CADTH Reimbursement Review
Cannabidiol (Epidiolex)
Sponsor: Jazz Pharmaceuticals Canada, Inc.
Therapeutic area: Seizures associated with tuberous sclerosis complex (TSC)
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine aminotransferase
ANCOVA
analysis of covariance
ASM
antiseizure medications
AST
aspartate aminotransferase
CEA
Canadian Epilepsy Alliance
CGIC
Caregiver Global Impression of Change
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
IQR
interquartile range
ITT
intention to treat
IVRS
interactive voice response system
LS
least squares
MID
minimally important difference
MMRM
mixed-effect model with repeated measures
mTOR
mammalian target of rapamycin
OLE
open-label extension
OR
odds ratio
PP
per protocol
QoL
quality of life
QOLCE
Quality of Life in Childhood Epilepsy
QOLIE-31-P
31-item Quality of Life in Epilepsy – Problems questionnaire
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SGIC
Subject Global Impression of Change
SUDEP
sudden unexpected death in epilepsy
TAND
TSC-associated neuropsychiatric disorders
TEAE
treatment-emergent adverse event
TSC
tuberous sclerosis complex
TSCST
Tuberous Sclerosis Canada Sclérose Tubéreuse
Vineland II
Vineland Adaptive Behaviour Scales, Second Edition
VNS
vagus nerve stimulation
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Cannabidiol (Epidiolex), 100 mg/mL, oral solution |
Sponsor | Jazz Pharmaceuticals Canada, Inc. |
Indication | Cannabidiol is indicated for use as adjunctive therapy for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome or TSC in patients 2 years of age and older |
Reimbursement request | Per the Health Canada indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 15, 2023 |
Recommended dose | Starting dose is 2.5 mg/kg twice daily (5 mg/kg per day). After 1 week, the dosage should be increased to 5 mg/kg twice daily (10 mg/kg per day) and the clinical response and tolerability should be assessed. Each dose can then be further increased in weekly increments of 2.5 mg/kg administered twice daily up to a maximum recommended dose of 12.5 mg/kg twice daily (25 mg/kg per day). |
NOC = Notice of Compliance; TSC = tuberous sclerosis complex.
Note: The reimbursement request for this review only pertains to the population of patients with TSC-associated seizures.
Introduction
Tuberous sclerosis complex (TSC) is a rare genetic disorder that results in the formation of benign tumours in many different organs, primarily in the brain, heart, lungs, kidneys, skin, and eyes.1 Although data specific to Canada are lacking, TSC is estimated to occur in 1 of every 5,000 to 10,000 live births and has a prevalence of 8.8 cases per 100,000 people.1-6 Epileptic seizures of various types are the most common neurologic manifestation of the disease, affecting upward of 70% of patients,7-12 and they are also a significant cause of morbidity and mortality in patients with TSC.11,13-16 Uncontrolled epilepsy is among the most common causes of death for patients with TSC, as a result of status epilepticus or sudden unexpected death in epilepsy (SUDEP).15 Clinically, the most effective prevention strategy for death related to epilepsy is to reduce the frequency of seizures.17,18
TSC-associated seizures generally begin in the first year of life for most patients (62.5% to 73.0%),10 beginning as infantile spasms, and are characterized by sudden and brief extension or flexion of the extremities. Other seizure types associated with TSC include focal seizures, which affect about two-thirds of patients and can present with variable symptoms and evolve into a more generalized seizure, including tonic (brief tonic extension of the extremities, sometimes resulting in a fall), atonic (sudden loss of muscle tone resulting in a fall), and tonic-clonic (involving both stiffening and twitching or jerking of extremities) seizures,19 which become refractory in two-thirds of patients.9-11,20,21 Seizure burden in patients with TSC can be high, with untreated patients reporting an average of 87 TSC-associated seizures per month.22 Patients with TSC-associated seizures often have severe impairment of daily functioning or a history of epilepsy-related injuries.23 As a result, TSC-associated epilepsy has a severe impact on a patient’s quality of life (QoL). Patients with TSC and the early onset of seizures experience greater impairment in intellectual development than those without seizures, and the early appearance of seizures usually results in severe forms of intellectual disability.10 TSC is a chronic, life-long condition, and although the prognosis for many people living with TSC has improved over the years and life expectancy has increased, careful monitoring of all organ systems and development is critical, with most patients requiring multidisciplinary care at tertiary institutions as a result of their seizures and/or aspects of TSC-associated neuropsychiatric disorders (TAND).
TSC may present at any age and is often diagnosed based on specific clinical criteria and/or genetic testing.24 Major clinical diagnostic criteria include 3 or more hypomelanotic macules at least 5 mm in diameter, 3 or more angiofibromas or fibrous cephalic plaques, 2 or more ungual fibromas, shagreen patch, multiple retinal hamartomas, multiple cortical tubers and/or radial migration lines, 2 or more subependymal nodules, subependymal giant cell astrocytoma, cardiac rhabdomyoma, lymphangioleiomyomatosis, and more than 2 angiomyolipomas. Minor diagnostic features of TSC include: confetti skin lesions, more than 3 dental enamel pits, more than 2 intraoral fibromas, retinal achromatic patch, multiple renal cysts, nonrenal hamartomas, and sclerotic bone lesions. Patients who have definite TSC have 2 major features or 1 major feature and 2 minor features. Possible TSC is considered in patients with either 1 major feature or 2 or minor features. Two genes have been identified that can cause TSC: TSC1 and TSC2. Only 1 pathogenic variant in either of these genes is required for TSC to be present.
The goal of treatment in patients with TSC-related seizures is to prevent or control seizures, which may improve cognitive neurodevelopment and enhance health-related quality of life (HRQoL).10 There are limited options for disease-modifying medical therapies in TSC, and no Canadian guidelines exist for the management of patients with TSC-related seizures. International guidelines broadly agree on the overall strategy, with antiepileptic drugs as the mainstay of current pharmacological treatment, consisting of sodium valproate, vigabatrin, levetiracetam, clobazam, lamotrigine, lacosamide, oxcarbazepine, topiramate, and carbamazepine in Canada.1,10,25 Additional nonpharmacological treatments for seizures related to TSC include a ketogenic diet, surgery for tumour removal, and vagus nerve stimulation (VNS).
The antiseizure mechanism of cannabidiol (Epidiolex) is unknown, although it is structurally distinct from other antiseizure medications (ASMs). Cannabidiol reduces neuronal hyperexcitability by modulating intracellular calcium via the G protein-coupled receptor 55 and transient receptor potential vanilloid cation channel subfamily V member 1, and by modulating adenosine-mediated signalling through the inhibition of adenosine transport via the equilibrative nucleoside transporter-1.26 The Health Canada Notice of Compliance for cannabidiol was issued on November 15, 2023. Cannabidiol has not previously been reviewed by CADTH, but it is currently being reviewed for use in 2 other indications: Dravet syndrome and Lennox-Gastaut syndrome.27
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol, oral solution (100 mg/mL), administered as adjunctive therapy along with other ASMs for the treatment of seizures associated with TSC in patients aged 2 years and older.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups provided input for this review: the Canadian Epilepsy Alliance (CEA), and Tuberous Sclerosis Canada Sclérose Tubéreuse (TSCST). The CEA collected input from its 24 member associations on the knowledge and experience of patients, caregivers, clinicians, volunteers, and supporters. The input from TSCST was gathered from a survey of 11 patient and caregiver members conducted in September 2023.
Both patient groups emphasized the catastrophic nature of uncontrolled seizures in infants and children, which are linked to cognitive delays, physical disabilities, and have a high correlation with mental illness, including depression and anxiety. Seizures occur so frequently that patients are unable to achieve milestones, learn, or even sleep. The patient groups noted that seizures associated with TSC are typically hard to control, and patients require constant monitoring and medication changes to try to get a combination that works to control, or at least reduce, the number of seizures. The patient groups noted that when someone has epilepsy, the whole family is affected, highlighting the tremendous burden of uncontrolled seizures on caregivers. Patients and caregivers experience anxiety around when and where the next seizure will occur, and what impact it will have. Caregivers are often sleep deprived and constantly fatigued due to sleep interruptions or anxiety. As well, caregivers are exposed to sometimes highly unpleasant side effects, including mood swings, sexual dysfunction, suicidal thoughts, memory loss, problems with concentration, fatigue, exhaustion, and depression, which are exacerbated by various medications.
Both patient groups emphasized the importance of total seizure freedom or reduction in seizure frequency to improved overall QoL. The patient groups noted that seizure control improves more than just developmental milestones; it also improves day-to-day life, leading to fewer postictal side effects, better sleep, and less fatigue, confusion, anxiety, and headaches, among other issues. Additionally, both patient groups highlighted the physical and emotional wellbeing of caregivers and patients, including the ability to get an education or find full-time employment, as well as the importance of social interactions because the disease is so isolating; which all could be improved with greater seizure control.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Given that TSC is a life-long disease, the experts noted that the main goals of treatment include seizure reduction and improved QoL, cognition, and behaviour, without side effects that worsen comorbidities. Other goals include the prevention of SUDEP, a reduction in caregiver burden, and greater independence for patients.
Current pharmacological treatment for TSC-associated seizures include ASMs, which the experts noted are generally directed at the specific types of seizure and are often age related. The experts highlighted that most patients present with infantile spasms, which are generally treated with first-line vigabatrin, followed by corticosteroids. Focal seizures are often treated with sodium channel blockers (e.g., carbamazepine, oxcarbazepine, eslicarbazepine, lamotrigine, phenytoin), whereas generalized seizures are often treated with broad-spectrum drugs (e.g., valproate, clobazam, lamotrigine, topiramate, levetiracetam, brivaracetam). Treatments targeting the mammalian target of rapamycin (mTOR) pathway, such as everolimus and sirolimus, are used to treat some of the tumours associated with TSC; however, there is controversy about whether they improve seizure frequency or neuropsychiatric comorbidities. Additionally, mTOR inhibitors require chronic use and have potential serious side effects that require close monitoring. Interruption of the use of mTOR inhibitors can lead to tumour regrowth or seizure worsening, and the long-term effects of mTOR inhibition on TSC are still uncertain. Despite the fact that there are many ASMs currently available, response is highly variable, and patients can continue to suffer from severe and debilitating seizures. The clinical experts explained that cannabidiol does not address the underlying disease process any more than other conventional ASMs; however, the distinct mechanism of action of cannabidiol could be complementary to other ASMs. Current treatments are often associated with side effects, including sedation, or liver toxicity that can worsen comorbidities, such as those related to behaviour and may require constant monitoring.
The clinical experts noted that patients with TSC-associated seizures most in need of intervention would be those whose seizures or behavioural issues remain uncontrolled with their current therapies. The experts considered that patients most likely to benefit from cannabidiol are those with intellectual disabilities and developmental delays. Additionally, patients with neuropsychiatric comorbidities could benefit from cannabidiol, as it may improve neuropsychiatric symptoms’ in contrast, other available ASMs may worsen these symptoms. The experts also noted that these patients would be easily identifiable by clinicians based on their seizures and comorbidities. The clinical experts emphasized that caution should be taken and patients with a history of depression and with liver disease should be monitored, particularly patients taking concomitant valproate. Additionally, a dose adjustment may be required for patients taking concomitant clobazam and mTOR inhibitors, due to changing levels of desmethylclobazam and increased levels of mTOR resulting from the administration of cannabidiol. There is also no established safety in pregnancy, which would be a consideration for patients of childbearing age.
The clinical experts highlighted the fact that measures of seizure frequency and severity remain the most important consideration of treatment. Additional assessments in real-world practice include hospitalizations, rescue medication use, and side effects of treatment. The clinical experts agreed that although important, QoL measurements, caregiver burden, increase in independence, and clinical global impression are not commonly used in clinical practice; the subjective experience of patients is used to inform treatment decisions. The clinical experts highlighted that despite the 50% responder threshold used in the trial, even a 25% to 30% reduction in seizure frequency may be beneficial if there is reduction in the most severe and disabling type of seizure (i.e., tonic-clonic seizures). Initially, patients with TSC-associated seizures visit a doctor (typically a specialist) as often as every 3 months to monitor treatment and perform any medication adjustments, although patients mostly visit a doctor every 6 months. For patients who are seizure free, annual assessments are conducted. The clinical experts agreed that treatment would be discontinued in patients who experience severe adverse events (AEs), such as an elevation in liver enzymes of more than 5 times the limit, severe sedation, nausea, and allergic reaction. Additionally, worsening of neuropsychiatric side effects, such as depression, should also be a reason for discontinuation. The clinical experts also stated that some medications can interact with cannabidiol (e.g., valproic acid and clobazam) and may need to be adjusted before discontinuation is considered. The experts noted that the use of additional rescue medication would not prompt the discontinuation of treatment, given that this is generally used to break a cluster of seizures or a continuous prolonged seizure.
Clinician Group Input
No clinician group input was received by CADTH for this review.
Drug Program Input
The drug programs identified the following jurisdictional implementation issues: relevant comparators, considerations for initiation of therapy, considerations for continuation or renewal of therapy, considerations for discontinuation of therapy, considerations for prescribing of therapy, generalizability, care provision issues, and system and economic issues. Refer to Table 3 for more details.
Clinical Evidence
Systematic Review
Description of Studies
One phase III, placebo-controlled, randomized controlled CARE6 trial (RCT) (N = 224) compared the reduction in seizure frequency with cannabidiol oral solution or placebo as adjunctive treatment for the management of seizures in children and adults with TSC that was not completely controlled by their current ASMs. Patients were randomized in a 2:2:1:1 ratio to cannabidiol 25 mg/kg per day (n = 75), cannabidiol 50 mg/kg per day (n = 73), and 2 matching dose-volume equivalent placebo groups (pooled n = 76; hereafter referred to as the placebo group) for 16 weeks.22 The 50 mg/kg per day dose of cannabidiol is not a recommended, per the Health Canada, and data for that group are not included in this report. After completion of the double-blind treatment period, patients had the option to enter the long-term, open-label extension (OLE) study.28
Baseline characteristics were generally balanced across treatment groups, with a mean age of 13.7 years (mean age was 14.1 years in the 25 mg/kg per day group and 13.9 years in the placebo group); there were a few baseline imbalances that were compatible with chance. All patients had TSC-associated seizures, with type 2 focal seizures occurring most frequently (25 mg/kg per day group versus placebo group) (46 [61.3%] versus 50 [65.8%]), followed by type 1 focal motor seizure (29 [38.7%] versus 33 [43.4%]). The mean number of TSC-associated seizures during the baseline period was 77.95 (standard deviation [SD] = 83.39; range, 7.7 to 427.7) in the cannabidiol 25 mg/kg per day group and 89.22 (SD = 101.78; range, 8.0 to 558.0) in the placebo group. The median number of concurrent ASMs in each treatment group was 3 (range, 0 to 5), and the median number of prior ASMs that were no longer being taken was 4 (range, 0 to 15).22
Efficacy Results
Percent Change From Baseline in Seizure Frequency
The primary end point of the CARE6 trial was the change from baseline in the number of TSC-associated seizures during the treatment period. The mean percent change from baseline with cannabidiol 25 mg/kg per day was 48.6% (95% confidence interval [CI], 40.4% to 55.8%) and with placebo was 26.5% (95% CI, 14.9% to 36.5%). The ratio of cannabidiol to placebo was 0.699 (95% CI, 0.567 to 0.861), which translated to an estimated relative reduction for cannabidiol 25 mg/kg per day compared to placebo of 31.0% (95% CI, 13.9% to 43.3%; P = 0.0009).22
Results of subgroup analyses were consistent with those from the primary analysis, although reductions in seizure frequency were larger in patients taking clobazam than in those not taking clobazam, and the 95% CIs overlap.22
Treatment Responders: Proportion of Patients With at Least a 25% Reduction in Seizure Frequency, at Least a 50% Reduction in Seizure Frequency, and Total Seizure Freedom
The proportion of patients with a reduction of greater than or equal to 50% from baseline in TSC-associated seizure frequency was the first key secondary end point in the CARE6 trial. During the double-blind treatment period, 27 (36.0%) patients in the cannabidiol 25 mg/kg per day group and 17 (22.4%) patients in the placebo group experienced a reduction of at least 50% in seizure frequency (odds ratio [OR], 1.95; 95% CI, 0.95 to 4.00; P = 0.0692). The difference in the proportion of patients achieving a reduction of at least 50% in TSC-associated seizure frequency between cannabidiol 25 mg/kg per day and placebo was 13.6% (95% CI, –0.7 to 28.0).22
The proportion of patients with a reduction in TSC-associated seizure frequency of at least 25% and seizure freedom (100% reduction in seizure frequency) were secondary end points of the CARE6 trial. During the treatment period, 43 (57.3%) and 33 (43.4%) patients in the cannabidiol 25 mg/kg per day and placebo groups, respectively, experienced a 25% or greater reduction in seizure frequency (OR, 1.75; 95% CI, 0.92 to 3.33). The difference in the proportion of patients achieving a 25% or greater reduction in TSC-associated seizure frequency between cannabidiol 25 mg/kg per day and placebo was 13.9% (95% CI, –1.9% to 29.7%). Only 1 (1.3%) patient in the cannabidiol 25 mg/kg per day group experienced seizure freedom during the treatment period.22
Health-Related Quality of Life
HRQoL was assessed using the Quality of Life in Childhood Epilepsy (QOLCE) questionnaire in patients aged 2 to 18 years and the 31-item Quality of Life in Epilepsy – Problems questionnaire (QOLIE)-31-P patients 19 years and older. For both measures, the overall scores ranged from 0 to 100, with higher scores indicating better HRQoL.
Change From Baseline in QOLCE Scores
An overall QoL score on the QOLCE was available for 45 patients in the cannabidiol 25 mg/kg per day group at baseline and for 42 patients at the end of treatment. In the placebo group, 50 patients had an overall QoL score on the QOLCE at baseline, as did 47 patients at the end of treatment. At the end of treatment, the least squares (LS) mean change from baseline was 3.1 points (95% CI, –0.6 to 6.7 points) and 1.6 points (95% CI, –1.8 to 4.9 points) in the cannabidiol and placebo groups, respectively. The LS mean difference between groups in change from baseline was 1.5 points (95% CI, –3.3 to 6.3 points).22
Change From Baseline in QOLIE-31-P Scores
The QOLIE-31-P was completed by 13 patients in the cannabidiol 25 mg/kg per day group and 10 patients in the placebo group at baseline, and by 14 patients in the cannabidiol 25 mg/kg per day group and 12 patients in the placebo group at the end of treatment. At the end of treatment, the LS mean change from baseline was –1.4 points (95% CI, –16.2 to 13.5) in the cannabidiol group and 2.3 points (95% CI, –15.0 to 19.7) in the placebo group. The LS mean difference between groups in change from baseline was –3.7 points (95% CI, –16.6 to 9.2 points).22
Rescue Medication Use
During the baseline period, the number of days of rescue medication use in the cannabidiol 25 mg/kg per day group and placebo group, respectively, was 2.14 days (SD = 2.187) and 2.32 days (SD = 3.200). The mean number of days of rescue medication use during the treatment period was 0.79 days (SD = 2.469) in the cannabidiol 25 mg/kg per day group and 0.55 days (SD = 1.395) in the placebo group, representing mean changes from baseline of 0.19 days (SD = 2.836) and –0.92 days (SD = 1.858), respectively. The mean difference in change from baseline in rescue medication use between the cannabidiol 25 mg/kg per day group and the placebo group was 0.96 days (95% CI, –0.65 to 2.56 days).22
Status Epilepticus
During the baseline period, no patients in the cannabidiol 25 mg/kg per day group had status epilepticus, whereas 3 (3.9%) patients in the placebo group did. The proportion of patients who reported episodes of status epilepticus during the treatment period was 6.7% in the cannabidiol 25 mg/kg per day group and 9.2% in the placebo group.22
Vineland Adaptive Behaviour Scales, Second Edition
At the end of treatment, the mean adaptive behaviour composite score in the cannabidiol 25 mg/kg per day group was 50.7 (SD = 22.24), and in the placebo group was 51.5 (SD = 25.57),, representing a LS mean change from baseline of –0.0 points (95% CI, –1.6 to 1.5 points) in cannabidiol 25 mg/kg per day and –0.0 points (95% CI, –1.6 to 1.5 points) in the placebo group. The difference in LS mean change from baseline was 0.0 points (95% CI, –2.2 to 2.1 points).22
Harms Results
At least 1 treatment-emergent adverse event (TEAE) was reported by 70 (93.3%) patients in the cannabidiol 25 mg/kg per day group and by 72 (94.7%) patients in the placebo group. The most frequently occurring TEAEs (10% of patients or more) in the cannabidiol 25 mg/kg per day group were diarrhea (23 [30.7%]); decreased appetite (15 [20.0%]); pyrexia (14 [18.7%]); vomiting (13 [17.3%]); increased levels of gamma-glutamyl transferase, alanine aminotransferase (ALT), and aspartate aminotransferase (AST) (12 [16.0%], 9 [12.0%], 8 [10.7%], respectively); somnolence (10 [13.3%]); and cough (8 [10.7%]). In the placebo group, the most frequently occurring TEAEs were diarrhea (13 [17.1%]), nasopharyngitis (12 [15.8%]), upper respiratory tract infection (10 [13.2%]), and decreased appetite (9 [11.8%]).22
A total of 28 (12.5%) patients in the CARE6 trial experienced a total of 44 serious adverse events (SAEs) (16 [21.3%] in the 25 mg/kg per day group and 2 [2.6%] in the placebo group). The most commonly reported individual SAEs in the cannabidiol 25 mg/kg per day group were increased levels of ALT (2 [2.7%]), increased levels of AST (2 [2.7%]), status epilepticus (2 [2.7%]), vomiting (2 [2.7%]), and viral gastroenteritis (2 [2.7%]). SAEs in the placebo group only occurred in 2 (2.6%) patients; 1 (1.3%) experienced pneumonia and 1 (1.3%) experienced status epilepticus.22
A total of 20 (8.9%) patients had TEAEs leading to the discontinuation of treatment (8 [10.7%] in the 25 mg/kg per day group and 2 [2.6%] in the pooled placebo group). The most common reason for the discontinuation of treatment in the cannabidiol group was rash (2 [2.7%]). All other reasons for discontinuation occurred in only 1 (1.3%) patient. Of the 2 patients in the placebo group who discontinued treatment due to TEAEs, 1 experienced ataxia and 1 experienced agitation.22
There were no deaths reported during the CARE6 trial.22
Notable Harms
AEs of special interest to this review consisted of hepatocellular injury and hypersensitivity reactions. In the cannabidiol 25 mg/kg per day group, liver injury and type IV hypersensitivity reactions occurred in 1 (1.3%) patient each and were listed as SAEs, and both led to the discontinuation of treatment.22
Critical Appraisal
The phase III CARE6 trial was the only study included in this review. Randomization was stratified by age; given the known interaction between clobazam and cannabidiol, failure to stratify by clobazam use was a limitation, although the CARE6 trial was initiated before the importance of this interaction was known. It remains unclear what impact this may have had on the distribution of patients in the trial, and how the results may have been impacted. There were some baseline imbalances, but the clinical experts consulted by CADTH noted that there is substantial disease heterogeneity in this population and agreed that the differences could be due to chance. There were also differences between the cannabidiol 25 mg/kg per day and placebo groups in discontinuation of study treatment (13.3% versus 1.3%); discontinuations were primarily due to AEs (10.7% versus 0.0%). Despite being a double-blind RCT, this may have revealed treatment assignment; however, it is unclear what effect this would have on the results of the study. Most outcomes in the CARE6 trial were related to seizure frequency, which was measured by countable seizures of various types. According to clinical experts, there is some subjectivity and error in they way patients and caregivers classify these; however, the seizure types defined for the trial are generally countable and should not ultimately bias the results. Subgroups of interest to this review included clobazam use and the number of concurrent and prior ASMs, based on discussion with the clinical experts consulted by CADTH. Results generally supported the primary analysis, although they were not statistically powered to detect within-group or between-group differences. Additionally, wide overlapping 95% CIs reflected uncertainty in the effect estimates and were likely due to the small sample sizes, so the results should be viewed as supportive evidence for the overall effect of cannabidiol. Outcomes related to HRQoL were considered important to patients and were captured as other secondary end points in the CARE6 trial. The QOLCE and QOLIE-31-P were considered reliable and valid measures for epilepsy in TSC, although the clinical experts consulted by CADTH noted that these are not used in routine clinical practice. The use of rescue medication and the change in rescue medication use days was an exploratory outcome in the CARE6 trial. Most patients required the use of rescue medication at some point during the treatment period, although rescue medication usage was not accounted for in the primary or key secondary end point analyses; thus, it remains unclear whether there was any impact of rescue medication on the results. As noted by the clinical experts, the use of rescue medication would not prompt the discontinuation of therapy.
Two dosages of cannabidiol were evaluated in the CARE6 trial: 25 mg/kg per day and 50 mg/kg per day; however, given that the maximum recommended Health Canada–approved dosage of cannabidiol for TSC-associated seizures is 12.5 mg/kg twice daily (25 mg/kg per day), the cannabidiol 50 mg/kg per day dose was not of interest to this review. The CARE6 trial was an international, multicentre study, but there were no Canadian sites. As part of the inclusion and exclusion criteria for the CARE6 trial, patients were required to have a clinical diagnosis of TSC. Genetic confirmation was not required, which was noted by the clinical experts consulted by CADTH to be consistent with clinical practice. The included population had a high seizure burden, and particularly had drug-resistant epilepsy, demonstrated by the baseline seizure frequency (range, 8 to 558), number of prior ASMs (range, 0 to 15), and number of concurrent ASMs (range, 0 to 5). The clinical experts consulted by CADTH noted that the included population was reflective of clinical practice, highlighting the fact that there is often variability in seizure burden across patients; however, they also noted that not all patients with TSC have such high disease burden, so the enrolled population may have been restrictive, selecting for patients with more refractory epilepsy and higher disease burden. Additionally, there was heterogeneity in the concomitant ASMs received by patients in the CARE6 trial, but the clinical experts consulted by CADTH noted that this is in line with clinical practice and varies by patient, based on response, intolerance, and various contraindications. Outcomes in the CARE6 trial were considered to be clinically relevant and important to patients, particularly measures of seizure frequency, which is the focus of epilepsy treatment in routine clinical practice. However, an additional consideration noted by patient groups and the clinical experts consulted by CADTH is the reduction in seizure severity, which was not explicitly measured in the CARE6 trial. The clinical experts consulted by CADTH explained that a reduction in the frequency of seizures may not necessarily be associated with a reduction in severity. The duration of the CARE6 trial, at 16 weeks, was considered to be appropriate for measuring response to treatment and observing changes in seizure frequency. However, given that the impacts of cannabidiol on HRQoL and on TANDs were outcomes of interest to this review, and given the secondary nature of these outcomes, the small sample sizes for various measures and the short duration of the CARE6 trial are difficult to interpret. As such, these outcomes should only be viewed as supportive of the overall effect of cannabidiol.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered to be most relevant to CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.29,30 With the GRADE approach, evidence from RCTs could start as high-certainty evidence and be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members: the percent change from baseline in the number of TSC-associated seizures at week 16; the proportion of patients considered treatment responders (i.e., achieving target reductions of at least 25% or 50%) or achieving seizure freedom (100% reduction in seizure frequency) at week 16; improved HRQoL, assessed by the change from baseline in QOLCE and QOLIE-31-P scores at week 16; the proportion of patients with status epilepticus at week 16; the change from baseline in rescue medication use days at week 16; the change from baseline in Vineland Adaptive Behaviour Scales, Second Edition (Vineland II) scores at week 16; the proportion of patients with at least 1 SAE; and the proportion of patients with hepatocellular injury.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence of a clinically important reduction in seizure frequency (percent change in seizure frequency) on thresholds informed from clinical expert opinion, treatment guidelines, and clinical trials, as well as HRQoL and patient-reported outcome (QOLCE, QOLIE-31-P, Vineland II) assessments informed by the literature, where available. Other targets for the certainty of evidence assessment were the presence or absence of any (nonnull) effect for the proportion of patients achieving 25%, 50%, or 100% reductions in seizure frequency, the proportion of patients with status epilepticus, and changes from baseline in rescue medication use.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for cannabidiol versus placebo for outcomes in the pivotal CARE6 trial.
Table 2: Summary of Findings for Cannabidiol Versus Placebo as an Adjunctive Treatment for Patients With TSC-Associated Seizures
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | Cannabidiol | Difference | |||||
Change in seizure frequency | |||||||
Percent change from baseline in TSC-associated seizure frequency Follow-up: 113 days | 151 (1 RCT) | Ratio 0.699 (0.57 to 0.86), expressed as % reduction: 31.0% (13.9 to 43.3%) | 26.5 per 100 (14.9 to 36.5 per 100) | 48.6 per 100 (40.4 to 55.8 per 100) | 22.1 per 100 fewer (NR) | Moderatea | Cannabidiol likely results in a clinically important decrease (improvement) in seizure frequency compared with placebo. |
Percent of patients with ≥ 50% reductions in TSC-associated seizure frequency Follow-up: 113 days | 151 (1 RCT) | OR = 1.95 (0.95 to 4.00) | 22.4 per 100 | 36.0 per 100 | 13.6 per 100 more (0.7 fewer to 28.0 more per 100) | Moderateb | Cannabidiol likely results in a greater proportion of patients achieving a 50% reduction in TSC-associated seizure frequency compared with placebo. The clinical importance of the reduction is unclear. |
Percent of patients with ≥ 25% reductions in TSC-associated seizure frequency Follow-up: 113 days | 151 (1 RCT) | OR = 1.75 (0.92 to 3.33) | 43.4 per 100 | 57.3 per 100 | 13.9 per 100 more (1.9 fewer to 29.7 more per 100) | Moderateb,c | Cannabidiol likely results in a greater proportion of patients achieving a 25% reduction in TSC-associated seizure frequency compared with placebo. The clinical importance of the reduction is unclear. |
Percent of patients with seizure freedom (100% reductions in TSC-associated seizure frequency) Follow-up: 113 days | 151 (1 RCT) | OR = NE | 0 per 100 | 1.3 per 100 | 1.3 per 100 (1.3 fewer to 3.9 more per 100) | Moderateb,c | Cannabidiol likely results in little to no difference in the proportion of patients achieving total TSC-associated seizure freedom (100% reduction in seizure frequency) compared with placebo. The clinical importance of the effects is uncertain. |
Status epilepticus and need for rescue medication | |||||||
Proportion of patients with status epilepticus Follow-up: 113 days | 151 (1 RCT) | NA | 9.2 per 100 | 6.7 per 100 | 2.5 fewer per 100 (11.2 fewer to 6.1 more per 100) | Lowc,d | Cannabidiol may result in little to no difference in the proportion of patients with status epilepticus compared with placebo. The clinical importance of the effects is uncertain. |
Mean change from baseline in rescue medication use days (per 28 days) Follow-up: 113 days | 151 (1 RCT) | NA | –0.92 (SD = 1.86) | 0.19 (SD = 2.84) | 0.96 (–0.65 to 2.56) | Lowc,d | Cannabidiol may result in little to no difference in the rescue medication use compared with placebo. The clinical importance of the effects is uncertain. |
QoL and adaptive behaviour | |||||||
Change from baseline in QOLCE overall QoL score, points Follow-up: 113 days | 82 (1 RCT) | NA | 1.6 (–1.8 to 4.9) | 3.1 (–0.6 to 6.7) | 1.5 (–3.3 to 6.3) | Very lowc,e | The effect of cannabidiol on QOLCE overall QoL score compared with placebo is very uncertain. |
Change from baseline in QOLIE-31-P total score, points Follow-up: 113 days | 22 (1 RCT) | NA | 2.3 (15.0 to 19.7) | –1.4 (–16.2 to 13.5) | –3.7 (–16.6, 9.2) | Very lowc,f | The effect of cannabidiol on QOLIE-31-P total score compared with placebo is very uncertain. |
Change from baseline in Vineland II composite score, points Follow-up: 113 days | 90 (1 RCT) | NA | 0.0 (–1.6 to 1.5) | 0.0 (–1.6 to 1.5) | 0.0 (–2.2 to 2.1) | Very lowc,g | The effect of cannabidiol on the Vineland II composite score compared with placebo is very uncertain. |
Harmsh | |||||||
Hepatocellular injury (safety end point) Follow-up: 113 days | 151 (1 RCT) | NA | 0 per 100 | 1 per 100 | 1.33 more per 100 (1.26 fewer to 3.93 more per 100) | Moderatei | Cannabidiol likely results in little to no difference in the proportion of patients with hepatocellular injury compared with placebo. The clinical importance of the effects is uncertain. |
SAEs Follow-up: 113 days | 151 (1 RCT) | NA | 3 per 100 | 21 per 100 | 18.7 more per 100 (8.76 to 28.65 more per 100) | Lowj | Cannabidiol may result in an increase in the proportion of patients with SAEs compared with placebo. The clinical importance of the difference is uncertain. |
CI = confidence interval; NA = not available; NE = not estimable; NR = not reported; OR = odds ratio; QoL = quality of life; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = 31-item Quality of Life in Epilepsy – Problems questionnaire; RCT = randomized controlled trial; SAE = serious adverse event; SD = standard deviation; TSC = tuberous sclerosis complex; Vineland II = Vineland Adaptive Behaviour Scales, Second Edition.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 1 level for serious imprecision. The 95% CI included the potential for no clinically meaningful benefit. Based on clinical expert opinion, a threshold of about a 25% reduction in seizure frequency could be considered meaningful, and any reduction not reaching this threshold would be difficult to quantify. The 95% CI on the relative effect suggests a wide range of effects, with the lower bound being potentially not clinically important.
bRated down 1 level for serious imprecision. Using the null as the threshold, the 95% CI is compatible with both a benefit and little to no difference.
cStatistical testing for this outcome was not adjusted for multiplicity in the trial and should be considered as supportive evidence.
dDid not rate down for risk of bias. Although there were notable and imbalanced withdrawals from the study, it is not clear at which time these patients stopped contributing to the analysis. Rated down 2 levels for imprecision. Using the null as the threshold, the 95% CI is compatible with both benefit and harm.
eRated down 2 levels for very serious risk of bias due to a large quantity of missing outcome data. Rated down 1 level for serious imprecision. Based on the reported minimally important difference (MID) of 2.9 to 6.0 points, the 95% CI is compatible with little to no difference and with benefit.
fRated down 2 levels for very serious risk of bias due to a large quantity of missing outcome data. Rated down 1 level for serious imprecision. Based on the reported MID of 7.1 to 11.0 points, the 95% CI is compatible with little to no difference and with harm.
gRated down 2 levels for very serious risk of bias due to a large quantity of missing outcome data. Rated down 2 levels for very serious imprecision. Using the null as the threshold, the 95% CI includes the potential for both benefit and harm. Rated down 1 level for serious indirectness due to an insufficient duration of follow-up to adequately assess this outcome, based on clinical expert opinion.
hThis result was not part of the sponsor's prespecified analysis plan and was requested by CADTH to assist in the interpretation of the findings.
iRated down 1 level for serious imprecision. Using the null as the threshold, the 95% CI is compatible with both little to no difference and with harm.
jRated down 2 levels for very serious imprecision. The effect is informed by a small number of events and may be unstable.
Source: CARE6 Clinical Study Report.22
Long-Term Extension Studies
Description of Studies
One open-label, single-arm, long-term extension of the CARE6 study (CARE6 OLE) was summarized to provide evidence regarding the long-term safety and efficacy of cannabidiol. Upon completion of the double-blind phase of the CARE6 study, 199 patients who had completed the double-blind phase were invited to receive open-label cannabidiol during the OLE period, for a maximum duration of 4 years (124 from the cannabidiol 25 mg/kg per day and 50 mg/kg per day groups and 75 from the placebo group). The primary outcome of the CARE6 OLE study was to evaluate the AE profile (long-term safety and tolerability) of cannabidiol. Secondary outcomes of interest to this review were in line with the outcomes evaluated during the double-blind period of the CARE6 trial.28
Efficacy Results
In the OLE study, maintenance of efficacy was assessed in 156 patients treated for 37 to 48 weeks to account for differences in sample sizes with increasing time. The median percent reduction in TSC-associated seizure frequency from baseline was –66.27% (interquartile range [IQR], –86.70% to –18.64%) during weeks 37 to 48 of treatment, and the median change during the entire OLE treatment period (n = 199) was –55.22% (IQR, –81.70% to –13.47%).28
The number of patients who achieved a reduction in TSC-associated seizure frequency of at least 50% at 37 to 48 weeks of treatment was 93 (60%), and during the entire OLE treatment phase was106 (53%). There were no notable differences in the proportion of patients achieving a reduction in TSC-associated seizure frequency of at least 50% between those treated with cannabidiol and those treated with placebo during the double-blind phase of the study (60.0% versus 59.0%).28
Patients experienced a reduction in the overall QOLIE-31-P (patients ≥ 19 years) total score relative to the prerandomization baseline of the double-blind phase, with a mean change from baseline of –9.0 points (SD = 17.99) for all patients (n = 9) and –7.4 (SD = 18.57) for patients 19 years and older (n = 8) at OLE end of treatment. Based on a change from double-blind phase baseline to OLE end of treatment, a reduction in the QOLIE-31-P total score was observed in the cannabidiol group (–14.8; SD = 20.60; n = 5) and in the placebo group (–1.8 [SD = 13.2]; n = 4). For patients 19 years and older (n = 8), QOLIE-31-P total score reduction was –13.1 (SD = 23.39; n = 4) in cannabidiol group and –1.8 (SD = 13.12; n = 4) in the placebo group.28
Based on a change from double-blind baseline to OLE end of treatment, the reduction in the mean number of days of rescue medication use was 0.44 (SD = 4.09) in total population (n = 55), 0.10 (SD = 4.73) in the cannabidiol group (n = 35), and 1.02 (SD = 2.64) in the placebo group (n = 20).28
The number of patients with status epilepticus was 5 (2.5%) during the baseline period and 20 (10.1%) during the OLE treatment period. The number of patients who experienced status epilepticus was similar for patients treated with cannabidiol and those treated with placebo during the double-blind phase of the CARE6 study.28
Harms Results
A total of 192 (96.5%) patients treated with cannabidiol had 1 or more AEs during the OLE study. Most common TEAEs were diarrhea (46.7%), seizure (29.6%), and pyrexia (24.1%). SAEs were reported in 56 (28.1%) participants with TSC, with the most common SAEs being seizure (8%), status epilepticus (5%), and dehydration (3%).28
There were 18 (9%) participants with TSC who stopped treatment due to AEs, with the most common AEs leading to discontinuation being seizure (2%) and diarrhea (2%). One patient died 2 months after starting the open-label treatment of cannabidiol, although the death was considered to be unrelated to cannabidiol.28
Critical Appraisal
There was no active comparator or placebo group in the CARE6 OLE study, so the safety and the efficacy data could not be used to draw any conclusion in relation to an appropriate comparator. Furthermore, the open-label design may bias the reporting of subjective end points, including AEs, SAEs, and TEAEs. Because completion of a pivotal trial was an eligibility criterion for the extension study, patients who discontinued either the trial or the OLE due to AEs or lack of response were excluded. This could result in a population of patients that were more tolerant of cannabidiol, which can lead to selection bias, as those not responding to treatment are less likely to continue it. Having a patient population more tolerant of cannabidiol can also lead to biased estimates related to AEs, potentially resulting in fewer and less severe AEs being reported. The sample size of the CARE6 OLE study (N = 199) may not be sufficient to detect rare AEs. Only 17.1% of patients completed the study, and there was wide variation among participants in follow-up duration. For several outcomes, the sample size was, therefore, very small and not representative of all patients who started the OLE period.
The CARE6 OLE study enrolled patients from multiple sites in different countries, although there were no study sites in Canada. No evidence indicating a difference between the study population and patients in Canada was identified after consultation with the clinical experts. Even though the median number of dosing days of 369.5 (range, 95.0 to 1,462 days) provides longer follow-up for AE assessment compared with the double-blind phase of the CARE6 study, the proportion of patients who adhered to cannabidiol during the longer follow-up was not reported. Thus, study drug exposure among the patients in the OLE study was uncertain. About half of the patients (46.7%) were taking the 50 mg/kg per day dose, which is not an approved dosing level and could have impacted the results. The remaining patients were taking the 25 mg/kg per day dose, which is the highest dose suggested in the product monograph.
Indirect Comparisons
No indirect evidence on the comparative efficacy or safety of cannabidiol in patients with TSC-associated seizures was submitted by the sponsor.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps in the systematic review evidence were submitted by the sponsor.
Conclusions
There is a need for new, safe, and effective treatments for TSC-associated seizures in patients with seizures that remain uncontrolled by current therapies and who require an additional reduction in seizure burden. The 1 study included in this review, CARE6, which was a phase III, double-blind, placebo-controlled study comparing the efficacy and safety of cannabidiol and placebo administered as adjunctive therapy along with other ASMs for the treatment of seizures associated with TSC in patients 2 years and older.
The CARE6 study demonstrated that cannabidiol likely results in a clinically important decrease (improvement) in seizure frequency compared with placebo around the 25% threshold of clinical importance defined by the clinical experts. Additionally, responder analyses using thresholds of 25% and 50% reductions in seizures showed a likely benefit of cannabidiol (i.e., a greater proportion of patients meeting the threshold than in the placebo group), but there was uncertainty in the clinical importance of these effects and they failed to reach statistical significance. Complete seizure freedom would be the most ideal response to treatment and is important to clinicians and patients; however, only 1 patient in the cannabidiol group of the CARE6 trial experienced seizure freedom. Results of the trial showed that cannabidiol may have little to no impact on status epilepticus or on the need for rescue medication. Effects on HRQoL and adaptive behaviour were very uncertain due to imprecision and risk of bias because of missing outcome data. The risk of SAEs was likely elevated in patients who received cannabidiol, and there was little to no difference in the risk of hepatocellular injury with cannabidiol in the short term. The included study had a short double-blind treatment duration of only 16 weeks, which was sufficient to address the primary outcome of change in the number of TSC-associated seizures, but precluded the ability to assess long-term efficacy and safety and HRQoL. The ongoing OLE phase of the CARE6 trial aims to address this gap, but is limited by the lack of a comparator group, selection bias, and losses to follow-up. Although considered to be an outcome of importance to patients, reduction in the severity of seizures was not expressly measured in the CARE6 trial. Seizure burden was higher in the CARE6 trial than in the overall population of patients with TSC-associated seizures and in the population with highly refractory epilepsy. The differences in patient populations, as well as the relatively short duration of follow-up for the randomized phase, may limit the generalizability of the study results to a broader population of patients with TSC-associated seizures.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol 100 mg/mL oral solution administered as adjunctive therapy along with other antiseizure medications for the treatment of seizures associated with TSC in patients 2 years and older.
Disease Background
The contents of this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the CADTH review team.
TSC is a rare, autosomal dominant, multisystemic disorder characterized by the formation of multiple benign tumours in different organs, primarily in the brain, heart, lungs, kidneys, skin, and eyes.1 TSC is a heterogenous disease, with presentation varying by tumour location. The central nervous system manifestations of TSC often lead to debilitating neurologic disorders, and include seizures, TANDs such as mental retardation, and behavioural disorders such as autism.1 Epileptic seizures of various types are the most common neurologic manifestation of the disease, affecting upward of 70% of patients,7-12 and are a significant cause of morbidity and mortality in patients with TSC.11,13-16 Uncontrolled epilepsy related to status epilepticus or SUDEP is among the most common causes of death in patients with TSC.15 Clinically, the most effective prevention strategy for death related to epilepsy is to reduce the frequency of seizures.17,18
Seizure burden in patients with TSC can be high; untreated patients report an average of 87 TSC-associated seizures per month.22 TSC-associated seizures generally begin in the first year of life in most patients (62.5% to 73.0%),10 beginning as infantile spasms that are characterized by sudden and brief extension or flexion of the extremities. Other seizure types associated with TSC include focal seizures, which affect about two-thirds of patients and can present with variable symptoms and evolve into a more generalized seizure, including tonic (brief tonic extension of the extremities, sometimes resulting in a fall), atonic (sudden loss of muscle tone resulting in a fall), and tonic-clonic (involving both stiffening and twitching or jerking of extremities) seizures,19 which become refractory in two-thirds of patients.9-11,20,21 The International League Against Epilepsy has defined refractory epilepsy as the failure to achieve sustained seizure freedom after 2 adequate trials of antiseizure medication.31
Aside from difficulty with seizure control, patients with TSC-associated seizures often have severe impairment of daily functioning or a history of epilepsy-related injuries.23 As a result, TSC-associated epilepsy has a severe impact on a patient’s QoL. Patients with TSC and an early onset of seizures experience greater impairment in intellectual development than those without seizures, and the early appearance of seizures usually results in severe forms of intellectual disability.10 As patients transition into adulthood, seizures may persist, and renal and pulmonary issues that can be associated with increased morbidity and mortality may surface.15 Patients may require constant supervision, often necessitating changes in virtually all aspects of the lives of caregivers and family members; caring for such patients dictates work schedules, family time, and leisure activities.32 TSC is a chronic, life-long condition, and although the prognosis for many people living with TSC has improved over the years and life expectancy has increased, careful monitoring of all organ systems and development is critical, with most patients requiring multidisciplinary care at tertiary institutions as a result of seizures and/or aspects of TAND.
Around 80% of patients with TSC-associated seizures have their epilepsy diagnosed when they are younger than 2 years,33 However, TSC can present at any age and is often diagnosed based on specific clinical criteria and/or genetic testing.24 Major clinical diagnostic criteria include 3 or more hypomelanotic macules at least 5 mm in diameter, 3 or more angiofibromas or fibrous cephalic plaques, 2 or more ungual fibromas, shagreen patch, multiple retinal hamartomas, multiple cortical tubers and/or radial migration lines, 2 or more subependymal nodules, subependymal giant cell astrocytoma, cardiac rhabdomyoma, lymphangioleiomyomatosis, and more than 2 angiomyolipomas. Minor diagnostic features of TSC include confetti skin lesions, more than 3 dental enamel pits, more than 2 intraoral fibromas, retinal achromatic patch, multiple renal cysts, nonrenal hamartomas, and sclerotic bone lesions. Patients who have definite TSC have 2 major features or 1 major feature and 2 minor features. Possible TSC is considered in patients with either 1 major feature or 2 or minor features. Two genes have been identified that cause TSC: TSC1 and TSC2. The TSC1 gene is located on chromosome 9 and directs production of the protein called hamartin, whereas the TSC2 gene, located on chromosome 16, directs production of the protein called tuberin. Both proteins act as tumour suppressors. Only 1 pathogenic variant in either of these genes is required for TSC to be present. Between 10% and 15% of patients with TSC meet the clinical diagnostic criteria but have no identified mutation on genetic testing.1
Although estimates specific to Canada are lacking, TSC is estimated to occur in 1 of every 5,000 to 10,000 live births and has a prevalence of 8.8 cases per 100,000 people.1-6
Standards of Therapy
The contents of this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the CADTH review team.
The goal of treatment in patients with TSC-related seizures is to prevent or control seizures as soon as possible after diagnosis, which may improve cognitive neurodevelopment and enhance HRQoL.10 There are limited options for disease-modifying medical therapies in TSC, and no Canadian guidelines exist for the management of TSC-related seizures.
International guidelines broadly agree on the overall strategy, with antiepileptic drugs as the mainstay of current pharmacological treatment, which in Canada consists of sodium valproate, vigabatrin, levetiracetam, clobazam, lamotrigine, lacosamide, oxcarbazepine, topiramate, and carbamazepine.1,10,25
The clinical experts consulted by CADTH highlighted the fact that the selection of treatment is generally guided by age and seizure type; infantile spams are generally initially treated with vigabatrin, followed by corticosteroids. Focal seizures are often treated with sodium channel blockers (e.g., carbamazepine, oxcarbazepine, eslicarbazepine, lamotrigine, phenytoin), and generalized seizures are often treated with broad-spectrum drugs (e.g., valproate, clobazam, lamotrigine, topiramate, levetiracetam, brivaracetam). The clinical experts also noted that mTOR inhibitors (everolimus and sirolimus) are used to treat some of the tumours associated with TSC and can reduce seizure frequency; however, interruption of the use of mTOR inhibitors can lead to tumour regrowth or seizure worsening, and the long-term effects of mTOR inhibition on TSC are still uncertain.
Additional nonpharmacological treatment for seizures related to TSC include a ketogenic diet, surgery for tumour removal, and VNS.
Drug Under Review
Cannabidiol is administered orally at a recommended starting dosage of 2.5 mg/kg twice daily (5 mg/kg per day). After 1 week, that should be increased to a maintenance dosage of 5 mg/kg twice daily (10 mg/kg per day). Each dosage should be further increased in weekly increments of 2.5 mg/kg twice daily up to a maximum recommended dosage of 12.5 mg/kg twice daily (25 mg/kg per day). Each vial contains 100 mg/mL of cannabidiol solution, available in 60 mL or 100 mL bottles.26
The anticonvulsive mechanism of cannabidiol is unknown, although it is structurally distinct from other ASMs. Cannabidiol does not exert its antiseizure effect by interacting with cannabinoid receptors. Cannabidiol reduces neuronal hyperexcitability by modulating intracellular calcium via the G protein-coupled receptor 55 and transient receptor potential vanilloid cation channel subfamily V member 1, and by modulating adenosine-mediated signalling through the inhibition of adenosine transport via the equilibrative nucleoside transporter-1.26
The Health Canada indication and the reimbursement request for cannabidiol are as adjunctive therapy administered with other antiseizure medications for the treatment of seizures associated with TSC in patients 2 years and older.27
The Health Canada Notice of Compliance for cannabidiol was issued on November 15, 2023. Cannabidiol has not previously been reviewed by CADTH, but it is currently being reviewed for use in 2 other indications: Dravet syndrome and Lennox-Gastaut syndrome.27
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input(s) received by CADTH has been included in the Stakeholder section of this report.
Two patient groups provided input for this review: the CEA, and TSCST. The CEA is a network of organizations supporting and advocating for people living with epilepsy and their families, whereas TSCST is a voluntary, nonprofit, charitable organization that raises awareness and supports individuals living with TSC and their families. The CEA collected input from its 24 member associations on the knowledge and experience of patients, caregivers, clinicians, volunteers, and supporters. The input from TSCST was gathered from a survey of 11 patient and caregiver members conducted in September 2023.
Living with seizures severely affects patients and caregivers. Both patient groups emphasized the catastrophic nature of uncontrolled seizures in infants and children, which are linked to cognitive delays and physical disabilities, and have a high correlation with mental illness, including depression and anxiety. Seizures occur so frequently that patients are unable to achieve milestones, learn, and even sleep. The patient groups noted that seizures associated with TSC are typically hard to control, and patients require constant monitoring and medication changes to try to get a combination that works to control, or at least reduce, the number of seizures.
The patient groups noted that when someone has epilepsy, the whole family is affected, highlighting the tremendous burden of uncontrolled seizures on caregivers. Patients and caregivers experience anxiety about when and where the next seizure will occur and what impact it will have. Caregivers are often sleep-deprived and constantly fatigued due to sleep interruptions or anxiety. As well, caregivers are exposed to sometimes highly unpleasant side effects, including mood swings, sexual dysfunction, suicidal thoughts, memory loss, problems with concentration, fatigue, exhaustion, and depression, which are exacerbated by various medications.
According to CEA input, patients living with uncontrolled epilepsy can be socially isolated due to stigma and fear of rejection in social, work, and educational situations. Additionally, parents and caregivers often miss work, as patients require the care of many specialists, including neurologists, nephrologists, pulmonary specialists, cardiologists, psychiatrists, and occasionally dermatologists.
Although many treatments are available for epilepsy, seizures remain uncontrolled by 1 or a combination of existing therapies in 30% of patients. Additionally, the patient groups highlighted the fact that currently available treatments may not work for a prolonged period. Respondents to the TSCST survey reported that each ASM worked for a short time but then stopped working. Also, they noted that the side effects are “brutal,” particularly those that cause “impossible behaviours.” No patients who provided input had experience with cannabidiol, as there have been no clinical trials conducted in Canada thus far; however, both patient groups emphasized the need for this medication to be brought to patients in Canada, emphasizing that patients without seizure control are constantly hopeful for new, effective therapies without side effects.
Both patient groups emphasized the importance of total seizure freedom or reduction in seizure frequency to improving overall QoL. The patient groups stated that seizure control improves more than just developmental milestones; it also improves day-to-day life, leading to fewer postictal side effects, better sleep, and less fatigue, confusion, anxiety, and headaches, among others. Additionally, both patient groups highlighted the physical and emotional wellbeing of caregivers and patients, including the ability to get an education or find full-time employment, as well as the importance of social interactions because the disease is so isolating; which all could be improved with greater seizure control.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of TSC-associated seizures.
Unmet Needs
Many individuals with TSC experience drug-resistant epilepsy and significant cognitive and behavioural comorbidities, known as TANDs. Despite many currently available ASMs, response is highly variable, and patients continue to suffer from severe and debilitating seizures. Moreover, treatments are often associated with side effects, including sedation, and liver toxicity that can worsen comorbidities such as those related to behaviour and may require constant monitoring.
Given that TSC is a life-long disease, the main goals of treatment include seizure reduction, and improved QoL, cognition, and behaviour, without side effects that worsen comorbidities. Other goals include the prevention of SUDEP, a reduction in caregiver burden, and greater independence for patients.
Place in Therapy
Current pharmacological treatment for TSC-associated seizures include ASMs, which the experts noted are generally guided by age and seizure type. Infantile spasms, which most patients present with, are generally treated with first-line vigabatrin, followed by corticosteroids. Focal seizures are often treated with sodium channel blockers (e.g., carbamazepine, oxcarbazepine, eslicarbazepine, lamotrigine, phenytoin), whereas generalized seizures are often treated with broad-spectrum drugs (e.g., valproate, clobazam, lamotrigine, topiramate, levetiracetam, brivaracetam). Treatments targeting the mTOR pathway, such as everolimus and sirolimus, are used to treat some of the tumours associated with TSC; however, there is controversy about whether they improve seizure frequency or neuropsychiatric comorbidities. Additionally, some treatments require chronic use and have potential serious side effects that require close monitoring. Interruption of the use of mTOR inhibitors can lead to tumour regrowth or seizure worsening, and the long-term effects of mTOR inhibition on TSC are still uncertain.
Nondrug seizure treatments consist of neuromodulation and a ketogenic diet; most patients become refractory to multiple ASMs. Although not fully understood, cannabidiol has a mechanism distinct from other ASMs and a proposed mechanism related to the mTOR pathway.
The clinical experts highlighted that cannabidiol does not address the underlying disease process any more than other conventional ASMs, but the distinct mechanism of action of cannabidiol could be complementary to other ASMs. Given the heterogeneity of seizure types in patients with TSC, treatment approaches vary and there is no specific treatment sequencing. The clinical experts noted that cannabidiol should be considered early in the treatment of TSC-associated seizures, as early as the second line; however, it would be reasonable to recommend that patients try other ASMs before trying cannabidiol, despite the fact that other available treatments often lead to limiting side effects and have not shown good efficacy.
Patient Population
Patients with TSC-associated seizures are undergoing treatment with a number of ASMs. Although the indication for cannabidiol specifies its use as adjunctive therapy to other ASMs, the clinical experts explained than any patient with TSC could be considered for treatment, regardless of the line of therapy (i.e., no matter how many ASMs have been used). The clinical expert noted that patients with TSC-associated seizures most in need of intervention would be those whose seizures or behavioural issues remain uncontrolled by their current therapies. Patients most likely to benefit from cannabidiol are those with intellectual disabilities and developmental delays, according to the experts. Additionally, patients with neuropsychiatric comorbidities could benefit from cannabidiol, as it may improve neuropsychiatric symptoms; in contrast, other available ASMs may worsen these symptoms. The experts also noted that these patients would be easily identifiable by clinicians based on their seizures and comorbidities.
The clinical experts emphasized that caution should be taken and patients with history of depression and with liver disease should be monitored, particularly those taking concomitant valproate. Additionally, a dose adjustment may be required in patients taking concomitant clobazam and mTOR inhibitors, due to changing levels of desmethylclobazam and increased levels of mTOR resulting from the administration of cannabidiol. There is also no established safety in pregnancy, which would be a consideration for patients of childbearing age.
Assessing the Response Treatment
The clinical experts highlighted that many outcome measures used in clinical trials are not normally used in clinical practice, although measures of seizure frequency and severity remain the most important consideration of treatment. Additional assessments in real-world practice include hospitalizations, rescue medication use, and side effects of treatment. The clinical experts agreed that although important, QoL measurements, caregiver burden, increase in independence, and clinical global impression are not commonly used in clinical practice; the subjective experience of patients is used to inform treatment decisions.
The clinical experts noted that the magnitude of response likely varies by physician, depending on treatment experience and comfort with dose increases. Despite the 50% responder threshold used in the trial, even a 25% to 30% reduction in seizure frequency may be beneficial if there is reduction in the most severe and disabling type of seizure (i.e., tonic-clonic seizures), the clinical experts explain.
Response to treatment would be assessed at each visit, but the frequency of visits is dependent on how well seizures are controlled. Initially, patients with TSC-associated seizures would visit a doctor (typically a specialist) as often as every 3 months to monitor treatment and perform any medication adjustments, although patients mostly visit a doctor every 6 months. For patients who are seizure free, annual assessments would be conducted. Recently, virtual care has aided the timely assessments of treatment response and is often more convenient for patients and caregivers, the clinical experts noted.
As previously noted, some patients experience side effects and/or drug interactions that require constant monitoring and may impact the response to treatment and rate of discontinuation. The clinical experts suggested that patients are more likely to stay on treatment if physicians are readily available to manage side effects and other issues with dose reductions in other ASMs.
Discontinuing Treatment
The clinical experts agreed that treatment would be discontinued in patients who experience severe AEs, such as an elevation of liver enzymes more than 5 times the upper limit of normal, severe sedation, nausea, and allergic reaction. Additionally, a worsening of neuropsychiatric side effects, such as depression, should also be a reason for discontinuation.
The clinical experts stated that some medications can interact with cannabidiol (e.g., valproic acid and clobazam) and may need to be adjusted before discontinuation is considered. They also noted that the use of additional rescue medication, generally used to break a cluster of seizures or a continuous prolonged seizure, would not prompt the discontinuation of treatment.
Additionally, the experts noted that pregnancy, or contemplation of pregnancy, would be a consideration for discontinuation, as there is no evidence available for patients considering childbearing.
Prescribing Considerations
Patients with TSC are under the care of neurologists who specialize in epilepsy, and would be qualified for cannabidiol, regardless of the practice setting (i.e., in tertiary academic centres or in the community).
Clinician Group Input
No clinician group input was received by CADTH for this review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The phase III, double-blind CARE6 trial evaluated the efficacy and safety of cannabidiol plus usual care vs. usual care alone (i.e., placebo). Currently, everolimus is the only drug indicated for TSC-associated seizures in Canada and it was approved by Health Canada for the adjunctive treatment of seizures associated with TSC in patients 2 years and older with a definite diagnosis of TSC who are not satisfactorily controlled with current therapies. However, everolimus for TSC-associated epilepsy has not been reviewed by CADTH. Everolimus was not included as a comparator in the submission, and patients receiving mTOR inhibitors were excluded from the CARE6 trial. Should everolimus be considered a comparator for cannabidiol? | Although everolimus has Health Canada approval for the adjunctive treatment of seizures associated with TSC in patients 2 years and older, the primary indication and use of this therapy is as a chemotherapy for tumour shrinkage and it is fundamentally a different class of treatment. As a chemotherapy, patients must remain on therapy, otherwise tubers can regrow. Despite some evidence of seizure frequency reduction, it would not be solely used for seizure control. |
Considerations for initiation of therapy | |
TSC can be diagnosed based on clinical findings (e.g., cutaneous manifestations) or genetic testing, although genetic testing was not a requirement in the CARE6 trial to diagnose TSC. Pathogenic variants of TSC1 and TSC2 provide a definite diagnosis in 85% to 90% of patients. How accessible is genetic testing for TSC across Canada, and is genetic testing typically conducted in Canada to confirm the diagnosis? | Genetic testing for TSC is widely available to patients in Canada; however, confirmation of a diagnosis by genetic testing is not necessary for TSC. TSC is most commonly diagnosed by various clinical markers, including the presence of tubers, skin lesions, and confirmed by imaging (e.g., CT or MRI). Although genetic testing is widely available, some families choose not to proceed with genetic testing for personal, ethical, or other reasons. Regardless, the results of genetic testing would not affect treatment decisions for patients with TSC-associated seizures. |
Patients in the CARE6 trial were required to have a documented history of epilepsy, which was not completely controlled by their current ASMs, and patients were required to be taking at least 1 ASM at a dose that had been stable for at least 4 weeks. The inclusion criteria for the CARE6 trial did not require patients to have failed 1 or more ASM before enrolment. Oxcarbazepine has a higher threshold for the initiation of coverage, requiring 1 to 3 ASMs to have failed. Would you initiate cannabidiol in patients who are currently undergoing treatment with only 1 ASM? | By definition, cannabidiol used as adjunctive treatment would be at least the second therapy attempted. The current standard of care requires careful consideration of treatment sequencing to optimize the balance of harms and effects. Other ASMs may be restricted to 2 or 3 prior attempts to control seizures; thus, a precedent for this has been set, and it would be reasonable to have similar limitations in place for cannabidiol. The current criteria of 3 prior ASM failures for oxcarbazepine is a barrier, as this could be high for some patients who are less refractory. Although no guidance exists on this issue, prescribers may initiate cannabidiol after at least 2 ASMs have been tried. |
Considerations for continuation or renewal of therapy | |
Most ASMs are open benefit, and no specific guidance is provided in terms of renewal criteria. A reduction in seizures is a relevant and clinically meaningful outcome for patients with TSC-associated epilepsy, and successful therapy is determined by a reduction in seizure frequency. What objective measures are used in routine clinical practice to assess therapeutic response in patients with TSC-associated seizures? | In clinical practice, therapeutic response is measured by seizure count and seizure severity. Quantifying seizure severity is difficult and not routinely done in clinical trials. The QoL of patients is another metric that is considered by treating physicians, although, generally, no specific QoL tools are used in practice; rather, patients and caregivers provide their own overall assessment of how their QoL has changed (e.g., increase or decrease in seizure frequency and/or severity, increase in alertness). |
Considerations for discontinuation of therapy | |
How would loss of response or absence of clinical benefit be defined in patients with TSC-associated seizures? | Loss or lack of response are also measured by seizure count and severity as reported by patients. |
Most of the patients in the CARE6 trial experienced side effects. There were no defined metrics provided for the discontinuation of the drug. In what circumstances would cannabidiol be discontinued? | Cannabidiol should be discontinued in patients who experience intolerable side effects from treatment, including but not limited to significant elevations in liver enzymes, sedation, significant GI side effects, and hypersensitivity reactions. |
Considerations for prescribing of therapy | |
The dosing of cannabidiol in the CARE6 trial (25 mg/kg per day and 50 mg/kg per day) was not reflective of the dosing criteria for TSC (10 mg/kg per day to 25 mg/kg per day) in the product monograph. There is potential for prescribers to increase the dose to those used in the clinical trials, impacting cost. Would you prescribe cannabidiol beyond the indicated dosage? | The CARE6 trial evaluated the dose of 50 mg/kg per day, which is not currently indicated for this population and is notably high for this type of medication. No observable dose-response relationship was observed in terms of efficacy; thus, it is unlikely that cannabidiol would be prescribed beyond the indicated dosage. If prescribed, dosing beyond the Health Canada–approved dosage of 25 mg/kg per day would be dependent on tolerability of treatment. |
It is expected that cannabidiol would be prescribed by neurologists with expertise in managing seizures. There may be limited access to neurologists in some regions. How could patients without access to specialized care receive treatment with cannabidiol? | Patients with TSC-associated seizures are under the care of neurologists with expertise in the treatment of epilepsy. Patients are required to visit a specialist to be prescribed treatment for TSC-associated seizures, although the administration of treatment is not a concern and does not need to be done in a specialized centre. Recently, virtual care has become more common and should assist with treatment monitoring. |
Cannabidiol is available as an amber liquid with 100 mg/mL in a 100 mL bottle. Patients are titrated to an effective therapeutic dose during the first 2 weeks of therapy. The patient or caregiver is required to measure the dose. | No response required. For CDEC consideration. |
This product is intended to be used as adjunctive therapy to current ASMs. Cannabidiol is a potent CYP3A4 and CYP2C19 inhibitor. It is known to increase drug levels of clobazam, rufinamide, and topiramate. More information about drug interactions would be beneficial. | No response required. For CDEC consideration. |
Generalizability | |
The CARE6 trial was a multisite, randomized, double-blind, placebo-controlled trial. Patients on mTOR inhibitors (everolimus), and patients who already were taking (medical) cannabis products were excluded from the trial. Would you consider using cannabidiol in these patients? | There is no evidence to support the use of cannabidiol in these patients. |
Medical cannabis is used to treat refractory or drug-resistant epilepsy. It is expected that patients would prefer to switch to a pharmaceutical-grade alternative for various reasons (consistent product availability and/or quality, pharmacist involvement and/or medication review, and coverage by public and/or private insurers [currently only Veterans Affairs Canada and some private insurers cover medical cannabis products]). Are there any challenges related to using the medical cannabis pathway supported by Health Canada? Do you foresee other patients with drug-resistant epilepsy wanting access to cannabidiol? | Most patients with TSC-associated seizures who use medical cannabis incur significant out-of-pocket costs, as it is not generally covered by most plans. As such, if there is no coverage available for cannabidiol, patients are unlikely to switch. However, some patients and/or caregivers may be interested in switching to cannabidiol because it is a natural product, although this perception may shift because it is a pharmaceutical product. |
Care provision issues | |
In the CARE6 trial, 94% to 100% of patients experienced AEs, most commonly diarrhea, decreased appetite, somnolence, and vomiting, which were largely resolved by the end of the study and did not result in many patients discontinuing the drug. The most common reason for discontinuation was elevated transaminases and rash. Other noteworthy harms included a greater than 5% decrease in weight in nearly 31% of patients in the cannabidiol 25 mg/kg per day group, compared to 8.4% in the placebo group. How significant are the side effects of cannabidiol relative to alternative ASMs? Are there any concerns with cannabidiol that may impact growth or development, and do patients with TSC-associated seizures already have challenges with nutritional intake (i.e., requiring nutritional support, such as meal replacements, tube feeds, or TPN), given the weight loss observed in the trial? | Overall, the distribution of AEs in the CARE6 trial was not notably different than the AE profile of other ASMs. The key consideration with the individual AEs experienced in the CARE6 trial is whether they led to the discontinuation of treatment. Considering that overall discontinuation due to GI events was low, the instance of this in clinical practice may not be a concern. Regarding weight loss, a 5% decrease in weight is likely not actionable and wouldn’t prompt the discontinuation of treatment. There is a concern about the impact of cannabidiol on the developing brain; however, the mechanism and impact of this is not fully understood, so patients would be carefully monitored. Additionally, these patients already have a significant brain disorder, so the advantages of cannabidiol currently outweigh the risks. |
System and economic issues | |
The submitted list price is $1,424.5400 per 100 mL bottle, extrapolated to an annual cost of $102,200 for an adult at the maximum recommended therapeutic dose. Note that the study dose went to a maximum of 50 mg/kg per day. The sponsor’s BIA estimated that the reimbursement of cannabidiol will result in an incremental cost of $911,156 in year 1, $2,022,989 in year 2, and $3,397,821 in year 3, for a cumulative 3-year budget impact of $6,331,966. It assumed an 85% compliance rate and did not account for wastage when a multidose bottle was used. | No response required. For CDEC consideration. |
Cannabidiol is an adjunctive therapy and, therefore, there are other ASM medication costs to be considered. There was no information provided with regard to changes in usual care (dose reductions or discontinuation of current ASMs). | No response required. For CDEC consideration. |
AE = adverse event; ASM = antiseizure medication; BIA = budget impact analysis; CDEC = CADTH Canadian Drug Expert Committee; GI = gastrointestinal; mTOR = mammalian target of rapamycin; QoL = quality of life; TPN = total parenteral nutrition; TSC = tuberous sclerosis complex.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of cannabidiol, 100 mg/mL, oral solution as adjunctive therapy for the treatment of seizures associated with TSC in patients 2 years and older. The focus will be placed on comparing cannabidiol to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of cannabidiol is presented in 4 sections, with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the Systematic Review, includes pivotal studies and RCTs that were selected in accordance with the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. The third and fourth sections include indirect evidence and additional studies that were considered by the sponsor to address important gaps in the systematic review evidence; however, no indirect treatment comparisons or additional studies were submitted by the sponsor.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
1 pivotal study or RCT identified in the systematic review (CARE6)
1 long-term, OLE study of CARE6.
Systematic Review
The contents of this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included study are summarized in Table 4.
Table 4: Details of the Study Included in the Systematic Review
Detail | CARE6 |
|---|---|
Designs and populations | |
Study design | Phase III, double-blind, placebo-controlled RCT |
Locations | 49 trial sites in 6 countries (the US, Spain, Poland, Australia, the UK, and the Netherlands) |
Patient enrolment dates | Start date: April 6, 2016 End date: August 31, 2018 |
Randomized (N) | Cannabidiol 25 mg/kg per day: n = 75 Cannabidiol 50 mg/kg per day: n = 73 Placebo: n = 76 Total: N = 224 Note that cannabidiol 50 mg/kg per day is not a Health Canada–approved dosage and is not included in the report. |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Cannabidiol 25 mg/kg per day or 50 mg/kg per day orally |
Comparator(s) | Placebo |
Study duration | |
Screening phase | 7 days |
Run-in phase | 28 days |
Treatment phase | 16 weeks (113 days) |
Follow-up phase | 10-day taper period + 28-day follow-up (patients were invited to continue in an OLE immediately after treatment phase) |
Outcomes | |
Primary end point | Change from baseline in the number of TSC-associated seizures (per 28 days) during the treatment period |
Secondary and exploratory end points | Key secondary:
Other secondary:
Exploratory:
|
Publication status | |
Publications | Reports: Sponsor’s Clinical Study Report Trial ID Numbers: EudraCT number: 2015 to 002154 to 12 ClinicalTrials.gov identifier: NCT02544763 |
ALT = alanine aminotransferase; ASM = antiseizure medication; AST = aspartate aminotransferase; CGIC = Caregiver Global Impression of Change; CGICSD = Caregiver Global Impression of Change in Seizure Duration; C-SSRS = Columbia-Suicide Severity Rating Scale; ECG = electrocardiogram; IMP = investigational medicinal product; INR = international normalized ratio; mTOR = mammalian target of rapamycin; OLE = open-label extension; PGIC = Physician Global Impression of Change; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = 31-item Quality of Life in Epilepsy – Problems questionnaire; RCT = randomized controlled trial; SGIC = Subject Global Impression of Change; SGICSD = Subject Global Impression of Change in Seizure Duration; TBL = total bilirubin; TSC = tuberous sclerosis complex; ULN = upper limit of normal.
Source: CARE6 Clinical Study Report.22
One study was included in the review. The CARE6 trial was a phase III, placebo-controlled RCT that evaluated the efficacy and safety of cannabidiol oral solution as an adjunctive treatment in children and adults with TSC that is not completely controlled by their current ASMs. The CARE6 trial consisted of a 7-day screening period followed by a 28-day baseline period to capture eligibility criteria related to seizure frequency and type. To be included, patients had to have experienced at least 8 seizures during the first 28 days of the baseline period, with at least 1 seizure occurring in at least 3 of the 4 weeks. A total of 224 patients were randomized in a 2:2:1:1 ratio using the interactive voice response system (IVRS), to cannabidiol 25 mg/kg per day (n = 75), cannabidiol 50 mg/kg per day (n = 73), and 2 matching dose-volume equivalent placebo groups for 16 weeks. The placebo groups were pooled for the analyses of efficacy (total n = 76).22 Because cannabidiol 50 mg/kg per day is not a recommended dosage, per Health Canada, data from that group are not included in this report.
Randomization was stratified by age group (1 to 6 years, 7 to 11 years, 12 to 17 years, and 18 to 65 years). The CARE6 trial was conducted in 49 centres in 6 countries: the US, Spain, Poland, Australia, the UK, and the Netherlands. No patients from Canada were enrolled. After completion of the double-blind treatment period, patients had the option to enter the long-term OLE study. Patients who did not enter the OLE trial had their treatment tapered 10% per day over 10 days.22 The overall study design of the CARE6 study is depicted in Figure 1.
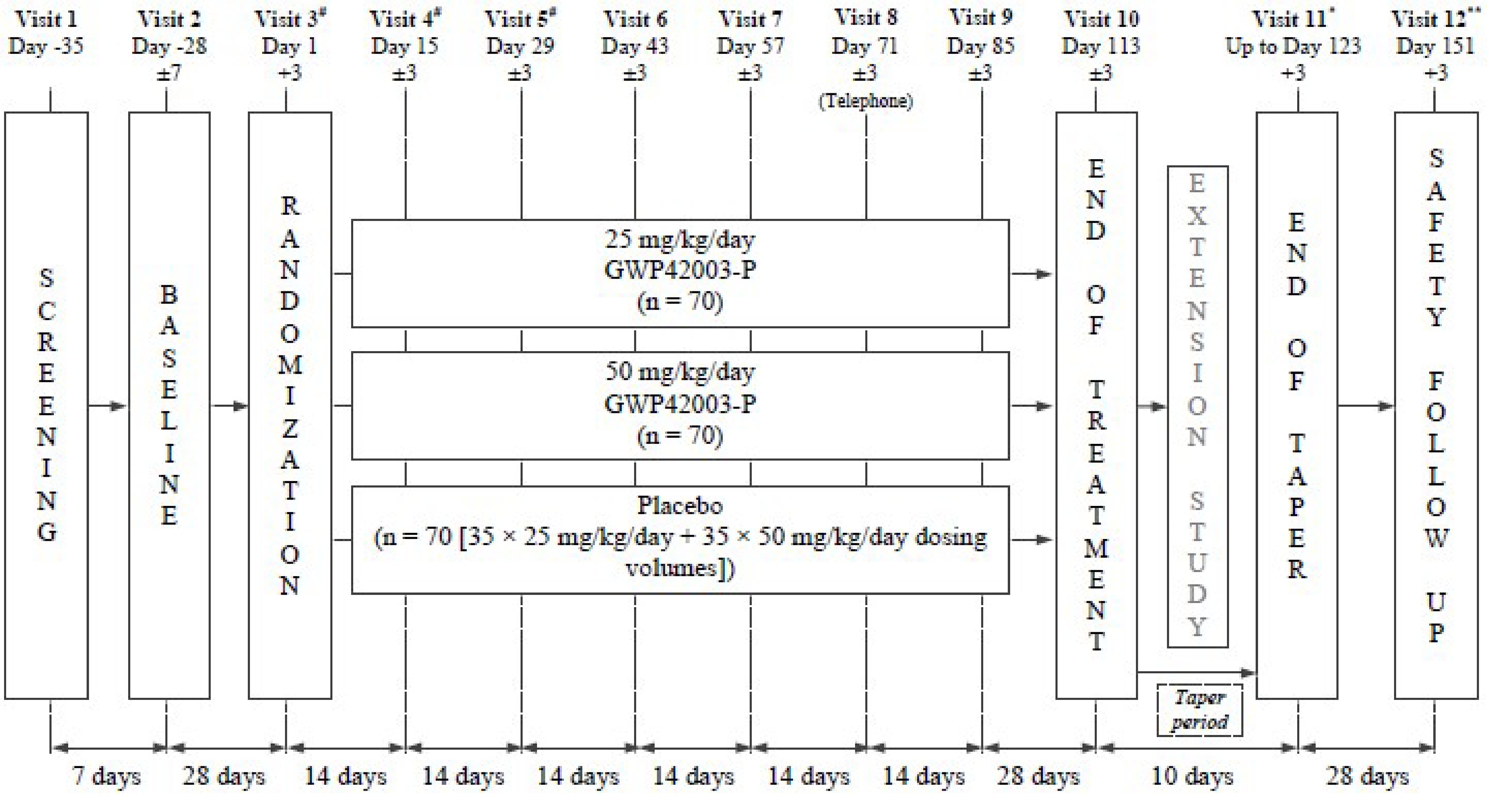
GWP42003-P = cannabidiol.
* For patients not entering the open-label extension on day 113.
** For patients not entering the open-label extension; could be conducted by telephone.
Source: CARE6 Clinical Study Report.22
Populations
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria for the CARE6 trial are summarized in Table 5. Briefly, eligible patients included male and female patients aged 1 to 65 years with a clinical diagnosis of TSC in accordance with the criteria agreed upon at the 2012 International TSC Consensus Conference and a well-documented history of epilepsy that is not adequately controlled by current ASMs. Patients also had to be taking at least 1 stable dose of ASM for at least 1 month. Additionally, patients had to have experienced at least 8 seizures during the baseline period. Patients were excluded if they had unstable medical conditions in the 4 weeks before screening, a history of alcohol or substance abuse, used recreational or medical cannabis in the previous 3 months, received general anesthetic in the 4 weeks before screening or randomization, or undergone surgery for epilepsy in the 6 months before screening.22
Interventions
Eligible patients were randomized in a 2:2:1:1 ratio to receive cannabidiol 25 mg/kg per day, 50 mg/kg per day, placebo 25 mg/kg per day, or placebo 50 mg/kg per day. The 2 doses were selected based on data from multiple investigational new drug studies and to allow demonstration of a possible dose-response in patients with TSC.22
The study drug was provided in 100 mL vials as an oral solution, containing either 0 mg/mL cannabidiol (i.e., placebo) or 100 mg/mL cannabidiol in sesame oil and anhydrous ethanol (79 mg/mL) with added sweetener (0.5 mg/mL sucralose) and strawberry flavouring (0.2 mg/mL). All doses of the study drug were administered orally twice each day (morning and evening). Cannabidiol was titrated as follows: on days 1 and 2, patients in the 25 mg/kg per day group received 5.0 mg/kg cannabidiol. Dosages were increased by 5.0 mg/kg every 2 days until the dose of 25.0 mg/kg was reached on days 9 and 10, which was continued until the end of treatment.22
Randomized patients were weighed on day 1, and the daily volumes of the study drug to be taken during the 4-week titration period and for the remainder of the trial were calculated and provided to the patient or caregiver. Each patient took the first dose of the study drug on day 1 and the final maintenance dose of the study drug on day 113 (end of treatment visit) or on the day of early withdrawal.22
Patients entering the OLE study transitioned to OLE treatment over a period of 2 weeks. Patients who did not enter the OLE study on day 113 or who withdrew early had their study drug dose tapered 10% each day over a period of 10 days, unless continued dosing was not possible due to an AE. Patients participating in the taper period returned the used and unused study drug vials to the investigative site on day 123 (end of taper period visit).22
Prior and Concomitant Therapy
Patients were required to be taking 1 or more ASMs at a stable dose for at least 4 weeks. Any nonpharmacological interventions for epilepsy were also required to be stable for 1 month before screening. For the duration of the trial, doses of concomitant ASMs and any nonpharmacological regimens for epilepsy were to remain stable. Concomitant ASM dose reductions were permitted on clinical grounds (e.g., due to AEs or transaminase elevations not meeting protocol-specified withdrawal criteria), not plasma levels of ASMs. Additional new ASMs could not be added during the randomized phase of the trial. The use of rescue medication was allowed when necessary.22
The following were prohibited during the trial:22
any new medications or interventions for epilepsy (including a ketogenic diet and VNS) or changes in dosage
recreational or medicinal cannabis or synthetic cannabinoid-based medications (including nabiximols [Sativex]) in the 3 months before or during the trial
any other investigational product taken as part of a clinical trial
felbamate if taken for less than 1 year before screening
oral mTOR inhibitors.
However, any patients taking these medications after randomization were not withdrawn from the trial unless there were safety concerns.22
Treatment Discontinuation
All patients were able to withdraw from the study at any point during treatment. The investigator could discontinue any patient at any time if medically necessary.22
Unless inadvisable (e.g., continued dosing was not possible due to an AE), patients who were withdrawn had their dose of the study drug tapered gradually (10% each day), beginning at the time the decision was made to discontinue. All withdrawn patients who had their study drug tapered were assessed 10 days after the last on-treatment dose for the evaluation of safety. Patients who began to taper but were withdrawn during the taper period underwent a safety assessment on the final day of dosing, or as soon as possible after this date. After the end of the taper assessment, telephone calls were made weekly for additional safety evaluation. A final safety assessment took place 28 days after the final dose of study drug (including tapered doses).22
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 5, and is followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review by the clinical experts consulted by CADTH and from stakeholder input from patient groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be most relevant to CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select harms outcomes considered important for CADTH’s expert committee deliberations were also assessed using GRADE (SAEs, hepatocellular injury).
According to all stakeholder inputs, a reduction in seizure frequency is the hallmark of treatment for patients with TSC-associated seizures, with the aim of slowing or halting downstream complications. Therefore, outcomes related to a reduction in seizure frequency were included as outcomes to be assessed using GRADE. In the CARE6 trial, this included the percent change from baseline in the number of TSC-associated seizures, as well as the proportion of patients considered to be treatment responders (i.e., achieving target reductions of 25% or 50% more) or achieving seizure freedom (100% reduction in seizure frequency). Additional outcomes related to seizure frequency or severity included the proportion of patients with status epilepticus and the proportion of patients requiring rescue medication.
The clinical experts consulted by CADTH and patient groups highlighted the importance of improved QoL as a result of a reduced seizure burden. As such, HRQoL outcomes from the CARE6 trial (i.e., change from baseline in QOLCE score, QOLIE-31-P score) were included in the GRADE assessment. Last, the clinical experts noted that neuropsychiatric outcomes are of importance to this population, although they would not necessarily be realized in the short duration of a clinical trial. Regardless, the change from baseline in Vineland II score was included in the GRADE assessment.
A complete list of the primary and secondary end points in the CARE6 trial is summarized in Table 5.
Table 5: Outcomes Summarized From the Study Included in the Systematic Review
Outcome measure | Time point | CARE6 |
|---|---|---|
Percentage change in TSC-associated seizures during the treatment period from baseline | End of treatment period (visit 10, day 113) | Primarya |
Proportion of patients considered to be treatment responders, defined as those with a ≥ 50% reduction from baseline in TSC-associated seizure frequency | End of treatment period (visit 10, day 113) | Key secondarya |
Proportion of patients with a ≥ 25% reduction from baseline in TSC-associated seizure frequency | End of treatment period (visit 10, day 113) | Secondary |
TSC-associated seizure freedom (100% reduction from baseline) | End of treatment period (visit 10, day 113) | Secondary |
Change from baseline in QOLCE scores | End of treatment period (visit 10, day 113) | Secondary |
Change from baseline in QOLIE-31-P scores | End of treatment period (visit 10, day 113) | Secondary |
Number of patients with status epilepticus | End of treatment period (visit 10, day 113) | Exploratory |
Rescue medication use | End of treatment period (visit 10, day 113) | Exploratory |
Change from baseline in Vineland II score | End of treatment period (visit 10, day 113) | Exploratory |
Hepatocellular injury, SAEs | End of treatment period (visit 10, day 113) | Secondary |
QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = 31-item Quality of Life in Epilepsy – Problems questionnaire, SAE = serious adverse event; TSC = tuberous sclerosis complex; Vineland II = Vineland Adaptive Behaviour Scales, Second Edition.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Source: CARE6 Clinical Study Report.22
Efficacy Outcomes
For all seizure-related outcomes, patients or their caregivers recorded the number and type of seizures, as well as the severity of focal seizures and the number of episodes of status epilepticus, each day from baseline (visit 2, day –28) until completion of dosing (as applicable: visit 10, day 113; end of treatment and/or withdrawal visit; or visit 11, day 123, end of taper). Data on seizure subtypes were collected daily. For the purposes of calculating the composite seizure score, the severity of focal seizures was assessed according to type:22
type 1 — focal motor seizures without impairment of consciousness or awareness
type 2 — focal seizures with impairment of consciousness or awareness
type 3 — focal seizures evolving into bilateral convulsive seizures
generalized seizures (tonic-clonic, tonic, clonic, atonic)
other seizures (absence seizures, myoclonic seizures, focal sensory seizures, infantile and/or epileptic spasms)
episodes of status epilepticus.
Primary End Point
The primary end point of the CARE6 study was the change in the number of TSC-associated seizures during the treatment period of the trial (day 1 to day 113) from baseline (from the day of visit 2 [day –28] to day 1) in patients taking cannabidiol or placebo.22
TSC-associated seizures are defined as focal motor seizures without impairment of consciousness or awareness, focal seizures with impairment of consciousness or awareness, focal seizures evolving into bilateral generalized convulsive seizures, and generalized seizures (tonic-clonic, tonic, clonic, and atonic) that are countable.22
Key Secondary End points
There were 3 key secondary efficacy end points evaluated in the CARE6 trial, 1 of which was of interest to this review: the proportion of patients considered to be treatment responders, defined as those with a reduction of at least 50% from baseline to the end of the treatment period (visit 10, day 113) in TSC-associated seizure frequency. Other key secondary end points included the change from baseline in Subject Global Impression of Change (SGIC) and Caregiver Global Impression of Change (CGIC) scores and the change in total seizure frequency.22
Other Secondary and Exploratory End Points
Other secondary and exploratory end points of the CARE6 trial of interest to this review included:22
the number of patients considered to be treatment responders, defined as those experiencing a reduction in TSC-associated seizure frequency of at least 25% and those experiencing a 100% reduction
the change from baseline to visit 10 (day 113) in HRQoL, using the QOLCE34 and QOLIE-31-P35
change in the number of patients with episodes of status epilepticus from baseline to visit 10 (day 113)
change in the use of rescue medication from baseline to visit 10 (day 113)
evaluation of the effect of cannabidiol from baseline to visit 10 (day 113) on TANDs, including cognitive and behavioural function using Vineland II.
TSC-Associated Seizure Treatment Responders and TSC-Associated Seizure Freedom
In addition to the key secondary end point, the proportion of patients considered to be treatment responders was also defined as those experiencing a reduction in TSC-associated seizure frequency of at least 25% or at least 75%, and the proportion of patients considered to be free of TSC-associated seizure was defined as those with a 100% reduction in TSC-associated seizure frequency.22 The proportion of patients with a 75% or greater reduction in seizure frequency was not evaluated in this report.
Quality of Life in Childhood Epilepsy for Patients Aged 2 to 18 Years
The QOLCE is a parent-reported questionnaire that can be used to evaluate HRQoL in children aged 2 to 18 years. It contains 76 items on 16 subscales covering 7 domains of life function: physical activities, social activities, cognition, emotional wellbeing, behaviour, general health, and general QoL. All items were rated on a 5-point or 6-point categorical scale. Based on responses to the items in each domain, scores for the 16 subscales are derived. Items within each subscale were transformed to a score of 0 to 100, where 0 represents the lowest or poorest category and 100 represents the highest level of HRQoL. The overall QoL score is calculated as the mean of the subscale scores.22
Quality of Life in Epilepsy – Problems for Patients 19 Years and Older
The QOLIE-31-P is a self-reported survey that can be used to measure HRQoL in adults with epilepsy and consists of 38 questions about health and daily activities and includes questions designed to evaluate how much distress the patient feels about problems and worries related to epilepsy. The tool is an adaptation of the original QOLIE, with items about distress related to epilepsy added. The QOLIE-31-P was administered to patients 19 years or older. The questionnaire consists of 7 subscales: energy, mood, daily activities, cognition, medication effects, seizure worry, and overall QoL. Each subscale consists of several questions in addition to a distress item. The raw score for each question and the distress item were converted to a final weighted score from 0 to 100, with higher scores reflecting better HRQoL.22
Status Epilepticus
The number of patients with status epilepticus, defined as any seizure lasting 30 minutes or longer, was recorded throughout the trial using an IVRS telephone diary.22
Rescue Medication Usage
The number of patients requiring the use of rescue medication was recorded throughout the trial on a paper diary and reviewed at scheduled visits and during safety telephone calls.22
Vineland Adaptive Behaviour Scales, Second Edition
Vineland II is an individually administered instrument that assesses adaptive behaviours in the domains of communication, daily living skills, socialization, and motor skills.36 Vineland II assessments were performed for all patients but were completed by caregivers. Using the raw score and the participant’s age, a v-scale score (1 to 24) with 90% CI, adaptive level, and age equivalent can be obtained. From this, the adaptive behaviour composite score (20 to 160) can be calculated. A higher score suggests a higher level of adaptive functioning.22
Table 6: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
QOLIE-31-Pa (≥ 18 years) | A self-administered, disease-specific survey of HRQoL for adults with epilepsy. The items in QOLIE-31-P encompass 7 subscales: energy/fatigue, emotional wellbeing, social function, cognitive functioning, medication effects, seizure worry, and overall QoL. The QOLIE-31-P includes an additional item assessing the degree of overall distress.35,37 Items are measured on 3- to 6-point Likert scales. Each subscale and the total score range from 0 to 100, with higher scores indicating better function. Recall period is the past 4 week for some items. | Posthoc analyses of psychometric properties have been performed for patients (n = 67) with TSC and refractory partial-onset seizures from the EXIST-3 trial.38 Validity: Item discriminant validity was demonstrated for all items (item-to-scale correlation, r < 0.40). Item convergent validity was demonstrated (item-to-scale correlation, r ≥ 0.40) for all items in the subscales except for medication effects and social function. Reliability: Internal consistency for total score and all domains, except for social function domain, was acceptable (alpha = 0.70 to 0.92) at baseline and end of core phase. Responsiveness: Mean changes from baseline in total score, cognitive domain, and seizure worry were higher for responders than nonresponders (P < 0.05). Other scales showed a similar relationship but were not statistically significant. | Based on the distribution-based method, MID has been estimated to be 7.1 (SD = 0.5) to 11.0 (SEM) in patients with TSC.38 |
QOLCE (4 to 18 years)b | A disease-specific, parent-reported measure of HRQoL for children and adolescents with epilepsy. The US version consists of 76 items, grouped into 7 domains (physical activities, cognition, function, emotional wellbeing, social activities, behaviour, general health, and general QoL), which are grouped into 16 subscales.39 All items were rated on a 5- or 6-point scale. An overall QoL score is calculated by taking the mean of the subscale scores. The score ranges from 0 to 100, with higher scores representing better QoL. Recall period is the past 4 weeks. | Posthoc analyses of psychometric properties have been performed in patients (n = 197) with TSC and refractory partial-onset seizures from EXIST-3 trial.38 Validity: Based on a WNV score cut-off of 70, individuals with normal intellectual ability at baseline demonstrated higher overall HRQoL scores with moderate effect size (–0.62) than those in the control group (P < 0.007). Item discriminant validity was demonstrated for all items (item-to-scale correlation, r < 0.40). Item convergent validity was demonstrated for the majority of items, but 14 items from various subscales and/or domains had item-to-scale correlation, r < 0.40. Reliability: Except for the self-esteem subscale and the anxiety, social interactions, control/helplessness, and depression subscales, internal consistency for overall QoL and other subscale scores was acceptable (alpha = 0.70 to 0.95). Responsiveness: Mean changes from baseline in overall QoL score were higher in responders than nonresponders (P = 0.016). There was a similar, but not significant, relationship for other domains. | Based on a distribution-based method, MID has been estimated to be 2.9 (SD = 0.5) to 6.0 (SEM) in patients with TSC.38 |
Vinland II | Caregiver-administered rating scale to evaluate adaptive behaviours of individuals from birth to 90 years. It consists of 4 adaptive behaviour domains (communication, daily living skills, socialization, and motor skills) and a maladaptive behaviour domain (optional).40 Using the raw score and the participant’s age, v-scale score (1 to 24) with 90% CI, adaptive level, and age equivalent can be obtained. From this, the adaptive behaviour composite (20 to 160) can be calculated. A higher score suggests a higher level of adaptive functioning. | No evidence of psychometric properties in patients with TSC has been found in literature. Validity: Test development followed procedures to ensure content validity.41 Convergent validity has been noted with ABAS-II in 197 individuals (r = 0.70) and similar subscales of the BASC-2 parent rating form (r = 0.34 to 0.74). Maladaptive scales were correlated with the behaviour symptoms index on the BASC-2 (r = 0.69 to 0.80). Divergent validity has also been noted with WAIS-III (r = near 0), as well as between the adaptive behaviour composite score and WAIS-III full-scale IQ score (r = 0.20).40 Reliability: Internal consistency for adaptive behaviour composite (Cronbach alpha = 0.93 to 0.97) and for the maladaptive behaviour index (alpha = 0.85 to 0.91) are acceptable across age groups. Test-retest reliability with an interval of 13 to 34 days was demonstrated in 414 respondents. Interinterviewer reliability (n = 148) and interrater reliability (except for maladaptive behaviour subscales and index) across domains and/or subdomains and ages have been demonstrated.40 Responsiveness: No evidence has been identified. | Unknown |
ABAS-II = Adaptive Behaviour Assessment System – Second Edition; BASC-2 = Behaviour Assessment System for Children, Second Edition; CI = confidence interval; HRQoL = health-related quality of life; IQ = intelligent quotient; MID = minimally important difference; QoL = quality of life; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = 31-item Quality of Life in Epilepsy – Problems questionnaire; SD = standard deviation; SEM = standard error of mean; TSC = tuberous sclerosis complex; Vinland II = Vineland Adaptive Behaviour Scales, Second Edition; WAIS-III = Wechsler Intelligence Scales for Children – Third Edition; WNV = Wechsler Non-Verbal.
aIn the CARE6 trial, QOLIE-31-P was administered to patients aged ≥ 19 years.
bIn the CARE6 trial, QOLCE was administered to patients aged 2 to 18 years.
Sources: Sponsor’s Clinical Evidence Summary (2023),27 Crudgington et al. (2020),39 Community-University Partnership (2011),40 Cramer et al. (1998),37 Cramer and van Hammee (2023),35 de Vries et al. (2015).42
Harms Outcomes
An AE was defined as any new unfavourable, unintended signs and/or symptoms (including abnormal laboratory findings), or a diagnosis or worsening of a preexisting condition, which was present after screening for the posttreatment, safety follow-up visit (visit 12), which may or may not have been related to the study drug. Any event that was the result of a trial procedure was recorded as an AE.22
Surgical and/or investigational procedures were not AEs. The medical reason for the procedure was the AE. Elective hospitalizations for pretrial existing conditions or elective procedures were not AEs. The exception was if the patient had an AE during hospitalization that prolonged the scheduled hospital stay, in which case it was considered an SAE. If reporting a fatal event, the SAE term was the underlying cause of the death (e.g., disease or medical condition leading to death).22
Statistical Analysis
Sample Size and Power Calculation
For the primary efficacy outcome of reduction in seizure frequency, sample size calculations were performed under the assumption that patients in the placebo group would experience a mean reduction in seizure frequency of 15% (from baseline), and patients receiving cannabidiol would experience at least a 50% reduction in seizures and a common standard deviation of 60%. As such, a sample size of 70 patients per group would be sufficient to detect a difference in response distributions with 90% power. This test was based on a 2-sided nonparametric Mann–Whitney-Wilcoxon test for continuous response data, with a 5% significance level.22
A total of 210 patients were planned for randomization across 4 treatment groups (25 mg/kg per day cannabidiol, 50 mg/kg per day cannabidiol, 25 mg/kg per day dose-volume equivalent placebo, or 50 mg/kg per day dose-volume equivalent placebo) at a 2:2:1:1 ratio.22
Multiple Testing Procedure
The primary and key secondary end points were tested with their type I error controlled at 5% with the use of a hierarchical gate-keeping procedure, in the following sequence:22
change in number of TSC-associated seizures; cannabidiol 25 mg/kg per day versus placebo.
number of patients with at least a 50% reduction in TSC-associated seizure frequency; cannabidiol 25 mg/kg per day versus placebo.
change in number of TSC-associated seizures; cannabidiol 50 mg/kg per day versus placebo.
number of patients with at least a 50% reduction in TSC-associated seizure frequency; cannabidiol 50 mg/kg per day versus placebo.
change in CGIC or SGIC score; cannabidiol 25 mg/kg per day versus placebo.
change in total seizures; cannabidiol 25 mg/kg per day versus placebo.
change in CGIC or SGIC score; cannabidiol 50 mg/kg per day versus placebo.
change in total seizures; cannabidiol 50 mg/kg per day versus placebo.
The null hypothesis of an end point was rejected at the level of 0.05 (2-sided) to test the hypothesis of the subsequent end point in the sequence at the level of 0.05 (2-sided). If a null hypothesis was not rejected, testing was stopped and all subsequent analyses were declared not statistically significant.22
Within the hierarchical testing sequence, only the primary and first key secondary end points were of interest to this review, and the cannabidiol 50 mg/kg per day group was not included in this report.
Statistical and Analytical Plans
Each end point had 2 comparisons against placebo (cannabidiol 25 mg/kg per day and cannabidiol 50 mg/kg per day). A summary of statistical analyses conducted in the CARE6 trial is included in Table 7.
Primary Efficacy Analysis
The primary efficacy analysis was performed using the intention-to-treat (ITT) analysis set. The percentage change from baseline in TSC-associated seizure frequency was calculated as:22

The primary end point was analyzed using a negative binomial regression model, with the total number of TSC-associated seizures during the baseline period and treatment period as the response variables. A mixed-effect model with repeated measures (MMRM) was performed, modelling the observed number of TSC-associated seizures in the baseline period and treatment period implemented within the framework of general linear models using the negative binomial response distribution. The model included stratified age group (1 to 6 years, 7 to 11 years, 12 to 17 years, and 18 to 65 years), time, treatment group, and treatment group by time interaction as fixed effects and the patient as a random effect. The log-transformed number of days in which seizure data were reported was included as an offset.22
The estimated LS mean seizure rate for each period and the estimated ratio of LS means for the treatment period to baseline period and 95% CI were presented for each treatment group. In addition, the estimated ratio of each cannabidiol group to placebo and 95% CI were presented along with the P value testing the null hypothesis that this ratio was 1. For each ratio and upper and lower bound of the 95% CI, the percentage reduction was also presented.22
Sensitivity Analysis
A total of 9 sensitivity analyses were conducted for the primary end point and are described in Table 7.
Posthoc Sensitivity Analysis
Additional posthoc analyses were performed in accordance with the statistical analysis plan addendum (November 28, 2019). Posthoc sensitivity analyses of interest to this review included:22
cumulative distribution plots depicting the percent reduction against the cumulative proportion of patients achieving that level of reduction for patients taking clobazam and for those not taking clobazam.
Secondary Efficacy Analysis
Key secondary end points of interest to this review were analyzed as described in the following sections.22
TSC-Associated Treatment Responders (≥ 50% Reduction in TSC-Associated Seizure Frequency)
The proportion of patients considered to be treatment responders, for patients who had not withdrawn from the trial, was summarized by treatment group for the ITT analysis set and repeated for the per-protocol (PP) analysis set. The proportion of patients considered to be treatment responders, the difference in proportions along with the 95% CIs, the estimated OR, the 95% CI for the OR, and the P value for the Cochran-Mantel Haenszel test stratified by age group were presented. If no patients in a treatment group were considered responders, then the OR and the 95% CI for the OR were not calculated.22
Subgroup Analysis
To assess the degree of effect heterogeneity, effect modifier analyses were performed for the primary efficacy end point and the key secondary efficacy end point of a reduction of at least 50% in TSC-associated seizure frequency. The following subgroups were of interest to this review: clobazam use (yes or no), number of concurrent ASMs (< 3 or ≥ 3), and number of prior ASMs (< 5 or ≥ 5).22
For the primary efficacy end point, the effect modifier analysis was performed in a manner identical to that in the primary analysis (negative binomial regression analysis), although the model was updated to include covariates for each level of the effect being tested (excluding a reference level), individually and with interactions with time, interactions with treatment group, and interactions with time and treatment. A separate model was used for testing each effect. The treatment ratios, percent reduction, and 95% CI were presented.22
For the key secondary efficacy end point of a 50% or greater reduction in TSC-associated seizure frequency, patients with a 50% or greater reduction in seizure frequency were modelled using logistic regression that included stratified age group and treatment group as covariates. The model also included covariates for each level of the effect being tested (excluding a reference level), individually and with interactions with treatment group. A separate model was used for testing each effect. The number and percent of responders and the ORs and 95% CIs were presented for each level of the effect. In addition, the effect by treatment group interaction P value, testing the hypothesis that the effect level ORs are homogeneous, was presented.22
Other Secondary and Exploratory End Points
TSC-Associated Seizure Treatment Responders and TSC-Associated Seizure Freedom
In addition to the key secondary end point, the proportion of patients with a 25% or greater reduction in seizure frequency and the proportion of patients who were free of TSC-associated seizures during the treatment period, for patients who had not withdrawn from the trial during the treatment period, was summarized by treatment group. The difference between groups was tested using the Cochran-Manel Haenszel test stratified by age.22
Quality of Life in Childhood Epilepsy for Patients Aged 2 to 18 Years
Changes from baseline to the end of treatment visit (visit 10) in QOLCE (overall QoL score and the attention/concentration, memory, language, other cognitive, social interactions, and behaviour subscale scores only) were summarized by treatment group. The primary analysis was based on all patients with a completed questionnaire, regardless of age. Summaries and analyses were repeated using questionnaires only from patients aged 2 to 18 years at the time of informed consent. The estimated LS means and treatment difference, 95% CIs, and P values were presented.22
Quality of Life in Epilepsy for Patients19 Years and Older
The QOLIE-31-P was to be completed for patients 19 years and older only. The primary analysis is based on all patients who have a completed questionnaire, regardless of age. Summaries and analyses were repeated using questionnaires only from patients who were 19 years or older at the time of informed consent. Only individual items of the QOLIE-31-P were listed. The weighted subscale scores, the total score recorded at each visit, and the change from baseline scores were summarized on a continuous scale by treatment group.22
Status Epilepticus
The number of patients with status epilepticus was presented for the baseline and treatment periods.22 No formal analysis was done.
Rescue Medication Usage
The number of days that rescue medication was taken since the previous visit was recorded for the baseline and treatment periods. The average number of days rescue medication was taken per 28 days within a period was calculated as follows:22

The treatment period refers to the period between visit 3 and visit 10. The change from the baseline period to the treatment period was analyzed using analysis of covariance (ANCOVA). The model included the baseline period and age group as covariates and the treatment arm as fixed factor. The estimated LS means and treatment difference, together with the 95% CIs and P values were presented.22
Vineland Adaptive Behaviour Scales, Second Edition
The 4 adaptive behaviour domains, the adaptive behaviour composite, and the maladaptive behaviour index only were analyzed for the change from baseline to the end of treatment. The adaptive behaviour composite and the maladaptive behaviour index only were analyzed using an ANCOVA model, with the baseline period and age group as covariates and the treatment group as a fixed factor. Factors for treatment and age group were included, along with the baseline adaptive level as a covariate. The estimated ORs, 95% CIs, and the P values were presented.22
Table 7: Statistical Analysis of Efficacy End Points in the CARE6 Trial
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Change in number of TSC-associated seizures during the treatment period from baseline | Negative binomial regression MMRM | Model included stratified age group, time, treatment arm, and treatment arm by time interaction as fixed effects, and patient as a random effect. The log-transformed number of days with seizure data reported was included as an offset. | Implicit via MMRM. If a patient withdrew during the treatment period, the primary analysis variable was calculated from all the available data during the treatment period, including any data available after the patient withdrew. | Primary end point analysis repeated using the PP analysis set. Wilcoxon rank sum test on percentage change from baseline in TSC-associated seizure frequency during the treatment period. ANCOVA on percentage change from baseline in TSC-associated seizure frequency during the treatment period. ANCOVA of log-transformed TSC-associated seizure frequency during the treatment period. ANCOVA of percentage change from baseline in TSC-associated seizure frequency during the treatment period, including baseline and stratified age group as covariates and treatment group as a fixed factor. Primary end point analysis repeated using the maintenance period. Primary end point analysis repeated using the titration period (days 1 to 28) and each 4-week period of the maintenance period (weeks 1 to 4, weeks 5 to 8, and weeks 9 to12 of the 12-week maintenance period). Primary end point analysis repeated using the worst case of LOCF, NOCB, and the daily mean from the nonmissing data for each patient (rounded up to the nearest integer) to impute missing data arising from unreported days in the IVRS during the treatment period only (not the baseline period). Primary end point analysis repeated using MI to impute data under the MNAR assumption. |
Proportion of patients considered to be treatment responders (≥ 25%, 50%, or 100% reduction from baseline in TSC-associated seizure frequency) | CMH test | Age group included as a stratification factor. | Patients who had withdrawn were considered to be nonresponders. | Analysis repeated on the PP set. CMH test was repeated for the ITT analysis set using data for the maintenance period only and during each 4-week period of the maintenance period (weeks 1 to 4, weeks 5 to 8, weeks 9 to 12). |
QOLCE scores | ANCOVA | Model included baseline and stratified age group as covariates and treatment group as a fixed factor. | Complete case. If less than 50% of the items in the subscale were missing, then the subscale score was calculated using the mean of the nonmissing items. If 50% or more of the items in the subscale were missing, then the subscale score was not calculated and was missing. | NR |
QOLIE-31-P scores | ANCOVA | Model included baseline and stratified age group as covariates and treatment group as a fixed factor. | Complete case. If less than 50% of the items within the subscale were missing, then the subscale score was calculated using the mean of the nonmissing items. If 50% or more of the items within the subscale were missing, then the subscale score was not calculated and was missing. | NR |
Status epilepticus | Descriptive statistics | NA | NR | NR |
Rescue medication use | ANCOVA | Model included the baseline period and stratified age group as covariates and treatment group as a fixed factor. | NR | NR |
Vineland Adaptive Behaviour Scales | ANCOVA | Factors for treatment and age group were included, along with the baseline adaptive level as a covariate. | Complete case. | NR |
ANCOVA = analysis of covariance; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; IVRS = interactive voice response system; LOCF = last observation carried forward; MI = multiple imputation; MMRM = mixed-effect model with repeated measures; MNAR = missing not at random; NA = not applicable; NOCB = next observation carried backward; NR = not reported; PP = per protocol; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = 31-item Quality of Life in Epilepsy – Problems questionnaire; TSC = tuberous sclerosis complex.
Sources: Sponsors clinical evidence summary;27 CARE6 Clinical Study Report.22
Harms Analysis
Safety analyses were conducted on the safety analysis set. All reported AEs were classified by system organ class, preferred term, and lower-level term, using Medical Dictionary for Regulatory Activities (MedDRA), version 19.1. Summaries were presented by treatment group and included an overall summary of AEs, TEAEs, TEAEs leading to withdrawal, and serious TEAEs. If patients had multiple occurrences of a TEAE, the TEAE was counted for the first occurrence only.22
Analysis Populations
A description of the analysis populations in the CARE6 study can be found in Table 8.
Table 8: Analysis Populations of the CARE6 Trial
Population | Definition | Application |
|---|---|---|
Safety analysis set | All patients randomized to treatment who received at least 1 dose of IMP. Patient data were analyzed according to the treatment they received. | Analysis of safety data and adverse effects. |
ITT analysis set | All patients who were randomized and dosed with IMP in the trial and had postbaseline efficacy data. Patient data were analyzed according to the treatment group to which they were randomized. | Primary analysis set for all efficacy end points. |
PP analysis set | All patients who completed the trial with no protocol deviations deemed to compromise the assessment of efficacy. Patient data were analyzed according to the treatment they received. | Sensitivity analyses of the percentage change from baseline in TSC-associated seizure frequency, total seizure frequency, proportion of treatment responders during the treatment period, and SGIC and CGIC scores. |
CGIC = Caregiver Global Impression of Change; IMP = investigational medicinal product; ITT = intention to treat; PP = per protocol; SGIC = Subject Global Impression of Change; TSC = tuberous sclerosis complex.
Source: CARE6 Clinical Study Report.22
Results
Patient Disposition
Table 9 summarizes the disposition of patients enrolled in the randomized, double-blind, placebo-controlled, phase III CARE6 trial. A total of 255 patients were screened for eligibility, and 224 were randomized in a 2:2:1:1 ratio to receive cannabidiol 25 mg/kg per day (n = 75), cannabidiol 50 mg/kg per day (n = 73), or to 1 of 2 matched placebo groups (n = 38 each) that were pooled for all analyses (n = 76).22
More patients in the cannabidiol 25 mg/kg per day group discontinued the study than in placebo group (10 [13.3%] versus 1 [1.3%]). The main reason for study discontinuation was AEs. Nearly all patients in the placebo group completed the study (99%), whereas just 87% of patients in the cannabidiol 25 mg/kg per day group completed the study.22
Table 9: Summary of Patient Disposition From the CARE6 Trial
Patient disposition | CARE6a | |
|---|---|---|
Cannabidiol 25 mg/kg per day (N = 75) | Placebo (N = 76) | |
Screened, N | 255 | |
Screening failure, n (%)b | 31 (12.2) | |
Did not meet inclusion criteria | 14 (45.2) | |
Met exclusion criteria | 3 (9.7) | |
Other reason | 8 (25.8) | |
Withdrew or withdrawn by parent or guardian | 5 (16.1) | |
Investigator decision | 2 (6.5) | |
Randomized, N | 75 | 76 |
Discontinued from study, n (%) | 10 (13.3) | 1 (1.3) |
Adverse events | 8 (10.7) | 0 |
Withdrawn by parent or guardian | 1 (1.3) | 1 (1.3) |
Met withdrawal criteria | 0 | 0 |
Physician decision | 0 | 0 |
Other | 1 (1.3) | 0 |
Completed treatment, N | 65 | 75 |
Entered open-label extension, N | 64 | 75 |
Safety, N | 75 | 76 |
ITT, N | 75 | 76 |
PP, N | 62 | 74 |
ITT = intention to treat; PP = per protocol.
aThe cannabidiol 50 mg/kg per day group was not included, as it is not a Health Canada–approved dose.
bPatients could have more than 1 reason for screen failure.
Source: CARE6 Clinical Study Report.22
Baseline Characteristics
The baseline characteristics for the CARE6 trial are summarized in Table 10. Generally, baseline characteristics were well balanced across treatment groups. The mean age in the CARE6 trial was 13.7 years (14.1 years in the 25 mg/kg per day group and 13.9 years in the placebo group). Across groups, there were more male patients (58.1%) than female patients, and most patients were white (89.6%). All patients had TSC-associated seizures, with type 2 focal seizures occurring most frequently in each group (46 [61.3%] in the 25 mg/kg per day group and 50 [65.8%] in the placebo group), followed by type 1 focal motor seizures (29 [38.7%] in the 25 mg/kg per day group and 33 [43.4%] in the placebo group).22
The mean number of seizures during the baseline period was 77.95 (SD = 83.39) in the cannabidiol 25 mg/kg per day group and 89.22 (SD = 101.78) in the placebo group. All patients were taking ASMs throughout the trial. The median number of concurrent ASMs in each treatment group was 3 (range, 0 to 5), whereas the median number of prior ASMs that were no longer being taken was 4 (range, 0 to 15).22
Table 10: Summary of Baseline Characteristics in the CARE6 Trial (Safety Analysis Set)a
Characteristic | Cannabidiol 25 mg/kg per day (N = 75) | Placebo (N = 76) |
|---|---|---|
Age, years | ||
Mean (SD) | 14.1 (10.8) | 13.9 (10.6) |
Median (range) | 11.6 (1.1 to 56.8) | 11.1 (1.2 to 55.8) |
Age group, n (%) | ||
1 to 6 years | 21 (28.0) | 22 (28.9) |
7 to 11 years | 18 (24.0) | 18 (23.7) |
12 to 17 years | 16 (21.3) | 16 (21.1) |
18 to 65 years | 20 (26.7) | 20 (26.3) |
Sex, n (%) | ||
Female | 32 (42.7) | 31 (41.3) |
Male | 43 (57.3) | 44 (58.7) |
Race, n (%) | ||
American Indian or Alaska Native | 1 (1.3) | 0 |
Asian | 1 (1.3) | 3 (4.0) |
Black or African American | 2 (2.7) | 0 |
Other | 3 (4.0) | 6 (8.0) |
White or Caucasian | 68 (90.7) | 66 (88.0) |
BMI (kg/m2) | ||
Mean (SD) | 19.7 (5.8) | 20.9 (6.3) |
Median (range) | 18.4 (8.4 to 44.4) | 19.2 (13.2 to 40.5) |
TSC-associated seizure types during baseline period, n (%) | ||
Type 1 focal motor | 29 (38.7) | 33 (43.4) |
Type 2 focal | 46 (61.3) | 50 (65.8) |
Type 3 focal | 17 (22.7) | 24 (31.6) |
Generalized seizures | ||
Atonic | 10 (13.3) | 13 (17.1) |
Clonic | 3 (4.0) | 2 (2.6) |
Tonic | 27 (36.0) | 15 (19.7) |
Tonic-Clonic | 22 (29.3) | 14 (18.4) |
Other seizures | 12 (16.0) | 15 (19.7) |
Absence | 5 (6.7) | 7 (9.2) |
Infantile or epileptic spasms | 5 (6.7) | 3 (3.9) |
Myoclonic | 3 (4.0) | 4 (5.3) |
Partial (focal) sensory | 2 (2.7) | 3 (3.9) |
Number of current ASMs | ||
Mean (SD) | 2.7 (1.0) | 2.6 (0.9) |
Median (range) | 3 (0 to 4) | 3 (1 to 5) |
Number of prior ASMs | ||
Mean (SD) | 4.8 (3.2) | 4.6 (3.3) |
Median (range) | 4 (0, 13) | 4 (0, 15) |
Number of TSC-associated seizures per 28 days at baseline | ||
Mean (SD) | 77.95 (83.390) | 89.22 (101.78) |
Median (range) | 56.00 (7.7 to 427.7) | 54.05 (8.0 to 558.0) |
ASM = antiseizure medication; BMI = body mass index; SD = standard deviation; TSC = tuberous sclerosis complex.
aThe cannabidiol 50 mg/kg per day group was not included, as it is not a Health Canada–approved dose.
Note that 1 patient from the pooled placebo group was excluded from the summary of demographic data because their height at screening was measured in inches but was recorded in cm. This meant that the calculated BMI for each patient at screening was incorrect.
Source: CARE6 Clinical Study Report.22
Concomitant Medications and Cointerventions
Nearly all patients in each treatment group were receiving concomitant ASMs (74 [98.7%] in the 25 mg/kg per day group and 76 [100.0%] in the placebo group). The most frequent concomitant ASMs in the CARE6 trial are summarized in Table 11. There were some imbalances across groups in the ASMs received by patients. By therapeutic class, more patients in the 25 mg/kg per day group than in the placebo group received carboxamide derivatives (40.0% versus 31.6%). Conversely, more patients in the placebo group than in the 25 mg/kg per day group were taking benzodiazepines (42.1% versus 33.3%). Across groups, the most common ASMs included valproic acid (44.6%), vigabatrin (33.0%), levetiracetam (29.0%), and clobazam (27.2%).22
A total of 27 patients received concomitant nonpharmacological therapies during the trial. Of these patients, 2 (2.6%) in the placebo group adhered to a ketogenic diet and 18 used VNS (10 [13.3%] in the 25 mg/kg per day group and 8 [10.5%] in the placebo group). Ten patients (4 [5.3%] in the 25 mg/kg per day group and 6 [7.9%] in the placebo group) had previously used cannabis.22
Table 11: Concomitant ASMs Used in the CARE6 Trial (Safety Analysis Set)a
Therapeutic class and preferred term | Cannabidiol 25 mg/kg per day (N = 75) | Placebo (N = 76) |
|---|---|---|
Benzodiazepine derivatives | 25 (33.3) | 32 (42.1) |
Clobazam | 17 (22.7) | 25 (32.9) |
Clonazepam | 6 (8.0) | 4 (5.3) |
Carboxamide derivatives | 30 (40.0) | 24 (31.6) |
Oxcarbazepine | 13 (17.3) | 10 (13.2) |
Carbamazepine | 11 (14.7) | 6 (7.9) |
Rufinamide | 7 (9.3) | 8 (10.5) |
Fatty acid derivatives | 42 (56.0) | 46 (60.5) |
Valproic acid | 29 (38.7) | 35 (46.1) |
Vigabatrin | 28 (37.3) | 17 (22.4) |
Other antiepileptics | 56 (74.7) | 58 (76.3) |
Levetiracetam | 19 (25.3) | 24 (31.6) |
Lamotrigine | 17 (22.7) | 18 (23.7) |
Lacosamide | 16 (21.3) | 12 (15.8) |
Topiramate | 7 (9.3) | 12 (15.8) |
Zonisamide | 9 (12.0) | 7 (9.2) |
Felbamate | 6 (8.0) | 4 (5.3) |
Perampanel | 4 (5.3) | 1 (1.3) |
Note: Frequencies greater than or equal to 5% are reported.
aThe cannabidiol 50 mg/kg per day group was not included, as it is not a Health Canada–approved dose.
Source: CARE6 Clinical Study Report.22
Exposure to Study Treatments
Exposure to study treatments during the CARE6 study is summarized in Table 12. The median duration of exposure across groups was 113.0 days, with the shortest duration of exposure being 9 days, recorded by 1 patient in the 25 mg/kg per day group who achieved a dose of 20 mg/kg per day but was then withdrawn due to TEAEs. Nearly all patients in the 25 mg/kg per day group achieved their target dose (98.7%).22
Table 12: Summary of Patient Exposure From the CARE6 Trial (Safety Analysis Set)a
Exposure | Cannabidiol 25 mg/kg per day (N = 75) | Placebo (N = 76) |
|---|---|---|
Dosing days | ||
Mean (SD) | 102.6 (28.68) | 113.4 (2.66) |
Median (range) | 113.0 (9 to121) | 113.0 (106 to 123) |
Target dose | ||
Achieved target dose, n (%) | 74 (98.7) | NR |
Maximum dose achieved (mg/kg per day), mean (SD) | 24.93 (0.577) | NR |
Adherence | ||
Adherence to study treatment, % | 96.4 | 99.7 |
NR = not reported; SD = standard deviation.
aThe cannabidiol 50 mg/kg per day group was not included as it is not a Health Canada–approved dose.
Source: CARE6 Clinical Study Report22
Efficacy
Efficacy results of interest to this review from the CARE6 trial are summarized in Table 13. Note that results for the cannabidiol 50 mg/kg per day group were not included, as it is not a Health Canada–approved dose.
Percent Change From Baseline in Seizure Frequency
The primary end point of CARE6 was the change from baseline in the number of TSC-associated seizures during the treatment period. Using negative binomial regression, the mean percent change from baseline for cannabidiol 25 mg/kg per day was 48.6% (95% CI, 40.4% to 55.8%) and for placebo was 26.5% (95% CI, 14.9% to 36.5%) for placebo. The ratio of cannabidiol to placebo was 0.699 (95% CI, 0.567 to 0.861), which translated to an estimated relative difference in mean percent reduction of 31.0% (95% CI, 13.9% to 43.3%; P = 0.0009).22
Figure 2: Negative Binomial Regression Analysis of TSC-Associated Seizure Count During the Baseline and Treatment Periods (ITT Analysis Set)a
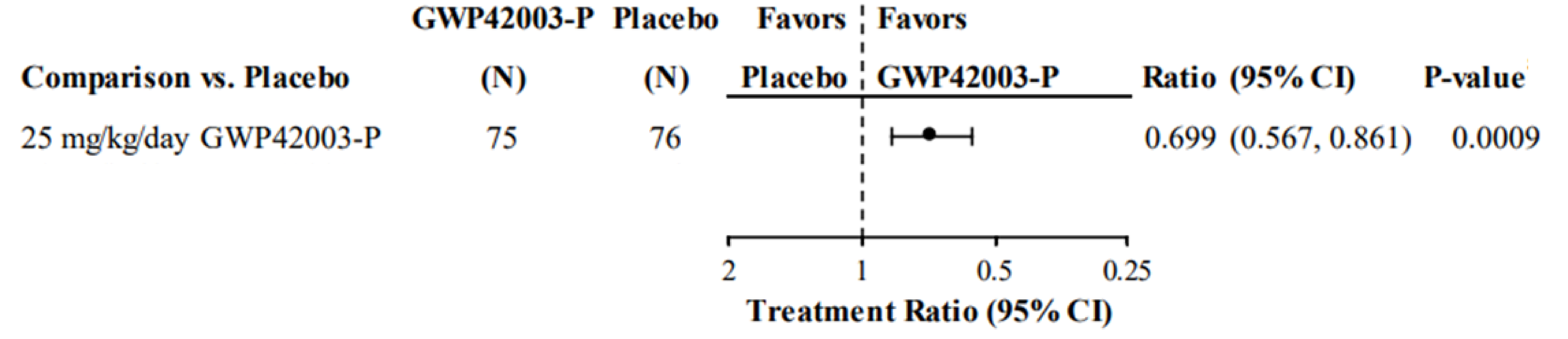
CI = confidence interval; GWP42003-P = cannabidiol; ITT = intention to treat; TSC = tuberous sclerosis complex.
Note: The model includes the total number of seizures as a response variable, age group, time (baseline and treatment period), treatment, and treatment-by-time interaction as fixed effects, and the patient as a random effect. The log-transformed number of days in which seizures were reported by period is included as an offset.
a Results for the cannabidiol 50 mg/kg per day group were not included, as it is not a Health Canada–approved dose.
Source: CARE6 Clinical Study Report.22
Sensitivity Analyses
Sensitivity analyses of the primary end point using the PP analysis set, the Wilcoxon rank sum test, ANCOVA, rank ANCOVA, and log-transformed ANCOVA are summarized in Table 20 of Appendix 1. The results of the sensitivity analyses were generally consistent with the primary analysis for the 25 mg/kg per day group. A sensitivity analysis imputing missing values as the worst of (highest number of seizures), the last observation carried forward, the next observation carried backward, and the mean daily number of seizures during the period also showed results generally consistent with the primary analysis.22
Subgroup Analysis
Subgroup analyses of interest to this review for the primary end point are summarized in Table 21. In the subgroup analyses of cannabidiol 25 mg/kg per day versus placebo, results were consistent with the primary analysis, although the reductions in seizure frequency observed in patients currently taking clobazam (ratio of 25 mg/kg per day to placebo, 0.53; 95% CI, 0.36 to 0.80) appeared larger than those not taking clobazam (ratio, 0.75; 95% CI, 0.59 to 0.96); however, the interaction P Value was nonsignificant (P = 0.1535) and the 95% CIs overlap.22
Treatment Responders: Proportion of Patients With a Reduction of at Least 50% in Seizure Frequency
The proportion of patients with a reduction of at least 50% from baseline in TSC-associated seizure frequency was the first key secondary end point of the CARE6 trial. In the double-blind treatment period, 27 (36.0%) patients in the cannabidiol 25 mg/kg per day group and 17 (22.4%) patients in the placebo group experienced a reduction of 50% or more in seizure frequency (OR, 1.95;95% CI, 0.95 to 4.00; P = 0.0692). The difference in the proportion of patients achieving a reduction of at least 50%in TSC-associated seizure frequency between the cannabidiol 25 mg/kg per day group and the placebo group was 13.6% (95% CI, –0.7% to 28.0%).22
Sensitivity Analyses
Sensitivity analyses of the first key secondary end point using the PP analysis set were consistent with the primary analysis, with 26 of 62 (41.9%) patients in the cannabidiol 25 mg/kg per day and 17 of 74 (23.0%) patients in the placebo group reporting a reduction of at least 50% in TSC-associated seizure frequency from baseline in favour of cannabidiol 25 mg/kg per day (OR, 2.42; 95% CI, 1.16 to 5.08).22
Subgroup Analysis
Subgroup analyses of interest to this review for the key secondary end point are summarized in Table 21. In the subgroup analyses comparing cannabidiol 25 mg/kg per day with placebo, results were consistent with the primary analysis, with intersecting 95% CIs, although the point estimates varied, with ORs ranging from 1.42 (95% CI, 0.55 to 3.66) for patients with less than 4 prior ASMs to 3.39 (95% CI, 0.86 to 13.38) for patients currently taking clobazam.22
Treatment Responders: Proportion of Patients With a Reduction in Seizure Frequency of at Least 50% or of 100%
The proportion of patients with reductions of 25% or more in TSC-associated seizure frequency and seizure freedom (100% reduction in seizure frequency) were secondary end points of the CARE6 trial. During the treatment period, 43 (57.3%) patients in the cannabidiol 25 mg/kg per day group and 33 (43.4%) in the placebo group experienced a 25% or greater reduction in seizure frequency (OR, 1.75; 95% CI, 0.92 to 3.33).22
Only 1 (1.3%) patient in the cannabidiol 25 mg/kg per day group and none in the placebo group experienced seizure freedom during the treatment period (relative effect not calculated).22
Sensitivity Analysis
Sensitivity analyses of the proportion of patients with seizure frequency reductions of 25% or more using the PP analysis set were consistent with the primary analysis, although the effect was slightly larger. In all, 42 of 62 (67.7%) patients in the cannabidiol 25 mg/kg per day group and 33 of 74 (44.6%) patients in the placebo group reported a reduction of 25% or greater in TSC-associated seizure frequency in favour of cannabidiol 25 mg/kg per day (OR, 2.61; 95% CI, 1.29 to 5.27). Sensitivity analysis results for total seizure freedom were identical to the primary analysis.22
Change from Baseline in QOLCE and QOLIE-31-P Scores
Quality of Life in Childhood Epilepsy Questionnaire
Results for the overall QoL in all patients who completed the QOLCE, regardless of age, are summarized in Table 13. In the cannabidiol 25 mg/kg per day group, an overall QoL score was available for 45 patients at baseline and 42 patients at the end of treatment. In the placebo group, an overall QoL score was available for 50 patients at baseline and 47 at the end of treatment. At the end of treatment, the LS mean change from baseline was 3.1 points (95% CI, –0.6 to 6.7 points) in the cannabidiol 25 mg/kg per day group and 1.6 points (95% CI, –1.8 to 4.9 points) in the placebo group. The LS mean difference in change from baseline was 1.5 points (95% CI, –3.3 to 6.3 points).22
Results for patients aged 2 to 18 years at the time the informed consent was signed are summarized in Table 22. Overall, although fewer patients were included in this analysis (n = 73), the results were consistent with the primary analysis of QOLCE, with an LS mean change from baseline of 2.9 points (95% CI, –1.3 to 7.0 points) for cannabidiol 25 mg/kg per day and 2.4 points (95% CI, –1.6 to 6.4 points) for placebo. The LS mean difference in change from baseline was 0.5 points (95% CI, –4.7 to 5.6 points).22
31-Item Quality of Life in Epilepsy – Problems Questionnaire
Results for the total score for all patients who completed the QOLIE-31-P, regardless of age, are summarized in Table 13. In total, the QOLIE-31-P was completed by 13 patients in the cannabidiol 25 mg/kg per day group and 10 patients in the placebo group at baseline, and by 14 patients in the cannabidiol 25 mg/kg per day group and 12 patients in the placebo group at the end of treatment. At the end of treatment, the LS mean change from baseline was –1.4 points (95% CI, –16.2 to 13.5 points) for cannabidiol 25 mg/kg per day and 2.3 points (95% CI, –15.0 to 19.7 points) for placebo. The LS mean difference in change from baseline was –3.7 points (95% CI, –16.6 to 9.2 points).22
Results for patients 19 years and older at the time the informed consent was signed (n = 20) are summarized in Table 22. Overall, results were consistent with the primary analysis of QOLIE-31-P, with LS mean changes from baseline of –1.2 points (95% CI, –10.8 to 8.5 points) for cannabidiol 25 mg/kg per day and 1.7 points (95% CI, –7.6 to 11.1 points) for placebo. The LS mean difference in change from baseline was –2.9 points (95% CI, –16.8 to 10.9 points).22
Although not specified as an outcome of interest to this review, the results for the CGIC and SGIC scales have been included in Table 23 of Appendix 1 to add context to the HRQoL end points.
Rescue Medication Use
During the baseline period, the mean number of days of rescue medication use in the cannabidiol 25 mg/kg per day group and the placebo group was 2.14 days (SD = 2.187) and 2.32 (SD = 3.200), respectively. The mean number of days of rescue medication use per 28 days during the treatment period was 0.79 days (SD = 2.469) in the cannabidiol 25 mg/kg per day group and 0.55 days (SD = 1.395) in the placebo group, representing mean changes from baseline of 0.19 days (SD = 2.836) and –0.92 days (SD = 1.858), respectively. The mean difference in rescue medication use days per 28-day period between cannabidiol 25 mg/kg per day and placebo was 0.96 (95% CI, –0.65 to 2.56).22
Status Epilepticus
During the baseline period, no patients in the cannabidiol 25 mg/kg per day group had status epilepticus, compared to 3 (3.9%) patients in the placebo group. The proportion of patients who reported episodes of status epilepticus during the treatment period was 6.7% (5 of 75 patients) in the cannabidiol 25 mg/kg per day group and 9.2% (7 of 76 patients) in the placebo group.22
Vineland Adaptive Behaviour Scales, Second Edition
In the cannabidiol 25 mg/kg per day group, 50 patients were included in the adaptive behaviour composite score of Vineland II at baseline and 51 patients were included at the end of treatment, whereas in the placebo group, 58 patients were included at baseline and 50 patients were included at the end of treatment. At the end of treatment, the mean adaptive behaviour composite score for the LS mean change from baseline was 0.0 points (95% CI, –1.6 to 1.5 points) for cannabidiol 25 mg/kg per day and 0.0 points (95% CI, –1.6 to 1.5 points) for placebo. The LS mean difference in change from baseline was 0.0 points (95% CI, –2.2 to 2.1 points).22
Table 13: Summary of Key Efficacy Results From the CARE6 Trial (ITT Analysis Set)a
Efficacy outcome | Cannabidiol 25 mg/kg per day (N = 75) | Placebo (N = 76) |
|---|---|---|
Change from baseline in TSC-associated seizures per 28 days | ||
Number of TSC-associated seizures during the baseline period | ||
Mean (SD) | 77.95 (83.390) | 89.22 (101.78) |
Number of seizures during the treatment period | ||
Mean (SD) | 46.07 (58.15) | 74.45 (105.21) |
Median (range) | 32.3 (0.0 to 286.9) | 41.1 (3.8 to 583.5) |
Percent change from baseline in TSC-associated seizures during the treatment periodb | ||
Mean (SD) | –35.22 (46.02) | –20.20 (33.88) |
Median (range) | –43.36 (–100.0 to 120.8) | –20.08 (–73.3 to 86.1) |
Negative binomial regression analysis | ||
Estimated baseline seizure rate, mean (95% CI) | 51.6 (40.8 to 65.3) | 54.8 (43.4 to 69.3) |
Treatment period seizure rate, mean (95% CI) | 26.5 (21.0 to 33.5) | 40.3 (31.9 to 50.8) |
Estimated rate ratio (treatment/baseline) | ||
Rate ratio (95% CI) | 0.514 (0.442 to 0.596) | 0.735 (0.635 to 0.851) |
Reduction between treatment and baseline, % (95% CI) | 48.6 (40.4 to 55.8) | 26.5 (14.9 to 36.5) |
Absolute treatment difference vs. placebo (95% CI) | NR | — |
Relative treatment difference (vs. placebo) | ||
Relative treatment ratio vs. placebo (95% CI) | 0.699 (0.57 to 0.86) | — |
Percent reduction vs. placebo, LS mean (95% CI) | 31.0 (13.9 to 43.3) | — |
P value | 0.0009 | — |
The proportion of patients with a ≥ 50% reduction from baseline in TSC-associated seizure frequencyc | ||
N (%)d | 27 (36.0) | 17 (22.4) |
Difference in proportions, % (95% CI) | 13.6 (–0.7 to 28.0) | — |
OR (95% CI) | 1.95 (0.95 to 4.00) | — |
P valuee | 0.0692 | — |
TSC-associated seizure treatment responders (≥ 25% reduction) and seizure freedom (100% reduction) | ||
≥ 25% reduction in TSC-associated seizure frequency from baseline | ||
N (%)d | 43 (57.3) | 33 (43.4) |
Difference in proportions, % (95% CI) | 13.9 (–1.9 to 29.7) | — |
OR (95% CI) | 1.75 (0.92 to 3.33) | — |
100% reduction in TSC-associated seizure frequency from baseline | ||
N (%)d | 1 (1.3) | 0 (0.0) |
Difference in proportions (95% CI) | 1.3 (–1.3 to 3.9) | — |
OR (95% CI) | NA | — |
QOLCE scores, overall quality of life (all patients)f | ||
Day 1 | ||
N | 45 | 50 |
Mean (SD) points | 50.8 (12.99) | 47.7 (13.85) |
End of treatment | ||
N | 42 | 47 |
Mean (SD) points | 54.3 (14.89) | 51.0 (15.52) |
Change from baseline | ||
N | 37 | 45 |
Mean (SD) points | 2.7 (10.82) | 1.8 (9.44) |
LS mean (95% CI) points | 3.1 (–0.6 to 6.7) | 1.6 (–1.8 to 4.9) |
Treatment difference, points (95% CI) | 1.5 (–3.3 to 6.3) | — |
QOLIE-31-P scores, total score (all patients)f | ||
Day 1 | ||
N | 13 | 10 |
Mean (SD) points | 68.3 (16.03) | 58.0 (13.26) |
End of treatment | ||
N | 14 | 12 |
Mean (SD) points | 64.5 (18.46) | 64.5 (16.89) |
Change from baseline | ||
N | 12 | 10 |
Mean (SD) points | –3.1 (17.64) | 3.1 (8.09) |
LS mean (95% CI) points | –1.4 (–16.2 to 13.5) | 2.3 (–15.0 to 19.7) |
Treatment difference, points (95% CI) | –3.7 (–16.6 to 9.2) | — |
Rescue medication use days per 28-day periodg | ||
Baseline period | ||
Number of patients using rescue medication | 16 | 20 |
Number of days, mean (SD) | 2.14 (2.187) | 2.32 (3.200) |
Treatment period | ||
Number of patients using rescue medication | 68 | 73 |
Number of days, mean (SD) | 0.79 (2.469) | 0.55 (1.395) |
Change from baseline in rescue medication use days, mean (SD) | 0.19 (2.836) | –0.92 (1.858) |
Treatment difference, days (95% CI) | 0.96 (−0.65 to 2.56) | — |
Status epilepticus | ||
Number of patients with status epilepticus, baseline period (%) | 0 | 3 (3.9) |
Number of patients with status epilepticus, treatment period (%) | 5 (6.7) | 7 (9.2) |
Vineland II scores | ||
Adaptive behaviour composite standard score | ||
Day 1 | ||
N | 50 | 58 |
Mean (SD) points | 50.4 (21.36) | 49.7 (23.66) |
End of treatment | ||
N | 51 | 50 |
Mean (SD) points | 50.7 (22.24) | 51.5 (25.57) |
Change from baselineh | ||
N | 43 | 47 |
Mean (SD) points | 0.3 (4.43) | 0.2 (5.30) |
LS mean points (95% CI) | 0.0 (–1.6 to 1.5) | 0.0 (–1.6 to 1.5) |
Treatment difference, mean points (95% CI) | 0.0 (–2.2 to 2.1) | — |
Treatment difference, OR (95% CI) | 1.19 (0.28 to 5.09) | — |
CI = confidence interval; ITT = intention to treat; LS = least squares; NR = not reported; OR = odds ratio; QOLCE = Quality of Life in Childhood Epilepsy; QOLIE-31-P = 31-item Quality of Life in Epilepsy – Problems questionnaire; SD = standard deviation; TSC = tuberous sclerosis complex; Vineland II = Vineland Adaptive Behaviour Scales, Second Edition.
aResults for the cannabidiol 50 mg/kg per day group were not included, as it is not a Health Canada–approved dose.
bModel includes total number of seizures as a response variable, and age group, time (baseline and treatment period), treatment, and treatment by time interaction as fixed effects, and the patient as a random effect. The log-transformed number of days seizures were reported by period is included as an offset.
cFirst key secondary end point controlled for multiplicity.
dPatients who withdrew from the trial during the treatment period were considered nonresponders.
eP value calculated from a Cochran-Mantel-Haenszel test stratified by age group (1 to 6 years, 7 to 11 years, 12 to 17 years, and 18 to 65 years).
fThe change from baseline is analyzed using an ANCOVA model with baseline and age group (1 to 6 years, 7 to 11 years, 12 to 17 years, and 18 to 65 years) as covariates and treatment group as a fixed factor.
gThe change from baseline period in number of days rescue medication was taken per 28 days is analyzed using an ANCOVA model with baseline period and age group (1 to 6 years, 7 to 11 years, 12 to 17 years, and 18 to 65 years) as covariates and treatment group as a fixed factor.
hThe change from baseline in adaptive behaviour domains and the adaptive behaviour composite are analyzed using an ANCOVA model with baseline and age group (1 to 6 years, 7 to 11 years, 12 to 17 years, and 18 to 65 years) as covariates and treatment group as a fixed factor. Higher scores represent greater levels of functioning.
Source: CARE6 Clinical Study Report.22
Harms
Safety results were presented for the safety analysis set for the cannabidiol 25 mg/kg per day and placebo groups only (n = 151). Refer to Table 14 for harms data.
Adverse Events
At least 1 TEAE was reported by 70 (93.3%) patients in the cannabidiol 25 mg/kg per day group and 72 (94.7%) patients in the placebo group. The most frequently occurring (10% of patients or more) TEAEs in the cannabidiol 25 mg/kg per day group were diarrhea (23 [30.7%]), decreased appetite (15 [20.0%]), pyrexia (14 [18.7%]), vomiting (13 [17.3%]), increased gamma-glutamyl transferase, ALT, and AST (12 [16.0%], 9 [12.0%]), and 8 [10.7%], respectively), somnolence (10 [13.3%]), and cough (8 [10.7%]). In the placebo group, the most frequently occurring TEAEs were diarrhea (13 [17.1%]), nasopharyngitis (12 [15.8%]), upper respiratory tract infection (10 [13.2%]), and decreased appetite (9 [11.8%]).22
The first occurrence of a TEAE was most commonly reported during the dose-escalation period in the 25 mg/kg per day group (46 [61.3%] patients) and in the placebo group (41 [53.9%] patients).22
Serious Adverse Events
In the CARE6 trial, 28 (12.5%) patients experienced a total of 44 SAEs, including 16 patients (21.3%) in the 25 mg/kg per day group and 2 patients (2.6%) in the placebo group. The most commonly reported individual SAEs in the cannabidiol 25 mg/kg per day group were increased ALT, increased AST, status epilepticus, vomiting, and viral gastroenteritis (2 [2.7%] patients each). SAEs in the placebo group only occurred in 2 (2.6%) patients and included pneumonia and status epilepticus (1 [1.3%] each).22
Withdrawal Due to Adverse Events
TEAEs leading to the discontinuation of treatment occurred in 8 (10.7%) patients in the 25 mg/kg per day group and 2 (2.6%) patients in the placebo group. The most common reason for discontinuing treatment in the cannabidiol group was rash (2 [2.7%]). All other reasons for discontinuation occurred in only 1 (1.3%) patient. In the placebo group, 1 patient discontinued treatment due to ataxia and 1 patient discontinued due to agitation.22
A total of 17 (22.7%) and 4 (5.3%) patients experienced TEAEs that led to dose reductions in the cannabidiol 25 mg/kg per day and placebo groups, respectively. The most frequent reasons for dose reductions were diarrhea (4 [5.3%] patients in the 25 mg/kg per day group and 1 [1.3%] patient in the placebo group), somnolence (1 [1.3%] patient versus 2 [2.6%] patients), and decreased appetite (4 [5.3%] patients versus 1 [1.3%] patient).22
Mortality
There were no deaths reported during the CARE6 trial.22
Notable Harms
AEs of special interest to this review consisted of hepatocellular injury and hypersensitivity reactions. Liver injury and type IV hypersensitivity reactions occurred in 1 (1.3%) patient each in the cannabidiol 25 mg/kg per day group, were listed as SAEs, and both led to the discontinuation of treatment.22
Table 14: Summary of Harms Results From the Study Included in the Systematic Review
Adverse events | CARE6a | |
|---|---|---|
Cannabidiol 25 mg/kg (N = 75) | Placebo (N = 76) | |
Most common AEs, n (%)b | ||
Number of patients with any AE | 70 (93.3) | 72 (94.7) |
Gastrointestinal disorders | 37 (49.3) | 27 (35.5) |
Diarrhea | 23 (30.7) | 13 (17.1) |
Vomiting | 13 (17.3) | 2 (2.6) |
Constipation | 8 (10.7) | 6 (7.9) |
General disorders and administration site conditions | 21 (28.0) | 11 (14.5) |
Pyrexia | 14 (18.7) | 6 (7.9) |
Infections and infestations | 41 (54.7) | 37 (48.7) |
Nasopharyngitis | 11 (14.7) | 12 (15.8) |
Upper respiratory tract infection | 7 (9.3) | 10 (13.2) |
Investigations | 30 (40.0) | 11 (14.5) |
Increased ALT | 9 (12.0) | 0 (0.0) |
Increased AST | 8 (10.7) | 0 (0.0) |
Increased GGT | 12 (16.0) | 0 (0.0) |
Metabolism and nutrition disorders | 20 (26.7) | 13 (17.1) |
Decreased appetite | 15 (20.0) | 9 (11.8) |
Nervous system disorders | 27 (36.0) | 32 (42.1) |
Somnolence | 10 (13.3) | 7 (9.2) |
Seizure | 5 (6.7) | 5 (6.6) |
Respiratory, thoracic, and mediastinal disorders | 15 (20.0) | 11 (14.5) |
Cough | 8 (10.7) | 5 (6.6) |
SAEs, n (%)c | ||
Number of patients with any SAE | 16 (21.3) | 2 (2.6) |
Gastrointestinal disorders | 2 (2.7) | 0 (0.0) |
Vomiting | 2 (2.7) | 0 (0.0) |
Infections and infestations | 4 (5.3) | 1 (1.3) |
Gastroenteritis viral | 2 (2.7) | 0 (0.0) |
Investigations | 2 (2.7) | 0 (0.0) |
Increased ALT | 2 (2.7) | 0 (0.0) |
Increased AST | 2 (2.7) | 0 (0.0) |
Nervous system disorders | 3 (4.0) | 1 (1.3) |
Status epilepticus | 2 (2.7) | 1 (1.3) |
Respiratory, thoracic, and mediastinal disorders | 2 (2.7) | 0 (0.0) |
Skin and subcutaneous tissue disorders | 2 (2.7) | 0 (0.0) |
Patients who stopped treatment due to adverse events, n (%)c | ||
Total WDAEs | 8 (10.7) | 2 (2.6) |
Gastrointestinal disorders | 1 (1.3) | 0 (0.0) |
Investigations | 3 (4.0) | 0 (0.0) |
Nervous system disorders | 0 (0.0) | 1 (1.3) |
Skin and subcutaneous tissue disorders | 4 (5.3) | 0 (0.0) |
Rash | 2 (2.7) | 0 (0.0) |
AEs of special interest, n (%) | ||
Hepatocellular injury | 1 (1.3) | 0 (0.0) |
Type IV hypersensitivity reactions | 1 (1.3) | 0 (0.0) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; GGT = gamma-glutamyl transferase; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
aResults for the cannabidiol 50 mg/kg per day group were not included, as it is not a Health Canada–approved dose.
bFrequency greater than or equal to 10%.
cFrequency greater than or equal to 2%.
Source: CARE6 Clinical Study Report.22
Critical Appraisal
Internal Validity
The phase III CARE6 trial was the only study included in this review. The methods of randomization, treatment allocation, and stratification employed using IVRS were appropriate, reducing the risk of selection bias. Acceptably, randomization was stratified by age, but, given the known interaction between clobazam and cannabidiol, stratification by clobazam use could have also been conducted, although the CARE6 trial was initiated before the importance of this interaction was known. Concomitant clobazam use was reported in 17 (22.7%) patients in the cannabidiol 25 mg/kg per day group and in 25 (32.9%) in the placebo group. It remains unclear what impact this may have had on the results. There was some variation in characteristics across groups, particularly for the number of TSC-associated seizures and seizure type during the baseline period, as well as the proportion of patients using various concomitant ASMs. However, given the relatively small sample size and the fact that the imbalances did not universally favour either treatment group, it is likely that these are the result of chance. Additionally, the clinical experts consulted by CADTH noted that there is substantial disease heterogeneity in this population, and they agreed that the differences could be due to chance.
The sample size calculation for the CARE6 study was considered appropriate; however, it was assumed that the proportion of patients in the placebo group would experience a mean reduction in seizure frequency of 15%, which may be considered low compared to what was observed in the CARE6 study (26.5%). It remains unclear how a larger placebo response would have affected the results of the sample size calculation. Overall, a small number of patients were included in the primary efficacy population for each treatment arm (25 mg/kg per day, n = 75; 50 mg/kg per day, n = 73; placebo, n = 76), although the study was powered to detect differences across populations. Two individual placebo arms consisting of 38 patients each were pooled for comparisons. Despite the appropriate use of the sample size estimation, the magnitude of the treatment-effect estimates observed in a small study sample may not be replicable in a larger sample.
There were differences between the cannabidiol 25 mg/kg per day and placebo groups in discontinuation from the study (13.3% versus 1.3%), primarily due to AEs; 10.7% of patients in the cannabidiol 25 mg/kg per day group discontinued the study due to AEs compared to 0 patients in the placebo group. Further, although not a dosage approved by Health Canada, 32.9% of patients in the cannabidiol 50 mg/kg per day group did not achieve their target maintenance dose during the titration phase, primarily due to TEAEs. Despite being a double-blind RCT, this may have revealed treatment assignment; however, it is unclear what effect this would have on the results of the study.
Outcomes evaluated in the CARE6 study were clinically relevant in the treatment of TSC-associated seizures. Most outcomes in the CARE6 trial were related to seizure frequency, which was measured by countable seizures of various types reported via IVRS. In consultation with clinical experts, it was determined that there is some subjectivity and error in the way patients and caregivers classify these; however, the seizure types defined for the CARE6 trial are generally countable and should not ultimately bias the results, per the clinical experts consulted by CADTH. The primary end point of the CARE6 trial was analyzed with negative binomial regression and MMRM. The main result of the primary analysis arises from the inverse of the ratio of the ratios for change from baseline, however, no absolute difference in the percent change from baseline in seizure frequency was available from this analysis. Numerous predefined sensitivity analyses were conducted to evaluate the robustness of the primary end point using different modelling methods and imputation methods that used different assumptions to account for missing data. Overall, the results of the primary analyses and sensitivity analyses were consistent, supporting the results of the primary analysis. For response outcomes (25%, 50%, and 100%), patients who withdrew were considered to be nonresponders, which is likely to be a conservative assumption. For the analyses of rescue medication use and status epilepticus, it appears that all patients were included, although not all would have completed follow-up (i.e., there would be missing data for those who withdrew early), which may result in the risk of bias due to missing outcome data, but the direction and extent is not clear. For HRQoL (QOLCE and QOLIE-31-P) and adaptive behaviour (Vineland II), the extent of missing data was large, resulting in a high risk of bias, although the direction is uncertain.
Various prespecified subgroup analyses based on various disease characteristics were conducted in the CARE6 trial to examine the consistency of the primary and secondary analyses results across subgroup levels. Subgroups of interest to this review included clobazam use and the number of concurrent and prior ASMs, based on discussion with the clinical experts consulted by CADTH. Again, the results of subgroup analyses generally supported the primary analysis, though they were not statistically powered to detect within-group or between-group differences. Additionally, wide overlapping 95% CIs reflected uncertainty in the effect estimates and were likely due to the small sample sizes of most subgroups. As such, the results should be interpreted as supportive evidence only for the overall effect of cannabidiol and do not provide strong evidence about the use of cannabidiol concomitantly with clobazam.
The methods used to account for multiplicity in the CARE6 trial were considered appropriate. The primary end point (percent change from baseline in seizure frequency) and key secondary end points (proportion of patients with a ≥ 50% reduction from baseline in TSC-associated seizure frequency, change from baseline in SGIC and CGIC scores, and change in total seizure frequency) were controlled for multiplicity for both dosages at the 0.05 level using a hierarchical gate-keeping procedure. However, only the first key secondary end point was of interest to this review, and results for other key secondary end points were not reported. No hierarchical testing procedure or multiplicity adjustments were implemented for the other secondary end points, and the results did not reach statistical significance.
As part of the CARE6 trial, exploratory end points included the use of rescue medication and the change in rescue medication use days. The use of rescue medication was not accounted for in any analyses of the primary or key secondary end points, so it remains unclear whether there was any impact of rescue medication on the results, considering that most patients required the use of rescue medication at some point during the treatment period. Although, as noted by the clinical experts, the use of rescue medication would not prompt the discontinuation of therapy.
Outcomes related to HRQoL were considered important to patients and were captured as other secondary end points of the CARE6 trial and analyzed using ANCOVA. The measures of interest to this review, QOLCE and QOLIE-31-P scores, were considered reliable and valid measures for epilepsy in TSC, with specific minimally important differences (MIDs) noted in the sponsors submission. The clinical experts consulted by CADTH noted that specific HRQoL measures are not used in routine clinical practice. Evidence of validity and reliability were available for Vineland II, although no evidence was located on responsiveness or to inform the MID. Although familiar with the included measures, the clinical experts consulted could not comment on what constitutes clinically meaningful differences in scores.
External Validity
Two dosages of cannabidiol were evaluated in the CARE6 trial: 25 mg/kg per day and 50 mg/kg per day. However, given that the maximum recommended Health Canada–approved dosage of cannabidiol for TSC-associated seizures is 12.5 mg/kg twice daily (25 mg/kg per day), the cannabidiol 50 mg/kg per day dose was not of interest to this review. Additionally, lower doses of cannabidiol (e.g., 10 mg/kg per day) were not studied in the CARE6 trial. CARE6 was an international, multicentre study, but there were no Canadian sites included. The clinical experts consulted by CADTH indicated that the inclusion and exclusion criteria for the CARE6 trial were appropriate to identify patients with TSC-associated epilepsy who should receive treatment with cannabidiol. As part of the inclusion and exclusion criteria for the CARE6 trial, patients were required to have a clinical diagnosis of TSC. Genetic confirmation was not required, as clinical markers of TSC are well established and can provide sufficient evidence for a diagnosis, which was corroborated by the clinical experts consulted by CADTH.
Patients enrolled in the CARE6 trial were required to be taking at least 1 ASM and to have experienced at least 8 seizures during the baseline period. Despite the modest thresholds outlined in the eligibility criteria, the mean number of prior ASMs and concurrent ASMs was 4.56 (maximum, 15) and 2.67 (maximum, 5), respectively, suggesting a highly refractive population. Additionally, the enrolled patients experienced 8 to 558 TSC-associated seizures over the 28-day baseline period, which suggested that the included population had a very high seizure burden. The clinical experts consulted by CADTH noted that the included population was reflective of clinical practice, highlighting the variability in seizure burden across patients; however, it was noted that not all patients with TSC have such a high disease burden, so the enrolled population may have been restrictive, selecting for patients with more refractory epilepsy and higher disease burden.
There was notable heterogeneity in the concomitant ASMs received by patients in the CARE6 trial; however, the clinical experts consulted by CADTH noted that this is in line with clinical practice and varies by patient based on response, intolerance, and various contraindications. The clinical experts highlighted the known interaction with benzodiazepines (e.g., clobazam), which requires dose adjustments in the event of hepatocellular injury.
Outcomes in the CARE6 trial were considered clinically relevant and important to patients, mainly focusing on measures of seizure frequency, which is the focus of epilepsy treatment in routine clinical practice. However, an additional consideration, as noted by patient groups and the clinical experts consulted by CADTH, is the reduction in seizure severity, which was not explicitly measured in the CARE6 trial but instead was measured in conjunction with seizure type and overall frequency. The clinical experts consulted by CADTH highlighted that a reduction in the frequency of seizures may not necessarily be associated with a reduction in severity. However, the clinical experts also noted a direct relationship between severity and type of seizure, stating that, of the seizure types defined by the sponsor, type 3 focal seizures are the most disabling. An exploratory analysis by individual TSC-associated seizure type was conducted in the CARE6 trial; however, the results were not included in this report, given the exploratory nature of the outcome, variation across groups, and small sample sizes.
The duration of the CARE6 trial, at 16 weeks, was considered appropriate for measuring response to treatment and observing changes in seizure frequency. However, given that the impact of cannabidiol on HRQoL and TANDs were also outcomes of interest to this review, the secondary nature of these outcomes, the small sample sizes for completion of various measures, and the short duration of the CARE6 trial make interpretation of the results difficult, and they should only be viewed as supportive of the overall effect of cannabidiol.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal study and RCT identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.29,30
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word likely for evidence of moderate certainty (e.g., X intervention likely results in Y outcome).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word may for evidence of low certainty (e.g., X intervention may result in Y outcome).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of the effect. We describe evidence of very low certainty as very uncertain.
Following the GRADE approach, evidence from RCTs starts as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence of a clinically important reduction in seizure frequency (percent change in seizure frequency) on thresholds informed by clinical expert opinion, treatment guidelines, and clinical trials, as well as HRQoL and patient-reported outcomes (QOLCE, QOLIE-31-P, Vineland II) assessments informed by the literature, where available. Other targets for the certainty of evidence assessment were the presence or absence of any (nonnull) effect for the proportion of patients achieving 25%, 50%, or 100% reductions in seizure frequency, the proportion of patients with status epilepticus, and changes from baseline in rescue medication use.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for outcomes in the cannabidiol and placebo groups in the pivotal CARE6 trial.
Long-Term Extension Studies
The contents of this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
Description of Studies
One open-label, single-arm, long-term extension of the CARE6 study (CARE6 OLE) has been summarized to provide evidence regarding the long-term safety and efficacy of cannabidiol. Upon completion of the double-blind phase of the CARE6 study, patients in both the cannabidiol and placebo treatment groups were invited to receive open-label cannabidiol during the OLE period for a maximum duration of 1 year. The OLE phase was extended to a duration of 4 years in the US and 3 years in Poland after protocol amendments. The OLE study included 199 of the 201 patients who had completed the double-blind phase at 43 study sites in Australia, the Netherlands, Poland, Spain, the UK, and the US. The study was initiated on August 31, 2016, and was completed on June 11, 2021.28
The primary objective of the CARE6 OLE study was to evaluate the long-term safety and tolerability of cannabidiol as add-on therapy in children and adults with TSC and inadequately controlled seizures. The secondary objectives were to evaluate the long-term effects of cannabidiol as an add-on therapy on antiepileptic measures, growth, development (in patients younger than 18 years), and QoL, and to evaluate the long-term safety and tolerability of cannabidiol. The exploratory objective was to evaluate the long-term effect of cannabidiol on TANDs, including cognitive and behavioural function and autistic features.28
Populations
The baseline demographic and clinical characteristics of the CARE6 OLE study are provided in Table 15. All patients who wished to continue cannabidiol after the double-blind phase of the CARE6 study were eligible for inclusion. Overall, there were more male patients (59.3%) than female patients (40.7%). Most patients were white (88.9%). Approximately half of all patients were from the US (51.8%). The mean age was 13.15 (SD = 10.02) years, with 76.9% of patients being younger than 18 years. The mean body mass index at baseline was 21.02 (SD = 10.63) kg/m2. The demographic characteristics were similar in the cannabidiol and placebo groups. The most common seizure types that participants had at baseline were tonic (28.6%), tonic-clonic (21.1%), and atonic (12.6%). The cannabidiol and placebo groups were similar in terms of the type of seizure patients had at baseline (tonic, 33.9% versus 20.0%; clonic, 4.0% versus 2.7%; atonic, 9.7% versus 17.3%) . The median number of ASMs at baseline was 3 (range, 0 to 5), with 30.7% of patients taking 2 ASMs and 41.7% of patients taking 3 ASMs at baseline.28
Table 15: Summary of Baseline Characteristics of the CARE6 OLE Study (Safety Analysis Set)
Characteristic | Patients who received cannabidiol during double-blind phase (N = 124) | Patients who received placebo during double-blind phase (N = 75) | Total (N = 199) |
|---|---|---|---|
Age, years | |||
Mean (SD) | 12.69 (9.64) | 13.92 (10.63) | 13.15 (10.02) |
Median (minimum to maximum) | 10.03 (1.1 to 56.8) | 11.06 (1.2 to 55.8) | 10.74 (1.1 to 6.8) |
Age group, n (%) | |||
1 to 6 years | 38 (30.6) | 21 (28.0) | 59 (29.6) |
7 to 11 years | 32 (25.8) | 18 (24.0) | 50 (25.1) |
12 to 17 years | 28 (22.6) | 16 (21.3) | 44 (22.1) |
18 to 65 years | 26 (21.0) | 20 (26.7) | 46 (23.1) |
Sex, n (%) | |||
Female | 51 (41.1) | 30 (40.0) | 81 (40.7) |
Male | 73 (58.9) | 45 (60.0) | 118 (59.3) |
Race, n (%) | |||
White or Caucasian | 111 (89.5) | 66 (88.0) | 177 (88.9) |
Black or African American | 4 (3.2) | 0 | 4 (2.0) |
American Indian or Alaska Native | 1 (0.8) | 0 | 1 (0.5) |
Asian | 1 (0.8) | 3 (4.0) | 4 (2.0) |
Other | 7 (5.6) | 6 (8.0) | 13 (6.5) |
Country, n (%) | |||
Australia | 12 (9.7) | 10 (13.3) | 22 (11.1) |
Netherlands | 4 (3.2) | 3 (4.0) | 7 (3.5) |
Poland | 35 (28.2) | 16 (21.3) | 51 (25.6) |
Spain | 8 (6.5) | 2 (2.7) | 10 (5.0) |
US | 62 (50.0) | 41 (54.7) | 103 (51.8) |
UK | 3 (2.4) | 3 (4.0) | 6 (3.0) |
Weight at baseline, kg | |||
Mean (SD) | 40.46 (22.53) | 44.91 (27.97) | 42.14 (24.74) |
Median (minimum to maximum) | 34.10 (12.1 to 130.0) | 36.90 (10.4 to 115.7) | 36.30 (10.4 to 130.0) |
Height at baseline, cm | |||
n | 122 | 75 | 197 |
Mean (SD) | 137.23 (28.66) | 137.8 (31.36) | 137.45 (29.64) |
Median (minimum to maximum) | 139.55 (43.0 to 196.0) | 140.60 (41.5 to 182.0) | 140.0 (41.5 to 196.0) |
BMI at baseline, kg/m2 | |||
n | 122 | 75 | 197 |
Mean (SD) | 20.32 (9.59) | 22.16 (12.11) | 21.02 (10.63) |
Median (minimum to maximum) | 18.49 (8.4 to 108.7) | 19.28 (13.2 to 110.3) | 18.71 (8.4 to 110.3) |
Seizure types during baseline, n (%) | |||
Tonic-clonic seizures | 28 (22.6) | 14 (18.7) | 42 (21.1) |
Tonic seizures | 42 (33.9) | 15 (20.0) | 57 (28.6) |
Clonic seizures | 5 (4.0) | 2 (2.7) | 7 (3.5) |
Atonic seizures | 12 (9.7) | 13 (17.3) | 25 (12.6) |
Absence seizures | 15 (12.1) | 7 (9.3) | 22 (11.1) |
Myoclonic seizures | 8 (6.5) | 4 (5.3) | 12 (6.0) |
Partial sensory seizures | 2 (1.6) | 3 (4.0) | 5 (2.5) |
Infantile or epileptic spasms | 10 (8.1) | 3 (4.0) | 13 (6.5) |
Number of ASMs a patient currently takinga | |||
Mean (SD) | 2.62 (0.99) | 2.6 (0.9) | 2.61 (0.96) |
Median (minimum to maximum) | 3.0 (0 to 5.0) | 3.0 (1.0 to 5.0) | 3.0 (0 to 5.0) |
Number of ASMs a patient currently taking, n (%)a | |||
0 | 1 (0.8) | 0 | 1 (0.5) |
1 | 16 (12.9) | 8 (10.7) | 24 (12.1) |
2 | 36 (29.0) | 25 (33.3) | 61 (30.7) |
3 | 50 (40.3) | 33 (44.0) | 83 (41.7) |
4 | 18 (14.5) | 7 (9.3) | 25 (12.6) |
5 | 3 (2.4) | 2 (2.7) | 5 (2.5) |
ASM = antiseizure medication; BMI = body mass index; OLE = open-label extension; SD = standard deviation.
aCurrent ASM use refers to the double-blind phase.
Source: CARE6 OLE CSR.28
Interventions
The OLE consisted of a 3-week titration period followed by a maintenance period and a 10-day taper period. After the end of the treatment visit or the decision to withdraw, cannabidiol was tapered down (10% per day for 10 days) at home until the end of the taper visit.28
During the titration period, cannabidiol was titrated up to 25 mg/kg per day, whereas blinded treatment (i.e., either cannabidiol or placebo taken by patients during the CARE6 double-blind phase) was simultaneously tapered down to 0 to accommodate patients who had been randomized to placebo during the double-blind phase. Patients administered 50 mg/kg per day during the double-blind phase were tapered (10% per day for 5 days) to 25 mg/kg per day. All patients completed the transition and entered the OLE, taking 25 mg/kg per day cannabidiol. After titration from the double-blind phase to the OLE phase, patients continued with their optimal cannabidiol dose during the maintenance period. However, investigators could adjust dosing, either to decrease the dose if a patient experienced intolerance or increase the dose to a maximum of 50 mg/kg per day if required for better seizure control until the optimal dose was found. If seizure freedom was achieved with the use of cannabidiol during the study, the investigator could consider reducing the dose of concomitant ASMs after 6 months of seizure freedom. Cannabidiol was to be administered by the patient or their caregiver twice each day (half the daily dose in the morning and half in the evening) using the syringe provided.28
Concomitant medication use, excluding rescue medications, is summarized in Table 16. A total of 198 (99.5%) patients took 1 or more concomitant ASMs during the study. The most commonly used ASMs were valproic acid (86 [43.2%] patients), vigabatrin (73 [36.7%] patients), and clobazam (70 [35.2%] patients). A total of 178 (89.4%) patients were recorded as taking concomitant medications aside from ASMs. The most common other concomitant medication reported was paracetamol (74 [37.2%] patients). As for nonpharmacological measures, 5 (2.5%) patients were on a ketogenic diet and 24 (12.1%) patients had received VNS.28
Table 16: Concomitant Medications Used in the CARE6 OLE Study (Safety Analysis Set)
Exposure | Patients who took cannabidiol during double-blind phase (N = 124) | Patients who took placebo during double-blind phase (N = 75) | Total (N = 199) |
|---|---|---|---|
Received 1 or more concomitant ASMs during the study, n (%) | 123 (99.2) | 75 (100.0) | 198 (99.5) |
Barbiturates and derivatives | 5 (4.0) | 2 (2.7) | 7 (3.5) |
Phenobarbital | 4 (3.2) | 1 (1.3) | 5 (2.5) |
Primidone | 1 (0.8) | 1 (1.3) | 2 (1.0) |
Benzodiazepine derivatives | 50 (40.3) | 40 (53.3) | 90 (45.2) |
Clobazam | 37 (29.8) | 33 (44.0) | 70 (35.2) |
Clonazepam | 10 (8.1) | 5 (6.7) | 15 (7.5) |
Lorazepam | 4 (3.2) | 2 (2.7) | 6 (3.0) |
Midazolam | 1 (0.8) | 2 (2.7) | 3 (1.5) |
Clorazepate dipotassium | 2 (1.6) | 0 | 2 (1.0) |
Nitrazepam | 1 (0.8) | 0 | 1 (0.5) |
Carboxamide derivatives | 52 (41.9) | 26 (34.7) | 78 (39.2) |
Oxcarbazepine | 24 (19.4) | 10 (13.3) | 34 (17.1) |
Carbamazepine | 19 (15.3) | 9 (12.0) | 28 (14.1) |
Rufinamide | 11 (8.9) | 8 (10.7) | 19 (9.5) |
Eslicarbazepine acetate | 2 (1.6) | 1 (1.3) | 3 (1.5) |
Fatty acid derivatives | 78 (62.9) | 48 (64.0) | 126 (63.3) |
Valproic acida | 50 (40.3) | 36 (48.0) | 86 (43.2) |
Vigabatrin | 55 (44.4) | 18 (24.0) | 73 (36.7) |
Tiagabine hydrochloride | 0 | 1 (1.3) | 1 (0.5) |
Hydantoin derivatives | 3 (2.4) | 3 (4.0) | 6 (3.0) |
Phenytoin | 3 (2.4) | 3 (4.0) | 6 (3.0) |
Other antiepileptics | 94 (75.8) | 63 (84.0) | 157 (78.9) |
Levetiracetam | 34 (27.4) | 25 (33.3) | 59 (29.6) |
Lacosamide | 23 (18.5) | 18 (24.0) | 51 (25.6) |
Lamotrigine | 26 (21.0) | 19 (25.3) | 45 (22.6) |
Topiramate | 18 (14.5) | 13 (17.3) | 31 (15.6) |
Zonisamide | 14 (11.3) | 8 (10.7) | 22 (11.1) |
Perampanel | 11 (8.9) | 5 (6.7) | 16 (8.0) |
Felbamate | 11 (8.9) | 4 (5.3) | 15 (7.5) |
Brivaracetam | 3 (2.4) | 2 (2.7) | 5 (2.5) |
Gabapentin | 2 (1.6) | 1 (1.3) | 3 (1.5) |
Pregabalin | 2 (1.6) | 1 (1.3) | 3 (1.5) |
Acetazolamide | 1 (0.8) | 0 | 1 (0.5) |
Selective immunosuppressants | 6 (4.8) | 2 (2.7) | 8 (4.0) |
Everolimus | 6 (4.8) | 2 (2.7) | 8 (4.0) |
Succinimide derivatives | 1 (0.8) | 0 | 1 (0.5) |
Ethosuximide | 1 (0.8) | 0 | 1 (0.5) |
Unspecified herbal and traditional medicine | 1 (0.8) | 0 | 1 (0.5) |
Cannabis sativa oil | 1 (0.8) | 0 | 1 (0.5) |
ASM = antiseizure medication; OLE = open-label extension.
Note: A medication is considered concomitant for each phase if it has a start date on or after the first dose of cannabidiol for the corresponding phase or if it was started before the first dose of cannabidiol and was ongoing.
aPreferred terms of Ergenyl chrono, valproate semisodium, valproate sodium, and valproate magnesium have been combined with the preferred term of valproic acid.
Source: CARE6 OLE CSR.28
Outcomes
The primary objective was to evaluate the long-term safety and tolerability of cannabidiol as add-on therapy in children and adults with TSC who experience inadequately controlled seizures through the primary end points of the incidence of AEs, type of AEs, and severity of AEs.28
The long-term effect of cannabidiol on antiepileptic measures was a secondary objective evaluated with various end points. The following end points selected from key and other secondary end points, as well as exploratory end points, are presented in this report: percentage change in the number of TSC-associated seizures (average per 28 days), number of patients considered to be treatment responders (defined as those with a ≥ 50% reduction in TSC-associated seizure frequency), number of patients achieving TSC-associated seizure freedom (100% reduction), QOLIE-31-P scores, rescue medications, and status epilepticus.28
Statistical Analysis
All patients who received at least 1 dose of cannabidiol in the OLE phase of the study were included in the analyses (safety analysis set). Neither formal sample size calculation nor formal hypothesis testing was done. Of note, seizure information was collected daily during the double-blind phase, but weekly during the OLE phase.28
All data collected during this phase were summarized across time, using descriptive statistical methods. Efficacy measures and patient-reported outcomes were evaluated relative to the 28-day prerandomization baseline period of the phase III, double-blind, placebo-controlled CARE6 trial. For the efficacy end points reported, when a patient withdrew during the treatment period, the primary analysis variable was calculated from all the available data during the treatment period, including any data available after the patient withdrew. Missing and/or incomplete dates and/or times for AEs were imputed in a manner that resulted in the earliest onset or the longest duration during the treatment period, considering that the start date and/or time should not be after the stop date and/or time. Stop dates and/or times were not imputed if the AE was ongoing. The imputation method was only used to determine treatment emergence, and imputed dates and/or times were not presented in AE outputs. A worst-case approach was followed in the event of missing severity or causality data. If the severity is missing, severe was imputed. If causality data were missing, yes was imputed for the question: Plausible relationship to study medication? Missing concomitant medication dates were handled in a manner similar to that described for AEs.28
Results
Patient Disposition
Patient disposition for the CARE6 OLE study (safety analysis set) is summarized in Table 17. Of the 199 OLE patients (100%) rolled over from the CARE6 study, 17.1% completed treatment. The most common reasons for withdrawal from study were other (54.3%), AE (9%), and withdrawal by parent or guardian (7.5%). Of the 108 (54.3%) patients who withdrew for an other reason, 92 (46.2%) patients transitioned to the commercial product and 11 (5.5%) patients discontinued due to a lack of efficacy. The proportion of patients in each category of reason for withdrawal were similar, except for AEs, there fewer patients in the cannabidiol group than in the placebo group (6.5% versus 13.3%).28
Table 17: Patient Disposition of the CARE6 OLE Study (Safety Analysis Set)
Patient disposition | Patients who took cannabidiol during double-blind phase (N = 124) | Patients who took placebo during double-blind phase (N = 75) | Overall (N = 199) |
|---|---|---|---|
Screened, N | 199 | ||
Enrolled, N (%) | 124 (100.0) | 75 (100.0) | 199 (100.0) |
Completed study, N (%) | 22 (17.7) | 12 (16.0) | 34 (17.1) |
Withdrawal, n | 102 (82.3) | 63 (84.0) | 165 (82.9)a |
Other | 69 (55.6) | 39 (52.0) | 108 (54.3) |
AE | 8 (6.5) | 10 (13.3) | 18 (9.0) |
Withdrawal by parent or guardian | 8 (6.5) | 7 (9.3) | 15 (7.5) |
Withdrawal by patient | 10 (8.1) | 4 (5.3) | 14 (7.0) |
Physician decision | 3 (2.4) | 1 (1.3) | 4 (2.0) |
Met withdrawal criteria | 2 (1.6) | 2 (2.7) | 4 (2.0) |
Transition to commercial product | 1 (0.8) | 0 | 1 (0.5) |
Lost to follow-up | 1 (0.8) | 0 | 1 (0.5) |
Safety analysis set,b N | 124 | 75 | 199 |
AE = adverse event; OLE = open-label extension.
aWithdrawals are shown according to the primary reason reported for each patient. Among the 108 patients who fell into the other reason category for withdrawal, 92 were withdrawn because they transitioned to a commercial product, 11 were withdrawn due to lack of efficacy, 2 were withdrawn due to advice from the medical monitor or their neurologist, 1 withdrew due to difficulties with compliance, 1 withdrew because the study completed, and 1 was due to parent and investigator decision.
bAll patients who received at least 1 dose of cannabidiol in the OLE phase of the study. Only patients confirmed to have not taken any cannabidiol during the OLE phase were excluded from this safety analysis set.
Source: CARE6 OLE CSR.28
Exposure to Study Treatments
Exposure information for the CARE6 OLE safety analysis set is described in Table 18. Of the 34 patients (17.1%) who completed the OLE treatment phase, the number of patients (17 [8.5%]) treated with a maximum recorded cannabidiol dosage of 25 mg/kg per day or less was the same as the number of patients treated with more than 25 mg/kg per day of cannabidiol. The mean number of dosing days reported during the OLE treatment period was 487.68 (SD = 360.98) days. The cannabidiol group showed a slightly higher number of dosing days (502.95; SD = 390.23) than placebo group (459.67; SD = 314.47). The median number of dosing days for the total population was 369.5 (range, 95.0 to 1,462.0) days. The median number of dosing days was similar for patients treated with cannabidiol (368.5; range, 95.1 to 1,462.0 days) and placebo (371.0; range, 361.0 to 1,458.0 days) during the double-blind phase.28
Overall, 95 (47.7%) patients were recorded as taking rescue medications; the proportion of patients was similar during the double-blind phase in the cannabidiol and placebo groups (58 [46.8%] versus 37[49.3%] patients). The most common rescue medication reported was diazepam (60 [30.2%] patients). Information on subsequent treatment and adherence was not captured in the CARE6 OLE study.28
Table 18: Patient Exposure in the CARE6 OLE Study (Safety Analysis Set)
Exposure | Patients who took cannabidiol during double-blind phase (N = 124) | Patients who took placebo during double-blind phase (N = 75) | Total (N = 199) |
|---|---|---|---|
Total number of dosing days, all patients | |||
Mean (SD) | 672.02 (402.97) | 585.2 (383.16) | 639.3 (396.89) |
Median (minimum to maximum) | 676.5 (29.0 to 1,462.0) | 581.0 (18.0 to 1,458.0) | 631.0 (18.0 to 1,462.0) |
Total number of dosing days, patients who completed the OLE treatment phase | |||
N (%) | 22 (17.7) | 12 (16.0) | 34 (17.1) |
Mean (SD) | 502.95 (390.23) | 459.67 (314.47) | 487.68 (360.98) |
Median (minimum to maximum) | 368.5 (95.0 to 1,462.0) | 371.0 (361.0 to 1,458.0) | 369.5 (95.0 to 1,462.0) |
Pooled maximum OLE dose, all patients, n (%) | |||
≤ 25 mg/kg per day | 71 (57.3) | 35 (46.7) | 106 (53.3) |
> 25 mg/kg per day | 53 (42.7) | 40 (53.3) | 93 (46.7) |
Pooled maximum OLE dose, patients who completed the OLE treatment phase, n (%) | |||
N (%) | 22 (17.7) | 12 (16.0) | 34 (17.1) |
≤ 25 mg/kg per day | 13 (10.5) | 4 (5.3) | 17 (8.5) |
> 25 mg/kg per day | 9 (7.3) | 8 (10.6) | 17 (8.5) |
OLE = open-label extension; SD = standard deviation.
Source: CARE6 OLE CSR.28
Efficacy
Percent Change From Baseline in Seizure Frequency
Patients experienced a median change of –66.27% (IQR, –86.70% to –18.64%) in weeks 37 to 48 of treatment (n = 156) and a median change of –55.22% (IQR, –81.70% to –13.47%) during the entire OLE treatment period (n = 199) from prerandomization baseline in TSC-associated seizure frequency.28 Reductions in TSC-associated seizure frequency were similar in patients treated with cannabidiol and those treated with placebo during the double-blind phase of the study, and were sustained over time.
Treatment Responders: Proportion of Patients With a Reduction of at Least 50% in Seizure Frequency
The number of patients who achieved a reduction of at least 50% in TSC-associated seizure frequency was 93 (60%) in weeks 37 to 48 of the treatment phase (n = 156) and 106 (53%) during the entire OLE treatment phase. There were no notable differences in the proportion of patients achieving a reduction of at least 50% in TSC-associated seizure frequency in patients treated with cannabidiol and those treated with placebo during the double-blind phase of the study.28
Health-Related Quality of Life
The 31-Item Quality of Life in Epilepsy– Problems Questionnaire
Patients experienced a reduction in the overall QOLIE-31-P (patients ≥ 19 years) total score relative to the prerandomization baseline of the double-blind phase, with a mean change from baseline of –9.0 (SD = 17.99) for all patients (n = 9) and –7.4 (SD = 18.57) for patients 19 years and older (n = 8) at OLE end of treatment. Based on a change from the double-blind phase baseline to OLE end of treatment, a reduction in the QOLIE-31-P total score was observed in the cannabidiol group (–14.8; SD = 20.60; n = 5) and the placebo group (–1.8; SD = 13.2; n = 4). For patients 19 years and older (n = 8), the QOLIE-31-P total score change was –13.1 (SD = 23.39; n = 4) in the cannabidiol group and –1.8 (SD = 13.12; n = 4) in the placebo group.28
Rescue Medication Use
The change in the mean number of days of rescue medication use from double-blind baseline to OLE end of treatment was –0.44 (SD = 4.09) in the total population (n = 55), –0.10 (SD = 4.73) in the cannabidiol group (n = 35), and –1.02 (SD = 2.64) in the placebo group (n = 20).28
Status Epilepticus
The number of patients with status epilepticus was 5 (2.5%) at the baseline period and 20 (10.1%) during the OLE treatment period. The number of patients who experienced status epilepticus was similar in patients treated with cannabidiol and those treated with placebo during the double-blind phase of the CARE6 study.28
Table 19: Summary of Harms Results From the CARE6 OLE Study (Safety Analysis Set)
Adverse events | Patients who took cannabidiol during double-blind phase (N = 124) | Patients who took placebo during double-blind phase (N = 75) | Total (N = 199) |
|---|---|---|---|
Most common adverse events, n (%) | |||
≥ 1 adverse eventa | 117 (94.4) | 75 (100.0) | 192 (96.5) |
Diarrhea | 50 (40.3) | 43 (57.3) | 93 (46.7) |
Seizure | 40 (32.3) | 19 (25.3) | 59 (29.6) |
Pyrexia | 33 (26.6) | 15 (20.0) | 48 (24.1) |
Decreased appetite | 23 (18.5) | 24 (32.0) | 47 (23.6) |
Vomiting | 27 (21.8) | 13 (17.3) | 40 (20.1) |
Somnolence | 15 (12.1) | 24 (32.0) | 39 (19.6) |
Nasopharyngitis | 19 (15.3) | 16 (21.3) | 35 (17.6) |
URTI | 22 (17.7) | 10 (13.3) | 32 (16.1) |
Cough | 13 (10.5) | 13 (17.3) | 26 (13.1) |
Constipation | 12 (9.7) | 9 (12.0) | 21 (10.6) |
Fall | 13 (10.5) | 8 (10.7) | 21 (10.6) |
Influenza | 16 (12.9) | 4 (5.3) | 20 (10.1) |
Serious adverse events, n (%) | |||
Patients with ≥ 1 serious adverse eventb | 38 (30.6) | 18 (24.0) | 56 (28.1) |
Seizure | 12 (9.7) | 4 (5.3) | 16 (8.0) |
Status epilepticus | 9 (7.3) | 1 (1.3) | 10 (5.0) |
Dehydration | 4 (3.2) | 2 (2.7) | 6 (3.0) |
Influenza | 5 (4.0) | 0 | 5 (2.5) |
Pneumonia | 4 (3.2) | 1 (1.3) | 5 (2.5) |
Patients who stopped treatment due to adverse events, n (%) | |||
Patients who stoppedc | 11 (8.9) | 7 (9.3) | 18 (9.0) |
Seizure | 3 (2.4) | 1 (1.3) | 4 (2.0) |
Diarrhea | 2 (1.6) | 2 (2.7) | 4 (2.0) |
Increased liver function test | 1 (0.8) | 1 (1.3) | 2 (1.0) |
Decreased appetite | 2 (1.6) | 0 | 2 (1.0) |
Deaths, n (%) | |||
Patients who died | 1 (0.8) | 0 | 1 (0.5) |
Cardiopulmonary failure | 1 (0.8) | 0 | 1 (0.5) |
OLE = open-label extension; URTI = upper respiratory infection.
aFrequency > 10% of the total population.
bFrequency > 2% of the total population.
cFrequency > 1% of the total population.
Source: CARE6 OLE CSR.28
Harms
Harms data from the CARE6 OLE study are summarized in Table 19. A total of 192 (96.5%) patients treated with cannabidiol had 1 or more AEs during the OLE study, with 51 (25.6%) patients reporting AEs of mild severity, 111 (55.8%) patients reporting AEs of moderate severity, and 30 (15.1%) patients reporting severe AEs. The most common TEAEs were diarrhea (46.7%), seizure (29.6%), and pyrexia (24.1%). SAEs were reported in 56 (28.1%) participants with TSC, with the most common SAEs being seizure (8%), status epilepticus (5%), and dehydration (3%).28
There were 18 (9%) participants with TSC who stopped treatment due to AEs; the most common AEs leading to discontinuation were seizure (2%) and diarrhea (2%).28
One patient died 2 months after starting the open-label treatment of cannabidiol. The patient died in their sleep, and no immediate cause of death (SUDEP) was noted. This fatal TEAE of cardiopulmonary failure due to TSC was considered by the investigator to be unrelated to cannabidiol. There were no meaningful differences between the cannabidiol and placebo groups in terms of AEs.28
Critical Appraisal
Internal Validity
There was no active comparator or placebo group in the CARE6 OLE study, so the safety and efficacy data from the CARE6 OLE could not be used to draw any conclusions about appropriate comparators. Furthermore, the open-label design of the study may have biased the reporting of subjective end points, including AEs, SAEs, and TEAEs. Because completion of a pivotal trial was an eligibility criterion for the extension study, patients who discontinued those trials due to AEs or lack of response were excluded. This could result in a population of patients that was more tolerant of cannabidiol, which could have led to selection bias, as those not responding to treatment are less likely to continue. Having a patient population more tolerant of cannabidiol can also lead to biased estimates related to AEs, potentially resulting in fewer and less severe AEs being reported.
The sample size of the CARE6 OLE study (N = 199) may not be sufficient to detect rare AEs. Only 17.1% of patients completed the study, and there was wide variation in follow-up duration among individuals. This resulted in a small sample size for several outcomes and a population that is not representative of all who began the OLE phase.
External Validity
The CARE6 OLE study enrolled patients from multiple sites in different countries, but there were no study sites in Canada. No evidence indicating a difference between the study population and patients in Canada was identified, according to the clinical experts. Even though the median number of dosing days — 369.5 (range, 95.0 days to 1,462 days) — provides longer follow-up for AE assessment than did the double-blind phase of the CARE6 study, the proportion of patients who adhered to the cannabidiol during the longer follow-up was not reported. Thus, study drug exposure among the patients in the OLE study was uncertain. About half the patients (46.7%) were taking the 50 mg/kg per day dose, which is not an approved dosing level and could have impacted the results. The remaining patients were taking the 25 mg/kg per day dose, which is the highest dose suggested in the product monograph.
Indirect Evidence
No indirect evidence on the comparative efficacy or safety of cannabidiol in patients with TSC-associated seizures was submitted by the sponsor.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the systematic review evidence were submitted by the sponsor.
Discussion
Summary of Available Evidence
The evidence included in this review consisted of 1 pivotal study identified by the sponsor’s systematic review (CARE6), and 1 long-term extension study of the pivotal trial. No indirect treatment comparisons or studies addressing gaps in the literature were included.
The CARE6 study was a phase III, placebo-controlled, RCT in patients aged 1 to 65 years with a clinical diagnosis of TSC and a history of epilepsy that was not controlled by current ASMs. Patients were randomized in a 2:2:1:1 ratio to cannabidiol 25 mg/kg per day (n = 75), cannabidiol 50 mg/kg per day (n = 73), or 2 matching pooled placebo (n = 76) groups for 16 weeks. Upon completion of the double-blind treatment period of the CARE6 study, patients were invited to enrol in the OLE study to receive cannabidiol at a dose of 25 mg/kg per day for a maximum duration of 1 year, which was subsequently extended to 4 years in the US and 3 years in Poland. Only the 25 mg/kg per day cannabidiol group was relevant to this report because this is the highest dose level suggested in the product monograph.
The primary end point of the CARE6 study was the change from baseline in the number of TSC-associated seizures during the treatment period; there were 3 key secondary end points, 1 of which was of interest to this review: the proportion of patients with a 50% or greater reduction from baseline in TSC-associated seizure frequency. Other secondary end points of interest to this review included the proportion of patients with a 25% or greater reduction from baseline in TSC-associated seizure frequency, total seizure freedom (100% reduction in TSC-associated seizures), HRQoL assessed by the QOLCE and QOLIE-31-P, change in the proportion of patients with status epilepticus during the treatment period, change in the use of rescue medication during the treatment period, and the effect of cannabidiol on TANDs assessed by Vineland II. The primary objective of the OLE study was to evaluate the long-term safety and tolerability of cannabidiol, and the secondary end points were in line with those in the CARE6 trial.
Generally, baseline characteristics were well balanced across treatment groups in the CARE6 study, although there were some differences with regard to seizure type and frequency that were likely due to chance. Most patients experienced type 2 focal seizures (61.3% versus 65.8%), followed by type 1 focal motor seizures (38.7% versus 43.4%), and type 3 focal seizures (22.7% versus 31.6%); greater variation was observed for generalized seizure types (tonic, 36.0% versus 19.7%; tonic-clonic, 29.3 versus 18.4%). Patients were highly refractory, having attempted a median of 4.0 (range, 0 to 15) prior ASMs, and currently taking a median of 3 (range, 0 to 5) ASMs. Baseline characteristics of the patients in the OLE study were similar to the combined characteristics of patients in the 25 mg/kg per day and 50 mg/kg per day cannabidiol groups in the double-blind treatment phase of the CARE6 study.
Interpretation of Results
Efficacy
There is a significant unmet need for new therapies for TSC. Current treatment for TSC-associated seizures is mostly limited to ASMs, which generally aim to control seizures associated with TSC rather than to cure the underlying disease. Generally, combinations of ASMs are used to reduce seizure frequency, as seizure freedom is seldom achieved with 1 ASM. However, there are notable complications related to and interactions with current ASMs, often requiring a medication change. Cannabidiol represents a novel add-on treatment for refractory TSC-associated epilepsy with a different mechanism of action. The efficacy of cannabidiol 25 mg/kg per day relative to placebo in patients with TSC-associated seizures was informed by the CARE6 study. This is the highest recommended dose for cannabidiol, and no evidence was submitted to inform the efficacy of lower doses that may be used in practice. As noted, patients randomized in the CARE6 study were considered to be representative of a highly refractory patient population with a high seizure burden, which may not reflect the entire population of patients with TSC-associated seizures in Canada. There is a potential for increased treatment effects in a population with a higher seizure burden, as it may be easier to observe mean changes in seizure frequency when the baseline seizure rate is higher. However, patients who are taking a greater number of prior or concurrent ASMs are also likely be living with more treatment-resistant epilepsy and may have a less favourable response to cannabidiol.
As noted, a reduction in seizure frequency is the most important outcome of treatment, given the immediate relief of seizure burden on patients and caregivers, as well as the downstream effects on behaviour and cognition. Outcomes included in the GRADE assessment were generally considered imprecise because they had 95% CIs that were compatible with benefits and effects that might not be considered clinically important (or null). The key secondary end point in the CARE6 trial assessed treatment responders, defined as the proportion of patients who experienced a 50% reduction in the frequency of TSC-associated seizures. The clinical experts consulted by CADTH noted that this definition of treatment response is typical of clinical trials, but that a placebo-adjusted reduction in seizure frequency of about 25% may also represent a significant and clinically meaningful response to treatment. This would be particularly true if there is a reduction in the most severe and disabling types of seizures, as reductions in frequency may not be associated with reductions in severity, or vice versa, which the clinical experts noted is a common limitation of clinical trials of epilepsy. The experts also noted that anything below a 25% response would be difficult to observe or measure, given the individual heterogeneity in seizure frequency and seizure type across patients, many of which are difficult to quantify. However, it was also noted by the clinical experts that the importance of changes in seizure frequency are subjective, depending on the perspective of patients and caregivers, as there may be improvements in other facets of the disease (e.g., seizure severity, duration).
The primary end point of the CARE6 study was the reduction in TSC-associated seizure frequency. The mean percent reduction in seizure frequency from baseline was 48.6% (95% CI, 40.4% to 55.8%) in the cannabidiol group and 26.5% (95% CI, 14.9% to 36.5%) in the placebo group (absolute difference not reported). The mean difference (22%) approaches the 25% threshold suggested by the clinical experts consulted by CADTH, and, therefore, could be considered clinically important. However, the CI of the relative effect, expressed as a percentage difference in the reductions from baseline in each group (31.0%; 95% CI, 13.9% to 43.3%), introduces uncertainty because it includes effects that are smaller and may not be considered clinically important. As mentioned, the primary result of this analysis is a ratio of ratios, which challenges the interpretation as an absolute change from baseline.
Results for other measures of seizure frequency, including the key secondary end point of the proportion of patients meeting the threshold of a 50% or greater reduction in seizure frequency at week 16 and the proportion of patients achieving a 25% or greater reduction in seizure frequency at week 16 had point estimates that were directionally aligned with the primary end point, but did not reach statistical significance. The clinical experts consulted by CADTH suggested that 20% to 30% of patients are expected to have a strong response to treatment (i.e., a 50% reduction). In the CARE6 trial, 36.0% of patients in the cannabidiol 25 mg/kg per day group had a 50% reduction in seizure frequency; however, 22.4% of patients in the placebo group also experienced a strong response, so the comparative results were not statistically significant (OR, 1.95; 95% CI, 0.95 to 4.00) and the clinical meaningfulness is uncertain. For the threshold of a 25% reduction in seizures, 57.3% and 43.4% of patients in the cannabidiol and placebo groups, respectively, experienced a response. The clinical experts noted that a robust placebo response is often observed in this population because of the substantial heterogeneity and natural history of the disease, as well as the particularly high seizure burden of the enrolled population. Complete seizure freedom is the ultimate (ideal) goal of treatment but was achieved by only 1 patient in the cannabidiol group during the trial.
The clinical experts consulted by CADTH and the patient groups highlighted the importance of reducing seizure severity in patients with TSC-associated epilepsy. Although seizure severity was captured as part of the primary outcome in the CARE6 study as reported by patients and used to classify seizures as type 1, type 2, or type 3 focal seizures, this measurement is highly subjective and difficult to quantify, which may result in some detection biases (i.e., in reporting of the outcome). An additional outcome of importance to patients and caregivers was the measurement of HRQoL, which was appropriately captured in the CARE6 trial. The results of HRQoL and patient-reported outcome assessments suggested no detriment or improvement in QoL or behaviour and did not meet the defined thresholds for the MID specified in the literature (refer to Table 6); however, they were subject to limited sample sizes and completion rates that resulted in a risk of bias, which reduces the certainty of the results. As previously noted, the clinical experts consulted by CADTH emphasized that specific HRQoL measures are not routinely used in clinical practice; rather, an informal assessment of change is conducted through discussion. Overall, the impact of cannabidiol on HRQoL and TANDs remains unknown.
Other outcomes of interest to this review included the incidence of status epilepticus and the use of rescue medication, which were exploratory in the CARE6 study. The number of status epilepticus events and rescue medication use was higher during the treatment period than the baseline period, which was expected, considering the treatment period was longer; however, minimal differences were observed between groups for both outcomes. The use of rescue medication was high during the CARE6 trial, but as noted by the clinical experts, did not prompt discontinuation of treatment. Specific lists of rescue medications used in the CARE6 trial were not provided, although rescue medication generally consists of ASMs, such as short-acting benzodiazepines, which are unsuitable for use as maintenance therapy because they are highly sedating.
Results of the ongoing OLE of the CARE6 study were generally consistent with results in the double-blind treatment period; however, nearly half of the enrolled patients (46.7%) received the cannabidiol 50 mg/kg per day dose during the double-blind treatment period, which is not an approved dosing level and could have impacted the results.
No indirect evidence was submitted for this review; as such, the comparative efficacy of cannabidiol remains unknown.
Harms
The incidence of harms reported in the CARE6 trial was well balanced in the cannabidiol and placebo groups, with nearly all patients experiencing TEAEs (93.3% versus 94.7%%). Although not reported, there was a higher frequency of TEAEs in the cannabidiol 50 mg/kg per day group, which, according to the clinical experts consulted by CADTH, was not unexpected. Generally, gastrointestinal AEs are common in this population, per the clinical experts, and their rate of occurrence in the CARE6 study was as expected. The clinical experts consulted by CADTH highlighted that the main safety concerns would be those that resulted in treatment withdrawal or discontinuation. Although discontinuation from treatment and from the study due to AEs were greater in the cannabidiol treatment group than in the placebo group, the total number of discontinuations due to AEs was consistent with clinical expectations and not a major safety concern. As noted in the patient group input, underlying behavioural issues can be aggravated by current ASMs causing impossible behaviours, although this was not captured in the present study; however, somnolence was experienced by 13.3% of patients in the cannabidiol group, which the experts noted was an important consideration that could have an impact on HRQoL.
Evidence from the trial showed that the risk of SAEs may be increased with cannabidiol, but this was informed by a small number of events. Notable harms of interest to this review included hepatocellular injury and hypersensitivity reactions. The clinical experts consulted by CADTH highlighted that hepatocellular injury was likely the most important notable harm associated with cannabidiol use, as it can cause dose-related elevations in liver transaminases (ALT and/or AST), which may be further increased by concomitant medications and require monitoring and dose reductions or discontinuation of treatment. Evidence from the trial showed that cannabidiol is not likely to increase the risk of hepatocellular injury over 16 weeks (there was 1 event in the trial). In general, although considered to be an important contraindication and consideration in dosing, increases in ALT and AST occurred in only 9 (12.0%) and 8 (10.7%) patients in the cannabidiol 25 mg/kg per day group, respectively.
Although there were no deaths reported during the CARE6 trial, it should be emphasized that TSC and the associated epilepsy is a life-long condition, and the short duration of the CARE6 trial limits the ability to assess the long-term safety of cannabidiol. The ongoing OLE of the CARE6 study aimed to address this gap and provide additional long-term safety data for cannabidiol up to a maximum of 4 years. The results of the OLE trial appeared to be consistent with the double-blind phase in the CARE6 study, but were limited by selection bias, losses to follow-up, and the lack of a relevant comparator.
Given that no indirect treatment comparisons were included in this review, the safety of cannabidiol relative to other relevant treatments for TSC-associated seizures remains unknown.
Conclusion
There is a need for new, safe, and effective treatments for TSC-associated seizures in patients with seizures that remain uncontrolled by current therapies and require an additional reduction in seizure burden. The 1 study included in this review — CARE6 —was a phase III, double-blind, placebo-controlled study evaluating the efficacy and safety of cannabidiol compared to placebo as adjunctive therapy with other ASMs for the treatment of seizures associated with TSC in patients 2 years of age and older.
The CARE6 study demonstrated that cannabidiol likely results in a clinically important decrease (improvement) in seizure frequency compared with placebo around the 25% threshold of clinical importance defined by the clinical experts. Additionally, responder analyses using seizure reduction thresholds of 25% and 50% showed a likely benefit of cannabidiol (i.e., a greater proportion of patients meeting the threshold than in the placebo group), but there was uncertainty in the clinical importance of these effects and they failed to reach statistical significance. Complete seizure freedom would be the most ideal response to treatment and is important to clinicians and patients; however, only 1 patient in the cannabidiol group in the CARE6 trial experienced seizure freedom. Results of the trial showed that cannabidiol may have little to no impact on status epilepticus or the need for rescue medication. Effects on HRQoL and adaptive behaviour were very uncertain because of imprecision and the risk of bias due to missing outcome data. The risk of SAEs was likely elevated in patients who received cannabidiol, but there was little to no difference in the risk of hepatocellular injury with cannabidiol in the short term. The included study had a short double-blind treatment duration of only 16 weeks, which was sufficient to address the primary outcome of change in the number of TSC-associated seizures but precluded the ability to assess long-term efficacy, safety, and HRQoL. The ongoing OLE phase of the CARE6 trial aims to address this gap but is limited by the lack of a comparator group, selection bias, and losses to follow-up. Although considered an outcome of importance to patients, reduction in the severity of seizures was not expressly measured in the CARE6 trial. Patients in the CARE6 trial had a higher seizure burden than those in the overall population with TSC-associated seizures and with highly refractory epilepsy. The differences in patient populations and the relatively short duration of follow-up during the randomized phase may limit the generalizability of the study results to a broader population of patients with TSC-associated seizures.
References
1.Northrup H, Aronow ME, Bebin EM, et al. Updated International Tuberous Sclerosis Complex Diagnostic Criteria and Surveillance and Management Recommendations. Pediatr Neurol. 2021;123:50-66. PubMed
2.Curatolo P, Bombardieri R, Jozwiak S. Tuberous sclerosis. Lancet. 2008;372(9639):657-668. PubMed
3.Hallett L, Foster T, Liu Z, Blieden M, Valentim J. Burden of disease and unmet needs in tuberous sclerosis complex with neurological manifestations: systematic review. Curr Med Res Opin. 2011;27(8):1571-1583. PubMed
4.Hong CH, Tu HP, Lin JR, Lee CH. An estimation of the incidence of tuberous sclerosis complex in a nationwide retrospective cohort study (1997-2010). Br J Dermatol. 2016;174(6):1282-1289. PubMed
5.O'Callaghan FJ. Tuberous sclerosis. BMJ. 1999;318(7190):1019-1020. PubMed
6.O'Callaghan FJ, Shiell AW, Osborne JP, Martyn CN. Prevalence of tuberous sclerosis estimated by capture-recapture analysis. Lancet. 1998;351(9114):1490. PubMed
7.European Public Assessment Report (EPAR): Kigabeq (vigabatrin). Amsterdam (NL): European Medicines Agency; 2021: https://www.ema.europa.eu/en/medicines/human/EPAR/kigabeq. Accessed 2022 Dec.
8.Hernandez A, Perry MS. Tuberous Sclerosis Complex (TSC). Epilepsy Foundation 2016; https://www.epilepsy.com/causes/structural/tuberous-sclerosis-complex. Accessed 2023 Oct.
9.Chu-Shore CJ, Major P, Camposano S, Muzykewicz D, Thiele EA. The natural history of epilepsy in tuberous sclerosis complex. Epilepsia. 2010;51(7):1236-1241. PubMed
10.Curatolo P, Nabbout R, Lagae L, et al. Management of epilepsy associated with tuberous sclerosis complex: Updated clinical recommendations. Eur J Paediatr Neurol. 2018;22(5):738-748. PubMed
11.Jeong A, Wong M. Systemic disease manifestations associated with epilepsy in tuberous sclerosis complex. Epilepsia. 2016;57(9):1443-1449. PubMed
12.Kingswood JC, d'Augeres GB, Belousova E, et al. TuberOus SClerosis registry to increase disease Awareness (TOSCA) - baseline data on 2093 patients. Orphanet J Rare Dis. 2017;12(1):2. PubMed
13.Amin S, Lux A, Calder N, Laugharne M, Osborne J, O'Callaghan F. Causes of mortality in individuals with tuberous sclerosis complex. Dev Med Child Neurol. 2017;59(6):612-617. PubMed
14.Shepherd CW, Gomez MR, Lie JT, Crowson CS. Causes of death in patients with tuberous sclerosis. Mayo Clin Proc. 1991;66(8):792-796. PubMed
15.Zollner JP, Franz DN, Hertzberg C, et al. A systematic review on the burden of illness in individuals with tuberous sclerosis complex (TSC). Orphanet J Rare Dis. 2020;15(1):23. PubMed
16.Webb DW, Fryer AE, Osborne JP. Morbidity associated with tuberous sclerosis: a population study. Dev Med Child Neurol. 1996;38(2):146-155. PubMed
17.Donner EJ, Camfield P, Brooks L, et al. Understanding Death in Children With Epilepsy. Pediatr Neurol. 2017;70:7-15. PubMed
18.Ruthirago D, Julayanont P, Karukote A, Shehabeldin M, Nugent K. Sudden unexpected death in epilepsy: ongoing challenges in finding mechanisms and prevention. Int J Neurosci. 2018;128(11):1052-1060. PubMed
19.Curatolo P, Moavero R, de Vries PJ. Neurological and neuropsychiatric aspects of tuberous sclerosis complex. Lancet Neurol. 2015;14(7):733-745. PubMed
20.Bachour K, House AA, Andrade DM, et al. Adults with tuberous sclerosis complex: A distinct patient population. Epilepsia. 2022;63(3):663-671. PubMed
21.Randle S. Tuberous sclerosis complex: Management and prognosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: https://www.uptodate.com/. Accessed 2023 Oct 4.
22.Clinical Study Report: GWEP1521. A double-blind, randomized, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P, CBD) as add-on therapy in patients with tuberous sclerosis complex who experience inadequately-controlled seizures [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2019 Dec 23.
23.Vergeer M, de Ranitz-Greven WL, Neary MP, et al. Epilepsy, impaired functioning, and quality of life in patients with tuberous sclerosis complex. Epilepsia Open. 2019;4(4):581-592. PubMed
24.2021 Tuberous sclerosis complex: Diagnostic criteria, surveillance and management recommendations. Silver Spring (MD): TSC Alliance; 2021: https://www.tscalliance.org/wp-content/uploads/2022/01/2021-TSC-Diagnostic-Criteria-Surveillance-and-Management-Recommendations.pdf. Accessed 2023 Oct.
25.Schubert-Bast S, Strzelczyk A. Review of the treatment options for epilepsy in tuberous sclerosis complex: towards precision medicine. Ther Adv Neurol Disord. 2021;14:17562864211031100. PubMed
26.Epidiolex (cannabidiol): 100 mg/mL, oral solution [product monograph]. Cambridge (UK): GW Research Ltd.; 2023 Nov 15.
27.Sponsor's clinical summary report: EPIDIOLEX (cannabidiol) as adjunctive treatment of seizures associated with tuberous sclerosis complex (TSC) in patients two years of age or older [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: cannabidiol, 100 mg/mL oral solution. Mississauga (ON): Jazz Pharmaceuticals; 2023 Sep.
28.Clinical Study Report: GWEP1521. A double-blind, randomized, placebo-controlled study to Investigate the efficacy and safety of cannabidiol (GWP42003-P, CBD) as add-on therapy in patients with tuberous sclerosis complex who experience inadequately-controlled seizures (open-label extension) [internal sponsor's report]. Cambridge (UK): GW Research Ltd; 2021 Nov 24.
29.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
30.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
31.Kwan P, Arzimanoglou A, Berg AT, et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51(6):1069-1077. PubMed
32.McDonald A, Goodwin J, Roberts S, et al. 'We've made the best of it. But we do not have a normal life': families' experiences of tuberous sclerosis complex and seizure management. J Intellect Disabil Res. 2019;63(8):947-956. PubMed
33.Nabbout R, Belousova E, Benedik MP, et al. Epilepsy in tuberous sclerosis complex: Findings from the TOSCA Study. Epilepsia Open. 2019;4(1):73-84. PubMed
34.Sabaz M, Cairns DR, Lawson JA, Nheu N, Bleasel AF, Bye AM. Validation of a new quality of life measure for children with epilepsy. Epilepsia. 2000;41(6):765-774. PubMed
35.Cramer JA, Van Hammée G. Maintenance of improvement in health-related quality of life during long-term treatment with levetiracetam. Epilepsy Behav. 2003;4(2):118-123. PubMed
36.Sparrow S, Cicchetti DV, Balla DA. Vineland Adaptive Behavior Scales: (Vineland II), Survey Interview Form/Caregiver Rating Form. Livonia (MN): Pearson Assessments; 2005.
37.Cramer JA, Perrine K, Devinsky O, Bryant-Comstock L, Meador K, Hermann B. Development and cross-cultural translations of a 31-item quality of life in epilepsy inventory. Epilepsia. 1998;39(1):81-88. PubMed
38.de Vries PJ, Franz DN, Curatolo P, et al. Measuring Health-Related Quality of Life in Tuberous Sclerosis Complex - Psychometric Evaluation of Three Instruments in Individuals With Refractory Epilepsy. Front Pharmacol. 2018;9:964. PubMed
39.Crudgington H, Rogers M, Morris H, Gringras P, Pal DK, Morris C. Epilepsy-specific patient-reported outcome measures of children's health-related quality of life: A systematic review of measurement properties. Epilepsia. 2020;61(2):230-248. PubMed
40.Community-University Partnership for the Study of Children, Youth, and Families. Review of the Vineland Adaptive Behavior Scales-Second Edition (Vineland-II). Edmonton (AB): University of Alberta; 2011: https://www.ualberta.ca/community-university-partnership/media-library/community-university-partnership/resources/tools—assessment/vinelandjune-2012.pdf. Accessed 2023 Oct.
41.Pepperdine CR, McCrimmon AW. Test Review: Vineland Adaptive Behavior Scales, Third Edition (Vineland-3) by Sparrow, S. S., Cicchetti, D. V., & Saulnier, C. A. Canadian Journal of School Psychology. 2018;33(2):157-163.
42.de Vries PJ, Whittemore VH, Leclezio L, et al. Tuberous sclerosis associated neuropsychiatric disorders (TAND) and the TAND Checklist. Pediatr Neurol. 2015;52(1):25-35. PubMed
Appendix 1: Detailed Outcome Data
Note this appendix has not been copy-edited.
Table 20: Sensitivity Analyses of the Primary End Point in the CARE6 Triala
Comparison vs. placebo | Cannabidiol 25 mg/kg per day | Pooled placebo |
|---|---|---|
Sensitivity Analysis: Change in TSC-Associated Seizures Compared to Baseline (PP Analysis Set) | ||
N | 62 | 74 |
Percent CFB, Mean (SD) | −35.07 (42.951) | −20.68 (34.063) |
Negative Binomial Regression Analysis Percent CFB, Mean (95% CI)b | −48.2 (−39.2, −55.8) | −27.0 (−15.6, −36.9) |
Treatment Ratio (95% CI) | 0.710 (0.572, 0.882)c | — |
Percent Reduction vs. Placebo, LS Mean (95% CI) | 29.0 (11.8, 42.8) | — |
P value | 0.0021 | — |
Sensitivity Analysis: Percent CFB in TSC-associated Seizure Frequency – Wilcoxon rank sum test (ITT Analysis Set) | ||
N | 75 | 76 |
Hodges-Lehmann Treatment Difference, Median (95% CI) | −18.77 (−31.32, −6.28)d | — |
p value | 0.0038b | — |
Sensitivity Analysis: Percentage CFB in TSC-associated Seizure Frequency – Rank ANCOVA (ITT Analysis Set)e | ||
N | 75 | 76 |
LS Mean Difference (95% CI) | −30.4 (−50.8, −10.0)f | — |
P value | 0.0037 | — |
Sensitivity Analysis: TSC-associated Seizure Frequency – Log-transformed ANCOVA (ITT Analysis Set)g | ||
N | 75 | 76 |
Treatment Ratio (95% CI) | 0.675 (0.531, 0.858)h | — |
P value | 0.0015 | — |
Sensitivity Analysis: Percent CFB in TSC-associated Seizure Frequency – ANCOVA (ITT Analysis Set)i | ||
N | 75 | 76 |
LS Mean Difference (95% CI) | −15.13 (−28.38, −1.88)f | — |
P value | 0.0254 | — |
Sensitivity Analysis: Negative Binomial Regression Analysis of TSC-Associated Seizure Count During Baseline and Treatment Periods After Imputing Unreported Days in IVRS (ITT Analysis Set)b, j | ||
N | 75 | 76 |
Treatment Ratio (95% CI) | 0.704 (0.576, 0.860) | — |
P value | 0.0007 | — |
CFB = change from baseline; CI = confidence interval; ITT = intent-to-treat; IVRS = interactive voice response system; PP = per protocol; TSC = tuberous sclerosis complex.
aResults for the cannabidiol 50 mg/kg per day group were not included as it is not a Health Canada–approved dose.
bModel includes total number of seizures as a response variable, age group, time (baseline and treatment period), treatment, and treatment by time interaction as fixed effects, and subject as a random effect. Log-transformed number of days in which seizures were reported by period is included as an offset.
cTreatment ratio (95% CI) of the difference in cannabidiol vs. Placebo from the binomial regression analysis.
dMedian difference between cannabidiol and placebo. Estimated median difference and 95% CI calculated using the Hodges-Lehmann approach, P value calculated from a Wilcoxon rank sum test.
eThe rank of the percent change from baseline TSC-associated seizure frequency is analyzed using an ANCOVA model with the rank of the baseline TSC-associated seizure frequency and age group (1 to 6, 7 to 11, 12–and 13 to 18 years) as covariates and treatment as a fixed factor. Lower ranks indicate a lower baseline seizure frequency or a smaller percent change from baseline TSC-associated seizure frequency.
fLeast squares mean difference between cannabidiol and placebo.
gThe log-transformed TSC-associated seizure frequency is analyzed using an ANCOVA model with the log-transformed baseline TSC-associated seizure frequency and age group (1 to 6, 7 to 11, 12 to 17 and 18 to 65 years) as covariates and treatment group as a fixed factor. A value of 1 is added to the TSC-associated seizure frequency for all patients before log-transformation. The LS means, treatment ratio, and 95% CI have been back-transformed.
hTreatment ratio (95% CI) of the difference in cannabidiol vs. placebo from the ANCOVA analysis.
iThe rank of the percent change from baseline TSC-associated seizure frequency is analyzed using an ANCOVA model with baseline TSC-associated seizure frequency and age group (1 to 6, 7 to 11, 12 to 17 and 18 to 65 years) as covariates and treatment as a fixed factor.
jMissing data from the treatment period arising from unreported days in the IVRS are imputed using the worst (highest number of seizures) of the following for each patient: last observation carried forward, next observation carried backward, and the mean daily number of seizures during the treatment period (using the nonmissing data).
Source: CARE6 Clinical Study Report.22
Table 21: Subgroup Analyses of the Primary and Key Secondary End Point in the CARE6 Trial (ITT Analysis Set)a
Subgroup | Cannabidiol 25 mg/kg per day vs. placebo | |||
|---|---|---|---|---|
Interaction P value | Cannabidiol N | Placebo N | Ratio (95% CI) | |
Subgroup Analysis: Primary End point (Reduction in Seizure Frequency)b | ||||
Overall | — | 75 | 76 | 0.699 (0.57, 0.86) |
Clobazam Use | ||||
Not currently taking | 0.1535 | 58 | 51 | 0.75 (0.59, 0.96) |
Currently taking | 17 | 25 | 0.53 (0.36, 0.80) | |
Number of Concurrent ASMs | ||||
< 3 | 0.8761 | 30 | 35 | 0.68 (0.50, 0.94) |
≥ 3 | 45 | 41 | 0.71 (0.54, 0.93) | |
Number of Prior ASMs | ||||
< 4 | 0.5938 | 41 | 42 | 0.74 (0.56, 0.98) |
≥ 4 | 34 | 34 | 0.66 (0.48, 0.90) | |
Subgroup Analysis: Key Secondary End point (At least 50% Reduction in Seizure Frequency)c | ||||
Overall | — | 27/75 | 17/76 | 1.96 (0.96, 4.03) |
Clobazam Use | ||||
Not currently taking | 0.3704 | 19/58 | 12/51 | 1.62 (0.69, 3.79) |
Currently taking | 8/17 | 5/25 | 3.39 (0.86, 13.38) | |
Number of Concurrent ASMs | ||||
< 3 | 0.8292 | 13/30 | 9/35 | 2.20 (0.77, 6.34) |
≥ 3 | 14/45 | 8/41 | 1.87 (0.69, 5.12) | |
Number of Prior ASMs | ||||
< 4 | 0.3147 | 14/41 | 11/42 | 1.42 (0.55, 3.66) |
≥ 4 | 13/34 | 6/34 | 3.03 (0.98, 9.37) | |
ASM = antiseizure medication; CI = confidence interval.
aResults for the cannabidiol 50 mg/kg per day group were not included as it is not a Health Canada–approved dose.
bModel includes total number of seizures as a response variable and age group (only when age is not the factor being tested), time (baseline and treatment period), treatment, factor, treatment by time interaction, factor by treatment interaction, factor by time interaction, and factor by time by treatment interaction as fixed effects, and subject as a random effect. Log-transformed number of days in which seizures were reported by period is included as an offset.
cResponders are analyzed using a logistic regression model with age group (only when age is not the factor being tested), treatment, factor, and factor by treatment interaction as covariates.
Source: CARE6 Clinical Study Report22
Table 22: Additional Analyses of HRQoL End Points (ITT Analysis Set)
HRQoL assessment | CARE6a | |
|---|---|---|
25 mg/kg per day Cannabidiol N = 75 | Placeboa N = 76 | |
QOLCE Scores – Overall Quality of Life (Patients Aged 2 to 18 Years at Signing of Consent)b | ||
Day 1 | ||
N | 41 | 41 |
Mean (SD) | 51.0 (12.59) | 46.9 (14.07) |
End of Treatment | ||
N | 39 | 40 |
Mean (SD) | 54.0 (14.67) | 51.0 (15.45) |
Change from Baseline | ||
N | 35 | 38 |
Mean (SD) | 2.2 (10.93) | 2.6 (9.32) |
LS Mean (95% CI) | 2.9 (−1.3, 7.0) | 2.4 (−1.6, 6.4) |
Treatment difference (95% CI) | 0.5 (−4.7, 5.6) | — |
QOLIE-31-P Scores – Total Score (Patients Aged 19 and Older at Signing of Consent)c | ||
Day 1 | ||
N | 11 | 10 |
Mean (SD) | 70.6 (15.56) | 58.0 (13.26) |
End of Treatment | ||
N | 12 | 11 |
Mean (SD) | 66.4 (18.74) | 62.2 (15.47) |
Change from baseline | ||
N | 10 | 10 |
Mean (SD) | −3.3 (19.50) | 3.1 (8.09) |
LS Mean (95% CI) | −1.2 (−10.8, 8.5) | 1.7 (−7.6, 11.1) |
Treatment difference (95% CI) | −2.9 (−16.8, 10.9) | - |
CI = confidence interval; HRQoL = health-related quality of life; LS = least squares; QOLCE = quality of life in childhood epilepsy; QOLIE = quality of life in epilepsy; SD = standard deviation
aResults for the cannabidiol 50 mg/kg per day group were not included as it is not a Health Canada–approved dose.
bEach score can range from 0 to 100, where 0 represents the lowest or poorest category and 100 represents the highest level of functioning. The overall quality of life score is calculated by taking the mean of the subscale scores.
cEach subscale consists of a number of questions in addition to a ‘distress’ item. The raw score for each question and the ‘distress’ item are converted to a 0 to 100 score. A final subscale weighted score is calculated where higher scores reflect a better quality of life; lower ones a worse quality of life. The overall quality of life score is calculated by taking the mean of the subscale scores. The total score is calculated as: (Sum of all subscale weighted scores ÷ Sum of all subscale ‘distress’ item converted scores) × 100.
Source: CARE6 Clinical Study Report22
Table 23: Results for SGIC and CGIC in the CARE6 Trial (ITT Analysis Set)
Efficacy outcome | 25 mg/kg per day Cannabidiol N = 75 | Placebo N = 76 |
|---|---|---|
Subject/Caregiver Global Impression of Change | ||
End of Treatment | ||
N | 70 | 76 |
Very Much Improved | 10 (14.3) | 3 (3.9) |
Much Improved | 13 (18.6) | 10 (13.2) |
Slightly Improved | 25 (35.7) | 17 (22.4) |
No Change | 14 (20.0) | 42 (55.3) |
Slightly Worse | 4 (5.7) | 3 (3.9) |
Much Worse | 3 (4.3) | 1 (1.3) |
Very Much Worse | 1 (1.4) | 0 |
Mean (SD) scorea | 3.0 (1.35) | 3.5 (0.96) |
Median (range) scorea | 3.0 (1, 7) | 4.0 (1, 6) |
OR (95% CI) | 2.25 (1.24, 4.07) | — |
P value | 0.0074 | — |
CI = confidence interval; OR = odds ratio; SD = standard deviation.
a1 = very much improved; 7 = very much worse.
Note: The combined caregiver and subject summary used either the caregiver or subject version if only one version was completed, or the caregiver version if both a caregiver and subject versions were completed.
Note: The global impression of change is analyzed using an ordinal logistic regression model with the treatment group as a fixed factor.
Source: CARE6 Clinical Study Report.22
Pharmacoeconomic Review
Abbreviations
AE
adverse event
ASM
antiseizure medication
BIA
budget impact analysis
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
LGS
Lennox-Gastaut syndrome
OLE
open-label extension
QALY
quality-adjusted life-year
SUDEP
sudden unexpected death in epilepsy
TAND
TSC-associated neuropsychiatric disorders
TEAE
treatment-emergent adverse event
TSC
tuberous sclerosis complex
WTP
willingness-to-pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Cannabidiol (Epidiolex), 100 mg/mL oral solution (100 mL) |
Submitted price | Cannabidiol, 100 mg/mL oral solution: $1,424.54 per 100 mL bottle |
Indication | For use as adjunctive therapy for seizures associated with Lennox-Gastaut syndrome, Dravet syndrome, or TSC in patients aged 2 years and older |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 15, 2023 |
Reimbursement request | For use as adjunctive therapy for the treatment of seizures associated with TSC in patients aged 2 years and older |
Sponsor | Jazz Pharmaceuticals Canada, Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance; TSC = tuberous sclerosis complex.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients aged 2 years and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM (i.e., patients who experience at least 8 seizures during a 28-day baseline period). |
Treatment | Cannabidiol, in combination with usual care. Usual care was defined as a variety of ASMs, including sodium valproate, vigabatrin, levetiracetam, clobazam, lamotrigine, lacosamide, oxcarbazepine, topiramate, and carbamazepine. |
Comparator | Usual care |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (100 years) |
Key data source | CARE6, a phase III, randomized, double-blind, placebo-controlled trial (data cut-off: February 26, 2019). |
Submitted results | ICER vs. usual care = $43,095 per QALY gained (incremental costs = $98,823; incremental QALYs = 2.29). |
Key limitations |
|
CADTH reanalysis results |
|
ASM = antiseizure medication; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; TSC = tuberous sclerosis complex.
Conclusions
CADTH’s review of the evidence from the CARE6 study suggests that cannabidiol (Epidiolex) likely resulted in a statistically significant and clinically important improvement in seizure frequency compared with usual care in patients aged 2 years and older with tuberous sclerosis complex (TSC) and a history of epilepsy that is inadequately controlled by their current antiseizure medication (ASM). The CADTH clinical review noted that the CARE6 study had a short double-blind treatment duration of 16 weeks, which was sufficient to address the primary outcome of change in number of TSC-associated seizures, but precluded the ability to assess long-term efficacy, safety, and health-related quality of life (HRQoL). Therefore, CADTH’s ability to draw any conclusions regarding the long-term efficacy of cannabidiol from the CARE6 study is limited. This uncertainty is propagated into the submitted economic model, given the underlying assumption that patient distribution across seizure frequency health states predicted16 weeks after treatment initiation would be maintained throughout the lifetime horizon of the model, while patients are receiving treatment.
In addition to the aforementioned limitations with the clinical evidence, CADTH identified several limitations with the sponsor’s economic submission. These limitations included a misalignment between the target population of the submitted model and the Health Canada–indicated population; the inability of the model structure to adequately reflect TSC in clinical practice and represent homogeneous health states; uncertainty regarding the impact of cannabidiol plus usual care on the HRQoL of patients with TSC; uncertainty regarding the inclusion of caregiver disutilities in the base-case analysis; uncertainty regarding the impact of cannabidiol on the long-term reduction in seizure frequency; a misalignment between the modelled and studied maintenance dose of cannabidiol; and poor modelling practices. As part of the base-case reanalysis, CADTH removed caregiver disutilities to align the analysis of HRQoL with the target patient population, and revised the mean maintenance dose of cannabidiol to 23 mg/kg per day, based on the mean maintenance dose observed among patients enrolled in the 25 mg/kg per day arm of the CARE6 trial.
As adjunctive therapy for seizures associated with TSC in patients aged 2 years and older, cannabidiol plus usual care was associated with an incremental cost-effectiveness ratio (ICER) of $295,503 per quality-adjusted life-year (QALY) gained compared to usual care alone. The probability that cannabidiol plus usual care was cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY was 3%. The estimated ICER was higher than the sponsor’s base-case value, driven by the exclusion of caregiver disutilities and the revision of the mean maintenance dose of cannabidiol. Compared to the sponsor’s analysis, the CADTH base case estimated a reduced QALY benefit with cannabidiol plus usual care (i.e., incremental QALYs = 0.94 [CADTH’s base case] versus 2.29 [sponsor’s analysis]) at a higher cost (i.e., incremental costs = $277,023 [CADTH’s base case] versus $98,823 [sponsor’s analysis]). A price reduction of 63% for cannabidiol would be required for cannabidiol plus usual care to be cost-effective compared to usual care alone at a WTP threshold of $50,000 per QALY gained. This would reduce the price of cannabidiol from $1,425 to $530 per 100 mL bottle.
The cost-effectiveness of cannabidiol plus usual care was sensitive to the inclusion of caregiver disutilities. In the sponsor’s base case, caregiver utilities were associated with the majority (59%) of incremental QALYs gained. The method for estimating these caregiver-associated QALYs produced a high degree of uncertainty within the analysis. The model was also highly sensitive to assumptions about the long-term efficacy of treatment, with 97% of incremental QALYs estimated through extrapolation beyond the submitted trial evidence. Given the extent of these and other methodological limitations associated with the sponsor’s submitted model, there remains considerable uncertainty about the cost-effectiveness results and an additional price reduction may be warranted.
The sponsor-submitted pharmacoeconomic analysis considers patients aged 2 years and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM (i.e., patients who experience at least 8 seizures during a 28-day baseline period). The cost-effectiveness of cannabidiol as adjunctive therapy in the full Health Canada–indicated population, which is not restricted to a particular level of seizure control, is thus unknown.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups and drug plans that participated in the CADTH review process. No registered clinician input was received for this review.
Two patient groups — Tuberous Sclerosis Canada Sclérose Tubéreuse and the Canadian Epilepsy Alliance — provided input for this review. Tuberous Sclerosis Canada Sclérose Tubéreuse collected data from patients and caregivers living in Canada with a survey conducted in September 2023 (n = 11), whereas the Canadian Epilepsy Alliance gathered information from firsthand experiences with patients, caregivers, and clinicians. The most important outcome for patients with TSC was improved seizure control, with the ultimate objective of preserving cognitive function and improving quality of life. Overall, patients’ disease experience was influenced by the physical symptoms associated with TSC (e.g., frequent seizures, specifically, infantile spasms; headaches; difficulty sleeping; and fatigue), as well as the psychosocial effects associated with the disease (i.e., depression associated with fear of rejection, anxiety associated with uncertainty about seizure frequency and severity, social isolation, irritability, difficulty concentrating, and loss of independence). In regard to experience with current treatment options, 72% of respondents reported having tried more than 4 different seizure medications or therapies, and none reported having achieved full seizure control. Patients noted that currently available ASMs tended to be ineffective (or effective for just a short period of time), indicating that important side effects included irritability. Patients additionally noted that the majority of them did not qualify for brain resection surgery. Patients did not have experience with cannabidiol.
Participating drug plans were interested in obtaining clarification as to whether genetic testing would typically be conducted to determine a diagnosis of TSC in clinical practice in Canada, as well as whether clinicians may be inclined to prescribe cannabidiol without the requirement of failure under current ASM. Drug plans further indicated that in the CARE6 trial, there was no requirement to have failed 1 or more ASMs before enrolment. Moreover, the drug plans inquired about the potential for renewal criteria and the objective measures that may be used by practising physicians to monitor therapeutic response and assess clinical benefit in practice. The drug plans explained that the recommended maintenance dosage for patients with TSC in the product monograph (10 mg/kg per day to 25 mg/kg per day) is substantially lower than the maximum maintenance dose used by patients in the CARE6 trial (25 mg/kg per day and 50 mg/kg per day). Consequently, the drug plans expressed concern regarding the potential for prescribers to increase the maximum dose to that observed in the clinical trial. Finally, the drug plans indicated that there is potential for patients with drug-resistant epilepsy who fall outside the Health Canada indication to switch from currently available medical cannabis to a pharmaceutical-grade alternative like cannabidiol for reasons such as barriers to access to medical cannabis, coverage by public and private insurers, and consistent product availability.
Several of these concerns were addressed in the sponsor’s model:
The impact of disease and treatment on a patient’s quality of life was captured with utility values.
Adverse events (AEs) were incorporated as disutilities within the analyses.
In addition, CADTH addressed some of these concerns, as follows:
CADTH assumed that patients would receive the mean maintenance dose of received by patients enrolled in the 25 mg/kg per day arm of the CARE6 trial.
CADTH was unable to address the following concerns raised from stakeholder input:
The cost-effectiveness of cannabidiol among patients who have already tried medical cannabis could not be addressed, owing to the lack of clinical data for this population.
Economic Review
The current review is for cannabidiol for patients aged 2 years and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM (i.e., patients who experience at least 8 seizures during a 28-day baseline period).
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of cannabidiol in combination with usual care compared with usual care alone.1 The modelled population comprised patients aged 2 years and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM (i.e., patients who experience at least 8 seizures during a 28-day baseline period). The target population of the economic evaluation is consistent with the enrolled population of the CARE6 clinical trial.1 However, the Health Canada indication does not restrict usage based on seizure frequency. The sponsor’s modelled population is narrower than the Health Canada–indicated population, as it does not consider patients with TSC who have fewer than 8 seizures over a 28-day period.
Epidiolex is a plant-derived pharmaceutical formulation of cannabidiol that reduces neuronal hyperexcitability by modulating intracellular calcium via the G protein-coupled receptor-55 (GPR55) and transient receptor potential vanilloid-1 (TRPV1) channels.1 Cannabidiol is available as a 100 mg/mL oral solution. The recommended dose of cannabidiol is 5 mg/kg per day for 1 week, followed by a maintenance dosage of 10 mg/kg per day, up to a maximum of 25 mg/kg per day, depending on individual response and tolerability.2 The submitted price of cannabidiol is $1,424.54 per 100 mL bottle.1 In the model, the sponsor applied a mean maintenance dose of 12 mg/kg per day for children and adults. Additionally, the sponsor separately calculated the costs of treatment for patients aged 2 to 6 years, 7 to 11 years, 12 to 17 years, and older than 18 years, based on weight-based dosing (20.30 kg, 32.20 kg, 52.60 kg, 73.40 kg, respectively), resulting in an annual per-patient cost of $12,631, $20,036, $32,730, and $45,672, respectively.1 The sponsor’s annual per-patient cost of usual care was similarly weight-based, and ranged from $1,238 to $2,540.1 Patients receiving cannabidiol plus usual care were assumed to use the same amount of other ASMs as those in the usual care group.
The clinical outcomes modelled were seizure frequency and seizure-free days.1 The economic outcomes of interest were QALYs and life-years. The economic evaluation was conducted over a lifetime time horizon (i.e., 100 years), from the perspective of the Canadian public health care payer. Costs and outcomes were discounted at 1.5% per annum.1
Model Structure
The sponsor submitted a Markov cohort-level model composed of 3 health states: alive (cannabidiol plus usual care), alive (usual care)’, and dead (Figure 1).1 Patients receiving cannabidiol plus usual care entered the model in the alive (cannabidiol plus usual care) health state, whereas patients receiving usual care alone entered the model in the alive (usual care) health state. The sponsor divided each alive health state into 4 weekly seizure frequency subhealth states, which were further divided into 5 daily seizure frequency subhealth states (Table 10).1 The weekly seizure frequency subhealth states were used to calculate health care resource use, whereas the daily seizure frequency subhealth states were used to calculate HRQoL (Figure 2). Patients enter the model in 1 of 5 daily seizure frequency subhealth states encompassed within 1 of 4 weekly seizure frequency subhealth states.1 The proportion of patients in each daily and weekly seizure frequency subhealth state was derived from regression models, using individual patient-level data from the CARE6 trial.1 Patients in the alive (cannabidiol plus usual care) health state could permanently discontinue cannabidiol treatment at any point during the lifetime horizon of the model and transition to the alive (usual care) health state in the cycle immediately after treatment discontinuation. Of note, patients transition to the same seizure frequency subhealth state and follow the usual care trajectory with associated costs and QALYs for the remainder of the model horizon. In contrast, patients receiving usual care were assumed to remain on treatment throughout the lifetime horizon of the model. Transitions between health states and subhealth states occur on a weekly cycle length, and patients accrue life-years, QALYs, and costs during each cycle. Patients may die at any time and from any health state, at which point they are considered to have transitioned to the death state and are removed from the model.
Model Inputs
Baseline patient characteristics were derived from the CARE6 trial, a phase III, randomized, placebo-controlled trial investigating the efficacy and safety of cannabidiol as adjunctive therapy among patients with TSC who experience inadequately controlled seizures (defined as at least 8 seizures during the 28-day baseline period) (n = 148).1 The target population of the economic model was split into 4 age categories (i.e., 2 to 6 years, 7 to 11 years, 12 to 17 years, and older than 18 years), which the sponsor assumed reflected the patient population in Canada. The main patient characteristics of each age group, including mean age, sex distribution, and mean weight, are presented in Table 11.1 These characteristics were derived from the enrolled patient population of the CARE6 trial and were used to inform the drug dosage regimens and the age-specific and sex-specific distribution of the general-population mortality risk.
The sponsor applied 2 independent mixed-effects regression models sequentially to the CARE6 individual patient-level data to predict the number of seizure-free days per week and the number of seizures on the remaining seizure days per week associated with each treatment.1 Given that seizure frequency is only estimated for the days in each cycle when patients are expected to have seizures, the sequential approach allowed for the correlation between seizure frequency and seizure-free days to be captured in the model. The fixed-effects parameters included treatment, treatment cycle, baseline seizure frequency, and an interaction term between treatment and treatment cycle to captures treatment effect over time.1 In addition, regression models incorporated random effects to account for the inherent correlation between observations from the same individuals. The sponsor selected models with 2 levels of random effects, thereby assuming that each patient may have a different intercept value (random intercept) and that the rate of change may vary per patient (random slope).1 The sponsor selected the fixed- and random-effect parameters used in the models based on Akaike information criterion and Bayesian information criterion goodness-of-fit statistics. Regression coefficients were applied to each patient’s baseline seizure frequency at the start of each 7-day model cycle to predict seizure-free days and seizure frequency distributions. The sponsor calculated the mean number of seizures per day using predicted seizure-free days and frequency per week. These individual calculations were used to distribute the modelled cohort among subhealth states representing different seizure frequency categories within the alive (on treatment) health states. The model assumed that the patient distribution predicted across seizure frequency health states at 16 weeks after treatment initiation is consistent and was maintained throughout the 100-year lifetime horizon of the model, while patients were receiving treatment. Hence, from cycle 16 onward, patients were assumed to remain in the same seizure frequency subhealth state until discontinuation or death.
Manifestations of TSC-associated neuropsychiatric disorders (TAND) are common in patients with TSC and are strongly associated with refractory epilepsy.3,4 The sponsor did not formally demonstrate the impact that a reduction in seizure frequency could have on TAND manifestation, so the relationship between seizure frequency and TAND was incorporated in the model based on clinical expert opinion. The sponsor did not formally demonstrate the impact that a reduction in seizure frequency can have on TAND manifestation, but the relationship between seizure frequency and TAND was incorporated in the model based on clinical expert opinion.1 The prevalence of 6 aspects of TAND (i.e., delayed developments, behavioural issues, intellectual disability, autism spectrum disorder, attention-deficit/hyperactivity disorder, and anxiety disorders) was sourced from a natural history study of patients with TSC-associated epilepsy from the TOSCA registry,3-5 and was matched to age categories used in the economic analysis. The model assumed that children (aged 2 to 6 years) who experienced a 50% reduction in seizure frequency would benefit from delaying TAND progression, which was implemented as a 50% reduction in TAND management costs and corresponding utility increments associated with prevention.
Background mortality was included to reflect the age-adjusted mortality risk for all patients in the model. General population survival was modelled using life tables from Statistics Canada to estimate the average survival of the general population with the same age distribution.6 Given that patients with TSC have an elevated mortality risk compared with the general population,6,7 the sponsor sourced an excess TSC mortality rate of 0.736% per year from the study by Zollner et al. (2020).8 Additionally, the background sudden unexpected death in epilepsy (SUDEP)–related mortality rate was estimated to be 0.176% per year from the study by Amin et al. (2017).9
The sponsor applied a per-cycle discontinuation rate of 0.67% (from week 1 to week 16) for all patients treated with cannabidiol plus usual care irrespective of seizure frequency, which reflected the withdrawal from treatment due AEs observed in the CARE6 blinded trial phase.10 From week 17 to week 48, per-cycle discontinuation rates ranging from 0.04% to 0.44% were applied according to seizure frequency, which reflected discontinuation for any cause observed in the CARE6 open-label extension (OLE) study.10 From week 89 onward, per-cycle discontinuation rates ranging from 0.04% to 0.77% were applied according to seizure frequency, based on the long-term discontinuation rates agreed to during the National Institute for Health and Care Excellence (NICE) appraisal of Lennox-Gastaut syndrome (LGS).11 After discontinuation, 5% of patients treated with cannabidiol plus usual care were assumed to receive everolimus, whereas the same proportion of patients treated with usual care were assumed to start treatment with everolimus 2.3 years after treatment initiation.
The sponsor’s model included health state utility values for patients, as well as utility decrements for caregivers (Table 12). The valuation of health effects associated with each treatment is based on the seizure frequency per day and seizure-free days. Utility gains (and caregiver decrements) corresponding to changes in seizure frequency and changes in seizure-free days were assumed to be the same irrespective of treatment. The sponsor conducted a vignette study that enrolled members of the general population in the UK (100 interviews that valued patient vignettes and 100 interviews that valued caregiver vignettes) to capture the HRQoL profile of people with TSC-associated epilepsy and their caregivers.1,12 Participants were asked to evaluate vignettes describing various seizure-related health states in terms of seizure frequency and severity on seizure days from the perspective of patients and caregivers, using the time trade-off methodology.1,12 Seizure severity proportions across seizure frequency per day categories observed in the CARE6 study were used to estimate the proportion of patients who experience either generalized seizures, focal seizures with impairment, or a combination of both.1 Utility values used in the model are the product of the seizure severity utility values derived in the vignette study and the seizure severity proportions observed in the CARE6 study. Table 13 presents the mean utility values derived from the vignette study by seizure frequency and severity on seizure days. Each patient was assumed to have 2 caregivers, based on a publication by Lagae et al. (2019).13 Table 14 presents the mean utility values derived for caregivers by seizure frequency and severity on seizure days. Caregiver utility decrements were applied additively.1 The burden of care is expected to be similar across patient age groups. Additionally, utility increments were derived for each TAND aspect from studies identified in the literature.14-17
All serious treatment-emergent adverse events (TEAEs) occurring during the 16-week CARE6 blinded trial were included in the model. Mean exposure in the CARE6 trial was used to calculate the per-cycle rate for each AE.10 Modelled AEs included vomiting, nausea, fatigue, malaise, liver injury, hypersensitivity reaction, rash erythematous, and electrolyte imbalance. A study by de Kinderen et al. (2020)18 reported a monthly disutility (–0.061) for epilepsy treatment-related side effects from a convenience sample of the Dutch general population, which the sponsor adjusted to a per-cycle disutility (–0.0001), assuming it would be similar across TEAEs.
Costs captured in the model included those associated with drug acquisition, disease monitoring and medical follow-up, subsequent treatment, TAND treatment, and the management of AEs.1 Drug-acquisition costs for cannabidiol were based on the sponsor’s submitted price.1 As described in the Overview section, the sponsor applied a mean maintenance dose of 12 mg/kg per day for children and adults receiving cannabidiol. The acquisition costs for ASMs were obtained from the Ontario Drug Benefit Formulary.19 The cost of the usual care basket of treatments was weighted based on the proportion of patients receiving each ASM in the CARE6 trial. The annual subsequent treatment cost of everolimus ranged by age group (from $9,995 to $21,035), and was applied as a one-off cost corresponding to 2 years of treatment. Costs associated with TAND management were sourced from a pan-European study reporting brain disorder costs by Gustavsson et al. (2011).20 The model considered health care resource use associated with routine patient monitoring, including physician visits, hospitalization, rescue medications, imaging, and long-term residential care.1 Health care resource use was assumed to vary by weekly seizure frequency subhealth state and age group (i.e., pediatric versus adult), with the frequency of resource use based on a UK clinical expert survey. The sponsor assumed that 50% of patients older than 18 years would incur costs associated with long-term residential care, based on clinical expert opinion. Unit costs for physician visits were obtained from the Ontario Schedule of Benefits for Physician Services.21 Unit costs for visiting nurses, occupational therapists, physiotherapy visits, and speech and language therapists were based on the Canadian median hourly wage obtained from the Government of Canada Job Bank.22-26 Costs for disease-specific hospitalizations were obtained from the Canadian Institute of Health Information Patient Cost Estimator.27 Direct medical costs for adults living in long-term residential care facilities were based on the Ontario Ministry of Health long-term care homes level-of-care per diem funding.28 AEs were assumed to be managed by neurologist, nurse, and emergency room visits, as well as by hospitalization.27,29
Summary of Sponsor’s Economic Evaluation Results
The sponsor-conducted the base case using a probabilistic sensitivity analysis with 1,000 simulations. The deterministic and probabilistic results were similar. The probabilistic findings are presented here.
Base-Case Results
Compared with usual care, cannabidiol plus usual care was associated with an incremental QALY gain of 2.29 and an incremental cost of $98,823, resulting in an ICER of $43,095 per QALY (Table 3). Given the duration of follow-up required to analyze a change in the number of TSC-associated seizures from baseline in the CARE6 blinded trial (i.e., 16 weeks), in contrast to the model’s time horizon (i.e., 100 years), it is important to note that 97% of the QALY benefit realized by patients receiving cannabidiol plus usual care was derived from the period beyond which there is observed trial data (i.e., extrapolated period).
Most of the incremental QALY gain associated with cannabidiol plus usual care relative to usual care was realized through improvements in caregiver utility (59%) rather than through HRQoL improvements experienced by patients with TSC. The key cost driver among patients receiving cannabidiol plus usual care was the cost of health care resource use associated with the highest seizure frequency (i.e., more than 7 seizures per week), which accounted for 42% of the total cost incurred by the public payer. Likewise, the main cost driver among patients receiving usual care was the cost of health care resource use in the highest seizure frequency category, which accounted for 49% of the total estimated cost.
Cannabidiol plus usual care was cost-effective at a WTP threshold of $50,000 per QALY in 51% of the simulations, compared to usual care. The sponsor’s submitted analysis is based on publicly available prices for all drug treatments. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. usual care ($/QALY) |
|---|---|---|---|---|---|
Usual care | 2,433,925 | Reference | 3.67 | Reference | Reference |
Cannabidiol + usual care | 2,532,749 | 98,823 | 5.96 | 2.29 | 43,095 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analyses Results
The sponsor assessed several model parameters and assumptions in its probabilistic scenario analyses, such as applying shorter lifetime horizons of 50 years and 75 years, excluding caregiver disutilities, including stopping rules, adopting a maintenance dose of 25 mg/kg per day for cannabidiol, assuming alternative estimates for utility values, and setting negative utility values to 0. The most influential parameters were alternative assumptions regarding the maintenance dose of cannabidiol and the exclusion of caregiver disutilities. When a maintenance dose of 25 mg/kg per day for cannabidiol was adopted, the ICER increased to $134,604 per QALY gained. Moreover, when caregiver disutilities were excluded, the ICER increased to $105,180 per QALY gained. All other scenarios resulted in ICERs that ranged between $33,104 and $51,832 per QALY gained.
The sponsor conducted a scenario analysis from a societal perspective. This analysis included additional costs associated with work absenteeism among caregivers. The sponsor assumed that 50% of caregivers to patients with TSC would be unable to work, based on clinical expert opinion, and estimated that caregivers would lose 20 hours per week from work. In this analysis, the ICER for cannabidiol plus usual care was $27,931 per QALY gained, relative to usual care. This was lower than the sponsor’s base-case analysis using a health care payer perspective.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations of the sponsor’s analysis that have notable implications for the economic analysis:
The submitted model does not align with the Health Canada–indicated population: The proposed reimbursement request for cannabidiol is for use as adjunctive therapy for the treatment of seizures associated with TSC in patients aged 2 years and older. The CARE6 trial was restricted to patients with TSC who were inadequately controlled by current ASMs. The clinical trials defined inadequate control as patients experiencing at least 8 seizures during a 28-day baseline period. As such, the sponsor’s modelled population does not consider patients with TSC who have fewer than 8 seizures over a 28-day period. Clinical expert input stated that, in clinical practice, inadequate control is defined more broadly and includes patients who experience 1 or more seizures per 28-day period, as well as patients who experience clusters of seizures over a 24-hour period and are subsequently seizure-free for months. Moreover, expert input highlighted that the definition of inadequate control may be subjective among patients and caregivers, as some may perceive, for instance, that 1 seizure every 3 months is inadequate control. Additionally, clinical experts noted that experiencing 3 or more generalized tonic-clonic seizures per month increases the risk of SUDEP, which is among the most common causes of death in patients with TSC. The increased risk of SUDEP is supported by a study by Wicker and Cole.30 Expert input noted that, given the likelihood of an elevated risk of SUDEP among patients who experience 3 or more seizures per month, coupled with the variability in the definition of inadequate control among patients, the sponsor’s modelled population could be perceived as restrictive and may not entirely align with the Health Canada–indicated population.
CADTH was unable to address this limitation, owing to a lack of clinical data on the efficacy of cannabidiol plus usual care in patients with TSC who experienced fewer than 8 seizures over a 28-day period. As such, the cost-effectiveness of cannabidiol plus usual care in this population is unknown, as is the cost-effectiveness of cannabidiol plus usual care in the full Health Canada–indicated population.
The model structure does not adequately reflect patient and clinician experience of TSC: The sponsor submitted a Markov model composed of 3 health states: alive (cannabidiol plus usual care), alive (usual care), and dead. The sponsor divided each alive health state into 4 weekly seizure frequency subhealth states, which were further divided into 5 daily seizure frequency subhealth states. The weekly seizure frequency subhealth states were used to calculate health care resource use, whereas the daily seizure frequency subhealth states were used to calculate HRQoL. Clinical expert input received by CADTH noted that the thresholds used by the sponsor for the daily seizure frequency subhealth states do not accurately capture the HRQoL associated with a seizure day, which is partly due to the heterogeneity between patients in the highest daily seizure frequency subhealth state (i.e., > 4 seizures per day). Notably, patient group input received by CADTH for this review described the experience of patients who may have upward of 100 seizures per day. Given that patients who experience more than 4 seizures per day are grouped together in 1 subhealth state, there is a potential for patients with high seizure burdens to experience a clinically meaningful reduction in seizures yet remain in the same daily seizure frequency subhealth state. For instance, a patient who experiences 10 seizures at baseline and has a 50% reduction in daily seizure frequency after initiating treatment would experience a clinically meaningful reduction in seizures, but the HRQoL implications of their improvement would not be captured in the submitted model. Hence, the sponsor could have explored more granular seizure frequency subhealth states to capture the HRQoL of patients with the highest seizure burden. Moreover, clinical expert input noted that the impact that seizure frequency has on a patient’s HRQoL will differ based on the length of a seizure (e.g., 30 seconds versus 1 hour). As such, daily seizure frequency subhealth states that do not also consider seizure length may not adequately capture changes in HRQoL. This is because there is a potential for patients to experience a clinically meaningful reduction in seizure length after initiating treatment yet remain in the same daily seizure frequency subhealth state. From a methodological perspective, health states in an economic model should represent a homogenous group of patients who have similar expected quality-of-life considerations31,32 and should be based on the clinical or care pathway for the condition of interest; this is not captured by the modelled health states. The implications of heterogeneity in health states have been well documented in the literature.33
CADTH was unable to address limitations related to the model structure, and the direction and magnitude of the impact of the model structure not adequately reflecting clinical practice is unknown.
The impact of cannabidiol plus usual care on the quality of life of patients with TSC is highly uncertain. The sponsor’s base case predicts an incremental gain of 2.29 QALYs with cannabidiol plus usual care compared to usual care alone (Table 3). As noted in the CADTH clinical review, no meaningful difference in HRQoL was observed. CADTH noted that the effect associated with cannabidiol plus usual care on the HRQoL of patients with TSC has not been shown in clinical trials, and is, thus, highly uncertain.
The sponsor derived mean utility values from a vignette study that enrolled members of the general population in the UK (n = 100) to capture the HRQoL profile of patients with TSC.12 Participants were asked to adopt the perspective of a patient and to evaluate vignettes describing various seizure-related health states using time trade-off and visual analogue scale methodologies.12 CADTH noted that there is a high degree of uncertainty around the values estimated in the vignette study. This is evident in the wide 95% confidence intervals, which overlap across a number of severity states, as a result of the relatively large variability in valuations given by participants and the study sample size. CADTH notes that the vignettes were designed to depict a typical patient experience by describing the clinical manifestations that are most commonly found to affect 13-year-old patients with TSC. By focusing on patients of an age at which seizures are expected to be a significant contributing factor to the patient burden,4 the vignettes portrayed a limited depiction of the condition, which in fact varies greatly across the lifespan.8,34 Although vignette-based utilities may be a useful approximation of patient HRQoL, its alignment with utilities derived from preference-based measures involving actual patients with TSC remains highly uncertain. Moreover, the accuracy and reliability of vignette-based utilities rely on the precision and comprehensiveness of the health state descriptions, which inevitably fall short of encompassing all potential facets of the patient experience with TSC.35 As vignettes cannot capture the entirety of patient experiences with TSC within a seizure severity category, the resulting utilities may underestimate the variability associated with the disease.35 Vignettes that concentrate solely on a particular aspect of seizure severity without offering a broader context of the lived experience of patients with TSC may lead general-population respondents to overemphasize the significance of minor attributes of TSC without taking into account other aspects of health and well-being. CADTH further noted that the perception of TSC by members of the general public may vary among cultures and contexts. Because no patients or members of the general public in Canada were included in this study, it is uncertain whether these utilities reflect the preferences of patients with TSC in Canada.
CADTH further noted that the vignette study conducted by the sponsor produced negative utility values for 2 seizure severity categories: generalized 3 to 14; and generalized 3 to 14, focal 5 to 14. These represent states of health that are worse than death. Given the limitations of the vignette-based study, utilities derived from general-population respondents, whose understanding of the disease is inherently incomplete, likely underestimate the quality of life of patients with TSC. Differences between hypothetical valuations mirrored in the vignette-based study and actual self-reported life satisfaction may depend on the fact that general-population respondents may not readily understand the adaptation that patients with TSC make to live with their condition over time.36-38 Clinical experts observed that utilities indicating a quality of life considered worse than death were severe. Experts further noted that, throughout their professional experience, they had not encountered a patient with TSC who had sought medical assistance in dying. Although it is clear that TSC is a condition with strong negative impacts on a patient’s quality of life, the evidence provided by the sponsor is not sufficient to support the extraordinary and consequential claim that is implied by the use of utility values below 0. Hence, it is unknown to what extent seizure severity categories valued worse than death by general-population respondents are reasonable from the perspective of patients with TSC.
CADTH was unable to address this limitation, owing to the lack of suitable data informing the HRQoL of patients with TSC.
The inclusion of caregiver disutilities in the base-case analysis is highly uncertain. The sponsor applied a disutility value representing quality-of-life decrements due to caregiver burden in the base case. The sponsor indicated that the inclusion of a caregiver utility in the model’s base case was justified, given that TSC is a complex disease with a substantial unmet need and burden on caregivers. As noted in the CADTH economic guidelines,39 the analysis of HRQoL must be focused on the target population, which is patients aged 2 years and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM. Hence, any spillover effects that fall outside the target population should be incorporated in a nonbase-case analysis. CADTH noted that, of the 2.29 incremental QALYs predicted by the sponsor’s model to be gained with cannabidiol plus usual care, the majority (59%) were accrued by caregivers. This finding is subject to the same methodological concerns identified in the limitations described previously in the vignette study, and is thus highly uncertain. The impact of cannabidiol on the HRQoL of caregivers has not been assessed in clinical trials. Further, the sponsor’s assumption that each patient with TSC would have 2 caregivers for the duration of their life and that each caregiver would have the same HRQoL decrement was deemed to be inappropriate by the clinical experts consulted by CADTH for this review. That is, not all patients with TSC will have 2 caregivers, and for patients with multiple caregivers, the individual burden of care (i.e., as described in the vignette study) would likely be shared rather than doubled.
In the CADTH base case, QALY decrements accrued by caregivers were excluded, such that the CADTH ICER reflects the cost-effectiveness of cannabidiol plus usual care for patients with TSC.
CADTH explored the impact of additionally including the effect of cannabidiol on caregivers in a scenario analysis. CADTH adjusted the number of caregivers per patient to 1, applicable to both pediatric and adult patients.
The impact of cannabidiol on the long-term reduction in seizure frequency is highly uncertain: The model assumed that the predicted patient distribution across seizure frequency health states 16 weeks after treatment initiation is consistent and maintained throughout the 100-year lifetime horizon of the model, while patients are receiving treatment. Hence, from cycle 16 onward, patients were assumed to remain in the same seizure frequency subhealth state until discontinuation or death. CADTH noted that no data supporting the effectiveness of cannabidiol are available beyond the duration of the CARE6 OLE study (5 years), and there are no comparative effectiveness data for cannabidiol plus usual care relative to usual care alone beyond the duration of the CARE6 trial (16 weeks). As such, it is uncertain whether the reduction in seizure frequency observed in the CARE6 and CARE6 OLE studies will be maintained indefinitely or whether treatment effectiveness may wane. CADTH additionally noted that the sponsor attempted to incorporate loss of response to cannabidiol over time with discontinuation assumptions in the economic analysis. Specifically, the sponsor assumed discontinuation rates due to nonresponse and other factors using evidence from the CARE6 (up to week 16) and CARE6 OLE (from week 17 to week 88) studies. However, long-term discontinuation rates (i.e., from week 89 until the end of the modelled lifetime horizon) were extrapolated from patients with LGS and assumed to be generalizable to patients with TSC. CADTH acknowledged that evidence-based discontinuation rates due to nonresponse may capture some of the potential treatment waning that may be experienced by patients with TSC receiving cannabidiol. However, given that the long-term discontinuation rates are not informed by evidence derived from the relevant patient population, there remains a high degree of uncertainty regarding the impact of cannabidiol on the long-term reduction in seizure frequency. Approximately 97% of the incremental QALYs realized by patients treated with cannabidiol plus usual care, relative to usual care alone, were accrued on the basis of extrapolation (i.e., in the posttrial period), highlighting the importance of assumptions related to the long-term relative treatment effectiveness.
CADTH was unable to explore the impact of the potential waning of cannabidiol treatment effect due to the structure of the submitted model.
The maintenance dosage of cannabidiol is underestimated. The recommended maintenance dosage of cannabidiol is 10 mg/kg per day up to a maximum of 25 mg/kg per day, depending on individual response and tolerability. In the submitted model, the sponsor applied a mean maintenance dose of 12 mg/kg per day to pediatric and adult patients. The sponsor assumed that a number of patients would not be expected to titrate up to the maximum dose of 25 mg/kg per day in clinical practice, based on evidence from a dispensing database in Germany, which reported 12 mg/kg per day and 8 mg/kg per day median doses among pediatric and adult patients with TSC (n = 118), respectively.40 CADTH noted that patients in the real-world-evidence database were not matched to the patient population enrolled in the CARE6 trial on the basis of disease severity. If patients enrolled in the CARE6 trial had more severe disease (e.g., higher seizure frequency and/or severity) relative to patients in the real-world-evidence study, it would not be reasonable to assume the same maintenance dose. Hence, using a maintenance dose derived from a real-world patient population with unknown seizure burden risks introducing substantial bias in the economic analysis. CADTH additionally noted that the recommended maintenance dosage in the product monograph (10 mg/kg per day to 25 mg/kg per day) is substantially lower than the maximum maintenance dose used by patients in the CARE6 trial (25 mg/kg per day and 50 mg/kg per day). CADTH further noted that the efficacy of cannabidiol was modelled using data from patients in the CARE6 trial who were randomized to receive a maximum dose of 25 mg/kg per day (n = 75). In this group, the mean maintenance dose at the end of treatment (week 16) was 23 mg/kg per day. CADTH noted that because the mean maintenance dose modelled for cannabidiol (12 mg/kg per day) is lower than the mean dose studied in patients enrolled in the 25 mg/kg per day arm of the CARE6 trial (whose outcomes were used to model the efficacy of cannabidiol plus usual care), so misalignment between modelled and studied doses may have important cost-effectiveness implications. That is, the sponsor assumed that the average patient treated with cannabidiol plus usual care would be prescribed a lower dose than that studied in the CARE6 trial (12 mg/kg per day versus 23 mg/kg per day), while experiencing the full extent of the treatment benefit associated with the studied maintenance dose. At CADTH’s request, the sponsor offered descriptive evidence showing that there is no clear dose response above doses of 10 mg/kg per day in patients with LGS or DS (Figure 3). However, it is uncertain whether efficacy results from patients with LGS or DS may be extrapolated to patients with TSC. This assumption may reduce the incremental cost and increase the incremental benefit of cannabidiol plus usual care relative to usual care alone, thereby introducing a cost-effectiveness bias in favour of cannabidiol.
CADTH conducted a reanalysis that adjusted the maintenance dose modelled for cannabidiol among pediatric and adult patients by using the mean maintenance dose observed in patients with TSC enrolled in the 25 mg/kg per day arm of the CARE6 trial.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, resulting in situations in which the parameter value was overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements rendered thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model ran inappropriately by overriding errors.
CADTH was unable to address this limitation, noting that a thorough validation of the submitted model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Excess TSC-related mortality is applied equally to patients receiving cannabidiol + usual care and patients receiving usual care alone. | Acceptable. Patients with TSC have significant morbidity and mortality. As data on mortality could not be collected within the time frame of the CARE6 trial, the sponsor assumed that the use of cannabidiol would have no impact on any of the aspects of TSC mortality. |
SUDEP mortality risk is applied equally across health states. | Acceptable. As data on mortality could not be collected within the time frame of the CARE6 trial, the sponsor assumed that the use of cannabidiol would have no impact on SUDEP-related mortality. |
A utility increment and a 50% reduction in management costs is applied for a lifetime to patients (aged 1 to 6 years) who, after 6 months of treatment, have at least a 50% reduction in seizure frequency from baseline. | Acceptable. This assumption is based on clinical expert input obtained by the sponsor that a reduction in seizure frequency is likely to lead to a reduction in TAND symptoms. TAND aspects, age from which it is better to start treatment, and required reduction in seizure frequency were informed by a Delphi panel study that involved 10 clinical experts and was validated by clinicians in Canada. |
The model does not distinguish between caregivers of patients who reside in long-term care institutions and caregivers of patients who do not in terms of the HRQoL impact. | Uncertain. CADTH notes that it is improbable for adults with TSC to consistently maintain 2 informal caregivers throughout their lifetimes. Eventually, the demise or incapacitation of the caregivers will necessitate transition of care to either another family member or, more probably, an institutional setting. The sponsor assumed that 50% of patients older than 18 years would incur costs associated with long-term residential care. It is plausible that caregivers of patients living in long-term residential care facilities experience the same quality-of-life decrements as caregivers of patients who do not. The sponsor explained that this is an appropriate assumption, given that each caregiver worries about the patient being at risk of injury from a seizure without being able to provide support when this happens. The sponsor further explained that even if the patient lives in a long-term care institution, caregivers are invested in patient care and are often responsible for managing medical appointments and visits to the emergency room. |
HRQoL = health-related quality of life; SUDEP = sudden unexpected death in epilepsy; TAND = TSC-associated neuropsychiatric disorders; TSC = tuberous sclerosis complex.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH’s reanalyses addressed several limitations within the economic model. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. These included removing caregiver disutilities to align the analysis of HRQoL with the target patient population and revising the mean maintenance dose of cannabidiol to 23 mg/kg per day, based on the mean maintenance dose observed for patients enrolled in the 25 mg/kg per day arm of the CARE6 trial. These changes are summarized in Table 5.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Caregiver utility decrements | Included | Excluded |
2. Maintenance dosage of cannabidiol | Mean maintenance dose of 12 mg/kg per day for pediatric and adult patients | Mean maintenance dose of 23 mg/kg per day for pediatric and adult patients |
CADTH base case | Reanalyses 1 + 2 | |
In the CADTH base case, cannabidiol plus usual care was associated with an ICER of $295,503 per QALY gained compared to usual care (incremental costs = $277,023; incremental QALYs = 0.94) (Table 6). There was a 3% probability that cannabidiol plus usual care was cost-effective at a WTP threshold of $50,000 per QALY gained.
CADTH’s estimated ICER was higher than the sponsor’s base-case value, driven by the exclusion of caregiver disutilities and the revision of the mean maintenance dose of cannabidiol. Consistent with the sponsor’s analysis, the CADTH reanalysis estimates that the near entirety (97%) of the incremental QALYs were accrued in the posttrial period of the model on the basis of extrapolation.
The CADTH base case is based on publicly available prices of the comparator treatments. A detailed breakdown of the disaggregated results is available in Appendix 4.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (deterministic) | Usual care | 2,280,917 | 1.64 | Reference |
Cannabidiol + usual care | 2,380,544 | 3.85 | 45,153 | |
CADTH reanalysis 1: caregiver disutility excluded | Usual care | 2,280,917 | 14.45 | Reference |
Cannabidiol + usual care | 2,380,544 | 15.44 | 100,620 | |
CADTH reanalysis 2: maintenance dosage revised | Usual care | 2,280,917 | 1.64 | Reference |
Cannabidiol + usual care | 2,539,451 | 3.85 | 117,173 | |
CADTH base case (deterministic) | Usual care | 2,280,917 | 14.45 | Reference |
Cannabidiol + usual care | 2,539,451 | 15.44 | 261,110 | |
CADTH base case (probabilistic) | Usual care | 2,435,144 | 16.54 | Reference |
Cannabidiol + usual care | 2,712,168 | 17.48 | 295,503 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s results and CADTH’s base case. The CADTH base case suggests that a 63% price reduction for cannabidiol would be required for cannabidiol plus usual care to be considered cost-effective at a WTP threshold of $50,000 per QALY gained relative to usual care alone (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for cannabidiol plus usual care vs. usual care | |
|---|---|---|
Price reduction | Sponsor base case ($/QALY) | CADTH reanalysis ($/QALY) |
No price reduction | 45,162 | 261,093 |
10% | 37,273 | 227,470 |
20% | 29,384 | 193,848 |
30% | 21,495 | 160,225 |
40% | 13,606 | 126,603 |
50% | 5,717 | 92,980 |
60% | DUR is dominant | 59,358 |
70% | DUR is dominant | 25,735 |
80% | DUR is dominant | DUR is dominant |
90% | DUR is dominant | DUR is dominant |
100% | DUR is dominant | DUR is dominant |
DUR = drug under review; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CADTH conducted a series of scenario analyses to explore the impact of alternative assumptions on the cost-effectiveness of cannabidiol plus usual care, as follows:
One included caregiver QALYs in the calculation of the ICER, such that the ICER reflects the cost-effectiveness of cannabidiol plus usual care compared with usual care alone in patients with TSC and their caregivers. One caregiver was included per patient in this scenario, which may reflect the caregiver burden experienced by a single person or the burden shared by multiple people.
Another implemented a stopping rule, using the sponsor-provided option to do so, such that patients who did not experience a 30% reduction in seizure frequency after the use of cannabidiol for 6 months, 1 year, 18 months, and 2 years were assumed to discontinue cannabidiol.
The results of these scenarios are presented in Appendix 4 (Table 17). When including caregiver QALYs, the ICER of cannabidiol plus usual care decreased to $169,662 per QALY gained relative to usual care alone. When implementing a stopping rule, the ICER of cannabidiol plus usual care decreased to $239,133 per QALY gained relative to usual care alone.
Issues for Consideration
Medical cannabis products are available in Canada but are generally not reimbursed by public drug plans: Patients with TSC in Canada may already use or have tried cannabis for medical purposes, including cannabidiol products accessed through federally licensed sellers operating under the Cannabis Act. The clinical experts consulted by CADTH indicated that patients who are currently using medical cannabis may be likely to switch to cannabidiol, owing to its higher dosage, a lack of private insurance coverage, and the out-of-pocket cost of medical cannabis to patients. The cost-effectiveness of cannabidiol plus usual care in patients who have previously responded to other forms of cannabidiol is unknown.
There is a potential for increased dosing, notwithstanding the product monograph: The clinical experts consulted by CADTH for this review noted that there is a potential for clinicians in Canada to increase the dose of cannabidiol to the maximum studied dose (50 mg/kg per day). That is, if cannabidiol were reimbursed, some patients may be prescribed doses that are higher than recommended, but aligned with doses used in the CARE6 trial. This would increase the cost of treatment with cannabidiol by an unknown amount, and would have an unknown effect on the incremental effectiveness.
Overall Conclusions
Evidence from the CARE6 trial suggests that cannabidiol likely resulted in a statistically significant and clinically important improvement in seizure frequency, compared with usual care, in patients aged 2 years and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM. The CADTH clinical review noted that the CARE6 trial had a short double-blind treatment duration of 16 weeks, which was sufficient to address the primary outcome of change in the number of TSC-associated seizures, but precluded the ability to assess long-term efficacy, safety, and HRQoL. The CADTH clinical review further noted that the potential selection bias for patients with a higher seizure burden and highly refractory epilepsy limits the generalizability of the findings to the broader population of patients with TSC-associated seizures. Therefore, CADTH’s ability to draw any conclusions regarding the long-term efficacy of cannabidiol from the CARE6 trial is limited. This uncertainty is propagated into the submitted economic model, given the underlying assumption that the predicted patient distribution across seizure frequency health states 16 weeks after treatment initiation would be maintained throughout the lifetime horizon of the model, while patients are receiving treatment.
In addition to the aforementioned limitations with the clinical evidence, CADTH identified several limitations of the sponsor’s economic submission. These limitations included misalignment between the target population of the submitted model and the Health Canada–indicated population; inability of the model structure to adequately reflect TSC in clinical practice and represent homogeneous health states; uncertainty regarding the impact of cannabidiol plus usual care on the HRQoL of patients with TSC; uncertainty regarding the inclusion of caregiver disutilities in the base-case analysis; uncertainty regarding the impact of cannabidiol on long-term reduction in seizure frequency; misalignment between the modelled and studied maintenance doses of cannabidiol; and poor modelling practices. As part of the base-case reanalysis, CADTH removed caregiver disutilities to align the analysis of HRQoL with the target patient population; and revised the mean maintenance dose of cannabidiol to 23 mg/kg per day, based on the mean maintenance dose observed in patients enrolled in the 25 mg/kg per day arm of the CARE6 trial.
The sponsor-submitted pharmacoeconomic analysis compared cannabidiol plus usual care with usual care alone in patients aged 2 years and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM (i.e., patients who experience at least 8 seizures during a 28-day baseline period). The efficacy of cannabidiol plus usual care was informed by individual patient data from the CARE6 clinical trial. As such, the pharmacoeconomic analyses reflect the cost-effectiveness of cannabidiol in patients with 8 or more seizures over a 28-day period who are inadequately controlled on their current ASMs. The cost-effectiveness of cannabidiol as adjunctive therapy in the full Health Canada–indicated population, which is not restricted to a particular level of seizure control, is thus unknown.
As adjunctive therapy for seizures associated with TSC in patients aged 2 years and older, cannabidiol plus usual care was associated with an ICER of $295,503 per QALY gained compared to usual care alone (incremental costs = $277,023; incremental QALYs = 0.94). The probability that cannabidiol plus usual care was cost-effective at a WTP threshold of $50,000 per QALY was 3%. The estimated ICER was higher than the sponsor’s base-case value, driven by the exclusion of caregiver disutilities and the revision of the mean maintenance dose of cannabidiol. Compared to the sponsor’s analysis, the CADTH base case estimated a reduced QALY benefit with cannabidiol plus usual care (i.e., incremental QALYs = 0.94 [CADTH’s base case] versus 2.29 [sponsor’s analysis]) at a higher cost (i.e., incremental costs = $277,023 [CADTH’s base case] versus $98,823 [sponsor’s analysis]). A price reduction of 63% for cannabidiol would be required for cannabidiol plus usual care to be cost-effective relative to usual care alone at a WTP threshold of $50,000 per QALY gained. This would reduce the price of cannabidiol from $1,425 to $530 (per 100 mL bottle).
The cost-effectiveness of cannabidiol plus usual care was sensitive to the inclusion of caregiver disutilities. When spillover quality-of-life decrements due to caregiver burden were accounted for, the ICER of cannabidiol plus usual care decreased to $169,662 per QALY gained (incremental costs = $278,484; incremental QALYs = 1.64) relative to usual care alone. CADTH was unable to address limitations related to the sponsor’s modelling approach, uncertainty about long-term efficacy, and the HRQoL impact associated with the use of cannabidiol plus usual care in patients with TSC. Given the extent of the limitations associated with the sponsor’s submitted model, there remains considerable uncertainty about the cost-effectiveness results. Moreover, when comparing the duration of follow-up in the CARE6 trial to the model’s time horizon (16 weeks versus 100 years), it is important to note that 97% of the QALY benefit realized by patients in the CADTH base case was accrued during the posttrial period of the model on the basis of extrapolation. In the absence of long-term evidence, the true comparative impact of cannabidiol on improvement in seizure frequency relative to usual care remains highly uncertain. Given the model’s underlying assumption that the efficacy of cannabidiol would be maintained indefinitely, the estimates presented in the CADTH base case likely represent the upper bounds of the incremental efficacy gains that may be realized from this therapy.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Epidiolex (cannabidiol), 100 mg/mL oral solution. Mississauga (ON): Jazz Pharmaceuticals; 2023 Sep 29.
2.Epidiolex (cannabidiol): 100 mg/mL, oral solution [product monograph]. Cambridge (UK): GW Research Ltd.; 2023 Nov 15.
3.National Institute for Health and Care Excellence. Cannabidiol with clobazam for treating seizures associated with Dravet syndrome [sponsor-submitted reference]. (Technology appraisal guidance TA614) 2019; https://www.nice.org.uk/guidance/TA614. Accessed 2023 May.
4.Rentz AM, Skalicky AM, Liu Z, et al. Tuberous sclerosis complex: a survey of health care resource use and health burden. Pediatr Neurol. 2015;52(4):435-441. PubMed
5.de Vries PJ, Belousova E, Benedik MP, et al. TSC-associated neuropsychiatric disorders (TAND): findings from the TOSCA natural history study. Orphanet J Rare Dis. 2018;13(1):157. PubMed
6.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2023 Dec 11.
7.Kingswood C, Bolton P, Crawford P, et al. The clinical profile of tuberous sclerosis complex (TSC) in the United Kingdom: A retrospective cohort study in the Clinical Practice Research Datalink (CPRD). Eur J Paediatr Neurol. 2016;20(2):296-308. PubMed
8.Zollner JP, Franz DN, Hertzberg C, et al. A systematic review on the burden of illness in individuals with tuberous sclerosis complex (TSC). Orphanet J Rare Dis. 2020;15(1):23. PubMed
9.Amin S, Lux A, Calder N, Laugharne M, Osborne J, O'Callaghan F. Causes of mortality in individuals with tuberous sclerosis complex. Dev Med Child Neurol. 2017;59(6):612-617. PubMed
10.A double-blind, randomized, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P, CBD) as add-on therapy in patients with tuberous sclerosis complex who experience inadequately-controlled seizures [sponsor-submitted reference]. Cambridge (UK): GW Research Ltd; 2019.
11.National Institute for Health and Care Excellence. Cannabidiol with clobazam for treating seizures associated with Lennox–Gastaut syndrome [sponsor-submitted reference]. (Technology appraisal guidance TA615) 2019; https://www.nice.org.uk/guidance/ta615/. Accessed 2023 May.
12.Acaster Lloyd Consulting Ltd. Patient and caregiver health state utilities in Tuberous Sclerosis Complex (TSC): Study report [internal sponsor's report]. Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2020 Oct 8.
13.Lagae L, Irwin J, Gibson E, Battersby A. Caregiver impact and health service use in high and low severity Dravet syndrome: A multinational cohort study. Seizure. 2019;65:72-79. PubMed
14.Johansson R, Carlbring P, Heedman A, Paxling B, Andersson G. Depression, anxiety and their comorbidity in the Swedish general population: point prevalence and the effect on health-related quality of life. PeerJ. 2013;1:e98. PubMed
15.van der Kolk A, Bouwmans CA, Schawo SJ, Buitelaar JK, van Agthoven M, Hakkaart-van Roijen L. Association between societal costs and treatment response in children and adolescents with ADHD and their parents. A cross-sectional study in the Netherlands. Springerplus. 2015;4:224. PubMed
16.Ten Hoopen LW, de Nijs PFA, Duvekot J, et al. Children with an Autism Spectrum Disorder and Their Caregivers: Capturing Health-Related and Care-Related Quality of Life. J Autism Dev Disord. 2020;50(1):263-277. PubMed
17.Kirkham FJ, Vigevano F, Raspall-Chaure M, et al. Health-related quality of life and the burden of prolonged seizures in noninstitutionalized children with epilepsy. Epilepsy Behav. 2020;102:106340. PubMed
18.de Kinderen RJ, Wijnen BF, van Breukelen G, et al. From clinically relevant outcome measures to quality of life in epilepsy: A time trade-off study. Epilepsy Res. 2016;125:24-31. PubMed
19.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index [sponsor-submitted reference]. 2023; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Apr.
20.Gustavsson A, Svensson M, Jacobi F, et al. Cost of disorders of the brain in Europe 2010. Eur Neuropsychopharmacol. 2011;21(10):718-779. PubMed
21.Schedule of benefits for physician services under the Health Insurance Act: (January 25, 2022 (effective July 1, 2022)). Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2023 Dec 12.
22.Government of Canada. Labour Market Information: Wages for Registered nurses and registered psychiatric nurses [sponsor-submitted reference]. https://www.jobbank.gc.ca/wagereport/occupation/993. Accessed 2023 Apr.
23.Government of Canada. Labour Market Information: Wages for Physiotherapists [sponsor-submitted reference]. https://www.jobbank.gc.ca/wagereport/occupation/18214. Accessed 2023 Apr.
24.Government of Canada. Labour Market Information: Wages for Occupational Therapists [sponsor-submitted reference]. https://www.jobbank.gc.ca/wagereport/occupation/4168. Accessed 2023 Apr.
25.Government of Canada. Labour Market Information: Wages for Audiologists and speech-language pathologists [sponsor-submitted reference]. https://www.jobbank.gc.ca/wagereport/occupation/22734. Accessed 2023 Apr.
26.Government of Canada. Labour Market Information: Wages for Home support workers, caregivers and related occupations [sponsor-submitted reference]. https://www.jobbank.gc.ca/wagereport/occupation/24584. Accessed 2023 May.
27.Canadian Institute for Health Information. Patient Cost Estimator [sponsor-submitted reference]. 2020: https://www.cihi.ca/en/patient-cost-estimator. Accessed 2023 May.
28.Government of Ontario. Long-term care homes level-of-care per diem funding summary [sponsor-submitted reference]. https://www.ontario.ca/page/long-term-care-home-level-care-diem-funding-summary. Accessed 2023 Jul.
29.Schedule of benefits for physician services under the Health Insurance Act: (January 25, 2022 (effective July 1, 2022)) [sponsor-submitted reference]. Toronto (ON): Ontario Ministry of Health; 2023: https://health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2023 Apr.
30.Wicker E, Cole JW. Sudden Unexpected Death in Epilepsy (SUDEP): A Review of Risk Factors and Possible Interventions in Children. J Pediatr Pharmacol Ther. 2021;26(6):556-564. PubMed
31.Sculpher M. Subgroups and heterogeneity in cost-effectiveness analysis. Pharmacoeconomics. 2008;26(9):799-806. PubMed
32.Phelps CE. Good technologies gone bad: how and why the cost-effectiveness of a medical intervention changes for different populations. Med Decis Making. 1997;17(1):107-117. PubMed
33.Zaric GS. The impact of ignoring population heterogeneity when Markov models are used in cost-effectiveness analysis. Med Decis Making. 2003;23(5):379-396. PubMed
34.McDonald A, Goodwin J, Roberts S, et al. 'We've made the best of it. But we do not have a normal life': families' experiences of tuberous sclerosis complex and seizure management. J Intellect Disabil Res. 2019;63(8):947-956. PubMed
35.Matza LS, Stewart KD, Lloyd AJ, Rowen D, Brazier JE. Vignette-Based Utilities: Usefulness, Limitations, and Methodological Recommendations. Value Health. 2021;24(6):812-821. PubMed
36.Tyc VL. Psychosocial adaptation of children and adolescents with limb deficiencies: A review. Clin Psychol Rev. 1992;12:275-291.
37.Wu S. Adapting to heart conditions: a test of the hedonic treadmill. J Health Econ. 2001;20(4):495-508. PubMed
38.Brickman P, Coates D, Janoff-Bulman R. Lottery winners and accident victims: is happiness relative? J Pers Soc Psychol. 1978;36(8):917-927. PubMed
39.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2024 Jan 10.
40.Jazz Pharmaceuticals Inc. VV-MED-29431 - Epidiolex Daily Dose in TSC - Patient INSIGHTS (INSIGHT Health) Germany [sponsor-submitted reference]. 2022.
41.Jazz Pharmaceuticals Canada Inc. response to November 15, 2023 CADTH request for additional information regarding Epidiolex (cannabidiol) CADTH review [internal sponsor's report]. Mississauga (ON): Jazz Pharmaceuticals Canada Inc.; 2023 Nov 21.
42.O'Callaghan FJ, Shiell AW, Osborne JP, Martyn CN. Prevalence of tuberous sclerosis estimated by capture-recapture analysis. Lancet. 1998;351(9114):1490. PubMed
43.Wilbur C, Sanguansermsri C, Chable H, Anghelina M, Peinhof S. Manifestations of Tuberous Sclerosis Complex: The Experience of a Provincial Clinic. Can J Neurol Sci. 2017;44(1):35-43. PubMed
44.Bachour K, House AA, Andrade DM, Connolly M, Debicki DB. Adults with tuberous sclerosis complex: A distinct patient population. Epilepsia. 2022;63(3):663-671. PubMed
45.Alsowat D, Whitney R, Hewson S, et al. The Phenotypic Spectrum of Tuberous Sclerosis Complex: A Canadian Cohort. Child Neurol Open. 2021;8(8 2329048x211012817):2329048X211012817.
46.Statistics Canada. Table 17-10-0005-01 Population estimates on July 1st, by age and sex. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2024 Jan 10.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison for the Treatment of Seizures Associated With TSC
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily maintenance cost ($) | Annual maintenance cost ($) |
|---|---|---|---|---|---|---|
Cannabidiol (Epidiolex) | 100 mg/mL | Oral solution in 100 mL bottles | 1,424.5400a | 10 mg/kg per day, up to a maximum of 25 mg/kg per day. | 17.42 to 260 | 6,242 to 94,923 |
Antiseizure medications | ||||||
Carbamazepine (generics) | 100 mg 200 mg | Tablet | 0.1702 0.3302 | 6 to 12 years: 100 mg/day, up to a maximum of 1,000 mg/day. > 12 years: 100 to 400 mg/day, up to a maximum of 800 to 1,200 mg/day. | 0.17 to 1.98 | 62 to 723 |
Clobazam (generics) | 10 mg | Tablet | 0.2197 | < 2 years: 0.5 to 1 mg/kg per day. 2 to 16 years: 5 mg/day, up to a maximum of 40 mg/day. ≥ 16 years: 5 to 15 mg/day, up to a maximum of 80 mg/day. | 0.11 to 1.76 | 40 to 642 |
Lacosamide (generics) | 50 mg 100 mg 150 mg 200 mg | Tablet | 0.6313 0.8750 1.1763 1.4500 | 200 to 600 mg/day. | 1.75 to 4.65 | 639 to 1,697 |
Lamotrigine (Lamictal, generics) | 5 mg 25 mg 100 mg 150 mg | Chewable Tablet Tablet Tablet Tablet | 0.2070 0.0698 0.2787 0.4107 | ≥ 9 kg: 1 to 5 mg/kg per day, maximum 200 mg. ≥ 12 years: 100 to 200 mg/day. | Chewable tablets: 0.41 to 8.28 Regular tablets: 0.28 to 0.56 | Chewable tablets: 151 to 3,022 Regular tablets: 102 to 203 |
Levetiracetam (generics) | 250 mg 500 mg 750 mg | Tablet | 0.3210 0.3911 0.5416 | < 18 years: up to a maximum of 100 mg/kg per day.b ≥ 18 years: 1,000 mg/day up to a maximum of 3,000 mg/day. | 0.78 to 2.17 | 286 to 791 |
Oxcarbazepine (generics) | 150 mg 300 mg 600 mg | Tablet | 0.6209 0.9102 1.8204 | 6 to 16 years: 900 mg/day (20 to 29 kg); 1,200 mg/day (29.1 to 39 kg); 1,800 mg/day (> 39 kg). > 16 years: 600 mg/day up to a maximum of 2,400 mg/day. | 2.73 to 7.28 | 996 to 2,657 |
Sodium valproate (generics) | 250 mg 500 mg 50 mg/mL | Capsule Enteric capsule Oral solution | 0.2905 0.8102 0.0398 per mL | 15 mg/kg/d up to a maximum of mg/d 60 mg/kg per day. | 0.46 to 1.35 | 44 to 2,957 |
Topiramate (generics) | 25 mg 100 mg 200 mg | Tablet | 0.2433 0.4583 0.6748 | ≥ 6 years: 100 mg/day up to a maximum of 400 mg/day. | 0.46 to 1.35 | 167 to 493 |
Vigabatrin (Sabril) | 500 mg | Tablet | 0.9566 | 2 to 16 years: 500 mg/day, up to a maximum of 3,000 mg/day. ≥ 16 years: 1,000 mg/day, up to a maximum of 3,000 mg/day. | 0.96 to 5.74 | 350 to 2,095 |
TSC = tuberous sclerosis complex.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed December 2023), unless otherwise indicated, and do not include dispensing fees. CADTH notes that there are currently no antiseizure medications (ASMs) specifically indicated for patients with TSC, and most patients use a combination of ASMs that are generally indicated for epilepsy.
aSponsor’s submitted price.1
bRecommended dosage is based on clinical expert opinion elicited by CADTH.
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The modelled population comprised patients 2 years of age and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM (i.e., patients who experience at least 8 seizures during a 28-day baseline period). The target population of the economic evaluation is consistent with the enrolled population of the CARE6 clinical trial. However, the Health Canada indication does not restrict usage based on seizure frequency. The sponsor’s modelled population is narrower than the Health Canada–indicated population as it does not consider patients with TSC who have fewer than 8 seizures over a 28-day period. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | No | The model structure did not adequately reflect TSC in clinical practice. Clinical experts noted that the thresholds used by the sponsor for the daily seizure frequency subhealth states do not accurately capture the HRQoL associated with a seizure day, which is partly due to remaining heterogeneity between patients in the highest daily seizure frequency subhealth state (i.e., > 4 seizures per day). Given that patients who experience greater than 4 seizures per day are grouped together in 1 subhealth state, there is potential for patients with high seizure burdens to experience a clinically meaningful reduction in seizures yet remain in the same daily seizure frequency subhealth state. Further, clinical experts noted that the HRQoL impact that seizure frequency may have on patients will differ based on the length of a seizure (e.g., 30 seconds vs. 1 hour). As such, daily seizure frequency subhealth state that do not also consider seizure length may not adequately capture changes in HRQoL. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The model was complex and lacked transparency, containing numerous IFERROR statements making validation difficult. The sponsor did not include the vignette study in their original submission, making the validation of critical health state utility values difficult. |
ASM = antiseizure medication; HRQoL = health-related quality of life; TSC = tuberous sclerosis complex.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
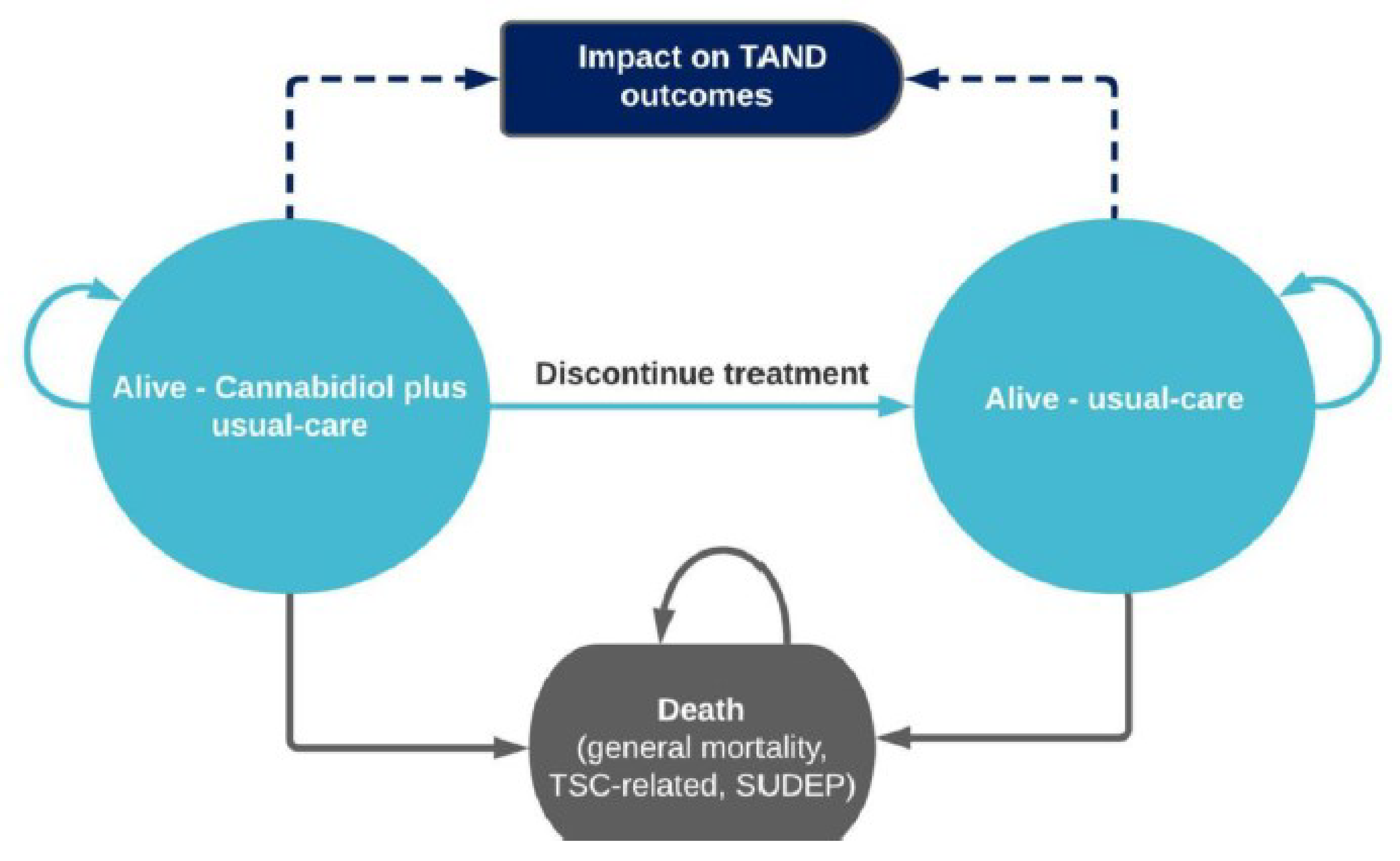
TSC = tuberous sclerosis complex; SUDEP = sudden unexpected death in epilepsy
Source: Sponsor’s Pharmacoeconomic Submission.1
Figure 2: Model Structure With Subhealth States Used for HCRU and HRQoL Calculations
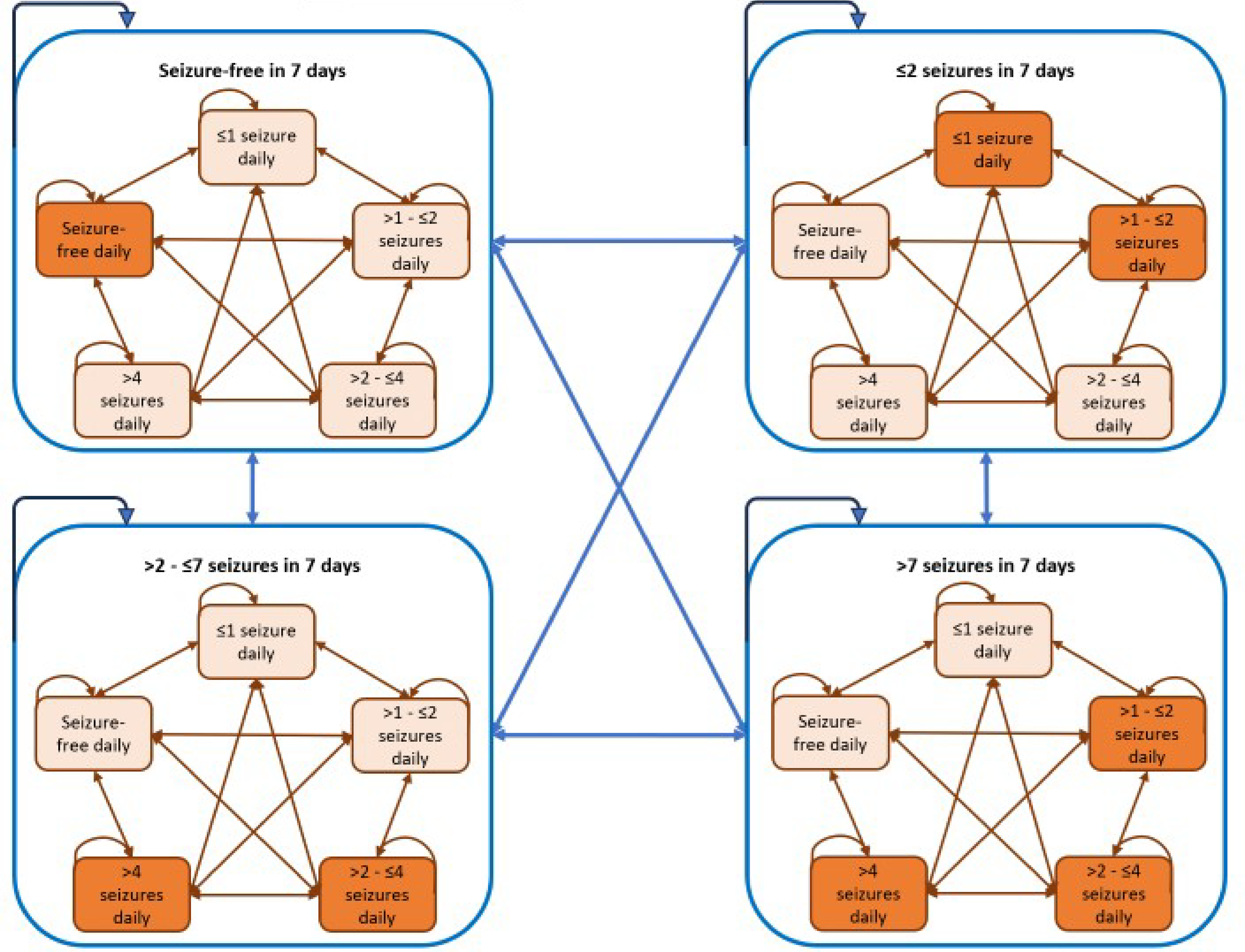
HCRU = health care resource use; HRQoL = health-related quality of life.
Graphical representation of the submitted economic model created by CADTH based on the sponsor’s Pharmacoeconomic Submission.1
Figure 3: Dose-Response Relationship Between Cannabidiol Dose and Seizure Severity in Patients With Dravet Syndrome and Lennox-Gastaut Syndrome From the CARE5 Trial
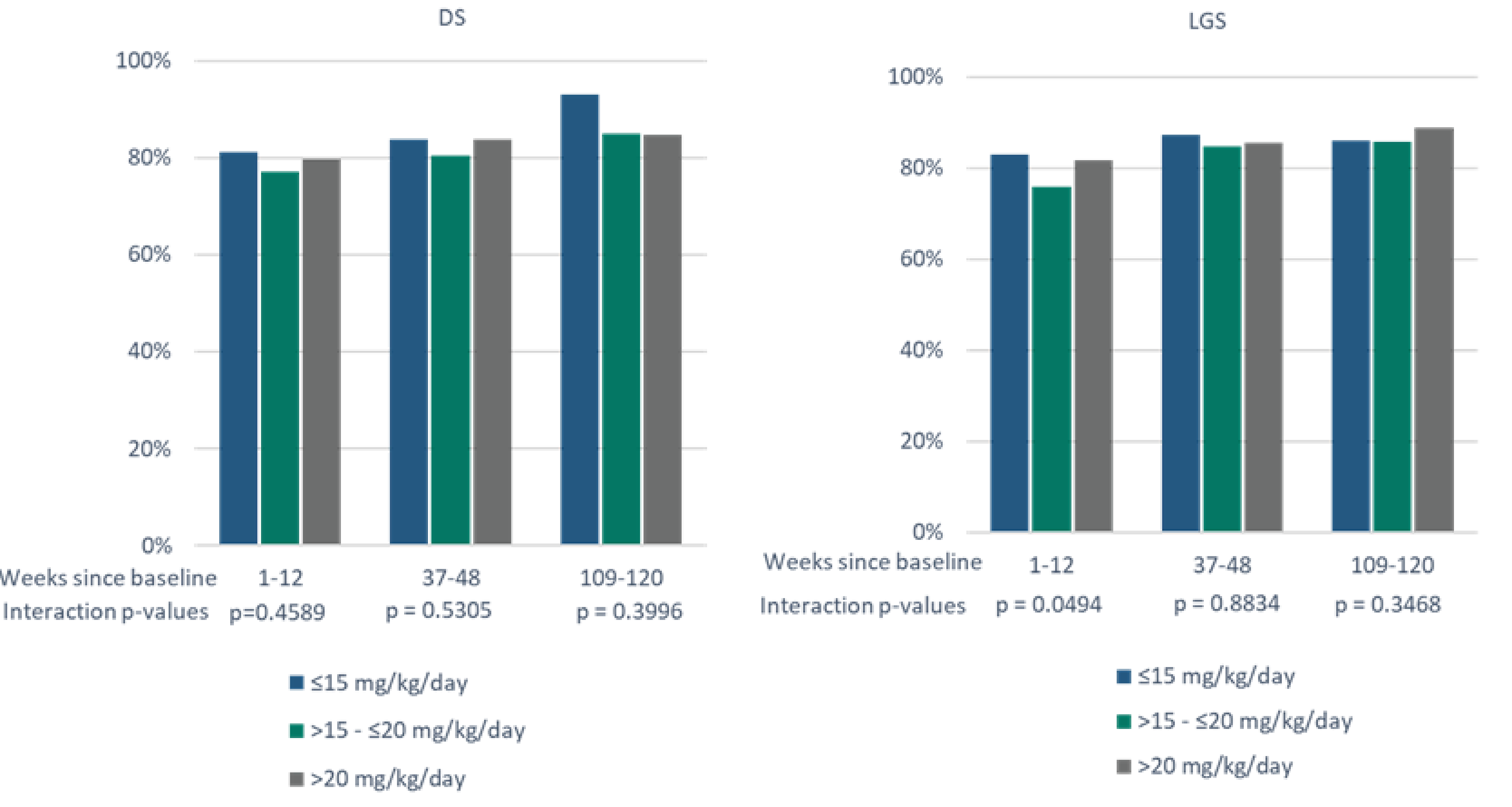
DS = Dravet Syndrome; LGS = Lennox-Gastaut Syndrome.
Source: provided to CADTH by the sponsor in response to a request for additional information.41
Table 10: Summary of Subhealth States Used for HCRU and HRQoL Calculations
HCRU health states | HRQoL health states |
|---|---|
Seizure-free per week | Seizure-free per day |
≤ 2 seizures per week | ≤ 1 seizure per day |
> 2 to ≤ 7 seizures per week | > 1 to ≤ 2 seizures per day |
> 7 seizures per week | > 2 to ≤ 4 seizures per day |
— | > 4 seizures per day |
HCRU = health care resource use; HRQoL = health-related quality of life.
Source: Sponsor’s Pharmacoeconomic Submission.1
Table 11: Patient Characteristics in the CARE6 Trial
Parameter | 2 to 6 years | 7 to 11 years | 12 to 17 years | ≥ 18 years | Total CARE6 population |
|---|---|---|---|---|---|
Mean age, years | 4.46 | 9.37 | 14.90 | 28.10 | 13.70 |
Proportion females, % | 38.20 | 41.70 | 53.10 | 35.00 | 41.90 |
Mean weight, kg | 20.30 | 32.20 | 52.60 | 73.40 | 43.37 |
Age distribution (%) of cohort at baseline | 23.94% | 25.35% | 22.54% | 28.17% | NA |
kg = kilogram; NA = not applicable.
Source: Sponsor’s Pharmacoeconomic Submission.1
Table 12: Subhealth State Utility Values Used in the Model
Subhealth state | Utility value |
|---|---|
Patient utility | |
Seizure-free per day | 0.73 |
≤ 1 seizure per day | 0.33 |
> 1 to ≤ 2 seizures per day | 0.27 |
> 2 to ≤ 4 seizures per day | 0.11 |
> 4 seizures per day | −0.09 |
Caregiver utility decrement | |
Seizure-free per day | 0.00 |
≤ 1 seizure per day | −0.25 |
> 1 to ≤ 2 seizures per day | −0.30 |
> 2 to ≤ 4 seizures per day | −0.40 |
> 4 seizures per day | −0.57 |
Source: Sponsor’s Pharmacoeconomic Submission.1
Table 13: Mean Utility Values for Patients by Seizure Type and Frequency
Seizure frequency per day | Mean utility value | Source | Calculation |
|---|---|---|---|
Seizure-free day | 0.725 | Vignette study | a |
Focal seizures | |||
1 or 2 | 0.504 | Vignette study | b |
3 or 4 | 0.282 | Vignette study | c |
5 and 14 | 0.074 | Vignette study | d |
Generalized seizures | |||
1 | 0.183 | Vignette study | e |
2 | 0.089 | Vignette study | f |
3 and 14 | −0.113 | Vignette study | g |
Combined seizures | |||
1 G, 1 and 4 F | 0.123 | Calculation | = e-(g-h)/2 |
2 G, 1 and 4 F | 0.029 | Calculation | = f-(g-h)/2 |
3 and 14 G, 1 and 2 F | −0.113 | Calculation | = g |
3 and 14 G, 3 or 4 F | −0.174 | Calculation | = (g+h)/2 |
1 G, 5 and 14 F | 0.062 | Calculation | = e-(g-h) |
2 G, 5 and 14 F | −0.174 | Calculation | = f-(g-h) |
3 and 14 G, 5 and 14 F | −0.234 | Vignette study | h |
F = focal seizures with impairment of consciousness or awareness; G = generalized seizures (tonic-clonic, tonic, clonic, and atonic)
Source: Sponsor’s Pharmacoeconomic Submission.1
Table 14: Mean Utility Values for Caregivers by Seizure Type and Frequency
Seizure frequency per day | Mean utility value | Source | Calculation |
|---|---|---|---|
Seizure-free day | 0.867 | Vignette study | a |
Focal seizures | |||
1 or 2 | 0.791 | Vignette study | b |
3 or 4 | 0.638 | Vignette study | c |
5 and 14 | 0.431 | Vignette study | d |
Generalized seizures | |||
1 | 0.546 | Vignette study | e |
2 | 0.476 | Vignette study | f |
3 and 14 | 0.319 | Vignette study | g |
Combined seizures | |||
1 G, 1 and 4 F | 0.427 | Calculation | = e-(g-h)/2 |
2 G, 1 and 4 F | 0.427 | Calculation | = f-(g-h)/2 |
3 and 14 G, 1 and 2 F | 0.319 | Calculation | = g |
3 and 14 G, 3 or 4 F | 0.270 | Calculation | = (g+h)/2 |
1 G, 5 and 14 F | 0.448 | Calculation | = e-(g-h) |
2 G, 5 and 14 F | 0.340 | Calculation | = f-(g-h) |
3 and 14 G, 5 and 14 F | 0.221 | Vignette study | h |
F = focal seizures with impairment of consciousness or awareness; G = generalized seizures (tonic-clonic, tonic, clonic, and atonic)
Source: Sponsor’s Pharmacoeconomic Submission.1
Detailed Results of the Sponsor’s Base Case
Table 15: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Cannabidiol + usual care | Usual care | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 35.98 | 35.98 | 0.00 |
Seizure-free per week | 2.84 | 0.00 | 2.84 |
With seizures (any day per week) | 33.14 | 35.98 | −2.84 |
Discounted QALYs (Patient) | |||
Total | 17.66 | 16.72 | 0.94 |
Seizure-free per day | 14.11 | 12.77 | 1.34 |
1 seizure per day | 0.03 | 0.00 | 0.03 |
> 1 - ≤ 2 seizures per day | 1.50 | 1.66 | −0.16 |
> 2 - ≤ 4 seizures per day | 1.70 | 1.91 | −0.21 |
> 4 seizures per day | 0.31 | 0.35 | −0.04 |
Adverse event disutility | −0.03 | 0.00 | −0.03 |
TAND delay increment | 0.04 | 0.02 | 0.02 |
Discounted QALYs (Caregiver) | |||
Total | −11.70 | −13.05 | 1.35 |
Seizure-free per day | 0.00 | 0.00 | 0.00 |
1 seizure per day | −0.03 | 0.00 | −0.03 |
> 1 - ≤ 2 seizures per day | −2.97 | −3.29 | 0.32 |
> 2 - ≤ 4 seizures per day | −6.05 | −6.81 | 0.76 |
> 4 seizures per day | −2.65 | −2.96 | 0.31 |
Discounted costs ($) | |||
Total | 2,532,749 | 2,433,925 | 98,823 |
Drug-acquisition costs | 194,352 | 0 | 194,352 |
Usual care costs | 54,487 | 54,487 | 0 |
Adverse events | 1,940 | 0 | 1,940 |
Monitoring costs | 35 | 0 | 35 |
Subsequent treatment | 12,731 | 14,994 | −2,263 |
TAND related cost | 234,304 | 234,808 | −504 |
HCRU costs | |||
Seizure free over 7 days | 92,372 | 0 | 92,372 |
≤ 2 seizures | 119,421 | 114,056 | 5,365 |
> 2 - ≤ 7 seizures | 748,172 | 826,004 | −77,832 |
> 7 seizures | 1,074,935 | 1,189,576 | −114,641 |
ICER ($/QALY) | 43,095 | ||
HCRU = health care resource use; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; TAND = TSC-associated neuropsychiatric disorders.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Detailed Results of CADTH Base Case
Table 16: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Cannabidiol + usual care | Usual care | Incremental |
|---|---|---|---|
Discounted Life-years | |||
Total | 35.97 | 35.97 | 0.00 |
Seizure-free per week | 2.87 | 0.00 | 2.87 |
With seizures (any day per week) | 33.11 | 35.97 | −2.87 |
Discounted QALYs | |||
Total | 17.48 | 16.54 | 0.94 |
Seizure-free per day | 14.01 | 12.69 | 1.33 |
≤ 1 seizure per day | 0.03 | 0.00 | 0.03 |
> 1 - ≤ 2 seizures per day | 1.43 | 1.58 | −0.15 |
> 2 - ≤ 4 seizures per day | 1.67 | 1.88 | −0.21 |
> 4 seizures per day | 0.33 | 0.37 | −0.04 |
Adverse event disutility | −0.03 | 0.00 | −0.03 |
TAND delay increment | 0.04 | 0.02 | 0.02 |
Discounted costs ($) | |||
Total | 2,712,168 | 2,435,144 | 277,023 |
Drug-acquisition costs | 372,613 | 0 | 372,613 |
Usual care costs | 54,476 | 54,476 | 0 |
Adverse events | 1,945 | 0 | 1,945 |
Monitoring costs | 35 | 0 | 35 |
Subsequent treatment | 12,714 | 14,987 | −2,274 |
TAND related cost | 234,784 | 235,287 | −503 |
HCRU costs | |||
Seizure free over 7 days | 92,306 | 0 | 92,306 |
≤ 2 seizures | 119,533 | 114,787 | 4,746 |
> 2 - ≤ 7 seizures | 746,496 | 824,885 | −78,389 |
> 7 seizures | 1,077,267 | 1,190,722 | −113,455 |
ICER ($/QALY) | 295,503 | ||
HCRU = health care resource use; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; TAND = TSC-associated neuropsychiatric disorders.
Note this table has not been copy-edited.
Scenario Analyses
Table 17: Scenario Analyses Conducted on the CADTH Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | Usual care | 2,433,925 | 3.67 | Ref. |
Cannabidiol + usual care | 2,532,749 | 5.96 | 43,095 | |
CADTH base case (probabilistic) | Usual care | 2,435,144 | 16.54 | Ref. |
Cannabidiol + usual care | 2,712,168 | 17.48 | 295,503 | |
CADTH Scenario 1: Caregiver disutility included | Usual care | 2,433,785 | 10.12 | Ref. |
Cannabidiol + usual care | 2,712,269 | 11.76 | 169,662 | |
CADTH Scenario 2: Stopping rule | Usual care | 2,477,766 | 16.78 | Ref. |
Cannabidiol + usual care | 2,698,393 | 17.71 | 239,133 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Note this table has not been copy-edited.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 18: Summary of Key Takeaways
Key Takeaways of the BIA |
|---|
|
ASM = antiseizure medication; BIA = budget impact analysis; NIHB = Non-Insured Health Benefits; TSC = tuberous sclerosis complex; WTP = willingness to pay.
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) to estimate the incremental 3-year budget impact of reimbursing cannabidiol as adjunctive therapy for the treatment of patients 2 years of age and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM, as per its reimbursement request. The analysis was performed from the perspective of the Canadian public drug plan formulary. The sponsor estimated the budget impact by comparing 2 scenarios: a reference scenario that estimated the total costs associated with usual care for the treatment of patients 2 years of age and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM; and a new drug scenario, where adjunctive treatment with cannabidiol is funded. Usual care was composed of a variety of ASMs, including sodium valproate, vigabatrin, levetiracetam, clobazam, lamotrigine, lacosamide, oxcarbazepine, topiramate, and carbamazepine. The sponsor estimated the eligible population using an epidemiology-based approach, leveraging data from multiple sources in the scientific literature42-45 and assumptions based on clinical expert input. Drug acquisition costs were the only costs considered in the model. The dosing modelled for cannabidiol reflected the product monograph. Key inputs to the BIA are documented in Table 19.
Key assumptions made by the sponsor include:
100% of pediatric and adult patients were assumed to be titrated up to 12 mg/kg per day as a maintenance dose for cannabidiol.
Distribution of pediatric (72%) and adult patients (28%) was obtained from CARE6 and assumed to be reflective of the real-world patient population with TSC in Canada.10
The 15.2% discontinuation rate observed in the CARE2 trial, which investigated the efficacy of cannabidiol among patients with DS, was assumed to be reflective of patients with TSC in Canada, and applied to patients treated with cannabidiol in Years 2 and 3 of the model.10
85% compliance rate was assumed for treated patients, and alternate rates were explored in scenario analyses.
In pediatric patients, uptake for cannabidiol was assumed to be 5%, 12%, and 21% in Year 1, 2, and 3, respectively.
In adult patients, uptake for cannabidiol was assumed to be 5%, 11%, and 18% in Year 1, 2, and 3, respectively.
Table 19: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target Population | |
Pan-Canadian population (ages 2 years and older) | 30,905,445 |
Prevalence of TSC42 | 0.0088% |
% Pediatric patients10 | 72% |
% with epilepsy43 | 87% |
% with refractory epilepsy45 | 56% |
% Eligible for public coverage | 60% |
% Adult patients10 | 28% |
% with epilepsy44 | 76% |
% with refractory epilepsy44 | 43% |
% Eligible for public coverage | 80% |
Number of patients eligible for drug under review | 780 / 788 / 797 |
Market uptake (3 years) | |
Uptake (reference scenario) | |
Usual care | 100% / 100% / 100% |
Uptake in pediatric population (new drug scenario) | |
Cannabidiol + usual care | 5% / 12% / 21% |
Usual care | 95% / 88% / 79% |
Uptake in adult population (new drug scenario) | |
Cannabidiol + usual care | 5% / 11% / 18% |
Usual care | 95% / 89% / 82% |
Cost of treatment | |
Annual cost of treatment (per pediatric patient) | |
Cannabidiol + usual care | $18,136 to $18,400a |
Usual care | $2,661 |
Annual cost of treatment (per adult patient) | |
Cannabidiol + usual care | $38,395 to $38,955a |
Usual care | $1,740 |
aWeighted average cost of the starting and maintenance doses are applied in year 1, while maintenance doses are applied in years 2 and 3.
TSC = tuberous sclerosis complex.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base case BIA suggest that the incremental expenditures associated with the reimbursement of cannabidiol for the treatment of patients 2 years of age and older with TSC and a history of epilepsy that is inadequately controlled by their current ASM, as per its reimbursement request, would be $911,156 in year 1, $2,022,989 in year 2, and $3,397,821 in year 3, for a 3-year cumulative total of $6,331,966.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The full indicated population for TSC was not modelled: In the BIA, the sponsor assumed that patients with TSC whose seizures are refractory to ASMs would be eligible for cannabidiol, whereas the Health Canada indication for cannabidiol does not specify that it may only be used in an ASM-refractory subgroup. Clinical expert input received by CADTH suggests that cannabidiol will most likely be prescribed for patients whose seizures are refractory to other ASMs; however, if cannabidiol is reimbursed for its full indication, it is possible that the number of patients who receive cannabidiol will be higher than estimated by the sponsor.
In the CADTH base case, the number of eligible patients was assumed to align with the full Health Canada indication. The impact of restricting the eligible population to an ASM-refractory subgroup was explored in scenario analyses.
The NIHB population was inappropriately calculated: The sponsor calculated the total population of CADTH-participating drug plans by adding the population of the provinces as reported by Statistics Canada,46 excluding Quebec, to the population of NIHB clients. NIHB clients living within the borders of a province are counted within provincial population data, thus the NIHB population was double counted in the sponsor’s analysis. Additionally, while the sponsor appropriately limited the included provincial populations to those aged 2 years and older, all clients of the NIHB were included without removing those under 2 years of age, overcounting the potentially eligible NIHB population. Finally, NIHB clients residing within Ontario who are under 25 or over 65 years of age are eligible for reimbursement by ODB and thus should be counted as ODB clients rather than NIHB clients for the purposes of modelling the budgetary impact of reimbursing cannabidiol.
CADTH did not adjust for this limitation in reanalysis. The impact on the pan-Canadian model results is expected to be minimal.
Cannabidiol drug costs are uncertain and likely underestimated: The sponsor assumed that all patients would receive a cannabidiol maintenance dose of 12 mg/kg per day. As noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, this assumption is not aligned with the monograph dosage, which allows for a maintenance dose of up to 25 mg/kg per day depending on “individual clinical response and tolerability.”2 CADTH additionally notes that the recommended maintenance dosage in the product monograph (10 mg/kg per day to 25 mg/kg per day) is substantially lower than the maximum maintenance dose used by patients in the CARE6 trial (25mg/kg per day and 50mg/kg per day). Given the misalignment between the recommended and the studied maintenance dose in CARE6, clinical experts noted that there is potential for clinicians in Canada to increase the dose of cannabidiol to the maximum studied dose (50 mg/kg per day). That is, if cannabidiol were reimbursed, some patients may be prescribed doses that are higher than recommended, but aligned with CARE6.
Finally, the sponsor assumed 85% adherence to cannabidiol, and thus reduced the drug-acquisition costs for cannabidiol by 15%. This is inconsistent with assumptions made in the pharmacoeconomic model, where adherence was not considered. The impact of reduced adherence on the clinical or cost-effectiveness of cannabidiol has not been explored. Furthermore, prescriptions for cannabidiol may be filled and reimbursed regardless of treatment adherence, thus the consideration of adherence of less than 100% may inappropriately reduce the cost of cannabidiol.
CADTH conducted a reanalysis that assumed that all patients would adhere to their prescribed dosage regimen and adopted an average cannabidiol dose of 23 mg/kg per day (aligned with the CADTH base case pharmacoeconomic evaluation), based on the mean maintenance dose observed in patients with TSC enrolled in the 25 mg/kg per day arm of the CARE6 trial.
The proportion of patients eligible for public drug plan coverage is uncertain and may be underestimated: The sponsor assumed that 60% of pediatric and 80% of adult patients with TSC are eligible for public reimbursement. No rationale supporting these assumptions was provided by the sponsor. While it is likely that many pediatric patients will have access to private insurance coverage through their parents’ employers, patients eventually age out of such coverage, and the proportion of adults with TSC who have their own employer-sponsored health insurance is likely small. Additionally, as described in the caregiver vignettes within the sponsor-conducted utility study,41 caregivers of people with TSC may leave full time employment to care for their family member, thus reducing the likelihood of private insurance coverage. As such, the sponsor’s assumptions on the proportion of patients eligible for public funding may be underestimated.
This limitation could not be addressed by CADTH owing to a lack of available data.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analyses by aligning the eligible population with the Health Canada indication for TSC, adopting a maintenance dose of 23 mg/kg per day, and using 100% adherence in the calculation of drug costs. The changes made to derive the CADTH base case are described in Table 20.
Table 20: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Eligible population | Assumed that only patients with drug-resistant TSC-associated epilepsy would be eligible for cannabidiol. | Aligned with the Health Canada indication for TSC. |
2. Maintenance dose of cannabidiol | 12 mg/kg per day | 23 mg/kg per day |
3. Adherence to cannabidiol | 85% | 100% |
CADTH base case | Reanalysis 1 + 2 + 3 | |
BIA = budget impact analysis; TSC = tuberous sclerosis complex.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 21 and a more detailed breakdown is presented in Table 22. In the CADTH base case, the 3-year budget impact of reimbursing cannabidiol as adjunctive therapy for the treatment of seizures associated with TSC is expected to be $28,340,500 (Year 1: $3,930,164; Year 2: $9,134,576; Year 3: $15,275,760).
Table 21: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 6,331,966 |
CADTH reanalysis 1: Full Health Canada population (for TSC) | 12,661,121 |
CADTH reanalysis 2: 23 mg/kg/d maintenance dose of cannabidiol | 12,048,053 |
CADTH reanalysis 3: 100% adherence | 7,449,372 |
CADTH base case (reanalyses 1 + 2 + 3) | 28,340,500 |
BIA = budget impact analysis; TSC = tuberous sclerosis complex.
CADTH conducted additional scenario analyses to explore remaining uncertainty associated with the potential budget impact, using the CADTH base case. Results are provided in Table 22.
Assuming only patients with drug-resistant TSC-associated epilepsy would be eligible for cannabidiol, estimated by the sponsor to be 56% of pediatric and 43% of adult patients with TSC.
Assuming that the price of cannabidiol is reduced by 63%, the price reduction at which cannabidiol + usual care would be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
Table 22: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysisa | Year 0 (current situation) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|
Submitted base case | 0 | 911,156 | 2,022,989 | 3,397,821 | 6,331,966 |
CADTH base case | 0 | 3,930,164 | 9,134,576 | 15,275,760 | 28,340,500 |
CADTH Scenario 1: Drug-resistant TSC only | 0 | 1,950,785 | 4,561,641 | 7,661,754 | 14,174,180 |
CADTH Scenario 2: 63% price reduction for cannabidiol | 0 | 1,462,021 | 3,398,062 | 5,682,583 | 10,542,666 |
BIA = budget impact analysis; TSC = tuberous sclerosis complex.
aAs usual care is not being displaced, costs for usual care are assumed to be $0. The cost of the reference case scenario is $0 in all years and the budget impact of cannabidiol is equal to the cost of the new drug scenario. Therefore, only the budget impact for each analysis is presented in this table.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.