CADTH Reimbursement Review
Cannabidiol (Epidiolex)
Sponsor: Jazz Pharmaceuticals Canada, Inc.
Therapeutic area: Lennox-Gastaut syndrome
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine transaminase
ASM
antiseizure medication
AST
aspartate transaminase
CEA
Canadian Epilepsy Alliance
CI
confidence interval
EEG
electroencephalogram
GRADE
Grading of Recommendations, Assessment, Development, and Evaluations
HRQoL
health-related quality of life
IQR
interquartile range
IVRS
interactive voice response system
LGS
Lennox-Gastaut syndrome
MID
minimally important difference
MNAR
missing not at random
OLE
open-label extension
QOLCE
Quality of Life in Childhood Epilepsy
QOLIE-31-P
Quality of Life in Epilepsy, version 2
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SUDEP
sudden unexpected death in epilepsy
VNS
vagus nerve stimulation
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Cannabidiol (Epidiolex), 100 mg/mL, oral solution |
Sponsor | Jazz Pharmaceuticals Canada |
Indication | As adjunctive therapy for seizures associated with LGS, DS, or TSC in patients 2 years of age and older |
Reimbursement requesta | Adjunctive therapy for the treatment of seizures associated with LGS in patients 2 years of age and older |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 15, 2023 |
Recommended dose | Up to a maximum recommended dosage of 10 mg/kg twice daily (20 mg/kg/day). Recommended dosing adjustments for notable subpopulations per the product monograph. |
DS = Dravet syndrome; LGS = Lennox-Gastaut syndrome; NOC = Notice of Compliance; TSC = tuberous sclerosis complex.
aDeviation requests for this reimbursement request were accepted on June 21, 2023, and September 15, 2023.
Introduction
Lennox-Gastaut syndrome (LGS) is a lifelong, complex epilepsy syndrome associated with multiple seizure types that vary across patients. LGS presents in the first 4 years of life (peak age of onset: 3 to 5 years) in children who had otherwise experienced age-appropriate development and is associated with refractory and multiple treatment-resistant seizure types, cognitive and behavioural impairments, and poor outcomes into adulthood.1-4 LGS has various etiologies, and patients experience multiple seizure types with distinctive electroencephalogram (EEG) features, which include tonic seizures (stiffening of the body, upward eye gaze, dilated pupils, and altered breathing patterns) and atypical absence seizures (staring spells), myoclonic jerks (sudden muscle jerks), tonic or atonic “drops” (brief loss of muscle tone), generalized tonic-clonic seizures (muscle stiffness and rhythmic jerking), and focal seizures.3 Atonic and tonic seizures can be accompanied by dangerous falls or “drop seizures” that often lead to injury.5 Indeed, LGS is considered a life-threatening condition associated with high rates of sudden unexpected death in epilepsy (SUDEP) and a risk of death among children 14 times higher than among the US general population.5-7 Currently, LGS is diagnosed using clinical criteria; there is no specific diagnostic test and no specific biologic markers for the diagnosis of LGS.6,8 LGS affects between 3% and 10% of children with epilepsy, more commonly males. The peak age for onset is 3 to 5 years, with extreme incidence occurring in the first and 10th years of life.9 The prevalence of LGS in Canada, as estimated by the sponsor, is 12 in 100,000 people.10
The goal of treatment is to achieve seizure freedom.3,6,8,11 In Canada, the only drugs currently indicated specifically for LGS are rufinamide12 and lamotrigine,13 both as add-on treatments to other antiseizure medications (ASMs). While lamotrigine is available through the Ontario Drug Benefit program, rufinamide must be obtained through the Exceptional Access Program.14 In addition to ASMs, most patients use enteral medications; dietary therapies such as ketogenic, modified Atkins, or low–glycemic index diets; neuromodulation with vagus nerve stimulation (VNS) or deep brain stimulation; and nonresective surgeries such as corpus callosotomy. Patients can benefit from surgical resection when the source of seizure activity can be identified. The clinical experts consulted by CADTH noted that purified cannabidiol from a licensed producer (“artisanal CBD” or medical cannabis) is available in Canada and has been used extensively for the treatment of drug-resistant LGS in children and adults, albeit at lower doses than were used in clinical trials of cannabidiol.
Cannabidiol received a Notice of Compliance from Health Canada on November 15, 2023, through the standard review pathway. The Health Canada indication for cannabidiol is for use as adjunctive therapy for the treatment of seizures associated with LGS, Dravet syndrome, or tuberous sclerosis complex in patients aged 2 years and older. The sponsor requested that CADTH review each neurologic disorder as a separate submission.
The product monograph–recommended starting dosage of cannabidiol is 2.5 mg/kg twice daily.15 After 1 week, the dosage should be increased to a maintenance dosage of 5 mg/kg twice daily. Based on individual clinical response and tolerability, each dose can be increased in weekly increments of 2.5 mg/kg, administered twice daily, up to a maximum recommended dosage of 10 mg/kg twice daily (20 mg/kg/day). For patients in whom a more rapid titration from 10 mg/kg/day to 20 mg/kg/day is warranted, the dose may be increased no more frequently than every other day. The product monograph also provides a dosing adjustment for patients with moderate or severe hepatic impairment, due to the risk of hepatocellular injury related to cannabidiol.15
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol 100 mg/mL oral solution for use as adjunctive therapy for the treatment of seizures associated with LGS in patients aged 2 years and older.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from the clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Patient group input was provided by the Canadian Epilepsy Alliance (CEA). The CEA is a network of organizations supporting and advocating for people living with epilepsy and their families. Patient input was sourced from the knowledge and experiences of patients, caregivers, clinicians, volunteers, donors, and funders, collected from 24 member associations. According to input from the CEA, current treatments may fail in 30% of patients with epilepsy. According to the input, people living with uncontrolled epilepsy are often socially isolated due to stigma and to fear of rejection in social, work, and educational settings. Patients often experience depression and anxiety upon initial diagnosis and often continuously experience these conditions if ASMs stop working. Caregivers and family members are also impacted by epilepsy as their lives revolve around the seizures experienced by patients under their care. Anxiety among caregivers is common as they worry about when the next seizure will occur, the consequences of the epilepsy, and how to navigate social gatherings (e.g., a young person with epilepsy gets invited to a birthday party). In addition, caregivers often experience compassion fatigue since they cannot leave the person with epilepsy alone, are often sleep deprived due to sleep interruptions or anxiety, and can be affected by side effects the patient may experience from medications (e.g., mood swings, sexual dysfunction, suicidal thoughts, memory loss, fatigue, exhaustion). Both patients and caregivers emphasized the importance of treatment that results in seizure freedom. However, patients and caregivers noted that they would accept a treatment that resulted in a reduction in the absolute number of seizures, as even a reduction in seizure frequency could improve overall quality of life. Because people with intractable epilepsy are very often unemployed or underemployed, not covered under employer-funded insurance plans, and/or have restricted income, most drugs to treat their epilepsy are inaccessible. Accordingly, the CEA stressed the importance of new medications being placed on the provincial formulary so that patients with intractable epilepsy have access to novel treatments. Input provided by the CEA did not include experience with cannabidiol.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of LGS.
The clinical experts consulted by CADTH for the purpose of this review noted that, despite the multiple treatment options available, there are currently no treatments available to reverse the course of LGS. Moreover, the overall prognosis of LGS remains unfavourable, and not all patients experience response to the available treatments. The clinical experts added that there is a need for treatment that can meaningfully improve quality of life for patients and their caregivers. The clinical experts noted that, despite its novel mechanism of action compared to available therapies, cannabidiol does not address the underlying disease process any more than other available treatments. Accordingly, the clinical experts suggest that cannabidiol would complement other available treatments as a symptom management treatment. The clinical experts opined that cannabidiol could be combined with 1 or 2 first-line ASM. The clinical experts also felt that it would be reasonable to require adequate trials of 1 or 2 other ASMs before the use of cannabidiol. The clinical experts expected that the approval of cannabidiol would lead to a shift away from the use of medical cannabidiol in jurisdictions where cannabidiol is reimbursed by either public or private drug insurance plans. According to input from the clinical experts, it is difficult to predict which patients with LGS are most likely to benefit from cannabidiol. Patients who have not experienced response with multiple ASMs are generally less likely to experience response to the next ASM; however, these are the patients who are most in need of novel therapies. The clinical experts suggested that patients should be screened for treatment according to clinician judgment based on seizure characterization and frequency, etiology investigation, and previous ASMs trialled, along with EEG interpretation. According to the clinical experts’ input, a clinically meaningful response to treatment in epilepsy is assessed in terms of the median reduction in seizure frequency over 28-day periods, a reduction in the number of seizures of 50% or more, and seizure freedom rates (i.e., reduction of total seizures per day and seizure-free days per month). The clinical experts added that seizure frequency should be assessed every 4 weeks. The clinical experts also noted that improved quality of life for both patients and caregivers is an important secondary outcome. According to the clinical experts’ input, treatment with cannabidiol should be discontinued if patients develop persistent and progressive elevation of transaminases or recurrent vomiting and diarrhea, which would compromise the absorption of ASMs. In addition, treatment with cannabidiol should be reassessed if a patient develops status epilepticus with no other reasonable explanation. The clinical experts noted that the prescribing and monitoring of cannabidiol for LGS should be limited to neurologists who have special expertise in the management of epilepsy in pediatric or adult patients.
Clinician Group Input
No clinician group input was received with this submission.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for cannabidiol:
relevant comparators
considerations for initiation of therapy
considerations for continuation or renewal of therapy
considerations for discontinuation of therapy
considerations for prescribing of therapy
generalizability
care provision issues
system and economic issues.
Clinical Evidence
Systematic Review
Description of Studies
Two studies were included in the sponsor-conducted systematic review: the CARE 3 and CARE 4 trials.16,17
Both the CARE 3 and CARE 4 trials were multicentre, double-blind, phase III randomized controlled trials (RCTs) evaluating the efficacy of cannabidiol as adjunctive treatment in reducing drop seizure frequency in patients aged 2 to 55 years with a clinical diagnosis of LGS.
In the CARE 3 trial, 225 patients across 29 sites in 4 countries (US, Spain, France, and UK) were randomized 1:1:1 to receive treatment with cannabidiol 20 mg/kg/day (n = 76), cannabidiol 10 mg/kg/day (n = 73), or volume-matched placebo (n = 76). Patients in the placebo group were split into 2 equivalent cohorts: half receiving 10 mg/kg/day (n = 38), and half receiving 20 mg/kg/day (n = 38). In the CARE 4 trial, 171 patients across 24 sites in 3 countries (US, Netherlands, and Poland) were randomized to receive treatment with either cannabidiol 20 mg/kg/day (n = 86) or volume-matched placebo (n = 86). The randomization in both the CARE 3 and CARE 4 trials was stratified by age group (2 to 5 years, 6 to 11 years, 12 to 17 years, and 18 to 55 years). Patients were titrated from a starting dosage of 2.5 mg/kg/day up to 10 mg/kg/day over 7 days, or up to 20 mg/kg/day over 11 days, and remained at this dosage level for the duration of the treatment period. Assigned treatments were add-ons to 1 or more background ASMs.
The primary efficacy end point for both the CARE 3 and CARE 4 trials was reduction in the number of drop seizures (per 28 days), compared with placebo, in patients with LGS. A “drop seizure” was defined as an attack or spell (atonic, tonic, or tonic-clonic) involving the entire body, trunk, or head that led or could have led to a fall, an injury, slumping in a chair, or the patient’s head hitting a surface. The key secondary outcome of interest was the number of patients who experienced a 50% reduction in the number of drop seizures at the end of the treatment period. Other outcomes that were assessed in the CARE 3 and CARE 4 trials included the following: proportions of patients who experienced at least a 25%, at least a 75%, or a 100% reduction in the number of drop seizures at the end of the treatment period; number of inpatient hospitalizations due to epilepsy; and health-related quality of life (HRQoL) as assessed by the Quality of Life in Childhood Epilepsy (QOLCE) questionnaire, for patients aged 2 to 18 years, or the Quality of Life in Epilepsy, version 2 (QOLIE-31-P) questionnaire, for patients aged 19 years and older, and by the number of drop seizure–free days.
In the CARE 3 trial, the mean age of the patients enrolled in the trial was 16.01 years (standard deviation [SD] = 10.77 years) in the cannabidiol 20 mg/kg/day group, 15.43 years (SD = 9.48 years) in the cannabidiol 10 mg/kg/day group, and 15.29 years (SD = 9.26 years) in the pooled placebo group. In the CARE 3 trial, the median number of drop seizures per 28 days at baseline was higher in the cannabidiol 10 mg/kg/day group (median = 86.90; interquartile range [IQR], 14.0 to 7,494.0) than in the cannabidiol 20 mg/kg/day group (median = 85.53; IQR, 13.0 to 1,092.0) and the pooled placebo group (median = 80.25; IQR, 8.7 to 1,278.3). The proportion of patients reporting convulsive seizures lasting longer than 30 minutes was higher in the cannabidiol 20 mg/kg/day group (10.5%) than in the cannabidiol 10 mg/kg/day group (2.7%) and the pooled placebo group (3.9%). Across all treatment groups, the mean number of prior ASMs used by patients was approximately 7 and the mean number of current ASMs being used at baseline was almost 3.
In the CARE 4 trial, the mean age of patients enrolled in the trial was 15.3 years (SD = 9.8 years) and 15.6 years (SD = 8.7 years) in the cannabidiol 20 mg/kg/day and the volume-matched placebo groups, respectively. The median number of drop seizures at baseline was higher in the volume-matched placebo group (median = 74.67; IQR, 11.2 to 3,174.6) than in the cannabidiol 20 mg/kg/day group (median = 71.43; IQR, 10.3 to 855.9). In both treatment groups, the mean number of prior ASMs used by patients was approximately 7 and the mean number of current ASMs being used at baseline was almost 3.
Efficacy Results
Percent Change From Baseline in Drop Seizure Frequency
At the end of the 14-week treatment period in the CARE 3 trial, a reduction in the median percent change in drop seizure frequency was associated with treatment with cannabidiol 20 mg/kg/day (median difference = –21.6%; 95% confidence interval [CI], –34.8 to –6.7; P = 0.0047) and cannabidiol 10 mg/kg/day (median difference = –19.2; 95% CI, –31.2 to –7.7; P = 0.0016) compared to the pooled placebo group.
At the end of the treatment period in the CARE 4 trial, a reduction in the median percent change in drop seizure frequency was associated with treatment with cannabidiol 20 mg/kg/day compared to volume-matched placebo (median difference = –17.2%; 95% CI, –30.3 to –4.1; P = 0.0135).
Reduction in the Number of Drop Seizures From Baseline of Greater Than or Equal to 50%
In the CARE 3 trial, during the treatment period, the difference in the proportion of patients who experienced at least a 50% reduction in the number of drop seizures from baseline between the cannabidiol 20 mg/kg/day group and the pooled placebo group was 25.0% (95% CI, 11.5% to 38.5%) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 21.1% (95% CI, 7.6% to 34.7%).
In the CARE 4 trial, the difference in the proportion of patients who experienced at least a 50% reduction in drop seizure frequency from baseline between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group was 20.7% (95% CI, 6.8% to 34.5%).
Reduction in the number of Drop Seizures From Baseline of Greater Than or Equal to 25%
In the CARE 3 trial, during the treatment period, the difference in the proportion of patients who experienced at least a 25% reduction in the number of drop seizure frequency from baseline between the cannabidiol 20 mg/kg/day group and the pooled placebo group was 18.4% (95% CI, 2.8% to 34.0%) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 19.6% (95% CI, 3.9% to 35.3%).
In the CARE 4 trial, the difference in the proportion of patients who experienced at least a 25% reduction in drop seizure frequency from baseline between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group was 20.4% (95% CI, 5.8% to 35.1%).
Reduction in the Number of Drop Seizures From Baseline of Greater Than or Equal to 75%
In the CARE 3 trial, during the treatment period, the difference in the proportion of patients who experienced at least a 75% reduction in the number of drop seizures from baseline between the cannabidiol 20 mg/kg/day group and the pooled placebo group was 22.4% (95% CI, 12.0% to 55.13%) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 8.3% (95% CI, 0.3% to 16.3%).
In the CARE 4 trial, the difference in the proportion of patients who experienced at least a 75% reduction in the number of drop seizures from baseline during the treatment period between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group was 11.5% (95% CI, 1.3% to 21.8%).
Reduction in the Number of Drop Seizures From Baseline of 100%
No patient experienced a 100% reduction in the number of drop seizures during the treatment period in either the CARE 3 or the CARE 4 trial.
Number of Inpatient Hospitalizations due to Epilepsy
In the CARE 3 trial, the number of patients who experienced 1 or more inpatient hospitalizations due to epilepsy was 7 (9.2%) in the cannabidiol 20 mg/kg/day group, 6 (8.2%) in the cannabidiol 10 mg/kg/day group, and 6 (7.9%) in the pooled placebo group.
In the CARE 4 trial, the number of patients who experienced 1 or more inpatient hospitalizations due to epilepsy was 10 (11.6%) and 5 (5.9%) in the cannabidiol 20 mg/kg/day and volumed-matched placebo groups, respectively.
QOLCE for Patients Aged 2 to 18 Years
In the CARE 3 trial, overall QOLCE scores were available for 33 patients (43.4%) in the cannabidiol 20 mg/kg/day group, 36 patients (49.3%) in the cannabidiol 10 mg/kg/day group, and 38 patients (50%) in the pooled placebo group. At baseline, the overall mean QOLCE scores were comparable across the cannabidiol 20 mg/kg/day group, the cannabidiol 10 mg/kg/day group, and the pooled placebo group, at 41.6 (SD = 15.6), 40.6 (SD = 15.4), and 41.4 (SD = 16.1), respectively. The adjusted mean treatment difference in change from baseline in overall QOLCE scores between the cannabidiol 20 mg/kg/day group and the pooled placebo group was –5.1 (95% CI, –11.4 to 1.2) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 1.6 (95% CI, –4.5 to 7.8).
In the CARE 4 trial, overall QOLCE scores were available for 26 patients (30.2%) and 38 patients (44.7%) in the cannabidiol 20 mg/kg/day group and the volumed-matched placebo group, respectively. At baseline, the overall mean QOLCE scores were comparable between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group, at 39.5 (SD = 12.6) and 39.1 (SD = 15.2), respectively. The adjusted mean treatment difference in change from baseline in overall QOLCE scores between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group was 3.7 (95% CI, –3.3 to 10.7).
QOLIE-31-P for Patients Aged 19 Years and Older
In the CARE 3 trial, total QOLIE-31-P scores were available for 13 patients in the cannabidiol 20 mg/kg/day group, 14 patients in the cannabidiol 10 mg/kg/day group, and 10 patients in the pooled placebo group. At baseline, the total mean QOLIE-31-P scores were 50.2 (SD = 16.6) in the cannabidiol 20 mg/kg/day group, 56.0 (SD = 19.2) in the cannabidiol 10 mg/kg/day group, and 62.5 (SD = 13.6) in the pooled placebo group. The adjusted mean treatment difference in change from baseline in total QOLIE-31-P scores between the cannabidiol 20 mg/kg/day group and the pooled placebo group was 2.9 (95% CI, –7.3 to 13.1) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 3.6 (95% CI, –7.0 to 14.3).
In the CARE 4 trial, total QOLIE-31-P scores were available for 14 patients (16.3%) in the cannabidiol 20 mg/kg/day group and 14 patients (16.5%) in the volume-matched placebo group. At baseline, the total QOLIE-31-P scores were comparable between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group at 55.8 (SD = 13.5) and 57.3 (SD = 19.5), respectively. The adjusted mean treatment difference in total QOLIE-31-P scores was not calculated due to the low number of patients who completed the assessment.
Drop Seizure–Free Days
In the CARE 3 trial, the mean number of drop seizure–free days had increased in all treatment groups at the end of the treatment period. Compared to placebo, treatment with cannabidiol 20 mg/kg/day was associated with an increase in the mean number of drop seizure–free days of 4.6 days (95% CI, 2.5 days to 6.8 days), while treatment with cannabidiol 10 mg/kg/day was associated with an increase of 3.3 days (95% CI, 1.2 days to 5.5 days).
In the CARE 4 trial, the mean number of drop seizure–free days had increased in both treatment groups at the end of the treatment period. Compared to volume-matched placebo, treatment with cannabidiol 20 mg/kg/day was associated with a mean increase in drop seizure–free days of 2.7 days (95% CI, 0.7 days to 4.7 days).
Other Outcomes
The following outcomes were noted as being meaningful by the patient group and the clinical experts consulted by CADTH but were not assessed in either the CARE 3 or CARE 4 trial: SUDEP rate, employment, and caregiver quality of life.
Harms Results
Adverse Events
In the CARE 3 trial, at least 1 adverse event (AE) was reported by 93.9% of patients in the cannabidiol 20 mg/kg/day group, 83.6% of patients in the cannabidiol 10 mg/kg/day group, and 72.4% of patients in the pooled placebo group.
In the CARE 4 trial, at least 1 AE was reported by 86.0% and 69.4% of patients in the cannabidiol 20 mg/kg/day and the volume-matched placebo group, respectively.
Serious Adverse Events
In the CARE 3 trial, at least 1 serious AE (SAE) was reported by 15.9% of patients in the cannabidiol 20 mg/kg/day group, 19.4% of patients in the cannabidiol 10 mg/kg/day group, and 10.5% of patients in the pooled placebo group.
In the CARE 4 trial, at least 1 SAE was reported by 23.3% and 4.7% of patients in the cannabidiol 20 mg/kg/day and the volume-matched placebo groups, respectively.
Treatment Discontinuation due to AEs
In the CARE 3 trial, discontinuation of treatment due to AEs was reported by 7.3% of patients in the cannabidiol 20 mg/kg/day group, 1.5% of patients in the cannabidiol 10 mg/kg/day group, and 1.3% of patients in the pooled placebo group.
In the CARE 4 trial, discontinuation of treatment due to AEs was reported by 14.0% and 1.2% of patients in the cannabidiol 20 mg/kg/day group and the volume-matched placebo group, respectively.
Mortality
There were no reported deaths in the CARE 3 trial. In the CARE 4 trial, 1 death was recorded (1.2% of patients) due to acute respiratory distress syndrome in the cannabidiol 20 mg/kg/day group.
Notable Harms
Notable harms of interest were related to nervous system disorders (i.e., somnolence, status epilepticus, and sedation), hepatocellular injury or investigation (i.e., increased levels of alanine transaminase [ALT] and aspartate transaminase [AST], bilirubin elevation, and serum transaminase elevation), and gastrointestinal disorders (i.e., diarrhea, vomiting, and constipation).
In the CARE 3 trial, somnolence, status epilepticus, and sedation were reported in 30.5%, 4.9%, and 3.7% of patients, respectively, in the cannabidiol 20 mg/kg/day group; in 20.9%, 10.4%, and 3.0% of patients, respectively, in the cannabidiol 10 mg/kg/day group; and in 5.3%, 3.9%, and 1.3% of patients, respectively, in the pooled placebo group. Increased levels of ALT, AST, and serum transaminase were reported in 4.9%, 3.7%, and 1.2% of patients, respectively, in the cannabidiol 20 mg/kg/day group; in 4.5%, 3.7%, and 1.5% of patients, respectively, in the cannabidiol 10 mg/kg/day group; and in 1.3%, 1.3%, and 0% of patients, respectively, in the pooled placebo group. The following investigations were not reported in the CARE 3 trial: abnormal liver function test, acute hepatic failure, and hepatotoxicity. Diarrhea, vomiting, and constipation were reported in 14.6%, 12.2%, and 4.9% of patients, respectively, in the cannabidiol 20 mg/kg/day group; in 10.4%, 6.0%, and 4.5% of patients, respectively, in the cannabidiol 10 mg/kg/day group; and in 7.9%, 11.8%, and 3.9% of patients, respectively, in the pooled placebo group.
In the CARE 4 trial, somnolence, sedation, and status epilepticus were reported in 15.1%, 8.1%, and 1.2% of patients, respectively, in the cannabidiol 20 mg/kg/day group and in 9.4%, 1.2%, and 1.2% of patients, respectively, in the volume-matched placebo group. The following hepatocellular injury or investigation AEs were reported in the cannabidiol 20 mg/kg/day group: increased ALT (9.3%), increased AST (7.0%), abnormal liver function test (4.7%), acute hepatic failure (3.5%), serum transaminase elevation (2.3%), hepatic failure (1.2%), and hepatotoxicity (1.2%). In the volume-matched placebo group, increased levels of ALT and AST were reported in 2.4% and 1.2% of patients, respectively. Diarrhea, vomiting, and constipation were reported in 18.6%, 10.5%, and 7.0% of patients, respectively, in the cannabidiol 20 mg/kg/day group and in 8.2%, 16.5%, and 4.7% of patients, respectively, in the volume-matched placebo group.
Critical Appraisal
Both the CARE 3 and CARE 4 trials were multicentre, double-blind phase III RCTs, designed in accordance with the European Medicines Agency Guideline on Clinical Investigation of Medicine Products in the Treatment of Epileptic Disorders and the FDA Guidelines for the Clinical Evaluation of Antiepileptic Drugs (Adults and Children).
In both trials, patients were randomized centrally using interactive voice response system (IVRS) technology, which is typically adequate for concealing allocation until treatment assignment. IVRS technology was also used to dispense the investigational product, allowing the treatment concealment for both patients and investigators. Although the CARE 3 trial included 4 treatment types (cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, volume-matched placebo 20 mg/kg/day, and volume-matched placebo 10 mg/kg/day), the study participants were randomized using a 1:1:1 randomization ratio to the cannabidiol 20 mg/kg/day treatment group, the cannabidiol 10 mg/kg/day treatment group, and the placebo treatment group. Patients in the placebo group were split in half to receive either the 20 mg/kg/day placebo or the 10 mg/kg/day placebo, and the study results were reported based on the pooled placebo group. While this approach is acceptable, it relies on the assumption that randomization was successful in each group. Differences in baseline characteristics between patients in the cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, and pooled placebo groups were noted in the following: proportion of patients reporting convulsive seizures longer than 30 minutes and reporting concomitant use of benzodiazepine derivatives. According to the clinical experts consulted by CADTH for the purpose of this review, because of the rarity of LGS, it is unknown if these differences in baseline characteristics could influence treatment response. At CADTH’s request, the sponsor reported that the assumptions related to splitting the placebo group and pooling results for analyses were not formally tested. However, the sponsor noted, as described in Clinical Study Report for the CARE 3 trial, that posthoc sensitivity analyses were conducted on the primary end point to determine if pooling the placebo group had an effect on the results. The analyses indicated that the comparisons of the efficacy response when cannabidiol 20 mg/kg/day and 10 mg/kg/day dosages were compared to their corresponding placebo dosages (i.e., 20 mg/kg/day (10 mg/kg/day, respectively) were consistent with the results of similar comparisons in the pooled analyses. In the CARE 4 trial, the 1:1 randomization ratio and the randomization stratification factors appeared appropriate, and no notable baseline imbalances were observed between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group.
In the CARE 3 trial, a higher proportion of patients in the cannabidiol 20 mg/kg/day group discontinued the study than in the cannabidiol 10 mg/kg/day and pooled placebo groups (approximately 12% versus approximately 3%). The higher discontinuation rate in the cannabidiol 20 mg/kg/day group appeared to be driven by AEs. In the CARE 4 trial, a higher proportion of patients in the cannabidiol 20 mg/kg/day group discontinued the study than in the volume-matched placebo group (9.3% versus 1.2%). The higher discontinuation rate in the cannabidiol 20 mg/kg/day group appeared to be driven by AEs. The application of the missing not at random (MNAR) assumption and sensitivity analysis exploring missing efficacy results due to treatment discontinuation suggest that bias due to uneven discontinuation was unlikely.
In both the CARE 3 and CARE 4 trials, all efficacy outcome questionnaires and assessments were to be completed by a caregiver. To maintain consistency, the same caregiver, if the patient had multiple caregivers, was to complete and answer the questionnaire and assessment. Seizure information in both studies was ascertained using an IVRS diary, while paper diaries were used to capture use of the investigational product, use of concomitant medications, and occurrence of AEs. According to input from the clinical experts, patient and parent or caregiver reports of seizures tend to be accurate for motor seizures but are not very reliable or accurate for nonmotor seizures. However, seizure diaries are the standard method of collecting data for clinical trials, and the International League Against Epilepsy recommends the use of dairies for collecting seizure frequency data.18 Both the CARE 3 and CARE 4 trials assessed HRQoL — outcomes deemed important by the patients and clinicians — using validated and reliable instruments: the QOLCE and QOLIE-31-P questionnaires. The double-blind nature of the trials minimized the risk of bias in the measurement of subjective items on the QOLCE and QOLIE-31-P questionnaires. However, comparative efficacy conclusions based on the HRQoL outcomes are limited since the QOLCE and QOLIE-31-P questionnaires were not part of the hierarchical testing procedure and because of the low completion rates across the treatment groups. Total QOLCE scores were available for 47.6% and 36.3% of patients in the CARE 3 and CARE 4 trials, respectively, while total QOLIE-31-P scores were available for 16.5% and 16.4% of patients in the CARE 3 and CARE 4 trials, respectively. Consequently, the assessment of HRQoL in both trials is at high risk of attrition bias, although the extent and direction of the bias cannot be determined since it is not clear if the patients who completed the questionnaires were systematically different from the patients who did not. As the completion rates were similar between the treatment groups within the CARE 3 and CARE 4 trials, there is little risk that attrition bias favoured any 1 treatment group.
The analysis of efficacy results in the CARE 3 and CARE 4 trials followed a defined statistical analysis plan. The primary and key secondary end points were addressed using a hierarchical gate-keeping procedure that controlled for type I errors. The sponsor conducted additional sensitivity analyses of the primary efficacy end point using the per-protocol analysis set and testing the MNAR assumption. In all scenarios, the sensitivity analyses were consistent with the primary efficacy analysis.
The clinical experts consulted by CADTH for the purpose of this review were unable to assess if the results of the CARE 3 and CARE 4 trials were applicable to the patients seen in the Canadian clinical setting. However, the clinical experts did note trial details that were applicable to the Canadian clinical setting and others that were not representative of the Canadian clinical setting. The clinical experts noted that the treatment periods in the CARE 3 and CARE 4 trials were long enough to detect a meaningful treatment response on seizures in patients with LGS; however, the clinical experts were uncertain if the treatment response observed could be sustained in the long-term. Moreover, a longer study period would be required to detect a treatment response on cognitive functioning. In the Canadian setting, where medicinal cannabis as adjunctive treatment for seizures associated with LGS can be accessed through the medical cannabis pathway supported by Health Canada, the clinical experts would not impose any sort of washout period before initiating pharmaceutical cannabidiol.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) assessment was based on the sponsor’s summary of clinical evidence, consultation with clinical experts, and input received from patient groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
change from baseline in number of drop seizures during the treatment period; proportion of patients who experienced a greater than or equal to 25%, greater than or equal to 50%, greater than or equal to 75%, or 100% reduction in the number of drop seizures from baseline
number of drop seizure–free days; and number of inpatient hospitalizations due to epilepsy
change from baseline in quality of life as measured by the QOLCE questionnaire (for patients aged 2 to 18 years) or the QOLIE-31-P questionnaire (for patients aged 19 years and older)
notable harms, including serious adverse events and hepatocellular injury.
For the pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for the outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.19,20
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The presence or absence of an important effect were based on thresholds informed by the clinical experts consulted for this review.
For the GRADE assessments, findings from the CARE 3 and CARE 4 trials were considered together and summarized narratively per outcome, because these studies were similar in population, interventions, design, and outcome measures.21
Table 2 presents the GRADE summary of findings for cannabidiol versus placebo.
Long-Term Extension Studies
To inform the longer-term safety and tolerability of cannabidiol as an adjunctive treatment in children and adults with inadequately controlled LGS, the results of 1 open-label extension (OLE) study — the CARE 5 trial — were summarized.22
Description of Study
The CARE 5 trial was a multicentre, single-arm, OLE, phase III study with the primary objective of evaluating the longer-term safety and tolerability of cannabidiol as adjunctive treatment in patients aged 2 years and older with LGS (N = 366) who had completed the CARE 3 and CARE 4 trials (the “core studies”). The long-term efficacy of cannabidiol as adjunctive treatment in patients aged 2 years and older with LGS was evaluated as the secondary objective of the CARE 5 trial. Patients enrolled in the CARE 5 trial received adjunctive cannabidiol in addition to their usual treatment; the trial consisted of a 2-week titration period, a maintenance period, and a 10-day taper period. Patients were titrated up to 10 mg/kg/day to 20 mg/kg/day cannabidiol using the recommended titration schedule. The patients continued at their 10 mg/kg/day to 20 mg/kg/day dosage throughout the maintenance period. During the maintenance period, dosing adjustments by the investigators were permitted should a patient experience intolerance (dose decrease) or require better seizure control (dose increase) until the optimal dose was achieved. A maximum dosage of 30 mg/kg/day was permitted, if deemed necessary by the investigator. For patients whose dose had been decreased, subsequent dose increases were considered provided the treatment was adequately tolerated. Following the end-of-treatment or withdrawal visit, doses were tapered at home (10% per day for 10 days) until the end-of-taper visit. Patients could receive treatment for up to 6 years (312 weeks after visit 1), depending on the
Table 2: Summary of Findings for Cannabidiol 10 mg/kg/day and Cannabidiol 20 mg/kg/day Versus Volume-Matched Placebo for Patients With Seizures Associated With
Outcome and follow-up | Patients, N (studies, N) | Effect | Certainty | What happens |
|---|---|---|---|---|
Reduction in the number of drop seizures | ||||
Median percent change from baseline in the number of drop seizures during the treatment period per 28-day cycle (95% CI) Follow-up: 14 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Moderatea | Cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day may result in little to no clinically important reduction in the median percent change from baseline for frequency of drop seizures during the treatment period when compared to placebo. |
Proportion of patients with ≥ 50% reduction in the number of drop seizures from baseline during the treatment period (95% CI) Follow-up: 14 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Moderateb | Cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day may result in a greater proportion of patients reporting a 50% or more reduction in drop seizures during the treatment period compared to placebo. |
Proportion of patients with ≥ 25% reduction in the number of drop seizures from baseline during the treatment period (95% CI)c Follow-up: 14 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Moderated | Cannabidiol 20 mg/kg/day may result in a greater proportion of patients reporting a 25% or more reduction in the number of drop seizures during the treatment period compared to placebo. Cannabidiol 10 mg/kg/day may result in little to no increase in the proportion of patients reporting a 25% or more reduction in number of drop seizures during the treatment period compared to placebo. |
Proportion of patients with ≥ 75% reduction in drop seizures from baseline during the treatment period (95% CI)c Follow-up: 14 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Lowe | Cannabidiol 20 mg/kg/day may result in a greater proportion of patients reporting a 75% or more reduction in number of drop seizures during the treatment period compared to placebo. Cannabidiol 10 mg/kg/day may result in little to no increase in the proportion of patients reporting a 75% or more reduction in number of drop seizures of during the treatment period compared to placebo. |
Proportion of patients with a 100% reduction in drop seizures from baseline during the treatment period (95% CI)c Follow-up: 14 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Lowf | Cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day may result in no difference in the proportion of patients reporting a 100% reduction in number of drop seizures during the treatment period compared to placebo. |
Seizure freedom | ||||
Change in the mean number of drop seizure–free days during the treatment periodc Follow-up: 14 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Moderateg | Cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day may result in a greater number of drop seizure–free days during the treatment period compared to placebo. |
HRQoL | ||||
Change in mean overall QOLCE score from baseline to end of treatmentc Follow-up: 14 weeks | 171 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Very lowh | Cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day likely result in little to no difference in HRQoL during the treatment period compared to placebo. |
Change in mean total QOLIE-31-P scores from baseline to end of treatmentc Follow-up: 14 weeks | 65 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Very lowi | Cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day likely result in little to no difference in HRQoL during the treatment period compared to placebo. |
Inpatient hospitalization due to epilepsy | ||||
Number of patients (%) reporting 1 or more inpatient hospitalizations for seizure during the treatment periodc Follow-up: 14 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Lowj | It is uncertain if cannabidiol 10 mg/kg/day or cannabidiol 20 mg/kg/day result in a difference in inpatient hospitalizations due to epilepsy during the treatment period compared to placebo. |
Harmsk | ||||
Serious adverse events, n (%) Follow-up: 20 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Moderatel | Cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day may result in an increase in severe adverse events compared with placebo. |
Hepatocellular injury, n (%) Follow-up: 20 weeks | 396 (2 RCTs) | CARE 3 trial
CARE 4 trial
| Moderatem | Cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day may result in an increase in hepatocellular injury compared with placebo. |
CI = confidence interval; HRQoL = health-related quality of life; LGS = Lennox-Gastaut syndrome; MID = minimally important difference; NE = not estimated; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = Quality of Life in Epilepsy, version 2; RCT = randomized controlled trial; SD = standard deviation.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the level of certainty being rated down are documented in the table footnotes.
aRated down 1 level for serious imprecision. In the CARE 3 trial, the 95% CI included the potential for no clinically meaningful benefit. In the absence of an empirically derived MID, a between-group difference of 25% was used as the clinically meaningful threshold, based on clinical expert input. Any increase (improvement) not reaching this threshold indicates there is uncertainty in the clinically meaningful treatment effect of cannabidiol compared with placebo. In the CARE 4 trial, the treatment effect estimates and the lower bounds of the 95% CI for the difference between groups included the possibility of a trivial effect (little to no difference) compared with placebo. In the absence of an empirically derived MID, a between-group difference of 25% was used as the clinically meaningful threshold, based on clinical expert input. Any increase (improvement) not reaching this threshold indicates there is uncertainty in the clinically meaningful treatment effect of cannabidiol compared with placebo. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
bRated down 1 level for serious imprecision. A 20% to 30% difference in the proportion of patients reporting a reduction in drop seizure from baseline of at least 50% was considered meaningful, based on the input from the clinical experts. The observed point estimate just met the lower bounds of the MID suggested by the clinical experts. The 95% CIs of the point estimates were wide. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
cStatistical testing for this outcome was not adjusted for multiplicity. The results are considered supportive evidence.
dRated down 1 level for serious imprecision. In the absence of an empirically derived MID, a 20% to 30% difference was used as the clinically meaningful threshold, based on clinical expert input. Any increase (improvement) not reaching this threshold indicates there is uncertainty in the clinically meaningful treatment effect of cannabidiol compared with placebo. In the CARE 3 trial, the point estimate and 95% CI are less than the 20% threshold. In the CARE 4 trial, the point estimate just meets the 20% threshold, while the lower bounds of the 95% CI fall under the threshold. Potential to rate down for serious inconsistency. The results of the CARE 3 and CARE 4 trials are different, with the effect estimate and lower 95% CI found under the threshold in the CARE 3 trial. Given that the estimate is close to the 20% threshold provided by the clinical experts, there was no rating down for inconsistency. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
eRated down 1 level for serious inconsistency. The point estimate in the CARE 4 trial is lower than that estimated in the CARE 3 trial. Rated down 1 level for serious imprecision. In the absence of an empirically derived MID, a between-group difference of 15% to 20% was used as the clinically meaningful threshold, based on clinical expert input. Any increase (improvement) not reaching this threshold indicates there is uncertainty in the clinically meaningful treatment effect of cannabidiol compared with placebo. In the CARE 4 trial, the point estimate and 95% CI are less than the 15% threshold. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
fRated down 2 levels for serious imprecision, based on there being zero events in both treatment groups. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
gRated down 1 level for serious imprecision. The 95% CI of the treatment difference included the point estimate for placebo response. In the absence of an empirically derived MID and no suggested MID from the clinical experts, the null was employed. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
hRated down 1 level for serious study limitation. Risk of bias (attrition) due to missing outcome data as results were available for less than 50% of randomized patients in the CARE 3 and CARE 4 trials. Rated down 1 level for serious imprecision. No MID estimate specific to the LGS population was identified or provided by the sponsor. Using the null, the treatment effect and the lower bound of the 95% CI included the potential for decrease (worsening) HRQoL. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. Clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
IRated down 2 levels for serious study limitation. Risk of bias due to missing outcome data as results were available for only 16% of randomized patients in the CARE 3 and CARE 4 trials. Rated down 1 level for serious imprecision. No MID estimate specific to the LGS population was identified or provided by the sponsor. Applying the MID of 5.19 established for patients with partial-onset seizure,, the treatment effect and the lower bound of the 95% CI included the potential for decrease (worsening) HRQoL. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
jRated down 2 levels for serious imprecision. In the absence of an empirically derived MID, a between-group difference of 10% was used as the clinically meaningful threshold, based on clinical expert input. Any increase (improvement) not reaching this threshold indicates there is uncertainty in the clinically meaningful treatment effect of cannabidiol compared with placebo. Difference of treatment effect could not be estimated due to the small number of events. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
kBetween-group differences in harms were not statistically tested.
lRated down 1 level for serious imprecision. There were important concerns about the small number of events that precluded estimating a treatment effect. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
mRated down 1 level for serious imprecision. There were important concerns about the small number of events that precluded estimating a treatment effect. Potential to rate down for serious indirectness. Although the certainty of evidence was not rated down for serious indirectness, important concerns regarding how well the evidence applies to patients with LGS in Canada were noted by CADTH. These concerns included the lack of study sites in Canada and the lack of representation of patients who had experience with medicinally sourced cannabis. The clinical experts advised that the generalizability of the CARE 3 and CARE 4 trials is difficult to determine because of the rarity of LGS and the variability in individual patient clinical characteristics.
Sources: Clinical Study Reports for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
protocols used in the country of enrolment. The end-of-treatment visit occurred after a maximum of 6 years’ treatment [312 weeks after visit 1], following early withdrawal from the study, or following an unscheduled “end-of-treatment visit” conducted no earlier than 730 days after visit 1.
The CARE 5 trial was conducted across 75 sites in 8 countries (Australia, Spain, France, Israel, Netherlands, Poland, the UK, and the US). Approximately 78% of patients were from the US. On average, patients were aged 15.9 years (SD = 9.5) and were concurrently taking 3.4 ASMs (SD = 1.38) at the time of enrollment. Of the 366 patients with LGS enrolled, 66.4% completed the treatment period, 20.5% continued to the taper phase, and 18.3% completed the taper phase.
Efficacy Results
Efficacy end points were analyzed in the safety analysis set. The retention rates for the safety analysis set at weeks 37 to 48 (12 months), weeks 85 to 96, weeks 133 to 144 (36 months), weeks 181 to 192, and weeks 241 to 252 were 82% (299 of 366 patients), 64% (236 of 366 patients), 59% (216 of 366 patients), 6% (22 of 366 patients), and 2% (8 of 366 patients), respectively. Missing data were addressed using the last observation carried forward method.
The proportion of patients experiencing drop seizure–free status at weeks 37 to 48 (12 months), weeks 133 to 144 (36 months), and weeks 253 to 264 (66 months) were 7% (24 of 364 patients), 8% (30 of 364 patients), and 9% (34 of 364 patients), respectively. The median percent change from baseline in drop seizure frequency during the same OLE periods from baseline of the core studies were –55.3% (IQR, –83.8% to –16.6%; n = 364), –59.1% (IQR, –85.7% to –15.2%; n = 364), and –59.4% (IQR, –87.1% to –16.0%; n = 364), respectively. The mean percent change in drop seizure frequency during the same OLE periods from baseline of the core studies were –34.9% (SD = 82.77; n = 364), –32.3% (SD = 106.11; n = 364), and –30.9% (SD = 127.21; n = 364), respectively. The proportion of patients who experienced a reduction in drop seizure frequency of 50% or greater during the same periods in the CARE 5 trial was 53.8% (196 of 364 patients), 56.3% (205 of 364 patients), and 58% (211 of 364 patients), respectively.
Among patients aged between 2 years and 18 years, the mean change in overall HRQoL score, as measured from the QOLCE score at baseline to last visit, was 5.5 (SD = 13.71; n = 152). Among patients aged 19 years and older, the mean change in the overall quality-of-life subscale weighted score (QOLIE-31-P) from baseline to last visit was 6.4 (SD = 28.63; n = 55).
Harms Results
A total of 353 patients with LGS (96.4%) reported experiencing 1 or more AEs during the CARE 5 trial. The most common treatment-emergent AEs were convulsion (38.5%), diarrhea (38.3%), and pyrexia (34.4%). SAEs were reported by 157 patients with LGS (42.9%). The most commonly reported SAEs were convulsion (12%), status epilepticus (11.5%), and pneumonia (7.1%). Discontinuation of treatment due to AEs was reported in 43 patients with LGS (11.7%). The most common reasons for treatment discontinuation due to AEs were convulsion (1.9%), diarrhea (1.6%), and vomiting (1.4%). Twelve patients with LGS (3.3%) died during the study. SUDEP as the cause of death was recorded in 4 patients (1.1%).
Critical Appraisal
The single-group, open-label, nonrandomized design of the CARE 5 OLE study makes interpretation of the long-term efficacy and safety of cannabidiol challenging. The lack of comparison with an active comparator and/or placebo precludes the ability to draw causal inference to assess the relative long-term therapeutic benefit or safety of cannabidiol. Although patient and caregiver self-counts of drop seizures and motor seizures were noted to be reliable by the clinical experts consulted by CADTH for the purpose of this review, self-counting of other types of seizures is not considered accurate. The results for caregiver-reported and patient-reported outcomes were inconclusive due to the open-label design of the trial and the substantial decline in the number of patients available to provide these assessments over time. Moreover, it is uncertain if the sample size (N = 366) was sufficient to detect rare AEs. As enrolment in the CARE 5 trial was contingent on the completion of a core study, thereby excluding patients who discontinued the CARE 3 or CARE 4 trials due to AEs or lack of response, it is possible that patients in the CARE 5 trial represent a select population that is more tolerant of cannabidiol. Therefore, response bias cannot be ruled out. Finally, the results may be biased due to attrition, as approximately a third of patients did not complete the study and there was wide variance in the follow-up duration for individuals. None of the CARE 5 trial sites were in Canada. Due to the rarity of LGS and a lack of robust population-based studies on LGS in Canada, the clinical experts were unable to determine if the patient population included in the CARE 5 trial was reflective of patients seen in the clinical practice setting across Canada. One clinical expert added that they would not, however, expect patients with LGS living in Canada to differ from patients with LGS living elsewhere. Adherence to the treatment regimen was not reported on and, as such, overall exposure to cannabidiol during the OLE study period is uncertain.
Indirect Comparisons
No indirect treatment comparisons were included in this submission.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps in the evidence from the systematic review were included in this submission.
Conclusions
LGS is a rare and complex epilepsy syndrome associated with multiple and concurrent seizure types that vary across people with the condition. Seizures associated with LGS can be difficult to treat and often become resistant to ASMs. Evidence of moderate certainty from 2 randomized, double-blind, placebo-controlled phase III trials (the CARE 3 and CARE 4 trials) in patients aged between 2 years and 55 years with LGS suggests that adjunctive treatment with cannabidiol 10 mg/kg/day or 20 mg/kg/day may result in a reduction in drop seizure frequency (primary analysis) for certain patients compared with placebo, when added to usual care, with a greater proportion of patients treated with cannabidiol reporting a reduction in drop seizure frequency of 50% or more (key secondary outcome). Although a median treatment difference in drop seizure frequency reduction of between 17% and 21% did not meet the threshold for clinical relevance, as identified by the clinical experts consulted by CADTH for the purpose of this review, the primary analysis was supported by key secondary analysis. No patients were reported at the end of the 14-week treatment period to have experienced a 100% reduction in drop seizures, and the clinical significance of the number of drop seizure–free days was uncertain. The included trials were limited to patients who reported having 2 or more drop seizures per week during the 28-day baseline period. According to input from the clinical experts, it is reasonable to expect that improvement in seizure frequency would translate to improved HRQoL. However, the ability of the CARE 3 and CARE 4 trials to assess the treatment effect of cannabidiol on HRQoL was limited due to low completion rates of the QOLCE and QOLIE-31-P questionnaires. The long-term safety, tolerability, and efficacy of cannabidiol was assessed in the CARE 5 OLE study. Confidence in the effect estimates from the OLE study was limited, primarily due to the CARE 5 trial not being designed to assess the efficacy of cannabidiol compared with an active treatment or placebo, a diminishing sample size over the study period, and the open-label design, which may have biased outcomes such as HRQoL and harms. As patients with LGS have limited treatment options for seizure control, both the patient group and the clinical expert input emphasized that there is an unmet need for new medications to achieve seizure control, and ideally seizure freedom, in patients with seizures associated with LGS.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol 100 mg/mL oral solution for use as adjunctive therapy for the treatment of seizures associated with LGS in patients aged 2 years and older.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CADTH review team.
LGS is a complex epilepsy syndrome associated with multiple seizure types that vary across people with the condition. LGS is a rare and lifelong condition that presents in the first 4 years of life (peak age of onset: 3 to 5 years) in in children who had otherwise experienced age-appropriate development. LGS is associated with refractory and multiple treatment-resistant seizure types, cognitive and behavioural impairments, and poor outcomes into adulthood.1-4 According to the clinical experts consulted by CADTH, LGS has various etiologies and people with LGS exhibit multiple seizure types with distinctive EEG features. The most prominent seizure types in LGS are tonic seizures (stiffening of the body, and sometimes upward eye gaze, dilated pupils, and altered breathing patterns) and atypical absence seizures (staring spells with distinctive EEG pattern), followed by myoclonic jerks (sudden muscle jerks), tonic or atonic drops (brief loss of muscle tone), generalized tonic-clonic seizures (muscle stiffness and rhythmic jerking), and focal seizures.3 Atonic and tonic seizures can be accompanied by dangerous falls or “drop seizures” that often lead to injury.5 High seizure frequency is an independent predictor of early death in people with chronic epilepsy.23 Indeed, LGS is considered a life-threatening condition associated with high rates of SUDEP and a risk of death among children 14 times higher than that of children, adolescents, and young adults in the US general population.6,7 For children with LGS, the reported mortality ratio is 13.92, compared to 3.11 for any kind of epilepsy,7 and the risk of death from neurologic causes (e.g., prolonged seizures, status epilepticus) is 179 greater in children with LGS compared to the general population.7 Clinical consensus suggests that the best prevention strategy for death related to epilepsy is to reduce the frequency of seizures through effective treatments.3,6,8,11
Refractory epilepsy (i.e., epilepsy for which the patient, after adequate trials of 2 appropriately chosen and used ASMs, as monotherapies or in combination, does not experience sustained seizure freedom)24 is associated with poor prognosis in people with LGS. Approximately 80% to 90% of people with LGS continue having seizures into adulthood, and nearly all have cognitive and behavioural impairments along with intellectual functioning and developmental delays within 5 years of diagnosis.3,6,8 As a result, people with LGS often require lifelong round-the-clock care that demands adjustments in virtually all aspects of the lives of their caregivers and family members. The high seizure burden associated with LGS therefore negatively impacts HRQoL for both people with the condition and their caregivers, as well as siblings and other household members.3,25-27 These impacts include high caregiver anxiety driven by the potential for injury, cognitive decline, or death of the person with LGS; financial burden; and, in applicable household environments, sibling psychological distress from witnessing seizures, not getting as much attention from parents, and experiencing concern for their parents’ stress or unhappiness.26,27
Currently, there are no specific diagnostic tests or biological markers for the diagnosis for LGS.6,8 Instead, LGS is diagnosed clinically, based on the presence of multiple seizure types, moderate to severe cognitive and behavioural impairment, and an abnormal EEG pattern of slow spike-wave complexes.28,29 LGS presentation is diverse, and symptoms can evolve over time, resulting in a delay between initial symptom onset and emergence of the full triad of clinical features.29 The clinical experts consulted by CADTH also noted that part of the diagnostic process and management involves the examination of underlying structural abnormalities. In some cases, enhanced access to advanced genetic testing, including epilepsy gene panels and whole exome or genome sequencing, has identified genetic etiologies for patients who would have previously had unknown causes of LGS.
LGS affects between 3% and 10% of children with epilepsy, more commonly males. The peak age for onset is 3 to 5 years, with extreme incidence occurring in the first and 10th years of life.9 Estimates of the incidence and prevalence rates of LGS from studies worldwide are highly variable due to variability in diagnosis criteria, the size of the study populations, the ages of the enrolled patients, and the length of the follow-up period: prevalence ranged from 4.2 to 60.8 per 100,000 people across studies for “probably” LGS and 2.9 to 28 per 100,000 for a confirmed and narrow definition of LGS.30 Approximately 48,000 children and adults in the US are estimated to have LGS.31 The prevalence of LGS in Canada, as estimated by the sponsor, is 12 in 100,000 people.10
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CADTH review team.
Based on clinical expert input solicited by CADTH for the purpose of this review, the primary objective in managing LGS is the reduction of seizures through the administration of ASM. Although available pharmacological treatments for LGS primarily target seizure frequency, the clinical experts noted that there is growing emphasis on measuring the impact of therapies on nonseizure outcomes (e.g., behaviour, independence in activities of daily living, patient and caregiver quality of life) in developmental and epileptic encephalopathies such as LGS.
The current ASMs that have been evaluated in the context of randomized trials and are available for patients with LGS are sodium valproate ordivalproex sodium (expert panel recommendation),32 lamotrigine and topiramate (level A evidence for drop attacks),33 rufinamide (effective add-on treatment for motor and nonmotor seizures as per 3 class I studies with level A evidence),33 clobazam (probably an effective add-on treatment for motor and nonmotor seizures per 2 class II studies),33 felbamate (adjunctive therapy as per the American Academy of Neurology and the American Epilepsy Society; FDA approved, but not available in Canada),33,34 fenfluramine (recently approved in the US after the OLE phase III trial NCT 03355209, but not available in Canada), and cannabidiol (FDA approved).35-38 Other ASMs commonly used, in the absence of randomized trial evaluations, include valproic acid ordivalproex sodium (first treatment option by expert panel),32 levetiracetam, ethosuximide, perampanel, brivaracetam, and zonisamide (unavailable in Canada).39,40 In Canada, the only drugs currently indicated specifically for LGS are rufinamide12 (to be taken in conjunction with 2 or more ASMs) and lamotrigine13 (to be taken with other ASMs). While lamotrigine is available through the Ontario Drug Benefit program, rufinamide must be obtained through the Exceptional Access Program.14 In addition to ASMs, other therapeutic options include dietary therapies such as ketogenic, modified Atkins, or low–glycemic index diets; neuromodulation including VNS and deep brain stimulations; and nonresective surgeries such as corpus callosotomy. In some cases, although uncommon, patients may benefit from surgical resection if the source of seizure activity can be identified.
Based on the Ontario Epilepsy Guidelines, first-line ASMs for LGS are rufinamide and valproic acid (indicated generally for epilepsy), while clobazam, lamotrigine, topiramate, and perampanel are recommended as adjunctive treatment.41 The clinical experts consulted by CADTH, however, suggested valproate as first-line therapy, followed by lamotrigine (adjunctive), rufinamide (second adjunctive), and then topiramate or clobazam or felbamate (subsequent adjunctives) in accordance with the treatment algorithm proposed by Cross et al.32 Recently, the LGS Transition of Care Advisory Board outlined a 3-tier model in which valproate, clobazam, lamotrigine, rufinamide, topiramate, and cannabidiol are considered tier 1 therapies; levetiracetam, perampanel, and zonisamide are considered tier 2 therapies; and felbamate, lacosamide, brivaracetam, and cenobamate are considered tier 3 therapies.38 If the LGS becomes refractory, however, there are no specific recommended combinations of ASMs; instead, a heterogeneous combination of ASMs is used to optimize seizure control.37
The clinical experts consulted by CADTH noted that purified cannabidiol from a licensed producer (“artisanal CBD” or medical cannabis) has been available in Canada for years and has been used extensively for the treatment of drug-resistant epilepsy in children and adults, including patients with LGS, albeit often at considerably lower doses than those used in clinical trials of cannabidiol.
Drug Under Review
The key characteristics of cannabidiol are summarized in Table 3, alongside other treatments available for seizures associated with LGS.
The exact mechanism of action of cannabidiol is unknown.15 Cannabidiol reduces neuronal hyperexcitability through the modulation of intracellular calcium via the GPR55 and TRPV1 receptors and the modulation of adenosine-mediated signalling through the inhibition of adenosine transport via the ENT1 transporter.15
Cannabidiol received a Notice of Compliance from Health Canada on November 15, 2023, through the standard review pathway as adjunctive therapy for the treatment of seizures associated with LGS, Dravet syndrome, or tuberous sclerosis complex in patients aged 2 years and older. The sponsor requested that CADTH review each neurologic disorder as a separate submission. CADTH accepted the sponsor’s request on June 21, 2023. Accordingly, the indication of focus for the current review of cannabidiol is for use as adjunctive therapy for the treatment of seizures associated with LGS in patients aged 2 years and older.
The product monograph–recommended starting dosage of cannabidiol is 2.5 mg/kg twice daily.15 After 1 week, the dosage should be increased to a maintenance dosage of 5 mg/kg twice daily (10 mg/kg/day). Based on individual clinical response and tolerability, each dose can be increased in weekly increments of 2.5 mg/kg, administered twice daily (5 mg/kg/day), up to a maximum recommended dosage of 10 mg/kg twice daily (20 mg/kg/day). For patients in whom a more rapid titration from 10 mg/kg/day to 20 mg/kg/day is warranted, the dose may be increased no more frequently than every other day. The product monograph also provides a dosing adjustment for patients with moderate or severe hepatic impairment, due to risk of hepatocellular injury related to cannabidiol.15
According to the product monograph, cannabidiol can cause somnolence and sedation. Other common adverse reactions associated with cannabidiol use are decreased appetite; diarrhea; transaminase elevations and liver impairment and toxicity; fatigue, malaise, and asthenia; rash; insomnia, sleep disorders and poor-quality sleep; and infections.15
Table 3: Key Characteristics of Cannabidiol and Other ASMs That Constitute Usual Care
Drug | Mechanism of action | Indication(s)a | Route and dose | Serious adverse effects or safety issues | Other |
|---|---|---|---|---|---|
Cannabidiol + usual care | Unknown mechanism of action; known to reduce neuronal excitability by modulating ENT1, GPR55, and TRPV1 channels | Adjunctive therapy for the treatment of seizures associated with LGS, Dravet syndrome, or TSC in patients aged 2 years and older. | Starting dosage: 5 mg/kg/day for 1 week Maintenance dosage: 10 mg/kg/day Maximum dosage: 20 mg/kg/day | Diarrhea, reduced appetite, fatigue, somnolence, insomnia, infections, transaminase elevations, hypersensitivity, CNS depression, suicidal ideation | Monitor liver enzymes (AST, ALT, bilirubin). Potential for multiple drug interactions with other ASMs. |
Usual care (combination of 1 or more of the following) | |||||
Rufinamide | Unknown mechanisms of action; may prolong the inactive state of plasma membrane sodium channels | Adjunctive treatment of seizures associated with LGS in children aged 4 years and older and in adults. | Maintenance dosage (pediatric): 200 mg/day Maximum dosage (pediatric): 1,300 mg/day Maintenance dosage (adult): 400 mg/day Maximum dosage (adult): 3,200 mg/day | QTc interval shortening, ataxia, somnolence, ophthalmological effects, DRESS, suicidal ideation and behaviour | Available through the Exceptional Access Program. First line for LGS.b One of 2 ASMs officially indicated for LGS in Canada. As per 3 class I studies with level A evidence, effective add-on treatment for motor and nonmotor seizures (modest benefit).33 |
Valproic acid or valproate | Multiple (GABA potentiation, glutamate inhibition, sodium channel, and T-type voltage-gated calcium channel blockade) | Use as sole or adjunctive therapy in the treatment of simple or complex absence seizures, including petit mal, and is useful in primary generalized seizures with tonic-clonic manifestations. Use adjunctively in patients with multiple seizure types which include either absence or tonic-clonic seizures. | Maintenance dosage: 15 mg/kg/day Maximum dosage: 60 mg/kg/day | Enzyme inhibitor, substantial teratogenicity, weight gain, tremors | First line for LGS.b Expert panel recommendation without randomized trials.32 |
Clobazam | GABA potentiation | Adjunctive therapy in patients with epilepsy who are not adequately stabilized with their current anticonvulsant therapy. | Maintenance dosage (pediatric): 5 mg/day Maximum dosage (pediatric): 40 mg/day Maintenance dosage (adult): 5 to 15 mg/day Maximum dosage (adult): 80 mg/day | Sedative, substantial tolerance (loss of efficacy) | As per 2 class II studies, probably effective add-on treatment for motor and nonmotor seizures.33 |
Lamotrigine | Voltage-gated sodium channel blocker | Adjunctive therapy for the management of the seizures associated with LGS. | Maintenance dose (with valproate; pediatric): 1 to 5 mg/kg Maximum dose (with valproate; pediatric): 200 mg/kg Maintenance dose (without valproate; pediatric): 1 to 5 mg/kg Maximum dose (without valproate; pediatric): 5 to 15 mg/kg Maintenance dosage (without valproate; patients aged > 12 years): 300 to 500 mg/day Maintenance dosage (with valproate; patients aged > 12 years): 100 to 200 mg/day | Enzyme inducer, skin hypersensitivity | 1 of 2 ASMs officially indicated for LGS in Canada. Level A evidence for drop seizures.34 |
Levetiracetam | SV2A modulation | Adjunctive therapy in the management of adult (aged > 18 years) patients with epilepsy that is not satisfactorily controlled by conventional therapy. Off-label use for pediatric patients. | Maintenance dosage: 1,000 mg/day Maximum dosage: 3,000 mg/day | Psychiatric side effects (irritability and other neuropsychiatric effects) | Pediatrics (patients aged < 18 years): Health Canada has not authorized an indication for pediatric use. |
Topiramate | Multiple (GABA potentiation, glutamate inhibition, sodium, and calcium channel blockade) | Adjunctive therapy for the management of patients (adults and children aged 2 years and older) with epilepsy that is not satisfactorily controlled with conventional therapy. | Loading dosage (pediatric): 25 mg/day Maintenance dosage (pediatric): 5 to 9 mg/kg/day Maintenance dosage (adult): 200 mg/day Maximum dosage (adult): 400 mg/day | Cognitive side effects, kidney stones, speech and other cognitive problems, weight loss | Level A evidence for drop seizures.34 Monotherapy for pediatric patients was only conducted in clinical trials with a limited number of patients. |
Perampanel | Glutamate antagonist | Adjunctive therapy in the management of partial-onset seizures in patients aged 7 years and older that are not satisfactorily controlled with conventional therapy. Adjunctive therapy in the management of primary generalized tonic-clonic seizures in patients aged 12 years and older with epilepsy that is not satisfactorily controlled with conventional therapy. | Maintenance dosage: 2, 4, 6, 8, 10, or 12 mg/day Maximum dosage: 12 mg/day | Boxed warning: serious psychiatric and behavioural reactions (aggression and hostility: incidence 20% at a dose of 12 mg/day) | Currently for adjunctive use only. |
Lacosamide | Enhanced slow inactivation of voltage-gated sodium channels | Adjunctive therapy in the management of partial-onset seizures in adult patients with epilepsy that is not satisfactorily controlled with conventional therapy. Off-label use for pediatric patients (aged < 18 years). | Starting dosage: 100 mg/day Maximum dosage: 400 mg/day | Most common: dizziness, headache, nausea, vomiting, diplopia, fatigue, and sedation (more common at higher doses; more likely when used in conjunction with other sodium channel blockers) | Pediatrics (patients aged < 18 years): the efficacy and safety of lacosamide have not been established. |
Brivaracetam | SV2A modulation | Adjunctive therapy in the management of partial-onset seizures in patients aged ≥ 4 years with epilepsy that is not satisfactorily controlled with conventional therapy. | Adults: initial 100 mg/day titrated up to a maximum dosage of 200 mg/day Children aged ≥ 4 years and adolescents: weight-based dosing | Hematologic abnormalities, bronchospasm, angioedema, serious dermatologic reactions, somnolence, fatigue, behavioural disorders, suicidal ideation and behaviours | Pediatrics (patients aged < 4 years): the efficacy and safety of brivaracetam have not been established. |
ALT = alanine transaminase; ASM = antiseizure medication; AST = aspartate transaminase; CNS = central nervous system; DRESS = drug reaction with eosinophilia and systemic symptoms; GABA = gamma-aminobutyric acid; LGS = Lennox-Gastaut syndrome; TSC = tuberous sclerosis complex.
aHealth Canada–approved indication.
bAs recommended by the Ontario Epilepsy Guidelines.
Sources: Sponsor’s clinical evidence summary;42 Health Canada–approved product monographs for rufinamide, valproic acid, clobazam, lamotrigine, levetiracetam, topiramate, perampanel, lacosamide, and brivaracetam;43-52 sponsor-submitted proposed product monograph for cannabidiol;15 American Academy of Neurology–American Epilepsy Society Guidelines 2004 and 2018;33,53 Ontario Epilepsy Guidelines 2020.41
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the Stakeholder section of this report.
The CEA provided patient group input. The CEA is a network of organizations supporting and advocating for people living with epilepsy and their families. Patient input was sourced from the knowledge and experiences of patients, caregivers, clinicians, volunteers, donors, and funders, collected from 24 member associations. According to input from the CEA, current treatments may fail in 30% of patients with epilepsy. According to the input, people living with uncontrolled epilepsy are often socially isolated due to stigma and to fear of rejection in social, work, and educational settings. Patients often experience depression and anxiety upon initial diagnosis and often continuously experience these conditions if ASMs stop working. Caregivers and family members are also impacted by epilepsy as their lives revolve around the seizures experienced by patients under their care. Anxiety among caregivers is common as they worry about when the next seizure will occur, the consequences of the epilepsy, and how to navigate social gatherings (e.g., a young person with epilepsy gets invited to a birthday party). In addition, caregivers often experience compassion fatigue since they cannot leave the person with epilepsy alone, are often sleep deprived due to sleep interruptions or anxiety, and can be affected by side effects the patient may experience from medications (e.g., mood swings, sexual dysfunction, suicidal thoughts, memory loss, fatigue, exhaustion). Both patients and caregivers emphasized the importance of treatment that results in seizure freedom. However, patients and caregivers noted that they would accept a treatment that resulted in a reduction in the absolute number of seizures, as even a reduction in seizure frequency could improve overall quality of life. Because people with intractable epilepsy are very often unemployed or underemployed, not covered under employer-funded insurance plans, and/or have restricted income, most drugs to treat their epilepsy are inaccessible. Accordingly, the CEA stressed the importance of new medications being placed on the provincial formulary so that patients with intractable epilepsy have access to novel treatments. Input provided by the CEA did not include experience with cannabidiol.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of LGS.
Unmet Needs
The clinical experts consulted by CADTH for the purpose of this review noted that, despite the multiple treatment options available, there are currently no treatments available to reverse the course of LGS. Moreover, the overall prognosis of LGS remains unfavourable, and not all patients experience response to the available treatments. LGS often becomes refractory to current options and requires multiple medication adjustments and combinations. In addition, the side effects of taking multiple ASMs (e.g., sedation, cognitive slowing) are associated with reduced quality of life, to the point where treatment becomes intolerable and must be discontinued. This challenge is further exacerbated by drug-drug interactions, which are complex and require close clinical monitoring and periodic bloodwork for drug levels, including to guard against incipient hepatotoxicity or bone marrow suppression. The clinical experts added that there is a need for treatment that can meaningfully improve quality of life for both patients and their caregivers.
Place in Therapy
The clinical experts explained that rational polytherapy involves combining ASMs with different mechanisms of action to ensure better seizure control and fewer AEs. While the mechanisms of action of currently available therapies for LGS mostly involve modulating the sodium and calcium channel, gamma-aminobutyric acid, or glutamate receptors, it is hypothesized that cannabidiol works through the endocannabinoid system, which regulates neural excitability. The clinical experts noted that despite its novel mechanism of action compared to available therapies, cannabidiol does not address the underlying disease process any more than other available treatments. Accordingly, the clinical experts suggest that cannabidiol would complement other available treatments as a symptom management treatment. The clinical experts opined that cannabidiol could be combined with 1 or 2 first-line ASMs. The clinical experts also felt that it would be reasonable to require adequate trials of 1 or 2 other ASMs before the use of cannabidiol.
The clinical experts noted that purified cannabidiol, referred to as cannabis for medical purposes, has been available in Canada for several years from licensed producers and has been used extensively (although often at lower doses) for the treatment of drug-resistant epilepsy in children and adults, including patients with LGS. These artisanal cannabidiol treatments are generally not covered by provincial formularies or most private drug insurance plans. The clinical experts expected that the approval of cannabidiol would lead to a shift away from the use of artisanal cannabidiol in jurisdictions where cannabidiol is reimbursed by either public or private drug insurance plans.
Patient Population
According to input from the clinical experts, it is difficult to predict which patients with LGS would be most likely to benefit from cannabidiol. According to the clinical experts, there have been no studies exploring antiseizure treatment response based on LGS etiology. Patients who have not experienced response with multiple ASMs are generally less likely to experience response to the next ASM; however, these are the patients who are most in need of novel therapies. As noted by the clinical experts, idiopathic cases of LGS, with no neurologic impairment before the onset of seizures, tend to respond better to treatment, whereas LGS cases converted from West syndrome or caused by extensive brain malformations or acquired brain lesions will often have less favourable outcomes.
The clinical experts suggest that patients should be screened for treatment according to clinician judgment based on seizure characterization and frequency, etiology investigation, and previous ASMs trialled, along with EEG interpretation.
Assessing the Response to Treatment
According to the clinical experts’ input, a clinically meaningful response to treatment in epilepsy is assessed in terms of the median reduction in seizure frequency over 28-day periods, a reduction in the frequency of seizures of 50% or more, and seizure freedom rates (i.e., reduction of total seizures per day and seizure-free days per month). The clinical experts added that seizure frequency should be assessed every 4 weeks. One clinical expert also added that assessing the frequency of motor and nonmotor seizures rather than drop seizures (i.e., motor seizures that could result in a fall) would be more meaningful. The clinical experts noted that improved quality of life for both patients and caregivers is an important secondary outcome.
Discontinuing Treatment
According to the clinical experts’ input, treatment with cannabidiol should be discontinued if patients develop persistent and progressive elevation of transaminases or recurrent vomiting and diarrhea, which would compromise the absorption of ASMs. In addition, treatment with cannabidiol should be reassessed if a patient develops status epilepticus with no other reasonable explanation. The clinical experts noted that concomitant use of cannabidiol and clobazam requires careful monitoring of clobazam and its metabolite (desmethylclobazam) levels, which are common causes of toxicity and may require clobazam dosing adjustments due to the risk of persistent somnolence.54,55
Prescribing Considerations
According to input received from the clinical experts, the prescribing and monitoring of cannabidiol for LGS should be limited to neurologists who have special expertise in the management of epilepsy in pediatric or adult patients. The clinical experts’ reasoning for this criterion is that specialized expertise is required for accurate LGS diagnosis and for the surveillance and management of drug-drug interactions.
Clinician Group Input
No clinician group input was received for this submission.
Drug Program Input
The drug programs provide input on each drug reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The 2 pivotal trials – the CARE 3 and CARE 4 trials – evaluated the efficacy and safety of cannabidiol plus usual care against usual care. From the submitted comparator table,, lamotrigine was missing. Lamotrigine is listed as 1 of 2 medications approved for seizure management in patients with LGS, with the other being rufinamide. The cost of lamotrigine is significantly less than rufinamide. | Comment from the drug programs to inform CDEC deliberations. The CADTH review team notes that lamotrigine is specially indicated for LGS and is reimbursed by at least 1 jurisdiction, thereby meeting CADTH’s criteria as a comparator. The current CADTH evaluation of cannabidiol includes lamotrigine in the economic evaluation. In the CADTH evaluation of rufinamide, also indicated for LGS, lamotrigine was considered a relevant comparator. |
Rufinamide is an ASM indicated for adjunctive treatment of seizures associated with LGS. CDEC recommends the following criteria for public drug coverage:
Health Canada is currently reviewing a generic submission for rufinamide. For enrolment in the CARE 3 and CARE 4 trials, patients had to have not experienced response with more than 1 ASM. Patients had to also be experiencing stability on 1 or more ASMs. A task force of the International League Against Epilepsy recommended replacing the term “intractable” with “drug-resistant” epilepsy and proposed that “drug resistant” be defined as the failure of adequate trials of 2 tolerated and appropriately chosen and administered ASMs (whether as monotherapy or in combination) to achieve seizure freedom. | Comment from the drug programs to inform CDEC deliberations. |
Considerations for initiation of therapy | |
Should all 3 abovementioned characteristics be present to confirm a diagnosis of LGS. Should a minimum number of drop seizures per month be applied to diagnose LGS? | The clinical experts noted that the alignment of the diagnosis of LGS with the clinical presentations of multiple seizure types; abnormal EEG patterns of slow spike-wave complexes and paroxysmal fast activity; and moderate to severe cognitive impairments is reasonable. The clinical experts believed that the diagnosis of LGS should not be contingent on a minimum number of drop seizures per 28-day period, as there is no minimum number of drop seizures related to the diagnosis of LGS. |
For enrolment in the CARE 3 and CARE 4 trials, patients were required to have not experienced response on more than 1 ASM and to currently be experiencing stability on 1 or more ASMs. To be eligible for cannabidiol, should patients be required to meet the definition of having treatment-resistant epilepsy (failure of 2 or more ASMs), similar to rufinamide? | The clinical experts consulted by CADTH agreed that the definition of treatment-resistant epilepsy involves the failure of 2 or more ASMs, which aligns with the definition used in the CARE 3 and CARE 4 trials. This is also the threshold used to refer patients with LGS for epilepsy surgery. However, the threshold for defining treatment-resistant epilepsy may be set higher or lower depending on the circumstances. As noted by the clinical experts, some special conditions that prevent clinicians from prescribing traditional ASMs, such as the presence of mitochondrial disorders or previous documented allergy to sodium channel blockers, should be carefully assessed for the possibility of prescribing cannabidiol in patients who did not respond to one previous ASM. |
Consider alignment with the reimbursement criteria for rufinamide, if appropriate. | Comment from the drug programs to inform CDEC deliberations. |
Considerations for continuation or renewal of therapy | |
What objective measures are used to assess and monitor therapeutic response in clinical practice? | Patient and/or caregiver feedback and clinical assessment are used to assess and monitor therapeutic response to treatment for seizures associated with LGS in the clinical practice setting. In some special circumstances, an EEG should also be considered as part of therapeutic response for LGS patients, as per clinician judgment. |
In most jurisdictions, rufinamide receives indefinite coverage once approved. No renewal criteria were provided in the submission. | Comment from the drug programs to inform CDEC deliberations. |
Considerations for discontinuation of therapy | |
How would you define treatment failure? | The clinical experts indicated that the following events could be indictive of treatment failure in LGS:
|
There are no discontinuation criteria identified in the CDR recommendations for rufinamide. | Comment from the drug programs to inform CDEC deliberations. |
Considerations for prescribing of therapy | |
The dosing schedule for cannabidiol, as per the sponsor is:
How frequently do patients require the maximum recommended dosage of 20 mg/kg/day? | The clinical experts stated that, in clinical practice, the maximum dose of any ASMs will always be attempted; however, many patients experience tolerability issues at the maximum dose. As clinical experience with cannabidiol in patients with LGS is limited, the clinical experts were unable to comment on how frequently the maximum dosage of 20 mg/kg/day may be required or tolerated. |
Cannabidiol is available as an amber liquid with 100 mg/mL of cannabidiol in a 100 mL bottle. Patients are titrated to an effective therapeutic dose during the first 2 weeks of therapy. The patient or caregiver is required to measure the dose. Frequency of administration and volume of liquid (small quantities) has the potential to result in wastage. | Comment from the drug programs to inform CDEC deliberations. |
There may be limited access to neurologists within some regions. | Comment from the drug programs to inform CDEC deliberations. The clinical experts agreed with this comment and added that virtual consultation may be a way to improve access. |
Patients were excluded from the CARE 3 and CARE 4 trials if they were taking more than 4 concurrent ASMs. As cannabidiol is intended to be used as adjunctive therapy, more information about drug interactions would be beneficial. Cannabidiol is a potent CYP3A4 and CYP2C19 inhibitor and is known to increase drug levels of clobazam, rufinamide, and topiramate. | Comment from the drug programs to inform CDEC deliberations. |
Consider aligning prescribing criteria with rufinamide, if appropriate. | Comment from the drug programs to inform CDEC deliberations. The clinical experts consulted by CADTH for the purpose of this review agreed with this comment. |
Generalizability | |
Refractory epilepsy is a challenging medical condition to treat. Medical cannabis is used in this space. There will be interest in patients with refractory or drug-resistant epilepsy switching to a pharmaceutical grade alternative for many reasons, including:
In clinical practice, do you have challenges related to using the medical cannabis pathway supported by Health Canada? Do you foresee other patients with drug-resistant epilepsy pursuing access to cannabidiol? | The clinical experts noted that there are several challenges in navigating the medical cannabis pathway supported by Health Canada, including a lack of physician comfort with the paperwork involved with authorizing medical cannabis. The clinical experts believed that it would be fair to assume that patients with other types of treatment-resistant epilepsy would pursue access to cannabidiol. |
Care provision issues | |
The indication population is vulnerable, often presenting with intellectual and physical disabilities. Communicating and reporting of side effects may be challenging in this population. Patients in the CARE 3 and CARE 4 trials were taking on average 3 ASMs concomitantly with cannabidiol, which can create uncertainty in the root cause of side effects. | Comment from the drug programs to inform CDEC deliberations. |
System and economic issues | |
The submitted list price for cannabidiol is $1,424.54 per 100 mL bottle. Cannabidiol is dosed according to weight, as such there is a substantial cost increase with heavier and/or older patients. The price of cannabidiol by weight is as follows:
The price for the comparator drugs:
| Comment from the drug programs to inform CDEC deliberations. |
Cannabidiol is an adjunctive therapy, and therefore the cost of other ASMs need to be considered. | Comment from the drug programs to inform CDEC deliberations. |
The cost of cannabidiol submitted by the sponsor is considerably higher than the medical cannabis (cannabidiol predominant) products. Patients who cannot afford upfront costs of this medication may resort to alternative pathways. Cannabidiol could have potential equity implications. | Comment from the drug programs to inform CDEC deliberations. The clinical experts consulted by CADTH for the purpose of this review agreed with this comment. |
ASM = antiseizure medication; CDR = CADTH Common Drug Review; CDEC = Canadian Drug Expert Committee; EEG = electroencephalogram; LGS = Lennox-Gastaut syndrome.
aCurrently only Veterans Affairs Canada and some private insurers cover medical cannabis products.
bHealth Canada is currently reviewing a generic submission for rufinamide.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol 100 mg/mL oral solution for use as adjunctive therapy in the treatment of seizures in patients with LGS. The focus will be placed on comparing cannabidiol to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of cannabidiol is presented in 2 main sections, with CADTH’s critical appraisal of the evidence included at the end of each section. The first main section, the systematic review, includes RCTs that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second main section details 1 sponsor-submitted long-term extension study. No indirect evidence or additional studies that were considered to address important gaps in the systematic review evidence were submitted by the sponsor.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
2 RCTs identified in systematic review (the CARE 3 and CARE 4 trials)16,17
1 long-term extension study (the CARE 5 trial).22
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 5.
Table 5: Details of Studies Included in the Systematic Review
Detail | CARE 3 | CARE 4 |
|---|---|---|
Designs and populations | ||
Study design | Multicentre, phase III, placebo-controlled, double-blind RCT | |
Locations | 29 sites across 4 countries: US, Spain, France, and UK | 24 sites across 3 countries: US, Netherlands, and Poland |
Patient enrolment dates | Start date: June 8, 2015 End date: May 19, 2016 | Start date: April 26, 2015 End date: March 18, 2016 |
Randomized (N) | N = 225
| N = 171
|
Inclusion criteria |
| |
Exclusion criteria |
| |
Drugs | ||
Intervention | Cannabidiol 20 mg/kg/day administered orally, half in the morning and half in the evening
| Cannabidiol 20 mg/kg/day administered orally, half in the morning and half in the evening
|
Comparator(s) | Matched 20 mg/kg/day or 10 mg/kg/day dosing volumes of placebo, administered orally, half in the morning and half in the evening | Matched 20 mg/kg/day dosing volumes of placebo, administered orally, half in the morning and half in the evening |
Study duration | ||
Screening phase | 28 days | |
Treatment phase | 14 weeks (2 weeks dose titration and 12 weeks dose maintenance) | |
Follow-up phase | 28 days | |
Outcomes | ||
Primary end point | Percent change from baseline in number of drop seizures (average per 28 days) during the treatment period of the study (day 1 to the end of the evaluable period) | |
Secondary and exploratory end points | Key secondary:
Other secondary:
Exploratory:
| |
Publication status | ||
Publications First author (Year) | Auvin (2023),56 Cross (2021),57 Devinsky (2018),58 Mazurkiewicz-Beldzinska (2019),59 Morrison (2018), Nabbout (2021),60 Privitera (2021),61 Wirrell (2017),62 Wirrell (2018),63 Wirrell (2022),64 Patel (2017)65 | Auvin (2023),56 Cross (2021),57 Joshi (2017),{Joshi, 2017 #72} Mazurkiewicz-Beldzinska (2019),59 Morrison (2018),66 Nabbout (2021),60 Privitera (2021),61 Thiele (2018),67 Wirrell (2018),63 Patel (2017)65 |
CTR number | NCT02224560 | NCT02224690 |
ASM = antiseizure medication; CTR = Clinical Trial Record; EEG = electroencephalogram; LGS = Lennox-Gastaut syndrome; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = Quality of Life in Epilepsy, version 2; RCT = randomized controlled trial; S/CGIC = Subject/Caregiver Global Impression of Change; S/CGICSD = Subject/Caregiver Global Impression of Change in Seizure Duration; VNS = vagus nerve stimulation.
Note: Health Canada reviewer’s report was included.68
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
Two sponsor-conducted studies were included in the systematic review: the CARE 3 and CARE 4 trials.16,17
Both the CARE 3 and CARE 4 trials were multicentre, randomized, double-blind, phase III RCTs evaluating the efficacy of cannabidiol as adjunctive treatment in reducing drop seizure frequency in patients with LGS.
In the CARE 3 trial, 225 patients across 29 sites in 4 countries (US, Spain, France, and UK) were randomized to receive treatment with either cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, or placebo. A schematic of the CARE 3 study design is presented in Figure 1. Prior to randomization in the CARE 3 trial, patients entered (at visit 1) a 28-day screening period that included tests to detect the presence of delta-9-tetrahydrocannabinol metabolites to confirm that cannabis was not taken immediately before entering the trial and to ensure that medications or interventions for epilepsy were stable for 4 weeks before screening. This period was also used to establish the baseline number and type of drop and nondrop seizures. To ensure the correct trial population was randomized, an independent review by the Epilepsy Study Consortium was conducted to verify the seizure types experienced by screened patients. Confirmation of seizure types from the Epilepsy Study Consortium was required before randomization at visit 2. Eligible patients were randomly allocated with a 1:1:1 ratio to 1 of the 3 treatment arms using an IVRS. Patients in the placebo group were split into 2 equivalent cohorts: half receiving 10 mg/kg/day dosing volumes, and half receiving 20 mg/kg/day dosing volumes. The allocation of investigational medicinal product was done according to randomization schedules produced by an independent statistician. The randomization was stratified by age group (2 to 5 years, 6 to 11 years, 12 to 17 years, and 18 to 55 years). The IVRS identified the pack number to be dispensed to the patient at each visit according to the treatment assigned in the randomization schedule. Patients returned to the clinic for an end-of-treatment visit after the 14-week treatment period on day 99 (visit 8), or earlier if they withdrew prematurely. Patients were invited to continue to receive cannabidiol in an OLE trial under a separate protocol immediately following visit 8.
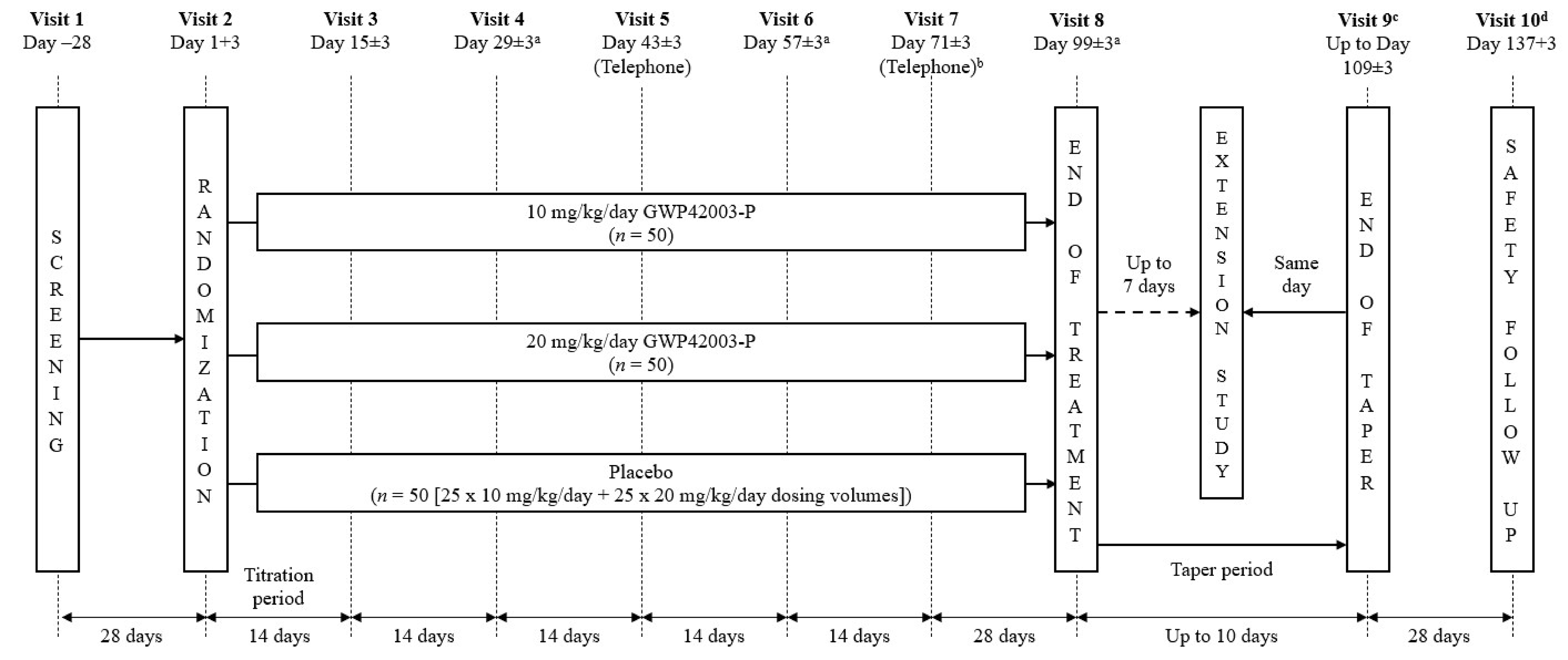
GWP42003-P = cannabidiol; OLE = open-label extension.
a For patients in France only, the visit window was fewer than 3 days rather than at least 3 days.
b For patients in France only, visit 7 was completed at the clinic and was not conducted by telephone.
c Visit 9 was for patients who did not enter the OLE trial or who withdrew from the study early; could be conducted by telephone.
d Visit 10 was for patients who did not enter the OLE trial at visit 8 or for those who withdrew early and tapered the investigational product. Patients who completed treatment but opted not to enter the OLE trial, or who withdrew from the trial early, had weekly (± 3 days) safety telephone calls from visit 9 (or date of final dosing) until visit 10.
Sources: Clinical Study Report for CARE 3 trial;16 sponsor’s summary of clinical evidence.
In the CARE 4 trial, 171 patients across 24 sites in 3 countries (US, Netherlands, and Poland) were randomized to receive treatment with either cannabidiol 20 mg/kg/day or placebo. A schematic of the CARE 4 study design is presented in Figure 2. Similar to the CARE 3 trial, a 28-day screening period was included to perform tests to detect the presence of delta-9-tetrahydrocannabinol metabolites, to ensure that all patients’ medications or interventions for epilepsy were stable for 4 weeks before screening, and to establish the baseline number and type of drop and nondrop seizures. Eligible patients were randomly allocated to 20 mg/kg/day cannabidiol or an equivalent volume of placebo in a 1:1 ratio using an IVRS. The allocation of investigational medicinal product, randomization stratification factors, and dispensing of treatment were done in the same manner as described for the CARE 3 trial.
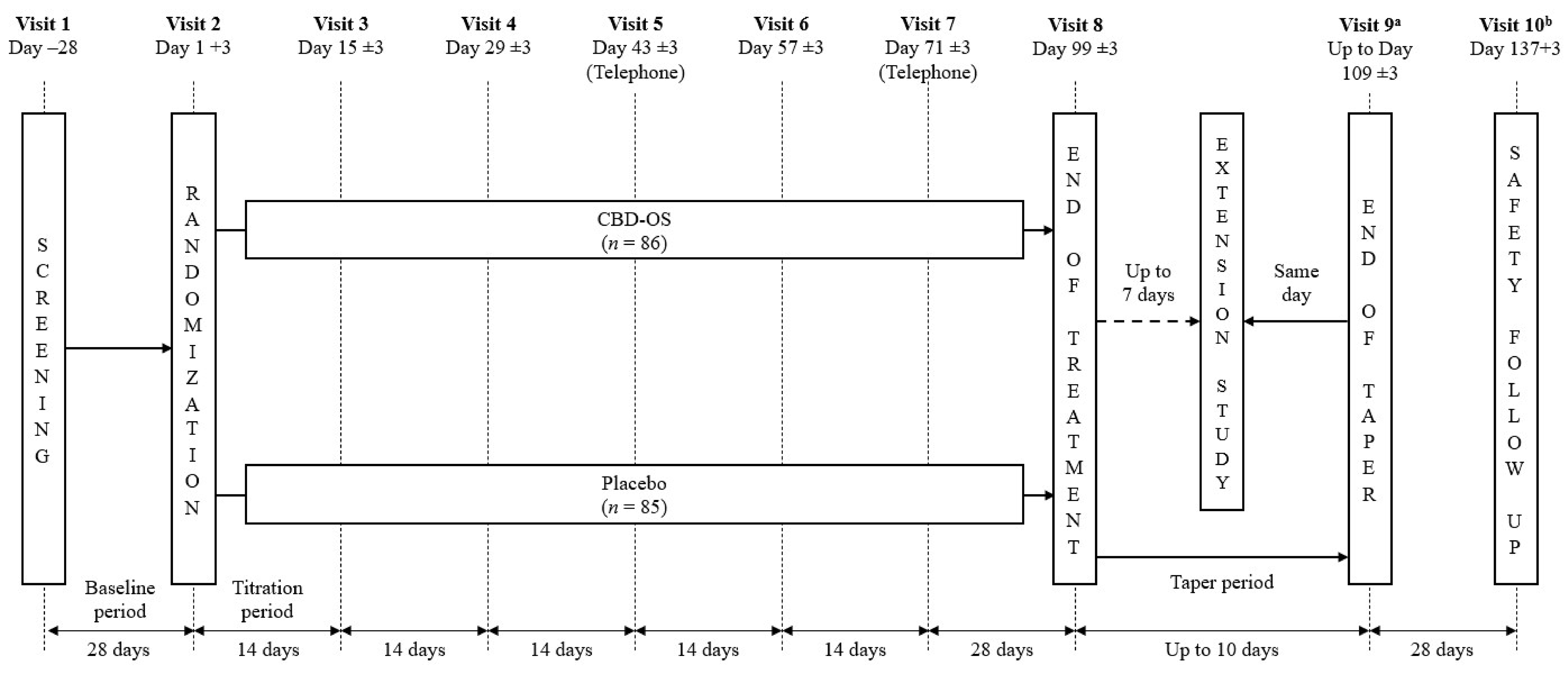
CBD-OS = cannabidiol; OLE = open-label extension.
a Visit 9 was for patients who did not enter the OLE trial at visit 8 or for those who withdrew early and tapered the investigation product. Patients who completed treatment but opted not to enter the OLE trial, or who withdrew from the trial early, had weekly (± 3 days) safety telephone calls from visit 9 (or date of final dosing) until visit 10.
b Visit 10 was for patients who did not enter the OLE trial or who withdrew from the study early; could be conducted by telephone.
Sources: Clinical Study Report and CARE 4 trials;17 sponsor’s summary of clinical evidence.
Protocol Amendments
The CARE 3 and CARE 4 trials underwent 7 and 4 protocol amendments, respectively.
In the CARE 3 trial, the intention-to-treat analysis set was revised per FDA request; statistical analysis testing of the primary end point and additional statistical analysis of the secondary end points were modified; and the statistical methods related to the handling of missing data were changed in amendment 4 (February 17, 2015). Statistical analysis for the primary and secondary end points was amended again in amendment 5 (March 27, 2015) and amendment 6 (June 11, 2015). Other amendments were mostly administrative changes and clarifications.
In the CARE 4 trial, recommendations received from the FDA were incorporated at the time of protocol amendment 3 (June 3, 2015) and included adding stratification by age across treatment arms, follow-up procedures for potential cases of drug-induced liver injury, and updated recommended target doses and titration regimens based on the recommendations of the data safety monitoring committee of the CARE 3 trial. Other amendments were mostly administrative changes and clarifications.
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria for the CARE 3 and CARE 4 trials are summarized in Table 5. Patients eligible for inclusion in the CARE 3 and CARE 4 trials were aged 2 to 55 years and had a clinical diagnosis of LGS, which included written documentation of having a history of a slow (< 3.0 Hz) spike-and-wave pattern in an EEG before their enrolment into the baseline period and evidence of more than 1 generalized seizure, including drop seizures (atonic, tonic, or tonic-clonic), for at least 6 months. During screening, care was taken not to include patients with benign myoclonic epilepsy of infancy, atypical benign partial epilepsy (pseudo-Lennox syndrome), or continuous spike-waves of slow sleep. In addition, patients eligible for study inclusion were required to have experienced at least 2 drop seizures each week during the first 28 days of the baseline period; to have experienced documented treatment failures on more than 1 ASM; and to be taking 1 or more ASMs at a dose that had been stable for at least 4 weeks before screening. All medications or interventions for epilepsy, including ketogenic diet and VNS, must have been stable for 4 weeks before screening, and the patient had to be willing to maintain a stable regimen throughout the trial. The key exclusion criteria were the etiology of the patient’s seizures being a progressive neurologic disease, the patient taking more than 4 concurrent ASMs, or the patient having taken corticotropins in the 6 months before screening. Any patients who were currently using or had used recreational or medicinal cannabis or synthetic cannabinoid-based medications within the 3 months before trial entry and were unwilling to abstain for the duration for the study were also excluded.
Interventions
Definition of Treatment and Maintenance Period
In both the CARE 3 and CARE 4 trials, the treatment period was defined as day 1 to day 99, or the date of last dose as recorded on the “end of treatment study outcome” case report form, whichever occurred earlier. The maintenance period was defined as day 15 to day 99, or the date of the last dose as recorded on the case report form.
Investigational Product
Cannabidiol
Patients randomized to receive cannabidiol received the treatment at a dosage of either 10 mg/kg/day (CARE 3 trial) or 20 mg/kg/day (CARE 3 and CARE 4 trials), administered orally by the patient or their caregiver twice each day: half in the morning and half in the evening. Patients were titrated from a starting dosage of 2.5 mg/kg/day up to 10 mg/kg/day over 7 days, or up to 20 mg/kg/day over 11 days, and remained at this dosage for the duration of the treatment period.
The dosage titration for cannabidiol 10 mg/kg/day was as follows:
2.5 mg/kg/day on days 1 and 2
5.0 mg/kg/day on days 3 and 4
7.5 mg/kg/day on days 5 and 6
10.0 mg/kg/day from day 7 onward for maintenance.
The dose titration for cannabidiol 20 mg/kg/day was as follows:
2.5 mg/kg/day on days 1 and 2
5.0 mg/kg/day on days 3 and 4
7.5 mg/kg/day on days 5 and 6
10.0 mg/kg/day on days 7 and 8
15.0 mg/kg/day on days 9 and 10
20 mg/kg/day from day 11 onward for maintenance.
The first dose and last dose of the cannabidiol were taken at visit 2 (day 1) and visit 8, respectively. Following the end of the treatment period, treatment with cannabidiol was gradually tapered by 10% each day over a 10-day taper period for patients who did not immediately enter the OLE trial. The taper period was interrupted if the patient requested to enter the OLE trial within a 7-day time frame. For patients who withdrew from the CARE 3 and CARE 4 trials early, the taper period followed the withdrawal visit unless continued dosing was not possible due to an AE.
Placebo
Patients randomized to the control group in both studies received volume-matched placebo treatment following the same titration schedule up to 7 or 10 days, depending on whether treatment with placebo was being compared to cannabidiol 10 mg/kg/day or 20 mg/kg/day.
Withdrawal From Treatment
All patients had the right to withdraw at any point during the treatment. In addition, any patients meeting the following criteria were withdrawn from the trial:
administrative decision by the investigator, sponsor, or a regulatory authority
pregnancy
protocol deviation considered to potentially compromise the safety of the patients
withdrawal of patient consent or assent or withdrawal of parent or legal representative consent
lost to follow-up
ALT or AST more than 3 times the upper limit of normal and total bilirubin greater than 2 times the upper limit of normal or with an international normalized ratio greater than 1.5
ALT or AST greater than 3 times the upper limit of normal with the appearance of fatigue, nausea, vomiting, right upper quadrant pain or tenderness, fever, rash, and/or eosinophilia (> 5%)
ALT or AST greater than 8 times the upper limit of normal
ALT or AST greater than 5 times the upper limit of normal for more than 2 weeks.
Patients may have also been withdrawn from the trial if they met or experienced any of the following criteria: patient noncompliance; an AE that would compromise the continued safe participation of the patient in the trial based on the opinion of the investigator; evidence of drug abuse or diversion; suicidal ideation or behaviour of type 4 or 5 during the treatment period as evaluated with the Columbia–Suicide Severity Rating Scale.
Prior, Concomitant, and Prohibited Medications
Prior Medications
Prior to screening, patients were required to be taking 1 or more ASMs at a dose that had been stable for at least 4 weeks. Although nonpharmacological interventions for epilepsy (e.g., ketogenic diet, VSN) were not counted as ASMs, their use must also have been stable for 4 weeks before screening.
Concomitant Medications
Throughout the study period, dosing of concomitant ASMs and any nonpharmacological regimens for epilepsy was to remain stable. However, due to potential pharmacological interactions between cannabidiol and other concurrently administered medication, the dosage for concomitant ASMs was permitted to be modified based on patients’ clinical symptoms or changes in plasma levels following the administration of cannabidiol. Any modifications of the dosage of concomitant ASMs were based on clinical need following discussion with the medical advisors.
The use of rescue medication was permitted when necessary.
Prohibited Therapy
The following medications were not permitted during the study period, starting from the acquisition of patient consent or assent:
Any new medications or interventions for epilepsy, including ketogenic diets and VSN, or change in dosing.
Recreational or medicinal cannabis or synthetic cannabinoid-based medications within 3 months before or during the trial.
Any other investigational products taken as part of a clinical trial within 6 months before or during, the trial.
Long-term systemic steroids, excluding inhaled medication for asthma treatment, or any other daily medications known to exacerbate epilepsy. Exceptions were made for prophylactic medication, for example for idiopathic nephrotic syndrome or asthma.
Outcomes
The primary, key secondary, other secondary, and exploratory outcomes for both the CARE 3 and CARE 4 trials were the same (Table 5).
A list of the efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review according to the clinical experts consulted by CADTH and stakeholder input from patient and public drug plans. Using the same considerations, the CADTH review team selected the end points that were considered most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE, and they included percent change in number of drop seizures; proportion of patients who experienced at least a 25%, at least a 50%, at least a 75%, or a 100% reduction in drop seizures from baseline; number of inpatient hospitalizations due to epilepsy; and number of drop seizure–free days. Patient-reported outcomes that reflected a patient’s quality of life or burden from disease and treatment were considered important by the patient groups and the clinical experts consulted by CADTH for the purpose of this review. While impression of change, as measured by Subject/Caregiver Global Impression Change score as a key secondary outcome, was considered by the clinical experts consulted by CADTH to be a practical measure of HRQoL in the clinical practice setting, the clinical experts added that other measures of HRQoL better captured and quantified the multiple domains of quality of life. According to input from the clinical experts, the QOLCE and QOLIE-31-P scores captured the multiple domains that affect patient’s quality of life (e.g., sleep, cognition, and patient or caregiver assessment) and were therefore assessed using GRADE. Select notable harms outcomes considered important for informing CADTH’s expert committee deliberations were also assessed using GRADE. The following notable harms were recognized as important based on the product monograph and according to the clinical experts consulted by CADTH and could be associated with treatment discontinuation SAE and hepatocellular injury.
Efficacy outcomes that were not assessed using GRADE are summarized in Appendix 1 (Table 26).
Drop Seizures
A drop seizure was defined as an attack or spell (atonic, tonic, or tonic-clonic) involving the entire body, trunk, or head that led or could have led to a fall, an injury, slumping in a chair, or the patient’s head hitting a surface. Drop seizures were the basis of several study end points, including the primary end point: the percent change from baseline in the number of drop seizures during the treatment period. Patients or their caregivers were instructed to record the number and type of drop seizures (atonic, tonic, tonic-clonic) and nondrop seizures from the screening (visit 1) until the completion of dosing (visit 8 or withdrawal visit) using the IVRS diary.
Table 6: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome | Time point | CARE 3 | CARE 4 |
|---|---|---|---|
Per cent change from baseline in number of drop seizuresa | Per 28 days, visit 2 (day 1 + 3) to visit 8 (day 99 ± 3) [treatment period] | Primary | Primary |
Number of patients who experienced a ≥ 50% reduction in drop seizures from baselinea | Visit 1 (day 1 + 3) to visit 8 (day 99 ± 3) [treatment period] | Key secondary | Key secondary |
Number of patients who experienced a ≥ 25%, ≥ 50%, ≥ 75%, or 100% reduction in drop seizures from baseline | Per 28 days, visit 2 (day 1 + 3) to visit 8 (day 99 ± 3) | Secondary | Secondary |
Number of inpatient hospitalizations due to epilepsy | Visit 2 (day 1 + 3) to visit 10 (day 137 + 3) | Secondary | Secondary |
QOLCE (for patients aged 2 to 18 years) or QOLIE-31-P (for patients aged 19 years and older) score | Visit 2 (day 1 + 3) to visit 8 (day 99 ± 3) | Secondary | Secondary |
Number of drop seizure–free days | Per 28 days, visit 2 (day 1 + 3) to visit 8 (day 99 ± 3) | Exploratory | Exploratory |
Notable harms (SAE and hepatocellular injury) | Visit 1 (day –28) to visit 10 (day 137 + 3) | Safety | Safety |
QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = Quality of Life in Epilepsy, version 2; SAE = serious adverse events.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
The frequency of drop seizures was based on a 28-day average. Percent change from baseline in drop seizure frequency, averaged per 28 days, during the treatment period was calculated as follows:

The frequency during each period was based on 28-day averages, calculated as follows:

A minimally important difference (MID) for the reduction of seizure frequency from baseline in patients with milder forms of epilepsy was considered by the sponsor to be at least 50% based on historical regulatory approval processes from the European Medicines Agency and the FDA. Currently, there is no empirically estimated MID for seizure reduction specifically for patients with LGS who experience more severe forms of seizures that are treatment refractory and who may benefit from a modest reduction in seizure frequency.69 According to input from the clinical experts consulted by CADTH, a 25% to 30% reduction in mean or median drop seizure frequency over the placebo response would be considered clinically meaningful.
The number of drop seizure–free days was assessed as an exploratory outcome. The number of drop seizure–free days during each period was based on 28-day averages and calculated as:

The clinical experts could not estimate a threshold of how many additional drop seizure–free days over the placebo response may be considered clinically meaningful.
Treatment Response
The key secondary outcome was the number of patients who experienced at least a 50% reduction in drop seizures from baseline during the treatment periods. Other response thresholds were examined: patients who experienced at least a 25%, at least a75%, or 100% reduction in drop seizures from baseline were assessed as secondary outcomes. As previously mentioned, there are not empirically estimated MIDs for each threshold of response or for which of the thresholds defines a clinically important change or difference. According to input from the clinical experts consulted by CADTH for the purpose of this review, the following clinically meaningful differences in patients who experienced treatment response between the cannabidiol and placebo treatment groups may be considered:
A between-group difference of 20% to 30% in patients who experienced treatment response at the greater than or equal to 25% and greater than or equal to 50% thresholds.
A between-group difference of 15% to 20% in patients who experienced treatment response at the greater than or equal to 75% threshold.
A between-group difference of 10% in patients who experienced treatment response at the 100% threshold.
Inpatient Hospitalization due to Epilepsy
Inpatient hospitalization due to epilepsy was a secondary outcome in both trials. Whether hospitalization was due to epilepsy was based on investigator opinion. According to input from the clinical experts consulted by CADTH for the purpose of this review, a 10% reduction in the number of hospitalizations due to epilepsy between the cannabidiol and placebo treatment groups would be considered clinically meaningful.
Health-Related Quality of Life
HRQoL as measured by the QOLCE or the QOLIE-31-P score was a secondary outcome in the included pivotal trials.
The QOLCE score is a disease-specific, parent-reported measure of HRQoL for children and adolescents with epilepsy. The QOLCE score captures the following domains of HRQoL: physical activities, well-being, cognition, social activities, behaviour, general health, and quality of life, which are grouped into 16 subscales. The subscale and overall quality-of-life scores range from 0 to 100, with a higher score indicative of better quality of life. There is no established MID for QOLCE score for patients with LGS or other seizure disorders.
The QOLIE-31-P is a self-administered, disease-specific survey of HRQoL in adults aged 18 years and older with epilepsy. The scale consists of 31 items related to a patient’s perception of their health and daily activities, which are grouped into 7 subscales: energy/fatigue, emotional well-being, social function, cognitive function, medication effects, seizure worry, and overall quality of life. The subscale and total scores range from 0 to 100, with a higher score indicative of better functioning. The last item of the QOLIE-31-P, which does not contribute to the total or subscale scores, asks patients to rank the importance of each subscale topic from 1 (the most important topic) to 7 (the least important topic). There is no established MID for QOLIE-31-P score in patients with LGS. However, an MID of 5.19 points in change in the total score for partial-onset seizures has been reported (refer to Table 7).70
The QOLCE questionnaire was completed by the parent or caregiver of patients aged 2 to 18 years at visits 2 and 8. The QOLIE-31-P questionnaire was completed by patients aged 19 years or older at visits 2 and 8. For patients who were unable to complete the QOLIE-31-P independently, caregiver assistance was allowed.
Harms
An AE was defined as any new, unfavourable, unintended signs of symptoms (including abnormal laboratory findings) or diagnosis or worsening of a preexisting condition that was present following screening (visit 1) and at the posttreatment, safety follow-up visit (visit 10) and that may or may not have been considered to be related to the investigational product. All AEs were coded by system organ class, preferred term, and lowest level term using MedDRA, version 17.1. The number of patients who had the following AEs were summarized by treatment group as well as system organ class and preferred term: all-causality AEs; treatment-emergent AEs; serious treatment-emergent AEs; discontinuation of investigational product due to treatment-emergent AEs; and deaths. The following notable harms were of interest to the CADTH clinical review team: SAEs and hepatocellular injury.
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
QOLIE-31-P (≥ 18 years) | The QOLIE-31-P is a self-administered, disease-specific survey of HRQoL for adults with epilepsy. The items included in the QOLIE-31-P were derived from the longer version QOLIE-89.70,71 The QOLIE-31-P consist of 31 items assessing a patient’s perception of their health and daily activities as it relates to 2 factors (emotional/psychological and medical/social effects). The recall period is the past 4 week for some items. The 31 items are grouped into 7 subscales:
Items are measured on 3 to 6 point Likert scales. Scores range from 0 to 100 for each subscale and the total score, with higher scores indicating better function. The QOLIE-31-P expands on the original QOLIE-31 questionnaire by including an additional item on each of the subscales to assess the degree of overall distress.71,72 This final item, which does not contribute to the subscale or total score, asks patients to rank the importance of each subscale topic from 1 (the most important topic) to 7 (the least important topic).72 | Validity: The content validity of the QOLIE-31 was determined during the developmental phase in 304 adult patients with epilepsy.71 No information regarding the validity of the QOLIE-31-P specifically in patients with LGS was identified. There was no evidence to suggest the validity estimates for the original QOLIE-31 are applicable to the QOLIE-31-P. Reliability: Based on data from 304 adults with epilepsy, the QOLIE-31 demonstrates adequate to high internal consistency within each subscale, as demonstrated by a Cronbach alpha value ranging from 0.77 (social functioning) to 0.85 (cognitive functioning).71 The intrarater reliability was determined to be adequate to high, as demonstrated by Pearson correlation coefficient values ranging from 0.64 (medication effects) to 0.85 (cognitive functioning).71 No information regarding the reliability of the QOLIE-31-P specifically in patients with LGS was identified. | No MID was identified for patients with LGS. In patients with treatment-resistant POS, a change of 5.19 points in the total score, with the threshold for subscales ranging from 3.95 to 7.42 was considered a MIC.70 |
QOLCE (4 to 18 years)a | The QOLCE score is a disease-specific, parent-reported measure of HRQoL for children and adolescents between the ages of 8 and 18 years with epilepsy. The recall period of the instrument is the past 4 weeks. The US version of the QOLCE questionnaire consists of 76 items, grouped into 7 domains:
The 76 items are grouped into 16 subscales,73 which are rated on a 5-point or 6-point scale. Subscale scores are calculated by computing the mean of all the items included within a specific subscale. In addition, the QOLCE includes an overall quality-of-life score based on the mean of the subscale scores. All scale scores range from 0 to 100, with higher scores indicative of better quality of life. | Validity: Convergent validity of the QOLCE score was established by being moderately to highly correlated to the subscales of the generic CHQ for 63 parents of children aged 4 to 18 years with refractory epilepsy (P < 0.01).74 Concurrent validity of the QOLCE score was established by having moderate to high correlations between similar subscales of CHQ in 71 parents of children aged 4 to 18 years with epilepsy (r = 0.46 to 0.70).75 Independent of a child’s age, gender, age at seizure onset, and IQ, seizure severity over the past 6 months was negatively correlated with all HRQoL subscales (r ≥ –0.3; P < 0.05), except for depression, self-esteem, attention, and behaviour in 63 parents of children aged 4 to 18 years with refractory epilepsy.74 After controlling for age at seizure onset, IQ, family income, and number of ASMs taken, high correlations were found between the stigma (r = –0.59), social activities (r = –0.53), and general health (r = –0.50) subscales and the parental rating of seizure severity.75 No information regarding the validity of the QOLCE score specifically in patients with LGS was identified. Reliability: The internal consistency of 13 multi-item scales of the QOLCE questionnaire was determined to be adequate based on reliable group comparisons (Cronbach alpha = 0.72 to 0.93) in a study including 63 parents of children with refractory epilepsy (aged 4 to 18 years).74 A reliability assessment of the QOLCE score in 71 families living in North America with children diagnosed with epilepsy found that the internal consistency of the subscales was acceptable (range alpha, 0.76 to 0.97).75 | No MID was identified for patients with LGS or other seizure disorders. |
CHQ = Child Health Questionnaire; HRQoL = health-related quality of life; LGS = Lennox-Gastaut syndrome; MIC = minimally important change; MID = minimally important difference; POS = partial-onset seizure; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = Quality of Life in Epilepsy, version 2.
aIn the CARE 3 and CARE 4 trials, the QOLCE questionnaire was administered to patients aged 2 to 18 years.
Sources: Sponsor’s clinical evidence summary;42 Sabaz et al. (2002); Sabaz et al. (2003); Cramer et al. (1998); Cramer et al. (2003); Borghs et al.(Borghs, 2012 #162).
Statistical Analysis
Sample Size Determination
Sample size determination in the CARE 3 trial was based on a 1:1:1 randomization ratio, stratification of age into 4 categories, and the assumption that patients in the placebo group would experience a mean reduction in drop seizure frequency of 18% (from baseline). In addition, it was assumed that although patients in the placebo group were split into 2 equivalent cohorts, 25 patients receiving 10 mg/kg/day dosing volumes and 25 patients receiving 20 mg/kg/day dosing volumes, the 2 cohorts could be pooled for the analyses of efficacy. Accordingly, a sample size of 50 patients per treatment group was determined to be sufficient to detect a difference of 32% between treatments (i.e., patients receiving cannabidiol would experience a reduction in drop seizure frequency of at least 50%) based on an SD of 56%, using a 2-tailed significance level of 0.05 and 80% power.
Sample size determination in the CARE 4 trial was based on a 1:1 randomization ratio and stratification of age into 4 categories. Using the assumptions and sample size and power calculation described in the CARE 3 trial, it was determined that a total of 100 patients would be sufficient.
Control of Type I Error
In both the CARE 3 and CARE 4 studies, type I error of the primary and key secondary efficacy end points was controlled using a hierarchical gate-keeping procedure. All statistical tests were conducted assuming a 2-sided significance level of 0.05. The null hypothesis of an end point was required to be rejected at the 2-sided significance level of 0.05 to test the hypothesis of the subsequent end point in the sequence. If a null hypothesis was not rejected, testing was stopped, and all subsequent analyses were declared not statistically significant. In both the CARE 3 and CARE 4 trials, the primary efficacy end point was tested first, and if positive, the key secondary end points were tested in sequential order. In the CARE 3 trial, each efficacy end point had 2 comparisons against placebo (cannabidiol 20 mg/kg/day and cannabidiol 10mg/kg/day). Of the outcomes reported in the clinical report, the first key secondary outcome – percent change from baseline in number of total seizures during the treatment period – was part of the testing order.
Statistical Methods
A summary of the statistical analysis employed in the CARE 3 and CARE 4 trials is presented in Table 8. In the CARE 3 trial, each end point had 2 comparisons against placebo (20 mg/kg/day cannabidiol and 10 mg/kg/day cannabidiol).
Seizure Frequency
The percent changes from baseline in drop seizure frequency, averaged per 28 days, were analyzed using a Wilcoxon rank sum test. An estimate of median difference between cannabidiol and placebo and an approximate 95% CI were calculated using the Hodges-Lehmann approach.
Patients with no seizures during the baseline period for a particular seizure type were excluded from the analysis of that seizure type.
Treatment Response
The Cochran-Mantel-Haenszel test, stratified by age group, was used to analyze the following outcomes:
The proportion of patients who experienced a greater than or equal to 50% reduction in drop seizure frequency from baseline during the treatment period
The proportion of patients who experienced a greater than or equal to 25% or greater than or equal to 75% reduction in drop seizure frequency from baseline
The proportion of patients who experienced a 100% reduction in drop seizure frequency
The following statistics were presented: the proportion of patients who experienced at least a 25%, at least a 50%, at least a 75%, or a 100% reduction in drop seizure frequency; the difference in proportion with 95% CI; the estimated odds ratio (cannabidiol versus placebo) with 95% CI; and the P value from the Cochran-Mantel-Haenszel test. If no patients in a particular treatment group experienced at least a 25%, at least a 50%, at least a 75%, or a 100% reduction in drop seizure frequency, then the odds ratio and its associated 95% CI were not calculated.
HRQoL Outcomes
QOLCE and QOLIE-31-P scores were analyzed using an analysis of covariance, with baseline score and age group as covariates and treatment group as a fixed factor in the CARE 3 trial. In the CARE 4 trial, no statistical analysis of the QOLIE-31-P score was performed due to the limited number of patients who completed the questionnaire.
Inpatient Hospitalization
The number of inpatient hospitalizations due to epilepsy was analyzed using the analysis of covariance approach, with baseline number and age group as covariates and treatment group as a fixed factor.
Missing Data
Missing data were handled under the MNAR assumption. The impact of the MNAR assumption on the efficacy results — that missing data were systematic — was explored by multiple imputation on drop seizure frequency, based on time point, corresponding to each of the 14 days of the treatment period.
Sensitivity Analysis
Several nonparametric and regression-based sensitivity analyses were conducted for the primary efficacy end point to assess the various assumptions related to the distribution of the outcome measures and missing data. These analyses are summarized in Table 8.
Subgroup Analyses
In both the CARE 3 and CARE 4 trials, subgroup analyses were performed on the intention-to-treatment analysis set for the primary efficacy end point and on the secondary efficacy end points of proportion of patients who experienced at least a 25%, at least a 50%, at least a 75%, or a 100% reduction in drop seizure frequency and drop seizure freedom. All statistical significance was tested at the 0.05 level without formal adjustment for multiplicity. Subgroup analysis on just the treatment period was performed as described for the primary efficacy end point. Subgroup analyses for proportion of patients who experienced at least a 25%, at least a 50%, at least a 75%, or a 100% reduction in drop seizure frequency and for drop seizure freedom were performed using the Fisher exact test.
The following subgroups analyzed in both the CARE 3 and CARE 4 trials were of interest to CADTH:
clobazam use (yes, no)
baseline average drop seizure frequency per 28 days (≤ observed tertile 1, > observed tertile 1 to ≤ observed tertile 2, > observed tertile 2; the observed tertile values were rounded to the nearest 5)
number of current ASMs (< 3 to ≥ 3)
number of prior ASMs (< 6, ≥ 6).
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
CARE 3 and CARE 4 trials | ||||
Mean percent change from baseline in number of drop seizures (during treatment period) |
| NA | Imputation using MCMC method | Wilcoxon rank sum test on:
ANCOVA on:
|
Number of patients who experienced a ≥ 50% reduction in the number of drop seizures from baseline (during treatment period) | CMH test | Age | NR |
|
Number of patients who experienced a ≥ 25%, ≥ 50%, ≥ 75%, or 100% reduction in the number of drop seizures from baseline | CMH test | Age | NR |
|
Number of inpatient hospitalizations due to epilepsy | ANCOVA |
| NR | NR |
QOLCE (for patients aged 2 to 18 years) or QOLIE-31-P (for patients aged 19 years and older) score | ANCOVA |
| QOLCE:
Following approaches used:
QOLIE-31-P:
| NR |
Number of drop seizure–free days | ANCOVA |
| NR | NR |
ANCOVA = analysis of covariance; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; LOCF = last observation carried forward; MCMC = Markov chain Monte Carlo; MI = multiple imputation; MNAR = missing not at random; NA = not applicable; NOCB = next observation carried backward; NR = not reported; PP = per protocol; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = Quality of Life in Epilepsy, version 2.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
Analysis Populations
A summary of the analysis sets used in the CARE 3 and CARE 4 trials is presented in Table 9.
Table 9: Analysis Populations of the CARE 3 and CARE 4 Trials
Study | Population | Definition | Application |
|---|---|---|---|
CARE 3 | ITT | All patients who were randomized and received the IMP in the trial and had postbaseline efficacy data. Patient data were analyzed according to the treatment group to which the patients were randomized. | Primary analysis set for all efficacy end points |
PP | All patients who completed the trial with no protocol deviations deemed to compromise the assessment of efficacy. Patient data were analyzed according to the treatment group to which the patients were randomized. | Efficacy analyses | |
Safety | All patients randomized to treatment who received at least 1 dose of the IMP. Patient data were analyzed according to the treatment the patient received. | Safety data and AE | |
CARE 4 | ITT | All patients who were randomized and received at least 1 dose of the IMP in the trial and had postbaseline efficacy data. Patient data were analyzed according to the treatment group to which the patients were randomized. | Primary analysis set for all efficacy end points |
PP | All patients who completed the trial with no protocol deviations deemed to compromise the assessment of efficacy. Patient data were analyzed according to the treatment group to which the patients were randomized. | Efficacy analyses | |
Safety | All patients randomized to treatment who received at least 1 dose of the IMP. Patient data were analyzed according to the treatment the patient received. | Safety data and AE |
AE = adverse event; IMP = investigational medicinal product; ITT = intention to treat; PP = per protocol.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
Results
Patient Disposition
Patient disposition for the CARE 3 and CARE 4 trials is summarized in Table 10.
Table 10: Summary of Patient Disposition From Studies Included in the Systematic Review
Patient disposition | CARE 3 | CARE 4 | ||||
|---|---|---|---|---|---|---|
Cannabidiol 20 mg/kg/day | Cannabidiol 10 mg/kg/day | Placebo 20 mg/kg/day | Placebo 10 mg/kg/day | Cannabidiol 20 mg/kg/day | Placebo 20 mg/kg/day | |
Screened, N | 293 | 200 | ||||
Screen failure, N (%) | 68 (23.2) | 29 (14.5) | ||||
Reason for screening failure, n (%) | ||||||
Did not meet inclusion criteria | 32 (47.1) | 20 (69.0) | ||||
Met exclusion criteria | 6 (8.8) | 1 (3.4) | ||||
Other reason | 23 (33.8) | 5 (17.2) | ||||
Withdrawal by patient or parent/guardian | 4 (5.9) | 3 (10.3) | ||||
Investigator decision | 3 (4.4) | 1 (3.4) | ||||
Patients enrolled, N (%) | 225 (76.8) | 171 (85.5) | ||||
Randomized, N (%) | 76 (33.8) | 73 (32.4)a | 38 (16.9) | 38 (16.9)a | 86 (50.3) | 85 (49.7) |
Discontinued from study, n (%) | 9 (11.8) | 2 (2.7) | 1 (2.6) | 1 (2.6) | 14 (16.3) | 1 (1.2) |
Reason for discontinuation, n (%) | ||||||
Adverse events | 4 (5.3) | 1 (1.4) | 0 | 1 (2.6) | 8 (9.3) | 1 (1.2) |
Met withdrawal criteria | 1 (1.3) | 0 | 0 | 0 | 4 (4.7) | 0 |
Protocol deviation | 1 (1.3) | 0 | 0 | 0 | NA | NA |
Withdrawal by patient or parent/guardian | 2 (2.6) | 0 | 1 (2.6) | 0 | NA | NA |
Withdrawn by investigator | 1 (1.3) | 1 (1.4) | 0 | 0 | NA | NA |
Other | NA | NA | NA | NA | 2 (2.3) | 0 |
ITT, N | 76 | 73 | 38 | 38 | 86 | 85 |
PP, N | 65 | 63 | 73 | 72 | 84 | |
Safety, N | 82b | 67 | 76b | 86 | 85 | |
ITT = intention to treat; NA = not applicable; PP = per protocol.
aSix patients randomized to receive cannabidiol 10 mg/kg/day and 3 patients randomized to receive placebo 10 mg/kg/day were given dosing schedules for 20 mg/kg/day patients and received greater than 10 mg/kg/day dosing volumes before the mistake was corrected. These patients are analyzed according to the treatment group to which they were randomized, unless otherwise stated.
bWithin the safety analysis set, the patients who mistakenly received greater than 10 mg/kg/day dosing volumes (refer to footnote “a”) are analyzed within the 20 mg/kg/day dose groups.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
In the CARE 3 trial, approximately 23% of the 293 patients screened were not randomized into the trial. The reasons for screen failure were not meeting the trial’s inclusion criteria (47.1%), other reasons (33.8%), meeting 1 or more exclusion criteria (8.8%), withdrawal from the study by patient or parent or guardian (5.9%), and investigator decision (4.4%). Of the 225 patients enrolled into the CARE 3 trial, 76 (33.8%) were randomized to receive cannabidiol 20 mg/day/day; 73 (32.4%) to receive cannabidiol 10 mg/kg/day; 38 (16.9%) to receive placebo 20 mg/kg/day; and 38 (16.9%) to receive placebo 10 mg/kg/day. All randomized patients received at least 1 dose of an investigational product and were thus included in the safety analysis set. Of those randomized, approximately 3% of patients in the cannabidiol 10 mg/kg/day and the 2 placebo groups discontinued the study. In the cannabidiol 20 mg/kg/day group, approximately 12% of patients discontinued the study, mainly due to AEs (5.3%) and withdrawal by the patient or their parent or guardian (2.6%).
In the CARE 4 trial, approximately 14.5% of the 200 patients screened were not randomized into the trial. The reasons for screen failure were not meeting the trial’s inclusion criteria (69.0%), other reasons (17.2%), withdrawal from study by patient or parent or guardian (10.3%), and investigator decision (3.4%). Of the 171 patients enrolled into the CARE 4 trial, 86 (50.3%) were randomized to receive cannabidiol 20 mg/kg/day and 85 (49.7%) to receive the volume-matched placebo. Approximately 16% of patients in the cannabidiol 20 mg/kg/day treatment group discontinued the study, mainly due to AEs (9.3%) and to meeting the withdrawal criteria (4.7%). In the volume-matched placebo group, 1 patient (1.2%) discontinued the study due to AEs.
Protocol Deviation
Protocol deviations in the CARE 3 and CARE 4 trials are summarized in Table 11.
In the CARE 3 trial, important deviations were recorded in 35.4% of patients in the cannabidiol 20 mg/kg/day group, 26.7% of patients in the cannabidiol 10 mg/kg/day group, and 34.2% of patients in the pooled placebo group. The most recorded protocol deviation was receipt of the wrong treatment or incorrect dose, which occurred more frequently in the cannabidiol 20 mg/kg/day group (23.2%) than in the cannabidiol 10 mg/kg/day group (14.9%) and the pooled placebo group (17.1%).
In the CARE 4 trial, important deviations were recorded in 8.1% of patients in the cannabidiol 20 mg/kg/day group and 10.6% of patients in the volume-matched placebo group. The most recorded protocol deviation was the receipt of the wrong treatment or incorrect dose, which occurred in 5.8% and 7.1% of patients in the cannabidiol 20 mg/kg/day treatment group and the volume-matched placebo group, respectively.
Table 11: Summary of Protocol Deviations From the CARE 3 and CARE 4 Trials
Protocol deviations | CARE 3 | CARE 4 | |||
|---|---|---|---|---|---|
Cannabidiol 20 mg/kg/day (n = 82) | Cannabidiol 10 mg/kg/day (n = 67) | Pooled placebo (n = 76) | Cannabidiol 20 mg/kg/day (n = 86) | Placebo 20 mg/kg/day (n = 85) | |
Patients with at least 1 important protocol deviation, N (%) | 22 (26.8) | 15 (22.4) | 15 (19.7) | 7 (8.1) | 8 (9.4) |
Total number of important deviations, N (%)a | 29 (35.4) | 18 (26.7) | 26 (34.2) | 7 (8.1) | 9 (10.6) |
Patients who entered study even though entry criteria were not satisfied, n (%) | 2 (2.4) | 1 (1.5) | 0 (0) | 0 (0) | 1 (1.2) |
Deviations related to patient assessment, n (%) | 2 (2.4) | 2 (3.0) | 5 (6.6) | 0 (0) | 0 (0) |
Absence of THC testing | 1 (1.2) | 1 (1.2) | 3 (3.9) | 0 (0) | 0 (0) |
Inadvertent completion of the study medication use and behaviour surveyb | 1 (1.2) | 1 (1.2) | 2 (3.0) | 0 (0) | 0 (0) |
Patients receiving wrong treatment or incorrect dose, n (%) | 19 (23.2) | 10 (14.9) | 13 (17.1) | 5 (5.8) | 6 (7.1) |
Deviations related to laboratory results, n (%) | 1 (1.2)c | 1 (1.5)c | 0 (0.0) | 2 (2.3) | 1 (1.2) |
Randomized without laboratory results | 1 (1.2)c | 1 (1.5)c | 0 (0) | 0 (0) | 0 (0) |
Deviation in PK sampling times | 0 (0) | 0 (0) | 0 (0) | 2 (2.3)d | 1 (1.2)d |
Patients adjusting concomitant AED dose without prior discussion, n (%) | 0 (0) | 2 (3.0) | 0 (0) | 0 (0) | 0 (0) |
AED = antiepileptic drug; PK = pharmacokinetic; THC = tetrahydrocannabinol.
aEach occurrence is counted, including multiple events of the same important protocol deviation for a single patient.
bAmong patients younger than 12 years.
cPatient was randomized without the laboratory results of visit 2 because the principal investigator did not receive the reports in a timely manner. The results were received after visit 3 and confirmed that hepatic enzymes were within permitted ranges at visit 1 and visit 2.
dPatient was identified as having deviations relating to PK sampling times at visit 2 or visit 8, which may have affected cannabidiol (and major metabolite) PK summary statistics.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 additional information received from sponsor (November 28, 2023).
Baseline Characteristics
The baseline characteristics outlined in Table 12 are limited to those that are most relevant to this review or were considered by the review team to affect the outcomes or interpretation of the study results.
In the CARE 3 trial, the mean age of patients enrolled in the trial was 16.01 years (SD = 10.77 years) in the cannabidiol 20 mg/kg/day group, 15.43 years (SD = 9.48 years) in the cannabidiol 10 mg/kg/day group, and 15.29 years (SD = 9.26 years) in the pooled placebo group. Approximately 11.5% of the patients in the CARE 3 trial were aged 2 to 5 years, 32.4% were aged 6 to 11 years, 26.2% were aged 12 to 17 years, and 29.8% were aged 18 to 55 years. The mean patient weight at baseline was 41.0 kg (SD = 20.6 kg), 44.25 kg (SD = 26.2 kg), and 45.7 kg (SD = 23.2 kg) in the cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, and pooled placebo groups, respectively. In terms of patient seizure history at baseline, the median number of drop seizures varied from 80.25 (range, 8.7 to 1,278.3) to 86.9 (range, 14.0 to 7,494.0) per 28 days. Overall, 8.4% and 23.6% of patients were reported to be on a ketogenic diet or have had a VNS, respectively, at baseline. In the CARE 3 trial, the mean number of drop seizures at baseline was higher in the cannabidiol 10 mg/kg/day group (mean = 277.8; SD = 902.4) than in the cannabidiol 20 mg/kg/day group (mean = 142.4; SD = 174.3) and the pooled placebo group (mean = 192.9; SD = 313.0), and the proportion of patients reporting convulsive seizures longer than 30 minutes was higher in the cannabidiol 20 mg/kg/day group (10.5%) than in the cannabidiol 10 mg/kg/day group (2.7%) and the pooled placebo group (3.9%).
In the CARE 4 trial, the mean age of patients enrolled was 15.5 years (SD = 8.7 years) and 15.3 years (SD = 9.8 years) in the cannabidiol 20 mg/kg/day and the volume-matched placebo groups, respectively. Approximately 13.4% of patients in the CARE 4 trial were aged 2 to 5 years, 31.0% were aged 6 to 11 years, 21.6% were aged 12 to 17 years, and 33.9% were aged 18 to 55 years. The mean patient weight at baseline was 42.7 kg (SD = 22.6 kg) and 43.0 kg (SD = 23.0 kg) in the cannabidiol 20 mg/kg/day and the volume-matched placebo groups, respectively. In terms of seizure history, the median number of drop seizures was 71.4 (range, 10.3 to 855.9) and 74.7 (range, 11.2 to 3174.6) in the cannabidiol 20 mg/kg/day and the volume-matched placebo groups, respectively. Overall, 8.2% and 29.8% of patients were reported to be on a ketogenic diet or to have had a VNS, respectively, at baseline.
Table 12: Summary of Baseline Characteristics From the CARE 3 and CARE 4 Trials (ITT Population)
Characteristic | CARE 3 | CARE 4 | |||
|---|---|---|---|---|---|
Cannabidiol 20 mg/kg/day (n = 76) | Cannabidiol 10 mg/kg/day (n = 73) | Pooled placebo (n = 76) | Cannabidiol 20 mg/kg/day (n = 86) | Placebo (n = 85) | |
Demographics | |||||
Age (years) | |||||
Mean (SD) | 16.01 (10.7664) | 15.43 (9.48) | 15.29 (9.26) | 15.48 (8.69) | 15.28 (9.79) |
Median | 13.36 | 12.73 | 12.74 | 14.20 | 13.28 |
Range | 2.62 to 47.98 | 2.61 to 42.56 | 2.60 to 43.35 | 2.72 to 38.96 | 2.81 to 45.09 |
Age group, n (%) | |||||
2 to 5 years | 9 (11.8) | 8 (11.0) | 9 (11.8) | 11 (12.8) | 12 (14.1) |
6 to 11 years | 25 (32.9) | 24 (32.9) | 24 (31.6) | 26 (30.2) | 27 (31.8) |
12 to 17 years | 20 (26.3) | 19 (26.0) | 20 (26.3) | 19 (22.1) | 18 (21.2) |
18 to 55 years | 22 (28.9) | 22 (30.1) | 23 (30.3) | 30 (34.9) | 28 (32.9) |
Sex, n (%) | |||||
Female | 31 (40.8) | 33 (45.2) | 32 (42.1) | 41 (47.7) | 42 (49.4) |
Male | 45 (59.2) | 40 (54.8) | 44 (57.9) | 45 (52.3) | 43 (50.6) |
Weight at baseline (kg) | |||||
Mean (SD) | 40.95 (20.646) | 44.25 (26.16) | 45.65 (23.17) | 42.74 (22.56) | 42.96 (22.96) |
Median | 38.20 | 35.80 | 40.90 | 36.90 | 36.30 |
Range | 10.8 to 104.3 | 12.8 to 140.2 | 11.9 to 112.6 | 13.6 to 98.7 | 13.4 to 106.0 |
Seizure history | |||||
Baseline drop seizures per 28 days | |||||
Mean (SD) | 142.4 (174.3) | 277.8 (902.4) | 192.9 (313.0) | 134.1 (170.3) | 161.1 (365.4) |
Median | 85.53 | 86.90 | 80.25 | 71.43 | 74.67 |
Range | 13.0 to 1,092.0 | 14.0 to 7,494.0 | 8.7 to 1,278.3 | 10.3 to 855.9 | 11.2 to 3,174.6 |
Seizure types during baseline period, n (%) | |||||
Drop | 76 (100) | 73 (100) | 76 (100) | 86 (100) | 85 (100) |
Tonic | 59 (77.6) | 56 (76.7) | 57 (75.0) | 71 (82.6) | 65 (76.5) |
Clonic | 3 (3.9) | 8 (11.0) | 5 (6.6) | 7 (8.1) | 12 (14.1) |
Tonic-clonic | 41 (53.9) | 37 (50.7) | 34 (44.7) | 49 (57.0) | 53 (62.4) |
Atonic | 50 (65.8) | 40 (54.8) | 41 (53.9) | 47 (54.7) | 59 (69.4) |
Myoclonic | 33 (43.4) | 22 (30.1) | 30 (39.5) | 38 (44.2) | 41 (48.2) |
Countable partial | 17 (22.4) | 18 (24.7) | 19 (25.0) | 20 (23.3) | 19 (22.4) |
Other partial | 5 (6.6) | 6 (8.2) | 4 (5.3) | 4 (4.7) | 2 (2.4) |
Absence | 40 (52.6) | 28 (38.4) | 37 (48.7) | 42 (48.8) | 40 (47.1) |
Convulsive seizures > 30 minutes | 8 (10.5) | 2 (2.7) | 3 (3.9) | 2 (2.3) | 1 (1.2) |
Nonconvulsive seizures > 30 minutes | 3 (3.9) | 3 (4.1) | 6 (7.9) | 3 (3.5) | 2 (2.4) |
ASMs at baseline | |||||
Number of prior ASMs no longer taking | |||||
Mean (SD) | 6.61 (3.68) | 7.01 (4.63) | 7.18 (4.37) | 6.40 (3.49) | 6.45 (4.62) |
Median | 6.00 | 6.00 | 6.00 | 6.00 | 6.00 |
Range | 1.0 to 18.0 | 0.0 to 21.0 | 1.0 to 22.0 | 1.0 to 18.0 | 0.0 to 28.0 |
Number of ASMs currently taking | |||||
Mean (SD) | 2.84 (0.93) | 2.93 (0.92) | 2.91 (0.93) | 2.88 (0.94) | 2.94 (0.86) |
Median | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 |
Range | 0.0 to 5.0 | 1.0 to 5.0 | 1.0 to 5.0 | 1.0 to 5.0 | 1.0 to 4.0 |
Nonpharmacological antiepileptic therapies at baseline, n (%) | |||||
Ketogenic diet | 6 (7.3) | 7 (10.4) | 6 (7.9) | 4 (4.7) | 10 (11.8) |
VNS | 18 (22.0) | 14 (20.9) | 21 (27.6) | 26 (30.2) | 25 (29.4) |
ASM = antiseizure medication; ITT = intention to treat; SD = standard deviation; VNS = vagus nerve stimulation.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence; exposure to Study Treatments.
Exposure and treatment adherence to the investigational products are summarized in Table 13.
Exposure
In the CARE 3 trial, the mean daily dose of the investigational products was 8 mL (SD = 4.1 mL) in the cannabidiol 20 mg/kg/day group, 4.4 mL (SD = 2.7 mL) in the cannabidiol 10 mg/kg/day group, and 6.9 mL (SD = 4.4 mL) in the pooled placebo group.
In the CARE 4 trial, the mean daily dose of the investigational products was 8.57 mL (SD = 4.50 mL) in the cannabidiol 20 mg/kg/day group and 8.59 mL (SD = 4.60 mL) in the volume-matched placebo group.
Treatment Adherence
Overall adherence to the investigational products in CARE3 was 89% in the cannabidiol 20 mg/kg/day group, 95% in the cannabidiol 10 mg/kg/day group and 95% in the pooled placebo group. In the CARE 3 trial, a missed dose (morning or evening) was reported more often in the cannabidiol 20 mg/kg/day group (17.1%) than in the cannabidiol 10 mg/kg/day group (9%) and the pooled placebo group (5.3%). Missed days (neither the morning nor evening dose taken) were reported more often in the cannabidiol 20 mg/kg/day group (6.1%) than in the cannabidiol 10 mg/kg/day group (3.0%) and the pooled placebo group (1.3%).
Overall adherence to the investigational products in CARE4 was 84% and 99% in the cannabidiol 20 mg/kg/day group and volume-matched placebo group, respectively. In the CARE 4 trial, a missed dose was reported more often in the cannabidiol 20 mg/kg/day group (15.1%) than in the volume-matched placebo group (9.4%), and missed days were also reported more often in the cannabidiol 20 mg/kg/day group (7.0%) than in the volume-matched placebo groups (2.4%).
Table 13: Summary of Patient Exposure From the CARE 3 and CARE 4 Trials (Safety Analysis Set)
Exposure details | CARE 3 | CARE 4 | ||||
|---|---|---|---|---|---|---|
Cannabidiol 20 mg/kg/day (n = 82) | Cannabidiol 10 mg/kg/day (n = 67) | Placebo 20 mg/kg/day (n = 41) | Placebo 10 mg/kg/day (n = 35) | Cannabidiol 20 mg/kg/day (n = 86) | Placebo 20 mg/kg/day (n = 85) | |
Exposure | ||||||
Total patient-days | 99 | 99 | ||||
Duration (days) | ||||||
Mean (SD) | 92.8 (19.67) | 98.4 (9.27) | 97.2 (14.12) | 99.9 (3.09) | 87.9 (25.97) | 98.3 (8.72) |
Median (range) | 99.0 (19 to 110) | 99.0 (42 to 111) | 99.0 (17 to 108) | 99.0 (95 to 107) | 99.0 (10 to 109) | 99.0 (22 to 108) |
Daily dose (mL)a | ||||||
Mean (SD) | 8 (4.1) | 4.4 (2.7) | 6.9 (4.4)b | 8.57 (4.50) | 8.59 (4.60) | |
Range | 2.2 to 20.8 | 1.2 to 14.0 | 1.6 to 21.0b | 2.8 to 19.8 | 2.6 to 21.2 | |
Adherence | ||||||
Adherence, n (%) | 73 (89) | 65 (97) | 39 (95) | 35 (100) | 72 (84) | 84 (99) |
Mean (SD) | 99.0 (4.68) | 99.8 (1.21) | 99.5 (3.43) | 100 (0.18) | 99.6 (2.0) | 99.2 (2.3) |
Range | 64 to 100 | 90 to 100 | 78 to 100 | 99 to 100 | 86.2 to 100 | 87.5 to 100 |
SD = standard deviation.
aDaily dose post-titration.
bDaily doses are for the pooled placebo (20 mg/kg/day and 10 mg/kg/day) group.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
Concomitant Medications and Co-Interventions
Concomitant medications, therapies, and rescue medications used in the CARE 3 and CARE 4 trials are summarized in Table 14. Only concomitant medications, therapies, and rescue medications used by 10% of patients in any treatment group are presented. According to input from the clinical experts consulted by CADTH, zonisamide and felbamate are not available in Canada.
Concomitant Medications
In the CARE 3 trial, 224 patients (99.6%) reported taking 1 or more ASMs during the trial. The use of benzodiazepine derivatives was reported in 65% of patients, of which clobazam (48.9%) and clonazepam (12.9%) were the most commonly used (≥ 10% of patients). Carboxamide derivatives were used in approximately a third of all patients, with the most commonly used being rufinamide (28.9%). Fatty acid derivates were used in 44.1% of patients, with valproic acid reported as the most used derivative (37.8%). The use of other antiepileptics was reported in 83.1% of patients in the CARE 3 trial and included the use of levetiracetam (30.7%), lamotrigine (29.8%), zonisamide (14.2%), topiramate (15.1%), lacosamide (13.4%), and felbamate (12.4%).
In the CARE 4 trial, all 171 patients (100%) reported taking 1 or more ASMs during the trial. The use of benzodiazepine derivatives was reported in 63.2% of patients, of which clobazam (49.1%) and clonazepam (12.9%) were the most commonly used (≥ 10% of patients). Carboxamide derivatives were used in approximately a third of all patients, with the most commonly used being rufinamide (26.0%). Fatty acid derivates were used in 43.9% of patients, with valproic acid reported as the most used derivative (40.4%). The use of other antiepileptics was reported in 81.3% of patients in the CARE 4 trial and included the use of levetiracetam (33.9%), lamotrigine (37.4%), zonisamide (9.4%), topiramate (14.6%), lacosamide (12.9%), and felbamate (11.7%).
The overall use of concomitant ASMs was generally balanced between the CARE 3 and CARE 4 trials. In the CARE 3 trial, the use of benzodiazepine derivatives was higher in the cannabidiol 10 mg/kg/day group (77.6%) than in the cannabidiol 20 mg/kg/day group (59.8%) and the pooled placebo group (60.5%). In the CARE 4 trial, the use of phenobarbital was greater in the cannabidiol 20 mg/kg/day group than in the volume-matched placebo group (11.6% versus 2.4%), while the use of levetiracetam was greater in the volume-matched placebo group than in the cannabidiol 20 mg/kg/day group (40.0% versus 27.9%).
Concomitant Antiepileptic Therapies
Overall use of ketogenic diets or VNS in the CARE 3 trial was reported in 8.4% and 23.6% of patients, respectively. The proportion of patients using a ketogenic diet in the cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, and pooled placebo groups was 7.3%, 10.4%, and 7.9%, respectively. VNS use was reported in 22.0%, 20.9%, and 27.6% of patients in the cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, and pooled placebo groups, respectively.
In the CARE 4 trial, overall use of ketogenic diets and VNS was reported in 8.2% and 29.8% of patients, respectively. Use of a ketogenic diet or VNS was reported in 4.7% and 30.2% of patients in the cannabidiol 20 mg/kg/day group and in 11.8% and 29.4% of patients in the pooled placebo group, respectively.
Rescue Medication
In the CARE 3 trial, 120 patients (53.3%) used rescue medications during the trial. The most frequently used rescue medication was diazepam (35.6%). The proportion of patients requiring rescue medications in the cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, and pooled placebo groups was 56.1%, 49.3%, and 53.9%, respectively.
In the CARE 4 trial, 103 patients (60.2%) used rescue medications during the trial. The most frequently used rescue medication was diazepam (42.7%). The proportion of patients requiring rescue medications in the cannabidiol 20 mg/kg/day and volume-matched placebo groups was 61.6% and 58.8%, respectively.
Table 14: Summary of Concomitant Antiseizure Medications, Therapies, and Rescue Medications Used in the CARE 3 and CARE 4 Trials (Safety Analysis Set)
Exposure | CARE 3 | CARE 4 | |||||
|---|---|---|---|---|---|---|---|
Cannabidiol 20 mg/kg/day (n = 82) | Cannabidiol 10 mg/kg/day (n = 67) | Placebo 20 mg/kg/day (n = 41) | Placebo 10 mg/kg/day (n = 35) | Pooled placebo (n = 76) | Cannabidiol 20 mg/kg/day (n = 86) | Placebo 20 mg/kg/day (n = 85) | |
Concomitant antiseizure medication, n (%) | |||||||
Antiepileptic medications | 81 (98.8) | 67 (100) | 41 (100) | 35 (100) | 76 (100) | 86 (100) | 85 (100) |
Barbiturates and derivativesa | 4 (4.9) | 5 (7.5) | 4 (9.8) | 2 (5.7) | 6 (7.9) | 10 (11.6) | 2 (2.4) |
Phenobarbital | 4 (4.9) | 4 (6.0) | 3 (7.3) | 2 (5.7) | 5 (6.6) | 10 (11.6) | 2 (2.4) |
Benzodiazepine derivativesa | 49 (59.8) | 52 (77.6) | 23 (56.1) | 23 (65.7) | 46 (60.5) | 53 (61.6) | 55 (64.7) |
Clobazam | 38 (46.3) | 35 (52.2) | 17 (41.5) | 20 (57.1) | 37 (48.7) | 41 (47.7) | 43 (50.6) |
Clonazepam | 10 (12.2) | 10 (14.9) | 5 (12.2) | 4 (11.4) | 9 (11.8) | 10 (11.6) | 12 (14.1) |
Carboxamide derivativesa | 28 (34.1) | 22 (32.8) | 14 (34.1) | 11 (31.4) | 25 (32.9) | 29 (33.7) | 27 (31.8) |
Rufinamide | 27 (32.9) | 18 (26.9) | 11 (26.8) | 9 (25.7) | 20 (26.3) | 24 (27.9) | 22 (25.9) |
Fatty acid derivativesa | 35 (42.7) | 29 (43.3) | 16 (39.0) | 17 (48.6) | 33 (43.4) | 38 (44.2) | 37 (43.5) |
Valproic acid | 32 (39.0) | 23 (34.3) | 15 (36.6) | 15 (42.9) | 30 (39.5) | 36 (41.9) | 33 (38.8) |
Other antiepilepticsa | 68 (82.9) | 51 (76.1) | 37 (90.2) | 31 (88.6) | 68 (89.5) | 68 (79.1) | 71 (83.5) |
Levetiracetam | 27 (32.9) | 19 (28.4) | 11 (26.8) | 12 (34.3) | 23 (30.3) | 24 (27.9) | 34 (40.0) |
Lamotrigine | 23 (28.0) | 19 (28.4) | 15 (36.6) | 10 (28.6) | 25 (32.9) | 33 (38.4) | 31 (36.5) |
Zonisamideb | 15 (18.3) | 8 (11.9) | 3 (7.3) | 6 (17.1) | 9 (11.8) | 8 (9.3) | 8 (9.4) |
Topiramate | 11 (13.4) | 13 (19.4) | 6 (14.6) | 4 (11.4) | 10 (13.2) | 11 (12.8) | 14 (16.5) |
Lacosamide | 11 (13.4) | 9 (13.4) | 6 (14.6) | 4 (11.4) | 10 (13.2) | 11 (12.8) | 11 (12.9) |
Felbamateb | 9 (11.0) | 6 (9.0) | 8 (19.5) | 5 (14.3) | 13 (17.1) | 9 (10.5) | 11 (12.9) |
Concomitant antiepileptic therapies, n (%) | |||||||
Ketogenic diet | 6 (7.3) | 7 (10.4) | 2 (4.9) | 4 (11.4) | 6 (7.9) | 4 (4.7) | 10 (11.8) |
VNS | 18 (22.0) | 14 (20.9) | 11 (26.8) | 10 (28.6) | 21 (27.6) | 26 (30.2) | 25 (29.4) |
Rescue medications, n (%) | |||||||
Rescue medication use | 46 (56.1) | 33 (49.3) | 21 (51.2) | 20 (57.1) | 41 (53.9) | 53 (61.6) | 50 (58.8) |
Benzodiazepine derivativesa | 45 (54.9) | 33 (49.3) | 21 (51.2) | 20 (57.1) | 41 (53.9) | 53 (61.6) | 50 (58.8) |
Diazepam | 24 (29.3) | 26 (38.9) | 13 (31.7) | 17 (48.6) | 30 (39.5) | 38 (44.2) | 35 (41.2) |
Clonazepam | 11 (13.4) | 4 (6.0) | 4 (9.8) | 1 (2.9) | 5 (6.6) | 6 (7.0) | 8 (9.4) |
Lorazepam | 9 (11.0) | 4 (6.0) | 3 (7.3) | 3 (8.6) | 6 (7.9) | 7 (8.1) | 6 (7.1) |
Midazolam | 7 (8.5) | 8 (11.9) | 2 (4.9) | 2 (5.7) | 4 (5.3) | 8 (9.3) | 5 (5.9) |
VNS = vagus nerve stimulation.
aRescue medication used by > 5% of patients in any treatment group reported.
bAntiseizure medications that are not available in Canada.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
Efficacy
Summary of key efficacy results from the CARE 3 and CARE 4 trials are presented in Table 15.
Percent Change From Baseline in Drop Seizure Frequency
At the end of the treatment period in the CARE 3 trial, a reduction in median percent change in drop seizure frequency was associated with treatment with cannabidiol 20 mg/kg/day (median difference = –21.6%; 95% CI, –34.8 to –6.7; P = 0.0047) and cannabidiol 10 mg/kg/day (median difference = –19.2%; 95% CI, –31.2 to –7.7; P = 0.0016) compared to placebo.
At the end of the treatment period in the CARE 4 trial, a reduction in the median percent change in drop seizure frequency was associated with treatment with cannabidiol 20 mg/kg/day compared to volume-matched placebo (median difference = –17.2%; 95% CI, –30.3 to –4.1; P = 0.0135).
Sensitivity Analysis
In both the CARE 3 and CARE 4 trials, sensitivity analyses using the per-protocol analysis set, and during the maintenance period using the intention-to-treat analysis set, were consistent with the primary analysis. The results of the sensitivity analyses that used imputed data for unreported days in the IVRS (using the worst case of the last observation carried forward, the next observation carried backward, and the mean daily number of seizures during the treatment period) and for MNAR (using a model with multiple imputations) were consistent with the primary analysis. The assumption of data MNAR did also not alter the results of the primary analysis.
Subgroup Analysis
The results of the subgroup analysis of percent change from baseline in drop seizure frequency are presented in Appendix 1. The treatment effect estimates generally favoured cannabidiol, compared with placebo, in the CARE 3 trial (Table 24) and the CARE 4 trial (Table 25).
Treatment Response
Reduction in Drop Seizures From Baseline of Greater Than or Equal to 50%
In the CARE 3 trial, during the treatment period, the difference in the proportion of patients who experienced at least a 50% reduction in drop seizure frequency from baseline between the cannabidiol 20 mg/kg/day group and the pooled placebo group was 25.0% (95% CI, 11.5% to 38.5%) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 21.1% (95% CI, 7.6% to 34.5%).
In the CARE 4 trial, the difference in the proportion of patients who experienced at least a 50% reduction in drop seizure frequency from baseline between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group was 20.7% (95% CI, 6.8% to 34.5%).
Reduction in Drop Seizures From Baseline of Greater Than or Equal to 25%
In the CARE 3 trial, during the treatment period, the difference in the proportion of patients who experienced at least a 25% reduction in drop seizure frequency from baseline between the cannabidiol 20 mg/kg/day group and the pooled placebo group was 18.4% (95% CI, 2.8% to 34.0%) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 19.6% (95% CI, 3.9% to 35.3%).
In the CARE 4 trial, the difference in the proportion of patients who experienced at least a 25% reduction in drop seizure frequency from baseline between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group was 20.4% (95% CI, 5.8% to 35.1%).
Reduction in Drop Seizures From Baseline of Greater Than or Equal to 75%
In the CARE 3 trial, during the treatment period, the difference in the proportion of patients who experienced at least a 75% reduction in drop seizure frequency from baseline between the cannabidiol 20 mg/kg/day group and the pooled placebo group was 22.4% (95% CI, 12.0% to 32.7%) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 8.3% (95% CI, 0.3% to 16.3%).
In the CARE 4 trial, the difference in the proportion of patients who experienced at least a 75% reduction in drop seizure frequency from baseline .during the treatment period between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group was 11.5% (95% CI, 1.3% to 21.8%).
Reduction in Drop Seizures From Baseline of 100%
No patient experienced a 100% reduction in drop seizure frequency during the treatment period in either the CARE 3 or CARE 4 trial.
Number of Inpatient Hospitalizations due to Epilepsy
In the CARE 3 trial, the number of patients who experienced 1 or more inpatient hospitalizations due to epilepsy was 7 (9.2%) in the cannabidiol 20 mg/kg/day group, 6 (8.2%) in the cannabidiol 10 mg/kg/day group, and 6 (7.9%) in the pooled placebo group.
In the CARE 4 trial, the number of patients who experienced 1 or more inpatient hospitalizations due to epilepsy was 10 (11.6%) and 5 (5.9%) in the cannabidiol 20 mg/kg/day and volumed-matched placebo groups, respectively.
Health-Related Quality of Life
QOLCE for Patients Aged 2 to 18 Years
In the CARE 3 trial, overall QOLCE scores were available for 33 patients (43.4%) in the cannabidiol 20 mg/kg/day group, 36 patients (49.3%) in the cannabidiol 10 mg/kg/day group, and in 38 patients (50%) in the pooled placebo group. At baseline, the overall mean QOLCE scores were comparable across the cannabidiol 20 mg/kg/day group, the cannabidiol 10 mg/kg/day group, and the pooled placebo group at 41.6 (SD = 16.5), 40.6 (SD = 15.4), and 41.4 (SD = 16.1), respectively. The adjusted mean treatment difference in change from baseline in overall QOLCE scores between the cannabidiol 20 mg/kg/day group and the pooled placebo group was –5.1 (95% CI, –11.4 to 1.2) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 1.6 (95% CI, –4.5 to 7.8).
In the CARE 4 trial, overall QOLCE scores were available for 26 (30.2%) and 38 (44.7%) patients in the cannabidiol 20 mg/kg/day group and the volumed-matched placebo group, respectively. At baseline, the overall mean QOLCE scores were comparable between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group at 39.5 (SD = 12.6) and 39.1 (SD = 15.2), respectively. The adjusted mean treatment difference in change from baseline in overall QOLCE scores between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group was 3.7 (95% CI, –3.3 to 10.7).
QOLIE-31-P for Patients Aged 19 Years and Older
In the CARE 3 trial, total QOLIE-31-P scores were available for 13 patients in the cannabidiol 20 mg/kg/day group, 14 patients in the cannabidiol 10 mg/kg/day group, and 10 patients in the pooled placebo group. At baseline, the total mean QOLIE-31-P scores were 50.2 (SD = 16.6) in the cannabidiol 20 mg/kg/day group, 56.0 (SD = 19.2) in the cannabidiol 10 mg/kg/day group, and 62.5 (SD = 13.6) in the pooled placebo group. The adjusted mean treatment difference in change from baseline in total QOLIE-31-P scores between the cannabidiol 20 mg/kg/day group and the pooled placebo group was 2.9 (95% CI, –7.3 to 13.1) and between the cannabidiol 10 mg/kg/day group and the pooled placebo group was 3.6 (95% CI, –7.0 to 14.3).
In the CARE 4 trial, total QOLIE-31-P scores were available for 14 patients (16.3%) in the cannabidiol 20 mg/kg/day group and 14 patients (16.5%) in the volume-matched placebo group. At baseline, the total QOLIE-31-P scores were comparable between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group at 55.8 (SD = 13.5) and 57.3 (SD = 19.5), respectively. The adjusted mean treatment difference in total QOLIE-31-P scores was not calculated due to the low number of patients who completed the assessment.
Drop Seizure–Free Days
In the CARE 3 trial, the mean number of drop seizure–free days at baseline was 5.3 (SD = 6.4) in the cannabidiol 20 mg/kg/day group, 5.3 (SD = 5.9) in the 10 mg/kg/day group, and 4.6 (SD = 5.5) in the pooled placebo group. The mean number of drop seizure–free days had increased in all treatment groups at the end of the treatment period. The change in the mean number of drop seizure–free days was 6.8 days (SD = 8.2) in the cannabidiol 20 mg/kg/day group, 5.5 days (SD = 6.7) in the cannabidiol 10 mg/kg/day group, and 2.3 days (SD = 5.1) in the pooled placebo group. Compared to placebo, treatment with cannabidiol 20 mg/kg/day was associated with an increase in the mean number of drop seizure–free days of 4.6 days (95% CI, 2.5 days to 6.8 days), while treatment with cannabidiol 10 mg/kg/day was associated with an increase of 3.3 days (95% CI, 1.2 days to 5.5 days).
In the CARE 4 trial, the mean number of drop seizure–free days at baseline was 6.4 (SD = 6.1) and 5.1 (SD = 5.5) in the cannabidiol 20 mg/kg/day group and the volume-matched placebo group, respectively. The mean number of drop seizure–free days had increased in both treatment groups at the end of the treatment period. The change in the mean number of drop seizure–free days was 5.8 days (SD = 7.4) in the cannabidiol 20 mg/kg/day group and 3.1 (SD, 5.4) days in the volume-matched placebo group. Compared to volume-matched placebo, treatment with cannabidiol 20 mg/kg/day was associated with a mean increase in drop seizure–free days of 2.7 days (95% CI, 0.7 days to 4.7 days).
Other Outcomes
The following outcomes were noted as being meaningful by the patient group and by the clinical experts consulted by CADTH but were not assessed in either the CARE 3 or CARE 4 trial: SUDEP rate, employment, and caregiver quality of life.
Table 15: Summary of Key Efficacy Results From the CARE 3 and CARE 4 Trials
Variable | CARE 3 | CARE 4 | |||
|---|---|---|---|---|---|
Cannabidiol 20 mg/kg/day (n = 76) | Cannabidiol 10 mg/kg/day (n = 73) | Pooled placebo (n = 76) | Cannabidiol 20 mg/kg/day (n = 86) | Placebo 20 mg/kg/day (n = 85) | |
Primary end point | |||||
Percent change from baseline in the number of seizures drop seizures during the treatment period (per 28 days)a | |||||
Baseline period median (Q1 to Q3) | 85.5 (38.3 to 161.5) | 86.9 (40.6 to 190.0) | 80.3 (47.8 to 148.0) | 71.4 (27.0 to 156.0) | 74.7 (47.3 to 144.0) |
Treatment period median (Q1 to Q3) | 44.9 (14.4 to 117.4) | 50.0 (20.5 to 113.2) | 72.7 (35.3 to 125.0) | 31.4 (14.4 to 92.0) | 56.3 (29.7 to 129.3) |
Median percent change (Q1 to Q3) | –41.9 (–72.4 to –1.3) | –37.2 (–63.8 to –5.6) | –17.2 (–37.1 to 0.9) | –43.9 (−69.6 to −1.9) | –21.8 (–45.7 to 1.7) |
Estimated median difference (95% CI)b | –21.6 (–34.8 to –6.7) | –19.2 (–31.2 to –7.7) | Reference | –17.2 (–30.3 to –4.1) | Reference |
P valuec | 0.0047 | 0.0016 | Reference | 0.0135 | Reference |
Key secondary end points | |||||
Proportion of patients who experienced a ≥ 50% reduction in the number | |||||
Yes, n (%) | 30 (39.5) | 26 (35.6) | 11 (14.5) | 38 (44.2) | 20 (23.5) |
No, n (%) | 46 (60.5) | 47 (64.4) | 65 (85.5) | 48 (55.8) | 65 (76.5) |
Difference in proportions (95% CI) | 0.250 (0.115 to 0.385) | 0.211 (0.076 to 0.345) | Reference | 0.207 (0.068 to 0.345) | Reference |
Odds ratio (95% CI) | 3.85 (1.75 to 8.47) | 3.27 (1.47 to 7.26) | Reference | 2.57 (1.33 to 4.97) | Reference |
P valuec | 0.0006 | 0.0030 | Reference | 0.0043 | Reference |
Other secondary end points | |||||
Proportion of patients who experienced a reduction in the number of drop seizures from baseline | |||||
Patients who experienced a ≥ 25% reduction in drop seizure frequency during the treatment periodd | |||||
Yes, n (%) | 47 (61.8) | 46 (63.0) | 33 (43.4) | 55 (64.0) | 37 (43.5) |
Difference in proportions (95% CI) | 0.184 (0.028 to 0.340) | 0.196 (0.039 to 0.353) | Reference | 0.204 (0.058 to 0.351) | Reference |
Odds ratio (95% CI) | 2.11 (1.10 to 4.04) | 2.22 (1.15 to 4.28) | Reference | 2.30 (1.24 to 4.26) | Reference |
P valuec | 0.0229 | 0.0149 | Reference | 0.0081 | Reference |
Patients who experienced a ≥ 75% reduction in the number of drop seizures during the treatment periodd | |||||
Yes, n (%) | 19 (25.0) | 8 (11.0) | 2 (2.6) | 17 (19.8) | 7 (8.2) |
Difference in proportions (95% CI) | 0.224 (0.120 to 0.327) | 0.083 (0.003 to 0.163) | Reference | 0.115 (0.013 to 0.218) | Reference |
Odds ratio (95% CI) | 12.33 (2.76 to 55.13) | 4.55 (0.93 to 22.22) | Reference | 2.75 (1.07 to 7.01) | Reference |
P valuec | < 0.0001 | 0.0453 | Reference | 0.0273 | Reference |
Patients who experienced a 100% reduction in the number of drop seizures during the treatment periodd | |||||
Yes, n (%) | 0 | 0 | 0 | 0 | 0 |
Inpatient hospitalizations due to epilepsy during treatment periodd | |||||
1 or more, n (%) | 7 (9.2) | 6 (8.2) | 6 (7.9) | 10 (11.6) | 5 (5.9) |
Change in QOLCE scores from baseline to end of treatmentd | |||||
Overall quality of life score | |||||
Patients, n | 33 | 36 | 38 | 26 | 38 |
Day 1, mean (SD) | 41.6 (16.5) | 40.6 (15.4) | 41.4 (16.1) | 39.5 (12.6) | 39.1 (15.2) |
End of treatment, mean (SD) | 43.6 (16.4) | 49.9 (15.4) | 50.5 (17.6) | 46.2 (14.8) | 40.5 (15.0) |
Change from baseline (SD) | 1.0 (11.9) | 7.7 (12.9) | 6.1 (14.9) | 7.1 (16.9) | 3.9 (11.5) |
Adjusted mean treatment difference (95% CI)e | –5.1 (–11.4 to 1.2) | 1.6 (–4.5 to 7.8) | Reference | 3.7 (–3.3 to 10.7) | Reference |
P valuee | 0.1141 | 0.6006 | Reference | 0.2925 | Reference |
Attention/concentration subscale score | |||||
Patients, n | 30 | 32 | 35 | 24 | 34 |
Day 1, mean (SD) | 25.4 (27.9) | 21.4 (20.9) | 26.0 (26.4) | 29.2 (23.4) | 26.6 (25.9) |
End of treatment, mean (SD) | 26.8 (26.5) | 30.8 (25.9) | 45.5 (32.3) | 33.0 (24.5) | 27.9 (23.0) |
Change from baseline (SD) | 4.3 (15.9) | 7.4 (19.0) | 16.3 (30.1) | 6.5 (22.2) | 4.3 (18.4) |
Adjusted mean treatment difference (95% CI)e | –12.2 (–23.6 to –0.8) | –8.2 (–19.5 to 3.0) | Reference | 3.7 (–6.9 to 14.4) | Reference |
P valuee | 0.0360 | 0.1486 | Reference | 0.4834 | Reference |
Memory subscale score | |||||
Patients, n | 19 | 17 | 16 | 14 | 15 |
Day 1, mean (SD) | 39.1 (33.2) | 33.1 (23.7) | 34.0 (28.6) | 28.3 (20.2) | 38.0 (27.9) |
End of treatment, mean (SD) | 38.8 (30.5) | 43.3 (34.1) | 51.2 (36.2) | 36.6 (26.6) | 45.1 (25.2) |
Change from baseline (SD) | 3.3 (22.5) | 9.6 (23.4) | 14.6 (33.1) | 17.6 (16.7) | –0.7 (20.3) |
Adjusted mean treatment difference (95% CI)e | –5.0 (–21.9 to 11.8) | –0.2 (–17.3 to 17.0) | Reference | 20.6 (7.2 to 33.9) | Reference |
P valuee | 0.5503 | 0.9838 | Reference | 0.0040 | Reference |
Language subscale score | |||||
Patients, n | 21 | 19 | 20 | 19 | 17 |
Day 1, mean (SD) | 31.4 (28.6) | 24.9 (21.1) | 31.5 (23.3) | 14.8 (15.3) | 28.7 (23.0) |
End of treatment, mean (SD) | 34.9 (30.6) | 33.1 (26.8) | 46.7 (32.7) | 22.4 (21.7) | 25.9 (19.5) |
Change from baseline (SD) | 1.4 (18.5) | 11.3 (24.0) | 12.6 (28.8) | 13.0 (15.1) | –5.5 (15.5) |
Adjusted mean treatment difference (95% CI)e | –8.6 (–23.4 to 6.2) | 2.3 (–12.9 to 17.4) | Reference | 18.6 (8.7 to 28.4) | Reference |
P valuee | 0.2508 | 0.7669 | Reference | 0.0005 | Reference |
Other cognitive subscale score | |||||
Patients, n | 31 | 29 | 33 | 22 | 28 |
Day 1, mean (SD) | 23.9 (28.2) | 20.0 (21.9) | 20.2 (22.6) | 21.2 (20.6) | 21.7 (23.9) |
End of treatment, mean (SD) | 23.8 (25.6) | 29.3 (28.7) | 40.4 (31.8) | 26.8 (25.0) | 20.0 (19.7) |
Change from baseline (SD) | 0.4 (18.7) | 6.6 (15.6) | 11.7 (28.5) | 11.9 (22.7) | –2.4 (16.2) |
Adjusted mean treatment difference (95% CI)e | –10.8 (–21.8 to 0.2) | –4.4 (–15.6 to 6.8) | Reference | 16.4 (5.8 to 27.1) | Reference |
P valuee | 0.0538 | 0.4338 | Reference | 0.0033 | Reference |
Social interactions subscale score | |||||
Patients, n | 35 | 36 | 37 | 32 | 46 |
Day 1, mean (SD) | 33.5 (29.9) | 34.0 (30.1) | 34.9 (30.6) | 32.3 (32.3) | 38.1 (33.1) |
End of treatment, mean (SD) | 44.1 (37.5) | 40.9 (32.8) | 50.9 (37.1) | 48.6 (35.8) | 35.9 (28.4) |
Change from baseline (SD) | 7.0 (32.4) | 4.4 (35.9) | 11.9 (29.9) | 13.9 (30.2) | 4.3 (25.0) |
Adjusted mean treatment difference (95% CI)e | –4.9 (–20.5 to 10.7) | –7.4 (–22.8 to 8.0) | Reference | 8.2 (–4.4 to 20.7) | Reference |
P valuee | 0.5325 | 0.3437 | Reference | 0.1981 | Reference |
Behaviour subscale score | |||||
Patients, n | 34 | 35 | 38 | 29 | 41 |
Day 1, mean (SD) | 58.2 (15.2) | 48.7 (16.7) | 57.8 (15.3) | 52.0 (16.2) | 51.0 (11.3) |
End of treatment, mean (SD) | 54.7 (13.7) | 57.7 (14.0) | 61.0 (14.0) | 52.5 (13.7) | 52.1 (13.4) |
Change from baseline (SD) | –2.0 (9.6) | 6.1 (15.8) | 2.8 (12.9) | 2.7 (10.6) | 1.5 (10.4) |
Adjusted mean treatment difference (95% CI)e | –4.9 (–11.0 to 1.3) | 3.3 (–2.8 to 9.4) | Reference | 1.6 (–3.6 to 6.8) | NA |
P valuee | 0.1186 | 0.2836 | Reference | 0.5387 | NA |
Change in QOLIE-31-P scores from baseline to end of treatmentd | |||||
Total score | |||||
Patients, n | 13 | 14 | 10 | 14 | 14 |
Day 1, mean (SD) | 50.2 (16.6) | 56.0 (19.2) | 62.5 (13.6) | 55.8 (13.5) | 57.3 (19.5) |
End of treatment, mean (SD) | 56.5 (14.5) | 61.8 (13.3) | 56.8 (16.2) | 60.0 (19.2) | 63.2 (12.9) |
Change from baseline to end of treatment, mean (SD)f | 2.7 (8.07) | 5.7 (13.17) | –0.2 (14.67) | 3.5 (15.34) | 1.9 (12.08) |
Adjusted mean treatment difference (95% CI)e | 2.9 (–7.3 to 13.1) | 3.6 (–7.0 to 14.3) | Reference | NE | NE |
P valuee | 0.5701 | 0.4907 | Reference | NE | NE |
Overall quality of life subscale weighted score | |||||
Patients, n | 12 | 14 | 9 | 13 | 12 |
Day 1, mean (SD) | 40.7 (29.0) | 32.9 (30.5) | 39.2 (23.0) | 26.3 (18.8) | 43.9 (31.3) |
End of treatment, mean (SD) | 33.2 (23.7) | 39.1 (20.0) | 27.4 (28.9) | 38.3 (33.2) | 44.5 (19.0) |
Change from baseline to end of treatment, mean (SD)f | –2.0 (12.66) | 7.8 (28.20) | –8.4 (24.71) | 9.5 (27.23) | –6.2 (17.36) |
Adjusted mean treatment difference (95% CI)e | 6.4 (–12.8 to 25.6) | 8.8 (–10.8 to 28.3) | Reference | NE | NE |
P valuee | 0.4988 | 0.3685 | Reference | NE | NE |
Energy subscale weighted score | |||||
Patients, n | 13 | 15 | 11 | 15 | 14 |
Day 1, mean (SD) | 32.8 (22.4) | 37.8 (26.5) | 43.1 (28.2) | 33.0 (20.1) | 34.0 (23.1) |
End of treatment, mean (SD) | 37.0 (20.7) | 51.5 (27.9) | 32.7 (27.7) | 30.0 (19.4) | 32.8 (23.9) |
Change from baseline to end of treatment, mean (SD)f | 4.6 (22.82) | 14.4 (18.79) | –6.2 (33.47) | –0.3 (23.60) | –7.4 (28.38) |
Adjusted mean treatment difference (95% CI)e | 12.9 (–7.5 to 33.2) | 18.0 (–1.8 to 37.8) | Reference | NE | NE |
P valuee | 0.2084 | 0.0732 | Reference | NE | NE |
Mood subscale weighted score | |||||
Patients, n | 13 | 15 | 11 | 14 | 15 |
Day 1, mean (SD) | 59.3 (30.1) | 66.0 (26.9) | 72.6 (17.8) | 49.5 (25.3) | 60.1 (27.8) |
End of treatment, mean (SD) | 61.7 (23.6) | 74.8 (23.9) | 57.4 (31.2) | 52.6 (29.5) | 58.4 (25.3) |
Change from baseline to end of treatment, mean (SD)f | 1.2 (17.99) | 12.7 (15.10) | –10.7 (25.30) | 8.7 (35.01) | –7.0 (18.08) |
Adjusted mean treatment difference (95% CI)e | 12.5 (–3.9 to 28.8) | 22.6 (6.7 to 38.5) | Reference | NE | NE |
P valuee | 0.1303 | 0.0067 | Reference | NE | NE |
Daily activities subscale weighted score | |||||
Patients, n | 13 | 14 | 10 | 14 | 15 |
Day 1, mean (SD) | 33.8 (26.0) | 41.1 (31.1) | 40.2 (31.4) | 33.9 (28.7) | 42.8 (31.3) |
End of treatment, mean (SD) | 42.9 (32.8) | 49.7 (28.1) | 32.4 (27.1) | 42.6 (35.2) | 58.9 (31.5) |
Change from baseline to end of treatment, mean (SD)f | 4.6 (28.05) | 8.1 (33.32) | –4.3 (40.57) | 12.4 (23.56) | 8.1 (40.77) |
Adjusted mean treatment difference (95% CI)e | 8.9 (–20.0 to 37.9) | 9.1 (–20.3 to 38.6) | Reference | NE | NE |
P valuee | 0.5349 | 0.5321 | Reference | NE | NE |
Cognition subscale weighted score | |||||
Patients, n | 11 | 14 | 9 | 13 | 15 |
Day 1, mean (SD) | 34.8 (31.3) | 37.3 (31.3) | 46.7 (35.9) | 35.2 (37.1) | 36.3 (32.9) |
End of treatment, mean (SD) | 37.8 (28.6) | 47.5 (31.7) | 27.2 (28.5) | 41.7 (29.1) | 44.0 (25.7) |
Change from baseline to end of treatment, mean (SD)f | 11.5 (16.14) | 6.4 (15.84) | −5.2 (29.10) | 20.6 (39.83) | 1.5 (30.61) |
Adjusted mean treatment difference (95% CI)e | 16.7 (–2.0 to 35.4) | 9.7 (–9.0 to 28.4) | Reference | NE | NE |
P valuee | 0.0782 | 0.2996 | Reference | NE | NE |
Medication effects subscale weighted score | |||||
Patients, n | 12 | 14 | 10 | 14 | 14 |
Day 1, mean (SD) | 30.8 (24.8) | 36.4 (35.0) | 49.5 (38.1) | 38.2 (32.8) | 47.0 (38.1) |
End of treatment, mean (SD) | 34.9 (33.5) | 41.0 (23.6) | 47.9 (36.5) | 62.2 (43.4) | 71.4 (32.7) |
Change from baseline to end of treatment, mean (SD)f | –2.1 (13.26) | 7.7 (34.01) | 0.0 (42.78) | 22.9 (26.44) | 16.7 (38.63) |
Adjusted mean treatment difference (95% CI)e | –2.1 (–29.6 to 25.4) | 2.2 (–25.9 to 30.2) | Reference | NE | NE |
P valuee | 0.8765 | 0.8765 | Reference | NE | NE |
Seizure worry subscale weighted score | |||||
Patients, n | 12 | 14 | 10 | 14 | 14 |
Day 1, mean (SD) | 30.7 (33.3) | 30.8 (34.3) | 40.6 (30.5) | 27.6 (37.0) | 48.6 (45.3) |
End of treatment, mean (SD) | 30.9 (34.3) | 39.8 (32.6) | 46.5 (44.6) | 38.1 (39.8) | 47.2 (36.5) |
Change from baseline to end of treatment, mean (SD)f | 1.8 (35.92) | 13.0 (33.25) | 7.7 (41.66) | 14.1 (27.20) | –11.8 (56.36) |
Adjusted mean treatment difference (95% CI)e | –5.9 (–35.4 to 23.6) | –6.8 (–36.9 to 23.3) | Reference | NE | NE |
P valuee | 0.6872 | 0.6482 | Reference | NE | NE |
Exploratory end points | |||||
Number of drop seizure–free days during the treatment periodd | |||||
Baseline period | |||||
Mean (SD) | 5.3 (6.4) | 5.3 (5.9) | 4.6 (5.5) | 6.4 (6.1) | 5.1 (5.5) |
Median (range) | 2.90 (0.0 to 21.7) | 1.93 (0.0 to 19.3) | 1.93 (0.0 to 19.3) | 4.41 (0.0 to 21.0) | 3.23 (0.0 to 19.3) |
Treatment period | |||||
Mean (SD) | 12.1 (9.0) | 10.8 (8.6) | 6.9 (7.4) | 12.2 (9.4) | 82 (7.8) |
Median (range) | 13.42 (0.0 to 27.7) | 10 0.0 (0.0 to 27.7) | 3.77 (0.0 to 27.4) | 11.90 (0.0 to 27.7) | 5.77 (0.0 to 25.4) |
Change from baseline | |||||
Mean (SD) | 6.8 (8.2) | 5.5 (6.7) | 2.3 (5.1) | 5.8 (7.4) | 3.1 (5.4) |
Median (range) | 4.16 (–17.2 to 24.5) | 4.23 (–7.4 to 26.7) | 0.46 (–9.5 to 27.4) | 4.76 (–10.9 to 26.2) | 1.41 (–6.4 to 22.0) |
Mean treatment difference (95% CI)e | 4.6 (2.5 to 6.8) | 3.3 (1.2 to 5.5) | Reference | 2.7 (0.7 to 4.7) | Reference |
P valuee | < 0.0001 | 0.0030 | Reference | 0.0075 | Reference |
CI = confidence interval; NA = not available; NE = not estimated; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = Quality of Life in Epilepsy, version 2; Q1 = lower quartile; Q3 = upper quartile; SD = standard deviation.
aAdjusted for multiplicity using a hierarchical gate-keeping procedure.
bThe P value from the Wilcoxon rank sum test is presented.
cThe P value calculated from a Cochran-Mantel-Haenszel test is presented.
dThis outcome was outside the adjustment for multiplicity.
eThe 95% CI and the P value from the analysis of covariance model are presented.
fThe change from baseline was presented for QOLIE-31-P because in the CARE 4 trial, the mean difference between groups was not assessed due to the small number of patients completing the questionnaire.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
Harms
A summary of the harms results in the CARE 3 and CARE 4 trials is presented in Table 16.
Adverse Events
In the CARE 3 trial, at least 1 AE was reported by 93.9% of patients in the cannabidiol 20 mg/kg/day group, 83.6% of patients in the cannabidiol 10 mg/kg/day group, and 72.4% of patients in the pooled placebo group. The most common AEs (reported in > 10% of patients) in the cannabidiol 20 mg/kg/day group were somnolence (30.5%), decreased appetite (25.6%), diarrhea (14.6%), upper respiratory tract infection (13.4%), pyrexia (12.2%), vomiting (12.2%), and nasopharyngitis (11.0%). In the cannabidiol 10 mg/kg/day group, the most common AEs reported were somnolence (20.9%), decreased appetite (16.4%), upper respiratory tract infection (16.4%), diarrhea (10.4%), and status epilepticus (10.4%). In the pooled placebo group, the most common AEs reported were pyrexia (15.8%), upper respiratory tract infection (14.5%), and vomiting (11.8%).
In the CARE 4 trial, at least 1 AE was reported by 86.0% and 69.4% of patients in the cannabidiol 20 mg/kg/day and the volume-matched placebo groups, respectively. Among patients randomized to receive cannabidiol 20 mg/kg/day, the most common AEs (reported in > 10% of patients) were diarrhea (18.6%), somnolence (15.1%), decreased appetite (12.8%), pyrexia (12.8%), and vomiting (10.5%). In the volume-matched placebo group, the most common AE reported was vomiting (16.5%).
Table 16: Summary of Harms Results From the CARE 3 and CARE 4 Trials
Harms | CARE 3 | CARE 4 | |||
|---|---|---|---|---|---|
Cannabidiol 20 mg/kg/day (n = 82) | Cannabidiol 10 mg/kg/day (n = 67) | Pooled placebo (n = 76) | Cannabidiol 20 mg/kg/day (n = 86) | Placebo 20 mg/kg/day (n = 85) | |
AEs, n (%) | |||||
≥ 1 AE | 77 (93.9) | 56 (83.6) | 55 (72.4) | 74 (86.0) | 59 (69.4) |
Most common AEsa | |||||
Somnolence | 25 (30.5) | 14 (20.9) | 4 (5.3) | 13 (15.1) | 8 (9.4) |
Decreased appetite | 21 (25.6) | 11 (16.4) | 6 (7.9) | 11 (12.8) | 2 (2.4) |
Diarrhea | 12 (14.6) | 7 (10.4) | 6 (7.9) | 16 (18.6) | 7 (8.2) |
Upper respiratory tract infection | 11 (13.4) | 11 (16.4) | 11 (14.5) | NA | NA |
Pyrexia | 10 (12.2) | 6 (9.0) | 12 (15.8) | 11 (12.8) | 7 (8.2) |
Vomiting | 10 (12.2) | 4 (6.0) | 9 (11.8) | 9 (10.5) | 14 (16.5) |
Nasopharyngitis | 9 (11.0) | 3 (4.5) | 5 (6.6) | NA | NA |
Status epilepticus | 4 (4.9) | 7 (10.4) | 3 (3.9) | NA | NA |
SAEs, n (%) | |||||
≥ 1 SAE | 13 (15.9) | 13 (19.4) | 8 (10.5) | 20 (23.3) | 4 (4.7) |
Most common SAEsb | |||||
Pneumonia | 2 (2.4) | 3 (4.5) | 0 | 3 (3.5) | 0 |
Viral infection | NA | NA | NA | 2 (2.3) | 0 |
AST increased | 1 (1.2) | 1 (1.5) | 0 | 4 (4.7) | 0 |
ALT increased | 1 (1.2) | 0 | 0 | 4 (4.7) | 0 |
Gamma-glutamyltransferase increased | 1 (1.2) | 0 | 0 | 3 (3.5) | 0 |
Dehydration | 0 | 1 (1.5) | 0 | 0 | 2 (2.4) |
Status epilepticus | 4 (4.9) | 7 (10.4) | 3 (3.9) | 1 (1.2) | 1 (1.2) |
Convulsion | 2 (2.4) | 0 | 0 | 2 (2.3) | 0 |
Hypoxia | 0 | 1 (1.5) | 1 (1.3) | 2 (2.3) | 0 |
Acute respiratory failure | NA | NA | NA | 3 (3.5) | 0 |
Treatment discontinuation due to AEs, n (%) | |||||
Patients who discontinued | 6 (7.3) | 1 (1.5) | 1 (1.3) | 12 (14.0) | 1 (1.2) |
Reason for discontinuationb | |||||
ALT increased | 3 (3.7) | 1 (1.5) | 0 | 3 (3.5) | 0 |
AST increased | 2 (2.4) | 1 (1.5) | 0 | 3 (3.5) | 0 |
Gamma-glutamyltransferase increased | 2 (2.4) | 0 | 0 | 2 (2.3) | 0 |
Deaths, n (%) | |||||
Patients who died | 0 | 0 | 0 | 1 (1.2) | 0 |
Reasons for death | |||||
Acute respiratory distress syndrome | 0 | 0 | 0 | 1 (1.2) | 0 |
Notable harms, n (%) | |||||
Nervous system disorders | 48 (58.5) | 28 (41.8) | 20 (26.3) | 33 (38.4) | 25 (29.4) |
Somnolence | 25 (30.5) | 14 (20.9) | 4 (5.3) | 13 (15.1) | 8 (9.4) |
Status epilepticus | 4 (4.9) | 7 (10.4) | 3 (3.9) | 1 (1.2) | 1 (1.2) |
Sedation | 3 (3.7) | 2 (3.0) | 1 (1.3) | 7 (8.1) | 1 (1.2) |
Hepatocellular injury | 17 (20.7) | 16 (23.9) | 12 (17.1) | 24 (27.9) | 13 (15.3) |
ALT increased | 4 (4.9) | 3 (4.5) | 1 (1.3) | 8 (9.3) | 2 (2.4) |
AST increased | 3 (3.7) | 3 (3.7) | 1 (1.3) | 6 (7.0) | 1 (1.2) |
Bilirubin elevation | NR | NR | NR | NR | NR |
Serum transaminase elevation | 1 (1.2) | 1 (1.5) | 0 | 2 (2.3) | 0 |
Liver function test abnormal | NR | NR | NR | 4 (4.7) | 0 |
Acute hepatic failure | NR | NR | NR | 3 (3.5) | 0 |
Hepatic failure | NR | NR | NR | 1 (1.2) | 0 |
Hepatotoxicity | NR | NR | NR | 1 (1.2) | 0 |
Gastrointestinal disorders | 27 (32.9) | 15 (22.4) | 21 (27.6) | 30 (34.9) | 23 (27.1) |
Diarrhea | 12 (14.6) | 7 (10.4) | 6 (7.9) | 16 (18.6) | 7 (8.2) |
Vomiting | 10 (12.2) | 4 (6.0) | 9 (11.8) | 9 (10.5) | 14 (16.5) |
Constipation | 4 (4.9) | 3 (4.5) | 3 (3.9) | 6 (7.0) | 4 (4.7) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; NA = not available; NR = not reported; SAE = serious adverse event.
aOccurring in more than 10% of patients in any treatment group.
bOccurring in at least 2% of patients in any treatment group.
Sources: Clinical Study Report for CARE 316 and CARE 4 trials;17 sponsor’s summary of clinical evidence.
Serious AEs
In the CARE 3 trial, at least 1 SAE was reported by 15.9% of patients in the cannabidiol 20 mg/kg/day group, 19.4% of patients in the cannabidiol 10 mg/kg/day group, and 10.5% of patients in the pooled placebo group. The most common SAEs (reported in > 2% of patients) in the cannabidiol 20 mg/kg/day group were status epilepticus (4.9%), convulsion (2.4%), and pneumonia (2.4%). In the cannabidiol 10 mg/kg/day group, the most common SAEs were status epilepticus (10.4%) and pneumonia (4.5%). In the pooled placebo group, the most common SAE was status epilepticus (3.9%).
In the CARE 4 trial, at least 1 SAE was reported by 23.3% and 4.7% of patients in the cannabidiol 20 mg/kg/day and the volume-matched placebo groups, respectively. Among patients randomized to receive cannabidiol 20 mg/kg/day, the most common SAEs were increased AST (4.7%), increased ALT (4.7%), acute respiratory failure (3.5%), increased gamma-glutamyltransferase (3.5%), pneumonia (3.5%), viral infection (2.3%), convulsion (2.3%), and hypoxia (2.3%). In the volume-matched placebo group, the most common SAE was dehydration (2.4%).
Treatment Discontinuation Due to AEs
In the CARE 3 trial, discontinuation of treatment due to AEs was reported by 7.3% of patients in the cannabidiol 20 mg/kg/day group, 1.5% of patients in the cannabidiol 10 mg/kg/day group, and 1.3% of patients in the pooled placebo group. The most common reasons for treatment discontinuation due to AEs (reported in more than 2% of patients) were all reported in the cannabidiol 20 mg/kg/day group: increased levels of ALT (3.7%), AST (2.4%), and gamma-glutamyltransferase (2.4%).
In the CARE 4 trial, discontinuation of treatment due to AEs was reported in 14.0% and 1.2% of patients in the cannabidiol 20 mg/kg/day group and the volume-matched placebo group, respectively. The most common reasons for treatment discontinuation due to AEs (reported in more than 2% of patients) were all reported in the cannabidiol 20 mg/kg/day group: increased levels of ALT (3.5%), AST (3.5%), and gamma-glutamyltransferase (2.3%).
Mortality
There were no reported deaths in the CARE 3 trial. In the CARE 4 trial, 1 death was recorded by investigators (1.2% of patients) due to acute respiratory distress syndrome in the cannabidiol 20 mg/kg/day group.
Notable Harms
Notable harms of interest were related to nervous system disorders (i.e., somnolence, status epilepticus, and sedation), hepatocellular injury or investigation (i.e., increased levels of ALT and AST, bilirubin elevation, and serum transaminase elevation), and gastrointestinal disorders (i.e., diarrhea, vomiting, and constipation).
In the CARE 3 trial, somnolence, status epilepticus, and sedation were reported in 30.5%, 4.9%, and 3.7% of patients, respectively, in the cannabidiol 20 mg/kg/day group; in 20.9%, 10.4%, and 3.0% of patients, respectively, in the cannabidiol 10 mg/kg/day group; and in 5.3%, 3.9%, and 1.3% of patients, respectively, in the pooled placebo group. Increased levels of ALT, AST, and serum transaminase were reported in 4.9%, 3.7%, and 1.2% of patients, respectively, in the cannabidiol 20 mg/kg/day group; in 4.5%, 3.7%, and 1.5% of patients, respectively, in the cannabidiol 10 mg/kg/day group; and in 1.3%, 1.3%, and 0% of patients, respectively, in the pooled placebo group. The following investigations were not reported in the CARE 3 trial: abnormal liver function test, acute hepatic failure, bilirubin elevation, and hepatotoxicity. Diarrhea, vomiting, and constipation were reported in 14.6%, 12.2%, and 4.9% of patients, respectively, in the cannabidiol 20 mg/kg/day group; in 10.4%, 6.0%, and 4.5% of patients, respectively, in the cannabidiol 10 mg/kg/day group; and in 7.9%, 11.8%, and 3.9% of patients, respectively, in the pooled placebo group.
In the CARE 4 trial, somnolence, sedation, and status epilepticus were reported in 15.1%, 8.1%, and 1.2% of patients, respectively, in the cannabidiol 20 mg/kg/day group and in 9.4%, 1.2%, and 1.2% of patients, respectively, in the volume-matched placebo group. The following hepatocellular injury and investigation AEs were reported in the cannabidiol 20 mg/kg/day group: increased ALT (9.3%), increased AST (7.0%), abnormal liver function test (4.7%), acute hepatic failure (3.5%), serum transaminase elevation (2.3%), hepatic failure (1.2%), and hepatotoxicity (1.2%). In the volume-matched placebo group, increased levels of ALT and AST were reported in 2.4% and 1.2% of patients, respectively. Diarrhea, vomiting, and constipation were reported in 18.6%, 10.5%, and 7.0% of patients, respectively, in the cannabidiol 20 mg/kg/day group and in 8.2%, 16.5%, and 4.7% of patients in the volume-matched placebo group.
Critical Appraisal
Internal Validity
Both the CARE 3 and CARE 4 trials were multicentre, randomized, double-blind phase III trials, designed in accordance with the European Medicines Agency Guideline on Clinical Investigation of Medicine Products in the Treatment of Epileptic Disorders and the FDA Guidelines for the Clinical Evaluation of Antiepileptic Drugs (Adults and Children). The treatment period (including the titration period), 10-day taper period, and 28-day follow-up period employed in the trial were chosen in consultation with an external advisory board and the FDA Center for Drug Evaluation and Research.76,77 Patients were randomized centrally using IVRS technology, which is typically adequate for concealing allocation until treatment assignment. IVRS technology was also used to dispense the investigational product, allowing the treatment concealment for both patients and the investigators.
Although the CARE 3 trial included 4 treatment types (cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, volume-matched placebo 20 mg/kg/day, and volume-matched placebo 10 mg/kg/day), the study participants were randomized using a 1:1:1 randomization ratio to the cannabidiol 20 mg/kg/day treatment group, the cannabidiol 10 mg/kg/day treatment group, and the placebo treatment group. Patients in the placebo group were split in half to receive either the 20 mg/kg/day placebo or the 10 mg/kg/day placebo, and the study results were reported based on the pooled placebo group. While this approach is acceptable, it relies on the assumption that randomization was successful in each group. Differences in baseline characteristics between patients in the cannabidiol 20 mg/kg/day, cannabidiol 10 mg/kg/day, and pooled placebo groups were noted in the following: proportion of patients reporting convulsive seizures longer than 30 minutes and reporting concomitant use of benzodiazepine derivatives at baseline. According to the clinical experts consulted by CADTH for the purpose of this review, benzodiazepine derivates, such as clobazam, could strengthen the treatment effect of cannabidiol due to synergism; they did not anticipate any significant effect modification through the use of the other concomitant ASMs. The clinical experts, however, were uncertain if the other imbalances could influence treatment response.
At CADTH’s request, the sponsor reported that the assumptions related to splitting the placebo group and pooling results for analyses were not formally tested. However, the sponsor noted, as described in the Clinical Study Report for the CARE 3 trial, that posthoc sensitivity analyses were conducted on the primary outcome to determine if pooling the placebo group had an effect on the results. The analyses indicated that the efficacy response when cannabidiol 20 mg/kg/day and 10 mg/kg/day dosages were compared to their corresponding placebo dosages (i.e., 20 mg/kg/day and 10 mg/kg/day, respectively) were consistent with the results of similar comparisons in the pooled analyses. In the CARE 4 trial, the 1:1 randomization ratio and the randomization stratification factors appeared appropriate, and no notable baseline imbalances were observed between the cannabidiol 20 mg/kg/day group and the volume-matched placebo group.
In the CARE 3 trial, 23.2% of patients screened for entry into the trial did not meet the screening criteria; the reason they did not meet the screening criteria was listed as “other reason” for approximately a third of these patients. Moreover, a higher proportion of patients in the cannabidiol 20 mg/kg/day group discontinued the study than in the cannabidiol 10 mg/kg/day and pooled placebo groups (approximately 12% versus approximately 3%). The higher discontinuation rate in the cannabidiol 20 mg/kg/day group appeared to be driven by AEs. In addition, 6 patients randomized to the cannabidiol 10 mg/kg/day group and 3 patients randomized to receive volume-matched placebo at 10 mg/kg/day were accidentally titrated to 20 mg/kg/day. This error was detected and, by day 42, those patients were returned to the 10 mg/kg/day dosage. For the purpose of the safety analysis, these patients were moved to their respective 20 mg/kg/day dosage groups. In the CARE 4 trial, a higher proportion of patients in the cannabidiol 20 mg/kg/day group discontinued the study than in the volume-matched placebo group (9.3% versus 1.2%). The higher discontinuation rate in the cannabidiol 20 mg/kg/day group appeared to be driven by AEs. The application of the MNAR assumption and sensitivity analysis exploring missing efficacy results due to treatment discontinuation suggest that bias due to uneven discontinuation was unlikely.
In both the CARE 3 and CARE 4 trials, all efficacy outcome questionnaires and assessments were to be completed by the caregiver. To maintain consistency, the same caregiver, if the patients had multiple caregivers, was to complete and answer the questionnaire and assessment. Seizure information in both studies was ascertained using an IVRS diary, while paper diaries were used to capture use of the investigational product, use of concomitant medications, and occurrence of AEs. A review of clinical outcomes used in LGS-focused research noted that while diaries enable day-to-day reporting, without a standardized questionnaire that can serve a prompt for the diary, the daily entry may be biased.78 According to input from the clinical experts, patient and parent or caregiver reports of seizures tend to be accurate for motor seizures but are not very reliable or accurate for nonmotor seizures. Indeed, studies examining the accuracy of clinical reports of seizures found that while absence seizures were least accurately identified (14%) compared to myoclonic seizures (48%) and complex or simple partial seizures (63%), all atonic and generalized tonic seizures were correctly identified by parents.79 Accordingly, it may be assumed that the frequencies of drop seizures reported by patients and/or caregivers in the CARE 3 and CARE 4 trials are reliable estimates of the true frequency experienced by patients. Seizure diaries are the standard method of collecting data for clinical trials, and the International League Against Epilepsy recommends the use of dairies for collecting seizure frequency data.18
Both the CARE 3 and CARE 4 trials assessed HRQoL — outcomes deemed important by the patients and clinicians — using validated and reliable instruments: the QOLCE and the QOLIE-31-P questionnaires. The double-blind nature of the trials minimized the risk of bias in the measurement of subjective items on the QOLCE and QOLIE-31-P questionnaires. However, comparative efficacy conclusions based on the HRQoL outcomes are limited since the QOLCE and the QOLIE-31-P questionnaires were not part of the hierarchical testing procedure and because of the low completion rate across the treatment groups. Total QOLCE scores were available for 47.6% and 36.3% of patients in the CARE 3 and CARE 4 trials, respectively, while total QOLIE-31-P scores were available for 16.5% and 16.4% of patients in the CARE 3 and CARE 4 trials, respectively. Consequently, the assessment of HRQoL in both trials is at high risk of attrition bias, although the extent and direction of the bias cannot be determined since it is not clear if the patients who completed the questionnaires were systematically different from those who did not. As the completion rates were similar between the treatment groups within the CARE 3 and CARE 4 trials, there is little risk that attrition bias favoured any 1 treatment group.
The analysis of efficacy results in the CARE 3 and CARE 4 trials followed a defined statistical analysis plan. The primary and key secondary end points were addressed using a hierarchical gate-keeping procedure that controlled for type I errors. The sponsor conducted additional sensitivity analysis of the primary efficacy end point using the per-protocol analysis set and testing the MNAR assumption. In all scenarios, the sensitivity analyses were consistent with the primary efficacy analysis. Subgroup analyses were performed in both the CARE 3 and CARE 4 trials for the primary efficacy end point to examine the consistency of the treatment effect observed. Although the subgroups were prespecified, strong conclusions could not be drawn due to the small sample size and the absence of statistical testing for interaction effects.
External Validity
Due to the rarity of the LGS and a lack of population-based data on LGS, the clinical experts consulted by CADTH for the purpose of this review were unable to assess if the results of the CARE 3 and CARE 4 trials were applicable to the patients seen in the Canadian clinical setting. One clinical expert added that they do not, however, expect patients with LGS living in Canada to differ from such patients elsewhere. The clinical experts did note trial details that were applicable to the Canadian clinical setting, and others that were not representative of Canadian clinical practice. The generalizability of the evidence, including the clinical expert input, is summarized in Table 17.
Table 17: Assessment of Generalizability of Evidence for Cannabidiol
Domain | Factor | Evidence | Assessment of generalizability |
|---|---|---|---|
Population | Baseline drop seizure rate | To be eligible for inclusion in the CARE 3 and CARE 4 trials, patients must have had at least 2 drop seizures each week during the 28 days of the baseline period. | According to the clinical experts, diagnosis of LGS is not dependent on a minimum number of drop seizures per week. The clinical experts agreed that minimum number of drop seizures should not be used for the consideration of initiating adjunctive treatment with cannabidiol in patients with LGS. |
Intervention | Washout period | Patients were excluded from the CARE 3 and CARE 4 trials if they were currently using or had used recreational or medicinal cannabis or synthetic cannabinoid (e.g., Sativex) within the 3 months before trial entry. | In the Canadian practice setting, medicinal cannabis for adjunctive treatment for seizure associated with LGS may be accessed through the medical cannabis pathways supported by Health Canada. While the clinical experts agreed that they would require eligible patients to stop use of recreational or medicinal cannabis before initiating pharmaceutical cannabis, they would not impose any sort of washout period. |
Length of treatment | The treatment period in the CARE 3 and CARE 4 trials was 14 weeks: 2 weeks dose titration and 12 weeks dose maintenance. | According to the clinical experts, response to treatment in patients with LGS, who often experience seizures daily, is usually apparent 1 to 2 months after achieving the target dose of ASM. Accordingly, the clinical experts agreed that the treatment period in the CARE 3 and CARE 4 trials was long enough to detect a meaningful treatment response in patients with LGS. The clinical experts did note, however, that it is uncertain if response to cannabidiol can be sustained in the long term.80 | |
Co-interventions | Limitation on use of concurrent ASMs | In the CARE 3 and CARE 4 trials, the inclusion criteria limited the use of ASMs to no more than 4 concurrent ASMs. | According to the clinical experts, limiting the number of concurrent ASMs for access to cannabidiol is not a reasonable expectation. The clinical experts explained that this limitation was likely put in place due to the lack of efficacy of ASMs after 3 ongoing agents and therefore to exclude patients from the trial who would be unlikely to respond to cannabidiol. According to the clinical experts, there have been no studies to date demonstrating significant reduction of seizures with a fourth or fifth drug added to the regimen of patients with refractory disease. |
Use of ketogenic diet and VNS | In the CARE 3 trial, overall use of ketogenic diets or VNS was reported in 8.4% and 23.6% of patients, respectively. In the CARE 4 trial, overall use of ketogenic diets and VNS was reported in 8.2% and 29.8% of patients, respectively. | According to the clinical experts, ketogenic diet and VNS are considered acceptable background therapy. The clinical experts noted the proportion of patients using VNS therapy in the CARE 3 and CARE 4 trials is higher than would be seen in the Canadian practice setting as VNS is not as readily available in Canada. | |
Comparator | Usual care | In the CARE 3 and CARE 4 trials, cannabidiol was compared to volume-matched placebo control groups. | The clinical experts noted that medical cannabis has been available to patients with LGS in Canada for a number of years now, although seldom at the dose indicated for cannabidiol. They are uncertain how pharmaceutical-grade cannabidiol would compare to medicinal cannabis when added to background ASM vs. the placebo response. |
Outcomes | Reduction in drop seizure frequency | Percent change from baseline in drop seizure frequency was the primary efficacy outcome in both the CARE 3 and CARE 4 trials. | According to the clinical experts, the reduction of seizure frequency is the main goal of treatment in patients with LGS. The clinical experts added that it is reasonable to expect that improvement in seizure frequency would translate to improved HRQoL. However, according to input from the patient group and the clinical experts, focusing exclusively on seizure counts does not directly capture the range of seizure burden that impacts both patients and their caregivers and families, which would include nonmotor seizures, severity of seizures, and inability to engage in activities of daily living. |
HRQoL | HRQoL was assessed in the CARE 3 and CARE 4 trials using the QOLCE and the QOLIE-31-P scores. | Input from the clinical experts and patient group emphasized that HRQoL is an important outcome. The clinical experts added that the QOLCE and the QOLIE-31-P questionnaires are not practical for clinical practice due to the special training required to administer the instrument. According to input from the clinical experts, patients and parents or caregivers are instead asked how they are feeling and whether there has been in improvement in their condition. | |
Setting | Multinational, multicentre study | No Canadian trial sites were included in either the CARE 3 or the CARE 4 trial. | The clinical experts were unable to comment on whether the trial results were generalizable to the Canadian setting. |
ASM = antiseizure medication; HRQoL = health-related quality of life; LGS = Lennox-Gastaut syndrome; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = Quality of Life in Epilepsy, version 2; VNS = vagus nerve stimulation.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for the outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:19,20
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of the effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and/or publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when such a threshold was available) or to the null. The presence or absence of an important effect were based on thresholds informed by the clinical experts consulted for this review.
For the GRADE assessments, findings from the CARE 3 and CARE 4 trials were considered together and summarized narratively per outcome because these studies were similar in population, interventions, design, and outcome measures.21
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for cannabidiol versus placebo.
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
To inform the long-term safety and tolerability of cannabidiol as an adjunctive treatment in children and adults with inadequately controlled LGS, the results of 1 sponsor-conducted OLE study — the CARE 5 trial — were summarized.22
Description of Studies
The CARE 5 trial was a multicentre, single-arm, OLE, phase III study with the primary objective of evaluating the long-term safety and tolerability of cannabidiol as adjunctive treatment in patients aged 2 years and older with LGS (N = 366) who had completed the CARE 3 and CARE 4 trials (the “core studies”). The long-term efficacy of cannabidiol as adjunctive treatment in patients aged 2 years and older with LGS was the secondary objective of the CARE 5 trial.
The CARE 5 trial was conducted across 75 sites in 8 countries (Australia, Spain, France, Israel, Netherlands, Poland, UK, and US); approximately 78% of patients were living in the US. A schematic of the CARE 5 study design is presented in Figure 3. The CARE 5 trial consisted of a titration period and a maintenance period, followed by a 10-day taper period. Between visits, safety telephone calls were made every 4 weeks starting at visit 2, with additional safety telephone calls made every 7 days for patients who were titrated to dosages above 20 mg/kg/day, until stable dosing was achieved. All safety telephone calls assessed AEs, epilepsy-related hospitalization, concomitant medications, and/or changes to medications. The end-of-treatment visit occurred either after a maximum duration of 6 years (312 weeks after visit 1), depending on the country of residence; following early withdrawal from the study; or following an unscheduled end-of-treatment visit conducted no earlier than 730 days after visit 1. A safety telephone call was made 2 weeks after the end-of-taper visit, or the date of final dosing, to administer the Cannabis Withdrawal Scale or the Pediatric Cannabinoid Withdrawal Scale surveys.
Populations
Patients eligible for inclusion in the CARE 5 trial were required to have completed all scheduled visits in the treatment phase of the CARE 3 and CARE 4 trials. Patients were excluded from entering the CARE 5 trial if they met any of the following exclusion criteria:
currently using or has used recreational or medicinal cannabis or synthetic cannabinoid-based medications within the 3 months before study entry, not including cannabidiol received during the core study
unwilling to abstain from using recreational or medicinal cannabis or synthetic cannabinoid-based medications during the study
a history of symptoms (e.g., dizziness, light-headedness, blurred vision, palpitations, weakness, syncope) related to a drop in blood pressure due to postural changes
any history of suicidal behaviour or any suicidal ideation of type 4 or 5 on the Columbia–Suicide Severity Rating Scale at visit 1
significantly impaired hepatic function at the end-of-treatment visit of the core study or at visit 1 of the CARE 5 trial if reassessed
is of childbearing potential or has a partner of childbearing potential, unless willing to ensure that they or their partner use highly effective contraception for the duration of the study and for 3 months thereafter.
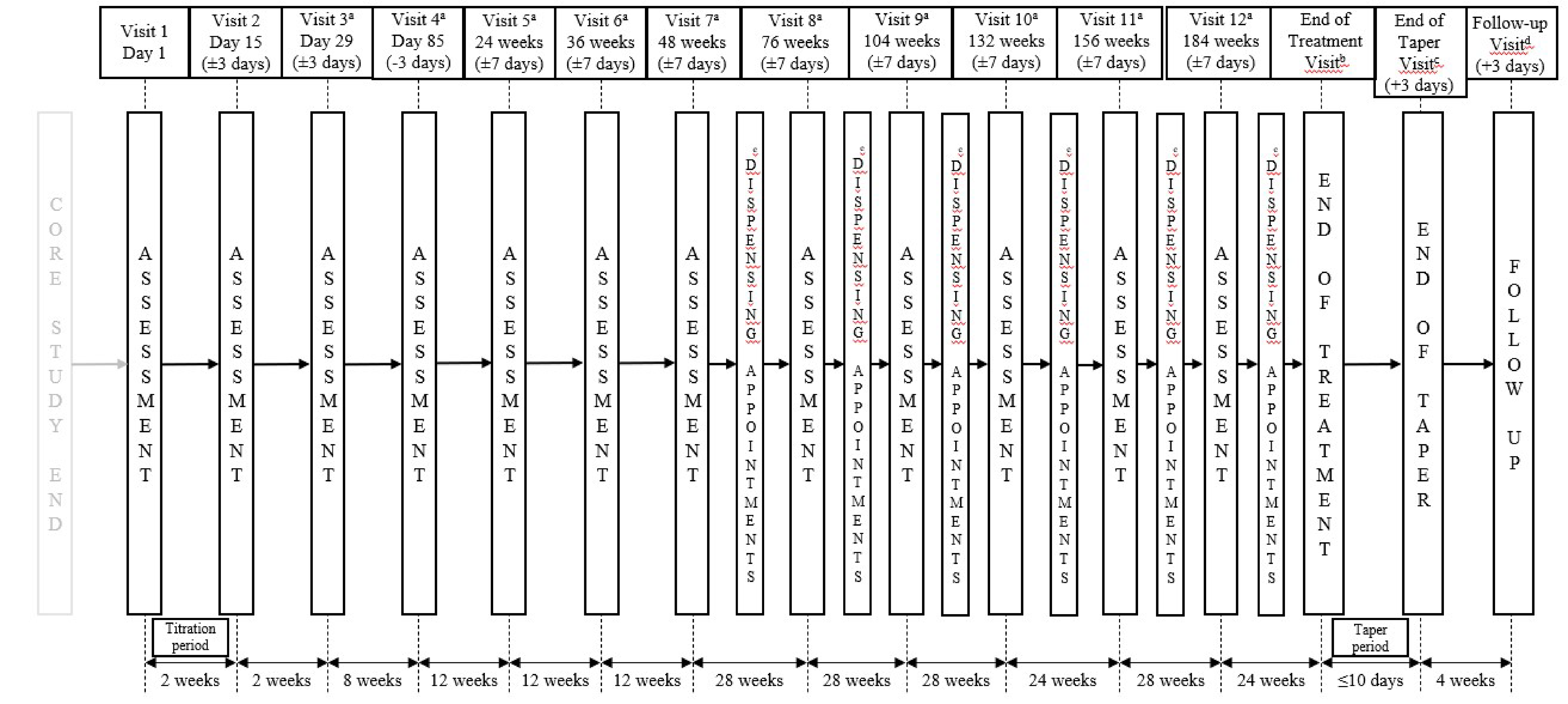
Notes: All participants were instructed to begin titration of the OLE IMP on the evening of visit 1 (day 1). Participants with no gap in IMP dosing between the core study and the OLE (including tapered dosing) took their final dose of core study IMP on the morning of visit 1. The maximum duration of the OLE study at the Poland site was 6 years (312 weeks after visit 1).
a Between visits, safety telephone calls were made every 4 weeks (± 7 days). In addition, during titration of dosages above 20 mg/kg/day, safety telephone calls were made every 7 days (± 3 days) until stable dosing was achieved. All safety telephone calls assessed adverse events, epilepsy-related hospitalizations, concomitant medications, and/or changes to medication.
b The end-of-treatment visit occurred after a maximum of 6 years’ treatment (312 weeks after visit 1), following early withdrawal from the study, or following an unscheduled end-of-treatment visit conducted no earlier than 730 days after visit 1.
c A safety telephone call was made 2 weeks (± 3 days) after the end-of-taper visit (or the date of final dosing) to collect seizure information, to administer the Cannabis Withdrawal Scale or Pediatric Cannabinoid Withdrawal Scale surveys, and to assess adverse events, epilepsy-related hospitalization, concomitant medications, and/or changes to medication.
d Could be conducted by telephone.
e IMP dispensing appointments took place between all visits after visit 7, 14 weeks after the previous visit.
Source: Sponsor’s summary of clinical evidence.42
Interventions
All patients enrolled in the CARE 5 trial received adjunctive treatment with cannabidiol, which consisted of a 2-week titration period, a maintenance period, and a 10-day taper period. Patients were instructed to begin titration of the investigational product on the evening of visit 1. Patients with no gaps in investigational dosing between the core studies and the OLE, including tapered dosing, took their final dose of core study investigational product on the morning of OLE visit 1. Patients were instructed to take cannabidiol twice daily (morning and evening) immediately after their usual ASM administration, or as otherwise specified by the investigator. Patients were titrated up to 10 mg/kg/day to 20 mg/kg/day cannabidiol using a titration schedule. In the event of intolerance during titration, the patient was maintained on a dosage below 10 mg/kg/day or 20 mg/kg/day. A titration rate faster than recommended was considered if there was an increase in seizures, following consultation with the medical monitor. The patients continued at their 10 mg/kg/day to 20 mg/kg/day dosage during the maintenance period. During the maintenance period, dosing adjustments by the investigators were permitted should a patient experience intolerance (dose decrease) or require better seizure control (dose increase) until the optimal dose was achieved. If deemed necessary by the investigator, a maximum dosage of 30 mg/kg/day was permitted. Dosage increases above 20 mg/kg/day were recommended to be done slowly, with maximum increments of 2.5 mg/kg every 5 to 7 days. Among patients whose dosage had been decreased, dosage increases were still considered, provided there was adequate tolerance. Following the end-of-treatment or withdrawal visit, doses were tapered at home (10% per day for 10 days) until the end-of-taper visit. Patients could receive treatment for up to a maximum of 6 years (312 weeks after visit 1), depending on the country of enrolment.
Outcomes
Primary End Point
The primary end point in the CARE 5 trial was the frequency of AEs.
Secondary End Points
The following seizure information was evaluated as secondary efficacy end points: drop seizure frequency, nondrop seizure frequency, number of patients who were drop seizure free, and response rate (defined in terms of a ≥ 25%, ≥ 50%, ≥ 75%, or 100% reduction of in drop seizure frequency).
The secondary efficacy end points evaluated in the CARE 5 trial that were also relevant to this review were:
HRQoL (as measured by the QOLCE and QOLIE-31-P scores)
need for hospitalization due to epilepsy.
Statistical Analysis
No formal sample size calculation was performed.
Safety and efficacy outcomes were summarized using descriptive statistical methods. Changes from baseline were presented where baseline data were available from the core studies. Efficacy end points were analyzed in the safety analysis set. Missing data were addressed using the last observation carried forward method.
There was no formal hypothesis testing.
Results
Patient Disposition
Patient disposition for the CARE 5 OLE study is summarized in Table 18.
Of the 681 patients screened and enrolled in the study, 366 (100%) were patients with LGS. Of these 366 patients, one-third (33.6%) discontinued the study, mainly due to withdrawal by patient or parent or guardian (13.1%), AEs (10.4%), and “other reasons” (4.9%). Most of the patients with LGS (79.5%) did not continue to the taper phase, which lasted up to 10 days. However, the majority of patients with LGS who did continue to the taper phase (20.5%) completed the taper phase (18.3%). All enrolled patients received at least 1 dose of cannabidiol and were included in the safety analysis set.
The retention rates for the safety analysis set at weeks 37 to 48 (12 months), weeks 85 to 96, weeks 133 to 144 (36 months), weeks 181 to 192, and weeks 241 to 252 were 82% (299 of 366 patients), 64% (236 of 366 patients), 59% (216 of 366 patients), 6% (22 of 366 patients), and 2% (8 of 366 patients), respectively.
Table 18: Patient Disposition in CARE 5 Open-Label Extension Study
Patient disposition | CARE 5 |
|---|---|
Total patients screened, N | 681 |
Total patients enrolled, N | 681 |
Patients with LGS | |
Patients with LGS enrolled to treatment phase, N (%) | 366 (100) |
Completed study, n (%) | 243 (66.4) |
Discontinued study, n (%) | 123 (33.6) |
Withdrawal by patient or parent/guardian | 48 (13.1) |
AE | 38 (10.4) |
Other | 18 (4.9) |
Withdrawn by the investigator | 11 (3.0) |
Met withdrawal criteria | 7 (1.9) |
Lost to follow-up | 1 (0.3) |
Continued to taper phase, n (%) | |
No | 291 (79.5) |
Yes | 75 (20.5) |
Withdrawal due to AE | 1 (0.3) |
Withdrawal by patient or parent/guardian | 3 (0.8) |
Not reported | 4 (1.1) |
Completed taper phase, n (%) | 67 (18.3) |
Safety analysis set, N | 366 |
AE = adverse event; LGS = Lennox-Gastaut syndrome.
Source: Clinical Study Report for CARE 5 trial.22
Baseline Characteristics
The baseline demographic and clinical characteristics of the CARE 5 OLE study for patients with LGS are summarized in Table 19.
The mean age of the patients with LGS was 15.9 years (SD = 9.5): 36 patients (9.8%) were aged 2 to 5 years, 121 patients (33.1%) were aged 6 to 11 years, 89 patients (24.3%) were aged 12 to 17 years, and 120 patients (32.8%) were aged 18 years or older. The proportion of male patients was 54.1%. The majority of patients (88.8%) were white. The median number of currently used ASMs was 3 (range, 1 to 13).
Table 19: Summary of Baseline Characteristics of Patients With LGS (Safety Analysis Set) in CARE 5 OLE Study
Characteristic | CARE 5 (N = 366) |
|---|---|
Age (years) | |
Mean (SD) | 15.9 (9.5) |
Median (range) | 13.7 (3.0 to 48.3) |
Sex, n (%) | |
Female | 168 (45.9) |
Male | 198 (54.1) |
Race, n (%) | |
White/Caucasian | 325 (88.8) |
Black/African American | 15 (4.1) |
Asian | 10 (2.7) |
American Indian/Alaska Native | 0 (0.0) |
Not applicablea | 1 (0.3) |
Other | 15 (4.1) |
Weight at baseline | |
Patients, n | 347 |
Mean, kg(SD) | 43.7 (23.2) |
Median (range) | 38.5 (11.2 to 142.1) |
Height at baseline (cm) | |
Patients, n | 344 |
Mean kg (SD) | 142.3 (23.0) |
Median (range) | 146.5 (89.0 to 190.5) |
BMI at baseline (kg/m2) | |
Patients, n | 344 |
Mean kg (SD) | 20.18 (6.3) |
Median (range) | 18.5 (10.4 to 52.3) |
Number of ASMs patient currently taking | |
Mean (SD) | 3.40 (1.383) |
Median (range) | 3.00 (1.0 to 13.0) |
ASM = antiseizure medication; BMI = body mass index; LGS = Lennox-Gastaut syndrome; OLE = open-label extension; SD = standard deviation.
aNot applicable as per country-specific data protection law.
Source: Clinical Study Report for CARE 5 trial.22
Exposure to Study Treatments
Exposure information for the 366 patients with LGS in the CARE 5 OLE study is described in Table 20.
The mean number of dosing days during the treatment period was 838 (SD = 464.85). The median number of dosing days was 1,090, with a minimum of 3 days and a maximum of 1,711 days. The maximum total daily dose of cannabidiol taken by patients with LGS was as follows: 45% of patients took 30 mg/kg or more, 41.2% of patients took more than 20 mg/kg but less than 30 mg/kg, and 13.8% of patients took 20 mg/kg or less. Rescue medications were taken by 258 patients (70.5%), with benzodiazepine derivatives being the most common therapeutic class (70.2% of patients) and diazepam being the most common rescue medicine (54.4% of patients).
Table 20: Exposure of Patients With LGS (Safety Analysis Set) in CARE 5 OLE Study
Exposure | CARE 5 (N = 366) |
|---|---|
Treatment phase (all patients) | — |
Duration, mean patient-days (SD) | 838.0 (464.85) |
Duration, median patient-days (range) | 1,090.0 (3 to 1,711) |
Maximum dose, n (%) | — |
20 mg/kg/day or less | 44 (13.8) |
> 20 mg/kg/day to < 30 mg/kg/day | 131 (41.2) |
30 mg/kg/day or more | 143 (45.0) |
Missing/unknown | 48 (13.1) |
LGS = Lennox-Gastaut syndrome; OLE = open-label extension; SD = standard deviation.
Source: Clinical Study Report for CARE 5 trial.22
Concomitant Medications and Co-Interventions
The concomitant medications used by at least 10% of the 366 patients with LGS during the CARE 5 trial are presented in Table 21.
All 366 patients with LGS (100%) took 1 or more concomitant ASMs during the study. If seizure freedom was achieved with the use of cannabidiol during the study, the investigator considered reducing the dose of concomitant ASMs after consultation with the medical monitor.
Table 21: Concomitant ASMs Taken by Patients With LGS (Safety Analysis Set) in CARE 5 OLE Study
Exposure | CARE 5 (N = 366) |
|---|---|
Number of patients who received 1 or more concomitant ASMs during the study, n (%) | 366 (100.0) |
Other antiepileptics, n (%) | 315 (86.1) |
Levetiracetam | 128 (35.0) |
Topiramate | 60 (16.4) |
Lamotrigine | 134 (36.6) |
Zonisamidea | 45 (12.3) |
Lacosamide | 68 (18.6) |
Felbamatea | 56 (15.3) |
Benzodiazepine derivatives, n (%) | 258 (70.5) |
Clobazam | 199 (54.4) |
Clonazepam | 58 (15.8) |
Fatty acid derivatives, n (%) | 162 (44.3) |
Valproic acid | 148 (40.4) |
Carboxamide derivatives, n (%) | 133 (36.3) |
Rufinamide | 109 (29.8) |
ASM = antiseizure medication; LGS = Lennox-Gastaut syndrome; OLE = open-label extension.
Note: Only those ASMs used in > 10% of patients are presented.
aNot available in Canada.
Source: Clinical Study Report for CARE 5 trial.22
Efficacy
Key efficacy outcomes for CARE 5 are presented in Table 22.
The proportion of patients experiencing drop seizure–free status at weeks 37 to 48 (12 months), weeks 133 to 144 (36 months), and weeks 253 to 264 (66 months) was 7% (24 of 364 patients), 8% (30 of 364 patients), and 9% (34 of 364 patients), respectively. The median percent change from baseline in drop seizure frequency during the same OLE periods from baseline of the core studies were –55.3% (IQR, –83.8% to –16.6%; n = 364), –59.1% (IQR, –85.7% to –15.2%; n = 364), and –59.4% (IQR, –87.1% to –16.0%; n = 364), respectively. The mean percent change in drop seizure frequency during the same periods of the OLE from baseline of the core studies were –34.9% (SD = 82.77; n = 364), –32.3% (SD = 106.11; n = 364), and –30.9% (SD = 127.21; n = 364), respectively. The proportion of patients who experienced a reduction in drop seizure frequency of 50% or greater during the same periods in the CARE 5 trial was 53.8% (196 of 364 patients), 56.3% (205 of 364 patients), and 58% (211 of 364 patients), respectively.
Table 22: Key Efficacy Outcomes for Patients With LGS (Safety Analysis Set) in CARE 5 OLE Study
Outcome | CARE 5 (N = 364) |
|---|---|
Proportion of patients experiencing drop seizure–free status, n (%)a | |
Weeks 37 to 48 (12 months) | 24 (7) |
Weeks 133 to 144 (36 months) | 30 (8) |
Weeks 253 to 264 (66 months) | 34 (9) |
Median change in drop seizure frequency from baseline of the core studies, % (IQR)a | |
Weeks 37 to 48 (12 months) | –55.3 (–83.8 to –16.6) |
Weeks 133 to 144 (36 months) | –59.1 (–85.7 to –15.2) |
Weeks 253 to 264 (66 months) | –59.4 (–87.1 to –16.0) |
Mean change in drop seizure frequency from baseline of the core studies, % (SD)a | |
Weeks 37 to 48 (12 months) | –34.9 (82.77) |
Weeks 133 to 144 (36 months) | –32.3 (106.11) |
Weeks 253 to 264 (66 months) | –30.9 (127.21) |
Proportion of patients who experienced a reduction in drop seizure frequency ≥ 50%, n (%)a | |
Weeks 37 to 48 (12 months) | 196 (53.8) |
Weeks 133 to 144 (36 months) | 205 (56.3) |
Weeks 253 to 264 (66 months) | 211 (58) |
IQR = interquartile range; LGS = Lennox-Gastaut syndrome; OLE = open-label extension; SD = standard deviation.
aAll the efficacy outcomes were analyzed using the last observation carried forward method to account for missing data.
Sources: Clinical Study Report for CARE 5 trial;22 sponsor’s summary of clinical evidence.42
Among patients aged 2 to 18 years, the mean change in overall quality-of-life score as measured by the QOLCE from baseline to last visit was 5.5 (SD = 13.71; n = 152). Among patients aged 19 years and older, the mean change in overall quality-of-life subscale weighted score on the QOLIE-31-P from baseline to last visit was 6.4 (SD = 28.63; n = 55). The mean change in adaptive behaviour composite standard score on the Vineland Adaptive Behaviour Scales-2 questionnaire from baseline to last visit was –2.5 (SD = 8.78; n = 179).
Harms
Harms reported during the CARE 5 trial are summarized in Table 23.
A total of 353 patients with LGS (96.4%) reported experiencing 1 or more AEs during the CARE 5 trial. The most common treatment-emergent AEs were convulsion (38.5%), diarrhea (38.3%), and pyrexia (34.4%). SAEs were reported by 157 patients with LGS (42.9%). The most commonly reported SAEs were convulsion (12%), status epilepticus (11.5%), and pneumonia (7.1%). Discontinuation of treatment due to AEs was reported in 43 patients with LGS (11.7%). The most common reasons for treatment discontinuation due to AEs were convulsion (1.9%), diarrhea (1.6%), and vomiting (1.4%). Twelve patients with LGS (3.3%) died during the study. Cause of death due to SUDEP was recorded in 4 patients (1.1%).
Table 23: Summary of Harms Results for Patients With LGS (Safety Analysis Set) From CARE 5 OLE Study
Adverse events | CARE 5 (N = 366) |
|---|---|
Most common adverse events,a n (%) | |
≥ 1 adverse event | 353 (96.4) |
Convulsion | 141 (38.5) |
Diarrhea | 140 (38.3) |
Pyrexia | 126 (34.4) |
Vomiting | 107 (29.2) |
Somnolence | 107 (29.2) |
Upper respiratory tract infection | 104 (28.4) |
Decreased appetite | 93 (25.4) |
Cough | 63 (17.2) |
Weight decreased | 61 (16.7) |
Nasopharyngitis | 58 (15.8) |
Urinary tract infection | 51 (13.9) |
Pneumonia | 51 (13.9) |
Ear infection | 50 (13.7) |
Sinusitis | 49 (13.4) |
Nasal congestion | 46 (12.6) |
Influenza | 45 (12.3) |
Constipation | 43 (11.7) |
Status epilepticus | 42 (11.5) |
Insomnia | 40 (10.9) |
Fatigue | 38 (10.4) |
Serious adverse events,b n (%) | |
Patients with ≥ 1 serious adverse event | 157 (42.9) |
Convulsion | 44 (12.0) |
Status epilepticus | 42 (11.5) |
Pneumonia | 26 (7.1) |
Stopping treatment due to adverse events,c n (%) | |
Patients who stopped | 43 (11.7) |
Convulsion | 7 (1.9) |
Diarrhea | 6 (1.6) |
Vomiting | 5 (1.4) |
Somnolence | 4 (1.1) |
Alanine aminotransferase increased | 4 (1.1) |
Hepatic enzyme increased | 4 (1.1) |
Deaths,c n (%) | |
Patients who died | 12 (3.3) |
SUDEP | 4 (1.1) |
LGS = Lennox-Gastaut syndrome; OLE = open-label extension; SAE = serious adverse event; SUDEP = sudden unexplained death in epilepsy.
aFrequency > 10%.
bFrequency > 5%.
cFrequency > 1%.
Sources: Clinical Study Report for CARE 5 trial;22 sponsor’s summary of clinical evidence.
Critical Appraisal
Internal Validity
The single-group, open-label, nonrandomized design of the CARE 5 OLE study makes interpretation of the comparative long-term efficacy and safety of cannabidiol challenging. The lack of comparison with an active comparator and/or placebo precludes the ability to draw causal inference to assess the relative long-term therapeutic benefit of cannabidiol. Although patient and caregiver self-counts of drop seizures and motor seizures were noted to be reliable by the clinical experts consulted by CADTH for the purpose of this review, patient or caregiver self-counting of other types of seizures may not be accurate. The results for patient-reported outcomes were inconclusive due to the open-label design of the trial and the substantial decline in the number of patients available to provide assessments over time. Moreover, it is uncertain if the sample size (N = 366) was sufficient to detect rare AEs. As enrolment in the CARE 5 trial was contingent on the completion of a core study, thereby excluding patients who discontinued the CARE 3 or CARE 4 trials due to AEs or lack of response, it is possible that patients in the CARE 5 trial represent an enriched population that is more tolerant of, and receives greater benefit from, cannabidiol. Therefore, response bias cannot be ruled out. Finally, results may be biased due to attrition as approximately a third of patients did not complete the study and there was wide variance in the follow-up duration for individuals.
External Validity
None of the CARE 5 trial sites were in Canada. Due to the rarity of LGS and the lack of population-based data on LGS in Canada, the clinical experts were unable to determine if the patient population included in the CARE 5 trial was reflective of patients seen in the clinical practice setting across Canada. One clinical expert added that they would not, however, expect patients with LGS living in Canada to differ from patients with LGS living elsewhere. Adherence to the treatment regimen was not reported on and, as such, overall exposure to cannabidiol during the OLE study period is uncertain.
Indirect Evidence
No indirect treatment comparisons were included in this submission.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the evidence from the systematic review were included in this submission.
Discussion
Summary of Available Evidence
Two studies were included in the sponsor-conducted systematic review: the CARE 3 and CARE 4 trials.
The CARE 3 and CARE 4 trials were multicentre, double-blind, placebo-controlled, randomized phase III studies evaluating the efficacy and safety of cannabidiol as adjunctive treatment in patients aged 2 years and older with seizures associated with LGS. In the CARE 3 trial, 225 patients were randomized to receive treatment with either cannabidiol 20 mg/kg/day (n = 76), cannabidiol 10 mg/kg/day (n = 73), or volume-matched placebo (n = 76). In the CARE 4 trial, 171 patients were randomized to receive treatment with either cannabidiol 20 mg/kg/day (n = 86) or volume-matched placebo (n = 85). The primary efficacy end points for both the CARE 3 and CARE 4 trials was the reduction in the number of drop seizures (per 28 days).
Due to the rarity of LGS and the individual variability in symptoms and clinical presentation of the condition, the clinical experts consulted by CADTH stated that it was difficult to say whether the study participants were similar to patients they typically meet with in clinical practice in Canada. In the CARE 3 trial, the mean number of drop seizures at baseline was higher in the cannabidiol 10 mg/kg/day group than in the cannabidiol 20 mg/kg/day group and the pooled placebo group, although the medians were similar between the groups. The proportion of patients reporting convulsive seizures longer than 30 minutes was higher in the cannabidiol 20 mg/kg/day group than in the cannabidiol 10 mg/kg/day and pooled placebo groups, while the use of benzodiazepine derivatives was higher in the cannabidiol 10 mg/kg/day group than in the cannabidiol 20 mg/kg/day and pooled placebo groups. In the CARE 4 trial, the use of phenobarbital was greater in the cannabidiol 20 mg/kg/day group than in the volume-matched placebo group, while the use of levetiracetam was greater in the volume-matched placebo group than in the cannabidiol 20 mg/kg/day group. The clinical experts consulted by CADTH for the purpose of this review were uncertain if these differences could influence treatment response. The baseline characteristics of the patients enrolled in the CARE 4 trial were generally similar between treatment groups.
To inform the longer-term safety and tolerability of cannabidiol as an adjunctive treatment in children and adults with inadequately controlled LGS, the results of 1 OLE study — the CARE 5 trial — were summarized.22 The CARE 5 trial was a multicentre, single-arm, OLE, phase III study that included 366 patients with LGS who had completed the CARE 3 and CARE 4 trials. The CARE 5 trial consisted of a titration, maintenance, and 10-day taper period. All participants were titrated up to 10 mg/kg/day to 20 mg/kg/day cannabidiol, with a potential for a maximum dose of 30 mg/kg/day. However, due to limitations in the design and reporting of the OLE study, the CADTH team was unable to complete a robust appraisal of the internal and external validity of the results. Moreover, due to the lack of randomized comparator, no causal conclusions regarding the comparative effectiveness of cannabidiol could be drawn from this study.
Interpretation of Results
Efficacy
Evidence from the pivotal phase III trials — the CARE 3 and CARE 4 trials — showed that treatment with cannabidiol as adjunctive therapy in patients aged 2 to 55 years with seizures associated with LGS reduced the drop seizure frequency from baseline during the 14-week treatment period compared with placebo. Similarly, a larger proportion of patients treated with cannabidiol experienced a reduction in drop seizure frequency from baseline of 50% or greater during the 14-week treatment period. The results from the subgroup analyses were consistent with the overall results of the trials, where cannabidiol in both doses was favoured over placebo. The change in drop seizure frequency and the proportion of patients experiencing at least a 50% reduction in drop seizure frequency during the treatment period were assessed as the primary and key secondary end points, respectively, in both the CARE 3 and CARE 4 trials and, as such, were considered in the sample size calculation and included in the hierarchical gate-keeping procedure to control for type I error. All other outcomes were other secondary outcomes (i.e., treatment response at various thresholds in reduction of drop seizures; quality of life; and inpatient hospitalization) or exploratory end points (i.e., drop seizure-free days) without adjustment for multiplicity and were therefore considered supportive evidence for the assessment of certainty in effect estimates.
According to input from the clinical experts, the goal of treatment for seizures associated with LGS is seizure freedom. However, nonmotor seizures can be difficult to detect, and therefore the frequency of motor-related seizures, including drop seizures, which are easier to identify, are more objective for assessing the effects of ASMs. The mean number of drop seizure–free days ranged from 2.7 days to 4.6 days in favour of treatment with cannabidiol versus placebo in both studies. However, as this outcome was only exploratory, it was not included in the statistical hierarchy to control for type I error. Furthermore, whether the treatment effect on drop seizure–free days is clinically meaningful is uncertain due to the lack of a MID. Similarly, the proportion of patients who experienced at least a 75% or a 100% reduction in seizure frequency, assessed as other secondary outcomes, were also not part of the statistical hierarchy to control for type I error. No patients were reported as having experienced a 100% reduction in seizure frequency from baseline at the end of the 14-week treatment period in either study.
The clinical significance of the reductions in drop seizure frequency from baseline to week 14 are difficult to determine. Epilepsy guidelines81 suggest that a primary efficacy end point in this patient population should dichotomize the data into patients who experience a certain predefined percentage reduction in seizure frequency (e.g., a 50% reduction) and patients who do not experience this percentage reduction. The sponsor, however, made the decision to use percent change from baseline in number of drop seizures as the primary end point instead. Given that patients with LGS can experience multiple seizures daily, the clinical experts stated that a decrease in drop seizure frequency from baseline of 25% can be considered clinically meaningful, although it is acknowledged that there is not any formally estimated MID for the change in LGS seizure frequency. While within-group reductions in drop seizure frequency (a median percent change from baseline) in patients randomized to receive treatment with cannabidiol 20 mg/kg/day was 42% to 49% and cannabidiol 10 mg/kg/day was 37during the treatment period, the comparative efficacy of cannabidiol was attenuated due to the placebo response in both the CARE 3 and CARE 4 trials. The median percent change from baseline in drop seizure frequency in the placebo groups ranged from 17% to 22%. Similarly, the proportions of patients who received placebo and experienced reductions of at least 25% from baseline in reduction in drop seizure frequency was 43%and among those who experienced reductions of at least 50% from baseline in drop seizure frequency 14% to 24% (cannabidiol responses ranged from 61% to 64% for reductions of at least 25% and from 35% to 44% for reductions of at least 50%, respectively). The reason for the observed placebo response is unclear. The placebo response may reflect many factors, including patient and caregiver expectations of treatment effects or the more frequent monitoring conducted under the study protocol.82 It may also be reflective of the overall trend of increasing placebo response across epilepsy trials in general.83
For all the seizure frequency and response outcomes, except for the proportion of patients who experienced at least a 50% reduction in drop seizure frequency, the cannabidiol 10 mg/kg/day treatment effect versus placebo was lower than the clinician-suggested thresholds, indicating little to no meaningful effect. The same was true of the cannabidiol 20 mg/kg/day treatment effect compared with placebo, except for the proportion of patients who experienced at least a 50% reduction in drop seizure frequency in the CARE 3 and CARE 4 trials, the proportion of patients who experienced at least a 25% reduction in drop seizure frequency in the CARE 4 trial, and the proportion of patients who experienced at least a 75% reduction in drop seizure frequency in the CARE 3 trial. For these outcomes, the treatment effect indicated that cannabidiol may improve (decrease) drop seizure frequency in a clinically meaningful way versus placebo. Additionally, there was notable imprecision in the between-group differences in drop seizure frequency and response. In all comparisons, the upper limit of the 95% CI exceeded the thresholds suggested by the clinical experts. But the lower limits of the 95% CIs were lower than the suggested thresholds for clinical significance for all the outcomes, including some that approached the threshold for harm (e.g., the lower limit for the between-group difference for cannabidiol 20 mg/kg/day and placebo for the proportion of patients who experienced at least a 25% reduction in drop seizure frequency from baseline was 5.8%). As with any treatment, there will be a distribution of responses, but the distribution of responses observed in the CARE 3 and CARE 4 trials was considered by CADTH reviewers, with clinician input, to be notably wide. The clinical experts consulted by CADTH emphasized the individual variation in responses to ASMs in LGS and noted that the distribution observed in the trials may reflect the real world in this regard. In addition to the absence of an active comparator other than placebo added-on to usual care, the degree of imprecision in the between-group treatment effect estimates resulted in CADTH reviewers determining the certainty in the evidence to be low to moderate that cannabidiol results in a meaningful reduction in drop seizure frequency after 14 weeks of treatment. As mentioned, however, there were responses to cannabidiol compared with placebo that exceeded the thresholds used for clinical significance based on the upper 95% CI limit. The available evidence, such as results from subgroup analyses, did not provide additional details on the characteristics of these patients.
Improvement in seizure outcomes (e.g., seizures frequency, seizure-free days) have been shown to be associated with improvement in nonseizure outcomes such as cognition, executive function, emotional functioning, sleep problems, and HRQoL.63,64 The HRQoL measures used in the CARE 3 and CARE 4 trials — QOLCE and QOLIE-31-P scores — captured many of the domains considered important to the patient group, including cognitive functioning, energy, mood, and behaviour. However, no significant treatment effect of cannabidiol 20 mg/kg/day or cannabidiol 10 mg/kg/day versus volume-matched placebo was observed on overall QOLCE and QOLIE-31-P scores in the CARE 3 and CARE 4 trials. According to input from the clinical experts, although the length of the CARE 3 and CARE 4 trials was sufficient to detect reduction in seizure frequency, a longer follow-up time was required to detect meaningful changes in HRQoL domains related to cognitive functioning, concentration, and behaviour. Regardless, conclusions about the effect of cannabidiol on HRQoL outcomes is limited due to the low number of patients who completed the QOLCE and QOLIE-31-P questionnaires.
Several evidence gaps were identified. First, according to the clinical experts consulted by CADTH, benzodiazepine derivates, such as clobazam, could strengthen the treatment effect of cannabidiol due to synergism. However, the opportunity to explore potential drug-drug interactions was limited due to patients taking up to 4 concomitant ASMs. Second, the trial eligibility criteria (i.e., a minimum of 2 drop seizures per week during the 28-day baseline period) resulted in a study population that may be considered to have very refractory epilepsy. Indeed, the baseline number of drop seizures per 28 days ranged from 8.7 to 7,494.0 in the CARE 3 trial and from 10.3 to 3,174.6 in the CARE 4 trial. To date, there is no evidence for the efficacy of cannabidiol among patients with fewer than 2 drop seizures per week.
The longer-term study of cannabidiol in children and adults with seizures associated in LGS (the CARE 5 trial) showed that cannabidiol is safe and effective in maintaining a reduction in total seizure frequency and drop seizure frequency. However, conclusions could not be drawn from the CARE 5 trial due to its noncomparative design.
Caregiver HRQoL, as well as employment and SUDEP, were identified as important outcomes by patients and the clinical experts consulted by CADTH but were not evaluated in the CARE 3, CARE 4, or CARE 5 trials. According to input from the patient group, caregivers often experience compassion fatigue and are often sleep deprived due to sleep interruptions or anxiety. Moreover, because patients with refractory epilepsy and their caregivers are very often unemployed or underemployed, not covered under employer-funded insurance plans, and/or have restricted income, most drugs to treat the patient’s epilepsy are inaccessible. Given that patients with LGS have limited treatment options for seizure control, both the patient group and the clinical experts consulted by CADTH for the purpose of this review noted the need for new medications to be publicly reimbursed so that patients with refractory seizure associated with LGS have access to treatments that may provide benefit.
Harms
Treatments with fewer side effects were identified in the patient input for this review as important for patients with LGS. In the CARE 3 and CARE 4 trials, AEs were more frequently reported in the cannabidiol treatment groups than in the placebo group. A greater proportion of patients in the cannabidiol 20 mg/kg/day group in the CARE3 trial reported AEs (93.9%), whereas reported AEs were similar in the cannabidiol 10 mg/kg/day group (83.6%) in the CARE 3 trial and the cannabidiol 20 mg/kg/day group (69.4%) in the CARE 4 trial. No deaths were reported in any of the cannabidiol treatment groups during the study period. Cannabidiol was used as adjunctive therapy to conventional ASM in the CARE 3 and CARE 4 trials. Most patients in the CARE 3 and CARE 4 trials reported taking multiple ASMs. The potential for drug-drug interactions was not explored.
Safety data from the OLE study appeared consistent with those observed in the CARE 3 and CARE 4 trials, with no new safety signals reported.
The product monograph for cannabidiol included serious warnings and precautions for hepatocellular injury, including transaminase elevation, and somnolence and sedation. Other common AEs associated with cannabidiol noted in the product monograph included decreased appetite, diarrhea, fatigue, malaise, asthenia, and infections.
According to the clinical experts’ input, treatment with cannabidiol should be discontinued if patients develop persistent and progressive elevation of transaminases or recurrent vomiting and diarrhea, which would compromise the absorption of antiseizure agents. In addition, treatment with cannabidiol should be reassessed if patients develop status epilepticus with no other reasonable explanation.
Conclusions
LGS is a rare and complex epilepsy syndrome associated with multiple and concurrent seizure types that vary across people with the condition. Seizures associated with LGS can be difficult to treat, and the seizures often become resistant to ASMs. Evidence of moderate certainty from 2 randomized, double-blind, placebo-controlled phase III trials (the CARE 3 and CARE 4 trials) in patients aged 2 to 55 years with LGS suggest that adjunctive treatment with cannabidiol 10 mg/kg/day and cannabidiol 20 mg/kg/day may result in a reduction in drop seizure frequencies (primary analysis) for certain patients compared with placebo added to usual care, with a greater proportion of patients treated with cannabidiol reporting a 50% or more reduction in the number of drop seizures (key secondary outcome), when compared to those who received placebo. Although a median treatment difference in drop seizure frequency reduction between 17% and 21% did not meet the threshold for clinical relevance identified by the clinical experts consulted by CADTH for the purpose of this review, the primary analysis was supported by key secondary analysis. No patients were reported at the end of the 14-week treatment period to have experienced a 100% reduction in drop seizures, and the clinical significance of the number of drop seizure–free days was uncertain. The included trials were limited to patients who reported having 2 or more drop seizures per week during the 28-day baseline period. According to input from clinical experts, it is reasonable to expect that improvement in seizure frequency would translate to improved HRQoL. However, the ability of the CARE 3 and CARE 4 trials to assess the treatment effect of cannabidiol on HRQoL was limited due to low completion rates of the QOLCE and QOLIE-31-P questionnaires. The long-term safety, tolerability, and efficacy of cannabidiol was assessed in the OLE study, the CARE 5 trial. Confidence in the effect estimates from the OLE study was limited, primarily due to the CARE 5 trial not being designed to assess the comparator efficacy of cannabidiol to an active treatment or placebo, the diminishing sample size over the study period, and the open-label design, which may have biased outcomes such as HRQoL and harms. As patients with LGS have limited treatment options for seizure control, both the patient group and the clinical experts emphasized that there is an unmet need for new medications to achieve seizure control, and ideally seizure freedom, in patients with seizures associated with LGS.
References
1.Heiskala H. Community-based study of Lennox-Gastaut syndrome. Epilepsia. 1997;38(5):526-531.PubMed
2.Hollenack KA, Story TJ, Acs A, Tran O, Krol J, Stockl KM. PND34 Economic burden of probable Lennox-Gastaut syndrome, probable Dravet syndrome, and other refractory epilepsies for United States Medicaid health plans. Value Health. 2019;22(suppl 2):S276.
3.Camfield PR. Definition and natural history of Lennox-Gastaut syndrome. Epilepsia. 2011;52(suppl 5):3-9.PubMed
4.Specchio N, Wirrell EC, Scheffer IE, et al. International League Against Epilepsy classification and definition of epilepsy syndromes with onset in childhood: Position paper by the ILAE Task Force on Nosology and Definitions. Epilepsia. 2022;63(6):1398-1442.PubMed
5.Nashef L, Hindocha N, Makoff A. Risk factors in sudden death in epilepsy (SUDEP): the quest for mechanisms. Epilepsia. 2007;48(5):859-871.PubMed
6.Bourgeois BF, Douglass LM, Sankar R. Lennox-Gastaut syndrome: a consensus approach to differential diagnosis. Epilepsia. 2014;55(suppl 4):4-9.PubMed
7.Autry AR, Trevathan E, Van Naarden Braun K, Yeargin-Allsopp M. Increased risk of death among children with Lennox-Gastaut syndrome and infantile spasms. J Child Neurol. 2010;25(4):441-447.PubMed
8.Arzimanoglou A, French J, Blume WT, et al. Lennox-Gastaut syndrome: a consensus approach on diagnosis, assessment, management, and trial methodology. Lancet Neurol. 2009;8(1):82-93.PubMed
9.Ontario E. Lennox-Gastaut Syndrome. 2011; https://epilepsyontario.org/lennox-gastaut-syndrome/. Accessed 2023 Oct 13.
10.Committee for Orphan Medicinal Products. Orphan Maintenance Assessment Report: Epidyolex (cannabidiol). Amsterdam (NL): European Medicines Agency; 2019: https://www.ema.europa.eu/en/documents/orphan-maintenance-report/epidyolex-orphan-maintenance-assessment-report-initial-authorisation_en.pdf. Accessed by sponsor, no date privded.
11.Ruthirago D, Julayanont P, Karukote A, Shehabeldin M, Nugent K. Sudden unexpected death in epilepsy: ongoing challenges in finding mechanisms and prevention. Int J Neurosci. 2018;128(11):1052-1060.PubMed
12.CADTH Drug Reimbursement Expert Review Committee final recommendation: rufinamide (Banzel – Eisai Limited). Ottawa (ON): CADTH; 2012 Feb 15: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_Banzel_March-19-12_e.pdf. Accessed 2023 Sep 22.
13.Ontario E. Lennox-Gastaut syndrome. 2018; https://epilepsyontario.org/about-epilepsy/types-of-seizures/lennox-gastaut-syndrome. Accessed 2023 Jul 26.
14.Ontario Drug Benefit Formulary, Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; 2024: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2023 May 05.
15.Epidiolex (cannabidiol): 100 mg/ml oral solution [product monograph]. Cambridge (UK): GW Research Ltd.; 2023 Nov 15.
16.Clinical Study Report: GWEP1414 (GWPCARE3). A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P; CBD) as adjunctive treatment for seizures associated with Lennox–Gastaut syndrome in children and adults [internal sponsor's report]. Cambridge (UK): GW Research Ltd.; 2017 Jul 19.
17.Clinical Study Report: GWEP1423 (GWPCARE4). A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P; CBD) as adjunctive treatment for seizures associated with Lennox–Gastaut syndrome in children and adults [internal sponsor's report]. Cambridge (UK): GW Research Ltd.; 2017 Feb 24.
18.Baker GA, Camfield C, Camfield P, et al. Commission on Outcome Measurement in Epilepsy, 1994-1997: final report. Epilepsia. 1998;39(2):213-231.PubMed
19.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406.PubMed
20.Santesso N, Glenton C, Dahm P, et al; GRADE Working Group. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135.PubMed
21.Popay J, Roberts HM, Sowden AJ, et al. Guidance on the conduct of narrative synthesis in systematic reviews: a product from the ESRC Methods Programme, version 1. 2006. https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf. Accessed 2023 Nov 29.
22.Clinical Study Report: GWEP1415 (GWPCARE5). An open-label extension study to investigate the safety of cannabidiol (GWP42003-P; CBD) in children and adults with inadequately controlled Dravet or Lennox-Gastaut Syndromes [internal sponsor's report]. Cambridge (UK): GW Research Ltd.; 2021 Feb 25.
23.Novy J, Belluzzo M, Caboclo LO, et al. The lifelong course of chronic epilepsy: the Chalfont experience. Brain. 2013;136(Pt 10):3187-3199.PubMed
24.Kwan P, Arzimanoglou A, Berg AT, et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51(6):1069-1077.PubMed
25.Gallop K, Wild D, Nixon A, Verdian L, Cramer JA. Impact of Lennox-Gastaut Syndrome (LGS) on health-related quality of life (HRQL) of patients and caregivers: literature review. Seizure. 2009;18(8):554-558.PubMed
26.Gibson PA. Lennox-Gastaut syndrome: impact on the caregivers and families of patients. J Multidiscip Healthc. 2014;7:441-448.PubMed
27.Bailey LD, Schwartz L, Dixon-Salazar T, et al. Psychosocial impact on siblings of patients with developmental and epileptic encephalopathies. Epilepsy Behav. 2020;112:107377.PubMed
28.Donner E. Clinical opinion. 2023. [sponsor supplied reference].
29.Resnick T, Sheth RD. Early diagnosis and treatment of Lennox-Gastaut syndrome. J Child Neurol. 2017;32(11):947-955.PubMed
30.Strzelczyk A, Zuberi SM, Striano P, Rosenow F, Schubert-Bast S. The burden of illness in Lennox-Gastaut syndrome: a systematic literature review. Orphanet J Rare Dis. 2023;18(1):42.PubMed
31.Foundation LGS. How many people have LGS. 2024; https://www.lgsfoundation.org/about-lgs-2/how-many-people-have-lgs/. Accessed 2023 Oct 13.
32.Cross JH, Auvin S, Falip M, Striano P, Arzimanoglou A. Expert opinion on the management of Lennox-Gastaut syndrome: treatment algorithms and practical considerations. Front Neurol. 2017;8:505.PubMed
33.Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs II: Treatment-resistant epilepsy: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2018;91(2):82-90.PubMed
34.French JA, Kanner AM, Bautista J, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology; Quality Standards Subcommittee of the American Academy of Neurology; American Epilepsy Society. Efficacy and tolerability of the new antiepileptic drugs II: treatment of refractory epilepsy: report of the Therapeutics and Technology Assessment Subcommittee and Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2004;62(8):1261-1273.PubMed
35.Jazz Pharms Res. Prescribing information: Epidiolex (cannabidiol) oral solution. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2018: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/210365lbl.pdf. Accessed 2023 Oct 13.
36.UCB INC. Prescribing information: Fintepla (fenfluramine) oral solution, CIV. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2022: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/212102s003lbl.pdf. Accessed 2023 Nov 29.
37.Brigo F, Jones K, Eltze C, Matricardi S. Anti-seizure medications for Lennox-Gastaut syndrome. Cochrane Database Syst Rev. 2021;4(4):CD003277.PubMed
38.Montouris G, Aboumatar S, Burdette D, et al. Expert opinion: Proposed diagnostic and treatment algorithms for Lennox-Gastaut syndrome in adult patients. Epilepsy Behav. 2020;110:107146.PubMed
39.Strzelczyk A, Schubert-Bast S. Expanding the treatment landscape for Lennox-Gastaut syndrome: current and future strategies. CNS Drugs. 2021;35(1):61-83.PubMed
40.Johannessen Landmark C, Potschka H, Auvin S, et al. The role of new medical treatments for the management of developmental and epileptic encephalopathies: Novel concepts and results. Epilepsia. 2021;62(4):857-873.PubMed
41.Guidelines OE. Clinical guidelines for the management of epilepsy in adults and children, version 2.0. Toronto, ON: The Epilepsy Research Program of the Ontario Brain Institute; 2020, https://clinictocommunity.ca/wp-content/uploads/2021/01/ManagementGuidelines_Nov2020.pdf. Accessed May 08, 2023.
42.Epidiolex (cannabidiol) as adjunctive treatment of seizures associated with Lennox-Gastaut syndrome (LGS) in patients two years of age and older: sponsor summary of clinical evidence. [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Epidiolex (cannabidiol), 100 mg/mL, oral solution. Mississauga, ON: Jazz Pharmaceuticals Canada Inc; 2023 Sep 19.
43.Banzel (rufinamide): 100 mg, 200 mg and 400 mg, oral tablets [product monograph]. Mississauga (ON): Eisai Limited; 2020 Oct 14: https://pdf.hres.ca/dpd_pm/00058487.PDF. Accessed 2023 Oct 16.
44.Apo-Valproic Acid (valpric acid): 250 mg oral capsules; Valproic Acid Oral Solution (valproic acid oral solution): 250 mg/5 mL valproic acid (as sodium valproate), oral solution [product monograph]. Toronto (ON): Apotex Inc.; 2023 Oct 05: https://pdf.hres.ca/dpd_pm/00072687.PDF. Accessed 2023 Oct 16.
45.Apo-Clobazam (clobazam): 10 mg oral tablets [product monograph]. Toronto (ON): Apotex Inc.; 2021 May 06: https://pdf.hres.ca/dpd_pm/00060946.PDF. Accessed 2023 Oct 16.
46.Apo-Lamotrigine (lamotrigine): 25 mg, 100 mg, and 150 mg oral tablets [product monograph]. Toronto (ON): Apotex Inc.; 2023 Apr 18: https://pdf.hres.ca/dpd_pm/00071067.PDF. Accessed 2023 Oct 16.
47.Apo-Levetiracetam (levetiracetam): 250 mg, 500 mg, and 750 mg oral tablets [product monograph]. Toronto (ON): Apotex Inc.; 2023 May 01: https://pdf.hres.ca/dpd_pm/00070544.PDF. Accessed 2023 Oct 16.
48.Ach-Topiramate (topiramate): 25 mg, 100 mg, and 200 mg oral tablets [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2022 Mar 07: https://pdf.hres.ca/dpd_pm/00064988.PDF. Accessed 2023 Oct 16.
49.Apo-Clonazepam (clonazepam): 0.5 mg and 2 mg, oral tablets [product monograph]. Toronto (ON): Apotex Inc.; 2023 Sep 15: https://pdf.hres.ca/dpd_pm/00072497.PDF. Accessed 2023 Oct 16.
50.Fycompa (perampanel): 2 mg, 4 mg, 6 mg, 8 mg, 10 mg, and 12 mg tablets [product monograph]. Mississauga (ON): Eisai Limited; 2023 Nov 16: https://pdf.hres.ca/dpd_pm/00073371.PDF. Accessed 2024 Apr 12.
51.pharma-Lacosamide (lacosamide): 50 mg, 100 mg, 150 mg, and 200 mg film-coated oral tablets [product monograph]. Montreal (QC): Pharmascience Inc.; 2023 Apr 14: https://pdf.hres.ca/dpd_pm/00070337.PDF. Accessed 2023 Nov 28.
52.Brivlera (brivaracetam): 10 mg, 25 mg, 50 mg, 75 mg, and 100 mg tablets; 10 mg/mL oral solution; and 10 mg/mL intravenous injection [product monograph]. Oakville (ON): UCB Canada Inc.; 2020 May 01: https://pdf.hres.ca/dpd_pm/00056430.PDF. Accessed 2023 Nov 28.
53.Sankar R. Initial treatment of epilepsy with antiepileptic drugs: pediatric issues. Neurology. 2004;63(10)(suppl 4):S30-S39.PubMed
54.Geffrey AL, Pollack SF, Bruno PL, Thiele EA. Drug-drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Epilepsia. 2015;56(8):1246-1251.PubMed
55.Morrison G, Crockett J, Blakey G, Sommerville K. A phase 1, open-label, pharmacokinetic trial to investigate possible drug-drug interactions between clobazam, stiripentol, or valproate and cannabidiol in healthy subjects. Clin Pharmacol Drug Dev. 2019;8(8):1009-1031.PubMed
56.Auvin S, Nortvedt C, Fuller DS, Sahekbar F. Poster 040: Seizure-free days as a novel and meaningful outcome in patients with Lennox-Gastaut Syndrome: post hoc analysis of patients receiving cannabidiol (CBD) in GWPCARE3 and GWPCARE4. Dev Med Child Neurol. 2023;65(suppl 1):34.
57.Cross H, Vyas K, Sahebkar F, Schreiber A, Mazurkiewicz-Beldzinska A. Abstract 137: Cannabidiol (CBD) in patients with Lennox-Gastaut syndrome (LGS) and Dravet syndrome (DS) on a ketogenic diet therapy (KDT) in four phase 3 trials. Virtual Congress: 34th International Epilepsy Congress; 2021 Aug 28 - Sep 01.
58.Devinsky O, Patel AD, Cross JH, et al; GWPCARE3 Study Group. Effect of cannabidiol on drop seizures in the Lennox-Gastaut syndrome. N Engl J Med. 2018;378(20):1888-1897.PubMed
59.Mazurkiewicz-Beldzinska M, Privitera M, Marsh E, et al. Time to onset of efficacy of cannabidiol (CBD) during titration in patients with Lennox-Gastaut syndrome and Dravet syndrome enrolled in three randomized controlled trials (S48.009). Neurology. 2019;92(15)(suppl).
60.Nabbout R, Bhathal H, Zolnowska M, et al. Abstract 245: Diarrhoea in patients with Lennox-Gastaut syndrome (LGS) or Dravet syndrome (DS) enrolled in four phase 3 clinical trials of cannabidiol (CBD). Virtual Congress: 34th International Epilepsy Congress; 2021 Aug 28 - Sep 01.
61.Privitera M, Bhathal H, Wong M, et al. Time to onset of cannabidiol (CBD) treatment effect in Lennox-Gastaut syndrome: Analysis from two randomized controlled trials. Epilepsia. 2021;62(5):1130-1140.PubMed
62.Wirrell E, Devinsky O, Patel A, et al. Cannabidiol (CBD) significantly reduces drop and total seizure frequency in Lennox Gastaut syndrome (LGS): results of a dose ranging, multicenter, randomized, double blind, placebo controlled trial (GWPCARE3). Ann Neurol. 2017;82(S21):S279.
63.Wirrell EC, Privitera M, Bhathal H, Wong MH, Cross JH, Sommerville K. Cannabidiol (CBD) treatment effect and adverse events (AEs) by time in patients with Lennox-Gastaut syndrome (LGS): pooled results from 2 trials (S19.006). Neurology. 2018;90(15)(suppl).
64.Wirrell EC, Schreiber A, Saurer TB, Wechsler RT. Efficacy and safety of cannabidiol (CBD) dose adjustment in patients with Lennox-Gastaut syndrome (LGS): post hoc analysis of phase 3 randomized controlled trial (RCT) GWPCARE3 and open-label extension (OLE) trial GWPCARE5 (P128.007). Neurology. 2022;98(18)(suppl).
65.Patel A, Wilfong A, Joshi C, Zuberi S. Cannabidiol (CBD) significantly reduces drop-seizure frequency in Lennox-Gastaut syndrome (LGS): pooled efficacy and safety results from two randomized controlled trials. American Epilepsy Society. 2017;59(suppl 4):18. sponsor provided reference.
66.Morrison G, Sardu ML, Rasmussen CH, Sommerville K, Roberts C, Blakey GE. Exposure-response analysis of cannabidiol (CBD) oral solution for the treatment of Lennox–Gastaut syndrome (P1.271). 2018;90(15 Supplement).
67.Thiele EA, Marsh ED, French JA, et al; GWPCARE4 Study Group. Cannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391(10125):1085-1096.PubMed
68.Health Canada reviewer’s report: Epidiolex (cannabidiol). [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Epidiolex (cannabidiol), 100 mg/mL, oral solution. Mississauga, ON: Jazz Pharmaceuticals Canada Inc; 2023 Nov.
69.van der Kop ML. The need for an individualized approach to what is considered a clinically significant reduction in seizure frequency: A patient’s perspective. Epilepsia. 2023;64(6):1469-1471.PubMed
70.Borghs S, de la Loge C, Cramer JA. Defining minimally important change in QOLIE-31 scores: estimates from three placebo-controlled lacosamide trials in patients with partial-onset seizures. Epilepsy Behav. 2012;23(3):230-234.PubMed
71.Cramer JA, Perrine K, Devinsky O, Bryant-Comstock L, Meador K, Hermann B. Development and cross-cultural translations of a 31-item quality of life in epilepsy inventory. Epilepsia. 1998;39(1):81-88.PubMed
72.Cramer JA, Van Hammée G; N132 Study Group. Maintenance of improvement in health-related quality of life during long-term treatment with levetiracetam. Epilepsy Behav. 2003;4(2):118-123.PubMed
73.Crudgington H, Rogers M, Morris H, Gringras P, Pal DK, Morris C. Epilepsy-specific patient-reported outcome measures of children’s health-related quality of life: A systematic review of measurement properties. Epilepsia. 2020;61(2):230-248.PubMed
74.Sabaz M, Cairns DR, Lawson JA, Nheu N, Bleasel AF, Bye AM. Validation of a new quality of life measure for children with epilepsy. Epilepsia. 2000;41(6):765-774.PubMed
75.Sabaz M, Lawson JA, Cairns DR, et al. Validation of the quality of life in childhood epilepsy questionnaire in American epilepsy patients. Epilepsy Behav. 2003;4(6):680-691.PubMed
76.Committee For Medicinal Products For Human Use. Guideline on clinical investigation of medicinal products in the treatment of epileptic disorders. London (UK): European Medicines Agency; 2010: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-epileptic-disorders-revision-2_en.pdf. Accessed 2023 Jan 12.
77.Guidelines for the clinical evaluation of antiepileptic drugs (adults and children). Rockville (MD): U.S. Food and Drug Administration (FDA); 1981: https://www.fda.gov/media/71165/download. Accessed 2023 Jan 12.
78.Danan V, Anup P, Jules B, et al. Clinical Trial Outcome Measurements in Lennox-Gastaut Syndrome and Their Application to the Development of Targeted Treatments. Curr Treat Options Neurol. 2021;23(9).
79.Akman CI, Montenegro MA, Jacob S, Eck K, Chiriboga C, Gilliam F. Seizure frequency in children with epilepsy: factors influencing accuracy and parental awareness. Seizure. 2009;18(7):524-529.PubMed
80.Tzadok M, Gur-Pollack R, Florh H, et al. Real-life experience with purified cannabidiol treatment for refractory epilepsy: a multicenter retrospective study. Pediatr Neurol. 2024;150:91-96.PubMed
81.Committee for Medicinal Products for Human Use. Guideline on clinical investigation of medicinal products in the treatment of epileptic disorders, draft. Amsterdam (NL): European Medicines Agency; 2023: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-epileptic-disorders-revision-3_en.pdf. Accessed 2023 Dec 14.
82.Goldenholz DM, Goldenholz SR. Response to placebo in clinical epilepsy trials--Old ideas and new insights. Epilepsy Res. 2016;122:15-25.PubMed
83.Rheims S, Perucca E, Cucherat M, Ryvlin P. Factors determining response to antiepileptic drugs in randomized controlled trials. A systematic review and meta-analysis. Epilepsia. 2011;52(2):219-233.PubMed
Appendix 1: Detailed Outcome Data
Note this appendix has not been copy-edited.
Table 24: Subgroup Analysis for Percent Change From Baseline in Drop Seizure Frequency in CARE 3 (ITT Analysis Set)
Subgroup | Cannabidiol 20 mg/kg/day vs. placebo | Cannabidiol 10 mg/kg/day vs. placebo | ||
|---|---|---|---|---|
N | Difference (95% CI) | N | Difference (95% CI) | |
Clobazam use | ||||
Yes | 73 | –34.0 (–51.8 to –15.6) | 74 | –17.6 (–36.8 to –1.27) |
No | 79 | –4.63 (–25.68 to 12.85) | 75 | –20.3 (–35.3 to –5.2) |
Baseline drop seizure frequency | ||||
≤ 55 | 47 | –28.4 (–54.3 to 2.09) | 48 | –15.4 (–40.6 to 5.75) |
> 55 to ≤ 125 | 59 | –17.98 (–36.0 to 6.40) | 50 | –24.9 (–42.9 to –7.7) |
> 125 | 46 | –18.6 (–46.9 to 6.9) | 51 | –15.4 (–38.7 to 5.8) |
Number of current ASMs | ||||
< 3 | 50 | –17.7 (–41.1 to 7.38) | 49 | –16.1 (–37.1 to 6.3) |
≥ 3 | 102 | –23.5 (–40.5 to –4.8) | 100 | –20.5 (–35.1 to –7.3) |
Number of prior ASMs | ||||
< 6 | 61 | –23.7 (–42.6 to –3.0) | 62 | –9.1 (–28.6 to 10.1) |
≥ 6 | 90 | –18.9 (–37.8 to 1.54) | 87 | –26.6 (–40.1 to –10.9) |
ASM = antiseizure medications; CI = confidence interval.
Note: Hodges-Lehmann median difference and 95% CI are presented.
Table 25: Subgroup Analysis for Percent Change From Baseline in Drop Seizure Frequency in CARE 4 (ITT Analysis Set)
Subgroup | Cannabidiol 20 mg/kg/day vs. placebo | |
|---|---|---|
N | Difference (95% CI) | |
Clobazam use | ||
Yes | 84 | –28 (–46.85 to –10.05) |
No | 87 | –6.04 (–25.25 to 15.46) |
Baseline drop seizure frequency | ||
≤ 45 | 56 | –15.84 (–40.70 to 11.42) |
> 45 to ≤ 110 | 57 | –26.00 (–45.51 to –2.73) |
> 110 | 58 | –11.08 (–34.71 to 13.71) |
Number of current ASMs | ||
< 3 | 57 | –31.22 (–51.83 to –6.78) |
≥ 3 | 114 | –9.64 (–26.76 to 7.48) |
Number of prior ASMs | ||
< 6 | 78 | –18.63 (–38.18 to 1.60) |
≥ 6 | 93 | –16.25 (–33.78 to 2.64) |
ASM = antiseizure medications; CI = confidence interval.
Note: Hodges-Lehmann median difference and 95% CI are presented.
Table 26: Summary of Efficacy Outcomes in the CARE 3 and CARE 4 Trials That Were Not Assessed by GRADE
Variable | CARE 3 | CARE 4 | |||
|---|---|---|---|---|---|
Cannabidiol 20 mg/kg/day (n = 76) | Cannabidiol 10 mg/kg/day (n = 73) | Pooled placebo (n = 76) | Cannabidiol 20 mg/kg/day (n = 86) | Placebo 20 mg/kg/day (n = 85) | |
Key secondary end points | |||||
Percent change from baseline in total seizure frequency during the treatment period | |||||
Patients analyzed, n | 76 | 73 | 76 | 86 | 85 |
Baseline, median (Q1, Q3) | 174.29 (82.7 to 392.4) | 165.00 (81.3 to 359.0) | 180.63 (90.4 to 431.3) | 144.56 (72.0 to 385.7) | 176.69 (68.6 to 359.5) |
End of treatment, median (Q1, Q3) | 90.33 (28.7 to 234.0) | 76.08 (38.5 to 188.4) | 138.91 (65.2 to 403.4) | 83.75 (27.4 to 255.4) | 128.68 (59.3 to 337.4) |
Median change during treatment, % (Q1, Q3) | –38.4 (–64.6 to –0.7) | –36.4 (–64.5 to –10.8) | –18.5 (–39.0 to 0.5) | –41.2 (–62.8 to –13.0) | –13.7 (–45.0 to 7.3) |
Estimated median difference (CI)a | –18.8 (–31.8 to –4.4) | –19.5 (–30.4 to –7.5) | NA | –21.1 (–33.4 to –9.4) | NA |
P valueb | 0.0091 | 0.0015 | NA | 0.0005 | NA |
Change from baseline in the S/CGIC at last visit | |||||
Combined caregiver and patient; category, n (%) | |||||
Patients analyzed, n | 75 | 73 | 75 | 84 | 85 |
Very much improved | 6 (8.0) | 9 (12.3) | 1 (1.3) | 15 (17.9) | 5 (5.9) |
Much improved | 15 (20.0) | 14 (19.2) | 8 (10.7) | 14 (16.7) | 9 (10.6) |
Slightly improved | 22 (29.3) | 25 (34.2) | 24 (32.0) | 20 (23.8) | 15 (17.6) |
No change | 25 (33.3) | 21 (28.8) | 35 (46.7) | 27 (32.1) | 43 (50.6) |
Slightly worse | 6 (8.0) | 3 (4.1) | 4 (5.3) | 7 (8.3) | 9 (10.6) |
Much worse | 1 (1.3) | 1 (1.4) | 3 (4.0) | 1 (1.2) | 2 (2.4) |
Very much worse | 0 | 0 | 0 | 0 | 2 (2.4) |
Median, last visit (range) | 3.0 (1 to 6) | 3.0 (1 to 6) | 4.0 (1 to 6) | 3.0 (1 to 6) | 4.0 (1 to 7) |
Odds ratio (95% CI)d | 1.83 (1.02 to 3.30) | 2.57 (1.41 to 4.66) | NA | 2.54 (1.45 to 4.47) | NA |
P valued | 0.0439 | 0.0020 | NA | 0.0012 | NA |
Other secondary end points | |||||
Percent change from baseline in drop seizure frequency during the maintenance period | |||||
Patients analyzed, n | 76 | 73 | 76 | 85 | 85 |
Median percent change during maintenance (Q1, Q3) | –47.2 (–78.8 to 1.7) | –40.0 (–67.4 to –2.2) | –18.7 (–40.6 to –1.2) | –48.8 (–74.6 to 2.2) | –20.5 (–48.5 to –0.3) |
Estimated median difference (CI)a | –21.2 (–36.4 to –6.2) | –19.5 (–32.2 to –6.5) | NA | –19.45 (–33.1 to –4.7) | NA |
P valueb | 0.0067 | 0.0033 | NA | 0.0096 | NA |
Percent change in drop seizure frequency during week 1 – week 4 of the maintenance period | |||||
Patients analyzed, n | 75 | 73 | 75 | 82 | 85 |
Median percent change during maintenance (Q1, Q3): week 1 to 4 | –39.7 (–85.6 to –0.5) | –41.7 (–61.1 to –10.0) | –20.0 (–37.1 to 0.0) | –51.3 (–81.5 to –21.4) | –23.3 (–51.9 to 0.0) |
Estimated median difference (CI)a | –25.2 (–40.9 to –9.0) | –20.4 (–31.8 to –8.3) | NA | –23.6 (–37.2 to –11.0) | NA |
P valueb | 0.0015 | 0.0017 | NA | 0.0005 | NA |
Percent change in drop seizure frequency during week 5 – week 8 of the maintenance period | |||||
Patients analyzed, n | 68 | 72 | 75 | 73 | 84 |
Median percent change during maintenance (Q1, Q3): week 5 to 8 | –53.5 (–89.9 to –5.4) | –44.1 (–71.9 to –0.4) | –22.2 (–45.6 to –1.9) | –45.4 (–70.8 to –17.4) | –23.5 (–53.8 to 0.0) |
Estimated median difference (CI)a | –29.1 (–43.6 to –12.9) | –17.1 (–31.7 to –1.8) | NA | –16.6 (–30.9 to –2.6) | NA |
P valueb | 0.0008 | 0.0255 | NA | 0.0205 | NA |
Percent change in drop seizure frequency during week 9 – week 12 of the maintenance period | |||||
Patients analyzed, n | 67 | 71 | 74 | 72 | 84 |
Median percent change during maintenance (Q1, Q3): week 9 to 12 | –36.4 (–76.6 to 10.1) | –49.0 (–79.6 to –6.3) | –22.8 (–46.0 to 0.0) | –52.6 (–77.9 to –13.1) | –27.0 (–46.9 to 5.1) |
Estimated median difference (CI)a | –14.8 (–32.1 to 2.1) | –22.0 (–35.6 to –6.6) | NA | –23.6 (–38.4 to –6.8) | NA |
P valueb | 0.0848 | 0.0068 | NA | 0.0062 | NA |
Proportion of Patients with Reduction in Drop Seizure Frequency from Baseline During maintenance Period | |||||
Patients analyzed, n | 76 | 73 | 76 | 86 | 85 |
Patients with ≥ 25% reduction | |||||
Yes (%) | 47 (61.8) | 47 (64.4) | 34 (44.7) | 54 (63.5) | 40 (47.1) |
Difference in Proportions (95% CI) | 0.171 (0.015 to 0.327) | 0.196 (0.040 to 0.353) | NA | 0.165 (0.017 to 0.312) | NA |
Odds Ratio (CI) | 2.00 (1.05 to 3.82) | 2.23 (1.16 to 4.31) | NA | 1.96 (1.06 to 3.62) | NA |
P valuec | 0.0337 | 0.0152 | NA | 0.0347 | NA |
Patients with ≥ 50% reduction | |||||
Yes (%) | 34 (44.7) | 29 (39.7) | 10 (13.2) | 39 (45.9) | 20 (23.5) |
Difference in Proportions (95% CI) | 0.316 (0.181 to 0.451) | 0.266 (0.130 to 0.401) | NA | 0.224 (0.084 to 0.363) | NA |
Odds Ratio (CI) | 5.34 (2.39 to 11.94) | 4.35 (1.93 to 9.81) | NA | 2.76 (1.43 to 5.32) | NA |
P valuec | < 0.0001 | 0.0002 | NA | 0.0020 | NA |
Patients with ≥ 75% reduction | |||||
Yes (%) | 20 (26.3) | 11 (15.1) | 3 (3.9) | 20 (23.5) | 7 (8.2) |
Difference in Proportions (95% CI) | 0.224 (0.115 to 0.332) | 0.111 (0.018 to 0.204) | NA | 0.153 (0.045 to 0.260) | NA |
Odds Ratio (CI) | 8.69 (2.46 to 30.71) | 4.32 (1.15 to 16.17) | NA | 3.43 (1.36 to 8.62) | NA |
P valuec | 0.0001 | 0.0208 | NA | 0.0056 | NA |
100% reduction in drop seizure frequency during the maintenance period | |||||
Yes (%) | 5 (6.6) | 3 (4.1) | 1 (1.3) | 5 (5.9%) | 0 |
Difference in Proportions (95% CI) | 0.053 (–0.009 to 0.114) | 0.028 (–0.024 to 0.080) | NA | 0.059 (0.009 to 0.109) | NA |
Odds Ratio (CI) | 5.28 (0.60 to 46.32) | 3.21 (0.33 to 31.63) | NA | NA | NA |
P valuec | 0.0994 | 0.2879 | NA | 0.0246 | NA |
Patients experiencing worsening, no change, or improvements in drop seizure | |||||
Patients analyzed, n | 76 | 73 | 76 | 86 | 85 |
No baseline period seizures, n (%) | 0 | 0 | 0 | 0 | 0 |
> 25% (Worsening), n (%) | 10 (13.2) | 7 (9.6) | 7 (9.2) | 12 (14.0) | 9 (10.6) |
≥ 0% to ≤ 25% (No change), n (%) | 8 (10.5) | 7 (9.6) | 15 (19.7) | 10 (11.6) | 13 (15.3) |
> –25% to < 0% (No change), n (%) | 11 (14.5) | 13 (17.8) | 21 (27.6) | 9 (10.5) | 26 (30.6) |
> –50% to ≤ –25% (Improvement), n (%) | 17 (22.4) | 20 (27.4) | 22 (28.9) | 17 (19.8) | 17 (20.0) |
> –75% to ≤ –50% (Improvement), n (%) | 11 (14.5) | 18 (24.7) | 9 (11.8) | 21 (24.4) | 13 (15.3) |
≤ –75% (improvement), n (%) | 19 (25.0) | 8 (11.0) | 2 (2.6) | 17 (19.8) | 7 (8.2) |
Percent change from baseline in seizure frequency by individual seizure type during the treatment period (per 28 days) | |||||
Nondrop seizures | |||||
Patients analyzed, n | 64 | 55 | 70 | 77 | 79 |
Baseline period, Median (Q1, Q3) | 93.7 (22.2 to 278.4) | 95.7 (14.0 to 280.0) | 78.0 (22.0 to 216.0) | 94.0 (19.8 to 311.0) | 85.0 (20.5 to 220.0) |
Treatment period, Median (Q1, Q3) | 24.2 (4.9 to 113.5) | 16.3 (5.7 to 121.1) | 54.9 (9.7 to 201.4) | 39.4 (4.7 to 136.2) | 57.7 (11.3 to 186.4) |
Median percent change during treatment (Q1, Q3) | –54.6 (–86.0 to –10.1) | –61.1 (–85.0 to –23.2) | –34.3 (–56.0 to 13.0) | –49.4 (–81.6 to –25.3) | –22.9 (–67.8 to 31.7) |
Estimated median difference (CI)a | −22.4 (−40.1, −2.2) | −28.31 (−43.8, −10.5) | NA | −26.1 (−46.1, −8.3) | NA |
P valueb | 0.0255 | 0.0028 | NA | 0.0044 | NA |
Convulsive seizures | |||||
Patients analyzed, n | 76 | 73 | 76 | 86 | 85 |
Baseline period, median (Q1, Q3) | 108.5 (60.9 to 185.4) | 102.9 (48.0 to 262.0) | 102.8 (59.9 to 184.3) | 87.0 (38.0 to 209.2) | 99.8 (51.2 to 189.0) |
Treatment period, median (Q1, Q3) | 55.4 (22.4 to 127.1) | 56.6 (21.5 to 164.0) | 88.7 (37.4 to 177.6) | 40.9 (16.9 to 92.0) | 72.4 (33.3 to 166.3) |
Median percent change during treatment (Q1, Q3) | –38.4 (–63.2 to –1.3) | –43.4 (–64.5 to –7.9) | –16.4 (–37.3 to 0.8) | –42.3 (–69.4 to –7.6) | –20.7 (–41.9 to 4.9) |
Estimated median difference (CI)a | −18.6 (−31.1, −5.5) | −22.1 (−33.5, −10.4) | NA | −21.3 (−33.4, −8.7) | NA |
P valueb | 0.0065 | 0.0004 | NA | 0.0010 | NA |
Nonconvulsive seizures | |||||
Patients analyzed, n | 59 | 45 | 60 | 67 | 67 |
Baseline period, median (Q1, Q3) | 71.0 (14.0 to 248.8) | 79.5 (21.0 to 160.3) | 62.24 (12.0 to 213.7) | 89.0 (16.0 to 297.0) | 59.0 (13.5 to 178.8) |
Treatment period, median (Q1, Q3) | 13.7 (2.9 to 115.1) | 18.6 (8.9 to 97.3) | 42.9 (4.2 to 215.2) | 30.9 (3.5 to 140.3) | 30.7 (10.0 to 156.3) |
Median percent change during treatment (Q1, Q3) | –58.3 (–91.3 to 0.3) | –57.5 (–85.5 to –8.0) | –32.2 (–60.0 to 4.1) | –50.8 (–85.7 to –24.6) | –18.6 (–64.6 to 26.2) |
Estimated median difference (CI)a | −18.9 (−40.2 to 0.00) | −16.6 (−37.8 to 3.4) | NA | −27.4 (−45.7, −9.4) | NA |
P valueb | 0.0530 | 0.1083 | NA | 0.0025 | NA |
Tonic seizures | |||||
Patients analyzed, n | 59 | 56 | 57 | 71 | 65 |
Baseline period, median (Q1, Q3) | 55.0 (22.0 to 113.7) | 47.3 (18.2 to 115.4) | 54.0 (27.0 to 103.3) | 39.7 (14.4 to 112.0) | 54.3 (30.0 to 102.3) |
Treatment period, median (Q1, Q3) | 30.6 (7.1 to 77.7) | 28.7 (9.1 to 72.1) | 44.5 (22.6 to 90.1) | 17.9 (4.6 to 69.1) | 40.4 (17.1 to 92.9) |
Median percent change during treatment (Q1, Q3) | –41.4 (–68.0 to –1.2) | –37.6 (–61.9 to –14.3) | –16.2 (–44.0 to 4.5) | –53.3 (–75.8 to –11.6) | –19.5 (–51.8 to 4.8) |
Estimated median difference (CI)a | −18.7 (−35.0, −1.6) | −21.8 (−35.9, −7.4) | NA | −25.8 (−40.8, −9.8) | NA |
P valueb | 0.0319 | 0.0039 | NA | 0.0015 | NA |
Atonic seizures | |||||
Patients analyzed, n | 50 | 40 | 41 | 47 | 59 |
Baseline period, median (Q1, Q3) | 36.5 (11.0 to 109.9) | 114.4 (22.6 to 335.0) | 75.6 (22.2 to 143.3) | 23.2 (13.0 to 90.8) | 44.4 (12.0 to 97.5) |
Treatment period, median (Q1, Q3) | 19.7 (4.5 to 79.3) | 33.0 (7.9 to 272.3) | 49.9 (10.0 to 113.3) | 11.0 (2.7 to 30.9) | 20.9 (9.1 to 62.9) |
Median percent change during treatment (Q1, Q3) | –49.6 (–74.4 to 12.3) | –59.5 (–76.2 to –10.5) | –28.0 (–46.5 to –2.7) | –45.8 (–88.7 to –9.0) | –41.9 (–73.6 to 14.3) |
Estimated median difference (CI)a | −17.0 (−37.8 to 8.5) | −28.8 (−45.6, −7.1) | NA | −12.2 (−31.3 to 6.2) | NA |
P valueb | 0.2090 | 0.0112 | NA | 0.2055 | NA |
Tonic-clonic seizures | |||||
Patients analyzed, n | 41 | 37 | 34 | 49 | 53 |
Baseline period, median (Q1, Q3) | 20.8 (7.7 to 51.6) | 25.3 (12.3 to 52.1) | 14.0 (7.5 to 36.4) | 23.0 (9.0 to 59.9) | 18.3 (6.0 to 55.0) |
Treatment period, median (Q1, Q3) | 11.0 (4.3 to 23.5) | 12.4 (3.7 to 31.2) | 12.1 (4.8 to 37.4) | 11.2 (3.4 to 28.9) | 13.6 (6.1 to 40.8) |
Median percent change during treatment (Q1, Q3) | –41.7 (–68.4 to –6.9) | –53.3 (–79.0 to –28.4) | –10.51 (–48.0 to 32.0) | –54.7 (–80.9 to 4.2) | –18.9 (–51.0 to 18.4) |
Estimated median difference (CI)a | −28.0 (−52.0, −2.9) | −39.9 (−64.6, −19.7) | NA | −22.8 (−44.9 to 0.4) | NA |
P valueb | 0.0244 | 0.0004 | NA | 0.0571 | NA |
Absence seizures | |||||
Patients analyzed, n | 40 | 28 | 37 | 42 | 40 |
Baseline period, median (Q1, Q3) | 37.3 (9.0 to 104.7) | 23.0 (5.4 to 75.7) | 47.5 (5.8 to 94.0) | 28.5 (7.0 to 120.0) | 43.3 (12.6 to 147.0) |
Treatment period, median (Q1, Q3) | 5.6 (1.4 to 25.1) | 9.5 (3.9 to 21.2) | 10.5 (1.4 to 82.9) | 5.8 (0.9 to 47.1) | 19.1 (1.8 to 84.8) |
Median percent change during treatment (Q1, Q3) | –81.7 (–95.0 to 15.3) | –58.8 (–87.7 to –15.9) | –52.2 (–78.2 to –15.6) | –66.7 (–96.4 to –31.6) | –45.7 (–83.9, –9.5) |
Estimated median difference (CI)a | –9.5 (–30.4 to 10.4) | –0.1 (–23.4 to 22.2) | NA | –12.9 (–34.6 to 3.8) | NA |
P valueb | 0.3326 | 0.9630 | NA | 0.1374 | NA |
Myoclonic seizures | |||||
Patients analyzed, n | 33 | 22 | 30 | 38 | 41 |
Baseline period, median (Q1, Q3) | 99.8 (5.0 to 284.0) | 62.9 (16.0 to 139.0) | 56.9 (14.9 to 224.0) | 62.2 (12.0 to 252.0) | 33.0 (9.7 to 143.0) |
Treatment period, median (Q1, Q3) | 38.8 (1.4 to 170.7) | 17.1 (2.8 to 48.3) | 38.1 (5.4 to 224.0) | 35.6 (10.7 to 123.3) | 33.1 (7.8 to 84.0) |
Median percent change during treatment (Q1, Q3) | –54.3 (–91.5 to –19.5) | –68.1 (–85.5 to –8.0) | –35.3 (–80.6 to –7.6) | –45.8 (–70.8 to –13.8) | –32.0 (–68.6 to 31.7) |
Estimated median difference (CI)a | –11.6 (–41.6 to 9.8) | –16.4 (–46.8 to 9.0) | NA | –15.7 (–48.7 to 11.8) | NA |
P valueb | 0.2529 | 0.2744 | NA | 0.2568 | NA |
Countable partial/focal seizures | |||||
Patients analyzed, n | 17 | 18 | 19 | 20 | 19 |
Baseline period, median (Q1, Q3) | 21.2 (5.0 to 43.9) | 36.5 (9.6 to 90.1) | 34.5 (4.0 to 78.2) | 26.5 (4.4 to 58.9) | 10.0 (5.4 to 21.2) |
Treatment period, median (Q1, Q3) | 9.4 (1.8 to 16.5) | 11.0 (2.7 to 59.1) | 25.4 (2.9 to 87.4) | 10.2 (0.8 to 26.6) | 6.1 (2.8 to 11.1) |
Median percent change during treatment (Q1, Q3) | –56.2 (–82.5 to –16.4) | –57.9 (–86.2 to –6.7) | –14.6 (–56.5 to 45.8) | –44.6 (–93.3 to –25.6) | –6.3 (–80.2 to 57.0) |
Estimated median difference (CI)a | –37.8 (–85.4 to 9.2) | –31.7 (–73.6 to 11.5) | NA | –34.0 (–91.8 to 4.7) | NA |
P valueb | 0.1165 | 0.1576 | NA | 0.0699 | NA |
Clonic seizures | |||||
Patients analyzed, n | 3 | 8 | 5 | 7 | 12 |
Baseline period, median (Q1, Q3) | 4.0 (1.0 to 30.1) | 38.9 (6.7 to 112.7) | 20.0 (3.0 to 22.8) | 18.0 (4.0 to 75.0) | 40.9 (8.0 to 129.4) |
Treatment period, median (Q1, Q3) | 0.3 (0.0 to 33.7) | 3.6 (2.2 to 22.7) | 9.1 (0.0 to 9.1) | 2.8 (0.0 to 4.9) | 11.0 (0.0 to 134.9) |
Median percent change during treatment (Q1, Q3) | –99.0 (–100.0 to 3392.5) | –73.1 (–84.6 to –61.3) | –59.8 (–100.0 to –54.7) | –92.5 (–100.0 to –84.4) | –74.1 (–100.0 to 27.2) |
Estimated median difference (CI)a | 0.0 (–282.2 to 3492.5) | –4.3 (–252.4 to 29.8) | NA | –6.4 (–120.0 to 7.5) | NA |
P valueb | 1.0000 | 1.0000 | NA | 0.4656 | NA |
Other partial seizures | |||||
Patients analyzed, n | 5 | 6 | 4 | 4 | 2 |
Baseline period, median (Q1, Q3) | 7.8 (1.0 to 23.2) | 6.9 (5.4 to 25.0) | 74.0 (2.5 to 180.0) | 107.9 (32.0 to 443.8) | 41.8 (1.9 to 81.6) |
Treatment period, median (Q1, Q3) | 3.1 (2.9 to 4.2) | 2.0 (0.6 to 10.2) | 121.9 (0.0 to 344.9) | 21.7 (1.0 to 213.0) | 51.0 (2.3 to 99.8) |
Median percent change during treatment (Q1, Q3) | –87.7 (–97.2 to 165.5) | –51.1 (–96.7 to 4.3) | –43.6 (–100.0 to 111.3) | –73.1 (–99.4 to –39.8) | 19.7 (17.2 to 22.2) |
Estimated median difference (CI)a | 2.1 (–306.9 to 311.1) | 0.00 (–306.4 to 151.0) | NA | –92.81 (–122.2 to –49.3) | NA |
P valueb | 0.7086 | 1.0000 | NA | 0.1052 | NA |
S/CGICSD Combined caregiver and patient; category, n (%) | |||||
Tonic-clonic seizures | |||||
Patients analyzed, n | 34 | 34 | 33 | 38 | 46 |
Decrease in average duration | 16 (47.1) | 19 (55.9) | 12 (36.4) | 14 (36.8) | 13 (28.3) |
No change in average duration | 16 (47.1) | 15 (44.1) | 17 (51.5) | 21 (55.3) | 29 (63.0) |
Increase in average duration | 2 (5.9) | 0 | 4 (12.1) | 3 (7.9) | 4 (8.7) |
Odds ratio (95% CI)d | 1.79 (0.67 to 4.74) | 2.74 (1.03 to 7.32) | NA | 1.42 (0.60 to 3.37) | NA |
Risk difference (95% CI) | NR | NR | NA | NR | NA |
P valued | 0.2424 | 0.0444 | NA | 0.4270 | NA |
Tonic seizures | |||||
Patients analyzed, n | 50 | 49 | 48 | 62 | 64 |
Decrease in average duration | 20 (40.0) | 28 (57.1) | 17 (35.4) | 29 (46.8) | 19 (29.7) |
No change in average duration | 28 (56.0) | 20 (40.8) | 28 (58.3) | 31 (50.0) | 39 (60.9) |
Increase in average duration | 2 (4.0) | 1 (2.0) | 3 (6.3) | 2 (3.2) | 6 (9.4) |
Odds ratio (95% CI)d | 1.38 (0.62 to 3.09) | 2.75 (1.20 to 6.30) | NA | 2.12 (1.04 to 4.30) | NA |
Risk difference (95% CI) | NR | NR | NA | NR | NA |
P valued | 0.4308 | 0.0172 | NA | 0.0379 | NA |
Clonic seizures | |||||
Patients analyzed, n | 3 | 8 | 5 | 8 | 7 |
Decrease in average duration | 1 (33.3) | 7 (87.5) | 1 (20.0) | 1 (12.5) | 2 (28.6) |
No change in average duration | 1 (33.3) | 1 (12.5) | 4 (80.0) | 7 (87.5) | 5 (71.4) |
Increase in average duration | 1 (33.3) | 0 | 0 | 0 | 0 |
Odds ratio (95% CI)d | 0.66 (0.03 to 15.20) | 13.81 (0.70 to 272.63) | NA | 0.25 (0.01 to 5.54) | NA |
Risk difference (95% CI) | NR | NR | NA | NR | NA |
P valued | 0.7945 | 0.0845 | NA | 0.3806 | NA |
Atonic seizures | |||||
Patients analyzed, n | 43 | 38 | 35 | 43 | 54 |
Decrease in average duration | 21 (48.8) | 22 (57.9) | 13 (37.1) | 18 (41.9) | 18 (33.3) |
No change in average duration | 20 (46.5) | 15 (39.5) | 16 (45.7) | 24 (55.8) | 32 (59.3) |
Increase in average duration | 2 (4.7) | 1 (2.6) | 6 (17.1) | 1 (2.3) | 4 (7.4) |
Odds ratio (95% CI)d | 1.90 (0.79 to 4.55) | 2.78 (1.11 to 6.96) | NA | 1.54 (0.68 to 3.46) | NA |
Risk difference (95% CI) | NR | NR | NA | NR | NA |
P valued | 0.1504 | 0.0293 | NA | 0.3000 | NA |
Myoclonic seizures | |||||
Patients analyzed, n | 27 | 17 | 25 | 31 | 41 |
Decrease in average duration | 9 (33.3) | 7 (41.2) | 6 (24.0) | 12 (38.7) | 11 (26.8) |
No change in average duration | 18 (66.7) | 10 (58.8) | 17 (68.0) | 19 (61.3) | 28 (68.3) |
Increase in average duration | 0 | 0 | 2 (8.0) | 0 | 2 (4.9) |
Odds ratio (95% CI)d | 1.84 (0.53 to 6.36) | 2.51 (0.65 to 9.68) | NA | 1.89 (0.70 to 5.04) | NA |
Risk difference (95% CI) | NR | NR | NA | NR | NA |
P valued | 0.3384 | 0.1806 | NA | 0.2066 | NA |
Countable partial seizures | |||||
Patients analyzed, n | 16 | 16 | 15 | 17 | 17 |
Decrease in average duration | 5 (31.3) | 8 (50.0) | 6 (40.0) | 5 (29.4) | 7 (41.2) |
No change in average duration | 10 (62.5) | 8 (50.0) | 7 (46.7) | 10 (58.8) | 9 (52.9) |
Increase in average duration | 1 (6.3) | 0 | 2 (13.3) | 2 (11.8) | 1 (5.9) |
Odds ratio (95% CI)d | 0.65 (0.15 to 2.88) | 1.54 (0.36 to 6.58) | NA | 0.41 (0.10 to 1.73) | NA |
Risk difference (95% CI) | NR | NR | NA | NR | NA |
P valued | 0.5746 | 0.5584 | NA | 0.2268 | NA |
Other partial seizures | |||||
Patients analyzed, n | 8 | 3 | 4 | 3 | 0 |
Decrease in average duration | 3 (37.5) | 1 (33.3) | 1 (25.0) | 2 (66.7) | 0 |
No change in average duration | 5 (62.5) | 2 (66.7) | 3 (75.0) | 1 (33.3) | 0 |
Increase in average duration | 0 | 0 | 0 | 0 | 0 |
Odds ratio (95% CI)d | 1.00 (0.04 to 27.24) | 1.46 (0.05 to 41.09) | NA | NA | NA |
Risk difference (95% CI) | NR | NR | NA | NR | NA |
P valued | 1.0000 | 0.8255 | NA | NA | NA |
Absence seizures | |||||
Patients analyzed, n | 34 | 26 | 32 | 37 | 39 |
Decrease in average duration | 18 (52.9) | 11 (42.3) | 8 (25.0) | 16 (43.2) | 9 (23.1) |
No change in average duration | 16 (47.1) | 15 (57.7) | 23 (71.9) | 19 (51.4) | 28 (71.8) |
Increase in average duration | 0 | 0 | 1 (3.1) | 2 (5.4) | 2 (5.1) |
Odds ratio (95% CI) | 3.41 (1.17 to 9.95) | 2.62 (0.84 to 8.15) | NA | 2.06 (0.80 to 5.34) | NA |
Risk difference (95% CI) | NR | NR | NA | NR | NA |
P value | 0.0247 | 0.0973 | NA | 0.1361 | NA |
Patients with status epilepticus | |||||
Number of patients with convulsive seizures greater than 30 minutes in duration, n (%) | |||||
Baseline period | 8 (10.5) | 2 (2.7) | 3 (3.9) | 2 (2.3) | 1 (1.2) |
Treatment period | 2 (2.6) | 1 (1.4) | 2 (2.6) | 1 (1.2) | 1 (1.2) |
Number of patients with nonconvulsive seizures greater than 30 minutes in duration, n (%) | |||||
Baseline period | 3 (3.9) | 3 (4.1) | 6 (7.9) | 3 (3.5) | 2 (2.4) |
Treatment period | 2 (2.6) | 3 (4.1) | 3 (3.9) | 1 (1.2) | 1 (1.2) |
Change in vineland-II scores from baseline to last visit | |||||
Communication domain standard score, n | 42 | 27 | 48 | 52 | 56 |
Day 1, mean (SD) | 41.0 (17.2) | 41.0 (13.6) | 38.8 (14.9) | 41.6 (17.2) | 39.9 (12.0) |
Last Visit, mean (SD) | 40.1 (16.1) | 41.4 (17.0) | 41.1 (17.3) | 38.8 (15.4) | 37.9 (12.7) |
Change from baseline (SD) | 0.7 (3.2) | 0.7 (3.7) | 0.2 (4.8) | –0.6 (6.7) | –2.0 (6.8) |
Adjusted mean treatment difference (95% CI)e | 0.6 (−1.1 to 2.3) | 0.6 (−1.3 to 2.5) | NA | 1.4 (−1.2 to 3.9) | NA |
P valuee | 0.4845 | 0.5235 | NA | 0.2887 | NA |
Daily living skills domain standard score, n | 47 | 38 | 52 | 54 | 58 |
Day 1, mean (SD) | 40.6 (17.5) | 41.6 (11.8) | 38.8 (14.5) | 40.5 (19.4) | 38.2 (12.1) |
Last visit, mean (SD) | 39.9 (17.6) | 40.0 (13.7) | 39.5 (17.8) | 38.2 (14.9) | 37.1 (12.0) |
Change from baseline (SD) | –0.6 (3.8) | 0.4 (4.4) | –0.6 (2.8) | –0.7 (6.5) | –0.3 (3.7) |
Adjusted mean treatment difference (95% CI)e | 0.0 (−1.4 to 1.5) | 1.1 (−0.5 to 2.6) | NA | −0.5 (−2.5 to 1.5) | NA |
P valuee | 0.9609 | 0.1816 | NA | 0.607 | NA |
Socialization domain standard score, n | 42 | 25 | 47 | 50 | 49 |
Day 1, mean (SD) | 44.8 (17.4) | 48.0 (15.9) | 43.2 (15.8) | 44.7 (16.6) | 47.2 (13.7) |
Last visit, mean (SD) | 44.6 (17.0) | 49.3 (15.9) | 46.0 (19.2) | 44.4 (18.0) | 42.8 (13.5) |
Change from baseline (SD) | 0.5 (4.2) | 1.6 (6.8) | 1.7 (6.7) | 0.3 (4.6) | –1.4 (3.4) |
Adjusted mean treatment difference (95% CI)e | −1.0 (−3.6 to 1.5) | 0.0 (−2.9 to 3.0) | NA | 1.7 (0.1 to 3.4) | NA |
P valuee | 0.4151 | 0.9777 | NA | 0.0380 | NA |
Motor skills domain standard score, n | 41 | 34 | 47 | 46 | 56 |
Day 1, mean (SD) | 42.6 (18.0) | 48.7 (22.2) | 43.5 (19.5) | 45.3 (21.8) | 47.7 (20.6) |
Last visit, mean (SD) | 43.1 (19.3) | 50.4 (25.2) | 46.0 (21.8) | 45.5 (22.3) | 45.0 (19.8) |
Change from baseline (SD) | 0.8 (5.4) | 2.8 (10.4) | 0.1 (4.9) | –0.7 (5.9) | 0.1 (6.3) |
Adjusted mean treatment difference (95% CI)e | 0.7 (−2.3 to 3.7) | 2.7 (−0.4 to 5.9) | NA | −0.9 (−3.3 to 1.6) | NA |
P valuee | 0.6303 | 0.0884 | NA | 0.4816 | NA |
Adaptive behaviour composite standard score, n | 39 | 23 | 45 | 46 | 48 |
Day 1, mean (SD) | 39.0 (17.7) | 41.0 (14.1) | 37.2 (14.8) | 38.9 (16.1) | 38.8 (11.3) |
Last visit, mean (SD) | 39.5 (16.8) | 40.3 (15.0) | 38.7 (16.1) | 37.9 (14.9) | 37.4 (12.0) |
Change from baseline (SD) | 0.3 (2.9) | 0.7 (4.1) | 0.4 (3.7) | –0.7 (3.9) | –1.1 (3.0) |
Adjusted mean treatment difference (95% CI)e | 0.1 (−1.4 to 1.6) | 0.5 (−1.3 to 2.3) | NA | 0.5 (−0.9 to 1.9) | NA |
P valuee | 0.8983 | 0.5960 | NA | 0.4986 | NA |
Maladaptive behaviour index V-scale score, n | 50 | 55 | 60 | 58 | 55 |
Day 1, mean (SD) | 18.9 (2.7) | 18.8 (2.4) | 18.2 (2.7) | 18.9 (2.2) | 19.0 (1.9) |
Last visit, mean (SD) | 18.7 (2.2) | 18.8 (2.0) | 18.0 (2.5) | 18.7 (2.3) | 18.8 (2.1) |
Change from baseline (SD) | –0.4 (2.2) | –0.2 (1.9) | –0.3 (1.9) | –0.3 (1.2) | –0.7 (1.6) |
Adjusted mean treatment difference (95% CI)e | −0.1 (−0.9 to 0.6) | 0.1 (−0.7 to 0.8) | NA | 0.4 (−0.2 to 0.9) | NA |
P valuee | 0.7012 | 0.8877 | NA | 0.1752 | NA |
Sleep disruption 0 to 10 NRS at last visit | |||||
Patients analyzed, n | 74 | 73 | 75 | 83 | 84 |
Day 1, mean (SD) | 3.7 (2.6) | 3.7 (2.4) | 3.6 (2.7) | 3.5 (2.4) | 4.0 (2.7) |
Last visit, mean (SD) | 3.2 (2.7) | 2.8 (2.4) | 3.4 (2.6) | 3.1 (2.6) | 3.7 (2.6) |
Change from baseline (SD) | –0.4 (2.7) | –0.9 (2.8) | –0.1 (2.9) | –0.4 (2.9) | –0.3 (3.0) |
Adjusted mean treatment difference (95% CI)e | –0.3 (–1.2 to 0.6) | –0.8 (–1.7 to 0.1) | NA | −0.2 (−1.1 to 0.7) | NA |
P valuee | 0.4998 | 0.0956 | NA | 0.7176 | NA |
ESS at last visit | |||||
Patients analyzed, n | 72 | 71 | 74 | 83 | 84 |
Day 1, mean (SD) | 11.1 (5.5) | 9.7 (5.8) | 10.1 (5.9) | 10.4 (5.3) | 10.9 (6.2) |
Last visit, mean (SD) | 11.0 (5.9) | 9.7 (6.2) | 10.0 (5.8) | 10.0 (6.1) | 9.9 (6.2) |
Change from baseline (SD) | –0.2 (4.9) | –0.1 (4.5) | –0.2 (4.0) | –0.3 (5.1) | –0.9 (4.6) |
Adjusted mean treatment difference (95% CI)e | 0.0 (−1.5 to 1.5) | 0.1 (−1.4 to 1.6) | NA | 0.6 (−0.8 to 2.1) | NA |
P valuee | 0.9909 | 0.9003 | NA | 0.3909 | NA |
Exploratory end points | |||||
Time to baseline drop seizure frequency during the treatment period | |||||
Estimated median number of days (95% CI)g | 48.0 (40.0 to 67.0) | 47.0 (38.0 to 55.0) | 36.0 (30.0 to 38.0) | 53.0 (44.0 to 68.0) | 35.0 (32.0 to 39.0) |
P valueg | < 0.0001 | 0.0001 | NA | 0.0005 | NA |
CI = confidence interval, ESS = Epworth Sleepiness Scale, mg/kg/day = milligrams per kilogram per day, n = number of patients, NA = not applicable, NR = not reported, 0 to 10 NRS = Sleep Disruption 0 to 10 Numerical Rating Scale, QOLCE = Quality of Life in Childhood Epilepsy, QOLIE-31-P = Quality of Life in Epilepsy, version 2, Q1 = lower quartile, Q3 = upper quartile, SD = standard deviation, S/CGIC = Subject/Caregiver Global Impression of Change, S/CGICSD = Subject/Caregiver Global Impression of Change in Seizure Duration, Vineland-II = Vineland Adaptive Behaviour Scales Second Edition.
aThe Hodges-Lehmann median difference and 95% CI is presented.
bThe P value from the Wilcoxon rank sum test is presented.
cThe P value calculated from a Cochran-Mantel-Haenszel test is presented.
dThe ordinal logistic regression result is presented.
eThe 95% CI and the P value from the ANCOVA model are presented.
fThe change from baseline was presented for QOLIE-31-P because in the CARE 4 trial, the mean difference between groups was not assessed due to a small number of patients completing the questionnaire.
gThe Kaplan-Meier Estimate and log rank test P value are presented.
Source: Clinical Study Report for CARE 316 and CARE 4.17 Details included in the table are from the sponsor’s summary of clinical evidence.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
ASM
antiseizure medication
BIA
budget impact analysis
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
LGS
Lennox-Gastaut syndrome
NICE
National Institute for Health and Care Excellence
NIHB
Non-Insured Health Benefits
QALY
quality-adjusted life-year
SUDEP
sudden unexpected death in epilepsy
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Cannabidiol (Epidiolex), 100 mg/mL oral solution |
Submitted price | Cannabidiol, 100 mg/mL oral solution: $1,424.54 per 100 mL bottle |
Indication | As adjunctive therapy for the treatment of seizures associated with LGS, DS or TSC in patients 2 years of age and older |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 15, 2023 |
Reimbursement request | As adjunctive therapy for the treatment of seizures associated with LGS in patients 2 years of age and older |
Sponsor | Jazz Pharmaceuticals Canada |
Submission history | Previously reviewed: In progress. Indication: As adjunctive therapy for the treatment of seizures associated with DS in patients 2 years of age or older. Recommendation: TBD. Previously reviewed: In progress. Indication: As adjunctive therapy for the treatment of seizures associated with TSC in patients 2 years of age or older. Recommendation: TBD. |
DS = Dravet syndrome; LGS = Lennox-Gastaut syndrome; NOC = Notice of Compliance; TBD = to be determined; TSC = tuberous sclerosis complex.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients aged 2 years or older with LGS inadequately controlled by their current usual care (i.e., patients taking at least 1 ASM who experience 2 or more drop seizures each week over a 28-day period) |
Treatment | Cannabidiol plus usual care (assumed to comprise 1 or more ASMsa) |
Comparator | Usual care |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (90 years) |
Key data source | CARE 3 and CARE 4 clinical trials; CARE 5 extension study |
Submitted results | ICER = $35,257 per QALY gained (incremental costs: $101,074; incremental QALYs: 2.867). |
Key limitations |
|
CADTH reanalysis results |
|
AE = adverse event; ASM = antiseizure medication; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; LGS = Lennox-Gastaut syndrome; LY = life-year; QALY = quality-adjusted life-year; RCT = randomized controlled trial.
aUsual care was assumed by the sponsor to the following ASMs: clobazam, valproic acid, levetiracetam, topiramate, clonazepam, rufinamide, lamotrigine, perampanel, or lacosamide.
Conclusions
Based on data from the CARE 3 and CARE 4 trials, the CADTH clinical review concluded that the use of cannabidiol may result in a reduction in drop seizures compared with placebo on a background of usual care antiseizure medications (ASMs). No patients were reported to have a 100% reduction in drop seizures at the end of the 14-week treatment period, and the clinical significance of the number of drop seizure–free days observed is uncertain. As noted in the CADTH clinical review, despite a reduction in drop seizures with cannabidiol in the CARE 3 and CARE 4 trials, cannabidiol likely results in little to no difference in health-related quality of life (HRQoL), as assessed over the 14-week CARE 3 and CARE 4 treatment phase; however, longer follow-up times and higher participant completion rates may be required to detect changes in HRQoL. Limited conclusions about the long-term benefit of cannabidiol can be made based on the CARE 5 extension study owing to its single-group, open-label design and enriched population. CADTH additionally notes that the magnitude of any treatment benefit between cannabidiol plus usual care versus usual care alone among patients with fewer than 2 drop seizures a week is unknown due to a lack of clinical data. As such, the cost-effectiveness of cannabidiol in this subgroup, and thus for the full reimbursement population, is highly uncertain.
CADTH undertook reanalyses to address limitations in the sponsor’s analysis, which included adopting alternative health state utility values, excluding quality-adjusted life-years (QALYs) accrued by caregivers, adopting a higher mean dose of cannabidiol, using mean patient weight in the calculation of drug costs, and assuming that the long-term rate of discontinuation for patients experiencing drop seizures would be equivalent to that observed in the CARE 5 study. The CADTH base case suggests that, at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained, cannabidiol plus usual care is not a cost-effective treatment option for seizures associated with Lennox-Gastaut syndrome (LGS) compared with usual care alone. A price reduction of 71% for cannabidiol would be required for cannabidiol plus usual care to be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
Although the CADTH base case estimated a gain in QALYs with cannabidiol plus usual care compared to usual care alone (incremental QALYs = 1.07), 99% of the incremental benefit was gained in the extrapolated period (i.e., after 14 weeks). In the absence of comparative evidence beyond 14 weeks, the incremental QALYs for cannabidiol plus usual care predicted in CADTH’s base case are highly uncertain and may be overestimated, and additional price reductions may be required.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received 1 patient input submission from the Canadian Epilepsy Alliance, which was not specific to LGS. The input was based on the knowledge and experience of the submitter and the lived experiences of the patients, caregivers, clinicians, volunteers, and supporters of the Canadian Epilepsy Alliance’s 24 member associations. According to this input, people with uncontrolled epilepsy may feel socially isolated due to stigma and fear of rejection in social, work, and educational situations and the person’s family can be affected by the unpredictable seizures and associated anxiety. Caregivers may be afraid to leave someone with frequent seizures alone, leading to a loss of independence and self-esteem for the person with epilepsy and potentially to compassion fatigue and sleep deprivation for the caregiver. A reduction in the absolute number of seizures experienced may improve the overall quality of life of the person with epilepsy; however, ASMs may be associated with side effects such as mood swings, sexual dysfunction, suicidal thoughts, memory loss, problems with concentration, fatigue, or depression, which can impact both patients and their caregivers. The Canadian Epilepsy Alliance input further noted that people with drug-resistant epilepsy are often unemployed or underemployed and are thus less likely to be covered by employer-funded insurance plans. Additionally, some people with epilepsy may take alternative substances, including cannabis.
No clinician group input was received for this review.
CADTH-participating drug plans noted that the CARE 3 and CARE 4 trials included patients whose seizures had failed to respond to more than 1 ASM, which differs from the International League Against Epilepsy’s definition of drug-resistant epilepsy (the failure of adequate trials of 2 or more tolerated, appropriately chosen and administered ASMs [as monotherapy or in combination] to achieve seizure freedom). The plans additionally noted that the CARE 3 and CARE 4 trials enrolled patients with at least 8 drop seizures per 28-day period and questioned whether there should be a minimum number of drop seizures experienced by a patient per month for cannabidiol to be reimbursed. The plans noted that rufinamide is less costly than the submitted price of cannabidiol and is reimbursed for patients who meet the International League Against Epilepsy definition of drug-resistant epilepsy. The plans noted that cannabidiol is dosed by weight and that the cost is considerably greater for those using higher doses and at higher body weight. Additionally, the frequency of administration and the small volumes involved when administering cannabidiol led to the drug plans considering that product wastage might become an issue. Finally, the plans indicated that the price submitted by the sponsor is considerably higher than that of medical cannabis and thus patients who cannot afford the upfront costs associated with the submitted product may seek alternate pathways, which may lead to equity implications.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s model considered the impact of reducing seizure frequency on patient HRQoL.
HRQoL was included in the model, both for patients with LGS and for caregivers.
The costs and consequences of adverse events (AEs) were included in the model; however, the HRQoL impacts of serious AEs were not adequately considered.
In scenario analyses, the sponsor considered the impact of adopting a stopping rule for patients who have not experienced at least a 30% reduction in seizure frequency after treatment for 6, 12, and 24 months.
In addition, CADTH addressed some of these concerns as follows:
CADTH assumed that not all patients would receive the minimum recommended maintenance dose of cannabidiol.
CADTH was unable to address the following concerns raised from stakeholder input:
The cost-effectiveness of cannabidiol among patients who meet the International League Against Epilepsy definition for drug-resistant epilepsy, owing to a lack of clinical information.
The cost-effectiveness of cannabidiol among patients who have previously used medical cannabis, owing to the lack of clinical data for this population.
Economic Review
The current review is for cannabidiol (Epidiolex) for use as adjunctive therapy for seizures associated with LGS in patients aged 2 years and older.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Cannabidiol is indicated for use as adjunctive therapy for seizures associated with LGS, Dravet syndrome, or tuberous sclerosis complex in patients aged 2 years and older,1 while the sponsor’s reimbursement request relevant to this review is for use as adjunctive therapy for the treatment of seizures associated with LGS in patients aged 2 years and older.2 The sponsor submitted a cost-utility analysis of cannabidiol plus usual care compared to usual care alone in the reimbursement population, with usual care assumed to comprise ASMs including clobazam, valproic acid, levetiracetam, topiramate, clonazepam, rufinamide, lamotrigine, perampanel, and lacosamide.3,4 The modelled population was aligned with patients enrolled in the CARE 3 and CARE 4 trials.
Cannabidiol is available as a 100 mg/mL oral solution. The recommended dosage of cannabidiol is 2.5 mg/kg twice daily (5 mg/kg/day) for 1 week, then increased to 5 mg/kg twice daily (10 mg/kg/day) to a maximum of 10 mg/kg twice daily (20 mg/kg/day), depending on individual response and tolerability.1 The submitted price of cannabidiol is $1,424.54 per 100 mL bottle.
In the model, the sponsor separately calculated costs of treatment for patients aged 2 to 5 years, 6 to 11 years, 12 to 17 years, and 18 years and older, based on weight-based dosing (16.25 kg, 25.65 kg, 45.50 kg, and 63.10 kg, respectively), resulting in an annual per-patient cost of $9,321, $14,712, $26,098, and $36,314, respectively. The sponsor’s annual per-patient cost of usual care was similarly weight based and ranged from $894 to $3,595. Patients receiving cannabidiol in addition to usual care were assumed to use the same amount of other ASMs as those in the usual care group.
The clinical outcomes of interest were life-years and QALYs. The sponsor adopted a lifetime horizon (90 years), with the analyses conducted from the perspective of a publicly funded health care payer. Future costs and benefits were discounted at a rate of 1.5% per year, and the model cycle length was 3 months.
Model Structure
The sponsor submitted a Markov model with 4 main health states based on the frequency of drop seizures per 28 days (drop seizure-free, ≤ 45 drop seizures, > 45 to ≤ 110 drop seizures, > 110 drop seizures) and death (Figure 1).5 Additionally, each seizure-based health state was further divided into 3 substates based on the number of days per 28-day period that patients were free of drop seizures (≤ 3 days, > 3 to ≤ 15 days, > 15 days) (Figure 2). Patients entered the model distributed across the main seizure-based health states, with the exception of the drop seizure-free state, based on the baseline number of drop seizures and drop seizure-free days per 28-day period of patients in the CARE 3 and CARE 4 trials. In the first cycle, patients could transition into other main health states based on individual patient data observed in the CARE 3 and CARE 4 trial. Thereafter, patients receiving usual care alone were assumed to remain in the same health state for the remainder of their lives. In cycles 2 to 9, patients receiving cannabidiol plus usual care continued to transition between the main health states based on individual patient data from the CARE 5 long-term extension study, which were specifically from patients who had previously received cannabidiol within the CARE 3 and CARE 4 trials. From cycle 10 onward, patients receiving cannabidiol plus usual care were assumed to remain in the same health state until they discontinued cannabidiol treatment or died. The distributions of patients among the drop seizure-free day substates after the first cycle were derived from the cannabidiol and placebo groups of patients in the CARE 3 and CARE 4 studies who continued into the CARE 5 trial, and differed by treatment group.
Patients could discontinue cannabidiol at any point in the time horizon. In the first model cycle, discontinuation was based on the withdrawal rate observed in the CARE 3 and CARE 4 trials. In cycles 2 through 9, discontinuation rates were estimated for each health state based on patients across all cannabidiol plus usual care and usual care alone treatment groups of the CARE 3 and CARE 4 trials (those who later enrolled in the CARE 5 trial). From cycle 10 onward, patients in the drop seizure-free state were assumed to discontinue cannabidiol at a rate of 0.5% per cycle, while a discontinuation rate of 10% per cycle was applied to patients who were not seizure free, based on a review of cannabidiol for LGS by the National Institute for Health and Care Excellence (NICE), UK.6 When patients discontinued cannabidiol, they were assumed to follow the seizure frequency distribution observed in the usual care group at the end of cycle 1. No stopping rule for cannabidiol was assumed in the base case.
Model Inputs
The pharmacoeconomic model was informed by inputs from the phase III randomized CARE 33 and CARE 4 trials,4 which enrolled patients with LGS (aged 2 to 55 years) who experienced at least 2 drop seizures per week and were taking 1 or more ASMs at baseline. Although the sponsor indicated that the mean age of the modelled cohort was 13.76 years, the sponsor assumed that the modelled cohort comprised 4 age groups at baseline (2 to 5 years: 11.48% of patients; 6 to 11 years: 33.24% of patients; 12 to 17 years: 24.59% of patients; ≥ 18 years: 31.69% of patients), with median body weight adapted for each cohort (2 to 5 years: 16.25 kg; 6 to 11 years: 25.65 kg; 12 to 17 years: 45.50 kg; ≥ 18 years: 63.10 kg). Patients moved into higher age and weight categories as they progressed through the model. The baseline distribution of patients across drop seizure–based health states was as follows: 0% in the drop seizure-free health state, 28.14% in the less than or equal to 45 drop seizures health state, 34.97% in the greater than 45 to less than or equal to 110 drop seizures health state, and 36.89% in the greater than 110 drop seizures health state.
Movement between seizure-based health states in the pharmacoeconomic model for cycle 1 was informed by pooled individual patient data from the CARE 3 and CARE 4 trials for patients receiving cannabidiol plus usual care or usual care alone. For cycles 2 through 9, the movement was informed by pooled individual patient data from the CARE 5 trial for patients receiving cannabidiol plus usual care, as described in the Model Structure section.
Treatment-emergent AEs were included in the model for the first 9 cycles based on observations from the CARE 3 and CARE 4 trials. Costs were incorporated for all AEs, while disutilities were included for AEs deemed to be serious and experienced by at least 3% of patients who received cannabidiol and at least 1% of patients who received placebo. Modelled AEs included rash, somnolence, fatigue, lethargy, sedation, diarrhea, decreased appetite, aggression, and irritability. No AEs were included from cycle 10 onward.
Mortality in the model included all-cause mortality (based on age- and gender-specific rates from Statistics Canada for the general population),7 sudden unexpected death in epilepsy (SUDEP), and non-SUDEP. Rates for SUDEP and non-SUDEP were obtained from the literature for patients with Dravet syndrome8 and were assumed to be equivalent for patients with LGS. The sponsor assumed that patients in the drop seizure-free health state would have a 29% reduction in the risk of death for both SUDEP and non-SUDEP based on a prospective cohort study9 that reported a risk reduction of 58% for seizure-free patients and on input from NICE, which suggested that this value was overestimated.6
The sponsor’s model included health state utility values for patients, as well as utility decrements for caregivers. Patient utility values and caregiver utility decrements were obtained from a study that enrolled members of the general population in the UK and Sweden.10 For model health states that did not correspond to those reported in the utility study, the sponsor adopted the average of adjacent health states (Table 11).5 In the model, each patient was assumed to have 2 caregivers, and caregiver utility decrements were applied linearly such that each caregiver had the same decrement per health state regardless of the number of caregivers. Disutilities for all severe AEs were assigned a value of –0.120 based on a 2016 utility study11 reporting such a decrement for “severe side effects” and were assumed to last for 1 model cycle (3 months).
Costs in the model included those associated with drug acquisition, AEs, health care resource use (general practitioner, neurologist, nurse, and therapy visits; emergency department visits; hospital stays; and rescue medication [buccal midazolam]), and end-of-life care (for deaths not attributed to SUDEP). Costs associated with long-term care were included for a proportion of patients older than 18 years. Drug acquisition costs for cannabidiol were based on the sponsor’s submitted price, with an assumed dosage of 10 mg/kg/day (cost per cycle based on patient weight). The acquisition costs of ASMs and buccal midazolam were obtained from the Ontario Drug Benefit Formulary and the Exceptional Access Program.12,13 The cost of usual care was based on the proportion of use for each ASM included within the usual care basket, derived from the proportion of use reported in the CARE 3 and CARE 4 trials. Health care resource use was assumed to vary by health state and age group (pediatric versus adult), with resource use frequency based on use in previous cost-effectiveness studies of treatments for Dravet syndrome.14,15 Unit costs for pediatrician and neurologist visits were obtained from the Ontario Schedule of Benefits for Physician Services16 and informed by the median hourly wages for nurses, occupational therapists, physiotherapists, and speech therapists in the Government of Canada Job Bank.17,18 Deaths not attributed to SUDEP were assumed to require an emergency department visit and 7 days in the intensive care unit, with hospitalization and intensive care unit costs obtained from the Canadian Institute for Health Information.19,20 In the absence of data on the proportion of patients requiring long-term care in adulthood, the sponsor assumed that 3% of adult patients who were seizure free and 13% of adult patients experiencing seizures would require long-term care, with the cost based on Ontario level-of-care per diem funding.21,22 AEs were assumed to be managed by a single neurologist visit. All costs were reported in 2023 Canadian dollars.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations) for the base-case and scenario analyses. The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following sections. All results are based on publicly available list prices. Additional results from the sponsor’s economic evaluation are presented in Appendix 3.
Base-Case Results
In the sponsor’s base case, cannabidiol plus usual care was associated with higher costs (incremental costs = $101,074) and QALYs (incremental QALYs = 2.87) compared to usual care alone, resulting in an incremental cost-effectiveness ratio (ICER) of $35,257 per QALY gained (Table 3). In this analysis, cannabidiol had a 98% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained.
Results were driven by the drug acquisition costs of cannabidiol plus usual care (incremental costs = $119,667), the predicted gain in life-years (incremental life-years = 0.16), and the predicted gain in QALYs (incremental QALYs = 2.87). The sponsor’s model estimated that less than 2% of the incremental benefits were accrued during the CARE 3 and CARE 4 trial period.
The total QALYs predicted by the sponsor’s model for both cannabidiol plus usual care and usual care alone are negative (Table 3) due to the sponsor’s incorporation of utility decrements for caregivers (Table 11); that is, the total QALYs gained by patients who receive cannabidiol plus usual care (6.17) or usual care (4.96) are greatly outweighed by the QALY loss experienced by their caregivers (–21.61 and –23.27 QALYs, respectively). Of the 2.87 incremental QALYs gained with cannabidiol plus usual care, 58% were accrued by caregivers, suggesting that the majority of incremental benefit predicted by the sponsor’s model will be experienced by caregivers, not patients. Additionally, the sponsor’s model suggests that cannabidiol plus usual care will be associated with an additional 0.16 life-years compared to usual care alone. At the end of the time horizon, 0% of patients were still alive.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYsa | Incremental QALYs | ICER vs. usual care ($/QALY) |
|---|---|---|---|---|---|---|---|
Usual care | 505,764 | Reference | 28.62 | Reference | –18.30 | Reference | Reference |
Cannabidiol plus usual care | 606,838 | 101,074 | 28.77 | 0.16 | –15.44 | 2.87 | 35,257 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: Usual care was assumed by the sponsor to consist of a basket of ASMs, including clobazam, valproic acid, levetiracetam, topiramate, clonazepam, rufinamide, lamotrigine, perampanel, and lacosamide.
aThe total QALYs attributed to usual care (–18.30) comprise 4.96 QALYs accrued by patients and –23.27 QALYs accrued by caregivers. The total QALYs attributed to cannabidiol plus usual care (–15.44) comprise 6.17 QALYs from patients and –21.61 QALYs from caregivers. The negative QALYs accrued by caregivers reflect the modelling of the impact on caregivers as utility decrements.
Source: Sponsor’s pharmacoeconomic submission.5
Sensitivity and Scenario Analysis Results
The sponsor provided several scenario analyses, including adopting an alternative time horizon (40 years, 65 years), excluding caregiver disutilities, implementing a stopping rule (i.e., patients who had not experienced a 30% reduction in drop seizures from baseline at 6, 12, and 24 months discontinued cannabidiol treatment), assuming patients in the usual care group would revert to their baseline health states after cycle 1, assuming SUDEP or non-SUDEP-related mortality was equal across health states, including utility decrements for other seizure types, assuming higher maintenance doses of cannabidiol (15 mg/kg/day, 20 mg/kg/day), adopting alternate utility value sets, excluding AEs, and adopting a societal perspective.
The scenarios with the greatest impact on the ICER were those excluding caregiver utility values (ICER = $83,580), increasing the maintenance dose of cannabidiol (15 mg/kg/day: ICER = $56,031; 20 mg/kg/day: ICER = $76,805), and using alternate utility value sets (range of ICERs, $47,930 to $60,938).
The sponsor also conducted a scenario analysis from a societal perspective, which included additional costs associated with hospital travel, caregiver loss of productivity, and out-of-pocket expenses for professional care. In this analysis, the ICER for cannabidiol plus usual care was $21,422 per QALY gained versus usual care alone. This value is lower than the sponsor’s base-case analysis using a health care payer perspective.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The full indicated population for LGS was not modelled: The sponsor-submitted analyses intended to reflect the cost-effectiveness of cannabidiol plus usual care for the treatment of seizures associated with LGS in patients aged 2 years and older, which is aligned with the approved Health Canada indication.1 Effectiveness in the sponsor’s model was informed by observations from the CARE 3 and CARE 4 trials, which enrolled patients with LGS whose seizures were inadequately controlled by current ASMs,4 which the sponsor defined as experiencing 2 or more drop seizures per week over a 28-day period. While the Health Canada indication is for use of cannabidiol as adjunctive therapy, it does not restrict usage based on seizure frequency. As such, the sponsor’s modelled population is narrower than the Health Canada–indicated population in that it does not consider patients with LGS who have fewer than 8 seizures over a 28-day period.
CADTH was unable to address this limitation owing to a lack of clinical data pertaining to patients with fewer than 2 drop seizures per week over a 28-day period. As such, the cost-effectiveness of cannabidiol plus usual care in this subgroup of patients is unknown, as is the cost-effectiveness of cannabidiol plus usual care in the full Health Canada–indicated population for LGS.
The model structure does not adequately reflect LGS in clinical practice: The sponsor submitted a Markov model with 4 main health states based on the number of drop seizures (Figure 1) and 3 substates based on the number of drop seizure–free days per 28 days (Figure 2).5 The sponsor adopted the upper and lower bounds for each main health state and substate such that patients enrolled in the CARE 3 and CARE 4 trials would be divided into 3 approximately equal groups.5 There are several limitations associated with this approach. First, the health states were based on observed data from the CARE 3 and CARE 4 trials. If the distribution of seizures among patients in clinical practice differs from those enrolled in these studies, the model health states may not reflect patients seen in clinical practice.
Second, health states in an economic model should represent a homogenous group of patients who have similar expected costs and quality-of-life considerations and should be based on the clinical or care pathway for the condition of interest;23 this is not captured by the modelled health states. The clinical expert input received by CADTH indicated that there is no clinical consensus regarding what seizure thresholds would adequately capture changes in HRQoL and costs; this was acknowledged by the sponsor.5 The clinical expert input further noted that relative reductions in seizure frequency may be important aspects in determining quality of life for patients and that a 25% to 30% reduction in seizures may be meaningful for patients. Using the sponsor’s cut-off points for the main seizure-based health states, patients who have, for example, 100 drop seizures per 28 days at baseline and experience a 50% reduction after initiating treatment (i.e., twice what clinical experts deemed meaningful) would remain in their initial health state of greater than 45 to less than or equal to 110 drop seizures per 28 days. These patients would thus experience the same quality of life and costs as patients who have 100 drop seizures every 28 days and did not improve. Additionally, the sponsor’s modelled substates for number of days of drop seizure freedom may not adequately reflect patient quality of life. The clinical expert input noted that the impact of the number of seizure-free days on quality of life will vary among patients and that some patients who were previously experiencing daily seizures may find even a few days of seizure freedom per month to be impactful. In the sponsor’s model, patients who experience, for example, 5 drop seizure-free days per 28 days are assumed to have the same quality of life as someone who experiences 14 days of drop seizure freedom, which clinical experts deemed unlikely. As such, narrower health states may have been more reflective of patient experience.
CADTH was unable to address limitations related to the model structure. The direction and magnitude of the impact of the model structure not adequately reflecting clinical practice is unknown.
The model lacked face validity and transparency: In assessing the internal validity of the sponsor’s submitted model, CADTH identified that the sponsor’s model did not return the expected results. Specifically, when the effectiveness and safety inputs (i.e., transition probabilities, days without drop seizures, AE incidence rates) were set to be equivalent for cannabidiol plus usual care and usual care alone, the sponsor’s model predicted an incremental QALY gain of 0.28 for cannabidiol plus usual care, rather than 0 as would be expected if cannabidiol plus usual care and usual care alone were clinically equivalent. CADTH requested that the sponsor submit a revised version of the model in which incremental QALYs were 0 when the effectiveness and safety parameters were set to be equivalent; the sponsor declined this request. The sponsor justified the residual incremental QALYs gained with cannabidiol as follows: “Patients discontinuing Epidiolex would be unlikely to experience the same seizure burden as patients who have never been on the treatment… patients who discontinue Epidiolex are assumed to follow the disease severity distribution as observed in the usual care arm at the end of cycle 1. This assumption was made because there are no data on seizure outcomes following withdrawal of Epidiolex.”24 CADTH notes that this assumption implicitly assumes that there will be residual benefit from cannabidiol after discontinuation, which has not been demonstrated in clinical trials. CADTH notes that this modelling issue was previously described by NICE in its appraisal of cannabidiol.6
CADTH additionally notes that the sponsor’s model included numerous IFERROR statements, resulting in situations where the parameter value was overwritten with an alternative value without alerting the user to the automatized overwriting. Due to the lack of transparency and the complexity of the model, CADTH was unable to fully validate the model or to identify the underlying cause of the unexpected results within the time frame of this review.
CADTH could not fully address this limitation and notes that a thorough validation of the sponsor’s model was not possible. As such, the results of the sponsor’s submitted base case and CADTH’s revised base case are associated with considerable uncertainty and overestimate the incremental QALYs between treatments. Consequently, the ICERs reported from these analyses are likely underestimated, and a higher price reduction may be required for cannabidiol to be cost-effective at a WTP threshold of $50,000 per QALY.
The long-term effectiveness of cannabidiol is highly uncertain: In the model, the efficacy of cannabidiol plus usual care in cycles 2 through 9 was based on individual patient data from the CARE 5 long-term extension study for patients who entered the CARE 5 trial after completing the CARE 3 or CARE 4 trials. As noted in the CADTH clinical review, the CARE 5 study population is considered to be enriched, as patients who discontinued the CARE 3 or CARE 4 trials (e.g., owing to lack of treatment response or AEs) were not eligible for the CARE 5 trial. From cycle 10 onward, the sponsor assumed that patients who receive cannabidiol plus usual care will remain in the same health state until death or discontinuation, while patients in the usual care group remain in the same health states from cycle 2 until death. No data supporting the long-term effectiveness of cannabidiol are available beyond the duration of the CARE 5 study (mean treatment duration [dosing days] = 838 days), and there are no comparative effectiveness data for cannabidiol plus usual care relative to usual care alone beyond the duration of the CARE 3 and CARE 4 trials (14 weeks). As such, it is uncertain whether the observed reduction in drop seizure frequency will be maintained indefinitely or whether treatment effectiveness may wane. Approximately 98% of the incremental QALYs gained with cannabidiol plus usual care relative to usual care alone were accrued on the basis of extrapolation (i.e., in the post–randomized controlled trial period), highlighting the importance of assumptions related to the long-term relative treatment effectiveness.
CADTH additionally notes that the sponsor assumed that, after cycle 9, patients who are not drop seizure free would discontinue cannabidiol at a rate of 10% per cycle (i.e., 3 months). In contrast, the discontinuation rates for patients experiencing seizures in cycles 2 through 9 were based on observations from the CARE 5 trial, assumed to reflect “insufficient treatment effect”; these rates are considerably lower than 10% (range, 2.45% to 7.75%). While the sponsor indicates that the assumption of 10% discontinuation was to account for “real world persistence on treatment,” the clinical experts consulted by CADTH did not find it plausible that patients who had been using cannabidiol for over 2 years would be more likely to discontinue cannabidiol than those with a shorter duration of use.
In the CADTH base case, from cycle 10 onward, CADTH adopted the rates of treatment discontinuation from the CARE 5 trial for patients experiencing seizures, consistent with the rates used for cycles 2 to 9. Due to the structure of the sponsor’s model and a lack of clinical data, CADTH was unable to explore the impact of potential waning of cannabidiol treatment effect. Basing the efficacy of cannabidiol plus usual care from cycle 10 onwards on data from the CARE 5 trial may bias the ICER in favour of cannabidiol.
Cannabidiol drug costs were underestimated: The Health Canada–recommended maintenance dosage of cannabidiol when used as adjunctive therapy for seizures associated with LGS is 10 mg/kg/day, which may be increased to a maximum of 20 mg/kg/day depending on “individual clinical response and tolerability.”1 In the submitted model, the sponsor assumed that all patients would receive a maintenance dosage of 10 mg/kg/day, implicitly assuming that no patients will receive a maintenance dosage greater than the minimum recommended. CADTH notes that both the CARE 3 and CARE 4 trials included 20 mg/kg/day groups3,4 and that 45% of patients in the CARE 5 long-term extension study received a maximum daily dose of more than 30 mg/kg (mean modal dosage = 24 mg/kg/day).25 There is therefore misalignment between the sponsor’s assumption that all patients will receive 10 mg/kg/day and the dosages used in the clinical studies. As noted in the product monograph, patients may increase dose based on tolerability and clinical response. The clinical experts consulted by CADTH further indicated that it is plausible that some patients who experience an initial treatment response but still experience seizures might trial a higher dose in an attempt to reach seizure freedom. Finally, the sponsor used the median baseline patient body weight reported in the CARE 3 and CARE 4 trials in the calculation of drug costs. CADTH considers it more appropriate to use the mean patient body weight rather than median in this calculation.
In the CADTH base case, CADTH assumed an average cannabidiol dose of 12 mg/kg/day, based on clinical expert input suggesting that approximately 20% of patients with LGS may receive the maximum recommended maintenance dosage of cannabidiol (20 mg/kg/day) while the remainder receive 10 mg/kg/day. CADTH additionally used the mean patient body weight to calculate drug costs rather than the median.
The impact of cannabidiol on patient quality of life is highly uncertain: The sponsor’s model predicts an incremental gain of 1.21 QALYs among patients with LGS who receive cannabidiol plus usual care (Table 12). According to the clinical expert input received by CADTH, it is plausible that a reduction in seizures may lead to improved patient HRQoL. However, as noted in the CADTH clinical review, despite a reduction in drop seizures with cannabidiol in the CARE 3 and CARE 4 trials, cannabidiol likely resulted in little to no difference in HRQoL over the 14-week treatment period of those trials; however, the CADTH clinical review noted that a longer follow-up time and higher participant completion rate of quality-of-life measures may be needed to detect changes in HRQoL. Whether the use of cannabidiol in clinical practice will lead to improved patient HRQoL is therefore uncertain.
Additionally, there is uncertainty associated with the utility values adopted by the sponsor, which were derived from a sponsor-funded vignette study10 that enrolled members of the general population in the UK and Sweden. In this study, participants were asked to adopt the perspective of a patient or caregiver and to evaluate vignettes describing various seizure-related health states using time trade-off and visual analogue scale methodologies. CADTH notes that the perception of LGS by members of the general public may be different from that of people with LGS and that public perception may vary between cultures and contexts. For example, there were substantial differences in the utility values derived for the same health states between respondents from the UK and Sweden.10 Since no people with LGS or members of the general public from Canada were included in this study, it is uncertain whether these utility values reflect the preferences of people with LGS in Canada.
Finally, CADTH notes that the sponsor’s vignette study produced utility values that were below 0 for several seizure severity categories (Table 11), implying that the HRQoL of these people is viewed as being worse than death. No evidence was submitted by the sponsor to support the assumption that people with LGS would consider their HRQoL worse than death, regardless of their seizure frequency, and the clinical experts consulted by CADTH indicated that this was not consistent with their clinical experience with this patient population. CADTH, in consultation with the clinical experts, considered the utility values derived from an alternate vignette study26 used in a scenario analysis conducted by the sponsor to better reflect the expected impact of seizure frequency on patient HRQoL.
In the CADTH base case, CADTH adopted an alternative set of health state utility values provided by the sponsor.26
The impact of cannabidiol on the HRQoL of caregivers is uncertain: Of the 2.87 incremental QALYs predicted by the sponsor’s model to be gained with cannabidiol plus usual care, 58% were accrued by caregivers (i.e., not by patients with LGS). As noted in the CADTH economic guidelines,23 any spillover in costs or treatment effects beyond the target population (i.e., patients with LGS) should be addressed in a non-base-case analysis. CADTH additionally notes that in the sponsor’s base case, the total QALYs gained by patients who receive cannabidiol plus usual care (6.17) or usual care (4.96) are greatly outweighed by the QALY loss experienced by their caregivers (–21.61 and –23.27 QALYs, respectively). This finding lacks face validity and may be related to the use of the utility values derived from members of the general public and the description of the health states in the vignette study,10 as described in the previous bullet point. The impact of cannabidiol on the HRQoL of caregivers has not been assessed in clinical trials. Further, the sponsor’s assumption that each patient with LGS would have 2 caregivers for the duration of their life and that each caregiver would have the same HRQoL decrement was deemed to be inappropriate by clinical experts consulted by CADTH for this review. That is, not all patients with LGS will have 2 caregivers and, for patients with multiple caregivers, the individual burden of care (as described in the vignette study) would likely be shared rather than doubled. Additionally, should a patient transition into a long-term care facility, the impact on caregiver quality of life is likely to be meaningfully different than that measured in the vignette study.
In the CADTH base case, QALY decrements accrued by caregivers were excluded, such that the CADTH ICER reflects the cost-effectiveness of cannabidiol plus usual care for patients with LGS. CADTH explored the impact of additionally including the effect of cannabidiol on caregivers in scenario analyses.
Uncertainty in the efficacy of cannabidiol was not modelled appropriately: Although the sponsor undertook probabilistic analyses, no uncertainty was incorporated for transition probabilities, which were based on individual patient data from the CARE 3, CARE 4, and CARE 5 trials, as described in the Summary of the Sponsor’s Economic Evaluation section.. Not incorporating uncertainty implicitly assumes that there is no uncertainty associated with the probability of moving between health states and that such transitions are fully reflected by observations from the CARE 3 and CARE 4 trials. As noted in the CADTH economic guidelines, “uncertainty regarding the value of each parameter should be examined through probabilistic analysis.” At CADTH’s request, the sponsor provided instructions to adopt Dirichlet distributions for these inputs; however, doing so disabled the model’s ability to appropriately report deterministic results. Owing to the lack of transparency and the complexity of the sponsor’s model, CADTH was unable to correct the underlying cause of this issue and was thus unable to implement uncertainty for transition probabilities within the time frame of this review.
The sponsor additionally assumed that any transitions between health states that were not observed within the clinical studies could not occur within the model (and, implicitly, within clinical practice). For example, in the first model cycle, patients using cannabidiol were assumed to be unable to move from the greater than 45 to less than or equal to 110 seizures per 28 days health state to the drop seizure-free state, but patients who started in the greater than 110 seizures per 28 days health state could become seizure free. This assumption does not meet face validity, nor does it adequately reflect the uncertainty inherent in extrapolating clinical trial observations to whole populations.
CADTH was unable to address this limitation. As uncertainty in the clinical evidence has not been adequately captured in the sponsor’s model, CADTH is unable to accurately estimate the probability of cannabidiol plus usual care being cost-effective compared to usual care alone; however, CADTH estimates this probability to be approximately 0%.
The impact of AEs was not adequately considered: The impact of AEs is uncertain for several reasons. First, in the economic model, the sponsor assumed that all serious AEs (i.e., rash, somnolence, fatigue, lethargy, sedation, diarrhea, decreased appetite, aggression, irritability) would have the same impact on quality of life (–0.12) and the same duration (3 months). Clinical expert input indicated that for patients with LGS, some AEs, such as aggression and irritability, are likely to have a greater impact on quality of life. Second, the sponsor calculated the incidence rates of serious AEs based on events reported by at least 3% of patients who received 10 mg/kg/day of cannabidiol in the CARE 3 trial and at least 1% of patients in the placebo arms of the CARE 3 and CARE 4 trials. Using different thresholds to calculate the incidence rates of AEs is inappropriate. Finally, the sponsor considered only AEs experienced by patients who received 10 mg/kg/day of cannabidiol (from the CARE 3 trial), whereas efficacy data were used from patients who received either 10 mg/kg/day or 20 mg/kg/day (from the CARE 3 and CARE 4 trials). As noted in the CADTH clinical review, 23% of patients in the 20 mg/kg/day group of the CARE 4 trial reported at least 1 serious AE, while serious AEs were reported by 19.4% and 15.9% of patients in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups of the CARE 3 trials, respectively. Discontinuation due to serious AEs was higher among patients who received 20 mg/kg/day of cannabidiol in the CARE 3 trial (7.3%) and the CARE 4 trial (14.0%) than among patients who received 10 mg/kg/day in the CARE 3 trial (1.5%).27,28
CADTH was unable to address limitations related to the AEs; the direction and magnitude of the impact on ICER is unknown.
Impact of cannabidiol on survival is uncertain: The sponsor’s base case predicts a survival advantage with cannabidiol plus usual care relative to usual care alone (incremental life-years = 0.16), which has not been shown in clinical trials. Survival was not an outcome in the CARE 3 or CARE 4 trials. CADTH notes that decreased seizure frequency has been correlated to decreased risk of SUDEP in the literature.29,30 CADTH additionally notes that, in the absence of mortality data for patients with LGS, the sponsor used SUDEP and non-SUDEP mortality rates reported for children with Dravet syndrome as a proxy for LGS mortality rates.8 In the sponsor’s model, the average lifespan of patients was greater than that expected by the clinical experts consulted by CADTH; that is, more than half the modelled patients remained alive when the average age of the cohort reached 55 years and 24% remained alive when the average age of the cohort reached 80 years. Finally, the sponsor assumed that patients who were seizure free would have a 0.71 risk ratio of mortality compared to those having seizures, based on a 2013 cohort study of patients with epilepsy enrolled in an outpatient clinic between 1970 and 1999.9 The sponsor halved the risk reduction associated with being seizure free reported within this study due to feedback from the NICE review of cannabidiol in LGS.6 However, it remains unclear whether patients with LGS who previously had seizures and subsequently became seizure free with treatment would follow the same trajectory as those observed in the Trinka et al. study,9 which was not specific to patients with LGS.
The survival benefit predicted by the sponsor’s model for cannabidiol plus usual care is uncertain. In scenario analyses, CADTH assumed equivalent mortality across health states, which ensured that there was no relative mortality effect of treatment with cannabidiol.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Background ASMs used in the CARE 3 and CARE 4 trials were assumed to represent usual care in Canada. | Uncertain. The CARE 3 and CARE 4 trials compared cannabidiol to placebo on a background of various ASMs considered to compose usual care. However, as this concomitant usual care was required to remain stable throughout the trial, background ASMs in the placebo groups of these trials may not reflect the use of ASMs in clinical practice, where ASMs (dosage and mix) are altered based on patients’ symptoms and other needs. As such, the cost-effectiveness of cannabidiol compared to usual care in the clinical context is uncertain, as is the cost-effectiveness of cannabidiol compared to any individual ASM or combination of ASMs. |
Dosing of ASMs was calculated by weight, regardless of patient age. | Inappropriate. According to clinical expert input and the relevant product monographs, most ASMs are typically dosed within a therapeutic range and based on treatment response, tolerance, and concomitant ASM use, rather than only by weight, particularly for adult patients. As such, some of the doses assumed by the sponsor overestimate or underestimate typical use in clinical practice. The sponsor additionally assumed that ASMs could be prescribed in partial amounts, whereas most ASMs are tablets or capsules and are unlikely to be prescribed in partial amounts. However, as cannabidiol was assumed by the sponsor to not displace or alter the dosing of ASMs composing usual care, the impact of these assumptions on the ICER is expected to be minor. |
Patients with lower frequencies of drop seizures were assumed to use fewer health care resources (e.g., clinician visits, hospitalizations, long-term care), with resource use estimates derived from clinical experts in the UK. | Uncertain. The sponsor applied Canadian costs to resource use estimated in the UK context. Whether these inputs are generalizable to the Canadian context is uncertain. According to clinical experts consulted by CADTH, it is plausible that patients who have a lower frequency of drop seizures would use fewer health care resources, but the magnitude of such effects is unknown. Health care resource use was not assessed as part of the CARE 3 and CARE 4 trials, with the exception of hospital admissions due to epilepsy. As noted in the CADTH clinical review, based on data from the CARE 3 and CARE 4 trials, it is uncertain whether cannabidiol results in a difference in hospital admissions due to epilepsy. CADTH, therefore, considers the magnitude of potential reductions in health care resource use to be highly uncertain. |
A proportion of adult patients with LGS will reside in a long-term care facility (3% of adults who are seizure free; 13% of adults who are not seizure free). | Uncertain. Clinical expert input received by CADTH indicated that the proportion of adults with LGS who reside in a group home or long-term care facility is likely higher than 13% and that the proportion likely increases with patient age. That is, as patients with LGS age, it becomes less likely that their parents or other family members are able to fully provide their care. As the sponsor’s model predicts that 24% of patients remain alive when the average age of the cohort reaches 80 years, the proportion of patients requiring long-term care is highly likely to be underestimated. In addition to health care resource use, this may additionally impact caregiver utility decrements. |
The impact of seizure types other than drop seizures was not adequately considered. | Uncertain. Clinical experts consulted by CADTH noted that the number of nondrop seizures experienced by patients would impact quality of life and potentially mortality risk; however, experts acknowledged that nondrop seizures are difficult to assess in clinical trials. Although the sponsor included a scenario that included disutilities for increasing frequencies of nondrop seizures, these disutilities were not specific to LGS and were obtained from a utility study not associated with drop seizures;11 these disutilities were applied to the model’s health states, which were defined by the frequency of drop seizures and drop seizure–free days. As such, this scenario may double count the benefit of reducing drop seizures, and the resulting ICER is therefore considered highly uncertain. |
ASM = antiseizure medication; ICER = incremental cost-effectiveness ratio; LGS = Lennox-Gastaut syndrome.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH undertook reanalyses that addressed key limitations within the submitted model, as summarized in Table 5. The CADTH base case was derived by making changes to model parameter values and assumptions in consultation with clinical experts. CADTH was unable to address the other limitations of the model, including the full Health Canada–indicated population for LGS not being fully modelled, limitations related to the sponsor’s modelling approach (e.g., model structure, transparency), uncertainty in the comparative clinical data, uncertainty in long-term efficacy, uncertainty in the potential effect of cannabidiol on survival, and uncertainty in AE rates and effect on quality of life.
CADTH undertook a stepped analysis, incorporating each change proposed in Table 5 to the sponsor’s base case to highlight the impact of each change (Table 6; disaggregated results are presented in Table 13). All CADTH probabilistic reanalyses were run for 1,000 iterations.
The results from the CADTH base case suggest that cannabidiol plus usual care was associated with higher costs (incremental costs = $200,241) and higher QALYs (incremental QALYs = 1.07) when compared to usual care alone, resulting in an ICER of $186,373 per QALY gained. The probability of cannabidiol plus usual care being cost-effective at a WTP threshold of $50,000 per QALY gained is approximately 0%.
The results were driven by the drug acquisition cost of cannabidiol plus usual care (incremental costs = $225,829; Table 13), as well as the predicted incremental gain of 1.07 QALYs with cannabidiol plus usual care. Consistent with the sponsor’s analysis, the CADTH reanalysis estimates that the majority (99%) of incremental QALYs were accrued in the posttrial period of the model on the basis of extrapolation.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Utility values | Derived from Lo et al.10 Utility value range, –0.186 to 0.754 | Derived from Radu et al.26 Utility value range, 0.235 to 0.833a |
2. Caregiver disutility values | Included (2 caregivers per patient) | Excluded |
3. Maintenance dosage of cannabidiol | 10 mg/kg/day | 12 mg/kg/dayb |
4. Patient weight | Pooled median patient weight by age group from the CARE 3 and CARE 4 trials | Pooled mean patient weight by age group from the CARE 3 and CARE 4 trials |
5. Discontinuation rates (cycle 10 onward) | Discontinuation per 3-month cycle:
| Discontinuation per 3-month cycle:c
|
CADTH base case | 1 + 2 + 3 + 4 + 5 | |
aUtility values derived from Radu et al.26 were as estimated by the sponsor except for the drop seizure-free health state, for which the utility value was corrected by CADTH to 0.833 to reflect the value for this health state reported for patients with LGS in the publication.
bBased on clinical expert input suggesting that approximately 20% of patients with LGS may receive the maximum recommended maintenance dosage of cannabidiol (20 mg/kg/day) while the remainder receive 10 mg/kg/day.
cPatients who are seizure free were assumed to discontinue cannabidiol at a rate of 0.5% per cycle, as per the sponsor’s assumption. Patients in the remaining seizure states (i.e., patients experiencing seizures) were assumed to discontinue cannabidiol at the same rates as in cycles 2 through 9, based on data from the CARE 5 study.31
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | Usual care | 505,764 | –18.30 | Reference |
Cannabidiol plus usual care | 606,838 | –15.44 | 35,257 | |
Sponsor’s base case | Usual care | 502,485 | –20.18 | Reference |
Cannabidiol plus usual care | 601,921 | –17.25 | 33,952 | |
CADTH reanalysis 1: Alternate utility values | Usual care | 502,485 | –13.65 | Reference |
Cannabidiol plus usual care | 601,921 | –11.08 | 38,636 | |
CADTH reanalysis 2: Caregiver disutilities excluded | Usual care | 502,485 | 4.90 | Reference |
Cannabidiol plus usual care | 601,921 | 6.09 | 83,225 | |
CADTH reanalysis 3: Cannabidiol dosage = 12 mg/kg/day | Usual care | 502,485 | –20.18 | Reference |
Cannabidiol plus usual care | 625,350 | –17.25 | 41,952 | |
CADTH reanalysis 4: Mean patient weight | Usual care | 504,705 | –21.18 | Reference |
Cannabidiol plus usual care | 608,442 | –17.25 | 35,421 | |
CADTH reanalysis 5: Discontinuation after cycle 9 | Usual care | 502,485 | –20.18 | Reference |
Cannabidiol plus usual care | 655,785 | –15.70 | 34,259 | |
CADTH base case (1 + 2 + 3 + 4 + 5) | Usual care | 504,705 | 11.42 | Reference |
Cannabidiol plus usual care | 700,818 | 12.48 | 184,763 | |
CADTH base case (1 + 2 + 3 + 4 + 5) (probabilistic) | Usual care | 504,169 | 11.47 | Reference |
Cannabidiol plus usual care | 704,410 | 12.54 | 186,373 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aDeterministic analysis, unless otherwise stated.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s results and CADTH’s base case. The CADTH base case suggests that a 71% price reduction for cannabidiol would be required for cannabidiol plus usual care to be considered cost-effective at a WTP threshold of $50,000 per QALY relative to usual care alone (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for cannabidiol plus usual care vs. usual care | |
|---|---|---|
Price reduction | Sponsor base case ($/QALY) | CADTH reanalysis ($/QALY) |
No price reduction | 35,257 | 186,373 |
10% | 31,102 | 167,185 |
20% | 26,948 | 147,997 |
30% | 22,793 | 128,809 |
40% | 18,638 | 109,621 |
50% | 14,483 | 90,433 |
60% | 10,328 | 71,245 |
70% | 6,174 | 52,058 |
80% | 2,019 | 32,870 |
90% | Dominant | 13,682 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CADTH conducted a series of scenario analyses to explore the impact of alternative assumptions on the cost-effectiveness of cannabidiol plus usual care:
Removing the mortality benefit associated with cannabidiol. Risk of death was assumed to be the same across all health states, which ensured that there were no relative mortality effects of the treatments.
Implementing a stopping rule, using the sponsor-provided option to do so, such that patients who do not experience a 30% reduction in the frequency of drop seizures after use of cannabidiol for 6 months, 1 year, and 2 years are assumed to discontinue cannabidiol.
Including caregiver QALYs in the calculation of the ICER, such that the ICER reflects the cost-effectiveness of cannabidiol plus usual care compared with usual care alone among patients with LGS and their caregivers. One caregiver was included per patient in this scenario, which may reflect the caregiver burden experienced by a single person or the burden shared by multiple people.
Results of these scenarios are presented in Appendix 4 (Table 14). The scenarios with the largest impact on the ICER were removing the survival benefit predicted by the model for cannabidiol plus usual care (ICER = $201,640 per QALY gained) and including QALYs accrued by caregivers (ICER = $83,264 per QALY gained).
Issues for Consideration
Medical cannabis products are available in Canada but are generally not reimbursed by public drug plans. Patients with LGS in Canada may already use or have tried cannabis for medical purposes, including cannabidiol products accessed through federally licensed sellers via the Cannabis Act. The clinical experts consulted by CADTH indicated that patients who are currently using medical cannabis may be likely to switch to Epidiolex owing to its higher dose, a lack of private insurance coverage, and the out-of-pocket cost of medical cannabis to patients. The cost-effectiveness of Epidiolex in patients who have previously responded to other forms of cannabidiol is unknown.
A generic version of rufinamide is under review by Health Canada. Input from CADTH-participating drug plans noted that branded rufinamide is substantially less expensive than cannabidiol at the submitted price. Should a generic version of rufinamide become available, the incremental cost difference between cannabidiol and rufinamide will be greater.
Overall Conclusions
Based on data from the CARE 3 and CARE 4 trials, the CADTH clinical review concluded that the use of cannabidiol may result in a reduction in drop seizures compared with placebo on a background of usual care ASMs. No patients were reported to have a 100% reduction in drop seizures at the end of the 14-week treatment period, and the clinical significance of the number of drop seizure–free days observed is uncertain. As noted in the CADTH clinical review, despite a reduction in drop seizures with cannabidiol in the CARE 3 and CARE 4 trials, cannabidiol likely resulted in little to no difference in HRQoL over the 14-week CARE 3 and CARE 4 treatment phase; however, longer follow-up and higher participant completion rates may be required to detect changes in HRQoL. Limited conclusions about the long-term benefit of cannabidiol can be made based on the CARE 5 extension study owing to its single-group, open-label design and enriched population. CADTH additionally notes that the magnitude of any treatment benefit between cannabidiol plus usual care versus usual care alone among patients with fewer than 2 convulsive seizures a week is unknown due to a lack of clinical data.
The sponsor submitted an economic analysis comparing the cost-effectiveness of cannabidiol plus usual care with usual care alone in patients with LGS, based on individual patient data from the CARE 3, CARE 4, and CARE 5 trials. The CARE 3 and CARE 4 trials enrolled patients who experienced 2 or more drop seizures each week over a 28-day period, despite taking 1 or more ASMs, while the CARE 5 long-term extension study enrolled patients who had completed the CARE 3 or CARE 4 trials. The Health Canada indication for cannabidiol is for use as adjunctive treatment for seizures associated with LGS and is not restricted based on inadequate control with ASMs or the number of drop seizures per week. As such, the cost-effectiveness of cannabidiol for the full Health Canada–indicated population for LGS is unknown.
CADTH identified additional limitations with the sponsor’s economic submission, including those related to the model structure and assumptions, the long-term effectiveness of cannabidiol plus usual care, impact of AEs, cannabidiol drug costs, health state utility values, and impact on survival. Notably, no uncertainty was incorporated by the sponsor for transition probabilities, which were based on individual patient data from the CARE 3, CARE 4, and CARE 5 studies, which implicitly assumes that there is no uncertainty associated with the probability of moving between health states and that such transitions are fully reflected by observations from the CARE 3, CARE 4, and CARE 5 trials.
CADTH undertook reanalyses to address limitations in the sponsor’s analysis, which included adopting alternative health state utility values, excluding QALYs accrued by caregivers, adopting a higher mean dose of cannabidiol, using mean patient weight in the calculation of drug costs, and assuming that the long-term rate of discontinuation for patients experiencing drop seizures would be equal to that observed in the CARE 5 study. The CADTH base case suggests that, at a WTP threshold of $50,000 per QALY gained, cannabidiol plus usual care is not a cost-effective treatment option for seizures associated with LGS compared with usual care alone. A price reduction of 71% for cannabidiol would be required for cannabidiol plus usual care to be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
The CADTH reanalysis attempted to address the identified limitations of the sponsor’s economic submission; however, a high degree of uncertainty remains. CADTH notes that, although the CADTH base case estimated a gain in QALYs with cannabidiol plus usual care compared to usual care alone (incremental QALYs = 1.07), 99% of the incremental benefit was gained after the duration of the pivotal randomized controlled trials (i.e., after 14 weeks). In the absence of comparative evidence beyond 14 weeks, the incremental QALYs for cannabidiol plus usual care predicted in CADTH’s base case are highly uncertain and may be overestimated, and additional price reductions may be required.
References
1.Epidiolex (cannabidiol): 100 mg/mL oral solution [product monograph]. Cambridge (UK): GW Research Ltd.; 2023 Nov 15.
2.Drug Reimbursement Review sponsor submission: Epidiolex (cannabidiol), 100 mg/mL oral solution [internal sponsor's package]. Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2023 Sep 19.
3.Devinsky O, Patel AD, Cross JH, et al. Effect of cannabidiol on drop seizures in the Lennox-Gastaut syndrome. N Engl J Med. 2018;378(20):1888-1897. PubMed
4.Thiele EA, Marsh ED, French JA, et al. Cannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE 4): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391(10125):1085-1096. PubMed
5.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Epidiolex (cannabidiol), 100 mg/mL oral solution. Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2023 Sep 19.
6.National Institute for Health and Care Excellence. Cannabidiol with clobazam for treating seizures associated with Lennox–Gastaut syndrome. (Technology appraisal guidance TA615) 2019; https://www.nice.org.uk/guidance/ta615. Accessed by sponsor, no date provided.
7.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2023 May 17.
8.Cooper MS, McIntosh A, Crompton DE, et al. Mortality in Dravet syndrome. Epilepsy Res. 2016;128:43-47. PubMed
9.Trinka E, Bauer G, Oberaigner W, Ndayisaba JP, Seppi K, Granbichler CA. Cause-specific mortality among patients with epilepsy: results from a 30-year cohort study. Epilepsia. 2013;54(3):495-501. PubMed
10.Lo SH, Lloyd A, Marshall J, Vyas K. Patient and caregiver health state utilities in Lennox-Gastaut syndrome and Dravet syndrome. Clin Ther. 2021;43(11):1861-1876 e1816.
11.de Kinderen RJ, Wijnen BF, van Breukelen G, et al. From clinically relevant outcome measures to quality of life in epilepsy: a time trade-off study. Epilepsy Res. 2016;125:24-31. PubMed
12.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2023: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2023 May 05 [sponsor accessed].
13.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2023; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 May 05 [sponsor accessed].
14.Elliott J, McCoy B, Clifford T, Potter BK, Wells GA, Coyle D. Economic evaluation of cannabinoid oil for Dravet syndrome: a cost-utility analysis. Pharmacoeconomics. 2020;38(9):971-980. PubMed
15.Elliott J, McCoy B, Clifford T, Wells GA, Coyle D. Economic evaluation of stiripentol for Dravet syndrome: a cost-utility analysis. Pharmacoeconomics. 2018;36(10):1253-1261. PubMed
16.Schedule of benefits, physician services under the Health Insurances Act (May 9, 2023 (effective April 1, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2023 May 17.
17.Job Bank. Wages for Registered nurses and registered psychiatric nurses. Ottawa (ON): Government of Canada; 2024: https://www.jobbank.gc.ca/wagereport/occupation/993. Accessed 2023 May 17.
18.Job Bank. Wages for Home support workers, caregivers and related occupations. Ottawa (ON): Government of Canada; 2024: https://www.jobbank.gc.ca/wagereport/occupation/24584. Accessed 2023 May 17.
19.Canadian Institute for Health Information. Care in Canadian ICUs. Ottawa (ON): CIHI; 2016: https://secure.cihi.ca/free_products/ICU_Report_EN.pdf. Accessed 2023 May 17.
20.Canadian Institute for Health Information. Patient Cost Estimator. 2020; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2023 May 17.
21.Long-term care homes level-of-care per diem funding summary. Toronto (ON): Ontario Ministry of Long-Term Care; 2023: https://www.ontario.ca/page/long-term-care-home-level-care-diem-funding-summary. Accessed 2023 Jul 25.
22.Paying for long-term care. Toronto (ON): Ontario Ministry of Long-Term Care; 2023: https://www.ontario.ca/page/paying-long-term-care. Accessed 2023 Jul 25.
23.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2024 Apr 12.
24.Jazz Pharmaceuticals Canada, Inc. response to November 22, 2023 CADTH request for additional information regarding Epidiolex LGS CADTH review [internal additional sponsor's information]. Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2023 Nov 27.
25.Jazz Pharmaceuticals Canada, Inc. response to November 02, 2023 CADTH request for additional information regarding Epidiolex LGS CADTH review [internal additional sponsor's information]. Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2023 Nov 09.
26.Radu X, Damera V, Martin M, Simontacchi K, Holland R. Pro58 Quality of life in patients with Dravet syndrome or Lennox Gastaut syndrome in the UK: higher seizure frequency has a substantial negative impact on quality of life. Value Health. 2019;22:S346.
27.Clinical Study Report: GWEP1423 (GWPCARE 4). A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P; CBD) as adjunctive treatment for seizures associated with Lennox–Gastaut syndrome in children and adults [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2017 Feb 24.
28.Clinical Study Report: GWEP1414 (GWPCARE 3). A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P; CBD) as adjunctive treatment for seizures associated with Lennox–Gastaut syndrome in children and adults [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2017 Jul 19.
29.Myland M, Buysse B, Tsong W, Power GS, Nordli D, Chin RFM. Seizure frequency, healthcare resource utilisation and mortality in childhood epilepsy: a retrospective cohort study using the THIN database. Arch Dis Child. 2019;104(11):1070-1076. PubMed
30.Ruthirago D, Julayanont P, Karukote A, Shehabeldin M, Nugent K. Sudden unexpected death in epilepsy: ongoing challenges in finding mechanisms and prevention. Int J Neurosci. 2018;128(11):1052-1060. PubMed
31.Clinical Study Report: GWEP1415 (GWPCARE 5). An open-label extension study to investigate the safety of cannabidiol (GWP42003-P; CBD) in children and adults with inadequately controlled Dravet or Lennox-Gastaut Syndromes [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2021 Feb 25.
32.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2023; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Nov 30 [CADTH accessed].
33.Table 17-10-0005-01. Population estimates on July 1st, by age and sex. Ottawa (ON): Statistics Canada; 2023: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed by sponsor, no date provided.
34.Non-Insured Health Benefits program: First Nations and Inuit Health Branch: annual report 2021 to 2022. Ottawa (ON): Indigenous Services Canada; 2023: https://www.sac-isc.gc.ca/eng/1683039690813/1683039973755. Accessed 2023 Aug 15 [sponsor accessed].
35.Ostendorf AP, Ng YT. Treatment-resistant Lennox-Gastaut syndrome: therapeutic trends, challenges and future directions. Neuropsychiatr Dis Treat. 2017;13:1131-1140. PubMed
36.Jazz Pharmaceuticals Inc. Data on File. Canadian Clinical Expert Survey. 2023 [sponsor provided reference].
37.Committee for Orphan Medicinal Products. Orphan Maintenance Assessment Report: Epidyolex (cannabidiol). Amsterdam (NL): European Medicines Agency; 2019: https://www.ema.europa.eu/en/documents/orphan-maintenance-report/epidyolex-orphan-maintenance-assessment-report-initial-authorisation_en.pdf. Accessed by sponsor, no date provided.
38.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Epidiolex (cannabidiol), 100 mg/mL oral solution. Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2023 Sep 19.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for the Treatment of Lennox-Gastaut Syndrome
Treatment | Strength / concentration | Form | Price ($) | Recommended maintenance dosagea | Daily maintenance cost ($) | Annual maintenance cost ($) |
|---|---|---|---|---|---|---|
Cannabidiol (Epidiolex) | 100 mg/mL | Oral solution in 100 mL bottles | 1,424.5400b | 10 mg/kg/d, up to a maximum of 20 mg/kg/d | 14.25 to 227.93 | 5,200 to 83,193 |
Clonazepam (generics) | 0.5 mg 2 mg | Tablet | 0.0418 0.0721 | < 10 years or < 30 kg: 0.1 to 0.2 mg/kg/d 10+ years: up to a maximum of 20 mg/d | 0.08 to 0.72 | 31 to 263 |
Lamotrigine (Lamictal, generics) | 5 mg 25 mg 100 mg 150 mg | Chewable Tablet Tablet Tablet Tablet | 0.2070 0.0698 0.2787 0.4107 | ≥ 9 kg: 1 to 5 mg/kg/day, maximum 200 mg ≥ 12 years: 50 to 100 mg twice daily | Chewable tablets: 0.41 to 8.28 Regular tablets: 0.28 to 0.56 | Chewable tablets: 151 to 3,022 Regular tablets: 102 to 203 |
Rufinamide (Banzel) | 100 mg 200 mg 400 mg | Tablet | 0.8730 1.7459 3.8043 | < 30 kg: 200 mg/d in 2 divided doses up to a maximum of 1,300 mg/d 30 to 50 kg: 400 mg/d in 2 divided doses up to a maximum of 1,800 mg/d 50.1 to 70 kg: 400 mg/d in 2 divided doses up to a maximum of 2,400 mg/d > 70 kg: 400 mg/d in 2 divided doses up to a maximum of 3,200 mg/d | 1.75 to 30.43 | 637 to 11,109 |
Note: All prices are from the Ontario Exceptional Access Program (accessed November 2023),12,32 unless otherwise indicated, and do not include dispensing fees. Doses are from the respective product monographs. For dosing that depends on weight, CADTH assumed a patient weight range of 10 kg to 80 kg. Daily and annual maintenance costs represent the range of potential costs (e.g., from 10 kg patients receiving the lowest recommended dose to 80 kg patients receiving the highest recommended dose).
aWhen used as monotherapy. Recommended dose ranges may change when used in combination with other ASMs, particularly when the combination includes lamotrigine and/or valproic acid.
bSponsor’s submitted price.
Table 9: CADTH Cost Comparison Table for Antiepileptic Agents Used for the Treatment of Lennox-Gastaut Syndrome (Nonindicated)
Treatment | Strength / concentration | Form | Price ($) | Recommended maintenance dosagea | Daily maintenance cost ($) | Annual maintenance cost ($) |
|---|---|---|---|---|---|---|
Clobazam (generics) | 10 mg | Tablet | 0.2197 | ≤ 2 years: 0.5 to 1 mg/kg/d 2 to 16 years: 5 mg/d, up to a maximum of 40 mg/d 16+ years: 5 to 15 mg/d, up to a maximum of 80 mg/d | 0.11 to 1.76 | 40 to 642 |
Lacosamide (generics) | 50 mg 100 mg 150 mg 200 mg | Tablet | 0.6313 0.8750 1.1763 1.4500 | 100 to 300 mg twice daily | 1.75 to 4.65 | 639 to 1,697 |
Levetiracetam (generics) | 250 mg 500 mg 750 mg | Tablet | 0.3210 0.3911 0.5416 | < 18 years: up to a maximum of 100 mg/kg/db 18+ years: 1,000 mg/d up to a maximum of 3,000 mg/d | 0.78 to 2.17 | 286 to 791 |
Perampanel (Fycompa) | 2 mg 4 mg 6 mg 8 mg 10 mg 12 mg | Tablet | 10.3869 | ≥ 7 years: 4 to 12 mg daily | 10.38 | 3,791 |
Topiramate (generics) | 25 mg 100 mg 200 mg | Tablet | 0.2433 0.4583 0.6748 | ≥ 6 years: 100 mg/d up to a maximum of 400 mg/d | 0.46 to 1.35 | 167 to 493 |
Valproic acid (generics) | 250 mg 500 mg 50 mg/mL | Capsule Enteric capsule Oral solution | 0.2905 0.8102 0.0398 per mL | 15 mg/kg/d up to a maximum of mg/d 60 mg/kg/d | 0.46 to 1.35 | 44 to 2,957 |
Note: All prices are from the Ontario Drug Benefit Formulary or the Ontario Exceptional Access Program (accessed November 2023),12,32 unless otherwise indicated, and do not include dispensing fees. Doses are from the respective product monographs. For dosing that depends on weight, CADTH assumed a patient weight range of 10 kg to 80 kg. Daily and annual maintenance costs represent the range of potential costs (e.g., from 10 kg patients receiving the lowest recommended dose to 80 kg patients receiving the highest recommended dose).
aWhen used as monotherapy. Recommended dose ranges may change when used in combination with other ASMs, particularly when the combination includes lamotrigine and/or valproic acid.
bRecommended dosage is based on clinical expert opinion elicited by CADTH.
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The modelled population is based on the CARE 3 and CARE 4 trial which enrolled patients with LGS whose seizures were inadequately controlled by current ASMs, which the sponsor defined as experiencing 2 or more drop seizures per week over a 28-day period. While the Health Canada indication is for use of cannabidiol as adjunctive therapy, it does not restrict usage based on seizure frequency. |
Model has been adequately programmed and has sufficient face validity | No | Individual patient data underlying the transition probabilities between seizure-based health states could not be validated by CADTH. Setting all efficacy and safety parameters to equal usual care resulted in residual QALY benefit for cannabidiol that the sponsor was unable to adequately explain.24 |
Model structure is adequate for decision problem | No | The model structure does not adequately reflect LGS in clinical practice. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Uncertainty was not incorporated into transition probabilities derived from individual patient data. Transitions between health states that were not observed from individual patients within the CARE 3 and CARE 4 trials were assumed to be impossible (i.e., transition probability assumed to be 0) which may not reflect the probability within a larger population. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to previous row regarding data incorporation into the model. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The model was complex and lacked transparency, containing numerous IFERROR statements making validation difficult. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Figure 1: Main Model Structure
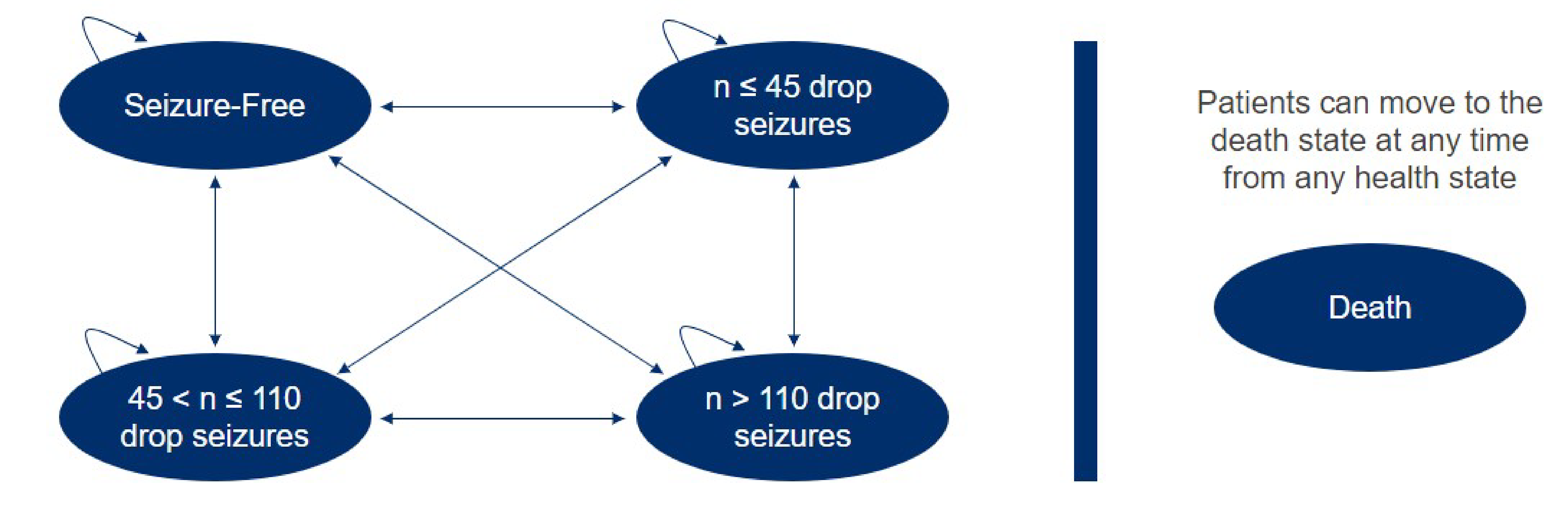
Note: Seizure numbers in each health state are per 28 days, while the cycle length is 3 months.
Source: Sponsor’s pharmacoeconomic submission.5
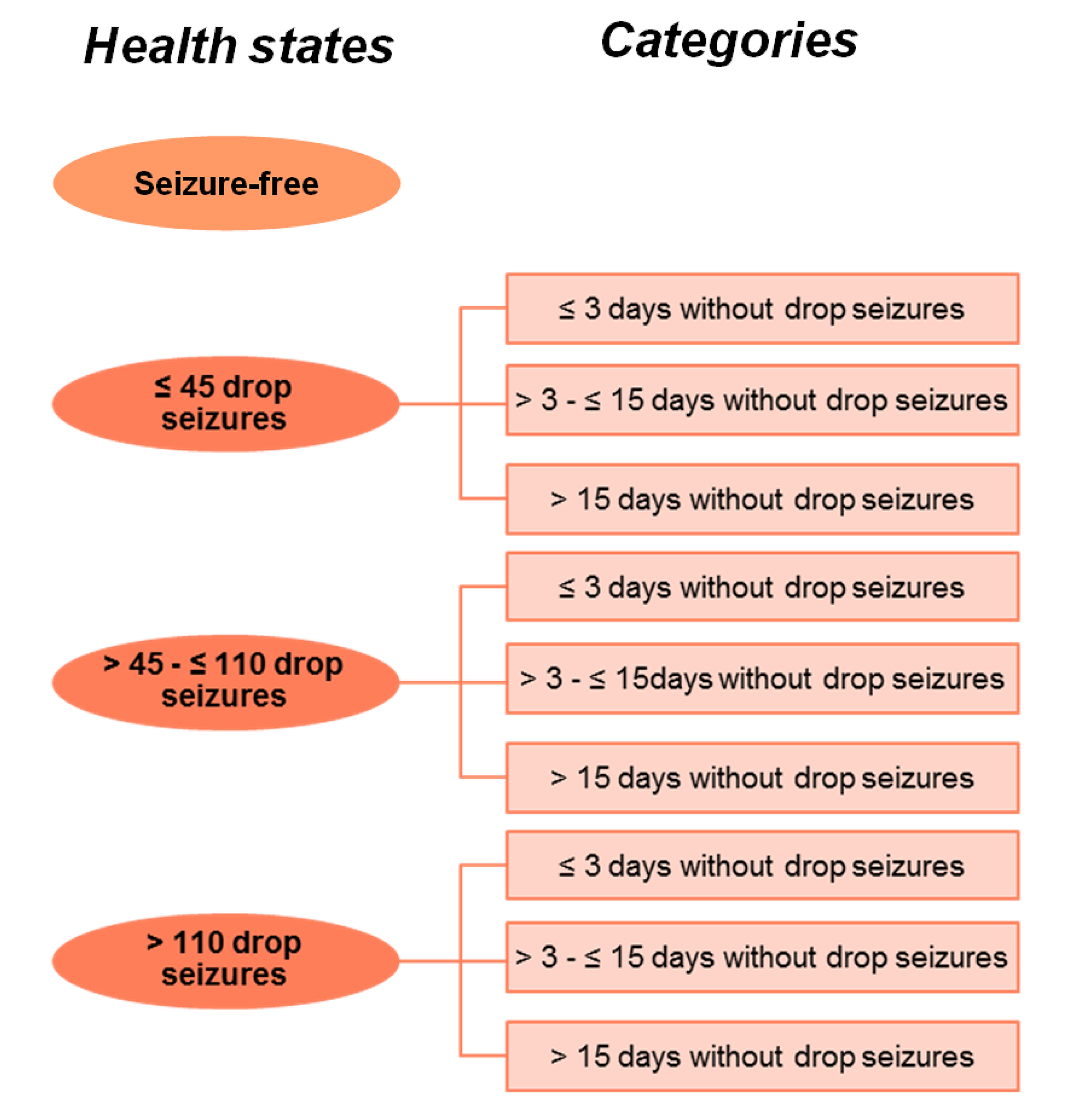
Table 11: Sponsor’s Base Case Health State Utility Values
Parameter | Utility value (SE) | ||
|---|---|---|---|
≤ 3 days without seizures | > 3 to ≤ 15 days without seizures | > 15 days without seizures | |
Patient utility values | |||
Seizure free | NA | NA | 0.754 (0.037) |
≤ 45 drop seizures per month | 0a | 0.375 (0.057) | 0.565 (0.047)a |
> 45 to ≤ 110 drop seizures per month | –0.008 (0.061) | 0.110 (0.061)a | 0.228 (0.060) |
> 110 drop seizures per month | –0.186 (0.062) | –0.077(0.063)a | 0.032 (0.063) |
Caregiver utility decrementsb | |||
Seizure free | NA | NA | 0 |
≤ 45 drop seizures per month | 0a | –0.238 (0.048) | –0.119 (0.024) |
> 45 to ≤ 110 drop seizures per month | –0.605 (0.058) | –0.496 (0.058) | –0.386 (0.058) |
> 110 drop seizures per month | –0.778 (0.067) | –0.635 (0.067) | –0.492 (0.067) |
NA = not applicable; SE = standard error.
aUtility values for these health states were not captured in the study by Lo et al.10 and were estimated by the sponsor.
bEach patient was assumed by the sponsor to have 2 caregivers.
Source: Adapted from sponsor’s pharmacoeconomic submission,5 and derived from Lo et al.10
Detailed Results of the Sponsor’s Base Case
Table 12: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Cannabidiol + usual care | Usual care alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 28.773 | 28.616 | 0.16 |
Seizure free | 1.435 | 0.000 | 1.44 |
≤ 45 drop seizures | 1.660 | 11.491 | –9.83 |
> 45 to ≤ 110 drop seizures | 0.838 | 8.076 | –7.24 |
> 110 seizures | 0.676 | 9.050 | –8.37 |
Discontinuation seizure free | 0.000 | 0.000 | 0.00 |
Discontinuation ≤ 45 drop seizures | 9.742 | 0.000 | 9.74 |
Discontinuation > 45 to ≤ 110 drop seizures | 6.798 | 0.000 | 6.80 |
Discontinuation > 110 seizures | 7.625 | 0.000 | 7.63 |
Discounted QALYs (QALYs accrued by patients and caregivers) | |||
Total | –15.436 | –18.303 | 2.87 |
Seizure free | 1.082 | 0.000 | 1.08 |
≤ 45 drop seizures | 0.523 | 3.315 | –2.79 |
> 45 to ≤ 110 drop seizures | –0.672 | –7.347 | 6.68 |
> 110 seizures | –0.987 | –14.271 | 13.29 |
Discontinuation seizure free | 0.000 | 0.000 | 0.00 |
Discontinuation ≤ 45 drop seizures | 2.815 | 0.000 | 2.82 |
Discontinuation > 45 to ≤ 110 drop seizures | –6.177 | 0.000 | –6.18 |
Discontinuation > 110 seizures | –12.020 | 0.000 | –12.02 |
Discounted QALYs (QALYs accrued by patients only) | |||
Total | 6.172 | 4.962 | 1.21 |
Seizure free | 1.082 | 0.000 | 1.08 |
≤ 45 drop seizures | 0.849 | 5.649 | –4.80 |
> 45 to ≤ 110 drop seizures | 0.103 | 0.687 | –0.58 |
> 110 seizures | –0.080 | –1.373 | 1.29 |
Discontinuation seizure free | 0.000 | 0.000 | 0.00 |
Discontinuation ≤ 45 drop seizures | 4.793 | 0.000 | 4.79 |
Discontinuation > 45 to ≤ 110 drop seizures | 0.581 | 0.000 | 0.58 |
Discontinuation > 110 seizures | –1.156 | 0.000 | –1.16 |
Discounted costs ($) | |||
Total | 606,838 | 505,764 | 101,074 |
Treatment cost | 215,380 | 95,713 | 119,667 |
Health state cost | 391,056 | 409,879 | –18,823 |
Adverse event cost | 402 | 172 | 230 |
ICER ($/QALY)a | 35,257 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
aIncludes QALYs accrued by both patients with LGS and caregivers (2 per patient).
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Cannabidiol + usual care | Usual care alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 28.74 | 28.59 | 0.16 |
Seizure free | 1.43 | 0.00 | 1.43 |
≤ 45 drop seizures | 3.42 | 11.48 | –8.06 |
> 45 to ≤ 110 drop seizures | 1.11 | 8.07 | –6.96 |
> 110 seizures | 0.74 | 9.04 | –8.30 |
Discontinuation seizure free | 0.00 | 0.00 | 0.00 |
Discontinuation ≤ 45 drop seizures | 8.88 | 0.00 | 8.88 |
Discontinuation > 45 to ≤ 110 drop seizures | 6.20 | 0.00 | 6.20 |
Discontinuation > 110 seizures | 6.95 | 0.00 | 6.95 |
Discounted QALYsa | |||
Total | 12.54 | 11.47 | 1.07 |
Seizure free | 1.19 | 0.00 | 1.19 |
≤ 45 drop seizures | 1.82 | 5.97 | –4.15 |
> 45 to ≤ 110 drop seizures | 0.44 | 2.99 | –2.55 |
> 110 seizures | 0.23 | 2.50 | –2.27 |
Discontinuation seizure free | 0.00 | 0.00 | 0.00 |
Discontinuation ≤ 45 drop seizures | 4.62 | 0.00 | 4.62 |
Discontinuation > 45 to ≤ 110 drop seizures | 2.30 | 0.00 | 2.30 |
Discontinuation > 110 seizures | 1.93 | 0.00 | 1.93 |
Discounted costs ($) | |||
Total | 704,410 | 504,169 | 200,241 |
Treatment cost | 323,548 | 97,719 | 225,829 |
Health state cost | 380,460 | 406,276 | –25,817 |
Adverse event cost | 403 | 173 | 229 |
ICER ($/QALY) | 186,373 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
aQALYs accrued by patients. The impact of including QALYs decrements to caregivers was explored in scenario analysis.
Scenario Analyses
Table 14: Scenario Analyses Conducted on the CADTH Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | UC | 505,764 | –18.30 | Reference |
Cannabidiol plus UC | 606,838 | –15.44 | 35,257 | |
CADTH base case (probabilistic) | UC | 504,169 | 11.47 | Reference |
Cannabidiol plus UC | 704,410 | 12.54 | 186,373 | |
CADTH scenario 1: no survival benefit with cannabidiol | UC | 503,865 | 11.56 | Reference |
Cannabidiol plus UC | 697,925 | 12.53 | 201,640 | |
CADTH scenario 2: stopping rule for cannabidiol implementeda | UC | 507,548 | 11.42 | Reference |
Cannabidiol plus UC | 635,602 | 12.21 | 167,823 | |
CADTH scenario 3: caregiver disutilities included (1 caregiver per patient) | UC | 503,996 | –0.04 | Reference |
Cannabidiol plus UC | 703,901 | 2.36 | 83,264 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; UC = usual care.
aBased on the sponsor’s scenario in which patients using cannabidiol who have not experienced at least a 30% reduction in seizure frequency are assumed to discontinue cannabidiol at 6 months, 1 year, and 2 years.
Appendix 5: Submitted BIA Budget Impact Analysis and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 15: Summary of Key Takeaways
Key takeaways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of cannabidiol for the adjunctive treatment of seizures associated with LGS in patients 2 year of age and older. The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2025 to 2027) using an epidemiological approach. The sponsor compared a reference scenario in which patients received usual care for the treatment of seizures associated with LGS to a new drug scenario in which cannabidiol was reimbursed for use in combination with usual care. The sponsor’s analysis included the drug acquisition cost of cannabidiol; dispensing fees and markups were not included in the base case. Data for the model were obtained from various sources including Statistics Canada,33 Non-Insured Health Benefits (NIHB) program annual reports,34 the CARE 3 and CARE 4 clinical trials,27,28 published literature,35 clinical expert opinion elicited by the sponsor,36 the sponsor’s internal market research, and assumptions.
Key assumptions by the sponsor included the following: The prevalence of LGS in Canada is similar to that reported in Europe; cannabidiol will only be used by patients whose seizures are refractory to ASMs; patients in clinical practice will have the same age and body weight distribution as those enrolled in the CARE 3 and CARE 4 trials; the addition of cannabidiol will not impact the usage of ASMs; all patients will initiate cannabidiol at 5 mg/kg/d for 7 days, followed by a maintenance dose of 10 mg/kg/d; and adherence to cannabidiol will be 85%. Key inputs to the BIA are documented in Table 16.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1 / year 2 / year 3) | |
|---|---|---|
Pediatric patients (2 to 17 years) | Adult patients (18+ years) | |
Target population | ||
Population of CADTH-participating jurisdictions who are aged 2 years and older | 31,244,786 / 31,584,127 / 31,923,469a | |
Prevalence of LGS | 0.012%b | |
Proportion of patients with LGS within each age group | ||
Proportion of patients with LGS who receive ASMs | 95%c | |
Proportion of patients with LGS whose seizures are refractory to ASMs | 90%35 | |
Proportion of patients eligible for public funding | 60%d | 80%d |
Number of patients eligible for cannabidiol | 2,129 / 2,152 / 2,175 | |
Market uptake (reference scenario, 3 years) | ||
Cannabidiol plus usual care | 0% / 0% / 0% | |
Usual care | 100% / 100% / 100% | |
Market uptake (new drug scenarioe) | ||
Cannabidiol plus usual care | 7.5% / 18.0% / 28.0% | 5.0% / 16.0% / 22.0% |
Usual care | 92.5% / 82.0% / 72.0% | 95.0% / 84.0% / 78.0% |
Annual cost of treatment per patient (first year / subsequent years) | ||
Cannabidiol plus usual care | $13,673 / $13,806 | $27,640 / $27,907 |
Usual care | $0 | $0 |
ASM = antiseizure medication; LGS = Lennox-Gastaut syndrome.
Note: Usual care consists of a basket of ASMs, including: clobazam, valproic acid, levetiracetam, topiramate, clonazepam, rufinamide, lamotrigine, perampanel, and lacosamide.
aSum of the populations aged 2 years and older of Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and Labrador, Nova Scotia, Ontario, Prince Edward Island, and Saskatchewan as well as clients of the Non-Insured Health Benefits program who are aged 2 years and older.33,34
bBased on average of prevalence rates reported for European countries from 1978 to 2015.37
cBased on assumption validated by 4 key opinion leaders in Canada as reported by the sponsor.36,38
dBased on assumption, rationale not provided.38
eBased on the sponsor’s internal market research, not provided.38
fThe sponsor assumed that the dosage of cannabidiol would be 5 mg/kg/d for 7 days, followed by 10 mg/kg/d for the remainder of the BIA horizon, with an adherence rate of 85%. Costs for pediatric patients (aged 2 to 17 years) assume a weighted average median body weight of 31.22 kg while adult patients (aged 18+ years) are assumed to have a median body weight of 63.10 kg based on the CARE 3 and CARE 4 trials.27,28 The sponsor assumed that usual care costs would be the same regardless of use of cannabidiol and thus assigned a cost of $0 to usual care.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing cannabidiol for use as adjunctive therapy to usual care among patients with LGS aged 2 years and older would be $18,867,870 (year 1: $2,475,430; year 2: $6,749,759; year 3: $9,642,681).
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The full indicated population for LGS was not modelled: In the BIA, the sponsor assumed that LGS patients whose seizures are refractory to other ASMs would be eligible for cannabidiol, whereas the Health Canada indication for cannabidiol does not specify that it may only be used in an ASM-refractory subgroup. Clinical expert input received by CADTH suggests that cannabidiol will most likely be prescribed for patients whose seizures are refractory to other ASMs; however, if cannabidiol is reimbursed for its full indication, it is possible that the number of patients who receive cannabidiol will be higher than estimated by the sponsor.
In the CADTH base case, the eligible population was aligned with the full Health Canada indication. The impact of restricting the eligible population to an ASM-refractory subgroup was explored in scenario analyses.
The NIHB population was inappropriately calculated: The sponsor calculated the total population of CADTH-participating drug plans by adding the population of the provinces as reported by Statistics Canada,33 excluding Quebec, to the population of NIHB clients. NIHB clients living within the borders of a province are counted within provincial population data, thus the NIHB population was double counted in the sponsor’s analysis. Additionally, while the sponsor appropriately limited the included provincial populations to those aged 2 years and older, all clients of the NIHB were included without removing those under 2 years of age, overcounting the potentially eligible NIHB population.34 Finally, NIHB clients residing within Ontario who are under 25 or over 65 years of age are eligible for reimbursement by the Ontario Drug Benefit plan, and thus should be counted as ODB clients rather than NIHB clients for the purposes of the modelling the budgetary impact of reimbursing cannabidiol.
CADTH did not adjust for this limitation in reanalysis. The impact on the pan-Canadian model results is expected to be minimal.
The proportion of patients eligible for public drug plan coverage is uncertain and may be underestimated: The sponsor assumed that 60% of pediatric and 80% of adult patients with LGS are eligible for public reimbursement.38 No rationale supporting these assumptions was provided by the sponsor. While it is likely that many pediatric patients will have access to private insurance coverage through their parents’ employers, patients eventually age out of such coverage, and the proportion of adults with LGS who have their own employer-sponsored health insurance is likely small. Additionally, as described in the caregiver vignettes within the sponsor-conducted utility study,10 caregivers of people with LGS may leave full time employment to care for their family member, thus reducing the likelihood of private insurance coverage. As such, the sponsor’s assumptions on the proportion of patients eligible for public funding may be underestimated.
This limitation could not be addressed by CADTH owing to a lack of available data.
Cannabidiol drug costs are uncertain and likely underestimated: The sponsor assumed that all patients would receive a cannabidiol maintenance dose of 10 mg/kg/d. As noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, this assumption is not aligned with the monograph dosage, which allows for a maintenance dose of up to 20 mg/kg/day depending on “individual clinical response and tolerability.”1 Clinical experts consulted by CADTH indicated that in clinical practice, some patients may trial a dosage above 10 mg/kg/d (e.g., those who do not experience an initial treatment response or who experience an initial response but wish to further attempt to reach seizure freedom). Additionally, as also noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, the sponsor used median body weights for adult and pediatric patients in the CARE 3 and CARE 4 trials, rather than mean body weights, which is inappropriate.
Finally, the sponsor assumed 85% adherence to cannabidiol, and thus reduced the drug acquisition costs for cannabidiol by 15%. This is inconsistent with assumptions made in the pharmacoeconomic model, where adherence was not considered. The impact of reduced adherence on the clinical or cost-effectiveness of cannabidiol has not been explored. Furthermore, prescriptions for cannabidiol may be filled and reimbursed regardless of treatment adherence, thus the consideration of adherence of less than 100% may inappropriately reduce the cost of cannabidiol in the sponsor’s BIA.
In the CADTH base case, CADTH assumed that all patients will adhere to their prescribed dosage regimen and adopted an average cannabidiol dosage of 12 mg/kg/d (aligned with the CADTH base-case pharmacoeconomic evaluation), based on expert input that approximately 20% of patients with LGS may receive a maintenance dose of 20 mg/kg/day. CADTH additionally used mean body weights, rather than medians, for each included age group from the CARE 3 and CARE 4 trials, as provided by the sponsor,24 in the calculation of drug acquisition costs.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analyses by aligning the eligible population with the Health Canada indication for LGS, adopting a maintenance dose of 12 mg/kg/day, and using mean body weight and 100% adherence in the calculation of drug costs. The changes made to derive the CADTH base case are described in Table 17.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19. In the CADTH base case, the 3-year budget impact of reimbursing cannabidiol as adjunctive therapy for the treatment of seizures associated with LGS is expected to be $29,429,895 (year 1: $3,868,277; year 2: $10,489,767; year 3: $15,071,851).
Table 17: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Eligible population | Assumed that only patients with drug-resistant LGS would be eligible for cannabidiol | Aligned with the Health Canada indication for LGS |
2. Maintenance dose of cannabidiol | 10 mg/kg/day | 12 mg/kg/daya |
3. Patient body weight | Pooled median patient weight by age group from CARE 3 and CARE 4 | Pooled mean patient weight by age group from CARE 3 and CARE 4 |
4. Adherence to cannabidiol | 85% | 100% |
CADTH base case | 1 + 2 + 3 + 4 | |
BIA = budget impact analysis.
aBased on clinical expert input, CADTH assumed that 80% of patients will receive a cannabidiol maintenance dose of 10 mg/kg/day and 20% will a maintenance dose of 20 mg/kg/day. The reanalysis also assumed that year 1 costs for patients who receive 20 mg/kg/day will incur all titration phase costs (i.e., 7 days at 5 mg/kg/day, 7 days at 10 mg/kg/day, 7 days at 15 mg/kg/day, and 344.25 days at 20 mg/kg/day).
Table 18: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | 3-year total |
|---|---|
Submitted base case | $18,867,870 |
CADTH reanalysis 1: Full Health Canada population (for LGS) | $20,964,300 |
CADTH reanalysis 2: 12 mg/kg/day maintenance dose of cannabidiol | $22,622,284 |
CADTH reanalysis 3: Mean body weight used in calculation of drug costs | $19,746,235 |
CADTH reanalysis 4: 100% adherence | $22,197,494 |
CADTH base case (reanalysis 1 + 2 + 3 + 4) | $29,429,895 |
BIA = budget impact analysis; LGS = Lennox-Gastaut syndrome.
CADTH conducted additional scenario analyses to explore remaining uncertainty associated with the potential budget impact, using the CADTH base case. Results are provided in Table 19.
Assuming only patients with drug-resistant LGS will be eligible for cannabidiol, assumed by the sponsor to be 90% of patients with LGS.
Assuming that the price of cannabidiol is reduced by 71%, the price reduction at which cannabidiol plus usual care would be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
Table 19: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysisa | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|
Submitted base case | $0 | $2,475,430 | $6,749,759 | $9,642,681 | $18,867,870 |
CADTH base case | $0 | $3,868,277 | $10,489,767 | $15,071,851 | $29,429,895 |
CADTH scenario 1: drug-resistant LGS only | $0 | $3,643,304 | $9,957,056 | $14,253,026 | $27,853,385 |
CADTH scenario 2: 71% price reduction for cannabidiol | $0 | $1,121,800 | $3,042,032 | $4,370,837 | $8,534,670 |
BIA = budget impact analysis; LGS = Lennox-Gastaut syndrome.
aAs usual care is not being displaced, costs associated with usual care were assumed by the sponsor to be $0. The cost of the reference case scenario is $0 in all years and the budget impact of cannabidiol is equal to the cost of the new drug scenario. Therefore, only the budget impact for each analysis is presented in this table.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.