CADTH Reimbursement Review
Nirmatrelvir-Ritonavir (Paxlovid)
Sponsor: Pfizer Canada ULC
Therapeutic area: Mild-to-moderate COVID-19
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
aOR
adjusted odds ratio
CEV
clinically extremely vulnerable
CI
confidence interval
DB
double blind
HR
hazard ratio
ICU
intensive care unit
KPSC
Kaiser Permanente Southern California
mITT
modified intention to treat
NNT
number needed to treat
OR
odds ratio
PCR
polymerase chain reaction
RCT
randomized controlled trial
RR
relative risk
SAE
serious adverse event
SARS-CoV-2
severe acute respiratory syndrome coronavirus 2
SD
standard deviation
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Nirmatrelvir-ritonavir (Paxlovid), 150 mg nirmatrelvir; 100 mg ritonavir, tablets, co-packaged for oral use |
Sponsor | Pfizer Canada ULC |
Indication | For the treatment of mild-to-moderate COVID-19 in adults with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | January 17, 2022 |
Recommended dose | The recommended dosage is 300 mg nirmatrelvir (two 150 mg tablets) with 100 mg ritonavir (one 100 mg tablet) with all 3 tablets taken together orally twice daily for 5 days. Nirmatrelvir-ritonavir should be given as soon as possible after positive results of direct SARS-CoV-2 viral testing and within 5 days of symptom onset. In patients with moderate renal impairment (eGFR ≥ 30 to < 60 mL/min), reduce the dosage of nirmatrelvir-ritonavir to 150 mg of nirmatrelvir (one 150 mg tablet) and 100 mg ritonavir (one 100 mg tablet) twice daily for 5 days. |
eGFR = estimated glomerular filtration rate; NOC = Notice of Compliance; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Introduction
COVID-19 is an illness caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 The rapid global spread of the virus led to a pandemic, as declared by WHO on March 11, 2020. In Canada, as of August 19, 2023, the cumulative count of documented COVID-19 cases had reached 4,706,450; however, serologic data suggest that approximately 80% of the population has contracted the infection at some point.2 The cumulative death toll since the beginning of the pandemic is 53,345.3
Patients with COVID-19 exhibit a broad spectrum of symptoms, varying from mild in the majority of cases (e.g., fever and malaise) to occasionally severe hypoxia with acute respiratory distress syndrome. In some patients, mild to moderate COVID-19 can lead to severe medical complications or progress into severe or critical states which are associated with a high morbidity and mortality rate.4
Several risk factors have been involved in the progression to severe COVID-19. Earlier in the pandemic, a wide range of risk factors were identified and included older age, cardiovascular disease, diabetes mellitus, hypertension, cerebrovascular disease, dementia, neurodevelopmental disorders, and chronic kidney disease.5 At the time of this review, the relevance of these risk factors for progressing to severe disease is not the same as it was during the pandemic,6 as population immunity has been building up over time and the proportion and characteristics of patients being hospitalized due to COVID-19 are now changing. The 2 clinical experts consulted by CADTH for this review agreed that, at the time of this review, the most relevant risk factors for progression to severe COVID-19 are older age (> 80 years), frailty, underprotection from SARS-CoV-2 (patients who were unvaccinated and who have not had a prior infection), and severe immunosuppression. This would encompass a larger population of patients than recommendations from the recently updated WHO living guideline, which states that patients at high risk of hospitalization are those with diagnosed immunodeficiency syndromes, patients who have undergone solid organ transplant and receive immunosuppressants, as well as patients with autoimmune illness receiving immunosuppressants.6 The guideline indicates that patients in the high-risk category have a 6% rate of hospitalization.6 The guideline also highlights characteristics which are now associated with only a moderate risk of progressing to severe disease, a category of patients who have a 3% rate of hospitalization: patients aged older than 65 years, patients with obesity, diabetes and/or chronic cardiopulmonary disease, chronic kidney or liver disease, active cancer, with disabilities, and those with comorbidities of chronic disease.6
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of nirmatrelvir-ritonavir, 150 mg (nirmatrelvir) and 100 mg (ritonavir) oral tablets, in the treatment of mild to moderate COVID-19 in adults with positive SARS-CoV-2 viral testing who are at high risk for progression to severe COVID-19.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Patient input was submitted by 7 patient groups: Arthritis Consumer Experts, the Canadian Breast Cancer Network, the Gastrointestinal Society, the Lung Health Foundation, the Save Your Skin Foundation, the Sickle Cell Awareness Group of Ontario, and the International Federation on Ageing.
The inputs were mostly gathered directly from patients through online surveys, focus groups, or by email. Most patients represented by the patient groups highlighted that because of their condition, they were at higher risk of worst outcome from COVID-19 than the general population, and that COVID-19 complications also posed a risk of worsening their baseline condition. Several patients described serious symptoms from contracting COVID-19 and shared their experience with the use of nirmatrelvir-ritonavir. Preventing hospitalizations was highlighted as a main goal of treatment. One patient group focused on the need to have treatment options for post–COVID-19 condition. The patient groups highlighted that nirmatrelvir-ritonavir needs to be safe, effective, and accessible on uniform terms and conditions across the country. Indeed, some reported that the administrative process required for approval can be lengthy, and the criteria for eligibility varies by jurisdiction, with some enforcing stricter parameters for access.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The current treatment paradigm for mild to moderate COVID-19 in Canada is to prevent hospitalization and death among patients at high risk for these outcomes. Risk factors for hospitalization and death can be determined from control groups in observational studies or from provincial outcomes data. Typically, age older than 70 years, unvaccinated status, and multiple comorbidities leading to frailty are considered the main risk factors. In addition, patients who are severely immunosuppressed, and those with a prior disease trajectory of worsening in the first 5 days or not starting to improve within 5 days, have a high likelihood of hospitalization. However, provincial outcomes data show that even in the highest-risk subgroups, the hospitalization rate remains low, averaging 2.5%.7
SARS-CoV-2 has evolved significantly since the beginning of the pandemic, and the current risk of hospitalization or death is very low. Therefore, the vast majority of mild to moderate COVID-19 requires no specific treatment, symptoms being mild and self-limited. First-line therapy for the vast majority of the population with COVID-19 is supportive care. If required to prevent hospitalization, benefits of treatment must be balanced against the risks and adverse events (AEs), including drug-drug interactions, that jeopardize patient well-being.
Nirmatrelvir-ritonavir is the first and only approved oral treatment for COVID-19 in Canada, through an emergency use authorization. One of the main caveats of the pivotal trial informing approval is that it was performed at a time when the Delta SARS-CoV-2 variant was circulating. Ongoing clinical trials are currently being performed; when results become available, these trials may provide evidence on the use of nirmatrelvir-ritonavir in other variants of SARS-CoV-2. In the meantime, additional evidence is available in the form of observational studies; however, its use to inform policy-making has limitations.
The role of nirmatrelvir-ritonavir in the long term is likely to evolve around the small number of individuals who were highly compromised who remain at high risk of negative outcomes because of a failure to fight infection or physiologic frailty. Treatment must be based on a positive diagnostic test since many viral upper respiratory tract infections present similarly, and nirmatrelvir-ritonavir can cause significant and potentially dangerous drug-drug interactions.
Nirmatrelvir-ritonavir should ideally be prescribed in primary care, by a clinician able to evaluate symptoms, disease trajectory, and risk for progression. This could be either a generalist clinician or a specialist in relevant fields for patients with high-risk conditions (e.g., oncologist, rheumatologist). To offer easy and rapid access, some jurisdictions use a decentralized model (no designated prescribers, availability through any participating pharmacy), while some permit pharmacists to write the prescription. In the stage of the pandemic at the time of this review, clinical experts suggested re-evaluating whether there is still a need for such decentralized models, including pharmacist prescribing, with a shift toward better selection and identification of patients who are likely to benefit the most from treatment.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. For the CADTH review of nirmatrelvir-ritonavir, the drug plans provided questions pertaining to existence of alternatives to nirmatrelvir-ritonavir, criteria to determine eligibility, definitions for high risk of progression to severe COVID-19, the role of vaccination within eligibility criteria, and various prescribing considerations. These questions were addressed by the clinical experts consulted for the CADTH review. Clinical expert responses have been included in the Drug Program Input section (Table 4).
Clinical Evidence
Systematic Review
Description of Studies
One multicentre, double-blind (DB), randomized controlled trial (RCT) was the primary source of evidence for the efficacy and safety of nirmatrelvir-ritonavir. The EPIC-HR study (N = 2,246) evaluated the superiority of nirmatrelvir-ritonavir compared with placebo for the treatment of adult symptomatic outpatients with mild to moderate COVID-19 who were not vaccinated against SARS-CoV-2 and who were considered at high risk for progression to severe disease and/or hospitalization at the time the study was performed, based on a wide range of prespecified patient characteristics. The primary outcome of the EPIC-HR study was a combined outcome of the proportion of patients with COVID-19–related hospitalization or who died from any cause through day 28.
Efficacy Results
Nirmatrelvir-ritonavir reduced the incidence of COVID-19–related hospitalization or death from any cause through day 28 compared with placebo; in the overall population of patients treated as per the product monograph (within 5 days of symptom onset), the absolute reduction was –5.5% (95% confidence interval [CI], –7.2% to –4.0%; P < 0.001). The proportion of patients experiencing a primary outcome event (0.9% with treatment and 6.3% with control) demonstrates the incidence of COVID-19–related hospitalization or death from any cause in the EPIC-HR study population was low. Overall, the magnitude of effect with nirmatrelvir-ritonavir was considered relatively small. In 1 subgroup analysis performed in patients aged 65 years and older, nirmatrelvir-ritonavir reduced the primary outcome incidence by 13.9% compared with placebo (modified intention to treat [mITT] 1 population, 0.8% versus 14.6%, respectively; 95% CI, –20.1% to –7.8%; P < 0.0001), suggesting that there might be subgroups of patients where the treatment effect is more pronounced, especially in the presence of a higher risk of worst outcome. However, the use of nirmatrelvir-ritonavir in the EPIC-HR study did not yield clinically meaningful differences compared with placebo on outcomes assessing duration or severity of COVID-19 signs and symptoms.
Harms Results
Nirmatrelvir-ritonavir was relatively well tolerated in the EPIC-HR study. Similar proportions of patients experienced AEs between treatment groups; however, numerically more patients reported AEs of higher severity and serious AEs (SAEs) in the placebo group than in the treatment group. Discontinuation of treatment due to AEs was low. No patient died in the nirmatrelvir-ritonavir group and 15 patients (1.3%) died in the placebo group, with most causes of death being related to COVID-19.
There is a lack of evidence on the safety of nirmatrelvir-ritonavir, especially in older adults and patients who are frail, who may be at increased risk of experiencing harms outcomes. Of note, the use of nirmatrelvir-ritonavir is associated with CYP3A inhibition, resulting in a number of drug-drug interactions; patients with significant drug-drug interactions were excluded from the EPIC-HR study.
The safety of nirmatrelvir-ritonavir was not assessed in observational studies.
Critical Appraisal
The overall risk of bias for the EPIC-HR study was low.
However, the most significant issue with the EPIC-HR study is that the findings of the trial cannot be generalized to the population of patients living in Canada at high risk for progression to severe COVID-19, as defined in clinical practice at the time of this review. Patients included in the EPIC-HR trial were relatively young, limiting conclusions on the efficacy and safety of nirmatrelvir-ritonavir in an older adult population, who are considered at increased risk. As per the study’s selection criteria, the EPIC-HR study did not include patients who were vaccinated or patients who had COVID-19 in the past. This is an important gap since according to the most recent data, at least 80% of the population of people living in Canada has completed a primary series of the COVID-19 vaccine,8 and approximately 80% of the population has contracted a SARS-CoV-2 infection at some point.3 Finally, patients included in the study presented with various comorbidities which, at the time the trial was performed, were considered risk factors for severe illness from COVID-19; however, these concomitant conditions are no longer considered to significantly increase the risk of worst outcomes. The 2 clinical experts consulted by CADTH for this review agreed that the most relevant risk factors for progressing to severe disease and hospitalization are currently older age (> 80 years), frailty, underprotection from SARS-CoV-2 (patients who are unvaccinated and those who have not had a prior infection), and severe immunosuppression.
In addition to the population issues, the primary variant observed in the trial population was Delta; however, this SARS-CoV-2 variant was no longer circulating at the time of this review, as the main variant of concern is Omicron and its subsequent subvariants, which are substantially less virulent.
Table 2: Summary of Key Results From the Pivotal Study and RCT Evidence
Key results | EPIC-HR | |
|---|---|---|
Nirmatrelvir-ritonavir | Placebo | |
Proportion of patients with COVID-19–related hospitalization or death from any cause, mITTa | ||
Number of patients in the analysis set | 697 | 682 |
Patients with event (death or hospitalization), n (%) | 5 (0.717) | 44 (6.452) |
Average time at risk for eventb (days) | 27.296 | 26.189 |
Average study follow-upc (days) | 27.455 | 27.284 |
Estimated event rate of COVID-19–related hospitalization or death, % (95% CI) | 0.723 (0.302 to 1.729) | 6.531 (4.901 to 8.676) |
Event rate difference from placebo, % (SE) | –5.807 (1.005) | |
95% CI of event rate difference | –7.777 to –3.837 | |
P value | < 0.001 | |
Proportion of patients with COVID-19–related hospitalization or death from any cause, mITT1d | ||
Number of patients in the analysis set | 1,039 | 1,046 |
Patients with event (death or hospitalization), n (%) | 9 (0.866) | 66 (6.310) |
Average time at risk for eventb (days) | 27.033 | 25.974 |
Average study follow-upc (days) | 27.213 | 27.098 |
Estimated event rate of COVID-19–related hospitalization or death, % (95% CI) | 0.878 (0.458 to 1.680) | 6.400 (5.063 to 8.075) |
Event rate difference from placebo, % (SE) | –5.522 (0.816) | |
95% CI of event rate difference | –7.122 to –3.923 | |
P value | < 0.001 | |
Proportion of patients with severe signs or symptoms attributed to COVID-19; mITTe | ||
Number of patients in the analysis set | 686 | 674 |
Patients with event (severe signs or symptoms), n (%) | 123 (17.93) | 137 (20.33) |
OR (95% CI) | 0.88 (0.66 to 1.17) | |
P value | 0.3872 | |
Proportion of patients who died from any cause; mITTe | ||
Number of patients in the analysis set | 697 | 682 |
Patients with event, n (%) | 0 | 11 (1.6) |
P value | 0.0004 | |
Harms outcomes | ||
Population, n | 1,109 | 1,115 |
≥ 1 AE, n (%) | 256 (23.1) | 270 (24.2) |
≥ 1 SAE, n (%) | 19 (1.7) | 74 (6.6) |
≥ 1 discontinuation of treatment due to AEs, n (%) | 23 (2.1) | 47 (4.2) |
Deaths, n | 0 | 15 (1.3) |
AE = adverse event; CI = confidence interval; mITT = modified intention to treat; OR = odds ratio; RCT = randomized controlled trial; SAE = serious adverse event; SE = standard error.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aThe mITT population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had at least 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment and were treated within 3 days following COVID-19 symptom onset.
bAverage time at risk for event is computed as time to first event, time to last day of participation, or day 28, whichever is earliest.
cAverage study follow-up is computed as time to last day of participation or day 28, whichever is earlier.
dThe mITT1 population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had at least 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment (treated within 5 days following COVID-19 symptom onset). Participants were analyzed according to the study intervention to which they were randomized.
eThe mITT population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had at least 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment and were treated within 3 days following COVID-19 symptom onset.
Source: EPIC-HR Clinical Study Report.9
Studies Addressing Gaps in the Evidence From the Systematic Review
Observational studies were submitted by the sponsor and reviewed by CADTH to bridge the evidence gaps from the EPIC-HR study. CADTH also considered a prior Health Technology Review of Nirmatrelvir-Ritonavir for the Treatment of COVID-19.10 With the help of clinical experts, observational studies within the report for which the populations are particularly relevant to Canadian clinical practice were selected and described in detail in this report. As part of the overall body of evidence, their findings can inform decision-making regarding the optimal use of nirmatrelvir-ritonavir in specific populations of real-world patients who would be considered more vulnerable to worst outcomes with COVID-19 and who could not be included in the pivotal EPIC-HR RCT. Overall, 1 additional RCT and 6 observational cohort studies contributed to the evidence.
EPIC-SR Study
EPIC-SR (N = 1,153) was a multicentre, DB, placebo-controlled RCT comparing nirmatrelvir-ritonavir to placebo for the treatment of nonhospitalized, symptomatic, adult patients with COVID-19 who were at low risk of progression to severe illness,11 which is outside of the Health Canada indication for nirmatrelvir-ritonavir. Patients were excluded if they had an underlying medical condition associated with an increased risk of developing severe illness from COVID-19 (unless the patient was vaccinated) or a prior COVID-19 infection. A subgroup of patients who were vaccinated with at least 1 risk factor for severe COVID-19 (n = 721) was submitted by the sponsor as evidence for the efficacy of nirmatrelvir-ritonavir in patients who were vaccinated during the Omicron wave. Enrolment was terminated early due to very low rates of hospitalization or death observed. The EPIC-SR study did not meet its primary objective, failing to demonstrate a difference between nirmatrelvir-ritonavir and placebo for COVID-19–related hospitalization or death from any cause, as well as for the primary outcome of time to sustained alleviation of all targeted COVID-19 signs and symptoms, in both the overall population of patients at standard risk of progressing to severe disease and in a subgroup of patients with an underlying medical condition who were vaccinated. Therefore, the EPIC-SR study is not informative with regard to the evidence gaps.
Lewnard et al. Study12
The study by Lewnard et al. (2023)12 (n = 7,274 treated with nirmatrelvir-ritonavir; n = 126,152 not treated with nirmatrelvir-ritonavir) was a retrospective cohort study using a matched cohort framework that was performed in California, US. Patients were included if they were aged 12 years or older, enrolled in the Kaiser Permanente Southern California (KPSC) health plans, and had a positive SARS-CoV-2 polymerase chain reaction (PCR) test result between April 8, 2022, and October 7, 2022. The primary end point of this study was hospital admission or death from any cause within 30 days. The included population was mostly vaccinated, with characteristics that were consistent with standard risk of progressing to severe COVID-19. The study resulted in those patients who were treated with nirmatrelvir-ritonavir having a clinically similar hospitalization and mortality rate compared to patients who did not receive this treatment. The study by Lewnard et al.12 has limited impact in addressing gaps in the evidence, mainly due to the presence of substantial confounding and the included population not having the characteristics of patients currently considered at high risk for progressing to severe COVID-19.
Schwartz et al. Study13
The study by Schwartz et al. (2023)13 (n = 8,876 treated with nirmatrelvir-ritonavir; n = 168,669 not treated with nirmatrelvir-ritonavir) was a population-based cohort study with propensity score-derived inverse probability of treatment weighting that was performed in Ontario. Patients were included in the study if they were Ontario residents aged between 18 and 110 years who had a positive PCR test for SARS-CoV-2 between April 4, 2022, and August 31, 2022. Patients who received nirmatrelvir-ritonavir were highly vaccinated (85% had received at least 3 doses of the SARS-CoV-2 vaccine); 42% were considered at high risk for progressing to severe disease. Overall, 2.1% of patients who received nirmatrelvir-ritonavir had a hospital admission due to COVID-19 or all-cause death within 30 days, compared with 3.7% for patients who did not receive this treatment, resulting in a weighted odds ratio (OR) of 0.56 (95% CI, 0.47 to 0.67) and a number needed to treat (NNT) to prevent 1 case of severe COVID-19 of 62 (95% CI, 44 to 77). This suggests a statistically significant but clinically small effectiveness of nirmatrelvir-ritonavir in a real-world population. The Schwartz et al. study may inform gaps in the evidence for the efficacy of nirmatrelvir-ritonavir in patients who were vaccinated during the Omicron wave, especially as it was performed in a population of people living in Canada. However, the population was not consistent with current definitions for being high risk of progressing to severe COVID-19. In the study, the impact of nirmatrelvir-ritonavir to prevent hospitalization and death was considered modest. Because of potential issues with selection and confounding, findings should be interpreted with caution, as there is uncertainty surrounding the true treatment effect.
Kaboré et al. Study14
The study by Kaboré et al. (2023)14 (n = 8,402 treated with nirmatrelvir-ritonavir; n = 8,402 not treated with nirmatrelvir-ritonavir) was a retrospective cohort study using nearest-neighbour propensity score matching performed in Quebec. Patients were included if they were covered by the Quebec public health insurance plan in 2022 and had either a prescription for nirmatrelvir-ritonavir (treated group) or a positive SARS-CoV-2 PCR result (control group) between March 15, 2022, and October 15, 2022. The study showed a benefit of nirmatrelvir-ritonavir compared to no such treatment on the primary outcome of COVID-19–related hospitalizations within 30 days (3.6% in the nirmatrelvir-ritonavir treatment group versus 11.5% in the control group; relative risk [RR] = 0.31; 95% CI, 0.28 to 0.36; P < 0.001). This yielded an NNT of 13, as calculated by CADTH. The magnitude of treatment effect observed with nirmatrelvir-ritonavir on preventing hospitalization should, however, be interpreted with caution, as the natural incidence of COVID-19–related hospitalizations in the control group was higher than would be expected in clinical practice; the estimates may have been affected by confounding factors, resulting in bias in favour of treatment with nirmatrelvir-ritonavir. The Kaboré et al. study may inform on subpopulations who are more likely to benefit from treatment. According to subgroup analyses, the magnitude of treatment effect was greater in patients who were unvaccinated than in the overall population and was also greater in patients aged 70 years and older (versus aged younger than 70 years) and in patients whose last vaccine dose was before the prior 6 months (versus within prior 6 months). Results also favoured nirmatrelvir-ritonavir versus no such treatment in a subgroup of patients who were severely immunocompromised.
Dryden-Peterson et al. Study15
The study by Dryden-Peterson et al. (2023)15 (n = 12,541 treated with nirmatrelvir-ritonavir; n = 32,010 not treated with nirmatrelvir-ritonavir) was a population-based cohort study using inverse probability-weighted analysis performed in Massachusetts and southern New Hampshire, US. The study was assessed as having a moderate risk of bias.10 Patients were included if they were aged 50 years or older and had a COVID-19 diagnosis between January 1, 2022, and July 17, 2022. Patients who received nirmatrelvir-ritonavir were highly vaccinated (79% vaccinated and boosted), half of the population was aged at least 65 years, 36% of patients were immunocompromised, and 23% had a solid tumour. The study showed a small benefit for nirmatrelvir-ritonavir compared to no such treatment on the primary outcome of hospitalization within 14 days or death within 28 days (0.5% versus 0.9%, respectively; absolute risk difference = –0.4%; RR = 0.56; 95% CI, 0.42 to 0.75). This yielded an NNT of 250, as calculated by CADTH. Findings were consistent across subgroups; however, vaccination status affected the magnitude of treatment effect, which was higher in patients who were not fully vaccinated (NNT = 50 as calculated by CADTH) or whose last vaccine was greater than 20 weeks before the study (NNT = 196 as calculated by CADTH).
Dormuth et al. Study16
The study by Dormuth et al.16 (n = 3,433 treated with nirmatrelvir-ritonavir; n = 3,433 not treated with nirmatrelvir-ritonavir) was a retrospective cohort study of patients at increased vulnerability to complications from COVID-19 performed in British Columbia. Inclusion of this study was suggested by clinical experts due to the high representativity of the population and sound methodology. High-dimensional propensity score models were used to minimize confounding and the nearest-neighbour method was used for matching patients. The study was performed between February 1, 2022, and February 3, 2023. The study assessed the effectiveness of nirmatrelvir-ritonavir on death from any cause and COVID-19–related hospitalization compared to no such treatment in different cohorts of patients who are clinically extremely vulnerable (CEV) at high risk for complications from COVID-19, as follows.
CEV1: aged at least 18 years and severely immunocompromised
CEV2: aged at least 18 years and moderately immunocompromised
CEV3: patients with selected medical conditions (severe respiratory disorders; insulin-dependent diabetes; or certain blood disorders, metabolic disorders, and cancers not captured in other groups)
Expanded eligibility: patients at lower risk than CEV but at higher risk than general population.
Hospitalization rates were low and aligned with clinical practice; in spite of this, patients who were severely immunocompromised (CEV1 cohort) and received nirmatrelvir-ritonavir had a –2.5% absolute risk difference (95% CI, –4.8% to –0.2%) of experiencing the primary outcome compared to control, yielding an NNT of 40. The corresponding risk difference was –1.7% (95% CI, –2.9% to –0.5%) for patients who were moderately immunocompromised (CEV2 cohort) and –1.3% (95% CI, –2.8% to 0.1%) for patients with selected medical conditions (CEV3 cohort), yielding NNTs of 60 and 75, respectively.
Hedvat et al. Study17
The study by Hedvat et al. (2022)17 (n = 28 treated with nirmatrelvir-ritonavir; n = 75 not treated with nirmatrelvir-ritonavir) was a retrospective study of all adult patients who received solid organ transplants and had a positive SARS-CoV-2 PCR test at a research hospital between December 16, 2021, and January 19, 2022. The study was performed in New York City, US, and was assessed as having a moderate risk of bias.10 The use of nirmatrelvir-ritonavir was associated with a reduction, compared with no treatment, in the incidence of hospitalization or death from any cause (14.3% versus 33.3%, respectively; adjusted risk ratio for organ transplant type = 0.21; 95% CI, 0.06 to 0.71; NNT = 6 as calculated by CADTH), and hospitalization or death from COVID-19 (10.7% versus 30.7%, respectively; adjusted risk ratio for organ transplant type = 0.17; 95% CI, 0.04 to 0.67; NNT = 5 as calculated by CADTH). According to the clinical experts consulted by CADTH, hospitalization rates in this study were higher than what is seen in clinical practice in similar populations with organ transplants; therefore, although the findings are consistent with the known vulnerability of this patient group, generalizability of the findings is uncertain.
Discussion of Evidence Gaps
Findings for the observational studies can inform decision-making regarding the optimal use of nirmatrelvir-ritonavir in specific populations of real-world patients who would be considered more vulnerable to worse COVID-19 outcomes and who could not be included in the pivotal RCT EPIC-HR.
Results from 5 observational studies discussed in this review13-17 show that nirmatrelvir-ritonavir is effective compared to no such treatments against the Omicron SARS-CoV-2 variant of concern among high-risk populations.
Observational studies also suggest that the effectiveness of nirmatrelvir-ritonavir in high-risk populations, as clinically defined in clinical practice in Canada, is likely to vary among the various categories of populations.
In 2 studies with subgroup analyses according to age group,14,16 there was a greater magnitude of effect with nirmatrelvir-ritonavir treatment versus no treatment in patients aged 70 years or older, compared with patients who were younger than 70 years. The overall incidence of hospitalization was also greater in both the treatment and control groups in patients who were older.
In 3 studies13,15,16 where the population consisted of patients who were highly vaccinated and in subgroup analyses of patients who had received prior vaccination, overall, nirmatrelvir-ritonavir was associated with a smaller magnitude of treatment effect when compared to patients who were vaccinated. In these studies or subgroup analyses, the incidence of hospitalization was typically small for both treatment and control arms, as would be expected in clinical practice, suggesting that patients who are vaccinated have an overall lower risk of progressing to severe COVID-19, regardless of whether or not they received treatment.
In 2 studies16,17 that included patients who were severely and/or moderately immunocompromised, nirmatrelvir-ritonavir was effective in preventing hospitalization and death compared with no such treatment; the magnitude of effect varied across the studies. In a large observational study conducted in Canada, the magnitude of treatment effect was proportional to the level of immunosuppression, being at its highest in the severely immunocompromised cohort.
Issues were noted in the observational studies with selection and confounding; this introduces uncertainty around the true treatment effect, which was addressed to a varying degree through the weighting models and use of covariates. Though findings should be interpretated with caution, as part of the overall body of evidence, they remain informative regarding the optimal use of nirmatrelvir-ritonavir in clinical practice.
Conclusions
Findings from the EPIC-HR study suggest that nirmatrelvir-ritonavir may contribute to preventing COVID-19–related hospitalization or death compared with placebo, in a population that was not considered at high risk for progressing to severe disease as defined by clinical practice at the time of this review. The incidence of hospitalization in the study was low, and the magnitude of treatment effect with nirmatrelvir-ritonavir was considered small in this patient population. Generalizability issues with the trial include that it was performed in patients who were unvaccinated, which is not representative of the highly vaccinated population of people living in Canada, and at a time when the Delta variant was in circulation. Therefore, additional evidence from the EPIC-SR study and observational studies were reviewed to bridge the evidence gaps from the EPIC-HR study. This supplementary evidence to the pivotal RCT suggests that nirmatrelvir-ritonavir retained efficacy against the Omicron variant of concern, but that the effectiveness of the drug was considerably reduced in adequately vaccinated populations. Observational cohort studies performed in specific populations suggest that the magnitude of effect with nirmatrelvir-ritonavir treatment may be greater in individuals of older age, unvaccinated, or severely immunosuppressed; these are all characteristics of patients who would be considered at high risk of progressing to severe disease and more vulnerable to worst COVID-19 outcomes, according to clinical experts consulted by CADTH for this review. Issues were noted in the observational studies with selection of patients and confounding; this introduces uncertainty around the true treatment effect, which was addressed to a varying degree through the weighting models and use of covariates. Though findings should be interpretated with caution, as part of the overall body of evidence, they inform on the optimal use of nirmatrelvir-ritonavir in clinical practice. Nirmatrelvir-ritonavir was relatively well tolerated in the EPIC-HR study; however, there is a lack of evidence in older adults and patients who are frail who may be at increased risk of experiencing harms outcomes. The use of nirmatrelvir-ritonavir poses additional issues in patients receiving medication metabolized through CYP3A, due to its inhibition by the drug, which results in a number of interactions.
Introduction
At the time of this review, the federal government, specifically the Public Health Agency of Canada, was responsible for overseeing the procurement and allocation of nirmatrelvir-ritonavir to ensure availability for federal, provincial, and territorial health care systems. Current provincial eligibility criteria for nirmatrelvir-ritonavir vary considerably between provinces and are presented in Appendix 1. Most jurisdictions elected to set a minimum age, and most require the presence of risk factors regardless of vaccination status.
The objective of this report Is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of nirmatrelvir-ritonavir, 150 mg (nirmatrelvir) and 100 mg (ritonavir) oral tablets, in the treatment of mild to moderate COVID-19 in adults with positive SARS-CoV-2 viral testing who are at high risk for progression to severe COVID-19.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
COVID-19 is an illness caused by SARS-CoV-2.1 The rapid global spread of the virus led to a pandemic, as declared by WHO on March 11, 2020. Despite the continuous countermeasures implemented worldwide, the COVID-19 pandemic was marked by successive waves across the world, characterized by exponential increases in case numbers. In Canada, as of August 19, 2023, the cumulative count of documented COVID-19 cases had reached 4,706,450, with a weekly percentage of 11.6% positive cases of the total tests conducted; however, serologic data suggest that approximately 80% of the population has contracted the infection at some point.3 The cumulative death toll since the beginning of the pandemic is 53,345.3
The global incidence of COVID-19 has begun to decline gradually starting early 2023. This gradual decline can also be seen in Canada since March 2023 with fluctuations in some jurisdictions reporting increases in percent positivity or new cases.3
Patients with COVID-19 exhibit a broad spectrum of symptoms, varying from asymptomatic or mild in the majority of cases (e.g., fever and malaise) to occasionally severe hypoxia with acute respiratory distress syndrome. In symptomatic patients, a report of 72,314 cases found that 81% developed mild disease, 14% developed severe disease requiring oxygen support, and 5% had critical disease with respiratory, cardiac, or multiorgan complications.18 Therefore, in some patients, mild to moderate COVID-19 can lead to severe medical complications or progress into severe or critical states which are associated with a high morbidity and mortality rate.4
Several risk factors have been involved in the progression to severe COVID-19. Earlier in the pandemic, a wide range of risk factors were identified and included older age, cardiovascular disease, diabetes mellitus, hypertension, cerebrovascular disease, dementia, neurodevelopmental disorders, and chronic kidney disease.5 At the time of this review, the relevance of these risk factors for progressing to severe disease is not the same as it was during the pandemic,6 as population immunity has been building up over time and the characteristics of patients being hospitalized due to COVID-19 are now changing. According to the recently updated WHO living guideline,6 the following characteristics are now associated with only a moderate risk of progressing to severe disease, based on the risk of hospitalization: patients aged older than 65 years, patients with obesity, diabetes and/or chronic cardiopulmonary disease, chronic kidney or liver disease, active cancer, with disabilities, and those with comorbidities of chronic disease.6
The 2 clinical experts consulted by CADTH for this review agreed that at the time of this review, the most relevant risk factors to progress to severe COVID-19 are older age (> 80 years), frailty, underprotection from SARS-CoV-2 (patients who were unvaccinated and who have not had a prior infection), and severe immunosuppression. This would encompass a larger population of patients than recommendations from the WHO living guideline, which states that patients at high risk of hospitalization are those with diagnosed immunodeficiency syndromes, patients who have undergone solid organ transplant and receive immunosuppressants, as well as patients with autoimmune illness receiving immunosuppressants.6 The guideline indicates that patients in the high-risk category have a 6% rate of hospitalization.6
Since the first symptoms of COVID-19 are similar to other respiratory infections, a confirmed diagnosis is essential to effectively manage the spread of the virus while minimizing the burden on the health care system. Antigen tests are valuable and robust to diagnose SARS-CoV-2 in symptomatic individuals, are typically self-administered at home, and provide rapid results (typically within 15 to 30 minutes), allowing quick action should access to a treatment be needed.19
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Since the approval of the first COVID-19 vaccine by Health Canada in December 2020, 83.2% of the population has received at least 1 dose (initial vaccination series) and vaccination remains the first line of defence to prevent SARS-CoV-2 infection.8
Currently, each province and territory adapt and implement the currently authorized treatments for adults with mild to moderate COVID-19 within their own health care systems considering local context and resources. Treatment approaches are essentially based on a patient’s severity of illness and risk level of progressing to severe disease, the assessment of which varies across jurisdictions. Patients with mild to moderate COVID-19 who are not hospitalized and who are at high risk of disease progression are usually first treated with oral nirmatrelvir-ritonavir, or alternatively, in some specific cases which vary by jurisdiction, with remdesivir. The use of tixagevimab-cilgavimab, sotrovimab, and casirivimab-imdevimab is limited due to lack of neutralizing activity against variants of concern including alpha, gamma, and/or Omicron, as well as several subvariants and sublineages.20-22
Drug Under Review
Nirmatrelvir is an orally administered medication for the treatment of COVID-19. It is a peptidomimetic inhibitor of the SARS-CoV-2 3C-like protease. The use of nirmatrelvir renders the virus incapable of processing polyprotein precursors, thus preventing viral replication.16 Nirmatrelvir is administered in combination with ritonavir, which is not active against SARS-CoV-2. The role of ritonavir is to inhibit the CYP3A-mediated metabolism of nirmatrelvir, resulting in increased plasma concentrations of nirmatrelvir.16
Nirmatrelvir-ritonavir has a Health Canada indication for the treatment of mild to moderate COVID-19 in adults with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death. Nirmatrelvir-ritonavir is not authorized for initiation of treatment in patients requiring hospitalization due to severe or critical COVID-19, for pre-exposure or postexposure prophylaxis for prevention of COVID-19, and/or use for longer than 5 consecutive days.
The recommended dosage is 300 mg nirmatrelvir (two 150 mg tablets) with 100 mg ritonavir (one 100 mg tablet) with all 3 tablets taken together orally twice daily for 5 days. Nirmatrelvir-ritonavir should be given as soon as possible after positive results of direct SARS-CoV-2 viral testing and within 5 days of symptom onset. In patients with moderate renal impairment (estimated glomerular filtration rate [eGFR] ≥ 30 to < 60 mL/min), reduce the dosage of nirmatrelvir-ritonavir to 150 mg of nirmatrelvir (one 150 mg tablet) and 100 mg ritonavir (one 100 mg tablet) twice daily for 5 days. Nirmatrelvir-ritonavir is not recommended in patients with severe renal impairment (eGFR < 30 mL/min). The product monograph provides a list of medical conditions and other factors placing patients at high risk for progression to severe COVID-19;23 however, the 2 clinical experts consulted by CADTH for this review agreed that these were no longer representative of patients with mild to moderate COVID-19 who progress to severe disease at the time of this review. Nirmatrelvir-ritonavir is currently accessible across all provinces and territories in Canada.
Key characteristics of nirmatrelvir-ritonavir are summarized in Table 3 with other treatments available for the treatment of mild to moderate COVID-19.
Table 3: Key Characteristics of Treatments for Mild to Moderate COVID-19
Drug class | Mechanism of action | Treatment | Indicationa |
|---|---|---|---|
Protease inhibitors | Inhibit viral replication and transcription | Nirmatrelvir-ritonavir (Paxlovid) | For the treatment of mild to moderate COVID-19 in adults with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death. |
Polymerase inhibitors | Act on RNA replication | Remdesivir (Veklury) | For the treatment of COVID-19 in:
|
Monoclonal antibodies | Bind to SARS-CoV-2 S protein to prevent entry into host cell | Tixagevimab-cilgavimab (Evusheld) |
|
Sotrovimab (Xevudy) | For the treatment of mild to moderate COVID-19, confirmed by direct SARS-CoV-2 viral testing, in adults and adolescents (aged ≥ 12 years, weighing at least 40 kg) who are at high risk for progressing to hospitalization and/or death. | ||
Casirivimab-imdevimab (REGEN-COV) | For the treatment of mild to moderate COVID-19, confirmed by direct SARS-CoV-2 viral testing, in adults and adolescents (aged ≥ 12 years, weighing at least 40 kg) who are at high risk for progressing to hospitalization and/or death. |
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aHealth Canada–approved indication.
Sources: Health Canada Drug Product Monograph for nirmatrelvir-ritonavir,23 remdesivir,24 tixagevimab-cilgavimab,25 sotrovimab,26 and casirivimab-imdevimab.27
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient inputs received by CADTH have been included in the stakeholder section of this report.
Patient input was submitted by 7 patient groups: Arthritis Consumer Experts, the Canadian Breast Cancer Network, the Gastrointestinal Society, the Lung Health Foundation, the Save Your Skin Foundation, the Sickle Cell Awareness Group of Ontario, and the International Federation on Ageing.
Arthritis Consumer Experts is Canada’s largest, longest running national arthritis patient organization and provides free, science-based information and education programs in both official languages to people with arthritis. The input was gathered from patients who shared their feedback by email. Several patients, most living with rheumatoid arthritis, described serious symptoms from contracting COVID-19, and shared their experience with the use of nirmatrelvir-ritonavir. Preventing hospitalizations was highlighted as a main goal of treatment. As it is frequent for patients with rheumatoid arthritis to receive immunocompromising medications, patients considered themselves vulnerable to complications from COVID-19 and expressed the need to have access to nirmatrelvir-ritonavir.
The Canadian Breast Cancer Network is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all Canadians affected by breast cancer through the promotion of information, education, and advocacy activities. The input received outlines that individuals with breast cancer may be considered high risk, especially because of weakened immune systems from cancer and cancer treatments. Preventing secondary illness, which poses a risk of worsening cancer care, is important because those with breast cancer already experience a severe disease with complex treatments. The patient group highlighted that nirmatrelvir-ritonavir needs to be safe, effective, and accessible on uniform terms and conditions across the country.
The Gastrointestinal Society is a national charity committed to improving the lives of people with gastrointestinal and liver conditions, supporting research, advocating for appropriate patient access to health care, and promoting gastrointestinal and liver health. The input was gathered primarily through meetings and discussions with health care professionals, researchers, academics, and first-hand experiences among staff who were affected by COVID-19. The input highlights the impact of COVID-19 on the digestive tract, which occurs in 2 primary ways. First, the virus attacks the body by interacting with the angiotensin-converting enzyme 2 receptor, causing damage and affecting the intestinal lining, leading to diarrhea, stomach upset, vomiting, and inflammation. Severe cases may even lead to obstructions, coinfections, or intestinal necrosis and organ failure. The virus also modifies the microbiome in the gastrointestinal tract, which can lead to opportunistic infections, severe gastrointestinal symptoms (pain, nausea, diarrhea), and even anxiety and depression. According to the input, access to nirmatrelvir-ritonavir needs to be improved, especially in a timely manner. The administrative process required can be lengthy, and the criterion for eligibility varies by jurisdiction, with some enforcing stricter parameters for access.
The Lung Health Foundation is a registered charity that provides programs and services to patients and health care providers, invests in lung research, and advocates for improved policies in lung health. It is a recognized leader, voice, and primary resource in the prevention and control of respiratory illness, tobacco cessation and prevention, and its effects on lung health. The input received was mostly obtained from an online survey, and concerns post–COVID-19 condition specifically. Patients expressed difficulty in coping with post–COVID-19 condition on a daily basis, which effects were debilitating at times. The most common symptoms reported were extreme tiredness and fatigue that interfered significantly with daily life, followed by difficulty thinking or concentrating, headaches, and muscle or joint pain. Depression and anxiety were other themes that came up repeatedly for several patients. Therefore, patients expressed the need for an accessible and affordable treatment for post–COVID-19 condition.
The Save Your Skin Foundation is a national, patient-led, not-for-profit group dedicated to the “fight against nonmelanoma skin cancers, melanoma, and ocular melanoma through nationwide education, advocacy, and awareness initiatives.” The Foundation provides a community of support for oncology patients and their caregivers throughout the entire continuum of care. The patient input was gathered through an online survey and is supported by the following patient groups: the Colorectal Cancer Resource & Action Network, the Leukemia & Lymphoma Society of Canada, Kidney Cancer Canada, Lung Cancer Canada, the Canadian Cancer Survivor Network, CanCertainty, the Canadian Skin Patient Alliance, and the Canadian Psoriasis Network. All patients who participated in the survey indicated that their symptoms had some degree of impact on their day-to-day lives. The patient group suggests improving access to COVID-19 treatments, as the survey suggests that there is a gap in this area, for reasons that include test availability and tight timeline for treatment initiation. The survey results also outline the experience of patients who received nirmatrelvir-ritonavir.
The Sickle Cell Awareness Group of Ontario is a leading charitable patient organization providing evidence-based support to patients and families living with sickle cell disease across the province. It supports clinical and psycho-social research, health promotion, patient and care providers education, community awareness, and the development of best practices guidelines. The input has been gathered through focus group interviews and surveys, webinars, and peer support meetings. Sickle cell disease is a life-threatening disorder where patients face debilitating complications, as the disease affects every organ of the body. As infection is very common with the disease, every precaution must be taken to ensure patients do not contract unnecessary infections or suffer preventable complications. With patients being at increased risk of worst outcome, the patient group insists that having a treatment with the potential to reduce COVID-19 complications including hospital admission, should they contract the disease, would allow more patients to have improved outcomes and quality of life.
The International Federation on Ageing acts to advance the agenda for the world’s aging population. The International Federation on Ageing is a non-State actor in official relations with WHO. The group noted that with strict and varying eligibility criteria across provinces, barriers to accessing nirmatrelvir-ritonavir aggravate the burden of an already strained health system in Canada that is impacting the degree to which health care professionals can respond to patients’ needs. Ensuring standardization of eligibility criteria (specifically adults aged 60 years and older and people who are at high risk with underlying medical conditions, regardless of vaccination status), universal ease of access, and affordability of nirmatrelvir-ritonavir will warrant that millions of people who are at the highest risk of severe illness and least able to afford and access the drug, are protected to receive the lifesaving treatment.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of mild to moderate COVID-19 in adults with positive SARS-CoV-2 viral testing who are at high risk for progression to severe COVID-19.
Unmet Needs
The current treatment options for COVID-19 include the combination of nirmatrelvir and ritonavir which, as oral medications, are relatively easy to administer, but together have substantial drug interactions that limit their use. Remdesivir, as an IV medication, is more challenging to administer, but has few contraindications to its use. In clinical practice, clinicians observe that the efficacy of both these treatments is decreasing over time, as the general population continues to develop immunity. However, this differs in people who are severely immunosuppressed, as both treatments help support the immune response but are not able to fully clear the infection. It is also difficult to treat patients who are physiologically fragile, as the infection worsens pre-existing comorbidities (e.g., heart failure).
Place in Therapy
The current treatment paradigm for mild to moderate COVID-19 in Canada is to prevent hospitalization or death among patients at high risk for these outcomes. The virus has evolved significantly since the beginning of the pandemic, and the current risk of these outcomes is very low. Therefore, the vast majority of mild to moderate COVID-19 requires no specific treatment, with symptoms being mild and self-limiting. First-line therapy for the vast majority of the population with COVID-19 is supportive care.
Treatments are guided by provincial guidelines. If required to prevent hospitalization, benefits of treatment must be balanced against the risks and AEs, including drug-drug interactions that jeopardize patient well-being. Nirmatrelvir-ritonavir is the first and only approved oral treatment in Canada. While it has been particularly useful earlier in the pandemic, populations are now becoming immune to SARS-CoV-2. The role of nirmatrelvir-ritonavir in the long term is likely to evolve around the small number of individuals who remain with a high risk of hospitalization because of a failure to fight infection or physiologic frailty.
Nirmatrelvir-ritonavir is the first and only approved oral treatment in Canada, through an emergency use authorization. One of the main caveats of the pivotal trial informing approval is that it was performed at a time when the Delta SARS-CoV-2 variant was circulating. Ongoing clinical trials are currently being performed; when results become available, these trials may provide evidence on the use of nirmatrelvir-ritonavir in other variants of SARS-CoV-2. In the meantime, additional evidence is available in the form of observational studies; however, their use to inform policy-making has limitations.
IV treatments are available but less feasible for outpatient administration.
Patient Population
Most COVID-19 infections will go completely unnoticed or produce mild symptoms that can be ignored. Treatment is unlikely to improve these infections. Even for patients who are at high risk of progression to severe disease, the vast majority will have self-limited symptoms that do not require treatment. Patients following an improving disease trajectory are not likely to benefit from treatment.
Risk factors for hospitalization and death can be determined from control groups in observational studies or from provincial outcomes data. Typically, age older than 70 years, unvaccinated status, and multiple comorbidities leading to frailty are considered the main risk factors. In addition, patients who are severely immunosuppressed, and those with a prior disease trajectory of worsening in the first 5 days or no improvement within 5 days have a high likelihood of hospitalization. However, provincial outcome data show that even in the highest-risk subgroups, the hospitalization rate remains low, averaging 2.5%.
It Is not clear If those whose symptoms are attributable to other disease states that are exacerbated by Infection benefit from treatment; further data are needed.
Assessing the Response to Treatment
The clearest indicator of improved outcome is hospitalization (yes or no) and duration (days) of hospitalization as well as survival for 30 days following infection. The caveat is that death in patients who are frail or in older adults needs to be evaluated compared to expected survivability as many inevitable deaths in older adults are preceded by a viral infection, which, while possibly contributory, is not the cause of death. Deaths and hospitalizations when considered for evaluating efficacy should be attributable, not merely associated.
Prescribing Considerations
Treatment must be based on a positive diagnostic test since many viral upper respiratory tract infections present similarly, and nirmatrelvir-ritonavir can cause significant AEs and potentially dangerous drug-drug interactions. This is an enormous challenge as respiratory virus diagnostics are difficult to access, even for patients who are at high risk. The rapid antigen tests are faster and more accessible; however, they are problematic from a quality management perspective, and have a relatively low sensitivity early in infection, at a time when treatment is likely to offer benefit. There is certainly value in strengthening provincial molecular diagnostic programs for respiratory viruses.
Nirmatrelvir-ritonavir should ideally be prescribed in primary care, by a clinician able to evaluate symptoms, disease trajectory, and risk for progression. This could be either a generalist clinician or a specialist in relevant fields for patients with high-risk conditions (e.g., oncologist, rheumatologist). To offer easy and rapid access, some jurisdictions use a decentralized model (no designated prescribers, availability through any participating pharmacy), while some permit pharmacists to write the prescription. In the stage of the pandemic at the time of this review, clinical experts suggested re-evaluating whether there is still a need for such decentralized models, including pharmacist prescribing, with a shift toward better selection and identification of patients who are likely to benefit the most from treatment.
There is a set duration of therapy for nirmatrelvir-ritonavir of 5 days. This has been shown equivalent to longer durations and should be the only duration routinely provided.
Clinician Group Input
No clinician group input submission was received for this review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical experts’ response |
|---|---|
Relevant comparators | |
Remdesivir is indicated for the same patient population and is generally used as a second-line treatment for patients who cannot take nirmatrelvir-ritonavir due to contraindication or drug interaction. In addition to contraindication or drug interaction to nirmatrelvir-ritonavir, is there any other scenario where you would use remdesivir instead of nirmatrelvir-ritonavir? | The clinical experts highlighted that the use of remdesivir is severely limited in outpatients because its route of administration is IV. However, they mentioned it could be used in a very small population of patients who already have IV access established. |
Some jurisdictions use a centralized access model (centralized intake with designated prescribers and dispensing pharmacies) while other provinces use a decentralized model (no designated prescribers, availability through any participating pharmacy). Additionally, some jurisdictions permit pharmacists to prescribe nirmatrelvir-ritonavir. In your opinion, which model should be used? | The clinical experts Indicated that there are advantages and disadvantages to both centralized and decentralized models, and that it is the prerogative of each jurisdiction to decide what model works best for them. A centralized model is likely to offer more control of use according to the appropriate criteria and surveillance data, while a decentralized model is likely to offer rapid and easy access to the drug for patients. |
Considerations for initiation of therapy | |
Eligibility criteria for the pivotal trial required patients to have:
The FDA has removed the positive viral test requirement from the indication, which could open access to many individuals who do not actually have COVID-19.
| The clinical experts highlighted that most of the risk factors for progressing to severe disease that were used in trials performed earlier in the pandemic are no longer relevant. The 2 clinical experts consulted by CADTH for this review agreed that the most relevant risk factors are currently older age (> 80 years), frailty, underprotection from SARS-CoV-2 (patients who are unvaccinated and who have not had a prior infection), and severe immunosuppression. The trajectory of the disease would also be important to consider (e.g., whether a patient's condition is worsening, course of prior infections). The clinical experts emphasized the need to have a positive viral test result to ensure the patient is infected with SARS-CoV-2. There was no consensus as to whether the testing method should be rapid testing or PCR. However, they noted self-administered COVID-19 tests are widely accessible and convenient to use. |
How should “high risk of progression to severe COVID-19” be defined to maximize safety and cost-effectiveness? | The 2 clinical experts consulted by CADTH for this review agreed that the most relevant risk factors are currently older age (> 80 years), frailty, underprotection from SARS-CoV-2 (patients who are unvaccinated and who have not had a prior infection), and severe immunosuppression. The trajectory of the disease would also be important to consider (e.g., whether a patient’s condition is worsening, course of prior infections). |
How soon after receiving a course of nirmatrelvir-ritonavir should individuals be eligible to receive another course if they are reinfected and/or have relapse? | The clinical experts discussed this issue; however, there is no evidence at this time to inform this question. |
Vaccinated individuals were excluded from the pivotal study; however, some real-world evidence confirms benefits of nirmatrelvir-ritonavir in these individuals. Should vaccinated patients be eligible to nirmatrelvir-ritonavir? | The clinical experts discussed this issue; however, there is only limited evidence at this time to inform this question. The clinical experts felt that vaccination itself should not be an exclusion criterion for receiving nirmatrelvir-ritonavir, but rather the criteria should focus on other risk factors as well. |
Considerations for prescribing of therapy | |
The National Institutes of Health guidelines do not officially recommend extending nirmatrelvir-ritonavir treatment beyond 5 days but acknowledge that some prescribers may choose to prolong treatment duration for certain patients (i.e., patients who are immunocompromised and have prolonged COVID-19 symptoms and evidence of ongoing viral replication).
| The clinical experts agreed that they would use a 10-day duration of treatment in few to no patients. One expert said this may be considered for patients at extreme risk who are expected to have very poor outcomes. There may be a niche use for patients who are chronically infected, although the data are limited to case reports and series, so no firm conclusions can be made. |
Generalizability | |
Should nirmatrelvir-ritonavir be used for prophylaxis of COVID-19 in any outbreak settings? | The clinical experts strongly disagreed with the use of nirmatrelvir-ritonavir for prophylaxis of COVID-19. |
Should nirmatrelvir-ritonavir be prescribed for patients planning to travel out of country so that it can be taken in the event of illness while travelling? | The clinical experts strongly disagreed with such use of nirmatrelvir-ritonavir. |
Care provision issues | |
Nirmatrelvir-ritonavir has the potential to cause significant, life-threatening drug interactions. Many sources of information on drug interactions are available to help prescribers determine whether nirmatrelvir-ritonavir is appropriate for their patients and how to mitigate significant interactions with other drugs. | This was a comment from the drug programs to inform CDEC deliberations. |
Patients on drug therapies that interact with nirmatrelvir-ritonavir (e.g., patients with solid organ transplant taking calcineurin inhibitors) may require active drug concentration monitoring if nirmatrelvir-ritonavir is administered. | This was a comment from the drug programs to inform CDEC deliberations. |
System and economic issues | |
Given that nirmatrelvir-ritonavir has a limited treatment window, some jurisdictions may not be able to implement restrictive criteria and still ensure timely access to the drug, given how provincial adjudication systems are designed. This will be a larger issue if the cost and/or utilization is high, and restrictive criteria are required to ensure appropriate use. Do you have any advice for jurisdictions that would not be able to implement any proposed criteria and still ensure timely access to therapy? | The clinical experts provided insights at the prescriber level regarding how to grant effective access to the drug through family physicians and other health care professionals such as pharmacists; however, they could not advise on issues surrounding the internal adjudication process from drug plans. |
CDEC = Canadian Drug Expert Committee; PCR = polymerase chain reaction; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of nirmatrelvir-ritonavir, 150 mg (nirmatrelvir) and 100 mg (ritonavir) oral tablets, in the treatment of mild to moderate COVID-19 in adults with positive SARS-CoV-2 viral testing who are at high risk for progression to severe COVID-19. The focus will be placed on comparing nirmatrelvir-ritonavir to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of nirmatrelvir-ritonavir is presented in 4 sections with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second section includes additional studies that were considered by the sponsor and/or CADTH to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
1 pivotal study (RCT) identified in systematic review
4 additional studies addressing gaps in evidence.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 5.
Table 5: Details of the Study Included in the Systematic Review
Detail | EPIC-HR |
|---|---|
Designs and populations | |
Study design | Phase II/III randomized, double-blind, placebo-controlled, multicentre, multinational study |
Locations | 343 sites: Argentina, Brazil, Bulgaria, Colombia, Czech Republic, Hungary, India, Japan, Malaysia, Mexico, Poland, Puerto Rico, Russia, South Africa, South Korea, Spain, Taiwan, Thailand, Turkey, Ukraine, US |
Patient enrolment dates | Start date: July 16, 2021 End date: April 25, 2022 |
Randomized (N) | Nirmatrelvir-ritonavir, N = 1,120 Placebo, N = 1,126 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Nirmatrelvir 300 mg (i.e., 2 tablets of 150 mg) and ritonavir 100 mg (i.e., 1 capsule of 100 mg) every 12 hours orally for 5 days |
Comparator(s) | Placebo for nirmatrelvir (2 tablets) and placebo for ritonavir (1 capsule) every 12 hours orally for 5 days |
Study duration | |
Screening phase | 3 days (days –1 to 1) |
Treatment phase | 5 to 6 days (days 1 to 5 or 6) |
Follow-up phase | Through week 24 |
Outcomes | |
Primary end point | Proportion of patients with COVID-19–related hospitalization or death from any cause through day 28 (mITT population)a |
Secondary | Secondary end points:
|
Publication status | |
Publications |
|
AE = adverse event; ICU = intensive care unit; mITT = modified intention to treat; RT-PCR = reverse transcription polymerase chain reaction; SAE = serious adverse event; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; TEAE = treatment-related adverse event.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aThe mITT population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had at least 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment and were treated within 3 days following COVID-19 symptom onset. Participants were analyzed according to the study intervention to which they were randomized.
bThe mITT1 population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had at least 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment and were treated within 5 days following COVID-19 symptom onset. Participants were analyzed according to the study intervention to which they were randomized.
Sources: EPIC-HR Clinical Study Report,9 Hammond et al. (2022),28 and ClinicalTrials.gov.29
One multicentre, phase II/III, DB RCT was the primary source of evidence for the efficacy and safety of nirmatrelvir-ritonavir. The EPIC-HR trial (N = 2,246) evaluated the superiority of the combination of nirmatrelvir and ritonavir compared with placebo for the treatment of adult symptomatic outpatients with mild to moderate COVID-19 who were not vaccinated against SARS-CoV-2 and who were considered at high risk for progression to severe disease and/or hospitalization at the time the study was performed, based on a wide range of prespecified patient characteristics. The primary outcome of the EPIC-HR trial was a combined outcome of the proportion of patients with COVID-19–related hospitalization or who died from any cause through day 28 (efficacy assessment). Subgroup analyses were reported for some populations of patients, which were stratified by time from symptom onset, baseline demographics, selected comorbidities, baseline antibody status, and baseline viral load.
Populations
Inclusion and Exclusion Criteria
Patients were eligible for the EPIC-HR study if they were adult outpatients (aged ≥ 18 years) with a confirmed SARS-CoV-2 infection based on the presence of at least 1 symptom and positive molecular test result. Initial onset of symptoms and molecular testing were required to have occurred within 5 days of randomization, and 1 or more symptoms had to also be present on the day of randomization.
Patients needed to have at least 1 characteristic or underlying medical condition associated with an increased risk of developing severe illness from COVID-19 at the time the study was performed. Risk factors for disease progression in the trial included the following: aged 60 years or older, body mass index greater than 25 kg/m2, current smoker with 100 or more lifetime cigarettes, immunosuppressive disease, prolonged use of immune-weakening medications, active cancer (other than localized skin cancer), chronic lung disease (including asthma requiring daily therapy), hypertension, cardiovascular disease (defined as history of any of the following: myocardial infarction, stroke, transient ischemic attack, heart failure, angina requiring nitroglycerin, coronary artery bypass grafting, percutaneous coronary intervention, carotid endarterectomy, or aortic bypass), type 1 or 2 diabetes, chronic kidney disease, sickle cell disease, neurodevelopmental disorders (e.g., cerebral palsy, Down syndrome) or other conditions that confer medical complexity (e.g., genetic or metabolic syndromes and severe congenital anomalies), or medical-related technology dependence.
Patients were excluded if they had a prior COVID-19 infection confirmed by molecular test, prior hospitalization or treatment for COVID-19, prior or planned vaccination against COVID-19, likely need for hospitalization within 48 hours, or any number of specific comorbidities.
Interventions
In the EPIC-HR study, nirmatrelvir-ritonavir was administered at the dosage recommended in the product monograph. Patients were randomized in a 1:1 ratio to 1 of 2 treatment groups in the study:
nirmatrelvir 300 mg (2 tablets of 150 mg) and ritonavir 100 mg (1 capsule of 100 mg) every 12 hours orally for 5 days
placebo for nirmatrelvir (2 tablets) and placebo for ritonavir (1 capsule) every 12 hours orally for 5 days.
All participants could receive standard of care therapy for COVID-19 in addition to study intervention, unless listed as prohibited medication. Standard of care therapy for COVID-19 was defined as any therapy that was approved and used as indicated by the local regulatory authorities (including approvals for emergency use, compassionate use, or through similar regulatory guidance), or any therapy as recommended by a relevant national or a reputable international scientific body. In addition, standard medical supportive care could be provided to manage AEs.
In countries in which monoclonal antibodies were authorized or approved and considered the standard of care, all participants were referred locally for treatment when deemed appropriate by the investigator and local guidelines, and this referral was documented.
Participants could not receive convalescent COVID-19 plasma treatment for COVID-19, during the study period. However, COVID-19 vaccinations were permitted after the day 34 visit.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical experts consulted by CADTH and stakeholder input from patient and clinician groups and public drug plans.
Table 6: Outcomes Summarized From the EPIC-HR Study
Outcome measure | Time point | EPIC-HR |
|---|---|---|
Proportion of patients with COVID-19–related hospitalization or death from any cause (mITT population)a | Through day 28 | Primary |
Proportion of patients with COVID-19–related hospitalization or death from any cause (mITT1 population)b | Through day 28 | Key secondary |
Time to sustained alleviation of all targeted signs or symptoms | Through day 28 | Secondary |
Time to sustained resolution of all targeted signs or symptoms | Through day 28 | Secondary |
Proportion of patients with severe signs or symptoms attributed to COVID-19 | Through day 28 | Secondary |
Duration of each targeted COVID-19 sign or symptom | Through day 28 | Secondary |
Progression to a worsening status in ≥ 1 self-reported COVID-19–associated symptoms | Through day 28 | Secondary |
Proportion of patients with a resting peripheral oxygen saturation ≥ 95% | Days 1 and 5 | Secondary |
Proportion of patients who died from any cause | Through week 24 | Secondary |
Viral loads measured via RT-PCR in nasal or nasopharyngeal swabs | Days 1, 3, 5, 10, 14 | Secondary |
Number of COVID-19–related medical visits | Through day 34 | Secondary |
Number of days in hospital and ICU stay in patients with COVID-19–related hospitalization | Through day 34 | Secondary |
Incidence of TEAEs | Through day 34 | Secondary |
Incidence of SAEs and AEs leading to discontinuations | Through day 34 | Secondary |
AE = adverse event; ICU = intensive care unit; mITT = modified intention to treat; RT-PCR = reverse transcription polymerase chain reaction; SAE = serious adverse event; TEAE = treatment-related adverse event.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aThe mITT population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had at least 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment and were treated within 3 days following COVID-19 symptom onset. Participants were analyzed according to the study intervention to which they were randomized.
bThe mITT1 population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had at least 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment and were treated within 5 days following COVID-19 symptom onset. Participants were analyzed according to the study intervention to which they were randomized.
Sources: EPIC-HR Clinical Study Report,9 Hammond et al. (2022),28 ClinicalTrials.gov.29
The primary outcome of the EPIC-HR trial was a combined outcome of the proportion of patients with COVID-19–related hospitalization or who died from any cause through day 28. Hospitalization was defined as greater than 24 hours of acute care, in a hospital or similar acute care facility, including emergency rooms or temporary facilities instituted to address medical needs of those with severe COVID-19 during the COVID-19 pandemic. This included specialized acute medical care units within an assisted living facility or nursing home and did not include hospitalization for the purposes of public health and/or clinical trial execution.
Statistical Analysis
Summary of statistical analysis for all efficacy end points is presented in Table 7.
The cumulative proportion of patients hospitalized for the treatment of COVID-19 or dying during the first 28 days of the study was estimated for each treatment group using the Kaplan-Meier method to take account of losses to follow-up and summarized graphically for each treatment group. The analysis was conducted for the planned interim analysis as well. Two-sided 95% CI (adjusted for the planned interim analysis) and associated P value for the null hypothesis of no difference between treatment groups were presented. Significance level was determined using the O’Brien-Fleming approach at the interim analysis and the final analysis. The overall significance level is set at 5% (2-sided).
The proportion of patients who died from any cause through week 24 was summarized by treatment group. Treatment comparison between the groups was presented as OR and its 95% CI using logistic regression including treatment and region effect as independent variables. In addition, depending on the analysis population, stratification variables were added to the model analyses as follows.
mITT: Baseline viral load, baseline serology status, geographic region
mITT1: Baseline viral load, baseline serology status, geographic region, and symptom onset days to first dose date (≤ 3 days, > 3 days)
mITT2: Baseline viral load, baseline serology status, geographic region, received or were expected to receive a monoclonal antibody treatment (yes or no), and symptom onset days to first dose date (≤ 3 days, > 3 days)
Sample Size and Power Calculation
The study was designed to have 90% statistical power to show a difference of 3.5% between the treatment arms (nirmatrelvir-ritonavir versus placebo), in the proportion of patients hospitalized or dying who did not receive COVID-19 therapeutic monoclonal antibody using a 2-sided type I error rate of 5%. Based on the BLAZE study, the proportion of hospitalizations or deaths in the placebo arm was assumed to be 7%.30 Using EAST (version 6.5) for a 2-sample proportion test, the sample size needed based on these considerations was determined to be 1,717 randomized patients.
Enrolment of patients who at baseline had received or were expected to receive COVID-19 therapeutic monoclonal antibody treatment was estimated to be approximately 20% and limited or capped to 25% enrolment. Therefore, the sample size was adjusted to 2,146 randomized patients. Assuming a dropout rate of approximately 5%, the total sample size for this study was approximately 2,260 patients.
Study enrolment was stopped once 1,717 patients were available for primary analysis.
Statistical Testing
For binary end points (i.e., proportion of patients with COVID-19–related hospitalization or death from any cause through day 28, proportion of patients with severe signs or symptoms attributed to COVID-19 through day 28, worsening status in 1 or more self-reported COVID-19–associated symptoms through day 28, and proportion of patients who died from any cause through week 24), the proportion of patients with the event was summarized for each group. Treatment comparison between the groups was presented as the difference of proportions with its 95% CI using a similar analysis method as the primary end point.
For continuous end points (i.e., viral titres measured via RT-PCR in nasal or nasopharyngeal swabs over time), a mixed effect model with repeated measures analysis of the covariance model was used to analyze change from baseline over time. Estimated mean differences between treatments and their respective 95% CIs and P values were calculated.
For categorical end points (i.e., proportion of patients with a resting peripheral oxygen saturation ≥ 95% at days 1 and 5), the proportion of patients for each category was summarized for each group and a test for homogeneity of OR using the Breslow-Day test was summarized.
For count end points (i.e., number of COVID-19–related medical visits through day 28 and number of hospitalizations or intensive care unit [ICU] visits), a negative-binomial regression model analysis, using the log-total number of days of data collection as the patient offset variable, was conducted and the difference in estimated rate was provided.
For time-to-event end points (i.e., time [days] to sustained alleviation or resolution of all targeted signs or symptoms through day 28 and duration of each targeted COVID-19 sign or symptom), 2 analyses were provided: a Cox proportional hazard regression model where the estimate of the hazard ratio (HR) for treatment (nirmatrelvir-ritonavir versus placebo) and its CI and P value were provided; and a Kaplan-Meier analysis where tabular summaries of the Kaplan-Meier curves providing the median, quartiles, mean, standard error of the mean, and range were provided for each treatment group. In addition, the Kaplan-Meier curves were presented graphically.
Multiple Testing Procedure
There was no method used to adjust for multiple testing or control of the type I error rate for analysis of the individual components of the composite end points.
Subgroup Analyses
The protocol-prespecified subgroup analyses of the primary end point include the following:
age group (< 65 years, ≥ 65 years)
sex (female, male)
race and ethnicity (Asian, Black or African American, white, others)
baseline serology status (positive, negative)
baseline viral load (< 104 copies/mL, ≥ 104 copies/mL and < 107 copies/mL, ≥ 107 copies/mL)
number of baseline comorbidities present (0 to 1, 2 to 3, ≥ 4)
viral strain or lineage at day 1, if appropriate
body mass index category (< 25 kg/m2, ≥ 25 and < 30 kg/m2, ≥ 30 kg/m2)
presence of any of these baseline comorbidities or risk factors:
smoking (yes, no)
diabetes mellitus (yes, no)
chronic lung disease (yes, no)
hypertension (yes, no)
cardiovascular disorder (yes, no)
chronic kidney disease (yes, no)
device dependence (yes, no)
HIV infection
sickle cell disease
neurodevelopmental disorder (yes, no)
cancer (yes, no)
These subgroup analyses did not account for multiplicity of testing.
Table 7: Statistical Analysis of Efficacy End Points in the EPIC-HR Study
End point | Statistical model | Adjustment factors | Handling of missing data | Relevant sensitivity analyses |
|---|---|---|---|---|
Proportion of patients with COVID-19–related hospitalization or death from any cause (mITT population) | Kaplan-Meier method | None | All data collected included regardless of intercurrent events. Kaplan-Meier method to take account of losses to follow-up. |
|
Proportion of patients with COVID-19–related hospitalization or death from any cause (mITT1 population) | NA | |||
Time to sustained resolution of all targeted signs or symptoms | Cox proportional hazard model | mITT: Baseline viral load, baseline serology status, geographic region mITT1: Baseline viral load, baseline serology status, geographic region, and symptom onset days to first dose date (≤ 3 days, > 3 days) mITT2: Baseline viral load, baseline serology status, geographic region, received or were expected to receive mAb treatment (yes or no), and symptom onset days to first dose date (≤ 3 days, > 3 days) | All data collected included regardless of intercurrent events. Missing severity at baseline will be treated as mild. | NA |
Proportion of patients with severe signs or symptoms attributed to COVID-19 | Logistic regression | All data collected included regardless of intercurrent events. Use BOCF or LOCF for missing data. | NA | |
Duration of each targeted COVID-19 sign or symptom | Descriptive statistics | None | All data collected were included regardless of intercurrent events. Missing data were not imputed. | NA |
Progression to a worsening status in ≥ 1 self-reported COVID-19–associated symptoms | Logistic regression | mITT: Baseline viral load, baseline serology status, geographic region mITT1: Baseline viral load, baseline serology status, geographic region, and symptom onset days to first dose date (≤ 3 days, > 3 days) mITT2: Baseline viral load, baseline serology status, geographic region, received or were expected to receive mAb treatment (yes or no), and symptom onset days to first dose date (≤ 3 days, > 3 days) | All data collected were included regardless of intercurrent events. Use BOCF or LOCF for missing data. | NA |
Proportion of patients with a resting peripheral oxygen saturation ≥ 95% | Breslow-Day test for Homogeneity of the Odds Ratios | None | All data collected included regardless of intercurrent events. Missing data were not imputed. | NA |
Proportion of patients who died from any cause | Logistic regression or Fisher exact test (if appropriate) | mITT: Baseline viral load, baseline serology status, geographic region mITT1: Baseline viral load, baseline serology status, geographic region, and symptom onset days to first dose date (≤ 3 days, > 3 days) mITT2: Baseline viral load, baseline serology status, geographic region, received or were expected to receive mAb treatment (yes or no), and symptom onset days to first dose date (≤ 3 days, > 3 days). | All data collected included regardless of intercurrent events. Missing data were not imputed. | NA |
Viral titres measured via RT-PCR in nasal swabs over time | MMRM analysis | None | All data collected included regardless of intercurrent events. For missing data, baseline viral load (continuous). | Viral titres measured via RT-PCR in nasopharyngeal samples at day 1 and day 5. |
Number of COVID-19–related medical visits | Descriptive statistics | None | All data collected were included regardless of intercurrent events. Missing data were not imputed. | NA |
Number of days in hospital and ICU stay in patients with COVID-19–related hospitalization |
BOCF = baseline observation carried forward; ICU = intensive care unit; LOCF = last observation carried forward; mAb = monoclonal antibody; mITT = modified intention to treat; MMRM = mixed effect model for repeated measures; NA = not applicable; RT-PCR = reverse transcription polymerase chain reaction.
Source: EPIC-HR Clinical Study Report.9
Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Analysis Populations
The primary analysis was conducted in the mITT analysis set, consisting of all treated patients with onset of symptoms within 3 days who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment. Secondary analyses were also conducted in the mITT1 analysis set, consisting of all treated patients with onset of symptoms within 5 days who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment. The mITT2 analysis set consisted of all treated patients with onset of symptoms within 5 days.
Table 8: Analysis Populations From the EPIC-HR Study
Population | Definition | Application |
|---|---|---|
FAS | All patients randomly assigned to study intervention regardless of whether or not study intervention was administered. | Baseline demographic and other characteristics |
SAS | All patients who received at least 1 dose of study intervention. | All safety outcomes |
mITT | All patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had ≥ 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic mAb treatment and were treated ≤ 3 days following COVID-19 symptom onset. | All efficacy analyses |
mITT1 | All patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had ≥ 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic mAb treatment (treated ≤ 5 days following COVID-19 symptom onset). | All efficacy analyses |
mITT2 | All patients randomly assigned to study intervention, who took at least 1 dose of study intervention, and who had ≥ 1 postbaseline visit through day 28 visit (regardless of COVID-19 therapeutic mAb treatment). | All efficacy analyses except primary efficacy outcome |
PP | All patients in the mITT1 set without important protocol deviations considered to impact the interpretation of the primary efficacy end point. | Primary efficacy outcome |
FAS = full analysis set; mAb = monoclonal antibody, mITT = modified intention to treat; PP = per protocol; SAS = safety analysis set.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Source: EPIC-HR Clinical Study Report.9
Results
Patient Disposition
The proportions of patients who discontinued the study were similar between treatment groups. Overall, 2,246 patients were randomized; of these, 6.0% of patients receiving nirmatrelvir-ritonavir and 7.7% of patients receiving placebo discontinued from the study. The most frequent reason for discontinuation was withdrawal by patient, followed by AEs.
Table 9: Summary of Patient Disposition From the EPIC-HR Study
Patient disposition | EPIC-HR | |
|---|---|---|
Nirmatrelvir-ritonavir N = 1,120 | Placebo N = 1,126 | |
Screened, n | 2,396 | |
Screening failure, n | 137 | |
Reasons | NR | NR |
Randomized, n (%) | 1,120 (100) | 1,126 (100) |
Discontinued from study, n (%) | 67 (6.0) | 87 (7.7) |
Reason for discontinuation, n (%) | ||
AE | 23 (2.1) | 47 (4.2) |
Withdrawal by participant | 32 (2.9) | 27 (2.4) |
Medication error | 0 | 1 (< 0.1) |
No longer meets eligibility criteria | 3 (0.3) | 1 (< 0.1) |
Other | 9 (0.8) | 11 (1.0) |
FAS, n (%) | 1,120 (100) | 1,126 (100) |
PP, n (%) | 670 (59.8) | 649 (57.6) |
SAS, n (%) | 1,109 (99.0) | 1,115 (99.0) |
AE = adverse event; FAS = full analysis set; NR = not reported; PP = per protocol; SAS = safety analysis set.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Source: EPIC-HR Clinical Study Report.9
Baseline Characteristics
Baseline characteristics are outlined in Table 10 and were generally comparable between treatment groups.
Some patient characteristics other than those presented in the Table 10 were considered particularly relevant to this review and were felt to affect the outcomes or interpretation of the study results. A total of 3% of patients included in the trial were aged 75 years or older. Among the comorbidities and risk factors for severe illness from COVID-19, immunosuppression was listed for 0.6% of the trial population, while cancer was listed for 0.5% of the population.9 Patients in the study were not vaccinated for COVID-19 and those with prior confirmed SARS-CoV2 infection were excluded for the trial; however, 51% were found to have a positive SARS-CoV-2 baseline antibody status. The dominating variant across both treatment arms was Delta.31
Exposure to Study Treatments
Exposure to study treatments is described in Table 11.
Table 10: Summary of Baseline Characteristics From the EPIC-HR Study
Characteristic | EPIC-HR | |
|---|---|---|
Nirmatrelvir-ritonavir N = 1,120 | Placebo N = 1,126 | |
Age at screening (years), mean (SD)a | 45.33 (15.40) | 46.34 (15.51) |
Age range (years), n (%) | ||
18 to 44 | 556 (49.6) | 517 (45.9) |
45 to 59 | 338 (30.2) | 349 (31.0) |
60 to 64 | 86 (7.7) | 112 (9.9) |
≥ 65 | 140 (12.5) | 148 (13.2) |
Sex, n (%) | ||
Female | 554 (49.5) | 544 (48.3) |
Male | 566 (50.5) | 582 (51.7) |
Race, n (%) | ||
American Indian or Alaska Native | 96 (8.6) | 95 (8.4) |
Asian | 154 (13.8) | 160 (14.2) |
Black or African American | 60 (5.4) | 50 (4.4) |
Multiracial | 1 (< 0.1) | 2 (0.2) |
White | 800 (71.4) | 808 (71.8) |
Not reported | 8 (0.7) | 9 (0.8) |
Unknown | 1 (< 0.1) | 2 (0.2) |
Ethnicity, n (%) | ||
Hispanic or Latino | 499 (44.6) | 505 (44.8) |
Not Hispanic or Latino | 616 (55.0) | 614 (54.5) |
Not reported or unknown | 5 (0.4) | 7 (0.6) |
BMI at screening (kg/m2), n (%) | ||
< 25.0 | 220 (19.6) | 217 (19.3) |
25.0 to < 30.0 | 492 (43.9) | 489 (43.4) |
> 30.0 | 407 (36.3) | 419 (37.2) |
Duration since first diagnosis, n (%)b,c | ||
≤ 3 days | 1,044 (93.2) | 1,071 (95.1) |
> 3 days | 76 (6.8) | 55 (4.9) |
Duration since first symptoms, n (%)c | ||
≤ 3 days | 754 (67.3) | 735 (65.3) |
> 3 days | 366 (32.7) | 391 (34.7) |
Number of risk factors of interest, n (%)d | ||
0 | 2 (0.2) | 0 |
1 | 449 (40.1) | 424 (37.7) |
2 | 392 (35.0) | 409 (36.3) |
3 | 184 (16.4) | 192 (17.1) |
4 | 77 (6.9) | 75 (6.7) |
> 4 | 16 (1.4) | 26 (2.3) |
COVID-19 mAb treatment, n (%) | ||
Received or expected to receive | 70 (6.3) | 70 (6.2) |
Not received or not expected to receive | 1,050 (93.8) | 1,056 (93.8) |
Viral load and serology status | ||
Negative serology, n (%) | 518 (46.3) | 537 (47.7) |
Positive serology, n (%) | 581 (51.9) | 568 (50.4) |
Viral load (log10 copies/mL), mean (SD) | 4.67 (2.88) | 4.59 (2.86) |
BMI = body mass index; mAb = monoclonal antibody; SD = standard deviation.
Note: Full analysis set population. Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aAge at screening (years) = (date of given informed consent – date of birth + 1) / 365.25.
bDuration since first diagnosis is days from qualifying positive SARS-CoV-2 test.
cDuration since first diagnosis and duration since first symptom are computed from the start of dosing.
dRisk factors include age ≥ 60 years, BMI > 25, and verbatims from prespecified medical history (cigarette smoker, immunosuppression, chronic sickle cell disease, neurodevelopmental disorder, cancer, and device dependence).
Source: EPIC-HR Clinical Study Report.9
Table 11: Summary of Patient Exposure From the EPIC-HR Study
Exposure | EPIC-HR | |
|---|---|---|
Nirmatrelvir-ritonavir N = 1,109 | Placebo N = 1,126 | |
Duration of treatment (days), mean (SD) | 5.03 (0.77) | 5.01 (0.83) |
Duration of treatment (days), median (range) | 5.00 (1.00 to 6.00) | 5.00 (1.00 to 7.00) |
Compliance, n (%)a | ||
< 80% | 54 (4.9) | 66 (5.9) |
≥ 80% to ≤ 115% | 1,043 (94.0) | 1,033 (92.6) |
> 115% | 12 (1.1) | 16 (1.4) |
SD = standard deviation.
Note: Safety analysis set population. Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aDrug compliance is defined as the ratio of actual number of tablets to expected number of tablets. Actual number of tablets was taken from the dosing record case report form added over the entire treatment duration.
Source: EPIC-HR Clinical Study Report.9
All patients were allowed to receive standard of care therapy for COVID-19, as previously defined in the interventions section, in addition to study drug, unless listed as prohibited medication. As such, the majority of patients in the trial received concomitant medications (77%). These are outlined in Table 12.
The proportion of patients who used concomitant antivirals for systemic use was 4.0% in the nirmatrelvir-ritonavir arm and 7.4% in the placebo arm; the corresponding proportion of patients who used concomitant corticosteroids for systemic use was 6.3% and 10.6%, respectively. Corticosteroids could be administered for any reason, including for the treatment of any underlying conditions (e.g., rheumatoid arthritis or asthma).
In addition to the medications reported in Table 12, 40 (1.8%) patients received monoclonal antibodies for COVID-19 treatment (bamlanivimab-etesevimab, casirivimab-imdevimab, and regdanvimab), which is less than the number of patients who were expected to receive monoclonal antibodies at the time of randomization (baseline). The proportion of patients who took a prohibited concomitant medication or vaccine was higher in the placebo group compared with the nirmatrelvir-ritonavir group (1.5% and 0.7%, respectively).
Table 12: Summary of Exposure to Concomitant Medication From the EPIC-HR Study
Exposure | EPIC-HR | |
|---|---|---|
Nirmatrelvir-ritonavir N = 1,109 | Placebo N = 1,126 | |
Received concomitant medications, n (%) | 854 (77.0) | 868 (77.8) |
Antivirals for systemic use, n (%) | 44 (4.0) | 82 (7.4) |
Acyclovir | 0 | 4 (0.4) |
Bamlanivimab-etesevimab | 0 | 1 (0.1) |
Casirivimab | 3 (0.3) | 7 (0.6) |
Casirivimab-imdevimab | 8 (0.7) | 17 (1.5) |
Efavirenz-emtricitabine-tenofovir disoproxil fumarate | 0 | 1 (0.1) |
Enisamium iodide | 2 (0.2) | 0 |
Favipiravir | 27 (2.4) | 34 (3.0) |
Imdevimab | 3 (0.3) | 7 (0.6) |
Inosine pranobex | 0 | 5 (0.4) |
Oseltamivir | 1 (0.1) | 0 |
Regdanvimab | 1 (0.1) | 1 (0.1) |
Remdesivir | 3 (0.3) | 17 (1.5) |
Valacyclovir | 0 | 1 (0.1) |
Corticosteroids for systemic use, n (%) | 10 (6.3) | 118 (10.6) |
Betamethasone | 1 (0.1) | 1 (0.1) |
Betamethasone dipropionate | 0 | 1 (0.1) |
Betamethasone, loratadine | 3 (0.3) | 4 (0.4) |
Corticosteroids | 0 | 1 (0.1) |
Deflazacort | 0 | 1 (0.1) |
Dexamethasone | 23 (2.1) | 59 (5.3) |
Dexamethasone phosphate | 2 (0.2) | 2 (0.2) |
Dexamethasone sodium phosphate | 0 | 1 (0.1) |
Hydrocortisone | 2 (0.2) | 2 (0.2) |
Hydrocortisone sodium succinate | 0 | 2 (0.2) |
Methylprednisolone | 19 (1.7) | 32 (2.9) |
Methylprednisolone sodium succinate | 0 | 1 (0.1) |
Prednisolone | 5 (0.5) | 16 (1.4) |
Prednisone | 21 (1.9) | 23 (2.1) |
Steroids | 0 | 1 (0.1) |
Triamcinolone | 0 | 1 (0.1) |
Triamcinolone acetonide | 0 | 1 (0.1) |
Other medication taken by at least 5% of patients in 1 arm, n (%) | ||
Acetylsalicylic acid | 141 (12.7) | 136 (12.2) |
Ascorbic acid | 160 (14.4) | 167 (15.0) |
Levofloxacin | 57 (5.1) | 55 (4.9) |
Ibuprofen | 83 (7.5) | 100 (9.0) |
Note: Safety analysis set population. Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Source: EPIC-HR Clinical Study Report.9
Efficacy
Proportion of Patients With COVID-19–Related Hospitalization or Death From Any Cause
The use of nirmatrelvir, in combination with ritonavir, was associated with an absolute reduction of 5.8% in the incidence of COVID-19–related hospitalization or death from any cause through day 28 compared with placebo in patients treated within 3 days of symptoms onset (mITT population: –5.8%; 95% CI, –7.8% to –3.8%; P < 0.0001). This yielded an NNT of 18, as calculated by CADTH. This was consistent with the results of secondary analyses obtained in patients treated within 5 days of symptoms onset (mITT1 population: –5.5%; 95% CI, –7.2% to –4.0%; P < 0.001). This yielded an NNT of 19, as calculated by CADTH.
In subgroup analyses performed in patients aged 65 years and older, the absolute risk reduction associated with the use of nirmatrelvir-ritonavir compared to placebo was –15.3% when treatment was initiated within 3 days of symptom onset (mITT population: –15.3%; 95% CI, –22.9% to –7.7%; P < 0.0001) and –13.9% when treatment was initiated within 5 days of symptoms onset (mITT1 population: –13.9%; 95% CI, –20.1% to –7.8%; P < 0.0001).
Time to Sustained Alleviation of All Targeted Signs or Symptoms
The use of nirmatrelvir-ritonavir was associated with a HR of 1.27 (95% CI, 1.12 to 1.44; P = 0.0003) versus placebo; for time to sustained alleviation of symptoms, a shorter time to event is considered a better outcome. The median was 12 days (95% CI, 12 to 13 days) in the treatment group and 15 days (95% CI, 13 to 16 days) in the placebo group. The analysis was performed in patients treated within 3 days of symptoms onset (mITT population).
Time to Sustained Resolution of All Targeted Signs or Symptoms
The use of nirmatrelvir-ritonavir was associated with a HR of 1.20 (95% CI, 1.05 to 1.37; P = 0.0088) versus placebo; for time to sustained resolution of symptoms, a shorter time to event is considered a better outcome. The median was 16 days (95% CI, 15 to 17 days) in the treatment group and 18 days (95% CI, 17 to 20 days) in the placebo group. The analysis was performed in patients treated within 3 days of symptoms onset (mITT population).
Proportion of Patients With Severe Signs or Symptoms Attributed to COVID-19
The proportion of patients with severe signs or symptoms attributed to COVID-19 through day 28 were 17.9% in the nirmatrelvir-ritonavir arm and 20.3% in the placebo arm. The use of nirmatrelvir-ritonavir was associated with an OR of 0.88 (95% CI, 0.66 to 1.17; P = 0.3872) versus placebo.
Progression to a Worsening Status in 1 or More Self-Reported COVID-19 Associated Symptoms
The proportion of patients progressing to a worsening status in 1 or more self-reported COVID-19 associated symptoms through day 28 was 76.2% in the nirmatrelvir-ritonavir arm and 74.7% in the placebo arm. The use of nirmatrelvir-ritonavir was associated with an OR of 1.11 (95% CI, 0.86 to 1.44; P = 0.4374) versus placebo.
Proportion of Patients With a Resting Peripheral Oxygen Saturation of 95% or Greater at Day 1 and Day 5
The use of nirmatrelvir-ritonavir was associated with an OR of 19.58 (95% CI, 7.88 to 48.67) for having a resting peripheral oxygen saturation of 95% or greater at day 5 versus day 1. The corresponding OR for the use of placebo was 9.54 (95% CI, 4.44 to 20.52); testing of the homogeneity of OR across treatment groups yielded a P value of 0.2331.
Proportion of Patients Who Died From Any Cause
There was no event of death from any cause in the nirmatrelvir-ritonavir arm. In the placebo arm, 11 patients (1.6%) died throughout study follow-up; of these, 9 deaths occurred through day 28, and the other 2 deaths occurred during the long-term follow-up period. The use of nirmatrelvir-ritonavir was associated with a P value of 0.0004 versus placebo.
Number of COVID-19–Related Medical Visits
The proportion of patients with COVID-19–related medical visits was 1.4% in the nirmatrelvir-ritonavir arm (10 patients; 22 visits) and 7.6% in the placebo arm (52 patients; 81 visits). The use of nirmatrelvir-ritonavir was associated with a least squares mean ratio of number of medical visits per day of 0.27 (95% CI, 0.13 to 0.54; P = 0.0002) versus placebo.
Number of Days in Hospital and ICU Stay in Patients With COVID-19–Related Hospitalization
The mean duration of hospitalization visits was 0.09 days (standard deviation [SD] = 1.03) in the nirmatrelvir-ritonavir arm and 0.80 days (SD = 4.42) in the placebo arm. No patients in the nirmatrelvir-ritonavir arm reported an ICU visit; the mean duration of ICU visits was 0.17 days (SD = 2.33) in the placebo arm.
In the nirmatrelvir-ritonavir arm, 9 patients received oxygen therapy for COVID-19; however, none of these patients received mechanical ventilation. In the placebo arm, 54 patients received oxygen therapy for COVID-19, and 3 patients received mechanical ventilation.
No between-group comparison was reported for this outcome.
Table 13: Summary of Key Efficacy Results From the EPIC-HR Study
Results | EPIC-HR | |
|---|---|---|
Nirmatrelvir-ritonavir | Placebo | |
Proportion of patients with COVID-19–related hospitalization or death from any cause, mITTa | ||
Number of patients in the analysis set | 697 | 682 |
Patients with event (death or hospitalization), n (%) | 5 (0.717) | 44 (6.452) |
Average time at risk for event (days)b | 27.296 | 26.189 |
Average study follow-up (days)c | 27.455 | 27.284 |
Estimated event rate of COVID-19–related hospitalization or death, % (95% CI) | 0.723 (0.302 to 1.729) | 6.531 (4.901 to 8.676) |
Event rate difference from placebo, % (SE) | –5.807 (1.005) | |
95% CI of event rate difference | –7.777 to –3.837 | |
P value | < 0.0001 | |
NNT = 1 divided by the reported absolute risk difference (approximation calculated by CADTH) | 17.4 | |
Proportion of patients with COVID-19–related hospitalization or death from any cause, mITT1d | ||
Number of patients in the analysis set | 1,039 | 1,046 |
Patients with event (death or hospitalization), n (%) | 9 (0.866) | 66 (6.310) |
Average time at risk for event (days)b | 27.033 | 25.974 |
Average study follow-up (days),c mean | 27.213 | 27.098 |
Estimated event rate of COVID-19–related hospitalization or death, % (95% CI) | 0.878 (0.458 to 1.680) | 6.400 (5.063 to 8.075) |
Event rate difference from placebo, % (SE) | –5.522 (0.816) | |
95% CI of event rate difference | –7.122 to –3.923 | |
P value | < 0.001 | |
NNT = 1 divided by the reported absolute risk difference (approximation calculated by CADTH) | 18.4 | |
Time to sustained alleviation of all targeted signs or symptoms, mITTa | ||
Number of patients in the analysis set | 686 | 674 |
Patients with event (sustained alleviation of all targeted signs or symptoms), n (%) | 526 (76.676) | 464 (68.843) |
Time to sustained alleviation (days), median (95% CI) | 12.000 (12.000 to 13.000) | 15.000 (13.000 to 16.000) |
HR (95% CI) | 1.267 (1.115 to 1.439) | |
P value | 0.0003 | |
Time to sustained resolution of all targeted signs or symptoms, mITTa | ||
Number of patients in the analysis set | 686 | 674 |
Patients with event (sustained resolution of all targeted signs or symptoms), n (%) | 464 (67.638) | 415 (61.573) |
Time to sustained resolution (days), median (95% CI) | 16.000 (15.000 to 17.000) | 18.00 (17.000 to 20.000) |
HR (95% CI) | 1.198 (1.047 to 1.371) | |
P value | 0.0088 | |
Proportion of patients with severe signs or symptoms attributed to COVID-19, mITTa | ||
Number of patients in the analysis set | 686 | 674 |
Patients with event (severe signs or symptoms), n (%) | 123 (17.93) | 137 (20.33) |
OR (95% CI) | 0.88 (0.66 to 1.17) | |
P value | 0.3872 | |
Progression to a worsening status in ≥ 1 self-reported COVID-19 associated symptoms, mITTa | ||
Number of patients in the analysis set | 686 | 674 |
Patients with event (worsening status), n (%) | 523 (76.229) | 504 (74.777) |
OR (95% CI) | 1.108 (0.855 to 1.435) | |
P value | 0.4374 | |
Proportion of patients with a resting peripheral oxygen saturation ≥ 95%, mITTa | ||
Number of patients in the analysis set | 697 | 682 |
OR for day 5 vs. day 1 (95% CI) | 19.581 (7.879 to 48.661) | 9.539 (4.435 to 20.518) |
P value from Breslow-Day test for testing the homogeneity of ORs across treatment groups | 0.2331 | |
Proportion of patients who died from any cause, mITTa | ||
Number of patients in the analysis set | 697 | 682 |
Patients with event, n (%) | 0 | 11 (1.6) |
P value | 0.0004 | |
Number of COVID-19–related medical visits, mITTa | ||
Number of patients in the analysis set | 697 | 682 |
Proportion of patients with COVID-19–related medical visits,e n (%) | 10 (1.435) | 52 (7.625) |
Total number of medical visits across all patients | 22 | 81 |
LS mean number of medical visits per day,f (95% CI) | 0.0007 (0.0004 to 0.0013) | 0.0027 (0.0016 to 0.0045) |
LS mean ratio of number of medical visits per day vs. placebo (95% CI) | 0.270 (0.134 to 0.544) | |
P value | 0.0002 | |
Number of days in hospital and ICU stay in patients with COVID-19–related hospitalization, mITTa | ||
Number of patients in the analysis set | 697 | 682 |
Duration of hospitalization visits (days), mean (SD) | 0.085 (1.030) | 0.801 (4.421) |
Duration of ICU visits (days), mean (SD) | 0.000 (0.000) | 0.170 (2.327) |
Duration of non-ICU visits (days), mean (SD) | 0.085 (1.030) | 0.632 (3.616) |
CI = confidence interval; HR = hazard ratio; ICU = intensive care unit; LS = least squares; mITT = modified intention to treat; NNT = number needed to treat; OR = odds ratio; SD = standard deviation; SE = standard error; vs. = versus.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aThe mITT population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had ≥ 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment and were treated ≤ 3 days following COVID-19 symptom onset.
bAverage time at risk for event is computed as time to first event, or time to last day of participation, or day 28, whichever is earlier.
cAverage study follow-up is computed as time to last day of participation, or day 28, whichever is earlier.
dThe mITT1 population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had ≥ 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment (treated ≤ 5 days following COVID-19 symptom onset). All participants randomly assigned to study intervention, who took at least 1 dose of study intervention. Participants were analyzed according to the study intervention to which they were randomized.
eThe mITT population included all patients randomly assigned to study intervention, who took at least 1 dose of study intervention, who had ≥ 1 postbaseline visit through day 28 visit, and who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody treatment and were treated ≤ 3 days following COVID-19 symptom onset.
fMedical visits include emergency department, practitioner’s office, home health care services, urgent care, telephone consultation, outpatient infusion centre, other, COVID-19–related-hospitalization (ICU and non-ICU stays). The medical visits and hospitalization events are limited through day 34 visit.
g.Number of medical visits per day = number of medical visits/number of days follow-up limited to day 37. The negative-binomial regression model includes main effects of treatment, geographic region, baseline severe acute respiratory syndrome coronavirus 2 serology status and baseline viral load (< 4 log10 copies/mL, ≥ 4 log10 copies/mL), and the log number of days of follow-up as the participant offset variable.
Source: EPIC-HR Clinical Study Report.9
Harms
Harms data are outlined in Table 14. Incidence data for each treatment group were provided within the safety analysis population, which included all patients who received at least 1 dose of the drug or placebo. Safety information was actively collected by investigators up to day 34.
Adverse Events
In the EPIC-HR trial, 23.1% and 24.2% of the patients in the nirmatrelvir-ritonavir and placebo groups reported at least 1 AE, respectively. The most common treatment-emergent AEs in the nirmatrelvir-ritonavir group versus placebo included dysgeusia (5.6% versus 0.3%), diarrhea (3.1% versus 1.6%), fibrin D-dimer increased (2.0% versus 2.8%), alanine aminotransferase increased (1.5% versus 2.4%), headache (1.4% versus 1.3%), creatinine clearance decreased (1.4% versus 1.6%), nausea (1.4% versus 1.7%), and vomiting (1.1% versus 0.8%).
Serious Adverse Events
Overall, 1.7% of patients in the nirmatrelvir-ritonavir arm and 6.6% of patients in the placebo arm reported at least 1 SAE. The most common SAEs in the nirmatrelvir-ritonavir group versus placebo were COVID-19 pneumonia (0.6% versus 3.3%), COVID-19 (0.2% versus 0.7%), and creatinine clearance decreased (0.1% and 0.3%).
Mortality
No deaths were reported in the nirmatrelvir-ritonavir group; in the placebo group, 15 patients died throughout study follow-up; none of the deaths were considered related to study treatment.
Table 14: Summary of Harms Results From the EPIC-HR Study
AEs | Nirmatrelvir-ritonavir N = 1,109 | Placebo N = 1,115 |
|---|---|---|
TEAEs by system organ class and preferred term ≥ 1%, n (%)a,b | ||
≥ 1 AE | 256 (23.1) | 270 (24.2) |
Patients with maximum grade 3 or 4 AEs | 47 (4.2) | 94 (8.4) |
Patients with maximum grade 5 AEs | 0 | 13 (1.2) |
Investigations | 90 (8.1) | 106 (9.5) |
Activated partial thromboplastin time prolonged | 9 (0.8) | 12 (1.1) |
Alanine aminotransferase increased | 17 (1.5) | 27 (2.4) |
Aspartate aminotransferase increased | 10 (0.9) | 14 (1.3) |
C-reactive protein increased | 10 (0.9) | 13 (1.2) |
Creatinine renal clearance decreased | 16 (1.4) | 18 (1.6) |
Fibrin D-dimer increased | 22 (2.0) | 31 (2.8) |
Nervous system disorders | 80 (7.2) | 25 (2.4) |
Dysgeusia | 62 (5.6) | 3 (0.3) |
Headache | 15 (1.4) | 15 (1.3) |
Gastrointestinal disorders | 66 (6.0) | 53 (4.8) |
Diarrhea | 34 (3.1) | 18 (1.6) |
Nausea | 16 (1.4) | 19 (1.7) |
Vomiting | 12 (1.1) | 9 (0.8) |
Infections and infestations | 25 (2.3) | 76 (6.8) |
COVID-19 | 3 (0.3) | 14 (1.3) |
COVID-19 pneumonia | 8 (0.7) | 41 (3.7) |
Pneumonia | 2 (0.2) | 15 (1.3) |
SAEs, n (%)c | ||
Patients with ≥ 1 SAE | 19 (1.7) | 74 (6.6) |
COVID-19 pneumonia | 7 (0.6) | 37 (3.3) |
COVID-19 | 2 (0.2) | 8 (0.7) |
Creatinine renal clearance decreased | 1 (0.1) | 3 (0.3) |
Abscess | 1 (0.1) | 0 |
Brain stem stroke | 1 (0.1) | 0 |
Chest discomfort | 1 (0.1) | 0 |
Dyspnea | 1 (0.1) | 3 (0.3) |
Facial paralysis | 1 (0.1) | 0 |
Hemoglobin decreased | 1 (0.1) | 0 |
Hypertensive crisis | 1 (0.1) | 0 |
Oxygen saturation decreased | 1 (0.1) | 0 |
Palpitations | 1 (0.1) | 0 |
Pneumonia | 1 (0.1) | 11 (1.0) |
Sepsis | 1 (0.1) | 0 |
Acute respiratory failure | 0 | 5 (0.4) |
Alanine aminotransferase increased | 0 | 1 (0.1) |
Anemia | 0 | 1 (0.1) |
Atypical pneumonia | 0 | 1 (0.1) |
Colon adenoma | 0 | 1 (0.1) |
Craniocerebral injury | 0 | 1 (0.1) |
Eye injury | 0 | 1 (0.1) |
Fibrin D-dimer increased | 0 | 1 (0.1) |
Hand fracture | 0 | 1 (0.1) |
Hypoxia | 0 | 2 (0.2) |
Interstitial lung disease | 0 | 2 (0.2) |
Pneumonitis | 0 | 5 (0.4) |
Pulmonary embolism | 0 | 2 (0.2) |
Rectal hemorrhage | 0 | 1 (0.1) |
Respiratory failure | 0 | 1 (0.1) |
Road traffic accident | 0 | 1 (0.1) |
Wrist fracture | 0 | 1 (0.1) |
Patients who discontinued treatment due to AEs, n (%)d | ||
Patients who discontinued | 23 (2.1) | 47 (4.2) |
Investigations | 9 (0.8) | 9 (0.8) |
Creatinine renal clearance decreased | 3 (0.3) | 4 (0.4) |
Glomerular filtration rate decreased | 2 (0.2) | 2 (0.2) |
White blood cell count decreased | 2 (0.2) | 0 |
Alanine aminotransferase increased | 1 (0.1) | 0 |
Aspartate aminotransferase increased | 1 (0.1) | 1 (0.1) |
Differential white blood cell count abnormal | 1 (0.1) | 0 |
Hemoglobin decreased | 1 (0.1) | 0 |
Oxygen saturation decreased | 1 (0.1) | 0 |
Blood glucose increased | 0 | 1 (0.1) |
Glomerular filtration rate abnormal | 0 | 1 (0.1) |
Gastrointestinal disorders | 7 (0.6) | 8 (0.7) |
Nausea | 5 (0.5) | 5 (0.4) |
Vomiting | 4 (0.4) | 2 (0.2) |
Abdominal pain lower | 1 (0.1) | 0 |
Colitis | 1 (0.1) | 0 |
Diarrhea | 1 (0.1) | 1 (0.1) |
Gastritis | 0 | 1 (0.1) |
Nervous system disorders | 4 (0.4) | 2 (0.2) |
Dysgeusia | 2 (0.2) | 0 |
Dizziness | 1 (0.1) | 1 (0.1) |
Headache | 1 (0.1) | 0 |
Restless leg syndrome | 0 | 1 (0.1) |
Infections and infestations | 2 (0.2) | 20 (1.8) |
COVID-19 | 1 (0.1) | 4 (0.4) |
COVID-19 pneumonia | 1 (0.1) | 13 (1.2) |
Pneumonia | 0 | 3 (0.3) |
Vascular disorders | 2 (0.2) | 0 |
Hypertension | 1 (0.1) | 0 |
Hypertensive crisis | 1 (0.1) | 0 |
Cardiac disorders | 1 (0.1) | 0 |
Palpitations | 1 (0.1) | 0 |
General disorders and administration site conditions | 1 (0.1) | 2 (0.2) |
Chest discomfort | 1 (0.1) | 0 |
Asthenia | 0 | 1 (0.1) |
Peripheral swelling | 0 | 1 (0.1) |
Musculoskeletal and connective tissue disorders | 1 (0.1) | 0 |
Myalgia | 1 (0.1) | 0 |
Reproductive system and breast disorders | 1 (0.1) | 0 |
Vaginal hemorrhage | 1 (0.1) | 0 |
Respiratory, thoracic, and mediastinal disorders | 1 (0.1) | 9 (0.8) |
Dyspnea | 1 (0.1) | 1 (0.1) |
Acute respiratory failure | 0 | 1 (0.1) |
Cough | 0 | 1 (0.1) |
Hypoxia | 0 | 1 (0.1) |
Interstitial lung disease | 0 | 1 (0.1) |
Pneumonitis | 0 | 3 (0.3) |
Respiratory failure | 0 | 1 (0.1) |
Skin and subcutaneous tissue disorders | 1 (0.1) | 1 (0.1) |
Rash maculo-papular | 1 (0.1) | 0 |
Rash | 0 | 1 (0.1) |
Psychiatric disorders | 0 | 1 (0.1) |
Insomnia | 0 | 1 (0.1) |
Renal and urinary disorders | 0 | 1 (0.1) |
Renal impairment | 0 | 1 (0.1) |
Deaths, n (%) | ||
Patients who died | 0 | 15 (1.3) |
COVID-19 pneumonia | 0 | 8 (0.7) |
COVID-19 | 0 | 3 (0.3) |
Pneumonitis | 0 | 2 (0.2) |
Acute respiratory failure | 0 | 1 (0.1) |
Sepsis with underlying relapsed acute myeloid leukemia | 0 | 1 (0.1) |
AEs of special interest, n (%) | ||
Hemodynamic AEs | 8 (0.7%) | 11 (1.0) |
Thyroid-related AEs | 7 (0.6) | 7 (0.6) |
Inflammatory AEs | 42 (3.8) | 46 (4.1) |
AE = adverse event; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aIncludes AEs that started on or before day 34 visit.
bPatients are counted only once per treatment in each row.
cSAEs were according to the investigator’s assessment.
dPatients who have an AE record that indicates that the AE caused the participant to be discontinued from the study.
Source: EPIC-HR Clinical Study Report.9
Critical Appraisal
Internal Validity
The overall risk of bias for the EPIC-HR study was low, as the risk of bias from all domains (including randomization, deviation, missing data, outcome measurement, and reporting) was low. Randomization, allocation concealment, and blinding were therefore considered adequate, baseline characteristics were balanced between treatment groups, and there was no evidence that discontinuation rates or missing data might introduce bias in the comparison. Outcomes were objective and appropriately measured; however, there was no method used to adjust for multiple testing or control of type I error rate for analysis of the individual components of the composite end points and for the otherwise prespecified subgroup analyses.
External Validity
The intervention, comparator, outcome measures, and setting in the study were all considered adequate and generalizable to clinical practice across the country.
However, the most significant issue with the EPIC-HR study is that the findings of the trial cannot be generalized to the population of patients living in Canada at high risk for progression to severe COVID-19, as defined in clinical practice at the time of this review. Indeed, the 2 clinical experts consulted by CADTH for this review agreed that the most relevant risk factors for progressing to severe disease and hospitalization are currently older age (> 80 years), frailty, underprotection from SARS-CoV-2 (patients who are unvaccinated and those who have not had a prior infection), and severe immunosuppression. It is worth noting that the sponsor disagreed with CADTH’s assessment regarding the generalizability of the study population. The sponsor noted in its comments that the EPIC-HR study was in line with the globally accepted clinical guidelines at the time the study was performed, and that the trial was the basis for the Health Canada–authorized indication.
Patients included in the EPIC-HR trial were relatively young, 87% being between the age of 18 years and 65 years, limiting conclusions on the efficacy and safety of nirmatrelvir-ritonavir in a population of older adults. As per the study’s selection criteria, the EPIC-HR study did not include patients who were vaccinated or patients who had COVID-19 in the past. Approximately 50% of patients were found to have a positive SARS-CoV-2 baseline antibody status; however, according to the clinical experts consulted by CADTH, seropositivity in itself, especially when acquired after an asymptomatic COVID-19 episode, is unlikely to offer an immune protection that would be comparable to that of the population of people living in Canada at this time. This is an important gap since according to the most recent data at the time of this review, at least 80% of the population of people living in Canada completed a primary series of COVID-19 vaccine,8 and approximately 80% of the population has contracted a SARS-CoV-2 infection at some point.3 It is likely that the magnitude of the treatment effect observed in the EPIC-HR study with nirmatrelvir-ritonavir would be smaller in patients who were vaccinated, who already have effective protection against SARS-CoV-2. Finally, patients included in the study presented with various comorbidities which, at the time the trial was performed, were considered risk factors for severe illness from COVID-19; however, the COVID-19 landscape is in constant and rapid evolution, and these concomitant conditions are no longer considered to significantly increase the risk of worst outcomes. The EPIC-HR study does not provide evidence on the use of nirmatrelvir-ritonavir in patients who are frail, or in those who are severely immunocompromised.
In addition, the primary variant observed in the trial population was Delta; however, this SARS-CoV-2 variant is no longer circulating at the time of this review, as the main variant of concern is Omicron and its subsequent subvariant, for which the effectiveness of nirmatrelvir-ritonavir has not been demonstrated in the context of an RCT in patients at high risk of severe disease.32
Long-Term Extension Studies
No long-term extension studies have been conducted.
Indirect Evidence
No long-term extension studies have been conducted. The sponsor provided an indirect treatment comparison comparing nirmatrelvir-ritonavir with remdesivir, however, that indirect treatment comparison was not considered in this review because remdesivir is not considered relevant comparator at the time of this review.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
A few gaps were identified in the evidence and concern the population and the type of COVID-19 variant studied. More specifically, the EPIC-HR study did not include patients who were vaccinated or patients who had COVID-19 in the past. In addition, nirmatrelvir-ritonavir was studied during a time period in which the Omicron variant was not yet circulating. Additional evidence is provided to address these gaps.
Table 15: Summary of Gaps in the Systematic Review Evidence
Gap in pivotal and RCT evidence | Studies that address gaps | |
|---|---|---|
Study description | Summary of key results | |
Vaccinated patients or patient with a prior diagnosis of COVID-19 were not included in the EPIC-HR RCT | EPIC-SR: multicentre phase II/III, double-blind, randomized placebo-controlled study in nonhospitalized symptomatic adult patients with COVID-19 who are at standard risk for developing severe COVID-19.11 EPIC-SR also included a subgroup of patients who had been vaccinated and had at least 1 risk factor for progression to severe COVID-19. Recruitment started on August 25, 2021, and was terminated early. | When restricted to a subgroup of patients who were vaccinated with at least 1 risk factor for severe COVID-19 (n = 721), there was a nonsignificant relative risk reduction of 57% for patients who received nirmatrelvir-ritonavir (n = 3 of 361) compared to those who received placebo (n = 7 of 360). For the same group of patients, reduction from baseline in viral RNA concentration was significantly (P < 0.0001) larger in the nirmatrelvir-ritonavir treatment group than in the placebo group. |
Lewnard et al.: Retrospective cohort study in California (US) within KPSC.12 This study aimed to estimate the effectiveness of nirmatrelvir-ritonavir in preventing severe outcomes of SARS-CoV-2 infection in an outpatient setting in a large, integrated US health care system between April 8, 2022, and October 7, 2022. | In this highly vaccinated US outpatient population, the administration of nirmatrelvir-ritonavir proved to be effective in reducing the occurrence of hospitalization or death within 30 days of a positive SARS-CoV-2 test when compared to not receiving this medication. The greatest clinical benefit was observed in early treatment, specifically when nirmatrelvir-ritonavir was given within 5 days of symptom onset. In these cases, the estimated effectiveness against the mentioned end point was 79.6% (95% CI, 33.9% to 93.8%) compared to 53.6% (95% CI, 6.6% to 77.0%) overall. | |
Schwartz et al.: Population-based cohort study in Ontario using linked databases available at ICES between April 4, 2022, and August 31, 2022.13 | Results from this study showed that nirmatrelvir-ritonavir was effective in reducing the risk of hospitalization or death in a population in majority vaccinated with weighted OR of 0.25 (95% CI, 0.12 to 0.50) for patients with 1 or 2 doses and 0.62 (95% CI, 0.51 to 0.75) for patients with 3 vaccine doses. | |
Kaboré et al.: Real-world effectiveness of nirmatrelvir-ritonavir on COVID-19–associated hospitalization prevention: a population-based cohort study in the province of Quebec.14 | Results from this study showed that regardless of vaccination status, nirmatrelvir-ritonavir–treated outpatients were associated with a statistically significant risk reduction when compared with untreated control patients. Outpatients had a 69% reduced relative risk of COVID-19–associated hospitalization (relative risk = 0.31; 95% CI, 0.28 to 0.36) when compared with control. A statistically significant relative risk reduction was also shown for each of the following subgroups: in patients with incomplete primary vaccination status, severely immunocompromised outpatients, and outpatients aged ≥ 70 years. | |
Nirmatrelvir-ritonavir was not studied with the Omicron variant which is currently circulating in Canada | Schwartz et al.: Population-based cohort study in Ontario (Canada) using linked databases available at ICES between April 4, 2022, and August 31, 2022.13 | Results from this study showed that nirmatrelvir-ritonavir was effective in reducing the risk of hospitalization or death in a population of people living in Canada during the spread of Omicron and its subvariants. Patients who received nirmatrelvir-ritonavir and those who did not had a 2.1% and 3.7% risk of hospital admission or death, respectively. The weighted OR of hospital admission or death within 30 days was 0.56 (95% CI, 0.47 to 0.67; P < 0.001). |
CI = confidence interval; ICES = Institute for Clinical Evaluative Sciences; KPSC = Kaiser Permanente Southern California; OR = odds ratio; RCT = randomized controlled trial; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
EPIC-SR Study
EPIC-SR (N = 1,153) was a multicentre, phase II/III, DB, randomized placebo-controlled study aiming to describe and compare the safety and tolerability of nirmatrelvir-ritonavir to placebo for the treatment of nonhospitalized, symptomatic, adult participants with COVID-19 who were at low risk of progression to severe illness.11 Patients were enrolled in 226 sites in Argentina, Brazil, Bulgaria, Colombia, Czech Republic, Hungary, Japan, Malaysia, Mexico, Poland, Puerto Rico, Romania, Slovakia, South Africa, South Korea, Spain, Thailand, Turkey, Ukraine, and the US starting August 25, 2021. This study had no sites in Canada.
The EPIC-SR study included outpatient adults (aged ≥ 18 years) with a confirmed SARS-CoV-2 infection 5 days before randomization and who had the initial onset of COVID-19 signs or symptoms within 5 days of randomization. Patients who were unvaccinated were only included if they did not have an underlying condition associated with an increased risk of developing severe illness from COVID-19. A subgroup of patients who were vaccinated with at least 1 risk factor for progression was also included in this study. Patients were excluded if they had a prior COVID-19 infection, had at least 1 underlying medical condition associated with an increased risk of developing severe illness from COVID-19 (unless the patient was vaccinated as previously mentioned), prior hospitalization or treatment for COVID-19, or any number of a list of specific comorbidities.
Patients enrolled in the EPIC-SR study were randomized in a 1:1 ratio to receive treatment with either:
nirmatrelvir 300 mg and ritonavir 100 mg every 12 hours given orally for 5 days
placebo for nirmatrelvir and placebo for ritonavir every 12 hours given orally for 5 days.
The study primary end point was the time to sustained alleviation of all targeted COVID-19 signs and symptoms from baseline through day 28. The key secondary outcome was the proportion of patients with COVID-19–related hospitalization or death from any cause. The primary and key secondary end points were evaluated using the mITT1 population, (i.e., all participants randomly assigned to study intervention, who took at least 1 dose of study intervention; participants were analyzed according to the study intervention they were randomized) and were summarized with Kaplan-Meier curves. Log-rank test was also used to compare the time to sustained alleviation of all targeted signs or symptoms through day 28 between the treatment groups. For efficacy end points related to COVID-19 signs or symptoms, missing data at baseline were treated as mild.
Subgroup analyses for the primary end point and key secondary end point was planned to only be performed for vaccination status. The prespecified subgroup analyses for vaccination status were, however, replaced for risk status as follows.
High risk: Participants enrolled before Protocol Amendment 5 (January 21, 2022) who were vaccinated and had at least 1 risk factor.
Standard risk: Participants who did not have risk factors and were either vaccinated or not vaccinated.
Other: For the 11 participants who did not meet the definition of high risk or standard risk. This category included 7 participants who enrolled before Protocol Amendment 5 who were not vaccinated but had at least 1 risk factor as well as the 4 participants enrolled after Protocol Amendment 5 (2 participants who were not vaccinated but had at least 1 risk factor and 2 participants with at least 1 risk factor and who were vaccinated more than 12 months before screening).
The total study duration was up to 24 weeks and study visits were conducted at the patient’s home or at another nonclinic location.33,34 The EPIC-SR study enrolment was early terminated on July 25, 2022, due to a very low rate of hospitalization or death observed in the patient population who are at standard risk.
Results
Patient Disposition
Table 16: Summary of Patient Disposition in the EPIC-SR Study
Patient disposition | EPIC-SR | |
|---|---|---|
Nirmatrelvir-ritonavir | Placebo | |
Screened, N | 1,407 | |
Screening failure, N (%) | 102 | |
Randomized, N (%) | 658 | 638 |
Discontinued from study, n (%) | 23 (4.2) | 21 (4.0) |
Reason for discontinuation, n (%) | ||
AE | 16 (2.4) | 5 (0.8) |
Withdrawal by participant | 9 (1.4) | 12 (1.9) |
No longer meets eligibility criteria | 2 (0.3) | 3 (0.5) |
Other | 4 (0.6) | 3 (0.5) |
AE = adverse event.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Source: EPIC-SR Clinical Study Report.11
Baseline Characteristics
Baseline characteristics were balanced between treatment groups and are presented in Table 17.
All patients had a laboratory-confirmed SARS-CoV-2 diagnosis, with 96.0% of participants having a qualifying SARS-CoV-2 positive test collected within 3 days of first dose of study intervention. Overall, 50.2% of patients had no risk factors for progression to severe COVID-19 and 56.9% were vaccinated for COVID-19. A total of 47.7% of patients reported a moderate intensity for their worst sign or symptom severity at baseline. At baseline, 74.2% of patients were SARS-CoV-2 seropositive and the proportions were balanced between treatment groups.
Table 17: Summary of Baseline Characteristics in the EPIC-SR Study
Characteristic | EPIC-SR | |
|---|---|---|
Nirmatrelvir-ritonavir N = 654 | Placebo N = 634 | |
Age at screening (years), mean (SD) | 41.76 (13.47) | 42.63 (13.13) |
Age range (years), n (%) | ||
18 to 44 | 394 (60.2) | 362 (57.1) |
45 to 59 | 193 (29.5) | 207 (32.6) |
60 to 64 | 31 (4.7) | 36 (5.7) |
65 to 74 | 30 (4.6) | 19 (3.0) |
≥ 75 | 6 (0.9) | 10 (1.6) |
Sex, n (%) | ||
Female | 344 (52.6) | 352 (55.5) |
Male | 310 (47.4) | 282 (44.5) |
Race, n (%) | ||
American Indian or Alaska Native | 39 (6.0) | 32 (5.0) |
Asian | 69 (10.6) | 72 (11.4) |
Black or African American | 28 (4.3) | 23 (3.6) |
Native Hawaiian or other Pacific Islander | 0 | 0 |
Multiracial | 0 | 0 |
White | 512 (78.3) | 498 (78.5) |
Other | 0 | 0 |
Not reported or unknown | 6 (1.0) | 9 (1.4) |
Ethnicity, n (%) | ||
Hispanic or Latino | 272 (41.6) | 261 (41.2) |
Not Hispanic or Latino | 378 (57.8) | 367 (57.9) |
Not reported or unknown | 4 (0.6) | 6 (0.9) |
BMI at screening (kg/m2), n (%) | ||
< 25.0 | 338 (51.7) | 323 (50.9) |
25.0 to < 30.0 | 207 (31.7) | 189 (29.8) |
> 30.0 | 109 (16.7) | 121 (19.1) |
Vaccination status | ||
Vaccinated | 372 (56.9) | 361 (56.9) |
Not vaccinated | 282 (43.1) | 273 (43.1) |
Risk statusa | ||
High risk | 317 (48.5) | 314 (49.5) |
Standard risk | 333 (50.9) | 313 (49.4) |
Other | 4 (0.6) | 7 (1.1) |
BMI = body mass index; SD = standard deviation.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aRisk factors include age 60 years and older (≥ 65 years for 2022 enrollees), BMI greater than 25 kg/m2 (≥ 30 kg/m2 for 2022 enrollees), and verbatim from prespecified medical history (cigarette smoker, chronic kidney disease, hypertension, diabetes mellitus, cardiovascular disorder, chronic lung disease, HIV Infection, sickle cell disease, neurodevelopmental disorder, cancer, and device dependence).
Source: EPIC-SR Clinical Study Report.11
Exposure to Study Treatments
Table 18: Summary of Exposure to Study Treatments in the EPIC-SR Study
Exposure | EPIC-SR | |
|---|---|---|
Nirmatrelvir-ritonavir N = 654 | Placebo N = 634 | |
Duration of treatment, mean (SD)a | 5.00 (0.72) | 5.05 (0.59) |
Duration of treatment, median (range) | 5.00 (1.00 to 6.00) | 5.00 (1.00 to 6.00) |
Compliance, n (%)a | ||
< 80% | 24 (3.7) | 17 (2.7) |
≥ 80% to ≤ 115% | 620 (94.8) | 612 (96.5) |
> 115% | 10 (1.5) | 5 (0.8) |
SD = standard deviation.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aStudy drug compliance is defined as the ratio of actual number of tablets to expected number of tablets.
Source: EPIC-SR Clinical Study Report.11
The most commonly reported concomitant medication (≥ 10%) in either treatment group was paracetamol (128 [19.6%] participants in the nirmatrelvir-ritonavir group and 177 [27.9%] participants in the placebo group).11
Efficacy
The EPIC-SR study did not meet its primary objective, failing to demonstrate a difference between nirmatrelvir-ritonavir and placebo on the primary outcome of time to sustained alleviation of all targeted COVID-19 signs and symptoms, as well as on the secondary outcome of COVID-19–related hospitalization or death from any cause.
In a post hoc subgroup analysis of patients who were considered as standard risk for progressing to severe COVID-19, the use of nirmatrelvir-ritonavir was associated with a 0.4% reduction in the proportion of patients with COVID-19–related hospitalization or death from any cause through day 28 versus placebo. For patients who were considered as high risk, the corresponding risk reduction associated with was nirmatrelvir-ritonavir 1.3% versus placebo.
Table 19: Summary of Proportion of Patients With COVID-19–Related Hospitalization or Death From Any Cause by Risk Subgroup in the EPIC-SR Study
Result | EPIC-SR | |
|---|---|---|
Nirmatrelvir-ritonavir | Placebo | |
Standard risk — mITT1 | ||
N | 333 | 313 |
Patients with event (hospitalization or death), n (%) | 2 (0.601) | 3 (0.958) |
COVID-19–related hospitalization | 2 (0.601) | 3 (0.958) |
Death | 0 | 0 |
Average time at risk for event (days) | 26.964 | 27.479 |
Average study follow-up (days) | 27.042 | 27.684 |
Estimated proportion, % (95% CI) | 0.608 (0.152 to 2.409) | 0.964 (0.312 to 2.958) |
Proportion difference from placebo, % (95% CI of difference) | –0.356 (–1.728 to 1.017) | |
P value | 0.6114 | |
High risk — mITT1 | ||
N | 317 | 314 |
Patients with event (hospitalization or death), n (%) | 3 (0.946) | 7 (2.229) |
COVID-19–related hospitalization | 3 (0.946) | 7 (2.229) |
Death | 0 | 1 (0.318) |
Average time at risk for event (days) | 27.621 | 27.105 |
Average study follow-up (days) | 27.820 | 27.564 |
Estimated proportion, % (95% CI) | 0.952 (0.308 to 2.924) | 2.245 (1.076 to 4.651) |
Proportion difference from placebo, % (95% CI of difference) | –1.292 (–3.255 to 0.671) | |
P value | 0.1970 | |
CI = confidence interval; mITT = modified intention to treat.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Source: EPIC-SR Clinical Study Report.11
Harms
Safety results for the subgroup of patients at high risk of progressing to severe COVID-19, as per the indication, was not reported.
Critical Appraisal
The EPIC-SR study was submitted by the sponsor to address gaps in the evidence, and to provide evidence for the efficacy of nirmatrelvir-ritonavir in patients who were vaccinated during the Omicron wave. However, patients included in the trial and in the subgroup of patients vaccinated with an underlying medical condition, do not fall within the category of patients at high risk of progressing to severe disease. Therefore, the EPIC-SR study is not informative with regard to the evidence gaps, if only to confirm the low hospitalization rates and the absence of benefits from nirmatrelvir-ritonavir treatment in patients who are not at high risk of disease progression according to current standards.
Observational Studies
A total of 3 observational studies have been summarized to provide evidence regarding the real-world efficacy of nirmatrelvir-ritonavir in patients who are vaccinated or have had prior SARS-CoV-2 infections, those who are at high risk of progressing to severe disease according to current clinical practice standards, and at a time period in which the Omicron variant was the main variant circulating. Safety was not assessed in any of the studies.
Observational studies allow the evaluation of an intervention in a large population of real-world patients; in this particular case, interest is in patients who would be considered at high risk of progressing to severe COVID-19, based on current clinical practice. According to the clinical experts consulted by CADTH, these would include older age (> 80 years), frailty, underprotection against SARS-CoV-2 (patients who are unvaccinated or patients with no prior SARS-CoV-2 infection), and patients who are immunosuppressed. However, observational studies can be subject to biases, especially confounding bias and selection bias. Although various methods are used to adjust for the differences between treatment groups, both known confounders are not captured in the electronic health care records, nor are unknown potential confounders, and this could affect the validity of the comparison and introduce bias for which the direction is unknown. As such, results should be interpretated with caution. Findings of observational studies should be viewed as complementary to those from RCTs.
Table 20: Details of Studies Addressing Gaps in the Systematic Review Evidence
Detail | Lewnard et al. | Schwartz et al. | Kaboré et al. |
|---|---|---|---|
Designs and populations | |||
Study design | Retrospective cohort study | Population-based cohort study | Retrospective cohort study |
Location | California, US | Ontario | Quebec |
Enrolled, N | Nirmatrelvir-ritonavir: n = 7,274 No nirmatrelvir-ritonavir: n = 126,152 | Nirmatrelvir-ritonavir: n = 8,876 No nirmatrelvir-ritonavir: n = 168,669 | Nirmatrelvir-ritonavir: n = 8,402 No nirmatrelvir-ritonavir: n = 8,402 |
Key inclusion criteria | At least 12 years of age; positive SARS-CoV-2 PCR result April and October 2022. Enrolled in KPSC health plans for at least 1 year. | Between 18 and 110 years; positive PCR test for SARS-CoV-2 between April and August 2022. | Individuals covered by the Quebec public health insurance plan between March and October 2022. |
Key exclusion criteria | No other positive test result within prior 90 days, no hospitalization within prior 7 days. | Patients hospitalized or with a nosocomial infection before or on the testing day. | Patients hospitalized or living in long-term care facilities. |
Drugs | |||
Intervention | Outpatient nirmatrelvir-ritonavir, 300 mg nirmatrelvir and 100 mg ritonavir orally twice daily for 5 days. | Nirmatrelvir-ritonavir dispensed through community pharmacies in Ontario. | Nirmatrelvir-ritonavir prescriptions from the Quebec administrative claims databases. |
Comparator(s) | No nirmatrelvir-ritonavir | No nirmatrelvir-ritonavir | No nirmatrelvir-ritonavir |
Outcomes | |||
Primary end point | Hospital admission or death within 30 days of the initial positive SARS-CoV-2 test. | Composite of hospital admission due to COVID-19 or all-cause death that occurred 1 day to 30 days after the date when nirmatrelvir-ritonavir was dispensed. | COVID-19–related hospitalization in the 30 days following the date of dispensing of nirmatrelvir-ritonavir for the treatment group and date of positive RT-PCR test for the control group. |
Notes | |||
Publications | Lewnard et al. (2023)35 | Schwartz et al. (2023)13 | Kaboré et al. (2023)14 |
KPSC = Kaiser Permanente Southern California; PCR = polymerase chain reaction; RT = reverse transcription; SARS-Cov-2 = severe acute respiratory syndrome coronavirus 2.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Description of the Lewnard et al. Study
The Lewnard et al. study was a retrospective cohort study in California, US, within KPSC. KPSC is a comprehensive health care system that provides integrated care across outpatient, inpatient, emergency department, and virtual settings. KPSC was linked to the California Immunization Registry, and with other health systems using the same electronic health record system to capture care received outside KPSC. This study aimed to estimate the effectiveness of nirmatrelvir-ritonavir in preventing severe outcomes of SARS-CoV-2 infection in an outpatient setting in a large, integrated US health care system. The primary end point of this study was hospital admission or death from any cause within 30 days of the index positive SARS-CoV-2 test.
Populations
KPSC patients had to be aged 12 years or older when they took the index test. The index test, which was a positive SARS-CoV-2 PCR result, had to be conducted between April 8 and October 7, 2022. Moreover, eligible patients should not have received another positive test result within the 90 days before this index test, nor were they hospitalized during their index test or within the preceding 7 days. Additionally, to be eligible, they had to be enrolled in KPSC health plans for at least 1 year before taking the index test.
Interventions
The primary exposures were outpatient receipt of nirmatrelvir-ritonavir (300 mg nirmatrelvir and 100 mg ritonavir taken orally twice daily for 5 days) within 5 days of symptom onset, and outpatient receipt of nirmatrelvir-ritonavir at any time after testing positive for SARS-CoV-2 (irrespective of the presence or timing of symptoms). Patients were exposed to nirmatrelvir-ritonavir from the date of dispensing, as recorded in KPSC pharmacy records or adjudicated out-of-network insurance claims. People who received nirmatrelvir-ritonavir 1 day or more after their index test were considered unexposed during the time between their index test and the dispensing date. Other antiviral or monoclonal antibody treatments for COVID-19 were used sparingly.
Outcomes
The main objective of this study was to investigate hospital admission or death within 30 days of the initial positive SARS-CoV-2 test. Additionally, as a secondary end point, admission to ICUs, the need for mechanical ventilation, or death within 60 days of the index test date were evaluated to indicate progression to severe disease.
Statistical Analysis
The effect of nirmatrelvir-ritonavir on clinical outcomes was accessed using a matched cohort framework. Patients were monitored from their initial SARS-CoV-2 test to the occurrence of each study end point or until censoring (i.e., due to the end of follow-up, study completion, or disenrollment from the KPSC health system). The patients' treatment assignments were updated on the date of treatment dispensing.
To compare outcomes between individuals who received nirmatrelvir-ritonavir and those who did not, an adjusted HR and their associated 95% CI were calculated using Cox proportional hazards models. To account for multiple observations from individuals whose treatment status changed during follow-up, the cluster-robust standard errors was employed. To evaluate the appropriateness of the proportional hazards assumption, the study tested for nonzero slopes of Schoenfeld residuals.
To determine the treatment effectiveness of nirmatrelvir-ritonavir for each end point, the adjusted HR was used, calculating it as follows: treatment effectiveness = (1 – adjusted HR) × 100%. When considering confounding driven by factors associated with both the likelihood of receiving nirmatrelvir-ritonavir and experiencing severe clinical outcomes, a minimal set of covariates was identified for statistical adjustment using a directed acyclic graph.
People with COVID-19 were grouped into regression strata (matches) based on their week of SARS-CoV-2 testing, age, sex, time of symptom onset relative to testing, health care use during the previous year, number of COVID-19 vaccine doses received, presence of comorbidities, and body mass index. This approach allowed for differing baseline hazards across all combinations of the listed covariates, considering interactions between risk factors affecting the likelihood of severe disease.
Other variables were included as model covariates for adjustment. To account for missing data on smoking status, body mass index, and neighbourhood deprivation index, multiple imputation was used with 5 completed pseudo-datasets, pooling parameter estimates across analyses.
Additional analyses were conducted in subgroups based on the number of COVID-19 vaccine doses received (at least 2 or at least 3 doses) and among individuals who met criteria for receiving nirmatrelvir-ritonavir due to being at high risk of COVID-19 progression, as defined in the US Emergency Use Authorization guidelines.
Exploratory analyses were performed within subgroups to understand the potential association of the timing of treatment initiation with clinical outcomes. These subgroups included people treated 0 days to 3 days after symptom onset, those treated 6 or more days after symptom onset or in the absence of documented acute COVID-19 symptoms, and those treated at any time after symptom onset.
Results
Patient Disposition
During the study period, a total of 197,484 individuals who had not tested positive for SARS-CoV-2 infection within the past 90 days were found to test positive for the infection. Of these, 166,980 individuals (84.6%) were eligible to be included in the study. Within this eligible population, 12,574 individuals (7.5%) received nirmatrelvir-ritonavir at some point during their clinical course.
Baseline Characteristics
Baseline characteristics, outlined in Table 21, show that patients included in the study were relatively young, highly vaccinated, and had a limited number of comorbidities. This is consistent with a population at standard risk of progressing to severe COVID-19.
Table 21: Baseline Characteristics for the Lewnard et al. Study
Characteristic | Lewnard et al. | |
|---|---|---|
Received nirmatrelvir-ritonavir N = 7,274 | Did not received nirmatrelvir-ritonavir N = 126,152 | |
Age range (years), n (%) | ||
12 to 19 | 11 (0.2) | 11,054 (8.8) |
20 to 29 | 170 (2.3) | 13,047 (10.3) |
30 to 39 | 505 (2.3) | 20,761 (16.5) |
40 to 49 | 1,103 (15.2) | 26,122 (20.7) |
50 to 59 | 1,556 (21.4) | 23,742 (18.8) |
60 to 69 | 1,674 (23.0) | 18,117 (14.4) |
70 to 79 | 1,503 (20.7) | 9,213 (7.3) |
80 to 89 | 602 (8.3) | 3,325 (2.6) |
≥ 90 | 150 (2.1) | 770 (0.6) |
Sex, n (%) | ||
Female | 4,196 (57.7) | 69,795 (55.3) |
Male | 3,080 (42.3) | 56,357 (44.7) |
BMI (kg/m2), n (%) | ||
< 18.5 | 38 (0.5) | 5,663 (4.5) |
18.5 to 24.9 | 1,240 (17.0) | 26,550 (21.0) |
25.0 to 29.9 | 2,190 (30.1) | 33,131 (26.3) |
30.0 to 39.9 | 2,703 (37.2) | 33,418 (26.5) |
≥ 40.0 | 550 (7.6) | 6,064 (4.8) |
Days from symptom onset to testing, n (%) | ||
0 to 5 | 5,472 (75.2) | 84,657 (67.1) |
6 to 14 | 1,290 (17.7) | 20,070 (15.9) |
No acute symptoms at point of testing | 512 (7.0) | 21,425 (17.0) |
Charlson Comorbidity Index, n (%) | ||
0 | 3,740 (51.4) | 99,516 (78.9) |
1 to 2 | 2,728 (37.5) | 22,055 (17.5) |
3 to 5 | 634 (8.7) | 3,434 (2.7) |
≥ 6 | 172 (2.4) | 1,147 (0.9) |
COVID-19 vaccine doses received, n (%) | ||
0 | 394 (5.4) | 16,759 (13.3) |
1 | 49 (0.7) | 2,016 (1.6) |
2 | 965 (13.3) | 31,504 (25.0) |
3 | 4,433 (60.9) | 66,738 (52.9) |
4 | 1,433 (19.7) | 9,135 (7.2) |
BMI = body mass index.
Source: Lewnard et al. (2023).12 Copyright 2023. This work is licensed under the Attribution 4.0 International Licence. Full text available here: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(23)00118-4/fulltext
Exposure to Study Treatments
During the study, nirmatrelvir-ritonavir was available to KPSC patients who received a positive SARS-CoV-2 test result in any outpatient setting or reported a positive at-home antigen test after consulting with a health care provider. This included outpatient visits, virtual appointments, or telephone consultations.
Eligible patients who did not receive nirmatrelvir-ritonavir for COVID-19 at KPSC were largely untreated; of a total of 166,908 eligible patients, 64 patients (< 0.1%) received outpatient molnupiravir and 11,075 patients (6.6%) received inpatient monoclonal antibodies.
Efficacy
In the analysis of treatment effectiveness, 7,274 of 12,574 eligible nirmatrelvir-ritonavir recipients (57.8%) and 126,152 of 154,406 eligible nonrecipients (81.7%) were included because they had at least 1 eligible match.
Among the nirmatrelvir-ritonavir recipients, the primary outcome of hospitalization or death from any cause within 30 days from the index test occurred in 51 individuals (0.7%). In comparison, among the nonrecipients, the primary outcome occurred in 695 individuals (0.6%).
The overall estimated effectiveness was reported as 1 minus the HR of nirmatrelvir-ritonavir in preventing hospital admission or death within 30 days of a positive test. After accounting for differences between individuals who received nirmatrelvir-ritonavir and those who did not, the estimated effectiveness of receiving nirmatrelvir-ritonavir within 5 days of COVID-19 symptom onset was 79.6% (95% CI, 33.9% to 93.8%; P = 0.0080) against progressing to hospital admission or death from any cause within 30 days. For the courses of nirmatrelvir-ritonavir administered at any time, regardless of the presence or timing of symptoms, the estimated effectiveness against progression to the same end point was 53.6% (95% CI, 6.6% to 77.0%). The estimated effectiveness of nirmatrelvir-ritonavir varies among subgroups. Overall, the absolute differences between the nirmatrelvir-ritonavir and control arms were considered small. Results are outlined in Table 22.
Table 22: Key Efficacy Results From the Lewnard et al. Study
Key results | Lewnard et al. | |
|---|---|---|
Received nirmatrelvir-ritonavir N = 7,274 | Did not receive nirmatrelvir-ritonavir N = 126,152 | |
All-cause hospital admission or death within 30 days of positive SARS-CoV-2 test | ||
Hospitalizations or deaths, n (%) | 51 (0.7) | 695 (0.5) |
Follow-up (days), median (IQR) | 13 (5 to 20) | 12 (5 to 21) |
Analysis: estimated effectiveness (%)a (95% CI); P value | ||
Within 5 days of symptom onset | 79.6 (33.9 to 93.8); 0.0080 | |
Any time (regardless of symptoms) | 53.6 (6.6 to 77.0); 0.031 | |
Subgroup analyses: estimated effectiveness (%)a (95% CI); P value | ||
Patients with ≥ 2 COVID-19 vaccines and outcome within 5 days of symptom onset | 83.1 (30.4 to 95.9); 0.014 | |
Patients with ≥ 3 COVID-19 vaccines and outcome within 5 days of symptom onset | 92.2 (52.0 to 98.7); 0.059 | |
Patients considered to be high risk and outcome within 5 days of symptom onset | 81.2 (35.6 to 94.6); 0.0078 | |
All-cause ICU admission, mechanical ventilation, or death within 60 days of positive SARS-CoV-2 test | ||
ICU admissions, mechanical ventilation, or death, n (%) | 17 (0.2) | 257 (0.2) |
Follow-up (days), median (IQR) | 20 (16 to 30) | 19 (5 to 35) |
Analysis: estimated effectiveness (%)a (95% CI); P value | ||
Within 5 days of symptom onset | 89.2 (–25 to 99.3); 0.075 | |
Clinical outcomes, n (%) | ||
Any hospital admission within 30 days | 46 (0.6) | 641 (0.5) |
Any ICU admission within 60 days | 9 (0.1) | 164 (0.1) |
Mechanical ventilation within 60 days | 1 (< 0.1) | 41 (< 0.1) |
Death within 60 days | 10 (0.1) | 124 (0.1) |
CI = confidence interval; ICU = intensive care unit; IQR = interquartile range; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
aEstimated effectiveness was reported as (1 – hazard ratio) of nirmatrelvir-ritonavir versus control.
Source: Lewnard et al.12 Copyright 2023. This work is licensed under the Attribution 4.0 International Licence. Full text available here: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(23)00118-4/fulltext
Critical Appraisal
Internal Validity
The Lewnard et al. study was assessed as having a moderate risk of bias. Details for the risk of bias assessment are outlined in the prior Health Technology Review of Nirmatrelvir-Ritonavir for the Treatment of COVID-19.10
More specifically, there were some differences between groups in the study. The use of a strict matching approach likely resulted in the exclusion of a large portion of the sample, which is likely to affect generalizability and may introduce selection bias. Differences can be observed between groups in terms of baseline characteristics even after matching, which was minimally addressed through covariate adjustment in the model. Therefore, there is a meaningful risk of bias due to confounding. As such, the inconsistency in subgroup results, which suggest a higher efficacy of nirmatrelvir-ritonavir proportional to the higher number of vaccine doses received, is likely to point to a systematic difference between treated and untreated patients rather than a true treatment effect.
External Validity
The study by Lewnard et al. included patients who were vaccinated or who had a prior SARS-CoV-2 infection. It was performed during a time period in which the Omicron variant was the main variant circulating; however, characteristics of the eligible population were not consistent with clinical practice standards for identification of patients who were at high risk. In addition, the effect reported has no meaningful clinical interpretation, which limits our ability to determine whether the estimated effects are clinically important.
Impact on Evidence Gaps
The CADTH review team, with the input provided by clinical experts, considers that the Lewnard et al. study has limited impact in addressing gaps in the evidence, due to the presence of confounding and to the included population, which did not have the characteristics of patients currently considered at high risk for progressing to severe COVID-19.
Description of the Schwartz et al. Study
The Schwartz et al. study was a population-based cohort study in Ontario. The data were hosted and analyzed at the Institute for Clinical Evaluation Sciences using unique encoded identifiers. The Institute for Clinical Evaluation Sciences is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. The databases available at the Institute for Clinical Evaluation Sciences and used in this study included the Ontario Drug Benefit database, COVID-19 Integrated Testing database, COVAXON database, Canadian Institute for Health Information database, and Ontario Health Insurance Plan database. All these databases were linked with Institute for Clinical Evaluation Sciences unique encoded identifiers. The population of Ontario aged between 18 years and 110 years who had a positive PCR test for SARS-CoV-2 between April 4, 2022, and August 31, 2022, were identified using the COVID-19 Integrated Testing database. The objective was to evaluate the effectiveness of nirmatrelvir-ritonavir in preventing severe COVID-19, while Omicron and its subvariants predominate.36
Populations
All people in Ontario between the ages of 18 years and 110 years who had a positive PCR test for SARS-CoV-2 between April 4, 2022, and August 31, 2022, were eligible for study inclusion. Non-Ontario residents or individuals that had invalid identifiers such as missing date of birth or death before the test date were excluded. Patients who were hospitalized or with a nosocomial infection before or on the testing day were also excluded.36
Interventions
Only nirmatrelvir-ritonavir dispensed through community pharmacies in Ontario was studied.36
Outcomes
The primary outcome was the composite of hospital admission due to COVID-19 or all-cause death that occurred 1 day to 30 days after the index date. The index date was defined as the date when nirmatrelvir-ritonavir was dispensed. Hospital admissions were determined from the Case and Contact Management database (Public Health Ontario).36
Statistical Analysis
To control for confounding, a propensity score-based weighting approach using inverse probability of treatment was used in weighted logistic regression models for the composite of hospital admission due to COVID-19 or all-cause death with nirmatrelvir-ritonavir use as the only covariate, to ascertain the treatment effect. Weights were incorporated into the model by weighting patients who were treated with nirmatrelvir-ritonavir by the inverse probability of not receiving nirmatrelvir-ritonavir and weighting patients who were not treated by the inverse probability of receiving nirmatrelvir-ritonavir. The estimated treatment effect was presented as weighted ORs along with 95% CIs. Statistically significant results were identified by considering P values less than 0.05. To calculate the NNT with 95% CIs, the estimated probabilities of outcomes for both the treated and untreated groups were obtained from weighted logistic regression models.
The analysis included prespecified covariates that were identified based on a literature review of the most important predictors of severe COVID-19. The identified list of variables to include were age (≥ 70 or < 70 years), vaccination status (0, 1 to 2, or ≥ 3 vaccine doses), potential drug-drug interactions in individuals aged older than 70 years (level 1, level 2, or no drug-drug interactions identified), number of comorbidities (≥ 3 or < 3), long-term care residents, and high or standard-risk categories as defined by the Ontario COVID-19 Science Advisory Table. Stabilized weights were used to reduce variability of the estimated treatment effect. Standardized differences were used to assess imbalances in both unweighted and weighted covariates, with a value of less than 0.1 reflecting a clinically important difference. The difference between the 2 periods of April 2022 to June 2022, and July 2022 to August 2022, was also evaluated.
The time since the last vaccination (14 to 179 or > 179 days) was added as a post hoc analysis in the stratified analyses.
Results
Baseline Characteristics
Before applying propensity score-derived inverse probability of treatment weighting, major between-group differences were observed across most variables. Patients receiving nirmatrelvir-ritonavir had a mean age of 74 years; patients who did not receive nirmatrelvir-ritonavir were younger, with a mean age of 52 years. A total of 84.8% of patients in the treatment arm had at least 3 doses of SARS-CoV-2 vaccine; this proportion was 75.8% for patients in the control arm. Overall, 41.9% of patients who were treated were considered at high risk and 58.1% were considered at standard risk; the risk profile for patients who were not treated differed, with 15.1% considered at high risk and 84.9% considered at standard risk.
However, after applying propensity score-derived inverse probability of treatment weighting, observed differences were reduced below the prespecified threshold for a clinically important difference (standardized mean difference ≤ 0.1).
Table 23: Baseline Characteristics for the Schwartz et al. Study
Characteristic | Schwartz et al. | |
|---|---|---|
Nirmatrelvir-ritonavir N = 8,876 | Did not receive nirmatrelvir-ritonavir N = 168,669 | |
Age (years), mean (SD) | 74.3 (16.3) | 52.4 (21.0) |
Gender and sex, n (%) | ||
Female | 5,261 (59.3) | 106,899 (63.4) |
Male | 3,617 (40.7) | 61,770 (36.6) |
Number of vaccine doses, n (%) | ||
0 | 467 (5.3) | 10,434 (6.2) |
1 | 87 (1.0) | 1,625 (1.0) |
2 | 798 (9.0) | 28,704 (17.0) |
≥ 3 | 7,524 (84.8) | 127,906 (75.8) |
Previous SARS-CoV-2 infection, n (%) | 412 (4.6) | 11 670 (6.9) |
Days since last vaccine dose, n (%) | ||
14 to 89 | 1,453 (16.4) | 17,438 (10.3) |
90 to 179 | 3,759 (42.4) | 72,705 (43.1) |
180 to 269 | 2,405 (27.1) | 46,190 (27.4) |
≥ 270 | 1,259 (14.2) | 32,336 (19.2) |
Ontario COVID-19 Science Advisory Table risk group, n (%) | ||
High risk | 3,720 (41.9) | 25,499 (15.1) |
Standard risk | 5,156 (58.1) | 143,170 (84.9) |
Comorbidity, n (%) | ||
Chronic respiratory disease | 3,128 (35.2) | 40,813 (24.2) |
Chronic heart disease | 2,249 (25.3) | 18,910 (11.2) |
Diabetes | 2,996 (33.8) | 27,954 (16.8) |
Immune compromised | 1,412 (15.9) | 10,102 (6.0) |
Hypertension | 6,071 (68.4) | 54,549 (32.3) |
Dementia | 2,659 (30.0) | 15,714 (9.3) |
Autoimmune disease | 1,150 (13.0) | 8,504 (5.0) |
Chronic kidney disease | 1,108 (12.5) | 9,867 (5.9) |
Advanced liver disease | 209 (2.4) | 2,110 (1.3) |
Long-term care resident, n (%) | 2,795 (31.5) | 12,806 (7.6) |
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; SD = standard deviation.
Source: Schwartz et al.36 Population-based evaluation of the effectiveness of nirmatrelvir-ritonavir for reducing hospital admissions and mortality from COVID-19. CMAJ. 2023;195(6):E220-E226. Copyright 2023. This work is licensed under the Attribution-NonCommercial-NoDerivs 4.0 International Licence. Full text available here: https://www.cmaj.ca/content/195/6/E220
Patient Disposition
Figure 1: Cohort Flow Chart for the Schwartz et al. Study
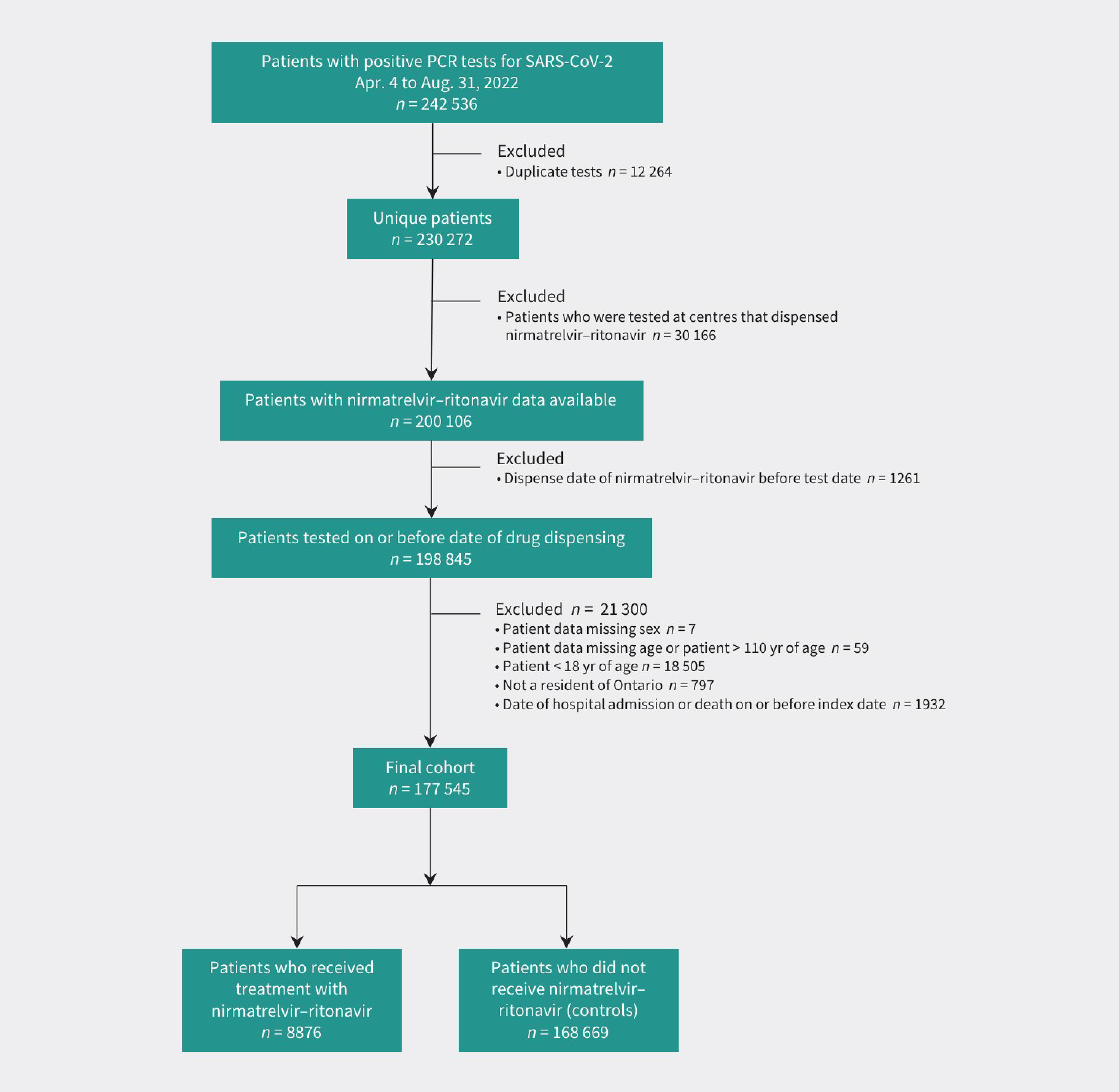
PCR = polymerase chain reaction; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; yr = years.
Source: Schwartz et al. 2023.36 Population-based evaluation of the effectiveness of nirmatrelvir-ritonavir for reducing hospital admissions and mortality from COVID-19. CMAJ. 2023;195(6):E220-E226. Copyright 2023. This work is licensed under the Attribution-NonCommercial-NoDerivs 4.0 International Licence. Full text available here: https://www.cmaj.ca/content/195/6/E220
Exposure to Study Treatments
A total of 177,545 people constituted the final cohort of 8,876 patients who received nirmatrelvir-ritonavir and 168,669 who did not receive this treatment.36
The exposure to concomitant medication, co-intervention, or confounding treatments was not presented for the whole cohort, but drug-drug interaction was evaluated in patients aged older than 70 years. Drugs were identified from Ontario Drug Benefit database. Potential drug-drug interaction was defined as any co-medications with a drug-drug interaction of severity level 1 or 2 through an Ontario Drug Benefit claim with an overlap in days supplied and the dispense date of nirmatrelvir-ritonavir, where level 1 included any co-medications contraindicated with nirmatrelvir-ritonavir and level 2 included co-medications with clinically significant drug-drug interactions that require a mitigation strategy while on nirmatrelvir-ritonavir according to the Ontario COVID-19 Science Advisory Table guideline.36
Efficacy
In the weighted primary analysis, patients who received nirmatrelvir-ritonavir, and those who did not, had a 2.1% and 3.7% risk of hospital admission or death, respectively. The weighted OR of hospital admission or death within 30 days was 0.56 (95% CI, 0.47 to 0.67; P < 0.001) and the weighted OR of death alone was 0.49 (95% CI, 0.40 to 0.60; P < 0.001).
Table 24: Key Efficacy Results From the Schwartz et al. Study
Key results | Nirmatrelvir-ritonavir N = 8,876 | Did not receive nirmatrelvir-ritonavir N = 168,669 |
|---|---|---|
Hospitalization or death | ||
Weighted % | 2.1 | 3.7 |
OR (95% CI) | 0.56 (0.47 to 0.67) | |
NNT (95% CI) | 62 (43 to 80) | |
Death | ||
Weighted % | 1.6 | 3.3 |
OR (95% CI) | 0.49 (0.40 to 0.60) | |
NNT (95% CI) | 60 (44 to 77) | |
CI = confidence interval; NNT = number needed to treat; OR = odds ratio.
Source: Schwartz et al. 2023.36 Population-based evaluation of the effectiveness of nirmatrelvir-ritonavir for reducing hospital admissions and mortality from COVID-19. CMAJ. 2023;195(6):E220-E226. Copyright 2023. This work is licensed under the Attribution-NonCommercial-NoDerivs 4.0 International Licence. Full text available here: https://www.cmaj.ca/content/195/6/E220
Overall results were similar in the stratified analyses when analyzed according to age, vaccination status, comorbidities, drug-drug interactions, and risk status (Figure 2).
The NNT was 62 (95% CI, 43 to 80) people treated with nirmatrelvir-ritonavir to prevent 1 hospital admission or death from COVID-19. There was substantial variability in absolute risk reductions by strata, with NNT ranging from 28 (95% CI, 7 to 49) for unvaccinated people to 181 (95% CI, 50 to 312) for those aged younger than 70 years.36
Figure 2: Forest Plot of Weighted ORs for Hospital Admission Related to COVID-19 or All-Cause Death and NNT at 30 Days — Schwartz et al. Study
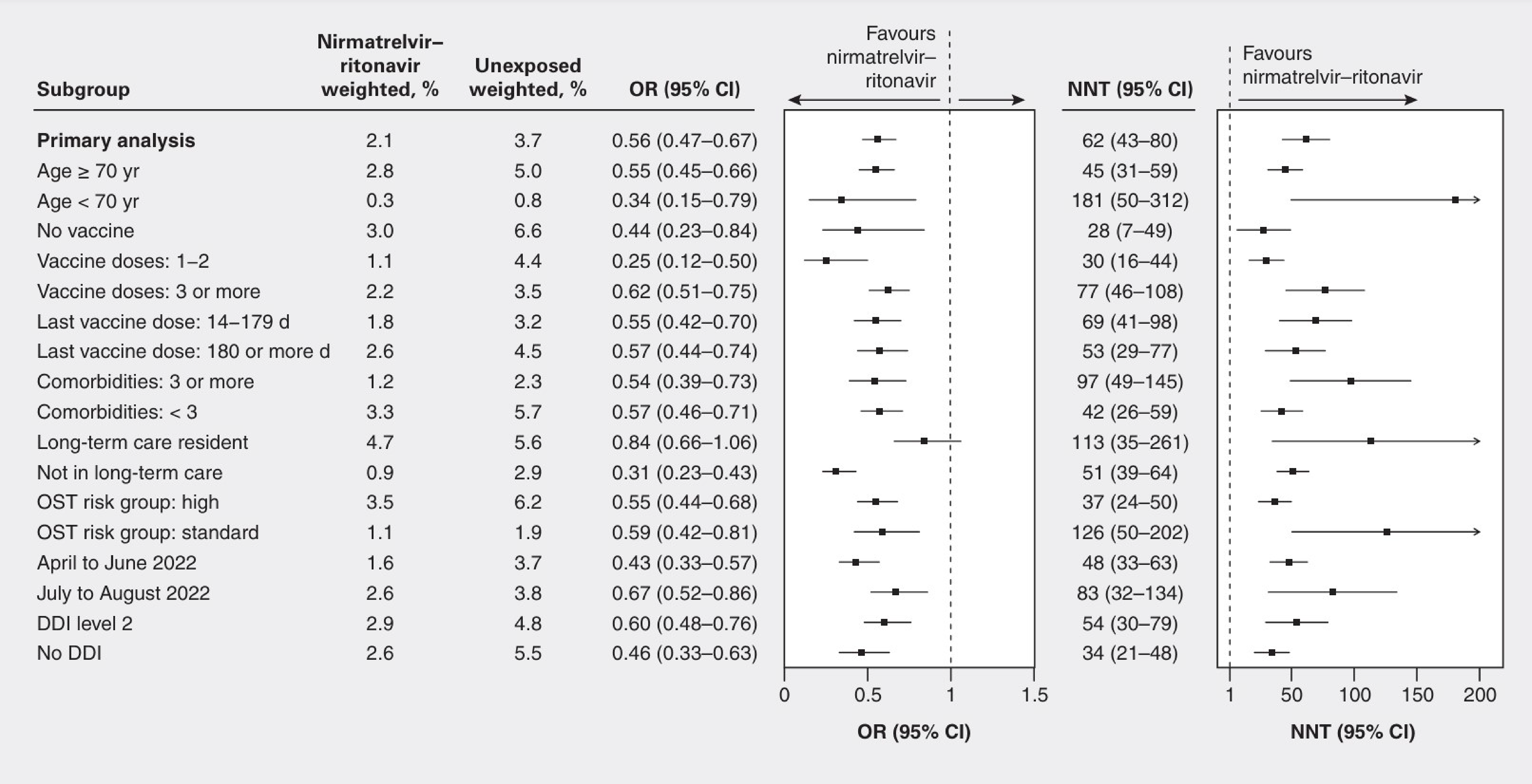
CI = confidence interval; d = days; DDI = drug-drug interaction; NNT = number needed to treat; OR = odds ratio; OST = Ontario COVID-19 Science Advisory Table; yr = years.
Source: Schwartz et al. (2023).36 Population-based evaluation of the effectiveness of nirmatrelvir-ritonavir for reducing hospital admissions and mortality from COVID-19. CMAJ. 2023;195(6):E220-E226. Copyright 2023. This work is licensed under the Attribution-NonCommercial-NoDerivs 4.0 International Licence. Full text available here: https://www.cmaj.ca/content/195/6/E220
Critical Appraisal
Internal Validity
The Schwartz et al. study was assessed as having a moderate risk of bias. Details for the risk of bias assessment are outlined in the prior Health Technology Review of Nirmatrelvir-Ritonavir for the Treatment of COVID-19.10
More specifically, there is an issue with selecting patients. Before weights were incorporated into the statistical model, major differences could be observed between treatment groups in terms of baseline characteristics. The weighting scheme used in the study was consistent with an average treatment effect among the overlap estimate, which means that patients were selected from the entire sample based on who could likely have received either treatment according to the study demographics. This results in not only a more restrictive subgroup of the study sample than the entire population, but also in an efficacy estimate that is likely to differ substantially from the average treatment effect among everyone. Based on the observed difference between treatment groups in the overall population sample, the estimated effect is likely to vary greatly according to the population selected, and this introduces uncertainty in the findings.37
External Validity
The study by Schwartz et al. included patients who were vaccinated or had a prior SARS-CoV-2 infection. It was performed during a time period in which the Omicron variant was the main variant circulating; however, characteristics of the eligible population were not consistent with clinical practice standards for identification of patients who are at high risk.
Impact on Evidence Gaps
The CADTH review team, with the input provided by clinical experts, considers that the Schwartz et al. study may inform gaps in the evidence for the efficacy of nirmatrelvir-ritonavir in patients who were vaccinated during an Omicron wave, especially as it was performed in a population of people living in Canada; however, this was not consistent with current definitions at the time of this review for patients at high risk for progressing to severe COVID-19. In the study, the impact of nirmatrelvir-ritonavir to prevent hospitalization and death was considered modest. Because of potential issues with selection and confounding, findings should be interpreted with caution, as there is uncertainty surrounding the true treatment effect.
Description of the Kaboré et al. Study
The Kaboré et al. study was a retrospective cohort study using data from the Quebec administrative claims databases. The data came from the Quebec Public Health Insurance provincial insurance plan and from the Ministry of Health and Social Services. The study aimed to assess whether nirmatrelvir-ritonavir reduces the risk of COVID-19–associated hospitalization among high-risk outpatients. The primary end point of this study was COVID-19–related hospitalization in the 30 days following the index date (date of dispensing of nirmatrelvir-ritonavir for the treatment group and date of positive RT-PCR test for the control group).
Populations
Patients included in this study encompassed individuals covered by the Quebec public health insurance plan in 2022 and were divided into 2 groups (treatment and control). The treatment group included outpatients who had received at least 1 dispensing of nirmatrelvir-ritonavir between March 15, 2022, and October 15, 2022, in community pharmacies. The control group included outpatients who tested positive for COVID-19 via RT-PCR test between March 15, 2022, and October 15, 2022, but who did not receive a prescription of nirmatrelvir-ritonavir during the study period. The index date was the start date of the follow-up period and was defined as the date of the first dispensing of nirmatrelvir-ritonavir for the treatment group, or as the date of the COVID-19–positive test for the control group. Patients were excluded if they had a short follow-up duration (< 30 days), were hospitalized or deceased at the index date, or were a long-term care resident and had missing data on certain key variables. Treated outpatients were matched to controls using a 1:1 ratio and nearest-neighbour propensity score matching (refer to statistical analysis for additional information).
Interventions
The intervention of interest was the receipt of a nirmatrelvir-ritonavir dispensing during the study period. The intervention was received by patients in the treatment group whereas it was not received by patients in the control group.
Outcomes
The main objective of this study was to investigate the effectiveness of nirmatrelvir-ritonavir for the prevention of COVID-19–related hospitalization at 1 month after treatment initiation in patients infected by COVID-19. Additionally, the objective was to evaluate the treatment effectiveness in the following subgroups by vaccination status (number of vaccine doses), time since last vaccine dose (≤ 6 months versus > 6 months), age (< 70 years versus ≥ 70 years), and severely immunocompromised status.
Statistical Analysis
Descriptive statistics were used to describe the treatment group and hospitalized cases at index date. For the purposes of regression analyses, individuals with missing data were excluded, as they represented a small subset of patients (1.7%). Treated outpatients were matched to controls using 1-to-1 nearest-neighbour propensity score matching without replacement with a caliper of 10−5 (a caliper of 10−2 was used to optimize number of matched outpatients for analysis among severely immunocompromised individuals). The propensity score was calculated through a logistic regression with the nirmatrelvir-ritonavir prescription as the outcome (yes or no). Covariates included in the propensity score model were number of vaccine doses; time since last vaccine dose; COVID-19 waves; age; sex; region of residence; number of health conditions; cardiovascular, respiratory, and other health condition; immunosuppression; and cancer.
The RR of hospitalization in the treatment group compared with the control group was estimated using a multivariable Poisson regression with robust error variance,38 which included the variables used for the propensity score to further adjust for potential confounding. The same method was repeated for each subgroup analysis (according to vaccination status, age [< 70 and ≥ 70 years], and among individuals with severe immunosuppression).39
Sensitivity analyses were conducted afterwards to confirm the findings. These analyses comprised a multivariate regression including overall individuals (not only matched individuals) and analysis considering only hospitalizations for which the main cause of admission was COVID-19 as the outcome, as well as another analysis considering both COVID-19–associated hospitalization and death as the outcome. Analyses were performed using Stata/SE 15.1 for Windows (StataCorp).
Results
Patient Disposition
A total of 18,120 patients were initially identified who received nirmatrelvir-ritonavir and 299,024 patients who were untreated; the final cohort comprised 16,601 patients receiving nirmatrelvir-ritonavir and 242,341 patients not receiving this treatment. The most frequent reasons for exclusion of patients from the cohort was hospitalization at index date (n = 242 and n = 16,059, respectively), long-term care setting residents (n = 86 and n = 13,668, respectively), and missing data on health conditions (n = 201 and n = 5,550, respectively).
Baseline Characteristics
Limited information was reported in the publication to assess the level of risk for progressing to severe disease. Most patients (83%) were younger than 80 years of age and 56% had incomplete primary vaccination. A total of 44% of patients had 1 to 4 concomitant health conditions, 32% had 5 to 9 concomitant health conditions, and 11% had 10 to 14 concomitant health conditions. Cardiovascular and/or respiratory conditions were reported in 46% of patients. A total of 18% of patients were considered immunosuppressed and 17% of patients had cancer. Full details regarding baseline characteristics are provided in the Kaboré et al. study.14
Exposure to Study Treatments
Dispensing of nirmatrelvir-ritonavir recorded between March 15, 2022, and October 15, 2022, was identified in the administrative claims databases using the drug identification number of the drug. Concomitant medications were not used in this analysis and were not adjusted for.
Efficacy
Of the 258,942 eligible outpatients, 16,804 (6.5%) were left after the propensity score matching which is equivalent to 8,402 in each group. Full efficacy results are provided in the Kaboré et al. study.14
In the total population, regardless of vaccination status, the primary outcome of hospitalization within 30 days following the index date occurred in 299 patients (3.56%) treated with nirmatrelvir-ritonavir. In comparison, among the untreated, the primary outcome occurred in 966 patients (11.50%). As a result, treatment with nirmatrelvir-ritonavir was associated with a RR of 0.31 (95% CI, 0.28 to 0.36; P < 0.001) for COVID-19–associated hospitalization. The NNT as calculated by CADTH (NNT = 1 / reported absolute risk difference) was approximately 13.
Subgroup analyses indicate that the effectiveness of nirmatrelvir-ritonavir was greater in patients with incomplete vaccination, with 27 patients (n = 4,101; 0.57%) in the nirmatrelvir-ritonavir group and 631 patients (n = 4,701; 13.42%) in the control group hospitalized due to COVID-19 (RR = 0.04; 95% CI, 0.03 to 0.06; P < 0.001). The NNT as calculated by CADTH was approximately 8. On the other hand, the magnitude of the results was smaller in patients who had a complete primary vaccination, with 276 patients (n = 3,665; 7.53%) in the nirmatrelvir-ritonavir group and 309 patients (n = 3,665; 8.43%) in the control group hospitalized due to COVID-19 (RR = 0.93; 95% CI, 0.78 to 1.08; P = 0.321). The NNT as calculated by CADTH was approximately 112.
Within subgroups of patients with complete primary vaccination, the effectiveness of nirmatrelvir-ritonavir also appeared to be the greatest in patients who were aged 70 years and older and who had their last vaccine dose before the prior 6 months, with 30 patients (n = 253; 11.9%) in the nirmatrelvir-ritonavir group and 58 patients (n = 253; 22.9%) in the control group hospitalized due to COVID-19 (RR = 0.50; 95% CI, 0.34 to 0.74; P < 0.001). The NNT as calculated by CADTH was approximately 10.
Critical Appraisal
Internal Validity
The study by Kaboré et al. was assessed as having a moderate risk of bias. Details for the risk of bias assessment are outlined in the prior Health Technology Review of Nirmatrelvir-Ritonavir for the Treatment of COVID-19.10
The study was considered methodologically sound, including the matching approach used, which was consistent with estimating the average treatment effect among the treated. It is possible however, despite the measure used to control for confounding, that the 2 groups had inherent differences that confounded the results. More specifically, patients treated with nirmatrelvir-ritonavir had to meet the specific eligibility criteria for accessing the drug in Quebec, while the control group did not; in addition, patients receiving nirmatrelvir-ritonavir included both outpatients with and without positive reverse transcription PCR tests, while the population of the control group was limited to only individuals with positive PCR tests. The COVID-19–related hospitalization rate in the group who did not receive treatment was substantially higher than what would be expected in clinical practice; therefore, the magnitude of the between-group difference should be interpreted with caution.
External Validity
The study by Kaboré et al. included patients who were vaccinated or had a prior SARS-CoV-2 infection. It was performed during a time period in which the Omicron variant was the main variant circulating; however, characteristics of the eligible population were not consistent with the current clinical practice standards for identification of patients who were at high risk at the time of this review.
Impact on Evidence Gaps
The CADTH review team, with the input provided by clinical experts, considers that the Kaboré et al. study may inform gaps in the evidence for the efficacy of nirmatrelvir-ritonavir in patients who were vaccinated during an Omicron wave, especially as it was performed in a population of people living in Canada. However, in the study, the magnitude of treatment effect observed with nirmatrelvir-ritonavir on preventing hospitalization should be interpreted with caution, as it may have been affected by confounding factors, resulting in bias in favour of treatment with nirmatrelvir-ritonavir. Although the population in the study was not consistent with current definitions for being high risk of progressing to severe COVID-19, subgroup analyses may inform on subpopulations who are more likely to benefit from treatment, as the magnitude of effect was greater in patients who were unvaccinated, in patients aged 70 years and older, in patients whose last vaccine dose was before the prior 6 months, and in patients who were severely immunocompromised.
Discussion
At the time of the review, the federal government, specifically the Public Health Agency of Canada, is responsible for overseeing the procurement and allocation of nirmatrelvir-ritonavir to ensure availability for federal, provincial, and territorial health care systems. Current provincial eligibility criteria for nirmatrelvir-ritonavir vary considerably between provinces and are presented in Appendix 1. Most jurisdictions elected to set a minimal age, as well as require the presence of risk factors, most regardless of vaccination status. As federal procurement ended in March 2024, there is a need for a CADTH reimbursement review.
The 2 clinical experts consulted by CADTH for this review agreed that at the time of this review, the most relevant risk factors to progress to severe COVID-19 are older age (> 80 years), frailty, underprotection from SARS-CoV-2 (patients who are unvaccinated and who have not had a prior infection), and severe immunosuppression. This would encompass a larger population of patients than recommendations from the recently updated WHO living guideline, which states that patients at high risk of hospitalization are those with diagnosed immunodeficiency syndromes, patients who have undergone solid organ transplant and receive immunosuppressants, as well as patients with autoimmune illness receiving immunosuppressants.6 The WHO living guideline strongly recommends the use of nirmatrelvir-ritonavir for these patients with nonsevere COVID-19 at high risk of hospitalization (patients in this high-risk category have a 6% rate of hospitalization).6
The guideline also highlights characteristics which are now associated with only a moderate risk of progressing to severe disease, a category of patients who have a 3% rate of hospitalization: patients aged older than 65 years, patients with obesity, diabetes and/or chronic cardiopulmonary disease, chronic kidney or liver disease, active cancer, with disabilities, and those with comorbidities of chronic disease.6 The guideline issued a moderate recommendation for the use of nirmatrelvir-ritonavir in patients with nonsevere COVID-19 at moderate risk of hospitalization.6 Although nirmatrelvir-ritonavir had a similar relative effect on patient-important outcomes of interest in both patients at moderate and high risk of progressing to severe disease, absolute effects were smaller in patients at moderate risk, because these patients have substantially lower hospitalization rates. In particular, the best estimate of reduction in hospitalization was 25 per 1,000 patients (2.5%).6
The National Advisory Committee on Immunization40 states that there is a spectrum of COVID-19 disease severity, ranging from asymptomatic to mild, moderate, severe, and critical disease. Severe disease more often occurs in those with increasing age and those with underlying medical conditions, with the risk increasing with the number of underlying conditions. A list of underlying medical conditions associated with more severe COVID-19 disease can be found in the Government of Canada’s clinician guide, “COVID-19 Signs, Symptoms, and Severity of Disease.” This guide states that the underlying medical conditions associated with more severe COVID-19 disease are: cancer; cerebrovascular disease; chronic kidney disease; chronic liver diseases (limited to cirrhosis, nonalcoholic fatty liver disease, alcoholic liver disease, and autoimmune hepatitis); chronic lung diseases (limited to bronchiectasis, chronic obstructive pulmonary disease, interstitial lung disease, pulmonary hypertension, and pulmonary embolism); cystic fibrosis; diabetes mellitus, type 1 and type 2; disabilities (e.g., Down syndrome; learning, intellectual, or developmental disabilities; attention-deficit/hyperactivity disorder; cerebral palsy; congenital disabilities; spinal cord injuries); heart conditions (e.g., cardiomyopathies, coronary artery disease, heart failure, and so forth); HIV infection; mental health disorders (limited to mood disorders, including depression, schizophrenia spectrum disorders); obesity; pregnancy and recent pregnancy; primary immunodeficiency diseases; smoking, current or former; solid organ or blood stem cell transplant; tuberculosis; and use of corticosteroids or other immunosuppressive medication.41 However, it is worth noting that the webpage was last updated on June 1, 2022, and the clinical experts consulted by CADTH indicated that based on their experience, these criteria may no longer be relevant and noted that the most relevant risk factors to progress to severe COVID-19 are older age (> 80 years), frailty, underprotection from SARS-CoV-2 (patients who are unvaccinated and who have not had a prior infection), and severe immunosuppression.
Summary of Available Evidence
One multicentre, DB, RCT was the primary source of evidence for the efficacy and safety of nirmatrelvir-ritonavir. The EPIC-HR study (N = 2,246)28 evaluated the superiority of nirmatrelvir-ritonavir compared with placebo for the treatment of adult symptomatic outpatients with mild to moderate COVID-19 who were not vaccinated against SARS-CoV-2 and who were considered at high risk for progression to severe disease and/or hospitalization at the time the study was performed, based on a wide range of prespecified patient characteristics. The primary outcome of the EPIC-HR trial was the composite of COVID-19–related hospitalization or death from any cause through day 28. The study was considered overall at low risk of bias.
Additional studies were provided by the sponsor to address evidence gaps because the EPIC-HR study did not include patients who were vaccinated or patients who had COVID-19 in the past, and it was performed at a time when the Omicron variant was not yet circulating. The EPIC-SR study (N = 1,153)11 was a multicentre, DB, placebo-controlled RCT comparing nirmatrelvir-ritonavir to placebo for the treatment of nonhospitalized, symptomatic, adult patients with COVID-19 who were at low risk of progression to severe illness. Patients were excluded if they had an underlying medical condition associated with an increased risk of developing severe illness from COVID-19 (unless the patient was vaccinated) or a prior COVID-19 infection. The primary end point was the time to sustained alleviation of all targeted COVID-19 signs and symptoms from baseline through day 28. Enrolment was terminated early due to a very low rate of hospitalization or death observed in the patient population who are at standard risk.
Other evidence submitted by the sponsor included 3 observational studies (Lewnard et al.,35 Schwartz et al.,13 and Kaboré et al.14), all of which were performed at a time when Omicron was the prevalent SARS-CoV-2 variant in circulation. These are discussed in greater detail in the following.
Finally, CADTH also considered a prior Health Technology Review of Nirmatrelvir-Ritonavir for the Treatment of COVID-19.10 With the help of clinical experts, 3 additional observational studies within the report were selected (Dryden-Peterson et al.,15 Dormuth et al.,16 and Hedvat et al.17), for which the populations were particularly relevant to clinical practice in Canada. As part of the overall body of evidence, their findings can inform decision-making regarding the optimal use of nirmatrelvir-ritonavir in specific populations of real-world patients who would be considered more vulnerable to worst outcomes with COVID-19 and who could not be included in the pivotal EPIC-HR RCT.
Interpretation of Results
Efficacy
Pivotal RCT
Stakeholder input outlined that the treatment goal with nirmatrelvir-ritonavir is to prevent progression to severe COVID-19, including COVID-19–related hospitalizations and mortality, in patients with mild to moderate disease. In the EPIC-HR pivotal RCT, nirmatrelvir-ritonavir reduced the incidence of COVID-19–related hospitalization or death from any cause through day 28 compared with placebo; in the overall population of patients treated as per the product monograph (within 5 days of symptoms onset), the absolute reduction was –5.5% (95% CI, –7.2% to –4.0%; P < 0.001). This yielded an NNT of 19, as calculated by CADTH. The proportions of patients experiencing a primary outcome event (0.9% with treatment and 6.3% with control) show that the incidence of COVID-19–related hospitalization or death from any cause in the EPIC-HR study population is low. Overall, the magnitude of effect with nirmatrelvir-ritonavir was considered small. In 1 subgroup analysis performed in patients aged 65 years and older, nirmatrelvir-ritonavir reduced the primary outcome incidence by –13.9% compared with placebo (mITT1 population, 0.8% versus 14.6%, respectively; 95% CI, –20.1% to –7.8%; P < 0.0001), suggesting that there might be subgroups of patients where the treatment effect is more pronounced, especially in the presence of a higher risk of worst outcomes. The use of nirmatrelvir-ritonavir in the EPIC-HR study did not yield clinically meaningful differences compared with placebo on outcomes assessing duration or severity of COVID-19 signs and symptoms.
Sponsor-Provided Additional Evidence
The EPIC-SR study, an RCT comparing nirmatrelvir-ritonavir to placebo for the treatment of nonhospitalized, symptomatic, adult patients with COVID-19 who were at low risk of progression to severe illness, was provided by the sponsor as evidence for the efficacy of nirmatrelvir-ritonavir in patients who were vaccinated during the Omicron wave. The study did not meet its primary objective, failing to demonstrate a difference between nirmatrelvir-ritonavir and placebo on the primary outcome of time to sustained alleviation of all targeted COVID-19 signs and symptoms. In a post hoc subgroup analysis of patients who were vaccinated and with an underlying medical condition, the use of nirmatrelvir-ritonavir was associated with a 1.29% reduction in the proportion of patients with COVID-19–related hospitalization or death from any cause through day 28 versus placebo (95% CI, –3.26 to 0.67). However, this patient population does not fall within the category of patients at high risk of progressing to severe disease. Therefore, the EPIC-SR study is not informative with regard to the evidence gaps.
The sponsor-submitted studies addressing gaps in the evidence included the following:
The study by Lewnard et al. (n = 7,274 treated with nirmatrelvir-ritonavir; n = 126,152 not treated with nirmatrelvir-ritonavir)35 was a retrospective cohort study using a matched cohort framework performed in California, US. Patients were included if they were aged at least 12 years, enrolled in KPSC health plans, and had a positive SARS-CoV-2 PCR result between April 8, 2022, and October 7, 2022. The primary end point of this study was hospital admission or death from any cause within 30 days. The included population was mostly vaccinated, with characteristics that were consistent with a standard risk of progressing to severe COVID-19. The study resulted in patients treated with nirmatrelvir-ritonavir having a clinically similar hospitalization and mortality rate compared to patients who did not receive this treatment. The Lewnard et al. study has limited impact in addressing gaps in the evidence, mainly due to the presence of substantial confounding and the included population not having the characteristics of patients considered at high risk for progressing to severe COVID-19 at the time of this review.
The study by Schwartz et al. (n = 8,876 treated with nirmatrelvir-ritonavir; n = 168,669 not treated with nirmatrelvir-ritonavir)13 was a population-based cohort study with propensity score-derived inverse probability of treatment weighting performed in Ontario. Patients were included in the study if they were Ontario residents aged between 18 years and 110 years who had a positive PCR test for SARS-CoV-2 between April 4, 2022, and August 31, 2022. Patients who received nirmatrelvir-ritonavir were highly vaccinated (85% had received at least 3 doses of SARS-CoV-2 vaccine); 42% were considered at high risk for progressing to severe disease. Overall, 2.1% of patients who received nirmatrelvir-ritonavir had a hospital admission due to COVID-19 or all-cause death within 30 days, compared with 3.7% for patients who did not receive this treatment, resulting in a weighted OR of 0.56 (95% CI, 0.47 to 0.67) and an NNT to prevent 1 case of severe COVID-19 of 62 (95% CI, 44 to 77). This confirms the statistically significant but clinically small effectiveness of nirmatrelvir-ritonavir in a real-world population. The Schwartz et al. study may inform gaps in the evidence for the efficacy of nirmatrelvir-ritonavir in patients who were vaccinated during the Omicron wave, especially as it was performed in a population of people living in Canada. However, this population is not consistent with current definitions for being high risk for progressing to severe COVID-19 at the time of this review. In the study, the impact of nirmatrelvir-ritonavir to prevent hospitalization and death was considered modest. Because of potential issues with selection and confounding, findings should be interpreted with caution, as there is uncertainty surrounding the true treatment effect.
The study by Kaboré et al. (n = 8,402 treated with nirmatrelvir-ritonavir; n = 8,402 not treated with nirmatrelvir-ritonavir)14 was a retrospective cohort study using nearest-neighbour propensity score matching performed in Quebec. Patients were included if they were covered by the Quebec public health insurance plan in 2022 and had either a prescription for nirmatrelvir-ritonavir (treated group) or a positive SARS-CoV-2 PCR result, but who did not receive a prescription for nirmatrelvir-ritonavir (control group) between March 15, 2022, and October 15, 2022. The study showed a benefit of nirmatrelvir-ritonavir compared to no such treatment on the primary outcome of COVID-19–related hospitalizations within 30 days (3.6% in the nirmatrelvir-ritonavir treatment group versus 11.5% in the control group; RR = 0.31; 95% CI, 0.28 to 0.36; P < 0.001). This yielded an NNT of 13, as calculated by CADTH. The magnitude of treatment effect observed with nirmatrelvir-ritonavir on preventing hospitalization should however be interpreted with caution, as the natural incidence of COVID-19–related hospitalizations in the control group was higher than would be expected in clinical practice; the estimates may have been affected by confounding factors, resulting in bias in favour of treatment with nirmatrelvir-ritonavir. The Kaboré et al. study may inform on subpopulations who are more likely to benefit from treatment. According to subgroup analyses, the magnitude of treatment effect was greater in patients who were not vaccinated than in the overall population and was also greater in patients aged 70 years and older (versus younger than 70 years) and in patients whose last vaccine dose was before the prior 6 months (versus within prior 6 months). Results also favoured nirmatrelvir-ritonavir versus no such treatment in a subgroup of patients who were severely immunocompromised.
Additional Evidence From CADTH
The most significant issue with these studies, including the EPIC-HR study, is that the findings cannot be generalized to the population of patients living in Canada at high risk for progression to severe COVID-19, as defined in clinical practice at the time of this review. The 2 clinical experts consulted by CADTH for this review agreed that the most relevant risk factors for progressing to severe disease and hospitalization are currently:
older age (> 80 years)
frailty
underprotection from SARS-CoV-2 (patients who are unvaccinated and those who have not had a prior infection)
severe immunosuppression.
To bridge this evidence gap, 3 additional observational studies have been selected, with the help of clinical experts, to inform on the use of nirmatrelvir-ritonavir in specific populations. All the studies included both a high-risk population and an incidence of hospitalization that was considered representative of, and relevant to, clinical practice in Canada. In addition, all the studies were performed at a time when Omicron was the prevalent variant of concern. Therefore, they inform on the efficacy of nirmatrelvir-ritonavir in real-world high-risk patients. Findings from the observational studies should be viewed as supplementary to those from the RCTs. This evidence was evaluated in a prior CADTH Health Technology Review of Nirmatrelvir-Ritonavir for the Treatment of COVID-19.10
The study by Dryden-Peterson et al. (n = 12,541 treated with nirmatrelvir-ritonavir; n = 32,010 not treated with nirmatrelvir-ritonavir)15 was a population-based cohort study using inverse probability-weighted analysis performed in Massachusetts and southern New Hampshire, US. The study was assessed as having a moderate risk of bias.10 Patients were included if they were aged 50 years or older and had a COVID-19 diagnosis between January 1, 2022, and July 17, 2022. Patients who received nirmatrelvir-ritonavir were highly vaccinated (79% vaccinated and boosted), half of the population was at least 65 years or older, 36% of patients were immunocompromised, and 23% had a solid tumour. The study showed a small benefit of nirmatrelvir-ritonavir compared to no such treatment on the primary outcome of hospitalization within 14 days or death within 28 days (0.5% versus 0.9%, respectively; absolute risk difference = –0.4%; RR = 0.56; 95% CI, 0.42 to 0.75; NNT = 250 as calculated by CADTH). Findings were consistent across subgroups; however, vaccination status affected the magnitude of treatment effect, which was higher in patients who were not fully vaccinated (NNT = 50 as calculated by CADTH), or whose last vaccine was more than 20 weeks before the study (NNT = 196 as calculated by CADTH).
The study by Dormuth et al. (n = 3,433 treated with nirmatrelvir-ritonavir; n = 3,433 not treated with nirmatrelvir-ritonavir)16 was a retrospective cohort study of patients at increased vulnerability to complications from COVID-19 performed in British Columbia. Inclusion of the study was suggested by the clinical experts, due to the high representativity of the population and sound methodology. High-dimensional propensity score models were used to minimize confounding and the nearest-neighbour method was used for matching patients. The study was performed between February 1, 2022, and February 3, 2023. The study assessed the effectiveness of nirmatrelvir-ritonavir on death from any cause and COVID-19–related hospitalization compared to no such treatment in different cohorts of patients deemed CEV at high risk for complications from COVID-19, as follows.
CEV1: at least 18 years and severely immunocompromised
CEV2: at least 18 years and moderately immunocompromised
CEV3: patients with selected medical conditions (severe respiratory disorders; insulin-dependent diabetes; or certain blood disorders, metabolic disorders, and cancers not captured in other groups)
Expanded eligibility: patients at lower risk than CEV but at higher risk than general population.
Hospitalization rates were low and aligned with clinical practice. Patients who were severely immunocompromised (CEV1 cohort) and who received nirmatrelvir-ritonavir had a –2.5% absolute risk difference (95% CI, –4.8 to –0.2) of experiencing the primary outcome compared to control, yielding an NNT of 40. The corresponding risk difference was –1.7% (95% CI, –2.9% to –0.5%) for patients who were moderately immunocompromised (CEV2 cohort) and –1.3% (95% CI, –2.8% to 0.1%) for patients with selected medical conditions (CEV3 cohort), yielding NNTs of 60 and 75, respectively.
The study by Hedvat et al. (n = 28 treated with nirmatrelvir-ritonavir; n = 75 not treated with nirmatrelvir-ritonavir)17 was a retrospective study of all adult patients who were solid organ transplant recipients and who had a positive SARS-CoV-2 PCR test within the research hospital between December 16, 2021, and January 19, 2022. The study was performed in New York City, US, and was assessed as having a moderate risk of bias.10 The use of nirmatrelvir-ritonavir was associated with a reduction, compared with no treatment, in the incidence of hospitalization or death from any cause (14.3% versus 33.3%, respectively; adjusted risk ratio for organ transplant type = 0.21; 95% CI, 0.06 to 0.71; NNT = 6 as calculated by CADTH), and hospitalization or death from COVID-19 (10.7% versus 30.7%, respectively; adjusted risk ratio for organ transplant type = 0.17; 95% CI, 0.04 to 0.67; NNT = 5 as calculated by CADTH). According to the clinical experts consulted by CADTH, hospitalization rates in this study were higher than what is seen in clinical practice in similar populations with organ transplants; therefore, although the findings are consistent with the known vulnerability of this patient group, generalizability of the findings is uncertain.
Discussion of Evidence Gaps
Results from 5 observational studies discussed in this review13-17 show that nirmatrelvir-ritonavir is effective compared to no such treatment against the prevalent Omicron SARS-CoV-2 variant of concern.
The observational studies also suggest that the effectiveness of nirmatrelvir-ritonavir in high-risk populations, as clinically defined in clinical practice in Canada, is likely to vary among categories of populations:
In 2 studies with subgroup analyses according to age group,14,16 there was a greater magnitude of effect with nirmatrelvir-ritonavir treatment versus no treatment in patients aged 70 years or older, compared with patients who were younger than 70 years. The overall incidence of hospitalization was also greater in both treatment and control groups in patients with older age.
In 3 studies13,15,16 where the population consisted of patients who were highly vaccinated and in subgroups analyses of patients who received prior vaccination, nirmatrelvir-ritonavir was overall associated a smaller magnitude of treatment effect when compared to patients who were vaccinated. In these studies or subgroup analyses, the incidence of hospitalization was typically small for both treatment and control arms, as would be expected in clinical practice, suggesting that patients who are vaccinated have overall a lower risk of progressing to severe COVID-19, regardless of whether or not they received treatment.
In 2 studies16,17 that included patients who were severely and/or moderately immunocompromised, nirmatrelvir-ritonavir was effective in preventing hospitalization and death compared with no such treatment; the magnitude of effect varied among the 2 studies. In a large, methodologically sound observational study conducted in Canada, the magnitude of treatment effect was proportional to the level of immunosuppression, being at its highest in the severely immunocompromised cohort.
Issues were noted in the observational studies with selection and confounding; this introduces uncertainty around the true treatment effect, which was addressed in a varying level of soundness through the weighting models and use of covariates. Though findings should be interpretated with caution, as part of the overall body of evidence, they remain informative regarding the optimal use of nirmatrelvir-ritonavir in real-world patients.
Harms
Nirmatrelvir-ritonavir was relatively well tolerated in the EPIC-HR study. Similar proportions of patients experienced AEs between treatment groups; however, numerically more patients reported AEs of higher severity and SAEs in the placebo group than in the treatment group. Discontinuation of treatment due to AEs was low. No patients died in the nirmatrelvir-ritonavir group and 15 patients (1.3%) died in the placebo group, with most reasons being related to COVID-19.
There is a lack of evidence on the safety of nirmatrelvir-ritonavir, especially in older adults and patients who are frail, who may be at increased risk of experiencing harms outcomes. Of note, additional safety considerations also guide the use of nirmatrelvir-ritonavir, which is associated with CYP3A inhibition, resulting in a number of drug-drug interactions. Nirmatrelvir-ritonavir is also not recommended in patients with severe renal or hepatic impairment.
The safety of nirmatrelvir-ritonavir was not assessed in observational studies.
Conclusion
Findings from the EPIC-HR study suggest that nirmatrelvir-ritonavir may contribute to preventing COVID-19–related hospitalization or death compared with placebo; however, this was in a population that was not considered at high risk for progressing to severe disease as defined by clinical practice at the time of this review. The incidence of hospitalization in the study was low, and the magnitude of treatment effect with nirmatrelvir-ritonavir was considered small in this patient population. Generalizability issues with the trial include that it was performed in patients who were unvaccinated, which is not representative of the highly vaccinated population of people living in Canada, and at a time when the Delta variant was in circulation. Therefore, additional evidence from the EPIC-SR study and observational studies were reviewed to bridge the evidence gaps from the EPIC-HR study. This supplementary evidence to the pivotal RCT suggests that nirmatrelvir-ritonavir retained efficacy against the Omicron variant of concern, but that the effectiveness of the drug was considerably reduced in adequately vaccinated populations. Observational cohort studies performed in specific populations suggest that the magnitude of effect with nirmatrelvir-ritonavir treatment may be greater in individuals of older age, or those who are unvaccinated or severely immunosuppressed. These are all characteristics of patients who would be considered at high risk of progressing to severe disease and more vulnerable to worse COVID-19 outcomes, according to clinical experts consulted by CADTH for this review. Issues were noted in the observational studies with selection of patients and confounding; this introduces uncertainty around the true treatment effect, which was addressed to a varying degree through the weighting models and use of covariates. Though findings should be interpretated with caution, as part of the overall body of evidence, they inform on the optimal use of nirmatrelvir-ritonavir in clinical practice. Nirmatrelvir-ritonavir was relatively well tolerated in the EPIC-HR study; however, there is a lack of evidence in older adults and patients who are frail who may be at increased risk of experiencing harms outcomes. The use of nirmatrelvir-ritonavir poses additional issues in patients receiving medication metabolized through CYP3A, due to its inhibition by the drug, which results in a number of interactions.
References
1.Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924. PubMed
2.Government of Canada. COVID-19 epidemiology update: Summary [sponsor supplied reference]. July 25, 2023: https://health-infobase.canada.ca/covid-19/.
3.Government of Canada. COVID-19 epidemiology. - Cases and death [sponsor supplied reference]. July 25, 2023: https://health-infobase.canada.ca/covid-19/.
4.Gebru AA, Birhanu T, Wendimu E, et al. Global burden of COVID-19: Situational analyis and review. Hum Antibodies. 2021;29(2):139-148. PubMed
5.World Health Organization. Living guidance for clinical management of COVID-19 [sponsor supplied reference]. Geneva: World Health Organization; November 23, 2021: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2.
6.World Health Organization. Therapeutics and COVID-19: living guideline, 10 November 2023 Geneva: World Health Organization; 2023.
7.Dormuth CR, Kim JD, Fisher A, Piszczek J, Kuo IF. Nirmatrelvir-Ritonavir and COVID-19 Mortality and Hospitalization Among Patients With Vulnerability to COVID-19 Complications. JAMA Netw Open. 2023;6(10):e2336678. PubMed
8.Public Health Agency of Canada. Canadian COVID-19 vaccination coverage report. Ottawa: Public Health Agency of Canada [sponsor supplied reference]. 2023; https://health-infobase.canada.ca/covid-19/vaccination-coverage/. Accessed August 2023.
9.Pfizer Inc. EPIC-HR Final CSR v1.0: An Interventional Efficacy and Safety, Phase 2/3, Double-Blind, 2-Arm Study to Investigate Orally Administered PF-07321332/Ritonavir Compared With Placebo in Nonhospitalized Symptomatic Adult Participants With COVID-19 Who are at Increased Risk of Progressing to Severe Illness [sponsor supplied reference]. 06 June 2022.
10.Eze N, Asante B, Spry C, Clement F. Nirmatrelvir-Ritonavir for the Treatment of COVID-19. 2023: https://www.cadth.ca/sites/default/files/covid-19/Bundle%20covid%2019/nirmatrelvir_ritonavir_for_treatment_of_covid-19_systematic%20review.pdf. Accessed June 26, 2024.
11.Pfizer Inc. EPIC-SR Final CSR v1.0: An Interventional Efficacy and Safety, Phase 2/3, Double-Blind, 2-Arm Study to Investigate Orally Administered PF-07321332/Ritonavir Compared With Placebo in Nonhospitalized Symptomatic Adult Participants With COVID-19 Who are at Low Risk of Progressing to Severe Illness [sponsor supplied reference]. 09 March 2023.
12.Lewnard JA, McLaughlin JM, Malden D, et al. Effectiveness of nirmatrelvir-ritonavir in preventing hospital admissions and deaths in people with COVID-19: a cohort study in a large US health-care system. Lancet Infect Dis. 2023;23(7):806-815. PubMed
13.Schwartz KL, Wang J, Tadrous M, et al. Population-based evaluation of the effectiveness of nirmatrelvir-ritonavir for reducing hospital admissions and mortality from COVID-19. Cmaj. 2023;195(6):E220-E226. PubMed
14.Kaboré. Real-World Effectiveness of Nirmatrelvir/Ritonavir on Coronavirus Disease 2019–Associated Hospitalization Prevention: A Population-based Cohort Study in the Province of Quebec, Canada [sponsor supplied reference]. Clinical Infectious Diseases® 2023;77(6):805–152023. PubMed
15.Dryden-Peterson S, Kim A, Kim AY, et al. Nirmatrelvir Plus Ritonavir for Early COVID-19 in a Large U.S. Health System: A Population-Based Cohort Study. Ann Intern Med. 2023;176(1):77-84. PubMed
16.Dormuth. Nirmatrelvir-Ritonavir and COVID-19 Mortality and Hospitalization Among Patients With Vulnerability to COVID-19 Complications. JAMA Network Open. 2023;6(10):e2336678.2023.
17.Hedvat J, Lange NW, Salerno DM, et al. COVID-19 therapeutics and outcomes among solid organ transplant recipients during the Omicron BA.1 era. Am J Transplant. 2022;22(11):2682-2688. PubMed
18.Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. Jama. 2020;323(13):1239-1242. PubMed
19.Government of Canada. Interim guidance on the use of rapid antigen detection tests for the identification of SARS-CoV-2 infection [sponsor supplied reference]. July 2022; https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/use-rapid-antigen-detection-tests.html. Accessed September 6, 2023.
20.Government of Canada. Health professional risk communication. EVUSHELD (tixagevimab and cilgavimab for injection) - Risk of Prophylaxis or Treatment Failure due to Antiviral Resistance to specific SARS-CoV-2 Subvariants [sponsor supplied reference]. 2023; https://recalls-rappels.canada.ca/en/alert-recall/evusheld-tixagevimab-and-cilgavimab-injection-risk-prophylaxis-or-treatment-failure-0. Accessed July 13, 2023.
21.Government of Canada. Health professional risk communication. Casirivimab and Imdevimab – High Risk of Treatment Failure Due to Circulation of SARS-CoV-2 Omicron Variant [sponsor supplied reference]. 2022; https://recalls-rappels.canada.ca/en/alert-recall/evusheld-tixagevimab-and-cilgavimab-injection-risk-prophylaxis-or-treatment-failure-0. Accessed July 13, 2023.
22.Government of Canada. Health professional risk communication: Sotrovimab for Injection - Risk of Treatment Failure due to Circulation of SARS-CoV-2 Omicron BA.2 Subvariant [sponsor supplied reference]. 2022; https://recalls-rappels.canada.ca/en/alert-recall/sotrovimab-injection-risk-treatment-failure-due-circulation-sars-cov-2-omicron-ba2. Accessed September 6, 2023.
23.PrPAXLOVID™ nirmatrelvir tablets; ritonavir tablets. Tablets, 150 mg nirmatrelvir; 100 mg ritonavir co-packaged for oral use [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2023: https://pdf.hres.ca/dpd_pm/00072200.PDF.
24.PrVEKLURY® (remdesivir) for injection, powder for solution for infusion, 100 mg/vial (5 mg/mL when reconstituted) [product monograph]. Mississauga (ON): Gilead Sciences Canada, Inc.; 2023: https://pdf.hres.ca/dpd_pm/00071267.PDF.
25.PrEVUSHELDTM tixagevimab and cilgavimab injection solution, 100 mg/mL (tixagevimab) and 100 mg/mL (cilgavimab), intramuscular use [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2023: https://pdf.hres.ca/dpd_pm/00071063.PDF.
26.PrSotrovimab for injection, solution for infusion, 500 mg/8 mL (62.5 mg/mL) single use vial [product monograph]. Mississauga (ON): GlaxoSmithKline Inc.; 2023: https://pdf.hres.ca/dpd_pm/00069318.PDF.
27.PrCasirivimab and imdevimab for injection, solutions for infusion, each available as 1332 mg/11.1 mL and 300 mg/2.5 mL (120mg/mL) single-use vials [product monograph]. 2022. https://pdf.hres.ca/dpd_pm/00066206.PDF.
28.Hammond J, Leister-Tebbe H, Gardner A, et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19. N Engl J Med. 2022;386(15):1397-1408. PubMed
29.ClinicalTrials.gov. EPIC-HR: Study of Oral PF-07321332/Ritonavir Compared With Placebo in Nonhospitalized High Risk Adults With COVID-19 [sponsor supplied reference]. 2022; https://clinicaltrials.gov/ct2/show/NCT04960202.
30.New data show treatment with Lilly's neutralizing antibodies bamlanivimab (LYCoV555) and etesevimab (LY-CoV016) together reduced risk of COVID-19 hospitalizations and death by 70 percent [sponsor supplied reference]. 2021; https://lilly.mediaroom.com/2021-01-26-New-data-show-treatment-with-Lillysneutralizing-antibodies-bamlanivimab-LY-CoV555-and-etesevimab-LY-CoV016-together-reduced-risk-of-COVID-19-hospitalizations-and-death-by-70-percent.
31.CADTH. CADTH drug implementation advice: Nirmatrelvir and ritonavir (Paxlovid). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/HD0007%20Paxlovid_Final.pdf.
32.Government of Canada. COVID-19 epidemiology update: Testing and variants. Ottawa: Government of Canada; 2023: https://health-infobase.canada.ca/covid-19/testing-variants.html.
33.ClinicalTrials.gov. Evaluation of Protease Inhibition for COVID-19 in Standard-Risk Patients (EPIC-SR). https://clinicaltrials.gov/ct2/show/NCT05011513 [sponsor supplied reference]. 2022.
34.Pfizer. Pfizer Reports Additional Data on PAXLOVID™ Supporting Upcoming New Drug Application Submission to U.S. FDA. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-reports-additional-data-paxlovidtm-supporting [sponsor supplied reference]. 2022.
35.Lewnard JA, McLaughlin JM, Malden D, et al. Effectiveness of nirmatrelvir-ritonavir against hospital admission or death: a cohort study in a large US healthcare system [preprint]. medRxiv. 2023:10.
36.Schwartz KL, Wang J, Tadrous M, et al. Population-based evaluation of the effectiveness of nirmatrelvir-ritonavir for reducing hospital admissions and mortality from COVID-19. CMAJ. 2023;195(6):E220-e226. PubMed
37.Desai RJ, Franklin JM. Alternative approaches for confounding adjustment in observational studies using weighting based on the propensity score: a primer for practitioners. BMJ (Clinical research ed). 2019;367:I5657. PubMed
38.Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159(7):702-706. PubMed
39.Furukawa TA, Guyatt GH, Griffith LE. Can we individualize the 'number needed to treat'? An empirical study of summary effect measures in meta-analyses. Int J Epidemiol. 2002;31(1):72-76. PubMed
40.Government of Canada. COVID-19 vaccines: Canadian Immunization Guide Ottawa: Government of Canada; 2023: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines/page-26-covid-19-vaccine.html.
41.Government of Canada. COVID-19 signs, symptoms and severity of disease: A clinician guide. Ottawa: Government of Canada; 2022: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/signs-symptoms-severity.html#a3.
Appendix 1: Current Provincial Eligibility Criteria of Nirmatrelvir-Ritonavir Summarized
Note that this appendix has not been copy-edited.
The following table summarizes current provincial eligibility criteria of nirmatrelvir-ritonavir. These criteria were provided by the sponsor and have not been validated.
Table 25: Provincial Eligibility Criteria of Nirmatrelvir-Ritonavir at the Time of the Review
Province | Eligibility criteria | Vaccination doses |
|---|---|---|
British Columbia | ≥ 70, 1 risk factors (unvaccinated or chronic condition is a risk factor) Special cases for Indigenous (≥ 60) | 70+ unvaccinated as 1 risk factor or not received 2 vaccines plus booster in past year or 1 or more serious medical condition |
Alberta | ≥ 60, + 1 risk factor; ≥ 50, + 2 or more risk factors Special cases for First Nations/LTC | Regardless of vaccination status |
Saskatchewan | ≥ 70 with risk factor; 18+ immunocompromised | Regardless of vaccination status |
Manitoba | ≥ 18 with risk factor including age | Regardless of vaccination status |
Ontario | ≥ 60; 18 to 59 at high risk of severe outcomes | Regardless of vaccination status |
Quebec | ≥ 60; fewer than 2 vaccine doses; 18+ fewer than 2 doses + 1 risk factor; HCPs can also use AZ code | Fewer than 2 doses or HCPs authorize using AZ code |
New Brunswick | ≥ 18 with risk factor including age | Regardless of vaccination status |
Nova Scotia | ≥ 70 with 1 risk factor | 2 doses or less |
Prince Edward Island | ≥ 50; 18+ with high risk factors; 18+ Indigenous | Regardless of vaccination status |
Newfoundland and Labrador | ≥ 60 or immunocompromised adult | Regardless of vaccination status |
Pharmacoeconomic Review
Abbreviations
ACE
Arthritis Consumer Experts
AE
adverse event
BIA
budget impact analysis
ICER
incremental cost-effectiveness ratio
ICU
intensive care unit
MV
mechanical ventilation
NNT
number needed to treat
QALY
quality-adjusted life-year
SARS-CoV-2
severe acute respiratory syndrome coronavirus 2
SoC
standard of care
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Nirmatrelvir-ritonavir (Paxlovid), tablets |
Submitted price | $1,288.89 per 5-day treatment course, consisting either of:
|
Indication | For the treatment of mild-to-moderate COVID-19 in adults with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | January 17, 2022 |
Reimbursement request | As per indication |
Sponsor | Pfizer Canada ULC |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision tree followed by Markov model |
Target population | Adult patients with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death |
Treatment | Nirmatrelvir-ritonavir |
Comparator | SoC basket comparator comprising over-the-counter and off-label steroid medications |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 10 years |
Key data source | EPIC-HR, a phase II/III double-blind, placebo-controlled randomized controlled trial in nonhospitalized symptomatic adult patients with a confirmed diagnosis of SARS-CoV-2 infection |
Submitted results (corrected) | Nirmatrelvir-ritonavir was dominant (incremental costs: –$42; incremental QALYs: 0.020 or 7 days of perfect health) compared to SoC |
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; LY = life-year; NNT = number needed to treat; QALY = quality-adjusted life-year; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; SoC = standard of care.
Conclusions
In the EPIC-HR pivotal randomized controlled trial, nirmatrelvir-ritonavir reduced the incidence of COVID-19–related hospitalization or death from any cause through day 28 compared with placebo. While the results were statistically significant, overall, the magnitude of effect with nirmatrelvir-ritonavir was considered relatively small. In addition, as noted in the clinical review, the EPIC-HR study did not include patients who were vaccinated or patients who had COVID-19 in the past, and it was performed at a time when the Omicron variant was not yet circulating. Finally, the trial was performed in a population that is not considered at high risk for progressing to severe disease, as defined in clinical practice, at the time of this review. These differences represent a fundamental challenge in interpreting the results from the sponsor’s submitted evidence dossier and accompanying pharmacoeconomic model which are based on the EPIC-HR study.
CADTH made 1 base case change, in consultation with clinical experts, and fixed a programming error in the sponsor’s model. CADTH used the efficacy data from an observational study, Schwartz et al., rather than the EPIC-HR study to inform the base case, as this study more accurately reflected the state of the population at risk for COVID-19 at the time of this review (e.g., vaccination and exposure to COVID-19). The CADTH base case resulted in incremental costs of $897 and a benefit in quality-adjusted life-years (QALYs) of 0.002 (or < 1 day of perfect health), an incremental cost-effectiveness ratio (ICER) of $442,082 per QALY gained for nirmatrelvir-ritonavir compared to standard of care (SoC). In CADTH’s base case, for nirmatrelvir-ritonavir to be considered cost-effective at a $50,000 per QALY gained threshold, the drug cost of nirmatrelvir-ritonavir would need to be $494 per treatment course, reflecting a price reduction of approximately 62%.
CADTH included an alternative approach considering the various numbers needed to treat (NNTs) to avoid 1 severe case of COVID-19 (hospitalization or death) as reported by the CADTH clinical review, to reflect the variability across the clinical studies. When considering the study by Schwartz et al., which best reflects the state of COVID-19 at the time of this review, the NNT is 62. When compared to the cost of a general ward admission for COVID-19 ($20,000), CADTH calculated a price reduction of 75% would be required to ensure minimal financial impact to the health care system. Other NNTs are reported in Table 8.
Results of this analysis are driven by the source of efficacy data used. Since the majority of patients (> 90%) in both the sponsor’s and CADTH’s analysis will not require hospitalization, even while receiving SoC, the effectiveness of nirmatrelvir-ritonavir is limited to patients who potentially would require hospitalization. Although the CADTH base case predicts incremental QALY gains of 0.002 per patient, this is an average of the cohort, and it is unlikely that 1 individual patient would experience this magnitude of benefit. In reality, it is more likely that a small percentage of patients who are frail and immunocompromised will derive a large benefit (e.g., preventing an intensive care unit [ICU] admission) while the vast majority of patients will experience minimal or no benefit. Identifying and treating only those patients at highest risk of hospitalization is therefore critical to maximizing the clinical benefit and cost-effectiveness of nirmatrelvir-ritonavir.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received patient input from the following patient groups: Gastrointestinal Society, Arthritis Consumer Experts (ACE), the Canadian Breast Cancer Network, Lung Health Foundation, Sickle Cell Awareness Group of Ontario, the International Federation on Ageing, and Save Your Skin Foundation. Information was gathered from patients mainly through online surveys and emails, along with focus groups and 1 phone interview. The survey conducted by the Save Your Skin Foundation included 38 patients with cancer from Canada, 18 of whom had received nirmatrelvir-ritonavir. The survey conducted by ACE included 12 patients with arthritis who had experience with nirmatrelvir-ritonavir. The Lung Health Foundation conducted a survey of 160 patients with various lung and respiratory conditions; demographic data were not collected in this survey or the survey conducted by ACE. The surveys did not provide information on patients’ experiences with alternate available COVID-19–specific pharmacologic treatments other than nirmatrelvir-ritonavir, and general difficulty accessing pharmacologic COVID-19 treatments was noted. It was suggested that those experiencing post–COVID-19 condition (also known as “long COVID,” meaning symptoms that continue or emerge after initial infection) may be prescribed puffers which patients reported as disruptive to daily activities. Most patients surveyed by ACE reported improved symptoms with nirmatrelvir-ritonavir within a few days of initiating therapy. Patients additionally reported side effects of diarrhea, nausea, and an unpleasant metallic taste.
No clinician input was received for this review.
Several points of consideration were provided by the drug plan input regarding drug eligibility, re-treatment, treatment duration, the potential for drug interactions, and resource use considerations. The plans sought clarification on the recommended eligibility for nirmatrelvir-ritonavir, specifically regarding the definition of “high risk of progression to severe COVID-19” and “confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.” The plans questioned whether patients would ever be eligible for a longer treatment duration (i.e., 10 days) or re-treatment with nirmatrelvir-ritonavir. Lastly, the plans expressed concerns surrounding the costs of testing to confirm infection, and the costs of laboratory monitoring for potential drug interactions.
Several of these concerns were addressed in the sponsor’s model.
The costs and quality of life impacts of post–COVID-19 condition were captured in the sponsor’s model.
Diarrhea was included as an adverse event (AE).
In addition, CADTH addressed some of these concerns as follows.
In the budget impact analysis, CADTH sought to align the eligible population (i.e., those at high risk of progression) with expert input and clinical practice guidelines.
CADTH was unable to address the following concerns raised from stakeholder input.
Re-treatment with nirmatrelvir-ritonavir was not considered in the sponsor’s or CADTH’s base case.
The costs of confirmatory COVID-19 testing were not considered.
Laboratory monitoring for potential drug interactions was not considered.
Economic Review
The current review is for nirmatrelvir-ritonavir (Paxlovid) for mild to moderate COVID-19.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of nirmatrelvir-ritonavir compared with SoC; SoC was a basket comparator comprising over-the-counter and off-label steroid medications (no specific treatment for COVID-19). The modelled population comprised adult patients with positive results of direct SARS-CoV-2 viral testing, who were at high risk for progression to severe COVID-19, including hospitalization or death. The modelled population is consistent with the Health Canada indication and reimbursement request, and is aligned with the EPIC-HR trial.1,2 As per the EPIC-HR trial, high risk was defined as having 1 or more of the following characteristics: aged 60 years or older; body mass index greater than 25 kg/m2; cigarette smoking; immunosuppressive disease (including HIV infection with CD4 cell count < 200 mm3 and viral load < 400 copies/mL) or prolonged iatrogenic immunosuppression; chronic lung, cardiovascular, kidney, or sickle cell disease; hypertension; diabetes, cancer, neurodevelopmental disorders, or other medically complex conditions; or medical-related technological dependence.2
Nirmatrelvir and ritonavir are co-packaged in cartons supplying a 5-day dose (the maximum treatment course). The recommended dose is 300 mg nirmatrelvir (two 150 mg tablets) and 100 mg ritonavir (one 100 mg tablet) with all 3 tablets taken together orally twice daily for 5 days.1 For patients with renal impairment, the dose is 150 mg nirmatrelvir and 100 mg ritonavir twice daily for 5 days.1 The sponsor-submitted cost for nirmatrelvir-ritonavir was $1,288.88 for the full 5-day treatment course.3 The comparator was SoC, consisting of a basket of over-the-counter and off-label steroid medications (no specific treatment for COVID-19). No cost was assumed for SoC.
The clinical outcomes of interest were QALYs and life-years over a 10-year time horizon. Discounting (1.5% per annum) was applied to both costs and outcomes and a monthly cycle length was used. The base-case perspective was that of the Canadian publicly funded health care payer.
Model Structure
The sponsor submitted a short-term acute care decision tree followed by a postdischarge Markov model. All patients entered the model in the decision tree (acute care) and the outcomes of their inpatient hospitalization (if necessary), were modelled according to outcomes from the EPIC-HR trial.4 Patients were allocated to the decision tree according to the highest level of care received in hospital (emergency department, general ward, ICU with or without mechanical ventilation [MV]) or remained outpatients. From hospital, patients were either cured, transitioned to post–COVID-19 condition, or died. The sponsor’s decision tree is presented in Figure 2.
The Markov model was used to capture outcomes for patients still alive postinfection. Patients were treated differently depending on if they had received MV in hospital, if they had transitioned to post–COVID-19 condition, or if both had occurred. The sponsor’s Markov model is presented in Figure 3.
Model Inputs
Patient baseline characteristics were informed by the EPIC-HR study, which enrolled 2,246 outpatients with symptomatic COVID-19 who were at high risk for progression to severe COVID-19. The median age in the trial was 46 years, with 48.9% of participants being female and 100% being unvaccinated.4
Allocation into the decision tree for patients receiving nirmatrelvir-ritonavir or SoC was based on the results of the EPIC-HR study in patients who were treated for COVID-19 within 5 days of symptom onset. As noted previously, patients could require emergency department visits, hospitalizations with varying levels of care, be managed as an outpatient, or die. As the EPIC-HR study did not provide information on the highest level of care received by those dying, this information was derived from published sources.5,6 post–COVID-19 condition, characterized by symptoms of COVID-19 such as fatigue, shortness of breath, general pain and discomfort, trouble sleeping, and cognitive disruptions lasting for more than 12 weeks after infection was assumed to occur in 15% of adults who were not hospitalized for their COVID-19 infection.7 A systematic review published in 2023 found an increased odds ratio of developing post–COVID-19 condition in those who were hospitalized.8
The probability of death for cured individuals not receiving MV was similar to the general population of people living in Canada.9 Patients who had received MV at any point were assumed to be at a 33% increased risk of death due to respiratory muscle weakness and other post-MV complications.10,11
The sponsor’s model included all-grade treatment-emergent AEs occurring in greater than 2% of patients in at least 1 treatment arm. The AEs included were diarrhea, dysgeusia, increased fibrin D-dimer, increased alanine aminotransferase, and pneumonia.4
The baseline utility value in the model for the average patient was according to that of the population of people living in Canada, calculated as 0.888 based on Guertin et al.12 Disutilities were also applied due to COVID-19 symptoms, hospitalization, and natural aging. The disutility for COVID-19 symptoms was –0.27, and for hospitalization in the ward, ICU without MV, and ICU with MV there were additional disutilities of –0.11, –0.36, and –0.56, respectively.11,13 An additional annual disutility of –0.097 was applied for post–COVID-19 condition symptoms and decreasing disutilities were applied for 5 years post-MV.11,14 One-time utility decrements were applied for AEs.15
The model included drug acquisition costs, COVID-19–related health care resources, and costs to manage AEs. Drug acquisition costs have been previously described. The costs of COVID-19 hospitalizations were obtained from the Canadian Institute for Health Information data, with published sources used to determine cost per type of hospitalization.5,16 The cost for a general ward, ICU without MV, and ICU with MV hospital stay was $20,097, $45,755, and $68,633, respectively, which reflects data up to March 2023.5 The cost of an emergency department visit was $348.17 The costs to manage AEs were weighted by their frequency and were negligible.3
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar.
CADTH identified an error in the sponsor’s pharmacoeconomic model which affected the results (described in more detail in the Critical Appraisal section). CADTH corrected this error in the sponsor’s base case. The probabilistic findings of the corrected sponsor’s model are presented in the following.
Base-Case Results
In the sponsor’s base-case analysis, treatment with nirmatrelvir-ritonavir was associated with fewer costs (–$42) and higher QALYs (0.020) than SoC (Table 3). Nirmatrelvir-ritonavir was dominant and cost-effective at a $50,000 per QALY gained threshold in 100% of iterations compared to SoC. However, less than 1% of incremental QALYs were gained during the trial period (i.e., 28 days) while the remainder were accrued afterwards. Full disaggregated results of the sponsor’s economic evaluation are available in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results (Corrected)
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SoC ($/QALY) |
|---|---|---|---|---|---|
SoC | 1,672 | Reference | 8.017 | Reference | Reference |
Nirmatrelvir-ritonavir | 1,630 | –42 | 8.036 | 0.020 | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SoC = standard of care; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.3
Sensitivity and Scenario Analysis Results
The sponsor included several scenario analyses involving alternate assumptions for the time horizon, discount rate, duration of MV and post–COVID-19 condition, and number of days before treatment. All these scenarios had minimal impact on the results; nirmatrelvir-ritonavir remained dominant or cost-effective at a $50,000 per QALY gained threshold. The sponsor also conducted a scenario including remdesivir as a treatment option. In this scenario, nirmatrelvir-ritonavir was less costly (incremental costs: –$1,776) and equally effective than remdesivir (incremental QALYs: less than –0.0001).
The sponsor included a scenario analysis from a societal perspective in which patients were assumed to miss work due to COVID-19. For nonhospitalized patients, 1 week of work loss was assumed and for hospitalized patients, the work time lost was assumed equal to the hospitalization length of stay. Employment rate and average weekly earnings were obtained from Statistics Canada.18 Results of this analysis were similar to the sponsor’s base case as nirmatrelvir-ritonavir was associated with fewer costs and higher QALYs than SoC. The incremental cost savings in the societal perspective were higher than in the base case from the payer perspective due to fewer inpatients missing work in the nirmatrelvir-ritonavir treatment group.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
The submitted evidence base does not reflect the treatment landscape for COVID-19 at the time of this review. The primary basis for the economic model was the EPIC-HR study, a phase II/III randomized controlled trial conducted from July 2021 to April 2022. During this time the Delta variant was most prominent which is biologically distinct from the variant of COVID-19 circulating at present.19,20 This difference was emphasized by the clinical experts consulted by CADTH, who highlighted that data from the EPIC-HR trial are not externally generalizable to patients infected with Omicron and later variants of COVID-19. Furthermore, the EPIC-HR trial was conducted in patients who were unvaccinated, which is also not reflective of the state of public health in Canada at the time of this review in which 81% of people have received a primary course of vaccines.21 As noted in the CADTH clinical review, while it appears that nirmatrelvir-ritonavir remained effective throughout the Omicron wave, the effectiveness of treatment was considerably reduced in patients who were vaccinated. In addition, data from Ontario from February 2021 to April 2023 indicate that COVID-19–related hospitalizations (and deaths) were highest among individuals who were unvaccinated compared to those who had completed their primary vaccine series with or without additional boosters.22 Thus, the benefits of nirmatrelvir-ritonavir are expected to be lower in the vaccinated population at the time of this review. These differences represent a fundamental challenge in interpreting the results from the sponsor’s submitted evidence dossier and accompanying pharmacoeconomic model which are based on the EPIC-HR study. The clinical experts strongly emphasized that an economic model based on EPIC-HR trial data is unable to meaningfully answer the research question of whether nirmatrelvir-ritonavir is cost-effective for the treatment of mild to moderate COVID-19 at the time of this review.
The sponsor provided 3 observational studies to supplement data gaps for individuals who are vaccinated, which are also included in the Health Canada indication for nirmatrelvir-ritonavir.23-25 CADTH identified additional observational studies through grey literature searches and consultation with clinical experts.20,26 Strengths of these studies included more recent data relevant to an Omicron variant of COVID-19, along with including significant numbers of individuals who were vaccinated. However, due to the observational nature of these studies they are subject to limitations, primarily a volunteer bias. The experts noted that patients most likely to seek out pharmacological treatment with nirmatrelvir-ritonavir are likely more health conscious and adherent than those managing COVID-19 symptoms with bedrest or over-the-counter medications. Despite these limitations, clinical experts supported the use of more recent observational studies to help inform the pharmacoeconomic model rather than the EPIC-HR study, which studied nirmatrelvir-ritonavir in a strain of the virus that is no longer circulating.
As part of the base case, in consultation with clinical experts, CADTH used data from Schwartz et al. to inform the decision tree in the economic model, using the sponsor-provided option to do so.25 Compared to the other submitted observational studies, this study was conducted in Ontario (a CADTH-participating jurisdiction) and was composed of a highly vaccinated population (> 90% of patients had received ≥ 2 vaccine doses).25
The sponsor’s model incorrectly linked AE disutilities to health state resource utilization costs. When calculating the disutility due to AEs, the sponsor’s model included an erroneous formula which referenced the health state health care utilization costs. The presence of this transcription error was acknowledged by the sponsor.
CADTH corrected this programming error in the sponsor’s base case. The sponsor’s results presented in this report reflect the updated pharmacoeconomic model. Accordingly, the CADTH base case was derived using this corrected model as a starting point.
Additional limitations were identified but were not considered to be key limitations. These limitations are outlined subsequently.
Potential for misclassification of hospitalization. Clinical experts noted that anecdotal evidence suggests individuals who were frail presenting to hospital between 2020 and 2023 for reasons other than COVID-19, but who are subsequently found to be infected with COVID-19 at the time of admission, may have their reason for hospitalization misclassified as being due to COVID-19 instead of the primary cause in hospital registries. Thus, the true hospitalization rate and length of stay for a COVID-19 infection may be influenced by the length of stay required to treat the underlying condition (e.g., pneumonia). This has an unknown effect on the cost-effectiveness results, as these individuals might have otherwise had their COVID-19 infection remain undiagnosed and therefore, not treated with nirmatrelvir-ritonavir.
The sponsor’s Markov structure did not allocate patients correctly. The sponsor’s model structure was based on a decision tree, informed by the EPIC-HR study, followed by a Markov model. In this model, patients who were allocated to the emergency department arm of the decision tree were assumed to remain there for the duration of the model time horizon, and only exited this state to the death state via transition probabilities associated with background mortality. In reality, patients who visit the emergency department for any reason would eventually be discharged as outpatients, and therefore should have transitioned to the outpatient state in the model. This does not appear to have affected the model results, however, as the cost for an emergency department visit was only applied once and utilities were the same between this and the outpatient health state.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients having once received MV are at increased risk of mortality thereafter. | Appropriate, aligns with published literature. |
Utilities and disutilities related to post–COVID-19 condition and various health states were derived from different sources. | Not appropriate. However, disutilities due to hospitalizations, ICU stays, MV, and post–COVID-19 condition do not substantially impact the results of the economic evaluation. |
ICU = intensive care unit; MV = mechanical ventilation.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. These changes, summarized in Table 5, included changing the source of efficacy data and fixing a modelling formula.
The CADTH base-case analysis found that nirmatrelvir-ritonavir was associated with 0.002 additional QALYs at an additional cost of $897. Therefore, the ICER of nirmatrelvir-ritonavir was $442,082 per QALY gained compared to SoC. A summary of the CADTH stepped analysis and base-case results can be found in Table 6.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s base case and the CADTH base case (Table 7). This analysis demonstrated that a price reduction of 62% would be necessary to achieve cost-effectiveness at a $50,000 per QALY gained threshold in the CADTH base case.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Programming error | AE disutilities linked to health care resource utilization costs | AE disutilities linked to health state occupancy |
Changes to derive the CADTH base case | ||
1. Source of efficacy data | EPIC-HR trial27 | Schwartz et al.25 |
CADTH base case | Correction 1 + reanalysis 1 | |
AE = adverse event.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results (Deterministic)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (corrected) | SoC | 1,674 | 8.0424 | Reference |
Nirmatrelvir-ritonavir | 1,631 | 8.0622 | Dominant | |
CADTH reanalysis 1 and base case | SoC | 1,092 | 8.0595 | Reference |
Nirmatrelvir-ritonavir | 1,988 | 8.0615 | 437,093 | |
CADTH reanalysis 1 and base case (probabilistic) | SoC | 1,089 | 8.0406 | Reference |
Nirmatrelvir-ritonavir | 1,986 | 8.0427 | 442,082 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SoC = standard of care.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for nirmatrelvir-ritonavir vs. SoC ($/QALY) | |
|---|---|---|
Price reduction (cost per treatment course) | Sponsor base case | CADTH reanalysis |
No price reduction ($1,289) | Dominant | $442,082 |
10% ($1,160) | Dominant | $378,484 |
20% ($1,031) | Dominant | $314,887 |
30% ($902) | Dominant | $251,289 |
40% ($773) | Dominant | $187,691 |
50% ($644) | Dominant | $124,093 |
60% ($516) | Dominant | $60,496 |
70% ($387) | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SoC = standard of care; vs. = versus.
Additionally, CADTH explored the inclusion of remdesivir in scenario analysis, as was done in the sponsor’s original submission. Results were similar to the analysis performed by the sponsor: nirmatrelvir-ritonavir was less costly (incremental costs: –$1,418) and equally effective as remdesivir (incremental QALYs: < –0.0007).
Additionally, the CADTH clinical review indicated an NNT of 62 (95% confidence interval, 44 to 77) to prevent 1 case of severe COVID-19, based on Schwartz et al.25 By multiplying the NNT by the cost of nirmatrelvir-ritonavir ($1,288.88) a cost of $79,911 is obtained — the cost to prevent 1 case of severe COVID-19. If this is compared to the cost of a general ward hospital stay ($20,097),5 a price reduction of approximately 75% is required to achieve cost neutrality. Other studies assessed in the CADTH clinical report are included in Table 8.
The CADTH clinical review also highlighted Dormuth et al. as a relevant observational study.26 This was a retrospective cohort study of patients at increased vulnerability to complications from COVID-19 performed in British Columbia, Canada. Clinical experts indicated that the inclusion criteria for this study were representative of a high-risk population. In this study, patients were categorized into different cohorts based on their clinical vulnerability. The NNT from this study ranged from 40 (patients who were severely immunocompromised) to 75 (patients with selected medical conditions such as severe respiratory and metabolic disorders) to avoid a COVID-19–related hospitalization or death from any cause. This results in price reductions ranging from approximately 61% to 79% for the cost of nirmatrelvir-ritonavir to be equivalent to 1 general ward stay.
The CADTH clinical review also reported an NNT of 19 from the EPIC-HR study to avoid a COVID-19–related hospitalization or death from any cause.4 CADTH has already highlighted the external generalizability issues with the EPIC-HR study that limit the applicability of this estimate.
Table 8: Characteristics of Studies and NNTs Assessed in the CADTH Clinical Report
Study characteristics | EPIC-HR2 | Dryden-Peterson et al.28 | Hedvat et al.29 | Schwartz et al.25 | Dormuth et al. — CEV126 | Dormuth et al. — CEV226 | Dormuth et al. — CEV326 |
|---|---|---|---|---|---|---|---|
Population | Unvaccinated, at high risk for progression | Vaccinated, Omicron predominant | Solid organ transplant recipients | Vaccinated, Omicron predominant | Vaccinated, increased vulnerability to COVID-19 complications | ||
Region | International | Massachusetts and New Hampshire | New York | Ontario | British Columbia | ||
Proportion vaccinated | 0% | 92% | 82% | 93% | 98% | 95% | 94% |
NNT | 19 | 250 | 5 | 62 | 40 | 60 | 75 |
Definition of NNT | COVID-19–related hospitalization or death from any cause | Hospitalization within 14 days or death within 28 days | COVID-19–related hospitalization or death | COVID-19–related hospitalization or death from any cause within 30 days | COVID-19–related hospitalization or death from any cause | ||
Total cost ($1,289 × NNT) | $24,489 | $322,221 | $6,444 | $79,911 | $51,555 | $77,333 | $96,666 |
CEV1 = clinically extremely vulnerable 1 (severely immunocompromised); CEV2 = clinically extremely vulnerable 2 (moderately immunocompromised); CEV3 = clinically extremely vulnerable 3 (not immunocompromised but have medical conditions that place them at higher risk for complications from COVID-19 infection); NNT = number needed to treat.
Given the uncertainty of the true NNT, CADTH explored the impact of different assumptions versus the cost of different levels of care in hospital. Figure 1 presents the total drug acquisition cost of nirmatrelvir-ritonavir based on different NNTs. As the NNT increases, so does the total cost of nirmatrelvir-ritonavir. For context, the average cost of different hospitalizations (i.e., ward or ICU) were included and are represented by the horizontal lines. For example, a general ward admission ($20,097 – highlighted by the bottom yellow line) is cost equivalent to an NNT of approximately 16 (i.e., treating 16 individuals with nirmatrelvir-ritonavir). An ICU stay without MV ($45,755 – highlighted by the middle orange line) is cost equivalent at an NNT of approximately 36, and an ICU stay with MV ($68,633 – highlighted by the top red line) is cost equivalent at an NNT of approximately 53. When the cost for a given NNT (represented by blue shading) is lower than the cost of a given hospitalization (i.e., the horizontal lines), this suggests nirmatrelvir-ritonavir may lead to cost savings in the health care system, when considering the cost of nirmatrelvir-ritonavir and hospital admissions only. When the cost for a given NNT is higher than that of the hospitalization, this suggests the use of nirmatrelvir-ritonavir will result in increased costs, without price reductions.
Figure 1: Total Drug Acquisition Cost of Nirmatrelvir-Ritonavir Based on Different NNT Thresholds
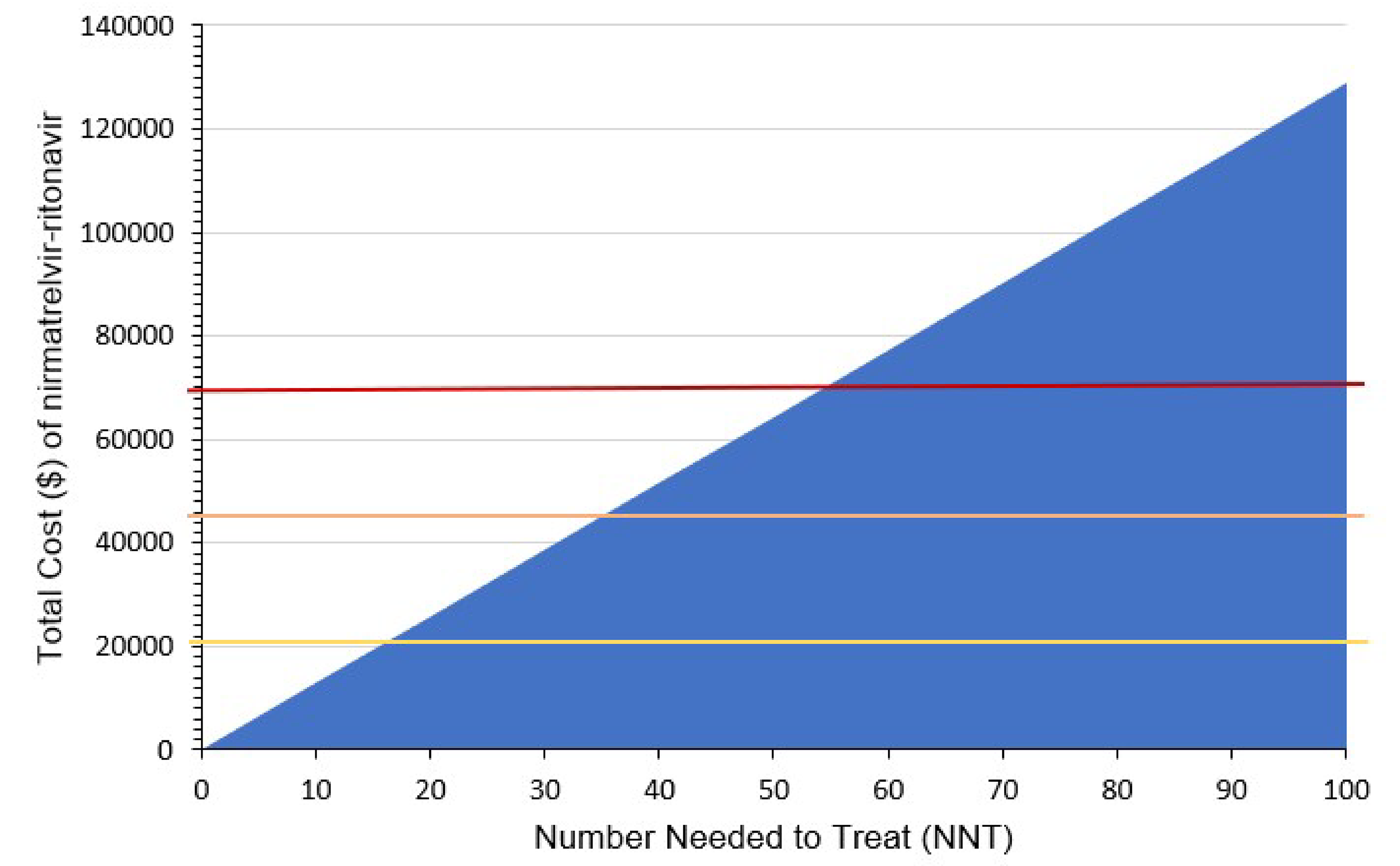
NNT = number needed to treat.
Note: The bottom yellow line is for a general ward admission, the middle orange line is for an ICU stay without mechanical ventilation, and the top red line is for ICU stay with mechanical ventilation.
Issues for Consideration
The CADTH base case predicts 0.002 incremental QALYs (or 18.4 quality-adjusted life-hours) with the use of nirmatrelvir-ritonavir compared to SoC for mild to moderate COVID-19, which is an average across all patients. In reality, it is more likely that a small percentage of patients who are frail and immunocompromised will derive a large benefit (e.g., preventing an ICU hospitalization) while the vast majority of patients will experience no benefit. As the economic analysis considers the full population, preferentially treating the individuals at highest risk of progression and death will improve the cost-effectiveness of nirmatrelvir-ritonavir, as will foregoing treatment in those unlikely to derive any benefit.
The product monograph for nirmatrelvir-ritonavir requires patients to have had a positive result of direct SARS-CoV-2 viral testing.1 However, the availability of tests is decreasing with decreasing rates of COVID-19 and tests are not as accessible as they were during the height of the pandemic. For example, Ontario has discontinued distribution of free rapid antigen tests.30 In addition, clinical experts consulted by CADTH suggested that results of rapid antigen tests be confirmed with polymerase chain reaction testing to minimize treating any false positives with nirmatrelvir-ritonavir. However, this would result in increased health care and laboratory resources.
Overall Conclusions
In the EPIC-HR pivotal randomized controlled trial, nirmatrelvir-ritonavir reduced the incidence of COVID-19–related hospitalization or death from any cause through day 28 compared with placebo. While the results were statistically significant, overall, the magnitude of effect with nirmatrelvir-ritonavir was considered relatively small. In addition, as noted in the clinical review, the EPIC-HR study did not include patients who were vaccinated or patients who had COVID-19 in the past, and it was performed at a time when the Omicron variant was not yet circulating. Finally, the trial was performed in a population that is not considered at high risk for progressing to severe disease, as defined in clinical practice, at the time of this review. These differences represent a fundamental challenge in interpreting the results from the sponsor’s submitted evidence dossier and accompanying pharmacoeconomic model which are based on the EPIC-HR study. The sponsor submitted 3 observational studies to bridge the evidence gap from the EPIC-HR study. These studies suggested that nirmatrelvir-ritonavir retained efficacy against the Omicron variant of concern, but that the effectiveness of the drug was considerably reduced in adequately vaccinated populations.
CADTH made 1 base case change, in consultation with clinical experts, and fixed a programming error in the sponsor’s model. CADTH used the efficacy data from an observational study, Schwartz et al., rather than the EPIC-HR study to inform the base case, as this study more accurately reflected the state of the population at risk for COVID-19 today (e.g., vaccination and exposure to COVID-19 infections). The CADTH base case resulted in incremental costs of $897 and a benefit in QALYs of 0.002 (or < 1 day of perfect health), an ICER of $442,082 per QALY gained for nirmatrelvir-ritonavir compared to SoC. In CADTH’s base case, for nirmatrelvir-ritonavir to be considered cost-effective at a $50,000 per QALY gained threshold, the drug cost of nirmatrelvir-ritonavir would need to be $494 per treatment course, reflecting a price reduction of approximately 62%.
The findings of CADTH’s base case differ from the sponsor’s due to the choice of clinical efficacy sources which better reflect the understanding and experience with COVID-19 at the time of this review. Since the effectiveness of the drug was considerably reduced in adequately vaccinated populations, nirmatrelvir-ritonavir was no longer cost-saving in CADTH’s base case because the cost of the treatment course itself is no longer offset by cost savings in hospitalizations, as was the case in the sponsor’s analysis. Thus, a price reduction is required to achieve cost-effectiveness at conventionally accepted thresholds. An alternative approach is to consider the NNT to avoid 1 hospitalization, 62 as reported by Schwartz et al. Compared to the cost of a general ward admission, CADTH calculated a price reduction of 75% would be required to ensure cost neutrality to health systems budgets.
Results of this analysis are driven by the source of efficacy data used. Since the majority of patients (> 90%) in both the sponsor’s and CADTH’s analysis will not require hospitalization, even on SoC, the effectiveness of nirmatrelvir-ritonavir is limited to patients who potentially would require hospitalization. Though the CADTH base case predicts incremental QALY gains of 0.002 per patient, this is an average of the cohort, and it is unlikely that 1 single patient would experience this magnitude of benefit. In reality, it is more likely that a small percentage of patients who are frail and immunocompromised will derive a large benefit (e.g., preventing an ICU hospitalization) while the vast majority of patients will experience minimal or no benefit. Identifying and treating only those patients at highest risk of hospitalization is therefore critical to maximizing the clinical benefit and cost-effectiveness of nirmatrelvir-ritonavir.
References
1.PrPAXLOVID™ (nirmatrelvir tablets; ritonavir tablets): tablets, 150 mg nirmatrelvir; 100 mg ritonavir co-packaged for oral use [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2023.
2.Hammond J, Leister-Tebbe H, Gardner A, et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19. New Engl J Med. 2022;386(15):1397-1408. PubMed
3.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: PAXLOVID™ (nirmatrelvir tablets; ritonavir tablets), 150 mg nirmatrelvir; 100 mg ritonavir co-packaged for oral use. Kirkland (QC): Pfizer; 2023.
4.Pfizer. Final Full Clinical Study Report (Protocol C4671005) - Data on file [sponsor supplied reference]. 2022.
5.Canadian Institute for Health Information. COVID-19 hospitalization and emergency department statistics [sponsor supplied reference]. 2023; https://www.cihi.ca/en/covid-19-hospitalization-and-emergency-department-statistics__;!!H9nueQsQ!9pVTjIDS7lJSXAp6t_RQyCoGp-oZ6qp1oXLmintMkE1ksEanqrPBVa0Gr3a2D482AM4QY-JKCcQZKZlzBkKSvdQ21pn1JmGNXg$. Accessed September 12, 2023.
6.Murthy S, Archambault PM, Atique A, et al. Characteristics and outcomes of patients with COVID-19 admitted to hospital and intensive care in the first phase of the pandemic in Canada: a national cohort study. CMAJ Open. 2021;9(1):E181-E188. PubMed
7.Government of Canada. Post COVID-19 condition (long COVID) [sponsor supplied reference]. 2023; https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/symptoms/post-covid-19-condition.html__;!!H9nueQsQ!9pVTjIDS7lJSXAp6t_RQyCoGp-oZ6qp1oXLmintMkE1ksEanqrPBVa0Gr3a2D482AM4QY-JKCcQZKZlzBkKSvdQ21pl6Fm3w8A$. Accessed September 12, 2023.
8.Tsampasian V, Elghazaly H, Chattopadhyay R, et al. Risk Factors Associated With Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern Med. 2023;183(6):566-580. PubMed
9.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2023 Sep 12.
10.Lone NI, Gillies MA, Haddow C, et al. Five-Year Mortality and Hospital Costs Associated with Surviving Intensive Care. Am J Respir Crit Care Med. 2016;194(2):198-208. PubMed
11.Sheinson D, Dang J, Shah A, Meng Y, Elsea D, Kowal S. A Cost-Effectiveness Framework for COVID-19 Treatments for Hospitalized Patients in the United States. Adv Ther. 2021;38(4):1811-1831. PubMed
12.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
13.Padula WV, Malaviya S, Reid NM, et al. Economic value of vaccines to address the COVID-19 pandemic: a U.S. cost-effectiveness and budget impact analysis. J Med Econ. 2021;24(1):1060-1069. PubMed
14.UpToDate. Clinical and physiologic complications of mechanical ventilation: Overview [sponsor supplied reference]. 2023; https://www.uptodate.com/contents/clinical-and-physiologic-complications-of-mechanical-ventilation-overview . Accessed September 12, 2023.
15.Sullivan PW, Ghushchyan V. Preference-Based EQ-5D index scores for chronic conditions in the United States. Med Decis Making. 2006;26(4):410-420. PubMed
16.Dasta JF, McLaughlin TP, Mody SH, Piech CT. Daily cost of an intensive care unit day: the contribution of mechanical ventilation. Crit Care Med. 2005;33(6):1266-1271. PubMed
17.Canadian Institute for Health Information. Hospital spending - Focus on the emergency department [sponsor supplied reference]. 2020; https://www.cihi.ca/sites/default/files/document/hospital-spending-highlights-2020-en.pdf. Accessed September 12, 2023.
18.Statistics Canada. Table 14-10-0222-01 Employment, average hourly and weekly earnings (including overtime), and average weekly hours for the industrial aggregate excluding unclassified businesses, monthly, seasonally adjusted [sponsor supplied reference]. 2023; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410022201. Accessed September 12, 2023.
19.Centers for Disease Control and Prevention. CDC Museum COVID-19 Timeline. Atlanta (GA): Centers for Disease Control and Prevention; 2023: https://www.cdc.gov/museum/timeline/covid19.html.
20.Lin D, Fadel F, Huang S, Milinovich A, Sacha G, Bartley P. Nirmatrelvir or Molnupiravir Use and Severe Outcomes From Omicron Infections. JAMA Netw Open. 2023;6(9):e2335077. PubMed
21.Government of Canada. COVID-19 vaccination: Vaccination coverage. 2023; https://health-infobase.canada.ca/covid-19/vaccination-coverage/.
22.Public Health Ontario. Severe Outcomes among Confirmed Cases of COVID-19 Following Vaccination in Ontario: December 14, 2020 to April 23, 2023. Toronto (ON): Public Health Ontario; 2023: https://www.publichealthontario.ca/-/media/Documents/nCoV/epi/covid-19-epi-confirmed-cases-post-vaccination.pdf?rev=3a3ead21e75640499dc626cc5283d141&sc_lang=en.
23.Kaboré JL, Laffont B, Diop M, et al. Real-World Effectiveness of Nirmatrelvir/Ritonavir on Covid-19-Associated Hospitalization Prevention: A Population-Based Cohort Study in the Province of Québec, Canada. Clin Infect Dis. 2023.
24.Lewnard JA, McLaughlin JM, Malden D, et al. Effectiveness of nirmatrelvir-ritonavir in preventing hospital admissions and deaths in people with COVID-19: a cohort study in a large US health-care system. Lancet Infect Dis. 2023;23(7):806-815. PubMed
25.Schwartz KL, Wang J, Tadrous M, et al. Population-based evaluation of the effectiveness of nirmatrelvir-ritonavir for reducing hospital admissions and mortality from COVID-19. CMAJ. 2023;195(6):E220-E226. PubMed
26.Dormuth C, Kim J, Fisher A, Piszczek J, Kuo I. Nirmatrelvir-ritonavir and COVID-19 mortality and hospitalization among patients with vulnerability to COVID-19 complications. JAMA Netw Open. 2023;6(10):e2336678. PubMed
27.Hammond J, Leister-Tebbe H, Gardner A, et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19. N Engl J Med. 2022;386(15):1397-1408. PubMed
28.Dryden-Peterson S, Kim A, Kim A, al e. Nirmatrelvir plus ritonavir for early COVID-19 in a Large US Health System. Ann Intern Med. 2023.
29.Hedvat J, Lange N, Salerno D, al. e. COVID-19 therapeutics and outcomes among solid organ transplant recipients during the Omicron BA.1 era. Am J Transplantation. 2022;22(11):2682-2688. PubMed
30.City of Toronto. COVID-19: Testing. 2023; https://www.toronto.ca/community-people/health-wellness-care/health-programs-advice/respiratory-viruses/covid-19/covid-19-what-you-should-do/covid-19-testing/. Accessed Nov 1, 2023.
31.DeltaPA. [Ottawa (ON)]: IQVIA; 2023: https://www.iqvia.com/. Accessed 2023 Oct.
32.Gilead Sciences Canada I. Press Releases: An Open Letter from Daniel O'Day, Chairman & CEO, Gilead Sciences. 2020; https://www.publichealthontario.ca/-/media/Documents/nCoV/epi/covid-19-epi-confirmed-cases-post-vaccination.pdf?rev=3a3ead21e75640499dc626cc5283d141&sc_lang=en. Accessed October 19, 2023.
33.Lau VI, Fowler R, Pinto R, et al. Cost-effectiveness of remdesivir plus usual care versus usual care alone for hospitalized patients with COVID-19: an economic evaluation as part of the Canadian Treatments for COVID-19 (CATCO) randomized clinical trial. CMAJ Open. 2022;10(3):E807-E817. PubMed
34.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: PAXLOVID™ (nirmatrelvir tablets; ritonavir tablets), 150 mg nirmatrelvir; 100 mg ritonavir co-packaged for oral use. Kirkland (QC): Pfizer; 2023.
35.Ramage-Morin PL, Polsky JY. Health-related concerns and precautions during the COVID-19 pandemic: A comparison of Canadians with and without underlying health conditions [sponsor supplied reference]. Ottawa: Statistics Canada; 2020: https://www.doi.org/10.25318/82-003-x202000500001-eng.
36.The Conference Board of Canada. Understanding the Gap: A Pan-Canadian Analysis of Prescription Drug Insurance Coverage [sponsor supplied reference]. 2017.
37.Statistics Canada. Table 17-10-0005-01 Population estimates on July 1st, by age and sex [sponsor supplied reference]. 2023:
38.Statistics Canada. Table 13-10-0114-01 Life expectancy and other elements of the complete life table, three-year estimates, Canada, all provinces except Prince Edward Island [sponsor supplied reference]. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed September 12, 2023.
39.Ipsos. Market research Wave 5: Latest 3/12 months confirmed, symptomatic infection rate; fielded Jan4-17 - Data on file [sponsor supplied reference]. 2023.
40.World Health Organization. Living guidance for clinical management of COVID-19 [sponsor supplied reference]. 2021: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2.
41.BC Covid Therapeutics Committee. Clinical Practice Guide for Therapeutics in Patients with Mild-Moderate COVID-19 [sponsor supplied reference]. 2023.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in Table 9 have been deemed to be appropriate based on feedback from clinical experts and CADTH-participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 9: CADTH Cost Comparison Table for the Treatment of COVID-19
Treatment | Strength | Form | Price | Recommended dosage | Treatment course | Cost per treatment course |
|---|---|---|---|---|---|---|
Nirmatrelvir-ritonavir (Paxlovid) | 150 mg / 100 mg | 10 or 20 tablets nirmatrelvir (depending on patient’s renal status) 10 tablets ritonavir One carton per treatment course containing 5 daily-dose blister cards (2 or 4 tablets nirmatrelvir and 2 tablets ritonavir each) | $1,288.8848a | 300 mg nirmatrelvir with 100 mg ritonavir twice daily for 5 days For renal impairment: 150 mg nirmatrelvir with 100 mg ritonavir twice daily for 5 days | 5 days | $1,289 |
Polymerase inhibitors | ||||||
Remdesivir (Veklury) | 5 mg/mL | 100 mg Powder for solution for infusion | $515.4600b | 200 mg on day 1, 100 mg daily thereafter | 3 to 10 days | $1,546 to $5,155 |
aSponsor’s submitted price.3
bPrice obtained from IQVIA DeltaPA (accessed October 2023).31 However, data from DeltaPA indicate this price may be out-of-date, with no current price provided. The cost per course provided here aligns with a published press release on the cost of remdesivir, $2,340 US dollars per 5-day course.32 This is also the cost assumed by the sponsor (after converting to Canadian dollars), who cited a Canadian economic evaluation of remdesivir.33
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The population studied in the EPIC-HR trial does not reflect the population eligible for nirmatrelvir-ritonavir at present due to differences in baseline risk, vaccination status, and COVID-19 variant. The population studied in the pivotal trial is not relevant. |
Model has been adequately programmed and has sufficient face validity | No | CADTH identified errors in the sponsor’s pharmacoeconomic model which are described in the Critical Appraisal section. |
Model structure is adequate for decision problem | No | Refer to the first limitation. The decision problem has not been addressed. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
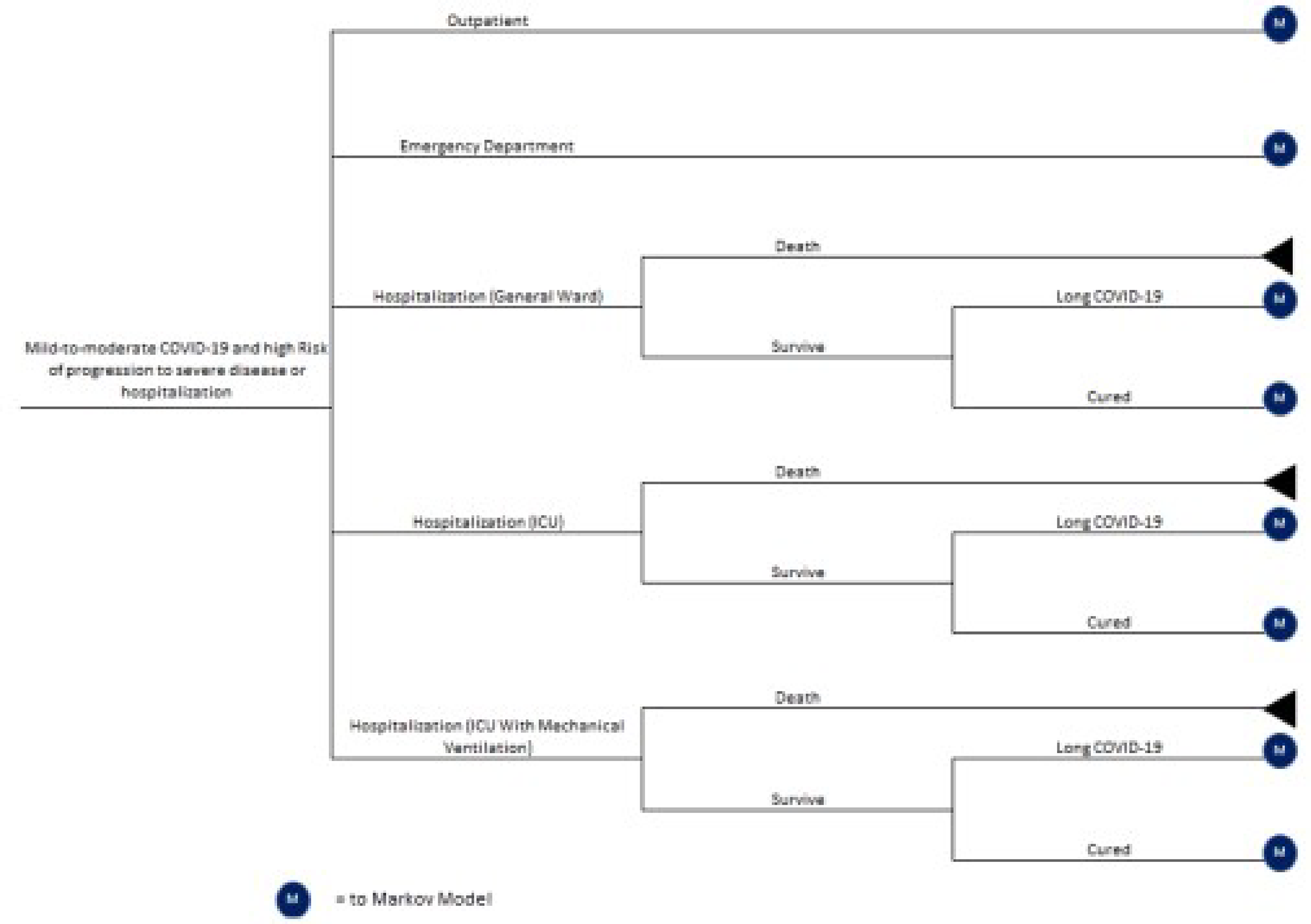
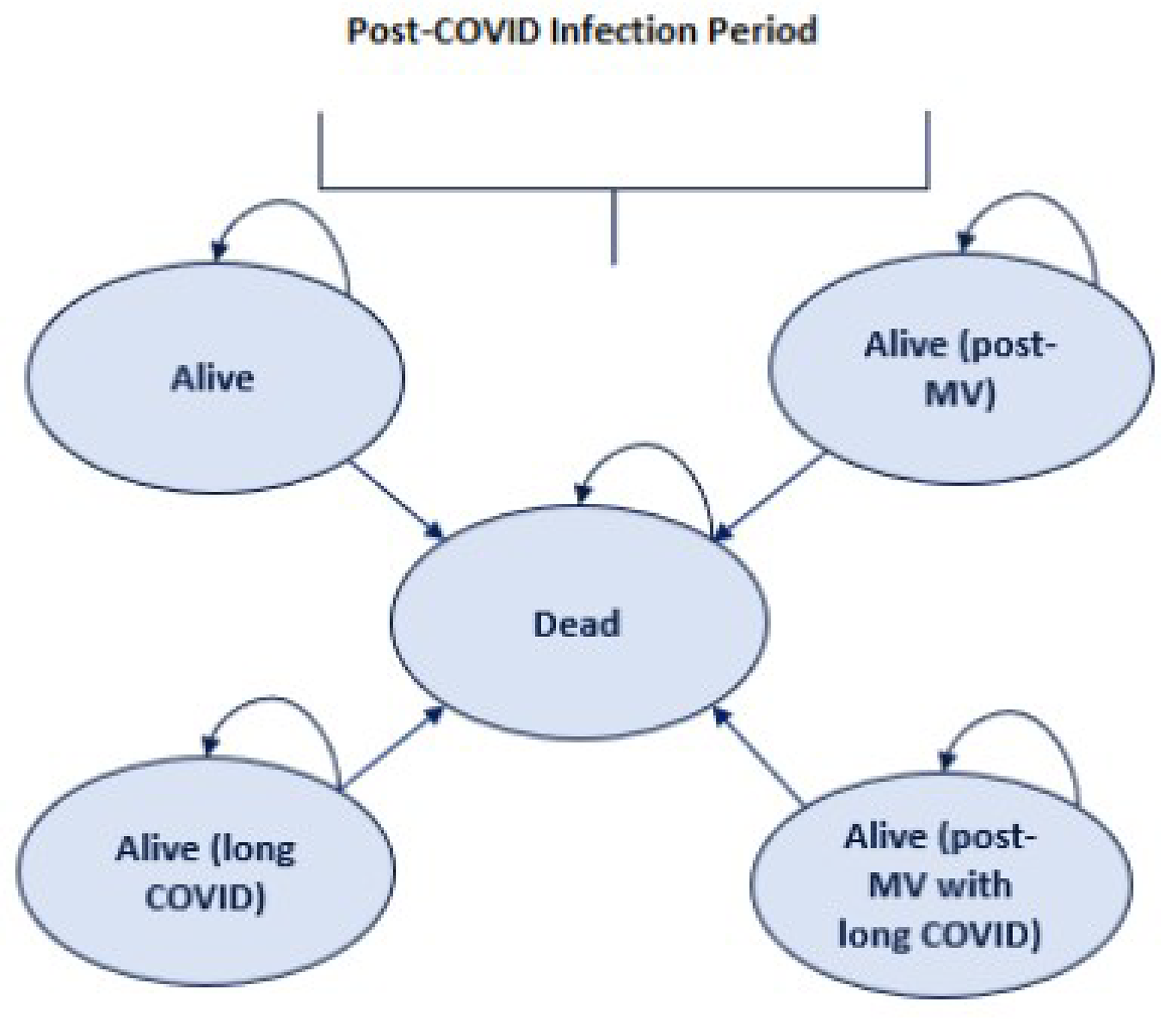
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of the Sponsor’s Economic Evaluation Results (Corrected)
Parameter | Nirmatrelvir-ritonavir | SoC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 9.173 | 9.153 | 0.020 |
Outpatient | 9.049 | 8.427 | 0.622 |
ED visit | 0.053 | 0.175 | −0.122 |
Hospitalization (general ward) | 0.071 | 0.477 | −0.406 |
Hospitalization (ICU/no MV) | 0.000 | 0.041 | −0.041 |
Hospitalization (ICU/MV) | 0.000 | 0.032 | −0.032 |
Discounted QALYs | |||
Total | 8.036 | 8.017 | 0.020 |
Outpatient | 7.929 | 7.384 | 0.545 |
ED visit | 0.046 | 0.154 | −0.107 |
Hospitalization (general ward) | 0.062 | 0.418 | −0.356 |
Hospitalization (ICU/no MV) | 0.000 | 0.036 | −0.036 |
Hospitalization (ICU/MV) | 0.000 | 0.028 | −0.028 |
Disutility in health states | −0.001 | −0.003 | 0.002 |
Disutility due to AEs | 0.000a | 0.000a | 0.000 |
Discounted costs ($) | |||
Total | 1,630 | 1,672 | -42 |
Acquisition | 1,289 | 0 | 1,289 |
Outpatient | 181 | 168 | 12 |
ED visit | 2 | 7 | −5 |
Hospitalization (general ward) | 154 | 1,042 | −888 |
Hospitalization (ICU/no MV) | 0 | 205 | −205 |
Hospitalization (ICU/MV) | 0 | 239 | −239 |
AEs | 4 | 11 | −7 |
ICER ($/QALY) | Dominant | ||
AE = adverse event; ICER = incremental cost-effectiveness ratio; ICU = intensive care unit; LY = life-year; MV = mechanical ventilation; QALY = quality-adjusted life-year; SoC = standard of care.
aThe disutility due to AEs for nirmatrelvir-ritonavir and SoC is less than 0.0001 for both treatments.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Nirmatrelvir-ritonavir | SoC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 9.172 | 9.171 | 0.002 |
Outpatient | 8.980 | 8.833 | 0.147 |
ED visit | 0.000 | 0.000 | 0.000 |
Hospitalization (general ward) | 0.167 | 0.293 | −0.126 |
Hospitalization (ICU/no MV) | 0.015 | 0.027 | −0.012 |
Hospitalization (ICU/MV) | 0.010 | 0.017 | −0.007 |
Discounted QALYs | |||
Total | 8.043 | 8.041 | 0.002 |
Outpatient | 7.875 | 7.746 | 0.129 |
ED visit | 0.000 | 0.000 | 0.000 |
Hospitalization (general ward) | 0.146 | 0.257 | −0.111 |
Hospitalization (ICU/no MV) | 0.013 | 0.024 | −0.010 |
Hospitalization (ICU/MV) | 0.009 | 0.015 | −0.006 |
Disutility in health states | −0.001 | −0.002 | 0.001 |
Disutility due to AEs | 0.000 | 0.000 | 0.000 |
Discounted costs ($) | |||
Total | 1,986 | 1,089 | 897 |
Acquisition | 1,289 | 0 | 1,289 |
Outpatient | 179 | 176 | 3 |
ED visit | 0 | 0 | 0 |
Hospitalization (general ward) | 364 | 640 | −276 |
Hospitalization (ICU/no MV) | 77 | 134 | −58 |
Hospitalization (ICU/MV) | 73 | 128 | −55 |
AEs | 4 | 11 | −7 |
ICER ($/QALY) | 442,082 | ||
Scenario Analyses
CADTH has described the results of the scenario analysis with remdesivir in the main text of this report.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The submitted budget impact analysis (BIA) assessed the introduction of nirmatrelvir-ritonavir for the treatment of adult patients with COVID-19 at high risk of disease progression.34 The analysis was undertaken from the perspective of the Canadian public drug plans using an epidemiologic-based approach. The analysis used a 3-year time horizon (2024 to 2026) with 2023 as a base year. The sponsor’s base-case analysis included drug acquisition costs only.
The reference case included SoC only while the new drug scenario included nirmatrelvir-ritonavir and SoC. Nirmatrelvir-ritonavir was assumed to capture 100% of market share if reimbursed. Key inputs to the BIA are documented in Table 14.
Key assumptions included:
All patients 60 years of age and older were assumed to be eligible for nirmatrelvir-ritonavir.1,34
18% of patients aged 18 to 59 were assumed to be immunocompromised or with a chronic condition and were therefore eligible for nirmatrelvir-ritonavir.35
Of confirmed COVID-19 cases in Canada, 27% occurred in those 60 years of age and older and 73% occurred in those aged 18 to 59. Public coverage rates of 98.48% for those 65 and older and 62.76% for those aged 18 to 64 were assumed to apply to these age groups despite a slight discrepancy in age categorization (i.e., 60 versus 65 years and older).36
Remdesivir was included in a scenario analysis only.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Population size of CADTH-participating jurisdictions (18+) | 25,632,301 / 26,055,233 / 26,476,77237 |
Proportion of adults 60 years of age and older | 30.88%38 |
Proportion of adults aged 18 to 59 | 69.12%38 |
Proportion immunocompromised or with a chronic condition | 18%35 |
Symptomatic COVID-19 infection rate | 26% / 27% / 28%39 |
Proportion of patients with mild to moderate symptoms | 80%40 |
Proportion of patients seeking treatment | 11%39 |
Public coverage in those aged 65 years of age and older | 98.48%36 |
Public coverage in those aged 18 to 64 | 62.76%36 |
Number of patients eligible for drug under review | 183,741 / 193,956 / 204,394 |
Market uptake (3 years) | |
Uptake (reference scenario) SoC | 100% / 100% / 100% |
Uptake (new drug scenario) Nirmatrelvir-ritonavir SoC | 100% / 100% / 100% 0% / 0% / 0% |
Cost of treatment (per patient) | |
Cost per treatment course Nirmatrelvir-ritonavir SoC Remdesivir | $1,289 $0 $2,925 |
COVID-19 = coronavirus 2019; SoC = standard of care.
Summary of the Sponsor’s BIA Results
The estimated budget impact of the introduction of nirmatrelvir-ritonavir for the treatment of COVID-19 in adult patients at high risk for progression was $247,088,096 in year 1, $261,040,638 in year 2, and $275,333,908 in year 3, for a 3-year total of $783,462,642.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The size of the eligible population is highly uncertain. As noted in the CADTH appraisal of the cost-utility analysis, the population studied in the EPIC-HR trial was mostly unvaccinated, and not representative of the population eligible for nirmatrelvir-ritonavir today. The product monograph for nirmatrelvir-ritonavir was based on the EPIC-HR trial and lists numerous risk factors for progression to severe COVID-19 including age greater than 60, various chronic diseases (e.g., diabetes), immunosuppressive disease or treatment, and active cancer.1 In the sponsor’s base case, 18% of those aged 18 to 59 and 100% of those aged 60 and older were eligible for nirmatrelvir-ritonavir. The 18% represents the proportion of adults aged 35 to 49 with either a compromised immune system or a chronic condition, retrieved from a Statistics Canada Health Report.35 However, this number is uncertain due to a mismatch in age categorization; 12% of those aged 15 to 34 and 28% of those aged 50 to 64 also met these criteria.35
The clinical experts indicated that, in clinical practice, eligibility for nirmatrelvir-ritonavir would be much more restrictive due to serious drug-drug interactions with ritonavir, the risks of which must be balanced against the potential for benefit with the treatment. The experts suggested a minimum age of 70 would be more appropriate and that, for those under 70, treatment would be restricted to transplant recipients and those with depleted B-cells, which are expected to make up a minority of those less than 70 years old.41
CADTH sought to align the eligible population with expert opinion, clinical practice guidelines, and published observational data.25,41 In the sponsor’s base case, those aged 60 and older were automatically eligible for nirmatrelvir-ritonavir; CADTH changed the minimum age for automatic eligibility to 70. For those less than 70 years old, CADTH referred to the study by Schwartz et al. which found that 27.5% of patients who had received nirmatrelvir-ritonavir were less than 70 years of age.25 Using this percentage, CADTH adjusted the proportion of patients less than 70 years old with a chronic or immunocompromised condition (8.72%) until the COVID-19 case breakdown reflected that of the Schwartz study (27.5% less than 70, 72.5% greater than 70).
As part of the CADTH analysis, inputs were modified to estimate the eligible population size in the manner outlined previously.
The proportion of patients seeking treatment is uncertain. The sponsor assumed that 11% of patients with mild to moderate COVID-19 at high risk of progression would seek pharmacologic treatment, based on confidential market access research.39 This number is uncertain, as the proportion of patients seeking treatment will likely be linked to disease severity, which fluctuates over time based on vaccination rates, prior exposure, and COVID-19 variant. The clinical experts consulted by CADTH felt this number was overestimated, and suggested that the proportion of patients receiving nirmatrelvir-ritonavir in the study by Schwartz et al. (2023) could be used to estimate this rate. This observational study conducted in Ontario included 177,545 patients for whom data on their use of nirmatrelvir-ritonavir were available.25 And while the cost of nirmatrelvir-ritonavir was covered for all Ontarians at risk in this study, only 8,876 (5%) received the drug, which may be more reflective of a vaccinated patient population in which previous COVID-19 infection may also have occurred.
CADTH acknowledges the limitations of this estimate, particularly because the Schwartz study enrolled any patient with COVID-19 regardless of their risk of progression to severe disease. However, 42% of patients who received nirmatrelvir-ritonavir and 15% of those who did not receive the drug were classified as high risk by the Ontario COVID-19 Science Advisory Table, and, as mentioned above, the majority were greater than 70 years of age.25 Ultimately, the proportion of patients seeking treatment is uncertain and directly proportional to the estimate of budget impact.
In scenario analysis, CADTH reduced the proportion of patients seeking treatment to 5%.
CADTH did not include the cost of testing to confirm COVID-19 diagnosis.
The symptomatic COVID-19 infection rate is uncertain. The sponsor used a symptomatic COVID-19 infection rate of 25% in the baseline year, based on confidential market access research.39 Data informing this assumption were provided to CADTH but were limited, and ‘symptomatic COVID-19’ was not defined. The clinical experts consulted by CADTH were unable to validate this estimate or provide an alternate source for the rate of COVID-19 infection and indicated that this estimate could change with new variants.
In scenario analysis, CADTH tested symptomatic infection rates of 15% and 35%.
CADTH Reanalyses of the BIA
Based on the identified considerations, CADTH explored different population sizes in reanalyses.
Table 15: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH reanalyses | ||
1. Eligible population size | 60+: 100% eligible 18 to 59: 18% eligible | 70+: 100% eligible 18 to 69: 8.72% eligible |
CADTH reanalysis | Reanalysis | |
The results of the CADTH stepwise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17. Based on the CADTH reanalysis, the estimated budget impact of the introduction of nirmatrelvir-ritonavir for the treatment of mild to moderate COVID-19 in patients at high risk of progression, where the population can be restricted, is $125,207,708 in year 1, $132,323,111 in year 2, and $139,617,714 in year 3, for a 3-year total of $397,148,534.
CADTH performed several scenario analyses to explore uncertainty in the eligible population estimates, particularly as it pertained to symptomatic infection rate and the proportion of patients seeking treatment. Results of CADTH’s scenario analyses indicate that the true 3-year budget impact of the reimbursement of nirmatrelvir-ritonavir is likely between $180,522,061 and $544,177,374.
Table 16: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $783,462,642 |
CADTH reanalysis | $397,148,534 |
BIA = budget impact analysis.
Table 17: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $247,088,096 | $261,040,638 | $275,333,908 | $783,462,642 | |
Budget impact | $0 | $247,088,096 | $261,040,638 | $275,333,908 | $783,462,642 | |
CADTH reanalysis | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $125,207,708 | $132,323,111 | $139,617,714 | $397,148,534 | |
Budget impact | $0 | $125,207,708 | $132,323,111 | $139,617,714 | $397,148,534 | |
CADTH scenario analysis: 5% seeking treatment | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $56,912,595 | $60,146,869 | $63,462,597 | $180,522,061 | |
Budget impact | $0 | $56,912,595 | $60,146,869 | $63,462,597 | $180,522,061 | |
CADTH scenario analysis: 15% infection rate | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $77,050,897 | $83,314,551 | $89,754,245 | $250,119,694 | |
Budget impact | $0 | $77,050,897 | $83,314,551 | $89,754,245 | $250,119,694 | |
CADTH scenario analysis: 35% infection rate | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $173,364,519 | $181,331,671 | $189,481,184 | $544,177,374 | |
Budget impact | $0 | $173,364,519 | $181,331,671 | $189,481,184 | $544,177,374 |
BIA = budget impact analysis.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.