not be evaluated against a placebo control beyond the 36-week double-blind treatment phase because of discontinuation of the placebo in nonresponders. As such, there is limited evidence for the effect of baricitinib 2 mg or baricitinib 4 mg on these outcomes for time points after 36 weeks (including for patients who up-titrated or down-titrated). Despite longer follow-up for harms, some rare harms (e.g., malignancies) may still not be fully captured.
Indirect Comparisons
No indirect comparative evidence was submitted by the sponsor. The sponsor noted that before the regulatory approval of baricitinib for severe AA in Canada, the standard of care included off-label therapies and nonpharmacological options. The sponsor further noted that the pivotal trials of baricitinib were placebo-controlled and given that no approved comparator drugs were available at the time of the phase III clinical development conduct, there is no indirect comparative efficacy evidence to present in this section.
Studies Addressing Gaps in the Evidence From the Systematic Review
Description of Studies
Additional insights into the effects of baricitinib in patients with AA were sought for males older than 60 years and females older than 70 years that were not included in the pivotal trials. A retrospective chart study (n = 14) by Tang et al. (2024)12 describing baricitinib treatment in patients older than 65 years was included. A retrospective chart review of 36 patients conducted by Moreno-Vilchez et al. (2024)13 and a retrospective chart review of 95 patients in Japan by Numata et al. (2024)14 provided additional data about the effects of baricitinib.
Efficacy Results
Tang et al. (2024)
After a mean (SD) duration of 18.5 (11.9) months, a 72.0% reduction in the mean SALT score from baseline was observed. Moreover, 11 of 14 (78.6%) patients attained a SALT score of less than 10 after a mean duration of 18.6 months where SD is not reported.
Numata et al. (2024)
The percentage of patients in the entire cohort who attained a SALT score of 20 or less at week 12, week 24, and week 36 was 6.4% (6 of 94) of patients, 35.4% (28 of 79) of patients, and 46.7% (21 of 45) of patients, respectively.
The complete response rate (a SALT score of 0) at week 24 and week 36 was 1.3% (1 of 79) of patients and 6.7% (3 of 45) of patients, respectively.
Moreno-Vilchez et al. (2024)
In this study, 58.8% of patients attained a SALT score of 20 or less at week 24. The response continued for 52 weeks, with 66.6% of patients classified as responders. Additionally, the study compared the SALT scores between patients treated with monotherapy and those who received adjuvant treatment.
Harms Results
Tang et al. (2024)
Adverse effects of baricitinib were moderate and included the reactivation of herpes zoster (n = 1), elevated creatine kinase (n = 1), and grade 2 neutropenia (n = 1). Only 1 patient required a reduction in the dose of baricitinib because of grade 2 neutropenia. No cases of venous thromboembolism, MACE, or malignancy were reported.
Numata et al. (2024)
Infectious complications occurred in 6 patients during the initial 12 weeks. Herpes simplex and COVID-19 (severe acute respiratory syndrome coronavirus 2) occurred in 1 patient and 5 patients, respectively. No other severe complications occurred during the entire 36-week course.
Moreno-Vilchez et al. (2024)
Overall, AEs were mild. Three patients were discontinued because of inadequate treatment response: 2 patients at week 52 and 1 patient at week 76. Additionally, 1 patient had temporary lymphopenia with methotrexate treatment.
Critical Appraisal
Limitations of the 3 studies included their retrospective designs and small sample sizes. Moreover, most patients were treated with concomitant treatments, and without a randomized comparison group, it is not possible to attribute the observed effects to baricitinib with certainty. Furthermore, information such as treatment exposure and concomitant treatments in Numata et al. were not reported. Both Tang et al. and Numata et al. included patients with moderate-to-severe AA; however, patients with moderate AA would not be candidates for baricitinib treatment in Canada. The results of these studies may not be generalizable to patients with severe or very severe AA, which may be more difficult to treat compared with moderate AA. The study by Numata et al. included patients exclusively from Japan whereas the study by Moreno-Vilchez et al. included patients exclusively from Spain (in 2 centres). It is uncertain whether results from small samples of patients treated in these countries would be generalizable to patients living in Canada, given the potential for differences in standard of care in these countries.
Conclusions
Direct comparative evidence from 2 pivotal double-blind RCTs (Study BRAVE-AA1 and Study BRAVE-AA2) demonstrated that 36 weeks of baricitinib 4 mg treatment resulted in the clinically important regrowth of scalp hair compared with placebo in adults with severe or very severe AA. Benefits of the regrowth of EB and EL hair were shown but were less certain because of study limitations. Results also favoured baricitinib 2 mg treatment with respect to the regrowth of scalp and EB hair, although there was some uncertainty on whether the magnitude of change was clinically important because of imprecision. No definitive conclusion can be drawn regarding the direction and magnitude of the effects of baricitinib treatment on anxiety, depression, and HRQoL because of important methodological limitations (potential attrition bias and a lack of evidence supporting the validity of the instruments used in patients with AA) and concerns with indirectness (for anxiety and depression outcomes). The benefits of baricitinib in hair regrowth appeared to be sustained through week 104 in the trials, although analyses beyond week 36 were noncomparative, which precluded firm conclusions. No conclusions can be drawn regarding the clinical benefits of baricitinib in older adults with severe AA from a sponsor-submitted retrospective chart review study (Tang et al. [2024]) because of a small sample size and single-arm study design. No notable concerns with the safety profile of baricitinib were identified based on results from the pivotal trials through week 104. No direct or indirect comparative evidence for baricitinib versus systemic treatments currently reimbursed by the public drug plans (immunosuppressants) were submitted.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of baricitinib 2 mg and baricitinib 4 mg oral tablets in the treatment of adult patients with severe AA.
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
AA is a chronic autoimmune disease characterized by nonscarring hair loss at the scalp as well as the loss of EB, EL, beard, pubic, or axillary hair. AA is a relapsing and remitting condition where spontaneous hair regrowth has been reported at the beginning of the disease (mild disease) progressing to extensive, chronic hair loss that does not remit without treatment.1 Up to 50% of patients will recover within 1 year even without treatment, but as many as 85% of individuals experience multiple episodes of hair loss.15 Progression from patchy AA to more severe forms (i.e., total hair loss at the scalp or body) occurs in 14% to 25% of patients, with full recovery in less than 10% of patients.1,16,17
The onset of hair loss in AA is typically rapid and the progression is unpredictable.1 In a systematic review of the epidemiology and burden of AA, the mean age of onset was found to range between 25.2 years and 36.3 years across studies. A total of 83% to 88% of individuals experienced disease onset by aged 40 years and 40.2% of individuals by aged 20 years.18
Involvement of other body areas (aside from the scalp) may occur as AA progresses or may occur as an isolated incident.19 AA sometimes manifests as a partial or complete loss of EB, EL, beard, pubic, or axillary hair, all of which can present unique challenges to patients.20,21 The loss of EBs or ELs or both may result in a dramatically altered appearance and eye irritation because of the loss of the physical barrier that helps prevent sweat and foreign particles from entering the eyes.22 Other ophthalmological issues secondary to EB or EL loss include ocular surface inflammation, dryness, and blepharitis. Since ELs and EBs also serve to define nonverbal communication and self-expression, their loss may have both a functional and psychological impact on patients’ quality of life.21,23 The skin in AA lesions does not typically show signs of inflammation or symptoms, although slight redness in the affected area or pruritus during periods of active hair loss have been reported.24,25
While the etiology of AA is unknown, it has been suggested that a triggering factor leads to the collapse of hair follicle immune privilege (IP), where functioning IP protects hair follicles from unwanted immune responses. In genetically predisposed individuals, the loss of IP results in characteristic hair loss.1,19 Since hair follicles are not destroyed by the disease process, the potential for hair regrowth is in theory retained in patients with AA.1
At present, there are no Canadian epidemiology data. When considering lifetime prevalence, approximately 2% (based on data from 1990 to 2009) of the general population will develop AA at some point in their lives, affecting men and women of all ages and races.1,4,26,27 Data on the prevalence of AA by severity are very limited. The cross-sectional study by Benigno et al. (2020) in a representative sample of the US population showed that the overall prevalence of AA was 0.21%, with 0.12% for mild disease (a SALT score of 50 or less), 0.09% for severe disease (a SALT score greater than 50), and 0.04% for total or near-total scalp or all-body hair loss subgroup in moderate-to-severe patients.2 From this data, it was estimated that among patients living with AA in Canada, 43% are living with severe disease.
AA is diagnosed based on presenting features and once other causes of hair loss have been excluded.25 Typical clinical features of AA that support a diagnosis include patches of hair loss and the presence of so-called “exclamation mark” hairs that are short and broken, and taper proximally.19 In addition, the pull test (the examiner grasping approximately 40 hairs to 60 hairs between their thumb, index, and middle fingers, and gently pulling them away from the scalp) can be used to diagnose hair loss. A positive result is attained if greater than 10% of the hairs are pulled out, indicating hair shedding. It is, however, hard to standardize this test, and a negative result does not always rule out an AA diagnosis.28 While further testing is often not required beyond careful evaluation of the patients’ clinical history and physical examination, additional investigations such as a dermoscopy or histopathology may sometimes be used to confirm the diagnosis.1,29 It has been suggested that standardized and objective measures be used to describe disease severity.30 However, there is no unique definition of disease severity for AA and the driver for the definition of AA severity is the extent of scalp hair loss.31 The main prognostic factor in patients with AA appears to be the extent of hair loss, especially at presentation.19,31 There is a tendency for severe patterns of AA to worsen over time.19,31 Additionally, an earlier age of disease onset corresponds to an increased lifetime risk of extensive disease (i.e., onset in the first 2 decades is often associated with severe AA).1,18 The prognosis of patients with severe AA is poor, even on therapy.25,31-34
Standards of Therapy
Canadian clinical practice guidelines for AA are not available to date. As per input from the clinical experts we consulted, in Canada, clinicians consider systemic drugs for the treatment of adults with severe AA. These include conventional immunosuppressants (cyclosporine, methotrexate, azathioprine, and mycophenolate mofetil) and JAK inhibitors. Ritlecitinib is a JAK inhibitor recently approved by Health Canada for the treatment of adults and adolescents aged 12 years and older with severe AA. Tofacitinib, upadacitinib, and abrocitinib are off-label JAK inhibitor treatments for severe AA; upadacitinib and abrocitinib are approved for the treatment of AD and may be used in patients with concurrent atopic dermatitis, as per clinical expert input. Conventional immunosuppressants are off-label treatments that are currently reimbursed by the public drug plans for the treatment of severe AA while ritlecitinib, tofacitinib, upadacitinib, and abrocitinib are currently not. The clinical experts noted that systemic treatments target the underlying immune mechanisms of AA, although they do not cure the condition and are associated with a high risk of relapse upon treatment discontinuation or dose reduction. In addition, oral corticosteroids (prednisone) may be used for short-term treatment in patients with AA that is rapidly progressing.
The clinical experts noted that, before the initiation of systemic therapy, patients with severe AA would typically have already received off-label topical medications (potent corticosteroids, minoxidil, a calcineurin inhibitor for EBs and beard specifically, and prostaglandin analogue for ELs specifically) and/or intralesional corticosteroids, and would continue to do so while on systemic therapy. While topical medications and intralesional corticosteroids are effective treatments in some patients with mild or localized AA, they are not effective in patients with severe AA when used alone and are reserved as an adjunct treatment to systemic drugs. Other treatments such as topical anthralin and contact immunotherapy with diphenylcyclopropenone are no longer commonly used in adults with severe AA in clinical practice because of low efficacy, difficult application, and the need for long-term treatment, according to the clinical experts. Phototherapy is not part of standard of care in Canada, as per clinical expert input. Nonpharmacological intervention with camouflage techniques (e.g., wig, hairpiece, EB tattooing) are commonly used to help patients cope with the impact of AA on altered body appearance.
According to the clinical experts, the treatment goals for severe AA are to attain a cosmetically meaningful regrowth of hair, improve HRQoL, avoid serious AEs, and if possible, reduce the risk for relapse with dose reduction or discontinuation of the systemic drug.
Drug Under Review
Key characteristics of baricitinib are summarized in Table 4 with other treatments available for severe AA in adult patients.
Baricitinib is available as 2 mg and 4 mg oral tablets and is approved by Health Canada for the treatment of adult patients with severe AA (the Notice of Compliance date was January 26, 2024). Baricitinib is a selective and reversible inhibitor of Janus kinase 1 and Janus kinase 2. JAKs are enzymes that transduce intracellular signals from a cell surface receptor for a number of growth factors involved in hematopoiesis, inflammation, and immune function. Within the intracellular signalling pathway, JAKs phosphorylate and activate signal transducers and activators of transcription, which modulate intracellular activity, including gene expression. Baricitinib modulates these signalling pathways, thereby reducing the phosphorylation and activation of signal transducers and activators of transcription thought to be involved in the pathogenesis of AA.35 The sponsor’s reimbursement request aligns with the Health Canada–approved indication. Baricitinib is also indicated for the treatment of adults with rheumatoid arthritis. Baricitinib has not been previously reviewed by CDA-AMC for the treatment of AA. However, baricitinib was previously reviewed by us for the treatment of rheumatoid arthritis and received a recommendation to reimburse with conditions on August 2, 2019. The recommended dose is 2 mg once daily and, if the response to treatment is not adequate, the dose may be increased to 4 mg once daily. For patients with nearly complete or complete scalp hair loss, and/or substantial EL or EB hair loss, a starting dose of 4 mg once daily may be considered. Once a patient attains an adequate response to treatment with 4 mg, a decrease in dose to 2 mg once daily may be considered. When clinically advisable, the lowest effective dose should be used to minimize AEs. The discontinuation of therapy should be considered if patients do not show evidence of therapeutic benefit after 36 weeks of treatment. Dose adjustment for baricitinib in patients with renal impairment is recommended. A combined use with other JAK inhibitors, biologic immunomodulators, or potent immunosuppressants such as azathioprine and cyclosporine is not recommended.35
Table 4: Key Characteristics of Baricitinib, Minoxidil, Corticosteroids, and Immunosuppressants
Characteristic | Baricitinib | Minoxidil | Corticosteroid | Immunosuppressant |
|---|---|---|---|---|
Examples | NA | NA | Mometasone, triamcinolone acetonide, prednisolone | Cyclosporine, methotrexate, azathioprine, mycophenolate mofetil |
Mechanism of action | Selectively and reversibly inhibits JAK, which in turn reduces phosphorylation and the activation of STATs that are involved in gene expression. It attenuates proinflammatory response and cytokine production. | Unknown May cause vasodilation and stimulate hair follicles | All: Anti-inflammatory Mometasone: Antipruritic, vasoconstrictive Triamcinolone acetonide: Modifies immune response Prednisolone: Immunosuppressive. | Cyclosporine, azathioprine: Unknown Methotrexate: Inhibits DHFR, the enzyme that reduces folic acid to tetrahydrofolic acid, thereby interfering with DNA synthesis, repair, and cellular replication Mycophenolate mofetil: Selectively and reversibly inhibits IMPDH, thereby interfering with the cytokine-mediated signalling pathway to DNA synthesis and proliferation |
Indicationa | Treatment of adult patients with severe alopecia areata. | 2% solution: Treatment of male androgenetic alopecia (male pattern hair loss) on the top of the scalp 5% foam: Same indication as for both males and females Oral: Off-label | Triamcinolone acetonide: Intradermal/ intralesional administration is indicated for alopecia areata. Mometasone, prednisolone: None (off-label) | None (off-label) |
Route of administration | Oral | Topical and oral | Topical (mometasone), intralesional injection (triamcinolone acetonide), oral (prednisolone) | Oral |
Recommended dose | 2 mg once daily; up to 4 mg once daily if inadequate response May start with 4 mg once daily for patients with (nearly) complete hair loss and/or substantial eyelash hair loss or eyebrow hair loss. Renal impairment:
| 2% solution: 1 mL applied twice daily to the scalp 5% foam: Half capful (1 g) applied to the scalp once (female) or twice (male) daily Oral: 20 mg once daily | Triamcinolone acetonide: Varies depending on the specific disease but limited to 1 mg (0.1 mL) per injection site Mometasone, prednisolone: Not available for these | Cyclosporine: 4 mg/kg once daily Azathioprine: 2 mg/kg once daily for 1 year Methotrexate: 20 mg per week Mycophenolate mofetil: 1,000 mg b.i.d., for 1 year |
Serious adverse effects or safety issues | Serious warning and precaution for serious infections, malignancies, MACE, and thrombosis | Rash, tachycardia, hyperventilation, bronchitis, pharyngitis, sinusitis, flu syndrome, pyrexia | Skin thinning, long-term side effects such as endocrine, metabolic, cardiovascular, ophthalmologic, and immune-related adverse events, as well as carcinogenesis and mutagenesis | Carcinogenesis and mutagenesis Increased susceptibility to infections Effects on reproduction and pregnancy Cardiovascular, endocrine, metabolic, immune, neurologic, hepatic, renal, and dermatologic side effects |
Other | Combined use with other JAK inhibitors, biologic immunomodulators, or potent immunosuppressants such as azathioprine and cyclosporine is not recommended. Lab monitoring is required. | Patients with known CVD or cardiac arrhythmia should contact a physician before using. | Contraindicated in systemic infections. | Should be used under the supervision of physicians experienced in immunosuppressive therapy Lab monitoring is required. |
b.i.d. = twice a day; CVD = cardiovascular disease; DHFR = dihydrofolate reductase; eGFR = estimated glomerular filtration rate; IMPDH = inosine monophosphate dehydrogenase; JAK = Janus kinase; MACE = major adverse cardiac event; NA = not applicable.
aThis is a Health Canada–approved indication that is relevant to the reimbursement request.
Sources: Sponsor’s Summary of Clinical Evidence, and Health Canada–approved product monographs for baricitinib, minoxidil, and triamcinolone acetonide.9,35-37
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full original patient input that we received has been included in the Perspectives of Patients, Clinicians, and Drug Programs section of this report.
We received 1 patient group submission from CANAAF. CANAAF was registered as a charitable organization in 2010 and is described as the voice for all patients and families affected by AA living in Canada. CANAAF collected data on the psychosocial and emotional impact of AA from peer-reviewed literature, as well as patient perspectives on AA from patient reports and support sessions.
CANAAF commented that AA is incredibly burdensome on a patient’s mental health and quality of life, and the disease causes disfiguring hair loss that occurs unexpectedly and can progress rapidly. Based on a patient report, CANAAF further stated that the anxiety, depression, and other resultant psychological conditions are not minor in nature; therefore, the loss of hair can create layers of stigma and misunderstandings. Short hair or baldness may be associated with a preference for an “edgy” look or having a certain sexuality, which may not be accurate. Those with this disease may feel less feminine or less masculine without hair. Children and teenagers may experience bullying. In addition, CANAAF revealed that there is a significant financial burden associated with AA; this was supported by the findings of a CANAAF community alopecia patient focus group conducted in 2023. The most significant cost item was wig purchase and maintenance, which can cost more than $2,500 a year. Some patients experienced significant impacts on their ability to work.
Based on the literature, CANAAF identified limitations of the currently available treatments for AA, including topical corticosteroids (limited effectiveness, only effective for patients with very limited AA, difficult product application, and scalp irritation), intralesional corticosteroids (painful injections and limited drug coverage by drug plans), oral corticosteroids (variable success rates, high relapse rate, limited drug coverage, and unfavourable side effects), topical minoxidil (nondurable benefits for very mild AA, and AEs such as excessive hair growth on body parts other than the site of application, irritation, and allergic contact dermatitis), oral minoxidil (systemic AEs relating to its antihypertensive property and limited drug coverage), and systemic immunosuppressants (variable effectiveness; a risk of organ toxicity, infection, and malignancy; concomitant administration of oral corticosteroids required for some drugs; and limited drug coverage).
CANAAF identified a need for an effective treatment option that could result in full and sustained hair growth and alleviate anxiety and depression associated with AA. CANAAF believed that baricitinib may fulfill this need by serving as an effective treatment that has a favourable side effect profile and is easy to administer. The group noted that most patients regrew all their hair with baricitinib treatment. CANAAF also noted that the side effect profile of baricitinib is much more favourable compared to existing treatments. Baricitinib is a much easier treatment option for patients as it only requires that they take 1 pill once a day. This is in comparison to other treatments that must be applied topically, injected (often by a health care professional), or taken orally more than once a day.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All our review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of AA.
Unmet Needs
According to the clinical experts we consulted, currently available systemic therapies for severe AA are associated with poor efficacy and, thus, fail to attain cosmetically meaningful hair regrowth and improvement in HRQoL in patients with severe AA. As well, the clinical experts noted that the existing systemic treatments are associated with a risk of relapse with dose reduction and/or discontinuation, as well as AEs. In particular, SAEs from the long-term use of conventional systemic immunosuppressants is a notable concern. Also, patient access to emerging therapies, such as ritlecitinib, is currently limited, as per clinical expert input.
Place in Therapy
The clinical experts noted that JAK inhibitors, such as baricitinib, bring a novel approach and mechanism of action to the treatment of severe AA; although similar to other systemic immunomodulators, baricitinib is not a curative treatment. The clinical experts noted that because of the limited efficacy of older systemic immunomodulators (e.g., methotrexate, cyclosporine), it is rational to use baricitinib (and JAK inhibitors in general) as a first-line systemic therapy in severe AA, rather than as the last line of treatment after the failure of older systemic immunomodulators. This is based on their clinical experience with the effectiveness of JAK inhibitors relative to conventional immunosuppressants and the paucity of published data on immunosuppressants in patients with severe AA. There may be exceptions where an immunosuppressant is chosen ahead of a JAK inhibitor — for example, in patients with comorbid conditions such as psoriasis — but in the clinical experts’ opinion, most patients should receive baricitinib as a first-line systemic treatment.
The clinical experts noted that baricitinib is not the first JAK inhibitor used by clinicians in Canada for the treatment of severe AA. Tofacitinib is used off-label and ritlecitinib is another treatment for severe AA that has been recently approved by Health Canada. At present, the treatment choice would be determined based on patient access to and reimbursement for a JAK inhibitor rather than on patient-specific clinical characteristics, as per clinical expert input. The clinical experts anticipated that over time, as the reimbursement environment evolves and as comparative efficacy and safety data accumulate, the decision would become a clinical one.
The clinical experts noted that it would be appropriate to use baricitinib in combination with topical treatments and/or intralesional corticosteroids but not in combination with other immunomodulators, except for prednisone where concomitant use with baricitinib may be appropriate.
Patient Population
The clinical experts noted that at present, disease severity is evaluated based on a global assessment and that no specific clinical tools are used; however, this may change as new treatments are adopted in clinical practice and SALT scores become a requirement for reimbursement. In the clinical experts’ opinion, patients who have severe AA with scalp involvement as reflected by a SALT score of 50 or more and who have a current episode of AA with a duration of greater than 1 year, but less than 10 years are potential candidates for baricitinib treatment. The clinical experts noted that the diagnosis of AA is readily made by a dermatologist, typically involving, for example, the use of the hair-pull test, trichoscopy, and/or biopsy; misdiagnosis is frequent among nondermatologists. They noted that there is no uniformly accepted definition of severe AA, although they considered a SALT score of 50 or more to be reflective of severe AA and noted that this definition has been used in clinical trials of other JAK inhibitors for the treatment of AA. They also noted that adhering to the inclusion criterion on the duration of a current episode that was used in the pivotal trials (i.e., more than 6 months and less than 8 years in duration) would be reasonable when selecting treatment candidates.
In terms of eligible age group, the clinical experts recognized that baricitinib is currently approved only in the adult population (aged 18 years or older), although they noted that the off-label use of baricitinib in the adolescent population (aged 12 years to 17 years) may also be reasonable from a clinical perspective. They anticipated that most clinicians would not prescribe baricitinib to adolescents until regulatory approval is granted in this population. The clinical experts also discussed the use of baricitinib in older adults (i.e., older than 60 years for males or older than 70 years for females, categories that were excluded from the pivotal trials). One clinical expert considered the use of baricitinib in this age group to be reasonable. The other clinical expert suggested restricting the use of baricitinib as per age restriction in the pivotal trials because of a lack of clinical trial data and unknown treatment benefits. This clinical expert anticipated that the older adults would not benefit from baricitinib treatment as much as younger patients since older adult patients tend to have other concurrent causes of hair loss that are not expected to be responsive to baricitinib treatment. Also, this clinical expert noted that AA has less impact on the HRQoL of older adults since camouflage management is typically more acceptable in this age group and most older adults have learned to adapt to AA.
Assessing the Response Treatment
The clinical experts noted that the outcome measures used in clinical trials are not aligned with clinical practice. The clinical experts noted that currently, a SALT score is typically not calculated in clinical practice; instead, a clinical judgment is made based on a global assessment by the clinician and the patient to determine whether cosmetically meaningful hair regrowth has occurred following treatment. The clinical experts noted that what constitutes cosmetically meaningful regrowth of hair varies from patient to patient. As well, in patients with rapidly progressing severe AA, the stabilization or cessation of further hair loss could be a clinically meaningful response to treatment, according to the clinical experts. For drug reimbursement, the clinical experts felt that it is reasonable to define meaningful response to treatment as attainment of a SALT score of 20 or less at week 36, consistent with the pivotal trials of baricitinib.
Discontinuing Treatment
The clinical experts noted that it would be reasonable to consider the discontinuation of baricitinib treatment in patients who fail to achieve cosmetically acceptable hair regrowth at 36 weeks, have further loss of hair at 36 weeks, experience severe AEs deemed to be related to the use of a JAK inhibitor (e.g., infection, hematologic abnormality, biochemical abnormality, hypersensitivity), or develop an intercurrent condition that makes the discontinuation of a JAK inhibitor advisable (e.g., malignancy).
Prescribing Considerations
Clinical experts noted that baricitinib treatment could be prescribed by dermatologists with experience in diagnosing, treating, and monitoring patients with severe AA. The clinical experts felt that it would not be appropriate for family physicians to prescribe baricitinib treatment at this time because of the risks of misdiagnosis and the inappropriate selection of patients for treatment, and the need for routine monitoring associated with JAK inhibitor use. The starting dose would likely be determined based on clinical judgment as per clinical expert input.
Clinician Group Input
We received no clinician group input for the drug under review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CDA-AMC reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts we consulted are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
There is currently no approved standard of care treatment for severe AA. Off-label treatments include intralesional corticosteroids, potent topical corticosteroids, systemic corticosteroids, conventional immunosuppressants, and minoxidil. Baricitinib treatment was compared with placebo in patients with severe AA in the phase II and phase III Study BRAVE-AA1 and the phase III Study BRAVE-AA2. These were multicentre, randomized, double-blind, placebo-controlled trials with primary efficacy analysis at 36 weeks and extension phases up to a total of 200 weeks (about 4 years). Question for clinical experts: What is the appropriate comparator for patients with severe AA? | The clinical experts noted that systemic treatments are relevant comparators of baricitinib. They noted that from a clinical perspective, oral JAK inhibitors, including ritlecitinib (a recently approved JAK inhibitor for the treatment of severe AA) and tofacitinib (an off-label treatment for severe AA) are the most appropriate comparators for baricitinib. As well, upadacitinib and abrocitinib may be used off-label for the treatment of severe AA in patients with coexisting atopic dermatitis. However, these treatments are not currently reimbursed by the public drug plans for the treatment of severe AA in Canada. Conventional immunosuppressants (e.g., methotrexate, azathioprine, mycophenolate mofetil, cyclosporine) are currently used by clinicians as off-label treatments for severe AA and are currently reimbursed by public drug plans. The clinical experts did not consider oral minoxidil as a relevant comparator of baricitinib since it is not used as monotherapy in the treatment of severe AA. The clinical expert did not consider systemic corticosteroids as relevant comparators since they are used for short-term treatment. The CDA-AMC team considered input from the clinical experts and noted that systemic treatments currently reimbursed by public drug plans (i.e., immunosuppressants including cyclosporine, methotrexate, azathioprine, and mycophenolate mofetil) are relevant comparators of baricitinib for the purpose of this review. These systemic drugs may be used with or without topical corticosteroids, intralesional corticosteroids, and/or oral minoxidil, as adjunctive treatments. |
This is the first reimbursement review for a medication indicated for severe AA. Some jurisdictions may have formulary exclusions for cosmetic drugs and/or hair growth stimulants. Question for clinical experts: Have you encountered any barriers in access to medications for your patients within the jurisdictions? | The clinical experts noted that in their practice, patients have not encountered significant barriers in access to medications used to treat AA. According to the clinical experts, currently, access to ritlecitinib is limited to patients who participated in clinical trials or are eligible for a support program offered by the drug sponsor at the request of their dermatologists. One clinical expert further noted that access to a dermatologist could be difficult in their province since many practices are closed to all patients with hair disorders. |
Considerations for the initiation of therapy | |
Severe AA is defined as ≥ 50% scalp hair loss. The BRAVE-AA1 and BRAVE-AA2 trials included patients with a current episode of severe AA of > 6 month in duration as measured by the SALT scale. The severity of disorders ranges from small patches of alopecia on any hair-bearing area to the complete loss of scalp, eyebrow, eyelash, and body hair. Questions for clinical experts: 1. Is the severity definition provided previously the standard for eligibility for the initiation of baricitinib in clinical practice? 2. Would you be able to comment on ≥ 50% scalp hair loss vs. ≥ 50% hair loss as an eligibility requirement for patients? | 1. According to the clinical experts, it is the standard to require ≥ 50% scalp hair loss for the initiation of systemic treatment (e.g., baricitinib) in clinical practice. 2. The clinical experts favoured the use of ≥ 50% scalp hair loss as a reimbursement criterion for treatment initiation. The clinical experts noted that focusing on scalp hair loss would capture most patients who would be treated with baricitinib since scalp hair is generally the treatment target. The clinical experts did not favour the use of ≥ 50% hair loss (without regard to the site of hair loss) as a reimbursement criterion since it would include a lot of patients who would not be offered systemic treatment routinely in clinical practice (e.g., patients with eyebrow and/or eyelash involvement whose SALT score is less than 50, patients with hair loss restricted to the body, patients with beard hair loss). |
Inclusion criteria of the pivotal trials included the following:
Questions for clinical experts:
|
|
Question for clinical experts: Should patients receive prior systemic therapies including corticosteroids, methotrexate, and cyclosporine before accessing baricitinib? | In the clinical experts’ opinion, JAK inhibitors should be positioned as a first-line systemic therapy in patients with severe AA, based on their clinical experience in the effectiveness of JAK inhibitors relative to conventional immunosuppressants and the paucity of published data on immunosuppressants in patients with severe AA. |
Question for clinical experts: If the treatment was interrupted and the patient relapsed, would the patient restart treatment immediately? | The clinical experts noted that relapse of the condition following dose reduction, or the interruption of treatment is a significant risk with all systemic treatments. In the case of relapse, patients and clinicians would be motivated to restart treatment immediately; however, the recapture of clinical benefit is not guaranteed, as per the clinical experts. |
Considerations for the continuation or renewal of therapy | |
Questions for clinical experts:
| 1 and 2: The clinical experts noted that refractory disease and the absence of clinical benefit are established when the patient shows no evidence of cosmetically acceptable hair regrowth at 36 weeks or the progression of hair loss at 36 weeks. For drug reimbursement, the clinical experts felt that it is reasonable to define response to treatment as attaining a SALT score of 20 or less at week 36, consistent with the pivotal trials of baricitinib. 3. The clinical experts noted that it would be reasonable to define disease progression as any increase in the SALT score and/or the development of new sites of hair loss, particularly with eyebrow and eyelash involvement. |
Considerations for the discontinuation of therapy | |
Questions for clinical experts:
|
|
Considerations for the prescribing of therapy | |
Question for clinical experts: Which prescriber specialty would initiate medication for severe AA? | The clinical experts noted that it would be appropriate for dermatologists with experience in diagnosing, treating, and monitoring patients with severe AA to prescribe baricitinib treatment. |
This relates to the consideration of what medications are not to be used in combination with baricitinib. As per the product monograph, the use of baricitinib in combination with other JAK inhibitors, biologic immunomodulators, or with potent immunosuppressants such as azathioprine and cyclosporine is not recommended. | For CDEC consideration. Our review team noted that the use of other JAK inhibitors and systemic immunosuppressants or immunomodulators was prohibited in the pivotal trials. In addition, the use of corticosteroids (systemic, intralesional, or topical) was prohibited, although as per clinical expert input, the use of corticosteroids concomitantly with baricitinib is reasonable from a clinical perspective. |
Generalizability | |
Question for clinical experts: If the disease severity is < 50% scalp hair loss or < 50% hair loss, would baricitinib have a role or place in therapy? At what point would you consider patients with this disease severity to be eligible for baricitinib therapy? | The clinical experts anticipated that over time, as more data accumulated, it is likely that baricitinib would have a role in therapy in patients with a SALT score of less than 50%; however, it is likely not a consideration at this time. |
Care provision issues | |
Baricitinib is associated with potential costs to the health care system: assessing patients with viral hepatitis, latent tuberculosis, renal insufficiency, or pregnancy before the start of therapy; doing baseline and periodic monitoring of CBC with differential, platelets, liver enzymes, and lipid levels; doing periodic assessments of the signs and symptoms of infection, skin examination (in patients with an increased risk of skin cancer), and abdominal symptoms (for patients at risk of gastrointestinal perforation). | For CDEC consideration. |
System and economic issues | |
The provision of this drug in the first-line setting may translate into an increased budget impact ($1,716.17 per 30 tablets for baricitinib 2 mg, $3,432.34 per 30 tablets for baricitinib 4 mg, $20,400 to $40,800 per year) relative to other off-label systemic therapy × number of patients. | For CDEC consideration. |
Baricitinib concluded with a successful LOI for rheumatoid arthritis. | For CDEC consideration. |
AA = alopecia areata; CBC = complete blood count; CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; LOI = letter of intent; JAK = Janus kinase; SALT = Severity of Alopecia Tool; vs. = versus.
Clinical Evidence
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of baricitinib 2 mg and baricitinib 4 mg oral tablets in the treatment of adult patients with severe AA. The focus has been placed on comparing baricitinib to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of baricitinib is typically presented in 4 sections with our critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. Our assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. The third section typically includes indirect evidence from the sponsor; however, such evidence was not submitted for this review. The fourth section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following is included in our review and appraised in this document:
2 pivotal RCTs identified in the sponsor-conducted systematic review (Study BRAVE-AA1 and Study BRAVE-AA2)6
long-term extension results of Study BRAVE-AA1 and Study BRAVE-AA238
3 additional studies addressing gaps in evidence (Tang et al. [2024],12 Numata et al. [2024],14 and Moreno-Vilchez et al. [2024]13).
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
Characteristics of the included studies are summarized in Table 6.
Two pivotal, multicentre, double-blind RCTs (Study BRAVE-AA1, N = 654; Study BRAVE-AA2, N = 546)6 aiming to assess the efficacy and safety of baricitinib relative to placebo in adult patients with severe or very severe AA were identified by the systematic review conducted by the sponsor. Study BRAVE-AA1 was an adaptive phase II and phase III trial; the phase II portion of Study BRAVE-AA1 was designed to determine the doses of baricitinib for use in the phase III portion of the study and in the phase III BRAVE-AA2 trial. Study BRAVE-AA1 was conducted in 70 study sites in North America and Asia. Study BRAVE-AA2 was conducted in 84 sites in North America, South America, Asia, and Australia. None of the trials included sites in Canada. The studies are ongoing; patient enrolment began in September 2018 in Study BRAVE-AA1 and in July 2019 in Study BRAVE-AA2. The analyses presented in this report are based on a database lock date of February 2, 2021, for Study BRAVE-AA1 and February 19, 2021, for Study BRAVE-AA2.
Study BRAVE-AA1
As shown in Figure 1, the phase III portion of the Study BRAVE-AA1 consisted of the following 5 periods.
A 5-week screening period (day –3 to day –35): This was for study eligibility assessment.
A 36-week double-blind, placebo-controlled treatment period (week 0 to week 36): Enrolled patients were randomized in a 2:2:3 ratio to receive either placebo, baricitinib 2 mg, or baricitinib 4 mg once daily for 36 weeks. Randomization was conducted in a blinded manner using an interactive web response system and was stratified by geographic region (North America, Asia, and the rest of the world) and duration of the current AA episode at baseline (less than 4 years versus at least 4 years). Patients, investigators, and study personnel were blinded to treatment assignment.
A 68-week long-term extension period (week 36 to week 104): Double-blinding was maintained throughout this treatment period.
At week 36:
Patients with a SALT score greater than 20 (hereinafter referred to as nonresponders as per the Clinical Study Report submitted by the sponsor) receiving placebo at week 36 were rescued to receive a baricitinib 4 mg or baricitinib 2 mg regimen by randomized assignment (1:1) for the remainder of the trial. Patients with a SALT score of 20 or less (hereinafter referred to as responders as per the Clinical Study Report submitted by the sponsor) receiving placebo continued the regimen with placebo for the remainder of the trial, regardless of whether relapse occurred later in the trial.
Baricitinib-treated patients continued treatment regardless of response at week 36 and were reassessed for response to treatment at week 52.
At week 52:
Responders: Patients who had stayed on the same dose of baricitinib from initial randomization and were responders at week 52 underwent randomized withdrawal (randomization not stratified), where they were randomized in a 3:1 ratio to either stay on their existing dose of baricitinib or transition to placebo. Patients in the placebo group at week 52 who were responders remained on placebo. Responders who experienced a loss of treatment benefit after week 52 (defined as greater than a 20-point absolute worsening in the total SALT score) and:
who were randomized to placebo at week 52 (randomized withdrawal) were re-treated with their baricitinib dose, as randomized at baseline
who remained on baricitinib at week 52 continued to receive the same dose of baricitinib
who were randomized to placebo at baseline remained on placebo.
Nonresponders:
patients who had been in the baricitinib 4 mg group from baseline, had never attained a response to treatment by week 52, and did not have an improvement of 2 points or more from baseline in a ClinRO measure for EB or EL hair loss at week 52 were transitioned to placebo
patients who had been in the baricitinib 4 mg group had attained a response to treatment before week 52, and had lost response remained on the baricitinib 4 mg dose
those who had been in the baricitinib 2 mg group from baseline were rescued to receive baricitinib 4 mg
those who were rescued to baricitinib at week 36 continued in their current treatment group at week 52.
At week 76:
Nonresponders at week 52 and week 76 were discontinued from the study unless they had at least a 2-point improvement from baseline in a ClinRO measure for EB or EL hair loss.
A 96-week bridging extension period (week 104 to week 200): Patients who completed week 104 and did not meet criteria for permanent discontinuation could continue to receive the same treatment they received during the long-term extension period in a double-blinded manner.
A 4-week post-treatment follow-up period (week 200 to week 204): A post-treatment follow-up visit was scheduled approximately 4 weeks after the bridging extension period.
Figure 1: Study BRAVE-AA1 Study Design
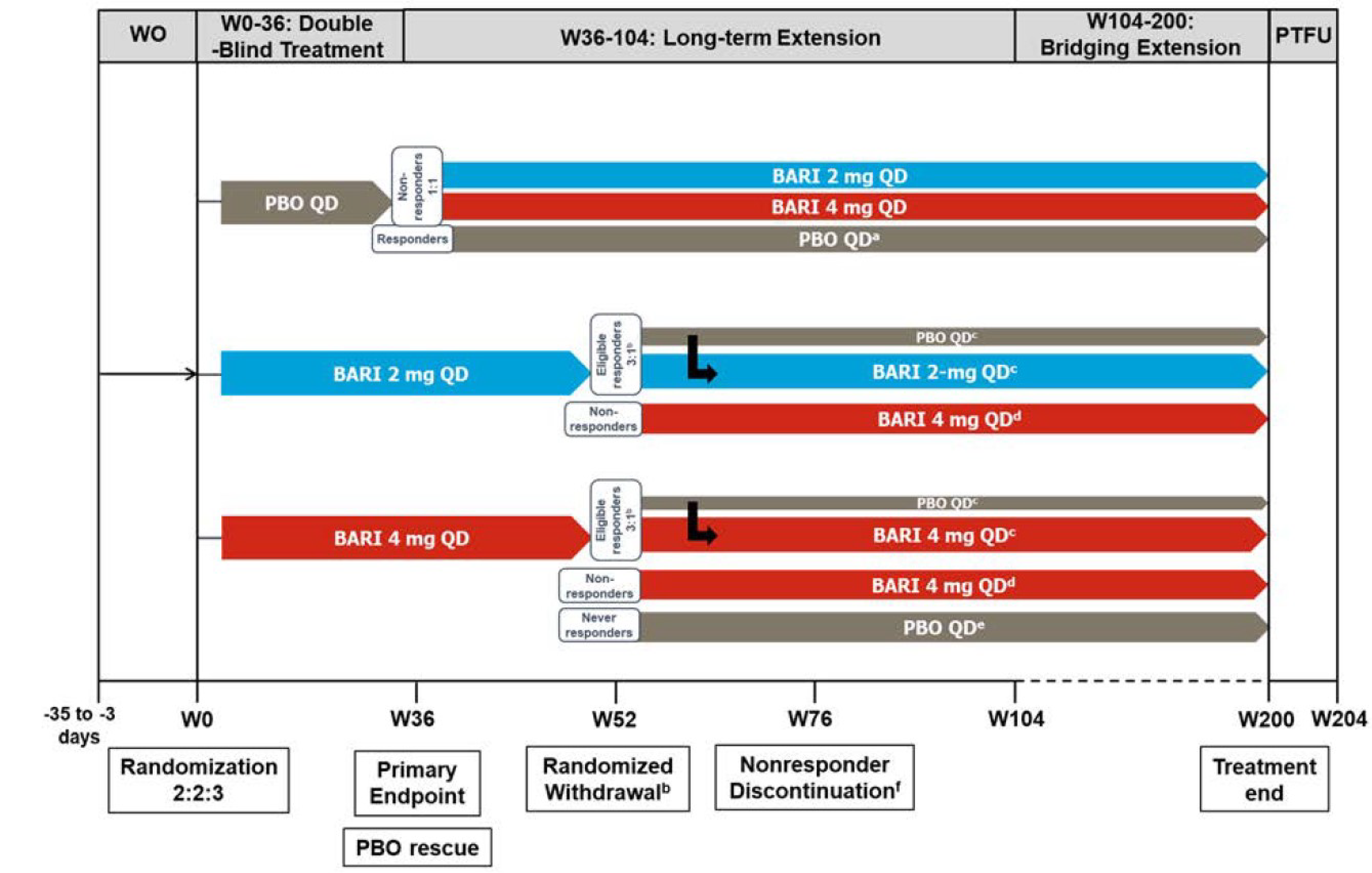
BARI = baricitinib; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; PBO = placebo; PTFU = post-treatment follow-up; QD = every day; SALT = Severity of Alopecia Tool; W = week; WO = washout.
a Placebo responders stayed on placebo for the remainder of the trial, even if relapse was observed later.
b Patients with a SALT score of 20 or less who stayed on the same dose of baricitinib from week 0 were randomized to stay on the existing baricitinib dose or transitioned to placebo.
c Responders participating in randomized withdrawal who experienced more than a 20-point absolute worsening in their total SALT score after week 52 were re-treated with the baricitinib dose to which they were originally randomized if they were randomized to placebo at week 52, or continued to receive the same dose of baricitinib if they were randomized to remain on baricitinib at week 52.
d Nonresponders at week 52 were rescued to baricitinib 4 mg if receiving baricitinib 2 mg from baseline or remained on baricitinib 4 mg if they were in the 4 mg group and attained a SALT score of 20 or less before week 52.
e Never-responders (those who never attained a SALT score of ≤ 20 by week 52 despite being in the baricitinib 4 mg group from baseline and had not experienced a ≥ 2-point improvement from baseline in ClinRO measures for EB or EL hair loss) were automatically transitioned to placebo.
f Nonresponders at week 52 and week 76 were automatically discontinued at week 76 unless they had an improvement of 2 points or more from baseline in ClinRO measures for EB or EL hair loss.
Source: Study BRAVE-AA1 Clinical Study Report.7
Study BRAVE-AA2
As shown in Figure 2, the study design of Study BRAVE-AA2 is nearly identical to that of Study BRAVE-AA1 (as previously described), except that the 68-week long-term extension period was conducted as described as follows. Note that the double-blinding of patients, investigators, and study personnel was maintained throughout this treatment period.
At week 36:
Placebo-treated nonresponders at week 36 were rescued to receive baricitinib 2 mg or baricitinib 4 mg by randomized assignment (1:1). Patients in the placebo group who attained a response at week 36 remained on placebo. Those patients who experienced spontaneous regrowth remained on placebo until week 52, even if a relapse was observed between week 36 and week 52.
Baricitinib-treated patients continued treatment regardless of response at week 36 and were reassessed at week 52.
At week 52:
Responders: Patients who had been in the baricitinib 4 mg group from baseline and attained a response at week 52 underwent randomized down-titration where they were randomized in a 1:1 ratio to either stay on their existing 4 mg dose of baricitinib or transition to a 2 mg dose of baricitinib. Patients who were rescued to baricitinib at week 36 and patients randomized to a 2 mg dose of baricitinib were not eligible for randomized down-titration and remained in their same treatment group. Patients in the placebo group at week 52 who attained a response remained on placebo. Responders who experienced a loss of treatment benefit after week 52 and:
who were randomized to baricitinib 2 mg at week 52 (randomized down-titration) were re-treated with the 4 mg dose of baricitinib as randomized at baseline
who remained on a 4 mg dose of baricitinib at week 52 (randomized down-titration) continued to receive the same dose of baricitinib
who were randomized to a 2 mg dose of baricitinib at baseline were rescued to a 4 mg dose of baricitinib
who had remained on placebo since baseline were rescued to baricitinib 2 mg.
Nonresponders:
Patients who had been in the baricitinib 4 mg dose group from baseline, had never attained a response by week 52, and had not had at least a 2-point improvement from baseline in a ClinRO measure for EB or EL hair loss at week 52 were transitioned to placebo.
Patients who had been in the baricitinib 4 mg dose treatment group, had attained a response before week 52, and had lost response remained on the baricitinib 4 mg dose.
Those who had been in the baricitinib 2 mg dose treatment group from baseline were rescued to the baricitinib 4 mg dose.
Those who were rescued to baricitinib at week 36 continued in their current treatment group at week 52.
Those who were randomized to placebo at baseline and were not eligible for rescue to baricitinib at week 36 (spontaneous remission) were rescued to baricitinib 2 mg.
At week 76:
Patients who were nonresponders at both week 52 and week 76 were discontinued from the study at week 76, unless they had at least a 2-point improvement from baseline in a ClinRO measure for EB or EL hair loss.
This section summarizes the 36-week double-blind, placebo-controlled treatment period of Study BRAVE-AA1 (the phase III portion only) and Study BRAVE-AA2. The long-term extension period and bridging extension period and their results are summarized in the long term Extension Studies section.
Figure 2: Study Design of Study BRAVE-AA2
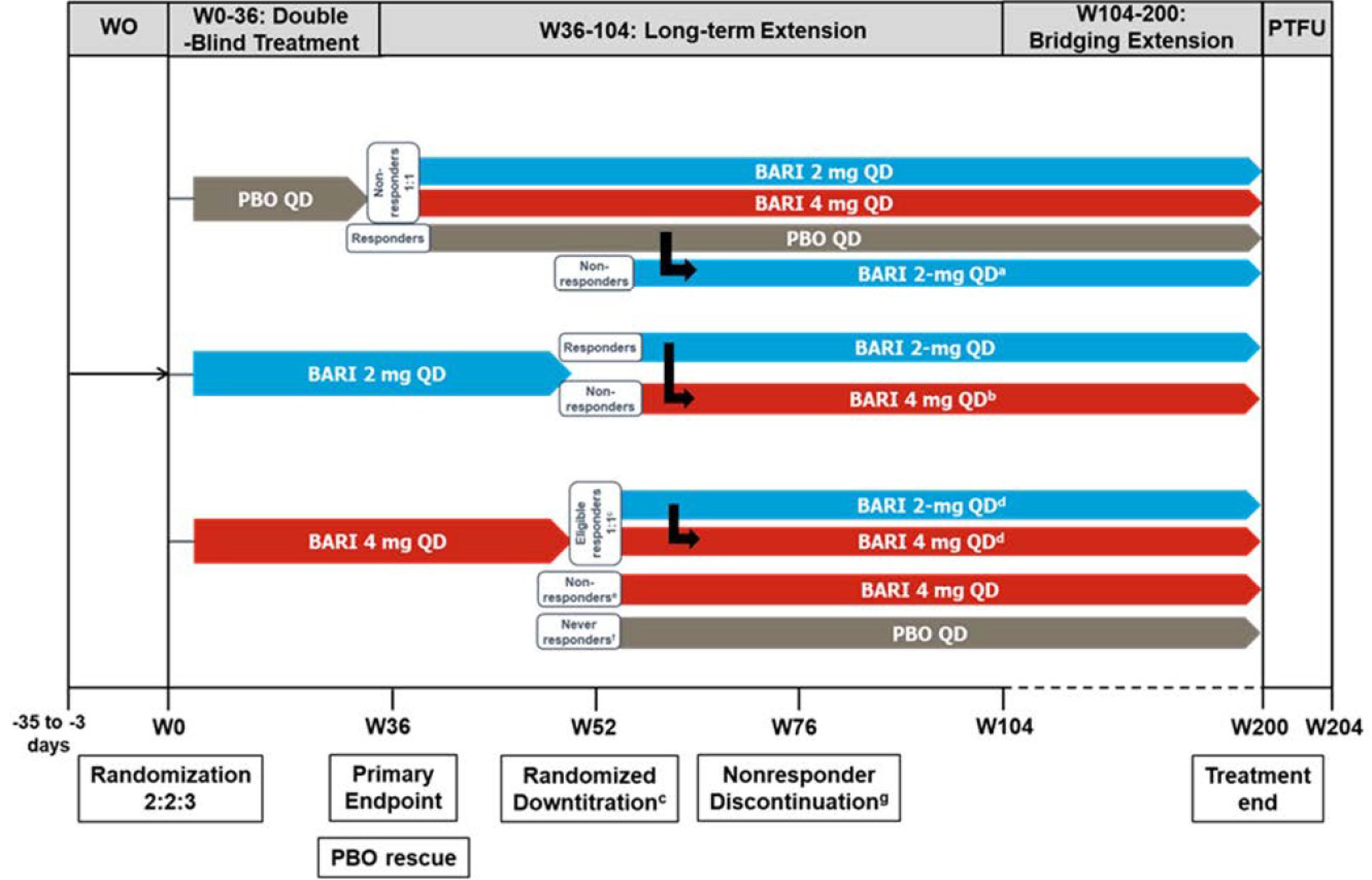
BARI = baricitinib; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; PBO = placebo; PTFU = post-treatment follow-up; QD = every day; SALT = Severity of Alopecia Tool; W = week; WO = washout.
a Placebo-treated patients not eligible for rescue to baricitinib at week 36 (because of spontaneous remission) were rescued to baricitinib if they were nonresponders at week 52, or if they experienced a loss of treatment benefit after week 52.
b Patients randomized to baricitinib 2 mg at week 0 were rescued to the baricitinib 4 mg dose if they were nonresponders at week 52 or were responders at week 52 but experienced more than a 20-point worsening in their SALT score after week 52.
c Responders in the baricitinib 4 mg group (patients with a SALT score ≤ 20 who stayed on baricitinib 4 mg from week 0) were randomized to either stay on 4 mg or transition to baricitinib 2 mg.
d Responders participating in the randomized down-titration who experienced a loss of treatment benefit after week 52 were re-treated with baricitinib 4 mg if they were randomized to the baricitinib 2 mg dose at week 52, or continued to receive baricitinib 4 mg if they were randomized to remain on the 4 mg dose at week 52.
e At week 52, nonresponders (patients with a SALT score > 20) in the baricitinib 4 mg group since baseline who attained a SALT score of 20 or less before week 52 remained on 4 mg.
f Never-responders (those who never attained a SALT score of ≤ 20 by week 52 despite being in the baricitinib 4 mg group from baseline and had not experienced a ≥ 2-point improvement from baseline in ClinRO measures for EB or EL hair loss) were automatically transitioned to placebo.
g Nonresponders at both week 52 and week 76 were automatically discontinued at week 76 unless they had an improvement of 2 points or more from baseline in ClinRO measures for EB or EL hair loss.
Source: Study BRAVE-AA2 Clinical Study Report.8
Table 6: Details of Studies Included in the Systematic Review
Detail | Study BRAVE-AA1a | Study BRAVE-AA2 |
|---|---|---|
Designs and populations | ||
Study design | Phase II and phase III, multicentre, double-blind RCT | Phase III, multicentre, double-blind RCT |
Locations | 70 sites in North America and Asia | 84 sites in North America and South America, Asia, and Australia |
Patient enrolment dates | Start date: September 24, 2018 End date: February 2, 2021 (database lock) | Start date: July 8, 2019 End date: February 19, 2021 (database lock) |
Randomized (N) | Total: 654 patients Baricitinib 2 mg: 184 patients Baricitinib 4 mg: 281 patients Placebo: 189 patients | Total: 546 patients Baricitinib 2 mg: 156 patients Baricitinib 4 mg: 234 patients Placebo: 156 patients |
Inclusion criteria |
| |
Exclusion criteria |
| |
Drugs | ||
Intervention | Baricitinib 2 mg or 4 mg oral tablet once daily | |
Comparator(s) | Placebo oral tablet once daily | |
Study duration | ||
Screening phase | Between 3 days and 35 days | |
Treatment phase | Double-blind treatment period: 36 weeks Long-term extension period: 68 weeks Bridging extension period: 96 weeks | |
Follow-up phase | Post-treatment follow-up: 4 weeks | |
Outcomes | ||
Primary end point | Proportion of patients attaining a SALT score ≤ 20 at week 36 | |
Secondary and exploratory end points | Secondary end points Key secondary end points:
Other secondary end points:
Exploratory end points
| |
Publication status | ||
Publications | King et al. (2022),6 Kwon et al. (2023),39 and Senna et al. (2024)38 (Study BRAVE-AA1 [NCT03570749]; Study BRAVE-AA2 [NCT03899259]) | |
AA = alopecia areata; AA-IGA = Alopecia Areata Investigator’s Global Assessment; ClinRO = clinician-reported outcome; EB = eyebrow; EI = eye irritation; EL = eyelash; EQ VAS = EQ visual analogue scale; HADS-A = Hospital Anxiety and Depression Scale-Anxiety; HADS-D = Hospital Anxiety and Depression Scale-Depression; MCS = mental component score; PCS = physical component score; PRO = patient-reported outcome; RCT = randomized controlled trial; SALT = Severity of Alopecia Tool; SALT30 = at least a 30% improvement from baseline in the Severity of Alopecia Tool score; SALT50 = at least a 50% improvement from baseline in the Severity of Alopecia Tool score; SALT75 = at least a 75% improvement from baseline in the Severity of Alopecia Tool score; SALT90 = at least a 90% improvement from baseline in the Severity of Alopecia Tool score; SALT100 = a 100% improvement from baseline in the Severity of Alopecia Tool score; SF-36 = Short Form (36) Health Survey; Skindex-16 for AA = Skindex-16 for Alopecia Areata.
Note: Details included in Table 6 are from the sponsor’s Summary of Clinical Evidence.9
aOnly details of the phase III portion of Study BRAVE-AA1 are reported in this table.
bThis is as assessed at screening and baseline.
cThis includes but is not limited to androgenetic alopecia, trichotillomania, and telogen effluvium.
dExamples are tinea capitis, psoriasis, lupus erythematosus, or secondary syphilis.
eThis was as clinically judged by the investigator to be at risk for suicide, or have suicidal ideation or behaviour as indicated by the Columbia-Suicide Severity Rating Scale, and ideation or behaviour that occurred within 2 months of the first visit in the study.
fThis was as assessed among patients with a score of 2 or more at baseline.
gThis was as assessed among patients with a score of 3 or more at baseline.
hThis was a component of the SF-36.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria of the BRAVE-AA1 and BRAVE-AA2 trials are presented in Table 6. The trials included patients who were aged at least 18 years and no more than 60 years for males (aged no more than 70 years for females), and had a current AA episode of more than 6 months’ duration that was severe or very severe in nature (i.e., hair loss encompassing at least 50% of the scalp as measured by SALT [the Alopecia Areata Investigator’s Global Assessment scale score of 3 or 4, corresponding to a SALT score of between 50 and 94 and a SALT score of between 95 and 100, respectively]). Eligible patients had no spontaneous improvement over the past 6 months (i.e., no more than 10 points in spontaneous reduction in the SALT score) and had a current episode of severe or very severe AA of less than 8 years’ duration. Patients were excluded if they had a primarily diffuse type of AA (characterized by diffuse hair shedding) or had significant uncontrolled neuropsychiatric disorder (e.g., suicidal ideation or behaviour).
Interventions
All study interventions were given once daily by oral means: baricitinib 2 mg, baricitinib 4 mg, and placebo. The baricitinib dose for patients randomized to the 4 mg daily treatment group who had renal impairment (defined as an estimated glomerular filtration rate less than 60 mL per minute per 1.73 m2) was 2 mg daily.
Each strength of a baricitinib tablet had a distinctive shape and colour, 4 mg versus 2 mg, and each tablet strength had a matching placebo. Patients received 2 tablets per day as follows:
baricitinib 4 mg daily regimen — baricitinib 4 mg tablet and placebo tablet (matching baricitinib 2 mg); 1 each
baricitinib 2 mg daily regimen — baricitinib 2 mg tablet and placebo tablet (matching baricitinib 4 mg); 1 each
placebo daily regimen — placebo tablet (matching baricitinib 2 mg) and placebo tablet (matching baricitinib 4 mg); 1 each.
Double-blinding was in place to minimize bias. All study assessments were performed by study personnel who were blinded to patients’ treatment groups. Patients, investigators, and any other personnel interacting directly with patients or investigative sites remained blinded to intervention assignment until after completion of the study. Dose adjustment for renal impairment, if required, was managed by an interactive web response system to ensure the maintenance of blinding.
The following medications were permitted during the study: topical corticosteroids and topical calcineurin inhibitors (except on the scalp, EBs, and eyelids); intranasal, ophthalmic, or inhaled steroid; intra-articular or soft tissue corticosteroid injections (a maximum of 2 injections until week 36, no limit thereafter); nonlive vaccinations; bimatoprost ophthalmic solution (if on a stable dose for 8 weeks before randomization); 5-alpha reductase inhibitors, or oral or topical minoxidil (if on a stable dose for 12 months before randomization); statins; and ezetimibe.
The temporary interruption of treatment intervention occurred when any of the following prohibited medications was received by patients: live vaccines, probenecid, systemic corticosteroids, and phototherapy. The permanent discontinuation of treatment intervention occurred when any of the following prohibited medications was taken by patients: corticosteroids (systemic, intralesional, or topical on the scalp, EBs, and/or eyelids) for the treatment of AA; topical JAK inhibitors applied to the scalp, EBs, and eyelids; other oral JAK inhibitors; systemic immunosuppressants or immunomodulators; and any other AA treatment.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical experts we consulted and input from patient and clinician groups and public drug plans. Using the same considerations, our review team selected end points that were considered to be most relevant to inform our expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using the GRADE tool. SAEs were also assessed using GRADE.
Considerations that informed the selection of outcomes to be summarized and assessed using GRADE include the following.
SALT scores are used to assess the extent of scalp hair loss, which is an important outcome according to input from a patient group and the clinical experts. A SALT score of 20 or less was considered to be a reasonable threshold for clinically meaningful improvement in patients with severe AA based on literature identified by the sponsor40 and clinical expert input. A brief description of the percentage change from baseline in SALT score results (GRADE not applied) is also provided in the Results section of this report.
The proportion of patients attaining a SALT50 response was an outcome that informs the sponsor’s pharmacoeconomic model and was included in the GRADE assessment. A brief description of the degree of alignment between SALT75 (GRADE not applied) and SALT50 responses is provided in the text.
The loss of EB hair and EL hair is distressing to patients with AA as per clinical expert input. ClinRO measure-based outcomes were included in the GRADE assessment. A brief description of the degree of alignment between PRO measure-based results (GRADE not applied) and ClinRO measure-based results is provided in the text.
The impact of AA on anxiety and depression was identified as an important outcome by a patient group and was assessed by the change from baseline in HADS anxiety and depression domain scores in the trials.
HRQoL was identified as an important outcome in patients with AA, as per input from a patient group and the clinical experts. Of those HRQoL measures included in the trials, Skindex-16 for AA, which is an AA-specific measure, was included in the GRADE assessment. The Short Form (36) Health Survey (SF-36) and the EQ-5D-5L are generic HRQoL measures and were not included in the GRADE assessment. Results of these generic HRQoL measures are summarized in Appendix 1 given that they inform the sponsor’s pharmacoeconomic model.
Clinical expert input noted that 36 weeks is a reasonable time frame in which to assess response to baricitinib treatment.
Harms were considered important outcomes according to input from a patient group and the clinical experts. SAE was selected for the GRADE assessment. The 36-week time point was selected, as it was the latest follow-up time where the randomized placebo comparison was maintained.
Table 7: Outcomes Summarized From Study BRAVE-AA1 and Study BRAVE-AA2
Outcome | Time point | Study BRAVE-AA1 | Study BRAVE-AA2 |
|---|---|---|---|
SALT score | |||
Proportion of patients attaining a SALT score ≤ 20 | At week 36 | Primarya | Primarya |
Proportion of patients attaining a SALT50 response | At week 36 | Secondary | Secondary |
ClinRO measure for EB hair loss and EL hair loss | |||
Proportion of patients attaining a ClinRO measure for EB hair loss score of 0 or 1 with ≥ 2-point improvement from baseline (among patients with a ClinRO measure for EB hair loss score of ≥ 2 at baseline). | At week 36 | Key secondarya | Key secondarya |
Proportion of patients attaining a ClinRO measure for EL hair loss score of 0 or 1 with ≥ 2-point improvement from baseline (among patients with a ClinRO measure for EL hair loss score of ≥ 2 at baseline). | At week 36 | Key secondarya | Key secondarya |
HADS-A domain and HADS-D domain | |||
Mean change from baseline in HADS-A and HADS-D domain total scores | At week 36 | Secondary | Secondary |
HRQoL | |||
Mean change from baseline in Skindex-16 for AA domain scores (symptoms, emotions, and functioning) | At week 36 | Exploratory | Secondary |
Harms | |||
Serious adverse event | At week 36 | Safety | Safety |
ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; HADS-A = Hospital Anxiety and Depression Scale-Anxiety; HADS-D = Hospital Anxiety and Depression Scale-Depression; HRQoL = health-related quality of life; SALT = Severity of Alopecia Tool; Skindex-16 for AA = Skindex-16 for Alopecia Areata.
Note: Details included in Table 7 are from the sponsor’s Summary of Clinical Evidence.9
aStatistical testing for these end points was adjusted for multiple comparisons.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Severity of Alopecia Tool
The SALT is an investigator-reported assessment tool used to assess the extent of scalp hair loss in AA.30,41 The SALT uses a visual aid that helps visualize the amount of terminal hair loss in each of the 4 quadrants of the scalp and then, upon the summing of these, generates a SALT score (i.e., the total percentage of scalp hair loss), which ranges from 0 (no scalp hair loss) to 100 (complete scalp hair loss).30 Evidence for the validity, reliability, and responsiveness of this instrument in patients with AA is summarized in Table 8. Attaining 80% or more scalp hair (a SALT score of 20 or less) has been shown to be a threshold for clinically meaningful improvement in patients with at least 50% scalp hair loss.40 SALT50 corresponds to at least 50% reduction (i.e., improvement) from baseline in the SALT score. Evidence for a MID in percentage change from baseline in the SALT score was not identified by the sponsor. Based on input from the clinical experts we consulted, a difference of at least 10% between the baricitinib group and the placebo group is likely to be clinically important with respect to the proportion of patients attaining a SALT score of 20 or less and the proportion of patients attaining SALT50.
ClinRO Measures for EB and EL Hair Loss
The ClinRO assessments are novel clinician-administered instruments developed by the sponsor and are used to assess the extent of EB hair loss (ClinRO measure for EB hair loss) and EL hair loss (ClinRO measure for EL hair loss).42 The instruments use a 4-point categorical scale, ranging from 0 to 3; a higher score indicates more hair loss. Evidence for validity, reliability, responsiveness, and MID in patients with AA is summarized in Table 8. Based on input from the clinical experts we consulted, a difference of at least 10% between the baricitinib group and the placebo group with respect to the proportion of patients attaining a ClinRO measure for EB (or EL) hair loss score of 0 or 1 with at least a 2-point improvement from baseline is likely to be clinically important.
Hospital Anxiety and Depression Scale
The HADS is a 14-item patient-administered instrument that is used to assess the levels of anxiety and depression that a patient has experienced over the past week.43,44 The HADS uses a 4-point Likert scale (0 to 3) for each question and is intended for patients aged between 12 years and 65 years.43,44 Scores for each domain (anxiety and depression) range from 0 to 21, with higher scores indicating greater anxiety or depression.44,45 Evidence for the validity, reliability, responsiveness, and MID of this instrument in patients with AA was not identified by the sponsor. The clinical experts we consulted did not suggest a reasonable MID estimate with certainty; therefore, the null was selected as the threshold when applying the GRADE assessment for these outcomes.
Skindex-16 for AA
The Skindex-16 questionnaire has been used to assess the HRQoL in patients with skin diseases. The Skindex-16 for AA is a version of the Skindex-16 that was adapted for use among adults with AA.9 It examines the degree to which patients are bothered by alopecia and associated symptoms. It is composed of 16 items grouped under 3 domains: symptoms, emotions, and functioning. Domain scores range from 0 (no effect) to 100 (effect experienced all the time), with higher scores indicating greater impact on quality of life.9 Evidence for the validity, reliability, responsiveness, and MID of this instrument in patients with AA was not identified by the sponsor. The clinical experts we consulted did not suggest a reasonable MID estimate with certainty; therefore, the null was selected as the threshold when applying the GRADE assessment for these outcomes.
Harms Outcomes
Harms outcomes included TEAEs, SAEs, WDAEs, death, and notable harms (infections, malignancies, gastrointestinal perforations, major adverse cardiac events [MACEs], and thromboembolic events). Based on clinical expert input, a difference of at least 5% between the baricitinib group and the placebo group in the proportion of patients experiencing SAEs is likely clinically important.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
SALT | A visual aid shows the division of the scalp hair into 4 areas, with the left side and right side of scalp being 18% each, the top constituting 40% of the total surface, and the posterior or back constituting 24%. The percentage of hair loss in each area is determined and is multiplied by the percentage of scalp covered by that area. The total sum of the 4 products of each area will give the SALT score, as developed by the National Alopecia Areata Foundation Working Committee. The SALT is scored from 0 (absence of hair loss) to 100 (complete hair loss).16 | Validity Content validity was confirmed via interviews with 10 dermatologists with expertise in AA and 45 patients with ≥ 50% AA-related scalp hair loss. Known-groups, convergent, and discriminant validity were evaluated based on data from the BRAVE-AA1 and BRAVE-AA2 studies. Known-groups validity: Patients with a Scalp Hair Assessment PRO score of 4 had worse scores than those reporting less severe hair loss (Scalp Hair Assessment PRO score ≤ 3). Convergent validity: Pearson and Spearman rank correlations at baseline and week 36 with the Scalp Hair Assessment PRO were ≥ 0.5. Discriminant validity: ███████ ███ ████████ ████ ████████████ ██ ████████ ███ ████ ██ ████ ███ █████ ████ ██████████ ███ ██████ ████ ██ █████ ████ ███████ ██ █████████ ████ ████████████ ████ ██████ ███████ ███ ████ ███████████ ████████ ███████████ █████ ████ ██ ██████46 Reliability Inter-rater reliability was examined with 24 clinicians via an online test using 5 patient photosets. The resulting ICC reliability estimates indicated near-perfect agreement.47 An intrarater reliability investigation was conducted in a subset of clinicians, and the resulting estimates indicated near-perfect agreement.47 ███ ████ ██████ ████ ████ ██ █████ ██████████ ████ ████ ███████████ ███████████ █████ ██████ █████████46 Responsiveness █████ ██ ████ ████ ███ █████████ ███ █████████ ███████ █████ ████ ███████ ██ █████ ████████████ ███████ ███████ ██ ████ █████ ███ ██ █████ ████ ██████████ ███ ████ ████████ ██ ████ ██ ████████ ███████████ ████ ██ ██████ █████ ████ ████████ ████████████ ███████ ███████ ██ ████ █████ ███ ███████ ██ ██████████ ████████ ██████ ██████ ██ ████ ████████ ███████ ██ █████ ███████ ████████████ ███████████ ███████████████ ███ ████████ ███ ███ ████████ ██ ██ ██████ ██████ ██ █████ ██ █████ ████ ██████████ ███ █████ ████ ████████ ██ ████ ███46 | Attaining 80% or more scalp hair (a SALT score ≤ 20) has been shown to be a threshold, indicating clinically meaningful improvement for patients with ≥ 50% scalp hair loss.40 |
ClinRO measure for EB hair loss | ClinRO measures use a 4-point response scale. An EB score ranges from 0 (full coverage and no areas of hair loss) to 3 (no notable EB hair).42 | Validity The content validity was confirmed via interviews with 10 dermatologists with expertise in AA and 45 patients with ≥ 50% AA-related scalp hair loss, including 35 patients with EB and/or EL involvement. Known-groups, convergent, and discriminant validity were evaluated based on data from the BRAVE-AA1 and BRAVE-AA2 studies. Known-groups validity: Patients with a PRO measure for EBs score of 2 or 3 had worse scores on the ClinRO measure for EB hair loss than those reporting less severe hair loss (a PRO measure for EBs score of 0 or 1). Convergent validity: Pearson and Spearman rank correlations at baseline and week 36 with the PRO measure for EBs were ≥ 0.5 at baseline and week 36 in both studies. Discriminant validity: ███████ ███ ████████ ██████████ ████████████ ██ ████████ ███ ████ ██ ████ ███ ███ ███████ ███ ████████ ████████ ███████████ █████ ████ ██ █████ ████ ███████ ██ █████████ ████ ████████████ ████ ███ ███ ███████ ███ ████ ██████████ ██ ████ ████████48 Reliability Test-retest reliability was examined using data from the BRAVE-AA1 and BRAVE-AA2 studies among patients who had stable disease. ███ ████ ██████ ████ ████ ██ █████ ██████████ ████ ███████████ ███████████ █████ ██████ █████████48 Responsiveness ██████████████ ███ █████████ █████ ████ ████ ███ █████████ ███ █████████ ██ ███████████ ███ ███████████ ███████ ██████ ██ ██████ ███████ ███ ███████ ████ ████ █████ ███ ██████ ██ █████ ██ ███ ███ ███████ ███ ████████ ███ ██ █████ ██████ ████ ███ ████ ████████ ██ ████ ████████ ████████ ██ █████ ████████████ ████ ████████ ███████ ███████ ██ ██████ ███████ ███ ███████ ████ ████ █████ ███ ███ ███████ ███ ████████ ██████ ████ ████████ ██ ████ ███ ██ ███ ██████ █████████ █ █████ ██ ███ █████████ ███ ████████ ██ ██████ ███████ ███ ███████ ████ ████ █████ ███ █████████ ██ ████████ ██ ███ ███████ ███ ███████ ████ ████ █████ ██ ████ ████████48 | ██████████ ███████████ ███ ██████████ ██ █ ███ ██ ████████48 |
ClinRO measure for EL hair loss | ClinRO measures use a 4-point response scale. An EL score ranges from 0 (ELs form a continuous line along the rim of eyelids on both eyes) to 3 (no notable ELs).42 | Validity Content validity was confirmed via interviews with 10 dermatologists with expertise in AA and 45 patients with ≥ 50% AA-related scalp hair loss, including 35 patients with EB and/or EL involvement. Known-groups, convergent, and discriminant validity were evaluated based on data from the BRAVE-AA1 and BRAVE-AA2 studies. Known-groups validity: Patients with a PRO measure for ELs score of 2 or 3 had worse scores on the ClinRO measure for EL hair loss than those reporting less severe hair loss (a PRO measure for ELs score of 0 or 1). Convergent validity: Pearson and Spearman rank correlations at baseline and week 36 with the PRO measure for ELs were ≥ 0.5 in both studies. Discriminant validity: ███████ ███ ████████ ████ ████████████ ████████████ ██ ████████ ███ ████ ██ ████ ███ ███ ███████ ███ █████████ ████ ███████ ██ █████████ ████ ████████████ ████ ███ ███████ ████ ████ ███ ███ ███████ ███ ████ ██████████ ██ ████ ████████49 Reliability Test-retest reliability was examined in patients who had stable disease. ███ ████ ██████ ████ ████ ██ █████ ██████████ ████ ███████████ ███████████ █████ ██████ █████████49 Responsiveness ██████████████ ███ █████████ ████ ████ ███ █████████ ███ █████████ ███████ ██ ███████████ ███ ██████ ██ ███████████ ███████ ██████ ██ ██████ ███████ ███ ███████ ████ ████ █████ ███ ██████ ██ █████ ██ ███ ███ ███████ ███ █████████ ███ ██ █████ ██████ ████ ███ ████ ████████ ██ ████ ████████ ████████ ██ █████ ████████████ ████ ████████ ███████ ███████ ██ ███ ██████ ███████ ███ ███████ ████ ████ █████ ███ ███ ███████ ███ █████████ ██████ ████ ████████ ██ ████ ███ ██ ███ ██████ █████████ █ █████ ██ ███ █████████ ███ ████████ ██ ██████ ███████ ███ ███████ ████ ████ █████ ███ █████████ ██ ████████ ██ ███ ███████ ███ █████████ █████ ██ ████ ████████49 | ██████████ ███████████ ███ ██████████ ██ █ ███ ██ ████████49 |
HADS | A 14-item self-assessment scale determines the levels of anxiety and depression that a patient is experiencing over the past week. The HADS uses a 4-point Likert scale (for example, 0 to 3) for each question and is intended for those aged 12 years to 65 years.43,44 Scores for each domain (anxiety and depression) can range from 0 to 21, with higher scores indicating greater anxiety or depression.44,45 | Evidence supporting the validity, reliability, and responsiveness of this instrument was not identified by the sponsor. | There is no known MID in patients with AA. |
Skindex-16 for AA domain scores | A total of 16 items are grouped under 3 domains: symptoms (4 items), emotions (7 items), and functioning (5 items). The score of each item ranges from 0 (never bothered) to 6 (always bothered). Scores are transformed to a linear scale ranging from 0 (no effect) to 100 (an effect is experienced all the time), with higher scores indicating greater impact on quality of life.9 | Evidence supporting the validity, reliability, and responsiveness of this instrument was not identified by the sponsor. | There is no known MID in patients with AA. |
AA = alopecia areata; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; HADS = Hospital Anxiety and Depression Scale; ICC = intraclass correlation coefficient; MID = minimal important difference, PRO = patient-reported outcome; SALT = Severity of Alopecia Tool; Skindex-16 for AA = Skindex-16 for alopecia areata.
Statistical Analysis
Table 9 summarizes the statistical analysis methods of the efficacy end points in the BRAVE-AA1 and BRAVE-AA2 trials. Baseline was defined as the last nonmissing measurement recorded on or before the first dose of treatment.
Sample Size and Power Calculation
A sample size calculation determined that approximately 625 randomized patients were required in the BRAVE-AA1 trial to demonstrate a statistically significant difference between each of the 2 treatment groups (baricitinib 2 mg and baricitinib 4 mg) and placebo with respect to the primary end point of proportion of patients attaining a SALT score of 20 or less at week 36, at a 2-sided significance level of 0.04 for baricitinib 4 mg and 0.01 for baricitinib 2 mg, with more than 90% power. This assumes that the response rates for baricitinib 4 mg, baricitinib 2 mg, and placebo are 30%, 20%, and 5%, respectively. In the BRAVE-AA2 trial, it was determined that 476 randomized patients were required to provide approximately 90% power to detect a statistically significant difference in the primary outcome based on the same assumptions. There was no sample size consideration for patients who entered randomized withdrawal (Study BRAVE-AA1) or randomized down-titration (Study BRAVE-AA2) at week 52.
Statistical Model
All efficacy analyses in the BRAVE-AA1 and BRAVE-AA2 trials were based upon the full analysis set population (Table 10). The difference between baricitinib and placebo with respect to the primary and key secondary end points were analyzed at an overall 2-sided significance level of 0.05. Categorical end points were tested using a logistic regression model, including geographic region, duration of the current episode of AA at baseline, baseline value, and treatment group as adjustment factors, except for outcomes related to HADS where baseline value was not included. Continuous efficacy end points were analyzed using an analysis of covariance model, including geographic region, duration of the current episode of AA at baseline, baseline value, and treatment group as adjustment factors.
Harms outcomes were assessed in the safety population (Table 10) and presented descriptively.
Multiple Testing Procedure
In both trials, a graphical procedure with a gatekeeping testing strategy for the primary and key secondary end points was implemented to control for type I error at a 2-sided significance level of 0.05. An overview of the testing procedure for Study BRAVE-AA1 and Study BRAVE-AA2 is outlined in Figure 3. Figure 4 further illustrates the testing scheme used within the tier 1 group for the testing procedure for Study BRAVE-AA2. Other secondary end points and exploratory end points were not controlled for type I error.
Handling of Missing Data and Imputation
Missing data for categorical efficacy outcomes were imputed using the nonresponder imputation (NRI) method, where patients were considered nonresponders if they did not meet clinical response criteria, permanently discontinued study treatment, or discontinued from the study at any time before the time point of interest for any reason. Missing data for continuous efficacy outcomes were imputed using the mLOCF method, where the most recent nonmissing postbaseline assessment was used and data after permanent study treatment discontinuation were not carried forward.
Subgroup Analyses
In consultation with the clinical experts we consulted, the CDA-AMC review team determined that the prespecified subgroup analyses of interest to this review included the duration of the current episode of AA category (less than 4 years and at least 4 years) and baseline SALT category (the severe category was a SALT score of 50 to 94 and the very severe category was a SALT score of 95 to 100). In both studies, to assess whether the treatment effect was similar across subgroups for the primary efficacy outcome, a logistic regression model was used and included treatment, baseline value, stratification variables, the subgroup variable, and the subgroup-by-treatment interaction. If the interaction was statistically significant at a significance level of 0.10, the treatment effect was estimated within each subgroup. There were no sample size considerations and no control for multiplicity in subgroup analyses.
Figure 3: Overview of the Graphical Testing Procedure for Study BRAVE-AA1 and Study Design BRAVE-AA2
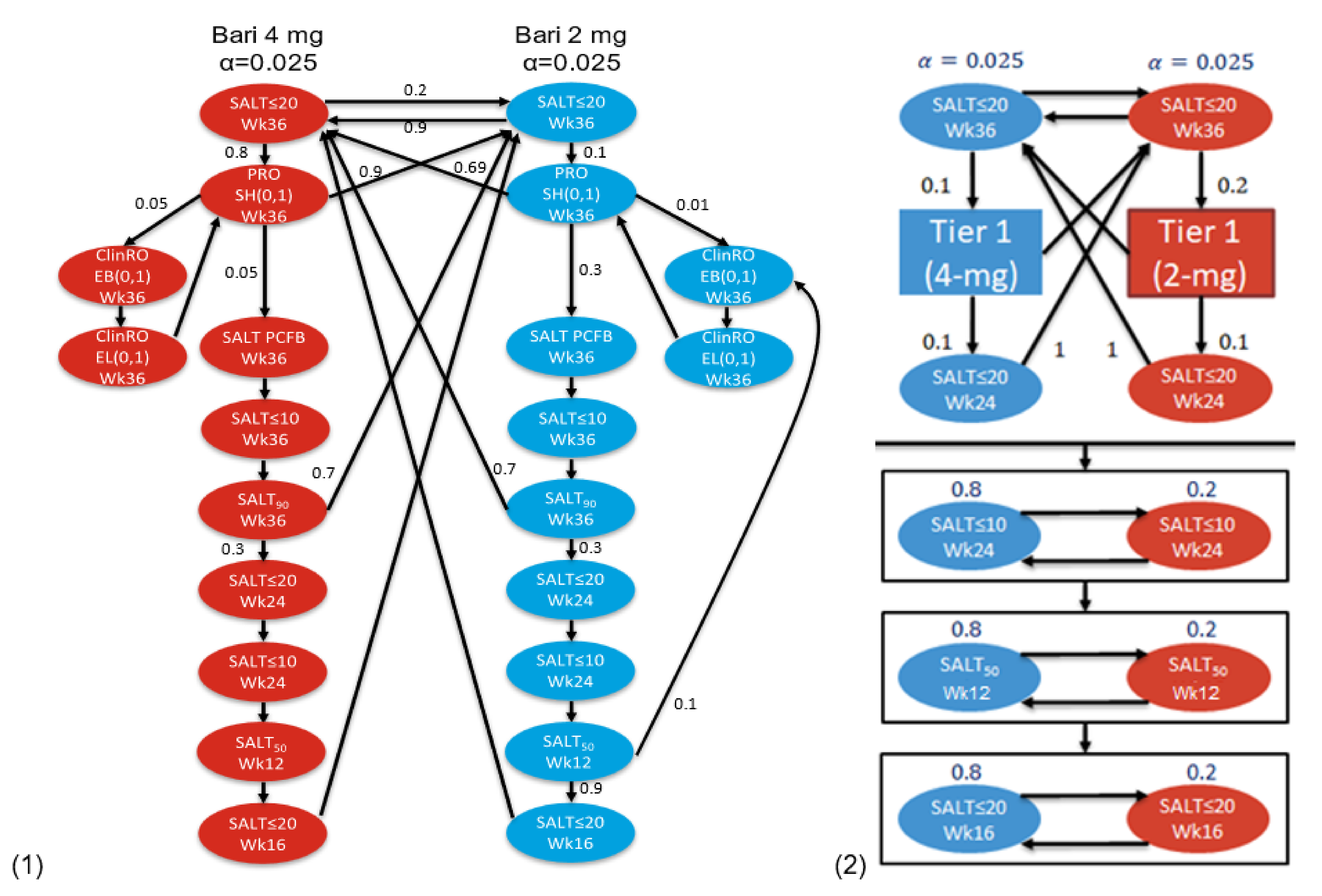
Bari = baricitinib; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; PCFB = percentage change from baseline; PRO = patient-reported outcome; SALT = Severity of Alopecia Tool; SALT50 = at least a 50% improvement from baseline in SALT score; SALT90 = at least a 90% improvement from baseline in SALT score; SH = Scalp Hair Assessment; Wk = week.
Note: Details included in Figure 3 are from the sponsor’s Summary of Clinical Evidence.9
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Figure 4: Graphical Testing Procedure Within Tier 1 Group of End Points for Study BRAVE-AA2
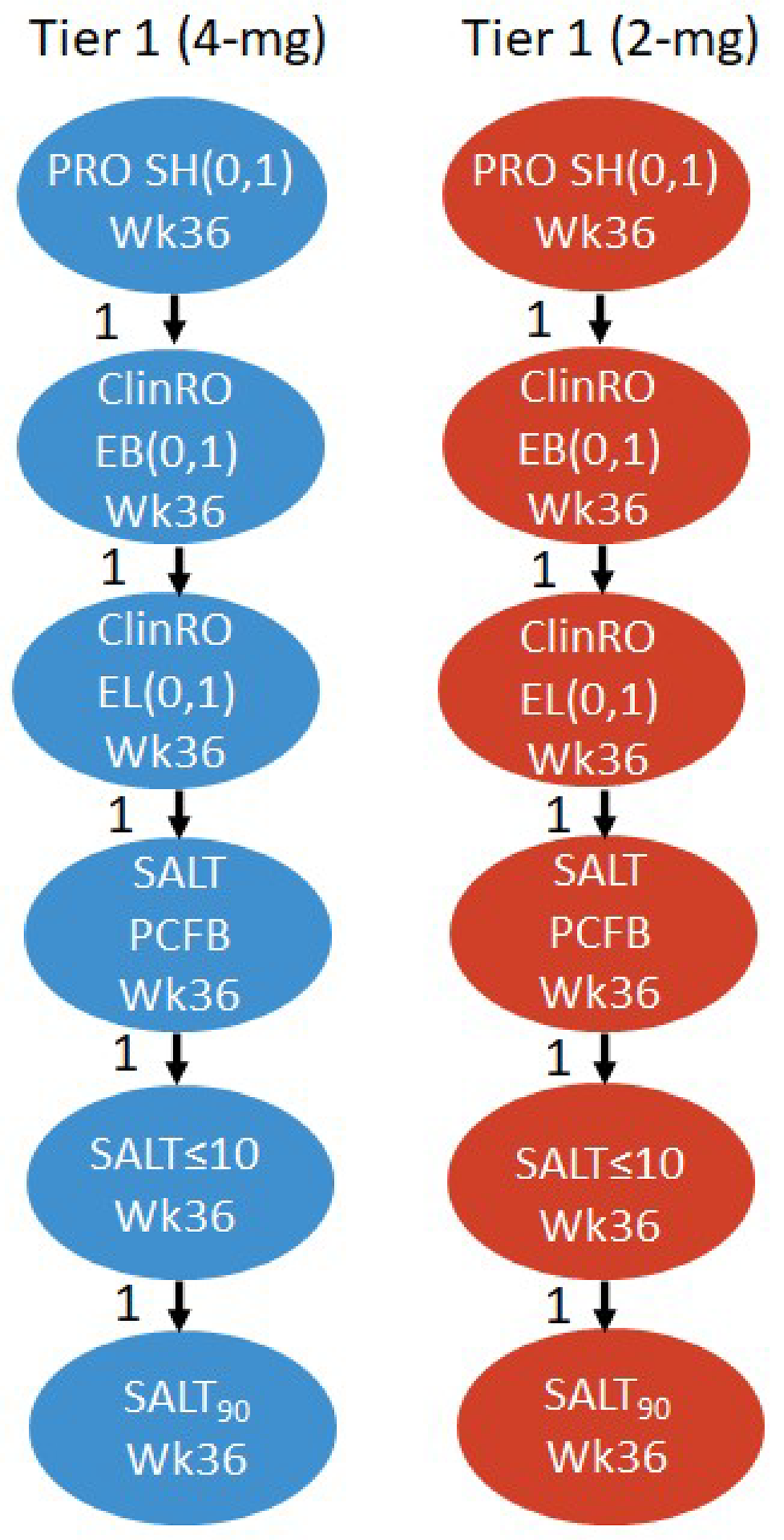
ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; PCFB = percentage change from baseline; PRO = patient-reported outcome; SALT = Severity of Alopecia Tool; SALT90 = at least a 90% improvement from baseline in SALT score; SH = Scalp Hair Assessment; Wk = week.
Note: Details included in Figure 4 are from the sponsor’s Summary of Clinical Evidence.9
Source: Study BRAVE-AA2 Clinical Study Report.8
Sensitivity Analyses
Hybrid imputation (primary and key secondary end points): Earlier in the COVID-19 pandemic, data were considered missing when the assessments were collected at remote visits or the whole visit was missed because of the pandemic. A sensitivity analysis using a hybrid imputation method was conducted to determine the effect of missing data because of the COVID-19 pandemic. For categorical end points, data that were missing because of COVID-19 were imputed using multiple imputation, while other data that were missing for reasons other than COVID-19 were imputed by NRI. This imputation procedure assumed that the effects of treatments would have been the same had patients not experienced any intercurrent event related to COVID-19 (i.e., a remote visit or missed visit) or that the effect would disappear after any intercurrent event unrelated to COVID-19. For continuous end points, data that were missing because of COVID-19 were imputed by multiple imputation, while other data that were missing for reasons other than COVID-19 were imputed by mLOCF. This imputation procedure assumed that the effects of treatments would remain the same had patients not experienced any intercurrent event related to COVID-19 or would remain the same after the event that caused data to be missing for reasons other than COVID-19.
Analysis Populations
Analysis populations of the BRAVE-AA1 and BRAVE-AA2 trials are summarized in Table 10.
Table 9: Statistical Analysis of Efficacy End Points in Study BRAVE-AA1 and Study BRAVE-AA2
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analysis |
|---|---|---|---|---|
Proportion of patients attaining the following at week 36:
| Logistic regression | Geographic region, duration of current episode at baseline, baseline value, and treatment group | NRIb | Hybrid imputation model: MI and NRI (primary and key secondary end points only) |
Mean change from baseline in HADS-A domain and HADS-D domain total scores at week 36 | ANCOVA | Geographic region, duration of current episode at baseline, and treatment group | mLOCFc | NA |
Mean change from baseline at week 36 in Skindex-16 for AA domain scores (symptoms, emotions, and functioning) | ANCOVA | Geographic region, duration of current episode at baseline, baseline value, and treatment group | LOCFd | NA |
ANCOVA = analysis of covariance; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; HADS-A = Hospital Anxiety and Depression Scale-Anxiety; HADS-D = Hospital Anxiety and Depression Scale-Depression; LOCF = last observation carried forward; MI = multiple imputation; mLOCF = modified last observation carried forward; NA = not applicable; NRI = nonresponder imputation; SALT = Severity of Alopecia Tool; SALT50 = at least a 50% improvement from baseline in the Severity of Alopecia Tool score; Skindex-16 for AA = Skindex-16 for Alopecia Areata.
Note: Details included in Table 9 are from the sponsor’s Summary of Clinical Evidence.9
aThis was among patients with a score of 2 or more at baseline.
bPatients were considered nonresponders if they did not meet clinical response criteria or if they permanently discontinued study treatment or discontinued from the study at any time before the time point of interest for any reason.
cThe most recent nonmissing postbaseline assessment was used. Data after permanent study treatment discontinuation were not carried forward.
dThe most recent nonmissing postbaseline assessment was used.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Table 10: Analysis Populations of Study BRAVE-AA1 and Study BRAVE-AA2
Population | Definition | Application |
|---|---|---|
Full analysis set | This included all randomized patients. Specifically for Study BRAVE-AA1, only randomized patients enrolled in the phase III portion were included. Patients were analyzed according to the intervention to which they were randomized at baseline. | Efficacy analyses, baseline patient characteristics, patient disposition, concomitant medications |
Safety population | This included all randomized patients who received at least 1 dose of study intervention and who did not discontinue from the study for the reason “lost to follow-up” at the first postbaseline visit. Patients were analyzed according to the intervention to which they were assigned. | Safety analyses |
Notes: Details included in Table 10 are from the sponsor’s Summary of Clinical Evidence.9
The trials included 2 additional analysis sets (a modified full analysis set and a per-protocol set). They were not of interest to this review and not summarized.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Results
Results of the 36-week, double-blind, placebo-controlled treatment phase of Study BRAVE-AA1 (the phase III portion only) and Study BRAVE-AA2 are summarized in this section.
Patient Disposition
Patient disposition in the BRAVE-AA1 and BRAVE-AA2 trials in the double-blind treatment period are summarized in Table 11.
In Study BRAVE-AA1 and Study BRAVE-AA2, 21.1% and 24.9% of patients were excluded during the screening period, respectively, mostly because they did not meet eligibility criteria. In Study BRAVE-AA1, a total of 654 patients were randomized to placebo (n = 189), baricitinib 2 mg (n = 184), and baricitinib 4 mg (n = 281). In Study BRAVE-AA2, a total of 546 patients were randomized to placebo (n = 156), baricitinib 2 mg (n = 156), and baricitinib 4 mg (n = 234). In both trials, study treatment discontinuation in the placebo group was higher numerically (11.1% in Study BRAVE-AA1 and 13.5% in Study BRAVE-AA2) compared with the baricitinib groups (2 mg [8.7%] and 4 mg [6.8%] in Study BRAVE-AA1 and 2 mg [10.9%] and 4 mg [7.7%] in Study BRAVE-AA2), with withdrawal by patient being the most common reason for treatment discontinuation in the placebo group.
In both trials, the full analysis set population consisted of all randomized patients in the treatment groups and the safety population consisted of all or close to all randomized patients (98.7% to 100%) in the treatment groups.
Table 11: Patient Disposition in Study BRAVE-AA1 and Study BRAVE-AA2 — DB Treatment Period
Patient disposition | Study BRAVE-AA1 | Study BRAVE-AA2 | ||||
|---|---|---|---|---|---|---|
Placebo | BARI 2 mg | BARI 4 mg | Placebo | BARI 2 mg | BARI 4 mg | |
Screened, N | 829 | 727 | ||||
Reason for exclusion during screening period, N (%) | 175 (21.1) | 181 (24.9) | ||||
Eligibility criteria | 140 (80.0) | 145 (80.1) | ||||
Withdrawal by patient | 27 (15.4) | 21 (11.6) | ||||
Adverse event | 1 (0.6) | 0 (0) | ||||
Physician decision | 2 (1.1) | 5 (2.8) | ||||
Other | 5 (2.9) | 11 (6.1) | ||||
Randomized, N | 189 | 184 | 281 | 156 | 156 | 234 |
Discontinued treatment before week 36 visit, n (%) | 21 (11.1) | 16 (8.7) | 19 (6.8) | 21 (13.5) | 17 (10.9) | 18 (7.7) |
Reason for study treatment discontinuation, n (%) | ||||||
Adverse event | 2 (1.1) | 2 (1.1) | 3 (1.1) | 4 (2.6) | 4 (2.6) | 6 (2.6) |
Lack of efficacy | 1 (0.5) | 0 (0) | 2 (0.7) | 1 (0.6) | 0 (0) | 2 (0.9) |
Pregnancy | 0 (0) | 0 (0) | 1 (0.4) | 1 (0.6) | 0 (0) | 0 (0) |
Protocol deviation | 0 (0) | 1 (0.5) | 0 (0) | 1 (0.6) | 1 (0.6) | 1 (0.4) |
Withdrawal by patient | 12 (6.3) | 5 (2.7) | 9 (3.2) | 7 (4.5) | 6 (3.8) | 7 (3.0) |
Lost to follow-up | 5 (2.6) | 6 (3.3) | 3 (1.1) | 5 (3.2) | 5 (3.2) | 2 (0.9) |
Physician decision | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.6) | 0 (0) |
Did not advance past screening | 0 (0) | 0 (0) | 1 (0.4) | 0 (0) | 0 (0) | 0 (0) |
Other | 1 (0.5) | 2 (1.1) | 0 (0) | 2 (1.3) | 0 (0) | 0 (0) |
FAS, n (%) | 189 (100) | 184 (100) | 281 (100) | 156 (100) | 156 (100) | 234 (100) |
Safety population, n (%) | 189 (100) | 183 (99.5) | 280 (99.6) | 154 (98.7) | 155 (99.4) | 233 (99.6) |
BARI = baricitinib; DB = double-blind; FAS = full analysis set.
Note: Details included in Table 11 are from the sponsor’s Summary of Clinical Evidence.9
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Baseline Characteristics
Patient baseline demographics, disease characteristics, and the history of treatment for AA of Study BRAVE-AA1 and Study BRAVE-AA2 are summarized in Table 12. The baseline characteristics outlined in the table are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
The baseline characteristics of the enrolled patients in general were similar between the BRAVE-AA1 and BRAVE-AA2 trials. The mean age of patients was 37.1 (SD = 13.0) years and 38.0 (SD = 12.7) years in Study BRAVE-AA1 and Study BRAVE-AA2, respectively. Compared to Study BRAVE-AA1, Study BRAVE-AA2 had proportionally more patients who were female (58.6% in Study BRAVE-AA1 and 63.2% in Study BRAVE-AA2) and white (45.9% in Study BRAVE-AA1 and 58.8% in Study BRAVE-AA2), and fewer patients who were Asian (41.2% in Study BRAVE-AA1 and 30.6% in Study BRAVE-AA2). In Study BRAVE-AA1 and Study BRAVE-AA2, patients had a mean duration of the current AA episode of 3.6 (SD = 3.9) years and 4.3 (SD = 4.9) years, respectively. Both trials consisted of a slightly higher proportion of patients with very severe AA (53.8% in Study BRAVE-AA1 and 52.5% in Study BRAVE-AA2) compared with those with severe AA (46.2% in Study BRAVE-AA1 and 47.5% in Study BRAVE-AA2). Approximately 90% of patients in the trials received prior AA treatment, with the most common treatments (reported in at least 40% of patients) being topical therapies, intralesional therapy, and systemic immunosuppressants and immunomodulators for AA.
Several between-group imbalances in baseline characteristics were identified in the trials. In Study BRAVE-AA1, compared with the placebo group, the baricitinib 2 mg group had a higher proportion of patients who were white (44.1% in the placebo group and 50.8% in the baricitinib 2 mg group), had very severe AA (51.3% in the placebo group and 58.2% in the baricitinib 2 mg group), and had adult onset of AA (59.3% in the placebo group and 67.9% in the baricitinib 2 mg group), as well as a lower proportion of patients who had received prior systemic immunosuppressive and immunomodulating treatments (53.4% in the placebo group and 45.7% in the baricitinib 2 mg group). A higher proportion of patients in the baricitinib 2 mg and baricitinib 4 mg groups compared to the placebo group had beforepical immunotherapy (31.0% in the baricitinib 2 mg group, 29.9% in the baricitinib 4 mg group, and 23.8% in the placebo group), phototherapy (18.5% in the baricitinib 2 mg group, 19.2% in the baricitinib 4 mg group, and 12.2% in the placebo group), and procedures for treating AA (22.3% in the baricitinib 2 mg group, 23.1% in the baricitinib 4 mg group, and 15.9% in the placebo group). In Study BRAVE-AA2, the baricitinib 2 mg and baricitinib 4 mg groups had a higher proportion of patients compared to the placebo group who were white (59.0% in the baricitinib 2 mg group, 61.5% in the baricitinib 4 mg group, and 54.5% in the placebo group) and a lower proportion of patients who had received prior systemic immunosuppressants and immunomodulators (57.1% in the baricitinib 2 mg group, 53.0% in the baricitinib 4 mg group, and 62.2% in the placebo group), and prior intralesional therapy (52.6% in the baricitinib 2 mg group, 44.4% in the baricitinib 4 mg group, and 56.4% in the placebo group). Also, a lower proportion of patients in the baricitinib 2 mg group (19.9%) had received beforepical immunotherapy compared to the placebo group (26.3%). No other notable between-group imbalances were observed for other baseline characteristics in the trials.
Table 12: Patient Baseline Characteristics in Study BRAVE-AA1 and Study BRAVE-AA2 — DB Treatment Period (FAS)
Characteristic | Study BRAVE-AA1 | Study BRAVE-AA2 | ||||
|---|---|---|---|---|---|---|
Placebo (N = 189) | BARI 2 mg (N = 184) | BARI 4 mg (N = 281) | Placebo (N = 156) | BARI 2 mg (N = 156) | BARI 4 mg (N = 234) | |
Demographics | ||||||
Age (years), mean (SD) | 37.4 (12.9) | 38.0 (12.8) | 36.3 (13.3) | 37.1 (12.4) | 39.0 (13.0) | 38.0 (12.7) |
Female, n (%) | 109 (57.5) | 109 (59.2) | 165 (58.7) | 98 (62.8) | 103 (66.0) | 144 (61.5) |
Male, n (%) | 80 (42.3) | 75 (40.8) | 116 (41.3) | 58 (37.2) | 53 (34.0) | 90 (38.5) |
Race, n (%) | ||||||
American Indian or Alaska Native | 8 (4.3) | 5 (2.7) | 8 (2.9) | 0 | 0 | 0 |
Asian | 78 (41.5) | 76 (41.5) | 114 (40.7) | 51 (32.7) | 49 (31.4) | 67 (28.6) |
Black or African American | 17 (9.0) | 7 (3.8) | 28 (10.0) | 16 (10.3) | 12 (7.7) | 18 (7.7) |
Native Hawaiian or other Pacific Islander | 1 (0.5) | 1 (0.5) | 1 (0.4) | 0 | 1 (0.6) | 0 |
White | 83 (44.1) | 93 (50.8) | 123 (43.9) | 85 (54.5) | 92 (59.0) | 144 (61.5) |
Disease characteristics | ||||||
Duration from onset of AA (years), mean (SD) | 12.6 (11.2) | 12.1 (9.8) | 11.8 (11.1) | 11.8 (10.2) | 13.1 (11.8) | 11.9 (11.1) |
Duration of the current episode of AA (years), mean (SD) | 3.5 (3.7) | 3.9 (4.7) | 3.5 (3.4) | 4.7 (5.5) | 4.4 (6.1) | 3.9 (3.4) |
Age of onset of AA in years, n (%) | ||||||
< 18 | 77 (40.7) | 59 (32.1) | 108 (38.4) | 57 (36.5) | 55 (35.3) | 74 (31.6) |
≥ 18 | 112 (59.3) | 125 (67.9) | 173 (61.6) | 99 (63.5) | 101 (64.7) | 160 (68.4) |
Disease severity, n (%) | ||||||
Severe (a SALT score of 50 to 94) | 92 (48.7) | 77 (41.8) | 133 (47.3) | 74 (47.7) | 70 (44.9) | 115 (49.1) |
Very severe (a SALT score of 95 to 100) | 97 (51.3) | 107 (58.2) | 148 (52.7) | 81 (52.3) | 86 (55.1) | 119 (50.9) |
AA treatment history | ||||||
Prior AA treatment, n (%) | 173 (91.5) | 163 (88.6) | 247 (87.9) | 149 (95.5) | 144 (92.3) | 211 (90.2) |
Topical therapiesa | 108 (57.1) | 102 (55.4) | 173 (61.6) | 98 (62.8) | 97 (62.2) | 148 (63.2) |
Topical immunotherapy | 45 (23.8) | 57 (31.0) | 84 (29.9) | 41 (26.3) | 31 (19.9) | 63 (26.9) |
Intralesional therapy | 101 (53.4) | 92 (50.0) | 152 (54.1) | 88 (56.4) | 82 (52.6) | 104 (44.4) |
Systemic immunosuppressive and immunomodulating drugs | 101 (53.4) | 84 (45.7) | 138 (49.1) | 97 (62.2) | 89 (57.1) | 124 (53.0) |
Corticosteroids | 68 (36.0) | 51 (27.7) | 103 (36.7) | 77 (49.4) | 77 (49.4) | 102 (43.6) |
JAK inhibitor | 12 (6.3) | 7 (3.8) | 15 (5.3) | 9 (5.8) | 6 (3.8) | 10 (4.3) |
Others | 57 (30.2) | 55 (29.9) | 88 (31.3) | 54 (34.6) | 32 (20.5) | 52 (22.2) |
Nonimmunosuppressive systemic treatments | 17 (9.0) | 20 (10.9) | 28 (10.0) | 15 (9.6) | 16 (10.3) | 18 (7.7) |
Phototherapy | 23 (12.2) | 34 (18.5) | 54 (19.2) | 28 (17.9) | 24 (15.4) | 37 (15.8) |
Proceduresb | 30 (15.9) | 41 (22.3) | 65 (23.1) | 35 (22.4) | 31 (19.9) | 47 (20.1) |
AA = alopecia areata; BARI = baricitinib; DB = double-blind; FAS = full analysis set; JAK = Janus kinase; SALT = Severity of Alopecia Tool; SD = standard deviation.
Note: Details included in Table 12 are from the sponsor’s Summary of Clinical Evidence.9
aThis excludes topical immunotherapy.
bThis includes cryotherapy, microneedling, and platelet-rich plasma injections.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Exposure to Interventions
Study Treatments
Patient exposure to study treatment in the double-blind treatment period of Study BRAVE-AA1 and Study BRAVE-AA2 are summarized in Table 13. No notable between-group difference was observed in the mean duration of exposure in both trials. The median treatment adherence rate varied from 98.4% to 99.2% across the treatment groups in the trials. One patient in the baricitinib 4 mg group of the BRAVE-AA1 trial had renal impairment requiring a dose adjustment to baricitinib 2 mg.
Concomitant Medications
The use of concomitant medications for AA in the double-blind treatment period of Study BRAVE-AA1 and Study BRAVE-AA2 are summarized in Table 14. In both trials, a small proportion of patients used at least 1 concomitant medication for AA (3.2% to 5.7% for Study BRAVE-AA1 and 3.2% to 5.1% for Study BRAVE-AA2). No notable imbalance was observed between treatment groups.
Table 13: Patient Exposure to Study Treatment in Study BRAVE-AA1 and Study BRAVE-AA2 — DB Treatment Period (Safety Population)
Exposure | Study BRAVE-AA1 | Study BRAVE-AA2 | ||||
|---|---|---|---|---|---|---|
Placebo | BARI 2 mg | BARI 4 mg | Placebo | BARI 2 mg | BARI 4 mg | |
Total, patient-yearsa | 124.0 | 121.2 | 188.7 | 100.6 | 101.5 | 156.4 |
Patient weeks of exposureb | ||||||
N | 189 | 183 | 280 | 154 | 155 | 233 |
Mean (SD) | 34.2 (7.5) | 34.6 (7.3) | 35.2 (5.8) | 34.1 (6.7) | 34.2 (7.0) | 35.0 (5.5) |
Patient adherence to treatment (%) | ||||||
N | 189 | 184 | 280 | 155 | 156 | 234 |
Mean (SD) | 99.4 (16.4) | 110.6 (90.7) | 99.9 (9.3) | 117.5 (281.9) | 120.1 (280.6) | 113.9 (229.5) |
Median (IQR) | 98.8 (95.5 to 100.2) | 99.2 (96.4 to 100.7) | 99.1 (96.9 to 100.4) | 98.4 (93.7 to 100) | 99.2 (95.6 to 100) | 99.2 (96.4 to 100) |
Range | 63.2 to 252.1 | 70.8 to 1,200 | 75.2 to 165.1 | 14.4 to 3,600 | 34.4 to 3,600 | 41.7 to 3,600 |
BARI = baricitinib; DB = double-blind; IQR = interquartile range; SD = standard deviation.
Note: Details included in Table 13 are from the sponsor’s Summary of Clinical Evidence.9
aTotal patient-years was calculated in the safety population as the sum of the duration of exposure in days for all patients in the dosing regimen divided by 365.25.
bThe duration of exposure was calculated in the full analysis set population as the date of the last dose of the study drug through week 36 – the date of the first dose of the study drug + 1.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Table 14: Concomitant AA Medications in Study BRAVE-AA1 and Study BRAVE-AA2 — DB Treatment Period (FAS)
Concomitant AA medication | Study BRAVE-AA1 | Study BRAVE-AA2 | ||||
|---|---|---|---|---|---|---|
Placebo (N = 189) | BARI 2 mg (N = 184) | BARI 4 mg (N = 281) | Placebo (N = 156) | BARI 2 mg (N = 156) | BARI 4 mg (N = 234) | |
Patients with ≥ 1 medication for AA, n (%) | 6 (3.2) | 6 (3.3) | 16 (5.7) | 5 (3.2) | 6 (3.8) | 12 (5.1) |
Most common medication,a n (%) | ||||||
Minoxidil (topical) | 2 (1.1) | 0 (0) | 6 (2.1) | 1 (0.6) | 1 (0.6) | 5 (2.1) |
Finasteride | 0 (0) | 0 (0) | 4 (1.4) | 0 (0) | 0 (0) | 1 (0.4) |
Glucosamine | 0 (0) | 1 (0.5) | 2 (0.7) | 0 (0) | 0 (0) | 0 (0) |
Bimatoprost | 2 (1.1) | 2 (1.1) | 1 (0.4) | 1 (0.6) | 0 (0) | 1 (0.4) |
Biotin | 1 (0.5) | 1 (0.5) | 1 (0.4) | 1 (0.6) | 0 (0) | 2 (0.9) |
AA = alopecia areata; BARI = baricitinib; DB = double-blind; FAS = full analysis set.
Note: Details included in Table 14 are from the sponsor’s Summary of Clinical Evidence.9
aThese medications were reported in 2 or more patients in any treatment group.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Efficacy
Key efficacy results from the double-blind treatment period of Study BRAVE-AA1 and Study BRAVE-AA2 are summarized in Table 15.
SALT Score
Proportion of Patients Attaining SALT Score of 20 or Less
The proportion of patients attaining a SALT score of 20 or less at week 36 was the primary end point in both trials. At week 36, the between-group difference comparing the baricitinib 2 mg group versus the placebo group was 16.4% (95% CI, 9.7% to 23.4%; P < 0.001) in Study BRAVE-AA1 and 14.7% (95% CI, 8.3% to 21.6%; P < 0.001) in Study BRAVE-AA2. The between-group difference comparing the baricitinib 4 mg group and the placebo group was 29.9% (95% CI, 23.2% to 36.2%; P < 0.001) in Study BRAVE-AA1 and 29.9% (95% CI, 23.1% to 36.3%; P < 0.001) in Study BRAVE-AA2. Results of the primary analysis were in favour of both regimens of baricitinib and the sensitivity analysis (accounting for missing data because of the COVID-19 pandemic) showed consistent results. In both trials, subgroup analyses by baseline disease severity and duration of the current episode of AA were consistent with the primary analysis (Appendix 1, Table 28).
The percentage change from baseline in the SALT score was assessed at week 36 (a key secondary end point) in both trials. In both trials, the between-group difference comparing baricitinib and placebo was in favour of baricitinib for both the 2 mg regimen (–23.1% [95% CI, –30.6% to –15.6%; P < 0.001] in Study BRAVE-AA1 and –25.3% [95% CI, –32.8% to –17.7%] in Study BRAVE-AA2) and the 4 mg regimen (–37.7% [95% CI, –44.4% to –30.9%; P < 0.001] in Study BRAVE-AA1 and 44.5% [95% CI, –51.3% to –37.7%; P < 0.001] in Study BRAVE-AA2).
Proportion of Patients Attaining SALT50
The between-group difference in the proportion of patients attaining a SALT50 response at week 36 (a secondary end point) comparing the baricitinib 2 mg group versus the placebo group was 17.7% (95% CI, 9.5% to 25.8%; P < 0.001) in Study BRAVE-AA1 and 23.1% (95% CI, 15.1% to 31.0%; P < 0.001) in Study BRAVE-AA2. The between-group difference comparing the baricitinib 4 mg group with the placebo group was 33.6% (95% CI, 25.6% to 40.7%; P < 0.001) in Study BRAVE-AA1 and 41.9% (95% CI, 34.0% to 48.7%; P < 0.001) in Study BRAVE-AA2. Results of the SALT75 responder analysis were consistent with the SALT50 responder analysis (Table 29 in Appendix 1). Neither end point was adjusted for multiplicity in the trials. Analyses using a lower threshold (e.g., at least a 30% improvement from baseline in the SALT score) were not conducted.
ClinRO Measures for EB and EL Hair Loss
Proportion of Patients Attaining ClinRO Measure for EB Hair Loss Score of 0 or 1 With Improvement of 2 Points or More From Baseline Among Patients With ClinRO Measure for EB Hair Loss Score of 2 or More at Baseline
Between 66.3% and 73.9% of all randomized patients had a ClinRO measure for EB hair loss score of at least 2 at baseline in the trials and contributed to the analysis of the proportion of patients who had a ClinRO measure for EB hair loss score of 0 or 1 with at least a 2-point improvement from baseline at week 36 (a key secondary end point).
The between-group difference comparing baricitinib 2 mg versus placebo was 15.9% (95% CI, 8.4% to 23.6%; P < 0.001) in favour of baricitinib 2 mg in Study BRAVE-AA1. In Study BRAVE-AA2, the between-group difference comparing baricitinib 2 mg versus placebo was 7.1% (95% CI, –0.3% to 15.0%; P = 0.08); because of the failure of this end point, no formal testing was conducted for subsequent end points in the statistical hierarchy in this study. The between-group difference was in favour of baricitinib 4 mg over placebo in both trials (28.2% [95% CI, 20.3% to 35.4%; P < 0.001] in Study BRAVE-AA1 and 30.3% [95% CI, 21.4% to 38.4%; P < 0.001] in Study BRAVE-AA2). Results based on the PRO measure showed consistent results.
Proportion of Patients Attaining ClinRO Measure for EL Hair Loss Score of 0 or 1 With Improvement of 2 Points or More From Baseline Among Patients With ClinRO Measure for EL Hair Loss Score of 2 or More at Baseline
Between 51.3% and 60.3% of all randomized patients had a ClinRO measure for EL hair loss score of at least 2 at baseline in the trials and contributed to the analysis of the proportion of patients who had a ClinRO measure for EL hair loss score of 0 or 1 with at least a 2-point improvement from baseline at week 36 (a key secondary end point).
The between-group difference comparing baricitinib 2 mg and placebo was 10.4% (95% CI, 2.7% to 18.3%) in Study BRAVE-AA1 and 4.6% (95% CI, –3.7% to 13.2%) in Study BRAVE-AA2, neither of which was formally tested for statistical significance because of a prior failure of an outcome in the statistical hierarchy. The between-group difference favoured baricitinib 4 mg treatment over placebo in both trials (30.4% [95% CI, 21.6% to 38.1%; P < 0.001] in Study BRAVE-AA1 and 28.7% [95% CI, 18.7% to 37.5%; P < 0.001] in Study BRAVE-AA2). Results based on the PRO measure showed consistent results.
HADS Anxiety and HADS Depression Domain Scores
The mean changes from baseline in HADS anxiety and HADS depression domain scores were secondary end points and not adjusted for multiplicity in both trials.
Change From Baseline in HADS Anxiety Domain Score
The between-group difference comparing baricitinib 2 mg and placebo with respect to change from baseline in the HADS anxiety domain score at week 36 favoured baricitinib 2 mg in Study BRAVE-AA1 at –0.8 (95% CI, –1.4 to –0.3; P ≤ 0.01) and at –0.2 (95% CI, –0.8 to 0.4; P = 0.5) in Study BRAVE-AA2. The between-group difference comparing baricitinib 4 mg and placebo favoured baricitinib 4 mg in both trials (–0.5 [95% CI, –1.1 to 0.0; P = 0.04] in Study BRAVE-AA1 and –0.7 [95% CI, –1.3 to –0.2; P = 0.01] in Study BRAVE-AA2).
Change From Baseline in HADS Depression Domain Score
The between-group difference comparing baricitinib 2 mg and placebo with respect to change from baseline in the HADS depression domain score at week 36 was –0.4 (95% CI, –0.9 to 0.1; P = 0.1) in Study BRAVE-AA1 and –0.5 (95% CI, –1.1 to 0.1; P = 0.08) in Study BRAVE-AA2. The between-group difference comparing baricitinib 4 mg and placebo favoured baricitinib 4 mg in Study BRAVE-AA2 at –0.7 (95% CI, –1.2 to –0.2; P = 0.01) and at –0.3 (95% CI, –0.8 to 0.1; P = 0.2) in Study BRAVE-AA1.
Skindex-16 for AA
The mean changes from baseline in Skindex-16 for AA domain scores (symptoms, emotions, and functioning) were exploratory end points in Study BRAVE-AA1 and secondary end points in Study BRAVE-AA2. These end points were not adjusted for multiplicity.
Change From Baseline in Skindex-16 for AA Symptoms Domain Score
The difference between the baricitinib 2 mg group and the placebo group with respect to change from baseline in the Skindex-16 for AA symptoms domain score at week 36 favoured the baricitinib 2 mg group in Study BRAVE-AA1 at –4.76 (95% CI, –9.13 to –0.40; P = 0.033) and at –3.02 (95% CI, –6.91 to 0.88; P = 0.129) in Study BRAVE-AA2. The difference between the baricitinib 4 mg group and the placebo group favoured the baricitinib 4 mg group in Study BRAVE-AA2 at –4.21 (95% CI, –7.75 to –0.68; P = 0.020) and at –2.75 (95% CI, –6.67 to 1.17; P = 0.168) in Study BRAVE-AA1.
Change From Baseline in Skindex-16 for AA Emotions Domain Score
The between-group difference with respect to change from baseline in the Skindex-16 for AA emotions domain score at week 36 was in favour of baricitinib over placebo in both trials for both the baricitinib 2 mg regimen (–11.50 [95% CI, –17.71 to –5.30; P < 0.001] in Study BRAVE-AA1 and –6.75 [95% CI, –12.68 to –0.82; P = 0.026] in Study BRAVE-AA2) and the baricitinib 4 mg regimen (–11.01 [95% CI, –16.57 to –5.45; P < 0.001] in Study BRAVE-AA1 and –13.42 [95% CI, –18.80 to –0.84; P < 0.001] in Study BRAVE-AA2).
Change From Baseline in Skindex-16 for AA Functioning Domain Score
The difference between the baricitinib 2 mg group and the placebo group with respect to change from baseline in the Skindex-16 for AA functioning domain score at week 36 was –5.07 (95% CI, –10.94 to 0.80; P = 0.090) in Study BRAVE-AA1 and –4.38 (95% CI, –9.65 to 0.88; P = 0.103) in Study BRAVE-AA2. The difference between the baricitinib 4 mg group and the placebo group favoured the baricitinib 4 mg group in both trials (–7.04 [95% CI, –12.31 to –1.77; P = 0.009] in Study BRAVE-AA1 and –8.33 [95% CI, –13.10 to –3.56; P < 0.001] in Study BRAVE-AA2).
Table 15: Key Efficacy Results From Study BRAVE-AA1 and Study BRAVE-AA2 — DB Treatment Period (FAS)
Outcome | Study BRAVE-AA1 | Study BRAVE-AA2 | ||||
|---|---|---|---|---|---|---|
PBO (N = 189) | BARI 2 mg (N = 184) | BARI 4 mg (N = 281) | PBO (N = 156) | BARI 2 mg (N = 156) | BARI 4 mg (N = 234) | |
Proportion of patients attaining a SALT score ≤ 20 at week 36 | ||||||
Response, n (%) (95% CI)a | 10 (5.3) (2.9 to 9.5) | 40 (21.7) (16.4 to 28.2) | 99 (35.2) (29.9 to 41.0) | 4 (2.6) (1.0 to 6.4) | 27 (17.3) (12.2 to 24.0) | 76 (32.5) (26.8 to 38.7) |
Difference vs. PBO % (95% CI)a | Reference | 16.4 (9.7 to 23.4) | 29.9 (23.2 to 36.2) | Reference | 14.7 (8.3 to 21.6) | 29.9 (23.1 to 36.3) |
P value | Reference | < 0.001 | < 0.001 | Reference | < 0.001 | < 0.001 |
Proportion of patients attaining a SALT50 response at week 36 | ||||||
Response, n (%) (95% CI) | 24 (12.7) (8.7 to 18.2) | 56 (30.4) (24.2 to 37.4) | 130 (46.3) (40.5 to 52.1) | 8 (5.1) (2.6 to 9.8) | 44 (28.2) (21.7 to 35.7) | 110 (47.0) (40.7 to 53.4) |
Difference vs. PBO % (95% CI)a | Reference | 17.7 (9.5 to 25.8) | 33.6 (25.6 to 40.7) | Reference | 23.1 | 41.9 |
P valueb | Reference | < 0.001b | < 0.001b | Reference | < 0.001b | < 0.001b |
Proportion of patients attaining a ClinRO measure for EB hair loss score of 0 or 1 with ≥ 2-point improvement from baseline at week 36 (among patients with a ClinRO measure for EB hair loss score of ≥ 2 at baseline) | ||||||
Number of patients included in the analysis, n (%) | 124 (65.6) | 136 (73.9) | 188 (66.9) | 112 (71.8) | 104 (66.7) | 161 (68.8) |
Response, n (%) (95% CI) | 4 (3.2) (1.3 to 8.0) | 26 (19.1) (13.4 to 26.5) | 59 (31.4) (25.2 to 38.3) | 5 (4.5) (1.9 to 10.0) | 12 (11.5) (6.7 to 19.1) | 56 (34.8) (27.9 to 42.4) |
Difference vs. PBO % (95% CI)a | Reference | 15.9 (8.4 to 23.6) | 28.2 (20.3 to 35.4) | Reference | 7.1 (–0.3 to 15.0) | 30.3 (21.4 to 38.4) |
P value | Reference | < 0.001 | < 0.001 | Reference | 0.08 | < 0.001 |
Proportion of patients attaining a ClinRO measure for EL hair loss score of 0 or 1 with ≥ 2-point improvement from baseline at week 36 (among patients with a ClinRO measure for EL hair loss score of ≥ 2 at baseline) | ||||||
Number of patients included in the analysis, n (%) | 96 (50.8) | 111 (60.3) | 167 (59.4) | 90 (57.7) | 89 (57.1) | 140 (59.8) |
Response, n (%) (95% CI) | 3 (3.1) (1.1 to 8.8) | 15 (13.5) (8.4 to 21.1) | 56 (33.5) (26.8 to 41.0) | 5 (5.6) (2.4 to 12.4) | 9 (10.1) (5.4 to 18.1) | 48 (34.3) (26.9 to 42.5) |
Difference vs. PBO % (95% CI)a | NA | 10.4 (2.7 to 18.3) | 30.4 (21.6 to 38.1) | NA | 4.6 (–3.7 to 13.2) | 28.7 (18.7 to 37.5) |
P value | NA | 0.012c | < 0.001 | NA | 0.260c | < 0.001 |
HADS anxiety domain total score | ||||||
Number of patients who contributed to the analysis, n (%) | 155 (82.0) | 162 (88.0) | 245 (87.2) | 129 (82.7) | 134 (85.9) | 211 (90.2) |
Baseline, mean | 6.74 | 6.22 | 6.12 | 5.90 | 6.22 | 6.37 |
Change from baseline in score at week 36, LSM (SE) | –0.40 (0.23) | –1.22 (0.24) | –0.93 (0.20) | –0.47 (0.23) | –0.67 (0.23) | –1.19 (0.18) |
Difference vs. PBO, LSM (95% CI)d | Reference | –0.8 (–1.4 to –0.3) | –0.5 (–1.1 to –0.0) | Reference | –0.2 (–0.8 to 0.4) | –0.7 (–1.3 to –0.2) |
P value | Reference | P ≤ 0.01b | 0.04b | Reference | 0.5b | 0.01b |
HADS depression domain total score | ||||||
Number of patients who contributed to the analysis, n (%) | 155 (82.0) | 162 (88.0) | 245 (87.2) | 129 (82.7) | 134 (85.9) | 211 (90.2) |
Baseline, mean | 3.96 | 4.21 | 3.95 | 3.69 | 3.78 | 3.83 |
Change from baseline in score at week 36, LSM (SE) | 0.04 (0.21) | –0.38 (0.21) | –0.28 (0.18) | 0.29 (0.21) | –0.22 (0.21) | –0.39 (0.17) |
Difference vs. PBO, LSM (95% CI)d | Reference | –0.4 (–0.9 to 0.1) | –0.3 (–0.8 to 0.1) | Reference | –0.5 (–1.1 to 0.1) | –0.7 (–1.2 to –0.12) |
P value | Reference | 0.1b | 0.2b | Reference | 0.08b | 0.01b |
Skindex-16 for AA domain scores | ||||||
Symptoms domain | ||||||
Number of patients who contributed to the analysis, n (%) | 92 (48.7) | 94 (51.1) | 147 (52.3) | 129 (82.7) | 134 (85.9) | 211 (90.2) |
Baseline, mean | 20.80 | 19.64 | 18.42 | 18.80 | 18.03 | 16.42 |
Change from baseline in score at week 36, LSM (SE) | 0.02 (1.67) | –4.74 (1.74) | –2.73 (1.39) | 1.17 (1.42) | –1.85 (1.43) | –3.04 (1.14) |
Difference vs. PBO, LSM (95% CI)d | Reference | –4.76 (–9.13 to –0.40) | –2.75 (–6.67 to 1.17) | Reference | –3.02 (–6.91 to 0.88) | –4.21 (–7.75 to –0.68) |
P value | Reference | 0.033b | 0.168b | Reference | 0.129b | 0.020b |
Emotions domain | ||||||
Number of patients who contributed to the analysis, n (%) | 92 (48.7) | 94 (51.1) | 147 (52.3) | 129 (82.7) | 134 (85.9) | 211 (90.2) |
Baseline, mean | 67.29 | 66.40 | 66.07 | 69.56 | 70.45 | 68.03 |
Change from baseline in score at week 36, LSM (SE) | –11.96 (2.38) | –23.46 (2.48) | –22.97 (1.99) | –11.98 (2.15) | –18.73 (2.17) | –25.40 (1.73) |
Difference vs. PBO, LSM (95% CI)d | Reference | –11.50 (–17.71 to –5.30) | –11.01 (–16.57 to –5.45) | Reference | –6.75 (–12.68 to –0.82) | –13.42 (–18.80 to –8.04) |
P value | Reference | < 0.001b | < 0.001b | Reference | 0.026b | < 0.001b |
Functioning domain | ||||||
Number of patients who contributed to the analysis, n (%) | 92 (48.7) | 94 (51.1) | 147 (52.3) | 129 (82.7) | 134 (85.9) | 211 (90.2) |
Baseline, mean | 48.18 | 49.10 | 53.98 | 52.88 | 48.40 | 49.13 |
Change from baseline in score at week 36, LSM (SE) | –10.12 (2.25) | –15.19 (2.34) | –17.16 (1.87) | –9.67 (1.91) | –14.05 (1.93) | –18.00 (1.54) |
Difference vs. PBO, LSM (95% CI)d | Reference | –5.07 (–10.94 to 0.80) | –7.04 (–12.31 to –1.77) | Reference | –4.38 (–9.65 to 0.88) | –8.33 (–13.10 to –3.56) |
P value | Reference | 0.090b | 0.009b | Reference | 0.103b | < 0.001b |
ANCOVA = analysis of covariance; BARI = baricitinib; CI = confidence interval; ClinRO = clinician-reported outcome; DB = double-blind; EB = eyebrow; EL = eyelash; FAS = full analysis set; HADS = Hospital Anxiety and Depression Scale; LSM = least squares mean; NA = not applicable; PBO = placebo; SALT = Severity of Alopecia Tool; SALT50 = at least a 50% improvement from baseline in the Severity of Alopecia Tool score; SE = standard error; Skindex-16 for AA = Skindex-16 for Alopecia Areata; vs. = versus.
Note: Details included in Table 15 are from the sponsor’s Summary of Clinical Evidence.9
aThese between-group differences were analyzed using a logistic regression model, including geographic region, the duration of the current episode at baseline, baseline value, and treatment group as adjustment factors.
bThis end point was not adjusted for multiplicity and was at a higher risk of type I error (false-positive results).
cThis end point was not formally tested for statistical significance because of a prior failure in the statistical hierarchy.
dThese between-group differences were analyzed using an ANCOVA model, including geographic region, the duration of the current episode at baseline, baseline value, and treatment group as adjustment factors.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Harms
Harms results from the double-blind treatment period of the BRAVE-AA1 and BRAVE-AA2 trials are summarized in Table 16.
Treatment-Emergent Adverse Events
TEAEs were reported in 50.8% to 59.6% of patients across treatment groups in Study BRAVE-AA1; the frequency was slightly higher in the baricitinib 4 mg group (59.6%) compared with the placebo group (51.3%). TEAEs were reported in 63.0% to 68.4% of patients across treatment groups in Study BRAVE-AA2, with no notable between-group differences. In both trials, the most common TEAEs of baricitinib (reported in at least 5% of patients in either baricitinib group) were upper respiratory tract infection, headache, urinary tract infection, nasopharyngitis, acne, and increased blood creatine phosphokinase.
Serious Adverse Events
SAEs were reported at a low frequency, with no notable between-group differences in either trial (1.6% to 2.1% in Study BRAVE-AA1 and 1.9% to 3.4% in Study BRAVE-AA2).
Withdrawal Due to Adverse Events
WDAEs were reported at a low frequency, with no notable between-group differences in either trial (1.1% to 1.8% in Study BRAVE-AA1 and 2.6% in all groups in Study BRAVE-AA2).
Mortality
No deaths were reported in either trial.
Notable Harms
Infection
Treatment-emergent infection was reported in 25.1% to 31.4% of patients across treatment groups in Study BRAVE-AA1 and 29.2% to 37.4% of patients across treatment groups in Study BRAVE-AA2. In Study BRAVE-AA2, the frequency of infection was higher in the baricitinib 2 mg group (37.4%) compared with the placebo group (29.2%), but this was not observed in Study BRAVE-AA1. In Study BRAVE-AA1, none of the infections was reported to be serious or to have led to treatment discontinuation. In Study BRAVE-AA2, serious infection was reported in 2 (1.3%) patients and 1 (0.4%) patient in the baricitinib 2 mg and baricitinib 4 mg groups, respectively, and infection leading to treatment discontinuation was reported in 1 (0.6%) patient in the baricitinib 2 mg group. Infection leading to treatment interruption was reported in 1.1% to 5.2% of patients across the trials.
Cardiovascular and Thromboembolic Events
In Study BRAVE-AA1, myocardial infarction and coronary revascularization was reported in 1 (0.5%) patient in the baricitinib 2 mg group. Serious arrhythmia was reported in 1 (0.5%) patient in the baricitinib 4 mg group. There were no reports of cardiovascular events in Study BRAVE-AA2. There were no reports of venous or pulmonary thromboembolic events in either trial.
Other Notable Harms
No gastrointestinal perforations were reported in either trial. No nonmelanoma skin cancers were reported in either trial; 1 patient in each of the placebo group (0.6%) and the baricitinib 4 mg group (0.4%) reported other forms of malignancies in Study BRAVE-AA2.
Table 16: Harms Results from Study BRAVE-AA1 and Study BRAVE-AA2 — DB Treatment Period (Safety Population)
Adverse event | Study BRAVE-AA1 | Study BRAVE-AA2 | ||||
|---|---|---|---|---|---|---|
Placebo (N = 189) | BARI 2 mg (N = 183) | BARI 4 mg (N = 280) | Placebo (N = 154) | BARI 2 mg (N = 155) | BARI 4 mg (N = 233) | |
TEAEs, n (%) | ||||||
Patients with ≥ 1 TEAE | 97 (51.3) | 93 (50.8) | 167 (59.6) | 97 (63.0) | 106 (68.4) | 154 (66.1) |
Most common TEAEa | ||||||
Upper respiratory tract infection | 10 (5.3) | 9 (4.9) | 21 (7.5) | 11 (7.1) | 12 (7.7) | 15 (6.4) |
Headache | 9 (4.8) | 8 (4.4) | 14 (5.0) | 10 (6.5) | 12 (7.7) | 21 (9.0) |
Urinary tract infection | 3 (1.6) | 2 (1.1) | 7 (2.5) | 2 (1.3) | 12 (7.7) | 11 (4.7) |
Nasopharyngitis | 12 (6.3) | 12 (6.6) | 21 (7.5) | 7 (4.5) | 2 (1.3) | 15 (6.4) |
Acne | 1 (0.5) | 10 (5.5) | 16 (5.7) | 3 (1.9) | 9 (5.8) | 11 (4.7) |
Increased blood creatine phosphokinase | 3 (1.6) | 3 (1.6) | 16 (5.7) | 2 (1.3) | 0 (0) | 7 (3.0) |
SAEs, n (%) | ||||||
Patients with ≥ 1 SAEb | 3 (1.6) | 4 (2.2) | 6 (2.1) | 3 (1.9) | 4 (2.6) | 8 (3.4) |
WDAEs, n (%) | ||||||
WDAEsb | 2 (1.1) | 3 (1.6) | 5 (1.8) | 4 (2.6) | 4 (2.6) | 6 (2.6) |
Deaths, n (%) | ||||||
Death | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Adverse events of special interest, n (%) | ||||||
Infectionc | 53 (28.0) | 46 (25.1) | 88 (31.4) | 45 (29.2) | 58 (37.4) | 69 (29.6) |
Serious infection | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (1.3) | 1 (0.4) |
Serious infection leading to study drug interruption | 3 (1.6) | 2 (1.1) | 4 (1.4) | 7 (4.5) | 8 (5.2) | 6 (2.6) |
Serious infection leading to study drug discontinuation | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.6) | 0 (0) |
MACE events | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
MI | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
CV events other than MACE | 0 (0) | 1 (0.5) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) |
Coronary revascularization | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Serious arrhythmia | 0 (0) | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) |
Gastrointestinal perforation | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
NMSC | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Malignancies other than NMSC | 0 (0) | 0 (0) | 0 (0) | 1 (0.6) | 0 (0) | 1 (0.4) |
Venous and pulmonary thromboembolic events | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
BARI = baricitinib; CV = cardiovascular; DB = double-blind; MACE = major adverse cardiac event; MI = myocardial infarction; NMSC = nonmelanoma skin cancer; SAE = serious adverse event; TEAE = treatment-emergent adverse event; WDAE = withdrawal due to adverse event.
Note: Details included in Table 16 are from the sponsor’s Summary of Clinical Evidence.9
aThese occurred in at least 5% of patients in any group.
bNo adverse event occurred in more than 1 patient.
cThis was a TEAE.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Critical Appraisal
Internal Validity
Study BRAVE-AA1 and Study BRAVE-AA2 were randomized, double-blind, placebo-controlled trials. The method used for randomization consisted of an interactive web response system, which enabled the concealment of the allocation sequence. The baseline patient demographics and disease characteristics were in general balanced between treatment groups, except for race, the onset of AA, the proportion of patients with severe AA, and treatment history, where between-group differences were identified. The clinical experts noted that the impact of such imbalances on study results is likely to be insignificant.
The blinding of patients and study personnel was appropriately maintained. However, given that a placebo was used as a control in the trials, there is a possibility that patients may have been able to infer treatment assignment through improvement in hair loss over the study period, which could have introduced bias to the results in favour of baricitinib for efficacy outcomes that required subjective judgment (ClinRO measure, HADS, and Skindex-16 for AA). The risk of bias in the measurement of the outcome is low for the SALT tool, which was an objective measure assessed by the investigators. There is a risk of inflated subjective harms with baricitinib treatment because of potential unblinding.
An adequate sample size was attained in both trials based on the a priori sample size calculations for the primary end point. Efficacy analyses were conducted in the full analysis set population, which included all randomized patients in the group to which they were randomized (i.e., intention-to-treat); this is the ideal approach to assess the effect of assignment to the intervention. Responder analyses of ClinRO measures (EB and EL loss) were conducted in patients with specific baseline scores. In total, 30% to 50% of patients were excluded from these analyses because of not having the specified baseline score, which could impact the maintenance of randomization (i.e., prognostic imbalances between groups could arise). The extent and direction of the resulting bias is, however, unclear.
In both trials, study treatment discontinuation in the placebo group was higher numerically (11.1% in Study BRAVE-AA1 and 13.5% in Study BRAVE-AA2) compared with the baricitinib groups (8.7% [baricitinib 2 mg group] and 6.8% [baricitinib 4 mg group] in Study BRAVE-AA1 and 10.9% [baricitinib 2 mg group] and 7.7% [baricitinib 4 mg group] in Study BRAVE-AA2), primarily because of withdrawal by patient, which could potentially lead to attrition bias in favour of baricitinib. Missing data for binary outcomes (SALT and ClinRO measure-based responder analyses) were imputed using NRI, which was a conservative approach. Missing data for continuous secondary end points (change from baseline in the HADS anxiety and depression domain scores and Skindex-16 for AA domain scores) were imputed using LOCF (where the most recent nonmissing postbaseline assessment was used) or modified mLOCF (where, in addition, data after permanent study treatment discontinuation were not carried forward). The sponsor noted that very few patients experienced waxing and waning in scalp hair during treatment from the phase II portion of Study BRAVE-AA1 and several external studies on AA; therefore, they felt that the use of mLOCF or LOCF imputation for missing data was reasonable. Nonetheless, given the differential discontinuation rate, particularly between the baricitinib 4 mg group and the placebo group where a notable difference was consistently observed in both trials, potential bias in favour of baricitinib could not be ruled out. A sensitivity analysis (hybrid imputation) assessing the impact of COVID-19 was conducted on the primary end point and showed results consistent with the primary analysis.
A hierarchical testing procedure was appropriately used to account for multiplicity in the primary and key secondary end points. Analyses of other secondary and exploratory end points were not part of the statistical hierarchy. As such, statistically significant results are at an increased risk of type I error (false-positive results). In both studies, results of the ClinRO measure for EL hair loss responder analysis comparing the baricitinib 2 mg and placebo groups were not formally tested for statistical significance because of a prior failure in the statistical hierarchy but provided supportive evidence. Subgroup analyses of interest (by baseline disease severity and duration of the current episode of AA) were specified a priori; however, there was a lack of sample size consideration and control for multiplicity for these subgroup analyses, which precluded definitive conclusions on subgroup effects.
The primary end point was assessed using the SALT tool for which evidence for validity in patients with AA is available. The responder analysis was based on a threshold of a SALT score of less than 20, which was consistent with the literature-identified MID estimate of the instrument.40 Evidence supporting the choice of threshold in percentage reduction in the SALT score responder analysis (e.g., SALT50) was not identified by the sponsor. The validity of ClinRO measures, which are novel instruments developed by the sponsor, was demonstrated in patients with AA in a study.42 Evidence supporting the use of a ██████████ ███████████ ████ ████████ ██ ███ █████████ ████████ of ClinRO EB and EL scores was available.48,49 Evidence for the validity and MID estimate of HADS and Skindex-16 for AA outcomes in patients with AA was not identified by the sponsor. In the absence of an MID estimate, it is unclear if the treatment effects of baricitinib observed in the studies were clinically important to patients and clinicians.
External Validity
The clinical experts we consulted noted that the inclusion and exclusion criteria of the trials in general were reflective of the patient population eligible for baricitinib treatment in Canada, although patients with a diffuse type of AA (estimated to range from 5% to 10% of patients) would not necessarily be excluded from treatment in clinical practice. The trials excluded males older than 60 years and females older than 70 years. One clinical expert commented that older adults are reasonable candidates for baricitinib treatment while the other clinical expert noted that older adults are much less likely to benefit from baricitinib treatment compared with younger patients since older adults tend to have other concurrent causes of hair loss that are not expected to be responsive to baricitinib treatment. According to the clinical experts, the baseline characteristics of the trial population were in general aligned with the patient population expected to receive baricitinib treatment, except that the proportion of patients with very severe AA appeared to be higher than in clinical practice; the clinical experts noted that patients with very severe AA tend to be less responsive to treatment. As well, the mean baseline HADS scores suggested the trial population had a normal to low degree of anxiety and depression; according to the clinical experts, this did not align with clinical practice since severe AA is generally associated with significant psychological burden. The clinical experts commented that the exclusion of patients with significant uncontrolled neuropsychiatric disorder (e.g., suicidal ideation or behaviour) from the trials was appropriate since these patients would not be candidates for baricitinib treatment in clinical practice because of concerns with treatment adherence.
The dosing regimen of baricitinib in the trials generally aligns with the product monograph, although in the trials, the dosing of baricitinib was assigned by randomization without regard to disease severity. This is different from the recommended dose from the product monograph where the starting dose should be determined based on the severity of hair loss in patients. In addition, dose adjustment of baricitinib occurred at week 52 in the trials. According to the clinical experts, the decision to adjust the dose as per response to treatment would likely take place in clinical practice at an earlier time point than week 52 (e.g., week 36). With regard to concomitant medication use, corticosteroids (systemic, intralesional, and topical) were prohibited in the trials; however, the clinical experts expected that these treatments might be used in combination with baricitinib treatment in clinical practice.
The efficacy outcomes assessed in the study were of clinical importance to patients and clinicians, including the severity of hair loss (scalp, EBs, and ELs), psychological impacts (anxiety and depression), and HRQoL. The clinical experts noted that none of the outcome instruments used in the clinical trials are administered in clinical practice. According to the clinical experts, the duration of follow-up of 36 weeks was adequate for the assessment of the efficacy of baricitinib. However, the clinical experts felt that a longer follow-up would be required to capture the long-term safety of baricitinib, including potential rare AEs (e.g., MACE, malignancy, thrombosis), since baricitinib is expected to be a lifelong treatment for many patients with AA.
It should be noted that the BRAVE-AA1 and BRAVE-AA2 trials are the only phase III RCT evidence submitted for review and that they are placebo-controlled studies. No head-to-head evidence comparing baricitinib with systemic treatments for severe AA that are currently reimbursed by the public drug plans (conventional immunosuppressants) were submitted. In addition, the absence of evidence for baricitinib in older adults (males older than 60 years and females older than 70 years — categories that were excluded from the trials) was an evidence gap in the treatment of severe AA since some clinicians may be open to prescribing baricitinib treatment to patients in this age group. In an effort to address this treatment gap, a single-arm observational study (Tang et al. [2024]) assessing the efficacy of baricitinib treatment in older adults with AA was submitted by the sponsor. This study is summarized in the Studies Addressing Gaps in the Systematic Review Evidence section of this report.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform our expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.50,51
“High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word ‘likely’ for evidence of moderate certainty (e.g., ‘X intervention likely results in Y outcome’).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word ‘may’ for evidence of low certainty (e.g., ‘X intervention may result in Y outcome’).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as ‘very uncertain.’”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. For this review, the target of the certainty of evidence assessment was based on the presence or absence of an important effect as informed by thresholds identified based on clinical expert input (a SALT score of 20 or less, a SALT50 response, and ClinRO measures). For other outcomes of interest to this review (HADS and Skindex-16 for AA outcomes), the target of the certainty of evidence assessment was based on the null since there was uncertainty in the thresholds suggested by the clinical experts. Findings from Study BRAVE-AA1 and Study BRAVE-AA2 were considered together and summarized narratively per outcome because these studies were similar in population, interventions, design, and outcome measures.
Results of GRADE Assessments
Table 2 and Table 3 present the GRADE summary of findings for baricitinib versus placebo in patients with severe or very severe AA.
Long-Term Extension Studies
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
Study BRAVE-AA1
This is an ongoing long-term extension study (week 36 onward) of Study BRAVE-AA1 (the anticipated completion date is January 26, 2025). The purpose of this study is to provide safety and efficacy analyses through week 104 to support dosing recommendations in product labelling.
At week 52, patients initially randomized to baricitinib who were responders (with a SALT score of ≤ 20) were rerandomized at a 3:1 ratio to stay on their current dose of baricitinib or to transition to placebo (a randomized withdrawal). Responders who had been rerandomized to placebo and had experienced a loss of treatment benefit (defined as > a 20-point worsening in the SALT score from week 52) at any time after week 52 were re-treated with their original baricitinib dose and the efficacy of re-treatment was analyzed as part of the other secondary end points of Study BRAVE-AA1.
This extension study included week 0 to week 52 and week 52 to week 76 efficacy and safety data for patients whose treatment dose with baricitinib was titrated up at week 52 (the up-titration cohort). The up-titration cohort included ███ patients randomized to baricitinib 2 mg at week 0 who did not attain a SALT score of 20 or less at week 52. The baricitinib dose in all ███ patients was titrated up to 4 mg.
Study BRAVE-AA2
This is an ongoing long-term extension study (week 36 onward) of Study BRAVE-AA2 (the anticipated completion date is July 29, 2025). The purpose of this study is to provide efficacy and safety analyses to support dosing recommendations in product labelling.
At week 52, patients were divided into 2 cohorts. The randomized down-titration cohort included 82 patients randomized at week 0 to baricitinib 4 mg who attained a SALT score of 20 or less at week 52. Of these, 42 patients were randomly assigned to remain on baricitinib 4 mg and 40 patients were randomly assigned to the down-titration of baricitinib to 2 mg. The up-titration cohort included ██ patients randomized to baricitinib 2 mg at week 0 who did not attain a SALT score of 20 or less at week 52. The baricitinib dose in all ██ patients was titrated up to 4 mg.
Eligibility Criteria
The inclusion and exclusion criteria for the long-term extension studies were previously described in the Systematic Review section.
Statistical Analysis
Study BRAVE-AA1 and Study BRAVE-AA2
Efficacy
Efficacy analyses were descriptive without inferential treatment comparisons. The efficacy results were presented for 2 analysis periods — 1 from week 0 to week 52 and 1 from week 52 to week 76 — using data from the baricitinib 2 mg up-titration cohort. Baseline assessments for the study were conducted at the start of each trial.
For the efficacy analysis from week 0 through week 52, the primary censoring rule was implemented; that is, efficacy results after permanent study drug discontinuation or results that were collected during remote visits because of the COVID-19 pandemic were censored. The primary censoring rule along with NRI or mLOCF for missing data imputation was applied to the summary statistics.
For the efficacy analysis from week 52 through week 76, the primary censoring rule was also implemented. The primary censoring rule along with NRI or mLOCF for missing data imputation was applied to the summary statistics. The mLOCF method imputed missing values post–week 52 using the last nonmissing assessment after patients switched to baricitinib 4 mg. If no assessment was completed post–week 52, the mLOCF method was not applicable. Censoring rules in the long term studies are summarized in Table 17.
Table 17: Censoring Rules in the long term Extension Period of Study BRAVE-AA1 and Study BRAVE-AA2
Censoring rule | Event | Application |
|---|---|---|
Secondary censoring rule | Data after permanent study drug discontinuation | Re-treated populations of Study BRAVE-AA1 and Study BRAVE-AA2 |
Tertiary plus censoring rule |
| Study BRAVE-AA1 withdrawal substudy population |
Quaternary plus censoring rule |
| Study BRAVE-AA2 down-titration substudy population |
Source: Senna et al. (2024).38
Harms
Safety analyses were performed for 2 analysis periods: 1 from week 0 through week 52 and 1 from week 52 through week 76. Descriptive statistics were provided. No treatment comparison was made. These analyses were conducted for TEAEs, SAEs, and AEs leading to permanent study drug discontinuation, and AEs of special interest.
Populations
Baseline Characteristics
A summary of the baseline demographic and clinical characteristics of participants in the Study BRAVE-AA1 up-titration cohort are presented in Table 18. For the randomized down-titration cohort and up-titration cohort of Study BRAVE-AA2, baseline demographic and clinical characteristics are presented in Table 19 and Table 20, respectively.
Table 18: Summary of Baseline (Week 52) Demographic and AA Clinical Characteristics in the Up-Titration Population of Study BRAVE-AA1
Characteristic | BARI 2 mg to BARI 4 mg ██ █ ████ |
|---|---|
Age (years), mean (SD) | ████ ███████ |
Female, n (%) | ██ ██████ |
Race, n (%) | |
American Indian or Alaska Native | | █████ |
Asian | ██ ██████ |
Black or African American | | █████ |
Native Hawaiian or other Pacific Islander | | █████ |
White | ██ ██████ |
Multiple | | █████ |
Weight (kg), mean (SD) | █████ ████████ |
Country, n (%) | |
US | ██ ██████ |
Republic of Korea | ██ ██████ |
Mexico | | █████ |
Body mass index (kg/m2), mean (SD) | █████ ███████ |
Duration from onset of AA (years), mean (SD) | █████ ███████ |
Duration of the current episode of AA categories in years, n (%) | |
0.5 to < 4 | ██ ██████ |
4 to < 8 | ██ ██████ |
≥ 8 | ██ ██████ |
Age of onset of AA categories in years, n (%) | |
< 18 | ██ ██████ |
≥ 18 | ██ ██████ |
Atopic background,a n (%) | |
Yes | ██ ██████ |
No | ██ ██████ |
Disease severity | |
SALT score, mean (SD) | ████ ███████ |
Severe (a SALT score of 50 to 94), n (%) | ██ ██████ |
Very severe (a SALT score of 95 to 100), n (%) | ██ ██████ |
ClinRO measure for EB hair loss, n (%) | |
0 | ██ ██████ |
1 | | █████ |
2 | ██ ██████ |
3 | ██ ██████ |
ClinRO measure for EL hair loss, n (%) | |
0 | ██ ██████ |
1 | ██ ██████ |
2 | ██ ██████ |
3 | ██ ██████ |
HADS, mean (SD) | |
Anxiety domain scale | ███ ██████ |
Depression domain scale | ███ ██████ |
AA = alopecia areata, BARI = baricitinib; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; HADS = Hospital Anxiety and Depression Scale; PRO = patient-reported outcome; SALT = Severity of Alopecia Tool; SD = standard deviation.
aAtopic background is defined as a medical history of or ongoing atopic dermatitis, allergic rhinitis, or allergic asthma.
Source: Study BRAVE-AA1 Clinical Study Report Addendum.10
Table 19: Summary of Baseline Demographics and AA Clinical Characteristics in the Randomized Down-Titration Cohort in Study BRAVE-AA2
Characteristic | BARI 4 mg to BARI 4 mg N = 42 | BARI 4 mg to BARI 2 mg N = 40 |
|---|---|---|
Age (years), mean (SD) | ████ ███████ | ████ ███████ |
Female, n (%) | ██ ██████ | ██ ██████ |
Race, n (%) | ||
Asian | ██ ██████ | ██ ██████ |
Black or African American | | █████ | | █████ |
White | ██ ██████ | ██ ██████ |
Multiple | | █████ | | █████ |
Weight (kg), mean (SD) | █████ ████████ | █████ ████████ |
Country, n (%) | ||
US | ██ ██████ | ██ ██████ |
Japan | | █████ | | ██████ |
Taiwan | | █████ | | █████ |
Republic of Korea | | █████ | | ██████ |
Australia | | █████ | | ██████ |
Brazil | | █████ | | █████ |
Argentina | | ██████ | | █████ |
Israel | | █████ | | ██████ |
Body mass index (kg/m2), mean (SD) | █████ ███████ | █████ ███████ |
Duration from onset of AA (years), mean (SD) | █████ ████████ | ████ ████████ |
Duration of the current episode of AA categories in years, n (%) | ||
0.5 to < 4 | ██ ██████ | ██ ██████ |
4 to < 8 | | ██████ | | ██████ |
≥ 8 | | ██████ | | █████ |
Age of onset of AA categories in years, n (%) | ||
< 18 | ██ ██████ | ██ ██████ |
≥ 18 | ██ ██████ | ██ ██████ |
Atopic background,a n (%) | ||
Yes | ██ ██████ | ██ ██████ |
No | ██ ██████ | ██ ██████ |
Disease severity | ||
SALT score, mean (SD) | ████ ███████ | ████ ███████ |
Severe (a SALT score of 50 to 94), n (%) | ██ ██████ | ██ ██████ |
Very severe (a SALT score of 95 to 100), n (%) | ██ ██████ | ██ ██████ |
ClinRO measure for EB hair loss, n (%) | ||
0 | ██ ██████ | ██ ██████ |
1 | | ██████ | | ██████ |
2 | ██ ██████ | | ██████ |
3 | ██ ██████ | ██ ██████ |
ClinRO measure for EL hair loss, n (%) | ||
0 | ██ ██████ | ██ ██████ |
1 | | ██████ | | ██████ |
2 | | █████ | | ██████ |
3 | ██ ██████ | ██ ██████ |
HADS, mean (SD) | ||
Anxiety domain scale | ███ ██████ | ███ ██████ |
Depression domain scale | ███ ██████ | ███ ██████ |
AA = alopecia areata, BARI = baricitinib; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; HADS = Hospital Anxiety and Depression Scale; PRO = patient-reported outcome; SALT = Severity of Alopecia Tool; SD = standard deviation.
aAtopic background is defined as a medical history of or ongoing atopic dermatitis, allergic rhinitis, or allergic asthma.
Source: Study BRAVE-AA2 Clinical Study Report Addendum.11
Table 20: Summary of Baseline Demographics and AA Clinical Characteristics in the Titration Up Cohort in Study BRAVE-AA2
Characteristic | BARI 2 mg to BARI 4 mg | | ██ |
|---|---|
Age (years), mean (SD) | ████ ███████ |
Female, n (%) | ██ ██████ |
Race, n (%) | |
American Indian or Alaska Native | ███ |
Asian | ██ ██████ |
Black or African American | | █████ |
White | ██ ██████ |
Multiple | | █████ |
Weight (kg), mean (SD) | █████ ████████ |
Country, n (%) | |
US | ██ ██████ |
Japan | | █████ |
Taiwan | | █████ |
Republic of Korea | ██ ██████ |
Australia | ██ ██████ |
Brazil | | █████ |
Argentina | | █████ |
Israel | ██ ██████ |
Body mass index (kg/m2), mean (SD) | █████ ███████ |
Duration from onset of AA (years), mean (SD) | █████ ████████ |
Duration of the current episode of AA categories in years, n (%) | |
0.5 to < 4 | ██ ██████ |
4 to < 8 | ██ ██████ |
≥ 8 | | █████ |
Age of onset of AA categories in years, n (%) | |
< 18 | ██ ██████ |
≥ 18 | ██ ██████ |
Atopic background,a n (%) | |
Yes | ██ ██████ |
No | ██ ██████ |
Disease severity | |
SALT score, mean (SD) | ████ ███████ |
Severe (a SALT score of 50 to 94), n (%) | ██ ██████ |
Very severe (a SALT score of 95 to 100), n (%) | ██ ██████ |
ClinRO measure for EB hair loss, n (%) | |
0 | ██ ██████ |
1 | ██ ██████ |
2 | ██ ██████ |
3 | ██ ██████ |
ClinRO measure for EL hair loss, n (%) | |
0 | ██ ██████ |
1 | ██ ██████ |
2 | ██ ██████ |
3 | ██ ██████ |
HADS, mean (SD) | |
Anxiety domain scale | ███ ██████ |
Depression domain scale | ███ ██████ |
AA = alopecia areata, BARI = baricitinib; ClinRO = clinician-reported outcome; EB = eyebrow; EL = eyelash; HADS = Hospital Anxiety and Depression Scale; PRO = patient-reported outcome; SALT = Severity of Alopecia Tool; SD = standard deviation.
aAtopic background is defined as a medical history of or ongoing atopic dermatitis, allergic rhinitis, or allergic asthma.
Source: Study BRAVE-AA2 Clinical Study Report Addendum.11
Outcomes
Study BRAVE-AA1 and Study BRAVE-AA2
The main efficacy end point was the proportion of patients attaining a SALT score of 20 or less at week 52, week 76, and week 104.
Results
Patient Disposition
Study BRAVE-AA1
The baricitinib 2 mg up-titration cohort included ███ patients randomized at week 0 to baricitinib 2 mg who did not attain a SALT score of 20 or less at week 52. Of the ███ patients, ███ patients █████ completed week 76, and ███ patients █████ discontinued after week 52 and before week 76 because of AE ██ ████████ █████, lack of efficacy ██ █████████ █████, withdrawal by patient ██ █████████ █████, lost to follow-up ██ █████████ █████, and ██ ████████ ███████ included in the “other” category who were nonresponders at week 76.
Study BRAVE-AA2
Randomized Down-Titration Cohort
The randomized down-titration cohort included 82 patients randomized at week 0 to baricitinib 4 mg who attained a SALT score of 20 or less at week 52. Of these 82 patients, 42 patients were randomly assigned to remain on baricitinib 4 mg and 40 patients were randomly assigned to the titration down of baricitinib to 2 mg.
Of the 42 patients who remained on the baricitinib 4 mg dose, 100% of the patients completed week 76. Of the 40 patients whose treatment dose was down-titrated to baricitinib 2 mg, ███ patients █████ completed week 76, and ███ patients ████ discontinued before week 76 because of AE ██ ████████ █████, and withdrawal by patient ██ ████████ ██████
Up-Titration Cohort
The up-titration cohort included ███ patients randomized at week 0 to receive baricitinib 2 mg who did not attain a SALT score of 20 or less at week 52. Of these ███ patients, ███ patients █████ completed week 76, and ███ patients █████ discontinued before week 76 because of lack of efficacy ██ █████████ █████, withdrawal by patient ██ █████████ █████, and ██ ████████ ███████ included in the “other” category who were nonresponders at week 76.
Exposure to Study Treatments
A summary of the duration of exposure to baricitinib in Study BRAVE-AA1 and Study BRAVE-AA2 is presented in Table 21 and Table 22, respectively.
Table 21: Patient Exposure in Study BRAVE-AA1
Exposure | Study BRAVE-AA1 | ||||
|---|---|---|---|---|---|
Week 0 through week 52 | Week 52 through week 76 | ||||
BARI 2 mg ██ █ ████ | BARI 4 mg ██ █ ████ | BARI 2 mg to BARI 4 mg ██ █ ████ | BARI 4 mg to BARI 4 mg ██ █ ███ | BARI 4 mg to PBO ██ █ ███ | |
Total, patient-years | █████ | ███ | ████ | ███ | ███ |
Patient weeks of exposure | |||||
N | ███ | ███ | ███ | ███ | ███ |
Mean (SD) | ████ ████ | ███ | ████ ████ | ███ | ███ |
Patient adherence to treatment | |||||
N | ███ | ███ | ███ | ███ | ███ |
Median (IQR) | ████ ████ | ████ ████ | ████ █████ | ████ █████ | ████ █████ |
Mean (SD), % | ████ ████ | ███ █████ | ████ █████ | █████████ | ██ ███████ |
BARI = baricitinib; IQR = interquartile range; NR = not reported; PBO = placebo; SD = standard deviation.
Note: In Study BRAVE-AA1, patients were deemed nonadherent if their adherence was less than 80% or 120% or greater between week 0 and week 52.
Source: Study BRAVE-AA1 Clinical Study Report Addendum.10
Table 22: Patient Exposure in Study BRAVE-AA2
Exposure | Study BRAVE-AA2: Randomized down-titration cohort | Study BRAVE-AA2: Up-titration cohort | |||
|---|---|---|---|---|---|
Week 0 through | Week 52 through week 76 | Week 0 through week 52 | Week 52 through week 76 | ||
BARI 4 mg ██ █ ███ | BARI 4 mg to BARI 4 mg ██ █ ███ | BARI 4 mg to BARI 2 mg ██ █ ███ | BARI 2 mg ██ █ ███ | BARI 2 mg to BARI 4 mg ██ █ ███ | |
Total, patient-years | ████ | ████ | ████ | ████ | ████ |
Patient weeks of exposure | |||||
N | ███ | ███ | ███ | ███ | ███ |
Mean (SD) | ██ █████ | ████ █████ | ████ █████ | ████ ████ | ████ ██████ |
Patient adherence to treatment | |||||
N | ███ | ███ | ███ | ███ | ███ |
Median (IQR) | ████ ███ | ███ | ███ | ████ ████ | ████ ████ |
Mean (SD), % | ███ ████ | ████ █████ | ████ █████ | ████ ████ | ████ █████ |
BARI = baricitinib; IQR = interquartile range; SD = standard deviation.
Note: In Study BRAVE-AA2, patients are deemed nonadherent if their adherence was less than 80% or 120% or greater between week 0 and week 52.
Source: Study BRAVE-AA2 Clinical Study Report Addendum.11
Efficacy: Up to Week 76 (Data Cut-Off Date of February 2021)
Proportion of Patients Attaining SALT Score of 20 or Less
The proportion of patients attaining a SALT score of 20 or less continuously increased over the treatment period beyond 36 weeks for the baricitinib 4 mg cohort. At week 52, 40.9% and 21.2% of patients receiving baricitinib 4 mg (N = 281) and baricitinib 2 mg (N = 184), respectively, attained a SALT score of 20 or less in Study BRAVE-AA1. Similarly, 36.8% and 24.4% of patients receiving baricitinib 4 mg (N = 234) and baricitinib 2 mg (N = 156), respectively, attained a SALT score of 20 or less at week 52 in Study BRAVE-AA2.
Study BRAVE-AA1: Up-Titration Cohort
At week 52, ███ patients who were originally randomized to baricitinib 2 mg were considered nonresponders and were titrated up to baricitinib 4 mg. At week 76, following 24 weeks of treatment on baricitinib 4 mg, ███ of ███ patients (████ ███ ████████ ██ ██████ in the up-titration cohort attained a SALT score of 20 or less.
Study BRAVE-AA2: Randomized Down-Titration Cohort
At week 52, 82 patients who were originally randomized to baricitinib 4 mg were eligible for randomized down-titration to baricitinib 2 mg. At week 52, █████ ████ ███ █████ ██ ██████ of patients attained a SALT score of 20 or less. ███ ███████ ███ █ ███████ █████ ██ ████ ███ ███ ████████ ████ █████████ █████ ████ ██████ ███ █████████ ████ ███ ████████ ████ ██ ████ ██ ██ ███ ████.
Among patients receiving baricitinib 4 mg who attained a SALT score of 20 or less at week 52, this response was retained up to week 76 in 75% (30 of 40 | ███ ██ ██████ ██ █████) of patients who were down-titrated to baricitinib 2 mg, and 98% (41 of 42, ███ ███ █████ ██ █████) of patients who remained on baricitinib 4 mg.
Study BRAVE-AA2: Up-Titration Cohort
At week 52, ███ patients who were originally randomized to baricitinib 2 mg were considered nonresponders and their baricitinib dose was titrated up to 4 mg. At week 76, after 24 weeks of titration up treatment on baricitinib 4 mg, ███ of ███ patients ███████ ███ ██ ██████ ██████ attained a SALT score of 20 or less.
ClinRO Measures for EB and EL Hair Loss
At week 52, 39.4% and 27.9% of patients receiving baricitinib 4 mg (N = 188) and baricitinib 2 mg (N = 136), respectively, attained a ClinRO measure EB hair loss score of 0 or 1 (with ≥ 2-point improvement from baseline through week 52 among patients with a score of ≥ 2 at baseline) in Study BRAVE-AA1 (Figure 5). Similarly, 49.7% and 16.3% of patients receiving baricitinib 4 mg (N = 161) and baricitinib 2 mg (N = 104), respectively, attained a ClinRO measure EB hair loss score of 0 or 1 (with ≥ 2-point improvement from baseline through week 52 among patients with a score of ≥ 2 at baseline) at week 52 in Study BRAVE-AA2 (Figure 5).
At week 52, 40.7% and 21.6% of patients receiving baricitinib 4 mg (N = 167) and baricitinib 2 mg (N = 111), respectively, attained a ClinRO measure EL hair loss score of 0 or 1 (with ≥ 2-point improvement from baseline through week 52 among patients with a score of ≥ 2 at baseline) in Study BRAVE-AA1 (Figure 6). Similarly, 50.7% and 30.3% of patients receiving baricitinib 4 mg (N = 140) and baricitinib 2 mg (N = 89), respectively, attained a ClinRO measure EL hair loss score of 0 or 1 (with ≥ 2-point improvement from baseline through week 52 among patients with a score of ≥ 2 at baseline) at week 52 in Study BRAVE-AA2 (Figure 6).
Figure 5: Patients Attaining ClinRO Measure Eyebrow Hair Loss Score of 0 or 1 Through Week 52 in Study BRAVE-AA1 and Study BRAVE AA2
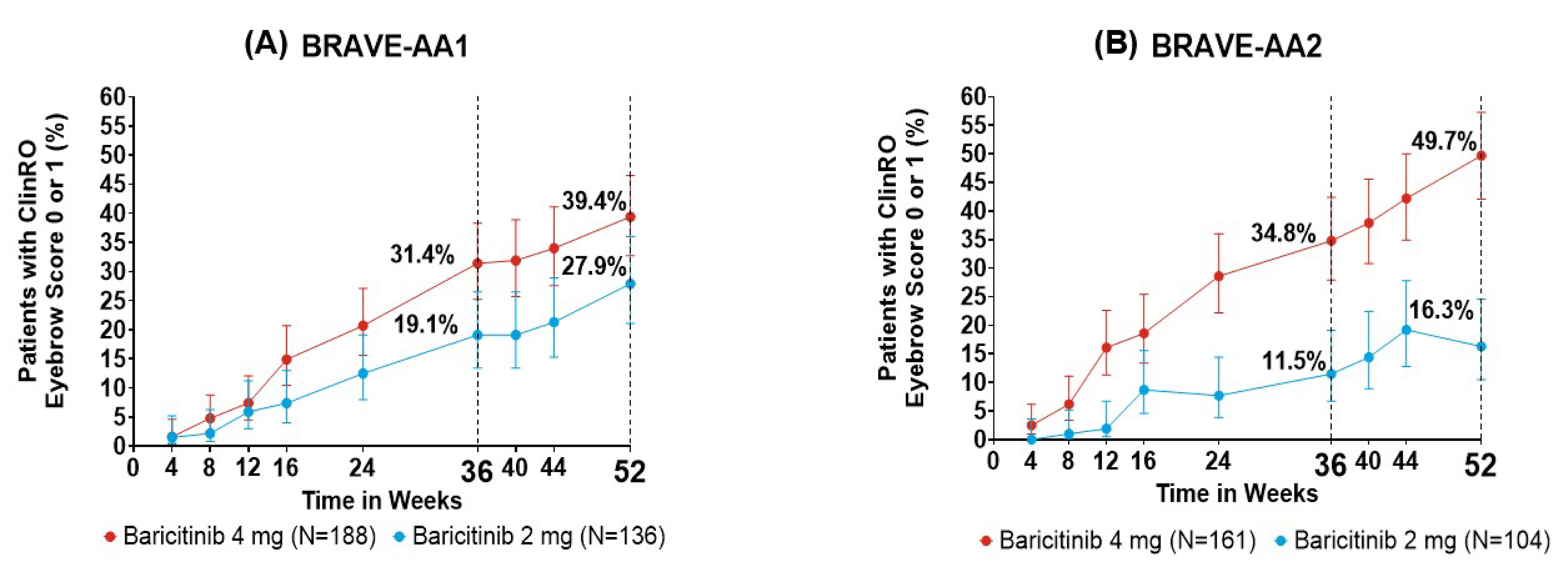
ClinRO = clinician-reported outcome; NRI = nonresponder imputation.
Note: Bars represent 95% confidence intervals. NRI was applied to missing data (prespecified analysis).
Source: Kwon et al. (2023).39
Figure 6: Patients Attaining ClinRO Measure Eyelash Hair Loss Score of 0 or 1 Through Week 52 in Study BRAVE-AA1 and Study BRAVE AA2
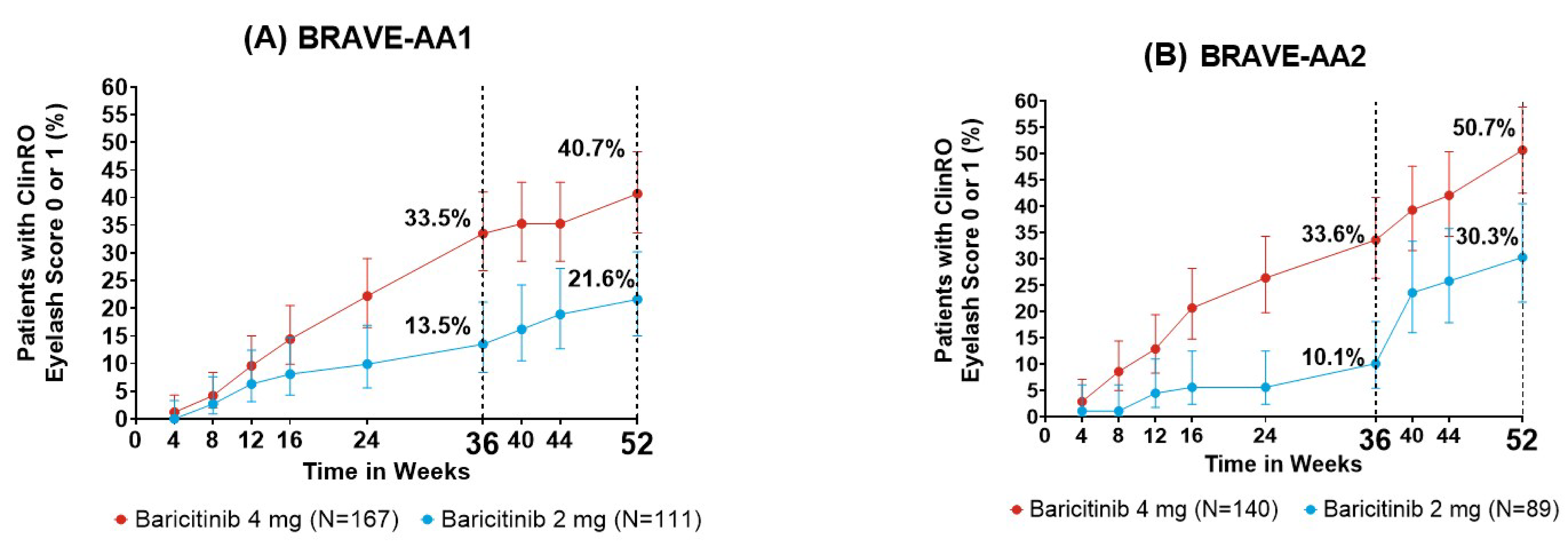
ClinRO = clinician-reported outcome; NRI = nonresponder imputation.
Note: Bars represent 95% confidence intervals. NRI was applied to missing data (prespecified analysis).
Source: Kwon et al. (2023).39
Efficacy (Updated): Up to Week 104 (Data Cut-Off Date of May 2022)
Clinically meaningful scalp hair regrowth was maintained through week 104 in nearly 90% of patients treated with baricitinib 4 mg or baricitinib 2 mg who responded at week 52 (Figure 7).
The proportion of patients attaining complete or nearly complete regrowth of EBs and ELs increased from week 52 through week 104 among week 52 responders (Figure 8).
Figure 7: Proportion of Week 52 Responders Who Attained SALT Score of 20 or Less Through Week 104
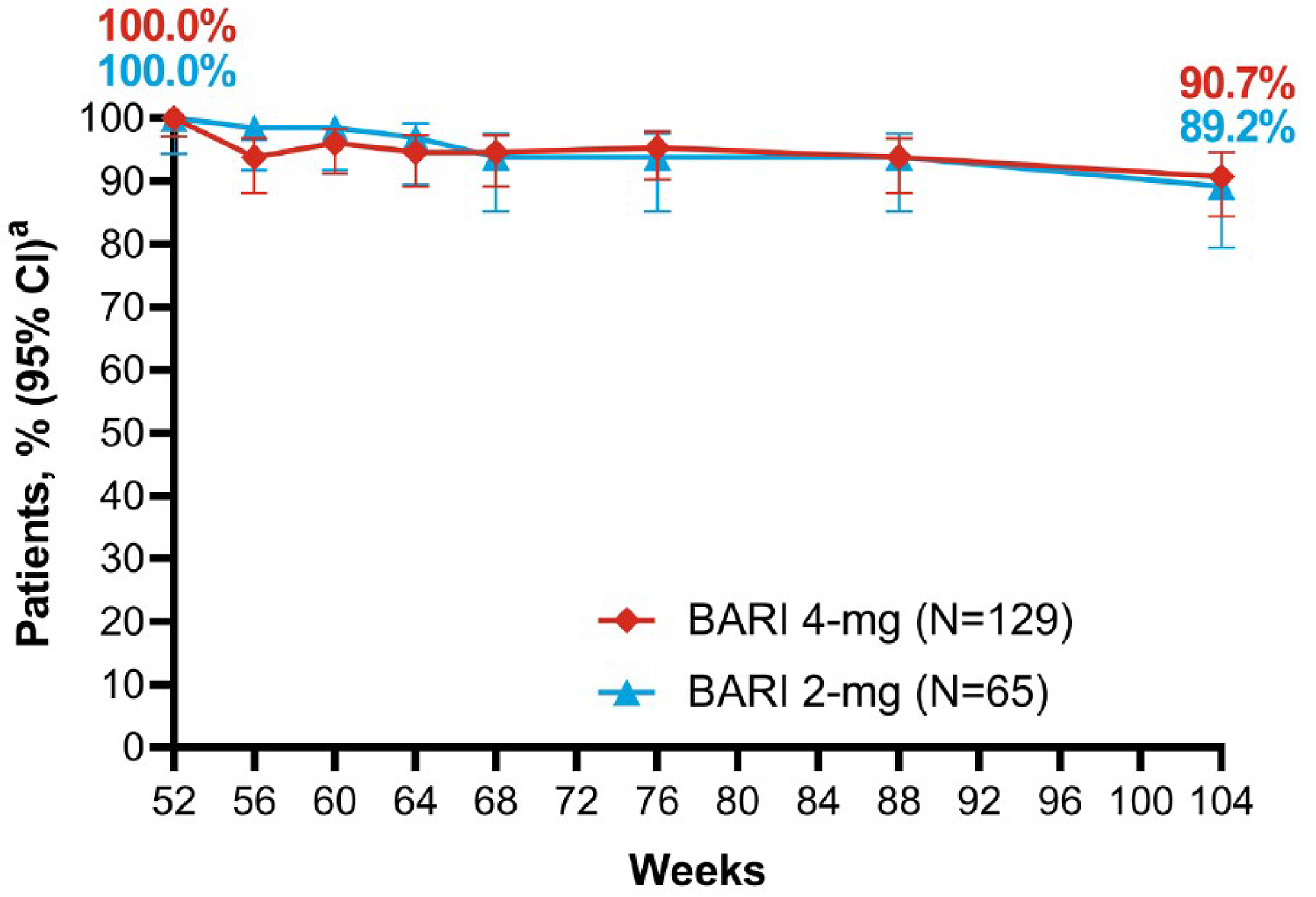
BARI = baricitinib; CI = confidence interval; mLOCF = modified LOCF; SALT = Severity of Alopecia Tool.
Note: Data were summarized with mLOCF imputation.
a These were patients who attained a SALT score of 20 or less at week 52.
Source: Senna et al. (2024).38
Figure 8: Proportion of Patients Attaining Complete or Nearly Complete Regrowth of Eyebrows and Eyelashes Through Week 104
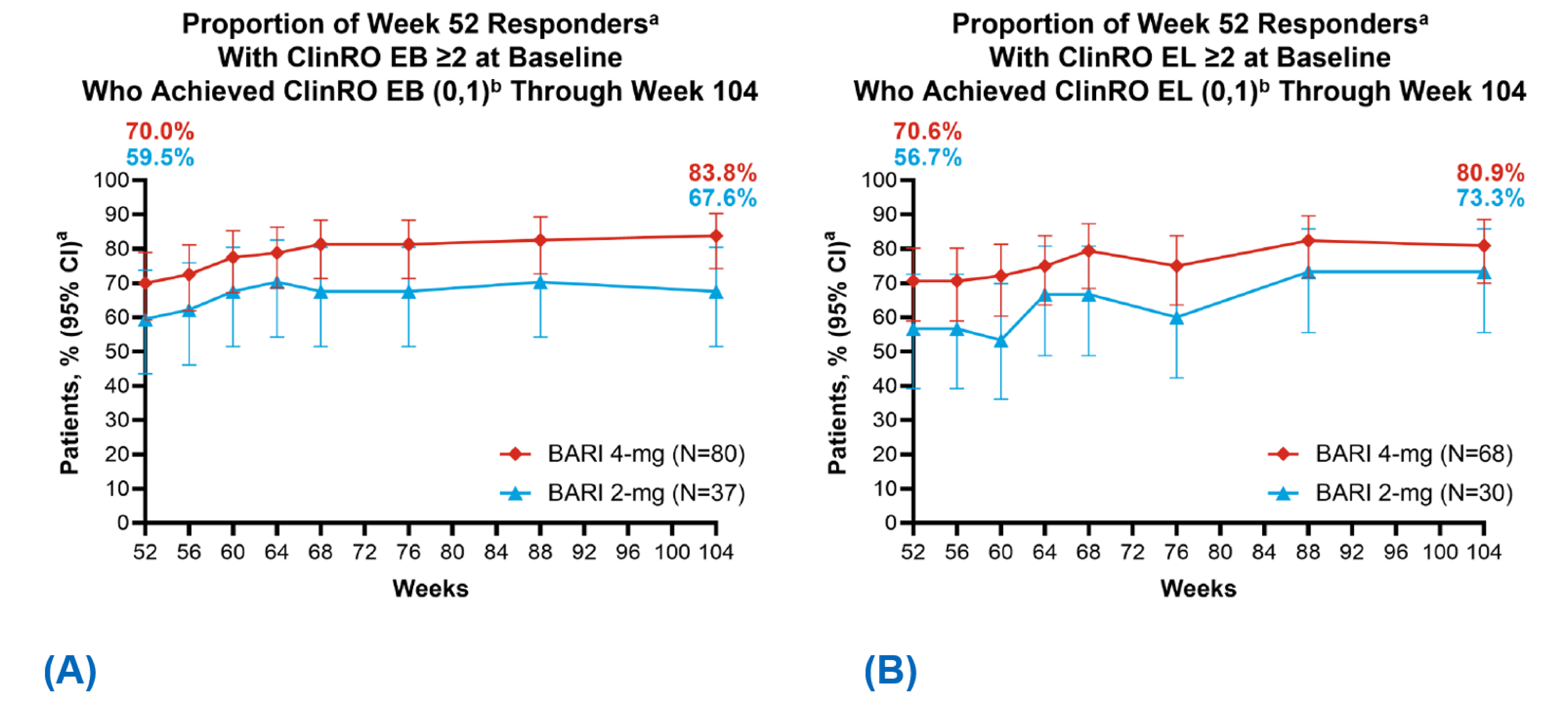
BARI = baricitinib; CI = confidence interval; ClinRO = clinician-reported outcome; EB = eyebrow; eyelash; mLOCF = modified LOCF; SALT = Severity of Alopecia Tool.
Note: Data were summarized with mLOCF imputation.
a These were BARI 4 mg–treated and BARI 2 mg–treated patients with a SALT score of 20 or less at week 52.
b This was with improvements of 2 points or more from baseline.
Source: Senna et al. (2024).38
Harms: Up to Week 76 (Data Cut-Off Date of February 2021)
Study BRAVE-AA1: Up-Titration Cohort
Week 0 Through Week 52
The overview of AEs between week 0 and week 52 for the ███ patients who were eligible for inclusion in the up-titration cohort are presented in Table 23. TEAEs were reported for █████ ███ ██ ████ of patients, and there ███ █ ███████ ███ ████████ ████ ████ ████ ██████ ██████
Week 52 Through Week 76
TEAEs were reported for ████ █ ███ ██ ████ of patients who up-titrated to baricitinib 4 mg. Most events were mild in severity. █████ ████ █ ████████ ███ ████████ ████ ████ ████ ██████ █████. ███ ███████ discontinued the study drug and study because of AEs of ██████ ████. There were no deaths in the up-titration cohort.
Study BRAVE-AA2: Randomized Down-Titration Cohort
Week 0 Through Week 52
The overview of AEs between week 0 and week 52 for the 82 patients who were eligible for inclusion in the down-titration cohort is presented in Table 24. TEAEs were reported for █████ ███ ██ ███ of patients, and there were | ████████ ███ ████████ ████ ████ ████ ██████ ██████
Week 52 Through Week 76
During the 24-week period, TEAEs were reported for █████ ███ ██ ███ of patients who remained on baricitinib 4 mg, and █████ ███ ██ ███ of patients who down-titrated to baricitinib 2 mg.
For both treatment groups, most events were mild or moderate in severity. Of the patients who remained on baricitinib 4 mg, |████████ ████████ ████ ███ ███ █ ███████ ████ █████ ███ █ ██████ █████
██ ████████ ████████ for patients who titrated down to baricitinib 2 mg.
██ ████████ ████████████ █████ ████ ██ █████ ███ ██ ███ ██ ███ ████ ██████
There were no deaths in the randomized down-titration cohort for all treatment groups.
Study BRAVE-AA2: Up-Titration Cohort
Week 0 Through Week 52
The overview of AEs between week 0 and week 52 for the ██ patients who were eligible for inclusion in the up-titration cohort is presented in Table 25. TEAEs were reported for █████ ███ ██ ███ of patients, and there were | ████████ ███ ████████ ████ ████ ████ ██████ ██████
Week 52 Through Week 76
TEAEs were reported for █████ ███ ██ ██ █████████ of patients who up-titrated to baricitinib 4 mg. Most events were mild or moderate in severity; | ███████ ████████ █ ██████ █████ ██ ████████ ████████ ████ ██ ████████████ █████ ████ ██ █████ ███ ██ ████ There were no deaths in the up-titration cohort in any treatment group.
Table 23: Summary of Harms of Study BRAVE-AA1—Titration Up Cohort
AE | Week 0 to week 52 | Week 52 to week 76 |
|---|---|---|
BARI 2 mg ██ █ ████ | BARI 2 mg to 4 mg | | ████ | |
Most common AEs, n (%) | ||
≥ 1 TEAEa | ██ ██████ | ██ ██████ |
SAEs,b n (%) | ||
Patients with ≥ 1 SAE | | █████ | | █████ |
Acute myocardial infarction | | █████ | | ███ |
Varicella | | ███ | | █████ |
Depression | | ███ | | █████ |
Patients who stopped treatment because of AEs, n (%) | ||
Patients with ≥ 1 AE | | ███ | | █████ |
Weight, increased | | ███ | | █████ |
Deaths, n (%) | ||
Patients who died | 0 (0) | 0 (0) |
AEs of special interest, n (%) | ||
Patients with ≥ 1 TEAE | ██ ██████ | | █████ |
Serious infections | | ███ | | █████ |
TE opportunistic infection | | ███ | | ███ |
TE herpes zoster | | █████ | | █████ |
TE herpes simplex | | █████ | | ███ |
TE tuberculosis | | ███ | | ███ |
TE viral hepatitis | | ███ | | ███ |
Led to study intervention interruption | | █████ | | █████ |
Led to study intervention discontinuation | | ███ | | ███ |
AE = adverse event; BARI = baricitinib; SAE = serious adverse event; TE = treatment-emergent; TEAE = treatment-emergent adverse event.
aPatients with multiple occurrences of the same event were counted under the highest severity category.
bThe denominator was adjusted because the event was specific to males; N = 49 (BARI 2 mg group [Study BRAVE-AA1]). In other cases, the denominator was adjusted because the event was specific to females; N = 63 (BARI 2 mg group [Study BRAVE-AA1]).
Source: Study BRAVE-AA1 Clinical Study Report Addendum.10
Table 24: Summary of Harms of Study BRAVE-AA2— Randomized Titration Down Cohort
AE | Week 0 through week 52 | Week 52 through week 76 | |
|---|---|---|---|
BARI 4 mg ██ █ ███ | BARI 4 mg to 4 mg ██ █ ███ | BARI 4 mg to 2 mg ██ █ ███ | |
Most common AEs, n (%) | |||
≥ 1 TEAEa | ██ ██████ | ██ ██████ | ██ ██████ |
SAEs,b n (%) | |||
Patients with ≥ 1 SAE | | █████ | | █████ | | ███ |
Herpes zoster | | █████ | | ███ | | ███ |
Appendicitis | | ███ | | █████ | | ███ |
Device dislocation | | █████ | | ███ | | ███ |
Uterine leiomyoma(s) | | ███ | | █████ | | ███ |
Patients who stopped treatment because of AEs, n (%) | |||
Patients who stopped treatment | | █████ | | ███ | | ███ |
Hepatic enzyme, increased | | █████ | | ███ | | ███ |
Deaths, n (%) | |||
Patients who died | 0 (0) | 0 (0) | 0 (0) |
AEs of special interest, n (%) | |||
Patients with ≥ 1 TEAE | ██ ██████ | | ██████ | | ██████ |
Serious infections | | █████ | | █████ | | ███ |
TE opportunistic infection | | ███ | | ███ | | ███ |
TE herpes zoster | | █████ | | █████ | | █████ |
TE herpes simplex | | █████ | | ███ | | █████ |
TE tuberculosis | | ███ | | ███ | | ███ |
TE viral hepatitis | | ███ | | ███ | | ███ |
Led to study intervention interruption | | █████ | | █████ | | █████ |
Led to study intervention discontinuation | | ███ | | ███ | | ███ |
AE = adverse event; BARI = baricitinib; SAE = serious adverse event; TE = treatment-emergent; TEAE = treatment-emergent adverse event.
aPatients with multiple occurrences of the same event were counted under the highest severity category.
bThe denominator was adjusted because the event was specific to males; N = 28 (BARI 4 mg group [Study BRAVE-AA2]). In other cases, the denominator was adjusted because the event was specific to females; N = 54 (BARI 4 mg group [Study BRAVE-AA2]).
Source: Study BRAVE-AA2 Clinical Study Report Addendum.11
Table 25: Summary of Harms of Study BRAVE-AA2 Extension — Titration Up Cohort
AE | Week 0 through week 52 | Week 52 through week 76 |
|---|---|---|
BARI 2 mg ██ █ ███ | BARI 2 mg to 4 mg ██ █ ███ | |
Most common AEs, n (%) | ||
≥ 1 TEAEa | ██ ██████ | ██ ██████ |
SAEs,b n (%) | ||
Patients with ≥ 1 SAE | | █████ | | ███ |
COVID-19 pneumonia | | █████ | | ███ |
Pyelonephritis | | █████ | | ███ |
Ankle fracture | | █████ | | ███ |
Patients who stopped treatment because of AEs, n (%) | ||
Patients who stopped treatment | | ███ | | ███ |
Deaths, n (%) | ||
Patients who died | 0 (0) | 0 (0) |
AEs of special interest, n (%) | ||
Patients with ≥ 1 TEAE | ██ ██████ | ██ ██████ |
Serious infections | | █████ | ███ |
TE herpes zoster | | █████ | | █████ |
TE herpes simplex | | █████ | ███ |
Led to study intervention interruption | | █████ | | █████ |
AE = adverse event; BARI = baricitinib; SAE = serious adverse event; TE = treatment-emergent; TEAE = treatment-emergent adverse event.
aPatients with multiple occurrences of the same event were counted under the highest severity category.
bThe denominator was adjusted because the event was specific to males; N = 27 (BARI 2 mg group [Study BRAVE-AA2]). In other cases, the denominator was adjusted because the event was specific to females; N = 57 (BARI 2 mg group [Study BRAVE-AA2]).
Source: Study BRAVE-AA2 Clinical Study Report Addendum.11
Harms (Updated): Up to Week 104 (Data Cut-Off Date of May 2022)
A pooled safety analysis was conducted, including data for all patients receiving baricitinib during Study BRAVE-AA1 and Study BRAVE-AA2 up to the data cut-off date (May 24, 2022, for Study BRAVE-AA1 and May 10, 2022, for Study BRAVE-AA2); this included the 36-week, placebo-controlled periods and long-term extension periods.38,52 Data were collected for 1,303 patients reflecting 2,218 patient-years of exposure (mean of 621.7 [SD = 303.8] days). The majority of TEAEs (93.2%) in the all-baricitinib dataset were mild to moderate in severity and the incidence rates (IRs) per 100 patient-years of SAEs (2.9) and treatment discontinuations because of AEs (1.9) were low. There was 1 opportunistic infection of multidermatomal herpes zoster (IR < 0.1), 44 cases of herpes zoster (IR = 2.0), 1 positively adjudicated MACE (a myocardial infarction [IR < 0.1]; this was in the baricitinib 2 mg group), 2 cases of pulmonary embolism (IR = 0.1; these cases were in the baricitinib 2 mg group), 4 malignancies other than nonmelanoma skin cancer (IR = 0.2; 2 malignancies were in the baricitinib 2 mg group and 2 malignancies were in the baricitinib 4 mg group), and 1 gastrointestinal perforation (IR < 0.1; this was in the baricitinib 4 mg group). The myocardial infarction was the same case that occurred in the placebo-controlled, 36-week treatment period. Meanwhile, in the 2 cases of pulmonary embolism, both patients had multiple risk factors for venous thromboembolism while 1 of these patients also had an identified deep venous thrombosis. No deaths were reported.
Critical Appraisal
Internal Validity
Both Study BRAVE-AA1 and Study BRAVE-AA2 extension studies were limited by their noncomparative design. At time points after 36 weeks, there remained no randomized comparison to placebo, challenging causal interpretations. Although the patients and investigators remained blinded to the assigned interventions, there is still the possibility that patients may be able to infer treatment assignment because of differences in efficacy (relative to placebo during the double-blind treatment phase). As such, there may be a risk of bias in the reporting of efficacy outcomes that required some level of subjective judgment by the evaluators (e.g., ClinRO), and harms outcomes, although the magnitude of bias cannot be predicted. It is unlikely that bias would be introduced for the SALT response since it is measured objectively. Finally, missing information such as pooling strategies for the 104-week results constrained a robust critical appraisal; hence, firm conclusions cannot be drawn on its long-term efficacy and safety.
External Validity
Since both Study BRAVE-AA1 and Study BRAVE-AA2 included rollover patients consistent with their characteristics at entry in the study, it is reasonable to expect similar limitations to the generalizability of the study results are relevant to the long-term extension phase. Further, some outcomes that are important to patients (e.g., HRQoL, anxiety, depression) could not be evaluated against a placebo control beyond the 36-week, double-blind treatment phase because of discontinuation of the placebo in nonresponders. As such, there is limited evidence for the effect of baricitinib 2 mg or baricitinib 4 mg on these outcomes for time points after 36 weeks (including for patients who up-titrated or down-titrated). Despite longer follow-up for harms, some rare harms (e.g., malignancies) may still not be fully captured.
Indirect Evidence
No indirect comparative evidence was submitted by the sponsor. The sponsor noted that before the regulatory approval of baricitinib for severe AA in Canada, the standard of care included off-label therapies and nonpharmacological options. The sponsor further noted that the pivotal trials of baricitinib were placebo-controlled and given that no approved comparator drugs were available at the time of the phase III clinical development conduct, there is no indirect comparative efficacy evidence to present in this section.
Studies Addressing Gaps in the Systematic Review Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
The sponsor submitted 1 study to provide evidence to address gaps in the systematic review evidence. The single-arm retrospective study by Tang et al. (2024)12 reported on baricitinib treatment among adult patients older than 65 years, as these older patients were excluded from the pivotal trials. Studies assessing the effects of baricitinib in patients in Japan (Numata et al. [2024])14 and in Spain along with evidence for adjuvant therapy among nonresponders (Moreno-Vilchez et al. [2024])13 were also submitted. However, our review team did not consider these studies to have addressed any identified gaps in evidence for the purpose of informing the reimbursement recommendation of baricitinib in the Canadian context. Table 26 summarizes the gaps in pivotal trials identified by the sponsor and the sponsor-submitted studies that could potentially address these gaps.
Table 26: Summary of Gaps in the Systematic Review Evidence
Sponsor-identified gap in pivotal and RCT evidence | Study that addresses the gap | |
|---|---|---|
Provided evidence for older adult patients ≥ 65 years with moderate-to-severe AA | Tang et al. (2024)12 | |
Study description | Summary of key results | |
Single-arm retrospective study that reviewed the records of 14 older adults aged ≥ 65 years with moderate-to-severe AA treated with baricitinib between April 2020 and September 2023 | After a mean (SD) treatment duration of 18.5 (11.9) months with baricitinib, a 72.0% reduction in the mean SALT score from baseline was observed. | |
Provided additional data among patients in Japan with moderate-to-severe AA | Numata et al. (2024)14 | |
Study description | Summary of key results | |
Retrospectively reviewed medical record data in 95 patients in Japan with moderate-to-severe AA | The percentage of patients in the entire cohort who attained a SALT score of 20 or less at week 12, week 24, and week 36 was 6.4% (6 of 94 patients), 35.4% (28 of 79 patients), and 46.7% (21 of 45 patients), respectively. | |
Provided longer-term evidence for adjuvant therapy among nonresponders to baricitinib | Moreno-Vilchez et al. (2024)13 | |
Study description | Summary of key results | |
Retrospectively reviewed medical records for patients with severe or very severe AA who were treated with baricitinib for at least 24 weeks at 2 university hospitals in Spain | In the study, 58.8% of patients attained a SALT score of ≤ 20 at week 24. Furthermore, in the study, patients who received adjuvant treatment had a similar initial SALT score but there were differences in the SALT scores between groups in subsequent weeks, suggesting that the use of adjuvant treatment — specifically, methotrexate in this case — could be a therapeutic alternative for patients who do not respond effectively to baricitinib monotherapy. | |
AA = alopecia areata; RCT = randomized controlled trial; SALT = Severity of Alopecia Tool; SD = standard deviation.
Note: Sources: Tang et al. (2024),12 Numata et al. (2024),14 and Moreno-Vilchez et al. (2024).13 Details included in Table 26 are from the sponsor’s Summary of Clinical Evidence.9
Description of Studies
Table 27 summarizes the Population, Intervention, Comparator, Outcome of the 3 sponsor-submitted observational studies included in this submission.
Tang et al. (2024)
The study investigators retrospectively reviewed the records of 14 patients aged 65 years or older with moderate-to-severe AA treated with baricitinib between April 2020 and September 2023. Hair loss before and after treatment was scored using the SALT tool based on standardized scalp photographs, with a SALT score of more than 20 representing moderate-to-severe AA. Patients were reviewed every 3 months to 4 months while on treatment.
The objective of this study was to evaluate the efficacy and safety of baricitinib in the treatment of moderate-to-severe AA in this older adult population (aged 65 years or older). All participants in the study received baricitinib. The mean dose of baricitinib was 3.52 (1.05) mg, with a mean (SD) duration of treatment of 18.5 (11.9) months. The study measured reduction in the mean SALT score from baseline in patients aged 65 years or older with moderate-to-severe AA.
Numata et al. (2024)
The study investigators retrospectively reviewed medical record data, including age, sex, age at AA onset, duration of the current episode of AA, AA subtype, prior treatments, nail involvement, trichoscopic findings (hair and scalp dermoscopy), and complications, among 95 patients in Japan with moderate-to-severe AA who were treated with baricitinib. Patients who had lost approximately 50% of their scalp hair for longer than 5 months were enrolled in the study, and all participants received baricitinib 4 mg between June 2022 and February 2023. The study measured the percentage of patients in the entire cohort who attained a SALT score of 20 or less at week 12, week 24, and week 36.
Moreno-Vilchez et al. (2024)
The study investigators retrospectively reviewed medical records for patients with severe or very severe AA who were treated with baricitinib 4 mg once daily for at least 24 weeks with participants on average being treated for 55.78 (range, 24 to 120) weeks. The study reported mean SALT scores as efficacy outcomes for the study.
Table 27: Details of Studies Addressing Gaps in the Systematic Review Evidence
Detail | Tang et al. (2024) | Numata et al. (2024) | Moreno-Vilchez et al. (2024) |
|---|---|---|---|
Designs and populations | |||
Study design | Single-arm retrospective study | Retrospectively reviewed medical records | Retrospectively reviewed medical records |
Enrolled, N | 14 | 95 | 36 |
Key inclusion criteria | Patients aged ≥ 65 years with moderate-to-severe AA | Patients with moderate-to-severe AA who had lost approximately 50% of their scalp hair for longer than 5 months were enrolled in the study. | Patients with severe or very severe AA who were treated with baricitinib 4 mg once daily for at least 24 weeks |
Drugs | |||
Intervention | Baricitinib | Baricitinib | Baricitinib |
Comparator(s) | None | None | None |
Outcomes | |||
Primary end point | Reduction in the mean SALT score from baseline | Percentage of patients in the entire cohort who attained a SALT score of 20 or less at week 12, week 24, and week 36 | Mean SALT scores |
Notes | |||
Publications | Tang et al. (2024) | Numata et al. (2024) | Moreno-Vilchez et al. (2024) |
AA = alopecia areata; SALT = Severity of Alopecia Tool.
Sources: Tang et al. (2024),12 Numata et al. (2024),14 and Moreno-Vilchez et al. (2024).13
Results
Baseline Characteristics
Tang et al. (2024)
Fourteen patients (3 males and 11 females) with a mean age of 72.1 (range, 65 to 87) years were included in the study. The median baseline SALT score was 59.8 (SD = 34.4) and the mean duration of the current episode of AA at baseline was 41.1 (SD = 59.8) months. Previous treatments included topical corticosteroids (n = 5), topical calcineurin inhibitors (n = 1), intralesional corticosteroids (n = 4), systemic corticosteroids (n = 5), diphenylcyclopropenone (n = 2), azathioprine (n = 1), cyclosporine (n = 1), methotrexate, (n = 1), and oral tofacitinib (n = 5). Concurrent treatments included topical corticosteroids (n = 1), intralesional corticosteroids (n = 2), and low-dose oral minoxidil (n = 13).
Numata et al. (2024)
The mean patient age was 38.7 (range, 18 to 65) years. The mean age at AA onset was 19.3 years where SD is not reported and the mean duration of the current episode of AA at baseline was 7.8 years where SD is not reported. The median baseline SALT score was 89.2. Previous treatments included topical corticosteroid (n = 2), intralesional corticosteroid (n = 4), oral corticosteroid (n = 3), dupilumab (n = 5), contact immunotherapy (n = 44), and phototherapy (n = 10). Twenty-seven previously untreated patients were enrolled.
Moreno-Vilchez et al. (2024)
The study involved 36 patients treated with baricitinib for an average of 55.78 (range, 24 to 120) weeks. The median baseline SALT score was 94.81 (SD = 9.759). Previous treatments included oral corticosteroid (n = 29), topical corticosteroid (n = 25), intralesional corticosteroid (n = 24), cyclosporine (n = 22), methotrexate (n = 19), and diphencyprone (n = 4).
Exposure to Study Treatments
Tang et al. (2024)
Treatments given in conjunction with baricitinib included corticosteroids (topical, n = 1; intralesional, n = 2) and low-dose oral minoxidil (n = 13). One patient applied a super-potent topical corticosteroid to his scalp in conjunction with baricitinib treatment. One patient with a baseline SALT score of 26.6 who still had residual bald patches on the scalp (with a SALT score of 15) despite baricitinib therapy received intralesional triamcinolone acetonide injections, resulting in a further reduction in the SALT score to 0. One 65-year-old male received intralesional corticosteroid injections in the EBs because of persistent gaps, resulting in complete hair regrowth.
Numata et al. (2024)
Information was not provided.
Moreno-Vilchez et al. (2024)
Out of the total cohort, 9 (25%) patients received combination therapy: 7 patients were treated with a combination of baricitinib and methotrexate (10 mg to 15 mg per week) while 2 patients received a combination of baricitinib and oral minoxidil (1 mg to 2 mg per day).
Efficacy
Tang et al. (2024)
After a mean (SD) duration of 18.5 (11.9) months, a 72.0% reduction in the mean SALT score from baseline was observed. Moreover, 11 (78.6%) patients attained a SALT score of less than 10 after a mean duration of 18.6 months where SD is not reported.
Numata et al. (2024)
The percentage of patients in the entire cohort who attained a SALT score of 20 or less at week 12, week 24, and week 36 was 6.4% (6 of 94 patients), 35.4% (28 of 79 patients), and 46.7% (21 of 45 patients), respectively. The complete response rate (a SALT score of 0) at week 24 and week 36 was 1.3% (1 of 79) of patients and 6.7% (3 of 45) of patients, respectively. Among these, the percentage of patients with patchy AA, alopecia totalis, alopecia universalis, or the ophiasis subtype of AA who attained a SALT score of 20 or less at week 36 was 75.0%, 48.0%, and 75.0%, respectively. The percentage of patients with a current AA episode of less than 4 years’ duration and a SALT score of 20 or lower at week 36 was greater than that of patients with an AA episode of 4 years’ duration or longer.
Moreno-Vilchez et al. (2024)
In the study, 58.8% of patients attained a SALT score of 20 or less at week 24. The response continued for 52 weeks, with 66.6% of patients classified as responders. Additionally, the study compared the SALT scores between patients treated with monotherapy and those who received adjuvant treatment.
Harms
Tang et al. (2024)
Adverse effects of baricitinib included the reactivation of herpes zoster (n = 1), elevated creatine kinase (n = 1), and grade 2 neutropenia (n = 1). One patient required a reduction in the dose of baricitinib because of grade 2 neutropenia. No cases of venous thromboembolism, MACE, or malignancy were reported.
Numata et al. (2024)
Infectious complications occurred in 6 patients during the initial 12 weeks. Herpes simplex and COVID-19 (severe acute respiratory syndrome coronavirus 2) occurred in 1 patient and 5 patients, respectively. No other complications occurred during the entire 36-week course.
Moreno-Vilchez et al. (2024)
Three patients discontinued baricitinib because of inadequate treatment response: 2 patients at week 52 and 1 patient at week 76. Additionally, 1 patient had temporary lymphopenia with methotrexate treatment.
Critical Appraisal
Internal Validity
Limitations of the 3 studies include their single-arm, retrospective designs and small sample sizes. Moreover, many patients in the studies were treated with concomitant treatments. Without a randomized comparison group, it is not possible to attribute the observed effects to baricitinib with certainty. Information such as treatment exposure and concomitant treatments in Numata et al. was not reported. Furthermore, there is a risk that what has been reported was among multiple analyses of the data because of lacking a priori protocols for these 3 studies. Lastly, there is also a risk of selection bias since information about how patients were selected for analysis was not presented.
External Validity
Both Tang et al. and Numata et al. included patients with moderate-to-severe AA; however, patients with moderate AA would not be candidates for baricitinib treatment in Canada. The results of these studies may not be generalizable to patients with severe or very severe AA, which may be more difficult to treat compared with moderate AA. The study by Numata et al. included patients exclusively from Japan whereas the study by Moreno-Vilchez et al. included patients exclusively from Spain (in 2 centres). It is uncertain whether results from small samples of patients treated in these countries would be generalizable to patients living in Canada, given the potential for differences in standard of care in these countries. Although the studies provided additional evidence among patients not included in the pivotal trials, many outcomes that are important to patients (e.g., HRQoL, EB and EL hair loss, anxiety, depression) were not measured or reported.
Discussion
This report summarizes the evidence for baricitinib in the treatment of adults with severe AA based on 2 phase III RCTs, results from the long-term extension period of the RCTs, and the findings of 3 retrospective, single-arm observational studies.
Summary of Available Evidence
Two studies, Study BRAVE-AA1 (N = 654) and Study BRAVE-AA2 (N = 546), met the inclusion criteria for the systematic review conducted by the sponsor. Study BRAVE-AA1 and Study BRAVE-AA2 were pivotal, double-blind, randomized, placebo-controlled trials that assessed the efficacy and safety of baricitinib 4 mg and baricitinib 2 mg relative to placebo in adult patients who had severe or very severe AA with at least 50% scalp involvement (i.e., a SALT score of at least 50) and had a current AA episode lasting more than 6 months and less than 8 years. The proportion of patients attaining a SALT score of 20 or less (the primary end point), a SALT50 response (a secondary end point), ClinRO measures for EB (and EL) hair loss scores of 0 or 1 with at least a 2-point reduction from baseline (key secondary end points), change from baseline in HADS anxiety and depression domain scores, and Skindex-16 for AA symptoms, emotions, and functioning domain scores (secondary or exploratory end points) at week 36 were of interest to this review. At baseline, there was about an equal proportion of patients with severe AA and very severe AA in both trials. Approximately 90% of patients received prior AA treatment, with the most common ones (reported in at least 40% of patients) being topical therapies, intralesional therapy, and systemic immunosuppressants and immunomodulators. Noncomparative efficacy and safety results of up to 104 weeks from the long-term extension period of the RCTs were also presented.
No indirect comparative evidence for baricitinib was submitted.
Three retrospective single-arm observational studies were submitted by the sponsor in an effort to address gaps in the evidence from the pivotal trials. Tang et al. [2024] provided evidence for the use of baricitinib in older adults with AA who were excluded from the pivotal studies. Studies assessing the effects of baricitinib in patients in Japan (Numata et al. [2024]) and in Spain along with evidence for adjuvant therapy among nonresponders (Moreno-Vilchez et al. [2024]) were also submitted. However, our review team did not consider these studies to have addressed any identified gaps in evidence for the purpose of informing the reimbursement recommendation of baricitinib in the Canadian context.
Interpretation of Results
Efficacy
Direct comparative evidence from the BRAVE-AA1 and BRAVE-AA2 trials supported the superiority of baricitinib to placebo with respect to the proportion of patients attaining a SALT score of 20 or less at week 36 in adults with severe AA or very severe AA, addressing a key treatment outcome of attaining a clinically meaningful regrowth of scalp hair noted by patients and clinicians. There is a high certainty that the magnitude of benefits of baricitinib 4 mg relative to placebo was clinically important, though evidence for baricitinib 2 mg is less certain because of imprecision (95% CI included the possibility of benefit and little to no difference in both trials). Prespecified subgroup analysis by duration of the current episode of AA and the severity of AA were consistent with the primary analysis; however, because of the lack of sample size consideration and control for multiplicity, no definitive conclusions can be drawn on subgroup effects. Responder analyses based on the percentage reduction in SALT score from baseline (secondary outcomes) were assessed as supporting evidence in the absence of the adjustment for multiplicity. Evidence for the MID in the percentage change from baseline in SALT scores was not identified by the sponsor. The trials conducted analyses using different thresholds. Results of the SALT50 responder analysis showed a clinically meaningful improvement in hair regrowth with baricitinib 4 mg and baricitinib 2 mg interventions compared with placebo in both trials. Results of the SALT75 responder analysis were similar.
Response to systemic treatments for severe AA is typically assessed based on scalp hair regrowth since scalp hair is the primary treatment target of systemic treatments, as per clinical expert input. EB and EL hair loss may also occur in some patients and could cause significant distress. In the trials, novel clinician-administered instruments developed by the sponsor (a ClinRO measure for EB hair loss and a ClinRO measure for EL hair loss) were used to assess the treatment effect of baricitinib on the regrowth of EB hair and ELs as key secondary end points. Evidence for the validity of these instruments in patients with AA was available. Results from the pivotal trials showed that baricitinib 4 mg likely resulted in clinically important benefits in the regrowth of EB hair and ELs. Evidence for baricitinib 2 mg was less certain because of imprecision (the point estimates from the trials were in different directions relative to the threshold of clinical importance and the 95% CIs included the possibility of benefit and no clinically important difference). Results based on the PRO measures (patient-administered assessment) were in general aligned with the ClinRO measures. Of note, the ClinRO measures were assessed in patients with a specific baseline score. Given that a large proportion of patients (between 31% and 42% of patients) was excluded because of not having the specified baseline score, there is a risk that randomization was impacted, which reduced the certainty of these findings. There is also a potential for bias in the measurement of this outcome since it required some level of subjective judgment by the evaluators, potentially resulting in the overestimated efficacy of baricitinib, though the impact on study results is unlikely to be significant.
The clinical experts and patient groups highlighted that hair loss is associated with significant psychological burden and that improvement of HRQoL is an important outcome in the treatment of AA. The HADS anxiety and depression domain scores (secondary outcomes), as well as scores of the Skindex-16 for AA disease-specific HRQoL instrument (an exploratory outcome in Study BRAVE-AA1 and a secondary outcome in Study BRAVE-AA2) were assessed as supporting evidence without control for multiplicity. No MID estimates for HADS and Skindex-16 for AA domains were identified from the literature by the sponsor. Results in change from baseline in HADS anxiety and depression domain scores at week 36 in general were very uncertain. Results in the Skindex-16 for AA domain scores were suggestive of benefits in HRQoL with baricitinib treatment but uncertain (or very uncertain). The uncertainty in HADS and Skindex-16 for AA outcomes was because of potential attribution bias in favour of baricitinib given the differential discontinuation of study treatment between treatment groups and because the imputation method used (mLOCF or LOCF) to account for missing data was not conservative. As well, the clinical experts noted that the trial population appeared to have a lower degree of anxiety and depression at baseline compared to patients in clinical practice, which limits the generalizability of the HADS outcomes. Evidence for the validity of the HADS and Skindex-16 for AA instruments for patients with severe AA was not available, which adds to the uncertainty of the results. Other HRQoL outcomes measured in the trials (the EQ-5D-5L and the SF-36 version 2 physical component and mental component scores) were similarly uncertain because of potential attrition bias from the differential treatment discontinuation between treatment groups that were not appropriately accounted for.
Overall, there are no major concerns with the generalizability of the pivotal trial results, although it should be noted that, as per clinical expert input, patients with a primarily diffuse type of AA may be eligible for treatment and that some clinicians may be open to prescribing baricitinib treatment to older adults with severe AA (i.e., males older than 60 years and females older than 70 years). The comparative treatment effects of baricitinib versus placebo in these patients are unknown since they were excluded from the pivotal trials. As well, the pivotal trials appeared to have enrolled a higher proportion of patients with very severe AA compared to clinical practice as per clinical expert input, though the concern is probably low given that patients with very severe AA are typically harder to treat than those with severe AA; the trial results may be more conservative than anticipated in clinical practice, on average.
Evidence from the long-term extension period of the BRAVE-AA1 and BRAVE-AA2 trials provided support for the up-titration and down-titration of the baricitinib dose according to response to treatment (as recommended by the product monograph). Results also suggested that the proportion of patients attaining a clinically meaningful regrowth of scalp hair increased or remained stable beyond week 36 and that the efficacy of baricitinib appeared to be sustained up to week 104 in most patients who were responders at week 52. However, for the long-term extension results up to week 104, no placebo control was available, limiting causal conclusions.
Older adults (i.e., males older than 60 years and females older than 70 years) were excluded from the BRAVE-AA1 and BRAVE-AA2 trials. To address this gap in evidence, the Tang et al. (2024) study — a single-arm, retrospective observational study in older adults aged 65 years or older with moderate-to-severe AA — was submitted by the sponsor. While evidence from the study suggested that baricitinib could improve scalp hair regrowth in older adults at approximately 18 months, results were uncertain because of the small sample size and the lack of a control group, which precluded a conclusion on whether the observed effects could be attributed to baricitinib. As well, the study included an unknown number of patients with moderate AA (baricitinib is currently approved for the treatment of severe AA only); this could potentially limit the generalizability of study findings.
The BRAVE-AA1 and BRAVE-AA2 trials were the only phase III RCTs of baricitinib to date. No indirect comparative evidence for baricitinib was submitted by the sponsor. Direct and indirect comparative evidence between baricitinib and systemic treatments for severe AA that are currently reimbursed by the public drug plans (conventional immunosuppressants) were not submitted; this represents an evidence gap in the treatment of severe AA.
Of note, the National Institute for Health and Care Excellence issued a recommendation to not reimburse baricitinib for the treatment of adults with severe AA. They stated in the rationale for the recommendation that baricitinib did not show a meaningful improvement in most of the HRQoL assessments done compared with placebo in the pivotal trials and that the cost-effectiveness of baricitinib is uncertain and is higher than normally considered acceptable by the organization.
Harms
Direct comparative evidence from the BRAVE-AA1 and BRAVE-AA2 trials showed that the safety profile of baricitinib was comparable to placebo in patients with severe AA at week 36. The most common TEAEs of baricitinib included upper respiratory tract infection, headache, urinary tract infection, and nasopharyngitis, all of which were reported at a low frequency (less than 10% of patients), as being not serious, and as not having led to treatment withdrawal or death. The clinical experts noted that the short-term safety profile of baricitinib is consistent with that of other JAK inhibitors, although a longer duration of follow-up is required to adequately capture the long-term safety of baricitinib, particularly the rare serious AEs noted in the product monograph as black box warnings (serious infections, malignancies, MACEs, and thromboses). Evidence from the long-term extension period of the pivotal trials showed that these rare serious AEs were uncommon and that there were no new safety signals with 104 weeks of baricitinib treatment. No notable safety concerns were identified from the 3 retrospective chart review studies. No direct or indirect comparative harms evidence for baricitinib versus systemic treatments currently reimbursed by the public drug plans were submitted.
Conclusion
Direct comparative evidence from 2 pivotal double-blind RCTs (Study BRAVE-AA1 and Study BRAVE-AA2) demonstrated that 36 weeks of baricitinib 4 mg treatment resulted in the clinically important regrowth of scalp hair compared with placebo in adults with severe or very severe AA; the benefits for the regrowth of EB and EL hair were shown but less certain because of study limitations. Results also favoured baricitinib 2 mg treatment with respect to the regrowth of scalp and EB hair, although there was some uncertainty about whether the magnitude of change was clinically important because of imprecision. No definitive conclusion can be drawn regarding the direction and magnitude of the effects of baricitinib treatment on anxiety, depression, and HRQoL because of important methodological limitations (potential attrition bias and the lack of evidence supporting the validity of the instruments used in patients with AA) and concerns with indirectness (for anxiety and depression outcomes). The benefits of baricitinib in hair regrowth appeared to be sustained through week 104 in the trials, although analyses beyond week 36 were noncomparative, which precluded firm conclusions. No conclusions can be drawn regarding the clinical benefits of baricitinib in older adults with severe AA from a sponsor-submitted retrospective chart review study (Tang et al. [2024]) because of a small sample size and single-arm study design. No notable concerns with the safety profile of baricitinib were identified based on results from the pivotal trials through week 104. No direct or indirect comparative evidence for baricitinib versus systemic treatments currently reimbursed by the public drug plans (i.e., immunosuppressants) was submitted.
References
1.Pratt CH, King LE, Jr., Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nat Rev Dis Primers. 2017;3:17011. PubMed
2.Benigno M, Anastassopoulos KP, Mostaghimi A, et al. A Large Cross-Sectional Survey Study of the Prevalence of Alopecia Areata in the United States. Clin Cosmet Investig Dermatol. 2020;13:259-266. PubMed
3.Harries M, Macbeth AE, Holmes S, et al. The epidemiology of alopecia areata: a population-based cohort study in UK primary care. Br J Dermatol. 2022;186(2):257-265. PubMed
4.Safavi K. Prevalence of alopecia areata in the First National Health and Nutrition Examination Survey. Arch Dermatol. 1992;128(5):702. PubMed
5.Soh BW, Kim SM, Kim YC, Choi GS, Choi JW. Increasing prevalence of alopecia areata in South Korea. J Dermatol. 2019;46(9):e331-e332. PubMed
6.King B, Ohyama M, Kwon O, et al. Two Phase 3 Trials of Baricitinib for Alopecia Areata. N Engl J Med. 2022;386(18):1687-1699. PubMed
7.Clinical Study Report: BRAVE-AA1. A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Operationally Seamless, Adaptive Phase 2/3 Study to Evaluate the Efficacy and Safety of Baricitinib in Adult Patients with Severe or Very Severe Alopecia Areata [internal sponsor's report]. Eli Lilly and Company; 2021 [sponsor submitted reference].
8.Clinical Study Report: BRAVE-AA2. A Multicenter, Randomized, Double-Blind, Placebo Controlled, Phase 3 Study to Evaluate the Efficacy and Safety of Baricitinib in Adult Patients with Severe or Very Severe Alopecia Areata [internal sponsor's report]. Eli Lilly and Company; 2021 [sponsor submitted reference].
9.Sponsor Summary of Clinical Evidence: Olumiant (baricitinib) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: baricitinib, 4 mg and 2 mg, oral tablets. Toronto (ON): Eli Lilly Canada Inc; 2024 Mar.
10.Clinical Study Report Addendum: BRAVE-AA1. A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Operationally Seamless, Adaptive Phase 2/3 Study to Evaluate the Efficacy and Safety of Baricitinib in Adult Patients with Severe or Very Severe Alopecia Areata [internal sponsor's report]. Eli Lilly and Company; 2022 [sponsor submitted reference].
11.Clinical Study Report Addendum: BRAVE-AA2. A Multicenter, Randomized, Double-Blind, Placebo Controlled, Phase 3 Study to Evaluate the Efficacy and Safety of Baricitinib in Adult Patients with Severe or Very Severe Alopecia Areata [internal sponsor's report]. Eli Lilly and Company; 2022 [sponsor submitted reference].
12.Tang GT, Triwongwaranat D, Sinclair R, et al. Treatment of moderate-to-severe alopecia areata in patients over the age of 65 with baricitinib. Clin Exp Dermatol. 2024. PubMed
13.Moreno-Vílchez C, Bonfill-Ortí M, Bauer-Alonso A, Notario J, Figueras-Nart I. Baricitinib for the treatment of alopecia areata in adults: Real-world analysis of 36 patients. J Am Acad Dermatol. 2024. PubMed
14.Numata T, Irisawa R, Miho M, Uchiyama M, Harada K. Baricitinib Therapy for Moderate to Severe Alopecia Areata: A Retrospective Review of 95 Japanese Patients. Acta Derm Venereol. 2024;104. PubMed
15.Alkhalifah A. Alopecia areata update. Dermatol Clin. 2013;31(1):93-108. PubMed
16.Olsen EA, Hordinsky MK, Price VH, et al. Alopecia areata investigational assessment guidelines--Part II. National Alopecia Areata Foundation. J Am Acad Dermatol. 2004;51(3):440-447. PubMed
17.Hordinsky M, Junqueira AL. Alopecia areata update. Semin Cutan Med Surg. 2015;34(2):72-75. PubMed
18.Villasante Fricke AC, Miteva M. Epidemiology and burden of alopecia areata: a systematic review. Clin Cosmet Investig Dermatol. 2015;8:397-403. PubMed
19.Lintzeri DA, Constantinou A, Hillmann K, Ghoreschi K, Vogt A, Blume-Peytavi U. Alopecia areata - Current understanding and management. J Dtsch Dermatol Ges. 2022;20(1):59-90.
20.Food and Drug Administration (FDA). The voice of the patient: Alopecia Areata. https://www.fda.gov/media/112100/download Accessed 2023 May 3.
21.Gilding AJ, Ho N, Pope E, Sibbald C. The Burden of Disease in Alopecia Areata: Canadian Online Survey of Patients and Caregivers. JMIR Dermatol. 2022;5(4):e39167. PubMed
22.Andersen YMF, Nymand L, DeLozier AM, Burge R, Edson-Heredia E, Egeberg A. Patient characteristics and disease burden of alopecia areata in the Danish Skin Cohort. BMJ Open. 2022;12(2):e053137. PubMed
23.Starace M, Cedirian S, Alessandrini AM, et al. Impact and Management of Loss of Eyebrows and Eyelashes. Dermatol Ther (Heidelb). 2023;13(6):1243-1253. PubMed
24.Yamakoshi T, Andoh T, Makino T, Kuraishi Y, Shimizu T. Clinical and histopathological features of itch in patients with alopecia areata. Acta Derm Venereol. 2013;93(5):575-576. PubMed
25.Messenger AG, McKillop J, Farrant P, McDonagh AJ, Sladden M. British Association of Dermatologists' guidelines for the management of alopecia areata 2012. Br J Dermatol. 2012;166(5):916-926. PubMed
26.Mirzoyev SA, Schrum AG, Davis MDP, Torgerson RR. Lifetime incidence risk of alopecia areata estimated at 2.1% by Rochester Epidemiology Project, 1990-2009. J Invest Dermatol. 2014;134(4):1141-1142. PubMed
27.Canadian Skin Patient Alliance (CSPA). Overview: What is alopecia? https://www.canadianskin.ca/alopecia/56-overview-what-is-alopecia#fast-facts Accessed 2023 May 3.
28.Phillips TG, Slomiany WP, Allison R. Hair Loss: Common Causes and Treatment. Am Fam Physician. 2017;96(6):371-378. PubMed
29.Spano F, Donovan JC. Alopecia areata: Part 1: pathogenesis, diagnosis, and prognosis. Can Fam Physician. 2015;61(9):751-755. PubMed
30.Olsen EA, Roberts J, Sperling L, et al. Objective outcome measures: Collecting meaningful data on alopecia areata. J Am Acad Dermatol. 2018;79(3):470-478.e473. PubMed
31.Meah N, Wall D, York K, et al. The Alopecia Areata Consensus of Experts (ACE) study part II: Results of an international expert opinion on diagnosis and laboratory evaluation for alopecia areata. J Am Acad Dermatol. 2021;84(6):1594-1601. PubMed
32.Delamere FM, Sladden MM, Dobbins HM, Leonardi-Bee J. Interventions for alopecia areata. Cochrane Database Syst Rev. 2008(2):Cd004413. PubMed
33.Vañó-Galván S, Fernández-Crehuet P, Grimalt R, et al. Alopecia areata totalis and universalis: a multicenter review of 132 patients in Spain. J Eur Acad Dermatol Venereol. 2017;31(3):550-556. PubMed
34.Trüeb RM, Dias M. Alopecia Areata: a Comprehensive Review of Pathogenesis and Management. Clin Rev Allergy Immunol. 2018;54(1):68-87. PubMed
35.Eli Lilly Canada Inc. Olumiant® (baricitinib). [product monograph] 2024. [sponsor submitted reference].
36.Rogain® (minoxidil): 2% topical solution and 5% topical foam [product monograph]. Markham (ON): Johnson & Johnson Inc; 2022 [sponsor submitted reference].
37.Kenalog® (triamcinolone acetonide): injectable suspension 10 mg/mL [product monograph]. Saint-Laurent (QC): Bristol-Myers Squibb Canada; 2023 [sponsor submitted reference].
38.Senna M, Mostaghimi A, Ohyama M, et al. Long‐term efficacy and safety of baricitinib in patients with severe alopecia areata: 104‐week results from BRAVE‐AA1 and BRAVE‐AA2. J Eur Acad Dermatol Venereol. 2024;38(3):583-593. PubMed
39.Kwon O, Senna MM, Sinclair R, et al. Efficacy and Safety of Baricitinib in Patients with Severe Alopecia Areata over 52 Weeks of Continuous Therapy in Two Phase III Trials (BRAVE-AA1 and BRAVE-AA2). Am J Clin Dermatol. 2023:1-9. PubMed
40.Wyrwich KW, Kitchen H, Knight S, et al. Using qualitative methods to establish the clinically meaningful threshold for treatment success in alopecia areata. Qual Life Res. 2023;32(5):1319-1327. PubMed
41.Wyrwich KW, Kitchen H, Knight S, et al. The Alopecia Areata Investigator Global Assessment scale: a measure for evaluating clinically meaningful success in clinical trials. Br J Dermatol. 2020;183(4):702-709. PubMed
42.Wyrwich KW, Kitchen H, Knight S, et al. Development of Clinician-Reported Outcome (ClinRO) and Patient-Reported Outcome (PRO) Measures for Eyebrow, Eyelash and Nail Assessment in Alopecia Areata. Am J Clin Dermatol. 2020;21(5):725-732. PubMed
43.White D, Leach C, Sims R, Atkinson M, Cottrell D. Validation of the Hospital Anxiety and Depression Scale for use with adolescents. Br J Psychiatry. 1999;175:452-454. PubMed
44.Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361-370. PubMed
45.Snaith RP. The Hospital Anxiety And Depression Scale. Health Qual Life Outcomes. 2003;1:29. PubMed
46.Clinician-Reported Outcomes Evidence Dossier. Severity of Alopecia Tool (SALT): A Measure of Scalp Hair Loss in Patients with Alopecia Areata [Sponsor's internal report]. Eli Lilly and Company; 2021 [sponsor submitted reference].
47.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. PubMed
48.Clinician-Reported Outcomes Evidence Dossier. Clinician-Reported Outcome (ClinRO) Measure for Eyebrow Hair Loss™ for Patients with AA [sponsor's internal report]. Eli Lilly and Company; 2021 [sponsor submitted reference].
49.Clinician-Reported Outcomes Evidence Dossier. Clinician-Reported Outcome (ClinRO) Measure for Eyelash Hair Loss™ for Patients with AA [sponsor's internal report]. Eli Lilly and Company; 2021 [sponsor submitted reference].
50.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
51.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
52.King B, Mostaghimi A, Shimomura Y, et al. Integrated safety analysis of baricitinib in adults with severe alopecia areata from two randomized clinical trials. Br J Dermatol. 2022;188(2):218-227. PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 28: Subgroup Analyses of Proportion of Patients Attaining SALT Score of 20 or Lower at Week 36 in Study BRAVE-AA1 and Study BRAVE-AA2
Subgroup | Study BRAVE-AA1 | Study BRAVE-AA2 | ||||
|---|---|---|---|---|---|---|
PBO | BARI 2 mg | BARI 4 mg | PBO | BARI 2 mg | BARI 4 mg | |
Duration of current episode of AA | ||||||
< 4 years | ||||||
Response at week 36 (%) | 9 (6.7) | 36 (28.3) | 76 (40.2) | 4 (4.3) | 21 (20.4) | 54 (38.6) |
Difference vs. PBO (%) (95% CI)a | Reference | 21.6 (12.6 to 30.6) | 33.5 (24.8 to 41.3) | Reference | 16.1 (7.1 to 25.3) | 34.3 (24.5 to 43.0) |
P value | Reference | < 0.001b | < 0.001b | Reference | < 0.001b | < 0.001b |
≥ 4 years | ||||||
Response at week 36 (%) | 1 (1.8) | 4 (7.0) | 23 (25.0) | 0 (0) | 6 (11.3) | 22 (23.4) |
Difference vs. PBO (%) (95% CI)a | Reference | 5.2 (–3.7 to 15.0) | 23.2 (12.2 to 33.0) | Reference | 11.3 (2.9 to 22.6) | 23.4 (14.0 to 32.9) |
P value | Reference | 0.364b | < 0.001b | Reference | 0.008b | < 0.001b |
Treatment-by-subgroup P value (Baricitinib pooled vs. PBO) | Reference | 0.339 | Reference | 0.838 | ||
Baseline disease severity | ||||||
Severe | ||||||
Response at week 36 (%) | 9 (9.8) | 28 (36.4) | 67 (50.4) | 4 (5.4) | 20 (28.6) | 51 (44.3) |
Difference vs. PBO (%) (95% CI)a | Reference | 26.6 (14.0 to 38.6) | 40.6 (29.2 to 50.1) | Reference | 23.2 (11.1 to 35.1) | 38.9 (27.3 to 48.6) |
P value | Reference | < 0.001b | < 0.001b | Reference | < 0.001b | < 0.001b |
Very severe | ||||||
Response at week 36 (%) (95% CI) | 1 (1.0) | 12 (11.2) | 32 (21.6) | 0 (0) | 7 (8.1) | 25 (21.0) |
Difference vs. PBO (%) (95% CI)a | Reference | 10.2 (3.6 to 17.6) | 20.6 (13.1 to 27.9) | Reference | 8.1 (2.0 to 15.9) | 21.0 (13.2 to 29.2) |
P value | Reference | 0.003b | < 0.001b | Reference | 0.014b | < 0.001b |
Treatment-by-subgroup P value (Baricitinib pooled vs. PBO) | Reference | 0.757 | Reference | 0.684 | ||
AA = alopecia areata; BARI = baricitinib; CI = confidence interval; PBO = placebo; vs. = versus.
Note: Details included in Table 28 are from the sponsor’s Summary of Clinical Evidence.9
aLogistic regression analysis with treatment, subgroup, and treatment-by-subgroup interaction and geographic region, duration of current episode at baseline (< 4 years vs. ≥ 4 years), and baseline total SALT score as factors.
bThis outcome was not adjusted for multiplicity and was at increased risk of type I error (false-positive results).
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Supportive outcome data at week 36 from the BRAVE-AA1 and BRAVE-AA2 trials are summarized in Table 29. Note that all end points described as follows were not adjusted for multiplicity. As such, statistically significant results were at an increased risk of type I error.
SALT75
The between-group difference in the proportion of patients attaining SALT75 at week 36 (secondary end point) comparing baricitinib 2 mg versus placebo was 14.3% (95% CI, 7.8% to 20.9%) in Study BRAVE-AA1 and 15.4% (95% CI, 9.4% to 22.1%) in Study BRAVE-AA2. The between-group difference comparing baricitinib 4 mg with placebo was 29.0% (95% CI, 22.4% to 35.2%) in Study BRAVE-AA1 and 30.8% (95% CI, 24.2% to 37.1%) in Study BRAVE-AA2. Results were in favour of baricitinib, consistent with the SALT50 responder analysis.
EQ-5D-5L Health State Index
The between-group difference with respect to change from baseline in EQ-5D-5L health state index at week 36 comparing baricitinib 4 mg and 2 mg versus placebo did not favour either intervention for both US algorithm-based and UK algorithm-based index (i.e., the point estimates and 95% CIs included effects close to the null), except for the comparison between 4 mg and placebo (based on the US algorithm) in Study BRAVE-AA2 where results marginally favoured baricitinib 4 mg (i.e., it is unclear whether the point estimate or upper bound of the 95% CI would be considered clinically important differences). Similar to HADS and Skindex-16 for AA outcomes, the EQ-5D-5L results are uncertain because of potential attrition bias given the differential discontinuation of study treatment between the baricitinib and placebo groups and the use of mLOCF imputation method to account for missing data.
SF-36 Version 2 Acute: Physical Component and Mental Component Scores
The between-group difference with respect to change from baseline in Physical Component Score at week 36 did not favour either baricitinib (both regimens) or placebo in both trials (i.e., the point estimates and 95% CIs included effects close to the null).
The between-group difference comparing baricitinib 2 mg versus placebo with respect to change from baseline in mental component score at week 36 did not favour either intervention in both trials (i.e., the point estimates were close to the null and the 95% CIs crossed the null). The between-group difference comparing baricitinib 4 mg and placebo favoured baricitinib 4 mg in Study BRAVE-AA2 but did not favour either intervention in Study BRAVE-AA1 (i.e., the point estimate was close to the null and the 95% CI crossed the null). Similar to HADS and Skindex-16 for AA outcomes, the SF-36 results are uncertain because of potential attrition bias given the differential discontinuation of study treatment between the baricitinib and placebo groups and the use of mLOCF imputation method to account for missing data.
Table 29: Supportive Outcome Data at Week 36 in Study BRAVE-AA1 and Study BRAVE-AA2 — DB Treatment Period (FAS)
Week 36 outcome | Study BRAVE-AA1 | Study BRAVE-AA2 | ||||
|---|---|---|---|---|---|---|
PBO (N = 189) | BARI 2 mg (N = 184) | BARI 4 mg (N = 281) | PBO (N = 156) | BARI 2 mg (N = 156) | BARI 4 mg (N = 234) | |
Proportion of patients attaining SALT75 at week 36 | ||||||
Response, n (%) (95% CI) | 9 (4.8) (2.5 to 8.8) | 35 (19.0) (14.0 to 25.3) | 95 (33.8) (28.5 to 39.5) | 2 (1.3) (0.4 to 4.6) | 26 (16.7) (11.6 to 23.3) | 75 (32.1) (26.4 to 38.3) |
Difference vs. PBO (%) (95% CI)a | Reference | 14.3 (7.8 to 20.9) | 29.0 (22.4 to 35.2) | Reference | 15.4 (9.4 to 22.1) | 30.8 (24.2 to 37.1) |
P value | Reference | < 0.001b | < 0.001b | Reference | < 0.001b | < 0.001b |
EQ-5D-5L health state index (US algorithm) | ||||||
Number of patients contributed to the analysis, n | 177 | 174 | 272 | 154 | 156 | 234 |
Baseline, mean (SD) | 0.90 (0.096) | 0.90 (0.100) | 0.91 (0.093) | 0.93 (0.090) | 0.91 (0.106) | 0.91 (0.101) |
Change from baseline in score at week 36, LSM (SE) | 0.00 (0.007) | 0.01 (0.007) | 0.00 (0.006) | –0.02 (0.007) | 0.00 (0.007) | 0.00 (0.006) |
Difference vs. PBO, LSM (95% CI)c | Reference | 0.00 (–0.01 to 0.02) | 0.00 (–0.01 to 0.02) | Reference | 0.02 (–0.00 to 0.04) | 0.02 (0.00 to 0.04) |
P value | Reference | 0.613b | 0.843b | Reference | 0.103b | 0.035b |
EQ-5D-5L health state index (UK algorithm) | ||||||
Number of patients contributed to the analysis, n | 177 | 174 | 272 | 154 | 156 | 234 |
Baseline, mean (SD) | 0.88 (0.124) | 0.89 (0.132) | 0.89 (0.120) | 0.92 (0.112) | 0.89 (0.143) | 0.89 (0.132) |
Change from baseline in score at week 36, LSM (SE) | 0.00 (0.009) | 0.00 (0.009) | 0.00 (0.008) | –0.02 (0.009) | 0.00 (0.009) | 0.00 (0.007) |
Difference vs. PBO, LSM (95% CI)c | Reference | 0.00 (–0.02 to 0.02) | 0.00 (–0.02 to 0.02) | Reference | 0.02 (–0.01 to 0.04) | 0.02 (–0.00 to 0.04) |
P value | Reference | 0.829b | 0.945b | Reference | 0.126b | 0.065b |
SF-36 version 2 acute: Physical component score | ||||||
Number of patients contributed to the analysis, n | 177 | 174 | 272 | 142 | 146 | 226 |
Baseline, mean (SD) | 55.56 | 55.81 | 55.91 | 56.84 | 56.16 | 56.61 |
Change from baseline in score at week 36, LSM (SE) | –0.49 (0.385) | 0.10 (0.391) | –0.08 (0.328) | –0.39 (0.431) | –0.64 (0.430) | –0.66 (0.342) |
Difference vs. PBO, LSM (95% CI)c | Reference | 0.58 (–0.35 to 1.52) | 0.40 (–0.44 to 1.25) | Reference | –0.25 (–1.43 to 0.93) | –0.26 (–1.34 to 0.81) |
P value | Reference | 0.220b | 0.349b | Reference | 0.678b | 0.628b |
SF-36 version 2 acute: Mental component score | ||||||
Number of patients contributed to the analysis, n | 177 | 174 | 272 | 142 | 146 | 226 |
Baseline, mean (SD) | 50.53 | 50.74 | 50.58 | 50.35 | 50.08 | 49.96 |
Change from baseline in score at week 36, LSM (SE) | –0.83 (0.620) | 0.18 (0.628) | –0.31 (0.528) | –0.91 (0.603) | 0.30 (0.601) | 0.90 (0.479) |
Difference vs. PBO, LSM (95% CI)c | Reference | 1.01 (–0.50 to 2.51) | 0.52 (–0.84 to 1.88) | Reference | 1.21 (–0.44 to 2.86) | 1.81 (0.32 to 3.31) |
P value | Reference | 0.189b | 0.452b | Reference | 0.150b | 0.018b |
BARI = baricitinib; CI = confidence interval; DB = double-blind; FAS = full analysis set; LSM = least squares mean; PBO = placebo; SALT = Severity of Alopecia Tool; SD = standard deviation, SE = standard error; SF-36 = Short Form (36) Health Survey; Skindex-16 for AA = Skindex-16 for Alopecia Areata; vs. = versus.
Note: Details included in Table 29 are from the sponsor’s Summary of Clinical Evidence.9
aLogistic regression analysis with treatment, subgroup, and treatment-by-subgroup interaction and geographic region, duration of current episode at baseline (< 4 years vs. ≥ 4 years), and baseline total SALT score as factors.
bThis outcome was not adjusted for multiplicity and was at risk of type I error (false-positive results).
cThis was analyzed using the analysis of covariance (ANCOVA) model including geographic region, duration of current episode at baseline, treatment group, and baseline value as fixed factors.
Sources: Study BRAVE-AA1 Clinical Study Report and Study BRAVE-AA2 Clinical Study Report.7,8
Pharmacoeconomic Review
Abbreviations
AA
alopecia areata
BIA
budget impact analysis
BSC
best supportive care
CDA-AMC
Canada’s Drug Agency
DSP
Disease Specific Programme
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
JAK
Janus kinase
QALY
quality-adjusted life-year
SALT
Severity of Alopecia Tool
SALT30
at least a 30% improvement from baseline in the Severity of Alopecia Tool score
SALT50
at least a 50% improvement from baseline in the Severity of Alopecia Tool score
SALT75
at least a 75% improvement from baseline in the Severity of Alopecia Tool score
SNRI
serotonin-norepinephrine reuptake inhibitor
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Baricitinib (Olumiant), 2 mg and 4 mg oral tablets |
Indication | For the treatment of adult patients with severe AA |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | January 26, 2024 |
Reimbursement request | As per indication |
Sponsor | Eli Lilly Canada Inc. |
Submission history | Previously reviewed: Yes Indication: Rheumatoid arthritis Recommendation date: August 2, 2019 Recommendation: Reimburse with clinical criteria and/or conditions |
AA = alopecia areata; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients with AA with a SALT score of 50 or higher at baseline (i.e., a SALT score of 50 to 100) |
Treatment | Baricitinib |
Dosage regimen | The recommended dose is baricitinib 2 mg daily, which may be increased to baricitinib 4 mg once daily if the response to treatment is not adequate. For patients with nearly complete or complete scalp hair loss and/or substantial eyelash or eyebrow hair loss, the recommended dose is baricitinib 4 mg once daily. Once patients attain an adequate response to treatment with baricitinib 4 mg, the dose may be decreased to 2 mg daily. |
Submitted prices | Baricitinib 2 mg: $57.21 per tablet 4 mg: $114.41 per tablet |
Submitted treatment cost | Baricitinib 2 mg daily: $20,894 per patient annually 4 mg daily: $41,789 per patient annually |
Comparator | No active treatment |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (63 years) |
Key data source | Pooled data from Study BRAVE-AA1 and Study BRAVE-AA2 were used to inform change from baseline in the SALT score (SALT50) and treatment discontinuation rates. |
Submitted results | Baricitinib 2 mg once daily:
Baricitinib 4 mg once daily:
|
Key limitations |
|
CDA-AMC reanalysis results |
|
AA = alopecia areata; BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SALT = Severity of Alopecia Tool; SALT30 = at least a 30% improvement from baseline in the Severity of Alopecia Tool score; SALT50 = at least a 50% improvement from baseline in the Severity of Alopecia Tool score; SALT75 = at least a 75% improvement from baseline in the Severity of Alopecia Tool score; WTP = willingness to pay.
Conclusions
Evidence from Study BRAVE-AA1 and Study BRAVE-AA2 — using a clinical response defined as achieving 80% or greater scalp hair coverage (a SALT score of ≤ 20) — demonstrated that 36 weeks of baricitinib 4 mg treatment resulted in the clinically important regrowth of scalp hair compared with no active treatment in patients with severe alopecia areata (AA). Results also favoured baricitinib 2 mg treatment for the regrowth of scalp hair, although there is uncertainty on whether the magnitude of change was clinically important. The clinical review by Canada’s Drug Agency (CDA-AMC) noted that while the benefits of baricitinib in hair regrowth appeared to be maintained through week 104 in the long term extension period of the trials, analyses beyond week 36 were noncomparative, limiting firm conclusions about the long-term comparative effectiveness of baricitinib. Additionally, our clinical review could not draw definitive conclusions regarding the effects of baricitinib on health-related quality of life (HRQoL) because of important methodological limitations, including potential attrition bias and lack of evidence supporting the validity of the psychometric instruments used in patients with AA. As part of the base-case reanalysis, CDA-AMC adopted the Severity of Alopecia Tool [SALT] and SALT30 (defined as at least a 30% improvement from baseline in the Severity of Alopecia Tool score) as the primary response outcome to determine treatment continuation based on clinical expert input; CDA-AMC assumed equal costs associated with drug acquisition, drug monitoring, and disease management for patients treated with baricitinib or no active treatment in the best supportive care (BSC) health state; and CDA-AMC used the EQ-5D utility values derived from Study BRAVE-AA1 and Study BRAVE-AA2.
In our base case, the use of baricitinib at the 2 mg dose was associated with an incremental cost-effectiveness ratio (ICER) of $5,465,503 per quality-adjusted life-year (QALY) gained compared to no active treatment (incremental costs = $62,457; incremental QALYs = 0.01). In addition, the use of baricitinib at the 4 mg dose was associated with an ICER of $6,803,200 per QALY gained compared to no active treatment (incremental costs = $203,814; incremental QALYs = 0.03). The estimated ICERs were higher than the sponsor’s base-case value. This increase was driven by aligning the response outcome with criteria likely to be used in Canadian clinical practice and by using EQ-5D utility estimates derived from the BRAVE-AA1 and BRAVE-AA2 trials. There is no price reduction upon which baricitinib would be considered cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained, irrespective of dose. Under these considerations, there remains considerable uncertainty in the cost-effectiveness results. Baricitinib is a relatively costly treatment ($20,000 to $41,000 per year) with a number of remaining areas of uncertainty, especially concerning the impact of baricitinib on the HRQoL of patients with severe AA (which, based on Study BRAVE-AA1 and Study BRAVE-AA2, may be lower than what was initially estimated), how treatment response will be defined in clinical practice, and consequently how treatment continuation will be determined. Moreover, when comparing the duration of the primary analysis of Study BRAVE-AA1 and Study BRAVE-AA2 to the model’s time horizon (36 weeks versus 63 years), it is important to note that the near entirety of the QALY benefit realized by patients receiving baricitinib was derived through extrapolation.
When adopting at least a 75% improvement from baseline in the Severity of Alopecia Tool score (SALT75) as an alternative response threshold to determine treatment continuation with baricitinib beyond 36 weeks, the ICER of baricitinib decreased to $346,345 per QALY gained for the 2 mg dose and $497,449 per QALY gained for the 4 mg dose, compared to no active treatment. In this scenario, a price reduction of 88% for the baricitinib 2 mg dose and 91% for the baricitinib 4 mg dose would be necessary for it to be cost-effective compared to no active treatment at a WTP threshold of $50,000 per QALY gained. CDA-AMC were unable to address the limitation concerning the exclusion of BSC as a relevant comparator owing to the absence of comparative clinical effectiveness data. Hence, the cost-effectiveness of baricitinib relative to BSC remains unknown.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
One patient group, the Canadian Alopecia Areata Foundation, provided input for this review. The Canadian Alopecia Areata Foundation collected data on the psychosocial and emotional impact of AA from peer-reviewed literature, as well as patient perspectives on AA from patient reports and support sessions conducted in Canada over the years. Overall, patients’ disease experience was influenced by the physical manifestations associated with AA (e.g., disfiguring hair loss), the psychological effects associated with this loss (e.g., anxiety, distress, depression), and the broader psychosocial impacts associated with feelings of grief, shame, and loss of identity, which often led to experiences of isolation, stigma, and bullying. Patient input highlighted the availability of various treatments for AA, each with distinct limitations. While topical corticosteroids offer limited effectiveness and may induce irritation, intralesional corticosteroids can effectively treat small hair loss patches but may not be covered by insurance. Oral corticosteroids exhibit variable success rates with common relapse and significant side effects. Minoxidil, effective for mild AA, may cause unwanted side effects. Treatments like platelet-rich plasma and topical calcineurin inhibitors lack solid efficacy data and insurance coverage. Systemic immunosuppressants like methotrexate, cyclosporine, and azathioprine offer modest effects but entail risks including organ toxicity, infection, and malignancy. Consequently, the modest benefits of the available treatments may not justify their risks, often leaving the cost uncovered for patients with severe AA. Patients noted that important outcomes of treatment include full and sustained hair growth, improving quality of life by alleviating the detrimental mental health effects associated with AA, and reducing treatment-emergent side effects. Most patients treated with baricitinib experienced complete hair regrowth and described mild to moderate side effects, including upper respiratory tract infections, headaches, and nasopharyngitis. Patients emphasized that the side effect profile of baricitinib is more favourable compared with existing therapies. Patients additionally highlighted that the once daily oral administration of baricitinib renders it a more convenient treatment option compared to therapies that involve topical application, injections, or multiple daily doses.
Our participating drug plans have highlighted concerns regarding the potential additional costs to the health care system associated with managing adverse events in patients undergoing treatment with baricitinib. These considerations encompass the assessment of viral hepatitis, latent tuberculosis, renal insufficiency, and pregnancy before initiating therapy. Additionally, it would be necessary to conduct baseline and periodic investigations, including those pertaining to full blood count, liver enzymes, and lipid levels, for patients receiving baricitinib. Moreover, routine assessments of signs and symptoms of infection, skin examination (particularly in patients with an elevated risk of skin cancer), and the evaluation of abdominal symptoms (in patients predisposed to gastrointestinal perforation) are likely to be required. Participating drug plans also observed that patients enrolled in Study BRAVE-AA1 and Study BRAVE-AA2 were permitted to continue their treatment with bimatoprost ophthalmic solution, 5-alpha reductase inhibitors (e.g., finasteride), and minoxidil under specific conditions. This raised questions about the likelihood of baricitinib being used in conjunction with other medications in clinical practice. Finally, the plans indicated that consideration should be given to discontinuing treatment in patients who show no evidence of therapeutic benefit after 36 weeks of treatment (as per product monograph), raising queries regarding the precise definition of a lack of clinical response that would justify discontinuing baricitinib in real-world clinical settings.
No clinician input was received for this review.
Several of these concerns were addressed in the sponsor’s model:
The primary clinical outcome incorporated in the model was the change from baseline in the SALT score measured at the end of the 36-week induction period.
The use of a cost-utility approach accounts for some issues related to HRQoL; however, it is unclear if all quality-of-life concerns noted to be important to patients were captured in the health state utility values adopted by the sponsor.
In addition, CDA-AMC addressed some of these concerns as follows:
Regarding the definition of response likely to be used in clinical practice, clinical experts CDA-AMC consulted expect that clinicians will continue prescribing baricitinib even if patients attain less than a 50% improvement from baseline at week 36. Consequently, CDA-AMC conducted a reanalysis that adopted SALT30 as the primary response outcome, aiming to capture the HRQoL benefit associated with achieving the reduced relative improvement in scalp hair loss that is likely to be acceptable in real-world clinical practice.
CDA-AMC were unable to address the following concerns raised from input:
The model's structure prevented the inclusion of relevant comparators such as BSC therapies available to patients with severe AA, including topical and intralesional corticosteroids, minoxidil, immunosuppressants, and systemic drugs.
Economic Review
The current review is for baricitinib (Olumiant) for the treatment of adult patients with severe AA.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of baricitinib compared with no active treatment.1 The model population comprised adult patients with severe AA.1 The patient cohort modelled in the sponsor’s base case is aligned with the Health Canada indicated population.
Baricitinib is a selective and reversible Janus kinase (JAK) inhibitor available as 2 mg and 4 mg oral tablets.1 The recommended dose of baricitinib is 2 mg once daily, which may be increased to 4 mg once daily if the response to treatment is not adequate.2 For patients with nearly complete or complete scalp hair loss and/or substantial eyelash or eyebrow hair loss, the recommended dose is 4 mg once daily.2 Once patients attain an adequate response to treatment with baricitinib 4 mg, the dose may be decreased to 2 mg once daily.2 At the sponsor’s submitted price of $57.2057 per 2 mg tablet and $114.4113 per 4 mg tablet,1 the annual cost of baricitinib is $20,894 per patient for those receiving the 2 mg daily dose and $41,789 per patient for those receiving the 4 mg daily dose. Wastage was not included in the submitted base case given the oral administration route of the intervention.
The clinical outcomes modelled were the proportion of patients who attained treatment response measured at week 36 (SALT50 [at least a 50% improvement from baseline in the Severity of Alopecia Tool score]) and the treatment discontinuation rates during the induction phase (week 1 to week 36) and the maintenance phase (week 37 onward).1 The economic outcomes of interest were QALYs and life-years. The economic evaluation was conducted over a lifetime model horizon of 63 years from the perspective of the Canadian public health care payer.1 Costs and outcomes were discounted at 1.5% per year.1
Model Structure
The sponsor submitted a Markov state transition model with a 4-week cycle length and 4 health states: induction, maintenance, BSC, and death (Figure 1).1 Patients enter the model in the induction health state, which is represented by a set of tunnel states, and receive baricitinib (2 mg or 4 mg) or no active treatment for 36 weeks. Patients who respond to treatment at the end of the induction period transition to the maintenance health state, where they remain on treatment. Patients in the maintenance health state who experience a loss of response transition to the BSC health state. Patients who do not respond to treatment at the end of the induction period, as well as patients who discontinue treatment with baricitinib or no active treatment before the end of the induction period, also transition to the BSC health state. Patients who do not respond to treatment with baricitinib are not considered for any additional BSC treatments and, hence, do not incur any additional costs corresponding to drug acquisition, drug monitoring, and disease management in the BSC health state. Conversely, patients who do not respond to treatment with no active treatment receive a basket of BSC therapies, including cyclosporine (1%), methotrexate (5%), intralesional steroids (50%), prednisolone (5%), and topical mometasone ointment (50%), and incur all the aforementioned costs. Patients may transition to the death state from any health state and at any time.
Model Inputs
Baseline patient characteristics were derived from the enrolled patient population in the Study BRAVE-AA1 and Study BRAVE-AA2 randomized phase III trials designed to evaluate the efficacy and safety of baricitinib versus no active treatment in adult patients with severe AA (a SALT score of 50 to 94) and very severe AA (a SALT score of 95 to 100) (n = 1,200).3,4 The average patient in the modelled cohort, which the sponsor assumed to reflect the Canadian patient population, is aged 38 years and is more likely to be female (61%) (i.e., male = 39%).
Clinical efficacy parameters used to characterize baricitinib and no active treatment, including change from baseline in SALT50 and treatment discontinuation rates, were derived from pooled data from Study BRAVE-AA1 and Study BRAVE-AA2 using the February 2, 2021, and February 19, 2021, data cut-off dates, respectively (maximum follow-up is 36 weeks).3,4 The sponsor used the proportion of patients who attained a SALT50 response at week 36 (baricitinib 2 mg = 29%; baricitinib 4 mg = 47%; and no active treatment = 9%) to extrapolate response maintenance for the lifetime horizon of the model. Hence, from week 36 onward, patients who transitioned to the maintenance health state were assumed to remain in that state until discontinuation or death.3,4 Notably, the model includes the option to alter the threshold value that defines response: SALT30, SALT50, or SALT75 (Table 13). The sponsor applied discontinuation rates per cycle with rates specific to the induction and maintenance periods (Table 14).3,4 Discontinuation during induction is defined to be because of all causes, excluding a lack of efficacy, while discontinuation during maintenance is defined to be because of all causes, including a lack of efficacy. The mortality risk of the modelled cohort is assumed to be equal to that of the age-matched and sex-matched Canadian general population.5
Health state utility values are derived from the Adelphi Disease Specific Programme (DSP), a real-world evidence study wherein patients diagnosed with AA provided EQ-5D-5L questionnaire responses. The sponsor employed a crosswalk value set methodology to convert the EQ-5D-5L estimates into EQ-5D-3L values. Patients in the induction health state are assigned a baseline utility value (0.781) while patients who respond to treatment enter the maintenance health state where they are assigned a utility value in accordance with the SALT50 response category (0.854). Patients who transition to the BSC health state because of nonresponse, loss of response, or treatment discontinuation revert to the baseline utility value (0.781). Notably, baseline utility varies according to the data source used to derive utility values (Table 15). Additionally, changes in utility that may be experienced in the maintenance health state vary according to the SALT response threshold used in the model (Table 15). The utility values from the final analysis of the Adelphi DSP study informing the economic model are as follows: the utility value for the severe subgroup in Adelphi DSP informed the induction health state, the utility value for the moderate severity subgroup in Adelphi DSP informed the maintenance health state for patients who responded to the SALT50 threshold, the utility value for the mild severity subgroup of the Adelphi DSP informed the maintenance health state for patients who responded to the SALT75 threshold, and the utility value for the severe subgroup of the Adelphi DSP study informed the BSC health state. The publication and poster for the Adelphi DSP study were provided by the sponsor in response to an additional information request from CDA-AMC.6,7 The sponsor did not explain the derivation of utility values used to inform the maintenance health state for patients who responded to the SALT30 threshold. Disutilities associated with treatment-emergent adverse events in patients treated with baricitinib and patients treated with BSC therapies are not included in the model. Furthermore, the sponsor estimated age-specific and sex-specific disutilities for each year, derived from general population utility values. This adjustment reflects the diminishing HRQoL associated with aging.
Costs captured in the model include those associated with drug acquisition, disease monitoring, and medical follow-up as well as the pharmacological treatment costs associated with managing the psychological burden of AA. Drug acquisition costs for baricitinib are based on the sponsor’s submitted price. The dosing modelled for baricitinib is consistent with that described in the Overview section. For patients in the induction and maintenance health states, health service resource use costs consist of dermatologist visits and investigations (including those pertaining to thyroid function, ferritin, full blood count, liver function, renal function, tuberculosis, and lipids). The frequency of these visits and investigations is determined by clinical expert input, and their costs are based on the Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act (June 29, 2023 (effective July 24, 2023)) and relevant literature sources.8,9 Pharmacological treatment costs associated with managing the psychological burden of AA encompass the 12-week acquisition cost of selective serotonin-norepinephrine reuptake inhibitors (SNRIs) (including sertraline, escitalopram, and duloxetine). These costs are only accrued in the induction period (i.e., patients who maintain response are assumed to no longer experience psychological burden because of AA). The proportion of patients requiring SNRIs is determined by clinical expert input and their costs are based on the Ontario Drug Benefit Formulary.10
Patients in the BSC health state receive additional therapy consisting of various BSC treatments: cyclosporine (1%), methotrexate (5%), intralesional steroids (50%), prednisolone (5%), and topical mometasone ointment (50%). The composition of the BSC basket and the proportion of patients assumed to receive each treatment is based on clinical expert input while unit costs are based on the Ontario Drug Benefit Formulary.10 In addition, patients in the BSC health state incur health service resource use costs consisting of investigations (including those pertaining to thyroid function, full blood count, liver function, renal function, lipids, electrolytes, and urinalysis), as well as drug monitoring costs consisting of dermatologist visits. The frequency of these visits and investigations is determined by clinical expert input, and their costs are based on the Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act (June 29, 2023 (effective July 24, 2023)) and relevant literature sources.8,9 Furthermore, patients in the BSC health state incur pharmacological treatment costs related to the acquisition of SNRIs, with the proportion necessitating SNRIs determined by clinical expert input and their costs referenced from the Ontario Drug Benefit Formulary.10 Notably, patients in the BSC health state who did not respond to no active treatment are assumed to bear all of the aforementioned costs ($2,427 annually), whereas patients who did not respond to baricitinib only accrue SNRI acquisition costs ($45 annually).
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted the base case via a probabilistic sensitivity analysis with 1,000 simulations.1 The deterministic and probabilistic results were similar. Both are presented as follows.
Base-Case Results
In the sponsor's probabilistic base case, the use of baricitinib at a 2 mg dose emerged as the dominant strategy. This indicates that baricitinib (2 mg dose) resulted in incremental cost savings of $13,562 and yielded an incremental QALY gain of 0.14 when compared to no active treatment. Conversely, the use of baricitinib at a 4 mg dose was associated with an incremental cost of $111,689 and an incremental QALY gain of 0.33 compared with no active treatment, resulting in an ICER of $342,410 per QALY gained.
The sponsor’s probabilistic analysis predicted that baricitinib was associated with improved quality of life compared with no active treatment. Given the duration of follow-up required to analyze the change from baseline in SALT scores in Study BRAVE-AA1 and Study BRAVE-AA2 (i.e., 36 weeks) in contrast to the model’s lifetime time horizon (i.e., 63 years), it is important to note that the near entirety (96%) of the QALY benefit realized by patients receiving baricitinib was derived beyond the primary analysis period of the pivotal trials (i.e., extrapolated period). CDA-AMC note that although the benefits of baricitinib in hair regrowth appeared to be sustained through week 104 in the long term extension period of the trials, analyses beyond week 36 were noncomparative, which preclude firm conclusions. Moreover, among patients receiving baricitinib, the primary cost driver was drug acquisition, which comprised 98% of the total cost incurred. In contrast, for patients receiving no active treatment, the primary cost driver was the cost associated with BSC drug monitoring, representing 63% of the total estimated cost.
The probability that the use of baricitinib at a 2 mg and 4 mg dose was cost-effective at a $50,000 per QALY gained WTP threshold was 77% and 0%, respectively. The sponsor’s submitted analysis is based on the publicly available prices for all drug treatments. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results, Baricitinib 2 mg Dose
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. no active treatment ($/QALY) |
|---|---|---|---|---|---|
Deterministic | |||||
No active treatment | 67,405 | Reference | 21.11 | Reference | Reference |
Baricitinib 2 mg | 53,770 | –13,635 | 21.25 | 0.14 | Dominant |
Probabilistic | |||||
No active treatment | 67,517 | Reference | 21.12 | Reference | Reference |
Baricitinib 2 mg | 53,955 | –13,562 | 21.27 | 0.14 | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Table 4: Summary of the Sponsor’s Economic Evaluation Results, Baricitinib 4 mg Dose
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. no active treatment ($/QALY) |
|---|---|---|---|---|---|
Deterministic | |||||
No active treatment | 67,405 | Reference | 21.11 | Reference | Reference |
Baricitinib 4 mg | 177,699 | 110,294 | 21.43 | 0.32 | 343,398 |
Probabilistic | |||||
No active treatment | 67,355 | Reference | 21.11 | Reference | Reference |
Baricitinib 4 mg | 179,044 | 111,689 | 21.43 | 0.33 | 342,410 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters and assumptions in probabilistic scenario analyses. These included implementing a 10-year time horizon, modelling different cohorts stratified by the baseline SALT score (i.e., a SALT score of 50 to 94 [severe] and a SALT score of 95 to 100 [very severe]), applying an alternative threshold for response to treatment based on the level of change from baseline (i.e., SALT75), and using alternative sources to inform health state utility estimates. When evaluating the 2 mg dose of baricitinib, the most influential parameter was the adoption of a 10-year time horizon wherein baricitinib transitioned from being the dominant strategy to yielding an ICER of $225,843 per QALY gained. All other scenarios resulted in ICERs ranging between $45,330 and $92,292 per QALY gained. When evaluating the 4 mg dose of baricitinib, the predominant parameter affecting outcomes was the use of alternative data sources for health state utility values. Employing EQ-5D-3L with the Hernandez algorithm resulted in an ICER of $3,466,609 per QALY gained while using the Brazier algorithm led to an ICER of $1,186,121 per QALY gained. All other scenarios resulted in ICERs ranging between $251,019 and $506,091 per QALY gained. No scenario analysis was conducted using a perspective other than that of the health care payer.
Our Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
Treatment response used in the model is inconsistent with the definition of response and discontinuation rules in the pivotal trials and it is uncertain whether it aligns with clinical practice. In the submitted economic model, the primary response outcome, SALT50, is defined as the proportion of patients achieving at least a 50% improvement from baseline in their SALT score. This measure is based on pooled data from Study BRAVE-AA1 and Study BRAVE-AA2. Consequently, in the economic model, patients who do not attain at least a 50% improvement at week 36 discontinue treatment. CDA-AMC note that the outcomes included in the economic model are relative measures of response whereas the primary end point in Study BRAVE-AA1 and Study BRAVE-AA2 was the proportion of patients achieving a SALT score of 20 or less, representing an absolute measure of response (i.e., less than or equal to 20% scalp hair loss). CDA-AMC further note that, in the BRAVE-AA1 and BRAVE-AA2 trials, baricitinib-treated patients continued treatment regardless of response at week 36 — that is, treatment was maintained even if the absolute improvement from baseline at week 36 did not meet the SALT score of 20 or less response threshold. Moreover, the product monograph for baricitinib indicates that consideration should be given to discontinuing treatment in patients who show no evidence of therapeutic benefit after 36 weeks of treatment. Consultation with clinical experts reveals that there is a lack of consensus as to whether the definition of response used in the economic model aligns with the response criteria that are likely to inform Canadian clinical practice. Some clinical experts who CDA-AMC consulted for this review anticipate that in real-world practice, clinicians are highly likely to continue prescribing baricitinib even if patients attain less than a 50% improvement from baseline at week 36. They explained that both clinician and patient assessments of clinically significant hair regrowth are generally expected to take precedence over the percentage improvement in the SALT score. For instance, should patients observe a regrowth of eyebrows and eyelashes, clinicians would be inclined to consider less than a 50% regrowth of scalp hair acceptable in real-world clinical practice, warranting the continuation of baricitinib treatment beyond the 36-week induction period. In response to this consideration, CDA-AMC conducted a reanalysis that adopted SALT30 (defined as at least 30% improvement from baseline in SALT score) as the primary response outcome, aiming to capture the HRQoL benefit associated with achieving the reduced relative improvement in scalp hair loss that is likely to be acceptable in real-world clinical practice. On the contrary, some clinical experts CDA-AMC consulted considered a SALT score of 20 or less to be a meaningful response outcome for patients with severe AA, given that it signified patients would attain at least 80% hair regrowth on the scalp. In response, CDA-AMC explored a scenario adopting SALT75 as the response outcome to capture the quality of life benefit akin to achieving the primary end point observed in Study BRAVE-AA1 and Study BRAVE-AA2, where patients with severe and very severe AA (i.e., baseline SALT scores ranging from 50 to 100) achieving a 75% improvement would attain SALT scores between 13 and 25, thus aligning with the pivotal trials’ primary end point of a SALT score of 20 or less.
CDA-AMC conducted a base-case reanalysis that adopted SALT30 as the response outcome.
CDA-AMC explored a scenario analysis that adopted SALT75 as the response outcome.
Differential access to BSC upon treatment failure between patients treated with baricitinib and no active treatment is inappropriate. In the sponsor’s submitted base case, patients who do not respond to treatment at the end of the induction period, as well as patients who discontinue treatment before the end of the induction period, transition to the BSC health state. Patients in the BSC health state undergo additional therapy, thereby incurring drug acquisition costs for a basket of BSC treatments, and drug monitoring costs consisting of investigations and dermatologist visits, along with pharmacological treatment costs associated with the acquisition of SNRIs. Notably, patients in the BSC health state who did not respond to no active treatment are assumed to bear all of the aforementioned costs ($2,427 annually), whereas patients who did not respond to baricitinib only accrue SNRI acquisition costs ($45 annually). CDA-AMC note that all patients enrolled in Study BRAVE-AA1 and Study BRAVE-AA2 had experience with prior BSC therapies for the treatment of severe AA.3,4 Our clinical review noted that treatment history in the pivotal trials included topical therapies, topical immunotherapy, intralesional therapy, and systemic immunosuppressive and immunomodulating drugs, as well as nonimmunosuppressive systemic treatments. Likewise, clinical experts who CDA-AMC consulted for this review noted that the indicated patient population with severe AA is likely to have prior experience with BSC. Hence, if response is not attained with baricitinib or no active treatment, patients who had exhausted all BSC therapy options would not receive further treatment while patients who were naive to certain BSC therapies would have an equal opportunity to access those treatments. Furthermore, in alignment with the literature, clinical expert input noted that a substantial proportion of patients may choose not to pursue treatment following its failure and instead opt for hairpieces and wigs as a means of managing their hair loss.11 Thus, CDA-AMC consider that drug acquisition, drug monitoring, and disease management costs in the BSC health state should be excluded in both model groups. Regarding the pharmacological treatments addressing the psychological ramifications of severe AA, clinical experts deemed the assumption that 5% to 16% of nonresponders would undergo an annual 12-week course of SNRIs to be reasonable. Hence, CDA-AMC retained this cost category in the BSC health state for patients who did not respond to baricitinib and no active treatment.
CDA-AMC further highlight the pivotal role of the sponsor's assumptions regarding the estimation and accrual of costs in the BSC health state in assessing the cost-effectiveness of baricitinib relative to no active treatment. This significance arises from the fact that patients in both model arms spend considerable time in this state, incurring costs without corresponding benefits, as the utility for this health state is maintained at baseline. As patients who received no active treatment are presumed to have comparatively greater access to additional therapies and health services post–treatment failure, this assumption inflates costs related to drug acquisition, ongoing management, and drug monitoring among these patients. Consequently, it biases the cost-effectiveness estimate in favour of baricitinib.
CDA-AMC conducted a base-case reanalysis by assuming equal costs for patients treated with baricitinib or no active treatment in the BSC health state. As such, drug acquisition, drug monitoring, and disease management costs incurred in the BSC health state were excluded for patients treated with baricitinib and patients treated with no active treatment alike. Costs associated with drug acquisition for SNRIs were retained for patients in both model arms.
The impact of baricitinib on the HRQoL of patients with severe AA is highly uncertain. The sponsor’s base case predicts an incremental gain of 0.14 QALY and 0.33 QALY with the baricitinib 2 mg and baricitinib 4 mg dose, respectively, compared to no active treatment over the 63-year lifetime horizon of the model (Table 3 and Table 4). As highlighted in our clinical review, there was no significant between-group difference observed in the change from baseline in the EQ-5D-5L health state index at week 36 when comparing the effects of baricitinib at doses of 4 mg and 2 mg versus no active treatment, according to both US and UK algorithm-based indices. The only exception was noted in the BRAVE-AA2 study, where a marginal preference for baricitinib 4 mg over no active treatment was observed based on the US algorithm. CDA-AMC note that the trial-based EQ-5D-5L findings may be affected by potential attrition bias because of differential discontinuation rates of study treatment between the baricitinib and no active treatment groups; thus, the effect associated with baricitinib on the HRQoL of patients with severe AA is highly uncertain.
The sponsor asserted that the utility values estimated during the trials were not sensitive to variations in the severity of AA and lacked content validity. This was attributed to the resulting baseline utility values being higher than the age-adjusted and sex-adjusted general population values in Canada. Hence, the utility values informing the economic model were sourced from the Adelphi DSP study, which collected EQ-5D-5L data from patients with AA in Europe (patients with severe and very severe AA [n = 184]).12 CDA-AMC note that the sponsor contributed to the funding of the Adelphi DSP study and collaborated on the data of relevance to be collected. CDA-AMC view the sponsor's rationale for not using pooled EQ-5D-5L data from Study BRAVE-AA1 and Study BRAVE-AA2 (attributing it to issues of sensitivity and content validity) as a critique of the EQ-5D tool itself rather than the methods employed to collect trial data. Consequently, CDA-AMC extend this criticism to the EQ-5D data obtained from the Adelphi DSP study. In seeking clarification during the review process, CDA-AMC inquired why the EQ-5D data from the Adelphi DSP study were deemed more suitable than those from Study BRAVE-AA1 and Study BRAVE-AA2. The sponsor noted that 46% of participants in the BRAVE-AA1 and BRAVE-AA2 trials had reported perfect health scores at baseline.12 Consequently, these patients would not experience any improvement in HRQoL by week 36 (i.e., “ceiling effect”). CDA-AMC note that the ceiling effect was also observed in the Adelphi DSP study, where 20% of patients reported perfect health at baseline.12
Moreover, the physician survey used in the Adelphi DSP study did not employ SALT scores to define severity. Instead, disease severity was determined by the physicians as requested in the survey question, “What is your overall assessment of severity of AA symptoms in this patient based on your own definition of the terms mild, moderate, and severe?”6 CDA-AMC interpret the severity categories from the Adelphi DSP study as indicative of absolute scalp hair coverage. It posits that the contrast between mild, moderate, and severe categories implies an assumed change in absolute hair regrowth, rather than the relative change from baseline assumed in the economic model (i.e., the percentage improvement from baseline in the SALT score). In fact, the pooled EQ-5D data from Study BRAVE-AA1 and Study BRAVE-AA2 only included patients with severe and very severe disease at baseline (defined as a SALT score of 50 to 100). The change from baseline at week 36, as estimated in the trials, reflects an observed score change from baseline among patients; this is substantially different from using baseline scores for patients with AA of mild and moderate severity, as derived in the Adelphi DSP study. Hence, the resulting utility values from the Adelphi DSP study are misaligned with the definition of disease severity used in the pivotal trials, as well as the relative change from baseline assumed in the economic model.
CDA-AMC further note that the age-matched general population utility value in Canada is 0.894 (95% confidence interval, 0.888 to 0.900).13 Contrary to the sponsor's assertion, the baseline utility value for patients with severe and very severe AA derived from data in Study BRAVE-AA1 and Study BRAVE-AA2 (0.892) is marginally lower than the general population value (0.894). Clinical experts who CDA-AMC consulted for this review remarked that a slightly lower baseline value is justifiable, considering that for most patients with severe AA, there is no substantial impact on HRQoL. Moreover, given that the sponsor collected extensive comparative data on the impact of baricitinib relative to no active treatment on HRQoL in Study BRAVE-AA1 and Study BRAVE-AA2, it is unclear what gap in the evidence is addressed by the use of external sources employing the same psychometric instrument. CDA-AMC underscore the limitations associated with real-world evidence, notably the potential for sampling, selection, and recall bias.6 These factors introduce additional uncertainty when deriving utility values from the Adelphi DSP study in contrast to trial-based estimates. Therefore, CDA-AMC consider that the BRAVE-AA1 and BRAVE-AA2 trials represent a more robust source of EQ-5D data to be used in the base-case cost-effectiveness analysis. This approach is reinforced by the methodological advantages of incorporating efficacy and HRQoL estimates generated from the same patient cohort.
CDA-AMC conducted a reanalysis using the EQ-5D values derived from Study BRAVE-AA1 and Study BRAVE-AA2.
CDA-AMC acknowledge the presence of conflicting evidence in the literature regarding the relationship between the severity of hair loss and the burden of AA on patient HRQoL.14-17 CDA-AMC conducted a scenario analysis using the EQ-5D values derived from the Adelphi DSP study, which implies that a patient with severe AA experiences a 15% lower quality of life compared to the average person of the same age in Canada.
The selection of relevant comparators is misaligned with current clinical practice. The sponsor omitted BSC therapies from the base-case analysis, despite evidence that BSC therapies are prescribed off-label in current Canadian clinical practice. During the review process, input from patient groups, participating drug plans, and the clinical expert panel that CDA-AMC convened revealed that BSC therapies are used off-label for the treatment of severe AA in adult patients in Canada. These therapies include antihypertensives (e.g., minoxidil), corticosteroids (e.g., mometasone, prednisolone, triamcinolone acetonide), and immunosuppressants and immunomodulators (e.g., cyclosporine, methotrexate, mycophenolate mofetil). According to our reimbursement review procedures, the base case must comprise all relevant comparators. These include treatments currently reimbursed by at least 1 participating drug plan for the indication under review, reimbursed treatments that are currently used off-label in Canadian practice, or treatments that have previously received a recommendation in favour of reimbursement from CDA-AMC for the indication under review. While BSC therapies are deemed suitable comparators for patients with severe AA, CDA-AMC note that their usage varies significantly and their efficacy is limited,18-22 which precludes them from being acknowledged as established standards of care. In the absence of comprehensive prescribing pattern data, as well as comparative effectiveness data concerning baricitinib, CDA-AMC consider no active treatment to be a suitable comparator for this patient population. However, the cost-effectiveness of baricitinib relative to BSC therapies used off-label for this indication remains unknown.
CDA-AMC could not address this limitation owing to the lack of comparative effectiveness data.
The results from the probabilistic sensitivity analysis lack transparency. In the sponsor’s model, the probabilistic results — that is, the total costs and total QALYs for each intervention, as well as the resulting ICER — are hard-coded. CDA-AMC specifically note that the sum of disaggregated QALYs resulting from the probabilistic sensitivity analysis does not correspond with the total QALYs presented in the summary of probabilistic results.
CDA-AMC could not address this limitation. Owing to the lack of transparency implicit in the calculation of the probabilistic ICER, our base case and scenario analyses are presented deterministically.
Additionally, the following key assumptions were made by the sponsor and have been appraised by us (refer to Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
AEs were not included in the model. | Acceptable. Because of the low incidence of serious AEs observed in Study BRAVE-AA1 and Study BRAVE-AA2 (less than 2.5% of patients experienced at least 1 serious AE), their influence was not factored into the economic model. CDA-AMC acknowledge that incorporating treatment-emergent AEs into the economic model has a negligible effect on the cost-effectiveness outcomes. |
Efficacy was assumed to occur at the end of the 36-week induction period. | Acceptable. The sponsor assumes that only patients entering the maintenance health state derive treatment benefits. CDA-AMC view this as conservative since patients receiving baricitinib incur drug acquisition costs during the induction period without the immediate benefits of treatment. It is probable that patients responding to treatment — thus staying in the induction health state for 36 weeks — experience improvements in HRQoL. |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; HRQoL = health-related quality of life.
Our Reanalyses of the Economic Evaluation
Base-Case Results
Our reanalyses addressed several limitations within the economic model. Our base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts. These included adopting SALT30 as the response threshold; assuming equal costs associated with drug acquisition, drug monitoring, and disease management for patients treated with baricitinib or no active treatment in the BSC health state; and using the EQ-5D utility values derived from Study BRAVE-AA1 and Study BRAVE-AA2. These changes are summarized in Table 6.
Table 6: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive CDA-AMC base case | ||
1. Treatment response threshold | SALT50 | SALT30 |
2. Proportion of patients in the BSC health state who incur BSC costsa |
|
|
3. Impact of baricitinib on HRQoL (mean HSUVs) | Induction: 0.781 Maintenance incremental change:
BSC: 0.781 | Induction: 0.892 Maintenance incremental change:b
BSC: 0.892 |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; HRQoL = health-related quality of life; HSUV = health state utility value; SALT30 = at least a 30% improvement from baseline in the Severity of Alopecia Tool score; SALT50 = at least a 50% improvement from baseline in the Severity of Alopecia Tool score; SALT75 = at least a 75% improvement from baseline in the Severity of Alopecia Tool score; SNRI = serotonin-norepinephrine reuptake inhibitor.
aThese are costs associated with drug acquisition, drug monitoring, and disease management in the BSC health state. Costs associated with drug acquisition for SNRIs were retained for patients in both model arms.
bThis was from the pooled data from Study BRAVE-AA1 and Study BRAVE-AA2 using a SALT30 response threshold.
In our base case, the use of baricitinib at the 2 mg dose was associated with an ICER of $5,465,503 per QALY gained compared to no active treatment (incremental costs = $62,457; incremental QALYs = 0.01) (Table 7). In addition, the use of baricitinib at the 4 mg dose was associated with an ICER of $6,803,200 per QALY gained compared to no active treatment (incremental costs = $203,814; incremental QALYs = 0.03) (Table 8). A detailed breakdown of the disaggregated results is available in Appendix 4.
Our reanalysis results are driven by the following base-case changes: aligning the response outcome with criteria likely to inform Canadian clinical practice and using EQ-5D utility estimates derived from Study BRAVE-AA1 and Study BRAVE-AA2. Consistent with the sponsor’s analysis, our reanalysis estimates that the near entirety (96%) of the QALY benefit realized by patients receiving baricitinib was derived beyond the primary analysis period of the pivotal trials (i.e., extrapolated period).
Table 7: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results, Baricitinib 2 mg Dose, Deterministic
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | No active treatment | 67,405 | 21.11 | Reference |
Baricitinib 2 mg | 53,770 | 21.25 | Dominant | |
CDA-AMC reanalysis 1: Treatment response (SALT30) | No active treatment | 66,982 | 21.11 | Reference |
Baricitinib 2 mg | 64,090 | 21.25 | Dominant | |
CDA-AMC reanalysis 2: Costs in BSC health state equal across arms | No active treatment | 1,575 | 21.11 | Reference |
Baricitinib 2 mg | 53,770 | 21.25 | 378,388 | |
CDA-AMC reanalysis 3: Trial-based utilities | No active treatment | 67,405 | 24.0683 | Reference |
Baricitinib 2 mg | 53,770 | 24.0825 | Dominant | |
CDA-AMC base case (reanalyses 1 + 2 + 3) | No active treatment | 1,633 | 24.0664 | Reference |
Baricitinib 2 mg | 64,090 | 24.0778 | 5,465,503 |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SALT30 = at least a 30% improvement from baseline in the Severity of Alopecia Tool score.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically. Our cumulative base case is presented deterministically owing to limitations with the sponsor’s probabilistic analysis.
Table 8: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results, Baricitinib 4 mg Dose, Deterministic
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | No active treatment | 67,405 | 21.11 | Reference |
Baricitinib 4 mg | 177,699 | 21.43 | 343,398 | |
CDA-AMC reanalysis 1: Treatment response (SALT30) | No active treatment | 66,982 | 21.11 | Reference |
Baricitinib 4 mg | 205,447 | 21.43 | 431,106 | |
CDA-AMC reanalysis 2: Costs in BSC health state equal across arms | No active treatment | 1,575 | 21.11 | Reference |
Baricitinib 4 mg | 177,699 | 21.43 | 548,356 | |
CDA-AMC reanalysis 3: Trial-based utilities | No active treatment | 67,405 | 24.0683 | Reference |
Baricitinib 4 mg | 177,699 | 24.1027 | 3,206,019 | |
CDA-AMC base case (reanalyses 1 + 2 + 3) | No active treatment | 1,633 | 24.0664 | Reference |
Baricitinib 4 mg | 205,447 | 24.0963 | 6,803,200 |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SALT30 = at least a 30% improvement from baseline in the Severity of Alopecia Tool score.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically. Our cumulative base case is presented deterministically owing to limitations with the sponsor’s probabilistic analysis.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s deterministic results and our deterministic base case. Our base case suggests that there is no price reduction upon which baricitinib would be considered cost-effective at a WTP threshold of $50,000 per QALY gained, irrespective of dose (Table 9 and Table 10). Even if baricitinib were provided at no cost, the ongoing management of patients treated with baricitinib necessitates additional tests and investigations, resulting in higher costs relative to no active treatment.
Table 9: CDA-AMC Price Reduction Analyses, Baricitinib 2 mg Dose
Analysis Price reduction | Unit drug cost $ | ICERs for baricitinib 2 mg vs. no active treatment ($/QALY) | |
|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | ||
No price reduction | 57.21 | Baricitinib 2 mg is dominant. | 5,465,503 |
10% | 51.49 | Baricitinib 2 mg is dominant. | 4,931,038 |
20% | 45.76 | Baricitinib 2 mg is dominant. | 4,396,573 |
30% | 40.04 | Baricitinib 2 mg is dominant. | 3,862,108 |
40% | 34.32 | Baricitinib 2 mg is dominant. | 3,327,643 |
50% | 28.60 | Baricitinib 2 mg is dominant. | 2,793,178 |
60% | 22.88 | Baricitinib 2 mg is dominant. | 2,258,713 |
70% | 17.16 | Baricitinib 2 mg is dominant. | 1,724,248 |
80% | 11.44 | Baricitinib 2 mg is dominant. | 1,189,783 |
90% | 5.72 | Baricitinib 2 mg is dominant. | 655,318 |
100% | 0 | Baricitinib 2 mg is dominant. | 120,853 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Table 10: CDA-AMC Price Reduction Analyses, Baricitinib 4 mg Dose
Analysis Price reduction | Unit drug cost $ | ICERs for baricitinib 4 mg vs. no active treatment ($/QALY) | |
|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | ||
No price reduction | 114.41 | 343,398 | 6,803,200 |
10% | 102.97 | 289,230 | 6,131,093 |
20% | 91.53 | 235,062 | 5,458,986 |
30% | 80.09 | 180,895 | 4,786,879 |
40% | 68.65 | 126,727 | 4,114,773 |
50% | 57.21 | 72,559 | 3,442,666 |
60% | 45.76 | 18,392 | 2,770,559 |
70% | 34.32 | Baricitinib 4 mg is dominant. | 2,098,453 |
80% | 22.88 | Baricitinib 4 mg is dominant. | 1,426,346 |
90% | 11.44 | Baricitinib 4 mg is dominant. | 754,239 |
100% | 0 | Baricitinib 4 mg is dominant. | 82,132 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
CDA-AMC conducted a series of scenario analyses to explore the impact of alternative assumptions on the cost-effectiveness of baricitinib, as follows:
CDA-AMC adopted SALT75 as an alternative response threshold
CDA-AMC used utility estimates from the EQ-5D data collected in the Adelphi DSP study
CDA-AMC employed weighted ICERs for our base case and scenario analyses, considering that 90% of patients with severe AA would receive the 4 mg dose while 10% of patients would receive the 2 mg dose (refer to the Issues for Consideration section).
Results of these scenarios are presented in Appendix 4 (Table 20).
When adopting SALT75 as an alternative response threshold, the ICER of baricitinib decreased to $346,345 per QALY gained for the 2 mg dose and $497,449 per QALY gained for the 4 mg dose compared to no active treatment. This result was expected given that patients who attained the SALT75 response threshold (i.e., at least a 75% improvement in SALT score from baseline) have a substantially higher HRQoL improvement (utility increment = 0.014) compared with patients who attained the SALT50 response threshold (utility increment = 0.003) and SALT30 response threshold (utility decrement = –0.010) in Study BRAVE-AA1 and Study BRAVE-AA2 (Table 15). In this scenario, a price reduction of 88% for the baricitinib 2 mg dose and 91% for the baricitinib 4 mg dose would be necessary for it to be cost-effective compared to no active treatment at a WTP threshold of $50,000 per QALY gained.
When using utility estimates from the EQ-5D data collected in the Adelphi DSP study, the ICER of baricitinib decreased to $452,788 per QALY gained for the 2 mg dose and $634,568 per QALY gained for the 4 mg dose compared to no active treatment. This result was expected because the HRQoL improvement associated with the SALT30 treatment response derived from the Adelphi DSP study (utility increment range, 0.000 to 0.115) is substantially higher than the HRQoL improvement associated with the SALT30 treatment response derived from Study BRAVE-AA1 and Study BRAVE-AA2 (utility increment range, –0.010 to 0.014). In this scenario, a price reduction of 91% for the baricitinib 2 mg dose and 93% for the baricitinib 4 mg dose would be necessary for it to be cost-effective compared to no active treatment at a WTP threshold of $50,000 per QALY gained.
CDA-AMC calculated weighted ICERs for our base case and scenario analyses based on clinical expert input, which indicated that most patients with severe AA are likely to have tried and not experienced improvement with both recommended and off-label therapies currently available; hence, physicians would be more likely to start with the higher dose of baricitinib and taper off where needed. Employing this approach, the weighted CDA-AMC base case suggests that baricitinib has an ICER of $6,748,810 per QALY gained relative to no active treatment. In the scenario adopting SALT75 as an alternative response threshold, the weighted ICER for baricitinib is $490,967 per QALY gained. Finally, in the scenario using utility estimates from the EQ-5D data collected in the Adelphi DSP study, the weighted ICER for baricitinib is $626,289 per QALY gained.
Issues for Consideration
Clinical experts who CDA-AMC consulted for this review indicated that the vast majority of patients with severe AA are likely to have tried and not experienced improvement with both recommended and off-label therapies currently available in Canada; hence, physicians would be more likely to start with the higher dose of baricitinib and taper off where needed. Clinical experts additionally noted that prescribers would be more likely to treat patients with the baricitinib 4 mg dose if it was found to be more efficacious than the baricitinib 2 mg dose in Study BRAVE-AA1 and Study BRAVE-AA2. Our clinical review noted that, in the pivotal trials, a greater proportion of patients treated with the 4 mg dose of baricitinib attained more than or equal to 80% scalp hair coverage (i.e., a SALT score ≤ 20) at week 36 compared with patients treated with the 2 mg dose of baricitinib versus no active treatment. As highlighted by clinical experts, such findings are likely to influence prescribers' decisions regarding the preferred starting dosage in Canadian clinical practice. CDA-AMC further note that the economic model submitted by the sponsor was not programmed with the functionality to explore assumptions regarding dose titration up and dose titration down. In light of this, CDA-AMC conducted a scenario analysis employing a weighted ICER, which considered that 90% of patients with severe AA would receive the baricitinib 4 mg dose while 10% of patients would receive the baricitinib 2 mg dose based on clinical expert input.
CDA-AMC previously reviewed baricitinib, in combination with methotrexate, for the treatment of signs and symptoms of moderate to severe rheumatoid arthritis in adult patients who have responded inadequately to 1 or more disease-modifying antirheumatic drug.23 The pan-Canadian Oncology Drug Review Expert Review Committee recommended that baricitinib be reimbursed for this indication with clinical criteria and conditions on August 2, 2019. The pan-Canadian Pharmaceutical Alliance concluded negotiations with a letter of intent for baricitinib regarding the aforementioned indication.24 As such, baricitinib has a confidential negotiated price and is currently funded by jurisdictional formularies.25,26 Our reanalyses are based on the publicly available price of baricitinib, which may be different than the confidential price and may influence the results of the cost-effectiveness and budget impact analyses.
Overall Conclusions
Evidence from Study BRAVE-AA1 and Study BRAVE-AA2 — using a clinical response defined as achieving a SALT score of 20 or less — demonstrated that 36 weeks of baricitinib 4 mg treatment resulted in the clinically important regrowth of scalp hair compared with no active treatment in patients with severe AA. Results also favoured baricitinib 2 mg treatment for the regrowth of scalp hair, although there is uncertainty on whether the magnitude of change was clinically important. Our clinical review noted that while the benefits of baricitinib in hair regrowth appeared to be maintained through week 104 in the long term extension period of the trials, analyses beyond week 36 were noncomparative, limiting firm conclusions about the long-term comparative effectiveness of baricitinib. Additionally, our clinical review could not draw definitive conclusions regarding the effects of baricitinib on HRQoL because of important methodological limitations, including potential attrition bias and lack of evidence supporting the validity of the psychometric instruments used in patients with AA.
In addition to the aforementioned limitations with the clinical evidence, CDA-AMC identified several limitations with the sponsor’s economic submission. These limitations included the fact that the primary response outcome used in the economic model (defined as SALT50) does not align with the response definition and continuation rules in Study BRAVE-AA1 and Study BRAVE-AA2, it is uncertain whether this threshold would be considered clinically meaningful in Canadian practice, the differential access to BSC therapies upon treatment failure between patients treated with baricitinib and patients treated with no active treatment is inappropriate, the impact of baricitinib on the HRQoL of patients with severe AA is highly uncertain, the selection of relevant comparators is misaligned with current clinical practice, and results from the probabilistic sensitivity analysis lack transparency. As part of the base-case reanalysis, CDA-AMC adopted SALT30 as the primary response outcome to determine treatment continuation based on clinical expert input, CDA-AMC assumed equal costs associated with drug acquisition, drug monitoring, and disease management for patients treated with baricitinib or no active treatment in the BSC health state, and CDA-AMC used the EQ-5D utility values derived from the BRAVE-AA1 and BRAVE-AA2 trials.
In our base case, the use of baricitinib at the 2 mg dose was associated with an ICER of $5,465,503 per QALY gained compared to no active treatment (incremental costs = $62,457; incremental QALYs = 0.01). In addition, the use of baricitinib at the 4 mg dose was associated with an ICER of $6,803,200 per QALY gained compared to no active treatment (incremental costs = $203,814; incremental QALYs = 0.03). The estimated ICERs were higher than the sponsor’s base-case value. This increase was driven by aligning the response outcome with criteria likely to be used in Canadian clinical practice and by using EQ-5D utility estimates derived from Study BRAVE-AA1 and Study BRAVE-AA2. When compared to the sponsor’s analysis, our base case estimated a reduced QALY benefit with the use of baricitinib at the 2 mg dose (i.e., incremental QALYs = 0.01 [our base case] versus 0.14 [sponsor’s analysis]) at a higher cost (i.e., incremental costs = $62,457 [our base case] versus –$13,635 [sponsor’s analysis]). Likewise, when compared to the sponsor’s analysis, our base case estimated a reduced QALY benefit with the use of baricitinib at the 4 mg dose (i.e., incremental QALYs = 0.03 [our base case] versus 0.32 [sponsor’s analysis]) at a higher cost (i.e., incremental costs = $203,814 [our base case] versus $110,294 [sponsor’s analysis]). Our base case suggests that there is no price reduction upon which baricitinib would be considered cost-effective at a WTP threshold of $50,000 per QALY gained, irrespective of dose. Even if baricitinib were provided at no cost, the ongoing management of patients treated with baricitinib would necessitate additional tests and investigations, resulting in higher costs relative to no active treatment. Under these considerations, there remains considerable uncertainty in the cost-effectiveness results. Baricitinib is a relatively costly treatment ($20,000 to $41,000 per year) with a number of remaining areas of uncertainty, especially concerning the impact of baricitinib on the HRQoL of patients with severe AA (which, based on Study BRAVE-AA1 and Study BRAVE-AA2, may be lower than what was initially estimated), how treatment response will be defined in clinical practice, and consequently how treatment continuation will be determined. Moreover, when comparing the duration of the primary analysis of the BRAVE-AA1 and BRAVE-AA2 trials to the model’s time horizon (36 weeks versus 63 years), it is important to note that the near entirety of the QALY benefit realized by patients receiving baricitinib was derived through extrapolation.
The cost-effectiveness of baricitinib was sensitive to the use of alternative response outcomes. When adopting SALT75 as an alternative response threshold to determine treatment continuation with baricitinib beyond 36 weeks, the ICER of baricitinib decreased to $346,345 per QALY gained for the 2 mg dose and $497,449 per QALY gained for the 4 mg dose, compared to no active treatment. This result is expected given that patients who attained the SALT75 response threshold had a higher HRQoL improvement compared with patients who attained the SALT50 or SALT30 response thresholds in Study BRAVE-AA1 and Study BRAVE-AA2. In this scenario, a price reduction of 88% for the baricitinib 2 mg dose and 91% for the baricitinib 4 mg dose would be necessary for it to be cost-effective compared to no active treatment at a WTP threshold of $50,000 per QALY gained. CDA-AMC were unable to address the limitation concerning the exclusion of BSC as a relevant comparator owing to the absence of comparative effectiveness data.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: baricitinib, 2 mg and 4 mg oral tablets: Toronto (ON): Eli Lilly Canada Inc.; 2024 Mar 4.
2.Eli Lilly Canada Inc. Olumiant® (baricitinib). [product monograph] 2024. [sponsor submitted reference].
3.Eli Lilly and Company. Clinical Study Report: A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Operationally Seamless, Adaptive Phase 2/3 Study to Evaluate the Efficacy and Safety of Baricitinib in Adult Patients with Severe or Very Severe Alopecia Areata (BRAVE-AA1). [sponsor submitted reference]. 2021 Feb 2.
4.Eli Lilly and Company. Clinical Study Report: A Multicenter, Randomized, Double-Blind, Placebo Controlled, Phase 3 Study to Evaluate the Efficacy and Safety of Baricitinib in Adult Patients with Severe or Very Severe Alopecia Areata (BRAVE-AA2). [sponsor submitted reference]. 2021 Feb 19.
5.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2023: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2024 May 10.
6.Vañó-Galván S, Blume-Peytavi U, Farrant P, et al. Physician- and Patient-Reported Severity and Quality of Life Impact of Alopecia Areata: Results from a Real-World Survey in Five European Countries. Dermatol Ther (Heidelb). 2023;13(12):3121-3135. PubMed
7.Anthony Bewley SVG, Erin Johansson, Jenny Austin, Frederick Durand, Helmut Petto, Bianca Maria Piraccini, Ulrike Blume Peytavi. Measuring the burden of Alopecia Areata with the European Quality of Life 5 Dimensions (EQ 5D): Results from a real world survey in 5 European countries. ISPOR EU; 2022.
8.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2024 May 10.
9.Hale I. Add to cart? Can Fam Phys. 2015(61):937. PubMed
10.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2024; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2024 May 10.
11.Davey L, Clarke V, Jenkinson E. Living with alopecia areata: an online qualitative survey study. Br J Dermatol. 2019;180(6):1377-1389. PubMed
12.Eli Lilly Response to April 17 2024 request for additional information regarding Olumiant (baricitinib) [internal sponsor's report]. Toronto (ON): Eli Lilly Canada Inc.; 2024 Mar 4.
13.Guertin JR, Feeny D, Tarride J-E. Age- and sex-specific Canadian utility norms, based on the 2013–2014 Canadian Community Health Survey. Can Med Assoc J. 2018;190(6):E155-E161. PubMed
14.Abedini R, Hallaji Z, Lajevardi V, Nasimi M, Karimi Khaledi M, Tohidinik HR. Quality of life in mild and severe alopecia areata patients. Int J Womens Dermatol. 2018;4(2):91-94. PubMed
15.Muntyanu A, Gabrielli S, Donovan J, et al. The burden of alopecia areata: A scoping review focusing on quality of life, mental health and work productivity. J Eur Acad Dermatol Venereol. 2023. PubMed
16.Reid EE, Haley AC, Borovicka JH, et al. Clinical severity does not reliably predict quality of life in women with alopecia areata, telogen effluvium, or androgenic alopecia. J Am Acad Dermatol. 2012;66(3):e97-102. PubMed
17.Senna M, Ko J, Glashofer M, et al. Predictors of QOL in Patients with Alopecia Areata. J Invest Dermatol. 2022;142(10):2646-2650.e2643. PubMed
18.Messenger AG, McKillop J, Farrant P, McDonagh AJ, Sladden M. British Association of Dermatologists' guidelines for the management of alopecia areata 2012. Br J Dermatol. 2012;166(5):916-926. PubMed
19.Delamere FM, Sladden MM, Dobbins HM, Leonardi-Bee J. Interventions for alopecia areata. Cochrane Database Syst Rev. 2008(2):Cd004413. PubMed
20.Meah N, Wall D, York K, et al. The Alopecia Areata Consensus of Experts (ACE) study part II: Results of an international expert opinion on diagnosis and laboratory evaluation for alopecia areata. J Am Acad Dermatol. 2021;84(6):1594-1601. PubMed
21.Pratt CH, King LE, Jr., Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nat Rev Dis Primers. 2017;3:17011. PubMed
22.Alkhalifah A, Alsantali A, Wang E, McElwee KJ, Shapiro J. Alopecia areata update: part II. Treatment. J Am Acad Dermatol. 2010;62(2):191-202, quiz 203-194. PubMed
23.CADTH Canadian Drug Expert Committee recommendation - baricitinib (Olumiant - Eli Lilly Canada Inc). Ottawa (ON)2019: https://www.cadth.ca/sites/default/files/cdr/complete/SR0597%20Olumiant%20-%20CDEC%20Final%20Recommendation_for%20posting.pdf. Accessed 2024 May 17.
24.pCPA. Olumiant (baricitinib). 2024; https://www.pcpacanada.ca/negotiation/21159. Accessed May 17 2024.
25.Ontario Drug Formulary. Baricitinib (Olumiant). 2023; https://www.formulary.health.gov.on.ca/formulary/results.xhtml?q=baricitinib&type=1. Accessed 2024 May 17.
26.Alberta Drug Formulary. Baricitinib (Olumiant). 2024; https://idbl.ab.bluecross.ca/idbl/drugsList;jsessionid=DsCIt3B8mrFu_t8h4TW-KBZlh7G_icN8fjizyOWVrc9xOPkcB6Y8!-373671022?searchTerm=baricitinib&category=&genericName=&ptc=&mfgCode=. Accessed 2024 May 17.
27.Products and Pricing on the Alberta Blue Cross Drug Price List (ABCDPL) Effective May 14, 2024. Edmonton (AB): Alberta Blue Cross; 2024: https://www.ab.bluecross.ca/dbl/pdfs/ABCDPL_2024_05_03.pdf. Accessed 2024 May 10.
28.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 May 8.
29.Harries M, Macbeth AE, Holmes S, et al. The epidemiology of alopecia areata: a population-based cohort study in UK primary care. Br J Dermatol. 2022;186(2):257-265. PubMed
30.Fenske C, Rosettie K, Lu T, et al. EE325 Budget Impact of Baricitinib for Patients with Severe Alopecia Areata. Value Health. 2022;25(7 Supplement):S397-S398.
31.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2024 May 17.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed appropriate based on feedback from clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 11: CDA-AMC Cost Comparison Table for the Treatment of Alopecia Areata
Treatment | Strength/ concentration | Form | Price | Recommended dosage | Daily cost ($) | Annual cost ($)a |
|---|---|---|---|---|---|---|
Baricitinib (Olumiant) | 2 mg 4 mg | Tablet | 57.2057b 114.4113b | 2 mg once daily, which may be increased to 4 mg once daily if response to treatment is not adequate. For patients with nearly complete or complete scalp hair loss, and/or substantial eyelash or eyebrow hair loss the recommended dose is 4 mg once daily. Once patients attain an adequate response to treatment with 4 mg, dosage may be decreased to 2 mg once daily.a | 57.21 to 114.41 | 20,894 to 41,789 |
Recommended practice | ||||||
JAK inhibitor | ||||||
Ritlecitinib (Litfulo) | 50 mg | Capsule | 49.6700c | 50 mg once daily | 49.67 | 18,142 |
Topical therapy | ||||||
Minoxidil (Generic) | 50 mg/mL (5% w/v) | Topical Foam | 0.5133d | 50 mg applied to the affected area twice daily | 1.03 | 375 |
Actual practice (off-label use) | ||||||
Antihypertensives | ||||||
Minoxidil (Loniten) | 2.5 mg 10 mg | Tablet | 0.5000 1.1030 | 5 mg per day in divided doses | 1.00 | 365 |
Corticosteroids | ||||||
Mometasone (Generic) | 0.1% in 15 g tube 0.1% in 50 g tube | Ointment | 0.2252 per gram | Application of a thin film of ointment to the affected area once daily.e | 0.28 | 103 |
Prednisolone (Generic) | 4 mg | Tablet | 0.5364 | Initial dose varies from 4 mg to 48 mg once daily. Maintenance is determined by decreasing the initial dose until the lowest dose that maintains adequate response is reached. | 0.54 to 6.44 | 196 to 2,351 |
Triamcinolone acetonide (Kenalog) | 10 mg/mL | Intralesional injection | 3.8900 | 1 mg applied weekly per injection site. Multiple sites may be injected.f | 0.56 | 29 |
Immunosuppressants and immunomodulators | ||||||
Azathioprine (Generic) | 50 mg | Tablet | 0.5185 | The initial dose is 1 mg/kg per day, which may be increased up to a maximum dose of 2.5 mg/kg per day.g | 1.04 to 2.07 | 379 to 758 |
Cyclosporine (Generic) | 25 mg 50 mg 100 mg | Capsule | 0.7870 1.5350 3.0720 | The initial dose is 2 mg/kg per day, which may be increased up to a maximum dose of 5 mg/kg per day.g | 4.61 to 11.54 | 1,683 to 4,214 |
Methotrexate (Generic) | 2.5 mg | Tablet | 0.2513 | 10 mg to 25 mg once weekly | 0.14 to 0.36 | 52 to 131 |
Mycophenolate mofetil (Generic) | 250 mg 500 mg | Capsule | 0.3712 0.7423 | 1,000 mg to 1,500 twice daily | 2.97 to 4.45 | 1,085 to 1,627 |
JAK inhibitors | ||||||
Tofacitinib (Generic) | 5 mg 10 mg | Tablet | 5.9897 21.1718 | 5 mg twice daily | 11.98 | 4,375 |
Topical prostaglandin analogues | ||||||
Latanoprost (Generic) | 50 mcg/mL | Ophthalmic solution | 9.5830 | 1 drop (equivalent to 0.05 mL) once daily on each eye | 0.96 | 350 |
Bimatoprost (Vistitan) | 2.5 mL (0.03% w/v) | Ophthalmic solution | 9.1936h | 1 drop (equivalent to 0.05 mL) once daily on each eye | 0.37 | 134 |
CDA-AMC = Canada’s Drug Agency.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed April 2024), unless otherwise indicated, and do not include dispensing fees.
aAssuming year is equal to 365.25 days.
bSponsor’s submitted price and recommended dosage.1,2
cPrice from the Alberta Blue Cross Drug Price List (effective May 14, 2024).27
dPrice per mL from IQVIA Delta PA (Accessed May 8, 2024).28
eAssuming 1.25 g ointment needed per day.
fAssuming 10 injection sites are needed, based on clinical expert input.
gAssuming 75 kg body weight for daily and annual cost calculations.
hPrice per 2.5 mL package.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to key limitation ‘Selection of relevant comparators is misaligned with current clinical practice.’ |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
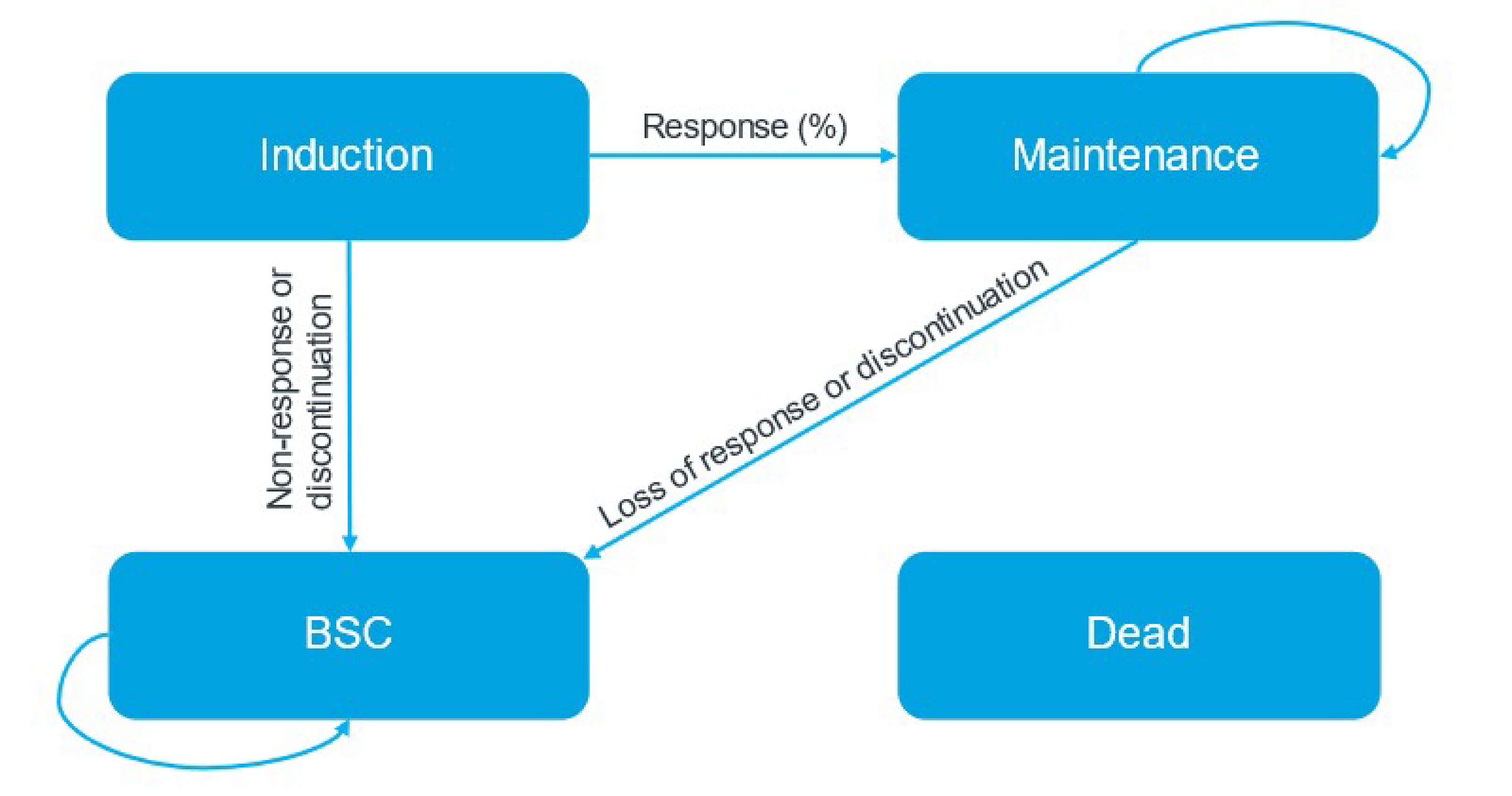
Table 13: Proportion of Patients With Severe AA Responding With Treatment After Induction Period (Week 36)
Intervention | SALT30 | SALT50 | SALT75 | |||
|---|---|---|---|---|---|---|
Efficacy | SE | Efficacy | SE | Efficacy | SE | |
Baricitinib 2 mg | ██████ | █████ | ██████ | █████ | ██████ | █████ |
Baricitinib 4 mg | ██████ | █████ | ██████ | █████ | ██████ | █████ |
No active treatment | ██████ | █████ | █████ | █████ | █████ | █████ |
SALT = Severity of Alopecia Tool; SALT30 = at least 30% improvement from baseline in the Severity of Alopecia Tool score; SALT50 = at least 50% improvement from baseline in the Severity of Alopecia Tool score; SALT75 = at least 75% improvement from baseline in the Severity of Alopecia Tool score; SE = standard error.
Table 14: Treatment Discontinuation Rates
Intervention | Induction | Maintenance | ||
|---|---|---|---|---|
Discontinuation | SE | Discontinuation | SE | |
Baricitinib 2 mg | █████ | █████ | ██████ | █████ |
Baricitinib 4 mg | █████ | █████ | ██████ | █████ |
No active treatment | ██████ | █████ | ██████ | █████ |
SE = standard error.
Table 15: Baseline Utility Values and Utility Increments in the Submitted Economic Model According to Source and Response Category
Response level | Adelphi DSP EQ-5D | Study BRAVE-AA1 and study BRAVE-AA2 EQ-5D | ||
|---|---|---|---|---|
Value | SE | Value | SE | |
Baseline | █████ | █████ | █████ | █████ |
CFB for SALT30 (increment) | █████ | █████ | ██████ | █████ |
CFB for SALT50 (increment) | █████ | █████ | █████ | █████ |
CFB for SALT75 (increment) | █████ | █████ | █████ | █████ |
CFB = change from baseline; DSP = Disease Specific Programme; SALT = Severity of Alopecia Tool; SALT30 = at least a 30% improvement from baseline in the Severity of Alopecia Tool score; SALT50 = at least a 50% improvement from baseline in the Severity of Alopecia Tool score; SALT75 = at least a 75% improvement from baseline in the Severity of Alopecia Tool score; SE = standard error.
Note: The utility values from the final analysis of the Adelphi DSP study informing the economic model are as follows: the utility value for the severe subgroup in Adelphi DSP informed the baseline utility value in the model, the utility value for the moderate severity subgroup in Adelphi DSP informed the CFB for SALT50, and the utility value for the mild severity subgroup of the Adelphi DSP informed the CFB for SALT75. The publication and poster for the Adelphi DSP study were provided by the sponsor in response to our additional information request.6,7 The sponsor did not offer an explanation for the derivation of the utility increment used to inform the CFB for SALT30.
Detailed Results of the Sponsor’s Base Case
Table 16: Disaggregated Summary of the Sponsor’s Economic Evaluation Results, Baricitinib 2 mg Dose
Parameter | Baricitinib 2 mg | No active treatment |
|---|---|---|
Discounted QALYs | ||
Total | 21.27 | 21.12 |
Less than SALT score of 50 | 19.72 | 20.76 |
SALT score of 50 to 75 | 0.59 | 0.24 |
SALT score of ≥ 75 | 0.96 | 0.13 |
Discounted costs ($) | ||
Total | 53,955 | 67,517 |
Drug acquisition costs | 51,211 | 2,663 |
Ongoing management costs | 1,529 | 21,004 |
Psychological support costs | 1,215 | 1,277 |
BSC drug monitoring costs | 0 | 42,574 |
QALY = quality-adjusted life-year; SALT = Severity of Alopecia Tool.
Source: Sponsor’s pharmacoeconomic submission.1
Table 17: Disaggregated Summary of the Sponsor’s Economic Evaluation Results, Baricitinib 4 mg Dose
Parameter | Baricitinib 4 mg | No active treatment |
|---|---|---|
Discounted QALYs | ||
Total | 21.43 | 21.11 |
Less than SALT score of 50 | 18.38 | 20.74 |
SALT score of 50 to 75 | 0.86 | 0.24 |
SALT score of ≥ 75 | 2.19 | 0.13 |
Discounted costs ($) | ||
Total | 179,044 | 67,355 |
Drug acquisition costs | 175,305 | 2,664 |
Ongoing management costs | 2,605 | 20,975 |
Psychological support costs | 1,134 | 1,273 |
BSC drug monitoring costs | 0 | 42,442 |
QALY = quality-adjusted life-year; SALT = Severity of Alopecia Tool.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of Our Base Case
Table 18: Disaggregated Summary of Economic Evaluation Results From CDA-AMC, Baricitinib 2 mg Dose, Deterministic
Parameter | Baricitinib 2 mg | Placebo |
|---|---|---|
Discounted QALYs | ||
Total | 24.08 | 24.07 |
Less than SALT score of 30 | 22.09 | 23.51 |
SALT score of 30 to 50 | 0.42 | 0.18 |
SALT score of 50 to 75 | 0.61 | 0.25 |
SALT score of ≥ 75 | 0.97 | 0.13 |
Discounted costs ($) | ||
Total | 64,090 | 1,633 |
Drug acquisition costs | 61,076 | 0 |
Ongoing management costs | 1,820 | 365 |
Psychological support costs | 1,194 | 1,267 |
BSC drug monitoring costs | 0 | 0 |
CDA-AMC = Canada’s Drug Agency; QALY = quality-adjusted life-year; SALT = Severity of Alopecia Tool.
Source: Sponsor’s pharmacoeconomic submission.1
Table 19: Disaggregated Summary of Economic Evaluation Results From CDA-AMC, Baricitinib 4 mg Dose, Deterministic
Parameter | Baricitinib 4 mg | Placebo |
|---|---|---|
Discounted QALYs | ||
Total | 24.10 | 24.07 |
Less than SALT 30 | 20.45 | 23.51 |
SALT score of 30 to 50 | 0.56 | 0.18 |
SALT score of 50 to 75 | 0.89 | 0.25 |
SALT score of ≥ 75 | 2.19 | 0.13 |
Discounted costs ($) | ||
Total | 205,447 | 1,633 |
Drug acquisition costs | 201,353 | 0 |
Ongoing management costs | 2,984 | 365 |
Psychological support costs | 1,109 | 1,267 |
BSC drug monitoring costs | 0 | 0 |
CDA-AMC = Canada’s Drug Agency; QALY = quality-adjusted life-year; SALT = Severity of Alopecia Tool.
Source: Sponsor’s pharmacoeconomic submission.1
Scenario Analyses
Table 20: Scenario Analyses Conducted on the CDA-AMC Base Case, Deterministic
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Baricitinib 2 mg | ||||
Sponsor’s base case (deterministic) | No active treatment | 67,405 | 21.11 | Reference |
Baricitinib 2 mg | 53,770 | 21.25 | Dominant | |
CDA-AMC base case (deterministic) | No active treatment | 1,633 | 24.07 | Reference |
Baricitinib 2 mg | 64,090 | 24.08 | 5,465,503 | |
CDA-AMC scenario 1: SALT75 | No active treatment | 1,495 | 21.09 | Reference |
Baricitinib 2 mg | 38,862 | 21.20 | 346,345 | |
CDA-AMC scenario 2: Adelphi DSP utilities | No active treatment | 1,633 | 21.11 | Reference |
Baricitinib 2 mg | 64,090 | 21.25 | 452,788 | |
Baricitinib 4 mg | ||||
Sponsor’s base case (deterministic) | No active treatment | 67,405 | 21.11 | Reference |
Baricitinib 4 mg | 177,699 | 21.43 | 343,398 | |
CDA-AMC base case (deterministic) | No active treatment | 1,633 | 24.07 | Reference |
Baricitinib 4 mg | 205,447 | 24.10 | 6,803,200 | |
CDA-AMC scenario 1: SALT75 | No active treatment | 1,495 | 21.09 | Reference |
Baricitinib 4 mg | 134,554 | 21.36 | 497,449 | |
CDA-AMC scenario 2: Adelphi DSP utilities | No active treatment | 1,633 | 21.11 | Reference |
Baricitinib 4 mg | 205,447 | 21.43 | 634,568 | |
Weighted ICER | ||||
CDA-AMC base case | No active treatment | 1,633 | 24.07 | Reference |
Baricitinib | 191,311 | 24.09 | 6,748,810 | |
CDA-AMC scenario 1: SALT75 | No active treatment | 1,495 | 21.09 | Reference |
Baricitinib | 124,985 | 21.34 | 490,967 | |
CDA-AMC scenario 2: Adelphi DSP utilities | No active treatment | 1,633 | 21.11 | Reference |
Baricitinib | 191,311 | 21.41 | 626,289 | |
CDA-AMC = Canada’s Drug Agency; DSP = Disease Specific Programme; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SALT = Severity of Alopecia Tool.
aSALT75 = proportion of patients achieving at least a 75% improvement from baseline in SALT score.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 21: Summary of Key Take Aways
Key take aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) to estimate the incremental 3-year budget impact of reimbursing baricitinib for the treatment of adult patients with severe AA, as per its Health Canada indication. The analysis was performed from the perspective of the Canadian public drug plan formulary. The sponsor estimated the budget impact by comparing 2 scenarios: a reference scenario that estimated the total costs associated with BSC for the treatment of patients with severe AA; and a new drug scenario, where baricitinib is funded. BSC was composed of topical corticosteroids (e.g., mometasone), intralesional corticosteroids (e.g., triamcinolone acetonide), minoxidil, immunosuppressants (e.g., azathioprine, mycophenolate mofetil), and other systemic drugs (e.g., cyclosporine, methotrexate). The sponsor estimated the eligible population using an epidemiology-based approach, leveraging data from multiple sources in the scientific literature29-31 and assumptions based on internal forecast estimates and clinical expert input. Drug acquisition costs were the only costs considered in the model. The dosing modelled for baricitinib reflected the product monograph. Key inputs to the BIA are documented in Table 22.
Key assumptions made by the sponsor include the following:
proportion of individuals diagnosed with AA was assumed to be 77% based on internal estimates
proportion of patients treated with JAK inhibitors was assumed to be 32% to 34% in years 1 to 3 based on internal estimates
distribution of BSC therapies, including cyclosporine (1%), methotrexate (5%), azathioprine (0%), triamcinolone acetonide (50%), prednisolone (5%), mometasone (50%), minoxidil (0%), mycophenolate mofetil (0%) was assumed based on Canadian clinical expert opinion
distribution across the 2 mg and 4 mg doses of baricitinib was assumed to be 50% each based on internal estimates
cost calculations for baricitinib were adjusted by a compliance factor of ██% based on internal estimates
uptake for baricitinib in the new drug scenario was assumed to be 10%, 20%, and 15% in year 1, year 2, and year 3, respectively. Baricitinib was assumed to displace all other therapeutic options equally
market share of baricitinib in year 3 was assumed to decrease from year 2 as therapeutic options in different drug classes (i.e., non-JAK inhibitors) are anticipated to enter the market at this time.
Table 22: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3 if appropriate) |
|---|---|
Target population | |
NIHB-adjusted pan-Canadian adult population | 26,187,322 |
Prevalence of AA29 | 0.58% |
Proportion of individuals diagnosed | 77% |
Proportion of patients with severe AA30 | 79% |
Proportion of patients treated with JAK inhibitors | 32% / 33% / 34% |
Proportion of patients eligible for public coverage31 | 28% to 100% |
Number of patients eligible for drug under review | 9,019 / 9,449 / 9,891 |
Market uptake (3 years) | |
Uptake (reference scenario) BSC | 100% / 100% / 100% |
Uptake (new drug scenario) Baricitinib BSC | 10% / 20% / 15% 90% / 80% / 85% |
Cost of treatment (per patient, per year) | |
Baricitinib BSC | $22,754 $247 |
AA = alopecia areata; BSC = best supportive care; NIHB = Non-Insured Health Benefits.
aThe NIHB-adjusted pan-Canadian population estimates were calculated by taking the Canadian population estimates for the applicable jurisdictions and removing the NIHB Program client population within the respective jurisdictions.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base-case BIA suggest that the incremental expenditures associated with the reimbursement of baricitinib for the treatment of adult patients with AA would be $20,298,600 in year 1, $42,532,871 in year 2, and $33,390,311 in year 3, for a 3-year cumulative total of $96,221,781.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Proportion of patients assumed to receive baricitinib 2 mg and 4 mg doses is highly uncertain. The sponsor assumed that the distribution across the 2 mg and 4 mg doses of baricitinib would be 50% each, based on internal estimates. Clinical experts who CDA-AMC consulted for this review indicated that the vast majority of patients with severe AA are likely to have tried and not experienced improvement with both recommended and off-label therapies currently available in Canada; hence, physicians would be more likely to start with the higher dose of baricitinib and taper off where needed. Clinical experts additionally noted that prescribers would be more likely to treat patients with the 4 mg dose if it were found to be more efficacious than the 2 mg dose in Study BRAVE-AA1 and Study BRAVE-AA2. Our clinical review noted that, in the pivotal trials, a greater proportion of patients treated with the 4 mg dose of baricitinib attained more than or equal to 80% scalp hair coverage (i.e., a SALT score ≤ 20) at week 36 compared with patients treated with the 2 mg dose, versus no active treatment. As highlighted by clinical experts, such findings are likely to influence prescribers' decisions regarding the preferred dosage in Canadian clinical practice.
CDA-AMC conducted a base-case reanalysis, which considered that 90% of patients with severe AA would receive the 4 mg dose while 10% would receive the 2 mg dose based on clinical expert input.
CDA-AMC conducted a scenario analysis that explored the budget impact of baricitinib if the 2 mg and 4 mg doses were prescribed equally (50% each) within the indicated population.
Assumptions regarding compliance underestimated drug acquisition costs. The sponsor adjusted cost calculations for baricitinib using a compliance factor of ██%. This implies that, on average, patients treated with baricitinib would be expected to miss approximately ██ daily doses every year. CDA-AMC note that, in the submitted economic model, the sponsor assumed ███% adherence to treatment,1 stating that the assumption appeared reasonable as it reflected the high compliance rates observed in Study BRAVE-AA1 and Study BRAVE-AA2. Indeed, our clinical review indicated that, in the BRAVE-AA1 and BRAVE-AA2 long-term extension studies, the near entirety of patients complied with the assigned baricitinib treatment at both 2 mg and 4 mg doses (median adherence ranging from ████ to ████ at week 52, and from ████ to ████ at week 72).3,4
CDA-AMC conducted a reanalysis by assuming 100% compliance among patients treated with baricitinib.
Projected market share of baricitinib is underestimated. The sponsor assumed that baricitinib would have a market share of 10%, 20% and 15% in year 1, year 2, and year 3, respectively. The sponsor explained that the market share of baricitinib in year 3 was assumed to decrease from year 2 as therapeutic options in different drug classes (i.e., non-JAK inhibitors) would be anticipated to enter the market at this time. Clinical experts CDA-AMC consulted indicated that while it is plausible for both JAK and non-JAK inhibitor comparators to enter the market in the future, it is highly uncertain whether and to what extent new comparators would capture market share from baricitinib, but certainly, the market share of BSC therapies would not increase if more JAK inhibitor options were available to treat patients with severe AA.
CDA-AMC conducted a reanalysis by adjusting the projected market share of baricitinib to 10%, 20% and 30% in year 1, year 2, and year 3, respectively, based on feedback sought from clinical experts.
Distribution of therapies in the BSC basket is highly uncertain. The sponsor assumed the following distribution of therapies in the BSC basket: cyclosporine (1%), methotrexate (5%), azathioprine (0%), triamcinolone acetonide (50%), prednisolone (5%), mometasone (50%), minoxidil (0%), mycophenolate mofetil (0%) based on clinical expert opinion. CDA-AMC note that the proportion of patients with severe AA that use each of these therapies is highly uncertain. Clinical experts CDA-AMC consulted for this review indicated that it is unlikely that no patients in Canada receive azathioprine, minoxidil, or mycophenolate mofetil. Experts additionally noted that the proportion of patients assumed by the sponsor to receive cyclosporine is underestimated.
CDA-AMC conducted a base-case reanalysis that revised the distribution of therapies in the BSC basket per clinical experts' input.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analysis by adjusting the proportion of patients that would receive the 2 mg and 4 mg doses of baricitinib; assuming 100% compliance in alignment with the cost-effectiveness model; modifying the projected market share of baricitinib; and revising the distribution of therapies in the BSC basket. The changes applied to derive our base case are described in Table 23.
Table 23: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive our base case | ||
1. Proportion of patients assumed to receive the 2 mg and 4 mg doses of baricitinib |
|
|
2. Compliance with baricitinib | ██% | 100% |
3. Market share of baricitinib |
|
|
4. Distribution of therapies in the BSC basket |
|
|
CDA-AMC base case | Reanalysis 1 + 2 + 3 + 4 | |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency.
The results of our stepwise reanalysis are presented in summary format in Table 24 and a more detailed breakdown is presented in Table 25. Our reanalysis suggests that reimbursing baricitinib for the treatment of severe AA would be associated with an incremental cost of $35,487,043 in year 1, $74,358,125 in year 2, and $116,749,276 in year 3, for a 3-year budgetary impact of $226,594,445.
Table 24: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | 3-year total ($) |
|---|---|
Submitted base case | 96,221,781 |
CDA-AMC reanalysis 1 | 122,162,895 |
CDA-AMC reanalysis 2 | 132,935,960 |
CDA-AMC reanalysis 3 | 129,612,092 |
CDA-AMC reanalysis 4 | 95,774,067 |
CDA-AMC base case | 226,594,445 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
CDA-AMC conducted the following scenario analysis to address remaining uncertainty, using our base case (results are provided in Table 25):
Assuming that the 2 mg and 4 mg doses of baricitinib would be prescribed equally (50% each) in the indicated population.
Table 25: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | 3-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 2,058,451 | 2,230,638 | 2,336,994 | 2,446,201 | 7,013,833 |
New drug | 2,058,451 | 22,529,238 | 44,869,865 | 35,836,512 | 103,235,615 | |
Budget impact | 0 | 20,298,600 | 42,532,871 | 33,390,311 | 96,221,781 | |
CDA-AMC base case | Reference | 2,930,037 | 3,175,125 | 3,326,510 | 3,481,951 | 9,983,586 |
New drug | 2,930,037 | 38,662,169 | 77,684,635 | 120,231,227 | 236,578,030 | |
Budget impact | 0 | 35,487,043 | 74,358,125 | 116,749,276 | 226,594,445 | |
CDA-AMC scenario analysis 1: Equal likelihood of patients receiving the 2 mg and 4 mg doses | Reference | 2,930,037 | 3,175,125 | 3,326,510 | 3,481,951 | 9,983,586 |
New drug | 2,930,037 | 31,124,367 | 61,890,229 | 95,432,519 | 188,447,116 | |
Budget impact | 0 | 27,949,242 | 58,563,720 | 91,950,569 | 178,463,530 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.