Drugs, Health Technologies, Health Systems
Reimbursement Review
Elexacaftor-Tezacaftor-Ivacaftor and Ivacaftor (Trikafta)
Sponsor: Vertex Pharmaceuticals (Canada) Incorporated
Therapeutic area: Cystic fibrosis, responsive CFTR mutations
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
BMI
body mass index
CanACT
Cystic Fibrosis Canada Accelerating Clinical Trials Network
CCFR
Canadian Cystic Fibrosis Registry
CDA-AMC
Canada's Drug Agency
CDEC
Canadian Drug Expert Committee
CF
cystic fibrosis
CF Canada
Cystic Fibrosis Canada
CFFPR
Cystic Fibrosis Foundation Patients Registry
CFQ-R
Cystic Fibrosis Questionnaire–Revised
CFQ-R (RD)
Cystic Fibrosis Questionnaire–Revised (respiratory domain)
CI
confidence interval
Cl−
chlorine ion
ELX
elexacaftor
ELX-TEZ-IVA
elexacaftor-tezacaftor-ivacaftor plus ivacaftor
FAS
full analysis set
FEV1
forced expiratory volume in 1 second
FRT
Fischer rat thyroid
GRADE
Grading of Recommendations Assessment, Development and Evaluation
IQR
interquartile range
ITC
indirect treatment comparison
IVA
ivacaftor
LUM-IVA
lumacaftor-ivacaftor plus ivacaftor
MID
minimal important difference
MMRM
mixed-effects model for repeated measures
LS
least squares
PEx
pulmonary exacerbation
ppFEV1
percent predicted forced expiratory volume in 1 second
RCT
randomized controlled trial
RF
residual function
SAE
serious adverse event
SD
standard deviation
SwCl
sweat chloride
TEZ
tezacaftor
TEZ-IVA
tezacaftor-ivacaftor plus ivacaftor
ULN
upper limit of normal
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Elexacaftor-tezacaftor-ivacaftor plus ivacaftor (Trikafta) Aged 2 to 5 years
Aged 6 years and older
|
Sponsor | Vertex Pharmaceuticals (Canada) Incorporated |
Indication | For the treatment of cystic fibrosis in patients aged 2 years and older who have at least 1 F508del mutation in the CFTR gene or a mutation in the CFTR gene that is responsive based on clinical and/or in vitro dataa |
Reimbursement request | As per indication |
Health Canada approval status | Approved |
Health Canada review pathway | Priority review |
NOC date | July 12, 2024 |
Recommended dose | Dosages recommended in the product monograph |
NOC = Notice of Compliance.
aThis review focuses only on non-F508del mutations, which are responsive to elexacaftor-tezacaftor-ivacaftor plus ivacaftor based on clinical and/or in vitro data.
Introduction
Trikafta (elexacaftor-tezacaftor-ivacaftor plus ivacaftor [ELX-TEZ-IVA]) is a fixed-dose combination product previously reviewed for the treatment of cystic fibrosis (CF) caused by F508del mutations of the CFTR gene. ELX-TEZ-IVA is available as both oral tablets and oral granules in the following dosage strengths:
tablets for patients 6 years and older:
elexacaftor (ELX) 50 mg, tezacaftor (TEZ) 25 mg, and ivacaftor (IVA) 37.5 mg co-packaged with a tablet containing IVA 75 mg
ELX 100 mg, TEZ 50 mg, and IVA 75 mg co-packaged with a tablet containing IVA 150 mg.
granules for patients aged 2 to less than 6 years:
ELX 100 mg, TEZ 50 mg, and IVA 75 mg (granules) plus IVA 75 mg (granules)
ELX 80 mg, TEZ 40 mg, and IVA 60 mg (granules) plus IVA 59.5 mg (granules), oral.
The current review is for an expanded indication that would include 152 additional non-F508del mutations in the CFTR gene. The sponsor has categorized the additional CFTR mutations as follows:
Fischer rat thyroid (FRT)-responsive mutations supported by clinical data (68 mutations)
FRT-responsive mutations with no available supporting clinical data (79 mutations)
noncanonical splice mutations (4 mutations): 4 CFTR mutations that result in small amounts of functional, normal CFTR protein. The sponsor has reported that these mutations cannot be evaluated in the FRT system, and it provided some form of clinical data for each of the mutations included in the application
N1303K mutation: A CFTR mutation that was initially identified as nonresponsive to ELX-TEZ-IVA in the FRT in vitro study that has subsequently been studied in a phase II clinical trial as well an investigator-sponsored real-world evidence study.
Figure 1: Additional CFTR Mutations Within the Expanded Indication
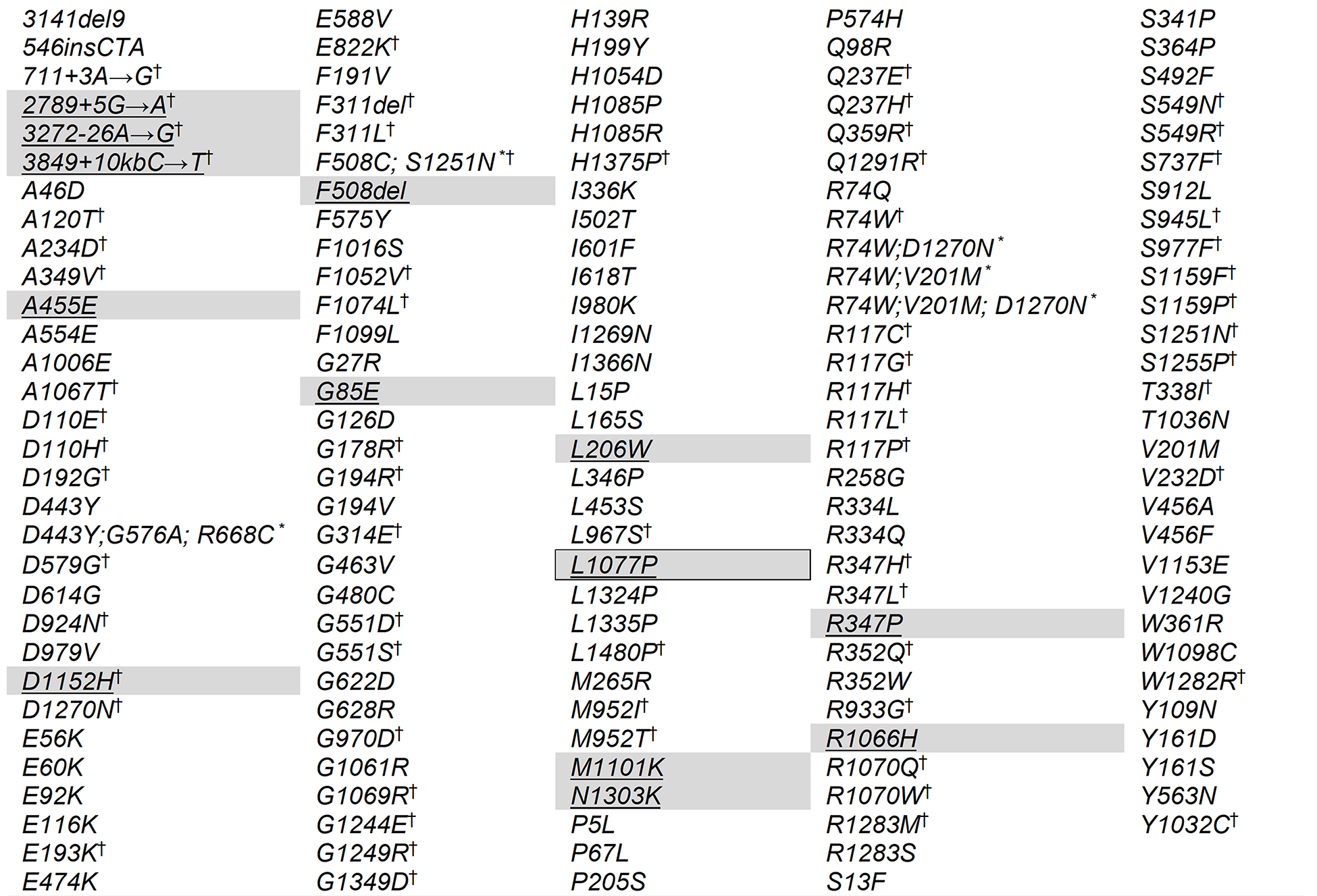
Note: CFTR mutations for which Health Canada concluded there is significant clinical evidence of efficacy in response to elexacaftor-tezacaftor-ivacaftor plus ivacaftor, independent of the mutation on the second allele, are underscored and shaded in grey.
* Complex and/or compound mutations where a single allele of the CFTR gene has multiple mutations; these exist independent of the presence of mutations on the other allele.
† CFTR mutations for which in vitro and/or clinical data supports some efficacy with ivacaftor monotherapy.
This is the fourth submission to Canada’s Drug Agency (CDA-AMC) for ELX-TEZ-IVA. We previously reviewed ELX-TEZ-IVA for the treatment of CF in patients aged 12 years and older who have 1 or more F508del mutations in the CFTR gene (final recommendation issued in August 2021); those aged 6 years and older (final recommendation issued in June 2022); and those aged 2 to 5 years (final recommendation issued in November 2023). For all of the previous reviews, the Canadian Drug Expert Committee (CDEC) recommended that ELX-TEZ-IVA be reimbursed with conditions. All of the indications for ELX-TEZ-IVA have been accepted as priority reviews by Health Canada.
The sponsor requested that the current submission for ELX-TEZ-IVA focus only on the expanded patient population (i.e., those aged 2 years and older with non-F508del mutations that are responsive to ELX-TEZ-IVA based on clinical and/or in vitro data). The drug combination comes in 2 dosage formats: orally administered tablets for those aged 6 years and older, and orally administered granules for those aged 2 to 5 years.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the call for input and from clinical experts consulted for the purpose of this review.
Patient Input
Two submissions were received from Cystic Fibrosis Canada (CF Canada). Information from CF Canada was based on a focus group of residents of Canada with rare mutations who are being treated with ELX-TEZ-IVA, those with rare mutations who do not have access to ELX-TEZ-IVA, and caregivers of patients with rare mutations that cause CF. In addition, data were retrieved from a survey of patients and caregivers with access to ELX-TEZ-IVA conducted in 2021, medical and scientific publications, as well as the Canadian Cystic Fibrosis Registry (CCFR). CF Canada also measured the burden of CF at the individual, family, health systems, and societal levels, using preliminary findings from phase I of the Burden of Disease Study, which is considered to be among the most comprehensive studies of the burden of CF in the world. The second input was authored by a patient with end-stage CF with a rare class II mutation (M1101K).
According to the patient group, although life-changing treatments are increasingly reaching the 4,445 people in Canada living with CF, and those born with CF today will live longer than those who came before them, many are still seriously ill and 1 in 7 living with the disease today is ineligible for the treatments that are making such a positive difference for others with CF.
The input stated that, from a health care and quality-of-life perspective, challenges remain for patients living with CF, including those who are unable to benefit from recent life-changing treatments. For example, in Canada, the 40 patients who died of CF in 2022 had a median age of 38; patients with CF collectively had 17,000 clinic visits, spent 10,000 days in hospital, and spent nearly 6,000 days on IV antibiotics in 2022 alone. For 1 in 5 adults with CF, depression or anxiety was recorded as a complication in the CCFR. As the disease progresses, more time and effort are needed for frequent clinic visits and hospital stays to manage the progressive and debilitating symptoms. This overwhelming treatment regimen has multiple side effects and a significant impact on patients’ and caregivers’ day-to-day activities and quality of life, and it creates a major financial burden for families.
Data from the CCFR on patients in Canada with CF who do not currently have a Health Canada indication for CFTR modulators show that 246 patients have rare mutations known to respond to ELX-TEZ-IVA. The patient input indicated that many of these patients come from diverse and often racialized backgrounds, they are already disadvantaged by health care systems that were not designed with them in mind, and they deserve the right to try ELX-TEZ-IVA, even when efficacy and safety evidence is limited.
Patients with rare mutations and their caregivers shared their hopes to access ELX-TEZ-IVA as they saw the benefits for those who are able to access it. Few patients in Canada with rare CF mutations have access to ELX-TEZ-IVA. Those who reported taking ELX-TEZ-IVA responded exceptionally well to therapy, even those who have mutations for which the clinical evidence of a therapeutic response is limited.
Clinician Input
Input From Clinical Experts
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). For this review of ELX-TEZ-IVA, a panel of 3 clinical experts provided input to characterize unmet therapeutic needs, helped identify and communicate gaps in the evidence that could be addressed through the collection of additional data, promoted the early identification of potential implementation challenges, gained further insights into the clinical management of patients living with CF, and explored the potential place in therapy of the drug combination. A summary of input from the clinical experts follows.
Unmet Needs
All patients living with CF have significant unmet therapeutic needs. No treatments are currently available that can effectively achieve the most important goals of therapy: prolong survival, prevent the need for a lung transplant, prevent an accelerated decline in lung function over time, or reverse the course of the disease. In addition, the current standard treatments are burdensome for patients and their caregivers. Patients may not respond or may stop responding over time to the currently available treatments. The majority of patients with a non-F508del mutation that is responsive to ELX-TEZ-IVA do not currently have access to therapy that involves a modulator of the CFTR protein.
Place in Therapy
ELX-TEZ-IVA is a modulator that functions by 2 mechanisms: ELE and TEZ increase the amount of CFTR protein at the cell surface while IVA improves the transport of chloride ions through the CFTR protein. ELX-TEZ-IVA is attractive because it acts directly on the CFTR protein to address the defects responsible for the CF phenotype. ELX-TEZ-IVA would be added to existing treatments such as physiotherapy, mucolytics, anti-infectives, and anti-inflammatory treatments (such as azithromycin). The clinical experts noted that ELX-TEZ-IVA has replaced earlier CFTR modulators that are significantly less effective (e.g., lumacaftor-ivacaftor [LUM-IVA] and IVA alone) for patients with 1 or more F508del mutations in the CFTR gene. For the current target patient population, the clinical specialists anticipated that all patients in the expanded population (i.e., those with a non-508del mutation that is responsive to ELX-TEZ-IVA) would be considered candidates for the therapy. This would include those with a gating mutation who are currently receiving treatment with IVA, provided they meet eligibility and age criteria.
It is anticipated that ELX-TEZ-IVA would be used as a preventive therapy, with treatment initiated before the patient develops significant lung disease. The current treatment paradigm would be significantly altered if ELX-TEZ-IVA can successfully prevent or delay progression to end-stage organ disease (e.g., lung transplant).
The indication currently under review is for patients aged 2 years or older. We previously recommended that ELX-TEZ-IVA be reimbursed for patients ages 2 to 5 years and those 6 years and older. The clinical experts consulted for this review and those who previously responded to the call for clinician input noted that children aged between 2 to 5 years will often have structural lung disease (e.g., bronchial wall thickening, mucus plugging, and/or bronchiectasis),1 but that detection is challenging using the tools available to evaluate lung function in clinical practice (i.e., spirometry) or as part of a research protocol (e.g., lung clearance index). However, despite younger patients with CF often exhibiting normal lung function, the early stages of lung abnormalities can be visualized using CT, and the underlying disease will continue to progress.1
Overall, all the clinicians who provided input for this review recommend initiating treatment with ELX-TEZ-IVA as soon as possible. This aligns with the previously published Canadian Clinical Consensus Guideline for Initiation, Monitoring and Discontinuation of CFTR Modulator Therapies for Patients with Cystic Fibrosis, which also recommends initiating CFTR modulators at the youngest age possible, with the goal of attenuating disease progression and improving clinical status. All contributors agreed that no data support withholding initiation of treatment with a CFTR modulator until clinical symptoms of CF have developed.
Patient Population
The diagnosis of CF is not challenging in routine clinical practice. As all provinces and territories are now screening newborns for CF, and most people with CF are identified at an early age and have a confirmed diagnosis by the age of 1 month (on average). Sweat chloride (SwCl) testing is available and can be used reliably to confirm the results of a screening test. The provinces and territories have slightly different testing algorithms and screening panels for CFTR mutations; however, all jurisdictions have effective processes. Almost 100% of newly diagnosed infants would have their CFTR mutations identified. Infants who are not identified via newborn screening (i.e., false negatives), are usually diagnosed before the age of 1 year after the development of clinical symptoms of CF. The diagnostic guidelines are clear and there is little variability in expert opinion. Misdiagnosis and underdiagnosis of CF is exceedingly rare in clinical practice in Canada.
Every patient who meets the Health Canada–approved indication could be treated with ELX-TEZ-IVA, regardless of their current or past treatment regimens. From a medical perspective, there is no rationale for requiring a patient to demonstrate an inadequate response or loss of response to prior therapies before initiating treatment with ELX-TEZ-IVA. It would be reasonable to require patients to complete important standard CF therapies in conjunction with ELX-TEZ-IVA. In clinical practice, eligible patients would be identified based on their CFTR genotype and all patients would be expected to respond to the treatment.
For the expanded indication (i.e., a non-F508del mutation that is responsive to ELX-TEZ-IVA), the clinical experts consulted for this review noted that nearly all patients would initiate therapy with ELX-TEZ-IVA as soon as possible, provided it is safe to start treatment. The clinical experts emphasized that ELX-TEZ-IVA has been a transformative and disease-modifying therapy for CF and that it would not be appropriate to wait until the patient shows worsening symptoms, more frequent exacerbations, or a decline in lung function to initiate treatment with ELX-TEZ-IVA.
Applicability of Existing Reimbursement Criteria to the Expanded Population
In discussions with the review team, the sponsor noted that nearly all patients in Canada aged 6 years and older who are eligible for treatment have initiated therapy with ELX-TEZ-IVA. (Some may have elected to discontinue treatment, but all who are interested have been given the opportunity to access the drug combination.) For those who have initiated treatment with ELX-TEZ-IVA, the sponsor noted that initial renewal criteria were met for all patients in Canada who started the therapy and wanted to continue (i.e., 100% of patients met the renewal criteria recommended by CDA-AMC and/or applied by the public drug programs). The clinical experts consulted for this review expressed general agreement with the sponsor’s position, noting that rates of initial access and renewal are high within their individual clinics. With nearly all patients currently achieving the recommended renewal criteria, the sponsor noted requiring these assessments consumes health care resources (e.g., the time required by health care practitioners to administer and document results for each of the required tests) without adding value to patients or the health care system.
The clinical experts consulted for this review support the application of the existing criteria recommended for the reimbursement of ELX-TEZ-IVA. Consistent with input from the participating drug programs, the clinical experts noted that a lack of alignment across CDA-AMC recommendations for the reimbursement of ELX-TEZ-IVA in patients with and without 1 or more F508del mutations could pose implementation challenges in clinical practice.
Clinician Group Input
Three groups of clinicians responded to the call for input: CF Canada Accelerating Clinical Trials Network (CanACT), the Edmonton Adult Cystic Fibrosis Clinic and Calgary Adult Cystic Fibrosis Clinic, and the CF Canada Health Care Advisory Council. The input from the clinician groups and the consulted clinical experts identified the same unmet medical needs for patients with CF and potential place in therapy for the drug under review. The clinician groups noted that there is a significant treatment gap in CF care. Of patients with CF in Canada with rare mutations who do not carry a copy of the F508del CFTR mutation but may be responsive to ELX-TEZ-IVA, 10% (n = 246) do not have access to the drug as no clinical trials have been conducted. The CF Canada Health Care Advisory Council added that recipients of lung transplants, particularly those with significant sinus disease, may still benefit from CFTR-modulator therapy; however, they were excluded from the clinical trials.
According to the clinician groups, any patient who carries 1 or more CFTR mutations that is responsive to ELX-TEZ-IVA should have access to this therapy. CanACT added that, for those with rare CFTR mutations for which data to support the use of ELX-TEZ-IVA are limited, it is incumbent on regulators to use all available evidence or generate the evidence needed to allow access to this life-saving drug, as each patient’s life may depend on access to this medication.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review processes. The following were identified as key factors that could affect the implementation of a recommendation for ELX-TEZ-IVA:
potential challenges with implementation if different reimbursement criteria were recommended for patients with non-F508del CFTR mutations compared with the existing recommendations for patients who have 1 or more F508del mutations in the CFTR gene
potential challenges with identifying objective reimbursement criteria for patients aged less than 6 years.
The clinical experts consulted for this review provided advice on the potential implementation issues raised by the drug programs (as detailed in the Drug Program Input section).
Evidence Included in Submission
The current review is for an expanded indication that would include 152 additional non-F508del mutations in the CFTR gene. The sponsor categorized the additional CFTR mutations as follows: 147 FRT-responsive mutations; 4 noncanonical splice mutations; and the N1303K mutation. Evidence supporting the use of ELX-TEZ-IVA in the expanded population consisted of the following: 1 double-blind, placebo-controlled randomized controlled trial (RCT) in FRT-responsive patients (Study 124; N = 307; 18 CFTR mutations); 1 long-term extension study (Study 125; same population as Study 124); 1 retrospective observational study (Study 14; N = 422; 64 CFTR mutations); 4 nonrandomized studies involving patients with 1 or more N1303K mutations (Solomon et al. [2024],2 N = 20; Burgel et al. [2023],3 N = 8; Burgel et al. [2024],4 N = 35; Sadras et al. [2023],14-16 N = 8). The sponsor reports that there are no clinical data for 79 FRT-responsive mutations (i.e., those considered responsive to ELX-TEZ-IVA in the in vitro model) and 1 of the noncanonical splice mutations.
████ ██████████████ █████ ██████████ | ████████████████ ███████ | |||
|---|---|---|---|---|
█████ ███ █████ | ████ ███████ ██████ | ████ █████████ | ████████ █████ █ ███ | |
███ ██████████ █████████ █████████ ██ ████████ ████ ███ ██████████ | ||||
██████ ███████ ████ ██████ ██████ ██████ ██████ ██████ ██████ ██████ ██████ | ████████ | ████████ | ███ ████ | ███ ███████ |
█████ ███████ ██████ | ████████ | ████████ | ████████ | |
███████ █████ ██████ █████ | ███ ██████ | ████████ | ███ ████████ | |
██████ ██████ ██████ ██████ ██████ █████ █████ ████████ ███████ ██████ ██████ ██████ ██████ ██████ ███████ ███████ ███████ █████ ██████ ██████ ██████ ██████ ███████ ██████ █████ ██████ ██████ ████ █████ ██████ ██████ ██████ ██████ ██████ ██████ ███████ ██████ ██████ █████ ██████ ██████ ███████ █████ ██████ ███████ █████ | ███ ███████ | ████████ | ███ ████████ | |
█████ █████ █████ █████ █████ | ███ █████ | ███ ██████ | ████████ | |
█████████████ ██████ █████████ ███ | ||||
███████████████████ █████████ | ████████ | ████████ | ███ █████ | ████████ |
████████ | ███ █████ | ███ █████ | ███ ██████ | |
█████ █████████ ███ | ||||
██████ | ███ ██████ | ███ ██████ | ████████ | ████████ |
██████████████ █████████ ████ ██ █████████ ████████ ████ ██ ███████ ████ | ||||
█████████ ██████████ █████ ██████ ██████ ██████ ██████ ███████ ███████ ██████ ██████ ██████████████████ ██████ ██████ █████ █████ █████ ██████ ██████ ██████ █████████████ ██████ ███████ ███████ █████ ██████ ██████ ██████ ██████ ██████ ██████ ██████ ██████ ███████ ███████ ██████ ███████ ███████ ███████ ██████ ██████ ██████ ███████ ███████ █████ ██████ ██████ ███████ ███████ ██████ ██████ ██████ ██████ ██████ ███████ ████████████ ███████████ ██████████████████ ██████ ██████ ██████ ██████ ███████ ███████ █████ ██████ ██████ ███████ ███████ ███████ ██████ ██████ ███████ ███████ ██████ ███████ ██████ ██████ █████
In Vitro Evidence
Overview of In Vitro Fischer Rat Thyroid Assay
The sponsor used an in vitro FRT-cell model to characterize individual CFTR mutations that produce at least some amount of full-length CFTR protein, for responsiveness to CFTR modulators. The model expresses a CFTR protein with a single mutation to test for responsiveness to CFTR modulators. Each FRT-cell line is engineered to express proteins with a specific CFTR mutation in a stable, epithelial-cell background. CFTR mutations selected for inclusion in the FRT assay study were those that were expected to produce full-length CFTR proteins. Protein-truncating CFTR mutations, whole or partial CFTR gene deletions, and noncanonical splice mutations were excluded from the in vitro study. Positive controls and negative controls were also included in the experiments.
The positive controls included G551D and R117H mutations that were IVA-responsive in previous FRT assays and have been demonstrated in clinical trials to provide clinical benefit for patients. (IVA is approved for use in the treatment of CF in patients who have a G551D and R117H CFTR mutation.)
The negative controls included G1061R, R1066C, N1303K mutations and untransfected FRT cells. These 3 CFTR mutations were identified as being nonresponsive to IVA or tezacaftor-ivacaftor plus ivacaftor (TEZ-IVA) in previous in vitro studies.
The function of CFTR at the cell surface was assessed in Ussing chamber studies, a procedure that quantifies the amount of CFTR-mediated chloride ion (Cl−) transport in FRT cells expressing each CFTR mutation as a fraction of the Cl− transport in FRT cells expressing normal CFTR (% normal).
Definition of In Vitro Responsive to ELX-TEZ-IVA
Responsive CFTR mutations were those that demonstrated an increase of 10% in Cl− transport over baseline when expressed as a percentage of normal CFTR Cl− transport. The sponsor selected this threshold because the analyses of CFTR activity and disease phenotype showed that a 10% increase in CFTR activity is associated with improved clinical status. The sponsor reported that patients with a severe CF phenotype generally have a CFTR function of less than 5% of normal, whereas the severity of CF begins to diminish in patients who have a CFTR function of 10% or more of normal. An increase in CFTR function of 10% or more is therefore expected to affect the disease phenotype for those living with CF.5
CFTR Mutations Identified as Responsive to ELX-TEZ-IVA
Using the in vitro FRT model, the sponsor identified 177 CFTR mutations as responsive to ELX-TEZ-IVA. These additional mutations do not include F508del, which has been studied in multiple clinical trials already reviewed by CDEC. Importantly, the sponsor notes that the 10% threshold should be considered conservative, citing the following additional mutations that have been included in this reimbursement review application:
The N1303K mutation did not meet the 10% threshold to be considered responsive to ELX-TEZ-IVA in the FRT model. (This mutation was chosen as 1 of the negative controls for the FRT model.) However, the sponsor has filed submissions with Health Canada and CDA-AMC citing real-world evidence that suggest these patients benefit from treatment with ELX-TEZ-IVA.
The R117C and S1255P mutations included in this reimbursement review application did not meet the 10% threshold in the FRT assay; however, previous in vitro FRT data and/or clinical data support the responsiveness of these mutations to IVA and/or TEZ-IVA (both of which are components of ELX-TEZ-IVA).
Regulatory Perspective
Health Canada considered the evidence derived from the FRT-cell model sufficient to warrant expanding the indication for ELX-TEZ-IVA to 152 additional mutations sought by the sponsor. The sponsor’s application was filed on a pre–Notice of Compliance basis and included an additional 31 CFTR mutations that were not approved by Health Canada for the following reasons:
Fifteen mutations were considered by Health Canada as not causative of CF, based on the CFTR2 and CFTR-France databases: D836Y, F508C, G576A, I148T, I807M, I1027T, L320V, L997F, R75Q, R170H, R668C, R1162L, T1053I, V562I, and V754M.
Ten mutations were excluded because of unknown clinical significance or were only reported as causing a CFTR-related disease (i.e., not CF), and which retain at least 50% of normal Cl− transport function: G178E, G576A;R668C, I1139V, K1060T, R31L, R553Q, R751L, R792G, V1293G, Y1014C.
Five mutations were excluded because they result in a cryptic splice mutation and insufficient full-length CFTR: H939R, I175V, M152V, E403D, and S589N.
One mutation was excluded because of the absence of in vitro or clinical data provided in the current submission: E831X.
Health Canada concluded that the CFTR mutations for which the sponsor has provided sufficient clinical evidence of efficacy are also among those more commonly harboured by patients with CF in Canada. As such, the requested indication for ELX-TEZ-IVA would be expected to significantly expand access to effective CF therapy in Canada. Health Canada noted that the inclusion of other CFTR variants to the product monograph as being responsive to ELX-TEZ-IVA treatment is based mainly on biological plausibility. In cases where the mutation is known to have the potential to cause CF because of the production of a dysfunctional full-length CFTR variant that has demonstrated in vitro responsiveness to ELX-TEZ-IVA (i.e., FRT-responsive mutations), or when a reduced amount of CFTR is produced and its function can be augmented (i.e., splicing mutations), ELX-TEZ-IVA treatment has the potential to provide clinically meaningful benefit to patients.
Clinical Expert Commentary on In Vitro Evidence
The clinical experts consulted for this review noted that responsiveness to ELX-TEZ-IVA using the in vitro model applied by Vertex in the clinical development program for patients with rare CFTR mutations is sufficient evidence to support prescribing it to these patients. In addition to regulatory approval (e.g., from the FDA) and based on this information, the clinical experts cited the following considerations that would support the use of ELX-TEZ-IVA in clinical practice:
Alternative treatment options are lacking for patients with a severe and progressive case of CF.
In vitro data demonstrating activity on the CFTR channel for patients with these rare mutations support extrapolation of the clinical benefit demonstrated in studies involving more common CF-causing mutations in the CFTR gene.
Concerns exist about equity for those living with CFTR mutations the incidence of which is sufficiently low to preclude the generation of robust clinical evidence. The clinical experts noted CF with a non-F508del mutation is more likely to be diagnosed in racial minorities who may already be encountering systemic disadvantages within the health care system. Based on the rarity of these “rarer” mutations, it would be impossible to include participants with each mutation in clinical trials. The current focus on clinical trial data alone for drug approval is resulting in ethnic and racial inequity in medication access. It is well known that patients from minority groups are underrepresented in clinical trials for a multitude of reasons (the accompanying Ethics Review Report discusses these issues in detail).
A mounting body of evidence from case reports, case series, and clinical experience indicates that ELX-TEZ-IVA can have a clinically meaningful impact on patients with rare CFTR mutations that in vitro data show are responsive to the drug combination.
In addition, the clinical experts noted that patients with CF in Canada are monitored in specialized clinics with well-organized and frequent clinical and laboratory evaluations to ensure treatment is used appropriately and safely in clinical practice. The clinical specialists emphasized that the in vitro data should not be viewed in insolation and that it is important to consider the large body of evidence demonstrating the clear and clinically important benefits of ELX-TEZ-IVA and the relatively few serious harms with the treatment (i.e., this is no longer a new drug in the management of CF). The specialists noted that the totality of information, including real-world experience with the drug for those with 1 or more F508del mutations, supports the expanded use of the drug for those with rare CFTR mutations.
Clinical Evidence
Systematic Review
Description of Studies
Evidence supporting the use of ELX-TEZ-IVA in the expanded population consisted of the following: 1 double-blind, placebo-controlled RCT in patients with FRT-responsive mutations (Study 124; N = 307; 17 Health Canada–approved CFTR mutations); 1 long-term extension study (Study 125; same population as Study 124); 1 retrospective observational study (Study 16; N = 422; 64 Health Canada–approved CFTR mutations); 4 nonrandomized studies involving patients with 1 or more N1303K mutations (Solomon et al. [2024],2 N = 20; Burgel et al. [2023],3 N = 8; Burgel et al. [2024],4 and N = 35; Sadras et al. [2023],14-16 N = 8). The sponsor reports that there are no clinical data for 79 FRT-responsive mutations approved by Health Canada (i.e., those that were considered responsive to ELX-TEZ-IVA in the in vitro model) and 1 of the noncanonical splice mutations.
The objective of Study 124 was to evaluate the efficacy, pharmacodynamics, and safety of ELX-TEZ-IVA in patients with a non-F508del ELX-TEZ-IVA–responsive CFTR mutation. This study was a phase III, double-blinded, randomized, placebo-controlled trial. Patients aged 6 years of age and older were recruited from 84 sites across Europe and Canada and randomized, with 205 patients enrolled in the ELX-TEZ-IVA treatment arm and 102 participants enrolled in the placebo-controlled arm.
Eligible participants included those with a non-F508del ELX-TEZ-IVA–responsive CFTR mutation based on the FRT assay with no exclusionary CFTR mutations (i.e., F508del, S549N, G551S, S1255P, R117H, S549R, G1244E, G1349D, G178R, G551D, and S1251N). The sponsor reported that 18 of the most prevalent CFTR mutations in Europe and Canada that are not currently indicated for a CFTR modulator were eligible (representing approximately 80% of the target patient population). The use of ELX-TEZ-IVA was approved by Health Canada for 17 of the 18 CFTR mutations included in Study 124 (1 mutation [L997F] was excluded by Health Canada on the basis that it has not been demonstrated to cause CF). Patients had to have a percent predicted forced expiratory volume in 1 second (ppFEV1) of 40% or greater, but no more than 100% of the predicted mean for age, sex, and height. Patients were excluded if they had an acute upper or lower respiratory infection, pulmonary exacerbation (PEx), change in therapy (including antibiotics) for sinopulmonary disease within 28 days before the first dose of the study drug, or lung infection with organisms associated with a more rapid decline in pulmonary status (including, but not limited to, Burkholderia cenocepacia, Burkholderia dolosa, and Mycobacterium abscessus).
ELX-TEZ-IVA was orally administered as fixed-dose combination tablets in the morning along with oral administration of IVA tablets in the evening. Placebo-arm treatments were matched to both ELX-TEZ-IVA and IVA administrations in dose and timing.
The primary end point was change from baseline in ppFEV1 through 24 weeks. Secondary end points included absolute change from baseline in SwCl (through 24 weeks), Cystic Fibrosis Questionnaire–Revised (respiratory domain) (CFQ-R [RD]) score (through 24 weeks), body mass index (BMI) and BMI z score (at 24 weeks), and body weight and body weight z score (at 24 weeks). The number of PEx events was also a secondary end point in Study 124.
Efficacy Results
Treatment with ELX-TEZ-IVA resulted in a statistically significant improvement in ppFEV1 compared with placebo through 24 weeks (least squares [LS] mean difference = 9.2%; 95% confidence interval [CI], 7.2 to 11.3; P < 0.0001). A reduction from baseline was observed at all postbaseline assessments (i.e., 2, 4, 8, 16, and 24 weeks).
Those in the ELX-TEZ-IVA group also demonstrated statistically significant improvement in CFQ-R (RD) scores compared with those in the placebo group (LS mean difference = 19.5 points; 95% CI, 15.5 to 23.5; P < 0.0001). This difference exceeded the minimally important difference (MID) for the CFQ-R (RD), which is typically cited as 4.0 points.
Patients in the ELX-TEZ-IVA group experienced an estimated 0.17 PEx events per year compared with 0.63 in the placebo group (rate ratio = 0.28; 95% CI, 0.15 to 0.51; P < 0.0001). Compared with placebo, treatment with ELX-TEZ-IVA also demonstrated statistically significant reductions in SwCl through 24 weeks (LS mean difference = −28.3 mmol/L; 95% CI, −32.1 to −24.5; P < 0.0001), increases in body weight at 24 weeks (LS mean difference = 1.3 kg; 95% CI, 0.6 to 1.9; P < 0.0001), and increases in BMI at 24 weeks (LS mean difference = 0.47 kg/m2; 95% CI, 0.24 to 0.69; P < 0.0001). In patients aged less than 20 years, there was no statistically significant difference between ELX-TEZ-IVA and placebo for the absolute change from baseline in body weight z score (LS mean difference = 0.06; 95% CI, −0.06 to 0.18) or BMI z score (LS mean difference = 0.08, 95% CI, −0.06 to 0.22).
Harms Results
The proportions of patients who experienced at least 1 AE were 94.1% in the ELX-TEZ-IVA group and 95.1% in the placebo group. The majority of adverse events (AEs) were mild or moderate in severity. Serious adverse events (SAEs) occurred in 18 patients (8.8%) in the ELX-TEZ-IVA group and 15 patients (14.7%) in the placebo group. SAEs that occurred in 2 or more patients in the ELX-TEZ-IVA group included infective PEx of CF (5 patients) and bronchopulmonary aspergillosis allergic (2 patients). The only SAE that occurred in 2 or more patients in the placebo group was infective PEx of CF (13 patients). Drug interruptions because of AEs were reported in 12.2% patients in the ELX-TEZ-IVA group and 1.0% in the placebo group.
Elevated transaminase was considered an adverse event of special interest (AESI) and occurred in | ██████ patients in the ELX-TEZ-IVA group and ██ patients in the placebo group. All elevated-transaminase events were mild or moderate in severity, and none were serious. Rash events, which were also considered AESIs, occurred in 55 patients (26.8%) in the ELX-TEZ-IVA group and 3 patients (2.9%) in the placebo group. The majority of rash events were mild or moderate in severity. One patient (0.5%) in the ELX-TEZ-IVA group had a serious rash event that was considered related to study drug treatment. Health Canada reviewers noted that long-term safety has already been established for ELX-TEZ-IVA and no data from the pivotal clinical study indicate the existence of CFTR genotype–dependent safety concerns.
Critical Appraisal
Baseline and demographic characteristics were generally well balanced across the ELX-TEZ-IVA and placebo groups in Study 124. Both study treatments (ELX-TEZ-IVA and placebo) were administered in a double-blind manner. The AE profile of ELX-TEZ-IVA was unlikely to compromise blinding in the study, except in patients who experienced a rash (a well-known AE associated with ELX-TEZ-IVA treatment) after initiating treatment (22% in the ELX-TEZ-IVA versus 1% in the placebo group). Patient disposition was thoroughly documented and well reported by the sponsor. Few patients discontinued the trials (the completion rate was 96.1% for ELX-TEZ-IVA and 100% for placebo). Adherence to study treatments was reported to be greater than 98.9%.
Study 124 evaluated the impact of ELX-TEZ-IVA on a range of different outcomes that are important in the management of CF. These included respiratory function (i.e., ppFEV1), nutritional status and growth (e.g., weight and BMI), health-related quality of life (Cystic Fibrosis Questionnaire–Revised [CFQ-R]), and clinical events (e.g., pulmonary exacerbations). As noted in the input from clinician groups, the end points in the clinical trials largely align with those that are evaluated in routine clinical practice. Spirometry measurements were standardized and performed according to American Thoracic Society guidelines (e.g., prebronchodilator and before dosing). There are no globally accepted definitions for PEx events in patients with CF. The definitions used in Study 124 were considered appropriate by regulatory authorities and the clinical experts consulted for this review. The key secondary end points were tested using a hierarchical approach to control the overall type I error rate at 0.05.
The diagnostic criteria used in the screening process for Study 124 were consistent with Canadian clinical practice for identifying patients with CF. The sponsor and clinical experts consulted for this review reported that all patients with CF in Canada have their genotype evaluated, and therefore identifying members of the expanded patient population would not be problematic in practice. As with previous CFTR-modulator studies, Study 124 excluded patients with a history of colonization with B. cenocepacia, B. dolosa, and/or M. abscessus. CDA-AMC committees have previously acknowledged the unmet need for these patients.
The use of placebo as the comparator in Study 124 is appropriate given CFTR modulators are not approved for the target patient population except for the subset of patients who have a CFTR gating mutation and are currently eligible for treatment with IVA. Study 124 investigated the use of ELX-TEZ-IVA at the dosage recommended in the Canadian product monograph. All studies compared the addition of the study treatments to ongoing standard CF-management therapies, which is reflective of how ELX-TEZ-IVA and other CFTR modulators would be administered in clinical practice. In general, the background therapies that were reported at baseline in the included studies were consistent with those used in Canadian clinical practice.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
Table 3: Summary of Findings for ELX-TEZ-IVA Versus Placebo From RCT
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | ELX-TEZ-IVA | Difference | |||||
Pulmonary function | |||||||
Absolute mean change from baseline in ppFEV1 Follow-up: 24 weeks | 290 (1 RCT) | NA | −0.4% (−2.0% to 1.3%) | 8.9% (7.7% to 10.0%) | 9.2% higher (7.2% to 11.3% higher) | Higha | ELX-TEZ-IVA results in an improvement in ppFEV1 compared with placebo |
Pulmonary exacerbations | |||||||
Annualized event rate of PEx Follow-up: 24 weeks | 307 (1 RCT) | Rate ratio: 0.28 (0.15 to 0.51) | 0.63 events per year (95% CI, NR) | 0.17 events per year (95% CI, NR) | Absolute effects not reported by sponsor | Cannot evaluateb | ELX-TEZ-IVA likely results in an improvement in frequency of PEx compared with placebo |
BMI | |||||||
Absolute mean change from baseline in BMI Follow-up: 24 weeks | 307 (1 RCT) | NA | 0.35 kg/m2 (0.16 to 0.53) | 0.81 kg/m2 (0.68 to 0.94) | 0.47 kg/m2 higher (0.24 to 0.69 higher) | Highc | ELX-TEZ-IVA results in an improvement in BMI compared with placebo |
Absolute mean change from baseline in BMI z score Follow-up: 24 weeks | 78 (1 RCT) | NA | 0.14 (0.03 to 0.25) | 0.22 (0.14 to 0.30) | 0.08 higher (−0.06 to 0.22) | Moderated | ELX-TEZ-IVA likely results in an improvement in BMI z score compared with placebo |
Health-related quality of life | |||||||
Absolute mean change from baseline in CFQ-R (RD) Follow-up: 24 weeks | 304 (1 RCT) | NA | −2.0 points (−5.2 to 1.3) | 17.5 points (15.2 to 19.8) | 19.5 points higher (15.5 to 23.5) | Highe | ELX-TEZ-IVA results in an improvement in CFQ-R (RD) compared with placebo |
Sweat chloride | |||||||
Absolute mean change from baseline in SwCl Follow-up: 24 weeks | 300 (1 RCT) | NA | 0.5 mmol/L (−2.6 to 3.6) | −27.8 mmol/L (−30.0 to −25.6) | −28.3 mmol/L lower (−32.1 to −24.5) | Moderatef | ELX-TEZ-IVA results in a reduction in SwCl compared with placebo |
Harms | |||||||
Elevated transaminase levels | 307 (1 RCT) | NA | | █████ | | █████ | NA | Moderateg | ELX-TEZ-IVA may increase in frequency of elevated transaminases compared with placeboh |
Rash | 307 (1 RCT) | NA | 3 (2.9%) | 55 (26.8%) | NA | Moderateg | ELX-TEZ-IVA may increase in the frequency of rash compared with placeboi |
BMI = body mass index; CF = cystic fibrosis; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised (respiratory domain); CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; MID = minimally important difference; NA = not applicable; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; SwCl = sweat chloride.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aWhile no published information on the MID in absolute change in ppFEV1 in CF was identified, the clinical experts consulted for this review noted that CF specialists would generally consider an absolute improvement in ppFEV1 of at least 5% to be clinically relevant.
bCertainty of evidence cannot be evaluated as the sponsor did not report the absolute difference between groups and did not provide this information upon request. While no published information on the MID for reducing PEx in CF was identified, the clinical experts consulted for this review noted that CF specialists would generally consider the reduction in PEx observed in the study to be clinically relevant.
cWhile no published information on the MID for absolute change in BMI in CF was identified, the clinical experts consulted for this review noted that CF specialists would generally consider the improvements observed in the study to be clinically relevant.
dRated down 1 level for imprecision because of the smaller sample size and wide CIs.
eA difference of at least 4 points in the respiratory domain score of the CFQ-R is commonly cited as the MID for patients with CF.
fRated down 1 level for indirectness because SwCl is a biomarker, and evidence for a relationship between SwCl and clinical outcomes is uncertain.
gBetween-group differences in harms were not statistically tested.
hThe product monograph provides recommendations for baseline assessment and ongoing monitoring of alanine transaminase and aspartate transaminase. The clinical experts consulted for this review noted that these recommendations for monitoring are typically followed in clinical practice and that patients in Canada are monitored in specialized clinics.
iStudy 124 found that discontinuations because of rash were uncommon, and the clinical experts consulted for the review similarly noted that these events do not typically result in long-term discontinuation of the treatment.
Source: Sponsor’s Summary of Clinical Evidence.
Long-Term Extension Studies
Description of Studies
Study 125 is an open-label long-term extension phase of Study 124 conducted to assess the long-term safety and efficacy of ELX-TEZ-IVA in patients with CF aged 6 years and older with non-F508del mutations in the CFTR gene that are responsive based on clinical and/or in vitro data. The data cut-off date in the submission to CDA-AMC is August 28, 2023, with results reported for the 4 weeks after the end of Study 124. Of the patients who were randomized to placebo in the parent study, 15 had been treated with ELX-TEZ-IVA for a total of 4 weeks, and those who were randomized to ELX-TEZ-IVA in Study 124 had been treated for 28 weeks.
Efficacy Results
Those who switched from placebo to ELX-TEZ-IVA demonstrated improvements in ppFEV1 (mean change = 7.1 percentage points; standard deviation [SD] = 7.3), SwCl (mean change = −27.4 mmol/L; SD = 18.9), and CFQ-R (RD) (mean change = 14.7 points; SD = 22.6) after receiving ELX-TEZ-IVA for 4 weeks. For those who received ELX-TEZ-IVA in the parent study, improvements in ppFEV1 (mean change = 10.1 percentage points; SD = 11.0), SwCl (mean change = −30.3 mmol/L; SD = 21.9), and CFQ-R RD (mean change = 20.1 points; SD = 20.7) were maintained after 4 additional weeks.
Harms Results
Harms data were not yet reported for Study 125.
Critical Appraisal
Study 125 is an ongoing, uncontrolled, open-label trial that enrolled patients who had completed Study 124. As this was an unblinded extension phase, patient’s expectations of treatment could influence the reporting of subjective outcomes, such as respiratory symptoms (as measured by the CFQ-R), or harms. Extension studies are often limited by selection bias, as only patients who are tolerant to treatment and complete the parent studies are eligible to enrol. For Study 125 and other ELX-TEZ-IVA studies, the risk of selection bias is generally low, given that nearly all patients from the primary study enrol in the extension study. Overall, there are limited data from the extension phase, as only 4 weeks of additional data were available. Issues with the generalizability of these data are the same as for Study 124 (e.g., a patient population reflective of those with mild to moderate disease, exclusion of patients with unstable disease or colonization with B. cepacia complex, and increased exposure to health care professionals).
Indirect Comparisons
The sponsor reported that an indirect treatment comparison (ITC) is not required for approximately 80% of the patients in the target patient population because no CFTR modulators are currently approved for use in these patients. The remaining 20% of patients in the target patient population could be eligible for treatment with IVA monotherapy. The sponsor conducted a feasibility assessment to determine whether an ITC could inform the comparative clinical benefits of ELX-TEZ-IVA versus IVA monotherapy. The sponsor concluded it was not feasible to conduct a robust ITC because of uncertainty in the degree of population overlap, low individual-patient-data sample sizes, incompatibility of outcomes, and different treatment histories and follow-up times.
The review team has no concerns regarding the absence of an ITC for the following reasons:
The dosage of ivacaftor administered as part of the ELX-TEZ-IVA combination regimen is the same as what patients would receive with IVA monotherapy (e.g., 150 mg in the morning and 150 mg in the evening).
Previous trials have demonstrated that patients with 1 or more F508del mutations and a gating mutation benefited from switching to ELX-TEZ-IVA from IVA monotherapy.
The submitted price for ELX-TEZ-IVA is the same as the current list price for IVA monotherapy.
Studies Addressing Gaps in the Evidence from the Systematic Review
Clinical evidence from 5 additional studies addressing gaps in evidence were included in the review:
1 study involving patients with 64 FRT-responsive CFTR mutations (Study 16 [N = 422])6
4 studies involving patients with 1 or more N1303K mutations (Solomon et al. [2024],2 N = 20); Burgel et al. [2023],3 N = 8) Burgel et al. [2024],4 N = 35); and Sadras et al. [2023],14-16 N = 8).
The sponsor included evidence from 3 additional abstracts and/or publications for patients with 1 or more N1303K mutations (Dreano et al. [2023],7 Livnat et al. [2023],8 and Pranke et al. [2022]9). These studies are not summarized in this report as the review team concluded that they do not address a gap in the evidence relative to the larger studies submitted in support of the expanded use of ELX-TEZ-IVA for patients with CF who have 1 or more N1303K mutations in the CFTR gene. In addition to the smaller sample sizes, the following additional concerns were noted: the reporting of these studies is insufficient for the review team to fully appraise the methodology used in the evaluation of patients; the publications by Dreano et al. (2023) and Pranke et al. (2022) refer to the same source of patients that was used in the larger studies reported by Burgel (2023) (N = 8) and Burgel et al. (2024) (N = 34). The sponsor was unable to confirm if there is overlap between the patient populations in these studies and the review team notes that these analyses were not included in the submission to Health Canada.
FRT-Responsive CFTR Mutations
Description of Study
Study 16 was a retrospective, observational, cohort study evaluating real-world clinical outcomes in patients with CF with non-F508del mutations that are responsive to ELX-TEZ-IVA. Data were sourced from the US Cystic Fibrosis Foundation Patients Registry (CFFPR). Index dates for patients were defined as the date of ELX-TEZ-IVA treatment initiation ranging from October 21, 2019, to December 1, 2022. Data from patients were evaluated for up to 2 years before the index date through December 31, 2022 (the follow-up period), or until loss to follow-up, death, treatment discontinuation, or lung transplant, whichever was earlier. The objective of Study 16 was to supplement Study 124 with respect to a further 64 mutations with data on the effectiveness of ELX-TEZ-IVA on lung function, PEx, and nutritional parameters in a real-world setting of patients with CF in the target population using data from the CFFPR patient registry.
Patients aged at least 6 years were included in the analysis if they had data recorded in the CFFPR; a select ELX-TEZ-IVA–responsive non-F508del CFTR genotype; received treatment with ELX-TEZ-IVA during the patient-accrual period; at least 1 ppFEV1 measurement in the 12 months before the index date; and at least 1 ppFEV1 measurement taken at least 4 weeks after the index date. Patients were excluded if they had received a lung transplant before the index date.
Efficacy Results
Change from baseline in ppFEV1 was the primary end point of Study 16. The overall patient population demonstrated a mean change from baseline of 4.53% (95% CI, 3.50 to 5.56). Study 16 included patients with and without prior exposure to a CFTR modulator (55.5% and 44.1%, respectively). The sponsor-reported subgroup analyses, which were based on prior CFTR-modulator exposure, found that the mean changes from baseline with ELX-TEZ-IVA were 6.11 (95% CI, 4.40 to 7.81) for those who were CFTR modulator–naive and 3.3% (95% CI, 2.06 to 4.58) for those who had prior exposure to a CFTR modulator.10
Change from baseline in BMI and body weight were secondary end points. The sponsor reported an increase from baseline in BMI and body weight after ELX-TEZ-IVA initiation (mean change = 0.65 kg/m2; 95% CI, 0.41 to 0.89; and 2.91 kg; 95% CI, 2.24 to 3.58, respectively) compared to baseline. Mean change from baseline in z scores for BMI and body weight were −0.05 (SD = 0.53) and −0.04 (SD = 0.48), respectively.
The number of PEx events and the annualized PEx rate were also assessed. The results suggest the PEx rate decreased by 53% (95% CI, 42% to 62%) after ELX-TEZ-IVA initiation. The annualized PEx rates were 0.43 in the pre-initiation period and 0.20 in the follow-up period.10
Harms Results
Adverse events were not investigated in Study 16.
Critical Appraisal
Study 16 was a retrospective observational study with no comparator treatment group. Given the real-world treatment setting, there was no blinded administration of ELX-TEZ-IVA (i.e., investigators, patients, and caregivers were aware of the treatment). Limitations common to observational studies apply to these data, including potential variability in timing of assessments for patients; no standardized definition for pulmonary exacerbations; variation in the duration of therapy; lack of information regarding adherence to ELX-TEZ-IVA during the treatment period; and the potential for missing data in the registry database. The index dates for patients spanned October 21, 2019, to December 1, 2022. This overlapped with the COVID-19 pandemic, which had a considerable impact on the baseline PEx rate for patients with CF. Because of isolation measures, the risk of pulmonary exacerbations was reduced during the pandemic period (from 0.70 to 0.31 events per year) making it challenging to interpret the overall pretreatment baseline rate (0.43 events per year) and the posttreatment rate of exacerbations (0.20 events per year). Overall, the number of patients with each of the individual mutations was variable and generally small across the population. The sponsor emphasized that, given the variability of the real-world data and the interpretability of data from small strata (e.g., mutation-level data), these analyses should be viewed with caution.
Patients evaluated in Study 16 were identified from the CFFPR. The clinical specialists consulted by the review team noted that baseline characteristics of patients with CF in the US are generally similar to those living in Canada and that the results would be considered generalizable to the target population in Canada. Study 16 included patients with and without prior exposure to a CFTR modulator. Given that treatment with a CFTR modulator is expected to improve the end points evaluated in clinical trials (e.g., baseline lung function, BMI, and SwCl), this prior exposure could bias the overall effective size reported for the study against ELX-TEZ-IVA for the target population in Canada (the majority of whom are expected to be CFTR-naive, except for those who have received IVA monotherapy). The sponsor reported results for patients with and without prior exposure to a CFTR modulator.
Health Canada reviewers noted that the differences between the mean and median change from baseline in ppFEV1 indicates that a few good responders may have skewed the average in favour of treatment (i.e., the mean change from baseline was 4.53 [SD = 9.84] and median change from baseline was 2.76 [range = −31.67 to 59.19]); however, definitive conclusions cannot be drawn because of variability in the timing of the baseline and posttreatment initiation spirometry tests. Health Canada concluded that data from Study 16 do not provide significant clinical evidence for ELX-TEZ-IVA responsiveness beyond providing some support for the efficacy of a few mutations, with sufficient evidence of efficacy already provided in Study 124.
N1303K CFTR Mutation
Description of Studies
This Clinical Review included 4 nonrandomized studies that investigated the use of ELX-TEZ-IVA in patients with 1 or more N1031K mutations in the CFTR gene. All of the studies were investigator-initiated (i.e., not sponsored by Vertex Pharmaceuticals).
Solomon et al. (2023)11,12 reported the results of a prospective, open-label trial assessing patients with 1 or more N1303K mutations (N = 20). Patients were treated with ELX-TEZ-IVA for 4 weeks. End points included change from baseline in ppFEV1, SwCl, CFQ-R scores, and body weight.
Burgel et al. (2024)4 reported the results of ELX-TEZ-IVA in patients with 1 or more N1303K mutations who received the treatment as part of a compassionate use program in France. The results were based on a retrospective observational cohort, pooled analyses from cohort studies, case reports, and unpublished data. The patients who received the treatment all had advanced lung disease (e.g., a ppFEV1 < 40%). The observational period ranged from 4 weeks to 8 weeks.
Burgel et al. (2023),3,13 similar to Burgel et al. (2024),4 this study investigated the use of ELX-TEZ-IVA in patients with 1 or more N1303K mutations who received the treatment as part of a compassionate use program in France. The study was a prospective observational cohort study with a treatment period of 4 to 6 weeks.
Sadras et al. (2023)14-16 was an observational prospective analysis from a multicentre registry in Israel investigating the use of ELX-TEZ-IVA in patients with CF who have 1 or more N1303K mutations in the CFTR gene. Patients were included if they had CF and carried 1 or more N1303K mutations on 1 allele and a nonsense or frameshift mutation on the other allele (i.e., a mutation that would not be expected to respond to ELX-TEZ-IVA for a period of 8 weeks). Efficacy end points included change from baseline in ppFEV1, SwCl, body weight, and the lung clearance index.
Efficacy Results
Key efficacy results from the nonrandomized studies for patients with 1 or more N1303K mutations in the CFTR gene are summarized in Table 4.
Solomon et al. (2023): After 4 weeks of treatment with ELX-TEZ-IVA, patients demonstrated statistically significant improvements from baseline in ppFEV1 (mean change = 9.5%; 95% CI, 6.7 to 12.3; P < 0.001), BMI (mean change = 0.4 kg/m2; 95% CI, 0.2 to 0.7; P = 0.002), and CFQ-R (RD) (mean change = 20.8; 95% CI, 11.9 to 29.8; P < 0.001). There was no statistically significant difference in change from baseline in SwCl (−1.1 mmol/L; 95% CI, −5.3 to 3.1; P = 0.61).11,12
Burgel et al. (2024): After 4 to 8 weeks of treatment with ELX-TEZ-IVA, patients demonstrated a statistically significant improvement in ppFEV1 from baseline (median change = 17.0%; interquartile range [IQR] = 10.0 to 25.0; P < 0.0001). Median body weight increased by 2.0 kg (IQR = 1.0 to 3.5) and median SwCl was reduced by −9.0 mmol/L (IQR = 3.5 to 21).4
Burgel et al. (2023): The authors reported that all patients with 1 or more N1303K mutations (N = 8) were considered ELX-TEZ-IVA responders. After 4 to 8 weeks of treatment with ELX-TEZ-IVA, the median change in ppFEV1 was 27.5% (IQR = 20.7% to 41.2%) and the median change in SwCl was –9 mmol/L (IQR = −5 to −36).3,13
Sadras et al. (2023): After 8 weeks of treatment, patients treated with ELX-TEZ-IVA demonstrated statistically significant improvements from baseline in ppFEV1 (mean change = 18.4; 95% CI, 12 to 24; P < 0.0001) and BMI (mean change = 0.79 kg/m2; 95% CI, 0.51 to 1.07; P < 0.0001). There was no statistically significant difference in change from baseline in SwCl (mean change = −7 mmol/L; 95% CI, not reported; P < 0.054).14-16
Harms Results
Adverse events were not investigated and/or reported in the studies by Solomon et al. (2023),11,12 Burgel et al. (2024),4 Burgel et al. (2023),3,13 or Sadras et al. (2023).14-16
Critical Appraisal
Overall, the 4 observational studies provided descriptive data on the effects of ELX-TEZ-IVA in patients with CF with 1 or more N1303K mutations at various stages of lung disease. The short-term results showed acute increases in ppFEV1 and weights that were comparable to or exceeded those reported in the clinical trials for ELX-TEZ-IVA conducted in patients with other CFTR mutations; however, these results should be interpreted with caution because of the uncontrolled, observational study designs, and the small sample sizes (N ranged from 8 to 35). All of studies had a short duration of treatment and follow-up. As all of the studies were investigator-sponsored, the available information regarding studies methods and results is limited to publications and abstracts.
Table 4: Summary of Findings for ELX-TEZ-IVA From Nonrandomized Studies
Study | Design | Patient group | Absolute change in ppFEV1 | Absolute change in BMI or body weight | Absolute change in SwCl | Absolute change in CFQR-RD |
|---|---|---|---|---|---|---|
FRT-responsive mutations (64 mutations not studied in Study 124) | ||||||
Study 166 | Retrospective, observational, cohort study | Total (N = 422) | Mean change: 4.53 (95% CI, 3.50 to 5.56) | BMI mean change: 0.65 (95% CI, 0.41 to 0.89) | NA | NA |
CFTRm-naive (n = 186) | Mean change: 6.11% (95% CI, 4.40 to 7.81) | NA | NA | NA | ||
Prior CFTRm (n = 234) | Mean change: 3.32% (95% CI, 2.06 to 4.58) | NA | NA | NA | ||
N1303K mutation | ||||||
Duration: 4 weeks | Prospective, open-label trial | N1303K (n = 20) | Mean change: 9.5 (95% CI, 6.7 to 12.3) P < 0.001 | BMI mean change: 0.4 (95% CI, 0.2 to 0.7) P = 0.002 | Mean change: −1.1 (95% CI, −5.3 to 3.1) P = 0.61 | Mean change: 20.8 (95% CI, 11.9 to 29.8) P < 0.001 |
Burgel et al. (2024)4 Duration: 4 to 8 weeks | Retrospective observational cohort; pooled analyses from cohort studies, case reports, and unpublished data | N1303K (N = 35) | Median change: 17.0% (IQR = 10.0 to 25.0) P < 0.0001 (n = 34) | Weight median change: 2.0 kg (IQR = 1.0 to 3.5) (n = 24) | Median change: −9.0 mmol/L (IQR = −3.5 to −21) P < 0.001 (n = 33) | NA |
Duration: 8 weeks | Observational prospective analysis | N1303K (N = 8) | Mean change: 18.4 (95% CI, 12 to 24) P < 0.0001 | BMI mean change: 0.79 kg/m2 (95% CI, 0.51 to 1.07) P < 0.0001 | Mean change: −7 mmol/L (NR) P < 0.054 | NA |
Duration: 4 to 6 weeks | Prospective observational cohort study | N1303K (n = 8) | Median change: 27.5% (IQR = 20.7 to 41.2) | NA | Median change: −9 mmol/L (IQR = –5 to –36) | NA |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTRm = CFTR modulator; CI = confidence interval; IQR = interquartile range; NA = not applicable; SwCl = sweat chloride.
Conclusions
The current review is for an expanded indication that would include 152 additional non-F508del of in the CFTR gene. The sponsor has categorized the additional CFTR mutations as follows: 147 FRT-responsive mutations; 4 noncanonical splice mutations; and the N1303K mutation. Evidence supporting the use of ELX-TEZ-IVA in the expanded population consisted of the following: 1 double-blind, placebo-controlled RCT of FRT-responsive patients (Study 124; N = 307; 18 CFTR mutations); 1 long-term extension study (Study 125; same population as Study 124); 1 retrospective observational study (Study 16; N = 422; 64 CFTR mutations); 4 nonrandomized studies involving patients with 1 or more N1303K mutations (Solomon et al. [2024], N = 20; Burgel et al. [2023], N = 8; Burgel et al. [2024], N = 35; and Sadras et al. [2023], N = 8). Evidence for 79 of the additional mutations is exclusively from the in vitro FRT model.
For the clinical studies in FRT-responsive mutations, Studies 124 and 16 demonstrated that ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function (an increase in ppFEV1), nutritional status (an increase in BMI), health-related quality of life (an increase in CFQ-R [RD] scores), CF biomarkers (a reduction in SwCl), and a reduced rate of pulmonary exacerbations. For the clinical studies in patients with 1 or more N1303K mutations, the short-term results showed acute increases in ppFEV1 and weight that were suggestive of a clinically meaningful benefit with ELX-TEZ-IVA in these patients; however, the results cannot be considered conclusive of a clinically important effect because of the limitations of the open-label, noncomparative, observational study designs, with relatively the small sample sizes (N ranged from 8 to 35), short durations, limited reporting of important information, and several potential sources of bias and uncertainty. For all of the mutations for which clinical data were available, the clinical specialists consulted for this review considered the results to be clinically meaningful and indicative that ELX-TEZ-IVA would benefit patients in the target population. The experts emphasized that there is a high level of unmet need among these patients as they currently do not have access to CFTR-modulator therapy in Canada (outside of enrolment in a clinical study).
For the 79 mutations that have been assessed exclusively from the in vitro FRT model, the sponsor defined responsive CFTR mutations as those that resulted in an increase of 10% in Cl− transport over baseline when expressed as a percentage of normal CFTR Cl− transport. The sponsor’s selection of a threshold increase in CFTR function of 10% or more is therefore expected to affect the disease phenotype for those living with CF. The CF specialists consulted by the review team pointed out that prescribers in Canada are not concerned about the absence of clinical data for patients with rare CFTR mutations. They noted the practical challenges in conducting clinical trials for patients with rare CFTR mutations and emphasized that there are important concerns regarding equity of access to CFTR modulators. Health Canada considered the data derived from the FRT-cell model to be acceptable evidence to warrant expanding the indication for ELX-TEZ-IVA. Health Canada concluded that the CFTR mutations for which the sponsor has provided sufficient clinical evidence of efficacy are also among those more commonly harboured by patients with CF in Canada. As such, expanding the indication for ELX-TEZ-IVA would be expected to significantly broaden access to effective CF therapy in Canada. They noted that inclusion of other CFTR variants to the product monograph because they are responsive to ELX-TEZ-IVA treatment is based mainly on biological plausibility. When the mutation is known to have the potential to cause CF because of the production of a dysfunctional full-length CFTR variant that has demonstrated in vitro responsiveness to ELX-TEZ-IVA (i.e., FRT-responsive mutations), or when a reduced amount of CFTR is produced and its function can be augmented (i.e., splicing mutations), ELX-TEZ-IVA treatment has the potential to provide clinically meaningful benefits to patients.
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., those aged at least 2 years with at least 1 mutation that is responsive to ELX-TEZ-IVA based on clinical and/or in vitro data). There have been no updates to the warnings and precautions section of ELX-TEZ-IVA product monograph since the previous CDA-AMC reviews.
Introduction
The objective of this review was to evaluate the beneficial and harmful effects of ELX-TEZ-IVA at recommended dosages for the treatment of patients aged 2 years and older with CF and who have at least 1 non-F50del mutation in the CFTR gene that is responsive to ELX-TEZ-IVA based on clinical and/or in vitro data.
Disease Background
Contents within this section were informed by materials submitted by the sponsor and clinical expert input. The following summary was validated by the review team.
Cystic fibrosis, an autosomal recessive condition, is the most common fatal genetic disease affecting children and young adults in Canada. It is caused by mutations in the CFTR gene, which is located on chromosome 7. The CFTR gene encodes a chloride channel that regulates ion and fluid transport across cell membranes. When the CFTR protein is dysfunctional, secretions become tenacious and sticky, resulting in pathology in multiple organs, including the lungs, large and small intestines, pancreatic and bile ducts, and the vas deferens. A deletion of phenylalanine 508 in the first nucleotide-binding domain (F508del) is the most common mutation that results in CF.17 The CCFR reported that 4,338 patients in Canada were living with CF in 2021. Of these, 87.6% carried 1 or more F508del mutations.18
More than 2,090 CFTR mutations have been identified among patients with CF.17 The mutations are classified as impaired biosynthesis (class I), defective protein maturation and accelerated degradation (class II), defective regulation of CFTR at the plasma membrane (class III), defective chloride conductance (class IV), diminished CFTR transcription (class V), and accelerated turnover at the cell surface (class VI).19 CFTR mutations within classes I to III are associated with severe CF as they are considered nonfunctional, while mutations in classes IV to VI may retain CFTR function.19,20 Genotyping for mutations in the CFTR gene is performed routinely on almost all patients with CF in Canada and is also part of the newborn screening process.17
Based on CF registry data, the sponsor estimates that there were 573 patients with non-F508del mutations in Canada, of whom 163 were responsive to ELX-TEZ-IVA (excluding Québec). The total target population for the current review represents an estimated 5% of the total CF population in Canada. The percentage of patients in Canada with CF in each province based on the 2021 CF registry was used to stratify patients by province (Table 5).
Table 5: Number of Patients in the Target Patient Population by Region
Region | Estimated number of patientsa |
|---|---|
Pan-Canadian (excluding Québec) | 163 |
Alberta | 31 |
British Columbia | 22 |
Manitoba | 7 |
New Brunswick | 3 |
Newfoundland and Labrador | 4 |
Northwest Territories | NA |
Nova Scotia | 13 |
Nunavut | NA |
Ontario | 74 |
Prince Edward Island | 1 |
Saskatchewan | 6 |
Yukon | NA |
Noninsured Health Benefits | 2 |
NA = not applicable.
aThe total number of patients included in the target patient population in each province for 2024 is based on 2023 numbers and assumes 1 year of growth in the CF population.
Source: Sponsor’s Summary of Clinical Evidence.
Cystic fibrosis results in airway obstruction, chronic endobronchial infection, and inflammation, which ultimately lead to destruction of lung tissue through development of bronchiectasis and loss of lung function.21 Although chronic pulmonary therapies instituted early in the disease have reduced the decline in lung function over time, patients who are homozygous for the F508del mutation will develop chronic infection with Pseudomonas and progressive bronchiectasis and airway obstruction. In a cohort of approximately 1,000 healthy young children with CF who did not have Pseudomonas infection at enrolment, there was a greater annual decline in forced expiratory volume in 1 second (FEV1) over the following 4 years in those who were homozygous for the F508del mutation.22 Chronic endobronchial infection of the airways with bacterial pathogens, such as Pseudomonas aeruginosa (reported in 34.6% of patients with CF in Canada in 2021),18 is associated with a more rapid loss of lung function.23 Acute or chronic endobronchial infections result in further destruction of lung tissue and are associated with respiratory morbidity. Lung disease accounts for the vast majority (> 80%) of deaths in patients with CF.17,24
Pulmonary exacerbations are associated with lung-function decline and mortality and may require treatment with IV antibiotics and hospitalization. The Cystic Fibrosis Foundation has reported that approximately a third of patients with CF will have at least 1 PEx per year requiring IV antibiotics.25
Maintenance of pulmonary function (higher FEV1) and fewer respiratory exacerbations are associated with increased survival.26 Pulmonary management of CF therefore aims to clear the airways of secretions and treat lung pathogens to minimize inflammation.
Patients typically have pancreatic, gastrointestinal, and nutritional disease as well as progressive pulmonary damage. Gastrointestinal and pancreatic involvement results in pancreatic exocrine insufficiency in most individuals with CF, causing malabsorption of fats and fat-soluble vitamins, which leads to malnutrition. Maintaining adequate nutrition is associated with improved clinical outcomes and longevity for patients with CF.27 Virtually all of these people will be pancreatic-insufficient and will need to take lifelong pancreatic enzyme replacement with every meal as well as fat-soluble vitamin therapy. With increasing age, these patients will develop CF-related diabetes and require therapy with insulin. In 2021, CF-related diabetes was reported in 22.0% of patients in Canada with CF (32.6% of adults and 2.8% of children).18
The median age of survival in Canada for a child born with CF is estimated to be 57.3 years.18 The CCFR has reported in increase in the median age of death for patients with CF in Canada since the year 2000.17 The median age of death was 38.7 years in 2021, compared to 26.6 years in 2002.18 There is a clear unmet need for improved CF therapies (as described in the Patient Group Input and Clinician Input sections).
Standards of Therapy
Contents within this section were informed by materials submitted by the sponsor and clinical expert input. The following summary was validated by the review team.
The goals of CF therapy include preservation of lung function by minimizing pulmonary infection and inflammation; restoration of baseline pulmonary function, symptoms, and level of inflammation after acute respiratory exacerbations; and maintenance of adequate nutrition. The choice of a therapeutic regimen for CF depends on organ involvement. The severity of lung function impairment and the presence of bacterial pathogens are deterministic factors when selecting chronic pulmonary therapy.
Treatments that are approved and/or available can be broadly classified as: therapies used to manage symptoms, complications, and comorbidities of CF; and therapies that aim to correct the underlying defects of the CFTR protein, known as CFTR modulators.
Management of Symptoms, Complications and Comorbidities
Respiratory treatments consist of physiotherapy and pharmacologic drugs such as inhaled antibiotics (e.g., tobramycin, aztreonam, colistin), anti-inflammatory agents, or mucolytics (e.g., hypertonic saline and/or dornase alfa).28 Nutritional treatments consist of high-calorie and high-fat diets and pancreatic enzyme replacement for those with pancreatic insufficiency.24,28 PEx events are treated with oral or IV antibiotics.29 These treatments do not halt, but only slow, the decline in lung function and the progression of disease.
CFTR Modulators
The CFTR modulators that are currently marketed in Canada or other jurisdictions are classified as: potentiators, which function by increasing the channel-open probability of the CFTR protein at the cell surface (IVA is a CFTR potentiator); or correctors, which function by improving the conformational stability of F508del-CFTR proteins, resulting in an increased expression of the F508del-CFTR protein at the cell surface. Lumacaftor, TEZ, and ELX are CFTR correctors.
Table 9 provides a summary of the CFTR modulators currently marketed or under review in Canada, the CFTR mutations and age ranges for which they been approved by Health Canada, and the reimbursement status within the public drug programs. The currently available CFTR modulators are not approved for use in all patients with 1 or more F508del mutations. The approved indications currently cover those who are homozygous for F508del mutations (LUM-IVA and TEZ-IVA), heterozygous for the 508del mutation and who also have a residual function mutation (TEZ-IVA), or a non-F508del gating mutation (IVA).
Drug Under Review
Trikafta is a fixed-dose combination product containing ELX, TEZ, and IVA co-packaged with IVA. ELX-TEZ-IVA is available as both oral tablets and oral granules in the following dosage strengths:
Tablets for patients 6 years and older:
ELX 50 mg, TEZ 25 mg, and IVA 37.5 mg co-packaged with IVA 75 mg
ELX 100 mg, TEZ 50 mg, and IVA 75 mg co-packaged with IVA 150 mg.
Granules for patients aged 2 to less than 6 years:
ELX 100 mg, TEZ 50 m, and IVA 75 mg co-packaged with IVA 75 mg
ELX 80 mg, TEZ 40 mg, and IVA 60 mg co-packaged with IVA 59.5 mg.
Indication Under Review
The current review is for an expanded indication that would include 152 additional non-F508del mutations of the CFTR gene (Figure 1). The sponsor categorized the additional CFTR mutations as follows:
FRT-responsive mutations supported by clinical data (68 mutations)
FRT-responsive mutations with no available clinical data to support (79 mutations)
Noncanonical splice mutations (4 mutations): mutations that result in small amounts of functional, normal CFTR protein; the sponsor has reported that these mutations cannot be evaluated in the FRT system and provided some form of clinical data for each of the mutations included in the application
N1303K mutation: A CFTR mutation that was initially identified as nonresponsive to ELX-TEZ-IVA in an FRT in vitro study that has subsequently been studied in a phase II clinical trial as well an investigator-sponsored real-world evidence study.
Sponsor’s Requested Reimbursement Criteria
The sponsor has requested reimbursement in accordance with the Health Canada–approved indication.
Table 6: Reimbursement Criteria Requested by the Sponsor
Category | Sponsor-requested conditions |
|---|---|
Initiation criteria |
|
First renewal | At least 1 of the following must be demonstrated after 12 monthsa of treatment:
|
Subsequent renewals annually |
|
BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second.
aThe sponsor has requested the initial renewal criteria be 12 months to align with patients aged 2 to 5 years according to the last CDA-AMC recommendation.
bThe sponsor requested this additional criterion (i.e., clinical judgment in the renewal process), citing the elimination of unnecessary burden to patients, CF specialists, and their administrative teams, and the need to ensure the renewal criteria remain consistent across Canada. The sponsor noted that Québec has removed the need for documentation and evaluation of ppFEV1, BMI, CFQ-R, and pulmonary exacerbation frequency from the reimbursement criteria for ELX-TEZ-IVA on the basis of a revised recommendation from the Institut national d'excellence en santé et services sociaux.
Mechanism of Action
ELX-TEZ-IVA is the third treatment specifically indicated for patients with CF who have 1 or more F508del mutations in the CFTR gene. This mutation is believed to be associated with misfolding of the CFTR protein, which reduces CFTR expression at the cell surface. In addition to the reduced quantity of the protein, the mutation results in CFTR that is less stable and has defective channel gating compared with wild-type CFTR. Treatment with ELX-TEZ-IVA results in an increased quantity and improved function of the F508del-CFTR protein at the cell surface, through the following mechanisms:30-32
ELX and TEZ improve the conformational stability of F508del-CFTR protein, resulting in an increased expression of the F508del-CFTR protein at the cell surface
IVA increases the channel-open probability of the CFTR protein at the cell surface.
Recommended Dosage
The recommended dosing of ELX-TEZ-IVA is summarized in Table 7. For patients aged 2 to less than 6 years who weigh less than 14 kg, the recommended dosage regimen is 1 packet of granules comprising ELX 80 mg, TEZ 40 mg, and IVA 60 mg in the morning and 1 packet of IVA 59.5 mg granules in the evening. For those who weigh at least 14 kg, the recommended dose is 1 packet of granules of ELX 100 mg, TEZ 50 mg, and IVA 75 mg in the morning and 1 packet of ivacaftor 75 mg granules in the evening.
Both tablets and granules are administered orally and should be taken approximately 12 hours apart with fat-containing food. Table 8 provides a summary of the recommended dose adjustments for patients with hepatic insufficiency or those receiving concomitant treatment with moderate CYP3A inhibitors (e.g., fluconazole, or erythromycin) or strong CYP3A inhibitors (e.g., ketoconazole, itraconazole, posaconazole, voriconazole, telithromycin, and clarithromycin).
Age (weight) | Morning dose (2 tablets) | Evening dose |
|---|---|---|
2 to < 6 years (< 14 kg) | 1 packet granules: ELX 80 mg, TEZ 40 mg, and IVA 60 mg | 1 packet granules: IVA 59.5 mg |
2 to < 6 years (≥ 14 kg) | 1 packet granules: ELX 100 mg, TEZ 50 mg, and IVA 75 mg | 1 packet granules: IVA 75 mg |
6 to < 12 years (< 30 kg) | 2 tablets: ELX 50 mg, TEZ 25 mg, and IVA 37.5 mg | 1 tablet: IVA 75 mg |
6 to < 12 years (≥ 30 kg) | 2 tablets: ELX 100 mg, TEZ 50 mg, and IVA 75 mg | 1 tablet: IVA 150 mg |
≥ 12 years | 2 tablets: ELX 100 mg, TEZ 50 mg, and IVA 75 mg | 1 tablet: IVA 150 mg |
ELX = elexacaftor; IVA = ivacaftor; TEZ = tezacaftor.
Source: Product monograph.30
Table 8: Recommended Dose Adjustments
Age | Condition | Dose adjustment |
|---|---|---|
Hepatic insufficiency | ||
Aged 2 to < 6 years | Mild (Child-Pugh Class A) | No dose adjustments |
Moderate (Child-Pugh Class B) | Use not recommended: Treatment should only be considered when there is a clear medical need, and the benefits are expected to outweigh the risks. If used, ELX-TEZ-IVA should be used with caution at a reduced dose, as follows:
Repeat dosing schedule each week. The evening dose of IVA should not be taken. | |
Severe (Child-Pugh Class C) | Should not be used | |
Aged 6 years and older | Mild (Child-Pugh Class A) | No dose adjustments |
Moderate (Child-Pugh Class B) | Use not recommended: Treatment should only be considered when there is a clear medical need and the benefits are expected to outweigh the risks; if used, ELX-TEZ-IVA should be used with caution at a reduced dose as follows: 2 ELX-TEZ-IVA tablets alternating with 1 ELX-TEZ-IVA tablet taken in the morning, on alternate days; the evening dose of IVA should not be taken | |
Severe (Child-Pugh Class C) | Should not be used | |
CYP3A inhibitors | ||
Aged 2 to < 6 years | Moderate CYP3A Inhibitors | Morning: 1 packet ELX-TEZ-IVA granules (day 1); 1 packet IVA granules (day 2) Evening: No dose |
Strong CYP3A Inhibitors | Morning: 1 packet ELX-TEZ-IVA granules (twice weekly; 3 to 4 days apart) Evening: No dose | |
Aged 6 years and older | Moderate CYP3A Inhibitors | Morning: Two ELX-TEZ-IVA tablets (day 1); 1 IVA tablet (day 2) Evening: no dose |
Strong CYP3A Inhibitors | Morning: Two ELX-TEZ-IVA tablets (twice weekly; 3 4 days apart) Evening: no dose | |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IVA = ivacaftor.
Source: Product monograph.30
Previous Reimbursement Reviews
This is the fourth reimbursement review submission for ELX-TEZ-IVA. We previously reviewed ELX-TEZ-IVA for the treatment of CF in patients who have 1 or more F508del mutations in the CFTR gene for those aged 12 years and older (final recommendation issued in August 2021); those aged 6 years and older (final recommendation issued in June 2022); and those aged 2 to 5 years (final recommendation issued in November 2023). For all of the previous reviews, CDEC recommended that ELX-TEZ-IVA be reimbursed with conditions.1,33,34 All of the indications for ELX-TEZ-IVA have been accepted as priority reviews by Health Canada.
In addition, we previously reviewed IVA alone for the following indications: patients aged 6 years and older who have a G551D mutation in the CFTR gene; patients aged 6 years and older who have 1 of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, S549R, or G970R; and patients aged 18 years and older who have an R117H mutation in the CFTR gene.35-37 For each of these indications, CDEC recommended that IVA be reimbursed with conditions. LUM-IVA was previously reviewed for the treatment of CF in patients who are homozygous for the F508del mutation in the CFTR gene and received do-not-reimburse recommendations in 2016 and 2018.38,39 CDA-AMC was unable to recommend reimbursement for TEZ-IVA as a submission was not filed by the sponsor.40
Key characteristics of ELX-TEZ-IVA and other CFTR modulators approved in Canada are summarized in Table 9.
Table 9: Key Characteristics of CFTR Modulators
Characteristics | Trikafta (ELX-TEZ-IVA + IVA) | Kalydeco (IVA) |
|---|---|---|
Mechanism of action | CFTR potentiator (IVA) and correctors (ELX and TEZ) | CFTR potentiator |
Indicationa | Patients aged 2 years and older who have 1 or more F508del mutations in the CFTR gene or a mutation in the CFTR gene that is responsive based on clinical and/or in vitro dataa | Granules (13.4 mg, 25 mg, 50 mg and 75 mg): Indicated for the treatment of children with CF aged 2 months and older and weighing 3 kg to less than 25 kg who have 1 of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, S549R, or R117H Tablets (150 mg) are indicated for the treatment of CF aged 6 years and older and weighing 25 kg or more who have 1 of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, S549R, or R117H |
Route of administration | Oral tablets and granules | Oral tablets and granules |
Recommended dose | Granules: 2 to < 6 years: < 14 kg: ELX 80 mg, TEZ 40 mg, and IVA 60 mg (morning); IVA 59.5 mg (evening) ≥ 14 kg: ELX 100 mg, TEZ 50 mg, and IVA 75 mg (morning); IVA 75 mg (evening) Tablets: 6 to < 12 years (< 30 kg): ELX 100 mg, TEZ 50 mg, and IVA 75 mg (morning); IVA 75 mg (evening) 6 to < 12 years (≥ 30 kg) or ≥ 12 years: ELX 200 mg, TEZ 100 mg, and IVA 150 mg (morning); IVA 150 mg (evening) | Tablets: IVA 150 mg q12h Granules: 7 to < 14 kg: IVA 50 mg every 12 hours 14 to < 25 kg: IVA 75 mg every 12 hours |
Serious adverse effects or safety issues | Product monographs of each of the products include a warning about the risk of elevated alanine transaminase and aspartate transaminase), and monitoring of liver function is recommended before initiating treatment, every 3 months during the first year of treatment, and annually thereafter5,30,41,42 The product monograph recommends that ELX-TEZ-IVA not be used in patients with severe hepatic impairment; dosage-reduction scenarios are provided in the product monographs for IVA, TEZ-IVA, and LUM-IVA5,30,41,42 | |
CDA-AMC reviews | Aged 2 to 5 years: Reimburse with conditions Aged ≥ 6 years: Reimburse with conditions34 Aged ≥ 12 years: Reimburse with conditions33 | |
CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IVA = ivacaftor; LUM-IVA = lumacaftor-ivacaftor; TEZ-IVA = tezacaftor-ivacaftor plus ivacaftor.
aHealth Canada–approved indications.
Sources: Product monographs for Trikafta and Kalydeco.5,30,41,42
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups. The full original patient inputs received by the team are included in the report.
Two submissions were received from CF Canada to the call for patient input for the current review of ELX-TEZ-IVA for the treatment of CF in patients aged 2 years and older who have 1 or more F508del mutations in the CFTR gene or a mutation in the CFTR gene that is responsive based on clinical and/or in vitro data. CF Canada is a national not-for-profit corporation committed to improving and lengthening the lives of people living with CF through treatments, research, information, and support.
Information from CF Canada was based on a focus group with individuals in Canada with rare mutations who are being treated with ELX-TEZ-IVA, those with rare mutations who do not have access to ELX-TEZ-IVA, and caregivers of those in Canada with rare mutations that cause CF. In addition, data were retrieved from a 2021 survey of patients and caregivers with access to ELX-TEZ-IVA, medical and scientific publications, as well as the CCFR. CF Canada also supplied preliminary findings from phase I of the Burden of Disease Study, which measured the burden of CF at the individual, family, health systems, and societal levels and is considered to be among the most comprehensive studies of the burden of CF in the world. The second input was authored by a patient with end-stage CF with a rare class II mutation (M1101K).
According to the patient group, although life-changing treatments are increasingly reaching the 4,445 patients with CF in Canada, and those born with CF today will live longer than those who came before them, many are still ill and 1 in 7 living with the disease today is ineligible for the treatments that are making such a positive difference for others with CF.
The input stated that, from a health care and quality-of-life perspective, there are continued challenges for those living with CF, including patients who are unable to benefit from recent life-changing treatments. For example, the 40 patients in Canada who died of CF in 2022 had a median age of 38; those with CF collectively made 17,000 clinic visits, spent 10,000 days in hospital, and spent nearly 6,000 days on IV antibiotics in 2022 alone; and for 1 in 5 adults with CF, depression or anxiety was recorded as a complication in the CCFR. As the disease progresses, more time, effort, frequent clinic visits, and hospital stays are needed to manage the progressive and debilitating symptoms. This overwhelming treatment regimen has many side effects and a significant impact on patients’ and caregivers’ day-to-day activities and quality of life and creates a huge financial burden for families.
Data from the CCFR on patients in Canada with CF who do not currently have a Health Canada indication for CFTR modulators show that 246 patients have rare mutations known to respond to ELX-TEZ-IVA. The patient input indicated that many of these patients come from diverse and often racialized backgrounds, they are already disadvantaged by health care systems that were not designed with them in mind, and they deserve the right to try ELX-TEZ-IVA, even when evidence of efficacy and safety is lacking.
According to the patient group input, patients with rare mutations and their caregivers shared their hopes to access ELX-TEZ-IVA, as they saw the benefits of the medications for those who were able to access it. Few Canadians with rare mutations that lead to CF have access to ELX-TEZ-IVA; all members of the focus groups who have rare mutations and are taking ELX-TEZ-IVA responded exceptionally well to therapy, even those who have mutations for which evidence is scarce.
Clinician Input
Input From Clinical Experts
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the review of ELX-TEZ-IVA, a panel of 3 clinical experts from across Canada was convened to characterize unmet therapeutic needs, help identify and communicate situations for which there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of input from this panel follows.
Unmet Needs
All patients living with CF have unmet therapeutic needs. No treatments are currently available that can effectively achieve the most important goals of therapy: prolong survival, prevent the need for a lung transplant, prevent an accelerated decline in lung function over time, and reverse the course of the disease. In addition, the current standard treatments are burdensome for patients and their caregivers. Patients may not respond or may stop responding over time to the currently available treatments. The majority of patients with non-F508del mutations that are responsive to ELX-TEZ-IVA do not currently have access to therapy with a CFTR modulator (only those who are currently eligible to receive IVA monotherapy).
Place in Therapy
ELX-TEZ-IVA is a CFTR modulator that functions through 2 mechanisms: ELX and TEZ increased the amount of CFTR protein at the cell surface and IVA improves the transport of chloride ions through the CFTR protein. The mechanism of action for ELX-TEZ-IVA is attractive because it acts directly on the CFTR protein to address the defects responsible for the CF phenotype. ELX-TEZ-IVA would be added to existing treatments, such as physiotherapy, mucolytics, anti-infectives, and anti-inflammatory treatments (such as azithromycin). The clinical experts noted that ELX-TEZ-IVA has replaced earlier CFTR modulators (e.g., LUM-IVA and IVA) that are, in their opinion, less effective for patients with 1 or more F508del mutations in the CFTR gene. For the current target patient population, the clinical specialists anticipated that all patients in the expanded population (i.e., those with a non-508del mutation that is responsive to ELX-TEZ-IVA) would be considered candidates for the therapy. This would include those with a gating mutation who are currently receiving treatment with IVA, provided they meet eligibility and age criteria.
It is anticipated that ELX-TEZ-IVA would be used as a preventive therapy with the goal of initiating treatment before the patient develops significant lung disease. The current treatment paradigm would be significantly altered if ELX-TEZ-IVA can successfully prevent or delay progression to end organ disease (e.g., lung transplant).
The indication currently under review is for patients aged 2 years or older. CDA-AMC has previously recommended that ELX-TEZ-IVA be reimbursed for patients aged 2 to 5 years and those 6 years and older. The clinical experts consulted for this review and those who previously responded to the call for clinician input noted that children aged between 2 and 5 years will often have structural lung disease (e.g., bronchial wall thickening, mucus plugging, bronchiectasis),1 but that detection is challenging using the tools available to evaluate lung function in clinical practice (i.e., spirometry) or as part of a research protocol (e.g., lung clearance index). These early stages of lung abnormalities can be visualized using CT; therefore, despite younger patients with CF often demonstrating normal lung function, the underlying disease will continue to progress.1
All the clinicians who provided input for this review recommend initiating treatment with ELX-TEZ-IVA as soon as possible. This is aligned with the previously published Canadian Clinical Consensus Guideline for Initiation, Monitoring and Discontinuation of CFTR Modulator Therapies for Patients with Cystic Fibrosis, which also recommends that CFTR modulators be initiated at the youngest age possible, with the goal of attenuating disease progression and improving clinical status. All contributors agreed that no data support withholding the initiation of CFTR-modulator treatment until clinical symptoms of CF develop.
Patient Population
The diagnosis of CF is not challenging in routine clinical practice. Because all provinces and territories screen newborns for CF, most people with CF have a confirmed diagnosis by the age of 1 month (on average). SwCl testing is available and can be used reliably to confirm the screening test. The provinces and territories have slightly different testing algorithms and CFTR-mutation-screening panels; however, all provinces and territories have effective processes. Almost 100% of newly diagnosed infants would have both CFTR mutations identified. Infants who are not identified via newborn screening (i.e., false negatives), are usually diagnosed before 1 year of age after the development of clinical symptoms of CF. The diagnostic guidelines are clear and there is little variability in expert opinion. Misdiagnosis and underdiagnosis of CF is exceedingly rare in Canadian clinical practice.
ELX-TEZ-IVA could be used in every patient who meets the Health Canada–approved indication, regardless of current or past treatment regimens. From a medical perspective, there is no rationale for requiring a patient to demonstrate an inadequate response or loss of response to prior therapies before initiating treatment with ELX-TEZ-IVA. It would be reasonable to require patients to complete important standard CF therapies at the same time as receiving treatment with ELX-TEZ-IVA. In clinical practice, eligible patients would be identified based on their CFTR genotype and all patients would be expected to respond to the treatment.
For the expanded indication (i.e., with a non-F508del mutation that is responsive to ELX-TEZ-IVA), the clinical experts consulted for this review noted that nearly all patients would initiate therapy with ELX-TEZ-IVA as soon as possible, provided it is safe to start to treatment. The clinical experts emphasized that ELX-TEZ-IVA has been a transformative and disease-modifying therapy for CF and that it would not be appropriate to wait until the patient shows worsening symptoms, more frequent exacerbations, or a decline in lung function to initiate treatment with ELX-TEZ-IVA.
Applicability of Existing Reimbursement Criteria to the Expanded Population
In discussions with the review team, the sponsor noted that nearly all patients in Canada aged 6 years and older who are eligible for treatment have initiated therapy with ELX-TEZ-IVA. (Some may have elected to discontinue, but all who are interested have been given the opportunity to access the drug.) For those who have initiated treatment, the sponsor noted that initial renewal criteria were met for all patients in Canada who started the therapy and wanted to continue (i.e., 100% of patients met the renewal criteria recommended by CDA-AMC and/or applied by the public drug programs). The clinical experts consulted for this review expressed general agreement with the sponsor’s position, noting that rates of initial access and renewal are high within their individual clinics. With nearly all patients currently achieving the CDA-AMC–recommended renewal criteria, the sponsor noted that requiring these assessments consumes health care resources (e.g., the time required by health care practitioners to administer and document results for each of the required tests) without adding value to patients or the health care system.
The clinical experts consulted for this review supported application of the existing criteria recommended for the reimbursement of ELX-TEZ-IVA. Consistent with input from the participating drug programs, the clinical experts noted that lack of alignment across CDA-AMC recommendations for the reimbursement of ELX-TEZ-IVA in patients with and without 1 or more F508del mutations could create implementation challenges in clinical practice.
Table 10: Current Recommended Reimbursement Conditions for Patients Aged 2 to 5 Years and 6 Years and Older
Patients aged 2 to 5 years | Patients aged 6 years and older |
|---|---|
Initiation | |
1. Confirmed diagnosis of CF with 1 or more F508del mutations in the CFTR gene 2. Aged 2 to 5 years 3. The following measurements must be completed before initiating treatment with ELX-TEZ-IVA:
| 1. Confirmed diagnosis of CF with 1 or more F508del mutations in the CFTR gene 2. Aged 6 years and older 3. The following measurements must be completed before initiating treatment with ELX-TEZ-IVA:
4. Patients should be optimized with best supportive care for their CF at the time of initiation 5. The maximum duration of initial reimbursement is for 6 months |
Renewal | |
4. For renewal after initial authorization, the physician must provide evidence of continuing benefit from treatment with ELZ-TEZ-IVA for subsequent renewal of reimbursement; patients on therapy should be monitored for response (e.g., no decrease in BMI z score) using clinical judgment and/or standard procedures 5. Assessment for clinical response should occur every 12 months | 6. For the first renewal, the physician must provide at least 1 of the following to demonstrate benefit after 6 months of treatment with ELX-TEZ-IVA:
7. Improvement by 4 points or more in the CFQ-R respiratory domain scale |
Discontinuation | |
6. Patient has undergone a lung transplant | 8. Patient has undergone a lung transplant |
Prescribing | |
7. Prescribing and monitoring of treatment response should be limited to CF specialists 8. ELX-TEZ-IVA should not be reimbursed in combination with other CFTR modulators | 9. Prescribing and monitoring of treatment response should be limited to CF specialists 10. ELX-TEZ-IVA should not be reimbursed in combination with other CFTR modulators |
BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor.
Clinician Group Input
This section was prepared by the Clinical Review team based on the input provided by clinician groups. The full original clinician group inputs received by the review team are included in the report.
Three groups of clinicians responded to call for input: CanACT (4 clinicians contributed to the input), Edmonton Adult Cystic Fibrosis Clinic and Calgary Adult Cystic Fibrosis Clinic (2 clinicians contributed to the input), and the CF Canada Health Care Advisory Council (5 clinicians contributed to the input). The input from the clinician groups identified the same unmet medical needs for patients with CF and potential place in therapy for the drug under review as the clinical experts consulted for this review.
According to clinician groups, the treatment paradigm in Canada for patients with CF aims to maintain health (delay disease progression, improve lung function, reduce the risk for pulmonary exacerbations, and prevent the need for organ transplant), maintain or improve quality of life, and prolong life. This includes nonpharmacological approaches such as nasal sinus saline irrigation, airway clearance, and high-protein, high-calorie nutrition. Medications commonly used in CF include antibiotics, mucolytics, bronchodilators, pancreatic enzymes, fat-soluble vitamins, anti-inflammatories, insulin for people with CF-related diabetes, ursodiol for liver disease, and chest physiotherapy. Oxygen, noninvasive positive-pressure ventilation, and lung transplant are treatments for those with end-stage CF lung disease. A transformational change was the introduction of CFTR modulators, which correct the basic defect in CF by improving the production and function of the abnormal CFTR protein. The first (IVA) and second-generation (LUM-IVA and IVA-TEZ) modulators had a modest but important clinical effect, but the response to the third-generation modulator (ELX-TEZ-IVA) is substantially greater.
Clinician groups noted that there is a significant treatment gap in CF care. Of patients with CF with rare mutations who do not carry a copy of the F508del CFTR mutation but may be responsive to ELX-TEZ-IVA, 10% (n = 246) do not have access to the drug as no clinical trials have been conducted. Benefit relies solely on reports of real-world evidence, in vitro data, or individual therapy trials. The CF Canada Health Care Advisory Council added that lung-transplant recipients, particularly those with significant sinus disease, may still benefit from CF modulator therapy; however, they were excluded from the clinical trials.
The 3 clinician groups noted that ELX-TEZ-IVA is an improvement on the existing CFTR modulators and the most effective. It addresses the underlying disease process and is complementary to the existing standard of care for CF that would improve adherence, potentially delay disease progression and therefore delay the need for other therapies, including lung transplants. The CF Canada Health Care Advisory Council stated that expanding access to those patients with other responsive CFTR mutations will give another 246 patients lifelong benefits and improve equitable access to those from marginalized communities in whom these rare mutations are often found.
According to the clinician groups, any patient who carries 1 or more CFTR mutations responsive to ELX-TEZ-IVA should have access to this therapy. CanACT added that, for those with rare CFTR mutations, for whom data to support the use of ELX-TEZ-IVA are limited, each patient’s life may depend on access to this medication, and it is incumbent on regulators to use all available evidence or generate the evidence needed to allow access to this life-saving drug.
All clinician groups indicated that the outcomes of interest include meaningful clinical responses such as improvement and stabilization in lung function as measured by FEV1 or lung clearance index (where available) obtained at a time of clinical stability, and for individuals aged 6 years or older, reduction of pulmonary exacerbations, reduction or stabilization of respiratory symptoms, stabilization or improvement in nutritional and growth status, improvement in quality-of-life scores, and reduction in SwCl.
The 3 clinician groups noted that discontinuation of therapy should be considered if there is a lack of clinical response following a therapy trial or if a severe side effect, allergy, or other AE occurs (e.g., elevation of liver function or allergic reaction). Clinician groups stated that treatment of patients with CF with ELX-TEZ-IVA should be performed by CF specialists practising at CF clinics.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 11.
Table 11: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
The participating drug programs noted that CDA-AMC has previously issued recommendations for ELX-TEZ-IVA for patients aged 2 to 5 years and patients aged 6 years and older who have 1 or more F508del mutations in the CFTR gene. The participating drug programs requested that the expert committee consider aligning with the initiation criteria for other ELX-TEZ-IVA recommendations, if appropriate. | This is a comment from the drug plans to inform CDEC deliberations. |
Considerations for continuation or renewal of therapy | |
The participating drug programs noted that CDA-AMC has previously issued recommendations for ELX-TEZ-IVA for patients aged 2 to 5 years and patients aged 6 years and older who have 1 or more F508del mutations in the CFTR gene. The participating drug programs requested that the expert committee consider aligning with the renewal criteria for other ELX-TEZ-IVA recommendations, if appropriate. | This is a comment from the drug plans to inform CDEC deliberations. |
The participating drug programs note that the sponsor has requested that “clinical benefit as determined by physician specializing in the treatment of CF” be included as 1 of the initial renewal criteria. Could the clinical experts and expert committed please comment on the appropriateness of this criterion? | This is a comment from the drug plans to inform CDEC deliberations. |
Considerations for discontinuation of therapy | |
The participating drug programs noted that CDA-AMC has previously issued recommendations for ELX-TEZ-IVA for patients aged 2 to 5 years and those aged 6 years and older who have 1 or more F508del mutations in the CFTR gene. The participating drug programs are requested that the expert committee consider aligning the discontinuation criteria with those of other ELX-TEZ-IVA recommendations, if appropriate. | This is a comment from the drug plans to inform CDEC deliberations. |
CDEC = Canadian Drug Expert Committee; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor.
In Vitro Evidence
This section of the clinical report provides a summary of the FRT in vitro data used to identify the CFTR mutations that are considered to be responsive to ELX-TEZ-IVA treatment. This data has not been appraised by the review team and commentary is limited to the opinion of Canadian and international regulatory authorities regarding the validity and relevance of the study results. Perspectives from CF clinical specialists regarding the absence of clinical data for many of the CFTR mutations in the target population are also included.
Overview of In Vitro Fischer Rat Thyroid Assays
The sponsor used an in vitro FRT-cell model to characterize individual CFTR mutations that produce at least some amount of full-length CFTR proteins, for responsiveness to CFTR modulators.43 The in vitro cell model uses FRT cells that express a CFTR gene with a single mutation to test for responsiveness to CFTR modulators. Each FRT-cell line is engineered to express a specific CFTR mutation in a stable, epithelial-cell background. DNA sequencing is performed on each cell line to confirm the presence of the specific CFTR mutation and quantitative polymerase chain reaction analysis is used to confirm the expression of mRNA.
The selection of CFTR mutations for inclusion in the in vitro study was based on a comprehensive understanding of CFTR mutations and the mechanism of action of CFTR modulators. Despite the occurrence of multiple CFTR mutation classes, the resulting functional abnormality is ultimately either a decreased quantity and/or decreased function of the CFTR protein. CFTR mutations selected for inclusion in the FRT assay study were based on evidence that the mutation caused CF, based on CFTR2 and/or scientific literature and in silico translation consistent with production of full-length CFTR proteins.5 Protein-truncating CFTR mutations, whole or partial CFTR gene deletions, and noncanonical splice mutations were excluded from the study. Positive controls and negative controls were also included in the experiments.
The positive controls included G551D and R117H that were found in previous FRT assays to be IVA-responsive and have been demonstrated in clinical trials to provide clinical benefit for patients. (IVA is approved for use in the treatment of CF in patients who have a G551D and R117H CFTR mutation.)
The negative controls included G1061R, R1066C, N1303K and untransfected FRT cells. These 3 CFTR mutations were identified as nonresponsive to IVA or TEZ-IVA in previous in vitro studies.
The function of CFTR at the cell surface was assessed in Ussing chamber studies, a procedure that quantifies the amount of CFTR-mediated Cl− transport in FRT cells expressing each CFTR mutation form as a fraction of the Cl− transport in FRT cells expressing normal CFTR (% normal).
Definition of In Vitro Response to ELX-TEZ-IVA
Responsive CFTR mutations were those that demonstrated an increase of 10% in Cl− transport over baseline when expressed as a percentage of normal CFTR Cl− transport. The sponsor selected this threshold because the analyses of CFTR activity and disease phenotype showed that a 10% increase in CFTR activity is associated with improved clinical status.44 The sponsor reported that patients with a severe CF phenotype generally have CFTR function of less than 5% of normal, whereas the sponsor reported that the severity of CF begins to diminish in patients who have CFTR function of 10% of normal or higher. An increase in CFTR function of 10% or more is therefore expected to affect the disease phenotype for those living with CF.
CFTR Mutations Identified as Responsive to ELX-TEZ-IVA
Using the in vitro FRT model, the sponsor identified 177 CFTR mutations as responsive to ELX-TEZ-IVA. These additional mutations do not include F508del, which has been studied in multiple clinical trials already reviewed by CDEC. Importantly, the sponsor noted that the 10% threshold for a response should be considered conservative, citing the following additional mutations that have been included in this reimbursement review application:
The N1303K mutation did not meet the 10% threshold in the FRT model to be considered responsive to ELX-TEZ-IVA (this mutation was chosen as 1 of the negative controls for the FRT model). However, the sponsor has filed submissions with Health Canada and CDA-AMC on the basis of real-world evidence that suggests that these patients benefit from treatment with ELX-TEZ-IVA.
The R117C and S1255P mutations included in this reimbursement review application did not meet the 10% threshold for the FRT assay; however, previous in vitro FRT data and/or clinical data support the responsiveness of these mutations to IVA and/or TEZ-IVA (both of which are components of ELX-TEZ-IVA).
Regulatory Perspectives and Approval History
FDA Conclusions
The FDA considered the evidence from the FRT-cell model sufficient to warrant expanding the indications for ELX-TEZ-IVA, TEZ-IVA, and IVA. The FDA was the first regulatory authority to expand the use of CFTR modulators (including ELX-TEZ-IVA) based on in vitro data from the FRT model. As shown in Table 12, the FDA initially expanded the use of IVA monotherapy based on in vitro data in May 2017. Subsequent approvals followed for TEZ-IVA in June 2019, and for ELX-TEZ-IVA, TEZ-IVA, and IVA monotherapy in December 2020. In total, the FDA has approved ELX-TEZ-IVA for 178 CFTR mutations, TEZ-IVA for 154 CFTR mutations, and IVA for 97 CFTR mutations.
Table 12: FDA Approvals for CFTR Modulators Based on In Vitro Evidence
Date | Indication expansions based on in vitro data |
|---|---|
December 21, 2020 |
|
June 21, 2019 |
|
May 17, 2017 |
|
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IVA = ivacaftor; TEZ-IVA = tezacaftor-ivacaftor plus ivacaftor.
Health Canada Conclusions
Health Canada–approved the use of ELX-TEZ-IVA for 147 of the 177 mutations that were responsive to ELX-TEZ-IVA in the FRT model, based on pivotal and/or supporting clinical data, the biological plausibility that the treatment would provide a substantive beneficial treatment effect, and the rarity of the CFTR mutations that are the subject of this review (i.e., clinical evidence collection would be challenging because of the small number of patients with each of the mutations). Of the 177 FRT-responsive CFTR mutations approved by the FDA and submitted for review to Health Canada and CDA-AMC, Health Canada did not authorize use for 30 of the mutations for the following reasons:
15 mutations were considered by Health Canada as not causative of CF, based on the CFTR2 and CFTR-France databases: D836Y, F508C, G576A, I148T, I807M, I1027T, L320V, L997F, R75Q, R170H, R668C, R1162L, T1053I, V562I, and V754M.
10 mutations were excluded because of unknown clinical significance, were only reported as causing a CFTR-related disease (i.e., not CF), and retain at least 50% of normal chloride-transport function: G178E, G576A;R668C, I1139V, K1060T, R31L, R553Q, R751L, R792G, V1293G, Y1014C.
5 mutations were excluded because they result in a cryptic splice mutation, and insufficient full-length CFTR: H939R, I175V, M152V, E403D, and S589N.
The Health Canada–approved product monograph states the following regarding the interpretation of the in vitro data: The in vitro CFTR-mediated chloride-transport response threshold was designated as a net increase of at least 10% of normal over baseline because it is predictive or is reasonably expected to predict clinical benefit. For individual mutations, the magnitude of the net change over baseline in CFTR-mediated Cl− transport in vitro is not correlated with the magnitude of clinical response. Not all mutations can be tested in the FRT system, but patients harbouring some mutations not amenable to testing in this system may demonstrate clinical benefit. Clinical outcomes were consistent with in vitro results and indicate that a single mutation responsive to ELX-TEZ-IVA is sufficient to generate a significant clinical response.
Perspectives of Cystic Fibrosis Specialists
The clinical experts consulted for this review noted that responsiveness to ELX-TEZ-IVA using the in vitro model applied by Vertex in the clinical development program for patients with rare CFTR mutations is sufficient evidence to support prescribing it to these patients. In addition to regulatory approval based on this information (e.g., FDA approvals), the clinical experts cited the following considerations that would support the use of ELX-TEZ-IVA in clinical practice:
There is a lack of alternative treatment options for these patients and the severe progressive nature of CF.
In vitro data demonstrating activity on the CFTR channel for patients with these rare mutations supports extrapolation of the clinical benefit demonstrated in studies involving more common CF-causing mutations in the CFTR gene.
There are concerns about equity for those living with CFTR mutations for which the incidence is sufficiently low to preclude the generation of robust clinical evidence. The clinical experts noted that CF with a non-F508del mutation is more likely to be diagnosed in racial minorities who may already be encountering systemic disadvantages within the health care system. Based on the rarity of these “rarer” mutations, it would be impossible to include participants with each mutation into clinical trials. The current focus on clinical trial data alone for drug approval is resulting in ethnic and racial inequity in medication access. It is well known that patients from minority groups are underrepresented in clinical trials for a multitude of reasons (as discussed in the Ethics Review Report).
There is a mounting body of evidence from case reports, case series, and clinical experience that ELX-TEZ-IVA can have a clinically meaningful impact on patients with rare CFTR mutations shown to be responsive based on in vitro data.
In addition, the clinical experts noted that patients with CF living in Canada are monitored in specialized clinics with well-organized and frequent clinical and laboratory evaluations to ensure the treatment is used appropriately and safely in clinical practice. The clinical specialists emphasized that the in vitro data should not be viewed in insolation and that is important to consider the large body of evidence demonstrating the clear and clinically important benefits of ELX-TEZ-IVA and the relatively few serious harms associated with the treatment (i.e., this is no longer a new drug in the management of CF). The specialists noted that the totality of information, including real-world experience with the drug, for those with 1 or more F508del mutations, supports the expanded use of the drug by those with rare CFTR mutations.
Clinical Evidence
The objective of the Clinical Review is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of ELX-TEZ-IVA in the treatment of CF in patients aged 2 years and older who have a non-F508del mutation in the CFTR gene that is responsive to ELX-TEZ-IVA based on in vitro and/or clinical data. The focus will be placed on comparing ELX-TEZ-IVA to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of ELX-TEZ-IVA is presented in 4 sections, with critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. The third section includes indirect evidence from the sponsor (not submitted). The fourth section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following studies are included in the review and appraised in this document:
1 RCT identified in systematic review (Study 124)
1 long-term extension study (Study 125)
5 additional studies addressing gaps in evidence:
1 study involving patients with FRT-responsive mutations (64 mutations)
4 studies involving patients with at least 1 N1303K mutation.
Systematic Review
Contents within this section were informed by materials submitted by the sponsor. The following summary was validated by the review team.
Description of Studies
Characteristics of the included studies are summarized in Table 13.
Table 13: Details of Studies Included in the Systematic Review
Detail | Study 124 |
|---|---|
Designs and populations | |
Study design | Phase III, double-blind, randomized, controlled trial |
Locations | 84 sites: Europe and Canada |
Study period: | Date first eligible subject signed the informed consent form: May 9, 2022 Date last subject completed the last visit: July 5, 2023 |
Randomized (N) | ELX-TEZ-IVA: N = 205 Placebo: N = 102 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | ELX-TEZ-IVA: fixed-dose combination tablets for oral administration in the morning IVA: tablet for oral administration in the evening |
Comparator(s) | Placebo matched to ELX-TEZ-IVA and IVA |
Study duration | |
Screening phase | Day −28 to day −1 |
Treatment phase | 24 weeks (day 1 to week 24) |
Follow-up phase | 28 days |
Outcomes | |
Primary end point | Absolute change from baseline in ppFEV1 through week 24 |
Secondary and exploratory end points | Secondary:
|
Publication status | |
Publications | NCT05274269 |
AE = adverse event; BMI = body mass index; CF = cystic fibrosis; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised (respiratory domain); ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IVA = ivacaftor; PEx = pulmonary exacerbations; ppFEV1 = percent predicted forced expiratory volume in 1 second; SAE = serious adverse event; SwCl = sweat chloride.
Source: Clinical Study Report.45
The objective of Study 124 was to evaluate the efficacy, pharmacodynamics, and safety of ELX-TEZ-IVA in patients with a non-F508del ELX-TEZ-IVA–responsive CFTR mutation. This study was a phase III double-blinded, randomized, placebo-controlled trial. Participants aged 6 years and older from 84 sites across Europe and Canada were recruited and randomized, with 205 participants enrolled in the ELX-TEZ-IVA treatment arm and 102 participants enrolled in the placebo-controlled arm. To achieve balanced treatment arms, randomization utilized stratification based on ppFEV1 at screening (< 70% versus ≥ 70%), age at screening (< 18 years versus ≥ 18 years), and mutation groups (≥ 1 residual function [RF]-like] mutation versus no RF-like mutation). A summary timeline of the study duration in available in Figure 2.
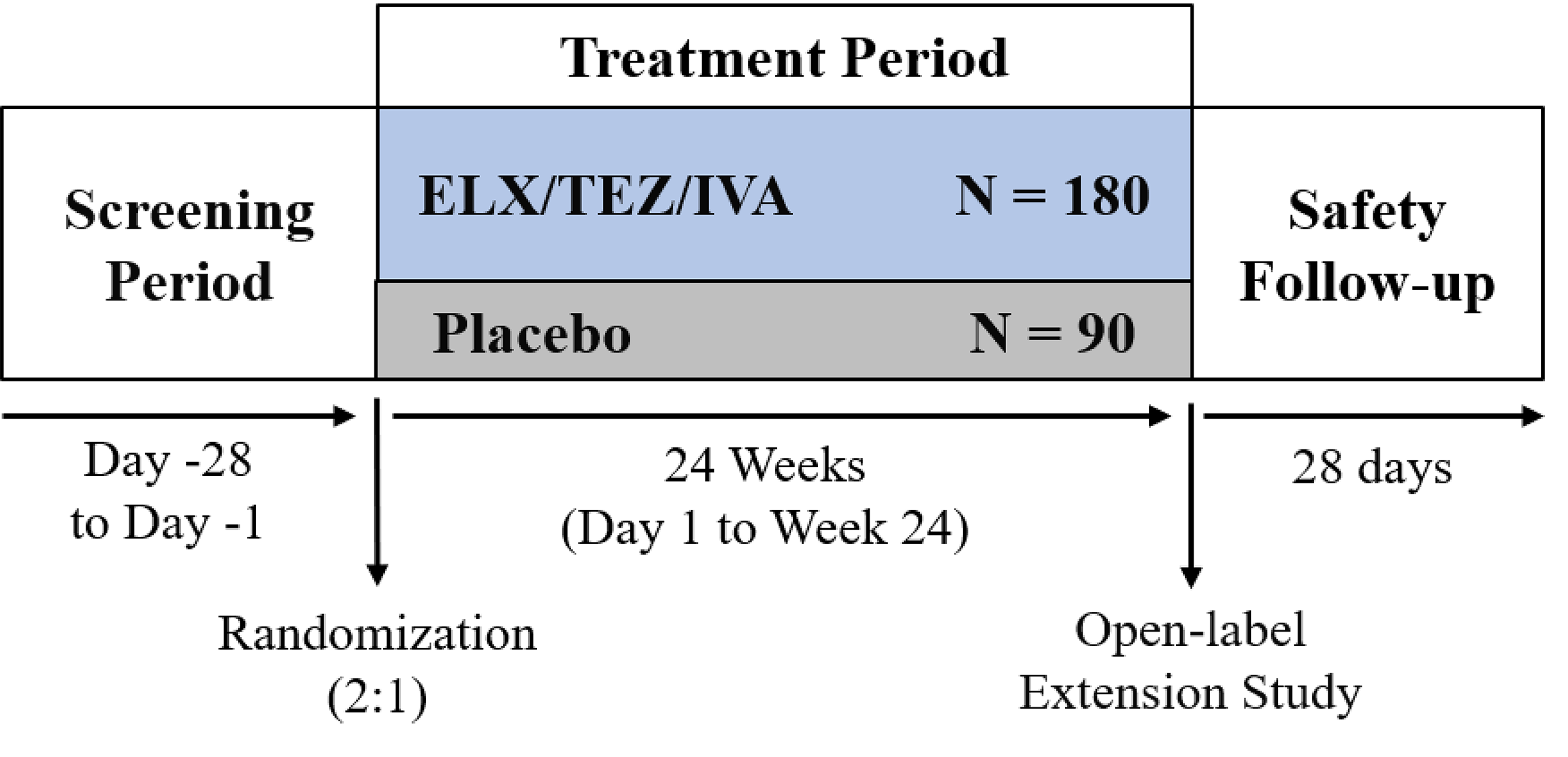
Populations
Inclusion and Exclusion Criteria
Eligible participants with stable CF, as judged by investigators, were at least 6 years of age with a non-F508del CFTR mutation responsive to ELX-TEZ-IVA based on the FRT assay with no exclusionary CFTR mutations (i.e., F508del, S549N, G551S, S1255P, R117H, S549R, G1244E, G1349D, G178R, G551D, and S1251N). The sponsor reported that 18 of the most prevalent CFTR mutations in Europe and Canada that are not currently indicated for a CFTR modulator were eligible (representing approximately 80% of the target patient population). The use of ELX-TEZ-IVA was approved by Health Canada for 17 of the 18 CFTR mutations included in Study 124 (1 mutation [L997F] was excluded by Health Canada on the basis that it has not been demonstrated to cause CF). Participants had to have a ppFEV1 value of between 40% and 100% of predicted mean for age, sex, and height.
Participants were excluded if they had an acute upper or lower respiratory infection, PEx, or change in therapy (including antibiotics) for sinopulmonary disease within 28 days before the first dose of the study drug, or a lung infection with organisms associated with a more rapid decline in pulmonary status (including, but not limited to, B. cenocepacia, B. dolosa, and M. abscessus). Participants with the following laboratory measures and illnesses were excluded: hemoglobin less than 10 g/dL; total bilirubin at least twice the upper limit of normal (ULN); aspartate transaminase, alanine transaminase, gamma-glutamyl transferase, or alkaline phosphatase at least 3 times the ULN; abnormal renal function was defined as glomerular filtration rate of up to 50 mL/min/1.73 m2 (calculated by the modification of diet in renal disease study equation) for patients aged 18 years of age or older and up to 45 mL/min/1.73 m2 (calculated by the Counahan-Barratt equation) for patients aged younger than 18 years.
Interventions
ELX-TEZ-IVA was orally administered as fixed-dose combination tablets in the morning along with an oral administration of IVA tablets in the evening. Placebo-arm treatments were matched to both ELX-TEZ-IVA and IVA administrations in dose and timing.
Outcomes
A list of efficacy end points assessed in this Clinical Review is provided in Table 14, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review by the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, the review team selected end points that were considered most relevant to inform the expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing the expert committee deliberations were also assessed using GRADE.
Percent Predicted FEV1
The ppFEV1 (in litres) was calculated using the ratio of FEV1 to the predicted FEV1. The ppFEV1 was calculated using the equations of the Global Lung Function Initiative. Absolute change from baseline was calculated as postbaseline value minus baseline value. Absolute change from baseline in ppFEV1 was the primary end point of Study 124 (evaluated through 24 weeks). The clinical experts consulted for this review noted that an absolute improvement of 5% is typically considered to be meaningful for acute changes in ppFEV1; however, they noted that even stabilization of ppFEV1 can be meaningful for patients, particularly those who are at risk of rapid decline.
Table 14: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | Study 124 |
|---|---|---|
Absolute change in ppFEV1 | Through 24 weeks | Primary end point |
Number of PEx | Through 24 weeks | Secondary end point |
Absolute change in BMI (kg/m2) | Through 24 weeks | Secondary end point |
Absolute change in weight (kg) | Through 24 weeks | Secondary end point |
Absolute change in CFQ-R (RD) score | Through 24 weeks | Secondary end point |
Absolute change in SwCl (mmol/L) | Through 24 weeks | Secondary end point |
Safety and tolerability as assessed by AEs and SAEs | Through 24 weeks | Secondary end point |
AE = adverse event; BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised (respiratory domain); PEx = pulmonary exacerbations; ppFEV1 = percent predicted forced expiratory volume in 1 second; SAE = serious adverse event; SwCl = sweat chloride.
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Sweat Chloride
As a biomarker of CFTR activity, SwCl testing is a standard diagnostic tool for CF. SwCl tests were conducted before administration of the morning dose of the study drug. Absolute change from baseline in SwCl through 24 weeks was a secondary end point in Study 124.
CFQ-R Respiratory Domain
The CFQ-R is a disease-specific, health-related quality-of-life instrument designed for patients with CF that is available in age-appropriate versions for children aged 6 to 13 years, parents who serve as a proxy for their child, and individuals 14 years of age and older.73 For children aged 6 to 11 years, the questionnaire is interviewer-administered, and for those aged 12 and 13 years, it is self-administered.74 The number of items and domains vary between versions; the children’s version includes 35 items within 8 domains, the parent version has 44 items and 11 domains, and the adolescent and adult version has 50 items within 12 domains.73,74 The domains in the adolescent and adult version have a health-related quality-of-life module that include physical functioning, vitality, emotional functioning, social or school functioning, role functioning, body image, eating problems, and treatment burden; a symptoms module that includes respiratory symptoms, digestive symptoms, and weight; and a health-perception module. A 4-point Likert scale is used to measure frequency (always, often, sometimes, or never), intensity (a great deal, somewhat, a little, or not at all), and true-false scales (very true, somewhat true, somewhat false, or very false). Items within domains are summed and standardized. Individual domain scores range from 0 to 100, with higher scores indicating better health-related quality of life. The scales are designed to measure symptoms and functioning during the 2-week period before administration of the questionnaire. A difference of at least 4 points in the respiratory domain score of the CFQ-R is commonly cited as the MID for patients with CF.
Pulmonary Exacerbations
PEx was defined as a new or change in antibiotic therapy (IV, inhaled, or oral) for any 4 or more of the following signs or symptoms:
change in sputum
new or increased hemoptysis
increased cough
increased dyspnea
malaise, fatigue, or lethargy
temperature above 38°C (equivalent to approximately 100.4°F)
anorexia or weight loss
sinus pain or tenderness
change in sinus discharge
change in physical examination of the chest
decrease in pulmonary function by 10%
radiographic changes indicative of pulmonary infection.
Adverse Events
An AE is defined as any untoward medical occurrence in a subject during the study; the event does not necessarily have a causal relationship with the treatment. This includes any newly occurring event or worsening of a pre-existing condition (e.g., an increase in its severity or frequency).
Statistical Analysis
Clinical Trial End Points
Primary End-Point Analysis (ppFEV1)
The primary analysis was performed using a mixed-effects model for repeated measures (MMRM) with change from baseline at day 15, week 4, week 8, week 16, and week 24 as the dependent variables. The model included treatment group, visit, and treatment by visit interaction as fixed effects, with continuous baseline ppFEV1, age at screening (< 18 versus ≥ 18 years), and mutation group (contains ≥ 1 RF-like mutation versus does not contain an RF-like mutation) as covariates.
Secondary Continuous End-Point Analysis (SwCl, CFQ-R [RD], BMI, and Weight)
The analysis of absolute change from baseline in SwCl, CFQ-R (RD), BMI, and weight was based on an MMRM similar to the analysis of the primary end point, with absolute change from baseline at day 15 (if applicable), week 4, week 8, week 16, and week 24 as the dependent variables. For SwCl and CFQ-R (RD), the primary result obtained from the model was the estimated treatment difference through week 24 defined as the averaged treatment effects estimated at week 4, week 8, week 16, and week 24.
Secondary End-Point Analysis (Number of PEx Events)
A PEx event was defined as new or change in antibiotic therapy (IV, inhaled, or oral) in 4 or more sinopulmonary signs and/or symptoms. The number of PEx events during the PEx analysis period for week 24 was performed using a negative binomial regression model with a fixed effect for treatment, as well as continuous baseline ppFEV1, age at screening (< 18 years versus ≥ 18 years), and mutation group (contains 1 or more RF-like mutations versus does not contain an RF-like mutation) as covariates. The logarithm of the subject-specific PEx analysis period duration (in years) was treated as the offset in the model. The estimated rate ratio and the associated 2-sided 95% CI and 2-sided P value were provided.
BMI Z Score and Weight Z Scores
The BMI and weight z scores were calculated by using Centers for Disease Control and Prevention growth charts.46 Analysis of BMI z scores and weight z scores were based on an MMRM similar to that of the analysis of the primary efficacy variable, excluding the covariate of age at screening (< 18 years versus ≥ 18 years), for patients aged 20 years or younger at baseline. Data obtained from visits at day 15, week 4, week 8, week 16, and week 24 were included in the model.
Safety Analyses
All safety analyses were based on data from the treatment-emergent period, which included the time from the date of the first dose of the study drug to 28 days after the last dose of the study drug or to the completion of study participation date, whichever occurred first.
Sample Size and Power Calculation
Approximately 270 patients were planned to be enrolled and randomized (2:1) to the ELX-TEZ-IVA or placebo groups. The primary end point was the absolute change from baseline in ppFEV1 through week 24. The primary null hypothesis to be tested was that the mean absolute change from baseline in ppFEV1 through week 24 is the same for the ELX-TEZ-IVA and placebo treatment groups. The null hypothesis was tested at a 2-sided significance level of 0.05. Assuming a within-group SD of 9 percentage points and a 10% dropout rate at week 24, a total sample size of 270 patients (180 patients in the ELX-TEZ-IVA group and 90 in placebo group) was estimated to have an approximately 90% power to detect a difference of 4.0 percentage points for the mean absolute change from baseline in ppFEV1 through week 24 between the 2 treatment groups, based on a 2-sided, 2-sample t test at a significance level of 0.05.
Statistical Test or Model
An MMRM approach was used to assess the primary and most secondary end points. The model was estimated using a restricted maximum likelihood. Denominator degrees of freedom for the F test for fixed effects were estimated using the Kenward-Roger approximation. An unstructured covariance structure was used to model the within-subject errors. If the model estimation did not converge, a compound symmetry covariance structure was used instead. Depending on the observed data and covariates, missing data were assumed to be missing at random.
Multiple Testing Procedure
The secondary end points were formally tested at an alpha of 0.05. A hierarchical testing procedure was used to control the type I error rate for the multiple secondary end points tested at an alpha of 0.05. For a test at any step to be considered statistically significant within the testing hierarchy, it must have been statistically significant, and all previous tests (if any) within the hierarchy must also have been statistically significant at the 0.05 level. The testing order of the secondary end points was as follows:
First secondary end point: absolute change in SwCl from baseline through week 24
Second secondary end point: absolute change in CFQ-R RD from baseline through week 24
Third secondary end point: absolute change in BMI from baseline at week 24
Fourth secondary end point: absolute change in weight from baseline at week 24
Fifth secondary end point: number of PEx events through week 24.
Subgroup Analyses
The MMRM used for the primary analysis was used for the subgroup analysis, with the same model applied to each category of the subgroup: age at screening (< 18 years versus ≥ 18 years), ppFEV1 (< 70 versus ≥ 70), and sex (male or female). For the subgroup analysis based on age, the covariate of age at screening (< 18 years versus ≥ 18 years) from the MMRM was removed. The adjusted means with 2-sided 95% CIs were provided. The estimated between-group difference through week 24 within a subgroup was also presented in a forest plot.
Analysis Populations
A summary of analysis sets defined in Study 124 is presented in Table 16.
Table 15: Statistical Analysis of Efficacy End Points of Study 124
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Absolute change in ppFEV1 | MMRM
| Models adjusted for covariates based on stratification factors | All data were assumed to be missing at random and were not imputed, unless otherwise specified Sensitivity analysis to evaluate the impact of missing at random assumption was conducted using multiple imputation | MMRM based on multiple imputation |
Absolute change in SwCL (mmol/L) | Same as primary end point | Same as primary end point | Same as primary end point | NR |
Absolute change in CFQ-R RD score | Same as primary end point | Same as primary end point | Same as primary end point | NR |
Absolute change in BMI (kg/m2) | Same as primary end point | Same as primary end point | Same as primary end point | NR |
Absolute change in weight (kg) | Same as primary end point | Same as primary end point | Same as primary end point | NR |
Number of PEx events |
| Same as primary end point | Same as primary end point | NR |
Safety analyses | Descriptive analysis | NR | NR | NR |
BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised (respiratory domain); CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; MMRM = mixed-effects model for repeated measures; NR = not reported; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride.
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Table 16: Analysis Populations of Study 124
Population | Definition | Application |
|---|---|---|
All patients set | All patients who were randomized or received ≥ 1 dose of study drug | Disposition summary tables, unless otherwise specified |
Full analysis set | All randomized patients who carry the intended mutation and received ≥ 1 dose of study drug | Analyses of all efficacy end points for which patients were analyzed according to randomized treatment group, unless otherwise specified |
Safety set | All patients who received ≥ 1 dose of study drug | All safety analyses where patients analyzed according to the treatment they received, unless otherwise specified |
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
A summary of patient dispositions for Study 124 is presented in Table 17.
Baseline Characteristics
The baseline characteristics outlined in Table 18 are limited to those that are most relevant to this review or were assumed to affect the outcomes or interpretation of the study results.
Table 17: Summary of Patient Disposition From Study 124
Patient disposition | ELX-TEZ-IVA (N = 205) | Placebo (N = 102) |
|---|---|---|
Screened, N | NR | NR |
Randomized, N (%) | 205 (100.0) | 102 (100.0) |
Discontinued from study, N (%) | 8 (3.9) | 0 (0.0) |
Reason for discontinuation, N (%) | ||
Adverse events | 3 (1.5) | 0 (0.0) |
Withdrawal of consent (not due to adverse event) | 2 (1.0) | 0 (0.0) |
Death | 1 (0.5) | 0 (0.0) |
Other | 2 (1.0) | 0 (0.0) |
Discontinued treatment, N (%) | 9 (4.4) | 0 (0.0) |
Reason for discontinuation, N (%) | ||
Adverse events | 5 (2.4) | 0 (0.0) |
Subject refused further dosing (not due to adverse event) | 2 (1.0) | 0 (0.0) |
Pregnancy (self or partner) | 2 (1.0) | 0 (0.0) |
Full analysis set, N | 205 | 102 |
Safety, N | 205 | 102 |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; NR = not reported.
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Table 18: Summary of Baseline Characteristics From Study 124
Characteristic | ELX-TEZ-IVA (N = 205) | Placebo (N = 102) |
|---|---|---|
Sex, N (%) | ||
Male | 92 (44.9) | 50 (49.0) |
Female | 113 (55.1) | 52 (51.0) |
Childbearing potential, n (%) | ||
Yes | 93 (82.3) | 37 (71.2) |
No | 20 (17.7) | 15 (28.8) |
CFTR mutation group, N (%) | ||
≥ 1 RF-like mutation | 151 (73.7) | 74 (72.5) |
No RF-like mutation | 54 (26.3) | 28 (27.5) |
Age group, N (%) | ||
Age (years), mean (SD) | 33.3 (15.9) | 33.9 (16.4) |
Age (years), median (minimum to maximum) | 33.4 (6.3 to 73.2) | 33.5 (7.0 to 87.3) |
Race, N (%) | ||
White | 172 (83.9) | 87 (85.3) |
Black or African American | 0 (0.0) | 0 (0.0) |
Asian | 4 (2.0) | 3 (2.9) |
American Indian or Alaska Native | 0 (0.0) | 0 (0.0) |
Native Hawaiian or other Pacific Islander | 0 (0.0) | 0 (0.0) |
Other | 3 (1.5) | 1 (1.0) |
Not collected per local regulations | 26 (12.7) | 12 (11.8) |
Geographic region, N (%) | ||
North America | 14 (6.8) | 10 (9.8) |
Europe | 191 (93.2) | 92 (90.2) |
ppFEV1 | ||
< 40 | 5 (2.4) | 5 (4.9) |
≥ 40 to < 70 | 99 (48.3) | 47 (46.1) |
≥ 70 to ≤ 90 | 78 (38.0) | (37.3) |
> 90 | 23 (11.2) | 12 (11.8) |
Mean (SD) | 67.5 (17.6) | 68.1 (18.1) |
Median (minimum to maximum) | 69.5 (35.8 to 108.7) | 69.2 (34.0 to 107.6) |
Sweat chloride (mmol/L) | ||
Mean (SD) | 79.5 (26.9) | 75.2 (28.7) |
Median (minimum to maximum) | 89.5 (10.0 to 126.0) | 79.5 (13.0 to 133.0) |
CFQ-R (RD) score | ||
Mean (SD) | 64.1 (20.7) | 65.8 (21.3) |
Median (minimum to maximum) | 66.7 (11.1 to 100.0) | 72.2 (0.0 to 100.0) |
BMI (kg/m2) | ||
Mean (SD) | 22.5 (4.6) | 22.5 (4.2) |
Median (minimum to maximum) | 21.9 (13.4 to 38.3) | 22.2 (13.9 to 38.9) |
BMI z score (patients ≤ 20 years old at baseline) | ||
Mean (SD) | −0.34 (1.04) | −0.22 (1.01) |
Median (minimum to maximum) | −0.35 (−2.68 to 1.79) | −0.21 (−2.58 to 1.63) |
Weight (kg) | ||
Mean (SD) | 61.9 (18.5) | 63.2 (16.7) |
Median (minimum to maximum) | 61.5 (19.0 to 109.5) | 63.9 (23.6 to 102.0) |
Weight z score (patients aged ≤ 20 years at baseline) | ||
Mean (SD) | −0.39 (1.18) | −0.29 (1.15) |
Median (minimum to maximum) | −0.32 (−4.44 to 1.63) | −0.01 (−2.37 to 1.80) |
Height (cm) | ||
Mean (SD) | 164.2 (14.7) | 166.2 (13.6) |
Median (minimum to maximum) | 165.5 (116.5 to 191.0) | 168.9 (118.0 to 187.0) |
BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire-Revised (respiratory domain); ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; RF = residual function; SD = standard deviation.
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
A summary of patient exposure to ELX-TEZ-IVA or placebo for Study 124 is presented in Table 19.
Concomitant Medications and Co-Interventions
Table 20 provides a summary of concomitant medications used among patients in Study 124.
Table 19: Summary of Patient Exposure From Study 124
Exposure | ELX-TEZ-IVA (N = 205) | Placebo (N = 102) |
|---|---|---|
Total, patient-weeks (patient-years) | 4,784.1 (99.7) | 2,453.7 (51.1) |
Duration, mean weeks (SD) | 23.3 (3.3) | 24.1 (0.5) |
Duration, median (range) | 24.0 (1.6 to 26.3) | 24.0 (22.6 to 25.9) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; SD = standard deviation.
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Table 20: Summary of Concomitant Medications From Study 124 (At Least 20% of Patients)
Preferred term | ELX-TEZ-IVA (N = 205) | Placebo (N = 102) |
|---|---|---|
Patients with any concomitant medication | 205 (100.0) | 102 (100.0) |
Dornase alfa | 124 (60.5) | 57 (55.9) |
Sodium chloride | 116 (56.6) | 63 (61.8) |
Salbutamol | 93 (45.4) | 47 (46.1) |
Azithromycin | 71 (34.6) | 41 (40.2) |
Paracetamol | 70 (34.1) | 40 (39.2) |
Cholecalciferol | 66 (32.2) | 29 (28.4) |
Pancreatin | 53 (25.9) | 27 (26.5) |
Ibuprofen | 53 (25.9) | 18 (17.6) |
Colistimethate sodium | 44 (21.5) | 26 (25.5) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor.
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Efficacy
Absolute Change in ppFEV1
In Study 124, totals of 192 and 98 patients in the full analysis set (FAS) were evaluated through week 24 in the ELX-TEZ-IVA and placebo arms, respectively. Results showed an LS absolute change from baseline in ppFEV1 of 8.9 (SD = 0.6) in the ELX-TEZ-IVA arm versus −0.4 (SD = 0.8) in the placebo arm (Figure 3). MMRM analysis of this primary end point showed an LS mean difference for ELX-TEZ-IVA versus placebo of 9.2% (95% CI, 7.2 to 11.3; P < 0.0001).
Figure 3: MMRM Analysis of Absolute Change From Baseline in ppFEV1 (Percentage Points) at Each Visit up to Week 24 (Full Analysis Set)
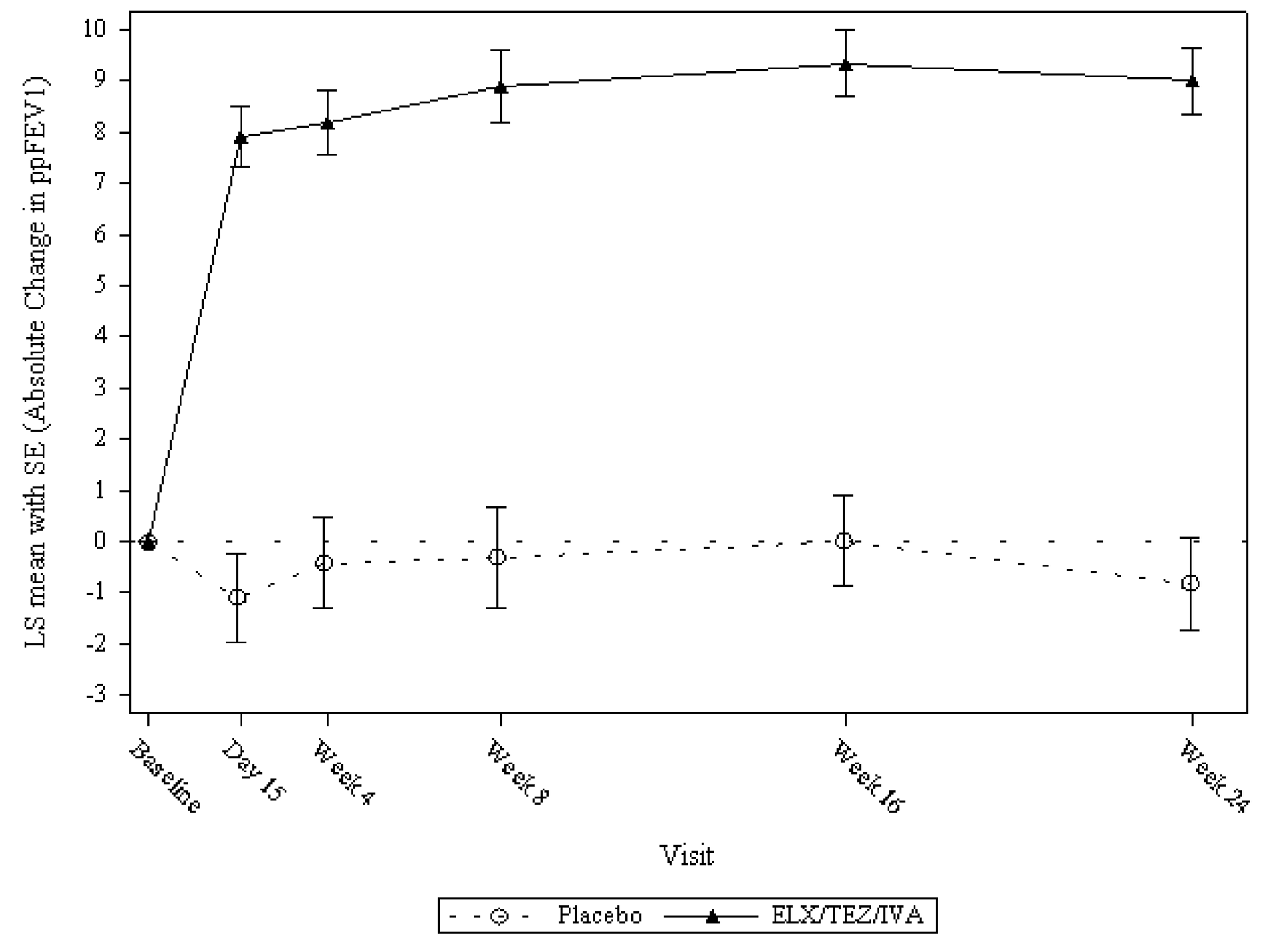
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; LS = least squares; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error.
Source: Clinical Study Report.45
Absolute Change in Sweat Chloride
In Study 124, totals of 200 and 100 patients in the FAS were evaluated through week 24 in the ELX-TEZ-IVA and placebo arms, respectively. Results showed an absolute change from baseline for SwCl, with an LS mean of −27.8 (SD = 1.1) in the ELX-TEZ-IVA arm versus 0.5 (SD = 1.6) in the placebo arm. An MMRM analysis of this secondary end point showed a statistically significant improvement (i.e., a reduction) in absolute change from baseline in SwCl for ELX-TEZ-IVA versus placebo, with an LS mean difference from placebo of −28.3 mmol/L (95% CI, −32.1 to −24.5; P < 0.0001).
Absolute Change in CFQ-R (RD) Score
In Study 124, totals of 202 and 102 patients in the FAS were evaluated through week 24 in the ELX-TEZ-IVA and placebo arms, respectively. Results showed an LS absolute change from baseline in CFQ-R (RD) score of 17.5 (SD = 1.2) in the ELX-TEZ-IVA arm versus −2.0 (SD = 1.6) in the placebo arm (Figure 4). MMRM analysis of this secondary end point showed a statistically significant LS mean difference for ELX-TEZ-IVA versus placebo of 19.5 points (95% CI, 15.5 to 23.5; P < 0.0001).
Figure 4: MMRM Analysis of Absolute Change From Baseline in CFQ-R (RD) Score at Each Visit up to Week 24 (Full Analysis Set)
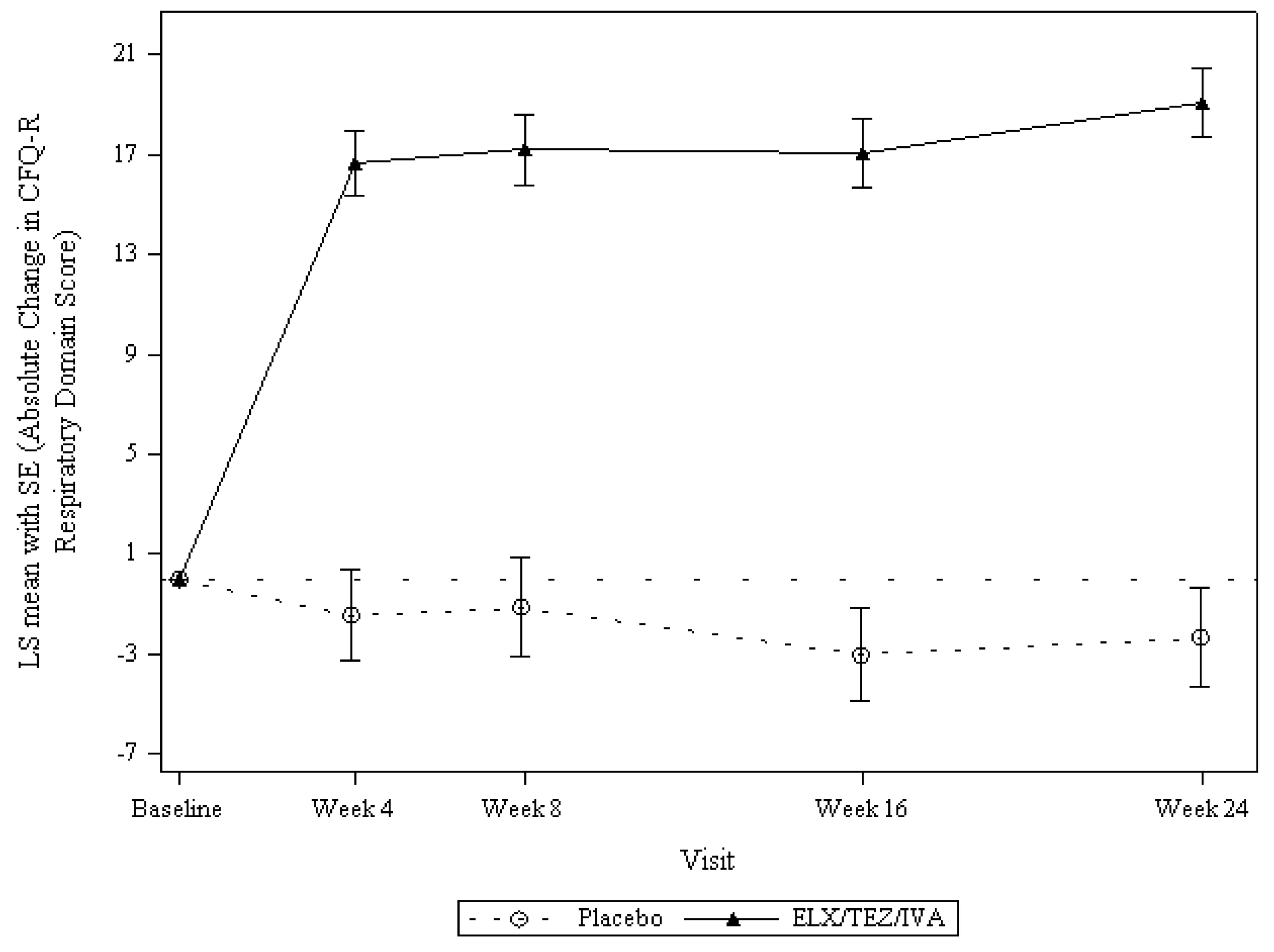
CFQ-R = Cystic Fibrosis Questionnaire-Revised; ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; LS = least squares; MMRM = mixed-effects model for repeated measures; SE = standard error.
Source: Clinical Study Report.45
Absolute Change in BMI
In Study 124, totals of 196 and 102 patients in the FAS were evaluated through week 24 in the ELX-TEZ-IVA and placebo arms, respectively. Results showed an absolute change from baseline for BMI with an LS mean of 0.81 (SD = 0.07) in the ELX-TEZ-IVA arm versus 0.35 (SD = 0.09) in the placebo arm (Figure 5). MMRM analysis of this secondary end point revealed a statistically significant change in absolute change from baseline in BMI for ELX-TEZ-IVA versus placebo, with an LS mean difference from placebo of 0.47 kg/m2 (95% CI, 0.24 to 0.69; P < 0.0001).
Figure 5: Absolute Change From Baseline in BMI at Each Visit up to Week 24 (FAS)
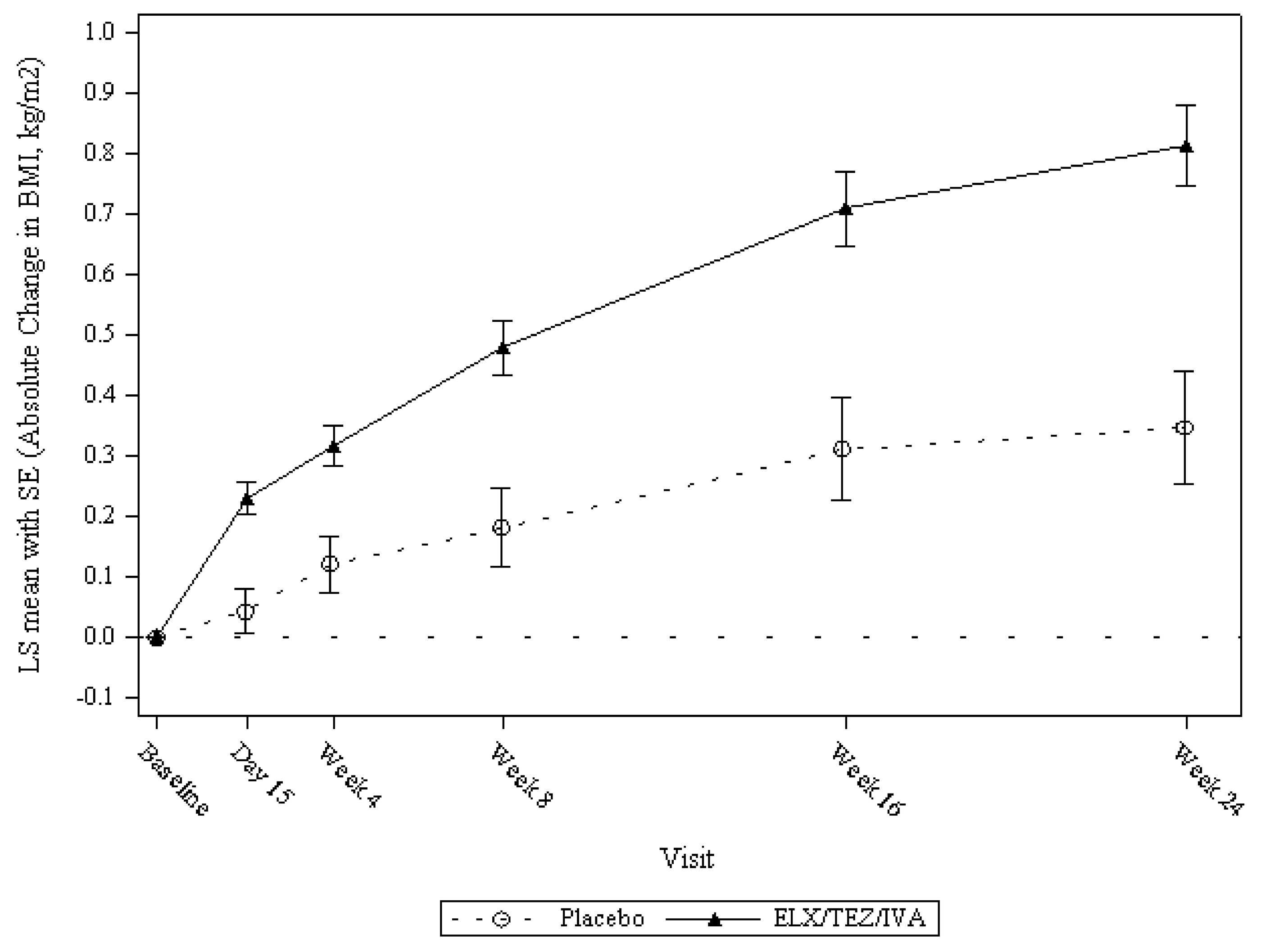
BMI = body mass index; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; FAS = Full Analysis Set; LS = least squares; SE = standard error.
Source: Clinical Study Report.45
Absolute Change in Weight
Results showed an absolute change from baseline for weight with an LS mean of 2.4 (SD = 0.2) in the ELX-TEZ-IVA arm versus 1.2 (SD = 0.3) in the placebo arm. MMRM analysis of this secondary end point showed a statistically significant change in absolute change from baseline in weight for ELX-TEZ-IVA versus placebo, with an LS mean difference from placebo of 1.3 kg (95% CI, 0.6 to 1.9; P < 0.0001).
Number of PEx Events
Results showed an estimated event rate per year of 0.17 in the ELX-TEZ-IVA arm versus 0.63 in the placebo arm. Analysis of this secondary end point showed a statistically significant reduction in PEx events through week 24, with a PEx rate that was 72% lower in the ELX-TEZ-IVA arm versus placebo (rate ratio = 0.28; 95% CI, 0.15 to 0.51; P < 0.0001).
Absolute Change in BMI Z Score (Patients Aged 20 Years or Younger)
Results showed an absolute change from baseline for BMI z score, with an LS mean of 0.22 (SD = 0.04) in the ELX-TEZ-IVA arm versus 0.14 (SD = 0.06) in the placebo arm. MMRM analysis of this end point showed a change in absolute change from baseline in BMI z score for ELX-TEZ-IVA versus placebo, with an LS mean difference from placebo of 0.08 (95% CI, −0.06 to 0.22).
Absolute Change in Body Weight Z Score (Patients Aged 20 Years or Younger)
Results showed an absolute change from baseline for weight z score, with an LS mean of 0.21 (SD = 0.03) in the ELX-TEZ-IVA arm versus 0.14 (SD = 0.05) in the placebo arm. MMRM analysis of this end point showed a change in absolute change from baseline in weight z score for ELX-TEZ-IVA versus placebo, with an LS mean difference from placebo of 0.06 (95% CI, −0.06 to 0.18).
Table 21: Summary of Results From Study 124 (Full Analysis Set)
Outcome | ELX-TEZ-IVA (N = 205) | Placebo (N = 102) |
|---|---|---|
Absolute change from baseline in ppFEV1 through week 24 | ||
Number of patients contributing to baseline evaluation | 205 | 102 |
Baseline, mean (SD) | 67.5% (17.6) | 68.1% (18.1) |
Number of patients contributing to the analysis | 192 | 98 |
LS mean change from baseline (95% CI) | 8.9% (7.7 to 10.0) | −0.4% (−2.0, 1.3) |
LS mean difference (95% CI), P value | 9.2 (7.2 to 11.3), < 0.0001 | |
Absolute change from baseline in SwCl (mmol/L) through week 24 | ||
Number of patients contributing to baseline evaluation | 202 | 100 |
Baseline, mean (SD) | 79.5 (26.9) | 75.2 (28.7) |
Number of patients contributing to the analysis | 200 | 100 |
LS mean change from baseline (95% CI) | −27.8 (−30.0 to −25.6) | 0.5 (−2.6 to 3.6) |
LS mean difference (95% CI), P value | −28.3 (−32.1 to −24.5), < 0.0001 | |
Absolute change from baseline in CFQ-R (RD) score through week 24 | ||
Number of patients contributing to baseline evaluation | 202 | 102 |
Baseline, mean (SD) | 64.1 (20.7) | 65.8 (21.3) |
Number of patients contributing to the analysis | 202 | 102 |
LS mean change from baseline (95% CI) | 17.5 (15.2 to 19.8) | −2.0 (−5.2 to 1.3) |
LS mean difference (95% CI), P value | 19.5 (15.5 to 23.5), < 0.0001 | |
Absolute change from baseline in in BMI (kg/m2) at week 24 | ||
Number of patients contributing to the baseline evaluation | 205 | 102 |
Baseline, mean (SD) | 22.5 (4.6) | 22.5 (4.2) |
Number of patients contributing to the analysis | 196 | 102 |
LS mean change from baseline (95% CI) | 0.8 (0.7 to 0.9) | 0.4 (0.2 to 0.5) |
LS mean difference (95% CI), P value | 0.5 (0.2 to 0.7), < 0.0001 | |
Absolute change from baseline in weight (kg) at week 24 | ||
Number of patients contributing to baseline evaluation | 205 | 102 |
Baseline, mean (SD) | 61.9 (18.5) | 63.2 (16.7) |
Number of patients contributing to the analysis | 196 | 102 |
LS mean change from baseline (95% CI) | 2.4 (2.1 to 2.8) | 1.2 (0.6 to 1.7) |
LS mean difference (95% CI), P value | 1.3 (0.6 to 1.9), < 0.0001 | |
Number of PEx events through week 24 | ||
Number of patients contributing to the analysis | 205 | 102 |
Number of patients with events, n (%) | 18 (8.8%) | 26 (25.5%) |
Number of events | 21 | 40 |
Estimated annualized event rate | 0.17 (95% CI, NR) | 0.63 (95% CI, NR) |
Rate ratio for ELX-TEZ-IVA vs. placebo (95% CI), P value | 0.3 (0.2 to 0.5), < 0.0001 | |
Absolute change from baseline in in BMI z score (kg/m2) at week 24 (patients aged ≤ 20 years at baseline) | ||
Number of patients contributing to the baseline evaluation | 52 | 26 |
Baseline, mean (SD) | −0.3 (1.0) | −0.2 (1.0) |
Number of patients contributing to the analysis | 48 | 24 |
LS mean change from baseline (95% CI) | 0.2 (0.1 to 0.3) | 0.1 (0.0 to 0.3) |
LS mean difference (95% CI), P value | 0.1 (−0.1 to 0.2) | |
Absolute change from baseline in in weight z score (kg/m2) at week 24 (patients ≤ 20 years of age at baseline) | ||
Number of patients contributing to the baseline evaluation | 52 | 26 |
Baseline, mean (SD) | −0.4 (1.2) | −0.3 (1.2) |
Number of patients contributing to the analysis | 48 | 24 |
LS mean change from baseline (95% CI) | 0.2 (0.1 to 0.3) | 0.1 (0.1 to 0.2) |
LS mean difference (95% CI), P value | 0.1 (−0.1 to 0.2) | |
BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised (respiratory domain); CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; LS = least squares; NR = not reported; PEx = pulmonary exacerbations; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SwCl = sweat chloride.
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Subgroup Analyses for Noncanonical Splice Mutations
Study 124 enrolled patients with 3 of the 5 noncanonical splice mutations in the target patient population for this review (2789 + 5G > A, 3272 to 26A > G, and 3849 + 10kbC > T). The sponsor conducted subgroup analyses for absolute change from baseline through 24 weeks in ppFEV1, SwCl, and CFQ-R (RD) (Table 22). Results of these analyses were consistent with the primary analyses.
Table 22: Results of Splicing Mutation Subgroup from Study 124 (Full Analysis Set)
Outcome | Placebo (N = 82) | ELX-TEZ-IVA (N = 34) |
|---|---|---|
ppFEV1 (percentage points) | ||
Baseline | ||
n | 34 | 82 |
mean (SD) | 61.6 (19.8) | 64.0 (17.0) |
Average change through week 24 | ||
n | 33 | 79 |
Mean (95% CI) | 0.1 (−2.4 to 2.6) | 8.9 (6.9 to 10.8) |
SwCl (mmol/L) | ||
Baseline | ||
n | 34 | 81 |
Mean (SD) | 76.0 (30.0) | 79.3 (26.4) |
Average change through week 24 | ||
n | 34 | 80 |
Mean (95% CI) | −0.8 (−2.8 to 1.2) | −15.4 (−17.7 to −13.1) |
CFQ-R RD (points) | ||
Baseline | ||
n | 34 | 81 |
Mean (SD) | 62.4 (24.6) | 62.4 (21.4) |
Average change through week 24 | ||
n | 34 | 81 |
Mean (95% CI) | −0.5 (−5.7 to 4.7) | 17.7 (13.5 to 22.0) |
CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised (respiratory domain); CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SwCl = sweat chloride.
Source: Clinical Study Report.45
Subgroup Analyses for Patients With Only 1 Responsive Mutation
The majority of patients enrolled in Study 124 were heterozygous for the CFTR mutations and some patients carried complex alleles (i.e., multiple mutations on 1 allele), Health Canada requested that the sponsor provide additional analyses for Study 124 showing a by-mutation analysis for patients who have only a single potentially responsive target mutation on 1 allele, and either the same single mutation on the second allele or a mutation expected to be nonresponsive (e.g., a frameshift, large deletion, or premature stop codon). The results are summarized in Table 23, with the majority showing within-group improvements comparable to the primary analysis Comparisons for these subgroups were not provided versus placebo. The sample sizes were small for these subgroups and baseline values varied, which may affect the magnitude of change observed after the 24-week treatment period.
█████ | ██████████ | █████| ███ | ████ ████████ | █████ ██ █████ |
|---|---|---|---|---|
████████ █ ███ | █████████ █ ███ | █████████ █ ███ | ||
████ █ ███████ | ||||
████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ████ ██████ | ████ ██████ | |
█████ █████ ████ ████ ██ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
█████████ | ||||
████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ████ █████ | ████ ██████ | |
██████████ ████ ██ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
██████████ | ||||
████████ | ███ | ██ | ██ | ███ |
████ ████ | ████ ██████ | ████ ██████ | ████ ██████ | |
██████ █████ █████ ████ ██ | ███ | ███ | ███ | ██ |
████ ████ | ███ █████ | █████ █████ | ████ ██████ | |
████ | ||||
████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ████ █████ | ████ ██████ | |
█████ ██████ █████ ████ ██ | ███ | ███ | ███ | ███ |
████ ████ | ███ ██████ | █████ ██████ | ████ ██████ | |
█████ | ||||
████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ████ ██████ | ████ ██████ | |
████ ████ ████ ████ ██ | ███ | ███ | ███ | ███ |
████ ████ | ███ ██████ | █████ ██████ | ████ ██████ | |
██████ | ||||
████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ████ █████ | ████ ██████ | |
██████ █████ ██████ ███ ██ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | ████ █████ | ████ ██████ | |
█████ | ||||
████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ████ ██████ | ████ ██████ | |
██████ █████ █████ ████ ██ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
█████ | ||||
████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ████ ██████ | ████ ██████ | |
█████ ████ ████ ████ ██ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
██████ | ||||
████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ████ █████ | ████ ██████ | |
██████ █████ ██████ ███ ██ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
█████ ███ ██████ ████████ █████████████████████ ███████████ ███████ ████ ████████████ ████ ████ ████████ ████ ████ ██████████ ██ ████ ██ ██████████ ██ █████ ██████ █████ ███████ ███████ █████████ ██████ ██████████ ██████ ██ █ ███████ ███ ████████ ██████████ █████ █████ █████████ ████ █████████████████ ████████ ███ ███████ ██ ███ ████ ██████ ███████████ ███████████ ██████ ███ █████ ████ ██ █████ ████ ██ ███ █████████ ███████ █ ████████ ██ █████████ ██ █████ ███ ██ ███████████ ███████ ██████ ████ ████████ ██████ ███ ████████ ███ ███ ██████████ ███ ███ ██████████ ████████ ██ ████ █ █████ █ ████████ ██ ███ ██████ ████████ ██ ███ ███████████ ███ ██████ ████ ██████████ ████ █████████ ████████████ ██ ███ ██ ████ ███ ████████ ██ ███ ███████████ ███ ███ ███████ ██████ ████ ████████ ███████ ████ ███████████ ██████ ██████ ████████
Harms
Table 24 provides a summary of harms data.
Adverse Events
The proportions of patients who experienced at least 1 AE were 94.1% in the ELX-TEZ-IVA group and 95.1% in the placebo group. The majority of AEs were mild or moderate in severity. Severe AEs occurred in 15 patients (7.3%) in the ELX-TEZ-IVA group and 12 patients (11.8%) in the placebo group.
Serious Adverse Events
Serious AEs occurred in 18 patients (8.8%) in the ELX-TEZ-IVA group and 15 patients (14.7%) in the placebo group. SAEs that occurred in 2 or more patients in the ELX-TEZ-IVA group included infective PEx of CF (5 patients) and bronchopulmonary aspergillosis allergic (2 patients). The only SAE that occurred in 2 or more patients in the placebo group was infective PEx of CF (13 patients).
Withdrawal Due to Adverse Events
Drug interruptions due to AEs were reported in 12.2% of patients in the ELX-TEZ-IVA group and 1.0% of the placebo group. AEs that led to treatment interruption for at least 1 patient in the ELX-TEZ-IVA group were rash (n = 14), increased alanine transaminase (n = 3), increased aspartate transaminase (n = 3), and increased gamma-glutamyl transferase (n = 3). Five (2.4%) patients in the ELX-TEZ-IVA group discontinued due to AEs (1 patient because of liver function test elevations, 1 patient due to AEs of lung adenocarcinoma and pneumonia, 1 patient because of diarrhea, 1 patient because of hepatic cytolysis, and 1 patient because of rash maculopapular). No patients in the placebo group discontinued due to an AE.
Mortality
One patient in the ELX-TEZ-IVA group (0.5%) died due to an SAE of lung adenocarcinoma that was not considered related to study drug treatment.
Notable Harms
Elevated transaminase events were considered AESIs and occurred in | ██████ patients in the ELX-TEZ-IVA group and no patients in the placebo group. All elevated transaminase events were mild or moderate in severity, and none were serious. Rash events were also considered AESIs and occurred in 55 patients in the ELX-TEZ-IVA group (26.8%) and 3 patients in the placebo group (2.9%). The majority of rash events were mild or moderate in severity. One subject in the ELX-TEZ-IVA group (0.5%) had a serious rash event that was considered related to study drug treatment.
Table 24: Summary of Harms Results From Studies Included in the Systematic Review
Adverse events | ELX-TEZ-IVA (N = 205) | Placebo (N = 102) |
|---|---|---|
At least 1 AE, n (%) | 193 (94.1) | 97 (95.1) |
AEs leading to study drug discontinuation, n (%) | 5 (2.4) | 0 (0.0) |
AEs leading to study drug interruption, n (%) | 25 (12.2) | 1 (1.0) |
Grade 3, 4, or 5 AEs, n (%) | 16 (7.8) | 12 (11.8) |
SAEs, n (%) | 18 (8.8) | 15 (14.7) |
AEs leading to death, n (%) | 1 (0.5) | 0 (0.0) |
Most common (≥ 5%) AE, n (%) | ||
Rasha | 45 (22.0) | 1 (1.0) |
Nasopharyngitis | 42 (20.5) | 20 (19.6) |
Headachea | 37 (18.0) | 13 (12.7) |
Cough | 36 (17.6) | 26 (25.5) |
Infective PEx of CF | 31 (15.1) | 37 (36.3) |
Pyrexia | 27 (13.2) | 14 (13.7) |
Diarrheaa | 26 (12.7) | 10 (9.8) |
Rhinitis | 20 (9.8) | 6 (5.9) |
Increased sputum increased | 20 (9.8) | 13 (12.7) |
COVID-19 | 19 (9.3) | 10 (9.8) |
Influenza | 18 (8.8) | 2 (2.0) |
Abdominal paina | 17 (8.3) | 13 (12.7) |
Oropharyngeal pain | 17 (8.3) | 10 (9.8) |
Upper respiratory tract infectiona | 17 (8.3) | 10 (9.8) |
Constipation | 15 (7.3) | 4 (3.9) |
Vomiting | 15 (7.3) | 7 (6.9) |
Hemoptysis | 12 (5.9) | 6 (5.9) |
Upper abdominal pain | 10 (4.9) | 7 (6.9) |
Nasal congestiona | 6 (2.9) | 8 (7.8) |
Productive cough | 6 (2.9) | 6 (5.9) |
SAEs in ≥ 2 patients, n (%) | ||
Patients with SAEs | 18 (8.8) | 15 (14.7) |
Infective PEx of CF | 5 (2.4) | 13 (12.7) |
Related SAEs | 2 (1.0) | 0 (0.0) |
Bronchopulmonary aspergillosis allergic | 0 (0.0) | 2 (1.0) |
AEs of special interest, n (%) | ||
Elevated transaminase levels | | █████ | | █████ |
Rash | 55 (26.8) | 3 (2.9) |
AE = adverse event; CF = cystic fibrosis; CK = creatine kinase; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; PEx = pulmonary expulsion; SAE = serious adverse event.
aLabelled in ELX-TEZ-IVA controlled-drug delivery system.
bAE belongs to 1 subject.
cAE belongs to 1 subject.
Sources: Clinical Study Report45 and the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
Randomization was performed using an appropriate methodology with adequate allocation concealment (i.e., an interactive web response system) and stratification based on relevant prognostic factors (i.e., age [aged < 18 years versus ≥ 18 years], baseline ppFEV1 [< 70% versus ≥ 70%], and CFTR genotype [contains ≥ 1 RF-like mutation versus does not contain an RF-like mutation]). Baseline and demographic characteristics were generally well balanced across the ELX-TEZ-IVA and placebo groups. Baseline BMI z scores and weight z scores were lower in the placebo group (−0.2 and −0.3, respectively) compared with the ELX-TEZ-IVA group (−0.3 and −0.4, respectively). The clinical experts consulted for this review noted these differences are unlikely to be clinically relevant.
Minor imbalances with the prior and concomitant medications were reported. A greater proportion of patients in the placebo group compared with the ELX-TEZ-IVA group reported prior use of inhaled hypertonic saline at baseline (52.0% versus 44.4%, respectively) and used inhaled hypertonic saline during the study (61.8% versus 56.6%, respectively). A greater proportion of patients in the ELX-TEZ-IVA group reported use of dornase alfa during the study compared with the placebo group (61.8% versus 56.6%, respectively). Any potential impact of these imbalances is uncertain (e.g., concomitant therapies could potentially benefit respiratory end points, or they could be indication that these patients had more severe disease that required additional treatment). The clinical experts consulted for this review noted that the differences are unlikely to be clinically relevant.
Study treatments were administered in a double-blind manner, with all groups issued the same number of tablets each day. The ELX-TEZ-IVA tablets were identical in appearance to the placebo tablets. The AE profile of ELX-TEZ-IVA was unlikely to compromise blinding in the study, except for those who experienced a rash after initiating treatment with ELX-TEZ-IVA (22% in the ELX-TEZ-IVA versus 1% in the placebo group). Rash is a well-known AE associated with ELX-TEZ-IVA treatment and is documented in the Canadian product monograph, which notes that the event is more common in females using hormonal contraceptive therapy. The observation of an elevated incidence of rash in the ELX-TEZ-IVA group is consistent with previous ELX-TEZ-IVA pivotal trials, although the proportion of patients affected in Study 124 (22%) is higher than in the other pivotal trials (approximately 10% for both the adolescent and adult and the pediatric trials). The clinical experts noted that these events would likely have compromised blinding for those affected but does not affect the overall interpretation of the results. The review team agreed that, given assessment of the efficacy outcomes investigated, and with the exception of health-related quality of life, the study’s results are relatively objective and less susceptible to bias from unblinding or patients or investigators.
Patient disposition was thoroughly documented and well reported by the sponsor in its application to CDA-AMC. Few patients discontinued the trials (the completion rate was 96.1% with ELX-TEZ-IVA and 100% with placebo), although the studies were relatively short in duration, which may in part explain the high percentage of patients who completed. Each FAS included all randomized patients.
Adherence to the study treatments, which was evaluated by counting the number of study drugs at each visit, was reported to exceed 98.9% in Study 124. In accordance with the study protocol, the use of concomitant medications remained stable throughout the treatment period.
There are no globally accepted definitions for PEx events in patients with CF. The definitions used in Study 124 were considered appropriate by regulatory authorities and the clinical experts consulted for this review. There was no independent adjudication of PEx events. When evaluated as an efficacy end point, fewer patients in Study 124 met the criteria for a PEx compared to the number of events reported as AEs (i.e., 36.3% versus 25.5% in the placebo group and 15.1% versus 8.8% in the ELX-TEZ-IVA group). Unlike previous ELX-TEZ-IVA clinical trials, Study 124 did not include a separate evaluation of PEx events that required the use of IV antibiotics and/or hospitalization. The clinical experts consulted for this review were not concerned about the absence of separate end points evaluating potential reductions in PEx events that required the use of IV antibiotics and/or hospitalization. The 24-week study period reduces the accuracy and variance of the point estimates for the PEx rates because of seasonal variation and other temporal factors that require longer follow-up to accurately estimate (ideally, at least 12 months of follow-up would account for these variables).
Statistical power calculations were reported for Study 124 and a sufficient number of patients were enrolled and completed the study. The number of withdrawals from the trials was well below the 10% proportion assumed in the sponsor’s statistical power calculations. The MMRM analyses for the primary and secondary evaluations assumed data were missing at random, which may not be a valid assumption. However, the amount of missing data in the trials was low and sensitivity analyses using multiple imputation were supportive of the primary analyses. The analyses in Study 124 were not true intention-to-treat analyses, although the majority of patients enrolled in the study were accounted for in the analyses (e.g., 95% of patients included in the primary analysis for change from baseline in ppFEV1).
In Study 124, the primary end point was the absolute change from baseline in ppFEV1 through 24 weeks. The key secondary end points were tested using a hierarchical approach to control the overall type I error rate at 0.05. All end points within the statistical testing hierarchies were statistically significant. Subgroup analyses and exploratory end points were tested without adjustment for multiple comparisons and all P values are considered nominal.
External Validity
The diagnostic criteria used in the screening process for Study 124 were consistent with Canadian clinical practice for identifying patients with CF. Because the sponsor reported that all patients with CF in Canada have their genotype evaluated, identification of those who could be considered candidates for ELX-TEZ-IVA based on the expanded patient population would not be problematic in practice. The clinical experts consulted for this review noted that prescribing ELX-TEZ-IVA to patients with these additional CFTR mutations would be integrated into Canadian clinical practice in the same manner as done for previous mutations (i.e., all patients would be considered candidates as there are no other potential disease-modifying therapies available for the target population).
Patients with CF with more severe lung disease (e.g., a ppFEV1 < 40% at screening) were excluded from Study 124; the results are therefore primarily applicable to patients with moderate (i.e., an FEV1 of 40% to 69%) to mild (i.e., FEV1 of 70% to 89%) lung disease. This is identical to the phase III trials previously conducted by the sponsor for ELX-TEZ-IVA and for other approved combination CFTR modulators (LUM-IVA and TEZ-IVA). The sponsor has previously reported that this population was selected because it was considered to be the most likely patient group to show an improvement in lung function in a clinical trial based on their experience with other therapies targeting CF lung disease. These screening criteria resulted in trial populations for which the proportion of patients with mild lung disease was generally similar to that of the adult CF population in Canada (approximately 27% of patients had mild lung disease in 2019).17 The proportion of patients with moderate lung disease in Study 124 was comparable to that of the overall adult CF population in Canada (approximately 38% in 2019).17 Previous CDA-AMC reviews evaluated data for the use of ELX-TEZ-IVA in patients with 1 or more F508del mutations who had more severe disease lung disease at the time of treatment initiation. Consistent with input from clinical specialists, these studies suggest that patients with advanced lung disease benefit from ELX-TEZ-IVA. In the current application, the sponsor has included 2 studies from a compassionate-access program in France that evaluated the use of ELX-TEZ-IVA in patients with advanced lung disease who have 1 or more N1303K mutations (Burgel et al. [2023]3,13 and Burgel et al. [2024]4 in the Studies Addressing Gaps in the Systematic Review Evidence section).
A majority of the participants in Study 124 were from Europe (92.2%) and the remaining patients were from sites in Canada (7.8%). Study 124 was conducted to support regulatory applications in Europe and Canada, which explains the absence of sites in the US (where ELX-TEZ-IVA has been approved for use in responsive nonF508del mutations since 2020). The clinical experts consulted noted that the results from centres in Europe would be generalizable to the Canadian setting. Study 124 was conducted at specialized CF clinics, which is consistent with Canadian clinical practice.
The Cystic Fibrosis Foundation clinical practice guidelines recommend that adult women and men (aged ≥ 20 years) maintain a BMI at or above 22 kg/m2 and 23 kg/m2, respectively. Mean baseline BMI was similar in Study 124 was 22.46 (SD = 4.45) which is similar to the estimated national median BMI for adult patients with CF (22.7 kg/m2) in Canada.17
As with previous CFTR-modulator studies, Study 124 excluded patients with a history of colonization with B. cenocepacia, B. dolosa, and/or M. abscessus. The CCFR indicated that 3.9% of patients with CF in Canada (88.4% of whom are adults) were infected with B. cepacia complex species in 2021.18 The clinical experts consulted for this review noted that the exclusion of such patients does not significantly lower the generalizability of the study results, given that these patients represent a small minority of those who could be eligible for ELX-TEZ-IVA and that the clinical management of such patients is more complex and variable than those without B. cepacia infection. CDA-AMC committees have previously acknowledged the unmet need for these patients.
The studies included excluded patients who had a respiratory infection, PEx, or changes in their therapy for pulmonary disease within 4 weeks before the first dose of the study drug. These are identical to the exclusion criteria used in the pivotal trials for the other CFTR modulators that are currently approved. The clinical experts consulted for this review noted that the exclusion of these patients is unlikely to limit the generalizability of the results to the broader population of patients with CF.
The use of placebo as the comparator in Study 124 is appropriate given CFTR modulators are not approved for the target patient population, except for the subset of patients who have a CFTR gating mutation and are currently eligible for treatment with IVA monotherapy. As noted in the Indirect Evidence section, the exclusion of an indirect comparison evaluating the comparative efficacy of ELX-TEZ-IVA versus IVA from the application is not considered an important limitation by the review team.
Study 124 investigated the use of ELX-TEZ-IVA at the dosage recommended in the Canadian product monograph. All studies compared the addition of the study treatments to ongoing standard CF-management therapies, which is reflective of how ELX-TEZ-IVA and other CFTR modulators would be administered in clinical practice. In general, the background therapies that were reported at baseline in the included studies were consistent with those used in Canadian clinical practice.
Similar to the pivotal trials for LUM-IVA47 and TEZ-IVA,48,49 patients in Study 124 were permitted to use inhaled hypertonic saline, which is commonly used in Canadian clinical practice. This feature improves the generalizability of the studies compared with the pivotal studies for ivacaftor (i.e., the STRIVE, ENVISION, and KONNECTION studies),50-52 during which patients were required to discontinue use of hypertonic saline. CDEC had previously noted that the exclusion of concomitant inhaled hypertonic saline was an important limitation of the IVA clinical study.35,36
Study 124 evaluated the impact of ELX-TEZ-IVA on a range of different outcomes that are important in the management of CF. These included respiratory function (ppFEV1), nutritional status and growth (e.g., weight and BMI), health-related quality of life (CFQ-R), and clinical events (PEx events). As noted in the input from clinician groups, the end points in the clinical trials largely align with those that are evaluated in routine clinical practice. Spirometry measurements were standardized and performed according to American Thoracic Society guidelines (e.g., prebronchodilator and before dosing).53,54
The 24-week treatment period used in Study 124 was sufficient for observing treatment differences in the primary and secondary end points; however, the duration was insufficient to determine whether treatment with ELX-TEZ-IVA has the potential to modify the course of disease for patients with CF. Previous CDA-AMC reviews of ELX-TEZ-IVA have evaluated evidence indicating that the impact of the treatment is durable; this is consistent with input from clinicians in Canada who have noted important long-term improvements in patients who initiate and continue with treatment. The reduction in PEx rates reported in Study 124 may not be observed to the same extent in clinical practice because of the relatively short duration of the trial and the effect on the accuracy of the rates (although the clinical specialists consulted during this review supported the effectiveness of ELX-TEZ-IVA for reducing exacerbations based on real-world use in their clinics for those with 1 or more 508del mutations in the CFTR gene).
As with the pivotal trials conducted for IVA, LUM-IVA, and TEZ-IVA, patients with CF who had received a lung transplant (or any organ or hematological transplant) were excluded from Study 124. According to the CF Canada registry, 7.8% of the Canadian CF population had received a lung transplant as of 2019;17 this is a relatively large subpopulation patients who were not studied in the clinical trials. The applications filed with CDA-AMC for ELX-TEZ-IVA have not included evidence regarding the use of the treatment in patients with CF who have had a lung transplant. The experts consulted for this review noted that ELX-TEZ-IVA would not likely be initiated in patients who have undergone a lung transplant. For those who have undergone a liver transplant, ELX-TEZ-IVA could be initiated as the drug may benefit the patient’s lung function. After a liver transplant, patients would likely receive additional monitoring for potential toxicity with a lower threshold for interrupting or discontinuing the drug (because of the potential risk of hepatic adverse events with ELX-TEZ-IVA). The sponsor expressed disagreement with this perspective and noted that input received from clinician groups (CF Canada Health Care Advisory Council and CanACT) suggests that patients who have undergone a lung transplant, particularly those who have significant sinus disease, could still benefit from ELX-TEZ-IVA. CanACT noted that, because ELX-TEZ-IVA could diminish the risk of developing chronic rejection after a lung transplant, ELX-TEV-IVA should be considered in those lung-transplant recipients with significant sinus disease. CanACT added that these patients see an improvement in their SwCl values and therefore avoid episodes of severe dehydration that can otherwise occur. Data for use in patients after a lung transplant have not been submitted for review by the sponsor.
As is common in clinical trial settings, patients enrolled in Study 124 received extensive contact with health professionals over the study period (e.g., 7 clinic visits and 1 telephone contact over a 6-month period). This level of contact is not reflective of routine care for patients with CF with relatively stable disease. The clinical experts consulted for this review and the clinician groups who provided input noted that patients with CF are typically seen once every 3 months. The experts noted that the level of contact in the clinical trials is typical for CF studies and would not affect the generalizability of the results to the target population in Canada.
Adherence to study treatment was high (> 99%) throughout the treatment periods of all studies. The clinical experts consulted for this review noted that the level of adherence observed in the included studies is typical of adults and adolescents with CF in Canada, where adherence with treatments, including orally administered treatments, is considerably lower.66
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform the expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:55,56
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 3 presents the GRADE summary of findings for ELX-TEZ-IVA versus placebo.
Long-Term Extension Studies
Contents within this section were informed by materials submitted by the sponsor. The following summary was validated by the review team.
Description of Studies
Study 125 is an open-label, long-term extension phase of Study 124 conducted to assess the long-term safety and efficacy of ELX-TEZ-IVA in patients with CF aged 6 years and older with non-F508del mutations in the CFTR gene that are responsive based on clinical and/or in vitro data. The data cut included in the submission to CDA-AMC is from August 28, 2023, and reports the results for 4 weeks after the end of Study 124. A timeline of the study time points and transitions is presented in Figure 6.
Figure 6: Duration of Study 125
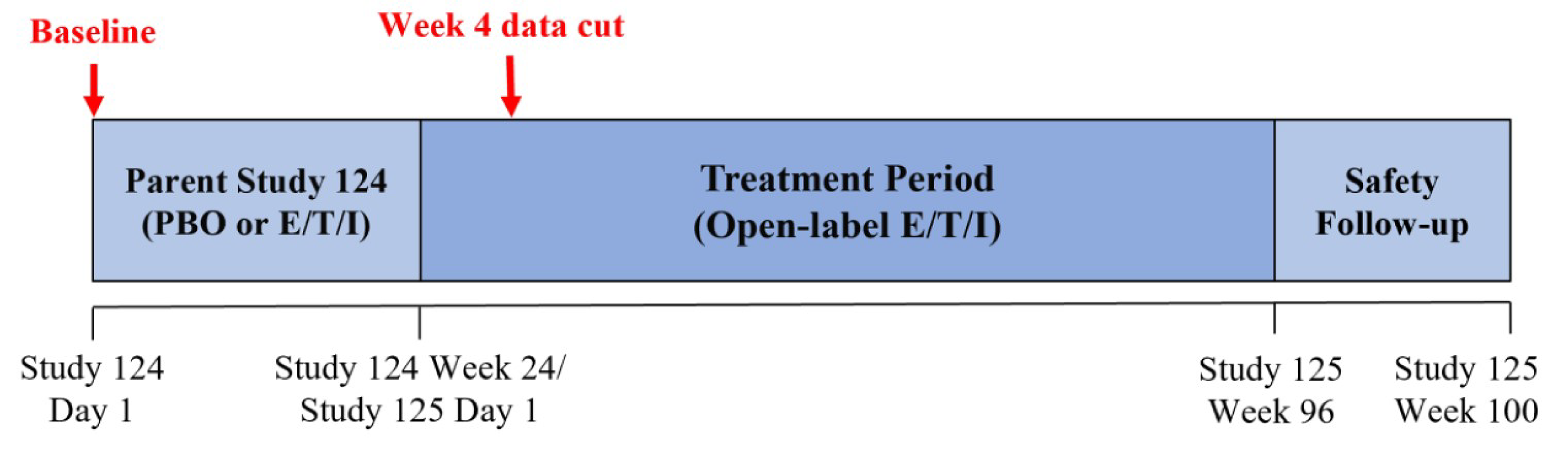
E/T/I = elexacaftor-tezacaftor-ivacaftor; PBO = placebo.
Source: Clinical Study Report.57
Populations
Patients were eligible for Study 125 if they were aged 6 years or older and completed study drug treatment in Study 124 or had study drug interruption(s) in the parent study but completed the study visits up to the last scheduled visit. Patients were excluded if they demonstrated intolerance to ELX-TEZ-IVA in Study 124.
Interventions
ELX-TEZ-IVA was administered at the same dosage as in Study 124. For those aged 12 years or younger, the doses were adjusted upwards if the patient increased in age and weight.
Outcomes
All AEs and SAEs are to be assessed as primary end points from baseline until week 100. Absolute changes from baseline for ppEV1, SwCl, CFQ-R (RD), BMI, weight, and number of PEx are all to be measured from baseline until week 96 as secondary end points of interest. Results are currently available and presented for ppEV1, SwCl, and CFQ-R (RD) for the 4-week data cut-off.
Statistical Analysis
Methods for statistical analysis were not reported.
Results
Patient Disposition
Only an additional 4 weeks of exposure was available for Study 125 and patient disposition was not reported.
Efficacy
A summary of efficacy results from Study 125 is presented in Table 25. Those who switched from placebo to ELX-TEZ-IVA demonstrated improvements in ppFEV1 (mean change = 7.1 percentage points [SD = 7.3]), SwCl (mean change = −27.4 mmol/L [SD = 18.9]), and CFQ-R RD (mean change = 14.7 points [SD = 22.6]) after receiving ELX-TEZ-IVA for 4 weeks. For those who received ELX-TEZ-IVA in the parent study, improvements in ppFEV1 (mean change = 10.1 percentage points [SD = 11.0]), SwCl (mean change = −30.3 mmol/L [SD = 21.9]), and CFQ-R (RD) (mean change = 20.1 points [SD = 20.7]) were maintained after 4 additional weeks.
Table 25: Summary of Efficacy Data
Outcome | ELX-TEZ-IVA (N = 195) | Placebo (N = 102) |
|---|---|---|
Absolute change from baseline in ppFEV1 through week 4a | ||
Patients in baseline evaluation | 195 | 102 |
Baseline, mean (SD) | 67.3 (17.4) | 68.1 (18.1) |
Patients contributing to the analysis | 170 | 86 |
Mean change from baseline (SD) | 10.1 (11.0) | 7.1 (7.3) |
Median change from baseline (minimum to maximum) | 8.8 (−14.2 to 42.0) | 4.9 (−4.2 to 25.5) |
Absolute change from baseline in SwCL (mmol/L) through week 4a | ||
Patients in baseline evaluation | 192 | 100 |
Baseline, mean (SD) | 79.9 (26.9) | 75.2 (28.7) |
Patients contributing to the analysis | 182 | 99 |
Mean change from baseline (SD) | −30.3 (21.9) | −27.4 (18.9) |
Median change from baseline (minimum to maximum) | −26.0 (−93.5 to 14.0) | −23.5 (−75.0 to 3.0) |
Absolute change from baseline in CFQ-R (RD) score through week 4a | ||
Patients in baseline evaluation | 192 | 102 |
Baseline, mean (SD) | 64.0 (20.5) | 65.8 (21.3) |
Patients contributing to the analysis | 188 | 102 |
Mean change from baseline (SD) | 20.1 (20.7) | 14.7 (22.6) |
Median change from baseline (minimum to maximum) | 16.7 (−50.0 to 66.7) | 11.1 (−50.0 to 66.7) |
CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised (respiratory domain); ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SwCl = sweat chloride.
aBaseline was defined as the most recent nonmissing measurement (scheduled or unscheduled) collected before the first dose of study drug in the parent study.
Source: Clinical Study Report.57
Harms
Harms data were not reported for Study 125.
Critical Appraisal
Internal Validity
Study 125 is an ongoing, uncontrolled, open-label trial that enrolled patients who had completed Study 124. Extension studies are often limited by selection bias, as only patients who are tolerant to treatment and complete the parent studies are eligible to enrol. For Study 125 and other ELX-TEZ-IVA studies, the risk of selection bias is generally low, given that nearly all patients enrol in the extension study. Overall, there are limited data from the extension phase as only 4 weeks of additional data were available, and the results are uninterpretable.
External Validity
Issues with the generalizability of these data are the same as for Study 124.
Indirect Evidence
Contents within this section were informed by materials submitted by the sponsor. The following summary was validated by the review team.
The sponsor reported that an ITC is not required for approximately 80% of the patients in the target patient population because no CFTR modulators are currently approved for use in these patients. The remaining 20% of patients in the target patient population could be eligible for treatment with IVA. The sponsor conducted a feasibility assessment to determine whether an ITC could be performed to inform the comparative clinical benefits of ELX-TEZ-IVA versus IVA monotherapy. The sponsor concluded that it was not feasible to conduct a robust ITC because of uncertainty in the degree of population overlap, low individual patient data sample sizes, incompatibility of outcomes, and differences in the treatment history and follow-up time.
The review team agrees with the sponsor that it would not have been feasible to conduct an ITC that would be interpretable for the target population, notably because of the small sample sizes that would result from comparing the patient population in Study 124 that would match that from the IVA trials, and the resulting breaking of randomization that could lead to biased estimates, as well as the differences in treatment history between the populations, among other likely sources of heterogeneity. As well:
The dosage of ivacaftor administered as part of the ELX-TEZ-IVA combination regimen is the same as what patients would receive with IVA monotherapy (e.g., 150 mg in the morning and 150 mg in the evening).
Previous trials have demonstrated that patients with 1 or more F508del mutations and a gating mutation benefited from switching to ELX-TEZ-IVA from IVA monotherapy.
The clinical experts consulted for this review noted that patients on IVA monotherapy would likely be switched to ELX-TEZ-IVA in Canadian practice.
The submitted price for ELX-TEZ-IVA is the same as the current list price for IVA monotherapy.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section were informed by materials submitted by the sponsor. The following summary was validated by the review team.
Study for FRT-Responsive CFTR Mutations
Detail | Study 16 |
|---|---|
Designs and populations | |
Study design | Retrospective, observational, cohort study (data from US CFFPR) |
Enrolled, N | N = 422 |
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention | ELX-TEZ-IVA at recommended doses |
Comparator(s) | No comparator |
Outcomes | |
Primary end point | Change from baseline for ppFEV1 (percentage points) |
Secondary end points |
|
Notes | |
Publications | None |
BMI = body mass index; CFFPR = Cystic Fibrosis Foundation Patients Registry; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Study 16
Study Description
Study 16 was a retrospective, observational, cohort study evaluating real-world clinical outcomes in patients with CF with non-F508del mutations that are responsive to ELX-TEZ-IVA based on in vitro testing.6 Data were sourced from the CFFPR. Index dates for patients were defined as the date of ELX-TEZ-IVA treatment initiation ranging from 21 October 2019 to 01 December 2022. Data from patients were evaluated for up to 2 years before the index date through December 31, 2022 (follow-up period), or until loss of follow-up, death, treatment discontinuation, or lung transplant, whichever was earlier. A summary of the study timeline is presented in Figure 7. The objective of Study 16 was to supplement Study 124 in a further 64 mutations with data on the effectiveness of ELX-TEZ-IVA on lung function, PEx, and nutritional parameters in a real-world setting of patients with CF in the target patient population using data from the CFFPR patient registry.
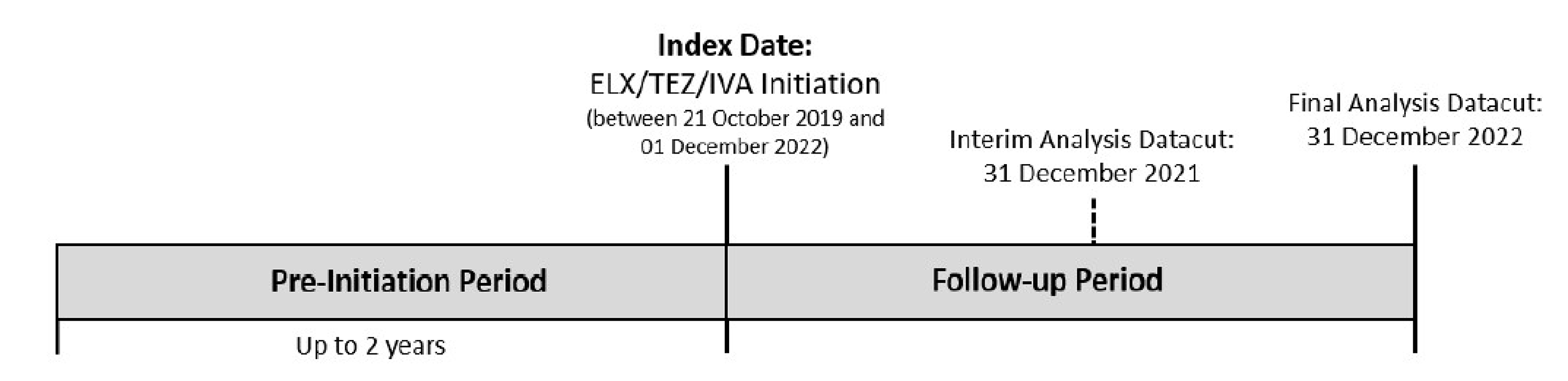
Populations
Patients aged 6 years or older were included in the analysis if they had data recorded in the CFFPR; a select ELX-TEZ-IVA–responsive non-F508del CFTR genotype; received treatment with ELX-TEZ-IVA during the patient-accrual period; at least 1 ppFEV1 measurement in the 12 months before the index date; and at least 1 ppFEV1 measurement taken at least 4 weeks after the index date. Patients were excluded if they had a history of lung transplant before the index date.
Interventions
ELX-TEZ-IVA was administered at recommended doses.
Outcomes
The primary efficacy end point was change in ppFEV1. Nutritional parameters (BMI, weight and associated z scores) from before and after ELX-TEZ-IVA initiation, and exposure-adjusted PEx rate were also assessed.
Statistical Analysis
Continuous variables were summarized using the number of observations (n), mean (SD), median (minimum to maximum), and 95% CI. Precision of measurement for each outcome was used to determine the number of decimal places to present. Categorical variables were summarized using counts and percentages, and 95% CIs. Percentages were presented to 2 decimal places unless specified otherwise.
The pre-initiation period was defined as up to 2 years before the index dates for each patient based on available registry data. If a patient had no encounter data outside of the 2-year period before the index date, then the pre-initiation period was from the first encounter within the 2-year period through the index date. If a patient had encounter data outside of the 2-year period before the index date, then the pre-initiation period was the 2 years before the index date.
For continuous end points, the baseline year was defined as up to the 12 months immediately preceding the index date. The baseline year was used to define the baseline value for ppFEV1 and nutritional parameters. For PEx, the pre-initiation period was further subdivided into the prepandemic and pandemic baseline periods, with March 13, 2020, as the cut-off date between the 2 periods. The follow-up period was defined as the date of ELX-TEZ-IVA treatment initiation (index date) through December 31, 2022.
Results
Patient Disposition
The selection process of patients from the CFFPR accounting for eligibility criteria is provided in Figure 8.
Figure 8: Study 16 Patient Flow Diagram

CF = cystic fibrosis; CFFPR = Cystic Fibrosis Foundation Patients Registry; ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Source: Study 16 Clinical Study Report.6
Baseline Characteristics
A summary of baseline characteristics for the included patients are presented in Table 27.
Table 27: Summary of Baseline Characteristics in Study 16
Characteristic | Overall (N = 422) |
|---|---|
Age at ELX-TEZ-IVA initiation (years) | |
Number of patients | 422 |
Mean (SD) | 29.81 (18.45) |
Median (minimum to maximum) | 24.88 (6.20 to 84.39) |
Age category at ELX-TEZ-IVA initiation, n (%) | |
Number of patients | 422 |
> 6 to < 12 years | 66 (15.64) |
≥ 12 to < 18 years | 82 (19.43) |
≥ 18 years | 274 (64.93) |
Gender, n (%) | |
Number of patients | 422 |
Male | 176 (41.71) |
Female | 246 (58.29) |
Prior CFTRm-treated, n (%) | |
Number of patients | 422 |
Missing | 2 (0.47) |
No | 186 (44.08) |
Yes | 234 (55.45) |
Weight (kg) | |
Number of patients | 416 |
Mean (SD) | 60.84 (21.15) |
Median (minimum to maximum) | 59.00 (19.80 to 145.10) |
Weight-for-age z score | |
Number of patients | 169 |
Mean (SD) | 0.16 (1.17) |
Median (minimum to maximum) | 0.11 (−3.46 to 3.34) |
BMI (kg/m2) | |
Number of patients | 416 |
Mean (SD) | 23.37 (5.91) |
Median (minimum to maximum) | 22.57 (14.06 to 57.16) |
BMI-for-age z score | |
Number of patients | 169 |
Mean (SD) | 0.36 (1.09) |
Median (minimum to maximum) | 0.42 (−2.27 to 2.99) |
ppFEV1 | |
Number of patients | 422 |
Mean (SD) | 74.15 (18.82) |
Median (minimum to maximum) | 78.93 (30.64 to 99.99) |
BMI = body mass index; CFTRm = CFTR modulator; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation.
Source: Study 16 Clinical Study Report.6
Exposure to Study Treatments
The mean ELX-TEZ-IVA exposure in Study 16 was 1.27 years (SD = 0.58).
Efficacy
Detailed efficacy results are presented in Table 28.
Change in ppFEV1
The ppFEV1 was assessed as a primary end point, with the overall patient population demonstrating a mean change of 4.53% (95% CI, 3.50 to 5.56) compared to baseline. Study 16 included patients with and without prior exposure to a CFTR modulator (55.5% and 44.1%, respectively). The sponsor reported subgroup analyses based on prior CFTR modulator exposure and reported that the mean change from baseline with ELX-TEZ-IVA was 6.11 (95% CI, 4.40 to 7.81) for those who were CFTR modulator–naive and 3.3% (95% CI, 2.06 to 4.58) for those who had prior exposure to a CFTR modulator.10
Change in Weight
Weight was assessed as a secondary end point, with results suggesting an increase in weight after ELX-TEZ-IVA initiation in the form of a mean change of 2.91 kg (95% CI, 2.24 to 3.58) compared to baseline. The z score for weight for age remained stable, with a mean change of −0.04 (SD = 0.48) compared to baseline.10
Change in Body Mass Index
The BMI was assessed as a secondary end point, with results suggesting an increase in BMI after ELX-TEZ-IVA initiation in the form of a mean change of 0.65 kg/m2 (SD = 2.11) compared to baseline. Z scores for BMI for age remained stable, with a mean change of −0.05 (SD = 0.53) compared to baseline.10
Summary of PEx Events
The number of PEx events and the annualized PEx rate were also assessed. The results suggest the PEx rate decreased by 53% (95% CI, 42% to 62%) after ELX-TEZ-IVA initiation. The annualized PEx rates were 0.43 in the pre-initiation period and 0.20 in the follow-up period.10
Table 28: Summary of Efficacy Results From Study 16
Characteristic | Overall (N = 422) |
|---|---|
Change from baseline for ppFEV1 (percentage points) | |
Number of patients | 352 |
Mean (95% CI) | 4.53 (3.50 to 5.56) |
Median (minimum to maximum) | 2.76 (−31.67 to 59.19) |
Change from baseline for weight (kg) | |
Number of patients | 298 |
Mean (95% CI) | 2.91 (2.24 to 3.58) |
Median (minimum to maximum) | 2.55 (−20.00 to 27.10) |
Change from baseline for weight-for-age z score | |
Number of patients | 135 |
Mean (95% CI) | −0.04 (−0.12 to 0.04) |
Median (minimum to maximum) | −0.04 (−2.15 to 1.61) |
Change from baseline for BMI (kg/m2) | |
Number of patients | 298 |
Mean (95% CI) | 0.65 (0.41 to 0.89) |
Median (minimum to maximum) | 0.49 (−7.94 to 11.80) |
Change from baseline for BMI-for-age z score | |
Number of patients | 135 |
Mean (95% CI) | −0.05 (−0.14 to 0.04) |
Median (minimum to maximum) | −0.08 (−2.15 to 1.83) |
Summary PEx | |
Total number of patients with events, n (%) | Pre-initiation period: 147 (34.83) |
Pre-pandemic baseline period: 93 (22.04) | |
Pandemic baseline period: 97 (22.99) | |
Follow-up period: 57 (13.51) | |
Total number of days (years) | Pre-initiation period: 295,538 (809.14) |
Prepandemic baseline period: 96,718 (264.80) | |
Pandemic baseline period: 198,820 (544.34) | |
Follow-up period: 195,203 (534.44) | |
Total number of PEx events | Pre-initiation period: 347 |
Prepandemic baseline period: 185 | |
Pandemic baseline period: 167 | |
Follow-up period: 107 | |
Annualized event rate/year (95% CI) | Pre-initiation period: 0.43 (0.38 to 0.48) |
Prepandemic baseline period: 0.70 (0.60 to 0.81) | |
Pandemic baseline period: 0.31 (0.26 to 0.36) | |
Follow-up period: 0.20 (0.16 to 0.24) | |
Annualized event rate ratio for follow-up period to pre-initiation period (95% CI) | 0.47 (0.38 to 0.58) |
Annualized event rate ratio for follow-up period to prepandemic baseline period (95% CI) | 0.29 (0.23 to 0.36) |
Annualized event rate ratio for follow-up period to pandemic baseline period (95% CI) | 0.65 (0.51 to 0.83) |
BMI = body mass index; CI = confidence interval; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Source: Study 16 Clinical Study Report.6
Table 29: ppFEV1 Subgroup Based on Prior CFTR-Modulator Treatment
Outcome | CFTR modulator–naive (N = 186) | CFTR modulator–treated (N = 234) |
|---|---|---|
Number of patients contributing to the analysis | 154 | 197 |
Baseline, mean (SD) | 76.36 (17.50) | 75.45 (18.22) |
Change from baseline mean (SD) | 6.11 (10.72) | 3.32 (8.96) |
Change from median (minimum to maximum) [95% CI] | 4.37 (−20.40 to 59.19) [4.40 to 7.81] | 2.37 (−31.67 to 54.79) [2.06 to 4.58] |
ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation.
Source: Study 16 Clinical Study Report.6
Splicing Mutations
Study 16 reported subgroup analyses for individual CFTR mutations that had 5 or more patients enrolled in the trial. This included 2 of 5 the noncanonical splicing mutations (2789 + 5G→A [n = 7] and 3849 + 10kbC→T [n = 16]). Results for change from baseline in these subgroups were 3.6% (SD = 6.4) and 2.5% (SD = 6.4) for 2789 + 5G→A and 3849 + 10kbC→T, respectively.
████████ | ████████ | ██████ ████ ████████ |
|---|---|---|
█████████ | ||
███ | ███ | ███ |
████ ████ | ████ ██████ | ███ █████ |
████ █ ███████ | ||
███ | ███ | ███ |
████ ████ | ████ ██████ | ███ █████ |
██ █ ████████ ██████████
Critical Appraisal
Internal Validity
Study 16 was a retrospective observational study with no comparator treatment group. In general, the lack of an unexposed or other comparator group means any observed changes in patient outcomes cannot be definitively attributed to the treatment, as they could be because of other factors, including variation in the disease course or other unmeasured factors.
Limitations common to observational studies apply to this data, including:
lack of control over the timing of scheduled patient visits
lack of standardized timing for assessments
lack of standardized definitions for pulmonary exacerbations (e.g., this would be at the discretion of the treating physician in the real-world setting)
variation in the duration of therapy
lack of information regarding adherence to ELX-TEZ-IVA during the treatment period
potential for missing data in the registry database.
Key limitations with the CFFPR include the potential for selection bias as the data are only entered into the CFFPR for patients who are treated at accredited care centre programs and who consent to participate (estimated to be 81% to 84% of patients). In addition, missing data have been identified as a challenge with the dataset. The index dates for patients spanned October 21, 2019, to December 1, 2022. This overlapped with the COVID-19 pandemic, which had a considerable impact on the baseline rate PEx for patients with CF. Because of isolation measures, the risk of pulmonary exacerbations was reduced during the pandemic period (0.70 events per year before versus 0.31 after) making it challenging to interpret the overall pretreatment baseline rate (0.43 events per year) and the posttreatment rate of exacerbations (0.20 events per year).
The target patient population for this review spans 152 additional CFTR mutations; patients with 64 of these mutations were evaluated in Study 16 (clinical data for 46 Health Canada–approved mutations was exclusively from Study 16). The number of patients with each of the individual mutations was variable and generally small across the population. The sponsor noted that, given the variability of the real-world data and the interpretability of data from small strata (e.g., mutation-level data), these analyses should be viewed with caution. As shown in Table 28, the sample sizes varied across the different outcomes (e.g., n = 352 and n = 298 for change from baseline in for ppFEV1 and BMI, respectively).
Health Canada reviewers noted that the differences between the mean and median change from baseline in ppFEV1 suggests that a few good responders may have skewed the average in favour of treatment (i.e., the mean change from baseline was 4.53 [SD, 9.84] and the median change from baseline was 2.76 [range = −31.67 to 59.19]). However, definitive conclusions cannot be drawn because of variability in the timing of the baseline and posttreatment initiation spirometry tests. Health Canada concluded that data from Study 16 does not provide significant clinical evidence for ELX-TEZ-IVA responsiveness beyond providing some support for the efficacy of a few mutations with sufficient evidence of efficacy already provided in Study 124.
External Validity
Patients evaluated in Study 16 were identified from the CFFPR. As shown in Figure 8, this is a comprehensive patient registry that included 34,567 patients with CF during the study index period. The clinical specialists consulted for this review have noted that baseline characteristics of patients with CF in the US are generally similar to those living in Canada and that the results would be considered generalizable to the target population in Canada.
For the target population in Canada, the majority of patients do not currently have access to a CFTR modulator as ELX-TEZ-IVA, LUM-IVA, and TEZ-IVA are only approved for use in patients who are homozygous or heterozygous for the F508del mutation in the CFTR gene. The approved label for TEZ-IVA is broader in the US as the FDA has also approved that drug for use in patients who have at least 1 mutation in the CFTR gene that is responsive to TEZ-IVA based on in vitro data and/or clinical evidence. As such, Study 16 included patients with and without prior exposure to a CFTR modulator. Given that treatment with a CFTR modulator is expected to improve the end points evaluated in clinical trials (e.g., baseline lung function, BMI, and SwCl), this prior exposure could bias the overall effective size reported for the study against ELX-TEZ-IVA for the target population in Canada (the majority of whom are expected to be inexperienced with a CFTR modulator, except for those who have received IVA monotherapy). The sponsor has reported results for patients with and without prior exposure to a CFTR modulator. The subgroup of patients in Study 16 with prior CFTR-modulator exposure demonstrated an improvement from baseline in ppFEV1 of 3.3% (95% CI, 2.1% to 4.6%) which was lower than the improvement of 6.11% (95% CI, 4.40 to 7.81) for those who were CFTR modulator–naive. In both populations the results were lower than what was reported in Study 124. As noted previously, observational datasets may have important limitations that make it difficult to accurately quantify the impact of the treatment on patient outcomes and makes it challenging to evaluate the consistency of results across the 2 studies.
Studies for N1303K CFTR Mutation
The sponsor included evidence from 7 publications that described the use of ELX-TEZ-IVA in patients with 1 or more N1303K mutations of the CFTR gene. Following review of the publications, CDA-AMC included data from 4 of the publications in the Clinical Review (Solomon et al. [2024],2 N = 20; Burgel et al. [2023],3 N = 8; Burgel et al. [2024],4 N = 35; and Sadras et al. [2023],14-16 N = 8).
The 3 additional abstracts and/or publications for patients with 1 or more N1303K mutations (Dreano et al.,[2023];7 Livnat et al. [2023];8 and Pranke et al. [2022]9) have not been summarized in this report as the review team concluded that these studies do not address a gap in the evidence that is not already addressed by the other 4 studies submitted in support of the expanded use of ELX-TEZ-IVA for patients with CF who have 1 or more N1303K mutations in the CFTR gene. The additional reasons are:
The reporting of these studies is insufficient for CDA-AMC to conduct an appropriate appraisal of the methodology used in the evaluation of patients as information is only available in abstract format.
The publications by Dreano et al. (2023) and Pranke et al. (2022) refer to the same source of patients that was used in the studies by Burgel et al. (2023), N = 8; and Burgel et al. (2024), N = 34, which also had larger sample sizes. The sponsor was unable to confirm if there is overlap between the patient populations in these studies.
These analyses were not included in the submission to Health Canada.
The study population from Sadras et al. (2023)14-16 was included in the study by Burgel et al. (2024),4 but this was still reviewed and appraised because it was included as a separate additional study in the submission to Health Canada for ELX-TEZ-IVA.
A summary of the key results from Solomon et al. (2024),2 Burgel et al. (2023),3 Burgel et al. (2024),4 and Sadras et al. (2023)14-16 is provided in Table 4. A summary and appraisal of each of the individual studies is provided in the following section.
Solomon (2024)
Description
Solomon et al. (2024) was a prospective, open-label trial assessing patients with CF carrying partial function or N1303K mutations not currently approved for treatment by ELX-TEZ-IVA.2 The study was divided into 2 subsections, with 1 enrolling 22 patients with rare genotypes and the other enrolling 20 participants carrying 1 or more N1303K mutations. Both populations were treated with ELX-TEZ-IVA for 4 weeks and assessed for efficacy and health-related quality-of-life outcomes.
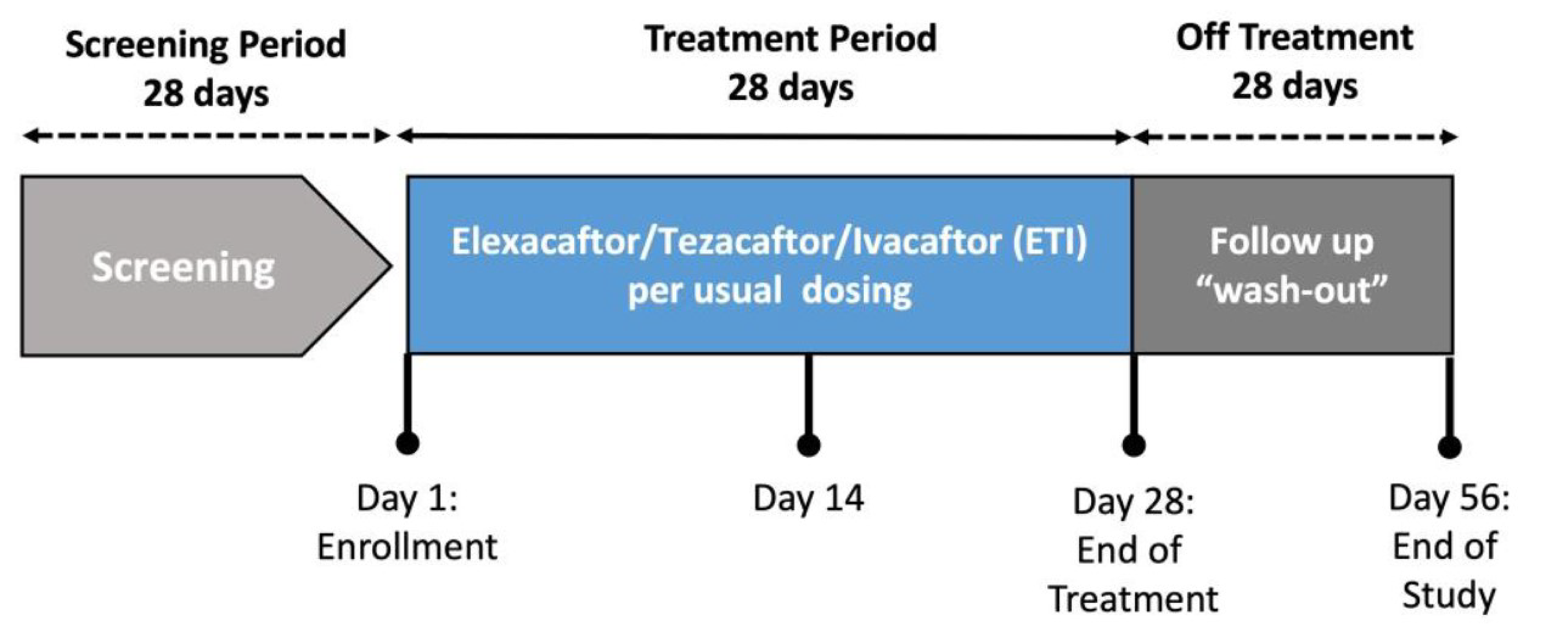
Populations
Patients were eligible if they were at least 12 years of age, had a diagnosis of CF, were clinically stable in the past 4 weeks with no evidence of CF exacerbation, and had 1 of the following: a partial function mutation not currently covered or likely to be covered for treatment with a CFTR modulator (Substudy 1); or an N1303K mutation and a minimal function mutation (Substudy 2). Key exclusion criteria included cirrhosis or elevated liver transaminases greater than 3 times the ULN; history of solid organ transplant; or treatment in the last 6 months with an approved CFTR modulator.10
Interventions
ELX-TEZ-IVA was taken for 28 days among patients with CF (tablets comprised 100 mg of ELX, 50 mg of TEZ, and 75 mg of IVA [2 tablets taken in the morning], and 150 mg of IVA taken in the evening).10
Outcomes
Changes in ppFEV1and SwCl were the primary clinical outcomes of interest and changes in CFQ-R scores and weight were secondary outcomes of interest.10
Statistical Analysis
Statistical methods were not reported as only abstracts were included in the application.
Results
Patient Disposition
Patient disposition was not reported.
Baseline Characteristics
Table provides a summary of the baseline and demographic characteristics from Solomon et al. (2023).12
Table 31: Summary of Baseline Characteristics in Solomon et al. (2023)
Baseline characteristics | ELX-TEZ-IVA (N = 20) |
|---|---|
Age distribution, n (%) | |
12 to < 18 years | 8 (40) |
≥ 18 years | 12 (60) |
CFTR genotype, n (%) | |
N1303K / MFa | 20 (100) |
CF medical history, n (%) | |
Pancreatic insufficiency | 20 (100) |
CF-related diabetes | 4 (20) |
Chronic sinusitis | 12 (60) |
ppFEV1 | |
Mean (SD) | 76 (20) |
Distribution, n (%) | |
< 50% | 4 (20) |
50 to < 75% | 3 (15) |
> 75% | 13 (65) |
Mean sweat chloride, mmol/L (SD) | 109 (9) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; CF = cystic fibrosis; MF = minimal function; ppFEV1 = percent predicted forced expiratory volume in 1 second.
aMF mutations included (n) W1282X (5), G542X (2), deltaI507 (2), E60X (1), 2490 + 1G > A (1), 3905insT (1), 1717 to 1 G > A (1), Q1100P (1), 2184delA (1), 2184insA (1), 711 + 1G > T (1), 11454insTC (1), 3120 + 1 G > A (1), and CFTRdele17a,17b (1).
Source: Common Technical Document.12
Efficacy
Table 32 provides a summary of efficacy results from Solomon et al. (2023).
Table 32: Summary of Results From Solomon et al. (2023)
End pointa | Baseline (day 1) | Treatment end (day 28) | LS differenceb | P value |
|---|---|---|---|---|
SwCl, mmol/L | 109 (105.6 to 112.4) | 107.9 (104.5 to 111.3) | −1.1 (−5.3 to 3.1) | 0.61 |
ppFEV1, % | 75.8 (73.3 to 78.3) | 85.3 (82.8 to 87.8) | 9.5 (6.7 to 12.3) | < 0.001 |
CFQ-R RD | 60.6 (54.6 to 66.5) | 81.4 (75.5 to 87.3) | 20.8 (11.9 to 29.8) | < 0.001 |
BMI, kg/m2 | 22.1 (21.9 to 22.3) | 22.5 (22.3 to 22.7) | 0.4 (0.2 to 0.7) | 0.002 |
Weight, kg | 57.5 (57.0 to 58.0) | 58.5 (58.0 to 59.1) | 1.0 (0.4 to 1.7) | 0.002 |
BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised (respiratory domain); LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride.
aResults presented are LS means with 95% confidence intervals.
bThe difference is the LS mean difference between day 1 and day 28 based on a mixed-effects model for repeated measures.
Source: Solomon et al. (2023).12
Internal Validity
Solomon et al. (2023) was a prospective cohort study that was investigator-initiated (i.e., it was not sponsored by Vertex Pharmaceuticals). As an investigator-initiated trial, no clinical study report was available to include in the application to CDA-AMC. Information available for the purposes of appraising and interpreting the evidence is limited to a conference abstract, a presentation, and information included by the sponsor in the regulatory submission (i.e., the Common Technical Document).
The use of a single-arm trial design is inconsistent with the design used for pivotal trials for ELX-TEZ-IVA in patients aged 12 years and older. This approach has been used for trials investigating ELX-TEZ-IVA in younger patients (for whom concerns regarding equipoise may preclude the use of a placebo comparator), but not for those aged 12 years and older. As a single-arm study, there is an increased risk of bias in the estimation of treatment effects because of the potential for confounding related to natural history and prognostic factors. The potential influence of selection bias is also difficult to determine in a single-arm study. As well, too few details about the inclusion (and exclusion) of patients into the study were provided to fully assess the potential for selection bias. No information was provided about concomitant therapies that may have influenced the results of the study.
As ELX-TEZ-IVA was administered in an open-label manner, the investigator and the study participants were aware of their treatment status, potentially increasing the risk of detection and performance biases. Open-label administration limits interpretability of the health-related quality-of-life end point (CFQ-R [RD]).
Insufficient information about the statistical analysis was provided to determine whether the evaluations were robust, including how potential confounders were handled.
External Validity
The study was conducted at centres in the US and (as noted for Study 16) the clinical experts consulted for this review had no concerns about generalizing the study results from US patients to a Canadian setting. The relatively small sample size made it difficult to evaluate the representativeness of the population based on baseline characteristics. The clinical experts noted that the baseline characteristics were a reasonable reflection of the target patient population in Canada. However, the relatively small sample size (N = 20) makes it difficult to determine if the distribution of patient characteristics could be informative for generalizing the results.
Although ELX-TEZ-IVA was administered at recommended dosages, the treatment duration was limited to 4 weeks (28 days), which is shorter than the 24-week duration used in the phase III clinical trials for ELX-TEZ-IVA.
Burgel (2023)
Burgel et al. (2023) reported a prospective observational cohort study from involving patients who received ELX-TEZ-IVA through a French compassionate-access program. Table 33 provides a summary of the study characteristics, results, and an appraisal of the internal and external validity.
Table 33: Summary of Burgel et al. (2023)
Study details | Description |
|---|---|
Population |
|
Interventions |
|
Outcomes |
|
Statistical analysis | Data on ppFEV1 and SwCl, and body weight before initiation and after 4 to 6 weeks were compared using a nonparametric Wilcoxon signed rank test. Results were reported as median or numbers (%), and statistical significance was considered for P < 0.05. |
Key characteristics (n = 84) | Mutations
Note: All other baseline and demographic characteristics were only reported for the full population (N = 84) and not for the population of interest (i.e., those with 1 or more N1303K mutations) |
Key findings at 4 to 6 weeks | ELX-TEZ-IVA treatment response for patients with 1 or more N1303K mutations (n = 8)
|
Critical appraisal | Internal validity
External validity
|
BMI = body mass index; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IQR = interquartile range; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride.
Source: Burgel et al. (2023).3
Burgel (2024)
Burgel et al. (2024) was a retrospective observational cohort study that employed pooled analyses drawn from various sources, including the French compassionate-access program's published reports, a study conducted in Israel (Sadras [2023]), 3 case reports, and unpublished data sourced from the French compassionate-access program. Table 34 provides a summary of the study characteristics, results, and an appraisal of the internal and external validity.
Table 34: Summary of Burgel et al. (2024)
Study Details | Description |
|---|---|
Population | Patients with CF with no F508del mutation and 1 or more N1303K mutations were included. Patients were selected from:
|
Interventions | ELX-TEZ-IVA at recommended doses for an individual trial of 4 to 8 weeks. |
Outcomes |
|
Statistical analysis |
|
Key characteristics (n = 35) | CFTR mutations
Demographics
Disease severity
|
Key findings | Overall population (N1303K/any) (n = 35)
N1303K/N1303K subgroup (n = 11)
N1303K/stop codon subgroup (n = 14)
N1303K or other subgroup (n = 10)
|
Critical appraisal | Internal validity
External validity
|
BMI = body mass index; CF = cystic fibrosis; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IQR = interquartile range; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride.
Source: Burgel et al. (2024).4
Sadras (2023)
Sadras et al. (2023) reported an observational prospective analysis from a multicentre registry in Israel, including in vitro evidence to report the clinical response and in vitro response to ELX-TEZ-IVA in patients who carry 1 or more N1303K mutations on 1 allele and a nonsense or frameshift mutation on the other. Table 35 provides a summary of the study characteristics, results, and an appraisal of the internal and external validity.
Table 35: Summary of Sadras et al. (2023)
Study details | Description |
|---|---|
Population | Patients were included if they had CF and carried 1 or more N1303K mutations on 1 allele and a nonsense or frameshift mutation on the other (not expected to respond to ELX-TEZ-IVA) |
Interventions | ELX-TEZ-IVA at recommended doses for 8 weeks |
Outcomes |
|
Statistical analysis |
|
Key characteristics (n = 8) | Mutations
Demographics
Comorbidities/ Disease Severity
|
Key findings at 8 weeks (n = 8) |
|
Critical appraisal | Internal validity
External validity
|
BMI = body mass index; CF = cystic fibrosis; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; NR = not reported; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride.
Source: Sadras et al. (2023).14-16
Discussion
Summary of Available Evidence
The current review is for an expanded indication that would include 152 additional non-F508del mutations of the CFTR gene. The sponsor has categorized the additional CFTR mutations as follows: 147 FRT-responsive mutations, 4 noncanonical splice mutations, and the N1303K mutation. Evidence supporting the use of ELX-TEZ-IVA in the expanded population consisted of the following: 1 double-blind, placebo-controlled RCT in patients with FRT-responsive CFTR mutations (Study 124; N = 307; 18 CFTR mutations); 1 long-term extension study (Study 125; same population as Study 124); 1 retrospective observational study (Study 14; N = 422; 64 CFTR mutations); 4 nonrandomized studies involving patients with 1 or more N1303K mutations (Solomon et al. [2024],2 N = 20; Burgel et al. [2023],3 N = 8; Burgel et al. [2024],4 N = 35; and Sadras et al. [2023],14-16 N = 8). The sponsor reports that there are no clinical data for 79 FRT-responsive mutations (i.e., those that were considered responsive to ELX-TEZ-IVA in the in vitro model) and 1 of the noncanonical splice mutations.
The sponsor’s application was filed on a pre–Notice of Compliance basis and included an additional 31 CFTR mutations that were not approved by Health Canada for the following reasons:
Fifteen mutations were considered by Health Canada as not causative of CF, based on the CFTR2 and CFTR-France databases: D836Y, F508C, G576A, I148T, I807M, I1027T, L320V, L997F, R75Q, R170H, R668C, R1162L, T1053I, V562I, and V754M.
Ten mutations were excluded because of unknown clinical significance or were only reported as causing a CFTR-related disease (i.e., not CF), and which retain at least 50% of normal chloride-transport function: G178E, G576A;R668C, I1139V, K1060T, R31L, R553Q, R751L, R792G, V1293G, Y1014C.
Five mutations were excluded because they result in a cryptic splice mutation, and insufficient full-length CFTR: H939R, I175V, M152V, E403D, and S589N.
One mutation was excluded because of the absence of in vitro or clinical data provided in the current submission: E831X.
Similar to the previous reviews for ELX-TEZ-IVA for those with an F508del mutation in the CFTR gene, the expanded indication only requires patients to have 1 mutation causing CF that is considered responsive to ELX-TEZ-IVA. As the majority of patients enrolled in Study 124 were heterozygous for the CFTR mutations and some patients carried complex alleles (i.e., multiple mutations on 1 allele), Health Canada requested that the sponsor provide additional analyses for Study 124 and Study 16 showing a by-mutation analysis for patients who have only a single potentially responsive target mutation on 1 allele, and either the same single mutation on the second allele or a mutation expected to be nonresponsive (e.g., a frameshift, large deletion, or premature stop codon). The sponsor provided the analyses for Study 124 but could not provide that level of detail for Study 16, citing the small sample size and the CFFPR’s restriction in providing data for subgroups with fewer than 5 patients. Health Canada concluded that there was sufficient evidence of efficacy that patients with 1 or more ELX-TEZ-IVA–responsive mutations will benefit from treatment, although a revision to the product monograph was required to identify the specific mutations for which the sponsor provided subgroup analyses demonstrative of efficacy for those who carried only 1 responsive mutation (i.e., those who were homozygous or carried a class I mutation on the other allele). The product monograph states that those specific CFTR mutations have “significant clinical evidence of efficacy for ELX-TEZ-IVA, independent of the mutation on the second allele.” This statement is simply intended to identify the mutations for which evidence has been generated and reported and is not meant to indicate that other mutations involving only a single responsive copy would be expected to show a reduced treatment effect (as this remains a gap in the evidence). Health Canada noted that the actual clinical responsiveness to ELX-TEZ-IVA for any individual patient with CF depends on multiple factors and cannot be predicted before treatment.
Indirect comparison: The sponsor reported that an ITC is not required for approximately 80% of the patients in the target patient population because no CFTR modulators are currently approved for use in these patients. The remaining 20% of patients in the target patient population could be eligible for treatment with IVA monotherapy. The sponsor conducted a feasibility assessment to determine whether an ITC could be performed to inform the comparative clinical benefits of ELX-TEZ-IVA versus IVA monotherapy. The sponsor concluded that it was not feasible to conduct a robust ITC because of uncertainty in the degree of population overlap, low individual-patient-data sample sizes, incompatibility of outcomes, and differences in the treatment history and follow-up time. The review team agreed with the sponsor that it would not have been feasible to conduct an ITC that would be interpretable for the target population, notably because of the small sample sizes that would result from comparing the patient population in Study 124 that would match that from the IVA trials, and the resulting breaking of randomization that could lead to biased estimates, as well as the differences in treatment history between the populations, among other likely sources of heterogeneity. In addition, the dosage of IVA administered as part of the ELX-TEZ-IVA combination regimen is the same that patients would receive with IVA monotherapy (e.g., 150 mg in the morning and 150 mg in the evening); previously reviewed trials have demonstrated that patients with 1 or more F508del mutations and a gating mutation benefited from switching to ELX-TEZ-IVA from ivacaftor monotherapy; the clinical experts consulted for this review noted that, in Canadian practice, patients on IVA monotherapy would likely be switched to ELX-TEZ-IVA; and the submitted price for ELX-TEZ-IVA is the same as the current list price for IVA monotherapy and the total costs of treatment would therefore be unlikely to change.
Interpretation of Results
Prior exposure to a CFTR modulator: For the target population in Canada, the majority of patients do not currently have access to a CFTR modulator as ELX-TEZ-IVA, LUM-IVA, and TEZ-IVA are only approved for use in patients who are homozygous or heterozygous for the F508del mutation in the CFTR gene. The percentage of the population who could receive IVA monotherapy is expected to be relatively small (approximately 20% based on sponsor estimates). The approved label for TEZ-IVA is broader in the US as the FDA has already approved that drug for use in patients who have at least 1 mutation in the CFTR gene that is responsive to TEZ-IVA based on in vitro data and/or clinical evidence. As such, the clinical studies include patients with and without prior exposure to a CFTR modulator. Given that treatment with a CFTR modulator is expected to improve the end points evaluated in clinical trials (e.g., baseline lung function), the results for patients with and without prior exposure to a CFTR modulator are discussed separately.
Efficacy for FRT-Responsive CFTR Mutations — Clinical Data
Lung function: In Study 124, ELX-TEZ-IVA was associated with a clinically meaningful absolute improvement in ppFEV1 compared with placebo after 24 weeks of treatment (LS mean difference = 9.2%; 95% CI, 7.2% to 11.3%). While no published information on the MID in absolute change in ppFEV1 in CF was identified by the review team, the clinical experts consulted for this review noted that CF specialists would generally consider an absolute improvement in ppFEV1 of at least 5% to be clinically relevant. Improvements in ppFEV1 in patients receiving ELX-TEZ-IVA were observed at the first postbaseline assessment of Study 124 (i.e., day 15) and were higher at all time points throughout the study. The results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses. Similar results were reported for placebo-treated patients who were crossed over to ELX-TEZ-IVA in Study 125, which demonstrated an absolute increase from baseline in ppFEV1 of 7.1% (SD = 7.3) after 4 weeks. Health Canada reviewers concluded that the primary analysis in Study 124 for change in ppFEV1 produced results comparable to those reported in the studies conducted with F508del patients for the initial approval of ELX-TEZ-IVA and support a significant benefit to lung function in responsive patients.
Patients in Study 16 demonstrated smaller improvements from baseline, with changes in ppFEV1 of 6.11% (95% CI, 4.40 to 7.81) for those who were CFTR modulator–naive. The subgroup of patients in Study 16 with prior CFTR-modulator exposure demonstrated an improvement from baseline in ppFEV1 of 3.3% (95% CI, 2.1% to 4.6%). The magnitude of improvement from switching to ELX-TEZ-IVA from TEZ-IVA or IVA was previously reviewed by CDA-AMC in the submission for patients aged 12 years and older (i.e., Study 103 and Study 109 in patients homozygous for the F508del mutation and Study 104 for patients with a single F508del mutation and either an RF or a gating mutation in the CFTR allele). The magnitude of improvement reported in Study 16 is similar to what was reported for those who switch from TEZ-IVA or IVA to ELX-TEZ-IVA in Study 104 (LS mean difference = 3.5%; 95% CI, 2.2 to 4.7; P < 0.0001) and lower than what was reported in the switching studies for patients who were homozygous for the F508del mutation (10.0%; 95% CI, 7.4 to 12.6 and 10.2%; 95% CI, 8.2 to 12.1).
Health Canada reviewers noted that the data from Study 16 did not provide significant support for any individual mutation, citing insufficient information. Health Canada further noted that use of CCFR data (instead of US CFFPR data) would be even less likely to provide clarity, given the rarity of the mutations and the size of the relevant population. Based on this assessment, Study 16 was not considered to be the basis of regulatory approval for the revised indication and the results of this study were removed from the Canadian product monograph.
Pulmonary exacerbations: PEx events are currently the most common reason for hospitalization of patients with CF58 and, accordingly, these events were identified as an outcome of interest by the patient groups and clinician groups who provided input for this review. PEx events are clinically significant for patients with CF and are correlated with increased mortality, greater decline in lung function, reduced quality of life, and increased health costs.59-63 In addition, it has been estimated that many patients with CF experience a permanent reduction in lung function following an exacerbation (i.e., their lung function will not recovery to the level it was before the exacerbation). In a large sample of patients with CF (N = 8,479), Sanders et al. (2010)64 estimated that 25% of patients with CF who experienced a PEx failed to recover to their baseline FEV1. A similar observation has been made in an analysis in pediatric patients with CF, of whom 23% failed to recover to their baseline FEV1 after being treated with IV antibiotics for a PEx.65
Treatment with ELX-TEZ-IVA was associated with a reduction in the risk of PEx events in the 24-week placebo-controlled trial (Study 124). The sponsor also reported a 53% reduction in the risk of a PEx after ELX-TEZ-IVA initiation in Study 16; however, the onset of the COVID-19 pandemic altered the baseline frequency of exacerbations (from 0.70 to 0.31 events per year) making it challenging to interpret the overall pretreatment baseline rate (0.43 events per year) and the posttreatment rate of exacerbations (0.20 events per year). The clinical experts consulted for this review noted that the reduction in PEx events in Study 124 is clinically meaningful. The 24-week study period reduced the accuracy and variance of the point estimates for the PEx rates because of seasonal variation and other temporal factors that require longer follow-up to accurately estimate (ideally at least 12 months of follow-up to account for these variables). Health Canada reviewers noted that the reduction in the number of PEx events in Study 124 was substantiative, albeit over a short 24-week study period. Similar to CDA-AMC, Health Canada noted that the reduction in PEx events observed in Study 16 was confounded by isolation measures that occurred during the COVID-19 pandemic and that the results are challenging to interpret.
There are no globally accepted definitions for a PEx in patients with CF. The definitions used in Study 124 were considered appropriate by regulatory authorities and the clinical experts consulted for this review, who noted there would be some variation in routine clinical practice in the threshold for diagnosing and treating pulmonary exacerbations across different CF clinics and/or physicians. This was also evident in Study 124, in which fewer patients met the criteria for a PEx when evaluated as an efficacy end point compared to the number of exacerbations reported as AEs (25.5% versus 36.3% in the placebo group). Although no standard definitions are currently uses in Canadian clinical practice, the clinical experts consulted for this review noted that the number of exacerbation events experienced by patients with CF is currently tracked in CF clinics.
Nutritional end points: Given that CF affects multiple organ systems, including those in the digestive system, and that CFTR modulators are systemic treatments, the pivotal studies for ELX-TEZ-IVA included BMI and body weight end points to evaluate the effect of treatment on the nutritional status of patients with CF. Treatment with ELX-TEZ-IVA was associated with statistically significant improvements in BMI compared with placebo at 24 weeks in Study 124 (LS mean difference = 0.47 kg/m2; 95% CI, 0.24 to 0.69). Previous CDA-AMC reviews of CFTR modulators noted that 24 weeks is a short period of time to evaluate changes in BMI. As shown in Figure 5, it is unclear if the posttreatment BMI for patients in the ELX-TEZ-IVA had stabilized at the time of the 24-week measurement, and additional data were available from the extension phase (Study 125) at the time of submission to CDA-AMC. The clinical experts noted that the improvements in BMI demonstrate that ELX-TEZ-IVA improves nutritional end points for the target patient population.
Health-related quality of life: As stated in the patient group input, CF has a major impact on the quality of life of patients and their caregivers. Treatment with ELX-TEZ-IVA demonstrated statistically significant and clinically meaningful improvements in health-related quality of life (i.e., CFQ-R) in each of the included studies. The magnitude of improvement in the CFQ-R (RD) scores with ELX-TEZ-IVA was 19.5 (95% CI, 15.5 to 23.5) at 24 weeks compared with placebo in Study 124. This exceeded the MID for the CFQ-R (RD), which is typically cited as 4.0 points. The clinical experts consulted for this review considered the results clinically relevant. Health Canada reviewers similarly concluded that results in Study 124 for change in CFQ-R (RD) scores were comparable to those reported in the studies conducted with F508del.
The patient input emphasized that the therapeutic regimen for patients with CF requires considerable time each day and is both physically and mentally demanding for those living with CF and their caregivers. Patients have expressed interest in therapeutic options that could help alleviate their existing treatment burden. The clinical experts consulted for this review and the clinician groups who provided input all noted that ELX-TEZ-IVA should be used as an add-on therapy. A large RCT (the SIMPLIFY trial) recently reported that patients whose disease is well controlled do not experience a decline in lung function after discontinuation of dornase or inhaled hypertonic saline after stabilization with ELX-TEZ-IVA.66,67
Efficacy for Noncanonical Splicing Mutations
The target patient population of the current review includes 5 noncanonical splicing mutations in the CFTR gene. These mutations result in small amounts of functional, normal CFTR protein. The sponsor has reported that these mutations cannot be evaluated in the FRT system and provided clinical data for each of the mutations included in the application. The sponsor reported that 4 of the 5 splicing mutations are supported by clinical data while clinical data are currently unavailable for 1 mutation (711 + 3A > G). The sponsor stated that, because CFTR modulators work through the same mechanism associated with all noncanonical splice mutations (i.e., by enhancing the activity of the small amount of full-length CFTR produced by noncanonical splice mutations) the response observed for noncanonical splice mutations with clinical data provides evidence that the additional noncanonical splice mutation will also be clinically responsive.
Study 124 enrolled patients with 3 of the 5 noncanonical splice mutations in the target patient population for this review (i.e., 2789 + 5G > A, 3272 to 26A > G, and 3849 + 10kbC > T). Subgroup analyses for absolute change from baseline through 24 weeks in ppFEV1, SwCl, and CFQ-R (RD) produced results consistent with those of the primary analyses. Study 16 reported subgroup analyses for individual CFTR mutations that had 5 or more patients enrolled in the trial. This included 2 of 5 of the noncanonical splicing mutations: 2789 + 5G→A (n = 7) and 3849 + 10kbC→T (n = 16). Although the changes from baseline appear lower than what was observed in Study 124 (absolute change from baseline of 3.6% [SD = 6.4]) and 2.5% [SD = 6.4] for 2789 + 5G→A and 3849 + 10kbC→T, respectively), making such judgments is challenging given the uncertainty as to the similarity of the study populations, the much smaller sample size in Study 16, and the aforementioned important limitations of the study and reporting of information. There may be inconsistency across studies in the effects of ELX-TEZ-IVA in patients with noncanonical splice mutations, but the limitations of the available evidence make it difficult to determine the accuracy and precision of the estimated treatment effects. The sponsor reported that clinical data were available for E831X, but no subgroup results were reported in Study 16 (in addition, the sample size would be problematically small). The experts emphasized that these patients have a high level of unmet need as they have no access to CFTR-modulator therapy in Canada (outside of enrolment in a clinical study).
Efficacy for N1303K CFTR Mutations
The N1303K mutation was identified as nonresponsive to ELX-TEZ-IVA in the FRT in vitro test that has subsequently been evaluated in investigator-sponsored studies. The sponsor included evidence from 7 publications that described the use of ELX-TEZ-IVA in patients with 1 or more N1303K mutations on the CFTR gene. Following a review of the publications, we included data from 4 of the publications in the Clinical Review (Solomon et al. [2023],2 N = 20; Burgel et al. [2023],3 N = 8; Burgel et al. [2024],4 N = 35; and Sadras et al. [2023],14-16 N = 4).
All of the studies reported an increase in ppFEV1 following between 4 to 8 weeks of treatment with ELX-TEZ-IVA. The improvement from baseline in ppFEV1 across studies ranged from 9.5% (95% CI, 6.7 to 12.3; P < 0.001) in Solomon et al. (2023) (N = 20),11,12 a study that enrolled patients who had moderate lung disease at baseline (i.e., the mean baseline FEV1 was 76% [SD = 20]). The largest improvements in ppFEV1 were reported in the publication by Burgel et al. (2023)3 (N = 8), in which only patients with advanced lung disease were evaluated. These patients had a median baseline ppFEV1 of 32% (95% CI, 26 to 39) and showed a median improvement of 27.5% (IQR = 20.7 to 41.2) after 4 to 6 weeks of treatment with ELX-TEZ-IVA. The clinical specialists consulted for this review considered the results to be clinically meaningful and indicate that ELX-TEZ-IVA would benefit patients with 1 or more N1303K mutations. The experts emphasized that there is a high level of unmet need for these patients as they currently do not have access to CFTR-modulator therapy in Canada (outside of enrolment in a clinical study).
Three studies (Solomon et al. [2023],11,12 Burgel et al. [2024], and Sadras et al. [2023]14-16) included change from baseline in BMI or body weight and all reported statistically significant increases from baseline over the short study periods. As with the other clinical studies, the clinical specialists consulted for this review noted that the duration of these studies is too short to accurately evaluate the impact of ELX-TEZ-IVA on increasing the nutritional status of patients with the N1303K mutation. However, the CF specialists emphasized that the results support a finding that ELX-TEZ-IVA is effective for these patients and likely to have a long-term effect on improving BMI and body weight for patients who may be underweight.
Only 1 of the N1303K studies investigated change from baseline in health-related quality of life. Solomon et al. (2023)11,12 reported a mean increase from baseline in the CFQ-R (RD) score of 20.8 (95% CI, 11.9 to 29.8; P < 0.001). As noted previously, the MID for this instrument is typically cited as a change of 4 units, which was far exceeded in this trial. Similar to the interpretation of the results from Study 124, the clinical specialists consulted by CDA-AMC described this as clinically relevant for patients.
The investigator-sponsored studies failed to consistently demonstrate that ELZ-TEZ-IVA treatment reduced SwCl in the patients with 1 or more N1303K mutations in the CFTR gene (i.e., no statistically significant difference in Solomon et al. [2023] or Sadras et al. [2023]) and the studies that did demonstrate a statistically significant reduction showed a lower magnitude in response in comparison with other mutations that have been studied (median change of –9 mmol/L in both Burgel et al. [2023] and Burgel et al. [2024]). The clinical experts consulted for this review were not concerned about the lack of improvements in SwCl in these trials, as this is more a reflective of mechanism of action of ELX-TEZ-IVA and is not considered a clinically meaningful end point for the evaluation of treatment response. The study authors speculated that ELX-TEZ-IVA may have a different mechanism of action for CFTR proteins with an N1303K mutation and emphasized the need for patients to be evaluated by a range of end points to determine response to treatment. Health Canada noted that alternative approaches to in vitro cell modelling (using human nasal epithelial cells and induced pluripotent stem cell-derived epithelial cells) have shown that ELX-TEZ-IVA can increase Cl− transport in patients with an N1303K or minimal function genotype. Given that the studies involving the N3103K mutation demonstrated consistent improvements in ppFEV1, but a lack of improvement in SwCl, Health Canada noted that ELX-TEZ-IVA appears to promote CFTR activity in the lungs, but not necessarily in the sweat glands for patients with an N1303K mutation. Health Canada noted that the exact mechanism responsible for the differences in the effects of ELX-TEZ-IVA in those with an N1303K mutation compared with those that were shown to be responsive in the FRT-cell model is unclear. However, Health Canada pointed out that the N1303K CFTR protein is degraded by the autophagy cellular pathway, which is a different than the F508del CFTR protein, and that this could result in different levels of CFTR expression at the cellular membrane of cellular types. In this instance, it has been hypothesized that the CFTR correctors (i.e., ELX and TEZ) may facilitate escape from the endoplasmic reticulum and trafficking to the plasma membrane more efficiently in epithelial cells of the respiratory tract compared to epithelial cells in other parts of the body, such as the skin.
The 4 observational studies have important limitations that make it challenging to determine whether the observed effects of ELX-TEZ-IVA in patients with CF who have 1 or more N1303K mutations at various stages of lung disease are because of the treatment or other factors. The sample sizes of the studies were relatively small (N ranged from 8 to 35). This has implications for the internal validity (e.g., key assumptions of statistical tests may be invalidated) and external validity (representativeness of the results to a wider population) of the studies. There were concerns regarding the selection of patients in all 4 studies and an increased risk of selection bias, as they enrolled patients who were more likely to show larger treatment effects. This partly results from the limited information provided in the description of patient eligibility, recruitment, and insufficient reporting of patient characteristics at baseline. Further, the absence of a comparator (concurrent or external) in the studies precludes the ability to interpret the magnitude of therapeutic benefit in terms of whether the effect was attributable to ELX-TEZ-IVA or other factors. There were several unanswerable questions, in part based on the limited reporting of the methods and analyses in the studies, related to the assessment of bias, particularly how well potentially relevant confounders and/or effect modifiers were accounted for. All of studies had a short duration of treatment and follow-up. None of the studies evaluated the rates of PEx. As all of the studies were investigator-sponsored, the available information regarding studies methods and results is limited to publications and abstracts. Overall, the studies are suggestive of a clinically important benefit with ELX-TEZ-IVA in patients with 1 or more N1303K mutations, but they are not conclusive.
Harms
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., aged at least 2 years with at least 1 mutation that is responsive to ELX-TEZ-IVA based on clinical and/or in vitro data). The warnings and precautions section of ELX-TEZ-IVA product monograph has not been updated since the previous CDA-AMC reviews. Health Canada reviewers noted that long-term safety has already been established for ELX-TEZ-IVA, and no data from the pivotal clinical study indicate the existence of CFTR genotype–dependent safety concerns.
As with previous CDA-AMC reviews of ELX-TEZ-IVA, SAEs and withdrawals because of AEs were rare in the included studies. The clinical experts consulted for this review noted that intolerance to ELX-TEZ-IVA among adolescents and adults has been rare in clinical practice. The clinical experts noted that patients who experience significant AEs following initial treatment with ELX-TEZ-IVA would not likely be completely discontinued from treatment; rather, treatment with ELX-TEZ-IVA would likely be interrupted and the patient would be rechallenged with the drug following resolution of the event(s). This is consistent with the input received from the 3 clinician groups that noted that discontinuation of therapy should be considered in patients who have clinically significant adverse effects that persist and recur after stopping and re-initiating therapy.
Similar to the development programs for the other CFTR modulators (IVA, LUM-IVA, and TEZ-IVA), patients with abnormal liver function were excluded from the phase III trials of ELX-TEZ-IVA. The clinical experts consulted for this review noted that most patients who could be eligible for ELX-TEZ-IVA would not have hepatic impairment. The product monograph recommends that the dosage of ELX-TEZ-IVA should be adjusted in patients with moderate hepatic impairment and that the drug should not be used in patients with severe hepatic impairment.30 These recommendations are more restrictive than those in the product monographs for IVA, LUM-IVA, or TEZ-IVA,30,41,42 all of which provide dosage-reduction scenarios for patients with CF who have severe hepatic impairment. The clinical experts suggested that clinicians may attempt to treat those with severe hepatic impairment using ELX-TEZ-IVA at a reduced dosage, as opposed to using the reduced dosages of the alternative CFTR modulators, which are unlikely to provide the same level of clinical benefit.
The product monograph notes that elevated transaminases have been observed in patients treated with ELX-TEZ-IVA and recommends assessing alanine transaminase and aspartate transaminase before initiating treatment with ELX-TEZ-IVA every 3 months during the first year of treatment and annually thereafter.30 The clinical experts consulted for this review noted that the recommendations for monitoring would likely be followed by the clinical community. The clinical experts and the clinician groups who provided input noted that patients with CF are typically seen once every 3 months (although visits have been less frequent in some cases because of COVID-19). As such, the recommended monitoring regimen for ELX-TEZ-IVA was not anticipated to result in a substantial increase in the number of the clinic visits for patients with CF (particularly after the first year of initiating the treatment).
Similar to IVA, LUM-IVA, and TEZ-IVA, the product monograph for ELX-TEZ-IVA notes that cases of noncongenital cataracts without impact on vision have been reported in pediatric patients who were treated with IVA-containing regimens.30,41,42,68 The product monograph states that the patients who demonstrated these events had other risk factors (e.g., corticosteroid use or exposure to radiation); however, a possible risk attributable to treatment with IVA cannot be excluded. As such, it is recommended that pediatric patients initiating treatment with ELX-TEZ-IVA received baseline and follow-up ophthalmological examinations.30 The clinical experts consulted during this review noted that children with CF currently have an ophthalmological examination before starting treatment with a CFTR modulator and are monitored on an ongoing basis thereafter.
No indirect comparison investigating the comparative safety of ELX-TEZ-IVA versus IVA for the subset of patients with an eligible gating mutation was included in this submission.69,70 Health Canada noted that some patients could have CFTR mutations that are responsive to IVA monotherapy and that these patients may not experience additional clinical benefit through exposure to the CFTR correctors (i.e., ELX and TEZ), although they could be at an increased risk of AEs.
Other Considerations
Health Canada reviewers noted that patients with many of the included CFTR mutations are potentially treatable with IVA monotherapy. The 2789 + 5G > A, 3272 to 26A > G, 3849 + 10kbC > T, R117C, L206W, V232D, T338I, R347H, A455E, S945L, L997F, and D1152H mutations are all listed as being IVA-responsive in the US product label for Kalydeco, and in vitro data provided in the current submission provides some support for use of IVA monotherapy in patients with these mutations. ██ ████████ ██ ██ ███████ ████ ██████ ███████ ███ ███████ ██████ ████ ████ ███ ███ █████████ ████████ ██ ██████ █ ██████████ ██ ████ ███ ████████ ███████████ ███ ████████ ███████ ██ █████ █████ █████████ ████████ ██ ███ ██████ ███████
Health Canada noted that application for ELX-TEZ-IVA did not specifically identify the patients with CFTR mutations that would benefit the most from receiving a combination therapy (ELX-TEZ-IVA) that includes the CFTR-corrector molecules as opposed to simply receiving monotherapy with a CFTR potentiator (i.e., IVA). This may be important for some patients who are intolerant to the triple-combination therapy, as the monotherapy could offer similar clinical benefit with reduced harms. Data protection for IVA ended on May 26, 2021. Should there be interest from public drug programs and CF clinical community, this product could be eligible for review through the Non-Sponsored Reimbursement Review Procedures.
Conclusion
The current review is for an expanded indication that would include 152 additional non-F508del mutations of the CFTR gene. The sponsor has categorized these mutations as follows: 147 FRT-responsive mutations; 4 noncanonical splice mutations; and the N1303K mutation. Evidence supporting the use of ELX-TEZ-IVA in the expanded population consisted of the following: 1 double-blind, placebo-controlled RCT in patients with FRT-responsive mutations (Study 124; N = 307; 18 CFTR mutations); 1 long-term extension study (Study 125; same population as Study 124); 1 retrospective observational study (Study 14; N = 422; 64 CFTR mutations); 4 nonrandomized studies involving patients with 1 or more N1303K mutations (Solomon et al., [2024], N = 20; Burgel et al. [2023], N = 8; Burgel et al. [2024], N = 35; and Sadras et al. [2023], N = 8). Evidence for 79 of the additional mutations is exclusively from the in vitro FRT model.
With respect to FRT-responsive mutations, Studies 124 and 16 demonstrated that ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function (an increase in ppFEV1), nutritional status (an increase in BMI), health-related quality of life (an increase in CFQ-R [RD] scores), CF biomarkers (a reduction in SwCl), and a reduced rate of PEx events. For the clinical studies in patients with 1 or more N1303K mutations, the short-term results showed acute increases in ppFEV1 and weight that were suggestive of a clinically meaningful benefit with ELX-TEZ-IVA in these patients; but the results cannot be considered conclusive of a clinically important effect because of the limitations of the open-label, noncomparative, observational study designs, with relatively small sample sizes (N ranged from 8 to 35), short durations, limited reporting of important information, and several potential sources of bias and uncertainty. For all of the mutations with clinical data, the clinical specialists consulted for this review described the results as clinically meaningful and indicative that ELX-TEZ-IVA would benefit patients in the target population. The experts emphasized the high level of unmet needs for these patients as they currently do not have access to CFTR-modulator therapy in Canada (outside of enrolment in a clinical study).
For the 79 mutations assessed exclusively by the in vitro FRT model, the sponsor defined responsive CFTR mutations as those that demonstrated an increase of 10% in Cl− transport over baseline when expressed as a percentage of normal CFTR Cl− transport. The sponsor’s selection of this threshold is therefore expected to affect the disease phenotype for those living with CF. The CF specialists consulted for this review reported that prescribers in Canada are not concerned about the absence of clinical data for patients with rare CFTR mutations. They noted the practical challenges in conducting clinical trials for patients with rare CFTR mutations and emphasized that there are important concerns regarding equity of access to CFTR modulators. Health Canada considered the evidence from the FRT-cell model sufficient to warrant the indication for ELX-TEZ-IVA. Health Canada concluded that the CFTR mutations for which the sponsor has provided sufficient clinical evidence of efficacy are also among those more commonly harboured by patients with CF in Canada. As such, expansion of the indication for ELX-TEZ-IVA would be expected to significantly increase access to effective CF therapy in Canada. Health Canada noted that the inclusion of other CFTR variants to the product monograph because they are responsive to ELX-TEZ-IVA treatment is based mainly on biological plausibility. In cases where the mutation is known to have the potential to cause CF because of the production of a dysfunctional full-length CFTR variant that has demonstrated in vitro responsiveness to ELX-TEZ-IVA (i.e., FRT-responsive mutations), or when a reduced amount of CFTR is produced and its function can be augmented (i.e., splicing mutations), ELX-TEZ-IVA treatment has the potential to provide clinically meaningful benefit to patients.
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., those aged at least 2 years with at least 1 mutation that is responsive to ELX-TEZ-IVA based on clinical and/or in vitro data). The warnings and precautions section of ELX-TEZ-IVA product monograph has not been updated since the previous CDA-AMC reviews.
References
1.Drug Reimbursement Expert Review Committee draft recommendation: elexacaftor-tezacaftor-ivacaftor and ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Incorporated). Ottawa (ON): CADTH; 2023 Oct: https://www.cda-amc.ca/sites/default/files/DRR/2023/SR0776%20Trikafta%20-%20Draft%20CADTH%20Recommendation%20October%2026%2C%202023%20-%20For%20posting.pdf. Accessed by sponsor, no date provided.
2.Solomon G, Linnemann R, Rich R, et al. 252 Interim results of an open-label trial to evaluate elexacaftor-tezacaftorivacaftor in individuals with cystic fibrosis and an N1303K mutation who are not eligible for modulator treatment. J Cyst Fibros. 2023;22(Supplement 3):S128.
3.Burgel PR, Sermet-Gaudelus I, Durieu I, et al. The French Compassionate Program of elexacaftor-tezacaftor-ivacaftor in people with cystic fibrosis with advanced lung disease and no F508del CFTR variant. Eur Respir J. 2023;61(5):2202437. PubMed
4.Burgel PR, Sermet-Gaudelus I, Girodon E, et al. Gathering real-world compassionate data to expand eligibility for elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis with N1303K or other rare CFTR variants: a viewpoint. Eur Respir J. 2024;63(1):2301959. PubMed
5.Nonclinical Study Report: VXMA-US-20-2000703, v.1. In vitro pharmacological profiling of CFTR mutations in FRT cells using VX-445, TEZ, and IVA: effects on processing and trafficking, and chloride transport. San Diego (CA): Vertex Pharmaceuticals Incorporated; 2020 Dec.
6.Clinical Study Report: VX22-CFD-016. An observational study evaluating real-world clinical outcomes of elexacaftor/tezacaftor/ivacaftor treatment in people with cystic fibrosis who have an elexacaftor/tezacaftor/ivacaftor-responsive non-F508del CFTR genotype [internal sponsor's report]. Boston (MA): Vertex Pharmaceuticals Incorporated; 2023 Oct 16.
7.Dreano E, Burgel PR, Hatton A, et al. Theratyping cystic fibrosis patients to guide elexacaftor/tezacaftor/ivacaftor out-of-label prescription. Eur Respir J. 2023;62(4):2300110. PubMed
8.Livnat G, Dagan A, Heching M, et al. Treatment effects of elexacaftor/tezacaftor/ivacaftor in people with CF carrying non-F508del mutations. J Cyst Fibros. 2023;22(3):450-455. PubMed
9.Pranke I, Dreano E, Hatton A, et al. 673 Elexacaftor/tezacaftor/ivacaftor corrects function of H1085R-, N1303K-, and R334W-cystic fibrosis transmembrane conductance regulator and improves clinical status of patients. J Cyst Fibros. 2022;21(Supplement 2):S368-S369.
10.Drug Reimbursement Review sponsor submission: Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg, oral tablets; Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 75 mg or 80mg/40mg/60mg and 59.5 mg, oral granules [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024 Mar 05.
11.Solomon G, Suzuki S, Hathorne H, et al. 606 Focused clinical trials of modulator response for rare cystic fibrosis genotypes. J Cyst Fibros. 2022;21(Supplement 2):S336.
12.Common Technical Document section 2.7.3: summary of clinical efficacy [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg oral tablets; Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 75 mg or 80mg/40mg/60mg and 59.5 mg oral granules. Vertex Pharmaceuticals (Canada) Incorporated: Sponsor name; 2024 Mar 05.
13.Burgel PR, Sermet-Gaudelus I, Durieu I, et al. WS10.01 The French Compassionate Programme of elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis with advanced lung disease and no F508del CFTR variant. J Cyst Fibros. 2023;22(Supplement 2):S20.
14.Cohen-Cymberknoh M, Sadras I, Kerem E, et al. P077 Clinical and functional efficacy of elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis carrying the N1303K mutation. J Cyst Fibros. 2023;22(Supplement 2):S87.
15.Sadras I, Kerem E, Livnat G, et al. Clinical and functional efficacy of elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis carrying the N1303K mutation. J Cyst Fibros. 2023;22(6):1062-1069. PubMed
16.Sadras I, Kerem E, Livnat G, et al. 133 Clinical response to elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis with the N1303K and non-modulator responsive mutation. J Cyst Fibros. 2022;21(Supplement 2):S78-S79.
17.Cystic Fibrosis Canada. The Canadian Cystic Fibrosis registry: 2019 annual data report. Toronto (ON): Cystic Fibrosis Canada; 2020: https://www.cysticfibrosis.ca/registry/2019AnnualDataReport.pdf. Accessed 2023 Nov 15.
18.Cystic Fibrosis Canada. The Canadian Cystic Fibrosis Patient Registry 2021 annual data report. Toronto (ON): Cystic Fibrosis Canada; 2023: https://www.cysticfibrosis.ca/uploads/2021-Annual-Data-Report-WEB-AODA.pdf. Accessed by sponsor, no date provided.
19.Rowe SM, Miller S, Sorscher EJ. Cystic fibrosis. N Engl J Med. 2005;352(19):1992-2001. PubMed
20.Veit G, Avramescu RG, Chiang AN, et al. From CFTR biology toward combinatorial pharmacotherapy: expanded classification of cystic fibrosis mutations. Mol Biol Cell. 2016;27(3):424-433. PubMed
21.Flume PA, O'Sullivan BP, Robinson KA, et al. Cystic fibrosis pulmonary guidelines: chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2007;176(10):957-969. PubMed
22.Cogen J, Emerson J, Sanders DB, et al. Risk factors for lung function decline in a large cohort of young cystic fibrosis patients. Pediatr Pulmonol. 2015;50(8):763-770. PubMed
23.Emerson J, Rosenfeld M, McNamara S, Ramsey B, Gibson RL. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatr Pulmonol. 2002;34(2):91-100. PubMed
24.Canadian consensus statement on aerosolized antibiotic use in cystic fibrosis. Toronto (ON): Cystic Fibrosis Canada; 2020: https://www.cysticfibrosis.ca/uploads/About%20Us/CFC005%20AEROSOLIZED%20ANTIBIOTIC%20_englishFinal.pdf. Accessed 2023 Nov 15.
25.Committee for Medicinal Products for Human Use. Assessment report: Kaftrio (ivacaftor/tezacaftor/elexacaftor). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2020: https://www.ema.europa.eu/en/documents/assessment-report/kaftrio-epar-public-assessment-report_en.pdf. Accessed 2020 Dec 17.
26.Liou TG, Adler FR, Fitzsimmons SC, Cahill BC, Hibbs JR, Marshall BC. Predictive 5-year survivorship model of cystic fibrosis. Am J Epidemiol. 2001;153(4):345-352. PubMed
27.Corey M, McLaughlin FJ, Williams M, Levison H. A comparison of survival, growth, and pulmonary function in patients with cystic fibrosis in Boston and Toronto. J Clin Epidemiol. 1988;41(6):583-591. PubMed
28.Mogayzel PJ, Jr., Naureckas ET, Robinson KA, et al. Cystic fibrosis pulmonary guidelines. Chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2013;187(7):680-689. PubMed
29.Flume PA, Mogayzel PJ, Jr., Robinson KA, et al. Cystic fibrosis pulmonary guidelines: treatment of pulmonary exacerbations. Am J Respir Crit Care Med. 2009;180(9):802-808. PubMed
30.Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor): 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg oral tablets; Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor): 100 mg/50 mg/75 mg and 75 mg or 80mg/40mg/60mg and 59.5 mg oral granules [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024 Jul 12.
31.Center for Drug Evaluation and Research. Multi-discipline review(s). Trikafta (elexacaftor, tezacaftor and ivacaftor tablets; ivacaftor) tablets. Company: Vertex Pharmaceuticals Incorporated. Application No.: 212273. Approval date: 10/21/2019 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2019: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2019/212273Orig1s000MultidisciplineR.pdf. Accessed 2020 Dec 17.
32.Vertex Pharmaceuticals Incorporated. Prescribing information: Trikafta (elexacaftor, tezacaftor and ivacaftor; ivacaftor) tablets. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2019: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212273s000lbl.pdf. Accessed 2023 Nov 15.
33.Drug Reimbursement Expert Review Committee final recommendation: elexacaftor-tezacaftor-ivacaftor and ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Inc.). Can J Health Technol. 2021;1(9). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/sr0673/sr0673. Accessed 2023 Dec 15.
34.Drug Reimbursement Expert Review Committee final recommendation: elexacaftor-tezacaftor-ivacaftor and ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Inc.). Can J Health Technol. 2022;2(7). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/SR0710/SR0710. Accessed 2023 Dec 15.
35.Drug Reimbursement Expert Review Committee final recommendation: ivacaftor (Kalydeco - Vertex Pharmaceuticals (Canada) Incorporated). Ottawa (ON): CADTH; 2013 Mar 22: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_Kalydeco_March-25-13_e.pdf. Accessed 2023 Nov 15.
36.Drug Reimbursement Expert Review Committee final recommendation: ivacaftor (Kalydeco — Vertex Pharmaceuticals Inc.). Ottawa (ON): CADTH; 2014 Dec 19: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_SR0379_Kalydeco_Dec-23-14.pdf. Accessed 2023 Nov 15.
37.Drug Reimbursement Expert Review Committee final recommendation: ivacaftor (Kalydeco — Vertex Pharmaceuticals Inc.). Ottawa (ON): CADTH; 2015 Nov 19: https://www.cadth.ca/sites/default/files/cdr/complete/SR0430_complete_Kalydeco_R117H_Nov-23-15_e.pdf. Accessed 2023 Nov 15.
38.Drug Reimbursement Expert Review Committee final recommendation: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Inc.). Ottawa (ON): CADTH; 2016 Oct 26: https://www.cadth.ca/sites/default/files/cdr/complete/SR0471_complete_Orkambi-Oct-28-16.pdf. Accessed 2023 Nov 15.
39.Drug Reimbursement Review clinical guidance report: lumacaftor/ivacaftor (Orkambi) for the treatment of cystic fibrosis in patients aged six years and older who are homozygous for the F508del mutation in the cystic fibrosis transmembrane conductance regulator gene. Ottawa (ON): CADTH; 2018 Oct: https://www.cadth.ca/sites/default/files/cdr/clinical/SR0559_Orkambi_CL_Report.pdf. Accessed 2023 Nov 15.
40.Drug Reimbursement Review: tezacaftor/ivacaftor (Symdeko). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/tezacaftorivacaftor. Accessed 2023 Nov 15.
41.Orkambi (lumacaftor/ivacaftor): 100 mg/125mg or 200 mg/125 mg, oral tablets; Orkambi (lumacaftor/ivacaftor): 100 mg/125mg or 150 mg/188mg, oral granules [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2018 Dec 11: https://pdf.hres.ca/dpd_pm/00048664.PDF. Accessed 2023 Nov 15.
42.Kalydeco (ivacaftor): 150 mg oral tablets, or 50 mg per packet or 75 mg per packet, oral granules [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2019 Jan 25: https://pdf.hres.ca/dpd_pm/00049400.PDF. Accessed 2023 Nov 15.
43.Van Goor F, Yu H, Burton B, Hoffman BJ. Effect of ivacaftor on CFTR forms with missense mutations associated with defects in protein processing or function. J Cyst Fibros. 2014;13(1):29-36. PubMed
44.Accurso FJ, Van Goor F, Zha J, et al. Sweat chloride as a biomarker of CFTR activity: proof of concept and ivacaftor clinical trial data. J Cyst Fibros. 2014;13(2):139-147. PubMed
45.Clinical Study Report: VX21-445-124. A phase 3 double-blind, randomized, placebo-controlled study evaluating the efficacy and safety of ELX/TEZ/IVA in cystic fibrosis subjects 6 years of age and older with a non-F508del ELX/TEZ/IVA-responsive CFTR mutation [internal sponsor's report]. Boston (MA): Vertex Pharmaceuticals Incorporated; 2023 Oct 06.
46.National Center for Health Statistics. CDC growth charts: percentile data files with LMS values. Hyattsville (MD): Centers for Disease Control and Prevention (CDC); 2009: https://www.cdc.gov/growthcharts/percentile_data_files.htm. Accessed 2022 Mar 21.
47.Wainwright CE, Elborn JS, Ramsey BW, et al. Lumacaftor-Ivacaftor in Patients with Cystic Fibrosis Homozygous for Phe508del CFTR. N Engl J Med. 2015;373(3):220-231. PubMed
48.Vertex Pharmaceuticals Incorporated. NCT02412111: A phase 3 study of tezacaftor (VX-661) in combination with ivacaftor (VX-770) in subjects aged 12 years and older with cystic fibrosis (CF), who have one F508del-CFTR mutation and a second mutation that has been demonstrated to be clinically responsive to ivacaftor. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2019: https://clinicaltrials.gov/ct2/show/NCT02412111. Accessed 2021 Dec 1.
49.Vertex Pharmaceuticals Incorporated. NCT02392234: A phase 3 study to evaluate the efficacy and safety of ivacaftor and VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the F508del-cystic fibrosis transmembrane conductance regulator (CFTR) mutation. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2018: https://clinicaltrials.gov/ct2/show/NCT02392234. Accessed 2021 Dec 1.
50.Vertex Pharmaceuticals Incorporated. NCT01614470: Study of ivacaftor in subjects with cystic fibrosis (CF) who have a non-G551D CF transmembrane conductance regulator (CFTR) gating mutation (KONNECTION). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2014: https://clinicaltrials.gov/ct2/show/NCT01614470. Accessed 2021 Dec 1.
51.Ramsey BW, Davies J, McElvaney NG, et al. A CFTR potentiator in patients with cystic fibrosis and the G551D mutation. N Engl J Med. 2011;365(18):1663-1672. PubMed
52.Davies JC, Wainwright CE, Canny GJ, et al. Efficacy and safety of ivacaftor in patients aged 6 to 11 years with cystic fibrosis with a G551D mutation. Am J Respir Crit Care Med. 2013;187(11):1219-1225. PubMed
53.Miller MR, Crapo R, Hankinson J, et al. General considerations for lung function testing. Eur Respir J. 2005;26(1):153-161. PubMed
54.Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319-338. PubMed
55.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
56.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
57.Clinical Study Report: VX21-445-125 Week 4 Data Cut. A phase 3 open-label study evaluating the long-term safety and efficacy of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis subjects with non-F508del CFTR genotypes [internal sponsor's report]. Boston (MA): Vertex Pharmaceuticals Incorporated; 2023 Oct 12.
58.The Canadian Cystic Fibrosis registry: 2013 annual report. Toronto (ON): Cystic Fibrosis Canada; 2015: https://www.cysticfibrosis.ca/uploads/cf%20care/Canadian-CF-Registry-2013-FINAL.pdf. Accessed 2020 Dec 17.
59.Bhatt JM. Treatment of pulmonary exacerbations in cystic fibrosis. Eur Respir Rev. 2013;22(129):205-216. PubMed
60.de Boer K, Vandemheen KL, Tullis E, et al. Exacerbation frequency and clinical outcomes in adult patients with cystic fibrosis. Thorax. 2011;66(8):680-685. PubMed
61.Solem CT, Vera-Llonch M, Liu S, Botteman M, Castiglione B. Impact of pulmonary exacerbations and lung function on generic health-related quality of life in patients with cystic fibrosis. Health Qual Life Outcomes. 2016;14:63. PubMed
62.Waters V, Atenafu EG, Salazar JG, et al. Chronic Stenotrophomonas maltophilia infection and exacerbation outcomes in cystic fibrosis. J Cyst Fibros. 2012;11(1):8-13. PubMed
63.Waters V, Stanojevic S, Atenafu EG, et al. Effect of pulmonary exacerbations on long-term lung function decline in cystic fibrosis. Eur Respir J. 2012;40(1):61-66. PubMed
64.Sanders DB, Bittner RC, Rosenfeld M, Hoffman LR, Redding GJ, Goss CH. Failure to recover to baseline pulmonary function after cystic fibrosis pulmonary exacerbation. Am J Respir Crit Care Med. 2010;182(5):627-632. PubMed
65.Sanders DB, Hoffman LR, Emerson J, et al. Return of FEV1 after pulmonary exacerbation in children with cystic fibrosis. Pediatr Pulmonol. 2010;45(2):127-134. PubMed
66.Mayer-Hamblett N, Nichols DP, Odem-Davis K, et al. Evaluating the impact of stopping chronic therapies after modulator drug therapy in cystic fibrosis: the SIMPLIFY clinical trial study design. Ann Am Thorac Soc. 2021;18(8):1397-1405. PubMed
67.Nicole Hamblett. NCT04378153: Impact of discontinuing chronic therapies in people with cystic fibrosis on highly effective CFTR modulator therapy (SIMPLIFY). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2024: https://clinicaltrials.gov/ct2/show/NCT04378153. Accessed 2024 Oct 09.
68.Clinical Study Report: VX18-445-106. A phase 3 study evaluating the pharmacokinetics, safety, and tolerability of VX-445/TEZ/IVA triple combination therapy in cystic fibrosis subjects 6 through 11 years of age [internal sponsor's report]. Boston (MA): Vertex Pharmaceuticals Incorporated; 2020 Nov 11.
69.Drug Reimbursement Review sponsor submission: Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg, oral tablets [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Jan 21.
70.Drug Reimbursement Review sponsor submission: Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), or 50 mg/25 mg/37.5 mg and 75 mg or 100 mg/50 mg/75 mg and 150 mg, oral tablets [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Nov 05.
Appendix 1: Excluded Studies
Please note that this appendix has not been copy-edited.
Dreano et al. (2023)
The study reported by Dreano et al., 2023 was a prospective observational cohort study from the French compassionate use program, a multicentre registry aimed to examine whether the pharmacological rescue of CFTR activity by ELX-TEZ-IVA in human nasal epithelial cells carrying various CFTR genotypes was predictive of an improvement in respiratory function and SwCl among patients with CF with no F508del CFTR mutation and with advanced lung disease.
The sponsor included an analysis from the publication by Dreano et al., 2023 that included 39 patients (18 of whom had a mutation in the CFTR gene that reflected the TPP for this review). The sponsor subsequently extracted data from 4 patients with at least 1 N1303K mutation from the overall population and reported a post hoc analysis. CDA-AMC reviewed the study by Dreano et al., 2023 and the sponsors rationale for including the information and concluded that the study should not be included in the review:
Does not address a gap in the evidence: The analysis from Dreano et al., 2023 reflects 4 patients with at least 1 N1303K mutation. However, the patients included in Dreano et al., had advanced lung disease and were enrolled in a compassionate use program in France. This is the same source of patients used in the larger studies reported by Burgel 2023 (N = 8)3,13 and Burgel et al. (2024) (N = 34). The sponsor was unable to confirm if there is overlap between the patient populations in these studies.
Population: The majority of patients included in the overall analyses had a genotype that is not relevant for the current review (21/38 [55%]). The patients selected for the subgroup analysis do not reflect all patients in the study with at least 1 N1303K mutation.
Methodology: There were no details reported regarding how the statistical analyses were conducted for the subgroup of patients with at least 1 N1303K mutation.
Absence from Canadian regulatory submission: CDA-AMC notes that these analyses were not included in the submission to Health Canada.
Pranke et al. (2022)
The sponsor included an abstract by Pranke et al., 2022 that reported a study evaluating the efficacy of ELX-TEZ-IVA in correcting activity of non-F508del-CFTR mutations in a human nasal epithelial cell primary model among patients with CF with severe respiratory insufficiency and no F508del mutations. The abstract reported the results for 3 patients with the following genotypes N1303K/N1303K (n = 1), N1303K/H1085R (n = 1), and other non-F508del mutations (n = 1). CDA-AMC reviewed the abstract and the sponsors’ rationale for including the information and concluded that the study should not be included:
Does not address a gap in the evidence: The analysis from Pranke et al., 2022 reflects 2 patients with at least 1 N1303K mutation. However, similar to the situation with the publication by Dreano et al., 2023, these are patients with advanced lung disease who were enrolled in a compassionate use program in France. This is the same source of patients used in the larger studies reported by Burgel 2023 (N = 8)3,13 and Burgel et al. (2024) (N = 34). The sponsor was unable to confirm if there is overlap between the patient populations in these studies.
Publication format: In accordance with CDA-AMC procedures, the sponsor must provide the additional information in a format that allows the review team to complete a detailed review and appraisal of the data (e.g., in accordance with the CONSORT reporting guidelines or Guidance for Reporting Real-World Evidence, as applicable). A single conference abstract is not an appropriate format for the submission of clinical data for the purposes of informing reimbursement recommendations.
Methodology: There were no details reported regarding how the statistical analyses were conducted for the subgroup of patients with at least 1 N1303K mutation.
Absence from Canadian regulatory submission: CDA-AMC notes that these analyses were not included in the submission to Health Canada.
Appendix 2: Detailed Outcome Data [Redacted]
Please note that this appendix has not been copy-edited.
████████ | █████████ | █████████████ █ ███ | ||
|---|---|---|---|---|
██████ ████████████ ███████ | ████ █████████ | █████ ██ █████████ | ||
███████████ | ███ | ███ | ███ | ███ |
████ ████ | ████ █████ | █████ █████ | ████ ██████ | |
████ | ███ | ██ | ███ | ███ |
████ ████ | ████ ██████ | █████ ██████ | ████ ██████ | |
█████████ | ███ | ██ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
██████████ | ███ | ██ | ███ | ███ |
████ ████ | ███ █████ | █████ █████ | ████ ██████ | |
██████ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | ████ █████ | ████ ██████ | |
█████ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
█████ | ███ | ███ | ███ | ██ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
█████ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
██████ | ███ | ███ | ███ | ███ |
████ ████ | ████ █████ | █████ ██████ | ████ ██████ | |
██████ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ ██████ | ████ ██████ | |
█████ | ███ | ███ | ███ | ███ |
████ ████ | ███ █████ | █████ █████ | ███ ██████ | |
██████ | ███ | ███ | ███ | ███ |
████ ████ | ████ ██████ | ███ | ███ | |
████████ | █████████ | ██████████████ █ ████ |
|---|---|---|
█████ | ███ | ███ |
████ ████ | ███ ██████ | |
█████ | ███ | ███ |
████ ████ | ███ █████ | |
██████ | ███ | ███ |
████ ████ | ███ █████ | |
████ | ███ | ███ |
████ ████ | ███ █████ | |
████ █ ████ ███ | ███ | ███ |
████ ████ | ███ █████ | |
█████ | ███ | ███ |
████ ████ | ███ ██████ | |
█████ | ███ | ███ |
████ ████ | ███ █████ | |
█████ | ███ | ███ |
████ ████ | ███ ██████ | |
██████ | ███ | ███ |
████ ████ | ████ ██████ | |
█████ | ███ | ███ |
████ ████ | ███ █████ | |
█████ | ███ | ███ |
████ ████ | ███ █████ | |
█████ | ███ | ███ |
████ ████ | ███ █████ | |
████ | ███ | ███ |
████ ████ | ███ ██████ | |
█████ | ███ | ███ |
████ ████ | ███ █████ | |
████ | ███ | ███ |
████ ████ | ████ █████ | |
██████ | ███ | ███ |
████ ████ | ███ █████ | |
████ █ ████ | ███ | ███ |
████ ████ | ███ █████ | |
█████ | ███ | ███ |
████ ████ | ███ █████ | |
██████ | ███ | ███ |
████ ████ | ████ ██████ | |
██████ | ███ | ███ |
████ ████ | | ███ ██████ |
Appendix 3: Summary of In Vitro Data [Redacted]
Please note that this appendix has not been copy-edited.
Table 38: Summary of In Vitro Data [Redacted]
████ ████ | ████████ █████████ ████████ | ████████ █████████ ██ ███████ | ██████ ████ ████████ ████ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
██ | ███ | ████ | ██ | ██ | ███ | ████ | ███ | ███ | ███ | ██ | |
████████ | |||||||||||
██████ | ███ | █████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | █████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | █████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
███ █████████ | |||||||||||
███ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
███ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
███ | ███ | ███ | ████ | ████ | ███ | ██ | ███ | ███ | ██ | ██ | ███ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ██ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ████ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ██ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ██ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ██ | ██ | ██ | ███ |
█████ | ███ | ████ | ███ | ████ | ███ | ███ | ██ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ██ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ████ | ███ | ██ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ██ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ██ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ██ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ██ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ██ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | || | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ██ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ██ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
██████ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ███ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | || |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ████ | ███ | ██ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | █████ | ███ | ███ | ██ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ███ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | || | ██ | ██ |
██████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ███ | █████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ███ | || | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ███ | ███ | █████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ ██ ███ ██ ███ ████ | |||||||||||
██████ | ███ | ███ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ███ | ███ |
█████ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ████ | ████ | ████ | ██ | ███ | ███ | ███ | ███ | ██ | ███ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ██ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
█████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
█████ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ██ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
██████ | ███ | ████ | ████ | ████ | ███ | ███ | ███ | ███ | ██ | ██ | ███ |
███ █████████ ███ ████████ ██████████ ███ ██████████ ██████ ███████ ████████ ███ ████████ █████ ██ ██ ████ ██ ██ ███ ███ █ ██ ███ ███ ██████ ████████ ████ ███ ████ █ ██ ███ | | | ███████████ ███████████ ███ ████ █████ ████████ ██████ ███ ██████████ ██ ████████ ██ ████████ ████ ██████ ████ ████ ████████ ███████ ████ ████████ ██████ █ ██████ █████ █████ ██████████ █████ █ ██████ █████ █████ ████ ██ ██ ███ ██████ ██████ ██ ██ ████ ████ █████ ██ █ ██████ ███████ ██████ ███ ██ ███████████ ██████ ███ █████████ ████████ ██████ ███████████ ██████ ███████ █████████ ████████ █████ ████ █████████ ███ ████████ ██ ███████ ██████ ████████ █████ ██ ███ ████ ██ ████ ███████ ██ ████ ████ ██ █████████ ███ █████████ ██ ████ ████ ██ █████████ ███ ████████ ██ █ ███████ ████ ████ ███ ██████ ██ ███████ ████████ ██ ██ █████ ███ ████ ██ █ ██████████████████ ████████ ██ ██ █████████ ███ ████████ ██ █████████████████ █████████ ██ ███████████ ████████ █ ███████ ██████ ██████ ████████ █████ ███ ███ ██ █ ███ ██████ █████ ███████ █████████ ████████ █████ ██ ███ ██████████ ████ ███████ ██████████████ ██ ███ ██████ ██ ████ ██ ███ ███████████ ██ ██ ██████ ███████████ ██ ███████ ██████ █████████ ██ ████████ ███ █ █████████ ██ ███ █████ ███████ ██████ ██████ ██████ ██████ ███ ███████ ██ ██████ ██████ | | █████ ████ ████ ████████ ███ ██ █ ███████ ██████ ██████ ██████████ ███ ███ ███ ██████ ████ █████ ███ █████████ ██████████ ██████ ████ ███ █ ██ ████████ ███ ███████ █████ ██████████████ ██ ████████ ██ ███ █████████████ ███████ ████ ████████ ████████ ████ █████████ ████ ████████ ███ ████████ ███ ███ █████████████ █████████ ████ ████████ █████████
███ ████ ██ ████ █████████ ██████ ███████ ███████ ██ ███ █████ ███ ███ ████ ██████████ ████████ ███ ██ ███ ████ ██████ ██ ████████ ██ █████ ████████ ███ ████ ██ ████████ ███ ████████████ ████████ █████
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
BSC
best supportive care
CDA-AMC
Canada's Drug Agency
CF
cystic fibrosis
CF Canada
Cystic Fibrosis Canada
CFRD
cystic fibrosis–related diabetes
ELX
elexacaftor
ELX-TEZ-IVA
elexacaftor-tezacaftor-ivacaftor plus ivacaftor
ICER
incremental cost-effectiveness ratio
IVA
ivacaftor
PEx
pulmonary exacerbations
ppFEV1
percent predicted forced expiratory volume in 1 second
QALY
quality-adjusted life-year
TEZ
tezacaftor
WFAZ
weight-for-age z score
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Elexacaftor-tezacaftor-ivacaftor plus ivacaftor (Trikafta) Aged 2 to 5 years:
Aged 6 years and older:
|
Indication | Proposed: For the treatment of cystic fibrosis in patients aged 2 years and older who have 1 or more F508del mutations in the CFTR gene or a mutation in the CFTR gene that is responsive based on in vitro and/or clinical dataa |
Health Canada approval status | Under review (pre-NOC) |
Health Canada review pathway | Priority |
NOC date | Anticipated: July 14, 2024 |
Reimbursement request | As per indication |
Sponsor | Vertex Pharmaceuticals (Canada) Incorporated |
Submission history | Previously reviewed: Yes Indication: Cystic fibrosis, F508del CFTR mutation in patients aged 12 years and older, 6 years and older, and 2 to 5 years Recommendation dates: August 2021, June 2022, and November 2023 Recommendation: List with criteria and conditions, including a substantial reduction in price |
CF = cystic fibrosis; NOC = Notice of Compliance.
aThis review focuses only on non-F508del mutations that are responsive to ELX-TEZ-IVA based on in vitro and/or clinical data.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Microsimulation |
Target population | Patients with CF aged 2 years and older who have a mutation in the CFTR gene that is responsive based on in vitro and/or clinical data |
Treatment | ELX-TEZ-IVA plus BSC BSC defined as recommended medications (such as mucolytics, inhaled and oral antibiotics, inhaled hypertonic saline, nutritional supplements, enteral tube feeding, pancreatic enzymes, antifungal agents, and corticosteroids) and physiotherapy |
Dose regimen | Based on patient weight
|
Submitted price | ELX-TEZ-IVA (Trikafta), 100 mg, 50 mg, and 75 mg plus IVA 150 mg tablets; 50 mg, 25 mg, and 37.5 mg and IVA 75 mg tablets; or 100 mg, 50 mg, and 75 mg plus IVA 75 mg granules; 80 mg, 40 mg, and 60 mg plus IVA 59.5 mg granules: $280.00 per tablet, $420.00 per granules packet |
Submitted treatment cost | $306,810 annually per patient, regardless of strength or form |
Comparators | SOC
SOC comprises a treatment mix of IVA and BSC, estimated by a weighting factor based on prevalence of IVA-eligible (20%) and IVA-ineligible patients (80%) and comparator market shares (10% BSC and 90% IVA in those who are IVA-eligible; 100% BSC in those who are IVA-ineligible) The final estimated SOC treatment mix is 82% BSC and 18% IVA |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs and life-years |
Time horizon | Lifetime (69 years) |
Key data sources | ELX-TEZ-IVA: Study 124 comprising patients with non-F508del mutations (24 weeks); Study VX17-445-105 comprising patients with F508del mutations (192 weeks) IVA: meta-analysis of Studies VX08-770-102, VX08-770-103, and VX-11-770-110 |
Submitted results | ICER vs. SOC = $306,901 per QALY gained (incremental costs = $3,707,909; incremental QALYs = 12.08) For IVA-eligible patients: ICER vs. IVA = $167,809 per QALY gained (incremental costs = $930,856; incremental QALYs = 5.55) For the full indicated population (i.e., irrespective of IVA eligibility): ICER vs. BSC = $319,432 per QALY gained (incremental costs = $4,317,506; incremental QALYs = 13.52) |
Key limitations |
|
CDA-AMC reanalysis results |
|
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; CF = cystic fibrosis; ELX = elexacaftor; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; QALY = quality-adjusted life-year; SOC = standard of care; TEZ = tezacaftor; vs. = versus.
Conclusions
Based on the Clinical Review, results from the 24-week phase II Study 124 suggest that treatment with elexacaftor-tezacaftor-ivacaftor plus ivacaftor (ELX-TEZ-IVA) resulted in statistically significant and clinically meaningful improvement in percent predicted forced expiratory volume in 1 second (ppFEV1) and reduction in risk of pulmonary exacerbation (PEx) compared with placebo after 24 weeks of treatment. The current review is for an expanded indication that would include 183 additional non-F508del mutations in the CFTR gene, of which only 18 were included in the Study 124 patient population. The sponsor provided additional clinical data in the form of a retrospective observational study, nonrandomized studies, and in vitro data; however, the sponsor reports that there are no clinical data for 94 Fischer rat thyroid (FRT)-responsive mutations (i.e., those that were considered responsive to ELX-TEZ-IVA in the in vitro model) and 1 of the noncanonical splice mutations. Furthermore, the comparative clinical benefit of ELX-TEZ-IVA compared to ivacaftor (IVA) is unknown because of a lack of head-to-head trial data. The Clinical Review did not raise concerns regarding this lack of data for the following reasons: the dosage of IVA administered as part of the ELX-TEZ-IVA combination regimen is the same as what patients would receive with IVA monotherapy (e.g., 150 mg in the morning and 150 mg in the evening); previous trials have demonstrated that patients with 1 or more F508del mutations and a gating mutation benefited from switching to ELX-TEZ-IVA from IVA monotherapy; and the submitted price for ELX-TEZ-IVA is the same as the current list price for IVA monotherapy.
The clinical experts consulted for the current review noted that, given the mechanism of action and compelling efficacy data in patients with F508del mutations, ELX-TEZ-IVA is expected to similarly benefit patients with non-F508del mutations. However, these conclusions are based on a pivotal study of patients with non-F508del mutations with a follow-up time of 24 weeks and studies in patients with F508del mutations with a maximum follow-up time of 192 weeks. No evidence is available on the long-term impact of ELX-TEZ-IVA on the rate of decline of ppFEV1 or PEx rates beyond the trial periods for any mutation or age group.
In addition to uncertainty in the long term clinical efficacy of ELX-TEZ-IVA, the review team identified several major limitations with the submitted economic evaluation. The CDA-AMC addressed these issues in its reanalysis through removal of an additional benefit of CFTR modulators on the long-term rate of decline in ppFEV1 and PEx; removal of dynamic pricing of CFTR modulators; inclusion of costs for ELX-TEZ-IVA for the period in which a survival benefit was achieved in comparison to best supportive care (BSC); removal of an adjustment to drug acquisition costs by patient adherence; and removal of a treatment-specific utility increment for patients on ELX-TEZ-IVA. Results of the CDA-AMC reanalysis were aligned with the sponsor’s in that ELX-TEZ-IVA was not cost-effective at conventionally acceptable incremental cost-effectiveness (ICER) thresholds. In the CDA-AMC base-case analyses, ELX-TEZ-IVA was associated with an ICER of $1,122,823 per quality-adjusted life-year (QALY) gained compared to standard of care (SOC) in the overall patient population with non-F508del mutations.
The key drivers in the analyses are drug acquisition costs, and assumptions in the long term benefits with ELX-TEZ-IVA, which were uncertain. Treatment with ELX-TEZ-IVA was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained in any scenario conducted by CDA-AMC. A price reduction of greater than 79% is required for ELX-TEZ-IVA to be considered cost-effective at this threshold when compared with SOC — the annual cost of ELX-TEZ-IVA would need be reduced to $65,351 per patient (from $306,810). The near entirety of expected incremental survival was estimated beyond the 24-week period of the Study 124. In the absence of robust, long-term clinical evidence in patients with non-F508del mutations, the extent of the treatment benefit is highly uncertain. Consequently, the CDA-AMC base case may overestimate the clinical benefits associated with ELX-TEZ-IVA and higher price reductions may be required for ELX-TEZ-IVA to be cost-effective.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient group input was submitted by Cystic Fibrosis Canada (CF Canada), informed by Canadian focus groups of patients with rare mutations and their caregivers, along with input from 1 patient with an M1101K mutation. Data from the CF Canada 2021 patient and caregiver survey (1,200 responses) on access to ELX-TEZ-IVA along with the Canadian Cystic Fibrosis Registry and findings from a burden-of-disease study conducted by Dalhousie University and CF Canada were also used to inform the patient group input. Patients and caregivers reported that living with cystic fibrosis (CF) has a tremendous impact on the physical, psychological, social, and financial components of their lives. When asked about disease management, patients noted that managing CF requires a demanding treatment routine that requires much time and effort, while frequent clinic visits and hospital stays are needed to manage the progressive and debilitating symptoms. Data from the Canadian Cystic Fibrosis Registry on patients in Canada with CF who do not currently have a Health Canada indication for modulators show that 246 patients have rare mutations known to respond to ELX-TEZ-IVA. Patients with rare mutations and their caregivers shared their hopes to access ELX-TEZ-IVA as they saw the benefits of the medications for those who are able to access it. Patient group input indicated that, based on clinical trials, published real-world evidence, and a limited number of patients who have accessed ELX-TEZ-IVA, patients were noted to have responded exceptionally well to therapy, even those who have mutations for which evidence is scarce.
Clinician input was received from the CF Canada Accelerating Clinical Trials Network, the CF Canada Health Care Advisory Council, and the Edmonton and Calgary Adult Cystic Fibrosis Clinics. Clinicians noted that the treatment paradigm for patients is lifelong. Patients are prescribed a multitude of treatments consisting of nonmodulator treatments and medications, many of which start at the time of diagnosis (including in infancy) and continue every day throughout life. The clinician input noted that, while not a cure, CFTR modulators are the first available therapies targeted at correcting the basic defect in CF. A gap in care exists for patients in Canada with CF who have non-F508del mutations that are responsive to ELX-TEZ-IVA who can currently only access treatments that target the downstream effects of dysfunctional CFTR proteins. In a subset of patients, IVA can be used to treat patients with specific non-F508del mutations but it is not effective in the majority of patients with non-F508del mutations. However, clinician input stated that patients with non-F508del mutations that are responsive to treatment should not be required to try other CFTR-modulator therapies such as IVA, lumacaftor-ivacaftor plus ivacaftor (LUM-IVA), or tezacaftor-ivacaftor plus ivacaftor before initiating treatment with ELX-TEZ-IVA because of the superior clinical results with the triple therapy. Clinician input stated that ELX-TEZ-IVA would become the SOC if it were made available. All the clinicians who provided input for this review recommend initiating treatment with ELX-TEZ-IVA as soon as possible. All contributors agreed that no data support withholding the initiation of CFTR-modulator treatment until clinical symptoms of CF develop.
Feedback from the drug plans indicated that alignment with initiation criteria for F508del mutations in different age groups (e.g., 2 to 5 years and 6 years and older) may be considered. They also expressed concerns regarding assessment and monitoring of therapeutic response, given that clinical benefit is determined by physicians specializing in treating CF in the absence of clinical data.
Two of these concerns were addressed in the sponsor’s model:
Relevant comparators were included for CF patients aged 2 years and older who have at least 1 mutation in the CFTR gene that is responsive based on in vitro and/or clinical data.
All patients were assumed to receive SOC, consisting of antibiotics, mucolytics, and pancreatic enzymes.
In addition, CDA-AMC’s analysis included disease-management costs for patients on CFTR modulators for the entire time horizon.
CDA-AMC was unable to address the concern raised in the input relevant to the economic review regarding switching treatment from IVA to ELX-TEZ-IVA in the cost-utility analysis.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing ELX-TEZ-IVA in combination with BSC for the treatment of CF in patients aged 2 years and older who have 1 or more non-F508del mutations in the CFTR gene that are responsive based on in vitro and/or clinical data. The sponsor compared the submitted drug regimen with SOC comprising IVA plus BSC or BSC alone in IVA-eligible patients (an estimated 20% of the total patient population) with gating mutations (G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, S549R, and G970R) inclusive of R117H, as well as BSC alone in the remainder of patients with non-F508del mutations that are ineligible for IVA (estimated 80%).1 The modelled population is aligned with a subset of the Health Canada indication, which had been not previously submitted to CDA-AMC, specifically patients aged 2 years and older with at least 1 non-F508del mutation in the CFTR gene. CDA-AMC previously reviewed ELX-TEZ-IVA for the treatment of CF in patients who have 1 or more F508del mutations in the CFTR gene for those aged 12 years and older;2 those aged 6 years and older;3 and those aged 2 to 5 years.4 The sponsor requested that the current submission for ELX-TEZ-IVA focus only on the expanded patient population (i.e., those aged 2 years and older with non-F508del mutations that are responsive to ELX-TEZ-IVA based on in vitro and/or clinical data).5
The recommended dosage of ELX-TEZ-IVA is age- and weight-dependent. Patients aged 2 to 5 years weighing less than 14 kg are to take 1 packet of elexacaftor (ELX) 80 mg, tezacaftor (TEZ) 40 mg, and IVA 60 mg granules in the morning and 1 packet of IVA 59.5 mg granules in the evening.6 Patients aged 2 to 5 weighing more than 14 kg are to take 1 packet of ELX 100 mg, TEZ 50 mg, and IVA 75 mg granules in the morning and 1 packet of IVA 75 mg granules in the evening.6 Patients aged 6 to 11 weighing less than 30 kg are to take 2 tablets, each containing ELX 50 mg, TEZ 25 mg, and IVA 37.5 mg in the morning and 1 tablet of IVA 75 mg in the evening.6 All other patients have a recommended dosage of 2 tablets, each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg in the morning and 1 tablet of IVA 150 mg in the evening.6 All morning and evening doses are to be taken approximately 12 hours apart with fat-containing food.6 The daily cost of treatment is $840.00, for an annual cost of $306,810, based on its list price, regardless of the strength or form.1
The SOC comprised different comparator treatments depending on IVA eligibility. For IVA-eligible patients with gating mutations inclusive of R117H, comparators were IVA plus BSC or BSC alone. For IVA-ineligible patients, the comparator treatment was BSC alone. BSC was defined as recommended medications (such as mucolytics, inhaled and oral antibiotics, inhaled hypertonic saline, nutritional supplements, enteral tube feeding, pancreatic enzymes, antifungal agents, and corticosteroids) and physiotherapy.1 All patients on CFTR-modulator therapies also received BSC.
Outcomes of the model included QALYs and life-years over a lifetime horizon of approximately 69 years. The analysis was undertaken from the perspective of the Canadian public health care payer. Discounting at 1.5% per year was applied for both costs and outcomes, and the cycle length was 4 weeks for the first 2 years and then annually for the remainder of the model time horizon.
Model Structure
The sponsor submitted a patient-level microsimulation model used to track CF disease progression and treatment benefits for a typical patient profile informed by Study 124 (Figure 1).1 In the sponsor’s probabilistic base case, 250 average patients were simulated and the expected costs and clinical effects of ELX-TEZ-IVA, BSC, and IVA (for the 20% of patients who are IVA-eligible only) were calculated.1 This process was repeated 80 times.
At the beginning of each cycle, the model calculated a patient’s mortality risk based on a Cox proportional hazards model that linked a CF patient’s survival to 9 risk factors, including age, gender, ppFEV1, annual number of PEx events, respiratory infections (Staphylococcus aureus and Burkholderia cepacia), cystic fibrosis–related diabetes (CFRD), weight-for-age z score (WFAZ), and pancreatic sufficiency status.1 For each cycle a patient remained alive, patient characteristics were updated, including age, ppFEV1, WFAZ, PEx rate, eligibility and occurrence of lung transplant, development of CFRD, and treatment discontinuation. Long-term health impacts because of treatment were predicted using clinical outcomes such as median predicted survival, mean time spent in ppFEV1 states, cumulative change in ppFEV1, annual and lifetime PEx rates, and proportion of patients receiving a lung transplant.1 During each cycle, patients would accrue life-years and QALYs, whereas costs were applied at the end of each run of 250 patients for efficiency gains.
Model Inputs
Baseline age-specific risk of death in the model was derived from a cohort-based survival analysis of the Canadian CF Registry reported by Stephenson et al.7 Kaplan-Meier curves from this analysis were digitized and fitted using parametric survival analysis to generate a mortality risk for the lifetime time horizon. In the sponsor’s base case, a Gompertz curve was selected as the best-fitting curve.1 Mortality was recalculated for each cycle using the Cox proportional hazards model developed by Liou et al.8 to account for the factors indicated in the Model Structure section. The hazard of mortality in the model was assumed to be no lower than that of the general population of Canada.1
Patient characteristics used to inform the mortality risk in the model were derived from mean baseline characteristics of individual patients from Study 124.9 The average patient profile was estimated to be 30.6 years on average, with females accounting for 53.7% of patients.1 The baseline rate of PEx requiring IV antibiotics and/or hospitalization was informed by Whiting et al.10 CFRD status at baseline was based on UK CF registry data.11 It was assumed that the risk of developing CFRD was equal for patients receiving a CFTR modulator and those receiving BSC alone.
Age, ppFEV1, PEx rate, and WFAZ were updated at the beginning of each model cycle. Clinical efficacy inputs were derived from Study 124 for ELX-TEZ-IVA9 for patients who are IVA-ineligible (80% of the full indicated population) and from a meta-analysis for IVA for patients who are IVA-eligible (20% of the full indicated population).12 The meta-analysis for IVA included the STRIVE, ENVISION, and KONDUCT trials (Studies VX08-770-102, VX08-770-103, and VX11-770-110).12 An indirect treatment comparison between ELX-TEZ-IVA and IVA was not included in the analysis for the 20% of patients who are IVA-eligible because of feasibility limitations.
Based on the results of the pivotal trial and meta-analysis, CFTR modulators were assumed to be associated with an acute increase in ppFEV1 that was CFTR modulator–specific. The acute increase in ppFEV1 for patients receiving ELX-TEZ-IVA was based on the placebo-adjusted change in ppFEV1 from baseline through 24 weeks in Study 124.9 The acute increase in ppFEV1 for patients receiving IVA was based on the placebo-adjusted change in ppFEV1 from baseline through 24 weeks from the sponsor-conducted meta-analysis.12 Patients on BSC alone were not expected to experience any acute increases in ppFEV1 and were assumed to experience a long-term decline in ppFEV1 based on an analysis of age-specific annual rates of ppFEV1 for patients with non-508del mutations.13,14 Patients receiving ELX-TEZ-IVA during the maintenance period were assumed to sustain their acute improvements for 192 weeks, based on the results of Study 105.15 There was no maintenance period for IVA. During the postacute maintenance period, patients on ELX-TEZ-IVA were modelled with an 90.0% reduction in the rate of ppFEV1 decline when compared with BSC alone.15 Patients on IVA were assumed to experience a 47.1% reduction in their rate of ppFEV1 decline compared to BSC alone based on an open-label extension study.16
The baseline rate of occurrence of PEx each cycle was based on the patient’s ppFEV1 and age, according to a formula derived by Goss et al.17 The rate of PEx events for patients on CFTR modulators was adjusted by a rate ratio derived by the sponsor. This was based on an assumed additional treatment impact on PEx beyond those explained by the improvements in ppFEV1 in patients treated with a CFTR modulator as captured in the Goss et al. formula. To account for the potential double-counting of the benefit because of better ppFEV1 observed with CFTR modulators, the sponsor attempted to calibrate the PEx rate ratio for patients on a CFTR modulator. These patients had their rate of PEx adjusted such that the resulting relative rate of PEx events between patients receiving a CFTR-modulator and those receiving BSC alone matched the treatment effect on PEx events requiring IV antibiotics and/or hospitalizations observed in their respective pivotal trials.
Patients treated with a CFTR modulator were assumed to experience an acute change in WFAZ from baseline. The magnitude and duration of the acute change were informed by Study 124 for ELX-TEZ-IVA9 and by the meta-analysis for IVA.12 Patients on BSC alone were expected to not experience any acute increases in WFAZ.
The sponsor’s model also accounted for treatment discontinuation and adherence. Discontinuation rates for ELX-TEZ-IVA corresponding to the trial duration period were obtained from Study VX21-445-104 for the first 24 weeks of the model.9 The model assumes no discontinuation of ELX-TEZ-IVA because of adverse events (AEs) or other reasons that occur after 24 weeks, with exception of patients discontinuing treatment upon receiving a lung transplant. For IVA, discontinuation was not applied for the first 24 weeks of the model based on data from the meta-analysis,12 and discontinuation was applied for IVA after 24 weeks based on Studies 770-105 and 770-112.15,18 The model assumes no discontinuation of IVA after the first 104 weeks of treatment.19 Upon CFTR-modulator discontinuation, patients were modelled to no longer receive benefits; however they retained the acute increase in ppFEV1 and WFAZ they achieved up until the point of discontinuation. The sponsor further considered treatment adherence to inform treatment costs over the acute period (first 24 weeks) based on data from Study VX21-445-104 for ELX-TEZ-IVA9 and the submitted meta-analysis for IVA.12 Treatment adherence in the postacute period was set to 93% across all CFTR modulators, aligned with real-world data for patients receiving LUM-IVA.1 Adherence was assumed to have no impact on treatment efficacy, and only affected the costs associated with CFTR modulators.
The sponsor-submitted economic model also considered lung transplants and AEs. The sponsor aligned the rate of lung transplant and mortality risk following a transplant with those of the previous CDA-AMC submission.20 In the base-case analysis, patients with a ppFEV1 threshold of 30% were eligible for a lung transplant and the probability of receiving a transplant was 4.6%.1 AEs in the model were based on data from Study VX21-445-104 for ELX-TEZ-IVA and the submitted meta-analysis for IVA.9,12
In the absence of utilities based on a generic instrument (e.g., EQ-5D), the sponsor used an equation developed by Solem et al. that included ppFEV1 and PEx events as predictors of an EQ-5D index utility score.21 For this calculation, each pulmonary exacerbation was assumed to last 21.7 days, based on the TRAFFIC and TRANSPORT trials.21 The sponsor also included a treatment-specific utility increment only for patients receiving ELX-TEZ-IVA, as the equation by Solem et al., did not appear to capture the impact of treatment on nonrespiratory outcomes. Post–lung transplant utility values were obtained from a study by Whiting et al.10 No disutilities related to AEs were included in the model, as they were assumed to have minimal impact on patient quality of life.
Costs considered in the model included those associated with drug acquisition, monitoring, disease management, pharmacotherapy, diagnostics, PEx events, AEs, and lung transplants. The cost of ELX-TEZ-IVA was submitted by the sponsor,1 whereas the prices of IVA were obtained from the Ontario Exceptional Access Program formulary.22 For CFTR modulators, including ELX-TEZ-IVA, the sponsor employed a dynamic pricing approach, whereby the introduction of a first generic into the market after loss of patent exclusivity would lead to a 25% reduction in the prices of all drugs, followed by a second generic entry reducing their prices by another 50%. These assumptions were based on a pan-Canadian Pharmaceutical Alliance office framework for pricing expectations upon generic entry. Additional costs associated with the use of CFTR modulators described in their product monographs included monitoring costs consisting of liver-function tests and ophthalmologist visits, with costs obtained from the Ontario Schedule of Benefits.23
Annual CFTR-modulator monitoring costs were applied as indicated in each CFTR’s associated product monograph.6,24 Disease-management costs were also captured to include clinician visits, hospitalizations, infection prevention, and management of comorbidities. Such costs were applied in the model by disease severity (defined by ppFEV1 thresholds) and were further divided into PEx and non-PEx event costs. Health care resource use associated with routine disease-management costs was informed by a sponsor-commissioned burden-of-illness study and supplemental data from the 2014 CF Canada patient registry.1 Physician and laboratory unit costs were informed by the Ontario Schedule of Benefits, whereas hospitalization costs were derived from a study by Skolnik et al.23,25,26 Informed by published literature suggesting patients on CFTR modulators have reduced CF-related inpatient admission and outpatient IV and antibiotic use, the sponsor adjusted disease-management costs for patients on CFTR modulators.27,28 As a result, differential annual inpatient costs and annual pharmacotherapy costs were estimated for patients on BSC alone and those on CFTR modulators. The sponsor also excluded disease-management costs for patients on CFTR modulators after a similar patient on BSC alone had died in a given simulation, while only incurring CFTR modulator–therapy costs for the remainder of the time horizon. Lung transplant costs were obtained from Alberta Health Services, with follow-up costs obtained from the literature.29,30 The cost of each AE was assumed to be equal to the cost of a single assessment by a general practitioner.23 All costs were reported in 2023 Canadian dollars.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically, with 250 average patients individually simulated for 80 iterations for the base-case and scenario analyses. The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section. The sponsor’s base case is based on publicly available list prices for comparators.
Base-Case Results
The sponsor presented weighted results for ELX-TEZ-IVA versus current SOC. Current SOC represents the current treatment mix of IVA and BSC alone weighted by the prevalence of patients in the target population who are IVA-eligible (20%) and IVA-ineligible (80%). The weighting factor also considers comparator market shares in the IVA-eligible population (10% receiving BSC alone and 90% receiving IVA) and IVA-ineligible population (100% receiving BSC alone). The final SOC comparator mix was therefore estimated to consist of 18% receiving IVA and the remaining 82% receiving BSC alone. ELX-TEZ-IVA was associated with an incremental cost of $3,707,909 and 12.08 incremental QALYs when compared to current SOC, resulting in a weighted ICER of $306,901 per QALY gained.
The sponsor also presented results separately for ELX-TEZ-IVA versus IVA and ELX-TEZ-IVA versus BSC alone. In the IVA-eligible population, ELX-TEZ-IVA was associated with $930,856 in incremental costs and 5.55 incremental QALYs when compared to IVA, resulting in an ICER of $167,809 per QALY gained. In the full indicated population (i.e., irrespective of IVA eligibility), ELX-TEZ-IVA was associated with $4,317,506 in incremental costs and 13.52 incremental QALYs when compared to BSC alone, resulting in an ICER of $319,432 per QALY gained.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($ per QALY) |
|---|---|---|---|---|---|
SOC | 1,605,106 | Reference | 15.11 | Reference | Reference |
ELX-TEZ-IVA | 5,313,015 | 3,707,909 | 27.19 | 12.08 | 306,901 |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Note: SOC comprises a treatment mix of IVA and BSC, estimated by a weighting factor based on prevalence of IVA-eligible (20%) and IVA-ineligible patients (80%) and comparator market shares (10% BSC and 90% IVA in those who are IVA-eligible; 100% BSC in those who are IVA-ineligible).
Source: Sponsor’s pharmacoeconomic submission.1
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses pertaining to different discounting values, pricing scenarios for CFTR modulators, and use of individual patient data. The scenario with the largest impact was that which assumed static pricing for IVA and ELX-TEZ-IVA compared to the sponsor’s dynamic pricing assumption, in which price reductions for CFTR-modulator therapies occurred at the end of patent exclusivity in the base case. Results of this scenario analysis resulted in a weighted ICER of $474,309.
The sponsor conducted a scenario analysis from a societal perspective. This analysis included additional costs associated with productivity loss because of PEx events and considered caregiver utility increments. In this analysis, the weighted ICER was $300,866 per QALY gained, relative to SOC. This was similar to the sponsor’s base-case analysis using a health care payer perspective.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The long-term impact of treatment with ELX-TEZ-IVA or IVA on ppFEV1 rate of decline is uncertain. In addition to the acute increase in ppFEV1 from treatment with a CFTR modulator, the sponsor assumed that treatment with ELX-TEZ-IVA would result in a 192-week maintenance period of ppFEV1 following this acute increase, based on data from Study 105. The sponsor further assumed that treatment with a CFTR modulator would slow the long-term rate of decline of ppFEV1 when compared with the rate of decline of patients on BSC alone following this 192-week maintenance period. This assumption was informed by the estimated annualized rate of change in ppFEV1 among patients aged 12 years and older with 1 or more F508del CFTR mutations treated with ELX-TEZ-IVA for up to 120 weeks in Study 105 matched via a propensity sore to untreated registry control patients from the US Cystic Fibrosis Foundation Patient Registry.31 While clinical expert feedback received for this review noted that there may be a long-term benefit of treatment with a CFTR modulator beyond the maintenance period, the likelihood of this possibility remains uncertain in the absence of data to support it. This uncertainty is compounded by applying long-term data from patients aged 12 years and older to patients expected to initiate treatment as early as 2 years of age for the entirety of the model time horizon after 192 weeks. The sponsor’s model was not flexible enough to change this relative rate reduction over time, meaning the assumption was applied for nearly 65 years. Overall, these issues resulted in uncertainty surrounding the benefit of ELX-TEZ-IVA on long-term ppFEV1, which may overestimate of the total QALYs and underestimate of the costs associated with ELX-TEZ-IVA in the sponsor’s base case.
CDA-AMC removed the long-term relative reduction in the rate of ppFEV1 decline for all CFTR modulators after 192 weeks from the CDA-AMC base case. Inclusion of the long-term relative reduction in the rate of ppFEV1 decline for all CFTR modulators, as included by the sponsor, was explored in a scenario analysis.
The assumption of an impact of CFTR-modulator therapy on PEx rates beyond its impact mediated by improvements in ppFEV1 is highly uncertain. The sponsor used a relationship identified in the literature to determine the PEx rate according to ppFEV1 and age. The sponsor calibrated the first 2 years of PEx rates in the model with the values from Study 124 to determine an additional relative reduction in PEx with ELX-TEZ-IVA beyond its impact mediated by changes in ppFEV1. This rate ratio was applied to patients of all ages in the model. While the clinical experts consulted for this review acknowledged this assumption was plausible, they were uncertain how long this additional benefit would be observed. The sponsor assumed the additional impact on PEx would be applicable for the entire modelled time horizon despite having data for only up to week 24 from the pivotal study. This potentially underestimates the number of PEx events that patients may experience when on ELX-TEZ-IVA, overestimates the total QALYs, and underestimates ELX-TEZ-IVA costs, creating a bias that favours ELX-TEZ-IVA.
CDA-AMC removed the additional reduction in PEx beyond the impact mediated by ppFEV1 in the CDA-AMC base case for all CFTR modulators for all patients in the period for which there were no observed data. An additional reduction in PEx beyond the impact mediated by ppFEV1, included as submitted by the sponsor, was explored in a scenario analysis.
The submitted model was not accurately programmed to retain this benefit in those aged 6 to 11 years; however, the impact on the ICER is expected to be minimal.
Dynamic pricing for CFTR-modulator therapies is uncertain and underestimates drug acquisition costs with ELX-TEZ-IVA and IVA. In the sponsor’s submitted base-case analysis, dynamic pricing was employed for CFTR modulars, including ELX-TEZ-IVA and IVA. It was assumed that generics would be introduced to the market following the loss of patent exclusivity, resulting in a 25% price reduction for CFTR modulators after the first introduction and a 50% price reduction in subsequent years after the launch of a second generic. While price reductions arising from the availability of generic entrants is possible, there is uncertainty as to if and when price reductions for patent-protected therapies would occur. Patents are frequently extended (i.e., evergreened), leading to uncertainty in the exact timing of entry of a generic, and there is no guaranteed number of generic entries in the market. CDA-AMC guidance states that full costs for a drug at its submitted price for the entire time horizon should be accounted for. In the sponsor’s base case, dynamic pricing reduces the total drug acquisition costs associated with the CFTR modulators, biasing results in their favour.
CDA-AMC excluded dynamic pricing from the CDA-AMC base-case analysis.
Adherence-adjusted drug costs underestimate the total costs associated with ELX-TEZ-IVA and other CFTR modulators. In the submitted economic evaluation, the sponsor adjusted the price of the CFTR modulators by the assumed adherence rate (93%) in the postacute period of the model (i.e., the period for which there were no observed data), with the assumption that savings would be incurred by the health care system based on a lack of adherence. There is limited evidence to support the real-world adherence rate and the sponsor did not adjust treatment efficacy in the model to align accordingly. Additionally, because the drugs would be dispensed regardless of whether the patients were adherent, the public health care payer would bear the full costs of drug acquisition. This adjustment resulted in an underestimate of the drug acquisition costs associated with CFTR modulators, biasing results in favour of ELX-TEZ-IVA when compared to BSC alone.
The CDA-AMC reanalysis assumed patients were 100% adherent to ensure all drug acquisition costs were accounted for.
Exclusion of health care costs in the period over which there is a gain in survival leads to an underestimation of the costs associated with ELX-TEZ-IVA. The sponsor failed to consider costs associated with CF care for patients on CFTR modulators after a similar patient on BSC alone had died and only considered CFTR-modulator therapy costs for the remainder of the time horizon. This assumption was based on the sponsor asserting that accounting for the costs borne by the health care system for the additional period of survival associated with ELX-TEZ-IVA does not align with how society values treatment. This exclusion of costs incurred by the health care system does not reflect the perspective of the public health care payer. This assumption led to an underestimate of the total costs associated with ELX-TEZ-IVA.
CDA-AMC included all costs relevant to the public health care payer in the additional survival period for patients on ELX-TEZ-IVA in the CDA-AMC base case.
The impact of ELX-TEZ-IVA on health care resource use beyond its impact mediated through improving lung function is uncertain. Health-state costs in the sponsor’s submitted model were primarily based on ppFEV1, with greater costs for patients with a lower ppFEV1. The sponsor included costs associated with inpatient and outpatient hospitalizations, routine antibiotics, and diagnostics. The sponsor adjusted the disease-management costs specific to inpatient hospital visits and pharmacotherapy for patients on CFTR modulators, based on studies in the literature that indicated a reduction in CF-related inpatient admissions and outpatient IV and antibiotic use.27,28 As a result, the annual inpatient costs and annual pharmacotherapy costs for patients on BSC alone differed from those of patients on CFTR modulators. Upon review of the sponsor’s sources for the reductions in costs associated with inpatient hospital visits and pharmacotherapy, CDA-AMC noted that the studies cited by the sponsor were observational before-and-after studies, assessing the impact of CFTR modulator use on relevant costs. These studies did not indicate whether they controlled for patient ppFEV1 or any other factors. As a result, it is difficult to determine whether the magnitude of difference in costs before and after use of CFTR modulators observed in these studies was because of ppFEV1 (which was already factored into the sponsor’s submitted model via treatment efficacy) or another factor, as asserted by the sponsor. The sponsor’s approach likely underestimated the inpatient hospital visit and outpatient antibiotic-use costs associated with CFTR modulator use, biasing results in favour of ELX-TEZ-IVA.
CDA-AMC assumed inpatient hospital costs and annual pharmacotherapy costs were the same for all patients in the model with a similar ppFEV1, regardless of whether they were receiving a CFTR modulator.
Treatment-specific utility increment for patients on ELX-TEZ-IVA leads to potential overestimation of total benefit. The sponsor based the utility values in the submitted model on an equation by Solem et al. that determines a utility based on the EQ-5D according to a patient’s ppFEV1 and whether they experienced a PEx.21 The sponsor included an additional utility increment for patients on ELX-TEZ-IVA based on an analysis comparing the utility scores, according to the 8-dimension Cystic Fibrosis Questionnaire–Revised of patients on ELX-TEZ-IVA versus those on placebo in Study 124, adjusting for ppFEV1. This analysis revealed a difference in utility scores for patients on ELX-TEZ-IVA in comparison with those on BSC that was not explained by ppFEV1. The sponsor’s analysis comparing Cystic Fibrosis Questionnaire–Revised scores from the trials did not account for PEx rates, which were already included in the sponsor’s utility estimate, meaning the difference observed in the sponsor’s analysis may be explained by PEx. It is difficult to know what proportion of the difference in utility scores from the trial is attributable to PEx, although the Solem et al. equation accounted for PEx. The sponsor should have explicitly modelled other events it assumed contribute to quality of life not captured by Solem et al. to allow for greater transparency with respect to what contributes to the quality-of-life estimates and to what extent. The inclusion of a treatment-specific utility increment for patients on ELX-TEZ-IVA potentially leads to double-counting of utility gains, likely biasing results in favour of ELX-TEZ-IVA.
CDA-AMC removed the treatment-specific utility increment with ELX-TEZ-IVA in the CDA-AMC base-case analysis. Treatment-specific utility increments with ELX-TEZ-IVA were explored in a scenario analysis.
The survival benefit with ELX-TEZ-IVA is potentially overestimated and the model estimate of median predicted survival does not meet face validity. The outputs of the sponsor’s model indicate the median predicted survival for patients on ELX-TEZ-IVA is 74.4 years. In addition, the comparison to BSC alone resulted in approximately 21 undiscounted, incremental life-years gained for ELX-TEZ-IVA. This result is highly uncertain given the limitations of the long-term efficacy of ELX-TEZ-IVA and other CFTR modulators. Furthermore, the survival results suggest a similar survival outcome for CF patients on ELX-TEZ-IVA compared with the general population. While the clinical experts consulted for this review indicated that ELX-TEZ-IVA treatment would likely significantly improve patient survival versus BSC alone, they noted that it would likely still not be equal to those of the general population. As such, the sponsor’s base-case results overestimated the survival benefit of ELX-TEZ-IVA based on the evidence currently available and do not meet face validity.
While CDA-AMC was unable to directly modify the survival assumptions for ELX-TEZ-IVA, the base-case changes in treatment efficacy corresponded to survival results in the CDA-AMC base case that more accurately reflected clinical expert opinion.
The model lacked transparency and its programming prevented a full exploration of the associated uncertainties. The sponsor’s submitted model was programmed with limited transparency, with many inputs and outputs being the result of coding in Visual Basic for Applications rather than using formula-based operations. CDA-AMC was unable to fully explore the uncertainty with parameters in the model, although results of the deterministic stepwise analysis met face validity.
CDA-AMC was unable to address this limitation in reanalysis.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Long-term clinical data used to inform parameters after the 24-week trial period of Study 124 were derived from patients with F508del mutations and were assumed to be reflective of patients with non-F508del mutations. | Reasonable. Lung function decline and pulmonary exacerbations are not likely to differ in severity or frequency between patients with F508del mutations vs. non-F508del mutations. |
The risk of developing CFRD for patients on CFTR modulators and BSC is the same. | Reasonable. |
The rate of lung transplants for patients with ppFEV1 < 40% is 4.6%. | Reasonable. Lung transplant rates have decreased in recent years. |
CDA-AMC = Canada’s Drug Agency; CFRD = cystic fibrosis–related diabetes; ppFEV1 = percent predicted forced expiratory volume in 1 second; vs. = versus.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. CDA-AMC undertook a stepped analysis, incorporating each change detailed in Table 6 into the sponsor’s model to highlight the impact of each change. The summary results of the CDA-AMC reanalyses for the weighted population are presented in Table 7.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Reduction in rate of ppFEV1 decline compared with BSC (after 192 weeks) | ELX-TEZ-IVA: 90.0% IVA: 47.1% | No reduction in rate of decline of ppFEV1 |
2. PEx rate ratio with CFTR modulators compared to BSC | ELX-TEZ-IVA: 0.20 IVA: 0 | 1 for all CFTR modulators |
3. Dynamic pricing of CFTR modulators | 25% price reduction after 15 years for ELX-TEZ-IVA and 5 years for IVA 50% price reduction after 16 years for ELX-TEZ-IVA and 6 years for IVA | No price reduction over model time horizon |
4. Patient adherence rate in postacute period | 93% | 100% |
5. Disease-management costs during period of survival benefit while on ELX-TEZ-IVA | Not included | Included |
6. ELX-TEZ-IVA impact on inpatient and pharmacotherapy costs (beyond impact on ppFEV1) | Annual inpatient costs BSC
CFTR modulator
Annual pharmacotherapy costs BSC
CFTR modulator
| Annual inpatient costs All comparators
Annual pharmacotherapy costs All comparators
|
7. Treatment-specific utility increment for ELX-TEZ-IVA | Increment of 0.05 included | No utility increment |
CDA-AMC base case | Reanalysis 1 + 2 + 3 + 4 + 5 + 6 + 7 | |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IVA = ivacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Results from the CDA-AMC base case estimated that ELX-TEZ-IVA was associated with incremental costs of $4,857,190 and an incremental QALY gain of 4.33 versus SOC, resulting in an ICER of $1,122,823 per QALY gained. The probability that ELX-TEZ-IVA was cost-effective at a threshold of $50,000 per QALY gained was 0%. The CDA-AMC base case presents weighted results comparing ELX-TEZ-IVA with SOC, which comprises the current treatment mix of IVA and BSC alone and is subject to a weighting factor (82% BSC, 18% IVA) using prevalence and market shares based on patient eligibility and ineligibility for IVA as described previously.
The sponsor’s model also produced separate ICERs for ELX-TEZ-IVA versus IVA for those who are eligible for IVA. In the IVA-eligible population, ELX-TEZ-IVA was associated with an ICER of $137,999 per QALY gained compared to IVA. In the full indicated population, ELX-TEZ-IVA was associated with an ICER of $1,175,160 per QALY gained compared to BSC. The change to the sponsor’s base case that had the greatest impact on the results was the removal of dynamic pricing because of the introduction of generic options, emphasizing the impact of drug acquisition costs as a key driver of the model.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case | SOC | 1,649,912 | 15.13 | Reference |
ELX-TEZ-IVA | 5,354,974 | 27.60 | 297,211 | |
CDA-AMC reanalysis 1 — ppFEV1 decline | SOC | 1,543,801 | 14.41 | Reference |
ELX-TEZ-IVA | 4,460,106 | 20.86 | 452,452 | |
CDA-AMC reanalysis 2 — PEx rate ratio | SOC | 1,656,240 | 15.07 | Reference |
ELX-TEZ-IVA | 5,282,984 | 26.70 | 311,881 | |
CDA-AMC reanalysis 3 — dynamic pricing | SOC | 2,115,850 | 15.13 | Reference |
ELX-TEZ-IVA | 8,028,635 | 27.60 | 474,309 | |
CDA-AMC reanalysis 4 — adherence in the postacute phase | SOC | 1,702,160 | 15.13 | Reference |
ELX-TEZ-IVA | 5,726,058 | 27.60 | 322,787 | |
CDA-AMC reanalysis 5 — disease-management costs during survival benefit period | SOC | 1,649,912 | 15.13 | Reference |
ELX-TEZ-IVA | 5,433,338 | 27.60 | 303,497 | |
CDA-AMC reanalysis 6 — inpatient and pharmacotherapy costs | SOC | 1,680,816 | 15.13 | Reference |
ELX-TEZ-IVA | 5,447,450 | 27.60 | 302,150 | |
CDA-AMC reanalysis 7 — treatment-specific utility for ELX-TEZ-IVA | SOC | 1,649,912 | 15.13 | Reference |
ELX-TEZ-IVA | 5,354,974 | 26.16 | 335,852 | |
CDA-AMC base case (reanalysis 1 + 2 + 3 + 4 + 5 + 6 + 7) | SOC | 1,998,395 | 14.35 | Reference |
ELX-TEZ-IVA | 6,814,259 | 18.41 | 1,186,224 | |
CDA-AMC base case (reanalysis 1 + 2 + 3 + 4 + 5 + 6 + 7) (probabilistic) | SOC | 2,024,984 | 14.36 | Reference |
ELX-TEZ-IVA | 6,882,174 | 18.68 | 1,122,823 |
CDA-AMC = Canada’s Drug Agency; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ICER = incremental cost-effectiveness ratio; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; QALY = quality-adjusted life-year; SOC = standard of care.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is presented both deterministically and probabilistically. SOC comprises a treatment mix of IVA and BSC, estimated by a weighting factor based on the prevalence of IVA-eligible (20%) and IVA-ineligible patients (80%) and comparator market shares (10% BSC and 90% IVA in those who are IVA-eligible; 100% BSC in those who are IVA-ineligible).
Scenario Analysis Results
CDA-AMC undertook price-reduction analyses based on the sponsor’s submitted results and the CDA-AMC base-case reanalysis. The base-case reanalysis presents results for the entire population combined and is weighted by prevalence and market shares based on IVA eligibility and ineligibility. The CDA-AMC base case suggests that a 79% price reduction is required for ELX-TEZ-IVA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained versus SOC. The annual drug acquisition costs of ELX-TEZ-IVA would be $65,351 per patient at a 79% price reduction.
Table 7: CDA-AMC Price-Reduction Analyses
Price reduction | Unit drug cost ($) | ICERs for ELX-TEZ-IVA vs. SOC ($ per QALY) | |
|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | ||
No price reduction | 420 | 306,901 | 1,122,823 |
10% | 378 | 264,803 | 986,452 |
20% | 336 | 222,706 | 850,081 |
30% | 294 | 180,608 | 713,710 |
40% | 252 | 138,511 | 577,338 |
50% | 210 | 96,413 | 440,967 |
60% | 168 | 54,316 | 304,596 |
70% | 126 | 12,218 | 168,225 |
80% | 84 | ELX-TEZ-IVA is dominant | 31,854 |
90% | 42 | ELX-TEZ-IVA is dominant | ELX-TEZ-IVA is dominant |
100% | 0 | ELX-TEZ-IVA is dominant | ELX-TEZ-IVA is dominant |
CDA-AMC = Canada's Drug Agency; BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; PEx = pulmonary exacerbation; QALY = quality-adjust life-year; SOC = standard of care; vs. = versus.
Note: SOC comprises a treatment mix of IVA and BSC, estimated by a weighting factor based on prevalence of IVA-eligible (20%) and IVA-ineligible patients (80%) and comparator market shares (10% BSC and 90% IVA in those who are IVA-eligible; 100% BSC in those who are IVA-ineligible). CDA-AMC also undertook a series of scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of ELX-TEZ-IVA. These included: long-term relative reduction of rates of ppFEV1 with ELX-TEZ-IVA (90.0%) and IVA (47.1%), in comparison with BSC, according to the sponsor’s base case assumption; a reduction in the rate of PEx observed with ELX-TEZ-IVA and IVA based on observed trial data was applied in the postmaintenance phase for the entire time horizon, according to the sponsor’s base case assumption; and a treatment-specific utility increment from benefits beyond improvements in lung function and PEx for patients on ELX-TEZ-IVA were included, according to the sponsor’s base-case assumption. Results of the CDA-AMC scenario analyses are available in Table 12 of Appendix 4. These scenarios highlighted the impact of assuming additional benefit with ELX-TEZ-IVA despite a lack of supporting evidence and resulted in ICERs ranging from $627,728 to $948,843 per QALY gained compared to SOC. These scenario analyses are driven by the high drug acquisition costs of ELX-TEZ-IVA that offset the estimated QALY gains.
Issues for Consideration
The estimated 79% price reduction for the current review of ELX-TEZ-IVA appears to be lower than that of previous reviews for ELX-TEZ-IVA, which were in excess of 90%. The difference in price reductions does not appear to be because of a difference in the clinical efficacy of ELX-TEZ-IVA relative to comparators. Instead, it may be because of the difference in patient populations, where patients are initiating treatment potentially at older ages (2 years or older) in the current review versus between 2 to 5 years of age in the most recent F508del submission. Because of the limitations identified in this report, particularly the uncertainty within the clinical evidence informing the model, the estimates of cost-effectiveness are highly uncertain and additional price reduction may be warranted.
CDA-AMC previously reviewed ELX-TEZ-IVA for the treatment of CF in patients with 1 or more F508del-CFTR mutations who were aged 12 and older, those aged 6 years and older, and those age 2 to 5 years. The submitted price in all previous reviews is consistent with the current submission, with a daily cost of $840 regardless of treatment strength or form. The committee recommended reimbursement of ELX-TEZ-IVA with conditions, including a price reduction greater than 90%, which is consistent across all previous reviews. Results from the current review of ELX-TEZ-IVA for non-F508del mutations were similar, indicating that this drug is not cost-effective at the submitted price and would require a substantial price reduction.
Overall Conclusions
Based on the CDA-AMC Clinical Review, results from the 24-week phase III Study 124 suggest that treatment with ELX-TEZ-IVA resulted in statistically significant and clinically meaningful improvement in ppFEV1 and a reduction in the risk of PEx events compared with placebo after 24 weeks of treatment. The current review is for an expanded indication that would include 183 additional non-F508del mutations in the CFTR gene, of which only 18 were included in the Study 124 patient population. The sponsor provided additional clinical data in the form of a retrospective observational study, nonrandomized studies, and in vitro data. However, the sponsor reports that there are no clinical data for 94 FRT-responsive mutations (i.e., those that were considered responsive to ELX-TEZ-IVA in the in vitro model) and 1 noncanonical splice mutation. Furthermore, the comparative clinical benefit of ELX-TEZ-IVA compared to IVA is unknown because of a lack of head-to-head trial data. The Clinical Review did not raise concerns regarding this lack of data because the dosage of IVA administered as part of the ELX-TEZ-IVA combination regimen is the same dosage that patients would receive with IVA monotherapy (e.g., 150 mg in the morning and 150 mg in the evening); previous trials have demonstrated that patients with 1 or more F508del mutations and a gating mutation benefited from switching to ELX-TEZ-IVA from IVA monotherapy; and the submitted price for ELX-TEZ-IVA is the same as the current list price for IVA monotherapy.
The clinical experts consulted for this review noted that, given the mechanism of action and compelling efficacy data from studies of patients with F508del mutations, ELX-TEZ-IVA is expected to similarly benefit patients with non-F508del mutations. However, these conclusions are based on a pivotal study of patients with non-F508del mutations with a follow-up time of 24 weeks and studies in patients with F508del mutations with a maximum follow-up time of 192 weeks. No evidence is available on the long-term impact of ELX-TEZ-IVA on the rate of decline of ppFEV1 or PEx rates beyond the trial periods for any mutation or age group.
Beyond uncertainty in the long term clinical efficacy of ELX-TEZ-IVA, CDA-AMC identified several major limitations with the submitted economic evaluation. The following were addressed in the CDA-AMC reanalysis: the removal of an additional benefit of CFTR modulators on the long-term rate of decline in ppFEV1 and PEx; the removal of dynamic pricing of CFTR modulators; the inclusion of costs for ELX-TEZ-IVA for the period in which a survival benefit was achieved in comparison to BSC; the removal of an adjustment to drug acquisition costs by patient adherence; and the removal of a treatment-specific utility increment for patients on ELX-TEZ-IVA. The results of the CDA-AMC reanalysis were aligned with the sponsor’s, in that ELX-TEZ-IVA was not cost-effective at conventionally acceptable ICER thresholds. In the CDA-AMC base-case analyses, ELX-TEZ-IVA was associated with an ICER of $1,122,823 per QALY gained compared to SOC in the overall patient population with non-F508del mutations.
The key drivers in the analyses are drug acquisition costs and assumptions in the long term benefits with ELX-TEZ-IVA, which were uncertain. Treatment with ELX-TEZ-IVA was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained in any scenario conducted by CDA-AMC. A price reduction of greater than 79% for ELX-TEZ-IVA is required for ELX-TEZ-IVA to be considered cost-effective at this threshold when compared with SOC — the annual cost of ELX-TEZ-IVA would need be reduced to $65,351 per patient (from $306,810). The near entirety of expected incremental survival was estimated beyond the 24-week period of the Study 124. In the absence of robust, long-term clinical evidence in patients with non-F508del mutations, the extent of any treatment benefit is associated with a high degree of uncertainty. Consequently, the CDA-AMC base case may overestimate the clinical benefits associated with ELX-TEZ-IVA and greater price reductions may be required for ELX-TEZ-IVA to be cost-effective.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg oral tablets; Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 75 mg or 80mg/40mg/60mg and 59.5 mg oral granules. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024 Mar 05.
2.Drug Reimbursement Expert Review Committee final recommendation: elexacaftor-tezacaftor-ivacaftor plus ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Inc.). Can J Health Technol. 2021;1(9). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/sr0673/sr0673. Accessed by sponsor, no date provided.
3.Drug Reimbursement Expert Review Committee final recommendation: elexacaftor-tezacaftor-ivacaftor plus ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Inc.). Can J Health Technol. 2022;2(7). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/SR0710/SR0710. Accessed by sponsor, no date provided.
4.Drug Reimbursement Expert Review Committee draft recommendation: elexacaftor-tezacaftor-ivacaftor plus ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Incorporated). Ottawa (ON): CADTH; 2023 Oct: https://www.cadth.ca/sites/default/files/DRR/2023/SR0776%20Trikafta%20-%20Draft%20CADTH%20Recommendation%20October%2026%2C%202023%20-%20For%20posting.pdf. Accessed by sponsor, no date provided.
5.Request for deviation [internal sponsor's document]. In: Drug Reimbursement Review sponsor submission: Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg oral tablets; Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 75 mg or 80mg/40mg/60mg and 59.5 mg oral granules. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024 Jan 19.
6.Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor): 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg, oral tablets; Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor): 100 mg/50 mg/75 mg and 75 mg or 80mg/40mg/60mg and 59.5 mg, oral granules [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024 Jul 12.
7.Stephenson AL, Tom M, Berthiaume Y, et al. A contemporary survival analysis of individuals with cystic fibrosis: a cohort study. Eur Respir J. 2015;45(3):670-679. PubMed
8.Liou TG, Adler FR, Fitzsimmons SC, Cahill BC, Hibbs JR, Marshall BC. Predictive 5-year survivorship model of cystic fibrosis. Am J Epidemiol. 2001;153(4):345-352. PubMed
9.Clinical Study Report: 124. A phase 3 double-blind, randomized, placebo-controlled study evaluating the efficacy and safety of ELX-TEZ-IVA in cystic fibrosis subjects 6 years of age and older with a non-F508del ELX-TEZ-IVA-responsive CFTR mutation [internal sponsor's report]. Boston (MA): Vertex Pharmaceuticals Incorporated; 2023 Oct 06.
10.Whiting P, Al M, Burgers L, et al. Ivacaftor for the treatment of patients with cystic fibrosis and the G551D mutation: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2014;18(18):1-106. PubMed
11.Adler AI, Shine BS, Chamnan P, Haworth CS, Bilton D. Genetic determinants and epidemiology of cystic fibrosis-related diabetes: results from a British cohort of children and adults. Diabetes Care. 2008;31(9):1789-1794. PubMed
12.Meta-analysis of participants aged 6 years and older without an F508del genotype from IVA RCTs for the ELX/TEZ/IVA 2+ Global Cost Effectiveness Model [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg oral tablets; Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 75 mg or 80mg/40mg/60mg and 59.5 mg oral granules. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024 Jan 31.
13.Konstan MW, Morgan WJ, Butler SM, et al. Risk factors for rate of decline in forced expiratory volume in one second in children and adolescents with cystic fibrosis. J Pediatr. 2007;151(2):134-139, 139.e131.
14.Konstan MW, Wagener JS, Vandevanter DR, et al. Risk factors for rate of decline in FEV1 in adults with cystic fibrosis. J Cyst Fibros. 2012;11(5):405-411. PubMed
15.McKone EF, Borowitz D, Drevinek P, et al. Long-term safety and efficacy of ivacaftor in patients with cystic fibrosis who have the Gly551Asp-CFTR mutation: a phase 3, open-label extension study (PERSIST). Lancet Respir Med. 2014;2(11):902-910. PubMed
16.Sawicki GS, McKone EF, Pasta DJ, et al. Sustained Benefit from ivacaftor demonstrated by combining clinical trial and cystic fibrosis patient registry data. Am J Respir Crit Care Med. 2015;192(7):836-842. PubMed
17.Goss CH, Burns JL. Exacerbations in cystic fibrosis. 1: epidemiology and pathogenesis. Thorax. 2007;62(4):360-367. PubMed
18.Vertex Pharmaceuticals Incorporated. Rollover Study of ivacaftor in subjects with cystic fibrosis and a non G551D CFTR mutation (KONTINUE). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2017: https://clinicaltrials.gov/study/NCT01707290. Accessed 2024 Jan 16.
19.Hoppe JE, Chilvers M, Ratjen F, et al. Long-term safety of lumacaftor-ivacaftor in children aged 2-5 years with cystic fibrosis homozygous for the F508del-CFTR mutation: a multicentre, phase 3, open-label, extension study. Lancet Respir Med. 2021;9(9):977-988. PubMed
20.Drug Reimbursement Review clinical, pharmacoeconomic, and ethics reports, and stakeholder input: elexacaftor-tezacaftor-ivacaftor plus ivacaftor (Trikafta) for cystic fibrosis, F508del CFTR mutation, 2 to 5 years. Can J Health Technol. 2024;4(2). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/SR0776r/SR0776r. Accessed 2024 Apr 15.
21.Solem C, Vera-Llonch M, Tai M, O'Callaghan L. PRS40: Pulmonary exacerbations, lung dysfunction, and EQ-5D measures in adolescents and adults with cystic fibrosis homozygous for the F508del-CFTR mutation. Washington (DC): Poster session presented at: ISPOR 21st Annual International Meeting; 2016 May 21-25.
22.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2024: http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2024 April 15.
23.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-2024-01-24.pdf. Accessed by sponsor, no date provided.
24.Kalydeco (ivacaftor): 150 mg oral tablets, or 50 mg per packet or 75 mg per packet, oral granules [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2019. Accessed by sponsor.
25.Skolnik K, Ronksley P, Pendharkar S, Wick J, Quon BS, Williamson T. 788 Hospitalization-related costs for Canadian cystic fibrosis patients. Pediatr Pulmonol. 2018;53(S2):S451.
26.Schedule of benefits for laboratory services. (Effective July 24, 2023). Toronto (ON): Ontario Ministry of Health; 2023: https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf. Accessed by sponsor, no date provided.
27.Feng LB, Grosse SD, Green RF, Fink AK, Sawicki GS. Precision medicine in action: the impact of ivacaftor on cystic fibrosis-related hospitalizations. Health Aff (Millwood). 2018;37(5):773-779. PubMed
28.Hassan M, Bonafede M, Limone B, Hodgkins P, Suthoff ED, Sawicki GS. 28 Reduction in pulmonary exacerbations (PEx) after initiation of ivacaftor: a retrospective cohort study among patients with cystic fibrosis (CF) treated in real-world settings. J Cyst Fibros. 2016;15(Supplement 1):S58.
29.Vasiliadis HM, Collet JP, Penrod JR, Ferraro P, Poirier C. A cost-effectiveness and cost-utility study of lung transplantation. J Heart Lung Transplant. 2005;24(9):1275-1283. PubMed
30.Government of Alberta. Alberta interactive health data application. Average cost of lung transplant procedure in 2017/2018. 2019 [sponsor provided reference].
31.Lee T, Sawicki GS, Altenburg J, et al. Effect of elexacaftor/tezacaftor/ivacaftor on annual rate of lung function decline in people with cystic fibrosis. J Cyst Fibros. 2023;22(3):402-406. PubMed
32.Kalydeco (ivacaftor): 150 mg oral tablets, or 25 mg per packet, 50 mg per packet, or 75 mg per packet, oral granules [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2022. Accessed by sponsor.
33.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 150 mg or 50 mg/25 mg/37.5 mg and 75 mg oral tablets; Trikafta (elexacaftor/tezacaftor/ivacaftor and ivacaftor), 100 mg/50 mg/75 mg and 75 mg or 80mg/40mg/60mg and 59.5 mg oral granules. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024 Mar 05.
Appendix 1: Cost-Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison for CFTR-Modulator Therapies for Cystic Fibrosis for Patients Aged 2 to 5 Years Old With Non-F508del Mutations in the CFTR Gene
Treatment | Strength / concentration | Form | Price | Recommended dosagea | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Elexacaftor/ tezacaftor/ ivacaftor and ivacaftor (Trikafta) | 100 mg/ 50 mg/ 75 mg and 75 mg 80 mg/ 40 mg/ 60 mg and 59.5 mg | Granules Packet | 420.0000b | One granule packet (containing elexacaftor 100 mg/ tezacaftor 50 mg /ivacaftor 75 mg or elexacaftor 80 mg/tezacaftor 40 mg/ivacaftor 60 mg) taken in the morning and 1 granule packet (ivacaftor 75 mg or ivacaftor 59.5 mg) taken in the evening approximately 12 hours apart, with fat-containing food | 840.00 | 306,810 |
100 mg/ 50 mg/ 75 mg and 150 mg 50 mg/ 25 mg/ 37.5 and 75 mg | Tablet | 280.0000b | Two tablets (each containing elexacaftor 100 mg/ tezacaftor 50 mg /ivacaftor 75 mg or elexacaftor 50 mg/tezacaftor 25 mg/ivacaftor 37.5 mg) taken in the morning and 1 tablet (ivacaftor 150 mg or ivacaftor 75 mg) taken in the evening approximately 12 hours apart, with fat-containing food | 840.00 | 306,810 | |
CFTR-modulator therapies | ||||||
Ivacaftor (Kalydeco) | 25 mg 50 mg 75 mg | Granules Packet | 420.0000 | ≥ 5 kg to < 7 kg: One granule packet (ivacaftor 25 mg) taken in the morning and 1 granule packet (ivacaftor 25 mg) taken in the evening approximately 12 hours apart, with fat-containing food ≥ 7 kg to < 14 kg: One granule packet (ivacaftor 50 mg) taken in the morning and 1 granule packet (ivacaftor 50 mg) taken in the evening approximately 12 hours apart, with fat-containing food ≥ 14 kg to < 25 kg: One granule packet (ivacaftor 75 mg) taken in the morning and 1 granule packet (ivacaftor 75 mg) taken in the evening approximately 12 hours apart, with fat-containing food | 840.00 | 306,810 |
150 mg | Tablet | 420.0000 | ≥ 25 kg: One tablet taken in the morning and 1 tablet taken in the evening approximately 12 hours apart, with fat-containing food | 840.00 | 306,810 | |
CDA-AMC = Canada’s Drug Agency.
Note: All prices are from the Ontario Exceptional Access Program formulary (accessed April 2024) unless otherwise indicated,22 and do not include dispensing fees. Annual costs are based on 365.25 days per year.
aRecommended dosages are from the respective product monographs.6,32
bSponsor-submitted price.1
Appendix 2: Submission Quality
Please note that this appendix table has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | Model lacks transparency with regards to programming; details in the CDA-AMC limitations section |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
CDA-AMC = Canada’s Drug Agency.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
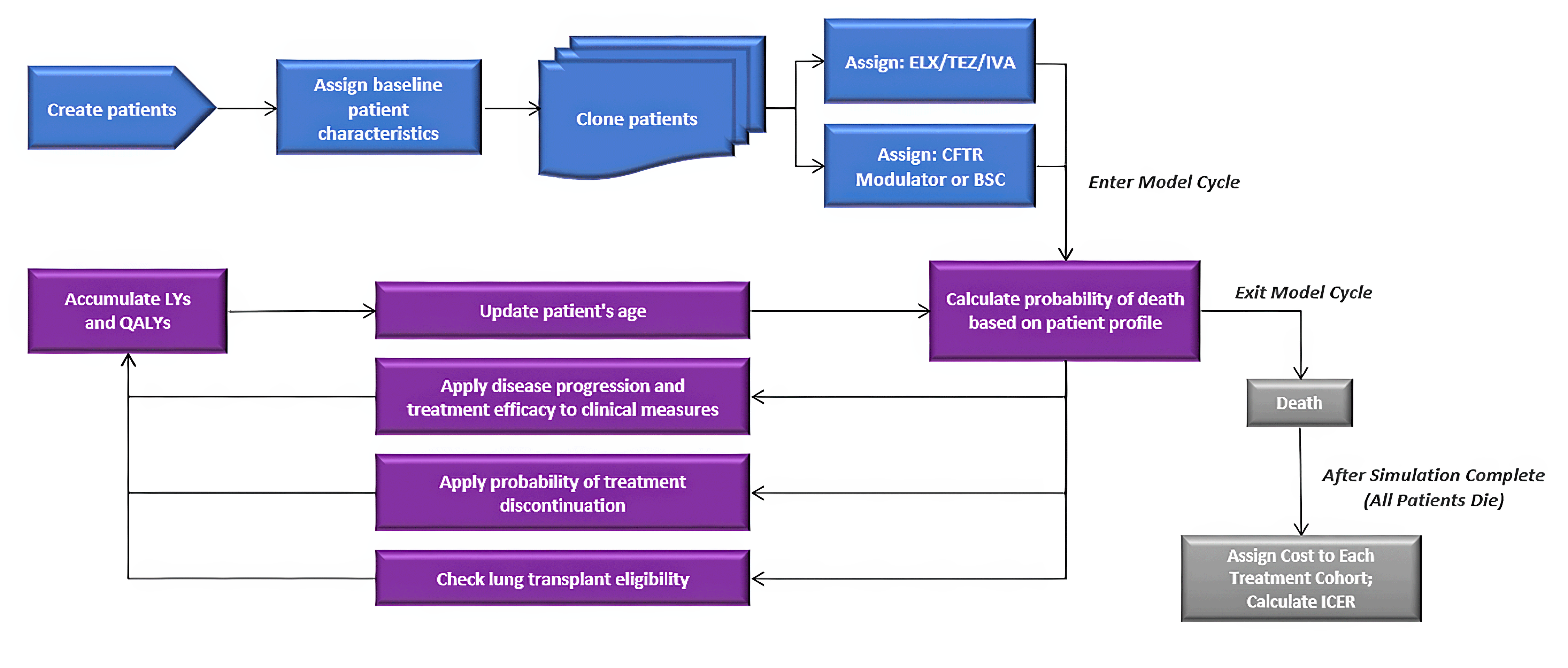
BSC = best supportive care; ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 10: Disaggregated Summary of the CDA-AMC Economic Evaluation Results (Weighted)
Parameter | ELX-TEZ-IVA | SOC |
|---|---|---|
Discounted LYs | ||
Total | 20.34 | 15.91 |
Discounted QALYs | ||
Total | 18.68 | 14.36 |
Discounted costs ($) | ||
Total | 6,882,174 | 2,024,984 |
Drug acquisition cost | 5,964,524 | 1,034,238 |
Non-PEx–related disease-management costs | 376,314 | 329,258 |
PEx-related costs | 538,165 | 658,255 |
Lung transplant costs | 966 | 1,991 |
Adverse event costs | 2,017 | 1,208 |
Monitoring costs | 189 | 35 |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; PEx = pulmonary exacerbations; QALY = quality-adjusted life-year; SOC = standard of care.
Note: SOC comprises a treatment mix of IVA and BSC, estimated by a weighting factor based on prevalence of IVA-eligible (20%) and IVA-ineligible patients (80%) and comparator market shares (10% BSC and 90% IVA in those who are IVA-eligible; 100% BSC in those who are IVA-ineligible).
Table 11: Disaggregated Summary of the CDA-AMC Economic Evaluation Results By Comparator
Parameter | ELX-TEZ-IVA | IVA | BSC |
|---|---|---|---|
Discounted LYs | |||
Total | 20.34 | 19.24 | 15.18 |
Discounted QALYs | |||
Total | 18.68 | 17.47 | 13.67 |
Discounted costs ($) | |||
Total | 6,882,174 | 6,714,817 | 995,509 |
Drug acquisition cost | 5,964,524 | 5,745,765 | 0 |
Non-PEx-related disease-management costs | 376,314 | 369,590 | 320,404 |
PEx-related costs | 538,165 | 596,126 | 671,893 |
Lung transplant costs | 966 | 1,487 | 2,102 |
Adverse event cost | 2,017 | 1,656 | 1,109 |
Monitoring cost | 189 | 192 | 0 |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ICER = incremental cost-effectiveness ratio; LY = life-year; PEx = pulmonary exacerbations; QALY = quality-adjusted life-year.
Note: SOC comprises a treatment mix of IVA and BSC, estimated by a weighting factor based on prevalence of IVA-eligible (20%) and IVA-ineligible patients (80%) and comparator market shares (10% BSC and 90% IVA in those who are IVA-eligible; 100% BSC in those who are IVA-ineligible).
Scenario Analyses
Table 12: CDA-AMC Scenario Analysis Summary
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
1. Slower rate of decline in ppFEV1 | SOC | 2,229,399 | 15.07 | Reference |
ELX-TEZ-IVA | 8,657,893 | 25.31 | 627,728 | |
2. Long-term reduction in PEx included for CFTR modulators | SOC | 2,003,118 | 14.41 | Reference |
ELX-TEZ-IVA | 6,920,937 | 19.76 | 919,031 | |
3. Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | SOC | 1,998,395 | 14.35 | Reference |
ELX-TEZ-IVA | 6,814,259 | 19.43 | 948,843 |
CDA-AMC = Canada’s Drug Agency; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; ICER = incremental cost-effectiveness ratio; PEx = pulmonary exacerbation; QALY = quality-adjusted life-year; SOC = standard of care.
Note: All results presented deterministically. SOC comprises a treatment mix of IVA and BSC, estimated by a weighting factor based on prevalence of IVA-eligible (20%) and IVA-ineligible patients (80%) and comparator market shares (10% BSC and 90% IVA in those who are IVA-eligible; 100% BSC in those who are IVA-ineligible).
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted an epidemiology-based budget impact analysis (BIA), assessing the expected budgetary impact of reimbursing ELX-TEZ-IVA plus BSC for the treatment of CF in patients 2 years and older who have at least 1 non-F508del mutation in the CFTR gene that is responsive based on in vitro and/or clinical data.33 The analysis was conducted from the perspective of the Canadian public drug plans over a 3-year time horizon (from 2025 to 2027, with 2024 as the base year). Only drug acquisition costs were included. The BIA considered a reference scenario where IVA and BSC alone were available for the estimated 20% of IVA-eligible patients with gating mutations (G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, S549R, and G970R) inclusive of R117H, while the remaining 80% of IVA-ineligible patients received BSC alone. The new drug scenario included ELX-TEZ-IVA, IVA, and BSC alone for IVA-eligible patients and ELX-TEZ-IVA and BSC alone for IVA-ineligible patients. All patients were assumed to receive background BSC, therefore costs associated with BSC were not considered. The sponsor’s estimates of expected ELX-TEZ-IVA utilization were based on internal estimates, whereas the market size was primarily based on data generated from the CF Canada patient registry and further reduced based on the proportion of patients covered by provincial formularies. Key inputs to the BIA are documented in key inputs to the BIA are documented in Table 16.
Additionally, the sponsor made the following key assumptions:
55% of indicated patients would be covered by provincial drug programs.
The adherence rate for CFTR modulators was assumed to be 93%.
Drug mark-up and dispensing fees were excluded in the base-case analysis.
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
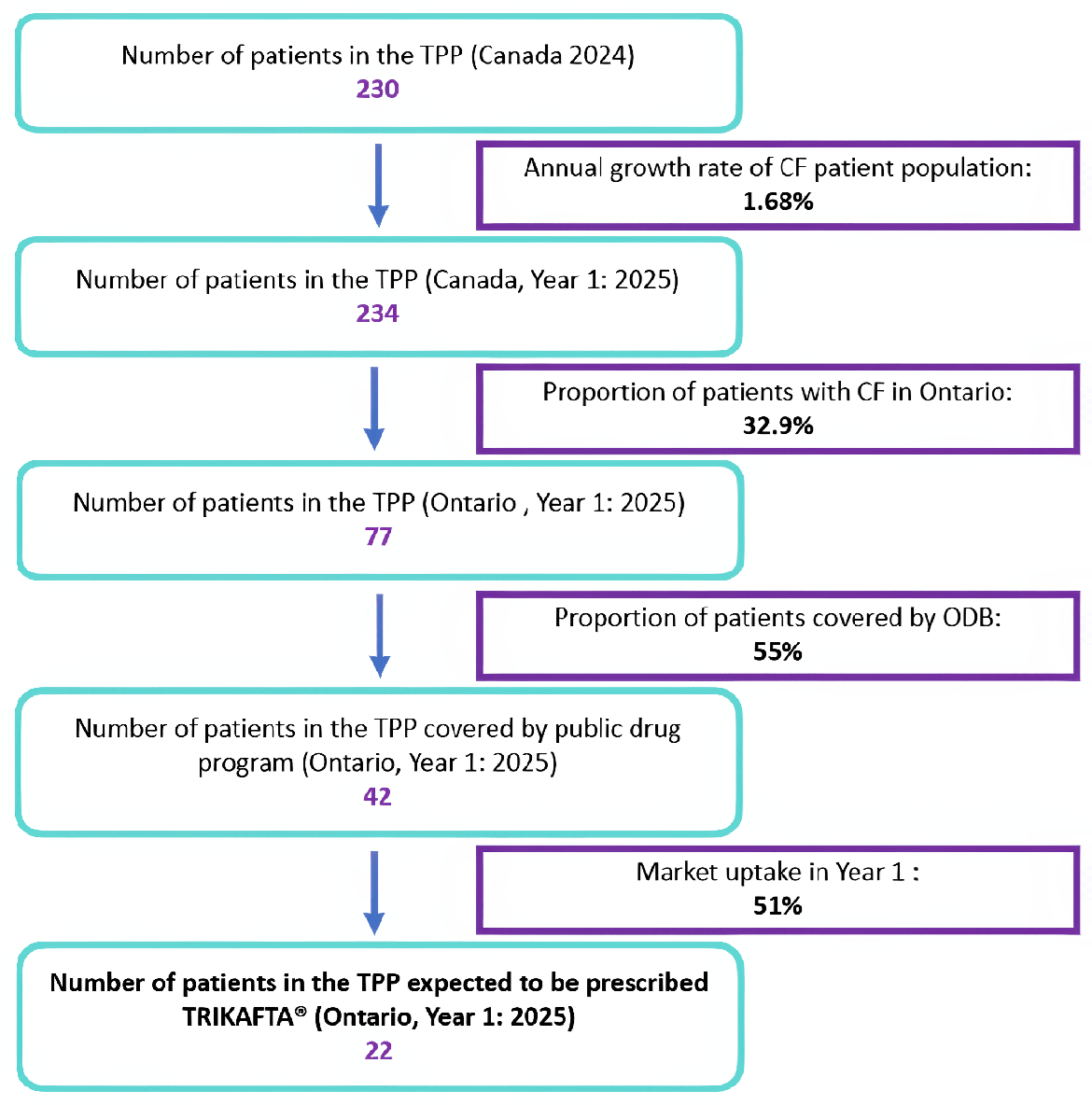
Source: Sponsor’s budget impact submission.33
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 234 / 238 / 242 |
Market uptake (3 years) | |
Uptake (reference scenario) | |
IVA-eligible population (20%) | |
IVA | 90% / 90% / 90% |
BSC | 10% / 10% / 10% |
IVA-ineligible population (80%) | |
BSC | 100% / 100% / 100% |
Uptake (new drug scenario) | |
IVA-eligible population (20%) | |
ELX-TEZ-IVA | 15% / 30% / 45% |
IVA | 75% / 60% / 45% |
BSC | 10% / 10% / 10% |
IVA-ineligible population (80%) | |
ELX-TEZ-IVA | 60% / 85% / 93% |
BSC | 40% / 15% / 7% |
Cost of treatment (per patient, per year) | |
Annual treatment cost, adjusted for 93% adherence | |
ELX-TEZ-IVA | $285,333 |
IVA | $285,333 |
BSC | $0 |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IVA = ivacaftor.
Note: Values may not sum to 100% because of rounding.
Summary of the Sponsor’s Budget Impact Analysis Results
Results from the sponsor’s base case BIA estimated that the reimbursement of ELX-TEZ-IVA for the treatment of CF in patients 2 years and older who have at least 1 non-F508del mutation in the CFTR gene that is responsive based on in vitro and/or clinical data would be $12,515,883 in Year 1, $18,028,802 in Year 2, and $20,057,120 in Year 3, resulting in a 3-year total budget impact of $50,601,806.
CDA-AMC Appraisal of the Sponsor’s Budget Impact Analysis
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The market uptake of ELX-TEZ-IVA is underestimated: The sponsor’s submitted budget impact analysis indicated that ELX-TEZ-IVA would result in a market uptake of 15% in Year 1, 30% in Year 2, and 45% in Year 3 for patients who are IVA-eligible and 60% in Year 1, 85% in Year 2, and 93% in Year 3 for patients who are IVA-ineligible based on the sponsor’s internal estimates. However, CDA-AMC obtained clinical expert feedback indicating that the market uptake of ELX-TEZ-IVA would be higher in the IVA-eligible population and more rapid in the overall patient population than that estimated by the sponsor. The sponsor’s market shares do not align with clinical expectations and clinical expert feedback indicated the sponsor likely underestimated ELX-TEZ-IVA uptake overall. Clinical expert feedback advised that uptake would be rapid and high given the use of ELX-TEZ-IVA in current clinical practice for patients with F508del mutations as well as the expectation that most IVA-eligible patients receiving IVA would also switch to ELX-TEZ-IVA. Clinical expert feedback noted that, because of the high unmet need in the non-F508del patient population, it is expected that the majority of patients would receive ELX-TEZ-IVA and a very small number of patients (approximately 5% or less) may remain on BSC only because of patient barriers and concerns with long-term side effects.
To address this limitation, CDA-AMC undertook a reanalysis by revising the market shares for ELX-TEZ-IVA in the new drug scenario to be 90% in Year 1, 92% in Year 2, and 95% in Year 3 for patients who are IVA-eligible and 80% in Year 1, 90% in Year 2, and 93% in Year 3 for patients who are IVA-ineligible.
Adherence-adjusted drug costs underestimate the total costs associated with ELX-TEZ-IVA and other CFTR modulators to public drug plans. In alignment with the submitted CEA, the sponsor adjusted the price of CFTR modulators by the assumed adherence rate of 93% claiming that savings would be incurred by public drug plans because of patients not being 100% adherent. As the real-world adherence rate with ELX-TEZ-IVA or IVA for patients aged 2 and older is not available, the sponsor used adherence data from another CFTR modulator, LUM-IVA, which is associated with uncertainty as ELX-TEZ-IVA and IVA may have a different adherence rates.33 Additionally, the full complement of ELX-TEZ-IVA would be dispensed, regardless of whether the patient was compliant, thus resulting in the full costs of treatment being incurred by the public drug payer. This underestimated the total costs associated with ELX-TEZ-IVA and its total budget impact.
CDA-AMC assumed patients were 100% adherent in reanalyses, in alignment with the CDA-AMC pharmacoeconomic base case.
Estimated proportion of patients with public coverage for CFTR-modulator therapy is uncertain. The sponsor assumed 55% of the population indicated for ELX-TEZ-IVA would have public coverage, thus reducing the total eligible population size by 45%. The evidence cited by the sponsor for this assumption was internal data not available to CDA-AMC, and uncertainty remains as to the proportion of the indicated population who would be covered by public drug plans. There is uncertainty in the proportion of patients with public versus private insurance. If more than 55% of the population would be covered, the anticipated budget impact associated with ELX-TEZ-IVA would be higher. If fewer are covered, the anticipated budget impact would be lower.
CDA-AMC assumed 55% coverage in the base-case analysis, and tested scenarios of 40% coverage and 100% coverage.
CDA-AMC Reanalyses of the Budget Impact Analysis
Table 15: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Market shares of ELX-TEZ-IVA | IVA-eligible population: ELX-TEZ-IVA: 15% / 30% / 45% IVA: 75% / 60% / 45% BSC: 10% / 10% / 10% IVA-ineligible population: ELX-TEZ-IVA: 60% / 85% / 93% BSC: 40% / 15% / 7% | IVA-eligible population: ELX-TEZ-IVA: 90% / 92% / 95% IVA: 5% / 3%% / 0% BSC: 5% / 5% / 5% IVA-ineligible population: ELX-TEZ-IVA: 80% / 90% / 93% BSC: 20% / 10% / 7% |
2. Patient adherence | 93% | 100% |
CDA-AMC base case | Reanalysis 1 + 2 | |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor plus ivacaftor; IVA = ivacaftor.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17.
Based on the CDA-AMC base case, the budget impact of the reimbursement of ELX-TEZ-IVA for the treatment of CF in patients 2 years and older who have at least 1 non-F508del mutation in the CFTR gene that is responsive based on in vitro and/or clinical data is expected to be $18,224,293 in Year 1, $20,811,236 in Year 2, and $21,856,672 in Year 3, for a three-year total of $60,892,201.
Table 16: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 50,601,806 |
CDA-AMC reanalysis 1 – market shares | 56,629,747 |
CDA-AMC reanalysis 2 – adherence | 54,410,544 |
CDA-AMC base case | 60,892,201 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 17:
Assuming 50% of patients have public coverage
Assuming 100% of patients have public coverage
Assuming that the price of DUR is reduced by 79% (the CDA-AMC estimated price reduction from the cost-utility analysis)
Table 17: Detailed Breakdown of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 4,615,886 | 4,693,456 | 4,772,330 | 4,852,529 | 14,318,315 |
New drug | 4,615,886 | 17,209,340 | 22,801,132 | 24,909,649 | 64,920,121 | |
Budget impact | 0 | 12,515,883 | 18,028,802 | 20,057,120 | 50,601,806 | |
CDA-AMC base case | Reference | 4,963,318 | 5,046,727 | 5,131,538 | 5,217,773 | 15,396,038 |
New drug | 4,963,318 | 23,271,020 | 25,942,773 | 27,074,446 | 76,288,239 | |
Budget impact | 0 | 18,224,293 | 20,811,236 | 21,856,672 | 60,892,201 | |
CDA-AMC scenario analysis 1: 50% public coverage | Reference | 4,512,108 | 4,587,934 | 4,665,034 | 4,743,430 | 13,996,398 |
New drug | 4,512,108 | 21,155,473 | 23,584,339 | 24,613,132 | 69,352,944 | |
Budget impact | 0 | 16,567,539 | 18,919,305 | 19,869,702 | 55,356,546 | |
CDA-AMC scenario analysis 1: 100% public coverage | Reference | 9,024,215 | 9,175,868 | 9,330,068 | 9,486,860 | 27,992,796 |
New drug | 9,024,215 | 42,310,945 | 47,168,679 | 49,226,265 | 138,705,889 | |
Budget impact | 0 | 33,135,077 | 37,838,611 | 39,739,404 | 110,713,092 | |
CDA-AMC scenario analysis 3: 79% price reduction | Reference | 1,057,187 | 1,074,953 | 1,093,018 | 1,111,386 | 3,279,356 |
New drug | 1,057,187 | 4,956,727 | 5,525,811 | 5,766,857 | 16,249,395 | |
Budget impact | 0 | 3,881,774 | 4,432,793 | 4,655,471 | 12,970,039 |
CDA-AMC = Canada’s Drug Agency.
Ethics Review
Abbreviations
CF
cystic fibrosis
ELX-TEZ-IVA
elexacaftor-tezacaftor-ivacaftor and ivacaftor
FRT
Fischer rat thyroid
IVA
ivacaftor
Summary
Cystic fibrosis (CF) is a rare, life-limiting genetic disorder caused by mutations in the CFTR gene, leading to progressive lung damage and multi-organ dysfunction. This report describes the ethical considerations posed by the use of elexacaftor-tezacaftor-ivacaftor plus ivacaftor (ELX-TEZ-IVA) for the treatment of CF in patients aged 2 years and older who have a mutation in the CFTR gene that, based on clinical and/or in vitro data, is responsive to the therapy. This report is informed by published literature as well as patient group, clinician group, clinical expert, and drug program input.
The ethical considerations identified in this review include:
Diagnosis, treatment, and experiences of non-F508del CF variants: ELX-TEZ-IVA has come to be understood as an effective treatment in the clinical management of people living with CF and carrying 1 or more F508del mutations in the CFTR gene. Ethnic minorities and racialized peoples are more likely to carry non-F508del variants than are their non-Hispanic white counterparts of European descent. People with rare, or ultrarare, non-F508del variants are currently ineligible to receive ELX-TEZ-IVA, resulting in substantial disparities in clinical outcomes and quality of life between individuals eligible for the treatment and those who are not. Lack of access to disease-modifying therapy has caused significant psychological distress among those with non-F508del variants. The lack of access also has the potential to exacerbate existing health inequities.
Clinical evidence used in the evaluation of ELX-TEZ-IVA: For people living with at least 1 of the 72 non-F508del variants supported by some form of clinical data, evidence indicates that treatment with ELX-TEZ-IVA may result in clinically meaningful improvements to lung function. However, there is some uncertainty regarding the durability of the effect in this population. There are only in vitro data, but no clinical data support the efficacy or safety for the use of ELX-TEZ-IVA in people carrying 1 of 79 further variants included in the expanded population. Neither clinical nor in vitro data are available for 1 variant. Although the generalizability of in vitro FRT-cell model data to real-world applications is uncertain, clinical experts were comfortable with relying on this data to prescribe ELX-TEZ-IVA given the absence of alternative treatment options; their experience with, and the mounting evidence for, ELX-TEZ-IVA in people with 1 or more F508del variants; and clinical data for other rare variants included in this review. Additionally, the clinical experts consulted for this review noted that relying on in vitro data in patients with rare, or ultrarare, non-F508del variants is justified as clinical trials may not be feasible.
Clinical use and implementation of ELX-TEZ-IVA: Given that individuals with non-F508del variants may be from historically disadvantaged groups, expanding access to ELX-TEZ-IVA has the potential to benefit these communities and lessen health inequities associated with access to effective therapy and improved treatment outcomes. The clinical experts consulted for this review noted that members of Canada’s Hutterite population with CF may also benefit from expanded access to ELX-TEZ-IV because of the high prevalence of non-F508del mutations in this group. The clinical experts are reportedly ready to prescribe ELX-TEZ-IVA to the expanded population as they believe the potential benefits outweigh the potential risks, given the lack of alternatives and mounting evidence supporting its safety and efficacy in people with F508del mutations. However, it is important to have a robust informed-consent process in which health care providers transparently communicate the absence of clinical evidence for the 79 variants supported solely by in vitro data and prepare patients for the uncertainties surrounding treatment safety and effectiveness.
Health systems: Expensive drugs for rare diseases raise ethical considerations related to distributive justice and equitable access, the sustainability of health care budgets and consideration of opportunity costs, and fair pricing of pharmaceuticals. As ELX-TEZ-IVA is a highly expensive medication, expanding access to it could present challenges for provincial drug budgets as the reimbursement of ELX-TEZ-IVA may have a disproportionately large budget impact.
Objective and Research Questions
The objective of this Ethics Review is to identify and describe ethical considerations associated with the use of ELX-TEZ-IVA for the treatment of CF in patients aged 2 years and older who have a mutation in the CFTR gene that is responsive based on clinical and/or in vitro data, including considerations related to the disease context, evidentiary basis, the use of ELX-TEZ-IVA, and impact on health systems.
To address this objective, this review addresses the following research questions:
What ethical considerations arise in the context of CF caused by rare, or ultrarare, non-F508del variants to the CFTR gene, including considerations related to diagnosis, treatment, and outcomes?
What ethical considerations are posed by the evidence (e.g., clinical and economic data) used to evaluate ELX-TEZ-IVA in the expanded population?
What ethical considerations arise in relation to the use of ELX-TEZ-IVA for patients, their caregivers, and their clinicians?
What are the ethical considerations for health systems related to ELX-TEZ-IVA?
Methods
Guiding questions identified in the EUnetHTA Core Model 3.0, Ethics Analysis Domain,1 supplemented by relevant questions from the Equity Checklist for Health Technology Assessments,2 drive the identification of ethical considerations relevant to the use of ELX-TEZ-IVA in the treatment of CF caused by rare, or ultrarare, non-F508del variants to the CFTR gene in this Ethics Review. These guiding questions are organized to respond to the research questions and to investigate ethical considerations related to:
patients living with CF caused by rare, or ultrarare, non-F508del variants to the CFTR gene and their caregivers (i.e., disparities in incidence, treatment, or outcomes; challenges or burdens related to diagnosis or clinical care; factors that might prevent patients from gaining access to therapies)
the evidence used to demonstrate the benefits, harms, and value of ELX-TEZ-IVA (i.e., ethical considerations in relevant clinical trials, including their representativeness, the choice of outcome measures, the appropriateness of the analytical methods and models used to all population groups; ethical considerations related to the data or assumptions in the economic evaluation)
the use of ELX-TEZ-IVA, including considerations related to benefits and harms to patients, relatives, caregivers, clinicians, and society, as well as considerations related to access to these therapies
the uptake of ELX-TEZ-IVA in health systems, including considerations related to the distribution of health care resources.
Review of Project Inputs
A single reviewer collected and considered input from 7 main sources of data related to ethical considerations relevant to the research questions guiding this Ethics Review. The reviewer considered:
evidence from a search of published literature
the sponsor’s submission, noting relevant information and external references or sources relevant to each of the research questions driving this report
clinician group input received from Cystic Fibrosis Canada’s Accelerating Clinical Trials Network, the Edmonton Adult Cystic Fibrosis Clinic and Calgary Adult Cystic Fibrosis Clinic, and the CF Canada Health Care Advisory Council
patient input received from Cystic Fibrosis Canada
drug program input from drug programs participating in the CDA-AMC reimbursement review process
discussions with clinical experts (n = 3) directly engaged over the course of this reimbursement review, including through a clinical consultation meetings involving 2 experts, and written input provided by all 3 experts; during this meeting, the reviewer asked the clinical experts targeted questions related to ethical considerations corresponding to the research questions driving this report; all the clinical experts are practising CF specialists. with 1 specializing in pediatrics and the other 2 in adults; all 3 had experience using ELX-TEZ-IVA in CF patients with F508del variants
engagement with clinical and economic reviewers to identify domains of ethical interest arising from their respective reviews and to identify relevant questions and sources to further pursue in this report.
Details on the Published Literature Search
An information specialist conducted a literature search on key resources, including MEDLINE via Ovid, Philosopher’s Index via Ovid, PsycInfo via Ovid, the Cumulative Index to Nursing and Allied Health Literature via EBSCO, and Scopus. Google Scholar was searched to find additional materials not captured in the major bibliographic databases. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Trikafta along with searches for CF and the F508del gene.
Search filters were applied to limit retrieval to citations related to ethical concepts or considerations, equity concepts or considerations, or qualitative studies. No filters were applied to the searches conducted in Philosopher’s Index. Duplicates were removed by manual deduplication in EndNote. Retrieval was limited to the English language. The search was completed on April 3, 2024.
Literature Screening and Selection
A single reviewer screened literature in 2 stages. First, the reviewer screened the titles and abstracts of the retrieved citations and identified and retrieved articles for full-text review if their titles or abstracts identified ethical considerations, or provided normative analyses (i.e., focusing on “what ought to be” through argumentation), or empirical research (i.e., focusing on “what is” through observation) of ethical considerations related to: the experiences, incidence, diagnosis, treatment, or outcomes of CF caused by rare, or ultrarare, non-F508del variants to the CFTR gene; or the evidence on, use of, or implications of ELX-TEZ-IVA for patients with CF caused by rare, or ultrarare, non-F508del variants to the CFTR gene. In the second stage, the same reviewer reviewed full-text publications categorized as “retrieve.” The reviewer included texts that included substantive information meeting the aforementioned criteria. Additionally, the reviewer retrieved and reviewed select sources drawn from relevant bibliographies, relevant key concepts, and consultation with experts, or other reviewers using the selection criteria listed previously.
Data Analysis
The 4 research questions driving this review guided the collection, coding, and thematic analysis of data. The reviewer conducted 2 iterative cycles of coding and analysis to abstract, identify, and synthesize relevant ethical considerations from the literature and from relevant project inputs. In the initial coding phase, the reviewer read the publications and input sources for ethical content (e.g., claims related to potential harms, benefits, equity, justice, and resource allocation as well as ethical issues in the evidentiary basis). The reviewer coded the identified claims related to ethical content using methods of qualitative description.3 In the second coding phase, the reviewer identified major themes and subcodes through repeated readings of the data,3 and summarized them into thematic categories within each guiding domain or research question. The reviewer noted if the ethical content did not fit into these categories or into the domains outlined in the research questions, or if there were discrepancies or conflicts between the ethical considerations or values identified between project sources or within thematic categories. The data analysis was iterative, and the reviewer used themes identified in the literature, in project inputs, and arising from consultations with clinical experts to further refine and re-interpret the ethical considerations identified. Finally, the reviewer thematically organized and described the data according to the 4 research questions and domains driving this Ethics Review. The results, limitations, and conclusions of this analysis are described in the following sections.
Results
Key Ethical Considerations
As highlighted by the Clinical Review, this submission represents the fourth time the Canadian Drug Expert Committee has considered ELX-TEZ-IVA since 2021. The previous 3 submissions were concerned specifically with people carrying at least 1 copy of the most common CFTR variant, the F508del mutation, and gradually expanded the indicated population from those aged 12 years or older4 to 6 years or older5 and finally to 2 years and older.6 All 3 received recommendations to reimburse with conditions, and ELX-TEZ-IVA is now reimbursed across Canada for people with CF aged 2 years and older carrying 1 or more F508del mutations in the CFTR gene.
The current review is for an expanded indication for ELX-TEZ-IVA for people with CF aged 2 years and older carrying at least 1 copy of an additional 152 rare, or ultrarare, non-F508del CFTR variants. This Ethics Review focuses on identifying ethical considerations relevant to deliberation on, or decision-making for, public reimbursement of the expanded indication.
Diagnosis, Treatment, and Experiences of Non-F508del CF
Cystic fibrosis is a rare genetic disorder caused by mutations in the CFTR gene, leading to progressive lung damage and multi-organ dysfunction. While more than 2,000 distinct variants of the CFTR gene have been identified, the F508del variant is the most common, both in Canada and globally.7 Slightly less than 87% of people with CF in Canada carry at least 1 copy of the F508del variant.7 As such, most people with CF in Canada are already eligible for ELX-TEZ-IVA. The sponsor expects that an additional 5% (n = 226) of the total CF population in Canada would become eligible for ELX-TEZ-IVA if the variants in the expanded indication are recommended for reimbursement. For people with certain non-F508del gating variants (i.e., G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, S549R, or R117H), CFTR-modulator therapy in the form of the single modulatory drug, ivacaftor (IVA) may also be reimbursed.
Current Treatment Options for Expanded Population
Clinical experts, clinician and patient group input, and published literature indicate that the introduction of ELX-TEZ-IVA into CF care regimens has dramatically altered the course of disease for people living with 1 or more F508del variants.8-12 ELX-TEZ-IVA delays disease progression, and improves survival, and people using ELX-TEZ-IVA report improvements in their quality of life.8 However, for those carrying rare, or ultrarare, non-F508del variants (outside of those specified for IVA eligibility), no CFTR-modulator therapy is currently available in Canada. While the modulator therapies IVA and ELX-TEZ-IVA are described as a paradigm shift8 in the care of people with a copy of the F508del mutation, standard of care for those ineligible for IVA because they carry a rare or ultrarare variant of the CFTR gene remains focused on symptom management.7,8
Patient and clinician group input highlight that symptom management is not only challenging to maintain for people with CF and their care providers, but that it is also less effective than modulator therapies. This has led to a significant disparity in clinical outcomes and quality of life between people who have access to modulator therapy, ELX-TEZ-IVA in particular, and those whose variants are currently ineligible for access to ELX-TEZ-IVA.8,12 The disparity is so acute that patient input stated that people with access to ELX-TEZ-IVA “will overwhelmingly live longer. [Those without] overwhelmingly won’t.” Beyond clinical outcomes, people who are ineligible for modulator therapy, namely ELX-TEZ-IVA, have reported experiences of significant emotional distress, feeling hopeless, “left behind,” and “desperate” for new treatment options.9-11
Although CF occurs in all races,12 the commonality of the F508del mutation broadly, and its increased prevalence in non-Hispanic white populations (approximately 90%),13 has led to CF being largely characterized as a “white people’s disease.”12-14 Indeed, in Canada, 92% of the CF population are identified as white.7 Racialized peoples of non-European descent are less likely to be eligible for CFTR modulators in Canada and therefore face disparities in access to care12,13,15,16 and may experience worse clinical outcomes as a result. Studies in the US report that racialized peoples and ethnic minorities experience higher rates of delayed diagnosis, reduced access to multidisciplinary care, lower lung-transplant referrals, and worse overall outcomes compared to their white counterparts.12,15,17 Systemic barriers such as racism, socioeconomic disadvantages, and geographic inaccessibility of specialized CF centres contribute to these disparities.12,16 The clinical experts consulted for this review indicated that, in Canada, disparities in outcomes and access to CFTR modulators extend to the Hutterite population in the Prairie provinces. They noted that only 52% of Hutterites living with CF are currently eligible for ELX-TEZ-IVA because many carry a non-F508del variant.
Diagnosis
Clinical experts indicated that newborn screening programs for CF vary across provinces and territories and that advanced diagnostics (i.e., full gene sequencing) may not be available, or utilized, across all jurisdictions.16 As a result, individuals with rare, ultrarare, or unclassified variants may experience varying degrees of diagnostic delay, particularly among racialized peoples or ethnic minorities whose variants are less likely to be included in standard panel tests optimized for white, European populations.16 However, clinical experts emphasized that such cases are rare in Canada and may be attributable to people living with less severe forms of non-F508del CF. While rates of missed diagnosis are low, addressing systemic barriers to timely access to diagnosis is important to ensuring equitable access to ELX-TEZ-IVA if reimbursed.
Ethics of Evidence and Evaluation of ELX-TEZ-IVA in the Expanded Population
The evidence used to assess ELX-TEZ-IVA for the expanded population is drawn from: 1 randomized control trial with an extension phase (Study 124) assessing clinical efficacy and safety in patients with 17 of the most common Health Canada–approved non-F508del variants; 1 prospective cohort study (Study 16) assessing clinical efficacy in patients with an additional 51 Health Canada–approved non-F508del variants; and 4 additional real-world-evidence studies assessing clinical efficacy in patients with another 5 Health Canada–approved non-F508del variants. Together, these clinical studies assessed the efficacy of using ELX-TEZ-IVA to treat patients with 73 of the 152 Health Canada–approved variants being considered in the expanded indication. For patients with 79 of the remaining variants, efficacy is determined exclusively based on in vitro Fischer rat thyroid (FRT) modelling. No in vitro or clinical data are available for the 711 + 3A > G variant. The Clinical Review Report describes the Health Canada–approved variants in detail.
The clinical evidence is discussed in detail in the Clinical and Pharmacoeconomic Review reports.
Ethical Considerations of Representativeness of Clinical Data
Clinical evidence indicates that treatment with ELX-TEZ-IVA may result in clinically meaningful improvements to the primary end point of percent predicted forced expiratory volume in 1 second. Only 17 of the Health Canada–approved variants included in Study 124 have safety data, which did not indicate CFTR genotype–dependent safety concerns. The remaining 135 variants under review lack safety data. However, the clinical experts consulted for this review expressed a general sense of comfort with the safety profile of ELX-TEZ-IVA based on evidence and experience prescribing it to patients with F508del mutations. Given limited long-term efficacy data, there is uncertainty regarding the durability of the effect of ELX-TEZ-IVA and risk of harm in the expanded population. This uncertainty has implications for consent conversations to support informed decision-making and the need for ongoing monitoring and data collection to understand benefits in practice and mitigate risks of harm.
Racialized peoples and ethnic minorities have a history of underrepresentation in CF research.16,18 It is difficult to verify the representativeness of the evidence used to assess ELX-TEZ-IVA in the expanded population as limited demographic data were reported for participants in Study 16 or the 4 real-world-evidence studies included in the sponsor’s submission. As only 3.5% of the active treatment population were identified as belonging to a racialized group or ethnic minority (i.e., “Asian”), it is possible that these results are underrepresentative of racialized populations and ethnic minorities in Canada. Including racialized populations in clinical trials is essential for addressing health disparities and understanding potential benefit or risk of harm in a diverse population.16
Ethical Considerations of the In Vitro FRT-Cell Model
Published literature noted some uncertainty regarding the ability of data collected through in vitro modelling to inform reimbursement decisions.19 While mounting evidence supports the effectiveness of ELX-TEZ-IVA for people with F508del variants, and in vitro data supports its potential in patients with non-F508del variants, questions remain about the extrapolation of in vitro results to those with non-F508del variants. Published literature indicated some concerns regarding the reliability of FRT-cell models, as utilized in the sponsor’s submission, in assessing the efficacy of CFTR correctors, such as elexacaftor-tezacaftor in ELX-TEZ-IVA.19-21
Despite the uncertainty regarding extrapolation based on in vitro data, the clinical experts suggested that the absence of alternative treatment options as well as growing evidence regarding the safety and efficacy of ELX-TEZ-IVA for patients with 1 or more F508del mutations warranted acceptance of this data to inform prescribing decisions for the extended population. Further, the clinical experts, as well as clinician and patient group input, highlighted how conducting clinical trials to assess the efficacy of ELX-TEZ-IVA for rare or extremely rare variants may not be feasible. The clinical experts noted that reimbursement based on in vitro data may be the only way for individuals with these rare variants to access treatment and understand real-world effectiveness in practice.
If recommended for reimbursement, ongoing data collection will be important to help minimize the potential risk of harm arising from the absence of clinical data. In addition to supporting collection of long-term effectiveness data, ongoing data collection or surveillance could support rapid responses to any potential harm arising in this population.22 The clinical experts indicated that the current practice of frequent clinical and lab follow-up following ELX-TEZ-IVA initiation supports ongoing data collection and allows them to closely monitor patients for clinical response and adverse events.
Ethical Considerations in the Use of ELX-TEZ-IVA in the Expanded Population
The use of ELX-TEZ-IVA in the expanded population raises ethical considerations related to the weighting of potential benefits and harms in the context of limited clinical data and, when data are available, limited certainty regarding long-term effectiveness and safety.
The sponsor is basing its argument for expanding the indication for ELX-TEZ-IVA on the growing disparity in clinical outcomes and quality of life between those with access to the therapy and those without. Despite evidentiary uncertainty or absence of clinical evidence (in the case of variants for which only in vitro evidence is available), the clinical experts indicated a clear readiness to prescribe ELX-TEZ-IVA for the expanded population. They suggested that the potential for benefits outweighed the risks of harm because of the absence of disease-modifying treatment alternatives for this population and mounting evidence supporting the safety and effectiveness of ELX-TEZ-IVA in people with F508del variants. While the level of risk is largely unknown in the proposed population given the limited or (in the case of variants with only in vitro evidence) absent safety data provided as part of its submission, the sponsor noted that frequent follow-up visits and lab testing provide the opportunity for CF specialists to closely monitor patients for treatment response and signs of adverse events.
The clinical experts also noted that expanding access to ELX-TEZ-IVA has the potential to benefit historically disadvantaged groups and improve equitable access to treatment for CF (given their higher likelihood of carrying non-F508del variants). However, it will also be important to remain mindful of broader structural determinants of health affecting health equity for these groups.12,13,15,23,24
The clinical experts noted that transparent communication regarding the absence of clinical data for 79 variants supported solely by in vitro data will be essential to ensuring informed decision-making by patients and their caregivers. This highlights the need for robust informed-consent processes, which must effectively communicate the uncertainty associated with treatment effectiveness for variants lacking clinical data and continue to inform patients as the evidence base develops. Ensuring transparency and thorough communication about the limitations of available data are crucial in empowering patients to actively participate in their treatment decisions and in managing expectations and potential psychological harm if the treatment is ineffective.
Health Systems Considerations
The reimbursement of ELX-TEZ-IVA for CF raises ethical considerations for health systems related to shifting use of health care resources, the sustainability of Canadian health care budgets, and opportunity costs. As identified by the clinical experts consulted for a previous ethics review of ELX-TEZ-IVA, the implementation of ELX-TEZ-IVA may result in an initial increase in the use of health care resources (e.g., frequent clinic visits, additional blood work, extended time for treatment education, more examinations, follow-up appointments, and associated treatment costs). However, the burden on health systems may be expected to gradually diminish because of the reduction in other required treatments and a decrease in pulmonary exacerbations and associated hospitalization costs.6 How ELX-TEZ-IVA is implemented may have additional resource implications. For example, the sponsor has indicated that the initial renewal criteria currently required for people aged 6 years or older with 1 or more F508del mutations, who are currently eligible for ELX-TEZ-IVA, are resource-intensive and burdensome for CF specialists and administrative teams and distressing for patients and caregivers.
Expensive drugs such as ELX-TEZ-IVA for rare diseases also raise ethical considerations related to distributive justice and equitable access, the sustainability of health care budgets, and the fair pricing of pharmaceuticals.25 Reimbursing high-cost drugs for rare diseases raises considerations about the opportunity costs associated with reimbursement and implementation, which can have implications for understanding the fair and equitable allocation of scarce health care resources.26 The assessment of the opportunity costs of implementing ELX-TEZ-IVA for people with 1 of the 79 variants currently supported through in vitro data alone is further complicated by the uncertainty about its effectiveness in practice. Published literature notes that outcomes-based agreements may be warranted for reimbursing ELX-TEZ-IVA for people with mutations with only in vitro data because of the greater evidentiary uncertainty and associated risk to payers in the absence of clinical evidence of efficacy.16,19 Clinical experts expressed confidence in the ability of providers to exercise responsible resource stewardship, including by carefully evaluating the risk-benefit of prescribing, continuing or discontinuing ELX-TEZ-IVA.
Limitations
Little published literature discusses the ethical considerations related to the use of ELX-TEZ-IVA for the treatment of people living with rare, or ultrarare, non-F508del CF variants, given both the rarity of these variants and the limited use of ELX-TEZ-IVA in these variants to date. This does not imply the absence of ethical considerations in the context of ELX-TEZ-IVA for people with non-F508del CF variants. Drawing on input received during this reimbursement review from patient groups, clinicians, and drug programs, and discussion with clinical experts, as well as engagement with other members of the review team, provides a more comprehensive understanding of the ethical considerations related to the use of ELX-TEZ-IVA for the treatment of rare, or ultrarare, non-F508del variants. More direct engagement (e.g., through direct interviews) with patients, their caregivers and family members, and decision-makers on their specific experiences with rare or ultrarare CF variants and/or ELX-TEZ-IVA may offer additional relevant perspectives or domains of ethical analysis.
Conclusion
This report considers input from patient groups, clinician groups, and provincial drug programs, as well as direct engagement with clinical experts and examination of the published literature to identify ethical considerations relevant to the use of ELX-TEZ-IVA in people with 1 of the 152 Health Canada–approved non-F508del variants under review. Lack of access to effective disease-modifying therapy contributes to significant disparities in clinical outcomes and quality of life between people with CF who have 1 or more F508del variants and those with non-F508del variants. This has not only resulted in significant psychological distress for those currently ineligible for ELX-TEZ-IVA, but it may also exacerbate existing health inequities for racialized peoples and ethnic minorities who are less likely to carry F508del mutations. While clinical studies have included promising results for patients with some non-F508del variants, the efficacy and risk of harm of ELX-TEZ-IVA in the proposed population remain uncertain, particularly for those with variants the efficacy and safety of which are supported solely by in vitro data. However, the clinical experts consulted for this review were willing to prescribe ELX-TEZ-IVA to the expanded population because of the absence of effective alternative treatments, growing evidence of its safety and efficacy in patients with F508del variants, and their belief that the potential benefits outweigh potential harms. Prescribing ELX-TEZ-IVA to the expanded population would require a robust informed-consent process in which providers transparently communicate the lack of clinical evidence for the 79 Health Canada–approved variants that are supported only by in vitro data and prepare patients for uncertainties regarding treatment safety and effectiveness. The potential budget impacts and ethical considerations surrounding the pricing and reimbursement of ELX-TEZ-IVA underscore the need for careful evaluation and decision-making to ensure fair and equitable access to this potentially transformative therapy for the expanded population. The sponsor has proposed clinician-guided renewal criteria on the basis that current criteria pose an unnecessary burden on providers, patients, and systems. This is supported by clinical experts who are confident that specialists are capable of being good stewards of scarce health care resources and their judgment could be informed by outcome measures taken at standard CF visits.
References
1.EUnetHTA Joint Action 2 Work Package 8, HTA Core Model version 3.0. Diemen (NL): EUnetHTA; 2016: https://www.eunethta.eu/wp-content/uploads/2018/03/HTACoreModel3.0-1.pdf. Accessed 2024 Mar 07.
2.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37:e17. PubMed
3.Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-340. PubMed
4.Drug Reimbursement Expert Review Committee final recommendation: elexacaftor-tezacaftor-ivacaftor and ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Inc.). Can J Health Technol. 2021;1(9). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/sr0673/sr0673. Accessed 2024 May 24.
5.Drug Reimbursement Expert Review Committee final recommendation: elexacaftor-tezacaftor-ivacaftor and ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Inc.). Can J Health Technol. 2022;2(7). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/SR0710/SR0710. Accessed 2024 May 24.
6.Drug Reimbursement Expert Review Committee final recommendation: elexacaftor-tezacaftor-ivacaftor and ivacaftor (Trikafta - Vertex Pharmaceuticals (Canada) Inc.). Can J Health Technol. 2023;3(12). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/SR0776/SR0776. Accessed 2024 May 24.
7.Cystic Fibrosis Canada. The Canadian Cystic Fibrosis Registry 2022 annual data report. Toronto (ON): Cystic Fibrosis Canada; 2023: https://www.cysticfibrosis.ca/uploads/2022-Annual-Data-Report-WEB-AODA.pdf. Accessed 2024 May 05.
8.Chun SW, Somers ME, Burgener EB. Highly effective cystic fibrosis transmembrane conductance (regulator) modulator therapy: shifting the curve for most while leaving some further behind. Curr Opin Pediatr. 2024;36(3):290-295. PubMed
9.Kramer-Golinkoff E, Camacho A, Kramer L, Taylor-Cousar JL. A survey: understanding the health and perspectives of people with CF not benefiting from CFTR modulators. Pediatr Pulmonol. 2022;57(5):1253-1261. PubMed
10.Milo F, Ciciriello F, Alghisi F, Tabarini P. Lived experiences of people with cystic fibrosis that were not eligible for elexacaftor-tezacaftor-ivacaftor (ETI): a qualitative study. J Cyst Fibros. 2023;22(3):414-419. PubMed
11.Landess L, Prieur MG, Brown AR, Dellon EP. Exploring perceptions of and decision-making about CFTR modulators. Pediatr Pulmonol. 2024;59(6):1614-1621. PubMed
12.McGarry ME, Gibb ER, Oates GR, Schechter MS. Left behind: the potential impact of CFTR modulators on racial and ethnic disparities in cystic fibrosis. Paediatr Respir Rev. 2022;42:35-42. PubMed
13.Vaidyanathan S, Trumbull AM, Bar L, Rao M, Yu Y, Sellers ZM. CFTR genotype analysis of Asians in international registries highlights disparities in the diagnosis and treatment of Asian patients with cystic fibrosis. Genet Med. 2022;24(10):2180-2186. PubMed
14.Rubin R. Tackling the misconception that cystic fibrosis is a “White people's disease”. JAMA. 2021;325(23):2330-2332. PubMed
15.Ladores S, Woods BM, Pitts LN, Belay D, Washington L, Bray LA. The lived experience of African American persons with cystic fibrosis. Creat Nurs. 2023;29(4):374-382. PubMed
16.Shemie G, Nguyen MT, Wallenburg J, Ratjen F, Knoppers BM. The equitable implementation of cystic fibrosis personalized medicines in Canada. J Pers Med. 2021;11(5):382. PubMed
17.Wright M, Wright T. Health disparity in CF: perspectives from a lived experience. Pediatr Pulmonol. 2022;57 Suppl 1:S13-S16. PubMed
18.McGarry ME, McColley SA. Cystic fibrosis patients of minority race and ethnicity less likely eligible for CFTR modulators based on CFTR genotype. Pediatr Pulmonol. 2021;56(6):1496-1503. PubMed
19.Costa E, Girotti S, Pauro F, Leufkens HGM, Cipolli M. The impact of FDA and EMA regulatory decision-making process on the access to CFTR modulators for the treatment of cystic fibrosis. Orphanet J Rare Dis. 2022;17(1):188. PubMed
20.Amaral MD, de Boeck K, Davies JC, et al. Theranostics by testing CFTR modulators in patient-derived materials: the current status and a proposal for subjects with rare CFTR mutations. J Cyst Fibros. 2019;18(5):685-692. PubMed
21.Clancy JP, Cotton CU, Donaldson SH, et al. CFTR modulator theratyping: current status, gaps and future directions. J Cyst Fibros. 2019;18(1):22-34. PubMed
22.Smith MJ, Komparic A, Thompson A. Deploying the precautionary principle to protect vulnerable populations in Canadian post-market drug surveillance. Can J Bioeth. 2020;3(1):110-118.
23.Rosenfeld M, Cromwell EA, Schechter MS, et al. The impact of switching to race-neutral reference equations on FEV1 percent predicted among people with cystic fibrosis. J Cyst Fibros. 2024;23(3):443-449. PubMed
24.Hutchins K, Barr E, Bellcross C, Ali N, Hunt WR. Evaluating differences in the disease experiences of minority adults with cystic fibrosis. J Patient Exp. 2022;9:23743735221112629. PubMed
25.Kacetl J, Marešová P, Maskuriy R, Selamat A. Ethical questions linked to rare diseases and orphan drugs - a systematic review. Risk Manag Healthc Policy. 2020;13:2125-2148. PubMed
26.Zampoli M, Morrow BM, Paul G. Real-world disparities and ethical considerations with access to CFTR modulator drugs: mind the gap! Front Pharmacol. 2023;14:1163391. PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.