Drugs, Health Technologies, Health Systems
Reimbursement Review
Atogepant (Qulipta)
Sponsor: AbbVie Corporation
Therapeutic area: Migraine, prevention
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AIM-D
Activity Impairment in Migraine-Diary
ALT
alanine aminotransferase
ANSG
Atlantic Neurology Specialist Group
AST
aspartate aminotransferase
CGRP
calcitonin gene–related peptide
CHS
Canadian Headache Society
CI
confidence interval
CrI
credible interval
eDiary
electronic diary
GP
general practitioner
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HIT-6
Headache Impact Test
HRQoL
health-related quality of life
ICHD-3
International Classification of Headache Disorders, third edition
ITC
indirect treatment comparison
LSM
least squares mean
LSMD
least squares mean difference
MAAP
market access analysis plan
mAb
monoclonal antibody
MHD
monthly headache day
MID
minimal important difference
MIDAS
Migraine Disability Assessment
mITT
modified intention-to-treat
MMD
monthly migraine day
MMRM
mixed model of repeated measures
MSQ
Migraine-Specific Quality-of-Life Questionnaire
NMA
network meta-analysis
NSAID
nonsteroidal anti-inflammatory drugs
OR
odds ratio
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SE
standard error
TEAE
treatment-emergent adverse event
TF
treatment failure
ULN
upper limit of normal
WPAI:Migraine
Work Productivity and Activity Impairment: Migraine
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Atogepant (Qulipta), tablets, 10 mg, 30 mg, and 60 mg, oral |
Sponsor | AbbVie Corporation |
Indication | For the prevention of migraine in adults who have at least 4 migraine days per month |
Reimbursement request | AbbVie is requesting that atogepant be reimbursed for the prevention of CM in adults with ≥ 15 headache days per month (among which 8 days are considered to be migraine days) and who have previously failed, are intolerant to, or have a contraindication to at least 2 oral prophylactic migraine medications. |
Health Canada approval status | Approved |
Health Canada review pathway | Standard review |
NOC date | May 2, 2024 |
Recommended dosage | CM: The recommended dosage is 60 mg orally once daily. |
CM = chronic migraine; NOC = Notice of Compliance.
Introduction
Migraine is a multifactorial, disabling neurologic disease characterized by recurrent and often debilitating headaches of moderate to severe intensity accompanied by neurologic symptoms.1 The Headache Classification Committee of the International Headache Society defines migraine as a recurrent primary headache disorder resulting in attacks that last 4 hours to 72 hours.1 In addition to severe headache pain, migraine attacks are associated with a wide range of nonheadache symptoms, including sensitivity to light, sound, and smells, and nausea and vomiting.2-4 Migraine is commonly categorized according to the frequency of attacks as episodic migraine or chronic migraine.1 People with migraine who have fewer than 15 migraine headache days are commonly referred to as having episodic migraine, a term that has been recently adopted in the Definition of Terms in International Classification of Headache Disorders, fourth edition alpha, and is widely used by clinicians and in migraine publications.5 Chronic migraine has been defined by the International Classification of Headache Disorders, third edition (ICHD-3), as headaches occurring on 15 or more days per month for more than 3 months, of which at least 8 days per month have the features of migraine attacks.1 As attack frequency or severity increases, migraine management requires the use of both acute and preventive treatments.6,7 Multiple pharmacologic options for migraine prevention are currently available in Canada for patients with chronic migraine, including established oral preventive treatments, injectable onabotulinumtoxin A, or self-injectable and infusion calcitonin gene–related peptide (CGRP) monoclonal antibodies (mAbs).
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of atogepant 60 mg once daily oral tablets for the prevention of chronic migraine in adults with 15 or more headache days per month (of which 8 days are considered to be migraine days) and who have experienced an inadequate response, intolerance, or contraindication to at least 2 oral prophylactic migraine medications.
On June 14, 2023, atogepant received a recommendation to reimburse with conditions by the Canadian Drug Expert Committee for the prevention of episodic migraine in adults with fewer than 15 migraine days per month who have experienced an inadequate response, intolerance, or contraindication to at least 2 oral prophylactic migraine medications.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to the Canada’s Drug Agency’s (CDA-AMC’s) call for input and from clinical expert(s) consulted by CDA-AMC for the purpose of this review.
Patient Input
CDA-AMC received 2 patient group submissions — 1 from the Canadian Migraine Society and a second from Migraine Canada and Migraine Quebec. Data were gathered by the Canadian Migraine Society from 3 perspectives: experience from support groups with 3,200 members, personal disease experience, and email interviews with 19 patients currently on atogepant conducted from November 1 to December 12, 2023. The information provided by Migraine Canada and Migraine Quebec was collected through a quality-of-life online survey that was launched in the late fall of 2021. In total, 1,165 adults living in Canada with migraine and their caregivers responded to the online survey. Migraine Canada launched an additional survey in November 2023 to gather further insights, seeking input from patients with experience with atogepant. In total, 230 adults with migraine responded to the survey.
Most of the patients from the 2 patient groups shared similar symptoms and acknowledged the impact of symptoms on their day-to-day lives and employment. The Canadian Migraine Society reported that migraine — and especially chronic migraine — affects every single facet of a person’s life. In both surveys conducted by Migraine Canada and Migraine Quebec, the 3 outcomes reported to be most valuable to patients when trying a preventive treatment were effects in headache intensity, headache frequency, and symptoms other than pain such as sensitivity to light, sound, nausea, or brain fog. The Canadian Migraine Society further stated that the desired outcome should be an increase in quality of life.
Both groups agreed that patients with chronic migraine need access to different options for effective medications (both preventive and acute), because patients with migraine do not respond equally to the same medication or treatment. Migraine Canada and Migraine Quebec also highlighted that considering the opioid crisis, new medications should play a role in a national plan to better manage pain and alleviate the need for opioids.
Clinician Input
The clinical expert consulted by CDA-AMC identified several unmet needs in the treatment of chronic migraine, including poor adherence to medication, often due to common side effects even when treatments are effective. Additionally, accessibility issues, such as the requirement for the specialized administration of certain medications like onabotulinumtoxin A, contribute to the need for treatments that are more easily accessible. The expert considered that in their opinion, atogepant shows promise as a first-line treatment option due to its effectiveness and low side-effects profile, but cost considerations may limit its initial prescription, potentially restricting it to patients who have already tried multiple medications.
The clinical expert advised caution for patients with certain medical histories such as stroke or other cardiac diseases, as well as special considerations that are necessary for patients of childbearing age.
According to the clinical expert, assessing treatment response relies on reductions in headache frequency or severity, with no standardized criteria for discontinuing an established treatment, though a minimum trial period of 6 months was recommended before considering the discontinuation of atogepant.
The clinical expert also mentioned that atogepant offers potential benefits for patients with migraine, particularly a reduction in migraine and headache frequency in those with treatment-resistant or frequent episodic migraine and can be prescribed by primary care providers without requiring specialized monitoring. However, cost considerations and the need for further research into long-term efficacy and discontinuation criteria remain significant factors in its clinical use.
Clinician Group Input
CDA-AMC received 2 clinician group submissions from the Atlantic Neurology Specialist Group (ANSG) and the Canadian Headache Society (CHS). ANSG held 2 professional meetings on October 5 and December 18, 2023, to discuss the migraine treatment landscape, and identify barriers to treatment access and the role of atogepant in fulfilling unmet patient needs. CHS gathered information from published clinical evidence and expert opinions from headache specialists in Canada and internationally. ANSG identified what it termed the top 3 unmet treatment needs for migraine in Canada: adverse events (AEs) and inadequate response to acute and preventive treatments, the fact that general practitioners (GPs) depend on specialists for prescribing preventive treatments, and restrictive reimbursement criteria that prevent patient access to the care they need. CHS also found similar treatment gaps and some additional ones such as the wearing off in effectiveness of current available treatments, contraindication to some patient populations, and patients’ preference for oral formulations over injectables and infusions. ANSG stated that atogepant is the first oral small-molecule CGRP antagonist approved for the preventive treatment of migraine in Canada. CHS also commented that atogepant could be combined with drugs with a different mechanism, though evidence to support the effectiveness of such combinations is lacking. ANSG believed that specialists, GPs, and nurse practitioners with experience diagnosing migraine could prescribe the product and monitor the patients. CHS further stated that atogepant prescription should not be restricted to neurologists or specialists due to the belief that it is well tolerated and safe compared to many other drugs prescribed in primary care.
Drug Program Input
The drug programs conveyed comments and questions for experts and committee members to be applied during the evaluation of the evidence and the deliberations.
The first comment was about relevant comparators. The pivotal PROGRESS trial only examined Qulipta at varying doses against a placebo, lacking direct comparisons of relevant migraine prevention treatments. Botox coverage for migraine prevention varies among drug plans, necessitating clarification of its role in therapy. Injectable CGRP inhibitors feature prominently across jurisdictions, suggesting a potential avenue for treatment. Harmonizing initiation criteria for atogepant with other CGRP inhibitors, where applicable, could streamline treatment protocols.
For initiation criteria, the number and type of prophylactic medications tried before initiation should be discussed. As noted earlier, the criteria for atogepant should align with other similar recommendations, if feasible. Members of the drug programs asked about Botox and other CGRP inhibitor medications before initiating atogepant (i.e., they wanted it clarified which and how many of these [prophylactic] medications should be tried first). According to the clinical expert, there is no evidence for establishing a specific order of medications. For example, some patients may need Botox first due to their initial symptoms. This also applies when assessing the new gepants drugs versus mAbs, where — according to the clinical expert — there is even less of a difference in terms of efficacy between these groups of drugs to establish a specific order of therapy. The clinical expert mentioned that any drug tried before atogepant will be adequate to include in the considerations for initiation. Furthermore, the clinical expert explained that there is no specific timing in the case of patients who discontinue the therapy due to benefit and then relapse with symptoms (i.e., if physicians consider giving the drug again). The clinical expert would recommend observing patients during the first 3 months off therapy; this is the time during which symptoms may come back.
For renewal and discontinuation criteria, the drug plans suggested consistency in the criteria with other similar drugs for this indication. Similarly, for prescribing criteria, the drug plans considered and evaluated the approved Health Canada dosage (60 mg every day).
Clinical Evidence
Systematic Review
Description of Studies
One pivotal randomized controlled trial (RCT) (the PROGRESS study) was included, assessing atogepant for the treatment of patients with chronic migraine. The PROGRESS study was a randomized, placebo-controlled trial that assessed the effects of atogepant 60 mg every day against placebo in adult patients with chronic migraine. The study included a subgroup of patients who had experienced an inadequate response, intolerance, or contraindication to at least 2 oral prophylactic migraine medications. There was a prespecified subgroup of patients with 2 or more treatment failures (TFs) ███ ███ █████████. The study assessed efficacy outcomes (monthly migraine days [MMDs], monthly headache days [MHDs], and monthly acute medication use), function or disability outcomes (the performance of daily activities, missed school days or workdays, and the impact of headaches in daily function), health-related quality of life (HRQoL), health resource use, and harms.
Efficacy Results
Change From Baseline in Mean MMDs
The primary efficacy end point in the PROGRESS study was the change from baseline in mean MMDs across the 12-week treatment period. In patients who had previously not experienced improvement with 2 or more migraine prevention medications with different mechanism of actions (2+ TFs population | | | ███), the least squares mean (LSM) change from baseline as measured by the mean MMDs across the 12-week treatment period was █████ ████ ████ ███ █████ ██ █████ █████ for atogepant 60 mg every day compared with █████ ████ ████ ███ █████ ██ █████ █████ for placebo. The least squares mean difference (LSMD) in change from baseline in mean MMD was █████ ████ ████ ███ █████ ██ █████ █████ | | ████████ favouring atogepant 60 mg every day.
Reduction of 50% or More in 3-Month Average of MMDs
In the 2 or more TFs population, the proportion of patients who had a 50% or greater reduction in the 3-month average of MMDs with atogepant 60 mg every day was █████ ████████ ██ █████ with placebo. The adjusted absolute between-group difference was ██████ ████ ███ ████ ██ ████████ The odds ratio (OR) for the proportion of patients who demonstrated a 50% or greater reduction in the 3-month average of MMDs was ████ ████ ███ ████ ██ █████ | | ███████, favouring atogepant 60 mg every day.
Change From Baseline in Mean MHDs
In the 2 or more TFs population, the LSM change from baseline in the number of mean MHDs across the 12-week treatment period was █████ ████ ████ ███ █████ ██ █████ █████ with atogepant 60 mg every day compared to █████ ████ ████ ███ █████ ██ █████ █████ with placebo. The LSMD in change from baseline in mean ███ █████ ████ ████ ███ █████ ██ █████ █████ | | ███████, favouring atogepant 60 mg taken every day.
Change From Baseline in Mean Monthly Acute Medication Use Days
In the 2 or more TFs population, the LSM change from baseline in the number of mean acute medication use days across the 12-week treatment period was █████ ████ ████ ███ █████ ██ █████ █████ for atogepant 60 mg every day compared to █████ ████ ███ █████ ██ █████ █████ with placebo. The LSMD in change from baseline in mean acute medication use days between atogepant 60 mg every day and placebo was █████ ████ ████ ███ █████ ██ █████ █████ | | ███████, favouring atogepant 60 mg taken every day.
Change From Baseline in Mean Monthly Performance of Daily Activities Domain Score of the Activity Impairment in Migraine-Diary Tool
In the 2 or more TFs population, the LSM change from baseline in the mean monthly performance of daily activities domain score of the Activity Impairment in Migraine-Diary (AIM-D) tool across the 12-week treatment period was ██████ ███ █ █████ for atogepant 60 mg every day compared with █████ ███ █ █████ for placebo, where negative values imply improvements from baseline. The LSMD in change from baseline in the mean monthly performance of daily activities domain score of AIM-D across the 12-week treatment period was █████ ██████ ████ ███ █████ ██ █████ ███████ | | ███████, favouring atogepant 60 mg every day.
Change From Baseline in the Migraine Disability Assessment Total Score
This end point was not available for the 2 or more TFs population; hence, it was only assessed in the overall modified intention-to-treat (mITT) population, where the LSM change from baseline in the Migraine Disability Assessment (MIDAS) total score at week 12 was ██████ ██████ ████ ███ ██████ ██ ██████ ██████) for atogepant 60 mg every day (improvement) as compared to ██████ ██████ ████ ███ ██████ ██ ██████ ███████ with placebo. The LSMD in change from baseline was ██████ ██████ ███████ ██████ ██ █████ ███████ | | ████████ favouring atogepant 60 mg every day.
Change From Baseline in Headache Impact Test Total Score
In the 2 or more TFs population, the LSM change from baseline in the Headache Impact Test (HIT-6) total score at week 12 ███ █████ ██████ ████ ███ █████ ██ █████ ███████ for atogepant 60 mg every day (with negative numbers implying improvement) and █████ ██████ ████ ███ █████ ██ █████ ███████ in the placebo group. The LSMD in change from baseline was █████ ██████ ████ ███ █████ ██ █████ ███████ | | ████████ favouring atogepant 60 mg every day.
Change From Baseline in Migraine-Specific Quality-of-Life Questionnaire Version 2.1 Role Function-Restrictive Domain Score
In the 2 or more TFs patient population, the LSM change from baseline in the Migraine-Specific Quality-of-Life Questionnaire (MSQ) Version 2.1 role function-restrictive domain score at week 12 was █████ ██████ ████ ██ █████ ██ █████ ███████ higher for atogepant 60 mg every day while the placebo group had an increase of █████ ██████ ████ ██ ████ ██ █████ ██████), where higher values suggest an improvement in patients’ functioning with daily social and work-related activities. The LSMD in change from baseline in the mean monthly MSQ Version 2.1 role function-restrictive domain score at week 12 was █████ ██████ ██████ ████ ███ ████ ██ █████ ███████ | | ███████ in the atogepant 60 mg every day group when compared to placebo.
Change From Baseline in Percentage of Work Time Missed Assessed by Work Productivity and Activity Impairment: Migraine Version 2.0
This was only evaluated in the subset of the overall (mITT) population and no information was provided for the 2 or more TFs subgroup. In the overall (mITT) population, the LSM change from baseline in the percentage of work time missed assessed with the Work Productivity and Activity Impairment: Migraine (WPAI:Migraine) at week 12 was █████ ██████ ████ ███ ██████ ██ █████ ███████ for atogepant 60 mg every day (negative values imply improvement) compared to █████ ██████ ████ ███ █████ ██ █████ ███████ with placebo. The LSMD in change from baseline in the percentage of work time missed at week 12 was █████ ██████ ████ ███ █████ ██ █████ ███████ | | ██████), favouring atogepant 60 mg every day.
Harms Results
The most frequently reported AEs (≥ 5% of patients in the safety population) in the atogepant treatment group were constipation (10%) and nausea (9.6%). In the 2 or more TFs population, patients also experienced more cases of ████████████████
In the 2 or more TFs population, ████████████ was reported in █████ of patients in the atogepant 60 mg every day treatment group and ████ of patients in the placebo treatment group. ██████ ███ ████████ ██ ████ of patients in the atogepant 60 mg every day treatment group, and ████ of patients in the placebo treatment group. ███████████████ was reported in ████ of patients in the atogepant 60 mg every day treatment group, and ████ of patients in the placebo treatment group.
In the 2 or more TFs patient population, serious adverse events (SAEs) were infrequent in the atogepant 60 mg every day treatment group and placebo group. In the overall patient population, SAEs were infrequent in the atogepant 60 mg every day treatment group and placebo group. There were no clinically meaningful differences of SAEs between the atogepant 60 mg every day treatment group and the placebo group.
AEs leading to treatment discontinuation were infrequent in the atogepant 60 mg every day treatment group and placebo group, in both the overall and 2 or more TFs populations. All AEs leading to treatment discontinuation in the atogepant 60 mg every day group occurred in less than 1% of patients.
No deaths were reported in the PROGRESS trial.
AEs of special interest were reported at low rates. A total of 1 patient in the placebo treatment group of the overall population reported an AE of suicidal ideation. No patients in the atogepant group reported an AE of suicidal ideation. A total of 3 patients had an elevated alanine aminotransferase (ALT) or aspartate aminotransferase (AST) laboratory value that was 3 or greater multiplied by the upper limit of normal (ULN) value; these patients were subject to blinded adjudication by then Adjudication Committee of the study.
Critical Appraisal
The PROGRESS trial was an RCT investigating the efficacy and safety of atogepant 60 mg every day (the dose of interest for this review) compared to placebo. The study involved a randomization and allocation concealment process that was judged to be properly implemented, ensuring an overall balanced distribution of participants to either the atogepant 60 mg every day arm or the placebo arm. The number of prior migraine prevention medications that did not yield improvement was a stratification factor in the randomization, which should ensure that the randomization is upheld in the 2 or more TFs subgroup. Some minor baseline imbalances were observed for the WPAI: Migraine end point, obtained from a subset of the population, with imbalances between groups. However, these were judged to have an overall low risk for introducing bias or to have suggested problems in the randomization process. In the study, patients maintained good adherence to the intended intervention. Concomitant medication use was comparable across the placebo and atogepant 60 mg every day treatment groups.
The 2 or more TFs subgroup, which represents █████ ███████ of the total mITT population, is of interest for this CDA-AMC report because it is the focus of the sponsor’s reimbursement request. However, the sample size (power) calculation did not consider this subgroup separately; therefore, it is unknown whether there was enough statistical power to detect any differences in treatment effect between the intervention and comparator arms in this subgroup. However, greater effect sizes for the 2 or more TFs subgroup were consistent across all key clinical end points (change from baseline in MMDs, MHDs, and monthly acute medication use days, and a reduction of ≥ 50% in 3-month average of MMDs) compared to the mITT population. There were no instances of meaningful missing outcome data, except ███ █ ██████ patients in the atogepant 60 mg group and ██ ████ in the placebo group for the main outcomes in the mITT population, which was unlikely to significantly affect the results. In the PROGRESS study, measurements of the outcomes were appropriate. The blinding of participants and clinical investigators was kept throughout the conduct of the study, and there is no evidence that patients or personnel became unblinded. The results were reported in accordance with predefined protocols, including the results from the subgroup of 2 or more TFs; this reduced the likelihood of selective reporting bias.
Overall, the study appears to have minimized risks across all domains assessed for risk of bias for the outcomes addressed when comparing atogepant to placebo.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal study identified in the sponsor’s systematic review, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool was used to assess the certainty of the evidence for outcomes considered most relevant to inform CDA-AMC’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.8,9
Following the GRADE approach, evidence from RCTs start as high-certainty evidence and can be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effect estimates, and publication bias.
When possible, certainty is rated in the context of the presence of an important effect (i.e., how certain it is that the effect is a nontrivial treatment effect). To determine what an important effect is, GRADE suggests using thresholds of clinical importance (minimal important difference [MID]); if the threshold is not possible to obtain, the certainty is rated in the context of the presence of any treatment effect (i.e., how certain are we that there is any — beneficial or harmful — effect). In this case, the clinical importance of any effect remains unclear. In all cases, the target of the certainty of evidence assessment is based on the point estimate of each outcome and where it is located relative to the chosen threshold for a clinically important effect (when a threshold is available) or to the null (when there is no threshold).
A GRADE summary of findings for the body of evidence for this review included the evaluation of the main outcomes considered important by clinicians, patient groups, and stakeholders. These assessments are presented in Table 2 for each outcome included.
Table 2: Summary of Findings for Atogepant 60 mg q.d. vs. Placebo for Patients With Chronic Migraine and 2 or More Treatment Failures
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | Atogepant 60 mg | Difference | |||||
Migraines, headaches, and acute medication use | |||||||
LSM change from baseline in MMDs Follow-up: 12 weeks | ███ (1 RCT) | NA | █████ | █████ ███████ ██ ██████ | ████ fewer (███ to ███ fewer) | Moderatea | Atogepant 60 mg q.d. likely results in a clinically important reduction in the mean MMDs when compared to placebo. |
Reduction of ≥ 50% of 3-month MMDs Follow-up: 12 weeks | ███ (1 RCT) | OR = ████ █████ ██ █████ | ███ per 1,000 | ███ per 1,000 (NR) | ███ more per 1,000 (██ ██ ███ more per 1,000) | Moderatea | Atogepant 60 mg q.d. likely results in an increase in the proportion of patients achieving a ≥ 50% reduction in MMDs when compared to placebo. There is uncertainty about the clinical importance of the increase. |
LSM change from baseline in MHDs Follow-up: 12 weeks | ███ (1 RCT) | NA | █████ | █████ ██████ ██ █████ | ████ fewer (████ ██ ████ fewer) | Moderatea | Atogepant 60 mg q.d. likely results in a clinically important reduction in the mean MHDs when compared to placebo. |
LSM change from baseline in monthly acute medication use days Follow-up: 12 weeks | ███ (1 RCT) | NA | █████ | █████ ██████ ██ █████ | ████ fewer █████ ██ ████ fewer) | Moderatea | Atogepant 60 mg q.d. likely reduces the monthly acute medication use days when compared to placebo. There is uncertainty about the clinical importance of the reduction. |
Function or disability | |||||||
LSM change from baseline in mean monthly performance of daily activities domain score of the AIM-D (0 [best] to 100 [worst]), points Follow-up: 12 weeks | ███ (1 RCT) | NA | █████ | █████ ████████ ██ ██████ | ███ lower points (████ to ████ lower) | Moderateb | Atogepant 60 mg q.d. likely reduces (improves) the monthly performance of daily activities score of the AIM-D when compared to placebo. There is uncertainty about the clinical importance of the improvement. |
LSM change from baseline in MIDAS total score (0 [no disability] to > 40 [very severe disability]), points Follow-up: 12 weeks | ███ (1 RCT) | NA | ██████ | ██████ ███████ ██ ██████ | ████ lower points █████ lower to ███ lower) | Moderatec, d | Atogepant 60 mg q.d. likely reduces (improves) the MIDAS total score when compared to placebo. There is uncertainty about the clinical importance of the improvement. |
LSM change from baseline in HIT-6 total score (36 [best] to 78 [worst]), points Follow-up: 12 weeks | ███ (1 RCT) | NA | █████ | █████ █████ to ██████ | ████ lower (████ to ████ lower) | Moderatea, e | Atogepant 60 mg q.d. likely results in a clinically important reduction (improvement) in the impact of headaches in daily function as measured by the HIT-6 scale when compared to placebo. |
HRQoL | |||||||
LSM change from baseline in monthly MSQ Version 2.1, RFR domain (0 [worst] to 100 [best]), points Follow-up: 12 weeks | ███ (1 RCT) | NA | █████ | █████ (█████ to ████) | █████ higher (████ to ████ higher) | Moderatea, f | Atogepant 60 mg q.d. likely results in a clinically important increase in HRQoL (work-related activities and daily social activities) when compared to placebo. |
Resource use | |||||||
Change from baseline in percentage of work time missed using WPAI: Migraine version 2.0 (0% [best] to 100% [worst]), % Follow-up: 12 weeks | ███ (1 RCT) | NA | █████ | ████████████ ██ █████ | ███ % lower (████ lower to ███ higher) | Lowg, h | Atogepant 60 mg q.d. may reduce the percentage of work time missed. The clinical relevance of the effect size is unclear. |
Harms | |||||||
AEs, SAEs, WDAEs, deaths Follow-up: 12 weeks | ███ (1 RCT) | NA | AEs were similar overall (█████ and ███████ Only ████████████ was deemed numerically increased in atogepant (██████ vs. placebo (██████ SAEs were reported by ||| patients in the atogepant group and ████ in the placebo group. WDAEs were reported in ||| patients in each group. No deaths were reported in any group. | Moderatea | Atogepant 60 mg q.d. likely results in little to no difference in AEs, SAEs, and WDAEs. Atogepant likely increases the number of mild or moderate constipation cases; the clinical importance is uncertain. | ||
AE = adverse event; AIM-D = Activity Impairment in Migraine-Diary; CI = confidence interval; HIT-6 = Headache Impact Test; HRQoL = health-related quality of life; LSM = least squares mean; LSMD = least squares mean difference; MHD = monthly headache day; MID = minimal important difference; MIDAS = Migraine Disability Assessment; MMD = monthly migraine day; MSQ = Migraine-Specific Quality-of-Life Questionnaire; NA = not applicable; NR = not reported; OIS = optimal information size; OR = odds ratio; q.d. = every day; RCT = randomized controlled trial; RFR = role function-restrictive; SAE = serious adverse event; TF = treatment failure; vs. = versus; WDAE = withdrawal due to adverse event; WPAI:Migraine = Work Productivity and Activity Impairment: Migraine.
Note: Analyses were unadjusted for multiplicity. The absolute difference (95% CI) in the change from baseline in a reduction of 50% or more of 3-month MMDs was requested from the sponsor for interpretation purposes.
aRated down 1 level for imprecision. The population was composed of those patients meeting the reimbursement criteria (2 or more TFs); the sample size and OIS for this subgroup were not reached. One day was defined as the threshold for a small but important benefit (or harm) for the change from baseline of MMD. For AEs, the number of events was small.
bRated down 1 level for imprecision. No MID was available for this measure; therefore, the effect was judged vs. the null. The OIS was not reached, but sample size was greater than 30% of the OIS.
cThe information was obtained from the overall 2 or more TFs population. The within-group MID (change from baseline) was estimated to be 4.5 points.
dRated down 1 level for imprecision.
eThe within-patient and between-group MID for patients with chronic migraine was estimated to be 6 points and 2.3 points, respectively.
fThe within-group MID was estimated to be 11 points. A lenient threshold of 5.5 points would lead to not rating down for imprecision; however, the OIS was not reached and the imprecision remained rated down 1 level.
gRated down 1 level for imprecision. The 95% CI excluded the null but may have included an important benefit and a trivial effect. Since there was no threshold of between-group clinical importance, the clinical relevance of the effect remained unclear. Furthermore, the sample size on this outcome did not reach the OIS.
hRated down 1 level due to the risk of bias as this outcome was assessed in a subset of the target population; the prognostic balance was not ensured.
Long-Term Extension Studies
Description of Studies
Study 3101 to 312 to 002 (Study 312) is a multicentre, open-label, 156-week, long-term safety extension study conducted in all eligible patients who completed the PROGRESS or ELEVATE study. (The ELEVATE study is a phase III, multicentre, randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy, safety, and tolerability of oral atogepant for the prophylaxis of migraine in participants with episodic migraine who have previously not experienced improvement with 2 classes to 4 classes of oral prophylactic treatments.) Study 312 consists of a 156-week, open-label treatment period, and a safety follow-up period of 4 weeks. The primary objective of the study is to assess the safety and tolerability of the long-term use of atogepant 60 mg every day treatment in patients with chronic migraine or episodic migraine. Efficacy end points for long-term evaluation were included; however, they were considered exploratory. An interim analysis (November 2023) is presented here, including only patients from the PROGRESS study. Patients were instructed to take atogepant 60 mg orally at approximately the same time each day for 156 weeks. Patients were followed for 4 weeks following completion or discontinuation of atogepant. All analyses were performed for the full population in the extension study, and no analyses specific to the 2 or more TFs population were presented.
Efficacy Results
Overall, reductions in mean MMDs, mean MHDs, and mean monthly acute medication use days relative to the lead-in study baseline were observed during the open-label treatment period. The proportion of patients with a 50% or greater improvement in MMDs was 41.0% across the 12-week treatment period in the PROGRESS study, and 67.0% for week 13 to week 16, and remained similar for week 29 to week 32, and week 45 to week 48. The change from baseline in the monthly performance of daily activities domain score of the AIM-D tool remained relatively consistent across week 13 to week 16, week 29 to week 32, and week 45 to week 48. Moreover, the change from baseline in the MSQ Version 2.1 role function-restrictive domain score at week 12, week 20, week 28, week 36, week 44, and week 52 remained similar across all weeks.
Harms Results
At the time of the interim analysis, ████ of patients had completed Study 312 and █████ were still ongoing. Of the 325 patients enrolled in Study 312 from the PROGRESS trial, █████ discontinued treatment, with ███████ ██████████ ███████ being the most common reason for discontinuation. Treatment-emergent AEs were reported by 265 (81.5%) patients. The most frequently reported AEs included COVID-19 (30.8%), constipation (10.2%), nasopharyngitis (9.8%), urinary tract infection (6.2%), and insomnia (5.5%). Treatment-emergent SAEs were reported by 20 (6.2%) patients. The following SAEs were reported by 1 patient each: ████████ █████████████ █████████ ███████ ██████████ █████████████ ██████████████ ██████ ████████████ ██████████████ ████ █████████ ████████ █████████████ ███████████████ ███████ ████ █████████ ██████ █████ ██████████ ███████ ███████ ███████████ █████████████ ██████ ███████ ██████████ ███████ █████████ ███████ ████████ ███████ █████████████ ███████ █████ ███████ ██████ █████████ █████████ █████████ ███ ████████ █████ AEs leading to study drug discontinuation were reported in 27 (8.3%) patients. AEs leading to any study drug discontinuation included █████████ █ ████████ ████████ ██ ██████████ ████████████ ████ ██████ ████ ███████ ████████████████ █████████ ████ █████████ ████████████████ █████████ ████ ███ █████████████████████ ████
Critical Appraisal
Study 312 was limited by its open-label and noncomparative design; since there is no comparator, it cannot be confirmed whether the results observed may be attributable to the effects of the drug or the natural history of the condition. Furthermore, the mITT population analyzed excluded ███ of patients, and the large missing outcome data (more than ████ introduces a risk of bias. The open-label and nonblinding nature of the study increases the risk of bias and because the outcome measures are generally self-reported, they are subjective, and it is uncertain if they can be replicated in another population beyond that included in the study. No information was provided on the 2 or more TFs population (the reimbursement requested population). It is therefore not possible to know whether the effects observed in the full population would be similar in that group. Because the patients who took part in the open-label, long-term safety extension phase were originally from the pivotal PROGRESS trial, it is reasonable to expect that the same limitations to generalizability are relevant to the open-label, long-term safety extension phase. Given the nature of noncomparative study design, it is not possible to compare the effectiveness and tolerability of atogepant as a prophylactic treatment of chronic migraine against other preventive treatment.
Indirect Comparisons
Description of Studies
The indirect treatment comparison (ITC) submitted is a network meta-analysis (NMA) conducted by the sponsor. The objective of the NMA was to evaluate the efficacy, safety, and tolerability of atogepant compared with CGRP inhibitors (i.e., the comparators of interest that are approved medications for the treatment of chronic migraine in Canada [atogepant, onabotulinumtoxin A, eptinezumab, erenumab, fremanezumab, or galcanezumab]).
A clinical systematic literature review was performed using the population, interventions, comparators, outcomes, and study design criteria previously established for the reimbursement request. ██ ██ ███████ ██████████ ██ ███ ████ ██ ███████ ███ ███ █████████ ████████ ███ ███ ████
Efficacy Results
Baseline characteristics of patients (age, sex, race) involved in all comparisons were, overall, similar across studies. ██ ███ ███████ ██ ██████████ ███ ███ ████████ ██ ██ ██ ███████████ █████████ ██ ██ ██ ██████ ████████ ██████ █████████ ████ ███████ ███████ █████████ ██ ██████ ████ ████████ ██ ████ ████ ███ █████ ███████████ █████ ████ █████████ ███ ██████ █████████ ██ █████████ ██ ██ ██ ████████ ██ ███ ████ ██ ███ ██████████████ █████ ████ ████ ████████ █████████ ███████ █████████ ███ ████ █████. These wide credible intervals (CrIs) denote imprecise estimates for any comparison of atogepant 60 mg every day to all active treatments. These wide CrIs were observed whether the analysis was made in the fixed effects or random effects models.
███ ███ ██ ██ ██ ███████████ █████ ███████ ████ ████ ████████ ████ █████████ ███ ████ ██ █ ███ █████████ ██ ███████ ████ ██ ███ ██ ██████ █████████ ████ ██ ██████ ██ ███████████ ██ ███ ████ ██ █████████ █ ███ ████████ ██ ████ ███ ████ ███████ ███████ ██████ █████ ████████ ███ ██████ ██ ███ ██ ██████ ███ ███████ ██ ████ ██ █████████ █ ███ ████████ ██ ████ ███ ████████ ██ █████████ ██ ██ ██ ██████ ████ ████ ██████ █████ ███████████ ███████████.
In the 2 or more TFs analysis, CrIs for atogepant 60 mg every day versus all treatments for evaluating the monthly acute medications used daily were also wide and included the null (except versus placebo) in both the fixed effects and random effects models.
████████ ███ ███ ██████ ████ █████████ ██ ██ ██ ██ ███ ██████████ ██ ████████ ██████ ██ ██████ ████████ ██ ███████ ███ ███ ████████ ██ █████ █████ ███ █████ ██████████ ████ ███ ██████ ███ ████████ ██ ███ ██ ███ █████ ██████████ █████████ ██████████████ █████████████ █████████ ██████ ██ █████████████ The effect estimates had wide CrIs (imprecision) that conveyed important uncertainty, inhibiting the drawing of definite conclusions for these comparisons.
Harms Results
Within the evidence from the NMA, only the overall chronic migraine population was assessed for harms. In this, █████████ ██ ██ ██ ██████ ██ █████████ ██████ ██ ███ ████ ████████ ██ ███████ ███ ███████████ ███ ███
For the rest of the comparisons, the hazard ratios were also accompanied by wide CrIs that carried uncertainty due to imprecision in the hazard rates between atogepant and all relevant comparators.
Critical Appraisal
The systematic review and NMA aimed to evaluate the efficacy and harms of atogepant 60 mg every day compared to relevant comparators for chronic migraine treatment, identified based on drugs licensed and approved in Canada. While the identification and inclusion of relevant trials for the specific population and comparators were appropriately executed, details regarding the screening process were lacking. Despite well-described study designs, there was a notable absence of information on data extraction and risk-of-bias assessment procedures. Some head-to-head trials were excluded due to strict criteria; to address this, a sensitivity analysis was conducted to address effects based on excluded populations. This ensured robustness in the final estimates. Some differences, however, were observed between fixed effects and random effects models, implying possible issues of inconsistencies between the included trials.
The construction of networks was thorough, assessing model fit, consistency, convergence, and heterogeneity, establishing comparability among populations included in each network, and upholding the transitivity assumption. However, there was no formal assessment of publication bias, and imprecise effect estimates for several end points posed challenges in drawing definitive conclusions.
Overall, the populations in individual studies were deemed generalizable to the Canadian population, with no significant concerns regarding the applicability of the results detected. However, the NMA did not include several relevant outcomes of interest (e.g., MIDAS, HIT-6, MSQ, WPAI: Migraine, SAE). Also, of relevance to this submission, there was a short length of follow-up. The lack of comparison to eptinezumab was considered important to note for the Canadian landscape as well as the few comparisons available for the 2 or more TFs population.
Overall, while the systematic review and NMA effectively synthesized existing evidence, some methodological gaps and imprecisions in effect estimates warrant cautious interpretation of the findings.
Conclusions
The body of evidence assessing the effects of atogepant 60 mg every day in patients with chronic migraine and at least 2 prior preventive TFs consisted of 1 pivotal RCT comparing atogepant 60 mg every day to placebo; a single-arm, open-label extension study (███████ ███████████ ██ ███ ████████ ██ ████ ████████); and 1 ITC that compared atogepant 60 mg every day to relevant treatments for chronic migraine in Canada. The body of evidence informed on clinical efficacy end points (MMDs, MHDs, acute medication use), function and disability outcomes, HRQoL, resource use, and harms; all of these were considered important outcomes for decision-making by clinical experts, patient groups, and stakeholders.
The available evidence shows that the use of atogepant, when compared to placebo, likely results in a clinically important reduction from baseline in mean MMDs and MHDs, and that a greater proportion of patients using atogepant 60 mg every day attain reductions of 50% or more in MMDs. Atogepant 60 mg every day likely decreases the effect chronic migraines have on daily activities, and missed workdays or school days, and the impact headaches have on patients in their ability to function at school, home, or in social situations. Some uncertainty remains on the effects of atogepant on long-term outcomes due to a relatively low sample size of patients with 2 or more TFs.
When assessing atogepant 60 mg taken every day against relevant comparators in Canada, 1 included NMA showed that there is still high uncertainty when compared to other interventions used to treat chronic migraine in Canada (galcanezumab, fremanezumab, erenumab, onabotulinumtoxin A, or eptinezumab) due to highly imprecise estimates (wide CrIs) that limit the ability to draw conclusions.
The assessed body of evidence, including that from an open-label extension study, suggests that atogepant is generally well tolerated and likely results in little to no increase in the proportion of patients with AEs, SAEs, and discontinuations due to AEs when compared to placebo or the relevant comparators in the NMA.
Overall, the use of atogepant 60 mg every day in patients with chronic migraine and 2 or more TFs provides clinical benefits in reducing migraine symptoms, and improving function and HRQoL, with an adequate safety profile when compared to placebo. However, the evidence from the NMA was inadequate to inform any conclusive decision about the comparative effectiveness of atogepant 60 mg every day versus the other currently funded treatment options.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of atogepant 60 mg taken every day as oral tablets in the prevention of chronic migraine in adults.
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
Migraine is a multifactorial, disabling neurologic disease characterized by recurrent and often debilitating headaches of moderate to severe intensity accompanied by neurologic symptoms.1 The Headache Classification Committee of the International Headache Society defines migraine as a recurrent primary headache disorder resulting in attacks that last 4 hours to 72 hours.1 In addition to severe headache pain, migraine attacks are associated with a wide range of nonheadache symptoms, including sensitivity to light, sound, and smells, and nausea and vomiting.2-4
Migraine typically has multiple phases (prodrome, aura, migraine attack, and postdrome phases).1,10,11 Attacks may begin with warning signs (prodromes), such as fatigue, excessive yawning, cravings for particular foods, and mood changes (hyperactivity or hypoactivity), which can last from a few hours up to 72 hours.1,12 Aura, a transient focal neurologic symptom consisting of visual, sensory, and language or brainstem disturbances,13 occurs most often before the headache component, but may occur during or after the headache. Most commonly, the aura consists of visual manifestations, such as scotomas, photophobia, or visual scintillations (e.g., bright zigzag lines).14 Attacks may conclude with a postdrome phase characterized by psychological, general, and autonomic symptoms, such as fatigue, the inability to concentrate, and mood changes. This is followed by an interictal phase, where patients are free of symptoms until the next migraine attack.
Migraine is commonly categorized according to the frequency of attacks as episodic migraine or chronic migraine.1 People with migraine who have fewer than 15 migraine headache days are commonly referred to as having episodic migraine, a term that has been recently adopted in the Definition of Terms in International Classification of Headache Disorders, fourth edition alpha, and is widely used by clinicians and in migraine publications.5 Chronic migraine has been defined by ICHD-3 as headaches occurring on 15 or more days per month for more than 3 months, of which at least 8 days per month have the features of migraine attacks.1
The natural history of migraine is complex; it has been conceptualized as a continuum from episodic migraine to chronic migraine with variations in symptoms and headache frequency that may increase, remit, or fluctuate over time.15,16 An increased frequency of migraine attacks with fewer pain-free days in between can indicate progression from episodic migraine to chronic migraine.15 Within an individual, there is a natural variation in headache-day frequency and progression of the disease, meaning a person can fluctuate between episodic migraine and chronic migraine at different points in time over the course of the disease.17,18
Each year, approximately 2.5% to 3% of patients with episodic migraine progress to chronic migraine.7,19 The mechanisms underlying the progression of episodic migraine to chronic migraine are complex and not fully understood; however, modifiable risk factors for progression include poor migraine attack management, the frequency of stress, high caffeine intake, and obesity.15,19-21 The overuse of acute migraine nonspecific and migraine-specific medications and ineffective acute treatment leading to medication overuse have been shown to increase the risk for migraine chronification.7,22,23
Migraine affects 8.3% of the population in Canada, with a higher prevalence in women than men, and a higher prevalence among the working population.24 The mean age of diagnosis is 26.2 years, 3.6 years after symptoms are first experienced. For both sexes, the prevalence of migraine is highest among those aged 30 years to 49 years, with female patients more than twice as likely as males to report migraine (11.8% versus 4.7%), which is consistent with studies in the global population.25
Worldwide migraine is highly prevalent, affecting more than 1 billion people,25-27 or approximately 1 in 7 individuals (14% of the population). Among those with migraine, the prevalence of chronic migraine ranges from approximately 5% to approximately 12%.28-30 Among the general population, the prevalence of chronic migraine ranges from 0.9% to 5.1%, with estimates typically in the range of 1.4% to 2.2%.31 The annual incidence of migraine in the general population from prospective cohort studies ranges from less than 1% to 2% or approximately 8 to 15 per 1,000 person-years.28
Migraine is the second leading cause of disability worldwide and the leading cause of disability among neurologic diseases, greatly affecting daily functioning and significantly impacting HRQoL.30
Standards of Therapy
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
As attack frequency or severity increases, migraine management requires the use of both acute and preventive treatments.6,7
Preventive pharmacotherapies are used to reduce the frequency, duration, and severity of migraine attacks, thereby reducing the need for acute medications.32 They are recommended in people with a high frequency of migraine attacks to improve function and HRQoL.33,34 The early initiation of preventive treatment can reduce the risk of migraine evolving from episodic migraine to chronic migraine.35,36
Multiple pharmacologic options for migraine prevention are currently available in Canada for patients with chronic migraine, including established oral preventive treatments, injectable onabotulinumtoxin A, or self-injectable and infusion CGRP mAbs.
Currently, the first-line therapy for managing chronic migraine is the established oral medications (e.g., topiramate, propranolol), which come from a variety of therapeutic classes (e.g., antidepressants, antiepileptics, antihypertensives).22 Health Canada–approved oral therapies for chronic migraine include anticonvulsants (e.g., topiramate), beta blockers (e.g., propranolol), and calcium channel antagonists (e.g., flunarizine).
CGRP mAbs are a disease-specific treatment class for migraine.6 They are indicated for the preventive treatment of episodic migraine or chronic migraine in adults, are administered via a subcutaneous injection or IV infusion, and have half-lives ranging from 27 days to 31 days. CGRP mAbs currently approved by Health Canada include erenumab, galcanezumab, fremanezumab, and eptinezumab. CGRP mAbs may have limitations affecting their use, including declining effectiveness over time, the need for self-injection or infusion, slow rates of clearance, and high discontinuation rates. Recent guidelines recommend the use of CGRP mAbs in people with migraine who are intolerant to established oral preventive treatments or in whom prior established oral preventive treatments have failed.6,37-39
Drug Under Review
Key characteristics of atogepant are summarized in Table 3 with other treatments available for chronic migraine.
Atogepant (Qulipta) tablets (10 mg, 30 mg, and 60 mg) are an orally administrated CGRP antagonist currently indicated for the treatment of adult patients (18 years and older) for the prevention of episodic migraine (< 15 migraine days per month). The sponsor is requesting that atogepant be reimbursed for the prevention of chronic migraine in adults with 15 or more headache days per month (of which 8 days are migraine days) and who have experienced an inadequate response, intolerance, or contraindication to at least 2 oral prophylactic migraine medications.
Atogepant was approved by Health Canada with a Notice of Compliance on May 2, 2024, to expand the indication to the prevention of migraine in adults who have at least 4 migraine days per month.
On June 14, 2023, atogepant received a recommendation to reimburse with conditions by the Canadian Drug Expert Committee for the prevention of episodic migraine in adults with fewer than 15 migraine days per month who have experienced an inadequate response, intolerance, or contraindication to at least 2 oral prophylactic migraine medications.
Dosing and Administration
For patients with chronic migraine, the recommended dose is 60 mg orally once daily.
Mechanism of Action
CGRP is a vasodilator and neuromodulator that plays a key role in migraine pathophysiology.40,41 Serum CGRP levels are elevated during migraine attacks and selective CGRP antagonists offer their clinical effects, inhibiting this pathway in patients with migraine.42-44 The first CGRP antagonists for migraine prevention were CGRP mAbs, which require subcutaneous injection or IV administration. Atogepant is a selective, oral, small-molecule, CGRP receptor antagonist that blocks the binding of the CGRP to the receptor and antagonizes CGRP receptor function.45
Table 3: Key Characteristics of Atogepant and Other Relevant Comparators
Drug | Mechanism of action | Indicationa | Route of administration | Recommended dosage | Serious adverse effects or safety issues |
|---|---|---|---|---|---|
Atogepant (Qulipta), 10 mg, 30 mg, 60 mg | CGRP mAb | Prevention of episodic migraine in adults | Oral | 60 mg once daily orally | Not reported |
Erenumab (Aimovig), 70 mg/mL, 140 mg/mL | CGRP mAb | Prevention of migraine in adults who have at least 4 migraine days per month | SC | 70 mg SC q.m.; some patients may benefit from 140 mg SC q.m. | Constipation with serious complications |
Galcanezumab (Emgality), 120 mg/mL | CGRP mAb | Prevention of migraine in adults who have at least 4 migraine days per month | SC | 240 mg SC loading dose followed by 120 mg SC q.m. | Serious hypersensitivity reactions |
Fremanezumab (Ajovy), 150 mg/mL | CGRP mAb | Prevention of migraine in adults who have at least 4 migraine days per month | SC | 225 mg SC q.m. or 675 mg SC q.3.m. | Serious hypersensitivity reactions |
Eptinezumab (Vyepti), 100 mg/mL | CGRP mAb | Prevention of migraine in adults who have at least 4 migraine days per month | IV | 100 mg or 300 mg IV over 30 minutes q.3.m. | Unknown effect in pregnancy and in patients with cardiovascular disease |
Topiramate | Antiepileptic | Prevention of migraine Epilepsy | Oral | 100 mg daily divided in 2 doses | Drowsiness, hyperammonemia, suicidal ideations |
Amitriptyline | Tricyclic antidepressant | Depression Off-label use for chronic migraine | Oral | 25 mg 3 times a day depending on response | Drug interactions, suicidal ideation, contraindicated in pregnancy, drowsiness |
Propranolol | Antihypertensive | Hypertension Prophylaxis of chronic migraine | Oral | 40 mg twice daily | Cardiac failure, oculomucocutaneous syndrome, bronchospasm |
Onabotulinumtoxin A (Botox) | Neuromuscular paralytic drug | Chronic migraine | IM injection | Varies. Start at 155 units IM. | Allergic reactions, muscle weakness, vision problems, difficulty breathing |
CGRP = calcitonin gene–related peptide; IM = intramuscular; mAb = monoclonal antibody; q.3.m. = every 3 months; q.m. = every month; SC = subcutaneous.
aHealth Canada–approved indication.
Sources: Product monographs of atogepant (Qulipta),46 amitriptyline,47 eptinezumab (Vyepti),48 erenumab (Aimovig),49 fremanezumab (Ajovy),50 galcanezumab (Emgality),51 onabotulinumtoxin A (Botox),52 topiramate,53 and propranolol.54
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full original patient input received by CDA-AMC have been included in the Stakeholder section of this report.
CDA-AMC received 2 patient group submissions — 1 from the Canadian Migraine Society and a second from Migraine Canada and Migraine Quebec.
The Canadian Migraine Society is an advocacy group focused on improving the quality of life of people in Canada living with migraine and has 3 main focuses: empathy (offered through 2 robust online support groups with almost 4,000 members), education (provided through a patient-centric website), and empowerment (realized by advocating with various stakeholders such as health care professionals, pharmaceutical companies, and government bodies).
Migraine Canada is a federally registered national charity founded in 2018 with the mission of providing support and education and raising awareness about the impact of migraines. Migraine Quebec is a provincial nonprofit patient organization founded in 2014 whose mission is to provide support and information to people with migraine, as well as to educate the public about the repercussions of the disease. Both groups advocate for optimal care for those living with migraines and support research to find treatments to improve the quality of life of patients with this chronic disease.
The Canadian Migraine Society gathered data from 3 perspectives: experience from support groups with 3,200 members, personal disease experience, and email interviews conducted from November 1 to December 12, 2023, with 19 patients currently on atogepant. The information provided by Migraine Canada and Migraine Quebec was collected through a quality-of-life online survey that was launched in the late fall of 2021. In total, 1,165 adults with migraine living in Canada and their caregivers responded to the online survey. Migraine Canada launched an additional survey in November 2023 to gather further insights, seeking input from patients with experience with atogepant. In total, 230 adults with migraine responded to the survey.
Most of the patients from the 2 patient group submissions shared similar symptoms and acknowledged the impact of symptoms on their day-to-day lives and employment. The Canadian Migraine Society reported that migraine — and especially chronic migraine — affects every single facet of a person’s life. As in the rest of the world, 85% of patients with chronic migraine are women, and the greatest prevalence of the disease occurs between the ages of 30 years to 39 years, the most productive years of many women’s lives. Furthermore, chronic migraine means having a migraine attack almost every other day, with migraine cycles and phases often lasting more than a day, implying that people experiencing this severity level are almost never without pain. Based the quality-of-life online survey conducted by Migraine Canada and Migraine Quebec, more than 52% of respondents had difficulty keeping a daily routine or schedule and 39% of patients were unable to do usual household chores. A significant number of people (55%) experienced feeling lack of control over their life because of the frequency of their migraine symptoms ranging from always (25 days to 30 days per month) to often (11 days to 15 days per month). In terms of employment, the quality-of-life online survey showed that only 46% of patients reported to work full-time while 11% of patients were able to work part-time. More than 20% of the respondents were on short- or long-term disability or retired early due to their migraine condition. Some respondents (3%) shared that they were unemployed and not able to have any support through disability programs. When asked about sleep issues, only 7% of patients reported no issues with their sleep patterns while 38% of patients always or regularly had sleep disrupted due to their migraine. Regarding mental health, 48% of patients said migraine has caused them to become depressed and/or anxious but not to the point where counselling or medication was required. Moreover, because of their migraine, 50% of patients worried about their family’s financial stability.
Most people (54%) indicated migraine has had a negative impact on their relationship with their partners. One of the patient testimonials on impact of quality of life from the November 2023 survey conducted by Migraine Canada and Migraine Quebec stated, “I have been having migraines since I was around 19/20 years old.” “Now I have 19-24 days per month of migraine. It’s debilitating. It makes it hard to live a ‘normal’ life. I can’t do many of the chores at home when I have a migraine, and I definitely cannot go socialize. It makes doing my job- I have my own small business- really difficult. Chronic pain from migraines causes all sorts of mental health issues too.”
Both patient groups remarked that the currently available treatments for migraine are not adequate, and more than 85% of respondents from the quality-of-life online survey by Migraine Canada and Migraine Quebec believe there is a need for a new oral daily preventive medication. The Canadian Migraine Society mentioned that most daily oral preventive medications, like Topamax, propranolol, and amitriptyline, are used off-label since they were not designed specifically for migraine. The side effects of current treatments include weight gain, depression, anxiety, brain fog, dizziness, numbness, and tingling, to name a few. Botox has a high success rate but for many, the 31 injection sites are not tolerable, and in terms of cost, it is publicly reimbursed on 2 provincial formularies (Alberta and Ontario). The Canadian Migraine Society further commented that CGRP mAbs like Aimovig, Emgality, Ajovy, and Vyepti have been designed specifically to treat migraine and have been life-changing for many. In terms of side effects, CGRP mAbs have a lower side-effects profile but due to the long half-lives, remain in a patient’s system for an average of 5 months to 6 months after treatment cessation. Monthly injections can be hard for some, and IV infusions can be very hard to access in smaller communities. Input from the November 2023 survey conducted by Migraine Canada and Migraine Quebec showed that there were 4 common themes about unmet needs: to have no side effects, to have symptom-free days to enjoy life, to have fewer migraine symptoms every day, and to have a treatment that is efficacious and affordable with few side effects.
In both surveys conducted by Migraine Canada and Migraine Quebec, the 3 outcomes that would be most valuable to patients when trying a preventive treatment were a decrease in headache intensity, a decrease in headache frequency, and a decrease in symptoms other than pain such as sensitivity to light and sound, and nausea and brain fog. The Canadian Migraine Society further stated that the desired outcome should be an increase in quality of life.
A total of 19 patients from the Canadian Migraine Society were receiving atogepant through either private insurance, the patient support program provided by AbbVie Corporation, or an 80 to 20 combination of the 2. These patients mention that “atogepant works much more quickly than other preventives,” and that “it is much easier to take than an injection or IV, and by reducing migraine frequency…are able to significantly lower their risk of medication overuse headache/rebound headaches from needing to treat so many attacks with acute medications.” Additionally, there was a total of 26 people who have had experience on atogepant from Migraine Canada and Migraine Quebec, and the majority (68%) perceived a benefit. More than 70% of patients responded that atogepant was easier or more convenient to use compared to other therapies.
All groups agreed that patients with chronic migraine need access to new options for other medications (both preventive and acute), because not everybody who lives with migraine responds to the same medication or treatment. Migraine Canada and Migraine Quebec also highlighted that considering the opioid crisis, these new medications can and should play a role in a national crisis by better managing pain and alleviating the need for opioids.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of chronic migraine.
Unmet Needs
The clinical expert consulted by CDA-AMC referred to poor adherence as an important unmet need, mentioning that the adherence at the 1-year mark is low — probably around 20% — among patients with chronic migraine. Also, side effects of current medications are common even when these medications are being effective, which leads to discontinuation or poor adherence to treatment.
The type of administration was mentioned as an important unmet need to be considered. For instance, onabotulinumtoxin A is a well-tolerated (and with very few side effects) medication for chronic migraine; however, patients must travel to clinical facilities and health professionals with experience in injecting the treatment and this is often not readily available.
Place in Therapy
According to the clinical expert, atogepant could be, under normal circumstances, a first-line treatment due to its effectiveness and low side-effects profile; however, it is possible that other circumstances (like costs) will cause a restriction of the indication to patients who try at least 2 prior medications first. Atogepant could be added to or replace a treatment such as onabotulinumtoxin A in people receiving only partial benefit from Botox because they work by slightly different mechanisms.
Atogepant addresses the underlying migraine disease process. The clinical expert suggested that because of its shorter half-life, it could be a better choice among patients contemplating pregnancy or in patients in whom there are concerns about vascular issues.
Hence, the cost factor would be the main reason patients try other medications before atogepant. Overall, the clinical expert noted that the gepants drugs tend to be better tolerated with good safety profiles.
Patient Population
The clinical expert mentioned that it is difficult to predict the likelihood of response to atogepant based on specific factors from patients. According to the clinical expert, patients would mostly be identified by history and physical examination by a primary care physician or a nurse practitioner. This would not require a headache specialist to make the diagnosis; hence, in the expert’s opinion, there is no need for diagnostic tests in clinical practice.
The clinical expert mentioned that patients with a history of stroke, transient ischemic attacks, ischemic cardiac disease, or peripheral vascular disease should be stable for 6 months before trying atogepant. Patients should be cautioned about getting pregnant and if they become pregnant, the medication should be stopped. Using atogepant while breastfeeding should be avoided, and the medication should be used only in those aged 18 years and older.
Assessing the Response Treatment
According to the clinical expert, physicians would like a reduction in the number of headache days or a reduction in the severity of headaches to determine an appropriate response to treatment. Some patients may continue to have severe headaches but have fewer of them in number. Other patients may continue to have a daily headache, but with less intensity. Primary care physicians and nurse practitioners typically do not use headache diaries or tools like the MIDAS and HIT-6 to assess patients’ headaches but rather to ask them such questions as how they are doing or if their medications are making them feel better. Furthermore, a minimum trial of 6 months is needed before assessing effectiveness.
Discontinuing Treatment
The clinical expert mentioned that there are no established criteria to discontinue treatment. Most physicians would assess if patients had 9 months with 4 or fewer headache days per month and if patients respond readily to acute treatment, then the medication could be stopped and reassessed.
Prescribing Considerations
Atogepant is suitable for prescription by primary care physicians and nurse practitioners. No special monitoring is required.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups. The full original clinician group input received by CDA-AMC has been included in the Stakeholder section of this report.
CDA-AMC received 2 clinician group submissions from the ANSG and CHS. ANSG consists of neurology specialists from Atlantic Canada who have significant experience in diagnosing, managing, and treating migraine in Canada. CHS is a scientific society of health care professionals founded in 1988 that is dedicated to headache medicine, with goals including research, the education of residents and physicians, and the promotion of better care for patients experiencing headache disorders.
ANSG held 2 professional meetings on October 5 and December 18, 2023, to discuss the migraine treatment landscape, and identify barriers to treatment access and the role of atogepant in fulfilling unmet patient needs. CHS gathered information from published clinical evidence and expert opinions from headache specialists in Canada and internationally.
ANSG emphasized that migraine is a debilitating disease that has substantial health and economic impacts and significantly affects the quality of life of patients; migraine can be categorized either as episodic or chronic. Patients who experience 4 headache days to 14 headache days a month are diagnosed with episodic migraine, while those who experience 15 or more headache days with 8 or more being migraine days a month are diagnosed with chronic migraine. In terms of treatment for migraines, both clinician groups agreed that there are nonpharmacologic treatments such as cognitive behavioural therapy and lifestyle changes, including regular diet and sleep, hydration, stress management, aerobic exercise, pacing, trigger management, and pharmacologic treatments consisting of acute and preventive medication. There are many options for acute migraine treatments, including triptans, nonsteroidal anti-inflammatory drugs (NSAIDs), nonopioid analgesics, antiemetics, and opioids. The goal of acute medication is to alleviate the symptoms of migraines and to return to function as quickly as possible and with no or minimal side effects. Preventive treatments for migraines may be oral and injectable medications. Oral preventives include antihypertensives, antiepileptics, and antidepressants, which are considered nonspecific to migraine because their mechanism of action is usually not well understood. Onabotulinumtoxin A has been approved in Canada since 2011 as an injectable preventive for the preventive treatment of chronic migraine. It requires injections at 31 sites to 39 sites on the head and neck of the patient every 3 months, administered by a physician trained in the injection procedure. More recently, CGRP mAbs have been approved for the treatment of chronic migraine (erenumab, galcanezumab, fremanezumab, and eptinezumab). However, CHS highlighted that access to onabotulinumtoxin A and CGRP antibodies varies significantly between provinces and territories depending on public coverage policies. Criteria for coverage also vary from 1 province to the other even for the same product.
ANSG believes that realistic treatment goals for patients living with chronic migraine are to attain a 50% reduction in migraine days from baseline with an increase in social activities, decreased time off work, and less health care use. CHS further commented that the goals of therapy should include improved HRQoL, improved function, reduced disability, reduced headache attack frequency, severity, and duration, a decreased need for acute medications that brings the risk of medication overuse headache, as well as reduced indirect costs associated with migraine (absenteeism and presenteeism).
ANSG prioritized 3 unmet treatment needs for migraine in Canada: the existence of AEs and inadequate response to acute and preventive treatments, the fact that GPs depend on specialists for prescribing preventive treatments, and the fact that restrictive reimbursement criteria prevent patient access to the care that they need. CHS also found similar treatment gaps and some additional ones, such as the effectiveness of current available treatments wearing off over time, contraindication to some patient populations, and patients’ preference for oral formulations.
CHS commented that atogepant could be combined with drugs with a different mechanism, though evidence to support the effectiveness of such combinations is lacking. CHS further highlighted that atogepant is the first oral drug of this class and provides unique advantages for patients who prefer a pill over an injection. ANSG agreed that the patients who are most suited for atogepant would be those who did not experience improvement with or have contraindications to other preventive medications, as well as those with needle phobia. On the other hand, CHS believed that atogepant, with its high efficacy and tolerability rates, is a reasonable first-line treatment from a medical perspective, and only financial arguments justify a second-line place requiring the trial of other oral preventives. Both clinician groups agreed that a reduction in migraine days, decreased severity, and/or improved response to rescue or acute therapies after 8 weeks to 12 weeks of daily atogepant should be used to determine response, and treatment should be discontinued if atogepant fails to display a reduction in migraine days, decreased severity, and/or improved response to rescue or acute therapies after 8 weeks to 12 weeks. ANSG believed that specialists, GPs, and nurse practitioners with experience diagnosing migraine could prescribe the product and monitor the patients. CHS stated that atogepant prescription should not be restricted to neurologists or specialists because it is well tolerated and safe compared to many other drugs prescribed in primary care.
CHS also emphasized that migraine is underdiagnosed and undertreated, particularly in primary care, due to a lack of education as well as a lack of effective, specific, and tolerated options for prevention. Moreover, access to specialized migraine care is limited across the country. According to CHS, atogepant could be a good migraine preventive in primary care if cost allowed it. Access to different migraine treatments, both acute and preventives such as triptans, onabotulinumtoxin A (drug and injection fee codes), and CGRP antibodies, vary from 1 province or territory to another.
Drug Program Input
The drug programs provide input on each drug being reviewed through CDA-AMC’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The PROGRESS trial compared atogepant (Qulipta) 30 mg b.i.d. to 60 mg q.d. to placebo over 12 weeks. There are no head-to-head comparisons of the relevant comparators in migraine prevention. | This is a comment from the drug programs to inform CDEC deliberations. |
Not all drug plans cover Botox for migraine prevention, but some do. The place in therapy is important to clarify. Injectable CGRP inhibitor medications are listed in many jurisdictions. If needed and applicable, the initiation criteria for atogepant should be aligned with other CGRP inhibitor medications for this indication. | This is a comment from the drug programs to inform CDEC deliberations. |
Considerations for initiation of therapy | |
The number and type of prophylactic medications tried before initiation should be discussed. As noted earlier, the criteria for atogepant should align with other similar recommendations, if feasible. | This is a comment from the drug programs to inform CDEC deliberations. |
Prior therapies: Considering Botox and other CGRP inhibitor medications before initiating atogepant, how many of these (prophylactic) medications should be tried first? Can it be specified as to which medications should be tried? | According to the clinical expert consulted by CDA-AMC, there is no evidence for establishing a specific order of medications. For example, some patients may need Botox first due to their initial symptoms. This also applies when assessing the new gepants drugs vs. monoclonal antibodies, where there is even less of a difference in terms of efficacy between these groups of drugs to establish a specific order of therapy. The clinical expert mentioned that any drug tried before atogepant will be adequate to include in the considerations for initiation. |
Eligibility to re-treatment: Can patients be re-treated? Namely, if patients discontinue the therapy due to benefit and then relapse with symptoms, can the drug be given again? If so, what would be the appropriate timing of re-treatment? | The clinical expert explained that there are no compelling reasons why clinicians and patients would not consider or try this maneuver. No specific timing can be addressed with certainty, but the clinical expert would recommend observing patients during the first 3 months off therapy, which is the time during which symptoms may come back. |
Consistency with initiation criteria associated with other drugs reviewed by CDA-AMC in the same therapeutic space: Consider alignment with other CGRP inhibitor recommendations for this indication. | This is a comment from the drug programs to inform CDEC deliberations. |
Considerations for continuation or renewal of therapy | |
Consistency with renewal criteria associated with other drugs reviewed by CDA-AMC in the same therapeutic space: Consider alignment with other CGRP inhibitor recommendations for this indication. | This is a comment from the drug programs to inform CDEC deliberations. |
Considerations for discontinuation of therapy | |
Consider alignment with other CGRP inhibitor recommendations for this indication. | This is a comment from the drug programs to inform CDEC deliberations. |
Considerations for prescribing of therapy | |
In the pivotal trial, the 30 mg b.i.d. and 60 mg q.d. dosage schemes were studied. However, the 60 mg q.d. is the only dosage recommended for this indication (based on the monograph).
| The clinical expert mentioned the lack of evidence for going over 60 mg daily; hence, there is uncertainty in this regard. The clinical expert also mentioned that the 30 mg b.i.d. is not needed in clinical practice as the 60 mg q.d. is more acceptable and feasible since it provides the same level of efficacy and with easier delivery and possibly better adherence to treatment. |
Consider “prescriber with experience in migraine therapy” to align with other recommendations and improve access in areas where neurologists may be difficult to meet with. | This is a comment from the drug programs to inform CDEC deliberations. |
There were comments on combining atogepant with Botox and possibly with other injectable CGRP inhibitor medications. | According to the clinical expert, these interventions can be combined by the treating physician if there is adequate, close clinical monitoring. In the clinical expert’s experience, using Botox and monoclonal antibodies is common in clinical practice. If there are no specific contraindications or drug interactions, the combination is allowed. |
Generalizability | |
Populations of interest matching the indication but with insufficient data:
| This is a comment from the drug programs to inform CDEC deliberations. |
Patients on active treatment with a time-limited opportunity to switch to the drug(s) under review:
| The clinical expert confirmed that it is feasible for patients to switch, and no specific regimen is needed to accomplish this strategy. |
System and economic issues | |
Presence of confidential negotiated prices for comparators:
| This is a comment from the drug programs to inform CDEC deliberations. |
B.i.d. = twice a day; CDEC = Canadian Drug Expert Committee; CGRP = calcitonin gene–related peptide; q.d. = every day; vs. = versus.
Clinical Evidence
The objective of CDA-AMC’s Clinical Review Report was to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of atogepant 60 mg once daily orally in the prevention of chronic migraine in adults. The focus was placed on comparing atogepant to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of atogepant is presented in 3 sections with CDA-AMC’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CDA-AMC’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. A third section includes the ITC and studies addressing gaps (when applicable).
Included Studies
Clinical evidence from the following is included in the CDA-AMC review and appraised in this document:
1 pivotal study (RCT) identified in the systematic review process
1 long-term extension study
1 ITC.
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
Only 1 double-blind, placebo-controlled RCT (Study 3101 to 303 to 002, known as the PROGRESS trial) was included from the systematic literature review. Characteristics of the included study are summarized in Table 5.
Table 5: Details of Study Included in the Systematic Review
PROGRESS trial (Study 3101 to 303 to 002) | |
|---|---|
Designs and populations | |
Study design | Multicentre, randomized, double-blind, placebo-controlled, parallel-group, phase III study |
Locations | Patients were screened for eligibility at 142 sites in the following countries: the US, the UK, Canada, China, Czech Republic, Denmark, France, Germany, Italy, Japan, Republic of Korea, Poland, Russia, Spain, Sweden, and Taiwan |
Patient enrolment dates | Start date: March 11, 2019 End date: January 20, 2022 |
Randomized (N) | Total N = 778 Atogepant 60 mg q.d. (N = 262; N | ███ in the 2+ TFs population) Atogepant 30 mg b.i.d. (N = 257) Placebo (N = 259; | | ██ in the 2+ TFs population) |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Atogepant 60 mg orally q.d. + placebo q.d. Atogepant 30 mg orally b.i.d. |
Comparator(s) | Matching oral placebo b.i.d. |
Study duration | |
Screening phase | 4 weeks |
Double-blind treatment period | 12 weeks |
Follow-up phase | 4 weeks |
Outcomes | |
Primary end point | Change from baseline in mean MMDs through 12 weeks |
Secondary and additional end points | Secondary end points (through 12 weeks)
Additional end points
|
Publication status | |
Publications | Pozo-Rosich et al.55 |
AIM-D = Activity Impairment in Migraine-Diary; b.i.d. = twice a day; CM = chronic migraine; eDiary = electronic diary; EQ VAS = EQ visual analogue scale; HIT-6 = Headache Impact Test; ICHD-3 = International Classification of Headache Disorders, third edition; MHD = monthly headache day; MIDAS = Migraine Disability Assessment; MMD = monthly migraine day; MSQ = Migraine-Specific Quality-of-Life Questionnaire; PGI-C = Patient Global Impression–Change; PGI-S = Patient Global Impression–Severity of Illness; PHQ-9 = Patient Health Questionnaire-9; PROMIS Short Form v1.1 - Pain Interference 6a = Patient-Reported Outcomes Measurement Information System - Short Form version 1.1 - Pain Interference 6a; q.d. = every day; TF = treatment failure; WPAI:Migraine = Work Productivity and Activity Impairment: Migraine.
Note: Details included in Table 5 are from the sponsor’s Summary of Clinical Evidence.
Sources: PROGRESS Clinical Study Report (2022).55
The PROGRESS study assessed the safety, tolerability, and efficacy of atogepant 30 mg twice a day and atogepant 60 mg every day compared with placebo in the prevention of chronic migraine. The objectives of the study were as follows:
to evaluate the safety and tolerability of atogepant 30 mg twice a day and atogepant 60 mg every day for the prevention of chronic migraine
to prospectively test for the superiority of atogepant 30 mg twice a day and atogepant 60 mg every day versus placebo for the prevention of chronic migraine.
In this report, results from the atogepant 30 mg twice a day group are not presented as it will not be an approved dosing regimen for the chronic migraine population. The study includes 778 initial patients who were randomized to 1 of 3 treatment arms (placebo, atogepant 30 mg twice a day, or atogepant 60 mg every day) in a 1:1:1 ratio. The randomization was stratified by acute headache medication overuse during the baseline period, migraine prevention medication exposure with proven efficacy, and region. Patients with current or past use were further stratified based on the number of medications that did not yield improvement with unique mechanisms of action: “failed 0 medications or failed 1 or more medication(s) with the same mechanism of action” or “failed 2 to 4 medications with different mechanisms of action.”
The study consisted of a 4-week screening and baseline period, a 12-week double-blind treatment period, and a 4-week follow-up period, for a total duration of 20 weeks (Figure 1). The follow-up visit (visit 8) must have been completed for all patients who took at least 1 dose of study medication, except for patients rolling over into Study 312 (a long-term safety extension study in regions excluding Japan and China), Study 3101 to 306 to 002 (a long-term safety extension study in Japan), or Study 3101 to 311 to 002 (an open-label safety extension study in China). For these rollover patients, visit 8 of the PROGRESS trial was not required because the follow-up visit was to be performed after the open-label treatment in the respective extension safety study. For patients who did not meet the screening criteria for the safety extension study, the follow-up visit (visit 8) of the PROGRESS trial must have been completed.
Figure 1: Design Schematic of the PROGRESS Study
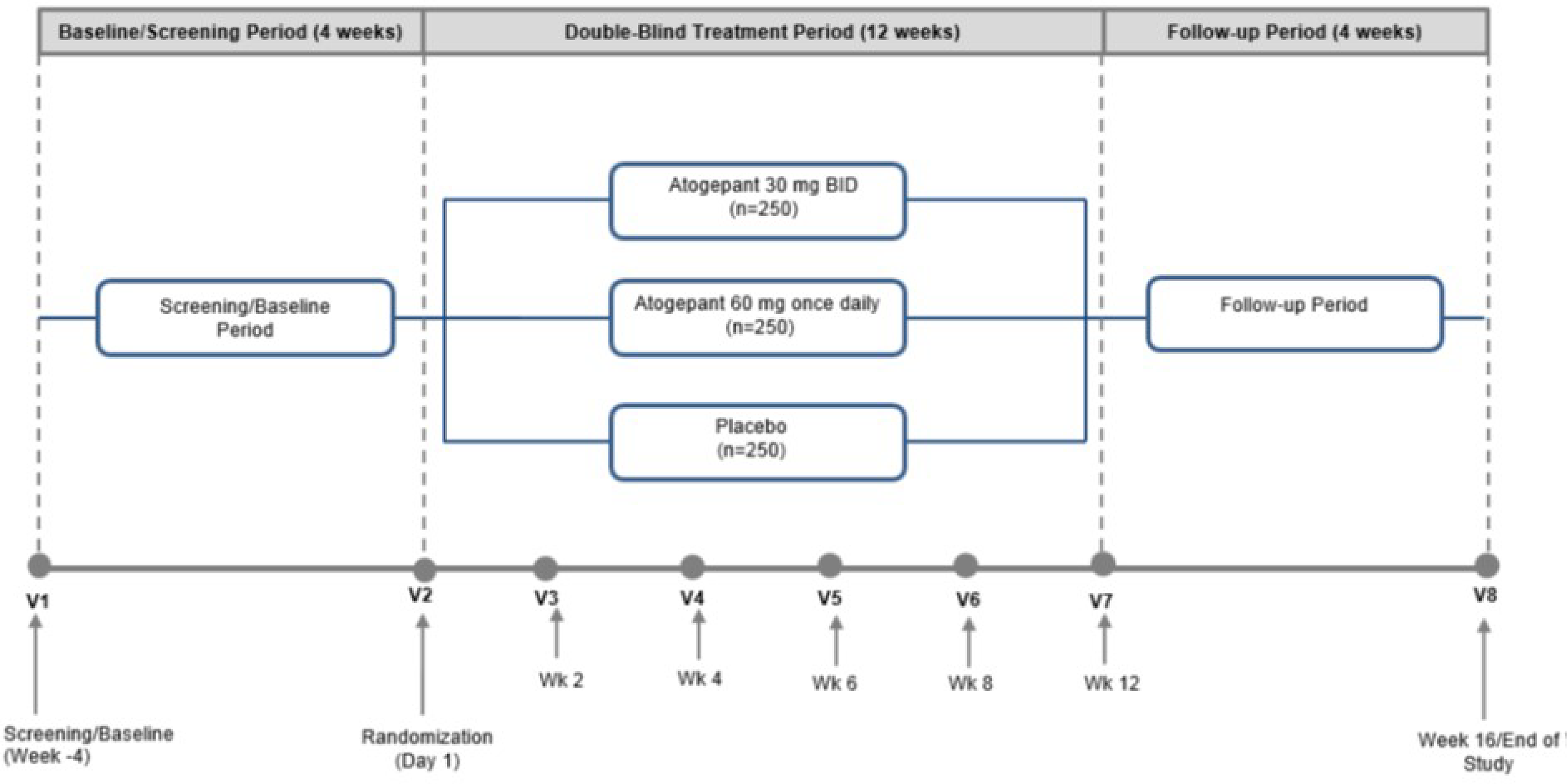
BID = twice a day; v = visit; wk = week.
Source: PROGRESS Clinical Study Report (2022).55
Populations
Inclusion and Exclusion Criteria
For the PROGRESS study, patients aged 18 years to 80 years who had a migraine onset before 50 years and had at least a 1-year history of chronic migraine, a diagnosis according to the ICHD-3, were included. Patients also must have reported 15 or more migraine headache days on average in the 3 months before visit 1, 15 or more headache days during the 4-week baseline period per an electronic diary (eDiary), and 8 or more migraine days during the 4-week baseline period per eDiary.
Patients were excluded from the PROGRESS study if they experienced an inadequate response to more than 4 preventive medications, were taking more than 1 preventive medication (if 1 medication was used, then the exclusion criteria were that the dose was not stable and/or well tolerated for more than 12 weeks before visit 1, or that the patient was unwilling or unable to maintain a stable dose and/or regimen during the trial), used opioids or barbiturates more than 4 days per month in the 3 months before visit 1, experienced clinically significant cardiovascular, cerebrovascular, hematologic, endocrine, pulmonary, renal, hepatic, gastrointestinal, or neurologic disease, laboratory values, or psychiatric conditions, dementia, or epilepsy. Patients were also excluded if they posed a significant risk of harm to self or others or had a concurrent pain condition and had difficulty distinguishing migraine headaches from other types.
For the purposes of this CDA-AMC submission, the population with 2 or more TFs was assessed as part of the analysis of the main outcomes.
Interventions
At the time of randomization, eligible patients were randomized in a 1:1:1 ratio into the following treatment arms: placebo, atogepant 30 mg twice a day, or atogepant 60 mg every day. Patients who met all the study entry criteria were randomized and provided with a study intervention to be taken on an outpatient basis. Sites subsequently dispensed the study intervention to patients at visit 3, visit 4, visit 5, and visit 6 (Figure 1). Patients took their first dose of the study intervention at the clinic at visit 2. The study intervention was administered orally for 12 weeks, and patients were followed for 4 weeks following study completion or discontinuation of the study intervention. All patients were instructed to take their study intervention twice daily (i.e., 2 tablets in the morning and 2 tablets in the evening) at approximately the same times each day. Patients, therefore, received either placebo twice a day, atogepant 30 mg twice a day, or a morning dose of atogepant 60 mg with an evening dose of placebo. A double-dummy design was used to maintain blinding. All study interventions were provided in identical blister cards to maintain masking of the study.
Patients using 1 concomitant migraine prevention medication were allowed to enrol, as were patients with an overuse of acute headache medication. Specifically, allowed medications for the acute treatment of migraines were triptans, ergots, opioids, analgesics (including acetaminophen), NSAIDs (including Aspirin), and antiemetics. Aspirin was allowed for cardiac prophylaxis at a dose of up to 325 mg per day, and selective serotonin reuptake inhibitors or selective norepinephrine reuptake inhibitors were also permitted so long as the treatment was stable for at least 60 days before the screening visit and did not change during the study.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. These outcomes were obtained from those included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical expert consulted by CDA-AMC and stakeholder input from patient groups, clinician groups, and public drug plans. Using the same considerations, the CDA-AMC review team crafted a list of selected end points that were most relevant in informing CDA-AMC’s expert committee deliberations and finalized this list of end points in an iterative consultation with members of the expert committee. The summarized efficacy end points were assessed and included in the GRADE evaluation of the body of evidence. Select notable harms outcomes considered important for informing CDA-AMC’s expert committee deliberations were also assessed using GRADE. Outcomes or different measurements of the same outcome not selected for inclusion in the GRADE summary of findings but noted as important can be included and described in the text of this report and/or the appendix.
Table 6: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | PROGRESS study |
|---|---|---|
Efficacy measures | ||
CFB in mean MMDsa | At 12 weeks | Primary |
Reduction of ≥ 50% in 3-month average of MMDsa | At 12 weeks | Secondary |
CFB in mean MHDsa | At 12 weeks | Secondary |
CFB in mean monthly acute medication use daysa | At 12 weeks | Secondary |
Function and disability: Health outcome measures | ||
AIM-D | ||
CFB in mean monthly performance of daily activities domain score of the AIM-Da | At 12 weeks | Secondary |
MIDAS | ||
CFB in the MIDAS total score | At week 12 | Additional |
HIT-6 | ||
CFB in the HIT-6 total scorea | At 12 weeks | Secondary |
Health-related quality of life | ||
MSQ Version 2.1 | ||
CFB in MSQ Version 2.1 role function-restrictive domain scorea | At 12 weeks | Secondary |
Resource use | ||
WPAI:Migraine version 2.0 | ||
CFB in percentage of work time missed | At 12 weeks | Additional |
AIM-D = Activity Impairment in Migraine-Diary; CFB = change from baseline; HIT-6 = Headache Impact Test; MHD = monthly headache day; MMD = monthly migraine day; MSQ = Migraine-Specific Quality-of-Life Questionnaire; WPAI:Migraine = Work Productivity and Activity Impairment: Migraine.
aStatistical testing for these end points was adjusted for multiple comparisons.
Source: PROGRESS study statistical analysis plan (2021).56
After an iterative discussion with relevant stakeholders and the expert committee members, what follows is a description of the outcomes finally included in this report.
Efficacy Outcomes
Change From Baseline in Mean Migraine Days (MMDs)
This was the primary end point measured in the PROGRESS pivotal trial. A migraine day was defined as any calendar day on which a headache occurred that met criteria A, B, and C, or met criteria D and E, listed as follows, as per patient eDiary.
Criteria A: A headache had at least 2 of the following 4 characteristics:
unilateral location
pulsating quality
moderate or severe pain intensity
was aggravated by or causing avoidance of routine physical activity (e.g., walking, climbing stairs).
Criteria B: A patient had at least 1 of the following:
nausea and/or vomiting
photophobia and phonophobia
typical aura (i.e., visual, sensory, or speech and/or language) accompanying or within 60 minutes before a headache begins.
Criteria C: The duration of a headache was 2 hours or longer on a calendar day unless an acute, migraine-specific medication (i.e., triptan or ergot derivative) was used after the start of the headache, in which case no minimum duration was to be specified.
Criteria D: The patient had any headache that fulfilled 1 criterion from the headache characteristics and at least 1 criterion from the symptoms or fulfilled at least 2 criteria from headache characteristic and 0 criterion from symptoms.
Headache characteristics were as follow:
unilateral location
pulsating quality
moderate or severe pain intensity
was aggravated by or causing avoidance of routine physical activity (e.g., walking, climbing stairs).
Symptoms were as follows:
nausea and/or vomiting
photophobia and phonophobia
a typical aura (i.e., visual, sensory, or speech and/or language) accompanied or occurred within 60 minutes before a headache began.
Criteria E: The duration of a headache was 2 hours or longer on a calendar day unless an acute, migraine-specific medication (i.e., triptan or ergot derivative) was used after the start of the headache, in which case no minimum duration was to be specified.
Clinical literature suggests that a 1-day reduction per month in headache frequency is a clinically meaningful response in chronic migraine.57 Moreover, the clinical expert consulted by CDA-AMC for this review agreed on this effect size as a reasonable threshold of clinical importance (beyond a trivial effect).
Reduction of 50% or More in 3-Month Average of MMDs
This outcome was assessed as a secondary end point in the PROGRESS study. Migraine days were defined in the same way as described in the change from baseline in mean migraine days as noted earlier. This outcome analyzes the proportion of patients with at least a 50% reduction from baseline in the 3-month average of MMDs across the 12-week treatment period. No threshold of clinically important difference between groups was determined.
Change From Baseline in MHDs
A headache day was defined as any calendar day on which headache pain lasting 2 hours or longer occurs unless an acute headache medication (e.g., ibuprofen, triptan) was used after the start of the headache, in which case no minimum duration was specified. Antiemetics were not counted as an acute headache medication for headache-day identification. Like the previous outcome, clinical literature and the clinical expert consulted by CDA-AMC suggested that a 1-day reduction per month in headache frequency is a sensible threshold for a clinically meaningful response in chronic migraine.57
Change From Baseline in Mean Monthly Acute Medication Use Days
An acute medication use day was defined as any day on which a patient reports, per eDiary, the intake of allowed medication(s) to treat an acute migraine. The allowed medications included the following categories of drugs: triptans, ergots, opioids, analgesics (including acetaminophen), NSAIDs (including Aspirin), and antiemetics. No threshold of minimal importance is available for change in monthly acute medication use days in the literature or from the clinical expert consulted by CDA-AMC.
Function and Disability Outcomes
Change From Baseline in Mean Monthly Performance of Daily Activities Domain Score of the AIM-D
AIM-D is an 11-item daily eDiary measure that is used to assess the impact of migraine; it comprises 2 domains that evaluate performance of daily activities (7 items) and physical impairment (4 items). Patients were asked to rate the level of difficulty experienced in the past 24 hours with the performance of daily activities (i.e., difficulty with household chores, errands, leisure activities at home, leisure or social activities outside the home, strenuous physical activities, concentrating, and thinking clearly) and physical impairment (i.e., difficulty walking, moving one’s body, bending forward, and/or moving one’s head) using this 6-point rating scale: “not difficult at all,” “a little difficult,” “somewhat difficult,” “very difficult,” “extremely difficult,” and “I could not do it at all.” The same set of questions are administered in headache and nonheadache versions. Each raw daily domain score, as well as the raw daily total score, are transformed to a 0 to 100 scale, with higher scores indicating a greater impact of migraine (i.e., higher disease burden).
The AIM-D tool was developed in accordance with the US FDA patient-reported outcome guidance58,59 with input from patients with chronic migraine and episodic migraine, clinical experts, and patient-reported outcome instrument development experts as a comprehensive measure of activity impairment due to migraine. It was specifically designed to evaluate the impact of migraine on patients' daily functioning. The content validity of the AIM-D was initially established through a prospective, observational, noninterventional study60 and other psychometric testing was conducted in the PROGRESS study. No MID for the AIM-D has been identified for migraine.
MIDAS Scale
MIDAS is a self-reported, valid, and reliable 7-item questionnaire designed to quantify headache-related disability over a 3-month period.61-63 The MIDAS score is the sum of missed workdays or school days, days at work or school plus days of household work where productivity was reduced by half or more, missed household workdays, and missed nonwork activity days due to headaches and in the last 3 months. The score is calculated by adding the number of days that the patient reported being unable to perform their usual activities due to migraine. The (within-group) MID in chronic migraine reported in the literature is 4.5 points.61-63
Headache Impact Test
HIT-6 is a valid, reliable, and responsive 6-question assessment used to measure the impact headaches have on a patient's daily life and ability to function on the job, at school, at home, and in social situations.64-66 Responses are based on frequency using a 5-point scale ranging from “never” (assigned a score of 6 points) to “always” (assigned a score of 13 points). The HIT-6 total score, which ranges from 36 points to 78 points, is the sum of the responses. Higher scores indicate a greater impact on daily life. Within-patient and between-group MIDs for patients with chronic migraine are estimated to be 6 points and 2.3 points, respectively.67,68
Health-Related Quality of Life
MSQ Version 2.1: Role Function-Restrictive Domain
MSQ Version 2.1 is a widely used valid, reliable, and responsive 14-item patient-reported outcome questionnaire designed to assess the impact of migraine in the past 4 weeks.65,69,70 It is divided into 3 domains: role function-restrictive, role function-preventive, and emotional function. The role function-restrictive domain assesses how migraines limit one’s daily social and work-related activities, the role function-preventive domain assesses how migraines prevent these activities, and the emotional function domain assesses the emotions associated with migraines. In this report, the role function-restrictive domain is assessed.
Patients responded to items using a 6-point scale ranging from “none of the time” to “all of the time.” Raw dimension scores were computed as a sum of item responses and rescaled to a 0 to 100 scale, where higher scores indicated better quality of life.
The estimated within-group MIDs for the MSQ Version 2.1 domains are 10.9 for role function-restrictive, 8.3 for role function-preventive, and 12.2 for emotional function.71
Resource Use and Work Productivity
WPAI: Migraine Version 2.0 Questionnaire
The WPAI: Migraine version 2.0 questionnaire is used to assess work productivity specific to migraine.72 The measure uses a 1-week recall and contains 6 questions related to work productivity. The 6 questions each contribute to different components of the overall score, which is calculated to quantify the impact of migraines on work productivity. WPAI: Migraine is used to measure both presenteeism and absenteeism. The measure yields 4 scores expressed as impairment in percentages ranging from 0 to 100%: the percentage of work time missed, the percentage of impairment while working, the percentage of overall work impairment, and the percentage of activity impairment due to migraine.
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusion about measurement properties | MID |
|---|---|---|---|
Change from baseline in mean monthly performance of daily activities domain score of the AIM-D | Generic 11-item daily electronic diary measure | Internal consistency of a Cronbach alpha of 0.97 Test-retest reliability intraclass correlation coefficient > 0.6 with evidence of responsiveness60 | No MID was identified. |
Migraine Disability Assessment Scale | Generic 7-item ordinal scale | Good validity and internal consistency (a Cronbach alpha of 0.82)62,73 | |
Headache Impact Test | Generic 6-item questionnaire | Internal consistency of 0.83 with intraclass correlation coefficient of 0.7766 | The within-patient and between-group MID was estimated to be 6 points and 2.3 points, respectively.67,68 |
Migraine-Specific Quality-of-Life Questionnaire Version 2.1; role function-restrictive domain | Generic 14-item instrument across 3 domains | Internal consistency of 0.96 and intraclass correlation coefficient of 0.6374 | There was an estimated within-group MID of 10.9 points for the role function-restrictive domain.71 |
Work Productivity and Activity Impairment: Migraine version 2.0 questionnaire | Generic 6-item questionnaire | Intraclass correlation coefficient of 0.8872 | An MID (within-patient change) of –20 points for overall work productivity loss was identified. |
AIM-D = Activity Impairment in Migraine Dairy; MID = minimal important difference.
Harms
Patient AEs were collected from the time of consent through to the last visit. For all AEs, the investigator provided an assessment of the severity, the causal relationship to atogepant, the start and stop date, and the seriousness of the event (e.g., SAE).
The sponsor defined treatment-emergent adverse events (TEAEs) as AEs that began or worsened (increased in severity or became serious) on or after the date of the first dose of double-blind study treatment. AEs that occurred more than 30 days after the last dose of double-blind study treatment or visit 8, whichever was later, were not counted as TEAEs. All TEAEs were summarized using Medical Dictionary for Regulatory Activities (version 24.0). TEAEs that started after the date of the last dose of study treatment were considered as newly emergent. In this report, TEAEs are reported as AEs (Table 32).
Selected nonserious AEs and SAEs were of special interest and required immediate reporting, recording, and follow-up. The following events were monitored:
treatment-emergent suicidal ideations with intent, with or without a plan (i.e., type 4 or type 5 on the Columbia-Suicide Severity Rating Scale), or any suicidal behaviours
a treatment-emergent elevated ALT or AST laboratory value that was 3 or greater multiplied by ULN
potential Hy’s law cases — an elevated ALT or AST laboratory value that was 3 or greater multiplied by ULN and an elevated total bilirubin laboratory value that was 2 or greater multiplied by ULN and, at the same time, an alkaline phosphatase laboratory value that was less than 2 multiplied by ULN.
Statistical Analysis
In the PROGRESS pivotal trial included in this report, the primary comparison between–treatment groups for the change from baseline in mean MMDs across the 12-week treatment period was done by a mixed model of repeated measures (MMRM) model. The statistical model included treatment group, visit, the stratification of region, the stratification of acute medication overuse, the stratification of migraine prevention medication uses and number of failures, and treatment-group-by-visit interaction as categorical fixed effects. The statistical model also included the baseline score and baseline-by-visit interaction as covariates. The analysis was performed based on all postbaseline values using only the observed cases without imputation of missing values. Pairwise contrasts in the MMRM model were used to make the pairwise comparisons of each atogepant dose to placebo. All treatment effects and treatment comparisons were estimated by the LSM and their differences in LSM, along with their standard error (SE) and 95% confidence intervals (CIs), and the P value corresponding to the between–treatment group difference. The impact of dropouts was explored graphically by plotting the response profiles by the dropout reason. Only data collected during the double-blind period were included in the analysis. The primary efficacy analyses were based on the mITT population.56
Multiple sensitivity analyses for missing data handling were conducted and are described as follows.
A supportive analysis was performed on the primary end point using an analysis of covariance model. The analysis of covariance model included terms for treatment, region, acute medications during the baseline period (medication overuse [yes or no]), current or past use of migraine prevention medications and the number of medications failed with unique mechanisms of action, and baseline score. The treatment difference for atogepant doses versus placebo was estimated and reported along with the corresponding 95% CI and nominal P value for superiority testing.
A sensitivity analysis was also performed based on within-group imputation using patients from the same treatment group with observed data under the missing-at-random assumption. Missing data for patients who prematurely discontinued were assumed to copy the profile of patients in the same treatment group with observed data. Additionally, a copy-reference approach was performed on the primary end point to assess the robustness of the MMRM analysis to possible violation of the missing-at-random assumption. In this approach, a pattern mixture model was used under which data could be missing not at random, with repeated analyses combined via the reference-based multiple imputation procedure.
The normality test was performed on the residuals generated by the same MMRM as was used for the primary efficacy analysis. If the normality test was rejected, the sensitivity analysis used multiple imputation in conjunction with robust regression to assess the robustness of the primary MMRM analysis to the possible violation of normality assumption.
The secondary end points for headache days, acute medication use days, the MSQ Version 2.1 role function-restrictive domain score, the performance of daily activities domain score of the AIM-D, the physical impairment domain score of the AIM-D, and the HIT-6 total score were analyzed in the same manner as the primary end point.
A logistic regression model was used to analyze 50% responders across the 12-week treatment period. The analysis model included treatment group, region, acute medications during the baseline period (medication overuse [yes or no]), and the current and past use of migraine prevention medications and the number of medications failed with unique mechanisms of action as categorical fixed effects; baseline value was included as a covariate. The analysis was performed using only the observed cases without imputation of missing values. The OR between each atogepant dose group and placebo was estimated and tested.56
For variables with a continuous response range, analyses were performed similarly to that used for the primary analysis. For variables where the data were essentially binary, comparisons between–treatment groups were done with logistic regression for variables with only 1 postbaseline assessment or using a generalized linear mixed model for variables with multiple postbaseline assessments. Table 8 provides an overview of the statistical analysis of the PROGRESS study’s primary and secondary end points.
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
PROGRESS study | ||||
Change from baseline in mean MMDsa, b | CFB MMRM | Group, visit, stratification of region, stratification of acute medication overuse, stratification of migraine prevention medication uses and number of failures, and treatment-group-by-visit interaction | Analysis was performed based on all evaluable postbaseline values using only the observed cases without imputation of missing values. | ANCOVA within-group imputation Copy-reference approach Multiple imputation with robust regression |
Change from baseline in mean MHDsc | CFB MMRM | As noted earlier | As noted earlier | None |
Change from baseline in mean monthly acute medication use daysb | CFB MMRM | As noted earlier | As noted earlier | None |
Change from baseline in MSQ Version 2.1 role function-restrictive domain scoreb | CFB MMRM | As noted earlier | As noted earlier | None |
Change from baseline in mean monthly performance of daily activities domain score of the AIM-Db | CFB MMRM | As noted earlier | As noted earlier | None |
Change from baseline in mean monthly physical impairment domain score of the AIM-Db | CFB MMRM | As noted earlier | As noted earlier | None |
Change from baseline in HIT-6 total scoreb | CFB MMRM | As noted earlier | As noted earlier | None |
Reduction of ≥ 50% in 3-month average of MMDsb | Logistic regression | Treatment group, region, acute medications during the baseline period (medication overuse [yes or no]), current and past use of migraine prevention medications, and the number of medications failed with unique mechanisms of action | As noted earlier | None |
AIM-D = Activity Impairment in Migraine-Diary; ANCOVA = analysis of covariance; CFB = change from baseline; HIT-6 = Headache Impact Test; MHD = monthly headache day; MMD = monthly migraine day; MMRM = mixed model of repeated measures; MSQ = Migraine-Specific Quality-of-Life Questionnaire; TF = treatment failure.
aSensitivity analyses were not run on the 2 or more TFs population.
bThis was a primary end point.
cThis was a secondary end point.
Source: PROGRESS study statistical analysis plan (2021).56
Sample Size and Power Calculation
It was estimated that a sample size of 250 patients randomized per treatment group would provide at least 96% power to detect the treatment difference between each of the atogepant 30 mg and 60 mg doses (assumed equally effective) and placebo for the primary efficacy end point. The sample size of this study was selected to provide sufficient power for the first 3 secondary end points. The power calculations were based on the following assumptions.
The treatment difference from placebo would be similar to the average value across the chronic migraine prevention studies for onabotulinumtoxin A and TEV-48125.75-77 The assumed treatment difference from placebo in change from baseline in mean MMDs across the 12-week treatment period is –2 days and the standard deviation (SD) is 5.5 days.
The PROGRESS study’s statistical testing plan controls the overall type I error at 5%. The power calculations of the primary and secondary end points accounted for multiple comparisons by testing each dose versus placebo at a 0.025 significance level, 2-sided. Once the primary end point for each dose was significant at 0.025, 2-sided, the secondary end points were tested sequentially.
Multiple Testing Procedure
A graphical weighted Bonferroni procedure was used to control the overall type I error rate at 0.05 for each set of primary end points and secondary end points between each atogepant group versus placebo. The initial testing allocated half of the alpha to the primary end point (change from baseline in mean MMD) for each dose. Within each dose, the testing of secondary end points occurred subsequently in a prespecified order. If the null hypotheses for both the primary end points and the first 3 secondary end points (i.e., change from baseline in mean MHD, change from baseline in mean monthly acute medication use day, and at least a 50% reduction in the 3-month average of MMDs) were rejected for 1 of the doses, one-third of the associated alpha was passed to the other dose and the remaining two-thirds of the associated alpha was reserved for testing null hypotheses of end points within the same dose. If hypotheses for 3 null hypotheses end points were rejected within a dose based on remaining alpha, the alpha for this dose was propagated to the other dose to make full use of the alpha. Additional efficacy end points and health outcome end points were tested at the nominal significance level, without adjusting for multiplicity. Analyses in the 2 or more TFs population (i.e., reimbursement requested population) were unadjusted for multiplicity.
Subgroup Analyses by Number of Migraine Prevention Medication Failures
A market access analysis plan (MAAP) was developed to conduct several prespecified subgroup analyses based on the mITT population. These subgroups included but were not limited to the following: baseline MMDs, acute medication overuse, prevention medication current use, prior exposure to a migraine prevention medication with proven efficacy, migraine prevention medication use and number of failures (past use only), and number of migraine prevention medication failures (current use or past use).
The subgroup analysis of interest for this submission that supports the requested reimbursement criteria is for “subjects with previous or current migraine prevention medication failure.” This subgroup was further stratified into the following subsets:
never used
had current or past use and “failed 0 medications”
had current or past use and “failed 1 or more medication(s) with the same mechanism of action”
requested reimbursement criteria — had current or past use and “failed 2 or more medications with different mechanisms of action” (2+ TFs population).
A separate analysis was performed for each of the mutually exclusive subsets and point estimates (with 95% CIs) were provided for all end points analyzed.
End points evaluated for patients with current or past use and who “failed 2 or more medications with different mechanisms of action” (the 2+ TFs population) included:
change from baseline in mean MMDs across the 12-week treatment period (Statistical Analysis Plan [SAP])
change from baseline in mean MHDs across the 12-week treatment period (SAP)
change from baseline in mean monthly acute medication use days across the 12-week treatment period (SAP)
at least a 50% reduction in the 3-month average of MMDs (SAP)
change from baseline in the MSQ Version 2.1 role function-restrictive domain score (MAAP)
change from baseline in the mean monthly performance of daily activities domain score of the AIM-D (MAAP)
change from baseline in the mean monthly physical impairment domain score of the AIM-D (MAAP)
change from baseline in the HIT-6 total score (MAAP).
For subgroup analyses of the continuous outcome variables, repeated measures analyses were conducted using a mixed model including observed measurements (MMRM) at all visits over the treatment period.78
Analysis Populations
The analysis populations and their applications used in the PROGRESS study are described in Table 9.
Table 9: Analysis Populations in the PROGRESS Study
Population | Definition | Application |
|---|---|---|
ITT population | All randomized patients | Study population not used in efficacy and safety analyses |
Safety population | All patients who received at least 1 dose of study intervention | All safety analyses |
mITT population | All randomized patients who received at least 1 dose of study intervention, had an evaluable baseline period of eDiary data, and had at least 1 evaluable postbaseline 4-week period (week 1 to week 4, week 5 to week 8, and week 9 to week 12) of eDiary data during the double-blind treatment period | All efficacy analyses were performed using the mITT population. Patients were analyzed according to the randomization assignment, regardless of actual treatment received. |
Off-treatment hypothetical estimand | All randomized patients who received at least 1 dose of study treatment, had an evaluable baseline period of eDiary data, and had at least 1 evaluable postbaseline 4-week period (week 1 to week 4, week 5 to week 8, and week 9 to week 12) of eDiary data, regardless of whether they were on study treatment or off study treatment | Used for the primary estimand in support of EU filing |
eDiary = electronic diary; EU = European Union; ITT = intention-to-treat; mITT = modified intention-to-treat.
Note: Details included in Table 9 are from the sponsor’s Summary of Clinical Evidence.
Source: PROGRESS study statistical analysis plan (2021).56
Results
Patient Disposition
Overall, 1,489 patients were screened for eligibility; 714 patients did not enter the PROGRESS study before randomization, primarily due to not meeting screening criteria (n = 661).55
Table 10 presents patient disposition in the intention-to-treat population in the atogepant 60 mg every day arm and the placebo arm.
Most randomized patients (88.9% and 88.8% in the atogepant 60 mg every day and the placebo arms, respectively) completed the double-blind treatment period. The main reasons for discontinuation reported during the double-blind treatment period were AEs and withdrawal by patient. Most randomized patients entered and completed the safety follow-up period (63% and 62.2% in the atogepant 60 mg every day and the placebo arms, respectively). The main reason for discontinuation during the safety follow-up period was the presence of AEs.
Table 10: Summary of Patient Disposition From Studies Included in the Systematic Review
Variable | PROGRESS study | |
|---|---|---|
Atogepant 60 mg q.d. (N = 262) | Placebo (N = 259) | |
Screened, N | 1,492 | |
Randomized, N (%) | 262 (100) | 259 (100) |
Double-blind treatment period | ||
Number of patients entered, N (%) | 262 (100) | 259 (100) |
Completed double-blind treatment period, N (%) | 233 (88.9) | 230 (88.8) |
Discontinued from double-blind treatment period, N (%) | 29 (11.1) | 29 (11.2) |
Reason for discontinuation, N (%) | ||
Adverse event | 9 (3.4) | 10 (3.9) |
Lack of efficacy | 1 (0.4) | 5 (1.9) |
Withdrawal by patient of consent | 14 (5.3) | 8 (3.1) |
Lost to follow-up | 3 (1.1) | 0 (0.0) |
Pregnancy | 0 (0.0) | 0 (0.0) |
Protocol deviation or violation | 2 (0.8) | 5 (1.9) |
Noncompliance with study drug | 0 (0.0) | 1 (0.4) |
Study terminated by sponsor | 0 (0.0) | 0 (0.0) |
Site terminated by sponsor | 0 (0.0) | 0 (0.0) |
Other | 0 (0.0) | 0 (0.0) |
Follow-up period | ||
Number of patients entered, N (%) | ███ ██████ | ███ ██████ |
Number of patients completed, N (%) | ███ ██████ | ███ ██████ |
Number of patients discontinued, N (%) | | █████ | | █████ |
Reason for discontinuation, N (%) | ||
Adverse event | ███ | ███ |
Withdrawal by patient | | █████ | | █████ |
Lost to follow-up | | █████ | | █████ |
Pregnancy | | █████ | | █████ |
Protocol deviation | | █████ | | █████ |
Study terminated by sponsor | | █████ | | █████ |
Site terminated by sponsor | | █████ | | █████ |
Other | | █████ | | █████ |
ITT, N (%) | ███ █████ | ███ █████ |
mITT, N (%) | ███ | ███ |
Safety, N (%) | ███ | ███ |
ITT = intention-to-treat; mITT = modified intention-to-treat; q.d. = every day.
Note: Details included in Table 10 are from the sponsor’s Summary of Clinical Evidence.
Source: PROGRESS Clinical Study Report (2022).55
Baseline Characteristics
The demographics and disease characteristics for the PROGRESS study in the overall and 2 or more TFs populations are presented in Table 11 and Table 12, respectively. Overall, there were no clinically meaningful differences between the placebo group and the atogepant 60 mg every day treatment group in either the overall or 2 or more TFs population. The baseline characteristics outlined are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
Table 11: Summary of Baseline Characteristics of PROGRESS Study in the Overall Population
Characteristic | Atogepant 60 mg q.d. (N = 261) | Placebo (N = 255) |
|---|---|---|
Demographic | ||
Age, years | ||
Mean (SD) | 41.7 (12.31) | 42.0 (12.43) |
Median (minimum to maximum) | 43.0 (18 to 70) | 42.0 (18 to 74) |
Sex, n (%) | ||
Male | 36 (13.8) | 30 (11.8) |
Female | 225 (86.2) | 225 (88.2) |
Race, n (%) | ||
White | 157 (60.2) | 151 (59.2) |
Black or African American | 9 (3.4) | 7 (2.7) |
Asian | 92 (35.2) | 94 (36.9) |
Other | 3 (1.1) | 3 (1.2) |
Weight, kg | ||
Mean (SD) | 68.7 (19.2) | 68.8 (17.2) |
Median (minimum to maximum) | 64.0 (41.7 to 171.9) | 65.4 (41.4 to 133.8) |
Height, cm | ||
Mean (SD) | 165.0 (8.5) | 164.1 (7.7) |
Median (minimum to maximum) | 164.5 (144.0 to 200.0) | 164.0 (141.8 to 187.0) |
BMI, kg/m2 | ||
Mean (SD) | 25.0 (5.5) | 25.5 (6.0) |
Median (minimum to maximum) | 23.5 (16.9 to 48.6) | 23.7 (15.8 to 48.7) |
Disease | ||
Migraine diagnosis, n (%) | ||
With aura | 34 (13.0) | 35 (13.7) |
Without aura | 158 (60.5) | 151 (59.2) |
Both | 69 (26.4) | 69 (27.1) |
Migraine disorder duration in years | ||
Mean (SD) | 21.2 (11.91) | 20.7 (12.32) |
Median (minimum to maximum) | 20.0 (2 to 55) | 19.3 (1 to 60) |
Past use of migraine prevention medication, n (%) | ||
Yes | 214 (82.0) | 212 (83.1) |
No | 47 (18.0) | 43 (16.9) |
Number of migraine days per month in last 3 months | ||
Mean (SD) | 16.6 (6.5) | 15.7 (5.7) |
Median (minimum to maximum) | 15 (8 to 30) | 15 (5 to 30) |
Number of headache days per month in last 3 months | ||
Mean (SD) | 21.7 (6.2) | 20.8 (5.0) |
Median (minimum to maximum) | 20 (15 to 78) | 20 (15 to 30) |
Acute medication treatment, n (%) | ||
Triptan | 184 (70.5) | 189 (74.1) |
Ergots or ergot combinations | 10 (3.8) | 1 (0.4) |
NSAID | 181 (69.3) | 189 (74.1) |
Opiates or opiate combination | 8 (3.1) | 9 (3.5) |
Antiemetic drug | 42 (16.1) | 36 (14.1) |
Barbiturates | 1 (0.4) | 0 |
Other | 87 (33.3) | 84 (32.9) |
Baseline efficacy parameters (mITT population) | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
N (% of ITT) | ||
Number of migraine days | ||
Mean (SD) | 19.2 (5.3) | 18.9 (4.8) |
Median (minimum to maximum) | 19 (9 to 28) | 18 (8 to 28) |
Number of headache days | ||
Mean (SD) | 21.5 (4.3) | 21.4 (4.1) |
Median (minimum to maximum) | 21 (10 to 28) | 21 (13 to 28) |
Number of acute medication use days | ||
Mean (SD) | 15.5 (7.4) | 15.4 (7.0) |
Median (minimum to maximum) | 16 (0 to 28) | 16 (0 to 28) |
MSQ Version 2.1 role function-restrictive domain score | ||
Mean (SD) | 43.4 (18.6) | 43.9 (19.1) |
Median (minimum to maximum) | 42.9 (0 to 97) | 42.9 (0 to 100) |
Performance of daily activities domain score of the AIM-D | ||
Mean (SD) | 31.1 (16.2) | 29.4 (13.7) |
Median (minimum to maximum) | 30.4 (0 to 87) | 28.3 (0 to 72) |
Physical impairment domain score of the AIM-D | ||
Mean (SD) | 27.0 (16.5) | 25.2 (13.6) |
Median (minimum to maximum) | 25.4 (0 to 82) | 23.7 (0 to 73) |
HIT-6 total score | ||
Mean (SD) | 64.4 (5.0) | 63.8 (4.9) |
Median (minimum to maximum) | 64.0 (45 to 78) | 64.0 (48 to 76) |
AIM-D = Activity Impairment in Migraine-Diary; BMI = body mass index; HIT-6 = Headache Impact Test; ITT = intention-to-treat; mITT = modified intention-to-treat; MSQ = Migraine-Specific Quality-of-Life Questionnaire; NSAID = nonsteroidal anti-inflammatory drug; q.d. = every day; SD = standard deviation.
Source: PROGRESS Clinical Study Report (2022).55
Table 12: Summary of Baseline Characteristics of PROGRESS Study in the 2 or More TFs Population
Characteristic | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Demographic | ||
Age, years | ||
Mean (SD) | ████ ███████ | ████ ███████ |
Median (minimum to maximum) | ████ ████ ███ | ████ ████ ███ |
Sex, n (%) | ||
Male | ██ █████ | ██ ██████ |
Female | ██ ██████ | ██ ██████ |
Race, n (%) | ||
White | ██ ██████ | ██ ██████ |
Black or African American | | █████ | | █████ |
Asian | ██ ██████ | ██ ██████ |
Other | | █████ | | █████ |
Weight, kg | ||
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ ████ ████ | █████ ████ ████ |
Height, cm | ||
Mean (SD) | ██████ ██████ | ██████ ██████ |
Median (minimum to maximum) | ███ █████ ████ | ███ █████ ████ |
BMI, kg/m2 | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | █████ ████ ███ | █████ ████ ███ |
Disease | ||
Migraine diagnosis, n (%) | ||
With aura | ██ ███████ | ██ ███████ |
Without aura | ██ ███████ | ██ ███████ |
Both | ██ ███████ | ██ ███████ |
Migraine disorder duration in years | ||
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ ███ ███ | █████ ███ ███ |
Past use of migraine prevention medication, n (%) | ||
Yes | ███ ███████ | ██ ███████ |
No | ███ | ███ |
Number of migraine days per month in last 3 months | ||
Mean (SD) | ████ ██████ | ████ ██████ |
Median (minimum to maximum) | ████ ███ ███ | ████ ███ ███ |
Number of headache days per month in last 3 months | ||
Mean (SD) | ████ ██████ | ████ ██████ |
Median (minimum to maximum) | ████ ████ ███ | ████ ████ ███ |
Acute medication treatment, n (%) | ||
Triptan | ██ ██████ | ██ ██████ |
Ergots or ergot combinations | | █████ | | █████ |
NSAID | ██ ██████ | ██ ██████ |
Opiates or opiate combination | | █████ | | █████ |
Antiemetic drug | ██ ██████ | ██ ██████ |
Barbiturates | ███ | ███ |
Other | ██ ██████ | ██ ██████ |
Baseline efficacy parameters | Atogepant 60 mg q.d. (N = 104) | Placebo (N = 94) |
Number of migraine days | ||
n (%) | ███ █████ | ██ █████ |
Mean (SD) | ████ ██████ | ████ ██████ |
Median (minimum to maximum) | ████ ███ ███ | ████ ███ ███ |
Number of headache days | ||
n (%) | ███ █████ | ██ █████ |
Mean (SD) | ████ ██████ | ████ ██████ |
Median (minimum to maximum) | ████ ███ ███ | ████ ████ ███ |
Number of acute medication use days | ||
n (%) | ███ █████ | ██ █████ |
Mean (SD) | ████ ██████ | ████ ██████ |
Median (minimum to maximum) | ████ ███ ███ | ████ ███ ███ |
MSQ Version 2.1 role function-restrictive domain score | ||
n (%) | ███ █████ | ██ █████ |
Mean (SD) | ████ ███████ | ████ ███████ |
Median (minimum to maximum) | ████ ███ ███ | ████ ███ ███ |
Performance of daily activities domain score of the AIM-D | ||
n (%) | ██ ███████ | ██ ███████ |
Mean (SD) | ████ ███████ | ████ ███████ |
Median (minimum to maximum) | ████ ███ ███ | ████ ███ ███ |
Physical impairment domain score of the AIM-D | ||
n (%) | ██ ███████ | ██ ███████ |
Mean (SD) | ████ ███████ | ████ ███████ |
Median (minimum to maximum) | ████ ███ ███ | ████ ███ ███ |
HIT-6 total score | ||
n (%) | ███ █████ | ██ █████ |
Mean (SD) | ████ ██████ | ████ ██████ |
Median (minimum to maximum) | ████ ████ ███ | ████ ████ ███ |
AIM-D = Activity Impairment in Migraine-Diary; BMI = body mass index; HIT-6 = Headache Impact Test; ITT = intention-to-treat; NSAID = nonsteroidal anti-inflammatory drug; MSQ = Migraine-Specific Quality-of-Life Questionnaire; q.d. = every day; SD = standard deviation; TF = treatment failure.
Note: Details included in Table 12 are from the sponsor’s Summary of Clinical Evidence.
Source: Market Access Analysis Plan Raw Output Tables.78
Exposure to Study Treatments
Study Treatments
Table 13 presents treatment duration within the safety population. Mean (SD) treatment duration was ████ ██████ ████ in the placebo treatment group and ████ ██████ days in the atogepant 60 mg every day treatment group. The mean (SD) overall adherence during the double-blind treatment period was 97.3% (7.0%) in the atogepant 60 mg every day treatment group and 97.2% (5.7%) in the placebo group.
Concomitant Medications and Cointerventions
Also from the safety population, concomitant medication use was comparable across the placebo treatment group (99.6%) and the atogepant 60 mg every day treatment group (100%) | ███ ████ ████████ ███████████ ███████████ ██████ ███ ████████████ █████████ ██████ ████ █████████ ██████ ██ ███████ ███ █████ ██ █████████ ██ ██ ████ ███████████ ██████ ███ ███████ ███ ███████████ ██████ ███ ███████
Table 13: Summary of Treatment Duration (Patient Exposure) in the Safety Population of the PROGRESS Study
Variable | Atogepant 60 mg q.d. (N = 261) | Placebo (N = 255) |
|---|---|---|
Mean (SD), days | ████ ██████ | ████ ██████ |
Median (minimum to maximum), days | ██ ███ ████ | ██ ███ ████ |
Patient-years | ████ | ████ |
q.d. = every day; SD = standard deviation.
Source: PROGRESS Clinical Study Report (2022).55
Efficacy
Change From Baseline in Mean MMDs
The primary efficacy end point in the PROGRESS study was the change from baseline in mean MMDs across the 12-week treatment period; it was considered of importance for decisions by stakeholders consulted by CDA-AMC.
In patients who had previously not experienced improvement with 2 or more migraine prevention medications with different mechanism of actions (2+ TFs population, n = ███), the LSM change from baseline as measured by the mean MMDs across the 12-week treatment period was █████ ████ ████ ███ █████ ██ █████ █████ for atogepant 60 mg every day compared with █████ ████ ████ ███ █████ ██ █████ █████ for placebo as shown in Table 14. The LSMD in change from baseline in mean MMD was █████ ████████ ███ █████ ██ █████ █████ | | ████████ favouring atogepant 60 mg every day. A forest plot of subgroup analyses by number of migraine prevention medication failures for change from baseline in mean MMD is presented in ██████ |.
In the overall (mITT) population (Table 15), the LSM change from baseline in the number of mean MMDs across the 12-week treatment period was –6.88 days (95% CI, –7.67 days to –6.08 days) for atogepant 60 mg every day compared to –5.05 days (95% CI, –5.86 days to –4.25 days) with placebo. The LSMD in change from baseline in mean MMDs was –1.82 days (95% CI, –2.89 days to –0.75 days; P = 0.0009), favouring atogepant 60 mg taken every day.
The sensitivity analyses supported the findings of the primary analysis approach in the overall population.
Table 14: Change From Baseline in Mean MMDs Across the 12-Week Treatment Period in the 2 or More TFs Population
Variable | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Baseline | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | ██ █████ ███ | ████ ████ ███ |
Postbaseline (month 1 to month 3) | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | ██ ███ ███ | ████ █████ ███ |
CFB | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | ████ ███████ █████ | ████ ███████ ████ |
MMRMa | ||
LSM | █████ | █████ |
95% CI | ██████ █████ | ██████ █████ |
Atogepant vs. placebo | ||
LSMD (SE of the least squares) | █████ ██████ | Reference |
95% CI | ██████ █████ | Reference |
P valueb | ██████ | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMD = monthly migraine day; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; SE = standard error; TF = treatment failure; vs. = versus.
Note: Postbaseline (month 1 to month 3) is the average of MMDs across the 12-week treatment period.
aAn MMRM was used for CFB.
bNot adjusted for multiple comparisons.
Source: PROGRESS Clinical Study Report (2022).55

BID = twice a day; mITT = modified intention-to-treat; QD = every day.
Source: PROGRESS Clinical Study Report (2022).55
Table 15: Change From Baseline in Mean MMDs Across the 12-Week Treatment Period in the Overall Population (mITT Population)
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
Mean (SD) | 19.16 (5.28) | 18.95 (4.78) |
Median (minimum to maximum) | 19 (8 to 28) | 18 (8 to 28) |
Postbaseline (month 1 to month 3) | ||
Mean (SD) | 12.04 (8.08) | 13.76 (6.51) |
Median (minimum to maximum) | 10.64 (0 to 28) | 13.00 (1 to 28) |
CFB | ||
Mean (SD) | –7.13 (6.23) | –5.19 (6.08) |
Median (minimum to maximum) | –7.27 (–22.3 to 12.9) | –4.63 (–21.9 to 9.7) |
MMRMa | ||
LSM (SE of the least squares) | –6.88 (0.41) | –5.05 (0.41) |
95% CI | –7.67 to –6.08 | –5.86 to –4.25 |
Atogepant vs. placebo | ||
LSMD (SE of the least squares) | –1.82 (0.55) | Reference |
95% CI | (–2.89 to –0.75) | Reference |
Adjusted P valueb | 0.0009 | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMD = monthly migraine day; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; SE = standard error; vs. = versus.
Notes: Details included in Table 15 are from the sponsor’s Summary of Clinical Evidence.
Postbaseline (month 1 to month 3) is the average of MMDs across the 12-week treatment period.
aAn MMRM was used for CFB. The response variable is the CFB to each postbaseline month in MMDs. The statistical model included treatment group, visit, the stratification of acute medication overuse, the stratification of migraine prevention medication uses and number of failures, the stratification of region, and treatment-group-by-visit interaction as categorical fixed effects. The statistical model included the baseline MMDs and baseline-by-visit interaction as covariates. The P values were from the test between the atogepant dose group and placebo.
bThe P value was adjusted for multiple testing.
Source: PROGRESS Clinical Study Report (2022).55
Reduction of 50% or More in 3-Month Average of MMDs
In the 2 or more TFs population, the proportion of patients who had a 50% or greater reduction in the 3-month average of MMDs with atogepant 60 mg every day was █████ compared to █████ with placebo, as shown in Table 16. The adjusted absolute between-group difference was ██████ ████ ███ ████ ██ ████████ The OR for the proportion of patients who demonstrated a 50% or greater reduction in the 3-month average of MMDs was ████ ████ ███ ████ ██ █████ | ████████ favouring atogepant 60 mg every day.
Table 16: Reduction of 50% or More in 3-Month Average of Monthly Migraine Days in the 2 or More TFs Population
Characteristic | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
50% responders | ||
Responders, n (%) | ██ ██████ | ██ ██████ |
Nonresponses, n (%) | ██ ██████ | ██ ██████ |
Adjusted risk difference, % (95% CI)a | █████ █████ ██ ██████ | Reference |
OR vs. placebo (95% CI)b | ████ ██████ █████ | Reference |
P valuec | ██████ | Reference |
CI = confidence interval; mITT = modified intention-to-treat; OR = odds ratio; q.d. = every day; TF = treatment failure; vs. = versus.
Note: Nonresponders included patients who had not met responder criteria.
a95% CIs for adjusted risk difference were calculated according to the Cochran-Mantel-Haenszel test adjusted for the stratification of region and acute medication overuse.
bThe population-level summary for this end point is the OR from a logistic regression for each atogepant group relative to placebo with baseline monthly migraine days as a covariate, and the stratification of region, acute medication overuse, migraine prevention medication and number of failures, and treatment group as fixed factors.
cNot adjusted for multiple comparisons.
Source: PROGRESS Clinical Study Report (2022).55
Similarly, in the overall (mITT) population, the proportion of patients with a 50% or greater reduction in the 3-month average of MMDs was 41.0% with atogepant 60 mg every day compared to 26.0% with placebo as shown in Table 17. The adjusted absolute between-group difference was 14.09% (95% CI, 5.93% to 22.25%). The OR for the proportion of patients who demonstrated a 50% or greater reduction in the 3-month average of MMDs was 2.04 (95% CI, 1.38 to 3.00; P = 0.0009), favouring atogepant 60 mg every day.
Table 17: Reduction of 50% or More in 3-Month Average of Monthly Migraine Days in the Overall Population (mITT Population)
Characteristic | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
50% responders | ||
Responders, n (%) | 105 (41.0) | 64 (26.0) |
Nonresponders, n (%) | 151 (59.0) | 182 (74.0) |
Adjusted risk difference, % (95% CI) a | 14.09 (5.93 to 22.25) | Reference |
OR vs. placebo (95% CI) b | 2.04 (1.38 to 3.00) | Reference |
Model P value | 0.0003 | Reference |
Adjusted P valuec | 0.0009 | Reference |
CI = confidence interval; mITT = modified intention-to-treat; OR = odds ratio; q.d. = every day; vs. = versus.
Note: Nonresponders included patients who had not met responder criteria.
a95% CIs for adjusted risk difference were calculated according to the Cochran-Mantel-Haenszel test adjusted for the stratification of region, acute medication overuse, and migraine prevention medication and number of failures.
bThe population-level summary for this end point is the OR from a logistic regression for each atogepant group relative to placebo with baseline monthly migraine days as a covariate, and the stratification of region, acute medication overuse, migraine prevention medication and number of failures, and treatment group as fixed factors.
cThe P value was adjusted for multiple testing.
Source: PROGRESS Clinical Study Report (2022).55
Change From Baseline in Mean MHDs
In the 2 or more TFs population, the LSM change from baseline in the number of mean MHDs across the 12-week treatment period was █████ ████ ████ ███ █████ ██ █████ ████) with atogepant 60 mg every day compared to █████ ████ ████ ███ █████ ██ █████ █████ with placebo as shown in Table 18. The LSMD in change from baseline in mean MHDs was █████ ████ ████ ███ ███████ █████ █████ | | ████████ favouring atogepant 60 mg every day. A forest plot of subgroup analyses by number of migraine prevention medication failures for change from baseline in mean MHDs is shown in ██████ |.
Table 18: Change From Baseline in Monthly Headache Days Across the 12-Week Treatment Period in the 2 or More TFs Population
Variable | Atogepant 60 mg q.d. | Placebo (N = 91) |
|---|---|---|
Baseline | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | ████ ████ ███ | ████ ██████ ███ |
Postbaseline (month 1 to month 3) | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | ████ █████ ███ | ████ █████ ███ |
CFB | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | █████ ███████ ████ | █████ ███████ ████ |
MMRMa | ||
LSM | █████ | █████ |
95% CI | ██████ █████ | ██████ █████ |
Atogepant vs. placebo | ||
LSMD | █████ | Reference |
95% CI | ██████ █████ | Reference |
P valueb | ██████ | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; TF = treatment failure; vs. = versus.
aAn MMRM was used for CFB.
bNot adjusted for multiple comparisons.
Source: PROGRESS Clinical Study Report (2022).55

BID = twice a day; mITT = modified intention-to-treat; QD = once a day.
Source: PROGRESS Clinical Study Report (2022).55
In the overall (mITT) population, the LSM change from baseline in the number of mean MHDs across the 12-week treatment period was –7.00 days (95% CI, –7.78 days to –6.21 days) for atogepant 60 mg every day compared to –5.13 (95% CI, –5.92 days to –4.33 days) for placebo (Table 19). The LSMD in change from baseline in mean MHD was –1.87 days (95% CI, –2.93 days to –0.81 days; P = 0.0009), favouring atogepant 60 mg every day.
Table 19: Change From Baseline in Monthly Headache Days Across the 12-Week Treatment Period in the Overall Population (mITT Population)
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
Mean (SD) | 21.52 (4.32) | 21.40 (4.10) |
Median (minimum to maximum) | 21.0 (9.7 to 28.0) | 21.0 (12.7 to 28.0) |
Postbaseline (month 1 to month 3) | ||
Mean (SD) | 14.38 (8.35) | 16.17 (6.77) |
Median (minimum to maximum) | 13.8 (0.3 to 28.0) | 15.0 (1.5 to 28.0) |
CFB | ||
Mean (SD) | –7.14 (6.24) | –5.23 (5.65) |
Median (minimum to maximum) | –6.71 (–22.3 to 9.0) | –4.26 (–23.7 to 6.7) |
MMRMa | ||
LSM (SE of the least squares) | –7.00 (0.40) | –5.13 (0.41) |
95% CI | –7.78 to –6.21 | –5.92 to –4.33 |
Atogepant vs. placebo | ||
LSMD (SE of the least squares) | –1.87 (0.54) | Reference |
95% CI | –2.93 to –0.81 | Reference |
Adjusted P valueb | 0.0009 | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; SE = standard error; vs. = versus.
aAn MMRM was used for CFB.
bThe P value was adjusted for multiple testing.
Source: PROGRESS Clinical Study Report (2022).55
Change From Baseline in Mean Monthly Acute Medication Use Days
In the 2 or more TFs population, the LSM change from baseline in the number of mean acute medication use days across the 12-week treatment period was █████ ████ ████ ███ █████ ██ █████ █████ for atogepant 60 mg every day compared to █████ ████ ███ █████ ██ █████ ████) with placebo as shown in Table 20. The LSMD in change from baseline in mean acute medication use days between atogepant 60 mg every day and placebo was █████ ████ ████ ███ █████ ██ █████ █████ | | ████████ favouring atogepant 60 mg every day.
Table 20: Change From Baseline in Monthly Acute Medication Use Days Across the 12-Week Treatment Period in the 2 or More TFs Population
Variable | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Baseline | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | ██ ███ ███ | ██ ███ ███ |
Postbaseline (month 1 to month 3) | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | ███ ███ ███ | ██ ███ ███ |
CFB | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | █████ █████ ██ | █████ ██████ ███ |
MMRMa | ||
LSM | █████ | █████ |
95% CI | ██████ █████ | ██████ █████ |
Atogepant vs. placebo | ||
LSMD | █████ | Reference |
95% CI | ██████ █████ | Reference |
P valueb | ██████ | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; TF = treatment failure; vs. = versus.
aAn MMRM was used for CFB.
bNot adjusted for multiple comparisons.
Source: PROGRESS Clinical Study Report (2022).55
In the overall (mITT) population, the LSM change from baseline in the number of mean acute medication use days across the 12-week treatment period was –6.23 days (95% CI, –6.98 days to –5.47 days) with atogepant 60 mg every day compared to –4.10 days (95% CI, –4.86 days to –3.33 days) with placebo (Table 21). The LSMD in change from baseline in mean acute medication use days between–treatment groups was –2.13 days (95% CI, –3.13 days to –1.13 days; P = 0.0009), favouring atogepant 60 mg every day.
Table 21: Change From Baseline in Monthly Acute Medication Use Days Across the 12-Week Treatment Period in the Overall Population (mITT Population)
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
Mean (SD) | 15.46 (7.38) | 15.42 (6.99) |
Median (minimum to maximum) | 16 (0 to 28) | 16 (0 to 28) |
Postbaseline (month 1 to month 3) | ||
Mean (SD) | 9.01 (7.84) | 11.19 (7.22) |
Median (minimum to maximum) | 6.5 (0 to 28) | 10.0 (0 to 28) |
CFB | ||
Mean (SD) | –6.45 (6.65) | –4.23 (6.12) |
Median (minimum to maximum) | –6.33 (–26.0 to 14.2) | –3.57 (–23.7 to 20.7) |
MMRMa | ||
LSM | –6.23 | –4.10 |
95% CI | –6.98 to –5.47 | –4.86 to –3.33 |
Atogepant vs. placebo | ||
LSMD | –2.13 | Reference |
95% CI | –3.13 to –1.13 | Reference |
Model P value | < 0.0001 | Reference |
Adjusted P valueb | 0.0009 | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; vs. = versus.
aAn MMRM was used for CFB.
bThe P value was adjusted for multiple testing.
Source: PROGRESS Clinical Study Report (2022).55
Change From Baseline in Mean Monthly Performance of Daily Activities Domain Score of the AIM-D
In the 2 or more TFs population, the LSM change from baseline (SD) in the mean monthly performance of daily activities domain score of AIM-D across the 12-week treatment period was ██████ ███████ for atogepant 60 mg every day compared with █████ ███████ for placebo (Table 22). The LSMD in change from baseline in mean monthly performance of daily activities domain score of AIM-D across the 12-week treatment period was █████ ██████ ████ ███ █████ ██ █████ ███████ | | ██████), favouring atogepant 60 mg every day.
Table 22: Change From Baseline in Mean Monthly Performance of Daily Activities Domain Score of AIM-D Across the 12-Week Treatment Period in the 2 or More TFs Population
Variable | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Baseline | ||
n | ███ | ███ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ ███ ███ | █████ ███ ███ |
Postbaseline (month 1 to month 3) | ||
n | ███ | ███ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ ███ ███ | █████ ███ ███ |
CFB | ||
n | ███ | ███ |
Mean (SD) | ██████ ███████ | █████ ███████ |
Median (minimum to maximum) | ██████ █████ ███ | █████ █████ ███ |
MMRMa | ||
LSM | ██████ | █████ |
95% CI | ███████ █████ | ███████ █████ |
Atogepant vs. placebo | ||
LSMD | █████ | Reference |
95% CI | ██████ █████ | Reference |
P valueb | ██████ | Reference |
AIM-D = Activity Impairment in Migraine-Diary; CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; TF = treatment failure; vs. = versus.
Note: Postbaseline (month 1 to month 3) is the average monthly performance of daily activities domain score of AIM-D across the 12-week treatment period.
aAn MMRM was used for CFB.
bNot adjusted for multiple comparisons.
Source: Market Access Analysis Plan Raw Output Tables.78
In the overall (mITT) population, the LSM change from baseline in the mean monthly performance of daily activities domain score of AIM-D across the 12-week treatment period was –12.92 points (95% CI, –14.23 points to –11.41 points) for atogepant 60 mg every day compared to –9.44 points (95% CI, –10.86 points to –8.03 points) with placebo (Table 23). The LSMD in change from baseline in mean monthly performance of daily activities domain score of AIM-D across the 12-week treatment period was –3.38 points (95% CI, –5.27 points to –1.49 points; P = 0.0009), favouring atogepant 60 mg every day.
Table 23: Change From Baseline in Mean Monthly Performance of Daily Activities Domain Score of AIM-D Across the 12-Week Treatment Period in the Overall Population (mITT Population)
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
n | 231 | 226 |
Mean (SD) | 31.18 (16.47) | 29.50 (13.73) |
Median (minimum to maximum) | 30.48 (0.0 to 86.9) | 28.27 (0.2 to 72.4) |
Postbaseline (month 1 to month 3) | ||
n | 231 | 226 |
Mean (SD) | 17.29 (15.60) | 19.70 (12.43) |
Median (minimum to maximum) | 12.87 (0.0 to 78.4) | 17.36 (0.1 to 75.9) |
CFB | ||
n | 231 | 226 |
Mean (SD) | –13.90 (12.63) | –9.80 (11.31) |
Median (minimum to maximum) | –12.69 (–60.5 to 26.8) | –8.60 (–47.9 to 25.5) |
MMRMa | ||
LSM (SE of the least squares) | –12.82 (0.72) | –9.44 (0.72) |
95% CI | –14.23 to –11.41 | –10.86 to –8.03 |
Atogepant vs. placebo | ||
LSMD (SE of the least squares) | –3.38 (0.96) | Reference |
95% CI | –5.27 to –1.49 | Reference |
Model P value | 0.0005 | Reference |
Adjusted P valueb | 0.0009 | Reference |
AIM-D = Activity Impairment in Migraine-Diary; CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; SE = standard error; vs. = versus.
Note: Postbaseline (month 1 to month 3) is the average monthly performance of daily activities domain score of AIM-D across the 12-week treatment period.
aAn MMRM was used for CFB.
bThe P value was adjusted for multiple testing.
Source: PROGRESS Clinical Study Report (2022).55
Change From Baseline in the MIDAS Total Score
In the 2 or more TFs population, the LSM change from baseline in MIDAS total score at week 12 (Table 24) was ██████ ██████ ████ ██ ██████ ██████ ██ ███████ for atogepant 60 mg every day compared to ██████ ██████ ████ ██ ██████ ██ █████ ███████ with placebo. The LSMD in change from baseline was ██████ ██████ ███████ ██████ ██ █████ ███████ | | ███████, in favour of atogepant 60 mg every day.
Table 24: Change From Baseline in MIDAS Total Score at Week 12 in the 2 or More TFs Population
Variable | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Baseline | ||
n | ███ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | ██ ████ ████ | ██ ████ ████ |
Postbaseline | ||
n | ███ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ ███ ████ | ██ ███ ████ |
CFB | ||
n | ███ | ██ |
Mean (SD) | ██████ ███████ | ██████ ███████ |
Median (minimum to maximum) | █████ ██████ ████ | █████ ██████ ████ |
ANCOVAa | ||
LSM | ██████ | ██████ |
95% CI | ███████ ██████ | ███████ █████ |
Atogepant vs. placebo | ||
LSMD | ██████ | Reference |
95% CI | ███████ █████ | Reference |
P valueb | █████ | Reference |
ANCOVA = analysis of covariance; CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; MIDAS = Migraine Disability Assessment; mITT = modified intention-to-treat; q.d. = every day; SD = standard deviation; TF = treatment failure.
aAn ANCOVA model was used for CFB. The model included treatment group, the stratification of acute medication overuse, the stratification of migraine prevention medication uses and number of failures, the stratification of region, and baseline.
bNot adjusted for multiple comparisons.
Source: Market Access Analysis Plan Raw Output Tables.78
In the overall (mITT) population, the LSM change from baseline in MIDAS total score at week 12 was ██████ ██████ ████ ███ ██████ ██ ██████ ███████ for atogepant 60 mg every day compared to ██████ ██████ ████ ███ ██████ ██ ██████ ██████) with placebo (Table 25). The LSMD in change from baseline was ██████ ██████ ███████ ██████ ██ █████ ███████ | | ████████ favouring atogepant 60 mg every day.
Table 25: Change From Baseline in MIDAS Total Score at Week 12 in the mITT Population
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
n | ███ | ███ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | ████ ███ ████ | ██ ████ ████ |
Postbaseline | ||
n | ███ | ███ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | ████ ███ ████ | ████ ███ ████ |
CFB | ||
n | ███ | ███ |
Mean (SD) | ██████ ███████ | ██████ ███████ |
Median (minimum to maximum) | █████ ██████ ████ | █████ ██████ ████ |
ANCOVAa | ||
LSM | ██████ | ██████ |
95% CI | ███████ ██████ | ███████ ██████ |
Atogepant vs. placebo | ||
LSMD | ██████ | Reference |
95% CI | ███████ █████ | Reference |
P valueb | ██████ | Reference |
ANCOVA = analysis of covariance; CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; MIDAS = Migraine Disability Assessment; mITT = modified intention-to-treat; SD = standard deviation.
aAn ANCOVA model was used for CFB. The model included treatment group, the stratification of acute medication overuse, the stratification of migraine prevention medication uses and number of failures, the stratification of region, and baseline.
bNot adjusted for multiple comparisons.
Source: Market Access Analysis Plan Raw Output Tables.78
Change From Baseline in HIT-6 Total Score
In the 2 or more TFs population, the LSM change from baseline in the HIT-6 total score at week 12 was █████ ██████ ████ ███ █████ ██ █████ ███████ for atogepant 60 mg every day compared with █████ ██████ ████ ███ █████ ██ ███████████) with placebo as shown in Table 26. The LSMD in change from baseline was █████ ██████ ████ ███ █████ ██ █████ ███████ | | ████████ favouring atogepant 60 mg every day.
Table 26: Change From Baseline in HIT-6 Total Score Across the 12-Week Treatment Period in the 2 or More TFs Population
Variable | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Baseline | ||
n | ██ | ██ |
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | █████ ████ ███ | ████ ████ ███ |
Postbaseline | ||
n | ██ | ██ |
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | █████ ████ ███ | █████ ████ ███ |
CFB | ||
n | ██ | ██ |
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | █████ █████ ██ | █████ █████ ███ |
MMRMa | ||
LSM | █████ | █████ |
95% CI | ██████ █████ | ██████ █████ |
Atogepant vs. placebo | ||
LSMD | █████ | Reference |
95% CI | ██████ █████ | Reference |
P valueb | ███████ | Reference |
CFB = change from baseline; CI = confidence interval; HIT-6 = Headache Impact Test; LSM = least squares mean; LSMD = least squares mean difference; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; TF = treatment failure.
Note: n is the number of patients with evaluable value at both baseline and a specific time point in the modified intention-to-treat population.
aAn MMRM was used for CFB.
Source: Market Access Analysis Plan Raw Output Tables.78
In the overall (mITT) population, the LSM change from baseline in the HIT-6 total score at week 12 was –7.94 points (95% CI, –8.94 points to –6.93 points) for atogepant 60 mg every day compared to –5.17 points (95% CI, –6.19 points to –4.15 points) with placebo, shown in Table 27. The LSMD in change from baseline was –2.77 points (95% CI, –4.14 points to –1.40; P = 0.0009), favouring atogepant 60 mg every day.
Table 27: Change From Baseline in HIT-6 Total Score at Week 12 (mITT Population)
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
n | 233 | 226 |
Mean (SD) | 64.26 (5.01) | 64.08 (4.77) |
Median (minimum to maximum) | 64.00 (45.0 to 78.0) | 65.00 (48.0 to 76.0) |
Postbaseline (month 1 to month 3) | ||
n | 233 | 226 |
Mean (SD) | 56.06 (8.60) | 58.83 (7.27) |
Median (minimum to maximum) | 57.00 (36.0 to 74.0) | 60.00 (36.0 to 76.0) |
CFB | ||
n | 233 | 226 |
Mean (SD) | –8.20 (8.45) | –5.25 (6.72) |
Median (minimum to maximum) | –6.00 (–38.0 to 7.0) | –4.00 (–30.0 to 12.0) |
MMRMa | ||
LSM | –7.94 | –5.17 |
95% CI | –8.94 to –6.93 | –6.19 to –4.15 |
Atogepant vs. placebo | ||
LSMD | –2.77 | Reference |
95% CI | –4.14 to –1.40 | Reference |
Model P value | < 0.0001 | Reference |
Adjusted P valueb | 0.0009 | Reference |
CFB = change from baseline; CI = confidence interval; HIT-6 = Headache Impact Test; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation.
aAn MMRM was used for CFB.
bThe P value was adjusted for multiple testing.
Source: PROGRESS Clinical Study Report (2022).55
Change From Baseline in MSQ Version 2.1 Role Function-Restrictive Domain Score
In the 2 or more TFs patient population, the LSM change from baseline in the MSQ Version 2.1 role function-restrictive domain score at week 12 was █████ ██████ ████ ██ █████ ██ █████ ███████ for atogepant 60 mg every day compared to █████ ██████ ████ ██ ████ ██ █████ ██████) with placebo, where higher values suggest an improvement in patients’ functioning with daily social and work-related activities (Table 28). The LSMD in change from baseline in the mean monthly MSQ Version 2.1 role function-restrictive domain score at week 12 was █████ ██████ ████ ███ ████ ██ █████ ███████ | | ████████ favouring atogepant 60 mg every day.
Table 28: Change From Baseline in Mean Monthly MSQ Version 2.1 Role Function-Restrictive Domain Score at Week 12 in the 2 or More TFs Population
Variable | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Baseline | ||
n | ██ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ ███ ███ | █████ ███ ███ |
Postbaseline | ||
n | ██ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ ████ ████ | █████ ███ ███ |
CFB | ||
n | ██ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ █████ ███ | █████ █████ ███ |
MMRMa | ||
LSM | █████ | █████ |
95% CI | ██████ █████ | █████ █████ |
Atogepant vs. placebo | ||
LSMD | █████ | Reference |
95% CI | █████ █████ | Reference |
P valueb | ███████ | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; MSQ = Migraine-Specific Quality-of-Life Questionnaire; q.d. = every day; SD = standard deviation; TF = treatment failure; vs. = versus.
Note: n is the number of patients with evaluable value at both baseline and a specific time point in the mITT population.
aAn MMRM was used for CFB.
bNot adjusted for multiple comparisons.
Source: Market Access Analysis Plan Raw Output Tables.78
In the overall (mITT) population, the LSM change from baseline in the MSQ Version 2.1 role function-restrictive domain score at week 12 was 23.33 points (95% CI, 20.65 points to 26.01 points) with atogepant 60 mg every day compared to 17.18 points (95% CI, 14.47 points to 19.89 points) with placebo (Table 29). The LSMD in change from baseline in the mean monthly MSQ Version 2.1 role function-restrictive domain score at week 12 was 6.15 points (95% CI, 2.51 points to 9.79 points; P = 0.0009), favouring atogepant 60 mg every day.
Table 29: Change From Baseline in Mean Monthly MSQ Version 2.1 Role Function-Restrictive Domain Score at Week 12 (mITT Population)
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
n | 233 | 226 |
Mean (SD) | 43.56 (18.91) | 43.55 (19.05) |
Median (minimum to maximum) | 42.86 (0.0 to 97.1) | 42.86 (0.0 to 91.4) |
Postbaseline (month 1 to month 3) | ||
n | 233 | 226 |
Mean (SD) | 67.80 (21.82) | 61.24 (21.85) |
Median (minimum to maximum) | 71.43 (11.4 to 100.0) | 60.00 (5.7 to 100.0) |
CFB | ||
n | 233 | 226 |
Mean (SD) | 24.24 (24.72) | 17.69 (22.15) |
Median (minimum to maximum) | 22.86 (–37.1 to 91.4) | 14.29 (–28.6 to 85.7) |
MMRMa | ||
LSM | 23.33 | 17.18 |
95% CI | 20.65 to 26.01 | 14.47 to 19.89 |
Atogepant vs. placebo | ||
LSMD | 6.15 | Reference |
95% CI | 2.51 to 9.79 | Reference |
Model P value | 0.0009 | Reference |
Adjusted P valueb | 0.0009 | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; MSQ = Migraine-Specific Quality-of-Life Questionnaire; q.d. = every day; SD = standard deviation; SE = standard error; vs. = versus.
aAn MMRM was used for CFB.
bThe P value was adjusted for multiple testing.
Source: PROGRESS Clinical Study Report (2022).55
Change From Baseline in Percentage of Work Time Missed Assessed by WPAI: Migraine Version 2.0
In the 2 or more TFs subgroup, the LSM change from baseline in the percentage of work time missed assessed by the WPAI:Migraine tool at week 12 (Table 30) ██ ███ █████ ██████ ████ ███ ██████ ██ ████████████ for atogepant 60 mg every day compared to █████ ██████ ████ ███ █████ ██ ████ ██████) with placebo. The LSMD in change from baseline in percentage of work time missed at week 12 was █████ ██████ ████ ███ ██████ ██ ████ ███████ | | ███████
Table 30: Change From Baseline in Percentage of Work Time Missed Assessed by WPAI:Migraine Version 2.0 at Week 12 (2+ TFs Population)
Variable | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Baseline | ||
n | ██ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | | ███ ████ | ████ ███ █████ |
Postbaseline | ||
n | ██ | ██ |
Mean (SD) | ████ ███████ | █████ ███████ |
Median (minimum to maximum) | | ███ ████ | | ███ ████ |
CFB | ||
n | ██ | ██ |
Mean (SD) | █████ ███████ | ████ ███████ |
Median (minimum to maximum) | | ███████ █████ | | ███████ ████ |
MMRMa | ||
LSM | █████ | █████ |
95% CI | ███████ █████ | ██████ ████ |
Atogepant vs. placebo | ||
LSMD | █████ | Reference |
95% CI | ███████ ████ | Reference |
P valueb | █████ | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; SE = standard error; TF = treatment failure; vs. = versus; WPAI:Migraine = Work Productivity and Activity Impairment: Migraine.
aAn MMRM was used for CFB.
bNot adjusted for multiple comparisons.
Source: PROGRESS Clinical Study Report (2022).55
In the overall (mITT) population, the LSM change from baseline in the percentage of work time missed assessed by the WPAI:Migraine tool at week 12 was █████ ██████ ████ ███ ██████ ██ █████ ███████ for atogepant 60 mg every day compared to █████ ██████ ████ ███ █████ ██ █████ ███████ ████ ███████ (Table 31). The LSMD in change from baseline in percentage of work time missed at week 12 was ████ ██████ ████ ███ █████ ██ █████ ██████████████, favouring atogepant 60 mg every day.
Table 31: Change From Baseline in Percentage of Work Time Missed Assessed by WPAI:Migraine at Week 12 (mITT Population)
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
n | ███ | ███ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | | ███ ████ | | ███████ |
Postbaseline | ||
n | ███ | ███ |
Mean (SD) | ████ ███████ | █████ ███████ |
Median (minimum to maximum) | | ███████ | | ███████ |
CFB | ||
n | ███ | ███ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | | ███████ ██████ | | ███████ ████ |
MMRMa | ||
LSM | █████ | █████ |
95% CI | ███████ █████ | ██████ █████ |
Atogepant vs. placebo | ||
LSMD | █████ | Reference |
95% CI | ██████ █████ | Reference |
P valueb | ██████ | Reference |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; SE = standard error; vs. = versus; WPAI:Migraine = Work Productivity and Activity Impairment: Migraine.
aAn MMRM was used for CFB.
bNot adjusted for multiple comparisons.
Source: PROGRESS Clinical Study Report (2022).55
Harms
Overview of Safety
A summary of harms for the PROGRESS study is presented in Table 32 for the overall population and in Table 33 for the 2 or more TFs population.
Adverse Events
In the overall population, 17.2% of patients in the atogepant 60 mg every day group and 13.3% of patients in the placebo group had at least 1 AE. The incidence was similar in the 2 or more TFs subgroup (14.4% versus 12.8%). The 2 AEs most frequently reported (≥ 5% of patients) in the atogepant treatment group ██ ████ ███ ███████ ███ ████ ███████████ were constipation and nausea ██ ███ ████ ███████████ ████████ ████ ███████████ ████ █████ ██ ████████████████
In the overall population, constipation was reported in 10.0% of patients in the atogepant 60 mg every day treatment group and 3.1% of patients in the placebo treatment group. Nausea was reported in 9.6% of patients in the atogepant 60 mg every day treatment group and 3.5% of patients in the placebo treatment group. None of the constipation or nausea events were serious.
In the 2 or more TFs population, ████████████ was reported in █████ of patients in the atogepant 60 mg every day treatment group and ████ of patients in the placebo treatment group. ██████ was reported in ████ of patients in the atogepant 60 mg every day treatment group and ████ of patients in the placebo treatment group. ███████████████ was reported in ████ of patients in the atogepant 60 mg every day treatment group and ████ of patients in the placebo treatment group.
Serious Adverse Events
In the overall patient population, SAEs were infrequent in the atogepant 60 mg every day treatment group (2.4%) and placebo treatment group (1.2%). There were no clinically meaningful differences of SAEs between the atogepant 60 mg every day treatment group and the placebo group.
In the 2 or more TFs patient population, SAEs were infrequent in the atogepant 60 mg every day treatment group ██████ and there were ████ in the placebo treatment group.
Withdrawals Due to AEs
AEs leading to treatment discontinuation were infrequent in the atogepant 60 mg every day treatment group (3.4%) and placebo treatment group (3.9%) in the overall population as well as the 2 or more TFs population █████ ███ ██████
In the overall patient population, the most common AE leading to treatment discontinuation (≥ 1% of patients) was migraine in the placebo treatment group (1.6%) versus none in the atogepant 60 mg every day treatment group. All AEs leading to treatment discontinuation in the atogepant 60 mg every day group occurred in less than 1% of patients.
██ ███ ████ ███████ ███████████ █████ ███ ███ ████ ████ ██ ████████ ████████ ███ ████████ ██ ███ █████████ ██ ██ ██ █████████ ██████ █████ ████ ███ ████████ ██ ███ ███████ ██████ ██ ███ ███████ ██████ ███ ████████ ███████████ ████████ ██████ ████ ██ ███ █████████ ██ ██ ██ ██████
Mortality
No deaths were reported in the PROGRESS trial.
Notable Harms
AEs of special interest were reported at low rates (measured in the mITT population). A total of 1 patient in the placebo treatment group reported an AE of suicidal ideation. No patients in the atogepant treatment group reported an AE of suicidal ideation. A total of 2 (0.8%) patients had an elevated ALT or AST laboratory value that was 3 or greater multiplied by ULN in the atogepant 60 mg every day group compared to 1 (0.4%) patient in the placebo group.
Table 32: Summary of Harms (Safety Population)
Preferred term | Atogepant 60 mg q.d. (N = 261) | Placebo (N = 255) |
|---|---|---|
Patients with at least 1 AE (≥ 2%), n (%) | ||
Overall | 45 (17.2) | 34 (13.3) |
Constipation | 26 (10.0) | 8 (3.1) |
Nausea | 25 (9.6) | 9 (3.5) |
Dizziness | 12 (4.6) | 8 (3.1) |
Nasopharyngitis | 11 (4.2) | 11 (4.3) |
Decreased appetite | 9 (3.4) | 0 |
Fatigue | 8 (3.1) | 7 (2.7) |
Pyrexia | 8 (3.1) | 3 (1.2) |
Urinary tract infection | 6 (2.3) | 3 (1.2) |
Diarrhea | 5 (1.9) | 6 (2.4) |
Insomnia | 5 (1.9) | 5 (2.0) |
COVID-19 | 4 (1.5) | 5 (2.0) |
Migraine | 4 (1.5) | 5 (2.0) |
Abdominal pain, upper | 3 (1.1) | 5 (2.0) |
Arthralgia | 3 (1.1) | 6 (2.4) |
Upper respiratory tract infection | 2 (0.8) | 6 (2.4) |
Patients with at least 1 SAE, n (%) | ||
Overall | 7 (2.4) | 3 (1.2) |
Cholecystitis | 1 (0.4) | 0 |
COVID-19 | 1 (0.4) | 0 |
Fall | 1 (0.4) | 0 |
Hip fracture | 1 (0.4) | 0 |
Road traffic accident | 1 (0.4) | 0 |
Vaccination complication | 1 (0.4) | 0 |
Epicondylitis | 0 | 1 (0.4) |
Spinal pain | 1 (0.4) | 0 |
Spinal cord neoplasm | 1 (0.4) | 0 |
Plasma cell myeloma | 1 (0.4) | 0 |
Suicide attempt | 1 (0.4) | 0 |
Nasal septum deviation | 1 (0.4) | 0 |
Treatment discontinuations due to AEs, n (%) | ||
Overall | 9 (3.4) | 10 (3.9) |
Nausea | 2 (0.8) | 2 (0.8) |
Abdominal pain | 0 (0.0) | 2 (0.8) |
Constipation | 0 (0.0) | 2 (0.8) |
Diarrhea | 0 (0.0) | 1 (0.4) |
Dyspepsia | 0 (0.0) | 1 (0.4) |
Asthenia | 1 (0.4) | 0 |
Malaise | 1 (0.4) | 0 |
Hip fracture | 1 (0.4) | 0 |
Glomerular filtration rate, decreased | 1 (0.4) | 0 |
Spinal cord neoplasm | 1 (0.4) | 0 |
Dizziness | 1 (0.4) | 1 (0.4) |
Migraine | 4 (1.6) | 1 (0.4) |
Disturbance in attention | 1 (0.4) | 0 |
Headache | 1 (0.4) | 0 |
Anxiety | 1 (0.4) | 1 (0.4) |
Pruritus | 1 (0.4) | 1 (0.4) |
Patients with at least 1 AESI, n (%) | ||
Suicidal ideation | 0 (0.0) | 1 (0.4) |
ALT or AST ≥ 3 × ULN | 2 (0.8) | 1 (0.4) |
AE = adverse event; AESI = adverse event of special interest; ALT = alanine aminotransferase; AST = aspartate aminotransferase; q.d. = every day; SAE = serious adverse event; ULN = upper limit of normal.
Note: Patients are counted only once within each preferred term.
Source: PROGRESS Clinical Study Report (2022).55
Table 33: Summary of Harms of the 2 or More TFs Population (Safety Population)
Preferred term | Atogepant 60 mg q.d. (N = 104) | Placebo (N = 94) |
|---|---|---|
Patients with at least 1 AE (≥ 2%), n (%) | ||
███████ | ██ ██████ | ██ ██████ |
████████████ | ██ ██████ | | █████ |
██████ | | █████ | | █████ |
███████████████ | | █████ | | █████ |
█████████ | | █████ | | █████ |
█████████ ████ | | █████ | ███ |
█████████ ████████ | | █████ | ███ |
█████████████ | | █████ | ███ |
████████ | | █████ | | █████ |
███████ | | █████ | ███ |
██████████ | | █████ | | █████ |
███████ | | █████ | | █████ |
███████ | | █████ | | █████ |
██████████ | | █████ | | █████ |
████████ | | █████ | | █████ |
████████ | | █████ | | █████ |
███████████████ █████ | | █████ | | █████ |
████████ | | █████ | | █████ |
████ ██ █████████ | | █████ | | █████ |
███████ █████ █████████ | | █████ | | █████ |
███ █████ | ███ | | █████ |
███ ████ | ███ | | █████ |
█████ ███████████ █████ ████ | ███ | | █████ |
████████ ████ ██ █████ █ ████ █ ███ | ||
███████ | | █████ | ███ |
████████ █████████ | ███ | ███ |
████ ███████ ████████ | | █████ | ███ |
██████ ████ | | █████ | ███ |
█████████ ████████████████ ███ ██ ████ █ ███ | ||
███████ | | █████ | | █████ |
████████ | | █████ | ███ |
████████ | ███ | | █████ |
███████ | | █████ | ███ |
████████ | | █████ | ███ |
AE = adverse event; AESI = adverse event of special interest; ALT = alanine aminotransferase; AST = aspartate aminotransferase; q.d. = every day; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event; TF = treatment failure; ULN = upper limit of normal; WDAE = withdrawal due to adverse event.
Sources: PROGRESS Clinical Study Report55 and Market Access Analysis Plan Raw Output Tables.78
Critical Appraisal
Internal Validity
The PROGRESS trial is an RCT investigating the efficacy and safety of atogepant 60 mg every day (the dosage of interest for this review) compared to placebo. The study involved a randomization and allocation concealment process that was judged to be properly implemented, ensuring an overall balanced distribution of participants to either the atogepant 60 mg every day arm or the placebo arm. The number of prior migraine prevention medications that did not yield improvement was a stratification factor in the randomization, which should have ensured that the randomization was upheld in the 2 or more TFs subgroup. Some minor baseline imbalances were observed in both populations. However, these were judged to have an overall low risk for introducing bias or to have suggested problems in the randomization process. Only for 1 outcome, the WPAI:Migraine, a subset of the population, was used which presented possible imbalances between groups.
In the PROGRESS study, patients maintained good adherence to the intended intervention, with a reported 97% rate of adherence in both arms and an adequate flow of participants throughout the study showing no important imbalances in the adherence to atogepant. Concomitant medication use was comparable across the placebo and atogepant 60 mg every day treatment groups.
The 2 or more TFs subgroup, for which the sponsor is requesting reimbursement, was not considered separately in the sample size (power) calculation for the PROGRESS study. Therefore, it is unknown whether there was enough statistical power to detect any differences in treatment effect between the intervention and comparator arms in this subgroup. However, greater effect sizes for the 2 or more TFs subgroup were consistent across all key clinical end points (change from baseline in MMDs, MHDs, and monthly acute medication use days, and a reduction of 50% or more in the 3-month average of MMDs) compared to the mITT population.
There were no instances of meaningful missing outcome data. A small number of patients were lost to follow-up ██ ██████ patients in the atogepant 60 mg group and ██ ████ in the placebo group for the main outcomes in the mITT population) — hence, reducing the risk of bias in this domain.
In the PROGRESS study, the measurements of the outcomes were appropriate. Although some of the end points ascertained (such as HRQoL and HIT-6) can be considered subjective (patient perception and measure), all measurements were recorded by blind assessors using validated and reliable instruments. The blinding of participants and clinical investigators was kept throughout the conduct of the study, and there is no evidence that patients or personnel became unblinded.
The results were reported in accordance with predefined protocols, including the results from the subgroup of 2 or more TFs, reducing the likelihood of selective reporting bias.
Overall, the study appears to have minimized risks across all domains assessed for risk of bias for the outcomes addressed when comparing atogepant to placebo.
External Validity
The population of interest for this submission is the 2 or more TFs population, composed by █████ ██████ █████████ of the total mITT (N = 502) population. The effects observed from this population (an international group of patients, including from Canada) are directly applicable to the review question of interest (i.e., the reimbursement criteria) and to the population of patients in Canada. The clinical expert consulted by CDA-AMC considered that the effect estimates observed in the 2 or more TFs population should be similar to the response in the overall (mITT) population. This assumption is supported by the data from the PROGRESS study in at least the 2 main outcomes (MMD, MHD) where results from the 2 or more TFs and mITT are, overall, similar.
The baseline characteristics and prognostic factors observed in the PROGRESS study are, overall, similar to those encountered in the population of Canada with chronic migraine, according to the clinical expert consulted by CDA-AMC. The clinical expert further noted that patient responses might take up to 6 months, and 12 weeks could be a short time frame in which to evaluate the full effects of benefit or evaluate rare harms. No other issues of generalizability were detected in the body of evidence.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CDA-AMC’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:8,9
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word likely for evidence of moderate certainty (e.g., ‘X intervention likely results in Y outcome’).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word may for evidence of low certainty (e.g., ‘X intervention may result in Y outcome’).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as ‘very uncertain.’”
Following the GRADE approach, evidence from RCTs start as high-certainty evidence and can be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effect estimates, and publication bias.
When possible, certainty is rated in the context of the presence of an important effect (i.e., how certain is CDA-AMC that the effect is a nontrivial treatment effect). To determine what an important effect is, GRADE suggests using thresholds of clinical importance (MID); if the threshold is not possible to obtain, the certainty is rated in the context of the presence of any treatment effect (i.e., how certain is CDA-AMC that there is any — beneficial or harmful — effect). In this case, the clinical importance of any effect remains unclear. In all cases, the target of the certainty of evidence assessment is based on the point estimate of each outcome and where it is located relative to the chosen threshold for a clinically important effect (when a threshold is available) or to the null (when there is no threshold).
Results of GRADE Assessments
A GRADE summary of findings for the body of evidence for this review included the evaluation of the main outcomes considered important by clinicians, patient groups, and stakeholders. These assessments are presented in Table 2 for each outcome included.
Long-Term Extension Studies
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
Study 312 is a multicentre, open-label, 156-week, long-term safety extension study conducted in all eligible patients who completed the PROGRESS or ELEVATE study, where the ELEVATE study is a phase III, multicentre, randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy, safety, and tolerability of oral atogepant for the prophylaxis of migraine in participants with episodic migraine who have previously not experienced improvement with 2 classes to 4 classes of oral prophylactic treatments. The study consists of a 156-week, open-label treatment period and a safety follow-up period of 4 weeks.
Patients who directly roll over from the PROGRESS or ELEVATE study will have visit 7 from their respective lead-in study function as visit 1 for Study 312. For patients who complete visit 7 before the initiation of Study 312, visit 8 and/or end of study should be completed per the schedule of assessments of their respective lead-in study and visit 8 and/or EOS will function as visit 1 for Study 312.
The primary objective of the study is to assess the safety and tolerability of the long-term use of atogepant 60 mg every day treatment in patients with chronic migraine or episodic migraine. Efficacy end points for long-term efficacy evaluation were included; however, they were considered exploratory. An interim analysis (from November 2023) is presented here, including only patients from the PROGRESS study.
Populations
Eligibility Criteria
Patients eligible to participate in this study, from either the atogepant 60 mg every day arm or the placebo arm, will have completed visit 7, and visit 8 (if applicable), of the PROGRESS or ELEVATE study without significant protocol deviations (e.g., noncompliance to protocol-required procedures) and without having experienced an AE that, in the investigator’s opinion, may indicate an unacceptable safety risk. Patients must be using a medically acceptable and effective method of birth control during the entire study.
Patients were excluded if they met the following criteria: had an electrocardiogram with clinically significant abnormalities at visit 1; had hypertension as defined by sitting systolic ██ █ ███ ██ ██ or sitting diastolic ██ █ ███ ██ ██ at visit 1; were at significant risk of self-harm or harm to others based on a clinical interview and responses on the Columbia-Suicide Severity Rating Scale; had clinically significant hematologic, endocrine, cardiovascular, pulmonary, renal, hepatic, gastrointestinal, or neurologic disease; had a history of acute hepatitis or chronic liver disease within 6 months of screening; or had any condition or medical reason that, in the investigator’s opinion, may confound study results or interfere significantly with participation in the study.
Interventions
Patients are treated with atogepant 60 mg every day. Patients are instructed to take their atogepant at approximately the same time each day. Atogepant is administered orally for 156 weeks, and patients are being followed for 4 weeks following completion or discontinuation of atogepant.
For the acute treatment of migraine, the following medications are allowed during the study: ████████ ██████ █████ ████████████ ████████ █████ █████ ██ █████████ ██████████ ███████████████ █████ ███████ ██████████ ███████ ███ ██████████ ████████ █████ ████ ██ ███ ██ ███ █████ ███████████ █████████ ███ ████████ █████ █████████ ███ █████ ██████████ ████ ████████████ ███ ██████ █ ████████ ███████ ██ █████████ ██ ███ █████ █████ ██████████ ██ ███ ████████ ███████ ███ ███ ██████████ ████████████████ ██ ██ ███ ██████ ██ ███████ ███ ███████ ████████████ ████ ██ ████ ███ ██████████ ████████ ████ █████████ ██ ██████ ███ ██ █████ ██ ████ █████ ██ █████ █ ███ █████████ ███████ ██████ ██ ████ ██████████ ███ ██████
Outcomes
Efficacy Measures
End points for the long-term efficacy evaluation at each monthly period (week 13 to week 16, week 29 to week 32, and week 45 to week 48) are listed as follows:
change from baseline in MMDs
change from baseline in MHDs
change from baseline in monthly acute medication use days at each monthly period
50% or greater improvement (decrease) of MMDs
change from baseline in monthly performance of daily activities domain score of the AIM-D.
End points for the long-term efficacy evaluation at week 12, week 20, week 28, week 36, week 44, and week 52 are listed as follows:
change from baseline in the MSQ Version 2.1 role function-restrictive domain score.
Safety Measures
The safety measures include:
Monitoring for AEs.
Statistical Analysis
All safety analyses were performed using the safety population, consisting of all patients who received at least 1 dose of study intervention (atogepant) in the extension study. For each of the clinical, laboratory, vital sign, and electrocardiogram parameters, the baseline value as defined for the lead-in study was used as the baseline in this extension study.
All efficacy analyses were performed using the mITT population, consisting of patients who received at least 1 dose of study intervention (atogepant) in the study, and had at least 1 evaluable postbaseline 4-week period of eDiary data in this extension study. For each of the efficacy end points, the baseline value as defined for the lead-in study was used as the baseline in the extension study. Descriptive statistics were provided by visit for all efficacy end points based on the mITT population. No inferential statistical analyses were performed.
Continuous variables were summarized by the number of patients, and mean, SD, median, minimum, and maximum values. Categorical variables were summarized by the number and percentage of patients.
No analyses specific to the 2 or more TFs population were presented.
Results
Only results for the overall mITT population were provided, with no subgroup data for the 2 or more TFs population presented.
Patient Disposition
Table 34 provides a summary of the patient disposition among those enrolled in Study 312 from the PROGRESS study. At the time of the interim analysis, 6.2% of patients had completed the study and 62.8% of patients were still ongoing. Of the 325 patients enrolled in Study 312 from the PROGRESS trial, 32.6% of patients discontinued treatment, with patient withdrawal (12.3%) being the most common reason for discontinuation.
Table 34: Patient Disposition in Study 312
Patient disposition | Atogepant 60 mg q.d. (N = 325) |
|---|---|
Screened, N (%) | 325 (100) |
Number of patients treated from the PROGRESS study, N (%) | 325 (100) |
Number of patients ongoing, N (%) | ███ ██████ |
Number of patients who completed, N (%) | ██ █████ |
1-year period | ██ █████ |
2-year period | | █████ |
3-year period | ███ |
Number of patients who discontinued, N (%) | ███ ██████ |
Reason for discontinuation, N (%) | |
Adverse event | ██ █████ |
Lost to follow-up | | █████ |
Lack of efficacy | | █████ |
Withdrawal by patients | ██ ██████ |
Pregnancy | | █████ |
Protocol deviation | ███ |
Noncompliance with study drug | | █████ |
Other | ██ █████ |
mITT, N (%) | ███ ██████ |
Safety, N (%) | ███ █████ |
ITT = intention-to-treat; mITT = modified intention-to-treat; q.d. = every day.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Exposure to Study Treatments
Study Treatments
In Table 35, the treatment duration in the safety population among the patients enrolled from the PROGRESS study is presented. The mean (SD) treatment duration was █████ ███████ days.
Table 35: Drug Exposure (Safety Population)
Variable | Patients From PROGRESS study (N = 325) |
|---|---|
Mean (SD), days | █████ ███████ |
Median (minimum to maximum), days | ███ ███ ████ |
Patient-years | █████ |
Q.d. = every day; SD = standard deviation.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Efficacy
Currently available efficacy results for Study 312 are presented as follows and include the change from lead-in baseline for each monthly period (week 13 to week 16, week 29 to week 32, and week 45 to week 48) in MMDs (Table 36), MHDs (Table 37), and the change from baseline in monthly acute medication use days at each monthly period (Table 38). The proportion of patients for each monthly period with a 50% or greater improvement in MMDs is presented in Table 39 and the monthly performance of daily activities domain score of the AIM-D is presented in Table 40.The change from baseline in the MSQ Version 2.1 role function-restrictive domain score at week 12, week 20, week 28, week 36, week 44, and week 52 is presented in Table 41.
Overall, reductions in mean MMDs, mean MHDs, and mean monthly acute medication use days relative to the lead-in study baseline were observed during the open-label treatment period. The proportion of patients with a 50% or greater improvement in MMDs was 41.0% across the 12-week treatment period in the PROGRESS study, █████ for week 13 to week 16, and ████████ ███████ for week 29 to week 32 and week 45 to week 48. The change from baseline in monthly performance of daily activities domain score of the AIM-D ████████ ██████████ ██████████ ██████ week 13 to week 16, week 29 to week 32, and week 45 to week 48. Moreover, the change from baseline in the MSQ Version 2.1 role function-restrictive domain score at week 12, week 20, week 28, week 36, week 44, and week 52 ████████ ███████ across all weeks.
Change From Baseline in Mean MMDs
Table 36: Change From Lead-In Baseline in Monthly Migraine Days for Each Monthly Period (mITT Population)
Variable | Patients From PROGRESS study ██ █ ████ |
|---|---|
Lead-in baseline | |
Mean (SD) | █████ ███████ |
Week 13 to week 16, CFB | |
LSM (SE) | ██████ ███████ |
95% CI | ███████ ██████ |
Week 29 to week 32, CFB | |
LSM (SE) | ██████ ███████ |
95% CI | ███████ ██████ |
Week 45 to week 48, CFB | |
LSM (SE) | ██████ ███████ |
95% CI | ███████ ██████ |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; SD = standard deviation; SE = standard error.
Note: LSM, SE, and 95% CI were derived from an MMRM with visit as a categorical fixed effect, and baseline score and a baseline-by-visit interaction as covariates.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Change From Baseline in Mean MHDs
Table 37: Change From Lead-In Baseline in Monthly Headache Days for Each Monthly Period (mITT Population)
Variable | Patients From PROGRESS study ██ █ ████ |
|---|---|
Lead-in baseline | |
Mean (SD) | █████ ███████ |
Week 13 to week 16, CFB | |
LSM (SE) | ██████ ███████ |
95% CI | ███████ ██████ |
Week 29 to week 32, CFB | |
LSM (SE) | ██████ ███████ |
95% CI | ███████ ██████ |
Week 45 to week 48, CFB | |
LSM (SE) | ██████ ███████ |
95% CI | ███████ ██████ |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; SD = standard deviation; SE = standard error.
Note: LSM, SE, and 95% CI were derived from an MMRM with visit as a categorical fixed effect, and baseline score and a baseline-by-visit interaction as covariates.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Change From Baseline in Monthly Acute Medication Use Days
Table 38: Change From Lead-In Baseline in Monthly Acute Medication Use Days for Each Monthly Period (mITT Population)
Variable | Patients From PROGRESS study | | ████ |
|---|---|
Lead-in baseline | |
Mean (SD) | █████ ███████ |
Week 13 to week 16, CFB | |
LSM (SE) | █████ ███████ |
95% CI | ██████ █████ |
Week 29 to week 32, CFB | |
LSM (SE) | █████ ███████ |
95% CI | ███████ █████ |
Week 45 to week 48, CFB | |
LSM (SE) | █████ ███████ |
95% CI | ███████ █████ |
CFB = change from baseline; CI = confidence interval; LSM = least squares mean; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; SD = standard deviation; SE = standard error.
Note: LSM, SE, and 95% CI were derived from an MMRM with visit as a categorical fixed effect, and baseline score and a baseline-by-visit interaction as covariates.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Reduction of 50% or More in 3-Month Average of MMDs
Table 39: Reduction of 50% or More in Mean Monthly Migraine Days (mITT Population)
Variable | Patients From PROGRESS study (N = 284) |
|---|---|
Week 13 to week 16, CFB | |
Responder rate, n of N1 (%) | ███████ ██████ |
Week 29 to week 32, CFB | |
Responder rate, n of N1 (%) | ███████ ██████ |
Week 45 to week 48, CFB | |
Responder rate, n of N1 (%) | ███████ ██████ |
CFB = change from baseline; mITT = modified intention-to-treat.
Note: N1 is the observed data at baseline and at that time point.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Change From Baseline in Mean Monthly Performance of Daily Activities Domain Score of the AIM-D
Table 40: Change From Lead-In Baseline in Monthly Performance of Daily Activities Domain Score of the AIM-D for Each Monthly Period (mITT Population)
Variable | Patients From PROGRESS study ██ █ ████ |
|---|---|
Lead-in baseline | |
Mean (SD) | █████ ████████ |
Week 13 to week 16, CFB | |
Mean (SE) | ██████ ████████ |
Week 29 to week 32, CFB | |
Mean (SE) | ██████ ████████ |
Week 45 to week 48, CFB | |
Mean (SE) | ██████ ████████ |
AIM-D = Activity Impairment in Migraine-Diary; CFB = change from baseline; mITT = modified intention-to-treat; SD = standard deviation; SE = standard error.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Change From Baseline in MSQ Version 2.1 Role Function-Restrictive Domain Score
Table 41: Change From Lead-In Baseline in MSQ Version 2.1 Role Function-Restrictive Domain Score (mITT Population)
Variable | Patients From PROGRESS study (N = 284) |
|---|---|
Lead-in baseline | |
Mean (SD) | █████ ████████ |
Week 12, CFB | |
Mean (SD) | █████ ████████ |
Week 20, CFB | |
Mean (SD) | █████ ████████ |
Week 28, CFB | |
Mean (SD) | █████ ████████ |
Week 36, CFB | |
Mean (SD) | █████ ████████ |
Week 44, CFB | |
Mean (SD) | █████ ████████ |
Week 52, CFB | |
Mean (SD) | █████ ████████ |
CFB = change from baseline; mITT = modified intention-to-treat; MSQ = Migraine-Specific Quality-of-Life Questionnaire; SD = deviation.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Harms
A summary of safety measures for the PROGRESS study is presented in Table 42. Treatment-emergent AEs were reported by 265 (81.5%) patients. The most frequently reported AEs included COVID-19 (30.8%), constipation (10.2%), nasopharyngitis (9.8%), urinary tract infection (6.2%), and insomnia (5.5%).
Treatment-emergent SAEs were reported by 20 (6.2%) patients. None of the SAEs were noted as treatment-related, as assessed by the investigator. The following SAEs were reported by 1 patient each ████████ █████████████ █████████ ███████ ██████████ █████████████ ██████████████ ██████ ████████████ ██████████████ ████ █████████ ████████ █████████████ ███████████████ ███████ ████ █████████ ██████ █████ ██████████ ███████ ███████ ███████████ █████████████ ██████ ███████ ██████████ ███████ █████████ ███████ ████████ ███████ █████████████ ███████ █████ ███████ ██████ █████████ █████████ █████████ ███ ████████ ████.
AEs leading to study drug discontinuation were reported in 27 (8.3%) patients. ███ ███████ ██ ███ █████ ████ ███████████████ █████████ █████████ █ ████████ ████████ ██ ██████████ ████████████ ████ ██████ ████ ███████ ████████████████ █████████ ████ █████████ ████████████████ █████████ ████ ███ █████████████████████ ████
No patients on atogepant 60 mg every day were reported to have violated Hy’s law (having an elevated ALT or AST laboratory value of ≥ 3 × ULN and an elevated total bilirubin laboratory value of ≥ 2 × ULN and, at the same time, having an alkaline phosphatase laboratory value of < 2 × ULN).
Table 42: Summary of Harms (Safety Population)
Preferred term | Patients From PROGRESS study (N = 325) |
|---|---|
Patients with 1 or more AE (≥ 2%), n (%) | |
Overall | 265 (81.5) |
COVID-19 | 100 (30.8) |
Constipation | 33 (10.2) |
Nasopharyngitis | 32 (9.8) |
Urinary tract infection | 20 (6.2) |
Insomnia | 18 (5.5) |
Upper respiratory tract infection | 16 (4.9) |
Back pain | 15 (4.6) |
█████████ ████████ | | █████ |
██████ | ██ █████ |
█████████ ████ █████ | | █████ |
███████████ | | █████ |
█████████ | | █████ |
███████████ | | █████ |
███████████████ | | █████ |
██████████ | | █████ |
███████ | | █████ |
█████████ | | █████ |
████████████ | | █████ |
█████ █████████ | | █████ |
Patients with 1 or more SAE, n (%) | |
Overall | 20 (6.2) |
WDAEs, n (%) | |
Overall | ██ █████ |
█████████ █ ████████ ████████ | | █████ |
████████████ | | █████ |
██████ | | █████ |
███ █████████ | | █████ |
███ █████████ | | █████ |
████████████████████ | | █████ |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; SAE = serious adverse event; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event; WDAE = withdrawal due to adverse event.
Source: Topline Results of Study 3101 to 312 to 002 (2023).79
Critical Appraisal
Internal Validity
Study 312 is limited by its open-label and noncomparative design; since there is no comparator, it cannot be confirmed whether the results observed may be attributable to the effects of the drug or the natural history of the condition. Furthermore, the mITT population analyzed excluded ███ of patients, and the large amount of missing outcome data (more than ████ introduces a risk of bias. The open-label and nonblinding nature of the study increases the risk of bias and because the outcome measures are generally self-reported, they are subjective, and it is uncertain if they can be replicated in another population beyond that which was included in the study.
External Validity
No information was provided on the 2 or more TFs population (the reimbursement requested population). It is therefore not possible to know whether the effects observed in the full population would be similar in that group. Because the patients who took part in the open-label, long-term, safety extension phase were originally from the pivotal PROGRESS trial, it is reasonable to expect that the same limitations to generalizability are relevant to the open-label, long-term, safety extension phase. Given the nature of the noncomparative study design, it is not possible to compare the effectiveness and tolerability of atogepant as a prophylactic treatment of chronic migraine against other preventive treatment.
Indirect Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Objectives for the Summary of Indirect Evidence
███ ███████ ████████ █████ ████████ ███ ████████ ███ ██████ ██ █████████ ████████ ██ ███████ ██ ████████ ████ ███ ████████ █████ ███ █████ █████████ ███████ █████████ ███ ████ ███ ███ █████████ ██ ██ ███ █ ██████ ██████████ ███████ █████████ ███ █████ █████████████ ██ ████████ ███ ███████ ████ ████ ██ ████████ █████████ ██████████ ██ █████████ ███████ ████████ ███████████ ███ █████████ ███ █████████ ██ ███ ████████ ███ █████████ ███ ██ ████████ ███ ████████ █████████ ███████ ███ ████████████ ██ █████████ ████████ ████ █████████████ ██ █████ ████
Description of Indirect Comparison(s)
███ ███ █████████ ██ █ ███████ █████████████ █████ █████████ ███ █████████ ██ ███ ████████ ███ █████████ ████████ ███ ███ ███ ███ █████████ ██ █████ ███ ███ █████████ ██ ██ ████████ ███ █████████ ███████ ███ ████████████ ██ █████████ ████████ ████ ████ ██████████ ███ ███████████████████ █████ ███ ████████ ██ █████ ██ ██ ████████
Table 43: Study Selection Criteria for the Network Meta-analysis [Redacted]
██████████████ | █████████ ████████ |
|---|---|
██████████ | █████ ████ █ ██ ██████ ████████ ████ ██████████ ██ ████████ ███ ████ ██████████████████ █████████ ███████ |
█████████████ | ████████████ █████████ █████ ███ ███████████ ██ ███████ █████████████████████████████████████████████████████████████████████████████████████████████████████████████████████████████████████ |
███████████ | ████████████ ██████████ ████ ███████ ████████████ ██ ███ █████████████ ██████ ███████████ ████████████ ███████ ███████ ███ █████ ███████████ ██ ████████ ████ ████████ |
████████ | ████████ ████████████ █████████████████████████ █████████ ██████████ ███ █████████████ ████ ██████ ███ ███ ██████████████████████ ███████ █████████████████████████ ███████ █████████████ ███████ █████ ████████████████████████ ██████ ████████████████ ███████████████ |
█████ ███████ | ████ █████ ████████ ███ ████████████████████ ██████████ ███████ ███ █████████████ |
███████████ ███████████████ | ██ ██████ |
█████████ ████████ | ████████████████████ ███████████████ ███████████████████ ████████████████ ███████ █████ ████ ███████████████████████████████ ███ ██ ████████████████████████ ██████████████████████████████████████████████ █████████████████████████ ███ ██ ██████████████████████ █████████ ████████ ███ ████████ ██ ███ █████████████ ██████████████████ ████████████████ ████████ █████████ ███ ███████████████████ ███ █████████████ ███████ ███████████ ███████ █████ ██ ████████ ███ █████████████ ███████ |
███ █ █████ █████ ████ ██ █ ███████ █████████ █████ █ ██████████████ ███████ ██ █████ ██ █ ███████████ ███ █ ███████ ████████ ████ ███ █ ███████ ████████ ████ ███ █ ██████████ ██████████ ██████ ███ █ ██████████ ██████████ ███████ ████ █ █████████ ████████ ███████ █████████████ ███████ ████████ ████████ ███ █████████████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ ██████████
Indirect Treatment Comparison Design
Study Selection Methods
████████ ██████████ ██████████ ██████ █████ ███ █████████ █████ ███ ███████████ ██████████████ ████████████ █████████ ███ █████ ██████ ████████ ████████ ██ █████ ███ ████████ ████████ ███ ████ ██████ ████ █████████ ██ ███ ███ █████ ███ ████ ███████ ██ █████████ ██ █████ ████████ ████ ███ ██████████ ██ ███████████ ████ █████ ████ ███ ████ ███████████ ██ █████ ██████████ ███████████ ████ ████████ ███ ███ ████ ███ █████ ████ ███ ██████ █████ ██ ████████ █████████ ██ █████████ █████ ████████ ████ ███████ ██ ███ ██████████ ██████ ███████ ██ ████████ ███ █████ ███ ██ ██████ ████ ████ ███ ████ ████ ██ ███ ████████ █████████ ███ ██████ ████ ██ ██████ ███ ██████ ███████ ███ ███ █████████ ███ ██████ ██ ████ ██████████ ████ ███ ████████ ███████ ███ █████████ ██ ████ ██ ████ ████ ████ ███ ██████████
ITC Analysis Methods
███████ ██ ███ ███████████ ███ ███ ███ ██ █████████ ██ █████ ████
Table 44: Indirect Comparison Analysis Methods [Redacted]
███████ | ███████████ |
|---|---|
████████ ███████ | ████████ ████████ ██ ███████ ███ ███████████ ██ █████ ██████████ █████ ██████████ ███████████ ███████ █████████ ████████ ████████ ████████ ███ █████████ █████ █████████ ██████ ██████ █████ █████ ██████ ███ ████████ ████████ ██ ██ ███████████ ██ ███ █████████ █████ ██████████ ███ ███████████ ███████ ████ █████████ ███████ █████████ █████████ ███████ ████ █████████ █████ ████ ████████ ███ ███████ ███ ██████ ███████ ██████████ ███ ████ ███ █████████ ██ █████ ███ ████████ ████ ███ ████ ███ ███ ██████████ ████ ███████████ ███ ████ █████████ ██ ██████████ ██████ ██ ███████ ████ █████████ ████ ███ █████████ ████████████ ██ ████████ █████████ ███████ ███ ███████ ███ █████ █████ ████ ██████████ █████████ █ ██████ ██████████ ████ ██ ████████ ████ ████████ ███ ███ ██ ███ ██████████ ██ ████ ███ ████ ███ ███ ████████ ██ █████████ ████ ████ ██████ ████████ █████████ ██ ████████ ██ ████ ███ ██████████ ██ ████ ████████ █ ████████ ██████████ ████ █ █████ ████ ████████ ███ ███ ██ ███ █████ ██████ ██ ████████ ███ ███ ██████ ██ ████████ ████████████ ███ ████████ ██ █████████ ████ ███ ██████ ███ ████████████ █████████ ██ ████████ ██ ███████ ███ ██████████ █ ████████ ██████████ ████ █ ███████ ████ ███ ██████ ██ ███ █████ ██████ ██ █████████ ███ ██████ ██ ████████ ████████████ ███ ████████ ██ ████████ ███ ███ ████ █████ ███ ████ ███ █████████ |
██████ | ███ ████ ██ ███ ██ ███████ █ ███████████████ ███████ ███ ██ ████████████ ███ ████ ██ ███ █████ ████████████ ███ ███ ███████ █████ ███ ████ █████ ████████████ ███████ ████ ███ █████ ███████ █ ███ █ ███ ███████ █████████ |
██████████ ██ █████ ███ | ████ ██ ███ ██ ██████ ████ ██████ ██ ███ █████ ███ █████ ██████████ ████ █ █████ ███ █████ ███ █ ██████ ███████ █████ ██ ███ ████ █████ ████████ ███ ███████████ ████ ████ █ ██ █ ████ ███ ██████████ ███████████ ██ █████ ██████ ███ ██ █████ ███ ██████ ██ ███ █████████ █████ ███ ███ ███████ ██████████████ ██ ███ █████ |
██████████ ██ ███████████ | █████████████ ███ ███████ ██ ██ ████████ █████ █ █████████ ██████ ████████████████ █████████ ███ ██████ ██ ███ ██████████ ██ ███ ███████ ██ ███ ██ ███████ ████ ████ ██ ███ ████ ████ █████ █████ ████ ██ █████████ █████ ██ █████ ██ █████████████ ████████ ██ ████ ██████████████ █████ ████ ██ █████████ █████ ██ ███ ████████ ██ ████ █████████████ ██ ███ ██ ██ █████████ ███ ██ ███████ ████████ █████████ |
██████████ ██ ███████████ | ███████████ ███ ████████ █████ ███ ███████████████████ █████████ ███ █████ ██ █████████ ████████ |
██████████ ██ █████████████ | ███████████ ███████████ ██ █████████████ ████ █████ ██ █████ ███ ███████████ ██ ██ ███ ██ ██████ █████ ███ ███ █████ ████████ █████████ |
████████ | ██████████ ████ ██ ████ ███████ ██ ████ ███████ █████ ███████ ██ ████ ██████████ ██████ ███████ ████████ ██ ██████████ ███████ ████████ ██ █████████████ █████████████████████ |
███████ ████ ███████████ | ██ ██████████ ████ ████ ███ █████████ ██████████ ████ ██ █████████ █████ ████████ ███ █████████ ███ ████████ ███ ████ ███████ █████ ██ ████ ███ ███ █ █████████████ ████████ █████████ ██ █████████ ███ ████████ ████ ███████ ████ █████████ █████ |
████████ ████████ | ███ █████████ ████████ ████████ ████ ██████████ ██ ████████ ████ ████ ███ ██ ████████ ████ ████ |
██ █ ███████ █████████ ███ █ ████████ █████████ ███ █ ████████ ███████████ ██████████ ██ █ █████ ███████ ██ █ ██████ ██████ ██████ █ ████████ ████████ ████████████ ██ █████ ██ ████████ █████████ ████ █ ██████ █████ █████ ██████ ██ █ ████ ███████████ ███ █ ███████ ████████ ████ ███ █ ███████ ████████ ████ ███ █ ███████ █████ ██████████ ███ █████ ███ █ ███████ ██████████████ ██ █ ████ ██████ ██ █ ██████ ███████ ███ █ ██████████ ██████████ ██████ ██ █ ████████ ██████████ ██ █ ████████ ██████ ███ █ ██████████ ██████████ ███████ ████ █ █████████ ████████ ███████ ██████ ██ █ █████████ ████████ ███ █ █████████ ███████ █████████
Results of the ITC
███ ████████ ███ ██████████ ██ ██████████ ██████████ ██████ ██████ ███████ ███ █████████ █████████ ███ ███████ ██████████ ██ ███ ███ ████ █████████ ███████████ ██ █████ ████████ ██████ ██████ █████████ ███████ ████ ████████ ████ ███ ████ ████ █████████ ██ █████ ███ ███████ ████████ ██ ███ ███ █████ ███████ ███ ███████████████ █████ ███ █ ████ ████ ██████████ ██ ████████ █████ █████ █████████████████ ███████████ ██ ████████ ████████ ██ ███ █████ ████████ ███ █████ ███ █ ██████ ██████████ ██ █████████████ █████ ██ ███████████████████ ███████████ ███ ███ ██ █████ ██ ████ ██████████ ██ ███████████ ████████ ███ █████████ ██ ███ ████ █████ ██ ███ ███████████ ██ ████████ ███████████ ███████████████████ ████████████ █████████ █████████████ ██ ██████████████ █████ ████████ ███ █████████ ████ ████ ████ ███ ██ █████████ ████ ██ █████ ██ ██████ ████ ███ ███ █████████ ███ ████ █ ██████████ ██ ████████ ███ ████ ███ ████████ ██ ███ █████████ ██ ███ █████████ ██ ███████ ██ ████ ████████ ██ ███ ████ ████ ███ █████████ ████████ ████ █████ ██████ ████████ ████ ███ ███ ██ ██ ████████ █████████████
███████ ██ ████████ ████████
███ ██████████ ██ ████████ ███ ███ ████████ ██ ███ ██ ███ ███ ██████ ███ ████████████ ████████ ███ ██████████ ███████████████████ ████████████ █████████ █████████████ ████████████ ███ ████████ ████████ █████ ████ ██ ████ ███ ███ ██ ███ ██ █████████ ███████ ███████████ ███ ███████████ ██ ██ █████████ ████ ███ █████████████ ██ █████████████ █████████ ███ █████████ ███████ ███████ ████ █████████████ ██████████ ██ ██ █████ █████████ ████ ███ ████████ █████████ ██ ███ ████ ███ ███ ███ ██████████████ ████████ █████████ █████ ███ █████████ ██ ███ ███ ████ █████ ██ ███ █████████ ██ ███ ██████████ ██ ███ ██ ███ ███ ███ ████████ █████████ ██████ ██████ ██████ ███████ ████████ ██████ ███ ███ ████████████ ██ ████████ ████████ ████ ███ ███ ██ ███ ██ ██ ████████████ ███ ██ ██ ██ ██████████ ████████ ████████ ████████ ████ ██ █████ ███ █████ ██████████ █████████ █████████ ███ ███████████ ██████ ████████ ███ ███ ██████████ ████████ ██ ███ ███ █████████ ██ ████ ███ ███ ██████ ███ ██████ ██████ ███████ ██████████ ███ ███████████ ████████ ████ ███ ███ ██ ███████████ ███ ███ ████████ ████████████ ██████ ████████ ██ ███ ███ █████ ████ ███ ██████ ██ ████████ ██ ████ ███████ ███ ██ ██████████ ███ █████████ ██ █████ ███
Table 45: Treatments [Redacted]
█████ ████ | █████████ | ████ | █████████ | ███ ███ |
|---|---|---|---|---|
███████████ ███ ██ | █████████ | ██ ██ | ███ | ███ |
██ ██ | ██ | ███ | ||
███████ | ||| | ||| | ███ | |
█████ █████ ███ | ███████████ | ███ █ ████ | | ████ █████ █████ ██████ | ███ |
███████ | ||| | ||| | ███ | |
████ ██████ ████ | ███████████ | ███ █ █████ | ████ █████ █████ ██████ | ███ |
███████ | ||| | ||| | ███ | |
██████████ ████ | ███████████ | ███████ ██ | ████ █ █████ | ███ |
███████ | ||| | ||| | ███ | |
███████████ | ███████████ | ███ ██ | ████ █ █████ | ███ |
███ ██ | ████ █████ █████ | ███ | ||
███████ | ||| | ███ | ||
██████ ████ | ████████ | ██ ██ | ████ █ █████ | ███ |
███ ██ | ███ | |||
███████ | ||| | ||| | ███ | |
█████ ████ | ███████████ | ███ ██ | ████ █ █████ | ██ |
███████ | ||| | ||| | ██ | |
████████ ████ | ███████████ | ███ ██ | ████ █ █████ | ███ |
███ ██ | ████ █████ █████ | ███ | ||
███████ | ||| | ||| | ███ | |
██████████ ██ | ███████████ | ███████ ██ | ████ █ █████ | ██ |
███████ | ||| | ||| | ██ | |
██████ ████ | ███████████ | ███ ██ | ████ █████ █████ | ███ |
███ ██ | ████ █████ █████ | ███ | ||
███████ | ||| | ||| | ███ | |
██████████ █ | ███████████ | ███ ██ | ████ █████ █████ | ███ |
███ ██ | ████ █████ █████ | ███ | ||
███████ | ||| | ||| | ███ | |
█████ ████ | ███████████ | ███ ██ | ████ █ █████ | ███ |
███ ██ | ████ █████ █████ | ███ | ||
███████ | ||| | ||| | ███ | |
█████████ ███ | ████████ | ██ ██ | ████ █ █████ | ██ |
███████ | ||| | ||| | ██ |
████ █████ ██████ ███ ███████ █████████ ████ ███████████████████ ██ ███████ ███ ████ ████████████ ████████████ ███████ ███████ ██ █ ███ ██ ███████ ████ ████████ ██ ███ ██ ████ █ ████████████ ██████████ ██████ ████ ████████ ██ █ ████████ ████████ ███ ███ ██ ███ ████ █████████████ ███████ ████████ ████████ ███ ██████
Results
█ █████ ██ ████████ ████████████████ ███████ ████ ███████ ████████ ███ ██ ███████ ████████ ██ ███ ███████ ██████████ ████████ ████████ ██████████ █████████████ █████ ████████ █ ████████ ███ ██████ ████████ ████████ █ █████ █████ █ █████ ██ ███████ ███ ████████ ███████ ████ ████ ████████ ████ ███ ███████ ██████ ███ ██ ███ ███████ █ █████ ███████ ████ ████████ ███ ████ █ ████ ████████ █ ████ ██ ███████ ████ ████████ ████ █ ██████ █████ █████ ██ ███████ ███ ████ ████████ ████ █ ██████ █████ █ ████ ██ █████████ ███ ████ ███████████ █ █████ ██ █ ██████ ████ ███████████ ███████ ██████████ ██████ █████ ████████ ██████ ███████ █ ███████ ██████ ███████ █ ███████ ██████ ████████ ███████ ███ ██████ ██████ ██████ ██████ ███ ██████ ████ ██████ ██ ███ ██████ ███ █████ ██ ███ █ ███████ ███ ███ ██████ █████ ████ ███ ██ ██ ██ ████████ █████████████ ███████ █ ███ ███████ █ ████ ███████ ██ ██ ███ ████ ██ █████ ██████████ ███████ ███████████ ███ █████ ███ ███████ ██ ██ ███ ████ ██ ███ ███████ █████ ███ ███████ ███ ██████ ███ ██████ ██ █████████████ ████ ██████ ██ █████ ████████ ████ ███ ███████ ████ ██ ████ ████ █ ███ ██████ ████ ███ ████████ █████ ███ █████ ██████ ████ ████████ ████ ███████ ███ ██ ██ ██ ███████████ ██████ ████ █████ ██ █████ ██████ ██████ ███ ██████ █████████ ██████████ ██ █████ ██ █████ ████████ ████ █████████████ ██████ ███ ████████████ ███ ██████████ ███████████ ██████ ███ ██████ ████ ███████ ████ ██ ██████ ████ ██████ ██████ ████ ███ ██████ ███████ ████ ███ ███ ███ ███████ ███ ██████ ███ ██████ ██ █████████████ █████ ████|███████████ ████ ███ █████████ ███ ████████ ██ ████████ ███ ██ ███ █████ ██ ██ ██ ██ ██████ ████████ ████ ███ ███████ ████████ █ ███ █ ███ █████████ █████ ████████ ████████ ██ ██ █████ █████ ███ ████ ████████ ███ ████████ ██ ██ ████████████████ ████████ ████████ ███ ███ ████████ ████████ ███ ███ ███████ ███ ██ ██ ██████████ ██████████████ ████████ ███ █████████ █████ ██ ██████ █ ██ █████ ██████ ██ ██ ██████ ███ ████████████ ████ ████ █████████ ████ ████████ ███ ███ ███████ ███████████ █████████ ████████ ████████ ███ ███ ██████ ███ ████████████ █████████ ███████ ███████ ████████ ██████






████████████████ ████ ███ █████████ ██ ██ ███ █████ ███ ███ █████████ ██ ██ ████ ███ ██ █ ███████████ ██████ ███████ ███ ███ ██ ███████████ ███████ ███ ███ ██ ██ ██████████ ████ ██ ███████████ ██ ████ ██ ███████ ████ ███ █████████████ ███████ ███ █████████████████ ████ ████████ ██ ████ ███████ ████████ ████ ████████ ███ ███████ ██ ███████████ █████████ ██ ██ ██ █████ ████████ ██████ █████████ ████ ███████ ███████ █████████ ██ ██████ ████ ████████ ██ ████ ██ ████ ███ ██ ███ ██ ██████ ██████ ████ ████████ ████ ████████ ██ ███ ████ ██ ███ ██████████████ ███ ██████ █████████ ██ ████ ███████████ ███ ████ ████████ █████████ █████ ██ ███████ ████ ███ ████ ████ ██████████ ████ ██████ █████████ █████ ████████████ ███ ████ ███████████ ███████ ███████ ████ █████████ ████████ ███ ████████ ██████ ████ ████████ ██ ███████ ███ ████ ████████ ██ ███ ██ █████ ███ ███ ██ ███ ██ █████ ██████ ████ ████ █████████ ██ ██ ██ ███ ████████ ██ ███ █████ █████████████ ██ ███ ████ ████████████ ███ ██████ █████████ ████ ██████ ████ ████████ █████████ ██ ████ ███ ██ ███ ██ ███████ ██ ███ ██ ██ ███████████ ██ ████████ █████████ ██ ███████ █████████ ██ ██ ██ ██ ████████████ █████ █████████ ████████ █████████ ██ ██ ██ ████ ████████ ███ ██ ███ ████████████ ███ ██ ███ ███ ████████████ ███ ██ ███ ███████ ████ ████ ██ ██████ ████ ████ ██████████ ████ ███ ████ ██ ██████████ ██ ██████ ██████████ ███████ █████ █████████ ██████████ ███████ ███ ███████████ ███ ██ ███████████ ██ ███████████████████ ████████ ██ ██ ███ ███ ████████████ ███ ██ ██ ███ █████ █████████ ████ ████ ████ ██████████ ████ ███ ████ ██ ██████████ ██ ██████ ██████████ ███████ █████ █████████ ██ ██ ████ ████████ ██ ███ █████ ██████████████ ███ ███████████ ████ ██ ██████ ████ ███ ████ ████ ████████ ███ ████ ███████████ ██ ███ █████████
████████ ██ ██ ██ ██ | █████ | █████ ██ ████ | ██ ██ ██ ███ |
|---|---|---|---|
█████████ ██ ██ ██ ██ | █████ | ████ ██████████ ████ ████ | |
███████ | █████ | █████ ███████ ████████████ ███████ ██████ | █████ ███████ ████████████ ███████ █████ |
██████████████████ | █████ | ████ ███████ ██████████ ███████ █████ | ████ ███████ ██████████ ███████ █████ |
████████ ██ ██ ██ | █████ | ████ ███████ ██████████ ███████ █████ | ████ ███████ ██████████ ███████ █████ |
████████ ███ ██ ██ | █████ | ████ ███████ ██████████ ███████ █████ | ████ ███████ ██████████ ███████ █████ |
████████████ ███ ██ ██ | █████ | █████ ███████ ███████████ ███████ █████ | ████ ███████ ██████████ ███████ █████ |
████████████ ███ ██ ███ | █████ | █████ ███████ ███████████ ███████ █████ | ████ ███████ ██████████ ███████ █████ |
████████████ ███ ██ ██ | █████ | ████ ███████ ██████████ ███████ █████ | ████ ███████ ██████████ ███████ █████ |
███████████ ███ ██ ███ | █████ | ████ ███████ ██████████ ███████ █████ | ██ |
███████████ ███ ██ ███ | █████ | ████ ███████ ██████████ ███████ █████ | ██ |
████████ ████ ████████ ██ ████ ███████ ████████ ████ █████████ ████████ ████████ ███ ███ ███████ ███ ██████ ██ ████████ ███ ████ █████████ ████████ ██ █████ ██ ███ ███████ ██ ███████████ ███ ████ ███ █████████ ██ ██ ██████ █████ ██████████ ████ ████ ███ █████████ ███ ████ ███████ ████████ ██ ████ ███ ██ ███ ██ █████████ ██████████ ████ ███ ████ ██ ██████████ ██ ██████ ██████████ ███████████ ██ █████████ ███████ ███████ ███ ████████ █████████ ██████ ███████ ███ ██ ██ ██ ███████████ ████ ███ █████████ ██ ██ ██████ ████████████ ████ ████ ████ ███ ███ █████████ ████████████ █████ █████████ ██ ██ ████ ████████ ██ ████████████ ███ ███ ██ ███ ██████████ ███████ ████████ █████████ ██ ██ ██ ██████ ████████ ██████ █████████ ████ ████████ ██ ████████ ███ ████ ██ ███ ██ ███████
█████████ ██ ██ ██ ██ | █████ | █████ ██ █████ | ██ ██ ██ ██████ |
|---|---|---|---|
████ ██████████ ████ ████ | |||
███████ | █████ | █████ ███████ ████████████ ███████ ██████ | █████ ███████ ████████████ ███████ █████ |
██████████████████ | █████ | █████ ███████ ███████████ ███████ █████ | ██ |
████████ ██ ██ ██ | █████ | ██ | ██ |
████████ ███ ██ ██ | █████ | ██ | ██ |
████████████ ███ ██ ███ | █████ | ████ ███████ ██████████ ███████ █████ | ██ |
████████████ ███ ██ ███ | █████ | █████ ███████ ███████████ ███████ █████ | ██ |
█████████ ███ ██ ████ | █████ | █████ ███████ ███████████ ███████ █████ | ████ ███████ ██████████ ███████ ██████ |
█████████ ███ ██ ███ | █████ | █████ ███████ ███████████ ███████ █████ | ██ |
███████████ ███ ██ ███ | █████ | ████ ███████ ██████████ ███████ █████ | ██ |
███ █ ██████ ████ █████████ ██ █ ███████ █████████ ███ █ ████████ █████████ ██ █ █████ ███████ ███ █ ███████ ████████ ████ ██ █ ████ ███████████ ██ █ ███ ██████████ ██ █ ████ ██████ ██ █ ████ █ ██████ ███ █ ████ ███ ████████ ██ █ ██████ ███████ ██████ ██████ █████████ ████ ██████████ ████ ███ ████████ ████████ ██ █████████ ███ ███████████ ████ ██████ ██████ █████████████ ███████████ ███████ ██████ █████████ ████ ██ ███ ███████ ███ ██ ██ ███████ ██████████ ██ ██ ███████ ███████████ █████████████ ███████ ██ █ ████████ ████ ██ ███ ██ ████████ ██ ███ ██ ███ ██████████ ██████ ██████████████ ███████ ██ █ ███ ██ ███████ ████ ████████ ██ ███ ██ ████ █ ██████████████ ███████ ████████ ████████ ███ ████████████████ ███████ ████████ ██ ███████ ████████ ████████ ███ ███████ ██ ███████████ █████████ ██ ██ ██ ██████ ██████ ████ ██ ████████ ██████ ██ █████ █ ███ ████████ ██ ████ ████ ████████ ████ ████████ ██ ███████ ████ █████████ ███ ██ █████ ████ ███ ██ ███ ██ █████ ██████ ████ ███ █████████ ███████████ ████████ ███████████████████ ████████ ██ ██ ██ ███ ███ ██ ███ ████████████ ███ ██ ███ ███ ███████████ ███ ██ ███ ███ ██ ████ ██ ██████ ███ ██ ██████ ████ █████ ███ ███ ███████████ ███ ████ ██ ███ ██ ███████ ████ ████████ ███ █████ ██████████ ████ ███ ████ ██ ██████████ ██ ██████ ██████████ ███████████ ██ █████████ ███████ ███████ ███ ████████ █████████ ██████ ████████ ███ ██ ██ ██ ██████████ ███ █████████ ███████████ ████████ ███████████████████ █████████ █████████████ ███ █████████████ ██ █████ ████████████ ████ █████ █████████ ███ ████ ██████ ███████ ████ ███ █████████ ██ ███ █████████ ██ ██ ██ ██████ ███ ██████ █████████ ██ ███ ████ ██ █ ███ █████████ ██ ███████ ███ ██ ██████ █████████ ██████████ ███ ██ ██████████ ██ █████████ ███████ ██ ██████ ███████████ ██ ███ ██ ██████ ████ ███████ ███████ ███ █████████ ████ ██ ████ █ █████████████ ███████████ ███████████ ██ ███ ████ ██ █████████ █ ███ ████████ ██ ████ █████
████████ ██ ██ ██ ██ | █████ | ██████ ██ ███████ | ██ ██ ██ ████████ |
|---|---|---|---|
████ █████ ████ ████ | |||
███████ | █████ | ████ ██████ ██████████ ██████ █████ | ████ ██████ ██████████ ██████ ██████ |
██████████████████ | █████ | ████ ██████ ██████████ ██████ █████ | ████ ██████ ██████████ ██████ ██████ |
████████ ██ ██ ██ | █████ | ████ ██████ ██████████ ██████ █████ | ████ ██████ ██████████ ██████ ██████ |
████████ ███ ██ ██ | █████ | ████ ██████ ██████████ ██████ █████ | ████ ██████ ██████████ ██████ ██████ |
██████████ ███ ██ ██ | █████ | ██ | ████ ██████ ██████████ ██████ ██████ |
██████████ ███ ██ ███ | █████ | ██ | ████ ██████ ██████████ ██████ ██████ |
████████████ ███ ██ ██ | █████ | ████ ██████ ██████████ ██████ █████ | ████ ██████ ██████████ ██████ █████ |
███████████ ███ ██ ███ | █████ | ████ ██████ ██████████ ██████ █████ | ██ |
███████████ ███ ██ ███ | █████ | ████ ██████ ██████████ ██████ █████ | ██ |
███ █ ██████ ████ █████████ ██ █ ███████ █████████ ███ █ ████████ █████████ ██ █ █████ ███████ ███ █ ███████ ████████ ████ ██ █ ███ ██████████ ██ █ ████ ██████ ██ █ ████ █ ██████ ███ █ ████ ███ ████████ ██ █ ██████ ███████ ███████ ██████ ███████████ ████ █████ ████ ███ ████████ ████████ ██ █████████ ███ ███████████ ████ ██████ ██████ █████████████ ███████████ ███████ ██████ █████████ ████ ██ ███ ███████ ███████████████ ███████ ██ █ ████████ ████ ██ ███ ██ ████████ ██ ███ ██ ███ ██████████ ██████████████████ ███████ ██ █ ███ ██ ███████ ████ ████████ ██ ███ ██ ████ █ ██████████████ ███████ ████████ ████████ ███ ████████████████ ████ ████████ ██ ████ ███████ █████ ██████████ ███ █████████ ███ ███ ███████ ██ ███ ██ █████ ████ ██████ █████████████ ███████ █████████ ███████████ ██ █████ ████████ ██████████ ███ ███ █████ ██████████ ███ ███ ██ ███ ██████ █████████████ ███████ █████ ██████████ ███ ████ ███ ████████ ████████ ██████████ █████ ████ ███████ █████████ █████ ██████████ ███ ████ ████ ██ ███ █████████ █████████ ███████████ ███ ███ ███████ ██████████ ████ ███████ ████████ ███████████████████ ████████████ ███ ███ ████ █████ ██ ████████████ ████████ ██ ███ ████████████ ███ ███ ████████████ ███ ███ ███ ████████ ███ ████████ █████████ ███ ██████ ████ ████████ ██ ████ ███████ █████ ████ █████████ ██ ██ ██ ██████ ██████ ██████████ ██ ████ ███████ █████ ██████████ ███ ████ ████ ████████ ██ ███████ ██ ███ ███████ ███ ███ ████ ██████████ ██ ███ ██ █████ ████████ ████ ███ ██ ███ ██ █████ ██████ ███████ ███ ███████ ███████████ ███ ██████ █████████ ███ ███ ███████████ ███████ ████████ ███ ████ █████ ████ ████████ ███ ████ ██████ ██ ████ ██ █████████ ███████ ██ ██████ █████████ ████ █████████ ███ ██ ██ ██ ███████████ ████████ ███████ ███ ███ ██ ██ ████████ ███ ███ ███████ ███ ██████ ██ ████████████ ██ ████████ ███ ████ █████████ ██ ███ ██ ██ █████████ ████ ███ █████████ ██ ██ ██ ██████ ███ ██████████ ███████ ████████ ██ ███ ██ ███ ██ ██████ ████████ ███ ████ ███ ████ ████ ██████ ███ ██████ ████████ █████████ ███ ██ ███ ███████████ ██████████
████████ ██ ██ ██ ██ | █████ | ███████ ██ ███████ | ██ ██ ██ ███████ |
|---|---|---|---|
████ ██████████ ████ ████ | |||
███████ | █████ | █████ ███████ ████████████ ███████ █████ | █████ ███████ ████████████ ███████ █████ |
██████████████████ | █████ | █████ ███████ ███████████ ███████ █████ | █████ ███████ ███████████ ███████ █████ |
████████ ██ ██ ██ | █████ | █████ ███████ ███████████ ███████ █████ | ██ |
████████ ███ ██ ██ | █████ | ████ ███████ ██████████ ███████ █████ | ██ |
████████████ ███ ██ ██ | █████ | ████ ███████ ██████████ ███████ █████ | ██ |
██████████ ███ ██ ███ | █████ | █████ ███████ ███████████ ███████ █████ | ██ |
████████████ ███ ██ ██ | █████ | ████ ███████ ██████████ ███████ █████ | ████ ███████ ██████████ ███████ █████ |
███████████ ███ ██ ██ | █████ | █████ ███████ ███████████ ███████ █████ | ██ |
██████ ███ ██ ███ | █████ | █████ ███████ ███████████ ███████ █████ | ██ |
Harms
███████████████████████████
█████████ ██ ██ ██ ██ | █████ | ██ ████ ████ |
|---|---|---|
███████ | █████ | ████ █████ ██████ █████ █████ |
██████████████████ | █████ | ████ █████ ██████ █████ █████ |
████████ ██ ██ ██ | █████ | ████ █████ ██████ █████ █████ |
████████ ███ ██ ██ | █████ | ████ █████ ██████ █████ █████ |
████████████ ███ ██ ██ | █████ | ████ █████ ██████ █████ █████ |
████████████ ███ ██ ███ | █████ | ████ █████ ██████ █████ █████ |
████████████ ███ ██ ██ | █████ | ████ █████ ██████ █████ █████ |
███████████ ███ ██ ███ | █████ | ████ █████ ██████ █████ █████ |
███████████ ███ ██ ███ | █████ | ████ █████ ██████ █████ █████ |
████████ ███ ██████
█████████ ██ ██ ██ ██ | █████ | ██ ████ ████ |
|---|---|---|
███████ | █████ | ████ █████ ██████ █████ █████ |
██████████████████ | █████ | ████ █████ ██████ █████ █████ |
████████ ██ ██ ██ | █████ | ████ █████ ██████ █████ █████ |
████████ ███ ██ ██ | █████ | ████ █████ ██████ █████ █████ |
████████████ ███ ██ ██ | █████ | ████ █████ ██████ █████ █████ |
████████████ ███ ██ ███ | █████ | ████ █████ ██████ █████ █████ |
████████████ ███ ██ ██ | █████ | ████ █████ ██████ █████ █████ |
███████████ ███ ██ ███ | █████ | ████ █████ ██████ █████ █████ |
███████████ ███ ██ ███ | █████ | ████ █████ ██████ █████ █████ |
███ █ ██████ ████ █████████ ██ █ ███████ █████████ ███ █ ████████ █████████ ██ █ █████ ███████ ██ █ ██████ ██████ ███ █ ███████ ████████ ████ ██ █ ████ ███████████ ██ █ ███ ██████████ ██ █ ████ ██████ ██ █ ████ █ ██████ ███ █ ████ ███ ████████ ██ █ ██████ █████████████ ██████ █████████ ████ ██████████ ████ ███ ████████ ████████ ██ █████████ ███ ███████████ ████ ██████ ██████ █████████████ ███████████ ███████ ██████ █████████ ████ ██ ███ ███████ ████ ████████████ ███████ ██ █ ████████ ████ ██ ███ ██ ████████ ██ ███ ██ ███ ██████████ ██████ ██ ████████████ ███████ ██ █ ███ ██ ███████ ████ ████████ ██ ███ ██ ████ █ ██████████████ ███████ ████████ ████████ ███ ██████
Critical Appraisal of the ITC
The submitted systematic review and NMA were conducted to assess the effects and harms of atogepant 60 mg every day against relevant comparators. These comparators were identified through analysis of the drugs licensed and approved in Canada.
Based on the methods detailed in the technical report, the authors performed an updated search for the ITC (up to September 2022) to identify comparative studies, unrestricted by publication date other than for grey literature, in which conference proceedings were searched for the past 2 years from the search dates to identify abstracts of interest (the search strategy, however, is not depicted in the technical report). No a priori protocol was reported or published.
Overall, the researchers did an appropriate identification and inclusion of the relevant trials for the specific population and comparators for the submission. However, there are no specific details of how the screening was performed; therefore, the risk of bias and error in the process is unknown.
Although each study design is well described, there is no detail as to how the data extraction (i.e., by a single or multiple assessors) and assessment of the risk of bias for each of the included studies were conducted or reported. Therefore, it is unclear whether risk of bias and error would have been introduced via the data extraction methods, and the impact of the risk of bias of the included studies on the results cannot be ascertained.
Several head-to-head trials were excluded due to the strict inclusion criteria. ██ █████████ █ ██ ██ ████████ ██████ ████ ████████ ███ ███ ██████ █████████ ███████████ ██ ███ ██ ██ ████████. ██ █████ █████ ██ ██ █████████ █████████ ███ ████ ███ ██ ███████ ███████████ ██ ███ █████████. However, authors state the reasons for the exclusions. Sensitivity analysis (█████ █████████ █████ ███████████) indicate that this exclusion was unlikely to pose important bias in the final estimates. Furthermore, it’s unlikely that the 4 excluded studies would have provided further meaningful evidence for the 2+TF population.
The networks were adequately constructed with a suitable assessment of model fit, consistency, convergence, and heterogeneity evaluation, establishing the comparability of the populations included in each network for each outcome, which holds the transitivity assumption such as populations’ age, type of migraine, duration. Furthermore, the duration of follow-up was overall similar at 12 weeks and up to 24 weeks in 2 studies. ██ ████████ ████████ █████ ████ ███ █████████ ███████ ████████ ███ ████████.
The networks were sparse with closed loops only formed by single trials, which precluded assessments of consistency. There was no formal assessment of the risk of publication bias.
██████ █████████ ██ ████ ████ ██ ████████ ███ ███████ █████████ ███████ █████████ ████████████ ███ ██████████ ███ ████ ███ ███ ██████ ███████ ███████ █████ ███ ███████ █ ████ █████████ ██████████ █████ ███ ████████████ ████████ ███ ███ ███████████ ████ ███ ██ ██████ ███ ███ ████ █████ ██ ███ ███████ ████ ██ █████████ ██ ████ ████████ ████████████
Overall, the populations included in the individual studies of the network are generalizable to the Canadian population and no concerns on the applicability of the results were detected. ███ ███ ███ ███ ███████ ███████ ████████ ████████ ██ ████████ ██████ ██████ ██████ ████ █████ █████ Also, of relevance to this submission, there was a short length of follow-up if other long-term assessments are required such as rare AEs, and efficacy beyond 24 weeks. ███ ████ ██ ██████████ ██ ███████████ ███ ██████████ █████████ ██ ████ ███ ███ ████████ █████████ ███ ███ ██ ██ ███████████
Studies Addressing Gaps in the Systematic Review Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
No studies addressing gaps were submitted by the sponsor.
Discussion
Summary of Available Evidence
The body of evidence informing this submission consists of 1 RCT (the PROGRESS study) assessing atogepant as treatment of patients with chronic migraine. Within this RCT, there was a subgroup of patients (N = ███ patients) who had experienced an inadequate response, intolerance, or contraindication to at least 2 oral prophylactic migraine medications. The PROGRESS study assessed efficacy outcomes (MMDs, MHDs, and monthly acute medication use), function or disability outcomes (the performance of daily activities, missed school days or workdays, and the impact of headaches in daily function), HRQoL, health resource use (workdays missed), and harms.
A supplemental body of evidence was submitted in the form of a single-arm, long-term, open-label extension study (Study 312, N = 325, mITT = 284, in a 156-week open-label treatment period) to describe the long-term effects, safety, and tolerability of atogepant in the overall population. This long-term extension study did not provide information on the 2 or more TFs population for which the sponsor is requesting reimbursement. The sponsor also submitted an NMA of studies that included patients with 2 or more TFs as ITCs of atogepant 60 mg every day versus relevant comparators in Canada in that population (i.e., galcanezumab, fremanezumab, erenumab, onabotulinumtoxin A, or eptinezumab).
Interpretation of Results
Efficacy
Patients with chronic migraine, clinician and patient groups, and drug programs concurred that the reduction in MMDs and MHDs are outcomes of importance for treatment decisions, as well as HRQoL, function (or disability), and harms. The clinical experts agreed with these considerations and deemed these end points to be key factors for their decisions in clinical practice.
The change from baseline in MMDs was the primary outcome in the PROGRESS trial. In the study (N = ███ patients from the 2+ TFs population), patients taking placebo had an average reduction from baseline of ████ migraine days at 12 weeks. The reduction was greater in those taking atogepant █████ days from baseline). The difference between groups was of ███ fewer migraine days with the intervention; the 95% CI suggests that the data are compatible with a reduction of ███ fewer days up to ███ fewer days. The sponsor suggested that 1 day less would be a meaningful difference for stakeholders; based on a suggestion from the clinical expert, it was agreed that some patients might find a half-day (0.5 day less) reduction to be meaningful. In other words, this reduction would be the minimal effect that they would consider meaningful. The lower bound of the CI (███ ████) implies that the values exclude this threshold of minimal importance. Similarly, when evaluating the proportion of patients reaching a 50% or greater reduction of MMDs from baseline, an improvement favouring atogepant 60 mg every day was observed. For instance, in the placebo arm, █████ of patients reached the 50% or greater reduction threshold while in the atogepant group █████ of the patients reached this threshold (████████ █████ █████ ██████ Expressed as absolute effects, this means that approximately ███ more patients per 1,000 patients treated with atogepant 60 mg every day reached this threshold when compared to placebo, but due to chance (the 95% CI), this number can go from ██ more per 1,000 patients (likely of clinical importance and beyond a trivial effect) to ███ more per 1,000 patients.
The change from baseline in headache days (MHDs) had similar results, with a mean difference between groups of ████ fewer headache days with the use of atogepant when compared to placebo; the 95% CI suggests that the data are compatible with differences of ███ fewer days up to ███ fewer days. The clinical expert and other stakeholders considered that a half-day (0.5 day) reduction would be the minimal effect that they would consider meaningful.
The PROGRESS study also showed changes of likely improvement with atogepant in the outcomes of function or disability, as shown by the change from baseline in the mean monthly performance of daily activities score of the AIM-D (4.5 points lower with atogepant [95% CI, 7.17 points lower to 1.13 points lower]), the MIDAS total score (████ ████ █████ █████ █████ ██ ███ █████), and the HIT-6 scale (4.43 points lower with atogepant [95% CI, 6.58 lower to 2.27 lower]). These effects measured the improvements in patients’ daily function (AIM-D), headache-related disability as missed or reduced productivity at work or school (MIDAS), and the impact of headaches on daily functions (HIT-6). The effects measured with MIDAS and HIT-6 scores reached a meaningful difference between the atogepant and placebo groups (with a within-patient difference of 4.5 points for MIDAS and a between-group difference of 2.3 points for HIT-6); all these outcomes were deemed of moderate certainty due to imprecision.
HRQoL (as work-related and daily social activities) was evaluated in 180 patients, showing that atogepant provides improvements in the mean monthly MSQ, Version 2.1 scale (role function-restrictive domain), with the score being 12.16 points higher when compared to placebo (with a 95% CI going from 6.22 points higher to 18.9 points higher). This effect was considered likely clinically meaningful when assessing the within-patient MID of 10.9 points. The evidence about work time missed in the PROGRESS study (per WPAI: Migraine) was very uncertain.
Overall, the evidence from the study for these outcomes had uncertainty due to the sample size of the 2 or more TFs population being about 40% of the mITT population. Even though the effect sizes for the 2 or more TFs subgroup were consistent across all key clinical end points (change from baseline in MMDs, MHDs, and monthly acute medication use days, and a reduction of 50% or more in the 3-month average of MMDs) compared to the mITT population.
Supplementary evidence from a single-arm, long-term, open-label extension study (Study 312, with 325 patients) with a follow-up of 52 weeks showed that the effects of atogepant on MMDs, MHDs, the performance of daily activities, and HRQoL continued through the observation period, suggesting that the effects of atogepant can continue over longer periods of time. However, these results were presented for the overall population, and no subgroup analyses were presented for the 2 or more TFs population of interest. Due to the lack of a comparison arm at these time points, in addition to the open-label nature and important losses to follow-up, the counterfactual assessment (i.e., what would happen if the other intervention or comparison is used) is unclear.
To evaluate the effects of atogepant 60 mg every day in the same population of interest (2+ TFs) when compared to other interventions approved in Canada for chronic migraine, a systematic review and NMA showed that atogepant is superior to placebo (in agreement with the results of the PROGRESS study reported here) in the outcomes of MMDs, MHDs, and acute medication use, but not superior to any of the other treatments evaluated (galcanezumab, fremanezumab, erenumab, onabotulinumtoxin A, or eptinezumab). The effect estimates had imprecision (wide CrIs) that conveyed uncertainty about which treatment might be favoured.
Harms
Atogepant was generally well tolerated, with some of the AEs being of higher frequency in the atogepant 60 mg every day arm than in the placebo arm. When assessing the 2 or more TFs safety population ██████ ███ ██ ██ █████████ ███ ███████ ████ ██████████████ the number of AEs were similar overall (█████ ███ ███████ Only ████████████ was deemed numerically increased in the atogepant arm ███████ when compared to placebo ███████.
SAEs were reported in ██ patient in the atogepant group and ████ in the placebo group. Similarly, withdrawals due to AEs were reported in ██ patients in each group.
No difference in other effects of special interest were detected (elevated liver enzymes or suicidal ideation) and no deaths were reported in any group. The follow-up time of 12 weeks might not be sufficient to detect rare or long-term effects of atogepant.
The data on harms could be confirmed when observing the results of the open-label extension study (████████████ █████ █████ ███████ ██ ███ ██ ████████); however, no comparative evidence was available for later time points.
Within the evidence from the NMA, for the overall chronic migraine population, atogepant 60 mg every day showed an increased hazard of AEs compared to placebo and eptinezumab 100 mg. For the rest of comparisons, the hazard ratios were accompanied by wide CrIs that carried uncertainty due to imprecision in the hazard rates between atogepant and all relevant comparators.
Conclusion
The body of evidence assessing the effects of atogepant 60 mg every day in patients with chronic migraine and at least 2 prior preventive TFs consisted of 1 pivotal RCT comparing atogepant 60 mg taken every day to placebo, a single-arm, open-label extension study ████████ ███████████ ██ ███ ████████ ██ ████ ██████████ and 1 ITC that compared atogepant 60 mg taken every day to relevant treatments for chronic migraine in Canada. The body of evidence informed on clinical efficacy end points (MMDs, MHDs, acute medication use), function and disability outcomes, HRQoL, resource use, and harms — all considered important outcomes for decision-making by clinical experts, patient groups, and stakeholders.
The available evidence shows that the use of atogepant, when compared to placebo, likely results in a clinically important reduction from baseline in mean MMDs and MHDs, and that a greater proportion of patients using atogepant 60 mg every day attain reductions of 50% or more in MMDs. Atogepant 60 mg every day likely decreases the effect chronic migraines have on daily activities, and missed workdays or school days, and the impact headaches have on patients in their ability to function at school, home, or in social situations. Some uncertainty remains regarding the effects of atogepant on long-term outcomes due to a relatively low sample size of patients with 2 or more TFs.
When assessing atogepant 60 mg taken every day against relevant comparators in Canada, 1 included NMA showed that there is still high uncertainty when compared to other interventions used to treat chronic migraine in Canada (galcanezumab, fremanezumab, erenumab, onabotulinumtoxin A, or eptinezumab) due to highly imprecise estimates (wide CrIs) that limit the ability to draw conclusions.
The assessed body of evidence, including that from an open-label extension study, suggests that atogepant is generally well tolerated and likely results in little to no increase in the proportion of patients with AEs, SAEs, and discontinuations due to AEs when compared to placebo or the relevant comparators in the NMA.
Overall, the use of atogepant 60 mg every day in patients with chronic migraine and 2 or more TFs provides clinical benefits in reducing migraine symptoms, and improving function and HRQoL, with an adequate safety profile when compared to placebo. However, the evidence from the NMA was inadequate to inform any conclusive decision about the comparative effectiveness of atogepant 60 mg every day versus the other currently funded treatment options.
References
1.International Headache Society. The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211.
2.Buse DC, Loder EW, Gorman JA, et al. Sex differences in the prevalence, symptoms, and associated features of migraine, probable migraine and other severe headache: Results of the American Migraine prevalence and prevention (AMPP) study. Headache. 2013;53(8):1278-1299. PubMed
3.Silberstein SD. Migraine symptoms: results of a survey of self-reported migraineurs. Headache. 1995;35(7):387-396. PubMed
4.Health Union, LLC. Migraine in America 2012. Migraine is Not “Just a Headache” [sponsor-supplied reference]. 2012: https://migraine.com/mia2012/. Accessed 2021 Jan 18.
5.Goadsby PJ, Evers S. International Classification of Headache Disorders - ICHD-4 alpha. Cephalalgia. 2020;40(9):887-888. PubMed
6.American Headache Society. The American Headache Society position statement on integrating new migraine treatments into clinical practice. Headache. 2019;59(1):1-18. PubMed
7.Lipton RB, Fanning KM, Serrano D, Reed ML, Cady R, Buse DC. Ineffective acute treatment of episodic migraine is associated with new-onset chronic migraine. Neurology. 2015;84(7):688-695. PubMed
8.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
9.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
10.Kelman L. The postdrome of the acute migraine attack. Cephalalgia. 2006;26(2):214-220. PubMed
11.Ng-Mak DS, Fitzgerald KA, Norquist JM, et al. Key concepts of migraine postdrome: a qualitative study to develop a post-migraine questionnaire. Headache. 2011;51(1):105-117. PubMed
12.Migraine Buddy. The stages of a migraine - migraine attack. 2018; https://migrainebuddy.com/the-stages-of-a-migraine-migraine-attack/. Accessed 2021 Apr 26.
13.Dodick DW. A Phase-by-Phase Review of Migraine Pathophysiology. Headache. 2018;58 Suppl 1(S1):4-16.
14.Chawla J. Migraine headache [sponsor-supplied reference]. Medscape. 2019. https://emedicine.medscape.com/article/1142556-overview. Accessed Jul 23.
15.Lipton RB, Silberstein SD. Episodic and chronic migraine headache: breaking down barriers to optimal treatment and prevention. Headache. 2015;55 Suppl 2:103-122; quiz 123-106. PubMed
16.Agostoni EC, Barbanti P, Calabresi P, et al. Current and emerging evidence-based treatment options in chronic migraine: a narrative review. J Headache Pain. 2019;20(1):92. PubMed
17.Bigal ME, Lipton RB. Concepts and mechanisms of migraine chronification. Headache. 2008;48(1):7-15. PubMed
18.Serrano D, Lipton RB, Scher AI, et al. Fluctuations in episodic and chronic migraine status over the course of 1 year: implications for diagnosis, treatment and clinical trial design. J Headache Pain. 2017;18(1):101. PubMed
19.Bigal ME, Serrano D, Buse D, Scher A, Stewart WF, Lipton RB. Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache. 2008;48(8):1157-1168. PubMed
20.Bigal ME, Lipton RB. Modifiable risk factors for migraine progression. Headache. 2006;46(9):1334-1343. PubMed
21.Katsarava Z, Buse DC, Manack AN, Lipton RB. Defining the differences between episodic migraine and chronic migraine. Curr Pain Headache Rep. 2012;16(1):86-92. PubMed
22.Blumenfeld AM, Bloudek LM, Becker WJ, et al. Patterns of use and reasons for discontinuation of prophylactic medications for episodic migraine and chronic migraine: results from the second international burden of migraine study (IBMS-II). Headache. 2013;53(4):644-655. PubMed
23.Torres-Ferrus M, Ursitti F, Alpuente A, et al. From transformation to chronification of migraine: pathophysiological and clinical aspects. J Headache Pain. 2020;21(1):42. PubMed
24.Ramage-Morin PL, Gilmour H. Prevalence of migraine in the Canadian household population. Health Rep. 2014;25(6):10-16. PubMed
25.G. B. D. Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):954-976. PubMed
26.G. B. D. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211-1259. PubMed
27.Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163-2196. PubMed
28.Adams AM, Serrano D, Buse DC, et al. The impact of chronic migraine: The Chronic Migraine Epidemiology and Outcomes (CaMEO) Study methods and baseline results. Cephalalgia. 2015;35(7):563-578. PubMed
29.Buse D, Manack A, Serrano D, et al. Headache impact of chronic and episodic migraine: results from the American Migraine Prevalence and Prevention study. Headache. 2012;52(1):3-17. PubMed
30.Doane MJ, Gupta S, Fang J, Laflamme AK, Vo P. The humanistic and economic burden of migraine in Europe: A cross-sectional survey in five countries. Neurol Ther. 2020;9(2):535-549. PubMed
31.Monteith TS. Chronic Migraine: Epidemiology, Mechanisms, and Treatment. In: Green MW, Cowan R, Freitag FG, eds. Chronic Headache: A Comprehensive Guide to Evaluation and Management. Cham (CH): Springer International Publishing; 2019:37-62.
32.Weatherall MW. The diagnosis and treatment of chronic migraine. Ther Adv Chronic Dis. 2015;6(3):115-123. PubMed
33.Silberstein SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2000;55(6):754-762. PubMed
34.Antonaci F, Ghiotto N, Wu S, Pucci E, Costa A. Recent advances in migraine therapy. Springerplus. 2016;5:637. PubMed
35.Manzoni GC, Camarda C, Torelli P. Chronification of migraine: what clinical strategies to combat it? Neurol Sci. 2013;34 Suppl 1:S57-60. PubMed
36.May A, Schulte LH. Chronic migraine: risk factors, mechanisms and treatment. Nat Rev Neurol. 2016;12(8):455-464. PubMed
37.Sacco S, Bendtsen L, Ashina M, et al. European headache federation guideline on the use of monoclonal antibodies acting on the calcitonin gene related peptide or its receptor for migraine prevention. J Headache Pain. 2019;20(1):6. PubMed
38.Diener HC, Forderreuther S, Gaul C, et al. Prevention of migraine with monoclonal antibodies against CGRP or the CGRP receptor: Addition to the S1 guideline: Therapy of migraine attacks and prevention of migraine. Recommendations of the Germany Society of Neurology and the German Migraine and Headache Society. Neurol Res Pract. 2020;2:11. PubMed
39.National Institute for Health and Care Excellence (NICE). Management of migraine (with or without aura) [sponsor-supplied reference]. 2020; https://pathways.nice.org.uk/pathways/headaches/management-of-migraine-with-or-without-aura.
40.Goadsby PJ, Dodick DW, Ailani J, et al. Safety, tolerability, and efficacy of orally administered atogepant for the prevention of episodic migraine in adults: a double-blind, randomised phase 2b/3 trial. Lancet Neurol. 2020;19(9):727-737. PubMed
41.Edvinsson L, Haanes KA, Warfvinge K, Krause DN. CGRP as the target of new migraine therapies - successful translation from bench to clinic. Nat Rev Neurol. 2018;14(6):338-350. PubMed
42.Goadsby PJ, Reuter U, Hallstrom Y, et al. A Controlled Trial of Erenumab for Episodic Migraine. N Engl J Med. 2017;377(22):2123-2132. PubMed
43.Stauffer VL, Dodick DW, Zhang Q, Carter JN, Ailani J, Conley RR. Evaluation of galcanezumab for the prevention of episodic migraine: The EVOLVE-1 randomized clinical trial. JAMA Neurol. 2018;75(9):1080-1088. PubMed
44.Ferrari MD, Diener HC, Ning X, et al. Fremanezumab versus placebo for migraine prevention in patients with documented failure to up to four migraine preventive medication classes (FOCUS): a randomised, double-blind, placebo-controlled, phase 3b trial. Lancet. 2019;394(10203):1030-1040. PubMed
45.Atogepant DRAFT PI [sponsor-supplied reference]. 2020.
46.QULIPTA (atogepant tablets): 10 mg, 30 mg and 60 mg, oral [product monograph; sponsor-supplied reference]. Saint-Laurent (QC): AbbVie Corporation; 2022.
47.Amitriptyline Hydrochloride: 10 mg, 25 mg, 50 mg, 75 mg, oral tablets [product monograph]. Varennes (QC): Strides Pharma Canada Inc.; 2023 Apr 12: https://pdf.hres.ca/dpd_pm/00070370.PDF. Accessed 2024 Aug 9.
48.VYEPTI® (eptinezumab): 100 mg/mL, solution for intravenous infusion [product monograph; sponsor-supplied reference]. Saint-Laurent (QC): Lundbeck Canada, Inc; 2021 Jul 27.
49.AIMOVIG® (erenumab injection): 70 mg/mL and 140 mg/mL, subcutaneous [product monograph; sponsor-supplied reference]. Dorval (QC): Novartis Pharmaceuticals Canada, Inc; 2021 Mar 23.
50.AJOVY® (fremenezumab): 150 mg/mL, solution for subcutaneous injection [product monograph; sponsor-supplied reference]. Toronto (ON): Teva Canada, Limited; 2021 Aug 11.
51.EMGALITY® (galcanezumab injection): 100 mg/mL and 120 mg/mL solution for subcutaneous injection [product monograph; sponsor-supplied reference]. Toronto (ON): Eli Lilly Canada, Inc; 2020 Sept 17.
52.Botox (onabotulinumtoxinA): Intramuscular Injection, 50, 100 and 200 Allergan units per vial [product monograph; sponsor-supplied reference]. Saint-Laurent (QC): AbbVie Corporation; 2022 Nov 04.
53.ACH-Topiramate: tablets 25 mg, 100 mg, and 200 mg, oral [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2024 Mar 11: https://pdf.hres.ca/dpd_pm/00074880.PDF. Accessed 2024 Aug 9.
54.Teva-Propranolol (propranolol hydrochloride): 10, 20, 40 and 80 mg tablets [product monograph]. Toronto (ON): Teva Canada Limited; 2011 Sep 19: https://pdf.hres.ca/dpd_pm/00014382.PDF. Accessed 2024 Aug 9.
55.Clinical Study Report: 3101-303-002. A phase 3, multicenter, randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy, safety, and tolerability of atogepant for the prevention of chronic migraine (PROGRESS CSR) [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Qulipta (atogepant), tablets, 10 mg, 30 mg, and 60 mg, oral. Chicago (IL): AbbVie Inc.; 2022 Apr 21.
56.Statistical Analysis Plan – Amendment 1. A phase 3, multicenter, randomized, double-blind, placebo controlled, parallel-group study to evaluate the efficacy, safety, and tolerability of atogepant for the prevention of chronic migraine (PROGRESS SAP) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Qulipta (atogepant), tablets, 10 mg, 30 mg, and 60 mg, oral. Dublin (IE): Allergan plc; 2019 Apr 10.
57.Dodick DW, Turkel CC, DeGryse RE, et al. Assessing clinically meaningful treatment effects in controlled trials: chronic migraine as an example. J Pain. 2015;16(2):164-175. PubMed
58.U.S. Food and Drug Administration. GUIDANCE DOCUMENT: Patient Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. Guidance for Industry [sponsor-supplied reference]. 2019 Oct 17.
59.U.S. Food and Drug Administration. Guidance for Industry Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims [sponsor-supplied reference]. 2009 Dec.
60.Lipton RB, Gandhi P, Stokes J, et al. Development and validation of a novel patient-reported outcome measure in people with episodic migraine and chronic migraine: The Activity Impairment in Migraine Diary. Headache. 2022;62(1):89-105. PubMed
61.Stewart WF, Lipton RB, Dowson AJ, Sawyer J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology. 2001;56(6 Suppl 1):S20-28. PubMed
62.Stewart WF, Lipton RB, Kolodner K, Liberman J, Sawyer J. Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia. 1999;19(2):107-114; discussion 174. PubMed
63.Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain. 2000;88(1):41-52. PubMed
64.Houts CR, McGinley JS, Wirth RJ, Cady R, Lipton RB. Reliability and validity of the 6-item Headache Impact Test in chronic migraine from the PROMISE-2 study. Qual Life Res. 2021;30(3):931-943. PubMed
65.Rendas-Baum R, Bloudek LM, Maglinte GA, Varon SF. The psychometric properties of the Migraine-Specific Quality of Life Questionnaire version 2.1 (MSQ) in chronic migraine patients. Qual Life Res. 2013;22(5):1123-1133. PubMed
66.Yang M, Rendas-Baum R, Varon SF, Kosinski M. Validation of the Headache Impact Test (HIT-6) across episodic and chronic migraine. Cephalalgia. 2011;31(3):357-367. PubMed
67.Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59(4):374-380. PubMed
68.Houts CR, Wirth RJ, McGinley JS, Cady R, Lipton RB. Determining Thresholds for Meaningful Change for the Headache Impact Test (HIT-6) Total and Item-Specific Scores in Chronic Migraine. Headache. 2020;60(9):2003-2013. PubMed
69.Haywood KL, Mars TS, Potter R, Patel S, Matharu M, Underwood M. Assessing the impact of headaches and the outcomes of treatment: A systematic review of patient-reported outcome measures (PROMs). Cephalalgia. 2018;38(7):1374-1386. PubMed
70.Bagley CL, Rendas-Baum R, Maglinte GA, et al. Validating Migraine-Specific Quality of Life Questionnaire v2.1 in episodic and chronic migraine. Headache. 2012;52(3):409-421. PubMed
71.Dodick DW, Silberstein S, Saper J, et al. The impact of topiramate on health-related quality of life indicators in chronic migraine. Headache. 2007;47(10):1398-1408. PubMed
72.Ford JH, Ye W, Ayer DW, et al. Validation and meaningful within-patient change in work productivity and activity impairment questionnaire (WPAI) for episodic or chronic migraine. J Patient Rep Outcomes. 2023;7(1):34. PubMed
73.Stewart WF, Lipton RB, Kolodner K. Migraine disability assessment (MIDAS) score: relation to headache frequency, pain intensity, and headache symptoms. Headache. 2003;43(3):258-265. PubMed
74.Martin BC, Pathak DS, Sharfman MI, et al. Validity and reliability of the migraine-specific quality of life questionnaire (MSQ Version 2.1). Headache. 2000;40(3):204-215. PubMed
75.Aurora SK, Dodick DW, Turkel CC, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia. 2010;30(7):793-803. PubMed
76.Diener HC, Dodick DW, Aurora SK, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia. 2010;30(7):804-814. PubMed
77.Bigal ME, Dodick DW, Rapoport AM, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of high-frequency episodic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2b study. Lancet Neurol. 2015;14(11):1081-1090. PubMed
78.Market Access Analysis Plan (MAAP) Output Tables [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Qulipta (atogepant), tablets, 10 mg, 30 mg, and 60 mg, oral. Pointe-Claire (QC): Abbvie Corporation; 2022 Apr 19.
79.Topline Results (Interim Analysis) of Study 3101-312-002: A Phase 3, Multicenter, Open-label 156-week Extension Study To Evaluate The Long-term Safety And Tolerability Of Oral Atogepant For The Prevention Of Migraine In Participants With Chronic Or Episodic Migraine [sponsor-supplied reference]. 2023 Nov 13.
80.Statistical Analysis Report for Network Meta-Analyses for Atogepant in Chronic Migraine V1.4 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Qulipta (atogepant), tablets, 10 mg, 30 mg, and 60 mg, oral. Pointe-Claire (QC): Abbvie Corporation; 2023 Apr 26.
81.Sakai F, Suzuki N, Kim BK, et al. Efficacy and safety of fremanezumab for chronic migraine prevention: Multicenter, randomized, double-blind, placebo-controlled, parallel-group trial in Japanese and Korean patients. Headache. 2021;61(7):1092-1101. PubMed
82.Takeshima T, Sakai F, Hirata K, et al. Erenumab treatment for migraine prevention in Japanese patients: Efficacy and safety results from a Phase 3, randomized, double-blind, placebo-controlled study. Headache. 2021;61(6):927-935. PubMed
83.Detke HC, Goadsby PJ, Wang S, Friedman DI, Selzler KJ, Aurora SK. Galcanezumab in chronic migraine: The randomized, double-blind, placebo-controlled REGAIN study. Neurology. 2018;91(24):e2211-e2221. PubMed
84.Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the Preventive Treatment of Chronic Migraine. N Engl J Med. 2017;377(22):2113-2122. PubMed
85.Tepper S, Ashina M, Reuter U, et al. Safety and efficacy of erenumab for preventive treatment of chronic migraine: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. 2017;16(6):425-434. PubMed
86.Mulleners WM, Kim BK, Lainez MJA, et al. Safety and efficacy of galcanezumab in patients for whom previous migraine preventive medication from two to four categories had failed (CONQUER): a multicentre, randomised, double-blind, placebo-controlled, phase 3b trial. Lancet Neurol. 2020;19(10):814-825. PubMed
87.Dodick DW, Lipton RB, Silberstein S, et al. Eptinezumab for prevention of chronic migraine: A randomized phase 2b clinical trial. Cephalalgia. 2019;39(9):1075-1085. PubMed
88.Lipton RB, Goadsby PJ, Smith J, et al. Efficacy and safety of eptinezumab in patients with chronic migraine: PROMISE-2. Neurology. 2020;94(13):e1365-e1377. PubMed
Appendix 1: Additional Outcome Data
Please note this appendix has not been copy-edited.
Table 52: Change From Baseline in Mean Monthly Physical Impairment Domain Score of AIM-D Across the 12-Week Treatment Period in the 2 or More TFs Population
Variable | Atogepant 60 mg q.d. (N = 101) | Placebo (N = 91) |
|---|---|---|
Baseline | ||
n | ██ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median (minimum to maximum) | █████ ███ ███ | █████ ███ ███ |
Postbaseline (month 1 to month 3) | ||
n | ██ | ██ |
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | █████ ███ ███ | ████ ███ ███ |
CFB | ||
n | ██ | ██ |
Mean (SD) | ██████ ███████ | █████ ███████ |
Median (minimum to maximum) | ██████ █████ ███ | █████ █████ ███ |
MMRMa | ||
LSM (SE of the least squares) | ██████ ██████ | █████ ██████ |
95% CI | ███████ █████ | ██████ █████ |
Atogepant vs. placebo | ||
LSMD (SE of the least squares) | █████ ██████ | Reference |
95% CI | ██████ █████ | Reference |
Nominal P value | ██████ | Reference |
AIM-D = Activity Impairment in Migraine-Diary; CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; SE = standard error; SEM = standard error of the mean; vs. = versus.
Note: Postbaseline (month 1 to month 3) is the average of the monthly physical impairment domain score of AIM-D across the 12-week treatment period.
aAn MMRM was used for CFB.
Source: Market Access Analysis Plan Raw Output Tables.78
Table 53: Change From Baseline in Mean Monthly Physical Impairment Domain Score of AIM-D Across the 12-Week Treatment Period in the Overall Population (mITT Population)
Variable | Atogepant 60 mg q.d. (N = 256) | Placebo (N = 246) |
|---|---|---|
Baseline | ||
n | 231 | 226 |
Mean (SD) | 27.11 (16.63) | 13.52 (0.90) |
Median (minimum to maximum) | 25.37 (0.0, 81.7) | 23.75 (0.0, 73.3) |
Postbaseline (month 1 to month 3) | ||
n | 231 | 226 |
Mean (SD) | 15.47 (14.91) | 17.19 (11.51) |
Median (minimum to maximum) | 10.74 (0.0, 80.0) | 15.16 (0.0, 62.7) |
CFB | ||
n | 231 | 226 |
Mean (SD) | –11.65 (12.17) | –8.05 (10.92) |
Median (minimum to maximum) | –10.42 (–59.8 to 29.2) | –6.33 (–48.4 to 23.9) |
MMRM* | ||
LSM (SE of the least squares) | –10.63 (0.67) | –7.92 (0.67) |
95% CI | –11.94 to –9.33 | –9.23 to –6.61 |
Atogepant vs. placebo | ||
LSMD (SE of the least squares) | –2.71 (0.89) | Reference |
95% CI | –4.47 to –0.96 | Reference |
Model P value | 0.0025 | Reference |
Adjusted P value | 0.0025a | Reference |
AIM-D = Activity Impairment in Migraine-Diary; CFB = change from baseline; CI = confidence interval; LSM = least squares mean; LSMD = least squares mean difference; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; q.d. = every day; SD = standard deviation; SE = standard error; SEM = standard error of the mean; vs. = versus.
Note: Postbaseline (month 1 to month 3) is the average monthly physical impairment domain score of AIM-D across the 12-week treatment period.
aThe P value was adjusted for multiple testing.
*An MMRM was used for CFB.
Source: PROGRESS Clinical Study Report (2022).55
Additional Efficacy End Points
Monthly Triptan Use Days, Mean Monthly Cumulative Headache Hours, Mean Monthly Moderate or Severe Headache Days, and Mean Monthly Severe Headache Days
███████ ██████████ ████ ████████ ██████ ██ ███████ ███████ ███ ████ ███ ████ ███████ ██████ ████████ ████ ██ ███ █████ █ █████ ██████ █ ██ ██ ████ ████████████ ███ █████████ ██ ██ ██ ████████ ████ ███████ ██ ███ ████ ███████████
Greater reductions from baseline (MMRM) in monthly triptan use days, mean monthly cumulative headache hours, mean monthly moderate or severe headache days, and mean monthly severe headache days in each of the 4-week intervals assessed (week 1 to week 4, week 5 to week 8, and week 9 to week 12) were demonstrated for atogepant 60 mg every day compared with placebo in the mITT population, except the reduction from baseline (MMRM) in monthly moderate or severe and severe headache days was comparable at week 9 to week 12 for atogepant 60 mg every day and placebo.
HIT-6 (Change From Baseline in Total Score and 5-Point Improvement From Baseline in Total Score at Week 4, Week 8, Week 12, and Week 16)
Change from baseline in HIT-6 total score at week 12 was considered an additional efficacy end point for all regions except Europe and Canada and was considered a secondary efficacy end point for Canada.
███████ ██████████ █████████████ ████ ████████ ██ █████ █████ █████ ██████ ██ █████ █ ███ █ ████ ████ █████████████ ██ ████████ ██ ████ ███ ███ █████████ ██ ██ ██ ████████ ████ ███████ ██ ████ ███ ████ ███ ███████ ███████████
Higher proportions of HIT-6 responders (defined as those patients who had at least a 5-point improvement [decrease] from baseline in the HIT-6 total score) at week 4, week 8, and week 12 were demonstrated in the atogepant 60 mg every day treatment group compared with the placebo treatment group in the 2 or more TFs and overall population.
Work Absenteeism, Work Presenteeism, Overall Work Productivity Loss, Impairment of Activity Outside of Work, Patient Global Impression–Severity of Illness; Score, Mean Monthly Activity Limitation, Total Score for Patient-Reported Outcomes Measurement Information System - Short Form Version 1.1 - Pain Interference 6a, and PHQ-9 Score
███████████ ███████ ██████████ █████████████ ████ ████████ ██████ ██ ████ ████████████ ████ █████████████ ███████ ████ ████████████ █████ ██████████ ██ ████████ ███████ ██ █████ ████ ██████ ████ ███████ ████████ ███████████ █████████ █████ ██████ ███ █████ █████ ████████ ████ ████████████ ██ █████ ██ ██ ███ ██ ██ ███ █████████ ██ ██ ██ █████████ █████ ████████ ████ ███ ███████ █████████ █████ ██ ███ ████ ███████████
PGI-C
█████ ████ ██████ ███████████ ██ ████████ ████████ ██ ███ ████ ██ █████ ███████ ██ █████ ████ ███████ ██ ████ ██ ██ ███ █████████ ██ ██ ██ █████████ █████ ████████ ████ ███ ███████ █████████ █████ ██ ███ ████ ███████████
Patient Satisfaction With Study Medication
██████ ██████████ ██ ████████ ████████ █████ ███████████ ███ ██████████ ██████████ ████ █████ ██████████ ███ ████████ ██████████ ██ █████ ██ ██ ███ ██ ██ ███ █████████ ██ ██ ██ █████████ █████ ████████ ████ ███ ███████ █████████ █████ ██ ███ ████ ██████████.
MSQ Version 2.1 (Role Function-Restrictive Domain Score at Week 4, Week 8, and Week 16; Role Function-Preventive and Emotional Function Domain Scores at Week 4, Week 8, Week 12, and Week 16)
Greater improvement from baseline (MMRM) in the MSQ Version 2.1 role function-restrictive domain score at week 4 and week 8 was demonstrated for atogepant 60 mg every day compared with placebo, indicating an improvement in patients' functioning with daily social and work-related activities, in both the 2 or more TFs and mITT population.
Greater improvement from baseline (MMRM) was also observed in the MSQ Version 2.1 role function-preventive and emotional function domain scores at week 4, week 8, and week 12 for atogepant 60 mg every day compared with placebo in both populations (2+ TFs and overall). This demonstrates an observed reduction on the impact of migraines on preventing daily activities and a reduction in the emotional burden associated with having migraine.
AIM-D (Change From Baseline in Mean Monthly Performance of Daily Activities and Physical Impairment Domain Scores Across Week 1 to Week 4, Week 5 to Week 8, and Week 9 to Week 12)
The end points of change from baseline in mean monthly performance of daily activities domain score of the AIM-D across the 12-week treatment period and change from baseline in mean monthly Physical Impairment domain score of AIM-D across the 12-week treatment period were considered secondary efficacy end points for all regions except Europe and Canada and additional efficacy end points for Canada.
Numerically greater reductions (improvement) from baseline (MMRM) in monthly performance of daily activities domain score and physical impairment domain score of AIM-D at week 1 to week 4, week 5 to week 8, and week 9 to week 12 were demonstrated for atogepant 60 mg every day compared with placebo.
Activity Level
Improvement from baseline (MMRM) in mean monthly activity level across the 12-week treatment period was comparable across treatments in the mITT population.
EQ-5D-5L
Greater improvements from baseline (MMRM) in EQ-5D-5L descriptive system index score and EQ visual analogue scale score at week 1 to week 2, and at specified windows around week 4, week 6, week 8, and week 12 were demonstrated for atogepant 60 mg every day compared with placebo in the mITT population.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CGRP
calcitonin gene–related peptide
CM
chronic migraine
MMD
monthly migraine day
NIHB
Non-Insured Health Benefits
NMA
network meta-analysis
ODB
Ontario Drug Benefit
pCPA
pan-Canadian Pharmaceutical Alliance
TF
treatment failure
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Atogepant (Qulipta), 60 mg oral tablets |
Indication | For the prevention of migraine in adults who have at least 4 migraine days per month |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | May 2, 2024 |
Reimbursement request | For the prevention of CM in adults with > 15 headache days per month (of which 8 days are considered to be migraine days) and who have previously experienced an inadequate response, are intolerant, or have a contraindication to at least 2 migraine preventive therapies |
Sponsor | AbbVie Corporation |
Submission history | Previously reviewed: Yes Indication: For the prevention of episodic migraine (< 15 migraine days per month) in adults Recommendation date: June 14, 2023 Recommendation: Reimburse with clinical criteria and/or conditions |
CM = chronic migraine; NOC = Notice of Compliance.
Table 2: Summary of Economic Information
Component | Description |
|---|---|
Type of economic evaluation | Cost-minimization analysis |
Target population | Adults with > 15 headache days per month (of which 8 days are considered to be migraine days) and who have previously experienced an inadequate response, are intolerant, or have a contraindication to at least 2 migraine preventive therapies |
Treatment | Atogepant 60 mga |
Dose regimen | 60 mg once daily |
Submitted price | Atogepant: $18.44 per 60 mg tablet |
Submitted treatment cost | $6,735 per patient per year |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Time horizon | 5 years |
Key data sources | NMA, with the effectiveness of atogepant informed by the pivotal PROGRESS trial |
Costs considered | Drug acquisition costs, drug administration costs, health care resource use costs |
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
CM = chronic migraine; CGRP = calcitonin gene–related peptide; NMA = network meta-analysis.
aAtogepant is additionally available as 10 mg and 30 mg oral tablets. These strengths were not submitted to CDA-AMC as part of the current review of atogepant for the prevention of CM.
Conclusions
Assuming similar clinical efficacy and safety for atogepant compared to fremanezumab, galcanezumab, and eptinezumab, the sponsor submitted a cost-minimization analysis comparing drug acquisition and monitoring costs for the reimbursement population (i.e., adults with more than 15 headache days per month and who had had 2 or more prior treatment failures [TFs]). Based on CDA-AMC’s clinical review of the sponsor-submitted network meta-analysis (NMA), the assumption of comparable clinical efficacy and safety between atogepant and comparators is associated with high uncertainty due to wide credible intervals that include effect estimates both in favour of and against atogepant compared to other treatments. Notably, for the reimbursement population, no comparative data were provided by the sponsor for atogepant compared to eptinezumab. CDA-AMC additionally noted that health-related quality of life outcomes, which are of importance to patients and clinicians, were not included in the sponsor’s NMA. Overall, the CDA-AMC clinical review concluded that evidence from the submitted NMA is inadequate to inform whether atogepant will result in similar or different effects compared to other currently funded treatment options.
The CDA-AMC base case suggests that, in the reimbursement population, atogepant will be more costly than onabotulinumtoxin A (incremental costs = $2,479) during a 5-year period, but less costly than fremanezumab, eptinezumab, and galcanezumab (range of incremental savings, $15 to $741). The estimated incremental savings are based on publicly available list prices of comparators and may not reflect actual prices paid by public drug plans in Canada. If pan-Canadian Pharmaceutical Alliance (pCPA) negotiations conclude with price reductions for fremanezumab, galcanezumab, or eptinezumab, atogepant may no longer result in cost savings to the public drug plans. In jurisdictions where onabotulinumtoxin A is funded for the prevention of migraine, savings associated with the reimbursement of atogepant for the reimbursement population may be further reduced or eliminated.
This cost-minimization analysis is based on the assumption of clinical similarity between atogepant and fremanezumab, galcanezumab, eptinezumab, and onabotulinumtoxin A. If atogepant confers differential safety or efficacy compared to the other calcitonin gene–related peptide (CGRP) inhibitors or onabotulinumtoxin A, the cost-effectiveness of atogepant relative to other treatments used in the reimbursement request population is unknown. CDA-AMC also notes that the magnitude of cost savings associated with atogepant over 5 years is uncertain due to the exclusion of subsequent therapy costs from the sponsor’s analysis.
Economic Review
Economic Information
Summary of Sponsor’s Economic Information
The sponsor submitted a cost-minimization analysis1 comparing atogepant with CGRP inhibitors currently funded by public drug plans (i.e., eptinezumab, fremanezumab, and galcanezumab), and onabotulinumtoxin A (scenario only). Atogepant is indicated for the prevention of migraine in adults who have at least 4 migraine days per month, and the sponsor’s reimbursement request is for the prevention of chronic migraine (CM) in adults with more than 15 headache days per month (of which 8 days are considered to be migraine days) and who have previously had an inadequate response, are intolerant, or have a contraindication to at least 2 migraine preventive therapies (2 or more prior TFs). The modelled population is consistent with that of the sponsor’s reimbursement request but narrower than that of the Health Canada indication, which is not restricted by the number of previous TFs.2 CDA-AMC has previously reviewed atogepant for the prevention of episodic migraine in adults.3
Atogepant is available in 10 mg, 30 mg, and 60 mg tablets; however, only the 60 mg tablet was submitted to CDA-AMC for the indication currently under review. The recommended dosage of atogepant for CM is 60 mg once daily.2 At the submitted price of $18.44 per tablet, the annual cost of atogepant for CM is $6,735 per patient. The annual maintenance cost of eptinezumab, fremanezumab, and galcanezumab ranges from $6,732 per patient to $7,240 per patient, while the typical annual cost of onabotulinumtoxin A is $2,526 per patient to $3,178 per patient.
In the absence of head-to-head evidence comparing atogepant to relevant comparators, the sponsor conducted NMAs4 to support the assumption of similar clinical efficacy in the 2 or more TFs subgroup, with the efficacy of atogepant informed by the PROGRESS trial.5 Clinical efficacy in the economic model was informed by the proportion of patients achieving a 50% reduction in monthly migraine days (MMDs) from baseline. The probability of attaining a 50% reduction in MMDs was assumed by the sponsor to be equivalent for atogepant and comparators, based on the results for atogepant in the 2 or more TFs subgroup (30%) in the sponsor’s NMA. The sponsor assumed that treatment discontinuation would be equal across treatments, with a 1-time ███% risk of discontinuation before response assessment at 12 weeks based on the probability of discontinuation at 12 weeks for atogepant 60 mg in the overall CM population of the sponsor’s NMA. After 12 weeks, discontinuation was assumed to be ███% every 4 weeks thereafter for all treatments, based on all-cause discontinuation in the atogepant 60 mg group of the long-term extension study of the PROGRESS trial (Study 312) at the time of the November 2023 interim analysis.6
The sponsor’s analysis included drug acquisition costs, based on the sponsor’s submitted price for atogepant and list prices from the Ontario Drug Benefit (ODB) Formulary and the ODB Exceptional Access Program for comparators.7,8 Administration costs were not included as the sponsor assumed that patients would self-administer atogepant, galcanezumab, and fremanezumab, and that administration costs for eptinezumab and onabotulinumtoxin A (when applicable) would be funded by manufacturer support programs or patients, respectively. Health care resource use costs9,10 included those associated with visiting a general practitioner, neurologist, or nurse practitioner 3 times in the first year of therapy and twice annually thereafter, except for onabotulinumtoxin A, where patients were assumed to have 4 visits per year. The proportion of patients visiting each type of clinician differed by treatment, based on clinical expert opinion obtained by the sponsor.1
A summary of the sponsor’s base case is presented in Table 7. The sponsor’s submitted base case estimated that in the reimbursement population (i.e., patients with CM and more than 15 headache days per month who have previously experienced an inadequate response, are intolerant, or have a contraindication to at least 2 migraine preventive therapies), atogepant would be associated with cumulative costs of $6,633 per patient during a 5-year period, while the estimated total cost of eptinezumab, fremanezumab, and galcanezumab ranged from $6,648 per patient to $7,374 per patient. Thus, the use of atogepant was predicted by the sponsor to result in incremental savings of $15 per patient to $741 per patient.
The sponsor conducted a scenario analysis in which onabotulinumtoxin A was included as a comparator. In this analysis, atogepant was associated with an incremental cost of $2,479 per patient over 5 years compared to onabotulinumtoxin A.
CDA-AMC Appraisal of the Sponsor’s Economic Information
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
The clinical similarity of atogepant to relevant comparators is uncertain. There is a lack of direct head-to-head evidence comparing atogepant and relevant comparators, and the sponsor submitted an NMA to support the assumption of clinical equivalence in the reimbursement population (2+ TFs).4 Efficacy in the pharmacoeconomic model (i.e., a 50% reduction in MMDs) was assumed to be equivalent across treatments, based on the results of the sponsor’s NMA (a subgroup analysis for the 2+ TFs population). As noted in the CDA-AMC clinical review, there is high uncertainty in the results of this analysis, owing to wide credible intervals that include the potential for effect estimates both in favour of and against atogepant compared to other treatments. Although the sponsor-submitted NMA suggests that there may be no statistically significant difference in the odds of attaining a 50% reduction in MMDs between atogepant and other treatments for CM in the 2 or more TFs subgroup, the point estimates from the sponsor’s analysis suggest that atogepant may be associated ████ █████ ████ ██ █████████ | 50% reduction in MMDs ████████ ████ █████████ █████████████ ███ ████████████ ████ ██████ ████ ██ ██████████████████ ███ ████ ██ █████████ ████████ ██ █████████████ █ ███████ ███████ ███ noted for a 30% reduction in MMDs, where data were available. Notably, for the reimbursement population, no comparative data were provided by the sponsor for atogepant compared to eptinezumab.
Further, CDA-AMC notes that all efficacy outcomes in the sponsor’s NMA were assessed at 12 weeks, which does not align with clinical practice or the anticipated renewal criteria for atogepant (refer to the subsequent appraisal point). As well, the sponsor’s NMA did not include some outcomes of importance to patients (i.e., health-related quality of life) and CDA-AMC-participating public drug plans (i.e., Headache Impact Test, for the potential alignment of renewal criteria in some jurisdictions).11 Adverse events were assessed only for the overall CM population, not for the reimbursement population (2+ TFs).
Given the lack of direct evidence and limitations with the sponsor’s NMA, whether atogepant has similar clinical effects (i.e., benefits and harms) as other treatments reimbursed for the prevention of CM in the reimbursement population is uncertain. CDA-AMC was unable to address this limitation in reanalysis.
The timing of response assessment in the submitted model is not aligned with clinical practice or with public drug plan renewal criteria for CGRP inhibitors reimbursed for CM. In the submitted economic model, the sponsor assumed that patients who do not attain a 50% reduction in MMDs after 3 months of treatment would discontinue treatment with atogepant and comparators. Clinical expert input received by CDA-AMC for this review indicated that it is more likely that a 6-month trial of atogepant would be given before assessing response to treatment. Further, input from CDA-AMC-participating drug plans indicated that the renewal criteria for atogepant would likely be aligned with that of other CGRP inhibitors reimbursed for the treatment of CM, which is based on an initial approval period of 6 months across jurisdictions. CDA-AMC additionally notes that an initial trial of 6 months of atogepant for CM would be aligned with the initial approval period for atogepant when reimbursed for episodic migraine.
CDA-AMC was unable to address this limitation given the structure of the sponsor’s model. CDA-AMC notes that there is a lack of comparative clinical evidence to support the clinical similarity of atogepant to other reimbursed treatments for CM after 6 months of initial treatment.
Onabotulinumtoxin A was excluded from the sponsor’s base case. In the sponsor’s base case, atogepant was compared to eptinezumab, fremanezumab, and galcanezumab. Onabotulinumtoxin A was excluded by the sponsor in the submitted base case, despite a positive recommendation from the Canadian Drug Expert Committee for the prophylaxis of headaches in adults with CM who have had an inadequate response, intolerance, or contraindication to at least 3 oral prophylactic migraine medications, and reimbursement in some jurisdictions.11-13 According to clinical expert opinion obtained by CDA-AMC for this review, the current standard of care for the requested reimbursement population (adults with CM and 2+ TFs) includes CGRP inhibitors as well as onabotulinumtoxin A in some jurisdictions. Onabotulinumtoxin A is a regular benefit in Alberta12 and is reimbursed for patients with CM who have had an inadequate response to 3 or more oral preventive therapies in Ontario.7 As indicated in the procedures for CDA-AMC reimbursement reviews,14 relevant comparators include treatments reimbursed by at least 1 drug plan for the indication under review, those used off-label in practice in Canada, or those that have previously received a recommendation in favour of reimbursement from CDA-AMC for the indication under review. As such, the exclusion of onabotulinumtoxin A from the sponsor’s base case was inappropriate.
In the CDA-AMC base case, onabotulinumtoxin A was included as a comparator, using the sponsor-provided option to do so.
The structure of the sponsor’s analysis does not adequately reflect the management of migraine in clinical practice. The sponsor assumed that patients who discontinued treatment (i.e., patients did not attain a 50% reduction in MMDs at 12 weeks or later or who discontinued treatment after an initial response) would receive no further preventive therapy for CM for the duration of the time horizon. According to clinical experts consulted by CDA-AMC for this review, as well as noted in previous CDA-AMC reviews of migraine preventive therapies,3,15-17 patients who discontinue a preventive treatment for migraine are likely to continue to receive a preventive migraine treatment, which may consist of another CGRP inhibitor, an oral preventive treatment, or, in some jurisdictions, onabotulinumtoxin A. This is consistent with patient group input, as noted in the CDA-AMC Clinical Review Report, in which patients described having tried many lines of preventive treatment. Thus, patients who discontinue atogepant or a comparator are likely to receive an alternate preventive therapy thereafter.
The cost of migraine prevention therapy estimated by the sponsor for the 5-year analysis period is underestimated for atogepant and all comparators due to the exclusion of subsequent therapy costs. CDA-AMC was unable to address this limitation owing to the structure of the sponsor’s model and a lack of comparative discontinuation rates and use of subsequent treatments between atogepant and comparators. The impact of this limitation on the estimated costs of treatment is unknown.
Confidential pricing agreements are unknown. The sponsor’s analysis incorporated pricing available from the ODB Exceptional Access Program for the CGRP inhibitors.7 However, confidential pricing agreements exist for eptinezumab, fremanezumab, and galcanezumab for the prevention of migraine.18-20 Therefore, the submitted price of atogepant may require a price reduction to avoid incurring additional costs relative to its comparators. A confidential pricing agreement already exists for atogepant for the treatment of episodic migraine.21
CDA-AMC was unable to address this limitation in reanalysis, as the negotiated prices of the comparators are unknown.
CDA-AMC Reanalyses of the Economic Information
The CDA-AMC base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts. CDA-AMC undertook reanalyses that addressed key limitations within the submitted economic model (Table 3). All CDA-AMC reanalyses are presented deterministically.
Table 3: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Comparators | Onabotulinumtoxin A excluded | Onabotulinumtoxin A included |
CDA-AMC base case | Reanalysis 1 | |
Results from the CDA-AMC base case suggest that for the reimbursement request population (CM and 2+ TFs), the total cost of atogepant is $6,633 per patient during a 5-year period while the total cost of other CGRP inhibitors ranged from $6,648 per patient to $7,374 per patient and the total cost of onabotulinumtoxin A was $3,839 per patient. The use of atogepant is expected to result in incremental savings of $15 per patient to $741 per patient when compared to fremanezumab, galcanezumab, and eptinezumab and an incremental cost of $2,479 per patient compared to onabotulinumtoxin A (Table 4), assuming publicly available list prices for all comparators (Table 5). This analysis is consistent with the sponsor’s submitted scenario analysis that included onabotulinumtoxin A.
Table 4: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Drug | Total drug costs ($) | Incremental drug costs vs. atogepant ($) | Total costs ($) | Incremental costs vs. atogepant ($) |
|---|---|---|---|---|
Onabotulinumtoxin A | 3,839 | –2,656 | 4,154 | –2,479 |
Atogepant | 6,495 | Reference | 6,633 | Reference |
Eptinezumab | 6,982 | 486 | 7,156 | 523 |
Fremanezumab | 6,492 | –3 | 6,648 | 15 |
Galcanezumab | 7,218 | 723 | 7,374 | 741 |
vs. = versus.
Issues for Consideration
Health Canada indication for atogepant is broader than the sponsor’s requested reimbursement population: CDA-AMC accepted a deviation request from the sponsor to focus the current pharmacoeconomic submission on the requested reimbursement population (patients with CM and at least 2 prior TFs). CDA-AMC notes, however, that the Health Canada indication for atogepant is not restricted based on the number of prior preventive therapies.2 Clinical expert input received by CDA-AMC indicated that, among patients with CM and fewer than 2 prior TFs, it is possible that atogepant could displace less costly oral preventive therapies, thus resulting in additional costs to the public drug plans if funded beyond the reimbursement request population.
Use of erenumab for CM is uncertain: The Canadian Drug Expert Committee recommended that erenumab be reimbursed for the prevention of migraine in adult patients with CM (≥ 15 monthly headache days, of which at least 8 are migraine days) who have previously had an inadequate response, intolerance, or contraindication to 2 or 3 oral migraine preventives.22 Subsequent negotiations with the pCPA concluded without an agreement.23 At its current wholesale list price,24 the annual cost of erenumab would be less than that of atogepant (based on the submitted price).
Different mode of administration and half-life: Some patients may prefer an oral treatment, such as atogepant, over the injectable or infusible modes of administration associated with fremanezumab, galcanezumab, eptinezumab, and onabotulinumtoxin A. Clinical input received by CDA-AMC for this review noted that the shorter half-life of atogepant compared to injectable or infusible CGRP inhibitors may be preferred for patients considering pregnancy, as well as those with a history of cardiovascular disease, including stroke.
Conclusions
Assuming similar clinical efficacy and safety for atogepant compared to fremanezumab, galcanezumab, and eptinezumab, the sponsor submitted a cost-minimization analysis comparing drug acquisition and monitoring costs for the reimbursement population (i.e., adults with more than 15 headache days per month and who have had 2 or more prior TFs). Based on CDA-AMC’s clinical review of the sponsor-submitted NMA, the assumption of comparable clinical efficacy and safety between atogepant and comparators is associated with high uncertainty due to wide credible intervals that include effect estimates both in favour of and against atogepant compared to other treatments. Notably, for the reimbursement population, no comparative data were provided by the sponsor for atogepant compared to eptinezumab. CDA-AMC additionally noted that health-related quality of life outcomes, which are of importance to patients and clinicians, were not included in the sponsor’s NMA. Overall, the CDA-AMC clinical review concluded that evidence from the submitted NMA is inadequate to inform whether atogepant will result in similar or different effects compared to other currently funded treatment options.
The CDA-AMC base case suggests that, in the reimbursement population, atogepant will be more costly than onabotulinumtoxin A (incremental costs = $2,479 per patient) during a 5-year period, but less costly than fremanezumab, eptinezumab, and galcanezumab (range of incremental savings, $15 per patient to $741 per patient). The estimated incremental savings are based on publicly available list prices of comparators and may not reflect actual prices paid by public drug plans in Canada. If pCPA negotiations conclude with price reductions for fremanezumab, galcanezumab, or eptinezumab, atogepant may no longer result in cost savings to the public drug plans. In jurisdictions where onabotulinumtoxin A is funded for the prevention of migraine, savings associated with the reimbursement of atogepant for the reimbursement population may be further reduced or eliminated.
This cost-minimization analysis is based on the assumption of clinical similarity between atogepant and fremanezumab, galcanezumab, eptinezumab, and onabotulinumtoxin A. If atogepant confers differential safety or efficacy compared to the other CGRP inhibitors or onabotulinumtoxin A, the cost-effectiveness of atogepant relative to other treatments used in the reimbursement request population would be unknown. CDA-AMC also notes that the magnitude of cost savings associated with atogepant over 5 years is uncertain due to the exclusion of subsequent therapy costs from the sponsor’s analysis.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Qulipta (atogepant), 10 mg, 30 mg, and 60 mg oral tablets. Pointe-Claire (QC): AbbVie Corporation; 2023 Dec 21.
2.Qulipta (atogepant): 10 mg, 30 mg, and 60 mg oral tablets [product monograph]. Saint-Laurent (QC): AbbVie Corporation; 2023 Mar 17.
3.CADTH Reimbursement Review: Atogepant (Qulipta). Can J Health Technol. 2023;3(8). https://www.cadth.ca/sites/default//files/DRR/2023/SR0724-Qulipta_combined.pdf. Accessed 2024 Jan 29.
4.Statistical Analysis Report for Network Meta-Analyses for Atogepant in Chronic Migraine [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Qulipta (atogepant), 10 mg, 30 mg, and 60 mg oral tablets. Pointe-Claire (QC): Medical Decision Modeling Inc. for AbbVie Corporation; 2023 Apr 26.
5.AbbVie Inc. A phase 3, multicenter, randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy, safety, and tolerability of atogepant for the prevention of chronic migraine (PROGRESS CSR) [Confidential information; sponsor-supplied reference]. North Chicago (IL). Accessed 2022 Apr 21.
6.AbbVie. Topline Results (Interim Analysis) of Study 3101-312-002: A phase 3, multicenter, open-label 156-week extension study to evaluate the long-term safety and tolerability of oral atogepant for the prevention of migraine in participants with chronic or episodic migraine [sponsor-supplied reference]. Accessed 2023 Nov 13.
7.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2024: http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2024 Jan 29.
8.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2024; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2024 Mar 20.
9.Schedule of benefits for physician services under the Health Insurance Act: (January 25, 2022 (effective July 1, 2022)) [sponsor-supplied reference]. Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf.
10.Collective Agreement between the Ottawa Hospital and Ontario Nurses’ Association [sponsor-supplied reference]. Toronto (ON): Ontario Nurses' Association; 2023: https://www.ona.org/wp-content/uploads/cba/the_ottawa_hospital_202101660_expiry_march_31_2023.pdf.
11.Ontario Ministry of Health. Exceptional Access Program Reimbursement Criteria for Frequently Requested Drugs. 2023. Accessed 2024 Jan 29.
12.Government of Alberta. Interactive Drug Benefit List. 2024; https://idbl.ab.bluecross.ca/idbl/load.do. Accessed 2024 Mar 08.
13.CADTH Common Drug Review Pharmacoeconomic Review Report: OnabotulinumtoxinA (Botox) for the prophylaxis of headaches in adults with chronic migraine (≥ 15 days per month with headache lasting four hours a day or longer) [sponsor-supplied reference]. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0584-botox-pharmacoeconomic-review-report-resubmission.pdf.
14.CADTH. Procedures for CADTH Reimbursement Reviews [sponsor-supplied reference]. 2023: https://www.cadth.ca/sites/default/files/Drug_Review_Process/CADTH%20Drug%20Reimbursement%20Review%20Procedures.pdf. Accessed 2023 Sep.
15.CADTH Drug Reimbursement Review Pharmacoeconomic Report: Fremanezumab (AJOVY) for the prevention of migraine in adults who have at least 4 migraine days monthly [sponsor-supplied reference]. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/cdr/complete/sr0641-ajovy-pharmacoeconomic-review-report.pdf. Accessed 2024 Mar 24.
16.CADTH Reimbursement Review: Eptinezumab (Vyepti). Can J Health Technol. 2023;3(3). https://www.cadth.ca/sites/default/files/DRR/2023/SR0743-Vyepti-meta.pdf. Accessed 2024 Mar 24.
17.CADTH Reimbursement Review: Galcanezumab (Emgality) [sponsor-supplied reference]. Can J Health Technol. 2022;2(3). https://www.cadth.ca/sites/default/files/DRR/2022/SR0693-Emgality.pdf. Accessed 2024 Mar 24.
18.pan-Canadian Pharmaceutical Alliance. Ajovy (fremanezumab): Prevention of migraine in adults. 2021; https://www.pcpacanada.ca/negotiation/21431. Accessed 2024 Jan 29.
19.pan-Canadian Pharmaceutical Alliance. Emgality (galcanezumab): Prevention of migraine. 2022; https://www.pcpacanada.ca/negotiation/21690. Accessed 2024 Jan 29.
20.pan-Canadian Pharmaceutical Alliance. Vyepti (eptinezumab): Prevention of migraine. 2023; https://www.pcpacanada.ca/negotiation/22136. Accessed 2024 Jan 29.
21.pan-Canadian Pharmaceutical Alliance. Qulipta (atogepant): For the prevention of episodic migraine in adults. 2023; https://www.pcpacanada.ca/negotiation/22394. Accessed 2024 Jan 29.
22.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: Erenumab (Aimovig - Novartis Pharmaceuticals Canada Inc.). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/complete/SR0578%20Aimovig%20-%20CDEC%20Final%20Recommendation%20July%2024%2C%202020%20%28redacted%29_For%20Posting.pdf. Accessed 2024 Mar 07.
23.pan-Canadian Pharmaceutical Alliance. Aimovig (erenumab): migraine, chronic. 2021; https://www.pcpacanada.ca/negotiation/21286. Accessed 2024 Mar 07.
24.DeltaPA. [Ottawa (ON)]: IQVIA; 2024: https://www.iqvia.com/. Accessed 2024 Mar 20.
25.Pringsheim T, Davenport W, Mackie G, et al. Canadian Headache Society guideline for migraine prophylaxis. Can J Neurol Sci. 2012;39(2 Suppl 2):S1-59. PubMed
26.Osman N, Worthington I, Lagman-Bartolome AM. Headache in adults. In: Compendium of therapeutic choices. Ottawa (ON): Canadian Pharmacists Association; 2021: https://www.pharmacists.ca. Accessed 2024 Jan 30.
27.Saskatchewan Drug Plan: search formulary. 2022; http://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2024 Jan 29.
28.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Qulipta (atogepant), 10 mg, 30 mg, and 60 mg oral tablets. Pointe-Claire (QC): AbbVie Corporation; 2023 Dec 21.
29.Table: 17-10-0005-01 Population estimates on July 1st, by age and sex [sponsor-supplied reference]. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1710000501. Accessed 2023.
30.Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2021 to 2022 [sponsor-supplied reference]. 2023; https://www.sac-isc.gc.ca/eng/1683039690813/1683039973755.
31.Table: 17-10-0057-01 Projected population, by projection scenario, age and sex, as of July 1 (x 1,000) [sponsor-supplied reference]. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 2023.
32.Ramage-Morin PL, Gilmour H. Prevalence of migraine in the Canadian household population. Health Rep. 2014;25(6):10-16. PubMed
33.Buse DC, Manack AN, Fanning KM, et al. Chronic migraine prevalence, disability, and sociodemographic factors: results from the American Migraine Prevalence and Prevention Study. Headache. 2012;52(10):1456-1470. PubMed
34.Dodick DW, Loder EW, Manack Adams A, et al. Assessing Barriers to Chronic Migraine Consultation, Diagnosis, and Treatment: Results From the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study. Headache. 2016;56(5):821-834. PubMed
35.Burrell E MK, Xue F, Buse D, Lipton R, Chia V. Sizing of the Migraine Population Treated with Preventive Medications for Migraine. Value Health. 2018;21:S204.
Appendix 1: Additional Economic Information
Please note that this appendix has not been copy-edited.
Cost Comparison Table
The comparators presented in Table 5 have been deemed to be appropriate based on feedback from clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table. As such, Table 5 may not represent the actual costs to public drug plans.
Table 5: CDA-AMC Cost Comparison Table for Prevention of CM
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | Annual costa ($) |
|---|---|---|---|---|---|---|
Atogepant (Qulipta) | 10 mg 30 mg 60 mg | Tablet | $18.4400a | 60 mg once daily | 18.44 | 6,735 |
Anti–calcitonin gene–related peptide monoclonal antibodies | ||||||
Eptinezumab (Vyepti) | 100 mg | Solution for IV infusion | $1,665.00 | 100 or 300 mg infused every 12 weeks | 19.82 to 59.46b | 7,240 to 21,719b |
Erenumab (Aimovig) | 70 mg/mL 140 mg/mL | Autoinjector | 532.0000c | 70 mg or 140 mg subcutaneously monthly | 17.48 | 6,384 |
Fremanezumab (Ajovy) | 225 mg / 1.5 mL | Prefilled syringe | 560.9800 | 225 mg once a month or 675 mg every 3 months | 18.43 | 6,732 |
Galcanezumab (Emgality) | 120 mg/mL | 1 mL prefilled syringe or pen | 577.8000 | 240 mg initial loading dose, then 120 mg once monthly | Maintenance: 18.98 | First year: 7,511 Subsequent years: 6,934 |
Other treatments indicated for migraine prophylaxis | ||||||
Flunarizine (generics) | 5 mg | Capsule | 0.7348 | 10 mg once daily | 1.47 | 537 |
Onabotulinumtoxin A (Botox) | 50 U 100 U 200 U | Concentrate powder for solution for injection | 187.4250d 374.8500d 749.7000d | 155 U to 195 U every 12 weeks | 6.92 to 8.70 | 2,526 to 3,178 |
Pizotyline/Pizotifen (Sandomigran DS) | 1 mg | Tablet | 1.1026 | 1 mg to 6 mg per daye | 1.10 to 6.62 | 403 to 2,416 |
Topiramate (generics) | 25 mg 100 mg 200 mg | Tablet | 0.2433 0.4583 0.6748 | 100 mg per daye | 0.46 | 167 |
All prices are from the ODB Formulary or Exceptional Access Program (accessed March 2024)7,8 unless otherwise indicated and do not include dispensing fees. All recommended doses are sourced from respective product monographs. An average year is assumed to be 365.25 days.
aSponsor’s submitted price for the 60 mg strength. The Ontario Exceptional Access Program lists the same price for all available strengths.7
bCost of 300 mg dose assumes linear pricing (i.e., the use of 3 of the 100 mg vials).
cIQVIA DeltaPA wholesale price, accessed March 2024.24
dOnabotulinumtoxin A is funded for CM under the Ontario Exceptional Access program.11 The list price is from the ODB Formulary.8
eRecommended dosage as well as daily and annual drug costs assume post-titration maintenance dose.
Table 6: CDA-AMC Cost Comparison Table for Prevention of Migraine (Nonindicated)
Drug/comparator | Strength | Dosage form | Price ($) | Recommended dosage | Daily drug cost ($) | Annual drug cost ($) |
|---|---|---|---|---|---|---|
Antiepileptics | ||||||
Divalproex sodium (generics) | 125 mg 250 mg 500 mg | Enteric Tablet | 0.1539 0.2767 0.5537 | 500 mg to 1,500 mg per daya,b | 0.55 to 1.66 | 202 to 607 |
Valproic acid (generics) | 250 mg | Capsule | 0.2905 | 500 mg to 1,500 mg per daya, b | 0.58 to 1.74 | 212 to 637 |
50 mg/mL | Oral solution | 0.0398 | 0.40 to 1.19 | 145 to 436 | ||
500 mg | Enteric Capsule | 0.8102 | 0.81 to 2.43 | 296 to 887 | ||
Gabapentin (generics) | 100 mg 300 mg 400 mg | Capsule | 0.0416 0.1012 0.1206 | 1,200 mg to 1,800 mg per day in 3 dosesa | 0.36 to 0.61 | 132 to 222 |
Antidepressants | ||||||
Amitriptyline (generics) | 10 mg 25 mg 50 mg | Tablet | 0.0435 0.0829 0.1540 | 20 mg to 150 mg per daya, b | 0.09 to 0.46 | 32 to 169 |
Doxepin (Sinequan) | 10 mg 25 mg 50 mg 75 mg 100 mg | Capsule | 0.4075 0.5000 0.9274 1.2242c 1.6100c | 25 mg to 100 mg per dayb | 0.50 to 1.61 | 183 to 588 |
Nortriptyline (Aventyl) | 10 mg 25 mg | Capsule | 0.2995 0.6054 | 20 mg to 150 mg per daya, b | 0.60 to 3.63 | 219 to 1,327 |
Venlafaxine (generics) | 37.5 mg 75 mg 150 mg | Extended-release capsule | 0.0913 0.1825 0.1927 | 150 mg per daya, b | 0.19 | 70 |
Antihypertensives | ||||||
Atenolol (generics) | 50 mg 100 mg | Tablet | 0.0938 0.1543 | 100 to 150 mg per dayb | 0.15 to 0.0.25 | 56 to 91 |
Metoprolol (generics) | 50 mg 100 mg | Tablet | 0.0624 0.1361 | 100 mg to 200 mg per daya, b | 0.12 to 0.25 | 46 to 91 |
100 mg 200 mg | Sustained-release tablet | 0.1415 0.2568 | 0.14 to 0.26 | 52 to 94 | ||
Nadolol (generics) | 40 mg 80 mg 160 mg | Tablet | 0.2375 0.3410 1.2046 | 80 mg to 160 mg per daya, b | 0.34 to 0.68 | 125 to 249 |
Propranolol (generics) | 10 mg 20 mg 40 mg 80 mg | Tablet | 0.0774 0.1243 0.1377 0.2285 | 80 mg to 160 mg per day in 2 dosesa, b | 0.28 to 0.46 | 101 to 167 |
Verapamil (generics) | 80 mg 120 mg | Tablet | 0.2735 0.4250 | 240 mg to 320 mg per daya, b | 0.82 to 1.09 | 300 to 400 |
120 mg 180 mg 240 mg | Sustained-release tablet | 0.5078c 0.5204 1.7143 | 1.71d | 626 | ||
Candesartan (generics) | 4 mg 8 mg 16 mg 32 mg | Tablet | 0.1700 0.2281 0.2281 0.2281 | Up to 16 mg per daya, b | 0.17 to 0.23 | 62 to 83 |
Lisinopril (generics) | 5 mg 10 mg 20 mg | Tablet | 0.1347 0.1619 0.1945 | 20 mg per daya | 0.19 | 71 |
Antimanic/Mood Stabilizer | ||||||
Lithium carbonate (generics) | 150 mg 300 mg 600 mg | Capsule | 0.0667 0.0657 0.1988c | 300 mg 3 times dailyb | 0.20 | 72 |
Lithium carbonate (Lithmax) | 300 mg | Sustained-release tablet | 0.2880c | 0.86 | 316 | |
All prices are from the ODB Formulary (accessed January 2024)8 unless otherwise indicated and do not include dispensing fees. An average year is assumed to be 365.25 days.
aSource: 2012 Canadian Headache Society Guideline for Migraine Prophylaxis.25
bSource: Canadian Pharmacists Association Therapeutic Choices: Headache in Adults, Drugs Used for Migraine Prophylaxis (Accessed January 2024).26
cSaskatchewan Formulary list price (accessed January 2024).27
dAssumes 240 mg, as 320 mg is not a possible dose with sustained-release tablets.
Additional Details on the Sponsor’s Submission
Table 7: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total drug costs ($) | Incremental drug costs ($) | Total costs ($) | Incremental costs vs. atogepant ($) |
|---|---|---|---|---|
Atogepant | 6,495 | Reference | 6,633 | Reference |
Eptinezumab | 6,982 | 486 | 7,156 | 523 |
Fremanezumab | 6,492 | −3 | 6,648 | 15 |
Galcanezumab | 7,218 | 723 | 7,374 | 741 |
vs. = versus.
Source: Sponsor’s economic submission.1
Additional Details on the CDA-AMC Reanalyses and Additional Analyses
CDA-AMC did not conduct any additional pharmacoeconomic analyses in the review of atogepant.
Appendix 2: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 8: Summary of Key Take Aways
Key take aways of the BIA |
|---|
|
BIA = budget impact analysis.
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the expected incremental budgetary impact of reimbursing atogepant for the prevention of CM in adults who have previously experienced an inadequate response, are intolerant, or have a contraindication to at least 2 migraine preventive therapies.28 CDA-AMC approved a deviation request from the sponsor to focus the BIA on this population. The BIA was conducted from the perspective of the pan-Canadian public drug plans over a 3-year time horizon (July 2025 through June 2028; July 2024 through June 2025 as the base year). The sponsor estimated the eligible population using an epidemiological approach. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets, excluding Quebec, as well as the Non-Insured Health Benefits (NIHB) program. Adjustments were made to the provincial populations to remove NIHB clients when estimating provincial public plan populations. The sponsor’s base case included drug acquisition costs only. Market shares and uptake of atogepant were estimated based on internal sponsor data. In the base case, the sponsor assumed that atogepant would displace only eptinezumab, fremanezumab, and galcanezumab, while onabotulinumtoxin A displacement was considered in jurisdictions where it is currently reimbursed for CM (i.e., Alberta and Ontario) in a scenario analysis. Key inputs to the BIA are documented in Table 9.
Table 9: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3 if appropriate) |
|---|---|
Target population | |
Pan-Canadian adult population, base year | |
Annual population growth rate | 1.38%31 |
Migraine Prevalence | 9.17%32 |
Proportion of patients with migraine who have with chronic migraine | 7.68%33 |
Proportion of patients with chronic migraine using preventives | 44.4%34 |
Proportion of patients with 2+ prior treatment failures | 18.0%35 |
Proportion reimbursed by public plan | 30% to 100%, varies by jurisdiction |
Number of patients eligible for drug under review | 5,442 / 5,518 / 5,596 |
Market shares (3 years, reference scenario) | |
Atogepant | 0% / 0% / 0% |
Eptinezumab | 18.7% / 19.7% / 20.3% |
Fremanezumab | 57.5% / 56.1% / 54.9% |
Galcanezumab | 23.7% / 24.2% / 24.9% |
Onabotulinumtoxin A (scenario only, Alberta and Ontario only) | 13.5% / 12.0% / 10.5%a |
Market shares (3 years, new drug scenario) | |
Atogepant | 38.1% / 50.0% / 56.6% |
Eptinezumab | 11.6% / 9.9% / 8.8% |
Fremanezumab | 35.6% / 28.1% / 23.9% |
Galcanezumab | 14.7% / 12.1% / 10.8% |
Onabotulinumtoxin A (scenario only, Alberta and Ontario only) | 13.0% / 11.5% / 10.0%a |
Cost of treatment (per patient per year) | |
Atogepant | $6,735 |
Eptinezumab | $7,240 |
Fremanezumab | $6,732 |
Galcanezumab | $7,511 (initial year) / $6,934 (maintenance years) |
Onabotulinumtoxin A (scenario only, Alberta and Ontario only) | $3,260 |
aIn the scenario including onabotulinumtoxin A, the market shares of the other comparators were proportionally reduced so that the sum of all comparator shares equalled 100%.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s analysis suggest that the reimbursement of atogepant for the prevention of CM in the requested reimbursement population (i.e., adults with CM who have previously experienced an inadequate response, are intolerant, or have a contraindication to at least 2 migraine preventive therapies) will be associated with incremental savings of $1,244,127 (year 1: $313,863, year 2: $425,315, year 3: $504,949) when compared to other CGRP inhibitors.
In a scenario analysis that included onabotulinumtoxin A as a comparator in Ontario and Alberta, the reimbursement of atogepant was associated with a 3-year incremental budgetary savings of $994,373 (year 1: $235,229, year 2: $340,637, year 3: $418,507).
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Onabotulinumtoxin A was excluded from the sponsor’s base case: In the sponsor’s base case, atogepant was compared to eptinezumab, fremanezumab, and galcanezumab. As described in the CDA-AMC Appraisal of the Sponsor’s Economic Information, the exclusion of onabotulinumtoxin A from the sponsor’s base case was inappropriate, given that onabotulinumtoxin A is used in the requested reimbursement population as part of standard of care and is funded in some jurisdictions (Alberta: regular benefit; Ontario: patients with CM and at least 3 prior TFs). As such, onabotulinumtoxin A is a relevant comparator in these jurisdictions for the reimbursement request population. Clinical expert opinion obtained by CDA-AMC indicated that, if reimbursed, atogepant is likely to displace some use of onabotulinumtoxin A in these jurisdictions.
In the CDA-AMC base case, onabotulinumtoxin A was included as a relevant comparator in jurisdictions where it is currently funded (i.e., Ontario and Alberta). CDA-AMC explored uncertainty regarding displacement of onabotulinumtoxin A by atogepant in scenario analysis.
The NIHB population was inappropriately calculated: NIHB clients residing within Ontario who are aged younger than 25 years or 65 years or older are eligible for reimbursement by ODB and thus should be counted as ODB clients and included in the Ontario population estimates rather than as NIHB clients for the purposes of modelling the budget impact of reimbursing atogepant for the prevention of CM in the 2 or more TFs subgroup.
CDA-AMC did not adjust for this limitation in reanalysis. The impact of this limitation on the pan-Canadian model results is expected to be minimal.
The price of drugs paid by public plans is uncertain: Both the sponsor’s and CDA-AMC’s analyses are based on publicly available list prices for all comparators. As fremanezumab, galcanezumab, and eptinezumab have gone through negotiations by pCPA,18-20 the prices paid by public plans are unknown. CDA-AMC additionally notes that atogepant has been negotiated by pCPA for the use in the prevention of episodic migraine21 and is listed on public formularies (e.g., Ontario).7 As such, the price paid by the drug plans for atogepant and comparators may be lower than incorporated in the sponsor’s analysis.
CDA-AMC was unable to incorporate the presence of confidential negotiated prices in reanalysis. Confidential negotiated prices for comparators may reduce the potential cost savings for atogepant. As such, the cost savings realized by the drug plans may be lower than predicted by the sponsor’s and CDA-AMC’s base case.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s base case by including onabotulinumtoxin A as a relevant comparator in Ontario and Alberta, using the sponsor-provided option to do so. The change is described in Table 10.
Table 10: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Comparators | Onabotulinumtoxin A excluded | Onabotulinumtoxin A included in jurisdictions where reimbursed for CMa |
CDA-AMC base case | Reanalysis 1 | |
aMarket shares for the other comparators, including atogepant, were proportionally reduced to account for that of onabotulinumtoxin A, as programmed by the sponsor and reported in Table 9. Onabotulinumtoxin A was considered to be a comparator only in Ontario and Alberta.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 11 and a more detailed breakdown is presented in Table 12.
Based on the CDA-AMC base case, the budged impact associated with the reimbursement of atogepant for the prevention of CM in the requested reimbursement population (i.e., adults who have previously experienced an inadequate response, are intolerant, or have a contraindication to at least 2 migraine preventive therapies) is expected to be a 3-year incremental cost savings of $994,373 (year 1: $235,229, year 2: $340,637, year 3: $418,507).
Table 11: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | 3-year total ($) |
|---|---|
Submitted base case | –1,244,127 |
CDA-AMC reanalysis 1: Onabotulinumtoxin A included as a comparator | –994,373 |
CDA-AMC base case | –994,373 |
BIA = budget impact analysis.
CDA-AMC conducted a scenario analysis in which atogepant was assumed to displace only fremanezumab, galcanezumab, and eptinezumab (as assumed in the sponsor’s base case), limiting the eligible population size to patients who would have otherwise received these CGRP inhibitors in the absence of atogepant. Results are provided in Table 12.
Table 12: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | 3-year total ($) |
|---|---|---|---|---|---|---|
Submitted base casea | Reference | 36,853,457 | 37,432,181 | 37,994,336 | 38,563,613 | 113,990,130 |
New drug | 36,853,457 | 37,118,319 | 37,569,021 | 38,058,663 | 112,746,002 | |
Budget impact | 0 | –313,863 | –425,315 | –504,949 | –1,244,127 | |
CDA-AMC base case | Reference | 35,042,266 | 35,781,571 | 36,505,447 | 37,241,918 | 109,528,937 |
New drug | 35,042,266 | 35,546,342 | 36,164,811 | 36,823,411 | 108,534,564 | |
Budget impact | 0 | –235,229 | –340,637 | –418,507 | –994,373 | |
CDA-AMC scenario 1: OnaBotA has share but is not displacedb,c | Reference | 33,406,382 | 34,288,957 | 35,160,370 | 36,048,734 | 105,498,061 |
New drug | 33,406,382 | 33,994,829 | 34,759,935 | 35,569,624 | 104,324,389 | |
Budget impact | 0 | –294,128 | –400,435 | –479,110 | –1,173,673 |
BIA = budget impact analysis; OnaBotTA = onabotulinumtoxin A.
aSponsor’s model was adjusted by CDA-AMC to report the pan-Canadian totals for the reference and new drug scenarios.
bThis scenario is aligned with the sponsor’s base case assumption that onabotulinumtoxin A will not be displaced by atogepant; however, 13.5%. 12.0%, and 10.5% of the population in Alberta and Ontario is assumed to still use onabotulinumtoxin A in year 1, year 2, and year 3, respectively, and are therefore not included in the population that may switch to atogepant These proportions are consistent with those assumed in the sponsor’s scenario analysis and CDA-AMC’s base case.
cReference and new drug totals do not include the cost of onabotulinumtoxin A, as it is assumed to be equal between them.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.