Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Elexacaftor-Tezacaftor-Ivacaftor and Ivacaftor (Trikafta)
Indication: Treatment of cystic fibrosis in patients aged 2 years and older who have at least one mutation in the CFTR gene that is responsive based on clinical and/or in vitro data
Sponsor: Vertex Pharmaceuticals (Canada) Incorporated
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Trikafta?
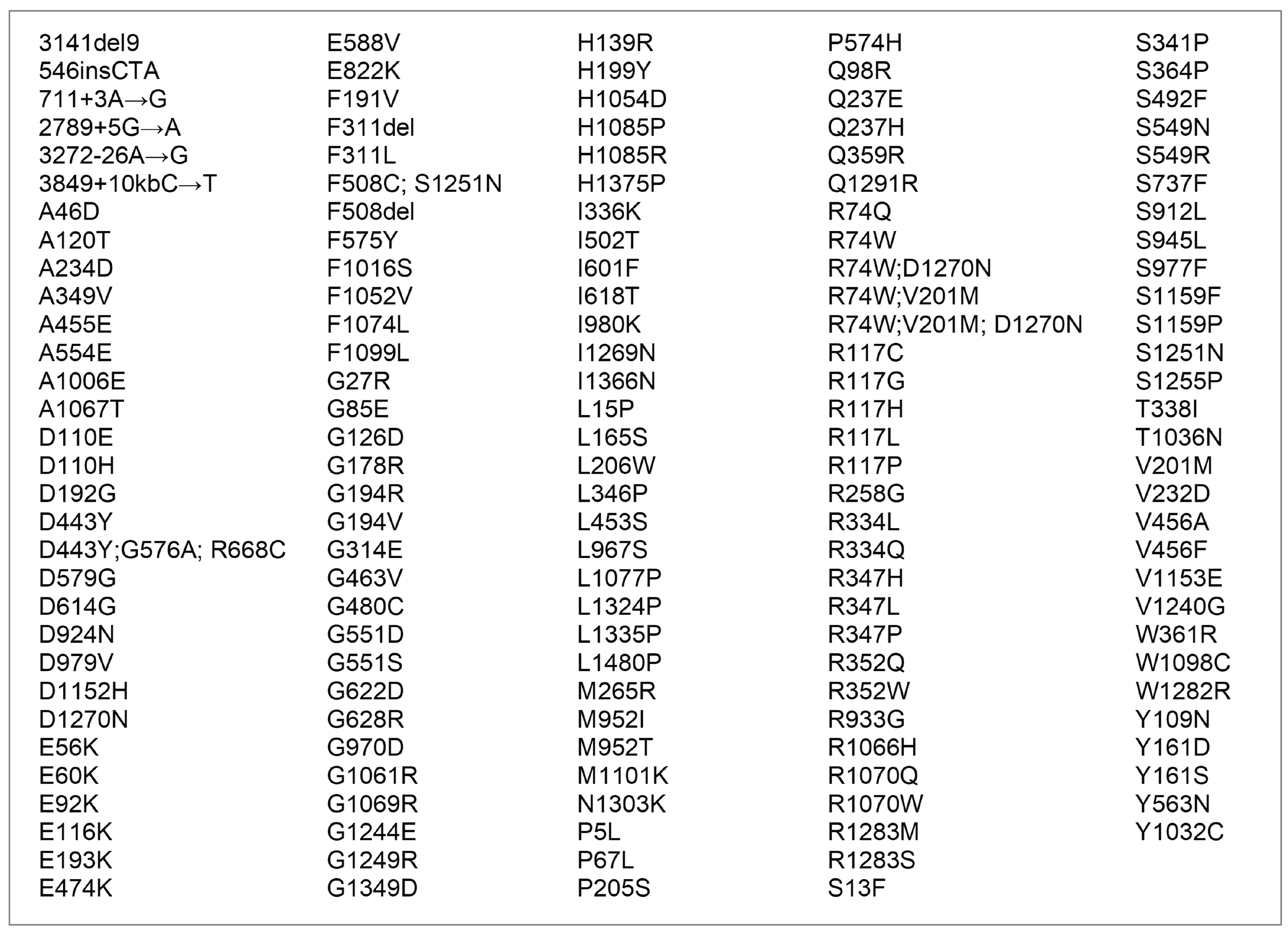
Canada’s Drug Agency (CDA-AMC) recommends that Trikafta be reimbursed by public drug plans for the treatment of cystic fibrosis (CF) in patients aged 2 years and older who have at least 1 of the 152 non-F508del mutations in the CFTR gene that are identified in Figure 1 of this document, if certain conditions are met.
What Are the Conditions for Reimbursement?
Patients aged 2 to 5 years who start treatment with Trikafta should be evaluated for response after 1 year, and those aged 6 years or older should be evaluated after 6 months. The physician must provide evidence that the patient is benefiting from the treatment. The cost of Trikafta must also be reduced.
Why Did CDA-AMC Make This Recommendation?
Six clinical studies demonstrated that Trikafta was well tolerated and resulted in clinically meaningful improvements in end points that are important for those living with CF (e.g., lung function, nutritional status, pulmonary exacerbations, and quality of life). For the rare CFTR mutations that have not been evaluated in clinical trials (i.e., those where the response to Trikafta has only been assessed in a laboratory), the committee acknowledged the practical challenges with generating clinical evidence. The committee concluded that Trikafta has the potential to provide clinically meaningful benefit for patients with CF caused by rare CFTR mutations, on the basis that the laboratory data were considered acceptable by Health Canada and that the biological plausibility of a beneficial treatment effect was supported by the CF specialists who provided input for this review.
Based on the CDA-AMC assessment of the health economic evidence, Trikafta does not represent good value to the health care system at the public list price. A price reduction is therefore required.
Based on public list prices, reimbursement of Trikafta for patients with at least 1 of the 152 non-F508del mutations in the CFTR gene that are identified in Figure 1 is estimated to cost the public drug plans approximately $61 million over the next 3 years.
Additional Information
What Is CF?
CF is a progressive, fatal, genetic disease that primarily affects the lungs and digestive system. Those living with CF lose the ability to breathe due to accumulated lung damage, caused by chronic lung infections and inflammation.
Unmet Needs in CF
There are significant unmet therapeutic needs for those living with CF. There are no treatments currently available that effectively meet the most important goals of CF therapy: prolonging survival, preventing the need for lung transplant, slowing the decline in lung function over time, and reversing the course of the disease.
How Much Does Trikafta Cost?
Treatment with Trikafta is expected to cost $306,810 per patient per year.
Recommendation
The Canadian Drug Expert Committee (CDEC) recommends that elexacaftor-tezacaftor-ivacaftor and ivacaftor (ELX-TEZ-IVA) be reimbursed for treatment of CF in patients aged 2 years and older who have at least 1 mutation in the CFTR gene that is responsive based on clinical and/or in vitro data (listed in Figure 1), only if the conditions listed in Table 1 are met.
Rationale for the Recommendation
CF is the most common fatal genetic disease affecting children and young adults in Canada. It is caused by mutations in the CFTR gene. Clinical expert input emphasized the importance of initiating treatment early in the disease course and that there is a significant unmet need for a treatment that would prevent disease progression and irreversible CF-related structural lung damage. Study 124 (N = 307; 18 CFTR mutations) and Study 16 (N = 422; 64 CFTR mutations) demonstrated that ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function (increase in ppFEV1), nutritional status (increase in body mass index [BMI]), health-related quality of life (HRQoL) (increase in Cystic Fibrosis Questionnaire – Revised [Respiratory Domain] [CFQ-R RD] scores), CF biomarkers (reduction in sweat chloride [SwCl]), and a reduced rate of pulmonary exacerbations. For the 4 clinical studies in patients with at least one N1303K mutation (Solomon et al. [2024] [N = 20], Burgel et al. [2023] [N = 8], Burgel et al. [2024] [N = 35], and Sadras et al. [2023] [N = 8]), the short-term results showed acute increases in ppFEV1 and weight that were suggestive of a clinically meaningful benefit with ELX-TEZ-IVA. For all of the mutations with clinical data, the clinical specialists consulted by CDA-AMC considered the results to be clinically meaningful and indicative that ELX-TEZ-IVA would benefit patients in the target population. The experts emphasized that there is a high-level of unmet need for these patients, as they currently do not have access to CFTR modulator therapy in Canada (outside of enrolment in a clinical study).
For the 79 mutations that have been assessed exclusively from the in vitro model, CDEC noted that the data were considered acceptable evidence by Health Canada to expand the indication for ELX-TEZ-IVA and that the sponsor had provided clinical evidence for those mutations that are more commonly harboured by patients with CF in Canada. The inclusion of CFTR mutations without clinical evidence in the approved indication was based primarily on biological plausibility and was supported by the CF specialists who provided input for this review. Given the rarity of these mutations, the committee acknowledged the practical challenges with generating clinical evidence for the CFTR mutations included in the expanded indication. Overall, CDEC concluded that ELX-TEZ-IVA has the potential to provide clinically meaningful benefit to those patients who have CFTR mutations that have been shown to be responsive to ELX-TEZ-IVA.
Using the sponsor-submitted price for ELX-TEZ-IVA and publicly listed prices for all other drug costs, the incremental cost-effectiveness ratio (ICER) for ELX-TEZ-IVA was $1,122,823 per quality-adjusted life-year (QALY) compared with best supportive care. At this ICER, ELX-TEZ-IVA is not cost-effective at a $50,000 per QALY willingness-to-pay (WTP) threshold for patients aged 2 years and older with non-F508del mutations that are responsive to ELX-TEZ-IVA, based on in vitro and/or clinical data. A price reduction is required for ELX-TEZ-IVA to be considered cost-effective at a $50,000 per QALY threshold.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Confirmed diagnosis of CF with at least 1 of the mutations in the CFTR gene listed in Figure 1 of this document | The indication approved by Health Canada for ELX-TEZ-IVA is limited to patients with at least 1 mutation in the CFTR gene that has been shown to be responsive to ELX-TZ-IVA based on in vitro and/or clinical data. | Figure 1 lists the 152 non-F508del mutations in the CFTR gene that are identified in the product monograph as being responsive to ELX-TEZ-IVA based on in vitro and/or clinical data. |
2. Aged 2 years and older | The indication approved by Health Canada for ELX-TEZ-IVA is limited to patients who are aged at least 2 years. | — |
3. For patients aged 2 to 5 years: The following measurements must be completed before initiating treatment with ELX-TEZ-IVA: • number of days treated with oral and IV antibiotics for pulmonary exacerbations in the previous 6 months or number of pulmonary exacerbations requiring oral and/or IV antibiotics in the previous 6 months • weight, height, and BMI. | This must be done to establish baseline values to be used for renewal of reimbursement for treatment with ELX-TEZ-IVA. | Weight, height, and BMI for pediatric patients are collected and reported as z scores or percentiles in clinical practice in Canada. |
4. For patients aged 6 years and older: The following measurements must be completed before initiating treatment with ELX-TEZ-IVA: • baseline spirometry measurements of FEV1 in litres and percent predicted (baseline lung function should be measured within a 3-month period before beginning treatment with ELX-TEZ-IVA) • number of days treated with oral and IV antibiotics for pulmonary exacerbations in the previous 6 months or number of pulmonary exacerbations requiring oral and/or IV antibiotics in the previous 6 months • number of CF-related hospitalizations in the previous 6 months • weight, height, and BMI • CFQ-R Respiratory Domain score. | This must be done to establish baseline values to be used for renewal of reimbursement for treatment with ELX-TEZ-IVA. | Weight, height, and BMI for pediatric patients are collected and reported as z scores or percentiles in clinical practice in Canada. The CFQ-R instrument comprises age-appropriate versions for children aged 6 to 13 years (CFQ-C); their parents (who serve as a proxy for their child) (CFQ-P); and individuals who are aged at least 14 years (CFQ-R teen or adult version). |
Renewal | ||
5. For patients aged 2 to 5 years: For renewal after initial authorization, the physician must provide evidence of continuing benefit from treatment with ELZ-TEZ-IVA for subsequent renewal of reimbursement. Patients on therapy should be monitored for response (e.g., no decrease in BMI z score) using clinical judgment and/or standard procedures. | Clinical experts have noted that it is difficult to obtain objective measurements to assess response to treatment in patients aged 2 to 5 years. | — |
6. For patients aged 6 years and older: For the first renewal, the physician must provide at least 1 of the following to demonstrate benefit after 6 months of treatment with ELX-TEZ-IVA: 6.1. improvement of lung function by 5% of predicted or more, relative to baseline 6.2. a decrease in the total number of days for which the patient received treatment with oral and/or IV antibiotics for pulmonary exacerbations compared with the 6-month period before initiating treatment or a decrease in the total number of pulmonary exacerbations requiring oral and/or IV antibiotics compared with the 6-month period before initiating treatment 6.3. decreased number of CF-related hospitalizations at 6 months compared with the 6-month period before initiating ELX-TEX-IVA treatment 6.4. no decline in BMI (BMI z score in children) at 6 months compared with the baseline BMI assessment 6.5. improvement by 4 points or more in the CFQ-R Respiratory Domain scale. | The studies demonstrated that treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in lung function (improvement in ppFEV1), nutritional status (increase in BMI or BMI z score), health-related quality of life (increase in CFQ-R respiratory domain scores), and a reduced rate of pulmonary exacerbations, including events that required IV antibiotics and/or hospitalization. | Clinically significant improvements from baseline in lung function (ppFEV1) and health-related quality of life (measured with the CFQ-R) are typically reported as at least 5% and 4 points, respectively. Validated thresholds for clinically relevant improvements in the frequency of exacerbations, total number of days in hospital for CF-related reasons, total number of days of treatment with oral and/or IV antibiotics for pulmonary exacerbations, and nutritional status were not identified. Clinical expert input indicated that the goal of therapy is to improve nutritional status (i.e., increase BMI into the healthy range for age and sex) and to reduce the frequency of exacerbations and related health care use (i.e., antibiotic use and hospitalization). |
7. Assessment for clinical response should occur every 12 months. | Annual assessments will help ensure the treatment is used for those benefiting from the therapy and would reduce the risk of unnecessary treatment. | — |
Discontinuation | ||
8. Patient has undergone lung transplant. | Patients who have had a solid organ transplant were excluded from the main studies of ELX-TEZ-IVA and clinical experts in Canada indicated that the treatment should be discontinued in patients who have received lung transplant. | — |
Prescribing | ||
9. Prescribing of ELX-TEZ-IVA and monitoring of treatment response should be limited to CF specialists. | Care for patients with CF is complex and is managed through specialized CF clinics in Canada. | — |
10. ELX-TEZ-IVA should not be reimbursed in combination with other CFTR modulators. | There is no evidence for the use of ELX-TEZ-IVA in combination with other available CFTR modulators. 1. ELX-TEZ-IVA is a combination product containing the same active components as Symdeko (TEZ-IVA) and Kalydeco (IVA). 2. IVA is also a component of Orkambi (LUM-IVA). | — |
Pricing | ||
11. A reduction in price | The ICER for ELX-TEZ-IVA is $1,122,823 when compared with BSC. A price reduction of at least 79% would be required for ELX-TEZ-IVA to achieve an ICER of $50,000 per QALY compared to BSC. | — |
BMI = body mass index; BSC = best supportive care; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire – Revised; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LUM = lumacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; QALY = quality-adjusted life-year; RCT = randomized controlled trial; TEZ = tezacaftor; WTP = willingness-to-pay.
Discussion Points
Criteria for significant unmet need are met: Given the uncertainty in the clinical evidence, CDEC deliberated on ELX-TEZ-IVA considering the criteria for significant unmet need described in section 9.3.1 of the Procedures for Reimbursement Reviews. Considering the rarity and severity of CF caused by rare mutations in the CFTR gene (i.e., non-F508del mutations) and the absence of clinically effective alternative treatments, CDEC concluded that the available evidence reasonably suggests that ELX-TEZ-IVA has the potential to reduce morbidity and/or mortality associated with the disease.
CDEC discussed that ELX-TEZ-IVA will potentially addresses some of the unmet needs among patients with rare mutations for whom approved CFTR modulator therapies had not been previously available. Patients with CF with rare mutations continue to deal with the impact of living with CF symptoms and the complexity of managing its therapy, which together affect all aspects of an individual’s life and the lives of those around them. Patient input highlighted the following expectations for new treatment for CF: stopping or slowing the progression of disease, reducing the frequency of exacerbations, reducing or avoiding the development of comorbidities and disease complications, improving digestive health (attaining and maintaining a healthy weight), longer life expectancy, avoiding hospitalizations and reducing the need for invasive procedures, reducing the burden of daily therapy, improved quality of life (especially wellness, well-being, and the ability to contribute to society), and minimizing side effects. Given this input and the available evidence, CDEC concluded that ELX-TEZ-IVA potentially meets some important unmet needs identified by patients.
Renewal criteria: The committee noted that nearly all patients in Canada who are eligible for treatment with ELX-TEZ-IVA have initiated therapy. For those who have initiated treatment with ELX-TEZ-IVA, the clinical experts consulted by CDA-AMC and the sponsor indicated that initial renewal criteria were met for all patients in Canada who started the therapy and wanted to continue (i.e., 100% of patients met the renewal criteria recommended by CDA-AMC and/or applied by the public drug programs). The committee agreed with the clinical experts consulted by CDA-AMC that renewal criteria can be beneficial for evaluating the response to ELX-TEZ-IVA. This was identified as particularly valuable for the current expanded patient population, where the sponsor has not submitted any clinical data for 79 of the 152 new CFTR mutations included in the indication approved by Health Canada.
Early initiation of treatment: The committee noted that input from patient groups, clinician groups, and the clinical experts consulted by CDA-AMC emphasized the importance of initiating treatment with ELX-TEZ-IVA early in the disease course, aiming to prevent disease progression and irreversible damage. The clinical experts consulted by CDA-AMC noted that many parents and caregivers would seek to initiate treatment for their child as early as possible (i.e., beginning at 2 years of age) and are anxiously awaiting access to ELX-TEZ-IVA for those who could be eligible based on the expanded approval by Health Canada.
Ethical and equity considerations: CDEC discussed ethical and equity considerations related to ELX-TEZ-IVA, including the significant burden of living with CF. The committee discussed how the absence of an effective disease-modifying therapy for people living with non-F508del mutations can contribute to psychological distress and significant disparities in clinical outcomes and quality of life when compared to people with at least one F508del mutation. CDEC acknowledged that differential access to ELX-TEZ-IVA may also exacerbate health inequities for racialized individuals and people of other ethnicities in equity-deserving groups who are less likely to carry F508del mutations. As a result, CDEC recognized that expanding access to ELX-TEZ-IVA can improve access to treatment among people experiencing health disparities associated with rare CF mutations. The committee also discussed how the pricing of ELX-TEZ-IVA highlights the ethical challenges for priority setting between the needs of the population and the needs of a small number of individuals under limited health system resources.
CFTR mutations without clinical evidence: CDEC discussed the use of in vitro data and acknowledged the practical challenges of conducting clinical trials in populations with rare CFTR mutations (e.g., challenges with patient recruitment for very rare mutations, potential concerns of patients and investigators with clinical equipoise given the widespread adoption of CFTR modulators). CDEC discussed the ethical and equity challenges of not extending access to people with a rare non-F508del mutation for whom there were in vitro data and the expectation of biological plausibility that ELX-TEZ-IVA would be responsive.
Background
Trikafta (ELX-TEZ-IVA) is a fixed-dose combination product containing elexacaftor, tezacaftor, and ivacaftor co-packaged with ivacaftor. This is the fourth submission to CDA-AMC for ELX-TEZ-IVA. CDA-AMC has previously reviewed ELX-TEZ-IVA for the treatment of CF in patients who have at least one F508del mutation in the CFTR gene for those aged 12 years and older (final recommendation issued in August 2021), those aged 6 years and older (final recommendation issued in June 2022), and those aged 2 to 5 years (final recommendation issued in November 2023). The current review is for an expanded indication that would include 152 additional non-F508del mutations in the CFTR gene. The sponsor has categorized the additional CFTR mutations as follows:
Fischer rat thyroid (FRT)-responsive mutations supported by clinical data (68 mutations)
FRT-responsive mutations with no supporting clinical data available (79 mutations)
noncanonical splice mutations (4 mutations): 4 CFTR mutations that result in small amounts of functional, normal CFTR protein; the sponsor has reported that these mutations cannot be evaluated in the FRT system and provided some form of clinical data for each of the mutations included in the application
N1303K mutation: A CFTR mutation that was initially identified as nonresponsive to ELX-TEZ-IVA in the FRT in vitro that has subsequently been studied in a phase II clinical trial as well as an investigator-sponsored RWE study.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information:
a review of 1 double-blind, placebo-controlled randomized controlled trial (RCT) in FRT-responsive patients (Study 124; N = 307; 18 CFTR mutations); 1 long-term extension study (Study 125; same population as Study 124); 1 retrospective observational study (Study 14; N = 422; 64 CFTR mutations); and 4 nonrandomized studies involving patients with at least one N1303K mutation (Solomon et al. [2024] [N = 20], Burgel et al. [2023] [N = 8], Burgel et al. [2024] [N = 35], and Sadras et al. [2023] [N = 8])
patients’ perspectives gathered by Cystic Fibrosis Canada
input from public drug plans that participate in the Reimbursement Review process
3 clinical specialists with expertise diagnosing and treating adults and children living with CF
input from 3 clinician groups (Cystic Fibrosis Canada’s Accelerating Clinical Trials Network [CF CanACT], the Edmonton Adult Cystic Fibrosis Clinic and Calgary Adult Cystic Fibrosis Clinic, and the CF Canada Health Care Advisory Council)
a review of the pharmacoeconomic model and report submitted by the sponsor
a review of relevant ethical issues related to ELX-TEZ-IVA and CF caused by rare mutations in the CFTR gene.
Perspectives of Patients, Clinicians, and Drug Programs
Patient Input
Two submissions were received from CF Canada. Information from CF Canada was based on a focus group with people in Canada with rare mutations who are being treated with ELX-TEZ-IVA, people in Canada with rare mutations who do not have access to ELX-TEZ-IVA, and caregivers of people in Canada with rare mutations that cause CF. In addition, data were retrieved from a survey of patients and caregivers with access to ELX-TEZ-IVA that was conducted in 2021, medical and scientific publications, as well as the Canadian Cystic Fibrosis Registry. CF Canada also measured the burden of CF at the individual, family, health systems, and societal levels, from preliminary findings from phase I of the Burden of Disease Study, which is considered 1 of the most comprehensive studies of the burden of CF in the world. The second input was authored by a patient with end-stage CF with a rare class II mutation (M1101K).
According to the patient group, life-changing treatments are increasingly reaching the 4,445 people in Canada living with CF. Those born with CF today will live longer than those who came before them; however, many are still very ill and 1 in 7 people living with the disease today is ineligible for the treatments that are making such a positive difference for others with CF.
The input indicated that there are continued challenges for individuals living with CF from a health care and quality-of-life perspective, including those who are unable to benefit from recent life-changing treatments. For example, 40 people who died of CF in Canada in 2022 had a median age of 38 years; people in Canada with CF collectively had 17,000 clinic visits, spent 10,000 days in hospital, and spent nearly 6,000 days on IV antibiotics in 2022; and 1 in 5 adults in Canada with CF has depression or anxiety recorded as a complication in the CF Registry. As the disease progresses, more time and effort are needed for frequent clinic visits and hospital stays to manage progressive and debilitating symptoms. This overwhelming treatment regimen has many side effects and a significant impact on patients’ and caregivers’ day-to-day activities and quality of life, and creates a substantial financial burden for families.
Data from the Canadian Cystic Fibrosis Registry on people in Canada with CF who do not currently have a Health Canada–based indication for modulators show that 246 patients have rare mutations known to respond to ELX-TEZ-IVA. The patient input indicated that many of these patients come from diverse and often racialized backgrounds, that they may already experience inequities in health care systems that were not designed with them in mind, and that they deserve the right to try ELX-TEZ-IVA (including those patients with mutations for which evidence is limited).
Patients with rare mutations and their caregivers shared their hopes to access ELX-TEZ-IVA as they saw the benefits of the medications for those who were able to access it. Very few people in Canada with CF rare mutations have access to ELX-TEZ-IVA. Those who reported taking ELX-TEZ-IVA responded exceptionally well to therapy, even those with mutations for which clinical evidence is scarce.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the review of ELX-TEZ-IVA, a panel of 3 clinical experts provided input to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with CF, and explore the potential place in therapy of the drug. A summary of input from the clinical experts follows.
Unmet Needs
There are significant unmet therapeutic needs for all patients living with CF. There are no treatments currently available that can effectively achieve the most important goals of therapy (prolonging survival, preventing the need for lung transplant, preventing an accelerated decline in lung function over time, and reversing the course of the disease). In addition, the current standard treatments are burdensome for patients and their caregivers. Patients may not experience a response or may stop experiencing a response over time to the currently available treatments. The majority of patients with a non-F508del mutation that is responsive to ELX-TEZ-IVA do not currently have access to therapy with a CFTR modulator.
Place in Therapy
ELX-TEZ-IVA is a CFTR modulator that functions by increasing the amount of CFTR protein at the cell surface (elexacaftor and tezacaftor) and by improving the transport of chloride through the CFTR protein (ivacaftor). The mechanism of action for ELX-TEZ-IVA is attractive because it acts directly on the CFTR protein to address the defects that are responsible for the CF phenotype. ELX-TEZ-IVA would be added to existing treatments such as physiotherapy, mucolytics, anti-infectives, and anti-inflammatory treatments (such as azithromycin). The clinical experts noted that ELX-TEZ-IVA has replaced earlier CFTR modulators that are significantly less effective (e.g., Orkambi and Kalydeco) for patients with at least one F508del mutation in the CFTR gene. For the current target patient population, the clinical specialists anticipate that all patients in the expanded population (i.e., with a non-508del mutation that is responsive to ELX-TEZ-IVA) would be considered candidates for the therapy. This would include those with a gating mutation who are currently receiving treatment with Kalydeco, provided they meet eligibility and age criteria.
It is anticipated that ELX-TEZ-IVA would be used as a preventive therapy with the goal of initiating treatment before the patient develops significant lung disease. The current treatment paradigm would be significantly altered if ELX-TEZ-IVA can successfully prevent or delay progression to end organ disease (e.g., lung transplant).
The indication currently under review is for patients aged 2 years or older. CDA-AMC has previously recommended that ELX-TEZ-IVA be reimbursed for patients aged 2 to 5 years and those aged 6 years or older. The clinical experts consulted for this review and those who previously responded to the call for clinician input noted that children aged between 2 and 5 years will often have structural lung disease (e.g., bronchial wall thickening, mucus plugging, bronchiectasis),1 but that detection is challenging using the tools that are available to evaluate lung function in clinical practice (i.e., spirometry) or as part of a research protocol (e.g., lung clearance index). However, despite younger patients with CF often demonstrating normal lung function, the early stages of lung abnormalities can be visualized using CT, and the underlying disease will continue to progress.1
All of the clinicians who provided input for this review recommended initiating treatment with ELX-TEZ-IVA as soon as possible. This is aligned with the previously published Canadian Clinical Consensus Guideline for Initiation, Monitoring and Discontinuation of CFTR Modulator Therapies for Patients with Cystic Fibrosis, which also recommended that CFTR modulators be initiated at the youngest age possible with the goal of attenuating disease progression and improving clinical status. All contributors agreed that there are no data to support withholding the initiation of CFTR modulator treatment until clinical symptoms of CF have developed.
Patient Population
The diagnosis of CF is not challenging in routine clinical practice. All provinces and territories have instituted newborn screening for CF, so most people with CF are now identified via newborn screening and have a confirmed diagnosis by 1 month of age (on average). Sweat chloride testing is available and reliably used to confirm the screening test. The provinces and territories have slightly different testing algorithms and CFTR mutation screening panels; however, all provinces and territories have effective processes. Almost 100% of newly diagnosed infants would have their CFTR mutations identified. Infants who are not identified via newborn screening (i.e., false negatives) are usually diagnosed before 1 year of age after the development of clinical symptoms of CF. There are clear diagnostic guidelines and very little variability in expert opinion. Misdiagnosis and underdiagnosis of CF is exceedingly rare in Canadian clinical practice.
ELX-TEZ-IVA could be used in every patient who meets the Health Canada–approved indication, regardless of their current or past treatment regimens. From a medical perspective, there is no rationale for a patient to demonstrate an inadequate response or loss of response to prior therapies before initiating treatment with ELX-TEZ-IVA. It would be reasonable to require patients to complete important standard CF therapies in conjunction with ELX-TEZ-IVA. In clinical practice, eligible patients would be identified based on their CFTR genotype, and all patients would be expected to respond to the treatment.
For the expanded indication (i.e., with a non-F508del mutation that is responsive to ELX-TEZ-IVA), the clinical experts consulted by CDA-AMC noted that nearly all patients would initiate therapy with ELX-TEZ-IVA as soon as possible, provided it is safe to start treatment. The clinical experts emphasized that ELX-TEZ-IVA has been a transformative and disease-modifying therapy for CF and that it would not be appropriate to wait until the patient shows worsening symptoms, more frequent exacerbations, or a decline in lung function to initiate treatment with ELX-TEZ-IVA.
Applicability of Existing Reimbursement Criteria to the Expanded Population
In discussions with CDA-AMC, the sponsor noted that nearly all patients in Canada aged 6 years or older who are eligible for treatment have initiated therapy with ELX-TEZ-IVA (some may have elected to discontinue, but all who are interested have been given the opportunity to access the drug). For those who have initiated treatment with ELX-TEZ-IVA, the sponsor noted that initial renewal criteria were met for all patients in Canada who started the therapy and wanted to continue (i.e., 100% of patients met the renewal criteria recommended by CDA-AMC and/or applied by the public drug programs). The clinical experts consulted expressed general agreement with the sponsor’s position, noting that rates of initial access and renewal are very high within their individual clinics. With nearly all patients currently meeting the renewal criteria recommended by CDA-AMC, the sponsor noted that the requirement for these assessments is consuming health care resources (e.g., time required by health care practitioners to administer and document results for each of the required tests) without adding value to patients or the health care system.
The clinical experts consulted by CDA-AMC supported the application of the existing criteria recommended for the reimbursement of ELX-TEZ-IVA. Consistent with input from the participating drug programs, the clinical experts noted that the lack of alignment across CDA-AMC recommendations for the reimbursement of ELX-TEZ-IVA in patients with and without at least one F508del mutation could generate implementation challenges in clinical practice.
Clinician Group Input
Three groups of clinicians responded to the call for input: CF CanACT, the Edmonton Adult Cystic Fibrosis Clinic and Calgary Adult Cystic Fibrosis Clinic, and the CF Canada Health Care Advisory Council. The input from the clinician groups identified the same unmet medical needs for patients with CF and potential place in therapy for the drug under review as the clinical experts consulted for this review. The clinician groups noted that there is a significant treatment gap in CF care. Ten percent (n = 246) of patients with CF in Canada with rare mutations who do not carry a copy of the F508del CFTR mutation but may be responsive to ELX-TEZ-IVA do not have access to the drug, as no clinical trials have been conducted. The CF Canada Health Care Advisory Council added that lung transplant recipients, especially those with significant sinus disease, may still benefit from CF modulator therapy; however, they were excluded from the clinical trials.
According to the clinician groups, any patient who carries at least 1 CFTR mutation that is responsive to ELX-TEZ-IVA should have access to this therapy. CF CanACT added that for those with rare CFTR mutations, for whom data to support the use of ELX-TEZ-IVA are very limited, it is incumbent on regulators to use all available evidence or to generate the evidence needed to allow access to this life-saving drug, as each patient’s life may depend on access to it.
Drug Program Input
The clinical experts consulted by CDA-AMC provided advice on the potential implementation issues raised by the drug programs.
Table 2: Responses to Questions From the Drug Programs
Drug program implementation questions | CDEC response |
|---|---|
Considerations for initiation of therapy | |
The participating drug programs noted that CDA-AMC has previously issued recommendations for ELX-TEZ-IVA for patients aged 2 to 5 years and patients aged 6 years or older who have at least one F508del mutation in the CFTR gene. The participating drug programs requested that the expert committee consider aligning with the initiation criteria for other ELX-TEZ-IVA recommendations, if appropriate. | The committee agreed that alignment with the criteria that were previously specified by CDEC in the recommendations issued for ELX-TEZ-IVA was appropriate for the current review. |
Considerations for continuation or renewal of therapy | |
The participating drug programs noted that CDA-AMC has previously issued recommendations for ELX-TEZ-IVA for patients aged 2 to 5 years and patients aged 6 years or older who have at least one F508del mutation in the CFTR gene. The participating drug programs requested that the expert committee consider aligning with the renewal criteria for other ELX-TEZ-IVA recommendations, if appropriate. | The committee agreed that alignment with the criteria that were previously specified by CDEC in the recommendations issued for ELX-TEZ-IVA was appropriate for the current review. |
The participating drug programs noted that the sponsor has requested that “clinical benefit as determined by physician specializing in the treatment of CF” be included as 1 of the initial renewal criteria. Could the clinical experts and expert committee comment on the appropriateness of this criterion? | The committee agreed with the clinical experts consulted by CDA-AMC that renewal criteria can be beneficial for evaluating the response to ELX-TEZ-IVA. This was identified as particularly valuable for the current expanded patient population, where the sponsor has not submitted any clinical data for 79 of the 152 new CFTR mutations included in the indication approved by Health Canada. |
Considerations for discontinuation of therapy | |
The participating drug programs noted that CDA-AMC has previously issued recommendations for ELX-TEZ-IVA for patients ages 2 to 5 years and patients ages 6 years and older who have at least 1 F508del mutation in the CFTR gene. The participating drug programs requested that the expert committee consider aligning with the discontinuation criteria for other ELX-TEZ-IVA recommendations, if appropriate. | The committee agreed that alignment with the criteria that were previously specified by CDEC in the recommendations issued for ELX-TEZ-IVA was appropriate for the current review. |
CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
In Vitro Evidence
Overview of In Vitro FRT Assay
The sponsor used an in vitro FRT cell model to characterize individual CFTR mutations that produce at least some amount of full-length CFTR protein, for responsiveness to CFTR modulators. The model expressed a CFTR gene with a single CFTR mutation to test for responsiveness to CFTR modulators. Each FRT cell line is engineered to express a specific CFTR mutation in a stable epithelial cell background. CFTR mutations selected for inclusion in the FRT assay study were those that were expected to produce full-length CFTR protein. Protein-truncating CFTR mutations, whole or partial CFTR gene deletions, and noncanonical splice mutations were excluded from the in vitro study. Positive controls and negative controls were also included in the experiments.
The positive controls included G551D and R117H, which were noted in previous FRT assays to be IVA-responsive and have been demonstrated in clinical trials to provide clinical benefit for patients (IVA is approved for use in the treatment of CF in patients who have a G551D and R117H CFTR mutation).
The negative controls included G1061R, R1066C, N1303K and untransfected FRT cells. These 3 CFTR mutations were identified as mutations that were nonresponsive to IVA or TEZ-IVA in previous in vitro assays.
The function of CFTR at the cell surface was assessed in an Ussing chamber study, a procedure that quantifies the amount of CFTR-mediated chloride transport in FRT cells expressing each mutation that CFTR forms as a fraction of the chloride transport in FRT cells expressing normal CFTR (% normal).
Definition of In Vitro Responsive to ELX-TEZ-IVA
Responsive CFTR mutations were those that demonstrated an increase of 10% in chloride transport over baseline when expressed as a percentage of normal CFTR chloride transport. The sponsor selected this threshold because the analyses of CFTR activity and disease phenotype showed that a 10% increase in CFTR activity is associated with improved clinical status. The sponsor reported that patients with a severe CF phenotype generally have CFTR function less than 5% of normal, whereas the severity of CF begins to diminish in patients who have CFTR function at least 10% of normal. An increase in CFTR function of 10% or more is therefore expected to affect the disease phenotype for those living with CF.2
CFTR Mutations Identified as Responsive to ELX-TEZ-IVA
Using the in vitro FRT model, the sponsor identified 177 CFTR mutations as responsive to ELX-TEZ-IVA. These additional mutations do not include F508del, which has been studied in multiple clinical trials already reviewed by CDEC. Importantly, the sponsor notes that the 10% threshold for responsive should be considered conservative, citing the following additional mutations that have been included in this Reimbursement Review application:
The N1303K mutation did not meet the 10% threshold in the FRT model to be considered responsive to ELX-TEZ-IVA (as noted above, this mutation was chosen as 1 of the negative controls for the FRT model). However, the sponsor has filed submissions with Health Canada and CDA-AMC on the basis of real-world evidence that has suggested that these patients benefit from treatment with ELX-TEZ-IVA.
The R117C and S1255P mutations included in this Reimbursement Review application did not meet the 10% threshold for the FRT assay; however, previous in vitro FRT data and/or clinical data support the responsiveness of these mutations to IVA and/or TEZ-IVA (both of which are components of ELX-TEZ-IVA).
Regulatory Perspective
The data derived from the FRT cell model were considered acceptable evidence by Health Canada to expand the indication for ELX-TEZ-IVA to 152 additional mutations sought by the sponsor. The sponsor’s application was filed on a pre-NOC basis and included an additional 31 CFTR mutations that were not approved by Health Canada for the following reasons.
There were 15 mutations considered by Health Canada not to be causative of CF, based on the CFTR2 and CFTR-France databases: D836Y, F508C, G576A, I148T, I807M, I1027T, L320V, L997F, R75Q, R170H, R668C, R1162L, T1053I, V562I, and V754M.
There were 10 mutations excluded due to unknown clinical significance, or only reported as causing a CFTR-related disease (i.e., not CF), and which retained at least 50% of normal chloride transport function: G178E, G576A;R668C, I1139V, K1060T, R31L, R553Q, R751L, R792G, V1293G, Y1014C.
There were 5 mutations excluded because they resulted in a cryptic splice mutation and insufficient full-length CFTR: H939R, I175V, M152V, E403D, and S589N.
There was 1 mutation excluded due to the absence of in vitro or clinical data provided in the current submission: E831X.
Health Canada concluded that the CFTR mutations for which the sponsor has provided sufficient clinical evidence of efficacy are also among those more commonly harboured by patients with CF in Canada. As such, the expansion of the indication for ELX-TEZ-IVA would be expected to significantly expand access to effective CF therapy in Canada. They noted that the inclusion of other CFTR variants to the product monograph as being responsive to ELX-TEZ-IVA treatment is based mainly on biological plausibility. In cases where the mutation is known to have the potential to cause CF due to the production of a dysfunctional full-length CFTR variant that has demonstrated in vitro responsiveness to ELX-TEZ-IVA (i.e., FRT-responsive mutations), or when a reduced amount of CFTR is produced and its function can be augmented (i.e., splicing mutations), ELX-TEZ-IVA treatment has the potential to provide clinically meaningful benefit to patients.
Clinical Expert Commentary on In Vitro Evidence
The clinical experts consulted by CDA-AMC noted that responsiveness to ELX-TEZ-IVA using the in vitro model applied by Vertex in the clinical development program for patients with rare CFTR mutations is sufficient evidence to support prescribing for these patients. In addition to regulatory approval based on this information (e.g., FDA approvals), the clinical experts cited the following considerations that would support the use of ELX-TEZ-IVA in clinical practice:
the lack of alternative treatment options for these patients and the severe progressive nature of CF
in vitro data demonstrating activity on the CFTR channel for patients with these rare mutations supports extrapolation of the clinical benefit demonstrated in studies involving more common CF-causing mutations in the CFTR gene
concerns about equity for those living with CFTR mutations where the incidence is sufficiently low to preclude the generation of robust clinical evidence. The clinical experts noted CF with a non-F508del mutation is more likely to be diagnosed in racialized individuals who may already be encountering systemic inequities within the health care system. Based on the rarity of these rarer mutations, it would be impossible to include participants with every mutation in clinical trials. The current focus on clinical trial data alone for drug approval is resulting in inequities based on race and ethnicity in medication access. It is well known that patients from equity-deserving groups are underrepresented in clinical trials for a multitude of reasons (refer to the Ethics Report for additional discussion on these issues)
the mounting body of evidence from case reports, case series, and clinical experience demonstrating that ELX-TEZ-IVA can have a clinically meaningful impact for patients with rare CFTR mutations shown to be responsive based on in vitro data.
In addition, the clinical experts noted that patients with CF living in Canada are monitored in specialized clinics with well-organized and frequent clinical and laboratory evaluations to ensure the treatment is used appropriately and safely in clinical practice. The clinical specialists emphasized that the in vitro data should not be viewed in insolation and that it is important to consider the large body of evidence demonstrating the clear clinically important benefits of ELX-TEZ-IVA and the relatively few serious harms with the treatment (i.e., this is no longer a new drug in the management of CF). Overall, the specialists noted that the totality of information, including real-world experience with the drug for those with at least one F508del mutation, supports the expanded use of the drug for those with rare CFTR mutations.
Clinical Evidence
Systematic Review
Description of Studies
Evidence supporting the use of ELX-TEZ-IVA in the expanded population consisted of the following: 1 double-blind, placebo-controlled RCT in patients with FRT-responsive mutations (Study 124; N = 307; 17 Health Canada–approved CFTR mutations); 1 long-term extension study (Study 125; same population as Study 124); 1 retrospective observational study (Study 16; N = 422; 64 Health Canada–approved CFTR mutations); 4 nonrandomized studies involving patients with at least one N1303K mutation (Solomon et al. [2024] [N = 20]; Burgel et al. [2023] [N = 8]; Burgel et al. [2024] [N = 35]; Sadras et al. [2023] [N = 8]). The sponsor reported that there were no clinical data for 79 FRT-responsive mutations approved by Health Canada (i.e., those that were considered responsive to ELX-TEZ-IVA in the in vitro model) and 1 of the noncanonical splice mutations.
The objective of Study 124 was to evaluate the efficacy, pharmacodynamics, and safety of ELX-TEZ-IVA in patients with a non-F508del ELX-TEZ-IVA-responsive CFTR mutation. This study was a phase III, double-blinded, randomized placebo-controlled trial. Patients aged 6 years or older were recruited from 84 sites across Europe and Canada and randomized, with 205 patients enrolled in the ELX-TEZ-IVA treatment arm and 102 participants enrolled in the placebo-controlled arm.
Eligible participants included those with a non-F508del ELX-TEZ-IVA-responsive CFTR mutation based on the FRT assay with no exclusionary CFTR mutations (i.e., F508del, S549N, G551S, S1255P, R117H, S549R, G1244E, G1349D, G178R, G551D, or S1251N). The sponsor reported that 18 of the most prevalent CFTR mutations in Europe and Canada that are not currently indicated for a CFTR modulator were eligible (representing approximately 80% of the target patient population). The use of ELX-TEZ-IVA was approved by Health Canada for 17 of the 18 CFTR mutations included in Study 124 (1 mutation [L997F] was excluded by Health Canada on the basis that it has not been demonstrated to be causative of CF). Patients had to have a percent predicted forced expiratory volume in 1 second (ppFEV1) value between 40% and 100% of the predicted mean for age, sex, and height. Patients were excluded if they had an acute upper or lower respiratory infection, pulmonary exacerbation (PEx), change in therapy (including antibiotics) for sinopulmonary disease within 28 days before the first dose of the study drug, or lung infection with organisms associated with a more rapid decline in pulmonary status (including, but not limited to, Burkholderia cenocepacia, B. dolosa, and Mycobacterium abscessus).
ELX-TEZ-IVA was orally administered as fixed-dose combination tablets in the morning along with an oral administration of IVA tablets taken in the evening. Placebo-arm treatments were matched to both ELX-TEZ-IVA and IVA administrations in dose and timing.
The primary end point was change from baseline in ppFEV1 through 24 weeks. Secondary end points included absolute change from baseline in SwCl (through 24 weeks), CFQ-R RD score (through 24 weeks), BMI and BMI z score (at 24 weeks), and body weight and body weight z score (at 24 weeks). PEx was also a secondary end point in Study 124.
Efficacy Results
Treatment with ELX-TEZ-IVA resulted in a statistically significant improvement in ppFEV1 compared with placebo through 24 weeks (least squares [LS] mean difference = 9.2% [95% CI, 7.2 to 11.3]; P < 0.0001). The reduction from baseline was observed at all postbaseline assessments (i.e., 2, 4, 8, 16, and 24 weeks).
Those in the ELX-TEZ-IVA group also demonstrated a statistically significant improvement in CFQ-R RD score compared with those in the placebo group (LS mean difference = 19.5 points [95% CI, 15.5 to 23.5]; P < 0.0001). This difference exceeded the minimally important difference (MID) for the CFQ-R RD, which is typically cited to be 4.0 points.
Patients in the ELX-TEZ-IVA group had estimated pulmonary exacerbation event rate per year of 0.17 compared with 0.63 in the placebo group (rate ratio = 0.28 [95%CI, 0.15 to 0.51]; P < 0.0001). Compared with placebo, treatment with ELX-TEZ-IVA also demonstrated statistically significant reductions in SwCl through 24 weeks (LS mean difference = −28.3 mmol/L [95% CI, −32.1 to −24.5]; P < 0.0001); an increase in body weight at 24 weeks (LS mean difference = 1.3 kg [95% CI, 0.6 to 1.9]; P < 0.0001); an increase in BMI at 24 weeks (LS mean difference = 0.47 kg/m2 [95% CI, 0.24 to 0.69]; P < 0.0001). In the subset of patients younger than 20 years, there was no statistically significant difference with ELX-TEZ-IVA compared with placebo for absolute change from baseline in body weight z score (LS mean difference = 0.06 [95% CI, −0.06 to 0.18]) or BMI z score (LS mean difference = 0.08 [95% CI, −0.06 to 0.22]).
Harms Results
The proportion of patients who experienced at least 1 adverse event (AE) was 94.1% in the ELX-TEZ-IVA group and 95.1% in the placebo group. The majority of AEs were mild or moderate in severity. Serious adverse events (SAEs) occurred in 18 patients (8.8%) in the ELX-TEZ-IVA group and 15 patients (14.7%) in the placebo group. SAEs that occurred in at least 2 patients in the ELX-TEZ-IVA group included infective PEx of CF (5 patients) and bronchopulmonary aspergillosis allergic (2 patients). The only SAE that occurred in at least 2 patients in the placebo group was infective PEx of CF (13 patients). Drug interruptions due to AEs were reported in 12.2% of patients in the ELX-TEZ-IVA group and 1.0% in the placebo group.
████████ ████████████ ██████ ████ ██████████ ██ ███████ █████ ██ ███████ ████████ ██████ ███ ████████ ██ █ ██████ ████████ ██ ███ ███████████ █████ ███ ██ ████████ ██ ███ ███████ █████. All elevated transaminase events were mild or moderate in severity, and none were serious. Rash events were also considered an adverse event of special interest (AESI) and occurred in 55 patients (26.8%) in the ELX-TEZ-IVA group and 3 patients (2.9%) in the placebo group. The majority of rash events were mild or moderate in severity. One patient (0.5%) in the ELX-TEZ-IVA group had a serious rash event that was considered related to the study drug treatment. Health Canada reviewers noted that long-term safety has already been established for ELX-TEZ-IVA and that there are no data from the pivotal clinical study to indicate the existence of CFTR genotype–dependent safety concerns.
Critical Appraisal
Baseline and demographic characteristics were generally well balanced across the ELX-TEZ-IVA and placebo groups in Study 124. Study treatments (ELX-TEZ-IVA and placebo) were administered in a double-blind manner. The AE profile of ELX-TEZ-IVA was unlikely to compromise blinding in the study, with the exception of those who experienced a rash (a well-known AE associated with ELX-TEZ-IVA treatment) after initiating treatment (22% in the ELX-TEZ-IVA group versus 1% in the placebo group). Patient disposition was thoroughly documented and well reported by the sponsor in their application to CDA-AMC. There were few patients who discontinued the trials (completion rate was 96.1% with ELX-TEZ-IVA and 100% with placebo). Adherence to the study treatments was reported to be more than 98.9%.
Study 124 evaluated the impact of ELX-TEZ-IVA on a range of different outcomes that are important in the management of CF. These included respiratory function (i.e., ppFEV1), nutritional status and growth (e.g., weight and BMI), HRQoL (CFQ-R), and clinical events (e.g., pulmonary exacerbations). As noted in the input from clinician groups, the end points that were in the clinical trials largely align with those that are evaluated in routine clinical practice. Spirometry measurements were standardized and performed according to the American Thoracic Society Guidelines (e.g., pre-bronchodilator and before dosing). There are no globally accepted definitions for pulmonary exacerbations in patients with CF. The definitions used in Study 124 were considered to be appropriate by regulatory authorities and the clinical experts consulted by CDA-AMC. The key secondary end points were tested using a hierarchical approach to control the overall type I error rate at 0.05.
The diagnostic criteria used in the screening process for Study 124 were consistent with Canadian clinical practice for identifying patients with CF. The sponsor and clinical experts consulted for this review reported that all patients with CF in Canada have their genotype evaluated, and hence the identification of those who could be considered candidates for ELX-TEZ-IVA based on the expanded patient population would not be problematic in practice. As with previous CFTR modulator studies, Study 124 excluded patients with a history of colonization with B. cenocepacia, B. dolosa, and/or M. abscessus. CDA-AMC committees have previously acknowledged the unmet need for these patients.
The use of placebo as the comparator in Study 124 is appropriate, given that CFTR modulators are not approved for the target patient population except for the subset of patients who have a CFTR gating mutation and are currently eligible for treatment with Kalydeco. Study 124 investigated the use of ELX-TEZ-IVA at the dosage recommended in the Canadian product monograph. All studies compared the addition of the study treatments to ongoing standard CF management therapies, which is reflective of how ELX-TEZ-IVA and other CFTR modulators would be administered in clinical practice. In general, the background therapies that were reported at baseline in the included studies were consistent with those used in Canadian clinical practice.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The list of outcomes shown in Table 3 was finalized in consultation with expert committee members.
Table 3: Summary of Findings for ELX-TEZ-IVA Versus Placebo From RCT
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | ELX-TEZ-IVA | Difference | |||||
Pulmonary function | |||||||
Absolute mean change from baseline in ppFEV1 Follow-up: 24 weeks | 290 (1 RCT) | NA | −0.4% (−2.0% to 1.3%) | 8.9% (7.7% to 10.0%) | 9.2% higher (7.2% to 11.3% higher) | Higha | ELX-TEZ-IVA results in an improvement in ppFEV1 compared with placebo. |
Pulmonary exacerbations | |||||||
Annualized event rate of PEx Follow-up: 24 weeks | 307 (1 RCT) | Rate ratio: 0.28 (0.15 to 0.51) | 0.63 events per year (95% CI, NR) | 0.17 events per year (95% CI, NR) | Absolute effects not reported by sponsor | Cannot evaluateb | ELX-TEZ-IVA likely results in an improvement in frequency of PEx compared with placebo. |
Body mass index | |||||||
Absolute mean change from baseline in BMI Follow-up: 24 weeks | 307 (1 RCT) | NA | 0.35 kg/m2 (0.16 to 0.53) | 0.81 kg/m2 (0.68 to 0.94) | 0.47 kg/m2 higher (0.24 to 0.69 higher) | Highc | ELX-TEZ-IVA results in an improvement in BMI compared with placebo. |
Absolute mean change from baseline in BMI z score Follow-up: 24 weeks | 78 (1 RCT) | NA | 0.14 (0.03 to 0.25) | 0.22 (0.14 to 0.30) | 0.08 higher (−0.06 to 0.22) | Moderated | ELX-TEZ-IVA likely results in an improvement in BMI z score compared with placebo. |
Health-related quality of life | |||||||
Absolute mean change from baseline in CFQ-R RD Follow-up: 24 weeks | 304 (1 RCT) | NA | −2.0 points (−5.2 to 1.3) | 17.5 points (15.2 to 19.8) | 19.5 points higher (15.5 to 23.5) | Highe | ELX-TEZ-IVA results in an improvement in CFQ-R RD compared with placebo. |
Sweat chloride | |||||||
Absolute mean change from baseline in SwCl Follow-up: 24 weeks | 300 (1 RCT) | NA | 0.5 mmol/L (−2.6 to 3.6) | −27.8 mmol/L (−30.0 to −25.6) | −28.3 mmol/L lower (−32.1 to −24.5) | Moderatef | ELX-TEZ-IVA results in a reduction in SwCl compared with placebo. |
Harms | |||||||
Elevated transaminase levels | 307 (1 RCT) | NA | █████ | █████ | NA | Moderateg | ELX-TEZ-IVA may increase in frequency of elevated transaminases compared with placebo.h |
Rash | 307 (1 RCT) | NA | 3 (2.9%) | 55 (26.8%) | NA | Moderateg | ELX-TEZ-IVA may increase in frequency of rash compared with placebo.i |
ALT = alanine transaminase; AST = aspartate transaminase; BMI = body mass index; CF = cystic fibrosis; CFQ-R RD = Cystic Fibrosis Questionnaire – Revised (Respiratory Domain); CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; MID = minimally important difference; NA = not applicable; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; SwCl = sweat chloride.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aWhile no published information on the MID in absolute change in ppFEV1 in CF was identified, the clinical experts consulted during this review noted that CF specialists would generally consider an absolute improvement in ppFEV1 of at least 5% to be clinically relevant.
bCertainty of evidence cannot be evaluated, as the sponsor did not report the absolute difference between groups and did not provide this information upon request. While no published information on the MID for reducing PEx in CF was identified, the clinical experts consulted during this review noted that CF specialists would generally consider the reduction in PEx observed in the study to be clinically relevant.
cWhile no published information on the MID for absolute change in BMI in CF was identified, the clinical experts consulted during this review noted that CF specialists would generally consider the improvements observed in the study to be clinically relevant.
dRated down 1 level for imprecision due to smaller sample size and wide CIs.
eA difference of at least 4 points in the respiratory domain score of the CFQ-R is commonly cited as the MID for patients with CF.
fRated down 1 level for indirectness because SwCl is a biomarker, and evidence for a relationship between SwCl and clinical outcomes is uncertain.
gBetween-group differences in harms were not statistically tested.
hThe product monograph provides recommendations for baseline assessment and ongoing monitoring of ALT and AST. The clinical experts consulted during this review noted that these recommendations for monitoring are typically followed in clinical practice and that patients in Canada are monitored in specialized clinics.
iStudy 124 demonstrated that discontinuations due to rash were uncommon and the clinical experts consulted during the review similarly noted that these events do not typically result in long-term discontinuation of the treatment.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Long-Term Extension Studies
Description of Studies
Study 125 is an open-label, long-term extension phase of Study 124 conducted to assess the long-term safety and efficacy of ELX-TEZ-IVA in patients with CF aged 6 years and older with non-F508del mutations in the CFTR gene that are responsive based on clinical and/or in vitro data. The data cut-off date included in the submission to CDA-AMC was August 28, 2023, and results were included for 4 weeks after the end of Study 124. Fifteen patients who were randomized to placebo in the parent study had been treated with ELX-TEZ-IVA for a total of 4 weeks, and those who were randomly assigned to ELX-TEZ-IVA in Study 124 had been treated for a total of 28 weeks.
Efficacy Results
Those who switched from placebo to ELX-TEZ-IVA demonstrated improvements in ppFEV1 (mean change = 7.1%; standard deviation [SD] = 7.3), SwCl (mean change = −27.4 mmol/L [SD = 18.9]), and CFQ-R RD (mean change = 14.7 points [SD = 22.6]) after receiving ELX-TEZ-IVA for 4 weeks. For those who received ELX-TEZ-IVA in the parent study, improvements in ppFEV1 (mean change = 10.1% [SD = 11.0]), SwCl (mean change = −30.3 mmol/L [SD = 21.9]), and CFQ-R RD (mean change = 20.1 points [SD = 20.7]) were maintained after 4 additional weeks.
Harms Results
Harms data were not yet reported for Study 125.
Critical Appraisal
Study 125 is an ongoing, uncontrolled, open-label trial that enrolled patients who had completed Study 124. As this is an unblinded extension phase, patients’ expectations of treatment could influence the reporting of subjective outcomes, such as respiratory symptoms (as measured by the CFQ-R) or harms. Extension studies are often limited by selection bias, as only patients who are tolerant to treatment and complete the parent studies are eligible to enroll. For Study 125 and other ELX-TEZ-IVA studies, the risk of selection bias is generally low, given that nearly all patients from the primary study enroll in the extension study. Overall, there are limited data from the extension phase, given that only 4 weeks of additional data were available. Issues with the generalizability of these data are the same as for Study 124 (e.g., patient population reflective of those with mild to moderate disease; exclusion of patients with unstable disease or colonization with B. cepacia complex; increased exposure to health care professionals).
Indirect Comparisons
The sponsor reported that an indirect treatment comparison (ITC) is not required for approximately 80% of the patients in the target patient population because no CFTR modulators are currently approved for use in these patients. The remaining 20% of patients in the target patient population could be eligible for treatment with ivacaftor monotherapy (Kalydeco). The sponsor conducted a feasibility assessment to determine whether an ITC could be performed to inform the comparative clinical benefits of ELX-TEZ-IVA versus ivacaftor monotherapy. The sponsor concluded that it was not feasible to conduct a robust ITC due to uncertainty in the degree of population overlap, low individual patient data sample sizes, incompatibility of outcomes, and differences in the treatment history and follow-up time.
CDA-AMC has no concerns regarding the absence of an ITC for the following reasons:
The dosage of ivacaftor administered as part of the ELX-TEZ-IVA combination regimen is the same as patients would receive with ivacaftor monotherapy (i.e., 150 mg in the morning and 150 mg in the evening).
Previous trials have demonstrated that patients with at least one F508del mutation and a gating mutation benefited from switching to ELX-TEZ-IVA from ivacaftor monotherapy.
The submitted price for ELX-TEZ-IVA is the same as the current list price for ivacaftor monotherapy.
Studies Addressing Gaps in the Evidence From the Systematic Review
Clinical evidence from 5 additional studies addressing gaps in evidence were included in the review:
1 study involving patients with 64 FRT-responsive CFTR mutations (Study 16 [N = 422])
4 studies involving patients with at least one N1303K mutation (Solomon et al. [2024] [N = 20], Burgel et al. [2023] [N = 8], Burgel et al. [2024] [N = 35], and Sadras et al. [2023] [N = 8]).
The sponsor included evidence from 3 additional abstracts and/or publications for patients with at least one N1303K mutation (Dreano et al. [2023], Livnat et al. [2023], and Pranke et al. [2022]). These studies have not been summarized in this report as CDA-AMC concluded that they do not address a gap in the evidence relative to the larger studies submitted in support of the expanded use of ELX-TEZ-IVA for patients with CF who have at least one N1303K mutation in the CFTR gene. In addition to the smaller sample sizes, the following additional concerns were noted:
The reporting of these studies is insufficient for CDA-AMC to full appraisal the methodology used in the evaluation of patients.
The publications by Dreano et al. (2023) and Pranke et al. (2022) refer to the same source of patients that was used in the larger studies reported by Burgel et al. (2023) (N = 8) and Burgel et al. (2024) (N = 34). The sponsor was unable to confirm if there was overlap between the patient populations in these studies.
These analyses were not included in the submission to Health Canada.
FRT-Responsive CFTR Mutations
Description of Study for FRT-Responsive CFTR Mutations
Study 16 was a retrospective, observational cohort study evaluating real-world clinical outcomes in patients with CF with non-F508del mutations that are responsive to ELX-TEZ-IVA. Data were sourced from the US Cystic Fibrosis Foundation Patient Registry (CFFPR). Index dates for patients were defined as the date of ELX-TEZ-IVA treatment initiation, ranging from October 21, 2019, to December 1, 2022. Data from patients were evaluated for up to 2 years before the index date through December 31, 2022 (follow-up period), or until loss of follow-up, death, treatment discontinuation, or lung transplant, whichever was earlier. The objective of Study 16 was to supplement Study 124 in a further 64 mutations with data on effectiveness of ELX-TEZ-IVA on lung function, PEx, and nutritional parameters in a real-world setting of patients with CF in the target patient population, using data from the US CFFPR patient registry.
Patients aged 6 years or older were included in the analysis if they had data recorded in the US CFFPR; had a select ELX-TEZ-IVA-responsive non-F508del CFTR genotype, had received treatment with ELX-TEZ-IVA during the patient accrual period, had at least 1 ppFEV1 measurement in the 12 months before the index date, and had at least 1 ppFEV1 measurement that occurred at least 4 weeks after the index date. Patients were excluded if they had a history of lung transplant before the index date.
Efficacy Results
Change from baseline in ppFEV1 was the primary end point of Study 16. The overall patient population demonstrated a mean change from baseline of 4.53% (95% CI, 3.50% to 5.56%). Study 16 included patients with and without prior exposure to a CFTR modulator (55.5% and 44.1%, respectively). The sponsor reported subgroup analyses based on prior CFTR modulator exposure, and reported that the mean change from baseline with ELX-TEZ-IVA was 6.11% (95% CI, 4.40% to 7.81%) for those who were naive to treatment with a CFTR modulator and 3.3% (95% CI, 2.06% to 4.58%) for those who had prior exposure to a CFTR modulator.
Change from baseline in BMI and body weight were secondary end points. The sponsor reported an increase from baseline in BMI and body weight after ELX-TEZ-IVA initiation (mean change = 0.65 kg/m2 [95% CI, 0.41 to 0.89] and 2.91 kg [95% CI, 2.24 to 3.58]) compared to baseline. Mean change from baseline in z scores for BMI and body weight were −0.05 (SD = 0.53) and −0.04 (SD = 0.48), respectively.
PEx and annualized PEx rate were also assessed, and results suggest PEx rate decreased by 53% (95% CI, 42% to 62%) after ELX-TEZ-IVA initiation. The annualized PEx rate was 0.43 in the preinitiation period and 0.20 in the follow-up period.
Harms Results
AEs were not investigated in Study 16.
Critical Appraisal
Study 16 was a retrospective observational study with no comparator treatment group. Given the real-world treatment setting, there was no blinded administration of ELX-TEZ-IVA (i.e., investigators, patients, and caregivers were aware of the treatment). Limitations that are common to observational studies apply to these data, including potential variability in timing of assessments for patients, no standardized definition for pulmonary exacerbations, variation in the duration of therapy, lack of information regarding adherence to ELX-TEZ-IVA during the treatment period, and the potential for missing data in the registry database. The index dates for patients spanned from October 21, 2019, to December 1, 2022. This overlapped with the COVID-19 pandemic, which had a considerable impact on the baseline PEx rate for patients with CF. Due to isolation measures during the pandemic, the risk of pulmonary exacerbations was reduced during the pandemic period (0.70 versus 0.31 events per year), making it challenging to interpret the overall pretreatment baseline rate (0.43 events per year) and the posttreatment rate of exacerbations (0.20 events per year). Overall, the number of patients with each of the individual mutations was variable and generally small across the population. The sponsor noted that, given the variability of the real-world data and the interpretability of data from small strata (e.g., mutation-level data), it is important to emphasize that these analyses should be viewed with caution.
Patients evaluated in Study 16 were identified from the US CFFPR. The clinical specialists consulted by CDA-AMC noted that baseline characteristics of patients with CF in the US are generally similar to those living in Canada, and that the results would be considered generalizable to the target population in Canada. Study 16 included patients with and without prior exposure to a CFTR modulator. Given that treatment with a CFTR modulator is expected to improve the end points evaluated in clinical trials (e.g., baseline lung function, BMI, SwCl, and so on), this prior exposure could bias the overall effective size reported for the study against ELX-TEZ-IVA for target population in Canada (the majority of whom are expected to be inexperienced with a CFTR modulator, except for those who have received IVA monotherapy). The sponsor has reported results for patients with and without prior exposure to a CFTR modulator.
Health Canada reviewers noted that the differences between the mean and median change from baseline in ppFEV1 indicate that a few good responders may have skewed the average in favour of treatment (i.e., mean change from baseline was 4.53 [SD = 9.84] and median change from baseline was 2.76 [range, −31.67 to 59.19]); however, definitive conclusions cannot be drawn due to variability in the timing of the baseline and posttreatment initiation spirometry tests. Health Canada concluded that the data from Study 16 do not provide significant clinical evidence for ELX-TEZ-IVA-responsiveness beyond providing some support for the efficacy of a few mutations, with sufficient evidence of efficacy already provided in Study 124.
N1303K CFTR Mutation
Description of Studies for N1303K Mutation
CDA-AMC included 4 nonrandomized studies that investigated the use of ELX-TEZ-IVA in patients with at least one N1031K mutation in the CFTR gene. All of the studies were investigator-initiated (i.e., not sponsored by Vertex Pharmaceuticals).
Solomon et al. (2023) reported the results of a prospective, open-label trial assessing patients with at least one N1303K mutation (N = 20). Patients were treated with ELX-TEZ-IVA for 4 weeks. End points included change from baseline in ppFEV1, SwCl, CFQ-R scores, and body weight.
Burgel et al. (2024) reported the results of ELX-TEZ-IVA in patients with at least one N1303K mutation who received the treatment as part of a compassionate use program (CUP) in France. The results reflect a retrospective observational cohort, pooled analyses from cohort studies, case reports, and unpublished data. The patients who received the treatment all had advanced lung disease (i.e., ppFEV1 less than 40%). The observational period ranged from 4 weeks to 8 weeks.
Burgel et al. (2023), similar to Burgel et al. (2024), investigated the use of ELX-TEZ-IVA in patients with at least one N1303K mutation who received the treatment as part of a CUP in France. The study was a prospective observational cohort study with a treatment period of 4 to 6 weeks.
Sadras et al. (2023) reported the results of an observational prospective analysis from a multicentre registry in Israel investigating the use of ELX-TEZ-IVA in patients with CF who had at least one N1303K mutation in the CFTR gene. Patients were included if they had CF and carried at least one N1303K mutation on 1 allele and a nonsense or frameshift mutation on the other allele (i.e., a mutation that would not be expected to respond to ELX-TEZ-IVA for a period of 8 weeks). Efficacy end points included change from baseline in ppFEV1, SwCl, body weight, and lung clearance index (LCI).
Efficacy Results
Key efficacy results from the nonrandomized studies for patients with at least one N1303K mutation in the CFTR gene are summarized as follows.
Solomon et al. (2023): After 4 weeks of treatment with ELX-TEZ-IVA, patients demonstrated statistically significant improvements from baseline in ppFEV1 (mean change = 9.5%; 95% CI, 6.7% to 12.3%; P < 0.001), BMI (mean change = 0.4 kg/m2; 95% CI, 0.2 to 0.7; P = 0.002), and CFQ-R RD (mean change = 20.8; 95% CI, 11.9 to 29.8; P < 0.001). There was no statistically significant difference in change from baseline in SwCl (−1.1 mmol/L; 95% CI, −5.3 to 3.1; P = 0.61).
Burgel et al. (2024): After 4 to 8 weeks of treatment with ELX-TEZ-IVA, patients demonstrated a statistically significant improvement in ppFEV1 from baseline (median change = 17.0%; interquartile range [IQR], 10.0% to 25.0%; P < 0.0001). Median body weight increased by 2.0 kg (IQR, 1.0 to 3.5) and median SwCl was reduced by −9.0 mmol/L (IQR, 3.5 to 21).
Burgel et al. (2023): The authors reported that all patients with at least one N1303K mutation (N = 8) were considered ELX-TEZ-IVA responders. After 4 to 8 weeks of treatment with ELX-TEZ-IVA, the median change in ppFEV1 was 27.5% (IQR, 20.7% to 41.2%) and the median change in SwCl was –9 mmol/L (IQR, –5 to –36).
Sadras et al. (2023): After 8 weeks of treatment, patients treated with ELX-TEZ-IVA demonstrated statistically significant improvements from baseline in ppFEV1 (mean change = 18.4; 95% CI, 12 to 24; P < 0.0001) and BMI (mean change = 0.79 kg/m2; 95% CI, 0.51 to 1.07; P < 0.0001). There was no statistically significant difference in change from baseline in SwCl (mean change = −7 mmol/L [95% CI was not reported]; P < 0.054).
Harms Results
AEs were not investigated and/or reported in the studies by Solomon et al., Burgel et al., or Sadras et al.
Critical Appraisal
Overall, the 4 observational studies provided descriptive data on the effects of ELX-TEZ-IVA in patients with CF who have at least one N1303K mutation at various stages of lung disease. The short-term results showed acute increases in ppFEV1 and weight that were comparable to or exceeded those reported in the clinical trials for ELX-TEZ-IVA conducted in patients with other CFTR mutations; however, these results should be interpreted with caution because of the uncontrolled, observational study designs and the small sample sizes (N ranging from 8 to 35). All of the studies had a short duration of treatment and follow-up. As all of the studies were investigator sponsored, the available information regarding the studies’ methods and results is limited to publications and abstracts.
Ethical Considerations
Patient group, clinical expert, and drug program input, as well as the relevant literature, were reviewed to identify ethical considerations relevant to the use of ELX-TEZ-IVA for the treatment of CF in patients aged 2 years or older who have a mutation in the CFTR gene that is responsive based on clinical and/or in vitro data.
The ethical considerations identified in this review included those related to the following: diagnosis, treatment, and experiences of non-F508del CF variants. ELX-TEZ-IVA has come to be understood as an effective treatment in the clinical management of people living with CF and carrying at least one F508del mutation in the CFTR gene. Racialized individuals and people of other ethnicities in equity-deserving groups are more likely to carry non-F508del variants than those identifying as non-Hispanic white individuals of European descent. People with rare or ultrarare non-F508del variants are currently ineligible to receive ELX-TEZ-IVA, resulting in substantial disparities in clinical outcomes and quality of life between individuals who are eligible for the treatment and those who are not. Lack of access to disease-modifying therapy has caused significant psychological distress among those with non-F508del variants. Lack of access also has the potential to exacerbate existing health inequities.
Clinical evidence used in the evaluation of ELX-TEZ-IVA: For people living with at least 1 of the 72 non-F508del variants supported by some form of clinical data, evidence indicated that treatment with ELX-TEZ-IVA may result in clinically meaningful improvements in lung function. However, there is some uncertainty regarding durability of effect in this population. There are only in vitro data (no clinical data) supporting the efficacy or safety for the use of ELX-TEZ-IVA in people carrying 1 of 79 further variants included in the expanded population. One variant has neither clinical nor in vitro data. Although the generalizability of in vitro FRT cell model data to a real-world application is uncertain, clinical experts were comfortable with relying on these data to prescribe ELX-TEZ-IVA, given the absence of alternative treatment options; their experience with and the mounting evidence for ELX-TEZ-IVA in people with at least one F508del variant; and clinical data for other rare variants included in this review. Additionally, clinical experts noted that relying on in vitro data in patients with rare or ultrarare non-F508del variants is justified, as clinical trials may not be feasible.
Clinical use and implementation of ELX-TEZ-IVA: Given that individuals with non-F508del variants may be from equity-deserving groups, expanding access to ELX-TEZ-IVA has the potential to benefit these communities and lessen health inequities associated with access to effective therapy and improved treatment outcomes. Given the high prevalence of a non-F508del mutations in the Hutterite population with CF in Canada, clinical experts noted that this group may also benefit from expanded access to ELX-TEZ-IV. Clinical experts expressed readiness to prescribe ELX-TEZ-IVA to the expanded population, as they believed the potential benefits would outweigh potential risks given the lack of alternatives and mounting evidence supporting its safety and efficacy in people with F508del mutations. However, it is important to have a robust informed consent process where health care providers transparently communicate the absence of clinical evidence for the 79 variants supported solely by in vitro data and prepare patients for uncertainties associated with treatment safety and effectiveness.
Health systems: Expensive drugs for rare diseases, such as ELX-TEZ-IVA, raise ethical considerations related to distributive justice and equitable access, the sustainability of health care budgets and consideration of opportunity costs, and fair pricing of pharmaceuticals. As a highly expensive medication, expanding access to ELX-TEZ-IVA could present challenges for provincial drug budgets as the reimbursement of ELX-TEZ-IVA may have a disproportionately large budget impact.
Economic Evidence
Cost and Cost-Effectiveness
Table 4: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Microsimulation |
Target population | Patients with CF aged 2 years or older who have a mutation in the CFTR gene that is responsive based on in vitro and/or clinical data |
Treatment | ELX-TEZ-IVA plus BSC BSC was defined as recommended medications (such as mucolytics, inhaled and oral antibiotics, inhaled hypertonic saline, nutritional supplements, enteral tube feeding, pancreatic enzymes, antifungal agents, and corticosteroids) and physiotherapy. |
Dose regimen | Based on patient weight
|
Submitted price | Elexacaftor-tezacaftor-ivacaftor (Trikafta),100 mg, 50 mg, 75 mg and ivacaftor 150 mg tablets, 50 mg, 25 mg, 37.5 mg and ivacaftor 75 mg tablets, or 100 mg, 50 mg, 75 mg and ivacaftor 75 mg granules, 80 mg, 40 mg, 60 mg and ivacaftor 59.5 mg granules: $280.00 per tablet, $420.00 per granule packet |
Submitted treatment cost | $306,810 annually per patient, regardless of strength or form |
Comparators | SoC
SoC comprises a treatment mix of IVA and BSC, estimated by a weighting factor based on prevalence of IVA-eligible (20%) and IVA-ineligible patients (80%) and comparator market shares (10% BSC and 90% IVA in those who are IVA-eligible; 100% BSC in those who are IVA-ineligible). The final estimated SoC treatment mix is 82% BSC and 18% IVA. |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (69 years) |
Key data sources | ELX-TEZ-IVA: Study VX21-445-124 comprising patients with non-F508del mutations (24 weeks); Study VX17-445-105 comprising patients with F508del mutations (192 weeks) IVA: Meta-analysis of Studies VX08-770-102, VX08-770-103, and VX-11-770-110 |
Key limitations |
|
CDA-AMC reanalysis results |
|
BSC = best supportive care; CF = cystic fibrosis; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; QALY = quality-adjusted life-year; SoC = standard of care; vs. = versus.
Budget Impact
CDA-AMC identified the following key limitations with the sponsor’s analysis: the sponsor’s estimate of the market uptake of ELX-TEZ-IVA is likely underestimated which underestimates the resulting budget impact, the sponsor’s adjustment of drug costs by an adherence rate for patients underestimates drug costs and the resulting budget impact, and there is uncertainty regarding the proportion of patients with public drug coverage. The reanalysis adjusted market shares and assumed 100% adherence for all drugs. In the base case, the reimbursement of ELX-TEZ-IVA for the treatment of CF in patients aged 2 years or older who have at least 1 non-F508del mutation in the CFTR gene that is responsive based on in vitro and/or clinical data is expected to be $18,224,293 in year 1, $20,811,236 in year 2, and $21,856,672 in year 3, for a 3-year total of $60,892,201. A scenario analysis by CDA-AMC found the budget impact to be sensitive to assumptions around the proportion of patients with public drug coverage.
CDEC Information
Members of the Committee
Dr. Peter Jamieson (Chair), Dr. James Silvius, Dr. Sally Bean, Dan Dunsky, Mr. Bob Gagne, Dr. Ran Goldman, Dr. Trudy Huyghebaert, Morris Joseph, Dr. Christine Leong, Dr. Kerry Mansell, Dr. Alicia McCallum, Dr. Srinivas Murthy, Dr. Danyaal Raza, Dr. Edward Xie, and Dr. Peter Zed.
Meeting date: August 29, 2024
Regrets: Two expert committee members did not attend.
Conflicts of interest: None
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up-to-date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.