Drugs, Health Technologies, Health Systems
Reimbursement Review
Risperidone (Longavo)
Sponsor: Teva Canada Innovation
Therapeutic area: Schizophrenia, adults
Combined Review
Abbreviations
AAP
atypical antipsychotic
AE
adverse event
BMI
body mass index
CDA-AMC
Canada’s Drug Agency
CGI-I
Clinical Global Impression–Improvement
CGI-S
Clinical Global Impression–Severity
CI
confidence interval
CrI
credible interval
D2
dopamine type 2
EPS
extrapyramidal symptoms
EQ
equivalent
ER
extended release
HR
hazard ratio
HRQoL
health-related quality of life
IAM
Institute for Advancements in Mental Health
ITC
indirect treatment comparison
ITT
intention to treat
LAI
long-acting injectable
NMA
network meta-analysis
PANSS
Positive and Negative Syndrome Scale
PSP
Personal and Social Performance
PP1M
paliperidone palmitate 1-month formulation
PP3M
paliperidone palmitate 3-month formulation
RR
relative risk
SE
standard error
SLR
systematic literature review
SQLS
Schizophrenia Quality of Life Scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Risperidone for extended-release injectable suspension (risperidone ER, Longavo), prefilled syringe, 50 mg, 75 mg, 100 mg, 125 mg, subcutaneous injection |
Sponsor | Teva Canada Innovation |
Indication | For the treatment of schizophrenia in adults |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | Received June 18, 2025 |
Recommended dose | Administered at 50 mg, 75 mg, 100 mg, or 125 mg once monthly |
ER = extended release; NOC = Notice of Compliance.
Introduction
Schizophrenia is a major severe, chronic, and disabling psychiatric syndrome. Schizophrenia represents a heterogeneous group of disorders that may differentially affect presentation, course, treatment response, and outcome.1-3 The positive symptoms reflect a distortion or abundance of normal functions (e.g., delusion, conceptual disorganization, hallucinatory behaviour); the negative symptoms reflect a loss or restriction of normal functioning (e.g., blunted affect, emotional withdrawal, poor rapport).4-6 Patients with schizophrenia are at an increased risk for death by suicide and substance use, homelessness, and unemployment.7,8 The prevalence of schizophrenia in Canada has been estimated to be approximately 0.95% of the population in 2016, with 1.08% in male and 0.82% in female.9 The incidence of schizophrenia in Canada has been estimated to be approximately 49 per 100,000 in 2016, with 58 per 100,000 in male and 41 per 100,000 in female.9 Antipsychotic medications form the cornerstone of treatment for schizophrenia as they target the characteristic symptoms of schizophrenia.4,10,11 The underlying principles for the administration of pharmacotherapy include the individualization of medication (including patient preferences), simple medication regimens, appropriate dosing, attention to side-effect profiles, regular evaluation of responses (including adverse events [AEs]), and short-term and long-term clinical efficacy, safety, and tolerability.8 One major obstacle to the effective treatment of schizophrenia is nonadherence to medication, resulting in cycles of relapse.12,13 Studies have found that continuing treatment with long-acting injectable (LAI) antipsychotic preparations in clinical practice outperforms oral antipsychotic medication in preventing rehospitalization.14
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of risperidone for extended-release (ER) injectable suspension (risperidone ER, or Longavo), prefilled syringe, 50 mg, 75 mg, 100 mg, and 125 mg subcutaneous injection, in the treatment of adults with schizophrenia. Risperidone ER was previously reviewed by CADTH in 2021.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s (now the Canada’s Drug Agency: CDA-AMC) call for input and from clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
No patient input was received for this review. Patient input received for a previous CADTH review (November 2021) on risperidone for ER injectable suspension for the same indication is reported in this section.
Patient group input was provided by the Institute for Advancements in Mental Health (IAM) and was obtained based on IAM’s 40-year history of serving adults with schizophrenia. IAM’s submission also draws on a survey of members of IAM’s client network conducted in 2018. Respondents to that survey self-described as “personally diagnosed” (12%), a caregiver (50%), a family member or friend of someone diagnosed with schizophrenia (63%), or working in the social services (18%).
The respondents indicated that many patients experience symptoms of psychosis, which have a significant impact on day-to-day functioning. Patient experiences vary widely but typically involve some levels of cognitive impairment, delusions, and hallucinations. Many patients also experience a lack of insight into their condition, which often affects their ability and motivation to access treatment and supports. This symptom can cause significant strain on relationships, including those with caregivers and family members, ultimately leading to social isolation and a lack of supports for the individual with the condition.
Patients indicated that the most common side effects of antipsychotic drugs were drowsiness (reported by 58%), dry mouth (50%), restlessness (50%), dizziness, muscle stiffness, constipation, and anxiety.
Twenty-three percent of patients identified the cost of medications as a significant barrier to access; 63% of respondents indicated that it is difficult to pay for health care bills, including for medication, visits to specialists, counselling, and so forth; 20% of patients indicated that not having their preferred medication covered by public drug programs is a challenge.
Patients expect new, quick, simple, convenient, and affordable access to a wide range of treatments and medications that suit their specific needs, which can improve adherence and allow for the highest level of daily functioning and symptom reduction while managing side effects.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Unmet Needs
The clinical expert noted that there are many aspects of schizophrenia treatment that constitute an unmet need. These include the 15% to 20% of patients whose schizophrenia does not respond to currently available treatments and the patients whose schizophrenia becomes refractory to current treatment options. Furthermore, no treatments are available that reverse the course of disease or improve negative or cognitive symptoms, which are correlated with poor functional outcomes. The clinical expert highlighted the need for better-tolerated treatments, noting the significant side effects including, but not limited to, sedation, weight gain and metabolic dysfunction, sexual side effects, motor side effects, and cognition-related and motivation-related problems. The clinical expert noted the need for treatments that improve adherence, such as, more convenient formulations, noting that many patients forget to take their oral medications.
Place in Therapy
The clinical expert noted that risperidone LAI does not differ from other LAI antipsychotics in reducing positive symptoms of schizophrenia and does not have a unique mechanism of action. Therefore, the clinical expert suggested that risperidone LAI could be used similarly as other LAI antipsychotics, often in the first-line or second-line setting.
Patient Population
The clinical expert suggested that all adult patients with schizophrenia would be suitable for treatment with risperidone LAI, and it should be prescribed in a manner similar to that of other LAI antipsychotics for schizophrenia.
Assessing the Response Treatment
The clinical expert stated that a 20% reduction in standard rating scale measures is usually considered an adequate response; however, it was noted that most clinicians do not use standardized measures when assessing patients. Once symptoms have stabilized, the clinical expert suggested that relapse prevention is a key goal and noted that there is less variability in what constitutes a clinical relapse.
The clinical expert suggested that response to treatment should be assessed every 3 months initially, and then once a year or at key decision points thereafter.
Discontinuing Treatment
The clinical expert noted that lack of efficacy in treating symptoms of psychosis or intolerable side effects, including neurologic (e.g., extrapyramidal symptoms [EPS]), metabolic, or sexual side effects that do not respond adequately to treatment strategies, would result in discontinuation of treatment. Prolonged stability can suggest dose reduction, and in rare cases, discontinuation.
Prescribing Considerations
The clinical expert suggested that it is appropriate for general practitioners to prescribe risperidone LAI, noting that it should not require a specialist. The clinical expert highlighted that treating psychosis early is paramount and that all general physicians should be able to prescribe risperidone LAI without specialist supervision to ensure wide access to all medication options.
Additional Considerations
The clinical expert highlighted that increasing the number of treatment and formulation options available to patients is of benefit. The clinical expert noted that LAIs have been shown to be superior to oral antipsychotics in relapse prevention. However, they are painful to receive as all of them are deep intramuscular injections. The clinical expert highlighted that longer-term LAIs are not available for risperidone, reducing options for patients with schizophrenia that has not been stabilized with oral risperidone treatment. A formulation that eliminates or reduces these barriers would be helpful.
Clinician Group Input
No clinician group input was received for this review.
Drug Program Input
The drug programs identified the following jurisdictional implementation issues: considerations for initiation of therapy, conditions for prescribing of therapy, care provision issues, and system and economic issues. Refer to Table 4 for more details.
Clinical Evidence
Systematic Review
Description of Studies
The RISE study (or Study TV46000-CNS-30072) was a phase III, multicentre, randomized, double-blind, placebo-controlled, relapse-prevention study of TV-46000 for the treatment of schizophrenia in adults and adolescents. The objective was to assess the efficacy, safety, and tolerability of 2 dose regimens of TV-46000 (risperidone ER injectable suspension; [Longavo]) given subcutaneously, versus placebo, as maintenance therapy for patients with schizophrenia (544 patients were randomized, 181received placebo, 183 received risperidone ER once monthly , and 180 received risperidone ER once every 2 months).
The SHINE study (or Study TV46000-CNS-30078) was a phase III, multicentre, randomized, double-blind, parallel-group study to evaluate the long-term safety, tolerability, and effectiveness of TV-46000 administered subcutaneously once monthly or once every 2 months at doses of 50 mg to 250 mg (comparable to 2 mg/day to 5 mg/day of oral risperidone) for up to 56 weeks in adult and adolescent patients with schizophrenia (n = 334 patients were randomized and treated). For new patients (who did not participate in the RISE study), the SHINE study consisted of a screening period (up to 4 weeks); a conversion or stabilization stage (12 weeks receiving oral risperidone), or stage 1; a double-blind, active-treatment maintenance stage (up to 56 weeks), or stage 2; and a follow-up period (8 weeks).
The primary outcome for the RISE study was time to impending relapse, while the primary end point for the SHINE study was frequency of AEs. In the RISE study, baseline patient characteristics and demographics were generally well balanced across treatment groups. The mean age of patients was approximately 49 years, 39% of patients were female and 61% were male. On average, patients in each group had schizophrenia for approximately 20 years, and the mean time since last relapse was approximately 10 months. In the SHINE study, the mean age of patients was 50.6 years, 36% were female and 64% were male, and the mean duration of disease was 21.1 years, with a mean of 21 months since last relapse. Only 3 adolescents were randomized and received at least 1 dose of TV-46000 in the study.
Efficacy Results (RISE Study)
To align with Health Canada–approved indication, only the findings regarding once-monthly dosing of risperidone ER are reported in this CADTH review.
Time to Impending Relapse
The number of patients in the placebo group with impending relapse was 53 (29%) and the number of patients in the TV-46000 once monthly group was 13 (7%), with a hazard ratio (HR) of 0.200 (95% confidence interval [CI], 0.109 to 0.367; P < 0.0001).
Impending Relapse Rate at Week 24
In the placebo group, the impending relapse rate at week 24 was 0.28 (95% CI, 0.205 to 0.347). The impending relapse rate at week 24 in the TV-46000 once monthly group was 0.07 (95% CI, 0.03 to 0.109; P < 0.0001).
Percentage of Patients Whose Symptoms Remained Stable at the End Point
The number of patients in the placebo group whose symptoms remained stable at the end point was 110 (61%). The number of patients in the TV-46000 once monthly group was 159 (87%; P < 0.0001).
Percentage of Patients Achieving Remission at the End Point
The percentage of patients who achieved remission at end point was 23% in the placebo group (N = 181) and 29% in the TV-46000 once monthly group (N = 183).
Drug Attitude Inventory 10-Item Version
In the placebo group the least squares mean change from baseline in Drug Attitude Inventory 10-Item Version total score was –0.55 (standard error [SE] = 0.38) at early termination and –0.59 (SE = 0.31) at end of treatment. In the TV-46000 once monthly group the least squares mean change from baseline was 0.25 (SE = 0.42) at early termination and 0.57 (SE = 0.28) at end of treatment.
Schizophrenia Quality of Life Scale
In the placebo group the least squares mean change from baseline in Schizophrenia Quality of Life Scale (SQLS) total score was 3.20 (SE = 1.58) at early termination and 1.14 (SE = 1.32) at end of treatment. In the TV-46000 once monthly group the least squares mean change in SQLS from baseline was –3.99 (SE = 1.74) at early termination and –5.40 (SE = 1.12) at end of treatment.
Table 2: Summary of Key Results From Pivotal Study
Characteristics | Placebo | TV-46000 once monthly | TV-46000 Overall (once monthly and once every 2 months) |
|---|---|---|---|
Primary end point: Time to impending relapse (weeks) by treatment group (ITT analysis set) | |||
N | 181 | 183 | 362 |
Patients with impending relapse, n (%)a | 53 (29) | 13 (7) | 36 (10) |
Hazard ratio (95% CI)b | — | 0.200 (0.109 to 0.367) | 0.283 (0.184 to 0.435) |
Log-rank test P value | — | < 0.0001c | < 0.0001 |
Proportional hazards test P valued | 0.7251 | — | — |
Key secondary end points | |||
Time to impending relapse (eITT analysis set) | |||
N | 181 | 183 | 363 |
Hazard ratio (95% CI) | — | — | 0.291 (0.190 to 0.446) |
P valuee | — | — | P < 0.0001 |
Impending relapse rate at week 24 (ITT analysis set) | |||
N | 181 | 183 | 362 |
Observed impending relapse rate at week 24 (95% CI) | 0.28 (0.205 to 0.347) | 0.07 (0.03 to 0.109) | 0.09 (0.059 to 0.123) |
Observed difference in impending relapse rates | — | –0.21 (–0.288 to –0.125) | –0.18 (–0.263 to –0.106) |
P value | — | < 0.0001 | < 0.0001e |
Percentage of patients with schizophrenia that remained stable at end point (ITT analysis set) | |||
N | 181 | 183 | 362 |
Overall Stability at end point, n (%)f | 110 (61) | 159 (87) | 302 (83) |
CMH P value | — | < 0.0001 | < 0.0001e |
Breslow and Day homogeneity P value | — | 0.9550 | 0.9338 |
Percentage of patients achieving remission at end point (ITT analysis set) | |||
N | 181 | 183 | 362 |
Percentage of patients achieving remission at end point (%) | 23 | 29 | 30 |
P value | — | — | P = 0.1214g |
Observed rate of impending relapse at end point (ITT analysis set)h | |||
N | 181 | 183 | 362 |
Observed rate of impending relapse at end point | 29% | 7% | 10% |
DAI-10 (ITT analysis set)h | |||
N | 181 | 183 | 362 |
Change from baseline in DAI-10 total score at early termination, LS mean (SE) | –0.55 (0.38) | 0.25 (0.42) | — |
Change from baseline in DAI-10 total score at end of treatment, LS mean (SE) | –0.59 (0.31) | 0.57 (0.28) | — |
SQLS (ITT analysis set)h | |||
N | 181 | 183 | 362 |
Change from baseline in SQLS total score at early termination, LS mean (SE) | 3.20 (1.58) | –3.99 (1.74) | — |
Change from baseline in SQLS total score at end of treatment, LS mean (SE) | 1.14 (1.32) | –5.40 (1.12) | — |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; DAI-10 = Drug Attitude Inventory 10-Item Version; eITT = extended intention to treat; ITT = intention to treat; LS = least squares; SE = standard error; SQLS = Schizophrenia Quality of Life Scale.
aA patient may have been counted in more than 1 relapse criterion.
bThe hazard ratio (95% CI) coming from the stratified Cox proportional hazard model, with treatment (placebo, TV-46000 once monthly and TV-46000 once every 2 months., or placebo and TV-46000 overall [including once monthly and once every 2 months]) as an exploratory variable and sex-dose as a stratification factor, and the stratified log-rank test P value (sex-dose as a stratification factor) refer to the comparison of TV-46000 with placebo.
cThe P values refer to the analyses of primary end points.
dThe proportional hazards test P value tests the overall proportional hazard assumption for the primary model.
eStatistical significance was met, and the next secondary end point was tested.
fStability is defined as meeting all of the following criteria for at least 4 consecutive weeks: outpatient status; Positive and Negative Syndrome Scale (PANSS) total score of 80; minimal presence of specific psychotic symptoms on the PANSS, as measured by a score of 4 on conceptual disorganization, suspiciousness, hallucinatory behaviour, and unusual thought content, each; Clinical Global Impression–Severity score of 4 (moderately ill); and Clinical Global Impression–Severity of Suicidality score of 2 (mildly suicidal) on part 1 and 5 (minimally worsened) on part 2 of the scale. The percentage was calculated as the number of patients who maintained stability at end point divided by the number of patients in each treatment group, using the last valid patient assessment as the end point. The patient population was limited to those treated with the investigational medicinal product for at least 4 weeks. The P value was from the CMH test adjusted for stratification factor of sex-dose for each pairwise comparison vs. placebo; P value of Breslow and Day test for homogeneity is also presented. Breslow and Day homogeneity test accompanies the results; its goal is to assess whether all the strata have the same odds ratio of patients maintaining stability at end point.
gThe difference did not reach statistical significance; therefore, the rest of the key secondary end points are descriptive.
hStatistical comparison was not performed because a previous end point in the hierarchy did not reach statistical significance.
Source: RISE Clinical Study Report.15
Harms Results (RISE and SHINE Studies)
The most commonly reported AE was injection site pain, with 5% of patients in the TV-46000 once monthly group and 6% in the placebo group reporting injection site pain. Another commonly reported AE was injection site nodule, reported by 6% of patients in the TV-46000 once monthly group and 3% in the placebo group. Serious AEs were reported by 4% in the TV-46000 once monthly group and 8% in the placebo group. AEs leading to treatment discontinuation were reported by 11% of patients in the TV-46000 once monthly group and 11% in the placebo group.
Critical Appraisal
The RISE and SHINE studies were phase III studies. The RISE study was a randomized, double-blind, placebo-controlled study and the SHINE study was a randomized, parallel-group study that allowed rollover enrolment from the RISE study. Limitations included the high number of protocol deviations, although the sponsor did note that sensitivity analyses were conducted in response to a request from the FDA regarding the protocol deviations. These sensitivity analyses indicated that the original results were robust. The primary end point of time to impending relapse was met by the once-monthly dosing group in comparison to placebo, as were several secondary end points. However, due to the hierarchal statistical testing in place to reduce the risk of type I error, important outcomes, such as health-related quality of life (HRQoL), were not statistically tested and thus no conclusions can be drawn with regard to the effect of risperidone ER once monthly on HRQoL.
According to the clinical expert consulted, the patient populations in the RISE and SHINE studies appear to be similar to the expected population of adult patients with schizophrenia in Canada; therefore, results should be generalizable to the population in Canada. The RISE and SHINE studies were conducted with patients with schizophrenia stabilized with oral risperidone treatment. While the clinical expert did not expect this to differ from the expected usage of risperidone ER, this is a more restricted population than that described in the indication and thus the generalizability of the study results to the broader indication is uncertain.
Indirect Comparisons
Description of Studies
A systematic literature review (SLR) and network meta-analyses (NMAs) were conducted to synthesize relevant literature and compare the efficacy and safety of risperidone ER (TV-46000) once monthly and once every 2 months with atypical LAIs approved in Canada and used for the maintenance treatment of schizophrenia. A total of 6 studies (including the RISE study) were eligible for inclusion in the NMA. Efficacy outcomes were relapse rate, time to relapse, and change in Personal and Social Performance (PSP) scale score. These outcomes were reported in 5 of the studies and include all interventions of interest within the network. Safety outcomes were AE-related discontinuation, significant weight gain, treatment-related AEs, and injection site pain. AE-related discontinuation and significant weight gain were reported in all the included studies. Treatment-related AEs were reported in 4 of the studies and injection site pain in 5 of the studies. Relative risk (RR) was used for the dichotomous outcome NMAs relapse rate at 6 months, AE-related discontinuation, significant weight gain, treatment-related AEs, and injection site pain. HR was used for the survival data NMA of time to relapse. Lastly, mean difference was used for the continuous outcome NMA of change from baseline in PSP scale score.
Efficacy Results
Relapse Rate at 6 Months
All active treatments, that is, TV-46000 once monthly, aripiprazole, paliperidone palmitate 1-month formulation (PP1M) 25 mg equivalent (EQ) to 100 mg EQ, paliperidone palmitate 3-month formulation (PP3M), TV-46000 once every 2 months, and PP1M 50 mg EQ to 150 mg EQ, were comparable and were significantly better than placebo.
Time to Relapse
All active treatments, that is, TV-46000 once monthly, aripiprazole, PP1M 25 mg EQ to 100 mg EQ, PP3M, TV-46000 once every 2 months, and PP1M 50 mg EQ to 150 mg EQ, were significantly better than placebo.
Change in Personal and Social Performance
All active treatments (i.e., TV-46000 once monthly, aripiprazole, PP1M 25 mg EQ to 100 mg EQ, PP3M, TV-46000 once every 2 months, and PP1M 50 mg EQ to 150 mg EQ) were comparable and significantly better than placebo.
Harms Results
AE-Related Discontinuation
TV-46000 once monthly and once every 2 months were comparable to PP1M and placebo.
Significant Weight Gain
TV-46000 once monthly, PP1M 25 mg EQ to 100 mg EQ, and TV-46000 once every 2 months were comparable to placebo and significantly better than both PP3M and PP1M 50 mg EQ to 150 mg EQ.
Treatment-Related AEs
PP1M 25 mg EQ to 100 mg EQ, TV-46000 once monthly, and TV-46000 once every 2 months were comparable to placebo. PP1M 25 mg EQ to 100 mg EQ, TV-46000 once monthly, and placebo were significantly better than PP3M and PP1M 50 mg EQ to 150 mg EQ. PP1M 25 mg EQ to 100 mg EQ and placebo were significantly better than PP1M 50 mg EQ to 150 mg EQ.
Injection Site Pain
All active treatments, that is, TV-46000 once monthly, aripiprazole, TV-46000 once every 2 months, PP3M, and PP1M, were comparable to placebo. Aripiprazole was significantly better than PP3M and PP1M.
Critical Appraisal
The sponsor-submitted indirect treatment comparison (ITC) was based on a well-described and appropriate SLR. The comparators in the included studies were appropriate to inform decision-making in the Canadian context. The outcomes included were appropriate; the exception was HRQoL, which was excluded for reasons of data availability. The baseline characteristics of the included studies were similar; the main differences were the older patient population and slightly higher Positive and Negative Syndrome Scale (PANSS) scores in the RISE study. However, the direction of bias introduced by these differences is unknown. Additional uncertainty results from the unknown censoring methodologies in the studies and the impact of these differences on the proportional hazard assumption.
Cost Information
At the submitted price of $456.18 for the 50 mg, 75 mg, 100 mg, and 125 mg doses, the annual drug cost of monthly risperidone ER (Longavo) is $5,930 per patient, with an annual administration cost of $51. Annual drug costs for the injectable comparators ranged from $2,394 to $9,939, with annual administration costs ranging from $17 to $101. The incremental cost of risperidone ER once monthly ranged from a savings of $4,060 annually to an additional cost of $3,486 annually, per patient, compared to risperidone 50 mg and 12.5 mg once every 2 weeks, respectively.
The sponsor’s cost comparison was associated with limitations including uncertainty in the assumption of clinical similarity between comparators and the exclusion of oral risperidone tablets as a comparator. The annual cost of risperidone ER is $5,486 to $5,634 more expensive than that of risperidone tablets ($297 to $444 per patient), not considering administration costs, or $5,537 to $5,685 per patient per year more expensive when administration costs are included. All incremental costs or savings are based on publicly available list prices and may not reflect actual prices paid by public drug plans in Canada.
Conclusions
Based on the summary of clinical evidence submitted by the sponsor, treatment with risperidone ER (TV-46000) once monthly showed statistically significant improvements in time to impending relapse compared to placebo. Conclusions on the effect of risperidone on HRQoL cannot be drawn because of the lack of statistical testing. The safety of the once-monthly dosing regimen appears to be consistent with the safety profile of oral and LAI risperidone once every 2 weeks The results of the submitted ITC, despite the methodological limitations, appear to be aligned with the clinical expert’s expectation that risperidone ER will have a similar clinical benefit to that of other LAI therapies used to treat schizophrenia in Canada. The inclusion of the long-term SHINE study, which allowed rollover of patients from the original RISE study, is aligned with the expected use of risperidone for long-term relapse avoidance.
At the submitted price, the annual drug cost of monthly risperidone ER is $5,930 per patient, with an annual administration cost of $51. When used once monthly, the incremental cost of risperidone ER ranged from an annual savings of $4,060 to an additional annual cost of $3,486 per patient compared to risperidone 50 mg and 12.5 mg once every 2 weeks, respectively. The sponsor’s cost comparison was associated with limitations including uncertainty in the assumption of clinical similarity between comparators and the exclusion of oral risperidone tablets as a comparator. The annual cost of risperidone ER is $5,537 to $5,685 per patient more expensive than oral risperidone tablets when administration costs are included. All incremental costs or savings are based on publicly available list prices and may not reflect actual prices paid by public drug plans in Canada.
Introduction
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CDA-AMC review team.
Schizophrenia is a major severe, chronic, and disabling psychiatric syndrome. Schizophrenia represents a heterogeneous group of disorders that may differentially affect presentation, course, treatment response, and outcome.1-3 The onset of schizophrenia typically occurs during middle to late adolescence or early adulthood. The diagnosis is based on specific signs and symptoms that prevent reality-based judgment.16,17 The most recent updated diagnostic criteria are defined in the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) (DSM-5).16,18 Schizophrenia is associated with hallucinations, delusions, cognitive impairment, disorganized thoughts, social withdrawal, and amotivation.10 Schizophrenia symptoms are often categorized as being either positive or negative.11 The positive symptoms reflect a distortion or abundance of normal functions (e.g., delusion, conceptual disorganization, hallucinatory behaviour); the negative symptoms reflect a loss or restriction of normal functioning (e.g., blunted affect, emotional withdrawal, poor rapport).4-6 Patients with schizophrenia are at an increased risk for death by suicide and substance use, homelessness, and unemployment.7,8 The Global Burden of Disease study reported that the age-standardized point prevalence of schizophrenia was 0.28% in 2016, with little variation across countries or regions.19 The prevalence of schizophrenia in Canada in 2016 was estimated to be approximately 0.95% of the population.9 The incidence of schizophrenia in Canada in 2016 was estimated to be approximately 49 per 100,000, including 41 per 100,000 in females and 58 per 100,000 in males.9 In 2018, schizophrenia was 1 of the top 20 causes of disability worldwide.18 Despite its low prevalence, the health, social, and economic burdens of schizophrenia are tremendous, not only for patients, but also for families, caregivers, and the wider society.20
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CDA-AMC review team.
Antipsychotic medications form the cornerstone of treatment for schizophrenia as they target the characteristic symptoms.4,10,11 The underlying principles for the administration of pharmacotherapy include the individualization of medication (including patient preferences), simple medication regimens, appropriate dosing, attention to side-effect profiles, and regular evaluation of responses (including AEs) and short- and long-term clinical efficacy, safety, and tolerability.8 The choice of antipsychotic medication should be made by the patient and physician together, taking into account caregivers’ views where appropriate.3 According to the clinical expert consulted by CDA-AMC, the medications are in oral and parenteral formulations and treat the positive symptoms of psychosis. The negative and cognitive symptoms, which are the most impairing for long-term function, have no approved medication treatments.
Based on input from the clinical expert consulted by CDA-AMC for this review, the ideal medication for schizophrenia would reduce both positive and negative symptoms, have rapid onset of action, would have minimal adverse effects, and be given once daily by mouth or monthly (or less often) as an injectable treatment. This medication would also be associated with improved daily function (such as improved social and occupational activities) and quality of life.
Existing antipsychotic therapies fall into 1 of 2 classes. The typical antipsychotics (also known as conventional antipsychotics or neuroleptics) are the first-generation antipsychotic class. These drugs have antagonistic activity at dopamine type 2 (D2) receptors21 and are associated with an increased incidence of EPS side effects.8 The second-generation or atypical antipsychotics (AAPs) have antagonistic activity at both D2 receptors and serotonin type 2A (5-HT2A) receptors. The risk of EPS incidence appears to be lower with AAPs, but differences between typical antipsychotics and AAP drugs can vary in this respect.22 Both typical antipsychotic and AAP classes are considered equally effective in the treatment of positive symptoms. However, treatment with AAPs increases the risk of weight gain and metabolic side effects.8
Risperidone, aripiprazole, and paliperidone belong to the AAP class of antipsychotic therapies.
One major obstacle to the effective treatment of schizophrenia is nonadherence to medication, resulting in cycles of relapse.12,13 Studies have found that continuing treatment with LAI antipsychotic preparations in clinical practice outperforms oral antipsychotic medication in preventing rehospitalization.14
LAI antipsychotics are usually used for patients with schizophrenia who have a history of good response to an oral antipsychotic but have adherence barriers.23 The 2021 American Psychiatric Association practice guidelines suggest that patients receive treatment with an LAI antipsychotic medication if they prefer such treatment or if they have a history of poor or uncertain adherence.18 The 2017 Canadian guidelines for schizophrenia pharmacotherapy recommend that LAIs be used earlier in the course of treatment and should not be restricted to only those patients who experience difficulty with adherence.3
In Canada, existing long-term atypical antipsychotic medications may be given as an intramuscular injection every 2 weeks to every 3 months, depending on the medication (Table 3).24 The LAI AAPs available in Canada include risperidone LAI (intramuscular, every 2 weeks),25 aripiprazole LAI (intramuscular, monthly),26 paliperidone LAI (intramuscular, monthly),27 and paliperidone LAI (intramuscular, every 3 months)28 (refer to Table 3). The Canadian guidelines for schizophrenia pharmacotherapy recommend that after a change of antipsychotic medication in response to acute exacerbation of schizophrenia, the medication should be continued for at least 4 weeks unless there are significant safety issues. If a partial response is observed at 4 weeks, the medication should be reassessed at 8 weeks unless there are significant safety concerns.3 Following resolution of positive symptoms of an acute episode of schizophrenia, patients should be offered antipsychotic maintenance treatment for up to 5 years or longer.3
Drug Under Review
Risperidone ER injectable suspension (Longavo, or TV-46000), prefilled syringe, 50 mg, 75 mg, 100 mg, and 125 mg, subcutaneous injection was approved by Health Canada in March 2024.29 Risperidone ER is indicated for the treatment of schizophrenia in adults.29 Like other AAPs, the exact mechanism of risperidone ER is unclear. The effect on schizophrenia could be mediated through a combination of D2 and 5-HT2 receptor antagonism. In addition, risperidone has a high affinity for alpha-adrenergic receptors. Antagonism at receptors other than D2 and 5-HT2 may explain some of the other effects of risperidone. Risperidone does not bind to dopamine type 1 (D1) and has no affinity (when tested at concentrations > 10 M to 5 M) for muscarinic cholinergic receptors.29
The Health Canada–recommended dose is once monthly — 50 mg, 75 mg, 100 mg, or 125 mg — by abdominal or upper arm subcutaneous injection. No loading dose is required. Similar to oral risperidone, risperidone LAI monthly, and other LAI AAPs, the main safety concern is increased mortality among older patients with dementia. Health Canada has not authorized risperidone ER for pediatric use.29 Risperidone ER should be administered only by a health care professional.
Risperidone tablets have been approved for the treatment of schizophrenia in Canada since 1993.30 Risperidone LAI for intramuscular administration every 2 weeks has been approved for the treatment of schizophrenia in Canada since 2004.31 The oral risperidone and risperidone LAI intramuscular, once every 2 weeks, have not been previously reviewed by CDA-AMC. Risperidone ER once monthly was reviewed by CADTH in 2021. Risperidone ER once monthly is a new formulation of risperidone.
The objective of this report is to review the beneficial and harmful effects of risperidone for ER injectable suspension, prefilled syringe, subcutaneous injection for the treatment of schizophrenia in adults.
Table 3: Key Characteristics of Risperidone and Other LAIs
Items | Risperidone | Aripiprazole | Paliperidone palmitate | ||||
|---|---|---|---|---|---|---|---|
ER | LAI | ORAL | |||||
Longavo | Perseris29 | Risperdal Consta25 | Oral32 | Abilify Maintena, IM)26 | Invega Sustenna, IM, monthly27 | Invega Trinza IM, every 3 months28 | |
Mechanism of action | Unclear. May be mediated through a combination of D2 and 5-HT2 receptor antagonism.a | A combination of D2 and 5-HT2 receptor antagonism.a | A combination of D2 and 5-HT2 receptor antagonism.a | A combination of D2 and 5-HT2 receptor antagonism.a | Unclear. May be mediated through a dose-dependent combination of partial agonist activity at D2 and 5-HT1A and antagonist activity at 5-HT2A receptors. | Unknown. May be mediated through a combination of D2 and 5-HT2A receptor antagonism. Antagonism at other receptors may explain some of the other effects. | Unknown. May be mediated through a combination of D2 and 5-HT2A receptor antagonism. Antagonism at other receptors may explain some of the other effects. |
Indicationb | For the treatment of schizophrenia in adults | For the treatment of schizophrenia in adults | For the management of schizophrenia | For the acute treatment and maintenance treatment of schizophrenia and related psychotic disorders | For the maintenance treatment of schizophrenia in stabilized adult patients | For the treatment of schizophrenia | For the treatment of schizophrenia in adult patients. Paliperidone palmitate, IM every 3 months is to be used only after paliperidone palmitate, IM monthly has been established as adequate treatment for at least 4 months |
Route of administration | Abdominal or upper arm SC injection | Abdominal SC injection | IM injection | Oral | IM injection | IM injection | IM injection |
Recommended dose | Once monthly: 50 mg, 75 mg, 100 mg, or 125 mg | Initial dose: risperidone ER at a dose of 90 mg or 120 mg once monthly by SC injection. Do not administer a loading dose. | 25 mg every 2 weeks | On a schedule of either once a day or twice a day, generally beginning with 1 mg to 2 mg per day. The dose should be adjusted gradually over several days based on the clinical response to a target dose of 4 mg to 6 mg per day. Some patients may benefit from lower initial doses or slower adjustment schedules. | 400 mg, once monthly | Initial dose: 150 mg on day 1 and 100 mg on day 8 (1 week later). Monthly maintenance dose: 75 mg (can be adjusted from 50 mg to 150 mg) | Initial dose: the equivalent 3.5-fold of a 1-month paliperidone palmitate dose. Following the initial dose, paliperidone palmitate should be administered every 3 months. If needed, the dose can be adjusted every 3 months in increments within the range of 175 mg to 525 mg based on individual patient tolerability and the efficacy of the medication. |
Serious side effects or safety issues | Increased mortality in older patients with dementia. | Increased mortality in older patients with dementia. | Increased mortality in older patients with dementia. | Increased mortality in older patients with dementia. | Increased mortality in older patients with dementia. | Increased mortality in older patients with dementia. | Increased mortality in older patients with dementia. |
D1 = dopamine type 1; D2 = dopamine type 2; ER = extended release; IM = intramuscular; LAI = long-acting injection; PP1M = paliperidone palmitate 1-month, PP3M = paliperidone palmitate 3-month; SC = subcutaneous; 5-HT1 = serotonin type 1; 5-HT2 = serotonin type 2.
aIn addition, risperidone has a high affinity for alpha-adrenergic receptors. Antagonism at receptors other than D2 and 5-HT2 may explain some of the other effects of risperidone. Risperidone does not bind to D1 receptors and has no affinity (when tested at concentrations > 10 M to 5 M) for muscarinic cholinergic receptors.
bHealth Canada indication.
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full original patient input received by CDA-AMC has been included in the Perspectives of Patients, Clinicians, and Drug Programs section of this report.
No patient input was received for this review.
Patient input received for a previous CADTH review (November 2021) on risperidone ER injectable suspension for the same indication is reported here.
About the Patient Groups and the Information Gathered
One patient group, IAM (formerly the Schizophrenia Society of Ontario), responded to the call for patient input for this Reimbursement Review. IAM is a solutions-driven organization that supports and drives change for better mental health.
IAM focuses on partnering and collaborating with communities to develop innovative mental health solutions. Historically serving those impacted by psychotic disorders such as schizophrenia and psychosis, IAM helps anyone affected by serious mental illness and their families, caregivers, and supports and their communities. IAM’s direct services include one-on-one and group counselling using cognitive behavioural therapy–based interventions, information and system navigation, training for front-line workers, community education, and more.
This submission was based on IAM’s 40-year history of serving adults with schizophrenia and other psychotic disorders and their families, service providers, and communities. Much of it came directly from IAM’s work with clients and the expertise of IAM front-line staff. IAM’s clients are primarily adults from the southern and central regions of Ontario, and include health service and social service providers who work with individuals with psychotic illnesses, including schizophrenia. A number of clients from northern regions of Ontario are served virtually.
IAM also drew on information from a survey of the IAM client network that was conducted by Ipsos in 2018. In the Ipsos survey, respondents self-described as personally diagnosed (12%), a caregiver (50%), a family member or friend of someone diagnosed (63%), or working in the social services (18%). Approximately 77% of survey respondents were born in Canada, and 83% described themselves as white. A total of 55% of respondents were from the Greater Toronto Area, while 20% were from southwestern Ontario, 14% from Eastern Ontario, 5% from Central Ontario, and 4% from Northern Ontario. An additional 2% came from outside Ontario.
The funding information for the patient group is included in the patient group input submission published on the CDA-AMC website.
Disease Experience
The IAM patient input submission included individuals with schizophrenia and other related disorders with psychosis as a main feature. It indicated that many of the patients experience symptoms of psychosis without having a formal diagnosis. Their symptoms often have a significant impact on day-to-day functioning. The patients’ experiences vary widely but typically involve some levels of cognitive impairment, delusions, and hallucinations. The cognitive impairment can range from being mild to severe, but is typically strongest in the cognitive domains of working and episodic memory, attention, processing speed, problem-solving, and social cognition. Many patients also experience anosognosia, a lack of insight into their condition, which often affects their ability and motivation to access treatment and supports. This symptom can cause significant strain on relationships, including those with caregivers and family members, ultimately leading to social isolation and a lack of supports for the individual with the condition.
Experience With Treatment
In the survey of the IAM client network, 55% of respondents were taking LAI medications or had taken them previously, while 98% were taking or had taken oral medications to manage their schizophrenia or psychosis symptoms. The most common side effects they reported were drowsiness (58%), dry mouth (50%), restlessness (50%), dizziness (45%), muscle stiffness (45%), constipation (43%), and anxiety (43%).
Of those taking LAI medications, the most common stated benefits were convenience and not needing to remember to take it every day. The most frequently described associated difficulties were pain at the injection site and the need for frequent travel to clinics.
While 63% of the IAM survey respondents said that they paid for their medications with government insurance, 23% paid out of pocket. A total of 63% of respondents agreed it is difficult to pay for health care bills, including medication, visits to specialists, counselling, and so forth.
Altogether 23% of respondents identified the cost of medications as a significant challenge to access. Other challenges identified included preferred medication not being covered by public drug programs (20%) and the wait times for approvals of certain medications under the Ontario Drug Benefit Exceptional Access Program and Health Canada Special Access Program (13%).
Patients expect new, quick, simple, convenient, and affordable access to a wide range of treatments and medications that suit their specific needs and allow for the highest level of daily functioning and symptom reduction while managing side effects, which could improve adherence.
Improved Outcomes
The patient group indicated that the right medication allows for the highest level of daily functioning while managing side effects. Finding this medication is often achieved through a process of trying several different medications and dosages to determine what works best. This trial-and-error process can make it difficult for patients to adhere to treatment. The process is exacerbated by additional challenges such as difficulty accessing psychiatrists, obtaining prescriptions, and understanding medication options; the cost of medications; and the wait times to access medications through public drug programs. When the right combination of therapy and medication is determined, individuals may still experience relapse and may require extensive supports to adhere to the treatment plan. This trial-and-error practice of finding the right medication for each individual would be improved by having quick, simple, and affordable access to a wide range of treatments and medications to suit unique needs.
Additional Information
The patient group indicated that the greater the variety and affordability of medications on the market, the easier it would be for patients with schizophrenia and psychosis to adhere to treatment and, by extension, have greater levels of recovery. IAM advocates for a wide selection of reimbursable medications in the Canadian marketplace.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug under review is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of schizophrenia.
Unmet Needs
The clinical expert noted that many aspects of schizophrenia treatment constitute an unmet need. In 15% to 20% of patients with schizophrenia, the disease does not respond to currently available treatments or it becomes refractory to current treatment options. Furthermore, none of the available treatments reverse the course of disease or improve negative or cognitive symptoms, which are correlated with poor functional outcomes. The clinical expert highlighted the need for better-tolerated treatments, noting the significant side effects. These side effects include, but are not limited to, sedation, weight gain, metabolic dysfunction, sexual side effects, motor side effects, and cognition-related and motivation-related problems. The clinical expert noted the need for treatments that improve adherence, including more convenient formulations, because many patients forget to take their oral medications.
Place in Therapy
The clinical expert noted that risperidone LAI does not differ from other LAI antipsychotics in reducing positive symptoms of schizophrenia and does not have a unique mechanism of action, and therefore would be used similarly to other LAI antipsychotics, often in the first-line or second-line setting.
Patient Population
The clinical expert suggested that all adult patients with schizophrenia would be eligible for treatment with risperidone LAI, and that risperidone LAI should be prescribed in a manner similar to that of other LAI antipsychotics prescribed for the treatment of schizophrenia.
Assessing the Response Treatment
The clinical expert noted that a 20% reduction in standard rating scale measures is usually considered adequate for a response; however, it was noted that most clinicians do not use standardized measures when assessing patients. The clinical expert suggested that, once schizophrenia symptoms have stabilized, relapse prevention is a key goal and noted that there is less variability in what constitutes a clinical relapse.
The clinical expert suggested that response should be assessed every 3 months initially, and then once a year or at key decision points thereafter.
Discontinuing Treatment
The clinical expert noted that lack of efficacy in treating symptoms of psychosis or intolerable side effects, including neurologic (e.g., EPS), metabolic, or sexual side effects that do not respond adequately to treatment strategies would result in discontinuation of treatment. Prolonged stability can suggest dose reduction, and in rare cases, discontinuation.
Prescribing Considerations
The clinical expert suggested that it is appropriate for general practitioners to prescribe risperidone LAI, noting that such prescriptions should not require a specialist. The clinical expert highlighted that treating psychosis early is paramount and that all general practitioners should be able to prescribe risperidone LAI without specialist supervision.
Additional Considerations
The clinical expert highlighted that increasing the number of treatment and formulation options available to patients would benefit them. The clinical expert noted that LAI medications have been shown to be superior to oral antipsychotics in relapse prevention. However, they are painful to receive. The clinical expert highlighted that longer-term LAI medications are not available for risperidone, reducing the options for patients with schizophrenia stabilized with oral risperidone treatment. A formulation that eliminates or reduces these barriers would be helpful.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups. The full original clinician group input(s) received by CDA-AMC have been included in the Perspectives of Patients, Clinicians, and Drug Programs section of this report.
No clinician group input was received.
Drug Program Input
The drug programs provide input on each drug being reviewed through CDA-AMC Reimbursement Review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
Other LAIs currently listed vary with regard to covered indications under the public drug plans. Some specifically state that they are covered for schizophrenia, plus or minus related psychotic disorders, and others do not specify the diagnosis needed for coverage. The sponsor’s request is that this be covered for adult patients with schizophrenia. As alluded to in the submission, this requires that the patient meet the diagnostic criteria for schizophrenia as detailed in the DSM-5. A diagnosis requires that the patient has continuous signs over a period of at least 6 months.
| Response from expert: The clinical expert noted that many patients present with schizophrenia spectrum disorders, so it would be beneficial to be able to prescribe to patients with schizophrenia spectrum disorders, including patients with a probable diagnosis. The clinical expert suggested that patients with brief psychotic disorder, substance use–induced psychotic disorder, and bipolar disorder would be unlikely to be prescribed risperidone. |
It is the sponsor’s intent that this be available for first-line use; however, that would misalign with other LAI criteria in various jurisdictions that require nonadherence to oral agents.
| The clinical expert highlighted that a treatment goal is to have patients receive LAIs if they can tolerate them because of the benefits of LAI over oral therapy. Therefore, the clinical expert did not support the requirement of nonadherence or intolerance before a patient could receive LAI risperidone. |
Listing criteria should be similar to that of Risperdal Consta, Invega Sustenna, Invega Trinza, and Abilify Maintena. | Note from the drug plans to inform CDEC deliberation. |
Considerations for prescribing of therapy | |
Dosing is to be done monthly or every second month. If there is relapse or inadequate symptom control on monthly dosing, would you expect that the dose frequency be increased (to every 3 weeks, for example)? | The clinical expert noted that there is no evidence to support increasing the frequency of dosing beyond the once monthly regimen. |
The sponsor noted that the dosing corresponds to the “the full range for maintenance treatment, as per oral risperidone product monograph.” Despite this, doses greater than 5 mg daily are seen in real-world practice with 1 reputable reference noting a maximum dose of 10 mg daily (8 mg max per single dose). It is unclear if patients who require greater than 5 mg oral daily will be eligible for this LAI. | The clinical expert noted that this is a small population of patients that may require more than 5 mg daily oral risperidone, and further noted the lack of evidence available to determine the benefit in these cases. |
In the case that they do receive the LAI, despite a maintenance oral risperidone dose > 5 mg daily, would it be expected that the dose be supplemented with oral risperidone? | While noting the difficulty of determining the appropriate management in this case, the clinical expert suggested they would supplement the patient with oral risperidone and then attempt to reduce the dose over time until the patient could be treated with LAI only. |
The RISE trial included patients stabilized on oral risperidone for 12 weeks before switching to the new LAI.
| The clinical expert noted that in the real-world setting, 4 to 8 weeks is an adequate time period to determine whether the patient will tolerate the treatment. As per the RISE study protocol, the oral conversion and stabilization stage 1 of the study was a total of 12 weeks. Patients had to be stabilized for 4 consecutive weeks. |
Although the study drug comes in a prefilled subcutaneous syringe, it does still require administration by a health care provider, as preparation for injection involves some professional skills. For example, it is a viscous solution that requires forceful motions when prepping the injection and also creates resistance during the injection administration. It is important to consider ease of access to health care professionals when determining eligibility for this medication. | Note from drug plans to inform CDEC deliberation. |
It is not uncommon to see various combinations of antipsychotic medications being used to treat patients.
| The clinical expert suggested that questions regarding the use of risperidone LAI in combination with other drugs should be handled in a manner similar to other LAI drugs. |
Care provision issues | |
This medication requires administration by a health care provider, and it also requires refrigeration until 30 minutes before administration. | Note from the drug plans to inform CDEC deliberations. |
System and economic issues | |
The 150 mg, 200 mg, and 250 mg PFS are double the price of the lower strengths. However, these 3 doses are only intended to be administered every 2 months, making them the same overall price as the lower strengths that are administered every month. Of note, the 100 mg PFS can also be dosed every 2 months (in lieu of 50 mg monthly), making the price of dosing 100 mg every 2 months half that of 50 mg monthly. The sponsor noted that the expected bimonthly use of the 100 mg dose is approximately 1%, so they only considered 100 mg monthly dosing for the purposes of their BIA. Comparably, the price of Consta increases with increased dose, despite frequency being maintained at every 2 weeks. In the sponsor’s BIA they expected that their LAI will displace market share differently in each province based on current usage of comparator treatments. Note Risperdal Consta is not a benefit in the Northwest Territories, and the 12.5 mg dose is not a benefit in Alberta. When comparing costs of the comparators (Risperdal Consta, Invega Sustenna/Trinza, and Abilify Maintena) the sponsor used dosing as recommended in each product monograph; however, in the real world, there are patients who require increased dosing or increased frequency of dosing, and these are not accounted for in the analysis. The sponsor anticipates a cumulative cost savings of $14,523,251 over 3 years. | Note from the drug plans to inform CDEC deliberation. |
Confidential pricing agreements are likely for Risperdal Consta, and they exist for Invega Sustenna, Invega Trinza, and Abilify Maintena. It is difficult, then, to directly compare the overall costs of using these previously listed options with the new risperidone LAI. | Note from the drug plans to inform CDEC deliberation. |
BIA = budget impact analysis; CDEC = Canadian Drug Expert Committee; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition); LAI = long-acting injectable; PFS = prefilled syringe.
Sponsor’s Summary of Clinical Evidence
Note that the clinical evidence summarized in this section was prepared by the sponsor in accordance with the CADTH tailored review process and has not been modified by CADTH.
Pivotal Studies
Table 5: Details of Included Studies
Characteristics | RISE | SHINE |
|---|---|---|
Study design | Phase 3, multicenter, randomized, double-blind, placebo-controlled study | Phase 3, multicenter, randomized, double-blind, parallel-group study |
Locations | 66 centers in the US and Bulgaria | 60 centers in the US and Bulgaria |
Patient enrolment dates | 01 Jun 2018 to 03 Dec 2020 | 17 April 2019 to 02 Dec 2021 |
Randomized (N) | 544 | 336 |
Inclusion criteria |
| Roll-over Patients from RISE Study
New Patients
|
Exclusion criteria |
|
|
Intervention | Stage 1: Oral risperidone 2-5 mg/d (max of 4 mg/d for adolescents) Stage 2: TV-46000 q1m SC injection, TV-46000 q2m SC injection TV-46000 dose for each patient was comparable to the patient’s oral dose in Stage 1 | Stage 1: Oral risperidone 2-5 mg/d (max of 4 mg/d for adolescents) Stage 2: TV-46000 q1m SC injection, TV-46000 q2m SC injection Roll-over patients began the study with the maintenance stage and continued the same dosing frequency. For new patients and roll-over patients who received placebo in RISE, TV-46000 dose for each patient was comparable to the patient’s oral dose in Stage 1. |
Comparator(s) | Stage 1: Oral risperidone 2-5 mg/d (max of 4 mg/d for adolescents) Stage 2: Placebo q1m SC injection | N/A |
Phase | ||
Run-in | Screening: 4 weeks Oral conversion & stabilization (Stage 1): 12 weeks | Screening: Up to 4 weeks Oral conversion & stabilization (Stage 1): 12 weeks |
Double-blind | Relapse prevention (Stage 2): Open-ended, variable length (up to 108 weeks) | Relapse prevention (Stage 2): Up to 56 weeks |
Follow-up | Study Exit: 8 weeks (note: eligible patients were offered to continue treatment by enrolling in SHINE) | Follow-up: 8 weeks |
Primary end point | Time to impending relapse | Frequency of all AEs, including serious AEs |
Secondary and exploratory end points | Key secondary endpoints:
Exploratory end points:
| Exploratory endpoints:
|
Publications | Publications: N/A ClinicalTrials.gov ID: NCT03503318 | Publications: N/A ClinicalTrials.gov ID: NCT03893825 |
AE=adverse event; BMI=body mass index; CGI-I= Clinical Global Impression – Improvement Scale; DAI-10=Drug Attitudes Inventory 10-Item Version; DSM-5=Diagnostic and Statistical Manual 5th Edition; ED=emergency department; EQ-5D-5L=5-Level EuroQol Five Dimensions Questionnaire; HBSAg= hepatitis B surface antigen; HIV= human immunodeficiency virus; PANSS=Positive and Negative Syndrome Scale; PFS=Pre-filled syringe; PSP= Personal and Social Performance scale; q1m=once monthly; q2m=once every 2 months; QoL=quality of life; RCT = randomized controlled trial; SQLSS=Schizophrenia Quality of Life Scale; US=United States
Sources: RISE CSR15; SHINE CSR33
Description of Studies
RISE
The RIsperidone Subcutaneous Extended-release (RISE) study (or Study TV46000-CNS-30072) was a Phase 3, multicenter, randomized, double-blind, placebo-controlled, relapse prevention study of TV-46000 for schizophrenia in adults and adolescents. The objective was to assess the efficacy, safety, and tolerability of 2 dose regimens of TV-46000 (risperidone extended-release injectable suspension; [Longavo]) given subcutaneously (SC) vs placebo as maintenance therapy for patients with schizophrenia. This study was conducted in the United States (US) and Bulgaria with initiation on April 27, 2018 and finalization on November 24, 2020.
The study consisted of a screening period and an oral conversion and stabilization period (Stage 1), a double-blind maintenance period (baseline + Stage 2), and a follow-up period. After the screening period (up to 4 weeks), patients’ medication therapy was converted to oral risperidone (2-5 mg daily; maximum of 4 mg daily for adolescents) during Stage 1 to ensure that they were able to tolerate risperidone and that the dose was sufficient to treat positive symptoms. During this stage, patients who were already treated with risperidone were stabilized with oral risperidone (2-5 mg daily; maximum of 4 mg daily for adolescents). Stabilization on oral risperidone was assessed at baseline prior to randomization.
Patients meeting randomization criteria were randomized in a 1:1:1 ratio to treatment with TV-46000 once monthly (q1m), TV-46000 once every 2 months (q2m), or placebo q1m, each of which were administered SC. The TV-46000 dose was comparable to the oral dose on which the patient was stabilized in Stage 1. Maximum doses of TV-46000 were comparable to 4-mg daily for adolescents and 5-mg daily for adults. During Stage 2, the study continued on an outpatient basis, and telephone contacts took place weekly between clinic visits. The double-blind maintenance stage varied in duration, with patients continuing until one of the following occurred: 1) relapse, 2) study discontinuation or withdrawal criteria were met; 3) remained relapse-free during the double-blind phase until study termination. TV-46000 and matching placebo were administered by SC injection to the abdomen (right or left of the umbilicus) or to the upper arm.
Figure 1: RISE Study Schematic Overview and Conversion Table From Oral Risperidone
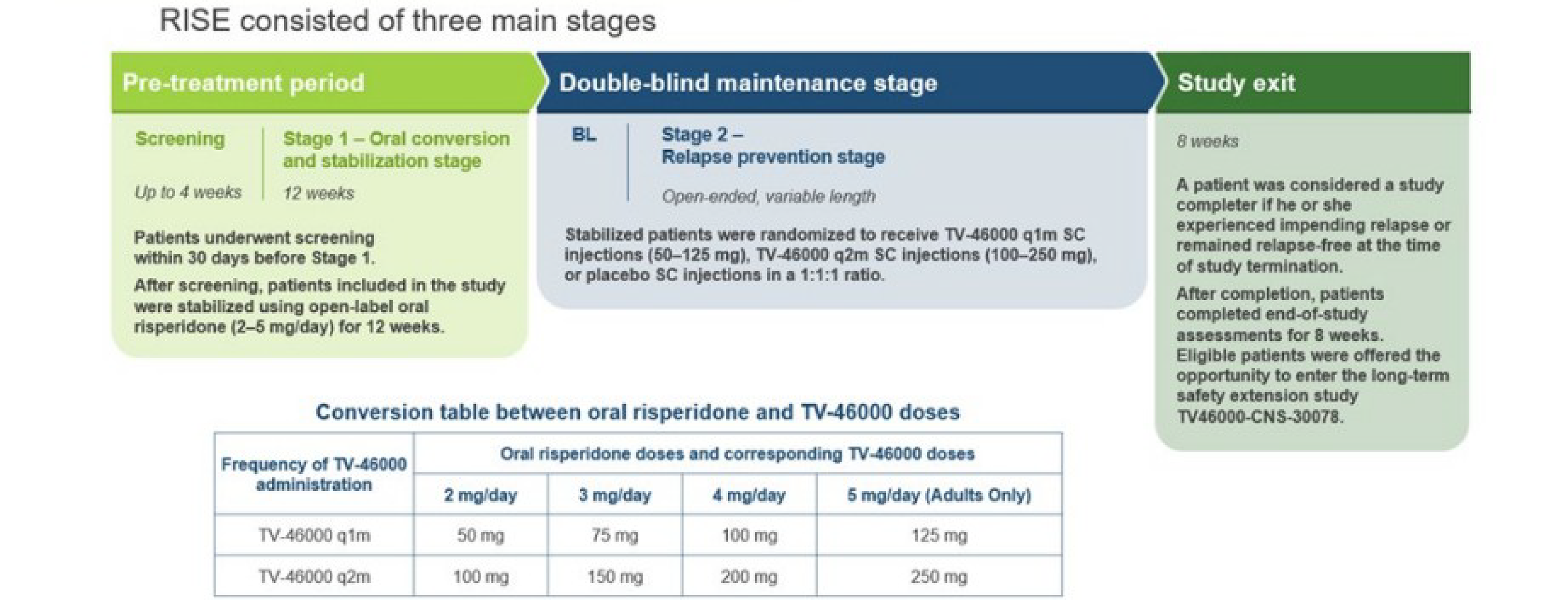
q1m = once monthly; q2m = once every 2 months; SC = subcutaneous
Source: Adapted from RISE CSR15
SHINE
The Safety in Humans of TV-46000 SC INjection Evaluation (SHINE) study (or Study TV46000-CNS-30078) was a Phase 3, multicenter, randomized, double-blind, parallel-group study to evaluate the long-term safety, tolerability, and effectiveness of TV-46000 administered q1m or q2m at doses of 50 to 250 mg SC (comparable to 2 to 5 mg/day of oral risperidone) for up to 56 weeks in adult and adolescent patients with schizophrenia (n=334 patients were randomized and treated). This study began in April 2019 and was completed in December 2021.
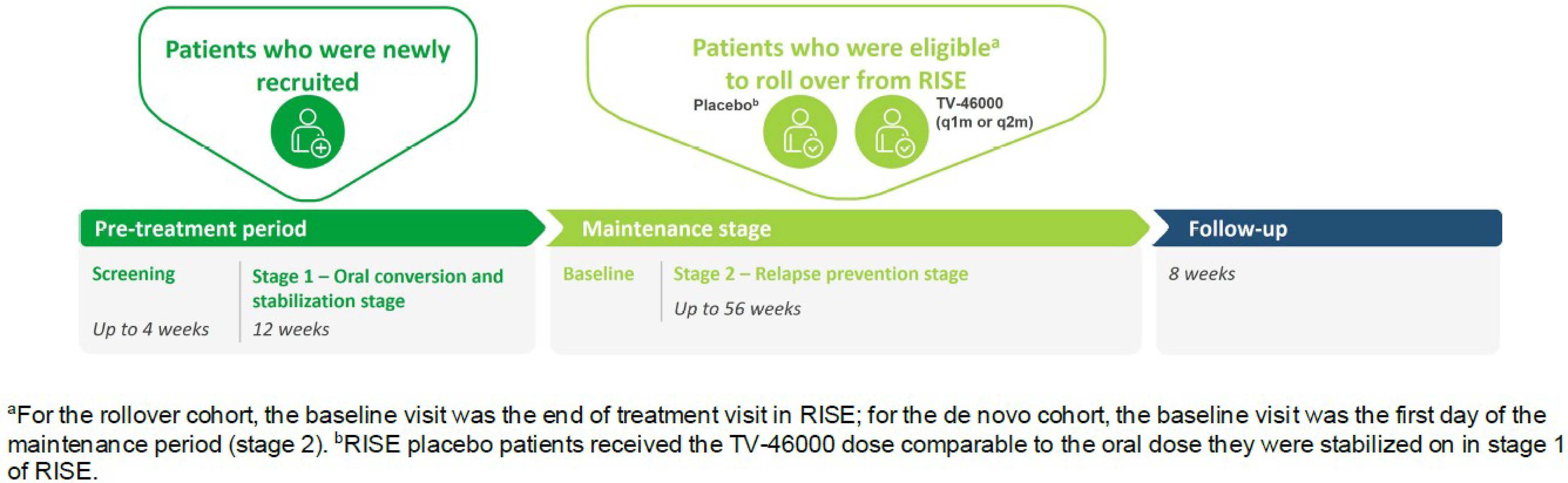
For new patients (who did not participate in the RISE study), the SHINE study consisted of a screening period (up to 4 weeks), a conversion/stabilization stage (12 weeks on oral risperidone, Stage 1), a double-blind, active-treatment maintenance stage (up to 56 weeks; Stage 2), and a follow-up period (8 weeks, Figure 2). New patients underwent screening procedures/assessment within 4 weeks before the start of Stage 1. At Stage 1, new patients on any oral antipsychotic except clozapine who could benefit from conversion to oral risperidone based on the investigator’s judgment were offered oral risperidone (dose of 2 to 5 mg daily) to stabilize the patients on treatment. Oral risperidone therapy continued for 12 weeks to ensure tolerability and that doses were adequate to treat positive symptoms for new patients.
At the baseline visit, new patients who met the stability criteria were randomized 1:1 to receive TV-46000 q1m or TV-46000 q2m SC at the dose comparable to the oral dose on which their disease was stabilized during Stage 1 (Figure 2). The same conversion from oral risperidone to TV-46000 for SC administration as used in the RISE study (Figure 1) was used in the SHINE study. In SHINE, the study drug was provided in ready-to-use, 1-mL Luer lock pre-filled syringe (PFS).
Unlike new patients, roll-over patients began the study at Stage 2. Roll-over patients who were treated with TV-46000 q1m or q2m SC during the RISE study continue their assigned dose from that study. Roll-over patients who were treated with placebo during RISE were randomized in a 1:1 manner to receive TV-46000 q1m or q2m SC injections at the TV-46000 dose comparable to the oral dose on which they were stabilized in Stage 1 of RISE.
During Stage 2, new and roll-over patients continued the study on an outpatient basis. Patients who completed all scheduled visits underwent early termination or end of treatment procedures and assessments at 4 and 8 weeks following the last TV-46000 dose in Stage 2.
Populations
Inclusion and Exclusion Criteria
RISE
The study included adults and adolescents with schizophrenia who had responded to antipsychotic treatments. Key inclusion and exclusion criteria are included in Table 5. In addition to the eligibility criteria to enter screening for the study, the following randomization criteria had to be fulfilled at the baseline visit before randomization:
No mental or physical deterioration that would have prevented participation in the study, per investigator judgment
Good compliance in following protocol requirements during Stage 1
Stabilized on oral risperidone therapy (i.e., met the following 4 criteria for ≥4 consecutive weeks before the baseline visit):
Outpatient status
Positive and Negative Syndrome Scale (PANSS) total score ≤80 and key PANSS items scores ≤4
Clinical Global Impression-Severity (CGI-S) score ≤4 (moderately ill)
Clinical Global Impression-Severity of Suicidality (CGI-SS) score ≤2 (mildly suicidal) on part 1 and ≤5 (minimally worsened) on part 2
SHINE
Eligible female and male patients with schizophrenia who did not experience a relapse and completed the RISE study (i.e., roll-over patients) and eligible new patients (i.e., those who did not participate in RISE) could enter this long-term study.
The specific key inclusion and exclusion criteria are outlined in Table 5. In addition to the eligibility criteria to enter screening for the study, the following randomization criteria had to be fulfilled by new patients at the baseline visit before randomization:
No mental or physical deterioration
Good compliance in following protocol requirements during Stage 1 (noncompliance was defined as total compliance <80% during Stage 1)
Stability of disease for ≥4 weeks as judged by:
Outpatient status
PANSS total score ≤80
Minimal presence of specific psychotic symptoms on PANSS (as measured by a score ≤4 on each of the following items: conceptual disorganization, suspiciousness, hallucinatory behavior, and unusual thought content)
CGI-S score ≤4
CGI-SS score ≤2 in Part 1 and ≤5 in Part 2
Baseline Characteristics
RISE
Baseline patient characteristics and demographics were generally well balanced across treatment groups. The mean age was approximately 49 years, 39% of patients were female, and 37%-39% were white. On average, patients in each group had schizophrenia for approximately 20 years, and the mean time since the last relapse was approximately 10 months.
Table 6: Summary of Baseline Characteristics in RISE
Characteristics | Placebo (N=181) | TV-46000 q1m (N=183) | TV-46000 q2m (N=180) |
|---|---|---|---|
Age, years, mean (SD) | 49.2 (11.43) | 50.6 (10.30) | 48.1 (11.09) |
Male, n (%) | 110 (61) | 112 (61) | 110 (61) |
Race, n (%) White Black or African American Asian Native Hawaiian or other Pacific Islander Not reported Other | 68 (38) 104 (57) 4 (2) 1 (<1) 2 (1) 2 (1) | 72 (39) 108 (59) 1 (<1) 1 (<1) 1 (<1) 0 | 66 (37) 110 (61) 2 (1) 0 0 2 (1) |
BMI, kg/m2, mean (SD) | 29.47 (5.10)* | 28.89 (4.87) | 29.72 (5.23) |
Oral risperidone at randomization, n(%) 2 mg 3 mg 4 mg 5 mg | 61 (34) 30 (17) 68 (38) 22 (12) | 47 (26) 46 (25) 68 (37) 22 (12) | 60 (33) 32 (18) 67 (37) 67 (37) |
Disease length, years, mean (SD) | 20.6 (12.21) | 22.9 (11.86) | 18.9 (12.31) |
Time since last relapse, months, mean (SD) | 10.5 (6.80) | 9.7 (6.67) | 10.2 (7.48)* |
Score at DB baseline, mean (SD) | |||
Overall PANSS score† | 61.0 (10.38)* | 61.5 (9.60) | 61.4 (10.29)* |
CGI-S, mean (SD)‡ | 3.3 (0.67)* | 3.3 (0.59) | 3.2 (0.66)* |
Injection site, n (%) Arm Abdomen Not treated | 49 (27) 130 (72) 2 (1) | 57 (31) 126 (69) 0 | 66 (37) 114 (63) 0 |
BMI = body mass index; CGI-S = Clinical Global Impression-Severity; DB = double-blind; PANSS = Positive and Negative Symptom Scale; SD = standard deviation;
*n=179; † Overall PANSS score at baseline was assessed using the ITT analysis set; ‡ CGI-S at baseline was assessed using the safety analysis set
Source: RISE CSR.
SHINE
Baseline demographics were similar across treatment groups (Table 7). Overall, 64% of patients were male, 54% were Black, the mean age was 50.6 years, and the mean length of disease was 21.1 years, with a mean of 21 months since last relapse. Only 3 adolescents were randomized and received at least one dose of TV-46000 in the study.
Table 7: Summary of Baseline Characteristics in SHINE
Characteristics | TV-46000 q1m (N=174) | TV-46000 q2m (N=162) | Total (N=336) |
|---|---|---|---|
Age, years, mean (SD) | 51.3 (10.28) | 49.8 (11.51) | 50.6 (10.90) |
Male, n (%) | 113 (65) | 103 (64) | 216 (64) |
Race, n (%) White Black or African American Asian American Indian or Alaska Native Native Hawaiian or other Pacific Islander Not reported Other | 80 (46) 91 (52) 1 (<1) 0 0 1 (<1) 1 (<1) | 67 (41) 90 (56) 2 (1) 0 1 (<1) 1 (<1) 1 (<1) | 147 (44) 181 (54) 3 (<1) 0 1 (<1) 1 (<1) 2 (1) |
BMI, kg/m2, mean (SD) | 29.78 (4.95) | 29.53 (5.28) | 29.66 (5.11) |
Oral risperidone at randomization, n(%) 2 mg 3 mg 4 mg 5 mg | 46 (26) 42 (24) 71 (41) 15 (9) | 57 (35) 22 (14) 67 (41) 16 (10) | 103 (31) 64 (19) 138 (41) 31 (9) |
Disease length, years, mean (SD) | 22.6 (12.23) | 19.4 (12.06) | 21.1 (12.23) |
Time since last relapse, months, mean (SD) | 20.7 (10.31) | 21.4 (10.83) | 21.0 (10.55) |
Injection site, n (%) Arm Abdomen Not treated | 49 (28) 123 (71) 2 (1) | 47 (29) 115 (71) 0 | 96 (29) 238 (71) 2 (<1) |
SD=standard deviation
Source: SHINE CSR33
Interventions
RISE
This was a double-blind study, all patients were randomly assigned to 1 of the 3 treatment groups (TV-46000 q1m, TV-46000 q2m, or placebo). Randomization was stratified by gender (male or female) and the dose of oral risperidone on which the patient was stabilized during Stage 1 (2/3 mg, 4 mg, or for adults only 5 mg). Due to the differences of appearance between the TV-46000 product and placebo, an unblinded nurse, not associated with rating the patient (including assessment of the injection site if needed) and independent from the study team, was required at each site to administer the study drug. The doses of TV-46000 to be evaluated in this study (50 to 125 mg q1m SC and 100 to 250 mg q2m SC) were selected based on data from the Phase 1 Study TV46000-SAD- 10055. As a result, the doses remained stable, and investigator was unable to optimize the dose of TV46000 during the trial.
In general, TV-46000 was administered to patients in the abdomen (except as indicated below) by SC injection, at intervals of q1m or q2m, at a dose comparable to oral risperidone 2 to 5 mg/day on which they were stabilized in Stage 1, per the conversion table in Figure 1. The maximal dose administered was comparable to an oral risperidone dose of 5 mg/day. Patients that required a stabilization dose below 2 mg/day were not randomized in the study. Also, as a precautionary measure, adolescent patients that required a stabilization dose of more than 4 mg during the oral conversion and stabilization stage were not randomized.
Several investigational centers were selected by the sponsor (based on the centers’ capabilities, sponsor’s considerations, and prior clinical experience with injectable medication) for injection of study drug into the back of the upper arm, instead of the abdomen, to all or some of the randomized patients at these sites. The injection site that was chosen for an individual patient remained consistent throughout the study.
Concomitant therapy or medication usage was monitored throughout the study. Medications most frequently used by patients before the study included psycholeptics (495 [91%] patients), psychoanaleptics (159 [29%] patients), and agents acting on the renin-angiotensin system (94 [17%] patients). Medications most frequently used by patients during the study included psycholeptics (66 [37%], 50 [27%], and 49 [27%] patients in the placebo, TV-46000 q1m, and TV-46000 q2m groups, respectively), psychoanaleptics (46 [26%], 37 [20%], and 50 [28%] patients, respectively), and agents acting on the renin-angiotensin system (30 [17%], 36 [20%], and 34 [19%] patients, respectively).
SHINE
This was a randomized, double-blind, parallel-group study. Patients were randomly assigned to receive 1 of the 2 treatment groups (TV-46000 q1m and TV-46000 q2m) at a 1:1 ratio. Patients and investigators remained blinded to treatment assignment during the study. Due to the differences between TV-46000 and placebo and the alternation between placebo and TV-46000 for the TV-46000 q2m arm, an unblinded nurse, who was not associated with rating the patient (including assessment of the injection site if needed) and was independent from the study team, was required at each site to administer the drug. Similar to RISE, the doses of TV-46000 to be evaluated in this study (50 to 125 mg q1m SC and 100 to 250 mg q2m SC) were selected based on data from the Phase 1 Study TV46000-SAD- 10055. As a result, the doses remained stable, and the investigator was unable to optimize the dose of TV46000 during the trial.
For new patients, TV-46000 was administered in the abdomen by SC injection, at intervals of q1m or q2m, at a dose comparable to the oral risperidone (2 to 5 mg/day) on which they were stabilized in Stage 1, per the conversion table in Figure 1 and per their assigned treatment arm. The maximal dose administered was comparable to an oral risperidone dose of 5 mg/day (adolescent patients received a maximal dose comparable to oral risperidone 4 mg/day). As a precautionary measure, adolescent patients who required oral risperidone stabilization dose of more than 4 mg/day during the stabilization stage were not randomized. Patients who required a stabilization dose below 2 mg/day were not randomized in the study.
Roll-over patients who were randomized to the q1m or q2m treatment arms in study 30072 continued to receive TV-46000 at the same frequency and dose in the current study. Patients randomized to the placebo arm in study 30072 were re-randomized to either the q1m or q2m arms in the current study and received TV-46000 at the dose equivalent to the oral dose on which they were stabilized in Stage 1 of study 30072. Dose presentation for all the roll-over patients was switched from vials and syringes to PFS so that all the patients in the current study were administered the investigational medicinal product (IMP) via PFS. The injection site that was chosen for an individual patient remained consistent throughout the study. If the chosen site was the arm, the injection was administered in an alternating manner between the right and the left arm. If the chosen site was the abdomen, the injection was administered in an alternating manner to the right and to the left of the umbilicus.
Concomitant therapy or medication usage was monitored throughout the study. Medications most frequently used by patients during the study included psycholeptics (138 [41%] patients), psychoanaleptics (112 [34%] patients), agents acting on the renin-angiotensin system (72 [22%] patients), lipid-modifying agents (61 [18%] patients), drugs used in diabetes (57 [17%] patients), anti-Parkinson drugs (56 [17%] patients), drugs for obstructive airway diseases (47 [14%] patients), anti-inflammatory and anti-rheumatic products (40 [12%] patients), and analgesics (36 [11%] patients).
Outcomes
Clinical Global Impression-Improvement (CGI-I)
The Clinical Global Impression-Improvement (CGI-I) scale assesses patient improvement from initiation of treatment and consists of a 7- point scale: 1=very much improved since the initiation of treatment; 2=much improved; 3=minimally improved; 4=no change from baseline (the initiation of treatment); 5=minimally worse; 6= much worse; 7=very much worse since the initiation of treatment.
Clinical Global Impression-Severity (CGI-S)
The CGI-S scale assesses illness severity over the past 7 days. It is based on the following question to the clinician “Considering your total clinical experience with this particular population, how mentally ill is the patient at this time?” which is rated on the following seven point scale: 1=normal, not at all ill; 2=borderline mentally ill; 3=mildly ill; 4=moderately ill; 5=markedly ill; 6=severely ill; 7=among the most extremely ill patients.
Clinical Global Impression-Severity of Suicidality (CGI-SS)
The CGI-SS scale provides an overall clinician-rated assessment of the risk of suicidality. The CGI-SS consists of a 5-point scale in Part 1 (the most severe level of suicidality experience) ranging from 1 (not at all suicidal) to 5 (attempted suicide) and a 7-point scale in Part 2 (change in participant suicidality) ranging from 1 (very much improved) to 7 (very much worse).
Positive and Negative Syndrome Scale (PANSS)
PANSS is widely used in clinical trials of schizophrenia and other disorders and is considered the “gold standard” for assessment of antipsychotic treatment efficacy. It is a 30-item, 7-point rating instrument with all 7 rating points representing increasing levels of psychopathology: 1=absent; 2=minimal; 3=mild; 4=moderate; 5=moderate-severe; 6=severe; 7=extreme. The scale is comprised of 7 items on the positive scale (delusions, conceptual disorganization, hallucinatory behavior, excitement, grandiosity, suspiciousness, hostility) and 7 items on the negative scale (blunted affect, emotional withdrawal, poor rapport, passive-apathetic social withdrawal, difficulty in abstract thinking, lack of spontaneity and flow of conversation, stereotyped thinking). The PANSS also includes a general psychopathology scale, which includes 16 items. Overall, higher PANSS scores indicate greater severity of psychopathology symptoms.
Drug Attitudes Inventory 10-Item Version (DAI-10)
The Drug Attitudes Inventory 10-Item Version (DAI-10) is a 10-item questionnaire to assess 1) subjective experience of drug and 2) attitudes and beliefs toward neuroleptics which may influence compliance in schizophrenia participants. The DAI-10 contains 6 items (1, 3, 4, 7, 9, and 10) that a participant who was fully adherent to the prescribed medication answered as “True” and 4 items (2, 5, 6, and 8) that a participant who was fully adherent to the prescribed medication answered as “False.” A correct answer was scored +1 and an incorrect answer was scored –1. The total score was the sum of the item scores. The total score ranges from –10 to +10. A positive total score indicates a positive attitude toward psychiatric medications and thus corresponds to a compliant response, and vice versa.
Schizophrenia Quality of Life Scale (SQLS)
The Schizophrenia Quality of Life Scale (SQLS) comprises 33 items categorized in 2 domains: psychosocial feelings (20 items) and cognition and vitality (13 items). The items were scored on a 5-point scale (1 - never, 2 - rarely, 3 - sometimes, 4 - often, 5 - always). Individual domain and total scores were standardized by scoring algorithm to a 0 (best health status) to 100 (worst health status) scale, with higher scores indicating comparatively lower quality of life (QoL). The last valid participant assessment was used as the endpoint.
Personal Social Performance (PSP)
The Personal Social Performance (PSP) evaluates functional status with higher PSP total scores indicating better personal and social functioning.
Statistical Analysis
In RISE, the primary efficacy endpoint was analyzed by fixed sequential testing (hierarchy). For the first primary endpoint hypothesis, TV-46000 q1m was compared with placebo with 2-sided test at alpha of 0.05. If the difference was found to be statistically significant, testing continued to the second primary hypothesis, which compared TV-46000 q2m to placebo with 2-sided test at alpha of 0.05. The study was stopped when 90 relapse events were observed. For key secondary endpoints, the TV-46000 q1m and q2m groups were pooled and analyzed vs placebo by using the fixed sequential (hierarchical) strategy. Note that while most key secondary endpoints were planned for the extended intention-to-treat (eITT) population, low enrollment of adolescent participants necessitated the use of the intention-to-treat (ITT) population for secondary endpoint evaluation, with the exception of time to impending relapse. For exploratory efficacy analyses, TV-46000 q1m and q2m groups were analyzed separately and pooled by using descriptive statistics.
In SHINE, the primary objective of the study was to evaluate the long-term safety and tolerability of TV-46000 administered in adult and adolescent patients with schizophrenia. As this was a safety-oriented study, there was no primary efficacy endpoint or analysis for this study, and efficacy data are summarized as descriptive statistics with 95% confidence interval (CI), as appropriate.
Primary Outcome(s) of the Studies
Power Calculation
In RISE, the total number of events was calculated to attain a statistical power of at least 90% in both comparisons of q1m and q2m versus placebo. A total of at least 90 relapse events needed to be observed during Stage 2 of the study in the ITT analysis set (adult patients) in the 3 treatment groups (combined) in order to attain at least 90% power to meet success criteria in both comparisons.
The SHINE study was safety-oriented in nature; therefore, no formal hypothesis testing was planned. Based on regulatory requirements, up to approximately 300 patients were planned to be enrolled in Stage 2 of this study in order to collect data on at least 100 patients exposed to TV-46000 for at least 1 year. Adolescent patients were only enrolled in the US.
Statistical Test or Model
In RISE, the ITT analysis set (employing while-on-treatment estimand) was used for all efficacy analyses during Stage 2 of the study unless otherwise specified. The primary efficacy analysis was compared using the stratified log-rank test. Kaplan-Meier (KM) curves were provided to present impending relapse rate data over time. In SHINE, the ITT analysis set was used for exploratory efficacy summaries during Stage 2 of the study (double-blind stage) unless otherwise specified.
Data Imputation Methods
In RISE, for all variables, only observed data from patients were used in the statistical analyses (i.e., no missing data were estimated). The only exception is the sensitivity analysis of the primary efficacy analysis due to potential informative censoring using a “tipping point” approach. In this analysis, time to event values were assigned to patients with suspected informative censoring using multiple imputation methodology.
In SHINE, for all variables, only observed data from patients were used in the statistical analyses (i.e., no missing data were estimated), unless otherwise specified. This analysis of observed data under the assumption of missing-at-random yields valid (unbiased) estimates of treatment effects. Ad hoc imputation for safety summary tables was performed only for the specific cases described in the statistical analysis plan (SAP). There was no imputation in the data listings (including ad hoc imputation); all values were displayed as recorded in the clinical database.
Subgroup Analyses
In RISE, subgroup analyses were performed for the primary efficacy endpoint according to the following categories, as applicable:
Gender
Race – in case of at least 15 patients per level-group
US versus outside of US
Time from diagnosis (<10 years, ≥10 years and <20 years, and ≥20 years).
Baseline PANSS (by quartiles)
The effect and its 2-sided 95% CI was estimated using Cox proportional hazard model and summarized in a forest plot.
In SHINE, no formal subgroup (e.g., race, sex) analyses were planned or conducted.
Sensitivity Analyses
In RISE, the primary analysis was repeated using the per-protocol (PP) analysis set to assess the robustness of the principal analysis results in the subpopulation of patients that completed the study without important protocol deviations. Other sensitivity analyses include interval censoring and using a “Tipping Point” approach.
As part of the US Food and Drug Administration (FDA) review, Teva applied both post-study monitoring by the Sponsor/Clinical Research Organization (CRO) and an independent third-party audit by Lachman Consulting Services to address issues raised for the RISE and SHINE studies. The activities were divided into three distinct elements of data collection, data auditing, and data analysis. Sensitivity analyses were then performed to evaluate whether dosing errors and lack of dosing documentation had any effect on the results and conclusions of the primary efficacy endpoint analysis.35
Secondary Outcomes of the Studies
In RISE, type-I error was controlled for the key secondary endpoints by employing a fixed sequential (hierarchical) testing strategy. Analyses of the key secondary endpoints were conducted on the pooled TV-46000 active treatment group (q1m and q2m) versus placebo. At the point where a comparison was found to be insignificant, the rest of the comparisons were made in an exploratory manner only; any p-value associated with these comparisons were considered as nominal and were not used for inference. The sequence of the secondary endpoint comparisons was as follows: 1) Time to impending relapse in the eITT analysis set; 2) Impending relapse rate at week 24; 3) Percentage of patients who maintain stability at endpoint; 4) Percentage of patients achieving remission at endpoint; 5) Observed rate of impending relapse at endpoint; 6) DAI-10 change from baseline to endpoint in adult patients; 7) SQLS change from baseline to endpoint in adult patients; 8) Time to impending relapse in adolescent patients
In SHINE, there were no primary efficacy endpoints in this study. Therefore, no adjustments were made for the preplanned multiple comparisons/endpoints.
Analysis Populations
In RISE the analysis sets included:
ITT population: all adult patients randomized to the double-blind maintenance stage (Stage 2), regardless of if they have received treatment or not. In the ITT analysis set, treatment was assigned based on the treatment to which patients were randomized, regardless of which treatment they actually received.
eITT population: all patients (adults and adolescents) randomized to the double-blind maintenance stage (Stage 2), regardless of if they received treatment or not. In the eITT analysis set, treatment was assigned based on the treatment to which patients were randomized, regardless of which treatment they actually received. Since the total number of adolescent patients in the study was less than 5, separate summary tables for adolescents and summary tables of the eITT analysis set were not presented, and the presentation for eITT was replaced with presentation for the ITT analysis set.
PP: all patients in the ITT analysis set who had no important protocol deviations that were deemed to be related to the primary analysis and to be excluded from the PP analysis; a case-by-case evaluation of which important protocol deviations deemed to be related to the primary endpoint was conducted before unblinding. In this analysis set, treatment was assigned based on the treatment patients actually received. If patients erroneously received a wrong drug assignment in some visits, a decision to which treatment group they were assigned was determined on a case-by-case manner before unblinding.
Safety population: all randomized patients who received at least 1 dose of study drug or placebo in the double-blind maintenance stage (Stage 2). In the safety analysis set, treatment was assigned based on the treatment patients actually received, regardless of the treatment to which they were randomized unless otherwise specified. If patients erroneously received a wrong drug assignment in some visits, a decision to which treatment group they were assigned was determined on a case-by-case manner before unblinding.
In SHINE the analysis sets included:
ITT population: all randomized patients who were randomized in SHINE. In the ITT analysis set, treatment was assigned based on the TV-46000 treatment to which the patients were randomized in this study, regardless of which treatment they actually received. The ITT analysis set includes all randomized patients, including new patients who did not take any IMP.
PP population: All patients in the safety analysis set who had no important protocol deviations. In this analysis set, treatment was assigned based on the treatment the patients actually received. If patients erroneously received a wrong drug assignment in some visits, a decision to which treatment group they were assigned was determined in a case-by-case manner before database lock.
Safety population: All patients who received at least 1 dose of TV-46000 in SHINE. In the safety analysis set, treatment was assigned based on the treatment the patients actually received, regardless of the treatment to which they were randomized, unless otherwise specified.
Sponsor’s Summary of the Results
Patient Disposition
RISE
A total of 1267 patients with schizophrenia were screened for enrollment into this study and 863 patients met entry criteria and were considered to be eligible for enrollment into Stage 1 of the study. Of the 404 patients who were not enrolled (screen failures), 231 were excluded on the basis of inclusion/exclusion criteria, 6 patients were excluded due to an adverse event, 98 patients withdrew consent, 52 patients were lost to follow-up before the enrollment visit, and 17 patients were not enrolled due to other reasons. Of the 319 patients who were enrolled but not randomized (randomization failures), 56 were excluded on the basis of inclusion/exclusion criteria, 24 patients were excluded due to an adverse event, 114 patients withdrew consent, 65 patients were lost to follow-up before the baseline visit, 51 patients failed to meet randomization criteria, and 9 patients were not randomized due to other reasons. Of the 544 patients randomized, 542 patients received at least 1 dose of study drug or placebo and were evaluated for safety in the study; 2 patients withdrew before taking any study drug.
A total of 205 (38%) patients discontinued study treatment (71 [39%] receiving TV-46000 q1m, 66 (37%) receiving TV-46000 q2m, and 68 [38%] receiving placebo treatment). The overall rate of withdrawal of the study treatment was balanced across the treatment groups. The most frequent reasons for withdrawal of study treatment were withdrawal of consent, adverse event, and being lost to follow-up.
SHINE
A total of 203 new patients with schizophrenia were screened for enrollment into this study. Of the 203 patients screened, 150 patients were considered to be eligible for enrollment into Stage 1 and received oral risperidone. In Stage 1, of the 150 new patients enrolled, 41 patients were not randomized to Stage 2, and 109 patients received at least 1 dose of study drug in Stage 2 and were evaluated for safety in the study. A total of 227 roll-over patients (172 from the active treatment group and 55 from the placebo group) were randomized. Two roll-over patients were randomized but not treated, thus, 225 rollover patients were evaluated for safety in the study.
In Stage 2, a total of 101 (30%) patients withdrew from treatment (48 [28%] receiving TV-46000 q1m treatment and 53 [33%] receiving TV-46000 q2m treatment). The highest overall rate of withdrawal was observed among new patients; 55 [50%]. The most frequent reason for withdrawal was withdrawal by patient, reported for 21 (12%) patients in the TV-46000 q1m treatment group and 25 (15%) patients in the TV-46000 q2m treatment group. Six patients, 3 (2%) in the TV-46000 q1m treatment group and 3 (2%) in the TV-46000 q2m treatment group, withdrew due to relapses. Only 7 adolescent patients volunteered for screening; 3 were screen failures; 4 enrolled in Stage 1, among these, 3 were randomized to Stage 2 of the study and received at least 1 injection of TV-46000.
Table 8: Table for Patient Disposition
Characteristics | RISE | SHINE | |||
|---|---|---|---|---|---|
Placebo | TV-46000 q1m | TV-46000 q2m | TV-46000 q1m | TV-46000 q2m | |
Screened, N | 1267 | 203 | |||
Randomized, N | 181 | 183 | 180 | 174 | 162 |
Discontinued, N (%) | 68 (38%) | 71 (39%) | 66 (37%) | 48 (28%) | 53 (33%) |
Reason for discontinuation, N (%) Adverse event Consent withdrawn Noncompliance with study drug Protocol deviation Lost to follow-up Lack of efficacy Death Relapse Other | 10 (6) 23 (13) 4 (2) 10 (6) 9 (5) 0 1(<1) NA 11 (6%) | 21 (11) 24 (13) 2 (1) 3 (2) 13 (7) 0 0 NA 8 (4) | 14 (8) 23 (13) 2 (1) 4 (2) 9 (5) 1 (<1) 4 (2) NA 9 (5) | 2 (1) 21 (12) 1 (<1) 2 (1) 5 (3) 1 (<1) 2 (1) 3 (2) 11 (6) | 5 (3) 25 (15) 0 1 (<1) 7 (4) 0 1 (<1) 3 (2) 11 (7) |
ITT, N | 181 (100) | 183 (100) | 179 (>99) | 174 (100%) | 162 (100%) |
eITT, N | 181 (100) | 183 (100) | 180 (100) | NA | NA |
PP, N | 179 (99) | 182 (>99) | 179 (>99) | 106 (61%) | 59 (36%) |
Safety, N (%) | 179 (99%) | 183 (100%) | 180 (100%) | 172 (99%) | 162 (100%) |
eITT=extended intention-to-treat; ITT = intention to treat); PP=per protocol; q1m=once monthly; q2m=once every 2 months
Sources: RISE CSR15, SHINE CSR33.
Exposure to Study Treatments
Study Treatments
RISE
A patient with total oral risperidone compliance of less than 80% in Stage 1 was considered noncompliant. Compliance with the study protocol was part of the determination for eligibility for randomization in Stage 2. A total of 6 (1%) patients in Stage 1 who were randomized in Stage 2 were ≥60% to <80% compliant, and no patients in Stage 1 who were randomized in Stage 2 were <60% compliant with study drug procedures in Stage 1. In Stage 2, among the 317 patients with protocol deviations, 107 (20%) had protocol deviations associated with the study drug and, of these, only 4 (<1%) resulted in treatment discontinuation.
In Stage 1, the mean duration of exposure to oral risperidone was 73.2 weeks (53.1 weeks for non-randomized patients and 84.9 weeks for randomized patients). In Stage 2, the mean duration of exposure to study drug was 30.9 weeks for patients in the placebo treatment group, 41.9 weeks for patients in the TV-46000 q1m treatment group, and 42.1 weeks for patients in the TV-46000 q2m treatment group.
SHINE
A patient with total oral risperidone compliance of less than 80% in Stage 1 was considered noncompliant. This was an important criterion in regard to compliance with the study protocol, which was required for the new patient to be eligible for randomization in Stage 2. Out of 150 patients in the enrollment patients set, 144 (96%) patients were compliant with study drug procedures during Stage 1. Out of 109 new patients who were subsequently randomized, only one was considered noncompliant (qualitative compliance ≥60% and <80%).
The majority (59%) of patients received treatment with study drug (TV-46000 q1m or TV-46000 q2m from PFS) for more than 26 weeks and less than or equal to 39 weeks. The mean duration of total patient exposure was more than 29 weeks (29.7 weeks for patients in the TV-46000 q1m treatment group and 33.7 weeks for patients in the TV-46000 q2m treatment group). The median number of weeks of treatment was 32.1 weeks for all treated patients. Twenty-seven patients completed at least one year of treatment. Three adolescent patients were randomized to Stage 2; one of them was exposed to TV-46000 for 4 weeks, the others were exposed for 16.7 weeks and 28.4 weeks. The overall cumulative exposure for the adolescent patients was 49.1 weeks.
Concomitant Medications
RISE
The majority (>95%) of patients in each treatment group received medications prior to study entry. In general, the medications taken were consistent with the patients’ known medical histories. Medications most frequently used by patients before the study included psycholeptics (495 [91%] patients), psychoanaleptics (159 [29%] patients), and agents acting on the renin-angiotensin system (94 [17%] patients).
A total of 210 (24%) patients were reported with use of prohibited concomitant medications in Stage 1. In Stage 2, use of prohibited concomitant medications was reported at a higher frequency of patients in the placebo group (48 [27%]) versus the pooled TV-46000 group (60 [17%] patients. In either stage, the most frequently used prohibited medications belonged to the therapeutic class of psycholeptics.
SHINE
The majority (>80%) of patients in each treatment group received medications prior to study entry. The most commonly used prior medications among the new patients prior to Stage 1 included psycholeptics (141 [94%] patients), psychoanaleptics (61 [41] patients), agents acting on the renin-angiotensin system (32 [21%] patients), lipid-modifying agents (26 [17%] patients), drugs used in diabetes (23 [15%] patients), anti-Parkinson drugs (20 [13%] patients), drugs for obstructive airway diseases (19 [13%] patients), anti-inflammatory and anti-rheumatic products (18 [12%] patients), and calcium channel blockers (17 [11%] patients).
Medications most frequently used by all patients before the study included psycholeptics (150 [45%] patients), psychoanaleptics (113 [34%] patients), agents acting on the renin-angiotensin system (72 [21%] patients), lipid-modifying agents (61 [18%] patients), drugs used in diabetes (54 [16%] patients), anti-Parkinson drugs (52 [15%] patients), and drugs for obstructive airway diseases (46 [14%] patients)
Medications most frequently used by patients during the study included psycholeptics (138 [41%] patients), psychoanaleptics (112 [34%] patients), agents acting on the renin-angiotensin system (72 [22%] patients), lipid-modifying agents (61 [18%] patients), drugs used in diabetes (57 [17%] patients), anti-Parkinson drugs (56 [17%] patients), drugs for obstructive airway diseases (47 [14%] patients), anti-inflammatory and anti-rheumatic products (40 [12%] patients), and analgesics (36 [11%] patients).
Efficacy
RISE
In Stage 2, the primary endpoint was met, with TV-46000 q1m and TV-46000 q2m having significantly prolonged the time to impending relapse relative to placebo. Thus, TV-46000 q1m significantly decreased the risk of relapse by 80.0% (log-rank p<0.0001; hazard ratio (HR) [95% CI]: 0.200 [0.109, 0.367]), and TV-46000 q2m significantly decreased the risk by 62.5% (log-rank p<0.0001; HR [95% CI] 0.375 [0.227, 0.618]) for the study duration (Table 9 and Figure 3). A smaller proportion of patients in the TV-46000 q1m and q2m groups vs the placebo group experienced relapse (7% [n=13] and 13% [n=23] vs 29% [n=53], respectively). Sensitivity analyses support the robustness of the primary analysis.
In response to issues raised by the FDA with respect to dosing deviations, sensitivity analyses were performed. The results of these sensitivity analyses of the primary efficacy endpoint in all the analysis subgroups based on the stratified log-rank test were consistent with the originally reported results regarding the effect of the active treatment (TV-46000) over placebo. As such, the effect of TV-46000 (q1m and q2m) over placebo is robust and the results of the original results of RISE can be considered reliable.35
Key secondary efficacy endpoints were assessed in hierarchical order and the TV-46000 treatment arms (q1m and q2m) were pooled and compared to placebo, based on the trial design. Clinical improvement was further demonstrated by the key secondary endpoints in an analysis on the pooled TV-46000 q1m and q2m dosing regimens compared with placebo. The impending relapse rate at week 24 was statistically significantly lower in patients treated with TV-46000 (9% [7% for q1m and 11% for q2m]) compared to placebo (28%). Further, the percentage of patients who maintained stability at endpoint was statistically significantly higher in patients treated with TV-46000 (83% [87% for q1m and 80% for q2m]) compared to placebo treatment (61%). The key secondary efficacy variable of percentage of patients achieving remission at endpoint did not reach statistical significance; as such, this endpoint and the remaining key secondary endpoints were descriptive. Of the 2 adolescent patients enrolled in the study, only 1 was randomized in the study; therefore, age-specific endpoints were not meaningful. The observed rate of impending relapse was 10% with TV-46000 treatment (7% for q1m and 13% for q2m) compared to 29% with placebo. In addition, patients who received TV-46000 showed ongoing improvement compared to placebo with regard to their attitude toward their medication (DAI-10 total score) and investigator-assessed psychopathology (PANSS total score) with ongoing treatment. Results of key secondary endpoints are provided in Table 9.
In the exploratory outcomes, QoL was evaluated via the 5-Level EuroQol Five Dimensions Questionnaire (EQ-5D-5L) score which showed differences from placebo in favor of pooled TV-46000 (q1m and q2m arms) at the end of treatment (least squares mean [LSM]: 2.28 vs –2.46 with placebo). The change from baseline in overall PANSS total score showed greater improvement with pooled TV-46000 than with placebo at the end of treatment (LSM: –4.10 vs 1.11, respectively), suggesting continuous improvement with TV-46000 even after stabilization with oral risperidone. The CGI-I score showed numerically greater improvement in the pooled TV-46000 group than in the placebo group at the end of treatment (LSM: 3.23 vs 3.85, respectively). Overall, the percentage of patients whose CGI-I scoring improved was higher in the pooled TV-46000 group than in the placebo group. Results of the PSP scale suggested patients in the pooled TV-46000 group had greater improvement in investigator-assessed personal and social functioning at the end of treatment vs placebo (LSM: 1.56 vs 0.11, respectively. Measures of healthcare utilization could not be evaluated due to small sample size of patients who used services over the course of the study.
An analysis of patient-centered endpoints in patients who completed the RISE study relapse-free was conducted.36 This analysis showed that both SQLS and EQ-5D-5L visual analog scale scores improved significantly from randomization to end of treatment for TV-46000 q1m, q2m, and combined groups (p<0.01), while the scores remained unchanged in the placebo group. Mean DAI-10 scores also improved significantly (p<0.01) from randomization to end of treatment in the TV-46000 q1m and TV-46000 combined treatment groups.
Table 9: Summary of Primary and Key Secondary Outcomes in RISE
Characteristics | Placebo | TV-46000 q1m | TV-46000 q2m | TV-46000 Overall |
|---|---|---|---|---|
Primary Endpoint: Time to Impending Relapse (Weeks) by Treatment Group (ITT Analysis Set) | ||||
N | 181 | 183 | 179 | 362 |
Patients with impending relapse* | 53 (29) | 13 (7) | 23 (13) | 36 (10) |
Hazard ratio (95% CI)† | - | 0.200 (0.109, 0.367) | 0.375 (0.227, 0.618) | 0.283 (0.184, 0.435) |
Log-rank test p-value | - | <0.0001‡ | <0.0001‡ | <0.0001 |
Proportional hazards test p-value** | 0.7251 | - | - | - |
Key Secondary Endpoints | ||||
Time to Impending Relapse (eITT Analysis Set) | ||||
N | 181 | 183 | 180 | 363 |
Hazard ratio (95% CI) | - | - | - | 0.291 (0.190, 0.446) |
p-value†† | - | - | - | p<0.0001 |
Impending Relapse Rate at Week 24 (ITT Analysis Set) | ||||
N | 181 | 183 | 179 | 362 |
Observed impending relapse rate at week 24 (95% CI) | 0.28 (0.205, 0.347 | 0.07 (0.03, 0.109) | 0.11 (0.065, 0.165) | 0.09 (0.059, 0.123) |
Observed difference in impending relapse rates | - | -0.21 (-0.288, -0.125) | -0.16 (-0.248, -0.074) | -0.18 (-0.263, -0.106) |
P-value | - | <0.0001 | 0.0001 | <0.0001†† |
Percentage of Patients Who Maintain Stability at Endpoint (ITT Analysis Set) | ||||
N | 181 | 183 | 179 | 362 |
Stability at endpoint, n (%)‡‡ Overall | 110 (61) | 159 (87) | 143 (80) | 302 (83 |
CMH p-value | - | <0.0001 | 0.0001 | <0.0001†† |
Berslow and Day homogeneity p-value | - | 0.9550 | 0.9585 | 0.9338 |
Percentage of Patients Achieving Remission at Endpoint (ITT Analysis Set) | ||||
N | 181 | 183 | 179 | 362 |
Percentage of patients achieving remission at endpoint | 23% | 29% | 32% | 30% |
p-value | - | - | - | p=0.1214*** |
Observed Rate of Impending Relapse at Endpoint (ITT Analysis Set)††† | ||||
N | 181 | 183 | 179 | 362 |
Observed rate of impending relapse at endpoint | 29% | 7% | 13% | 10% |
Drug Attitudes Inventory 10-Item Version (ITT Analysis Set) ††† | ||||
N s | 181 | 183 | 179 | 362 |
Change from baseline in DAI-10 total score at ET, LS mean (SE) | -0.55 (0.38) | 0.25 (0.42) | -0.40 (0.41) | - |
Change from baseline in DAI-10 total score at EoT, LS mean (SE) | -0.59 (0.31) | 0.57 (0.28) | 0.10 (0.29) | - |
Schizophrenia Quality of Life Scale (ITT Analysis Set) ††† | ||||
N | 181 | 183 | 179 | 362 |
Changes from baseline in SQLS total score at ET, LS mean (SE) | 3.20 (1.58) | -3.99 (1.74) | -1.58 (1.78) | - |
Changes from baseline in SQLS total score at EoT, LS mean (SE) | 1.14 (1.32) | -5.40 (1.12) | -4.54 (1.16) | - |
CI=confidence interval; CMH= Cochran-Mantel-Haenszel; DAI-10=Drugs Attitudes Inventory 10-Item Version; eITT=extended intention-to-treat; EoT=end of treatment; ET = early termination; ITT= intention-to-treat; LS=least squares; SE=standard error; SQLS= Schizophrenia Quality of Life Scale
*A patient may have been counted in more than 1 relapse criterion.
†The hazard ratio (95% CI) coming from the stratified Cox proportional hazard model, with treatment (placebo, TV-46000 q1m and TV-46000 q2m, or placebo and TV-46000 overall [including q1m and q2m]) as exploratory variable and sex-dose as a stratification factor, and the stratified log-rank test p-value (sex-dose as a stratification factor) refer to TV-46000/placebo comparison.
‡The p-values refer to the analyses of primary endpoint.
**The proportional hazards test p-value tests the overall proportional hazard assumption for the primary model.
††Statistical significance was met, and next secondary endpoint was tested.
‡‡Stability is defined as meeting all of the following criteria for at least 4 consecutive weeks: outpatient status; PANSS total score of 80; minimal presence of specific psychotic symptoms on the PANSS, as measured by a score of 4 on each of the following items: conceptual disorganization, suspiciousness, hallucinatory behavior, and unusual thought content; CGI-S score of 4 (moderately ill); and CGI-SS score of 2 (mildly suicidal) in Part 1 and 5 (minimally worsened) in Part 2. The percentage was calculated as the number of patients who maintained stability at endpoint divided by the number of patients in each treatment group, using the last valid patient assessment as the endpoint. The patient population was limited to those treated with the IMP for at least 4 weeks. The p-value was from the CMH test adjusted for stratification factor of sex-dose for each pairwise comparison versus placebo; p-value of Breslow and Day test for homogeneity is also presented. Breslow and Day homogeneity test accompanies the results; its goal is to assess whether all the strata have the same odds ratio of patients maintaining stability at endpoint.
***The difference did not reach statistical significance; therefore, the rest of the key secondary endpoints are descriptive.
†††Statistical comparison not performed because a previous endpoint in the hierarchy had not reached statistical significance.
Source: RISE CSR15
Figure 3: Kaplan-Meier Curves of Primary Efficacy Endpoint in RISE Study (ITT Analysis Set)
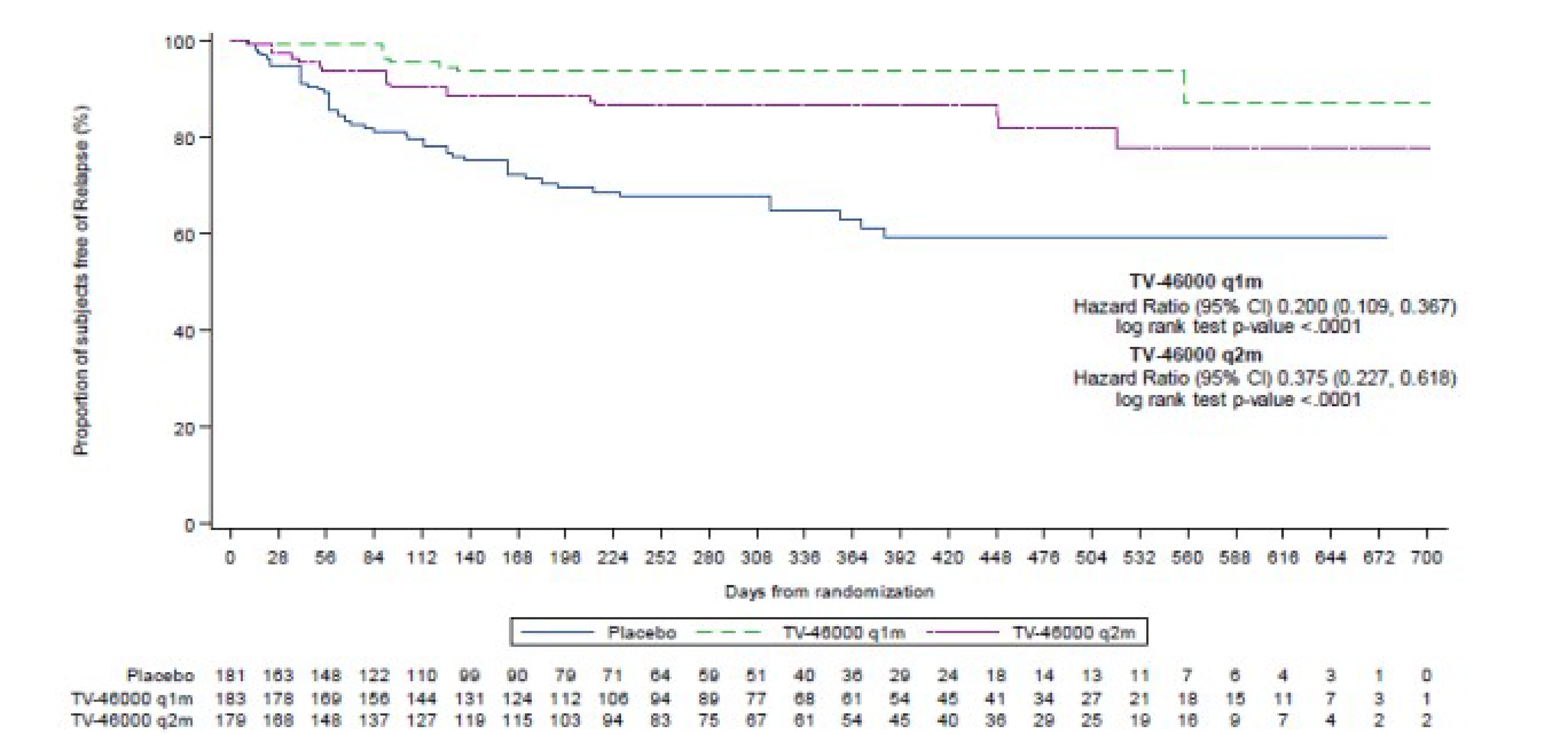
CI=confidence interval; ITT=intent-to-treat; q1m=once monthly; q2m=once every 2 months.
Source: RISE CSR15
SHINE
The primary objective of the study was to evaluate the long-term safety and tolerability of TV-46000 administered in adult and adolescent patients with schizophrenia. As such, efficacy analyses were exploratory. Overall, 6 patients (3 in each treatment group) met relapse criteria. In the TV-46000 q1m and q2m groups, the risk of relapse by Week 56 was 2% and 12%, respectively. Mean PANSS total scores decreased from baseline (indicating improvement) in both treatment groups (q1m, -0.45 and q2m, -1.59), with new and placebo roll-over patients experiencing slightly larger reductions in PANSS total scores. LSM CGI-I scores indicated patient perception of minimal improvement to no change. PSP total score showed minimal changes over time; however, a numeric improvement from baseline was observed in both treatment groups at the last assessment.
The long-term QoL and attitudes towards treatment in adult patients with schizophrenia either remained stable or improved with TV-46000. Reductions in SQLS (indicating improvement) were observed for both treatment groups at the last assessment compared with baseline, with the TV-46000 q2m group showing a slightly larger difference from baselines vs the q1m group (-2.16 vs -0.43, respectively). Changes from baseline to last assessment in EQ-5D-5L were minimal (<1.5) for all dimensions in both treatment groups. DAI-10 scores were positive (indicating favorable view of treatment) in both treatment groups at baseline with minimal change at last assessment.
A summary of select exploratory efficacy in SHINE results, which were key efficacy results in RISE, are provided in Table 10.
Table 10: Exploratory Effectiveness Analyses in SHINE
Characteristics | TV-46000 q1m (N=174) | TV-46000 q2m (N=162) | Total (N=336) |
|---|---|---|---|
Proportion of Patients Who Experienced a Relapse by Treatment Group – Stage 2 (ITT Analysis Set) | |||
Patients with impending relapse, n (%) | 3 (2) | 3 (2) | 6 (2) |
Patients early discontinued treatment without relapse, n (%) | 45 (26) | 50 (31) | 95 (28) |
Change in the Positive and Negative Syndrome Scale Total Score from Baseline – Stage 2 (ITT Analysis Set) | |||
Mean PANSS total score from baseline to last assessment, LS mean (SE) | -0.45 (0.66) | 1.59 (0.68) | - |
Drug Attitudes Inventory 10-Item Version - Stage 2 (ITT Analysis Subset for Adults) | |||
N | 173 | 160 | 333 |
DAI-10 total score change from baseline to EoT, mean (SD) | -0.1 (3.36) | -0.2 (3.40) | -0.1 (3.38) |
DAI-10 total score change from baseline to EoT, LS mean (SE) | -0.09 (0.27) | -0.14 (0.27) | - |
Schizophrenia Quality of Life Scale - Stage 2 (ITT Analysis Subset for Adults) | |||
N | 173 | 160 | 333 |
SQLS total score change from baseline to last assessment, mean (SE) | -0.9 (0.97) | -2.7 (0.95) | -1.8 (0.68) |
SQLS total score change from baseline to last assessment, LS mean (SE) | -0.43 (0.98) | -2.16 (0.98) | - |
CI=confidence interval; DAI-10=Drug Attitudes Inventory 10-Item Version; EoT=end of treatment; ITT=intent-to-treat; LS=least squares; PANSS= Positive and Negative Syndrome Scale; q1m=once monthly; q2m=once every 2 months; SD=standard deviation; SE=standard error; SQLS= Schizophrenia Quality of Life Scale
Source: SHINE CSR33
Harms
The following safety summary includes pooled safety populations from both RISE and SHINE, as prepared for Health Canada as part of the new drug submission.37
Safety Evaluation Plan
The safety of the doses selected for clinical studies was supported by nonclinical assessments. Nonclinical studies evaluated TV-46000 clinically relevant formulations and doses administered by SC injection using the highest dose of TV-46000 intended to be administered in humans using the clinical formulation. TV-46000 was well tolerated locally, and the injection site reaction was characterized by an expected foreign body reaction which is non-adverse, self-limiting, and is eventually resorbed. Altogether, the data obtained from nonclinical studies supported the transition into human studies including dose selection for the first-in-human study to which healthy subjects were exposed in the Phase 1 study. In the Phase 1 studies, 219 patients with schizophrenia and schizoaffective disorder received single and multiple doses of TV-46000.
Safety data herein pertain to the Phase 3 studies. In the Phase 3 studies, a total of 466 patients with schizophrenia were exposed to TV-46000, 363 patients were treated in Study 30072 and 103 new patients were treated in Study 30078. Overall, 258 patients were exposed to TV-46000 for 6 months; of these, 133 patients were exposed to TV-46000 for at least 12 months, with 65 patients exposed to q1m and 68 patients to q2m. The dose of TV-46000 was not modified for a given patient during the study. Narratives describing key safety results are provided in the following sections.
Overview of Safety
Overall, the TV-46000 safety profile was deemed favorable for all dose levels, was comparable between q1m and q2m dose regimens, and was consistent with other risperidone formulations. TV-46000 was well tolerated locally, and the injection site reaction was characterized by an expected foreign body reaction which is non-adverse, self-limiting, and is eventually resorbed.
Overall (for patients with at least 1 event), the exposure-adjusted event rate (EAER) was lower in the TV-46000 total group compared to the placebo group (234.16 and 293.17, respectively) in the Phase 3 trials (RISE & SHINE). The EAERs for the TV-46000 q1m and q2m dose regimens were comparable (237.01 and 231.37, respectively). The EAERs for certain adverse events tended to increase with increasing dose in each regimen. Such dose dependency is considered to be in line with other risperidone formulations.
An overview of the adverse events in the Phase 3 trials is provide in Table 11.
Table 11: Summary of Adverse Events – Safety Analysis Set (Pooled Data, RISE & SHINE)
Adverse events, n(%) | Placebo (N=179 PY=106.08) | TV-46000 q1m (N=235 PY=161.17) | TV-46000 q2m (N=231 PY=164.67) | TV-46000 Total (N=466 PY=325.85) |
|---|---|---|---|---|
Most Frequent (≥5% in Any Group) Adverse Events in the Relapse Prevention Period –Stage 2 | ||||
Patients with at least 1 AE | 92 (51) | 132 (56) | 137 (59) | 269 (58) |
Gastrointestinal disorders | 18 (10) | 23 (10) | 23 (10) | 46 (10) |
General disorders and administration site conditions | 26 (15) | 48 (20) | 43 (19) | 91 (20) |
Injection site pain | 11 (6) | 12 (5) | 16 (7) | 28 (6) |
Injection site nodule | 6 (3) | 13 (6) | 16 (7) | 29 (6) |
Injection site pruritus | 4 (2) | 12 (5) | 7 (3) | 19 (4) |
Infections and infestations | 19 (11) | 36 (15) | 29 (13) | 65 (14) |
Urinary tract infection | 4 (2) | 9 (4) | 11 (5) | 20 (4) |
Injury, poisoning and procedural complications | 8 (4) | 4 (2) | 9 (4) | 13 (3) |
Investigations | 15 (8) | 27 (11) | 27 (12) | 54 (12) |
Weight increased | 6 (3) | 13 (6) | 13 (6) | 26 (6) |
Metabolism and nutrition disorders | 15 (8) | 14 (6) | 14 (6) | 28 (6) |
Musculoskeletal and connective tissue disorders | 16 (9) | 15 (6) | 20 (9) | 35 (8) |
Nervous system disorders | 22 (12) | 50 (21) | 48 (21) | 98 (21) |
Headache | 10 (6) | 9 (4) | 11 (5) | 20 (4) |
Psychiatric disorders | 33 (18) | 27 (11) | 26 (11) | 53 (11) |
Insomnia | 10 (6) | 12 (5) | 7 (3) | 19 (4) |
Respiratory, thoracic and mediastinal disorders | 4 (2) | 12 (5) | 6 (3) | 18 (4) |
Skin and subcutaneous tissue disorders | 9 (5) | 9 (4) | 4 (2) | 13 (3) |
Serious Adverse Events (≥1% in Any Group) in the Relapse Prevention Period –Stage 2 | ||||
Patients with at least 1 serious AE | 14 (8) | 9 (4) | 13 (6) | 22 (5) |
Infections and infestations | 1 (<1) | 3 (1) | 3 (1) | 6 (1) |
Injury, poisoning and procedural complications | 0 | 0 | 3 (1) | 3 (<1) |
Psychiatric disorders | 9 (5) | 4 (2) | 6 (3) | 10 (2) |
Schizophrenia | 4 (2) | 0 | 3 (1) | 3 (<1) |
Psychotic disorder | 2 (1) | 0 | 1 (<1) | 1 (<1) |
Psychotic symptom | 2 (1) | 0 | 0 | 0 |
AEs Leading to Treatment Discontinuation (≥1% in Any Group) in the Relapse Prevention Period –Stage 2 | ||||
Patients with at least 1 AE leading to treatment discontinuation | 20 (11) | 25 (11) | 21 (9) | 46 (10) |
Gastrointestinal disorders | 1 (<1) | 3 (1) | 1 (<1) | 4 (<1) |
General disorders and administration site conditions | 0 | 3 (1) | 4 (2) | 7 (2) |
Injury, poisoning and procedural complications | 0 | 0 | 3 (1) | 3 (<1) |
Investigations | 2 (1) | 2 (<1) | 2 (<1) | 4 (<1) |
Nervous system disorders | 1 (<1) | 9 (4) | 4 (2) | 13 (3) |
Somnolence | 0 | 3 (1) | 2 (<1) | 5 (1) |
Psychiatric disorder | 15 (8) | 8 (3) | 5 (2) | 13 (3) |
Schizophrenia | 7 (4) | 4 (2) | 3 (1) | 7 (2) |
Psychotic disorder | 2 (1) | 0 | 1 (<1) | 1 (<1) |
AE=adverse event; CI=confidence interval; ITT=intent-to-treat; q1m=once monthly; q2m=once every 2 months.
Source: Health Canada CTD Module 2.7.4.37
Sensitivity analyses of safety were performed on the integrated safety dataset that excluded dually and triply enrolled patients, separately for the RISE and SHINE studies and for the integrated dataset from both studies, to assess the potential impact of the dosing deviations on the safety results reported in the original new drug submission. No new safety signals of concern were identified in the sensitivity analyses for any of the subgroups. The overall safety profile of TV-46000 in the different subgroup sensitivity analyses is consistent with the safety profile from the original new drug submission.35
Adverse Events
The most frequently reported adverse events were those associated with injection site reactions and other adverse events also reported following second-generation antipsychotic use and for other risperidone formulations (Table 11). Extrapyramidal symptoms and weight gain are commonly associated with the use of antipsychotics and are contributing factors for treatment discontinuation. Frequent extrapyramidal symptoms associated with risperidone use include akathisia, dystonia, tremors, tardive dyskinesia, and parkinsonism. These events occurred at a higher EAER in the TV-46000 total group compared to placebo, including weight increased, somnolence, extrapyramidal disorder, and tremor. Within the TV-46000 dose regimens, the EAERs were generally comparable between TV-46000 q1m and TV-46000 q2m for these same events. The EAERs for injection site reactions were generally similar between the TV-46000 q1m and q2m dose regimens, except for injection site pruritus, which occurred at a higher rate in the TV-46000 q1m group compared to the q2m group. There were no clear trends observed when examining the EAERs across the individual TV-46000 dose levels within the q1m and q2m TV-46000 dose regimens.
Serious Adverse Events
In the Phase 3 trials, the percentage of patients with severe adverse events was generally low (≤11%) across the individual TV-46000 dose levels and was reported at a higher frequency in the placebo group compared to the TV-46000 total group and at a slightly higher frequency in the TV-46000 q2m dose regimen compared to the q1m dose regimen. TV-46000 treatment led to 2 severe akathisia cases, both occurring in the TV-46000 q2m dose regimen. Extrapyramidal disorder was reported following TV-46000 treatment, and none were reported in placebo; all events were mild to moderate in severity.
For serious adverse events, the integrated analysis of the Phase 3 trials showed a higher EAER in the placebo group compared to the TV-46000 total group, with most events occurring in the Psychiatric Disorders system organ class (SOC) and related to the underlying disease (e.g., relapses). Between the TV-46000 dose regimens, there was a slightly increased event rate with TV-46000 q2m compared to TV-46000 q1m. A total of 5 patients had an adverse event leading to death in Cohort 1. Of these, 4 patients died in the TV-46000 groups. None of the deaths were assessed as related to study drug.
Withdrawals Due to Adverse Events
The most common adverse events leading to treatment discontinuation in the TV-46000 total group (i.e., with the highest EAERs) were schizophrenia (2.15), somnolence (1.53), injection site nodule (0.92), akathisia (0.92), suicidal ideation (0.92), dry mouth (0.61), weight increased (0.61), weight decreased (0.61), Type 2 diabetes mellitus (0.61), extrapyramidal disorder (0.61), and tremor (0.61). Since schizophrenia exacerbation is a possible outcome of the study, somnolence was considered the most frequent adverse event in the TV-46000 total group. The most common adverse events leading to treatment discontinuation in the placebo group were schizophrenia (6.60), psychotic disorder (1.89), and psychotic symptom (1.89).
Adverse Events of Special Interest
Weight gain is frequently observed following risperidone use and was reported following TV-46000 treatment compared to placebo for both the Phase 3 trials. Further assessments indicated that increases in weight and body mass index (BMI) were observed across all the TV-46000 dose levels at the last assessment, whereas both weight and BMI decreased in the placebo group. The change from baseline to the last assessment for weight and BMI were comparable between the TV-46000 q1m and q2m dose regimens. TV-46000 treatment resulted in a substantial difference in prolactin levels compared to placebo, consistent with other risperidone formulations. In the Phase 3 trials, 3 patients displayed galactorrhea following TV-46000 treatment. All were reported as mild in severity and were considered non-serious. Galactorrhea led to study withdrawal in 1 patient in the TV-46000 q2m group; this event did not resolve. One patient who displayed galactorrhea also developed gynecomastia; the event of gynecomastia did not resolve.
The safety profile was further assessed by injection site location (upper arm and abdomen). Overall (for patients with at least 1 event), the EAER was higher when TV-46000 was administered in the abdomen compared to the upper arm. There were no clear trends observed among the individual dose levels in either the q1m or q2m dose regimen when administered in the upper arm or the abdomen. The safety profiles of both injection site locations (abdomen and upper arm) were favorable, did not demonstrate any unexpected findings, and were consistent with other long-acting injectable (LAI) formulations of risperidone.
There was no evidence of dose dumping (i.e., rapid onset of adverse event pattern indicative of rapidly increasing plasma concentrations) in the clinical studies conducted with TV-46000. This is consistent with the safety data obtained from all clinical studies including Phase 1 and Phase 3 studies and is aligned with the formulation chemical attributes of risperidone and TV-46000.
Across the cohorts, there were no meaningful shifts from baseline in suicidal ideation or behavior related to treatment. There were no clinically meaningful trends in mean changes from baseline in Abnormal Involuntary Movement Scale (AIMS) total score, Simpson-Angus Scale (SAS) score, Calgary Depression Scale for Schizophrenia (CDSS) depression score, Barnes Akathisia Rating Scale (BARS) score, Columbia-Suicide Severity Rating Scale (C-SSRS), CGI-SS, and CGI-S values. There were no meaningful differences seen in the safety profile when examined by the planned intrinsic and extrinsic factors.
Bioequivalence
TV-46000 total active moiety (TAM) exposure parameters at steady-state (average plasma drug concentration at steady-state (Cavg,ss), trough plasma drug concentration at steady-state (Ctrough,ss) and maximum plasma drug concentration at steady-state (Cmax,ss)) were simulated at all doses and dosing regimens using the final population pharmacokinetics (PopPK) model. Oral risperidone (1 to16 mg/day) exposure was obtained from the following sources: noncompartmental observed data from TV-46000 Phase 1 studies; observed data reported by Eerdekens et al. (2004)38; and model predicted exposures reported by Korell et al (2017).39 The Phase 1 studies 10055 and 10148 were used to support the Health Canada new drug submission, both provided observed pharmacokinetic data which established a pharmacokinetic bridge between TV-46000 (100 mg) and the Reference Listed Drug (RLD), oral risperidone (4 mg/day).40,41 PopPK analysis was used to further strengthen the pharmacokinetic bridge between TV-46000 and oral risperidone. The PopPK modelling approach is a scientifically robust approach and provides additional support to the TV-46000 dose recommendation and PK comparability to oral risperidone.
The daily exposure (area under the plasma concentration-time curve [AUC]) of TV-46000 was comparable to the daily exposure of corresponding doses of oral risperidone. TV-46000 TAM concentrations across all doses and dose regimens were within the range of exposure (Ctrough,ss to Cmax,ss) of the approved dose range of oral risperidone (1 to 16 mg/day) (Table 12). Moreover, TV-46000 TAM exposure was within the range of exposures for the recommended daily dose range of oral risperidone for the treatment of schizophrenia (2 to 8 mg/day).
Additionally, average TAM Cavg,ss from TV-46000 administered q1m and q2m is comparable to the daily administration of oral risperidone at corresponding doses (Table 12). This outcome supports the recommended TV-46000 doses for q1m regimen and provides additional support to the pharmacokinetic bridge between TV-46000 and the RLD.
Table 12: Median Total Active Moiety Pharmacokinetic Parameters for TV-46000 (Model Predicted) and for Oral Risperidone (Observed, Simulated, and Literature Reported Values)
Data Source | Dose | N | AUC at ss (ng.h/mL) | Cmax ,ss (ng/mL) | Ctrough,ss (ng/mL) | Cavg,ss (ng/mL) |
|---|---|---|---|---|---|---|
||||| |||||| ||||| ||||| |||| ||||||||||| | |||||||| |||| | | |||||||| |||||||| |||||||| |||||||| |||||| | |||||||||| ||||||| | |||||||||||||||| ||||||||||||||||| | |||||||||||| ||| ||||| ||||||||| | |||||||||| |||| |||||| |||||||| | ||||||| |||||||| ||||||| ||||||| |
Korell et al 201739 Oral Risperidone – model simulated data | 1 mg/day 2 mg/day 3 mg/day 4 mg/day 5 mg/day 6 mg/day 8 mg/day 16 mg/day | 500 500 500 500 500 500 500 500 | 187.0 374.0 561.0 749.0 936.0 1120.0 1500.0 2990.0 | 12.3 24.7 37.0 49.3 61.6 74.0 98.6 197.0 | 4.5 9.0 13.5 17.9 22.4 26.9 35.9 71.8 | 7.8 15.6 23.4 31.2 39.0 46.8 62.4 125.0 |
Eerdekens et al 200438 Oral Risperidone – Observed data* | 2 mg/day 4 mg/day 6 mg/day | 21 31 26 | 428.3 859.1 1289.7 | 32.8 67.2 101.0 | 11.1 18.1 29.1 | 17.8 35.8 53.7 |
TV-46000 q1m – Model predicted, median daily AUC at ss | 50 mg 75 mg 100 mg 125 mg | 500 500 500 500 | 475.2 712.5 947.2 1183.6 | 25.1 36.4 47.5 58.7 | 12.1 19.5 26.8 34.2 | 19.8 29.7 39.5 49.3 |
|||||||| || | | ||||| |||||||||| |||||| ||||| ||| || || | ||| ||||| | |||||| |||| || || | || |||||||| ||||| | |||||||| ||||| ||||||||||| | |||| ||||||||| |||||| | |||||| ||||| ||||||| | ||| ||||||| ||||||||| |
AUC = area under the plasma concentration-time curve; Cavg,ss = average plasma drug concentration at steady-state; Cmax,ss= maximum plasma drug concentration at steady-state; CSR = clinical study report; Ctrough;ss = trough plasma drug concentration at steady-state; N = total number of subjects/patients; q1m = once monthly; q2m = once every 2 months; ss = steady-state.
*AUC,ss and Cavg,ss presented as least square mean values.
Source: Health Canada CTD Module 2.7.242
Sensitivity analyses of the population PK model, based on the results from the 3 individual Phase 1 clinical studies (Study RISPE1ZG15EU, Study 10055, and Study 10148) and the adjusted subsets for 2 Phase 3 studies (RISE and SHINE), following the audit were performed. No significant differences were identified, and it can be concluded that previous evaluations remain valid and that the exposure-response relationship of the safety findings were adequately characterized in the original new drug submission.
Critical Appraisal of the Clinical Evidence
CDA-AMC conducted a critical appraisal of the clinical study for risperidone ER (TV-46000) based on the summary of the evidence provided by the sponsor.
Internal Validity
The RISE study was a phase III, multicentre, randomized, double-blind, placebo-controlled study to evaluate treatment with risperidone ER (TV-46000) once monthly or once every 2 months in adults and adolescents with schizophrenia, and the SHINE study was a phase III, multicentre, randomized, parallel-group study that allowed rollover enrolment of participants in the RISE study. Participants in the SHINE study could either continue receiving their current dose or, if they were in the placebo group, to be randomized to receive either risperidone ER once monthly or risperidone ER once every 2 months. To align with the Health Canada–approved indication, the CDA-AMC review focused solely on data related to once-monthly dosing. Appropriate randomization and allocation concealment procedures were described. Comparisons with placebo of end points for each dose group was conducted using a hierarchal testing strategy to control type I error.
A high number of patients in the RISE study had protocol deviations; 317 of 544 patients (58%) had important protocol deviations, 107 (20%) of which were related to the study drug. A per-protocol analysis was conducted for patients with no important protocol deviations that might have been related to the primary analysis, but this was done on a subjective case-by-case basis. As such, bias due to the high number of protocol deviations may have affected the RISE study results. The sponsor noted in their summary that, in response to concerns raised by the FDA regarding dosing deviations, sensitivity analyses were performed; these indicated that the original results were robust to dosing deviations.
The primary end point of time to impending relapse and the secondary end points of impending relapse rate at week 24, the percentage of patients whose schizophrenia remained stable at the end point was statistically significant for once monthly risperidone ER compared with placebo. However, the results of the analysis on percentage of patients whose schizophrenia is in remission at end point, which compared pooled active treatment groups to placebo, did not show statistical significance. As a result, statistical comparisons for other outcomes prespecified in the sponsor’s testing hierarchy were not performed. Important end points, such as the Drug Attitude Inventory 10-Item Version and HRQoL measures, were descriptive in nature and no conclusions can be drawn.
Patients were enrolled into the SHINE study from the RISE study provided they met the study drug adherence criteria . New patients were also enrolled. All patients received risperidone ER either once monthly or once every 2 months. As a parallel-group study without a placebo comparator, the SHINE study assessed the long-term safety of risperidone ER with no formal hypothesis testing; hence, no conclusions can be drawn from the descriptive efficacy analysis provided, although nothing in the results suggests an increase in relapse rate compared to the placebo-controlled RISE study.
External Validity
According to the clinical expert consulted by CDA-AMC, the patient populations in the RISE and SHINE studies appear to be similar to the expected population of adult patients with schizophrenia in Canada, although the majority of the populations in the RISE and SHINE studies were Black, which differs from the population in Canada.
The doses of risperidone ER were not entirely aligned with the approved doses in Canada (once monthly) because the studies included dosing schedules of both once monthly and once every 2 months. The outpatient, longer-term design of the studies, with a primary end point of time to remission, is aligned with the expected use of risperidone ER in the patient population in Canada.
The RISE and SHINE studies were conducted with patients whose symptoms were stabilized on oral risperidone. In the RISE study, this meant that, for 4 consecutive weeks before the baseline visit, patients’ PANSS total scores were less than or equal to 80, key PANSS items scores were less than or equal to 4, Clinical Global Impression–Severity (CGI-S) scale scores were less than or equal to 4 (moderately ill), and Clinical Global Impression–Severity of Suicidality scale scores were less than or equal to 2 (mildly suicidal) on part 1 and less than or equal to 5 (minimally worsened) on part 2 of the scale. While the clinical expert did not expect this to differ from the expected usage of risperidone ER, this is nevertheless a more restricted population than the indication and thus the generalizability of the study results to the broader indication is uncertain.
Sponsor’s Summary of Indirect Evidence
Summary of Findings
A systematic literature review (SLR) and network meta-analyses (NMAs) were conducted to synthesize relevant literature and compare the efficacy and safety of TV-46000 q1m and q2m with atypical LAIs approved in Canada and used for the maintenance treatment of schizophrenia. The efficacy results demonstrated that both TV-46000 q1m and q2m were comparable to the other LAIs approved in Canada and were better than placebo. Specifically, for the primary analysis of relapse rate at six months, TV-46000 q1m and TV-46000 q2m were observed to have a 77% (relative risk [RR]: 0.23, 95% credible interval [CrI]: 0.11-0.43) and 60% (RR: 0.4, 95% CrI: 0.22-0.66) relative risk reduction (RRR), respectively, compared to placebo. For the analysis of time to relapse, TV-46000 q1m and TV-46000 q2m were observed to have an 80% (HR: 0.2, 95% CrI: 0.11-0.37) and 63% (HR: 0.37, 95% CrI: 0.23-0.62) reduction in risk of relapse, respectively, compared to placebo. Furthermore, for the third efficacy outcome of change in PSP, TV-46000 q1m and TV-46000 q2m were observed to have a mean difference of 3.54 (95% CrI: 1.35-5.75) and 3.16 (95% CrI: 0.92-5.39), respectively, compared to placebo.
The safety results demonstrated that both TV-46000 q1m and q2m were comparable to placebo, comparable to the active treatments (i.e., adverse event [AE]-related discontinuation and injection site pain), and sometimes better than the active treatments. Specifically, for significant weight gain, TV-46000 q1m and TV-46000 q2m were observed to have a 91% (RR: 0.09, 95% CrI: 0.01-0.43) and 94% (RR: 0.06, 95% CrI: 0.01-0.33) RRR, respectively, compared to paliperidone palmitate 1-month (PP3M), and a 92% (RR: 0.08, 95% CrI: 0.01-0.4) and 94% (RR: 0.06, 95% CrI: 0.01-0.31) RRR, respectively, compared to paliperidone palmitate 1-month (PP1M) 50-150 mg equivalent (EQ). Additionally, for treatment-related AEs, TV-46000 q1m was observed to have a 38% (RR: 0.62, 95% CrI: 0.38-0.98) risk reduction compared to PP3M.
Objectives
To assess the comparative efficacy and safety of TV-46000 compared with the LAIs approved in Canada and used for the maintenance treatment of schizophrenia.
Study Selection Methods
Systematic Literature Review
A search strategy was developed by an information specialist which was reviewed by a second information specialist according to the PRESSS checklist.43 The primary search was conducted May 11, 2023 using the Ovid platform (Ovid Technologies, New York City, NY) to search multiple databases including MEDLINE® (Epub ahead of print, in-process and other non-indexed citations), Embase, Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews.
Other sources for the literature search included grey literature. Specifically, the last two years of key congress databases that are not indexed in Embase, such as American Psychiatric Association (APA), European Psychiatric Association (EPA), and World Psychiatric Association (WPA) were searched. Additionally, manual reviews of health technology agency (HTA) websites including the Canadian Agency for Drugs and Technologies in Health (CADTH) and National Institute for Health and Care Excellence (NICE) were conducted, and the bibliographies of relevant SLR references from the primary literature search were used to validate searches and confirm complete literature retrieval. The clinical study reports (CSR) from the RISE and SHINE trials were used to provide data for risperidone extended-release injectable suspension (TV-46000). Information from ClinicalTrials.gov was also used to fill any data gaps where possible.
Studies were screened according to the inclusion and exclusion parameters (i.e., study eligibility criteria) outlined in Table 13.
Table 13: PICOS Inclusion and Exclusion Criteria
Domain | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
Population |
|
|
Intervention(s) |
|
|
Comparator(s) |
|
|
Outcomes |
|
|
Study Design |
|
|
Language |
|
|
Date |
|
|
AE = adverse event; CGI-S = Clinical Global Impression – Severity; EQ-5D = EuroQol 5 Dimension; ER = emergency room; PANSS = Positive and Negative Syndrome Scale
Source: EVERSANA NMA Report44
All identified articles were screened by two independent reviewers. Discrepancies for individual studies were resolved by consensus, with any disputes resolved by a third independent reviewer. Records retrieved from the grey literature searches were screened by a single independent reviewer and verified by a second independent reviewer. Discrepancies for individual records were resolved by a third independent reviewer. A total of 61 records from 24 unique studies were included in the SLR.
Network Meta-Analysis
Following screening for the SLR, included trials also underwent an additional review process to ensure that they were similar enough for inclusion in NMAs to assess the comparative efficacy and safety of TV-46000 and atypical LAIs approved in Canada. To be eligible for NMAs, studies were required to compare an atypical LAI of interest versus either placebo or another atypical LAI of interest. Studies that compared an intervention of interest to a comparator other than an atypical LAI, dosing studies, or studies that compared different administration locations for a single LAI of interest were excluded due to lack of connectivity in NMA networks. Studies were also excluded if they included non-stable patients based on a PANSS total score above 80 at randomization or mean CGI-S score greater than 4 at baseline. In schizophrenia trials, a patient is typically deemed as stable if they have a PANSS total score of ≤80 and CGI-S score ≤4.5,45,46 Furthermore, studies with identified limitations regarding study design or sample size were also considered for exclusion from NMAs. After the assessment of the 24 unique studies from the SLR, 18 unique studies were excluded, and a total of 6 studies (including RISE) were eligible for inclusion in the NMA.
The outcomes selected for the NMA were based on data availability, inclusivity of interventions in the network, and clinical significance. Efficacy outcomes were relapse rate, time to relapse, and change in PSP. Safety outcomes were AE-related discontinuation, significant weight gain, treatment-related AEs, and injection site pain.
Indirect Comparison Analysis Methods
Summary Measures
RR was used for the dichotomous outcome NMAs including relapse rate at six months, AE related discontinuation, significant weight gain, treatment-related AEs, and injection site pain. HR was used for the survival data NMA of time to relapse. Lastly, mean difference was used for the continuous outcome NMA of change from baseline in PSP score. All results are presented in league tables with pairwise comparisons as point estimates and 95% CrIs.
Geometry of the Network and Planned Methods of Analysis
Evidence network diagrams were developed for each outcome of interest. Within the networks, each treatment is represented by a node and comparisons between treatments are depicted by links between nodes. The size of a node reflects the sample size, and the width of the links reflects the number of studies connecting the treatments. It is also important to note that treatment with different doses were considered as separate nodes in the networks.
The NMAs were conducted in a Bayesian framework with fixed effect on the treatment parameters for the primary analyses of each outcome of interest. Fixed effect models were used as primary analyses due to the sparse networks with single study connections.47
Primary analyses for each outcome were selected based on data availability and on the results of the assessment of heterogeneity. Rationale for the primary analyses selected is provided below in the “Analysis Considerations” section of this report. NMA model specifications (burn-ins, iterations, and thinning) were adjusted to achieve convergence for each outcome (see Figure 8 - Figure 14).
Assessment of Heterogeneity and Inconsistency
The validity of an NMA requires that the included trials have similar study and patient characteristics. Heterogeneity across trials was assessed qualitatively by comparing trial design characteristics, patient eligibility criteria, and baseline patient characteristics. The following parameters were considered in the assessment of heterogeneity:
Study Design (i.e., blinding, randomization, and drug phases)
Intervention and Comparator Doses
Time of Drug Exposure
Eligibility Criteria (i.e., inclusion and exclusion criteria)
Randomization Criteria
Outcome Definition
Relevant Baseline Characteristics (i.e., age, sex, BMI, PANSS total score, CGI-S score, and prior psychotropic medications)
Tests for inconsistency were not appropriate for the NMAs conducted due to the sparse treatment networks and limited data available. When this is the case, inconsistency tests are underpowered and will nearly always fail to reject the null hypothesis of consistency (i.e., will fail to detect inconsistency).48
Sponsor’s Summary of the Results
Summary of Included Studies
A total of six studies were eligible for inclusion in the NMA (Table 14). Efficacy outcomes were relapse rate, time to relapse, and change in PSP. These outcomes were reported in five of the relevant studies captured and include all interventions of interest within the network. Safety outcomes were AE-related discontinuation, significant weight gain, treatment-related AEs, and injection site pain. AE-related discontinuation and significant weight gain were reported by all included studies. Treatment-related AEs and injection site pain were reported in four and five of the relevant studies, respectively. The data availability for the outcomes of interest is depicted in Table 15.
Table 14: Studies Included in Network Meta-Analyses
Intervention | Trial | Treatments Arms | Blinding | Study Duration | Key Outcomes | PANSS Randomization Criteria |
|---|---|---|---|---|---|---|
Risperidone | RISE | Risperidone SC (50-125mg; monthly) | Double-blind | 12 weeks + variable randomized phase | Time to relapse
| ≤80 |
Risperidone SC (100-250mg; bi-monthly) | ||||||
Placebo | ||||||
PP1M | Hough45 | PP1M IM (25, 50 or 100mg EQ; monthly) | Double-blind | 33 weeks + variable randomized phase | Time to relapse
| ≤75 |
Placebo | ||||||
Aripiprazole | ASPIRE-US | Aripiprazole IM (300 or 400mg; monthly) | Double-blind | 20-54 weeks + variable randomized phase | Time to relapse Change in PANSS and CGI-S Safety | ≤80 |
Placebo | ||||||
QUALIFY | Aripiprazole IM (400mg; monthly) | Open-label | 28 weeks | Change in QLS total score CGI-S | NR | |
PP1M IM (50-234mg; monthly) | ||||||
PP3M | Berwaerts 2015 | PP3M IM (175, 263, 350, or 525mg EQ; quarterly) | Double-blind | 29 weeks + variable randomized phase | Time to relapse Change in PANSS, CGI-S, and PSP Safety | <70 |
Placebo | ||||||
Savitz 2016 | PP3M IM (175, 263, 350, or 525mg EQ; quarterly) | Double-blind | 48 weeks | Rate of patients who remained relapse-free
| <70 | |
PP1M IM (50, 75, 100, or 150mg EQ; monthly) |
Bolded outcomes are the primary outcomes in each trial.
CGI-I = Clinical Global Impression – Improvement; CGI-S = Clinical Global Impression – Severity; CGI-SS = Clinical Global Impression of Severity of Suicidality; EQ = equivalent; IM = intramuscular; NR = not reported; PANSS = Positive and Negative Syndrome Scale; PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; PSP = Personal and Social Performance; QoL = quality of life; QLS = Quality of Life Scale; SC = subcutaneous.
Sources: RISE CSR,15 Hough (2010),49 Gopal (2011),50 Kozma (2011),51 Sliwa (2014),52 Markowitz (2013),53 Kane (2012),45 Fleischhacker (2013),54 NCT00705783 (2008),55 Kane (2015),56 Fleishhacker (2014),57 Naber (2015),58 Naber (2018),59 NCT01795547 (2013),60 EUCTR2012-002785-12-SE (2013),61 Berwaerts (2015),62 Bell (2019),63 NCT01529515 (2012),64 EUCTR2011-004676-11-RO (2017),65 Savitz (2019),66 Chirila (2017),67 Savitz. (2016),68 Gopal (2020),69 Kern (2018),70 Mathews (2018),71 Savitz (2019),72 Savitz (2017),73 Savitz (2017),74 NCT01515423 (2012),75 EUCTR2011-004889-15-PT (2012)76
Table 15: Data Availability for Network Meta-Analysis Outcomes
Intervention | Trial | Relapse Rate | Time to Relapse | Change in PSP | AE Related Discontinuation | Significant Weight Gain | Treatment- Related AEs | Injection Site Pain |
|---|---|---|---|---|---|---|---|---|
Risperidone | RISE | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
PP1M | Hough 2010 | Yes | Yes | Yes | Yes | Yes | Yes | No |
Aripiprazole | ASPIRE-US | Yes | Yes | Yes | Yes | Yes | No | Yes |
QUALIFY | No | No | No | Yes | Yes | No | Yes | |
PP3M | Berwaerts 2015 | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Savitz 2016 | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
AE = adverse event; PSP = Personal and Social Performance.
Sources: RISE CSR,15 Hough 2010,49 Kane 2012,45 Naber 2015,58 Berwaerts 2015,62 Savitz 201668
Heterogeneity Assessment
Trials were in alignment for several of the study and patient characteristics; however, there were also differences observed. Baseline characteristics including age, sex, BMI, mean PANSS score, and mean CGI-S score for including studies are depicted in Table 16. Key differences in study characteristics are presented in Table 17. Key differences in patient characteristics are presented in Table 18. Analytic approach based on the observed heterogeneity is discussed in the following section.
Table 16: Study and Patient Characteristics for Studies Included In NMA
Intervention | Trial | Treatments Arms | Treatment Exposure Duration (weeks) | Inclusion Criteria | Baseline Characteristics | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
Age (years) | Time Since Schizophrenia Diagnosis (years) | Previous Relapse Episodes | Number of Patients Randomized | Mean Age (years) | Male (%) | BMI (kg/m2) | Mean PANSS Total Score | Mean CGI-S Score | ||||
Risperidone | RISE | Risperidone SC (50-125mg; monthly) | 40a | 13-65c | ≥1 | ≥1 in the last 24 months | 183 | 50.6 | 61 | 28.9 | 61.5 | 3.3 |
Risperidone SC (100-250mg; bi-monthly) | 38.1a | 180 | 48.1 | 61 | 29.7 | 61.4 | 3.2 | |||||
Placebo | 24.3a | 181 | 49.2 | 61 | 29.5 | 61.0 | 3.3 | |||||
PP1M | Hough 2010 | PP1M IM (25, 50 or 100mg EQ; monthly) | 24.4a | 18-60 | ≥3 | NR | 205 | 38.8 | 53 | 27.3 | 52.1 | 3d |
Placebo | 15a | 203 | 39.4 | 55 | 27.2 | 53.1 | 3d | |||||
Aripiprazole | ASPIRE-US | Aripiprazole IM (300 or 400mg; monthly) | NR | 18-65 | ≥1 | NR | 269 | 40.1 | 60 | 28.1 | 54.5 | NR |
Placebo | NR | 134 | 41.7 | 59 | 29.5 | 54.4 | NR | |||||
QUALIFY | Aripiprazole IM (400mg; monthly) | NR | 18-60 | NR | NR | 148 | 42.6 | 60 | 29.9 | NR | 4 | |
PP1M IM (50-234mg; monthly) | NR | 147 | 41.2 | 60 | 29.1 | NR | 4 | |||||
PP3M | Berwaerts 2015 | PP3M IM (175, 263, 350, or 525mg EQ; quarterly) | 24.1a | 18-70 | ≥1 | NR | 160 | 37.1 | 74 | 26.2 | 54.9 | 2.7 |
Placebo | 20.9a | 145 | 38.5 | 76 | 26.2 | 54.2 | 2.8 | |||||
Savitz 2016 | PP3M IM (175, 263, 350, or 525mg EQ; quarterly) | 42.2b | 18-70 | ≥1 | NR | 483 | 39.2 | 51 | 26.6 | 57.3 | 2.9 | |
PP1M IM (50, 75, 100, or 150mg EQ; monthly) | 41b | 512 | 38.3 | 55 | 26.4 | 58.2 | 2.9 | |||||
aReported as median time of drug exposure.
bReported as mean time of drug exposure.
cRISE did not include adolescents (ages 13-17) in analyses.
dReported as median score.
BMI = body mass index; CGI-S = Clinical Global Impression – Severity; EQ = equivalent; IM = intramuscular; NR = not reported; PANSS = Positive and Negative Syndrome Scale; PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; SC = subcutaneous
Sources: RISE CSR,15 Hough 2010,49 Kane 2012,45 Naber 2015,58 Berwaerts 2015,62 Savitz 201668
Table 17: Differences in Study Characteristics
Outcome | Study Design | Intervention/ Comparator Doses | Time of Drug Exposure | Outcome Definition |
|---|---|---|---|---|
Relapse Rate | RISE was the only study that did not include a depot-drug phase before randomization | Differences in PP1M doses. PP1M dose in Hough 2010 was 25-100 mg EQ, whereas PP1M dose in Savitz 2016 was 50-150 mg EQ | No key differences observed | The definition of relapse varied across studies with RISE and ASPIRE-US having a lower threshold for relapse compared with Hough 2010 Berwaerts 2015, and Savitz 2016. Specifically, the PANSS criteria for Hough 2010/Berwaerts 2015/Savitz 2016 must be met for two consecutive visitsa, whereas for RISE/ASPIRE-US, it is only one visit. |
Time to Relapse | ||||
Change in PSP | Treatment exposure varied across studies, with randomized phases that were event driven for most studies and had different pre-planned number of events for analyses. Duration of exposure is presented in Table 16 | No key differences observed | ||
AE-Related Discontinuation | RISE and QUALIFY did not include a depot-drug phase before randomization. QUALIFY was also not a double-blind and patients were randomized before the oral medication phase | |||
Significant Weight Gain | ||||
Treatment-Related AEs | RISE was the only study that did not include a depot-drug phase before randomization | |||
Injection Site Pain | RISE and QUALIFY did not include a depot-drug phase before randomization. QUALIFY was also not a double-blind and patients were randomized before the oral medication phase | No key differences observed | No key differences observedb |
aTwo consecutive visits are between 3 and 7 days apart for Savitz 2016/Berwaerts 2015 (see Table 19 for relapse definition across all studies).
bAnalysis of injection site pain was based on the reported percentage of patients with injection site pain (regardless of time of drug exposure). Therefore, differences in time of drug exposure were not considered relevant for this outcome.
AE = adverse event; PP1M = paliperidone palmitate 1-month; PSP = Personal and Social Performance.
Table 18: Differences in Patient Characteristics
Outcome | Eligibility Criteria | Randomization Criteria | Relevant Baseline Characteristics |
|---|---|---|---|
Relapse Rate | No key differences observed | No key differences observed | RISE had a higher mean age and Berwaerts 2015 had a greater proportion of males |
Time to Relapse | |||
Change in PSP | |||
AE-Related Discontinuation | Differences in CGI-S scorea. RISE and ASPIRE-US requested ≤4, while QUALIFYb requested ≥3 and ≤5 | RISE had a higher mean age and QUALIFY had a higher mean CGI-S | |
Significant Weight Gain | RISE had a higher mean age, Berwaerts 2015 had a greater proportion of males, and QUALIFY had a higher mean CGI-S | ||
Treatment-Related AEs | No key differences observed | RISE had a higher mean age and Berwaerts 2015 had a greater proportion of males | |
Injection Site Pain | Differences in CGI-S scorea. RISE and ASPIRE-US requested ≤4, while QUALIFYb requested ≥3 and ≤5 | RISE had a higher mean age, Berwaerts 2015 had a greater proportion of males, and QUALIFY had a higher mean CGI-S |
aCGI-S not reported in Hough 2010, Berwaerts 2015, and Savitz 2016.
bFor QUALIFY, inclusion criteria correspond to randomization criteria. For this table, differences that involved the QUALIFY study were included only in the randomization criteria column.
AE = adverse event; CGI-S = Clinical Global Impression - Severity; PSP = Personal and Social Performance.
Sources: RISE CSR,15 Hough 2010,49 Kane 2012,45 Naber 2015,58 Berwaerts 2015,62 Savitz 201668
Study | Clinical Definition |
|---|---|
RISE | Relapse was defined as: 1) CGI-I of ≥5 (greater than or equal to minimally worse, i.e., minimally worse, much worse, or very much worse), AND an increase of any of the following individual PANSS items: conceptual disorganization, hallucinatory behavior, suspiciousness, and unusual thought content, to a score of >4 with an absolute increase of ≥2 on that specific item since randomization, OR an increase in any of the following 4 individual PANSS items: conceptual disorganization, hallucinatory behavior, suspiciousness, and unusual thought content, to a score of >4 and an absolute increase of ≥4 on the combined score of these 4 PANSS items (conceptual disorganization, hallucinatory behavior, suspiciousness, and unusual thought content) since randomization; 2) hospitalization due to worsening of psychotic symptoms (including partial hospitalization programs), excluding hospitalization for psychosocial reasons, 3) CGI-SS of 4 (severely suicidal) or 5 (attempted suicide) on Part 1 and/or 6 (much worse) or 7 (very much worse) on Part 2; 4) violent behavior resulting in clinically significant self-injury, injury to another person, or property damage |
ASPIRE-US | Relapse defined as meeting any or all of the following 4 criteria at any time during phase 4: 1) Clinical worsening as defined by CGI-I score of ≥5 and an increase on any of 4 individual PANSS items (conceptual disorganization, hallucinatory behavior, suspiciousness, or unusual thought content) to a score >4 with an absolute increase of ≥4 on the combined score of these items since randomization; 2) Hospitalization due to worsening of psychotic symptoms 3) Risk of suicide as defined by CGI-SS score of 4 (severely suicidal) or 5 (attempted suicide) on part 1 or a score of 6 (much worse) or 7 (very much worse) on part 2 4) Violent behavior resulting in clinically significant self-injury, injury to another person, or property damage |
Hough 2010 | Relapse was defined as one or more of the following: (1) hospitalization for symptoms of schizophrenia (involuntary or voluntary admission), (2) 25% increase in PANSS total score for two consecutive assessments for patients who scored >40 at randomization, or a 10-point increase for patients who scored ≤40 at randomization, (3) deliberate self-injury or aggressive behavior, or suicidal or homicidal ideation and aggressive behavior that was clinically significant, and (4) increase for two consecutive assessments in prespecified individual PANSS items scores (P1, P2, P3, P6, P7 and G8) to ≥5 for patients whose score was ≤3 at randomization, or to ≥6 for patients whose score was 4 at randomization. |
Berwaerts 2015 | Relapse defined as at least 1 of the following: 1) Hospitalization for schizophrenia symptoms (involuntary or voluntary admission); 2) 25% increase in PANSS total score from randomization for 2 consecutive assessments between 3 and 7 days apart for patients scoring higher than 40 at randomization or a 10-point increase for patients scoring 40 or lower at Randomization; 3) Increase in distinct PANSS item scores (P1 [delusions], P2 [conceptual disorganization], P3 [hallucinatory behavior], P6 [suspiciousness/persecution], P7 [hostility], or G8 [uncooperativeness]) for 2 consecutive assessments between 3 and 7 days apart; 4) Clinically significant deliberate self-injury or violent behavior resulting in suicide, injury, or significant damage; 5) Suicidal or homicidal ideation and aggressive behavior |
Savitz 2016 | Relapse defined as ≥1 of the following: (1) hospitalization for schizophrenia symptoms (involuntary or voluntary admission); (2) 25% increase in PANSS total score from randomization for 2 consecutive assessments between 3 and 7 days apart for patients scoring >40 at randomization, or a 10-point increase for patients scoring ≤40 at randomization; (3) increase in distinct PANSS item scores (P1, P2, P3, P6, P7, or G8) for 2 consecutive assessments between 3 and 7 days apart; (4) clinically significant, deliberate self-injury or violent behavior resulting in suicide, injury, or significant damage; or (5) suicidal or homicidal ideation and aggressive behavior. |
CGI-I = Clinical Global Impression-Improvement; CGI-SS = Clinical Global Impression-Severity of Suicidality; PANSS = Positive and Negative Symptom Scale
Sources: RISE CSR,15 Hough 2010,49 Kane 2012,45 Berwaerts 2015,62 Savitz 201668
Analysis Considerations
The primary networks for each of the seven outcomes of interest were selected based on data availability and the results of the heterogeneity assessment. Studies included in the primary networks accounted for the important differences between studies, where possible. Solutions based on the differences observed are described below.
All primary networks included PP1M 25-100 mg EQ49 and PP1M 50-150 mg EQ68 as separate nodes as the doses were not deemed comparable. The mean dose of PP1M in Savitz 2016 was 119 mg EQ, which is above the range of acceptable doses used in Hough 2010.
For change in PSP, despite the limitation of a lack of similar time-point of assessment, all relevant studies were included in the primary network and the analysis was based on the change in PSP from baseline to study endpoint.
Additionally, for the safety outcomes in which the differences in time of drug exposure were considered relevant (i.e., AE-related discontinuation, significant weight gain, and treatment-related AEs), the primary analyses adjusted for these differences by assuming a constant incidence rate and estimating the number of events at six months. Therefore, the primary analyses only included studies that reported time of drug exposure.
In addition, despite having a higher proportion of males, Berwaerts 201562 was included in the primary networks for change in PSP and significant weight gain because an analysis without Berwaerts 2015 would result in a loss of network connectivity, as it connects the PP3M node to the network, and therefore any comparison with PP3M and PP1M 50-150 mg EQ.
Furthermore, while the definition of relapse varied across studies with RISE15 and ASPIRE-US45 having a lower threshold for relapse compared with Hough 2010, Berwaerts 2015, and Savitz 2016, all relevant studies were included in the primary analyses. This approach was considered very conservative for TV-46000.
Lastly, as for the other differences observed for RISE, such as not including a depot-drug phase before randomization and having a higher mean age at baseline, no further adjustments were considered for the analyses. The lack of a depot drug phase in RISE was considered a conservative factor for TV-46000 within the analysis, given that RISE is most likely to be the study negatively impacted by this difference. As for RISE having a higher mean age, based on clinical expert opinion from a clinician actively treating patients with schizophrenia in Canada, consulted by the Sponsor, it was considered unlikely that these differences could bias the results in favor of TV-46000.
Evidence Networks
The primary networks for each selected outcome accounted for the analysis considerations described above. Firstly, for the primary analysis of relapse rate at six months, KM curves for time to relapse were digitized for each included study to estimate the relapse rate at six months and inform the respective NMA. The primary analysis for time to relapse included all studies that reported outcome data. Additionally, the primary analysis for change in PSP included all studies that reported outcome data. The primary analysis for AE-related discontinuation is with the calculated number of events at 26 weeks (assumed constant incidence rate) and with the two studies that reported outcome, time of drug exposure data, and achieved convergence. Furthermore, the primary analyses for significant weight gain and treatment-related AEs are with the calculated number of events at 26 weeks (assumed constant incidence rate) and with the four studies that reported outcome and time of drug exposure data. Lastly, the primary analysis for injection site pain is with the absolute incidence of events at study endpoint and with all studies that reported outcome data (including the QUALIFY study).
The network diagrams for the primary analyses for each outcome of interest are presented in the subsequent sections.
Relapse Rate, Time to Relapse, and Change in Personal and Social Performance
The studies included in the primary analysis for relapse rate at six months, time to relapse, and change in PSP are RISE, Hough 2010, ASPIRE-US, Berwaerts 2015, and Savitz 2016. Figure 4 depicts the network diagram for the five studies included in the NMAs.
Figure 4: Relapse Rate, Time to Relapse and Change in Personal and Social Performance Network Diagram
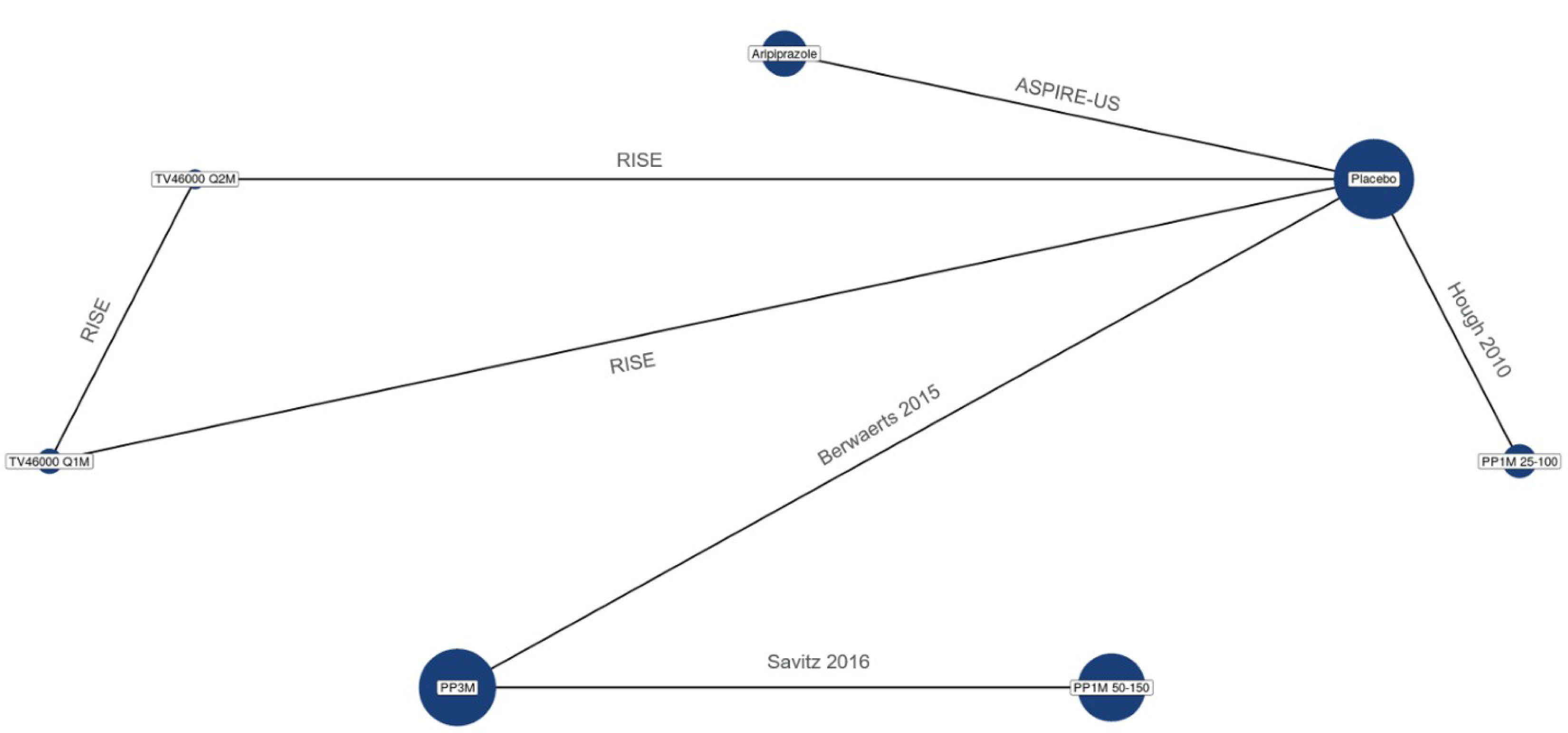
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Adverse Event Related Discontinuation
The studies included in the primary analysis for AE-related discontinuation are RISE21 and Hough 201038. Figure 5 depicts the network diagram for the two studies included in the NMA for AE-related discontinuation.
Figure 5: Adverse Event Related Discontinuation Network Diagram
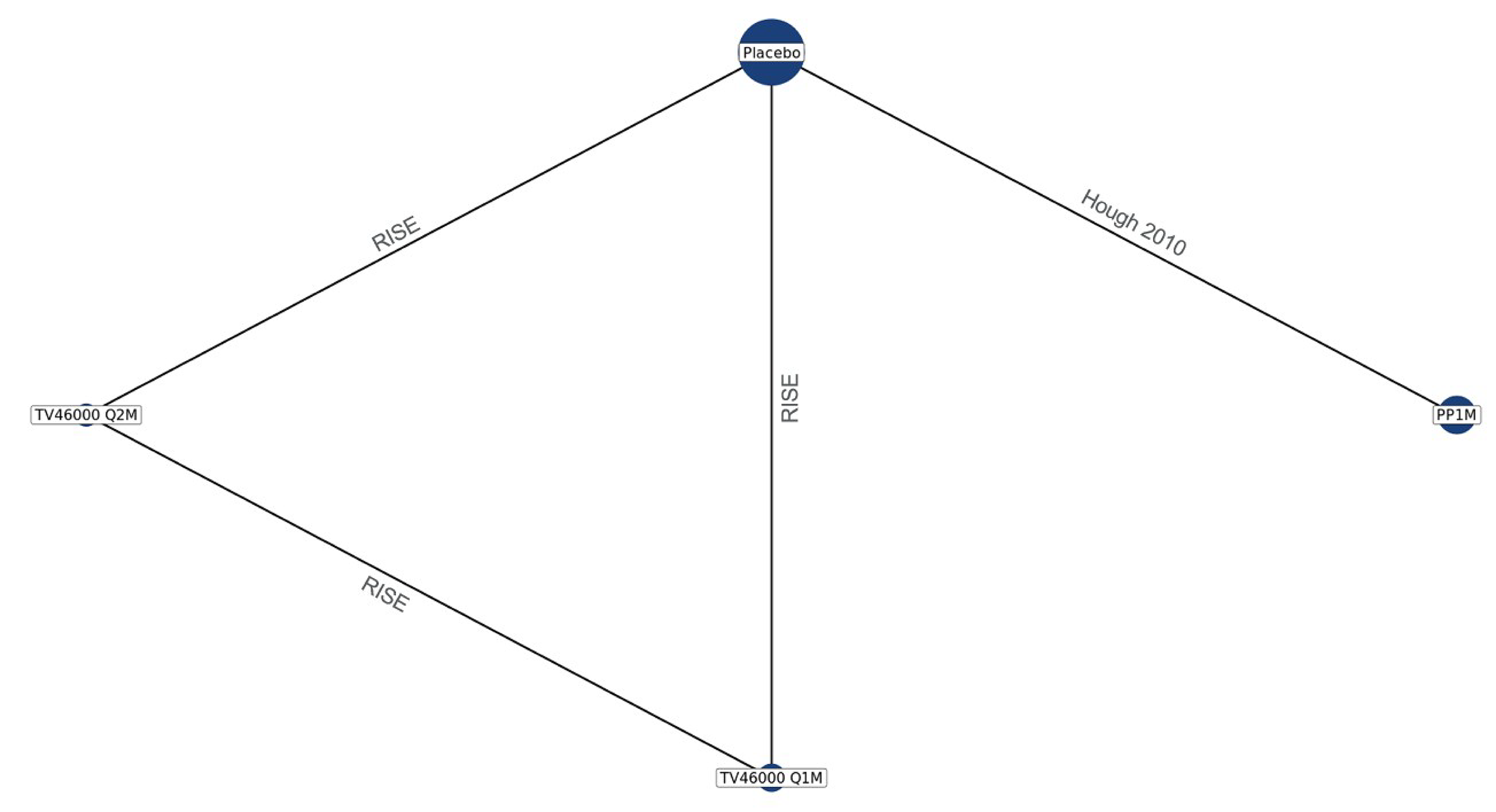
PP1M = paliperidone palmitate 1-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Significant Weight Gain, and Treatment-Related Adverse Events
The studies included in the primary analysis for significant weight gain and treatment-related AEs are RISE, Hough 2010, Berwaerts 2015, and Savitz 2016. Figure 6 depicts the network diagram for the four studies included in the NMAs.
Figure 6: Significant Weight Gain and Treatment-Related Adverse Events Network Diagram
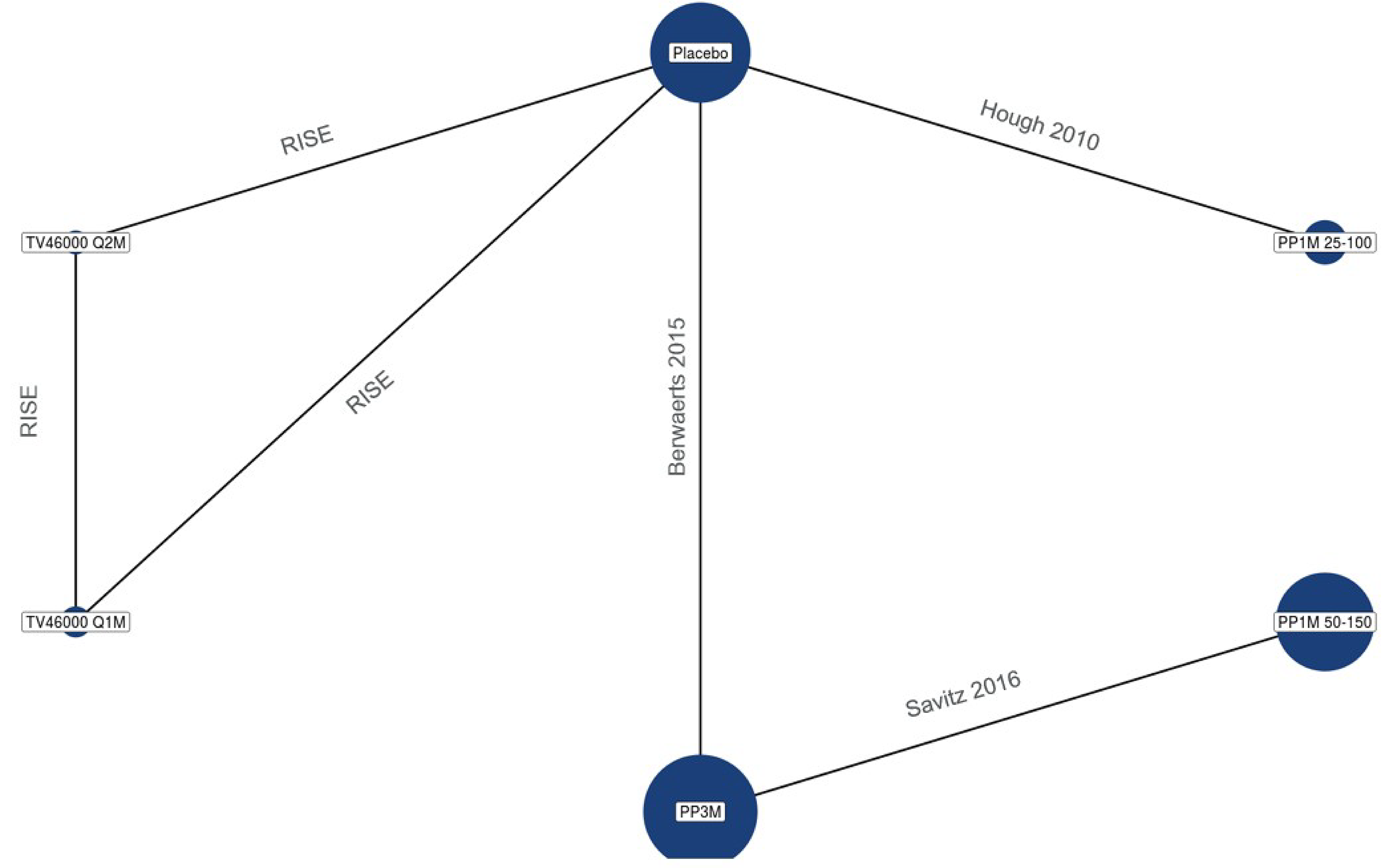
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly
Source: EVERSANA NMA Report44
Injection Site Pain
The studies included in the primary analysis for injection site pain are RISE, ASPIRE-US, Berwaerts 2015, Savitz 2016, and QUALIFY. Figure 7 depicts the network diagram for the five studies included in the NMA for injection site pain.
Figure 7: Injection Site Pain Network Diagram
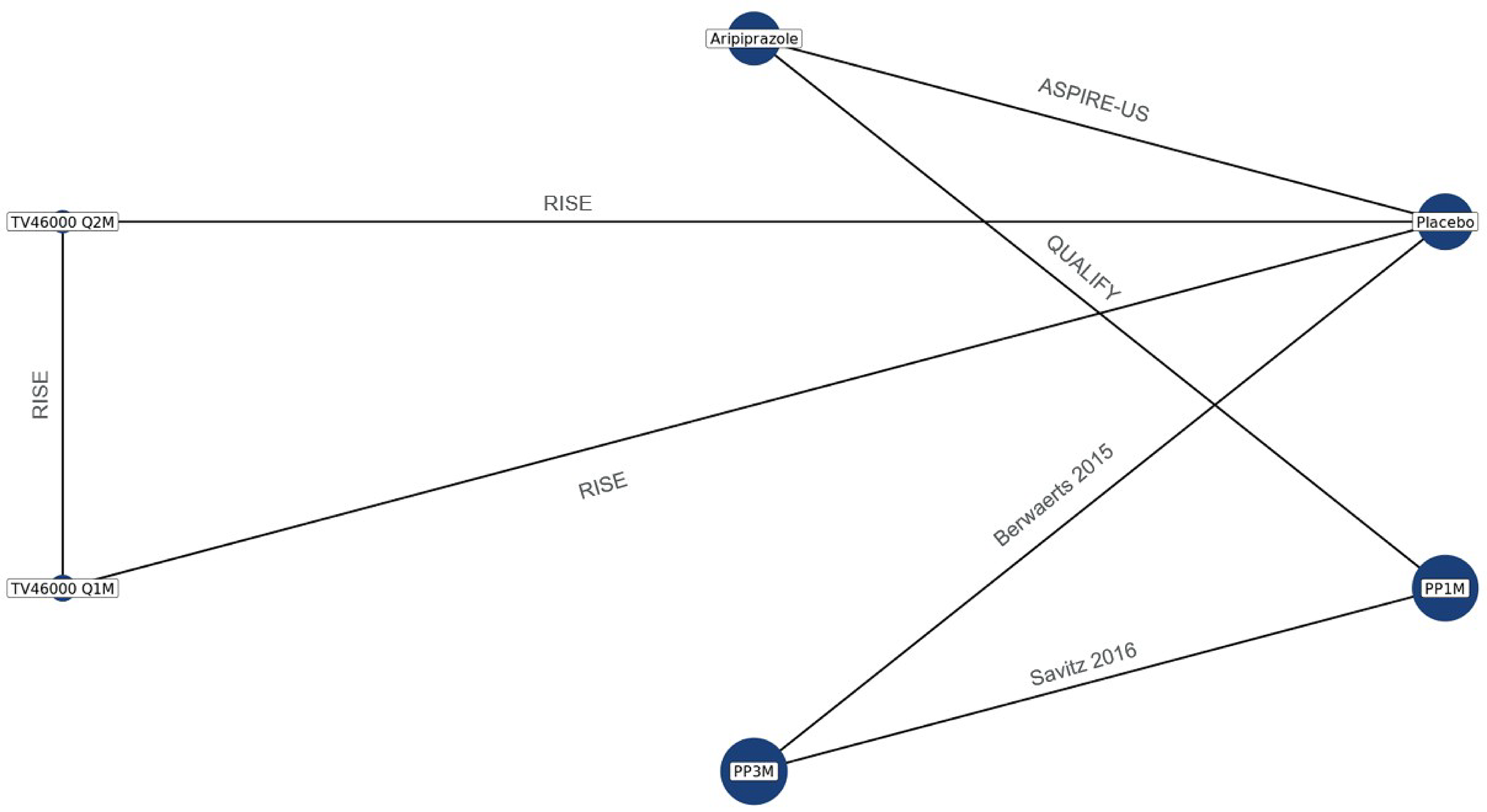
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Efficacy
Relapse Rate at Six Months
The fixed effects NMA results for relapse rate at six months is depicted in Figure 8. All active treatments (i.e., TV-46000 q1m, aripiprazole, PP1M 25-100 mg EQ, PP3M, TV-46000 q2m, and PP1M 50-150 mg EQ) were comparable, and were significantly better than placebo.
Figure 8: Relapse Rate at 6 Months - Fixed Effects NMA League Table
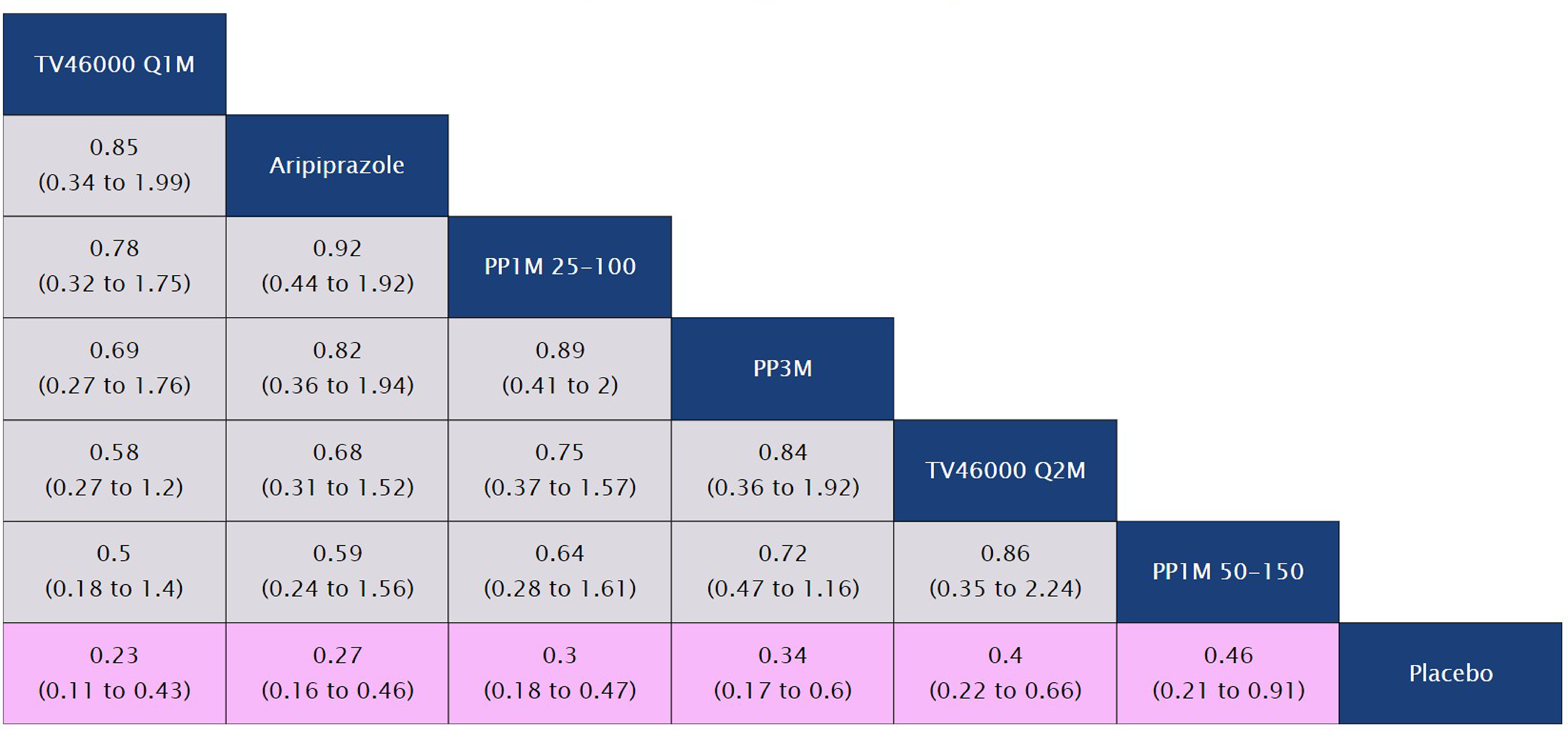
Note: Study sample size was the average sample size from baseline to six months (reported by KM curves)
Pairwise comparisons from the fixed-effect model are shown in terms of relative risk and 95% credible intervals (CrIs). Order on the table is determined by the average rank of a treatment. Treatments with the highest rank are found at the top left side of the table. Rank is determined by point estimates and does not indicate certainty of superiority or inferior. A credible interval overlapping 1 is indicative of treatments that are comparable (grey cells). A credible interval that does not contain 1 indicates that there are significant differences between treatments (pink cells).
Model specifications: 40,000 iterations, 40,000 burn-ins, 1 thinning.
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Time to Relapse
The fixed effects NMA results for time to relapse is depicted in Figure 9. All active treatments (i.e., TV-46000 q1m, aripiprazole, PP1M 25-100 mg EQ, PP3M, TV-46000 q2m, and PP1M 50-150 mg EQ) were significantly better than placebo.
Figure 9: Time to Relapse - Fixed Effects NMA League Table
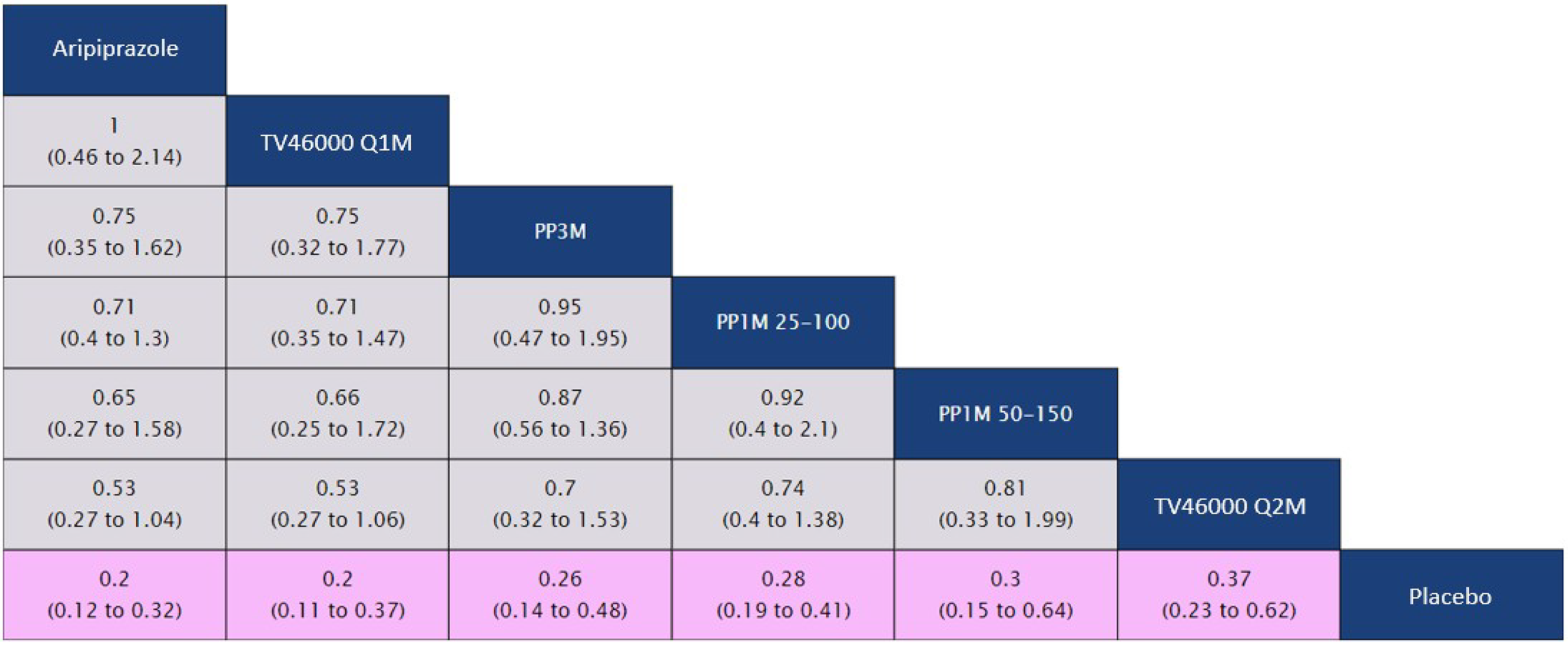
Pairwise comparisons from the fixed-effect model are shown in terms of hazard ratio and 95% credible intervals (CrIs). Order on the table is determined by the average rank of a treatment. Treatments with the highest rank are found at the top left side of the table. Rank is determined by point estimates and does not indicate certainty of superiority or inferior. A credible interval overlapping 1 is indicative of treatments that are comparable (grey cells). A credible interval that does not contain 1 indicates that there are significant differences between treatments (pink cells).
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Change in Personal and Social Performance
The fixed effects NMA results for change in PSP is depicted in Figure 10. All active treatments (i.e., TV-46000 q1m, aripiprazole, PP1M 25-100 mg EQ, PP3M, TV-46000 q2m, and PP1M 50-150 mg EQ) were comparable, and were significantly better than placebo.
Figure 10: Change in Personal and Social Performance - Fixed Effects NMA League Table
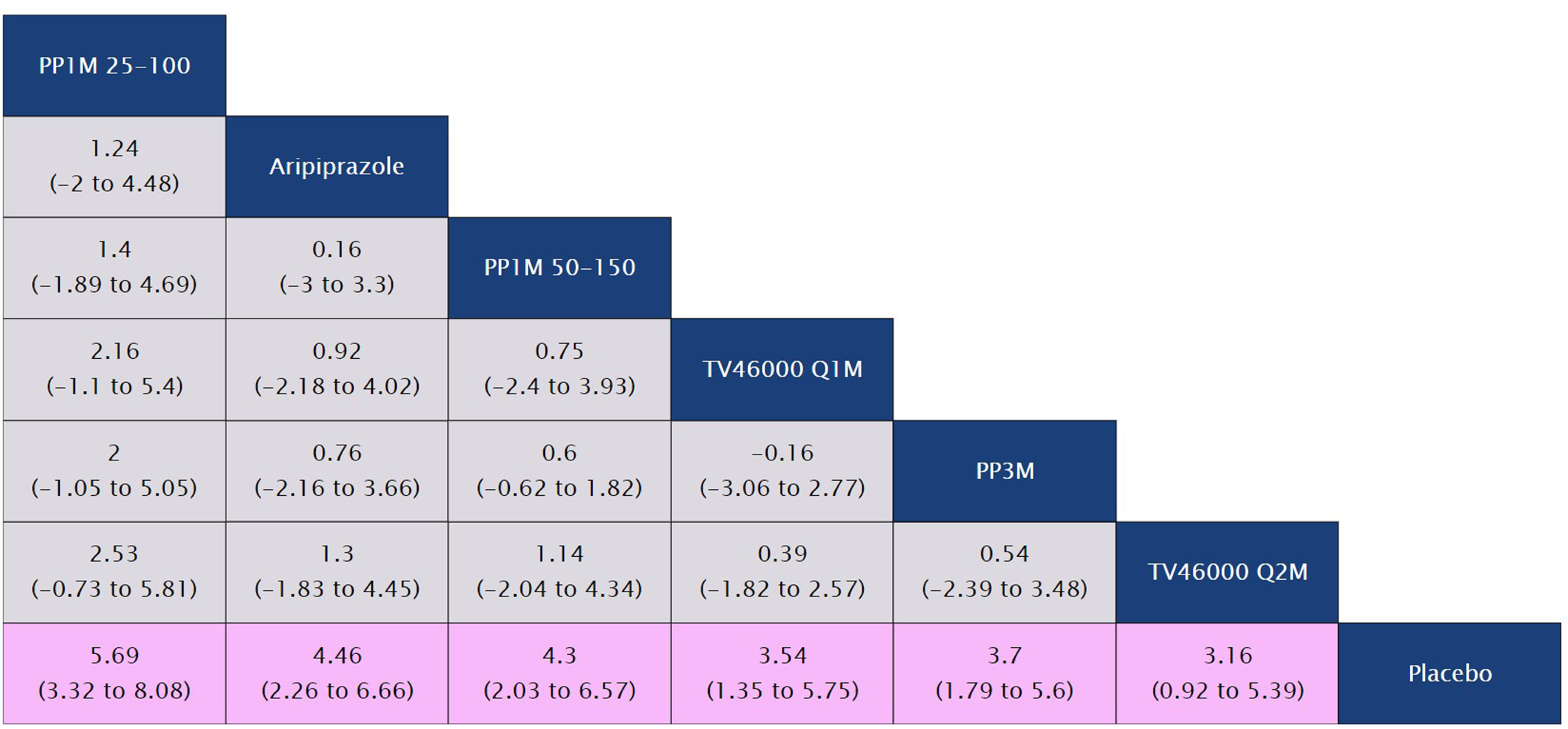
Pairwise comparisons from the fixed-effect model are shown in terms of mean difference and 95% credible intervals (CrIs). Order on the table is determined by the average rank of a treatment. Treatments with the highest rank are found at the top left side of the table. Rank is determined by point estimates and does not indicate certainty of superiority or inferior. A credible interval overlapping 0 is indicative of treatments that are comparable (grey cells). A credible interval that does not contain 0 indicates that there are significant differences between treatments (pink cells).
Model specifications: 40,000 iterations, 40,000 burn-ins, 1 thinning.
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Harms
Adverse Event Related Discontinuation
Results from a preliminary analysis with RISE, Hough 2010, Berwaerts 2015, and Savitz 2016 did not achieve convergence with a fixed effects model. Therefore, results are not interpretable. Berwaerts 2015 reported zero events for AE-related discontinuation for the PP3M arm, which creates challenges for model fit. If treatment effects are too different, a fixed effect model is not flexible enough to fit the data. A fixed effect model without Berwaerts 2015 was included as the primary analysis, with the caveat that Savitz 2016 was also not included in the network as there is a lack of network connection with Berwaerts 2015 removed.
The fixed effects NMA results for AE-related discontinuation is depicted in Figure 11. TV-46000 q1m and q2m were comparable to PP1M and placebo.
Figure 11: Adverse Event Related Discontinuation (At 26 Weeks) - Fixed Effects NMA League Table
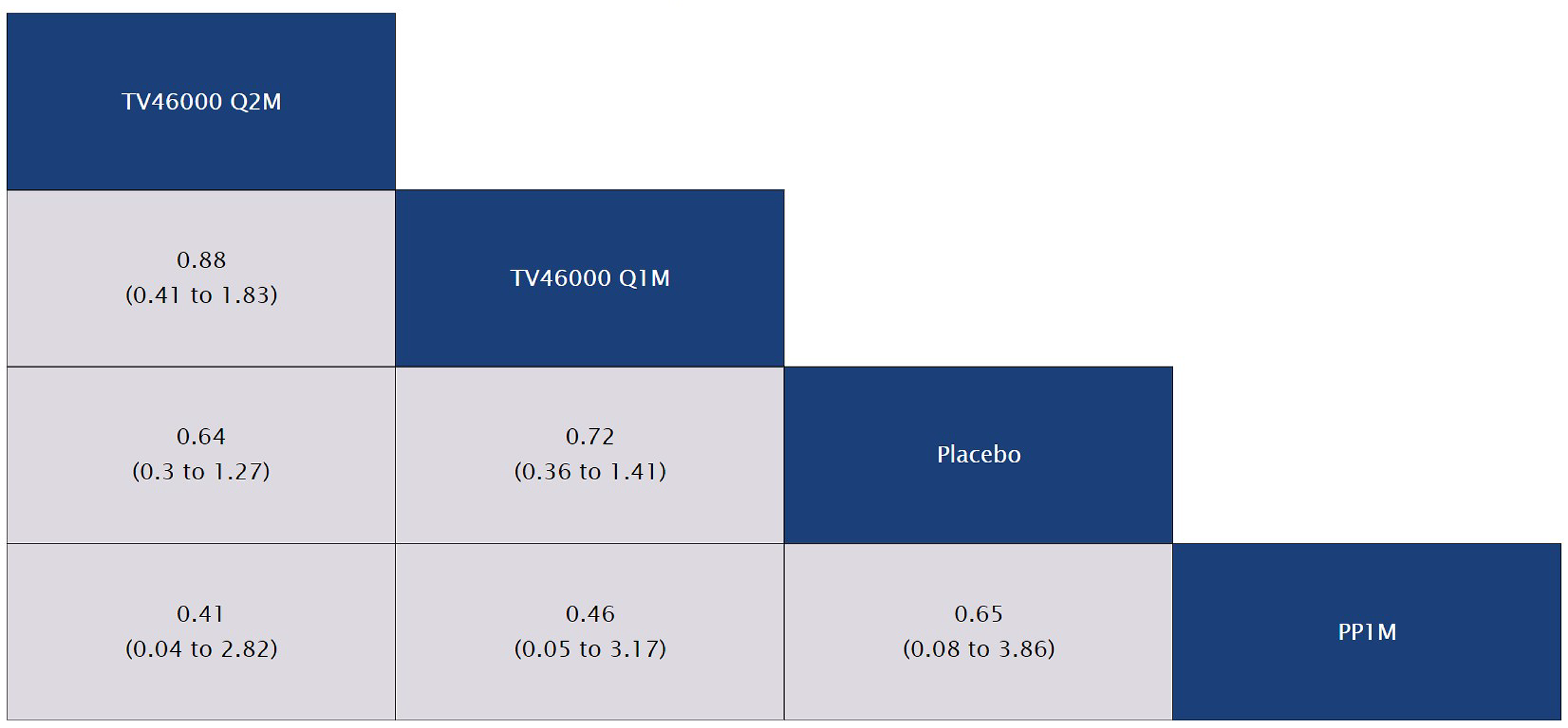
Pairwise comparisons from the fixed-effect model are shown in terms of relative risk and 95% credible intervals (CrIs). Order on the table is determined by the average rank of a treatment. Treatments with the highest rank are found at the top left side of the table. Rank is determined by point estimates and does not indicate certainty of superiority or inferior. A credible interval overlapping 1 is indicative of treatments that are comparable (grey cells). A credible interval that does not contain 1 indicates that there are significant differences between treatments (pink cells).
Model specifications: 80,000 iterations, 40,000 burn-ins, 2 thinning.
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Significant Weight Gain
The fixed effects NMA results for significant weight gain is depicted in Figure 12. TV-46000 q1m, PP1M 25-100 mg EQ, and TV-46000 q2m were comparable to placebo and significantly better than both PP3M and PP1M 50-150 mg EQ.
Figure 12: Significant Weight Gain (At 26 Weeks) - Fixed Effects NMA League Table
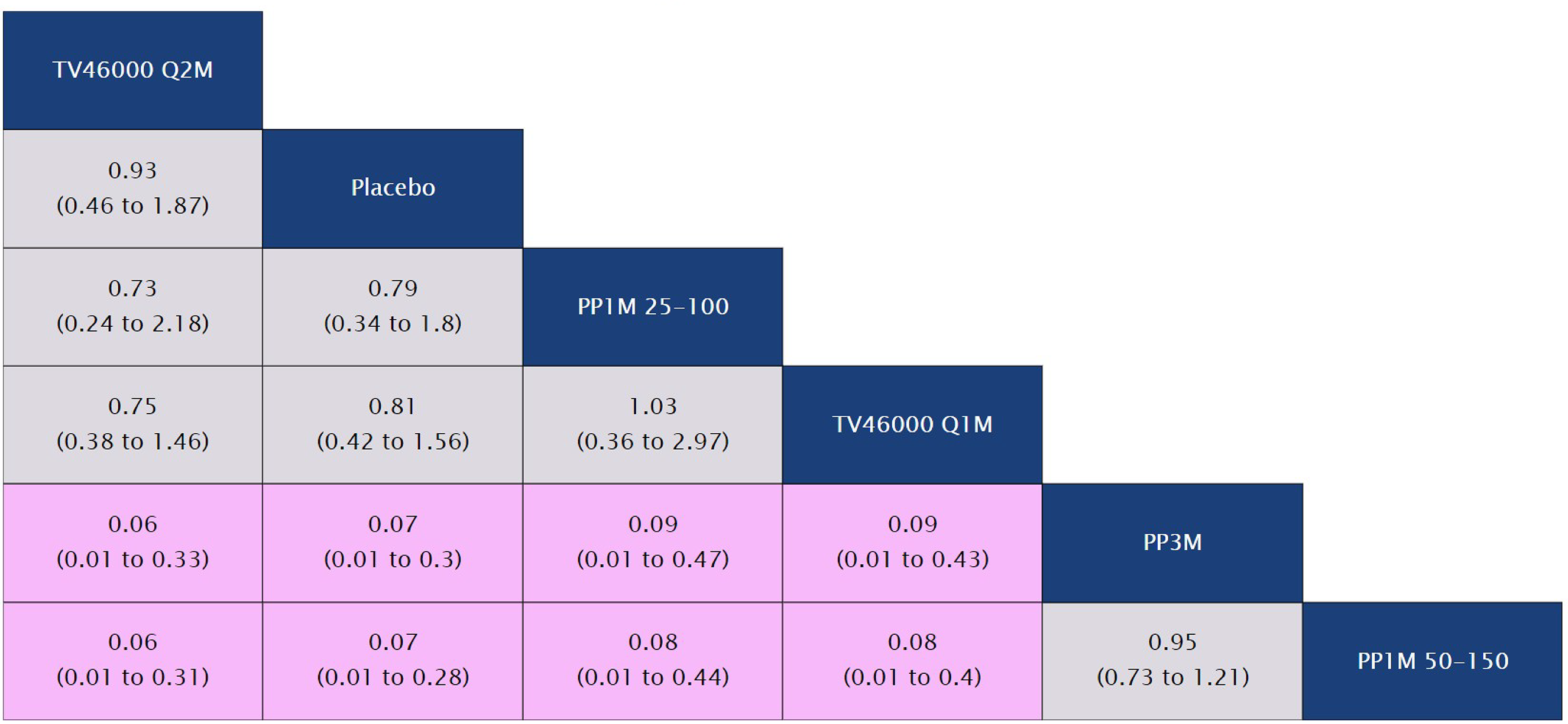
Pairwise comparisons from the fixed-effect model are shown in terms of relative risk and 95% credible intervals (CrIs). Order on the table is determined by the average rank of a treatment. Treatments with the highest rank are found at the top left side of the table. Rank is determined by point estimates and does not indicate certainty of superiority or inferior. A credible interval overlapping 1 is indicative of treatments that are comparable (grey cells). A credible interval that does not contain 1 indicates that there are significant differences between treatments (pink cells).
Model specifications: 80,000 iterations, 40,000 burn-ins, 2 thinning.
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Treatment-Related Adverse Events
The fixed effects NMA results for treatment-related adverse events is depicted in Figure 13. PP1M 25-100 mg EQ, TV-46000 q1m, and TV-46000 q2m were comparable to placebo. PP1M 25-100 mg EQ, TV-46000 q1m, and placebo were significantly better than PP3M and PP1M 50-150 mg EQ. PP1M 5-100 mg EQ and placebo were significantly better than PP1M 50-150 mg EQ.
Figure 13: Treatment-Related Adverse Events (At 26 Weeks) - Fixed Effects NMA League Table
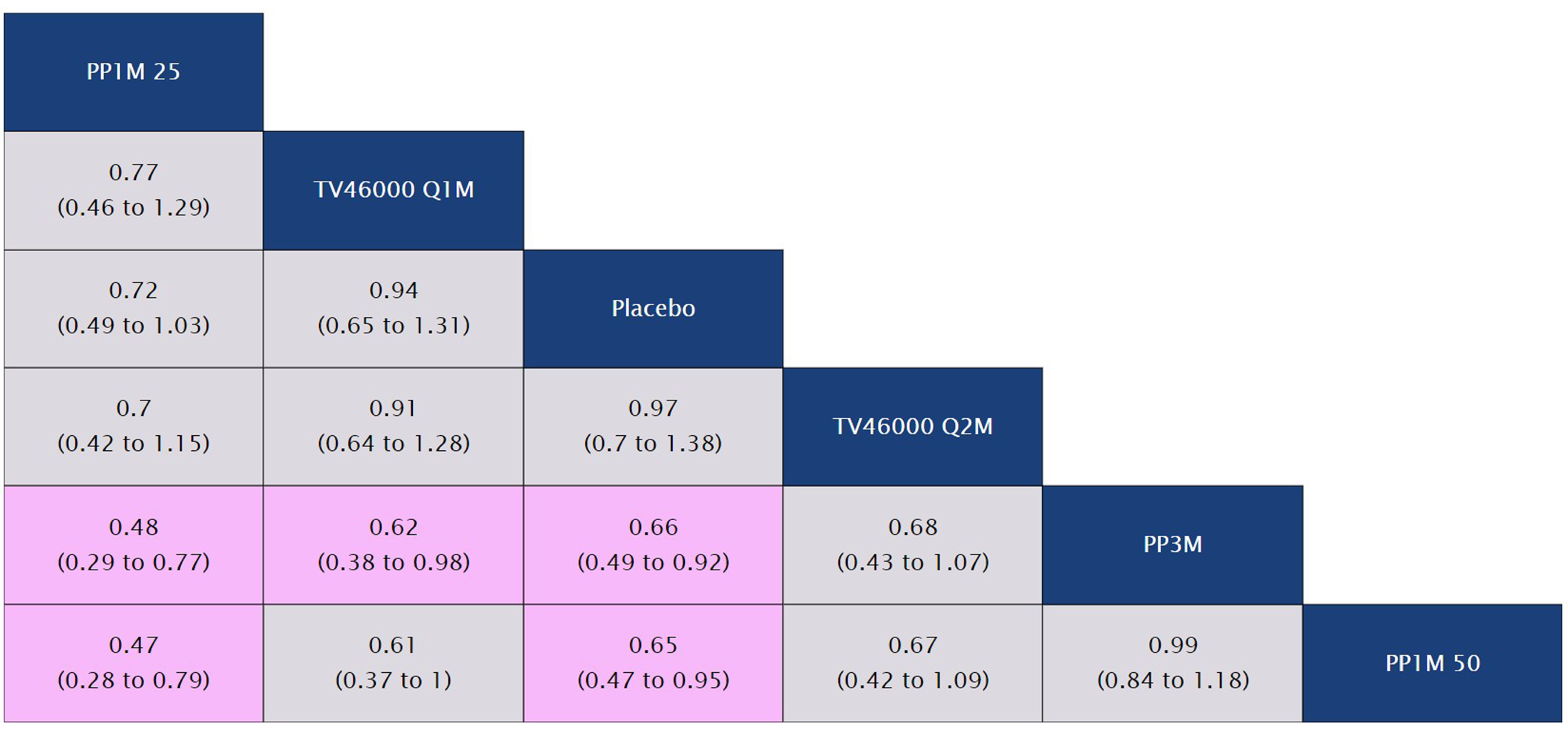
Pairwise comparisons from the fixed-effect model are shown in terms of relative risk and 95% credible intervals (CrIs). Order on the table is determined by the average rank of a treatment. Treatments with the highest rank are found at the top left side of the table. Rank is determined by point estimates and does not indicate certainty of superiority or inferior. A credible interval overlapping 1 is indicative of treatments that are comparable (grey cells). A credible interval that does not contain 1 indicates that there are significant differences between treatments (pink cells).
Model specifications: 40,000 iterations, 40,000 burn-ins, 1 thinning.
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Injection Site Pain
The fixed effects NMA results for injection site pain is depicted in Figure 14. All active treatments (TV-46000 q1m, aripiprazole, TV-46000 q2m, PP3M, and PP1M were comparable to placebo. Aripiprazole was significantly better than PP3M and PP1M.
Figure 14: Injection Site Pain - Fixed Effects NMA League Table
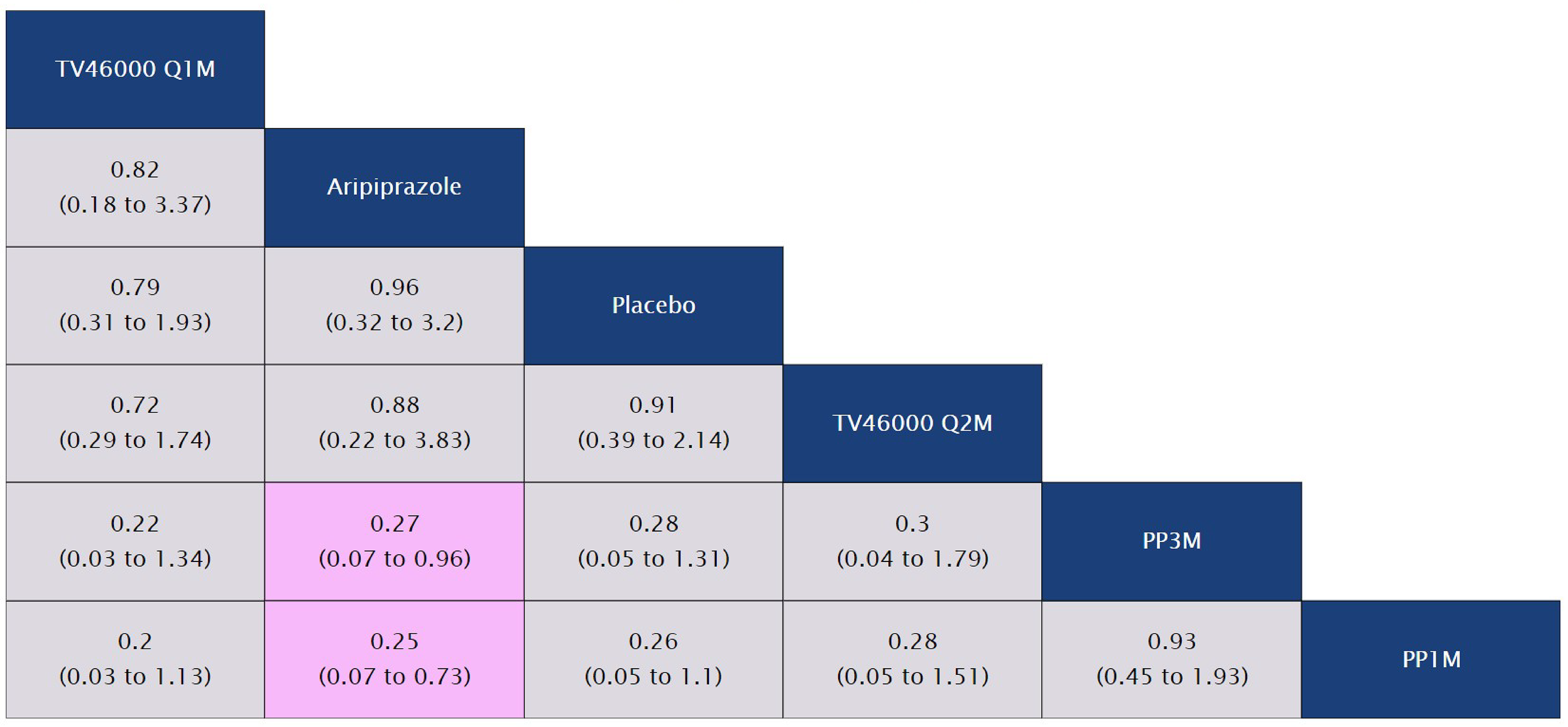
Pairwise comparisons from the fixed-effect model are shown in terms of relative risk and 95% credible intervals (CrIs). Order on the table is determined by the average rank of a treatment. Treatments with the highest rank are found at the top left side of the table. Rank is determined by point estimates and does not indicate certainty of superiority or inferior. A credible interval overlapping 1 is indicative of treatments that are comparable (grey cells). A credible interval that does not contain 1 indicates that there are significant differences between treatments (pink cells).
Model specifications: 200,000 iterations, 100,000 burn-ins, 5 thinning.
PP1M = paliperidone palmitate 1-month; PP3M = paliperidone palmitate 3-month; q1m = monthly; q2m = bi-monthly.
Source: EVERSANA NMA Report44
Key Sensitivity Analyses
The primary analysis of relapse rate at six months used the average sample size of population at risk from baseline to six months, as reported by the KM curves. Sensitivity analyses that used the sample size at study baseline and at last available time point before 6 months, were conducted. Additionally, for the safety outcomes in which the differences in time of drug exposure were considered relevant (i.e., AE-related discontinuation, significant weight gain, and treatment-related AEs), the primary analyses adjusted for these differences by assuming a constant incidence rate and estimating the number of events at six months. Sensitivity analyses using the absolute incidence of events at study endpoint (i.e., regardless of time of treatment exposure) were also conducted.
For relapse rate at six months, the significant difference between all active treatments and placebo remained regardless of the sample size used in this analysis, except for the comparison of PP1M 50-150 versus placebo when the sample size at last available time point before 6 months was used. For the safety outcome sensitivity analyses based on events at study endpoint, compared to the primary analyses, TV-46000 q1m and TV-46000 q2m kept the same ranking in relation to other active treatments in the league tables, and showed similar results for the statistical significance across those comparators, although with a difference for the NMA of treatment-related adverse events. In the primary analysis of treatment-related adverse events (which used the estimated number of events at six months), TV-46000 q1m was significantly better than PP3M; however, that statistical significance difference was not observed in the sensitivity analysis based on the absolute incidence of treatment-related adverse events at study endpoint.
Conclusions
In conclusion, the results of the NMAs demonstrate that TV-46000 q1m and TV 46000 q2m subcutaneous risperidone injections are generally comparable in terms of efficacy and safety to other LAIs used for the maintenance treatment of schizophrenia in Canada. For the efficacy outcomes of relapse rate, time to relapse, and change in PSP, TV-46000 was comparable to other active treatments and significantly better than placebo. Furthermore, for the safety outcomes of AE-related discontinuation, significant weight gain, treatment-related AEs, and injection site pain, TV-46000 was comparable to placebo, usually comparable to other active treatments, and sometimes significantly better than other active treatments. Specifically, for significant weight gain, TV-46000 q1m and q2m were significantly better than both PP3M and PP1M 50-150 mg EQ, and for treatment-related AEs, TV-46000 q1m was significantly better than PP3M.
Critical Appraisal of the Indirect Evidence
The sponsor-submitted NMA identified studies for inclusion through an SLR with clearly described and appropriate methods. A total of 61 records from 24 unique studies were screened for inclusion based on predefined criteria; 18 of the 24 studies were excluded and the remaining 6 (the RISE study among them) were included in the NMA. The outcomes included in the NMA were based on data availability, in addition to clinical significance, and therefore important outcomes such as HRQoL were not included.
The included studies had appropriate comparators for risperidone ER (TV-46000), according to the clinical expert consulted by CDA-AMC. The patients’ baseline characteristics were sufficiently similar to warrant inclusion in the NMA. However, patients included in the RISE study were on average a full decade older than the patients in the comparator trials. The clinical expert consulted noted that patients with schizophrenia tend to have their disease become more manageable as they age out of early adulthood. However, the PANSS scores suggested that the patients in the RISE study had slightly more severe symptoms compared to those in the comparator studies. These differences introduce uncertainty into the results. There were some differences in the definition of clinical relapse in the included studies, but the clinical expert consulted considered the definitions comparable and not likely to impact the interpretability of the results.
The NMAs used RR for the dichotomous outcomes of relapse rate at 6 months, discontinuation due to AEs, significant weight gain, treatment-related AEs, and injection site pain, which was considered appropriate. HR was used for the survival data NMA of time to relapse. The investigators did not report whether censoring was accounted for. Given the potential for censoring to impact the results due to patients lost to follow-up and the use of different censoring rules in the included studies, the potential for bias in the results cannot be ruled out. Furthermore, interpreting the proportional hazard is challenging when the model used is not specified. Comparison of HR across trials can be misleading because each HR is dependent on each trial’s specific hazard and each trial’s specific censoring methods. Overall, these statistical concerns increase the uncertainty of the overall results and could introduce bias (the direction of which is unknown) into the NMA estimates.
Economic Review
Sponsor-Submitted Cost Comparison
The sponsor submitted a cost comparison for risperidone ER once monthly (Longavo) compared with other LAI antipsychotics approved for the treatment of adults with schizophrenia, including risperidone once every 2 weeks (Risperdal Consta), another risperidone ER once monthly (Perseris), aripiprazole once monthly (Abilify Maintena), and paliperidone once monthly and once every 3 months (Invega Sustenna and Invega Trinza, respectively).
The sponsor reported an annual drug cost of risperidone ER once monthly of $5,930 per patient, and an annual administration cost of $51 (Table 20 and Table 21). Annual drug costs for the injectable comparators ranged from $2,394 to $9,939, with annual administration costs ranging from $17 to $101. The incremental cost of risperidone ER once monthly ranged from an annual savings of $4,060 per patient compared to risperidone intramuscular 50 mg to an additional annual cost of $3,486 per patient compared to risperidone intramuscular 12.5 mg once monthly (Table 22).
Critical Appraisal of Cost Information
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the cost comparison:
Assumption of clinical similarity is uncertain: The sponsor submitted a cost comparison of risperidone ER compared to other LAIs available for the treatment of schizophrenia in adult patients based on a sponsor-conducted ITC. In the submitted ITC, risperidone ER once monthly was generally comparable to aripiprazole once monthly, paliperidone once monthly, and paliperidone once every 3 months in terms of relapse rate at 6 months, time to relapse, change in PSP scale score, AE-related discontinuation, treatment-related AEs, and injection site pain, although some comparators were not included within the networks of all outcomes due to lack of data. Risperidone ER once monthly had significantly less risk of weight gain than both forms of paliperidone palmitate. However, the ITC was associated with limitations that increased uncertainty in the results, such as baseline differences in mean age and PANSS scores between the patient population in the RISE study and those in the comparator trials. Additionally, the lack of information on how censoring was accounted for in individual studies could potentially bias the results in an unknown direction. As such, the assumption of clinical similarity is uncertain.
CDA-AMC was unable to address this limitation in reanalyses.
Uncertainty in the comparators that may be displaced: In their submission,77 the sponsor noted that LAI AAPs are underutilized in Canada due to limitations related to complex initiation regimens; preparation steps, such as reconstitution; an intramuscular mode of administration that patients may find invasive and painful; and limited dosing, administration, and injection site flexibility. The sponsor also noted that some jurisdictions in Canada limit reimbursement of LAI AAPS to patients who experienced barriers to adherence or whose schizophrenia failed to respond to other antipsychotic options or who have intolerances or contraindications to other antipsychotic options. The sponsor further stated that risperidone ER was designed to facilitate acceptance of LAIs, improve adherence, and ease the transition from oral to LAI therapy. Clinical expert feedback obtained by CDA-AMC agreed that risperidone ER is intended to and likely will displace some use of oral antipsychotic drugs currently reimbursed in Canada, particularly oral risperidone.
CDA-AMC considered oral risperidone to be a relevant comparator because risperidone ER is expected to displace some of its use.
Confidential pricing agreements: Although the submitted price for risperidone ER is similar to the publicly available list prices of other LAI AAPs, these list prices are higher than the price paid by jurisdictional drug plans due to confidential pricing agreements for at least some of the comparators.78,79 Therefore, the submitted price of risperidone ER likely requires a price reduction to avoid incurring additional costs relative to its comparators.
CDA-AMC was unable to address this limitation in reanalyses because the negotiated prices of the comparators are unknown.
CDA-AMC Reanalyses
CDA-AMC reanalyses were derived by making changes in values and assumptions in consultation with clinical experts. The single change made by CDA-AMC was the inclusion of oral risperidone as a relevant comparator.
As reported by the sponsor, at the submitted price, the annual drug cost of risperidone ER once monthly ($5,930 per patient; Table 20) is equal to the annual drug cost of aripiprazole once monthly ($5,930 per patient) and within the range of annual costs for the various available doses of risperidone once every 2 weeks, paliperidone once monthly, and paliperidone once every 3 months ($2,394 to $8,779), when comparing public list prices for the comparators. The annual drug acquisition cost of risperidone ER is $5,486 to $5,634 higher per patient than the annual drug acquisition cost of oral risperidone. When administration costs are also considered, the annual total cost of risperidone ER once monthly is $5,537 to $5,685 higher per patient than the annual total cost of oral risperidone (Table 22).
Table 20: CDA-AMC Cost Comparison Table
Generic name (brand name) | Strength | Dosage form | Price ($) | Recommended dosage regimen | Annual drug cost ($) | Difference in annual drug cost ($) |
|---|---|---|---|---|---|---|
Risperidone ER (Longavo) | 50 mg/0.1 mL 75 mg/0.2 mL 100 mg/0.3 mL 125 mg/0.4 mL | 50 mg 75 mg 100 mg 125 mg prefilled syringes | 456.1800a 456.1800a 456.1800a 456.1800a | 50 mg, 75 mg, 100 mg, 125 mg once monthly | 5,930 | Reference |
Long-acting injectable comparators | ||||||
Risperidone ER (Perseris)b | 50 mg/mL | 90 mg 120 mg powder for injection | 456.1800c 608.2200c | 90 mg or 120 mg once monthly | 5,930 7,907 | 0 1,977 |
Risperidone (Risperdal Consta) | 6.25 mg/mL 12.5 mg/mL 18.75 mg/mL 25 mg/mL | 12.5 mg 25 mg 37.5 mg 50 mg powder for injection | 92.0600d 191.1500 286.7100 382.2800 | 25 mg to 50 mg once every 2 weeks | 2,394 4,970 7,454 9,939 | –3,537 –960 1,524 4,009 |
Aripiprazole (Abilify Maintena) | 200 mg/mL | 300 mg 400 mg powder for injection | 456.1800 456.1800 | 300 mg to 400 mg once monthly | 5,930 | 0 |
Paliperidone (Invega Sustenna) | 100 mg/mL | 50 mg 75 mg 100 mg 150 mg prefilled syringes | 327.4500 491.1800 506.4600 675.2700 | 50 mg to 150 mg once monthly | 4,257 6,385 6,584 8,779 | –1,673 455 654 2,848 |
Paliperidone (Invega Trinza) | 200 mg/mL | 175 mg 263 mg 350 mg 525 mg prefilled syringes | 953.7300 1,430.6100 1,430.6100 1,907.4900 | 175 mg to 525 mg once every 3 months | 4,130 6,195 6,195 8,259 | –1,801 264 264 2,329 |
Oral comparator | ||||||
Risperidone (generics) | 0.25 mg 0.5 mg 1 mg 2 mg 3 mg 4 mg | Tablets | 0.0878 0.1470 0.2031 0.4062 0.6083 0.8111 | 4 mg per day to 6 mg per day in 1 to 2 dosese | 297 to 444 | –5,486 to –5,634 |
ER = extended release.
Note: All prices are from the Ontario Drug Benefit Formulary, accessed January 2024 unless otherwise specified.80 Annual drug cost calculations assume 13 monthly injections, 26 biweekly (every 2 weeks) injections and 4.33 quarterly (once every 3 months) injections. Clinical expert input obtained by CDA-AMC considered these assumptions clinically appropriate.
aSponsor’s submitted price.77
bPerseris was a relevant comparator at the time of the original analysis, but it has since been removed from the market.
cCADTH Reimbursement Review “Risperidone for Extended-Release Injectable Suspension (Perseris),” published November 2021, accessed January 2024.81
dThe Saskatchewan Formulary, accessed January 2024.82
eThe product monograph for oral risperidone recommends a target dose range after titration of 4 mg per day to 6 mg per day, administered in 1 to 2 doses, with a maximum of 16 mg per day.32 The monograph for risperidone ER includes dose selection guidance when replacing oral risperidone doses of 2 mg per day to 5 mg per day.83
Source: Sponsor’s submission.77 Oral risperidone was added to the table by CDA-AMC.
Issues for Consideration
Lack of loading dose or cross-tapering requirement: As with other LAIs, patients initiating risperidone ER require an established tolerance to the oral form of their medication; however, risperidone ER does not require concomitant use with an oral antipsychotic therapy. In contrast, concomitant use of an oral antipsychotic drug is recommended during the initial 2 to 3 weeks of therapy with risperidone once every 2 weeks and aripiprazole once monthly. Risperidone ER also does not require an additional injection as a loading dose, while it is recommended when initiating paliperidone monthly injections or as an alternate to concomitant oral therapy when initiating aripiprazole.25-27,83 This benefit eliminates the costs associated with cross-tapering and loading doses and may be an advantage in reducing the intensity of monitoring required for outpatients or the length of stay required for inpatients when initiating LAI AAPs.
Subcutaneous administration may be preferable for some patients: While results of the submitted ITC did not demonstrate a substantial reduction in injection site pain for risperidone ER compared to other LAIs or placebo, clinical expert input obtained by CDA-AMC noted that the intramuscular injections associated with most other available LAI AAPs can be painful, which is a barrier to uptake for some patients. The expert noted that the availability and funding of risperidone ER, which is administered subcutaneously, would be likely to increase access to LAI AAPs and may thus also increase adherence to AAP therapy.
Discussion
Summary of Available Evidence
The CADTH clinical review was based on a summary of clinical evidence provided by the sponsor in accordance with the CDA-AMC tailored review process. The sponsor’s summary of evidence was based on 1 phase III, randomized, double-blind, placebo-controlled study (the RISE study) and 1 phase III, randomized, double-blind, parallel-group study (the SHINE study) that allowed rollover of participants from the RISE study. The objective of RISE was to compare the efficacy, safety, and tolerability, versus placebo, of 2 dose regimens (once monthly and once every 2 months) of risperidone ER given subcutaneously as maintenance therapy for patients with schizophrenia. The objective of the SHINE study was to evaluate the long-term safety, tolerability, and effectiveness of risperidone ER administered subcutaneously once monthly or once every 2 months at doses of 50 mg to 250 mg, comparable to 2 mg/day to 5 mg/day of oral risperidone, for up to 56 weeks in adult and adolescent patients with schizophrenia. The primary efficacy end point in the RISE study was time to impending relapse. As a safety-oriented study, the SHINE study did not include formal primary efficacy end points and provided only descriptive efficacy data.
Baseline demographics were generally well balanced in the RISE and SHINE studies. In the RISE study, the mean age of patients was approximately 49 years, 39% of patients were female and 61% were male. On average, patients in each treatment group had schizophrenia for approximately 20 years, and the mean time since last relapse was approximately 10 months. In the SHINE study, the mean age of patients was 50.6 years, 36% were female and 64% were male, and the mean duration of disease was 21.1 years, with a mean of 21 months since last relapse. Only 3 adolescents were randomized and received at least 1 dose of TV-46000 in the study.
The sponsor also submitted an ITC the aim of which was to provide estimates for comparative efficacy of risperidone ER compared to other LAI options for the treatment of schizophrenia. A total of 6 studies (including the RISE study) were eligible for inclusion in the NMA. Efficacy outcomes were relapse rate, time to relapse, and change in PSP scale score. Safety outcomes were AE-related discontinuation, significant weight gain, treatment-related AEs, and injection site pain.
Interpretation of Results
To align with the Health Canada–approved indication, this CDA-AMC review only reports the findings regarding once-monthly dosing with risperidone ER.
Efficacy
With regard to time to impending relapse (the primary outcome), risperidone ER (TV-46000) once monthly subcutaneously, demonstrated a benefit over placebo. In the group that received once monthly dosing, 7% of patients had impending relapse compared to 29% of patients in the group that received placebo (HR = 0.200; 95% CI, 0.109 to 0.367; P < 0.0001). The clinical expert consulted noted that the time to impending relapse is an appropriate end point given the expected use of risperidone ER for long-term relapse prevention. The clinical expert also suggested that the magnitude of benefit compared with placebo for risperidone is impressive but not beyond the expectations for other LAIs used to treat schizophrenia in Canada. This observation is aligned with the efficacy outcomes included in the sponsor-submitted ITC, which, despite the limitations outlined in the Critical Appraisal section in this report, found risperidone to be similar in efficacy to other LAI comparators in Canada.
One of the goals of treatment of schizophrenia is to maintain or restore HRQoL. The SQLS measure was used in the RISE pivotal study, but HRQoL was assessed as a secondary outcome and was not statistically tested due to earlier outcomes in the testing hierarchy did not reach statistical significance. Hence, no conclusions can be made regarding the effects of risperidone e ER on the HRQoL outcomes of patients with schizophrenia.
Harms
Safety analyses were conducted on pooled safety populations from both the RISE and SHINE studies. The most commonly report AEs were injection site pain (reported by 5% of patients in the risperidone ER once monthly group and 6% in the placebo group) and injection site nodule (6% in the once monthly group and 3% in the placebo group). Serious AEs were experienced by 4% of patients receiving risperidone once monthly and by 8% of patients receiving placebo. AEs leading to treatment discontinuation were reported by 11% of patients in the risperidone once monthly group and by 11% in the placebo group.
Overall, treatment with risperidone ER once monthly was generally well tolerated by adult patients with schizophrenia. There were no new safety signals compared with the known safety profile of oral risperidone products, except for the expected local injection site reactions that are observed with all LAI antipsychotics. The clinical expert consulted for this review indicated that the AEs reported in the included trials might be similar to that observed with risperidone (oral and LAIs) and paliperidone in clinical practice.
Other Considerations
Other formulations of risperidone are currently approved in Canada, including tablet (Risperdal) for once daily oral administration and an LAI formulation (Risperdal Consta) for intramuscular administration every 2 weeks. Risperidone ER (Perseris) subcutaneous LAI for administration once monthly was given a recommendation for reimbursement with conditions by CADTH in September 2021. (The conditions for reimbursement included the following: reimburse in similar manner to other LAI atypical antipsychotic drugs in adults with schizophrenia; with a total monthly dose not exceeding 120 mg; not used in combination with other antipsychotic LAIs; not costing more than other LAI atypical antipsychotic drugs.) However, the pan-Canadian Pharmaceutical Alliance (pCPA) negotiations were concluded without a listing agreement.
In addition, other existing LAIs for schizophrenia are administered intramuscularly and require oral supplementation or loading doses given either the same day or requiring additional office visits.25-28 The sponsor indicated that the risperidone LAI currently under review required no loading dose or supplemental oral risperidone dosing. The clinical expert consulted by CDA-AMC indicated that risperidone LAI is administered subcutaneously, which may cause less pain, although no evidence addressing this issue was provided in the sponsor’s summary of clinical evidence for this review.
Cost
At the submitted price of $456.18 for the 50 mg, 75 mg, 100 mg, and 125 mg doses once monthly, the annual drug cost of risperidone ER is $5,930 per patient, with an annual administration cost of $51. Annual drug costs for the injectable comparators ranged from $2,394 to $9,939, with annual administration costs ranging from $17 to $101. The incremental cost of risperidone ER once monthly ranged from a savings of $4,060 annually to an additional cost of $3,486 annually, per patient, compared to risperidone 50 mg and 12.5 mg once every 2 weeks, respectively.
The sponsor’s cost comparison was associated with limitations including uncertainty in the assumption of clinical similarity between comparators and the exclusion of oral risperidone tablets as a comparator. The annual cost of risperidone ER is $5,486 to $5,634 more expensive than that of risperidone tablets ($297 to $444 per patient), not considering administration costs, or $5,537 to $5,685 per patient per year more expensive when administration costs are included. All incremental costs or savings are based on publicly available list prices and may not reflect actual prices paid by Canadian public drug plans.
Conclusion
Based on the summary of clinical evidence submitted by the sponsor, risperidone ER once monthly showed statistically significant improvements in time to impending relapse compared to placebo. Evidence related to the effect of risperidone on HRQoL is uncertain because of the lack of statistical testing; therefore, conclusions cannot be drawn. The safety of the once-monthly dosing regimen appears to be consistent with the safety profile of risperidone oral and risperidone LAI once every 2 weeks. The results of the submitted ITCs, despite methodological limitations, appear to be aligned with the clinical expert’s expectation that risperidone ER will have a clinical benefit similar to that of other LAI therapies used to treat schizophrenia in Canada. The inclusion of the long-term SHINE study that allowed rollover of patients from the original RISE study is aligned with the expected use of risperidone for long-term relapse avoidance.
At the submitted price, the annual drug cost of risperidone ER once monthly is $5,930 per patient, with annual administration costs of $51. The incremental cost of risperidone ER once monthly ranged from an annual savings of $4,060 per patient compared to risperidone 50 mg every 2 weeks to an additional cost of $3,486 annually per patient compared to 12.5 mg once every 2 weeks. The sponsor’s cost comparison was associated with limitations including uncertainty in the assumption of clinical similarity between comparators and the exclusion of oral risperidone tablets as a comparator. The annual cost of risperidone ER is $5,537 to $5,685 per patient more expensive than oral risperidone tablets when administration costs are included. All incremental costs or savings are based on publicly available list prices and may not reflect actual prices paid by public drug plans in Canada.
References
1.Jablensky A, Sartorius N, Ernberg G, et al. Schizophrenia: manifestations, incidence and course in different cultures. A World Health Organization ten-country study. Psychol Med Monogr Suppl. 1992;20:1-97. doi: 10.1017/s0264180100000904 PubMed
2.Mc Glanaghy E, Turner D, Davis GA, et al. A network meta-analysis of psychological interventions for schizophrenia and psychosis: Impact on symptoms. Schizophr Res. 2021;228:447-459. doi: 10.1016/j.schres.2020.12.036 PubMed
3.Remington G, Addington D, Honer W, Ismail Z, Raedler T, Teehan M. Guidelines for the Pharmacotherapy of Schizophrenia in Adults. Can J Psychiatry. 2017;62(9):604-616. doi: 10.1177/0706743717720448 PubMed
4.O'Carroll R. Cognitive impairment in schizophrenia. Adv Psychiatr Treat. 2000;6(3):161-168.
5.Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261-76. doi: 10.1093/schbul/13.2.261 PubMed
6.Kay SR, Opler LA, Lindenmayer JP. Reliability and validity of the positive and negative syndrome scale for schizophrenics. Psychiatry Res. 1988;23(1):99-110. doi: 10.1016/0165-1781(88)90038-8 PubMed
7.Canadian Psychiatric Association. Clinical practice guidelines. Treatment of schizophrenia. Can J Psychiatry. 2005;50(13 Suppl 1):7s-57s. PubMed
8.Kasper S, Lerman MN, McQuade RD, et al. Efficacy and safety of aripiprazole vs. haloperidol for long-term maintenance treatment following acute relapse of schizophrenia. Int J Neuropsychopharmacol. 2003;6(4):325-37. doi: 10.1017/S1461145703003651 PubMed
9.Government of Canada. Canadian Chronic Disease Surveillance System (CCDSS). 2018. Accessed May 6, 2021. https://health-infobase.canada.ca/ccdss/data-tool/
10.Health Canada. A report on mental illnesses in Canada. 2002. Accessed December 7, 2023. https://www.phac-aspc.gc.ca/publicat/miic-mmac/pdf/men_ill_e.pdf
11.Diagnostic and statistical manual of mental disorders: DSM-IV-TR. American Psychiatric Association; 2000.
12.Ayuso-Gutierrez JL, del Rio Vega JM. Factors influencing relapse in the long-term course of schizophrenia. Schizophr Res. 1997;28(2-3):199-206. doi: 10.1016/s0920-9964(97)00131-x PubMed
13.Cramer JA, Rosenheck R. Compliance with medication regimens for mental and physical disorders. Psychiatr Serv. 1998;49(2):196-201. doi: 10.1176/ps.49.2.196 PubMed
14.Barnes TR, Drake R, Paton C, et al. Evidence-based guidelines for the pharmacological treatment of schizophrenia: Updated recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2020;34(1):3-78. doi: 10.1177/0269881119889296 PubMed
15.Teva Branded Pharmaceutical Products R&D Inc. Clinical Study Report: TV46000-CNS-30072. A Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Efficacy, Safety, and Tolerability of Risperidone Extended-Release Injectable Suspension (TV-46000) for Subcutaneous Use as Maintenance Treatment in Adult and Adolescent Patients with Schizophrenia (The RISE Study – The RIsperidone Subcutaneous Extended-release Study) [Confidential Information] [internal sponsor's report]. April 26, 2021.
16.American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5). 5th ed. American Psychiatric Publishing; 2013.
17.Lewis DA, Lieberman JA. Catching up on schizophrenia: natural history and neurobiology. Neuron. 2000;28(2):325-34. doi: 10.1016/s0896-6273(00)00111-2 PubMed
18.The American Psychiatric Association practice guideline for the treatment of patients with schizophrenia. 3rd ed. American Psychiatric Association; 2021. Accessed December 7, 2023. https://psychiatryonline.org/doi/pdf/10.1176/appi.books.9780890424841
19.Charlson FJ, Ferrari AJ, Santomauro DF, et al. Global Epidemiology and Burden of Schizophrenia: Findings From the Global Burden of Disease Study 2016. Schizophr Bull. 2018;44(6):1195-1203. doi: 10.1093/schbul/sby058 PubMed
20.Chong HY, Teoh SL, Wu DB, Kotirum S, Chiou CF, Chaiyakunapruk N. Global economic burden of schizophrenia: a systematic review. Neuropsychiatr Dis Treat. 2016;12:357-73. doi: 10.2147/NDT.S96649 PubMed
21.Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: safety and tolerability in short-term, placebo-controlled trials. Schizophr Res. 2003;61(2-3):123-36. doi: 10.1016/s0920-9964(03)00050-1 PubMed
22.Lehman AF, Kreyenbuhl J, Buchanan RW, et al. The Schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations 2003. Schizophr Bull. 2004;30(2):193-217. doi: 10.1093/oxfordjournals.schbul.a007071 PubMed
23.Lauriello J, Campbell AR. Post TW, ed. Pharmacotherapy for schizophrenia: Long-acting injectable antipsychotic drugs. UpToDate; 2021. Accessed May 6, 2021. www.uptodate.com
24.Schizophrenia Care in the Community for adults. Health Quality Ontario; 2018. Accessed May 6, 2021. https://www.hqontario.ca/Portals/0/documents/evidence/quality-standards/qs-schizophrenia-community-clinician-guide-en.pdf
25.Janssen Inc. Risperdal Consta® (risperidone powder for injectable prolonged-release suspension): 12.5 mg, 25 mg, 37.5 mg and 50 mg [product monograph]. Updated December 18, 2020. Accessed May 6, 2021. https://pdf.hres.ca/dpd_pm/00059290.PDF
26.Otsuka Canada Pharmaceutical Inc. Abilify Maintena® (aripiprazole for prolonged release injectable suspension): 300 mg and 400 mg vial, 300 mg and 400 mg dual chamber syringe [product monograph]. February 10, 2014. Updated December 21, 2020. Accessed November 17, 2023. https://pdf.hres.ca/dpd_pm/00059334.PDF
27.Janssen Inc. Invega Sustenna (paliperidone palmitate prolonged-release injectable suspension): pre-filled syringes containing 50 mg/0.5 mL, 75 mg/0.75 mL, 100 mg/1 mL, and 150 mg/1.5 mL [product monograph]. Updated December 17, 2020. Accessed November 17, 2023. https://pdf.hres.ca/dpd_pm/00059297.PDF
28.Janssen Inc. Invega Trinza (paliperidone palmitate prolonged-release injectable suspension): pre-filled syringes containing 175 mg/0.875 mL, 263 mg/1.315 mL, 350 mg/1.75 mL, and 525 mg/2.625 mL (3 months) [product monograph]. Updated December 17, 2020. Accessed November 17, 2023. https://pdf.hres.ca/dpd_pm/00059281.PDF
29.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
30.Health Canada. Notices of compliance: prescription products for human use. January - December, 1993. 1993. Accessed April 27, 2021. https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/dhp-mps/alt_formats/hpfb-dgpsa/txt/prodpharma/pre93et-eng.txt
31.Health Canada. Notice of compliance (NOC) for Risperdal Consta (risperidone powder for injectable prolonged-release suspension). July 16, 2004. Accessed April 26, 2021. https://health-products.canada.ca/noc-ac/info.do?lang=en&no=4799
32.Janssen Inc. Risperdal® (risperidone): tablets house standard 0.25, 0.5, 1, 2, 3 and 4 mg risperidone tartrate oral solution risperidone 1 mg/mL [product monograph]. April 14, 1993. Updated September 10, 2018. Accessed November 17, 2023. https://pdf.hres.ca/dpd_pm/00047330.PDF
33.Teva Branded Pharmaceutical Products R&D Inc. Clinical Study Report: TV46000-CNS-30078. A Study to Evaluate the Safety, Tolerability, and Effect of Risperidone Extended-Release Injectable Suspension (TV-46000) for Subcutaneous Use as Maintenance Treatment in Adult and Adolescent Patients with Schizophrenia (The SHINE Study – Safety in Humans of TV-46000 sc INjection Evaluation) [Confidential Information] [internal sponsor's report]. April 24, 2022.
34.Kane JM, Harary E, Tohami O, et al. Long-term Safety, Tolerability, and Effectiveness of TV-46000, a Long-Acting Subcutaneous Antipsychotic (LASCA), in Patients With Schizophrenia: A Phase 3, Randomized, Double-Blind Study (SHINE). presented at: Schizophrenia International Research Society 2023 Annual Congress; 2022 May 11-15 Toronto (ON).
35.Teva Canada Limited. Common Technical Document, Module 2.5 Clinical Overview Addendum 01 [sponsor supplied reference].
36.Citrome L, M S, Franzenburg K, et al. TV-46000, a long-acting subcutaneous risperidone injectable, demonstrated improved patient-centered outcomes in patients with schizophrenia. Poster presented at Psych Congress, San Antonio, TX. Oct 29-Nov 1 2021:
37.Teva Canada Limited. Common Technical Document, Module 2.7.4 Summary of Clinical Safety [sponsor supplied reference].
38.Eerdekens M, Van Hove I, Remmerie B, Mannaert E. Pharmacokinetics and tolerability of long-acting risperidone in schizophrenia. Schizophr Res. 2004;70(1):91-100. doi: 10.1016/j.schres.2003.11.001 PubMed
39.Korell J, Green B, Remmerie B, Vermeulen A. Determination of Plasma Concentration Reference Ranges for Risperidone and Paliperidone. CPT Pharmacometrics Syst Pharmacol. 2017;6(9):589-595. doi: 10.1002/psp4.12217 PubMed
40.Janssen Inc. RISPERDAL CONSTA® (risperidone): powder for Injectable Prolonged-Release Suspension 12.5 mg, 25 mg, 37.5 mg and 50 mg Intramuscular Injection [product monograph]. December 18, 2020.
41.Janssen Pharmaceuticals Inc. RISPERDAL CONSTA® (risperidone): long-acting injection [US prescribing information] [sponsor supplied reference]. Accessed February 2021.
42.Teva Canada Limited. Common Technical Document, Module 2.7.2 Summary of Clinical Pharmacology Studies [sponsor supplied reference].
43.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40-6. doi: 10.1016/j.jclinepi.2016.01.021 PubMed
44.Teva Canada. Systematic Literature Review and Network Meta-Analysis of the Atypical Long-Acting Injectable Antipsychotics Approved in Canada and Used for the Maintenance Treatment of Schizophrenia [sponsor supplied reference]. September 29, 2023.
45.Kane JM, Sanchez R, Perry PP, et al. Aripiprazole intramuscular depot as maintenance treatment in patients with schizophrenia: a 52-week, multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2012;73(5):617-24. doi: 10.4088/JCP.11m07530 PubMed
46.Lincoln J. Long-acting injectable aripiprazole for adult schizophrenia. Current Psychiatry. 2013 May;12(5):46-50.
47.Cameron C, Coyle D, Richter T, et al. Systematic review and network meta-analysis comparing antithrombotic agents for the prevention of stroke and major bleeding in patients with atrial fibrillation. BMJ Open. 2014;4(6):e004301. doi: 10.1136/bmjopen-2013-004301 PubMed
48.Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. NICE DSU Technical Support Document 4: Inconsistency in Networks of Evidence Based on Randomised Controlled Trials. Decision Support Unit, ScHARR, University of Sheffield; 2014. Accessed August 6, 2025. https://www.ncbi.nlm.nih.gov/pubmed/27466656
49.Hough D, Gopal S, Vijapurkar U, Lim P, Morozova M, Eerdekens M. Paliperidone palmitate maintenance treatment in delaying the time-to-relapse in patients with schizophrenia: a randomized, double-blind, placebo-controlled study. Schizophr Res. 2010;116(2-3):107-17. doi: 10.1016/j.schres.2009.10.026 PubMed
50.Gopal S, Vijapurkar U, Lim P, Morozova M, Eerdekens M, Hough D. A 52-week open-label study of the safety and tolerability of paliperidone palmitate in patients with schizophrenia. J Psychopharmacol. 2011;25(5):685-97. doi: 10.1177/0269881110372817 PubMed
51.Kozma CM, Slaton T, Dirani R, Fastenau J, Gopal S, Hough D. Changes in schizophrenia-related hospitalization and ER use among patients receiving paliperidone palmitate: results from a clinical trial with a 52-week open-label extension (OLE). Curr Med Res Opin. 2011;27(8):1603-11. doi: 10.1185/03007995.2011.595000 PubMed
52.Sliwa JK, Fu DJ, Bossie CA, Turkoz I, Alphs L. Body mass index and metabolic parameters in patients with schizophrenia during long-term treatment with paliperidone palmitate. BMC Psychiatry. 2014;14:52. doi: 10.1186/1471-244X-14-52 PubMed
53.Markowitz M, Fu DJ, Levitan B, Gopal S, Turkoz I, Alphs L. Long-acting injectable paliperidone palmitate versus oral paliperidone extended release: a comparative analysis from two placebo-controlled relapse prevention studies. Ann Gen Psychiatry. 2013;12(1):22. doi: 10.1186/1744-859X-12-22 PubMed
54.Fleischhacker WW, Sanchez R, Johnson B, et al. Long-term safety and tolerability of aripiprazole once-monthly in maintenance treatment of patients with schizophrenia. Int Clin Psychopharmacol. 2013;28(4):171-6. doi: 10.1097/YIC.0b013e3283615dba PubMed
55.Otsuka Pharmaceutical Development & Commercialization, Inc. NCT00705783: Intramuscular Depot Formulation of Aripiprazole as Maintenance Treatment in Patients With Schizophrenia (ASPIRE). ClinicalTrials.gov. Accessed September 18, 2023. https://classic.clinicaltrials.gov/ct2/show/NCT00705783
56.Kane JM, Sanchez R, Baker RA, et al. Patient-Centered Outcomes with Aripiprazole Once-Monthly for Maintenance Treatment in Patients with Schizophrenia: Results From Two Multicenter, Randomized, Double-Blind Studies. Clin Schizophr Relat Psychoses. 2015;9(2):79-87. doi: 10.3371/CSRP.KASA.022015 PubMed
57.Fleischhacker WW, Baker RA, Eramo A, et al. Effects of aripiprazole once-monthly on domains of personal and social performance: results from 2 multicenter, randomized, double-blind studies. Schizophr Res. 2014;159(2-3):415-20. doi: 10.1016/j.schres.2014.09.019 PubMed
58.Naber D, Hansen K, Forray C, et al. Qualify: a randomized head-to-head study of aripiprazole once-monthly and paliperidone palmitate in the treatment of schizophrenia. Schizophr Res. 2015;168(1-2):498-504. doi: 10.1016/j.schres.2015.07.007 PubMed
59.Naber D, Baker RA, Eramo A, et al. Long-term effectiveness of aripiprazole once-monthly for schizophrenia is maintained in the QUALIFY extension study. Schizophr Res. 2018;192:205-210. doi: 10.1016/j.schres.2017.04.013 PubMed
60.H. Lundbeck A/S. NCT01795547: Aripiprazole Once-monthly Versus Paliperidone Palmitate in Adult Patients With Schizophrenia. ClinicalTrials.gov. Accessed September 18, 2023. https://classic.clinicaltrials.gov/ct2/show/NCT01795547
61.H. Lundbeck A/S. EUCTR2012-002785-12-SE: A 28-week, randomised, open-label study evaluating the effectiveness of aripiprazole once-monthly versus paliperidone palmitate in adult patients with schizophrenia. World Health Organization. Accessed September 18, 2023. https://trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2012-002785-12-SE
62.Berwaerts J, Liu Y, Gopal S, et al. Efficacy and Safety of the 3-Month Formulation of Paliperidone Palmitate vs Placebo for Relapse Prevention of Schizophrenia: A Randomized Clinical Trial. JAMA Psychiatry. 2015;72(8):830-9. doi: 10.1001/jamapsychiatry.2015.0241 PubMed
63.Bell Lynum KS, Turkoz I, Kim E. Paliperidone palmitate once-every-3-months in adults with early illness schizophrenia. Early Interv Psychiatry. 2019;13(3):667-672. doi: 10.1111/eip.12685 PubMed
64.Janssen Research & Development, LLC. NCT01529515: A Study of Paliperidone Palmitate 3 Month Formulation for the Treatment of Patients With Schizophrenia. ClinicalTrials.gov. Accessed September 18, 2023. https://classic.clinicaltrials.gov/ct2/show/NCT01529515
65.Janssen-Cilag International N.V. EUCTR2011-004676-11-RO: A Randomized, Multicenter, Double-Blind, Relapse Prevention Study of Paliperidone Palmitate 3 Month Formulation for the Treatment of Subjects with Schizophrenia. World Health Organization. Accessed September 18, 2023. https://trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2011%E2%80%90004676%E2%80%9011%E2%80%90RO
66.Savitz AJ, Xu H, Gopal S, Nuamah I, Mathews M, Soares B. Efficacy and safety of paliperidone palmitate 3-month formulation in Latin American patients with schizophrenia: A subgroup analysis of data from two large phase 3 randomized, double-blind studies. Braz J Psychiatry. 2019;41(6):499-510. doi: 10.1590/1516-4446-2018-0153 PubMed
67.Chirila C, Nuamah I, Woodruff K. Health care resource use analysis of paliperidone palmitate 3 month injection from two phase 3 clinical trials. Curr Med Res Opin. 2017;33(6):1083-1090. doi: 10.1080/03007995.2017.1300144 PubMed
68.Savitz AJ, Xu H, Gopal S, et al. Efficacy and Safety of Paliperidone Palmitate 3-Month Formulation for Patients with Schizophrenia: A Randomized, Multicenter, Double-Blind, Noninferiority Study. Int J Neuropsychopharmacol. 2016;19(7). doi: 10.1093/ijnp/pyw018 PubMed
69.Gopal S, Gogate J, Pungor K, Kim E, Singh A, Mathews M. Improvement of Negative Symptoms in Schizophrenia with Paliperidone Palmitate 1-Month and 3-Month Long-Acting Injectables: Results from a Phase 3 Non-Inferiority Study. Neuropsychiatr Dis Treat. 2020;16:681-690. doi: 10.2147/NDT.S226296 PubMed
70.Kern Sliwa J, Savitz A, Nuamah I, et al. An assessment of injection site reaction and injection site pain of 1-month and 3-month long-acting injectable formulations of paliperidone palmitate. Perspect Psychiatr Care. 2018;54(4):530-538. doi: 10.1111/ppc.12267 PubMed
71.Mathews M, Pei H, Savitz A, et al. Paliperidone Palmitate 3-Monthly Versus 1-Monthly Injectable in Patients With Schizophrenia With or Without Prior Exposure to Oral Risperidone or Paliperidone: A Post Hoc, Subgroup Analysis. Clin Drug Investig. 2018;38(8):695-702. doi: 10.1007/s40261-018-0647-z PubMed
72.Savitz AJ, Xu H, Gopal S, et al. Efficacy and safety of paliperidone palmitate 3-month versus 1-month formulation in patients with schizophrenia: comparison between European and non-European population. Neuropsychiatr Dis Treat. 2019;15:587-602. doi: 10.2147/NDT.S189668 PubMed
73.Savitz AJ, Xu H, Gopal S, Nuamah I, Hough D, Mathews M. Paliperidone palmitate 3-month treatment results in symptomatic remission in patients with schizophrenia: a randomized, multicenter, double-blind, and noninferiority study. Int Clin Psychopharmacol. 2017;32(6):329-336. doi: 10.1097/YIC.0000000000000190 PubMed
74.Savitz AJ, Xu H, Gopal S, et al. Efficacy and safety of paliperidone palmitate three-monthly formulation in East Asian patients with schizophrenia: subgroup analysis of a global, randomized, double-blind, Phase III, noninferiority study. Neuropsychiatr Dis Treat. 2017;13:2193-2207. doi: 10.2147/NDT.S134287 PubMed
75.Janssen Research & Development, LLC. NCT01515423: Study of Paliperidone Palmitate 3 Month and 1 Month Formulations for the Treatment of Patients With Schizophrenia. ClinicalTrials.gov. Accessed September 18, 2023. https://classic.clinicaltrials.gov/ct2/show/NCT01515423
76.Janssen Research & Development, LLC. NCT01515423: A Randomized, Multicenter, Double-Blind, Non-inferiority Study of Paliperidone Palmitate 3 Month and 1 Month Formulations for the Treatment of Subjects With Schizophrenia. ClinicalTrials.gov. https://trialsearch.who.int/Trial2.aspx?TrialID=NCT01515423
77.Teva Canada Innovation. Drug Reimbursement Review sponsor submission: Risperidone extended-release injectable suspension, 50 mg, 75 mg, 100 mg, 125, 150 mg, 200 mg, 250 mg pre-filled syringes for subcutaneous injection [internal sponsor's package]. October 12, 2023.
78.pan-Canadian Pharmaceutical Alliance. Abilify Maintena (aripiprazole) for Schizophrenia. 2015. Accessed November 17, 2023. https://www.pcpacanada.ca/negotiation/20847
79.pan-Canadian Pharmaceutical Alliance. Invega Trinza (paliperidone) for Schizophrenia. 2018. Accessed November 17, 2023. https://www.pcpacanada.ca/negotiation/20996
80.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2023. Accessed January 3, 2024. https://www.formulary.health.gov.on.ca/formulary/
81.CADTH Drug Reimbursement Review: Risperidone for Extended Release Injectable Suspension (Perseris). Can J Health Technol. 2021;1(11). doi:10.51731/cjht.2021.195
82.Saskatchewan Drug Plan: search formulary. 2023. Accessed January 3, 2024. http://formulary.drugplan.ehealthsask.ca/SearchFormulary
83.Teva Canada Limited. Uzedy (risperidone extended-release injectable suspension): 50 mg, 75 mg, 100 mg, 125 mg, 150 mg, 200 mg, 250 mg pre-filled syringes for subcutaneous injection [draft product monograph]. January 30, 2023.
84.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 23, 2023)). Ontario Ministry of Health; 2023. Accessed November 16, 2023. https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf
85.Teva Canada Innovation. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Risperidone extended-release injectable suspension, 50 mg, 75 mg, 100 mg, 125, 150 mg, 200 mg, 250 mg pre-filled syringes for subcutaneous injection. October 12, 2023.
86.Teva Canada Innovation. Teva Canada response to CADTH request for additional information regarding Risperidone ER CADTH review on November 7, 2023 [internal additional sponsor's information]. November 14, 2023.
Appendix 1: Additional Economic Information
Please note that this appendix has not been copy-edited.
Additional Details on the Sponsor’s Submission
Table 21: Sponsor’s Estimated Health Care Costs
Generic name (brand name) | Number of injections per year | Aggregated health care cost per year ($)a | Difference in health care costs per year ($) |
|---|---|---|---|
Risperidone ER (Longavo) | 13 | 51 | Reference |
Long-acting injectable comparators | |||
Risperidone ER (Perseris) | 13 | 51 | 0 |
Risperidone (Risperdal Consta) | 26 | 101 | 51 |
Aripiprazole (Abilify Maintena) | 13 | 51 | 0 |
Paliperidone (Invega Sustenna) | 13 | 51 | 0 |
Paliperidone (Invega Trinza) | 4.33 | 17 | –34 |
Oral comparator | |||
Risperidone tablets (generics) | NA | 0 | –51 |
ER = extended release; NA = not applicable.
Note: CDA-AMC added oral risperidone as a comparator.
aBased on health care components included in the table. Health care costs assumed an administration fee of 3.89 per injection.84
Table 22: Sponsor’s Summary of Comparative Treatment Costs
Generic name (brand name) | Dosage form | Difference in drug acquisition costs per year ($) | Difference in health care costs per yearb ($) | Difference in total costs per year($) |
|---|---|---|---|---|
Risperidone ER (Longavo) | 50 mg 75 mg 100 mg 125 mg | Reference | Reference | Reference |
Long-acting injectable comparators | ||||
Risperidone ER (Perseris) | 90 mg 120 mg | 0 1,977 | 0 0 | 0 1,977 |
Risperidone (Risperdal Consta) | 12.5 mg 25 mg 37.5 mg 50 mg | –3,537 –960 1,524 4,009 | 51 51 51 51 | –3,486 –910 1,575 4,060 |
Aripiprazole (Abilify Maintena) | 300 mg 400 mg | 0 0 | 0 0 | 0 0 |
Paliperidone (Invega Sustenna) | 50 mg 75 mg 100 mg 150 mg | –1,673 455 654 2,848 | 0 0 0 0 | –1,673 455 654 2,848 |
Paliperidone (Invega Trinza) | 175 mg 263 mg 350 mg 525 mg | –1,801 264 264 2,329 | –34 –34 –34 –34 | –1,834 230 230 2,295 |
Oral comparator | ||||
Risperidone tablets (generics) | 2 mg to 6 mg daily | –5,486 to –5,634 | –51 | –5,537 to –5,685 |
ER = extended release.
Note: CDA-AMC added oral risperidone as a comparator.
Additional Details on the CDA-AMC Reanalyses and Additional Analyses
Except for adding oral risperidone as a comparator (in Table 20, Table 21, and Table 22), CDA-AMC did not conduct any additional pharmacoeconomic analyses in the review of risperidone ER.
Appendix 2: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 23: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
ER = extended release; LAI = long-acting injectable.
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a claims-based budget impact analysis (BIA)85 assessing the expected budgetary impact of introducing risperidone ER for the treatment of schizophrenia over a 3-year time horizon (Q3 2025 to Q2 2028) from the perspective of a drug plan payer in Canada. Dispensing fees, markups, and administration costs were not included.
Data for the model were obtained by the sponsor from PDCI public claims data for 2017 through 202285 and internal forecasting. Key inputs to the BIA are documented in Table 24, with Ontario inputs reported as an example.
Key assumptions included:
Risperidone ER will only displace other LAI AAPs.
Claims per year can be standardized to represent units displaced by comparators with different administration frequencies. Aripiprazole, paliperidone monthly, and paliperidone quarterly were assumed to have 1 unit per claim, while risperidone biweekly was calculated by dividing the number of units reimbursed by the number of claims.
Risperidone biweekly is used semimonthly, while aripiprazole (Abilify Maintena), paliperidone monthly (Invega Sustenna), and risperidone ER (Longavo) are used monthly, and paliperidone quarterly (Invega Trinza) is used quarterly.
Claims data from 2017 to 2022 can be linearly forecasted to the target time horizon.
Table 24: Summary of Key Model Parameters (Ontario as an Example)
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of monthly treatment equivalent claims eligible for drug under review | 262,574 / 277,243 / 291,912 |
Market uptake (reference scenario) | |
Risperidone ER (Longavo) | 0% / 0% / 0% |
Risperidone (Risperdal Consta) | 4.4% / 3.6% / 2.9% |
Aripiprazole (Abilify Maintena) | 35.0% / 35.8% / 36.6% |
Paliperidone monthly (Invega Sustenna) | 37.8% / 36.8% / 35.9% |
Paliperidone quarterly (Invega Trinza) | 22.8% / 23.7% / 24.6% |
Market uptake (new drug scenario) | |
Risperidone ER (Longavo) | ████ █ ████ █ ████ |
Risperidone (Risperdal Consta) | ████ █ ████ █ ████ |
Aripiprazole (Abilify Maintena) | █████ █ █████ █ █████ |
Paliperidone (Invega Sustenna) | █████ █ █████ █ █████ |
Paliperidone (Invega Trinza) | █████ █ █████ █ █████ |
Cost of treatment (per unit) | |
Risperidone ER (Longavo) | $456 |
Risperidone (Risperdal Consta) | $89 to $369, depending on the dose |
Aripiprazole (Abilify Maintena) | $456 |
Paliperidone (Invega Sustenna) | $327 to $675, depending on the dose |
Paliperidone (Invega Trinza) | $954 to $1,907, depending on the dose |
ER = extended release.
Source: Sponsor’s submitted budget impact analysis.85 Note that comparator claims, costs, and the projected uptake of risperidone ER varies by jurisdiction.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base case suggest that the incremental budget impact associated with the reimbursement of risperidone ER would be a savings of $3,046,667 in Year 1, $4,708,593 in year 2, and $6,767,990 in year 3, for a cumulative 3-year budgetary savings of $14,523,251.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Use of a claims-based approach to estimate market size introduces uncertainty with the anticipated budget impact of risperidone ER: The sponsor estimated market size based on public claims data for the comparator LAI AAPs. However, the included comparators are also indicated for schizoaffective disorder25,27,28 or bipolar disorder.25,26 Upon request, the sponsor clarified that risperidone ER’s single indication for schizophrenia is accounted for in its estimated market uptake while the claims included for comparators in the BIA represent all claims for those comparators without limitation by indication.86 Additionally, the sponsor did not convert the claims data to an estimated number of users, but instead standardized claims to “monthly dosing equivalents.” As the projected annual cost of each comparator is based on the total claims made for each product standardized to monthly dosing equivalents, there is uncertainty around whether the overall distribution and growth rate of doses within the dataset represent the distribution of doses used by patients with schizophrenia. Therefore, the relative costs and market shares of the comparators are uncertain.
CDA-AMC was unable to adjust for this limitation in reanalyses.
Health Canada product monograph indication only includes the monthly regimen: While the RISE trial included dose regimens for risperidone ER once monthly and once every 2 months, Health Canada only included the once monthly dosing in the product monograph. As such, once every 2 months doses of risperidone ER will not be available, and thus will not have the uptake originally estimated by the sponsor. The sponsor’s estimated market uptake for risperidone ER doses associated with once every 2 months usage (150 mg, 200 mg, and 250 mg).
CDA-AMC removed the market uptake for risperidone ER doses associated with usage once every 2 months.
Uncertainty in the comparators that may be displaced: In their submission, the sponsor notes that LAI AAPs are underutilized in Canada due to limitations related to complex initiation regimens, preparation steps such as reconstitution, an intramuscular mode of administration that patients may find invasive and painful, and limited dosing, administration, and injection site flexibility. In addition, the sponsor notes that some jurisdictions in Canada limited reimbursement of LAI AAPS to patients who experience difficultly with nonadherence or whose disease failed to respond to treatments or who experienced intolerances or contraindications to other antipsychotic options. The sponsor further states that risperidone ER was designed to facilitate acceptance of LAIs, improve adherence, and ease the transition from oral to LAI therapy. According to clinical expert input obtained by CDA-AMC, it is likely that risperidone ER is intended to and will also displace some use of oral antipsychotic drugs currently reimbursed in Canada as more patients are likely to accept LAIs due to the increased convenience and potential for reduced injection site pain. Clinical expert input obtained by CADTH estimated that as many as 10% more patients might use an LAI AAP rather than an oral AAP if risperidone ER was funded for its full indication.
CDA-AMC conducted a scenario analysis assuming that the LAI market would expand by 10% if risperidone ER was funded for its full indication, with these patients assumed to have previously been receiving oral risperidone.
Confidential pricing agreements: While the submitted price of risperidone ER is similar to the publicly available list prices of other LAI AAPs, as evidenced by pCPA negotiations which concluded with a Letter of Intent,78,79 confidential pricing agreements exist which lower the annual cost of the comparator products to the jurisdictional drug plans. The submitted price of risperidone ER would thus also have to be lowered to avoid incurring additional costs relative to its comparators.
CDA-AMC explored reanalysis scenarios where all comparators were 10% and 25% less expensive than estimated by the sponsor.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by removing the market uptake of risperidone ER doses associated exclusively with bimonthly dosing. (i.e., claims associated with uptake to bimonthly doses of risperidone ER in the sponsor’s base case were assumed to remain as their reference scenario LAI).
Table 25: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
| 50 mg, 75 mg, 100 mg, 125 mg, 150 mg, 200 mg, 250 mg Overall uptake: ████ █ ████ █ ████ (Ontario)a | 50 mg, 75 mg, 100 mg, 125 mg Overall uptake: 3.6% / 5.4% / 7.3% (Ontario)a |
CDA-AMC base case | 1 | |
BIA = budget impact analysis.
aRisperidone ER uptake percentages represent year 1 / year 2 / year 3 in the new drug scenario.
The results of the CDA-AMC base case reanalysis are presented in Table 26. The 3-year budget impact of reimbursing risperidone ER for the treatment of schizophrenia is expected to be a savings of $11,763,833 (Year 1 savings: $2,467,801, Year 2 savings: $3,813,961, Year 3 savings: $5,482,072).
Additionally, CADTH conducted several scenario analyses exploring limitations within the sponsor’s assumptions as follows, with results reported in Table 26:
CDA-AMC increased the number of monthly equivalent doses in each year by 10% to represent an additional 10% of eligible patients. CDA-AMC assumed these additional patients receive oral risperidone in the reference scenario. In the new drug scenario, 33%, 67%, and 100% of these additional patients instead received risperidone ER in years 1, 2, and 3, respectively. For simplicity, all patients receiving oral risperidone were assumed to receive 5 mg daily for $30.86 monthly, based on Ontario Drug Benefit list prices.80
All comparators were assumed to cost 10% less than their list prices.
All comparators were assumed to cost 25% less than their list prices.
A combination of Scenarios 1 and 3.
The CDA-AMC base case results may be considered the best-case scenario regarding the reimbursement of risperidone ER for the treatment of adults with schizophrenia, where risperidone ER is not expected to increase the LAI market and the cost of the comparator products is close to their respective list prices. In contrast, CADTH’s scenario 4 represents a scenario where risperidone ER expands access to LAIs and where the costs of the comparator products paid by public drug plans are substantially less expensive than their public list prices. The true budget impact of reimbursing risperidone ER for the treatment of schizophrenia in adults is likely to lie in between these 2 estimates.
Table 26: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $265,590,837 | $280,692,216 | $295,897,607 | $311,190,255 | $1,153,370,915 |
New drug | $265,590,837 | $277,645,548 | $291,189,013 | $304,422,265 | $1,138,847,664 | |
Budget impact | $0 | –$3,046,667 | –$4,708,593 | –$6,767,990 | –$14,523,251 | |
CDA-AMC base case: Risperidone ER uptake for bimonthly-only doses removed | Reference | $265,590,837 | $280,692,216 | $295,897,607 | $311,190,255 | $1,153,370,915 |
New drug | $265,590,837 | $278,224,415 | $292,083,646 | $305,708,183 | $1,141,607,081 | |
Budget impact | $0 | –$2,467,801 | -$3,813,961 | –$5,482,072 | –$11,763,833 | |
CDA-AMC Scenario 1: LAI market grows by 10% | Reference | $267,124,945 | $282,316,747 | $297,613,161 | $312,997,336 | $1,160,052,189 |
New drug | $267,124,945 | $277,166,449 | $307,552,539 | $331,874,669 | $1,183,718,602 | |
Budget impact | $0 | –$5,150,298 | $9,939,378 | $18,877,333 | $23,666,413 | |
CDA-AMC Scenario 2: Comparators cost 10% less | Reference | $239,630,425 | $253,217,995 | $266,901,127 | $280,664,417 | $1,040,413,964 |
New drug | $239,630,425 | $251,904,627 | $264,886,799 | $277,791,848 | $1,034,213,699 | |
Budget impact | $0 | –$1,313,367 | –$2,014,328 | –$2,872,569 | –$6,200,264 | |
CDA-AMC Scenario 3: Comparators cost 25% less | Reference | $199,692,021 | $211,014,996 | $222,417,606 | $233,887,014 | $867,011,637 |
New drug | $199,692,021 | $211,536,581 | $223,243,206 | $235,105,737 | $869,577,545 | |
Budget impact | $0 | $521,585 | $825,601 | $1,218,723 | $2,565,909 | |
CDA-AMC Scenario 4: LAI market grows and Comparators cost 25% less (1 + 3) | Reference | $200,842,602 | $212,233,394 | $223,704,272 | $235,242,325 | $872,022,593 |
New drug | $200,842,602 | $211,884,638 | $239,268,761 | $261,942,303 | $913,938,304 | |
Budget impact | $0 | –$348,756 | $15,564,490 | $26,699,977 | $41,915,711 |
BIA = budget impact analysis.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.