CADTH Reimbursement Review
Cannabidiol (Epidiolex)
Sponsor: Jazz Pharmaceuticals Canada Inc.
Therapeutic area: Dravet syndrome
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine aminotransferase
ASM
antiseizure medication
AST
aspartate aminotransferase
C-SSRS
Columbia-Suicide Severity Rating Scale
CaGIC
Caregiver Global Impression of Change
CEA
Canadian Epilepsy Alliance
CI
confidence interval
DS
Dravet syndrome
ESS
Epworth Sleepiness Scale
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
HRQoL
health-related quality of life
IMP
investigational medicinal product
ITT
intention to treat
LGS
Lennox-Gastaut syndrome
MID
minimal important difference
NRS
numerical rating scale
OLE
open-label extension
OR
odds ratio
QOLCE
Quality of Life in Childhood Epilepsy
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SUDEP
sudden unexpected death in epilepsy
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Cannabidiol (Epidiolex), 100 mg/mL, oral solution |
Sponsor | Jazz Pharmaceuticals Canada Inc. |
Indication | Use as adjunctive therapy for the treatment of seizures associated with Lennox-Gastaut syndrome, Dravet syndrome, or tuberous sclerosis complex in patients 2 years of age and older |
Reimbursement request | Epidiolex (cannabidiol) for the adjunctive therapy for the treatment of seizures associated with Dravet syndrome in patients 2 years of age and oldera |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 15, 2023 |
Recommended dosage | 2.5 mg/kg by mouth twice daily (5 mg/kg/day). After 1 week, the dosage can be increased to a recommended maintenance dosage of 5 mg/kg twice daily (10 mg/kg/day). Based on individual clinical response and tolerability, the dosage can be increased in weekly increments of 2.5 mg/kg administered twice daily (5 mg/kg/day) up to a maximum recommended dosage of 10 mg/kg twice daily (20 mg/kg/day). For patients in whom a more rapid titration from 10 mg/kg/day to 20 mg/kg/day is warranted, the dosage may be increased no more frequently than every other day. |
NOC = Notice of Compliance.
aDeviation requests for this reimbursement request were accepted on June 21, 2023, and September 15, 2023.
Introduction
Dravet syndrome (DS) is a very rare form of epilepsy associated with treatment-resistant, lifelong seizures and substantial comorbidities such as intellectual disability and behavioural, sleep, and gait problems. Epilepsy onset in DS usually occurs within the first year of life with febrile or afebrile clonic and tonic-clonic, generalized, and unilateral seizures in infants who have previously developed as expected.1 Approximately 70% to 85% of cases with clinical features of DS have mutations of the SCN1A gene.2-4 The most common causes of death in DS are sudden unexpected death in epilepsy (SUDEP) and status epilepticus. In 2011, the estimated incidence of DS was 1 in 33,000 live births worldwide, with a prevalence estimated at 1 in 45,700 children younger than 18 years of age.5 Epidemiological data specific to the Canadian landscape are scarce; however, Dravet Canada estimates that 1,000 individuals in Canada have DS, which accounts for 1% of the general epilepsy population.6 According to Orphanet, the estimated prevalence of DS in Canada is 1 in 40,000.7
The diagnosis of DS is based primarily on clinical observations. Confirmatory genetic testing for an SCN1A variant can be necessary when there is clinical uncertainty in the diagnosis. Treatment includes valproic acid and clobazam initially, but these are usually insufficient to control seizures. In patients with DS that is refractory to initial therapies, clinicians may add other antiseizure medications (ASMs), including stiripentol, topiramate, levetiracetam, clonazepam, and rufinamide. Cannabidiol is also recommended as an adjunctive treatment option for patients whose condition fails to respond to first-line ASMs.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol (Epidiolex) 100 mg/mL oral solution in the treatment of patients 2 years of age and older with seizures associated with DS.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from the clinical experts consulted by CADTH for the purpose of this review.
Patient Input
CADTH received 1 patient input, which was from the Canadian Epilepsy Alliance (CEA). CEA is dedicated to the promotion of independence and quality of life for people with epilepsy and their families by providing support services, information, and advocacy and increasing public awareness. Information for this submission was gathered by the president of the CEA through consultation with 24 member associations.
The CEA highlighted that individuals with uncontrolled epilepsy are at risk of social isolation and mental illness. The unpredictable nature of seizures and side effects of medications, such as anxiety, depression, mood swings, sexual dysfunction, suicidal thoughts, and exhaustion, have negative effects on patients and their family and caregivers. Currently available treatments do not control seizures in all patients. Lack of access to an approved treatment among patients with uncontrolled seizures can result in trying alternative practices and treatments such as cannabis and unregulated substances. The CEA input mentioned that any reduction in the frequency of seizures can improve quality of life among patients. Because of the frequent seizures, patients with epilepsy syndromes are often unemployed or underemployed with restricted income and without access to employer-funded insurance plans, which limit their access to drugs that are not on the provincial formulary.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
Two clinical specialists with expertise in the diagnosis and management of DS provided input to this submission. Both agreed that the treatment goals of any therapy for patients with DS include improving seizure control with the improvement of health-related quality of life (HRQoL), and decreasing seizure burden without affecting the mood, cognition, or behaviour of patients. Other goals include increasing the number of seizure-free days and decreasing visits to health care facilities and the need for rescue medications. The clinical experts mentioned that cannabidiol has the potential for fewer adverse effects when compared with other drugs indicated for this condition. Initially, it is anticipated that cannabidiol would be used after valproic acid and clobazam. The experts mentioned that cannabidiol may be useful in the treatment paradigm in adult patients, as they do not seem to tolerate stiripentol as well as children do; in both populations, the need exists for drugs with fewer side effects and greater benefits.
According to the clinical experts, the frequency and change over time in seizure frequency, number of seizure-free days, decrease in seizure duration and severity, reduction of status epilepticus, and decreased use of rescue medication are important end points when assessing response to treatment. The experts mentioned they would consider an inadequate improvement in seizure frequency (approximately less than a 50% decrease from baseline) and the presence of intolerable adverse events (AEs) as factors to determine the discontinuation of the medication.
Most patients taking cannabidiol will be treated in outpatient epilepsy clinics. The clinical experts suggested that epileptologists and/or neurologists with expertise in the treatment of DS should be the health care providers monitoring response in these patients.
Clinician Group Input
No clinician group input was received by CADTH.
Drug Program Input
The drug program input highlights that the diagnosis of DS is largely clinical, and genetic testing for variants (i.e., of the SCN1A gene) alone is not sufficient for diagnosis. The input also mentioned that the reimbursement criteria for stiripentol, the drug currently approved for DS in Canada, only include a diagnosis of DS (without specific criteria around a diagnosis). Cannabidiol would require similar criteria, if appropriate.
The Health Canada indication and reimbursement criteria for stiripentol include combination treatment with both valproate and clobazam. The drug programs asked if it would be appropriate to require patients to be on both valproate and clobazam before being eligible for reimbursement for cannabidiol (i.e., similar to the indication for stiripentol and aligned with current clinical guidelines). The clinical experts consider that it is possible, based on the current available evidence.
The drug programs also inquired about the objective measures used to assess and monitor therapeutic response in clinical practice. The experts mentioned that reduction in convulsive seizures, use of rescue medication, number of hospital and emergency department visits, and number of AEs are appropriate measures, and added that an inadequate reduction in total seizures (i.e., a reduction of less than 50%) would be an adequate measure to assess response.
The drug programs wanted to know how many patients the clinical experts think will use the dose of 20 mg/kg/day. The experts approximated that 30% of patients would require this higher dose.
The drug programs noted there may be limited access to neurologists within some regions of Canada. The stiripentol reimbursement criteria in most jurisdictions indicate that the drug “must be prescribed by or in consultation with,” or the patient “must be under the care of” a neurologist or general pediatrician; hence, the drug programs suggested considering alignment with the prescribing criteria for stiripentol where these practitioners can provide the needed care in these situations.
Also, the drug programs pointed out that patients currently using medicinal cannabis or synthetic cannabinoid-based medications and transitioning to pharmaceutical-grade cannabidiol were excluded from the CARE1 and CARE2 trials and need to be considered in the deliberations.
Finally, the drug programs recommended that due to the risk of hepatocellular injury, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin levels should be obtained at baseline and then at 1, 3, and 6 months after starting treatment — and periodically thereafter, as clinically indicated — or within 1 month of change in cannabidiol dosing or upon a change in other medications that affect liver function.
Clinical Evidence
Systematic Review
Description of Studies
The body of evidence informing this submission consists of 2 individual studies assessing cannabidiol in patients with DS.
First, the pivotal CARE1 Part B study (N = 120 patients) was a phase III, double-blind, placebo-controlled, multicentre, randomized trial evaluating cannabidiol 20 mg/kg/day (n = 61) against placebo (n = 59) as an adjunctive therapy in patients aged 2 to 18 years whose DS is not completely controlled with current ASMs. The study evaluated seizure frequency per month, proportion of patients with a 50% or greater reduction in convulsive-seizure frequency, number of seizure-free days, presence of status epilepticus, HRQoL scores, amount of sleep disruption, and harms. The time of treatment and assessment was 14 weeks.
Second, the pivotal CARE2 was a 3-arm study that evaluated cannabidiol 20 mg/kg/day (n = 67) and 10 mg/kg/day (n = 67) against a placebo group (n = 65). All patients in this study were also 2 to 18 years of age and were receiving multiple therapies for controlling their seizures. The study also evaluated seizure frequency per month, proportion of patients with a 50% or greater reduction in convulsive-seizure frequency, number of seizure-free days, presence of status epilepticus, HRQoL scores, amount of sleep disruption, and harms. The time of treatment and assessment was 14 weeks.
Efficacy Results
Percentage Change From Baseline in the Frequency of Convulsive Seizures During the Treatment Period
In the CARE1 Part B study, patients in the 20 mg/kg/day cannabidiol group achieved a median percentage change from baseline in convulsive-seizure frequency during the 14-week treatment period of –38.9% (95% confidence interval [CI], –69.5% to –4.8%) versus –13.3% (95% CI, –52.5% to 20.2%) for the placebo group. The estimated median difference between treatment arms was –22.8% (95% CI, –41.1% to –5.4%; P = 0.0123).
In the CARE2 study, the median percentage change from baseline during treatment was –41.2% (95% CI, –81% to 3.0%), –47.0% (95% CI, –71.4% to –10.5%), and –24.5% (95% CI, –51.9% to 4.6%) in the cannabidiol 10 mg/kg/day, cannabidiol 20 mg/kg/day, and placebo groups, respectively. The estimated median difference for cannabidiol 10 mg/kg/day versus placebo was –15.7% (95% CI, –31.3% to 3.7%; P = 0105) and –19.9% (95% CI, –33.9% to 5.3%; P = 0.008) for cannabidiol 20 mg/kg/day versus placebo.
Proportion of Patients With a 50% or Greater Reduction From Baseline in the Frequency of Convulsive Seizures During the Treatment Period
In the CARE1 Part B study, the proportion of patients with a reduction of 50% or more in their baseline convulsive-seizure frequency was greater in the cannabidiol group, with 26 of 61 patients (42.6%) experiencing this level of reduction versus 16 of 59 patients (27.1%) in the placebo group. The difference in proportions was 0.155 (95% CI, –0.013 to 0.323) in favour of the intervention. The odds of achieving this end point in the cannabidiol group were double the odds in the placebo group (odds ratio [OR] = 2.00; 95% CI, 0.93 to 4.30; P = 0.0784).
In the CARE2 study, the proportion of patients with a reduction of 50% or more from baseline in the frequency of convulsive seizures was greater in the 10 mg/kg/day group (29 of 66 patients; 43.9%) and in the 20 mg/kg/day group (33 of 67 patients; 49.3%) compared with placebo (17 of 65 patients; 26.2%). The difference in proportion versus placebo was 0.178 (95% CI, 0.017 to 0.338) in the 10 mg/kg/day group and 0.231 (95% CI, 0.071 to 0.391) in the 20 mg/kg/day group. The odds of achieving this end point were higher in both the 10 mg/kg/day group (OR = 2.21; 95% CI, 1.06 to 4.62; P = 0.0332) and the 20 mg/kg/day group (OR = 2.74; 95% CI, 1.32 to 5.70; P = 0.0069) compared with placebo.
Proportion of Patients With a 75% or Greater Reduction From Baseline in the Frequency of Convulsive Seizures During the Treatment Period
In the CARE1 Part B study, the proportion of patients with a reduction of 75% or more in their baseline convulsive-seizure frequency was greater in the 20 mg/kg/day cannabidiol group compared with placebo, with 14 of 61 patients (23%) and 7 of 59 patients (11.9%), respectively, experiencing this level of reduction. The difference in proportions was 0.111 (95% CI, –0.023 to 0.245) in favour of the intervention. The odds of achieving a 75% or greater reduction was 2.21 (95% CI, 0.82 to 5.95; P = 0.1121) in favour of the 20 mg/kg/day group.
In the CARE2 study, 12 of 67 patients (17.9%) in the 20 mg/kg/day cannabidiol group and 20 of 66 patients (30.3%) in the 10 mg/kg/day cannabidiol group achieved a 75% or greater reduction in convulsive-seizure frequency compared with 4 of 65 patients (6.2%) in the placebo group. The difference in proportion between the 10 mg/kg/day group and placebo was 0.241 (95% CI, 0.116 to 0.367) and 0.118 (95% CI, 0.009 to 0.226) in the 20 mg/kg/day group. Compared with placebo, the odds of achieving a 75% or greater reduction was 6.63 (95% CI, 2.12 to 20.73; P = 0.0004) in the 10 mg/kg/day group and 3.33 (95% CI, 1.01 to 10.92; P = 0.0468) in the 20 mg/kg/day group.
Number of Convulsive Seizure–Free Days
In the CARE2 study, the mean number of convulsive seizure–free days increased in all 3 treatment groups, although greater increases were seen in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups compared with placebo. The treatment difference was in favour of both cannabidiol doses, with a treatment difference of 2.4 (95% CI, 1.0 to 3.9; P = 0.0009) between the 10 mg/kg/day group and placebo, and 1.3 (95% CI, –0.1 to 2.8; P = 0.0683) between the 20 mg/kg/day group and placebo.
Percentage Change From Baseline in Total Seizure Frequency During the Treatment Period
In the CARE1 Part B study, a greater median percentage change in total seizure frequency was seen in the 20 mg/kg/day cannabidiol group (median difference of –28.6%; 95% CI, –70.4 to –4.0) compared with the placebo group (median difference of –9.0%; 95% CI, –51.4 to 19.6). The median difference between 20 mg/kg/day cannabidiol and placebo was –19.2 (95% CI, –39.3 to –1.2; P = 0.0335).
In the CARE2 study, the percentage reduction was 56.4 (95% CI, 47.8 to 63.6) in the 10 mg/kg/day and 47.3 (95% CI, 36.9 to 56.0) in the 20 mg/kg/day cannabidiol groups compared with 29.7 (95% CI, 16.0 to 41.1) in the placebo group.
Patients With Status Epilepticus
In both studies, there were few incidents of status epilepticus reported overall during the baseline and treatment periods, with similar rates across all treatment groups. In the CARE1 Part B study, there was only 1 case (1.6%) in the 20 mg/kg/day group versus 0 in the placebo group at the end of the treatment period. Similarly, patients in the CARE2 study presented with status epilepticus in numbers of 3 (4.5%), 9 (13.4%), and 8 (12.3%) in the cannabidiol 10 mg/kg/day, cannabidiol 20 mg/kg/day, and placebo groups, respectively, at the end of treatment.
Health-Related Quality of Life
Patients included in the CARE1 Part B and CARE2 studies had a poor quality of life based on the low mean overall Quality of Life in Childhood Epilepsy (QOLCE) scores at baseline. Nonetheless, the adjusted mean differences for all QOLCE scores in both studies were in favour of cannabidiol 20 mg/kg/day treatment in the CARE1 Part B study, with an adjusted mean difference of 1.5 points (95% CI, –3.8 to 6.8; P = 0.576) over placebo, and 3.8 points (95% CI, –0.1 to 7.8; P = 0.058) and 1.8 points (95% CI, –2.2 to 5.8; P = 0.382) points over placebo for the 10 mg/kg/day and 20 mg/kg/day doses, respectively, in the CARE2 study.
Sleep Disruption and Function
In both the CARE1 Part B and CARE2 studies, the mean baseline scores in the sleep disturbance numerical rating scale (NRS) were similar across the treatment groups. In the CARE1 Part B study, a mean treatment difference of –0.4 (95% CI, –1.5 to 0.7) in sleep disruption score was observed, with no evidence of a significant difference between the cannabidiol 20 mg/kg/day and placebo groups. Similarly, in the CARE2 study, the mean treatment difference in sleep disruption score between the 10 mg/kg/day cannabidiol and placebo groups was 0.0 (95% CI, –0.9 to 0.8), and was –0.1 (95% CI, –0.9 to 0.8) between the 20 mg/kg/day cannabidiol and placebo groups.
CADTH evaluated the mean scores at baseline for the Epworth Sleepiness Scale (ESS) and found them to be relatively high in both trials in all treatment groups (> 7.1 in the CARE1 Part B study; > 7.2 in the CARE2 study). In the CARE1 Part B study, the mean treatment difference in ESS score between the 20 mg/kg/day cannabidiol and placebo groups was 1.51 (95% CI, –0.18 to 3.19; P = 0.078) in favour of placebo. In the CARE2 study, the mean treatment difference in ESS score between the 10 mg/kg/day and placebo groups was –0.55 (95% CI, –1.86, 0.75; P = 0.404) and 0.74 (95% CI, –0.57, 2.05; P = 0.267) between the 20 mg/kg/day and placebo groups.
Resource Use
In the CARE1 Part B study, a total of 6 patients (5%) reported 1 or more inpatient hospitalizations due to epilepsy during the treatment period: 5 patients (8.2%) in the 20 mg/kg/day cannabidiol group and 1 patient (1.7%) in the placebo group. In the CARE2 study, a total of 26 patients (13.1%) reported 1 or more inpatient hospitalizations due to epilepsy: 8 patients (11.9%) in the 20 mg/kg/day cannabidiol group, 12 patients (18.2%) in the 10 mg/kg/day cannabidiol group, and 6 patients (9.2%) in the placebo group.
The number of patients using rescue medication was similar overall in both studies. In the CARE1 Part B study, 36 patients (59.0%) and 41 patients (69.5%) in the cannabidiol 20 mg/kg/day and placebo groups, respectively, used rescue medication, while in the CARE2 study, the numbers in the cannabidiol 10 mg/kg/day, cannabidiol 20 mg/kg/day, and placebo groups were 54 (84.4%), 58 (84.1%), and 54 (80%) patients, respectively.
Harms Results
In the CARE1 Part B study, 57 of 61 patients (93.4%) in the 20 mg/kg/day cannabidiol group and 44 of 59 patients (74.6%) in the placebo group reported 1 or more AEs. In the CARE2 study, 56 of 64 patients (87.5%) in the 10 mg/kg/day cannabidiol group, 62 of 69 patients (89.9%) in the 20 mg/kg/day cannabidiol group, and 58 of 65 patients (89.2%) in the placebo group reported 1 or more AEs. The most common AEs (more than 10% of patients in any treatment group) reported in both studies were somnolence, diarrhea, and decreased appetite.
In the CARE1 Part B study, 10 of 61 patients (16.4%) in the 20 mg/kg/day cannabidiol group and 3 of 59 patients (5.1%) in the placebo group reported 1 or more serious AEs (SAEs). In the CARE2 study, 13 of 64 patients (20.3%) in the 10 mg/kg/day cannabidiol group, 17 of 69 patients (24.6%) in the 20 mg/kg/day cannabidiol group, and 10 of 65 patients (15.4%) in the placebo group reported 1 or more SAEs. The most common SAEs reported in both studies were nervous system disorders, status epilepticus, somnolence, and convulsion. Pneumonia was also a common SAE reported in the CARE2 study. All SAEs were resolved in the CARE1 Part B study, while 3 patients in the 20 mg/kg/day cannabidiol group in the CARE2 study had 3 SAEs that were not resolved at the end of the trial.
Patient discontinuation from treatment due to AEs was relatively low, although higher in the 20 mg/kg/day cannabidiol groups in both studies. In the CARE1 Part B study, AEs that led to discontinuation of the medication occurred in 9 of 61 patients (14.8%) in the 20 mg/kg/day cannabidiol group and in 1 of 59 patients (1.7%) in the placebo group while, in CARE2, 5 of 69 patients (7.2%) in the 20 mg/kg/day cannabidiol group experienced AEs leading to discontinuation from the study. No patients in the 10 mg/kg/day cannabidiol group or placebo groups withdrew from the study due to AEs. No patient deaths occurred during either study.
Critical Appraisal
Both the CARE1 Part B and CARE2 studies are randomized controlled trials (RCTs) involving an adequate randomization process, with an overall balanced distribution of participants to either the cannabidiol or placebo arms. There were some observed baseline imbalances in both studies; however, these were judged to have a low risk of introducing bias. There was good adherence to the intended interventions. There were, however, some imbalances observed in the use different cointerventions; although these possible deviations could introduce bias, the impact and direction of the bias on the outcomes of interest are uncertain. Some modifying effects from variables were observed (i.e., use of stiripentol, use of clobazam, and geographical location); however, the low number of patients across subgroups in both studies warrants caution in attributing any credible effect modification from any of these variables. There were no instances of meaningful missing outcome data. In both studies, the measurements of the outcomes were appropriate. The blinding of the participants and clinical investigators that was maintained throughout the studies mitigates potential biases in this domain. Overall, both studies demonstrated adherence to methodological consistency and minimized risks across all of the domains assessed for risk of bias for most outcomes when comparing cannabidiol with placebo. Several secondary end points depicting statistically significant results lacked multiplicity control, carrying a risk of false-positives; hence, cautious interpretation is needed due to potential random error.
Overall, the patients included in the CARE1 Part B and CARE2 trials have baseline characteristics and prognostic factors similar to those encountered in the population of patients in Canada with DS, according to the clinical experts consulted by CADTH. There were some concerns of uncertainty on the applicability of the results to adult populations older than 18 years of age since no patients older than 18 years were included in either trial. However, according to the clinical experts consulted by CADTH, it is unlikely that the response observed in the CARE1 Part B and CARE2 studies will be different in terms of beneficial effects and possible harms. There is also uncertainty as to whether the results can be generalized to patients with fewer than 4 seizures per month, since patients with such characteristics were not included in these studies. The trials excluded patients using medicinal cannabis or synthetic cannabinoid-based medications and transitioning to cannabidiol (pharmaceutical). This would be a common situation in Canada; the clinical experts suggested that this is an important consideration, but it is unlikely to affect the generalizability of the results of the studies.
The question of whether cannabidiol is more efficacious than the other treatment available in Canada for patients with DS (i.e., stiripentol) when added to standard of care is still uncertain. There is no head-to-head comparison of cannabidiol against stiripentol. Furthermore, the standard-of-care treatments commonly used in patients with DS vary and make it difficult to assess this question using an indirect treatment comparison, since such differences may include issues of inconsistency or intransitivity. Given the lack of head-to-head comparisons and with the current evidence at hand, it is difficult to draw a strong conclusion on this issue.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) tool was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.
The selection of outcomes for the GRADE assessment was based on the sponsor’s summary of clinical evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
percentage change from baseline in convulsive-seizure frequency during the treatment period
patients with a 50% or greater reduction from baseline in convulsive-seizure frequency during the treatment period
patients with a 75% or greater reduction from baseline in convulsive-seizure frequency during the treatment period
number of convulsive seizure–free days
percentage change from baseline in total seizure frequency during the treatment period
patients with convulsive status epilepticus
HRQoL
sleep and sleep disruption (measured with ESS and 0 to 10 NRS scores)
resource utilization (use of rescue medication and inpatient hospitalizations due to epilepsy)
harms (AEs, SAEs, harms of special interest).
Results of GRADE Assessments
The GRADE assessments included an evaluation of the main outcomes considered important by clinicians, patient groups, and stakeholders. The comparisons evaluated in the GRADE assessments of this report compared cannabidiol 10 mg/kg/day against placebo and cannabidiol 20 mg/kg/day against placebo. In Table 2 and Table 3, we present the GRADE summary of findings for both comparisons, respectively.
Table 2: Summary of Findings for Cannabidiol 10 mg/kg/day Versus Placebo for Patients With DS
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | Cannabidiol 10 mg/kg/day | Difference | |||||
Seizure control | |||||||
Median % change from baseline in the frequency of convulsive seizures Follow-up: 14 weeks | 131 (1 RCT) | NA | –24.5% | –41.2% (95% CI, –81.0% to 3.0%) | 15.7% greater reduction (from a 3.7% lower reduction to a 31.3% greater reduction) | Moderatea | Cannabidiol 10 mg/kg/day likely reduces the frequency of convulsive seizures from baseline when compared with placebo. |
≥ 50% reduction from baseline in the frequency of convulsive seizures Follow-up: 14 weeks | 131 (1 RCT) | OR = 2.21 (1.06 to 4.62) | 17/65 (26.2%) | 29/66 (43.9%) | 178 more patients per 1,000 (from 17 more to 338 more patients) | Moderateb | Cannabidiol 10 mg/kg/day likely increases convulsive-seizure control (≥ 50% reduction in seizure frequency from baseline) when compared with placebo. |
≥ 75% reduction in convulsive-seizure frequency from baseline Follow-up: 14 weeks | 131 (1 RCT) | OR = 6.63 (2.12 to 20.73) | 12/67 (17.9%) | 20/66 (30.3%) | 241 more patients per 1,000 (from 116 more to 367 more patients) | High | Cannabidiol 10 mg/kg/day increases convulsive-seizure control (≥ 75% reduction in seizure frequency from baseline) when compared with placebo. |
Change from baseline in mean number of convulsive seizure–free days Follow-up: 14 weeks | 131 (1 RCT) | NA | 1.7 | 3.9 (SD = 4.8) | MD = 2.4 days more (from 1 day more to 3.9 days more) | High | Cannabidiol 10 mg/kg/day increases the mean number of convulsive seizure–free days from baseline when compared with placebo. |
Median % change from baseline in the frequency of total seizures Follow-up: 14 weeks | 131 (1 RCT) | NA | The change from baseline in the intervention group was –51.9% (95% CI, –79.3% to –14.5%) while, in the placebo group, it was –26.8%. The MD was not reported. | Moderatec | Cannabidiol 10 mg/kg/day likely reduces the frequency of total seizures from baseline when compared with placebo. | ||
Percentage of patients with convulsive status epilepticus change from baseline Follow-up: 14 weeks | 131 (1 RCT) | NA | The number of patients with status epilepticus went from 4 of 66 patients (6.1%) at baseline to 3 of 66 patients (4.5%) at end of treatment in the intervention group while, in the placebo group, the number went from 4 of 65 patients (6.2%) to 8 patients (12.3%). Changes from baseline and between-group differences were not reported. | Lowc | Cannabidiol 10 mg/kg/day may produce little to no difference in the frequency of status epilepticus from baseline when compared with placebo. | ||
HRQoL | |||||||
Adjusted mean change from baseline in QOLCE score Follow-up: 14 weeks | 110 (1 RCT) | NA | 2.6 | 6.4 (SD = 10.9) | MD = 3.8 points higher (0.1 point lower to 7.8 points higher) | Lowd | Cannabidiol 10 mg/kg/day may produce little to no difference in the HRQoL when compared with placebo. The clinical meaningfulness of the results is uncertain. |
Sleep disruption | |||||||
Change from baseline in mean ESS and 0 to 10 NRS scores Follow-up: 14 weeks | 131 (1 RCT) | NA | The MD in the sleep disturbance NRS 0 to 10 scale was 0 (95% CI, –0.9 to 0.8), while the MD in the ESS score was –0.55 (–1.86 to 0.75). | Lowd | Cannabidiol 10 mg/kg/day may produce little to no difference in the sleep disruption scales when compared with placebo. The clinical meaningfulness of the results is unclear. | ||
Resource utilization | |||||||
Rescue medication and hospital days Follow-up: 14 weeks | 131 (1 RCT) | NA | Fifty-four patients in each of the cannabidiol 10 mg/kg and placebo groups (84.4% vs. 80%, respectively) used rescue medications; meanwhile, 12 vs. 6 patients (18.2% vs. 9.2%, respectively) were hospitalized due to epilepsy. | Lowe | Cannabidiol 10 mg/kg/day may produce little to no difference in health resource utilization. The clinical meaningfulness of the results is unclear. | ||
Harms | |||||||
AEs, SAEs, and harms of special interest Follow-up: 14 weeks | 131 (1 RCT) | NA | In the cannabidiol 10 mg/kg/day and placebo groups, the number of patients experiencing AEs was 56 vs. 58 (87.5% vs. 89.2%), respectively, while 13 vs. 10 patients experienced SAEs (20.3% vs. 15.4%), respectively; no patients died. | Lowe | Cannabidiol 10 mg/kg/day may produce little to no difference in AEs and SAEs. The clinical meaningfulness of the results is unclear. | ||
AE = adverse event; CI = confidence interval; DS = Dravet syndrome; ESS = Epworth Sleepiness Scale; HRQoL = health-related quality of life; MD = mean difference; NA = not applicable; NRS = numerical rating scale; OR = odds ratio; QOLCE = Quality of Life in Childhood Epilepsy; RCT = randomized controlled trial; SAE = serious adverse event; SD = standard deviation; vs. = versus.
Note: This comparison was obtained from the CARE2 study assessing the 10 mg/kg/day arm vs. placebo.
aRated down 1 level for imprecision. The target of our certainty is on a nontrivial effect. The 95% CI includes the null and the threshold of a 5% meaningful difference between treatment and placebo, as informed by the clinical experts.
bRated down for imprecision. The target of our certainty is an important benefit. The 95% CI includes the threshold of meaningful difference between treatment and placebo for 20 patients more (or fewer) per 1,000 treated as considered by the clinical experts consulted by CADTH.
cRated down 2 levels for imprecision. No thresholds or CIs were assessed. Based on sample size, the number did not reach a plausible optimal information size.
dRated down 2 levels for imprecision. Based on the target of the certainty of a meaningful effect of the intervention, the 95% CI was considered wide and no threshold for a minimal important difference could be obtained.
eRated down for imprecision. No CIs could be assessed. Rated down due to small sample size that did not reach a plausible optimal information size.
Table 3: Summary of Findings for Cannabidiol 20 mg/kg/day Versus Placebo for Patients With DS
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects | Certainty | What happens |
|---|---|---|---|---|---|
Seizure control | |||||
Median % change from baseline of convulsive seizures frequency. Follow-up: 14 weeks. | 252 (2 RCTs) | NA |
| High | Cannabidiol 20 mg/kg/day reduces the frequency of convulsive seizures from baseline when compared with placebo. |
≥ 50% reduction in convulsive-seizure frequency from baseline. Follow-up: 14 weeks. | 252 (2 RCTs) |
|
| High | Cannabidiol 20 mg/kg/day increases convulsive-seizure control (≥ 50% reduction from baseline) when compared with placebo. |
≥ 75% reduction in convulsive-seizure frequency from baseline. Follow-up: 14 weeks. | 252 (2 RCTs) |
|
| Moderatea | Cannabidiol 20 mg/kg/day likely increases control of convulsive seizures (≥ 75% reduction from baseline) when compared with placebo. |
Mean number of convulsive seizure–free days, change from baseline. Follow-up: 14 weeks. | 132 (1 RCT) | NA |
| Moderateb | Cannabidiol 20 mg/kg/day likely increases the frequency of convulsive seizure–free days from baseline than placebo. |
Median % change in total seizures frequency change from baseline. Follow-up: 14 weeks. | 252 (2 RCTs) | NA |
| Moderatec | Cannabidiol 20 mg/kg/day likely reduces the frequency of total seizures from baseline when compared with placebo. |
Percentage of patients with convulsive status epilepticus, change from baseline. Follow-up: 14 weeks. | 252 (2 RCTs) | NA |
| Lowd | Cannabidiol 20 mg/kg/day may produce little to no difference in the frequency of status epilepticus from baseline compared with placebo. |
HRQoL | |||||
Adjusted mean change from baseline in QOLCE score. Follow-up: 14 weeks. | 193 (2 RCTs) | NA |
| Lowe | Cannabidiol 20 mg/kg/day may produce little to no difference in HRQoL when compared with placebo. The clinical meaningfulness of the results is uncertain. |
Sleep disruption | |||||
Change from baseline in mean ESS and NRS 0 to 10 scores. Follow-up: 14 weeks. | 252 (2 RCTs) | NA |
| Lowd | Cannabidiol 20 mg/kg/day may produce little to no difference in the sleep disruption scales when compared with placebo. The clinical meaningfulness of the results is uncertain. |
Resource utilization | |||||
Rescue medication and hospital days. Follow-up: 14 weeks. | 252 (2 RCTs) | NA |
| Lowd | Cannabidiol 20 mg/kg/day may produce little to no difference in health resource utilization. The clinical meaningfulness of the results is uncertain. |
Harms | |||||
AEs, SAEs, and harms of special interest. Follow-up: 14 weeks. | 252 (2 RCTs) | NA |
| Lowd | Cannabidiol 20 mg/kg/day may produce more AEs and SAEs as well as cases of somnolence and investigations of liver enzymes than placebo. The clinical meaningfulness of these results is uncertain. |
AE = adverse event; CI = confidence interval; DS = Dravet syndrome; ESS = Epworth Sleepiness Scale; HRQoL = health-related quality of life; MD = mean difference; NA = not applicable; NRS = numerical rating scale; OR = odds ratio; Q1 = lower quartile; Q3 = upper quartile; QOLCE = Quality of Life in Childhood Epilepsy; RCT = randomized controlled trial; SAE = serious adverse event; SD = standard deviation.
aRated down for imprecision. The target of our certainty is an important benefit. The CI crosses a threshold of 20 patients more (or fewer) per 1,000 treated, as considered by the clinical experts consulted by CADTH.
bRated down 1 for imprecision. The target of the certainty is that of any beneficial effect (based on the null). Only 1 study assesses this outcome. No thresholds or CIs were evaluated.
cThe target of the certainty is that of an important benefit. The lower bound of the CI could include a trivial effect, the threshold for which was considered to be 5%.
dNo thresholds or CIs were assessed. Numbers are not optimal to assess if the intervention provides a large or trivial effect; hence, it was rated down 2 levels for imprecision.
eBased on the target of the certainty of a meaningful effect of the intervention, the 95% CI was considered wide and no threshold for a minimal important difference could be obtained. Sample size was considered low in relation to a plausible optimal information size.
Source: CARE1 Part B and CARE2 studies.
Long-Term Extension Studies
Description of Studies
CARE5 was a multicentre, open-label extension (OLE) study for patients with DS or Lennox-Gastaut syndrome (LGS) who had completed the double-blind, placebo-controlled, clinical studies with cannabidiol (CARE1, CARE2, CARE3, and CARE4 trials). The objective of this OLE study was to evaluate cannabidiol’s long-term safety and tolerability and effect on seizures as an adjunctive treatment in children and adults with inadequately controlled DS or LGS.
Efficacy Results
During weeks 37 to 48 of treatment, patients with DS experienced a median percentage change of –62.6% in total seizure frequency from their original study baseline. The proportion of patients who achieved a 50% or greater reduction in total seizure frequency during weeks 37 to 48 of treatment was 59.3%. Out of all patients with DS, 70.1% experienced a 25% or greater reduction in total seizure frequency, 39.7% experienced a 75% or greater reduction in total seizure frequency, and 6.1% experienced total seizure freedom (100% reduction).
During weeks 37 to 48 of treatment, patients with DS experienced a median percentage change of –54.2% in the frequency of convulsive seizures compared with their baseline frequency from the original study. The proportion of patients who achieved a 50% or greater reduction from baseline in the frequency of convulsive seizures during weeks 37 to 48 of treatment was 52.3%. Out of all patients with DS, 67.8% experienced a 25% or greater reduction from baseline in the frequency of convulsive seizures, 34.6% experienced a 75% or greater reduction in the frequency of convulsive seizures, and 7.9% experienced convulsive-seizure freedom (100% reduction). During the last 12 weeks of treatment, 4.5% of patients with DS reported convulsive seizures greater than 30 minutes in duration compared with a baseline of 4.8% during their original study. The proportion of patients with DS with nonconvulsive seizures greater than 30 minutes in duration during the last 12 weeks of treatment was 4.8% compared with a baseline of 7.2% during their original study.
Harms Results
A total of 306 patients (97.1%) with DS had 1 or more AEs during the study, with 71 patients (22.5%) reporting AEs of mild severity, 157 patients (49.8%) reporting AEs of moderate severity, and 78 patients (24.8%) reporting severe AEs. SAEs were reported for 133 participants (42.2%) in the DS group, with the most common SAEs being status epilepticus, convulsion, and pneumonia. There were 28 patients (8.9%) with DS who stopped treatment due to AEs, with the most common AEs leading to discontinuation being convulsion, increased AST, and increased ALT. A total of 6 patients (1.9%) with DS died during the study.
Critical Appraisal
The CARE5 study is a nonrandomized, open-label, single-arm study. The lack of comparison with an active comparator precludes the ability to assess the relative long-term therapeutic benefits or safety of cannabidiol versus other ASMs. Furthermore, the lack of blinding in the CARE5 study may affect subjective measures such as patient-reported outcomes. The direction and magnitude of this potential bias remains unclear.
Since completion of the CARE1 and CARE2 studies was an eligibility criterion for enrolment into the CARE5 study, patients who discontinued from the CARE1 or CARE2 study for any reason, such as AEs, withdrawal by patient or parent, or withdrawal by investigator, were excluded from the CARE5 study. Thus, enrolment into the CARE5 study was limited to those who tolerated and whose condition responded to cannabidiol. Moreover, only 54% of patients completed the study; as such, there is a risk of bias due to missing outcomes data. The proportion of patients who adhered to the study drug during the longer follow-up was not reported.
Indirect Comparisons
No indirect treatment comparisons were submitted by the sponsor.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the systematic review evidence were submitted by the sponsor.
Conclusions
The body of evidence informing the effects of cannabidiol on patients with DS consisted of 2 pivotal RCTs comparing cannabidiol (at doses of 10 mg/kg/day and 20 mg/kg/day) versus placebo, and 1 single-arm OLE study. Both pivotal studies inform the effects of cannabidiol on the outcomes of convulsive and total seizure control, HRQoL, sleep disruption, resource utilization, and AEs. All of these are considered by the clinical experts, patient groups, and stakeholders to be critical outcomes for decision-making.
The evidence shows that the use of cannabidiol, when compared with placebo, results in a greater reduction from baseline in the number of convulsive seizures. A greater proportion of patients using cannabidiol achieved reductions from baseline of 50% or more in the frequency of convulsive seizures, and 75% or more compared with placebo. Cannabidiol also likely provides beneficial albeit smaller improvement effects in the number of convulsive seizure–free days and in total seizure frequency. There is still uncertainty in the effects of cannabidiol on status epilepticus, HRQoL, sleep disruption, and use of rescue medications and hospital use.
Cannabidiol was generally well tolerated. However, the evidence suggests that cannabidiol may have more AEs and SAEs when compared with placebo, although there is uncertainty on the clinical significance of these differences to inform decision-making. The performance of cannabidiol against the other comparator used in Canada for patients with DS (i.e., stiripentol) is still uncertain, as no head-to-head comparison is available. Similarly, there is no evidence on the effects of cannabidiol as a first-line adjunctive treatment in patients older than 18 years of age, nor for its use in patients with DS who experience fewer seizures (i.e., fewer than 4 seizures per month).
Overall, the use of cannabidiol yields better estimates of seizure control with an adequate safety profile when compared with placebo. The effects on long-term outcomes of behaviour and HRQoL are still uncertain.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol 100 mg/mL oral solution in the treatment of patients with seizures associated with DS.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
DS is a very rare form of epilepsy associated with treatment-resistant, lifelong seizures and substantial comorbidities, such as intellectual disability and behavioural, sleep, and gait problems.1 Epilepsy onset in DS usually occurs within the first year of life at between 5 and 8 months of age. It is characterized by febrile or afebrile clonic and tonic-clonic, generalized, and unilateral seizures that tend to be prolonged in infants who have previously developed as expected.8
Later on, multiple seizure types (mainly myoclonic, atypical absences, and focal seizures) and behavioural disorders may appear, and developmental and cognitive skills may slow.8 Convulsive seizures, consisting of generalized clonic, generalized tonic-clonic, or unilateral clonic seizures are present throughout the lifespan of patients with DS.8 The frequency of convulsions often gradually decreases over time, and status epilepticus rarely occurs after the age of 10.3
It has been reported that 70% to 85% of patients with clinical features of DS have mutations of the SCN1A gene that result in the dysfunction of voltage-gated sodium channels in neurons.2-4
The most common causes of mortality in DS are SUDEP (accounting for nearly half of the overall mortality) and status epilepticus (accounting for one-third of all deaths). Other causes include accidents, drowning, or infection.3
For patients with epilepsy of any cause, the main SUDEP risk factors include a high frequency of convulsions and antiepileptic polytherapy, which are related to the severity of epilepsy.3 The most important mechanisms of SUDEP are cardiac arrhythmias, respiratory dysfunction, and dysfunction of the brainstem arousal system. The only effective way to prevent SUDEP is through the control of seizures.9
DS is associated with several comorbidities that, cumulatively, have substantial and lifelong impacts on the HRQoL of both patients and caregivers.10 Having fewer seizures and additional seizure-free days have been linked to improved HRQoL in patients with DS and their caregivers.10 According to a survey of parents of children younger than 6 years of age living with DS (n = 36), reduction in severe seizures and communication issues were the most important aspects of the disease that need to be addressed with a potential new drug, identified by more than 90% of respondents.11
According to a population-based study in Sweden conducted between 2007 and 2011, the estimated incidence of DS was 1 in 33,000 live births, and the prevalence in 2011 was 1 in 45,700 children younger than 18 years of age.5 According to a retrospective cohort study of 355 patients with DS in the UK published in 2012, the estimated incidence of gene mutation–positive DS was at least 1 in 40,900 births.12
The diagnosis of DS is based primarily on clinical observations of tonic-clonic seizures during the first year of life, the occurrence of myoclonic seizures and ataxia later, impaired psychomotor development following the onset of seizures, and poor response to antiepileptic drugs. Confirmatory genetic testing for an SCN1A mutation in patients with suspected DS, especially those younger than 2 years of age (in whom a clinical diagnosis can be difficult), has been shown to decrease unnecessary testing and improve access to therapies and supportive-care services for families.13
The diagnosis of DS is largely clinical, as genetic testing for variants of the SCN1A gene alone is not sufficient for a diagnosis, since the variants can also be seen in other conditions.14
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Treatment goals for patients with DS are currently focused on balancing optimal seizure control with treatment side effects and patient quality of life.1 Control of convulsive seizures should also be prioritized over nonconvulsive seizures due to their stronger association with SUDEP and impact on HRQoL.1 An additional therapeutic goal is to minimize other nonseizure manifestations of DS such as cognitive disabilities, behavioural difficulties, and psychiatric issues.15 For patients with DS that is refractory to ASMs, it is challenging to optimize treatment regimens that will reduce the frequency of seizures. However, as every seizure increases the future risk of poor outcomes and reduced HRQoL, even a moderate improvement in seizure control can have cumulative benefits over a patient’s lifetime.1,16
Based on the Ontario Epilepsy Guidelines,17 DS-specific international guidelines,1,13,18,19 and Canadian clinical expert opinion,20 valproic acid and clobazam are often used initially, but these are usually insufficient to control seizures.18 Stiripentol in conjunction with clobazam and valproate is currently the only ASM specifically indicated for DS in Canada,21 with the other ASMs indicated for general epilepsy or prescribed off-label.22 Due to the intractability of the seizures in patients with DS, there is a tendency to place patients on multiple ASMs, with the typical patient on a median of 3 ASMs.1,20 However, some ASMs (e.g., carbamazepine, oxcarbazepine, lamotrigine, phenytoin) may exacerbate seizures and should be avoided.1 Clinicians treating patients with DS that is refractory to initial therapies can attempt to add other ASMs, including stiripentol, topiramate, levetiracetam, clonazepam, and rufinamide. Cannabidiol is also recommended as an adjunctive treatment option for patients whose condition fails to respond to first-line ASMs.1,19,23 Adjunctive nonpharmacological interventions, including a ketogenic diet and vagus nerve stimulation, may also be considered as another treatment option.1 In Canada, there is no standardized approach to treatment for patients with DS.20
Drug Under Review
The key characteristics of cannabidiol are summarized in Table 4 along with those of other therapies available for the treatment of seizures associated with DS.
The requested indication for cannabidiol under review by Health Canada is as adjunctive therapy for the treatment of seizures associated with LGS, DS, or tuberous sclerosis complex in patients 2 years of age and older.
Jazz Pharmaceuticals Canada requested that CADTH review each neurologic disorder (i.e., LGS, DS, and tuberous sclerosis complex) as a separate submission and this request was accepted on June 21, 2023. The specific requested listing for Epidiolex (cannabidiol) for this review is as adjunctive therapy for the treatment of seizures associated with DS in patients 2 years of age and older. A deviation request was accepted by CADTH on September 15, 2023, permitting the reimbursement request (i.e., for patients 2 years of age or older) to deviate from the anticipated Health Canada indication (i.e., for patients 1 year of age or older).
Dosing and Administration
The recommended starting dosage is 2.5 mg/kg by mouth twice daily (5 mg/kg/day).24 After 1 week, the dosage can be increased to a recommended maintenance dosage of 5 mg/kg twice daily (10 mg/kg/day). Based on individual clinical response and tolerability, the dosage can be increased in weekly increments of 2.5 mg/kg administered twice daily (5 mg/kg/day) up to a maximum recommended dosage of 10 mg/kg twice daily (20 mg/kg/day). For patients in whom a more rapid titration from 10 mg/kg/day to 20 mg/kg/day is warranted, the dosage may be increased no more frequently than every other day.
Mechanism of Action
Cannabidiol (Epidiolex) is a highly purified, plant-derived pharmaceutical formulation of cannabidiol administered as an oral solution. Although not fully elucidated, cannabidiol is thought to have novel mechanisms of action that are different from those of other ASMs.24
Table 4: Key Characteristics of Cannabidiol and Antiepileptic Medications Considered Usual Care Interventions
Drug | Indication(s)a | Route and dose | Serious adverse effects or safety issues |
|---|---|---|---|
Cannabidiol | Adjunctive therapy for the treatment of seizures associated with LGS or DS or TSC in patients 2 years of age and older. |
| Somnolence and/or sedation, diarrhea. |
Valproic acidb | Use as sole or adjunctive therapy in the treatment of simple or complex absence seizures, including petit mal; useful in primary generalized seizures with tonic-clonic manifestations. Use adjunctively in patients with multiple seizure types that include either absence or tonic-clonic seizures. |
| Teratogenicity, hepatotoxicity, pancreatitis, and acute liver failure in patients with mitochondrial disease. |
Clobazam | Adjunctive therapy in patients with epilepsy that is not adequately stabilized with their current anticonvulsant therapy. | Pediatric dose:
Adult dose:
|
|
Stiripentol | Use in conjunction with clobazam and valproate as adjunctive therapy of refractory generalized tonic-clonic seizures in patients with SMEI and DS whose seizures are not adequately controlled with clobazam and valproate alone. |
|
|
Levetiracetam | Adjunctive therapy in the management of adult patients (> 18 years of age) with epilepsy that is not satisfactorily controlled by conventional therapy. Off-label use for pediatric patients. |
| QT prolongation, somnolence, fatigue, reproductive toxicity, hematologic changes in hemoglobin and white blood cells (hepatitis and liver failure have been reported), suicidal ideation, mood changes, psychiatric reactions. |
Topiramate | Adjunctive therapy for the management of patients (adults and children 2 years of age and older) with epilepsy whose condition is not satisfactorily controlled with conventional therapy. | Pediatric dose:
Adult dose:
| Drug interactions, somnolence, hyperammonemia, encephalopathy, dysthermia, altered hepatic function, and neurologic effects or psychiatric effects, including suicidal ideation. |
Clonazepam | Alone or as an adjunct in the management of myoclonic and akinetic seizures and petit mal variant (LGS). In patients with absence spells (petit mal) whose condition has failed to respond to succinimides. | Pediatric dose:
Adult dose:
| Paradoxical seizure activity, withdrawal symptoms, dependence or tolerance, psychiatric or neurologic issues (psychosis, depression, amnesia, suicidal ideation), drug interactions (opioids). |
Rufinamide | Off-label use for patients with DS. | Pediatric dose:
Adult dose:
| QT shortening, dependence or tolerance, withdrawal symptoms. |
ASM = antiseizure medication; DS = Dravet syndrome; LGS = Lennox-Gastaut syndrome; NA = not applicable; SMEI = severe myoclonic epilepsy in infancy; TSC = tuberous sclerosis complex.
aHealth Canada–approved indication.
bIncludes valproate.
Sources: Product monographs for cannabidiol,24 valproic acid,25 clobazam,26 stiripentol,21 levetiracetam,27 topiramate,28 clonazepam,29 and rufinamide.30
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the stakeholder section of this report.
CADTH received 1 patient input, which was from the CEA. The CEA is dedicated to the promotion of independence and quality of life for people with epilepsy and their families by providing support services, information, advocacy, and increasing public awareness. Information for this submission was gathered by the president of the CEA. The input drew on the knowledge and experiences of the CEA’s 24 member associations and the lived experiences and first-hand knowledge of patients, caregivers, clinicians, volunteers, and supporters (donors and funders).
The CEA highlighted that individuals with uncontrolled epilepsy are at risk of social isolation and mental illness. The CEA noted that the unpredictable nature of seizures and side effects of medications, such as anxiety, depression, mood swings, sexual dysfunction, suicidal thoughts, and exhaustion, have negative effects on patients and their family and caregivers.
The CEA stated that currently available treatments do not control seizures in all patients and there is a percentage of patients with uncontrolled seizures. Lack of access to an approved treatment among patients with uncontrolled seizures will result in trying alternative practices and treatments such as cannabis and unregulated substances. The CEA noted that even a small reduction in the number of seizures can improve quality of life among patients.
According to the CEA input, because of the frequent seizures, patients with epilepsy are often unemployed or underemployed, with restricted income and without access to employer-funded insurance plans, which limit their access to the drugs that are not on the provincial formulary. Although the CEA could not comment on patient or caregiver experience with cannabidiol, it noted that each new drug that is brought to market offers hope to patients whose seizures are uncontrolled by 1 or a combination of existing therapies.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of DS.
Unmet Needs
Treatment goals, according to the clinical experts consulted by CADTH, include improving seizure control with the improvement of HRQoL and decreasing seizure burden without affecting the mood, cognition, or behaviour of patients. Other goals include increasing the number of seizure-free days and decreasing visits to health care facilities and the need for rescue medications.
Also, the clinical experts added that reducing the risk of sudden death and preventing status epilepticus with treatments that do not adversely affect behaviour or mood or cause excessive sedation, are important needs in patients with DS.
The experts mention that patients with DS, tuberous sclerosis complex, and LGS rarely become seizure free. Patients with DS would benefit from more ASM options that improve seizure control without adverse behavioural and cognitive effects. Currently, most ASMs are either effective with many adverse effects or largely ineffective with few side effects.
Place in Therapy
Cannabidiol has a unique mechanism of action not shared by any other ASM. According to the clinical experts, cannabidiol will likely complement other ASMs and could become an important inclusion in the therapeutic options for DS. The possible advantage of cannabidiol is that it may have fewer adverse effects when compared with other drugs indicated for this condition. The clinical experts anticipated that, initially, cannabidiol would be used after valproic acid and clobazam.
Patient Population
Both experts agreed that the decision to prescribe cannabidiol hinges on the judgment of the treating neurologist. There is no need for an electroencephalogram (EEG) or MRI biomarkers. The diagnosis is usually made by an epileptologist or neurologist with expertise in epilepsy, since the diagnosis can be missed by general neurologists.
The clinical experts commented that, in their experience, using cannabidiol would be considered when the patient’s condition has failed to respond to 2 or more appropriate ASMs, including valproic acid, clobazam, stiripentol, or topiramate. They stated that, in their clinical practice, they would opt for these interventions as early as feasible. Evaluating treatment response is part of a clinician’s routine practice, incurring no additional time cost.
Assessing the Response Treatment
In clinical practice, the clinical experts suggested that the frequency of seizures and change over time, the number of seizure-free days, a decrease in seizure duration and severity, a reduction of status epilepticus, and a decrease in the use of rescue medication are important when assessing response to treatment.
Discontinuing Treatment
In general, little or no improvement in seizure frequency (approximately less than a 50% in change from baseline), or AEs from the intervention that become intolerable for patients and caregivers, are factors the clinical experts would take into consideration to determine whether to discontinue the use of the medication.
Prescribing Considerations
An outpatient epilepsy clinic is an ideal setting for initiating cannabidiol treatment and monitoring patients with DS; a hospital admission would rarely be needed. It would also be ideal to have an epileptologist or neurologist with expertise in the treatment of DS monitor response to treatment in these patients.
Additional Considerations
The clinical experts considered that the use of cannabidiol would be appropriate in adults, even though the evidence from the clinical trials generally excludes the adult population.
Clinician Group Input
No clinician group input was received by CADTH.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The sponsor notes that the only relevant comparator in this population is usual care because no single combination of ASMs is effective for seizure control in DS. Most patients with DS require 2 or more drugs to achieve reasonable seizure control, and the choice of drugs is individualized based on efficacy, side effects, tolerability, and access. Diacomit (stiripentol) is the only ASM with a Health Canada indication for DS. In the CARE1 and CARE2 studies, 35% to 42% of patients took stiripentol concomitantly and 10% to 18% of patients had previously used stiripentol. Other ASMs used in DS are indicated for general epilepsy and are prescribed off-label. | For CDEC deliberations. |
Stiripentol is reimbursed in the majority of jurisdictions as a restricted benefit for refractory generalized tonic-clonic seizures in patients with DS. Reimbursement criteria include the use (addition) of stiripentol in combination with clobazam and valproate in patients whose seizures are not adequately controlled with these 2 drugs. British Columbia reimbursement criteria also require a documented inadequate response to levetiracetam or topiramate. | For CDEC deliberations. |
Considerations for initiation of therapy | |
Diagnosis of DS is largely clinical; genetic testing for variants (i.e., of the SCN1A gene) alone is not sufficient for the diagnosis. The reimbursement criteria for stiripentol only include having a diagnosis of DS (without specific criteria around diagnosis). Consider alignment of reimbursement criteria for stiripentol, if appropriate. | For CDEC deliberations. The clinical experts agreed with this assertion. |
Drug resistant epilepsy may be defined as failure of adequate trials of 2 tolerated and appropriately chosen and used antiepileptic drug schedules (whether as monotherapies or in combination) to achieve sustained seizure freedom. Inclusion criteria for the CARE1 and CARE2 studies included patients on 1 or more ASMs (patients were on approximately 3 ASMs). Based on the Ontario Epilepsy Guidelines, international Dravet-specific guidelines, and Canadian clinical expert opinion, valproate and clobazam are often used initially, but are usually insufficient to control seizures. Patients with DS that is refractory to initial therapies can attempt to add ASMs, including stiripentol, topiramate, levetiracetam, clonazepam, and rufinamide. Cannabidiol is also recommended as an adjunctive treatment option for patients whose condition fails first-line ASMs. The Health Canada indication and reimbursement criteria for stiripentol include combination treatment with both valproate and clobazam. | According to the clinical experts, this will be the case in most situations and based on the current available evidence. |
Question for CDEC and/or the clinical experts: Would it be appropriate to require patients to be on both valproate and clobazam before being eligible for reimbursement of cannabidiol (i.e., similar to stiripentol and aligned with current clinical guidelines)? | |
Considerations for continuation or renewal of therapy | |
Patients with uncontrolled DS typically experience dozens of convulsive seizures each month. Treatment goals focus on balancing optimal seizure control — reducing length and number of seizures (especially convulsive seizures which can be associated with sudden unexpected death in epilepsy) and preventing status epilepticus — with side effects and patient quality of life. The primary end point in the CARE1 and CARE2 trials was the percent change from baseline in convulsive-seizure frequency. In clinical practice, what objective measures are used to assess and/or monitor therapeutic response? | Reduction in convulsive seizures, use of rescue medication, hospital and emergency department visits, and adverse events. |
There are no specific renewal criteria for stiripentol. | For CDEC deliberations. |
Considerations for discontinuation of therapy | |
How would loss of response be defined? | Lack of response with a less than 50% reduction in seizures. |
There are no specific discontinuation criteria for stiripentol. | For CDEC deliberations. |
Considerations for prescribing of therapy | |
How frequently would patients require the maximum recommended dose of 20 mg/kg/day? | According to the clinical experts, approximately 30% would require this maximum dose. |
There may be limited access to neurologists in some regions. Stiripentol criteria in most jurisdictions indicate that the drug “must be prescribed by or in consultation with” or the patient “must be under the care of” a neurologist or pediatrician. Consider alignment with prescribing criteria for stiripentol. | For CDEC deliberations. |
Generalizability | |
Patients currently using medicinal cannabis or synthetic cannabinoid-based medications and transitioning to cannabidiol (pharmaceutical). They were excluded from the CARE1 and CARE2 trials. | For CDEC deliberations. |
Patients with other forms of treatment-resistant epilepsy who fall outside the Health Canada indications for cannabidiol. Jurisdictions could receive requests for coverage. | For CDEC deliberations. |
Care provision issues | |
Due to the risk of hepatocellular injury, ALT, AST, and total bilirubin levels should be obtained at baseline and then at 1, 3, and 6 months after starting treatment and periodically thereafter as clinically indicated, or within 1 month of change in cannabidiol dosing or with changes in other medications that affect liver function. | For CDEC deliberations. |
System and economic issues | |
Concerns regarding the anticipated budget impact and sustainability
| For CDEC deliberations. |
There is a confidential negotiated price for Diacomit (stiripentol). | For CDEC deliberations. |
ALT = alanine aminotransferase; ASM = antiseizure medication; AST = aspartate aminotransferase; BIA = budget impact analysis; CDEC = Canadian Drug Expert Committee; DS = Dravet syndrome.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol (Epidiolex) 100 mg/mL oral solution as an adjunctive treatment of seizures associated with DS in patients 2 years of age and older. The focus of this report is on comparing cannabidiol with relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of cannabidiol is presented in 4 sections, with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. The third and fourth sections would include indirect evidence and additional studies that were considered to address important gaps in the systematic review evidence, respectively; however, neither was submitted by the sponsor.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
2 pivotal RCTs identified in the systematic review
1 long-term extension study.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
Description of Studies
A total of 2 double-blind, placebo-controlled phase III RCTs were included in the systematic literature review. The characteristics of the included studies are summarized in Table 6.
Table 6: Details of Studies Included in the Systematic Review
Detail | CARE1 Part B study | CARE2 study |
|---|---|---|
Designs and populations | ||
Study design | Phase III, double-blind, placebo-controlled RCT | Phase III, double-blind, placebo-controlled RCT |
Locations | 23 trial sites in 4 countries:a France, Poland, UK, and US | 43 trial sites in 6 countries:b Australia, Israel, Netherlands, Poland, Spain, and US |
Patient enrolment dates | Start date: March 30, 2015 End date: November 26, 2015 | Start date: April 13, 2015 End date: April 9, 2018 |
Randomized (N) | N = 120:
| N = 199:
|
Key inclusion criteria |
| |
Key exclusion criteria |
| |
Drugs | ||
Intervention | Participants received 20 mg/kg/day of cannabidiol administered orally, half in the morning and half in the evening. Patients’ doses were titrated to the maintenance dose, receiving 2.5 mg/kg on days 1 and 2 of the treatment period, 5.0 mg/kg on days 3 and 4, 7.5 mg/kg on days 5 and 6, 10.0 mg/kg on days 7 and 8, 15.0 mg/kg on days 9 and 10, and 20 mg/kg from day 11 onward during the treatment period. | Participants were randomized to receive either 20 mg/kg/day or 10 mg/kg/day of cannabidiol administered orally, half in the morning and half in the evening. Patients’ doses in the 20 mg/kg/day cannabidiol group were titrated to the maintenance dose, receiving 2.5 mg/kg on days 1 and 2 of the treatment period, 5.0 mg/kg on days 3 and 4, 7.5 mg/kg on days 5 and 6, 10.0 mg/kg on days 7 and 8, 15.0 mg/kg on days 9 and 10, and 20 mg/kg from day 11 onward during the treatment period. Patients randomized to the 10 mg/kg/day cannabidiol group followed the same titration schedule but maintained the 10 mg/kg/day dose reached on day 7 until the end of the treatment period. |
Comparator(s) | Participants received placebo, volume-matched to the 20 mg/kg/day cannabidiol dose level, administered orally, half in the morning and half in the evening. Titration schedules were the same as the 20 mg/kg/day cannabidiol group. | Participants received placebo, volume-matched to either the 20 mg/kg/day or 10 mg/kg/day dose level, administered orally, half in the morning and half in the evening. Titration schedules were the same as the 20 mg/kg/day and 10 mg/kg/day cannabidiol groups. |
Study duration | ||
Screening phase | 28 days | 28 days |
Treatment phase | 98 days (14 weeks) | 98 days (14 weeks) |
Follow-up phase | 10-day taper period plus a 28-day follow-up (patients were invited to continue in an OLE immediately after treatment phase) | |
Outcomes | ||
Primary end point | Percentage change from baseline in total convulsive-seizure frequency (per 28 days) during the treatment period | |
Secondary and exploratory end points | Secondary:
Exploratory:
| Key secondary:
Other secondary:
Exploratory:
|
Publication status | ||
Publications | Cross (2021),31 Devinsky (2017),32 Madan Cohen (2021),33 Mazurkiewicz-Beldzinska (2019),34 Nabbout (2021)35 | Cross (2021),31 Madan Cohen (2021),33 Nabbout (2021),35 Miller (2019),36 Miller (2020),37 |
Clinical trial record number | NCT02091375 | NCT02224703 |
ASM = antiseizure medication; CaGIC = Caregiver Global Impression of Change; CaGICSD = Caregiver Global Impression of Change in Seizure Duration; DS = Dravet syndrome; ECG = electrocardiogram; ESS = Epworth Sleepiness Scale, NRS = numerical rating scale; OLE = open-label extension; QOLCE = Quality of Life in Childhood Epilepsy; RCT = randomized controlled trial; Vineland-2 = Vineland Adaptive Behavior Scales, 2nd Edition; VNS = vagus nerve stimulation.
aOut of 23 trial sites, 22 sites randomized patients into the CARE1 Part B study.
bOut of 43 trial sites, 38 sites randomized patients into the CARE2 study.
cFollowing advice from the European Medicines Agency on the protocol, the response analysis of the ≥ 50% reduction in convulsive-seizure frequency was considered a key secondary end point for European regulatory submissions only.
Sources: CARE138 and CARE2 Clinical Study Reports.39 Details included in the table are from the sponsor’s summary of clinical evidence.
CARE1 Part B Study
The objective of the CARE1 Part B study was to assess the efficacy and safety of cannabidiol as an adjunctive antiepileptic treatment compared with placebo with respect to the percentage change from baseline in convulsive-seizure frequency during the treatment period of the trial. This study was a multisite, randomized, double-blind, placebo-controlled trial. A total of 120 patients were randomized to double-blind treatment between March 30 and November 26, 2015. The trial was conducted at 23 trial sites in 4 countries: France, Poland, the UK, and the US. A 28-day screening period was included to perform tests to detect the presence of tetrahydrocannabinol metabolites (i.e., to confirm that the patient had not taken cannabis immediately before entering the trial) and ensure that all medications or interventions for epilepsy were stable for 4 weeks before screening. This period was also used to establish the baseline number and type of convulsive and nonconvulsive seizures. Eligible patients were randomized to 20 mg/kg/day of cannabidiol or an equivalent volume of placebo, titrating from a 2.5 mg/kg/day dose up to a 20 mg/kg/day maintenance dose over 11 days. Patients were randomly allocated to intervention or placebo groups using an interactive voice response system or interactive web response system. The allocation of investigational medicinal product (IMP) to patient identifier was done according to randomization schedules produced by an independent statistician. The randomization was stratified by age group (2 to 5 years, 6 to 12 years, and 13 to 18 years of age). The trial design of CARE1 Part B is summarized in Figure 1.
Figure 1: CARE1 Part B Trial Design
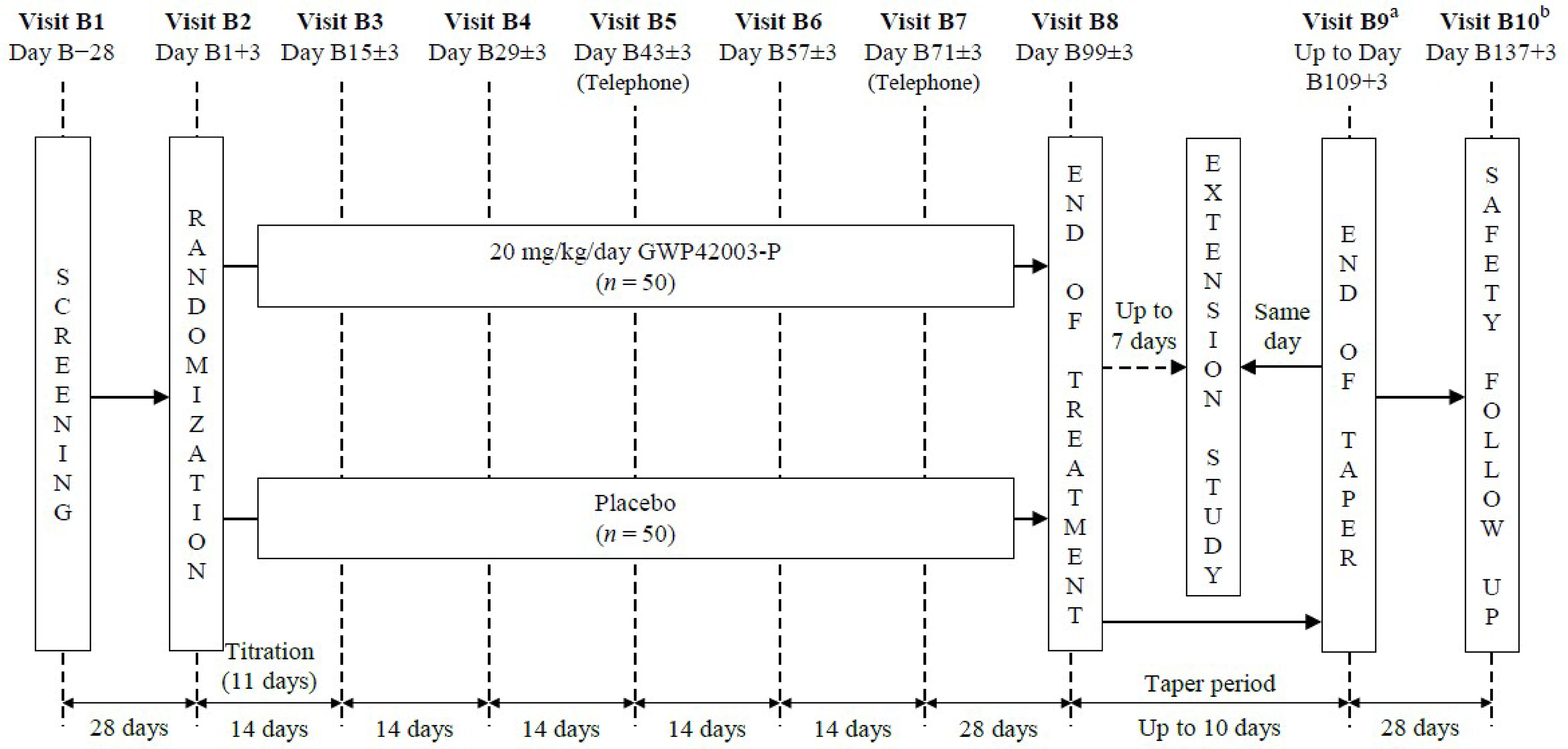
OLE = open-label extension.
a For patients who did not enter the OLE trial at visit B8 or for those who withdrew early and tapered the investigational medicinal product. Patients who completed treatment but opted not to enter the OLE trial, or who withdrew from the trial early, had weekly (± 3 days) safety telephone calls from visit B9 (or date of final dosing) until visit B10.
b For patients who did not enter the OLE trial or who withdrew from the trial early; could be conducted by telephone.
Source: CARE1 Clinical Study Report.38
CARE2 Study
The CARE2 study shared the same objective and study design as the CARE1 Part B trial. A total of 199 patients were randomized to double-blind treatment between April 13, 2016, and April 9, 2018. The trial was conducted at 43 sites in 6 countries: Australia, Israel, Netherlands, Poland, Spain, and the US. Of these, 38 sites randomized patients into the trial. A 28-day screening period was included that was similar to the CARE1 Part B study. Eligible patients were randomized to receive cannabidiol 10 mg/kg/day, cannabidiol 20 mg/kg/day, placebo 10 mg/kg/day dose-volume equivalent, or placebo 20 mg/kg/day dose-volume equivalent at a 2:2:1:1 ratio. Patients assigned to either dose level titrated from a 2.5 mg/kg dose up to the assigned 10 mg/kg or 20 mg/kg maintenance dose over 11 days. Patients were randomly allocated using an interactive web response system. The allocation of IMP to patient number identifier was done according to a randomization schedule produced by an independent statistician. The randomization was stratified by age group (2 to 5 years, 6 to 12 years, and 13 to 18 years of age). The trial design of CARE2 is summarized in Figure 2.
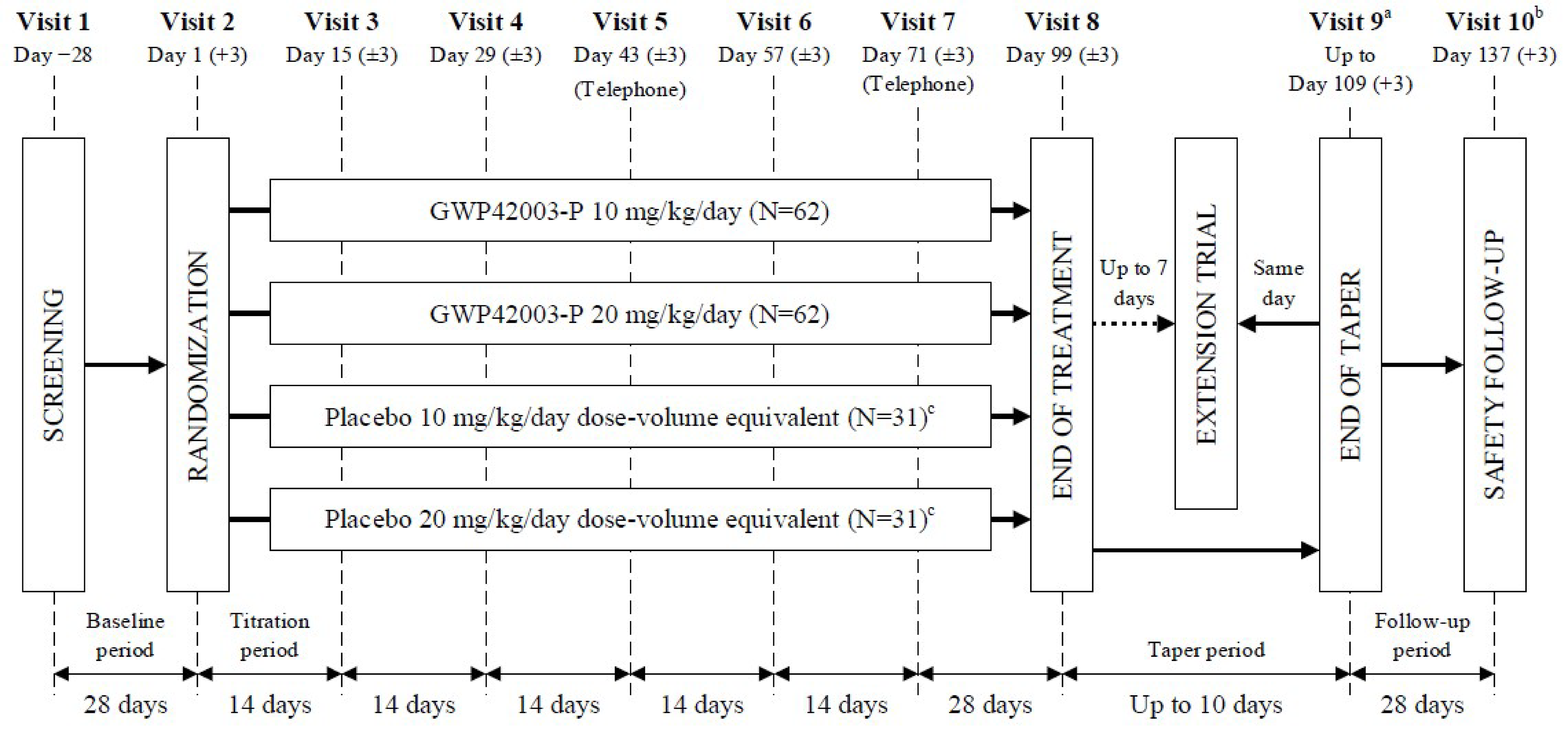
GWP42003-P = cannabidiol; OLE = open-label extension.
a For patients who did not enter the OLE trial at visit B8 or who withdrew early and tapered the investigational medicinal product. Patients who completed treatment but opted not to enter the OLE trial or who withdrew from the trial early had weekly (± 3 days) safety telephone calls from visit B9 (or date of final dosing) until visit B10.
b For patients who did not enter the OLE trial or who withdrew from the trial early; could be conducted by telephone.
c The placebo groups were pooled for the analyses of efficacy.
Source: CARE2 Clinical Study Report.39
Populations
Inclusion and Exclusion Criteria
Key inclusion criteria for the CARE1 Part B and CARE2 studies were patients who were aged 2 to 18 years (inclusive), had 4 or more convulsive seizures per 28 days, had a confirmed diagnosis of DS, had been taking 1 or more ASMs at a dose that had been stable for at least 4 weeks, and had seizures that were not completely controlled by their current ASMs. Key exclusion criteria were having unstable medical conditions in the 4 weeks before screening, a history of substance abuse (including alcohol), use of recreational or medical cannabis in the previous 3 months, and initiated use of felbamate within the past year. Overall, patient inclusion and exclusion criteria were the same for both studies and are reported in more detail in Table 6.
Interventions
Both the CARE1 Part B and CARE2 trials compared 20 mg/kg/day cannabidiol versus placebo as an adjunctive antiepileptic treatment, while CARE2 also included the 10 mg/kg/day cannabidiol arm. In both trials, the same titration period was followed. Patients in the 20 mg/kg/day cannabidiol and dose volume–equivalent placebo treatment arms followed a titration schedule starting with a 2.5 mg/kg dose on days 1 and 2 during the treatment period, a 5 mg/kg dose on days 3 and 4, a 7.5 mg/kg dose on days 5 and 6, a 10 mg/kg dose on days 7 and 8, a 15 mg/kg dose on days 9 and 10, and a maintenance dose of 20 mg/kg from day 11 onward. In the CARE2 study, the 10 mg/kg/day cannabidiol and dose volume–equivalent placebo treatment arms followed the same titration schedule up to day 7, when the maintenance 10 mg/kg/day dose was reached and was to remain constant throughout the rest of the treatment period. Throughout the duration of both trials, doses of concomitant ASMs and any nonpharmacological regimens for epilepsy were to remain stable. The doses of these drugs could be modified by the treating physician. The use of rescue medications was allowed and recorded by the investigators. Any new medications or interventions for epilepsy (including a ketogenic diet) or changes in dosage within 4 weeks before or during the trial were not allowed. Also, recreational medical cannabis and synthetic cannabinoid-based medications were not allowed during the trial.
Outcomes
A list of efficacy end points assessed in this report is provided in Table 7 followed in Table 8 by descriptions of the outcome measures and properties. The summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review, according to the clinical experts consulted by CADTH and the stakeholder input from the patient group and the public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All selected and summarized efficacy end points were assessed using GRADE. AEs and select notable harms outcomes considered important for informing CADTH’s expert committee deliberations were also assessed using GRADE. The outcomes selected included: frequency of total and convulsive seizures (change from baseline and as rates of total seizure reduction, e.g., ≥ 50% reduction), convulsive seizure–free days, and status epilepticus rates. Also, the HRQoL end point measured by the QOLCE scale, sleep disruption (ESS score and sleep disturbance NRS 0 to 10 score), and the use of rescue medications and hospitalizations due to epilepsy. Other outcomes not included in the GRADE framework are described in Appendix 1 (Table 23).
Outcomes in the Pivotal Trials
Both the CARE1 Part B and CARE2 studies had the same primary and secondary efficacy outcomes, with the exception of Cognitive Assessment Battery scores and number of convulsive seizure–free days, which were secondary end points assessed only in the CARE2 study. The outcomes assessed in the CARE1 Part B and CARE2 studies that were considered important for this review are summarized in Table 7.
The primary end point in both studies was the percentage change in convulsive seizures during the treatment period compared with baseline in patients taking cannabidiol compared with placebo. The clinical experts consulted by CADTH agreed this is a critical outcome for decision-making. In the pivotal trials, patients or their caregivers recorded the number and type of convulsive (tonic, clonic, tonic-clonic, or atonic) and nonconvulsive seizures (myoclonic, partial, or absence) each day from screening until completion of dosing using an interactive voice response diary. The seizure frequency during each period was based on 28-day averages. The proportion of patients with a reduction from baseline in convulsive-seizure frequency of 25% or greater, 50% or greater, 75% or greater, and 100% were reported as secondary end points in both studies. The percentage change for other individual seizure types, total seizure frequency, and status epilepticus were also reported as secondary end points. A minimal important difference (MID) for the reduction in seizure frequency is sometimes considered to be a relative reduction from baseline of 50% or greater,40 although this threshold is largely arbitrary based on historical European Medicines Agency and FDA regulatory approval processes in the mainly “general” (i.e., milder) forms of epilepsy.41 Patients with DS may have a more severe form of epilepsy that is treatment-refractory, and there may be more uncertainty around a threshold of important benefit.42
Sleep disruption (measured using the sleep disturbance NRS or the ESS) and HRQoL (assessed using the QOLCE questionnaire) were secondary end points assessed in both studies. For sleep disruption, caregivers were asked to indicate the number that best described their child’s sleep disruption in the past week from a scale of 0 to 10. Scores ranged from 0 (slept extremely well) to 10 (unable to sleep at all). The ESS is a self-reported questionnaire that was completed by each patient’s caregiver. The total score was based on the total of the 8 item scores in the assessment and could range from 0 to 24, with higher total scores representing greater levels of daytime sleepiness. The QOLCE questionnaire was completed by the parent or caregiver of patients aged 4 years and older. QOLCE scores ranged from 0 to 100 for each subscale, where 0 represents the lowest level of functioning and 100 represents the highest level of functioning. The overall quality-of-life score was calculated by taking the mean of the subscale scores. None of these measurements had a published MID value applicable to patients with DS or other measures of the validity, reliability, or responsiveness of the scales.
All AEs and inpatient hospitalizations due to epilepsy observed by the investigator or reported by the patient or caregiver were recorded on the patient’s case report form at all trial visits. An AE was defined as any new unfavourable or unintended signs or symptoms, or diagnosis or worsening of a pre-existing condition, that occurred following screening or at any point up to the posttreatment safety follow-up visit and that may or may not be considered related to the IMP. Any event that was the result of a trial procedure was to be recorded as an AE. Patients’ expected seizure types were not documented as AEs, but any worsening, including change in the pattern or severity of seizures, was to be documented as an AE. An AE was considered serious if it was: fatal, life-threatening, or required inpatient hospitalization or prolonged existing hospitalization; was persistently or significantly disabling or incapacitating; was a congenital anomaly or birth defect; or was a medically significant event that, based upon appropriate medical judgment, may have jeopardized the patient and may have required medical or surgical intervention to prevent 1 of the outcomes listed.
Table 7: Outcomes Summarized From the Pivotal Studies, CARE1 Part B and CARE2
Outcome measure | Time point | CARE1 Part B | CARE2a |
|---|---|---|---|
Percentage change from baseline in the frequency of convulsive seizures during the treatment period | Every 28 days from visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Primary | Primary |
Proportion of patients with a ≥ 50% reduction from baseline in the frequency of convulsive seizures during the treatment period | Visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Key secondary |
Proportion of patients with a ≥ 75% reduction from baseline in convulsive-seizure frequency during the treatment period | Visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Secondary |
Percentage change from baseline in the frequency of nonconvulsive seizures during the treatment period | Every 28 days from visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Secondary |
Percentage change from baseline in total seizures during the treatment period | Every 28 days from visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Key secondary |
Number of convulsive seizure–free days | Visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | NA | Exploratory |
Change from baseline in number of patients with episodes of status epilepticus during the treatment period | Visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Secondary |
Change from baseline in QOLCE score | Visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Secondary |
Change from baseline in ESS score | Visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Secondary |
Change from baseline in sleep disturbance NRS 0 to 10 score | Visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Secondary |
Use of rescue medication | Visit 2 (day 1 + 3) up to visit 8 (day 99 ± 3) | Secondary | Secondary |
Number of patients with inpatient hospitalizations due to epilepsy | Visit 2 (day 1 + 3) up to visit 10 (day 137 ± 3) | Secondary | Secondary |
ESS = Epworth Sleepiness Scale; NA = not applicable; NRS = numerical rating scale; QOLCE = Quality of Life in Childhood Epilepsy.
aOutcomes from both cannabidiol arms (10 mg/kg/day and 20 mg/kg/day) were compared with the placebo group.
Sources: CARE138 and CARE2 Clinical Study Reports.39 Details included in the table are from the sponsor’s summary of clinical evidence.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Reduction in seizure frequency | The percentage reduction from baseline in the number of seizures at different time points during treatment | Not applicable for validity, reliability, or responsiveness properties | Considered to be a ≥ 50% relative reduction from baseline, based on historical EMA and FDA regulatory approval processes in other forms of epilepsy. The clinical experts consulted by CADTH agreed on this threshold as significant. |
Change from baseline in ESS score | Higher scores mean higher levels of sleepiness. The range of values is typically from 0 to 24 with scores above 10 generally considered significant daytime sleepiness. | Not reported | Not reported |
Change from baseline in QOLCE score | Ranged from 0 to 100 for each subscale, where zero represents the lowest or poorest category and 100 represents the highest level of functioning. The overall quality-of-life score was calculated by taking the mean of the subscale scores. | Not reported | Not reported |
Change from baseline in sleep disturbance NRS 0 to 10 score | Number that best described their child’s sleep disruption in the past week on a scale from 0 to 10, where 0 = slept extremely well and 10 = unable to sleep at all. ESS was based on the total of the 8 item scores in the assessment and could range from 0 to 24, with higher total scores representing greater levels of daytime sleepiness. | Not reported | Not reported |
EMA = European Medicines Agency; ESS = Epworth Sleepiness Scale; MID = minimal important difference; NRS = numerical rating scale.
Sources: CARE138 and CARE239 Clinical Study Reports.
Statistical Analysis
Clinical Trial End Points
In the CARE1 Part B study, the primary end point and all other secondary end points related to seizure frequency were analyzed using a Wilcoxon rank sum test. The estimated median differences for all seizure frequency–related end points between the cannabidiol and placebo treatment arms, together with a 95% CI, were calculated using the Hodges-Lehmann approach. Wilcoxon rank sum tests were also conducted in seizure frequency–related end points in the CARE2 study but were treated as part of the sensitivity analyses. In the CARE2 study, the differences between the cannabidiol and placebo treatment arms were analyzed using a negative binomial regression analysis, with the estimated ratio of least squares means of each cannabidiol treatment group to placebo (with 95% CI) presented as the primary outcome. Primary analyses were performed using the intention-to-treat (ITT) analysis set. Analyses using the per-protocol analysis sets were performed for the primary and key secondary end points only.
In both the CARE1 Part B and CARE2 studies, the proportion of patients whose condition was considered to have responded to treatment (defined as those with a ≥ 25%, ≥ 50%, ≥ 75%, or 100% reduction from baseline in the frequency of convulsive seizures during the treatment period) was analyzed using a Cochran-Mantel-Haenszel test stratified by age group.
In both studies, an analysis of covariance (ANCOVA) with baseline and age group as covariates and treatment group as fixed factor was used to analyze sleep disruption in the sleep disturbance NRS (0 to 10 scale), ESS, and QOLCE scores. A summary of the statistical analyses is presented in Table 9 and Table 24.
Table 9: Statistical Analysis of Efficacy End Points in the Pivotal Trials
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
CARE1 Part B study | ||||
Percentage change from baseline in convulsive-seizure frequency | Wilcoxon rank sum test 95% CI with the Hodges-Lehmann method | NR |
|
|
Proportion of patients with a ≥ 50% reduction from baseline in convulsive-seizure frequency during the treatment period | CMH test | Age group included as a stratification factor | If a patient withdrew during the treatment period, then the primary analysis variable was calculated from all available data obtained during the treatment period before the patient withdrawing. | CMH tests were repeated on the ITT analysis set using data for the maintenance period only for each 4-week period during maintenance. |
Proportion of patients with a ≥ 25%, ≥ 75%, or 100% reduction from baseline in convulsive-seizure frequency during the treatment period | CMH test | Age group included as a stratification factor | If a patient withdrew during the treatment period, then the primary analysis variable was calculated from all available data obtained during the treatment period before the patient withdrawing. | CMH tests were repeated on the ITT analysis set using data for the maintenance period only and during each 4 weeks of the maintenance period. |
Change from baseline in number of patients with episodes of status epilepticus during the treatment period | Descriptive statistics only | NR | NR | NR |
Percentage change from baseline in total seizure frequency | Wilcoxon rank sum test 95% CI with the Hodges-Lehmann method | NR | If a patient withdrew during the treatment period, then the primary analysis variable was calculated from all available data obtained during the treatment period before the patient withdrawing. | Sensitivity analyses were repeated on the ITT analysis set using data for the maintenance period only and during each 4 weeks of the maintenance period. |
Change from baseline in seizure frequency by individual seizure type during the treatment period | Wilcoxon rank sum test 95% CI with the Hodges-Lehmann method | NR | If a patient withdrew during the treatment period, then the primary analysis variable was calculated from all available data obtained during the treatment period before the patient withdrawing. | Sensitivity analyses were repeated on the ITT analysis set using data for the maintenance period only and during each 4 weeks of the maintenance period. |
Use of rescue medication | Descriptive statistics only | NR | NR | NR |
Number of patients with inpatient hospitalizations due to epilepsy | ANCOVA | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | NR | NR |
Change from baseline in sleep disturbance NRS 0 to 10 score | ANCOVA | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | NR | NR |
Change from baseline in ESS score | ANCOVA | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | If scores for fewer than 4 of the 8 individual questions were missing, the mean of the remaining nonmissing scores was used for the calculation of the total score only; if the scores of 4 or more of the individual questions were missing, the patient data were not included in the summary or analysis for that visit. | NR |
Change from baseline in QOLCE score | ANCOVA | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | The calculations of subscale and overall scores treated responses of “not applicable” as missing values. For each subscale, if less than 50% of the items within the subscale were missing (including “not applicable”), then the subscale score was calculated using the mean of the nonmissing items. If 50% or more of the items within the subscale were missing, then the subscale score was not calculated and was missing. For the overall quality-of-life score, if fewer than 8 of the 16 subscale scores were missing, then the overall quality-of-life score was calculated using the mean of the nonmissing subscale scores. If 8 or more of the subscale scores were missing, then the overall quality-of-life score was not calculated and was missing. | NR |
CARE2 study | ||||
Change from baseline in total convulsive seizures | Negative binomial regression MMRM | Models included total number of seizures as a response variable; age group, time (baseline and treatment period), and treatment and treatment-by-time interaction as fixed effects; and patient as a random effect. Log-transformed number of days in which seizures were reported by period is included as an offset. |
|
|
Change from baseline in total seizures | Negative binomial regression MMRM | Models included total number of seizures as a response variable; age group, time (baseline and treatment period), and treatment and treatment-by-time interaction as fixed effects; and patient as a random effect. Log-transformed number of days in which seizures were reported by period is included as an offset. | NR | Sensitivity analyses were repeated on the ITT analysis set using data for the maintenance period only and during each 4 weeks of the maintenance period. |
Number of patients with a ≥ 50% reduction from baseline in convulsive-seizure frequency | CMH test | Age group included as a stratification factor. | NR | CMH tests were repeated for the PP analysis set and the ITT analysis set using data for the maintenance period only, and during each 4 weeks of the maintenance period. |
Number of patients with a ≥ 25%, ≥ 75%, or 100% reduction from baseline in convulsive-seizure frequency | CMH test | Age group included as a stratification factor | NR | CMH tests were repeated for the PP analysis set and the ITT analysis set using data for the maintenance period only, and during each 4 weeks of the maintenance period. |
Change from baseline in number of patients with episodes of status epilepticus during the treatment period | Descriptive statistics only | Models included total number of seizures as a response variable; age group, time (baseline and treatment period), and treatment and treatment-by-time interaction as fixed effects; and patient as a random effect. Log-transformed number of days in which seizures were reported by period is included as an offset. | NR | NR |
Use of rescue medication | Descriptive statistics only | NR | NR | NR |
Number of patients with inpatient hospitalizations due to epilepsy | Descriptive statistics only | NR | NR | NR |
Change from baseline in sleep disturbance NRS 0 to 10 score | ANCOVA | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | NR | NR |
Change from baseline in ESS score | ANCOVA | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | If scores for fewer than 4 of the 8 individual questions were missing, the mean of the remaining nonmissing scores was used for the calculation of the total score only. If the scores for 4 or more of the individual questions were missing, the patient was not included in the summary or analysis for that visit. | NR |
Change from baseline in QOLCE score | ANCOVA | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | Calculations of subscale and overall scores treated responses of “not applicable” as missing values. For each subscale, if less than 50% of the items within the subscale were missing (including “not applicable”), then the subscale score was calculated using the mean of the nonmissing items. If 50% or more of the items within the subscale were missing, then the subscale score was not calculated and was missing. For the overall quality-of-life score, if fewer than 8 of the 16 subscale scores were missing, then the overall quality-of-life score was calculated using the mean of the nonmissing subscale scores. If 8 or more of the subscale scores were missing, then the overall quality-of-life score was not calculated and was missing. | NR |
Number of convulsive seizure–free days | ANCOVA | NR | NR | NR |
ANCOVA = analysis of covariance; CaGIC = Caregiver Global Impression of Change; CaGICSD = Caregiver Global Impression of Change in Seizure Duration; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ESS = Epworth Sleepiness Scale; ITT = intention to treat; IVRS = interactive voice response system; LOCF = last observation carried forward; MI = multiple imputation; MMRM = mixed-model for repeated measures; MNAR = missing not at random; NOCB = next observation carried backward; NR = not reported; NRS = numerical rating scale; PP = per protocol; QOLCE = Quality of Life in Childhood Epilepsy; Vineland-2 = Vineland Adaptive Behavior Scales, 2nd Edition.
Sample Size and Power Calculation
The CARE1 Part B study planned to enrol 100 patients randomly allocated on a 1:1 basis (cannabidiol versus placebo) and stratified by age group (2 to 5 years, 6 to 12 years, and 13 to 18 years of age). The investigators assumed that patients in the placebo group would experience a mean reduction in convulsive-seizure frequency of 18% from baseline, for which a sample size of 50 patients per group would be sufficient to detect a difference of 32% in treatment effect between treatment groups. This was based on a standard deviation of 56% using a 2-sided 5% significance level and 80% power.
The CARE2 study planned to randomize a total of 186 patients across 4 treatment groups (cannabidiol 10 mg/kg/day, cannabidiol 20 mg/kg/day, placebo 10 mg/kg/day dose-volume equivalent, or placebo 20 mg/kg/day dose-volume equivalent) in a 2:2:1:1 ratio, stratified by age group (2 to 5 years, 6 to 12 years, and 13 to 18 years of age). The investigators determined that a sample size of 62 per group (after pooling the placebo groups) was required to obtain a power of at least 80% for a Wilcoxon-Mann–Whitney test comparing 2 distributions with a 2-sided significance level of 0.05. This was based on a gamma distribution for the cannabidiol groups with a scale parameter of 65.614 and a shape parameter of 1.0886, and a gamma distribution for the placebo group with a scale parameter of 40.887 and a shape parameter of 2.3059. Maximum likelihood estimates using the Newton-Raphson approximation were computed for the scale and shape parameters using data from the CARE1 Part B study.
Statistical Testing
In both the CARE1 Part B and CARE2 studies, all statistical tests were 2-sided with a 5% significance level. No formal adjustment of statistical significance for multiple testing was performed for the CARE1 Part B study.
In the CARE2 study, each end point had 2 comparisons against placebo (cannabidiol 20 mg/kg/day and 10 mg/kg/day versus placebo). The primary and key secondary end points were tested using a hierarchical gate-keeping procedure to control for type I error.
The key secondary end points were defined as follows:
First key secondary end point: percentage change from baseline in total seizure frequency during the treatment period
Second key secondary end point: number of patients with a 50% or greater reduction in convulsive-seizure frequency from baseline during the treatment period
Third key secondary end point: Caregiver Global Impression of Change (CaGIC) scores
The null hypothesis of an end point at the level of 0.05 (2-sided) must have been rejected to test the hypothesis of the subsequent end point in the sequence at the level of 0.05 (2-sided). If a null hypothesis was not rejected, then testing would stop and all subsequent analyses would be declared not statistically significant.
Subgroup Analyses
In both trials, subgroup analyses were performed for the primary efficacy end point and for patients with a 25% or greater, 50% or greater, 75% or greater, or 100% reduction in the frequency of convulsive seizures from baseline using the ITT analysis set. All statistical significance was to be tested at the 0.05 level without formal adjustment for multiplicity. The same analyses were performed as for the primary efficacy variable using data from the treatment period. In the CARE1 study, for patients with a 25% or greater, 50% or greater, 75% or greater, or 100% reduction in the frequency of convulsive seizures, analyses were performed using a Fisher exact test. In the CARE2 study, for the key secondary end point of a 50% or greater reduction in convulsive-seizure frequency, patients with a 50% or greater reduction in seizure frequency were modelled using logistic regression, including stratified age group and treatment arm as covariates. The model also included covariates for each level of the effect being tested (excluding a reference level), both individually and with interactions with the treatment arm. A separate model was used for testing each effect.
The following subgroups were used In both the CARE1 Part B and CARE2 studies:
age group (2 to 5 years, 6 to 12 years, and 13 to 18 years of age)
sex (male, female)
region (US, rest of the world)
clobazam use (yes, no)
valproic acid use (yes, no)
stiripentol use (yes, no)
baseline average convulsive-seizure frequency per 28 days (≤ observed tertile 1, > observed tertile 1 to ≤ observed tertile 2, > observed tertile 2)
number of current ASMs (< 3, ≥ 3)
number of prior ASMs (< 4, ≥ 4).
The CARE2 study also included the following subgroups:
clobazam use and stiripentol use (yes/yes, yes/no, no/yes, no/no)
levetiracetam use (yes, no)
topiramate use (yes, no)
number of prior and concurrent ASMs (< 8, ≥ 8).
Analysis Populations
A summary of study populations in the CARE1 Part B and CARE2 studies is presented in Table 10.
Table 10: Analysis Populations of the CARE1 Part B and CARE2 Studies
Study | Population | Definition | Application |
|---|---|---|---|
CARE1 Part B | Safety analysis set | All patients randomized to treatment who received at least 1 dose of the IMP. Patients were analyzed according to the treatment they received. | Analyses of safety data and adverse events. |
ITT analysis set | The ITT analysis set included all patients in the Part B safety analysis set who had postbaseline efficacy data. Patients were analyzed according to the treatment group to which they were randomized. | Primary analysis set for all efficacy end points. | |
PP analysis set | The PP analysis set included all patients in the Part B ITT analysis set who completed the treatment period of the trial. Patients were analyzed according to the treatment group to which they were randomized. | Sensitivity analyses of percentage change from baseline in convulsive-seizure frequency and proportion of treatment responders during the treatment period. | |
CARE2 | Safety analysis set | All patients randomized to treatment who received at least 1 dose of IMP. Patients were analyzed according to the treatment they received. | Analyses of safety data and adverse events. |
ITT analysis set | The ITT analysis set included all patients who were randomized and dosed with IMP in the trial and had postbaseline efficacy data. Patients were analyzed according to the treatment group to which they were randomized. | Primary analysis set for all efficacy end points. | |
PP analysis set | The PP analysis set included all patients who completed the trial with no protocol deviations deemed to compromise the assessment of efficacy. Patients were analyzed according to the treatment group to which they were randomized. | Sensitivity analyses of percentage change from baseline in convulsive-seizure frequency and proportion of treatment responders during the treatment period. |
IMP = investigational medicinal product; ITT = intention to treat; PP = per protocol.
Sources: CARE138 and CARE239 Clinical Study Reports. Details included in the table are from the sponsor’s summary of clinical evidence.
Results
Patient Disposition
In the CARE1 Part B and CARE2 studies, 32% and 30% of patients failed screening, respectively, most commonly due to not meeting the eligibility criteria or reported as “other reason” (not defined). After randomization, the discontinuation rates were higher in the cannabidiol 10 mg/kg/day and 20 mg/kg/day arms versus the placebo arms, the majority due to AEs (Table 11) when considering both studies.
Table 11: Summary of Patient Disposition From Studies Included in the Systematic Review
Patient disposition | CARE1 Part B study | CARE2 studya | |||
|---|---|---|---|---|---|
20 mg/kg/day cannabidiol (N = 61) | Placebo (N = 59) | 10 mg/kg/day cannabidiol (N = 67) | 20 mg/kg/day cannabidiol (N = 67) | Placebob (N = 65) | |
Screened, N | 177 | 285 | |||
Screening failure, N | 57 | 86 | |||
Reason for screening failure,c n (%) | |||||
Not meeting criteria | 26 (45.6) | 52 (60.5) | |||
Other reason | 24 (42.1) | 29 (33.7) | |||
Withdraw or withdrawn by parent or guardian | 4 (7.0) | 5 (5.8) | |||
Investigator decision | 4 (7.0) | 3 (3.5) | |||
Patients enrolled, N | 120 | 199 | |||
Randomized, N (%) | 61 (50.8) | 59 (49.2) | 67 (23.5) | 67 (23.5) | 65 (22.8) |
Discontinued from study, N (%) | 9 (14.8) | 3 (5.1) | 3 (4.5) | 6 (9.0) | 0 |
Reason for discontinuation, n (%) | |||||
AE | 8 (13.1) | 1 (1.7) | 0 | 5 (7.5) | 0 |
Lost to follow-up | 0 | 1 (1.7) | 0 | 0 | 0 |
Withdrawal by patient or parent or guardian | 0 | 1 (1.7) | 0 | 1 (1.5) | 0 |
Withdrawn by the investigator | 1 (1.6) | 0 | 1 (1.5) | 0 | 0 |
Other | 0 | 0 | 2 (3.0) | 0 | 0 |
Safety, N | 61 | 59 | 64 | 69 | 65 |
ITT, N | 61 | 59 | 66 | 67 | 65 |
PP, N | 52 | 56 | 61 | 59 | 62 |
AE = adverse event; ITT = intention to treat; PP = per protocol.
Note: Details included in the table are from the sponsor’s summary of clinical evidence.
aTwo patients randomized to receive 10 mg/kg/day cannabidiol were mistakenly given dosing schedules for patients receiving 20 mg/kg/day at visit 2 (day 1) and thus received > 10 mg/kg/day dosing volumes before the error was corrected. In 1 patient, the error was not identified and rectified until visit 6 (day 57), while the other continued at the higher dose throughout the trial. These patients were analyzed according to the treatment group to which they were randomized, unless otherwise stated.
bPooled results from the 10 mg/kg/day and 20 mg/kg/day dose volume–equivalent placebo groups from the CARE2 study are presented.
cPatients could have more than 1 reason for screen failure.
Source: CARE138 and CARE239 Clinical Study Reports.
Baseline Characteristics
The baseline characteristics outlined in Table 12 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. In general, the initial characteristics were evenly distributed among the groups in both studies. However, slight discrepancies were observed in the variables of sex and age. These disparities are likely attributable to random variation and the limited sample size evaluated.
Exposure to Study Treatments
Exposure and adherence information for the CARE1 Part B and CARE2 studies (safety analysis set) are summarized in Table 13. Lower mean patient-days of exposure in the CARE2 study in the 20 mg/kg/day group (93.9 patient-days versus 99.5 and 98.3 patient-days in the placebo and 10 mg/kg/day groups, respectively) were aligned with higher discontinuation rates due to AEs in this treatment group.
Table 12: Summary of Baseline Characteristics From Studies Included in the Systematic Review (Safety Analysis Set)
Characteristic | CARE1 Part B study | CARE2 study | |||
|---|---|---|---|---|---|
20 mg/kg/day cannabidiol (N = 61) | Placebo (N = 59) | 10 mg/kg/day cannabidiol (N = 64) | 20 mg/kg/day cannabidiol (N = 69) | Placeboa (N = 65) | |
Age (years) | |||||
n | 61 | 59 | 64 | 69 | 65 |
Mean (SD) | 9.7 (4.7) | 9.8 (4.9) | 9.2 (4.2) | 9.2 (4.4) | 9.6 (4.6) |
Median | 9.1 | 9.2 | 8.2 | 10.0 | 9.1 |
Range | 2.5 to 18.0 | 2.3 to 18.4 | 2.3 to 17.7 | 2.2 to 18.9 | 2.2, to 18.1 |
Age group, n (%) | |||||
2 to 5 years | 18 (29.5) | 17 (28.8) | 18 (28.1) | 21 (30.4) | 18 (27.7) |
6 to 12 years | 23 (37.7) | 24 (40.7) | 31 (48.4) | 31 (44.9) | 28 (43.1) |
13 to 18 years | 20 (32.8) | 18 (30.5) | 15 (23.4) | 17 (24.6) | 19 (29.2) |
Sex, n (%) | |||||
Female | 26 (42.6) | 32 (54.2) | 38 (59.4) | 32 (46.4) | 34 (52.3) |
Male | 35 (57.4) | 27 (45.8) | 26 (40.6) | 37 (53.6) | 31 (47.7) |
Race, n (%) | |||||
White or Caucasian | 44 (72.1) | 50 (84.7) | 55 (85.9) | 66 (95.7) | 55 (84.6) |
Black or African American | 2 (3.3) | 2 (3.4) | 1 (1.6) | 0 | 4 (6.2) |
American Indian or Alaska Native | NR | NR | 0 | 0 | 1 (1.5) |
Asian | 1 (1.6) | 0 | 0 | 1 (1.4) | 4 (6.2) |
NAb | 11 (18.0) | 6 (10.2) | NA | NA | NA |
Other | 3 (4.9) | 1 (1.7) | 8 (12.5) | 2 (2.9) | 1 (1.5) |
Height (cm) | |||||
n | 60 | 59 | 64 | 69 | 65 |
Mean (SD) | 132.2 (26.3) | 131.1 (24.4) | 129.2 (21.4) | 130.0 (23.5) | 131.5 (22.3) |
Median | 127.5 | 127.0 | 125.3 | 131.0 | 131.0 |
Range | 89.3 to 188.0 | 87.6 to 189.0 | 90.0 to 171.0 | 90.0 to 174.5 | 90.0 to 173.5 |
Weight (kg) | |||||
n | 61 | 59 | 64 | 69 | 65 |
Mean (SD) | 33.8 (16.6) | 35.1 (18.3) | 32.8(16.4) | 34.2 (19.3) | 34.0 (14.9) |
Median | 28.4 | 29.4 | 26.8 | 31.5 | 28.6 |
Range | 10.8 to 88.6 | 12.0 to 88.4 | 14.0 to 88.9 | 11.8 to 133.8 | 14.0 to 70.0 |
Body mass index (kg/m2) | |||||
n | 60 | 59 | 64 | 69 | 65 |
Mean (SD) | 18.3 (4.5) | 19.1 (4.7) | 18.5 (4.6) | 18.8 (4.6) | 18.8 (3.9) |
Median | 17.4 | 18.1 | 16.7 | 17.7 | 17.9 |
Range | 13.0 to 38.7 | 13.5 to 35.6 | 13.3 to 32.7 | 13.9 to 43.9 | 13.0 to 31.2 |
Seizure class, n (%) | |||||
n | 61 | 59 | 64 | 69 | 65 |
Tonic-clonic | 55 (90.2) | 52 (88.1) | 59 (92.2) | 64 (92.7) | 64 (98.5) |
Generalized tonic-clonic | NR | NR | 47 (73.4) | 49 (71.0) | 54 (83.1) |
Secondarily generalized tonic-clonic | NR | NR | 12 (18.8) | 15 (21.7) | 10 (15.4) |
Absence | 20 (32.8) | 23 (39.0) | 27 (42.2) | 33 (47.8) | 23 (35.4) |
Myoclonic | 18 (29.5) | 25 (42.4) | 27 (42.2) | 36 (52.2) | 37 (56.9) |
Tonic | 17 (27.9) | 12 (20.3) | 15 (23.4) | 19 (27.5) | 21 (32.3) |
Complex partial | NR | NR | 25 (39.1) | 29 (42.0) | 26 (40.0) |
Countable partial | 15 (24.6) | 14 (23.7) | NR | NR | NR |
Hemiclonic | NR | NR | 17 (26.6) | 12 (17.4) | 8 (12.3) |
Clonic | 14 (23.0) | 11 (18.6) | 5 (7.8) | 7 (10.1) | 13 (20.0) |
Atonic | 5 (8.2) | 11 (18.6) | 5 (7.8) | 12 (17.4) | 12 (18.5) |
Other partial | 3 (4.9) | 4 (6.8) | 0 | 3 (4.3) | 4 (6.2) |
Nonconvulsive seizures > 30 minutes in duration | 2 (3.3) | 3 (5.1) | 4 (6.3) | 5 (7.2) | 3 (4.6) |
Convulsive seizures > 30 minutes in duration | 0 | 1 (1.7) | 9 (14.1) | 14 (20.3) | 15 (23.1) |
Number of prior ASMs patient no longer taking | |||||
n | 61 | 59 | 64 | 69 | 65 |
Mean (SD) | 4.6 (4.3) | 4.6 (3.3) | 4.48 (3.2) | 4.49 (2.5) | 4.32 (2.5) |
Median | 4.0 | 4.0 | 4.0 | 4.0 | 4.0 |
Range | 0.0 to 26.0 | 0.0 to 14.0 | 0.0 to 19.0 | 0.0 to 11.0 | 0.0 to 11.0 |
Number of ASMs patient currently taking | |||||
n | 61 | 59 | 64 | 69 | 65 |
Mean (SD) | 3.0 (1.0) | 2.9 (0.9) | 2.70 (1.0) | 2.83 (0.9) | 3.03 (0.9) |
Median | 3.0 | 3.0 | 3.0 | 3.0 | 3.0 |
Range | 1.0 to 5.0 | 1.0 to 5.0 | 1.0 to 5.0 | 1.0 to 4.0 | 1.0 to 5.0 |
ASM = antiseizure medication; NA = not applicable, NR = not reported, SD = standard deviation.
aThe pooled results from the 10 mg/kg/day and 20 mg/kg/day dose volume–equivalent placebo groups from the CARE2 study are presented.
bThese patients were all from France, where identification of race is subject to a data-protection law.
Sources: CARE138 and CARE239 Clinical Study Reports. Details included in the table are from the sponsor’s summary of clinical evidence.
Table 13: Summary of Patient Exposure From Studies Included in the Systematic Review (Safety Analysis Set)
Exposure | CARE1 Part B Study | CARE2 study | |||
|---|---|---|---|---|---|
20 mg/kg/day cannabidiol (N = 61) | Placebo (N = 59) | 10 mg/kg/day cannabidiol (N = 64) | 20 mg/kg/day cannabidiol (N = 69) | Placebo (N = 65) | |
Total, patient-days | 99 | 99 | |||
Duration, mean patient-days (SD) | 90.2 (26.0) | 95.9 (16.3) | 98.3 (7.4) | 93.9 (22.0) | 99.5 (2.6) |
Duration, median patient-days (range) | 99.0 (11 to 131) | 99.0 (17 to 114) | 99.0 (57 to 120) | 99.0 (12 to 123) | 99.0 (92 to 109) |
Adherence, % | NR | NR | 99.8 | 98.5 | 99.8 |
NR = not reported; SD = standard deviation.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Concomitant Medications and Cointerventions
The use of concomitant medications (excluding rescue medications) in the safety populations of the CARE1 Part B and CARE2 studies is summarized in Table 14.
In the CARE1 Part B study, overall, the utilization of concurrent ASMs was evenly distributed among the groups, with stiripentol being the only exception, with 30 patients (49.2%) and 21 patients (35.6%) in the cannabidiol and placebo arms, respectively, using stiripentol. All 120 patients (100%) took 1 or more concomitant ASMs during the trial. The most common classes of ASMs used concomitantly (i.e., reported in more than 50% of patients overall) were other antiepileptics, which were used by 101 patients (84.2%); benzodiazepine derivatives, which were used by 98 patients (81.7%); and fatty acid derivatives, which were used by 71 patients (59.2%). The most commonly used concomitant ASM was clobazam, which was used by 78 patients (65.0%); followed by valproic acid, which was used by 68 patients (56.6%); and stiripentol, which was used by 51 patients (42.5%).
Similarly, in the CARE2 study, the utilization of concurrent ASMs was evenly distributed among the groups, with clonazepam and topiramate being the exception. All 198 patients (100.0%) took 1 or more concomitant ASMs during the trial. The most common classes of ASMs used concomitantly (i.e., reported in more than 50% of patients overall) were other antiepileptics, which were used by 161 patients (81.3%); benzodiazepine derivatives, which were used by 148 patients (74.7%); and fatty acid derivatives, which were used by 139 patients (70.2%). The most commonly used ASM was valproic acid, which was used by 139 patients (70.2%); clobazam, which was used by 126 patients (63.6%); stiripentol, which was used by 71 patients (35.9%); levetiracetam, which was used by 54 patients (27.3%); and topiramate, which was used by 46 patients (23.2%).
Table 14: Concomitant Antiseizure Medications Used in the CARE1 Part B and CARE2 Studies (Safety Analysis Set)
Exposure, n (%) | CARE1 Part B study | CARE2 study | |||
|---|---|---|---|---|---|
20 mg/kg/day cannabidiol (N = 61) | Placebo (N = 59) | 10 mg/kg/day cannabidiol (N = 64) | 20 mg/kg/day cannabidiol (N = 69) | Placebo (N = 65) | |
Barbiturates and derivatives | 1 (1.6) | 5 (8.5) | 2 (3.1) | 3 (4.3) | 5 (7.7) |
Phenobarbital | 1 (1.6) | 5 (8.5) | 2 (3.1) | 3 (4.3) | 4 (6.2) |
Primidone | NR | NR | 0 | 0 | 1 (1.5) |
Benzodiazepine | 51 (83.6) | 47 (79.7) | 48 (75.0) | 48 (69.6) | 52 (80.0) |
Clobazam | 40 (65.6) | 38 (64.4) | 44 (68.8) | 41 (59.4) | 41 (63.1) |
Clonazepam | 9 (14.8) | 9 (15.3) | 41 (63.1) | 8 (11.6) | 11 (16.9) |
Benzodiazepine derivatives | 3 (4.9) | 3 (5.1) | NR | NR | NR |
Diazepam | 2 (3.3) | 0 | 2 (3.1) | 1 (1.4) | 2 (3.1) |
Nitrazepam | 0 | 1 (1.7) | NA | NA | NA |
Midazolam | NA | NA | 1 (1.6) | 0 | 0 |
Clorazepate dipotassium | NA | NA | 0 | 0 | 1 (1.5) |
Benzodiazepine-related drugs | 0 | 1 (1.7) | NR | NR | NR |
Carboxamide derivatives | 4 (6.6) | 1 (1.7) | 2 (3.1) | 5 (7.2) | 2 (3.1) |
Rufinamide | 4 (6.6) | 1 (1.7) | 2 (3.1) | 5 (7.2) | 2 (3.1) |
Detoxifying drugs for antineoplastic treatment | 1 (1.6) | 0 | NR | NR | NR |
Calcium folinate | 1 (1.6) | 0 | NR | NR | NR |
Folinic acid | 1 (1.6) | 0 | NR | NR | NR |
Fatty acid derivatives | 37 (60.7) | 34 (57.6) | 43 (67.2) | 48 (69.6) | 48 (73.8) |
Valproate sodium | 18 (29.5) | 14 (23.7) | NRa | NRa | NRa |
Valproic acid | 10 (16.4) | 12 (20.3) | 43 (67.2) | 48 (69.6) | 48 (73.8) |
Valproate semisodium | 8 (13.1) | 6 (10.2) | NRa | NRa | NRa |
Vigabatrin | NR | NR | 0 | 0 | 1 (1.5) |
Ergenyl chronospheres | 1 (1.6) | 2 (3.4) | NR | NR | NR |
Hydantoin derivatives | 1 (1.6) | 1 (1.7) | 1 (1.6) | 1 (1.4) | 0 |
Phenytoin | 1 (1.6) | 1 (1.7) | 1 (1.6) | 1 (1.4) | 0 |
Multivitamins, plain | 1 (1.6) | 0 | NR | NR | NR |
Vitamins, nitric oxide supplements | 1 (1.6) | 0 | NR | NR | NR |
Other antiepileptics | 52 (85.2) | 49 (83.1) | 52 (81.3) | 57 (82.6) | 52 (80.0) |
Stiripentol | 30 (49.2) | 21 (35.6) | 23 (35.9) | 24 (34.8) | 24 (36.9) |
Levetiracetam | 16 (26.2) | 17 (28.8) | 18 (28.1) | 22 (31.9) | 14 (21.5) |
Topiramate | 16 (26.2) | 15 (25.4) | 10 (15.6) | 19 (27.5) | 17 (26.2) |
Zonisamide | 8 (13.1) | 9 (15.3) | 7 (10.9) | 6 (8.7) | 4 (6.2) |
Lamotrigine | 1 (1.6) | 2 (3.4) | 0 | 1 (1.4) | 3 (4.6) |
Felbamate | 0 | 2 (3.4) | 5 (7.8) | 2 (2.9) | 3 (4.6) |
Perampanel | NR | NR | 1 (1.6) | 0 | 3 (4.6) |
Pregabalin | NR | NR | 1 (1.6) | 0 | 2 (3.1) |
Acetazolamide | 1 (1.6) | 0 | 0 | 0 | 2 (3.1) |
Lacosamide | 0 | 1 (1.7) | 4 (6.3) | 5 (7.2) | 2 (3.1) |
Sultiame | NR | NR | 0 | 0 | 2 (3.1) |
Other hypnotics and sedatives | 4 (6.6) | 5 (8.5) | 2 (3.1) | 4 (5.8) | 5 (7.7) |
Bromides | 2 (3.3) | 5 (8.5) | 0 | 1 (1.4) | 3 (4.6) |
Potassium bromide | 2 (3.3) | 0 | 2 (3.1) | 3 (4.3) | 2 (3.1) |
Phenylalkylamine derivatives | 0 | 2 (3.4) | NR | NR | NR |
Verapamil | 0 | 2 (3.4) | NR | NR | NR |
Succinimide derivatives | 5 (8.2) | 2 (3.4) | 2 (3.1) | 5 (7.2) | 5 (7.7) |
Ethosuximide | 4 (6.6) | 1 (1.7) | 2 (3.1) | 4 (5.8) | 4 (5.8) |
Mesuximide | 1 (1.6) | 1 (1.7) | 0 | 1 (1.4) | 1 (1.5) |
Unspecified herbal and traditional medicine | 0 | 1 (1.7) | NR | NR | NR |
Cannabis sativa oil | 0 | 1 (1.7) | NR | NR | NR |
NA = not applicable; NR = not reported.
aFor the CARE2 study, the preferred terms of valproate semisodium and valproate sodium were combined with the preferred term of valproic acid.
Sources: CARE138 and CARE239 Clinical Study Reports.
Efficacy
The results of the main efficacy outcomes (from the ITT populations in the pivotal trials, CARE1 Part B and CARE2) are summarized in Table 15. These end points represent those considered important for decision-making by the clinical experts consulted by CADTH and other relevant stakeholders, such as committee members and patient representatives. These outcomes are also assessed in the GRADE framework and summary of findings. The rest of the end points submitted by the sponsor are reported in Table 23 in Appendix 1.
Table 15: Summary of Key Efficacy Results From Studies Included in the Systematic Review (ITT Analysis Set)
Variable | CARE1 Part B study | CARE2 study | |||
|---|---|---|---|---|---|
20 mg/kg/day cannabidiol (N = 61) | Placebo (N = 59) | 10 mg/kg/day cannabidiol (N = 66) | 20 mg/kg/day cannabidiol (N = 67) | Placebo (N = 65) | |
Seizure control | |||||
Percentage change from baseline in convulsive-seizure frequency during the treatment period | |||||
Number of patients analyzed | 61 | 59 | 66 | 67 | 65 |
Baseline period, median (Q1, Q3) | 12.4 (6.2, 28.0) | 14.9 (7.0, 36.0) | 13.5 (6.0, 31.2) | 9.0 (6.3, 21.2) | 16.6 (7.0, 51.1) |
Treatment period, median (Q1, Q3) | 5.9 (3.2, 17.3) | 14.1 (4.2, 31.1) | 6.3 (2.7, 18.6) | 4.8 (2.3, 21.8) | 14.0 (5.7, 49.3) |
Median percentage change during treatment (95% CI)a | –38.9 (–69.5 to –4.8) | –13.3 (–52.5 to 20.2) | –41.2 (–81.0 to –3.0) | –47.0 (–71.4 to –10.5) | –24.5 (–51.9 to 4.6) |
Estimated median difference (95% CI) | –22.8 (–41.1 to –5.4) | –15.7 (–31.3 to 3.7) | –19.9 (–33.9 to –5.3) | NA | |
P value | 0.0123 | 0.1051 | 0.0082 | NA | |
Patients with a ≥ 50% reduction from baseline in convulsive-seizure frequency during the treatment period | |||||
Number of patients analyzed | 61 | 59 | 66 | 67 | 65 |
Yes, n (%) | 26 (42.6) | 16 (27.1) | 29 (43.9) | 33 (49.3) | 17 (26.2) |
Difference in proportions (95% CI) | 0.155 (–0.013 to 0.323) | 0.178 (0.017 to 0.338) | 0.231 (0.071 to 0.391) | NA | |
Odds ratio (95% CI) | 2.00 (0.93 to 4.30) | 2.21 (1.06 to 4.62) | 2.74 (1.32 to 5.70) | NA | |
P value | 0.0784 | 0.0332 | 0.0069 | NA | |
Patients with a ≥ 75% or 100% reduction from baseline in convulsive-seizure frequency during the treatment period | |||||
Number of patients analyzed | 61 | 59 | 66 | 67 | 65 |
≥ 75% reduction in convulsive-seizure frequency from baseline | |||||
Yes, n (%) | 14 (23.0) | 7 (11.9) | 20 (30.3) | 12 (17.9) | 4 (6.2) |
Difference in proportions (95% CI) | 0.111 (–0.023 to 0.245) | 0.241 (0.116 to 0.367) | 0.118 (0.009 to 0.226) | NA | |
Odds ratio (95% CI) | 2.21 (0.82 to 5.95) | 6.63 (2.12 to 20.73) | 3.33 (1.01 to 10.92) | NA | |
P valueb | 0.1121 | 0.0004 | 0.0468 | NA | |
100% reduction in convulsive-seizure frequency from baseline | |||||
Yes, n (%) | 3 (4.9) | 0 | 2 (3.0) | 3 (4.5) | 1 (1.5) |
Difference in proportions (95% CI) | 0.049 (–0.005, 0.103) | 0.015 (–0.036, 0.066) | 0.029 (–0.028, 0.087) | NA | |
Odds ratio (95% CI) | NA | 2.00 (0.18, 22.61) | 3.00 (0.30, 29.61) | NA | |
P valueb | 0.0827 | 0.5600 | 0.3640 | NA | |
Number of convulsive seizure–free days | |||||
Baseline period, mean (SD) | NR | NR | 17.4 (7.8) | 17.7 (7.6) | 15.9 (8.3) |
Treatment period, mean (SD) | NR | NR | 21.3 (7.1) | 20.5 (7.9) | 17.6 (8.4) |
Change from baseline, mean (SD) | NR | NR | 3.9 (4.8) | 2.7 (4.0) | 1.7 (4.1) |
Treatment difference (95% CI) | NR | NR | 2.4 (1.0 to 3.9) | 1.3 (–0.1 to 2.8) | NA |
P valueb | NR | NR | 0.0009 | 0.0683 | NA |
Percentage change from baseline in total seizure frequency during the treatment period | |||||
Total seizures | |||||
Number of patients analyzed | 61 | 59 | 66 | 67 | 65 |
Baseline period, median (Q1, Q3) | 24.0 (10.4, 141.0) | 41.5 (12.0, 367.0) | 34.5 (10.4, 104.5) | 26.0 (10.0, 194.1) | 46.3 (16.0, 217.0) |
Treatment period, median (Q1, Q3) | 13.7 (4.8, 137.2) | 31.1 (7.7, 282.6) | 12.8 (3.7, 76.9) | 15.7 (4.4, 96.9) | 35.7 (10.2, 124.0) |
Median percentage change during treatment (Q1, Q3)a | –28.6 (–70.4, –4.0) | –9.0 (–51.4, 19.6) | –51.9 (–79.3, –14.5) | –52.7 (–67.1, –13.1) | –26.8 (–58.1, 7.0) |
Estimated median difference (95% CI) | –19.2 (–39.3 to –1.2) | NR | NR | NA | |
P valueb | 0.0335 | NA | NA | NA | |
Percentage reduction: Treatment period divided by baseline period, % (95% CI)c | NR | NR | 56.4 (47.8 to 63.6) | 47.3 (36.9 to 56.0) | 29.7 (16.0 to 41.1) |
Treatment ratio: Cannabidiol divided by placebo (95% CI) | NR | 0.620 (0.481 to 0.799) | 0.749 (0.581 to 0.965) | NA | |
P valueb | NR | 0.0003 | 0.0255 | NA | |
Patients with convulsive status epilepticus | |||||
Number of patients with convulsive seizures greater than 30 minutes in duration, n (%) | |||||
Baseline period | 0 | 1 (1.7) | 4 (6.1) | 6 (9.0) | 4 (6.2) |
Treatment period | 1 (1.6) | 0 | 3 (4.5) | 9 (13.4) | 8 (12.3) |
HRQoL | |||||
QOLCE scores, overall quality-of-life score | |||||
Patients included | n = 47 | n = 44 | n = 57 | n = 53 | n = 49 |
Day 1, mean (SD) | 44.1 (14.5) | 41.8 (13.1) | 43.7 (13.8) | 42.9 (14.6) | 43.2 (11.6) |
End of treatment, mean (SD) | 48.7 (13.5) | 46.3 (15.0) | 49.3 (12.0) | 48.4 (15.7) | 45.1 (15.3) |
Change from baseline, mean (SD) | 5.4 (14.6) | 3.8 (9.9) | 6.4 (10.9) | 4.0 (11.8) | 2.6 (9.7) |
Adjusted mean treatment difference (95% CI) | 1.5 (–3.8 to 6.8) | 3.8 (–0.1 to 7.8) | 1.8 (–2.2 to 5.8) | NA | |
P valueb | 0.5766 | 0.0581 | 0.3827 | NA | |
Sleep and sleep disruption | |||||
Sleep disturbance NRS 0 to 10 scale | |||||
Last visit, mean treatment difference (95% CI) | –0.4 (–1.5 to 0.7) | –0.0 (–0.9 to 0.8) | –0.1 (–0.9 to 0.8) | NA | |
P value | 0.453 | 0.951 | 0.840 | NA | |
ESS score | |||||
Last visit, mean treatment difference (95% CI) | 1.51 (–0.18 to 3.19) | –0.55 (–1.86 to 0.75) | 0.74 (–0.57 to 2.05) | NA | |
P valueb | 0.078 | 0.404 | 0.267 | NA | |
Resource utilization | |||||
Use of rescue medication, n (%) | |||||
Number of patients using rescue medication | 36 (59.0) | 41 (69.5) | 54 (84.4) | 58 (84.1) | 54 (80.0) |
Inpatient hospitalizations due to epilepsy, n (%) | |||||
Number of patients reporting 1 or more inpatient hospitalizations due to epilepsy during the treatment period | 5 (8.2) | 1 (1.7) | 12 (18.2) | 8 (11.9) | 6 (9.2) |
CI = confidence interval; ESS = Epworth Sleepiness Scale; HRQoL = health-related quality of life; ITT = intention to treat; NA = not applicable; NR = not reported; NRS = numerical rating scale; Q1 = lower quartile; Q3 = upper quartile; QOLCE = Quality of Life in Childhood Epilepsy; SD = standard deviation.
aAnalyzed using Wilcoxon rank sum test. This statistical test was used as a sensitivity analysis in the CARE2 study.
bNo multiplicity adjustment was made for this end point.
cAnalyzed using negative binomial regression. This statistical test was used in the primary analysis of the CARE2 study.
Sources: CARE138 and CARE239 Clinical Study Reports.
Seizure Control
Percentage Change From Baseline in Convulsive-Seizure Frequency During the Treatment Period
In the CARE1 Part B study, patients in the 20 mg/kg/day cannabidiol group achieved a median percentage change from baseline in convulsive-seizure frequency of –38.9% (95% CI, –69.5% to –4.8%) during the 14-week treatment period compared with –13.3% (95% CI, –52.5% to 20.2%) for the placebo group. The estimated median difference between treatment arms was –22.8% (95% CI, –41.1% to –5.4%; P = 0.0123).
In the CARE2 study, the percentage reduction in convulsive-seizure frequency from baseline was 48.7% (95% CI, 37.9% to 57.6%) for the 10 mg/kg/day cannabidiol group and 45.7% (95% CI, 34.2% to 55.2%) for the 20 mg/kg/day cannabidiol group versus 26.9% (95% CI, 11.9% to 39.4%) for the placebo group. The treatment ratio between the 10 mg/kg/day cannabidiol group and the placebo group was 0.702 (95% CI, 0.538 to 0.916; P = 0.0095), and between the 20 mg/kg/day cannabidiol group and the placebo group was 0.743 (95% CI, 0.568 to 0.971; P = 0.0299).
Proportion of Patients With a 50% or Greater Reduction in Convulsive-Seizure Frequency From Baseline During the Treatment Period
In the CARE1 Part B study, the proportion of patients with a reduction of 50% or greater in their baseline frequency of convulsive seizures was 42.6% in the 20 mg/kg/day cannabidiol group and 27.1% in the placebo group. The OR for achieving this end point in the 20 mg/kg/day cannabidiol group compared with placebo was 2.00 (95% CI, 0.93 to 4.30; P = 0.0784).
In the CARE2 study, the proportion of patients with a reduction of 50% or greater in their baseline frequency of convulsive seizures was 43.9% in the 10 mg/kg/day cannabidiol group and 49.3% in the 20 mg/kg/day cannabidiol group compared with 26.3% in the placebo group. The odds of achieving this end point was an OR of 2.21 (95% CI, 1.06 to 4.62; P = 0.0332) in the 10 mg/kg/day group and an OR of 2.74 (95% CI, 1.32 to 5.70; P = 0.0069) in the 20 mg/kg/day group compared with placebo.
Proportion of Patients With a 25% or Greater, 75% or Greater, or 100% Reduction From Baseline in Convulsive-Seizure Frequency During the Treatment Period
In the CARE1 Part B study, the proportion of patients with a reduction of 75% or greater in their baseline convulsive-seizure frequency was 23.0% in the 20 mg/kg/day cannabidiol group compared with 11.9% in the placebo group. The OR for achieving a 75% or greater reduction in the frequency of convulsive seizures was 2.21 (95% CI, 0.82 to 5.95; P = 0.1121) in the 20 mg/kg/day cannabidiol group compared with the placebo group. Three patients (4.9%) in the 20 mg/kg/day cannabidiol group experienced convulsive-seizure freedom (i.e., a 100% reduction in convulsive-seizure frequency) compared with no patients in the placebo group (treatment difference of 4.9%; 95% CI, –0.5 to 10.3; P = 0.0827).
In the CARE2 study, the proportion of patients with a 75% or greater reduction in the frequency of convulsive seizures was 17.9% in the 20 mg/kg/day cannabidiol group, 30.3% in the 10 mg/kg/day cannabidiol group, and 6.2% in the placebo group. The OR for a 75% or greater reduction in the frequency of convulsive seizures was 6.63 (95% CI, 2.12 to 20.73; P = 0.0004) in the 10 mg/kg/day cannabidiol group and 3.33 (95% CI, 1.01, 10.92; P = 0.0468) in the 20 mg/kg/day cannabidiol group compared with placebo. Five patients in the cannabidiol groups reached convulsive-seizure freedom (2 patients taking 10 mg/kg/day and 3 patients taking 20 mg/kg/day cannabidiol) compared with 1 patient in the placebo group, with an OR of 2.00 (95% CI, 0.18 to 22.61; P = 0.5600) for 10 mg/kg/day cannabidiol versus placebo and an OR of 3.00 (95% CI, 0.30 to 29.61; P = 0.3640) for 20 mg/kg/day cannabidiol versus placebo.
In the CARE2 study, the proportion of patients who experienced any improvement in the frequency of convulsive seizures was 75.8% in the 10 mg/kg/day and 82.1% in the 20 mg/kg/day cannabidiol groups, while it was 73.8% in the placebo group.
Number of Convulsive Seizure–Free Days
In the CARE2 study, the mean change from baseline in the number of convulsive seizure–free days during the treatment period was 3.9 days (standard deviation [SD] = 4.8) and 2.7 days (SD = 4.0) in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups, respectively, compared with 1.7 (SD = 4.1) in the placebo group. The mean difference in the change from baseline was 2.4 days (95% CI, 1.0 to 3.9; P = 0.0009) between the 10 mg/kg/day group and placebo, and 1.3 days (95% CI, –0.1 to 2.8; P = 0.0683) between the 20 mg/kg/day group and placebo. This outcome was not reported in the CARE1 Part B study.
Percentage Change From Baseline in Total Seizure Frequency During the Treatment Period
In the CARE1 Part B study, the median percentage change in total seizure frequency in the 20 mg/kg/day cannabidiol group was –28.6% (95% CI, –70.4% to –4.0%) compared with –9.0% (95% CI, –51.4% to 19.6%) in the placebo group. The median difference between 20 mg/kg/day cannabidiol and placebo was –19.2% (95% CI, –39.3% to –1.2%; P = 0.0335).
In the CARE2 study, the median percentage reduction in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups was –56.4% (95% CI, 47.8% to 63.6%) and –47.3% (95% CI, 36.9% to 56.0%), respectively, compared with –29.7% (95% CI, 16.0% to 41.1%) in the placebo group. The treatment ratios were 0.620 (95% CI, 0.481 to 0.799; P = 0.0003) for 10 mg/kg/day cannabidiol versus placebo and 0.749 (95% CI, 0.581 to 0.965; P = 0.0255) for 20 mg/kg/day cannabidiol versus placebo.
Percentage Change From Baseline in Seizure Frequency by Individual Seizure Type During the Treatment Period
In the CARE1 Part B study, of the individual convulsive-seizure types, tonic-clonic seizures were the most common type reported by patients during the baseline period (89.2% of patients) followed by tonic seizures (24.2%), clonic seizures (20.8%), and atonic seizures (13.3%). Reductions in the frequency of all 4 individual convulsive-seizure types were observed in every treatment group. Greater percentage reductions were seen in the cannabidiol treatment group for all convulsive-seizure types except for clonic seizures, where the placebo group experienced a greater percentage change than the cannabidiol treatment group. Treatment differences were in favour of cannabidiol over placebo for all seizure types except clonic seizures. For tonic-clonic seizures, the treatment difference was –22.0 (95% CI, –42.5 to –2.1; P = 0.0254), which was statistically significant.
In the CARE2 study, of the individual types of convulsive seizures reported by patients during the baseline period, tonic-clonic seizures were the most common (91.4% of all patients), followed by tonic seizures (40.9%), clonic seizures (24.7%), and atonic seizures (15.2%); the distribution of the individual convulsive-seizure types across the 3 treatment groups was similar during the baseline period. Reductions in the frequency of all 4 types of convulsive seizures were observed in every treatment group. In all cases, greater percentage reductions were seen in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups compared with the placebo groups. In all cases, the treatment ratios for individual convulsive-seizure analyses were numerically in favour of both doses of cannabidiol over placebo but were not statistically significant. Negative binomial regression analyses showed nominal statistical significance in favour of 10 mg/kg/day cannabidiol over placebo for the reduction of atonic seizures, although caution is advised with interpreting the data due to low patient numbers.
In the CARE1 Part B study, of the individual types of nonconvulsive seizures reported by patients during the baseline period, myoclonic and absence seizures were the most common (each type was experienced by 35.8% of patients), followed by countable partial seizures (24.2%) and other seizures (5.8%). Reductions in the frequency of all 4 types of nonconvulsive seizures were seen for both treatment groups, except in the case of countable partial seizures in the placebo group, where there was an increase in seizure frequency. Greater percentage reductions were seen in the cannabidiol treatment group for all types of nonconvulsive seizures, except for absence seizures. None of the treatment differences were statistically significant.
In the CARE2 study, of the individual types of nonconvulsive seizures reported by patients during the baseline period, myoclonic and absence seizures were the most common (42.4% of patients for each), followed by countable partial seizures (34.3%), and other partial seizures (9.1%). Reductions in the frequency of all 4 types of nonconvulsive seizures during the treatment period were observed across the treatment groups. Greater percentage reductions in the 20 mg/kg/day and 10 mg/kg/day cannabidiol groups were seen for myoclonic and absence seizures compared with the placebo group. For countable partial and other partial seizures, the treatment ratios were in favour of placebo over both cannabidiol doses; none of the treatment ratios were nominally statistically significant.
Patients With Status Epilepticus
In the CARE1 Part B study, there were 0 patients and 1 (1.7%) patient with status epilepticus during the baseline period in the 20 mg/kg/day cannabidiol and placebo groups, respectively. During the treatment period, there was 1 patient (1.6%) and 0 patients with status epilepticus in the 20 mg/kg/day cannabidiol and placebo groups, respectively. In the CARE2 study, there were 4 (6.1%) and 6 (90%) patients with status epilepticus during the baseline period in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups, respectively, compared with 4 patients (6.2%) in the placebo group. During the treatment period, there were 3 (4.5%) and 9 (13.4%) patients with status epilepticus during the baseline period in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups, respectively, compared with 8 patients (12.3%) in the placebo group. The changes from baseline and between-group differences were not reported in either study.
Health-Related Quality of Life
Change in QOLCE Scores From Baseline
In the CARE1 Part B study, the mean change from baseline in QOLCE scores among patients aged 4 years or older was 5.4 (SD = 14.6) in the 20 mg/kg/day cannabidiol group and 3.8 (SD = 9.9) in the placebo group. The adjusted mean difference in the change from baseline was 1.5 (95% CI, –3.8 to 6.8; P = 0.5766).
In the CARE2 study, the mean changes from baseline in QOLCE score among patients aged 4 years or older were 6.4 (SD = 10.9) and 4.0 (SD = 11.8) in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups, respectively, compared with 2.6 (SD = 9.7) in the placebo group. The adjusted mean differences in the change from baseline were 3.8 (95% CI, –0.1 to 7.8; P = 0.0581) for the 10 mg/kg/day cannabidiol group and 1.8 (95% CI, –2.2 to 5.8; P = 0.3827) for the 20 mg/kg/day cannabidiol group compared with placebo.
Sleep Disruption and Function
Change in the Sleep Disturbance NRS 0 to 10 Score at Last Visit
In the CARE1 Part B study, the mean difference in the change from baseline was –0.4 (95% CI, –1.5 to 0.7; P = 0.4543).
In the CARE2 study, the mean treatment difference in scores for the NRS 0 to 10 scale between the 10 mg/kg/day cannabidiol group and placebo group was 0.0 (95% CI, –0.9 to 0.8; P = 0.9510); between the 20 mg/kg/day cannabidiol and placebo groups, the between-treatment difference was –0.1 (95% CI, –0.9 to 0.8; P = 0.8407).
Change in ESS Score at Last Visit
In the CARE1 Part B study, the mean treatment difference in ESS score between the 20 mg/kg/day cannabidiol and placebo groups was 1.51 (95% CI, –0.18 to 3.19; P = 0.078).
In the CARE2 study, the mean treatment difference in ESS score between the 10 mg/kg/day cannabidiol and placebo groups was –0.55 (95% CI, –1.86 to 0.75; P = 0.4041) and 0.74 (95% CI, –0.57 to 2.05; P = 0.2676) between the 20 mg/kg/day group and placebo.
Resource Use
Hospitalizations Due to Epilepsy
In the CARE1 Part B study, a total of 5 patients in the 20 mg/kg/day cannabidiol group (8.2%) and 1 patient in the placebo group (1.7%) reported 1 or more inpatients hospitalizations due to epilepsy during the treatment period.
In the CARE2 study, 8 patients (11.9%) in the 20 mg/kg/day cannabidiol group, 12 patients (18.2%) in the 10 mg/kg/day cannabidiol group, and 6 patients (9.2%) in the placebo group reported 1 or more inpatient hospitalizations due to epilepsy during the treatment period. Although reported as epilepsy-related admissions, follow-up determined that a number of admissions were unlikely to be related to epilepsy. Overall, the numbers of patients for whom follow-up confirmed epilepsy-related hospitalizations were similar across treatment groups: 3 patients (4.5%) randomized to 20 mg/kg/day cannabidiol, 7 patients (10.4%) randomized to 10 mg/kg/day cannabidiol, and 4 patients (6.2%) randomized to placebo.
Use of Rescue Medications
In the CARE1 Part B study, 36 (59.0%) and 41 (69.5%) patients in the 20 mg/kg/day cannabidiol and placebo groups, respectively, used rescue medication. In the CARE2 study, the number of patients using rescue medications in the cannabidiol 10 mg/kg/day, 20 mg/kg/day, and placebo groups were 54 (84.4%), 58 (84.1%), and 54 (80.0%), respectively.
Subgroup Effects
When evaluating the subgroup effects of the primary end points (reduction from baseline in the frequency of convulsive seizures and reduction of more than 50% from baseline in the frequency of convulsive seizures) in both studies, the results were consistent with the overall effect in favour of cannabidiol for all variables with a few exceptions:
In the CARE1 Part B study, no use of clobazam favoured placebo.
In the CARE2 study, for most subgroups, the difference between treatments was in favour of cannabidiol (both 10 mg/kg/day and 20 mg/kg/day) over placebo. The modifiers with the most credible effects in the 20 mg/kg/day group were region of study and baseline frequency of convulsive seizures. In the 10 mg/kg/day group, only stiripentol use had a modifying effect on the interaction tests (P = 0.046).
Harms
A summary of AEs reported in patients during the CARE1 Part B and CARE2 trials can be found in Table 16. In the CARE1 Part B and CARE2 studies, safety analyses were conducted on the safety analysis set. In the CARE2 study, 2 patients randomized to receive 10 mg/kg/day cannabidiol were titrated above the target dose in error and were included in the 20 mg/kg/day treatment groups in the safety analysis set. One patient in the 10 mg/kg/day cannabidiol group was excluded from the safety analysis set because they were randomized in error and never received IMP.
The first occurrence of an AE was most commonly reported during the 2-week titration (dose escalation) period in each treatment group in both the CARE1 Part B and CARE2 studies. In the CARE1 Part B study, AEs were reported in 39 patients (63.9%) taking cannabidiol and 27 patients (45.8%) receiving placebo. In the CARE2 study, AEs were reported in 28 patients (50.0%) in the 10 mg/kg/day cannabidiol group, 38 patients (61.3%) in the 20 mg/kg/day cannabidiol group, and 33 patients (56.9%) in the pooled placebo group. Somnolence was the most commonly reported AE followed by diarrhea and decreased appetite across both studies. In the CARE1 Part B study, the proportion of patients who received cannabidiol who experienced AEs was 93.4% compared with 74.6% of patients in the placebo group; most AEs (89%) were mild or moderate in severity. In the CARE2 study, 87.5% of patients receiving 10 mg/kg/day cannabidiol, 89.9% of patients receiving 20 mg/kg/day cannabidiol, and 89.2% of patients in the pooled placebo group had 1 or more AEs during the trial; most AEs (92.0%) were of mild or moderate severity.
Adverse Events
In the CARE1 Part B study, 57 of 61 patients (93.4%) in the 20 mg/kg/day cannabidiol group and 44 of 59 patients (74.6%) in the placebo group reported 1 or more AEs. In the CARE2 study, 56 of 64 patients (87.5%) in the 10 mg/kg/day cannabidiol group, 62 of 69 patients (89.9%) in the 20 mg/kg/day cannabidiol group, and 58 of 65 patients (89.2%) in the placebo group reported 1 or more AEs. The most common AEs reported in both studies (> 10% of patients in any treatment group) were somnolence, diarrhea, and decreased appetite.
Serious Adverse Events
The most commonly reported serious AEs (SAEs) in both trials were nervous system disorders. All SAEs were resolved in the CARE1 Part B study, while 3 patients in the 20 mg/kg/day cannabidiol group in the CARE2 study collectively had 3 SAEs that were not resolved at the end of the trial.
In the CARE1 Part B study, 10 of 61 patients (16.4%) in the 20 mg/kg/day cannabidiol group and 3 of 59 patients (5.1%) in the placebo group reported 1 or more SAEs. In the CARE2 study, 13 of 64 patients (20.3%) in the 10 mg/kg/day cannabidiol group, 17 of 69 patients (24.6%) in the 20 mg/kg/day cannabidiol group, and 10 of 65 patients (15.4%) in the placebo group reported 1 or more SAEs. The most common SAEs reported in more than 2% of patients in both studies were status epilepticus, somnolence, and convulsion. Pneumonia was also a common SAE reported in the CARE2 study.
Withdrawals Due to Adverse Events
In the CARE1 Part B study, AEs that led to treatment discontinuation occurred in 9 of 61 patients (14.8%) in the 20 mg/kg/day cannabidiol group and in 1 of 59 patients (1.7%) in the placebo group. In the CARE2 study, 5 of 69 patients (7.2%) in the 20 mg/kg/day cannabidiol group experienced AEs leading to discontinuation from the study. No patients in the 10 mg/kg/day cannabidiol group or placebo groups discontinued treatment due to AEs.
Mortality
No patient deaths occurred during either study.
Notable Harms
Notable harms (AEs of special interest) were not specified in either the CARE1 Part B or CARE2 studies. However, the clinical experts consulted by CADTH suggested the occurrence of somnolence, hypotonia, lethargy, mood disorder, and increased liver enzymes as harms to explore more closely. Of these, only the total number of investigations related to liver function were increased in the 20 mg/kg/day arm of both studies (Table 16).
Table 16: Summary of Harms Results From the CARE1 Part B and CARE2 Studies (Safety Analysis Set)
AEs | CARE1 Part B study | CARE2 study | |||
|---|---|---|---|---|---|
20 mg/kg/day cannabidiol (N = 61) | Placebo (N = 59) | 10 mg/kg/day cannabidiol (N = 64) | 20 mg/kg/day cannabidiol (N = 69) | Placebo (N = 65) | |
Most common AEs,a n (%) | |||||
Patients with ≥ 1 AE | 57 (93.4) | 44 (74.6) | 56 (87.5) | 62 (89.9) | 58 (89.2) |
Gastrointestinal disorders | 29 (47.5) | 12 (20.3) | 14 (21.9) | 28 (40.6) | 16 (24.6) |
Diarrhea | 19 (31.1) | 6 (10.2) | 11 (17.2) | 18 (26.1) | 8 (12.3) |
Vomiting | 9 (14.8) | 3 (5.1) | 4 (6.3) | 11 (15.9) | 4 (6.2) |
General disorders and administration site conditions | 21 (34.4) | 8 (13.6) | 20 (31.3) | 27 (39.1) | 18 (27.9) |
Fatigue | 12 (19.7) | 2 (3.4) | 5 (7.8) | 15 (21.7) | 7 (10.8) |
Pyrexia | 9 (14.8) | 5 (8.5) | 15 (23.4) | 15 (21.7) | 11 (16.9) |
Infections and infestations | 26 (42.6) | 17 (28.8) | 27 (42.2) | 32 (46.4) | 25 (38.5) |
Nasopharyngitis | 3 (4.9) | 3 (5.1) | 4 (6.3) | 8 (11.6) | 5 (7.7) |
Upper respiratory tract infection | 7 (11.5) | 5 (8.5) | 3 (4.7) | 4 (5.8) | 3 (4.6) |
Investigations | 17 (27.9) | 7 (11.9) | 13 (20.3) | 25 (36.2) | 8 (12.3) |
Alanine aminotransferase increased | NR | NR | 3 (4.7) | 9 (13.0) | 0 |
Aspartate aminotransferase increased | 2 (3.3) | 0 | 3 (4.7) | 8 (11.6) | 0 |
Metabolism and nutrition disorders | 20 (32.8) | 3 (5.1) | 12 (18.8) | 21 (30.4) | 14 (21.5) |
Decreased appetite | 17 (27.9) | 3 (5.1) | 11 (17.2) | 20 (29.0) | 11 (16.9) |
Nervous system disorders | 32 (52.5) | 18 (30.5) | 28 (43.8) | 35 (50.7) | 30 (46.2) |
Convulsion | 7 (11.5) | 3 (5.1) | 6 (9.4) | 4 (5.8) | 5 (7.7) |
Lethargy | 8 (13.1) | 3 (5.1) | 1 (1.6) | 1 (1.4) | 2 (3.1) |
Somnolence | 22 (36.1) | 6 (10.2) | 16 (25.0) | 16 (23.2) | 9 (13.8) |
Status epilepticusb | 4 (6.6) | 3 (5.1) | 5 (7.8) | 7 (10.1) | 9 (13.8) |
SAEs,c n (%) | |||||
Patients with ≥ 1 SAE | 10 (16.4) | 3 (5.1) | 13 (20.3) | 17 (24.6) | 10 (15.4) |
Gastrointestinal disorders | 2 (3.3) | 0 | 0 | 1 (1.4) | 0 |
Pneumonia | 1 (1.6) | 0 | 3 (4.7) | 2 (2.9) | 0 |
Investigations | 3 (4.9) | 0 | 0 | 2 (2.9) | 0 |
Alanine aminotransferase increased | NR | NR | 0 | 1 (1.4) | 0 |
Aspartate aminotransferase increased | 1 (1.6) | 0 | 0 | 1 (1.4) | 0 |
Gamma-glutamyl transferase level abnormal | 1 (1.6) | 0 | NR | NR | NR |
Liver function test abnormal | 1 (1.6) | 0 | 0 | 1 (1.4) | 0 |
Platelet count abnormal | 1 (1.6) | 0 | NR | NR | NR |
Weight decreased | 1 (1.6) | 0 | NR | NR | NR |
Convulsion | 2 (3.3) | 1 (1.7) | 3 (4.7) | 0 | 1 (1.5) |
Seizure cluster | NR | NR | 1 (1.6) | 0 | 2 (3.1) |
Somnolence | 3 (4.9) | 0 | 2 (3.1) | 0 | 0 |
Status epilepticus | 3 (4.9) | 3 (5.1) | 5 (7.8) | 7 (10.1) | 8 (12.3) |
Pneumonia aspiration | NR | NR | 1 (1.6) | 2 (2.9) | 0 |
Patients who stopped treatment due to AEs, n (%) | |||||
Patients who stopped | 9 (14.8) | 1 (1.7) | 0 | 5 (7.2) | 0 |
Gastrointestinal disorders | 1 (1.6) | 0 | 0 | 2 (2.9) | 0 |
Abdominal distension | 1 (1.6) | 0 | NR | NR | NR |
Abdominal pain | 1 (1.6) | 0 | NR | NR | NR |
Diarrhea | NR | NR | 0 | 1 (1.4) | 0 |
Vomiting | NR | NR | 0 | 1 (1.4) | 0 |
General disorders and administration site conditions | 3 (4.9) | 0 | 0 | 3 (4.3) | 0 |
Asthenia | 1 (1.6) | 0 | NR | NR | NR |
Fatigue | 2 (3.3) | 0 | 0 | 3 (4.3) | 0 |
Pyrexia | 1 (1.6) | 0 | 0 | 1 (1.4) | 0 |
Investigations | 4 (6.6) | 1 (1.7) | 0 | 3 (4.3) | 0 |
Alanine aminotransferase increased | NR | NR | 0 | 2 (2.9) | 0 |
Aspartate aminotransferase increased | 2 (3.3) | 0 | 0 | 2 (2.9) | 0 |
Gamma-glutamyl transferase level abnormal | 1 (1.6) | 0 | NR | NR | NR |
Liver function test abnormal | 1 (1.6) | 1 (1.7) | 0 | 1 (1.4) | 0 |
Platelet count abnormal | 1 (1.6) | 0 | NR | NR | NR |
Transaminases increased | 1 (1.6) | 0 | NR | NR | NR |
Metabolism and nutrition disorders | 3 (4.9) | 0 | 0 | 2 (2.9) | 0 |
Decreased appetite | 3 (4.9) | 0 | 0 | 2 (2.9) | 0 |
Nervous system disorders | 6 (9.8) | 0 | 0 | 3 (4.3) | 0 |
Convulsion | 3 (4.9) | 0 | 0 | 1 (1.4) | 0 |
Coordination abnormal | NR | NR | 0 | 1 (1.4) | 0 |
Deaths, n (%) | |||||
Patients who died | 0 | 0 | 0 | 0 | 0 |
Harms of special interest | |||||
Hypotonia | 2 (3.3) | 0 | NR | NR | NR |
Lethargy | 1 (1.6) | 0 | NR | NR | NR |
Investigations related to liver function | 4 (6.6) | 1 (1.7) | 0 | 3 (4.3) | 0 |
Mood disorder: Aggression | 1 (1.6) | 0 | NR | NR | NR |
Somnolence | 5 (8.2) | 0 | 0 | 2 (2.9) | 0 |
AE = adverse event, IVRS = interactive voice response system, NR = not reported, SAE = serious adverse event.
aThe most common AEs included those reported in ≥ 10% of patients from the CARE1 Part B or CARE2 studies.
bIncidence of status epilepticus reported as an AE by the investigator may differ from the number of events of status epilepticus reported by patient caregivers using the IVRS.
cThose reported in ≥ 2% of patients in any group in any trial.
Sources: CARE138 and CARE239 Clinical Study Reports.
Critical Appraisal
Internal Validity
Both the CARE1 Part B and CARE2 studies are RCTs investigating the efficacy of cannabidiol compared with placebo. They both involved a randomization process that was properly implemented, ensuring an overall balanced distribution of participants to either the cannabidiol or placebo arms, reassured by the balanced distribution of the baseline characteristics among participants in the studies. There were some observed baseline imbalances in both studies. However, these were judged to have a low risk of introducing bias or to have suggested problems in the randomization process. The randomization lists from both studies were also properly generated and the allocation was successfully concealed from investigators and patients. The HRQoL assessment applied only to patients aged 4 years or older; however, since the randomization was stratified by age group, prognostic balance was likely to have been maintained for this subpopulation.
Both studies provided ground for patients to maintain good adherence to the intended interventions, confirmed by the flow of participants throughout the studies showing no important imbalances in the adherence to cannabidiol. There were, however, some imbalances observed in the use of different cointerventions. Although these possible deviations could introduce bias, the impact and direction of the bias on the outcomes of interest are uncertain. Although some modifying effects were observed (i.e., use of stiripentol and clobazam and geographical location), the low number of patients across subgroups in both studies warrants caution for stating any credible effect modification resulting from any of these variables. Further, the subgroup analyses were not adjusted for multiple comparisons, so there is an increased risk of type I error (false-positive results) for statistically significant findings.
There were no instances of meaningful missing outcome data. The low number of patients who were lost to follow-up as well as the low number of changes in doses or withdrawals confirm the completeness of the analysis, thus reducing the risk of bias in this domain. This is in addition to an ITT analysis of those patients with complete information.
In both studies, measurements of the outcomes were appropriate. Convulsive seizures are objective end points to measure by both clinicians and patients. Some nonconvulsive seizures may be challenging to detect and may lead to measurement error; however, the magnitude of this error is difficult to determine. The blinding of participants and clinical investigators that was maintained throughout the studies mitigates potential biases in this domain. Only a small difference in the mean number of patient-days of treatment was noticed in the 20 mg/kg/day cannabidiol group of the CARE2 study due to AEs, which could have opened the possibility of patients and clinicians knowing they were receiving the intervention. Similarly, other AEs such as somnolence and appetite changes may have signalled to patients and caregivers which treatment they were receiving.
The results were reported in accordance with predefined protocols, reducing the likelihood of selective reporting bias. Overall, both studies demonstrated adherence to methodological consistency and minimized risks across all of the domains that were assessed for risk of bias for most outcomes when comparing cannabidiol with placebo.
Several secondary end points depicting statistically significant results lacked multiplicity control (refer to Table 15), carrying a higher risk of false-positives; hence, cautious interpretation is needed due to potential random errors.
External Validity
Overall, patients included in the CARE1 Part B and CARE2 trials had baseline characteristics and prognostic factors that were similar to those encountered in the population of people in Canada with DS, according to the clinical experts consulted by CADTH. There were some concerns of uncertainty on the applicability of the results to adult populations older than 18 years of age, since no patients older than 18 years were included in either trial. According to the clinical experts consulted by CADTH, it is unlikely that the response observed in the CARE1 Part B and CARE2 studies would be different in terms of beneficial effects and possible harms; however, there are no trial data to confirm whether the efficacy and safety of cannabidiol would be equivalent in adults. As such, the generalizability of the data from the CARE1 Part B and CARE2 trials to adults older than 18 years of age is uncertain. Given that the severity and frequency of seizures differs between children and adults, the comparative efficacy of cannabidiol compared with usual care could differ between these groups; hence, any effect remains uncertain.
It is unknown whether the results can be generalized to patients with fewer than 4 seizures per month, since patients with such characteristics were not included in these studies.
The CARE1 Part B and CARE2 trials excluded patients using medicinal cannabis or synthetic cannabinoid-based medications and transitioning to cannabidiol (pharmaceutical). This would be a common situation in Canada, as noted by the drug programs. The clinical experts suggested that while this is an important consideration, it would not affect the generalizability of the results in such patients once they stop using other forms of medicinal cannabis.
The question as to whether cannabidiol is more efficacious than the other treatment available in Canada for patients with DS (i.e., stiripentol) when added to standard of care is still uncertain. There is no head-to-head comparison of cannabidiol against stiripentol. Furthermore, the standard-of-care treatments commonly used in patients with DS vary and make it difficult to assess this question using indirect comparison, since such differences may include issues of inconsistency or intransitivity. With the lack of head-to-head comparisons and the current evidence at hand, it is difficult to draw a strong conclusion on this issue.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined, as outlined by the GRADE Working Group.43,44
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of the evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
The GRADE assessments included an evaluation of the main outcomes considered important by clinicians, patient groups, and stakeholders. The comparisons evaluated in the GRADE assessments of this report were that of cannabidiol 10 mg/kg/day against placebo and cannabidiol 20 mg/kg/day versus placebo. In Table 2 and Table 3, we present the GRADE summary of findings, respectively, for each comparison.
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
To inform the long-term safety and tolerability of cannabidiol as an adjunctive treatment in children and adults with inadequately controlled DS, a summary of the results of 1 sponsor-conducted OLE study,45 GWPCARE5 (hereafter referred to as the CARE5 study), is provided subsequently.
The CARE5 trial was a multicentre, OLE study for patients with DS or LGS who had completed the double-blind, placebo-controlled, clinical studies of cannabidiol (the CARE1, CARE2, CARE3, and CARE4 trials). The objective of the CARE5 OLE study was to evaluate the long-term safety and tolerability and the effect on seizures of cannabidiol as adjunctive treatment in children and adults with inadequately controlled DS. The secondary objectives of the CARE5 OLE were to evaluate the effect of cannabidiol as adjunctive treatment on quality of life, adaptive behaviour, need for hospitalization due to epilepsy, usage of rescue medication, maintenance of seizure frequency reduction and freedom from seizures during the OLE study, frequency of total seizures, change in duration of subtypes of seizures, number of episodes of status epilepticus, growth and development, menstruation cycles (in females), and signals indicating drug abuse liability of cannabidiol. For patients with DS only, the effect on convulsive-seizure frequency, nonconvulsive-seizure frequency, number of participants who were convulsive seizure–free, and responder rate (defined in terms of percentage reduction in convulsive-seizure frequency) were also evaluated. The following information focuses on the patients with DS enrolled in the CARE5 study who had completed the CARE1 and CARE2 studies.
The study consisted of a titration period and a maintenance period followed by a 10-day taper period. During the 10 days of the titration period, all participants titrated up to 10 mg/kg/day to 20 mg/kg/day of cannabidiol. Thereafter, patients entered the maintenance period where the optimal dosage was maintained (although increases or decreases could occur if there was intolerance or seizures were not optimally controlled). Following the end-of treatment visit or withdrawal, the doses of the IMP were down-titrated at home (10% per day for 10 days) until the end-of-taper period visit.
The baseline period was defined as the 28-day period of the original study from screening to randomization, while the treatment period was defined as day 1 to the day of the last dose up to and including the end-of-treatment visit.
Populations
Patients who completed all scheduled visits in the treatment phase of the CARE1 and CARE2, CARE3, or CARE4 studies were included. Those who used cannabis or cannabinoid-based medication, had a history of postural hypotension symptoms, had a history of suicidal behaviour, had been part of a clinical trial involving an IMP, were of child-bearing potential as a patient or partner of the patient, were pregnant, had any disease or abnormalities that put them at risk, were unwilling to abstain from blood donation during the trial, or had impaired hepatic function were excluded.
Interventions
The CARE5 study consisted of a titration period and a maintenance period followed by a 10-day taper period. Participants could receive treatment for up to a maximum of 6 years (312 weeks after visit 1), depending on the country. Cannabidiol was to be taken twice daily (morning and evening) immediately after the patient’s usual ASM administration or as otherwise specified by the investigator. All patients were titrated up to 10 mg/kg/day to 20 mg/kg/day of cannabidiol. If there was intolerance during titration, the patient was maintained on a dose below 10 mg/kg/day to 20 mg/kg/day.
Patients were titrated up to 10 mg/kg/day to 20 mg/kg/day and then remained at this dose until the end-of-treatment visit, with the option for doses to be increased (up to a maximum of 30 mg/kg/day) or decreased, if deemed necessary by the investigator. Following the end-of-treatment visit, the doses of the IMP were down-titrated at home (10% per day for 10 days) until the end-of-taper period visit.
Outcomes
A summary of outcomes reported in the CARE5 study that were relevant to this review is presented in Table 17.
The safety of cannabidiol was assessed by the AE profile and by evaluating changes in the following, relative to the prerandomization baseline of the original study: vital signs, physical examination (including height and body weight), electrocardiograms (ECGs), Columbia-Suicide Severity Rating Scale (C-SSRS) score, Cannabis Withdrawal Scale score or Pediatric Cannabis Withdrawal Scale score, and clinical laboratory parameters. Participants aged 18 years and older were administered the Cannabis Withdrawal Scale, while participants aged 4 to 17 years (inclusive) were administered the Pediatric Cannabis Withdrawal Scale. The children’s C-SSRS was used for participants aged 6 to 18 years (inclusive), while the C-SSRS was used for participants aged 19 years and older.
Baseline Characteristics
The baseline demographic and clinical characteristics of the CARE5 OLE study for patients with DS (safety analysis set) are summarized in Table 18.
Table 17: Summary of Outcomes in the CARE5 Study
Outcome measure | Time point | Type of end point |
|---|---|---|
AE profile: Change in vital signs, physical examination findings, ECG result, C-SSRS score, CWS or PCWS score, and clinical laboratory parameters relative to the baseline prerandomization results from the original study | For vital signs, physical exam, ECG, and clinical laboratory parameters: Every visit window from visit 1 (day 1) to end-of-taper visit (± 3 days) or end-of-treatment visit (laboratory parameters) For C-SSRS: Visit 1 (day 1) and every visit window from visit 5 (24 weeks ± 7 days) to end-of-taper visit (± 3 days) CWS or PCWS score: End-of-taper visit (± 3 days), safety call (2 weeks after end-of-taper visit), and follow-up visit (± 3 days) | — |
Change in quality of life (QOLCE if 18 years of age or younger; QOLIE if 19 years of age or older) relative to the baseline prerandomization results from the original study, if assessed | Visit 1 (day 1) and every visit window from visit 5 (24 weeks ± 7 days) to end-of-treatment visit | Secondary |
Change in number of inpatient epilepsy-related hospitalizations relative to the prerandomization baseline from the original study, if assessed | Every visit window from visit 1 (day 1) to follow-up visit (± 3 days) | Secondary |
Change in the use of rescue medication relative to the prerandomization baseline from the original study | Every visit window from visit 1 (day 1) to follow-up visit (± 3 days) | Secondary |
Maintenance of reduction in seizure frequency and freedom from seizures | Every visit window from visit 1 (day 1) to follow-up visit (± 3 days) | Secondary |
Percentage change in the frequency of total seizures relative to the prerandomization baseline from the original study | Every visit window from visit 1 (day 1) to follow-up visit (± 3 days) | Secondary |
Change in the number of episodes of status epilepticus relative to the prerandomization baseline from the original study | Every visit window from visit 1 (day 1) to follow-up visit (± 3 days) | Secondary |
Percentage change in total convulsive-seizure frequency, relative to the prerandomization baseline from the original study | Every visit window from visit 1 (day 1) to follow-up visit (± 3 days) | Secondary |
AE = adverse event; CWS = Cannabis Withdrawal Scale; C-SSRS = Columbia-Suicide Severity Rating Scale; ECG = electrocardiogram; IGF-1 = insulin-like growth factor; PCWS = Pediatric Cannabis Withdrawal Scale; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE = Quality of Life in Epilepsy.
aSince the CARE1 and CARE2 studies only enrolled patients aged 2 to 18 years, no patients with Dravet syndrome were eligible to complete the QOLIE questionnaire.
Source: CARE5 Clinical Study Report.45
Table 18: Summary of Baseline Characteristics in the CARE5 Study (Safety Analysis Set)
Characteristic | CARE5 study dravet syndrome, cannabidiol 10 mg/kg/day to 20 mg/kg/day (N = 315) |
|---|---|
Age (years) | |
n | 315 |
Mean (SD) | 9.7 (4.4) |
Median | 9.3 |
Range | 2.5 to 19.3 |
Age group, n (%) | |
2 to 5 years | 82 (26.0) |
6 to 11 years | 134 (42.5) |
12 to 17 years | 90 (28.6) |
18 to 55 years | 9 (2.9) |
Sex, n (%) | |
Female | 159 (50.5) |
Male | 156 (49.5) |
Race, n (%) | |
White or Caucasian | 269 (85.4) |
Black or African American | 10 (3.2) |
American Indian or Alaska Native | 1 (0.3) |
Asian | 6 (1.9) |
Not applicable | 15 (4.8) |
Other | 14 (4.4) |
Region, n (%) | |
US | 176 (55.9) |
Rest of the world | 139 (44.1) |
Weight at baseline (kg) | |
n | 308 |
Mean (SD) | 34.0 (17.1) |
Median | 28.0 |
Range | 10.5 to 133.4 |
Height at baseline (cm) | |
n | 307 |
Mean (SD) | 131.2 (22.3) |
Median | 129.0 |
Range | 88.3 to 189.0 |
BMI at baseline (kg/m2) | |
n | 307 |
Mean (SD) | 18.7 (4.5) |
Median | 17.3 |
Range | 11.4 to 44.3 |
Number of ASMs currently being taken by patients | |
n | 315 |
Mean (SD) | 3.2 (1.1) |
Median | 3.00 |
Range | 1.0 to 8.0 |
Number of patients taking an ASM, n (%) | |
Clobazam | 215 (68.3) |
Valproic acid | 218 (69.2) |
Lamotrigine | 8 (2.5) |
Levetiracetam | 92 (29.2) |
Rufinamide | 15 (4.8) |
Topiramate | 83 (26.3) |
Felbamate | 14 (4.4) |
ASM = antiseizure medication; BMI = body mass index; SD = standard deviation.
Source: CARE5 Clinical Study Report.45
Statistical Analysis
All data collected during this study were summarized across time. Changes from baseline were also presented where data from the original studies were available. This included seizure information, C-SSRS assessments, quality-of-life assessments, and other measures of safety (e.g., vital signs, clinical laboratory samples). Descriptive statistical methods were used throughout. There was no formal hypothesis testing.
The safety analysis set is the only analysis set in this study and included all patients who received at least 1 dose of IMP in the study.
For the seizure outcomes, when a patient withdrew after they had taken their first dose in the OLE, seizure frequencies were calculated from the data available before the patient withdrawing. The last observation carried forward methodology was used to impute missing data.
Results
Patient Disposition
Patient disposition for the CARE5 OLE study (safety analysis set) is summarized in Table 19.
Exposure to Study Treatments
Exposure information for the CARE5 OLE study (safety analysis set) is described in Table 20.
Table 19: Patient Disposition (Safety Analysis Set)
Patient disposition | CARE5 study cannabidiol 10 mg/kg/day to 20 mg/kg/day (N = 315) |
|---|---|
Total patients screened, N | 681 |
Total patients enrolled, N (%) | 681 (100.0) |
Patients with DS enrolled in treatment phase, N (%)a | 315 (100.0) |
Completed, n (%)a | 170 (54.0) |
Withdrawn, n (%)a | 145 (46.0) |
Reason for discontinuing from treatment phase, n (%)a | |
AE | 26 (8.3) |
Lost to follow-up | 2 (0.6) |
Met withdrawal criteria | 5 (1.6) |
Withdrawal by patient or parent or guardian | 62 (19.7) |
Withdrawn by the investigator | 23 (7.3) |
Other | 27 (8.6) |
Continued to the taper phase, n (%)a | |
No | 233 (74.0) |
Yes | 82 (26.0) |
Completed | 76 (92.7) |
Withdrawn | 3 (3.7) |
Not reported | 3 (3.7) |
Reason for discontinuing from taper phase, n (%)a | |
AE | 1 (1.2) |
Withdrawal by participant or parent or guardian | 0 (0.0) |
Other | 2 (2.4) |
AE = adverse event; DS = Dravet syndrome.
aOnly patients with DS were included in these counts.
Source: CARE5 Clinical Study Report.45
Table 20: Patient Exposure in the CARE5 Study (Safety Analysis Set)
Exposure | CARE5 study cannabidiol 10 to 20 mg/kg/day (N = 315) |
|---|---|
Total planned patient-weeks | NR |
Duration, mean patient-days (SD) | 638.8 (462.0) |
Duration, median patient-days (range) | 444.0 (18 to 1,822) |
Adherence, % | NRa |
NR = not reported; SD = standard deviation.
aThe study tracked adherence to study intervention rather than adherence. The CARE5 Clinical Study Report contains individual patient-level data on compliance and/or drug concentration data.
Source: CARE5 Clinical Study Report.45
All 315 patients with DS (100%) took 1 or more concomitant ASMs during the study. The most common classes of ASMs (i.e., reported in > 50% of patients overall) used concomitantly by patients with DS were other antiepileptics, which were used by 266 participants (84.4%); benzodiazepine derivatives, which were used by 254 participants (80.6%); and fatty acid derivatives, which were used by 218 participants (69.2%). The most commonly used ASMs by patients with DS were valproic acid, used by 218 participants (69.2%); clobazam, used by 215 participants (68.3%); stiripentol, used by 120 participants (38.1%); and levetiracetam, used by 92 participants (29.2%).
Efficacy
The efficacy values of the CARE5 study are presented in Table 21.
Table 21: Summary of Key Efficacy Outcomes in the CARE5 Study (Safety Analysis Set)
Variables | CARE5 study cannabidiol 10 mg/kg/day to 20 mg/kg/day (N = 315) |
|---|---|
Change in the frequency of total seizures | |
Baseline period, n | 291 |
Baseline period, median (Q1, Q3) | 36.0 (10.6, 194.1) |
Treatment period (week 1 to 12), n | 288 |
Treatment period (week 1 to 12), median (Q1, Q3) | 13.3 (4.1, 78.9) |
Treatment period (week 37 to 48), n | 214 |
Treatment period (week 37 to 48), median (Q1, Q3)a | 12.5 (3.4, 67.2) |
Median percentage change from baseline (Q1, Q3) | –62.6 (–87.7, –6.4) |
Number of patients who were seizure free (week 37 to 48)a | 13 |
Response rates for total seizure frequency (week 37 to 48) | |
Number of patients | 214 |
≥ 50% reduction, n (%) | 127 (59.3) |
≥ 75% reduction, n (%) | 85 (39.7) |
100% reduction, n (%) | 13 (6.1) |
Change in the frequency of convulsive seizures | |
Baseline period, n | 291 |
Baseline period, median (Q1, Q3) | 12.4 (6.3, 33.4) |
Treatment period (week 1 to 12), n | 288 |
Treatment period (week 1 to 12), median (Q1, Q3) | 7.3 (2.9, 16.6) |
Treatment period (week 37 to 48), n | 214 |
Treatment period (week 37 to 48), median (Q1, Q3)a | 6.6 (2.0, 20.0) |
Median percentage change from baseline (Q1, Q3) | –54.2 (–83.1, –10.1) |
Number of convulsive seizure–free patients (week 37 to 48)a | 17 |
Responder rates for convulsive-seizure frequency (week 37 to 48) | |
Number of patients | 214 |
≥ 25% reduction, n (%) | 145 (67.8) |
≥ 50% reduction, n (%) | 112 (52.3) |
≥ 75% reduction, n (%) | 74 (34.6) |
100% reduction, n (%) | 17 (7.9) |
Change in the number of episodes of status epilepticus | |
Number of patients with convulsive seizures greater than 30 minutes in duration | |
Baseline period, n (%) | 14 (4.8) |
Treatment period (week 1 to 12), n (%) | 14 (4.9) |
Treatment period (week 37 to 48), n (%)a | 6 (2.8) |
Number of patients with nonconvulsive seizures greater than 30 minutes in duration | |
Baseline period, n (%) | 21 (7.2) |
Treatment period (week 1 to 12), n (%) | 9 (3.1) |
Treatment period (week 37 to 48), n (%)a | 6 (2.8) |
Change from baseline in QOLCE scores at last visitc | |
Overall quality-of-life score, n | 254 |
Core study baseline, mean (SD) | 43.2 (13.3) |
Last visit, mean (SD) | 47.9 (15.0) |
Change from baseline, mean (SD) | 4.6 (15.0) |
Inpatient hospitalizations due to epilepsy at last visit | |
Number of inpatient hospitalizations due to epilepsy since previous visit (%) | 14 (4.4) |
Use of rescue medications | |
Number of participants taking rescue medications (%) | 254 (80.6) |
Q1 = lower quartile; Q3 = upper quartile; QOLCE = Quality of Life in Childhood Epilepsy; SD = standard deviation.
aEfficacy results for time points up to weeks 253 to 264 are available in the CARE5 Clinical Study Report.
bCombined caregiver and patient scores are reported.
cQuestionnaire data reported for patients aged 2 to 18 years.
Source: CARE5 Clinical Study Report.45
Change in the Frequency of Total Seizures
During weeks 37 to 48 of treatment, patients with DS experienced a median percentage change from their original study baseline of –62.6% in total seizure frequency (interquartile range, –87.7 to –6.4).
Responder Rates for Total Seizure Frequency
The proportion of patients who achieved a 50% or greater reduction in total seizure frequency during weeks 37 to 48 of treatment was 59.3%. Out of all patients with DS, 70.1% experienced a 25% or greater reduction in total seizure frequency, 39.7% experienced a 75% or greater reduction in total seizure frequency, and 6.1% experienced total seizure freedom.
Change in the Frequency of Convulsive Seizures
During weeks 37 to 48 of treatment, patients with DS experienced a median percentage change from their original study baseline of –54.2% (interquartile range, –83.1 to –10.1) in convulsive-seizure frequency.
Responder Rates for Convulsive-Seizure Frequency
The proportion of patients who achieved a 50% or greater reduction in convulsive-seizure frequency during weeks 37 to 48 of treatment was 52.3%. Out of all patients with DS, 67.8% experienced a 25% or greater reduction in the frequency of convulsive seizures, 34.6% experienced a 75% or greater reduction in the frequency of convulsive seizures, and 7.9% experienced convulsive-seizure freedom (100% reduction).
Change in the Number of Episodes of Status Epilepticus
During the last 12 weeks of treatment, 4.5% of patients with DS reported convulsive seizures greater than 30 minutes in duration compared with 4.8% during the original study baseline. The proportion of patients with DS with nonconvulsive seizures greater than 30 minutes in duration during the last 12 weeks of treatment was 4.8% compared with 7.2% during the original study baseline.
Inpatient Hospitalizations Due to Epilepsy at Last Visit
During the study, 16 patients (6.4%) had 1 or more inpatient hospitalizations due to epilepsy.
Use of Rescue Medications
During the study, 258 patients (70.5%) were recorded as taking rescue medications.
Harms
A total of 306 patients with DS (97.1%) had 1 or more AEs during the study, with 71 patients (22.5%) reporting AEs of mild severity, 157 patients (49.8%) reporting AEs of moderate severity, and 78 patients (24.8%) reporting severe AEs. SAEs were reported for 133 patients (42.2%) with DS, with the most common SAEs experienced being status epilepticus, convulsion, and pneumonia. Twenty-eight patients (8.9%) with DS stopped treatment due to AEs. The most common AEs leading to discontinuation were convulsion, increased AST, and increased ALT. A total of 6 patients (1.9%) with DS died during the study, 4 (1.3%) due to SUDEP, and 1 (0.3) each due to drowning and convulsion (Table 22).
Table 22: Summary of Harms Results From CARE5 (Safety Analysis Set)
Adverse events | CARE5 study cannabidiol 10 mg/kg/day to 20 mg/kg/day (N = 315) |
|---|---|
≥ 1 adverse event | 306 (97.1) |
Most common adverse events,a n (%) | |
Blood and lymphatic system disorders | 21 (6.7) |
Anemia | 6 (1.9) |
Gastrointestinal disorders | 192 (61.0) |
Diarrhea | 135 (42.9) |
Vomiting | 63 (20.0) |
Constipation | 20 (6.3) |
Nausea | 16 (5.1) |
Abdominal pain upper | 11 (3.5) |
General disorders and administration site conditions | 162 (51.4) |
Pyrexia | 124 (39.4) |
Fatigue | 39 (12.4) |
Gait disturbance | 12 (3.8) |
Asthenia | 10 (3.2) |
Infections and infestations | 229 (72.7) |
Upper respiratory tract infection | 78 (24.8) |
Nasopharyngitis | 78 (24.8) |
Sinusitis | 38 (12.1) |
Pneumonia | 35 (11.1) |
Ear infection | 35 (11.1) |
Influenza | 37 (11.7) |
Urinary tract infection | 19 (6.0) |
Pharyngitis streptococcal | 26 (8.3) |
Gastroenteritis viral | 15 (4.8) |
Otitis media | 21 (6.7) |
Bronchitis | 15 (4.8) |
Viral upper respiratory tract infection | 11 (3.5) |
Viral infection | 12 (3.8) |
Pharyngitis | 15 (4.8) |
Gastroenteritis | 16 (5.1) |
Conjunctivitis | 5 (1.6) |
Respiratory tract infection | 13 (4.1) |
Injury, poisoning, and procedural complications | 80 (25.4) |
Fall | 22 (7.0) |
Laceration | 8 (2.5) |
Contusion | 15 (4.8) |
Skin abrasion | 2 (0.6) |
Investigations | 126 (40.0) |
Weight decreased | 21 (6.7) |
Alanine aminotransferase increased | 37 (11.7) |
Aspartate aminotransferase increased | 38 (12.1) |
Gamma glutamyltransferase increased | 32 (10.2) |
Liver function test abnormal | 13 (4.1) |
Weight increased | 5 (1.6) |
Metabolism and nutrition disorders | 127 (40.3) |
Decreased appetite | 99 (31.4) |
Dehydration | 8 (2.5) |
Increased appetite | 8 (2.5) |
Nervous system disorders | 214 (67.9) |
Convulsion | 79 (25.1) |
Somnolence | 87 (27.6) |
Status epilepticus | 47 (14.9) |
Lethargy | 21 (6.7) |
Headache | 18 (5.7) |
Sedation | 16 (5.1) |
Drooling | 11 (3.5) |
Balance disorder | 9 (2.9) |
Tremor | 14 (4.4) |
Psychiatric disorders | 108 (34.3) |
Abnormal behaviour | 34 (10.8) |
Insomnia | 16 (5.1) |
Irritability | 26 (8.3) |
Aggression | 20 (6.3) |
Agitation | 9 (2.9) |
Sleep disorder | 12 (3.8) |
Renal and urinary disorders | 17 (5.4) |
Respiratory, thoracic, and mediastinal disorders | 98 (31.1) |
Cough | 42 (13.3) |
Nasal congestion | 13 (4.1) |
Rhinorrhea | 20 (6.3) |
Pneumonia aspiration | 4 (1.3) |
Hypoxia | 2 (0.6) |
Oropharyngeal pain | 12 (3.8) |
Epistaxis | 13 (4.1) |
Acute respiratory failure | 3 (1.0) |
Upper respiratory tract congestion | 2 (0.6) |
Skin and subcutaneous tissue disorders | 51 (16.2) |
Rash | 14 (4.4) |
Alopecia | 10 (3.2) |
Erythema | 1 (0.3) |
Most common SAEs,b n (%) | |
Patients with ≥ 1 SAE | 133 (42.2) |
Gastrointestinal disorders | 6 (1.9) |
General disorders and administration site conditions | 24 (7.6) |
Pyrexia | 17 (5.4) |
Infections and infestations | 54 (17.1) |
Pneumonia | 20 (6.3) |
Influenza | 7 (2.2) |
Urinary tract infection | 1 (0.3) |
Investigations | 18 (5.7) |
Aspartate aminotransferase increased | 10 (3.2) |
Alanine aminotransferase increased | 7 (2.2) |
Nervous system disorders | 82 (26.0) |
Status epilepticus | 47 (14.9) |
Convulsion | 34 (10.8) |
Respiratory, thoracic, and mediastinal disorders | 11 (3.5) |
Pneumonia aspiration | 4 (1.3) |
Acute respiratory failure | 1 (0.3) |
Respiratory failure | 2 (0.6) |
Patients who stopped treatment due to adverse events,c n (%) | |
Patients who stopped | 28 (8.9) |
Gastrointestinal disorders | 5 (1.6) |
Vomiting | 1 (0.3) |
Investigations | 14 (4.4) |
Alanine aminotransferase increased | 7 (2.2) |
Aspartate aminotransferase increased | 8 (2.5) |
Hepatic enzyme increased | 1 (0.3) |
Liver function test abnormal | 3 (1.0) |
Nervous system disorders | 12 (3.8) |
Convulsion | 8 (2.5) |
Somnolence | 1 (0.3) |
Deaths, n (%) | |
Patients who died | 6 (1.9) |
General disorders and administration site conditions | 5 (1.6) |
Sudden unexplained death in epilepsy | 4 (1.3) |
Drowning | 1 (0.3) |
Nervous system disorders | 1 (0.3) |
Convulsion | 1 (0.3) |
Adverse events of special interest, n (%) | |
Patients with adverse events of special interest | NR |
SAE = serious adverse event.
aMost common adverse events included those reported in > 10% of patients in any treatment group from the CARE5 study.
bMost common SAEs included those reported in ≥ 2% of patients in any treatment group from the CARE5 study.
cMost common adverse events leading to discontinuation of the investigational medicinal product included those reported in > 1% of patients in any treatment group from the CARE5 study.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence and the CARE5 Clinical Study Report.45
Critical Appraisal
Internal Validity
The CARE5 study is a nonrandomized, open-label, single-arm extension study. The lack of a randomized comparator precludes the ability to draw strong conclusions regarding the long-term therapeutic benefits or safety of cannabidiol as an adjunctive therapy among patients with DS compared with other relevant therapies. It is also not possible to ascertain a causal relationship between cannabidiol and the observed effects.
Furthermore, the lack of blinding in the CARE5 study may affect the reporting of subjective measures such as patient-reported outcomes; the direction and magnitude of this potential bias cannot be ascertained. Moreover, only 54% of patients completed the study, so there is a risk of bias due to missing outcomes data. The median number of dosing days in the treatment phase for all participants was 444 days (range, 18 days to 1,822 days), which provided a longer follow-up time for assessment of AEs compared with the double-blind trials; however, the proportion of patients who adhered to the study drug during the longer follow-up was not reported. As such, it is not possible to determine whether there is a risk of bias due to deviations from the intended interventions.
External Validity
Completion of the CARE1 and CARE2 studies was an eligibility criterion for enrolment into the CARE5 study. As such, patients who discontinued from either the CARE1 or CARE2 study for any reason, such as AEs, withdrawal by patient or parent, or withdrawal by investigator, were excluded from the CARE5 study. Therefore, it is likely that the patients who were enrolled in the CARE5 study were those who tolerated cannabidiol better and/or had a more favourable response. The results may therefore not be generalized to all patients with DS who might be eligible for treatment with cannabidiol. Similar to the original trials, there were few patients older than 18 years of age; as such, it is not certain whether the results could be generalized to adults with DS. The outcomes reported included those that were identified as important by patients and clinicians.
Indirect Evidence
An indirect treatment comparison was not included in this submission. The reasoning provided by the sponsor was that usual care was considered the only appropriate comparator in the DS population. Patients with DS often cycle through numerous ASMs in attempts to control their seizures, but many have disease that is refractory to currently available ASMs and display heterogeneity in their response to therapies. The sponsor consulted clinical experts in Canada who confirmed that the usual care followed in the CARE trials is representative of Canadian clinical practice. Additionally, the sponsor formulated that in the real-world setting, cannabidiol will be administered as an add-on treatment. Therefore, the only comparator considered by the sponsor in this population was the established standard of care or clinical management. CADTH recognized that stiripentol is currently indicated for use in combination with clobazam and valproate to treat refractory generalized tonic-clonic seizures in patients with DS whose seizures are not adequately controlled with clobazam and valproate alone. The sponsor considered stiripentol to be a part of usual care; however, the efficacy and cost-effectiveness of cannabidiol compared with stiripentol is unknown due to a lack of published head-to-head comparisons. Indirect comparative evidence from the literature suggests that stiripentol may be associated with a higher seizure control rate than cannabidiol, but the certainty in the effect estimates remains to be determined due to the high heterogeneity in the comparisons assessed, increasing the possibility of intransitive assessments from a network meta-analysis.46
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the systematic review evidence were submitted by the sponsor.
Discussion
Summary of Available Evidence
The body of evidence informing this submission consists of 2 individual studies assessing cannabidiol as an adjunctive treatment in patients with DS. First, the pivotal CARE1 Part B study (N = 120 patients) evaluated cannabidiol 20 mg/kg/day against placebo in patients with DS. Second, the pivotal CARE2 study evaluated cannabidiol 20 mg/kg/day (n = 67) and cannabidiol 10 mg/kg/day (n = 67) therapy against a placebo group (n = 65). All patients in these studies were younger than 18 years of age and were receiving multiple therapies for controlling their seizures.
A supplemental body of evidence was submitted in the form of a single-arm, long-term, OLE study (CARE5) to inform the long-term safety and tolerability of cannabidiol as an adjunctive treatment in children and adults with inadequately controlled DS. No evidence from indirect treatment comparisons or studies addressing gaps in the systematic review evidence were submitted by the sponsor.
Interpretation of Results
Efficacy
For patients with DS, the end points of the studies — reduction in convulsive and total seizure frequency — are highly valued outcomes, as are those related to HRQoL, sleep disruption, medication and hospital use, and harms. The clinical experts agreed with these considerations and deemed these end points to be key factors that would inform their decisions in clinical practice.
Comparison of Cannabidiol 10 mg/kg/day Against Placebo
The reduction in the frequency of convulsive seizures (measured as number of seizures per month and then as either the percentage change from baseline or as the proportion of patients achieving a 50% or greater or 75% or greater reduction from baseline) was 1 of the main outcomes deemed relevant for decision-making. The CARE2 study (N = 131 patients) provided information on the 10 mg/kg/day dosage of cannabidiol. In this study, patients in the placebo arm had a 24.5% reduction in the frequency of seizures per month; in contrast, patients taking cannabidiol at 10 mg/kg/day had a reduction from baseline of 41.2%. This means that cannabidiol 10 mg/kg/day provides a 15.7% greater reduction than placebo. However, due to chance, this difference in reduction can go from a reduction of 31.3% to an increase of 3.7% (the 95% CI); this implies that the possible values still include a trivial effect.
Similarly, when evaluating the proportion of patients reaching a 50% or greater reduction from baseline in convulsive seizures, an improvement favouring cannabidiol was observed, although still with some uncertainty as to whether this effect can be clinically important due to imprecision in the effect estimate. For instance, in the placebo arm, 26.2% of patients reached the 50% or greater reduction threshold while, in the cannabidiol 10 mg/kg/day group, 43.9% of the patients reached this threshold (OR = 2.21; 95% CI, 1.06 to 4.62). Expressed as absolute effects, this means that 178 more patients per 1,000 treated with cannabidiol 10 mg/kg/day reached this threshold when compared with placebo; however, due to chance (the 95% CI), this number can go from 17 more patients per 1,000 (likely a trivial effect) to 338 more patients per 1,000 (a large effect). Since no MID for between-group difference could be obtained, the clinical experts consulted by CADTH considered that a difference between cannabidiol and placebo of at least 20 more patients per 1,000 achieving a 50% or greater reduction from baseline in convulsive seizures was considered a conservative threshold of meaningful clinical importance. Cannabidiol 10 mg/kg/day also had effects in increasing the control of convulsive seizures by 75% or more from baseline (deemed of higher certainty), and in increasing the number of convulsive seizure–free days by 2.4 days when compared with placebo. However, little to no difference was observed in the outcome of change in number of episodes of convulsive status epilepticus.
HRQoL was evaluated in 110 patients in the 10 mg/kg/day group of the CARE2 study and showed that cannabidiol provided improvement in the HRQoL measure, resulting in a QOLCE score that was 3.8 points higher compared with placebo, but the 95% CI was imprecise (0.1 lower to 7.8 higher), including the null effect. The clinical meaningfulness of this effect is uncertain also because no threshold of clinical benefit could be obtained.
Similarly, the ESS and the NRS 0 to 10 scores indicated the study did not provide evidence of differences between the cannabidiol and placebo arms in the sleep disruption outcome, an outcome considered relevant by patients and clinicians. Like HRQoL, thresholds of clinical importance were not possible to obtain; hence, the overall certainty for these end points was assessed based on any effect that would exclude the null. As a result, these end points were considered of low certainty due to imprecision.
The utilization of resources in the form of hospital and medication use was not meaningfully different between treatment with cannabidiol and placebo. The body of evidence also had uncertainty due to low sample size and no description of a specific effect estimate from the pivotal studies in both outcomes of resource utilization.
Comparison of Cannabidiol 20 mg/kg/day Against Placebo
Both the CARE1 Part B and CARE2 pivotal studies informed this comparison. Overall, the results were in agreement with the 10 mg/kg/day dose comparison against placebo, but with higher certainty on the effect estimates.
Reduction in convulsive-seizure frequency (measured as either the percentage change from baseline or as the proportion of patients achieving a 50% or greater or 75% or greater reduction from baseline) was the main outcome deemed relevant by experts for decision-making. Evidence from the 2 studies (N = 252 patients in total) showed that, on average, cannabidiol produces greater reductions from baseline in the frequency of seizures when compared with placebo, with cannabidiol 20 mg/kg/day providing 22.8% and 19.9% greater reductions from baseline than placebo in the CARE1 Part B and CARE2 studies, respectively.
Similarly, the proportion of patients reaching a 50% or greater reduction in seizures from baseline was higher in the intervention groups compared with the placebo group (CARE1 Part B study: OR = 2.0; 95% CI, 0.93 to 4.30; CARE2 study: OR = 2.74; 95% CI, 1.32 to 5.70). Compared with placebo, the number of patients who reached this threshold was 155 higher per 1,000 patients (from 13 fewer to 323 more patients) in the CARE1 Part B study and 231 more patients per 1,000 (from 71 more to 391 more patients) in the CARE2 study.
Similar effects were observed when assessing the outcome of a 75% or greater reduction in convulsive seizures from baseline, with an OR of 2.21 (95% CI, 0.82 to 5.95) in the CARE1 Part B study and an OR of 3.33 (75% CI, 1.01 to 10.92) in the CARE2 study. For the number of convulsive seizure–free days, total seizure frequency, and instances of convulsive status epilepticus, effect estimates in favour of cannabidiol were observed; however, the evidence was considered less certain due to imprecision in the effect estimates.
HRQoL was evaluated in 193 patients from both studies using the QOLCE score, where higher values imply better HRQoL. This was deemed a relevant outcome for clinicians and showed that cannabidiol provides a greater improvement in QOLCE score. However, the effect was considered imprecise due to a wide 95% CI ranging from a reduction to an increase in the scale points. The clinical meaningfulness of this effect is uncertain also because no MID or threshold of clinical benefit could be obtained.
The CARE1 Part B and CARE2 studies did not provide evidence of differences between the cannabidiol and placebo arms in sleep disruption outcomes in either the ESS or the NRS 0 to 10 scores, although the overall certainty was deemed low due to imprecision. When evaluating the utilization of resources in both pivotal studies, the rate of hospitalization and medication use was not meaningfully different between treatment and placebo. The body of evidence also had uncertainty due to imprecision (low sample size) from the pivotal studies.
CADTH could not establish enough evidence to support a dose-response effect of cannabidiol for any of the measured outcomes or harms due to the small number of observations and wide CIs. Although different effects between 20 mg/kg/day and 10 mg/kg/day were observed, the information is not sufficient to declare a dose response.
Other Considerations
CADTH recognizes that stiripentol is currently approved in Canada and indicated for use in combination with clobazam and valproate to treat refractory generalized tonic-clonic seizures in patients with DS whose seizures are not adequately controlled with these drugs alone. The sponsor considered stiripentol to be a part of usual care; however, clear evidence on the efficacy and cost-effectiveness of cannabidiol compared with stiripentol is lacking due to the absence of published head-to-head comparisons. Indirect comparative evidence from the literature suggests that stiripentol may be associated with a higher seizure control rate than cannabidiol,46 but the certainty in the effect estimates remains to be determined due to the high heterogeneity in the comparisons assessed in the published literature, increasing the possibility of intransitive assessments from a network meta-analysis.
Whether the effect estimates obtained from the body of evidence in this review can be generalized to adults older than 18 years of age remains uncertain, even though data from long-term observational studies and input from the clinical experts consulted by CADTH suggest that adults with DS might achieve comparable, adequate seizure control through the use of cannabidiol.
Harms
Cannabidiol, either as 10 mg/kg/day or 20 mg/kg/day, was generally well tolerated, with some of the AEs being of higher frequency in the 20 mg/kg/day group than in the 10 mg/kg/day and placebo groups. Some exceptions observed in certain events and investigations are noted subsequently.
In the cannabidiol 10 mg/kg/day versus placebo comparison, the proportion of patients with at least 1 AE was similar for the intervention when compared with the placebo group: 56 patients (87.5%) in the intervention arms versus 58 patients (89.2%) in the placebo group. Similarly, little difference was observed in the number of patients with at least 1 SAE, with 13 patients (20.3%) versus 10 patients (15.4%) in the intervention and placebo arms, respectively. A slight increase in the investigations of liver enzymes (ALT and/or AST) was observed in the CARE2 study, with 13 (20.3%) versus 8 (12.3) patients in the intervention and control groups undergoing these evaluations, respectively. According to the experts consulted by CADTH, these measurements are not a critical concern and typically do not necessitate additional assessment beyond routine checks. Also, the number of SAEs was slightly higher in the 10 mg/kg/day group (13 patients; 20.3%) versus placebo (10 patients; 15.4%), but the numbers were considered too small to draw definite conclusions.
In the 20 mg/kg/day versus placebo comparison, the proportion of patients with AEs increased in the CARE1 Part B study, with 57 patients (93.4%) and 44 patients (74.6%) having at least 1 AE in the intervention and placebo arms, respectively; this difference was not present in the CARE2 study. Looking at the most common AEs, more gastrointestinal disorders (diarrhea and vomiting), fatigue, pyrexia, somnolence, and investigations of liver enzymes were observed with the 20 mg/kg/day group versus placebo in both studies. Meanwhile, in total, SAEs were more common in the 20 mg/kg/day group, occurring in 10 patients (16.4%) and 3 patients (5.1%) in the CARE1 Part B study’s intervention and placebo arms, respectively, and in 17 patients (24.6%) and 10 patients (15.4%) in the CARE2 study. The clinical meaningfulness of these differences in AEs and SAEs is uncertain due to the relatively small number of patients assessed.
More harms of special interest occurred in the cannabidiol 20 mg/kg/day group when compared with the 10 mg/kg/day or placebo groups. Somnolence occurred in a total of 7 patients in the cannabidiol 20 mg/kg/day arms of both studies (5 in the CARE1 Part B study and 2 in the CARE2 study) while no events were reported in the placebo arms or in the 10 mg/kg/day arm (CARE2 study). Hypotonia, lethargy, and investigations of liver enzymes also followed this pattern. However, for all events of special interest, the numbers were considered too low to draw definite conclusions.
When comparing the cannabidiol 20 mg/kg/day dose with the 10 mg/kg/day dose and placebo, more discontinuations of the intervention due to AEs were observed with the 20 mg/kg/day dose than with the 10 mg/kg/day dose or placebo. This was also observed for some AEs, such as gastrointestinal disorders and somnolence.
The clinical experts and patient groups identified sudden death as an outcome of special interest to monitor. However, no deaths were reported in any of the pivotal studies. In the long term, open-label, single-arm CARE5 study, with a follow-up of up to 260 weeks, 6 deaths were reported among 315 patients (1.9%), 4 due to SUDEP.
Conclusion
The body of evidence informing the effects of cannabidiol on patients with DS consisted of 2 pivotal RCTs comparing cannabidiol (at doses of 10 mg/kg/day and 20 mg/kg/day) versus placebo, and 1 single-arm OLE study. Both pivotal studies inform the effects of cannabidiol on the outcomes of convulsive and total seizure control, HRQoL, sleep disruption, resource utilization, and AEs. All of these are considered by the clinical experts, patient groups, and stakeholders to be critical outcomes for decision-making.
The evidence shows that the use of cannabidiol, when compared with placebo, results in a greater reduction from baseline in the number of convulsive seizures. A greater proportion of patients using cannabidiol achieved reductions from baseline of 50% or more in the frequency of convulsive seizures, and 75% or more compared with placebo. Cannabidiol also likely provides beneficial albeit smaller improvement effects in the number of convulsive seizure–free days and in total seizure frequency. There is still uncertainty in the effects of cannabidiol on status epilepticus, HRQoL, sleep disruption, and use of rescue medications and hospital use.
Cannabidiol was generally well tolerated. However, the evidence suggests that cannabidiol may have more AEs and SAEs when compared with placebo, although there is uncertainty on the clinical significance of these differences to inform decision-making. The performance of cannabidiol against the other comparator used in Canada for patients with DS (i.e., stiripentol) is still uncertain, as no head-to-head comparison is available. Similarly, there is no evidence on the effects of cannabidiol as a first-line adjunctive treatment in patients older than 18 years of age, nor for its use in patients with DS who experience fewer seizures (i.e., fewer than 4 seizures per month).
Overall, the use of cannabidiol yields better estimates of seizure control with an adequate safety profile when compared with placebo. The effects on long-term outcomes of behaviour and HRQoL are still uncertain.
References
1.Wirrell EC, Hood V, Knupp KG, et al. International consensus on diagnosis and management of Dravet syndrome. Epilepsia. 2022;63(7):1761-1777. PubMed
2.Skluzacek JV, Watts KP, Parsy O, Wical B, Camfield P. Dravet syndrome and parent associations: the IDEA League experience with comorbid conditions, mortality, management, adaptation, and grief. Epilepsia. 2011;52 Suppl 2:95-101. PubMed
3.Shmuely S, Sisodiya SM, Gunning WB, Sander JW, Thijs RD. Mortality in Dravet syndrome: a review. Epilepsy Behav. 2016;64(Pt A):69-74.
4.Wirrell EC, Laux L, Donner E, et al. Optimizing the diagnosis and management of Dravet syndrome: recommendations from a North American consensus panel. Pediatr Neurol. 2017;68:18-34.e13. PubMed
5.Rosander C, Hallböök T. Dravet syndrome in Sweden: a population-based study. Dev Med Child Neurol. 2015;57(7):628-633. PubMed
6.Dravet Canada. What is Dravet? https://dravet.ca/what-is-dravet/. Accessed 2023 Jul 19.
7.Orpha.net. Dravet syndrome. 2021; https://www.orpha.net/en/disease/detail/33069#:~:text=Disease%20definition,with%20cognitive%20and%20motor%20impairment. Accessed 2023 Jul 11.
8.Dravet Canada. The core Dravet syndrome phenotype. Epilepsia. 2011;52 Suppl 2:3-9. PubMed
9.Ruthirago D, Julayanont P, Karukote A, Shehabeldin M, Nugent K. Sudden unexpected death in epilepsy: ongoing challenges in finding mechanisms and prevention. Int J Neurosci. 2018;128(11):1052-1060. PubMed
10.Auvin S, Damera V, Martin M, Holland R, Simontacchi K, Saich A. The impact of seizure frequency on quality of life in patients with Lennox-Gastaut syndrome or Dravet syndrome. Epilepsy Behav. 2021;123:108239. PubMed
11.Juandó-Prats C, James E, Bilder DA, et al. DRAVET ENGAGE. Parent caregivers of children with Dravet syndrome: perspectives, needs, and opportunities for clinical research. Epilepsy Behav. 2021;122:108198. PubMed
12.Brunklaus A, Ellis R, Reavey E, Forbes GH, Zuberi SM. Prognostic, clinical and demographic features in SCN1A mutation-positive Dravet syndrome. Brain. 2012;135(Pt 8):2329-2336. PubMed
13.Cross JH, Caraballo RH, Nabbout R, Vigevano F, Guerrini R, Lagae L. Dravet syndrome: treatment options and management of prolonged seizures. Epilepsia. 2019;60 Suppl 3:S39-s48. PubMed
14.Andrade DM, Berg AT, Hood V, et al. Dravet syndrome: a quick transition guide for the adult neurologist. Epilepsy Res. 2021;177:106743. PubMed
15.Schubert-Bast S, Kay L, Simon A, et al. Epidemiology, healthcare resource use, and mortality in patients with probable Dravet syndrome: a population-based study on German health insurance data. Epilepsy Behav. 2022;126:108442. PubMed
16.Strzelczyk A, Schubert-Bast S. Therapeutic advances in Dravet syndrome: a targeted literature review. Expert Rev Neurother. 2020;20(10):1065-1079. PubMed
17.Ontario Epilepsy Guidelines. Clinical guidelines for the management of epilepsy in adults and children, version 2.0. Toronto (ON): The Epilepsy Research Program of the Ontario Brain Institute; 2020: https://clinictocommunity.ca/wp-content/uploads/2021/01/ManagementGuidelines_Nov2020.pdf. Accessed 2023 May 08.
18.Strzelczyk A, Schubert-Bast S. A practical guide to the treatment of Dravet syndrome with anti-seizure medication. CNS Drugs. 2022;36(3):217-237. PubMed
19.Cardenal-Muñoz E, Auvin S, Villanueva V, et al. Guidance on Dravet syndrome from infant to adult care: road map for treatment planning in Europe. Epilepsia Open. 2022;7(1):11-26. PubMed
20.Jazz Pharmaceuticals Inc. Data on File. Canadian Clinical Expert Survey. 2023 [sponsor provided reference].
21.Diacomit (stiripentol): 250 mg and 500 mg oral capsules, or 250 mg and 500 mg oral powder for suspension [product monograph]. Newmarket (ON): Biocodex Canada Inc.; 2021 Jul 14: https://pdf.hres.ca/dpd_pm/00062850.PDF. Accessed 2023 Nov 20.
22.Health Canada. Summary basis of decision (SBD) for Diacomit. 2021; https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?linkID=SBD00181. Accessed 2023 Jul 19.
23.National Institute for Health and Care Excellence. Epilepsies in children, young people and adults. (NICE guideline NG217) 2022; https://www.nice.org.uk/guidance/ng217. Accessed 2023 Dec 18.
24.Epidiolex (cannabidiol): 100 mg/mL, oral solution [product monograph]. Cambridge (UK): GW Research Ltd.; 2023 Nov 15: https://pdf.hres.ca/dpd_pm/00073344.PDF. Accessed 2023 Nov 20.
25.Apo-Valproic Acid (valpric acid capsules): 250 mg oral capsules; Valproic Acid Oral Solution (valproic acid oral solution): 250 mg/5 mL valproic acid (as sodium valproate), oral solution [product monograph]. Toronto (ON): Apotex Inc.; 2023 Oct 05: https://pdf.hres.ca/dpd_pm/00072687.PDF. Accessed 2023 Oct 25.
26.Apo-Clonazepam (clonazepam): 10 mg, oral tablets [product monograph]. Toronto (ON): Apotex Inc.; 2021 May 06: https://pdf.hres.ca/dpd_pm/00060946.PDF. Accessed 2023 Oct 25.
27.Ach-Levetiracetam (levetiracetam): 250 mg, 500 mg, and 750 mg oral tablets [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2023 Aug 10: https://pdf.hres.ca/dpd_pm/00072037.PDF. Accessed 2023 Oct 25.
28.Ach-Topiramate (topiramate): 25 mg, 100 mg, and 200 mg oral tablets [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2022 Dec 12: https://pdf.hres.ca/dpd_pm/00068700.PDF. Accessed 2023 Oct 25.
29.Apo-Clonazepam (clonazepam tablets): 0.5 mg and 2 mg, oral tablets [product monograph]. Toronto (ON): Apotex Inc.; 2023 Sep 15: https://pdf.hres.ca/dpd_pm/00072497.PDF. Accessed 2023 Oct 25.
30.Banzel (rufinamide): 100 mg, 200 mg and 400 mg, oral tablets [product monograph]. Mississauga (ON): Eisai Limited; 2020 Oct 14: https://pdf.hres.ca/dpd_pm/00058487.PDF. Accessed 2023 Oct 25.
31.Cross H, Vyas K, Sahebkar F, Schreiber A, Mazurkiewicz-Beldzinska A. Abstract 137: Cannabidiol (CBD) in patients with Lennox-Gastaut syndrome (LGS) and Dravet syndrome (DS) on a ketogenic diet therapy (KDT) in four phase 3 trials. Virtual Congress: 34th International Epilepsy Congress; 2021 Aug 28 - Sep 01.
32.Devinsky O, Cross JH, Laux L, et al. Trial of cannabidiol for drug-resistant seizures in the Dravet syndrome. N Engl J Med. 2017;376(21):2011-2020. PubMed
33.Madan Cohen J, Checketts D, Dunayevich E, et al. Time to onset of cannabidiol treatment effects in Dravet syndrome: analysis from two randomized controlled trials. Epilepsia. 2021;62(9):2218-2227. PubMed
34.Mazurkiewicz-Beldzinska M, Privitera M, Marsh E, et al. Time to onset of efficacy of cannabidiol (CBD) during titration in patients with Lennox-Gastaut syndrome and Dravet syndrome enrolled in three randomized controlled trials (S48.009). Neurology. 2019;92:S48.009.
35.Nabbout R, Bhathal H, Zolnowska M, et al. Abstract 245: Diarrhoea in patients with Lennox-Gastaut syndrome (LGS) or Dravet syndrome (DS) enrolled in four phase 3 clinical trials of cannabidiol (CBD). Virtual Congress: 34th International Epilepsy Congress; 2021 Aug 28 - Sep 01.
36.Miller I, Scheffer I, Gunning B, et al. Abstract 79: Cannabidiol (10 and 20 mg/kg/d) significantly reduces convulsive seizure frequency in children and adolescents with Dravet syndrome: results of a dose-ranging, multicenter, randomized, double-blind, placebo-controlled trial (GWPCARE2). Philadelphia (PA): The 71st American Academy of Neurology Annual Meeting; 2019 May 04 - May 10.
37.Miller I, Scheffer IE, Gunning B, et al. Dose-ranging effect of adjunctive oral cannabidiol vs placebo on convulsive seizure frequency in Dravet syndrome: a randomized clinical trial. JAMA Neurol. 2020;77(5):613-621. PubMed
38.Clinical Study Report: GWEP1332, GWPCARE1 Part B. A double-blind, placebo-controlled, two-part study to investigate the dose-ranging safety and pharmacokinetics, followed by the efficacy and safety of cannabidiol (GWP42003-P) in children and young adults with Dravet syndrome [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2016 Nov 11.
39.Clinical Study Report: GWEP1424, GWPCARE2, amendment 1. A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P) in children and young adults with Dravet syndrome [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2019 Mar 15.
40.Nabbout R, Mistry A, Zuberi S, et al. Fenfluramine for treatment-resistant seizures in patients with Dravet syndrome receiving stiripentol-inclusive regimens: a randomized clinical trial. JAMA Neurol. 2020;77(3):300-308. PubMed
41.Committee For Medicinal Products For Human Use. Guideline on clinical investigation of medicinal products in the treatment of epileptic disorders, draft. Amsterdam (NL): European Medicines Agency; 2023: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-epileptic-disorders-revision-3_en.pdf. Accessed 2023 Dec 12.
42.van der Kop ML. The need for an individualized approach to what is considered a clinically significant reduction in seizure frequency: a patient's perspective. Epilepsia. 2023;64(6):1469-1471. PubMed
43.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
44.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
45.Clinical Study Report: GWEP1415, GWPCARE5. An open-label extension study to investigate the safety of cannabidiol (GWP42003-P; CBD) in children and adults with inadequately controlled Dravet or Lennox-Gastaut Syndromes [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2021 Feb 25.
46.Lattanzi S, Trinka E, Russo E, et al. Pharmacotherapy for Dravet syndrome: a systematic review and network meta-analysis of randomized controlled trials. Drugs. 2023;83(15):1409-1424. PubMed
47.Nabbout R, Sullivan J. Abstract 3.202: What defines “clinical meaningful changes in seizure frequency?” Analysis of data from a phase 3 clinical trial of ZX008 in Dravet syndrome. New Orleans (LA): 2018 AES Annual Meeting; 2018 Nov 30 - Dec 04.
Appendix 1: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 23: Summary of Additional Key Efficacy Results From Studies Included in the Systematic Review
Variable | CARE1 Part B study | CARE2 study | |||
|---|---|---|---|---|---|
20 mg/kg/day cannabidiol (N = 61) | Placebo (N = 59) | 10 mg/kg/day cannabidiol (N = 66) | 20 mg/kg/day cannabidiol (N = 67) | Placebo (N = 65) | |
Percentage change from baseline in convulsive frequency during the maintenance period | |||||
Number of patients analyzed | 60 | 59 | 66 | 63 | 65 |
Maintenance period, median (Q1, Q3) | n = 60 6.0 (2.0, 14.8) | n = 59 14.0 (4.3, 31.2) | 6.3 (2.7, 21.7) | 4.9 (2.1, 18.3) | 12.9 (5.1, 46.3) |
Maintenance period, median percentage reduction, % (95% CI)a | n = 60 –40.7 (–79.9 to –10.9) | n = 59 –16.0 (–54.9, 21.0) | n = 66 –37.8 (–81.3 to –8.3) | n = 63 –49.4 (–73.3 to –13.9) | n = 65 –25.8 (–52.4, 1.2) |
Estimated median difference (95% CI) | –26.1 (–45.1 to –8.2) P value = 0.0052 | NR | NR | NA | |
Maintenance period (weeks 1 to 4), median percentage change, % (Q1, Q3) | n = 57 –58.2 (–80.0, –19.0) | n = 58 –24.7 (–53.6, 29.5) | n = 66 –49.4 (–83.3, –7.9) | n = 63 –57.1 (–85.7, –14.3) | n = 65 –23.5 (–56.5, 7.1) |
Maintenance period (weeks 5 to 8), median percentage change, % (Q1, Q3) | n = 54 –49.2 (–82.3, –15.2) | n = 56 –25.0 (–56.4, 5.9) | n = 66 –32.9 (–85.7, 3.7) | n = 62 –46.3 (–74.7, –10.0) | n = 65 –33.3 (–58.5, 7.4) |
Maintenance period (weeks 9 to 12), median percentage change, % (Q1, Q3) | n = 52 –41.4 (87.9, 7.3) | n = 55 –21.7 (–64.1, 21.7) | n = 64 –48.9 (–81.8, –5.5) | n = 62 –42.5 (–76.2, 0.0) | n = 65 –28.3 (–57.2, –3.4) |
Maintenance period, percentage reduction, % (95% CI)c | NR | NR | n = 66 49.2 (38.1 to 58.3) | n = 63 48.6 (36.9 to 58.2) | n = 65 28.6 (13.3 to 41.2) |
Treatment ratio, cannabidiol vs. placebo (95% CI) | NR | n = 66 0.711 (0.539, 0.938) | n = 63 0.719 (0.542, 0.954) | NA | |
P value | NR | 0.0160 | 0.0224 | NA | |
Maintenance period (weeks 1 to 4), percentage reduction, % (95% CI) | NR | NR | n = 66 53.9 (43.2 to 62.6) | n = 63 48.5 (36.1 to 58.6) | n = 65 26.7 (10.6 to 39.9) |
Maintenance period (weeks 5 to 8), percentage reduction, % (95% CI) | NR | NR | n = 66 43.4 (29.6 to 54.5) | n = 62 46.5 (32.8 to 57.5) | n = 65 29.4 (12.7 to 42.9) |
Maintenance period (weeks 9 to 12), percentage reduction, % (95% CI) | NR | NR | n = 64 50.3 (38.7 to 59.7) | n = 62 45.8 (32.9 to 56.3) | n = 65 28.2 (12.7 to 41.0) |
Patients with nonconvulsive status epilepticus | |||||
Number of patients with nonconvulsive seizures greater than 30 minutes in duration | |||||
Baseline period | 2 (3.3) | 3 (5.1) | 7 (10.6) | 6 (9.0) | 5 (7.7) |
Treatment period | 2 (3.3) | 2 (3.4) | 3 (4.5) | 6 (9.0) | 2 (3.1) |
Percentage change from baseline in nonconvulsive-seizure frequency during the treatment period | |||||
Number of patients analyzed, n (%) | 37 (60.7) | 41 (69.5) | 50 (75.8) | 48 (71.6) | 51 (78.5) |
Baseline period, median (Q1, Q3) | 14.0 (6.0, 222.1) | 64.0 (9.7, 400.0) | 17.8 (6.0, 137.0) | 23.9 (5.4, 158.5) | 27.0 (3.0, 145.3) |
Treatment period, median (Q1, Q3) | 13.6 (0.6, 119.4) | 34.3 (1.2, 277.7) | 7.7 (0.6, 58.0) | 13.5 (0.6, 101.8) | 16.3 (1.5, 114.3) |
Median percentage change during treatment (Q1, Q3)a | –40.2 (–92.1, –3.6) | –34.7 (–97.5, –0.7) | –66.2 (–95.1, –26.2) | –60.7 (–79.0, –20.4) | –42.4 (–67.5, 10.7) |
Estimated median difference (95% CI) | 0 (–21.4 to 31.69) P value = 0.8803 | NR | NR | NA | |
Percentage reduction, treatment period divided by baseline period, % (95% CI)b | NR | NR | 66.2 (55.3 to 74.4) | 54.7 (39.6 to 66.0) | 42.9 (25.0 to 56.6) |
Treatment ratio, cannabidiol vs. placebo (95% CI) | NR | 0.593 (0.401 to 0.876) | 0.794 (0.534 to 1.181) | NA | |
P value | NR | 0.0091 | 0.2532 | NA | |
CaGICSD | |||||
Tonic-clonic seizures | |||||
Number of patients | 49 | 41 | 50 | 50 | 50 |
Decrease in average duration, n (%) | 17 (34.7) | 8 (19.5) | 29 (58.0) | 23 (46.0) | 15 (30.0) |
No change in average duration, n (%) | 32 (65.3) | 31 (75.6) | 20 (40.0) | 21 (42.0) | 30 (60.0) |
Increase in average duration, n (%) | 0 | 2 (4.9) | 1 (2.0) | 6 (12.0) | 5 (10.0) |
Odds ratio (95% CI) | 2.48 (0.94 to 6.51) | 3.27 (1.48 to 7.24) | 1.68 (0.78 to 3.62) | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
P value | 0.0657 | 0.0035 | 0.1874 | NA | |
Tonic seizures | |||||
Number of patients | 12 | 15 | 20 | 19 | 19 |
Decrease in average duration, n (%) | 4 (33.3) | 2 (13.3) | 9 (45.0) | 10 (52.6) | 6 (31.6) |
No change in average duration, n (%) | 8 (66.7) | 12 (80.0) | 11 (55.0) | 6 (31.6) | 12 (63.2) |
Increase in average duration, n (%) | 0 | 1 (6.7) | 0 | 3 (15.8) | 1 (5.3) |
Odds ratio (95% CI) | 3.40 (0.52 to 22.23) | 1.78 (0.51 to 6.16) | 1.67 (0.48 to 5.82) | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
P value | 0.2007 | 0.3630 | 0.4240 | NA | |
Clonic seizures | |||||
Number of patients | 11 | 7 | 17 | 15 | 15 |
Decrease in average duration, n (%) | 5 (45.5) | 3 (42.9) | 9 (52.9) | 9 (60.0) | 3 (20.0) |
No change in average duration, n (%) | 6 (54.5) | 3 (42.9) | 8 (47.1) | 5 (33.3) | 12 (80.0) |
Increase in average duration, n (%) | 0 | 1 (14.3) | 0 | 1 (6.7) | 0 |
Odds ratio (95% CI) | 1.25 (0.15 to 10.57) | 3.61 (0.80 to 16.31) | 4.53 (0.94 to 21.74) | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
P value | 0.8384 | 0.0958 | 0.0593 | NA | |
Atonic seizures | |||||
Number of patients | 3 | 7 | 5 | 9 | 11 |
Decrease in average duration, n (%) | 2 (66.7) | 2 (28.6) | 3 (60.0) | 3 (33.3) | 4 (36.4) |
No change in average duration, n (%) | 1 (33.3) | 3 (42.9) | 2 (40.0) | 5 (55.6) | 7 (63.6) |
Increase in average duration, n (%) | 0 | 2 (28.6) | 0 | 1 (11.1) | 0 |
Odds ratio (95% CI) | 7.44 (0.27 to 204.96) | 2.70 (0.29 to 25.03) | 0.76 (0.12 to 4.90) | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
P value | 0.2357 | 0.3827 | 0.7731 | NA | |
Myoclonic seizures | |||||
Number of patients | 14 | 18 | 24 | 21 | 29 |
Decrease in average duration, n (%) | 4 (28.6) | 3 (16.7) | 12 (50.0) | 9 (42.9) | 7 (24.1) |
No change in average duration, n (%) | 10 (71.4) | 12 (66.7) | 10 (41.7) | 11 (52.4) | 20 (69.0) |
Increase in average duration, n (%) | 0 | 3 (16.7) | 2 (8.3) | 1 (4.8) | 2 (6.9) |
Odds ratio (95% CI) | 2.89 (0.58 to 14.47) | 2.51 (0.83 to 7.60) | 2.20 (0.70 to 6.90) | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
P value | 0.1971 | 0.1031 | 0.1757 | NA | |
Countable partial seizures | |||||
Number of patients | 12 | 13 | 15 | 14 | 22 |
Decrease in average duration, n (%) | 5 (41.7) | 2 (15.4) | 5 (33.3) | 8 (57.1) | 9 (40.9) |
No change in average duration, n (%) | 7 (58.3) | 9 (69.2) | 10 (66.7) | 5 (35.7) | 12 (54.5) |
Increase in average duration, n (%) | 0 | 2 (15.4) | 0 | 1 (7.1) | 1 (4.5) |
Odds ratio (95% CI) | 6.01 (0.83, 43.21) | 0.84 (0.22, 3.17) | 1.70 (0.43, 6.67) | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
P value | 0.0750 | 0.7919 | 0.4464 | NA | |
Other partial seizures | |||||
Number of patients | 3 | 5 | 4 | 7 | 6 |
Decrease in average duration, n (%) | 0 | 3 (60.0) | 0 | 2 (28.6) | 2 (33.3) |
No change in average duration, n (%) | 3 (100.0) | 2 (40.0) | 4 (100.0) | 3 (42.9) | 2 (33.3) |
Increase in average duration, n (%) | 0 | 0 | 0 | 2 (28.6) | 2 (33.3) |
Odds ratio (95% CI) | 1.00 (< 0.01 to > 999.99) | 0.91 (0.08 to 10.68) | 0.96 (0.10 to 9.70) | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
P value | 1.0000 | 0.9423 | 0.9743 | NA | |
Absence seizures | |||||
Number of patients | 16 | 19 | 18 | 29 | 17 |
Decrease in average duration, n (%) | 4 (25.0) | 6 (31.6) | 7 (38.9) | 12 (41.4) | 2 (11.8) |
No change in average duration, n (%) | 11 (68.8) | 12 (63.2) | 11 (61.1) | 12 (41.4) | 11 (64.7) |
Increase in average duration, n (%) | 1 (6.3) | 1 (5.3) | 0 | 5 (17.2) | 4 (23.5) |
Odds ratio (95% CI) | 0.61 (0.14 to 2.62) | 4.44 (1.13 to 17.39) | 3.01 (0.88 to 10.30) | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
P value | 0.5028 | 0.0325 | 0.0784 | NA | |
Vineland-2 scores | |||||
Communication domain standard score | n = 17 | n = 19 | n = 36 | n = 32 | n = 43 |
Day 1, mean (SD) | 58.8 (17.3) | 56.2 (13.5) | 57.9 (17.1) | 54.6 (16.9) | 54.5 (17.7) |
Last visit, mean (SD) | 56.8 (18.4) | 57.1 (14.6) | 56.5 (17.6) | 57.0 (18.2) | 55.4 (18.4) |
Change from baseline, mean (SD) | –0.8 (4.2) | 2.8 (5.1) | –0.3 (5.1) | 2.1 (6.6) | 1.5 (5.6) |
Adjusted mean treatment difference (95% CI) | –3.8 (–7.1 to –0.6) | –1.8 (–4.4 to 0.8) | 0.7 (–2.0 to 3.3) | NA | |
P value | 0.0235 | 0.1718 | 0.6281 | NA | |
Daily living skills domain standard score | n = 20 | n = 19 | n = 39 | n = 34 | n = 42 |
Day 1, mean (SD) | 54.0 (16.2) | 53.0 (16.6) | 57.3 (19.3) | 55.2 (19.8) | 55.1 (19.6) |
Last visit, mean (SD) | 53.0 (18.8) | 51.1 (16.0) | 55.9 (19.5) | 53.0 (18.1) | 56.2 (20.9) |
Change from baseline, mean (SD) | –0.5 (4.8) | –1.4 (8.8) | –0.1 (4.8) | –2.7 (6.6) | 0.5 (5.6) |
Adjusted mean treatment difference (95% CI) | 0.0 (–4.7 to 4.7) | –0.6 (–3.1 to 1.9) | –3.2 (–5.7 to –0.6) | NA | |
P value | 0.9931 | 0.6146 | 0.0158 | NA | |
Socialization domain standard score | n = 12 | n = 16 | n = 34 | n = 30 | n = 37 |
Day 1, mean (SD) | 59.6 (16.3) | 58.4 (11.9) | 61.2 (17.5) | 60.1 (17.6) | 60.5 (16.2) |
Last visit, mean (SD) | 62.0 (18.2) | 58.0 (14.3) | 61.8 (19.2) | 60.6 (17.2) | 61.4 (19.0) |
Change from baseline, mean (SD) | 0.1 (3.6) | –0.8 (7.7) | 1.1 (6.7) | 0.4 (7.6) | –0.1 (6.2) |
Adjusted mean treatment difference (95% CI) | 0.1 (–5.3 to 5.4) | 1.2 (–2.1 to 4.4) | 0.5 (–2.9 to 3.9) | NA | |
P value | 0.9779 | 0.4800 | 0.7671 | NA | |
Motor skills domain standard score | n = 20 | n = 22 | n = 34 | n = 39 | n = 45 |
Day 1, mean (SD) | 66.0 (16.8) | 61.3 (13.8) | 64.3 (10.7) | 62.2 (15.2) | 64.6 (16.4) |
Last visit, mean (SD) | 64.3 (16.2) | 62.3 (14.0) | 64.3 (12.6) | 63.4 (11.8) | 64.5 (16.4) |
Change from baseline, mean (SD) | –0.9 (8.2) | 1.4 (5.9) | 0.2 (6.3) | 0.5 (5.4) | 0.1 (5.4) |
Adjusted mean treatment difference (95% CI) | –4.3 (–8.4 to –0.1) | 0.2 (–2.3 to 2.6) | 0.2 (–2.1 to 2.6) | NA | |
P value | 0.0460 | 0.8999 | 0.8373 | NA | |
Adaptive behaviour composite standard score | n = 12 | n = 15 | n = 32 | n = 27 | n = 37 |
Day 1, mean (SD) | 54.2 (16.9) | 53.6 (11.0) | 56.7 (17.5) | 53.5 (17.4) | 54.9 (17.5) |
Last visit, mean (SD) | 54.6 (17.6) | 52.6 (13.9) | 55.7 (17.3) | 54.4 (16.8) | 55.8 (18.9) |
Change from baseline, mean (SD) | –0.9 (5.0) | 0.2 (5.6) | –0.2 (4.1) | 0.2 (4.3) | 0.2 (4.3) |
Adjusted mean treatment difference (95% CI) | –2.6 (–6.8 to 1.6) | –0.4 (–2.5 to 1.7) | 0.0 (–2.2 to 2.2) | NA | |
P value | 0.2087 | 0.6970 | 0.9971 | NA | |
Maladaptive behaviour index v-scale score | n = 47 | n = 48 | n = 47 | n = 47 | n = 47 |
Day 1, mean (SD) | 18.7 (2.2) | 19.0 (1.9) | 19.3 (1.7) | 19.4 (1.5) | 19.6 (1.8) |
Last visit, mean (SD) | 18.5 (1.8) | 18.8 (2.0) | 19.0 (2.0) | 19.3 (1.5) | 19.3 (2.2) |
Change from baseline, mean (SD) | –0.3 (1.4) | –0.4 (1.3) | –0.3 (1.2) | –0.4 (1.1) | –0.4 (2.3) |
Adjusted mean treatment difference (95% CI) | 0.1 (–0.5 to 0.6) | 0.1 (–0.6 to 0.7) | 0.1 (–0.6 to 0.7) | NA | |
P value | 0.7768 | 0.8334 | 0.8652 | NA | |
CaGIC | |||||
CaGIC at last visit by category | n = 60 | n = 58 | n = 66 | n = 66 | n = 65 |
Very much improved | 9 (15.0) | 4 (6.9) | 13 (19.7) | 11 (16.7) | 1 (1.5) |
Much improved | 10 (16.7) | 4 (6.9) | 11 (16.7) | 10 (15.2) | 8 (12.3) |
Slightly improved | 18 (30.0) | 12 (20.7) | 21 (31.8) | 19 (28.8) | 18 (27.7) |
No change | 15 (25.0) | 31 (53.4) | 18 (27.3) | 17 (25.8) | 32 (49.2) |
Slightly worse | 3 (5.0) | 6 (10.3) | 2 (3.0) | 5 (7.6) | 4 (6.2) |
Much worse | 4 (6.7) | 1 (1.7) | 1 (1.5) | 3 (4.5) | 2 (3.1) |
Very much worse | 1 (1.7) | 0 | 0 | 1 (1.5) | 0 |
Last visit, median (Q1, Q3) | 3.0 (2.0, 4.0) | 4.0 (3.0, 4.0) | NR | NR | NR |
Estimated median difference (95% CI) | –1.0 (–1.0, 0.0) P value = 0.0166 | NR | NR | NA | |
Odds ratio for achieving an improvement (95% CI) | 2.29 (1.17 to 4.47) P value = 0.0155 | 2.93 (1.56 to 5.53) P value = 0.0009 | 2.02 (1.08 to 3.78) P value = 0.0279 | NA | |
Risk difference (95% CI) | NR | NR | NR | NA | |
Time to baseline convulsive-seizure frequency | |||||
Estimated median number of days (95% CI) | 46.0 (38.0 to 70.0) | 33.0 (29.0 to 37.0) | 52.5 (35.0 to 69.0) | 52.0 (39.0 to 64.0) | 35.0 (33.0 to 44.0) |
P value | 0.0065 | 0.0040 | 0.0203 | NA | |
BASC-2 = Behaviour Assessment System for Children, 2nd Edition; CI = confidence interval; CaGIC = Caregiver Global Impression of Change; CaGICSD = Caregiver Global Impression of Change in Seizure Duration; ESS = Epworth Sleepiness Scale; NEPSY-2 = A Developmental Neuropsychological Assessment; NRS = numerical rating scale; QOLCE = Quality of Life in Childhood Epilepsy; Q1 = lower quartile; Q3 = upper quartile; SD = standard deviation; Vineland-2 = Vineland Adaptive Behavior Scales, 2nd Edition; .
aAnalyzed using Wilcoxon rank sum test. This statistical test was used as a sensitivity analysis in the CARE2 study.
bAnalyzed using negative binomial regression. This statistical test was used in the primary analysis of the CARE2 study.
Sources: CARE138 and CARE239 Clinical Study Reports.
The Clinical Global Impression–Improvement (CGI-I) was deemed important but not critical for decision-making by the clinical experts consulted by CADTH. Nonetheless, the changes in convulsive-seizure frequency with a reduction in seizure frequency of 44% was associated with improvements in CGI-I scores and considered in other studies as clinically meaningful for DS.47 Similarly, the change from baseline in the CaGIC score was a secondary end point in both studies. The CaGIC was rated on a 7-point scale and comprised of the question: “Since your child started treatment, please assess the status of your child’s overall condition (comparing their condition now to their condition before treatment) using the scale below.” The markers were: “very much improved,” “much improved,” “slightly improved,” “no change,” “slightly worse,” “much worse,” “very much worse.”
On the same venue, the Caregiver Global Impression of Change in Seizure Duration scores were assessed in both studies and comprised the following question to be rated on a 3-point scare for each seizure subtype: “Since the patient started treatment, please assess the average duration of the patient’s seizures (comparing their condition now to their condition before treatment) using the scale below.” The markers were: “average duration of seizures has decreased,” “average duration of seizures has stayed the same,” “average duration of seizures has increased.”
Table 24: Statistical Analysis of Other Efficacy End Points in the Pivotal Trials
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
CARE1 Part B study | ||||
Number of patients experiencing worsening, no change, or improvements in convulsive-seizure frequency from baseline during the treatment period | Descriptive statistics only | NR | NR | NR |
Change in nonconvulsive-seizure frequency from baseline | Wilcoxon rank sum test; 95% CI with the Hodges-Lehmann method | NR | If a patient withdrew during the treatment period, then the primary analysis variable was calculated from all available data obtained during the treatment period before the patient withdrawing | Sensitivity analyses were repeated on the ITT analysis set using data for the maintenance period only and during each 4 weeks of the maintenance period |
CaGICSD | ANCOVA | Included age group as a covariate and treatment group as a factor in the model | NR | NR |
Change from baseline in Vineland-2 score | ANCOVA Ordinal logistic regression | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | NR | NR |
CaGIC at last visit | ANCOVA ordinal logistic regression Wilcoxon rank sum test | Included age group as a covariate and treatment group as a factor in the model | NR | NR |
Time to baseline convulsive-seizure frequency | Kaplan-Meier method | NR | Patients who completed the trial without experiencing greater than or equal to the number of seizures (per 28 days) experienced during the baseline period, or who withdrew from the trial, were censored at day 99 or the date of last dose as recorded, whichever occurred earliest | NR |
CARE2 study | ||||
CaGIC at last visit | Ordinal logistic regression | Treatment group included as a factor in the model | NR | Cochran-Armitage trend test |
Patients experiencing worsening, no change, or improvements in convulsive-seizure frequency from baseline | Descriptive statistics only | NR | NR | NR |
Change in nonconvulsive-seizure frequency from baseline | Negative binomial regression MMRM | Models included total number of seizures as a response variable; age group, time (baseline and treatment period), treatment and treatment-by-time interaction as fixed effects; and patient as a random effect. Log-transformed number of days in which seizures were reported by period is included as an offset | NR | Sensitivity analyses were repeated on the ITT analysis set using data for the maintenance period only and during each 4 weeks of the maintenance period |
Change in seizure frequency by individual seizure type from baseline | Negative binomial regression MMRM | Models included total number of seizures as a response variable; age group, time (baseline and treatment period), and treatment and treatment-by-time interaction as fixed effects; and subject as a random effect. Log-transformed number of days in which seizures were reported by period is included as an offset | NR | Sensitivity analyses were repeated on the ITT analysis set using data for the maintenance period only and during each 4 weeks of the maintenance period |
Use of rescue medication | Descriptive statistics only | NR | NR | NR |
CaGICSD | Ordinal logistic regression | NR | NR | NR |
Change from baseline in Vineland-2 score | ANCOVA Ordinal logistic regression | Included corresponding baseline value and age group as covariates and treatment group as a factor in the model | NR | NR |
Time to baseline convulsive-seizure frequency | Kaplan-Meier method | NR | Patients who completed the trial without experiencing greater than or equal to the number of seizures (per 28 days) experienced during the baseline period, or who withdrew from the trial, were censored at day 99 or the date of last dose as recorded, whichever occurred earliest | NR |
ANCOVA = analysis of covariance; CaGIC = Caregiver Global Impression of Change; CaGICSD = Caregiver Global Impression of Change in Seizure Duration; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ESS = Epworth Sleepiness Scale; ITT = intention to treat; IVRS = interactive voice response system; LOCF = last observation carried forward; MI = multiple imputation; MMRM = mixed-model for repeated measures; MNAR = missing not at random; NOCB = next observation carried backward; NR = not reported; NRS = numerical rating scale; PP = per protocol; QOLCE = Quality of Life in Childhood Epilepsy; Vineland-2 = Vineland Adaptive Behavior Scales, 2nd Edition.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
ASM
antiseizure medication
BIA
budget impact analysis
DS
Dravet syndrome
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
LGS
Lennox-Gastaut syndrome
NICE
National Institute for Health and Care Excellence
NIHB
Non-Insured Health Benefits
QALY
quality-adjusted life-year
SAE
severe adverse event
SUDEP
sudden unexpected death in epilepsy
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Cannabidiol (Epidiolex), oral solution |
Submitted price | Cannabidiol, 100 mg/mL oral solution: $1,424.54 per 100 mL bottle |
Indication | For use as adjunctive therapy for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome or tuberous sclerosis complex in patients 2 years of age and older. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 15, 2023 |
Reimbursement request | For use as adjunctive therapy for the treatment of seizures associated with Dravet syndrome in patients 2 years of age and older |
Sponsor | Jazz Pharmaceuticals Canada, Inc. |
Submission history | Previously reviewed: In progress Indication: Seizures associated with tuberous sclerosis complex Recommendation: TBD Indication: Seizures associated with Lennox-Gastaut syndrome Recommendation: TBD |
NOC = Notice of Compliance; TBD = to be determined.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients 2 years of age and older with DS that is inadequately controlled by their current usual care (i.e., patients taking at least 1 ASM who experienced 4 more convulsive seizures over a 28-day period) |
Treatment | Cannabidiol plus usual care (assumed to comprise 1 or more ASMsa) |
Comparator | Usual care |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (90 years) |
Key data sources | CARE1 and CARE2 clinical trials, CARE5 extension study |
Submitted results | ICER = $35,705 per QALY gained (incremental costs = $71,735; incremental QALYs = 2.01) |
Key limitations |
|
CADTH reanalysis results |
|
AE = adverse event; ASM = antiseizure medication; DS = Dravet syndrome; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SAE = serious adverse event.
aUsual care was assumed by the sponsor to include the following ASMs: clobazam, valproic acid, stiripentol, levetiracetam, topiramate, clonazepam, and rufinamide.
Conclusions
Based on data from the CARE1 and CARE2 trials, the CADTH Clinical Review concluded that the use of cannabidiol likely reduces the frequency of convulsive seizures and increases convulsive seizure-free days compared with placebo among patients with Dravet syndrome (DS). As noted in the CADTH Clinical Review, the impact of cannabidiol on health-related quality of life (HRQoL) and health care resource use is uncertain. Limited conclusions about the long-term benefit of cannabidiol can be made based on the CARE5 extension study owing to its single-group open-label design and enriched population. CADTH additionally notes that the magnitude of any treatment benefit between cannabidiol plus usual care versus usual care alone among patients with fewer than 4 convulsive seizures per 28-day period or among patients aged 18 years and older is unknown due to a lack of clinical data. As such, the cost-effectiveness of cannabidiol in these subgroups, and thus for the full reimbursement population, is highly uncertain.
CADTH undertook reanalyses to address several limitations in the sponsor’s analysis, which included excluding the quality-adjusted life-years (QALYs) accrued by caregivers, adopting a higher mean dose of cannabidiol, using mean patient body weights in the calculation of cannabidiol costs and adopting a higher mean weight for patients aged 18 to 55, and assuming that the long-term rate of discontinuation for patients experiencing convulsive seizures would be equivalent to that observed in the CARE5 study. The CADTH base case suggests that at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained, cannabidiol plus usual care is not a cost-effective treatment option for seizures associated with DS compared with usual care alone. A price reduction of at least 44% for cannabidiol would be required for cannabidiol plus usual care to be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
Although the CADTH base case estimated a gain in QALYs with cannabidiol plus usual care compared with usual care alone (incremental QALYs = 1.07), more than 99% of the incremental benefit was gained in the extrapolated period (i.e., after 14 weeks). In the absence of comparative evidence beyond 14 weeks and the uncertainty as to whether the clinical evidence from the CARE trials can be generalized to adult patients, the incremental QALYs for cannabidiol plus usual care predicted in CADTH’s base case are highly uncertain and may be overestimated. Additional price reductions may therefore be required.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient group input was received from the Canadian Epilepsy Alliance (CEA), which was not specific to DS. The input provided was based on the knowledge and experience of the submitter and the lived experiences of the patients, caregivers, clinicians, volunteers, and supporters of the CEA’s 24 member associations. The input noted that patients with uncontrolled epilepsy may feel socially isolated due to stigma and fear of rejection in social, work, and educational situations, and that the patient’s family can be affected by unpredictable seizures. It was noted that caregivers may be afraid to leave someone with frequent seizures alone and that caregivers may experience compassion fatigue and sleep deprivation. The input noted that antiseizure medications (ASMs) may be associated with side effects such as mood swings, sexual dysfunction, suicidal thoughts, memory loss, problems with concentration, fatigue, or depression, which can impact both patients and their caregivers, and that patients with intractable epilepsy are often unemployed or underemployed due to the frequency of their seizures. The input noted that a reduction in the absolute number of seizures experienced may improve the patient’s overall quality of life. It was additionally noted that some patients with epilepsy may take alternative substances, including cannabis.
No clinician group input was received for this review.
CADTH participating drug plans noted that stiripentol is the only ASM indicated for DS and that other ASMs used for DS are prescribed off-label. The plans noted that 35% to 42% of patients in the CARE1 and CARE2 studies were receiving stiripentol concomitantly. The plans questioned whether the prescribing criteria for cannabidiol should be aligned with stiripentol and noted there is a confidential negotiated price for stiripentol. The drug plans noted that, based on the Ontario Epilepsy Guidelines, international Dravet-specific guidelines, and Canadian clinical expert opinions, valproate and clobazam are used as initial treatment but that patients whose seizures are refractory to initial therapies may add other ASMs (e.g., stiripentol, topiramate, levetiracetam, clonazepam, rufinamide) or cannabidiol. The drug plans questioned how loss of treatment response would be defined and assessed in clinical practice, as this may be relevant for consideration for discontinuation of therapy. Additionally, the plans noted that while the minimum recommended maintenance dose for cannabidiol is 10 mg/kg/day, the cost of cannabidiol doubles if patients receive the maximum recommended dose.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s model considered the impact of reducing seizure frequency on patient HRQoL.
HRQoL was included in the model for both patients with DS and caregivers.
Costs of adverse events (AEs) and consequences of serious AEs (SAEs) were included in the model; however, the HRQoL impacts of SAEs were not adequately considered.
In a scenario analysis, the sponsor considered the impact of adopting a stopping rule for patients who have not achieved at least a 30% reduction in seizure frequency after treatment for 6, 12, and 24 months.
CADTH addressed some of these concerns as follows:
CADTH assumed that not all patients would receive the minimum recommended maintenance dose of cannabidiol.
CADTH was unable to address the following concerns raised from stakeholder input:
The sponsor considered stiripentol to be part of usual care; however, the cost-effectiveness of stiripentol relative to cannabidiol is uncertain owing to a lack of direct comparative evidence.
Economic Review
The current review is for cannabidiol (Epidiolex) for use as adjunctive therapy for seizures associated with DS in patients aged 2 years and older.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Cannabidiol is indicated for use as adjunctive therapy for seizures associated with Lennox-Gastaut syndrome (LGS), DS, or tuberous sclerosis complex in patients aged 2 years and older,1 while the sponsor’s reimbursement request is for use as adjunctive therapy for seizures associated with DS in patients 2 years of age and older.2 The sponsor submitted a cost-utility analysis of cannabidiol plus usual care compared with usual care alone in the reimbursement population.2 The modelled population was aligned with patients enrolled in the CARE1 and CARE2 trials.3,4 The sponsor assumed that usual care would consist of ASMs, including clobazam, valproic acid, stiripentol, levetiracetam, topiramate, clonazepam, and rufinamide.
Cannabidiol is available as a 100 mg/mL oral solution at a submitted price of $1,424.54 per 100 mL bottle.2 The recommended dose of cannabidiol is 5 mg/kg/day for 1 week, followed by a maintenance dosage of 10 mg/kg/day, up to a maximum of 20 mg/kg/day depending on individual response and tolerability.1
In the model, the sponsor separately calculated the costs of treatment for patients aged 2 to 5 years, 6 to 11 years, 12 to 17 years, and older than 18 years using weight-based dosing (17.3 kg, 27.2 kg, 49.9 kg, 50.8 kg, respectively), resulting in an annual per-patient cost of $11,110, $17,469, $32,047, and $36,128, respectively. The sponsor’s annual per-patient cost of usual care was similarly weight-based, ranging from $2,140 to $9,786. Patients receiving cannabidiol in addition to usual care were assumed to use the same amount of ASMs as those in the usual-care group.
The clinical outcomes of interest were life-years and QALYs. The sponsor adopted a lifetime horizon (90 years), with the analyses conducted from the perspective of a publicly funded health care payer. Future costs and benefits were discounted at a rate of 1.5% per year, and the model cycle length was 3 months.
Model Structure
The sponsor submitted a Markov model with 4 main health states based on the monthly frequency of convulsive seizures (seizure-free, ≤ 8 convulsive seizures, > 8 to ≤ 25 convulsive seizures, > 25 convulsive seizures) and death (Figure 1).2 Note that the sponsor assumed each month comprised 28 days (hereafter, 1 month refers to a 28-day cycle). Additionally, each seizure-based health state was further divided into 3 substates based on the number of days per month that patients were free of convulsive seizures (≤ 18 days, > 18 to ≤ 24 days, > 24 days) (Figure 2). Patients entered the model distributed across the 3 main health states with seizures (≤ 8 convulsive seizures, > 8 to ≤ 25 convulsive seizures, > 25 convulsive seizures) based on the baseline characteristics from the CARE1 and CARE2 trials. In the first cycle, patients could transition into other health states based on observations from the CARE1 and CARE2 studies. Thereafter, patients receiving usual care alone were assumed to remain in the same health state for the remainder of their lives (or time horizon). In cycles 2 to 9, patients receiving cannabidiol plus usual care continued to transition between health states. From cycle 10 onward, patients receiving cannabidiol plus usual care were assumed to remain in the same health state until they discontinued cannabidiol treatment or died.
Patients could permanently discontinue cannabidiol treatment throughout the time horizon. Patients receiving usual care alone were assumed to remain on treatment indefinitely. For the first cycle, discontinuation was assumed to be primarily driven by AEs; therefore, the overall treatment withdrawal rate observed in the CARE1 and CARE2 trials was applied. For cycles 2 through 9, discontinuation was assumed to be largely driven by insufficient treatment effect, and discontinuation rates were estimated for each health state based on patients across all cannabidiol plus usual care and usual care alone treatment groups of the CARE1 and CARE2 trials (those who later enrolled in the CARE5 study), adjusted to account for the 3-month cycle length. From cycle 10 onward, patients in the seizure-free state were assumed to discontinue cannabidiol at a rate of 0.5% per cycle, while a discontinuation rate of 10% per cycle was applied to patients who were not seizure-free, based on a review of cannabidiol for DS in the UK by the National Institute for Health and Care Excellence (NICE).5 When patients discontinued cannabidiol, they were assumed to follow the same seizure frequency distribution observed in the usual care–alone arm at the end of cycle 1. No stopping rules were implemented in the base case.
Model Inputs
The pharmacoeconomic model was informed by inputs from the phase III randomized CARE1 and CARE2 trials, which enrolled patients with DS (aged 2 to 55 years) taking at least 1 ASM who experienced 4 or more convulsive seizures over a 28-day period. Although the sponsor indicated that the mean age of the modelled cohort was 11.52 years, the sponsor assumed that the modelled cohort comprised 4 age groups at baseline (2 to 5 years, 29.21% of patients; 6 to 11 years, 37.80% of patients; 12 to 17 years, 30.93% of patients; ≥ 18 years, 2.06% of patients). The baseline distribution of patients across the 4 convulsive seizure–based health states was as follows: 0% in the seizure-free health state, 35.74% in the 8 or fewer convulsive seizures health state, 34.02% in the more than 8 up to 25 convulsive seizures health state, and 30.24% in the more than 25 convulsive seizures health state.
Movement between seizure-based health states in the pharmacoeconomic model was informed by pooled individual patient data based on observations from the CARE1 and CARE2 studies. In cycle 1, patients could transition into other health states based on observations from the CARE1 and CARE2 studies. For cannabidiol plus usual care, transitions between health states in cycles 2 to 9 were based on individual patient data from the CARE5 trial (which enrolled patients who had completed the CARE1 or CARE2 study). Patients in the usual-care group were assumed to remain in their cycle 1 health state for the remainder of the model horizon.
Treatment-emergent AEs were included in the model for the first 9 cycles based on the 10 mg/kg/day cannabidiol arm and the placebo arms of the CARE1 and CARE2 trials. Costs were incorporated for all AEs, while disutilities were included for AEs deemed to be serious and experienced by 3% or more of the patients who received cannabidiol and 1% or more of the patients who received placebo. Modelled AEs included rash, somnolence, fatigue, lethargy, sedation, diarrhea, decreased appetite, aggression, and irritability. No AEs were included in the model from cycle 10 onward.
Mortality in the model included all-cause mortality (based on age- and gender-specific rates for the general population from Statistics Canada), sudden unexpected death in epilepsy (SUDEP), and non-SUDEP. Rates for SUDEP and non-SUDEP were obtained from the literature for patients with DS.6 The sponsor assumed that patients in the seizure-free health state would have a 29% reduction in the risk of death from both SUDEP and non-SUDEP based on a prospective cohort study that reported a risk reduction of 58% for seizure-free patients and input from NICE that suggested this value was overestimated.
The sponsor’s model included health state utility values for patients as well as utility decrements for caregivers. Patient utility values and caregiver utility decrements were estimated by use of a study that enrolled members of the general population in the UK and Sweden who were asked to evaluate vignettes describing various seizure-related health states from the patient and caregiver perspective using both time trade-off and visual analogue scale methodology.7 For model health states that did not correspond to those reported in the utility study, the sponsor adopted the average of adjacent health states. In the model, each patient was assumed to have 2 caregivers, and caregiver utility decrements were applied linearly such that each caregiver had the same decrement per health state regardless of the number of caregivers. Disutilities for all SAEs were assigned a value of −0.120 and were assumed to last for 1 model cycle (3 months).8
Costs in the model included those associated with drug acquisition, AEs, health care resource use (general practitioner, specialist, nurse, and therapy visits; emergency department visits; hospital stays; rescue medication [buccal midazolam]), and end-of-life care (for deaths not attributed to SUDEP). Additionally, costs associated with long-term care were included for 2% of patients older than 18 years of age who were seizure-free and 10% of patients older than 18 years of age experiencing seizures.9 Drug acquisition costs for cannabidiol were based on the sponsor’s submitted price, while the acquisition costs of ASMs and buccal midazolam were obtained from the Ontario Drug Benefit Formulary and Exceptional Access Program list prices.10,11 The cost of usual care was based on the concomitant use of each ASM from the CARE1 and CARE2 trials. Health care resource use was assumed to vary by health state and age (pediatric versus adult), with resource use frequency based on a UK clinical expert survey. Unit costs for a general practitioner, pediatrician, and neurologist and emergency department visits were obtained from the Ontario Schedule of Benefits: Physician Services.12 Unit costs for visiting nurses, occupational therapists, physiotherapy visits, and speech and language therapists were based on the Canadian median hourly wage obtained from the Government of Canada Job Bank.13-15 Hospitalization and intensive care unit (ICU) costs were obtained from the Canadian Institute for Health Information.16,17 AEs were assumed to be managed by a single neurologist visit. Deaths not attributed to SUDEP were assumed to require an emergency department visit and 7 days in the ICU. All costs were reported in 2023 Canadian dollars.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations) for the base-case and scenario analyses. The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently. All results are based on publicly available list prices. Additional results from the sponsor’s economic evaluation are presented in Appendix 3.
Base-Case Results
In the sponsor’s base case, cannabidiol plus usual care was associated with higher costs (incremental costs = $74,735) and QALYs (incremental QALYs = 2.01) compared with usual care alone, resulting in an incremental cost-effectiveness ratio (ICER) of $35,705 per QALY gained (Table 3). Cannabidiol plus usual care had a 95% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained.
Results were driven by the drug acquisition costs of cannabidiol plus usual care (incremental costs = $119,431), the predicted gain in life-years (incremental life-years = 0.28), and the predicted gain in QALYs (incremental QALYs = 2.01) (Table 11). Of the incremental benefit compared with usual care alone (2.01 QALYs), more than 99% of benefit is predicted to be accrued after the first 3 months of treatment (i.e., beyond the treatment duration of the CARE1 and CARE2 trials). Of the 2.01 incremental QALYs gained with cannabidiol plus usual care, 52% were accrued by caregivers, suggesting that more than half of the incremental benefit predicted by the sponsor’s model will be experienced by caregivers, not patients. At the end of the time horizon, 0% of patients were still alive.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYsa | Incremental QALYs | ICER vs. UC ($/QALY) |
|---|---|---|---|---|---|---|---|
UC | 794,732 | Reference | 29.04 | Reference | 4.60 | Reference | Reference |
Cannabidiol plus UC | 866,467 | 71,735 | 29.33 | 0.28 | 6.61 | 2.01 | 35,705 |
ASM = antiseizure medication; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; UC = usual care.
Note: Usual care was assumed by the sponsor to include the following ASMs: clobazam, valproic acid, stiripentol, levetiracetam, topiramate, clonazepam, and rufinamide.
aThe total QALYs attributed to usual care (4.60) include 14.66 QALYs accrued by patients and −10.06 QALYs accrued by caregivers, The total QALYs attributed to cannabidiol plus usual care (6.661) include 15.64 QALYs from patients and −9.03 QALYs from caregivers. Negative QALYs accrued by caregivers reflect the modelling of the impact on caregivers as utility decrements.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor provided several scenario analyses, including adopting alternative time horizons (40 years and 60 years) and discount rates (0% and 3%), excluding caregiver disutilities, implementing a stopping rule for cannabidiol treatment, assuming that patients in the usual-care group would revert to their baseline health states after cycle 1, assuming that SUDEP and non-SUDEP mortality was equal across health states, including utility decrements for other seizure types, assuming a higher maintenance dose of cannabidiol (20 mg/kg/day), adopting alternate utility values, including utility decrements for nonconvulsive seizures, and excluding AEs. Scenarios with the greatest impact on the ICER were excluding caregiver utilities ($73,198 per QALY gained), increasing the maintenance dose of cannabidiol to 20 mg/kg/day ($93,813 per QALY gained), and using alternate utility values ($47,889 per QALY gained).
The sponsor also conducted a scenario analysis from a societal perspective that included additional costs associated with travel costs and productivity loss experienced by caregivers of patients with DS. In this analysis, relative to usual care, the ICER was $2,276 per QALY gained. This was lower than the sponsor’s base-case analysis using a health care payer perspective.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The full indicated population for DS was not modelled: The sponsor submitted analyses intended to reflect the cost-effectiveness of cannabidiol plus usual care for the treatment of seizures associated with DS in patients aged 2 years and older, which is aligned with the approved Health Canada indication.1 Effectiveness in the sponsor’s model was informed by observations from the CARE1 and CARE2 trials,3,4 which enrolled patients with DS whose seizures were inadequately controlled by current ASMs, which the sponsor defined as experiencing 4 or more convulsive seizures over a 28-day period. While the Health Canada indication is for the use of cannabidiol as adjunctive therapy, it does not restrict usage based on seizure frequency. As such, the sponsor’s modelled population is narrower than the Health Canada–indicated population in that it does not consider patients with DS who have fewer than 4 seizures over a 28-day period. CADTH additionally notes that the definition of inadequate control used by the sponsor (4 or more convulsive seizures over a 28-day period) is not aligned with the International League Against Epilepsy’s definition of drug-resistant epilepsy (failure of adequate trials of 2 or more tolerated and appropriately chosen and administered ASMs, as monotherapy or in combination, to achieve seizure freedom).18 However, the clinical expert input received by CADTH indicated that the definition of inadequate control may differ among patients and caregivers. Additionally, it was noted that experiencing 3 or more generalized tonic-clonic seizures per month increases the risk of SUDEP 15-fold and the risk of SUDEP in DS is approximately 20%. The increased risk of SUDEP is supported by Wicker et al.19 The expert input noted there is a documented increase in risk for patients who experience 3 or more seizures per month.
CADTH was unable to address this limitation owing to a lack of clinical data on the efficacy of cannabidiol plus usual care among patients who experienced fewer than 4 seizures over a 28-day period. As such, the cost-effectiveness of cannabidiol plus usual care in this population is unknown, as is the cost-effectiveness of cannabidiol plus usual care in the full Health Canada–indicated population.
The efficacy and safety inputs in the pharmacoeconomic model were derived from pediatric patients: The sponsor’s pharmacoeconomic analysis was informed by efficacy inputs from the CARE1, CARE2, and CARE5 studies, which enrolled patients aged 2 to 18 years. This is narrower than the Health Canada indication, which does not limit use to patients under 18 years of age. Although the clinical expert input received by CADTH suggested that the data from the CARE studies may be generalizable to adults, there is little evidence from trials (9 out of 315 patients were 18 to 19 years old in the extension study) to confirm whether the efficacy and safety of cannabidiol would be equivalent in adults. As such, the generalizability of the data from the CARE studies to adults older than 18 years of age is uncertain. Given that the severity and frequency of seizures differ between children and adults with DS,20 it is plausible that the effectiveness of cannabidiol compared with usual care would differ between these subgroups. CADTH notes that approximately 67% of the incremental QALYs are gained after the cohort reaches an average age of 18 years; thus, the majority of the incremental benefit relies on the assumption that the efficacy of cannabidiol is equivalent between pediatric and adult patients.
CADTH was unable to address this limitation owing to a lack of data on the drug’s effectiveness and safety among adults, and it is uncertain whether the magnitude of benefit associated with cannabidiol compared with usual care will be equivalent in adults. As such, the incremental QALYs predicted with the use of cannabidiol plus usual care compared with usual care alone are highly uncertain owing to the use of pediatric data to inform the model.
The model structure does not adequately reflect DS in clinical practice: The sponsor submitted a Markov model with 4 main health states based on the monthly frequency of convulsive seizures (Figure 1) and further divided each seizure-based health state into 3 substates based on the number of days per month that patients were free of convulsive seizures (Figure 2).2 The sponsor adopted the upper and lower bounds for each main health state and substate such that patients enrolled in the CARE1 and CARE2 trials would be divided into 3 approximately equal groups.3,4 There are several limitations associated with this approach. First, the health states were based on observed data from the CARE1 and CARE2 trials. If the distribution of seizures among patients in clinical practice differs from that of the patients enrolled in these studies, the model health states may not reflect patients treated in clinical practice.
Second, health states in an economic model should represent a homogenous group of patients who have similar expected costs and quality-of-life considerations and should be based on the clinical or care pathway for the condition of interest;21 this is not captured by the modelled health states. The clinical expert input received by CADTH indicated there is no clinical consensus regarding what seizure thresholds would adequately capture changes in HRQoL and costs; this was acknowledged by the sponsor.2 The expert input further noted that the thresholds used by the sponsor are not meaningful, as they do not adequately capture the quality-of-life change some patients experience after achieving a large reduction in seizures. Using the sponsor’s cut points for the main seizure-based health states, patients who have, for example, 100 convulsive seizures per 28 days at baseline and experience a 70% reduction after initiating treatment (i.e., higher than what the clinical experts deemed meaningful), would remain in their initial health state of greater than 25 convulsive seizures per 28 days. These patients would thus experience the same quality of life and costs as patients who have 100 convulsive seizures every 28 days and do not improve. Moreover, the clinical expert input noted that the quality-of-life impact that the number of convulsive seizures has on patients and their families likely differs based on the length of a seizure (e.g., 30 seconds versus 1 hour). Furthermore, the sponsor’s modelled substates for the number of days of seizure freedom may not adequately reflect patient quality of life. The clinical expert input noted that the impact of the number of seizure-free days on quality of life will vary among patients; for example, some patients who were previously experiencing daily seizures may find 5 days of seizure freedom per 28 days to be impactful. However, in the sponsor’s model, patients who experience 5 or 14 days of seizure freedom per 28 days are assumed to have the same quality of life, which the clinical experts deemed unlikely. As such, narrower health states may have been more reflective of patient experience.
CADTH was unable to address limitations related to the model structure, and the direction and magnitude of the impact of the model structure not adequately reflecting clinical practice is unknown.
The model lacked face validity and transparency: In assessing the internal validity of the sponsor’s submitted model, CADTH identified that the sponsor’s model did not return the expected results. Specifically, when the effectiveness and safety inputs (i.e., transition probabilities, days without convulsive seizures, SAE rates) were set to be equivalent for cannabidiol plus usual care versus usual care alone, the sponsor’s model predicted an incremental QALY gain of 0.30 for cannabidiol plus usual care, rather than 0.00, as would be expected if cannabidiol plus usual care and usual care alone were clinically equivalent. CADTH requested that the sponsor submit a revised version of the model in which incremental QALYs were zero when the effectiveness and safety parameters were set to be equivalent; the sponsor declined this request. The sponsor justified the residual incremental QALYs gained with cannabidiol as follows: “Patients discontinuing EPIDIOLEX would be unlikely to experience the same seizure burden as patients who have never been on the treatment…patients who discontinue EPIDIOLEX are assumed to follow the disease severity distribution as observed in the usual care arm at the end of cycle 1. This assumption was made because there are no data on seizure outcomes following withdrawal of EPIDIOLEX.”22 CADTH notes that this assumption implicitly assumes there will be residual benefit from cannabidiol after discontinuation, which has not been demonstrated in clinical trials. CADTH notes that this modelling issue was previously described by NICE in its appraisal of cannabidiol.5
CADTH additionally notes that the sponsor’s model included numerous IFERROR statements, resulting in situations where the parameter value was overwritten with an alternative value without alerting the user to the automatic overwriting. Due to the lack of transparency and complexity of the model, CADTH was unable to fully validate the model or to identify the underlying cause of the unexpected results within the time frame of this review. As such, the sponsor’s submitted base case as well as CADTH’s revised base case are associated with increased uncertainty, as well as an unexplained and unearned QALY benefit to cannabidiol when compared with usual care. As such, the ICERs reported from these analyses are likely underestimated.
CADTH could not fully address this limitation and notes that a thorough validation of the sponsor’s model was not possible. As such, the results of the sponsor’s submitted base case and CADTH’s revised base case are associated with considerable uncertainty and overestimate the incremental QALYs between treatments. Consequently, the ICERs reported from these analyses are likely underestimated, and a higher price reduction may be required for cannabidiol to be cost-effective at a WTP threshold of $50,000 per QALY.
The long-term effectiveness of cannabidiol is highly uncertain: In the model, the efficacy of cannabidiol plus usual care in cycles 2 through 9 was based on individual patient data from the CARE5 extension study for patients who entered CARE5 after completing the CARE1 or CARE2 study in a cannabidiol treatment group. As noted in the CADTH Clinical Review, the CARE5 study population is considered to be enriched, as patients who discontinued from the CARE1 or CARE2 study (e.g., owing to lack of treatment response or AEs) were not eligible for the CARE5 trial. From cycle 10 onward, the sponsor assumed that patients who receive cannabidiol plus usual care will remain in the same health state until death or discontinuation, while patients in the usual-care group remain in the same health states from cycle 2 until death. No data supporting the effectiveness of cannabidiol are available beyond the duration of the CARE5 study (mean treatment duration = 639 dosing days), and there are no comparative effectiveness data for cannabidiol plus usual care relative to usual care alone beyond the duration of the CARE1 and CARE2 trials (14 weeks). As such, it is uncertain whether the reduction in seizure frequency observed in the CARE studies will be maintained indefinitely or whether treatment effectiveness may wane. CADTH notes that more than 99% of the incremental QALYs gained with cannabidiol plus usual care relative to usual care alone were accrued on the basis of extrapolation (i.e., in the post-trial period), highlighting the uncertainty related to long-term relative treatment effectiveness.
CADTH additionally notes that the sponsor assumed that, after cycle 9, patients who are not seizure free would discontinue cannabidiol at a rate of 10% per cycle (i.e., 3 months). In contrast, the discontinuation rates for patients experiencing seizures in cycles 2 through 9 were based on observations from the CARE5 study and were assumed to reflect “insufficient treatment effect.” These rates are lower than the 10% assumed by the sponsor (range, 4.5% to 9.54%). While the sponsor indicated that the assumption of 10% discontinuation was to account for “real-world persistence on treatment,” the clinical experts consulted by CADTH did not find it plausible that patients who had been using cannabidiol for more than 2 years would be more likely to discontinue it thereafter.
In the CADTH base case, from cycle 10 onward, CADTH adopted the rates of treatment discontinuation from the CARE5 study for patients experiencing seizures, consistent with those used for cycles 2 to 9. Due to the structure of the sponsor’s model, CADTH was unable to explore the impact of the potential waning of the cannabidiol treatment effect. Basing the efficacy of cannabidiol plus usual care from cycle 10 onward on data from the CARE5 study may bias the ICER in favour of cannabidiol.
Cannabidiol drug costs were underestimated: The Health Canada–recommended maintenance dose of cannabidiol when used as adjunctive therapy for seizures associated with DS is 10 mg/kg/day, which may be increased to a maximum of 20 mg/kg/day depending on “individual clinical response and tolerability.”1 In the submitted model, the sponsor assumed that all patients would receive a maintenance dose of 10 mg/kg/day, thereby assuming that no patient would receive a maintenance dose greater than the minimum recommended dose. CADTH notes that both the CARE1 and CARE2 trials included 20 mg/kg/day groups3,4 and that 38% of patients in the long term extension study (CARE5) received a cannabidiol dose of 30 mg/kg/day or higher (mean dose of 22.18 mg/kg/day).22 Therefore, there is a misalignment between the sponsor’s assumption that all patients will receive 10 mg/kg/day and the doses used in the clinical trials. The clinical expert input received by CADTH noted that some patients who experience an initial treatment response but have not achieved seizure freedom may trial a higher dose in an attempt to achieve seizure freedom.
Additionally, the body weight used by the sponsor in the calculation of drug costs for patients aged 18 to 55 years (mean weight of 49.7 kg) was deemed by the clinical experts consulted by CADTH for this review to be inappropriately low for adult patients with DS. CADTH notes that the CARE1 and CARE 2 trials only enrolled patients aged 2 to 18 years, and the sponsor estimated that only 2% of patients with DS are over the age of 18, which underestimates the prevalence of adult patients with DS, according to the clinical expert input received by CADTH. Underestimating the prevalence of DS among adult patients underestimates the cost of drugs dosed by weight (including cannabidiol), given that adult patients are typically larger than pediatric ones. Finally, the sponsor used the median baseline weight reported in the CARE1 and CARE2 studies in the calculation of drug costs. CADTH considers it more appropriate to use the mean weight rather than the median in this calculation.
In the CADTH base case, CADTH assumed an average cannabidiol dose of 12 mg/kg/day, based on expert input suggesting that approximately 20% of patients with DS may receive the maximum recommended maintenance dose of cannabidiol (20 mg/kg/day) while the remainder receive 10 mg/kg/day. CADTH additionally used the mean patient weight in the calculation of drug costs instead of the median and, for patients aged 18 to 55 years, CADTH adopted the mean patient weight from the CARE3 and CARE4 trials for patients with LGS, based on expert input that the weight of adult patients with DS is expected to be similar to that of adult patients with LGS. CADTH was unable to adjust the proportion of adults with DS owing to a lack of data.
The impact of cannabidiol on patient quality of life is highly uncertain: The sponsor’s model predicts an incremental gain of 2.01 QALYs among patients with DS who receive cannabidiol plus usual care (Table 3). Based on the clinical expert input received by CADTH, it is plausible that a reduction in seizures may lead to improved patient HRQoL. As noted in the CADTH Clinical Review, cannabidiol may result in a numerical improvement from baseline in the adjusted mean score for the Quality of Life in Childhood Epilepsy questionnaire compared with placebo; however, the clinical meaningfulness of this reduction is uncertain. Whether the use of cannabidiol in clinical practice will lead to improved patient HRQoL over longer time frames is therefore uncertain.
Additionally, there is uncertainty associated with the utility values adopted by the sponsor, which were derived from a sponsor-funded vignette study that enrolled members of the general population in the UK and Sweden.23 In this study, adult participants were asked to adopt the perspective of a patient or caregiver and to evaluate vignettes describing various seizure-related health states using time trade-off and visual analogue scale methodologies. CADTH notes that the perception of DS by members of the general public may be different from that of patients with DS. As noted by Lo (2021), from the author’s perspective, the disease burden of DS is, on average, more severe than that of LGS. Yet, the derived utility values suggest that LGS has a greater impact on quality of life than DS, likely due to the general population’s comprehension of the relative impact of convulsive seizures versus drop seizures. Additionally, as no patients or members of the general public from Canada were included in this study, it is uncertain whether these utilities reflect the preferences of patients with DS in Canada.
CADTH was unable to address this limitation owing to a lack of alternative data.
The impact of cannabidiol on the HRQoL of caregivers was included in the base case: Of the 2.01 incremental QALYs to be gained with cannabidiol plus usual care predicted by the sponsor’s model, 52% were accrued by caregivers (i.e., not by patients with DS). As noted in CADTH’s Guidelines for the Economic Evaluation of Health Technologies: Canada,21 any spillover in costs or treatment effects beyond the target population (i.e., patients with DS) should be addressed in a non–base-case analysis. CADTH additionally notes that the impact of cannabidiol on the HRQoL of caregivers has not been assessed in clinical trials. Further, the sponsor’s assumption that each patient with DS would have 2 caregivers for the duration of their life and that each caregiver would have the same HRQoL decrement was deemed by the clinical experts consulted by CADTH for this review to be inappropriate; that is, not all patients with DS will have 2 caregivers, and, for patients with multiple caregivers, the individual burden of care (i.e., as described in the vignette study) would likely be shared between caregivers rather than doubled. Additionally, should a patient transition into a long-term care facility, the impact on caregiver quality of life is likely to be meaningfully different than measured in the vignette study.
In the CADTH base case, QALY decrements accrued by caregivers were excluded such that the CADTH ICER reflects the cost-effectiveness of cannabidiol plus usual care for patients with DS. CADTH explored the impact of additionally including the effect of cannabidiol on caregivers in a scenario analysis.
The uncertainty in the efficacy of cannabidiol was not modelled appropriately: Although the sponsor undertook probabilistic analyses, no uncertainty was incorporated for transition probabilities, which were based on individual patient data from the CARE1, CARE2, and CARE5 studies. As such, the sponsor assumed there is no uncertainty associated with the probability of moving between health states and that the probabilities of moving between health states (i.e., improving or worsening) in clinical practice will be exactly as observed in the CARE1 and CARE2 studies. As noted in the CADTH economic guidelines, “uncertainty regarding the value of each parameter should be examined through probabilistic analysis.” At CADTH’s request, the sponsor provided instructions for adopting Dirichlet distributions for these inputs; however, doing so disabled the model’s ability to appropriately report deterministic results, and adopting the Dirichlet distributions was not possible beyond cycle 9. Owing to the lack of transparency and the complexity of the sponsor’s model, CADTH was unable to correct the underlying cause of this issue and was thus unable to implement uncertainty for transition probabilities within the time frame required for this review.
The sponsor additionally assumed that any transitions between health states that were not observed within the clinical studies could not occur within the model (and implicitly, within clinical practice). For example, in cycle 5, patients using cannabidiol were assumed to be unable to move from the “greater than 8 to up to 25 convulsive seizures per 28 days” health state to the seizure-free state, but patients in the “greater than 25 convulsive seizures per 28 days” health state could become seizure free. This assumption does not meet face validity, nor does it adequately reflect the uncertainty inherent in extrapolating clinical trial observations to whole populations.
CADTH was unable to address this limitation. Additionally, as uncertainty in the clinical evidence for seizure frequency was not incorporated in the sponsor’s model, CADTH is unable to accurately estimate the probability of cannabidiol plus usual care being cost-effective relative to usual care alone. However, the impact of this limitation in CADTH’s base case is minor, as CADTH’s reanalysis predicts a 0% probability of cannabidiol plus usual care being cost-effective at a WTP threshold of $50,000 per QALY gained.
The impact of AEs was not adequately considered: The impact of AEs is uncertain for several reasons. First, in their economic model, the sponsor assumed that all SAEs (i.e., rash, somnolence, fatigue, lethargy, sedation, diarrhea, decreased appetite, aggression, irritability) would have the same impact on quality of life (−0.12) and the same duration (3 cycles). The clinical expert input indicated that for patients with DS, some AEs, such as aggression and irritability, are likely to have a greater impact on quality of life. Second, the sponsor calculated the incidence rates of SAEs based on events reported by at least 1% and 3% of patients who received placebo and 10 mg/kg/day of cannabidiol, respectively, in the CARE1 and CARE2 trials.3,4 Using different thresholds to calculate the incidence rates of AEs is inappropriate. Finally, the sponsor considered only SAEs experienced by patients who received 10 mg/kg/day of cannabidiol (in the CARE2 study), whereas the efficacy data were for patients who received either 10 mg/kg/day or 20 mg/kg/day (in the CARE1 and CARE2 studies). As noted in the CADTH Clinical Review, 16.4% of patients in the 20 mg/kg/day group of the CARE1 study reported at least 1 SAE, while SAEs were reported by 20.3% and 24.6% of patients in the 10 mg/kg/day and 20 mg/kg/day cannabidiol groups in the CARE2 study, respectively. Discontinuation due to SAEs was higher among patients who received 20 mg/kg/day of cannabidiol in the CARE1 study (14.8%) and the CARE2 study (7.2%) compared with the 10 mg/kg/day group in the CARE2 study, in which zero patients discontinued due to AEs.3,4
CADTH was unable to address limitations related to the AEs, and the direction and magnitude of the impact of AEs is unknown.
The impact of cannabidiol on survival is uncertain: The sponsor’s base case predicts a survival advantage with cannabidiol plus usual care relative to usual care alone (incremental life-years = 0.28), which has not been shown in clinical trials. Survival was not an outcome in the CARE1 or CARE2 trials. CADTH notes that decreased seizure frequency has been correlated in the literature to a decreased risk of SUDEP.24,25 Additionally, in the sponsor’s model, the average lifespan of patients was greater than that expected by the clinical experts consulted by CADTH; that is, more than half of the modelled patients remained alive when the average age of the cohort reached 50 years of age and 23.5% remained alive when the average age of the cohort reached 80 years. Finally, the sponsor assumed that patients who were seizure-free would have a 0.71 risk ratio of mortality compared with those having seizures, based on a 2013 cohort study of patients with epilepsy enrolled in an outpatient clinic between 1970 and 1999.26 The sponsor halved the risk reduction associated with being seizure-free reported within this study due to feedback from the NICE review of cannabidiol in DS.5 However, it remains unclear whether patients with DS who previously had seizures and became seizure free follow the same trajectory as those observed in the Trinka et al. (2013) study, which was not specific to patients with DS.
The survival benefit predicted by the sponsor’s model for cannabidiol plus usual care is uncertain. CADTH was unable to address this limitation in the absence of more robust clinical data. In a scenario analysis, equivalent mortality was assumed across health states, which ensured there was no relative mortality effect of treatment with cannabidiol.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The background ASMs used in the CARE1 and CARE2 trials were assumed to represent usual care in Canada. | Uncertain. The CARE1 and CARE2 trials compared cannabidiol with placebo on a background of various ASMs considered to comprise usual care. However, as this concomitant usual care had to remain stable throughout the trial, the background ASMs in the placebo groups of these trials may not reflect the usage of ASMs in clinical practice, where the dosages and mix of ASMs would be altered based on patient symptoms or other needs. Additionally, the clinical expert input received by CADTH highlighted that the use of specific ASMs may differ based on patient age (e.g., clonazepam is rarely used to treat seizures in pediatric patients in Canada). As such, the cost-effectiveness of cannabidiol compared with usual care in the clinical context is uncertain, as is the cost-effectiveness of cannabidiol compared with any individual ASM or combination of ASMs. |
Costs associated with AEs were only accumulated during cycles 1 to 9. | Reasonable. The clinical expert input received by CADTH noted that most AEs occur in the first 3 to 6 months that a patient is on treatment; however, the experts noted that AEs may recur if the patient’s dose increases. As such, the sponsor’s approach is likely conservative. |
Dosages of ASMs were calculated by patient weight, regardless of patient age. | Inappropriate. According to the clinical expert input and the relevant product monographs, most ASMs are typically dosed within a therapeutic range and based on treatment response, tolerance, and concomitant ASM use rather than only by weight, particularly for adult patients. As such, some of the doses assumed by the sponsor overestimated or underestimated typical use in Canadian clinical practice. The sponsor additionally assumed that ASMs could be prescribed in partial amounts, whereas most ASMs are tablets and capsules and unlikely to be prescribed in partial amounts. However, as cannabidiol was assumed by the sponsor to not displace or alter the dosage of ASMs comprising usual care, the impact of these assumptions on the ICER is expected to be minor. |
Patients with lower frequencies of convulsive seizures were assumed to use fewer health care resources (e.g., clinician visits, hospitalizations, long-term care), with resource use estimates derived from clinical experts in the UK. | Uncertain. The sponsor applied Canadian costs to resource use estimated in the UK context. Whether these inputs are generalizable to the Canadian context is uncertain. According to the clinical experts consulted by CADTH, it is plausible that patients who have a lower frequency of convulsive seizures would use fewer health care resources, but the magnitude of such effects is unknown. Health care resource use was not assessed as part of the CARE1 and CARE2 trials, with the exception of hospital admissions due to epilepsy. As noted in the CADTH Clinical Review, cannabidiol may result in little to no difference in hospitalizations due to epilepsy for patients who received cannabidiol vs. placebo. |
A proportion of adult patients were assumed to reside in a long-term care facility (2% of adults who are seizure free, 10% of adults who are not seizure free). | Uncertain. The clinical expert input received by CADTH indicated that the proportion of adults with DS who reside in a group home or long-term care facility is likely higher than 10% and that the proportion likely increases with patient age. That is, as patients with DS age, it becomes less likely that their parents or other family members would be able to fully provide their care. As the sponsor’s model predicts that 23.5% of patients remain alive when the average age of the cohort reaches 80 years, the proportion of patients requiring long-term care is highly likely to be underestimated. In addition to health care resource use, this may additionally impact caregiver utility decrements. |
AE = adverse event; ASM = antiseizure medication; DS = Dravet syndrome; ICER = incremental cost-effectiveness ratio; vs. = versus.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH undertook reanalyses that addressed key limitations within the submitted model, as summarized in Table 5. The CADTH base case was derived by making changes to model parameter values and assumptions in consultation with clinical experts. CADTH was unable to address the other limitations of the model, including the Health Canada–indicated population not being fully modelled, the use of pediatric data to inform the model, limitations related to the sponsor’s modelling approach (e.g., model structure, transparency), and uncertainty in the impact of cannabidiol on quality of life, long-term efficacy, survival, and AEs.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Caregiver disutility values | Included (2 caregivers per patient) | Excluded |
2. Maintenance dose of cannabidiol | 10 mg/kg/day | 12 mg/kg/daya |
3. Body weight | Pooled median patient weight by age group, sourced from the CARE1 and CARE2 trials. | Pooled mean patient weight by age group, sourced from the CARE1 and CARE2 trials for the < 18 age groups. For the 18 to 55 age group, the pooled mean weight was based on the corresponding age group from the CARE3 and CARE4 trials for LGS. |
4. Discontinuation rates (cycle 10+) | Discontinuation per 3-month cycle:
| Discontinuation per 3-month cycle:b
|
CADTH base case | Reanalysis 1 + 2 + 3 + 4 | |
DS = Dravet syndrome; LGS = Lennox-Gastaut syndrome.
aBased on expert input suggesting that approximately 20% of patients with DS may receive the maximum recommended maintenance dose of cannabidiol (20 mg/kg/day) while the remainder receive 10 mg/kg/day.
bPatients who are seizure-free were assumed to discontinue cannabidiol at a rate of 0.5% per cycle, as per the sponsor’s assumption. Patients in the remaining seizure states (i.e., patients experiencing seizures) were assumed to discontinue cannabidiol at the same rates as in cycles 2 through 9, based on data from the CARE5 study.27
CADTH undertook a stepped analysis, incorporating each change to the sponsor’s base case proposed in Table 5 to highlight the impact of each change (Table 6; disaggregated results are presented in Table 12). All of the CADTH probabilistic reanalyses were run for 1,000 iterations.
Results from the CADTH base case suggest that cannabidiol plus usual care was associated with higher costs (incremental costs = $136,593) and higher QALYs (incremental QALYs = 1.07) when compared with usual care alone, resulting in an ICER of $128,062 per QALY gained. In the CADTH base case, cannabidiol plus usual care had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained.
The results were driven by the drug acquisition cost of cannabidiol plus usual care (incremental costs = $187,558; Table 12), as well as the predicted incremental gain of 1.067 QALYs with cannabidiol plus usual care. Consistent with the sponsor’s analysis, the CADTH reanalysis estimates that more than 99% of the incremental QALYs were accrued in the post-trial period of the model on the basis of extrapolation. Similarly, CADTH notes that approximately 90% of the $52,479 in predicted savings in health care costs with cannabidiol plus usual care compared with usual care alone are expected to be realized in the post-trial period.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | UC | 790,968 | 4.33 | Reference |
Cannabidiol plus UC | 862,210 | 6.34 | 35,362 | |
CADTH reanalysis 1: Caregiver disutilities excluded | UC | 790,968 | 14.57 | Reference |
Cannabidiol plus UC | 862,210 | 15.54 | 73,388 | |
CADTH reanalysis 2: Cannabidiol dose = 12 mg/kg/day | UC | 790,968 | 4.33 | Reference |
Cannabidiol plus UC | 885,330 | 6.34 | 46,837 | |
CADTH reanalysis 3: Mean patient weight | UC | 847,910 | 4.33 | Reference |
Cannabidiol plus UC | 938,921 | 6.34 | 45,174 | |
CADTH reanalysis 4: Discontinuation after cycle 9 | UC | 790,968 | 4.33 | Reference |
Cannabidiol plus UC | 872,345 | 6.53 | 36,869 | |
CADTH base case (1 + 2 + 3 + 4) | UC | 847,910 | 14.57 | Reference |
Cannabidiol plus UC | 981,578 | 15.62 | 127,224 | |
CADTH base case (1 + 2 + 3 + 4) (Probabilistic) | UC | 849,156 | 14.62 | Reference |
Cannabidiol plus UC | 985,750 | 15.68 | 128,062 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; UC = usual care.
aDeterministic analysis, unless otherwise stated. The probabilistic and deterministic results of the sponsor’s base case were similar.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s results and CADTH’s base case. The CADTH base case suggests that a 44.8% price reduction for cannabidiol would be required for cannabidiol plus usual care to be considered cost-effective at a WTP threshold of $50,000 per QALY relative to usual care alone (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for cannabidiol plus usual care vs. usual care | |
|---|---|---|
Price reduction | Sponsor base case ($/QALY) | CADTH reanalysis ($/QALY) |
No price reduction | 35,362 | 127,224 |
10% | 29,624 | 109,976 |
20% | 23,886 | 92,727 |
30% | 18,184 | 75,478 |
40% | 12,410 | 58,229 |
50% | 6,672 | 40,980 |
60% | 934 | 23,731 |
70% | Dominant | 6,482 |
80% | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
CADTH conducted a series of scenario analyses to explore the impact of alternative assumptions on the cost-effectiveness of cannabidiol plus usual care:
Removing the mortality benefit associated with cannabidiol. The risk of death was assumed to be the same across all health states, which ensured there were no relative mortality effects of the treatments.
Implementing a stopping rule, using the sponsor-provided option to do so, such that patients who do not experience a 30% reduction in the frequency of drop seizures after use of cannabidiol for 6 months, 1 year, and 2 years are assumed to discontinue cannabidiol.
Including caregiver QALYs in the calculation of the ICER such that the ICER reflects the cost-effectiveness of cannabidiol plus usual care compared with usual care alone among patients with DS and their caregivers. One caregiver was included per patient in this scenario, which may reflect the caregiver burden experienced by a single person or the burden shared by multiple people.
Results of these scenarios are presented in Appendix 4 (Table 13). The scenarios with notable ICERs included removing the survival benefit predicted by the model for cannabidiol plus usual care (ICER of $140,547 per QALY gained) and including the QALYs accrued by caregivers (ICER of $83,771 per QALY gained).
Issues for Consideration
A ketogenic diet and vagus nerve stimulation may also be used to treat DS but were not considered as comparators in the submitted analysis. The cost-effectiveness of cannabidiol compared with either ketogenic diet or vagus nerve stimulation is unknown.
Stiripentol is indicated for use in combination with clobazam and valproate to treat refractory generalized tonic-clonic seizures in patients with DS whose seizures are not adequately controlled with clobazam and valproate alone. The sponsor considered stiripentol to be a part of usual care; however, the cost-effectiveness of cannabidiol compared with stiripentol is unknown. Indirect comparative evidence from the literature suggests that stiripentol may be associated with a higher seizure response rate than cannabidiol.28
Medical cannabis products are available in Canada but are generally not reimbursed by public drug plans; patients with DS in Canada may already use or have tried cannabis for medical purposes, including cannabidiol products accessed through federally licensed sellers via the Cannabis Act. The clinical expert input received by CADTH indicated that patients who are currently using medical cannabis may be likely to switch to Epidiolex, owing to its higher dosage, a lack of private insurance coverage, and the out-of-pocket cost of medical cannabis to patients. The cost-effectiveness of Epidiolex in patients who have previously responded to other forms of cannabidiol is unknown.
Overall Conclusions
Based on data from the CARE1 and CARE2 trials, the CADTH Clinical Review concluded that the use of cannabidiol likely reduces the frequency of convulsive seizures and increases convulsive seizure–free days compared with placebo among patients with DS. As noted in the CADTH Clinical Review, the impact of cannabidiol on HRQoL and health care resource use is uncertain. Limited conclusions about the long-term benefit of cannabidiol can be made based on the CARE5 extension study owing to its single-group open-label design and enriched population. CADTH additionally notes that the magnitude of any treatment benefit between cannabidiol plus usual care versus usual care alone among patients with fewer than 4 convulsive seizures per 28-day period or among patients aged 18 years and older is unknown due to a lack of clinical data.
The sponsor submitted an economic analysis comparing the cost-effectiveness of cannabidiol plus usual care with usual care alone in patients with DS, based on individual patient data from the CARE1, CARE2, and CARE5 studies. The CARE1 and CARE2 trials enrolled patients who experienced 4 or more convulsive seizures over a 28-day period despite taking 1 or more ASMs, while the CARE5 long-term extension study enrolled patients who had completed the CARE1 or CARE2 study. The Health Canada indication for cannabidiol is for use as adjunctive treatment of seizures associated with DS and is not restricted based on having inadequate control with ASMs or the number of convulsive seizures over a specified time period. As such, the cost-effectiveness of cannabidiol for the full Health Canada–indicated population for DS is unknown.
CADTH identified additional limitations with the sponsor’s economic submission, including those related to the model structure and assumptions, long-term effectiveness of cannabidiol plus usual care, impact of AEs, cannabidiol drug costs, health state utility values, and impact on survival. Notably, no uncertainty was incorporated by the sponsor for transition probabilities, which were based on individual patient data from the CARE1, CARE2, and CARE5 studies. This implicitly assumes there is no uncertainty associated with the probability of moving between health states and that such transitions are fully reflected by observations from the CARE1, CARE2, and CARE5 studies.
CADTH undertook reanalyses to address several limitations in the sponsor’s analysis, which included excluding QALYs accrued by caregivers, adopting a higher mean dose of cannabidiol, using mean patient body weights in the calculation of cannabidiol costs, adopting a higher mean weight for patients aged 18 to 55 years, and assuming that the long-term rate of discontinuation for patients experiencing convulsive seizures would be equivalent to that observed in the CARE5 study. The CADTH base case suggests that at a WTP threshold of $50,000 per QALY gained, cannabidiol plus usual care is not a cost-effective treatment option for seizures associated with DS compared with usual care alone. A price reduction of at least 44% for cannabidiol would be required for cannabidiol plus usual care to be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
Although the CADTH base case estimated a gain in QALYs with cannabidiol plus usual care compared with usual care alone (incremental QALYs = 1.07), more than 99% of the incremental benefit was gained in the extrapolated period (i.e., after 14 weeks). In the absence of comparative evidence beyond 14 weeks and uncertainty as to whether the clinical evidence from the CARE trials can be generalized to adult patients, the incremental QALYs for cannabidiol plus usual care predicted in CADTH’s base case are highly uncertain and may be overestimated. Additional price reductions may therefore be required.
References
1.Epidiolex (cannabidiol): 100 mg/mL oral solution [product monograph]. Cambridge (UK): GW Research Ltd; 2023 Nov 15.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Epidiolex (cannabidiol), 100 mg/mL, oral solution. Mississauga (ON): Jazz Pharmaceuticals Canada; 2023 Sep 25.
3.Clinical Study Report: GWEP1332, GWPCARE1. A double-blind, placebo-controlled, two-part study to investigate the dose-ranging safety and pharmacokinetics, followed by the efficacy and safety of cannabidiol (GWP42003-P) in children and young adults with Dravet syndrome [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2016 Nov 11.
4.Clinical Study Report: GWEP1424, GWPCARE2, amendment 1. A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P) in children and young adults with Dravet syndrome [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2019 Mar 15.
5.National Institute for Health Care Excellence. Cannabidiol with clobazam for treating seizures associated with Dravet syndrome. (Technology appraisal guidance TA614) 2019; https://www.nice.org.uk/guidance/ta614. Accessed by sponsor, no date provided.
6.Cooper MS, McIntosh A, Crompton DE, et al. Mortality in Dravet syndrome. Epilepsy Res. 2016;128:43-47. PubMed
7.Verdian L, Yi Y, Oyee J, Heyes A, Tolley K. Abstract 1.352: Eliciting utility scores for health states associated with Lennox-Gastaut syndrome (LGS). Seattle (WA): 62nd meeting of the American Epilepsy Society; 2008 Dec 05 - Dec 09.
8.de Kinderen RJ, Wijnen BF, van Breukelen G, et al. From clinically relevant outcome measures to quality of life in epilepsy: a time trade-off study. Epilepsy Res. 2016;125:24-31. PubMed
9.Long-term care homes level-of-care per diem funding summary. Toronto (ON): Ontario Ministry of Long-Term Care; 2023: https://www.ontario.ca/page/long-term-care-home-level-care-diem-funding-summary. Accessed 2023 Jul 25.
10.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 May 05 [sponsor accessed].
11.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2023: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2023 May 05 [sponsor accessed].
12.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: http://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2023 May 12.
13.Job Bank. Wages of Physiotherapists. Ottawa (ON): Government of Canada; 2023: https://www.jobbank.gc.ca/wagereport/occupation/18214. Accessed 2023 Aug 21.
14.Job Bank. Wages for Occupational therapists. Ottawa (ON): Government of Canada; 2022: https://www.jobbank.gc.ca/wagereport/occupation/4168. Accessed 2023 May 17.
15.Job Bank. Wages for Registered nurses and registered psychiatric nurses. Ottawa (ON): Government of Canada; 2022: https://www.jobbank.gc.ca/wagereport/occupation/993. Accessed 2023 May 17.
16.Canadian Institute for Health Information. Patient Cost Estimator. 2020; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2023 May 17.
17.Canadian Institute for Health Information. Care in Canadian ICUs. Ottawa (ON): CIHI; 2016: https://secure.cihi.ca/free_products/ICU_Report_EN.pdf. Accessed 2023 May 17.
18.Kwan P, Arzimanoglou A, Berg AT, et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51(6):1069-1077. PubMed
19.Wicker E, Cole JW. Sudden unexpected death in epilepsy (SUDEP): a review of risk factors and possible interventions in children. J Pediatr Pharmacol Ther. 2021;26(6):556-564. PubMed
20.Auvin S, Damera V, Martin M, Holland R, Simontacchi K, Saich A. The impact of seizure frequency on quality of life in patients with Lennox-Gastaut syndrome or Dravet syndrome. Epilepsy Behav. 2021;123:108239. PubMed
21.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed by sponsor, no date provided.
22.Jazz Pharmaceuticals Canada, Inc. response to November 16, 2023 CADTH request for additional information regarding Epidiolex DS CADTH review [internal additional sponsor's information]. Mississauga (ON): Jazz Pharmaceuticals Canada; 2023 Nov 23.
23.Lo SH, Lloyd A, Marshall J, Vyas K. Patient and caregiver health state utilities in Lennox-Gastaut syndrome and Dravet syndrome. Clin Ther. 2021;43(11):1861-1876.e1816.
24.Ruthirago D, Julayanont P, Karukote A, Shehabeldin M, Nugent K. Sudden unexpected death in epilepsy: ongoing challenges in finding mechanisms and prevention. Int J Neurosci. 2018;128(11):1052-1060. PubMed
25.Myland M, Buysse B, Tsong W, Power GS, Nordli D, Chin RFM. Seizure frequency, healthcare resource utilisation and mortality in childhood epilepsy: a retrospective cohort study using the THIN database. Arch Dis Child. 2019;104(11):1070-1076. PubMed
26.Trinka E, Bauer G, Oberaigner W, Ndayisaba JP, Seppi K, Granbichler CA. Cause-specific mortality among patients with epilepsy: results from a 30-year cohort study. Epilepsia. 2013;54(3):495-501. PubMed
27.Clinical Study Report: GWEP1415, GWPCARE5. An open-label extension study to investigate the safety of cannabidiol (GWP42003-P; CBD) in children and adults with inadequately controlled Dravet or Lennox-Gastaut Syndromes [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2021 Feb 25.
28.Lattanzi S, Trinka E, Russo E, et al. Pharmacotherapy for Dravet syndrome: a systematic review and network meta-analysis of randomized controlled trials. Drugs. 2023;83(15):1409-1424. PubMed
29.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2023: http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2023 Nov [CADTH accessed].
30.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2023; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Nov 30 [CADTH accessed].
31.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Epidiolex (cannabidiol), 100 mg/mL, oral solution. Mississauga (ON): Jazz Pharmaceuticals Canada; 2023 Sep 25.
32.Table: 17-10-0005-01. Population estimates on July 1st, by age and sex. Ottawa (ON): Statistics Canada: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed by sponsor no date provided.
33.Non-Insured Health Benefits program: First Nations and Inuit Health Branch: annual report 2021 to 2022. Ottawa (ON): Indigenous Services Canada; 2023: https://www.sac-isc.gc.ca/eng/1683039690813/1683039973755. Accessed 2023 Aug 15.
34.Orpha.net. Dravet syndrome. 2021; https://www.orpha.net/en/disease/detail/33069#:~:text=Disease%20definition,with%20cognitive%20and%20motor%20impairment. Accessed 2023 Jul 11.
35.Wirrell EC, Hood V, Knupp KG, et al. International consensus on diagnosis and management of Dravet syndrome. Epilepsia. 2022;63(7):1761-1777. PubMed
36.Jazz Pharmaceuticals. Data on File. Canadian Clinical Expert Survey. 2023 [sponsor provided reference].
37.Dravet Canada. What is Dravet? https://dravet.ca/what-is-dravet/. Accessed 2023 Dec 14.
38.Marshall J, Skrobanski H, Moore-Ramdin L, Kornalska K, Swinburn P, Bowditch S. Caregivers' perspectives on the impact of cannabidiol (CBD) treatment for Dravet and Lennox-Gastaut syndromes: a multinational qualitative study. J Child Neurol. 2023;38(6-7):394-406. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for the Treatment of Dravet Syndrome
Treatment | Strength / concentration | Form | Price ($) | Recommended maintenance dosage | Daily maintenance cost ($) | Annual maintenance cost ($) |
|---|---|---|---|---|---|---|
Cannabidiol (Epidiolex) | 100 mg/mL | Oral solution in 100 mL bottles | 1,424.5400a | 10 mg/kg/d, up to a maximum of 20 mg/kg/d | 14.25 to 227.93 | 5,200 to 83,193 |
Stiripentol (Diacomit) | 250 mg 500 mg | Capsule Oral solution | 5.8984 11.7783 | 50 mg/kg/d | 11.80 to 94.37 | 4,306 to 34,447 |
Note: All prices are from the Ontario Exceptional Access Program (accessed November 2023),29 unless otherwise indicated, and do not include dispensing fees. Doses are from the respective product monographs. For dosing that depends on weight, CADTH assumed a patient weight range of 10 kg to 80 kg. Daily and annual maintenance costs represent the range of potential costs (e.g., from 10 kg patients receiving the lowest recommended dose to 80 kg patients receiving the highest recommended dose).
aSponsor’s submitted price.2
Table 9: CADTH Cost Comparison Table for Antiepileptic Drugs Used in the Treatment of Dravet Syndrome
Treatment | Strength / concentration | Form | Price ($) | Recommended maintenance dosage | Daily maintenance cost ($) | Annual maintenance cost ($) |
|---|---|---|---|---|---|---|
Clobazam (generics) | 10 mg | Tablet | 0.2197 | ≤ 2 years: 0.5 mg/kg/day to 1 mg/kg/day; 2 to 16 years: 5 mg/d, up to a maximum of 40 mg/day; 16+ years: 5 mg/day to 15 mg/day, up to a maximum of 80 mg/day | 0.11 to 1.76 | 40 to 642 |
Clonazepam (generics) | 0.5 mg 2 mg | Tablet | 0.0418 0.0721 | < 10 years or < 30 kg: 0.1 mg/kg/day to 0.2 mg/kg/day; 10+ years: up to a maximum of 20 mg/day | 0.08 to 0.72 | 31 to 263 |
Levetiracetam (generics) | 250 mg 500 mg 750 mg | Tablet | 0.3210 0.3911 0.5416 | < 18 years: up to a maximum of 100 mg/kg/daya; 18+ years: 1,000 mg/day up to a maximum of 3,000 mg/day | 0.78 to 2.17 | 286 to 791 |
Rufinamide (Banzel) | 100 mg 200 mg 400 mg | Tablet | 0.8730b 1.7459b 3.8043b | < 30 kg: 200 mg/day up to a maximum of 1,300 mg/day; 30 kg to 50 kg: 400 mg/day up to a maximum of 1,800 mg/day; 50.1 kg to 70 kg: 400 mg/day up to a maximum of 2,400 mg/day; > 70 kg: 400 mg/day up to a maximum of 3,200 mg/day | 3.80 to 30.43 | 1,389 to 11,109 |
Topiramate (generics) | 25 mg 100 mg 200 mg | Tablet | 0.2433 0.4583 0.6748 | ≥ 6 years: 100 mg/day up to a maximum of 400 mg/dayb | 0.46 to 1.35 | 167 to 493 |
Valproic acid (generics) | 250 mg 500 mg 50 mg/mL | Capsule Enteric capsule Oral solution | 0.2905 0.8102 0.0398 per mL | 15 mg/kg/day up to a maximum of 60 mg/kg/day | 0.46 to 1.35 | 44 to 2,957 |
Note: All prices are from the Ontario Drug Benefit Formulary or the Ontario Exceptional Access Program (accessed November 2023)29,30 and do not include dispensing fees. Doses are from the respective product monographs. For dosing that depends on weight, CADTH assumed a patient weight range of 10 kg to 80 kg. Daily and annual maintenance costs represent the range of potential costs (e.g., from patients weighing 10 kg receiving the lowest recommended dose to patients weighing 80 kg receiving the highest recommended dose).
aRecommended dosage is based on clinical expert opinion elicited by CADTH.
bWhen used as monotherapy. Recommended dose ranges may change when used in combination with other antiseizure medications.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
The population is relevant, with no critical intervention missing, and no relevant outcome missing. | No | The modelled population is restricted to patients with DS who are inadequately controlled by their current usual care, while the indication is for the adjunctive treatment of seizures associated with DS. The clinical evidence to inform the sponsor’s pharmacoeconomic submission was derived from the CARE, and the generalizability of the findings to adult patients is unclear. |
The model has been adequately programmed and has sufficient face validity. | No | Individual patient data underlying the transition probabilities between seizure-based health states could not be validated. Setting all efficacy and safety parameters to equal usual care resulted in unearned residual QALY benefit for cannabidiol that the sponsor was unable to adequately explain.22 |
The model structure is adequate for the decision problem. | No | The model structure did not adequately reflect DS in clinical practice. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis). | No | Uncertainty was not incorporated into transition probabilities derived from individual patient data. Transitions between health states that were not observed from individual patients within the CARE studies were set to 0 without consideration for their probability within a larger population. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem. | No | Refer to previous row regarding data incorporation into the model. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough detail). | No | The model was complex and lacked transparency, containing numerous IFERROR statements making validation difficult. |
DS = Dravet syndrome; QALY = quality-adjusted life-year.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
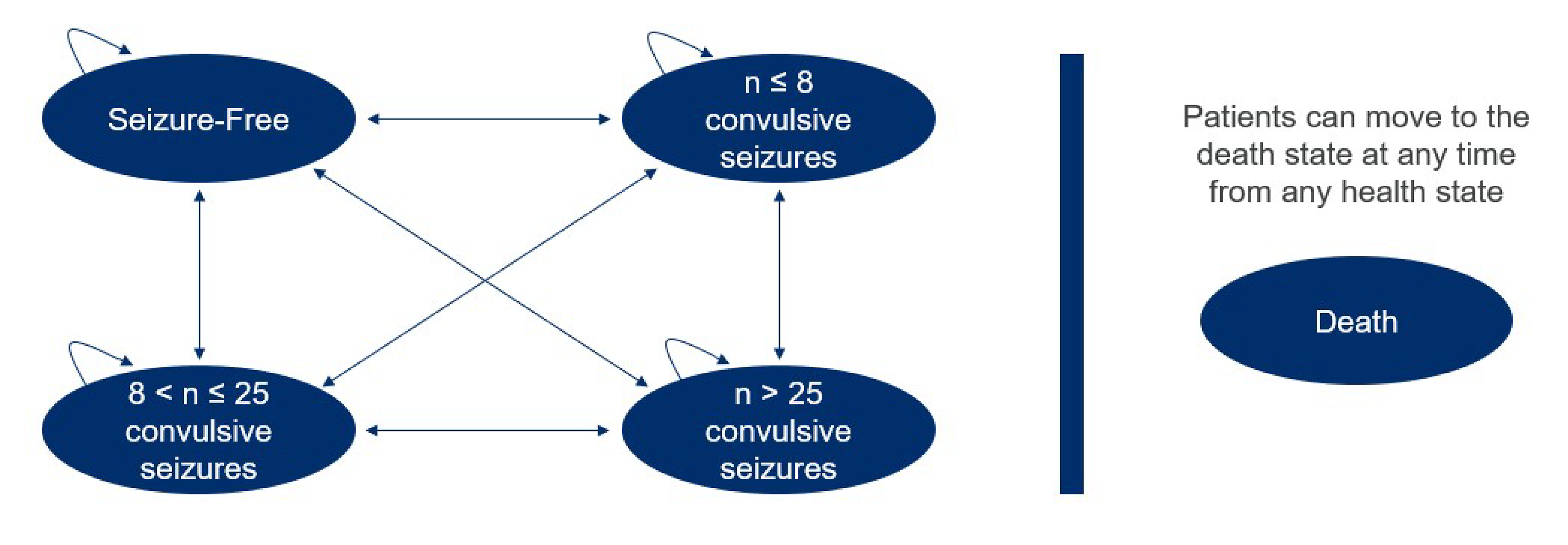
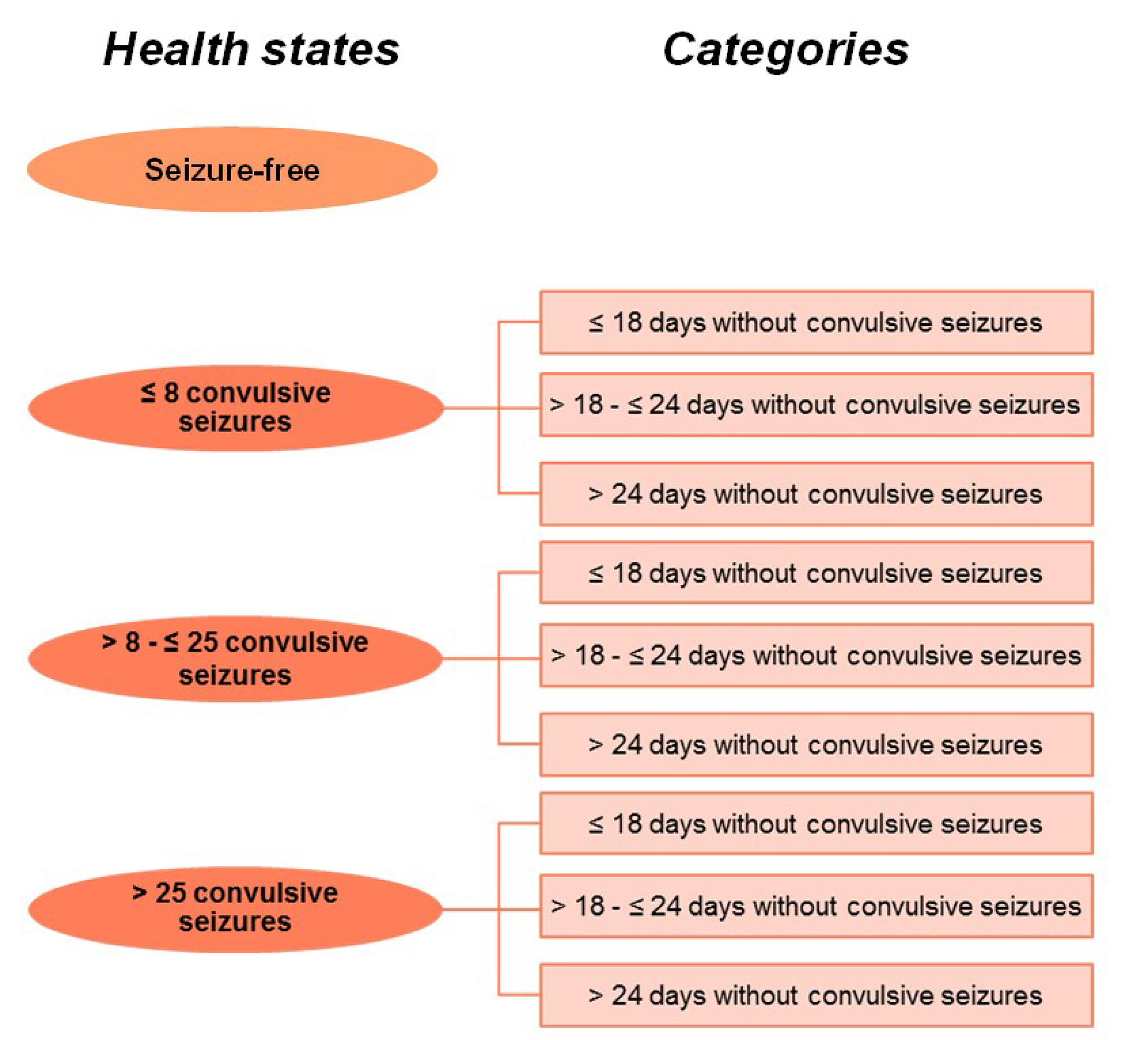
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of the Sponsor’s Economic Evaluation Results, Probabilistic
Parameter | Cannabidiol plus UC | UC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 29.33 | 29.05 | 0.28 |
Seizure-free | 2.79 | 1.46 | 1.33 |
≤ 8 seizures | 1.34 | 11.84 | −10.50 |
> 8 to ≤ 25 seizures | 0.72 | 7.55 | −6.83 |
> 25 seizures | 0.61 | 8.20 | −7.59 |
Discontinuation seizure-free | 1.21 | 0.00 | 1.21 |
Discontinuation ≤ 8 seizures | 9.75 | 0.00 | 9.75 |
Discontinuation > 8 to ≤ 25 seizures | 6.18 | 0.00 | 6.18 |
Discontinuation > 25 seizures | 6.74 | 0.00 | 6.74 |
Discounted QALYs (QALYs accrued by patients and caregivers) | |||
Total | 6.61 | 4.60 | 2.01 |
Seizure-free | 2.17 | 1.14 | 1.03 |
≤ 8 seizures | 0.75 | 6.53 | −5.78 |
> 8 to ≤ 25 seizures | 0.14 | 0.65 | −0.52 |
> 25 seizures | −0.26 | −3.72 | 3.46 |
Discontinuation seizure-free | 0.94 | 0.00 | 0.94 |
Discontinuation ≤ 8 seizures | 5.38 | 0.00 | 5.38 |
Discontinuation > 8 to ≤ 25 seizures | 0.54 | 0.00 | 0.54 |
Discontinuation > 25 seizures | −3.05 | 0.00 | −3.05 |
Discounted QALYs (QALYs accrued by patients only) | |||
Total | 15.64 | 14.66 | 0.98 |
Seizure-free | 2.17 | 1.14 | 1.03 |
≤ 8 seizures | 0.92 | 7.98 | −7.07 |
> 8 to ≤ 25 seizures | 0.39 | 3.75 | −3.36 |
> 25 seizures | 0.11 | 1.80 | −1.69 |
Discontinuation seizure-free | 0.94 | 0.00 | 0.94 |
Discontinuation ≤ 8 seizures | 6.57 | 0.00 | 6.57 |
Discontinuation > 8 to ≤ 25 seizures | 3.07 | 0.00 | 3.07 |
Discontinuation > 25 seizures | 1.48 | 0.00 | 1.48 |
Discounted costs ($) | |||
Total | 866,467 | 794,732 | 71,735 |
Treatment cost | 364,837 | 245,406 | 119,431 |
Health state cost | 501,213 | 549,036 | −47,822 |
Adverse event cost | 417 | 291 | 126 |
ICER ($/QALY) | 35,705 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; UC = usual care.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Cannabidiol plus UC | UC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 29.35 | 29.07 | 0.28 |
Seizure-free | 2.79 | 1.46 | 1.33 |
≤ 8 seizures | 1.88 | 11.85 | −9.96 |
> 8 to ≤ 25 seizures | 0.73 | 7.56 | −6.82 |
> 25 seizures | 0.66 | 8.21 | −7.56 |
Discontinuation seizure-free | 1.18 | 0.00 | 1.18 |
Discontinuation ≤ 8 seizures | 9.51 | 0.00 | 9.51 |
Discontinuation > 8 to ≤ 25 seizures | 6.03 | 0.00 | 6.03 |
Discontinuation > 25 seizures | 6.57 | 0.00 | 6.57 |
Discounted QALYs | |||
Total | 15.68 | 14.62 | 1.07 |
Seizure-free | 2.17 | 1.14 | 1.03 |
≤ 8 seizures | 1.29 | 7.97 | −6.68 |
> 8 to ≤ 25 seizures | 0.39 | 3.73 | −3.34 |
> 25 seizures | 0.11 | 1.78 | −1.66 |
Discontinuation seizure-free | 0.92 | 0.00 | 0.92 |
Discontinuation ≤ 8 seizures | 6.40 | 0.00 | 6.40 |
Discontinuation > 8 to ≤ 25 seizures | 2.98 | 0.00 | 2.98 |
Discontinuation > 25 seizures | 1.42 | 0.00 | 1.42 |
Discounted costs ($) | |||
Total | 985,750 | 849,156 | 136,593 |
Treatment cost | 490,887 | 303,329 | 187,558 |
Health state cost | 494,446 | 545,539 | −51,093 |
Adverse event cost | 417 | 289 | 128 |
ICER ($/QALY) | 128,062 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; UC = usual care.
Table 13: Summary of the Scenario Analyses Conducted on the CADTH Base Case
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | UC | 849,156 | 14.62 | Reference |
Cannabidiol plus UC | 985,750 | 15.68 | 128,062 | |
CADTH scenario 1: Mortality benefit removed | UC | 847,190 | 14.49 | Reference |
Cannabidiol plus UC | 970,064 | 15.36 | 140,547 | |
CADTH scenario 2: Stopping rule for cannabidiol implementedb | UC | 850,902 | 14.62 | Reference |
Cannabidiol plus UC | 922,303 | 15.29 | 107,698 | |
CADTH scenario 3: Caregiver disutilities included (1 caregiver per patient) | UC | 851,455 | 9.70 | Reference |
Cannabidiol plus UC | 986,887 | 11.32 | 83,771 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; UC = usual care.
aProbabilistic unless otherwise stated.
bBased on the sponsor’s scenario in which patients using cannabidiol who have not experienced at least a 30% reduction in seizure frequency are assumed to discontinue cannabidiol at 6 months, 1 year, and 2 years.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Takeaways
Key Takeaways of the BIA |
|---|
|
Summary of Sponsor’s BIA
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of cannabidiol for the adjunctive treatment of seizures associated with DS in patients 2 years of age and older.31 The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2025 to 2027) using an epidemiological approach (Table 15). The sponsor compared a reference scenario in which patients received usual care for the treatment of seizures associated with DS to a new drug scenario in which cannabidiol was reimbursed for use in combination with usual care. The sponsor’s analysis included the drug acquisition cost of cannabidiol; dispensing fees and markups were not included in the base case. Data for the model were obtained from various sources, including Statistics Canada,32 Non-Insured Health Benefits (NIHB) annual reports,33 the pivotal trials of cannabidiol in DS,3,4 the published literature,34,35 clinical expert opinion elicited by the sponsor,36 the sponsor’s internal market research, and assumptions. Key inputs to the BIA are documented in Table 16.
Key assumptions included:
The usage of cannabidiol will be restricted to patients whose seizures are refractory to ASMs.
The patients in clinical practice will have the same age and body weight distribution as those enrolled in the CARE1 and CARE2 trials.
The addition of cannabidiol will not impact the usage of ASMs.
All patients will initiate cannabidiol at 5 mg/kg/day for 7 days followed by a maintenance dose of 10 mg/kg/day.
Adherence to cannabidiol will be 85%.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1 / year 2 / year 3) | |
|---|---|---|
Pediatric patients (aged 2 to 17 years) | Adult (18+ years) | |
Target population | ||
Population of CADTH-participating jurisdictions aged 2 years and older | 30,905,44532 | |
Prevalence of DS | 0.0025%34 | |
Proportion of patients with DS in each age group | ||
Proportion of patients with DS who receive ASMs | 95%36 | |
Proportion of patients with DS whose seizures are refractory to ASMs | 90%a | |
Proportion of patients eligible for public coverage | 60%b | 80%b |
Number of patients eligible for cannabidiol | 403 / 408 / 412 | |
Market uptake (reference scenario, 3 years) | ||
Cannabidiol plus UC | 0% / 0% / 0% | |
UC | 100% / 100% / 100% | |
Uptake (new drug scenario) | ||
Cannabidiol plus UC | 10% / 22% / 30% | 8% / 20% / 26% |
UC | 90% / 78% / 70% | 92% / 80% / 74% |
Annual cost of treatment per patient (first year / subsequent years) | ||
Cannabidiol plus UCc | $13,761 / $13,894 | $22,252 / $22,467 |
UC | $0 | $0 |
ASM = antiseizure medication; DS = Dravet syndrome; UC = usual care.
Note: Usual care was assumed by the sponsor to include the following ASMs: clobazam, valproic acid, stiripentol, levetiracetam, topiramate, clonazepam, and rufinamide.
aBased on a survey of clinical experts conducted by the sponsor, which suggested that 90% to 96% of patients with DS have seizures that are refractory to ASMs.36
bBased on the sponsor’s internal market research.
cThe sponsor assumed that the dosage of cannabidiol costs would be 5 mg/kg for the first 5 days, followed by 10 mg/kg for the remainder of the BIA horizon, with an adherence rate of 85%. Costs for pediatric patients (aged 2 to 17 years) assume a weighted average median body weight of 31.42 kg while adult patients (aged 18+ years) are assumed to have a median body weight of 50.80 kg based on the CARE1 and CARE2 trials.3,4 The sponsor assumed that usual care costs would be the same regardless of use of cannabidiol and thus assigned a cost of $0 to usual care.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing cannabidiol for use as adjunctive therapy to usual care among patients with DS aged 2 years and older would be $3,281,628 (year 1: $559,663; year 2: $1,176,781; year 3: $1,545,184).
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The full indicated population for DS was not modelled: In the BIA, the sponsor assumed that patients with DS whose seizures are refractory to other ASMs would be eligible for cannabidiol, whereas the Health Canada indication for cannabidiol does not specify that it may only be used in an ASM-refractory subgroup. The clinical expert input received by CADTH suggests that cannabidiol will most likely be prescribed for patients whose seizures are refractory to other ASMs; however, if cannabidiol is reimbursed for its full indication, it is possible that the number of patients who receive cannabidiol will be higher than estimated by the sponsor. In their analysis, the sponsor assumed that 90% of patients with DS have drug-refractory seizures; however, a survey of clinical experts conducted by the sponsor suggests that this could be up to 96% of patients.31
In the CADTH base case, the eligible population was aligned with the full Health Canada indication. The impact of restricting the eligible population to an ASM-refractory subgroup was explored in scenario analyses.
The number of patients with DS in Canada is uncertain: The sponsor used an epidemiologic approach to estimate the number of patients eligible for cannabidiol, starting with the estimated prevalence of DS of 1/40,000. This estimate was obtained from the Orpha.net database for rare diseases. CADTH notes that this database estimates the average prevalence of DS at birth to be 1/30,000 with an estimated range between 1/15,000 and 1/40,000.34 Clinical experts consulted by CADTH agreed with the range published by Orpha.net, and Dravet Canada estimates that approximately 1,000 people in Canada have DS.37
CADTH explored uncertainty in the eligible population size in scenario analyses.
The NIHB population was inappropriately calculated: The sponsor calculated the total population of CADTH-participating drug plans by adding the population of the provinces as reported by Statistics Canada,32 excluding Quebec, to the population of NIHB clients. NIHB clients living within the borders of a province are counted within provincial population data, thus the NIHB population was double counted in the sponsor’s analysis. Additionally, while the sponsor appropriately limited the included provincial populations to those aged 2 years and older, all clients of the NIHB were included without removing those under 2 years of age, overcounting the potentially eligible NIHB population.33 Finally, NIHB clients residing within Ontario who are under 25 or over 65 years of age are eligible for reimbursement by the Ontario Drug Benefit (ODB) and thus should be counted as ODB clients rather than NIHB clients for the purposes of modelling the budgetary impact of reimbursing cannabidiol.
CADTH did not adjust for this limitation in reanalysis. The impact on the pan-Canadian model results is expected to be minimal.
The proportion of patients eligible for public drug plan coverage is uncertain and may be underestimated: The sponsor assumed that 60% of pediatric and 80% of adult patients with DS are eligible for public reimbursement.31 No rationale supporting these assumptions was provided by the sponsor. While it is likely that many pediatric patients will have access to private insurance coverage through their parents’ employers, patients eventually age out of such coverage. Additionally, as described in the sponsor’s submitted pharmacoeconomic evaluation, a recent caregiver study conducted in the US, UK, and Germany found that 79% of caregivers for patients with DS stopped working due to caring responsibilities,38 which may reduce the likelihood of private insurance coverage. Given the severity of DS, the proportion of adults with DS who have their own employer-sponsored health insurance is likely small. The clinical expert input received by CADTH suggests that 100% of adult patients with DS are likely eligible for public drug coverage in Canada. As such, the sponsor’s assumptions on the proportion of patients eligible for public funding may be underestimated.
This limitation could not be addressed by CADTH owing to a lack of available data.
Cannabidiol drug costs are uncertain and likely underestimated: The sponsor assumed that all patients would receive a cannabidiol maintenance dose of 10 mg/kg/day. As noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, this assumption is not aligned with the monograph dosage, which allows for a maintenance dose of up to 20 mg/kg/day depending on “individual clinical response and tolerability.”1 Clinical experts consulted by CADTH indicated that in clinical practice, some patients may trial a dosage above 10 mg/kg/day (e.g., those who do not experience an initial treatment response or who experience an initial response but wish to further attempt to reach seizure freedom). Additionally, as also noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, the sponsor used median body weights for adult and pediatric patients in the CARE1 and CARE2 trials, rather than mean body weights, which is inappropriate.
As noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, the use of weight estimates from the CARE1 and CARE2 trials, which enrolled patients aged 2 to 18 years, resulted in an underestimate of the weight of adult patients. This, combined with the sponsor’s estimate that only 2% of patients with DS are over the age of 18, further contributes to an underestimation of cannabidiol acquisition costs.
Finally, the sponsor assumed 85% adherence to cannabidiol and thus reduced the drug acquisition costs for cannabidiol by 15%. This is inconsistent with assumptions made in the pharmacoeconomic model, where adherence was not considered. The impact of reduced adherence on the clinical or cost-effectiveness of cannabidiol has not been explored. Furthermore, prescriptions for cannabidiol may be filled and reimbursed regardless of treatment adherence, thus the consideration of adherence of less than 100% may inappropriately reduce the cost of cannabidiol.
In the CADTH base case, CADTH assumed that all patients will adhere to their prescribed dosage regimen and adopted an average cannabidiol dose of 12 mg/kg/day (aligned with the CADTH base-case pharmacoeconomic evaluation), based on expert input suggesting that approximately 20% of patients with DS may receive a maintenance cannabidiol dose of 20 mg/kg/day (20 mg/kg/day). Additionally, CADTH used mean body weights, rather than median, in the calculation of drug costs. For patients aged 18 to 55 years, CADTH adopted mean patient weights from the corresponding age group in the CARE3 and CARE4 trials involving patients with LGS.
The market uptake of cannabidiol is uncertain: The sponsor’s submitted base case assumed that 10%, 22%, and 33% of eligible pediatric patients and 8%, 20%, and 26% of eligible adult patients would receive cannabidiol plus usual care in year 1, year 2, and year 3, respectively, based on the sponsor’s internal estimates and expert opinion. The clinician input received by CADTH for this review suggests that the sponsor’s estimates may underestimate the uptake of cannabidiol, with approximately 25%, 50%, and 75% of eligible patients potentially receiving cannabidiol in year 1, year 2, and year 3, respectively.
CADTH explored uncertainty in the uptake of cannabidiol in scenario analyses.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analyses by aligning the eligible population with the Health Canada indication for LGS, adopting a maintenance dose of 12 mg/kg/day, and using mean body weight and 100% adherence in the calculation of drug costs. The changes made to derive the CADTH base case are described in Table 16.
Table 16: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Eligible population | Assumed that only patients with drug-resistant DS would be eligible for cannabidiol | Aligned with the Health Canada indication for DS |
2. Maintenance dose of cannabidiol | 10 mg/kg/day | 12 mg/kg/daya |
3. Patient body weight | Pooled median patient weight by age group from the CARE1 and CARE2 trials | Patients aged 2 to 17 years: Pooled mean patient weight from the CARE1 and CARE2 trials. Patients aged 18+: Pooled mean patient weight for the corresponding age group from the CARE3 and CARE4 trials |
4. Adherence to cannabidiol | 85% | 100% |
CADTH base case | 1 + 2 + 3 + 4 | |
BIA = budget impact analysis.
aBased on clinical expert input, CADTH assumed that 80% of patients will receive a cannabidiol maintenance dose of 10 mg/kg/day and 20% will receive a maintenance dose of 20 mg/kg/day. The reanalysis also assumed that year 1 costs for patients who receive 20 mg/kg/day will incur all titration phase costs (i.e., 7 days at 5 mg/kg/day, 7 days at 10 mg/kg/day, 7 days at 15 mg/kg/day, and 344.25 days at 20 mg/kg/day).
The results of the CADTH stepwise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. In the CADTH base case, the 3-year budget impact of reimbursing cannabidiol as adjunctive therapy for the treatment of seizures associated with DS is expected to be $5,532,598 (year 1: $937,992; year 2: $1,986,853; year 3: $2,607,754).
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $3,281,628 |
CADTH reanalysis 1: Full Health Canada population (for DS) | $3,646,254 |
CADTH reanalysis 2: 12 mg/kg/day maintenance dose of cannabidiol | $3,933,622 |
CADTH reanalysis 3: Patient body weight | $6,530,913 |
CADTH reanalysis 4: 100% adherence | $3,860,739 |
CADTH base case (reanalysis 1 + 2 + 3 + 4) | $5,532,598 |
BIA = budget impact analysis.
CADTH conducted additional scenario analyses to explore remaining uncertainty associated with the potential budget impact, using the CADTH base case. Results are provided in Table 18.
Assuming only patients with drug-resistant DS will be eligible for cannabidiol, assumed by the sponsor to be 90% of patients with DS.
Assuming that the uptake of cannabidiol is 25%, 50%, and 75% in year 1, year 2, and year 3, respectively, for eligible patients (pediatric and adult).
Adopting a higher prevalence of DS (1/15,000).
Assuming that the price of cannabidiol is reduced by 44.8%, the price reduction at which cannabidiol plus usual care would be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 0 | 0 | 0 | 0 | 0 |
New drug | 0 | 559,663 | 1,176,781 | 1,545,184 | 3,281,628 | |
Budget impact | 0 | 559,663 | 1,176,781 | 1,545,184 | 3,281,628 | |
CADTH base case | Reference | 0 | 0 | 0 | 0 | 0 |
New drug | 0 | 937,992 | 1,986,853 | 2,607,754 | 5,532,598 | |
Budget impact | 0 | 937,992 | 1,986,853 | 2,607,754 | 5,532,598 | |
CADTH scenario 1: Drug-resistant DS only | Reference | 0 | 0 | 0 | 0 | 0 |
New drug | 0 | 844,192 | 1,788,168 | 2,346,978 | 4,979,339 | |
Budget impact | 0 | 844,192 | 1,788,168 | 2,346,978 | 4,979,339 | |
CADTH scenario 2: Increased cannabidiol uptake | Reference | 0 | 0 | 0 | 0 | 0 |
New drug | 0 | 2,369,098 | 4,501,445 | 6,639,688 | 13,510,230 | |
Budget impact | 0 | 2,369,098 | 4,501,445 | 6,639,688 | 13,510,230 | |
CADTH scenario 3: Higher prevalence of DS | Reference | 0 | 0 | 0 | 0 | 0 |
New drug | 0 | 2,501,311 | 5,298,275 | 6,954,010 | 14,753,596 | |
Budget impact | 0 | 2,501,311 | 5,298,275 | 6,954,010 | 14,753,596 | |
CADTH scenario 4: 44.8% price reduction for cannabidiol | Reference | 0 | 0 | 0 | 0 | 0 |
New drug | 0 | 517,771 | 1,096,743 | 1,439,480 | 3,053,994 | |
Budget impact | 0 | 517,771 | 1,096,743 | 1,439,480 | 3,053,994 |
BIA = budget impact analysis.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.